severe obstructive sleep apnea elicits concentric left ventricular geometry
TRANSCRIPT

CE: Namrta; HJH/201793; Total nos of Pages: 9;
HJH 201793
Severe obstructive sleep apnea elicits concentric leftventricular geometryGiovanni Cioffia, Tiziano Edoardo Russoa, Carlo Stefenellia, Alessandro Selmia,Francesco Furlanelloa, Dana Cramariucb, Eva Gerdtsb andGiovanni de Simonec
Background Obstructive sleep apnea (OSA) has several
negative effects on the heart including increase in
myocardial end-systolic stress, venous return and
sympathetic activity, all potential stimuli of left ventricular
(LV) hypertrophy. The impact of the severity of OSA on
LV geometry is unknown. We hypothesized that OSA is
related to concentric LV geometry.
Methods One hundred and fifty-seven patients with
suspected OSA underwent echocardiography, ambulatory
24-h blood pressure and ECG monitoring. On the basis of
the severity of OSA, patients were divided into controls, mild
OSA and moderate/severe OSA (apnea–hypopnea index
<5, 5–15 and >15/h, respectively). Patients with LV
hypertrophy were defined as LV mass at least 49.2 g/m2.7
for men and at least 46.7 for women. Relative wall thickness
of at least 0.43 identified patients with concentric LV
geometry.
Results Patients with moderate/severe OSA (n U 86) had a
higher body mass index and a higher prevalence of
paroxysmal atrial fibrillation than those (n U 51) with mild
OSA and controls (n U 20). Prevalence of hypertension,
diabetes, obesity, LV mass and blood pressure did not differ
between the groups. Relative wall thickness was positively
related to apnea–hypopnea index (r U 0.30; P U 0.003) and
the prevalence of concentric LV geometry was 20% in
controls, 12% in mild OSA and 58% in moderate/severe
OSA (P < 0.001). In logistic regression analysis concentric
LV geometry was associated with moderate/severe OSA
[odds ratio (OR) 7.6, P < 0.001], low stress-corrected midwal
shortening (OR 3.38, P U 0.004), and higher body mass
index (OR 1.09, P U 0.03).
Conclusions Moderate/severe OSA is associated with high
prevalence of concentric LV geometry. This increased
prevalence may in part explain the increased rate of
cardiovascular events in these patients. J Hypertens
28:000–000 Q 2010 Wolters Kluwer Health | Lippincott
Williams & Wilkins.
Journal of Hypertension 2010, 28:000–000
Keywords: apnea–hypopnea index, concentric hypertrophy, desaturations,left ventricular geometry, obstructive sleep apnea
Abbreviations: AHI, apnea–hypopnea index; ECG, electrocardiogram; LV,left ventricular; LVH, left ventricular hypertrophy; OSA, obstructive sleepapnea
aDepartment of Cardiology, Villa Bianca Hospital, Trento, Italy, bDepartment ofHeart Disease, Haukeland University, Bergen, Norway and cDepartment ofClinical and Experimental Medicine, Federico II, University Hospital, School ofMedicine, Naples, Italy
Correspondence to Giovanni Cioffi, MD, Echocardiography Laboratory,Villa Bianca Hospital, via Piave 78, 38100 Trento, ItalyTel: +39 0 461 916000; fax: +39 0 461 916874;e-mail: [email protected]
Received 12 August 2009 Revised 8 November 2009Accepted 18 December 2009
IntroductionObstructive sleep apnea (OSA) is a common under-
diagnosed pathological condition implicated in the
initiation and progression of cardiovascular diseases
[1,2]. OSA has several negative effects on the heart
including increase in left ventricular (LV) afterload,
venous return (influencing preload) and sympathetic
activity, all potential stimuli of LV hypertrophy (LVH)
[1,3,4]. The magnitude of these effects parallels the
severity of OSA. Patients with OSA have a high preva-
lence of arterial hypertension and, more importantly,
obesity, which represents the strongest predisposing
factor for the sleep abnormalities [5,6]. The relation
between hypertension and obesity and its impact on
LV geometry are known [7,8]. Less is known about
the impact of OSA on LV geometry. OSA should
hypothetically produce changes in LV geometry lead-
ing to a concentric remodeling through sympathetic
activation, vasoconstriction and elevation in blood
pressure.
Accordingly, we studied a group of patients with OSA to
test the hypothesis that higher degree of sleep disturb-
ance is related to concentric LV geometry.
MethodsStudy populationThe study group included participants above 18 years of
age with ascertained OSA by a formal sleep study, who
were addressed by their General Practitioners to our
center for a more precise stratification of their global
cardiovascular risk. All participants were free of symp-
toms and clinical signs of cardiac disease (New York
Heart Association functional class I). Recruitment period
Original article 1
0263-6352 � 2010 Wolters Kluwer Health | Lippincott Williams & Wilkins DOI:10.1097/HJH.0b013e328336c90a

CE: Namrta; HJH/201793; Total nos of Pages: 9;
HJH 201793
lasted from January 2007 to March 2008. Exclusion
criteria were presence of coronary heart disease (diag-
nosed by clinical, electrocardiographic and echocardio-
graphic evaluation at rest and by the results of exercise/
echo-stress test or coronary angiography), LV ejection
fraction less than 50%, LV wall motion abnormalities, or
more-than-mild valve regurgitation or any grade of
valve stenosis.
Study protocolAll patients underwent a complete clinical and echocar-
diographic evaluation which included Berlin question-
naire test [9], the measurement of body weight and
waist, arterial blood pressure, serum creatinine, hemo-
globin, haematocrit, microalbuminuria and reactive C
protein, polysomnography, transthoracic echocardiogra-
phy, maximal exercise test by cycloergometer, 24-h ECG
Holter monitoring and 24-h blood pressure Holter
monitoring. Physical and echocardiographic examin-
ations were performed the same morning blood samples
were collected. Polysomnography, exercise test, spirome-
try, 24-h ECG and blood pressure Holter monitoring
were performed within the next 3 days. Variables con-
sidered in the statistical analysis derived by 24-h blood
pressure Holter monitoring were mean day-time systolic
and diastolic blood pressure, mean nocturnal systolic
and diastolic blood pressure, mean diurnal systolic and
diastolic blood pressure, mean systolic and diastolic day/
night-time excursion. History of hypertension and num-
ber of antihypertension drugs were also considered in the
study analyses. As parameters of sympathetic activity
we considered baseline heart rate, mean day-time and
nocturnal heart rate and day-time night-time heart rate
excursion. The protocol of the present study was
approved by the local institutional review board and
written informed consent was obtained from all patients.
