pierre bordachar, laurent barandon service de cardiologie ... · pdf filel’extracteur et...
TRANSCRIPT

L’extracteur et le
chirurgien
Pierre Bordachar, Laurent Barandon
Service de cardiologie et de chirurgie cardiaque
Hôpital Cardiologique Haut-Lévèque

Pour les infections …
Une seule solution: l’extraction !!!
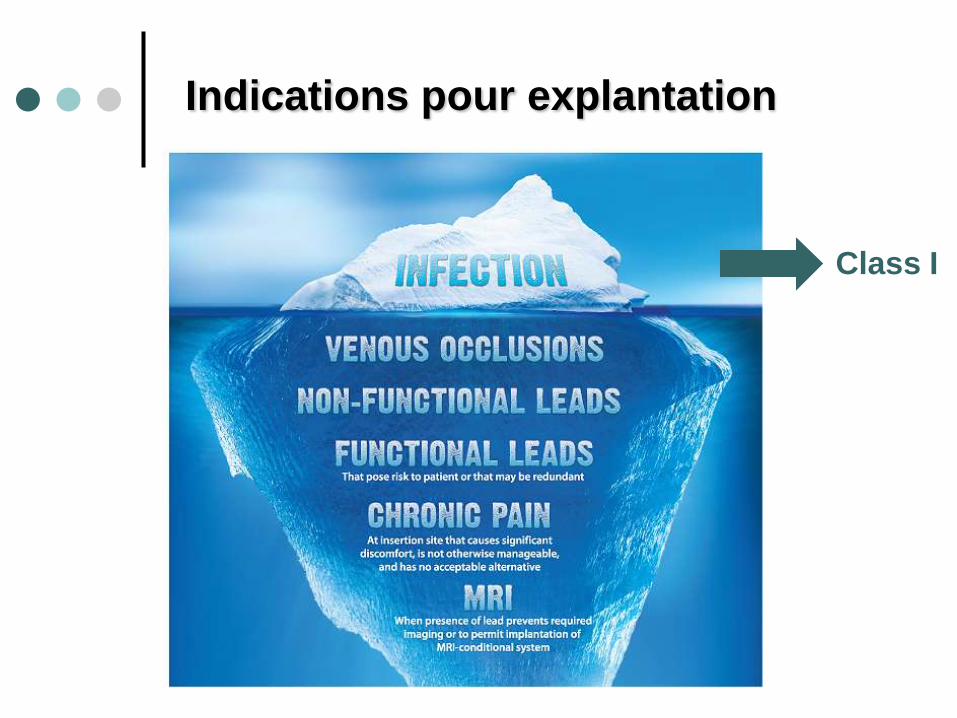
Indications pour explantation
Class I

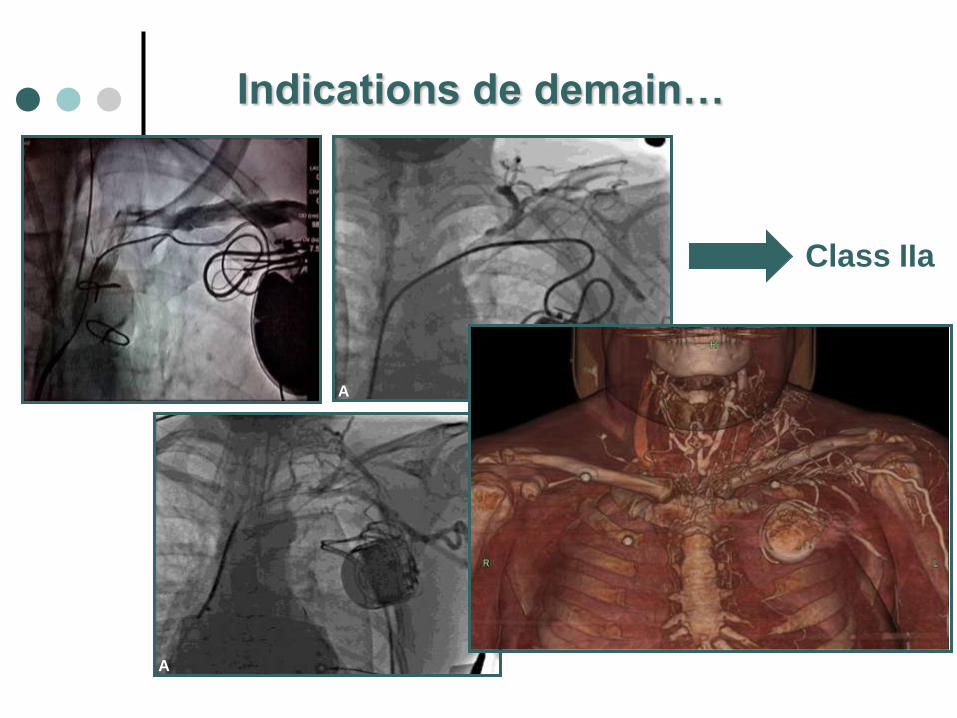
Indications de demain…
Class IIa
Class IIb
A
A
Photographs courtesy of Dr. Josh Cooper and Dr. Avi Fischer
Class IIa
Indications de demain…

