cardiovascular consequences of obstructive sleep apnea
TRANSCRIPT

Introduction
Obstructivesleepapnoea(OSA)ischaracterizedbyrepetitive interruption of ventilation during sleep dueto collapse of the pharyngeal airway. The inspiratoryairflow can be either reduced (hypopnoea) or completely absent(apnoea),andanapnoeathatlasts10secorlonger,associatedwithongoingventilatoryeffort,characterizesa patient with OSA. To establish a definitive diagnosis, a full polysomnography is required. The diagnosis of OSA is confirmed when a person has an apnoea-hypopnoea index (AHI; number of apnoeas and hypopnoeas per hour of sleep) > 5 events/h associated with symptoms of excessive daytime sleepiness1.
OSA is a public health issue due to its highprevalence in North American, European and Asian
Cardiovascular consequences of obstructive sleep apnoea
Fatima H. Sert Kuniyoshi, Snigdha Pusalavidyasagar*, Prachi Singh & Virend K. Somers
Division of Cardiovascular Diseases, Department of Internal Medicine, Mayo Clinic & Foundation, Rochester MN & *Division of Sleep Medicine, University of Minnesota Medical Center, Minneapolis, MN, USA
ReceivedFebruary26,2009
Obstructive sleep apnoea (OSA) is a form of sleep disordered breathing with a high prevalence rate and is often underdiagnosed. OSA is associated with hypertension, coronary artery disease, stroke, peripheral vascular disease, heart failure, and arrhythmias. The presence of OSA may be a strong predictor of fatal cardiovascular events in patients with cardiovascular disease (CVD). Increased sympathetic drive, activation of metabolic and inflammatory markers, and impaired vascular function are some of the proposed mechanisms that could explain the association between OSA and cardiovascular diseases. Understanding these mechanisms is important for identifying treatment strategies. The presence of OSA should be considered in clinical practice, especially in patients with CVD. Randomized intervention studies are needed to establish whether early identification and treatment of OSA patients reduces cardiovascular morbidity.
Key words Cardiac arrhythmias - cardiovascular risk - CPAP - ischaemia - myocardial infarction - OSA
nations. Epidemiologic data in the US population show that approximately 20 per cent of adults have at least mild OSA (AHI > 5 events/h) and about 7 per cent of adults have moderate to severe OSA (AHI > 15 events/h), affecting preferentially the male gender2. Home sleep studies suggest that 7.5 per cent of urban middle-aged Indian men have OSA3.Longitudinal data have confirmed that obesity and ageing increase the risk of OSA4. It has also beensuggested that the nocturnal pathophysiologicmechanisms activated in OSA patients might lead to cardiovasculardiseases5,6 (Fig.1).Thisreviewwillprovide insights into mechanisms that might link OSAtocardiovasculardiseases,andoutlineevidenceoftheassociationbetweenOSAandcardiovascularconditions.
196
Indian J Med Res 131, February 2010, pp 196-205
Review Article

Pathophysiological mechanisms linking OSA with cardiovascular risk
OSA patients experience intermittent hypoxaemia and CO2 retention that modify the autonomic and haemodynamic responses to sleep7.Althoughthere isnoconsistentevidenceofthecausalroleofOSA,thefrequent nocturnal cardiovascular stressors experienced by these patients over the years might contribute to the development of chronic cardiovascular diseases. Acute hypoxaemia activates pathophysiological responses that might also lead to acute nocturnal cardiac events8-11.
(i) Sympathetic activation and cardiovascular variability
InOSApatients, recurrentnocturnal apnoeas arefollowed by sympathetic activation. Interestingly, higher sympathetic drive persists during daytime wakefulness even in normoxic conditions9 (Fig. 2).Heightened muscle sympathetic activity to peripheral bloodvesselsinOSApatientsappearstobeindependentofobesity12.OSApatientsalsohavefasterheartratesduring resting wakefulness, suggesting that there is also an increased cardiac sympathetic drive13.
(ii) Inflammation
Hypoxaemic stress may also play a role in the activation of systemic inflammatory pathways14.In fact, OSA patients (who also have a combination of repetitive episodes of hypoxaemia and sleep deprivation) have increased levels of plasma cytokines, adhesion molecules15,16, serum amyloid-A17, and C-reactive protein (CRP)16,18-20. Increased CRP levels in OSApatientsappeartobeindependentofadiposity20.
Obstructive sleep apnoeic patients also haveenhanced leukocyte activation21,22. In vitro experiments showed that monocytes from OSA patients bind more actively to endothelial cells than do monocytes from control subjects, and this can be attenuated by treatment with continuous positive airway pressure (CPAP)21.
Insights from cell culture studies also provide evidence that intermittent hypoxia may promote different reactions when compared with sustained hypoxia, and might help to explain the association between OSA and the development of cardiovascular diseases. Intermittent hypoxia followed by complete reoxygenation selectively activates the pro-inflammatory transcription factor NFκB, and increases circulating tumour necrosis factor
Fig.1. Schematic outlining proposed pathophysiologic components of OSA, activation of cardiovascular disease mechanisms, with consequent development of established cardiovascular disease. [Reprinted with permission from Wolters Kluwer Health (Circulation2008;118 : 1080-111)].
Fig. 2. Recordings of sympathetic activity, respiration and intra-arterial blood pressure in a patient with sleep apnoea on no medications and free of other diseases. Measurements were obtained during wakefulness (top left), during obstructive sleep apnoea (OSA) in rapid eye movement (REM) sleep (bottom), and during REM sleep after treatment of OSA with continuous positive airway pressure (CPAP). During wakefulness, sympathetic activity was high and blood pressure was approximately 130/60 mmHg. During REM sleep, repetitive apnoea resulted in hypoxia and chemoreflex stimulation with consequent sympathetic activation. The vasoconstriction resulting from sympathetic activation causes marked surges in blood pressure to levels as high as 250/110 mmHg at the end of apnoea, because of increases in cardiac output attermination of apnoea. Treatment of sleep apnoea and elimination of apnoeic episodes by CPAP resulted in stabilization and lower levels of both blood pressure and sympathetic activity during REM sleep. [Reprinted with permission from The American Society for ClinicalInvestigaion(J Clin Invest1995;96 : 1897-904)].
KUNIyOSHI et al: OSA & CARDIOVASCULAR DISEASES 197
(TNF)-alpha in OSA patients. These effects can be reduced by the use of CPAP therapy23.
