adjunct armodafinil improves wakefulness and memory in obstructive sleep apnea/hypopnea syndrome
TRANSCRIPT

ARTICLE IN PRESS
Respiratory Medicine (2007) 101, 616–627
0954-6111/$ - see frdoi:10.1016/j.rmed.
�Corresponding au
E-mail address: m
Adjunct armodafinil improves wakefulnessand memory in obstructive sleepapnea/hypopnea syndrome
M. Hirshkowitza,�, J.E. Blackb, K. Wesnesc, G. Nieblerd, S. Arorad, T. Rothe
aMichael E. DeBakey VAMC Sleep Center, Baylor College of Medicine, Houston, TX 77030, USAbStanford University, Stanford, CA 94305, USAcCognitive Drug Research, Ltd, Goring-on-Thames, UK RG8 0ENdCephalon, Inc, Frazer, PA 19355, USAeSleep Disorders and Research Center, Henry Ford Hospital, Detroit, MI 48202, USA
Received 1 December 2005; accepted 9 June 2006
KEYWORDSArmodafinil;Obstructive sleepapnea/hypopneasyndrome;Wakefulness;Memory;Fatigue;Excessive sleepiness
ont matter & 20062006.06.007
thor. Tel.: 713 794
SummaryObjective: Armodafinil is the R-enantiomer of racemic modafinil and has a significantlylonger half-life than the S-enantiomer. This study evaluated armodafinil 150mg/day as anadjunct treatment for residual excessive sleepiness in patients with obstructive sleepapnea/hypopnea syndrome (OSA/HS) who were otherwise well controlled with nasalcontinuous positive airway pressure (nCPAP). We assessed the ability of armodafinil toimprove wakefulness and cognition and reduce fatigue in this population.Methods: In this 12-week, randomized, double-blind study, patients (n ¼ 259) receivedarmodafinil (150mg) or placebo once daily. Efficacy assessments at baseline and weeks 4,8, and 12 included the Maintenance of Wakefulness Test (MWT), Clinical Global Impressionof Change (CGI-C), Cognitive Drug Research battery, Epworth Sleepiness Scale, and BriefFatigue Inventory.Results: At final visit, mean (SD) MWT sleep latency increased from baseline by 2.3(7.8)min with armodafinil and decreased by 1.3 (7.1)min in the placebo group(P ¼ 0.0003). Armodafinil improved clinical condition (CGI-C, 71% vs. 53% for armodafiniland placebo, respectively; P ¼ 0.0069). Armodafinil significantly improved episodicsecondary memory (P ¼ 0.0102) and patient-estimated wakefulness (Po0.01) and reducedfatigue (Po0.05) compared with placebo. Armodafinil did not adversely affect nCPAP use.The most common adverse event associated with armodafinil was headache. Sleepmacroarchitecture was not altered by armodafinil.Conclusion: Adjunct treatment with armodafinil significantly improved alertness, overallclinical condition, and long-term memory. Armodafinil also reduced fatigue and the impact
Elsevier Ltd. All rights reserved.
7562; fax: 713 794 7558.
u (M. Hirshkowitz).

ARTICLE IN PRESS
Adjunct armodafinil in obstructive sleep apnea 617
of sleepiness on daily activities in patients with OSA/HS who have residual excessivesleepiness notwithstanding regular use of nCPAP. Armodafinil was well tolerated.& 2006 Elsevier Ltd. All rights reserved.
Introduction
Obstructive sleep apnea/hypopnea syndrome (OSA/HS)afflicts 7–20% of American adults.1 OSA/HS usually reducesan individual’s overall functioning; is associated withexcessive sleepiness (ES), fatigue, and lack of energy; andoften adversely affects memory, concentration, and atten-tion.2,3 Nasal continuous positive airway pressure (nCPAP) isthe standard of care for treating OSA/HS. It reducessleepiness,4,5 improves functioning,6 and improves self-reported health status.4,7 However, some patients whoregularly use nCPAP experience residual ES.8 Studies haveshown that modafinil improves wakefulness in patients withOSA/HS who have residual ES notwithstanding adequatenCPAP use.9,10 Modafinil is the only drug currently approvedfor the treatment of ES in this patient population.
Modafinil is a racemic compound containing equalamounts of R-modafinil and S-modafinil. The R-enantiomer,also known as armodafinil, has a half-life of 10–14 hcompared with 3–4 h for that of the S-enantiomer.11–13
Following chronic use of modafinil, the proportion ofcirculating R-modafinil can be as much as three timesgreater than that of circulating S-modafinil.11–13 Therefore,most of the wakefulness maintenance effects of racemicmodafinil could theoretically be attributable to armodafinil.This study assessed whether the therapeutically beneficialeffects of racemic modafinil for improving wakefulness9,10,14
could be replicated by administering armodafinil alone.This randomized, double-blind, placebo-controlled study
assessed the efficacy and tolerability of armodafinil 150mg/day as adjunct therapy to nCPAP for improving wakefulnessin patients with OSA/HS with residual ES notwithstandingregular and effective nCPAP therapy.
Methods
Patient selection
Eligible subjects included men and women, age 18–65 years,who were diagnosed with OSA/HS15 and complained ofresidual ES notwithstanding effective, regular, and adequateuse of nCPAP. The nCPAP criteria included stable therapy (forat least 4 weeks); effective therapy (an apnea-hypopneaindex [AHI]p10 during overnight polysomnography); andregular and adequate nCPAP use (X4 h per night on at least70% of the nights during a 2-week evaluation period). AClinical Global Impression of Severity of illness16 rating ofX4 (corresponding to moderately ill or worse) and anEpworth Sleepiness Scale (ESS)17 score of X10 wererequired. Female patients of childbearing potential wererequired to have a negative serum pregnancy test atscreening and use a medically accepted method of birthcontrol. Steroidal contraceptives had to be used inconjunction with a barrier method.
Individuals were excluded from the study if they had thefollowing: any clinically significant, uncontrolled psychiatricor medical conditions that could account for their ES; aprobable or confirmed diagnosis of another sleep disorder(other than OSA/HS); or any disorder that might interferewith drug absorption, distribution, metabolism, or excretionor produce daytime sleepiness. Other exclusion criteriaincluded pregnancy or lactation; consumption of 4600mg/day of caffeine; history of alcohol or drug abuse18; medicalrequirement for drugs disallowed by the protocol (modafinil,melatonin, sodium oxybate, lithium, St. John’s wort,methylphenidate, amphetamines, pemoline, antipsychoticagents, benzodiazepines, zolpidem, monoamine oxidaseinhibitors, anticoagulants, anticonvulsants, and barbitu-rates); use of clinically significant amounts of nonprescrip-tion drugs within 7 days of the screening visit; use ofinvestigational drugs within 1 month of the screening visit;or clinically significant drug sensitivity to stimulants ormodafinil. The study was conducted between March 26 andOctober 23, 2004.
