perioperatives management bei patientinnen mit alten und ... · vorstand: prim. prof. dr. b....
TRANSCRIPT

OÄ Dr. Sabine Heil DEAAAbteilung für Anästhesie und IntensivmedizinVorstand: Prim. Prof. Dr. B. Gustorff DEAA
Wien / [email protected]
Perioperatives Management bei PatientInnenmit alten und neuen Gerinnungshemmern
Fortbildung der Blutspendezentralefür Blutdepotbeauftragte12. Mai und 9. Juni 2009

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
0
1000000
2000000
3000000
4000000
5000000
6000000
Zytostatika 5520521,12
Diagnostika 2829318,53
Blutderivate 2428755,48
Antibio tika 2187691,29
Verbandstoffe 839641,34
Isotopen 797223,29
Blutbeeinflussende Arzneimittel 795289,92
Infusionslösungen 733364,46
Chirurgisches Nahtmaterial 678163,89
Antimycotika systemisch 655017,92
1
Anstaltsapotheke WilhelminenspitalLeistungsbericht 2008
Arzneimittel welche 2008 am meisten Kosten verursachten

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
EK FFP TK PPSB 500IE Fibrinogen 1g AT III 500IE rFVIIa 60KIE
2004 2005 2006 2007 2008
Anz
ahl P
rodu
ktei
nhei
t
WIL gesamt
0
200
400
600
800
1000
1200
EK FFP TK PPSB 500IE Fibrinogen 1g AT III 500IE rFVIIa 60KIE
Anästhesie n ~12.000
Statistik 2004-2008

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Paucity of studies to support that abnormal coagulation test results predictBleeding in the setting of invasive procedures: an evidense-based reviewSegal JB, Dzik WHTransfusion 2005;Vol 45:1413-1425
„… clinicians should not assume that mild to moderate prolongation of the INR or PT predicts a higher risk of bleeding or represents an indication for preprocedure
Transfusion of FFP or clotting factor concentrates.“

