midwives - who | world health organization
TRANSCRIPT
fltf, ()
\ eprinted from the
International Digest of Health Legislation, 1954, 5, 431-482
MIDWIVES
A survey of recent legislation
WORLD HEALTH ORGANIZATION
T'ALAJS DES NATIONS
GENEVA
1954
Price: 3/6 $0.50 Sw. fr. 2.-
The World Health Organization (WIIO ) is a specialized agency of the United Nations and represents the culmination of e!Toris to establish a single intergovernmental health agency. As such, it inherits the functions of antecedent organizations such as the Office International d'llygilme Publique, the Health Organization of the League of Nations, and the Health Division of UNRRA.
vYIIO had ils origin in the proposal made at the United Nations Conference held in San Francisco in 1945 that a specialized agency be created to deal with all matters relating to health. In 1946, representatives of 61 governments met al the International Health Conference, New York, drafted and signed the WHO Constitution, and established an Interim Commission to serve until the Constitution could be ratified by 26 Member States of the United Nations. The Constitution came into force on 7 April 1948, the first World Health Assembly met in Geneva in June 1948, and on I September l!J48 the permanent Organization was established.
The work of the Organization is curried out by three organs: the World Health Assembly, the supreme authority, to which all Member States send delegates; the Executive Board, the executive organ of the Health Assembly, consisting of 18 persons designatt'd by as many Member Slates; and a Secretariat under the Director-General.
The scope of WIIO's interests and activities exceeds that of any previous international health organization and includes programmes relating to a wide variety of public-health questions : malaria, tuberculosis, venereal diseases, other communicable diseuses, maternal and child health, menial health, social and occupational health, nutrition, nursing, environmental sanitation, public-health administration, professional education and training, and health education of the public. In addition, WHO undertakes or participates in certain technical work of international significance, such as the compilation of an international pharmacopoeia, the setting-up of biological standards and of standards for insecticides and insecticide-spraying equipment, the control of addiction-producing drugs, the exchange of scientific information, the drawing-up of international sanitary regulations, the revision of the international list of diseases and causes of death, the collection and dissemination of epidemiological information, and statistical studies on morbidity and mortality.
The comparative surveys of health legislation are based on health laws and regulations published in the International Digest of Health Legislation and, in the case of legislation enacted before 1947, in the Bulletin mensuel de l'Office International d'Hygiene Publique. Use has also been made of works mentioned in the Bibliographical Section of the Digest.
The sources used, then, are those available to the World Health Organization and, while in most instances sufficient to indicate the general tendencies of the legislation of different countries, are not exhaustive. Microfilm copies of original texts referred to in this survey may be obtained on application to the Editor.
-432-
MIDWIVES
A survey of recent legislation
Page
Introduction • . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 434
Definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 436
Professional training . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 439
1. Admission to training schools . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 439
2. Midwives training schools . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 440
3. Period of training . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 441
4. Number of labours to be witnessed or conducted during training 441
5. Examinations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 443
6. Refresher courses and further training courses . . . . . . . . . . . . . . . . 443
7. Maternity nurses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 444
Administrative regulations
1. Right to practise . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 445
2. Recognition of foreign diplomas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 449
3. Midwives boards . . . . . . . . . . . . . • . . . . . . . . . . . . . . . . . . . . . . . . . . . . 451
4. Membership of midwives boards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 453
5. Registration of midwives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 453
6. Removal from the register and suspension from practice . . . . . . . . 455
7. Protection of title, uniform, and insignia . . . . . . . . . . . . . . . . . . . . . 456
Professional regulations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 456
l. Requirements of practice : general rules . . . . . . . . . . . . . . . . . . . . . . 457
2. Calling in medical aid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 460
3. Drugs and instruments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 465
4. Supervision of midwives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 466
5. Records . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 466
6. Deliveries at a midwife's home . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 467
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 467
Appendix 1. Synoptic table of legal requirements concerning training, examinations, and refresher courses . . . . . . . . . . . . . . . . . . . . 470
Appendix 2. Drugs and instruments that may be employed by midwives 477
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 480
2 -433-
Introduction
No comprehensive study has yet been made of the various national laws and regulations governing the training of midwives, their establishment (intention to practise), and their professional obligations.
A comparative study embodying a general review of midwifery legislation today and an appraisal of its prevailing trends may therefore be of interest ;" the more so, in view of the attention paid to legislation by the international congresses of midwives held between 1930 and 1940.1
These congresses discussed and made recommendations on various problems affecting the profession, including that of lengthening the period of training, of making provision for refresher courses, of legalizing the use of certain drugs, of obtaining a better distribution of midwives in different countries, and of establishing a better method of selecting candidates for the profession.
By way of introduction to this study it may not be out of place to draw the attention of the reader to certain historical facts that illustrate the development the profession has undergone and its present importance in different countries of the world. Until the beginning of this century, the delivery of women in child-birth had been the almost exclusive preserve of midwives, the medical profession offering little or no competition.
In England in the seventeenth century, it was remarked that "midwifery was an act foreign to the habits of a gentleman". Towards the end of that century, however, physicians began to take up midwifery and were known as " men-midwives " or " extraordinary midwives ". 14
The rapid progress of medicine during the nineteenth century enabled physicians to outdistance midwives in obstetrical technique and thus to engage in larger number in the practice of midwifery. About the same time, the nurse began to receive public recognition owing to the activities of Florence Nightingale, but the public still did not become midwife-conscious. 5 It persisted in considering motherhood and its problems as a matter of essentially private concern ; and it has been stated that, even as late as the beginning of the present century, in the United Kingdom "in labour the doctor was called only in a grave emergency when the efforts of the midwife, in those days untrained and unregistered, had failed to effect delivery ". 8
The first Midwives Act was not, in fact, enacted in England and Wales until1902. These remarks are not, however, of general application, for in certain European countries the public authorities had already been exercising control over midwives for more than a hundred years ; legislation governing the registration and control of midwives was adopted in Austria, in Norway and in Sweden in 1801, in France
a A similar study on Nursing has been published in the Digest. 11
-434-
435
in 1803, in Belgium in 1818 and in Russia, in Holland and in Prussia in 1865.a, 15
The present situation may be summed up as follows : in countries where there is a shortage of physicians and of auxiliary medical workers, most women are still delivered by untrained midwives, whereas in countries which have well-developed public-health services a growing proportion of women (in the United States, almost all women 1 • 8 )
are delivered by physicians, midwives playing a less important part but providing nursing care before and after child-birth. There are, however, countries with well-developed public-health services where this is not so. In Sweden, almost all normal deliveries, whether domiciliary or institutional, are conducted by midwives. 13 In France and in England and Wales also, a large proportion of women are delivered by midwives.
