the work of who - who | world health organization
TRANSCRIPT
OFFICIAL RECORDSOF THE
WORLD HEALTH ORGANIZATION
No. 59
THE WORK OF WHO1954
ANNUAL REPORT OF THE DIRECTOR - GENERALTO THE
WORLD HEALTH ASSEMBLYAND TO THE
UNITED NATIONS
The Financial Report, 1 January -31 December 1954,which constitutes a supplement to this volume,is published separately as Official Records No. 62
WORLD HEALTH ORGANIZATIONPALAIS DES NATIONS
GENEVA
March 1955
ABBREVIATIONS
The following abbreviations are used in the Official Records of the World Health Organization:
ACC - Administrative Committee on Co-ordination
CIOMS - Council for International Organizations of Medical Sciences
ECAFE - Economic Commission for Asia and the Far East
ECE - Economic Commission for Europe
ECLA - Economic Commission for Latin America
FAO - Food and Agriculture Organization
ICAO - International Civil Aviation Organization
ICITO - Interim Commission of the International Trade Organization
ILO - International Labour Organisation (Office)
ITU - International Telecommunication Union
OIHP - Office International d'Hygiène Publique
PASB - Pan American Sanitary Bureau
PASO - Pan American Sanitary Organization
TAA Technical Assistance Administration
TAB - Technical Assistance Board
TAC - Technical Assistance Committee
UNESCO - United Nations Educational, Scientific and Cultural Organization
UNICEF - United Nations Children's Fund
UNKRA - United Nations Korean Reconstruction Agency
UNRWA United Nations Relief and Works Agency for Palestine Refugees in the Near East
WFUNA - World Federation of United Nations Associations
WMO World Meteorological Organization
PRINTED IN SWITZERLAND
Introduction
CONTENTS
PART I - GENERAL REVIEW
Page
V
Chapter 1. Communicable Diseases 3
Chapter 2. Public -Health Services 18
Chapter 3. Environmental Sanitation 31
Chapter 4. Education and Training 33
Chapter 5. Services in Epidemiology and Health Statistics 39
Chapter 6. Drugs and other Therapeutic Substances 46
Chapter 7. Procurement of Supplies 50
Chapter 8. Publications and Reference Services 52
Chapter 9. Public Information 56
Chapter 10. Constitutional, Financial and Administrative Developments 58
PART II - THE REGIONS
Chapter 11. African Region 63
Chapter 12. Region of the Americas 69
Chapter 13. South -East Asia Region 77
Chapter 14. European Region 83
Chapter 15. Eastern Mediterranean Region 95
Chapter 16. Western Pacific Region 103
PART III - CO- OPERATION WITH OTHER ORGANIZATIONS
Chapter 17. Co- ordination of Work with other Organizations 113
Chapter 18. Expanded Programme of Technical Assistance for Economic Development 120
PART IV - PROJECT LIST
Projects in Operation in 1954 127
ANNEXES
1. Membership of the World Health Organization 193
2. Membership of the Executive Board in 1954 194
3. Expert Advisory Panels and Committees 195
4. Organizational Meetings and Meetings of Expert Committees and Advisory Groups held in 1954 199
- III -
Page
5. Tentative Schedule of WHO Organizational Meetings in 1955 200
6. Non -Governmental Organizations in Official Relationship with WHO 2007. Regular Budget for 1954 201
8. Structure of the Headquarters Secretariat 202
9. Numbers and Distribution of Staff 203
10. Composition of Staff by Nationality 205
11. Fellowships awarded in 1954 206
MAPS
1. FAO /WHO Brucellosis Centres 11
2. WHO Influenza Centres 13
3. International Sanitary Regulations : Position at 31 December 1954 40
4. Regions and Offices of the World Health Organization 62
- IV -
INTRODUCTION
vIEWEDagainst the background of its basic functions and long -term objectives, the progress made
by the World Health Organization in 1954 should be measured less by any particular achievementthan by the development of the general attitude which, as a result of six years' experience, most
of its Members seem to be taking towards it. Indeed, in all parts of the world there has beennoticeable a better understanding of the real purposes pursued by the Organization. This evolution isclearly reflected by the very nature of the assistance WHO is asked to provide: there is a definite trendaway from requests for supplies and equipment towards requests for technical advice on virtually allaspects of public health. Authorities in many countries now realize that, to be truly effective, theresources of WHO should be utilized not so much for the temporary alleviation of their problems as forthe strengthening of the permanent foundations of their health services. The most encouraging aspect ofthe requests received by the Organization in 1954 is the active desire shown by many countries toobtain WHO's help in working out long -term plans for the progressive and orderly development oftheir public -health services. To provide this type of assistance has of course always been one of theessential aims of WHO, and in the coming years the machinery of the Organization will be geared tothe fullest possible extent to this task, which remains the sine qua non for any substantial success inendeavours to raise standards of health throughout the world.
The growing attachment of Member States to the idea of international co- operation -and theirincreasing readiness to undertake joint action in solving problems which affect more than one country -are demonstrated by the great number of inter -country and inter -regional projects which figure in thisReport. They are also reflected in the continued interest shown by countries in WHO's efforts to co-ordinate on a regional basis activities carried out on a national level. These methods are being effectivelyapplied in all areas and in practically all aspects of WHO's work ; during 1954, they were used in projectsfor the development of training facilities, for the exchange of scientific information, and also for the controlof communicable diseases and their vectors.
A few examples will indicate the very important role such regional projects played in the total pro-gramme of WHO during 1954.
In the field of education, the Inter -American Centre of Biostatistics in Chile is making a valuablecontribution to the improvement of vital and health statistics of all Latin American countries by trainingtechnical personnel for the various statistical services. The creation at Alexandria of a regional collegeof nursing is expected to go a long way towards raising the standards of nursing and nursing educationin the countries of the Eastern Mediterranean. Countries in Europe took advantage of the advancedtraining course for waterworks engineers, held in Belgium and the Netherlands, which was attended byengineers from eleven countries.
-- V
As far as exchange of scientific information is concerned, I should like particularly to mention theimportant seminar organized in Wellington (New Zealand) at which thirty -seven participants, from twenty -one countries of the Western Pacific, South -East Asia and Eastern Mediterranean Regions, discussedproblems relating to dental health. The conference on African onchocerciasis, convened at Leopoldvilleand attended by some thirty experts from three Regions, yielded valuable information for national andregional campaigns which are to be undertaken in Africa against that disease. The sanitary engineeringseminar held in Venezuela proved most effective in promoting inter- American co- operation in the fieldof sanitation and in integrating public- health engineering activities into the general health programmesof the countries concerned.
One outstanding example of the role being played by the Organization in the regional co- ordinationof national campaigns against specific diseases is the combined effort to be made towards the eradicationof malaria from the Americas as a whole. This campaign is to be based on the malaria- control work alreadybeing done by individual countries in that region, and on two inter- country programmes assisted by WHO,one for the Caribbeans and one for Central America.
The second Asian malaria conference, attended by representatives from fifteen countries of South -East Asia and the Western Pacific, which took place in the Philippines in November 1954, can be consideredas a preliminary step in organizing an inter- regional campaign against this disease. By the same token,the contacts arranged by the Regional Office for South -East Asia between health authorities of Thailandand of Indonesia are undoubtedly of help to the two countries in their great efforts to bring yaws undercontrol.
Thus, the patterns of inter- country and inter- regional co- operation have, by 1954, become an essentialfeature of the programmes of WHO. The results achieved in the last few years have shown that, throughthis type of work, the Organization is indeed fulfilling its primary objective of serving as an internationalclearing -house for the flow of scientific and medical information among countries. Moreover, the projectsI have just mentioned provide a powerful stimulus for the promotion of health improvement on the nationallevel. Taking the European Region as an example, there is no doubt that the intensification of efforts
for the care of handicapped children in Austria, Greece and Italy is largely due to a series of inter -countryactivities which dealt with that problem from 1951 onwards. Similarly, the emergence in 1954 of healtheducation programmes in several countries may be traced to the multi -disciplinary conference whichtook place on that subject in London in 1953.
The part of the Report dealing with assistance rendered by WHO in combating or preventing com-municable diseases underlines the growing importance attached by the Organization to research beingcarried out in the field of public health. Even a cursory examination of the results achieved during thelast few years serves to confirm that, through the research work internationally co- ordinated by WHO,more and more knowledge is being gained about a number of infectious diseases. At the same time, researchhelps us to acquire greater knowledge of the effectiveness of insecticides under varying local conditions,the efficacy of various vaccines and sera, and so on. It is hoped that, thanks to the close contacts establishedwith experts and institutions engaged in research work on the use of antibiotics, WHO will be able toassemble the available knowledge on the so- called " second -string " antibiotics, should any indicationbe found that penicillin resistance is developing in the treponemes.
There are many examples in the 1954 Report of the part WHO can play in promoting and especiallyin co- ordinating essential research work going on in various countries. I should like to mention here the

testing of sorbtion of non - volatile insecticides by certain types of mud wall, carried out by seven institutesin the Americas, Asia and Europe, and co- ordinated by WHO. There is also the programme startedby WHO to ensure collaboration among leading experts responsible for field epidemiology studies oftrachoma and associated conjunctivitises in different areas of the world. A meeting organized by WHOin Teheran brought together specialists from Iraq, Syria, Turkey and Iran for a useful exchange of informa-tion on the epidemiology of sylvatic plague. As a final example, I may mention the arrangements initiatedby WHO for the exchange of scientific workers between the Nutrition Research Unit in Kampala, thenational laboratories of the Indian Council of Medical Research, and the Institute of Nutrition of CentralAmerica and Panama.
In view of the fundamental importance of all types of research, much attention was given in 1954 tofilling the need for simplified equipment and to introducing more economical laboratory methods underfield conditions.
The discussions of the Seventh World Health Assembly and of the fourteenth session of the ExecutiveBoard, as well as those of practically all the regional committees, stressed the overwhelming importanceof environmental sanitation for the health programmes of the great majority of Member States. Thestatement made by the chairman of one of the regional committees, that " environmental sanitation isa key to the solution of many evils we are beset with in our Region ", holds equally true for most of theother areas where WHO is active. The Organization is determined to devote as much time and energyas possible to all aspects of sanitation everywhere. In addition to the advisory services in this field renderedduring 1954 by WHO to a number of countries, preliminary studies were begun with a view to developinginternational standards for the quality of drinking -water on the basis of information received from aboutseventy countries. At the same time, the preparation of material relating to rural water supplies and excretadisposal continued and it is hoped that this material will contribute to the improvement of sanitaryconditions in the rural areas where more than three -quarters of the world's population live.
The scarcity of qualified personnel in the field of sanitation remains acute, and the highest prioritywill continue to be given in future years to the training of sanitary engineers and related personnel.
The shortage of adequately trained personnel is not, of course, limited to any particular branch ofpublic health. It is true to say that, in all countries, health can be improved only to the extent to whichthe level of medical education is being raised, both in quantity and in quality. The scope of the assistancegiven by WHO in this field can be measured by the fact that, in 1954, about forty per cent. of the projectsin all regions were mainly concerned with education and training. In addition to the training of sanitaryengineers already mentioned, the entire question of medical education continued to occupy much of thetime of our experts. The study made of the situation in medical education in South -East Asia, followingupon visits made by teams of medical scientists to that region, deserves special mention. It is generallybelieved that the study will prove to be of great value to individual Member countries in their nationalassessment of the problem and the plans to be made for its solution.
Training and education were also at the very core of the efforts made by WHO to assist countriesto meet the many health needs of mothers and children, especially in rural areas. International teams,working side by side with national counterpart staff in twenty countries during the year, were principallyengaged in training activities. It is becoming abundantly clear that, even in countries which are fortunateenough to possess organized health services already, there is still an urgent need for adequate training inmaternal and child health for all types of personnel.
WHO's efforts to help relieve the continuing shortage of nurses all over the world are to a very largeextent centred on the improvement and extension of training facilities. Indeed in 1954, as in previousyears, we have given all possible assistance towards the provision of good basic training in nursing andmidwifery. In a number of countries, it has been decided to supplement the services of professional personnelby those of auxiliaries. These auxiliaries must of necessity be trained by professional nurses, and thisin turn makes it indispensable that already qualified or qualifying nurses receive additional instructionin teaching and supervision.
The year 1954 was the second during which the International Sanitary Regulations were in force.Reports received from health administrations show that these Regulations can be fitted without any greatdifficulty into national quarantine practices, and that the problems which do arise are being satisfactorilysettled, either nationally by changes in legislation, or internationally by negotiations leading to agreementsbetween the countries concerned. However, one subject of these Regulations, the provisions concerningyellow fever, is still under review by the Health Assembly.
Preparatory work, including meetings of groups of experts, was done for the Seventh DecennialRevision of the International Lists of Diseases and Causes of Death, the subject of an internationalconference to take place in February 1955.
The task of providing biological standards for preventive, diagnostic and therapeutic purposes continueduninterruptedly during the year.
In a related field, the network of institutions through which WHO is promoting research work wasfurther extended by the establishment of international shigella centres in London and Atlanta (Georgia,United States of America). The duties of these centres will be in particular to collect and identify strainsand supply material to designated national centres as well as to train workers.
The Spanish edition of the first volume of the Pharmacopoea Internationalis was published duringthe year. Final arrangements were made for the publication of the second volume of the Pharmacopoeaand, at the same time, work continued on the establishment and maintenance of suitable specificationsof safety and purity in pharmaceutical preparations.
Good progress was made during the year in yet another group of technical services made availableby WHO to Member States. The publications of the Organization were increasingly devoted to presentinggeneral reviews of subjects of importance to international health and medicine. Complete issues of theBulletin were devoted to single subjects such as malaria control, health statistics, rabies, syphilis, influenzaand poliomyelitis. The very favourable reception given to these issues is an encouragement to the Organi-zation to continue and develop this editorial policy.
Every effort will also be made to increase comparative studies in health legislation, which, in 1954,had definitely become a regular feature of the International Digest of Health Legislation.
In line with the decision made by the Seventh World Health Assembly, the first steps were takento expand the use of Spanish as a working language of the Organization.

The great number of inter- agency projects described in various chapters of this Report are a practicalexpression of the conviction firmly rooted in the Organization that, wherever possible, efforts to improvethe health of any country should be an integral part of the general endeavour to raise its social and economicstandards of living.
The most important projects through which a combined attack is being made on the causes of poverty,ill -health and ignorance are, of course, those being carried out by the United Nations and the specializedagencies under the Expanded Programme of Technical Assistance for Economic Development. Despitefinancial uncertainties and fluctuations, WHO succeeded in adjusting its Technical Assistance programmefor 1954 without any serious disruptions, in continuing all existing projects according to schedule andeven, in some instances, in meeting urgent new requests. Thus, by the end of the year, there were onehundred and twenty -eight WHO- assisted projects in operation under the Expanded Programme, as comparedwith one hundred and twenty -one at the end of 1953. The importance of this part of the work of the Organi-zation can be measured by the fact that, in December 1954, altogether two hundred and twenty -five expertsfrom thirty -six countries were working in fifty -one countries and territories, and that, during the sameyear, two hundred and seventeen fellowships were awarded to candidates from fifty countries and territories.
Joint work with UNICEF during 1954 continued to be progressively adapted to the basic policyof WHO. This means that in all fields relating to the health of children- including those of tuberculosis,treponematoses, malaria, environmental sanitation and, naturally, maternal and child health jointUNICEF/ WHO activities are being shifted from emergency campaigns and demonstration projects tothe development of services which can be carried out by countries as part of their general public- healthprogrammes, and also to the training of national staff for those services. On the financial side, the twoorganizations have explored the means for implementing the resolution of the Seventh World HealthAssembly recommending that WHO should assume the responsibility for the employment of the technicalpersonnel needed for joint activities.
As to other United Nations agencies, mention should be made of our co- operation with FAO onnutrition, meat hygiene and zoonoses; with UNESCO on fundamental education; with ILO on occupa-tional health activities and on the hygiene of seafarers; and, finally, with ICAO on the sanitation of airports.
Further efforts were made in 1954 to discharge adequately the responsibilities of the Organizationas " the directing and co- ordinating authority on international health work ". Co- ordination with theColombo Plan extended to the selection of fellows and to the provision of equipment needed for the carryingout of health projects. On several of these projects, experts assigned under the Colombo Plan are nowworking as members of teams otherwise composed of WHO advisers and their national colleagues. Inour relations with the United States Foreign Operations Administration, we are achieving increasing successin co- ordinating activities on the country level, with the obvious purpose of avoiding duplication.
The efficacy of our relationship with other organizations interested in promoting health -be theygovernmental or non -governmental -will depend to a significant extent on the information made availableto WHO on health conditions prevailing in Member States. A resolution passed in 1954 by theEconomic and Social Council on the organization of its own work underlines the urgent need for WHOto obtain such information. According to that resolution, the Council will in future concentrate its efforts
-rx -
on the study of the major economic and social problems of the world, and expects the representatives ofthe specialized agencies to take an active part in the discussion of these problems. It is obvious that inorder to contribute effectively to the work of the Economic and Social Council, WHO must be inpossession of the most accurate and up -to -date information available on the health situation in the world.
I cannot conclude these introductory remarks on WHO's work in 1954 without mentioningbriefly a new challenge which faces the Organization as a result of the modern discoveries of science andmedicine. It has indeed become increasingly clear in recent years that, sooner or later, WHO wouldhave to assume responsibility for assessing the possible effects on health of the unprecedented interferencewith natural processes now occurring over large areas of the world. For example, to what extent is thebalance of nature being affected by the wholesale destruction of insects? What will be the long -term resultsof the extensive use of antibiotics ? How will the disease patterns of a population be influenced by theintense efforts now being made to raise the standards of environmental sanitation and of hygiene in general ?How important is the contamination of the air, soil and water caused by the increased use of atomic energy ?
The study of this last problem acquired emphasis, by the end of 1954, as a result of a decision takenby the United Nations General Assembly to invite WHO to participate in an international conferencewhich is to examine the peaceful uses of atomic energy. Thanks to the contributions of four experts, whoadvised WHO on the role it could play in this field, I am confident that the plans submitted to the ExecutiveBoard and to the Eighth World Health Assembly will make it possible for the Organization fully to assumeits new responsibilities in the domain of atomic energy in relation to medicine and public health. In sodoing, the Organization will remain faithful to its constitutional obligations, the essence of which is toensure, through co- operation and mutual aid between countries, health, prosperity and peace to all mankind.
Director - General
--X-

PART I
GENERAL REVIEW

CHAPTER 1
COMMUNICABLE DISEASES
The work of WHO in assisting governments in field programmes against communicable diseases hascontinued along the lines already described in the Annual Report for 1953. For details of work donein individual regions in 1954, the reader is referred to Part II of this report and to Part IV, the list of projects.This chapter gives a general description of the work done on certain specific diseases.
Experience in applying preventive methods of communicable- disease control on a large scale has shownthat results cannot always be correctly forecast. Clinical and laboratory methods of proved efficacy in individualcases do not always yield the results expected when applied on a large scale to communities ; public -healthmeasures effective under certain epidemiological conditions may prove disappointing in others. In order tofacilitate objective valuation and to ascertain the reasons for unexpected results, scientific method must beused in planning field and laboratory studies. Staff who are to plan and carry out these studies require qualifica-tions different from those of field staff conducting large campaigns, and suitably qualified workers, trained inthe scientific method and with experience in the application of research methods to field studies, are not easyto find.
Some problems which have been encountered in WHO- assisted field activities are under study. Researchhas been undertaken into causes of apparent failures of DDT house -spraying in certain areas, now attributedto sorbtion of DDT in certain kinds of mud walls.
To investigate the reasons for variations in the results obtained in treating treponematoses in differentareas, immunological and other studies are being made in a central laboratory. These studies deal with therelationship between strains and types of treponemes, and have been combined with studies of thesensitivity of treponemes to various antibiotics.
The results of vaccination programmes have not always been satisfactory. Controlled field trials and co-ordinated laboratory research are necessary to determine the reasons, and studies of BCG vaccine (see page 9)and smallpox, rabies, typhoid, brucellosis, and combined diphtheria -pertussis vaccines are in progress. Theneed for means of relating the results of laboratory tests to the actual protection afforded by a vaccine has beenemphasized and, where necessary, appropriate studies have been planned.
The need for simplified equipment and economical laboratory methods for use under field conditions hasbeen recognized and appropriate studies are under way. In answer to many requests from governments, WHOhas advised on the organization of, and equipment for, public- health laboratories. The standardization ofdiagnostic procedures and laboratory reagents has proceeded. Methods of testing various biological productshave been studied in order to establish minimum requirements.
Through these and other studies, the need for which has generally become apparent in the course ofservices to governments, WHO is stimulating and co- ordinating research on many diseases of internationalpublic -health importance which present problems to which there is as yet no satisfactory solution -amongthem influenza, poliomyelitis, trachoma, onchocerciasis, bilharziasis and certain of the zoonoses. Some of theresearch programmes have been continued from previous years ; others, such as those on poliomyelitis andonchocerciasis, are new and rapidly developing activities. Much of this work, especially in co- ordinated research,has been made possible by the excellent response of governments, institutes and individual scientists all overthe world, and this in itself shows the growing appreciation of its value.
The pages which follow summarize the work accomplished during 1954 in malaria, venereal diseases,tuberculosis, veterinary public health and the zoonoses, virus diseases, and in other communicable diseases.
-3-
4 THE WORK OF WHO, 1954
JMalaria
The new facts which made 1953 a significant yearand, one might say, a turning point in WHO'spolicy in malaria control, have acquired greatertmportance in 1954. There are indications of a growingtendency for anopheline species to become resistantio insecticides (Anopheles superpictus, A. maculipennisin Greece ; A. sundaicus in Indonesia). More impor-tant still is the fact that in both Greece and Indonesiathe resistance to insecticides has actually interferedwith malaria control, and numerous cases of malariahave occurred in localities which had previouslybeen sprayed with insecticides. The development ofresistance of the local vectors in Lebanon and changesin insect behaviour in DDT -sprayed areas in Indo-nesia have also been described by WHO field per-sonnel. By supplying standard testing outfits fortests in the field, WHO has helped its field workersand various malaria institutes in attempts to deter-mine the susceptibility of local anopheline speciesto insecticides and any eventual variations in suchsusceptibility. It has also secured the collaborationof reference laboratories in London and in Romein this work.
Another disturbing problem which received furtherattention in 1954 was that of the rapid loss of effi-ciency that non -volatile insecticides seem to undergowhen sprayed on particular types of mud walls.WHO has co- ordinated research on this subject,which is being carried out by seven collaboratinginstitutes in the Americas, in Asia and in Europe.
At the end of 1953, projects in which WHOpersonnel assisted were in operation in the followingeighteen areas : Afghanistan, Bolivia, Burma, Cam-bodia, the Caribbean area, Dominican Republic,French Cameroons, Haiti, Indonesia, Iraq, Lebanon,Liberia, Paraguay, the Philippines, Sarawak, SaudiArabia, Syria and Taiwan (for details of the projectsin Afghanistan, Taiwan and the Eastern Mediter-ranean, see pages 79, 105 and 100). Of these theprojects in Lebanon and the Philippines endedin 1954. The projects in Bolivia and Haiti were trans-ferred to the budget of the Pan American SanitaryBureau. WHO's assistance to UNRWA in malariacontrol also continued. New projects were : asecond project of bilharziasis and malaria control inSyria ; a project which started in the second quarterof the year in Nepal ; one in Nigeria, which beganin August and to which WHO contributed an
entomologist, and one in East Africa, for whichthe personnel arrived during the fourth quarter ofthe year.
Personnel from Headquarters or expert consultantsvisited Burma, the Cameroons, Chile, Colombia,French Equatorial Africa, French West Africa,Greece, Guatemala, India, Indonesia, Iran, Kenya,Liberia, Mexico, Nicaragua, Taiwan, Tanganyika,Togoland, and the United States of America. Someof these governments were, on their request, presentedwith reports appraising the control measures in theState or territory for which they are responsible.
Malaria control was discussed in two conferencesduring the year. The XIV Pan American SanitaryConference, at Santiago, stressed the need for theintensification and co- ordination of antimalaria workin order to achieve the eradication of malaria fromthe Western Hemisphere. Member Governmentswere urged to convert all programmes for malariacontrol into eradication campaigns within the shortesttime possible, with the aim of eradicating the diseasebefore the appearance of anopheline resistance toinsecticides. The inter -regional conference onmalaria for the South -East Asia and Western PacificRegions held in the Philippines discussed the recentlydiscovered possibility of controlling malaria trans-mitted by vector species characteristic of the Asianand Australian areas, such as Anopheles minimusflavirostris, A. sundaicus, A. leucosphyrus group andA. puntulatus group. Formerly the last three of thesedid not seem very susceptible to control by residualspraying. The problem has been solved thanksto the co- operation of WHO expert personnel andtheir research work in the areas affected. The secondmain subject on the Conference's agenda was areview of current activities for malaria control in thetwo Regions and of the methods for planning long-term antimalaria programmes.
The WHO monograph, Terminologie du Palu-disme,1 which appeared in 1954, has been preparedfor the guidance of malaria workers in territorieswhere French is spoken. Its value lies in the standard-ization of nomenclature, and in its suggestions ofuniform methods which are now widely adoptedfor carrying out malaria surveys and for appraising
1 Vaucel, M., Roubaud, E. & Galliard, H. (1954) Termino-logie du paludisme, Genève (Organisation Mondiale de laSanté: Série de Monographies, No 25)
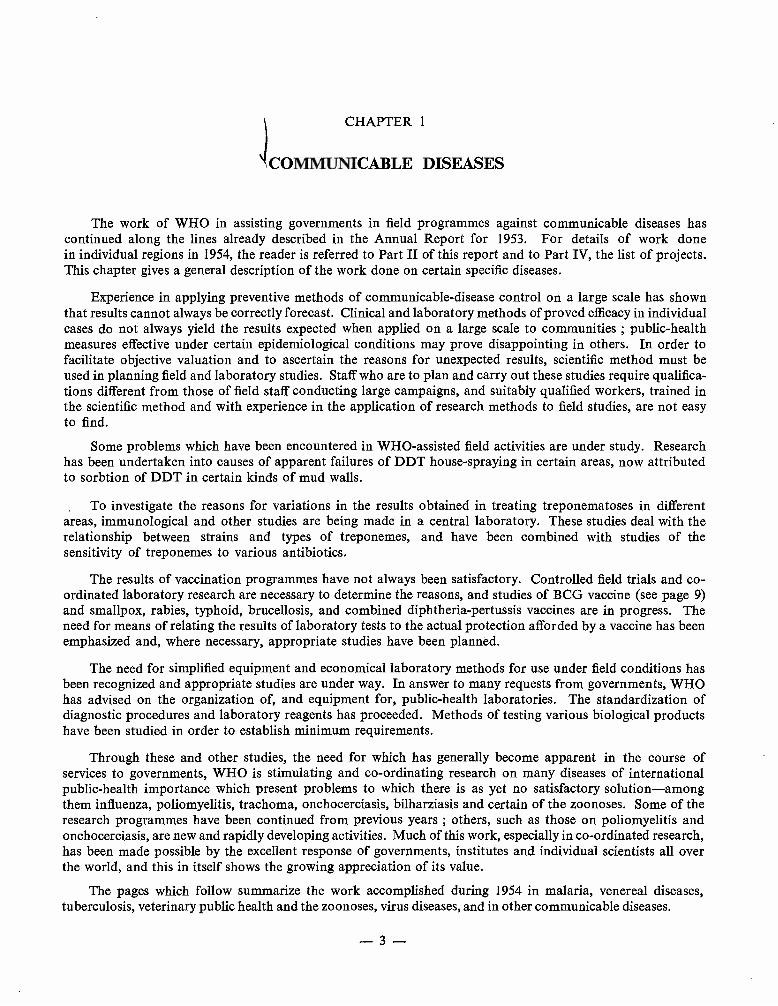
LAOS AND MALAYA
A team on its way to a remote village inMalaya leaves the main road and startsthe more difficult part of its journey.
On the arrival of the WHO team, a teacher at a village school in Malaya addresseshis pupils and invites their co- operation.
The Laotian team leader gives an injection to a small patient.
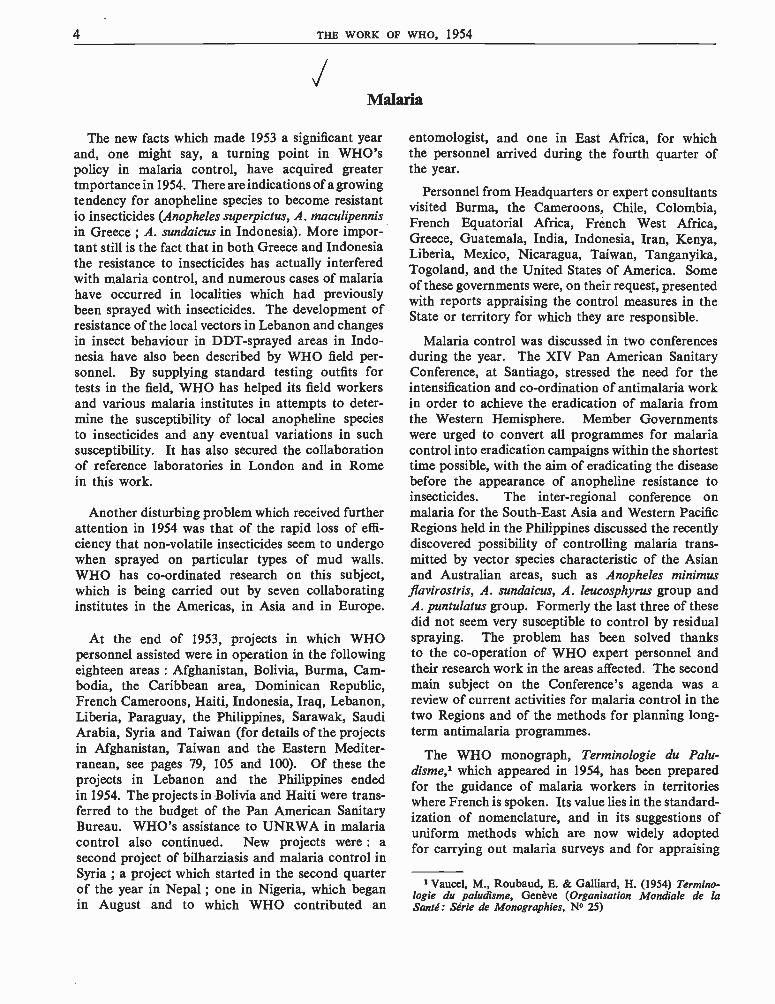
ENVIRONMENTAL SANITATION
The pictures -left -of back -yards and a side street in Yunnawa, Thailand, show conditionswhich constitute an obvious danger to health; the difficulties of refuse collection are evident.
The photograph above shows a WHO expert, accompanied by Thai "understudies ", ona tour of inspection.
Below is a house in the same neighbourhood, showing what can be done with relativelysimple resources and a little effort.
vxa r rá9T[?-?:S+ r,tr*rltrtira{i3a,c
w,,,rq,,:.0 0 . '(eTTtt'-
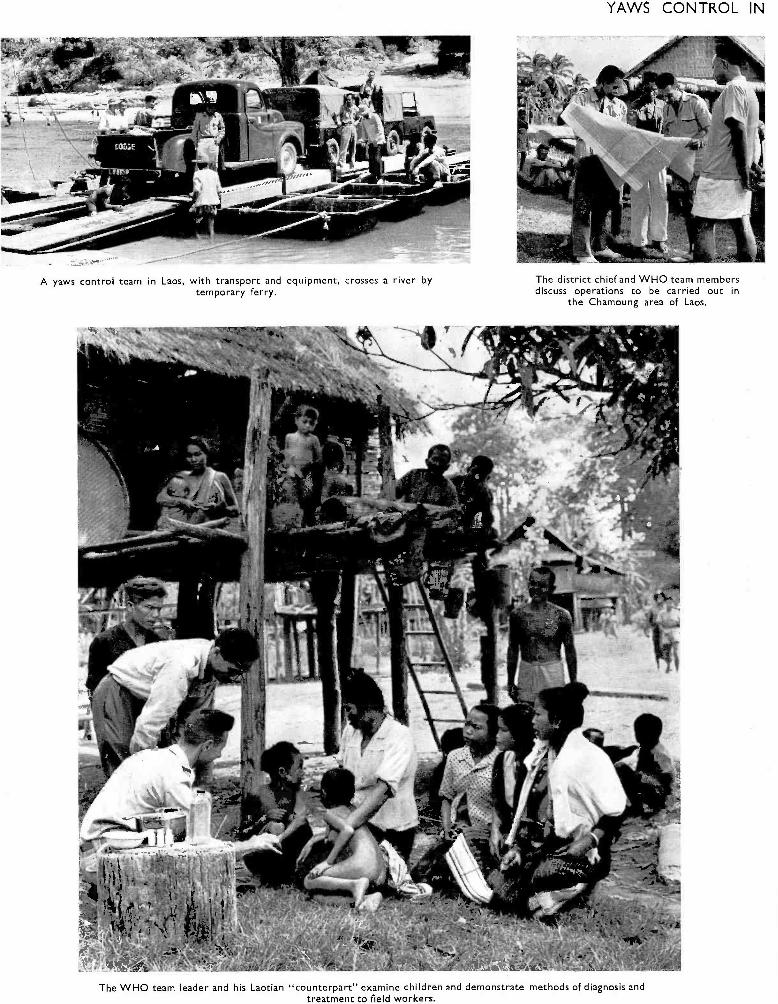
A yaws control team in Laos, with transport and equipment, crosses a river bytemporary ferry.
YAWS CONTROL IN
The district chief and WHO team membersdiscuss operations to be carried out in
the Chamoung area of Laos.
The WHO team leader and his Laotian "counterpart" examine children and demonstrate methods of diagnosis andtreatment to field workers.
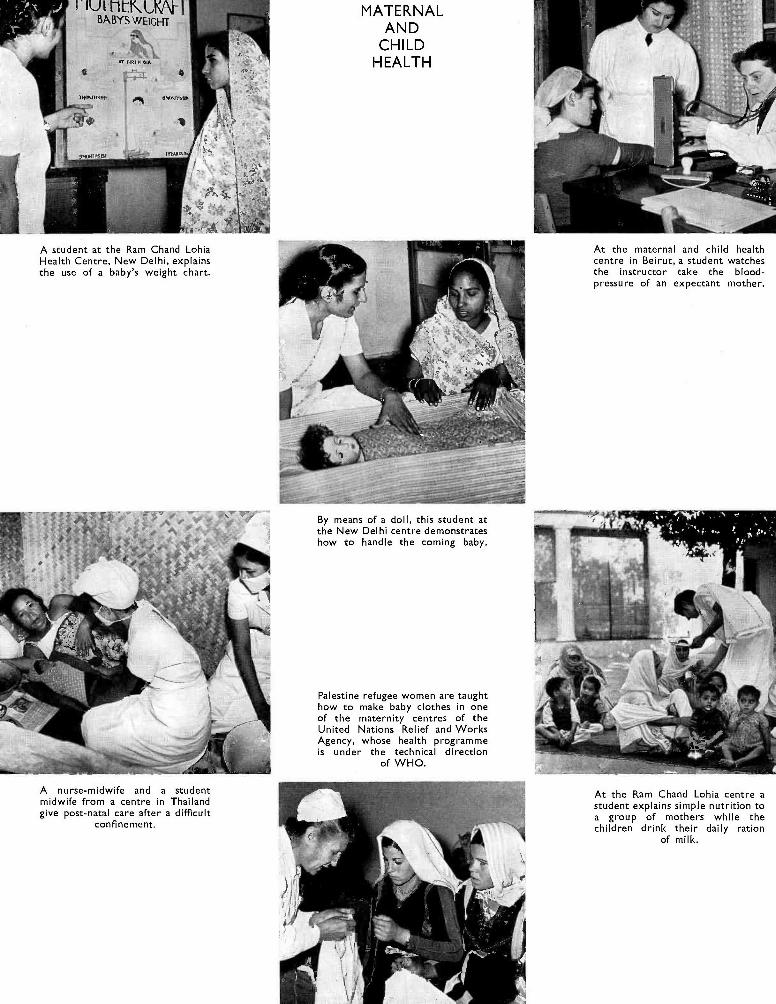
í'1V1 t1Cr rpBABYS WEIGHT
A student at the Ram Chand LohiaHealth Centre, New Delhi, explainsthe use of a baby's weight chart.
A nurse -midwife and a studentmidwife from a centre in Thailandgive post -natal care after a difficult
confinement.
MATERNALAND
CHILDHEALTH
By means of a doll, this student atthe New Delhi centre demonstrateshow to handle the coming baby.
Palestine refugee women are taughthow to make baby clothes in oneof the maternity centres of theUnited Nations Relief and WorksAgency, whose health programmeis under the technical direction
of WHO.
At the maternal and child healthcentre in Beirut, a student watchesthe instructor take the blood -pressure of an expectant mother.
At the Ram Chand Lohia centre astudent explains simple nutrition toa group of mothers while thechildren drink their daily ration
of milk.
COMMUNICABLE DISEASES 5
results of malaria control schemes. Another mono-graph, resulting from a recommendation of theExpert Committee on Malaria,1 on chemothera-peutics of malaria, was prepared for publication in1954. Hitherto the medical profession has not had
í
readily available concise information on the pro-perties of the antimalarial drugs now used andconsequently somewhat irrational treatment andprophylaxis with the new drugs has been a commonexperience.
Treponematoses and Venereal Infections
Unlike many other micro- organisms, the treponemeshave so far not developed penicillin resistance.However, it is possible that they may do so, as peni-cillin is now being used (and misused) in very largeamounts and on an increasingly wide scale through-out the world. WHO, to be prepared for such aneventuality, has maintained close contact withexperts and institutions carrying out research on theuse and value of several other antibiotics. Someof the investigations are being made at the Inter-national Treponematosis Laboratory Center inJohns Hopkins University, assisted by grants fromWHO. A similar precaution has been taken withregard to the non -treponemal venereal infections,which are still public -health problems in manyparts of the world.
Allergic and other reactions to certain penicillinsalts and to components of the vehicles of repositorypreparations have been observed in some countrieswhere penicillin has been widely used over longperiods. The effectiveness of some new penicillinsalts and preparations is therefore being tested inmany institutes, and research into the possibility ofapplying the new amine penicillin salts in masscampaigns for treponematoses control has beeninitiated by WHO in anticipation of future possibleneeds. It has been found that effective penicillinaemiacan be obtained for a longer period with a lowerdosage of these new salts after a single injection thanwith PAM. The question is being examined bymembers of the WHO Expert Advisory Panel andother investigators.
In connexion with the continued investigationsmade by the International Treponematosis Labo-ratory Center into the fundamental biology of trepo-nemal diseases (see the Annual Report for 1953 2),WHO arranged for the new treponemal agglutinationtest, developed at the centre, to undergo field trialsin several co- operating laboratories in differentregions. The practical consequences of the trials-if successful -could considerably simplify the
1 Wld Hlth Org. techn. Rep. Ser. 1951, 39, 232 Of Rec. Wld Hlth Org. 51, 8
work of all public- health laboratories in trepone-matoses control.
The collaborative study on the Treponema pallidumimmobilization (TPI) test was continued, and theparticipating laboratories exchanged information ontechniques and results. WHO distributed controlserum to the laboratories and evaluated the results.The Treponema pallidum immune adherence (TPIA)and the Treponema pallidum agglutination (TPA)tests were studied in some co- operating laboratories ;TPA antigen was distributed to laboratories in allsix WHO regions for comparison against lipoidaland cardiolipin antigens. Arrangements have beenmade to provide material for the first internationalreference preparations of sera from syphilitics, andto select reference antigens for tests used by WHOfield teams.
On the recommendation of the Sub -Committeeon Serology and Laboratory Aspects of the ExpertCommittee on Venereal Infections and Trepone-matoses, the WHO International Serological Refer-ence Laboratory in Copenhagen continued a studyon the reactivity of freeze -dried sera from syphiliticsand non- syphilitics (see Annual Report for 1953 3).The Laboratory also arranged for a study on thethermo -stability of freeze -dried sera from non -syphilitics. The Statistical Service in the StatensSeruminstitut, Copenhagen, is evaluating the resultsof these two studies. Since June 1954 the VenerealDisease Research Laboratory of the United StatesPublic Health Service, Chamblee, Georgia, has actedas another reference centre for WHO, and the workof the two reference centres (in Copenhagen and inGeorgia) is now being co- ordinated.
Following the recommendations of the WHOExpert Committee on Venereal Infections andTreponematoses, the Organization is inquiring intothe control and importance to public health indifferent countries of some of the non -treponemalvenereal infections, particularly donovanosis (lympho-granuloma venereum) and non -gonococcal urethritis,and work has proceeded on the revision of the
3 Of Rec. Wld Hlth Org. 51, 9
6 THE WORK OF WHO, 1954
International List of Venereal- Disease TreatmentCentres in Ports as a collateral to the Brussels Agree-ment of 1924.
In 1954, WHO assisted health administrations inlong -term projects with the double aim of eliminatingendemic treponematoses as a public- health problem,and strengthening rural health services. Newcampaigns against yaws and other non- venerealtreponematoses were started in Bechuanaland, Ma-laya, Nigeria and Syria, and planning of controlmeasures proceeded in tropical Africa and in thePacific and Caribbean areas. Projects continuedwere those for the control of yaws in Haiti, Indonesia,Liberia, the Philippines and Thailand, and that forthe control of endemic syphilis in Yugoslavia.WHO continued to assist with projects for venereal-disease control in Afghanistan, Burma, Ecuador,Ethiopia, Iran, Paraguay, Saudi Arabia and Taiwan ;the demonstration project in Karachi, Pakistan, wastaken over by the Government in June. A newmass campaign against syphilis was started inMorocco (French Zone).
By the end of the year more than twenty -fivemillion people had been examined and six milliontreated in the campaigns carried out in Haiti, Indo-nesia, Laos, the Philippines, Thailand and Yugo-slavia (the projects in Haiti and Indonesia aredescribed more fully on pages 73 and 81). The averagecost of treatment and examination in these campaignsfell below the figures given in the Annual Report for1953, to approximately $1.25 per patient or contacttreated with penicillin and $0.12 per person examined,including all national and international expenditures.
Internationally recruited advisory staff, who werewithdrawn by the end of the year from Burmaand from the demonstration and training centrein Pakistan, left behind much information onthe extent and nature of the treponematoses andvenereal infections, a wider appreciation of public -health methods for their control, trained personneland strengthened health services to develop the pro-grammes further.
UNICEF assisted materially in many of theprojects.
The general outlook for the control of trepone-matoses among the rural population in under-developed areas remains favourable. In Haiti,India and Yugoslavia it was shown that for yaws andendemic syphilis the infectious reservoir to be dealtwith after one year in follow -up surveys of the ruralpopulation could be less than one per cent. In themore highly developed countries, with active organi-
zation for the control of venereal disease, the preva-lence has remained low, although recent informa-tion suggests that the premature relaxation of controlmeasures may lead to a recrudescence of the disease :an increase in early infectious syphilis which showeditself in eighteen states of the United States ofAmerica in 1953,1 supports the view that long -termconsolidation of early results achieved in penicillinprogrammes is necessary. There is little evidencethat the incidence of gonorrhoea, chancroid, lympho-granuloma venereum and granuloma inguinale hasdecreased significantly in any country, and gonorrhoeain particular has remained at approximately thepre -war level. At the same time a significant increasehas been recorded in the number of cases of non-
gonococcal urethritis, which is considered a public -health problem in certain countries.
Various difficulties and problems have beenencountered in the WHO programme. Healthadministrations are not always taking full advantageof the accumulating experience acquired in masstreatment campaigns against treponematoses inrural areas and in projects for venereal- diseasecontrol in urban districts. Greater thoroughness incoverage, wider treatment of contacts and lowerpenicillin dosages would make the programmemore effective. Nor has it been fully appreciatedthat programmes for the control of endemic trepone-matoses offer an effective method of strengtheningrural health services. Further studies are needed inselected areas to develop simpler methods of con-solidation. Further efforts are also required toestablish simpler public- health indices in masscampaigns which can be applied to households andin communities and which will enable health adminis-trations to appraise more readily the effectivenessof the treponematoses- control programme.
A standard portable serological unit for use in thefield has been devised for areas in which there arepilot projects. It is used in mass campaigns to probereservoirs of infection on a sample basis and as ameans of evaluating the effectiveness of the pro-gramme.
Material is being collected for a field manual onyaws control which will provide interested healthadministrations with information accumulated frommany projects assisted by UNICEF and WHO andwhich will be valuable in the expanding work againsttreponematoses in all rural areas.
1 Erickson, H. M. et al (1954) Amer. J. Syph., 38, 161

COMMUNICABLE DISEASES 7
Several publications on venereal- disease and tre-ponematoses control were issued by WHO duringthe year. A monograph on donovanosis (granulomainguinale) was published ;1 an entire issue of theBulletin was devoted to the reorientation in the
treatment of venereal 'syphilis over the last decade,'and an issue of the Chronicle presented a review ofWHO activities in relation to the epidemiology andcontrol of the treponematoses throughout the worldfrom the public- health point of view.'
Tuberculosis
The steep decline in tuberculosis mortality thathas been reported in recent years in countries wherereliable statistics are available has created theimpression that tuberculosis might soon be broughtcompletely under control. But tuberculosis morbidityhas not decreased to the same extent, and in countrieswhere within five years the mortality has diminishedby about half, the number of reported cases oftuberculosis has dropped little, and the number ofknown infectious cases has sometimes even increased.
There is evidence that chemotherapy, oftenassociated with surgery, has had an effect on tuber-culosis mortality. The antimicrobial drugs have alsoundoubtedly been welcomed by clinicians, who haveseen some of their patients apparently cured, the lifeof others prolonged, and, in most cases, rapid andimpressive relief of symptoms. This has led toenormous quantities of drugs being used all over theworld in varying doses and combinations, and withwhat effect on the tuberculosis problem no oneknows at this time.
As a few examples will show, the public- healthadministrator is faced with a series of new problemswhen planning a programme of tuberculosis control :Mortality figures can no longer be used as an indexof the extent of the disease -other indices will haveto be adopted or devised and international agreementwill have to be sought upon the use of such indices,if comparisons between countries are to remainpossible ; The prolongation of life in patients withextensive disease may result in large numbers ofpartially or even totally disabled persons requiringmeasures of rehabilitation and assistance. Thuseconomic, social and administrative problems arecreated, which are of a more complex and generalnature than those pertaining to the control of tuber-culosis proper. The epidemiological impact ofwidespread chemotherapy is not yet known. It isa fact that the drugs have a sterilizing effect in alarge proportion of cases. This may be counter-
1 Rajam, R. V. & Rangiah, P. N. (1954) Donovanosis(granuloma inguinale, granuloma venereum), Geneva (WorldHealth Organization: Monograph Series, No. 24)
balanced by the unsatisfactory results in somepatients, whose survival rate is higher but whoremain infectious in spite of chemotherapy, andalso by the relapse of apparently successfully treatedcases into an infectious state. In regard to thislast point the question of drug resistance requiresfurther study and appraisal.
Such problems require investigation, and thosewhich are closely, related to the work of WHO arebeing given special attention. Among these, thequestion of ambulatory chemotherapy is of crucialimportance for areas where institutional facilities arenot, and cannot be, adequate to meet the need forisolation and treatment. Carefully controlled fieldinvestigations are required in such areas, where thecontrol of the disease may eventually be shown todepend on the treatment of infectious cases eitherwith the drugs which are now available or withnewer ones which are now being subjected to pre-liminary trials.
Most field projects, in which WHO is providingassistance to governments in tuberculosis control,fall into two main categories : mass BCG vaccination,and tuberculosis teaching and training centres. In1954, projects of one or the other of these categorieswere in operation in twenty -eight countries, mostlyin the tropical and subtropical zones. Some fortydifferent schemes were in operation -twenty -twoBCG vaccination projects and eighteen demonstra-tion centres. An account of the programme in Iraqand details of two projects in the Americas are givenon pages 98 and 73. The cost of the WHO fieldstaff and of the equipment and supplies for all theBCG campaigns, and the cost of the equipmentand supplies for some of the training centres, havebeen borne entirely by UNICEF. About 32 millionpersons were tested with tuberculin during the yearand about 11 million persons were given BCGvaccination. BCG vaccination, therefore, hascontinued to be an important part of the Organi-zation's field programme in tuberculosis control.
2 Bull. WId. Hlth Org. 1954, 10, 501-7023 Chron. Wld Hlth Org. 1954, 8, 37-114
8 THE WORK OF WHO, 1954
Gradually, however, there has been a change ofemphasis in the type of assistance given by WHO toBCG projects, and more attention is being devotedto planning and re- examining schemes, to determiningtechniques and to evaluating results, rather than toplaying a large part in the execution of mass pro-grammes.
Experience has shown that advice given during theoperation of projects should be based not only ongeneral experience or accepted technical principles,but also on data gathered from the actual projectarea. Care is needed to ensure that elements ofpersonal bias are excluded when information isrecorded from representative samples of the popu-lation concerned and the staff doing this work mustacquire particular skill. An interesting developmentin this regard during the year has been the creationof three regional BCG assessment teams : one inSouth -East Asia, one in the Western Pacific and onein the Eastern Mediterranean. The doctors andnurses working in these teams have all receivedprolonged training from the Tuberculosis ResearchOffice, which is also giving technical supervisionto their work and analysing and interpreting the datawhich are being gathered.
An attempt is thus being made to assess theoperation and immediate effects of the mass vaccina-tion programme : in particular, to determine howefficiently the prevaccination tuberculin test separatesinfected and uninfected children, and to ascertain theresults of post- vaccination testing.
The work already shows significant results, whichsuggest that such an assessment has not been startedtoo soon. Thus, it is evident that the high prevalenceof non -specific tuberculin sensitivity in many placesseriously interferes with the selection of children forvaccination, that many children are erroneouslybeing called positive reactors and hence are notvaccinated, and that changes should be made inprocedures for prevaccination tuberculin testing.Equally evident is the disturbing finding that inmany areas children have been and are beingvaccinated with weakened vaccines, or that there aredefects in the vaccination technique. There is noindication that children anywhere are incapable ofbecoming strongly allergic after vaccination.
For the first time it was possible, in 1954, to carryout a fact -finding pilot study in preparation for amass vaccination campaign. A team, following theprinciples outlined above, has been performingtuberculin tests and BCG vaccination on represen-tative groups in many parts of the Sudan. Oncethe data of a study of this kind are collected and
analysed, it will be possible to advise the governmentwhether or not a mass vaccination project shouldbe undertaken and, if so, what techniques shouldbe used and which age -groups included.
BCG vaccination mass campaigns usually coverspecific age -groups of the population and personsare vaccinated once only in such campaigns. Thequestion of revaccination has lost its immediateurgency because the results of field research showthat the allergy induced by BCG vaccination canpersist for several years. Efforts must, however, beintensified to ensure that satisfactory levels ofallergy are attained in routine mass campaign work.
The problem still remains of vaccinating groupswhich for some reason are not covered by a masscampaign, and, among these, the children added tothe population. Leaving these vaccinations to suchinstitutions as maternal and child health centres,tuberculosis dispensaries, etc., as has been done inthe past, has proved disappointing, particularly inregard to the number of children vaccinated, andother possible solutions to this problem are nowbeing studied.
In some countries the BCG campaign has been thefirst public- health activity, particularly in ruralareas, in which preventive measures have beenapplied effectively to large groups of people. Con-siderable experience has now been gained in masscampaign organization and techniques, and sincesimilar tactics have been used in the control of othercommunicable diseases -yaws for example- public-health administrators are asking whether severalpreventive measures cannot be applied at the sametime in one mass campaign. Simultaneous vaccina-tion against several diseases would permit thepooling of control activities and reduce costs, andmight contribute to the formation of a realisticpublic- health programme.
These problems have been under consideration forsome time and, during 1954, two new combinedprogrammes were started : the study of simultaneousvaccinations, including BCG, in population groups,and the study of BCG vaccination plus penicillintreatment for yaws. Both are designed to furnishpractical information for the communicable- diseaseservices of WHO.
Work in the training centres during the year hasconfirmed earlier impressions that some of themethods used were not suitable to the epidemio-logical, physical and economic conditions prevailingin most of the countries in which WHO is working.Attempts to obtain information and experience onwhich to base a more realistic approach to the
COMMUNICABLE DISEASES
tuberculosis problem have not yet met with successbecause a clinical concept of antituberculosis workhas been too often inherent in the administrativestructure of some centres. It is felt, however, that thisdifficulty may be overcome, although a decisiveshifting of the balance towards prevention may taketime and will call for specially trained personnel.
When the Tuberculosis Research Office wasestablished in 1949, it was assigned the task of super-vising the statistical work and of preparing andpublishing detailed statistical records of the massBCG- vaccination campaigns. That task is nowcompleted. Reports have been published on cam-paigns in sixteen countries and on the campaignconducted among the Palestine refugees ; theydocument the tuberculin testing of twenty -twomillion people and the vaccination of eleven millionby giving for each country the number (and per-centage) of persons tested and vaccinated, by age,sex and administrative divisions. Together, thereports furnish a permanent and detailed record ofwhat was undoubtedly the largest, most uniformlycarried out, immunization programme ever attempted.The value of the reports may well be expected toincrease with time : tuberculin sensitivity figuresand accurate statistics on the population vaccinatedat the time of the campaign will provide a basisfor epidemiological studies as well as for planningtuberculosis -control programmes in the countriesconcerned for years to come.
In 1951, when WHO and UNICEF joined forcesto assist governments in mass BCG campaigns, therecord keeping and the statistical documentationformerly used in the International TuberculosisCampaign were considerably simplified. Monthlysummary reports of the progress of the BCG pro-grammes are now issued and, as the programmes arecompleted, detailed final reports are prepared foreach country.
The long -range research programmes developed inco- operation with the national health services inFinland and in Denmark have begun to pay divi-dends. A report on tuberculosis mortality in Finland,undertaken to provide a background for comparingthe course of tuberculosis before and after the massvaccination campaign of 1948 -49, shows that therecent significant drop in mortality is, relatively, nogreater in Finland than in other countries wherepractically no BCG vaccination had been carriedout. This finding, plus the fact that the fall intuberculosis had started well before the mass BCG
programme and greatly affected the older membersof the population, who were not vaccinated, leadsto the view that other powerful influences haveoperated in Finland, as in other countries, to producethe downward plunge of tuberculosis mortality rates.
An important by- product of the preparation of theDanish National Tuberculosis Index -an individualrecord file of all persons who participated or wereinvited to participate in the Danish mass campaignof 1950 -52 -is a study of the value of duplicatereading of mass survey x -ray films of the chest.Nearly half a million films were read twice. Thesecond reading increased by 20 per cent. the numberof active cases discovered, at a cost per case of onlyabout one -tenth of that of finding cases by a singlereading. Mass x -ray surveys may not be practicableeverywhere, but where they are, the case for dualreading of the films seems established.
Studies on technical aspects of tuberculin testinghave continued during the year. One shows thatvariations in site and depth of the intracutaneousinjection have little bearing on the results, providedthe dose is accurately measured. The method ofgauging the dose by estimating the size of whealformed in the skin -a common practice in massprogrammes because of leaking syringes -is foundto be highly unreliable : the wheal varies not onlywith depth of injection but also with the age and sexof the person tested. Leaking syringes may thusaccount, indirectly, for considerable variations intuberculin testing and -in practice -in the selectionof children for vaccination. Another study showsthat tuberculin tests should not be given twice in thesame place on the arm, even though many monthsmay intervene between the two tests. If tests arerepeated in the same place, the second test will oftenresult in an abnormal bullous reaction that interfereswith the interpretation of the test : this is of particularimportance when tests are given to evaluate theallergy produced by BCG vaccination. Anotherstudy, using observations collected in the tropics,shows that sunlight severely reduces the potency,not only of BCG vaccine, but also of tuberculin.
Sufficient information has now been assembled toenable a number of general conclusions to be drawnabout the nature of BCG- induced tuberculin sensi-tivity. The sensitivity caused by intracutaneousBCG vaccination cannot be logically described interms of positive and negative tuberculin reactions.Intracutaneous vaccination always produces -orincreases -sensitivity to tuberculin, although, ac-
10 THE WORK OF WHO, 1954
cording to the vaccine used and the person vaccinated,it may be only a low degree of sensitivity. The degreevaries with the potency of the vaccine : it has beenshown, wherever carefully controlled studies havebeen made, that a potent vaccine causes allergy aboutas strong as that produced by natural infection. Thelower levels of allergy that have been (and are stillbeing) produced in much of the mass campaign worksuggest the use of weakened vaccines or point todefects in vaccination technique. Contrary to thegeneral impression, tuberculin sensitivity apparentlydoes not wane and is not lost, even up to five yearsafter vaccination : that it has seemed to do so mayoften have been due to ignoring the influence ofexperimental error in tuberculin testing and to thepractice of revaccinating persons called " negativetuberculin reactors ". If it is correct that the strongdegrees of allergy that may be produced by potentvaccines do not, in general, fade, it then becomespractically impossible to distinguish between allergyproduced by natural infection (or super -infection)and that produced by vaccination. Thus, contraryto what many workers have maintained, the tuber-culin test is lost as a diagnostic tool in clinicaltuberculosis work.
Co- operative laboratory work developed to supple-ment the field studies has made good progressduring the year. In the Tuberculosis ImmunizationResearch Centre, the laboratory jointly supportedby the Danish Government and WHO, the searchfor new and more practical methods for measuringresponses in tuberculosis has continued. Severalpapers report the result of these investigations, andplans have been made to determine whether thenew procedures apply to human beings as well as tolaboratory animals. In the United States Public
Health Service laboratory at Atlanta, Georgia,studies undertaken in co- operation with WHO haveproduced results of immediate practical value forvaccination programmes. By reproducing in animalswhat was being done with children in the BCGcampaigns, it was found that the more potent theBCG vaccine in producing allergy, the moreeffectively it protects animals against a challengeinfection with virulent tubercle bacilli. This resultlends support to the view that it may be desirablefor very potent vaccine in as large doses as can betolerated to be used for human vaccination work.The results also indicate that the use of vaccineweakened by exposure to sunlight, as was probablythe case in many of the earlier BCG campaigns,may have given little, if any, protection againsttuberculosis.
New -born children and infants are usually excludedfrom mass BCG campaigns because of the fear ofcomplications -enlarged axillary and cervical glandsand abscesses. Because of the very high tuberculosismorbidity and mortality in young children in somecountries, however, some attempts have been made tovaccinate them, in spite of the complications. Asystematic study of this problem has therefore beenbegun. Preliminary results show a striking increasein the frequency of complications with an increasein the dose of BCG. It appears that preventingcomplications may be largely a matter of preventinginexperienced and careless vaccinators from in-jecting too deeply and more than the prescribed doseinto the thin skin of young infants. Further study ofthis problem is urgently needed, but it seems likelythat techniques can be developed which will make itfeasible to include young children in the mass BCGwork.
JVeterinary Public Health and Zoonoses
The Seventh World Health Assembly, in thetechnical discussions, considered the problems oforganizing veterinary public- health services andcontrolling the zoonoses in rural areas, and exploredways in which countries could undertake zoonosescontrol -even with very limited resources in moneyand personnel -or could expand work alreadystarted.
Brucellosis
In order to increase the basic knowledge ofBrucella melitensis infection in sheep and goats,FAO, with the technical collaboration of WHO,organized in 1953 a series of experiments to study the
pathogenesis of the disease and to explore thepossibilities of developing an effective vaccine forthese animals. The experiments are being carried outin the FAO /WHO Brucellosis Centre at the InstitutPasteur, Tunis, with generous support from theauthorities. The results of the first year's work havegiven new and important information on the epi-demiology of Br. melitensis infection in sheep andgoats, which will undoubtedly change certain basiccontrol procedures hitherto used for these animals.Vaccine trials were begun towards the end of 1954,and some preliminary results are expected by 1956.It is planned to continue these studies for severalyears.
COMMUNICABLE DISEASES 11
MAP 1. FAO /WHO BRUCELLOSIS CENTRES
The FAO /WHO Brucellosis Centres (see Map 1)continued their activities as regional centres forresearch, diagnosis, training and control. Smallfinancial grants were made to assist several ofthe centres and brucellosis laboratories in theirwork.
A training course was held from 1 to 13 Marchat the Instituto de Investigaciones Pecuarias, PaloAlto, Mexico, for workers from the Caribbeanregion, from Central America and from Mexico.WHO consultants served as instructors to twenty -onephysicians, veterinarians and bacteriologists onlaboratory problems connected with the diagnosis ofbrucellosis (see also page 71).
Rabies
The publication in 1954 of a WHO monograph onlaboratory techniques in rabies has met an importantneed.' This monograph contains the latest informa-tion on diagnostic procedures and the production andpotency testing of rabies vaccine and hyperimmuneserum, and describes procedures applicable in areaswith limited facilities, and in the most advancedcountries. The second report of the WHO Expert
i World Health Organization, ed. (1954) Laboratory tech-niques in rabies, Geneva (World Health Organization: Mono-graph Series, No. 23)
Committee on Rabies 2 was also published during1954.
WHO continued its work of co- ordinating researchon several aspects of rabies, including the efficacyof serum and vaccines in the prophylaxis of rabiesin man, the local treatment of wounds, and the dura-tion of immunity conferred by the use of differentrabies vaccines in animals. Financial grants weremade to several laboratories engaged in this work.
Arrangements were made for the preparation of aprovisional international standard hyperimmuneserum against rabies. Serum was sent to differentcollaborating laboratories for tests. This work isexpected to be completed in 1955. Preliminarysteps were also taken to determine the possibility ofestablishing an international standard vaccine toserve as a basis of comparison in tests with locally-produced vaccines.
The appearance of rabies in non -haemophagousbats in the states of Texas, Florida and Penn-sylvania in the United States of America has beena disturbing complication in the known epidemiologyof rabies. Rabid bats in two of these states haveattacked human beings. WHO has closely followedthe problem of rabies in bats in Mexico for the pasttwo years and will further investigate this subject in
2 Wld Hlth Org. techo. Rep. Ser. 1954, 82
12 THE WORK OF WHO, 1954
collaboration with the United States and Mexicanauthorities.
An entire issue of the WHO Bulletin was devotedto rabies and published the results to date of thefield demonstration programmes of rabies control inIsrael and Malaya in which WHO assisted in formeryears.' Observations in these countries have beencontinued. The results in Malaya were again satis-factory in that no case of rabies in animals wasdiagnosed since June 1953. In Israel, however, therewas a recrudescence of the disease during the firsthalf of 1954, but no vaccinated dog contracted thedisease. This resurgence of rabies was undoubtedlycaused by the relaxation of government control ofstray dogs. The control has been resumed by theIsraeli government authorities.
WHO consultants visited Egypt, Israel, Lebanon,Mexico, Portugal, Spain and Yugoslavia during theyear to assist with problems of rabies control.
Q Fever
Work was continued on assessing the value ofdifferent serological diagnostic procedures used forthe detection of Q fever in man and animals, such asthe complement- fixation test, micro -agglutination andmacro -agglutination tests, and a macroscopic capil-lary tube agglutination test. As reported in 1953 (seethe Annual Report for that year 2) work was com-pleted on the International Standard for Anti -Q-Fever Serum, establishing unitage for this product.WHO has made small financial grants to laboratoriesto help them study effective diagnostic screeningprocedures for rickettsial diseases, including Q fever,and for research on antigen production.
Leptospirosis
Co- ordinated research was started on the use andstability of killed antigens for the diagnosis ofleptospirosis in man and animals. Batches of antigenwere prepared by different laboratories for trialin field surveys for the presence of this disease.
To clarify the identification of Leptospira strains,arrangements were made for specific antisera to beprepared for use in leptospirosis laboratories indifferent parts of the world.
' Bull. Wld Hlth Org. 1954, 10, 703-8662 Off. Rec. Wld _Filth Org. 51, 12, 50
A WHO consultant was sent to Spain to study theepidemiology of the disease there and to advise theGovernment.
Animal Tuberculosis
In a rural area in Egypt a study is being under-taken to correlate the prevalence of animal tuber-culosis and other zoonoses with human infection.The human population concerned is being givencareful individual, including x -ray, examinations,and the animal population has been surveyed bymeans of the tuberculin test. At the same time, theanimals are being examined serologically for Q fever,leptospirosis and brucellosis infection.
The examination by different laboratories of theprovisional International Standard for PurifiedProtein Derivative of Avian Tuberculin was com-pleted. This standard was established at the eighthsession of the WHO Expert Committee on BiologicalStandardization (see page 46).
Hydatidosis
WHO has assisted with hydatidosis -control studiesin Argentina, Chile and Uruguay, and a consultantalso visited Lebanon to advise on this problem andon that of other zoonoses.
A study of the efficacy of anthelminthics in dogsfor the removal of the tapeworm, Echinococcusgranulosis, was begun. By this study it is hopedto find ways of simplifying the present methods fortreating dogs in hydatidosis -control programmes sothat control of this disease can more easily beincorporated and combined with that of rabies.
Veterinary Biological Standards
In collaboration with FAO and the Office Inter-national des Epizooties WHO undertook work on theInternational Biological Standard for Swine Erysi-pelas Serum, Anti -N, and the International ReferencePreparations of Clostridium welchii antitoxins. Theywere established during the year (see page 46).
Food Hygiene
A WHO /FAO seminar on meat hygiene, organizedby the WHO Regional Office for Europe forEuropean countries, was held in Copenhagen inFebruary. About thirty veterinary and medicalofficers attended and the subjects considered includedpresent practices for the inspection of slaughter-houses, and the hygiene of meat handling and foodshops. Discussion leaders drew attention to advances

COMMUNICABLE DISEASES 13
in slaughterhouse hygiene, slaughter procedures, theprocessing and conservation of meat and meatproducts, meat inspection, laboratory tests, and thetraining of inspectors. A WHO /FAO Expert Com-mittee on Meat Hygiene met towards the end of theyear to formulate recommendations that can beapplied in all parts of the world.
The secretariat FAO /WHO /UNICEF inter- agencyworking group on milk and milk products continuedits work which, in 1954, included surveys in Yugo-slavia and Egypt for the purpose of advising theGovernments on their milk programmes. The groupalso held several meetings to prepare standards in
milk legislation and to consider the problems ofsterilizing milk (see also under EnvironmentalSanitation, page 32).
Other Zoonoses
During the year, WHO has also been concernedwith anthrax, trichinosis, toxoplasmosis, psittacosisand the arthropod -borne virus encephalitides. WHOhas closely followed research and field surveys in thesesubjects with a view to simplifying laboratorydiagnostic procedures and improving control pro-cedures.
Virus and Rickettsial Diseases
In 1954 work on virus diseases has been continuedon the principle, which was outlined in the AnnualReport for 1953, of broadening and integratingWHO's work on these diseases. Emphasis has beengiven to the need to bring virological techniques intopractical use for diagnosis and control of virusdiseases. The old conception that the study of virusesin the laboratory was both too difficult and tooexpensive to play any part in public -health or clinical
1 The work done on Q fever and rabies is described in thepreceding section, on zoonoses.
practice is now completely outdated. Many of thevirological techniques available are as simple asmany routine bacteriological procedures and littlemore expensive. Indeed, similarities between the twoare becoming increasingly apparent.
Influenza
The WHO influenza laboratories continued theirstudies on the epidemiology of influenza viruses (fornetwork of these laboratories, see Map 2). The finalreports on the 1952 -53 epidemic have been published.
MAP 2. WHO INFLUENZA CENTRES
14 THE WORK OF WHO, 1954
A study, carried out by the World Influenza Centre,of 212 viruses isolated by the WHO Influenza Centresall over the world has shed light on the epidemiologyof this disease. There was no widespread epidemicin the Northern Hemisphere during the winter of1953 -54, but both A and B viruses were isolatedin scattered outbreaks. In June and July outbreakswere reported in South Africa and Australia, both Aand B viruses being incriminated. The study ofoutbreaks on ships coming from South Africaresulted in the isolation in London of an A (Liver-pool) virus identical with strains isolated in Johannes-burg. This strain had not previously been detectedin the United Kingdom during 1954.
In April an informal meeting of a group of expertswas held at the World Influenza Centre to discussproblems connected with influenza vaccines. Parti-cular emphasis was placed on the problems that havearisen in the European Region, where provisions forthe control of influenza vaccines are less advancedthan in North America. The group recommendedstrains of virus for use in current vaccine production,and outlined a procedure for reviewing the recom-mendations in the future should changes in theprevalent influenza viruses make this necessary.Interim recommendations were made for the testingof vaccines, and standard reagents were preparedfor this purpose by the World Influenza Centre.The WHO Expert Committee on Biological Stand-ardization, which was informed of this development,asked that further studies should be made to correlatefield and laboratory results with a view to the eventualadoption of international reference preparations.
Poliomyelitis
A WHO programme for the study of poliomyelitishas been developed, based on the recommendationsof the WHO Expert Committee on Poliomyelitis.Progress was made in the organization of a networkof laboratories to carry out the laboratory part of theprogramme. In some regions laboratories weredesignated as WHO Regional Poliomyelitis Labo-ratories, to co- ordinate the work in the region. Inothers, where no suitable laboratory existed, assis-tance was given to selected laboratories to enablethem to undertake the more advanced work requiredin the programme. Considerable interest has beenshown by many national laboratories, a number ofwhich are already co- operating in the WHO influenzanetwork. The poliomyelitis network may thereforebe extended more rapidly than was originally planned.
The intensive research on the development ofpoliomyelitis vaccines which is in progress in many
parts of the world, particularly in the United Statesof America, has been carefully studied. Progress hasbeen rapid, and the prospects for eventual successare good. However, it is necessary to emphasize thatthe vaccines under study are still in the experimentalstage, and many problems remain to be solved beforethe vaccines can be accepted for routine public -health application.
The results of the prophylactic use of gamma -globulin for poliomyelitis control in the UnitedStates of America and elsewhere have been examined.The opinion of the WHO Expert Committee that thismeasure was likely to be of limited public- healthvalue has been confirmed. Recent experienceindicates that, as supplies of this expensive substanceare limited, it should be reserved for the prophylaxisof measles and infectious hepatitis, for which it ishighly effective.
The report of the WHO Expert Committee onPoliomyelitis 1 was published early in the year, and anumber of countries have adopted the recommenda-tions from the report as the basis of their nationalcontrol policies.
A monograph on poliomyelitis 2 was in press atthe end of the year. It contains reviews on epidemio-logical, virological and clinical aspects of polio-myelitis and on its therapy and control.
Also published was a study of the incidence ofpoliomyelitis in the world in 1953 which included,for the first time, information gathered from panelmembers and other co- operating workers on thetypes of virus responsible for outbreaks in a numberof countries. It is expected that such studies willbecome increasingly important as more and betterinformation becomes available by means of theWHO poliomyelitis programme.
Yellow Fever
The provisions of the International SanitaryRegulations relating to yellow fever were reviewedby the Committee on International Quarantine at itssecond session. Recommendations were made forthe revision of these provisions by the Eighth WorldHealth Assembly. This aspect of the work of theOrganization is described in Chapter 5 in the sectionon the International Sanitary Regulations (seepage 39).
1 Wid Hlth Org. techn. Rep. Ser. 1954, 812 Debré et al. (1955) Poliomyelitis, Geneva (World Health
Organization: Monograph Series, No. 26)
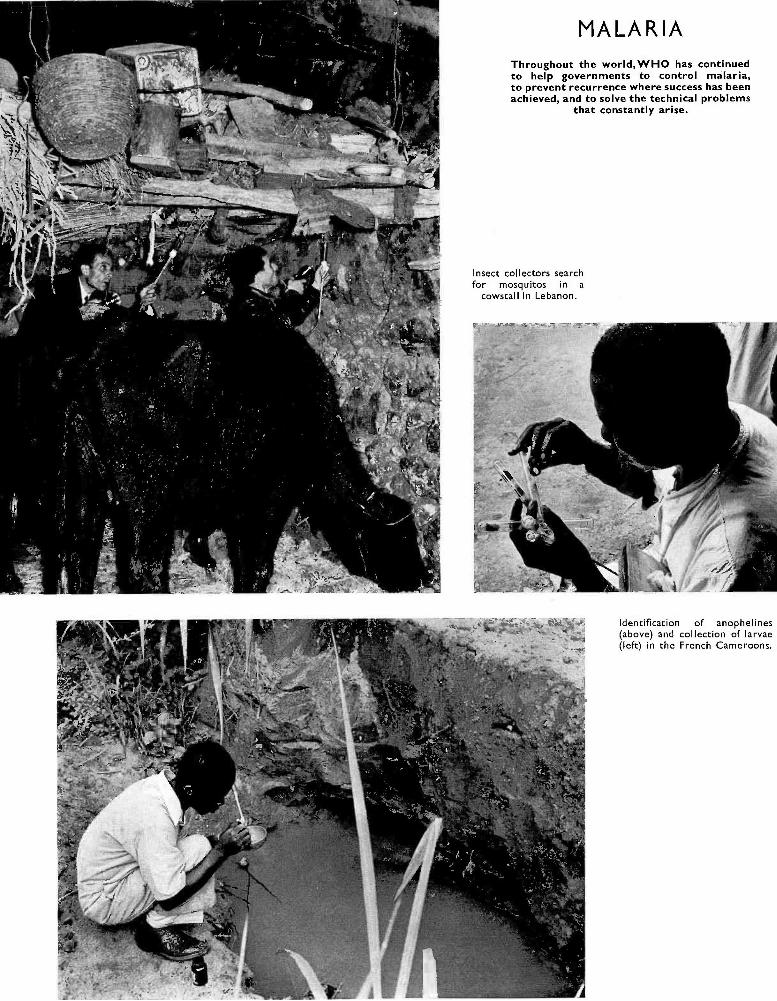
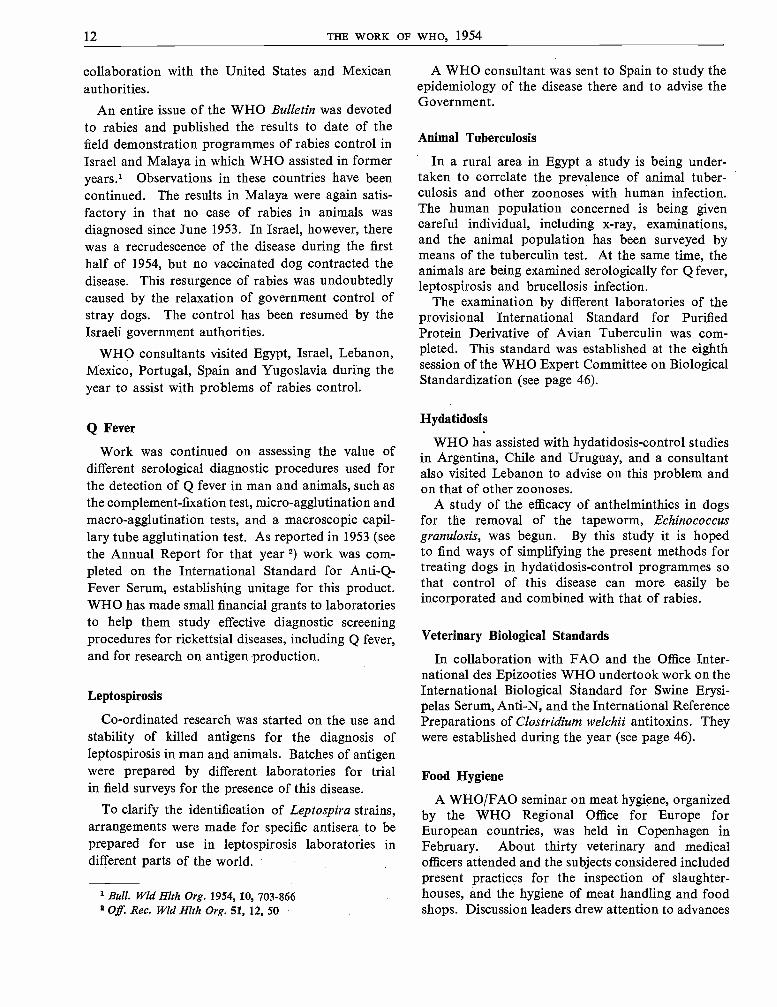
MALARIAThroughout the world,WHO has continuedto help governments to control malaria,to prevent recurrence where success has beenachieved, and to solve the technical problems
that constantly arise.
Insect collectors searchfor mosquitos in a
cowstall in Lebanon.
Identification of anophelines(above) and collection of larvae(left) in the French Cameroons.
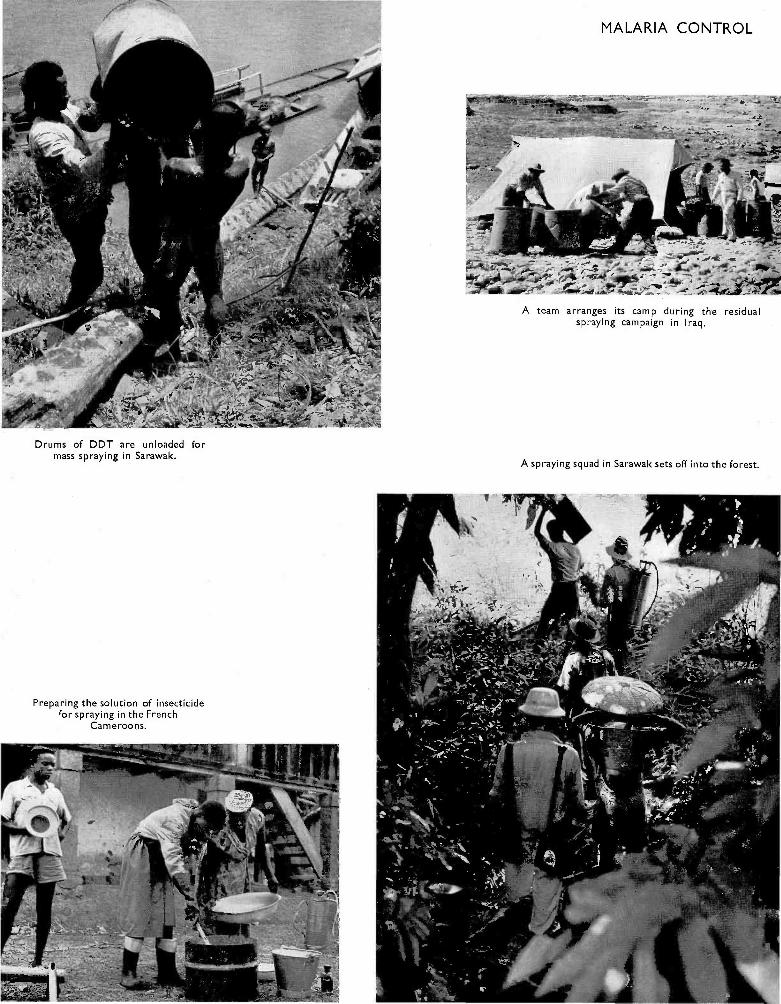
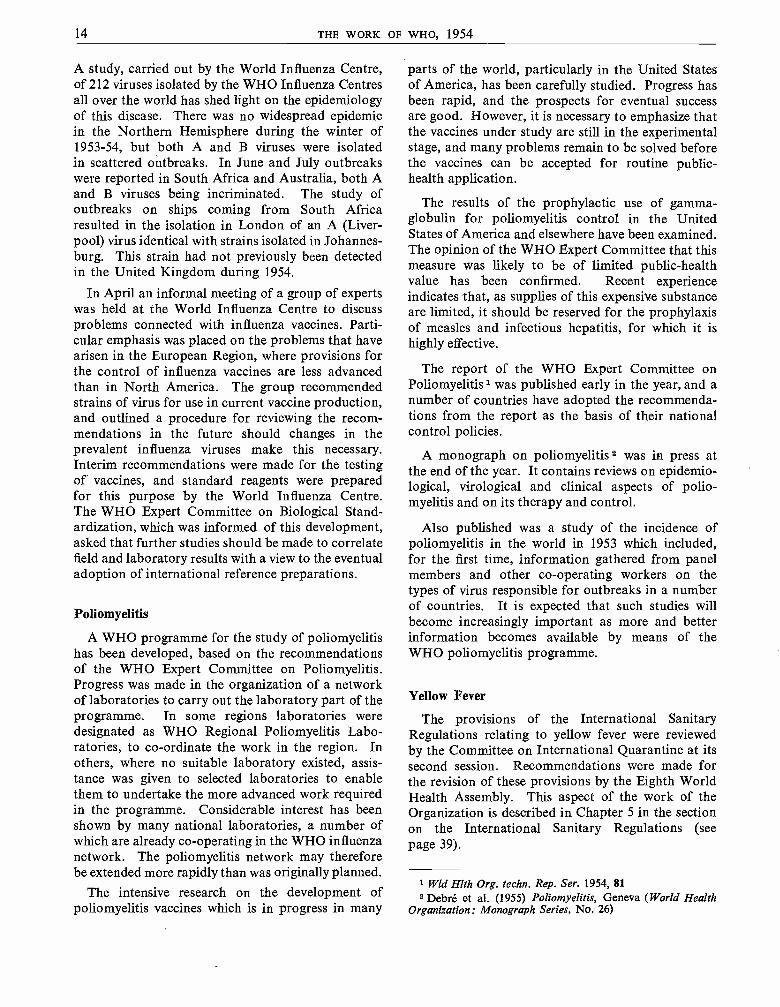
Drums of DDT are unloaded formass spraying in Sarawak.
Preparing the solution of insecticidefor spraying in the French
Cameroons.
MALARIA CONTROL
A team arranges its camp during the residualspraying campaign in Iraq.
A spraying squad in Sarawak sets off into the forest.
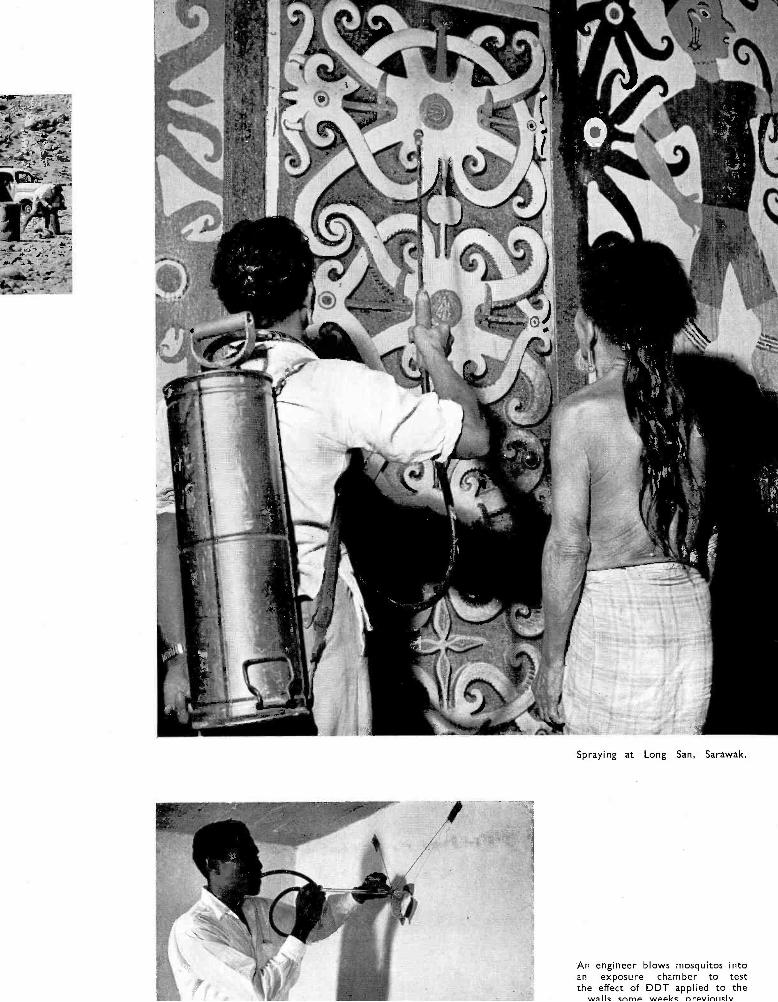
Spraying at Long San, Sarawak.
An engineer blows mosquitos intoan exposure chamber to testthe effect of DDT applied to the
walk cnrnp weekc nrevinlisly

Technicians examine blood samplesin Sarawak (above) and the French
Cameroons (right).
In the French Cameroons, a patient isexamined for enlarged spleen, one of the
indications of malarial infection.
To check the efficacy of control work in Lebanon, bloodsamples are taken in the unsprayed area just over the
Syrian frontier.Members of the control team take blood samples from
children in Maymyo, Burma.
COMMUNICABLE DISEASES 15
Epidemiological information about yellow feverin Africa was published in a special issue of theWHO Bulletin.1 Tables and maps illustrating thedistribution of yellow -fever cases and deaths, anddata on the results of sero -protection tests performedwith human sera, are being kept up to date by WHO.
Surveys undertaken under the aegis of, or inco- operation with, WHO were carried out in severalStates and territories in Africa -Ethiopia, the Fede-ration of Rhodesia and Nyasaland, the Union ofSouth Africa, South -West Africa and the Sudan-which are adjacent to recognized yellow -feverreservoir areas, for the purpose of determining thepresent position of these regions as regards yellowfever.
In accordance with recommendations made by theExpert Committee on Yellow Fever at its secondsession,' WHO has initiated studies on the co-ordination of yellow -fever research and also on thepossibility of carrying out an experimental Aëdesaegypti eradication scheme in a rural area of WestAfrica.
In the Americas, A. aegypti eradication campaignshave continued.
A new type of yellow -fever vaccine, prepared atYaba, Lagos, with a 17D strain, to be applied byscarification, was submitted to testing laboratorieswith a view to its approval by WHO for the issueof international certificates of vaccination againstyellow fever.
Smallpox
The laboratory investigation of four dried small-pox vaccines was completed during the year. Statis-tical analysis of the results is still in progress. It isalready clear that one of the four vaccines has givenresults markedly superior to the other three. Thisvaccine and a newly -developed dried vaccine ofcomparable temperature stability are being subjectedto strictly controlled field trials in humans under thesupervision of the Medical Research Council of theUnited Kingdom, which receives a grant from WHOtowards the cost of this work. These trials aredesigned to give information on the relationshipbetween the vaccine titres as measured by laboratorytests in the experimental animal and chick embryoand successful vaccination rates in humans ; theyalso are to measure the efficiency and protectivevalue of the vaccines after exposure to adverseconditions such as may be met with in tropicalclimates. These trials are likely to last at least two
1 Bull. Wld Hlth Org. 1954, 11, 315-5082 Off Rec. Wld Hlth Org. 56, 83
years, and may be followed by further trials inendemic areas.
A study was undertaken on the problems of small-pox control in the Western Pacific Region.
In accordance with resolution WHA7.5, WHOoffered its assistance to national administrations intheir smallpox -control programmes.
Studies were published on the endemicity of small-pox. A comparative study of the laws governingsmallpox vaccination was published in the Inter-national Digest of Health Legislation.3
Trachoma
More governments asked for assistance on tra-choma in 1954 ; new field projects were started, andrequests for information on the results of the pilotprojects in operation were received from manygovernments, non -governmental organizations andtrachomatologists. A preliminary assessment of theresults of pilot projects was discussed at the XVIIInternational Congress of Ophthalmology, at itsmeetings in Montreal and New York in September.
All the current field activities against trachomaform one part of a general plan of field research totest the efficacy of a proposed control method underdifferent epidemiological conditions prevailing invarious countries, and to ascertain the most efficientand economical methods suitable for differentconditions.
Important differences of opinion on fundamentalpoints related to the etiology, epidemiology andtherapy of trachoma exist among leading trachoma-tologists in different parts of the world. In order toclarify these differences, a programme of exchange ofinformation on trachoma was arranged, involvingtrachomatologists from Egypt, Iran, Japan, Morocco(French Zone) and Tunisia. The results, still underconsideration, have already proved valuable for theelaboration of future programmes. From theseexchanges, and from the data collected from thepilot field projects, it became evident that a co-ordinated programme was necessary involving(1) epidemiological field studies on trachoma andassociated conjunctivitis in different areas of theworld, (2) laboratory research aiming at the isolationand study of the local strains of the trachoma virus,and (3) studies on the etiology of non -trachomatousfollicular conjunctivitis and the other essential eyeinfections. Such activities have already been started incollaboration with members of the Expert AdvisoryPanel and other leading trachomatologists, and a
3 Int. Dig. Hlth Leg. 1954, 5, 223

16 THE WORK OF WHO, 1954
report is being prepared for the meeting of theExpert Committee on Trachoma to be held in 1955.
The pilot project in Taiwan, in accordance with thedecision of the Government in 1953, is being extendedto include the treatment of all the schoolchildrenof the island, and a survey was made for this purposein 1954. The pilot project in Morocco (FrenchZone) was successful in preventing the annualepidemic of seasonal conjunctivitis (see also page 90).New pilot projects were started in Egypt, Tunisia and
Yugoslavia, and surveys or planning activities havealso been carried out in India, Indonesia and Spain.
Other Virus and Rickettsial Diseases
Owing to pressure of other work, plans for co-ordinated research on virus hepatitis, the viruses ofthe lymphogranuloma -psittacosis- trachoma group,the virus encephalitides, and the rickettsioses havehad to be held in abeyance.
Other Communicable Diseases
Diphtheria and Pertussis
WHO made a grant to the Medical ResearchCouncil of the United Kingdom towards the costof their important field trials, which have beenextended to include combined diphtheria andpertussis vaccinations. Follow -up work is in progressbut the results are unlikely to be available before1956.
Typhoid Fever
The controlled field trials of typhoid vaccines inYugoslavia,Reports on the conduct of these trials and on thevaccines in use are highly satisfactory. The possibilitywas explored of organizing replicate laboratory testsof the vaccines with a view to developing an inter-national reference preparation and a report was madeto the WHO Expert Committee on BiologicalStandardization.
Onchocerciasis
The first report of an Expert Committee onOnchocerciasis, published at the end of the year,'describes the symptoms and pathology of the disease,suggests methods for standardizing epidemiologicalsurveys and reviews control measures under twoheads : therapy and vector control. Stress is laidon the need for detailed surveys to determine thegeographical distribution and epidemiological charac-teristics of onchocerciasis in Africa and the Americas.
A conference on African onchocerciasis wasorganized in Leopoldville in November, when agroup of experts from Europe, from African terri-tories and from various non -governmental organi-zations, made a review of the epidemiological dataat present available for Africa.
1 Wld Hlth Org. techn. Rep. Ser. 1954, 87
This was the first time that such a review had beenmade ; the data considered for some countries hadbeen collected by means of surveys made especiallyfor the Conference.
Leprosy
Activities in leprosy control are increasing in anumber of countries. Projects are being plannedin Indonesia, Iraq, and the Philippines. A surveywas made in Paraguay by the Pan American SanitaryBureau, and WHO started projects in Ceylon andNigeria. The project in Burma is being continuedby national staff after the end of WHO assistance.The preparation of guiding lines for the elaborationof future projects has continued.
A study " Leprosy, a Survey of Recent Legisla-tion ", appeared in the International Digest of HealthLegislation.2
The internationally co- ordinated study of histo-pathological material was continued.
Plague and Cholera
At the request of the Government of Iran, WHOassisted with a programme of co- ordination ofresearch with regard to the control of wild- rodentplague. A meeting for the co- ordination of researchand control activities on wild- rodent plague in thearea was convened by WHO in Teheran in October.It was attended by specialists representing theGovernments of Iran, Iraq, Syria and Turkey. Auseful exchange of information took place on theepidemiological conditions prevailing in the differentcountries.
Agreement was reached on a co- ordinated andprogressive plan for training local staff in antiplaguetechniques, and on collaboration for the delimitation
2 Int. Dig. Hlth Leg. 1954, 5, 3
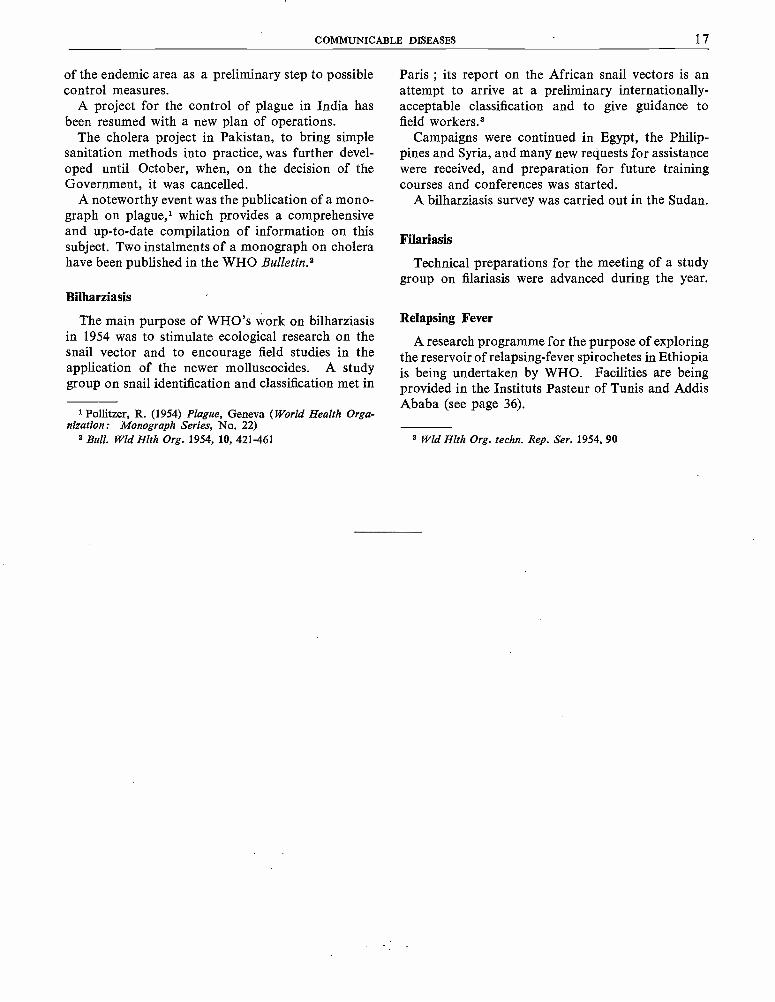
COMMUNICABLE DISEASES 17
of the endemic area as a preliminary step to possiblecontrol measures.
A project for the control of plague in India hasbeen resumed with a new plan of operations.
The cholera project in Pakistan, to bring simplesanitation methods into practice, was further devel-oped until October, when, on the decision of theGovernment, it was cancelled.
A noteworthy event was the publication of a mono-graph on plague,1 which provides a comprehensiveand up -to -date compilation of information on thissubject. Two instalments of a monograph on cholerahave been published in the WHO Bulletin.2
Bilharziasis
The main purpose of WHO's work on bilharziasisin 1954 was to stimulate ecological research on thesnail vector and to encourage field studies in theapplication of the newer molluscocides. A studygroup on snail identification and classification met in
1 Pollitzer, R. (1954) Plague, Geneva (World Health Orga-nization: Monograph Series, No. 22)
2 Bull. WId Hlth Org. 1954, 10, 421 -461
Paris ; its report on the African snail vectors is anattempt to arrive at a preliminary internationally -acceptable classification and to give guidance tofield workers.3
Campaigns were continued in Egypt, the Philip-pines and Syria, and many new requests for assistancewere received, and preparation for future trainingcourses and conferences was started.
A bilharziasis survey was carried out in the Sudan.
Filariasis
Technical preparations for the meeting of a studygroup on filariasis were advanced during the year.
Relapsing Fever
A research programme for the purpose of exploringthe reservoir of relapsing -fever spirochetes in Ethiopiais being undertaken by WHO. Facilities are beingprovided in the Instituts Pasteur of Tunis and AddisAbaba (see page 36).
3 Wld Hlth Org. techn. Rep. Ser. 1954, 90