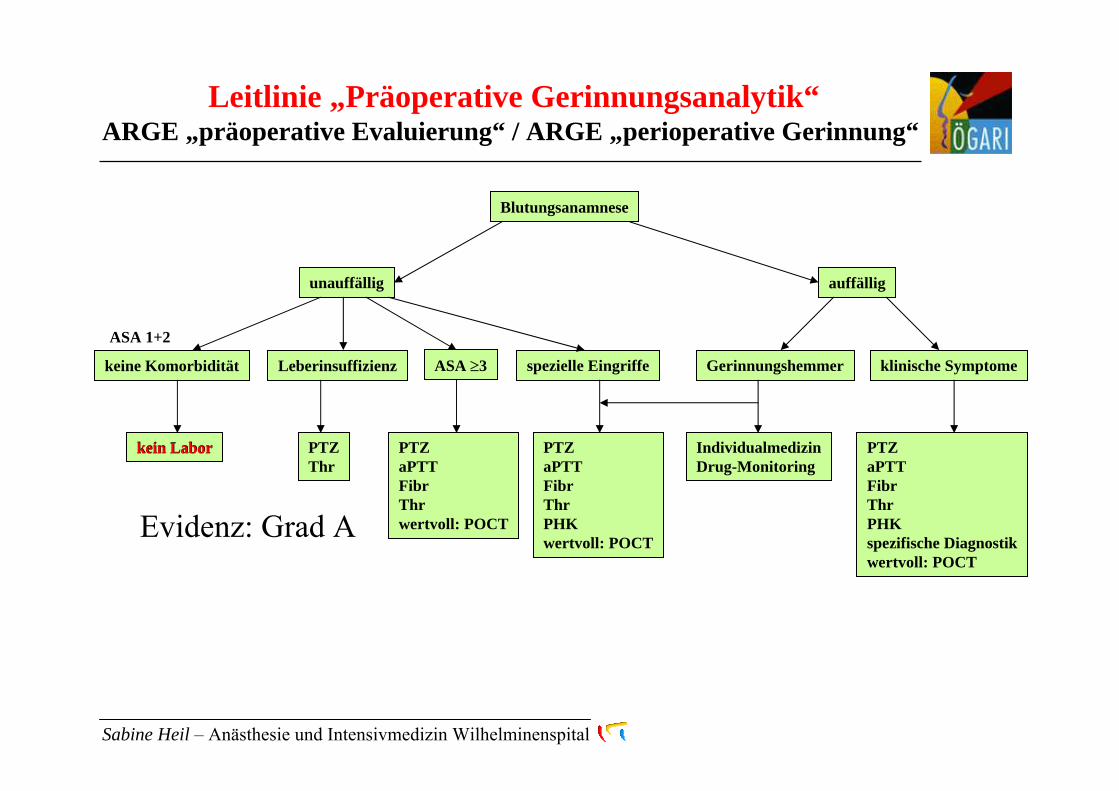
BlutungsanamneseBlutungsanamnese
unauffällig auffällig
keine Komorbidität Leberinsuffizienz ASA ≥ 3 spezielle Eingriffe Gerinnungshemmer klinische Symptome
kein Labor PTZThr
PTZaPTTFibrThrwertvoll: POCT
PTZaPTTFibrThrPHKwertvoll: POCT
IndividualmedizinDrug-Monitoring
PTZaPTTFibrThrPHKspezifische Diagnostikwertvoll: POCT
Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Leitlinie „Präoperative Gerinnungsanalytik“ARGE „präoperative Evaluierung“ / ARGE „perioperative Gerinnung“
www.oegari.at
„Präoperative Blutungsanamnese“– Empfehlungen der Arbeitsgruppe perioperative Gerinnung der Österreichischen Gesellschaft für Anästhesiologie, Reanimation und IntensivmedizinDer Anaesthesist 2007; 56:604-11
kein Labor
Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Blutungsanamnese
unauffällig
keine Komorbidität
kein Labor
auffällig
Leberinsuffizienz ASA ≥3 spezielle Eingriffe Gerinnungshemmer klinische Symptome
PTZThr
PTZaPTTFibrThrwertvoll: POCT
PTZaPTTFibrThrPHKwertvoll: POCT
IndividualmedizinDrug-Monitoring
PTZaPTTFibrThrPHKspezifische Diagnostikwertvoll: POCT
ASA 1+2
Evidenz: Grad A
Leitlinie „Präoperative Gerinnungsanalytik“ARGE „präoperative Evaluierung“ / ARGE „perioperative Gerinnung“

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Blutungsanamnese
auffällig
klinische Symptome
PTZaPTTFibrinogenThrombozytenzahlPHK*spezifische Diagnostikwertvoll: POCT
unauffällig
keine Komorbidität Leberinsuffizienz ASA ≥3 spezielle Eingriffe Gerinnungshemmer
kein Labor PTZThr
PTZaPTTFibrThrwertvoll: POCT
PTZaPTTFibrThrPHKwertvoll: POCT
IndividualmedizinDrug-Monitoring
* Primäre Hämostasekapazität
PHK: vWF:Ag, vWF:RCo, PFA-100 oder Aggregometrie
BA nicht erhebbar !!
Evidenz: Grad A
POCT = Point-of-care funktionelles Gerinnungsmonitoring: z.B. ROTEM
Leitlinie „Präoperative Gerinnungsanalytik“ARGE „präoperative Evaluierung“ / ARGE „perioperative Gerinnung“
PTZaPTTFibrinogenThrombozytenzahlPHK*spezifische Diagnostikwertvoll: POCT
PTZaPTTFibrinogenThrombozytenzahlPHK*spezifische Diagnostikwertvoll: POCT

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Preoperative identification of patients with impaired (primary) haemostasis –A practical conceptJ. Koscielny1, S. Ziemer, H. Radtke, M. Schmutzler, H. Kiesewetter1, A. Salama, G.-F. von TempelhoffHämostaseologie 2007;27(3):177-184
9382298+ PFA-100 (C/E)sBA + Quick (PT), aPTT, Thrombozytenzahl
61552773+ BlutungszeitsBA + Quick (PT), aPTT, Thrombozytenzahl
34228713sBA + Quick (PT), aPTT, Thrombozytenzahl
NPV bzgl. Ausschluss von Hämostase-störungen(%)
PPV bzgl. Erkennung von Hämostase-störungen(%)
nicht erkannte Hämostase-störungen(%)
erkannte Hämostase-störungen(%)
+ zusätzliche Screening-Tests
Klassisches präoperativesScreening mit standardisierter Blutungsanamnese (sBA)