(iii) Endothelial dysfunction
Increased oxidative stress and systemicinflammation together with reduced nitric oxide (NO) availabilityand cell apoptosis might contribute to the endothelial dysfunctionobservedinpatientswithOSA24,25.Althoughthere are conflicting results regarding the presence of endothelialdysfunctioninOSApatients26-28, recentdatashowedreducedendothelialnitricoxidesynthase(eNOS)and phosphorylated e-NOS (P-eNOS) expression in OSA, suggestive of endothelial dysfunction29. These changesare reversed after 4 wk of CPAP therapy. Moreover, this study showed an inverse relationship between eNOSand P-eNOS in venous endothelial cells and OSA severity29. Oxygen tension might play an important role in NO production30; in fact, it has been proposed thatconduitvesselendothelialdysfunctioninOSApatientsisproportional to the nocturnal hypoxaemia31.
Experimental data suggest that hypoxaemia induces endothelin-1 release in cultured human endothelium32.Phillips and colleagues33haveshownthatseveralhoursof untreated severe sleep apnoea results in increasedendothelin-1 levels, which correlated with the changes in blood pressure. Recent data support a role for endothelin-1inraisingbloodpressureinOSApatients34.
(iv) Intra-thoracic pressure changes
In patients with OSA, the abrupt and repetitiveinspiratoryeffortagainstaclosedupperairwayduringthe apnoeic episodes generate changes in negative intra-thoracic pressure that increase transmural gradients across the atria, ventricles and aorta35,36 and may disruptventricularfunction35. leading to autonomic and haemodynamic instability37.Moderate tosevereOSAis associated with impaired right and left ventricular function, increased left atrial volume, wall stress, and afterload38,39, and impaired diastolic function38,40.Thesecardiac changes may contribute to the development of atrial fibrillation and heart failure in OSA patients. Furthermore, Sampol and colleagues41suggestthattheincreased aortic transmural pressure may impose an additional risk of aortic dissection in OSA patients.
The Association between OSA and cardiovascular diseases
Myocardial ischaemia
Experimental data have shown that chronic intermittent hypoxia induces atherosclerosis in the presence of a high cholesterol diet42. Indeed OSA
patients who were free of co-morbidities presentedearly signsof atherosclerosis43. In a more recent study, Turmel et al44 showed a strong correlation betweenAHI and atherosclerotic plaque volume measured by intravascular ultrasound imaging. Chronic effects of OSA that might contribute to atherogenesis include systemic inflammation, oxidative stress, vascular smooth cell activation, lymphocyte activation, increased lipidlowering in macrophages, lipid peroxidation,high-density lipoproteindysfunction,andendothelialdysfunction45.
On the other hand acute effects of OSA thatcould potentially be a trigger for plaque rupture with consequent cardiac ischaemia include severe intermittent hypoxaemia, acidosis, increased blood pressure and sympathetic vasoconstriction, in conjunction with simultaneous changes in intra-thoracic and cardiac transmural pressures6.Nocturnalangina and ST depression have been described inOSA patients, and may be diminished after treatment with CPAP46,47. However, a later study48 did not find evidence of nocturnal myocardial injury detectable by measurements of cardiac troponin T in patients with established coronary artery disease and moderate/severeOSA,beforeandafterasinglenight’ssleep.
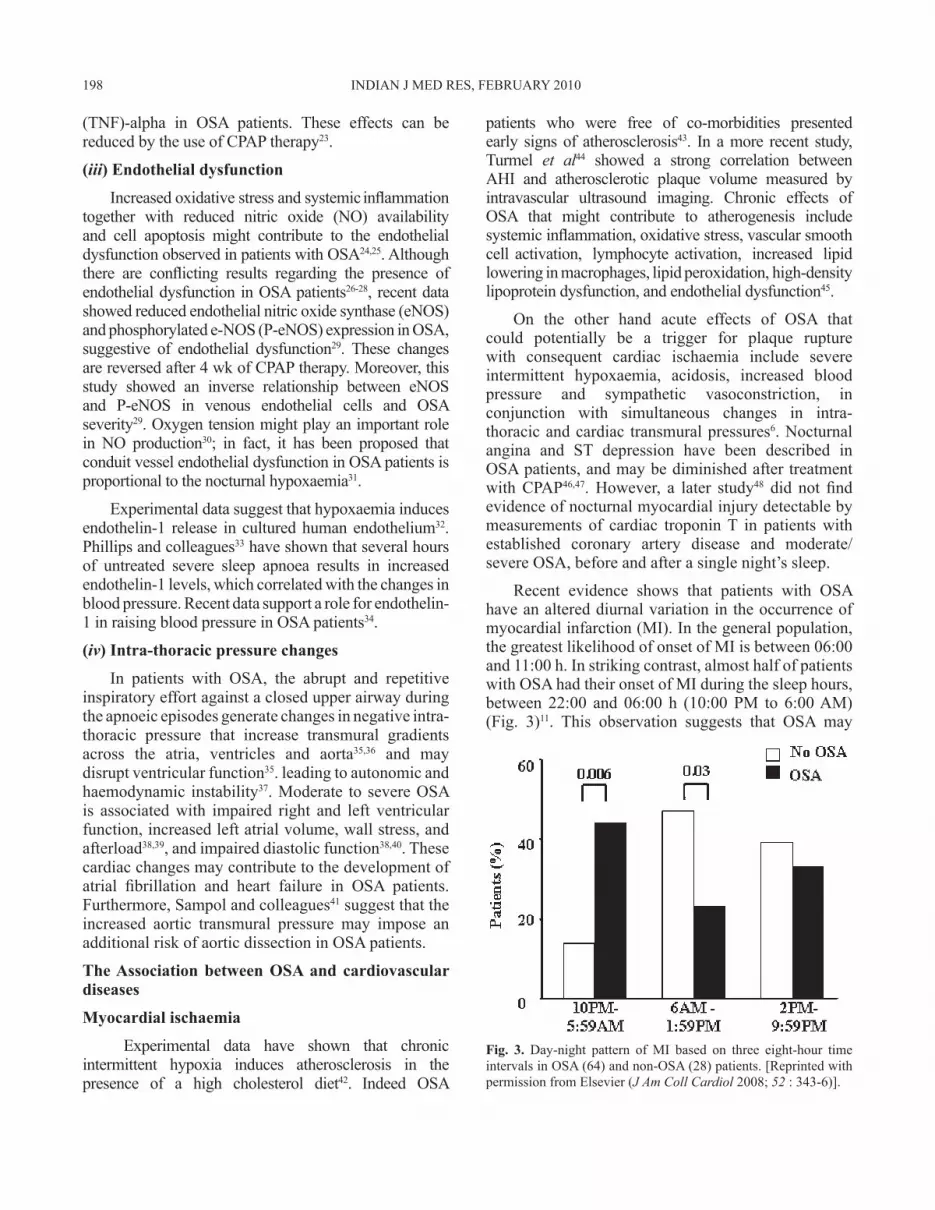
Recent evidence shows that patients with OSAhaveanaltereddiurnalvariationintheoccurrenceofmyocardial infarction (MI). In the general population, the greatest likelihood of onset of MI is between 06:00 and 11:00 h. In striking contrast, almost half of patients withOSAhadtheironsetofMIduringthesleephours,between 22:00 and 06:00 h (10:00 PM to 6:00 AM) (Fig. 3)11. This observation suggests that OSA may
Fig. 3. Day-night pattern of MI based on three eight-hour time intervals in OSA (64) and non-OSA (28) patients. [Reprinted with permission from Elsevier (J Am Coll Cardiol 2008;52 : 343-6)].