RV pacing lead after upgrade to ICD
Class IIa
Class IIb
Indications de demain…

Ce que l’on voit …

Ce que l’on ne voit pas …

Ce que l’on ne voit pas…
mais que l’on sait

Venous entry
Innominate /
SVC
RA
RV
RA tip
RV tip
Sites d’adhérences des sondes
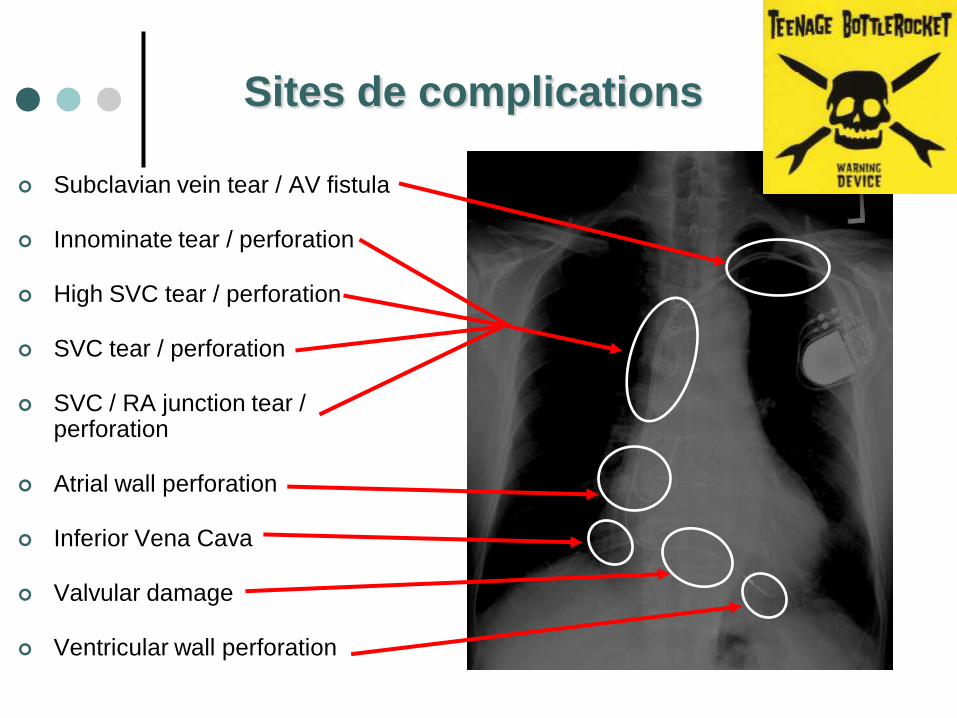
Subclavian vein tear / AV fistula
Innominate tear / perforation