Study design
This 12-week, randomized, double-blind, placebo-con-trolled, parallel-group study was conducted in 36 centersin the United States, Australia, Russia, Germany, andFrance. The protocol was approved by an IndependentEthics Committee or an Institutional Review Board at eachparticipating center. Furthermore, the study was conductedaccording to international, national, and local laws andregulations. Patients provided written informed consent.Screening assessments included a 2-week period of at-homenCPAP therapy using a REMstar Auto nCPAP System (Re-spironics, Murrysville, PA) to assess adherence and nighttimepolysomnography to determine nCPAP effectiveness. TheREMstar Auto nCPAP device was used in CPAP mode. Patientsreturned to the clinic for baseline assessments, randomiza-tion, and drug dispensation and for postbaseline assessments(weeks 4, 8, and 12) and nighttime polysomnography (week12 only).
Patients meeting inclusion, exclusion, and screeningcriteria were randomized (1:1) via an interactive voicerandomization system to receive armodafinil 150mg, for-mulated as film-coated 50-mg tablets, or a matchingplacebo. Because of the large number of planned centers,randomization was stratified by country. Patients assigned toarmodafinil received 50mg on the first day followed by anadditional 50mg/day for two consecutive days, with thefinal dosage reached on day 4. Patients assigned to placebowere titrated in the same manner. Study drug was packagedin child-resistant blister cards. At home, patients took studydrug once daily in the morning before 0800 h, approximately30min before breakfast. On clinic days, study drug wastaken at approximately 0700 h. Patients and investigators

ARTICLE IN PRESS
M. Hirshkowitz et al.618
remained blinded to treatment throughout the study. Ateach center, the investigator was responsible for monitoringpatient compliance. Compliance checks included comple-tion of study drug accountability records and reviews ofpatient diaries.
Assessments
Efficacy assessments were performed at screening or base-line and at weeks 4, 8, and 12. The Maintenance ofWakefulness Test (MWT), an objective measure of wakeful-ness that uses polysomnography to verify a patient’s abilityto remain awake19 was conducted as 30-min tests scheduledat 0900, 1100, 1300, 1500, 1700, and 1900. The use of 20-,30-, and 40-min sessions has been reported previously.19–22
In this study, 30-min tests were conducted to minimize thepotential for a ceiling effect with regard to the objectivelevel of ES in these nCPAP-treated patients with OSA/HS andto accommodate the timely administration of all theassessments used in the study. Sleep latency was definedas the time to onset of the first of three consecutive epochsof stage 1 sleep or the time to onset of any epoch of stages2, 3, and 4, or rapid eye movement sleep.23 Individualsfalling asleep during a testing session were awakened butrequired to remain in bed and were prevented from fallingasleep for the remainder of the 30-min test session. Patientswho did not fall asleep during a test session were assigned asleep latency of 30min. To distinguish between earlier andlater effects, MWT sleep latencies were averaged across thefirst 4 (0900, 1100, 1300, and 1500) and the last 3 (1500,1700, and 1900) tests.
The Clinical Global Impression of Change (CGI-C) assessedchanges from baseline in overall clinical condition. For theCGI-C, seven categories ranging from ‘‘very much im-proved’’ to ‘‘very much worse’’ were completed by theinvestigators.16
The Cognitive Drug Research (CDR) battery, a computer-ized battery of tests that assesses changes in cognitivefunction,24,25 was administered at 0930, 1130, 1330, 1530,1730, and 1930. The CDR battery included tests of memory(i.e., numeric working memory, word recognition, immedi-ate word recall, delayed word recall, and picture recogni-tion) and attention (i.e., simple reaction time, choicereaction time, and digit vigilance task). The entire batteryof tests took approximately 25min to complete. Compositefactors derived from the CDR included quality of episodicsecondary memory, which measures the ability to store andretrieve information while not actively rehearsing theinformation; speed of memory, which assesses the time ittakes to decide whether an item is held in memory; power ofattention, which measures the ability to focus attention andavoid distraction; and continuity of attention, whichmeasures the ability to sustain concentration. CDR factorscores were averaged across the first 4 (0930, 1130, 1330,and 1530) and the last 3 (1530, 1730, and 1930) tests.
At each visit, the ESS and Brief Fatigue Inventory (BFI)were assessed. The ESS, a subjective measure of the extentto which ES interferes with daily activities, assessed changesfrom baseline in patient-estimated sleepiness.17 Total scoresrange from 0 to 24, with higher scores indicating greatersleepiness. The BFI, a 9-item questionnaire that assesses the
severity and impact of fatigue on daily functioning,26 wasused to assess patient-rated fatigue based on changes inglobal fatigue (average of all questions) and worst fatigueduring the past 24 h (item number 3). It uses a numericrating scale ranging from 0 to 10, with higher scorescorresponding to greater fatigue. Both the ESS and BFI wereadministered before the first MWT at each visit. Electronicdiaries were completed by patients and contained questionsrelated to sleepiness and recorded the number of unin-tended sleep episodes, number of naps, and number ofmistakes/near misses/accidents. Diaries were distributed atscreening and reviewed at baseline and weeks 4, 8, and 12.
Primary efficacy variables included the change frombaseline to final visit (week 12 or termination) in meanMWT sleep latency averaged across the first 4 tests and theproportion of patients with at least minimal improvement onCGI-C, as related to clinical condition, at the final visit(week 12 or termination). Secondary efficacy assessmentsincluded changes in MWTsleep latencies averaged across thelast 3 tests, CDR factor scores, ESS total scores, and BFIscores (global and worst fatigue). All efficacy assessmentswere analyzed at weeks 4, 8, and 12 (using observed cases)and at final visit (using last observation carried forward).
Adverse events were monitored throughout the study,with severity and the relationship to study drug provided bythe investigator. Clinical laboratory tests (chemistry, hema-tology, urinalysis), vital sign measurements, and electro-cardiograms were performed at screening, baseline, andweeks 4, 8, and 12. Vital signs were assessed at approxi-mately 3 and 13 h post study drug administration. Physicalexaminations were conducted at screening, baseline, andweek 12. To assess whether armodafinil adversely affectednighttime sleep, polysomnography 23 was conducted for 8 h,starting within 30min of the patient’s habitual bedtime butno earlier than 2130, at screening, and at week 12 (after thedaytime MWT). Nasal CPAP use was objectively monitored atleast 2 weeks before baseline and throughout the study.
Statistical analysis
A sample size of 108 patients per treatment group wasrequired to provide at least 80% power to detect a 2.5-mindifference in the MWT mean sleep latency, assuming acommon SD of 6.5min, and a 25% difference in theproportion of patients reporting at least minimal improve-ment in CGI-C ratings, assuming 36% improvement in theplacebo group. An enrollment of approximately 240 patientswas planned to obtain 216 evaluable patients with at least 1postbaseline MWT and CGI-C assessment.