Until recent years, midwives were a strictly autonomous profession, but we may now discern a tendency to establish closer relations between midwives and nurses in many countries. The expansion of maternity services and developments in pre-natal and post-natal nursing care have extended the midwife's field of practice and made it necessary for her to possess a knowledge of nursing. More and more midwives are to be found who have received a basic nursing training ; in England and Wales approximately 96 per cent of the midwives are also trained nurses.1 The WHO Expert Committee on Nursing noted in its first report that " in some countries midwives complete basic nursing education before studying midwifery, and the trend in this direction is increasing ".18 In Japan and in Haiti, only persons who have completed a course of training in nursing may be trained as midwives ; and in most other countries, the period of midwifery training is reduced if students have completed a nursing course.
This tendency is also to be seen in the growing number of countries which have established a common board of control for midwives and nurses, and in the creation of titles such as " maternity nurse " and "nurse-midwife ".b
The steadily increasing proportion of cases confined in hospitals -in England and Wales, 15 per cent in 1922, 55 per cent in 1942 and approximately 67 per cent in 1952 '• 10-may also have affected the profession, for midwives in institutional practice are under medical supervision and are thus not independent practitioners as they are in domiciliary practice.
This survey covers the following countries ;c Austria ( 1925, 1928,
a The earliest midwifery law still in force appears to be the Norwegian law of 1687. It deals especially with professional ethics.l&
b In the United States of America, " nurse-midwife " means a graduate nurse who has completed a course of training in midwifery in an approved school. Up to 1945, only the State of New Mexico had enacted a law for the licensure of nurse-midwives. They are mostly employed as consultants or as supervisors of untrained midwives.11
c The dates indicate the year of the enactment of either the principal law or the latest amendment thereto. The sources used will be found in the table of bibliographical references under the name of the country.
436
1953), Belgian Congo (1951), Belgium (1951), Colombia (1938), Cyprus (1951), Denmark (1953), Egypt (1949, 1951), England and Wales (1949, 1951), Fiji (1948, 1951), Finland (1920, 1934), France (1943, 1945, 1952), Germany (Federal Republic of Germany (1938), German Democratic Republic (1950)), Haiti (1938), India (1947), Israel (1930), Italy (1936, 1940), Japan (1951), Kenya (1952), Netherlands (1953), New Zealand (1945, 1947, 1950), Pakistan (Punjab) (1932), Seychelles (1950), Somalia (1952), Southern Rhodesia (1952), Sweden (1919, 1953), Switzerland (Aargau (1948), St. Gallen (1940), Thurgau (1943), Vaud (1951), Zurich (1952)), Syria (1949, 1952), Uganda (1950, 1951), Union of South Africa (1944, 1949), United States of America (Alabama (1940), Arkansas (1947), Connecticut (1950), Georgia (1949), New York State (1950), New York City (1948), North Carolina (1943), South Carolina (1944), West Virginia (1950), VietNam (1953).
The subject matter is arranged under the following heads: a
Definitions
Professional training : admission to training schools ; midwives training schools ; period of training ; number of labours to be witnessed and conducted during training ; examinations ; refresher courses and further training courses ; maternity nurses.
Administrative regulations : right to practise ; recognition of foreign diplomas ; midwives boards ; membership of midwives boards; registration of midwives ; removal from the register and suspension from practice ; protection of title, uniform, and insignia.
Professional regulations : requirements of practice (general rules); calling in medical aid ; drugs and instruments ; supervision of midwives ; records; deliveries at a midwife's home.
Conclusion
Definitions
The terms " midwife " and " practice of midwifery " are defined in the laws of a certain number of countries. The aim of such definitions is to delimit the scope of a midwife's practice and thus to prevent her from performing, in connexion with child-birth, acts pertaining to the medical profession. The laws also stipulate that the practices defined may be performed by qualified midwives only and so reserve the practice of midwifery to such persons.
In the countries of the British Commonwealth the definition given is usually summary, to the effect that a midwife means a woman registered as such under the law, the effect of which is to protect the title of midwife. Nevertheless, these countries, like those whose laws attempt to define the practice of midwifery, specify the acts which
a Information is complete for most of the countries sturlied; in some instances, the sources used relate to training and to requirements of practice only.
437
a midwife must perform, as well as those from which she must abstain. This shows that definitions which aim at delimiting the scope of a midwife's practice in a single formula are, of necessity, incomplete. The different aspects of midwifery practice are dealt with below.
The difficulty of defining even the extent of a midwife's practice is shown by the Swedish regulations, as amended, of 21 November 1919. They state: "The practice of midwifery comprises in particular care of pregnant women in good health, normal deliveries, normal post-partum care and the care of infants in good health. Where any abnormality or illness occurs in a mother or her child, the midwife may not give assistance except where authorized by these regulations. " In a further section of the regulations these abnormal cases are enumerated, but even then it is stipulated that they must be dealt with as laid down in the midwife's textbook.
In the Swedish regulations, as in those of many other countries, there is a general provision to the effect that midwives shall only employ methods in which they have received instruction during their training or at refresher courses.
Definitions, like professional regulations, are of considerable importance to the midwife, for by delimiting the scope of her practice they define her responsibility at law.
Most laws stipulate that midwives shall concern themselves solely with normal delivery and post-partum. This broad restriction placed on the activities of a midwife is regularly mentioned in the literature on the subject; the Report of the Working Party on Midwives, for example, states that the midwife " should be the practitioner of normal midwifery : the expert in normal childbearing in all its varied aspects. " 8
The following definitions have been selected from the laws studied :
Austria: The Law of 1925 defines the practice of midwifery to include advice to pregnant women, assistance during delivery, care of lying-in women, of newly born babies and of infants, and co-operation with the maternal and child health services.