High SVC tear / perforation
SVC tear / perforation
SVC / RA junction tear / perforation
Atrial wall perforation
Inferior Vena Cava
Valvular damage
Ventricular wall perforation
Sites de complications
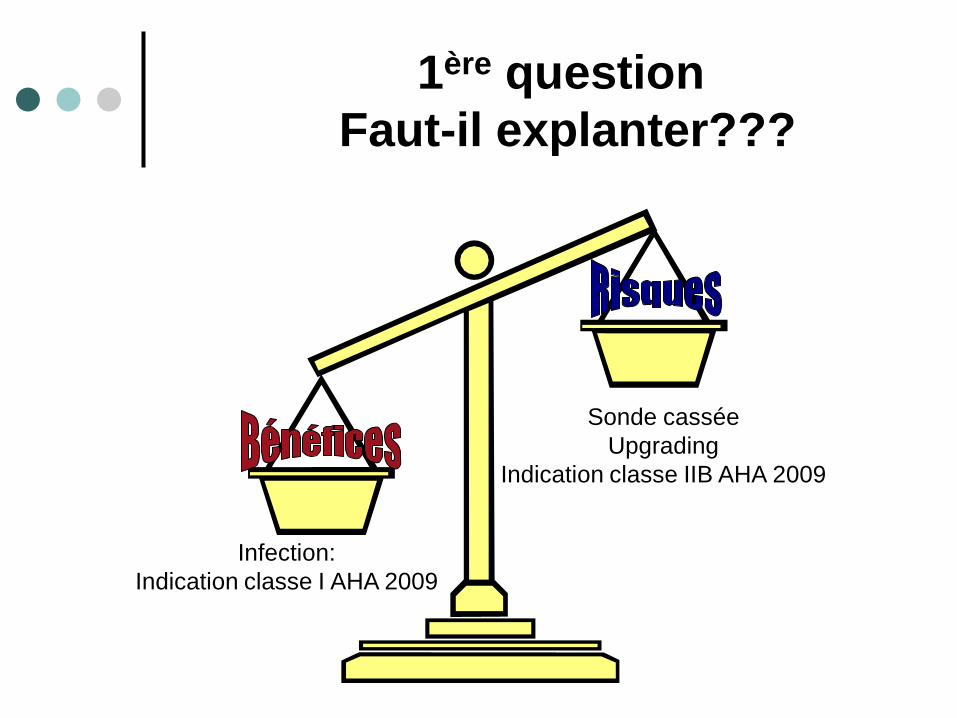
1ère question
Faut-il explanter???
Infection:
Indication classe I AHA 2009
Sonde cassée
Upgrading
Indication classe IIB AHA 2009