CHAPTER 2
v PUBLIC -HEALTH SERVICES
One of the aims of the Organization is to strengthen national health services by introducing needed measuresto become part of the permanent health organization of the country. The measures introduced in this waynaturally depend on the stage,of development of the health services. The methods adopted fall into three broadcategories : first, the use of field projects to demonstrate work on single health problems, in programmes thatcan be developed into national organized services ; secondly, the demonstration, usually in rural areas, ofintegrated health services that can be extended to cover the whole country ; and, thirdly, the stimulation, in avariety of ways, of the initiative of individuals, communities or professional groups in developing their ownhealth services.
(1) Demonstration of Single Health Services. Most of the projects in whichWHO is assisting, includingthose demonstrating the control of communicable diseases (described in the previous chapter) still fall into thefirst category and are gradually but steadily being transformed into organized health services. For many ofthem, officers with general public -health experience or training have been appointed team leaders who, on thecompletion of the original projects, have assisted the governments in planning a permanent health service in thesame locality. The projects in maternal and child health in Burma, India and Peru, which have been assistedby WHO and UNICEF, and the project in the Dominican Republic, assisted by the Pan American SanitaryBureau and UNICEF, are examples of such transformations which have already or will soon have taken place.Many others will be found throughout this report.
In Afghanistan, Burma, Cambodia, Ceylon, India, Indonesia, Iran and Saudi Arabia the various WHO -assisted projects of this type have been co- ordinated by public -health administrators or advisers whom WHOhas assigned to these countries.
(2) Demonstration of Integrated Health Services. In 1954, during the technical discussions at the SeventhWorld Health Assembly on the subject " Public- Health Problems in Rural Areas ", three aspects were givenparticular attention : the organization of public- health units in rural areas, rural sanitation and the zoo noses.It was agreed that the most effective and economical way of approaching these problems was to organizeintegrated health services in rural areas. The second report of the Expert Committee on Public- HealthAdministration, entitled the Methodology of Planning an Integrated Health Programme for Rural Areas"was published during the year.
In a number of countries in the Americas, and in Burma, Egypt, Ethiopia and Malaya, WHO has helpedwith pilot projects for developing integrated health services in certain rural areas.
The health demonstration area in El Salvador has developed further ; with the active participation of thepeople, the services are being decentralized to the village level. By applying the principle of self -help, theinhabitants have installed sewage disposal and water supply systems in several towns : Quezaltepeque, Nejapa,Apopa, Guazapa, Opico and El Paisnal (see also page 72).
Developments in Panama have been significant in that the Organization, after assisting a few local healthcentres (in La Chorrera, David, Chame, Ocu and Antón), was asked to advise on the reorganization of theCentral Health Department, which now includes a section responsible for the promotion of local health services(unidades sanitarias). An active programme of public- health training for doctors, sanitary inspectors, nursesand nursing aides (auxiliares sanitarias) has been carried out at the health centre in La Chorrera.
The public- health demonstration and training centre in Callao, Peru, is an example of the establishmentof such integrated health services in an urban area. This project was initiated late in 1952 with a preliminary
Wld Hlth Org. tecluz. Rep. Ser. 1954, 83
- 18 -
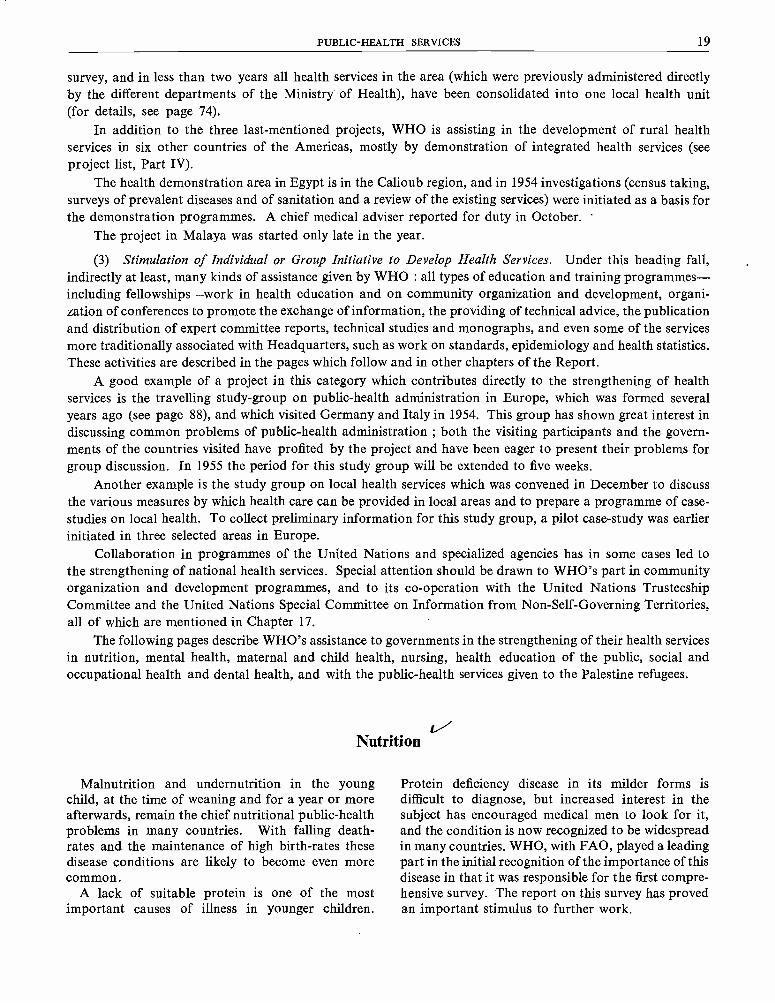
PUBLIC -HEALTH SERVICES 19
survey, and in less than two years all health services in the area (which were previously administered directlyby the different departments of the Ministry of Health), have been consolidated into one local health unit(for details, see page 74).
In addition to the three last -mentioned projects, WHO is assisting in the development of rural healthservices in six other countries of the Americas, mostly by demonstration of integrated health services (seeproject list, Part IV).
The health demonstration area in Egypt is in the Calioub region, and in 1954 investigations (census taking,surveys of prevalent diseases and of sanitation and a review of the existing services) were initiated as a basis forthe demonstration programmes. A chief medical adviser reported for duty in October.
The project in Malaya was started only late in the year.
(3) Stimulation of Individual or Group Initiative to Develop Health Services. Under this heading fall,indirectly at least, many kinds of assistance given by WHO : all types of education and training programmes -including fellowships -work in health education and on community organization and development, organi-zation of conferences to promote the exchange of information, the providing of technical advice, the publicationand distribution of expert committee reports, technical studies and monographs, and even some of the servicesmore traditionally associated with Headquarters, such as work on standards, epidemiology and health statistics.These activities are described in the pages which follow and in other chapters of the Report.
A good example of a project in this category which contributes directly to the strengthening of healthservices is the travelling study -group on public- health administration in Europe, which was formed severalyears ago (see page 88), and which visited Germany and Italy in 1954. This group has shown great interest indiscussing common problems of public- health administration ; both the visiting participants and the govern-ments of the countries visited have profited by the project and have been eager to present their problems forgroup discussion. In 1955 the period for this study group will be extended to five weeks.
Another example is the study group on local health services which was convened in December to discussthe various measures by which health care can be provided in local areas and to prepare a programme of case -studies on local health. To collect preliminary information for this study group, a pilot case -study was earlierinitiated in three selected areas in Europe.
Collaboration in programmes of the United Nations and specialized agencies has in some cases led tothe strengthening of national health services. Special attention should be drawn to WHO's part in communityorganization and development programmes, and to its co- operation with the United Nations TrusteeshipCommittee and the United Nations Special Committee on Information from Non -Self - Governing Territories,all of which are mentioned in Chapter 17..
The following pages describe WHO's assistance to governments in the strengthening of their health servicesin nutrition, mental health, maternal and child health, nursing, health education of the public, social andoccupational health and dental health, and with the public- health services given to the Palestine refugees.
Nutrition
Malnutrition and undernutrition in the youngchild, at the time of weaning and for a year or moreafterwards, remain the chief nutritional public- healthproblems in many countries. With falling death -rates and the maintenance of high birth -rates thesedisease conditions are likely to become even morecommon.
A lack of suitable protein is one of the mostimportant causes of illness in younger children.
Protein deficiency disease in its milder forms isdifficult to diagnose, but increased interest in thesubject has encouraged medical men to look for it,and the condition is now recognized to be widespreadin many countries. WHO, with FAO, played a leadingpart in the initial recognition of the importance of thisdisease in that it was responsible for the first compre-hensive survey. The report on this survey has provedan important stimulus to further work.
20 THE WORK OF WHO, 1954
Animal protein, particularly in the form of milk,will maintain growth and development in the child,but the total supply of milk is not sufficient for theworld's needs, and it does not appear likely that itwill ever be so. Plant protein, on the other hand,is cheap and can be produced in relatively largequantities, but does not maintain satisfactory growthand development in the child. If the reason for thiscan be established, it may be possible to developcheap processing to make proteins from plantsources approximate in value the scarce and moreexpensive animal proteins.
WHO's work in nutrition is, therefore, con-centrated on the prévention of protein malnutrition.The Organization has stimulated and co- ordinatedactivities in this subject and has assisted centresengaged in the study of plant proteins in relation totheir use for the young child. At the end of 1953, agrant was made to the British Medical ResearchCouncil Nutrition Research Unit in Kampala,Uganda, to assist in investigation into the proteinthat can be obtained from sunflower. An exchangeof scientific workers between this research unit and theInstitute of Nutrition of Central America and Panamain Guatemala, arranged in 1953, has ensured thatthe research in the two centres is now being conductedalong comparable lines. In 1954, WHO arrangeda similar exchange of scientific workers between theKampala Research Unit and the nutrition labora-tories of the Indian Council of Medical Research, andmade a grant to enable the latter to continue investiga-tions into the use of locally grown pulses for theprevention of child malnutrition in India. This workwill run parallel with the investigations being made inGuatemala and in Kampala. WHO will maintainclose contact between workers in these differentcentres by exchanges, and by organizing meetingswhich will also be attended by workers in alliedfields, competent to judge progress and advise onprinciples.
Biochemists, experimental nutritionists, paedia-tricians, and workers in other related fields areworking in each of these centres, and the results theyobtain will, it is hoped, have implications for otherparts of the world. Some standardization of themethods of testing the different forms of proteinto find out whether they can maintain adequategrowth and development is likely to be an earlyresult of their work. This in itself would be a con-
siderable advance ; the existence of standardizedmethods might encourage workers in other centresto attempt to apply them to local problems.
Although the total supply of protein suitable forfeeding the young and growing child is inadequateand means of increasing it must be found, there areother more complicated causes of protein mal-nutrition, since it occurs even when relativelyadequate supplies of protein are available. In suchcases the remedy lies in a reorientation -throughmodern methods of health education -of the people'sdietary customs -especially during weaning when thechild is highly vulnerable to deficiency disease.Choice of food is known to be influenced greatly bysocial conditions, beliefs and cultural practices andan understanding of such influences is a prerequisitefor the health education work.
During 1954 a first step was taken in a programmefor preventing protein malnutrition by improvededucation. A sociologist has been sent to a country inSouth -East Asia to inquire into the living conditionsof people among whom protein malnutrition inchildhood is common and yet who are not in thepoorest economic circumstances. This investigationincludes inquiries into the relative prevalence ofdisease in different ethnic groups ; whether it occursmostly in people moving from rural to urban areas,in adopted children or in families in which therehas been divorce ; and the nature of the attitudes andbeliefs towards mothers' and children's food.
The inquiry will, it is hoped, indicate the kind ofknowledge which is required if this problem is to besolved successfully.
The conclusions reached will be discussed at aseminar on nutrition education which is to beorganized, in 1955, with FAO. The future directionof the long -term plans for the prevention of childmalnutrition through education will depend largelyon this preliminary work.
Early in the year WHO received two reportsresulting from the survey of nutrition work made in1953 in maternal and child health centres in theEastern Mediterranean, South -East Asia and WesternPacific Regions. These reports dealt with (a) theeducation in nutrition which they give to mothers,and (b) the use of milk powder made available byUNICEF to the centres. Both reports were construc-tive and were widely circulated. The second question

PUBLIC -HEALTH SERVICES 21
was discussed by the UNICEF /WHO Joint Com-mittee on Health Policy, at its meeting in April.A report on child nutrition in the tropics and sub-tropics was written by the consultant who carriedout the survey.
During the year the Organization has made afurther study of the prevalence and prevention ofpellagra. Consultants sent by the regional officesvisited countries in the European and EasternMediterranean Regions to help to define and adviseon the prevention of the disease and went to Basuto-land and Southern Rhodesia to obtain informationon pellagra in that part of the world and to considerhow the techniques used for prevention elsewherecould be applied under the different conditionsobtaining there.
One of the first nutritional problems to be studiedby WHO was that of endemic goitre -a conditionof major importance socially, economically andmedically in large areas of the world. In manycountries the effective preventive measure of iodizingsalt has not been applied because of the difficultyof maintaining the necessary concentration of iodinein the crude salt that is in general use. It has beenestablished that iodates are relatively stable in crudesalt, are as effective in goitre prevention as iodides,are non -toxic in the dosage obtained from saltiodized to the higher levels recommended, and canbe introduced into crude salt by cheap apparatus
evolved for the purpose. In 1954, a consultant on thechemical and engineering aspect of salt iodizationwent to the Americas to advise on the developmentof plans to control endemic goitre ; he visited fifteencountries in Latin America, with a consultantappointed by the Regional Office.
At the fourth session of the Joint FAO /WHOExpert Committee on Nutrition, held in Geneva inlate October, the Committee considered requirementsfor calories and other nutrients and gave specialattention to various aspects of subjects which are ofimportance in present and future programmes ofboth organizations : chemical additives to food,pellagra, endemic goitre, education in nutrition,anthropometry applied to nutrition, nutrition anddegenerative diseases, and the enrichment of skimmilk with vitamins A and D.
WHO was represented at the twentieth session ofthe FAO Council, held in Rome in September, atthe Third International Congress of Nutrition, inSeptember in Amsterdam, and at a meeting of corres-pondents appointed by governments Members ofthe Commission for Technical Co- operation inAfrica South of the Sahara, on the subject ofnutrition, in Brussels, also in September. A represen-tative of the Organization served as member of astudy group, which met in October in Paris, toexamine the activities of the International Children'sCentre in tropical and sub -tropical countries.
Mental Health
WHO's mental health programme has continuedalong established lines. The comparative study ofnational legislation affecting the hospitalization ofmental patients, which was begun in 1953, wascompleted and is to be published in the InternationalDigest ofHealth Legislation early in 1955. Followingthe completion of this survey, the Expert Committeeon Mental Health was convened to consider allaspects of legislation affecting the care of psychiatriccases, and prepared a report containing recommen-dations with regard to the principles on whichfuture legislation of this type should be based.
In the light of the views expressed in the thirdreport of the Expert Committee (section 4.1 " TheCommunity Mental Hospital " 1), WHO has begun
1 Wld Hlth Org. teehn. Rep. Ser. 1953, 73, 16
a study of the influence of the architectural designof the mental hospital on the work of the hospital.The methods being used in surveys to assess theneeds to be filled by general hospitals 'are beingexamined with a view to applying similar methodsto the study and planning of mental hospitals. It isbelieved that by 1956 enough data will be assembledto allow the Expert Committee on Mental Health toconsider this subject at its next meeting.
During 1954 WHO convened a meeting of expertsdrawn from the Expert Advisory Panels on MentalHealth and on Drugs Liable to Produce Addictionto discuss certain aspects of the problem of alcoholand alcoholism. It had become evident from previousreports on alcoholism made by the Expert Committeeon Mental Health and from the report of the firstmeeting of the Expert Committee on Alcohol that
22 THE WORK OF WHO, 1954
there were certain aspects of this problem which couldbe dealt with only at a meeting which included bothclinicians and laboratory workers. The meeting led toconsiderable clarification of certain technical prob-lems in this field (see also page 49).
The preparation of a series of national studies ofalcohol problems continued.
A second meeting of the Study Group on thePsychobiological Development of the Child was heldearly in the year. The report of this meeting wascompleted, and preparations were started for athird meeting, to take place early in 1955. Also in1955, WHO will convene a new research study group,to consider the subject of juvenile epilepsy and studyall aspects of this important public -health problem,i.e., the neurological, pharmacological, psychologicaland social aspects, and preparations for this meetingare likewise being made. A critical survey of epi-demiological studies of psychiatric disorders has beenstarted. Work in this field has not aroused theinterest in public- health circles which its importancemerits, and the need for an up -to -date, critical andcomprehensive survey of the studies being undertakenor completed in different countries is urgent.
As in previous years, international seminars havebeen a particularly successful part of the Organi-zation's mental -health programme. At the thirdWHO seminar on alcoholism, held in the Nether-lands, attention was concentrated on the problems oftreatment (for details, see page 92). Sweden acted
Maternal and Child Health 1
as host to a regional study group on the relationshipbetween paediatrics and child psychiatry in the workof children's hospitals. During the year, as a follow -up of the second WHO seminar on alcoholism, heldin Argentina in 1953, the WHO consultant on thissubject went to different countries of the Americasfor discussions with groups of individuals who hadparticipated in the seminar.
Assistance to individual countries has continued.Short -term consultants visited Iran, Iraq andMalaya ; a child psychologist was recruited for theChild Mental Hygiene Unit in Bangkok, Thailand,and teachers in psychiatric nursing and in electro-physiology and neurology were recruited for theAll -India Institute of Mental Health in Bangalore,India. A mental health programme in the EasternMediterranean was begun in Jordan (page 96).The programme on alcoholism in Europe is describedon page 92.
Continued interest has been shown in certainstudies carried out in previous years at Headquarters.The monograph, Maternal Care and Mental Health,for instance, originally published in English andFrench, has now been translated and publishedcommercially in three other languages (see page 53).In addition to large sales of the original, over 25 000copies have been sold of an abridged version inEnglish, which has been published commerciallyand is soon to be translated into Dutch.
Shortage of trained personnel and administratorsis one of the main handicaps to the development ofpublic- health and medical services to meet the specialneeds of mothers and children. Assistance fromWHO, in collaboration with UNICEF, has thereforebeen directed mainly towards helping governmentsto develop their training programmes for bothprofessional and auxiliary personnel. During theyear, UNICEF /WHO teams were provided to workwith national counterpart staff in demonstrationand training projects in Ceylon, India, Jordan,Libya and Turkey. Similar assistance was continuedin twenty other demonstration and training centresin sixteen countries. In seven of them the teamswere withdrawn after they had completed theirassignments, and the national staff assumed fullresponsibility for the programme.
1 See also Nursing, p. 24.
In India, the state Governments of Bihar, Hy-derabad, Travancore -Cochin, Uttar Pradesh andWest Bengal initiated comprehensive programmesfor co- ordinating and expanding their health ser-vices for mothers and children, and for improvingthe basic training of workers in this field. WHOand UNICEF are participating in this work, andwill also provide assistance to three more statesin India for similar projects planned to start in 1955.Progress has also been made in the maternal and childhealth programme in Bangkok, Thailand (page 80).The development of these and other similar pro-grammes increases the need for specialized post-graduate training in maternal and child health, andin the organization and administration of maternaland child health services within the general public -health programme. Facilities for such training are atpresent very limited. However, the Government ofIndia, with assistance from UNICEF and WHO,
PUBLIC -HEALTH SERVICES 23
is expanding the Department of Maternal and ChildHealth at the All -India Institute of Hygiene andPublic Health in Calcutta, to provide for post-graduate training of this nature, which, as it isbased on conditions common to many areas, will beof particular value to the Region.
Sound undergraduate and post -graduate trainingin paediatrics is a prerequisite for the developmentof comprehensive child health services. The improve-ment of such training has been included as part ofthe general programme in maternal and child healthin some projects in which WHO is assisting. Thestudy of paediatric education sponsored jointlyby WHO and the International Paediatric Associa-tion was continued during the year in most of thecountries of Europe, and was extended to coverAustralia and New Zealand. It is concerned withcourses in paediatrics for medical students, post-graduate training for physicians wishing to specializein paediatrics, and refresher courses for generalpractitioners. The final report is expected to beavailable by the end of 1955.
In accordance with a recommendation of the ExpertCommittee on Maternity Care, a meeting of anExpert Committee on Midwifery Training was heldduring 1954, with participants selected from theExpert Advisory Panels on Maternal and ChildHealth and on Nursing. At this meeting the Com-mittee drew attention to the need for a further studyof the problems connected with pregnancy and child-birth in different areas of the world (see also page 25).
The special needs of school -age children and howinter- agency co- operation might help to meet themwere the main topics of discussion at the third meetingof the inter -secretariat Technical Working Groupon Long -Range Activities for Children, a co-ordinating body of the United Nations and specializedagencies.
In the development of school health programmes,including health services and health education, thepart that can be played by the schoolteacher, ifgiven adequate training, is receiving fuller recogni-tion. In Thailand, for example, a pilot teacher -training project initiated by the Ministry of Educa-tion with assistance from UNESCO was expandedduring the year by the addition of WHO advisersin school health, provided at the request of theMinistry of Health. In Burma, Cambodia, HongKong, India, Indonesia, Libya, Pakistan and Taiwan,
particular efforts are being made by the nationalhealth administrations to promote health pro-grammes for school -age children as part of thegeneral child health services. A European Con-ference on School Health Services, organized byWHO's Regional Office for Europe, was held in Juneand attended by twenty -six participants (see page 91).
WHO has continued to assist several countries indeveloping their services for handicapped children.For an account of the project for the rehabilitationof crippled children in Israel, see page 99. Consul-tants were also sent to Austria, Greece, Italy andJapan.
Programmes have been developed in severalcountries to provide services for the care of prematureinfants. To make these services available throughoutthe countries concerned, a number of " prematureinfant units " have been established, each with astaff of specialists and provided with emergencytransport facilities. It has been shown that a relation-ship exists between the development of retrolentalfibroplasia, often resulting in blindness, in the pre-mature infant, and excess of oxygen supply duringthe neo -natal period, although it is recognized thatother factors probably influence the onset andseverity of the condition. UNICEF is sendingportable incubators, used mainly for long- distancetransport, to several countries, and WHO providedUNICEF with the necessary technical advice.
Co- operation with UNICEF in programmes ofmilk distribution (see pages 20 and 32) has alsogone forward during the year.
The Organization has maintained a close workingrelationship with the International Children's Centrein Paris. A representative of WHO was a memberof the Technical Advisory Committee of the Centre,and other staff members have been invited to parti-cipate in the planning of training and researchprogrammes in their special fields of interest.
With the development of many national trainingand service programmes in maternal and childhealth, trained workers will need opportunitiesto meet and discuss their problems and experiences.In this respect WHO can assist by stimulatinginterest in the conferences and seminars organizedon a country or regional basis, and by encouragingand helping governments to provide refresher coursesfor auxiliary and professional staff.
24 THE WORK OF WHO, 1954
V
Nursing
During the year assistance was continued to seven-teen schools of nursing and was given for the firsttime to five others. In Cambodia, Nepal and NorthBorneo, students had their first opportunity to enrolin recognized nursing courses in their own country.An account of progress made in the national schoolof nursing in Bolivia, which WHO has assisted since1953, is given on page 71, and the school of nursingin Kandy, Ceylon, is described on page 80. WHOprovided nine countries with nurse -midwives toorganize and give basic courses of midwifery training,and continued to help with the first courses forpublic -health nurses in Indonesia, Malaya andThailand. Indonesia also held the first course forinstructors in midwifery, and in many other countriesplans were made to establish courses for nursingand midwifery instructors in 1955. In severalcountries where, for economic reasons and becauseof shortage of personnel, it has not been possibleto establish complete training courses, short courseshave been organized for teachers, supervisors andadministrators of nursing services. All the trainingprogrammes have included staff education and in-service training, both in order to improve the nurses'services to the patient and to provide the studentnurses with more suitable clinical practice.
In most countries the services of fully trainedpersonnel must be supplemented by the use of auxi-liaries, who need training in the specific duties theyare to perform. It is accepted that auxiliaries shouldbe trained and supervised by fully trained staff ;therefore instruction in teaching and in supervisionmust form part of even the basic training of nursesand midwives. Emphasis has been placed on theteam approach, with professional and auxiliarypersonnel working together to meet the service needs.
In one country the type of auxiliary chosen fortraining with WHO assistance is the " health visitor "who, after a one -year course, is able to give teachingon health matters. In another country longer courses,which include more instruction in nursing and mid-wifery, are being given to " community healthvisitors ". This type of course may be used as a basisfor training a recognized professional worker skilledin nursing, midwifery and public health. A trend in
this direction is already noticeable in several newlydeveloping schools.
A serious shortage of basic texts in nursing andmidwifery persists in many countries ; WHO isattempting to help with this problem in some areas.In Taiwan internationally recruited and nationalnursing instructors have prepared manuals ofmedical, surgical and paediatric nursing in Chinesewhich will serve as basic texts for use in Chinese-
speaking countries. Manuals of paediatric nursinghave been similarly prepared in Afghanistan and inIndia. In many WHO- assisted schools mimeo-graphed material used for teaching notes is beingrevised and will eventually serve as a basis for manualsor texts applicable to the needs of the countriesconcerned.
In areas where educational facilities are limitedand where the status of nursing is low, there arefew opportunities to enter nursing for the youngwoman who is interested in continuing with highereducation. To help remedy the situation in theEastern Mediterranean Region, a Regional Collegeof Nursing has been established in association withthe University of Alexandria. The college will serveseveral countries of the Region and give Arabic -
speaking girls their first opportunity to study in theirown language for a degree in nursing. In the WesternPacific, WHO is also helping to establish a universitycourse for nurses in the National Taiwan University.
In many of the training programmes there has beena welcome increase in the number of male nursingstudents enrolled. The shortage of woman -poweravailable for nursing, which results in many countriesfrom the demands of industrial development or fromtraditional limitation on the extent to which womencan be employed, makes it impossible to obtainenough nursing recruits among women. In manycountries also, because of custom or religious beliefs,nursing is done by men, who all too frequently havenot had proper training.
The Organization has continued to assist in thepreparation of legislation related to nursing. Asurvey, published in the International Digest of HealthLegislation,' of the midwifery legislation in some
1 Int. Dig. Hlth Leg. 1954, 5, 433
PUBLIC-HEALTH SERVICES 25
thirty countries, should be of value to administrationsconsidering new or revised legislation for the controlof midwifery practice.
The theme -" The Nurse, Pioneer of Health "-for World Health Day, 1954, stimulated the interestof the public and of potential nursing students inmany countries.
In 1956 the technical discussions at the WorldHealth Assembly will be on " Nurses -their Educa-tion and their Role in Health Programmes ", andarrangements are being made for nurses and otherhealth workers in Member countries to participateearly in the preparatory work so that the discussionsmay be closely related to the programmes and needsof the individual countries.
With the assistance of grants from WHO, theInternational Council of Nurses has published fordistribution to Member countries the two reportsprepared in 1953.1 In the first, " An InternationalList of Advanced Programmes in Nursing Educa-tion ", detailed information on the training pro-grammes in countries providing post -basic educationfor graduate nurses has been assembled and madeavailable for the first time in one volume. Thesecond " How to Survey a School of Nursing ",describes the techniques suggested by reference tostudies made of five of the schools included in thelist referred to above. The aim was to providenursing schools with an adaptable system forevaluating their own programmes as a preliminaryto any necessary improvements.
The Expert Committee on Nursing, at its thirdsession in London from 29 March to 3 April, studied
problems in the administration of public- healthnursing services and nursing services in hospitals.A preparatory analysis of the conditions that makenursing administration difficult revealed three mainsources of trouble : lack of good human relation-ships, inadequate in- service education and un-satisfactory personnel policies. The Committee'sreport outlines the principles of administration andgives examples of their application in public- healthand hospital nursing.
Five nurse -midwives were members of the ExpertCommittee on Midwifery Training, which met inThe Hague from 2 to 7 August (see page 23). Itsreport describes basic training for midwifery per-sonnel at all levels and in all countries, but parti-cularly in those where a shortage of fully trainedworkers makes it necessary to staff the midwiferyservice largely with auxiliary personnel.
In the Eastern Mediterranean Region, a seminarfor midwives was held in Lebanon during the year(see page 95), and the European Regional Officeorganized a seminar on nursing in Istanbul.
In the national nursing programmes with whichWHO is assisting certain trends are noticeable, ofwhich the following are the most significant : long-term programmes are being planned more carefully ;there is a greater readiness to experiment in methodsand techniques in order to find those that are mostsuitable to the particular situation ; the close inter-dependence of nursing education and nursing serviceis being recognized more fully ; and, finally, auxiliarypersonnel are being more widely accepted as membersof the health team.
Health Education of the Public
The Organization, in furthering its objective ofhelping to strengthen national health programmes,has co- operated with governments to establish morecomprehensive services in health education, appro-priate to the interests, needs and cultural charac-teristic of the people and to the resources andfacilities available.
In 1954, WHO assisted twenty -five governmentsin planning and developing local and national healtheducation services as an integral part of healthprogrammes. The assistance was given by Head-quarters and the regional offices and by the assigningof personnel to demonstration and training pro-
1 See Off. Rec. Wld Hlth Org. 51, 30.
grammes. The importance of cultural factors hasbeen recognized in the programmes in which theOrganization has co- operated with Member States ;three full -time cultural anthropologists have con-tinued to assist health administrations and healthworkers with field studies, training projects and theplanning of educational aspects of health pro-grammes.
Regional health education conferences, similar tothose held in 1953 in Mexico and the United King-dom, were planned. A meeting was held in Lyons(France) to prepare for a second European conferencein 1956 which will study training in health educationof the public for health workers and teachers. FAOand WHO together planned a regional conference

26 THE WORK OP WHO, 1954
on health education and nutrition to be held in theWestern Pacific in 1955. Follow -up work of previousregional conferences was initiated in two regions, andassistance was provided in planning and organizingseminars and conferences on other technical subjects,such as the regional nursing seminar held in Turkey(see page 91).
Largely as a result of interest aroused by regionalconferences, national seminars in health educationwere organized in six countries.
The Expert Committee on Health Education of thePublic, at its first session in Paris in December 1953,paid particular attention to the role that schoolscan play in health education. It recommended thatWHO, with UNESCO, should explore methodsfor developing training in health education in teacher -training institutions, colleges and universities.' Thetwo organizations have started to compile data onthe training in health education now given toteachers, as a preliminary to future study groups andconferences on this problem.
Much can be done through the existing channelsof WHO to foster the further development of soundhealth programmes for school -age children. Duringthe year, several health and education authorities-both national and local- conducted seminars,refresher courses and training programmes on theopportunities for health education in schools, theresponsibilities of school- teachers in regard to healtheducation, and the training they require.
Post -graduate training, such as that provided byinstitutes or schools of public health, affords avaluable opportunity for training health personnel inthe principles and procedures of health education ofthe public. The Organization has co- operated withthe Government of India in preparing, at the All -India Institute of Hygiene and Public Health inCalcutta, the courses on health education for diplomastudents in public- health administration, public -health nursing, maternal and child health andindustrial hygiene. At the University of Malaya, inSingapore, WHO's assistance in health educationended in July. The work is being continued under
the guidance of a trained worker appointed by theGovernment. At the School of Public Health inTurkey a consultant assisted with a training coursefor public- health medical officers.
WHO participated in a meeting on curriculumplanning at the University of London Institute ofEducation, where, during the autumn term a diplomacourse in health education was organized for thefirst time, in co- operation with the London Schoolof Hygiene and Tropical Medicine, the CentralCouncil for Health Education and the Institute ofChild Health (see also page 91).
Some Member States have expressed the need fortraining in health education a nucleus of professionalworkers who will then help with the training of healthand educational personnel and with the planningand organization of more comprehensive healtheducation services as part of the national healthprogrammes As in previous years, the Organizationhas granted fellowships for graduate study in healtheducation of the public for periods ranging from afew months to a year.
The Organization continued to assist the UnitedNations Relief and Works Agency for PalestineRefugees iñ the Near East in training a small groupof health education workers among the Arab refugees.The first course was satisfactory and a similar coursefor a second group of students was started inNovember -again with help from WHO.
WHO has continued its health education work inthe various programmes for community developmentand fundamental education being carried on by theUnited Nations, UNESCO and other specializedagencies.
The Organization was associated with planning forthe third international conference of the InternationalUnion for Health Education of the Public, to beconvened in Rome, Italy, in 1956. Representativesof WHO also took part in the meeting of the HealthAdvisory Committee of the League of Red CrossSocieties, held in Oslo, Norway, in May, wherehealth education of the public was one of the twomain subjects of discussion.
Social and Occupational Health
Because of the wide range of subjects dealt withunder this heading, the WHO Expert Advisory Panelon Social and Occupational Health was replacedin 1954 by four expert advisory panels ; one on the
1 Wld Hlth Org. techn. Rep. Ser. 1954, 89, 34
Organization of Medical Care, one on OccupationalHealth, one on Chronic Degenerative Diseases, andone on Rehabilitation. For the present, the ExpertAdvisory Panel on Occupational Health will beconcerned with the hygiene of seafarers ; that on theOrganization of Medical Care with hospital planning

PUBLIC -HEALTH SERVICES 27
and administration ; that on Chronic DegenerativeDiseases with the rheumatic group of diseases,cardiovascular diseases, etc., and that on Rehabilita-tion with prosthetics.
Organization of Medical Care
The organization of medical care is becomingmore and more important to a number of countrieswhere the health services are reaching new stagesof development. The considerable funds devoted tocurative medicine, even by low- income countries,might serve public- health purposes if advantage weretaken of the possibility of familiarizing hospitalpatients and their families with simple requirementsof health, and if out -patient departments alsoparticipated in preventive medicine. Much moneycan be saved by developing domiciliary medicalservices sufficiently to provide care in their homes-instead of in hospital -for all patients who do notdefinitely need hospital treatment.
WHO has continued its assistance to certaingovernments on various aspects of hospital planningand administration, for example, the project forreorganizing medical store management in Ceylon,and the project in Turkey on hospital constructionand administration. Similar programmes in othercountries are now at the planning stage.
Plans are being made to convene a meeting of anexpert committee on the organization of medicalcare in 1956. A WHO monograph L'hôpital rural'was published in French and an English edition isin preparation.
Occupational Health
By approving the Director -General's report on" Measures for strengthening occupational healthactivities " 2 the Executive Board laid down thelines for WHO's own programme and for its co-operation with ILO on this subject. WHO is concernedwith two aspects : stimulating the interest of nationaladministrations and the medical profession inproblems of occupational health, and trainingpersonnel for industrial health services. To staff anational programme of occupational health it isnecessary for physicians to be given a knowledgeof industrial problems, for engineers to have some
' Bridgman, R. F. (1954) L'hôpital rural, Genève (Organi-sation Mondiale de la Santé: Série de Monographies N° 21).
2 Of Rec. Wld Hlth Org. 52, 131
knowledge of requirements of health, and for nursesto be trained in human relations in industry. Totrain more personnel for industrial medical services,occupational health institutes are being establishedin various parts of the world, starting with Egypt,Indonesia and India.
The professor in industrial hygiene and physiologyprovided by WHO for the All -India Institute ofPublic Health in Calcutta finished his work inAugust 1954. This project laid the foundations for apermanent centre for teaching and research, operatingunder the responsibility of the national authority.
A report on the development of occupationalhealth services was completed by a WHO consultant.
An inter -agency working party, including represen-tatives of the secretariats of ILO and WHO, met inFebruary, at the request of the Universal PostalUnion (UPU) to discuss the occupational risks ofpostal workers, and prepared a questionnaire forcirculation by UPU to its Member States.
At the request of the Executive Board (resolutionEB 13. R54), WHO started a study of measures forprotecting workers and the general populationagainst x -rays and radiation from radioactiveisotopes. Member States were asked for informationon national legislation and regulations.
Hygiene of Seafarers
The Joint ILO /WHO Committee on the Hygieneof Seafarers agreed -at its second session in April -that the existing facilities for providing medicaladvice by radio to ships at sea were generally satis-factory ; nevertheless it recommended some furthermeasures for their improvement. It approved forthe guidance of governments standard recommenda-tions on the contents and uses of medicine chests onships not carrying doctors, and suggested a minimallist of medicaments. It also recommended that newentrants to merchant navies should be examined fortuberculosis, and that periodical re- examinationsshould be encouraged through a continuing campaignof health education. The great improvement in thecontrol of venereal diseases amongst seafarers wasnoted.
Medical Rehabilitation of the Physically Handicapped
WHO continued various activities relating to themedical rehabilitation of the physically handicapped,both at Headquarters and in the regions. In August
28 THE WORK OF WHO, 1954
a consultant group on prosthetics was convened, inwhich the United Nations, ILO, UNESCO andother interested agencies, such as the InternationalSociety for the Welfare of Cripples and the WorldVeterans Federation, were also invited to take part.This group, which met in Copenhagen, reviewedthe causes and prevention of amputations and theprinciples and practices for the rehabilitation of theamputee, with special reference to prosthetic appli-ances. Simplified artificial limbs for use in tech-nologically less advanced countries were also recom-mended. A report of the conference is being publishedin the Technical Report Series.
WHO also participated in the fifth session of thead hoc Technical Working Party on the Rehabilita-tion of the Physically Handicapped, set up by theAdministrative Committee on Co- ordination. Aninternational programme for the education andrehabilitation of the deaf and partially deaf wasamong the items discussed.
The Organization has continued to support fieldrehabilitation projects- sometimes with supplies andequipment provided by UNICEF -for physicallydisabled adults and children, in Greece, India, Israel(see also page 99), Italy and Japan. With the UnitedNations Technical Assistance Administration, WHOhas given advice on similar projects in Guatemala,Indonesia and Venezuela. A survey is being made
in Turkey as a preliminary to the preparation offuture rehabilitation programmes.
Rheumatic DiseasesThe Expert Committee on Rheumatic Diseases,
in its first report,' recommended that WHO shouldstudy the problem of preventing rheumatic feverand its implications. Preliminary steps have sincebeen taken to initiate a study of the epidemiology ofthis disease with reference to its cardiovascular andother implications ; the information available on thissubject will now be collected.
Other SubjectsWork on the medical aspects of migration was
also continued. WHO collaborated with ILO andthe Intergovernmental Committee for EuropeanMigration in preparing a report of the meeting ofexperts on the medical selection of migrants (seeAnnual Report for 1953 2), which was submittedto the fourteenth session of the Executive Board.In accordance with the decision of the Board (resolu-tion EB14.R18), the report was communicated toMember governments for consideration in connexionwith the medical examination of migrants who areto carry out ordinary or heavy work or work requiringspecial physical ability.
Dental Health
More governments have expressed interest inproblems of dental health and in the organizationof dental health services. Following a discussion onthis subject in the Health Assembly and the ExecutiveBoard, a meeting of a consultant group was convenedto consider the main problems in dental health, andto advise the Director - General on the lines alongwhich the World Health Organization's programmemight be developed. Representatives of the Fédéra-
tion dentaire internationale and the Kellogg Founda-tion participated in this meeting.
A dental health seminar organized by WHO inNew Zealand in September was attended by thirty -seven members from three regions (see also page 105).A final report of this seminar has been compiled.It is planned to send a consultant in 1955 to someof the countries represented at the seminar.
Health Work among Palestine Refugees 8
The Seventh World Health Assembly, in resolutionWHA7.11, extended the 1950 agreement with theUnited Nations Relief and Works Agency for
1 Wld Hlth Org. techn. Rep. Ser. 1954; 782 O$: Rec. Wld Hlth Org. 51, 31
Palestine Refugees in the Near East (UNRWA) to30 June 1955. The Organization has accordinglycontinued to plan and direct UNRWA's health
8 Full accounts of the health work of UNRWA can be foundin the annual report of its Health Division, obtainable fromits office in Beirut.
PUBLIC- HEALTH SERVICES 29
programme, as described in the Annual Reportfor 1953,1 and in addition to a full -time medicalofficer, malariologist, public- health engineer andconsultants, has, in 1954, under the terms of ajoint project referred to below, also provided ahealth educator. A grant of $42 857 was again made.
During the twelve months from 1 July 1953 to30 June 1954 the total cost to UNRWA of theprogrammes with which WHO has assisted was$5 064 626. This sum includes $1 975 691 in respectof general health services, personnel, supplies,clinics, institutions, etc., and $1 625 573 in respectof environmental sanitation, camp maintenance andnew housing. These figures show an increase ofapproximately $300 000 (mainly for housing) overthe previous year's expenditure. Responsibility forsupplementary feeding and milk distribution pro-grammes was transferred to the Health Divisionfor the first time and expenditure on these itemsamounted to $1 463 362.
The increase in the number of persons employedin the Health Division, from some 1800 persons inJune 1953 to 2900 in June 1954, was largely due tothe transfer of the workers in the various nutritionalprogrammes. Eighteen of these are internationalstaff members, the remainder local employees -mainly Palestine refugees.
The host governments and voluntary societies gavevaluable assistance in the running of hospitals, clinicsand maternity and child health services, and inorganizing and carrying out various trainingprogrammes.
The general health of the refugees remained goodthroughout the year. None of the quarantinablediseases was reported. There were, however, 88 casesof tick -borne relapsing fever, 84 of which occurredin Jordan, and 26 cases of poliomyelitis, 22 of whichwere in Jordan. Measles, pertussis and varicellaoutbreaks of moderate intensity occurred during theautumn and spring ; the incidence of diphtheria(77 cases) and of the enteric group of fevers (1010)was less than in the previous year, especially amongcamp residents. The decrease was due to the highproportion of persons protected by immunizationand to the control of water supplies. Trachoma wasstill widespread, and acute conjunctivitis was muchin evidence during the summer months. The numberof cases of tuberculosis reported again decreased-to about 64 per cent. of the number reportedduring the previous twelve months -but the incidenceof infections occurring among the close contacts ofopen cases remains high. Hospital facilities are still
1 Off Rec. Wld Hlth Org. 51, 33
inadequate, and satisfactory isolation of open casesis frequently impossible.
The joint UNRWA /WHO training project inhealth education (started in 1953) 2 progressedduring the year, and nine students completed theirsix months of academic training and their six monthsof field training. Eleven other students began theiryear's training course. In addition to the healtheducator, the Organization is providing funds forfellowships for trainees, teaching equipment andeducational supplies ; UNRWA is contributing fieldtraining allowances, administrative supplies andinstructors.
As a result of this joint training project, twentyhealth educators are expected to be available forservice in 1955, among the refugee communitiesand with local health authorities.
As in past years, the use of prophylactic immuniza-tion has been continued in order to maintain immunityto infectious diseases at as high a level as possible.During a 12 -month period some 244 000 smallpoxvaccinations, 286 000 TAB inoculations and 163 000diphtheria inoculations were carried out.
The malaria control programme was continuedduring the year. In the Gaza district, which hasbeen free from anophelines since their eradicationin 1947, antilarval measures were directed againstnuisance mosquitos. Elsewhere WHO has closelyco- operated with the governments in residualspraying campaigns of malarious areas. The Yarmuk-Jordan antimalaria project is being implementedjointly with the Jordanian Government under thetechnical direction of the UNRWA /WHO malario-logist, and with the help of an entomologist and agroup of malaria inspectors. It has now been inoperation for almost two years. Each year therehas been DDT- residual spraying of malarioussettlements in the spring and, for a period of eightmonths, an intensive weekly larvicidal campaigncovering the Yarmuk- Jordan Valleys. The successof these control measures has been shown by amarked decrease in the number of patients withsymptoms of clinical malaria. The agreementbetween UNRWA and the Government in respect ofthis project has recently been extended for afurther five years.
A survey by WHO and FAO consultants showedthat the nutritional level of the refugees was sub-stantially the same as in 1953. There was, however,some early evidence of vitamin -A deficiency amongschoolchildren. The enrichment with vitamin A ofthe reconstituted milk supplied to all the children
2 See Off. Rec. Wld Hlth Org. 51, 34.
30 THE WORK OF WHO, 1954
is being considered and experiments carried out.Much importance is being attached to the supple-mentary feeding and milk distribution programmes,as they are fundamental to the safeguarding of thenutritional status of vulnerable groups. The scalesof issue, for the basic food ration and for supple-mentary rations, have been modified in order tointroduce local foodstuffs, such as burghol (soakedoats), and to make more petty cash available forthe purchase of fresh food -meat, vegetables, fruitand eggs -to be used in the supplementary feedingof those selected by the camp doctors.
A school -health service was started at the beginningof the 1954 -55 scholastic year. It consists of sixhealth teams proportionately distributed throughoutthe various countries, to care for the 110 000 refugeechildren being educated in the Agency's schools.
The training of selected refugees as auxiliarymedical workers was continued. Courses were con-ducted for general nurses, public health, mentalhealth, and tuberculosis nurses, malaria inspectors,laboratory technicians, assistant pharmacists, sanitaryinspectors, medical orderlies and midwives. In 1954,204 refugees were trained or being trained in para-medical subjects, as compared with 147 in 1953.
Ninety UNRWA clinics -an increase of ninesince 1953 -now serve the refugees, and over 2000
hospital beds are available for their treatment. Thenumbers of refugees per available hospital bed inLebanon, Gaza, Syria and Jordan are now 313,327, 475 and 524 respectively.
The Sanitation and Camp Maintenance Branch ofthe Health Division has the responsibility for pro-viding an adequate water supply, ensuring safe wastedisposal and carrying on work in insect controlunder the direction of the epidemiologist. Thisbranch also maintains refugee shelters and UNRWAinstallations in camps. The gradual replacement ofpit latrines by septic tanks was successfully continuedduring the year. Routine bacteriological examina-tions of water supplies were conducted, and thenumber of chlorinated supplies increased. Tentaccommodation is gradually being replaced by hutsbuilt by UNRWA or the refugees themselves :only huts are being built as new shelters. Of thetotal refugee population of 884 700 in mid -1954,some 324 700 (i.e., 36.8 per cent. of the population)live in or around the fifty -eight UNRWA camps,the remainder being accommodated in villages andtowns.
During the year a procurement programme formedical and sanitation supplies in the amount of$680 000 was implemented through UNICEF.
CHAPTER 3
ENVIRONMENTAL SANITATION
The Seventh World Health Assembly, in resolutionWHA7.53, called for more leadership from WHOin environmental sanitation and suggested thatMember States should be encouraged to give dueprominence to sanitation in their health programmes.Some of the general problems to be dealt with are(1) the disposal of sewage, excreta and refuse in asafe and practical manner, both from communitiesand, more pressingly, from rural households ;(2) the development of supplies of safe and suitabledrinking -water ; (3) the supply of uncontaminatedmilk and other food, which involves suitable pro-visions for cleanliness in processing, storing, handling,preparing and serving ; (4) vector control, includingthe specification, handling and use of insecticides,rodenticides and molluscocides and the equipmentor methods for their application ; (5) the healthaspects of housing and town and country planning ;and (6) the protection of industrial workers and thegeneral public from atmospheric pollution orunhealthy industrial environment. The ExecutiveBoard, in resolution EB14.R21, focused attention onthe importance of safe water supplies and the dis-posal of human waste and refuse, and requested theDirector - General, through the regional organiza-tions, to study and report on ways of stimulatinglocal action on these problems. The study wassubmitted to the Executive Board at its fifteenthsession.
In 1954 WHO continued its work in environ-mental sanitation : it gave advisory services tocountries, collaborated with the United Nations,specialized agencies and other agencies workingin international public health, and made environ-mental sanitation an integral part of its work onother more specialized public- health problems,particularly on the control of communicable diseasesand the organization of public- health services.
The scarcity of qualified personnel in sanitationremains a pressing problem. Stress is, therefore,being laid on the training of sanitary engineers andother workers : two instructors are being recruitedto organize courses in sanitary engineering in Egypt
and India, seminars on sanitary engineering wereheld in Central and South America during the year(see page 71), and WHO is helping to extend theteaching of sanitation in medical schools. Specialattention has been given to this subject by theRegional Office for Europe ; its programme isdescribed in detail on page 92.
One of the most important advances of the yearwas the progress made in the UNICEF -aided pro-jects in environmental sanitation, for which WHOgives technical advice and assistance. In 1953 theUNICEF Executive Board, on the recommendationof the Joint Committee on Health Policy, agreedthat UNICEF should undertake work in environ-mental sanitation since in so doing it would becontributing directly to the protection of children'shealth. Environmental sanitation forms part ofprojects being undertaken or planned with the assis-tance of the two organizations in Colombia, Peru,Burma and Ceylon. Rural sanitation projectsinclude work on drinking -water and the properdisposal of excreta and refuse, and extend to healtheducation and the training of various classes ofpersonnel.
The importance of improving rural sanitationhas been emphasized by both the Health Assemblyand the Executive Board, and formed a part of thetopic for the technical discussions at the SeventhWorld Health Assembly. WHO has given directassistance to governments in preparing and advancingprojects in rural sanitation. It has also preparedin draft form manuals on rural water supply andexcreta disposal in rural areas which emphasize thefundamental principles of techniques and organi-zation and give examples of the application of theseprinciples under various conditions.
A similar manual on refuse disposal, also in pre-paration, deals with the theory and practice of theproduction and use of compost, and touches uponthe health and economic problems involved. Thetext has been discussed with FAO, and submit-ted in draft to experts in many parts of theworld.
- 31 -
32 THE WORK OF WHO, 1954
WHO continued the world -wide survey, startedin 1953, of current practices in the sanitary examina-tion of water and of standards of drinking -waterquality. Considerable interest has been shown. Theinformation provided by seventy -one countries hasbeen collected, analysed and distributed through theregional offices, for discussion by regional groups.The European Region has already held the firstmeeting, and meetings in other regions will followin 1955. After the regional discussions it is plannedto convene a group of experts to discuss the questionon a world -wide basis. It is hoped that the prepara-tion and distribution of a realistic and acceptable setof water -quality standards and an accompanyingseries of uniform methods for laboratory examina-tions may encourage their general acceptance.
Work on milk sanitation has gone forward duringthe year, particularly through the collaboration ofthe secretariats of FAO, UNICEF and WHO in aninter - agency working group. In drafting milklegislation, there have been several instances in thepast where countries have adhered closely to modelmilk laws developed for countries where milktechnology is more advanced. This had led to greatdifficulty in enforcement and FAO, UNICEF andWHO are working together to lay down basicprinciples that countries can safely follow in prepar-ing milk legislation that is applicable to their ownspecial situations. WHO has also appointed aconsultant on milk legislation to advise the healthauthorities of two countries in South -East Asia,and to assist with the regional programme. Otherresults of inter -agency collaboration were the milkstudy- course in Bombay on milk problems in tro-pical areas which was sponsored by FAO and theGovernment of India, with assistance from UNICEFand WHO, and the assistance given to the Govern-ment of Egypt in developing its own milkindustry.
Vector control, as a means of preventing the spreadof certain diseases, has been an important activity.The way in which the Expert Advisory Panel onInsecticides has participated in the work of WHO byundertaking research, evaluating results, givingscientific opinions and stimulating continual advancesin field activities, is a good example of how theworld's expert knowledge can be used in WHO'sprogrammes. Specific studies have dealt with theresistance of lice to DDT and other insecticides, thetoxicity of insecticides to man, and the effects oftropical storage on the physical characteristics ofinsecticide formulations. Much work has also beendone on the development and improvement ofequipment for dispersing or applying insecticides
and molluscocides in the field. The studies ofthe resistance of lice to DDT and certain otherinsecticides, begun in 1953, have already shownthat there are resistant strains in Egypt, Ethiopiaand South Africa. The field test kits mentionedin the Annual Report for 1953 are now beingdistributed to forty -six countries. The ExpertCommittee on Insecticides, at its fifth session, heldin Caracas (Venezuela), in September, for the firsttime included in its report specifications for a body -dusting powder to be used against lice which areresistant to chlorinated hydrocarbons.
In Egypt, Iran and Israel and in the refugee campsadministered by the United Nations Relief and WorksAgency for Palestine Refugees in the Near East,studies were made during the year of the work ininsect control, the co- ordination of WHO's workwith that of several entomological research andtraining institutions, and the use of new materials,new equipment and new techniques. These studieswere carried out by staff from Headquarters andthe Regional Office for the Eastern Mediterranean.
WHO has continued to pay attention to the healthaspects of housing by sending representatives tomeetings, and by preparing technical papers for theUnited Nations economic commissions.
In industrial hygiene, WHO works closely withILO, which has a long- established programme forimproving the industrial environment (see alsopage 27). Assistance was also given for the meetingof a Committee of Experts on the Transport ofDangerous Goods, a committee of the Economicand Social Council's Transport and CommunicationsCommission.
In the future, it is expected that WHO will be ablegreatly to advance its aims by continuing to assistgovernments to plan and develop effective servicesin urban and rural sanitation and to integratethese services into their expanding health organiza-tion. The great need for improved sanitation in allthe regions is stressed in Part II of this report.
The role that trained and experienced people canplay in improving environmental sanitation incountries is illustrated by the great influence thateven a single consultant has been shown to have onnational programmes. This influence has beenparticularly apparent in Burma, Ceylon and Indo-nesia where the Governments, on the basis of recom-mendations of an adviser from Headquarters, arestarting in 1955 large projects for the organizationof sanitation services and programmes for sanitationwork. WHO is assisting with similar programmesin North Borneo and Taiwan -also resulting fromthe advice of consultants.
CHAPTER 4
EDUCATION AND TRAINING
Work on education and training has continued to be guided by the Executive Board's organizationalstudy on this subject, which was discussed by the World Health Assembly in 1953. The two main aspectsof the work have been assistance to countries in solving their own training problems and promotion ofcertain principles in education which have emerged from international studies or are favoured by recenttrends and experience.
The Organization has continued to strengthen national training institutions by awarding fellowships,promoting the exchange of information, and providing visiting teaching personnel, teaching supplies andadvice -as described in more detail below. Such assistance has been given to medical, nursing, public -health and other schools for health workers in almost all the regions. In some cases, WHO has supportedinstitutions or courses which have been organized or are being maintained jointly by several countries :examples are the regional college for advanced nursing education in Egypt, the Inter -American Centre ofBiostatistics in Chile and the public- health training courses for Scandinavian countries. Assistance hasbeen given to international courses on such subjects as child health, health statistics, environmental sanitation,anaesthesiology, nursing and health education. Certain national courses have also been assisted. Anotherform of activity, particularly used in the European Region, has again been the international seminar orconference, which provides an opportunity for an exchange of experience among senior professional men.In 1954, about 200 projects -approximately 40 per cent. of all those in which the Organization assisted duringthe year -were mainly for training purposes (for list of projects, see Part IV). This figure does not includeprojects primarily concerned with other work, in which fellowships have been used as a supporting method,but only those of which training was one of the predominant objectives. In the Eastern MediterraneanRegion projects of this type made up some 25 per cent. of the total ; in South -East Asia they amounted to40 per cent. ; in Europe over 50 per cent., and they ranged between 25 and 35 per cent. in the other regions.
In order to analyse educational trends and formulate principles emerging from them, expert committeesof WHO have over the past few years reviewed medical education, nursing education and the training ofsanitary engineers, as well as problems of training in some of the more specialized subjects within these broadcategories. In November 1954, there was a meeting of an Expert Committee on Midwifery Training (seepage 25), and the report of the expert committee dealing with training in health education was published.1Progress was made in two studies : one on paediatric education undertaken jointly by WHO and the Inter-national Paediatric Association, part of which, relating to Europe, is expected to be completed in 1955 ; anda second resulting from the two conferences organized in 1952 and 1953, on the teaching of preventive medicine,hygiene and public health. WHO held informal discussions with the World Medical Association on possibleco- operation in their second world conference on medical education, which will discuss in 1959 some selectedproblems of post -graduate education.
In the light of the experience and knowledge gained from some international studies and from directco- operation with governments on their specific educational problems, WHO is undertaking an analysisof medical education on a regional basis, with suggestions for future developments. South -East Asia wasthe first region chosen because of the attention which it has given to the subject and the amount of informationavailable. A summary of the analysis of medical education in this region (described in detail on page 35)was discussed at the September session of the Regional Committee, which adopted a resolution recognizingand defining the urgent needs in training, and recommending certain action to be taken by WHO and bygovernments in the Region to meet them. The separate studies on medical education in the individualcountries of the Region, which are attached to this analysis, are being circulated to governments, agencies
1 Wld Hlth Org. techn. Rep. Ser. 1954, 89
- 33 -

34 THE WORK OF WHO, 1954
and interested persons to serve as a guide in the assessment of national problems and as a basis for co- operativeaction in developing medical education in these countries. This method of long -term planning may, ifsuccessful, be followed in other regions, with help from the governments of the countries concerned andfrom interested agencies.
Thé Fellowships Programme
Since the inception of the programme in 1947,WHO has awarded 4416 fellowships, of which 667were awarded in 1954 (for details, see Annex 11).
Again the tendency was to place a high proportionof the fellows for study in their own region : in 1954,regional fellowships accounted for 68 per cent. ofthe total awarded, while from 1947 to 1951 the percen-tage was only 55. This increase has been made possibleby a more systematic use of existing facilities and theestablishment of new courses, some of them per-manent. Regional fellowships, apart from theobvious saving in travel expenditure, have theadvantage of enabling fellows to study under condi-tions similar to those in their own countries, sothat the process of adapting their acquired knowledgeto their home environment is easier.
Of the fellowships awarded in 1954, 144 (or 22per cent.) were for 14 group training programmes(courses, etc.) organized or assisted by WHO.These figures do not include 13 educational meetings,where there was no formal differentiation betweenteachers and trainees, the 308 participants in suchmeetings, or the 5 national courses organized withthe assistance of WHO under resolution WHA6.35,which were attended by 79 nationals whose main-tenance and travel costs were paid by WHO. Thesespecial fellowships for national courses have beenawarded since 1951, and were first provided for inthe programme approved by the Third World HealthAssembly.'
WHO fellows studied in 72 countries, about four -fifths of the fellows being placed in the followingseventeen countries : the United Kingdom of GreatBritain and Northern Ireland, France, the UnitedStates of America, Sweden, Netherlands, Denmark,Chile, Switzerland, Egypt, Norway, India, Turkey,Italy, Federal Republic of Germany, Finland,Lebanon, Canada.
Most WHO fellows studied in 1954 subjectsrelated to public- health organization and allied
1 Off. Rec. Wld Hlth Org. 23, 162-163
services : public -health administration (17 per cent.),sanitation (7 per cent.), nursing (7 per cent.),maternal and child health (7 per cent.) and othermore specialized health services (16 per cent.),control of communicable diseases (33 per cent.).The studies of the remaining 13 per cent. were inmedical education, basic medical sciences and variousaspects of clinical medicine.
To assist the staff of the regional offices in helpingthe candidate and his administration to choose placesof study, a " Record of Training Facilities utilizedby 1,100 Fellows, 1951/1952 " was prepared. Thisrecord is being supplemented by current informationon training facilities, as data become available.
A review was begun of various procedures whichhave not been entirely satisfactory : this has includedconsideration of the timing of applications forfellowships in order to permit adequate planningand preparation ; methods of testing the candidate'sknowledge of the language of his prospective courseof study, and arrangements for visiting the fellowsduring their study period.
An earlier submission of applications for fellow-ships has facilitated the necessary planning for theinterviewing of candidates and the detailed discussionwith the fellow of plans for his study and futurework. Improved arrangements are being made forvisiting fellows -particularly those in one place forlong courses -during their period of study abroad,in order to smooth out difficulties and provide forany necessary adjustment in the programme ofstudy. Hitherto it has not been possible to dothis systematically and the responsibility has some-times been undertaken by a member of the nationalhealth administration of the country of study. In1954, however, the Regional Office for the Americasand the Foreign Operations Administration (FOA)-which has a large fellowship programme- agreedto make joint plans in order to ensure that as manyof their fellows as possible would be visited by repre-sentatives of either FOA or WHO.
EDUCATION AND TRAINING 35
Attention is again called to the extreme difficultyof assessing the value of fellowships in any preciseway. Joint efforts of the United Nations agenciesto arrive at some satisfactory criteria for a successfulfellowship are continuing.
In 1953, a first experimental attempt was madeby WHO to evaluate the fellowships awarded from1947 to 1949.1 Such an evaluation can be madeonly after a certain lapse of time, since it is basedon two annual reports by the fellow on his work inhis own country, and a statement by the govern-ment -two years after his return -on the use madeof his services.
In 1954 a further effort at evaluation was made.The required reports were obtained and other datacollected and evaluated by the regional offices ; and,with the co- operation of national health administra-tions, a consultant from Headquarters met about600 fellows in eleven countries -Austria, Egypt,Finland, Greece, Israel, Italy, Lebanon, Norway,Sweden, Syria and Yugoslavia.
A detailed report is being prepared on the basisof the information collected : in general, the findingsdiffer little from those of the preliminary study.The results of what can be classed as successfulfellowships differ considerably. Some fellows re-cognize that their specialized knowledge was formedmainly by their studies abroad. To the somewhat
more junior group of post -graduate fellows, oneyear of systematic studies, in public health, forinstance, has very often given decisive direction forthe rest of their careers. For a number of organizersand research workers the international contacts madeduring the fellowship have provided real initiationinto a broader outlook on their work. Fellows havebrought back many new techniques, have startedspecialized activities -often for the first time -intheir countries ; have trained personnel to take overthe work initiated by foreign specialists, and insome cases, have influenced the health legislation oftheir governments.
Relatively few fellowships can be classified aswholly unsuccessful : most WHO fellows are phy-sicians, nurses or sanitarians, already pre -selectedthrough long studies and vocational calling, andmany of them have long- standing professionalcareers. Only a few of the fellowships that mustbe classified as wasted on account of " forcemajeure "- death, sickness, political changes, etc.- or personal incompatibility could be prevented bybetter selection and more thorough medical examina-tion. It has been found that it is easier for govern-ments to use fellows effectively, on their return,when the fellowship has formed part of a plannedprogramme for the development of a particularaspect of the public -health services.
Exchange of Scientific
The exchange of scientific information is a pro-minent feature of virtually all the technical activitiesof WHO. It naturally develops whenever theOrganization establishes international scientific con-tacts in the course of its routine functions ; but itis more actively promoted by specifically designedprojects, such as the various kinds of scientificmeetings being organized on an increasing numberof subjects. The primary purpose of exchangingscientific information may differ in particularinstances : sometimes such exchange may aim atincreasing the available body of scientific knowledge ;sometimes it may aim at specific improvements inpublic- health practice and the care of the sick ;again, it may serve as an essential feature of medicaleducation aimed at improving the standards ofacademic teaching staffs. Only the medical educa-tional aspects of the exchange of scientific informa-tion are dealt with here.
1 See the Annual Report for that year, Of Rec. WldHith Org. 51, 38.
Information
Between 1950 and 1953 seminars, symposia, andvisiting teams of medical scientists were organized topromote the exchange of scientific information inthe basic medical sciences, in the clinical disciplinesand in the preventive, socio- medical and public -health specialties, by personal contacts among aca-demic teaching staffs and research workers. Exten-sive reports on these activities from consultants andstaff resulted in an accumulation of information onmany aspects of medical education in different partsof the world, and in the South -East Asia Region inparticular. In 1954 this material provided the basisfor a comprehensive analytical study of medicaleducation in South -East Asia.
The underlying purpose of this study is to assistin alleviating the shortage of medical manpower,which is believed to be one of the main obstacles-if not the main one -to the implementation ofotherwise feasible health programmes urgently neededin the Region. Since medical schools are the onlysource of trained medical personnel, the various
36 THE WORK OF WHO, 1954
problems of these schools are considered in relationto the national long -range health programme. Theshortage of teaching personnel, especially in thebasic medical sciences, is, for instance, shown as aproblem of far greater significance and urgency thanis generally recognized. The attention of govern-ments is called to the fact that without an increasein the teaching staffs the capacity and output ofthe existing medical schools cannot be increased,new schools cannot be founded, and the road to aquantitative solution of the medical manpowerproblem will remain blocked.
The qualitative aspect of the medical manpowerproblem is also treated, the premise being thatmedical education and training in any countryshould conform to its specific needs. It is proposedthat the desirable system of medical educationfor South -East Asia should give proper emphasisto the preventive aspects of medical work. Theprinciple stressed in this connexion is that inany part of the world where populations remainexposed to elementary public- health hazards, im-provements in individual curative care alone cannotbe expected to raise appreciably the general standardof health. Therefore the necessity for a certainreorientation of the medical schools and for re-adjustments of the medical curriculum is pointedout ; technical and organizational changes aresuggested ; the social and economic, as well asprofessional, aspects of such changes are explored,and detailed recommendations are made on what isthought to be a practical approach to overcomingadministrative difficulties and bringing about thesuggested reforms.
The general study will be complemented by aseries of detailed country studies, of which the oneon Burma was completed in 1954, and that onIndonesia almost completed. The country studiesoutline programmes, of from five to ten years, inmedical education which could be carried out by theco- ordinated efforts of governments and all foreignand international agencies concerned with medicaleducation. In this respect the study should make anappreciable contribution to programme planning.
By far the greater part of medical research isconducted in universities, in which teaching andresearch functions are inextricably interwoven ; andwithout facilities for medical research the standardof medical schools cannot be raised from the voca-tional to the academic level, particularly in countrieswhich have hitherto not had to rely on their ownresearch resources. The stimulation and promotionof research, therefore, have become an ever -growingconcern in educational programmes. WHO, besides
the attention it has given to this problem in theprogrammes of the visiting teams of medical scientistsand consequently in the study mentioned above,assisted the Council for the International Organiza-tion of Medical Sciences (see below) in organizingin London, in October, a first international conferenceof national research councils. The Conference'sreport on methods of selecting, training and usingresearch workers should, when published, prove ofconsiderable practical use to all countries.
For the same purpose, WHO also initiated a newscheme of exchange of research workers. Threeseparate projects were developed in this programme.The aim of the first, now completed, was to clarifydivergent views on some of the fundamentals in theunderstanding of the pathology of trachoma. Asmentioned in Chapter 1, page 15, specialists fromEgypt, Iran, Japan, Morocco (French Zone) andTunisia took part in the programme : they visitedone another's laboratories, reviewed the materialavailable, made joint field visits to trachoma controlprojects in their respective areas, and submittedreports on the results of their investigations.
The second project has for objective the com-parison of the methods and results of research intocancer of the liver in Africa, being conducted con-currently but independently at the Institut desHautes Etudes de Dakar (Ecole préparatoire deMédecine et de Pharmacie) and at the University ofWitwatersrand, Johannesburg.
The purpose of the third project, a co- operativeundertaking with the Instituts Pasteur of Tunis andof Addis Ababa, is to explore the reservoir of relaps-ing -fever spirochetes in Ethiopia, believed to beof key significance in the epidemiology of this disease.The outcome of this investigation will be circulatedto other interested scientists throughout the worldfor an exchange of their views or comments.
One of the important traditional means of ex-changing scientific information is provided by thelarge international congresses of medical sciences.WHO has consistently assisted these congresses bysponsoring the Council for International Organiza-tions of Medical Sciences (CIOMS), by closely co-operating with it and by granting it an annualsubsidy. Although the efforts of the CIOMStowards co- ordinating the time, place and subjectmatter of congresses have so far met with only verylimited success, some improvement has been madein congress techniques and the organization ofscientific symposia related to congresses, of which theSymposium on Glaucoma, conducted in connexionwith the XVII International Congress of Ophthal-mology in September, is the most recent example.

EDUCATION AND TRAINING 37
WHO co- operated actively in the InternationalCongress on Gynaecology and Obstetrics, in July,this being the first time that the proceedings of anentire congress were devoted to the preventiveaspects of a major clinical subject. Co- operationwas facilitated by the fact that the congress washeld in Geneva. A special meeting, arranged byWHO in the Palais des Nations, was attended byabout a thousand obstetricians and gynaecologistsfrom all over the world. WHO staff members readpapers on the main subject of the proceedings, andhelped to organize a symposium on " The Organiza-tion and Teaching of Prophylaxis in Gynaecologyand Obstetrics ", which was attended by aboutseventy professors.
With WHO's assistance, a microfilm reference
service is being established for the Eastern Mediter-ranean Region in the library of the AmericanUniversity of Beirut. This type of project, firstdeveloped in 1949 and 1950 for some Europeancountries at the Charles University Library inPrague,' was endorsed and recommended for furtherdevelopment by the Expert Committee for Profes-sional and Technical Education of Medical andAuxiliary Personnel at its first session.2
A small team of medical scientists was scheduledto visit the University of Damascus in Syria duringthe year to demonstrate how teaching of the pre-ventive aspects of clinical subjects can be introducedinto the curriculum for undergraduate students ofmedicine. The visit was cancelled for reasons overwhich the Organization had no control.
/Provision of Teaching Staff and other Assistance to Educational Institutions
The provision of teachers for short periods, ofteaching equipment, supplies and advice on variousaspects of medical education have been an importantpart of WHO's programme for assistance to edu-cational institutions. Information on curriculumplanning and content, teaching methods, staff andinstitutional administration, is being sought by anincreasing number of schools. In 1954 WHO wasable to begin to analyse the results of its experiencein this field and, in the hope of improving its advisoryservices, to try to determine the factors that influencethe rate and direction of the development of medicaltraining institutions.
The chief objective in assigning a visiting professorto an educational institution has always been thathe should ensure the continuing development of theteaching of his subject in the institution by training,from among local men, a professor and other teachersto take over the department when he leaves. Thisobjective has been reached in some cases, where thetraining given by the visitor has been supplementedby the award of fellowships to local candidates foradvanced study abroad. However, it has becomeclear that two or even three years are not longenough to permit a visiting professor to train asuccessor to carry out adequately the responsibleteaching, research and administrative duties of ahead of department. Consequently, it is now con-sidered that this kind of outside help should be,
not the first, but the last stage of a long and care-fully planned process. Measures by governmentsand educational institutions to train men for pro-fessorial posts early in their careers would contributeto the expansion of medical education which isneeded in many countries today. Because of theinfluence of general education on professionaleducation, long -term planning for such expansioncalls for collaboration with national educationauthorities and with the educational services ofUNESCO.
For obvious reasons, WHO teaching appointmentsshould be for at least two years, and it has beendifficult to find suitable candidates who can interrupttheir careers at home for so long. Few governmentsand institutions in the more advanced countrieshave yet been able to make arrangements to allowtheir best men to work abroad for a year or twowithout hindering their future advancement. Inspite of these difficulties, a roster is being drawn upof persons who are both well qualified and preparedto accept posts outside their own countries. In thiswork, WHO, again, has maintained liaison withUNESCO, each organization putting its lists ofpotential candidates at the disposal of the other.
' See Of Rec. Wld Hlth Org. 24, 40 ; 30, 112.2 WId Hlth Org. techa. Rep. Ser. 1950, 22, 15.
38 THE WORK OF WHO, 1954
During 1954, some thirty teachers provided byWHO were working in medical training institutionsin many countries. Seven of them began dutyduring the year : one in Afghanistan (in physiology),one in Burma (in the training of auxiliary personnel),two in Ethiopia (in the training of auxiliary per-sonnel and sanitation), two in India (in maternaland child health and social medicine) and one inIndonesia (in paediatrics). Among the eight whofinished their assignments during the year was theprincipal of a medical school in Trivandrum, India.When he left after his two -year appointment theschool was developing well along the lines he hadworked out in co- operation with his local colleagues.Of the six others who finished their appointments,three were in India (in pharmacology, physiology andindustrial hygiene, physiotherapy), one in Pakistan (inpathology), and two in Singapore (in applied nutritionand health education of the public). Lecturers inbacteriology, public- health administration and sani-tary engineering were provided for three months tothe University of the Philippines. The provision onsimilar lines of teaching staff in nursing and mid-wifery is discussed more fully in Chapter 2.
Experience in these projects enabled Headquartersand regional offices to give better and more realisticbriefing to visiting professors before they take uptheir appointments. The procedure whereby theprofessors visit Headquarters at the end of theirappointments was introduced as a routine and hasyielded much useful information for evaluating pasteducational projects and planning future ones. Thepractice, started some years ago, of providingequipment judged by the visiting professor to beneeded in his department has been continued.
In 1954 the Diploma of Public Health of theUniversity of Malaya, Singapore (which WHO hashelped by supplying lecturers in applied nutrition,applied physiology, health education and medicalstatistics) was recognized by the General MedicalCouncil of the United Kingdom (see also page 107).
The extensive programme in the Americas forimproving medical and public- health education byproviding teachers and fellowships is described onpage 70.
The special importance of auxiliary personnel inareas in which full professional health services are
not yet available has been emphasized in previousyears, and WHO has continued its study of thesubject. In Geneva, in July, an inter -agencymeeting was convened by the United Nations, onthe use, functions, responsibilities and training ofauxiliary personnel and community workers in anumber of technical fields. Principles were for-mulated which may help governments in planningto meet their needs in this respect. To promotefurther analysis and concentrated study of the ques-tion of auxiliary health workers, an expert com-mittee will be held in 1955.
Material has been gathered for the second editionof the World Directory of Medical Schools, firstpublished in 1953. In collaboration with the Inter-national Association of Universities, the informationin the first edition has been revised, supplementedand brought up to date. In the second edition, thedetailed information on the individual schools willbe preceded by descriptive accounts of the systemsof medical education in each country (about eightyin all) possessing medical schools. Information forthese has been collected during the year. Medicaleducators will thus have available both factualreference tables, as in the first edition, and basicinformation which may serve as a starting pointfor comparative studies in medical education.
Inventories of apparatus and materials for theundergraduate teaching of certain of the basicmedical sciences which were prepared by WHO, asdescribed in last year's Annual Report 1 have beenpublished by UNESCO. The material listed undereach subject represents the consensus of some twentywell -known teachers on the equipment needed forteaching the subject to medical students. The listsare both qualitative and quantitative (based onclasses of forty students) ; they contain roughindications of prices and are preceded by a shortdiscussion of teaching methods with special referenceto the organization of practical work. They areintended chiefly for new schools and schools whichare reorganizing their departments. A French editionwill soon be published ; the book will be publicizedin the medical press and presentation copies will besent to Member governments and to deans of medicalschools.
1 Off. Rec. Wld Hlth Org. 51, 41

J CHAPTER 5
SERVICES IN EPIDEMIOLOGY AND HEALTH STATISTICS
The Second Year of the International Sanitary Regulations
The second year of virtually world -wide applicationof the Regulations was completed on 1 October 1954.
Map 3 and its accompanying table show the Statesand territories which had accepted the Regulationsby 31 December 1954 and those which had not yetdone so. If due account is taken of the new procedureadopted for the entry- into -force of the Regulationsand of their effect on national legislation, the positionappears reasonably satisfactory. Moreover, healthadministrations of several of the States and territorieswhich have formally rejected the Regulations haveinformed the Organization that they are neverthelessconforming to their provisions as far as nationallegislation permits. There is good reason to hopethat the International Sanitary Regulations willeventually operate on a truly world -wide basis.
The main development of the year in this connexionwas undoubtedly the adoption by the Seventh WorldHealth Assembly of a series of decisions and recom-mendations which will solve many of the difficultieswhich States and territories have experienced in theday -to -day application of the Regulations. Thedecisions and recommendations arose from theHealth Assembly's examination of the first reportof the Committee on International Quarantine.Successive Health Assemblies will probably add tothe series and thus build over the years a valuableguide to the interpretation and practical applicationof the Regulations. In the light of the proceedingsof the Health Assembly, health administrationswill be able to modify those parts of their nationalquarantine legislation and services which are inconflict with the interpretations given. The pro-ceedings and reports of the Seventh World HealthAssembly relating to international quarantine, includ-ing the various reports and opinions on the delinea-tion of yellow -fever endemic zones, have beenpublished in a special volume in the Official Recordsseries.1
1O,ff. Rec. Wld Hlth Org. 56. This volume contains the
annual report of the Director - General on the working of theRegulations, the first report of the Committee on InternationalQuarantine and the relevant proceedings of the SeventhWorld Health Assembly.
Health administrations were again asked to informthe Organization (for the purpose of the annual reporton the working of the Regulations) of the difficultiesexperienced in the application of the Regulations.Not unexpectedly, fewer difficulties were reportedthan in 1953. Health administrations seem to befinding that, except for the provisions relating toyellow fever, the Regulations are fitting withoutgreat difficulty into their quarantine organizations,and that most of the problems that arise are beingsatisfactorily settled on a national basis by changein legislation, or, when a problem touches morethan one country, by negotiation and discussionleading to an agreement between the countriesconcerned. It can be said that on the whole theRegulations appear to be functioning satisfactorily.
As already stated, an exception must be made con-cerning the yellow -fever provisions. One of WHO'sresponsibilities under the Regulations is the deli-neation of yellow -fever endemic zones. The ExpertCommittee on Yellow Fever met in September 1953
and recommended delineations to the Committeeon International Quarantine. There was, howevera difference of opinion among the members of theExpert Committee. The Committee on InternationalQuarantine rejected the recommendations proposedby the Expert Committee on Yellow Fever in favourof a different delineation, against which some of itsown members put in a minority report. Subsequentconsultations with the States concerned on thedelineations proposed again revealed disagreements.The Seventh World Health Assembly was thus facedwith several conflicting views and recommendations.After considerable discussion, it decided to refer allthe yellow -fever provisions of the Regulations backto the Committee on International Quarantine forreview. Until the recommendations of that com-mittee are before the Eighth World Health Assemblyand the Assembly can take formal decisions on them,the delineations which were in operation before theapplication of the International Sanitary Regulationsremain in force.
Towards the end of the year the Committee onInternational Quarantine held its second session.
- 39 --
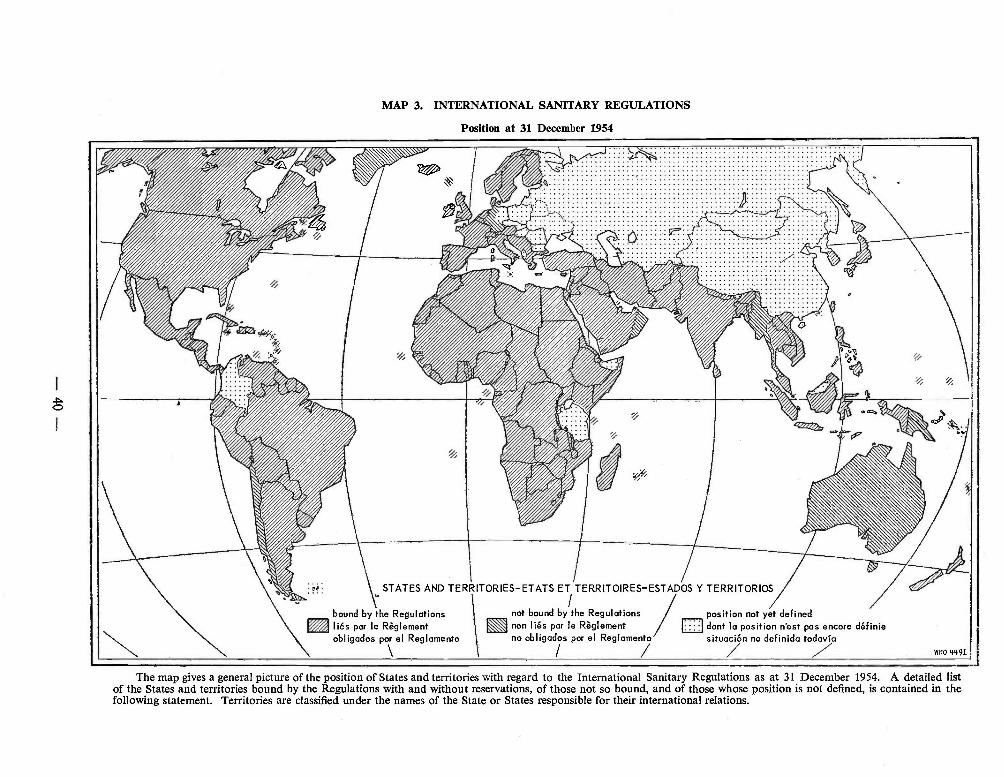
MAP 3. INTERNATIONAL SANITARY REGULATIONS
Position at 31 December 1954
ié: STATES AND TERRITORIES -ETATS ET TERRITOIRES - ESTADOS Y TERRITORIOS
bound by the Regulations not bound by the Regulations position not yet definedliés par le Règlement non liés par le Règlement n dont la position n'est pas encore définieobligados por el Reglamento no obligados por el Reglamento situación no definida todavía
WHO 4491
The map gives a general picture of the position of States and territories with regard to the International Sanitary Regulations as at 31 December 1954. A detailed listof the States and territories bound by the Regulations with and without reservations, of those not so bound, and of those whose position is not defined, is contained in thefollowing statement. Territories are classified under the names of the State or States responsible for their international relations.
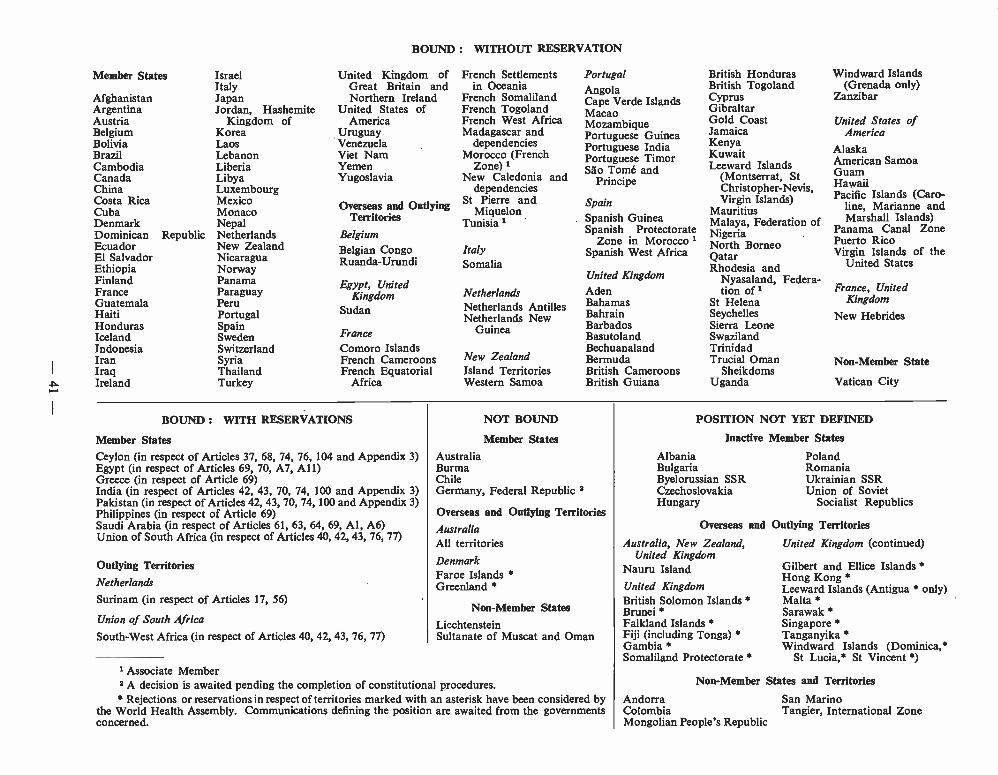
Member States
AfghanistanArgentinaAustriaBelgiumBoliviaBrazilCambodiaCanadaChinaCosta RicaCubaDenmarkDominicanEcuadorEl SalvadorEthiopiaFinlandFranceGuatemalaHaitiHondurasIcelandIndonesiaIranIraqIreland
IsraelItalyJapanJordan, Hashemite
Kingdom ofKoreaLaosLebanonLiberiaLibyaLuxembourgMexicoMonacoNepal
Republic NetherlandsNew ZealandNicaraguaNorwayPanamaParaguayPeruPortugalSpainSwedenSwitzerlandSyriaThailandTurkey
BOUND : WITHOUT RESERVATION
United Kingdom ofGreat Britain andNorthern Ireland
United States ofAmerica
UruguayVenezuelaViet NamYemenYugoslavia
Overseas and OutlyingTerritories
Belgium
Belgian CongoRuanda -Urundi
Egypt, UnitedKingdom
Sudan
FranceComoro IslandsFrench CameroonsFrench Equatorial
Africa
French Settlementsin Oceania
French SomalilandFrench TogolandFrench West AfricaMadagascar and
dependenciesMorocco (French
Zone) 1New Caledonia and
dependenciesSt Pierre and
MiquelonTunisia 1
ItalySomalia
NetherlandsNetherlands AntillesNetherlands New
Guinea
New ZealandIsland TerritoriesWestern Samoa
PortugalAngolaCape Verde IslandsMacaoMozambiquePortuguese GuineaPortuguese IndiaPortuguese TimorSao Tomé and
Principe
SpainSpanish GuineaSpanish Protectorate
Zone in Morocco 1Spanish West Africa
United KingdomAdenBahamasBahrainBarbadosBasutolandBechuanalandBermudaBritish CameroonsBritish Guiana
British HondurasBritish TogolandCyprusGibraltarGold CoastJamaicaKenyaKuwaitLeeward Islands
(Montserrat, StChristopher- Nevis,Virgin Islands)
MauritiusMalaya, Federation ofNigeriaNorth BorneoQatarRhodesia and
Nyasaland, Federa-tion of 1
St HelenaSeychellesSierra LeoneSwazilandTrinidadTrucial Oman
SheikdomsUganda
Windward Islands(Grenada only)
Zanzibar
United States ofAmerica
AlaskaAmerican SamoaGuamHawaiiPacific Islands (Caro-
line, Marianne andMarshall Islands)
Panama Canal ZonePuerto RicoVirgin Islands of the
United States
France, UnitedKingdom
New Hebrides
Non- Member State
Vatican City
BOUND : WITH RESERVATIONS
Member StatesCeylon (in respect of Articles 37, 68, 74, 76, 104 and Appendix 3)Egypt (in respect of Articles 69, 70, A7, All)Greece (in respect of Article 69)India (in respect of Articles 42, 43, 70, 74, 100 and Appendix 3)Pakistan (in respect of Articles 42, 43, 70, 74, 100 and Appendix 3)Philippines (in respect of Article 69)Saudi Arabia (in respect of Articles 61, 63, 64, 69, Al, A6)Union of South Africa (in respect of Articles 40, 42, 43, 76, 77)
Outlying Territories
Netherlands
Surinam (in respect of Articles 17, 56)
Union of South Africa
South -West Africa (in respect of Articles 40, 42, 43, 76, 77)
NOT BOUND
Member StatesAustraliaBurmaChileGermany, Federal Republic 8
Overseas and Outlying TerritoriesAustraliaAll territoriesDenmarkFaroe Islands *Greenland
Non -Member States
LiechtensteinSultanate of Muscat and Oman
1 Associate Member2 A decision is awaited pending the completion of constitutional procedures. Rejections or reservations in respect of territories marked with an asterisk have been considered by
the World Health Assembly. Communications defining the position are awaited from the governmentsconcerned.
POSITION NOT YET DEFINED
Inactive
AlbaniaBulgariaByelorussian SSRCzechoslovakiaHungary
Overseas and
Australia, New Zealand,United Kingdom
Nauru IslandUnited KingdomBritish Solomon Islands *Brunei *Falkland Islands *Fiji (including Tonga)GambiaSomaliland Protectorate *
Member States
PolandRomaniaUkrainian SSRUnion of Soviet
Socialist Republics
Outlying Territories
United Kingdom (continued)
Gilbert and Ellice Islands Hong Kong *Leeward Islands (Antigua * only)Malta SarawakSingapore *Tanganyika *Windward Islands (Dominica,*
St Lucia,* St Vincent )
Non- Member States and Territories
AndorraColombiaMongolian People's Republic
San MarinoTangier, International Zone
42 THE WORK OF WHO, 1954
Four members of the Expert Advisory Panel onYellow Fever attended for the discussions on yellow -fever matters. The most important item on theagenda was of course the revision of the yellow -feverprovisions of the Regulations. After careful consi-deration, a draft text to replace the existing provisionswas agreed on, for submission to the Eighth WorldHealth Assembly in May 1955. The QuarantineCommittee also examined comments and obser-vations submitted by Member States and those madeby the Director - General on the second year ofapplication of the Regulations, and considered thefollowing matters relating to the Mecca Pilgrimage,taking into account the views of the countriesconcerned : standards of hygiene for pilgrimstravelling by means other than by ship or aircraft,the general adoption of a " Carnet de Pèlerinage ",
J
and the adequacy of one injection for the purposeof issuing to pilgrims an international certificateof vaccination against choléra. The Committee, inaddition, discussed the responsibility in internationallaw for accidents during deratting operations ; thepossible exemption of infants from the requirementto possess certificates of vaccination against smallpoxand yellow fever ; and, finally, the loss of immunityafter vaccination and development of immunity afterrevaccination against smallpox. In each case infor-mation was obtained from experts on the subjectand, where appropriate, from the governmentsconcerned.
The Eighth World Health Assembly will considerthe new recommendations of the Committee onInternational Quarantine.
Epidemiological Information
The successful application of the InternationalSanitary Regulations can be ensured only if eachcountry has readily available knowledge of thepresence or absence of dangerous communicablediseases in other countries. The important positionwhich the epidemiological services of the Organiza-tion therefore occupy in assuring the success orfailure of the International Sanitary Regulations wasstressed in the Annual Report for 1953.
The Organization's epidemiological services arebeing continuously reviewed and changes are intro-duced as necessary to improve their efficiency indisseminating intelligence and information.
In many respects there has been an improvementin the regularity of the returns and reports sent tothe Organization. Nevertheless the position isnot yet entirely satisfactory and it is only whencomplete and regular returns are received that theOrganization will be able to carry out its respon-sibilities fully.
The Seventh World Health Assembly, on theadvice of the Committee on International Quarantine,decided that WHO should use the Weekly Epi-demiological Record and the daily radio broadcastfor officially transmitting to health administrationsthe epidemiological and other information receivedunder the Regulations and that in that way certainof the Organization's responsibilities under theRegulations would be held to be discharged. TheOrganization's epidemiological radio bulletins trans-mit important information on the incidence of thequarantinable diseases and other diseases of inter-national interest throughout the world. Bulletins
are broadcast daily from Geneva (on eight wave-lengths in English and two in French), weekly fromSingapore, twice weekly from Alexandria, and dailyover a wide network reaching the Indian Ocean andthe Western Pacific.
During the year an inquiry was made by circularletter into the value of WHO's epidemiological radiobulletins and the use made of them by States andterritories. Table I (opposite) states briefly theresults of this investigation.
The table shows that, of the States and territoriescontacted, 65 per cent. replied, but only 27 per cent.have formal administrative arrangements for receivingregularly one or more of the Organization's radiobulletins. The low proportion of States with sucharrangements may be regarded as disappointing.On the other hand, the broadcasts are also pickedup by local port and airport services, and by ships atsea and, moreover, health administrations which useonly the printed Weekly Epidemiological Record or itsregional equivalents during non -epidemic periods,make arrangements to pick up the epidemiologicalbroadcasts in time of epidemic emergency. Never-theless, such a restricted use of the radio bulletinsdoes not allow the health administration to takefull advantage of the protection which the WHOnetwork of telegraphic epidemiological informationprovides.
The discussions which took place at the SeventhWorld Health Assembly and the favourable com-ments received from a number of countries as to thevalue of the broadcasting services, were, on the otherhand, encouraging, and WHO will continue to use
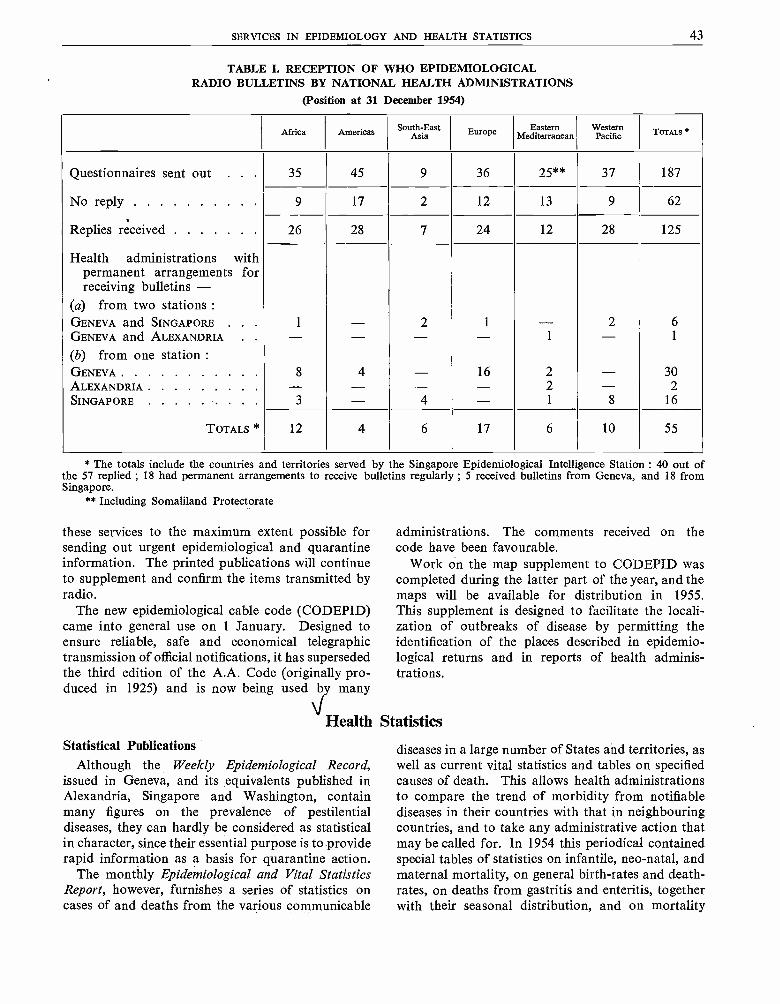
SERVICES IN EPIDEMIOLOGY AND HEALTH STATISTICS 43
TABLE I. RECEPTION OF WHO EPIDEMIOLOGICALRADIO BULLETINS BY NATIONAL HEALTH ADMINISTRATIONS
(Position at 31 December 1954)
Africa Americas South -EastAsia Euroep Eastern
MediterraneanWesternPacific TOTALS
Questionnaires sent out . . 35 45 9 36 25 ** 37 187
No reply 9 17 2 12 13 9 62
Replies received 26 28 7 24 12 28 125
Health administrations withpermanent arrangements forreceiving bulletins -
(a) from two stations :GENEVA and SINGAPORE . . . 1 - 2 1 - 2 6
GENEVA and ALEXANDRIA . .
(b) from one station :- - - - 1 - 1
GENEVA 8 4 - 16 2 - 30ALEXANDRIA - - - - 2 - 2SINGAPORE 3 - 4 - 1 8 16
TOTALS * 12 4 6 17 6 10 55
* The totals include the countries and territories served by the Singapore Epidemiological Intelligence Station : 40 out ofthe 57 replied ; 18 had permanent arrangements to receive bulletins regularly ; 5 received bulletins from Geneva, and 18 fromSingapore.
** Including Somaliland Protectorate
these services to the maximum extent possible forsending out urgent epidemiological and quarantineinformation. The printed publications will continueto supplement and confirm the items transmitted byradio.
The new epidemiological cable code (CODEPID)came into general use on 1 January. Designed toensure reliable, safe and economical telegraphictransmission of official notifications, it has supersededthe third edition of the A.A. Code (originally pro-duced in 1925) and is now being used by many
HealthStatistical Publications
Although the Weekly Epidemiological Record,issued in Geneva, and its equivalents published inAlexandria, Singapore and Washington, containmany figures on the prevalence of pestilentialdiseases, they can hardly be considered as statisticalin character, since their essential purpose is to providerapid information as a basis for quarantine action.
The monthly Epidemiological and Vital StatisticsReport, however, furnishes a series of statistics oncases of and deaths from the various communicable
administrations. The comments received on thecode have been favourable.
Work on the map supplement to CODEPID wascompleted during the latter part of the year, and themaps will be available for distribution in 1955.This supplement is designed to facilitate the locali-zation of outbreaks of disease by permitting theidentification of the places described in epidemio-logical returns and in reports of health adminis-trations.
Statistics
diseases in a large number of States and territories, aswell as current vital statistics and tables on specifiedcauses of death. This allows health administrationsto compare the trend of morbidity from notifiablediseases in their countries with that in neighbouringcountries, and to take any administrative action thatmay be called for. In 1954 this periodical containedspecial tables of statistics on infantile, neo- natal, andmaternal mortality, on general birth -rates and death -rates, on deaths from gastritis and enteritis, togetherwith their seasonal distribution, and on mortality
44 THE WORK OF WHO, 1954
from bronchitis, pneumonia, and tuberculosis, withcomparative figures for mortality from tuberculosisof the respiratory system since the beginning of thecentury. Some original tables on the main zoonosesand on venereal diseases were also published.
Two volumes of the Annual Epidemiological andVital Statistics were issued for the years 1950 and1951. Thus, since 1948, statistics relating to thirteenyears (1939 -51) have been published in this referenceseries and the period between the actual years coveredand the date of issue has been progressively reduced.Some interval is inevitable since, if this series is tobe a reliable work of reference, the data must alwaysbe revised before publication. The 1951 volumecontains tables on population, by age and sex whereavailable, on general vital statistics for selectedcountries, similar data by calendar months to showseasonal trends, and details of deaths of childrenunder five years of age. Deaths by age, sex and causeaccording to the International Abbreviated List aregiven for twenty -eight countries for which mortalitystatistics are particularly reliable. Detailed mortalitystatistics are also given by cause, age and sex forchildren under five ; and from tuberculosis andmalignant neoplasms according to site. For twenty -four communicable diseases showing a distinctseasonal distribution the statistics of cases anddeaths are given by monthly or by four -weeklyperiods, and, for others, they are given annually.A table of the diseases notifiable in each territory isappended to the volume.
Improvement of Mortality Statistics
An analysis of the information contained in anyvolume of Annual Epidemiological and Vital Sta-tistics shows the considerable differences in the degreeof completeness of reporting of notifiable diseasesin the various territories, the absence of othermorbidity data on a basis comparable internationally,and the lack of mortality data, even in the crudestform, for a large section of the world's population.This analysis points to directions in which healthstatistics should be improved. As regards the inter-national comparability of mortality statistics, for thelast sixty years steady efforts have been made toobtain reliable statistics for this purpose, culminatingin 1948 in the International Conference for the SixthDecennial Revision of the International Lists ofDiseases and Causes of Death, prepared by WHO.As a result of this conference, a detailed decimalInternational List was established for the first time.'
The Expert Committee on Health Statisticsrecommended that the next Revision Conferenceshould take place in 1955.2 The preparation for thisrevision began in 1951, when a WHO centre forproblems relating to the classification of disease wasset up under the General Register Office of Englandand Wales, to act as a laboratory for testing aseries of possible improvements in the InternationalLists and rules for tabulating deaths from multiplecauses. The results of the studies made at thiscentre were presented to an advisory group onclassification of diseases, which met in London,in February 1954, to consider possible technicalimprovements in the existing International Lists.The amendments recommended by this group werecommunicated to governments ; the commentsand suggestions of governments were, in turn,examined by the Expert Committee on HealthStatistics at its fourth session in September, andincorporated, in so far as practicable, in a documentwhich will serve as a basis for the work of the 1955Revision Conference. It was emphasized by theExpert Committee, as it had been by the advisorygroup, that only minor modifications would needto be introduced into the existing lists and classifica-tion in 1955 -a significant tribute to their value.
Morbidity Statistics
Studies for the improvement of morbidity statisticswere, on the recommendation of the 1951 Conferenceon Morbidity Statistics, entrusted to the nationalcommittees on vital and health statistics- improve-ment at the national level being a prerequisite tointernational comparability. Among the nationalcommittees that undertook studies in 1954 werethe national committee in the United States ofAmerica, which studied the relation between hospitalmorbidity data and general morbidity in communitiesat large and also drew up plans for detailed surveysof illness and medical care, and the French nationalcommittee, which dealt particularly with cancermorbidity and standard definitions applicable to thisfield.
The focal unit set up at Headquarters to act as aliaison agency with the national committees onvital and health statistics has distributed to thecommittees the studies mentioned above, and afurther series -dealing with the use of samplingmethods, statistics for mental hospitals, statisticaltraining of medical students, the Danish morbiditysurvey, and selections from the proceedings of
1 Published in 1948 as the Manual of the International 2 See the third report of the Expert Committee, Wld HlthStatistical Classification of Diseases, Injuries and Causes of Death Org. techn. Rep. Ser. 1952, 53, 36.
SERVICES IN EPIDEMIOLOGY AND HEALTH STATISTICS 45
various national committees. These papers werecirculated so that collaboration between the nationalcommittees, which was greatly stimulated by theconference of their representatives in London inOctober 1953, could continue most effectively.
Co- operation with International Organizations
Active co- operation has also been continuedwith international organizations concerned withstatistics. Apart from the routine implementationof arrangements with the United Nations, by whichWHO is supplied with population and vital statisticsand, in turn, furnishes data on medical personneland institutions, the Organization, with otherinternational agencies, was invited to contribute toa study on the measurement of levels of living,initiated by the Economic and Social Council. Itis noteworthy that all the participating agencies,when listing the components of the levels of livingin the preparatory papers for this study, placedhealth indicators at the head of their lists. Thehealth indicators considered by the United NationsStatistical Commission in April were referred to theWHO Expert Committee on Health Statistics, whichconsidered them in September 1954 and recom-mended research on the most significant healthindices that could be made available in a large numberof countries and territories.
WHO, at the request of the United Nations andin terms of its agreement with that body, took partin the World Population Conference held in Romein September. Certain papers dealing with statisticalaspects of mortality and morbidity were presentedat the Conference.
Training and Advice in Statistical Methods
Assistance to governments in training in healthand vital statistics has been one of the responsibilitieswhich WHO has exercised jointly with the UnitedNations. In September and October a member ofthe headquarters staff acted as technical organizerof a six weeks' training course in Afghanistan, heldin the Training Centre in Vital and Health Statistics,
Kabul, and jointly supported by the Government,the United Nations and WHO. Lectures were alsogiven at the United Nations Permanent Interna-tional Statistical Education Centre established inthe Indian Statistical Institute at Calcutta. Assistancewas continued to the Inter - American Centre ofBiostatistics (see page 75).
To provide governments with advice, WHO haseither placed statistical experts at the disposal ofcertain national administrations on a full -time basisor has made available its consultants on statisticsin the regional offices or at Headquarters. Statisticalspecialists from Headquarters have co- operated infield projects in yaws, malaria, sanitation and vitalregistration in tropical Africa, and in trachoma inNorth Africa.
The statistical services have been called uponincreasingly to provide technical units at Head-quarters, regional offices and field consultants withadvice on the statistical methods best suited to theirrespective problems, particularily on the sta-tistical evaluation of results obtained, and withassistance in the actual planning of operations. Suchstatistical planning is, of course, necessary if properstatistical analysis and evaluation are eventuallyto be made.
Epidemiological Studies
Officers of the epidemiological and statisticalservices have co- operated with specialists in commu-nicable diseases in preparing epidemiological studies,particularly on the virus diseases. Studies publishedin 1954 have covered the evolution of poliomyelitis inthe last thirty years, recent poliomyelitis epidemiologyand world distribution of cholera. Other studiesbased on statistical material, collected either byroutine or specially for the purpose by the epi-demiological and statistical services, dealt with snake-bite mortality throughout the world ; urban andrural health statistics ; and infant and childhoodmortality in areas of high death -rates. In addition,a number of short epidemiological notes of topicalinterest were published in the Weekly EpidemiologicalRecord.
CHAPTER 6
DRUGS AND OTHER THERAPEUTIC SUBSTANCES
JBiological Standardization
The International Biological Standards make itpossible to measure the biological activity of a sub-stance (i.e., its therapeutic, prophylactic or otherform of biological activity) in terms of InternationalUnits. An International Unit (say of diphtheriaantitoxin, or of insulin) is the activity of an agreedquantity of the International Standard for the par-ticular substance in question. The InternationalBiological Standards are therefore comparable withthe International Standards for weights and measures,which make it possible to describe the weight orlength of a substance in terms of internationalunits, i.e., in grams or metres -or in fractions ormultiples thereof.
There are, however, two important differencesbetween biological standards and standards forweights and measures ; whereas the standardsrequired for weights and measures are few andpractically indestructible, a separate standard pre-paration is required for each biological product,and these standards are constantly being depletedas portions of them are regularly removed by labo-ratories when comparing their own products withthe standard.
The double task of providing new standards fornew therapeutic and other biological substancesand of replacing those that are nearing depletionhas proceeded uninterruptedly during the year. Themain and exacting burden of the technical workcontinues to be carried, in co- operation with labo-ratories throughout the world, by the two Inter-national Centres for Biological Standards -theone in Copenhagen, for standards of an immunologi-cal nature, and that in London, for those that arenon -immunological.
Besides accepting the responsibility for most ofthe technical work, these centres store the standardswhen established and distribute them to the nationallaboratories for biological standards throughout theworld. The programme as a whole is conducted forthe World Health Organization in the light of advicegiven by its Expert Advisory Panel and ExpertCommittee on Biological Standardization.
The Expert Committee met again in 1954, andestablished the following nine new internationalstandards :
International Reference Preparations of Clostri-dium welchii (Type B) Antitoxin and of Clostridiumwelchii (Type D) Antitoxin. These will be useful tothe producers of therapeutic sera for both man anddomestic animals.
International Standards for Schick Test Toxin(Diphtheria). These will bring greater precision tothe detection of susceptibility to diphtheria. Mean-while, considerable progress has been made towardsproviding an International Standard for DiphtheriaToxoid, Adsorbed, which will enable the activityof diphtheria prophylactics to be measured withmuch greater accuracy than hitherto.
International Standard for Swine Erysipelas Serum,Anti -N. Like the new International ReferencePreparations for Clostridium welchii Antitoxinsreferred to above, this also will be useful to theproducers of therapeutic sera both for man and fordomestic animals, though its main use will be inveterinary rather than in medical practice.
International Standard for Purified Protein Deri-vative of Avian Tuberculin. There is already anInternational Standard for Purified Protein Derivativeof Mammalian Tuberculin, and the new standard forthe avian form of tuberculin will facilitate studies ofthe specificity of tuberculin reactions both in manand in bovines.
International Standard for Thyrotrophin. This willbe used for treatment and research in endocrinedisorder.
International Reference Preparation of Protamine.This preparation will facilitate the production ofbatches of protamine -zinc insulin of predictablepotency and of predictable duration of activity wheninjected into diabetics.
International Reference Preparation of Mel Band MSb. These substances are being increasinglyused and investigated for the treatment and pro-
--- 46 -
DRUGS AND OTHER THERAPEUTIC SUBSTANCES 47
phylaxis of African sleeping sickness, and theInternational Reference Preparations will enablethem to be more accurately controlled in respectof their therapeutic activity and toxicity, before beingused in man.
International Centres for Salmonella and Escherichia,for Shigella and for Blood GroupingThe international biological standards are essen-
tially quantitative -that is, they make it possible tocarry out accurate measurements of activity,` interms of international units. There is another typeof biological preparation, however, which is designedfor classification and identification rather than formeasurement -for example, the sera used foridentifying and classifying micro- organisms, as wellas those for typing or identifying the rarer bloodgroups.
International centres for identification and classi-fication have been established. The first was theInternational Salmonella and Escherichia Centrein Copenhagen, which has functioned under the
auspices of WHO since 1948. For similar workamong the dysentery bacteria, two InternationalShigella Centres were established by WHO in 1954
-in Atlanta, Georgia, United States of Americaand in London. A consultant was engaged to assistin co- ordinating the work of these two centres.International centres engaged on similar work inbrucellosis and influenza are shown in Maps 1 and 2respectively (pages 11 and 13).
The International Blood Group Reference Labo-ratory in London has continued its functions ofsupplying typing sera and giving advice to labora-tories throughout the world.
Publications on Biological Standardization
Experts have been encouraged to contributearticles for publication in the Bulletin of the WorldHealth Organization on the international biologicalstandards, and on various aspects of biologicalstandardization ; and in 1954 a special number ofthe Bulletin was devoted to articles on the subject.'
Pharmaceutical Specifications and Nomenclature
Just as important as WHO's work on the unitsof measurement for biological substances are itsactivities in relation to pharmaceutical preparations,such as the publication of an international phar-macopoeia and the establishment of internationalnon -proprietary names. In 1954 Volume II of thefirst edition of the Pharmacopoea Internationalis wasbeing printed and was available in proof form. Thisvolume, together with the Addendum being pre-pared, will complete the first edition, therebysupplying Member States with specifications ona large number of internationally used pharma-ceutical preparations. During the year, the text ofVolume II was submitted to the members of theExpert Advisory Panel on the International Pharma-copoeia and Pharmaceutical Preparations, whosecomments were then examined at the thirteenthsession of the Expert Committee on the InternationalPharmacopoeia, which was held from 28 June to3 July. In accordance with requests, proof copieswere also forwarded to Member States, and thesuggestions received from them will be examinedwith a view to their inclusion in the texts of themonographs and appendices of Volume II beforefinal publication, or for consideration in the prepa-ration of the second edition. The preface to Volume IIwill again emphasize that the Pharmacopoea Inter -nationalis constitutes only a series of recommenda-
tions and is not intended to be a legal pharma-copoeia in any country unless adopted by thatcountry's pharmacopoeial authorities.
Reports from various sources indicate that theauthorities responsible for the pharmacopoeias indifferent countries are examining the text of Volume Iand incorporating the specifications and nomen-clature as far as possible in their national pharma-copoeias. This volume thus appears to be of serviceto many national health administrations and phar-macopoeia commissions. The Spanish editionhas been published and sent to governments ofSpanish- speaking countries ; the German translationwas completed during the year and is being printed.
The preparation of a second edition is proceeding,with the help of technical and general advice fromthe members of the Panel and other specialists,expert committees, national organizations, manu-facturers, and pharmacopoeial and other com-missions in different countries. Consultations on aswide a basis as possible have been made on suchaspects of this work as : substances for whichspecifications should be included ; tables of dosesfor adults and children ; specifications for reagentssuitable for the tests of the pharmacopoeia ; andphysical, chemical and biological methods to be
Bull. Wld HIM Org. 1954, 10, 867 -1038