198 INDIAN J MED RES, FEBRUARy 2010
precipitate nocturnal MI and that nocturnal MI may contribute to the increased likelihood of nocturnal suddencardiacdeathobservedinOSApatients10.
Treatment of OSA was associated with a decrease in theoccurrenceofnewcardiovasculareventsinpatientswith combined OSA and coronary artery disease49.Doherty et al50observedthattotalcardiovasculardeathswere less common in CPAP-treated patients compared to CPAP intolerant patients.
Even though there is evidence of an association betweensleepapnoeaandcoronaryarterydisease51-54,thereisstillnoproofofcausality.
Heart failure
There is a high likelihood of OSA in patients with systolic heart failure and diastolic dysfunction55,56.About10percentofsystolicheartfailurepatientsarethought tohaveOSA.Theassociationbetween thesetwoconditionsisreinforcedbytheobservationthatbothsystolic and diastolic functions improve with adequate treatment of the sleep disorder of breathing40,57,58. While CPAP therapy seems to improve ejection fraction, there is as yet no evidence that treating OSA can reducemortality in heart failure patients.
Obstructive events, which may occur hundreds of times over the course of the night, and induce abrupt increases in left ventricule transmural pressure, could play an important role in the development of myocardial ischaemia, contractile dysfunction, and ventricular dilation59. The sympathetic surges and blood pressure increases may also be expected to worsen heart failure in patients with co-existent OSA46,60,61.
Heart failure may directly exacerbate OSA by oedema formation in the soft tissues of the neck. Reduction in the intravascular volume and attenuated venous congestion resulting from heart failure treatment couldpotentiallyreduceOSAseverity62.
Systemic hypertension
ThereisevidencethatOSAandhypertensionarecausally related63,64,withOSAoftenundiagnosed65-69.An apnoea-hypopnoea index of 15 events/h or more was independently associated with a 3-fold increased risk of developing hypertension70 in the Wisconsin cohort study. OSA patients tend to lack the sleep related nocturnal decrease in blood pressure (non-dippers). The attenuationofnocturnalbloodpressurereductionisanindependent risk factor for cardiovascular morbidity71.
Intermittent hypoxaemia, chemoreceptor stimulation, sympathetic activation, and the renin-angiotensin system are possible mechanisms by which OSA might leadtohypertension72,73.
Sleep disordered breathing and endothelialdysfunction are more likely to occur in patients with pre-eclamptic toxaemia74. The concept that pregnancy may exacerbatesleepapnea is supportedbyevidence thattheseverityofsleepapnoeaandtheassociatedbloodpressure responses as measured in the third trimester, improve significantly (P=0.03)afterparturition75.
Treatment of OSA may help decrease daytime blood pressure (BP), especially in patients with resistant hypertension (defined as a clinic BP of > 140/90 mmHg while taking a combination of three or more antihypertensive drugs, titrated to maximally recommended doses) and in patients with relatively mild hypertension76.
Pulmonary hypertension
The prevalence of pulmonary hypertension (PH) in OSA patients ranges from 17 to 53 per cent. The reason for this wide range may be due to methodological problems, such as selection bias77. Even though OSA patients experience frequent episodes of increased pulmonary artery pressure during sleep, the pulmonary hypertension is generally milder than in primary PH78.Patients with OSA in conjunction with PH tend to have higher BMI, left heart disease, parenchymal lung disease, and greater nocturnal oxygen desaturations. Hypoxicvasoconstriction with consequent vascular remodeling is thought to be the likely primary mechanism for any OSA-related pulmonary arterial hypertension79, 80.
Pulmonary arterial pressure and pulmonary vascular reactivity to hypoxia is reduced with continuouspositive airway pressure (CPAP) therapy81.
Stroke
Stroke has been linked to OSA in both cross-sectional and case-controlled studies, and sleep apnoea is highly prevalent in patients with stroke82-85. Patients at risk for OSA and at risk for stroke share common demographic features.
The fluctuations in blood pressure, reduction in cerebral blood flow, altered cerebral autoregulation, endothelial dysfunction, accelerated atherogenesis,and pro-thrombotic and pro-inflammatory states are some of the mechanisms that have been implicated in increased risk of stroke in OSA patients6.
KUNIyOSHI et al: OSA & CARDIOVASCULAR DISEASES 199

OSA in post-stroke patients may be associated with reduced motivation, cognitive impairment, increased risk of recurrent stroke, and death. A significant relationisalsoevidentbetweenAHIandthedegreeofmetabolic impairment in cerebral white matter86.Thesealterations may be associated with neuropsychological andcognitivedysfunctioninOSApatients.
The potential for rehabilitation post-stroke may be improved with positive airway pressure treatment among stroke patients. CPAP treatment in acute stroke can be started in about 50 per cent of patients withsleep-disordered breathing but can be chronically maintained in only a minority of patients83.Ontheotherhand, the percentage of continued CPAP usage among stroke patients with OSA was higher in another study87.ItisstillunclearwhetherOSAbyitself,independentofother factors, is a significant cause of stroke.
Arrhythmias
OSAisassociatedwithdifferent typesofcardiacarrhythmias. Their prevalence and complexity increase with the severity of the OSA and the associatedhypoxaemia88-91.