2ème question
Chirurgie ou percutanée ???

12% de mortalitéFrame R et al PACE 1993; 16: 2343-2348.
2ème question
Chirurgie ou percutanée ???

ETO
Taille des Végétations
<15 mm >15 mm
Ablation percutanée Ablation chirurgicale
20 mm ?
2ème question
Chirurgie ou percutanée ???
Co-morbidités
EXTRACTION MECANIQUE
PAR VOIE HAUTE

Libération des attaches
proximales

Left PARight PA
Libération des attaches
distales: mandrin métallique classique

1: close 2: open
Libération des attaches
distales: avec mandrin bloqueur

Libération des attaches
distales: avec mandrin bloqueur

Extraction de la sonde
EXTRACTION LASER
PAR VOIE HAUTE

Extraction de la sonde
Laser

Photochemical
Photothermal
Photomechanical
Breaking molecular
bonds
Producing thermal
energy
Creating
kinetic energy
Photoablation is the use of light to vaporize and
remove tissue
Three distinct mechanisms of action contribute to
excimer laser photoablation
Improvement in laser technology

Extraction de la sonde
Laser

Extraction de la sonde
Laser

EXTRACTION MECANIQUE
PAR VOIE BASSE

Extraction de la sonde
Voie basse

Comparison of laser sheath versus femoral
approach for extraction of old pacemaker or
defibrillator leads
A multicenter study
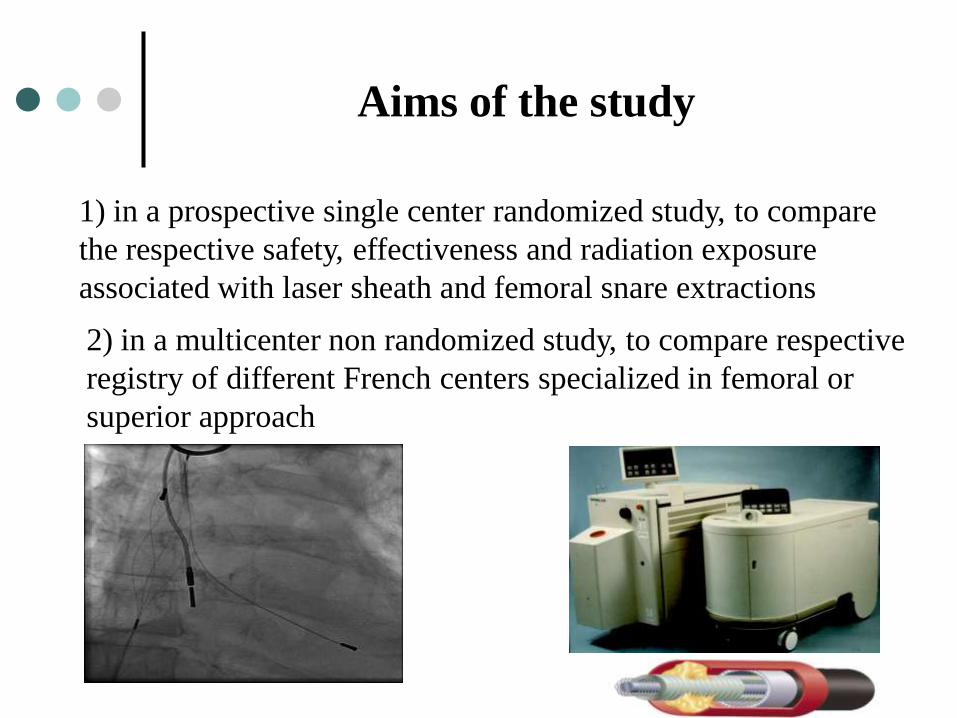
Aims of the study
2) in a multicenter non randomized study, to compare respective
registry of different French centers specialized in femoral or
superior approach
1) in a prospective single center randomized study, to compare
the respective safety, effectiveness and radiation exposure
associated with laser sheath and femoral snare extractions

Methods: single center study
101 consecutive patients were randomly and prospectively
assigned to extraction with:
- a laser sheath (group I: n=50)
- a Dotter™ helical basket (group II: n=51)

Single center study
Characteristics of the patients
Laser
(n=50)
Femoral
(n=51)
p value
Age (year) 69 ± 15 72 ± 15 0.46
Gender: male/female 38/12 40/11 0.77
Left ventricular EF (%) 57 ± 14 53 ± 14 0.25
Time from implantation (year) 12 ± 6 13 ± 6 0.73
Number of leads/patient (n) 2.3 ± 0.7 2.1 ± 0.6 0.23
Device 0.59
Pacemaker 44 (88%) 43 (84%)
ICD 6 (12%) 8 (16%)
Primary indication 0.63
Endocarditis 21 (42%) 19 (37%)
Pocket infection 25 (50%) 25 (49%)
Malfunction or upgrading 4 (8%) 7 (14%)

0%
20%
40%
60%
80%
100%
1 2
Failure
Incomplete
Complete
Laser Femoral
p = ns
Single center study: success rate
- Complete extraction: 88% versus 88%
- Partial extraction: 10% versus 10%
- Failed extraction: 2% versus 2%