Polysomnography and definitionsAll participants underwent a standard overnight poly-
somnography while breathing room air (Hypno PTT
machine - Tayco HealthCare). The following parameters
were considered: apneas; hypoapneas; duration of apneas/
hypopneas (s), oxygen saturation (%) and arousals.
Apneas were defined as an absence (<20% baseline) of
airflow for at least 10 s; hypoapneas as a reduction in
airflow (20–50% baseline) producing a reduction in O2
saturation at least 3%; desaturations were recognized in
presence of a reduction of oxygen saturation by at least
3% from baseline and expressed as total number/hours of
sleep [10]; arousals were identified from the signals
received from the electrodes positioned on the chest
and were expressed as total number/hours of sleep.
Obstructive and central events were discriminated by
the analysis of the respiratory effort and the typical
respiratory pattern. Mixed events were considered as
obstructive. OSA was identified by the apnea–hypopnea
index (AHI¼ rate of apneasþhypopneas per hour of
sleep), which was also used for classifying patients
according to the severity of the syndrome. Patients were
thus categorized in two groups according to suggested
cut-points [6]: ‘mild OSA’ (AHI between 5 and 15) and
‘moderate/severe OSA’ (AHI >15). Patients with AHI
less than 5 were retained to have not OSA and were
considered as control group.
Hypertension was defined as pharmacologically treated
high blood pressure or a resting blood pressure at least
140/90 mmHg. Overweight was diagnosed according to
the clinical guidelines of National Institute of Health [11]
in presence of a body mass index at least 27.8 kg/m2
in men and at least 27.3 kg/m2 in women; obesity
was defined as body mass index equal or greater than
30 kg/m2. Paroxysmal atrial fibrillation was diagnosed by
24-h Holter monitoring as the presence of a burst of atrial
arrhythmia lasting more than 30 s [12]. Functional
capacity was determined by maximal exercise test
(cycloergometer) and measured in watts.
EchocardiographyThe echocardiographic evaluations were performed by
transthoracic approach using a commercially available
instrument (MEGAS Esaote Biomedical System, Flor-
ence, Italy) equipped with a 2.5–3.5 Mhz annular-array
transducer. Echocardiographic measurements were
blinded to the presence and magnitude of OSA.
Left ventricular chamber dimensions (normalized for
height), interventricular septum, and posterior wall thick-
ness were measured from M-mode tracings according to
the American Society of Echocardiography [13] and LV
mass calculated using a necropsy validated formula [14].
LV mass was normalized for height to the 2.7 power and
LVH was defined as LV mass at least 49.2 g/m2.7 for men
and at least 46.7 for women [15]. Relative wall thickness
was calculated as the end-diastolic ratio posterior wall
thickness/LV diameter and indicated concentric LV geo-
metry if at least 0.43 (the 97.5 percentile in normal
population) [16].
Concentric geometry included concentric LVH (if LV
mass index was increased) or concentric remodeling (if
LV mass index was normal). Similarly, in patients without
concentric LV geometry (relative wall thickness <0.43),
two patterns of LV geometry were identified: eccentric
LVH (if LV mass index was increased) and normal (if LV
mass index was normal).
Left ventricular volumes were estimated by the
Z-derived formulas [17] and used to generate ejection
fraction and stroke volume. Stroke volume was normal-
ized for height at the allometric power of 2.04 to account
for its nonlinear variation with body size [18]. Myocardial
contractility was assessed by the midwall shortening and
by end-systolic stress-corrected midwall shortening
2 Journal of Hypertension 2010, Vol 00 No 00

CE: Namrta; HJH/201793; Total nos of Pages: 9;
HJH 201793
[19,20]. Stress-corrected midwall shortening less than
87% in men and less than 90% in women was indicative
of impaired LV myocardial contractility [21].
Statistical analysisData are reported as mean values� 1 standard deviation
for parametric variables and median and quartiles for
nonparametric variables (i.e. AHI and desaturations).
Between-group comparisons of categorical and continu-
ous variables were performed by x2 test and analysis of
variance (ANOVA), respectively. To assess whether
moderate/severe OSA was an independent determinant
of concentric LV geometry, the relations of concentric
LV geometry to severity of OSA, demographics, indexes
of LV systolic and diastolic function and measures of
hypertension were investigated by multiple logistic
regression analyses using a stepwise forward procedure
(SPSS/PC 11 Release, SPSS Inc. Chicago, IL). Measures
of hypertension were included in the model one by one to
avoid collinearity. A two-tailed value of P< 0.05 was used
to reject the null hypothesis.
ResultsDescription of the study populationThe study population consisted of 157 patients (mean age
of 61� 13 years, 17% women) and had a high prevalence
of arterial hypertension (72%), dyslipidemia (58%),
obesity (44%), and diabetes mellitus (18%). LVH was
detected in 45% of cases, and concentric geometry in
38%. LV myocardial contractility measured at midwall
level was impaired in 53% of patients. Spirometry results
were normal in 90% of patients, and the maximal func-
tional capacity to exercise test was 133� 40 watts. The
median AHI was 17 [9–31] and the median duration of
apnea–hypopnea episodes was 24 s [21–26]. OSA was
mild in 51 patients (32%) and moderate to severe in 86
patients (55%). Twenty patients (13%) had AHI less than
5 and formed the control group. The clinical character-
istics of these patients were similar to those with mild
OSA, but they were treated with a smaller number of
antihypertension drugs and less frequently received ACE
inhibitors/AT1-receptor blockers.
Clinical features of patients with mild andmoderate/severe obstructive sleep apneaPatients with moderate/severe OSA had a higher body
mass index and a higher prevalence of obesity and
paroxysmal atrial fibrillation than patients with mild
OSA, but had similar prevalence of dyslipidemia, dia-
betes mellitus and hypertension. Mean values of blood
pressure were not different between the groups both
when measured in the day-time and night-time but
patients with moderate/severe OSA patients used a
higher number of antihypertensive drugs and received
more frequently diuretics and vasodilators than those
with mild OSA (Table 1). Parameters of renal function,
inflammatory state, hematocrit, maximal functional
capacity and spirometric pattern were not different
between the groups (data not shown).