48 THE WORK OF WHO, 1954
included after laboratory investigation of the testsdescribed in Volume I on samples obtained invarious countries.
Members of the Expert Advisory Panel haveprepared reports on the establishment and main-tenance of suitable specifications of safety and purityin pharmaceutical preparations, for discussion at afuture expert committee meeting.
Good collaboration has been maintained withnational health administrations and authoritiesresponsible for naming drugs on the selection ofinternational non -proprietary names. In general,the international non -proprietary names whichhave been proposed have been accepted and intro-duced into national pharmacopoeias and otherrecent books of specifications. They are provingto be of practical assistance in preventing the con-fusion which arises from the use of a multiplicityof non- proprietary names for the same substancen different countries.
On many aspects of this work, pharmacopoeialcommissions have been consulted, either throughgovernments or members of the Expert AdvisoryPanel, or directly by questionnaires on such subjectsas the naming of barbituric acid derivatives. Thecomments received on the first list of proposedinternational non -proprietary names were carefullyexamined and dealt with by correspondence andat a session of the Sub -Committee on Non -Pro-prietary Names, held from 27 to 30 September, atwhich a supplementary list of proposed interna-tional non -proprietary names was selected. Theexperience gained in dealing with these names willbe useful in preparing a possible revision of theprocedure for selecting recommended internationalnon -proprietary names and the general principlesfor guidance in devising them, which were adoptedat the twelfth session of the Executive Board.' Withthe co- operation of Member States, care is beingtaken to prevent infringement of proprietary rights.
Drugs Liable to Produce Addiction
WHO, in meeting its technical and advisoryobligations with regard to the conventions on themanufacture and distribution of narcotic drugs, hascontinued its work on such drugs -collectinginformation, providing advice to governments ontheir request, convening the Expert Committee onthis subject, and forwarding advice to the UnitedNations on the liability of certain substances toproduce addiction.
In order to help decide whether a product whichis not itself an addiction -producing drug is or is notconvertible into one, an important feature of WHO'swork in 1954 was the interpretation, in so far asWHO's responsibilities are concerned, of the meaningof the word " convertible " in the 1931 Conventionfor Limiting the Manufacture and Regulating theDistribution of Narcotic Drugs (paragraphs 3 and4 of Article 11), as amended by the Protocol of1948. As a result of the discussions of the ExpertCommittee on Drugs Liable to Produce Addictionat its fourth session in June 1953, and the subsequentrecommendation of the Executive Board to theWorld Health Assembly (resolution EB13.R10), itwas decided by the Seventh World Health Assemblythat, in regard to functions conferred upon WHO bythe said Convention, WHO would consider asubstance as " convertible " where the ease ofconversion and the yield obtained constitute a riskto public health, and that in cases where there wasuncertainty as to whether a substance would fall
under this definition, the substance would also beconsidered as " convertible " rather than as " notconvertible " (resolution WHA7.7).
By another resolution (WHA7.6) the SeventhWorld Health Assembly determined more preciselythe exercise of functions conferred upon the Orga-nization under the various international agreementson addiction -producing drugs. By this resolutionthe Director -General is now empowered, uponreceipt of the appropriate expert advice, to takedecisions on the classification of substances undercertain international agreements ; the placing undercontrol of new addiction -producing drugs willconsequently be speeded up considerably -a stepclearly in the interests of the protection of publichealth. Decisions on the application or interpretationof the international agreements or on any changesin the functions of the Organization under the controlregime will continue to be taken by the HealthAssembly, or, in case of urgency, provisionally bythe Executive Board.
Collaboration with the United Nations Divisionof Narcotic Drugs has developed considerably.During the year, advice was given to this divisionon many subjects, and memoranda were preparedfor the ninth session of the Commission on Narcotic
1 Off Rec. Wld Hlth Org. 49, 7, 29
DRUGS AND OTHER THERAPEUTIC SUBSTANCES 49
Drugs of the Economic and Social Council. Thefirst paper- entitled " Chemical Aspects " -in theseries " Synthetic Drugs with Morphine -like Effect "was elaborated jointly by the United Nations andWHO in compliance with resolution 505 C (XVI)of the Economic and Social Council ; it waspublished in the Bulletin of the World HealthOrganization.' The second paper in the same seriesis being prepared.
Co- operation with the Permanent Central OpiumBoard and the Drug Supervisory Body of the UnitedNations continued as usual.
The Organization was represented at most of themeetings of the ninth session of the Commissionon Narcotic Drugs, held in New York from 19 Aprilto 14 May. As in earlier years, the representativeof WHO took part in discussions on diacetyl-morphine (heroin), the coca leaf, cannabis, syntheticnarcotic drugs, drug addiction, and the draft revisedform of annual reports of governments, which are sub-mitted in accordance with the 1931 Convention andwhich may in future provide important informationthat WHO is otherwise unable to obtain. TheCommission on Narcotic Drugs showed specialinterest in the opinion, expressed by the ExpertCommittee on Drugs Liable to Produce Addictionat its third and fourth sessions, that it would beadvisable to strengthen the control of amphetamineand its derivatives,2 and asked WHO's advice on thetherapeutic value and addiction -producing qualitiesof dihydrodesoxymorphine, and on special officialprescription forms for addiction - producing drugs.
A meeting of experts on mental health andalcohol was convened in Geneva from 27 Septemberto 2 October. At this meeting the classificationof alcohol made by the Expert Committee onDrugs Liable to Produce Addiction 3 and the ExpertCommittee on Alcohol4 as belonging to the group ofsubstances intermediate in kind and degree betweenthe " addiction -producing " and " habit -forming "drugs, was confirmed. The meeting is further de-scribed on page 21.
The fifth session of the Expert Committee onDrugs Liable to Produce Addiction was held inGeneva from 11 to 16 October. The Committee recog-nized six drugs, partly new morphine derivatives, partlysynthetic substances, as addiction -producing and
' Bull. Wld Hith Org. 1954, 10, 10032 Wld Hlth Org. techn. Rep. Ser. 1952,3 Wld Hlth Org. techn. Rep. Ser. 1952,4 Wld Hlth Org. techn. Rep. Ser. 1954,
57,57,84,
11 ;10
10
1954, 76, 11
one as convertible into such a drug, with a consider-able yield. It was therefore decided to submit all ofthem to international narcotics control, and theDirector -General, in accordance with the 1931
Convention and the 1948 Protocol, sent the corre-sponding notifications to the Secretary - General ofthe United Nations.
The situation concerning the abuse of pethidineamong physicians and members of the paramedicalprofessions was discussed, and note was taken ofthe high incidence of addiction to pethidine, observedin one country, among members of the medical,nursing, and associated professions. The Com-mittee was of the opinion that pethidine is as dan-gerous as morphine as a potential agent of addiction,and urged the Director- General to bring to theattention of governments and the medical professionthroughout the world, by whatever means he con-sidered appropriate, the danger of the addictionpotentiality of this drug and the need for exercisingthe same care with it as with morphine. Severalnew types of synthetic drugs with morphine -likeeffect, which are still in the early experimental stage,were also considered. The fact that new groups arestill being found by synthetic means confirms theopinion that there is promise of therapeutic progressin this field. The Committee also discussed pro-cedures for speeding up the selection of internationalnon -proprietary names for addiction -producingdrugs. Another important item considered was thesituation concerning Cannabis sativa. On the basisof a report from the Union of South Africa and oninformation from India and other countries, theCommittee, which had already considered thissubject in earlier sessions, expressed the opinionthat abuse of cannabis came definitely under theterms of its definition of addiction, that it was stilla serious problem in many parts of the world, andthat, far from any slackening of measures for itscontrol, greater effort should be made for its aboli-tion.
By means of discussions with authorities of severalgovernments information was exchanged duringthe year on such aspects of addiction -producingdrugs as the abuse of cannabis resin (marihuana) ;4, 4- diphenyl- 6- dimethylamino -hexanone-3 (containedin the cough- mixture Ticarda) ; dihydroisocodeine ;1- methyl-4-phenylpiperidine-4-carboxilic acid iso-propyl ester (i.e., the isopropyl analogue of pethi-dine), and present methods for the treatment of drugaddicts.
CHAPTER 7
PROCUREMENT OF SUPPLIES
Purchases of medical and other supplies andequipment for WHO projects financed from theregular budget and Technical Assistance fundsamounted to US $420 000 for the year 1 October1953 to 30 September 1954. Most of the purchaseswere made from non -dollar sources, with currenciescontributed to the Technical Assistance Programme.In the conduct of WHO's supply operations it isimportant for expenditures to be concentrated inone group of currencies or another, according tothe changes in the Organization's currency holdingsthroughout the year. The progressive relaxation ofexport controls and the increase in production rangein a number of European and other countries inrecent years has helped to make this possible.Additional non -dollar sources are becoming avail-able for DDT conforming to the recommendationsof the WHO Expert Committee on Insecticides.Experience in purchasing substitutes for certainproducts or alternative pieces of apparatus givingthe requisite performance, and the maintenance atHeadquarters and the regional offices of up -to -dateand readily accessible documentation on sources ofsupply in the more important medical supply markets,have also helped WHO to make advantageous useof its available cash resources.
Prices of supplies and equipment used in WHOprogrammes have, in most instances, not variedgreatly during the year. One exception has beenthe further reduction in the price of penicillin PAM,which should benefit countries undertaking masscampaigns with this product. There have also beendevelopments in the use of other repository penicillinpreparations, some of which are being tried out infield studies under the auspices of WHO. In someEuropean countries the suppliers are taking a some-what shorter time for deliveries than in previousyears.
The Organization has maintained close co-operation with the purchasing units of other UnitedNations agencies that have similar problems, andexchanges current information with them on supplysources, costs and performance.
The fluctuations, referred to in Chapters 10 and18, in the sums earmarked for WHO TechnicalAssistance expenditure during 1954 created diffi-culties in planning for and procuring supplies andequipment. At the beginning of 1954 it was neces-sary to reduce appreciably the expenditure plannedfor the year's operating projects ; then, during thesecond quarter, when the necessary adjustmentshad been completed, more changes had to be madebecause of two additional earmarkings by theTechnical Assistance Board. The regional officeswere obliged to revise some of their requirements insupplies and equipment several times, with conse-quent delays at Headquarters in placing orders andobtaining delivery for projects.
In 1954, the carry -over of obligations in suppliesand equipment for Technical Assistance projectspurchased but not delivered in 1953 was noticeablyheavier than in previous years, again largely becausethe uncertainties of the financial situation in 1953had delayed the placing of orders in that year.
X -ray Equipment for Tuberculosis Projects
Manufacturers of x -ray equipment have continuedtheir efforts to produce both mobile and staticunits capable of giving a more reliable performanceunder tropical conditions with a minimum need forrepairs.
Recent developments in mirror cameras havemade it possible to use lighter and simpler x -raygenerators with consequent reductions in bulk, costand maintenance. In addition, x -ray units can nowbe obtained affording greater protection againsttropical operating conditions, such as heat, humidityand dust. WHO has encouraged manufacturers toproduce equipment conforming as closely as possibleto the needs of tuberculosis control programmes inunder- developed tropical and sub -tropical areas.Particular attention has been paid to economy inpurchase cost and operation, simplicity of manipula-tion and maintenance, sturdiness and, where neces-sary, mobility. The Organization, in associationwith manufacturers, has also given consideration to
-50--
PROCUREMENT OF SUPPLIES 51
the design of mobile x -ray units for such areas.Completely self -contained mobile units built intosuitable vehicles appear to have certain advantagesover transportable units which need to be erectedand dismantled. In studying the design of suchunits and in selecting the vehicle, account must betaken of factors such as the kind of terrain in whichit is to be used, the type and output of the generatorand the method of housing it, the necessity foradequate ventilation and the provision of facilitiesfor emergency processing of film.
Performance and Suitability of Equipment
Efforts have been made to stimulate reportingfrom the field on the performance and suitability ofthe equipment supplied to WHO projects. Thesereports have been taken up with the manufacturersconcerned and in some cases modifications in designhave resulted.
Assistance to Member States and to other UnitedNations Agencies
All the medical supplies and equipment neededfor a medical school and teaching hospital and fora nursing training school, at a total cost of $280 000,were purchased for the United Nations KoreanReconstruction Agency (UNKRA), which providedthe currencies needed. WHO assisted in theestablishment of the detailed lists of requirements,and drew up the specifications subsequently used asthe basis of procurement. Purchases involvingthousands of separate items were made in many
countries ; the supplies were shipped by vesselsunder charter to UNKRA, by military transport,or by normal commercial shipping. Because it wasnecessary to synchronise deliveries of supplies withthe completion of the hospital building, the timefor establishing the final list of requirements and forprocurement and shipment was limited, whichplaced an unusually heavy burden on the staffconcerned. A number of visits had to be paid tosupply sources and to health authorities in thecountries of procurement, which gave valuableassistance.
Check Lists of Equipment for Field Projects
The preparation of standard lists of equipmentfor certain projects was continued. A check list ofbasic equipment for a nursing training centre wasdrawn up, and the list of equipment for a venereal -disease laboratory was revised in the light of fieldexperience. A similar list for projects in environ-mental sanitation was started. The lists are usedby WHO and UNICEF in planning new projects.
The Co- operative for American Remittances toEverywhere, Inc.
The agreement with the Co- operative for AmericanRemittances to Everywhere, Inc. (CARE) remainedin effect throughout the year. It is reported byCARE that new and used medical equipment andsupplies to an estimated value of $67 000 weredonated during the year, and that shipments to avalue of $7500 were made to institutions in fulfilmentof requests.

CHAPTER 8
PUBLICATIONS AND REFERENCE SERVICES
Continued emphasis has been laid on the need todevelop the Organization's publishing and referenceservices as media for advancing the general objectivesand activities in its programme. This has involvedconstant review of editorial policy in accordancewith varying requirements, of arrangements for paidand unpaid distribution of publications, and of theutilization of the WHO library and reference servicesat Headquarters and in the regions.
A major task in 1954 has been the detailed studyof the implications of the Seventh World HealthAssembly's decision to take further steps towardsthe adoption of Spanish as a working language.It was clear from this study that it would be essentialto recruit a nuclear staff of Spanish -speaking transla-tors and editors during the latter months of 1954in order to introduce at the beginning of 1955 theuse of Spanish to the full extent authorized by theHealth Assembly. An experienced translator- consul-tant was engaged to assist in the solution of thevarious problems connected with the recruitmentand training of the new personnel, and in the establish-ment of a suitable terminology. By the end of theyear a selection of translators and editorial staff hadbeen made from among a very large number ofapplicants.
Production of Publications
As early in the history of the Organization as 1948,the Interim Commission, in referring to the FirstWorld Health Assembly the " General Report onPublications " prepared by the Executive Secretary,particularly stressed " the importance of publishingsymposia and monographs on special subjects ",1and four years later, the Board, in its study of theOrganization's programme of publications, expresseditself in favour of publishing special numbers of theBulletin and monographs,2 thus endorsing the policyearlier formulated.
Although substantial progress can be recordedin the production of monographs and of specialissues of the Bulletin, an increase in the volume of
1 Off Rec. Wld Hith Org., 12, 182 Off Rec. Wld Hlth Org., 40, 54
such publications is clearly not an end in itself, andthe amount of material that is not, for reasons ofeditorial policy, accepted for publication has alsoincreased.
In the consideration of any manuscript, one ofthe main questions to be asked is : what objectiveis served by issuing this document under the imprintof an intergovernmental health organization ? Inthe case of contributions which are purely factual,in the sense that they report the author's directpersonal observations in the laboratory, the clinic,or in the field, publication by WHO serves a clearpurpose if the findings are considered to make asignificant contribution to knowledge and if thesubject is important to one of the Organization'sprogramme activities. However, in the case ofsubjects with broader social or administrativeimplications, factual reporting is often mingled withopinion or advocacy, which goes beyond, or is notnecessarily to be concluded from, the data presented.It is in such cases that difficulties, and sometimessharp differences of opinion, may arise in decidingwhether the manuscript should be published byWHO. Although examination of the WHO publica-tions issued to date might well show that a completejustification for publication by the Organizationcould not be made out retrospectively in all cases,there has been a growing awareness of the importanceof adhering to a well- defined publishing policy.
Of the numbers of the Bulletin published in 1954,eight were on special subjects : syphilis ; rabies ;therapeutic, prophylactic and diagnostic substances ;health statistics ; yellow fever in Africa ; malaria ;tuberculosis, and environmental sanitation. For thesix years 1949 to 1954 inclusive, the total numberof pages published in the Bulletin was approximately7000, and in 1954 rather more than 1800 pages werepublished.
Apart from the increasing tendency to publishspecial numbers of the Bulletin, as referred to above,a start has been made in developing the " Notesand Reports " section of this publication as avehicle for making more widely available in abridgedform a selection of the large quantity of technicalmaterial that is circulated in the form of workingpapers.
- 52 -
PUBLICATIONS AND REFERENCE SERVICES 53
By the end of 1954, twenty titles had been publishedin the Monograph Series in English, sixteen in French,and two in mixed- language editions.
The subjects of monographs published during theyear were as follows :
English editions: influenza ; biology of Ano-pheles gambiae ; plague ; laboratory techniquesin rabies ; donovanosis.
French editions: toxic hazards of certain pesti-cides to man ; the African mind in health anddisease ; design and operation of septic tanks ;advances in the control of zoonoses ; influenza ;the rural hospital ; plague ; milk pasteurization ;malaria terminology ; BCG vaccination.
The plans for improving the publishing scheduleof the International Digest of Health Legislation,referred to in the Annual Report for 1953, weresuccessfully carried out in 1954, when the whole ofVolume 5 was published in four quarterly parts, onepart appearing in the first half of each quarter.Comparative surveys of health legislation on leprosy,smallpox vaccination, and midwifery appeared inthis volume. Separate offprints of all these surveyshave been made available for sale, and for distributionto members of the corresponding expert advisorypanels.
Improvements in the Chronicle were effected start-ing with the eighth volume, published during theyear. The format was slightly changed to allow for awider page -area, and the text was printed in doublecolumns, thus giving at the same time a shorter linefor ease of reading and scope for more interestingpresentation of illustrative material. An attemptwas also made to improve the content of the Chroniclefrom the point of view of the health workers forwhom it is intended, by giving increased emphasisto the technical work of the Organization, andcorrespondingly reducing the amount of spaceallotted to organizational meetings and othersubjects of more internal interest. A further newdeparture was the publication of a whole numberdevoted to a general review of the Organization'swork in a special subject- treponematoses. Planswere made for publishing such special numbers atleast once, and possibly twice, each year.
In previous years, the indexes of the Bulletin andthe Chronicle were greatly in arrears, and this wasa cause of complaints from libraries wishing to bindtheir volumes. In 1954 these arrears were entirelyliquidated, and arrangements were made to produceindexes punctually after the issue of each volume.Regular monthly publication of the Chroniclein English and French has been maintained, but
with the Bulletin this is much more difficult toachieve, largely because of the necessity to sendproofs to authors in many lands.
It has now been arranged that the responsibilityfor publishing the Spanish edition of the Chroniclewill revert to Headquarters from the Regional Officefor the Americas, starting with the first number for1955. The Regional Office will continue to liquidatethe arrears of the previous volume, and in this wayit is hoped that the Spanish Chronicle will be main-tained up to date without lack of continuity.
In addition to the regular Official Records volumespublished during the year, a special volume (No. 56)on " Proceedings and Reports relating to Interna-tional Quarantine " was issued in the autumn.
Reception of WHO PublicationsIn general, the Monograph Series continues to be
the most salable of the Organization's publications.Of this series, the second, which was first publishedin early 1952- Maternal Care and Mental Health -has had the greatest sales, and there is still a smallbut steady demand for it. Since the original printing,there have been six new impressions of the Englishedition, financed from the Publications RevolvingFund, and by the end of the year nearly 12 000 copiesof this edition and 1000 copies of the French editionhad been sold. In addition, popular abridgedversions have been commercially published in theUnited Kingdom and the United States of America,and commercial or state publishing houses have,with the agreement of the Organization, publishedtranslations in the Danish, Swedish and Serbo -Croatlanguages.
The subject of this monograph was one of generalappeal to a wide variety of health and social workers,and the purely scientific monographs, such as thosepublished in 1954 on influenza and plague, naturallydo not sell in such large quantities. Nevertheless,the reception given in the professional and scientificpress to these more specialized monographs hasbeen uniformly excellent.
Distribution and SalesDuring the year, efforts to rationalize unpaid
distribution by revising the mailing lists havecontinued, and much attention has been paid to theproblems of developing sales. New or additionalsales agents have been appointed in the BelgianCongo, Federal Republic of Germany, Indonesia,Italy, Japan, Taiwan and Thailand. In four othercountries sales agents whose performance was notsatisfactory have been changed. By the end of the
54 THE WORK OF WHO, 1954
year, WHO publications were available againstpayment in local currency in forty -one countries.
There has been an increasing amount of cor-respondence with sales agents, both in respect ofinformation about new publications and of the useto which the catalogue of WHO publications andoccasional prospectuses can be put. After consulta-tion with agents representative of the English -language book trade, it was decided, in order toconform with the requirements of the market, thatas from 1955 English editions of WHO monographswould be placed on the market only in cloth -boundeditions, the paper -bound editions being reservedfor non- commercial distribution.
In the spring, 21 000 copies of the catalogue inEnglish and 9000 in French were distributed. Severalagents are now regularly including mention of WHOpublications in their own catalogues, announcementsor journals.
At the beginning of the year, global, block andother special subscription rates were introduced, andthe expectation that these would be of specialinterest to libraries has been fully justified. Theglobal subscription, which for the year 1954 wasset at $ 80, entitles subscribers to receive all WHOpublications in one of the working languages, andsixty such subscriptions were entered during the year.There were also forty block subscriptions at $52.50entitling subscribers to receive all the Organization'speriodicals and also the Official Records and TechnicalReport Series. Special rates were also offered forcombined subscriptions to the Bulletin and Chronicleand to the Epidemiological and Vital StatisticsReport and Weekly Epidemiological Record.
In the report on distribution and sale of WHOpublications submitted by the Director- General forthe consideration of the Executive Board at itseleventh session, it was stated : " The appointmentof depository libraries in some countries has beenon a generous scale, and this has led to some anoma-lies. At present some libraries that would have nospecial financial or currency difficulties to overcomein subscribing to WHO publications are receivingthem free of charge because they have been nominateddepository libraries. Similar libraries in the samecountry subscribe to some or all WHO publications."However, as soon as possible, arrangements weremade to offer global or block subscriptions as analternative to receiving WHO publications withoutpayment, and at the beginning of the year letterswere sent to thirty -three depository libraries inform-ing them that it would no longer be possible tocontinue a free service of WHO publications andat the same time pointing out the advantages of
the new special subscription rates. Of these libraries,twenty -three have since taken out global or blocksubscriptions, and none has complained of thediscontinuance of the free service.
Prepayment for WHO publications in the formof subscriptions has been very satisfactory. Atmid -year this represented a face -value of approxi-mately $23 000, which, after deducting trade discountsand the commission charged by the United NationsSales Service, represents a net income to the Publica-tions Revolving Fund of some $14 000. The totalreceipts in 1954 amounted to $ 31 222, representingsales to the face -value of approximately $ 63 000.
Library and Reference Services
The Organization was represented at three interna-tional meetings concerned with various aspects ofdocumentation -the UNESCO Advisory Committeefor Documentation in the Natural Sciences, theUNESCO International Advisory Committee onBibliography, and the UNESCO International Com-mittee for Social Sciences Documentation. At thelast of these, WHO submitted a paper on biblio-graphical contacts between the medical and socialsciences.
Improvements have been made in the arrangementsfor the handling and circulation of national statisticalpublications and in the procedure for dealing withorders for medical literature received from theregional offices. From the beginning of the yearLibrary News was issued in an improved form, withall accessions classified by the Barnard system,which had been put into use in the WHO Libraryin the previous year.
A complete rearrangement of the extensive WHOmaterials in the stacks of the United Nations librarywing, including the former Office Internationald'Hygiène Publique collection, was started in May1953 and completed in March 1954. This work hasinvolved the handling and arrangement of manythousands of volumes. As a result, much valuablematerial has become readily accessible.
While developing the current services to the WHOSecretariat in Geneva, the Library continued itsefforts during the year to extend them to the technicalstaff in the regional offices and in the field. So asto facilitate the use of microfilms, which are moreeconomical than Photostat copies as a method ofsupplying literature, microfilm readers were sent toBrazzaville and Manila ; duplicate material has beensent regularly as an addition to the libraries in theregional offices. Discussions were held with theRegional Office for Europe on the implications fromthe point of view of library and reference facilities,

PUBLICATIONS AND REFERENCE SERVICES 55
of the transfer of the Regional Office to Copenhagenand complete agreement was reached on the meansof avoiding duplication in holdings and services.
It is indicative of a growing recognition of theimportance of the Library's collection of currentmedical literature that serious consideration had tobe given during the year to the regulation of loans
to other medical and scientific libraries. Even so,nearly a thousand items were lent through the Swissinter -library loan service, and microfilms weresupplied on request to medical and scientific librariesin Czechoslovakia, Federal Republic of Germany,France, Italy, Japan, Norway, Poland, the Union ofSouth Africa and the United States of America.
JCHAPTER 9
PUBLIC INFORMATION
The year has been marked by progress in all typesof work in public information, both at Headquartersand in the regions. Encouraging reports of WHO'spublic- information programme were presented bythe directors of United Nations information centresin Europe, Asia and Africa, who attended thetwentieth session of the Consultative Committeeon Public Information, held at the end of June inGeneva, at the invitation of the World HealthOrganization.
Press and Publications
Press cuttings received from forty -eight countriesindicated that newspapers had made good use ofpress releases and special features, particularly thoseon penicillin and syphilis, world mortality fromsnakebite, the appearance of the WHO monographon plague, traffic accidents due to alcohol, the declinein infant mortality, deaths from transport accidentsand diseases transmitted from animals to man.
The material prepared by the members of thejoint UNICEF /UNESCO /WHO public informationteam which visited a number of Eastern Mediterra-nean countries in 1953 (see Annual Report for1953 1) was released during the year. A series ofarticles on this mission was published by Paris -Presse and in other publications in Europe.
The basic information folder WHO, What it is.. .What it does... How it works was made availablein ten different languages.
An illustrated booklet entitled A Strategy forWorld Health appeared at the end of the year inEnglish, French and Spanish. This replaces TheLamp is Lit, of which stocks were exhausted.
The Newsletter
In the first nine months of 1954, the total circula-tion of the Newsletter increased, through individualrequests alone, from 39 500 to 43 000 copies permonth, 35 000 of these being in English. The cir-
1 Off. Rec. Wld Hlth Org. 51, 59
culation of the French issue, as well as of the Englishedition, doubled in the last two years. The issues onalcoholism, the waterworks seminar in New Delhi,and mental health, had a particularly good reception.
An attempt is being made to increase the numberof articles originally written in French.
Radio
The supply of radio material to the United Nationsradio services at Geneva and New York was main-tained during the year. United Nations Radio,Geneva, devoted two weekly programmes to WHO.United Nations Radio, New York, included a talkon influenza in one of its feature programmes.
Early in 1954 the European Service of the BBCprepared a special broadcast on WHO, partlyproduced in Geneva, which was transmitted bythe BBC in eleven languages. The radio materialbrought back by the joint UNICEF /UNESCO /WHOmission from the Eastern Mediterranean was usedin three BBC broadcasts of one hour each.
Photographs and Exhibits
There has been an increase in the distribution ofphotographs and exhibits. Of the 31 000 standard -size and 500 exhibit -size prints produced in the WHOphotograph laboratory in 1954, 22 000 were dis-tributed either to regional information officers orto newspapers, photo- agencies, magazines or indivi-duals for publication and display.
The practice of issuing sets of a dozen or morepictures in the form of " picture- stories " with ashort accompanying text proved popular with photo -agencies and illustrated magazines : the six storiesalready distributed have been reproduced in morethan twenty countries. Further stories were startedon leprosy in Burma, yellow -fever in Latin America,poliomyelitis rehabilitation in Europe, and controlof yaws and malaria in the French Cameroons.
Seven new language adaptations of the travellingexhibit were made : in Arabic, Chinese, German,Hebrew, Italian, Swedish and Urdu.
- 56 -

PUBLIC INFORMATION 57
A new type of exhibit, consisting of a series ofsixteen enlarged photographs with printed text inblack- and -white, was produced with the title Healthis a Fundamental Human Right. Five thousandcopies were printed in five languagues, to meet partof the growing demand for exhibit materials in theregions.
Films and Filmstrips
A short newsreel made during the Seventh WorldHealth Assembly was shown, in cinemas and tele-vision programmes, in various parts of the worldand, according to estimates, may have been seen, inwhole or in part, by as many as forty million people.
Two film scripts were prepared in 1954 for pre-sentation to potential sponsors -one on mass cam-paigns against the treponemal diseases, and theother, for an animated cartoon, on alcoholism.
A filmstrip specially designed in colour to illustratethe structure and 'activities of WHO will serve forbriefing purposes and as a graphic accompanimentto talks and lectures.
World Health Day
National administrations and WHO regionaloffices made wide use of the " nursing " themechosen for World Health Day in 1954, in recognitionof the centenary of Florence Nightingale's workin the Crimean War. In many countries nursingassociations and nursing journals co- operated withnational and local health services in arranging forthe observance of this day.
The Director -General's World Health Day mes-sage was recorded and broadcast from a large num-ber of radio stations, including at least twenty -fivein Europe, frequently as part of feature or discussionprogrammes.
The BBC, in co- operation with WHO, produceda 60- minute documentary feature television pro -gramme, entitled World Nurse, which, according toBBC estimates, was seen by approximately fourmillion people in the United Kingdom.
The theme chosen by the Seventh World HealthAssembly for World Health Day for 1955 is theimportance of safe water for health.
CHAPTER 10
CONSTITUTIONAL, FINANCIAL AND ADMINISTRATIVE DEVELOPMENTS
Constitutional
Membership of the Organization
At the Seventh World Health Assembly, theFederation of Rhodesia and Nyasaland was admittedas an Associate Member of the Organization, theassociate membership of Southern Rhodesia con-sequently lapsing. The notice of acceptance ofassociate membership on behalf of the Federation,required under Rules 106 and 107 of the Rules ofProcedure of the World Health Assembly, was givenby the Chief Delegate of the United Kingdom ofGreat Britain and Northern Ireland at the sixthplenary meeting on 14 May 1954.
A list of the 84 Members and Associate Membersof the Organization 1 appears in Annex 1.
Agreements with Governments
Negotiations took place during the year with aview to the conclusion of :
(a) an agreement on further arrangements forthe Regional Office for Africa in Brazzaville ;(b) a host agreement with the Government ofDenmark, including provisions on the legal status,
privileges and immunities of the Organization, inconnexion with the establishment of the RegionalOffice for Europe in Copenhagen ; and(c) arrangements with the Government of Mexicofor the holding of the Eighth World HealthAssembly and the sixteenth session of the ExecutiveBoard in Mexico City.
Accessions to the Convention on Privileges andImmunities
Two Members acceded to the Convention on thePrivileges and Immunities of the Specialized Agenciesduring the year -Nepal on 23 February and Iraqon 9 July. The following twenty Member States havenow acceded to this convention (some with reser-vations), with respect to the World Health Organiza-tion : Austria, Belgium, Chile, Denmark, Ecuador,Egypt, Guatemala, Haiti, Hashemite Kingdom ofthe Jordan, India, Iraq, Italy, Luxembourg, Nepal,Netherlands, Norway, Philippines, Sweden, UnitedKingdom of Great Britain and Northern Ireland,and Yugoslavia.
The Financial Position
Although this section deals mainly with the finan-cial position relating to the regular budget of theOrganization -details of financial developmentsunder the Expanded Programme of TechnicalAssistance being given in Chapter 18 -some mentionof the latter in this chapter is unavoidable sincechanges in the availability of Technical Assistancefunds have repercussions on those of the regularbudget. Similarly the policy regarding the reimburse-ment by UNICEF of certain expenses of WHOrelating to jointly- assisted projects is mentioned hereas having implications for the regular funds.
During the first half of 1954, WHO was faced withfinancial difficulties similar to those experienced in
1 This figure includes nine inactive Members.
1953, as a result of the continued shortage of thefunds made available to the Organization under theExpanded Programme of Technical Assistance. Toensure the continuation of all projects already inoperation it was necessary to finance from regularfunds some continuing projects originally plannedunder the Technical Assistance programme and todefer some new projects planned for 1954 under theregular programme. A complete review of the 1954programme was therefore started with the purposeof adjusting it to the total resources available.Moreover, UNICEF was asked to give financialassistance in 1954 by reimbursing the costs of per-sonnel required for BCG and certain other jointly -assisted projects, and the UNICEF ExecutiveBoard agreed to allocate $828 000 for that purpose.
- 58 -
CONSTITUTIONAL, FINANCIAL AND ADMINISTRATIVE DEVELOPMENT 59
The Executive Board at its thirteenth session(resolution EB13.R39) approved the action taken orproposed by the Director - General to meet the situa-tion and asked him, inter alla, to report to the SeventhWorld Health Assembly the modifications made inthe 1954 programme as a result of his review, andany further developments in the financial situation.The Health Assembly approved the modificationsmade, which also took account of an increase in theamount earmarked for WHO by the TechnicalAssistance Board after the January session of theExecutive Board.
After the Seventh World Health Assembly afurther increase in the amount allocated from Techni-cal Assistance funds allowed the Director - Generalto resume financing under Technical Assistancesome of the continuing projects which had pre-viously been transferred to the regular budget. There- transfer of projects, a measure consistent withthe policy adopted by the Seventh World HealthAssembly for the 1955 programme, made it possibleto start work on some new activities, originallyplanned under the regular programme for 1954 butlater postponed. It was further found possible tofinance the costs of personnel in certain UNICEF/WHO jointly- assisted projects which the UNICEFExecutive Board had agreed to reimburse to WHO,and to inform UNICEF that WHO could returnapproximately $134 000 of the total amount thatits Executive Board had allocated for such costs in1954.
The Budget for 1954
The budget for 1954, as approved by the SixthWorld Health Assembly, was $9 838 000 ; this, lessa sum of $1 340 300 for the assessments of inactiveMembers, provided an effective working budget of$8 497 700.
Annex 7 shows the apportionment of the totalbudgetary provision for 1954 among the various
Structure and Staff
activities of the Organization and gives details ofthe transfers between sections of the AppropriationResolution made by the Director - General with theapproval of the Executive Board.
The actual obligations for the year will not beknown until the accounts to the end of the year areavailable. They will be published in the FinancialReport (a supplement to this volume), which willbe submitted, with the Report of the ExternalAuditor, to the Eighth World Health Assembly.
Contributions and the Working Capital Fund
In general, the payment of contributions inrespect of the current year was again satisfactory.Further progress was also made in the collectionof contributions due to the Organization for earlieryears ; hence it was possible to repay $104 032 tothe Working Capital Fund, thus liquidating advancesmade from the Fund pending the receipt of contri-butions for the 1952 budget. On the other hand, somegovernments became increasingly in arrears withtheir contributions to the Organization, even thoughtheir attention was drawn to the fact by the regularmonthly statements and by special letters and cables.
Tables showing the contributions received at31 December 1954, the comparative rate of collectionat the end of the years 1952, 1953 and 1954, and theadvances to the Working Capital Fund, will bepublished in the Financial Report.
WHO SealsThe issue of World Health Seals in 1955 was
approved by the Seventh World Health Assembly(resolution WHA7.23). The interest shown bygovernments in the sale of these seals has decreased,and in many cases the receipts have not covered thecost of printing. Eleven countries took part in thesales in 1952 ; only seven participated in 1953 andfive in 1954. Seven have asked for seals for sale in1955.
Administration
Some changes have been made in the structure ofthe Secretariat at Headquarters during the pastyear, either as a result of changed circumstances orin order to improve operating efficiency. Theorganization is shown in Annex 8.
In the Department of Central Technical Services,the Antibiotics and Insecticides Section was replacedby one on Health Laboratory Methods. Besides
providing advice on antibiotics in scientific fields ofresponsibility, as opposed to undertaking industrialactivities -a function which was transferred to theUnited Nations Technical Assistance Administration(see the Annual Reports for 1952 and 19531) -this section will give advice on methods andtechniques employed in health laboratories.
1 Off Rec. Wld Hlth Org. 45, 54; 51, 53

60 THE WORK OF WHO, 1954
In the Department of Administration and Finance,the Travel Unit was transferred from the Conferenceand Office Services Section to the Finance andAccounts Section, with the object of combining inone unit functions previously carried out separatelyand achieving more effective financial control.Another change in the Department was the placingof Supply Services, a unit which previously reporteddirectly to the Assistant Director -General, in theDivision of Administrative Management and Per-sonnel.
The size and geographical composition of the staffremained virtually constant throughout 1954. Detailsof the composition of the Secretariat as at 30 No-vember 1954 are given in Annexes 9 and 10.
Headquarters Accommodation
All questions relating to the new building have,as far as WHO is concerned, now been settled.
The total cost of the extension of the Palais desNations, subject to minor adjustments on receiptof final accounts from the United Nations, wasSw. fr. 4 424 613.97, of which Sw. fr. 3 000 000 wascontributed by the Swiss Confederation.
As the Fourth and Fifth World HealthAssemblies had voted a total amount of $362 975(Sw. fr. 1 553 533) for this purpose, there was a
surplus of Sw. fr. 128 919.03. An amount of$25 000 (Sw. fr. 107 000) having been previouslytransferred from the Building Fund to the AssemblySuspense Account, there remains a balance of$5 121.26 (Sw. fr. 21 919.03) which will be transferredwhen the final accounts have been received andagreed.
Place of the Eighth World Health Assembly
The Seventh World Health Assembly acceptedthe invitation of the Mexican Government to holdthe 1955 Health Assembly and the sixteenth sessionof the Board in Mexico City. A start was madeimmediately after the Health Assembly on theadministrative arrangements for these two meetings.
Site of the Regional Office for Europe
The Regional Committee for Europe held aspecial meeting during the Health Assembly toreconsider, at the request of the Executive Board,the question of the permanent location of the Re-gional Office in the light of new information thathad become available. The Committee's choice ofCopenhagen was approved by the Board in May,and negotiations were started with the Governmentof Denmark with regard to the host agreement andthe construction of an office building (see alsopage 83).
PART II
THE REGIONS

MAP 4. REGIONS AND OFFICES OF THE WORLD HEALTH ORGANIZATION
WHO HQ
ORegional Offices 1 as
eTemporary Regional Office
Q, Other Offices of the WHO
11111111
\L
African Region
Provisionally assignedto African Region
Region of the Americas
South -East Asia Region
ElEuropean Region
QProvisionally assignedto European Region
III111Eastern MediterraneanRegion
Provisionally assigned toEastern Mediterranean Region
© Western Pacific Region
Provisionally assigned to theWestern Pacific Region
ElStates and territoriesnot yet assigned to a region
WHO 4493
Owing to the small scale of this map, a precise delineation of the boundaries of each region cannot be given here.

/ CHAPTER 11
AFRICAN REGION t
The main aims of the programme in Africa and themethods which are being adopted to attain themhave been described in preceding annual reports.Some progress has been made, in co- operation withexisting health services and with UNICEF, inexpanding campaigns against communicable diseases,particularly malaria and the treponematoses. Pro-grammes for the control of tuberculosis, leprosy andother communicable diseases, and for the improve-ment of nutrition, nursing, maternal and child healthand environmental sanitation, are also under way.Surveys made in previous years are giving a solidbasis for beginning new projects and organizingtraining courses. Nevertheless, what has been doneso far represents only a very small fraction of whatstill remains to be accomplished. In view of thevery special conditions in the Region, studiesstill have to be carried out to determine the bestmethods to be used, before more extensive activitiescan be planned.
The Regional Committee
The Regional Committee for Africa held its fourthsession at Leopoldville, in the Belgian Congo, from20 to 25 September. This session was attended byrepresentatives of all Members and AssociateMembers in the Region : Belgium, France, Liberia,Portugal, Spain, the Union of South Africa, theUnited Kingdom of Great Britain and NorthernIreland, the Federation of Rhodesia and Nyasalandand the Spanish Protectorate Zone in Morocco.UNICEF, seven other intergovernmental organi-zations and eight non -governmental organizationssent representatives or observers. The Director -General was represented by an Assistant Director -General.
The Annual Report of the Regional Director wasdiscussed and noted with satisfaction.
1 This region comprises those parts of Africa not includedin the Eastern Mediterranean Region or among the FrenchTerritories of North Africa. It was delineated by the FirstWorld Health Assembly (see Off. Rec. Wld Hlth Org. 13, 80,330). In accordance with resolution WHA6.46, Ascension,Somaliland Protectorate, Mauritius, St Helena, Seychelles,Spanish Sahara (and its island dependencies), SpanishProtectorate Zone in Morocco, Tristan da Cunha andZanzibar were pro visionally assigned to this region.
The Regional Committee approved the draftprogramme and budget estimates for 1956 presentedby the Regional Director, subject to minor adjust-ments. It also approved the revised programme andbudget for 1955.
A discussion was held on campaigns againstsmallpox, on which, in accordance with a resolutionadopted by the Regional Committee at its thirdsession, health administrations in the Region hadbeen consulted. The information collected showedthat efforts to combat this disease were already beingmade by most of the governments in the Region andconfirmed that immediate practical assistance fromWHO was not required. The Regional Committeenevertheless reaffirmed its previous recommendationthat smallpox campaigns should be intensified, andsuggested that further studies should be made oftechniques and of types of vaccination.
Technical discussions were held on the subject ofpublic- health problems in rural areas. The RegionalCommittee reaffirmed its previous decision to havetechnical discussions each year on the topic discussedduring the previous World Health Assembly, andaccordingly decided that the topic for its discussionsat the next session should be " The health problemsof the pre -school child in Africa and the role of thepublic- health nurse in solving them ".
Particular attention was given to the developmentof relationships with the Commission for TechnicalCo- operation in Africa South of the Sahara (CCTA).The desirability of avoiding duplication of effortwas emphasized, and it was recommended that thefollowing points, among others, should be studiedwith the, CCTA : co- operation in organizing seminarsand conferences, joint research in the health field,and the allocation of responsibilities in the assistancebeing given to inter -country health programmes.
The Regional Committee considered the report ofan ad hoc committee that it had set up at its previoussession to consider the conditions of service forRegional Office staff (see Annual Report for 1953 2),and also a summary by the Regional Director ofdevelopments since the meeting of that committee.
2 Off Rec. Wld Hlth Org. 51, 68
- 63 -
64 THE WORK OF WHO, 1954
It was reported that progress had been made towardsimproving the conditions of service and in establish-ing provisions which would tend to make the staffingmore permanent. Notable developments had beenthe recruitment of larger numbers of local staff, andthe offer of the French Government to place a partof the Cité du Djoué at the disposal of the RegionalOffice to help solve the problem of office and livingaccommodation. The authorities of French Equato-rial Africa made arrangements for the RegionalCommittee to visit the Cité du Djoué. The RegionalCommittee was convinced that the negotiations beingundertaken would lead to satisfactory arrangementsand thanked the Government of France for itsassistance.
Finally, the Regional Committee confirmed itsdecision that its fifth session should be convened inTananarive, Madagascar, beginning on 19 September1955, and accepted an invitation from the Govern-ment of Portugal to hold the 1956 session in Luanda,Angola.
The Regional Office
In February, Dr F. Cambournac took over hisresponsibilities as the new Regional Director. Hevisited the Governments of all the Member countriesof the Region.
During the year the three administrative areas intowhich the Region had been divided were replaced byfour, constituted as follows :
Central area: Belgian Congo, Ruanda -Urundi,French Equatorial Africa, Angola, the Islands ofSão Tomé and Principe, and the Island of StHelena and its dependencies (Ascension, Tristanda Cunha).Western area: Liberia, Spanish Protectorate Zonein Morocco (North and South Zones), FrenchWest Africa, Cameroons (French), Togoland(French), Portuguese Guinea, Cape Verde Islands,Spanish Guinea (including Fernando Po, Annobón,Corisco, Little Elobey and Great Elobey), SpanishSahara (Rio de Oro and Sekia el Hamra), SidiIfni, Nigeria, the Gold Coast, Sierra Leone,Gambia, Togoland (British) and Cameroons(British).
Eastern area: Kenya, Uganda, Seychelles Islands,Somaliland Protectorate, Tanganyika, Zanzibarand Pemba.Southern area: Union of South Africa, the Federa-tion of Rhodesia and Nyasaland, Madagascarand dependencies, Reunion Island, Comoro Is-lands, Mozambique, Basutoland, Bechuanaland,Mauritius and dependencies, and Swaziland.
A public- health officer is to be assigned to each ofthe last three areas ; for the central area, the work willbe done by staff of the Regional Office. Two suchofficers were working in the Region at the end ofthe year.
The present policy followed in developing andstaffing the Regional Office is to expand it to approxi-mately the same size as that of the South -East AsiaRegion, because the needs of the Region suggestthat that is the appropriate size. At the end of theyear eleven internationally recruited and thirteenlocally recruited staff members were working in theRegional Office. There were difficulties in obtainingqualified personnel, and the post of Deputy RegionalDirector remained vacant. It was also difficult tofind enough project personnel : at the end of theyear there were fourteen field workers from ninedifferent countries, and four short -term consultants.
During the year technical officers in the RegionalOffice visited countries and territories of the Regionas much as possible, to obtain direct informationon health needs and the work already being carriedon. The public -health officer for the western areaspent part of the year at headquarters ; at the end of1953, he undertook journeys to Senegal, Liberia, theGold Coast, Nigeria and Leopoldville in connexionwith UNICEF /WHO assisted projects, and laterwent to the French Cameroons, Liberia and Nigeriafor discussions on projects for campaigns againstcommunicable diseases. The sanitary engineer fromthe Regional Office helped the health administrationin Nigeria to plan the distribution of potable waterin the Oudo Province (western area) and visitedLagos to give technical advice ; the sanitary techni-cian continued his work in the Seychelles.
Progress has been made in drawing up long -termplans. The sociologist attached to the RegionalOffice developed a method of sociological approachto health problems, and prepared commentaries onall the projects undertaken in the Region. Theresults obtained from these studies have shown thenecessity for advice of this type at all stages, andparticularly in the planning, of programmes forassistance to technically under -developed countries.
Since the appointment of the public informationofficer in September 1953, public- information acti-vities in the Region have developed considerably.Press releases and news items have been issued, andinformation on WHO is broadcast regularly byRadio Brazzaville in three programmes ; in 1954there were also a number of special broadcasts.World Health Day was observed in French EquatorialAfrica, the French Cameroons, Liberia, Nigeria,Northern Rhodesia and the Seychelles. Towards the

AFRICAN REGION 65
end of the year, the Regional Office was able tosupply information on existing visual media, tocirculate filmstrips and to prepare travelling exhibits.
Co- operation with other Organizations
The Regional Office has collaborated with UNICEFon numerous projects : from the list given in Part IVit may be seen that in Africa such joint projects haveconstituted a large proportion of the total.
Close relations have been maintained with FAO inconnexion with joint programmes and plans fororganizing training courses on nutrition.
As in the past, there were useful contacts withCCTA ; co- ordination was maintained on questionsof all conferences to be organized by one or the otherorganization, whether separately or jointly. Thisco- operation will be increased, by agreement withthe CCTA and in accordance with the resolution ofthe Regional Committee (see above). Plans have beenmade for holding a jointly sponsored training courseand seminar on rabies.
In Liberia there were frequent contacts with thepersonnel of the United States Foreign OperationsAdministration (FOA).
Regional Surveys and Research
Some of the surveys referred to in previous AnnualReports were continued in 1954. The survey oftuberculosis in western and central Africa wascompleted, and similar investigations were made inthe countries and territories of south and east Africa,including most of the islands in the Indian Oceanwhich form a part of the Region. The two reportsprepared on this subject will be sent to the govern-ments concerned.
The survey on health statistics, made by a consul-tant from Headquarters, who visited some of thecountries in the Region at the end of 1953, wasconcluded at the beginning of 1954. As there is agreat need for improving vital and health statisticsin Africa, WHO is conferring with the CCTA witha view to sponsoring a special project for this purposein 1955.
Finally, replies were received to a questionnaireconcerning mortality from serpent bites, on which asurvey was made, and to another on the epidemiologyand control of malaria.
As for the research sponsored by WHO within theRegion, the South African Institute for MedicalResearch has agreed to undertake investigations andtests on the resistance of body lice to insecticidesand negotiations are taking place with a view to itsacting as a regional research centre on poliomyelitis.WHO has also given subsidies to the Virus ResearchInstitute at Entebbe and the South African Institute
for Medical Research at Johannesburg for research onyellow fever immunity and epidemiology in Africa (forre earch on African cancer of the liver, see page 36).
Regional Conferences, Seminars and Training Courses
In October 1954, a conference on African oncho-cerciasis was convened in Leopoldville, all thenecessary facilities being provided by the BelgianGovernment. This conference, attended by somethirty experts from many countries and territories inAfrica, from countries of Europe and America andfrom several non -governmental organizations, washeld to exchange information on the seriousness andfrequency of this disease in Africa. Various aspectsof onchocerciasis were discussed : the factorsinfluencing the high incidence of blindness or otherserious eye complications in the various endemicareas, the connexion between onchocerciasis andvarious types of elephantiasis, onchocerciasis amongchildren, the economic and social importance of thedisease, the evolutionary cycle of the parasite worm,the biology and geographical distribution of theSimulium vectors in Africa, and the training ofspecialized sanitary personnel. The conference alsoconsidered general measures to be taken in controlcampaigns and the possibilities of organizingnational and international programmes againstonchocerciasis in Africa. It was agreed that thesuccess that had been obtained in vector controlprojects and the progress made in therapy justifiedundertaking such programmes, and suggestions weremade that the governments concerned should takeco- ordinated action on this problem, with assistancefrom the interested international organizations.
Preparations were made for a number of con-ferences, seminars and training courses to be heldin 1955 : a conference on malaria, a symposium onyaws, the seminar and course on rabies mentionedabove, a training course in malariology for physicians,to be given in the French language at the beginningof 1955 at Yaoundé, in co- operation with the FrenchGovernment, and a nutrition course in French, tobe organized jointly with FAO.
A conference, organized by the French Govern-ment and attended by a representative of WHO, washeld at Bobo -Dioulasso in French West Africa inDecember to prepare for the yaws symposium. Planswere also made for a conference on bilharziasis totake place in 1956, for the evaluation of materialaccumulated in the surveys conducted during thelast few years by the Snail Identification Centre,which continues to work in the Federation ofRhodesia and Nyasaland, and resulting from thework done in the various countries of the Region.
66 THE WORK OF WHO, 1954
Preparations were started for seminars in environ-mental sanitation and health education of the public,to take place in 1955 or 1956.
Fellowships
As an important step in strengthening the trainingprogrammes for health personnel and for the furtherdevelopment of health services, WHO has placedspecial emphasis on the fellowships programme inthe African Region.
For the first time in four years there was an increasein the yearly number of fellowships granted. Thetotal number of awards made in 1954 was 84, asagainst 27 in 1953.
Although most of the awards were again forindividual training (69), for the first time fellowshipswere also awarded for group training programmesorganized or assisted by WHO.
Sixty -three of the fellows received awards for studyin other regions, and twenty -one for study in theAfrican Region. The latter included fellowships forindividual training in the Union of South Africa,West Africa and Tanganyika.
Toward the end of the year the Regional Officetook over the administration of all its fellowships,which the Regional Office for Europe had previouslyassumed.
Selected Projects : Work on Communicable Diseases
As the Regional Office and most of the regionalprogrammes are still in the formative stage, it is notyet possible to describe any " typical " projects of theRegion. A complete list and brief description of allprojects current during the year are given in Part IVof the Report. Here it would perhaps be appropriateto say a few words about some of the campaignsagainst malaria and the treponematoses which arebeing carried out in countries in the Region, andsome of which have been going on for several years.
Non -Venereal Treponematoses in Bechuanaland
In Bechuanaland, a preliminary survey was madein September 1953 for a programme for the controlof the non -venereal treponematoses, known in thiscountry as " dichuchwa ". During the first yearthis project (Bechuanaland 1) was to consist of thesurvey and the training of personnel, who, during thesecond and third years, were to carry out masstreatment.
The national team was trained, and work began on23 November 1953. In 1954, the investigative stage wascompleted, and statistical and laboratory informationwere analysed to determine the symptomatology,endemicity and epidemiology of the disease and alsoits social repercussions. By the end of June, 18 438persons had been examined and 10 443 treated. Thework proceeded principally among the Bakwena,who number about 40 000. Much latent syphilis,especially in persons over fifteen years of age, and ahigh sero -positivity rate were detected, but littleactive treponematosis was found except in thepopulation of the desert fringe (Lelteking area).
The population distribution is different accordingto the time of year. As the area is situated on theedge of the desert, the population is concentratedin the villages during the dry period, especially inJuly and August, but during the rainy season and thefollowing months it is scattered over a very wide area.For this reason the activity of the teams variesaccording to the season.
Progress was more rapid than had been planned,and it is hoped to form a second national team in1955.
Full co- operation has at all times been given by theGovernment, the South African Institute for MedicalResearch, and the people, who have shown realenthusiasm for the assistance given.
Malaria Control in French Africa
Since November 1952, WHO and UNICEF haveassisted the French Government in an inter -countryproject on malaria control (French Africa 1).
Campaigns are being carried on by the FrenchGovernment itself in Senegal, Upper Volta, the IvoryCoast, Togoland, Dahomey and the northern partof the French Cameroons. WHO is assisting with apilot project in and around Yaoundé in the FrenchCameroons by providing personnel and technicaladvice. UNICEF is supplying insecticides, sprayingequipment and transport for the campaigns (exceptthe campaign on the Ivory Coast) and the pilotproject.
In the pilot project, which began in April 1953,various insecticides and methods have been tried witha view to deciding which will give the best results ina campaign for the control of malaria in this area.

AFRICAN REGION 67
In addition, the biology of anopheles found there isbeing studied, and the results obtained are beingassessed from the entomological point of viewand also from that of the incidence of the disease.
There are about 40 000 inhabitants in the pilotzone, distributed among about 200 villages. In thefirst round of spraying, which started on 24 Februaryand ended on 24 May 1954, 35 519 persons wereprotected and about 10 000 dwellings treated withinsecticides.
By the end of 1954, some 765 000 persons had beenprotected in the northern area (savannah) and in thesouthern area, which surrounds the pilot project andwhere the work is carried out exclusively by personnelemployed by the Government. The results from thepoint of view of malaria incidence are encouragingin both the pilot zone and the northern area. Noresults have yet been obtained for the southern areaas the work began there only recently.
There were again delays caused by the late arrivalof supplies, the inadequacy of the vehicles suppliedfor transportation, and failure to appoint matchingpersonnel. However, good progress was made in thepilot centre. Much is expected from the work ofthis centre, which is supplying useful scientificinformation on the epidemiology of malaria inAfrica, on anophelines, and on the most effectivemethods of control. Plans have been made for amalaria training course to be given in Yaoundé in1955.
Control of Yaws and Malaria in Liberia
In a combined project against yaws and malaria(Liberia 3 and 5), WHO has been assisting theLiberian Government since 1952.
From August 1953 to 30 June 1954 yaws surveyswere conducted in 134 villages. Operations developedin the early part of the year in the Gbarnga andSanniquellie districts, and a new survey was made inthe region of Bahn and Saklepea. On the basis ofthese surveys and resurveys, at the end of August1954, 40 239 people had been examined, and treat-ment given to 22 122 patients and 12 306 contacts.Progress was impeded, however, by lack of transport,penicillin, and fuel for the vehicles, the shortage andconstant turnover of local personnel, lack of co-operation by the population, and the difficulty ofrecruiting replacements for international staff. Theproject was without a WHO yaws adviser fromMarch and an administrator from September, but itis expected that replacements will arrive early in1955. Health education was undertaken by the male
public- health nurse, and serological surveys and masstreatment were continued.
In the malaria part of the project, three insecticidesare being used, as in the French Cameroons, in aneffort to determine which is the most effective.This work, too, was delayed by lack of transport,supplies and local personnel ; the internationallyrecruited staff also underwent many changes. By theend of 1954, about 55 000 persons had been protected.The policy governing spraying operations wasrevised : BHC spraying was limited to twice a year,and the area to be protected with dieldrin increased.It is expected that the area to be covered will beconsiderably expanded in 1955.
New Projects in Nigeria and East Africa
New projects against yaws and malaria (Nigeria 1and 2) were begun during 1954 with the assistance ofUNICEF and WHO. In the yaws project mobilefield units trained and staffed by the Governmentare conducting mass treatment campaigns withprocaine penicillin in each of the three regions ofNigeria, with especially good results in the easternregion. The medical officer provided by WHO isassisting in the eastern region and co- ordinating theactivities in all three regions. By September, thenational teams had examined 309 512 people,diagnosed and treated 206 712 cases, and treated96 427 latent cases and contacts. The rapid progressbeing made in this project is largely due to thebackground of knowledge and experience both ofthe doctors and field personnel. A new scheduleof penicillin dosage was adopted during the year.
The work in malaria, which is a pilot project todevelop measures adaptable to other areas of thecountry, has been begun by the Government. About50 000 persons have already been protected by theuse of dieldrin, DDT and BHC in three differentsectors. A fellowship was provided to the malario-logist in charge of the project, and WHO is recruitingan entomologist to assist with the work.
A further project with which WHO began toassist during the year is the strengthening of theEast Africa Malaria Unit in Amani (East Africa 1).This unit, which is being run by the British EastAfrica High Commission to serve Kenya, Uganda,Tanganyika, Zanzibar and Somaliland Protectorate,will be expanded into a malaria institute as a centrefor research and for planning and directing controlmeasures throughout East Africa. WHO is providingstaff, and UNICEF, supplies. The Director of theunit is operating a large pilot project in malariacontrol in the Pare Mountain area in Tanganyika,
68 THE WORK OF WHO, 1954
to be continued for four years. This pilot projectis rather different from other pilot projects : it is toassess the total effect of malaria control on thepopulation of a hyper -endemic area, and thereforeincludes an exhaustive survey of social, physical and
*
Present Trends and Future Developments
Particular attention is to be devoted to programmesfor developing environmental sanitation and healtheducation. The Regional Office is also continuing itsefforts to arrange for training larger numbers of per-sonnel as one of the principal means of strengthening
even mental conditions. About 54 000 persons willbe protected by the spraying of approximately 12 000dwellings with dieldrin, in an effort not so much tofind out how to protect the population as to deter-mine what the effects of this protection will be.
health services. Assistance in the control of the moreimportant communicable diseases will be continued,and new campaigns will be started, but only when thestudies referred to above have indicated the methodswhich can best be applied in the different conditionsexisting in the Region.
CHAPTER 12
REGION OF THE AMERICAS
In the Americas there has been considerableprogress in the development of public- health servicesduring recent years. This progress must, however,be assessed in relation to the expanding needs of apopulation which is increasing rapidly, especiallyin tropical areas. The population of Latin Americanow almost equals that of the United States ofAmerica and Canada and its rate of increase is high.A great effort is, consequently, required to raise thehealth services to a level which will not only meetpresent requirements but also provide for continuousexpansion commensurate with the growth of futureneeds. Leadership, energy, economic resourcesand trained personnel are required to develop public -health services ; at the same time it is of utmostimportance to continue assistance to governments inspecial campaigns against communicable diseasessusceptible to mass attack.
The specific health problems which have beenreported on in previous years have not changedsubstantially. The available statistical data show theseriousness of gastro -intestinal infections and para-sitic infestations and thus emphasize the need forenvironmental sanitation.
Well- trained, adequately paid and fully employedpersonnel continue to be required if efficient healthservices are to be developed throughout the Region.It is realized that standards of public -health ad-ministration- including personnel policies and con-ditions of employment in public -health services -are related to and dependent upon the standardsapplying to all government services. The Organi-zation obviously cannot offer advice on publicadministration as a whole ; but unless ways are foundto promote the employment of trained public -health
1 In accordance with the decision of the First World HealthAssembly (Of Rec. Wld Hlth Org. 13, 80, 331) this regioncomprises all the Americas. The following countries in theRegion are Members of WHO : Argentina, Bolivia, Brazil,Canada, Chile, Costa Rica, Cuba, the Dominican Republic,Ecuador, El Salvador, Guatemala, Haiti, Honduras, Mexico,Nicaragua, Panama, Paraguay, Peru, the United States ofAmerica, Uruguay and Venezuela. At the Sixth World HealthAssembly, the Falkland Islands and their Dependencies andHawaii were provisionally added to the Region (resolutionWHA6.46).
personnel on a full -time basis with adequate paytheir training will be wasted, the incentive for trainingmore personnel will be lost, and the health serviceswill be unable to meet demands made on them.
Regional Committee
The XIV Pan American Sanitary Conference,serving also as the sixth session of the RegionalCommittee of WHO, was held in Santiago, Chile,from 7 to 22 October. Meetings of the RegionalCommittee were attended by representatives of allMember States in the Region except Honduras(Canada was represented by an official observer) andof France, the Netherlands and the United Kingdomof Great Britain and Northern Ireland on behalf ofcertain territories in the Americas. Observers weresent by the United Nations and its specializedagencies, the Organization of American States, anda number of non -governmental organizations con-cerned with public health. The Director - Generalof WHO was present.
The Conference adopted for the Pan AmericanSanitary Bureau (PASB), which serves also as theRegional Office for the Americas, a programme for1955 in which emphasis is placed on strengtheningnational health services, and a budget of $2 100 000,the same amount as for 1954. Two million dollarsof this sum is to be financed by contributions fromMembers of the Pan American Sanitary Organization(PASO), and $100 000 by miscellaneous receiptsand contributions on behalf of the non -self-governing territories for which France, the Netherlandsand the United Kingdom are responsible. As the WHORegional Committee, the Conference approved aproposed programme and a budget of $1 158 255 forthe Region of the Americas for 1956, to be trans-mitted to the Director - General for his considerationin preparing the WHO budget for that year.
The Director of the Bureau, Dr Fred L. Soper,was re- elected by the Conference for a four -yearterm beginning on 1 February 1955, and the Con-ference, as Regional Committee, submitted his nameto the Executive Board of WHO for re- appointmentas Regional Director.
- 69 -
70 THE WORK OF WHO, 1954
Reports were presented on the public- healthconditions and the progress achieved in twenty -oneAmerican republics, Members of PASO, during thefour years between the XIII and XIV Pan AmericanSanitary Conferences. The Conference held technicaldiscussions and adopted resolutions on the eradica-tion of malaria and the treponematoses in theAmericas. With regard to malaria, attention wascalled to the experience of countries where eradica-tion has been achieved and to recent observationsindicating that some anopheline species havedeveloped resistance to certain insecticides. TheConference emphasized the urgency of carrying outthe terms of resolution XVIII of the XIII PanAmerican Sanitary Conference, in which it wasrecommended that the Pan American Sanitary Bureaushould promote the intensification and co- ordinationof antimalaria work, with a view to achieving theeradication of this disease in the Western Hemi-sphere. In another resolution the Conference author-ized the use of up to $100 000 of surplus fundsavailable as at 31 December 1954 for an increase ofthe Bureau's antimalaria activities, and decided toinclude an equal amount for that purpose abovethe 1954 budgetary level in the budget for 1956.
Technical discussions also took place on methodsof improving the reliability of raw statistical datarequired for health programmes, the control ofinfant diarrhoeas in the light of recent scientificprogress, and health education in rural areas inLatin America. It was decided that at the seventhsession of the Regional Committee the topics for thetechnical discussions would be (a) methods ofimproving the education of public -health personneland (b) medical care in rural areas.
The Executive Committee of PASO (also acting asa working party of the Regional Committee) metearlier in Washington, from 22 to 27 April, and inSantiago immediately before and after the Con-
Reports on Typical
A complete list of projects current during the yearwill be found in Part IV. The following have beenselected for fuller description.
1 The six zones are as follows : Zone I (Office, Washington,D.C.) for Alaska, Canada, the United States of America, andnon -self -governing territories except for British Honduras ;Zone II (Office, Mexico City) for Cuba, the DominicanRepublic, Haiti and Mexico ; Zone III (Office, GuatemalaCity) for British Honduras, Costa Rica, El Salvador, Guate-
ference. At the meeting preceding the Conference,it considered the regional budget for 1956. TheExecutive Committee will meet in Mexico City inApril, just before the Eighth World Health Assembly.
In 1955 the eighth meeting of the Directing Councilof PASO, which will be the seventh session of theRegional Committee, is to be held in Washington inOctober.
Administrative and Organizational Developments inthe Regional Office
A programme of economies and decentralization,begun in the Regional Office in 1951, had its greatesteffect the following year when the division of thecontinent into " zones " and the establishment ofzone offices was completed.1 Throughout 1952 and1953, efforts were continued to complete the staffingof all offices ; by early 1954, nearly all the seniorposts were filled, and by the end of the year therewere only a few important vacancies in Washington,in the zone offices, or in field projects. One significantdevelopment was the establishment of the post ofmedical adviser in the UNICEF Regional Office andthe nomination of an official to occupy it.
Amongst the factors affecting recruitment was asteady closing of normal sources of supply of skilledtechnicians. A number of Member States in theAmericas have shown increasing reluctance to releasepersonnel for service with international organizations,as they are convinced that these technicians are moreurgently needed in their own countries. Also someadministrative procedures established at the nationallevel have created delays in the recruitment of certainnationals. In spite of these difficulties, slow butdefinite progress has been made in completing thestaffing, and it is expected that most positions willsoon be capably filled.
Projects in the Region
Medical and Public -Health Education
To help countries to improve their standards ofbasic education in medicine and in public health,the Regional Office and zone offices, in collaboration
mala, Honduras, Nicaragua and Panama ; Zone IV (Office,Lima, Peru) for Bolivia, Colombia, Ecuador, Peru and Vene-zuela ; Zone V (Office, Rio de Janeiro) for Brazil ; and Zone VI(Office, Buenos Aires, Argentina) for Argentina, Chile,Paraguay and Uruguay.

REGION OF THE AMERICAS 71
with other interested agencies, are systematicallyaccumulating quantitative data about the medicalschools in Latin America. On the basis of thesedata fellowships are awarded to selected professorsfor training in other countries, and some schools arebeing provided with visiting professors and necessaryequipment (AMRO 18). During 1954 visits were paidto several of the schools for the purpose of assessingthe programmes and making plans for assistance overa period of years. One part of the programmeincludes plans for the award of travel grants to deansand senior officials of selected schools, to help themto re- appraise the curricula in the light of develop-ments in other countries. Unfortunately this part ofthe programme had little success in 1954, largelybecause of unexpected changes in the personnel at theschools for which such aid had been planned.
Greater progress can be reported in the programmefor schools of public health. Seven awards were madeto senior faculty members of North American schoolsfor visits to Latin America and six to senior facultymembers of Latin American schools (three in Chile,one in Argentina, one in Haiti and one in Mexico)for visits to both North and South America. Pro-vision has also been made for providing visitingprofessors and limited amounts of teaching equip-ment to some of these schools.
Seminars and Training Courses
Several seminars and training courses designed toimprove technical work in specialized fields of publichealth were organized in the Americas in 1954:among them a short training course in diagnosticmethods for brucellosis and a seminar in sanitaryengineering.
The former (AMRO 26.2) was held in Mexico Cityin March, with the collaboration of the FAO /WHOBrucellosis Centre and the Mexican Ministry ofHealth. A WHO consultant visited the variouscountries of Zones II and III to assist in selecting theparticipants -workers in brucellosis from tencountries. Two experts from the United States ofAmerica -one from the Public Health Service andone from the Department of Agriculture -helpedwith the instruction and collaborated with the staffof the Brucellosis Centre and the veterinary consul-tant for Zone II. This course was the second of aseries designed to raise the level of brucellosis
diagnostic procedures in government laboratoriesthroughout the Americas. Emphasis was placed onstandard performance and interpretation ofdiagnostic techniques, since many of the countriesin the area do not produce antigens.
The seminar on sanitary engineering (AMRO64.1), held in Caracas (Venezuela), in May, differedfrom the course on brucellosis in that it was attendedby senior personnel holding key posts in sanitaryengineering in the countries of Zones IV and V. Inaddition to an exchange of experience, there was adiscussion of possible methods of improving public -health engineering and of introducing work insanitary engineering into general health programmes.The Government of Venezuela acted as host, tookpart in the seminar, and will publish the proceedingswith assistance from WHO.
Nursing Education, Bolivia
Assistance is being given to Bolivia in nursingeducation as part of a long -term project (Bolivia 5)designed to raise nursing standards throughout thecountry. The immediate objective is to improve theNational School of Nursing. This is being done byrevising the programme of studies, training a facultyof nurses and improving the wards where the studentsobtain clinical experience. Two nurse educatorscollaborated in the project in 1954.
Entrance requirements for the school have pur-posely been kept high in order to obtain a nucleus ofgraduate nurses who may later serve as instructors inthe school and supervisors in the health services.After two years the school's advisory committeewill decide whether a full secondary education canbe maintained as an entrance requirement or whetherit is too high. The first class, which began the schoolyear in April 1954, had seventeen students, themajority of whom have their " bachillerato ".
To prepare a group of head nurses fully acquaintedwith the new programme, a refresher course in wardteaching and administration was given to seventeengraduate nurses, in January and February.
A faculty of nursing instructors is slowly beingformed. By the end of the year,, six nurses, three ofthem in 1954, had been sent to Chile for basicnursing preparation, and three graduate nurses havebeen given one -year fellowships to train them to

72 THE WORK OF WHO, 1954
teach certain specialties. For the first time a nursewas appointed Director of the school ; she began hernew duties in April.
Tuberculosis Teaching Centre, Ecuador
The project at the tuberculosis teaching centre inGuayaquil (Ecuador 5) was designed to assist withthe training of national students and, when possible,of some students from other countries with similarproblems and inadequate training facilities.
The Government of Ecuador has constructedliving quarters for the students, and the Organizationhas provided a pathologist, a short -term consultantand some financial support. In 1954 a six -weekcourse was attended by eleven students from Ecuadorand eight students from Bolivia, El Salvador, Guate-mala, Honduras, Panama and Paraguay. Specialemphasis has been placed on the development ofservices in pathology.
Health Demonstration Area, El Salvador
In August 1950 the Minister of Health of ElSalvador requested WHO's assistance in setting upa health demonstration area in the San Andrésvalley, an important agricultural area with a popu-lation of about a hundred thousand. An initialsurvey revealed that major health problems weremalaria, gastro -intestinal infections, tuberculosis andmalnutrition, which could not be dealt withadequately because of the lack of trained personnelto provide medical care and to improve hygiene andsanitation. The object of the project was to organizeand develop a programme of health services in aselected area, co- ordinated with programmes ofsocial and economic improvement (in agriculture,education, and labour relations), to demonstratepublic -health methods which could be applied else-where in the country, and to provide field training forpublic- health personnel. ILO, FAO and UNESCOalso co- operated in this project (El Salvador 5).
During the first year (1951) a planning committeewas set up, consisting of representatives from certainministries and international agencies giving technicalassistance. DDT spraying of the area was begun,and training programmes for sanitary inspectors,public -health nurses, and nursing auxiliaries wereorganized. A start was also made on renovating the
buildings to be used for health centres and fortraining.
In the next year, detailed surveys of the area weremade by sanitary inspectors, nurses and healtheducators, and a plan of operations was preparedby the Government. Activities were first started inthe health unit of Quezaltepeque, where centraloffices were established. In the following yearsthe work was gradually expanded, so that full healthservices are now available to two- thirds of thepopulation of the area and more limited services tothe other third.
Some of the population has become transient as aresult of the short -term employment which is charac-teristic of the sugar, coffee and cotton industries, andthis has created a special problem of housing and ofcontinuity of health services. The housing situationhas therefore received particular attention.
Health units and clinics have been built and arebeing operated in the main population centres, andsanitary posts are being set up to extend servicesto the rural areas. Services in medical care, maternaland child health care, and emergency treatment wereprovided from the outset. More recently they havebeen extended to cover school hygiene and the controlof communicable diseases such as tuberculosis andvenereal diseases. Emphasis has been placed through-out on the development of sanitation : the provisionof safe water, the building of privies, the constructionof sanitary premises for markets and slaughterhouses,the disposal of garbage and sewage and the controlof waste from the coffee and sugar industries. Thepublic has been encouraged to take part in all theseactivities. Assistance has also been given in thecollection of statistical data and in the organizationof an adequate records system.
National personnel are being trained in the countryand elsewhere so that they may eventually be ableto assume the entire responsibility for continuing thehealth services after the internationally recruitedpersonnel are withdrawn. In- service training is alsobeing carried out as a fundamental part of the pro-gramme. Training centres are being developed.Special orientation programmes have been arrangedfor workers already trained in public health. Fellow-ships have been awarded for study abroad in public -
health administration, statistics, nutrition, healtheducation, public -health nursing and sanitation.