Single center study: major complications
We did not observe any per or peri-procedural death
Major complications (p=ns) were observed in:
- 2 patients of group laser (superior vena cava perforation
requiring sternotomy; haemothorax requiring drainage)
- 1 patient of group femoral approach (right atrial
perforation requiring sternotomy)
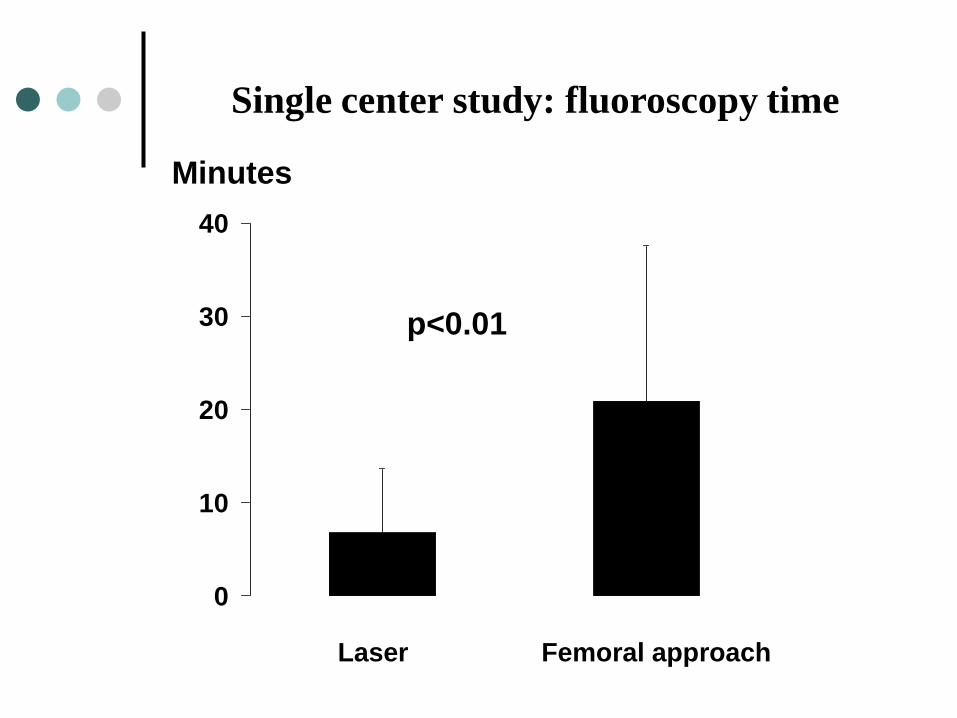
0
10
20
30
40
p<0.01
Laser Femoral approach
Minutes
Single center study: fluoroscopy time

0
40
80
120
160
200
p<0.01
Minutes
Single center study: procedure time
Laser Femoral approach

Methods: multicenter study
3 centers
Femoral approach
n = 138
3 centers
Superior approach
n = 218

Laser
(n=218)
Femoral
(n=138)
p value
Age (year) 71 ± 15 69 ± 15 ns
Gender: male/female 168/50 106/32 ns
LVEF (%) 53 ± 18 50 ± 13 ns
Time from implantation (year) 9 ± 5 10 ± 5 ns
Number of leads/patient (n) 2.1 ± 0.7 2.1 ± 0.8 ns
Device
Pacemaker 180 114
ICD 38 24
Primary indication
Endocarditis 88 50
Pocket infection 94 61
Malfunction or upgrading 36 27
Multicenter study
Characteristics of the patients

Multicenter study: success rate
0%
20%
40%
60%
80%
100%
1 2
Failure
Incomplete
Complete
Laser Femoral
p = ns
- Complete extraction: 85% versus 86%
- Partial extraction: 12% versus 11%
- Failed extraction: 3 % versus 3%

Multicenter study: major complications
We observed 2 per or peri procedure-related deaths in group laser versus 1 in
group femoral approach
Major procedural complications were observed in 4% of patients in group laser,
versus 3% of patients in group femoral approach (p=0.72)
In group laser, major complications included:
- 1 case of haemothorax and 2 cases of tamponade requiring drainage
- 1 case of superior vena cava perforation and one case of subclavian
vein injury requiring urgent surgery
- 1 case of important tricuspid regurgitation
In group femoral approach, major complications included:
- 1 case of tamponade and 1 case of haemothorax requiring drainage
- 2 cases of important tricuspid regurgitation.
Conclusion
- Old transvenous leads were similarly successfully
extracted by the femoral and superior approaches
- Rates of complete extraction and of complications
were similar
- The femoral approach was associated with longer
procedures, longer fluoroscopic times, and a higher
radiation exposure of patients and operators

Plus difficile à
extraire qu’à
implanter
Conclusion