By the Midwives Regulations of 1928, midwives are permitted to attend normal cases only.
Germany (Federal Republic) : The practice of midwifery includes advice and assistance to pregnant women, supervision and assistance during delivery or miscarriage, as well as care of lying-in women and newly born infants.
In the same law, the extent of a midwife's practice is restricted to personal supervision of normal pregnancy, delivery and postpartum and the care of normal children.
Israel: A person shall be deemed to practise midwifery who holds herself out, either directly or by implication, as being prepared to examine, diagnose, prescribe or treat or deliver any woman in connexion with child-birth.
Italy : A midwife, in addition to her specific competence with respect to assistance to a mother during normal pregnancy, delivery
438
and post-partum, and care of the new born, shall be responsible for the surveillance of a mother and her child until the latter has attained the age of three years.
Japan: "Midwife " shall mean the female who has been licensed by the Minister of Welfare and practises midwifery or guidance with respect to the health of pregnant women, women in child-birth and newly-born babies.
N elherlands : A midwife shall be competent to give advice and aid during normal childbirth. "Child-birth " means a delivery which takes place after a pregnancy of not less than 18 weeks in duration. It shall be the duty of a midwife to call in medical aid as soon as she ascertains that an obstetrical intervention is or may be necessary.
New Zealand: For the purposes of this Act (Act of 1945) the expression " to undertake the duties of a midwife ", or any like expression, means to attend a woman in child-birth or during the next succeeding ten days, in any case where a registered medical practitioner has not undertaken responsibility for the care of the patient ; and the expression " to undertake the duties of a maternity nurse ", or any like expression, means to attend a woman in child-birth or during the next succeeding ten days, in any case where a registered medical practitioner has undertaken responsibility for the care of a patient.
Sweden: The practice of midwifery comprises in particular care of pregnant women in good health, normal deliveries and normal post-partum care and the care of infants in good health. Where any abnormality or illness occurs in a mother or in her child, a midwife may not give assistance except where authorized by these regulations.
Switzerland (Zurich) : Midwifery includes advice to pregnant women, assistance at the request of a physician in the event of a miscarriage, conduction of labours, and care of lying-in women and of the new born.
United Stales of America (Connecticut): The practice of midwifery is defined as and limited to such assistance or offers of assistance as may be rendered by any person for compensation received, promised, or expected, to any one in normal child-birth, without using any instruments or artificial or forcible or mechanical means and without performing or attempting to perform any version, or removing or attempting to remove adherent placenta, and without prescribing or using or advising the use of any drug other than a disinfectant. Each licensed midwife may give not more than one teaspoon dose of the fluid extract of ergot and only after the expulsion of the intact placenta.
United Stales of America (Georgia) : The term "midwife" shall be held to mean and include any person, other than a regularly licensed physician, who shall attend or who shall bargain, contract, or agree to attend anyone at or during child-birth.
United Stales of America (West Virginia) : A midwife shall be any person at least 21 years of age, other than a physician, who shall
439
attend or agree to attend anyone at or during child-birth, and who shall accept any compensation or other remuneration for her services : provided, that nothing contained in this article shall prevent a neighbour or friend from rendering assistance in such cases in an emergency.
Professional training
Midwifery legislation usually contains detailed provisiOns relating to admission to training schools, including age of admission, period of training, examinations, recognition of training schools, approval of their curriculum a and teaching staff, and refresher courses, the last-mentioned being of special interest to midwives in certain countries. Appendix 1 contains a synoptic table of the provisions relating to these subjects in the legislation studied.
1. Admission to training schools
The age-limits prescribed for admission to a training school vary considerably ; the minimum lower age-limit encountered is 17 years (Seychelles), the maximum upper age-limit, 40 years (England and Wales). The health authorities in certain countries have the discretionary power to raise or lower the age-limits. Sometimes the age of admission to a training school is not specified in the law ; in its stead the law stipulates the minimum age for admission to the qualifying examination, as in Kenya 21 years, and in New Zealand 20 years (both for maternity nurses and for midwives); or the minimum age for registration, as in the Union of South Africa 21 years, and in Cyprus 20 years.
Applicants are usually required to present a certificate of physical andfor mental health and a certificate of good moral character. In France an applicant who has a negative tuberculin reaction or has not reached the age of 25 years is, in addition, required to be vaccinated with BGG. BGG vaccination is also a requirement for admission to a training school in Finland and in Norway, and is recommended in Austria.b
In France, applicants are required to sit for a competitive examination. They are required to pass an entrance examination in Somalia (examination of general education and of aptitude), in Bel-
a The curriculum of midwives training schools is set out in extenso in the legislation of the following countries: Austria, Belgian Congo, Belgium,* France, Germany (Federal Republic), Italy, Japan, Kenya,* the Netherlands, New Zealand, Somalia,* Switzerland (Vaud),* United States of America (New York City); in the case of the countries marked with an asterisk, the text in question has been published in the Digest. Other countries (Cyprus, England and Wales, the Netherlands, New Zealand, Union of South Africa) embody the examination syllabus in their legislation.
b A study of recent legislation on Tuberculosis has been published in the Digest.11
440
gium (examination of general education) and in the Netherlands (entrance examination). In Finland they may also be required to pass an entrance examination. In Germany (Federal Republic), before applying to a training school, an intending student of midwifery must report to the local medical officer of health [ Amtarzt ], who examines her as to her physical and mental health. She must also submit to him her birth certificate, vaccination certificate and a certificate of good moral character.
Where applicants have completed a course of training in nursing, the period of midwifery training is reduced in Cyprus, England and Wales, Finland, Italy, Kenya, Seychelles, Uganda, and the Union of South Africa (Appendix 1). In New Zealand, the training of midwives is of a special nature in that no woman may be accepted for such training unless she is already a registered maternity nurse. In Haiti and in Japan, only trained nurses are admitted to schools of midwifery, and in Sweden applicants must have completed two years of general nursing training.