Left ventricular systolic performance and functionEchocardiographic features of the study groups are shown
in Table 2. Parameters of LV performance and function
were similar between controls and patients with mild
OSA. Patients with moderate/severe OSA exhibited a
decreased LV myocardial contractility, as measured at the
midwall level, than patients with mild OSA and controls,
with a significantly greater prevalence of LV systolic
dysfunction. Moderate/severe OSA was mostly found
among patients with impaired LV myocardial contracti-
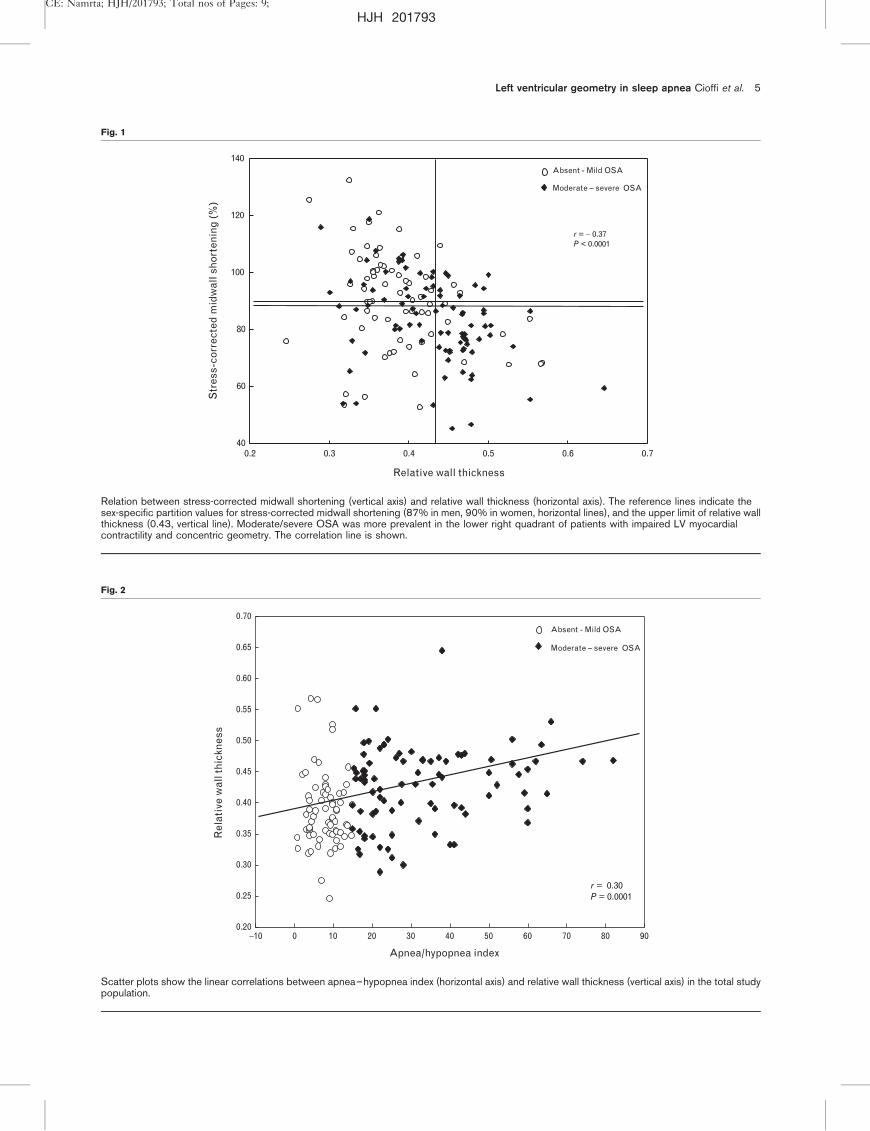
lity and concentric geometry (Fig. 1).
Left ventricular geometryThe study groups had similar LV mass and prevalence of
hypertrophy. The AHI was directly related with relative
wall thickness. This significant linear correlation was
found both in the total population (r¼ 0.30, SEE 16.4,
P¼ 0.003) (Fig. 2) and in the subgroup of patients with
normal LV geometry (r¼ 0.38, SEE 12.5, P¼ 0.001), who
were significantly younger (56� 16 vs. 65� 9 years,
P< 0.0001), had smaller LV volumes and left atrial size,
and less frequently impaired LV myocardial contractility
(30 vs. 68%, P< 0.0001) than patients with abnormal LV
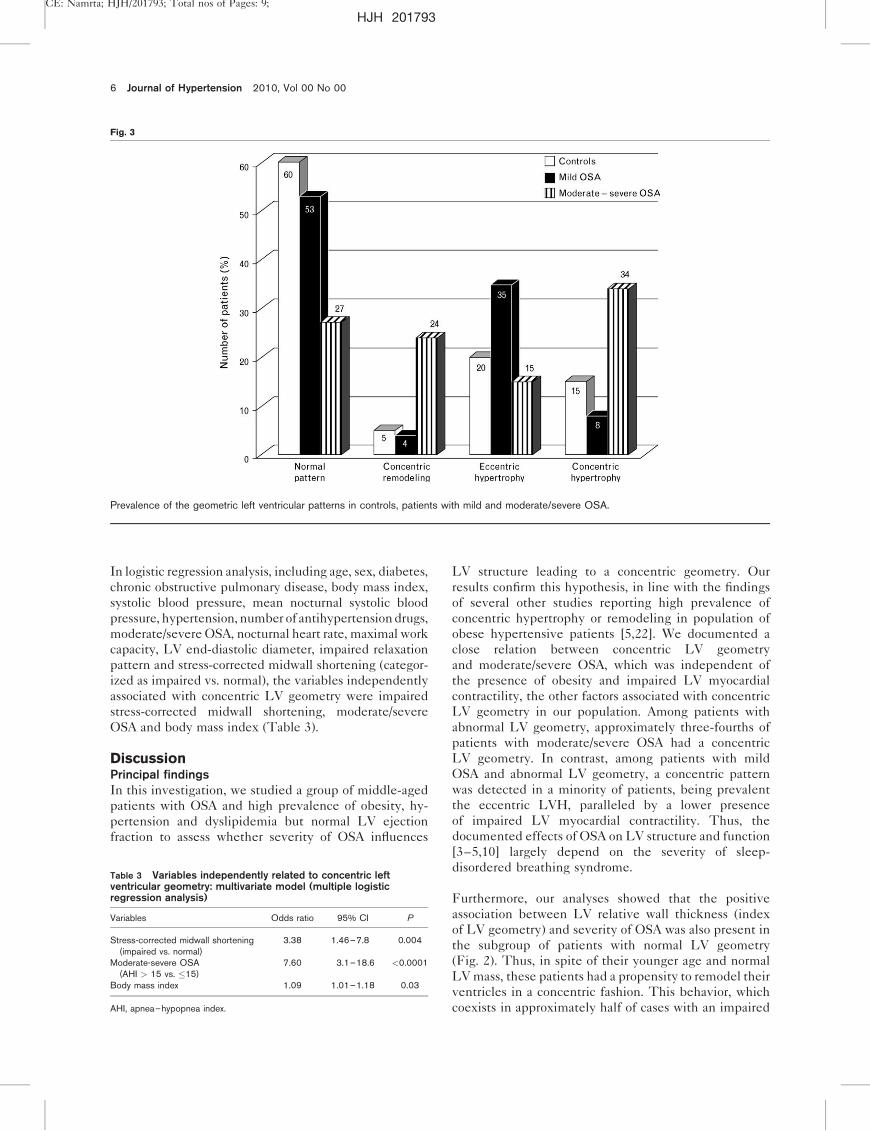
geometry. Figure 3 shows the prevalence of LV geo-
metric patterns in controls, in patients with mild and
moderate/severe OSA. Prevalence of concentric LV geo-
metry (concentric remodelingþ concentric LVH) was
similar in controls (four patients¼ 20%) and in patients
with mild OSA (six patients¼ 12%, P¼ns), whereas it
was significantly higher in patients with moderate/severe
OSA (50 patients¼ 58%, P< 0.0001). Approximately
two-thirds of these patients (80% with concentric remo-
deling and 74% with concentric LVH) had moderate/
severe OSA, which affected only 40% of patients with
nonconcentric LV geometry (38% with normal geometry
and 45% with eccentric LVH) (P¼ 0.007).
Determinants of concentric geometryConcentric LV geometry was positively associated in
univariate analysis with older age, female sex, obesity,
severity of OSA, number of antihypertension drugs and
reduced functional capacity. As expected, this condition
was closely related to smaller left ventricles, greater LV
mass and impaired diastolic and systolic function (data
not shown). Serum creatinine, protein C reactive,
parameters deriving from spirometry and 24-h ECG
and blood pressure monitoring were not related to con-