REGION OF THE AMERICAS 73
However, the responsibility for local training is beingassumed to an increasing extent by the personnel ofthe demonstration area : those trained in the areahave subsequently been employed there, or by theMinistry of Health for assignments in other parts ofthe country, where they apply the methods theyhave learned.
The administration of this project is being decen-tralized to the local units. Furture plans include theextension of all the health services throughout thearea, the training of further personnel, and theevaluation and consolidation of the activities.
Yaws Eradication and Syphilis Control, Haiti
Until 1950, yaws was undoubtedly the mostimportant public- health problem in Haiti. In spiteof an almost complete lack of statistical data, thedisease was known to be highly prevalent in therural areas ; it was estimated that it affected about athird of the rural population, reaching 50 to 70 percent. of the inhabitants in some areas. It incapacitatedand disfigured many persons and caused untoldsuffering.
In 1949 the Government asked for internationalhelp to combat yaws. In July 1950 the Government,UNICEF and WHO undertook to co- operate byorganizing an eradication campaign (Haiti 1) basedon mass treatment with penicillin (600 000 units forcases and 300 000 for contacts).
From July 1950 to October 1951 over 650 000persons were treated by the " daily clinic method ".When official census figures first became availablein 1951, it was apparent that this was a relatively lowproportion of the population of the areas covered.It was therefore necessary to change to the " house -to -house method ", whereby each house was visitedand all cases and contacts treated. By this method,from 27 October 1951 to 31 July 1954, treatment wasgiven to over two and a half million persons, makinga total of more than three millions, i.e., nearly 98per cent. of the population of the areas concerned.At present, one or other method of treatment has beenused in all rural areas. In spite of the high coverageobtained by the " house -to -house method ", smallfoci of the disease still remain throughout Haiti.
To evaluate the efficacy of both methods, surveyswere carried out in the Department of the South,from November 1953 to March 1954, and in theDepartments of the North and North -West, fromMarch to April 1954. In the Department of theSouth a sample of almost 40 000 persons (about
5 per cent. of the population) was examined ; therates of prevalence observed ranged from a maximumof 8 per cent. in one locality and 4.3 per cent. in onerural section to 0 per cent. in six rural sections,giving an average prevalence of 0.8 per cent. Thoserates show clearly the excellent results obtained in thisprogramme, even in regions previously thought of asdoubtfully treated. In the survey of the North andNorth -West a sample of about 5600 persons or 0.8per cent. of the population was examined. Therates of prevalence observed ranged from 0.8 per cent.(in two rural sections, one in each Department) to0 per cent. in one rural section, with an averageprevalence for both Departments of 0.35 per cent.The differences between these average prevalencescan be attributed in part to the different methods oftreatment, i.e., the " daily clinic method " used in theDepartment of the South and the " house -to -housemethod " in the Departments of the North andNorth -West.
Similar surveys are being carried out in the rest ofthe country in order to establish the present yawsprevalence.
The results of the surveys to determine residualinfected cases have been encouraging, and havegiven a firmer basis for expecting that yaws will beshortly eradicated from the entire country. It isbelieved that the present prevalence for all the ruralareas in Haiti is not above 0.5 per cent.
It is planned to broaden the yaws programme toinclude an intensive campaign against urban syphilis,by mass treatment techniques, which are justified bythe gravity of the problem. A recent study of urbansyphilis has confirmed the seriousness of the situationpreviously reported.
Tuberculosis Control and BCG Vaccination, Paraguay
In Paraguay the death -rate from tuberculosis _isexceeded only by that from the parasitic diseasesand enteritis of childhood.
In 1951, the Government requested WHO's helpin organizing a large -scale programme of tuberculosiscontrol and in training the local health personnel tocarry it out (Paraguay 2). This programme was tobe co- ordinated with other health services forwhich the Government had also requested WHO'said under the Technical Assistance Programme.
The Organization provided a tuberculosis adviser,a medical bacteriologist, a public- health nurse andan x -ray technician, together with the supplies and

74 THE WORK OF WHO, 1954
equipment (x -ray, laboratory, clinical, etc.) requiredto maintain this type of programme.
Progress was handicapped in 1952 by difficultiesin recruiting personnel and, particularly, in procuringand delivering equipment. In 1953 the main emphasiswas placed on training local personnel. With theassistance of the x -ray technician, four x -ray unitsprovided by the Organization were installed inAsunción, Villarrica, Paraguarí and San Bautista.
During 1954 the programme made good progress.The tuberculosis services already existing in Asunciónwere expanded, and new services were created inthe rural areas outside the capital city. Radiologicalsurveys were carried out in the capital and in some ofthe new dispensaries. Training of the nationalpersonnel assigned to the programme was continued.Norms for carrying out radiological surveys andinstructions for the clinical personnel of the dis-pensaries were prepared by the WHO x -ray techni-cian. A central registry of tuberculosis patients wasorganized in Asunción.
The clinical laboratories in Asunción and thosein the different dispensaries were equipped. Amember of the national staff received a WHOfellowship for study of the clinical and controlaspects of tuberculosis in Argentina.
A BCG vaccination campaign, assisted by UNICEFand WHO, has also been started (Paraguay 7).Regional advisers trained staff and helped to makegeneral plans for the campaign ; a physician and anurse were recruited by WHO (their cost reimbursedby UNICEF), and a BCG statistician spent severalweeks in Paraguay training personnel in the statis-tical aspects of the campaign.
Public Health Demonstration and Training Centre,Peru
In December 1950, the Minister of Health andSocial Assistance of Peru requested the help of WHOand UNICEF in integrating and expanding healthservices in the Municipality of Callao, an urban areabordering on Lima. In September 1952 WHO agreedto assist in a project for unifying and promotinghealth services in Callao in order to demonstrate thevalue of integrated activities in solving major healthproblems and to provide a pattern of administrationand public -health practices which could be appliedin other parts of the country (Peru 13).
An initial survey was carried out late in 1952 withthe help of two internationally recruited consultants.
According to the plan subsequently developed, allhealth services previously administered from centralservices in the Ministry of Health were to be con-solidated in a local health unit, with a directorresponsible only to the Division of Health Units ofthe Ministry. The services would also be co- ordinatedwith other medical and related services in the pro-vince, and would demonstrate modern public- healthmethods and procedures.
In 1953, a separate national budget for the CallaoHealth Unit was approved ; a co- ordinating com-mittee was organized, and unification of services wasbegun. Divisions of health education and public -
health nursing were set up ; work in environmentalsanitation was organized. A number of full -timecareer positions were created for trained public -health workers. Staff previously employed in thevarious central services were absorbed by the newlycreated unit, and in- service training was planned forthem and for new staff members.
In 1954, the integration and expansion of servicescontinued. Tuberculosis and venereal- disease case -
finding campaigns were carried out among selectedgroups, and methods were developed for the reportingof communicable diseases by physicians and hospitals.Although the local tuberculosis dispensary continuesto be administered by the appropriate department inthe Ministry of Health, progress has been madetowards integrating the dispensary services with thehealth unit.
The division of environmental sanitation in thehealth unit has taken over the former programmeof sanitary inspection of the municipality, and thework done in assuring safe water, food sanitation,and adequate garbage and refuse disposal is beginningto show results.
Maternal and child health and school healthservices have been expanded, with emphasis onpreventive measures. The interest and participationof parents and teachers in school health has beenespecially gratifying.
Activitic s in health education have been plannedand carried out as a part of all services and by allstaff members. The health unit is also being used forfield training of medical and nursing students, and itsprogramme has been studied by a number of physi-cians interested in learning about public -healthpractices.
It is planned to consolidate this programmefurther in 1955, with the assistance of an adviser in
REGION OF THE AMERICAS 75
maternal and child health and the award of twofellowships to candidates for study abroad. In- servicestaff training will be continued. Problems still to bedealt with are the limited space in the centre (buildingplans were halted for lack of funds), the need for astable budget, the improvement of personnel prac-tices and the fixing of adequate salary scales toensure full -time services.
Education and Training Programme in StatisticsTo improve health statistics throughout the
Americas a programme for training in health statisticsis being organized in a series of individual trainingprojects ; of the five projects for which assistance hasbeen given, four are described below.
One (AMRO 75, financed by PASB) is designed topromote professional training in statistics, and toprovide undergraduate and post -graduate educationfor statisticians, with the ultimate objective ofestablishing health statistics as a profession. Thisrequires the organization of regular courses inelementary statistics in national universities and theestablishment of a centre, or centres, for specializedpost -graduate training in health statistics, for adegree comparable to that of Master of Science. Theproject is to assist countries to provide universityeducation in statistics, and to improve the teachingof statistics in schools of public health. Fellowships,short -term consultants and supplies will be provided.Progress has been made during the year in the slowprocess of setting up these courses for undergraduatesand graduates within the present pattern of theuniversities.
In 1954, the Inter- American Centre of Biostatisticsin Chile (AMRO 10) organized a second course invital and health statistics for officials with importantresponsibilities in the registration, collection, com-pilation, analysis and teaching of vital and healthstatistics in Latin America. The nine -month course
(six months theoretical and three months practical)is designed for students with secondary education touniversity entrance standard and preferably withsome higher education : it is not for doctors or pro-fessional statisticians. Twenty -seven students fromfifteen countries attended in 1954. The faculty of theSchool of Public Health of Chile participates in theprogramme and in 1954 took more responsibility forthe administration and teaching of the courses. Ithas made its statistical offices available for the fieldtraining programme.
WHO is helping to provide courses to train statis-tical clerks in vital statistics, notifiable- diseasestatistics, and elementary statistical methods. Thefirst, a six -week training course in biostatistics(AMRO 79), held in Jamaica at the end of 1954, wasattended by seventeen students from Antigua,Barbados, Bermuda, British Guiana, Dominica,Grenada, Jamaica, Netherlands Antilles, St Kitts,St Lucia, St Vincent and Trinidad. The subjectstaught included vital statistics, elementary statisticalmethods, health statistics, the International StatisticalClassification of Diseases, Injuries and Causes ofDeath, hospital statistics, and statistics for healthand medical services.
To provide in- service training, plans have beenmade for a course on the International StatisticalClassification in Spanish for the Spanish- speakingcountries of the Americas (AMRO 85). It is to beheld in 1955 in the Centre for Classification ofDiseases of the Ministry of Health of Venezuela.
To stimulate the development of this programmein two zones of the Region, a health statistician is tobe added to the staff in 1955 (AMRO 86). He willassist with the education and training programmes instatistics, by helping to develop university educationand training courses in biostatistics and by selectingthe students for such training.
* * *
Trends and Future Developments
The planning of programmes by zone offices inconsultation with national health authorities and thesubsequent careful study of the programme andbudget by the Regional Committee have resulted in
widespread understanding and support of WHO'sprogramme. Public -health services in all countriesgain by the participation of governments in aninternational organization, and national health

76 THE WORK OF WHO, 1954
administrations are increasingly disposed to make useof the international machinery provided.
The large number of inter -country projects in theRegion clearly indicates the readiness of governmentsto take joint action in solving common problems.Some inter -country projects involve the control ofcommunicable diseases or of some disease vectors ;others are to establish and maintain special facilities- such as laboratories - which can be more eco-nomically and effectively operated by co- operativeeffort ; others, again, are to develop training facilitiesand the exchange of scientific information.
Health administrations are showing greaterappreciation of the value of and need for the technicaladvisory services of the Organization. With thewider use of modern techniques of public administra-tion and organization, frequent requests for suchservices are accepted as a normal and necessaryelement in growth and improvement : it is beingrealized that the use of consultant services is evidenceof a desire for growth and of a capacity to absorbnew ideas and techniques. Fortunately this attitudeis replacing the negative idea that a request fortechnical advice is an adverse reflection on existingservices.
In the last five years the budgets for health activitiesof many Member countries in the Region have sub-stantially increased. The trend toward the develop-ment of integrated national health programmes,reported in 1954, has continued : two projects ofassistance in integrating public- health services werestarted in 1954 in Guatemala and Nicaragua, andmore are planned for 1955 and 1956.
The activities in the field are consistent with thelong -range programme adopted by the Regional
Committee, so that no important changes from yearto year may now be expected. Developments willrather take the form of more precise definition ofobjectives, improving the quality of advisory services,emphasis on improving and increasing trainingfacilities, and more effective planning.
Work on communicable diseases will continue.Experience has indicated that there is a sound basisfor attempting to eradicate yaws from the Region.The malaria -control programmes undertaken bythe countries in the Region are to be developed intoprogrammes for the eradication of malaria, and at thesame time a special effort is to be made to rid theRegion of Aëdes aegypti in the shortest possible time.,Finally, special emphasis will probably be given tocampaigns against smallpox, the importance ofwhich has in past years been emphasized by theRegional Committee.
Efforts are being made to stimulate and improvepublic -health statistics : as mentioned on page 75, afield consultant to assist health administrations inthis task will start work in 1955 in a large area.Better planning of health programmes is also beingstimulated : basic information on each country isbeing collected for this purpose, and, as a part ofcertain projects with which WHO is assisting, thegovernments have included requests for help innational planning and in the establishment of officesfor such planning in their national health services.
Projects for the integration of all types of public-
health services provide an effective vehicle for thewidespread application of measures for environmentalsanitation, and more emphasis on this subject in theRegion is also to be expected.
CHAPTER 13
SOUTH -EAST ASIA REGION 1
Eighty -five per cent. of the people of the South -East Asia Region are in rural areas and have a verylow standard of living. The provision of healthservices for the people in these areas is consequentlythe basic need. As a step towards meeting it, variouskinds of rural health units are being organized by thegovernments. From a modest start, with emphasison environmental sanitation and on maternal andchild health, they will gradually be expanded asresources in money, material and manpower permit.
WHO- assisted programmes for maternal andchild health, control of communicable diseases andfor training health personnel are gradually beingintegrated into the general public -health services.These programmes are an important activity in theRegion, and some of them have been in operationfor a number of years.
For planning and supervising the expansion ofhealth services an administrative structure adequateat all levels is essential. To help strengthen thenational administrations in Afghanistan, Burma,Ceylon and Indonesia, internationally recruitedexperts have been or are to be attached to the healthdirectorates.
Basic environmental sanitation remains the mostimportant single problem, and plans have beenmade to give more assistance in sanitation to all thecountries in the Region.
The shortage of trained staff of almost all cate-gories- doctors, nurses, midwives, health assistants,sanitarians, health visitors, etc. -continues, andthere is also a great lack of auxiliary personnel.The Organization is therefore giving much attentionto helping governments in their training programmes.
For the achievement of these ends, it has becomemost important for the health efforts of the variousinternational organizations working in the Regionto be co- ordinated, and the responsibilities of the
1 The South -East Asia Region comprises Afghanistan,Burma, Ceylon, India, Indonesia, Nepal and Thailand (seeOff. Rec. Wld HIM Org. 13, 80, 330 ; resolution WHA3.118 ;and resolution WHA6.48). In accordance with resolutionWHA6.46, the Maldive Islands were added to the Regionprovisionally.
Regional Office in collaborating with other agenciesand advising governments have been very muchincreased. Health co- ordination committees havenow been established in all the countries of theRegion.
The Regional Committee
The Regional Committee for South -East Asiaheld its seventh session in New Delhi from 21 to25 September, at the seat of the Regional Office.Representatives of nine of the ten Member countriesof the Region were present (the United Kingdom ofGreat Britain and Northern Ireland was not re-presented). There were also representatives of theUnited Nations (including the United NationsTechnical Assistance Board and UNICEF), ILO,UNESCO, and fourteen intergovernmental andnon -governmental organizations, and observers fromother agencies. The Prime Minister of India waspresent at the opening of the session and addressedits first meeting.
The sixth annual report of the Regional Directorwas discussed at length, and the following pointsemerged : National health administrations are spend-ing a disproportionately large percentage of theirnational budgets on medical care institutions ascompared with the amount allocated for public -health activities such as sanitation and water supply ;much greater stress needs to be given to the adequatestaffing of national health administrations at thecentral and provincial levels in order, to ensurethe adequate supervision of planned programmes inpublic health ; experience has shown that nationalhealth co- ordination committees are useful andimportant ; in view of the rapid industrialization inthe Region, further attention should be given toindustrial health services ; work on improvingenvironmental sanitation, health education, andeducation and training services should continue tobe considered basic health activities in the Region ;without minimizing the importance of internationalfellowships, the Organization should continue toencourage regional and national fellowships ; andthe reports of the Regional Director should contain
- 77 -
78 THE WORK OF WHO, 1954
information not only on activities for which inter-national assistance is being given but also on thework of national health administrations in general.
The Regional Committee considered that anappropriate and satisfactory balance between majorsubject headings in the regional programme for 1955had been maintained, in spite of the modificationsmade necessary by budgetary reductions. A pro-posed programme and budget and a supplementaryprogramme of projects for 1956 were discussed andendorsed.
As a result of discussions on environmentalsanitation and medical education, Member States inthe Region were called upon to give top priority toenvironmental sanitation in their health programmes,and the Regional Director was requested to encouragethe convening of national conferences or studygroups of medical educators and administrators toexamine problems of the education of medicalundergraduates.
A number of useful recommendations arose fromthe technical discussion on nursing requirements inrelation to health programmes.
The Regional Committee noted with satisfactionthe recommendation of the Executive Board and thedecision of the World Health Assembly that Membergovernments should be exempted from providinglodging and other subsistence allowances (includingtravel per diem within the country) to expertsassigned to new projects planned to start in 1955and to all projects from 1956 onwards.
It was decided that whenever the subjects chosenfor the technical discussions held during the WorldHealth Assembly were of direct and immediateregional interest the Regional Committee wouldarrange for their discussion at the regional level.The subject chosen for the regional technical discus-sions in 1955 was a review of antituberculosismeasures in South -East Asia.
The Regional Committee expressed its apprecia-tion of the offer of the Government of India to placethe facilities of the Central Research Institute, inKasauli, at the disposal of the countries in theRegion, free of charge, to serve as a laboratory fortesting the quality and potency of biologicalsubstances and to train personnel.
The Regional Committee accepted an invitationfrom the Government of Indonesia for the holdingof its eighth session in Indonesia. The ninth sessionwill be held at the seat of the Regional Office inNew Delhi, and the tenth, on the invitation of the
Government of the Union of Burma, in that country.These sessions will be held in September of 1955,1956 and 1957 respectively.
Regional Office
There was little change in the structure of theRegional Office. A few local posts, such as that oftravel clerk, were suppressed as an economy measure.Other posts remained vacant because of the difficultyof securing suitable personnel. A regional adviserin venereal diseases was recruited, but the posts ofstatistician for the Epidemiology and Health StatisticsUnit, of regional advisers in environmental sanitationand health education, and of area representative forThailand remain unfilled. The difficulty of recruitingsuitable experts for field work was aggravated bythe uncertainty of the availability of funds underTechnical Assistance. In other cases successfulrecruitment could not be effected because of delaysby Member governments either in signing plans ofoperations or in clearing prospective candidates.
In public- information work closer relations weredeveloped with Member governments. Greateruse was made of World Health Day as an occasionfor stimulating public interest in national and localhealth programmes rather than merely for publicizingthe activities of the Organization. Six MemberStates have now appointed liaison officers to co-operate with the Regional Office in promoting abetter understanding among the general public ofWHO's aims and its work for the strengthening ofnational health services. A forty -page illustratedbooklet on Afghanistan's internationally -assistedhealth work was published, and the Regional Officewas able to stimulate interest among a number ofcommercial producers in the possible production ofdocumentary and educational films.
Co- operation with other Agencies
Relations between the Regional Office and theUnited Nations and specialized agencies have beenclose and cordial. The Regional Office took anactive part in the International Exhibition of Low -Cost Housing, and in the seminar on low -costhousing organized by the United Nations TechnicalAssistance Administration during the year. Aninter -secretariat working party on housing, underthe auspices of the Economic Commission for Asiaand the Far East, was held at the Regional Office.
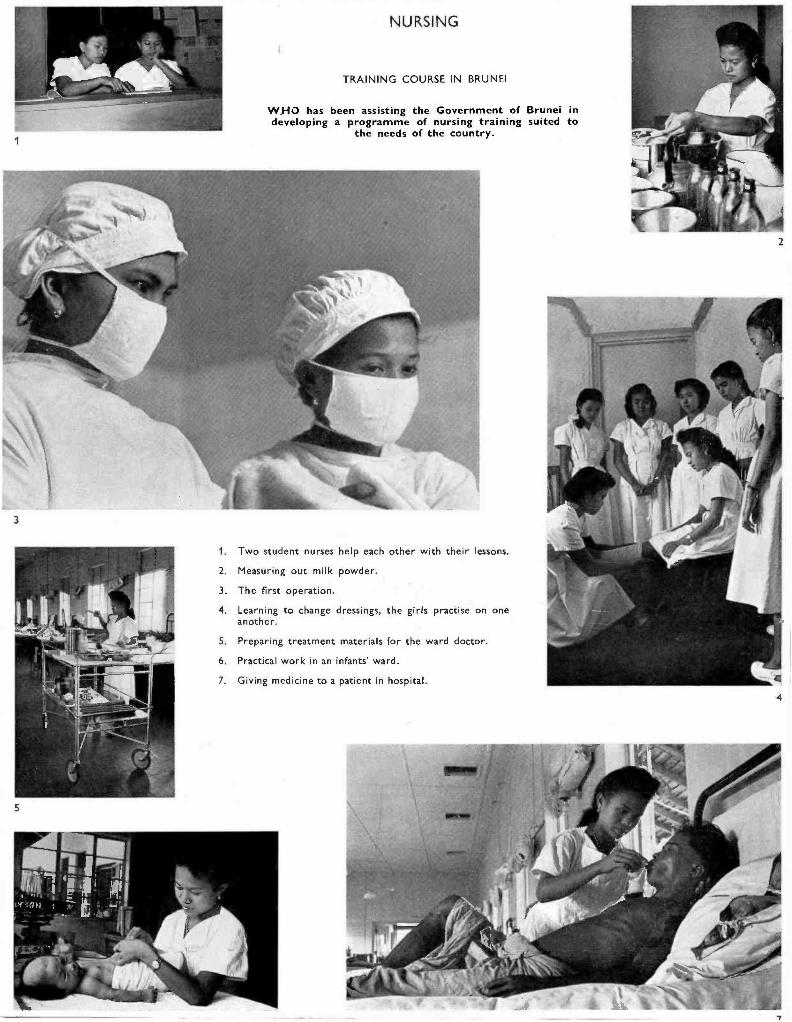
NURSING
TRAINING COURSE IN BRUNEI
WHO has been assisting the Government of Brunei indeveloping a programme of nursing training suited to
the needs of the country.
3
5
1. Two student nurses help each other with their lessons.
2. Measuring out milk powder.
3. The first operation.
4. Learning to change dressings, the girls practise on oneanother.
5. Preparing treatment materials for the ward doctor.
6. Practical work in an infants' ward.
7. Giving medicine to a patient in hospital.
2
4
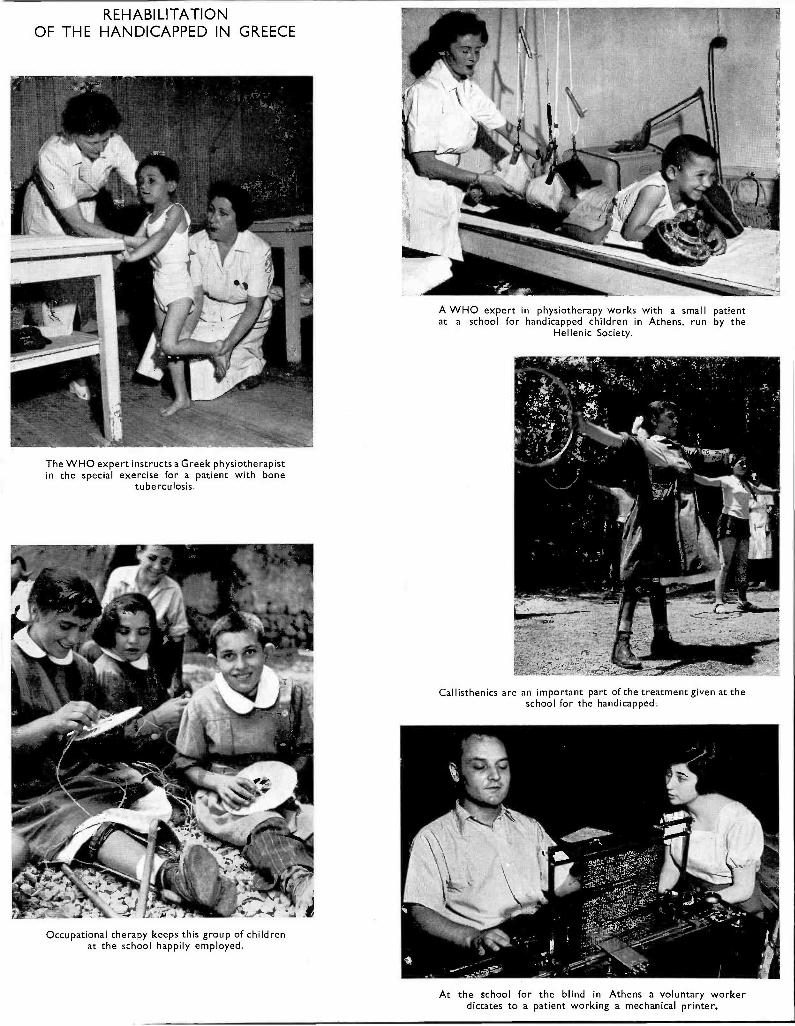
REHABILITATIONOF THE HANDICAPPED IN GREECE
The WHO expert instructs a Greek physiotherapistin the special exercise for a patient with bone
tuberculosis.
Occupational therapy keeps this group of childrenat the school happily employed.
A WHO expert in physiotherapy works with a small patientat a school for handicapped children in Athens, run by the
Hellenic Society.
Callisthenics are an important part of the treatment given at theschool for the handicapped.
At the school for the blind in Athens a voluntary workerdictates to a patient working a mechanical printer.
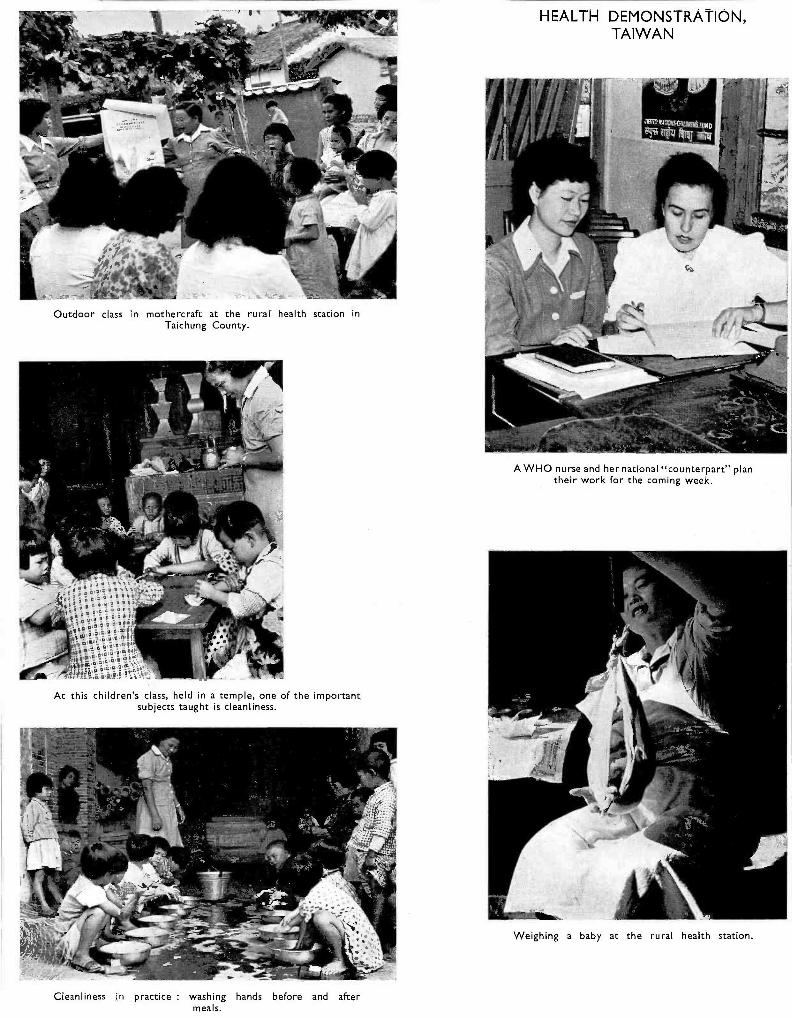
Outdoor class in mothercraft at the rural health station inTaichung County.
At this children's class, held in a temple, one of the importantsubjects taught is cleanliness.
Cleanliness in practice : washing hands before and aftermeals.
HEALTH DEMONSTRATION,TAIWAN
A WHO nurse and her national "counterpart" plantheir work for the coming week.
Weighing a baby at the rural health station.
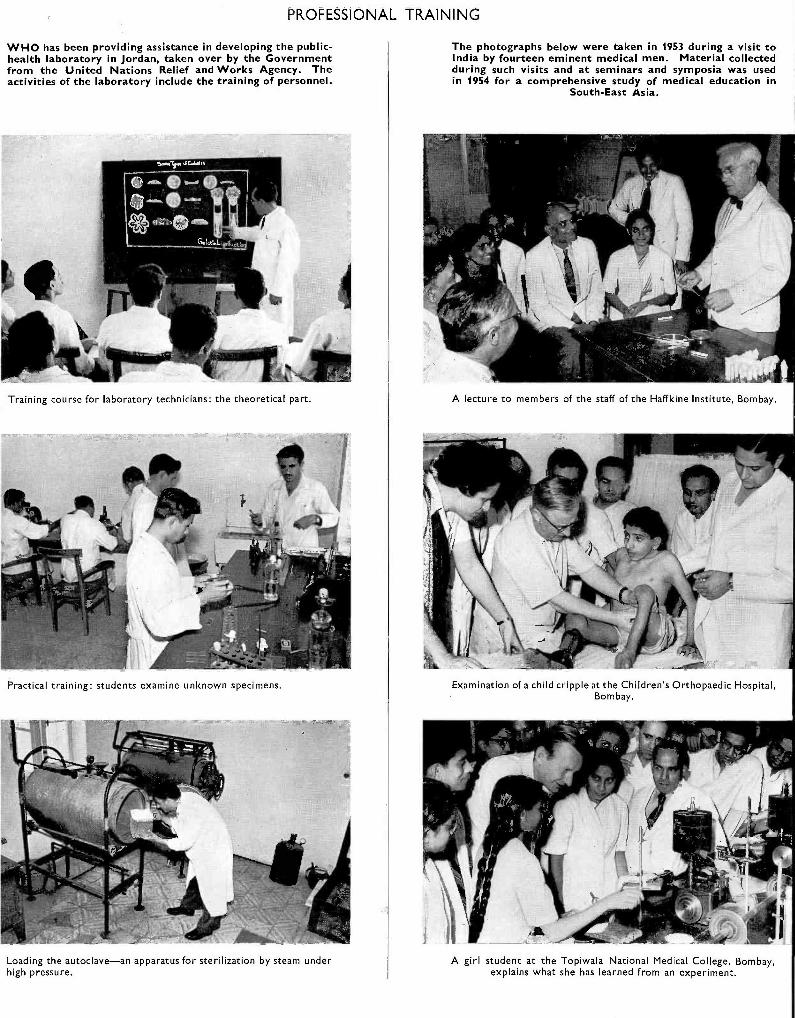
PROFESSIONAL TRAINING
WHO has been providing assistance in developing the public -health laboratory in Jordan, taken over by the Governmentfrom the United Nations Relief and Works Agency. Theactivities of the laboratory include the training of personnel.
Training course for laboratory technicians: the theoretical part.
Practical training: students examine unknown specimens.
e
Loading the autoclave -an apparatus for sterilization by steam underhigh pressure.
The photographs below were taken in 1953 during a visit toIndia by fourteen eminent medical men. Material collectedduring such visits and at seminars and symposia was usedin 1954 for a comprehensive study of medical education in
South -East Asia.
A lecture to members of the staff of the Haffkine Institute, Bombay.
Examination of a child cripple at the Children's Orthopaedic Hospital,Bombay.
A girl student at the Topiwala National Medical College, Bombay,explains what she has learned from an experiment.
SOUTH -EAST ASIA REGION 79
WHO was represented on the United Nations com-mission to survey community organization anddevelopment in India, Ceylon and Thailand. TheWHO area representatives played a very importantrole in facilitating the co- ordination of the planning ofhealth programmes at the country level, and main-tained close collaboration in all the countries of theRegion with the resident Technical Assistancerepresentatives.
Inter -agency collaboration on activities in indi-vidual countries has also been increased. In Burmaand Thailand, WHO assistance has been givenjointly with the Social Affairs Division of the UnitedNations on maternal and child health, and withFAO on nutrition. In Ceylon and Thailand threeUNESCO -assisted fundamental education projectswere actively supported by WHO. The Organizationtook part in the seminar on the teaching of thesocial sciences organized by UNESCO in India ;assistance was given to the Indian pilot studies onfamily planning in collaboration with the UnitedNations Population Division, and FAO and WHOco- operated in the work of the brucellosis centre atMukteswar.
Reports on Typical
A complete list of projects current during theyear will be found in Part IV. The following havebeen selected for fuller description.
Malaria and Insect Control, Afghanistan
Until recently, malaria was the chief public -healthproblem in Afghanistan. Out of a population oftwelve million, nearly two million people wereexposed. The problem was very severe in the rivervalleys, where rice cultivation and untidy irrigationare common, and was thus having a serious effecton the country's economy.
The WHO- assisted malaria project (Afghanistan11) has made remarkable progress during the fiveyears of its existence. Before 1950, there was nomalaria -control service for the country. In 1949, aWHO malaria consultant made a survey, after whicha pilot project was established in the Laghmandistrict. The results of this project were so strikingthat the Government made a formal request for afull demonstration team, with equipment, supplies,transport, etc., to operate for two years ; and a WHOteam of three experts began operations in theKunduz- Khanabad district early in 1950. Duringthe following two years, the internationalteam studied the local epidemiology of malaria
Relations with UNICEF continued to be verysatisfactory. To facilitate the smoother planningand operation of programmes, attempts weremade, in collaboration with UNICEF, to planprojects for longer periods. The two organizationsare giving joint assistance in several large scaleprojects, especially in maternal and child health andthe control of venereal diseases, tuberculosis andmalaria. In addition WHO is giving technicaladvice in a number of UNICEF projects which areneither completely reflected in WHO's programmeof work nor shown in the list of projects in Part IV.
Joint planning between WHO area representativesand the medical missions of the Foreign OperationsAdministration of the United States of America hascontinued.
WHO's collaboration with the Colombo Plan inthe field of health has become more active. Inaddition to offering technical advice, WHO hasfrequently taken the initiative in bringing togetherrepresentatives of the donor and recipient countries,and acting as a clearing house for programmeproposals under the Colombo Plan.
Projects in the Region
and the vector species responsible and intro-duced modern methods of malaria control byindoor DDT spraying. About 110 000 people wereprotected. The results not only convinced theauthorities of the feasibility of malaria control at avery low cost but also created a situation in whichthe affected communities began to make pressingdemands for protection against malaria and evenvolunteered donations to cover the expenses.Accordingly, the Government began a large -scaleexpansion of malaria control in 1952, with supportfrom UNICEF in supplies, equipment and transport,and with technical advice from WHO. Since then,the campaign has been carried forward steadilyuntil it now covers one and a fifth million people ;and by the end of 1956 it is hoped that all the peopleliving in the malarious areas will have receivedprotection.
The cost of the campaign has been twelve UnitedStates cents a head. In its health budget the Govern-ment has made substantial provision for malariacontrol ; in 1954 the appropriation amounted tothree and a third million afghanis. The economicbenefits of malaria control are already obvious : thetowns of Phulekhumri, Kunduz and Kandahar haveundergone a minor industrial revolution, and landvalues have increased beyond expectation.
80 THE WORK OF WHO, 1954
A national organization for malaria control hasbeen firmly established and is now staffed by eightmalaria officers, two entomologists and sixty -fourauxiliaries. A malaria institute, inaugurated bythe King of Afghanistan, was set up in Kabul totrain more personnel within the country itself andfor continued research in local malariology. Afghan-istan now having limited but well- staffed services,the two WHO malariologists were withdrawn at theend of the year. WHO will continue to furnishconsultant services throughout 1955 and 1956.
Nursing Education Programme, Kandy, Ceylon
Ceylon's second school of nursing was organizedin Kandy in 1952 ; WHO assisted by providing twonursing instructors, teaching equipment and supplies,and fellowships.
Ceylon, like many other countries, is short ofnurses. The one nursing school in Colombo, fromwhich approximately seventy -five nurses a yeargraduated, was inadequate to provide nursingservices of even minimal acceptable standard forthe island's population of more than seven million.
The main objectives of the project (Ceylon 15)are to assist the Government to increase the numberof trained nurses ; to ensure that the training givenat the Kandy Nursing School covers the preventiveand curative aspects of nursing and combinespractical training with the theoretical work ; andto advise the Government on the planning andpreparation of programmes in nursing education.
The first group of students was admitted in October1952. A preliminary three -month training pro-gramme was devoted mainly to class -room teaching,but practical experience was also given in the hospitalwards. A gradual transition from the emphasis onclass -room teaching to clinical teaching with expe-rience in wards and special departments has sincedeveloped very satisfactorily with the full co-operation of the entire staff.
Public- health aspects, including health education,have been stressed throughout the programme.
Each student is required to give health talks toexpectant mothers in the ante -natal wards or tomothers admitted with their sick children. Thestudents later visit some of the mothers in theirhomes, advise on infant care and undertake generalhealth teaching.
After two years, WHO's assistance to the projectwas redefined. The national paediatric nurse, who
had proved a capable teacher, was then ready totake over from the WHO peadiatric nurse, and aWHO public -health nursing instructor was appointedin her place. This had an important bearing on theteaching programme, as the public- health programmewas ready for further expansion, and from then onnursing training included experience in generalpublic- health work.
Fewer students were admitted to the school in 1954than had been planned, because of many unforeseendifficulties in accommodation, but the numberaimed at- 120-is likely to be reached in 1955.
In 1955, it is planned to make the school bilingual.Swabhasha instructors were appointed in the lastquarter of 1954 to prepare for the next class, whichwill be taught in Cingalese. The aim is to giveidentical teaching in both languages and to use thealternate English- speaking classes as control groups.The Cingalese teaching programme as developed atthe Kandy School of Nursing will serve as a guidefor other national schools, which are now only inthe planning stage.
The project has so far had the following results :It has increased the total number of nurses in thecountry. It has developed a sound education andtraining programme in which the preventive aspecthas been taught alongside the curative aspect ofnursing. Nursing education has been accepted inthe country, as shown by the Government's plan toestablish new nursing schools along the same lines,in which instruction will be given in the student'smother tongue. The students are showing pride intheir school and in their profession -an importantadvance in nursing in Ceylon.
Maternal and Child Health and Nursing, Bangkok
The objectives of this project (Thailand 6) were :to raise the standard of health of the people, par-ticularly of women and children, by improving andenlarging the existing health services and by pro-
viding better facilities for training all types of healthpersonnel engaged in maternal and child healthwork ; and to demonstrate in one urban and onesemi -rural area the pattern of community healthservices in which the preventive, curative and socialaspects of care are combined.
This project had assistance from WHO fromSeptember 1951 until 1954. The WHO staff includedan officer in maternal and child health, a public-
SOUTH -EAST ASIA REGION 81
health nurse, a sanitarian and an instructor inmidwifery. A social worker was provided by theUnited Nations.
The work was done in a number of units establishedunder this project. In addition to the traditionalmaternal and child health activities, such as ante-natal and post -natal care and infant care, paediatric,venereal- disease and tuberculosis clinics were heldon the premises. The local health workers and thepublic were thus shown how medical services couldbe centralized and unified. Immunizations andhealth education in the centres and homes alsoformed part of the service of these units.
There was close liaison between hospitals, theclinics and the maternal and child health project.A twenty -four hour domiciliary midwifery servicewas established for the first time, and over 800women were delivered in their homes between June1952 and May 1954. The integration of schoolhealth services into the general health services wasbegun by including one school in the project.
Trainees from the provinces who came to Bangkokfor refresher courses carried out, on their returnhome, the methods that had been demonstrated inthe project units.
During the period, infant mortality in the projectarea was nearly halved. The demand for all types ofmedical services has risen and there is pressure fromthe public for more centres to be established.
Yaws -Control Project, Indonesia
This WHO /UNICEF- assisted yaws -control pro-gramme (Indonesia 1), the largest of its kind, hasjust entered its fifth year of operation. Yaws is
Present Trends and Future Developments
The appointment of area representatives to thecountries of South -East Asia has contributed sub-stantially toward their understanding and acceptanceof WHO's role in helping governments to improvehealth services. Besides requests for assistancewith programmes, governments are tending to refer
recognized to be an extremely grave problem inIndonesia : it incapacitates much of the popula-tion and, by attacking the productive age -groups,hinders economic growth. The interest that theGovernment has shown and the support that hasbeen given by participating agencies from the begin-ning show the seriousness with which this public -health problem is regarded. The simplified systemof treatment used increasingly in the campaign overthe last two years has resulted in wider coverage.The teams, now operating with fewer personnel, havebeen increased in number so that the campaign caneventually be extended to the entire country. Bythe end of 1954, over fourteen million people hadbeen examined and over two million cases treated.An analysis of the data available shows that thecampaign has progressed steadily and rapidly eachyear since it began in 1950.
The laboratory at the headquarters of theproject has helped to maintain scientific controlof the campaign and to train specialized laboratorytechnicians. Attention is now being given to theultimate objective of integrating yaws treatmentinto the general public- health services, and alsoto research activities in techniques and operationalprocedures.
Though two million sufferers from yaws, who havehitherto caused a regular drain on the country'sresources, are now free from the disease, much workremains to be done. Approximately sixty millionpeople have yet to be examined, and a proportionatenumber, also in the millions, will require treatment.The plans for extending this campaign rapidly andcompletely throughout the country were under wayat the end of the year.
specific problems to the Organization for technicaladvice. An important link is being established withthe Colombo Plan authorities and the United Statesbilateral agencies for technical assistance.
In most countries of the Region, the budgetallocated to health has gradually increased, as isshown by the following table :
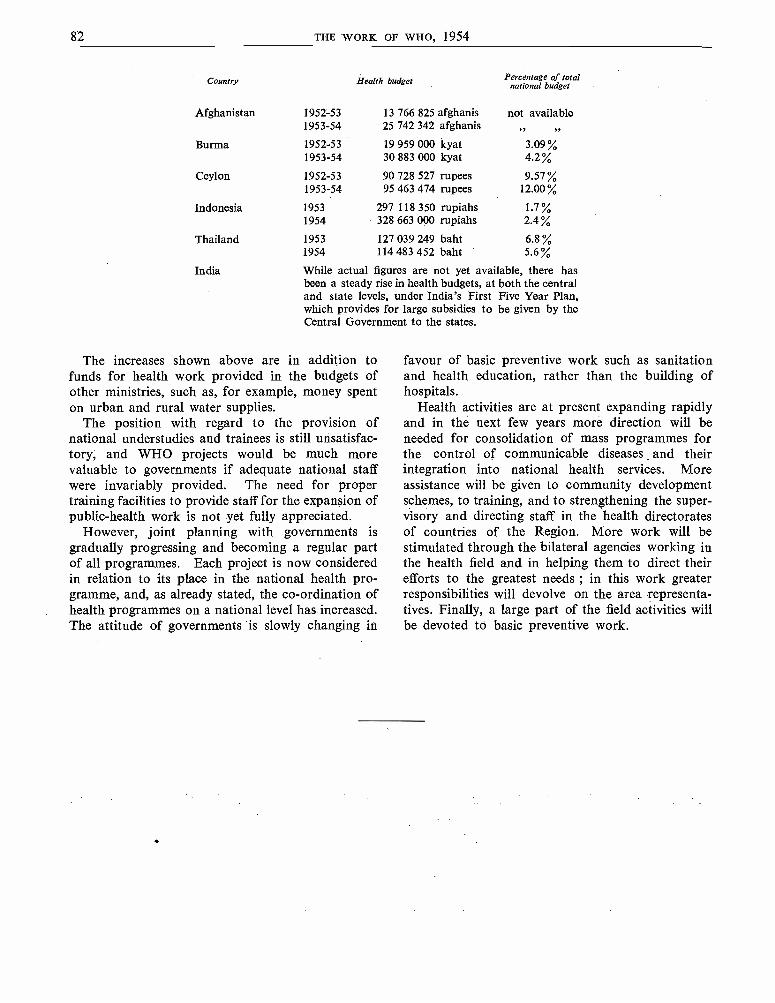
82
Country
Afghanistan
Burma
Ceylon
Indonesia
Thailand
India
THE WORK OF WHO, 1954
Health budget Percentage of totalnational budget
1952 -53 13 766 825 afghanis not available1953 -54 25 742 342 afghanis
1952 -53 19 959 000 kyat 3.091953 -54 30 883 000 kyat 4.2
1952 -53 90 728 527 rupees 9.571953 -54 95 463 474 rupees 12.00
1953 297 118 350 rupiahs 1.71954 328 663 000 rupiahs 2.4
1953 127 039 249 baht 6.81954 114 483 452 baht 5.6%
While actual figures are not yet available, there hasbeen a steady rise in health budgets, at both the centraland state levels, under India's First Five Year Plan,which provides for large subsidies to be given by theCentral Government to the states.
The increases shown above are in addition tofunds for health work provided in the budgets ofother ministries, such as, for example, money spenton urban and rural water supplies.
The position with regard to the provision ofnational understudies and trainees is still unsatisfac-tory, and WHO projects would be much morevaluable to governments if adequate national staffwere invariably provided. The need for propertraining facilities to provide staff for the expansion ofpublic -health work is not yet fully appreciated.
However, joint planning with governments isgradually progressing and becoming a regular partof all programmes. Each project is now consideredin relation to its place in the national health pro-gramme, and, as already stated, the co- ordination ofhealth programmes on a national level has increased.The attitude of governments is slowly changing in
favour of basic preventive work such as sanitationand health education, rather than the building ofhospitals.
Health activities are at present expanding rapidlyand in the next few years more direction will beneeded for consolidation of mass programmes forthe control of communicable diseases and theirintegration into national health services. Moreassistance will be given to community developmentschemes, to training, and to strengthening the super-visory and directing staff in the health directoratesof countries of the Region. More work will bestimulated through the bilateral agencies working inthe health field and in helping them to direct theirefforts to the greatest needs ; in this work greaterresponsibilities will devolve on the area representa-tives. Finally, a large part of the field activities willbe devoted to basic preventive work.
CHAPTER 14
EUROPEAN REGION
The countries of Europe, while varied in theirindividual patterns of health services and problemsand in their stages of economic development, yetform together a region which is probably moreuniform than any of the other WHO regions.
This has permitted the resources in expert per-sonnel and finances to be concentrated on activitieswhich interest simultaneously several or all of thecountries in the Region. It is to be regretted thatAlbania, Bulgaria, the Byelorussian SSR, Czecho-slovakia, Hungary, Poland, Romania, the UkrainianSSR and the Union of Soviet Socialist Republicshave not yet found it possible to resume their co-operation in the international health work of WHOin Europe. The numerous inter -country programmeswhich the Regional Office has sponsored during thepast years are a sign of the high level of co- operationin public health between Member States of theRegion.
The Regional Committee
The Regional Committee held two sessions in1954 -a special session in Geneva on 21 May and thefourth regular session in Opatija, Yugoslavia, from13 to 16 September. At the special session theRegional Committee gave further consideration tothe question of the permanent site of the RegionalOffice and recommended Copenhagen. This choicewas approved by the Executive Board at its fourteenthsession.
The fourth session of the Regional Committeewas attended by representatives of all twenty -threeactive Members and Associate Members, the United
1 This region, in accordance with the decision of the FirstWorld Health Assembly (Of Rec. Wld Hith Org. 13, 80, 330)comprises all Europe. Turkey, by resolution WHA5.46, wasadmitted to the Region while provisionally suspending itsactivities in the Eastern Mediterranean. By resolutionsWHA5.43 and WHA6.46, Algeria, Morocco (French Zone),Tunisia, Greenland, Gibraltar and Malta were also provi-sionally assigned to the European Region. In 1954 the follow-ing Members or Associate Members participated in the workof the Region : Austria, Belgium, Denmark, Finland, France,Germany (Federal Republic), Greece, Iceland, Ireland,Italy, Luxembourg, Monaco, Morocco (French Zone),Netherlands, Norway, Portugal, Spain, Sweden, Switzerland,Tunisia, Turkey, the United Kingdom of Great Britain andNorthern Ireland, and Yugoslavia.
Nations (and UNICEF), the International Children'sCentre, and interested intergovernmental organi-zations, and by observers for nine non- governmentalorganizations in official relations with WHO. TheDirector - General was represented by his deputy.
The Regional Committee endorsed modificationsin the programme for 1955 which had arisen mainlyfrom the reduced budget adopted by the SeventhWorld Health Assembly, but recommended theaddition to the programme of a training coursein the management of poliomyelitis patients withbulbar involvement, because of the urgency of thesituations which had arisen in connexion withpoliomyelitis in some countries in the Region. In itsdetailed review of programme proposals for 1956,the Regional Committee suggested improvements insome of the inter -country projects planned, andspecific activities for inclusion in future WHO
inThe possibility of augmenting the finances for
WHO's work in Europe was considered further, but,in the light of views expressed by Member govern-ments, the Regional Committee did not recommendthat Member States should be asked at the presenttime to contribute to a supplementary regionalbudget.
With regard to technical discussions, the RegionalCommittee favoured the choice of topics of particularregional interest and decided to discuss at its nextregular session " Changes in health services neces-sitated by the ageing of populations ".
The Regional Committee again expressed the viewthat each regional committee should be empoweredto grant its Associate Members full rights of vote atits meetings if it so desired, and invited the ExecutiveBoard to take account of that opinion in its recom-mendations to the Eighth World Health Assembly.
The Regional Committee decided to hold its fifthregular session in Vienna, Austria, its sixth in Rabat,Morocco (French Zone), and its seventh in Copen-hagen, Denmark.
The Regional Office
Following the Executive Board's decision on thesite of the Regional Office, negotiations proceededwith the Government of Denmark on the conclusion
- 83 -
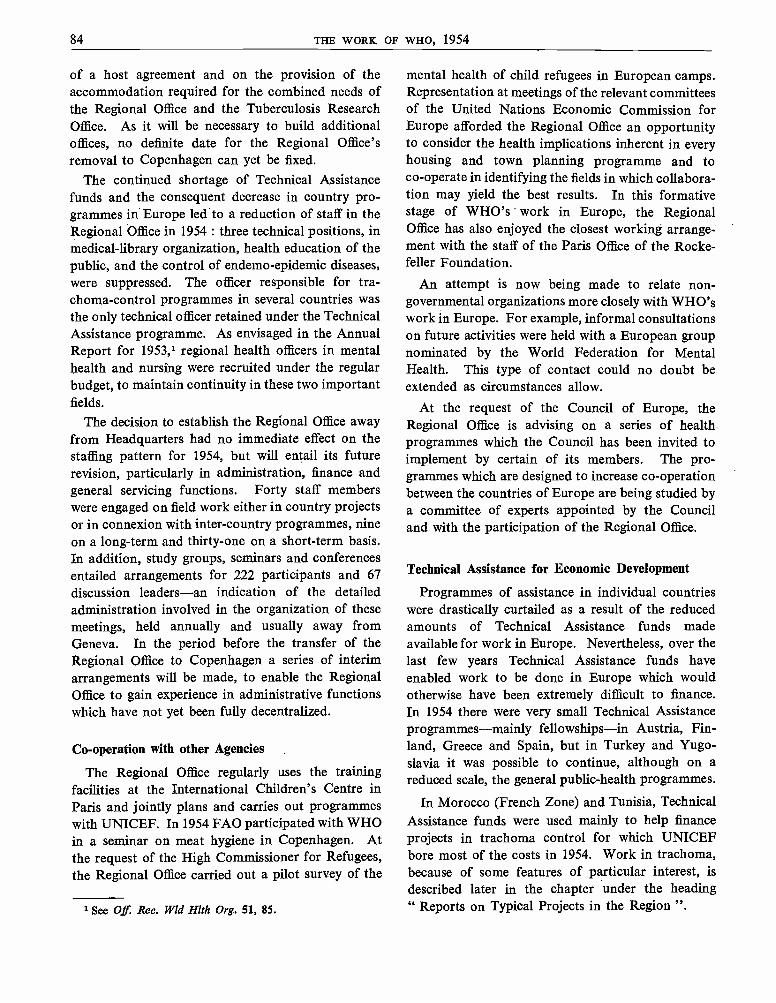
84 THE WORK OF WHO, 1954
of a host agreement and on the provision of theaccommodation required for the combined needs ofthe Regional Office and the Tuberculosis ResearchOffice. As it will be necessary to build additionaloffices, no definite date for the Regional Office'sremoval to Copenhagen can yet be fixed.
The continued shortage of Technical Assistancefunds and the consequent decrease in country pro-grammes in Europe led to a reduction of staff in theRegional Office in 1954 : three technical positions, inmedical -library organization, health education of thepublic, and the control of endemo- epidemic diseases,were suppressed. The officer responsible for tra-choma- control programmes in several countries wasthe only technical officer retained under the TechnicalAssistance programme. As envisaged in the AnnualReport for 1953,1 regional health officers in mentalhealth and nursing were recruited under the regularbudget, to maintain continuity in these two importantfields.
The decision to establish the Regional Office awayfrom Headquarters had no immediate effect on thestaffing pattern for 1954, but will entail its futurerevision, particularly in administration, finance andgeneral servicing functions. Forty staff memberswere engaged on field work either in country projectsor in connexion with inter -country programmes, nineon a long -term and thirty -one on a short -term basis.In addition, study groups, seminars and conferencesentailed arrangements for 222 participants and 67discussion leaders -an indication of the detailedadministration involved in the organization of thesemeetings, held annually and usually away fromGeneva. In the period before the transfer of theRegional Office to Copenhagen a series of interimarrangements will be made, to enable the RegionalOffice to gain experience in administrative functionswhich have not yet been fully decentralized.
Co- operation with other Agencies
The Regional Office regularly uses the trainingfacilities at the International Children's Centre inParis and jointly plans and carries out programmeswith UNICEF. In 1954 FAO participated with WHOin a seminar on meat hygiene in Copenhagen. Atthe request of the High Commissioner for Refugees,the Regional Office carried out a pilot survey of the
See Off. Rec. Wld Hith Org. 51, 85.
mental health of child refugees in European camps.Representation at meetings of the relevant committeesof the United Nations Economic Commission forEurope afforded the Regional Office an opportunityto consider the health implications inherent in everyhousing and town planning programme and toco- operate in identifying the fields in which collabora-tion may yield the best results. In this formativestage of WHO's work in Europe, the RegionalOffice has also enjoyed the closest working arrange-ment with the staff of the Paris Office of the Rocke-feller Foundation.
An attempt is now being made to relate non-governmental organizations more closely with WHO'swork in Europe. For example, informal consultationson future activities were held with a European groupnominated by the World Federation for MentalHealth. This type of contact could no doubt beextended as circumstances allow.
At the request of the Council of Europe, theRegional Office is advising on a series of healthprogrammes which the Council has been invited toimplement by certain of its members. The pro-grammes which are designed to increase co- operationbetween the countries of Europe are being studied bya committee of experts appointed by the Counciland with the participation of the Regional Office.
Technical Assistance for Economic Development
Programmes of assistance in individual countrieswere drastically curtailed as a result of the reducedamounts of Technical Assistance funds madeavailable for work in Europe. Nevertheless, over thelast few years Technical Assistance funds haveenabled work to be done in Europe which wouldotherwise have been extremely difficult to finance.In 1954 there were very small Technical Assistanceprogrammes -mainly fellowships -in Austria, Fin-land, Greece and Spain, but in Turkey and Yugo-slavia it was possible to continue, although on areduced scale, the general public- health programmes.
In Morocco (French Zone) and Tunisia, TechnicalAssistance funds were used mainly to help financeprojects in trachoma control for which UNICEFbore most of the costs in 1954. Work in trachoma,because of some features of particular interest, isdescribed later in the chapter under the heading" Reports on Typical Projects in the Region ".
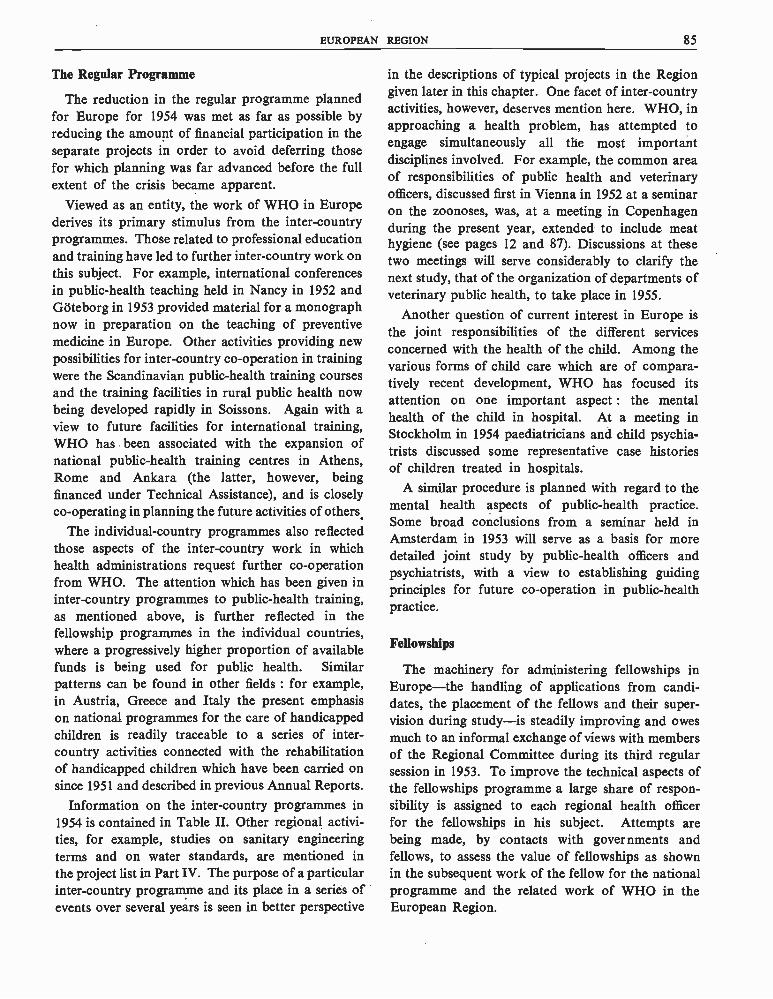
EUROPEAN REGION 85
The Regular Programme
The reduction in the regular programme plannedfor Europe for 1954 was met as far as possible byreducing the amount of financial participation in theseparate projects in order to avoid deferring thosefor which planning was far advanced before the fullextent of the crisis became apparent.
Viewed as an entity, the work of WHO in Europederives its primary stimulus from the inter -countryprogrammes. Those related to professional educationand training have led to further inter -country work onthis subject. For example, international conferencesin public- health teaching held in Nancy in 1952 andGoteborg in 1953 provided material for a monographnow in preparation on the teaching of preventivemedicine in Europe. Other activities providing newpossibilities for inter -country co- operation in trainingwere the Scandinavian public -health training coursesand the training facilities in rural public health nowbeing developed rapidly in Soissons. Again with aview to future facilities for international training,WHO has been associated with the expansion ofnational public -health training centres in Athens,Rome and Ankara (the latter, however, beingfinanced under Technical Assistance), and is closelyco- operating in planning the future activities of others.
The individual- country programmes also reflectedthose aspects of the inter -country work in whichhealth administrations request further co- operationfrom WHO. The attention which has been given ininter -country programmes to public -health training,as mentioned above, is further reflected in thefellowship programmes in the individual countries,where a progressively higher proportion of availablefunds is being used for public health. Similarpatterns can be found in other fields : for example,in Austria, Greece and Italy the present emphasison national programmes for the care of handicappedchildren is readily traceable to a series of inter -country activities connected with the rehabilitationof handicapped children which have been carried onsince 1951 and described in previous Annual Reports.
Information on the inter -country programmes in1954 is contained in Table II. Other regional activi-ties, for example, studies on sanitary engineeringterms and on water standards, are mentioned inthe project list in Part IV. The purpose of a particularinter -country programme and its place in a series ofevents over several years is seen in better perspective
in the descriptions of typical projects in the Regiongiven later in this chapter. One facet of inter -countryactivities, however, deserves mention here. WHO, inapproaching a health problem, has attempted toengage simultaneously all the most importantdisciplines involved. For example, the common areaof responsibilities of public health and veterinaryofficers, discussed first in Vienna in 1952 at a seminaron the zoonoses, was, at a meeting in Copenhagenduring the present year, extended to include meathygiene (see pages 12 and 87). Discussions at thesetwo meetings will serve considerably to clarify thenext study, that of the organization of departments ofveterinary public health, to take place in 1955.
Another question of current interest in Europe isthe joint responsibilities of the different servicesconcerned with the health of the child. Among thevarious forms of child care which are of compara-tively recent development, WHO has focused itsattention on one important aspect : the mentalhealth of the child in hospital. At a meeting inStockholm in 1954 paediatricians and child psychia-trists discussed some representative case historiesof children treated in hospitals.
A similar procedure is planned with regard to themental health aspects of public- health practice.Some broad conclusions from a seminar held inAmsterdam in 1953 will serve as a basis for moredetailed joint study by public- health officers andpsychiatrists, with a view to establishing guidingprinciples for future co- operation in public- healthpractice.
Fellowships
The machinery for administering fellowships inEurope -the handling of applications from candi-dates, the placement of the fellows and their super-vision during study -is steadily improving and owesmuch to an informal exchange of views with membersof the Regional Committee during its third regularsession in 1953. To improve the technical aspects ofthe fellowships programme a large share of respon-sibility is assigned to each regional health officerfor the fellowships in his subject. Attempts arebeing made, by contacts with governments andfellows, to assess the value of fellowships as shownin the subsequent work of the fellow for the nationalprogramme and the related work of WHO in theEuropean Region.
86 THE WORK OF WHO, 1954
The prospects of attaining a smoothly operatingfellowships programme, well integrated with the otheraspects of WHO's work in Europe, appear betternow than at any period in the development of theOrganization. Practically all the countries in Europetake part in the fellowships programme. Althoughthis means that the number of fellowships awarded
to any one country cannot be large, the total forthe Region in 1954 was 283 fellowships, includingtwo administered on behalf of UNICEF, comparedwith 287 for the previous year. One hundred andfive fellows from other regions studied in Europe.Sixteen per cent. of all fellowships granted by WHOhave been for study in Europe.
TABLE II. INTER- COUNTRY PROGRAMMES IN EUROPE
Description of programme DurationGovernment(s)
principallyconcerned
Other participating countriesParticipants
orfellows *
Participating agencies and roleof Regionala Office
AlcoholismA teaching seminar for physi- 2 weeks Netherlands Austria Ireland 26 Government of the Nether -
cians, public -health admin-istrators and psychiatricsocial workers actively en-gaged in the prevention andtreatment of alcoholism ;held in Noordwijk.
28 March-10 April
Belgium ItalyFrance SpainGermany, TurkeyFederal Republic United
Kingdom
lands and Regional Office,which provided a directorof studies and elevenfaculty members.
EURO 67
Anaesthesiology(a) Fifth basic post -graduate 1 year Denmark Austria Norway 9 University of Copenhagen
course for anaesthesiolo- Aug. 1954 - Germany, Portugal and Regional Office, whichgists ; held at the Anaes-thesiology Centre, Copen-hagen. t
July 1955 Federal Republic SpainGreece Turkey
Yugoslavia
provided outside lecturers.
EURO 52
(b) Training course for anaes- 1 year France Belgium Greece 6 University of Paris andthesiologists ; held at the May 1953- Germany, Spain Regional Office, whichAnaesthesiology Centre,Paris.EURO 62
April 1954 § Federal Republic SwitzerlandTurkey
provided a technical ad-viser, an outside lecturer,and some teaching equip-ment.
Environmental Sanitation(a) An advanced training 3 weeks Netherlands Austria Portugal 13 Governments of the Nether -
course for waterworks 22 March- Belgium Greece Spain lands and Belgium andengineers ; held in TheHague and Liége.EURO 45
10 April Ireland TunisiaMorocco Turkey
(French Zone) Yugoslavia
Regional Office, whichprovided a consultant tohelp organize the course.
(b) A conference of Europeansanitary engineers onwater pollution and waterchlorination ; held inOpatija.
10 days21 -30 April
Yugoslavia Austria LuxembourgBelgium MoroccoDenmark (FrenchFinland Zone)France Netherlands
36 Government of Yugoslavia,Rockefeller Foundationand Regional Office, whichprovided seven discussionleaders.
EURO 9.4 Germany, NorwayFederal Republic Portugal
Greece SwedenIceland SwitzerlandIreland TunisiaItaly Turkey
UnitedKingdom
* Regional participants or fellows sponsored by WHOt Although these European inter- country activities were open to participation from other regions, only European parti-
cipants and fellowships are recorded in this table.§ Although a further training course would have begun in 1954, the participation of WHO fellows had to be postponed
until January 1955 because of budgetary difficulties.

EUROPEAN REGION 87
INTER -COUNTRY PROGRAMMES IN EUROPE (continued)
Description of programme DurationGovernments)
principallyconcerned
Other participating countriesParticipants
orfellows
Participating agencies and roleof Regional Office
Health VisitorsPreparation of the report on 4 years France - - - Rockefeller Foundation and
the pilot study carried outin France and the UnitedKingdom from 1951 to 1953,to determine the kind ofworker best suited to meetfamily health and welfareneeds.
1951 -54 UnitedKingdom
Regional Office, whichjointly provided twoexperts to collaborate indrafting the report.
EURO 6
ImmunizationA conference for medical
officers on modern methods6 days15 -20 March
Germany,Federal
Austria NetherlandsBelgium Norway
31 Government of the FederalRepublic of Germany and
of immunization ; held inFrankfurt -am -Main.EURO 47
Republic Denmark PortugalFinland SpainFrance Sweden
Regional Office, whichprovided ten discussionleaders.
Greece SwitzerlandIceland TunisiaIreland TurkeyItaly UnitedLuxembourg KingdomMorocco Yugoslavia
(French Zone)
Meat HygieneA seminar for veterinarians 6 days Denmark Austria Netherlands 29 Government of Denmark
and medical officers ; heldin Copenhagen. tEURO 50
22 -27 Feb. Belgium NorwayFinland PortugalFrance SpainGermany, Sweden
Federal Republic Switzerland
and Regional Office, whichprovided ten discussionleaders and a consultantto help organize theseminar.
Greece TunisiaIreland TurkeyItaly UnitedMorocco Kingdom
(French Zone) Yugoslavia
Mental HealthA study conference of paedia- 10 days Sweden Austria Italy 21 Government of Sweden and
tricians and child psychia-trists on the care of childrenin hospitals ; held in Stock-holm.
2 -11 Sept. Belgium NetherlandsDenmark NorwayFinland PortugalFrance Switzerland
Regional Office, whichprovided a director ofstudies and six discussionleaders.
EURO 43 Germany, UnitedFederal Republic Kingdom
Greece Yugoslavia
Mother /Child Separation StudyA study of the effects on child Since France - - - International Children's
development of separationfrom the mother in the earlyyears of life.EURO 64
Nov. 1952 UnitedKingdom
Centre and RegionalOffice, which contributedto the cost of the studyteams working in Franceand the United Kingdom.
Regional participants or fellows sponsored by WHOt Although these European inter- country activities were open to participation from other regions, only European parti-
cipants and fellowships are recorded in this table.
88 THE WORK OF WHO, 1954
INTER- COUNTRY PROGRAMMES IN EUROPE (continued)
Description of programme DurationGovernment(s)
principallyconcerned
Other participating countriesParticipants
orfellows *
Participating agencies and roleof Regional Office
Public - Health Administration(a) Continuation of a study of
certain aspects of public-1 month15 March-
Germany,Federal
Austria NorwayBelgium Portugal
21 Regional Office, which pro -vided two leaders and an
health administration, in 15 April Republic Denmark Sweden administrative officer forGermany and Italy. Italy Finland Switzerland the travelling study group.EURO 12.3 France Spain
Greece TurkeyIceland UnitedIreland KingdomNetherlands Yugoslavia
(b) A group training course 2 months Sweden Denmark Iceland 21 Government of Sweden andfor Scandinavian public-health officers and veteri-narians ; held in Giste-borg.
1 Aug.-30 Sept.
Finland Norway Regional Office, whichprovided an internationallecturer and contributed tothe cost of the course.
EURO 60
Public -Health NursingA seminar on team work in 2 weeks Turkey Austria Morocco 37 Government of Turkey and
nursing services, for medicaladministrators and public-health and hospital nurses ;held in Istanbul.
17 -31 Oct. Germany, (FrenchFederal Republic Zone)
Greece PortugalItaly Spain
Regional Office, whichcontributed a director ofstudies and two discus -sion leaders.
EURO 72 SwitzerlandTunisiaYugoslavia
RehabilitationA group training course on 6 weeks France Italy Spain 6 International Children's
the rehabilitation of handi-capped children, for physi-cians, medical auxiliariesand social workers ; heldin Paris.
11 Jan.-21 Feb.
Portugal Yugoslavia Centre.
EURO 74.1
School HealthA conference on some selected 6 days France Austria Morocco 26 Government of France and
topics of school health ser-vices, for school physiciansand persons actively en-gaged in school health; heldin Grenoble.
14 -19 June Belgium (FrenchDenmark Zone)Finland NetherlandsGermany, NorwayFederal Republic Spain
Regional Office, which pro -vided a conference orga-nizer.
EURO 40.2 Greece SwedenIceland SwitzerlandIreland TunisiaItaly TurkeyLuxembourg UnitedMonaco Kingdom
Yugoslavia
* Regional participants or fellows sponsored by WHO
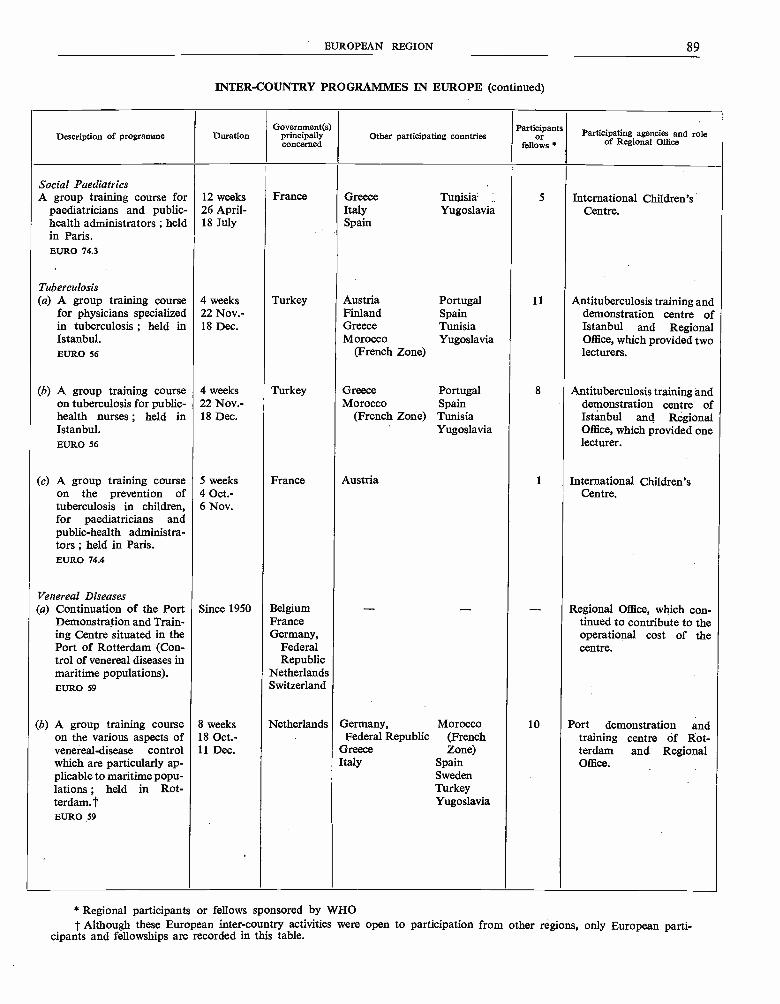
EUROPEAN REGION 89
INTER- COUNTRY PROGRAMMES IN EUROPE (continued)
Description of programme DurationGovernment(s)
principallyconcerned
Other participating countriesParticipants
orfellows *
Participating agencies and roleof Regional Office
Social PaediatricsA group training course for 12 weeks France Greece Tunisia 5 International Children's
paediatricians and public-health administrators ; heldin Paris.
26 April-18 July
Italy YugoslaviaSpain
Centre.
EURO 74.3
Tuberculosis(a) A group training course 4 weeks Turkey Austria Portugal 11 Antituberculosis training and
for physicians specialized 22 Nov: Finland Spain demonstration centre ofin tuberculosis ; held in 18 Dec. Greece Tunisia Istanbul and RegionalIstanbul.EURO 56
Morocco Yugoslavia(French Zone)
Office, which provided twolecturers.
(b) A group training course 4 weeks Turkey Greece Portugal 8 Antituberculosis training andon tuberculosis for public- 22 Nov.- Morocco Spain demonstration centre ofhealth nurses ; held in 18 Dec. (French Zone) Tunisia Istanbul and RegionalIstanbul.EURO 56
Yugoslavia Office, which provided onelecturer.
(c) A group training courseon the prevention oftuberculosis in children,for paediatricians andpublic- health administra-tors ; held in Paris.
5 weeks4 Oct:6 Nov.
France Austria 1 International Children'sCentre.
EURO 74.4
Venereal Diseases(a) Continuation of the Port
Demonstration and Train-ing Centre situated in thePort of Rotterdam (Con-trol of venereal diseases inmaritime populations).
Since 1950 BelgiumFranceGermany,
FederalRepublic
Netherlands
- - - Regional Office, which con -tinued to contribute to theoperational cost of thecentre.
EURO 59 Switzerland
(b) A group training course 8 weeks Netherlands Germany, Morocco 10 Port demonstration andon the various aspects of 18 Oct.- Federal Republic (French training centre of Rot -venereal- disease controlwhich are particularly ap-plicable to maritime popu-lations ; held in Rot-terdam.t
11 Dec. Greece Zone)Italy Spain
SwedenTurkeyYugoslavia
terdam and RegionalOffice.
EURO 59
* Regional participants or fellows sponsored by WHOt Although these European inter- country activities were open to participation from other regions, only European parti-
cipants and fellowships are recorded in this table.

90 THE WORK OF WHO, 1954
Reports on Typical Projects in the Region
A complete list of projects current during theyear will be found in Part IV. The followinghave been selected for fuller description.
Communicable Diseases
Smallpox, malaria and venereal diseases are nolonger major problems in Europe. Some countrieshave satisfactory programmes for preventing thecommon communicable diseases of childhood, butgenerally these diseases, though now capable ofcontrol, are not controlled adequately. For example,it is estimated that in 1953 European countries spentat least two million dollars on the medical care of60 663 reported diphtheria cases.
At a European conference held early in 1954 inFrankfurt -am -Main, public- health administrators,paediatricians, epidemiologists and bacteriologistsdiscussed recent advances in, and practical aspectsof, immunization for the control of diphtheria,pertussis, tetanus, measles, poliomyelitis, scarletfever, smallpox and tuberculosis. This arose out ofthe WHO technical conference, held at Dubrovnikin 1952, for heads of laboratories producing diph-theria and pertussis vaccines.' WHO, with UNICEF,has been assisting Austria in a project for the pro-duction and administration of prophylactics fordiphtheria, pertussis and tetanus. In Yugoslavia ateam of consultants gave courses in the control ofcommunicable diseases, and later a productionexpert spent some time in Yugoslav serum andvaccine laboratories. The United Nations TechnicalAssistance Administration has reported that theUNICEF /WHO project (later transferred to theUnited Nations) to develop and improve a penicillinplant in Yugoslavia has been completed, and thatproduction is greater than originally forecast.
Assistance to public -health laboratories continued,with the award of fellowships for study in bacterial,virus and rickettsial diseases. The shifting patternin communicable diseases in Europe has broughtvirus and rickettsial diseases more to the fore. In1956 a seminar is planned for directors of public -health laboratories and their bacteriologists andserologists, to discuss technical and administrative
1 The report of this conference has been published inWld Hlth Org. techn. Rep. Ser. 1953, 61.
aspects of public- health laboratory services in thisgroup of diseases.
Although the high epidemicity of trachoma andseasonal acute conjunctivitis in certain areas isrecognized as being due to environmental factors,attempts have been made recently to control theseinfections by mass chemotherapy and by antibiotics.In North Africa, where the two diseases coexist,the control of trachoma depends primarily on thatof seasonal conjunctivitis. From pilot projectsinitiated, with the assistance of WHO and UNICEF,in Morocco (French Zone) and in Tunisia, it isplanned to develop operations which will be ap-plicable on as large a scale as economic resourceswill permit. The first results have been encouraging.During 1954, 400 000 individuals were treated in thetwo project areas in field campaigns against seasonalconjunctivitis. As effective treatment of trachomain the early school years eliminates a source ofinfection and minimizes the risk of late complicationsof the disease, resulting in blindness, a programmeof systematic treatment of trachomatous childrenis being introduced into the schools ; approximately50 000 received antibiotic treatment in 1954. Modifiedprojects were planned, with technical advice fromWHO, for Spain, where seasonal conjunctivitis is lessof a problem than in North Africa, and for Yugo-slavia, where trachoma exists in a nearly pure form.WHO has made special efforts to standardizemethods of recording and evaluating results, inorder to facilitate the comparison of data andexperience between countries.
Nursing
The first conference for European nurses wasorganized at Noordwijk in 1950 with the co- opera-tion of the Government of the Netherlands.' Par-ticipants from ten countries in northern and westernEurope discussed together the everyday practicalproblems of the public -health nurse under the broadheadings of health education, mental health andnutrition. In subsequent contacts the participantshave emphasized how much their teaching andpractice were influenced by this first conference. Anexample of direct follow -up was a national conference
' See Of Rec. Wld Hith Org. 30, 29, 110.

EUROPEAN REGION 91
on similar lines organized by the Government of theNetherlands in 1952 with the participation of WHO.
At the second regional conference, at Mont -Pèlerin (Switzerland) in 1953, participation wasbroadened to include nurses from twenty -onecountries in Europe, the subjects for discussionbeing staff education and the co- ordination ofhospital and public- health nursing services. Par-ticular stress was placed on the need for a betterunderstanding of the nursing requirements of theindividual, family and community and on methodsdesigned better to use the available nursing resources.An additional feature of the Mont -Pèlerin conferencewas a practical demonstration of conference tech-niques requested by the participants for the purposeof follow -up meetings in their own countries.
During and after this second regional conference,the participants assisted the Regional Office inplanning the third step, which was designed prin-cipally for the countries of southern Europe. Thistook the form of a seminar on team work in nursingservices organized in Istanbul in 1954 (see Table II)with the participation of a medical officer, a public -health nurse and a hospital nurse from each ofeleven countries.
These three regional meetings have facilitated awide exchange of ideas and experience among thenursing profession in Europe, and it is evident fromcontacts maintained with the participants that theobjective of stimulating similar activities on anational level is being achieved. An additionalbenefit is the much clearer picture which has emergedof the nursing services- in the Region and of theparticular problems faced in the different countries.This information will guide WHO and serve tosharpen the focus of future work on nursing educa-tion which is planned in the Region as a whole andin individual countries such as Tunisia and Turkeywhere the co- operation of WHO is requested.
Health Education of the Public
The conference on health education of the publicheld in London in 1953 brought together membersof various professions -medical administrators,health officers, public -health nurses, educators,sanitarians and public relations officers -to considerthe present scope and future growth of healtheducation, and the role and opportunities of healthworkers in this field.
Various activities resulted from this conference.
National meetings and seminars were organized forgroup discussions of problems selected by theparticipants. A national health education programmewith long -range objectives was organized in Portugal.In Perugia, Italy, a health education project wasstarted under the leadership of the provincial healthofficer, with the co- operation of the national healthauthorities, and one of the participants from Yugo-slavia translated and published in book form articleson health education of the public. In severalcountries in the Region, the co- operation betweenpublic -health and educational agencies for healtheducation programmes has been closer. Anotherresult was that more fellowships were awarded tohealth personnel for the purpose of studying thepractice, methods and organization of healtheducation.
During the year plans have been made andpreparations started for a second conference, to beheld in 1956. An ad hoc committee has advisedon the organization of this conference, which willexplore needs, present facilities and potential re-sources for training in health education of thepublic.
A notable addition to training facilities in theRegion was the establishment, at the University ofLondon, of a diploma course in content andof health education, organized by the Institute ofEducation of the University, in co- operation withthe London School of Hygiene and Tropical Medi-cine and the Institute of Child Health ; the CentralCouncil for Health Education also takes part inthe teaching.
School Health Services
The organization of school health services hasbeen studied by WHO fellows in different countries.In 1953, a study tour was arranged for a group ofsenior school health officers from eighteen countriesin the Region, who were also accompanied byofficers from countries in the Eastern Mediter-ranean. For three weeks, members of this groupwere able to observe a full range of general andspecialized services in Denmark and the Netherlandsand exchange experiences on the organization ofschool health services in their own countries.
A development in 1954 was a European conferenceon school health services, which was convened inGrenoble and attended by observers from UNESCO.At this conference senior health officers from twenty -two countries in the Region, together with public-
92 THE WORK OF WHO, 1954
health and school -health nurses, a dental specialist,a teacher and a psychologist, discussed broad admin-istrative and legislative problems and, in particular,the character of services required by countries atdifferent levels of economic development. Specialattention was given to the way in which teachers,medical staff, non -teaching school staff and parentscan best collaborate to ensure the health of school-children. Health education in schools has at leastthree aspects : (1) the teaching of the basic sciences(e.g., anatomy and physiology) and social sciences,which would be entirely a matter for the teacher ;(2) instruction in general and personal hygiene andfirst aid, sports and physical education, which wouldalso appear to be chiefly the responsibility of theteacher ; and (3) instruction in preventive medicineand prophylaxis of social diseases, which would bechiefly the province of the doctor or of an experiencedschool nurse.
Considerable time was devoted to the effect ofschool work on health. The conference consideredthat it is not so much overwork as the combinationof a number of circumstances -very often a badlyorganized life, with tension and pressure of variouskinds -that leads to mental stress in schoolchildrenand adolescent students. An attempt was made toclassify the physical and mental causes of schoolfatigue. If suitable remedies are to be applied it wasfelt advisable for school health services in everycountry to be represented on educational boardsand in other bodies responsible for drawing upschool programmes. Dental care was cited as amost important part of school hygiene, and it wasconsidered that rational measures in this respectshould be taken urgently. Finally, the group sug-gested methods of furthering an internationalexchange of information on school health services.
This conference was not intended to cover allaspects of school health services and it will benecessary at a future meeting to study relatedquestions, such as vaccination in schools, the medicalsupervision of teaching personnel, food hygiene andment alhealth problems.
Alcoholism
The main activities of WHO,in Europe on alcoho-lism have followed the recommendations of theExpert Committee. One example is the seminarson the prevention and treatment of alcoholism,uch as the one held in 1951 in Copenhagen, the
repercussions from which have justified the con-tinuation of this specific activity. A second Europeanseminar on alcoholism was held in 1954 at Noord-wijk (Netherlands) in March and April, withAustria, Belgium, France, the Federal Republic ofGermany, Ireland, Italy, the Netherlands, Spain,Turkey and the United Kingdom participating(with observers from Chile and from the Union ofSouth Africa). In Belgium and the Netherlandsmeetings have recently been organized with the soleobject of studying and discussing the materialproduced by the Noordwijk seminar. Much interestcentred on the subject of " drinking patterns "in various countries, and it was recognized thatknowledge of this matter, although at presentinsufficient, is basic to the formulation of programmesfor the prevention of alcoholism. This pointstowards possible future activities of the RegionalOffice for Europe : it seems desirable to encouragesurveys of drinking patterns, organized so that theirresults may allow of comparison. Progress has alsobeen made in collecting data on the public care ofalcoholics and the nature of alcohol problems inEuropean countries.
Training of Personnel in Environmental Sanitation
The regional long -term programme in environ-mental sanitation consists of the developing of anexchange of technical information, the fostering ofcollaboration and understanding between engineersand other public- health workers, and certain formsof group training which supplement the individualtraining offered by the fellowships programme. Themain difficulties in expanding environmental sanita-tion programmes are the lack of funds and, whatis perhaps an even greater difficulty, scarcity oftrained personnel. Highly developed countrieswhere large -scale programmes for the essentialsanitary installations, such as water supply andsewerage systems, are nearly completed have nowto cope with new developments, e.g., growth of thepopulation, changes in its distribution, and strongdemands on the part of the public for higher stan-dards of sanitation in other respects, and are conse-quently always in need of more and better -trainedengineers. Other countries still struggling to com-plete vast schemes find themselves hampered intheir programmes by lack of the type of personnelwho combine a thorough understanding of thecountry's needs with sound experience of the progressmade in other more advanced areas.
EUROPEAN REGION 93
To meet this situation it has long been the practiceto send trainees to foreign institutions, mainly inthe United States of America, where they canobtain training in all the aspects required. However,even with outside help no country can afford tosend for training abroad all the personnel needed inenvironmental sanitation, and a tendency towardsEuropean and even national forms of training isdeveloping. Several institutions in the Region havestarted to draw up curricula and arrange facilitiesfor post- graduate training of engineers in environ-mental sanitation.
The Regional Office has co- operated with theHealth Division of the Rockefeller Foundation,which has long given financial assistance and fellow-ships to strengthen environmental sanitation pro-grammes in Europe.
To follow up the initiative taken in some countriesin this respect and to encourage new projects, theRegional Office has planned a symposium on thetraining of engineers engaged in environmentalcontrol work. This seminar is to be held in 1955 andaims at providing answers to a variety of questionsand giving guidance to the institutions or govern-ments which are sponsoring this pioneer work.
Other activities in the year under review haveincluded : (1) the organization of the fourth Euro-pean conference for sanitary engineers, which washeld at Opatija, Yugoslavia, in April, and at whichthe two main subjects of discussion were waterpollution and the disinfection of water by chlorina-tion ; (2) an advanced training course for water-works engineers, in late March and April, whichwas organized in collaboration with the Governmentsof Belgium and the Netherlands ; (3) co- operationwith the Government of Portugal in starting anational training course in environmental sanitationin Lisbon ; (4) continuation of the study on methodsof water analysis and criteria for water quality ;and (5) continuation of the study on French andEnglish terminology in sanitary engineering.
Present Trends and Future Developments
A review of the long -term objectives of WHOin Europe is soon to be made by the RegionalCommittee. This will not necessarily involve major
Anaesthesiology
The great majority of the countries of Europeemerged from the second World War noticeablyunder -developed as regards anaesthesiology, whichin many countries hardly existed as a separatespecialty. Programmes to meet the need for highlytrained anaesthesiologists were among the firstactivities undertaken by WHO in Europe. At therequest of the Danish Government and the Universityof Copenhagen, a centre was established in Denmarkin 1950, which immediately offered facilities forinternational training in this subject. Here, inaddition to the candidates attending at their ownexpense or sponsored by other health agencies,sixty -four WHO fellows, Europeans and non -Europeans, will have received one year's full -timetraining by the end of the training course now inprogress, the fifth of its kind.
Over the past four years this centre has had aninfluence in reducing the long period which wouldnormally be required for the importance of a com-paratively young specialty to be recognized and itstechniques to be brought to the level required bypresent -day surgery. Information about fellowsfrom European countries who were trained in thecentre indicates that some of them are now occupyingleading positions in their countries. In Yugoslavia,WHO has co- operated with a former fellow ininstituting national training in anaesthesiology inZagreb by providing an experienced foreign lecturerand meeting some of the needs for specializedequipment.
Later, the Organization co- operated in developinga second anaesthesiology centre at the Universityof Paris. This centre complements the one atCopenhagen by providing teaching in the Frenchlanguage and offering opportunities for advancedstudies in special techniques. So far six WHOfellows have attended the Paris centre, for whichWHO also provided a consultant during the firstyear.
A more detailed follow -up, designed to try toassess more precisely the relationship between theanaesthesiology training programmes and the ad-vances which have occurred in some countries inEurope, is now being prepared.
changes in general objectives but it may well callfor a careful selection of new activities. In recentyears, the full development of certain projectswhich had very modest beginnings, and the need for
94 THE WORK OF WHo, 1954
maintaining continuity and follow -up, have virtuallymade it impossible for the Office to undertake newtasks with the budget at its disposal. If new pro-grammes are to be begun, the only possibility, shortof finding some other solution to the problem offinance, is to withdraw gradually from certainprojects which have been in operation for manyyears and which no longer merit the highest priority,and possibly to space out other more standardprogrammes of a long -term character. In thisway, preliminary work could begin on other projectswhich have been waiting for many years and whichdeal with current problems of some magnitude inEurope. Among these are the public- health aspectsof some of the chronic killing and disabling diseases,the unification of health regulations in Europe(e.g., those on fond sanitation), the human factor
in traffic accidents, human relations in an expandingindustry, and many others.
At the same time, it will be necessary steadilyto improve the techniques for preparing and con-ducting inter -country programmes and to devisenew methods for disseminating the informationwhich they produce. Much also remains to bedone in establishing the fellowships programme on along -term basis and in bringing present and pastfellows into closer contact with the Regional Office.
With the continued co- operation of Membergovernments, it may be expected that the futurework of WHO in Europe will come to concentratemore and more on two primary objectives : theexpansion of co- operation in public- health workwithin Europe, and the promotion of educationand training programmes.

WILD- RODENT PLAGUE
During the meeting on wild- rodent plague held in Iran under the auspices of WHO, participantsvisited the district of Kurdistan, where a focus was known to exist, to demonstrate field research
techniques.
Searching for colonies of wild rodents (Meriones). Entrances to burrows of Meriones, with connecting tracks.
Discovery of winter grain provi-sions in a burrow.
Excavation of burrows in search of fleas that may be vectors of plague. Collecting fleas and other ecto-parasites from a capturedMeriones for laboratory research.

The team gathers data in thevillage of Mit Halfa for a survey of
enteric diseases.
Samples of water for chemicaland bacteriological analysis
are taken at each housevisited.
A pump is disinfected with ablowtorch.
HEALTH DEMONSTRATIONPROJECT IN THE RURAL
DISTRICT OF CALIOUB, EGYPT
Work on the survey continues at night, so asnot to miss the men who work in the
fields in the daytime.
This woman is telling a member of the teamthat her family finds canal water has a
better taste than the clean water of thepump outside her door.
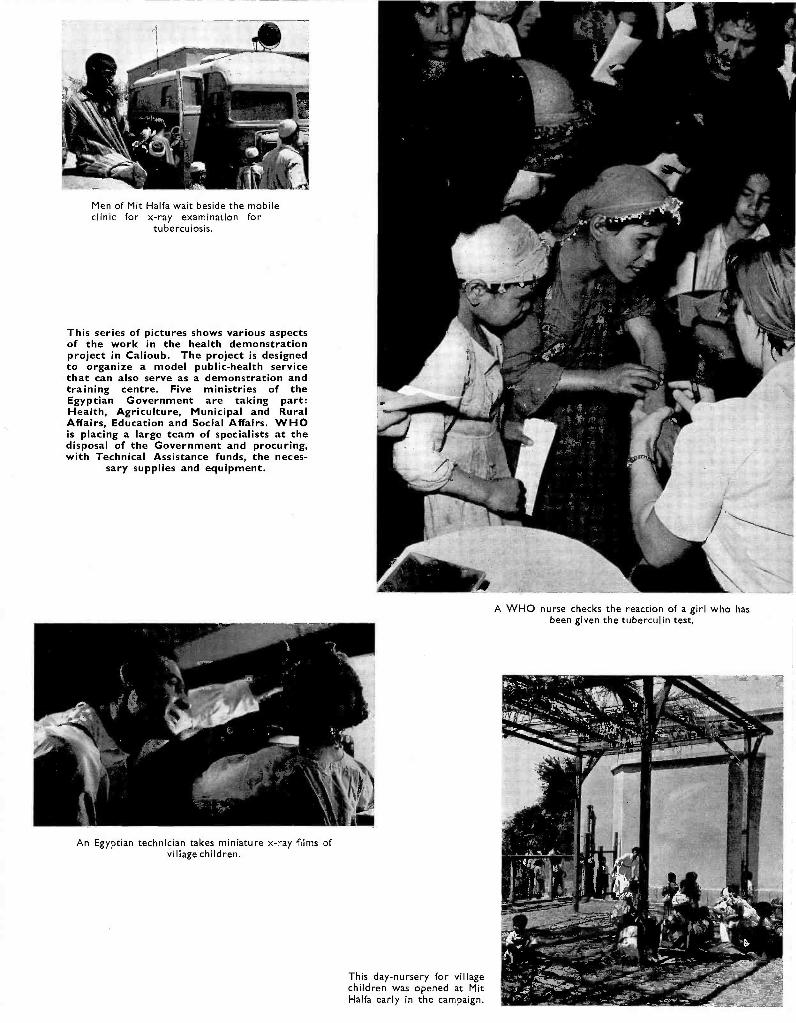
Men of Mit Haifa wait beside the mobileclinic for x -ray examination for
tuberculosis.
This series of pictures shows various aspectsof the work in the health demonstrationproject in Calioub. The project is designedto organize a model public -health servicethat can also serve as a demonstration andtraining centre. Five ministries of theEgyptian Government are taking part:Health, Agriculture, Municipal and RuralAffairs, Education and Social Affairs. WHOis placing a large team of specialists at thedisposal of the Government and procuring,with Technical Assistance funds, the neces-
sary supplies and equipment.
An Egyptian technician takes miniature x -ray films ofvillage children.
This day- nursery for villagechildren was opened at MitHaifa early in the campaign.
A WHO nurse checks the reaction of a girl who hasbeen given the tuberculin test.
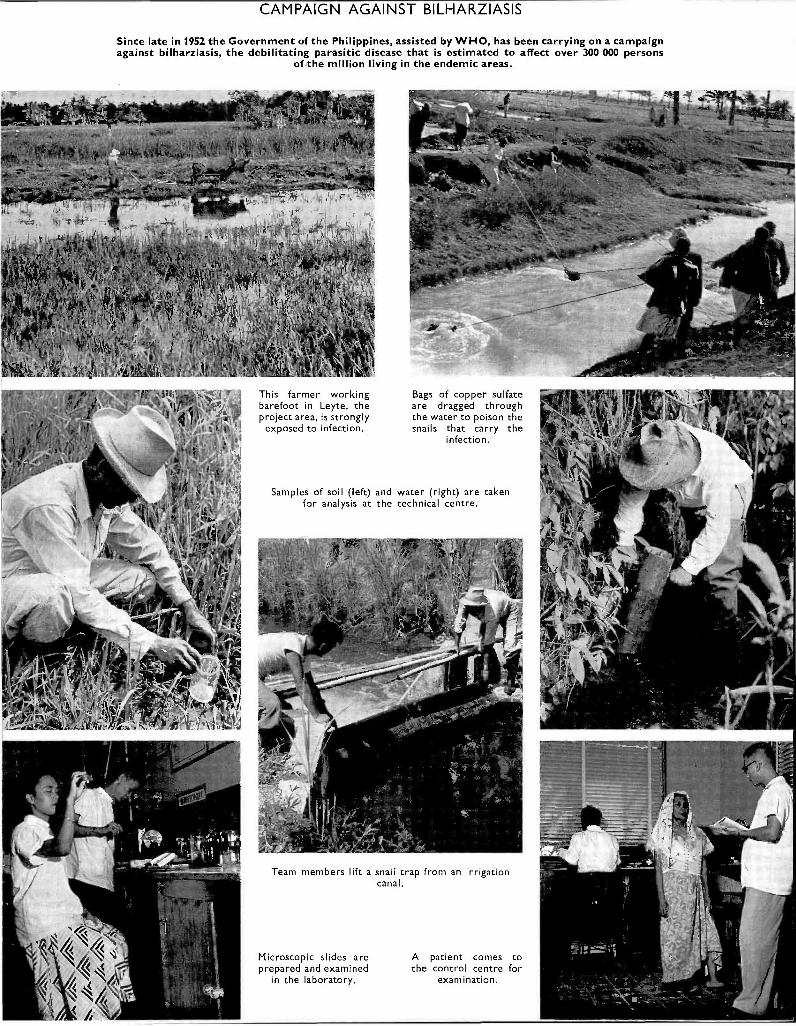
CAMPAIGN AGAINST BILHARZIASIS
Since late in 1952 the Government of the Philippines, assisted by WHO, has been carrying on a campaignagainst bilharziasis, the debilitating parasitic disease that is estimated to affect over 300 000 persons
of the million living in the endemic areas.
This farmer workingbarefoot in Leyte, theproject area, is strongly
exposed to infection.
Bags of copper sulfateare dragged throughthe water to poison thesnails that carry the
infection.
Samples of soil (left) and water (right) are takenfor analysis at the technical centre.
Team members lift a snail trap from an irrigationcanal.
Microscopic slides areprepared and examined
in the laboratory.
A patient comes tothe control centre for
examination.
JEASTERN
CHAPTER 15
MEDITERRANEAN REGION 1
WHO's regional programme in the EasternMediterranean Region consists of assistance togovernments for three main purposes : strengtheningnational health administration, controlling com-municable diseases, and improving the training ofhealth personnel -particularly by the developmentof training facilities within the Region.
Public- health administration. One of the greatestdeficiences in the Region is the shortage of trainedhealth administrators. Therefore a large proportionof the fellowships in the Region are being awardedto health administrators for study abroad to enablethem to see how problems similar to those in theircountries have been dealt with elsewhere.
The need for employing highly trained healthpersonnel on a full -time basis is not yet adequatelyappreciated in all countries of the Region, and thefailure of some governments to provide the necessarymatching personnel for training by the WHO expertshas complicated the efforts to strengthen nationalhealth services and has jeopardized the continuationof work after the departure of WHO staff.
Environmental sanitation has become an indis-pensable component of almost every WHO -assistedhealth project in the Region. The greatest need isfor regional training facilities, and WHO has assistedwith several schemes for training sanitarians inEgypt and Lebanon. Adequate remuneration andsecurity of tenure need to be offered to attract andhold the right type of person and to ensure the con-tinuity of services.
Many projects have been designed to convincepopulations of the benefits resulting from improve-
1 This region, according to the decisions of the First,Second and Fifth World Health Assemblies (O$. Rec. WldHlth Org. 13, 80, 330 ; 21, 17, 53 ; 42, 31), comprises Aden,Somaliland Protectorate, Cyprus, Egypt, Ethiopia, FrenchSomaliland, the Hashemite Kingdom of Jordan, Iran, Iraq,Israel, Lebanon, Libya, Pakistan, Saudi Arabia, Syria, Turkeyand Yemen. In accordance with resolutions WHA5.46 andWHA6.46, Turkey was temporarily transferred to the EuropeanRegion, Somaliland Protectorate to the African Region,and Somalia (Trusteeship), Bahrain, Kuwait, Qatar, and theTrucial Sheikdoms were provisionally assigned to the EasternMediterranean.
ments in sanitation and other conditions, and toinform them on health matters. The co- operationof representative village committees and school-teachers is being enlisted to promote this healtheducation of the public.
The number of programmes in maternal and childhealth assisted jointly by UNICEF and WHO hasincreased considerably. There have been demon-strations of modern domiciliary midwifery techniquesand of the care of the mother and child (from thepre -natal stage until the child is of school age) inmaternal and child health centres set up for thesepurposes. Although treatment is given to childrenfor minor ailments, every effort is made to preventthese centres from becoming ordinary paediatricdispensaries by stressing prevention as against cure.To maintain this distinction is easy enough in thelarge urban centres, but more difficult in rural areas.Training in maternal and child health work is beinggiven to a wide variety of personnel: doctors,medical students, student nurses, graduate nurses,trained and even sometimes untrained midwives,community health visitors (see page 97) andauxiliaries.
Another feature of this work has been the milkdistribution scheme, financed by governments andUNICEF and operated as a routine activity in eachcentre. From extensive surveys made by the regionaladviser it was learned that the complications ofpregnancy throughout the Region were mainly dueto malnutrition and lack of pre -natal care, and thatinfant mortality was mostly caused by malnutritionand ignorance of infant feeding, especially duringthe weaning period.
During the year, the Government of Lebanonsponsored and arranged a seven -day seminar formidwives, at which some twenty speakers addressedand held discussions with 120 participants.
The idea of a school medical service as an essentialbranch of preventive medicine is not yet fully under-stood in the Region. Some fellowships have beenawarded to promote developments in this field, inwhich further co- operation with UNICEF is alsoplanned.
-- 95 -

96 THE WORK OF WHO, 1954
Wide surveys of mental health have already beenconducted by consultants in Egypt, Iran, Iraq,Jordan, Lebanon, Sudan and Syria. Following thesurvey in Jordan, WHO provided the services of amental health consultant, who began his work inthat country early in 1954 on a project -the first ofits kind in the Region -to develop a full diagnosticand therapeutic service, occupational therapy andtraining. It also involves revising out -of -date lunacylaws and medical procedures, not only in Jordan butin most countries of the Region where a reorienta-tion of the public attitude to the problem, andtraining of expert staff, are required. AnotherWHO consultant is advising on the organization andoperation of a school for backward children whichis being established in Baghdad.
In order to improve the nursing services, it isnecessary to increase the number of adequatelytrained nurses by standardizing and upgrading theirtraining to the level of other countries, and makingthe nursing career attractive enough economicallyand socially to draw into it young women withdesirable qualifications. The support not only ofministries of health but of other government depart-ments is essential in securing for nurses conditionsof service as good as those of other competingoccupations.
In the Calioub health demonstration area WHO ishelping to develop a suitable pattern of healthservices for the rural areas of Egypt. Particularattention is given to the relations between healthand other services needed in rural communities, e.g.,in agriculture, veterinary public health, educationand social welfare. The United Nations is parti-cipating and the work is being co- ordinated withthat of an FAO programme in the area.
Control of Communicable Diseases. Work inmalaria control has hitherto been concentrated inthe adjoining countries of Iran, Iraq, Israel, Jordan,Lebanon and Syria, where the eradication of thedisease seems practicable in the foreseeable future(a special account of the work on malaria in thesecountries is given later in this chapter underthe heading " Reports on Typical Projects in theRegion "). It is planned to hold an inter -regionalconference with the European Region in 1955.Starting in 1955, it is also hoped to devote greaterattention to the control of malaria in those countriesof the Region which lie in Africa and in the Arabianpeninsula. In Egypt and Pakistan DDT -productionplants are being built with the assistance of UNICEFand Technical Assistance funds ; WHO is providing
advice on the use of the product. Similar pro-grammes have been requested by Iran and Iraq.
The incidence of the treponematoses varies widelyin the Region ; endemic forms are found in somecountries. In 1954 WHO- assisted demonstrationand training centres for the control of venerealdiseases were continued in Ethiopia, Iran and SaudiArabia, WHO personnel was withdrawn from thecentre in Pakistan, and work on a bejel- syphilisproject began in Syria. It is planned to continueassistance in combating this group of diseases.
Some problems have been met in controllingbilharziasis in the Region. The price of mollus-cocides makes the cost of controlling the intermediatehost almost prohibitive, but to achieve control byaltering the age -old habits of the people will obviouslytake a very long time. The project in Egypt is beingreconsidered in an attempt to solve some of theproblems and to evolve simpler and more effectivemethods.
The incidence of tuberculosis varies widely in theRegion. In most countries BCG campaigns arenow operating, and in many the time is coming toincorporate them into the regular health services(the work in Iraq is described on page 98). A BCGevaluation team has recently begun work in theRegion.
The problem of trachoma has always had theattention of the Regional Office. since the adventof sulfonamides and antibiotics, a regional cam-paign against the disease has been under considera-tion. A great deal of information has been obtainedfrom such sources as an experiment conductedamong the Palestine refugees, the recommendationsof the expert committee which met in Geneva in1952,1 and field operations being carried on inNorth Africa with the assistance of WHO andUNICEF. A pilot project is shortly to be startedin Egypt to devise a practical and effective methodsuitable for mass campaigns.
Finally, there is the great problem of gastro-intestinal diseases, which is closely linked withthose of environmental sanitation and the healtheducation of the public.
Education and Training. Teaching facilities varywidely from country to country, and WHO assistswith the training of several categories of personnel :administrators and instructors, who are awardedfellowships in such subjects as public -health admin-istration and nursing education ; doctors and nurses
1 Published in Wld H,'th Org. techn. Rep. Ser. 1952, 59.