Bradyarrhythmias are sometimes seen in OSA, in conjunction with obstructive apnoeas. Vagally mediated sinusbradycardiaoccursasaphysiologicalresponsetoapnoea and hypoxaemia. Various forms of nodal heart block are common and may occur even in the absence of any disease of the cardiac conduction system. Treatment of underlying OSA usually eliminates these arrhythmias92,93.
Atrial fibrillation is also common in people with OSA. The mechanisms that predispose to the development of atrial fibrillation in OSA patients are hypoxaemia, sympathetic activation, blood pressure surges, transmural pressure changes and systemic inflammation. Gami et al94 showed an increased risk of incident atrial fibrillation in younger patients with OSA. Kanagala et al95inaprospectivestudy,observedthat patients cardioverted for atrial fibrillation in the setting of untreated OSA had a high likelihood of recurrence of the atrial fibrillation compared to OSA patients treated with CPAP.
Ventricular arrhythmias varying from benign premature ventricular contractions (seen in up to two-thirds of patients with OSA) to fatal ventricular tachycardia have been reported in patients withOSA92,96. A significant link between sleep apnoea and nocturnalventricularectopywasevidentintheSleep
Heart Health Study91. Nocturnal arrhythmias in OSA patients are often attenuated by effective treatment of thedisorderedbreathing93,97-100.
Management of OSA patients
Continuous positive airway pressure (CPAP)
CPAP consists of an air-pressure source that keeps aconstantpositivepressureintheairwaythroughtherespiratory cycle. The airflow is delivered through a nasal or oronasal interface, and maintains patency of the upper airway. The optimal pressure level is determined during a sleep study and is intended to eliminate the respiratory events in all sleep stages and all sleeping positions. CPAP continues to be the primary therapy for patients with OSA101,102. Besidesimprovement in daytime sleepiness, and neurocognitive function103-108, there is also evidence that therapy might reduce cardiovascular risk in OSA patients. Reduction in sympathetic activity, blood pressure and arterial stiffness and improvement in baroreflex sensitivity and endothelial dysfunction are some of the proposed mechanisms by which CPAP therapy might reduce cardiovascular risk109.
Bi-level positive airway pressure (BiPAP) is also an option that maintains a constant positive pressure in the airway,butprovidestwopressurelevels,withalowerexpiratory pressure, which reduces work of breathing and might increase acceptance and compliance. This might be a better choice in patients with OSA associated with chronic obstructive pulmonary disease110.
Positional therapy
This refers to the use of sleep posture that might have a positive impact on breathing pattern during sleep. Since apnoea is often worse in the supineposture111,avoidanceof thispostureduringsleepcanbe achieved through a variety of means including body
belts, an uncomfortable object sewn into the back of the nightshirt, positional alarms and specially designed pillows.111 Cervical extension might be helpful since this positionisassociatedwithanincreaseinupperairwaycross-sectional sizeandreducedairwayresistance112.
Oral appliances
Mandibular advancement devices (MADs) are the most common oral appliance used for treatment of OSA. These devices increase the antero-posterior dimensions
of the oropharynx through mechanical advancement of themandible. While some studies have shown reduced AHIandsnoring113, improvement in sleep architecture,
200 INDIAN J MED RES, FEBRUARy 2010

oxidativestressandendothelialdysfunction114,thereisas yet no evidence of reduced cardiovascular risk after treatment with oral applicances115. However, MADs couldbeconsideredwhenpatientscannottolerate,orare not complaint with CPAP therapy.
Weight loss
Obesity plays a major role in the pathogenesis of sleep apnoea and probably also in the associatedcardiovascular risk116. A prospective cohort study ofmildly overweight individuals showed that a 10 per cent weight losspredicteda26percentdecrease insleepapnoeaseverity4. The exact mechanism of improvement is not completely understood, but might be related to improvement in airway structure, neurophysiologic regulation of respiration, and chemoreflex function117.
Surgery
The goal of surgical treatment in OSA patients is toincreaseairwaysizeandreduceairwayresistance118.Uvulopalatopharyngoplasty (UPPP) is the most common surgery for OSA, and is used to enlarge the retropalatal airway. The procedure is complex, and involves some amount of risk and discomfort, and long term efficacy needs to be better understood. Tracheostomy can be considered in patients with life-threatening OSA who fail or do not accept non-surgical treatment119.There is a lack of studies comparing the efficacy of CPAP versus surgery in cardiovascular risk reduction.
Conclusion
There is a high and rising prevalence of OSAdue to the rising incidenceofobesity.Therefore, thepresence of OSA should be considered in clinicalpractice, especially in obese patients with co-morbid cardiovascular disease. Whether treating OSA will reduce cardiovascular risk and improve outcomes is still controversial. Therefore randomized controlled trials are needed to assess the efficacy of OSA treatment in reducing cardiovascular morbidity and mortality.
Acknowledgment
Virend K. Somers is supported by NIH Grants HL65176 and M01-RR00585. Fatima H. Sert Kuniyoshi is supported by American Heart Association grant 09-20069G. Prachi Singh is supported by American Heart Association grant 07-257872Z.
Conflict of interest: VKS serves as a consultant for ResMed and Respironics, and has spoken at meetings sponsored by Respironics, ResMed and Medtronic. He has also served as consultant forGlaxoSmithKline, Sepracor, and Cardiac Concepts. He has been a principal investigator or co-investigator on research grants from
the ResMed Foundation, the Respironics Sleep and BreathingFoundation, Sorin, Inc., and Select Research, Inc. He also works with Mayo Health Solutions and iLife on intellectual propertyrelatedtosleepandtoobesity.
References1. The Report of an American Academy of Sleep Medicine
Task Force. Recommendations for syndrome definitive and measurement techniques in clinical research. Sleep1999; 22:667-89.
2. young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructivesleepapnea:apopulationhealthperspective.Am J Respir Crit Care Med2002;165 : 1217-39.
3. Udwadia ZF, Doshi AV, Lonkar SG, Singh CI. Prevalence of sleep-disordered breathing and sleep apnea in middle-aged urban Indian men. Am J Respir Crit Care Med 2004; 169 :168-73.
4. Peppard PE, young T, Palta M, Dempsey J, Skatrud J. Longitudinal study of moderate weight change and sleep-disorderedbreathing.JAMA2000;284 : 3015-21.
5. Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, Javier NietoF,et al. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study.Am J Respir Crit Care Med2001;163 : 19-25.