centric LV geometry. In particular, diurnal/nocturnal
systolic blood pressure excursion, diastolic blood pressure
excursion and heart rate excursion were 4.8� 5 mmHg,
6.5� 6 mmHg and 5.0� 5 b.p.m. vs. 4.9� 5 mmHg,
4.2� 4 mmHg and 4.3� 4 b.p.m. (all P¼ns), respect-
ively, in patients with and without concentric LV
geometry.
Left ventricular geometry in sleep apnea Cioffi et al. 3
CE: Namrta; HJH/201793; Total nos of Pages: 9;
HJH 201793
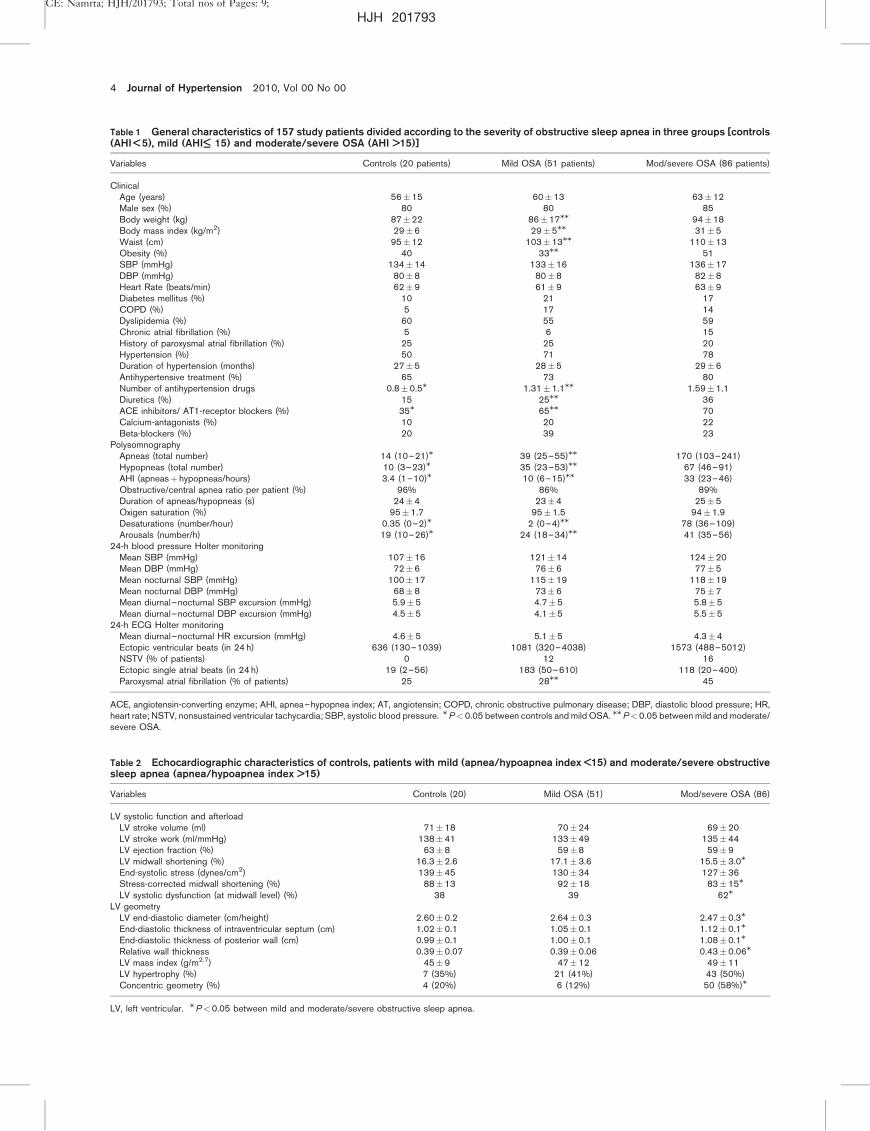
4 Journal of Hypertension 2010, Vol 00 No 00
Table 1 General characteristics of 157 study patients divided according to the severity of obstructive sleep apnea in three groups [controls(AHI < 5), mild (AHI<— 15) and moderate/severe OSA (AHI >15)]
Variables Controls (20 patients) Mild OSA (51 patients) Mod/severe OSA (86 patients)
ClinicalAge (years) 56�15 60�13 63�12Male sex (%) 80 80 85Body weight (kg) 87�22 86�17MM 94�18Body mass index (kg/m2) 29�6 29�5MM 31�5Waist (cm) 95�12 103�13MM 110�13Obesity (%) 40 33MM 51SBP (mmHg) 134�14 133�16 136�17DBP (mmHg) 80�8 80�8 82�8Heart Rate (beats/min) 62�9 61�9 63�9Diabetes mellitus (%) 10 21 17COPD (%) 5 17 14Dyslipidemia (%) 60 55 59Chronic atrial fibrillation (%) 5 6 15History of paroxysmal atrial fibrillation (%) 25 25 20Hypertension (%) 50 71 78Duration of hypertension (months) 27�5 28�5 29�6Antihypertensive treatment (%) 65 73 80Number of antihypertension drugs 0.8�0.5M 1.31�1.1MM 1.59�1.1Diuretics (%) 15 25MM 36ACE inhibitors/ AT1-receptor blockers (%) 35M 65MM 70Calcium-antagonists (%) 10 20 22Beta-blockers (%) 20 39 23
PolysomnographyApneas (total number) 14 (10–21)M 39 (25–55)MM 170 (103–241)Hypopneas (total number) 10 (3–23)M 35 (23–53)MM 67 (46–91)AHI (apneasþ hypopneas/hours) 3.4 (1–10)M 10 (6–15)MM 33 (23–46)Obstructive/central apnea ratio per patient (%) 96% 86% 89%Duration of apneas/hypopneas (s) 24�4 23�4 25�5Oxigen saturation (%) 95�1.7 95�1.5 94�1.9Desaturations (number/hour) 0.35 (0–2)M 2 (0–4)MM 78 (36–109)Arousals (number/h) 19 (10–26)M 24 (18–34)MM 41 (35–56)
24-h blood pressure Holter monitoringMean SBP (mmHg) 107�16 121�14 124�20Mean DBP (mmHg) 72�6 76�6 77�5Mean nocturnal SBP (mmHg) 100�17 115�19 118�19Mean nocturnal DBP (mmHg) 68�8 73�6 75�7Mean diurnal–nocturnal SBP excursion (mmHg) 5.9�5 4.7�5 5.8�5Mean diurnal–nocturnal DBP excursion (mmHg) 4.5�5 4.1�5 5.5�5