EASTERN MEDITERRANEAN REGION 97
who require post -graduate training, especially inpublic health and preventive medicine ; public -health engineers ; sanitarians ; nurses and midwives ;community health visitors and auxiliaries ; laboratorytechnicians, and others. The programme of fellow-ships in the Eastern Mediterranean is like that ofother regions except for the special emphasis that isgiven to long -term fellowships for undergraduatesfrom countries that have no medical schools.
There is still a general lack of appreciation of theneed to employ fellows in the specialties in whichthey are trained.
In the training of nurses throughout the Region,the public -health aspect of nursing is being stressed.The lack of instructors is a major obstacle to progress.The regional nursing college which is being estab-lished in Alexandria and which will start early in 1955will have an important function in this respect.In an effort to meet urgent needs, certain govern-ments are also establishing a special category of" community health -visitors ", for work in ruralcommunities. In continuous training courses, whichlast for twenty -seven months and which are beinggiven in ten maternal and child health centres ofthe Region, these workers are trained in generalnursing, midwifery and especially public -healthnursing. Full training in these subjects would nor-mally require four and a half years ; the shortercourses are intended to meet immediate needs.
Nursing auxiliaries are also being trained (forexample, in Syria) in courses of about twelve months'duration, in which emphasis is on maternal andchild health, tuberculosis, venereal diseases andsanitation. The purpose of this training is to supplystaff for the immediate expansion of health services,in which the auxiliaries will work under the super-vision of trained nurses.
The problem of the untrained midwife (dai) isstill largely unsolved : the gradual replacement ofthe dais by trained midwives will require manyyears, much greater expansion of training facilitiesand, if qualified midwives are to be induced to settlein rural areas, better conditions of service.
The Regional Committee
In resolution WHA7.33 the Seventh World HealthAssembly recommended that the Regional Commit-tee for the Eastern Mediterranean should provi-sionally carry out its duties through being dividedinto two sub -committees (referred to here as Sub -Committees A and B). However, only one of thesesub -committees was able to meet in 1954.
The Regional Director first asked the MemberStates of the Region whether they wished to attend
one or both of the sub -committees, and invitedsuggestions as to the place of meeting and how tofacilitate the satisfactory application of the provisionsof the resolution cited above. Eleven Members(Egypt, Ethiopia, Iran, Iraq, the Hashemite Kingdomof Jordan, Lebanon, Libya, Pakistan, SaudiArabia, Syria and Yemen) notified their intentionof participating in one sub -committee, and three(France, Italy and the United Kingdom of GreatBritain and Northern Ireland) elected to attend both.
At the same time, a majority of the Membersexpressed the wish that Sub -Committee A should beconvened in Alexandria, and arrangements weretherefore made for it to meet at the headquartersof the Regional Office from 27 September to1 October. The Government of Italy offeredMogadishu, in Somalia, for the site of the meetingof Sub -Committee B, and the Regional Directornotified the interested countries that this sub-committee would be convened there from 13 to16 October.
One Government (Israel), which had reserved itsposition, later reiterated its reserve, stating that itwas unable to participate.
The Regional Director notified all Members ofthe Region of this situation, and during the meetingof Sub -Committee A in Alexandria the representa-tives of France, Italy and the United Kingdom statedthat in the circumstances their Governments wouldnot be represented at the meeting of Sub -Committee B.
As a result of these decisions, the meeting ofSub -Committee B, convened in Mogadishu, couldnot take place at the date notified, and these threecountries decided that they would exercise their rightof vote in Sub -Committee A.
At the meeting of Sub -Committee A, fourteen ofthe fifteen Member countries were represented,Sudan sent an observer, and representatives orobservers were present for the United Nations,UNICEF, the United Nations Relief and WorksAgency for Palestine Refugees in the Near East(UNRWA), and several specialized agencies andother organizations. The Director - General wasrepresented by his deputy.
In accordance with the provisions of resolutionWHA7.33, the Sub - Committee adopted its own rulesof procedure.
The Sub -Committee commended the considerableprogress and development in WHO activities in theRegion which had taken place since the RegionalCommittee had met (in 1950), and supported themodifications proposed in the regional programmefor 1955. It reviewed and found adequate the
98 THE WORK OF WHO, 1954
proposed programme and budget estimates for 1956,as presented by the Regional Director, and gavespecial emphasis to the inter -country part of theprogramme. The importance of long -term plan-ning by health ministries, in conjunction with otherministries, such as those responsible for socialaffairs, agriculture, education and finance, wasstressed.
In the discussions on the programme, particularattention was given to the need for improvingenvironmental sanitation, as one of the first essentialson which most other public -health measures in theRegion depended, and to smallpox control. Countriesin the Region were called upon to plan programmesin both these subjects, and WHO was asked tocollaborate and to collect data on the immunityresulting from vaccination.
At a private meeting the Sub -Committee recom-mended the extension of the appointment ofDr A. T. Shousha as Regional Director.
The question of using Arabic as one of the workinglanguages in the Regional Organization was raised,and the Sub -Committee recommended that thematter be studied and a report made to a latersession.
Concern was expressed about the new policy forthe allocation of funds from the Expanded Pro-gramme of Technical Assistance for EconomicDevelopment, it being feared that health work wouldreceive a reduced allocation of funds under the newprocedure of country planning established by theEconomic and Social Council.
On the question of the payment of local costs bygovernments for internationally -assisted projects,the Regional Director was asked to pursue thequestion of harmonizing the policies in this matterbetween the regular and Technical Assistanceprogrammes.
The Sub -Committee expressed appreciation ofthe health work performed by UNICEF and
UNRWA, and noted with approval the work inepidemiological intelligence carried on by theRegional Office. The importance of developingprogrammes in the co- ordination of research wasalso stressed.
A technical discussion was held on the use andtraining of auxiliary health workers, a matter ofprimary importance to the Region, and it wassuggested that this question might be an appropriatetopic for discussions at the Health Assembly in 1956.In general, however, it was not considered that thesubjects of technical discussions at sessions ofregional committees should be the same as those tobe discussed at the World Health Assembly.
It was agreed that the next meeting should be heldin Lebanon.
Finally, even though the meeting of the other sub-committee had been cancelled, the Sub -Committeeappointed a representative and an alternate toconform with the provisions of resolution WHA7.33.1
The Regional Office
No changes have been made to the basic organiza-tion of the Regional Office during the past year, butthere have been some modifications in staffing.
In addition to one temporary appointment of aspecial consultant and the recall to the RegionalOffice of an area representative to help the officethrough a critical period, posts for a malaria adviserand for an adviser in education and training wererestored. The filling of these posts, as soon aspossible, by persons with a general training in publichealth and additional specialized experience, willhelp the work of the Regional Office considerably.
Similarly, on the administrative side, the appoint-ment of a budget analyst and the strengthening ofthe staff of the medical supplies unit has enabled theRegional Office to keep abreast of its work, despitethe additional strain resulting from fluctuations inTechnical Assistance funds.
Reports on Typical Projects in the Region
A complete list of projects current during theyear will be found in Part IV. The following havebeen selected for fuller description.
1 Subparagraph 2(8) of which reads :" in order to co- ordinate the opinions of the sub- commit-tees, the following procedure shall be adopted : a persondesignated by each sub -committee, with the authorizationof the respective sub -committees, shall meet together withthe Regional Director in order to harmonize as far as maybe necessary the decisions of the sub -committees and to
Tuberculosis in IraqThe tuberculosis vaccination project in Iraq
(Iraq 10) is an example of a mass BCG campaignwhich is being closely co- ordinated with other workon tuberculosis and successfully integrated into apermanent tuberculosis service.
present a final report, and the decisions arrived at shallbe forwarded to the Executive Board with the details ofvoting, if any. "
EASTERN MEDITERRANEAN REGION 99
Preliminary surveys by WHO advisers of conditionsamong a large section of the population suggestedthe possibility of a high incidence of the disease.An analysis of the findings of the subsequent BCGcampaign showed that 16 per cent. of children inthe 1 -6 age group, 40 per cent. in the 7 -14 age group,and 78 per cent. of children over fourteen gavepositive tuberculin reactions. The only tuberculosisservice which existed was a 300 -bed tuberculosissanatorium, with an out -patient clinic, in Baghdad.
With assistance from UNICEF, BCG field opera-tions began in May 1952, to provide some measureof immediate protection and lay the foundation ofa permanent BCG service combined with a nationalorganization for tuberculosis control. By August1954, 460 853 persons, mainly schoolchildren, hadbeen tested, and 175 723 negative reactors vaccinated,in a campaign extending over the greater part ofthe country.
In May 1953, the senior adviser of the BCG teamwas made responsible for the demonstration andtraining project in tuberculosis control (Iraq 7), whileretaining the general direction of the BCG activities.
A comprehensive three -year plan for the organiza-tion of tuberculosis control was drawn up. Itincluded the setting -up in the Ministry of Health ofa tuberculosis control section, in charge of policy,legislation, co- ordination and finance ; the establish-ment of a national training unit and diagnosticlaboratory at the centre in Baghdad ; and the creationof regional, provincial and rural organizations.Each administrative area (or "liwa ") is to have atuberculosis dispensary, staffed by a medical officer,a nurse, two health visitors, a laboratory technicianand an x -ray technician. Appropriate equipmentand facilities for diagnostic (clinical, x -ray andlaboratory) services, BCG vaccination, and treat-ment are to be provided. So far, two liwa dispen-saries, organized along the lines of this plan, havebeen established. The liwa organization is to bebased on regional tuberculosis sanatoria which willbe built in Basra, Mosul and Baghdad, to serve thenorthern, southern and central areas of the countryrespectively.
At the rural level the organization for tuberculosiscontrol is still in an experimental stage. Activitieswill be organized on the same lines as those of theliwa dispensaries, and will provisionally consist of astudy of certain control methods, to be carried outin selected villages.
Meanwhile, the tuberculosis centre in Baghdad istraining the staff required to serve in the nationalorganization -medical officers, nurses, health visitors,x -ray and laboratory technicians and registration
and statistical clerks. In addition, WHO hasprovided three fellowships in tuberculosis controland one in tuberculosis bacteriology.
This project was noteworthy for the smoothtransition from the mass campaign to the permanent -control- service phase, and for the public interest ithas aroused, leading to a demand for measures toprevent and control tuberculosis.
UNICEF aid for the BCG campaign has beenextended to mid -1955, and WHO's participation inthe control project is expected to continue with areduced staff until mid -1956.
Rehabilitation of Crippled Children, Israel
In 1951 Israel suffered from a severe epidemic ofpoliomyelitis, which was followed by recrudescencesof the disease in succeeding years. These outbreakswere characterized by an abnormally high incidenceof cases among children under one year of age andby a very high percentage of residual paralysis ; thetotal number of cases of paralysis was estimated atsome 1500 by the end of 1953. In addition, therewas a considerable influx of post -poliomyelitis casesamongst immigrants.
To deal with this serious problem Israel had onlyapproximately twenty trained physiotherapists, andan inadequate number of unqualified workerstrained only by apprenticeship. There was no schoolof physiotherapy.
In May 1951 the Government asked WHO forassistance in establishing a rehabilitation centre forphysically handicapped children and a nationalschool of physiotherapy. In 1953, WHO provided aphysiotherapist. Equipment, including raw materialsfor the manufacture of prosthetic appliances, wassupplied by UNICEF (Israel 8). The NationalSchool of Physiotherapists was opened in December1953 at the. Government Hospital in Sarafand, withseventeen students, and a three -year course wasstarted in accordance with the specifications of theWorld Confederation for Physical Therapy.
The project developed along lines which had notbeen foreseen but which were dictated and justifiedby circumstances. The number of trained physio-therapists was so very small in relation to the largenumber of paralysed children that it was foundequally impossible to keep the children indefinitelyin hospital, to deal with them as out -patients inhospitals (because of difficulties of transport), toopen physiotherapy clinics in outlying districts or toarrange for domiciliary treatment. The solution
100 THE WORK OF WHO, 1954
adopted was a scheme of simplified and standardizedtreatment to be carried out at home by the parentsunder the supervision of public- health nurses, whoreceive special training for that purpose.
Another interesting development was the exten-sion of the training to include the care of rheumaticcases, chronic nervous diseases, surgical cases andpre -natal and post -natal cases, as well as the re-habilitation of the aged.
The rehabilitation centre, also in Sarafand, wasslower in developing, but the buildings are nowcompleted, and comprise a fully equipped gymna-sium, a hydro- therapeutic unit and an occupationaltherapy department. Two wards opened in Julytook in forty -one post -poliomyelitis cases, while theout -patient department is dealing with both post -poliomyelitis and other orthopaedic surgical cases.
The orthopaedic workshop is to be developed tosupply and modify all the appliances required.
Inter- Country Malaria Control
During the last five years, the Organization hasassisted the Governments of Iran, Iraq, Lebanon andSyria to develop malaria control ; similar work hasbeen carried out amongst the Arab refugees, espe-cially under the auspices of UNRWA, andassistance has been given to Israel in the form oftechnical advice and fellowships.
This group of countries forms a more or lessisolated bloc stretching from the eastern shores ofthe Mediterranean to the desert and mountainousborder of Pakistan ; it is bounded on the north bymountains and the Caspian Sea, and on the southby desert and the Persian Gulf. Turkey, in theEuropean Region, has close links with this group.Generally speaking, there is free communicationamong most of these countries, with no great naturalbarriers, . and they have similar malaria -controlproblems. In ancient times much of this countrywas irrigated and very fertile and provided food forlarge populations. With the passage of centuriesthe irrigation systems have fallen into ruin, malariahas become severe and widespread, and there hasgenerally been extensive depopulation.
Present Trends and Future DevelopmentsThe statements by the government representatives
at the meeting of Sub -Committee A (see page 97)attested to an increased confidence in the work ofthe Organization and an understanding of its aims
In attacking the problem of malaria in this area,the first step taken jointly by most of the govern-ments and WHO has been to set up projects, withsurveys, demonstrations of modern methods ofmalaria control and the training of staff. In Iran,aid was also given in the establishment of a malariainstitute.
With the knowledge gained in the demonstrationprojects, control measures were introduced overincreasingly large areas. In Lebanon, such measuresnow extend to almost the entire country. In thiseffort towards nation -wide control the countrieshave also been aided by UNICEF and by the UnitedStates Foreign Operations Administration (FOA),which has made extensive grants for supplies, equip-ment and transport. Already some five and a halfmillion people are protected from malaria.
As control measures within neighbouring countriesexpand and reach the frontiers, there is an evidentneed for inter -country co- ordination. Moreover,experience in other regions has shown that if controlmeasures can be established to ensure completecoverage over wide areas for long enough to breakthe chain of transmission, it will probably in the endbe possible to suspend expensive spraying operationswithout a recrudescence of malaria.
Accordingly, an inter -regional conference hasbeen planned for representatives of the above -mentioned countries of the Eastern Mediterraneanand contiguous countries of Europe, and from otherorganizations, to discuss common problems andplan a co- ordinated campaign to free the areacompletely from malaria.
Much hard work remains to be done, and largefinancial contributions will be required both fromthe countries themselves and from the supportingorganizations. But the ultimate results, both econo-mically and in terms of human welfare, areincalculable. It is even possible that vast tracts ofthis area may eventually resume their ancient fertility.
Thus it is seen that demonstration projects whichare developing into country -wide control measuresand finally into inter -country programmes may lead,within the foreseeable future, to the elimination ofan ancient scourge from a group of countries whosepopulation totals some thirty -two million.
and purposes. This has also been reflected in thechanging nature of requests : governments now makefewer demands for large quantities of supplies andequipment and are more likely to ask for technicaladvice and assistance with education and training

EASTERN MEDITERRANEAN REGION 101
projects. This has justified the policy pursuedduring the years in which the Regional Committeehas not met.
The regional programme will probably becomeless dependent on demonstrations and field projectsand lean even more towards the development ofeducation and training facilities for both professionaland auxiliary workers. It is unlikely that the prob-lems of this region can be solved by attempting tosupply enough fully- trained professional workers ;the economy of towns and villages will not standit, and highly trained personnel will not work inlocalities with few amenities and low standards ofcomfort. However, properly trained auxiliaries,with reasonable supervision by personnel trained inpublic health, can and will do the work -probablybetter than the more highly trained workers.
Good results are expected from the technicaldiscussions on the use and training of auxiliarypersonnel which were held during the meeting ofSub -Committee A. This is an example of a subjectof wide interest, in which much experience has beenaccumulated but where there is remarkably littleagreement, even on basic terminology, and theexchange of experience among the countries of thisregion and other regions should help to co- ordinatethinking.
In connexion with the emphasis on education andtraining, the Regional Office, besides continuingwith the fellowships programmes, has planned forsome time to organize a series of regional seminars.Countries in the Region have taken part in inter-regional conferences, but, mainly owing to shortageof funds, there has so far been only one seminar-on mental health, in 1953. However, seminarson maternal and child health, environmental sanita-tion, and meat hygiene are scheduled for 1955 and1956, and plans have been made for a series of travellingseminars -the first in 1955 -in which senior public -health administrators will visit countries in theRegion, discuss problems of common interest andstudy methods of solving them. The first travellingseminar will visit Egypt, Iraq and the Sudan. It isexpected that the practice of bringing together public -health administrators and specialists with one or twovisiting specialists to discuss common problems willprove increasingly useful in years to come.
Demonstrations and field work will not of coursebe abandoned, but circumstances and long -termrequirements will dictate their relative importance.
Regional co- operative programmes will be empha-sized ; and it is planned that for specific tasks short-term consultants, whose services have becomeincreasingly popular with governments, will be usedmore widely.
A further welcome trend in a number of countriesin the Region has been the setting up of five- toten -year plans for developing health services, andefforts are being made to assist countries in suchlong -term planning. Greater stability in the financingof the regional programme should make it easierto develop plans for collaboration over longerperiods of time, not only for work in which WHOassists one particular country but also where morethan one country is involved. It is felt that thetime has come for more programmes of a trulyregional character. Several countries have estab-lished special funds, in addition to their normalrevenue, to finance these and other long -term plans.In addition to these extra -budgetary sources ofrevenue, the normal government expenditure forroutine health services is now approaching 10 percent. of the national budgets.
The development of integrated health programmesvaries widely from country to country. In somecountries, efforts are being made to achieve betterintegration, either by developing the co- ordinatingrole of the Ministry of Health or by combining allhealth services at the provincial level under oneunified direction, as is being done in the experimentaltraining and demonstration area in Calioub. Ingeneral, there is a gradual trend towards fusingcurative and preventive services, and closely co-ordinating those for health with other social services.
In one or two countries of the Region, however,health services are being set up separately -as, forexample, in workers' insurance schemes or by socialwelfare ministries -outside the jurisdiction of thehealth ministries, with all the disadvantages inherentin such decentralization. In this connexion, theOrganization, jointly with UNICEF, has begun toassist in several projects to develop rural healthunits in which integrated health services may beprovided and staff trained.
There have been important developments in thelast few years in the co- ordination of the work withUNICEF, the United Nations Technical AssistanceBoard and other international organizations andfoundations. With UNICEF in particular, now

102 THE WORK OF WHO, 1954
that it is no longer an " emergency " organization,and is increasingly preoccupied with long -termplans, co- operation and joint assistance to govern-ments will no doubt continue to increase.
The emphasis on programmes of environmentalsanitation which was called for by the Sub -Com-mittee will require considerable investments in
capital. Health departments should not be askedto carry the whole burden of the very large expen-diture necessary for any real results in this field ;and the cost for sanitation involved in any schemefor developments in, for example, agriculture, trans-port, power, or industry should be borne by thoseimplementing the scheme.

CHAPTER 16
VWESTERNPACIFIC REGION
As in other regions, the work of WHO in theWestern Pacific Region has one basic purpose : tostrengthen national health services. This can be doneonly if the supply of trained personnel is adequateand if their services are fully used. The acute shortageof trained personnel in some countries has had adetrimental effect on programmes : WHO staff havesometimes had to work without the promisednational.counterparts, with the result that the handingover of projects to national health workers has beendelayed, or that the appointments of the internationalstaff have ended before counterparts were sufficientlytrained to take over the responsibilities. Theincreasing number of requests from the governmentsfor assistance in education and training work-whether in the form of fellowships, the develop-ment of training centres, exchange programmes orseminars -shows that national health administrationsare aware of the seriousness of the problem.
Although countries in the Region are receptive tothe idea of health education, community participationin health work -the principle advocated by WHO-is slow to be understood. Many governments havenot yet appreciated the need for health educatorsand WHO, is, therefore, by practical demonstrations,endeavouring to emphasize health education activitiesin the Region by including them in all field projects.
Diseases susceptible of control by known techniquesof environmental sanitation are a considerableproblem in many countries. Only a few urbancommunities have water supplies which meetminimum public- health standards, and most in-habitants of rural areas use water which, if notobviously contaminated, is certainly suspect. Sani-
1 The Region, as delineated by the First World HealthAssembly (Off. Rec. Wld Hith Org. 13, 80, 330) and affectedby resolutions WHA3.118, WHA4.86 and WHA6.46, includesAustralia, Cambodia, China, Japan, Korea, Laos, NewZealand, the Philippines, Viet Nam and, provisionally, thefollowing territories : American Samoa, British SolomonIslands Protectorate, Brunei, Fiji, Gilbert and Ellice Islands,Guam, Hong Kong, Malaya, New Hebrides, New ZealandIsland Territories, North Borneo, Pacific Islands TrustTerritory, Sarawak, Singapore, Tonga, and other UnitedKingdom possessions in the South Pacific.
tary disposal of human excreta is practised in onlya few cities and towns. In many communities and inalmost all rural areas, soil pollution and contami-nation of drinking -water are evident, and few or nomeasures are taken to deal with other environmentalproblems, such as those connected with housing,refuse disposal, rodents and flies. Every effort hasbeen made to assist governments to define theirproblems and to study plans for improving environ-mental sanitation. The great importance of thiswork is being increasingly recognized.
Budgetary limitations have continued to restrictfield activities. Other difficulties arise from the weakeconomic situation of some of the countries as aresult of unsettled conditions and the problemscreated by the influx of refugees.
The Regional Committee
The fifth session of the Regional Committee washeld in Manila from 10 to 16 September and wasattended by representatives of all Member States inthe Region. The Governments of France, the Nether-lands, Portugal, the United Kingdom of GreatBritain and Northern Ireland, and the United Statesof America, responsible for territories in the Region,were represented by local health administrators.Representatives from the United Nations Children'sFund, the United Nations Technical AssistanceBoard, the United Nations Korean ReconstructionAgency, the International Labour Organisation, theWHO Epidemiological Intelligence Station in Singa-pore, and observers from other agencies and ofsixteen non -governmental organizations in officialrelations with WHO were also present. The Director -General was represented by an Assistant Director -General.
The Regional Committee endorsed certain modi-fications in the proposed programme and budget for1955 which were made necessary by the reduction inthe budget decided upon by the Seventh WorldHealth Assembly, and adopted a resolution proposingthat, if funds became available from budgetarysavings in 1954 and 1955, priority should be given
- 103 -
104 THE WORK OF WHO, 1954
to health projects requested by Cambodia, Laos andViet Nam as contained in the supplementary list ofprojects. In examining the proposals for 1956, theRegional Committee stressed the importance oforganizing regional conferences, lectures and studytours, which, it was believed, would foster cordialrelations and understanding among Member Statesin the Region, and requested that every effort shouldbe made to allocate funds for this purpose. Con-sideration was also given to establishing criteria forthe selection of projects to be financed from regularfunds, and the Regional Director was asked toprepare such criteria for the consideration of theRegional Committee at its sixth session.
The importance and control of insect -borne virusdiseases in the Western Pacific were discussed. TheRegional Committee recommended that experts inthe Region should be asked to prepare papers on thepublic- health aspects of this problem for considera-tion by members of the Expert Advisory Panel onVirus Diseases, and with a view to the holding of aseminar.
The Regional Committee approved the report ofthe Regional Director, expressed appreciation of thegrowth in the regional fellowship programme andrecommended the re- establishment of the post ofstatistician and programme evaluator (cancelledduring the year) so that governments might benefitfrom this form of assistance.
The subject of the technical discussions waspublic- health administration with particular referenceto the organization of health departments, anddiscussion was focused on (a) methods of obtainingsuitable workers for health departments ; (b) thebasic health unit in areas with limited or no healthservices ; and (c) the use of multi -lateral and bi-lateral assistance for health programmes. TheRegional Committee considered the discussions usefulbut felt that a more limited subject should be chosenfor the technical discussions at the sixth session.
The Regional Committee decided to hold the sixthsession in Singapore in 1955, and the seventh sessionin Manila, unless the Regional Director received aninvitation before the sixth session to hold it elsewhere.
The Regional Office
During the year a prefabricated building- for thelibrary, a conference room and two offices- was addedto the Regional Office. The possibility of obtaininga permanent building to house the Regional Officeand the offices of the United Nations and otherspecialized agencies in Manila is under consideration.
No major changes in personnel took place, althoughfor reasons of economy it was found necessary to
suppress the post of regional statistician and pro-gramme evaluator, those of the area representativesand some minor clerical posts. However, in- servicetraining, a clearer definition of responsibilities andthe very small turn -over of staff made for increasedefficiency of the Regional Office. Progress was madein the recruitment of project personnel during theyear, and a satisfactory geographical distributionwas maintained. The transfer of project staff betweenregions was beneficial in that the staff working onprojects had already been trained, and were accus-tomed to working in countries other than their ownand under field conditions. Twenty -seven inter-nationally recruited experts from ten countries wereassigned to field work, bringing the total number ofinternationally recruited staff working in the fieldup to sixty -one, from seventeen countries. Nineshort -term consultants were also recruited fromthree countries.
The stabilization of Technical Assistance funds andthe separation of activities under the regular budgetand Technical Assistance funds are already relievingthe Regional Office of the work entailed in thecontinuous review and recosting of projects that hashitherto been inevitable. Closer attention is beinggiven to reports on budget savings with the resultthat savings on one project are being diverted atthe earliest possible date to other projects so thefullest use is made of funds.
Co- ordination of Work with other Agencies
Work with other agencies operating within theRegion is being co- ordinated through local com-mittees established for the purpose. In the Philip-pines, sub -committees of the Public Health Pro-gramme Co- ordinating Committee have also beenset up to deal with bilharziasis, environmentalsanitation, health education, hospital rehabilitation,malaria, maternal and child health, mental health,rural health units and tuberculosis. Representativesof the Philippine Department of Health, WHO,UNICEF and the Foreign Operations Administra-tion have been appointed to each of the sub-committees, which meet to discuss the planning,implementation and progress of programmes. Rela-tions with the resident Technical Assistance repre-sentative of the United Nations Technical AssistanceBoard and with other United Nations agencies,such as UNICEF and UNESCO, continued to behighly satisfactory. Co- operation with UNICEFhas resulted in the extension of existing programmesand the implementation of new ones, bringing the
WESTERN PACIFIC REGION 105
total of WHO /UNICEF- assisted projects in theRegion up to eighteen.
Public Information
In most countries of the Region, World HealthDay was more widely observed in 1954 than inprevious years. The Regional Office producedposters, booklets, folders and pamphlets, andarranged for press interviews, radio talks and publicmeetings, cinema shows and school lectures. Theslogan " The Nurse, Pioneer of Health " was post-marked, mostly for one month, on all letters passingthrough the post offices of a number of countriesin the Region and also on all mail going out fromthe Regional Office.
The Public Information Office expanded its work.Over 65 000 pieces of information material weredistributed in four languages as compared with50 000 in 1953. A Japanese edition of 100 000 copiesof the WHO folder was published through the co-operation of the Japanese Government, whichprovided the translation and supervised the publica-tion. The series of radio broadcasts from Manila,begun early in 1952, was continued. The facilitiesof the television station in Manila were used, andlocal stations broadcast recordings on WHO sentby the United Nations Radio Division and WHOHeadquarters in Geneva. Films dealing with thework of WHO were given wide distribution in com-mercial cinemas.
Education and Training
An outstanding feature of the year has been theincreasing interest shown in exchange programmesbetween medical schools within the Region andoutside it. This interest arose largely from thesuccess of the exchange of professors arrangedbetween the Johns Hopkins University School ofPublic Health and the Institute of Hygiene of theUniversity of the Philippines. Three other similarprogrammes are now being planned. The Regional
Office acts as originator and co- ordinator of theprogrammes. Once they are established, WHO'ssupport will be withdrawn and directed to otherinstitutions with similar needs.
Another feature has been the larger number offellowships awarded for study in the Region (parti-cularly in Australia, Japan, New Zealand and thePhilippines) in pursuance of a resolution passed bythe Regional Committee during its fourth session.During the year 59 fellowships were awarded, 28 ofwhich were of this type.
A dental -health seminar was held in Wellington,New Zealand, from 4 to 21 May 1954 at the DominionTraining School for Dental Nurses, to provide anopportunity for an exchange of views betweenexperts on dental health on some of the importantdental -health problems in different parts of theworld. The following aspects were discussed :topical application of fluoride in the prevention ofdental caries ; dental- health services in less advancedcountries ; the modern concept of dental caries ;etiology, pathology and general prevention ; thetraining and use of personnel in public dental -healthservices ; the cause and prevalence of periodentaldiseases ; dental care as an integral part of modernpublic- health services, and the prevention of dentalcaries through oral cleanliness. The seminar wasattended by thirty -seven participants, from Australia,Fiji, Hong Kong, Japan, Korea, Malaya, NewZealand, North Borneo, the Philippines, Sarawak,Singapore, Territory of Papua and New Guinea,China (Taiwan) and Viet Nam in the WesternPacific Region ; from Burma, India, Indonesia andThailand in South -East Asia, and from Egypt andIran in the Eastern Mediterranean Region.
Two new schools of public health were establishedduring the year, the first in Korea as a result of theWHO /UNKRA Health Planning Mission, and thesecond in Taiwan, where the Institute of PublicHealth was opened in February after the Instituteof Tropical Medicine of the National Universityhad been reorganized.
Reports on Typical Projects in the Region
A complete list of projects current during theyear will be found in Part IV. The following havebeen selected for fuller description.
Malaria and Insect Control, Taiwan
In Taiwan, malaria is one of the most importantpublic- health problems. It is estimated that everyyear ten per cent. of the total population of over
eight million is affected with this disease. In May1952, upon the request of the Government, WHOsent an international team to advise and assist inimplementing an island -wide malaria -control pro-gramme, which, it was hoped, would serve eventuallyas the basis for a campaign to eradicate the diseasefrom the country. The team was composed of threemembers, a malariologist, an entomologist and apublic -health engineer. The Taiwan Provincial

106 THE WORK OF WHO, 1954
Malaria Research Institute was designated by theGovernment as the counterpart organization of theWHO team. The international staff and somelaboratory equipment and supplies were providedby WHO under the United Nations TechnicalAssistance Programme ; the greater part of theequipment and supplies was provided by the ForeignOperations Administration. This project (China 7),which was originally planned to last four years, wasextended for another year at the request of theGovernment.
After a preliminary survey in 1952, a demonstra-tion area with a population of 37 280 and a controlarea with a population of 21 370 were selected.Anopheles minimus, the chief vector, was found tohave a predilection for resting on certain parts ofhouses, and as the houses in rural areas follow ageneral pattern of construction, a selective sprayingscheme was introduced in certain areas. In 1952,the houses of more than 156 000 people were sprayedwith DDT. In 1953, field activities extended toalmost ten times the population covered in 1952 ;selective spraying was undertaken in a highly mala-rious area with a population of 244 770 ; check areaswere maintained for comparison, and additionalannual surveys of spleen, parasites, malaria morbidityand infant parasites, as well as entomologicalobservations, were organized. These activities werecontinued in 1954, when all the malarious areas ofTaiwan were included in the control programme, withthe aim of directly protecting a population of about5 400 000 -the total malarious population of theisland.
An interesting feature of the programme was thedecentralization of spraying operations. One or twotechnicians from each of the 365 health stations inTaiwan were trained and appointed supervisors of thespraying of the areas in which they worked. Thesetechnicians resume their normal duties after thespraying, which lasts from one to two months eachyear. This procedure has not only resulted in savingsand ensured the availability of trained personnel,but also in some cases has led to an integration ofmalaria control into the local health services.
The effectiveness of the control programme wasshown by the results of the infant parasite surveysin the sprayed and unsprayed areas. In June 1952,before the spraying operations, 9.6 per cent. of 833infants examined in the demonstration area, and 7.9per cent. of 491 infants in the check area, were foundpositive for malaria. The demonstration area wasfirst sprayed in September of the same year, and onemonth later only 0.4 per cent. of the 2487 infantsexamined in the sprayed area showed a positive
blood smear, while in the unsprayed area 2.5 per cent.of 1997 infants were found to be positive. Thesecond round of spraying in the demonstration areawas completed in October 1953, and an infant parasitesurvey conducted the following month showed thatnone of the 1725 infants examined had contractedmalaria. The check areas were sprayed for the firsttime in October 1953, and the following month onlytwo of the 1596 infants examined (0.13 per cent.)were positive. It was found that selective sprayingwas as effective in stopping malaria transmission ascomplete spraying. Equally significant reductions inthe spleen and parasite rates and in the indoor densityof the mosquito vector species were noted after thespraying operations.
With the development of the campaign, traininghas increased. By the end of 1954, more than 180supervisors, 870 foremen and 3490 operators hadcompleted training, and, with the policy of decentra-lization of spraying mentioned above, every townshipis able to be self -sufficient -a fact that has strength-ened the malaria services at all levels. The projecthas now entered the consolidation phase, duringwhich every effort will be made to maintain the resultsof the progress made, and to extend the work to thestudy and control of other insect -borne diseases,particularly those amenable to control by insecticides.
Bilharziasis- Control Pilot Project, Philippines
Bilharziasis, which is endemic in China, Japan andthe Celebes, is an important public -health andsocio- economic problem in the Philippines in that noefficient method has yet been found for treatingbilharziasis resulting from the infection with Schisto-soma japonicum and no control methods have beendeveloped that are both effective and economicallyfeasible.
Of the one million inhabitants in the twelve endemicareas so far delineated in the Philippines, more than300 000 are estimated as infected. No appraisal hasyet been made of the effects of this disease upon thegeneral health of the public.
At the request of the Philippine Government, aWHO bilharziasis team, consisting of a parasitolo-gist, a malacologist and a public- health engineer,made a survey and study of this disease in thePhilippines from 20 June to 30 September 1952.On the recommendations of the team, the Govern-ment set up a bilharziasis- control pilot project, forwhich WHO provided three experts and supplies andequipment. Additional supplies and equipmentwere furnished by the Foreign Operations Adminis-tration of the United States of America and the

WESTERN PACIFIC REGION 107
Philippine Council for United States Aid. Theproject (Philippines 9) is expected to last aboutfour years.
The primary objective is to determine the mosteffective and economical means of controllingbilharziasis in the Philippines. When this has beendone, professional and auxiliary personnel will betrained, and a national bilharziasis- control pro-gramme will be planned.
The area of operation is a part of the Island ofLeyte where the disease has long been known to behighly endemic. Much progress has been made todate : a fully -equipped new laboratory and buildingsfor project centres have been constructed andstaffed with national and internationally recruitedpersonnel ; considerable data have been collectedby means of studies on the human host, gastropodvectors and domestic and wild -animal reservoirs ;intensive field studies have been made on the ecolo-gical factors affecting the intermediate host, andselected methods of control have been given labo-ratory and field trials.
Surveys of two semi -rural communities on theisland, on the basis of a single stool examination,indicated that almost half the population is infected(47.7 per cent. in Palo and 46.1 per cent. in Tanauan).In one hyperendemic zone of Palo a study, in whichboth the single stool examination and intradermaltesting with adult fluke antigen were used, revealedthat 74.8 per cent. of the group of 171 adult indivi-duals were positive for ova and a further 19.8 percent. (for which one stool examination gave negativeresults) positive to the skin test. The possibility thusexists that 94.6 per cent. of the adult population ofthis zone could have been infected at some time withbilharziasis.
In tests on domestic animals, incidence of infectionwas found to range from 20 per cent. in cows tobelow 1 per cent. in water buffaloes. The averageprevalence in domestic animals in Palo was 11.3 percent. and in Tanauan, 10.6 per cent. In wild rats,an overall infection rate of 48 per cent. was shown.The infection rates in rats seemed to vary in such away as to indicate the proximity of infected snailcolonies. A study is being undertaken to determinewith what precision rodent infection rates can beused as indices to locate such colonies.
Ecological and biological studies of the gastropodvectors have yielded some useful information on thedistribution of colonies, population densities, eco-logical distribution of snails, sex ratios, sexual andage- specific differences in infection rates, growthrates, longevity of snails in relation to habitats,
and the effects of agricultural practices on snailpopulations.
Experimental control has included studies of theeffects of clearing vegetation from snail habitats, ofimproving agricultural practices and of the properdisposal of human excreta.
The experiment of giving assistance in the construc-tion of latrines to the people living in a hyperendemicarea was carried out so that the effects of the properdisposal of human excreta, bringing about aninterruption in the contamination of aquatic snailhabitats, could be measured in terms of the effectson densities of snail population and incidences ofinfection within snail colonies. It was found thatthough latrines were constructed by the majority ofthe households in the area, and in spite of the effortsof the project staff to encourage their use, they werenot used regularly and sometimes not at all. If thismethod of control is to be a success, a better under-standing is needed of the customs, beliefs and livinghabits of the people in order to discover ways toinduce them to use latrines.
The project cannot, of course, yet be assessed. Itcan be said that the plan of operations has thus farbeen substantially followed, and that, in spite ofminor setbacks, progress towards the primary objec-tive has been steady and sound.
Public -Health Education in the University of Malaya,Singapore
When the University of Malaya, Singapore, wasfounded in 1949, the long -established King Ed-ward VII College of Medicine became its Faculty ofMedicine. One of the first developments under thenew charter was the creation of a new Departmentof Social Medicine and Public Health, which wasestablished to promote the principles of socialmedicine in teaching and research and to provide, assoon as possible, medical officers of health withpost -graduate training in courses designed to suit theparticular needs of the country. They will thus be nolonger dependent on the metropolitan schools ofBritain and America for public -health training.
In 1950, the Government, in order to attain thisaim rapidly and to attract students of other countrieswhere no similar school existed, asked for help instrengthening the school in its early stages : theprovision of seven visiting lecturers (in health educa-tion, applied nutrition, medical statistics, industrialhealth, maternal and child health, public- healthengineering, and applied physiology) ; fellowshipsto train counterparts ; and supplies and equipment
108 THE WORK OF WHO, 1954
for each consultant. This project (Singapore 2) wasto be financed from Technical Assistance funds.
The first course for the Diploma in Public Health inthe University, originally planned to start in October1952, was postponed for a year by difficulties inrecruiting the consultants and delays in the applica-tion of candidates for admission. This delay wasnot without its compensation. It left time for morethorough planning of the courses and the erectionof buildings to accommodate staff and students.The University's own plans for training staff, inconjunction with the Government in Singapore,had so far progressed that, by the time the course wasdue to begin, trainees in maternal and child healthand public -health engineering had returned fromcourses overseas, and that there was in charge of theDepartment of Social Medicine a professor who wasalso an expert in industrial health. As a result, thethree visiting lecturers on these three subjects werenot required.
The first course for the post -graduate Diploma inPublic Health was officially opened by the Vice -Chancellor on 5 October 1953, with three Malayansas students. At this time WHO had recruited fourvisiting lecturers a professor in health educationfrom the United States of America, a reader inmedical statistics from the United Kingdom, a
applied physiology from the Philippines,and an Australian expert as lecturer in appliednutrition. These consultants reinforced the teachingstaff of the faculty and acted as advisers to thegovernment authorities in Singapore and the Federa-tion of Malaya. They have helped to teach under-graduate medical students, and students in education,adult education and social science, and also to trainsuch medical auxiliaries as statistical coders, sanitaryinspectors and medico -social workers.
The three students all qualified in June 1954, andthe second course began on 11 October, with sevenstudents -four from Malaya, two from the Philip-pines, and one from Netherlands New Guinea. Fivewere awarded fellowships. Although the numberof students is still small, the course is already inter-national in character.
When the present agreement ends, in July 1955,an institute of health or urban health centre,Adjoining the Medical School, will have been estab-lished by the Government with the assistance ofWHO, in association with the University and theCity Council. The institute, with the UniversityDepartment of Social Medicine, the health services ofthe district, the main school health clinic of Singaporeand other services, will together provide researchfacilities, training for all grades of health personnel,and health services to the community.
Demonstration and Training in Venereal- DiseaseControl, TaiwanIn August 1953, WHO, on the request of the
Government, sent a venereologist (as team leader)and a health educator to Taiwan to help organize anisland -wide programme of venereal -disease control(China 1) ; a serologist and a public- health nursewere assigned to the project early in 1954. Theproject was also supported by UNICEF, whichprovided supplies and equipment, and by the ForeignOperations Administration of the United States ofAmerica.
Venereal diseases were known to be a considerablepublic -health problem in Taiwan, although noprecise information was available as to their pre-valence. Therefore, a venereal -disease advisorycommittee was set up to prepare a comprehensiveplan for control. A demonstration and trainingcentre was established in the provincial Taipeihospital and a serological reference laboratory centrein the Taiwan serum and vaccine laboratory.
After the in- service training of a national team wascompleted, attention was concentrated on a long-term programme to train health personnel in thecontrol of venereal disease. Technicians -one fromeach of twenty selected laboratories -were trainedat the reference laboratory centre in groups of sixor seven. Doctors and nurses -one from each healthcentre on the island -were trained in groups of fouror five at the demonstration and training centre.Shorter courses of about a week were also arrangedfor doctors and nurses at health stations. Thetrained personnel formed the nucleus of workers onvenereal -disease control, and, under the supervisionof the directors of the health centres, carried outintensive training courses for the doctors and nursesof the local health stations, of which there are over350. Private practitioners and medical personnel ofclinics and hospitals in Taiwan also benefited fromthe training scheme. By the autumn of 1954, 681doctors, 38 medical students, 639 nurse /midwivesand 21 laboratory technicians had been trained inthis way, making a total of 1379 persons who havereceived some type of training since the beginning ofthe project in the autumn of 1953.
Parallel with the training programme, steps weretaken to establish and equip an island -wide labo-ratory service which would enable the whole popu-lation to be serologically examined free of charge.By the end of 1954 this programme had beenexpanded to cover twenty -two areas in the island, allof which now have active venereal- disease controlunits and fully- equipped serological laboratories.Every effort has been made to ensure that these
WESTERN PACIFIC REGION 109
laboratories maintain a high level of test performanceand that their staff is aware of the importance ofstandardizing techniques, reagents, records andreports, and of the need for research and specialstudies.
Plans have been completed for the periodic evalua-tion of test performance in all these laboratories,which have been designated as " collection sta-tions ", and negative and positive sera are being sentto the reference laboratory, where a series of 100" unknown " sera will be prepared for dispatch toeach of the laboratories in the island. The sera willbe tested with the routine procedures used in eachlaboratory, and the results will be statisticallyanalysed and evaluated by the main laboratory. Thisprogramme for the periodic evaluation of test per-formance is to be maintained on a yearly basis, andtechnicians who do not meet the requisite standardwill be invited to return to the reference laboratoryfor refresher training.
Serological screening surveys have been carriedout in different occupational and socio- economicgroups in order to provide a more realistic pictureof the prevalence of infection, so that attention canbe concentrated on the groups and areas which needit most. Because of the importance of congenitalsyphilis, special emphasis has been placed on theexamination and treatment of all children and
Present Trends and Future Developments
More active support to the WHO programme isnow being given by the highly developed countriesin the Region, which have placed their educationaland training institutions at the disposal of theOrganization.
Countries which have hitherto been more interestedin medical supply programmes are now realizing thatthe assistance given by international personnel canalso be extremely beneficial ; more importance,too, is being placed on the careful selection of fellowsso that their services can be used to the best advantageafter they have completed their studies.
The cessation of hostilities in certain areas hasmade it somewhat easier to carry on projects in ruralareas, but has likewise brought with it difficulties inaccommodation and local financing in the countriesconcerned. This situation is being closely watched,as it affects team members and has a bearing on thepossibility of implementing projects for which fundsare available.
pregnant women, and attention has been drawn intraining courses to this aspect of venereal- diseasecontrol. Maternal and child health centres through-out the island are co- operating in the programme.
Health education has also been stressed and specialteaching materials -manuals, filmstrips and charts-have been used in the training courses ; and posters,booklets and newsletters have been issued to thehealth personnel receiving training in venereal -disease control to pass on to their colleagues and tothe public. The UNESCO audio -visual educationexpert working in Taiwan has assisted in the pre-paration of filmstrips and other visual materials. Aneducation programme on venereal- disease controlhas been planned for certain sections of the popula-tion, and for the community as a whole.
Activities have been expanded in accordance withthe schedule established, and health workers at boththe health centre and in health stations now have thebasic knowledge necessary to carry out a satisfactoryprogramme of venereal- disease control. The intro-duction of follow -up measures and contact tracinghas awakened interest in the epidemiologicalapproach to venereal -disease control, and, afterfurther experience, it is expected that the objective ofintroducing a comprehensive venereal -disease controlprogramme for the whole of the island may berealized.
In the future, a greater proportion of fellowshipsawarded will be for study within the Region. Thispolicy will permit an expansion of the fellowshipprogramme as a result of savings in travel costs,and will also strengthen the educational and trainingcentres. The programme for the exchange of pro-fessors between medical schools in and outside theRegion will also be expanded, and it is hopedeventually to extend it to most of the institutions inthe Western Pacific which would benefit from thistype of assistance. Finally, every effort will be madeto carry out inter -country projects of the seminar orstudy group type, bringing together health officialsfrom different areas and all the countries of theRegion.
As there is a lack of basic statistical data, theattention of governments will be drawn to theimportance of organizing statistical services. Aregional seminar for this purpose is planned for theFrench -speaking countries in 1955.
Emphasis will continue to be given to environ-mental sanitation. Programmes resulting from
110 THE WORK- OF WHO, 1954
surveys will be implemented within the limits ofavailable funds. Should additional funds : beprovided, high priority will be given to the projectsin this field contained in the supplementary budget.
In programmes for the control of communicablediseases, attention will be directed to isolated, sparselypopulated islands in the South Pacific. Yaws isprevalent in these islands and WHO may assistin campaigns against the treponematoses. Towardsthe end of the year a yaws campaign was started in
Fiji which, it is expected, will awaken the interestof the authorities of other territories where nego-tiations are taking place for assistance in yawscampaigns and in other health work.
More attention will be paid to long -term planning.The completion of BCG programmes in somecountries, such as the Philippines and Taiwan, will,for example, be used as an incentive for establishingcountry -wide programmes aimed at broader servicesfor tuberculosis control.
PART III
CO- OPERATION WITH OTHER ORGANIZATIONS
CHAPTER 17
CO- ORDINATION OF WORK WITH OTHER ORGANIZATIONS
New developments in 1954 affecting WHO'sprogramme and its relationship with the UnitedNations organizations were the adoption by theEconomic and Social Council of a new plan fororganizing its work and the decision of the GeneralAssembly of the United Nations on peaceful usesof atomic energy. The first development resultsfrom eight years of experience in internationalco- operation, and the second breaks new groundfor international co- operation in a field of sciencewhich has great potentialities for health.
Reorganization of the Work of the Economic andSocial Council
For several years, governments have been seekingways of improving co- ordination in the UnitedNations system and making its work more realistic.The Economic and Social Council is the focus ofthis effort, but governments have also acted throughother United Nations organs and the directing bodiesof the specialized agencies. They have sought(1) to concentrate and strengthen the programmesand (2) to rationalize the work of the directingorgans.
In regard to programmes, the problem of theproliferation and overlapping of activities was raisedin 1949. Following discussions on the concentra-tion of efforts and resources the Council adopted,in 1950, criteria for use in determining priorities(resolution 324 (XI))1 and, in 1952, a list of priorityprogrammes in the economic and social fields(resolution 451A (XIV)). It also invited the agenciesto consult, through the Administrative Committeeon Co- ordination (ACC), on activities of commoninterest before presenting them for approval, and toformulate joint programmes.
In these discussions the Council considered thecommon objectives of the agencies as well as theiractivities. In 1950 it invited the ACC to indicatefrom time to time broad fields of activity and
1 Reproduced in part in Of Rec. Wld Hlth Org. 32, 48
objectives which might receive major emphasis(resolution 324 (XI)). In 1952, in order to definesocial objectives more realistically, it asked theSecretary - General of the United Nations to col-laborate with the specialized agencies and appro-priate non -governmental organizations in preparingreports on the world social situation and on pro-grammes of social development (resolution 434(XIV)). In 1953, it approved a programme ofconcerted practical action in the social field anddefined general principles and immediate objectivesfor this work (resolution 496 (XVI)).
The second line of effort was to make the Councila more effective instrument for discussion and deci-sion by governments. In 1951 the Council revisedsome of its procedures, discontinued certain sub-ordinate bodies and spaced out the meetings ofothers (resolution 414 (XIII)). In 1954 it adopted aresolution (557 (XVIII)) on the organization andoperation of the Council, concentrating its effortson the major economic and social problems -thatis, the substance of the programmes, which shoulddetermine the form of inter -agency consultations -and facilitating attendance by high -level representa-tives. It decided to concentrate in its two regularsessions each year on major economic and socialproblems and on human rights and, in one of them,to make a review of the development and co-ordination of United Nations programmes andactivities as a whole. The executive heads of thespecialized agencies were invited to take an activepart in the Council's discussions of the programmesof the United Nations and also, where appropriate,of the world economic and social situations.
The new procedures of the Council will enable itto bring together all the information available inthe United Nations and the specialized agencies andthus to consider programmes in the light of the jointdiscussion on each problem. This makes it neces-sary for WHO to provide information on the healthsituation and policies for use by the Council indetermining broad policies and programmes. WHO
- 113 -
114 THE WORK OF WHO, 1954
may need to review in the near future the place thatshould be given in its programme to periodicassessments of the health situation.
Peaceful Uses of Atomic Energy
The General Assembly, on 4 December 1954,expressed the hope that an international atomicenergy agency, with an appropriate form of agree-ment with the United Nations, would be establishedas soon as possible to facilitate the use of atomicenergy for peaceful purposes by the entire world andto encourage international co- operation in its furtherdevelopment and practical application for the benefitof mankind.
The General Assembly also called for an inter-national technical conference to be held under theauspices of the United Nations, not later thanAugust 1955, to explore means of developing thepeaceful uses of atomic energy through internationalco- operation and, in particular, to study the develop-ment of atomic power and consider other technicalsubjects -such as biology, medicine, radiation pro-tection and fundamental science -in which inter-national co- operation might be most effective. Itinvited all Member States of the United Nations orof the specialized agencies to participate in the con-ference. The specialized agencies themselves will alsoparticipate, and those most concerned, particularlyFAO, UNESCO and WHO, are to assist with theplanning.
WHO has for some time been considering theimplications of the new scientific advances for itsown programme. New scientific developments, suchas discoveries in the field of antibiotics and insecti-cides, have deeply influenced the work of theOrganization ; and though the ultimate effect of thediscoveries in the field of atomic energy and theirpossibilities for health work cannot be predicted,the present stage of scientific progress alreadywarrants study. In view of this and the resolutionof the General Assembly, the Director- Generalconvened a small consultant group in December 1954.The group, made up of international experts, dis-cussed two main topics : (1) the problems of thehealth protection of workers exposed to atomicradiations, disposal of radioactive waste material,nuclear reactor safety, definition of radiologicalunits and standardization or radioactive materials ;and (2) the use of atomic energy in biology, medicineand public health, particularly the present andpotential use of radioactive isotopes in biological
and medical research, diagnosis and treatment, andthe epidemiology and control of diseases.
Administrative Committee on Co- ordination
In 1954, the Administrative Committee on Co-ordination (ACC) concerned itself mainly with itscontribution to the work of the Economic and SocialCouncil, the development of international socialprogrammes and the co- ordination of its work withthat of the Technical Assistance Board. This lastsubject is dealt with in Chapter 18.
The extension of free and compulsory educationwas brought for the first time within the scope ofthe working group on long -range activities forchildren, and consultations on the training ofauxiliary and community workers, now to be relatedto community development, were renewed. Inaddition, the ACC has kept under review economicprogrammes of interest to several agencies, thevarious co- operative programmes in the social fieldand matters of administrative co- ordination. Theprincipal programmes approved by the ACC arenoted below.
International Social ProgrammesDuring the year, it was agreed that the heads of
departments responsible for the social programmesof the United Nations, ILO, FAO, UNESCO andWHO should meet yearly to exchange informationand co- ordinate their plans for carrying out theirprogrammes. As a result of an offer made byUNESCO at the 1954 meeting, the possibility thatthat organization might conduct certain social sciencestudies on behalf of WHO is being discussed.
WHO contributed to the international survey ofprogrammes of social development and continuedits participation in existing joint programmes in thesocial field.
Free, Compulsory EducationThe place of free, compulsory education in the
international social programme was considered bythe working group of the ACC on long -rangeactivities for children. Recognizing the contributionthat schools can make to economic and socialdevelopment, the ACC agreed that UNESCO shouldseek, and the other agencies concerned should give,the fullest co- operation in providing assistance toStates in appropriate activities to support the develop-ment of free, compulsory education, and in services

CO- ORDINATION OF WORK WITH OTHER ORGANIZATIONS 115
designed to encourage school attendance and toimprove the quality of education. In connexionwith such programmes, WHO has undertaken toprovide, on request, advice and assistance on thedevelopment of health services for schools and onthe teaching of hygiene.
Training of Auxiliary Workers
In 1954, at an ad hoc meeting, the United Nationsconsulted with other interested agencies on a reporton the training of auxiliary workers which is to besubmitted to the Social Commission. At thismeeting a statement of principles was drafted con-cerning the training of auxiliary and communityworkers for use by each organization to the extentrequired.
Community Development
WHO was represented at the regional conferenceon community development in South and South -East Asia convened by the United Nations in accord-ance with the resolution of the Economic and SocialCouncil on the programme of concerted action inthe social field. This is the first of a series of con-ferences to enable governments to exchange informa-tion and define the essential elements of a nationalprogramme of community development. At therequest of some. governments, WHO staff concernedwith projects of environmental sanitation, theorganization of local health units or health educationassisted in collecting and organizing information foruse at this conference.
Fundamental Education
Two WHO staff members worked, in 1954, in theArab States Fundamental Education Centre estab-lished by the Government of Egypt with assistancefrom UNESCO. WHO has been represented atmeetings of the newly formed advisory committee ofthis centre, and through the Regional Office for theAmericas maintains contact with the FundamentalEducation Centre for Latin America. WHO hasalso assisted with the national fundamental educationprojects assisted by UNESCO in Ceylon andThailand.
Long -Range Activities for Children
In Syria, the Regional O ffice for the EasternMediterranean co- operated in an assessment ofservices for children, one of a series of such assess-ments arranged under this joint programme.Consultations are going forward concerning further
collaboration in assistance to Syria and in similarassessments in other countries.
Rehabilitation of the Physically Handicapped
In connexion with this programme, WHO con -vened a conference on prostheses with the co-operation of the United Nations, ILO and UNESCOand of two non- governmental organizations (seepage 27). WHO has taken part in conferences onrehabilitation in Yugoslavia and Italy, has giventechnical advice in programmes assisted by theUnited Nations in Guatemala, Indonesia andVenezuela, and continues to co- operate withUNICEF in assistance to programmes for handi-capped children.
Other Joint Social Programmes
WHO has continued to take part in inter- agencyconsultations on migration convened by ILO, inwhich the Intergovernmental Committee for Euro-pean Migration . (ICEM) also co- operates (seepage 28), and has kept in touch with the work ofthe United Nations in housing and town planningthrough attendance at meetings and participation inthe seminar and exhibition organized by the Govern-ment of India in January 1954.
Standards of Living. In 1954 the Statistical Com-mission of the Economic and Social Council con-sidered the report of the committee of experts,convened in 1953 by the United Nations, ILO andUNESCO, on the international definition of stand-ards and levels of living. WHO provided com-ments on the committee's report and information onthe related work of the Organization. In responseto the Commission's recommendation that theUnited Nations and the specialized agencies con-cerned should study the adequacy of the indicatorsproposed by the experts and the availability andaccuracy of statistics relating to them, WHO sub-mitted the committee's report to its Expert Com-mittee on Health Statistics.
Water Resources. In 1954, the Council adoptedin resolution 533 (XVIII) a series of recommenda-tions to strengthen international co- operation inregard to the development and use of water resources..At an inter -secretariat meeting to co- ordinateactivities under this resolution, WHO expressedinterest in the question of stream pollution and waterquality in agricultural or industrial development,and of the risk of epidemics resulting from theconcentration of workers during construction projectsor the influx of population to newly developed areas.
116 THE WORK OF WHO, 1954
Administrative Co- ordination
Administrative co- ordination has been assured byWHO's participation in the International CivilService Advisory Board, the Consultative Committeeon Administrative Questions, the Joint Staff PensionBoard and various ad hoc committees convened tostudy administrative matters of common interest.In 1954 WHO received the report of the InternationalCivil Service Advisory Board on standards ofconduct in the international civil service, which is tobe distributed to all staff members. The Inter-national Civil Service Advisory Board has beenasked by the ACC to undertake in 1955 a study ofthe problems confronting international civil servantswith respect to the education of their children.Also during the year a representative of the Organiza-tion took part in a special meeting of the ConsultativeCommittee on Administrative Questions to definethe terms of reference of a committee of expertswhich will be convened early in 1955 to reviewcertain aspects of the remuneration of staff membersin the professional category.
Co- operation with other Organs of the United Nations
In response to requests from the Committee onInformation from Non - Self -Governing Territoriesand the Trusteeship Council, WHO has intensifiedits co- operation with these two bodies. It hasreported on projects assisted by the Organizationin the territories in question and has studied insome detail the health aspects of reports receivedby the Trusteeship Council.
Reference has been made in Chapters 5 and 6to the continued co- operation with the UnitedNations in the collection and publication of statisticsand in work in addiction- producing drugs. Thefirst of a series of joint technical studies on syntheticdrugs with morphine -like effect, requested by theCouncil in resolution 505 C (XVI), was completedby the United Nations and WHO in 1954, andpublished.' Further studies were begun.
WHO has co- operated with the Economic Com-mission for Europe and the Transport and Com-munications Commission in technical studies on thetransport of dangerous goods (see page 32).
Many of the activities in the social field in whichWHO and the United Nations collaborate are men-tioned above in connexion with the international
1 In Bull. Wld Hlth Org. 1954, 10, 1003
social programme. In Europe, WHO has takenpart in several technical conferences organized bythe United Nations in the general field of socialwelfare and particularly in child welfare. The twoorganizations are also co- operating in assistance tomaternal and child health projects in Burma andThailand.
WHO has continued to co- operate with the UnitedNations Relief and Works Agency for PalestineRefugees in the Near East (UNRWA), the UnitedNations Korean Reconstruction Agency (UNKRA)and the United Nations High Commissioner forRefugees. An account of the health work done inconnexion with UNRWA will be found on page 28.Medical supplies were purchased on behalf ofUNKRA (page 51). At the request of the UnitedNations High Commissioner for Refugees, WHOmade a pilot survey of the mental health of childrenliving in refugee camps in Europe.
UNICEF
In 1954, a number of maternal and child healthprogrammes assisted jointly by UNICEF and WHOwere expanded into integrated health units (seepage 18). UNICEF is increasing its assistance inenvironmental sanitation and particularly in pro-grammes for the provision of clean milk, which areplanned through the FAO /UNICEF /WHO secre-tariat working group on milk and milk products (seepages 13 and 32).
A representative of the Director- General is amember of the Advisory Committee of the Inter-national Children's Centre. WHO continues to usethe training facilities provided by the Centre and toco- operate in certain technical programmes (seepage 23 and Chapter 14).
The Seventh World Health Assembly re- affirmedthe principle that WHO should assume, subject toits financial resources, the responsibility for theemployment of the technical personnel needed forjoint activities. It declared that WHO must main-tain a balanced public- health programme andrequested the Director- General to include in futureprogrammes for joint UNICEF /WHO activitiesonly projects for which he is sure that the technicalpersonnel engaged by the Organization can beremunerated. In pursuance of this resolution, theexecutive heads of UNICEF and WHO have ex-amined together the conditions under which certainjoint projects could be implemented if the financesrequired exceeded the ordinary resources of WHO.
CO- ORDINATION OF WORK WITH OTHER ORGANIZATIONS 117
In the meantime, for some projects (listed inPart IV) UNICEF has continued to reimburse WHOfor the cost of the technical personnel (see page 58).
Co- operation with Individual Specialized Agencies
ILO
The Director -General's report on measures tostrengthen occupational health activities was ap-proved in 1954 by the policy -making bodies of ILOand WHO (see page 27). Joint work on internationalstandards continues, and collaboration in technicalstudies and in projects of assistance to governmentsis increasing.
The Joint ILO /WHO Committee on theHygieneof Seafarers met in 1954.
It was decided that the work of the InternationalAnti -Venereal- Disease Commission of the Rhine,with which ILO and WHO were associated, would betaken over by the participating governments as partof their normal programmes of medical care andsocial security. WHO took part in the UnitedNations /ILO /UNESCO field mission on indigenouspopulations in the Andean Highlands.
FAO
Work in nutrition, food hygiene and the controlof animal diseases communicable to man is plannedand carried out as part of the joint programme withFAO, and is described in Chapters 1 and 2. Twojoint expert committees were convened in 1954, oneon nutrition and one on meat hygiene. Referencehas already been made above to the UNICEF /FAO/WHO secretariat working group on milk and milkproducts. FAO was consulted on a study on thecomposting of organic wastes for sanitary disposaland reclamation (see page 31). Work on the inter-national reference preparations for several biologicalsubstances used in veterinary medicine (see pages 12and 46) has, as usual, been done in consultation withFAO and the Office International des Epizooties.
UNESCO
Co- operation with UNESCO in fundamentaleducation and in the extension of free and compulsoryeducation is mentioned above.
WHO took part in the first meeting of UNESCO'sInternational Advisory Committee for Documen-tation in the Natural Sciences, and the two organi-zations reached agreement on the relation betweenWHO's work for the co- ordination of research on
cancer and the international work in basic researchbeing undertaken by UNESCO on cell growthand related problems with a view to assisting inresearch on cancer.
In many other WHO programmes, there has beenclose co- operation with UNESCO : in professionaland technical education (see Chapter 4), in healtheducation of the public (page 26) and in school healthservices (page 23). WHO was represented atmeetings of the UNESCO Advisory Committee onArid Zone Research and at two regional conferencesof UNESCO on the teaching of the social sciences.
Other Specialized Agencies
ICAO made a valuable contribution to the workof the WHO Committee on International Quarantinein 1954, and the two organizations are collaboratingin the preparation of a manual on the sanitationof airports. At the request of UPU a workingparty of ILO and WHO was formed to advise onthe occupational risks of postal workers (page 27).
'Non- Governmental Organizations
Non -Governmental Organizations in Official Relationswith WHOIn 1954, at the thirteenth session of the Executive
Board, three non -governmental organizations -theInternational Committee of Catholic Nurses andMedico -Social Workers, the Medical Women's Inter-national Association, and the Union OSE -wereadmitted into official relations with WHO. Elevenother applications which had been submitted wereeither not accepted or postponed for considerationat the fifteenth session of the Board.
In connexion with the biennial review of thetwenty -seven non -governmental organizations alreadyin official relations, the Board, upon the recom-mendation of its Standing Committee on Non -Governmental Organizations, agreed to maintainrelations with twenty -five of them. It postponed thereview of the other two until its fifteenth session,when additional information regarding their activitieswill have been obtained.
In conformity with previous practice, all non-governmental organizations in official relations wereinvited to be represented at the Seventh WorldHealth Assembly, the thirteenth and fourteenthsessions of the Executive Board, and all the sessionsof the regional committees.
118 THE . WORK OF WHO, 1954
The following is a brief summary of developmentsin relations with some of these organizations.
The. Council for International Organizations ' ofMedical Sciences (CIOMS) (see also page 36) madea critical assessment of the usefulness and poten-tialities of large international congresses and othertypes of scientific meetings. It, continued its sub-sidies to international congresses and, in 1954,sponsored two smaller meetings under its ownauspices : a symposium on glaucoma in Canada inconnexion with the XVII International Congressof Ophthalmology, and a meeting of representativesof national research councils and institutes held inLondon, to discuss the selection, training and supportof research workers (see also page 36).
The Fédération dentaire internationale sent tworepresentatives to take part in the consultant groupon dental health, convened by WHO in September(see page 28). WHO is also starting to co- operatewith the Fédération on the collection of data onprofessional dental education.
Assisted by a grant from WHO, the InternationalCouncil of Nurses is making a study of educationalprinciples applicable to the education of nurses, andof the role of the nursing school in preparing nurses forthe increasing responsibilities resulting from changesin medical and public- health practice. The two reportspublished by the Council on a previous study aredescribed on page 25. The Council also assisted inthe collection of material on psychiatric nursing.
WHO has made a grant of $6000 to the Inter-national Paediatric Association for a survey of pae-diatric education in all the Western Europeancountries with which WHO is in active relationshipand, as far as possible, in selected countries of otherareas of the world. This survey, which began lastyear, is described on page 23.
Following requests from the International Associa-tion of Microbiological Societies, formerly known asthe International Association of Microbiologists,WHO established two international shigella centresduring the year (see page 47) and continued to collectinformation to facilitate the postal transmission ofbiological materials.
The relations with the World Federation of UnitedNations Associations (WFUNA) have been main-tained and strengthened during the year. The sixthseminar on world health organized by WFUNA washeld during the first two weeks of the Seventh WorldHealth Assembly and was attended by forty -eightdoctors, medical students, nurses and public- health
and social workers from fourteen countries. Theseminar was opened by the Director- General, andthe programme included talks on a wide range ofhealth problems by numerous WHO staff members,both from Headquarters and from the regionaloffices. Among the other meetings sponsored byWFUNA were : the Pacific Regional Seminar on" Teaching about the United Nations and Educationfor International Understanding ", held in Manila,at which a WHO representative gave an address ;a seminar on international organization andhealth problems, organized in Milan by theItalian United Nations Association and addressedby a senior official of the national health services ;and a conference on world health at Bad Gastein,organized by the Austrian United Nations Associa-tion, in which WHO took part and which wasattended by fifty -seven participants from twentycountries. Through its member associationsWFUNA has done excellent work in promoting theobservance of World Health Day, particularly inAustralia, Austria, Greece, Hong Kong, Israel andNigeria. The _United Kingdom Association waslargely responsible for arrangements for the WorldHealth Day meeting which was held at the RoyalCollege of Nursing in London.
The World Medical Association continued to co-operate with WHO in questions concerning the pre-paration of the Pharmacopoea Internationalis. Atthe sessions of its Council and General Assembly,which were held respectively in Zurich in April andin Rome in September, increasing interest was shownin medical education, occupational health and inter-national medical law.
WHO was represented at the following meetings ofthe three organizations admitted into official relationsduring the year : (1) the Fifth Congress of the Inter-national Committee of Catholic Nurses and Medico-Social Workers, held in Quebec in September, duringwhich the Board of Directors of the Committeediscussed ways of co- operating with WHO ; (2) theopening of the Seventh Congress of the MedicalWomen's International Association in Italy inSeptember, and (3) meetings of the Union OSE,which held its own world conference, together witha conference on the study of health problems amongJewish populations and the role of the OSE, inParis in July. The Organization was also representedat the meetings of practically all the other non-governmental organizations in official relations withWHO (a full list of these is given in Annex 6).
CO- ORDINATION OF WORK WITH OTHER ORGANIZATIONS 119
Non -governmental organizations were representedat or contributed to WHO meetings, assisted inselecting members of expert advisory panels orconsultants, gave or requested advice, and heldconsultations with a view to future possible co-operative enterprises.
Non -Governmental Organizations not in OfficialRelations
Some non -governmental organizations not inofficial relations with WHO have none the lesscontributed to its activities ; very often workingarrangements with them have proved to be of greatuse. In this connexion special mention may be madeof the activities in 1954 of the International Federationof Medical Student Associations, International Hy-datidological Association, International Blood Trans-fusion Society, International Organization for Stand-
ardization, International Union for Health Educa-tion of the Public, World Confederation for PhysicalTherapy, International Society of GeographicalPathology, International Association of Gerontology,International Association of Universities, Inter -national Dairy Federation, International Organiza-tion against Trachoma, International Society ofCriminology, International Union of Architects,Permanent Committee for the International Veteri-nary Congresses, Pacific Science Association andWorld Veterans Federation.
Other Organizations
WHO's co- operation with organizations such asthe Rockefeller Foundation, the Kellogg Foundationand CARE has continued, and is described, whereapplicable, in the report. Their co- operation inspecific projects is shown in the list in Part IV.

CHAPTER 18
EXPANDED PROGRAMME OF TECHNICAL ASSISTANCEFOR ECONOMIC DEVELOPMENT
In 1954 the financial resources for the fourthperiod of activities under the Expanded Programmeof Technical Assistance for Economic Developmentagain fell short of the requirements for the plannedprogramme. However, by slowing down the rate ofactivities, and even for a certain period borrowingfrom the Technical Assistance Board, WHO wasable to carry out its planned programme with nottoo serious a disruption, to continue all existingprojects according to schedule, and to undertake,in some instances, exceptionally urgent new requests.
In December 1954 there were 128 WHO -assistedprojects in operation under the Expanded Pro-gramme of Technical Assistance, as compared with121 at the end of 1953. Twenty -six projects werecompleted during the year and 39 new ones started(including those developed with governments aspart of a special effort to use some non -convertiblecurrencies), as against 34 and 9 respectively in 1953.One hundred and twenty -six experts from 30 coun-tries were recruited by WHO for services under theProgramme, compared with 150 experts in 1953.In December 1954 altogether 225 experts, as against239 in 1953, from 36 countries were engaged in51 countries and territories. In 1954 217 fellowships(238 in 1953) were awarded to candidates from50 countries and territories ; 142 fellows completedtheir training.
The principal type of work in which WHO wasengaged under the Technical Assistance Programmediffered little from that in 1953, although still furtheremphasis was laid on training projects and on thoseprojects having the most direct effect on economicand social developments.
The Technical Assistance Committee, in reviewingthe sixth annual report submitted by the TechnicalAssistance Board : (a) emphasized the desirabilityof concentrating the limited resources on projects ofmajor importance ; (b) noted the drop in the numberof fellowships provided and in the expenditure onsupplies and equipment but presumed that, as this
was mainly due to financial stringency during thelatter part of 1953, these important elements of theprogramme would continue to receive adequateattention ; (c) emphasized the importance of theevaluation of the programme being undertaken bythe participating agencies, not only with regard toits efficiency but also with regard to its influenceon economic development, cautioning against atheoretical approach and stating that the cost ofsuch activities should be kept to a minimum ;(d) again emphasized that the participating organiza-tions should make use of the national committeesfor technical assistance in recruiting experts andorganizing training seminars ; and finally (e) notingwith satisfaction that the Technical Assistance Boardand the participating organizations had both suc-ceeded in reducing the administrative and indirectoperational costs of the programme, expressed thewish that efforts towards further reduction shouldbe continued.
Financial Arrangements in 1954
At the Fourth Technical Assistance Conference,held on 12 and 13 November 1953, sixty govern-ments pledged a total of US $23 617 000 for the1954 programme, and by 30 November 1954 seventy -three governments had pledged $25 342 044.
The Technical Assistance Board, taking into con-sideration the estimated collection of pledges duringthe first six months, placed an " obligation ceiling "of twelve million dollars on the total programmeoperations up to 30 June 1954. This meant that,whereas the total cost of the WHO- assisted pro-gramme for 1954 approved by the Technical Assis-tance Board was $4 491 000, the amount actuallyavailable -including carry -over from 1953, reallottedto WHO -was $2,752,207. This situation wasbrought to the attention of the Executive Board andof the Seventh World Health Assembly, whichauthorized the Director - General to adjust the pro-gramme in such a way as to continue all projects and
- 120 -
EXPANDED PROGRAMME OF TECHNICAL ASSISTANCE FOR ECONOMIC DEVELOPMENT 121
activities already in operation and to start thosewhich were in an advanced stage of planning (orwhich were part of programmes designed in stages).This was done by (1) transferring some continuingTechnical Assistance projects to the regular budgetand postponing the implementation of new projects ;(2) requesting UNICEF to provide financial supportfor certain joint projects ; (3) exercising maximumeconomy in the entire programme ; and finally(4) obtaining a loan from Technical Assistance fundsagainst future allocations to WHO in 1954.
With the gradual payment of the contributionspledged by governments, the financial situationimproved during the year, and the Technical Assis-tance Board was able to raise the" obligation ceiling"from the twelve million dollars to fourteen and ahalf million in March, to sixteen million in May,and finally to eighteen million for the total pro-gramme operations in 1954. As a result WHO'sshare of the funds was eventually increased from$2 337 500 to $3 552 575. In the second half ofthe year it thus became possible to increase the rateof operations and to resume financing under theTechnical Assistance funds some of the projectswhich had been transferred to the regular budget.
Legislative Developments
Future Financing of the ProgrammeIt will be remembered that in 1953 the Technical
Assistance Committee, recognizing the desirabilityof providing a more stable financial basis for long-term planning, reviewed the financial procedures ofthe programme. The Executive Board at its sessionin January 1954 supported the principle that, becauseof fluctuations in the amount of Technical Assistancefunds available each year and in order to safeguardthe operational requirements of the programme, cashto complete the planned project should be availableand earmarked before project agreements weresigned with governments. The Technical AssistanceCommittee at its March meeting agreed that greaterfinancial security was necessary. Because of theprobable effect on the progress of the programme,it did not provide the full security advocated bythe Executive Board, but approved the followingmeasures as representing a reasonable compromise :each participating organization would keep itsobligations at all times within the limit of fundsearmarked for it by the Technical Assistance Board ;in each financial period, the amounts earmarkedwould initially be based on the most conservativeestimates of contributions likely to be availableduring the programme year, so that programmeauthorizations would not have to be withdrawn
because of shortage of funds, supplementary amountsbeing earmarked as and when justified by the receiptof contributions ; each participating organizationwould limit its forward contractual commitmentsand residual liquidating liabilities to its pro ratashare of the Working Capital and Reserve Fund,when that Fund was fully established ; the SpecialReserve Fund would be reconstituted as a WorkingCapital and Reserve Fund, increased to a normallevel of 50 per cent. of total pledges for the pre-ceding year, and the necessary funds would beretained for this programme from contributions tobe received in 1955 and 1956 at a level provisionallyfixed at $12 000 000 ; pending the full establishmentof the Working Capital and Reserve Fund, eachparticipating organization would limit its forwardcontractual commitments and residual liquidatingliabilities to its pro rata share of $12 000 000. Thisprocedure was approved by the General Assemblyon the recommendation of the Economic and SocialCouncil in its resolution 521 (XVII).
System of Allocation of Funds
One of the most important developments of theyear was the approval by the General Assembly ofthe recommendation of the Technical AssistanceCommittee adopted by the Economic and SocialCouncil to amend further the Council's resolution222 (IX), as revised by resolution 433 (XIV), with aview to closer intergovernmental control.
The Economic and Social Council, at its eigh-teenth session in July, after examining a reportfrom the Technical Assistance Committee and aspecial report of the Administrative Committee onCo- ordination, bringing to its attention a number offundamental considerations relating to the financialadministration of the programme, unanimouslyadopted resolution 542 B (XVIII), making an impor-tant change in the management of the programmeand in the method of allocation of funds.
This resolution provides that in 1956 and sub-sequent years the Technical Assistance Programmewill be drawn up at the country level, within thefigures established by the Technical Assistance Boardfor each country, by the government concerned inconsultation with the representative of the TechnicalAssistance Board. The participating organizationswill continue to be responsible for advising andassisting the appropriate governmental authoritiesin the technical planning of individual projects.
It also provides that, beginning with the 1956programme, the Technical Assistance Committeewill review and approve the overall programme inthe light of its importance for economic develop-
122 THE WORK OF WHO, 1954
ment. In this review the Committee will not dealwith the technical aspect of the programme or withcountry allocations, but will concern itself withoverall priorities, the evaluation of the projects andthe programme inter -relationships. The approvalof the Committee will be necessary before commit-ments can be made on implementing the programme.The Committee will also authorize the allocation offunds to each of the participating organizations inproportion to their part of the approved overallprogramme, it being provided that, to avoid toosharp a fluctuation, the amount allocated to each ofthem shall not be less than 85 per cent. of their shareof the allocations for the current year.
Consequently, for the programme for 1956 andsubsequent years, the funds of the Expanded Pro-gramme of Technical Assistance will no longer beallocated to the organizations participating in theprogramme on the basis of fixed percentages asestablished in the past by the Economic and SocialCouncil in resolution 222 (IX).
The amount of money received by WHO in 1956and subsequent years under the new system willtherefore be determined by the importance given tohealth activities in the integrated country programmesof individual governments (but will not be less than85 per cent. of the amount received the previousyear). It is now more important than ever for thenational health administrations of the receivingcountries to ensure that health activities receive theplace they deserve in the total economic and socialplans for their countries.
Collaboration with other Technical Assistance Pro-grammes
An encouraging development during the year wasthe closer and more fruitful collaboration with otherprogrammes of technical assistance. Earlier con-tacts and informal arrangements with other agenciesprepared the way for effective working relationshipsin countries receiving substantial aid in health workfrom other sources, particularly the Colombo Planand the Foreign Operations Administration of theUnited States of America (FOA). Co- ordinationon a high level with FOA was fostered by twomeetings of its Director and his senior officers withthe members of the Technical Assistance Board andrepresentatives of the participating organizations.
Further efforts have been made in 1954 to improveco- ordination of field work and prevent overlappingof the programme. Specific examples of jointprojects which are receiving assistance from various
sources of technical assistance will be found in thelist of projects in Part IV.
Plans for 1955
The Economic and Social Council at its eighteenthsession reviewed the programme for 1954 submittedby the Technical Assistance Board. It did not setany financial goal for 1955 but urged the govern-ments participating in the Expanded Programme togive it their continued and increased support.
The Fifth Technical Assistance Conference washeld on 26 November 1954, and 56 countries pledged$12 264 136.
New Local Costs and Waivers
By 31 December 1954 sixty -one governments hadagreed to implement the new system of local costs.During the year the Technical Assistance Boardconsidered the question of " country waivers "-a country waiver exempts a country from payinglocal costs in respect of all Technical Assistanceprojects -and " project waivers ", by which exemp-tion is given only for certain projects for whichgovernments are already providing extensive staff andother facilities. The Board decided to set up stan-dard criteria for the granting of country waivers, butfelt that the criteria for granting project waiverswere no longer applicable, and that, in view of theestablishment of the new local costs plan, thesewaivers should normally not be granted. It waspointed out by WHO, however, that the TechnicalAssistance Committee had authorized the grantingof project waivers in exceptional circumstances, evenwith the new local costs plan in operation. Pendinga ruling by the Technical Assistance Committee onthis question, all existing country and projectwaivers were extended until 30 June 1955. Mean-while no new project waivers will be granted.
Evaluation
The Technical Assistance Committee, after review-ing the report prepared by the Technical AssistanceBoard on techniques of evaluation by different par-ticipating organizations, and bearing in mind thatthe initial formative period of the ExpandedProgramme was nearly over, believed that it wastime to attempt to evaluate the effectiveness of theprogramme and its impact upon economic develop-ment. It set up a working group, consisting ofeleven members, to evaluate the results and effective-ness of ther pogramme. The Committee was unani-mous in its agreement that the approach to this

EXPANDED PROGRAMME OF TECHNICAL ASSISTANCE FOR ECONOMIC DEVELOPMENT 123
evaluation should be practical rather than theoreticaland that the study should be based primarily on theviews of the recipient governments. The group willalso take full advantage of the efforts of the TechnicalAssistance Board and the experience of participatingorganizations in evaluating the programme as awhole or in part and of the methods that they havedeveloped.
In undertaking this study the Technical AssistanceCommittee agreed that no additional expenditurewas to be contemplated at this stage.
European National Committees
A full report on the first two sessions of theEuropean National Committees was made to thethirteenth session of the Executive Board. TheExecutive Board considered the interest these com-mittees had shown in recruitment methods and therecommendations they had made for recruitingthrough them the experts employed under theExpanded Programme. As the Organization'ssources and procedure of recruitment, developed
over five years of experience, are particularly adaptedto its decentralized operations and the highly tech-nical character of its staff, the Executive Boardexpressed the belief that WHO's present arrangementsfor the recruitment and selection of project staffwere appropriate to its needs (resolution EB13.R43).
The third conference of European national com-mittees was held in Rome in September ; twentycountries were represented. It was noted withsatisfaction that some of the specialized agencies hadtaken the necessary steps to act in accordance withthe recommendations on recruitment made at theprevious conference, held in September 1953, and itwas hoped that the World Health Assembly wouldfind it possible to reconsider ways and means ofcarrying out the recommendations, notwithstandingthe resolution of the Executive Board.
The technical nature of WHO's experts and theOrganization's legislative requirements were onceagain explained to the conference. Some of thedelegates, still unsatisfied, indicated that they mightwish to bring this matter to the attention of theWorld Health Assembly.

PART IV
PROJECT LIST

PROJECTS IN OPERATION IN 1954
This part of the Report contains a list of projects which are recorded as having been in operation duringthe whole or part of 1954, and in which WHO is assisting governments by providing personnel, supplies ortechnical advice. A number of UNICEF projects for which WHO has given technical advice are not describedin the list, and fellowships are included only when they form part of a larger programme. (Tables showing thefellowships awarded during the year and the subjects of study appear in Annex 11.)
This list is considerably more detailed than that contained in the Annual Report for 1953. For some of thecompleted projects an attempt has again been made to summarize the results. This has been facilitated by thesystem of evaluation which was worked out in 1953, applied experimentally to a number of projects in 1954,and which will become a routine part of the Organization's work in planning, operating and assessing itsprojects of assistance to governments. However, it has not yet been possible to apply the system to all theprojects included in this list. Moreover, attention is again called to the difficulty of assessing the results of sometypes of project as soon as international help ends, since frequently the full effect cannot be apparent for someyears.
The projects are serially numbered and again grouped under the six WHO regions : Africa, the Americas,South -East Asia, Europe, the Eastern Mediterranean and the Western Pacific. Under each region, projects thatconcern several countries appear first and are lettered " AFRO ", " AMRO ", " SEARO ", " EURO "," EMRO " or " WPRO ". The other projects, in the alphabetical order of countries, follow. Inter -regionalprojects are given at the end of the list.
In the first column, " Project No., Source of Funds, Co- operating Agencies ", " R " means the regularbudget ; " TA " means Technical Assistance funds, and " UNICEF " the United Nations Children's Fund.Names of other co- operating agencies, whether or not they have contributed funds, are given in parentheses.When UNICEF has not only furnished supplies but has also reimbursed the cost of the personnel involved,this is stated in the description of the project.
In the second column, the finishing date is given as well as the starting date for projects completed duringthe year. A field project is considered to have started when a senior member of the international team arriveson the site, or, if no staff have been provided, when supplies are received ; it is considered to have finished wheninternational staff are withdrawn.
As the projects are those of governments, the " aim of the project ", which in most cases is briefly stateddirectly under the title in the third column, is the government's purpose in establishing it, irrespective of theamount of assistance given by WHO.
AFRICAProject No.Source of Funds Dates DescriptionCo- operating Agencies
AFRO Sl Oct. 1953- Tuberculosis SurveyR March 1954 Aim of the Project. To determine the distribution and intensity of tuberculosis in the
Region, as a preliminary to a control programme.
Assistance provided by WHO in 1954. Two consultants.
Work accomplished. Nearly all the countries of the Region, including the islands of theIndian Ocean, were visited by the two consultants ; one of them conducted a surveyin the western and central parts of Africa and the other in southern and eastern Africa.
As a result of the survey, a project was being planned at the end of 1954 forBechuanaland, for which a consultant in mass miniature radiography will be provided.Projects were also being planned for Nyasaland and Kenya ; a provisional scheme forinvestigating various forms of treatment of tuberculosis in Africa had been formulatedfor these projects and plans were being made for strengthening laboratory services andproviding consultants.
- 127 -
128 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
AFRO S10 Nov. 1953- Health and Vital Statistics SurveyR Feb. 1954 Aim of the Project. To improve health and vital statistics.
Work accomplished. An expert from Headquarters discussed health and vital statisticswith local authorities in Liberia, Nigeria, the French Cameroons, French EquatorialAfrica, the Belgian Congo, Southern Rhodesia, Kenya and the Seychelles.
He also advised on the statistical aspects of the yaws -control projects in Liberiaand Nigeria, on the malaria projects in Liberia and the French Cameroons, and on theenvironmental- sanitation project in the Seychelles.
AFRO 8 Oct. 1954 Onchocerciasis Conference, Leopoldville
R Aim of the Project. To study the prevalence, epidemiology and social and economicimplications of African onchocerciasis.
The conference, which was organized by the Regional Office and Headquarters,was attended by experts from territories of the Region, from the Americas and Europe,and from non -governmental organizations.
For details, see pages 16 and 65.
p/ Bechuanaland 1 Sept. 1953- Non -Venereal Treponematoses
R Aim of the Project. To investigate " dichuchwa " -a non -venereal treponematosis-UNICEF in the Bechuanaland Protectorate (etiology, epidemiology, clinical and laboratory
characteristics, response to therapy, biological relationships to other treponematoses) ;to carry out a mass treatment campaign (to begin in 1955), using procain penicillinaluminium monostearate ; to train local professional and auxiliary personnel.
Assistance provided by WHO in 1954. A venereologist.
Probable Duration of Assistance. Until the end of 1956.
Work in 1954. See page 66.
East Africa 1 Nov. 1954- Malaria Institute, Amani
TA Aim of the Project. To expand into a malaria institute the existing East Africa MalariaUNICEF Unit (run by the British East Africa High Commission to serve Kenya, Uganda,
Tanganyika, Zanzibar and the Somaliland Protectorate).
Assistance provided by WHO. An entomologist and a chemist (from November 1954).Two sanitarians will also be provided, one of whom will take up his duties in January1955.
Probable Duration of Assistance. Until the end of 1956 in the first instance.
Work in progress. The East Africa Malaria Unit is carrying out a pilot project formalaria control in Tanganyika, for which UNICEF is supplying insecticides, sprayingequipment and transport. UNICEF is also providing some laboratory equipment forthe Institute. For further details, see page 67.
v
,,French Africa 1 Nov. 1952- Malaria Control, French Cameroons
TA Aim of the Project. To determine, by a pilot project, the most efficacious methods ofUNICEF using residual insecticides for malaria control in the French Cameroons, and eventually
in other territories of equatorial Africa.
Assistance provided by WHO in 1954. A malariologist and a sanitarian.
Probable Duration of Assistance. Until the end of 1956.
Work accomplished. See page 66.
Kenya 3 1953- Education and Training of Midwives, Nurses and Medical AuxiliariesR March 1954 Aim of the Project. To strengthen training schools by provision of teaching equipment.
Twelve items were ordered in 1953 ; some were delivered in that year and theremainder in March 1954.
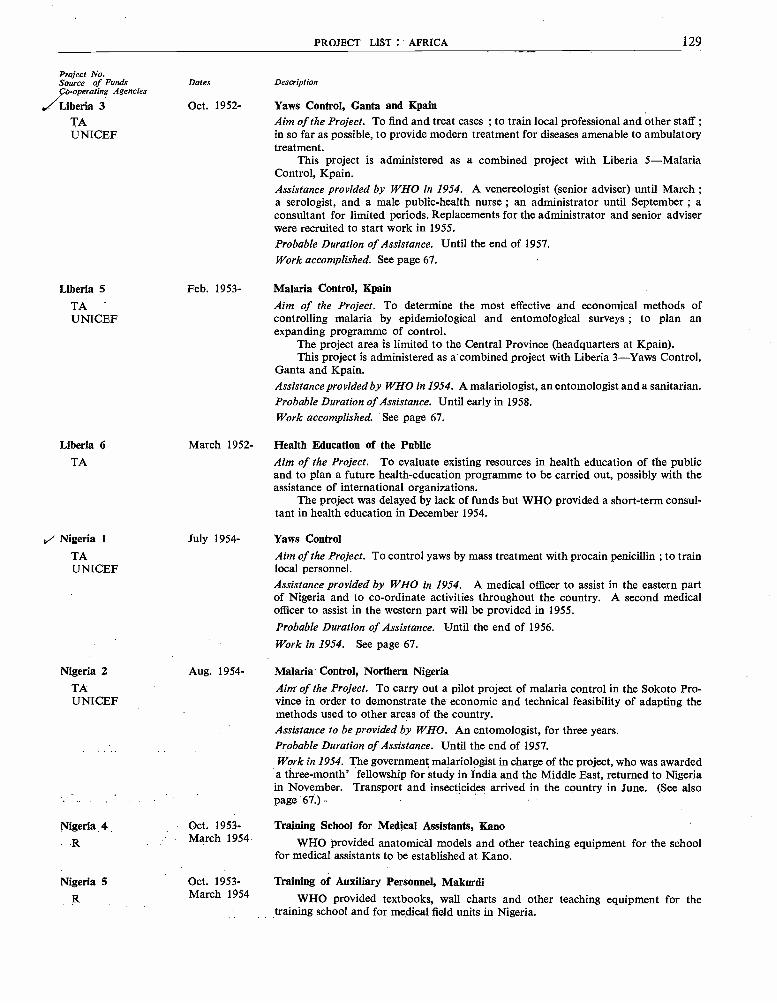
PROJECT LIST : AFRICA 129
Project No.Source of Funds Dates DescriptionCo- operating Agencies
/Liberia 3 Oct. 1952- Yaws Control, Ganta and KpainTA Aim of the Project. To find and treat cases ; to train local professional and other staff ;UNICEF in so far as possible, to provide modern treatment for diseases amenable to ambulatory
treatment.This project is administered as a combined project with Liberia 5- Malaria
Control, Kpain.Assistance provided by WHO in 1954. A venereologist (senior adviser) until March ;a serologist, and a male public -health nurse ; an administrator until September ; aconsultant for limited periods. Replacements for the administrator and senior adviserwere recruited to start work in 1955.Probable Duration of Assistance. Until the end of 1957.Work accomplished. See page 67.
Liberia 5 Feb. 1953- Malaria Control, KpainTA Aim of the Project. To determine the most effective and economical methods ofUNICEF controlling malaria by epidemiological and entomological surveys ; to plan an
expanding programme of control.The project area is limited to the Central Province (headquarters at Kpain).This project is administered as a combined project with Liberia 3 -Yaws Control,
Ganta and Kpain.Assistance provided by WHO in 1954. A malariologist, an entomologist and a sanitarian.Probable Duration of Assistance. Until early in 1958.Work accomplished. See page 67.
Liberia 6 March 1952- Health Education of the PublicTA Aim of the Project. To evaluate existing resources in health education of the public
and to plan a future health- education programme to be carried out, possibly with theassistance of international organizations.
The project was delayed by lack of funds but WHO provided a short -term consul-tant in health education in December 1954.
,i Nigeria 1 July 1954- Yaws Control
TA Aim of the Project. To control yaws by mass treatment with procain penicillin ; to trainUNICEF local personnel.
Assistance provided by WHO in 1954. A medical officer to assist in the eastern partof Nigeria and to co- ordinate activities throughout the country. A second medicalofficer to assist in the western part will be provided in 1955.Probable Duration of Assistance. Until the end of 1956.Work in 1954. See page 67.
Nigeria 2 Aug. 1954- Malaria Control, Northern NigeriaTA Aim of the Project. To carry out a pilot project of malaria control in the Sokoto Pro -UNICEF vine in order to demonstrate the economic and technical feasibility of adapting the
methods used to other areas of the country.Assistance to be provided by WHO. An entomologist, for three years.Probable Duration of Assistance. Until the end of 1957.Work in 1954. The government malariologist in charge of the project, who was awardeda three -month' fellowship for study in India and the Middle East, returned to Nigeriain November. Transport and insecticides arrived in the country in June. (See alsopage 67.)
Nigeria 4R
Nigeria 5
R
Oct. 1953 -March 1954
Oct. 1953 -March 1954
Training School for Medical Assistants, Kano
WHO provided anatomical models and other teaching equipment for the schoolfor medical assistants to be established at Kano.
Training of Auxiliary Personnel, Makurdi
WHO provided textbooks, wall charts and other teaching equipment for thetraining school and for medical field units in Nigeria.