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Case Report 02/08
56a, weiblichHemicolektomie rechts am Folgetag geplant
sBA positiv
x
xx
x
xx
xx
x
xx
x
Erweiterte Gerinnungsanalytik

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
OP verschoben
93.9F XIII Akt. %
76F VIII:C Akt. %
28.6vWF-Antigen %
>300PFA-ADP sec
>300PFA-Epinephrin sec
367Fibrinogen funktionell mg/dl
100AT III %
18.3TZ sec
31aPTT sec
96PTZ %
13vWF-Aktivität %
56a, weiblichHemicolektomie rechts am Folgetag geplant
sBA positiv
Erweiterte Gerinnungsanalytik
Case Report 02/08
Diagnose: angeborene VWD Typ 1
Therapie: DDAVP (1-Deamino-8-D-Arginin-Vasopressin)* FVIII/vWF-Konzentrat
*More on: platelet function analyzer (PFA)-100 closure time in the evaluation of platelet disorders and platelet function.Koscielny J, Kiesewetter H, von Tempelhoff GF; J Thromb Haemost 2006; 4:1426-1427

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Blutungsanamnese
auffällig
Gerinnungshemmer
PTZaPTTFibrThrPHKwertvoll: POCT
IndividualmedizinDrug-Monitoring
klinische Symptome
PTZaPTTFibrThrPHKspezifische Diagnostikwertvoll: POCT
unauffällig
keine Komorbidität Leberinsuffizienz ASA ≥3 spezielle Eingriffe
kein Labor PTZThr
PTZaPTTFibrThrwertvoll: POCT
Lokoregionalanästhesien unter gerinnungshemmender MedikationEmpfehlungen der AGPG der ÖGARIDer Anaesthesist 2005; 55:476-84Update 2009: www.oegari.at
Leitlinie „Präoperative Gerinnungsanalytik“ARGE „präoperative Evaluierung“ / ARGE „perioperative Gerinnung“

Substanzen Therapieende + Labortestwert Therapiebeginnvor Punktion / Katheterentfernung nach Punktion / Katheterentfernung
Unfraktionierte Heparineprophylaktische Dosis 3 h 1 htherapeutische Dosis aPTT oder ACT im Referenzbereich (> 3 h) 1 h (s.c.), 6-12 h (i.v.)
Niedermolekulare Heparineprophylaktische Dosis 11 h 2 htherapeutische Dosis 24 h + anti-Xa-Aktivität im Referenzbereich 2 h
Direkte ThrombininhibitorenDesirudin, Lepirudin 4,4 h + aPTT im Referenzbereich 4 hArgatroban 2 h + aPTT im Referenzbereich 4 hBivalirudin 1 h + aPTT im Referenzbereich 4 hDabigatran 26 h 3,5 h
Synthetisches PentasaccharidFondaparinux (≤ 2,5 mg/die) 34 h 4 h
Direkte Faktor-Xa-InhibitorenRivaroxaban 16 h 3 h
Heparinoide / Danaparoid anti-Xa-Aktivität im Referenzbereich 4 hVitamin K-Antagonisten INR < 1,4 sofortrekombinantes aktiviertes Protein C 2 h 4 hAdenosin Diphosphat (ADP) Rezeptor-Antagonisten
Clopidogrel 7 Tage sofortTiclopidin 10 Tage sofort
CyclooxygenasehemmerASS, NSAR, COX II-H. nicht erforderlich sofort
Glykoprotein IIb/IIIa-InhibitorenAbciximab 48 h 4 hTirofiban, Eptifibatid 8 h 4 h
Antiaggregatorische ProstaglandineIloprost 2 h sofortProstacyclin, Prostaglandin E1 0,5 h sofort
Lok
oreg
iona
lanä
sthe
sien
unt
er g
erin
nung
shem
men
der
Med
ikat
ion:
Em
pfeh
lung
en d
er A
GPG
der
ÖG
AR
IU
pdat
e 20
09: w
ww
.oeg
ari.a
t