24-h ECG Holter monitoringMean diurnal–nocturnal HR excursion (mmHg) 4.6�5 5.1�5 4.3�4Ectopic ventricular beats (in 24 h) 636 (130–1039) 1081 (320–4038) 1573 (488–5012)NSTV (% of patients) 0 12 16Ectopic single atrial beats (in 24 h) 19 (2–56) 183 (50–610) 118 (20–400)Paroxysmal atrial fibrillation (% of patients) 25 28MM 45
ACE, angiotensin-converting enzyme; AHI, apnea–hypopnea index; AT, angiotensin; COPD, chronic obstructive pulmonary disease; DBP, diastolic blood pressure; HR,heart rate; NSTV, nonsustained ventricular tachycardia; SBP, systolic blood pressure. MP<0.05 between controls and mild OSA. MMP<0.05 between mild and moderate/severe OSA.
Table 2 Echocardiographic characteristics of controls, patients with mild (apnea/hypoapnea index <15) and moderate/severe obstructivesleep apnea (apnea/hypoapnea index >15)
Variables Controls (20) Mild OSA (51) Mod/severe OSA (86)
LV systolic function and afterloadLV stroke volume (ml) 71�18 70�24 69�20LV stroke work (ml/mmHg) 138�41 133�49 135�44LV ejection fraction (%) 63�8 59�8 59�9LV midwall shortening (%) 16.3�2.6 17.1�3.6 15.5�3.0M
End-systolic stress (dynes/cm2) 139�45 130�34 127�36Stress-corrected midwall shortening (%) 88�13 92�18 83�15M
LV systolic dysfunction (at midwall level) (%) 38 39 62M
LV geometryLV end-diastolic diameter (cm/height) 2.60�0.2 2.64�0.3 2.47�0.3M
End-diastolic thickness of intraventricular septum (cm) 1.02�0.1 1.05�0.1 1.12�0.1M
End-diastolic thickness of posterior wall (cm) 0.99�0.1 1.00�0.1 1.08�0.1M
Relative wall thickness 0.39�0.07 0.39�0.06 0.43�0.06M
LV mass index (g/m2.7) 45�9 47�12 49�11LV hypertrophy (%) 7 (35%) 21 (41%) 43 (50%)Concentric geometry (%) 4 (20%) 6 (12%) 50 (58%)M
LV, left ventricular. MP<0.05 between mild and moderate/severe obstructive sleep apnea.
CE: Namrta; HJH/201793; Total nos of Pages: 9;
HJH 201793
Left ventricular geometry in sleep apnea Cioffi et al. 5
Fig. 1
0.2 0.3 0.4 0.5 0.6 0.740
60
80
100
120
140
Str
ess-
corr
ecte
d m
idw
all s
hort
enin
g (
%)
Relative wall thickness
r = − 0.37P < 0.0001
Absent - Mild OSA
Moderate – severe OSA
Relation between stress-corrected midwall shortening (vertical axis) and relative wall thickness (horizontal axis). The reference lines indicate thesex-specific partition values for stress-corrected midwall shortening (87% in men, 90% in women, horizontal lines), and the upper limit of relative wallthickness (0.43, vertical line). Moderate/severe OSA was more prevalent in the lower right quadrant of patients with impaired LV myocardialcontractility and concentric geometry. The correlation line is shown.