130 THE WORK OF WHO, 1954
Project No.Source of FundsCo- operating Agencies
Nyasaland 1R
Seychelles 1
` SomalilandProtectorate 1R
Southern
VRhodesia 1
R
t Tanganyika 1
R
/ Zanzibar 1VVV
R
AMR() 1R
AMR() 6(UN)(ILO)(UNESCO)
Dates
Dec. 1953 -June 1954
Aug. 1953-
Jan. -June 1954
Dec. 1953 -June 1954
Dec. 1953 -Dec. 1954
Feb. -Dec. 1954
Dec. 1952-
July 1952-
Description
Health Training School, ZombaWHO supplied teaching aids and equipment to the school for medical assistants at
Zomba.
Public Health and SanitationAim of the Project. To train auxiliary sanitary personnel.Assistance provided by WHO. (a) An adviser in environmental sanitation (from August1953) to start the project and continue until the appointment of a public- health officerand a sanitarian. A public -health nurse will take up duties in January 1955. (b) Afellowship for study in Tanganyika.Probable Duration of Assistance. Until August 1956.
Training of Auxiliary Personnel, HargeisaWHO provided teaching supplies and equipment for the school for nurses in
Hargeisa.
Teaching Equipment for Maternity HospitalsWHO supplied teaching equipment for the following hospitals : Harari Maternity
Hospital, Salisbury ; Salisbury Hospital ; Bulawayo Hospital ; Mpilo MaternityHospital, Bulawayo.
Training of Auxiliary PersonnelWHO provided teaching supplies for nurses' training schools at Kongwa, Dar-es -
Salaam, Mwanza, Bumbuli and Minaki.
Training of Auxiliary PersonnelWHO provided teaching and midwifery equipment for the Nurses' Training Centre.
THE AMERICAS
Training in Environmental Sanitation, Brazil, Chile and Mexico (to serve all countriesin the Americas)Aim of the Project. To train sanitary engineers and auxiliary personnel for staffingnational and local health departments ; to expand and strengthen facilities for trainingin environmental sanitation at the University of Sáo Paulo and the Schools of PublicHealth in Santiago and Mexico City.Assistance provided by WHO in 1954. (a) A short -term consultant and services ofWHO/PASB staff members.(b)Three sanitary engineers and two sanitary inspectors fromthree different countries received fellowships for training in Sao Paulo ; twelve sanitaryinspectors and one sanitary engineer from eight countries received fellowships fortraining in Santiago. (c) Fellowships were granted to two sanitary inspectors for studyin El Salvador and to one sanitary engineer for study in the United States of America.Probable Duration of Assistance. At least ten years.
Joint Field Mission on Indigenous Populations, Andean Highlands of Bolivia, Ecuadorand Peru
Aim of the Project. To promote educational and social development of indigenouspopulations of these areas with a view to facilitating their integration into their nationalcommunities.
Assistance provided in 1954. A short -term consultant in public health from Februaryto August (cost reimbursable by ILO).
Probable Duration of Assistance. Because of the good response of the people to servicesoffered, ILO plans to continue its assistance in 1955.
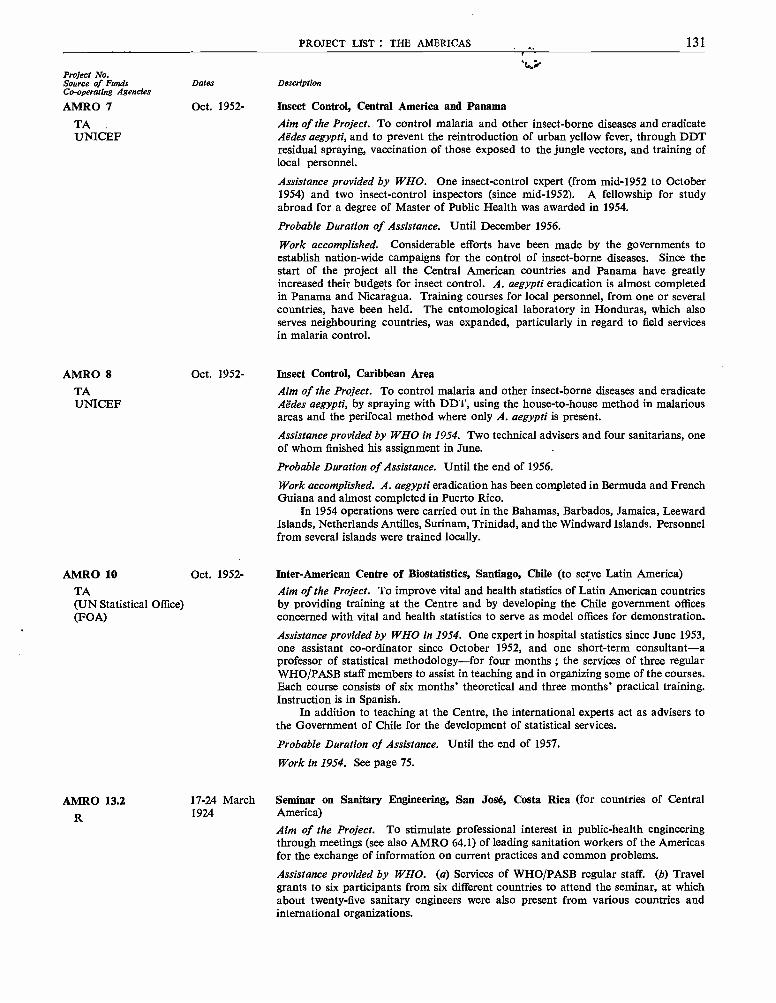
PROJECT LIST : THE AMERICAS 131
Project No.Source of Funds Dates DescriptionCo- operating Agencies
AMRO 7 Oct. 1952- Insect Control, Central America and Panama
TA Aim of the Project. To control malaria and other insect -borne diseases and eradicateUNICEF Aëdes aegypti, and to prevent the reintroduction of urban yellow fever, through DDT
residual spraying, vaccination of those exposed to the jungle vectors, and training oflocal personnel.
Assistance provided by WHO. One insect -control expert (from mid -1952 to October1954) and two insect -control inspectors (since mid -19521. A fellowship for studyabroad for a degree of Master of Public Health was awarded in 1954.
Probable Duration of Assistance. Until December 1956.
Work accomplished. Considerable efforts have been made by the governments toestablish nation -wide campaigns for the control of insect -borne diseases. Since thestart of the project all the Central American countries and Panama have greatlyincreased their budgets for insect control. A. aegypti eradication is almost completedin Panama and Nicaragua. Training courses for local personnel, from one or severalcountries, have been held. The entomological laboratory in Honduras, which alsoserves neighbouring countries, was expanded, particularly in regard to field servicesin malaria control.
AMRO 8 Oct. 1952- Insect Control, Caribbean Area
TA Aim of the Project. To control malaria and other insect -borne diseases and eradicateUNICEF Aëdes aegypti, by spraying with DDT, using the house -to -house method in malarious
areas and the perifocal method where only A. aegypti is present.
Assistance provided by WHO in 1954. Two technical advisers and four sanitarians, oneof whom finished his assignment in June.
Probable Duration of Assistance. Until the end of 1956.
Work accomplished. A. aegypti eradication has been completed in Bermuda and FrenchGuiana and almost completed in Puerto Rico.
In 1954 operations were carried out in the Bahamas, Barbados, Jamaica, LeewardIslands, Netherlands Antilles, Surinam, Trinidad, and the Windward Islands. Personnelfrom several islands were trained locally.
AMRO 10 Oct. 1952- Inter -American Centre of Biostatistics, Santiago, Chile (to serve Latin America)
TA Aim of the Project. To improve vital and health statistics of Latin American countries(UN Statistical Office) by providing training at the Centre and by developing the Chile government offices(FOA) concerned with vital and health statistics to serve as model offices for demonstration.
Assistance provided by WHO in 1954. One expert in hospital statistics since June 1953,one assistant co- ordinator since October 1952, and one short -term consultant -aprofessor of statistical methodology -for four months ; the services of three regularWHO /PASB staff members to assist in teaching and in organizing some of the courses.Each course consists of six months' theoretical and three months' practical training.Instruction is in Spanish.
In addition to teaching at the Centre, the international experts act as advisers tothe Government of Chile for the development of statistical services.
Probable Duration of Assistance. Until the end of 1957.
Work in 1954. See page 75.
AMRO 13.2R
17 -24 March Seminar on Sanitary Engineering, San José, Costa Rica (for countries of Central1924 America)
Aim of the Project. To stimulate professional interest in public -health engineeringthrough meetings (see also AMRO 64.1) of leading sanitation workers of the Americasfor the exchange of information on current practices and common problems.
Assistance provided by WHO. (a) Services of WHO /PASB regular staff. (b) Travelgrants to six participants from six different countries to attend the seminar, at whichabout twenty -five sanitary engineers were also present from various countries andinternational organizations.
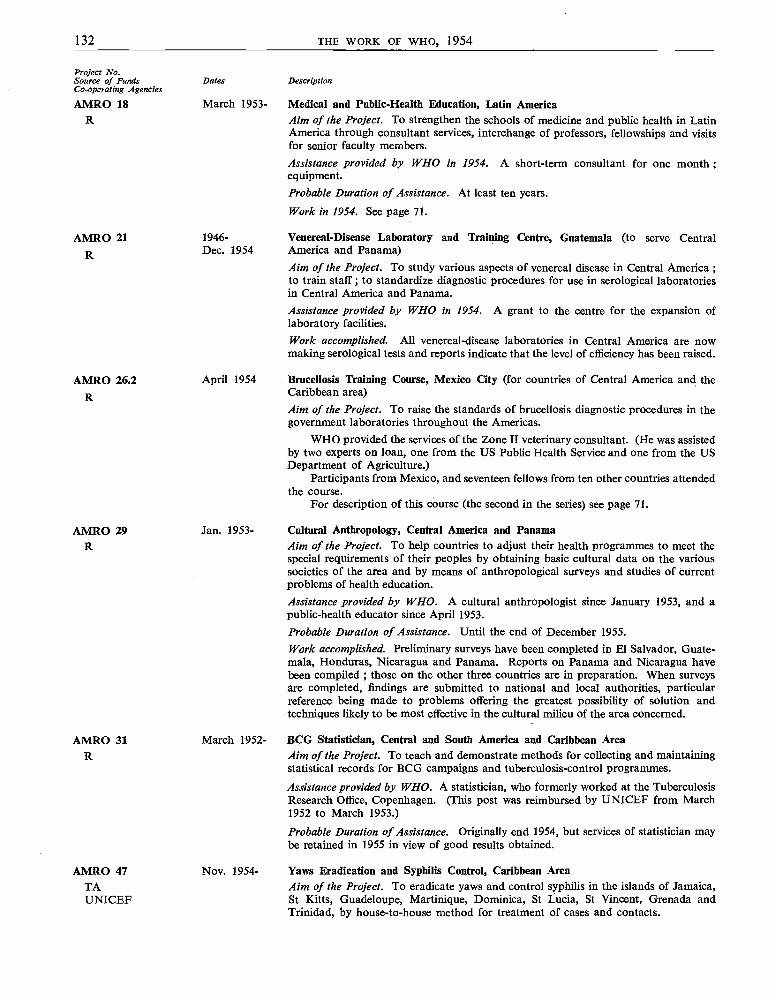
132 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
AMRO 18 March 1953- Medical and Public -Health Education, Latin AmericaR Aim of the Project. To strengthen the schools of medicine and public health in Latin
America through consultant services, interchange of professors, fellowships and visitsfor senior faculty members.
Assistance provided by WHO in 1954. A short -term consultant for one month ;equipment.
Probable Duration of Assistance. At least ten years.
Work in 1954. See page 71.
AMRO 21R
AMRO 26.2R
AMR() 29R
1946- Venereal- Disease Laboratory and Training Centre, Guatemala (to serve CentralDec. 1954 America and Panama)
Aim of the Project. To study various aspects of venereal disease in Central America ;to train staff ; to standardize diagnostic procedures for use in serological laboratoriesin Central America and Panama.Assistance provided by WHO in 1954. A grant to the centre for the expansion oflaboratory facilities.
Work accomplished. All venereal -disease laboratories in Central America are nowmaking serological tests and reports indicate that the level of efficiency has been raised.
April 1954
Jan. 1953-
Brucellosis Training Course, Mexico City (for countries of Central America and theCaribbean area)Aim of the Project. To raise the standards of brucellosis diagnostic procedures in thegovernment laboratories throughout the Americas.
WHO provided the services of the Zone II veterinary consultant. (He was assistedby two experts on loan, one from the US Public Health Service and one from the USDepartment of Agriculture.)
Participants from Mexico, and seventeen fellows from ten other countries attendedthe course.
For description of this course (the second in the series) see page 71.
Cultural Anthropology, Central America and PanamaAim of the Project. To help countries to adjust their health programmes to meet thespecial requirements of their peoples by obtaining basic cultural data on the varioussocieties of the area and by means of anthropological surveys and studies of currentproblems of health education.
Assistance provided by WHO. A cultural anthropologist since January 1953, and apublic -health educator since April 1953.
Probable Duration of Assistance. Until the end of December 1955.Work accomplished. Preliminary surveys have been completed in El Salvador, Guate-mala, Honduras, Nicaragua and Panama. Reports on Panama and Nicaragua havebeen compiled ; those on the other three countries are in preparation. When surveysare completed, findings are submitted to national and local authorities, particularreference being made to problems offering the greatest possibility of solution andtechniques likely to be most effective in the cultural milieu of the area concerned.
AMRO 31 March 1952- BCG Statistician, Central and South America and Caribbean AreaR Aim of the Project. To teach and demonstrate methods for collecting and maintaining
statistical records for BCG campaigns and tuberculosis -control programmes.
Assistance provided by WHO. A statistician, who formerly worked at the TuberculosisResearch Office, Copenhagen. (This post was reimbursed by UNICEF from March1952 to March 1953.)
Probable Duration of Assistance. Originally end 1954, but services of statistician maybe retained in 1955 in view of good results obtained.
AMRO 47 Nov. 1954- Yaws Eradication and Syphilis Control, Caribbean AreaTA Aim of the Project. To eradicate yaws and control syphilis in the islands of Jamaica,UNICEF St Kitts, Guadeloupe, Martinique, Dominica, St Lucia, St Vincent, Grenada and
Trinidad, by house -to -house method for treatment of cases and contacts.
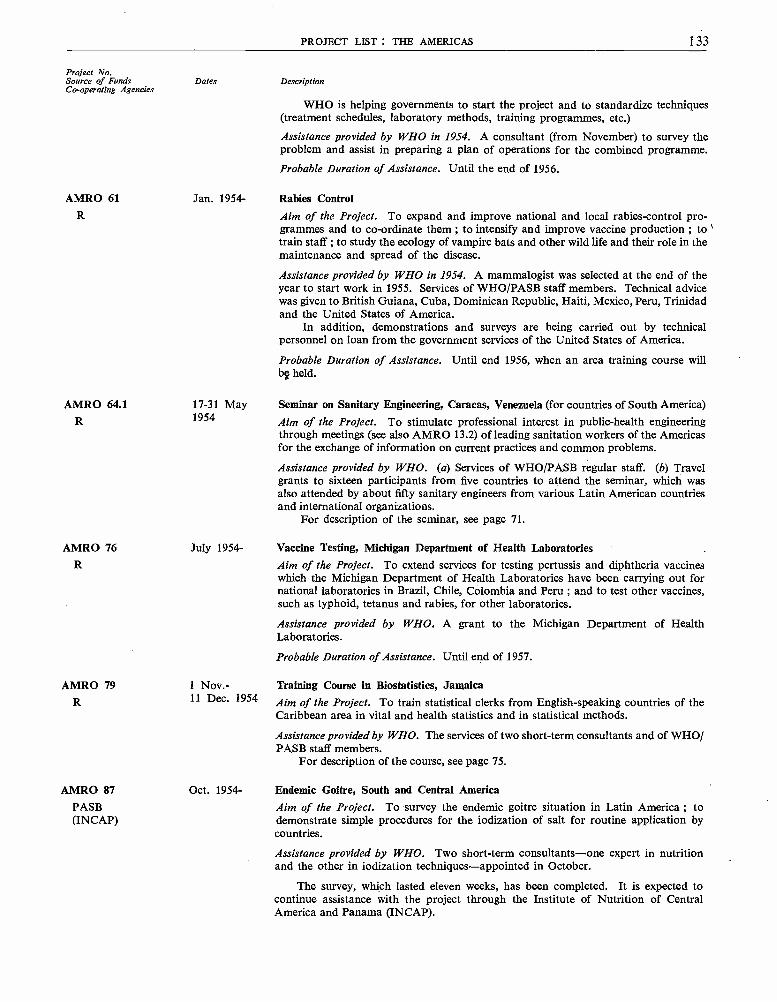
PROJECT LIST : THE AMERICAS 133
Project No.Source of Funds Dates DescriptionCo- operating Agencies
WHO is helping governments to start the project and to standardize techniques(treatment schedules, laboratory methods, training programmes, etc.)
Assistance provided by WHO in 1954. A consultant (from November) to survey theproblem and assist in preparing a plan of operations for the combined programme.
Probable Duration of Assistance. Until the end of 1956.
AMRO 61 Jan. 1954- Rabies ControlR Aim of the Project. To expand and improve national and local rabies -control pro-
grammes and to co- ordinate them ; to intensify and improve vaccine production ; totrain staff ; to study the ecology of vampire bats and other wild life and their role in themaintenance and spread of the disease.
Assistance provided by WHO in 1954. A mammalogist was selected at the end of theyear to start work in 1955. Services of WHO /PASB staff members. Technical advicewas given to British Guiana, Cuba, Dominican Republic, Haiti, Mexico, Peru, Trinidadand the United States of America.
In addition, demonstrations and surveys are being carried out by technicalpersonnel on loan from the government services of the United States of America.
Probable Duration of Assistance. Until end 1956, when an area training course willbe held.
AMR() 64.1R
17 -31 May1954
Seminar on Sanitary Engineering, Caracas, Venezuela (for countries of South America)
Aim of the Project. To stimulate professional interest in public -health engineeringthrough meetings (see also AMRO 13.2) of leading sanitation workers of the Americasfor the exchange of information on current practices and common problems.
Assistance provided by WHO. (a) Services of WHO /PASB regular staff. (b) Travelgrants to sixteen participants from five countries to attend the seminar, which wasalso attended by about fifty sanitary engineers from various Latin American countriesand international organizations.
For description of the seminar, see page 71.
AMRO 76 July 1954- Vaccine Testing, Michigan Department of Health LaboratoriesR Aim of the Project. To extend services for testing pertussis and diphtheria vaccines
which the Michigan Department of Health Laboratories have been carrying out fornational laboratories in Brazil, Chile, Colombia and Peru ; and to test other vaccines,such as typhoid, tetanus and rabies, for other laboratories.
Assistance provided by WHO. A grant to the Michigan Department of HealthLaboratories.
AMRO 79R
1 Nov. -11 Dec. 1954
Probable Duration of Assistance. Until end of 1957.
Training Course in Biostatistics, JamaicaAim of the Project. To train statistical clerks from English- speaking countries of theCaribbean area in vital and health statistics and in statistical methods.
Assistance provided by WHO. The services of two short -term consultants and of WHO/PASB staff members.
For description of the course, see page 75.
AMRO 87 Oct. 1954- Endemic Goitre, South and Central AmericaPASB Aim of the Project. To survey the endemic goitre situation in Latin America ; to(INCAP) demonstrate simple procedures for the iodization of salt for routine application by
countries.
Assistance provided by WHO. Two short -term consultants -one expert in nutritionand the other in iodization techniques- appointed in October.
The survey, which lasted eleven weeks, has been completed. It is expected tocontinue assistance with the project through the Institute of Nutrition of CentralAmerica and Panama ( INCAP).
V
134 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Bolivia 5 Aug. 1953- Nursing Education, La PazR Aim of the Project. To raise the standard of nursing throughout the country by
reorganization of the National School of Nursing.Assistance provided by WHO. Two nurse educators, since August 1953 and July 1954respectively.
Probable Duration of Assistance. Until the end of 1958.Work accomplished. See page 71.
Bolivia 6 July 1953- Study of Water Supply, La PazR March 1954 Aim of the Project. To improve the water -supply system of the city through study of
water -supply problems and training of national technicians.
Assistance provided by WHO in 1954. (a) The services of a consultant (an engineerspecialized in the chemical treatment of water) for three months ; (b) two fellowships- one awarded to an engineer who will later work on the water system, the secondfor studies in chemistry and pharmacy ; (c) equipment.
After 1954 WHO participation will be limited to the granting of fellowships.Work accomplished. During the first phase of the project (two weeks in 1953), an initialsurvey of the problems was made and a list of needed equipment was drawn up. Someof this equipment was provided by the Organization. The second phase of the projectconsisted of an analysis of the data collected, chemical studies of the water and pre-paration of a plan for obtaining and distributing a supply of water of adequate quantity
/and quality.
Brazil 4 Sept. 1951- Diphtheria and Pertussis Vaccine, Instituto Oswaldo CruzR Aim of the Project. To set up at the Instituto Oswaldo Cruz a laboratory for theUNICEF production of diphtheria and pertussis vaccine. (This project supplements the PASB
maternal and child health project -Brazil 3)Assistance provided by WHO in 1954. Zone Office staff provided services to thelaboratory.Work accomplished. Vaccine production did not begin until June 1953, when the initialoutput was 4000 doses per month. By the end of 1954 the laboratory was producingapproximately 10 000 doses per month.
All batches of vaccine are tested by the Michigan Department of HealthLaboratories under project AMRO 76- Vaccine Testing.
A systematic plan for mass immunization has been put into effect in Brazil.
4 British Guiana 1 March -July Tuberculosis Control (BCG)
R 1954 Aim of the Project. To carry out a BCG campaign.UNICEF Assistance provided. A BCG consultant (cost reimbursed by UNICEF). The
BCG statistician employed under project AMRO 31 spent some time on the recordingand retesting part of the project.Work accomplished. The project started in Georgetown, then was extended to outsideareas. After two weeks spent in publicizing the campaign, testing was carried out,first in schools, then in government offices and business houses. Initial testing andvaccination was completed and a start made on the follow -up work. Over 123 000persons had been tested and nearly 72 000 vaccinated by the end of September.
X -ray examination of tuberculin positives is under the direction of the existingtuberculosis service.
British Honduras 2RUNICEF
Sept. 1953 -Sept. 1954
BCG Vaccination
Aim of the Project. To tuberculin -test all persons under 30 in the territory and tovaccinate all negative reactors with BCG ; to train local professional and auxiliarypersonnel in testing and vaccination techniques, evaluation of results and maintenanceof records.
Assistance provided by WHO in 1954. Technical advice by the area supervisor and thestatistical consultant employed under project AMRO 31.Work accomplished. A high percentage of the population has been vaccinated.
PROJECT LIST THE AMERICAS 135
Project No.Source of Funds Dates DescriptionCo- operating Agencies
1 /Chile 10 May 1954- Tuberculosis Control (BCG)
R Aim of the Project. To test and vaccinate persons between 1 and 30 years of age in townsUNICEF with a population of under 5000 ; to train local personnel.
Assistance provided by WHO. Advisory services by staff of the zone office.
Chile 12 Oct. 1954- Care of Premature Infants, Calvo Mackenna Hospital, SantiagoR Aim of the Project. To lower mortality rates among prematurely born infants byUNICEF improved care -through the establishment, at the Calvo Mackenna Hospital, of
a demonstration and training centre for professional and auxiliary personnel ; thedevelopment of norms and procedures for care of premature infants ; the integrationof services for premature infants into the country's general health services ; and theextension of provision for such specialized care to all parts of the country.
Assistance provided by WHO in 1954. Fellowships.
Probable Duration of Assistance. Until the end of 1955.
Work accomplished. Fellowships were awarded for study in the United States ofAmerica to two physicians, for training in paediatrics and care of premature infants,and to the head nurse for attendance at courses on prematurity and visits to centres forthe care of premature infants.
,Colombia 4 Sept. 1951- Maternal and Child Health, BogotáR Aim of the Project. To organize training courses at the School of Public Health, Bogotá,UNICEF in order to form a nucleus of highly trained nurse -midwives to act as instructors and
supervisors.The San José Hospital, the National School of Nursing, and Health Centre No. 6
of the Municipality of Bogotá are co- operating with the Ministry of Health in theproject, which will later form part of a project for integrated public -health services.
Assistance provided by WHO. Two nurse educators since late 1952, one of whomfinished her assignment in September 1954.
Probable Duration of Assistance. Until the end of 1957.
Work accomplished. Three eight -month courses in nurse -midwifery had been held byMay 1954. WHO awarded fellowships to the top students of the first two courses forstudy abroad ; and they will, on their return, assume responsibility for training.
Colombia 5 April 1951- Insect Control
TA Aim of the Project. To eradicate Aëdes aegypti and control malaria and other insect-UNICEF borne diseases in the northern part of Colombia by spraying with DDT, using the house -
to -house method in malarious areas and the perifocal method where only A. aegyptiis present ; to train local professional and auxiliary personnel in the most effectivemethods of insect control.
Endemic yellow fever exists in the jungle region of Colombia and A. aegypti ispresent in various areas of the country, in many of which infestation is high. Thepresence of this vector makes it possible for jungle yellow fever to spread into theseareas.
Assistance provided by WHO. (a) An insect -control adviser since April 1951, anda sanitarian since January 1952 ; (b) in 1954, a fellowship in entomology for studyabroad.
Probable Duration of Assistance. Until the end of 1955, after which the project will besupervised by an insect -control adviser serving the countries in Zone IV.
Work accomplished. By April 1954, 694 localities had been inspected after DDTspraying and only one was found to be infested with A. aegypti, and, in the non -malariousareas, 462 localities out of 581 inspected had been treated against A. aegypti. Of these,438 were reinspected and only 8 were found to be still infested.
A study made by the Ministry of Health estimated that the reduction in malariacases was such as to save 14 000 000 pesos (calculated in terms of cost of treatmentand working time previously lost through illness).

136 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo-operating Agencies
Colombia 15 April 1954- Tuberculosis Control (BCG)
UNICEF Aim of the Project. To carry out a country-wide BCG campaign.Assistance provided. A technical adviser (cost reimbursed by UNICEF). The BCGstatistician employed under project AMRO 31 is spending time on the recordingand retesting part of the project. A short -term fellowship was awarded for studyabroad of BCG- vaccine production.Probable Duration of Assistance. Until the end of 1955.
Work accomplished. After the campaign had been publicized, testing was carried out,first in schools, then in government offices and business houses. By September 195460 479 persons had been vaccinated./ Costa Rica 3 June 1951- Nursing Education, San José
TA Aim of the Project. To strengthen the teaching facilities of the School of Nursingoperated by the Government in connexion with the San Juan de Dios Hospital ; toprepare a limited number of graduate nurses for teaching, for hospital nursing andpublic- health nursing ; to train nursing auxiliary personnel ; to establish a post-graduate course of one year for nurse -midwives.
Assistance provided by WHO. (a) Five nurse educators (one as educational director,four for psychiatry, midwifery, public -health nursing and training of auxiliariesrespectively). The educational director has been working on the project since 1951 ;the others started work between April 1953 and September 1954. (b) Four fellowshipsin 1954 for study abroad.
Probable Duration of Assistance. Until the end of 1956.
Work accomplished. A faculty of nursing instructors had been prepared through thefellowship programme. The first class under the organized curriculum graduated atthe end of 1954. The first class of approximately forty nursing auxiliaries graduatedin December 1953 and two more courses for this type of worker have been started.A post -graduate course for nurse -midwives started in July 1954.
Costa Rica 5RUNICEF
March 1952 -July 1954
BCG Vaccination
Aim of the project. To carry out a country -wide BCG campaign.Assistance provided by WHO. The BCG statistician employed under project AMRO 31spent some time on the recording and retesting part of the project.
Work accomplished. After the campaign had been publicized, testing was started inSan José and extended from thereto the outlying provinces. By June 1954, when themass campaign ended, 262 738 persons had been tested and 195 116 vaccinated. Planshave been made with the Government for continuation of the retesting work, and thenational team who will carry it out is well instructed in the procedure.
Dominican Sept 1952- Insect Controli/ Republic 2 Aim of the Project. To eradicate Aëdes aegypti and control malaria and other insect-
TA borne diseases in the whole country by spraying with DDT, using the house -to -houseUNICEF method in malarious areas and the perifocal method where only A. aegypti is present.
Assistance provided by WHO. A malariologist, since September 1952.Probable Duration of Assistance. Until the end of 1956.Work accomplished. More than a million persons (half the population) have beenprotected in the malarious areas and the eradication of A. aegypti is proceeding satis-factorily.
/ Ecuador 5 Sept. 1951- Tuberculosis Teaching Centre, National Institute of Health, Guayaquil
R Aim of the Project. To improve and extend the already existing diagnostic and thera-UNICEF peutic services and to provide training facilities for workers from Ecuador and other
countries in the Americas.Assistance provided by WHO. A pathologist since 1952, and a short-term consultant,both of whom act as key instructors.Probable Duration of Assistance. Until the end of 1955.Work accomplished. See page 72.
PROJECT LIST : THE AMERICAS 137
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Ecuador 6 Aug. 1952- BCG Laboratory, Guayaquil
R Aim of the Project. To give additional training in techniques of vaccine preparationUNICEF to the staff of the BCG -vaccine laboratory, Guayaquil, in order to bring the vaccine to
the standard necessary for approval for general use by the Expert Committee on Bio-logical Standardization ; the Laboratory, built by the Government, was opened inAugust 1952 as part of the WHO /UNICEF- assisted BCG programme which followedthe mass vaccination campaign carried out from June 1950 to July 1951.
Assistance provided by WHO in 1954. A short -term consultant since August.
Ecuador 7
TA
1951-April 1954
Venereal- Disease Control, Portoviejo (1951), Manta (1952) and Bahía (1953 -54)
Aim of the Project. To control syphilis by mass treatment techniques.
Assistance provided by WHO in 1954. A venereologist and a public -health nurse.
Work accomplished. In addition to the mass treatment campaign, two serologicalsurveys were carried out, followed by a re -check of the positive reactors found bythe survey.
Ecuador 11 Oct. 1952- National Institute of Health, Guayaquil
TA Aim of the Project. To improve the standards of the Institute, which is responsiblefor the control of drugs and foodstuffs imported into the country and which, as partof the Office of the Director- General of Health, produces vaccines for the controlof several communicable diseases, provides diagnostic services and conductsepidemiological investigations.Assistance provided by WHO. A virus specialist since August 1953 ; a fellowship inpublic- health administration, awarded for study abroad.Probable Duration of Assistance. Until the end of 1956.Work in 1954. By May the animal colony of the Institute had been reorganized and anew building erected to house it.
El Salvador 5 May 1951- Health Demonstration Area, San Andrés Valley
TA Aim of the Project. To provide integrated health services in a selected rural community ;(ILO) to develop effective methods of public -health administration ; to demonstrate methods(FAO) of integration of health programmes into programmes for social and economic im-(UNESCO) provement ; to provide field training.
Assistance provided by WHO in 1954. A medical officer, a statistician, a sanitaryengineer and two public -health nurses (the first two since 1952).
Probable Duration of Assistance. Until the end of 1956.Work accomplished. See page 72.
El Salvador 6 1952- Maternal and Child Health
R Aim of the Project. To improve maternal and child health services throughout theUNICEF country by : extending services in urban areas ; organizing maternal and child health
services in certain rural areas where none exist ; training professional and auxiliarypersonnel ; organizing domiciliary midwifery services and training courses for midwives;expanding health- education programmes in certain areas.Assistance provided by WHO in 1954. Staff of the Zone Office have given technicaladvice.
Probable Duration of Assistance. In 1955 the project is scheduled to continue as partof a rural health services programme.
%y' V Guatemala 8
RUNICEF
Aug. 1954- Rural Public -Health Services
Aim of the Project. To reorganize public -health services in rural areas throughout thecountry and develop rural health units ; to reorganize health services at all levels ; toestablish a demonstration health unit with subcentres ; to train personnel for medical,nursing and sanitation work.Assistance provided by WHO in 1954. A medical officer, from August ; two fellowshipsin public -health nursing for study abroad.
138 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Guatemala 10 Feb. 1953- Garbage Disposal, Guatemala CityAug. 1954
Aim of the Project. To reorganize the garbage collection and disposal system, which willbe used for demonstration and training purposes for other cities in Guatemala.
Assistance provided by WHO. A public -health engineer for the duration of the project.A fellowship was granted in 1953 to a local sanitary engineer who, on his return in1954, took charge of the service.
Work accomplished. A new collection system was planned and started ; a modernrecords system was established, and demonstrations were given in the use of newequipment. Fly control was carried out. Health education formed part of the project.
J Haiti 1 July 1950- Yaws Eradication and Syphilis Control
R Aim of the Project. To eradicate yaws and to control syphilis in urban and ruralPASB areas by mass- treatment methods, using antibiotics, by training local personnel andUNICEF educating the population in the benefits of treatment and control measures for yaws
and syphilis.Towards the end of 1954 plans were made to include in the programme an intensive
mass -treatment campaign for the control of syphilis in urban areas.
Assistance provided by WHO. Three medical officers, one since February 1950, onesince October 1952 and one since November 1954.
Probable Duration of Assistance. Until the end of 1957.
Work accomplished. See page 73.
Haiti 2 Sept. 1954- Local Health Services
TA Aim of the Project. To organize and develop rural health services throughout thecountry.
This project is to combine the PASB project Haiti 9 (public- health laboratory)and project Haiti 10 (training of non -professional midwives) with a proposed projectin maternal and child health and the project in Petit Goave for the demonstration oflocal health services.
ü Leeward Islands 1
RUNICEF
Nov. 1953 -March 1954
Work in 1954. As a first step, four fellowships were awarded for training abroad -onefor studies leading to a degree of Master of Public Health (twelve months), one inobstetrics (two months) and two in public -health administration (approximately twomonths each).
Later it is planned to provide consultants to advise the Government, and, withcounterparts, to demonstrate the value of rural health services, at first in selected areas.
BCG Vaccination, St Kitts, Nevis and Anguilla
Aim of the Project. To carry out a BCG campaign.
Assistance provided. A BCG consultant (cost reimbursed by UNICEF). The BCGstatistician employed under project AMRO 31 spent some time on the recording andretesting part of the project.
Work accomplished. After two weeks spent in publicizing the campaign, testing wascarried out, first in schools, then in Government offices and business houses. Thetotal number of persons tested was 37 533 and about 95 per cent. of these werevaccinated. X -ray examination of the tuberculin positives was organized and hadstarted by the end of 1954.
v Mexico 15 Sept. 1954- Rural Health Services
UNICEF Aim of the Project. To organize rural public- health services in eight states, and laterthroughout the country ; to provide in- service training for all categories of healthpersonnel.
Particular attention will be paid to maternal and child health services in all eightstates, and to environmental sanitation in Guanajuato.
PROJECT LIST : THE AMERICAS 139
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Assistance provided in 1954. A consultant for one month (cost reimbursed by UNICEF).Later it is planned to provide a public -health adviser, a sanitary engineer and apublic -health nurse.
Probable Duration of Assistance. Approximately five years.
Work in 1954. The consultant made a preliminary survey and his report was in pre-paration at the end of the year.
Mexico 53 July 1953- Insect ControlTA Aim of the Project. To eradicate Aëdes aegypti and to control malaria in the wholeUNICEF country by spraying with DDT, using the house -to -house method in malarious areas
and the perifocal method where only A. aegypti is present.Assistance provided by WHO in 1954. (a) Two insect -control advisers -one since Julyand the other since August ; services of WHO /PASB staff members. (b) Two travelgrants, one for attendance at a malaria course in Maracay, and one for visits to anti -malaria services in Argentina, Brazil, Uruguay and Venezuela.Probable Duration of Assistance. Until 1959.
Work in 1954. Field operations started in the south -east in mid -1954 and willbe extended progressively until the whole country has been covered (towards the endof 1956). Training of local personnel commenced.
N./ Nicaragua 3 Sept. 1954- Rural Public -health ServicesTA Aim of the Project. To reorganize and develop health services in rural areas throughoutPASB the country by : setting up a demonstration and training centre, extending localUNICEF services ; strengthening the central services, and undertaking environmental sanitation
work. This project is an extension of the PASB environmental sanitation project -Nicaragua 51.
Assistance provided by WHO in 1954. A public -health engineer since September, anda medical officer since October ; a fellowship in nursing for study abroad.Probable Duration of Assistance. Five years.Work in 1954. Organizing and planning.
v Panama 1 Aug. 1952- Rural Public -Health ServicesTA Aim of the Project. To co- ordinate and extend public -health services in selected ruralUNICEF communities ; to give in- service training to public- health personnel at a rural health
centre ; to develop methods of public -health administration better adapted to theneeds of the population.Assistance provided by WHO. (a) A medical officer, a public -health laboratory expert,a public- health engineer and two public -health nurses. Except for one of the public-health nurses, who commenced duty in November 1954, all have been working on theproject since 1952 or early 1953. (b) Two fellowships for study abroad.Probable Duration of Assistance. Until the end of 1957.Work accomplished. During the first phase of the project (1952 -53) a survey was madeof existing services, information was collected on health and related conditions in thecountry and a planning unit was established to co- ordinate the work. A demonstrationhealth unit was set up, in- service training was given to professional and auxiliarypersonnel and the Central Health Laboratory in Panama City was reorganized. Fellow-ships for study abroad were granted to nationals who returned to work on the project.
The second phase of the project started in 1954 with reorganization of rural healthservices in selected communities. Training of personnel continued. Progress was madewith the reorganization of the central department of health.
Paraguay 1
TAUNICEF
May 1951 -Dec. 1954
Insect Control
Aim of the Project. To eradicate Aëdes aegypti and to control malaria and other insect -borne diseases in the whole country by spraying with DDT, using the house -to -housemethod in malarious areas and the perifocal method where only A. aegypti is present.Assistance provided by WHO in 1954. A sanitary inspector from August 1952 to June1954 ; services of WHO /PASB staff members ; a fellowship for study abroad for adegree of Master of Public Health.
140 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Paraguay 2TA
Paraguay 3RUNICEF
Paraguay 4TA
June 1952 -Dec. 1954
Sept. 1951 -Dec. 1954
Dec. 1951 -Dec. 1954
Work accomplished. By 1954 Paraguay was free from A. aegypti. Malaria had not beencompletely eliminated by the control programme. Arrangements were therefore madefor an evaluation and analysis of the situation by the PASB malaria consultant. Theinformation in his report will determine the basis for further co- operation with theGovernment on malaria control.
Tuberculosis Control, Asunción and Rural Areas
Aim of the Project. To organize a large -scale tuberculosis -control programme inAsunción and rural areas and to co- ordinate tuberculosis control with other specializedwork in the Health Department.
The project includes radiological surveys, for which norms were established, andthe training of dispensary and other personnel.Assistance provided by WHO. (a) A medical officer, a medical bacteriologist, apublic -health nurse and an x -ray technician, all of whom have worked on the projectfrom two to two -and -a -half years. (b) Supplies and equipment.
Work accomplished. See page 73.In 1955 the project will become part of a general public- health project -
Paraguay 10.
Maternal and Child Health, Asunción- Villarrica AreaAim of the Project. To reduce maternal mortality and morbidity by improving andextending prenatal and post -natal services in existing health centres, creating newcentres and training personnel.
Assistance provided by WHO in 1954. A medical adviser and a public- health nurse/midwife ; fellowships.
Work accomplished. Maternal and child health programmes for the health centres were .planned and professional midwives and nurses and auxiliary personnel were trainedfor work in the centres. Auxiliary personnel (including nursing aides, sanitarians andlaboratory and x -ray technicians) were trained locally ; senior national officials weregiven fellowships for study abroad. A BCG programme began in August 1954.
Progress was made in forming the WHO staff of this and other projects into ateam to advise the Government.
In 1955 the project will become part of a general public -health project -Paraguay 10.
Venereal- Disease Control, Asunción- Villarrica Area
Aim of the Project. To determine the prevalence of venereal disease ; to demonstratemethods of control ; to develop services in the area.
Assistance provided by WHO. A serologist since May 1953 and a public -health nursesince December 1951 ; a fellowship for study abroad.
Work accomplished. Blood sampling, analyses, and clinical examinations were carriedout, and positive cases were treated. Laboratory services were improved and serologiststrained.
In 1955 the project will become part of a general public -health project -Paraguay 10.
Paraguay 5 Dec. 1951 - Hookworm and Smallpox Control, Asunción- Villarrica Area
TA Dec. 1954 Aim of the Project. To reduce mortality and morbidity from hookworm and smallpoxby a comprehensive control programme, first in the Asunción- Villarrica area, later inthe whole country, by demonstrating methods and techniques and training professionaland auxiliary personnel.
Assistance provided by WHO. (a) A public -health adviser, a health educator, a public-health engineer and a sanitary inspector. The first two have worked nearly three yearson the project, and the latter two nearly two years. (b) Two fellowships in 1954 forstudy abroad.
PROJECT LIST : THE AMERICAS 141
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Work accomplished: Mass treatment, environmental sanitation work, health education,and coprological surveys were carried out for control of hookworm. The environ-mental sanitation work was hampered at first by lack of local staff. In the smallpoxcampaign, conducted from June 1953 to March 1954, 74 527 persons were vaccinated.Dried smallpox vaccine provided by WHO was used.
In 1955 the project will become part of a general public -health project -Paraguay 10.
Paraguay 6 Jan. 1953- Department of Preventive Medicine, School of Medicine, AsunciónR Aim of the Project. To improve teaching of preventive medicine at the School of
Medicine of the National University of Paraguay ; to improve medical education as awhole by including study of preventive medicine in all phases of the curriculum.
Assistance provided by WHO. A professor of public health since January 1953.
Probable Duration of Assistance. Until the end of 1955, when the University will beable to continue the Department of Preventive Medicine as a permanent part of theMedical School.
Paraguay 7RUNICEF
Aug. 1954-
Work accomplished. The first full course was given in 1953, the second in 1954. Shortcourses for medical students and certain technicians were also given. Progress hasbeen made in including preventive medicine in the teaching of other subjects.
BCG Vaccination
Aim of the Project. To carry out a BCG campaign.
Assistance provided. A BCG adviser and a nurse (cost of both reimbursed by UNICEF).The BCG statistician employed under project AMRO 31 is spending some time on therecording and retesting part of the programme.
Probable Duration of Assistance. Until the end of 1955.
Work accomplished. See page 74.
Peru 10 Sept. 1952- Maternal and Child Health and Related Health Services, Rural Area Lima- Pativilca-TA Dec. 1954 Huaras - Callejón de Huaylas
UNICEF Aim of the Project. To establish, in a rural area, comprehensive public -health serviceswhich can also serve for training of public -health personnel.
Assistance provided by WHO. A medical officer since May 1953, a laboratory expertsince August 1953, and a public -health nurse since December 1952 ; fellowships.
Work accomplished. Maternal and child health clinics were organized, twelve being inoperation by the end of 1954. A start was made on organization of a public -healthlaboratory and on a tuberculosis control service, and nutrition and general sanitationprogrammes were begun. Courses were given for auxiliary personnel.
Because of financial problems, including that of providing adequate remunerationfor full -time staff, the Government has difficulty in continuing the project after with-drawal of international assistance.
Peru 13 Sept. 1952- Public - Health Demonstration and Training Centre, CallaoTA Aim of the Project. To co- ordinate and expand public -health services in the urbanUNICEF community of Callao bordering Lima, and establish a health centre which can be
used for training health personnel and serve as a model for similar activities in otherparts of the country.
Assistance provided by WHO. A medical officer specialized in venereal -disease controland a public -health nurse, both since late 1952.
Probable Duration of Assistance. Until the end of 1955.
Work accomplished. See page 74.
142 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Peru 14 1951- Ica Health Centre (to serve rural areas around the Centre)RUNICEF
Aim of the Project. To organize a programme of general public -health servicesincluding health education, provision of water supplies, arrangements for sewage andrefuse disposal, medical care, maternal and child health services at the Centre and in thehomes.
WHO assistance, advice from a nurse and an engineer attached to the staff ofZone Office IV, is to continue indefinitely.
By the end of 1954 units for maternal and child health services had been set upin Pisco, Chinela and Nazca, as well as in Ica itself.
Peru 16 Sept. 1953- Diphtheria and Pertussis Vaccination
R Aim of the Project. To protect children throughout the country against diphtheria andUNICEF pertussis, which are highly prevalent, and to ensure the effective continuation of the
programme.Execution of the programme is facilitated by the existence of a programme of mass
vaccination against smallpox carried out by the National Health and Social WelfareFund in various parts of the country.
Assistance provided by WHO in 1954. Advisory services of staff of Zone Office IV.
Work in 1954. By the end of June, 75 319 children had been vaccinated.
1 Trinidad 1 April 1952- BCG Vaccination, Trinidad and TobagoR May 1954 Aim of the Project. To carry out a BCG campaign.
UNICEF Assistance provided. A BCG consultant (cost reimbursed by UNICEF). The BCGstatistician employed under project AMRO 31 spent some time on the recording andretesting part of the project.
Work accomplished. After two weeks spent in publicizing the campaign, testing wascarried out, first in schools, then in government offices and business houses. The totalnumber of persons tested was 337 648, over 50 per cent. of the population, and 211 923of these were vaccinated. X -ray examination of the tuberculin positives was organizedand is being carried out by the Tuberculosis Service.
Windward Islands 1
RUNICEF
Jan.-March 1954
BCG Vaccination, GrenadaAim of the Project. To carry out a BCG campaign.
Assistance provided. A BCG consultant (cost reimbursed by UNICEF). The BCGstatistician employed under project AMRO 31 spent some time on the recordingand retesting part of the project.
Work accomplished. After two weeks spent in publicizing the campaign, testing wascarried out, first in schools, then in government offices and business houses. The totalnumber of persons tested was 60 471, and 39 579 of these were vaccinated. X -rayexamination of the tuberculin positives was organized and was being carried out at theend of 1954.
SOUTH -EAST ASIA
tf Afghanistan 1 and 11 July -Nov. Malaria Control, Whole Country1949R Aim of the Project. To carry out a malaria survey and a small-scale demonstration of
TA June 1950- malaria control in the Langhman district of the Eastern Province (1949).UNICEF Dec. 1954 To demonstrate modern methods of malaria control in the Kunduz- Khanabad
area (Kataghan Province) ; to evaluate results ; to train local professional and auxiliarypersonnel (1950 -51).
To expand malaria -control operations to the different malarious areas of thecountry ; to carry out a demonstration of malaria control in Kabul city ; to set up amalaria institute in Kabul (1952 -54).
PROJECT LIST : SOUTH -EAST ASIA 143
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Assistance provided by WHO in 1954. Two malariologists, withdrawn at the end of theyear.
(For the first part of the project (1949) WHO provided two experts from July toNovember ; for the second part (1950 -51) a malariologist, an entomologist, a public -health engineer, and a malaria inspector for four months.)
Probable Duration of Assistance. Until the end of 1956 -consultant services.
Work accomplished. See page 79.
Afghanistan 2 and 10 Sept. 1950- Maternal and Child Health and Venereal- Disease Control, Whole CountryTA Aim of the Project. (a) To carry out a pilot project in maternal and child health toUNICEF investigate : the causes of the high mortality rate among infants ; the training facilities
required for student nurses ; the need for extra milk ; the prevalence of syphilis.(b) To carry out an expanded programme, including a venereal- disease control pro-gramme, first in Kabul and Herat, later throughout the country ; to establish a modelclinic at Kabul to serve as a teaching centre ; to set up a laboratory service ; to surveypopulation groups for venereal disease ; to carry out routine testing of pregnant womenand contact investigation.
Assistance provided by WHO. (a) A venereologist until March 1954, a clinical patho-logist, a laboratory technician, two public -health nurses, a paediatrician, an obstetri-cian- gynaecologist, a paediatric nurse, a nursing instructor, a midwifery tutor, and adomiciliary midwifery instructor. (b) Supplies. (c) Fellowships.
Probable Duration of Assistance. Until April 1955 according to the original plan ofoperations ; the project was redefined at the end of 1954 and a new plan of operationsfor a comprehensive project in maternal and child health in 1955 and 1956 will beprepared.
Work in 1954. A nursing school has been established for the first time. A venereal -disease laboratory has been set up. Venereal- disease clinics and maternal and childhealth centres are developing. The training schools for nursing and midwifery have beenimproved.
Afghanistan 4 Oct. 1953- School for Male Nurses, Mi -Abad Hospital, KabulR Aim of the Project. To strengthen the teaching staff of the hospital and to supplemena
teaching in lecture -rooms and hospital wards.Assistance provided by WHO in 1954. A nursing instructor until September.
Probable Duration of Assistance. Until the end of 1956.Work in 1954. Difficulties arose in connexion with the carrying -out of this project.A school to train male health workers is being planned for which a male nurse instructorand a sanitarian are to be assigned in 1955.
Afghanistan 6 Nov. 1951- Public -Health Administration, Kabul
R Aim of the Project. To improve public -health administration through the aid of apublic -health adviser to survey existing medical and public -health conditions, to help indeveloping training programmes for medical and paramedical personnel, in formu-lating plans to improve health services and in organizing and co- ordinating thedifferent programmes begun by national and international organizations.Assistance provided by WHO. A public -health adviser to the Directorate of Health.
Afghanistan 9 Nov. 1953- Tuberculosis -Control Demonstration and TrainingR Aim of the Project. To establish an organized tuberculosis service ; to train local
personnel.
Assistance provided by WHO in 19.54. A senior adviser, a public -health nurse sinceJanuary, an x -ray technician since November 1953, and a laboratory technician sinceJanuary.Probable Duration of Assistance. Until the end of 1956.Work in 1954. A modern tuberculosis clinic has been set up for the first time, and asurvey started.
144 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Afghanistan 12 Dec. 1951- Environmental Sanitation, KabulR Nov. 1952 Aim of the Project. To improve environmental sanitation.
Jan. 1954-
Afghanistan 13
R
Afghanistan 18
R
Jan. -Aug.1952Sept. 1953-
Sept. -Oct.1954
Assistance provided by WHO. (a) A public -health engineer (from December 1951 toNovember 1952 and from January 1954), to carry out the following activitities : tostart a course of training at the Teachers' Training Centre ; to assist the Ministry ofHealth in matters relating to public health, environmental sanitation, sanitaryinspectors' services and surveys ; to lecture at the Faculty of Medicine ; to assist theMalaria Institute, Kabul, in developing sanitary installations and expanding anti -typhus campaigns ; to survey the design and execution of water -supply and sanitaryinstallations ; to collaborate with the malaria -control team. (b) Teaching aids andequipment.
Probable Duration of Assistance. Until the end of 1956.
Assistance to Faculty of Medicine, University of KabulAim of the Project. To develop departments in the Faculty of Medicine and to trainnational counterparts of the visiting professors.
Assistance provided by WHO. A professor of epidemiology and social medicine in1952 (part- time), a professor of anatomy since September 1953, and a professorof physiology since March 1954. In 1954 WHO supplied teaching equipment andawarded a fellowship to the national counterpart of the professor of physiology.
Probable Duration of Assistance. Until the end of 1956.
Training Course in Vital and Health Statistics, KabulAim of the Project. To improve national vital and health statistical services, througha six -week training course in elementary techniques in vital and health statistics.
Assistance provided by WHO. Two statistical experts ; funds for translation of lecturesinto Farsi ; some equipment and supplies ; maintenance costs and half the travel costsfor trainees who came from outside Kabul. Thirty -eight students attended the course.
Work accomplished. A nucleus of statistical workers has been created.
Burma 2 April 1951- Malaria Control, Lashio, then Maymyo
TA Aim of the Project. To set up a demonstration and training centre for malaria control ;to carry out a preliminary survey ; to demonstrate modern methods of malaria control ;to train national staff ; to set up a national malaria organization.
Assistance provided by WHO in 1954. A malariologist, an entomologist and a public -health engineer.
Probable Duration of Assistance. Until mid -1956.
Work accomplished. The results of the first two years' operations, as revealed bymalariometric surveys, were very satisfactory. Malaria has been controlled in thearea and many field workers have been trained. In April 1954 the WHO team beganoperations in Maymyo. Emphasis was shifted to training personnel required forcarrying out the Government's five -year plan, which aims at protecting seven- and -a-half million people.
Burma 3 and 18 July 1951- Tuberculosis- Control Demonstration and Training, Rangoon and MandalayTA Aim of the Project. To set up a demonstration and training centre in Rangoon and aUNICEF second one in Mandalay.
Assistance provided by WHO. (a) A senior adviser and a public -health nurse sinceJuly 1954, and a laboratory technician since September 1954. (An x -ray technician willbe recruited for 1955.) (b) Equipment and supplies. (c) Fellowships.
Probable Duration of Assistance. Until mid -1956.

PROJECT LIST : SOUTH -EAST ASIA 145
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Burma 4 and 6TAUNICEF(UN)
Burma 7R
Burma 11
UNICEF
Work accomplished. WHO assistance to the Rangoon centre ended in July 1954 andthe team moved to Mandalay, where the second centre has been set up. The Rangooncentre is being continued under national control. A tuberculosis clinic has beenestablished and local staff have been trained. An adviser to the Government is to beprovided to help plan a wider tuberculosis service.
Sept. 1950- Maternal and Child Health and Venereal- Disease Control, Rangoon and Mandalay
Aim of the Project. To improve maternal and child health through aid to preventive,curative and teaching services, with emphasis on diagnosis and treatment of syphilisin mothers and children ; to develop a long -term plan of action ; to establish a sero-logical laboratory ; to train post -graduate students in modern serological techniques.
The project was redefined at the end of 1954, although the original plan of opera-tions will remain valid until the end of 1955. After that, the nursing part of the projectwill be split into three -assistance to a post -graduate school of nursing in Rangoon,provision of a nursing adviser to the Division of Nursing, and assistance to the Schoolof Nursing in Mandalay. AIso from the end of 1955 the venereal- disease control partof the project will be expanded into a provincial health project.Assistance provided by WHO in 1954. A venereologist, a serologist, a paediatrician,two nursing instructors and four public -health nurses. (The venereologist will bereplaced by a public -health officer in 1955.)Probable Duration of Assistance. Until the end of 1956.
Work accomplished. Good training facilities for undergraduate nurses have beenestablished, as well as a well -organized maternal and child health service for Rangooncity, for which local staff have been trained.
March 1953 - School of Nursing, Dufferin Hospital, Rangoon
Aim of the Project. To strengthen the teaching staff of the Dufferin Hospital -thelargest training school for midwives in Burma ; to train nurses and midwives.Assistance provided by WHO in 1954. Two nursing instructors, since March 1953 andFebruary 1954 respectively.
Probable Duration of Assistance. Until the end of 1956.Work accomplished. A sound programme has been established for training midwivesand field instructors.
Nov. 1951 -Dec. 1954
BCG Vaccination, Whole Country
Aim of the Project. To strengthen services for the protection of children and adolescentsagainst tuberculosis, by integrating BCG services into the general prevention andcontrol programme of the tuberculosis services, expanding BCG vaccination from ademonstration activity into a mass campaign, and training local personnel.Assistance provided (cost reimbursed by UNICEF). A senior BCG medical officeruntil February 1954 and a BCG nurse until December 1954.Work accomplished. The BCG -vaccination demonstration took place from the end of1951 to June 1952 ; the mass campaign followed, from July 1952 to December 1954.Ten national teams are continuing the campaign as from the end of 1954.
Burma 20 Jan. 1954- School for Health Assistants, RangoonR Aim of the Project. To improve the training of paramedical personnel and their
conditions of service.Assistance provided by WHO. (a) A specialist in medical education to advise and assistthe director of the School for Health Assistants, Rangoon, in developing a programmeof instruction for paramedical personnel, and to advise the Ministry of Health in theemployment of such personnel and recommend any suitable changes in employmentand training practices. (b) Some initial supplies and equipment. (c) Fellowships.
Probable Duration of Assistance. Until the end of 1955.Work accomplished. One hundred and twenty health assistants graduated early in1954 and were placed in rural health centres for practical training. A new class wasadmitted.
146 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Burma 26 Aug. 1954- Nutrition, Rangoon
R(FAO)
Aim of the Project. To reorganize the nutrition services and nutrition educationprogramme ; to establish a nutrition laboratory in Rangoon ; to train national personnelto carry on the work after departure of the international staff.Assistance provided by WHO in 1954. (a) A nutritionist since August. (A biochemicaltechnician will be provided in 1955.) (b) Supplies and equipment. (c) Fellowships.Probable Duration of Assistance. Until the end of 1956.
Burma 29 July -Sept. Short -Term Refresher Course in Paediatric Nursing, Rangoon General Hospital
R 1954The WHO maternal and child health staff in Rangoon helped to run a course in
paediatric nursing for nurses from hospitals in Mandalay, Maymyo, Bassein, andTaunggyi. WHO also gave maintenance and travel grants to the students.
Burma 31
TA
Ceylon 2
TA(UNESCO)
Ceylon 4TAUNICEF
Ceylon 8R.
May 1954- Strengthening of Malaria Division, Harcourt Butler Institute, Rangoon
Aim of the Project. To strengthen the Malaria Division at the Harcourt Butler Institute ;to plan expansion of malaria control work on a country -wide basis and train thepersonnel required.Assistance provided by WHO. A malariologist ; fellowships.Probable Duration of Assistance. Until the end of 1956.
March 1952 -April 1953Sept. 1954-
April 1951 -Dec. 1953Sept. 1954
Health Education of the Public
WHO's contribution to the UNESCO Fundamental Education Centre inMinneriya -the services of a health educator -was unavoidably interrupted in 1953.In September 1954 a health educator was assigned to the Central Health Directorate tohelp the Government develop the national health- education programme and he willalso give advice to the Fundamental Education Project. WHO assistance is planned tocontinue until the end of 1956.
Maternal and Child Health Demonstration Centre, Colombo and Kalutara
Aim of the Project. To develop a midwifery training programme ; to improve thepaediatric nursing service ; to give training in paediatric nursing in the basic schoolof nursing ; to develop teaching of public- health nursing.Assistance provided by WHO. (a) Two midwifery instructors and two paediatric nursinginstructors from 1951 to December 1953. (b) Two public -health nurses from September1954. (c) Fellowships.Probable Duration of Assistance. Until the end of 1955.Work accomplished. A midwifery teaching programme was prepared ; three months'practical training in obstetrics was incorporated into the basic nursing curriculum ofgeneral nurses ; in- service training for midwives, emergency nurses and staff nurses wasestablished. Lectures in obstetrical nursing were given to medical students. Instructionin paediatric nursing was incorporated into the post -graduate public -health nursingcourse. Assistance was given in improving techniques for formula preparation andin teaching care of premature babies. Interest in paediatrics and in improvement ofmidwifery practice was stimulated among members of hospital staffs, public- healthnurses and auxiliary personnel.
Seven nurses trained in Ceylon, who were awarded fellowships for study abroad,returned and by the end of 1954 were in responsible positions carrying out theprogramme which had been developed.
Oct. 1951 - Nurses' Training School, Colombo
Atm of the Project. To improve training in the School of Nursing in the ColomboGeneral Hospital (associated with project Ceylon 4- Maternal and Child HealthDemonstration Centre, Colombo and Kalutara), to which nurses are assigned forinstruction in paediatrics and midwifery.Assistance provided by WHO in 1954. A nurse educator and a public -health nursinginstructor, to assist in the School of Nursing.Probable Duration of Assistance. Until mid -1956.
PROJECT LIST : SOUTH -EAST ASIA 147
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Ceylon 9 Nov. 1951- Control of Insect -Borne Diseases -Training Centre, KurunegalaTA Dec. 1954 Aim of the Project. To improve training facilities, especially in entomology, and raise
the scientific level of the malaria field- training centre ; to investigate and co- ordinateresearch in the control of all insect -borne diseases prevalent in the country.Assistance provided by WHO. An entomologist ; some supplies and equipment.Work accomplished. A research team was formed which has given good assistance(resulting in considerable financial savings) to the field programmes for malaria andfilariasis control.
Ceylon 10 June 1951- Tuberculosis Demonstration and Training Centre, ColomboTA Aim of the Project. To train personnel in modern methods of tuberculosis control,UNICEF with the ultimate objective of establishing nine similar centres in other parts of the
island, and staffing them with personnel trained in Colombo, in order to develop acountry -wide programme. (See also Ceylon 25.)Assistance provided by WHO. An x -ray technician and a laboratory technician ;some equipment and supplies.Probable Duration of Assistance. Until April 1955.
Ceylon 15 Jan. 1952- Nurses' Training School, KandyTA Aim of the Project. To improve training of nurses and midwives at the Kandy school
of nursing and to increase the number trained ; to plan nursing education and developnursing services. (See also page 80.)Assistance provided by WHO. A paediatric nurse (later replaced by a public -healthnursing instructor) and an instructor in nursing arts ; supplies and fellowships.Probable Duration of Assistance. Until the end of 1955.Work accomplished. See page 80.
Ceylon 22 Oct. 1953-R May 1954
Ceylon 23 Nov. 1952-R Sept. 1954
Medico -Legal Consultant, Medical and Sanitary Services, ColomboAim of the Project. To maintain a high standard of medico -legal work in Colombountil a national medical officer has been suitably trained to take over the work ; totrain medical officers to carry on medico -legal work in the provinces ; to improve thequality of medico -legal work throughout the island.Assistance provided by WHO. A medico -legal consultant.Work accomplished. A survey was completed and recommendations were made forthe organization of the medico -legal services.
Medical Stores ManagementAim of the Project. To study the system of purchasing, storekeeping and distributingthe equipment, supplies and drugs required by the Department of Medical and SanitaryServices ; to organize the work of the Civil Medical Stores in assessing requirements,and in purchasing, storekeeping and distribution ; to plan better distribution of equip-ment, supplies and drugs to medical institutions ; to train an understudy to the expertprovided by WHO, and other personne'.Assistance provided by WHO. An expert in medical stores management fromNovember 1952 to September 1954.Work accomplished. The medical supply system was reorganized with much resultingeconomy.
Ceylon 25 May 1953- Tuberculosis Demonstration and Training Centre, GalleTA Aim of the Project. To co- ordinate the work of the Galle centre with that of theUNICEF Colombo centre and to use it for the intensified antituberculosis campaign (see
project Ceylon 10) ; to make an epidemiological study of tuberculosis in theSouthern Province ; to train local personnel.Assistance provided by WHO in 1954. A senior adviser, a radiographer and a public -health nurse.Probable Duration of Assistance. Until April 1955.Work in 1954. A local tuberculosis service has been organized for which staff arebeing trained.
148 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Ceylon 26 July 1954- Leprosy Control
R Aim of the Project. To improve the leprosy -control programme and leprosy research ;to develop a central leprosy clinic into a training and research centre (which could beused for international purposes) for workers in leprosy control ; to organize a systemof occupational therapy for leprosy patients.Assistance provided by WHO. A leprosy specialist and an occupational therapist ;initial equipment and supplies ; a fellowship.
Probable Duration of Assistance. Until mid -1956.
Ceylon 32
UNICEF
May 1954- BCG Vaccination
Aim of the Project. To reorganize and expand the existing BCG campaign and inte-grate BCG vaccination into the planned expansion of tuberculosis control throughoutthe country. (The campaign, previously confined mainly to schoolchildren, will coverall children, adolescents and young adults.)Assistance provided (cost reimbursed by UNICEF). A BCG nurse to assist in improv-ing the technical standard of the campaign and in training local personnel.Probable Duration of Assistance. Until the end of 1955.
Ceylon 36 May 1954- Tuberculosis Specialist, Colombo
R Assistance provided by WHO. A tuberculosis specialist as adviser to the Government,to help with the technical aspects and organization of the tuberculosis campaign andto train a national counterpart.Probable Duration of Assistance. Initially, until mid -1956.
India 2UNICEF
India 15
UNICEF
June 1953- Maternal and Child Health Department, All-India Institute of Hygiene and PublicHealth, Calcutta
Aim of the Project. To develop the maternal and child welfare section of the All -India Institute of Hygiene and Public Health into a first -class Department of Maternaland Child Health, which will provide training for nationals of India and other Asiancountries.
Assistance provided (cost reimbursed by UNICEF). A paediatric nursing instructorand a public- health nursing instructor since June 1953, an administrative officer sinceFebruary 1954, and a specialist in social medicine, a paediatrician and a health educatorsince October 1954.
Probable Duration of Assistance. Until the end of 1956.
June 1952 Cardiolipin Production, All-India Institute of Hygiene and Public Health, Calcutta
Aim of the Project. To establish a plant for the production of cardiolipin antigen.Assistance provided by WHO. Technical advice.Work in 1954. Production was commenced under the supervision of the Governmentof India's serologist, the first batch of cardiolipin -lecithin products being expectedearly in 1955.
India 19 June 1952- Nursing, Calcutta
R Aim of the Project. To develop the basic school of nursing at the Medical CollegeHospital, Calcutta, particularly as regards training in midwifery and public -healthnursing, with organization of refresher courses and staff education.
Assistance provided by WHO in 1954. Four nurse educators.Probable Duration of Assistance. Until the end of 1956.Work in 1954. In October courses in mental health were included in the syllabus ofthe school. This completed the list of basic requirements for the syllabus suggestedby the Indian Nursing Council.
PROJECT LIST : SOUTH -EAST ASIA 149
Project No.Source of Funds Dates DescriptionCo- operating Agencies
India 24 Oct. 1952- Yaws Control, parts of the States of Madhya Pradesh, Hyderabad and AndhraR Aug. 1953 Aim of the Project. To reduce the incidence of yaws to a level at which the public -TA Feb. 1954- health programme can maintain control.UNICEF Assistance provided by WHO. Advice by the Regional Adviser. A consultant in
February 1954.
India 26TA
Aug. 1952 -June 1954
Medical College, Trivandrum
Aim of the Project. To develop the newly- established medical college at Trivandrumand plan the teaching programme on sound and proper lines.Assistance provided by WHO. A principal for the college from August 1952 to June1954.
Work accomplished. In spite of difficulties due to shortage of teaching personnel, itwas possible to build up the teaching staff with professors retired from other medicalcolleges. It is expected that in future medical men returning from training abroad willbe available for teaching.
India 28 July 1951- BCG Vaccination Mass Campaign
UNICEF Aim of the Project. To protect against tuberculosis children and adolescents by(a) continuing and extending the mass BCG campaigns, and (b) integrating the BCGservices into the general preventive and control programmes of the country's tuber-culosis services.Assistance provided in 1954 (cost reimbursed by UNICEF). A senior BCG adviser,three BCG nurses, a BCG medical officer and an administrative officer.Work accomplished. By the end of 1954 the project was expanding satisfactorily andin many states national teams were operating independently.
India 29 Oct. 1952- Pharmacology, School of Tropical Medicine, Calcutta
TA Aim of the Project. To train pharmacologists both for teaching and research ; todevelop a pharmacology teaching and research centre ; to train a suitable understudyto take over from the professor provided by WHO.Assistance provided by WHO. A professor of pharmacology from October 1952 toOctober 1954. A replacement for six months from November 1954.Work accomplished. Work proceeded satisfactorily in accordance with the aims ofthe project.
A much improved department of pharmacology has been developed with emphasison research.
India 30TA(UN)
Oct. 1951 -March 1954
Pilot Studies in Family Planning, Mysore State and New DelhiAim of the Project. To carry out pilot studies in the use of the rhythm method.Assistance provided by WHO. A consultant for the initial survey- October -December1951 -and two field workers for the studies -May 1952 -March 1954.Work accomplished. One study was made among educated lower -income civil servantsin New Delhi and the other among illiterate residents of fourteen villages in MysoreState. The United Nations assisted in the planning and statistical evaluation of thesestudies. The final report and recommendations on the project were forwarded to theGovernment. The studies should help the Government to determine the next appropriatestep for national action.
India 31 July 1952- Plague Control, Uttar Pradesh
R Aim of the Project. To supplement the existing survey system ; to study procedures(Institut in use ; to carry out control work in selected areas ; to train personnel.Pasteur, Assistance provided by WHO in 1954. A consultant in May and June ; a medicalTeheran) officer (consultant) from October.
Probable Duration of Assistance. Until the end of 1956.Work in 1954. Following the visit of the consultant in May and June the project wasreorganized as follows : The plague research project will be continued for two yearsby experts from the Institut Pasteur, Teheran ; the headquarters of the project will
150 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
India 34TA
be transferred to Dehra Dun, in the North -West District of Uttar Pradesh ; thenecessary material for completely autonomous functioning of the laboratory, togetherwith transport and other items for field work, will be supplied by WHO. Activeoperations were resumed in October, when the medical officer arrived. The projectis still at the investigation stage.
Sept. 1952- Physiological and Industrial Hygiene, All-India Institute of Hygiene and Public Health,Aug. 1954 Calcutta
Aim of the Project. To undertake teaching and research in physiology and industrialhygiene ; to promote the development on sound lines of the section of physiologyand industrial hygiene of the Institute ; to guide the research undertaken by theIndustrial Health Unit of the Indian Council of Medical Research ; to train an under-study for the WHO professor.Assistance provided by WHO. A professor of physiological and industrial hygienefrom September 1952 to August 1954. (His report has been submitted to the Govern-ment.)
Work accomplished. The Industrial Health Department of the Institute has beenconsiderably strengthened and is now a good teaching centre. Emphasis has beenlaid on research ; liaison has been established with industry.
India 38 June 1954- Nursing, Ludhiana
TA Aim of the Project. To develop basic nursing education ; to train health visitors andto establish a rural training centre.Assistance provided by WHO in 1954. A nurse educator from June (A second nurseeducator will be provided in 1955.)Probable Duration of Assistance. Until the end of 1956.
India 39 April 1954- Thoracic Surgery Centre, Delhi
R Aim of the Project. To set up and equip a modern chest surgery centre at the SilverJubilee Hospital, in order to provide surgical treatment of pulmonary tuberculosisand certain other diseases of the chest ; to train surgical and medical staff, nursesand technicians in the technique of thoracic surgery.Assistance provided by WHO in 1954. (a) A senior adviser, an anaesthesiologist andan operating -room nurse from April, and a physiotherapist from June. (b) Equipmentand supplies.Probable Duration of Assistance. Until mid -195.5.
Work in 1954. Satisfactory progress was made.
India 40 Sept. 1953- Nursing, Bombay
R Aim of the Project. To extend the nursing training programme in the J.J. groupof hospitals, including improving the further training of graduate nurses and midwives ;to develop in these hospitals nursing techniques and procedures suited to local con -ditions ; to correlate theoretical teaching with the teaching in the hospital wards andto demonstrate the public -health aspects of nursing along with the curative aspects.Assistance provided by WHO in 1954. A nurse educator (senior adviser), a nursingarts instructor, a paediatric nursing instructor and a midwifery instructor ; equipmentand supplies ; fellowships.Probable Duration of Assistance. Until the end of 1956.Work in 1954. Satisfactory progress was made.
India 41 Oct. 1952- School of Physiotherapy, Kem Hospital, Bombay
TA Aim of the Project. To establish a physiotherapy centre and school which will givetraining to students from all parts of India ; to train physiotherapists for the school.Assistance provided by WHO in 1954. Two physiotherapists -one for the wholeyear and one until March ; supplies and equipment.Probable Duration of Assistance. Until April 1955.Work accomplished. A teaching department on modern lines has been created for thefirst time ; there is still much difficulty in training adequate local staff.
PROJECT LIST : SOUTH -EAST ASIA 151
Project No.Source of FundsCo- operating Agencies
India 49UNICEF
India 52
R
Dates Description
March 1954- Maternal and Child Health /Nursing, Hyderabad
Aim of the Project. To improve and expand the facilities for graduate and under-graduate training of certain categories of health personnel at selected institutionsand in urban and rural practical- training areas, with emphasis on maternal and childhealth work.Assistance provided in 1954 (cost reimbursed by UNICEF). A senior medical officersince March, and a paediatric nurse and a midwifery instructor since May.Probable Duration of Assistance. Until mid -1956.
Feb. 1953- Pharmacology, Seth G.S. Medical College, Bombay
Aim of the Project. To train medical undergraduates in pharmacology ; to workout a training programme in accordance with the requirements of the Indian MedicalCouncil ; to develop research ; to improve the Department of Pharmacology of theCollege ; to train an understudy to take over from the WHO professor.Assistance provided by WHO. A professor of pharmacology since February 1953 ;supplies and equipment ; fellowships.
Probable Duration of Assistance. Until the end of 1955.
Work accomplished. The original object was limited to the training of medical under-graduates in pharmacology. When additional equipment was provided by the Rocke-feller Foundation the scope of the project was enlarged to include the teaching ofpharmacology to post -graduate students. By the end of 1954 three members of thestaff of the Department of Pharmacology were eligible to carry on the work of theWHO expert after his departure. A six -month international fellowship was awardedto one graduate student, and the senior understudy was given two years' study leaveand a stipend to enable him to work abroad.
India 55 Nov. 1954- Maternal and Child Health /Nursing, West Bengal
R Aim of the Project. To establish new maternal and child health centres with equipmentUNICEF and supplies from UNICEF ; to improve and expand the training of health personnel ;
to establish and organize one urban and one rural demonstration and training area forschool health.Assistance provided by WHO. A public -health nurse from November 1954.
Probable Duration of Assistance. Until the end of 1956.
India 69
UNICEF
Jan. 1954- BCG Re- testing and Assessment Team
Aim of the Project. To assess the results of BCG -vaccination campaigns.Assistance provided (cost reimbursed by UNICEF). A medical officer and two BCGnurses.
Probable Duration of Assistance. The team is to return to India for three monthsduring the second quarter of 1955.Work in 1954. The team was engaged mainly in re- testing schoolchildren previouslyvaccinated in various state campaigns. A field evaluation of six consecutive batchesof Indian BCG vaccine was carried out ; Danish vaccine was included in the evaluationso that a comparison between the two vaccines would be available. Studies were alsomade of post- vaccination allergy in groups vaccinated in small campaigns or by theteam. Tuberculin studies in vaccinated and non -vaccinated groups were developedalong the lines indicated by the Tuberculosis Research Office, Copenhagen. The teamworked in Madhya Pradesh, Delhi, Assam, West Bengal, Punjab, Pepsu, Travancore-Cochin, Mysore and Hyderabad.
Indonesia 1 June 1950- Yaws Control, Jakarta and Jogjakarta (later Whole Country)TA Aim of the Project. To establish a yaws -control scheme, combined with measures forUNICEF the prevention of congenital syphilis, limited to Jakarta and Jogjakarta ; later to
extend the scheme to the whole country, using a simplified method of yaws control.