VitK-Antagonist
II Thrombin
FVIIa/TF
Gewebefaktor =TF
X Xa X
VIIIa VIII
XIa XI
Va V
Ext
rins
isch
es S
yste
m
Intrinsisches System
Fibrinogen
Fibrinmonomere
Fibrinpolymere
Quervernetzte Fibrinpolymere
XIII XIIIa
UFH
NMWHDTI
HeparinoidPentasaccharid
Quick, PTZ, INRProthrombinzeitReagens: TF, Ca2+, Phospholipid
aPTT, aktivierte Pro-thrombinzeitReagens: Kaolin, Phospholipide
Antifaktor Xa Ecarin Clotting Time
Activated Clotting Time
Antikoagulatorische Substanzen - Monitoring
FVII
FVIIaIXa IX
Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
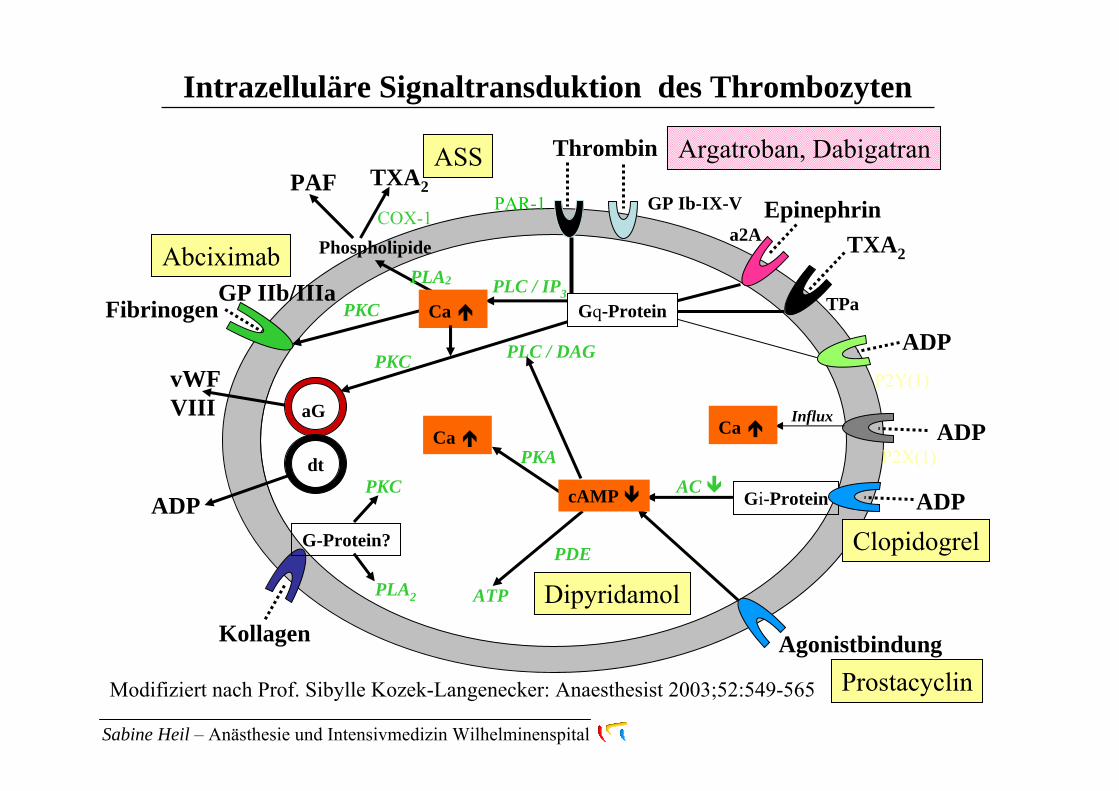
Intrazelluläre Signaltransduktion des Thrombozyten
PKA
Thrombin
PAR-1 GP Ib-IX-V
Phospholipide
GP IIb/IIIa
TXA2
ADP
Epinephrin
TPa
Gi-ProteinP2Y(12)
Ca
a2A
PAF TXA2
PLA2
COX-1
AC
ADPP2Y(1)
PKC
PLC / IP3
ADP
ADPP2X(1)
aGvWFVIII Influx
PLC / DAG
PKC
Agonistbindung
dt
Kollagen
PKC
G-Protein?
PLA2
Ca Ca
Clopidogrel
Abciximab
ASS
Dipyridamol
Prostacyclin
Fibrinogen
PDE
ATP
Modifiziert nach Prof. Sibylle Kozek-Langenecker: Anaesthesist 2003;52:549-565
cAMP
Gq-Protein
Argatroban, Dabigatran