Descriptive statistics were used to summarize continuousand categorical demographic variables. Continuous demo-graphic variables were compared between groups usinganalysis of variance (ANOVA), with treatment group as afactor. Categorical demographic variables were comparedusing Pearson’s w2 test or Fisher exact test. Efficacy analysesincluded randomized patients who received at least 1 doseof study drug and had a baseline measurement and at least 1postbaseline measurement on the MWT and at least 1assessment on the CGI-C. All continuous efficacy variableswas analyzed using ANOVA, with treatment and countryas factors and pairwise comparisons performed using

ARTICLE IN PRESS
Adjunct armodafinil in obstructive sleep apnea 619
appropriate contrasts. Categorical efficacy variables wereanalyzed using a Cochran–Mantel–Haenszel w2 adjusted forcountry; pairwise comparisons were performed using theappropriate subsets. All tests of treatment effect were2-sided and performed at the 0.05 significance level. Changefrom baseline to the final visit for data from patient diariesand vital signs was analyzed using the nonparametric test ofWilcoxon. The change in nCPAP use from baseline to on-treatment values was analyzed using a 1-way ANOVA withtreatment as factors. Data from nighttime polysomnographywere summarized using descriptive statistics. Safety ana-lyses included all randomized patients who received at least1 dose of study drug.
Results
Patients
Of 466 patients screened for the study, 263 (armodafinil,n ¼ 131; placebo, n ¼ 132) were randomized, and 259(armodafinil, n ¼ 129; placebo, n ¼ 130) received studydrug. Patient characteristics were comparable between thegroups (Table 1). With respect to illness severity, 57% ofpatients were rated by the investigator(s) as moderately ill,with the remaining 43% rated as markedly, severely, or
Table 1 Baseline/Screening Demographics.
Characteristic Placebo
Mean (SD) age, y 50.6 (8Range� 25–68
Sex, n (%)Men 93 (72)
Race, n (%)White 111 (85)Other 18 (14)Missing 1 (o1
Mean (SD) BMI, kg/m2 30.8 (7CGI-S, n (%)y
Moderately ill 75 (58)Markedly ill 39 (30)Severely ill 13 (10)Among the most extremely ill 3 (2)
Mean (SD) ESS total scorey 16.0 (3nCPAP, h/nightz 6.9 (1Mean (SD) MWT sleep latencyy 23.3 (8AHI at baseline during nCPAPz 1.4 (2
AHI ¼ apnea-hypopnea index; BMI ¼ body mass index; CGI-S ¼ CliSleepiness Scale; MWT ¼ Maintenance of Wakefulness Test; nCPAP ¼ n�As exceptions to the protocol, 1 patient receiving placebo and 2 pa
of age.yAt screening. ESS scores are for 120 patients receiving placebo and
pathologic sleepiness.zNasal CPAP data are for 126 patients receiving placebo and 128 pyMWT sleep latencies were averaged across the first 4 sessions (09
placebo and 116 patients receiving armodafinil 150mg/day.zAHI data are for 129 patients receiving placebo and 125 patients
extremely ill. Patients experienced ES before the start ofthe double-blind phase (as shown by mean ESS total scoresof 15.6 and 16.0 for the armodafinil and placebo groups,respectively) notwithstanding a high mean duration ofnightly nCPAP therapy of approximately 7 h and low meanAHI indices. At baseline, mean sleep latency on the MWTwassimilar between the groups. In accordance with entrycriteria, patients were receiving effective nCPAP therapybefore receiving armodafinil or placebo (mean [SD] AHI,armodafinil, 1.1 [2.1]; placebo, 1.4 [2.3]). One hundredfifty-three patients (59%) had a medical history of cardio-vascular disease. Cardiovascular disease included hyperten-sion, n ¼ 102 (39%); arrhythmias, n ¼ 11 (4%); chest pain,n ¼ 13 (5%); congestive heart failure, n ¼ 1 (o1%); andother, n ¼ 88 (34%).
Two hundred twenty-nine patients (armodafinil, n ¼ 111;placebo, n ¼ 118) (87%) completed the study. Twentypatients (15%) randomized to armodafinil discontinued thestudy for the following reasons: adverse event (n ¼ 5),consent withdrawn (n ¼ 5), noncompliance with studyprocedures (n ¼ 3), protocol violation (n ¼ 2), loss tofollow-up (n ¼ 2), other (n ¼ 2), and insufficient efficacy(n ¼ 1). Fourteen patients (11%) randomized to placebodiscontinued the study for the following reasons: adverseevent (n ¼ 6), consent withdrawn (n ¼ 3), protocol violation(n ¼ 3), and loss to follow-up (n ¼ 2).
n ¼ 130 Armodafinil 150mg n ¼ 129
.9) 50.7 (9.2)27–69
97 (75)
107 (83)22 (17)
) 0 (0).5) 36.3 (7.8)
72 (56)37 (29)18 (14)2 (2)
.5) 15.6 (3.5)
.0) 6.8 (1.3)
.2) 23.7 (8.6)
.3) 1.1 (2.1)
nical Global Impression of Severity of Illness; ESS ¼ Epworthasal continuous positive airway pressure; SD ¼ standard deviation.tients receiving armodafinil 150mg/day were older than 65 years
115 patients receiving armodafinil 150mg/day. ESSX10 indicates
atients receiving armodafinil 150mg/day.00, 1100, 1300, and 1500). Data are for 120 patients receiving
receiving armodafinil 150mg/day.