2. Midwives training schools
Schools of midwifery are usually public institutions, but in some countries public and private institutions exist side by side ; nevertheless, in all cases, they are subject to supervision by the public authorities. The approval and supervision of schools is one of the most important functions of the midwives boards (or nursing councils) in the countries of the British Commonwealth. In Austria, Colombia, Germany (Federal Republic), Haiti and Italy, some schools are attached to a university medical centre. They are under the control of the State or cantonal boards of health in Switzerland and the United States of America; of the State Medical Board in Finland and Sweden; of the Ministry of Education in Italy; and in Austria, Belgium and Japan under the joint control of the Ministries of Education and of Health.
Provision is usually made for the withdrawal of approval from a training school which does not meet the requirements relating to the number of maternity beds at the disposal of the training institution, teaching equipment, the qualifications and number of teaching staff, etc. Teaching staff is sometimes approved by the midwives board and sometimes appointed directly by the minister concerned.
The initial period of a midwife's training is often probationary; this probationary period extends over two weeks in the United States of America (New York City), one month in Sweden (student nurses who have completed two years of nursing training are exempt), three months in Germany (Federal Republic), and six months in England and Wales, in Finland and in the Seychelles. In these countries, as in the Netherlands, a student may be dismissed at the end of this period if she is found unsuitable or if her conduct has been unsatisfactory.
441
3. Period of training
The period of midwifery training varies from country to country. It is six months in Japan and 12 months in Haiti, but, as noted above midwifery training in these countries is open only to qualified nurses It is six months in New York City (United States of America) and in the Canton of St. Gallen (Switzerland) 12 months; in Germany (Federal Republic}, Austria, Seychelles, Canton of Aargau (Switzerland) and the Union of South Africa 18 months; in Uganda not less than 21 months; in Germany (German Democratic Republic}, Cyprus, Finland, Kenya, New Zealand,a England and Wales, Somalia and in the Canton of Vaud (Switzerland) two years; in the Belgian Congo,b Belgium, France, Italy and the Netherlands three years ;c in Fiji not less than three years and three months and not more than five years.b The period of training is usually reduced if students have been trained as nurses.
In South Carolina (United States of America) a woman is eligible to register as a midwife if she has attended a course of instruction of at least ten lessons to be given to midwifery classes in the countries by either State or county nurses, and has received a certificate of proficiency. In West Virginia, every applicant for a licence to practise must either possess a diploma from a recognized school of midwives or have attended under the instructions of a duly licensed and registered physician not fewer than five women and new-born infants during lying-in periods of at least ten days each and must present a written statement from this physician that she is reasonably skilful and competent.
4. Number of labours to be witnessed or conducted during training
Training is both theoretical and practical. The number of labours to be witnessed and conducted by a student midwife during her practical training is specified in certain laws.
In Germany (Federal Republic), a student is required to assist at not fewer than 50 labours and personally support the perineum in 30 cases. In addition she must conduct vaginal examinations on 50 women (30 during pregnancy and 20 during labour) and not fewer than 50 rectal examinations during labour.
In Cyprus, a student is required to examine and receive instruction in the ante-natal supervision of 30 pregnant women, witness not
a Only registered maternity nurses are admitted to training as midwives, the course in maternity nursing being of 18 months' duration.
b In the Belgian Congo, nurse-midwives [inflrmieres-accoucheuses indigenes] and in Fiji, Fiji Obstetric Nurses, are only allowed to practise under supervision.
c The International Congresses of Midwives, held between 1930-1940, recommended that the period of training should be 3 years. 1
3
442
less than 10 labours, attend and watch the progress, making abdominal and vaginal examinations during the course of 40 labours and personally delivering the patients (10 in their own homes), and nurse 40 lying-in patients and their infants during the ten days following labour (at least 10 in their own homes).
In England and Wales, a student who is a State-registered general or sick children's nurse is required, during the first part of her training, which extends over six months, to conduct ante-natal examinations on not less than 50 pregnant women, witness not less than 10 labours, attend not less than 10 labours within the approved institution, making full examination, including abdominal palpation during the course of labour and personally delivering the child and the afterbirth, and attend and nurse not less than 20 lying-in women and their children. For other students the first part of training extends over 18 months. After six months' general nursing they follow a similar course to that of the State-registered nurse, except that 20 labours must be witnessed instead of 10, and 40 lying-in women attended and nursed instead of 20. During the second period of training, which extends over six months in all cases, a student must attend and take responsibility for the ante-natal care of not less than 20 pregnant women and of 20 women during labour and subsequently attend and nurse 20 lying-in women and their children (at least 10 in their own homes).
In Japan and in the Netherlands, a student must deliver 10 women; in Uganda, a student must conduct the examination of 50 ante-natal patients, witness 10 labours, attend and watch the progress of not fewer than 20 labours, making the necessary examinations and personally delivering these women, and subsequently nurse 20 lying-in patients and their infants.
In Kenya, the requirements are the examination of 70 ante-natal patients, the witnessing of 20 labours and attendance on 30 women in labour, including full examination and personal delivery of the child and the afterbirth ( 10 patients in their own homes) and the care of not less than 60 lying-in women (10 in their own homes). For students who are already trained nurses, 10 labours must be witnessed
.. instead of 20 and 40 lying-in women attended and nursed instead of 60. In the Union of South Africa, a student must witness 20 labours
and examine 30 pregnant women (25 if the student is already a trained nurse), attend and watch, making abdominal and vaginal examinations of not less than 30 labours (25 is she is a trained nurse) and personally deliver 30 women (25 if she is a trained nurse), five of which are to be delivered in their own homes, nurse not less .than 30 lying-in women (25 if she is a trained nurse) and their infants.
In New York City (United States of America), a student must attend at least 20 cases of labour and have the care of at least 20 mothers and their children during the lying-in period.
443
5. Examinations
Examinations for midwives are sometimes organized by the training school itself (Finland, Sweden); sometimes by an examining board appointed by the nursing counoil or midwives board (most countries of the British Commonwealth); and sometimes by the ministry concerned. When the examination is organized by a ministry, it is a State examination ; and the examining board is composed of members of the teaching staff of the training school and of representatives of the ministry. In some countries students must first pass the examinations conducted by the training school in order to be eligible to sit for the qualifying examination conducted by the midwive[) board (Kenya).