6. Somers VK, White DP, Amin R, Abraham WT, Costa F, CulebrasA,et al.Sleepapneaandcardiovasculardisease:anAmerican Heart Association/American College Of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council On Cardiovascular Nursing.IncollaborationwiththeNationalHeart,Lung,andBlood Institute National Center on Sleep Disorders Research (NationalInstitutesofHealth).Circulation2008;118 : 1080-111.
7. Somers VK, Dyken ME, Mark AL, Abboud FM. Sympathetic-nerve activity during sleep in normal subjects. N Engl J Med 1993;328 : 303-7.
8. Somers VK, Mark AL, Zavala DC, Abboud FM. Influence of ventilation and hypocapnia on sympathetic nerve responses to hypoxia in normal humans. J Appl Physiol1989; 67 : 2095-100.
9. Somers VK, Dyken ME, Clary MP, Abboud FM. Sympathetic neural mechanisms in obstructive sleep apnea. J Clin Invest1995;96 : 1897-904.
10. Gami AS, Howard DE, Olson EJ, Somers VK. Day-night patternofsuddendeathinobstructivesleepapnea.N Engl J Med 2005;352 : 1206-14.
11. Kuniyoshi FH, Garcia-Touchard A, Gami AS, Romero-Corral A, van der Walt C, Pusalavidyasagar S, et al. Day-night variation of acute myocardial infarction in obstructive sleep apnea.J Am Coll Cardiol2008;52 : 343-6.
12. Narkiewicz K, van de Borne PJ, Cooley RL, Dyken ME, Somers VK. Sympathetic activity in obese subjects with and withoutobstructivesleepapnea.Circulation1998;98 : 772-6.
13. Narkiewicz K, Montano N, Cogliati C, van de Borne PJ, Dyken ME, Somers VK. Altered cardiovascular variability in obstructivesleepapnea.Circulation1998;98 : 1071-7.
KUNIyOSHI et al: OSA & CARDIOVASCULAR DISEASES 201

14. Hartmann G, Tschop M, Fischer R, Bidlingmaier C, Riepl R, Tschop K, et al. High altitude increases circulating interleukin-6, interleukin-1 receptor antagonist and C-reactive protein. Cytokine2000;12 : 246-52.
15. Ohga E, Tomita T, Wada H, yamamoto H, Nagase T, Ouchi y. Effects of obstructive sleep apnea on circulating ICAM-1, IL-8, and MCP-1. J Appl Physiol2003;94 : 179-84.
16. Minoguchi K, yokoe T, Tazaki T, Minoguchi H, Oda N, Tanaka A, et al.Silentbraininfarctionandplateletactivationinobstructivesleepapnea.Am J Respir Crit Care Med 2007; 175 : 612-7.
17. Svatikova A, Wolk R, Shamsuzzaman AS, Kara T, Olson EJ, Somers VK. Serum amyloid A in obstructive sleep apnea. Circulation2003;108 : 1451-4.
18. Shamsuzzaman AS, Winnicki M, Lanfranchi P, Wolk R, Kara T, Accurso V, et al. Elevated C-reactive protein in patients withobstructivesleepapnea.Circulation2002;105 : 2462-4.
19. Larkin EK, Rosen CL, Kirchner HL, Storfer-Isser A, Emancipator JL, Johnson NL, et al. Variation of C-reactive protein levels in adolescents: association with sleep-disordered breathingandsleepduration.Circulation2005;111 : 1978-84.
20. Punjabi NM, Beamer BA. C-reactive protein is associated with sleep disordered breathing independent of adiposity.Sleep 2007; 30 : 29-34.
21. Dyugovskaya L, Lavie P, Lavie L. Increased adhesion molecules expression and production of reactive oxygen species in leukocytes of sleep apnea patients. Am J Respir Crit Care Med2002;165 : 934-9.
22. Dyugovskaya L, Lavie P, Lavie L. Lymphocyte activation as a possible measure of atherosclerotic risk in patients with sleep apnea. Ann N Y Acad Sci2005; 1051 : 340-50.
23. Ryan S, Taylor CT, McNicholas WT. Selective activation of inflammatory pathways by intermittent hypoxia in obstructive sleep apnea syndrome. Circulation2005;112 : 2660-7.
24. El Solh AA, Akinnusi ME, Baddoura FH, Mankowski CR. Endothelial cell apoptosis in obstructive sleep apnea: a link toendothelialdysfunction.Am J Respir Crit Care Med 2007; 175 : 1186-91.
25. Ip MS, Tse HF, Lam B, Tsang KW, Lam WK. Endothelial function in obstructive sleep apnea and response to treatment. Am J Respir Crit Care Med2004;169 : 348-53.
26. Kato M, Roberts-Thomson P, Phillips BG, Haynes WG, Winnicki M, Accurso V, et al. Impairment of endothelium-dependentvasodilationofresistancevessels inpatientswithobstructivesleepapnea.Circulation2000;102 : 2607-10.
27. Carlson JT, Rangemark C, Hedner JA. Attenuated endothelium-dependentvascularrelaxationinpatientswithsleepapnoea.J Hypertens1996;14 : 577-84.
28. Kraiczi H, Hedner J, Peker y, Carlson J. Increased vasoconstrictorsensitivityinobstructivesleepapnea.J Appl Physiol2000;89 : 493-8.
29. Jelic S, Padeletti M, Kawut SM, Higgins C, Canfield SM, Onat D, et al. Inflammation, oxidative stress, and repair capacity of the vascular endothelium in obstructive sleep apnea.Circulation2008;117 : 2270-8.
30. Lavie L. Obstructive sleep apnoea syndrome--an oxidative stressdisorder.Sleep Med Rev2003;7 : 35-51.
31. Cross MD, Mills NL, Al-Abri M, Riha R, Vennelle M, Mackay TW, et al. Continuous positive airway pressure improves vascular function in obstructive sleep apnoea/hypopnoeasyndrome: a randomised controlled trial. Thorax 2008;63 :578-83.
32. Kourembanas S, Marsden PA, McQuillan LP, Faller DV. Hypoxiainducesendothelingeneexpressionandsecretionincultured human endothelium. J Clin Invest1991;88 : 1054-7.
33. Phillips BG, Narkiewicz K, Pesek CA, Haynes WG, Dyken ME, Somers VK. Effects of obstructive sleep apnea on endothelin-1 andbloodpressure.J Hypertens1999;17 : 61-6.