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Blutungsanamnese
auffällig
Gerinnungshemmer
PTZaPTTFibrThrPHKwertvoll: POCT
IndividualmedizinDrug-Monitoring
Phytopharmaka
Drugmonitoring wenn
keine präoperative Therapiepauseverminderte EleminationMedikamente mit klinisch relevanter Steigerung der Blutungsmenge
Evidenz: Grad C
Leitlinie „Präoperative Gerinnungsanalytik“ARGE „präoperative Evaluierung“ / ARGE „perioperative Gerinnung“
Multiplate®
Evidenz: Grad AManagement bei dualer Antiplättchentherapie
Metzler H et al.: Der Anaesthesist 2007; 56:401–12ACCP Chest 2008, 133:S71-105
PTZaPTTFibrThrPHKwertvoll: POCT

Empfehlungen des Arbeitskreises „Gerinnung Wilhelminenspital“: Perioperatives Management von Patienten mit koronarem Stent, nach akutem Koronarsyndrom (ACS) oder perkutaner koronarer Angioplastie (PTCA) unter dualer Plättchenhemmung mitAcetylsalizylsäure (ASS) und Clopidogrel beim nicht kardiochirurgischen Eingriff.
Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
0sehr hoch
hoch
gering
ASS
ASS + Clopidogrel
RisikoStentthrombose
hoch
geringDuale
Antiplättchen-therapie
Blutungsrisiko
Nicht kardiochirugischer Eingriff
Notfall Semi-elektiv und dringlich Elektiv
Freigabe zur OP „Case by case“Entscheidung
Beendigung der Therapiemit Clopidogrel abwarten
ASS wenn möglich belassen
*
* Evidenz: Grad A
Arbeitskreis
Gerinnung
Arbeitskreis
Gerinnung

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Bare Metall Stent 4 Wochen Drug Eluting Stent 12 Monate
Im Einzelfall kann eine kürzere Dauer der dualen Plättchenhemmung akzeptiert werden (3-) 6 Monate
Nach ACS 9-12 Monate
ASS soll lebenslang verabreicht werdenClopidogrel abhängig von der koronaren Situation wie folgt
Präoperative KarenzzeitenASS 2(-7) Tage / Clopidogrel 7(-10) Tage
Postoperatives WiedereinsetzenASS und Clopidogrel je nach Blutungsrisiko binnen24-48 Stunden mit Erhaltungsdosis
Empfehlungen des Arbeitskreises „Gerinnung Wilhelminenspital“: Perioperatives Management von Patienten mit koronarem Stent, nach akutem Koronarsyndrom (ACS) oder perkutaner koronarer Angioplastie (PTCA) unter dualer Plättchenhemmung mitAcetylsalizylsäure (ASS) und Clopidogrel beim nicht kardiochirurgischen Eingriff.
Arbeitskreis
Gerinnung
Arbeitskreis
Gerinnung

Argatroban - Argatra®direkter, monovalenter,reversibler TI
Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Thrombininhibitoren
Bivalirudin - Angiox®direkter, bivalenter,reversibler TI
Dabigatran Etexilat - Pradaxa®diekter, reversibler, kompetitiver TIoral, HWZ 14-17h, 85% renal
Lepirudin - Refludan®direkter, bivalenter TIirreversibler Komplex
i.v.