ARTICLE IN PRESS
M. Hirshkowitz et al.620
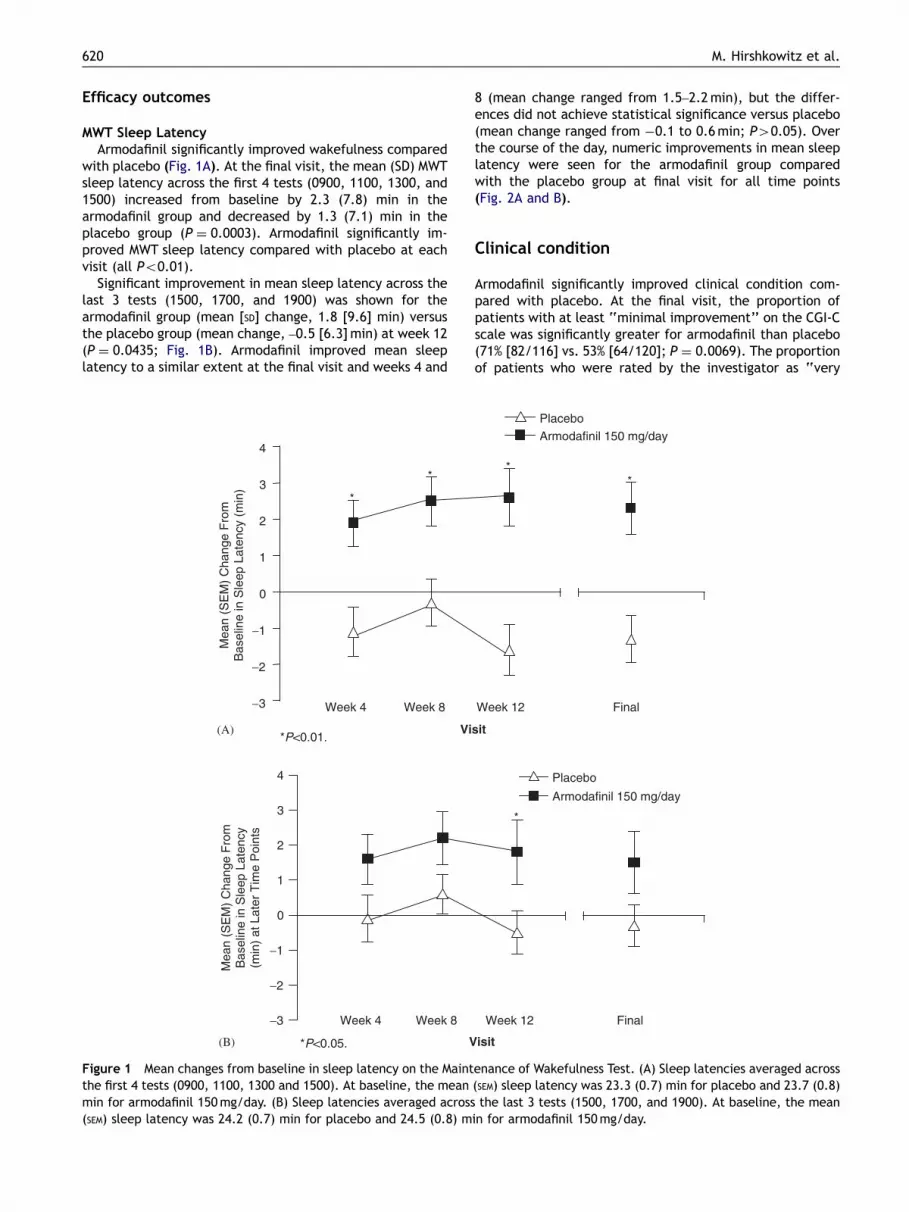
Efficacy outcomes
MWT Sleep LatencyArmodafinil significantly improved wakefulness compared
with placebo (Fig. 1A). At the final visit, the mean (SD) MWTsleep latency across the first 4 tests (0900, 1100, 1300, and1500) increased from baseline by 2.3 (7.8) min in thearmodafinil group and decreased by 1.3 (7.1) min in theplacebo group (P ¼ 0.0003). Armodafinil significantly im-proved MWT sleep latency compared with placebo at eachvisit (all Po0.01).
Significant improvement in mean sleep latency across thelast 3 tests (1500, 1700, and 1900) was shown for thearmodafinil group (mean [SD] change, 1.8 [9.6] min) versusthe placebo group (mean change, –0.5 [6.3]min) at week 12(P ¼ 0.0435; Fig. 1B). Armodafinil improved mean sleeplatency to a similar extent at the final visit and weeks 4 and
Week 4 Week 8−3
−2
−1
0
1
2
3
4
Mea
n (S
EM
) C
hang
e F
rom
Bas
elin
e in
Sle
ep L
aten
cy (
min
)
*
*
*P<0.01.Vi
Week 4 Week 8
0
1
2
3
4
Mea
n (S
EM
) C
hang
e F
rom
Bas
elin
e in
Sle
ep L
aten
cy(m
in)
at L
ater
Tim
e P
oint
s
*P<0.05. V
−3
−2
−1
(A)
(B)
Figure 1 Mean changes from baseline in sleep latency on the Maintthe first 4 tests (0900, 1100, 1300 and 1500). At baseline, the meanmin for armodafinil 150mg/day. (B) Sleep latencies averaged across(SEM) sleep latency was 24.2 (0.7) min for placebo and 24.5 (0.8) m
8 (mean change ranged from 1.5–2.2min), but the differ-ences did not achieve statistical significance versus placebo(mean change ranged from �0.1 to 0.6min; P40.05). Overthe course of the day, numeric improvements in mean sleeplatency were seen for the armodafinil group comparedwith the placebo group at final visit for all time points(Fig. 2A and B).
Clinical condition
Armodafinil significantly improved clinical condition com-pared with placebo. At the final visit, the proportion ofpatients with at least ‘‘minimal improvement’’ on the CGI-Cscale was significantly greater for armodafinil than placebo(71% [82/116] vs. 53% [64/120]; P ¼ 0.0069). The proportionof patients who were rated by the investigator as ‘‘very
Week 12
Placebo
Armodafinil 150 mg/day
**
Final
sit
*
Week 12
Placebo
Armodafinil 150 mg/day
Final
isit
enance of Wakefulness Test. (A) Sleep latencies averaged across(SEM) sleep latency was 23.3 (0.7) min for placebo and 23.7 (0.8)the last 3 tests (1500, 1700, and 1900). At baseline, the mean
in for armodafinil 150mg/day.

ARTICLE IN PRESS
Baseline
Final Visit
0
20
22
24
26
28
30
Mea
n (S
EM
) S
leep
Lat
ency
(m
in)
Mea
n (S
EM
) S
leep
Lat
ency
(m
in)
1100 1300 1700 1900
Time
15000900
1100 1300 1700
BaselineFinal Visit
1900
Time
150009000
20
22
24
26
28
30
(A)
(B)
Figure 2 Sleep latencies at individual time points for (A)armodafinil and (B) placebo.
Adjunct armodafinil in obstructive sleep apnea 621
much improved’’ and ‘‘much improved’’ at the final visitwere 22% and 25%, respectively, in the armodafinil groupcompared with 6% and 21%, respectively, in the placebogroup. Armodafinil significantly improved overall clinicalcondition compared with placebo at each study visit (allPo0.05).
Cognitive Drug Research battery
Armodafinil significantly improved quality of episodic sec-ondary memory compared with placebo. When averagedacross the first 4 tests (0930, 1130, 1330, and 1530), qualityof episodic secondary memory increased by 7.6 points frombaseline to the final visit for patients in the armodafinilgroup and decreased by 7.0 points for those in the placebogroup (P ¼ 0.0102 for the change from baseline vs. placebo;Fig. 3A). Significant improvement across the first 4 tests alsowas shown at week 12 for the armodafinil group versus theplacebo group (P ¼ 0.005), with numeric differences infavor of armodafinil observed at weeks 4 and 8. Numericimprovements from baseline in quality of episodic secondarymemory across the last 3 tests (1530, 1730, and 1930) wereobserved in the armodafinil group compared with theplacebo group; however, the difference versus placebo didnot achieve statistical significance (Fig. 3B). The numericimprovements from baseline in speed of memory, continuityof attention, or power of attention with armodafinil
treatment compared with placebo were not significant atany study visit or at the final visit (P40.05).