34. Gjorup PH, Sadauskiene L, Wessels J, Nyvad O, Strunge B, Pedersen EB. Abnormally increased endothelin-1 in plasma duringthenightinobstructivesleepapnea:relationtobloodpressure and severity of disease. Am J Hypertens 2007; 20:44-52.
35. Buda AJ, Pinsky MR, Ingels NB, Jr., Daughters GT, 2nd, Stinson EB, Alderman EL. Effect of intrathoracic pressure on left ventricular performance. N Engl J Med 1979; 301 : 453-9.
36. Floras JS, Bradley TD. Treating obstructive sleep apnea: is there more to the story than 2 millimeters of mercury? Hypertension 2007; 50 : 289-91.
37. Somers VK, Dyken ME, Skinner JL. Autonomic and hemodynamic responses and interactions during the Mueller maneuver in humans. J Auton Nerv Syst 1993;44 : 253-9.
38. Otto ME, Belohlavek M, Romero-Corral A, Gami AS, Gilman G, Svatikova A, et al. Comparison of cardiac structural and functional changes in obese otherwise healthy adults withversuswithoutobstructivesleepapnea.Am J Cardiol 2007; 99 : 1298-302.
39. Romero-Corral A, Somers VK, Pellikka PA, Olson EJ, Bailey KR, Korinek J, et al. Decreased right and left ventricular myocardial performance in obstructive sleep apnea. Chest2007; 132 : 1863-70.
40. Arias MA, Garcia-Rio F, Alonso-Fernandez A, Mediano O, Martinez I, Villamor J. Obstructive sleep apnea syndrome affects left ventricular diastolic function: effects of nasalcontinuous positive airway pressure in men. Circulation2005;112 : 375-83.
41. Sampol G, Romero O, Salas A, Tovar JL, Lloberes P, Sagales T,et al.Obstructivesleepapneaandthoracicaortadissection.Am J Respir Crit Care Med2003;168 : 1528-31.
42. Savransky V, Nanayakkara A, Li J, Bevans S, Smith PL, Rodriguez A, et al. Chronic intermittent hypoxia induces atherosclerosis.Am J Respir Crit Care Med 2007; 175 : 1290-7.
43. Drager LF, Bortolotto LA, Lorenzi MC, Figueiredo AC, Krieger EM, Lorenzi-Filho G. Early signs of atherosclerosis inobstructivesleepapnea.Am J Respir Crit Care Med2005;172 : 613-8.
44. Turmel J, Series F, Boulet LP, Poirier P, Tardif JC, Rodes-CabeauJ,et al.Relationshipbetweenatherosclerosisandthesleep apnea syndrome: an intravascular ultrasound study. Int J Cardiol2009;132 : 203-9.
45. Lorenzi-Filho G, Drager LF. Obstructive sleep apnea and atherosclerosis: a new paradigm. Am J Respir Crit Care Med2007; 175 : 1219-21.
202 INDIAN J MED RES, FEBRUARy 2010
46. Franklin KA, Nilsson JB, Sahlin C, Naslund U. Sleep apnoea andnocturnalangina.Lancet1995;345 : 1085-7.
47. Peled N, Abinader EG, Pillar G, Sharif D, Lavie P. Nocturnal ischemic events in patients with obstructive sleep apnea syndrome and ischemic heart disease: effects of continuous positive air pressure treatment. J Am Coll Cardiol1999;34:1744-9.
48. Gami AS, Svatikova A, Wolk R, Olson EJ, Duenwald CJ, Jaffe AS,et al.CardiactroponinTinobstructivesleepapnea.Chest 2004;125 : 2097-100.
49. Milleron O, Pilliere R, Foucher A, de Roquefeuil F, Aegerter P, Jondeau G, et al. Benefits of obstructive sleep apnoea treatment in coronary artery disease: a long-term follow-up study.Eur Heart J2004;25 : 728-34.
50. Doherty LS, Kiely JL, Swan V, McNicholas WT. Long-term effectsofnasalcontinuouspositiveairwaypressure therapyon cardiovascular outcomes in sleep apnea syndrome. Chest 2005;127 : 2076-84.
51. Mooe T, Rabben T, Wiklund U, Franklin KA, Eriksson P. Sleep-disordered breathing in men with coronary artery disease.Chest 1996;109 : 659-63.
52. Peker y, Kraiczi H, Hedner J, Loth S, Johansson A, Bende M. Anindependentassociationbetweenobstructivesleepapnoeaandcoronaryarterydisease.Eur Respir J1999;14 : 179-84.
53. Sanner BM, Konermann M, Doberauer C, Weiss T, Zidek W. Sleep-disordered breathing in patients referred for angina evaluation--association with left ventricular dysfunction. Clin Cardiol2001; 24 : 146-50.
54. Shafer H, Koehler U, Ewig S, Hosper E, Tasci S, Luderitz B. Obstructive sleep apnea as a risk marker in coronary artery disease.Cardiology1999;92 : 79-84.
55. Chan J, Sanderson J, Chan W, Lai C, Choy D, Ho A, et al.Prevalence of sleep-disordered breathing in diastolic heart failure.Chest 1997; 111 : 1488-93.
56. Fung JW, Li TS, Choy DK, yip GW, Ko FW, Sanderson JE, et al. Severe obstructive sleep apnea is associated with leftventriculardiastolicdysfunction.Chest 2002;121 : 422-9.
57. Kaneko y, Floras JS, Usui K, Plante J, Tkacova R, Kubo T, et al. Cardiovascular effects of continuous positive airwaypressure in patients with heart failure and obstructive sleepapnea.N Engl J Med 2003;348 : 1233-41.
58. Shivalkar B, Van de Heyning C, Kerremans M, Rinkevich D, Verbraecken J, De Backer W, et al.Obstructivesleepapneasyndrome: more insights on structural and functional cardiac alterations, and the effects of treatment with continuous positiveairwaypressure.J Am Coll Cardiol2006;47 : 1433-9.
59. Cohn JN, Ferrari R, Sharpe N. Cardiac remodeling--concepts and clinical implications: a consensus paper from an international forum on cardiac remodeling. Behalf of an International Forum on Cardiac Remodeling. J Am Coll Cardiol2000;35 : 569-82.
60. Bradley TD, Floras JS. Sleep apnea and heart failure: Part I: obstructivesleepapnea.Circulation2003;107 : 1671-8.
61. Tkacova R, Rankin F, Fitzgerald FS, Floras JS, Bradley TD. Effects of continuous positive airway pressure on obstructive sleepapneaandleftventricularafterloadinpatientswithheartfailure.Circulation1998;98 : 2269-75.