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
i.v. Thrombininhibitoren
nicht verfügbarnicht verfügbarnicht verfügbarAntidot
NeinNeinNeinKreuzreaktivität mit HIT-Antikörpern
Ja, starkJaJaEffekt auf INR
aPTT, (ECT), ACT aPTT, ACTaPTT, ECTDrug-Monitoring
MinimalJaJaUltrafiltration
überwiegend hepatischgeringfügig renal
enzymatische Proteolyse, geringfügig renalrenalElimination
54%keinegeringPlasmaproteinbindung
52719806980Molekulargewicht
52 ± 16 min25 min1,3 h (i.v.); 2 h (s.c.)Halbwertszeit
ArgatrobanBivalirudinLepirudinEigenschaften

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Ausgewählte Gerinnungshemmer zur Thromboseprophylaxe bei Hüft- und Kniegelenksersatz im Vergleich
Rivaroxaban - Xarelto®direkter Faktor-Xa-Hemmer
Fondaparinux Natrium - Arixtra®indirekter Faktor-Xa-Hemmer
Dabigatran Etexilat - Pradaxa®diekter, reversibler, kompetitiver TI
Postoperativer Beginn1x täglichKumulation bei NiereninsuffizienzKein Antidot
s.c.HWZ 17 hElemination 64-77% renalWeitere Indikationsgebiete
Superior gegenüber EnoxaparinoralHWZ 5-7hElemination 66% renal + 28% biliärSehr hohe EiweißbindungoralHWZ 14-17hElemination 85% renal

AGPG der ÖGARI: Anaesthesist 2005; 54:476-84S.A. Kozek-Langenecker: Anaesthesist 2008 · 57:597–606
Substanzen Antidot medikamentöse nicht-medikamentöse Antagonisierung Therapieoptionen Elimination
MEDIKAMENTE MIT ANGRIFFSPUNKT IN DER PLASMATISCHEN GERINNUNG
Unfraktionierte Heparine ProtaminNiedermolekulare Heparine (Protamin) Fondaparinux rVIIa PlasmaphereseDesirudin, Lepirudin PPSB, rVIIa, DDAVP Hämodialyse, -filtrationArgatroban FFP Hämodialyse?Bivalirudin FFP, PPSB, rFVIIa Ultrafiltration Dabigatran FFP, forcierte Diurese HämodialyseRivaroxapan Aktivkohle, rFVIIaDanaparoid FFP, PPSB, rVIIa PlasmaphereseKumarine Vitamin K PPSB, FEIBA
Frischplasma, rVIIa
MEDIKAMENTE MIT ANGRIFFSPUNKT IN DER ZELLULÄREN GERINNUNG
Acetylsalizylsäure DDAVP,TKClopidogrel, Ticlopidin DDAVP,TKPlasmapherese
Glukokortikoide, AprotininAbciximab Thrombozytenkonzentrat (TK)
rVIIa, GlukocorticoideTirofiban, Eptifibatid Glukocorticoide Hämodialyse, -filtration

FVIIa/TF
Gewebefaktor =TF
FVII
FVIIa
X Xa X
II
VIIIa VIII
XIa XI
Va V
IXa IX
Ext
rins
isch
es S
yste
m
Intrinsisches System
Fibrinogen
Fibrinmonomere
Fibrinpolymere
Quervernetzte Fibrinpolymere
XIII XIIIa
rFVIIa
Thrombin
TK
Fibrinogen
rFVIII
FIX
EK
FFP
DDAVP
FXIII
FIV = Calcium
AprotininTranexamsäure
Protamin
FVIII/vWFTherapie der Blutung
Azidose + Hypothermie korrigieren
PPSBII, VII, IX, X
Vitamin K
Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital

Sabine Heil – Anästhesie und Intensivmedizin Wilhelminenspital
Zusammenfassung
Bewusstsein für Kosten und Ressourcen
Standardisierte Blutungsanamnese
Sinnvolle Gerinnungsanalytik
Fundierte Kenntnis Gerinnung beeinflussender Medikamente
Karenzzeiten einhalten
Balance von Blutungs- und Thromboserisiko
Gezielte Therapie bei Blutung oder Thrombose

Vielen Dank für ihre Aufmerksamkeit!
Arbeitsgruppe „Perioperative Gerinnung“ derÖsterreichisch Gesellschaft für Anästhesie, Reanimation und Intensivmedizin