152 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Indonesia 2
TAUNICEF
Jan. 1952 -Dec. 1953Dec. 1954-
Assistance provided by WHO in 1954. A serologist for the laboratory at Jogjakarta ;a short -term consultant in February and a biostatician until August.Probable Duration of Assistance. Until the end of 1956.Work in 1954, The recommendations of the consultant, based on the evaluationsurvey which he carried out, were submitted to the Government. For further details,see page 81.
Maternal and Child Health, JogjakartaThe maternal and child health activities carried out by WHO in Jogjakarta were
suspended when the paediatrician employed under this project was withdrawn at theend of 1953. In December 1954 WHO provided a consultant in paediatrics to surveyfurther needs.
Indonesia 4 Aug. 1951- Malaria- Control Demonstration, TjilatjapTA Aim of the Project. To demonstrate malaria control (three phases- survey ; control
operations ; resurvey) ; to set up a research and demonstration centre ; to trainmedical officers, entomologists and auxiliary personnel.Assistance provided by WHO in 1954. A malariologist, an entomologist and a public-health engineer.Probable Duration of Assistance. Until the end of 1956.Work in 1954. Control measures have been established over an area with a populationof 175 000.
Indonesia 5 Jan. 1952- Institute of Nutrition, JakartaTA Aim of the Project. To organize effective programmes in nutrition education ; to
re- establish school feeding programmes ; to carry out nutrition surveys ; to carry outchemical analysis of Indonesian foodstuffs of biological material collectedin connexion with the assessment of the nutritional standards of the population.Assistance provided by WHO. A biochemical technician until June 1954, and amedical nutritionist until December 1954.Work in 1954. The training programme and research, especially on protein malnutri-tion, have continued.
Indonesia 8A Oct. 1952- BCG VaccinationTA Aim of the Project. To carry out BCG vaccination, as a preliminary for a massUNICEF campaign.
Assistance provided (cost reimbursed by UNICEF). A medical officer since October1952 and two BCG nurses since November 1953.Probable Duration of Assistance. Until the end of 1956.Work in 1954. The mass vaccination campaign was started and, by June 1954, nearlya million children had been tested by eight operating teams.
Indonesia 813 Sept. 1952- Tuberculosis- Control Demonstration and Training, BandungTA Aim of the Project. To set up a demonstration and training area for tuberculosisUNICEF control, at first in the city of Bandung but to be extended later by local personnel ; to
carry out a BCG demonstration and training programme.Assistance provided by WHO in 1954. A medical officer, a public -health nurse and alaboratory technician.Probable Duration of Assistance. Until the end of 1956.
Indonesia 13 Sept. 1953- Faculty of Medicine, Gadjah Mada University, Jogjakarta and SamarangR Aim of the Project. To develop the Faculty of Medicine on sound lines ; to train
national counterparts to take over teaching responsibilities from professors providedby WHO.
PROJECT LIST : SOUTH -EAST ASIA 153
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Assistance provided by WHO in 1954. An associate professor of biochemistry sinceSeptember 1953, a professor of pharmacy and pharmaceutical chemistry since October1953, and a professor of paediatrics since August 1954.Probable Duration of Assistance. Until the end of 1956.
Indonesia 15 Jan. 1954- Post -graduate School of Nursing, Bandung
R Aim of the Project. To organize post -graduate courses in teaching of midwifery andin public -health nursing at the Post -graduate School of Nursing, Bandung, and (forpractical training) at the Rantjabadak City Hospital.Assistance provided by WHO in 1954. (a) A public -health nurse since January, amidwifery instructor since June and a second public -health nurse since July ; (b) afellowship in midwifery ; (c) some teaching equipment and supplies.Probable Duration of Assistance. Until the end of 1956.
Nepal 1 June 1954- Malaria Control, Rhapati Valley
R Aim of the Project. To study the malaria situation and determine suitable control(FOA) techniques ; to carry out indoor spraying with DDT in areas not covered by the
Foreign Operations Administration ; to train nationals in malaria prevention.Assistance provided by WHO in 1954. A malariologist since June and an entomologistand auxiliary personnel since October.Probable Duration of Assistance. Until the end of 1956.Work in 1954. Rhimpedi in the Rhapati Valley was selected as headquarters for theproject. Progress was retarded by disruption of communications caused by heavyfloods.
Nepal 2
TA
Nov. 1954- Training of Nurses, KathmanduAim of the Project. To plan a nursing- education programme ; to set up a trainingschool for nurses.Assistance provided by WHO. Two nursing instructors since November 1954 ;teaching equipment and supplies ; fellowships.
Probable Duration of Assistance. Until the end of 1956.
Nepal 4 Oct. -Nov. Public -Health Administration Survey
R 1954 Aim of the Project. To plan a health administration in keeping with the developingneeds of the country.Assistance provided by WHO. A short -term consultant in October and November tohelp with a survey.
/ Thailand 2 Sept. 1950- Treponematoses Control
TA Aim of the Project. To carry out systematic control of yaws throughout the country ;UNICEF to reduce the reservoir of infection to a level at which the disease can be controlled by
rural health authorities ; to train local personnel ; to integrate yaws control into thepermanent public -health services. (Headquarters of the project are in Rajburi.)Assistance provided by WHO in 1954. A serologist until end of July, a public -healthnurse until September and a statistician for four months. The team leader, a venereo-logist, who was previously working on the project, left in January.Work in 1954. Satisfactory progress was made, although it was not possible to replacein 1954 the WHO team members.
Thailand 5 Feb. 1954- School Health, Chachoengsao
R Aim of the Project. To develop a comprehensive school health service in conjunction(UNESCO) with the UNESCO fundamental education project and teachers' training programme.
Assistance provided by WHO in 1954. A school -health physician since February anda school -health nurse since May.Probable Duration of Assistance. Until mid -1956.
Thailand 6 Aug. 1951- Maternal and Child Health, Bangkok
TA July 1954 Aim of the Project. To set up a public -health demonstration unit in an urban areaUNICEF to provide practical training for public -health nurses and midwives ; to provide(UN) facilities for training of undergraduate medical and nursing students and student
154 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Thailand 7
TAUNICEF
Oct. 1951 -June 1954
sanitary inspectors, and further training for medical officers of health ; to developschool health services.Assistance provided by WHO in 1954. A paediatrician, a public -health nurse, a mid-wifery supervisor and a sanitarian.Work accomplished. See page 80.
Tuberculosis Demonstration and Training Centre, Bangkok
Aim of the Project. To establish on modern lines a demonstration and trainingcentre which will serve as the nucleus of a future tuberculosis service covering diagnosis,prevention, epidemiological control and institutional isolation and treatment. To beachieved by : placing all facilities, existing and future, under one central direction ;providing a tuberculosis diagnostic laboratory, carrying out BCG vaccination ;training local personnel in modern control methods ; carrying out epidemiologicalsurveys by means of mobile and static mass radiography units.
Assistance provided by WHO in 1954. A senior adviser, an epidemiologist, an x -raytechnician, a laboratory technician and a public- health nurse.Work accomplished. Diagnostic, preventive, curative and epidemiological sectionswere established in the centre. Satisfactory progress was made with all the centre'sactivities, except in the home -visiting service, for which it became increasingly difficultto recruit national nursing staff. An extensive epidemiological survey was made,consisting partly of a house -to -house survey of certain areas of Bangkok. Radiologicalexaminations revealed a prevalence of lung tuberculosis of about five per cent., withan average of one per cent. sputum -positive cases. In connexion with the prevention oftuberculosis, emphasis was placed on isolation ; wherever space in the home permittedisolation of the patient at night, sleeping benches were set up ; where this was notpossible, other preventive measures were employed. Teaching and demonstrationprogrammes were implemented, both at the centre and at the Nonburi tuberculosishospital, for graduates and undergraduates. BCG vaccination was carried out underproject Thailand 15 (see below).
Thailand 13 Nov. 1951- Rural Health Centre, Chiengmai (Maternal and Child Health /Nursing)
TA Aim of the Project. To establish a rural health centre for improving general healthUNICEF conditions- particularly environmental sanitation and maternal and child health -
and for training local personnel.Assistance provided by WHO in 1954. A public -health adviser (specialized in maternaland child health), two public -health nurses and, since May, a sanitarian.Probable Duration of Assistance. Until the end of 1955.
Thailand 15 May 1953- BCG Vaccination
UNICEF Aim of the Project. To carry out a mass BCG- vaccination campaign, testing at leastfive million young persons and vaccinating negative reactors.Assistance provided (cost reimbursed by UNICEF). A medical officer and a BCGnurse from May 1953, and a second BCG nurse from September 1954.
The BCG assessment team (see India 69) also worked on the project for threemonths in 1954.
Thailand 21 April 1954- Post -graduate School of Nursing, Bangkok
TA Aim of the Project. To establish a post -graduate school for nurses ; to organizepost -graduate courses in public -health nursing.Assistance provided by WHO. A nursing instructor ; some teaching supplies andequipment ; two fellowships.
Probable Duration of Assistance. Until the end of 1956.
PROJECT LIST : EUROPE 155
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Thailand 24 June 1954- Rural Health ProgrammeR Aim of the Project. To develop rural health services, including nursing ; to provide(FOA) adequate guidance and supervision of nursing and midwifery services.
This project is closely associated with the UNICEF project for development andstrengthening of maternal and child welfare centres in Thailand.Assistance provided by WHO. A public -health nurse /midwife.
EUROPE
EURO 6 1951 -54 Study on Health Visitors (Family Health and Welfare Workers) *R(RockefellerFoundation)
EURO 9.4R(RockefellerFoundation)
EURO 9.5R
21 -30 April Conference on Water Pollution and Water Chlorination, Opatija *1954
12 -13 Oct.1954
Ad hoc Committee of Sanitary Engineers, BrusselsTo review the work of the conference on water pollution (EURO 9.4) and prepare
for the next meeting in Helsinki in 1956.
EURO 12.3 15 March- Public -Health Administration Study Tour, Germany and Italy *R 15 April
1954
EURO 25.2 11 -12 June Ad hoc Committee on Health Education, LyonsR 1954 Nine public -health experts met to prepare the Second European Conference on
Health Education of the Public (date of conference not yet determined).
EURO 40.2 14 -19 June Conference on School Health Services, Grenoble *R 1954
EURO 43 2 -11 Sept. Study- Conference on Care of Children in Hospitals, Stockholm *
R 1954
EURO 45 22 March- Training Course for Waterworks Engineers, The Hague and Liége *
R 10 April1954
EURO 47R
EURO 50R
EURO 52RTA
15 -20 March Conference on Immunization, Frankfurt -am -Main*1954
22 -27 Feb.1954
Seminar on Meat Hygiene, Copenhagen *
Aug. 1954- Fifth Basic Post -graduate Course for Anaesthesiologists, Copenhagen *
* For details, see Table II, p. 86.
156 THE WORK OF WHO, 1954
Project No.Source of FundsCo- operating Agencies
EURO 56TA
Dates Description
22 Nov. -18 Dec. 1954
Tuberculosis Training Courses, Istanbul *
EURO 59 1950- Port Demonstration and Training Centre for Control of Venereal Disease, Rotterdam *R
EURO 59R
EURO 60R
EURO 61R(InternationalChildren'sCentre)(RockefellerFoundation)
EURO 62R
EURO 63R(RockefellerFoundation)
18 Oct.- Training Course in Venereal Disease Control, Rotterdam *11 Dec. 1954
1 Aug. -30 Sept. 1954
Training Course for Scandinavian Public -Health Officers, Göteborg *
1950- Rural Public -Health Training Centre, SoissonsA new centre to provide facilities for national and international training.WHO has awarded fellowships to the staff of the centre, provided some teaching
supplies, and financed the statistical services.
May 1953 -April 1954
April 1952 -Dec. 1954
Training Course for Anaesthesiologists, Paris *
Morbidity Survey, DenmarkA pilot survey of international interest.WHO has provided consultant services, awarded fellowships for staff engaged in
statistical survey, and provided equipment.A final report on the survey is expected to be available in 1955.
EURO 64 Nov. 1952- Mother and Child Separation Study, France, United Kingdom *R(InternationalChildren'sCentre)
EURO 65R(UNESCO)
EURO 66R
EURO 67R
EURO 72TA
EURO 73R(HighCommissionerfor Refugees)
June 1953- Study of Sanitary Engineering TermsA study designed to develop an accepted terminology (in French and English)
for use in Europe.The project is expected to be completed in 1955.
26 Sept. -26 Oct. 1954
28 March -10 April1954
17 -31 Oct.1954
Aug. -Nov.1954
* For details, see Table II, p. 86.
Study on Water StandardsA WHO consultant prepared a report reviewing the situation with regard to
standards of water quality and methods of analysis, and containing proposals for futureaction.
Planning continued in 1954 for the second meeting of the Study Group on WaterStandards, to take place in 1955, for which a consultant will carry out technical pre-paratory work.
Seminar on Prevention and Treatment of Alcoholism, Noordwijk, Netherlands *
Seminar on Public -Health Nursing, Istanbul *
Pilot Study on Mental Health of Children living in Refugee Camps, AustriaA WHO team of four experts recruited by the Institute of Preventive Medicine,
Leyden, surveyed the situation in refugee camps. Their report has been submitted tothe High Commissioner for Refugees.
PROJECT LIST : EUROPE 157
Project No.Source of Funds Dates DescriptionCo- operating Agencies
EURO 74.1 11 Jan.- Training Course on Rehabilitation of Handicapped Children, Paris *R 21 Feb.(International 1954
Children'sCentre)
EURO 74.3R(InternationalChildren'sCentre)
EURO 74.4R(InternationalChildren'sCentre)
EURO 76R(UNESCO)
EURO 78R(TAA)
EURO 81R(TAA)
EURO 82R
EURO 94R
26 April -18 July 1954
4 Oct. -6 Nov. 1954
5 -10 April1954
26 May-5 June 1954
Training Course on Social Paediatrics, Paris *
Training Course on Prevention of Tuberculosis in Children, Paris *
Conference on Psychological Services for Schools, HamburgA conference on psychological services for schools and other institutions, held
for specialists in child psychology. WHO provided two lecturers.
Seminar on Foster -Home Care, ParisA WHO consultant lectured and took part in group discussions.
2 -12 Oct. Seminar on the Rehabilitation of Physically Handicapped Adults, Belgrade1954 WHO contributed a lecturer on the mental aspects of rehabilitation.
4 -5 June Ad hoc Committee on Mental -Health Aspects of Public- Health Practice, Geneva1954
19 Sept. -11 Dec. 1954
The committee advised on preparation for a study group which is to meet in 1955.
European Survey of Institutions for Training Sanitary EngineersA consultant surveyed European institutions for the training of sanitary engineers,
as a basis for a symposium on the training of sanitary engineers to be held in 1955.
n Austria 4.2 Dec. 1952- Tuberculosis Control
TA Aim of the Project. To strengthen tuberculosis -control services in order to reducethe relatively high morbidity rate in the country.Assistance provided by WHO. Fellowships for key personnel ; supplies and equip-ment.
Work in 1954. Three fellowships were completed (one of six months, for study ofclinical tuberculosis in the United States of America ; one of three months, for studyof tuberculosis bacteriology in Denmark ; one of two months, for study of thoracicsurgery in Germany). In October a fellow started a six -month study of tuberculosisrehabilitation in the United Kingdom. Two further fellowships, each of three months'duration, were awarded at the end of the year for studies in 1955 ; the project will endwhen the recipients have completed their studies.
Austria 4.5 Nov. 1952- Rehabilitation of Handicapped Children, Wiener Neustadt
R Aim of the Project. To strengthen and extend existing facilities for the care of physicallyUNICEF handicapped children ; to establish a rehabilitation centre in the Waldschule, in Wiener
Neustadt.Assistance provided by WHO. A consultant physiotherapist ; fellowships for membersof the staff of the centre.
* For details, see Table II, p. 86.
158 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo-operating Agencies
Work in 1954. In May a six -month fellowship for study of rehabilitation (poliomyelitisand other neurological conditions) in the United States of America and the UnitedKingdom was completed. A physician of the Wiener Neustadt Centre started a six -month fellowship for study of rehabilitation in the United Kingdom in November.A fellowship was awarded for study in 1955.
Austria 4.6 Nov. 1952- Mental Health, ViennaR Aim of the Project. Initially, to establish a new juvenile epilepsy diagnostic and treat -UNICEF ment centre in Vienna, equipped with UNICEF supplies and run by personnel trained
through WHO fellowships. (The project was subsequently expanded to include othermental -health services for children.)
Work in 1954. Two consultants each delivered lectures for one month at the ChildGuidance Clinic in Vienna. A fellowship for the study of neurology in the UnitedStates of America was completed in July. A second fellow completed a study ofpsychiatric nursing in the United Kingdom in October.
Austria 4.10 Sept. 1954- Sera and Vaccine ProductionTA Aim of the Project. To improve and increase production of sera and vaccines for theUNICEF protection of children from childhood diseases ; to reach the highest technical
standards of quality and to produce sufficient quantities to protect adequately allAustrian children.Assistance provided by WHO. Consultant services of experts in sera and vaccine pro-duction and in epidemiology ; fellowships.Work in 1954. A consultant visited Austria to advise on production of immunologicalsubstances and the use of the material provided by UNICEF. A fellowship was awardedto a member of the Austrian State Serum Institute.
Greece 3
RUNICEF(TAA)(ILO)
Sept. 1952 -Nov. 1954
Rehabilitation of Handicapped Children, Voula
Aim of the Project. To extend diagnostic, treatment and rehabilitation services forphysically handicapped children by co- ordinating and improving existing facilities ;increasing the number of trained personnel ; centralizing the direction of a programmeof services for physically handicapped children.Assistance provided by WHO in 1954. A medical- director consultant (from May toNovember) and a physiotherapist consultant (until the end of July).Work in 1954. The Voula Centre for physically handicapped children was officiallyopened in July and a number of children were admitted. The physiotherapist consultantassisted with teaching at a second training course in physiotherapy.
Greece 4 Sept. 1952- Maternal and Child Health, ThessalyTA Aim of the Project. To establish and expand maternal and child health services andUNICEF provide mobile units for rural areas, to be attached to permanent health centres in
Thessaly.
Assistance provided by WHO in 1954. A social paediatrician consultant for one month(October- November).
Probable Duration of Assistance. Until 1956.Work in 1954. The consultant submitted proposals on ways of using the expandingfacilities to the best advantage.
Greece 5 March 1954 - School of Hygiene, AthensR Aim of the Project. To develop post -graduate education in public health at the School
of Hygiene, Athens.Assistance provided by WHO in 1954. A consultant in March.Work in 1954. The consultant advised the Ministry of Health and the direction of theSchool of Hygiene on the development of post -graduate training.
PROJECT LIST : EUROPE 159
Project No.Source of FundsCo- operating Agencies
Greece 6.1
TA
Dates Description
June 1952- Tuberculosis Control
Aim of the Project. To develop a tuberculosis -control programme as part of thecountry's public -health service ; to establish regional control areas ; to develop theAthens Chest Institute as a national training centre for Greek tuberculosis workers.Assistance provided by WHO. In 1952, services of two consultants ; a small amount ofsupplies for the Athens Chest Institute. In 1954, further supplies, procurement of amobile x -ray unit ; two fellowships for studies to begin early in 1955.
A public -health tuberculosis officer will be assigned to the project early in 1955.
Italy 5 Sept. 1952- Rehabilitation of Handicapped Children, Rome and Parma
R Aim of the Project. To set up physiotherapy departments in Rome and Parma ; toUNICEF develop a general rehabilitation scheme.
Assistance provided in 1954. A consultant in physiotherapy (cost reimbursed byUNICEF) ; fellowships.Probable Duration of Assistance. Until 1956.Work in 1954. The consultant gave a course for sixteen physiotherapy students whichended in March. His final report was submitted to the Government. A fellowship wasawarded to a member of the Rizzolo Orthopaedic Institute, Bologna, for three months'study in the United Kingdom of problems related to the rehabilitation of crippledchildren.
Italy 9 Oct. 1952- Public -Health Training School, Rome
R Aim of the Project. To set up and develop a new school of public health in Rome forpost -graduate education and research in public -health fields.
Assistance provided by WHO. Since 1952, teaching equipment and medical literature.In 1954, further medical literature ; fellowships for two members of the teaching staff.
A visiting lecturer will be assigned to the project early in 1955.
Italy 15 Sept. 1953- Health Education, PerugiaR Aim of the Project. To improve health education by a demonstration centre in the
Perugia area.Assistance provided by WHO. Teaching equipment ; fellowships for staff membersholding responsible positions at the centre.
Probable Duration of Assistance. Until 1956.Work in 1954. The formal opening of the experimental centre took place in June.WHO gave technical advice for the project and supplied visual aids material.
1, Morocco 1 March 1953- Communicable Eye Diseases (Trachoma) Control
TA Aim of the Project. To control trachoma and communicable eye diseases by : an in-UNICEF tensive campaign, on an area basis, against seasonal acute conjunctivitis ; systematic
treatment of trachoma in schools ; health education of the public ; a programme fortreatment of complications of conjunctivitis and trachoma in existing health centres.Assistance provided in 1954 (cost reimbursed by UNICEF). An ophthalmologistand a sanitary engineer since January, and a statistician (from June to December) ;fellowships.
Probable Duration of Assistance. Until May 1955.Work in 1954. About 31 000 trachomatous children in schools (12 000 in Marrakechand 19 000 in Casablanca) were treated with antibiotics. A statistical evaluation of theresults of the operation was started towards the end of the year. A field campaignagainst seasonal acute conjunctivitis in the Tafilalet and Ouarzazate territories wasstarted in July. A group of sixteen villages in the Goulmina sector of Tafilalet wasselected for a detailed comparative study of three basic control measures-collectivechemotherapy of carriers during the pre- epidemic period, collective antibiotic treatmentduring the epidemic season, and fly control.
Five fellowships, of two or three months' duration, were awarded and three werecompleted during the year.
160 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Morocco 2
TAUNICEF
Aug. 1954- Venereal -Disease Control
Aim of the Project. To reduce the prevalence of syphilis generally and limit its spreadto the rural population.Assistance provided by WHO. Visiting experts and fellowships (in accordance with therecommendations of a WHO consultant who made a preliminary survey in 1953).Work in 1954. Two WHO fellows completed their studies (one month and two monthsrespectively.) A third fellowship was awarded for studies in 1955. The recruitment of aphysician serologist was postponed until 1955.
V' Netherlands 4 Oct. 1952- Public -Health Training Centre, Amsterdam and Leyden
R Aim of the Project. To develop the public- health training centre (grouping the Nether-lands Institute for Preventive Medicine, Leyden, the Institute for Tropical Hygiene ofthe University of Amsterdam, and the Institute for Tropical Medicine of the Universityof Leyden).
Assistance provided by WHO. Visiting lecturers, teaching supplies and fellowships formembers of the teaching staff of the centre.
Work in 1954. In April the Director of the Regional Office for the Eastern Mediter-ranean lectured and conducted seminars at the centre. Two members of the teachingstaff of the centre completed WHO fellowships. Supplies and medical literature wereprovided.
Portugal 10 Sept. 1954 Rabies Vaccine Production, Lisbon
R A WHO consultant spent September in Lisbon assisting Portuguese workers in theproduction and control of rabies vaccine. His report was submitted to the Government.
Portugal 12 Oct. 1954 Training Course in Sanitary Engineering, Lisbon
R To give additional training in sanitary engineering, particularly to municipalengineers responsible for sanitation services.
A two -week training course was held in October -November. WHO provided twolecturers, stipends for twenty trainees and some educational and training material.
\I Spain 1 May 1952- Endemo -epidemic Diseases
TA Aim of the Project. To reduce the prevalence of tuberculosis, the zoonoses and otherendemo -epidemic diseases.
Assistance provided by WHO. Consultant services ; supplies and equipment ; fellow-ships.
Work in 1954. A consultant visited the rice -fields in the south of Spain to assist indetermining the extent of leptospirosis. Fellowships were awarded for studies inbrucellosis, insect control, tuberculosis, malaria, venereal diseases, zoonoses andquarantine practice. Medical supplies were delivered.
Tunisia 3 Nov. 1953- Communicable Eye Diseases (Trachoma) Control
TA Aim of the Project. To undertake a campaign against seasonal acute conjunctivitis ;UNICEF to carry out systematic treatment of trachoma in schools.
Assistance provided in 1954 (cost reimbursed by UNICEF). An ophthalmologist-team leader -(since November 1953) and a bacteriologist (since Februar 1954).Probable Duration of Assistance. Until 1956.
Work in 1954. Treatment with antibiotics of about 9000 trachomatous children inschools on the Island of Djerba was completed in June. Results were evaluated inOctober and November.
The first phase of the mass campaign against seasonal acute conjunctivitis, inwhich 181 000 persons received treatment, was completed at the end of July. Thesecond phase began in September.
PROJECT LIST : EUROPE 161
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Turkey 6 Sept. 1952- Maternal and Child Health, AnkaraTAUNICEF
Turkey 8TA
Aug. 1952 -Aug. 1954
Aim of the Project. To train maternal and child health workers in a demonstration andteaching centre to be established in Ankara, as a first step towards the development ofmaternal and child health services in Turkey as part of the public -health service.
Assistance provided by WHO in 1954. A social paediatrician (team leader), a public -health nurse and a midwife (all since September) ; fellowships.
Probable Duration of Assistance. Until 1957.
Work in 1954. A WHO fellow began a twelve -month fellowship in maternal and childcare in April ; two further fellowships were awarded for studies to begin in 1955.
School of Nursing, AnkaraAim of the Project. To develop existing and establish new schools of nursing andmidwifery and to include public -health nursing in the curriculum ; to organize apost -graduate course for graduate nurses at the School of Nursing in Ankara.Assistance provided by WHO. A public -health nurse instructor and a midwiferyinstructor (August 1952 to August 1954) ; fellowships.
Work accomplished. The instructors gave two courses in nursing education and trainednurse educators, some of whom were in teaching posts by the end of 1954. Suppliesand equipment were provided. Except for continuing fellowships, the project endedwith the withdrawal of the team in August 1954.
Turkey 13 1952- BCG Vaccination
UNICEF Aim of the Project. To carry out a campaign of BCG vaccination of children and youngadults, and to establish an evaluation unit ; to lay the foundations for a permanentnational BCG -vaccination service by demonstration of methods and training localpersonnel.
Assistance provided in 1954 (cost reimbursed by UNICEF). A BCG nurse -adviser-until June.Probable Duration of Assistance. Until the end of 1955.
The WHO nursing adviser assisted the special evaluation team in its work inBursa, Balikesir, Aydin, Erzurum, Kastamonu, Sinop and Izmir.
Turkey 16 July 1953- Public -Health Training School, Ankara
TA Aim of the Project. To improve post -graduate training at the Public -Health TrainingSchool in Ankara.Assistance provided by WHO in 1954. Three lecturers -in epidemiology, environmentalsanitation and health education.Probable Duration of Assistance. Not determined.Work in 1954. A course for medical officers was held from 29 March to 26 June, atwhich a WHO consultant gave lectures and conducted seminars on epidemiology.A second course was held from 16 August to 27 October.
Turkey 22TA
Turkey 24TA(UN)(ILO)
June 1953 -Nov. 1954
Hospital Construction
Aim of the Project. To improve hospital planning, construction and installation.Assistance provided by WHO in 1954. A medical consultant and an architect for twomonths and an engineer for one month.Work in 1954. Advice was given to the Public Health Department and the TurkishWorkers' Medical Insurance on the construction of various hospitals.
Aug. 1953- Vital and Health StatisticsAim of the Project. To improve vital and health statistics.Assistance provided by WHO. A consultant statistician from September 1953 toSeptember 1954.
Probable Duration ofAssistance. Until 1956.
162 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Work in 1954. With the support of the Central Statistical Office, the consultant finishedsetting up vital statistics sample units. Some of the units had completed their initialsurveys by the end of May.
Yugoslavia 2 1950- Congenital Heart DiseaseR In 1954 WHO supplied x -ray films and awarded two fellowships for further training
in cardiology and radiology, as a continuation of the work of the WHO team which,in 1950, demonstrated new techniques for diagnosis and surgery of heart disease inchildren.
The project will end when the fellows have completed their studies.
Yugoslavia 16.1 1953- Endemo -epidemic Diseases
TA Aim of the Project. To reduce the prevalence of enteric diseases, typhus, Q fever,trachoma, pellagra, diphtheria and other endemo- epidemic diseases which still presenta serious problem in Yugoslavia.Assistance provided by WHO in 1954. A consultant on endemic goitre and pellagra, forone month ; fellowships.
Probable Duration of Assistance. Until 1956.
Work in 1954. The consultant visited areas where endemic goitre and pellagra areprevalent. His report was submitted to the Government.
Three WHO fellows started their studies during the year and four further fellow-ships were awarded for studies in 1955.
Yugoslavia 16.4 1953- Tuberculosis Control
TA Aim of the Project. To develop national antituberculosis services.Assistance provided by WHO. Consultant services (the visit of a consultant is plannedfor 1955) ; supplies and equipment ; fellowships.
Work in 1954. A WHO fellow started a six -month course of study in thoracic surgery.Three more fellowships were awarded for study in 1955 of tuberculosis control andrehabilitation, pulmonary tuberculosis and bone tuberculosis.
Yugoslavia 16.9 Dec. 1953- Maternal and Child HealthTA Aim of the Project. To expand the maternal and child health services, principally byUNICEF increasing the maternity consultation centres, infant -welfare centres and facilities for
training nurses and midwives.Assistance provided by WHO. Consultant services and fellowships (in accordance withthe recommendations of WHO consultants who made preliminary investigations in1952 and 1953). Visits of short -term lecturers for national training centres are plannedfor 1955.
Work in 1954. A paediatric nurse completed a three -month fellowship in public -healthnursing and a second fellowship was awarded for studies in 1955.
Yugoslavia 16.11 1954- Vital and Health StatisticsTA Aim of the Project. To improve vital and health statistics services.
Assistance provided by WHO. Two fellowships for studies in the United Kingdom.A consultant will be provided in 1955.
Yugoslavia 16.12 1954- Social and Occupational HealthTA Aim of the Project. To reduce accidents and raise the standard of the health of workers
in industry by introducing appropriate measures, improving safety and ventilationdevices, improving the diet of workers and establishing regional laboratories forindustrial hygiene.
Assistance provided by WHO. Fellowships, in accordance with the recommendationsof a WHO consultant who made a preliminary visit in 1952.Work in 1954. A WHO fellow started six months' training in the United Kingdom.Three further fellowships were awarded for studies in 1955.
PROJECT LIST : EASTERN MEDITERRANEAN 163
Project No.Source of Funds Dates DescriptionCo- operating Agencies
EASTERN MEDITERRANEAN
EMRO 5 Oct. 1953- Regional College of Nursing, Faculty of Medicine, University of Alexandria
TA Aim of the Project. To raise the standard of nursing and nursing education in Egyptand other countries of the Region by : establishing a college of nursing for studentsfrom Egypt and other countries of the Region ; promoting study and research in nursingin the Region ; and providing assistance in the solution of nursing problems.Assistance provided by WHO in 1954. A senior nurse educator as director of thecollege, since October 1953, and a public -health nursing instructor and a nursing artsinstructor since September 1954 ; a two -year fellowship for an Egyptian nursinginstructor for study in the United States of America. (Further staff and fellowships willbe provided in 1955.)Probable Duration of Assistance. Not yet determined, but is expected to last severalyears, staff being provided until the end of 1956.Future work. The College is expected to open in January 1955. The Organization willfill thirty per cent. of vacancies for students with suitably qualified candidates fromcountries in the Region.
EMRO 7 May 1953 - Arab States Fundamental Education Centre, Sirs -el- Layyan
TA Aim of the Project. A UNESCO project to train national staff from all Arab States in(UNESCO) the principles of fundamental education.
Assistance provided by WHO. (a) A medical officer since May 1953 and a healtheducator from September 1953 to August 1954, to provide instruction in health aspectsof fundamental education and in health education of the public. (b) Fellowships fornationals of five Arab countries in the Region.Probable Duration of Assistance. At least until May 1955.
EMRO 14 Oct. 1954- BCG Assessment Team, Libya, Egypt, Iran, Cyprus
UNICEF Aim of the Project. To assess the results of mass BCG- vaccination campaigns and toprovide information for future campaigns.Assistance provided (cost reimbursed by UNICEF). A BCG medical officer and twoBCG nurses.Work in 1954. First in Libya, then in Egypt, the team studied tuberculin allergy ofchildren vaccinated with BCG, in order to evaluate the results of the mass campaigns ;it also studied the difference in intensity of tuberculin allergy in unvaccinated childrenand adults, as a guide for future BCG- vaccination campaigns. In December the teammoved to Iran for five months.Future work. In Iran the team will collect information on : (a) allergy produced byBCG vaccination carried out in the mass campaign ; (b) the pattern and prevalence ofnaturally acquired tuberculin sensitivity in all age -groups ; (c) the capacity to react(allergy production and local lesion) of the population to BCG vaccination carried outby the team ; (d) tuberculin sensitivity in tuberculosis patients ; (e) special problemsconnected with tuberculin sensitivity ; (f) results of simultaneous vaccination againsttuberculosis and against smallpox (see also project Iran 11).
'Cyprus 1 Sept. 1954- Nursing Education, Nicosia
R Aim of the Project. To develop modern methods of nursing education in the school ofnursing to be set up in the General Hospital, Nicosia, in order to provide graduatenurses for the island's health services.Assistance provided by WHO. A nursing instructor from September 1954.Probable Duration of Assistance. Until September 1956.
164 THE WORK OF WHO, 1954
Project No.Source of FundsCo- operating Agencies
Egypt 5TA
Egypt 6R
Egypt 9UNICEF
Dates Description
Aug. 1953- Health Demonstration Area, CalioubAim of the Project. To organize a programme of health services in a selected ruralarea, to study and demonstrate methods of correlating them with services for social andeconomic development and to evaluate results in terms of the effect on health andsocial and economic status of the population ; to demonstrate methods of local healthadministration suited to the needs of the area ; to provide field training in rural healthto technical personnel from Egypt and other countries.Assistance provided by WHO in 1954. A public -health administrator, as senior adviser,since October, a public -health engineer since February, an epidemiologist since April1953, a health educator since January 1953, two public -health nurses since October 1953and a statistician since December 1953. (Additional staff will be provided in 1955.)The consultant on fly control employed on project Egypt 31 worked on the projectfrom September to December.Probable Duration of Assistance. Until the end of 1956.Work accomplished. A pilot census has been completed and analysed and a full censuswas being carried out at the end of 1954, and surveys of health conditions. Water -supply and excreta -disposal schemes have been started, the latter with the assistanceof the Foreign Operations Administration (FOA). FOA has also begun a healtheducation project, with which WHO assists by giving guidance to teachers. At the endof 1954 consideration was being given to co- ordinating the WHO- assisted work oncontrol of bilharziasis and communicable eye diseases with the FAO programme inthe area.
Dec. 1952 -Feb. 1954
July 1951 -March 1954
Trachoma Research, Memorial Ophthalmic Laboratory, GizaAim of the Project. To carry out research on trachoma and teaching at the MemorialOphthalmic Laboratory, Giza.Assistance provided by WHO. A virologist ; some equipment and supplies ; one fellow-ship.
Work accomplished. Research work was made difficult by a lack of equipment, butprogress was made in the reorganization of the laboratory. It was not possible forthe Government to provide a virologist as counterpart to the WHO expert ; however,two assistants were trained, one of whom was granted a fellowship for study abroad.
BCG VaccinationAim of the Project. To continue a mass BCG- vaccination campaign.Assistance provided in 1954. A BCG nurse since November 1953 (cost reimbursed byUNICEF).Work in 1954. From November 1953 to March 1954 the BCG nurse worked with theGovernment's BCG evaluation team and helped to train three Egyptian nurses in thetechnique of tuberculin re- testing.
Egypt 10 Nov. 1952- Bilharziasis Control, Calioub Province
TA Aim of the Project. To demonstrate the effect of co- ordinated effort in the control ofbilharziasis in a selected community in the south -west part of Calioub Province(measures include health education, sanitation, snail destruction and treatment of cases).
Assistance provided by WHO. A malacologist for certain periods each year sinceNovember 1952 and a full -time public -health engineer since December 1953.
Probable Duration of Assistance. Until the end of 1956.Work in 1954. Studies of the effect of copper sulfate in snail destruction and the ecologyof snail colonies were continued and an investigation was made into sanitation methodsin the area. Treatment of cases continued but results were poor.
As a result of this work it has been decided to redefine the project, selecting anew area and stressing field investigations.
PROJECT LIST : EASTERN MEDITERRANEAN 165
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Egypt 20 Aug. 1952- Tuberculosis -Control Demonstration and Training Centre, Cairo
TA
Egypt 21R
Egypt 31R
Feb. -April1954
Sept. -Dec.1954
Aim of the Project. To establish a regional demonstration and training centre for allaspects of prevention, diagnosis and treatment of tuberculosis, and to co- ordinateexisting tuberculosis -control services and provide new ones. The centre will teach anddemonstrate modern methods of tuberculosis control and assist in establishing adiagnostic laboratory service.Assistance provided by WHO in 1954. A tuberculosis specialist (team leader)and a laboratory technician, an epidemiologist until July, a bacteriologist until Augustand a public -health nurse and an administrative assistant until June. (A second public -health nurse was provided until December 1953.)
Probable Duration of Assistance. Until the end of June 1955.Work in 1954. The work of the centre was firmly established and WHO staff weregradually withdrawn, the team leader remaining in an advisory capacity. Reports onsurveys made in Cairo city and the Calioub demonstration area during the year willbe published in 1955.
Pellagra SurveyAim of the Project. To evaluate the different local factors which influence the courseand clinical manifestations of pellagra, in connexion with a comprehensive survey beingcarried out ; to determine suitable control measures.Assistance provided by WHO. Three consultants for three months.Work accomplished. From February to April 1954 the consultants made their survey.Their report and recommendations were submitted to the Government.
Insecticides and Insect ResistanceAim of the Project. To study resistance of certain insects to insecticides.Assistance provided by WHO. A consultant for three months.Work accomplished. The consultant carried out a study from September to December1954 ; his report was submitted to the Government.
1 'Ethiopia 3 Oct. 1952- Public -Health Administration, Addis Ababa
R Aim of the Project. To improve public -health administration generally (includinghospital administration, statistical services, epidemiology and epidemiological reportingand research, nutrition, control of infectious diseases, medical laboratories andresearch institutions, environmental sanitation in urban and rural areas) and in-corporate these and other services in a long -term basic health programme.Assistance provided by WHO. A public -health administrator since October 1952.
Probable Duration of Assistance. Until the end of 1955.
Ethiopia 4 June 1952- Venereal- Disease Control, Addis Ababa (later Whole Country)
TA Aim of the Project. To make available modern methods of venereal -disease controland investigate the epidemiology of venereal ',diseases throughout the country ; toevaluate the results of control work ; to train personnel and establish a centrallaboratory at one of the venereal -disease clinics in Addis Ababa.Assistance provided by WHO in 1954. A senior adviser and a serologist until May, anda public -health nurse ; a successor to the senior adviser was appointed in August.
Probable Duration of Assistance. Until the end of 1956.Work accomplished. Work was started in Addis Ababa. When sufficient personnelhave been trained they are to be sent to work in health centres in other parts of thecountry. The senior adviser appointed in August 1954 was mainly occupied inreorganizing the centre in Addis Ababa and in elaborating plans for 1955.Future work. It is hoped with the participation of UNICEF to start an expandedprogramme of treatment in 1955, starting with expectant mothers.

166 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Ethiopia 5 Jan. -Dec. Yellow -Fever Survey, Shoa Province
R 1954 Aim of the Project. (a) To organize and carry out a yellow -fever survey in the ShoaProvince and later in the parts of Ethiopia situated to the south and west of the pro-vince. (b) To extend the survey to the northern part of Ethiopia and to Eritrea. Thesurvey is being made by the staff of the Institut Pasteur, Addis Ababa.Assistance provided by WHO. A grant of $2000 to cover expenses.
Ethiopia 8 April 1953- BCG Vaccination
UNICEF Aim of the Project. To organize and carry out tuberculin testing of persons undertwenty and to vaccinate non -reactors with BCG ; to found a permanent BCG- vaccina-tion service within the general tuberculosis -control service by demonstrating methodsand training local personnel.Assistance provided in 1954 (cost reimbursed by UNICEF). A senior BCG adviser, anadministrative officer, two BCG nurses, a medical officer and a laboratory technician.In 1955 only a medical officer, a nurse and the administrative officer will be retained.Probable Duration of Assistance. Until the end of 1955.
Ethiopia 9 March 1954- Training of Auxiliary Health Workers, Gondar
R Aim ofthe Project. To train auxiliary personnel at a centre to be established at Gondar ;UNICEF to develop model health services for the Province of Begemeder and the town of
Gondar ; to determine the local pattern of diseases by epidemiological investiga-tions ; to extend health services throughout the country ; eventually to expand theteaching facilities of the centre at Gondar so that professional staff may be trainedthere.
Assistance provided by WHO in 1954. An epidemiologist (team leader) since March, apublic -health engineer since October, and a public -health nurse since May.
Probable Duration of Assistance. Until mid -1957.
Work in 1954. Training of health officers began in September.
Iran 2 Dec. 1952- Control of Insect -Borne Diseases, Sabzawar
TA Aim of the Project. To control insect -borne diseases in a selected area, by a pilotproject using modern insect -control methods.Assistance provided by WHO in 1954. A public -health engineer, an epidemiologist(team leader) since January, and a laboratory technician since April ; an entomologistfrom January to June.Probable Duration of Assistance. Until the end of 1955.Work accomplished. It was not possible to carry out the pilot project at the sitesoriginally selected (Rizaiyeh and Hamadan) and some months were spent searchingfor a suitable area, i.e., one in which several insect -borne diseases were prevalent andwhich had never been sprayed with residual insecticides. Sabzawar was chosen inMay 1954. A revised plan of operation was being negotiated at the end of 1954.
Iran 4 Nov. 1952- Venereal- Disease Control, Teheran
TA Aim of the Project. (a) To expand and intensify the control of venereal diseases inTeheran and the neighbourhood of the city by : establishing a venereal- disease centre inTeheran with a laboratory to perform serological tests and train serologists andtechnicians ; training professional and technical personnel (including a team to takeover from the WHO personnel) in modern control methods. (b) To intensify controlactivities in other parts of the country by establishing venereal -disease centres.(c) Eventually, to control venereal disease throughout the country by a mass campaign.
Assistance provided by WHO in 1954. A venereologist, a serologist and a public -healthnurse.
e
PROJECT LIST : EASTERN MEDITERRANEAN 167
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Probable Duration of Assistance. Until the end of 1955.Work in 1954. The work of the clinic at the Teheran centre was reorganized, a newrecords system was introduced, and the serological laboratory was firmly established.The venereologist and serologist began a series of visits to the provinces. A plan forcontrol of venereal disease throughout the country was drawn up and submitted to theMinistry of Health.
Iran 5 Nov. 1951- Public- Health Administration, Teheran
TA Aim of the Project. To develop the basic health administration, covering medical care,public health, and preventive medicine and welfare.
Assistance provided by WHO. A public -health adviser from November 1951 to the endof 1954 ; a public -health nurse from September 1952 to August 1954 ; and a statisticianfrom October 1954 to the end of 1955.Probable Duration of Assistance. Until the end of 1955.
Work accomplished. The team made valuable studies of the health services in Iran.One of the public -health adviser's main tasks was to advise the Government on thedevelopment of public -health administration and the co- ordination of curative andpreventive health services, a task complicated by the establishment of the Government/Point IV Public Health Co- operative. WHO's assistance with the project, which,except for the services of the statistician, ended in December 1954, has mainly providedinformation which can be used in the consideration of future technical assistanceprogrammes in health.
Iran 8 Nov. 1952- Nursing Education, Ashraf School of Nursing, Teheran
TA Aim of the Project. To raise the standard of nursing, which is lower than the standardof midwifery, by : training nurses ; staffing the school and wards of the Pahlevi Hospitalwith trained nurses ; providing trained personnel for provincial schools and hospitals.Assistance provided by WHO. Four nurse educators ; some teaching equipment ;fellowships.
Probable Duration of Assistance. Until the end of 1956.Work accomplished. Good progress has been made in establishing a sound basis fortraining of nurses and in revising the syllabus of the School.
Iran 9 March 1954- Tuberculosis -Control Demonstration and Training Centre, Teheran
TA Aim of the Project. To establish a tuberculosis -control centre which will train personnel,demonstrate modern methods of tuberculosis control and serve as a central tuberculosisdispensary for Teheran ; to establish a central diagnostic laboratory for tuberculosis,under the direction of the Institut Pasteur, Teheran ; to organize a mobile epidemio-logical team for surveys among selected population groups ; eventually to develop anational tuberculosis -control programme.Assistance provided by WHO in 1954. A senior adviser since March, an x -ray technicianand a laboratory technician since August, and a public -health nurse since September.Probable Duration of Assistance. Until mid -1956.
Work in 1954. Progress was retarded by delay in the completion of the Teheran centre.
Iran 10TAUNICEF
Dec. 1954- Maternal and Child Health Demonstration and Training Centre, TeheranAim of the Project. To establish a maternal and child health centre in Teheran, fordemonstrating methods of mother and child care and for training medical andauxiliary personnel ; to plan maternal and child health services throughout the country.
Assistance provided by WHO. A paediatrician (team leader) and a public -health nursesince December 1954. A second public -health nurse will be provided in 1955.
Probable Duration of Assistance. Until the end of 1956.
168 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Iran 11 Jan. 1952- BCG Vaccination
UNICEF
Iran 21
UNICEF
Aim of the Project. To extend the BCG production laboratory at the Institut Pasteur,Teheran, and to establish under the Institute's direction a vaccine- distribution serviceand a tuberculin -dilution laboratory ; to organize and carry out a mass BCG- vaccina-tion programme, combining the UNICEF /WHO- assisted BCG programme and thenational BCG -vaccination campaign into a single campaign for the whole country.Assistance provided in 1954 (cost reimbursed by UNICEF). A BCG nurse, an admini-strative officer and a transport officer. Most members of the international team werewithdrawn in 1953.
Probable Duration of Assistance. Until the end of 1955, the BCG nurse and the admi-nistrative officer being retained throughout the year.Work accomplished. Tuberculin testing showed a very low prevalence of tuberculousinfection in Iran -a finding so surprising that it was decided that the regional BCGassessment team (see project EMRO 14) should study the situation. The team beganwork in December 1954 and will stay five months in the country.
Nov. 1954- Midwifery School, Teheran
Aim of the Project. To re- establish the midwifery school at the University Women'sHospital in Teheran, with : a survey of existing teaching facilities ; organization ofrefresher courses for midwives and nurse -midwives, and a course of training to enablequalified nurses to graduate as nurse -midwives.Assistance provided in 1954 (cost reimbursed by UNICEF). A midwifery instructorfrom November. (Two further midwifery instructors will be provided if funds becomeavailable.) The staff will advise on the curriculum of the school and do some teaching.
Probable Duration of Assistance. Until the end of 1956.
. Iraq 7 Oct. 1953- Tuberculosis Control, Baghdad
TA Aim of the Project. To improve control of tuberculosis in Baghdad by establishing ademonstration centre which will work with other tuberculosis services, includingsanatorium services. Plans include training, maintaining statistical data, educatingthe public in ways in which infection is spread and the preventive measures to be taken.
Assistance provided by WHO. A senior adviser since October 1953, a public -healthnurse since September 1954, an x -ray technician since June 1954 and a laboratorytechnician from March to June 1954 ; equipment, transport and supplies ; fellowships.
Probable Duration of Assistance. Until mid -1956.
Work accomplished. See page 99.
Iraq 8
UNICEF
Oct. 1953 - Maternal and Child Health
Aim of the Project. To plan, develop and equip throughout the country, as a part ofthe national health services, a maternal and child health service comprising prenatalcare, midwifery and post -natal service and preventive care of infants and youngchildren, by : demonstrating methods best suited to Iraq ; training in maternal andchild health work various categories of personnel, including auxiliary health visitorsand community midwives.Assistance provided in 1954 (cost reimbursed by UNICEF). A senior medical officersince October 1953, two public -health nurses since November 1953, and a midwiferyinstructor since March 1954. (It is hoped to provide three more nurses in 1955.)Probable Duration of Assistance. Until the end of 1956.Work accomplished. The Sheik Omar Clinic in Baghdad was reorganized as a maternaland child health centre and a maternal and child health directorate was establishedin the Ministry of Health with the co- operation of the WHO team and a full nationalteam. Training of auxiliary health visitors began in May 1954 and in August a ruralhealth centre was opened in Dawra. The WHO team co- operated with the USForeign Operations Administration mission in Iraq.
PROJECT LIST : EASTERN MEDITERRANEAN 169
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Iraq 10 May 1952- BCG Vaccination
UNICEF Aim of the Project. To organize and carry out a mass BCG -vaccination programme ;to start a national BCG -vaccination service as part of the tuberculosis -control service.
Assistance provided in 1954 (cost reimbursed by UNICEF). A BCG adviser ; a BCGnurse from February to April and September to December ; a statistician's clerk fromJanuary to June.Probable Duration of Assistance. Until mid -1955 (medical officer only).
Work accomplished. See page 98.
Iraq 11 May 1952- Malaria Control, Tanjero Valley, Sulaimaniya Liwa
TA Aim of the Project. To continue malaria control in the Sulaimaniya Liwa and, possibly,to reduce the prevalence of other insect -borne diseases ; to train local personnel ;to assess the results of control in terms of malariometric data, especially on children,and entomological findings.Assistance provided by WHO in 1954. A malariologist and a sanitarian.
Probable Duration of Assistance. Until the end of 1956.Work in 1954. Spraying operations continued in the Sulaimaniya Liwa. The extensionof operations to adjacent areas in 1956 was planned and the necessary staff was trained.Entomological and malariometric indices were used for frequent comparisons madeof the situation in sprayed and unsprayed areas ; results show that DDT residualspraying was highly successful.
Iraq 17 Oct. -Dec. 1954 School for Backward Children, Baghdad
R Aim of the Project. To establish a school for backward children in Baghdad,and eventually similar schools in other parts of Iraq.Assistance provided by WHO in 1954. An expert for three months from October, tohelp prepare suitable curricula and supervise teaching activities.
Iraq 19R
Nov. 1953 -Feb. 1954
Ankylostomiasis Survey
Aim of the Project. To assess the prevalence of ankylostomiasis in Iraq.Assistance provided by WHO. A consultant, from November 1953 to February 1954,to carry out the survey.Work accomplished. The consultant's report and recommendations for controllingthe disease within five years have been submitted to the Government.
Israel 8 Oct. 1953- Rehabilitation of Handicapped Children, Sarafand
R Aim of the Project. To establish a general rehabilitation centre at Sarafand Hospital,UNICEF mainly for physically handicapped children ; to demonstrate modern methods of
physiotherapy in the treatment of handicapped children ; to establish a national schoolof physiotherapy.Assistance provided by WHO in 1954. An instructor in physiotherapy from October1953.
Probable Duration of Assistance. Until September 1955.
Work accomplished. See page 99.
Israel 11 July 1954- Tuberculosis -Control Demonstration and Training Centre, Jaffa
TA Aim of the Project. To establish a demonstration and training centre, with a modeltuberculosis dispensary and related services, to work with sanatorium services and toprovide : advice on tuberculosis control ; diagnosis by clinical, radiological and lab-oratory methods ; tracing, examination and follow -up of contacts ; treatment for
170 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
ambulatory cases : home visiting ; training of personnel ; statistical services ; educationof the public in the ways in which infection is spread and the preventive measuresto be taken.Assistance provided by WHO in 1954. A senior adviser in tuberculosis and a public -health nurse, both since July.Probable Duration of Assistance. The nurse until the end of 1955 ; the senior adviserwill be withdrawn in June.Work in 1954. The centre was officially opened in December.
Israel 16 Aug. 1952- Zoonoses
R Aim of the Project. To improve control of bovine tuberculosis, rabies and brucellosis.Assistance provided by WHO. Technical advice, usually by regular staff members.
Work in 1954. The veterinary medical officer from Headquarters went to Israel inAugust. His report has been submitted to the Government.
Israel 21 Nov. 1954- Care of Premature Infants, Tel -Aviv, Haifa and Tiberias
R Aim of the Project. To equip three centres for the care of premature infants, at Tel -Aviv,UNICEF Haifa and Tiberias.
Assistance provided by WHO in 1954. A consultant for three weeks (November -December) to advise on the equipment needed, which will be supplied by UNICEF.
Work in 1954. The consultant's report and recommendations were submitted to theGovernment and to UNICEF.
Jordan 3 June 1954- Maternal and Child Health Demonstration Centre, Amman, and West and East Jordan
TA Aim of the Project. To develop maternal and child care by improving eleven existingUNICEF maternal and child health centres (one in Amman and ten in west Jordan) and
establishing eleven new centres in east Jordan ; to co- ordinate and expand services ;demonstrate modern methods of care ; train community midwives ; provide refreshercourses for doctors and nurses.Assistance provided by WHO in 1954. A public -health nursing instructor since June, anda midwifery instructor since December. (A paediatrician -team leader -will beprovided early in 1955.)
Probable Duration of Assistance. Until mid -1956.
Jordan 8UNICEF
Jordan 9R
Nov. 1953- BCG Vaccination
Aim of the Project. To establish a permanent BCG- vaccination service as part of theantituberculosis programme, with : tuberculin testing of children, including refugees,throughout the country, and BCG vaccination of non -reactors ; studies of pre -vaccination tuberculin allergy in various age -groups, as a basis for future plans.Assistance provided in 1954 (cost reimbursed by UNICEF). A BCG medical officerand, since February, a BCG nurse.Probable Duration of Assistance. Until the end of 1955.Work accomplished. The campaign started in Amman in December 1953. By the endof September 1954 nearly 187 000 persons had been tested, and about 93 000 of themvaccinated. Ten vaccinators from the Ministry of Health, five from the Army, and onefrom UNRWA, completed training. The campaign in the Army started in March 1954.By the end of the year work, on the whole, was ahead of schedule and proceedingsatisfactorily.
July 1952 -June 1954
Public -Health Laboratory, Jerusalem
Aim of the Project. To operate the laboratory at the Augusta Victoria Hospital,Jerusalem, which has been taken over by the Government from UNRWA as a public -health laboratory, with : routine diagnostic services in public health ; production of
PROJECT LIST : EASTERN MEDITERRANEAN 171
Project No.Source of FundsCo- operating Agencies
Dates Description
vaccines and other antigenic substances or antisera ; training of laboratory technicians ;epidemiological investigations.Assistance provided by WHO. A laboratory technician.
Work in 1954. The laboratory technician submitted his final report, which was underconsideration at the end of the year.
Jordan 10 March 1954- Mental Health, Bethlehem, Amman, JerusalemR Aim of the Project. To improve and expand mental -health services within the general
public -health services with : immediate improvement and expansion of facilities at theBethlehem Mental Hospital ; early establishment of outpatient clinic facilities,especially in Amman and Jerusalem ; training of psychiatric nurses and other mental -health workers ; improvement of treatment facilities for the criminally insane and forprisoners suffering from minor psychiatric disorders.Assistance provided by WHO in 1954. A mental -health expert since March.Probable Duration of Assistance. Until mid -1956.
Jordan 12 July -Sept. Relapsing -Fever Survey
R 1954 Aim of the Project. To establish the epidemiology of relapsing fever in Jordan and toidentify the vector, by means of a survey.Assistance provided by WHO. A consultant from July to September 1954.Work accomplished. The consultant's interim report has been submitted to the Govern-ment. It states that relapsing fever in Jordan, which is tick -borne, occurs sporadicallythroughout the country, especially around Irbid and Nablus. The disease occursmainly in shepherds and seldom affects townspeople. Vector ticks are Ornithodorostholozani and O. coniceps ; the latter has not previously been identified as a vector.
Lebanon 6TAUNICEF
Lebanon 7TAUNICEF
Feb. 1952 -Aug. 1954
Aug. 1951 -Jan. 1954
Maternal and Child Health Demonstration and Training Centre, BeirutAim of the Project. To improve maternal and child health services in Beirut, by acentre which, among other things, would train casa nurses and provide a domiciliarymidwifery service.
Assistance provided by WHO. A medical officer, a public -health nurse and a nurse -midwife ; fellowships for two medical officers and one public -health nurse.
Work accomplished. Originally planned to last two years, the project was prolongedfor a third year and expanded to include the establishment of centres at Tripoli andTyre. The Government provided counterparts for the WHO staff and appointed thefellows, on completion of their post -graduate study of maternal and child health,to posts in the Ministry of Health, where a child -health department had been set up.
Increasing attendance at the Beirut centre showed that its services were appreciatedby the people.
Malaria ControlAim of the Project. (a) To make an epidemiological survey of malaria in a demonstra-tion area and in a control area ; to carry out malaria -control operations and to evaluatetheir results. (b) To set up a malaria -control service in the Ministry of Health, staffedby trained personnel, to organize extensive control measures with a view to the gradualelimination of malaria from the country.Assistance provided by WHO. A malariologist, an entomologist, a public -health nurseuntil April 1952, and a sanitary engineer.Work accomplished. The work of the various agencies interested in malaria controlwas co- ordinated. A national team, capable of carrying out malaria control in Lebanon,was trained. A complete malaria survey (the first in the country) was made and, forthe first time, control operations were extended to all malarious areas. The WHOteam was withdrawn at the end of January 1954 and its final report is underconsideration. UNICEF is continuing to supply DDT to the Government.
172 THE WORK OF WHO, 1954
Project NoSource of Funds Dates DescriptionCo- operating Agencies
Lebanon 11 1952- Microfilm Production Unit, American University, BeirutR
4 Libya 1TA(UN)
Jan. 1951 -Feb. 1954
Aim of the Project. To supply microfilm and related services to the Region by equippinga microfilm laboratory to be installed in the American University, Beirut.
Assistance provided by WHO. Supplies and equipment, to be imported into the countryfree of tax, duty, or other charge, and to remain the property of WHO.Work in 1954. The necessary legislation was passed to enable the equipment, held incustoms, to be released, and it is hoped that the equipment will be delivered earlyin 1955.
Public -Health Administration
Aim of the Project. To plan a health service.Assistance provided by WHO. A public- health administrator until February 1954 ;a sanitary engineer and a public -health nurse, both withdrawn in 1953.
Work in 1954. The report of the public -health administrator was submitted to theGovernment.
Libya 2 April 1954- Maternal and Child Health Demonstration and Training Centre, Suk el Juma, Tripolitania
R Aim of the Project. To establish a demonstration and training centre which will trainUNICEF community midwives, demonstrate to these and other workers modern methods of
mother and child care, and provide practical training under rural conditions.Assistance provided by WHO in 1954. A medical officer and a public -health nurse sinceApril. (A nurse -midwife will be provided early in 1955 ; a health educator employedunder project Libya 4 also works at the centre.)Probable Duration of Assistance. Until mid -1957.Work in 1954. UNICEF supplies were delivered to the centre and the WHO teamstarted clinical and domiciliary work in May. In July national counterpart staff wereappointed. Ten trainees began practical work in August and the theoretical course inSeptember (stipends for these trainees were paid by UNICEF).
Libya 4 June 1953- Health Education, Tripoli, Benghazi
R Aim of the Project. To improve the health of the individual and the communitythrough health education.Assistance provided by WHO in 1954. A health educator in Tripolitania (who alsoworks for the maternal and child health centre at Suk el Juma -see project Libya 2)and another in Cyrenaica.Probable Duration of Assistance. Until the end of 1955.
Libya 5 Jan. 1953- BCG Vaccination, Settled Population of Tripolitania, the Fezzan, and Cyrenaica
UNICEF Aim of the Project. To organize and carry out tuberculin testing of most of the popula-tion under eighteen and to vaccinate non -reactors with BCG ; to start a permanentBCG- vaccination service as part of the tuberculosis -control service.Assistance provided in 1954 (cost reimbursed by UNICEF). A BCG medical adviserand two BCG nurses -one of whom was withdrawn in February.Probable Duration of Assistance. Until the end of 1955. (For work of the regionalBCG -assessment team in Libya, see project EMRO 14.)
( Pakistan 2 Feb. 1951- Tuberculosis Control, Karachi, West Pakistan
TA Aim of the Project. (a) To establish in Karachi a tuberculosis- control demonstrationUNICEF and training centre to train doctors, nurses and technicians in modern methods of
tuberculosis control. (b) Ultimately to establish similar centres in other parts of thecountry, staffed by personnel trained in Karachi, thus gradually developing a country-wide programme of tuberculosis control.

PROJECT LIST: EASTERN MEDITERRANEAN 173
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Assistance provided by WHO in 1954. A senior adviser, a laboratory technician untilthe end of March, and a public -health nurse until the end of April.Probable Duration of Assistance. Until February 1955.
Work in 1954. The WHO team was withdrawn, except for the senior adviser, whoremained to advise the Pakistani staff of the centre in its routine work.
Pakistan 3 April 1952- Maternal and Child Health Demonstration and Training Centre, Peshawar, WestTA Dec. 1954 Pakistan
UNICEF Aim of the Project. To establish a centre for training community health visitors for theprovincial maternal and child health programme and demonstrating the value ofmaternal and child health services.Assistance provided by WHO in 1954. A medical officer (maternal and child health)until June, and a public -health nursing instructor and a midwifery instructor untilDecember.
Work accomplished. The main objective of this project has been achieved. By December1954 the first nine community midwives had been trained, and ten more were beingtrained at the end of the year. The lack of a national counterpart to the team leaderwas a serious handicap and the administrative difficulties in this project have beenconsiderable. Implementation of government and Red Cross plans for expandingmaternal and child health services in the provinces should provide posts for the com-munity midwives trained in the programme.
Pakistan 5TA
Pakistan 7TA
Aug. 1952 -Nov. 1954
Cholera Control, Jhalakati, East PakistanAim of the Project. To make extensive studies of the bacteriological aspects of theepidemiology of cholera ; to demonstrate environmental sanitation methods applicableto the control of cholera in East Pakistan.Assistance provided by WHO in 1954. A public -health engineer and a sanitarian.Work in 1954. Progress was retarded by physical and climatic conditions andadministrative difficulties, but work proceeded slowly on the installation of wells andlatrines, the improvement of water supplies, and on health education. It provedimpossible to recruit a health educator. After two years' search a bacteriologist wasfound who could withstand the unavoidable hardships ; however, after discussionswith the Government, it was decided to terminate the project. It was considered thatsanitation work connected with the control of cholera had been adequatelydemonstrated, although its effects on endemic cholera in the area had yet to bemeasured. The WHO team was withdrawn in November ; the way in which thesupplies and equipment provided are to be used was being considered at the end ofthe year.
Nov. 1952- Demonstration and Training Centre for Venereal- Disease Control, Karachi, WestJune 1954 Pakistan
Aim of the Project. To improve venereal -disease control in and around Karachi by :establishing a modern venereal- disease control centre in Karachi and expandingexisting facilities in the city and surrounding district, demonstrating modern methods oftreatment, and training personnel ; establishing a laboratory to carry out serologicaltests for Karachi and neighbourhood (including merchant seamen passing through theport) and to train serologists and laboratory personnel.Assistance provided by WHO in 1954. A venereologist, a serologist and a public -healthnurse, all until the end of June.
Work accomplished. At the end of June the national director of the centre took charge,with a national serologist to run the laboratory.
Pakistan 9 Oct. 1953- Maternal and Child Health Demonstration and Training Centre, Karachi, West PakistanR Aim of the Project. To establish a centre for demonstration of the value of maternalUNICEF and child health services and for training community health visitors and dais for the
provincial maternal and child health programme.
174 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Assistance provided by WHO in 1954. A social paediatrician (team leader) fromFebruary ; a public -health nurse ; a midwifery instructor ; a district midwife supervisorand a nurse educator.Probable Duration of Assistance. Until September 1956.Work in 1954. The team, which had previously worked on a similar project in Lahore,was in Karachi by November 1953 and the team leader arrived in February 1954.However, building delays held up work until May, when the prenatal clinic wasopened. Thenceforth rapid progress was made in all services provided by the centre.The first group of trainees was enrolled in May and the second in October but thetraining of dais was not started. At the end of the year provision was being made togive community health visitors practical training under rural or semi -rural conditions.
Pakistan 10 Feb. 1953- Maternal and Child Health Demonstration and Training Centre, Dacca, East PakistanTA Aim of the Project. To establish a centre for demonstrating the value of maternal andUNICEF child health services, for training community health visitors for the provincial maternal
and child health programme, and for training doctors, medical undergraduates, andgraduate and undergraduate nurses in maternal and child health work ; to improvethe teaching of paediatrics and paediatric care at the Medical College Hospital, Dacca,so that it may serve as a model for East Pakistan.
Assistance provided by WHO in 1954. A medical officer (maternal and child health)as team leader ; two public -health nursing instructors ; two midwifery instructors.Probable Duration of Assistance. Until March 1956.Work in 1954. The work of the centre was consolidated and expanded ; further traineeswere admitted to the preliminary- training school and senior students began theirtraining in midwifery and public health. A domiciliary midwifery service -wellreceived by the population -was established.
Pakistan 12 March 1953- Tuberculosis -Control Demonstration and Training Centre, Dacca, East PakistanTA Aim of the Project. (a) To establish a model tuberculosis -control clinic to serve as aUNICEF centre for training staff in modern methods of tuberculosis control. (b) To develop
a tuberculosis service for East Pakistan.Assistance provided by WHO in 1954. A senior adviser, a public -health nurse, an x -raytechnician and a laboratory technician.Probable Duration of Assistance. Until the end of 1956 (senior adviser and public -health nurse only).Work in 1954. Work continued satisfactorily throughout the year. The first basictraining course for home visitors and for laboratory and x -ray technicians began inJanuary and ended in July. At the end of the year a programme of chemotherapeuticcontrol of tuberculosis, with the participation of UNICEF, was under consideration.
Pakistan 13 Nov. 1951- BCG VaccinationUNICEF Aim of the Project. To continue and expand into a mass campaign the existing BCG -
vaccination programme ; to train personnel for a permanent BCG -vaccination service.
Assistance provided in 1954 (cost reimbursed by UNICEF). Three BCG medicalofficers, six BCG nurses (four until May and two until the end of December), astatistical adviser and an administrative officer.Probable Duration of Assistance. Until the end of 1956, with a reduced team.
Pakistan 19 Oct. 1952- Training of Nurses, Dacca, East PakistanR Aim of the Project. To increase the number of trained nurses in East Pakistan byUNICEF extending and improving facilities at the Medical College Hospital, Dacca, for training
student nurses, staff nurses, teachers, supervisors and auxiliaries. The curriculum of thehospital will be reviewed and teaching of public health included.Assistance provided by WHO in 1954. A senior nurse educator, a paediatric nursinginstructor and a surgical nursing instructor.Probable Duration of Assistance. Until the end of 1956.
PROJECT LIST : EASTERN MEDITERRANEAN 175
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Work in 1954. The team was brought up to full strength after many delays. Trainingcontinued with a larger number of students, who reached a higher standard than thoseof the previous year. There were still not enough adequately trained ward supervisorsand it will take some years before the deficiency is remedied.
Pakistan 20 April 1952- Assistance to Dow Medical College, Karachi, West PakistanR Aim of the Project. To improve the teaching of pathology and physiology at the Dow
Medical College, Karachi.
Assistance provided by WHO. A professor of pathology until January 1954, and aprofessor of physiology, to undertake the following work : to serve as heads of theDepartments of Pathology and Physiology ; to assist the Dean of the College in drawingup curricula ; to lecture and give practical teaching ; to develop the laboratories oftheir departments on modern lines ; to train university staff in the methodology ofpathology and physiology ; on request, to advise the Government of Pakistan or theprovincial government on the wider aspects of their specialties.Probable Duration of Assistance. The Government requested that the Professor ofPhysiology should stay until June 1956 in view of the difficulty of finding a Pakistanisuccessor.
Pakistan 21TA
Saudi Arabia 1R
July 1953-
Dec. 1952-
Work in 1954. The final report of the Professor of Pathology was submitted to theGovernment.
Nursing Adviser
Aim of the Project. To develop nursing services and training.Assistance provided by WHO. (a) A nursing adviser, assigned to the Office of theDirector -General of Health for Pakistan. (b) A fellowship to train a Pakistani nurse forthe post of nursing adviser when the WHO expert is withdrawn.Probable Duration of Assistance. Until the end of 1955.
Quarantine Station for Pilgrims, JeddahAim of the Project. To expand the quarantine station for pilgrims to Mecca.Assistance provided by WHO in 1954. An epidemiologist with specialized knowledgeof quarantine procedure ; supplies and equipment.Probable Duration of Assistance. Until September 1955 (end of the 1955 pilgrimageseason).
Work in 1954. Progress in the establishment of the new station has been slow and thework was not completed by the end of the year. The WHO epidemiologist will thereforeremain until after the 1955 pilgrimage season to advise the local authorities during thefirst year of operation of the station.
Saudi Arabia 2 Nov. 1952- Venereal- Disease Control, Mecca
TA Aim of the Project. To establish in Mecca a demonstration centre where local technicaland auxiliary staff can be trained in modern methods of diagnosis and treatment ofvenereal diseases ; to study the epidemiological aspects of venereal diseases in thecountry by field surveys.
Assistance provided by WHO in 1954. A medical officer, and a male public- healthnurse until the end of September.Probable Duration of Assistance. Until June 1956 -to consist of the services of a medicalofficer and some supplies.
Work accomplished. In Mecca a centre for venereal- disease control was established,comprising an outpatients' clinic, an in- patient ward, and a central laboratory. Alaboratory was set up in Asir and another in Medina. Field surveys were made in Asir,Taif and Medina. There were not enough local personnel available for training.
1 WHO gives technical advice and approval to nine UNICEF projects in Pakistan. These are concerned with : malaria control ;maternal and child health centres ; equipment for maternity hospitals ; school health services ; typhus control ; diphtheria toxoidproduction ; establishment of twelve hospitals -one in Karachi, one in Dacca, and ten (district hospitals) in the Punjab.
176 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Saudi Arabia 3 July 1953- Public -Health Administration
R Aim of the Project. To improve public -health services generally.
Assistance provided by WHO. A public -health adviser.
Work in 1954. Achievements included : the setting -up of a permanent committee todeal with all health matters relating to the Mecca Pilgrimage ; a plan for the reorgani-zation of the Ministry of Health ; improved methods of controlling infectious disease ;planning of measures to deal with the serious problem of stray dogs ; planning of anew law for licensing establishments where food is manufactured, cooked, or preparedand exposed for sale ; the opening in Jeddah of the first maternal and child welfareclinic in the country ; the construction at Taif of the first tuberculosis sanatorium ;vaccination against smallpox and yellow fever of port and airport personnel who arein contact with aircraft or ships.
Saudi Arabia 4 March 1952- Malaria Control
TA Aim of the Project. To make surveys, with a view to future insect -control operations,in the Gizan and other areas ; to control mosquitos in Jeddah town ; to train nationalpersonnel in malaria control.
Assistance provided by WHO in 1954. A malariologist, an entomologist and asanitarian.
Probable Duration of Assistance. Until mid -1956.
Work in 1954. The Gizan and Hasa areas were sprayed, and surveying and spraying wascarried out near Jeddah and in the southern coastal districts. The training programmecontinued on a small scale, although there were few students ; however, students fromthe class held earlier worked usefully on the project during the year. During thePilgrimage the team worked on fly control, but since basic sanitation measures arelacking, the cost is high and the results are inadequate and temporary. In Octoberand November a special malaria -control operation was carried out in Najran.
Sudan 3 March 1954- BCG Vaccination
UNICEF Aim of the Project. To establish a permanent BCG -vaccination service as part of theantituberculosis programme ; to study pre- vaccination tuberculin allergy on represen-tative samples of the population and to plan future action on the basis of the findings.
Assistance provided in 1954 (cost reimbursed by UNICEF). A BCG medical officer anda BCG nurse.
Sudan 4R
Sudan 5R
July 1954
July 1954
Probable Duration of Assistance. Until mid -1955.
Work in 1954. A pilot scheme was started in the sou thern provinces. National counter-parts to the WHO team were trained.
School of Pharmacy, KhartoumAim of the Project. To improve the teaching of pharmacy in the Sudan.
Assistance provided by WHO. A consultant to make a study, in July.
Work accomplished. The report of the consultant and his recommendations for raisingthe standard of training in pharmacy have been submitted to the Government.
Bilharziasis Control, Gezira Irrigated AreaA WHO consultant and a consultant from the Egyptian Government visited the
Sudan for discussions on the programme of bilharziasis control to be carried out in1955. Their report was submitted to the Government.
PROJECT LIST : EASTERN MEDITERRANEAN 177
Project No.Source of Funds Dates DescriptionCo- operating Agencies
/Syria 2 Oct. 1952- Malaria ControlTAUNICEF
Aim of the Project. To achieve complete and permanent control of malaria throughoutthe country by gradually extending insecticide spraying operations and maintainingcontrol measures until transmission has been effectively interrupted.
Assistance provided by WHO in 1954. A malariologist and a sanitarian.
Work in 1954. Malariometric and entomological surveys were made in the Horns -Hama and the Latakia -Baniyas areas and spraying operations were carried out in thecoastal (Latakia) area. Pre -operative surveys were made in north -west Syria and post-operative surveys were effected in areas where demonstration spraying operations hadbeen carried out. The Horns area was re- sprayed.
Syria 3 March 1954- Control of Bejel and Syphilis, Deir -ez -Zor
R Aim of the Project. To control bejel and syphilis in northern Syria and to train pro -UNICEF fessional and technical personnel in control methods.
Assistance provided by WHO in 1954. A senior medical officer, a serologist until August,and a male public -health nurse.
Probable Duration of Assistance. Until the end of 1955.
Work in 1954. A centre at Deir -ez -Zor was established. Steady progress was madewith clinical work, but serological work was delayed by the late delivery of someimportant items of laboratory equipment and by the departure of the serologist inAugust. A national serologist was appointed by the Government as a temporaryreplacement but his services were available only part -time. Extensive surveys weremade in the Euphrates and Khabour valleys.
Syria 4 Dec. 1953- Control of Bilharziasis and Malaria, JezireR Aim of the Project. To control bilharziasis and malaria in the Jezire area by : demonstra-
ting control methods in certain affected parts of the area and encouraging their applica-tion to the entire area ; training national personnel to continue the work after theWHO team leaves ; educating the local people in the value of control methods inorder to obtain their co- operation.
Assistance provided by WHO in 1954. A medical officer, a public -health engineer, asanitarian and a laboratory technician.
Probable Duration of Assistance. Until the end of 1956.
Work in 1954. Excessive rains during the winter of 1953 -54 and delay in delivery ofsupplies hindered operations. However, technical sections were formed, and personneltrained. The interest of the public in the control measures was obtained. As regardsbilharziasis, it is considered that suitable control measures will result from the experi-ments which were in progress at the end of the year.
Syria 5 Sept. 1952- Maternal and Child Health Demonstration and Training Centre, Damascus
TA Aim of the Project. To improve maternal and child health in Damascus by : establishingUNICEF a centre for demonstrating methods of mother and child care ; training local pro-
fessional personnel ; evaluating results on the basis of reduction in mortality anduse made of the services by the community ; advising on the extension of servicesto other parts of the country.
Assistance provided by WHO in 1954. A social paediatrician (team leader) until June,a public -health nursing instructor, a midwifery instructor.
Probable Duration of Assistance. Until mid -1955.
Work in 1954. Emphasis was placed on the training of public -health auxiliaries,particularly for staffing new maternal and child health centres, four of which wereopened during the year -in Aleppo, Latakia, Homs and Deraa. The local staff of theDamascus centre was increased and its clinical facilities expanded, but the domiciliarymidwifery service was handicapped by shortage of personnel.
178 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Syria 10 May 1952- Tuberculosis -Control Demonstration and Training Centre, Damascus
R Aim of the Project. To demonstrate effective methods of tuberculosis control, byestablishing a centre to work with other tuberculosis services.
Assistance provided by WHO in 1954. A senior medical adviser, an epidemiologistuntil May, a public -health nurse until August, and a laboratory technician and anx -ray technician until June.
Probable Duration of Assistance. Until June 1955 (senior medical adviser only).
Work accomplished. National action for the control of tuberculosis began with thecreation of two centres, at Damascus and Aleppo, and the drawing -up of a detailedcontrol programme, covering several years. By the end of 1954 Syrian personnel hadtaken over full responsibility for the programme and tuberculosis services, includingBCG vaccination and training of personnel, had been improved and extended. Duringthe team's work in Damascus existing personnel were given advanced training and newstaff trained to work on the project ; facilities were increased by equipment providedby WHO. Fellowships were awarded to persons working in the Damascus centre.
Syria 13 Sept. 1954- School Health Services (Favus Control)
R Aim of the Project. To establish, as part of the general health services, permanentUNICEF services for the control of mycotic infection of the scalp in children, with improvement
of control methods and training of personnel.
Assistance provided by WHO in 1954. A dermatologist (team leader) from September,and an x -ray technician from August.
Probable Duration of Assistance. Until September 1955.
Syria 14 June 1953- Nursing Education, Damascus
TA Aim of the Project. To improve the training of nurses and increase the number ofhospital nurses, public -health nurses and midwives by : developing teaching andpractice facilities at the School of Nursing of the Syrian University, Damascus ;revising the curriculum of the school to incorporate all aspects of nursing ; traininggraduate nurses as supervisors of hospital wards or health centres and as teachers andsupervisors of student nurses and local auxiliaries.
Assistance provided by WHO in 1954. A senior nursing adviser and a public -healthnursing instructor. (Provision in 1955 of a paediatric nursing instructor and a nurse -educator was being considered at the end of the year.)
Probable Duration of Assistance. Until the end of 1955.
Work in 1954. A new curriculum for the school was established and put into use.Public -health nursing was included in the basic course and public -health centres wereused for practical training of student nurses. A nursing section under a Syrian nursewas officially established by the Ministry of Health.
Yemen 3
R
Feb. 1954- Public -Health Administration
Aim of the Project. To survey existing national health services and determine mosturgent needs, with a view to planning the expansion of health facilities.
Assistance provided by WHO in 1954. A public -health adviser from February to March.A successor will be provided in January 1955.
Probable Duration of Assistance. Until the end of 1956.

PROJECT LIST : WESTERN PACIFIC 119
Project No.Source of Funds Dates DescriptionCo- operating Agencies
WPRO 12UNICEF
Jan. 1954-
WESTERN PACIFIC
BCG Assessment Team
Aim of the Project(1) In countries where a BCG - vaccination programme is contemplated but not started.To collect information on the prevalence of reactors to tuberculin in sample localities,in order to determine the areas and age -groups to be covered in BCG campaigns andthe appropriate techniques and procedures.(2) In countries where a BCG -vaccination campaign has been carried out. To determine,by sample methods, what has been achieved and provide information enablingtechniques and procedures to be altered and improved if necessary.Assistance provided in 1954 (cost reimbursed by UNICEF). A medical officer and twonurses.
Work accomplished. The team has made field checks of the vaccines produced in theAlabang Laboratory, Philippines (used in the Philippines, Indonesia, Sarawak, Bruneiand Hong Kong), and of those produced by the BCG laboratories in Taipei (used inTaiwan) and Saigon (used in Viet Nam and Cambodia).
After working in the Philippines, Viet Nam and Indonesia (in the South -East AsiaRegion), the team went to Taiwan in December. It is to go to Hong Kong and back tothe Philippines in 1955.
UNICEF has accepted financial responsibility for this project until the end ofApril 1955.
WPRO 16 July -Nov. Smallpox Survey
R 1954 Aim of the Project. To obtain information on the sources of infection, prevalence anddistribution of smallpox in certain countries of the Region with a view to planningnational and inter -country measures for the eradication of the disease.Assistance provided by WHO. A consultant for five months.Work accomplished. A survey was made in Cambodia, Hong Kong, Japan, Korea,Macao, Malaya, Philippines, Singapore, Taiwan and Viet Nam. The report on thesurvey will be submitted to the governments concerned.
WPRO 17R
Brunei 1
R
Brunei 3TA
4 -21 May Dental -Health Seminar, Wellington, New Zealand1954
Jan. 1950 -June 1954
Aim of the Project. To enable dental -health experts to discuss common problems,including methods of making dental -health programmes an effective part of public -health services and the selection and training of dental -health personnel.
The seminar was attended by thirty -seven participants from twenty countries ofthe Western Pacific, South -East Asia and Eastern Mediterranean Regions.
For description of the seminar, see page 105.
School of Nursing, Brunei
Aim of the Project. To provide training, including in- service training, for assistantnurses ; to evaluate the training programme in terms of local needs and resources.
Assistance provided by WHO in 1954. A public -health nurse.
Work accomplished. A training programme was established for assistant nurses,thirty of whom were trained. Plans were made to train selected students to becomefully -qualified nurses. In November 1953 a school feeding scheme was organized ;this was continued by the Government after withdrawal of the public -health nursein June.
Oct. 1953- Malaria and Insect Control Pilot ProjectSee description of Sarawak 5.
180 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Brunei 4 Aug. -Dec. Nutrition
R 1954 Aim of the Project. To review the school feeding scheme in Brunei with a view toextending it.
Assistance provided by WHO. A nutritionist for four months.Work accomplished. The school feeding scheme has been extended ; 4350 school-children were receiving free meals by 30 September 1954, about 60 per cent. morethan in May 1954. Community interest has grown as a result of decentralization ofthe scheme, which is running smoothly under the supervision of school committeesdirectly responsible to the Medical Department.
'1 Cambodia 1 Aug. 1951- Malaria Control
TA Aim of the Project. To organize antimalaria services ; to demonstrate methods ofmalaria control, by establishing demonstration and comparison areas and trainingnational personnel.
Assistance provided by WHO in 1954. A malariologist and a sanitarian.
Probable Duration of Assistance. Until the end of 1956.Work accomplished. In spite of restrictions on field activities owing to unsettled con-ditions, demonstration and comparison areas were established, infant -parasite andentomological surveys carried out and night capture work begun. Towards the end of1954 an improvement in field conditions enabled the work to proceed more satis-factorily.
Cambodia 2 Nov. 1953- Public- Health Administration
R Aim of the Project. To improve public -health administration by : co- ordinating healthprogrammes and planning long -term programmes ; surveying health conditions.
Assistance provided by WHO. A specialist in public -health administration, sinceNovember 1953, to help with the above work and co- ordinate the health work ofinternational agencies.
Probable Duration of Assistance. Until November 1956.
Cambodia 3 Sept. 1951- Nursing Education, Phnom -Penh
R Aim of the Project. To set up a school of nursing (the first in the country) in Phnom -Penh ; to develop nursing and midwifery training.
Assistance provided by WHO. A public -health nurse as team leader since September1951, and three nurse educators, one since November 1952 and two -in generalnursing and midwifery-since August 1954.
Probable Duration of Assistance. Until December 1956.
Work accomplished. Unsettled conditions and lack of suitable local counterparts retardedprogress initially. Nevertheless, in conjunction with the maternal and child healthproject, Cambodia 4, a health centre was established which serves about 1400 familiesand which is staffed by nurses who have completed either in- service training or a six -month supplementary course. It also provides practical training for other nurses.
Also in conjunction with the maternal and child health project, a paediatric wardof twenty -five beds was established, staffed by nurses trained by the team. Practicaltraining in paediatrics is now part of the nursing course.
Cambodia 4 Jan. 1952- Maternal and Child Health, Phnom -Penh
TA Aim of the Project. To teach modern methods of maternal and child care suitable to theUNICEF cultural background and financial resources of the country ; to improve teaching of
obstetrics and child care in the Phnom -Penh schools of nursing and midwifery ; toimprove teaching of paediatrics, obstetrics and gynaecology at the Royal School ofMedicine ; to demonstrate methods of combining the curative, preventive and educa-tional aspects of health services ; to extend maternal and child health services and makethem part of the country's general health services.
PROJECT LIST : WESTERN PACIFIC 181
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Assistance provided by WHO in 1954. A medical officer and a public -health nurse fromNovember.
Probable Duration of Assistance. Until the end of 1956.
Work accomplished. A health centre and a paediatric ward were established (seeCambodia 3).
At the end of 1954 the creation of a maternal and child health division in theMinistry of Health was being planned
Cambodia 5 July 1953- Royal School of Medicine, Phnom -Penh
TA Aim of the Project. To improve teaching facilities at the Royal School of Medicinewith the aid of supplies and medical literature and by providing lecturers to help theDirector organize certain departments and assist with teaching.
Assistance provided by WHO in 1954. A lecturer.
Probable Duration of Assistance. Until July 1956.
Cambodia 6
UNICEF
BCG Vaccination
See description of Viet Nam 4.
China 1 Aug. 1953- Venereal- Disease Control, Taiwan
R Aim of the Project. To control venereal diseases throughout the island by training localUNICEF personnel in case -finding, contact investigation, health education and modern methods
of diagnosis and treatment ; by improving laboratories and standardizing laboratorymethods ; and by surveys.Assistance provided by WHO in 1954. A venereologist, a serologist, a health educatorand a public -health nurse.Probable Duration of Assistance. Until August 1956.Work accomplished. See page 108.
China 3 Aug. 1952- Maternal and Child Health, Taiwan
TA Aim of the Project. To provide an efficient maternal and child health service throughoutUNICEF the island to train nursing and medical personnel in all aspects of public health relating
to mother and child ; to improve health education.Assistance provided by WHO in 1954. A medical officer, a nurse educator (midwifery)and a public -health nurse.
Probable Duration of Assistance. Until August 1956.
Work accomplished. By the end of 1954 ten supervisors, thirty -five student nurses andsixty staff -level trainees had completed training in maternal and child health work.Four -month training courses had been given at sixteen health centres.
More duties and responsibilities are being gradually transferred to the supervisors,who participate in lectures, in in- service training, and in supervision of maternaland child health work outside the Taichung area.
UNICEF is providing supplies and equipment for fifty maternal and child welfarecentres, from which staff is sent for in- service training to the centre established inTaichung.
China 6 May 1952- Nursing Education, Taiwan
TA Aim of the Project. To improve the standard of nursing education and the quality ofnursing services, through the establishment, at the University Hospital in Taipeh, of auniversity school of nursing.Assistance provided by WHO in 1954. A senior nurse educator and four other nursinginstructors.
Probable Duration of Assistance. Until May 1957.

182 `113E WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Work accomplished. Progress has been made with plans for raising the standard ofadmission to the school and for establishing a university course to train nurses forteaching, supervisory and administrative posts. Manuals for teaching of nursing arts,obstetrical nursing, paediatric nursing and surgical nursing have been compiled andtranslated into Chinese.
Fellowships were awarded to instructors for study abroad.
China 7 May 1952- Malaria Control, Taiwan
TA Aim of the Project. To control malaria, and eventually to eradicate it, throughout theisland, by use of insecticides with residual action.
Assistance provided by WHO in 1954. A malariologist, an entomologist and a public -health engineer.
Probable Duration of Assistance. Until 1957.
Work accomplished. See page 105.
China 13 Oct. 1954- Trachoma Mass Campaign, Taiwan
TA Aim of the Project. To control trachoma in a population of over a million school -UNICEF children and their families by a mass campaign ; to organize key centres in schools and
health stations to maintain a practically permanent scheme of prevention and treatment.This project follows the WHO /UNICEF- assisted trachoma pilot project which
ended in March 1953.Assistance provided by WHO in 1954. A consultant for one month.
Probable Duration of Assistance. Until October 1956.Work in 1954. The consultant assisted in a preliminary survey, in evaluating the resultsof the pilot project and in drawing up plans for the campaign.
China 14 Oct. 1954- Environmental Sanitation, Taiwan
R Aim of the Project. To survey the organization and functions of governmental agenciesTA concerned with environmental sanitation ; to evaluate major sanitation problems and
establish priorities for work ; to carry out a pilot project to demonstrate modern andeconomical sanitation procedures ; to train personnel.Assistance provided by WHO in 1954. (a) A consultant in environmental sanitationfor three months. (Later WHO will provide two public -health engineers for twoyears.) (b) A fellowship.Probable Duration of Assistance. Until December 1956.
Fiji 1 Nov. 1954- Treponematoses Control
R Aim of the Project. To reduce the prevalence of yaws by mass examination and treat -UNICEF ment with penicillin ; ultimately to eliminate the disease as a public -health problem ;
to train local personnel in the diagnosis, therapy and epidemiology of yaws.Assistance provided (cost reimbursed by UNICEF). A chief medical adviser and aserologist, for six months from November 1954, both of whom will also work on asimilar project in Western Samoa, planned for 1955.Probable Duration of Assistance. Until November 1956.
/Hong Kong 4 April 1953- Maternal and Child Health
TA Aim of the Project. To demonstrate modern maternal and child health services suitableto Hong Kong ; to strengthen infant -welfare and school health programmes anddomiciliary midwifery services ; to provide instruction in child health for school-teachers and parents, health education, and refresher courses for midwives; to improvetraining in paediatrics and promote post -graduate education in child health.Assistance provided by WHO. A medical officer from April 1953, and two nurseeducators from March and July 1954 respectively.
Probable Duration of Assistance. Until September 1955.Work accomplished. By the end of 1954 an in- service training programme for public -health nurses and midwives and a school health programme were in operation.
PROJECT LIST : WESTERN PACIFIC 183
Project No.Source of Funds Dates DescriptionCo- operating Agencies
, Japan 1 Nov. 1952- Poliomyelitis and Rehabilitation of Crippled Children, Tokyo
R Aim of the Project. To consolidate and expand existing services for the protection ofUNICEF children against crippling and deformities, and for the diagnosis, treatment and
rehabilitation of crippled children ; to train local professional and auxiliary personnel.Assistance provided by WHO in 1954. A short -term consultant in occupational therapy(September- October).
Probable Duration of Assistance. Until 1957.
Work accomplished. A short -term consultant went to Tokyo in November 1952 ;subsequently a plan for the organization of training courses was agreed upon andfellowships were awarded to national personnel who, on their return, were to beresponsible for the training courses.
The second phase of the project began in September 1954 with the arrival of aconsultant in occupational therapy. Recommendations were submitted to the Govern-ment at the end of October.
Japan 2 Nov. 1952- Premature Infants, Tokyo
R Aim of the Project. To investigate the causes of prematurity and to devise methods ofpreventing it ; to demonstrate modern methods of care of premature infants ; to trainlocal professional and auxiliary personnel.Assistance provided by WHO. A consultant for three months in 1953 ; fellowships ;supplies and equipment.Probable Duration of Assistance. Until 1957.Work accomplished. Following the visit of the consultant recommendations weresubmitted to the Government. WHO supplied equipment and awarded three fellow-ships in 1954.
By the end of 1954 the three fellows had returned to their previous posts and atraining unit had been established at the Red Cross Lying -in Hospital.
It is expected to open in 1955 a centre at the Sategaya Infants Home.
Japan 4 June 1953- National Institute of Mental Health, Tokyo
R Aim of the Project. To survey the needs and existing facilities for mental health anddraw up a mental -health programme ; to carry out research ; to train local professionaland auxiliary personnel.Assistance provided by WHO. Two consultants, each for one month, in 1953 ; a fellow-ship ; supplies and equipment.Probable Duration of Assistance. Until the end of 1955.Work accomplished. In the first phase of the project the consultants formulated recom-mendations which were accepted by the Government.
V Laos 2
TA
3 Malaya 1TA
Jan. 1953- Treponematoses Control, Thakhet, Savannakhet, Saravane and PakséAim of the Project. To survey the yaws situation ; to train local personnel in thediagnosis and treatment of yaws ; to carry out a mass campaign through healtheducation, house -to -house case -finding and treatment of all accessible clinical casesand contacts so as to reduce incidence to a level at which the public -health programmecan maintain control.Assistance provided by WHO in 1954. A senior medical adviser.
Probable Duration of Assistance. Until December 1956.
Work accomplished. In spite of unsettled conditions which hampered progress, anumber of areas had been surveyed by the end of 1954 and a high percentage of theirpopulation treated. Considerable data had been accumulated. Surveys were carriedout a second time in villages where prevalence had been found to be high.
June 1950- Nursing Education, Kuala Lumpur and Penang
Aim of the Project. To improve the standard of basic and graduate nursing educationand the quality of nursing services ; to prepare local nurses for administrative andteaching posts ; to adapt the nursing- education programme to local resources andneeds.
184 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Assistance provided by WHO. At Kuala Lumpur -a midwifery tutor until June 1955.At Penang -a senior nurse educator and a male tutor until the end of 1955, and apaediatric tutor and a nurse educator until August 1954.Probable Duration of Assistance. Until the end of 1955.
Work accomplished. By the end of 1954 a school had been set up for preliminary trainingand courses for nurses and midwives were being given. From 2 August to 8 September1954 a post -graduate course was held at Penang, in which particular attention was paidto medicine, medical nursing and teaching.
Later, midwifery- training schools will be established at Penang, Ipoh, KualaLumpur, Malacca and Johore Bharu, to form the basis of a midwifery service for thewhole of Malaya.
Malaya 3 Dec. 1953- Yaws Control, Kelantan and TrengganuR Aim of the Project. To reduce the prevalence of yaws in Kelantan and Trengganu byUNICEF mass treatment with penicillin and, ultimately, to achieve complete control of the
disease ; to train local professional and auxiliary personnel in the diagnosis, moderntherapy and epidemiology of yaws ; to encourage case -finding and treatment by theexisting dispensaries, clinics and hospitals.
Assistance provided by WHO in 1954. A serologist for two months (March -April) ;fellowships.
Probable Duration of Assistance. Until the end of 1955.
Work in 1954. The mass campaign started in April ; despite well -planned house -to-house surveys only about 75 per cent. of the population could be examined. About20 per cent, of the population in the areas covered are estimated to be suffering fromthe disease.
A fellowship was awarded to the medical officer selected as director of the project,to enable him to observe yaws -control projects in Thailand, Indonesia and the Philip-pines.
Malaya 9 Nov. 1954- Rural- Health Training Centre, Jitra, KedahR Aim of the Project. To establish a training centre at Jitra for assistant health nurses,UNICEF rural midwives, dispensers and sanitary overseers.
Staff trained at the centre will be assigned to the rural health centres to be set upunder project Malaya 5, due to start in 1955.Assistance provided by WHO in 1954. A medical officer and a public -health nurse fortwo years from November.Probable Duration of Assistance. Until the end of 1956.
Malaya 11R
Nov. -Dec.1954
Mental Health
Aim of the Project. To review existing facilities and needs in connexion with mentalhospitals, particularly with a view to developing a community mental hospital pro-gramme.
Assistance provided by WHO. A consultant, in November and December.Work accomplished. The consultant visited the two mental hospitals of the Federationand made recommendations on training of medical and nursing staff, on number ofbeds required, and on measures for prevention of mental illness. At least two mental -nursing tutors and a lecturer in psychological medicine at the University of Malayawere considered to be needed.
North Borneo 6 June 1950- Nursing Education, Jesselton and SandakanTA Aim of the Project. To establish a programme of basic nursing education, including
public -health nursing and midwifery.
Assistance provided by WHO in 1954. Two nurse educators and a public -health nurse.
Probable Duration of Assistance. Until the end of 1955.Work accomplished. By the end of 1954 five health clinics in the Jesselton area had beenorganized ; a school of nursing had been established in Sandakan and training ofmidwives, public -health nurses, students and dressers was in progress.
PROJECT LIST : WESTERN PACIFIC 185
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Progress was hampered by shortage of nursing staff, making it necessary to transferstudents to other centres and trained nurses to provide nursing services where mostneeded.
North Borneo 8 Dec. 1953- Environmental Sanitation
TA Aim of the Project. To study environmental sanitation problems, particularly collectionand disposal of sewage in Jesselton, Labuan, Kudat, Tawau, Sandakan, Papar andBeaufort, with a view to carrying out appropriate measures.Assistance provided by WHO. A consultant from December 1953 to February 1954, andtwo public- health engineers from July and November 1954 respectively.
Probable Duration of Assistance. Until the end of 1956.
Work in 1954. Surveys were carried out in various areas ; work started on the sewagescheme in Jesselton.
;,d'Philippines 9
TA
Philippines 12
June 1952- Bilharziasis Pilot Project, Leyte
Aim of the Project. To determine the most effective and economical means of controllingbilharziasis ; to train local professional and auxiliary personnel ; to conduct studies onthe human, domestic -animal and snail hosts of Schistosoma japonicum and on theparasite itself ; to make an epidemiological study of the disease in a highly epidemicarea ; to plan a control programme.Assistance provided by WHO in 1954. A parasitologist, a malacologist and a public -health engineer.Probable Duration of Assistance. Until the end of 1956.Work accomplished. See page 106.
July 1953- Institute of Hygiene, University of the Philippines, Manila
TA Aim of the Project. To provide further training to the faculty of the Institute of Hygiene(Johns Hopkins by an exchange programme between members of the teaching staff of the Institute andUniversity) the Johns Hopkins University School of Hygiene and Public Health.(Rockefeller The Johns Hopkins Professors of Public - Health Administration and of SanitaryFoundation) Engineering spent short periods at the Institute in 1953 and 1954 ; the Professor of
Microbiology went there in 1954. The Johns Hopkins Associate Professors of SanitaryEngineering, Parasitology and Microbiology joined the staff of the Institute for a year,and two members of the Institute staff were assigned to the Johns Hopkins School,also for a year.
The visiting experts participated in the teaching at the Institute of Hygiene, theSchool of Medicine and the School of Engineering, and, to a certain extent, in otherteaching programmes of the University. They also served as special consultants to theDepartment of Health.
The project is scheduled to continue until 1957.
Philippines 14
TA
Feb. 1952 -July 1954
Malaria Pilot Project, MindoroAim of the Project. To determine the most effective and economic means of controllingmalaria transmitted by Anopheles minimus flavirostris, the chief vector in the Philip-pines ; to train local personnel ; to carry out studies on the malaria vector species ;to plan an expanded malaria -control programme to cover the whole country.
Assistance provided by WHO. A malariologist and an entomologist ; suppliesand equipment.Work accomplished. The results of the pilot project were particularly significantbecause they demonstrated, for the first time, that it is possible to control by residualinsecticides malaria transmitted by A. minimus flavirostris. The project provided thebasis for planning the overall malaria -control programme, in which FOA is assistingthe Government.
186 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Philippines 15 Aug. 1951- Treponematoses Control
R Aim of the Project. To control yaws in selected areas (see below) ; to reduce its pre -UNICEF valence so that it can be kept under control by the local health authorities ; to train
personnel ; to plan a long -term programme to be integrated into the governmentservices.
Assistance provided by WHO. Technical advice. (UNICEF provides supplies andequipment.)
Probable Duration of Assistance. Until December 1955.
Work accomplished. A control demonstration carried out in the provinces of Samarand Leyte was completed in August 1953. It was followed by an expanded programmein the provinces of Surigao, Agusan, Davao, Cotabato, Zamboanga, Sulu and Catan-duanes. In other provinces, where the prevalence of yaws is estimated to be low, controlwas integrated into the provincial health services, with participation of local personnel.
Consolidation of the control work will be assured by a rural health bill providingfor the establishment of 1102 rural health units.
Philippines 29 Oct. 1953- Midwifery Training, Caloocan
UNICEF Aim of the Project. To study existing midwifery services and training facilities ;to train village midwives (hilots) ; to make a study of maternity -nursing needs andresources ; to formulate a midwifery practice act.Assistance provided in 1954. A nurse educator in midwifery (cost reimbursed byUNICEF).Probable Duration of Assistance. Until December 1956.Work accomplished. By the end of 1954 midwifery training had been started in severalareas. Nurses who had completed training were assisting in the organization of hilotclasses in their own towns.
Sarawak 5 July 1952- Malaria Pilot Project, Baram, Northern Sarawak
TA Aim of the Project. To control malaria by indoor spraying with residual insecticides inan experimental area to determine the efficacity of this control method in the country ;to train professional, auxiliary and ancillary personnel for malaria control throughoutthe country.Assistance provided by WHO in 1954. A malariologist and an entomologist.Probable Duration of Assistance. Until December 1956.
Work accomplished. By the end of 1954 the malaria situation in practically the wholecountry had been mapped, observations on the malaria transmission period made andthe bionomics of the vector species studied. Training of personnel was in progress.
In October 1953 the project was extended to Brunei -project Brunei 3.In February 1954 the team started to combine the surveys and spraying operations
in remote villages with a campaign against yaws and gonorrhoea, using penicillintreatment.
This project is important for the Region and the results of the experimental workwill be of great value to the whole of Borneo.
Singapore 2 Oct. 1953- University of Malaya
TA Aim of the Project. To develop the teaching of preventive and social medicine in theFaculty of Medicine of the University ; to establish a first -class post -graduate school ofpublic health.Assistance provided by WHO in 1954. A professor of health education (until July),a reader in medical statistics, a professor of applied physiology and a lecturer in appliednutrition.
Probable Duration of Assistance. Until mid -1955.
Work accomplished. See page 107.
PROJECT LIST : WESTERN PACIFIC 187
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Singapore 3 June 1952- Nursing Education, Singapore
TA
v Viet Nam 2R
Feb. 1951 -June 1953Oct. 1954-
Aim of the Project. To improve the standard of nursing education and the qualityof nursing services and health teaching ; to prepare local nurses for administrative andteaching posts ; to adapt the nursing- education programme to local needs and resources.
Assistance provided by WHO in 1954. Two nurse educators -to the Singapore GeneralHospital.Probable Duration of Assistance. Until 1956.
Work accomplished. By the end of 1954 courses in midwifery education had beenorganized, training programmes for undergraduate and graduate nurses established,and a domiciliary after -care service introduced.
Public -Health Administration
Aim of the Project. To draw up long -term plans for health services.Assistance provided by WHO. A specialist in public -health administration from February1951 to June 1953, and a second from November 1954.Probable Duration of Assistance. Until November 1956.
Viet Nam 3 Dec. 1954- Maternal and Child Health, Saigon, Hue and Dalat
TA Aim of the Project. To meet needs in preventive and curative paediatrics by reorgani-UNICEF zation of the three clinics in Saigon -Cholon ; to develop a programme of maternal
and child health services by: setting up prenatal and post -natal consultative services;establishing maternal and child health centres in the three Saigon clinics, in a hospitalat Hue and in one at Dalat ; introducing progressively a system of domiciliary healthvisiting.
Assistance provided by WHO. An expert in maternal and child health from December1954. A public -health nurse will be provided in 1955.Probable Duration of Assistance. Until the end of 1956.
Viet Nam 4 Jan. 1954- BCG Vaccination
UNICEF Assistance provided in 1954 (cost reimbursed by UNICEF). A BCG officer and twoBCG nurses.Probable Duration of Assistance. Until the end of 1956.Work in 1954. Unsettled conditions hampered the progress of the campaign, but threeteams had been organized by the end of the year and it was expected shortly to organizea fourth.
At the end of the year the work of the WHO team was extended to Cambodia(project Cambodia 6) and the team leader will divide his time between the two countries.
The BCG assessment team (see project WPRO 12) worked in Viet Nam during theyear.
Viet Nam 5UNICEF
Nov. -Dec.1952Jan. 1954-
Children's Hospital, Saigon -Cholon
Aim of the Project. To establish a teaching hospital of 260 beds in Saigon -Cholon,based on plans drawn up by the WHO consultant on hospital planning who visitedViet Nam for two months in 1952 and for a week at the beginning of 1954.Assistance provided by WHO. Technical advice by the maternal and child health teamworking in Viet Nam (see project Viet Nam 3).
It is expected that the hospital will be opened in March 1955.

188 THE WORK OF WHO, 1954
Project No.Source of Funds Dates DescriptionCo- operating Agencies
INTER -REGIONAL
Inter -regional 7 1952- Field Trials in Rabies TreatmentR A study, in which laboratories of five countries are collaborating, is being carried
out to determine the value of different methods of inoculation of rabies vaccine andhyperimmune serum. Studies are also being made on the effectiveness of hyperimmuneserum in human beings exposed to the bites of rabid wolves.
Inter -regional 8 1951- Brucellosis Centres
R Work in the fourteen FAO /WHO brucellosis centres throughout the world (see(FAO) Map I, page 11) is in progress on standardization of diagnostic tests, bacteriological
studies, investigations on human therapy, vaccines for the prevention of the disease inanimals and studies on the pathogenesis of brucellosis.
Inter -regional 10 1948- Influenza Centres
R The centres (see Map 2, page 13) collect and study strains of influenza virus fromdifferent parts of the world ; watch for outbreaks of influenza, and classify the type ofvirus so that the appropriate vaccine may be prepared in advance of the spread of theoutbreak to other countries.
Inter -regional 11
R
Aug. 1953- International Treponematosis Laboratory Center, Johns Hopkins University School ofHygiene and Public Health, Baltimore
This centre collects strains of treponemes, examines their antigenic structure andtheir sensitivity to penicillin, undertakes immunological studies of treponemes, developstests using treponemes. At present there are three tests -the Treponema pallidumimmobilization test (TPI), the Treponema pallidum immune adherence test (TPIA) andthe Treponema pallidum agglutination test (TPA).
A grant of $5000 was paid in 1954 to the Johns Hopkins University.
Inter -regional 13 Jan. 1954 - International Shigella Centres, United Kingdom and United States of America
R Two centres were established on 1 January 1954, one at the Central Public HealthLaboratory, London, and the other at the Communicable Disease Center, Atlanta,Georgia. Both these centres collect and identify Shigella strains, distribute strains andsera to national centres, and train workers from national centres. The following grantswere paid in 1954: $3500 to the Medical Research Council ; $10 000 to the US PublicHealth Service.
Inter -regional 14 1954- Poliomyelitis Centres
R These centres collect and study strains of poliovirus from different parts of theworld ; undertake epidemiological studies in preparation for the eventual use ofvaccines ; train virologists in the latest tissue -culture techniques.
Inter- regional 15 April 1954- Standardization of Virus and Rickettsial Tests
R Work is under way to simplify and make more accurate screening procedures to beused in public -health laboratory tests for various viral and rickettsial diseases. Labora-tories of many countries are collaborating in this work.
PROJECT LIST : INTER- REGIONAL 189
Project No.Source of Funds Dates DescriptionCo- operating Agencies
Inter -regional 16 15 -24 Nov. Malaria Conference WPRO /SEARO, Baguio City, Philippines
R 1954 This conference was attended by forty -two participants from thirteen differentcountries. After the conference, nineteen of the participants visited the malaria servicesand the antimalaria campaigns in Taiwan. One of the main subjects discussed at theconference was whether malaria control by spraying with residual insecticides could berecommended for areas where malaria is transmitted by vector species which, untilrecently, were thought not to be amenable to control by such methods.
Inter -regional 21
R
Nov. 1950 -andJune 1954-
WHO Reference Laboratories, Copenhagen and ChambleeThe WHO International Serological Reference Laboratory was established at the
Statens Seruminstitut, Copenhagen, in November 1950. It tests antigens and sera,examines reference preparations, studies serological methods and trains personnel.
A grant of $4000 was paid in 1954 to the Institute.The Venereal- Disease Research Laboratory was established in June 1954 at the
Communicable Disease Center, Chamblee, Georgia, United States of America. Itsfunctions are the same as those of the Copenhagen laboratory. No grant is made.