The diploma in midwifery is awarded in some countries after several examinations, according to the manner in which the curriculum is organized (Belgium, France, Netherlands); and in other countries after a single qualifying examination (Finland, Germany (Federal Republic of Germany, German Democratic Republic), Switzerland (Aargau, St. Gallen)). In no case is a student entitled to present herself for the qualifying ~xamination until she has completed the prescribed theoretical and practical training.
6. Refresher courses and further training courses
In many countries midwives are required to attend refresher courses, on termination of which an examination is held. In this respect midwives constitute an exception to the other medical and auxiliary medical professions. Such courses are compulsory in Austria, England and Wales, Finland, Germany (Federal Republic), Sweden, Switzerland (Aargau, Thurgau, Zurich).
In Germany (Federal Republic), a midwife is examined as to her knowledge every three years by the local medical officer of health, assisted by the director of a midwifery school. If the result of this examination is unsatisfactory, she is required to take the examination a second time within six months, and if she fails on that occasion, she may be required to follow the course of basic training once again either in full or in part, and even to sit for the qualifying examination. In addition, midwives are required to attend a two-week refresher course every five years ; the interval between such courses may be extended.
In Austria, all midwives other than those working in public institutions are required to attend refresher courses of three weeks' duration every five years ; those who have shown themselves to be incompetent in the course of practice may be required to attend at more frequent intervals and may be suspended from practice until they have successfully passed such a course ; and those who are especially competent may attend at less frequent intervals, namely every 10 years. A midwife's establishment permit may be withdrawn
444
if she fails to attend. A midwife who has interrupted her practice for two years may be required to follow such a course before resuming practice. On reaching the age of 55 years midwives who have already successfully passed the examinations held after three of such courses are excused.
In Finland, the State Medical Board designates each year the midwives who are required to attend refresher courses, which are of one month's duration. From time to time special courses are organized, the purpose of which is to instruct midwives in the use of forceps. Further training courses of six months' duration are organized for midwives who wish to become midwifery teachers.
Refresher courses of four weeks' duration are held in England and Wales, and midwives are required to attend them every seven years. Exemptions may, however, be granted by the Central Midwives Board. Where a midwife has not practised as a midwife or acted as a maternity nurse during the two years immediately preceding the year she intends to resume practice, she may be required to attend a course of instruction before doing so. At the request of the local supervising authority, the Central Midwives Board may make the interval between courses shorter than 7 years or the course of instruction longer than four weeks. Provision is also made for further training courses for candidates for the midwife teacher's diploma. Admission to such courses is limited to midwives of 25 years of age or more who have been certified for at least three years, have the prescribed teaching experience, and hold a nursing diploma.
In the Canton of Aargau (Switzerland), a midwife is required to attend refresher courses every 10 years, and her permit to practise, which is valid for the same period, is only renewed if she is successful at such a course. A midwife who has shown herself to be weak in practice may be required to attend a course at an earlier date. In the Canton of Thurgau, district midwives and midwives in private practice are required to follow an annual refresher course. Provision is also made for refresher courses in the Canton of Zurich.
In the Netherlands further training courses are organized for the purpose of instructing midwives in the ·technique of taking blood samples (midwives are entitled to take a blood sample from a pregnant woman for the purpose of detecting syphilis or ascertaining the rhesus factor). During these further training courses they are also taught how to suture superficial lacerations of the perineum.
7. Maternity nurses
Some midwifery laws also embody provisions relating to maternity nurses (New Zealand: maternity nurse; Germany (Federal Republic) : Wochenpflegerin; Netherlands : Kraamverpleegster). Except in emergencies, this category of medical auxiliary worker does not provide obstetric care ; her function is to attend women during
445
and after delivery in any case where a physician has undertaken responsibility for the care of the patient.
In New Zealand, the course of training for maternity nurses is of 18 months' duration (six months if the student is a trained nurse). In the Netherlands a diploma in maternity nursing is granted to general nurses who have successfully completed six months' special training in a recognized school or who have undertaken the duties of a maternity nurse for a period of three years in a recognized institution. In Germany (Federal Republic), the period of training is of six months' duration (three months if the student is a qualified nurse or children's nurse [Sauglings- und Kinderschwester ]).
In England and Wales, there is no title " maternity nurse " but a midwife is deemed to be acting as a maternity nurse if in any maternity case she is under the direction and personal supervision of a medical practitioner who has been engaged to deliver the patient, has been notified of the onset of labour, and continues to be in charge of and responsible for the case throughout the lying-in period (14-28 days).
Administrative regulations
1. Right to practise
The conditions which entitle midwives to practise are complex. Generally speaking a midwife is required initially to be registered or licensed. In addition she is usually required to notify the local authorities in the area in which she intends to practise (England and Wales) or obtain from them an establishment permit (Austria, Germany) or be enrolled in a list maintained by the designated authorities (France, United States of America). She may also be required to undergo a medical examination before commencing to practise (Austria, Union of South Africa). The right to continue in practice may be dependent on periodical medical examinations (Switzerland (Zurich)), attendance at refresher courses (Austria), or annual reregistration (New Zealand).
Apart from emergencies, in which any person may render aid to a woman in child-birth, the laws usually permit a student midwife to deliver women during her training, but such deliveries are, of course, supervised.
In order to prevent unqualified persons from acting as substitutes for certified midwives, it is sometimes stipulated that unqualified persons may only attend a woman in child-birth under the direction and personal supervision of a physician.
In most of the countries studied, the right to practise midwifery is reserved to qualified midwives. The only exceptions to this rule are countries in which there is a shortage of qualified midwives ; there, unqualified midwives may practise outside certain specified areas but where the number of qualified midwives in any locality reaches a figure deemed sufficient for local needs, such an area may be
446
prescribed and no further unqualified persons may engage therein in practise of midwifery. The exclusion of unqualified persons from the practise of midwifery is thus a very gradual process in most countries. In England and Wales, where midwifery legislation was first adopted in 1902, unqualified persons were not finally excluded from practice until 1926. Midwives who have not followed the prescribed course of training are still entitled to practise in Colombia, Fiji, Israel, Pakistan (Punjab), Southern Rhodesia, Switzerland (Thurgau), Syria, Union of South Africa and Viet Nam.