62. Kraiczi H, Hedner J, Peker y, Grote L. Comparison of atenolol, amlodipine, enalapril, hydrochlorothiazide, and losartan for antihypertensive treatment in patients with obstructive sleep apnea.Am J Respir Crit Care Med2000;161 : 1423-8.
63. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr., et al. The Seventh Report of the JointNational Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 Report.JAMA2003;289 : 2560-72.
64. Silverberg DS, Oksenberg A, Iaina A. Sleep-related breathing disorders as a major cause of essential hypertension: fact or fiction? Curr Opin Nephrol Hyperte1998;7 : 353-7.
65. Fletcher EC, DeBehnke RD, Lovoi MS, Gorin AB. Undiagnosed sleepapneainpatientswithessentialhypertension.Ann Intern Med1985;103 : 190-5.
66. Kales A, Bixler EO, Cadieux RJ, Schneck DW, Shaw III LC, Locke TW, et al.Sleepapnoeainahypertensivepopulation.Lancet1984;2 : 1005-8.
67. Lavie P, Ben -yosef R, Rubin AE. Prevalence of sleep apnea syndrome among patients with essential hypertension. Am Heart J1984;108 : 373-6.
68. Vardan S, Dunsky MH, Hill NE, Mookherjee S, Smulyan H, Warner RA. Systemic systolic hypertension in the elderly: correlation of hemodynamics, plasma volume, renin, aldosterone, urinary metanephrines and response to thiazide therapy.Am J Cardiol1986;58 : 1030-4.
69. Williams AJ, Houston D, Finberg S, Lam C, Kinney JL, Santiago S. Sleep apnea syndrome and essential hypertension. Am J Cardiol1985; 55 : 1019-22.
70. Peppard PE, young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension.N Engl J Med 2000;342 : 1378-84.
71. Pankow W, Nabe B, Lies A, Becker H, Kohler U, Kohl FV, et al. Influence of sleep apnea on 24-hour blood pressure. Chest 1997; 112 : 1253-8.
72. Fletcher EC, Lesske J, Culman J, Miller CC, Unger T. Sympathetic denervation blocks blood pressure elevation in episodichypoxia.Hypertension1992;20 : 612-9.
73. Lesske J, Fletcher EC, Bao G, Unger T. Hypertension caused by chronic intermittent hypoxia--influence of chemoreceptors and sympathetic nervous system. J Hypertens 1997; 15 : 1593-603.
74. yinon D, Lowenstein L, Suraya S, Beloosesky R, Zmora O, Malhotra A, et al. Pre-eclampsia is associated with sleep-disorderedbreathingandendothelialdysfunction.Eur Respir J2006;27 : 328-33.
75. Edwards N, Blyton DM, Hennessy A, Sullivan CE. Severity of sleep-disordered breathing improves following parturition. Sleep2005;28 : 737-41.
76. Logan AG, Tkacova R, Perlikowski SM, Leung RS, Tisler A, Floras JS, et al. Refractory hypertension and sleep apnoea:effect of CPAP on blood pressure and baroreflex. Eur Respir J 2003;21 : 241-7.
77. Atwood CW, Jr., McCrory D, Garcia JG, Abman SH, Ahearn GS. Pulmonary artery hypertension and sleep-disordered breathing: ACCP evidence-based clinical practice guidelines. Chest 2004;126 (1 Suppl) : 72S-7S.
KUNIyOSHI et al: OSA & CARDIOVASCULAR DISEASES 203

78. Chaouat A, Weitzenblum E, Krieger J, Oswald M, Kessler R. Pulmonary hemodynamics in the obstructive sleep apnea syndrome. Results in 220 consecutive patients. Chest 1996;109 : 380-6.
79. Motley HL, Cournand A, Werko L, Himmelstein A, Dresdale D. The influence of short periods of induced acute anoxia upon pulmonary artery pressures in man. Am J Physiol 1947; 150 : 315-20.
80. Voelkel NF. Mechanisms of hypoxic pulmonary vasoconstriction.Am Rev Respir Dis1986;133 : 1186-95.
81. Sajkov D, Wang T, Saunders NA, Bune AJ, McEvoy RD. Continuous positive airway pressure treatment improves pulmonary hemodynamics in patients with obstructive sleep apnea.Am J Respir Crit Care Med2002;165 : 152-8.
82. Bassetti C, Aldrich MS, Chervin RD, Quint D. Sleep apnea in patients with transient ischemic attack and stroke: a prospective studyof59patients.Neurology1996;47 : 1167-73.
83. Bassetti CL, Milanova M, Gugger M. Sleep-disordered breathing and acute ischemic stroke: diagnosis, risk factors, treatment, evolution, and long-term clinical outcome. Stroke 2006;37 : 967-72.
84. Good DC, Henkle JQ, Gelber D, Welsh J, Verhulst S. Sleep-disordered breathing and poor functional outcome after stroke. Stroke1996;27 : 252-9.
85. Wessendorf TE, Teschler H, Wang yM, Konietzko N, Thilmann AF. Sleep-disordered breathing among patients with first-ever stroke. J Neurol2000;247 : 41-7.
86. yaggi H, Mohsenin V. Obstructive sleep apnoea and stroke. LancetNeurol2004;3 : 333-42.
87. Wessendorf TE, Wang yM, Thilmann AF, Sorgenfrei U, Konietzko N, Teschler H. Treatment of obstructive sleep apnoea with nasal continuous positive airway pressure instroke. Eur Resp J 2001; 18 : 623-9.
88. Koehler U, Schafer H. Is obstructive sleep apnea (OSA) a risk factor for myocardial infarction and cardiac arrhythmias in patients with coronary heart disease (CHD)? Sleep 1996; 19:283-6.
89. Liston R, Deegan PC, McCreery C, McNicholas WT. Role of respiratory sleep disorders in the pathogenesis of nocturnalangina and arrhythmias. Postgrad Med J1994;70 : 275-80.
90. Shepard JW, Jr. Hypertension, cardiac arrhythmias, myocardial infarction, and stroke in relation to obstructive sleep apnea. Clin Chest Med 1992;13 : 437-58.
91. Mehra R, Benjamin EJ, Shahar E, Gottlieb DJ, Nawabit R, Kirchner HL, et al. Association of nocturnal arrhythmias with sleep-disordered breathing: The Sleep Heart Health Study. Am J Respir Crit Care Med2006;173 : 910-6.