Patient-reported wakefulness and reduction infatigue
Armodafinil significantly reduced the impact of ES on dailyactivities. At final visit and each study visit, the meanchange from baseline in ESS total score was significantlygreater for patients receiving armodafinil than for thosereceiving placebo (all Po0.01; Fig. 4A). Armodafinilsignificantly reduced global fatigue and worst fatigue inthe past 24 h at weeks 4 and 12 and at the final visitcompared with placebo (all Po0.05; Fig. 4B and C).
Diary data for daytime sleepiness
Significant differences were shown between the armodafiniland placebo groups in the number of unintended sleepepisodes and number of daily naps. At baseline, the mean(SD) number of unintended sleep episodes was 1.0 (1.1) forthe armodafinil group and 1.2 (1.2) for the placebo group.Post baseline, the percentage decrease from baseline in thenumber of unintended sleep episodes was 54.7% and 37.1%,respectively (overall treatment comparison, P ¼ 0.0002).The mean (SD) number of daily naps at baseline was 0.5 (0.5)for the armodafinil group and 0.5 (0.5) for the placebogroup. Post baseline, the percentage decrease from baselinewas 35.7% and 17.0%, respectively (overall treatmentcomparison, P ¼ 0.0016). No statistically significant differ-ences were observed between the armodafinil and placebogroups in the number of mistakes/near misses/accidents(percentage change from baseline, �29.2% and –12.8% forarmodafinil and placebo, respectively). Caffeine use wascomparable across all groups.
Safety outcomes
Headache, nausea, diarrhea, dizziness, and anxiety werethe most frequently reported adverse events (X5%) inpatients who received armodafinil (Table 2). Adverse eventswere generally mild or moderate in nature. No patientsreceiving armodafinil experienced a serious adverse event; 1patient receiving placebo experienced serious gastroeso-phageal reflux. Four percent (5/129) of patients randomizedto armodafinil discontinued the study because of an adverseevent compared with 5% (6/130) of patients receivingplacebo. Rash was the most frequent adverse event leadingto discontinuation (armodafinil, n ¼ 2; placebo, n ¼ 1).
There were no clinically meaningful changes from base-line to final visit in either group for laboratory values, vitalsign measurements, electrocardiographic parameters, orphysical examination findings. Small mean increases frombaseline to the final visit in gamma-glutamyl transpeptidase(armodafinil, 6.6 [11.2] U/L vs. placebo, 0.6 [12.8] U/L) andalkaline phosphatase (2.3 [9.7] U/L vs. –1.1 [9.4] U/L)observed in patients receiving armodafinil compared withthose receiving placebo were not considered clinicallymeaningful. There were no statistically or clinically mean-ingful changes in systolic and diastolic blood pressure or

ARTICLE IN PRESS
**
−15
−10
−5
0
5
10
15
Mea
n (S
EM
) C
hang
e F
rom
Bas
elin
e in
Qua
lity
of E
piso
dic
Sec
onda
ry M
emor
y (u
nits
)
*P=0.01.
Week 4 Week 8 Week 12 Final
Visit
Placebo
Armodafinil 150 mg/day
0
5
10
15
Mea
n (S
EM
) C
hang
eF
rom
Bas
elin
e in
Qua
lity
ofE
piso
dic
Sec
onda
ry M
emor
y(u
nits
) at
Lat
er T
ime
Poi
nts
Week 4 Week 8 Week 12 Final
Visit
Placebo
Armodafinil 150 mg/day
−15
−10
−5
(A)
(B)
Figure 3 Mean changes from baseline in quality of episodic secondary memory on the Cognitive Drug Research battery. (A) Scoreswere averaged across the first 4 tests (0930, 1130, 1330, and 1530). At baseline, the mean (SEM) episodic memory score was 161.9(4.0) units for placebo and 172.4 (3.7) units for armodafinil 150mg/day. (B) Scores were averaged across the last 3 tests (1530, 1730,and 1930). At baseline, the mean (SEM) episodic memory score was 150.5 (4.2) units for placebo and 162.6 (3.8) units for armodafinil150mg/day.
M. Hirshkowitz et al.622
pulse. There were no qualitative differences in electro-cardiography findings between armodafinil and placebo.
The duration of nCPAP therapy was high in both groups,approximately 7 h per night before the start of study drug,and remained high during the study. The mean (SD) durationof nCPAP decreased slightly from the baseline to postbase-line period for the armodafinil (–0.2 [0.7]) and placebo (–0.2[0.6]) groups. This small decrease in nCPAP use was notaccompanied by an increase in the AHI in either group (meanchange from baseline, armodafinil, 0.1 [1.4] vs. placebo, 0.2[2.9]).
Armodafinil had no adverse effects on nighttime sleep asdetermined by subjective and objective measures. Mean (SD)sleep efficiency from patient diaries increased by 2.6% (4.4)and 2.0% (5.2), and mean sleep latency decreased by 5.8(12.7) and by 4.1 (9.2) min for the armodafinil and placebogroups, respectively. No clinically meaningful changes in
polysomnographically defined sleep parameters were seenin either group (Table 3).
Discussion
Excessive sleepiness is a serious condition that is oftenundiagnosed.27 It is associated with high morbidity andaffects not only patients but also their families, coworkers,and the public at large. The true prevalence of residual ES inOSA/HS patients who use nCPAP is not known, and themechanisms that underlie residual sleepiness in thesepatients are poorly defined. Possible explanations includechronic partial sleep loss from sleeping less than 8 h pernight, fragmented sleep caused by persistent nighttimearousals, and alterations in sleep architecture that lead toless-than-adequate sleep. Alternatively, hypoxia-induced

ARTICLE IN PRESS
−6
−5
−4
−3
−2
−1
0
*
* * *
Mea
n (S
EM
) C
hang
eF
rom
Bas
elin
e in
Epw
orth
Sle
epin
ess
Sca
le T
otal
Sco
re
*P<0.01.
Week 4 Week 8 Week 12 Final
Visit
Placebo
Armodafinil 150 mg/day
−2.0
−1.5
−1.0
−0.5
0.0
* **
Mea
n (S
EM
) C
hang
eF
rom
Bas
elin
e in
Glo
bal F
atig
ue S
core
*P<0.05.
Week 4 Week 8 Week 12 Final
Visit
Placebo
Armodafinil 150 mg/day
−2.0
−1.5
−1.0
−0.5
0.0
* **
Mea
n (S
EM
) C
hang
eF
rom
Bas
elin
e in
Wor
st F
atig
ue S
core
*P<0.05.
Week 4 Week 8 Week 12 Final
Visit
Placebo
Armodafinil 150 mg/day
(A)
(B)
(C)
Figure 4 Mean changes from baseline in patient-reported wakefulness and fatigue. (A) Epworth Sleepiness Scale total score. Atbaseline, total scores were 16.0 (0.3) for placebo and 15.6 (0.3) for armodafinil 150mg/day. (B) Global fatigue score. At baseline,scores were 4.9 (0.2) for placebo and 4.7 (0.2) for armodafinil 150mg/day. (C) Worst fatigue in the past 24 h score. At baseline,scores were 7.1 (0.2) for placebo and 7.0 (0.2) for armodafinil 150mg/day.