In Syria, untrained midwives who were in practice before the adoption of the present law (1949) were given six months' grace in which to pass an examination in midwifery, success in which entitled them to practise in villages where there were no trained midwives.
In Colombia, the directors of health posts and health commissions may require untrained midwives practising in areas designated by the Departmental Director of Hygiene to follow a basic training course in midwifery. In Pakistan (Punjab), a person employed or practising as dai a on the entry into force of the present law ( 1932) was entitled to become registered and therefore legally entitled to practise if she made application to the registrar within three years, this period of grace being extended to five years in 1936. Any local authority has the power to make by-laws prohibiting unregistered persons from practising within the area subject to its authority ; and if they fail to make such by-laws, the Provincial Government may by notification prohibit unregistered persons from practising within the area subject to the jurisdiction of the local authority.
In the Union of South Africa, untrained midwives may practise outside the prescribed areas, i.e. areas in which facilities for obtaining attendance by medical practitioners or registered midwives are sufficient for all classes of population. They may use the title "midwife " but not the title "registered midwife ". They may even become registered and thus entitled to practise in a prescribed area if within two years of its being prescribed they submit (1) proof to the satisfaction of the South African Nursing Council that for at least three consecutive years immediately preceding the proclamation prescribing such an area they were in bona fide practice; and (2) a recommendation from one or more medical practitioners under whose supervision they have worked to the effect that they are fit and proper persons. The same provision exists in Southern Rhodesia.
No remuneration is recoverable in Southern Rhodesia in any court of law in respect of any act pertaining to the calling of a registered person when performed by a person who is prohibited from performing such an act for gain. Moreover, no unregistered midwife may hold any appointment in a public service or in any establishment, institution or body, whether public or private, if the appoint-
a " Dai " is defined as any person, whether following a hereditary occupation or not, who ordinarily practises midwifery for gain and who has not passed any of the examinations in midwifery recognized by the Council.
447
ment involves the performance of any act which is unlawful for any unregistered person to perform for gain.
In Israel, qualified midwives are licensed and only they may practise in the prescribed midwifery areas. Untrained midwives may practise outside such areas if they are registered in the register kept by the district medical officer ; they are then entitled to use the title "Registered Dayah ", and are granted a certificate of registration, valid for one year only. If in the area in which an untrained midwife proposes to practise a sufficient number of persons are registered, the district medical officer may refuse to register her. When an order is made prescribing an area, a registered dayah already in practice in the area may, if she applies to the Director of Medical Services within three months, be granted a permit to continue to practise provided she is a fit and proper person; she may, where necessary, be required to undergo a course of training before doing so.
In Viet Nam, the practice of midwifery is restricted to persons of Vietnamese nationality (or to nationals of a country in which Vietnamese midwives may practise) who hold a diploma in midwifery and are registered in the register of the midwives' corporation. Rural midwives [ accoucheuses rurales] may, however, practise in villages in which there are no qualified midwives ; and even continue to practise in villages in which there are qualified midwives if they do not use the title " State midwife " or " Indo-Chinese midwife ".
In countries where the powers relating to health matters are decentralized, the legislation varies from State to State (United States of America) or from canton to canton (Switzerland).
In the United States of America, there are no licensing laws for midwives in Alabama and North Carolina, and to become eligible to practise a midwife is required merely to be enrolled with the State Board of Health andfor the local registrar of vital statistics. In Connecticut, Georgia, New York, South Carolina, and West Virginia, on the other hand, persons are prohibited from practising unless they are licensed by the State Board of Health and, in addition, are enrolled either with the State Department of Health (Connecticut) or the registrar of vital statistics (Georgia, New York, South Carolina, West Virginia).
In the Swiss cantons of Aargau1 St. Gallen, Thurgau and Zurich, the health authorities grant a permit to practise to midwives who hold a recognized diploma. In each commune the authorities are required to make provision for a midwifery service in accordance with local needs. In the Canton of Thurgau, for example, a communal midwife must be appointed in every commune in which more than 30 women are delivered at home every year. These midwives may continue in practice until they reach the age of 65 years. An untrained midwife appointed as a communal midwife after the entry into force of this law (1943) was required by the public-health authorities to follow a course and pass an examination in an official training school, the costs incurred being equally shared between the commune and the canton.
448
In Germany (Federal Republic), the law requires every pregnant woman to be cared for by a midwife ; at delivery it is the duty of a physician to ensure that this condition is fulfilled. Only qualified midwives are granted official recognition [Anerkennung]; however, in order to engage in private practice a midwife must also obtain an establishment permit [Niederlassungserlaubnis] from the local authorities, who may refuse such a permit if there are sufficient midwives within the area subject to their authority. Before granting such a permit the medical officer of health must be consulted. A midwife may continue to practise until she attains the age of 70 years, or even later if she is approved by the higher administrative authorities.
In Austria, there are four categories of qualified midwife : district midwives [offentlich bestellte Hebamme], institutional midwives [ Anstaltshebamme ], independent midwives [ frei praktizierende Hebamme], and midwives practising in State maternity homes. Of these, the first three categories require an establishment permit, which is valid in the case of the first two only for the locality or institution in which they work; in the case of the third category it is valid throughout the whole country. The fourth category does not need an establishment permit.
Only qualified midwives may practise in Denrriark, Egypt, Finland, France, Haiti, Italy, the Netherlands, and Sweden. In Denmark, before commencing to practise in a medical district, a midwife must submit her licence to practise to the medical officer of health ; such a licence is granted on request to persons who have obtained a diploma in midwifery, but must be refused to persons suffering from physical defects or mental illness caused by sickness or intemperance in the use of alcohol or narcotic drugs.
In Finland, where each commune is required to make provision for the services of a qualified midwife, there is normally one midwife for every 5,000 inhabitants.
In the Netherlands, a midwife's certificate of proficiency must be endorsed by the medical inspector of the district before she commences to practise. It is interesting to note that, in the Netherlands, midwives, like physicians, do not normally nurse patients during the lyingin period ; such care is usually provided by a maternity nurse.