92. Guilleminault C, Connolly SJ, Winkle RA. Cardiac arrhythmia andconductiondisturbancesduringsleepin400patientswithsleep apnea syndrome. Am J Cardiol1983;52 : 490-4.
93. Koehler U, Fus E, Grimm W, Pankow W, Schafer H, Stammnitz A,et al. Heart block in patients with obstructive sleep apnoea: pathogenetic factors and effects of treatment. Eur Respir J 1998;11 : 434-9.
94. Gami AS, Hodge DO, Herges RM, Olson EJ, Nykodym J, Kara T,et al. Obstructive sleep apnea, obesity, and the risk of incident atrial fibrillation. J Am Coll Cardiol 2007; 49 : 565-71.
95. Kanagala R, Murali NS, Friedman PA, Ammash NM, Gersh BJ, Ballman KV, et al.Obstructivesleepapneaandtherecurrenceof atrial fibrillation. Circulation2003;107 : 2589-94.
96. Hoffstein V, Mateika S. Cardiac arrhythmias, snoring, and sleepapnea.Chest 1994;106 : 466-71.
97. Harbison J, O’Reilly P, McNicholas WT. Cardiac rhythm disturbances in the obstructive sleep apnea syndrome: effects of nasal continuous positive airway pressure therapy. Chest 2000;118 : 591-5.
98. Grimm W, Hoffmann J, Menz V, Kohler U, Heitmann J, Peter JH,et al. Electrophysiologic evaluation of sinus node function and atrioventricular conduction in patients with prolongedventricular asystole during obstructive sleep apnea. Am J Cardiol 1996; 77 : 1310-4.
99. Becker H, Brandenburg U, Peter JH, Von Wichert P. Reversal of sinus arrest and atrioventricular conduction block in patients with sleep apnea during nasal continuous positive airwaypressure.Am J Respir Crit Care Med1995;151 : 215-8.
100. Tilkian AG, Guilleminault C, Schroeder JS, Lehrman KL, Simmons FB, Dement WC. Sleep-induced apnea syndrome. Prevalence of cardiac arrhythmias and their reversal after tracheostomy. Am J Med 1977; 63 : 348-58.
101. Sullivan CE, Issa FG, Berthon-Jones M, Eves L. Reversal of obstructive sleep apnoea by continuous positive airwaypressureappliedthroughthenares.Lancet1981;1 : 862-5.
102.BasnerRC.Continuouspositiveairwaypressureforobstructivesleepapnea.N Engl J Med 2007; 356 : 1751-8.
103. Derderian SS, Bridenbaugh RH, Rajagopal KR. Neuropsychologic symptoms in obstructive sleep apnea improve after treatment with nasal continuous positive airway pressure.Chest 1988;94 : 1023-7.
104. Engleman HM, Cheshire KE, Deary IJ, Douglas NJ. Daytime sleepiness, congnitive performance and mood after continuous positive airway pressure for the sleep apnoea/hypopnoeasyndrome. Thorax1989;48 : 911-4.
105. Engleman HM, Martin SE, Deary IJ, Douglas NJ. Effect of continuous positive airway pressure treatment on daytime function in sleep apnoea/hypopnoea syndrome. Lancet1994;343 : 572-5.
106. Lamphere J, Roehrs T, Wittig R. Recovery of alertness after CPAP in apnea. Chest 1989;96 : 1364-7.
107. Rajagopal KR, Bennett LL, Dillard TA, Tellis CJ, Tenholder MF. Overnight nasal CPAP improves hypersomnolence in sleepapnea.Chest 1986;90 : 172-6.
108. Zimmerman ME, Arnedt JT, Stanchina M, Millman RP, Aloia MS. Normalization of memory performance and positive airway pressure adherence in memory-impaired patients with obstructivesleepapnea.Chest 2006;130 : 1772-8.
109. Kohler M, Pepperell JC, Casadei B, Craig S, Crosthwaite N, StradlingJR,et al. CPAP and measures of cardiovascular risk in males with OSAS. Eur Respir J 2008; 32 : 1488-96.
110. Resta O, Guido P, Picca V, Sabato R, Rizzi M, Scarpelli F, et al. Prescription of nCPAP and nBIPAP in obstructive sleep apnoea syndrome: Italian experience in 105 subjects. A prospectivetwocentrestudy.Respir Med 1998;92 : 820-7.
111. Cartwright RD. Effect of sleep position on sleep apnea severity.Sleep1984;7 : 110-4.
204 INDIAN J MED RES, FEBRUARy 2010

112. Kushida CA, Sherrill CM, Hong SC, Palombini L, Hyde P, Dement WC. Cervical positioning for reduction of sleep-disordered breathing in mild-to-moderate OSAS. Sleep Breath2001; 5 : 71-8.
113. Ferguson KA, Cartwright R, Rogers R, Schmidt-Nowara W. Oral appliances for snoring and obstructive sleep apnea: areview.Sleep 2006;29 : 244-62.
114. Itzhaki S, Dorchin H, Clark G, Lavie L, Lavie P, Pillar G. The effects of 1-year treatment with a herbst mandibular advancement splint on obstructive sleep apnea, oxidative stress,andendothelialfunction.Chest 2007; 131 : 740-9.
115. Chan AS, Lee RW, Cistulli PA. Non-positive airway pressure modalities: mandibular advancement devices/positional therapy.Proc Am Thorac Soc2008;5 : 179-84.
116. Vgontzas AN. Does obesity play a major role in the pathogenesis of sleep apnoea and its associated manifestations via inflammation, visceral adiposity, and insulin resistance? Arch Physiol Biochem 2008;114 : 211-23.
117. Carter R, 3rd, Watenpaugh DE. Obesity and obstructive sleep apnea: Or is it OSA and obesity? Pathophysiology2008;15:71-7.
118. Fleisher KE, Krieger AC. Current trends in the treatment of obstructive sleep apnea. J Oral Maxillofac Surg 2007; 65 :2056-68.
119. Lundkvist K, Januszkiewicz A, Friberg D. Uvulopalatopharyngoplasty in 158 OSAS patients failing non-surgical treatment. Acta Otolaryngol 2009;129 : 1-7.
Reprint requests: Dr Virend K. Somers, Mayo Clinic, Division of Cardiovascular Diseases, 200 1st St., SW, Rochester MN 55905-0001, USA e-mail: [email protected]
KUNIyOSHI et al: OSA & CARDIOVASCULAR DISEASES 205