Adjunct armodafinil in obstructive sleep apnea 623

ARTICLE IN PRESS
M. Hirshkowitz et al.624
cerebral dysfunction arising from chronic disease, residualupper airway abnormalities, suboptimal quantity or qualityof sleep arising from subtherapeutic nCPAP, or suboptimalsleep induced by nCPAP may be contributing factors.28
Interestingly, residual ES can be present even when sleepfragmentation and hypoxemia are well treated in patientswho adhere strictly to nCPAP therapy.8 Regardless of theunderlying cause, recognition and management of ES iscritical given its adverse effects on cognitive, occupational,and social functioning.29
By selection, patients in this study adhered well to nCPAPtherapy and used it for an adequate duration but stillreported ES. Inclusion criteria were based on a substantivecomplaint of ES, which was verified by the ESS. Nonetheless,some patients did not have substantial sleepiness at baselineas determined by the objective MWT measures. Mean sleeplatency for normal controls has been reported to be18.7(2.6) and 35.2(7.9) min on the 20- and 40-min MWT,
Table 2 Adverse Events Occurring in X5% of PatientsReceiving Armodafinil or Placebo.�
Adverse Event Number (%) of Patients
Placebon ¼ 130
Armodafinil150mg n ¼ 129
Headache 9 (7) 19 (15)Upper respiratorytract infection
8 (6) 5 (4)
Nasopharyngitis 6 (5) 5 (4)Nausea 4 (3) 6 (5)Diarrhea 3 (2) 6 (5)Dizziness 2 (2) 6 (5)Anxiety 0 (0) 6 (5)
�Includes randomized patients who received at least 1dose of study drug.
Table 3 Polysomnographic Parameters for Patients Receiving A
Parameter Placebo
Baseline�
Latency to persistent sleep, minz 23.3 (27.0)Number of arousalsz 18.6 (9.9)Number of awakeningsz 9.1 (5.6)Sleep efficiency, %z 80.7 (14.0)Wake after sleep onset (min)z 73.4 (57.8)Sleep stage percentagez
Stage 1 11.1 (6.4)Stage 2 59.4 (10.4)Stage 3/4 10.9 (9.7)REM 18.7 (7.8)
REM ¼ rapid eye movement.�Baseline: placebo, n ¼ 128; armodafinil, n ¼ 126.yFinal visit: placebo, n ¼ 115; armodafinil, n ¼ 105.zValues are the mean (SD).
respectively.30 In the absence of normative data for a 30-mintest, it would be plausible to suggest that normal meansleep latency on a 30-min test would fall between thesevalues, perhaps around 25–26min. The mean sleep latencyat baseline on the 30-min MWT in this study was approxi-mately 23min and may very well be representative of mildto moderate sleepiness. Armodafinil administered once dailysignificantly improved patients’ wakefulness as assessed bythe MWT and overall clinical condition compared withplacebo. These improvements were observed on the firstpostbaseline visit, were maintained throughout the 12weeks of the study, and were accompanied by improvementsin multiple patient-reported outcomes. Armodafinil reducedfatigue, the extent to which ES interfered with dailyactivities, and the number of naps and unintended sleepepisodes.
Previous studies9,10 did not evaluate the wake-promotingeffects of modafinil in the late afternoon in patients withOSA/HS. Pharmacokinetic and pharmacodynamic resultswith armodafinil and modafinil in healthy volunteers duringacute sleep loss show that a single dose of armodafinil200mg helps sustain wakefulness and attention longer thana single dose of modafinil 200mg.31 Thus, we anticipated inthe present study that armodafinil would improve late-dayalertness. Armodafinil significantly improved mean sleeplatency across the last 3 tests (1500–1900) at week 12(P ¼ 0.0435). At final visit, the MWT sleep latency data atlate-day time points showed an expected diurnal increase inwakefulness for both groups. Most of the between groupdifference in mean sleep latency came at the 1500 testsession. Although armodafinil increased mean sleep latencycompared with placebo later in the day, the circadian-related increase in wakefulness may have produced a ceilingeffect, thereby preventing discernment of a significantdifference between treatment groups during the individualMWT measurements in the late afternoon and early evening.Behavioral effects related to the last test of the day (lastnap effect) and high intertest variability in sleep latency(i.e., three tests may have been insufficient to show a
rmodafinil or Placebo.
Armodafinil 150mg
Finaly Baseline� Finaly
24.4 (25.9) 21.6 (22.8) 19.1 (15.4)18.8 (10.8) 20.0 (11.2) 18.4 (10.3)9.7 (5.4) 8.8 (4.3) 9.6 (5.3)
79.6 (12.9) 81.9 (9.5) 81.9 (9.1)74.2 (50.6) 70.5 (39.9) 71.5 (41.6)
11.3 (7.3) 11.2 (6.2) 10.4 (5.4)57.0 (12.5) 59.7 (9.3) 58.1 (10.3)11.2 (10.6) 10.9 (9.1) 11.3 (9.5)20.5 (9.1) 18.2 (7.3) 20.1 (6.5)

ARTICLE IN PRESS
Adjunct armodafinil in obstructive sleep apnea 625
treatment difference) may also have contributed to thisfinding. Moreover, the study was powered to detectthe difference in treatment effect for the first 4 testsessions.
The etiology of diminished cognitive functioning inpatients with OSA/HS is unknown. One hypothesis blameschronic intermittent hypoxia.32–34 However, some reportsindicate nCPAP-related improvement in memory and atten-tion in patients with OSA/HS, whereas others have docu-mented reduced sleepiness without improvedcognition.5,33–36 Findings from the CDR indicate thatarmodafinil significantly improved long-term memory (qual-ity of episodic secondary memory) at final visit comparedwith placebo. The factor score for quality of episodicsecondary memory combined the accuracy measures of 4classical tests of memory: immediate word recall, delayedword recall, word recognition, and picture recognition.Significant improvements in this score were seen at week 12and final visit, reflecting greater ability to store and retrieveverbal and pictorial information in episodic memory. Thesedata indicate that memory function can be improved in thisclinical group by armodafinil. A previous study of healthyvolunteers undergoing a period of acute sleep loss hasreported that armodafinil and modafinil showed similarability to sustain attention on the Psychomotor VigilanceTask when administered at similar doses.31 Because indirectcomparisons across studies are speculative, a head-to-headstudy of armodafinil and modafinil would be needed todirectly assess cognitive effects of the two compounds in apopulation with ES.
When ES is present, patients often report fatigue,tiredness, and lack of energy rather than sleepiness.37 Datafrom the current study show that, on average, patients withOSA/HS experienced severe fatigue at baseline even withadequate nCPAP therapy, as shown by a mean score of 47for the BFI worst fatigue item.26 Armodafinil significantlyreduced symptoms of fatigue for the duration of the study.