In Sweden, midwives in private practice may establish themselves anywhere in the country provided they give notice of their intention to practise to the medical officer of health ; district midwives, on the other hand, are appointed by the State Medical Board according to local needs.
In Japan, a licence to practise may not be granted to a midwife who is suffering from a physical or mental defect, is intemperate in the use of narcotic drugs, or has served a prison sentence. A midwife must notify the Governor concerned of her intention to practise. Licences to practise are granted by the Minister of Welfare, who also maintains the register of midwives.
In New Zealand, a registered midwife or maternity nurse may not
449
practice unless she is in possession of an annual practising certificate issued by the Nurses and Midwives Board. Before engaging in domiciliary practice, a midwife must inform the medical officer of health of her intention to do so.
In Uganda, a registered midwife must notify the Midwives Board of her intention to practise and, if in private practice, must report in person every year to the supervisory authority and submit her certificate for inspection. Any woman who practises midwifery habitually or for gain without being registered is liable on conviction to a fine.
This last-mentioned provision also exists in Cyprus and in Kenya. In the Seychelles, no unregistered person may attend a woman in
child-birth otherwise than under the direction and personal surpervision of a registered medical practitioner. A registered midwife may not employ an unregistered person as her substitute. In England and Wales, any person who is not a certified midwife who attends a woman in child-birth otherwise than under the direction and personal supervision of a duly qualified medical practitioner is, except in cases of urgency or necessity, liable on conviction to a fine. When the Minister of Health is satisfied that in the area of a local supervising authority that authority has secured the provision of a service, adequate for the needs of the area, of certified midwives who are available for attendance as midwives or maternity nurses on women in their own homes, he may by order make any person who is not a certified midwife nor registered nurse, or a male person, who receives any remuneration for attending as a nurse on a woman in child-birth or any time during the 10 days following child-birth liable on conviction to a fine. No midwife may employ as her substitute a woman who is not certified. Every certified midwife must inform the local supervising authority of her intention to practise before doing so and thereafter every year.
In France, a qualified midwife must, within one month of commencing to practise, register her diploma with the Prefect, who maintains the list of practising midwives.
2. Recognition of foreign diplomas
The recognition of foreign diplomas encompasses both the recognition of a diploma acquired abroad by a midwife who wishes to practise in her own country, and the recognition of a diploma acquired abroad or in the country in question by a midwife who is an alien.
In Austria, an alien holding an Austrian or a foreign diploma may be granted an establishment permit if she is a national of a country granting similar rights to Austrian nationals.
In Colombia, provision is made for the recognition of diplomas awarded in countries having a reciprocity agreement with Colombia ; midwives holding diplomas granted in countries which do not have such an agreement with Colombia are required to sit for a validation examination .
•
450
In Denmark, the health authorities may grant a permit to practise to a person holding a foreign diploma if they are satisfied that the training she has undergone is the equivalent of that prescribed m Denmark.
An alien cannot practise in Egypt unless she is a national of the country in which Egyptian midwives are entitled to practise, and, in addition, is registered in the register maintained by the Ministry of Health. To become registered she must successfully pass an examination before a medical board appointed by the Minister.
In France, only those aliens who were in practice before 1945 may practise midwifery. Where a reciprocity agreement exists, the holders of foreign diplomas may be authorized to practise in France by the Minister of Public Health and Population if the equivalence of their diplomas has been recognized by the Minister of Education. In other cases, the holder of a foreign diploma or any person who has completed the training prescribed for such a diploma and applies for a French State Diploma may be granted certain credits with respect to training, the extent of which varies according to the nature and duration of the training undergone abroad. The equivalence of diplomas, as well as exemption from training or examinations, is conferred by the Ministry of Education, after consultation with the Council for the Improvement of Midwifery Schools.
In Haiti, a person holding a foreign diploma is not allowed to practise until her diploma has been validated. First, a special committee must decide whether the application for validation can be entertained and thereupon the applicant is required to pass an examination ; where the person concerned is a Haitian national, she may be exempted from this examination.
An alien midwife may practise in Viet Nam if she is a national of a country in which Vietnamese midwives have similar rights. Other aliens who were engaged in the practice of midwifery before the present (1953) legislation was adopted may continue to practise for a period of five years if their diploma is approved by the National Council of the Midwives Corporation. Vietnamese nationals holding a foreign diploma may continue to practise without restriction if their diploma is approved ; if it is not approved, they may practise for five years only and if they wish to practise thereafter must obtain a French or Vietnamese diploma in midwifery. Henceforward, Vietnamese nationals who obtain foreign diplomas may only practise if their diploma is recognized.
In Cyprus, England and Wales, Fiji, New Zealand and Uganda, persons holding foreign qualifications may practise if registered. In England and Wales, the Central Midwives Board may enrol women who have successfully completed their training abroad in accordance with a scheme satisfactory to the Board ; where, however, such training is not in accordance with the scheme recognized by the Board, a midwife may be required to undergo further training and pass an examination before they enrol her. In Fiji, midwives may
451
be enrolled if they are registered in a country where the standard of training is not lower than that recognized in Fiji. In New Zealand, the Board has the power to register persons who satisfy them that they have undergone a course of training and passed an examination elsewhere which is equivalent to that required in New Zealand.
In Uganda, a woman is entitled to be registered if she has successfully passed the final examination of the Central Midwives Board of England and Wales or is certified or registered in any other country in which there is any law in force for the certification or registration of midwives, and the Director of Medical Services is satisfied that the training and examination required in that country is not inferior to the standard adopted by the Board ; provided that when the Director of Medical Services is not so satisfied she shall be required to pass such examination as he shall direct.
In Cyprus, the diploma of the Central Midwives Board of England and Wales is likewise recognized, as is that of any body or institution that may from time to time be approved by the Board.
3. Midwives boards
Powers relating to the training of midwives, approval of training schools, conditions of registration, regulation and supervision of practice, etc., are normally vested in the central authorities. In the countries of the British Commonwealth there is a tendency to delegate these powers to certain statutory bodies known as midwives boards or nursing councils. In other countries, the position varies. In Syria and in VietNam there is a midwives corporation responsible for registration and discipline. In France, Belgium and Japan, there is in addition a special body which advises the Ministry as to training programmes and the approval of training schools. In Egypt, there is no midwives corporation, but a committee dealing with disciplinary matters has been established in each province by the Ministry.