Fig. 2
−10 0 10 20 30 40 50 60 70 80 900.20
0.25
0.30
0.35
0.40
0.45
0.50
0.55
0.60
0.65
0.70
Rel
ativ
e w
all t
hick
ness
Apnea/hypopnea index
Absent - Mild OSA
Moderate – severe OSA
r = 0.30P = 0.0001
Scatter plots show the linear correlations between apnea–hypopnea index (horizontal axis) and relative wall thickness (vertical axis) in the total studypopulation.
CE: Namrta; HJH/201793; Total nos of Pages: 9;
HJH 201793
In logistic regression analysis, including age, sex, diabetes,
chronic obstructive pulmonary disease, body mass index,
systolic blood pressure, mean nocturnal systolic blood
pressure, hypertension, number of antihypertension drugs,
moderate/severe OSA, nocturnal heart rate, maximal work
capacity, LV end-diastolic diameter, impaired relaxation
pattern and stress-corrected midwall shortening (categor-
ized as impaired vs. normal), the variables independently
associated with concentric LV geometry were impaired
stress-corrected midwall shortening, moderate/severe
OSA and body mass index (Table 3).
DiscussionPrincipal findingsIn this investigation, we studied a group of middle-aged
patients with OSA and high prevalence of obesity, hy-
pertension and dyslipidemia but normal LV ejection
fraction to assess whether severity of OSA influences
LV structure leading to a concentric geometry. Our
results confirm this hypothesis, in line with the findings
of several other studies reporting high prevalence of
concentric hypertrophy or remodeling in population of
obese hypertensive patients [5,22]. We documented a
close relation between concentric LV geometry
and moderate/severe OSA, which was independent of
the presence of obesity and impaired LV myocardial
contractility, the other factors associated with concentric
LV geometry in our population. Among patients with
abnormal LV geometry, approximately three-fourths of
patients with moderate/severe OSA had a concentric
LV geometry. In contrast, among patients with mild
OSA and abnormal LV geometry, a concentric pattern
was detected in a minority of patients, being prevalent
the eccentric LVH, paralleled by a lower presence
of impaired LV myocardial contractility. Thus, the
documented effects of OSA on LV structure and function
[3–5,10] largely depend on the severity of sleep-
disordered breathing syndrome.
Furthermore, our analyses showed that the positive
association between LV relative wall thickness (index
of LV geometry) and severity of OSA was also present in
the subgroup of patients with normal LV geometry
(Fig. 2). Thus, in spite of their younger age and normal
LV mass, these patients had a propensity to remodel their
ventricles in a concentric fashion. This behavior, which
coexists in approximately half of cases with an impaired
6 Journal of Hypertension 2010, Vol 00 No 00
Fig. 3
Prevalence of the geometric left ventricular patterns in controls, patients with mild and moderate/severe OSA.
Table 3 Variables independently related to concentric leftventricular geometry: multivariate model (multiple logisticregression analysis)
Variables Odds ratio 95% CI P
Stress-corrected midwall shortening(impaired vs. normal)
3.38 1.46–7.8 0.004
Moderate-severe OSA(AHI > 15 vs. �15)
7.60 3.1–18.6 <0.0001
Body mass index 1.09 1.01–1.18 0.03
AHI, apnea–hypopnea index.

CE: Namrta; HJH/201793; Total nos of Pages: 9;
HJH 201793
LV myocardial contractility, evidently heralds overt
cardiac structural abnormalities and represents a
phenomenon ‘ab initio’, which might identify, at an early
stage, the concentric LV geometry phenotype.
Potential mechanismsAn important limitation to most of previous studies which
evaluated LV geometry in the various clinical settings is
their focus on the patients as they present while awake.
This approach assumes that any determinants contribut-
ing in the patho-physiology or progression of LV geome-
try are inactive during the sleep [23]. Unfortunately, OSA
produces a series of mechanical, hemodynamic, chemical,
neural, and inflammatory responses (i.e. intermittent
apnea-induced hypoxia, hypercapnia, rises in sympath-
etic drive and LV myocardial afterload, daytime hyper-
tension, loss of vagal heart rate regulation and systemic
vasculature remodeling) [1,5,10,24,25] which strongly
impact the cardiovascular system, being all potent stimuli
to myocyte necrosis and apoptosis, myocardial ischemia,
and finally, development of concentric LV geometry.
These conditions may explain the extremely high preva-
lence of concentric LV geometry found in our patients
with moderate/severe OSA as well as in those recently
studied by Drager et al. [26] who showed a close associ-
ation between OSA, increased arterial stiffness and
increased LV mass and concentric geometry in a small
group of 15 patients with severe OSA and hypertension.
In contrast, Mylinski et al. [27] found a predominance of
eccentric LVH in 108 newly-diagnosed OSA patients.
Such apparent discrepancy can be explained by the
younger age and duration of OSA of these patients
and, more importantly, by the severity of OSA, which
was mild in a considerable portion of patients included in
the analysis.
The associations between sleep-disordered breathing
and LV geometry have been previously investigated
in a lot of studies conducted on patients with obesity
and hypertension and the results are irreconciliable
[2,5,7,22,28–30]. Both overweight and increased blood
pressure determine a state of chronic myocardial LV
overload and represent two of the main predisposing
factors for LVH and systolic dysfunction. In theory,
the two conditions are hemodynamically different and
should lead to different LV geometric adaptations
[5,25,28–31]. In clinical practice, such dichotomy is
less evident, because obesity and hypertension lead to
heterogenic and unpredictable changes in LV geometry
[5,22–24].
In our patients neither the presence of hypertension
(highly prevalent in all our study subgroups), systolic
or diastolic blood pressure, average 24-h blood pressure,
or nocturnal hypertension were different between
patients with mild and those with severe OSA despite
the ascertainment of hypertension was appropriate,
measurements of blood pressure were accurate and cru-
cial selection bias were reasonably absent. These findings
are not totally unexpected being in line with those
observed by several studies conducted both in patients
with [10,26] or without OSA [32] which clearly evidenced
that changes in LV geometry and LVH may precede the
onset of hypertension. This phenomenon may be related
to some consequences of severe OSA including signifi-
cant hypoxiemia, increased sympathetic drive and/or
transmural pressure due to the respiratory effort during
an apneic/hypoapneic event. Furthermore, it is important
to underline that our patients with moderate/severe OSA
patients were using a higher number of antihypertensive
drugs and receiving more frequently diuretics and vaso-
dilators than those with mild OSA or controls. These
differences in pharmacological treatment could explain
why the measures of hypertension were not related to the
magnitude of OSA in our population. However, type and
number of antihypertension drugs were not related to the
presence of concentric geometry in the multivaried
analysis, suggesting that other factors had a more relevant
effect on LV structure. The present study was limited by
lack of a sub-analysis on patients with OSA without
concomitant hypertension (not doable for the small
sample size) which could remove the possible confound-
ing effect of pharmacological treatment in evaluating the
role of blood pressure in explaining the study results.