Armodafinil was generally well tolerated, with mostadverse events rated as mild to moderate in severity. Therate of study discontinuations attributable to adverse eventswas low and comparable to that shown with placebo.Armodafinil, taken once daily in the morning, had noadverse effect on the quality or quantity of nighttime sleep.The magnitude of change in the nightly duration of nCPAPuse was relatively small, and nCPAP use remained high (i.e.,at approximately 7 h per night), with no effect on arousals.In other studies, average nightly use of nCPAP has beenreported to range from 5 to 6.5 h.38 Although more than halfof the study population had cardiovascular disease and morethan one third of patients had hypertension at baseline,treatment with armodafinil was not associated with adversecardiovascular effects. Previous studies with racemic mod-afinil also failed to show heart rate and blood pressurealterations.9,10 This is noteworthy because untreated OSA/HS is an independent risk factor for heart disease39 andsystemic hypertension.40,41
The relatively short duration of treatment in this studylimits generalizability to long-term clinical use. The studywas conducted in patients who were receiving regular nCPAPtherapy yet had residual ES. These findings should not begeneralized to OSA/HS patients who are not receivingtherapeutic nCPAP. Armodafinil does not treat the under-
lying obstruction and is not a replacement for nCPAPtherapy.
In summary, once-daily administration of armodafinil150mg/day improved patients’ wakefulness and overallclinical condition when used as adjunct therapy for residualES associated with OSA/HS in patients who regularly usenCPAP therapy. Further research is warranted to follow upon findings that armodafinil may improve long-term memory.Additional studies should explore whether the reduction infatigue seen with armodafinil in this study affects daytimefunctioning and quality of life in this population. Theseresults support using armodafinil to treat residual ES inpatients with OSA/HS who adhere to nCPAP therapeutic useprescription, who are properly titrated to an effectivepressure, and who maintain an adequate sleep schedule.
Acknowledgment
This study was sponsored by Cephalon, Inc., Frazer, PA.The authors wish to acknowledge the following investi-
gators who enrolled patients in the United States: J. Aaron(Regional Pulmonary and Sleep Medicine, Elkton, MD), M.Ahmed (Southwest Cleveland Sleep Center, MiddleburgHeights, OH), G. Asnis (Montefiore Medical Center, Bronx,NY), M. Erman (Pacific Sleep Medicine Services, Inc., SanDiego, CA), F. Fakih (Sleep-Wake Disorder Center of SouthFlorida, Winter Park, FL), D. Fried (Omega MedicalResearch, Warwick, RI), Y. Furman (Pacific Sleep MedicineServices, Inc., Los Angeles, CA), J. Hudson (FutureSearchTrials, Austin, TX), J. Hansbrough (Graves Gilbert Clinic,Bowling Green, KY), S. Hull (Vince and Associates ClinicalResearch, Overland Park, KS), L. Jimenez (SomniCare SleepInstitute, San Juan, PR), T. Kaelin (Lowcountry Lung andCritical Care, Charleston, SC), S. Kriengkairut (St. AlexiusMedical Center, Bismarck, ND), D. Laman (ConsolidatedClinical Trials, Pittsburgh, PA), W. Leeds (Topeka Pulmonary,Topeka, KS), G. Leo (Allegiance Research Specialists,Wauwatosa, WI), D. Loewy (PsyPharma Clinical Research,Tucson, AZ), D. Lorch (PAB Clinical Research, Brandon, FL),D. Mayleben (Community Research, Crestview, KY), J.Medoff (Vital re:Search, Greensboro, NC), J. Murphy (South-western Research, Beverly Hills, CA), M. Scharf (Tri StateSleep Disorders Center, Cincinnati, OH), L. Sweer (CapitalRegion Sleep Disorders Center, Carlisle, PA), T. Swick(Houston Sleep Center, Houston, TX), P. Whitten (PeoriaPulmonary Associates, Peoria, IL); in France: Marie-Piad’Ortho (Hospital Henri-Mondor, Service d’ExplorationsFonctionnelles, Creteil); in Australia: R. Antic (RoyalAdelaide Hospital, Sleep Disorders Service, North Terrace,Adelaide), P. Cistulli (Centre for Sleep Disorders andRespiratory Failure, Kogarah, New South Wales), A. Desai(Royal Prince Alfred Hospital, Woolcock Institute of MedicalResearch, Camperdown, New South Wales), M. Ho (MonashMedical Center, Clayton, Victoria), J. Swieca (MelbourneSleep Disorders Centre, East Melbourne, Victoria), J.R.Wheatley (Department of Respiratory Medicine, WestmeadHospital, Westmead, New South Wales); in Germany: H.Becker (Klinikum der Philipps, Universitat Baldingerstr. 1,Marburg), P. Geisler (University of Regensburg, Regensburg);and in Russia: G. Oganesyan (Clinical Hospital Russian

ARTICLE IN PRESS
M. Hirshkowitz et al.626
Science Academy, Saint Petersburg), A. Kalinkin (CityClinical Hospital No. 83, Moscow).
References
1. Young T, Skatrud J, Peppard PE. Risk factors for obstructivesleep apnea in adults. JAMA 2004;291:2013–6.
2. Greenberg GD, Watson RK, Deptula D. Neuropsychologicaldysfunction in sleep apnea. Sleep 1987;10:254–62.
3. Bassiri A, Guilleminault C. Clinical features and evaluationof obstructive sleep apnea-hypopnea syndrome. In: Kryger M,Roth T, Dement W, editors. Principles and practice of sleepmedicine. Philadelphia, PA: W.B. Saunders Company; 2000.p. 869–78.
4. Jenkinson C, Davies RJ, Mullins R, Stradling JR. Comparison oftherapeutic and subtherapeutic nasal continuous positive air-way pressure for obstructive sleep apnoea: a randomisedprospective parallel trial. Lancet 1999;353:2100–5.
5. Engleman HM, Martin SE, Kingshott RN, Mackay TW, Deary IJ,Douglas NJ. Randomised placebo controlled trial of daytimefunction after continuous positive airway pressure (CPAP)therapy for the sleep apnoea/hypopnoea syndrome. Thorax1998;53:341–5.
6. Hack M, Davies RJ, Mullins R, et al. Randomised prospectiveparallel trial of therapeutic versus subtherapeutic nasal con-tinuous positive airway pressure on simulated steering perfor-mance in patients with obstructive sleep apnoea. Thorax2000;55:224–31.
7. Jenkinson C, Davies RJ, Mullins R, Stradling JR. Long-termbenefits in self-reported health status of nasal continuouspositive airway pressure therapy for obstructive sleep apnoea.QJM 2001;94:95–9.
8. Sforza E, Krieger J. Daytime sleepiness after long-termcontinuous positive airway pressure (CPAP) treatment inobstructive sleep apnea syndrome. J Neurol Sci 1992;110:21–6.