ANNEXES
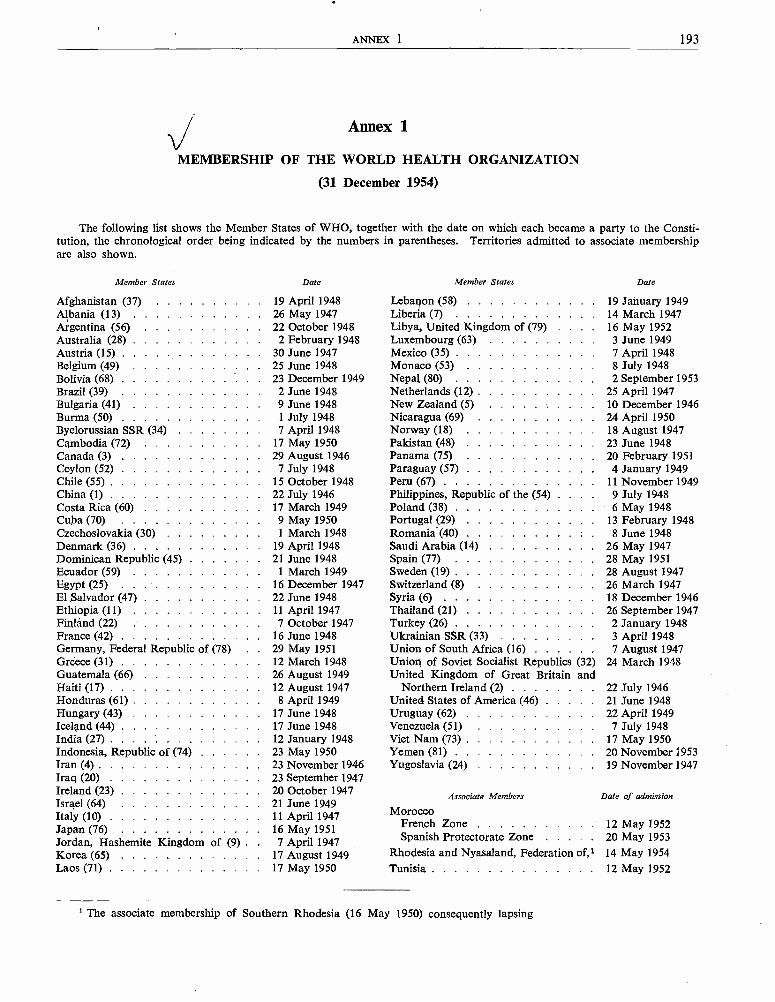
ANNEX 1 193
Annex 1
MEMBERSHIP OF THE WORLD HEALTH ORGANIZATION
(31 December 1954)
The following list shows the Member States of WHO, together with the date on which each became a party to the Consti-tution, the chronological order being indicated by the numbers in parentheses. Territories admitted to associate membershipare also shown.
Member States Date Member States Date
Afghanistan (37) 19 April 1948 Lebaion (58) 19 January 1949Albania (13) 26 May 1947 Liberia (7) 14 March 1947Argentina (56) 22 October 1948 Libya, United Kingdom of (79) 16 May 1952Australia (28) 2 February 1948 Luxembourg (63) 3 June 1949Austria (15) 30 June 1947 Mexico (35) 7 April 1948Belgium (49) 25 June 1948 Monaco (53) 8 July 1948Bolivia (68) 23 December 1949 Nepal (80) 2 September 1953Brazil (39) 2 June 1948 Netherlands (12) 25 April 1947Bulgaria (41) 9 June 1948 New Zealand (5) 10 December 1946Burma (50) 1 July 1948 Nicaragua (69) . .. 24 April 1950Byelorussian SSR (34) 7 April 1948 Norway (18) 18 August 1947Cambodia (72) 17 May 1950 Pakistan (48) 23 June 1948Canada (3) 29 August 1946 Panama (75) 20 February 1951Ceylon (52) 7 July 1948 Paraguay (57) 4 January 1949Chile (55) 15 October 1948 Peru (67) 11 November 1949China (1) 22 July 1946 Philippines, Republic of the (54) 9 July 1948Costa Rica (60) 17 March 1949 Poland (38) 6 May 1948Cuba (70) 9 May 1950 Portugal (29) 13 February 1948Czechoslovakia (30) 1 March 1948 Romania (40) 8 June 1948Denmark (36) 19 April 1948 Saudi Arabia (14) 26 May 1947Dominican Republic (45) 21 June 1948 Spain (77) 28 May 1951Ecuador (59) 1 March 1949 Sweden (19) 28 August 1947Egypt (25) 16 December 1947 Switzerland (8) 26 March 1947El Salvador (47) 22 June 1948 Syria (6) 18 December 1946Ethiopia (11) 11 April 1947 Thailand (21) 26 September 1947Finland (22) 7 October 1947 Turkey (26) 2 January 1948France (42) 16 June 1948 Ukrainian SSR (33) 3 April 1948Germany, Federal Republic of (78) 29 May 1951 Union of South Africa (16) 7 August 1947Greece (31) 12 March 1948 Union of Soviet Socialist Republics (32) 24 March 1948Guatemala (66) 26 August 1949 United Kingdom of Great Britain andHaiti (17) 12 August 1947 Northern Ireland (2) 22 July 1946Honduras (61) 8 April 1949 United States of America (46) 21 June 1948Hungary (43) 17 June 1948 Uruguay (62) 22 April 1949Iceland (44) 17 June 1948 Venezuela (51) 7 July 1948India (27) 12 January 1948 Viet Nam (73) 17 May 1950Indonesia, Republic of (74) 23 May 1950 Yemen (81) 20 November 1953Iran (4) 23 November 1946 Yugoslavia (24) 19 November 1947Iraq (20) 23 September 1947Ireland (23) 20 October 1947 Associate Members Date of admissionIsrael (64) 21 June 1949Italy (10) 11 April 1947 Morocco
Japan (76) 16 May 1951 French Zone 12 May 1952
Jordan, Hashemite Kingdom of (9) 7 April 1947 Spanish Protectorate Zone 20 May 1953
Korea (65) 17 August 1949 Rhodesia and Nyasaland, Federation of,' 14 May 1954Laos (71) 17 May 1950 Tunisia 12 May 1952
1 The associate membership of Southern Rhodesia (16 May 1950) consequently lapsing
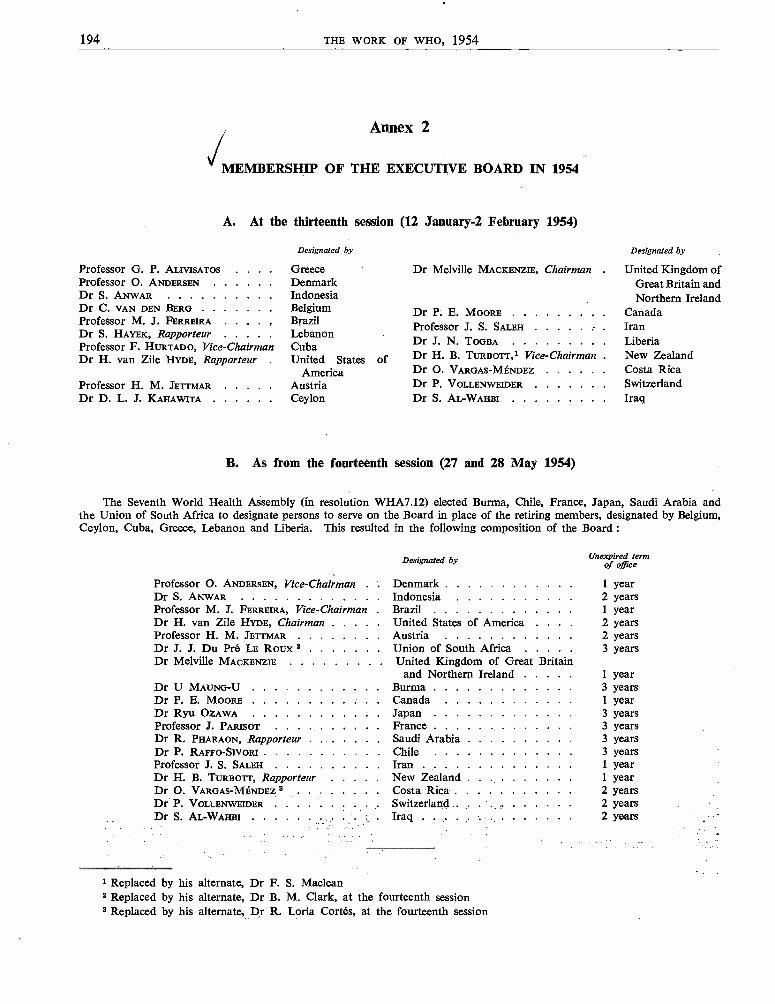
194 THE WORK OF WHO, 1954
Annex 2
MEMBERSHIP OF THE EXECUTIVE BOARD IN 1954
A. At the thirteenth session (12 January -2 February 1954)
Professor G. P. ALIVISATOSProfessor O. ANDERSENDr S. ANWARDr C. VAN DEN BERGProfessor M. J. FERREIRADr S. HAYEK, RapporteurProfessor F. HURTADO, Vice - ChairmanDr H. van Zile HYDE, Rapporteur
Professor H. M. JETTMARDr D. L. J. KAHAWITA
Designated by
GreeceDenmarkIndonesiaBelgiumBrazilLebanonCubaUnited States
AmericaAustriaCeylon
Dr Melville MACKENZIE, Chairman
Dr P. E. MOOREProfessor J. S. SALEHDr J. N. TOGBA
of Dr H. B. TURBOTT,1 Vice-ChairmanDr O. VARGAS-MÉNDEZDr P. VOLLENWEIDERDr S. AL-WAHBI
B. As from the fourteenth session (27 and 28 May 1954)
Designated by
United Kingdom ofGreat Britain andNorthern Ireland
CanadaIranLiberiaNew ZealandCosta RicaSwitzerlandIraq
The Seventh World Health Assembly (in resolution WHA7.12) elected Burma, Chile, France, Japan, Saudi Arabia andthe Union of South Africa to designate persons to serve on the Board in place of the retiring members, designated by Belgium,Ceylon, Cuba, Greece, Lebanon and Liberia. This resulted in the following composition of the Board :
Professor O. ANDERSEN, Vice - ChairmanDr S. ANWARProfessor M. J. FERREIRA, Vice - ChairmanDr H. van Zile HYDE, ChairmanProfessor H. M. JETTMARDr J. J. Du Pré LE Roux 2Dr Melville MACKENZIE
Dr U MAUNG-UDr P. E. MooREDr Ryu OZAWAProfessor J. PARISOTDr R. PHARAON, RapporteurDr P. RAFFO-SIVORIProfessor J. S. SALEH . . . .
Dr H. B. TURBOTT, RapporteurDr O. VARGAS-MÉNDEZ 3Dr P. VOLLENWEIDERDr S. AL-WAHBI
Designated by
DenmarkIndonesiaBrazilUnited States of America . .
AustriaUnion of South Africa . . .
United Kingdom of Great Britainand Northern Ireland
BurmaCanadaJapanFranceSaudi ArabiaChileIranNew ZealandCosta RicaSwitzerlandIraq . . . . . . . .
I Replaced by his alternate, Dr F. S. Maclean2 Replaced by his alternate, Dr B. M. Clark, at the fourteenth session3 Replaced by his alternate, Dr R. Loria Cortés, at the fourteenth session
Unexpired termof office
1 year2 years1 year2 years2 years3 years
1 year3 years1 year3 years3 years3 years3 years1 year1 year2 years2 years2 years

ANNEX 3 195
Annex 3
EXPERT ADVISORY PANELS AND COMMITTEES 1
1. EXPERT ADVISORY PANELS
To supply the Organization with technical advice by correspondence and to provide the membershipof its expert committees (and of the Committee on International Quarantine), panels of experts have beenestablished for each of the following subjects :
AntibioticsBiological standardizationBrucellosisCholeraChronic degenerative diseasesDrugs liable to produce addictionEnvironmental sanitationHealth education of the publicHealth statisticsInsecticidesInternational pharmacopoeia and pharmaceutical
preparationsInternational quarantineLeprosyMalariaMaternal and child healthMental healthNursing
NutritionOccupational healthOrganization of medical careParasitic diseasesPlagueProfessional and technical education of medical and
auxiliary personnelPublic -health administrationRabiesRehabilitationRickettsiosesTrachomaTuberculosisVenereal infections and treponematoses (including
serology and laboratory aspects)Virus diseasesYellow feverZoonoses
2. EXPERT COMMITTEES
The membership of the expert committees which met in
Expert Committee on Alcohol and Alcoholism
First SessionDr H. Duchêne, Chief, Mental Health Service, Département
de la Seine, Paris, FranceDr H. Isbell, Director of Research, Public Health Service
Hospital, Lexington, Ky., United States of AmericaDr G. A. R. Lundquist, Associate Professor of Psychiatry ;
Chief Physician, Lángbro Hospital, Stockholm, SwedenL. D. MacLeod, B.Sc., Burden Neurological Institute,
Stapleton, Bristol, EnglandDr J. Mardones Restat, Professor of Pharmacology, Faculty
of Medicine, University of Chile, Santiago, ChileProfessor J. E. Staehelin, University Psychiatric Clinic, Basle,
SwitzerlandDr H. M. Tiebout, Greenwich, Conn., United States of America
1954 was as follows :
Expert Committee on Biological Standardization
Eighth Session
Dr E. Grasset, Director, Institut d'Hygiène ; Professor ofBacteriology and Hygiene, University of Geneva, Switzerland
Dr O. Maaloe, Chief, Department of Biological Standards,Statens Seruminstitut, Copenhagen, Denmark
Professor A. A. Miles, Director, Lister Institute of PreventiveMedicine, London, England
Dr C. A. Morrell, Director, Food and Drug Divisions, Depart-ment of National Health and Welfare, Ottawa, Canada
Professor A. B. Nichols, Secretary, United States Pharmaco-poeial Convention Inc., New York, N.Y., United States ofAmerica
1 The Committee on International Quarantine, which has special functions defined by the Health Assembly in resolutionWHA6.20, is for convenience included in this annex, as section 3.
196 THE WORK OF WHO, 1954
Dr W. L. M. Perry, Director, Department of BiologicalStandards, National Institute for Medical Research, MillHill, London, England
Professor R. Prigge, Director, Paul- Ehrlich Institut, StaatlicheAnstalt für Experimentelle Therapie, Frankfurt -am -Main,Germany
Professor J. Tréfouel, Director, Institut Pasteur, Paris, France
Dr P. M. Wagle, Director, Haffkine Institute, Bombay, India
Dr W. G. Workman, Chief, Biologics Control Laboratory,National Microbiological Institute, National Institutes ofHealth (Public Health Service), Bethesda, Md., UnitedStates of America
Expert Committee on Drugs Liable to Produce Addiction
Fifth Session
Sir Ram Nath Chopra, M.D., Emeritus Professor, Director,Drug Research Laboratory, Srinagar, Kashmir
Dr N. B. Eddy, Chief, Section on Analgesics, Division ofChemistry, National Institute of Arthritis and MetabolicDiseases, National Institutes of Health (Public HealthService), Bethesda, Md., United States of America
Dr F. Eichholtz, Professor of Pharmacology, Faculty ofMedicine, University of Heidelberg, Germany
Dr G. Joachimoglu, Professor of Pharmacology ; Chairman,Superior Health Council, Ministry of Hygiene, Athens,Greece
Dr J. La Barre, Professor of Pharmacology, Faculty ofMedicine and Pharmacy, University of Brussels, Belgium
Dr B. Lorenzo -Velázquez, Professor of Pharmacology,Faculty of Medicine, University of Madrid, Spain
J. R. Nicholls, D.Sc., Department of the Government Chemist,London, England
Dr J. M. Watt, Professor of Pharmacology and Therapeutics,Medical School, University of Witwatersrand, Johannes-burg, Union of South Africa
Expert Committee on Health Statistics
Fourth Session
Dr M. J. Aubenque, Chief, Health Statistics Section, Institutnational de la Statistique et des Etudes économiques, Paris,France
Dr M. Grais, Director, Statistical Section, Ministry of PublicHealth, Cairo, Egypt
F. F. Harris, Director, Health and Welfare Division, DominionBureau of Statistics, Ottawa, Canada
Dr I. M. Moriyama, Chief, Mortality Analysis Branch,National Office of Vital Statistics, Department of Health,Education and Welfare, Washington, D.C., United Statesof America
Dr K. C. K. E. Raja, Ministry of Health, New Delhi, India
Dr Sadamu Watanabe, Division of Health and WelfareStatistics, Ministry of Health and Welfare, Tokyo, Japan
Expert Committee on Insecticides
Fifth Session
Dr A. W. A. Brown, Head, Department of Zoology, Uni-versity of Western Ontario, London, Canada
Dr R. A. E. Galley, Director, Colonial Products ResearchLaboratory, London, England
Dr H. L. Haller, Assistant Director, Crops Research, Agri-cultural Research Service, Department of Agriculture,Washington, D.C., United States of America
Dr H. Mazzarri, Chief, Chemical Laboratory, Division ofMalariology, Ministry of Health and Social Welfare,Maracay, Venezuela
Dr R. Pal, Assistant Director, Malaria Institute of India,New Delhi, India
Dr J. Treboux, Research Laboratory J. R. Geigy S.A., Basle,Switzerland
Expert Committee on the International Pharmacopoeia
Thirteenth Session
Dr H. Baggesgaard Rasmussen, Professor of Organic Che-mistry, Royal Danish School of Pharmacy, Copenhagen,Denmark ; Member of the Danish Pharmacopoeia Com-mission and of the Scandinavian Pharmacopoeial Council
Dr T. Canbáck, Director, Pharmaceutical Control Laboratory,Stockholm, Sweden ; Vice -Chairman of the SwedishPharmacopoeia Commission ; Member of the ScandinavianPharmacopoeial Council
Dr I. R. Fahmy, Professor of Pharmacognosy, Faculty ofMedicine, Cairo University, Egypt ; Secretary of theEgyptian Pharmacopoeia Commission
Dr H. Flück, Professor of Pharmacognosy, Federal Instituteof Technology, Zurich, Switzerland ; Member of the FederalPharmacopoeia Commission
Dr C. H. Hampshire, formerly Secretary, British Pharmaco-poeia Commission, General Medical Council Office,London, England
Dr R. Hazard, Professor of Pharmacology and Materiamedica, Faculty of Medicine, University of Paris, France ;Member of the French Pharmacopoeia Commission
Dr L. C. Miller, Director of Revision of the Pharmacopeiaof the United States of America, New York, N.Y., UnitedStates of America
Dr B. Mukerji, Director, Central Drug Research Institute,Lucknow, India ; Joint Secretary of the Co- ordinationCommittee, Indian Pharmacopoeia
Dr D. van Os, Professor of Pharmacy and Toxicology, Uni-versity of Groningen, Netherlands ; Chairman, NetherlandsPharmacopoeia Commission
Dr J. L. Powers, Chairman, Committee on National For-mulary, American Pharmaceutical Association, Washington,D.C., United States of America
Sub -Committee on Non -Proprietary Names
Sixth Session
Dr H. Baggesgaard Rasmussen, Professor of Organic Che-mistry, Royal Danish School of Pharmacy, Copenhagen,Denmark ; Member of the Danish Pharmacopoeia Com-mission and of the Scandinavian Pharmacopoeial Council

ANNEX 3 197
T. C. Denston, Secretary, British Pharmacopoeia Commission,London, England
Dr R. Hazard, Professor of Pharmacology and Materiamedica, Faculty of Medicine, University of Paris, France ;Member of the French Pharmacopoeia Commission
Dr E. Sellés, Professor of Galenical Pharmacy, Faculty ofPharmacy, University of Madrid, Spain ; Member ofthe Spanish Pharmacopoeia Commission
Dr R. T. Stormont, Secretary, Council on Pharmacy andChemistry, American Medical Association, Chicago, Ill.,United States of America
Expert Committee on Mental Health
Fourth Session
Dr J. V. Ashburner, Psychiatrist Superintendent, MentalHospital, Kew, Australia
Dr E. J. Aujaleu, Director of Social Health, Ministry ofHealth and Population, Paris, France
Dr A. Botelho, Director, National Service for Mental Diseases,Rio de Janeiro, Brazil
Dr R. Felix, Director, National Institute of Mental Health,National Institutes of Health (Public Health Service),Bethesda, Md., United States of America
Professor H. W. Gruhle, Director, University Neuro-Psychiatric Clinic, Bonn, Germany
Professor G. Kraus, University Psychiatric Clinic, Gronin-gen, Netherlands
Dr G. A. R. Lundquist, Associate Professor of Psychiatry ;Chief Physician, Lângbro Hospital, Stockholm, Sweden
Dr T. P. Rees, Medical Superintendent, Warlingham ParkHospital, Warlingham, Surrey, England
Dr Tigani el Mahi, Clinic for Nervous Diseases, KhartoumNorth, Sudan
Expert Committee on Midwifery Training
First SessionMiss A. Anderson, Nurse -Midwife Consultant, Royal Medical
Board, Stockholm, Sweden
Dr S. Bhatia, Adviser in Maternity and Child Welfare,Directorate- General of Health Services, New Delhi, India
Miss P. M. Dickens, Principal Matron, Medical Service,Ministry of Health, Sudan Government, Khartoum,Sudan
Dr N. J. Eastman, Professor of Obstetrics, Johns HopkinsUniversity, Baltimore, Md., United States of America
Miss N. Goffard, Midwifery Tutor, Institut Edith Cavell -Marie Depage, Brussels, Belgium
Dr J. H. de Haas, Head, Maternal and Child Health Depart-ment, National Public Health Service, The Hague ; Head,Health Department, Netherlands Institute of PreventiveMedicine, Leyden, Netherlands
Miss M. Kaneko, Chief, Nursing Section, Ministry of Healthand Welfare, Tokyo, Japan
Dr S. Prawirohardjo, Professor of Obstetrics and Gynaecology,University of Indonesia, Jakarta, Indonesia
Dr J. M. Sénécal, Professor of Paediatrics, Institut des HautesEtudes, Dakar, Senegal
Miss E. Stephenson, Chief Nursing Officer, Public HealthDepartment, Newcastle- upon -Tyne, England
Expert Committee on Nursing
Third Session
Miss Mei -yu Chow, Dean and Professor of Nursing, NursingDepartment, National Defense Medical Center, Taipeh,Taiwan
Miss E. Cockayne, Chief Nursing Officer, Ministry of Health,London, England
Miss M. M. Doctor, Superintendent of Nursing Services,Office of the Surgeon -General, Government of Bombay,India
Miss R. M. Morrison, Associate Professor, School of Nursing,University of British Columbia, Vancouver, Canada
Miss M. R. S. Pinheiro, Director, Nursing Division, SpecialPublic Health Service, Rio de Janeiro, D.F., Brazil
Miss R. Sleeper, Director, School of Nursing and NursingServices, Massachusetts. General Hospital, Boston, Mass.,United States of America
Joint Expert Committees
Joint WHO /FAO Expert Committee on Meat Hygiene
First Session
FAO
Professor A. Jepsen, Royal Veterinary and AgriculturalCollege, Copenhagen, Denmark
Dr A. R. Miller, Chief, Federal Inspection Service, Depart-ment of Agriculture, Washington, D.C., United States ofAmerica
Dr H. Thornton, Chief Veterinary Inspector, City of New-castle- upon -Tyne, England
WHO
Dr W. C. Cockburn, Central Public Health Laboratory,Public Health Laboratory Service, London, England
Professor G. M. Dack, Director, Food Research Institute,University of Chicago, Chicago, Ill., United States ofAmerica
N. A. Nilsson, Sveriges Slakteriforbund, Stockholm, Sweden
Professor F. Schonberg, Institut für Tierürztliche Lebens-mittelkunde and Milch Hygiene, Hanover, Germany
Dr A. A. Sidky, Director -General, Cairo Municipal HealthDepartment, Cairo, Egypt
Dr Takeo Matsui, Chief, Veterinary Department, Instituteof Public Health, Tokyo, Japan.

198 THE WORK OF WHO, 1954
Joint FAO /WHO Expert Committee on Nutrition
Fourth Session
FAO
Professor M. J. L. Dols, General Adviser, Ministry of Agri-culture, Fisheries and Food, The Hague, Netherlands
Professor A. Keys, Director, Laboratory of PhysiologicalHygiene, University of Minnesota, Minneapolis, Minn.,United States of America
Dr Hazel K. Stiebeling, Director, Bureau of Human Nutritionand Home Economics, Department of Agriculture,Washington, D.C., United States of America
Professor E. F. Terroine, Director, Centre national de Co-ordination des Etudes et Recherches sur la Nutrition etl'Alimentation, Centre national de la Recherche scienti-fique, Paris, France
Dr N. Wright, Chief Scientific Adviser, Ministry of Food,London, England
WHO
Dr J. M. Bengoa, Chief, Technical Section, National Institute ofNutrition, Caracas, Venezuela
Professor W. J. Darby, Director, Division of Nutrition,Vanderbilt University School of Medicine, Nashville, Tenn.,United States of America
Professor B. S. Platt, Director, Applied Nutrition Unit,London School of Hygiene and Tropical Medicine ;Director, Human Nutrition Research Unit, MedicalResearch Council, London, England
Dr M. V. Radhakrishna Rao, Chief, Department of Nutrition,Government of Bombay ; Haffkine Institute, Bombay,India
Second Session
Dr J. Salcedo, jr, Head, Department of Chemical Hygieneand Nutrition, Institute of Hygiene, University of thePhilippines, Manila, Philippines
Joint ILO /WHO Committee on the Hygiene of Seafarers
Second Session
ILO
Captain O. I. Loennechen, Vice -President, InternationalShipping Federation, Tonsberg, Norway
Sir Richard Snedden, General Manager, International Ship-ping Federation, London, England
Captain D. S. Tennant, General Secretary, Navigators andEngineer Officers Union, London, England
Tom Yates, General Secretary, National Union of Seamen,London, England
WHO
Dr P. R. Dutt, Deputy Assistant Director -General of HealthServices, New Delhi, India
Dr K. Evang, Director - General of Health Services, Oslo,Norway
Professor W. M. Frazer, Emeritus Professor of Public Health,University of Liverpool, England
Dr G. H. Hunt, Assistant Surgeon General ; Associate Chief,Bureau of Medical Services, Public Health Service, Depart-ment of Health, Education and Welfare, Washington, D.C.,United States of America
Dr J. Lembrez, Divisional Inspector of Health, Director ofthe Service de Contrôle sanitaire, Marseilles, France
3. COMMITTEE ON INTERNATIONAL QUARANTINE
Members
H. B. Calderwood, Office of the United Nations Economicand Social Affairs, Department of State, Washington, D.C.,United States of America
Dr A. Castro, formerly Director, National Anti -Plague Ser-vice, Ministry of Education and Health, Rio de Janeiro,D.F., Brazil
Professor A. Halawani, Director, Research Institute andHospital of Tropical Diseases, Cairo, Egypt
Dr M. Jafar, Director -General of Health ; Joint Secretary,Ministry of Health and Works, Karachi, Pakistan
Dr C. K. Lakshmanan, Director -General of Health Services,Ministry of Health, New Delhi, India
Dr M. T. Morgan, Medical Adviser, Ministry of Transport ;formerly Medical Officer of Health, Port of LondonAuthority, London, England
1 The Committee on International Quarantine is governedby special regulations adopted by the Seventh World HealthAssembly in resolution WHA7.56. (For text of the regulations,see O ff. Rec. Wld Hlth Org. 56, 70.)
Dr C. B. Spencer, Medical Director, Chief, Division ofForeign Quarantine, Public Health Service, Department ofHealth, Education and Welfare, Washington, D.C., UnitedStates of America
Dr O. Vargas -Méndez, Director- General of Health, San José,Costa Rica
Dr M. A. Vaucel, Inspecteur général des Instituts Pasteurd'Outre -Mer, Institut Pasteur, Paris, France
Additional Members (for yellow fever matters)
Dr A. F. Mahaffy, formerly Director, Virus Research Insti-tute, Entebbe, Uganda
Dr K. C. Smithbum, Division of Medicine and Public Health,Rockefeller Foundation, South African Institute for MedicalResearch, Johannesburg, Union of South Africa
Dr R. M. Taylor, Director, Department of Virology, USNaval Medical Research Unit No. 3, Cairo, Egypt
Dr B. Wilson, formerly of the Division of Medicine andPublic Health, Rockefeller Foundation, New York, N.Y.,United States of America
ANNEX 4 199
Annex 4
ORGANIZATIONAL MEETINGS AND MEETINGS OF EXPERT COMMITTEES
AND ADVISORY GROUPS HELD IN 19541
7 -13 Jan.
12 Jan. - 2 Feb.15 -20 Feb.
29 March - 3 April9 -12 April
29 April - 1 May
4 -21 May
21 May27 -28 May
28 June - 3 July2 -7 Aug.
23 -28 Aug.
2 -11 Sept.
6 -13 Sept.
13 -16 Sept.
Study Group on the Psychobiological Development of the ChildExecutive Board, thirteenth sessionAdvisory Group on Classification of DiseasesExpert Committee on Nursing, third sessionILO /WHO : Joint Committee on the Hygiene of Seafarers, second sessionUNICEF /WHO : Joint Committee on Health Policy, seventh sessionSeventh World Health AssemblyRegional Committee for Europe, special sessionExecutive Board, fourteenth sessionExpert CommitteeExpert CommitteeConsultant Group
on the International Pharmacopoeia, thirteenth sessionon Midwifery Training, first sessionon Prosthetics
Expert Committee on Insecticides, fifth session
Regional Committee for the Western Pacific, fifth sessionRegional Committee for Europe, fourth session
13 -18 Sept. Expert Committee on Health Statistics, fourth session20 -25 Sept. Consultant Group on Dental Health20 -25 Sept. Regional Committee for Africa, fourth session21 -25 Sept. Regional Committee for South -East Asia, seventh session
27 -30 Sept. Expert Committee on the International Pharmacopoeia, Sub -Committee on Non -Proprietary Names, sixth session
27 Sept. - 1 Oct. Regional Committee for the Eastern Mediterranean, fourth session : Sub -Com-mittee A
27 Sept. - 2 Oct. Expert Committee on Alcohol and Alcoholism7 -22 Oct. Regional Committee for the Americas, sixth session, and XIV Pan American
Sanitary Conference
11 -16 Oct. Expert Committee on Drugs Liable to Produce Addiction, fifth session18 -23 Oct. Expert Committee on Biological Standardization, eighth session25 Oct. - 2 Nov. Committee on International Quarantine, second session26 Oct. - 2 Nov. FAO /WHO : Joint Expert Committee on Nutrition, fourth session1 -6 Nov. Expert Committee on Mental Health, fourth session6 -11 Dec. WHO /FAO : Joint Expert Committee on Meat Hygiene, first session13 -15 Dec. Consultant Group on Atomic Energy in relation to Medicine and Public Health
LondonGeneva
London
London
Geneva
Geneva
Geneva
Geneva
Geneva
Geneva
The HagueCopenhagen
Maracay,Venezuela
Manila
Opatija,Yugoslavia
Geneva
Geneva
Leopoldville
New Delhi
Geneva
Alexandria
Geneva
Santiago, Chile
Geneva
Geneva
Geneva
Geneva
Geneva
Geneva
Geneva
Details of seminars, training courses and regional technical conferences organized by WHO in co- operation with governmentsor with organizations are given in the Project List in Part IV, and in Table II on p. 86.
200 THE WORK OF WHO, 1954
Annex 5
TENTATIVE SCHEDULE OF WHO ORGANIZATIONAL MEETINGS IN 1955
10 January
18 January10 MayBeginning of June19 September
September
September
September
September
October
Executive Board, fifteenth session, Standing Committee on Administration andFinance
Executive Board, fifteenth sessionEighth World Health AssemblyExecutive Board, sixteenth sessionRegional Committee for Africa, fifth sessionRegional Committee for South -East Asia, eighth sessionRegional Committee for Europe, fifth sessionRegional Committee for the Eastern Mediterranean, fifth session
Sub -Committee ASub -Committee B
Regional Committee for the Western Pacific, sixth sessionRegional Committee for the Americas, seventh session, and Directing Council
PASO, eighth meeting
Annex 6
Geneva
Geneva
Mexico CityMexico CityMadagascar
Indonesia
Vienna
Lebanon(Unscheduled)
Singapore
Washington, D.C.
NON -GOVERNMENTAL ORGANIZATIONS IN OFFICIAL RELATIONSHIP WITH WHO
(as at 31 December 1954)
American College of Chest Physicians,Chicago, Ill., United States of America
Biometric Society,New Haven, Conn., United States of America
Central Council for Health Education,London, England
Council for International Organizations of Medical Sciences,Paris, France
Fédération dentaire internationale,London, England
Inter -American Association of Sanitary Engineering,Rio de Janeiro, Brazil
International Academy ofBordeaux, France
International AssociationRome, Italy
International AssociationParis, France
International CommitteeSocial Workers,Paris, France
Forensic and Social Medicine,
of Microbiological
for the Prevention
Societies,
of Blindness,
of Catholic Nurses and Medico-
International Committee of the Red Cross,Geneva, Switzerland
International Conference of Social Work,Columbus, Ohio, United States of America
International Council of Nurses,London, England
International Federation for Housing and Town Planning,The Hague, Netherlands
International Hospital Federation,London, England
International League against Rheumatism,Philadelphia, Pa., United States of America
International Leprosy Association,London, England
International Paediatric Association,Zurich, Switzerland
International Pharmaceutical Federation,Amsterdam, Netherlands
International Society for the Welfare of Cripples,New York, N.Y., United States of America

ANNEX 7 201
International Union against Cancer,Paris, France
International Union for Child Welfare,Geneva, Switzerland
International Union against Tuberculosis,Paris, France
International Union against Venereal Diseases,Paris, France
League of Red Cross Societies,Geneva, Switzerland
Medical Women's International Association,London, England
Union OSE - World -wide Organization for Child Care,Health and Hygiene among Jews,Geneva, Switzerland
World Federation for Mental Health,London, England
World Federation of United Nations Associations,Geneva, Switzerland
World Medical Association,New York, N.Y., United States of America
Annex 7
REGULAR BUDGET FOR 1954
Appropriation Purpose of appropriationsection
PART I : ORGANIZATIONAL MEETINGS
Originalamountvoted I
US $
Transfersauthorized
by ExecutiveBoard 2US$
appropria-Revised
tion
US$
1. World Health Assembly 159 500 (2 200) 157 3002. Executive Board and its Committees 87 450 87 4503. Regional Committees 44 400 5 600 50 000
Total - Part I 291 350 3 400 294 750
PART II : OPERATING PROGRAMME
4. Central Technical Services 1 544 847 (33 116) 1 511 7315. Advisory Services 4 357 963 (45 862) 4 312 101
6. Regional Offices 1 149 277 75 578 1 224 8557. Expert Committees and Conferences 135 757 135 757
Total - Part II 7 187 844 (3 400) 7 184 444
PART III : ADMINISTRATIVE SERVICES
8. Administrative Services 1 018 506 1 018 506
Total - Part III 1 018 506 - 1 018 506
SUB -TOTAL - PARTS I TO III 8 497 700 8 497 700
PART IV : RESERVE
9. Undistributed Reserve 1 340 300 1 340 300
Total - Part IV 1 340 300 1 340 300
TOTAL - ALL PARTS 9 838 000 - 9 838 000
1 Voted by the Sixth World Health Assembly (resolution WHA6.28, Off. Rec. Wld Hlth Org. 48, 27)2 Transfers authorized by the Executive Board at its thirteenth and fourteenth sessions (resolutions EB13.R22, Off. Rec. Wld
filth Org. 52, 8 and EB14.R16, Off. Rec. Wld Hlth Org. 57, 4)

202 THE WORK OF WHO, 1954
Annex 8STRUCTURE OF THE HEADQUARTERS SECRETARIAT
THE DIRECTOR -GENERAL - Offices of the Director -General
Departments
-AdvisoryServices
-CentralTechnicalServices
Divisions
-Communicable- DiseaseServices
-Organization of Public -HealthServices
-Environmental Sanitation
-Education and Training Services
-Epidemiological and HealthStatistical Services
- -Therapeutic Substances
-Editorial and Reference Services -
-Administrationand Finance -
-Administrative Managementand Personnel
-Budget and Finance
-Division of Public Information-Office of External Relations-Office of Technical Assistance-Office of Reports and Analysis
Sections
-Malaria and Insect Control-Tuberculosis-Venereal Diseases and Treponematoses-Endemo- epidemic Diseases
-Maternal and Child Health-Mental Health-Nutrition-Public -Health Administration-Nursing-Health Education of the Public-Social and Occupational Health
-Fellowships-Exchange of Scientific Information-Assistance to Educational Institutions
-Epidemiological Information and MorbidityStatistics
-International Quarantine-Statistical Studies-International Classification of Diseases and
Causes of Death-Singapore Epidemiological Intelligence Station
-Biological Standardization-Pharmaceutical-Addiction -producing Drugs-Health Laboratory Methods-Tuberculosis Research Office, Copenhagen
-Technical Publications-Health Legislation-Documents and Official Records-Translation-Library and Reference Services
-Administrative Management-Personnel-Conference and Office Services-Supply Services
Legal Office-I-Office of Internal Audit
Budget-I- and Accounts
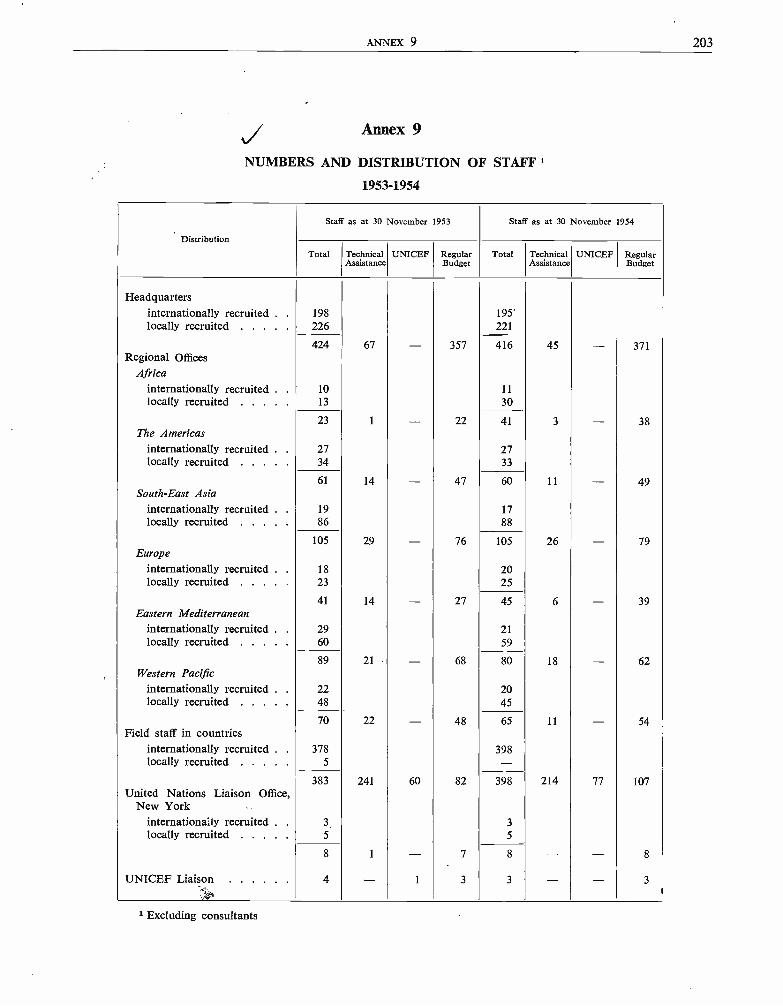
ANNEX 9 203
Annex 9
NUMBERS AND DISTRIBUTION OF STAFF
1953 -1954
Distribution
Staff as at 30 November 1953 Staff as at 30 November 1954
Total TechnicalAssistance
UNICEF RegularBudget
Total TechnicalAssistance
UNICEF RegularBudget
Headquartersinternationally recruited . 198 195'locally recruited 226 221
424 67 - 357 416 45 - 371Regional Offices
Africainternationally recruited . 10 11locally recruited 13 30
23 1 - 22 41 3 - 38The Americas
internationally recruited . 27 27locally recruited 34 33
61 14 - 47 60 11 - 49South -East Asia
internationally recruited . 19 17locally recruited 86 88
105 29 - 76 105 26 - 79Europe
internationally recruited . 18 20locally recruited 23 25
41 14 - 27 45 6 - 39Eastern Mediterranean
internationally recruited . 29 21locally recruited 60 59
89 21 - 68 80 18 - 62Western Pacific
internationally recruited . 22 20locally recruited 48 45
70 22 - 48 65 11 - 54Field staff in countries
internationally recruited . 378 398locally recruited 5 -
383 241 60 82 398 214 77 107United Nations Liaison Office,
New Yorkinternationally recruited . 3 3locally recruited 5 5
8 1 - 7 8 - - 8
UNICEF Liaison 4 - 1 3 3 - - 3
Excluding consultants
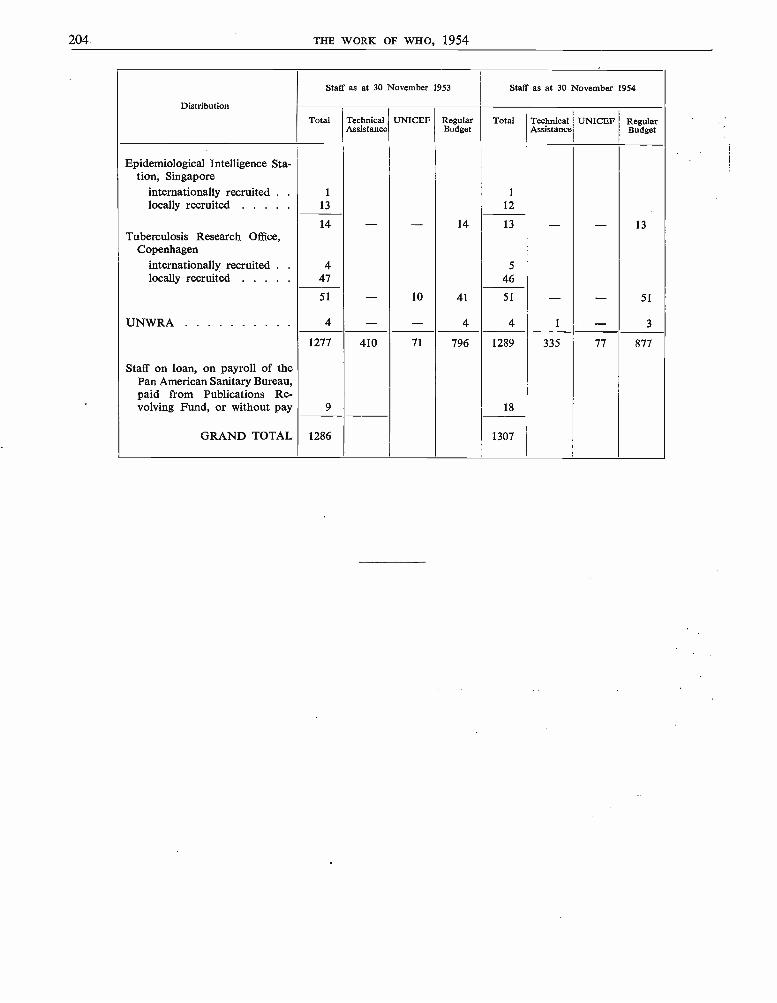
204 THE WORK OF WHO, 1954
Distribution
Staff as at 30 November 1953 Staff as at 30 November 1954
Total TechnicalAssistance
UNICEF RegularBudget
Total TechnicalAssistance
UNICEF RegularBudget
Epidemiological Intelligence Sta-tion, Singapore
internationally recruited . 1 1
locally recruited 13 12
14 - - 14 13 - - 13Tuberculosis Research Office,
Copenhageninternationally recruited . 4 5
locally recruited 47 46
51 - 10 41 51 - - 51
UNWRA 4 - - 4 4 1 - 3
1277 410 71 796 1289 335 77 877
Staff on loan, on payroll of thePan American Sanitary Bureau,paid from Publications Re-volving Fund, or without pay 9 18
GRAND TOTAL 1286 1307
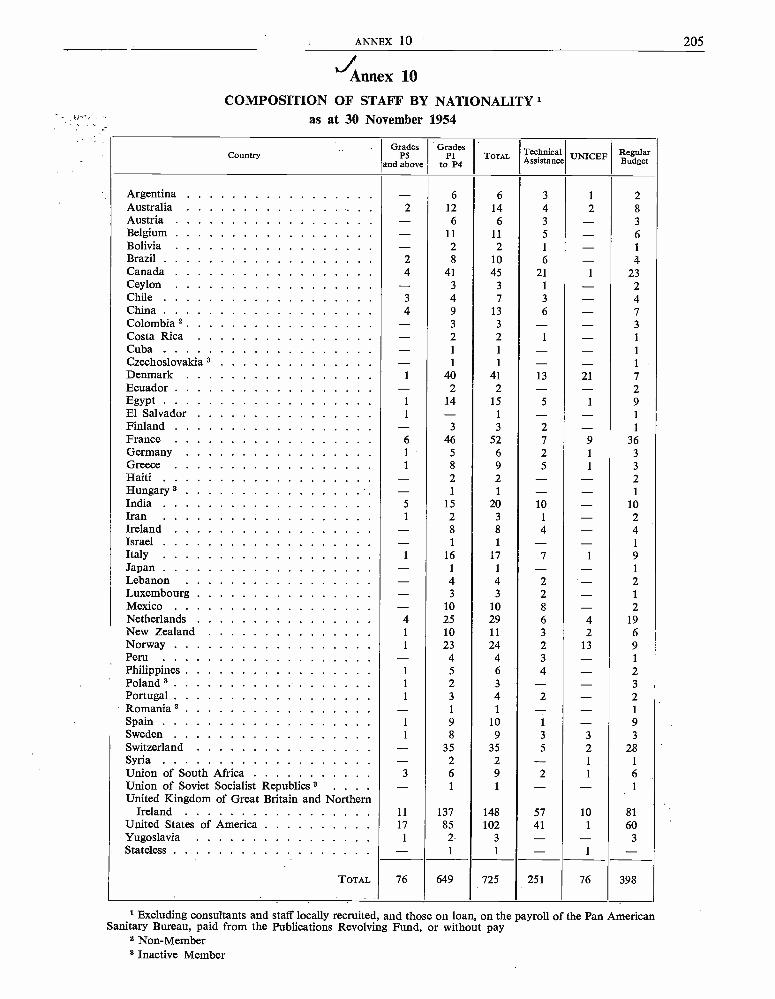
ANNEX 10 205t
*' Annex 10
COMPOSITION OF STAFF BY NATIONALITYas at 30 November 1954
CountryGrades
P5and above
GradesPl
to P4TOTAL Technical
Assistance UNICEF RegularBudget
Argentina - 6 6 3 1 2Australia 2 12 14 4 2 8Austria - 6 6 3 - 3Belgium - 11 11 5 - 6Bolivia - 2 2 1 - 1
Brazil 2 8 10 6 - 4Canada 4 41 45 21 1 23Ceylon - 3 3 1 - 2Chile 3 4 7 3 - 4China 4 9 13 6 - 7Colombia 2 - 3 3 - - 3
Costa Rica - 2 2 1 - 1
Cuba - 1 1 - - 1
Czechoslovakia 3 - 1 1 - - 1
Denmark 1 40 41 13 21 7Ecuador - 2 2 - - 2Egypt 1 14 15 5 1 9El Salvador 1 - 1 - - 1
Finland - 3 3 2 - 1
France 6 46 52 7 9 36Germany 1 5 6 2 1 3
Greece 1 8 9 5 1 3
Haiti - 2 2 - - 2Hungary 3 - 1 1 - - 1
India 5 15 20 10 - 10Iran 1 2 3 1 - 2Ireland - 8 8 4 - 4Israel - 1 1 - - 1
Italy 1 16 17 7 1 9Japan - 1 1 - - 1
Lebanon - 4 4 2 - 2Luxembourg - 3 3 2 - 1
Mexico - 10 10 8 - 2Netherlands 4 25 29 6 4 19New Zealand 1 10 11 3 2 6Norway 1 23 24 2 13 9Peru - 4 4 3 - 1
Philippines 1 5 6 4 - 2Poland 3 1 2 3 - - 3
Portugal 1 3 4 2 - 2Romania 3 - 1 1 - - 1
Spain 1 9 10 1 - 9Sweden 1 8 9 3 3 3
Switzerland - 35 35 5 2 28Syria - 2 2 - 1 1
Union of South Africa 3 6 9 2 1 6Union of Soviet Socialist Republics 3 . . . . - 1 1 - - 1
United Kingdom of Great Britain and NorthernIreland 11 137 148 57 10 81
United States of America 17 85 102 41 1 60Yugoslavia 1 2 3 - - 3Stateless - 1 1 - 1 -
TOTAL 76 649 725 251 76 398
i Excluding consultants and staff locally recruited, and those on loan, on the payroll of the Pan AmericanSanitary Bureau, paid from the Publications Revolving Fund, or without pay
2 Non -Member3 Inactive Member
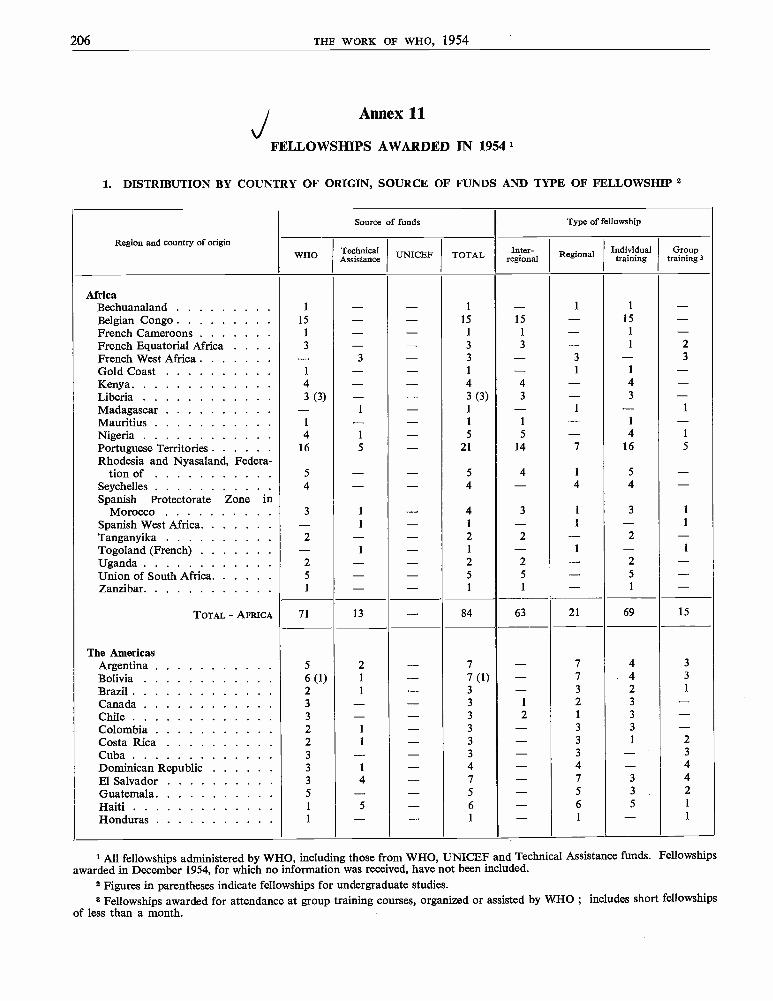
206 THE WORK OF WHO, 1954
Annex 11
FELLOWSHIPS AWARDED IN 19541
1. DISTRIBUTION BY COUNTRY OF ORIGIN, SOURCE OF FUNDS AND TYPE OF FELLOWSHIP 2
Region and country of origin
Source of funds Type of fellowship
WHO TechnicalAssistance UNICEF TOTAL Inter-
regional Regional Individualtraining
Grouptraining 3
AfricaBechuanaland 1 - - 1 - 1 1 -Belgian Congo 15 - - 15 15 - 15 -French Cameroons 1 - - 1 1 - 1 -French Equatorial Africa . . . . 3 - - 3 3 - 1 2
French West Africa - 3 - 3 - 3 - 3
Gold Coast 1 - - 1 - 1 1 -Kenya 4 - - 4 4 - 4 -Liberia 3 (3) - - 3 (3) 3 - 3 -Madagascar - 1 - 1 - 1 - 1
Mauritius 1 - - 1 1 - 1 -Nigeria 4 1 - 5 5 - 4 1
Portuguese Territories 16 5 - 21 14 7 16 5
Rhodesia and Nyasaland, Federa-tion of 5 - - 5 4 1 5 -
Seychelles 4 - - 4 - 4 4 -Spanish Protectorate Zone in
Morocco 3 1 - 4 3 1 3 1
Spanish West Africa - 1 - 1 - 1 - 1
Tanganyika 2 - - 2 2 - 2 -Togoland (French) - 1 - 1 - 1 - 1
Uganda 2 - - 2 2 - 2 -Union of South Africa 5 - - 5 5 - 5 -Zanzibar 1 - - 1 1 - 1 -
TOTAL - AFRICA 71 13 - 84 63 21 69 15
The AmericasArgentina 5 2 - 7 - 7 4 3
Bolivia 6 (1) 1 - 7 (1) - 7 4 3
Brazil 2 1 - 3 - 3 2 1
Canada 3 - - 3 1 2 3 -Chile 3 - - 3 2 1 3 -Colombia 2 1 - 3 - 3 3 -Costa Rica 2 1 - 3 - 3 1 2
Cuba 3 - - 3 - 3 - 3
Dominican Republic 3 1 - 4 - 4 - 4
El Salvador 3 4 - 7 - 7 3 4
Guatemala 5 - - 5 - 5 3 2
Haiti 1 5 - 6 - 6 5 1
Honduras 1 - - 1 - 1 - 1
1 All fellowships administered by WHO, including those from WHO, UNICEF and Technical Assistance funds. Fellowshipsawarded in December 1954, for which no information was received, have not been included.
2 Figures in parentheses indicate fellowships for undergraduate studies.3 Fellowships awarded for attendance at group training courses, organized or assisted by WHO ; includes short fellowships
of less than a month.
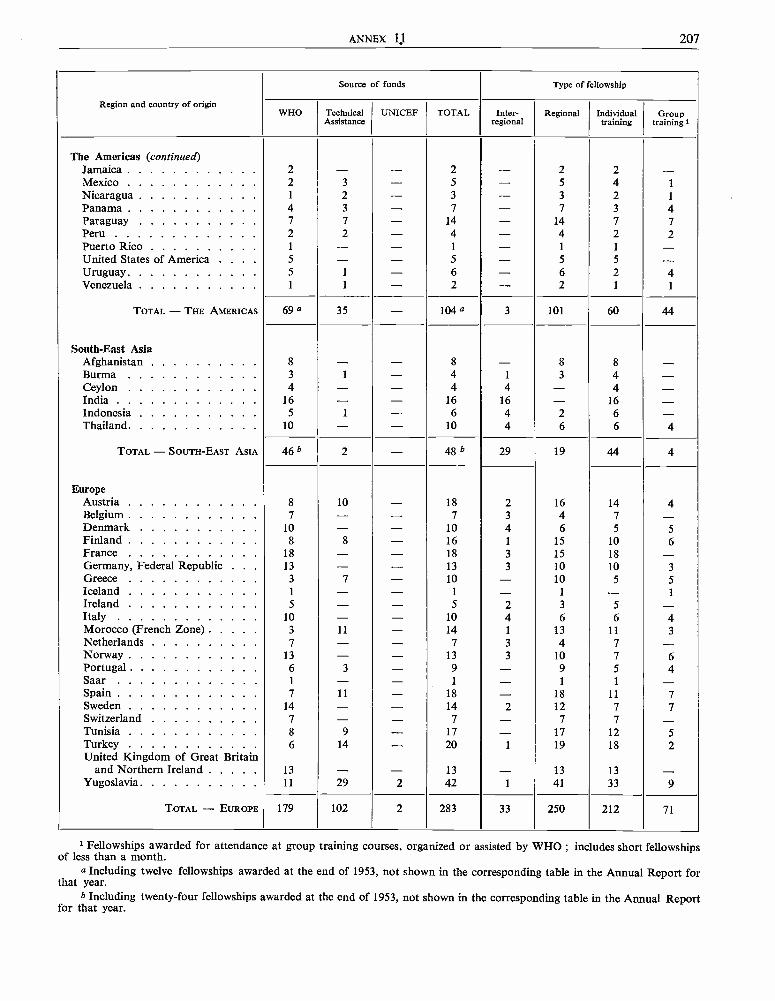
ANNEX 1,J 207
Region and country of origin
Source of funds Type of fellowship
WHO TechnicalAssistance
UNICEF TOTAL Inter-regional
Regional Individualtraining
Grouptraining 1
The Americas (continued)Jamaica 2 - - 2 - 2 2 -Mexico 2 3 - 5 - 5 4 1
Nicaragua 1 2 - 3 - 3 2 1
Panama 4 3 - 7 - 7 3 4Paraguay 7 7 - 14 - 14 7 7Peru 2 2 - 4 - 4 2 2Puerto Rico 1 - - 1 - 1 1 -United States of America . . . . 5 - - 5 - 5 5 -Uruguay 5 1 - 6 - 6 2 4Venezuela 1 1 - 2 - 2 1 1
TOTAL - THE AMERICAS 69 a 35 - 104 a 3 101 60 44
South -East AsiaAfghanistan 8 - - 8 - 8 8 -Burma 3 1 - 4 1 3 4 -Ceylon 4 - - 4 4 - 4 -India 16 - - 16 16 - 16 -Indonesia 5 I - 6 4 2 6 -Thailand 10 - - 10 4 6 6 4
TOTAL - SOUTH -EAST ASIA 46 b 2 - 48 b 29 19 44 4
EuropeAustria 8 10 - 18 2 16 14 4Belgium 7 - - 7 3 4 7 -Denmark 10 - - 10 4 6 5 5Finland 8 8 - 16 1 15 10 6France 18 - - 18 3 15 18 -Germany, Federal Republic . . . 13 - - 13 3 10 10 3Greece 3 7 - 10 - 10 5 5Iceland 1 - - 1 - 1 - 1
Ireland 5 - - 5 2 3 5 -Italy 10 - - 10 4 6 6 4Morocco (French Zone) 3 11 - 14 1 13 11 3Netherlands 7 - - 7 3 4 7 -Norway 13 - - 13 3 10 7 6Portugal 6 3 - 9 - 9 5 4Saar 1 - - 1 - 1 1 -Spain 7 11 - 18 - 18 11 7Sweden 14 - - 14 2 12 7 7Switzerland 7 - - 7 - 7 7 -Tunisia 8 9 - 17 - 17 12 5Turkey 6 14 - 20 1 19 18 2United Kingdom of Great Britain
and Northern Ireland 13 - - 13 - 13 13 -Yugoslavia 11 29 2 42 1 41 33 9
TOTAL - EUROPE 179 102 2 283 33 250 212 71
1 Fellowships awarded for attendance at group training courses, organized or assisted by WHO ; includes short fellowshipsof less than a month.
a Including twelve fellowships awarded at the end of 1953, not shown in the corresponding table in the Annual Report forthat year.
b Including twenty -four fellowships awarded at the end of 1953, not shown in the corresponding table in the Annual Reportfor that year.
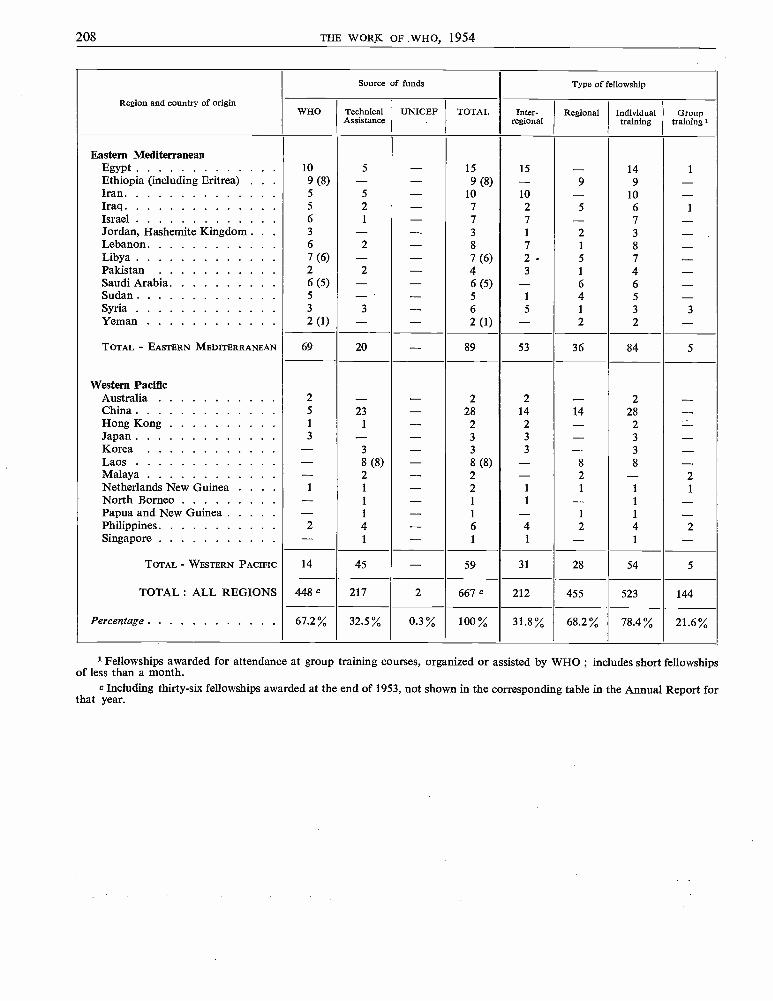
208 THE WORK OF WHO, 1954
Region and country of origin
Source of funds Type of fellowship
WHO TechnicalAssistance
UNICEF TOTAL Inter-regional
Regional Individualtraining
Grouptraining I
Eastern MediterraneanEgypt 10 5 - 15 15 - 14 1
Ethiopia (including Eritrea) . . . 9 (8) - -- 9 (8) - 9 9 -Iran 5 5 - 10 10 - 10 -Iraq 5 2 - 7 2 5 6 1
Israel 6 1 - 7 7 - 7Jordan, Hashemite Kingdom . . . 3 - - 3 1 2 3 -Lebanon 6 2 - 8 7 1 8 -Libya 7 (6) - - 7 (6) 2 - 5 7 -Pakistan 2 2 - 4 3 1 4 -Saudi Arabia 6 (5) - - 6 (5) - 6 6 -Sudan 5 - - 5 1 4 5 -Syria 3 3 - 6 5 1 3 3Yeman 2 (1) - - 2 (1) - 2 2 -TOTAL - EASTERN MEDITERRANEAN 69 20 - 89 53 36 84 5
Western PacificAustralia 2 - - 2 2 - 2 -China 5 23 - 28 14 14 28 -Hong Kong 1 1 - 2 2 - 2 -Japan 3 - - 3 3 - 3 -Korea - 3 - 3 3 - 3 -Laos - 8 (8) - 8 (8) - 8 8 -Malaya - 2 - 2 - 2 - 2Netherlands New Guinea 1 1 - 2 1 1 1 1
North Borneo - 1 - 1 1 - 1 -Papua and New Guinea - 1 - 1 - 1 1 -Philippines 2 4 - 6 4 2 4 2Singapore - 1 - 1 1 - 1 -
TOTAL - WESTERN PACIFIC 14 45 - 59 31 28 54 5
TOTAL : ALL REGIONS 448 C 217 2 667 c 212 455 523 144
Percentage 67.2% 32.5% 0.3 % 100 % 31.8 % 68.2% 78.4% 21.6%
1 Fellowships awarded for attendance at group training courses, organized or assisted by WHO ; includes short fellowshipsof less than a month.
c Including thirty -six fellowships awarded at the end of 1953, not shown in the corresponding table in the Annual Report forthat year.
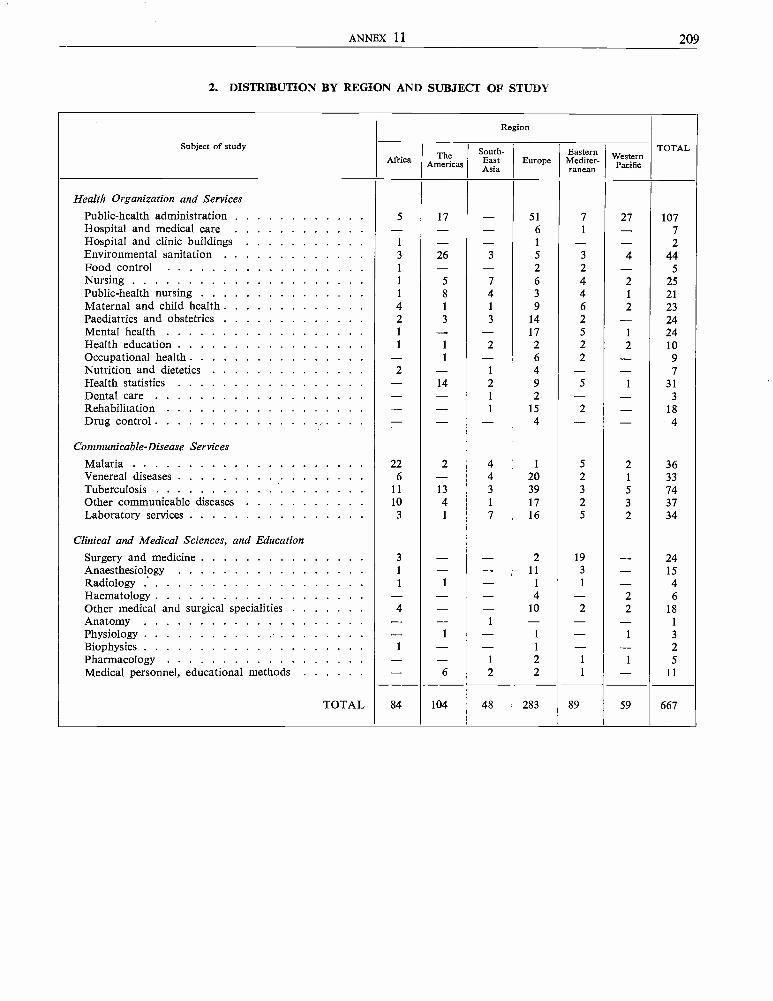
ANNEX 11 209
2. DISTRIBUTION BY REGION AND SUBJECT OF STUDY
Subject of study
Region
TOTALAfrica The
AmericasSouth-EastAsia
EuropeEastern
Mediter-ranean
WesternPacific
Health Organization and ServicesPublic -health administration 5 17 - 51 7 27 107Hospital and medical care - - - 6 1 - 7Hospital and clinic buildings 1 - - 1 - - 2Environmental sanitation 3 26 3 5 3 4 44Food control 1 - - 2 2 - 5Nursing 1 5 7 6 4 2 25Public -health nursing 1 8 4 3 4 1 21Maternal and child health 4 1 1 9 6 2 23Paediatrics and obstetrics 2 3 3 14 2 - 24Mental health 1 - - 17 5 1 24Health education 1 1 2 2 2 2 10Occupational health - 1 - 6 2 - 9Nutrition and dietetics 2 - 1 4 - - 7Health statistics - 14 2 9 5 1 31Dental care - - 1 2 - - 3
Rehabilitation - - 1 15 2 - 18Drug control - - - 4 - - 4
Communicable -Disease Services
Malaria 22 2 4 1 5 2 36Venereal diseases 6 - 4 20 2 1 33Tuberculosis 11 13 3 39 3 5 74Other communicable diseases 10 4 1 17 2 3 37Laboratory services 3 1 7 16 5 2 34
Clinical and Medical Sciences, and EducationSurgery and medicine 3 - - 2 19 - 24Anaesthesiology 1 - - 11 3 - 15Radiology . 1 1 - 1 1 - 4Haematology - - - 4 - 2 6Other medical and surgical specialities 4 - - 10 2 2 18Anatomy - - 1 - - - 1
Physiology - 1 - 1 - 1 3
Biophysics I - - 1 - - 2Pharmacology - - 1 2 1 1 5
Medical personnel, educational methods - 6 2 2 1 - 11
TOTAL 84 104 48 283 89 59 667

OFFICIAL RECORDS OF THE WORLD HEALTH ORGANIZATION No. 59
THE WORK OF WHO, 1954
ANNUAL REPORT OF THE DIRECTOR - GENERAL
TO THE
WORLD HEALTH ASSEMBLY AND TO THE UNITED NATIONS
INDEX
WORLD HEALTH ORGANIZATIONPALAIS DES NATIONS
GENEVA
INDEX
Main references by subject, and main references to the project list by country, are in heavy type.
Accommodation -Headquarters, 60Regional Office for Africa, 64Regional Office for Europe, 60, 84
Administrative Committee on Co- ordination, 113, 114, 116Advisory groups, meetings in 1954, 199Aëdes aegypti eradication -
Africa, 15 ; Americas, 15, 76, 131 ; Colombia, 135 ;Dominican Republic, 136 ; Mexico, 139 ; Panama, 131 ;Paraguay, 139
Afghanistan, 24, 79 -80, 142 -4African Region, 16, 36, 63 -8, 127 -30Agreements with governments, 58Alcohol and alcoholism, 21, 49
Europe, 22, 86, 92, 156Americas, see Region of the AmericasAnaesthesiology -
Europe, training courses, 86, 93, 155, 156 ; Yugoslavia, 93Andean Highlands Field Mission, 130Animal tuberculosis, 12Ankylostomiasis -
Iraq, 169 ; Paraguay, 140Annual Epidemiological and Vital Statistics, 44Anthropology, cultural, 25, 132Antibiotics research, 5Associate Members, 193
admission of Federation of Rhodesia and Nyasaland, 58rights and obligations in regional committees, 83
Atomic energy, peaceful uses, 113, 114Austria, 85, 90, 157 -8Auxiliary health workers, training, 24, 38, 114
Americas, 130 ; Burma, 145 ; Eastern Mediterranean, 97,98, 101 ; Ethiopia, 166 ; Kenya, 128 ; Nigeria, 129 ;Nyasaland, 130 ; Palestine refugees, 30 ; Paraguay, 140 ;Seychelles, 130 ; Somaliland Protectorate, 130 ; Syria,177, 178 ; Tanganyika, 130
Bahamas, 131Barbados, 131BCG -
assessment teams, 8, 151, 154, 163, 179statistician, Central and South America and Caribbean
area, 132vaccination campaigns, 7 -10
British Guiana, 134 ; British Honduras, 134 ; Burma,145 ; Cambodia, 181, 187 ; Ceylon, 148 ; Chile,135 ; Colombia, 136 ; Costa Rica, 136 ; Egypt,164 ; Ethiopia, 166 ; India, 149 ; Indonesia, 152 ;Iran, 168 ; Iraq, 98 -9, 169 ; Jordan, 170 ; LeewardIslands, 138 ; Libya, 172 ; Pakistan, 174 ; Para-guay, 74, 141 ; Sudan, 176 ; Thailand, 154 ; Tri-nidad and Tobago, 142 ; Turkey, 161 ; Viet Nam,187 ; Windward Islands, 142
vaccine production, Ecuador, 137Bechuanaland, 66, 128Bejel, Syria, 177
Bermuda, 131Bilharziasis, 17
Africa, 65 ; Eastern Mediterranean, 96 ; Egypt, 96, 164 ;Philippines, 106 -7, 185 ; Sudan, 176 ; Syria, 177
Biological standardization, 12, 46 -7See also Expert Committee on Biological Standardization
Biostatistics -Americas, 75, 133See also Inter -American Centre of Biostatistics ; Statistics
Bolivia, 71, 130, 134Brazil, 130, 133, 134British Guiana, 134British Honduras, 134Brucellosis, 10 -11, 188
training course, Mexico City, 71, 132Brunei, 179 -80, 186Budget -
for 1954, 59summary by appropriation section, 201
See also Programme and budgetBulletin of the World Health Organization, 7, 12, 15, 17, 47,
49, 52, 53Burma, 6, 144 -6
Cambodia, 24, 180 -1, 187Cancer research, 117
Africa, 36Cannabis, 49Cardiolipin production, India, 148Caribbean area, 75, 131, 132, 133Central America, 131, 132, 133Ceylon, 80, 146 -8Children -
backward, Iraq, 96, 169foster -home care, 157handicapped, see Rehabilitation of the handicappedmental health, studies, 22, 84, 85, 87, 155, 156services for, Syria, 115See also Maternal and child health ; School health services
Chile, 75, 130, 131, 135China, 181 -2
See also TaiwanCholera, 17
Pakistan, 17, 173Chronicle of the World Health Organization, 7, 53Classification of diseases, advisory group, 44CODEPID (epidemiological cable code), 43Colombia, 135 -6Colombo Plan, 79, 122Commission on Narcotic Drugs (United Nations), 49Commission for Technical Co- operation in Africa South of
the Sahara (CCTA), 21, 63, 65Committee of Experts on the Transport of Dangerous Goods
(Economic and Social Council), 32Committee on Information from Non -Self -Governing Ter-
ritories (United Nations), 116
- 1 -
2 INDEX
Committee on International Quarantine, 14, 39, 42membership in 1954, 198
Communicable diseases, 3 -17Eastern Mediterranean, 96 ; Europe, 90 ; Western
Pacific, 110See also Endemo -epidemic diseases
Community development, 115Community health visitors, 24
Eastern Mediterranean, 97Congenital heart disease, Yugoslavia, 162Conjunctivitis, acute -
Morocco (French Zone), 16, 90, 159 ; Spain, 90 ; Tunisia,90, 160
Consultative Committee on Administrative Questions, 116Contributions, status, 59Convention on Privileges and Immunities of the Specialized
Agencies, accessions, 58Co- operative for American Remittances to Everywhere, Inc.
(CARE), 51Costa Rica, 136Council of Europe, 84Council for International Organizations of Medical Sciences
(CIOMS), 36, 118Cyprus, 163
DDT -procurement, 50production, Eastern Mediterranean, 96
Denmark, 9, 58, 91Dental health, 28, 92, 118
seminar, Wellington, 105, 179Diphtheria, 16
Peru, 142vaccine production -
Austria, 90, 158 ; Brazil, 134Dominican Republic, 136Donovanosis, 5, 6, 7Drugs liable to produce addiction, 48 -9, 116
East Africa, Malaria Institute, Amani, 67 -8, 128Eastern Mediterranean Region, 24, 37, 95 -102, 163 -78Economic Commission for Europe, 84Economic and Social Council, 113, 121Ecuador, 72, 130, 136 -7Education and training, 33 -8
Americas, 70 -1, 130 ; Burma, 145 ; Eastern Mediter-ranean, 96 -7, 98, 101 ; Ethiopia, 166 ; Europe, 92 -3 ;Palestine refugees, 30 ; Seychelles, 130 ; South -EastAsia, 34, 35 -6, 77, 78 ; Western Pacific, 103
Educational institutions, assistance to, 37 -8Afghanistan, 143, 144 ; Africa, 128 -30 ; Americas, 71,
130, 132 ; Bolivia, 71 -2, 134 ; Burma, 145 ; Cambodia,181 ; Ceylon, 80, 146, 147 ; Costa Rica, 136 ; Ecuador,136 ; Greece, 158 ; India, 148, 149, 150 ; Indonesia,152 ; Iran, 167, 168 ; Netherlands, 160 ; Pakistan, 174,175 ; Paraguay, 141 ; Philippines, 185 ; Singapore, 26,38, 107 -8, 186 ; Syria, 178 ; Turkey, 161 ; WesternPacific, 105, 109
Egypt, 12, 19, 95, 96, 97, 164 -5Eighth World Health Assembly, place, 60El Salvador, 18, 72 -3, 132, 137Endemic goitre, 21
Central and South America, 133 ; Yugoslavia, 162
Endemo -epidemic diseases -Spain, 160 ; Yugoslavia, 162See also Communicable diseases
Environmental sanitation, 31 -2Afghanistan, 144 ; Americas, 130 ; Bolivia, 134 ; Eastern
Mediterranean, 95, 98, 102 ; El Salvador, 72 ; Europe,86, 92 -3, 155 ; Guatemala, 138 ; Mexico, 138 ; NorthBorneo, 185 ; Palestine refugees, 30 ; Peru, 74 ; Sey-chelles, 130 ; South -East Asia, 77, 78 ; Taiwan, 182 ;Thailand, 154 ; Western Pacific, 103, 109
See also Sanitary engineering ; Rural health servicesEpidemiological cable code (CODEPID), 43Epidemiological information, 42 -3Epidemiological studies, 45Epidemiological and Vital Statistics Report, 43Epilepsy, juvenile, 22, 158Ethiopia, 17, 36, 97, 165 -6European Region, 22, 83 -94, 155 -62Exchange of scientific information, 35 -7Executive Board, membership, 194Expanded Programme of Technical Assistance for Economic
Development, see Technical Assistance ProgrammeExpert Advisory Panel on Chronic Degenerative Diseases, 26Expert Advisory Panel on Insecticides, 32Expert Advisory Panel on the International Pharmacopoeia
and Pharmaceutical Preparations, 47, 48Expert Advisory Panel on Occupational Health, 26Expert Advisory Panel on the Organization of Medical Care, 26Expert Advisory Panel on Rehabilitation, 26Expert Advisory Panel on Yellow Fever, 42Expert advisory panels, list, 195Expert Committee on Alcohol and Alcoholism, 21, 49, 195Expert Committee on Biological Standardization, 12, 14,
46, 195Expert Committee on Drugs Liable to Produce Addiction,
49, 196Expert Committee on Health Education of the Public, 26Expert Committee on Health Statistics, 44, 45, 196Expert Committee on the International Pharmacopoeia, 47, 196Expert Committee on Mental Health, 21, 197Expert Committee on Midwifery Training, 23, 25, 197Expert Committee on Nursing, 25, 197Expert Committee on Onchocerciasis, 16Expert Committee on Poliomyelitis, 14Expert Committee on Public- Health Administration, 18Expert Committee on Rabies, 11Expert Committee on Rheumatic Diseases, 28Expert committees, meetings held in 1954, 199
membership, 195 -8
Family planning, India, 149FAO, 10, 21, 32, 65, 79, 84, 117FAO /WHO Brucellosis Centres, 10, 11, 188FAO /WHO /UNICEF inter -agency working group on milk
and milk products, 13, 32Federation of Rhodesia and Nyasaland, 58
See also Nyasaland ; Southern RhodesiaFédération dentaire internationale, 118Fellowships, 34 -5, 120, 206 -9
Africa, 66 ; Eastern Mediterranean, 97 ; Europe, 85 -6 ;South -East Asia, 77 ; Western Pacific, 104, 105, 109
Fiji, 110, 182Filariasis, 17
Ceylon, 147Finland, 9
INDEX 3
Food and Agriculture Organization, see FAOFood hygiene, 12 -13
See also Meat hygiene ; MilkForeign Operations Administration (FOA), 34, 65, 79, 100,
104, 106, 122, 164Foster -home care, seminar, 157French Africa, 66 -7, 128French Guiana, 131Fundamental education, 115
Ceylon, 146 ; Eastern Mediterranean, 163 ; Thailand, 153
Gamma -globulin, 14Garbage disposal, see Refuse disposalGermany, Federal Republic, 19, 155Glaucoma, symposium, 36Gonorrhoea, 6Greece, 85, 158 -9Guatemala, 132, 137 -8Gynaecology, 37
Haiti, 6, 73, 138Headquarters accommodation, 60Health demonstration areas -
Egypt, 19, 96, 164 ; El Salvador, 18, 72 -3, 137Health education of the public, 25 -6
Ceylon, 146 ; Europe, 25, 91, 155 ; Italy, 91, 159 ; Liberia,129 ; Libya, 172 ; Palestine refugees, 26, 29 ; Peru, 74 ;Singapore, 107, 186 ; Taiwan, 109 ; Western Pacific,103
Health statistics, see Biostatistics ; StatisticsHealth visitors, 24
pilot study, France and United Kingdom, 87, 155Heart disease, congenital, Yugoslavia, 162High Commissioner for Refugees, 84, 116Honduras, 131, 132Hong Kong, 182Hookworm, see AnkylostomiasisHospital construction, 21
Turkey, 161 ; Viet Nam, 187Housing and town planning, 84, 115Hydatidosis, 12Hygiene of seafarers, 27
See also Joint ILO /WHO Committee on the Hygiene ofSeafarers ; Venereal diseases
ICAO, 117ILO, 27, 28, 117Immunization conference, 87, 90, 155India, 6, 17, 22, 24, 148 -51Indonesia, 24, 81, 151 -3Industrial hygiene, 27, 32
India, 150Influenza, 13 -14, 188Insect -borne diseases -
Ceylon, 147 ; Iran, 166 ; Western Pacific, 104Insect control -
Afghanistan, 79 -80, 142 ; Americas, 131 ; Brunei, 179,186 ; Colombia, 135 ; Dominican Republic, 136 ; El
Salvador, 72 ; Mexico, 139 ; Panama, 131 ; Paraguay,139 ; Taiwan, 105 -6, 182
See also MalariaInsecticides, 32
resistance, 4, 32, 65Egypt, 165
sorbtion in mud walls, 3, 4Institute of Nutrition of Central America and Panama, 133
Inter -American Centre of Biostatistics, Chile, 75, 131Inter -country programmes, Europe, 85, 86 -9, 155 -7Intergovernmental Committee for European Migration, 28International Anti -Venereal- Disease Commission of the Rhine,
117International Association of Microbiological Societies, 118International Association of Universities, 38International biological standards, see Biological standardiza-
tionInternational Blood Group Reference Laboratory, London, 47International Children's Centre, 21, 23, 84International Civil Aviation Organization, see ICAOInternational Civil Service Advisory Board, 116International Committee of Catholic Nurses and Medico -
Social Workers, 117, 118International Congress on Gynaecology and Obstetrics, 37International Congress of Ophthalmology (XVII), 15, 36International Council of Nurses, 25, 118International Digest of Health Legislation, 15, 16, 21, 24, 53International Labour Organisation, see ILOInternational List of Venereal- Disease Treatment Centres in
Ports, 6International Paediatric Association, 23, 118International pharmacopoeia, see Pharmacopoea InternationalisInternational quarantine, 175
See also Committee on International Quarantine ; Inter-national Sanitary Regulations
International reference preparations, see Biological standar-dization
International Salmonella and Escherichia Centre, Copenhagen,47
International Sanitary Regulations, 14, 39 -42International Serological Reference Laboratories, Copen-
hagen and Chamblee, 5, 189International shigella centres, 47, 188International Treponematosis Laboratory Center, Baltimore,
5, 188International Union for Health Education, 26Inter- regional projects, 188 -9Iran, 16, 97, 166 -8Iraq, 96, 97, 98 -9, 168 -9Isotopes, radioactive, 27Israel, 12, 99 -100, 169 -70Italy, 19, 85, 91, 155, 159
Jamaica, 131, 132Japan, 183Joint FAO /WHO Expert Committee on Meat Hygiene, 13, 197Joint FAO /WHO Expert Committee on Nutrition, 21, 198Joint ILO /WHO Committee on the Hygiene of Seafarers, 27,
198Jordan, 96, 97, 170-1
Kenya, 128Korea, 105
Laos, 183League of Red Cross Societies'Lebanon, 95, 96, 97, 98, 100, 171 -2 yLeeward Islands, 131, 138Leprosy, 16
Ceylon, 148Leptospirosis, 12Liberia, 67, 129Library, WHO, 54 -5

4 INDEX
Libya, 97, 172Local health services, study group, 19
Malaria, 4 -5Afghanistan, 79 -80, 142 ; Africa, 65, 67 -8, 128 ; Americas,
70, 76, 131 ; Brunei, 179, 186 ; Burma, 144, 146 ;Cambodia, 180 ; Ceylon, 147 ; Colombia, 135 ; Domi-nican Republic, 136 ; Eastern Mediterranean, 96, 100 ;Indonesia, 152 ; Iraq, 169 ; Lebanon, 171 ; Liberia, 67,129 ; Mexico, 139 ; Nepal, 153 ; Nigeria, 67, 129 ;Palestine refugees, 29 ; Panama, 131 ; Paraguay, 139 ;Philippines, 185 ; Sarawak, 186 ; Saudi Arabia, 176 ;Syria, 177 ; Taiwan, 105 -6, 182conference, Philippines, 4, 189
Malaya, 12, 183 -4Maternal Care and Mental Health, 22, 53Maternal and child health, 22 -3
Afghanistan, 143 ; Burma, 145 ; Cambodia, 180 ; Ceylon,146 ; Chile, 135 ; Colombia, 135 ; Eastern Mediter-ranean, 95 ; El Salvador, 137 ; Europe, 156 ; Greece,158 ; Hong Kong, 182 ; India, 22, 148, 151 ; Indonesia,152 ; Iran, 167 ; Iraq, 168 ; Israel, 170 ; Japan, 183 ;Jordan, 170 ; Lebanon, 171 ; Libya, 172 ; Mexico, 138 ;Pakistan, 173, 174 ; Paraguay, 140 ; Peru, 74, 141 ;Syria, 115, 177 ; Taiwan, 181 ; Thailand, 80 -1, 153,154 ; Turkey, 161 ; Viet Nam, 187 ; Yugoslavia, 162
See also ChildrenMeat hygiene -
seminar, Copenhagen, 12, 87, 155See also Joint FAO /WHO Expert Committee on Meat
HygieneMecca Pilgrimage, 42, 175Medical care, 27Medical education, see Education and training; Educational
institutionsMedical Research Council, 15Medical schools, directory, 38Medical scientists, visiting team, 35, 37Medical stores management, Ceylon, 147Medical supplies, see SuppliesMedical Women's International Association, 117, 118Medico -legal work, Ceylon, 147Membership of WHO, 58, 193Mental health, 21 -2
Austria, 158 ; Eastern Mediterranean, 96 ; Europe, 84,85, 87, 156, 157 ; Japan, 183 ; Jordan, 96, 171 ; Malaya,184
See also ChildrenMental hospitals, 21
Malaya, 184Mexico, 11, 58, 130, 138 -9Microfilm reference service, Eastern Mediterranean, 37, 172Midwifery, 23, 24, 25
Burma, 145 ; Cambodia, 180 ; Ceylon, 146, 147 ; Colom-bia, 135 ; Costa Rica, 136 ; Eastern Mediterranean, 95,97 ; El Salvador, 137 ; Hong Kong, 182 ; India, 150 ;Indonesia, 24, 153 ; Iran, 168 ; Iraq, 168 ; Lebanon,171 ; Libya, 172 ; Malaya, 184 ; North Borneo, 184 ;Paraguay, 140 ; Philippines, 186 ; Singapore, 187 ;Syria, 178 ; Thailand, 153 -4 ; Turkey, 161 ; Yugoslavia,162
Migration, 28Milk -
distribution scheme, Eastern Mediterranean, 95powder, 20sanitation, 13, 32, 116
Monographs, see World Health Organization: MonographSeries
Morbidity statistics, 44 -5survey, Denmark, 156
Morocco (French Zone), 16, 90, 159 -60
Narcotic drugs, see Drugs liable to produce addictionNational committees on vital and health statistics, 44Nepal, 24, 153Netherlands, 91, 160Netherlands Antilles, 131Nicaragua, 131, 132, 139Nigeria, 67, 129Non -governmental organizations, 84, 117 -19, 200Non -proprietary names, 48North Borneo, 24, 184 -5Nursing, 24 -5, 118
Afghanistan, 24, 143 ; Bolivia, 71, 134 ; Brunei, 179 ;Burma, 145, 146 ; Cambodia, 24, 180 ; Ceylon, 80,146, 147 ; Costa Rica, 136 ; Cyprus, 163 ; EasternMediterranean, 24, 96, 97, 163 ; Europe, 88, 90 -1, 156 ;India, 24, 148, 150, 151 ; Indonesia, 153 ; Iran, 167 ;Malaya, 183 ; Nepal, 24, 153 ; North Borneo, 24, 184 ;Pakistan, 174, 175 ; Singapore, 187 ; Syria, 178 ;Taiwan, 24, 181 ; Thailand, 80 -1, 153 -4, 155 ; Turkey,161 ; Yugoslavia, 162
Nutrition, 19 -21Africa, 65 ; Brunei, 180 ; Burma, 146 ; Indonesia, 152 ;
Palestine refugees, 29Nyasaland, 130
See also Federation of Rhodesia and Nyasaland
Obstetrics, 37Occupational health, see Social and occupational healthOfficial Records of the World Health Organization, 53Onchocerciasis, 16
conference, Leopoldville, 16, 65, 128Organizational meetings -
held in 1954, 199scheduled for 1955, 200
Paediatric education, study, 23, 33Paediatrics, social, Europe, 89, 157Pakistan, 6, 17, 97, 172 -5Palestine refugees, see United Nations Relief and Works
Agency for Palestine Refugees in the Near EastPan American Sanitary Conference, 4, 69Panama, 18, 131, 132, 139Paraguay, 73 -4, 139 -41Pellagra, 21
Egypt, 165 ; Yugoslavia, 162Penicillin, 5, 50
production, Yugoslavia, 90Pertussis, 16
Peru, 142vaccine production -
Austria, 90, 158 ; Brazil, 134Peru, 18, 74, 130, 141 -2Pethidine, 49Pharmaceutical preparations, non -proprietary names, 48Pharmaceutical specifications and nomenclature, 47 -8Pharmacology, India, 149, 151Pharmacopoea Internationalis, 47Pharmacy training, Sudan, 176Philippines, 106 -7, 185 -6Physiological and industrial hygiene, India, 150
INDEX 5
Physiotherapy, India, 150Plague, 16 -17
India, 17, 149 ; Iran, 17Poliomyelitis, 14, 65, 188
Europe, 83 ; Japan, 183Portugal, 160Postal workers, occupational risks, 27Premature infants, care, 23
Chile, 135 ; Israel, 170 ; Japan, 183Preventive medicine -
Paraguay, 141 ; Singapore, 186Programme and budget, regional, 63, 69, 78, 83, 97, 103Prosthetics, consultant group, 28Protein malnutrition, 20Psychobiological development of the child, study group, 22Public -health administration, 18 -19
Afghanistan, 143 ; Cambodia, 180 ; Eastern Mediter-ranean, 95 ; Ethiopia, 165 ; Europe, 19, 88, 155, 156 ;Iran, 167 ; Libya, 172 ; Nepal, 153 ; Saudi Arabia, 176 ;Viet Nain, 187 ; Yemen, 178
Public -health demonstration and training centre, Peru, 18,74 -5, 141
Public -health laboratories -Ecuador, 137 ; Europe, 90 ; Jordan, 170
Public -health schools -Italy, 159 ; Korea, 105 ; Taiwan, 105 ; Turkey, 161
Public -health services, 18 -30Americas, 75, 76 ; Eastern Mediterranean, 101 ; South -
East Asia, 81 -2 ; Western Pacific, 104.Public information, 56 -7
Africa, 64 ; South -East Asia, 78 ; Western Pacific, 105Publications and reference services, 52 -5Puerto Rico, 131
Q fever, 12Quarantine -
station, Saudi Arabia, 175See also Committee on International Quarantine ; Inter-
national Sanitary Regulations
Rabies, 11 -12, 188Africa, 65 ; Americas, 11 -12, 133 ; Israel, 12 ; Malaya,
12 ; Portugal, 160Radioactive isotopes, 27Refuse disposal, 31
Guatemala, 138Region of the Americas, 11, 15, 69 -76, 130 -42Regional Committee for Africa, 63 -4Regional Committee for the Americas, 69 -70Regional Committee for the Eastern Mediterranean, 97 -8Regional Committee for Europe, 83Regional Committee for South -East Asia, 77 -8Regional Committee for the Western Pacific, 103 -4Regional Office for Africa, 64 -5Regional Office for the Americas, 70Regional Office for the Eastern Mediterranean, 98Regional Office for Europe, 60, 83 -4Regional Office for South -East Asia, 78Regional Office for the Western Pacific, 104Regions and offices of WHO, map, 62Rehabilitation of the handicapped, 23, 27 -8, 115
Austria, 85, 157 ; Europe, 88, 157 ; Greece, 85, 158 ;Israel, 99 -100, 169 ; Italy, 85, 159 ; Japan, 183
Relapsing fever, 17Ethiopia, 17, 36 ; Jordan, 171
Research co- ordination, 3, 5, 15, 65, 98Rheumatic diseases, 28Rickettsioses, 12, 16, 188Rockefeller Foundation, 84, 93, 151Rural health services, 18
Egypt, 96 ; El Salvador, 72, 137 ; Guatemala, 137 ;Haiti, 138 ; Malaya, 184 ; Mexico, 138 ; Nicaragua,139 ; Panama, 18, 139 ; Peru, 141 ; South -East Asia,77 ; Thailand, 154, 155
training centre, Soissons, 156See also Environmental sanitation ; Maternal and child
health
Sanitary engineering -study of terms, 156training, 31
Americas, 71, 130, 131, 133 ; Europe, 86, 155, 157 ;Portugal, 160
See also Environmental sanitationSarawak, 186Saudi Arabia, 97, 175 -6School health services, 23, 26, 115
Eastern Mediterranean, 95 ; Europe, 88, 91 -2, 155, 157 ;Hong Kong, 182 ; Palestine refugees, 30 ; Peru, 74 ;Syria, 178 ; Thailand, 23, 153
Scientific information, exchange, 35 -7Seafarers, see Hygiene of seafarersSecretariat, structure, 59 -60, 202Seychelles, 130Singapore, 26, 38, 107 -8, 186 -7Smallpox, 15
Africa, 63 ; Americas, 76 ; Eastern Mediterranean, 98 ;Paraguay, 140 ; Western Pacific, 179
Social development programmes, 113, 114, 115, 116Social and occupational health, 26 -8
Yugoslavia, 162Social paediatrics, Europe, 89, 157Somaliland Protectorate, 130South African Institute for Medical Research, Johannesburg,
65, 66South -East Asia Region, 77 -82, 142 -55
medical education study, 33, 35 -6Southern Rhodesia, 130
See also Federation of Rhodesia and NyasalandSpain, 12, 90, 160Staff -
composition by nationality, 205numbers and distribution, 203 -4regional, 63, 64, 70, 78, 84, 98, 104
Standards of living, study, 45, 115Statens Seruminstitut, Copenhagen, 5Statistician, BCG, Central and South America and Caribbean
area, 132Statistics -
health and vital, 43 -5Afghanistan, 144 ; Africa, 65, 128 ; Americas, 70,
75, 76, 133 ; Turkey, 161 ; Western Pacific, 109 ;Yugoslavia, 162
morbidity, 44 -5Denmark, 156
Strategy for World Health (A), 56Sub -Committee on Non -Proprietary Names, 48, 196Sudan, 176Supplies, procurement, 50 -1
Palestine refugees, 30Surinam, 131

6 INDEX
Syphilis, 6, 7Caribbean area, 132 ; Ecuador, 137 ; Haiti, 73, 138 ;
Morocco (French Zone), 160 ; Syria, 177See also Venereal diseases
Syria, 37, 97, 115, 177 -8
Taiwan, 16, 24, 105 -6, 108 -9, 181 -2Tanganyika, 130Teaching equipment, 38
Kenya, 128 ; Nigeria, 129 ; Nyasaland, 130 ; SomalilandProtectorate, 130 ; Southern Rhodesia, 130 ; Tanga-nyika, 130 ; Zanzibar, 130
Technical Assistance Board, 104, 120, 121, 122Technical Assistance Committee, 120, 121, 122Technical Assistance Programme, 58, 59, 84, 98, 104, 120 -3Technical discussions in regional committees, 63, 70, 78, 83,
98, 104Technical Working Group on Long -Range Activities for
Children, 23Technical Working Party on the Rehabilitation of the Phy-
sically Handicapped, 28Terminologie du Paludisme, 4Thailand, 23, 80 -1, 153 -5Thoracic surgery, India, 150Trachoma, 15 -16, 36
Eastern Mediterranean, 96 ; Egypt, 164 ; Morocco(French Zone), 16, 90, 159 ; Taiwan, 16, 182 ; Tunisia,90, 160 ; Yugoslavia, 90
Treponematoses, 3, 5 -7Bechuanaland, 66, 128 ; Eastern Mediterranean, 96See also Bejel ; Venereal diseases ; Yaws
Trinidad, 75, 131, 142Trusteeship Council, 116Tuberculin testing, studies, 9Tuberculosis, 7 -10
Afghanistan, 143 ; Africa, 65, 127 ; Austria, 157 ; Burma,144 ; Ceylon, 147, 148 ; Eastern Mediterranean, 96 ;Ecuador, 72, 136 ; Egypt, 165 ; Europe, 89, 156, 157 ;Finland, 9 ; Greece, 159 ; Indonesia, 152 ; Iran, 167 ;Iraq, 99, 168 ; Israel, 169 ; Pakistan, 172, 174 ; Para-guay, 73 -4, 140 ; Peru, 74 ; Syria, 178 ; Thailand, 154 ;Western Pacific, 110 ; Yugoslavia, 162
See also BCGTuberculosis Immunization Research Centre, Copenhagen, 10Tuberculosis Research Office, Copenhagen, 9Tunisia, 90, 160Turkey, 161Typhoid fever, 16
UNESCO, 37, 38, 79, 104, 109, 117UNICEF, 23, 31, 65, 79, 84, 98, 100, 101, 104, 116 -17
reimbursement of cost of project personnel, 58, 59, 116 -17,121
Union OSE, 117, 118United Nations, 45, 48, 49, 78, 79, 113, 114, 116
See also Economic and Social CouncilUnited Nations Children's Fund, see UNICEFUnited Nations Educational, Scientific and Cultural Organiza-
tion, see UNESCOUnited Nations Korean Reconstruction Agency, supplies, 51United Nations Relief and Works Agency for Palestine
Refugees in the Near East (UNRWA), 26, 28 -30, 98United States of America, 11, 14, 132, 133Universal Postal Union, 27
University of London Institute of Education, 91Urethritis, non -gonococcal, 5, 6
Vaccines -communicable diseases, studies, 3, 10, 11, 14, 15, 16production -
Austria, 90, 158 ; Brazil, 134 ; Portugal, 160testing, Michigan Department of Health Laboratories, 133yellow fever, approval for international certificate of
vaccination, 15Venereal diseases, 5 -7
Afghanistan, 143 ; Americas, 132 ; Burma, 6, 145 ;Ecuador, 137 ; Ethiopia, 165 ; Haiti, 73, 138 ; Iran,166 ; Morocco (French Zone), 160 ; Pakistan, 6, 173 ;Paraguay, 140 ; Peru, 74 ; Saudi Arabia, 175 ; Syria,177 ; Taiwan, 108 -9, 181
in maritime populations, 89, 156Veterinary biological standards, 12Veterinary public- health, 10 -13Viet Nam, 187Virus diseases, 13 -16, 188
Western Pacific, 104Virus Research Institute, Entebbe, 65Vital statistics, see Biostatistics ; Statistics
Water -pollution and chlorination, 86, 155resources, 115standards of quality, 32, 156supply, Bolivia, 134
Weekly Epidemiological Record, 42, 43, 45Western Pacific Region, 15, 24, 103 -10, 179 -87WHO Newsletter, 56WHO Seals, 59Windward Islands, 131, 142Working Capital Fund, advances to, 59World Directory of Medical Schools, 38World Federation of United Nations Associations, 118World Health Assembly, see Eighth World Health AssemblyWorld Health Day, 57, 64, 105, 118World Health Organization: Monograph Series, 4, 5, 7, 11,
17, 22, 27, 52, 53World Medical Association, 33, 118World Population Conference, Rome, 45
X -ray equipment for tuberculosis projects, 50-1X -rays, protection against radiation, 27
Yaws, 6, 8Africa, 65 ; Americas, 76, 132 ; Fiji, 182 ; Haiti, 6, 73,
138 ; India, 6, 149 ; Indonesia, 81, 151 ; Laos, 183 ;Liberia, 67, 129 ; Malaya, 184 ; Nigeria, 67, 129 ;Philippines, 186 ; Sarawak, 186 ; Thailand, 153
Yellow fever, 14 -15provisions of International Sanitary Regulations, revision,
14, 39, 42Yellow -fever endemic zones, delineation, 39
connected surveys, 65, 166Yemen, 97, 178Yugoslavia, 6, 90, 93, 162
Zanzibar, 130Zoonoses, 10 -13
Israel, 169 -70