Obesity was actually one of these factors. It was strongly
related to LV concentric geometry, independently of
severity of OSA in our population. In obese patients,
moderate/severe OSA may activate, more than in other
phenotypes, a variety of biological molecules including
lipids, proteins and DNA which can alter biological
functions such as myocardial energy metabolism [33],
endothelial dysfunction [34] and oxidative stress [35], all
stimuli leading to concentric LV geometry. Through
these mechanisms obesity may come undone from
OSA, representing both the main predisposing condition
for the sleep-disordered breathing and a primary deter-
minant of concentric LV geometry by itself.
Study limitation and clinical implicationsThe protocol of the present cross-sectional study did not
permit to generalize our results being in a selected
patient-based population with high prevalence of hyper-
tension, diabetes and dyslipidemia, and no conclusion
can be made on the causality of our findings. As
parameters of sympathetic activity we considered only
heart rate and its diurnal–nocturnal excursion. The
evaluation of plasma catecholamine levels, baroreflex
sensitivity or heart rate spectral analysis, not available
in our study, could be useful to better comprehend the
relations between LV geometry and OSA. However,
our hypothesis that OSA elicits concentric LVH could
be indirectly supported by the positive effects of
continuous positive airway pressure (CPAP) therapy on
Left ventricular geometry in sleep apnea Cioffi et al. 7

CE: Namrta; HJH/201793; Total nos of Pages: 9;
HJH 201793
LV geometry. Several studies, indeed, demonstrated that
the application of nasal CPAP produced at medium-term
follow-up a significant regression of LV mass [10,36]
which was probably due to the decreased LV afterload,
sympathetic drive and normalization of oxygenation, all
potential underlying causative factors of LVH activated
by OSA. On the basis of Framingham data (8), the
shift from concentric to normal LV geometry and the
regression of LV mass represent two of the main thera-
peutic targets for these patients.
Also the relatively small sample size leads to consider our
data as hypothesis-generating results, not conclusive. In
this view, our study suggests that the assessment of OSA
could be useful to investigate the determinants of
changes in LV structure, performance and function in
patients with risk factors for cardiovascular disease. The
heterogenic expression of LV geometric abnormalities
characterizing patients with obesity and hypertension is
lost in those who have moderate/severe OSA. In most of
these patients, indeed, concentric LV geometry is the
pathological pathway elicited by the sleep-disordered
breathing. This increased prevalence may in part explain
the increased rate of cardiovascular events in these
patients.
AcknowledgementsConception and design: Giovanni Cioffi, Carlo Stefenelli,
Tiziano Edoardo Russo, Francesco Furlanello, Alessan-
dro Selmi, Eva Gerdts, Dana Cramariuc, Giovanni de
Simone. Generation of clinical data: Giovanni Cioffi,
Carlo Stefenelli, Tiziano Edoardo Russo, Francesco Fur-
lanello, Alessandro Selmi. Analysis and interpretation of
data, or both: Giovanni Cioffi, Eva Gerdts, Dana Cramar-
iuc, Giovanni de Simone. Drafting of the manuscript or
revising it critically for important intellectual content:
Giovanni Cioffi, Dana Cramariuc, Eva Gerdts, Carlo
Stefenelli, Giovanni de Simone. Final approval of the
manuscript submitted: Giovanni Cioffi, Eva Gerdts,
Dana Cramariuc, Carlo Stefenelli, Giovanni de Simone,
Alessandro Selmi, Tiziano Edoardo Russo.
References1 Shamsuzzaman ASM, Gersh BJ, Somers VK. Obstructive sleep apnea:
implications for cardiac and vascular disease. J Am Med Assoc 2003;290:1906–1914.
2 Phillipson EA. Sleep apnea: a major public health problem. N Engl J Med1993; 328:1271–1273.
3 Hedner J, Ejnell H, Caidahl K. Left ventricular hypertrophy independent ofhypertension in patients with obstructive sleep apnea. J Hypertension1990; 8:941–946.
4 Noda A, Okada T, Yasuma F, Nakashima N, Yokota M. Cardiac hypertrophyin obstructive sleep apnea syndrome. Chest 1995; 107:1538–1544.
5 Avelar E, Cloward TV, Walker JM, Farney RJ, Strong M, Pendleton RC, et al.Left ventricular hypertrophy in severe obesity: interaction among bloodpressure, nocturnal hypoxemia and body mass. Hypertension 2007;49:34–39.
6 Peppard PE, Young T, Palta M, Skadrut J. Prospective study of theassociation between sleep-disordered breathing and hypertension. N EnglJ Med 2000; 19:1378–1384.
7 Savage DD, Garrison RJ, Kannel WB, Levy D, Anderson SJ, Stokes J 3rd,et al. The spectrum of left ventricular hypertrophy in a general populationsample: the Framingham Study. Circulation 1987; 75:I26–33.
8 Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP.Prognostic implications of echocardiographically determined leftventricular mass in the Framingham Heart Study. N Engl J Med 1990;323:1706–1707.
9 Hiestand DM, Britz P, Goldman M, Phillips B. Prevalence of symptomsand risk of sleep apnea in the US population: results from the nationalsleep foundation sleep in America 2005 poll. Chest 2006; 130:780–786.
10 Cloward TV, Walker JM, Farney RJ, Anderson JL. Left ventricularhypertrophy is a common echocardiographic abnormality in severeobstructive sleep apnea and reverses with nasal continuous positive airwaypressure. Chest 2003; 124:594–601.
11 Clinical guidelines on the identification, evaluation, and treatment ofoverweight and obesity in adults: the evidence report. National Institutes ofHealth. Obes Res 1998; Suppl 2:51–209.
12 Vincenti A, Brambilla R, Fumagalli MG, Merola R, Pedretti S. Onsetmechanism of paroxysmal atrial fibrillation detected by ambulatory Holtermonitoring. Europace 2006; 8:204–210.