9. Pack AI, Black JE, Schwartz JR, Matheson JK. Modafinil asadjunct therapy for daytime sleepiness in obstructive sleepapnea. Am J Respir Crit Care Med 2001;164:1675–81.
10. Black J, Hirshkowitz M. Modafinil for treatment of residualexcessive sleepiness in nasal continuous positive airwaypressure-treated obstructive sleep apnea/hypopnea syndrome.Sleep 2005;28:464–71.
11. Robertson Jr. P, Hellriegel ET. Clinical pharmacokinetic profileof modafinil. Clin Pharmacokinet 2003;42:123–37.
12. Wong YN, King SP, Simcoe D, et al. Open-label, single-dosepharmacokinetic study of modafinil tablets: influence of ageand gender in normal subjects. J Clin Pharmacol 1999;39:281–8.
13. Wong YN, Simcoe D, Hartman LN, et al. A double-blind,placebo-controlled, ascending-dose evaluation of the pharma-cokinetics and tolerability of modafinil tablets in healthy malevolunteers. J Clin Pharmacol 1999;39:30–40.
14. Kingshott RN, Vennelle M, Coleman EL, Engleman HM, MackayTW, Douglas NJ. Randomized, double-blind, placebo-controlledcrossover trial of modafinil in the treatment of residualexcessive daytime sleepiness in the sleep apnea/hypopneasyndrome. Am J Respir Crit Care Med 2001;163:918–23.
15. American Academy of Sleep Medicine. International Classifica-tion of Sleep Disorders, 2nd ed. Diagnostic and Coding Manual.Westchester, IL: American Academy of Sleep Medicine; 2005.
16. Guy W. clinical global impressions. In: ECDEU AssessmentManual for Psychopharmacology. Rockville, MD: US Dept ofHealth and Human Services, National Institute of Mental Health;1976. p. 218–22.
17. Johns MW. A new method for measuring daytime sleepiness: theEpworth sleepiness scale. Sleep 1991;14:540–5.
18. American Psychiatric Association. Diagnostic and statisticalmanual of mental disorders, fourth edition. Washington, DC:American Psychiatric Association; 1994.
19. Poceta JS, Timms RM, Jeong DU, Ho SL, Erman MK, Mitler MM.Maintenance of wakefulness test in obstructive sleep apneasyndrome. Chest 1992;101:893–7.
20. Mitler MM, Gujavarty KS, Browman CP. Maintenanceof wakefulness test: a polysomnographic technique for eva-luation treatment efficacy in patients with excessivesomnolence. Electroencephalogr Clin Neurophysiol 1982;53:658–61.
21. Schwartz JR, Feldman NT, Bogan RK, Nelson MT, Hughes RJ.Dosing regimen effects of modafinil for improving daytimewakefulness in patients with narcolepsy. Clin Neuropharmacol2003;26:252–7.
22. Schwartz JR, Nelson MT, Schwartz ER, Hughes RJ. Effects ofmodafinil on wakefulness and executive function in patientswith narcolepsy experiencing late-day sleepiness. Clin Neuro-pharmacol 2004;27:74–9.
23. Rechtschaffen A, Kales A. A manual of standardized terminol-ogy, techniques and scoring system for sleep stages of humansubjects. Los Angeles: UCLA Brain Information Service/BrainResearch Institute; 1968.
24. Keith MS, Stanislav SW, Wesnes KA. Validity of a cognitivecomputerized assessment system in brain-injured patients.Brain Inj 1998;12:1037–43.
25. Wesnes KA, McKeith IG, Ferrara R, et al. Effects of rivastigmineon cognitive function in dementia with Lewy bodies: arandomised placebo-controlled international study using thecognitive drug research computerised assessment system.Dement Geriatr Cogn Disord 2002;13:183–92.
26. Mendoza TR, Wang XS, Cleeland CS, et al. The rapid assessmentof fatigue severity in cancer patients: use of the Brief FatigueInventory. Cancer 1999;85:1186–96.
27. Young T, Evans L, Finn L, Palta M. Estimation of the clinicallydiagnosed proportion of sleep apnea syndrome in middle-agedmen and women. Sleep 1997;20:705–6.
28. Schmidt H, Berendts B. Narcolepsy and sleep disorderedbreathing: insights into sleep fragmentation and treatmentfailures. Sleep 1999;22(suppl 1):S64–5.
29. Roth T, Roehrs TA. Etiologies and sequelae of excessive daytimesleepiness. Clin Ther 1996;18:562–76.
30. Doghramji K, Mitler MM, Sangal RB, et al. A normative study ofthe maintenance of wakefulness test (MWT). Electroencepha-logr Clin Neurophysiol 1997;103:554–62.
31. Dinges DF, Arora S, Darwish M, Niebler GE. Pharmacodynamiceffects on alertness of single doses of armodafinil in healthysubjects during a nocturnal period of acute sleep loss. Curr MedRes Opin 2006;22:159–67.
32. Bartlett DJ, Rae C, Thompson CH, et al. Hippocampal areametabolites relate to severity and cognitive function inobstructive sleep apnea. Sleep Med 2004;5:593–6.
33. Kotterba S, Rasche K, Widdig W, et al. Neuropsychologicalinvestigations and event-related potentials in obstructive sleepapnea syndrome before and during CPAP-therapy. J Neurol Sci1998;159:45–50.
34. Sateia MJ. Neuropsychological impairment and quality of life inobstructive sleep apnea. Clin Chest Med 2003;24:249–59.
35. Ferini-Strambi L, Baietto C, Di Gioia MR, et al. Cognitivedysfunction in patients with obstructive sleep apnea (OSA):partial reversibility after continuous positive airway pressure(CPAP). Brain Res Bull 2003;61:87–92.
36. Barnes M, Houston D, Worsnop CJ, et al. A randomizedcontrolled trial of continuous positive airway pressure in mildobstructive sleep apnea. Am J Respir Crit Care Med 2002;165:773–80.
37. Chervin RD. Sleepiness, fatigue, tiredness, and lack of energy inobstructive sleep apnea. Chest 2000;118:372–9.

ARTICLE IN PRESS
Adjunct armodafinil in obstructive sleep apnea 627
38. Collard P, Pieters T, Aubert G, Delguste P, Rodenstein DO.Compliance with nasal CPAP in obstructive sleep apneapatients. Sleep Med Rev 1997;1:33–44.
39. Peker Y, Kraiczi H, Hedner J, Loth S, Johansson A, Bende M. Anindependent association between obstructive sleepapnoea and coronary artery disease. Eur Respir J 1999;14:179–84.
40. Peppard PE, Young T, Palta M, Skatrud J. Prospective study ofthe association between sleep-disordered breathing and hyper-tension. N Engl J Med 2000;342:1378–84.
41. Nieto FJ, Young TB, Lind BK, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in a largecommunity-based study. Sleep heart health study. JAMA2000;283:1829–36.