13 Sahn DJ, Demaria A, Kisslo J, Weyman A. The committee on M-Modestandardization on the American Society of Echocardiography:recommendations regarding quantitation in M-Mode echocardiography.Results of a survey study of echocardiographic measurements. Circulation1978; 58:1072–1083.
14 Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E,Sachs I, Reichek N. Echocardiographic assessment of left ventricularhypertrophy: comparison to necropsy findings. Am J Cardiol 1986;57:450–458.
15 de Simone G, Devereux RB, Daniels SR, Koren MJ, Meyer RA, Laragh JH.Effect of growth on variability of left ventricular mass: assessment ofallometric signals in adults and children and their capacity to predictcardiovascular risk. J Am Coll Cardiol 1995; 25:1056–1062.
16 Roman MJ, Pickering TG, Schwartz JE, Pini R, Devereux RB. Association ofcarotid atherosclerosis and left ventricular hypertrophy. J Am Coll Cardiol1995; 25:83–90.
17 de Simone G, Devereux RB, Ganau A, Ahn RT, Saba PS, Mureddu G, et al.Estimation of left ventricular chamber and stroke volume by limited M-modeechocardiography and validation by two-dimensional and Dopplerechocardiography. Am J Cardiol 1996; 78:801–807.
18 de Simone G, Devereux RB, Daniels SR, Mureddu G, Roman MJ, KimballTR, et al. Stroke volume and cardiac output in normotensive children andadults. Assessment of relations with body size and impact of overweight.Circulation 1997; 95:1837–1843.
19 de Simone G, Devereux RB, Roman MJ, Ganau A, Saba PS, Alderman MH,Laragh JH. Assessment of left ventricular function by the midwall fractionalshortening/end-systolic stress relation in human hypertension. J Am CollCardiol 1994; 23:1444–1451.
20 de Simone G, Devereux RB, Koren MJ, Mensah GA, Casale PN,Laragh JH. Midwall left ventricular mechanics. An independentpredictor of cardiovascular risk in arterial hypertension. Circulation 1996;93:259–265.
21 Bella JN, Palmieri V, Roman MJ, Paranicas MF, Welty TK, Lee ET,et al. Gender differences in left ventricular systolic function inAmerican Indians (from the Strong Heart Study). Am J Cardiol 2006;98:834–837.
22 de Simone G, Devereux RB, Roman MJ, Alderman MH, Laragh JH. Relationof obesity and gender to left ventricular hypertrophy in normotensive andhypertensive adults. Hypertension 1994; 23:600–606.
23 Bradley TD, Floras JS. Sleep apnea and heart failure. Part I: obstructivesleep apnea. Circulation 2003; 107:1671–1678.
24 Somers VK, Dyken ME, Mark AL, Abboud FM. Sympathetic-nerve activityduring sleep in normal subjects. N Engl J Med 1993; 328:303–307.
25 Khatri IM, Freis ED. Hemodynamic changes during sleep. J Appl Physiol1967; 22:867–873.
26 Drager LF, Bortolotto LA, Figuereido AC, Silva BC, Krieger EM,Lorenzi-Filho G. Obstructive sleep apnea, hypertensione and theirinteraction on arterial stiffness and heart remodeling. Chest 2007;131:1379–1386.
27 Mylinski W, Duchna HW, Rasche K, Dichmann M, Mosiewicz J, Schultze-Werninqhaus G. Left ventricular geometry in patients with obstructive sleepapnea coexisting with treated systemic hypertension. Respiration 2007;74:176–183.
28 Hedner JA, Wilcox I, Sullivan CE. Speculations on the interaction betweenvascular disease and obstructive sleep apnea. In: Saunders NA, SullivanCE, editors. sleep and breathing, 2nd ed. Rev. New York: Marcel Dekker;1994. pp. 823–846.
29 Lauer MS, Anderson KM, Kannel WB, Levy D. The impact of obesity on leftventricular mass and geometry. The Framingham Heart Study. J Am MedAssoc 1991; 266:231–236.
8 Journal of Hypertension 2010, Vol 00 No 00
CE: Namrta; HJH/201793; Total nos of Pages: 9;
HJH 201793
30 Sukhija R, Aronow WS, Sandhu R, Kakar P, Maquire GP, Ahn C, LehrmanSG. Prevalence of left ventricular hypertrophy in persons with and withoutobstructive sleep apnea. Cardiol Rev 2006; 14:170–172.
31 Messerli FH, Sundgaard-Riise K, Reisin ED, Dreslinski GR, Ventura HO,Oigman W, et al. Dimorphic cardiac adaptation to obesity and arterialhypertension. Ann Intern Med 1983; 99:757–761.
32 Post WS, Larson MG, Levy D. Impact of left ventricular structure on theincidence of hypertension: the Framingham Heart Study. Circulation 1994;90:179–185.
33 Ambrosio G, Zweier JL, Flaherty JT. The relationship between oxygenradical generation and impairment of myocardial energy metabolismfollowing postischemic reperfusion. J Mol Cell Cardiol 1991; 23:1359–1374.
34 Schulz R, Seeger W, Grimminger F. Serum nitrite/nitrate levels inobstructive apnea. Am J Resp Crit Care Med 2001; 164:1997–1998.
35 Suzuki YJ, Jain V, Park AM, Day RM. Oxidative stress and oxidant signalingin ostructive sleep apnea and associated diseases. Free Radic Biol Med2006; 40:1683–1692.
36 Duchna HW, Myslinski W, Dichmann M, Rasche K, Schultze-WerninghausG, Orth M. Cardiac structure and function in patients with obstructive sleepapnea syndrome and co-prevalent arterial hypertension. Influence of CPAPtherapy. Med Klin 2006; 101:1–8.
Left ventricular geometry in sleep apnea Cioffi et al. 9
HJH Journal of Hypertension Typeset by Thomson Digital
for Lippincott Williams & Wilkins Manuscript No. 201793 Dear Author, During the preparation of your manuscript for typesetting, some queries have arisen. These are listed below. Please check your typeset proof carefully and mark any corrections in the margin as neatly as possible or compile them as a separate list. This form should then be returned with your marked proof/list of corrections to the Production Editor.
QUERIES: to be answered by AUTHOR/EDITOR QUERY NO. QUERY DETAILS RESPONSE
NO QUERY