In England and Wales, New Zealand, and the Union of South Africa, one of the most important functions of the midwives board is to frame rules relating to the admission of midwives to the roll. This roll or register is maintained by a registrar or secretary, who issues a certificate of registration as proof that the midwife's name appears on the register. The board also has the power to remove the name of a midwife from the register or, as the case may be, to restore her name thereto. It may also determine the courses of training to be undergone and the examinations to be passed as a condition of the issue of the certificate of registration, approve training institutions, prescribe the conditions under which a midwife may be suspended from practice, require midwives to attend refresher courses, prescribe the conditions under which midwives teachers' diplomas are granted, make rules with respect to the uniform and badge which may be worn by certified midwives, and register midwives who have been
452
trained abroad. The removal of a midwife's name from the register does not necessarily prevent her from practising under another title, for in some countries all midwives, and in others a high proportion of midwives, are also nurses. In England and Wales and in Uganda, however, the midwives board may prohibit midwives whose names have been removed from the register from attending any woman during labour or the lying-in period in any other capacity.
In Egypt, the Ministry of Health is responsible for the various matters mentioned above, with the exception of disciplinary matters involving midwives not in the public service ; these fall within the competence of the disciplinary tribunals established in each province.
In the Union of South Africa, there exists side by side with the South African Nursing Council a body corporate styled the South African Nursing Association, the objects of which include that of providing an efficient and adequate midwifery service for the Union, and of raising the status, maintaining the integrity and promoting the interests of the midwifery profession. It may also establish and administer sick and provident and pension funds. Registered midwives, whether practising or not, and pupil midwives are admitted to membership of this Association.
In Austria, there is a midwives association [Hebammegrenium] with similar functions, in each province.
The body responsible for registration and discipline in France and in Viet Nam is the Midwives Corporation [Ordre des SagesFemmes] and in Syria the Midwives and Specialized Nurses Corporation [Ordre des Sages-Femmes et des Infirmieres specialisees ]. French regulations relating to discipline have been published in the form of a code of ethics for midwives; this code covers the general duties of midwives, their duties towards their patients, their duties in respect of social medicine, their duties towards colleagues, and towards members of the para-medical professions and medical auxiliaries. In France, there is also a Council for the Improvement of Midwifery Schools [Conseil de Perfectionnement des Ecoles des Sages-Femmes], which advises the Minister on matters relating to the organization and operation of midwifery schools, including the number of pupils to be admitted to each school annually, approval of schools and training programmes, and examinations. In Japan, there is a Council on Authorization of Schools, Training Schools, and Examination for Public-Health Nurses, Midwives and Nurses, with similar functions.
In England and Wales, in Uganda and in the Seychelles, the midwives boards are independent bodies but in many countries of the British Commonwealth nurses and midwives are controlled by the same body. In Ireland, there was formerly both a Central Midwives Board and a General Nursing Council, but in 1950 these two bodies were amalgamated. In Southern Rhodesia, midwives as well as other para-medical professions come under the jurisdiction of the Medical Council. In the Union of South Africa, a Nursing Council was estab-
453
lished in 1944 to take charge of the affairs of nurses and midwives, independent of the Medical Council under which they had formerly fallen.
4. Membership of midwives boards or nursing councils
The bodies which exercise delegated powers with respect to the regulation and control of midwives often comprise public-health officials, medical practitioners, representatives of hospitals, as well as midwives and/or nurses. In England and Wales, in Uganda and in the Seychelles the midwives' boards are independent bodies. The representation of midwives in England and Wales is fixed at at least six out of a total membership of 16. In the Seychelles and in Uganda, out of seven members of the board, at least four may be either midwives or medical practitioners.
The number of midwives represented on councils which regulate both n;J.idwives and nurses is naturally smaller. In Pakistan (Punjab), out of a council of 23 members there is at least one midwife ; in Fiji, one midwife on a council of six members; in New Zealand one midwife on a council of nine members. In Southern Rhodesia, where midwives fall under the Medical Council, they are represented by at least one midwife out of 17 members. In Kenya, where the council comprises 17 members, there may be at least six persons with midwifery qualifications. In Cyprus, there are two midwives on a council of nine. Of the 25 persons composing the South African Nursing Council, at least four hold qualifications in midwifery, and of the council of the South African Nursing Association at least three of the 10 members have qualifications in midwifery. In France all members of the regional and in Viet Nam all members of the departmental councils of the midwives corporation [Ordre des Sages-Femmes] are midwives, with the exception of the chairman who is an obstetrician. The national council of the midwives corporation includes three physicians appointed by the medical corporation and six midwives elected by the regional or departmental councils. In Syria, the five members of the council of the midwives and specialized nurses corporation may be either all midwives or all specialized nurses.
5. Registration of midwives
In a previous study 18 it was pointed out that laws relating to nursing fall into two well-defined categories : the first is mandatory and restricts the practice of nursing to registered or licensed nurses ; the second does not restrict the practice of nursing but aims at protecting the title, uniform, and insignia of registered or licensed nurses. There is no such distinction in so far as the laws relating to midwives are concerned. In the legislation covered by ·this study the practice of midwifery is reserved to registered or licensed midwives. Even in countries where unregistered midwives may practise this general principle holds good. In other words, registration is a guarantee that the person concerned has undergone the prescribed training. The
454
protection of the title, uniform, and insignia of registered nurses aims at protecting the status of such nurses in countries where the unqualified may practise ; in so far as midwives are concerned, it is of only secondary importance.
In most of the countries of the British Commonwealth a person seeking registration must satisfy the midwives board or nursing council that she has undergone the training and passed the examinations prescribed, and is of good moral character. In most of these countries midwives trained abroad may be registered if the board recognizes their qualifications. When a law concerning the registration of midwives is first adopted, it usually specifies a period of grace within which persons already practising midwifery may be registered subject to certain conditions being fulfilled. The right to practise is conferred by registration. Persons whose application for registration has been refused may appeal.
In some States of the United States of America, on the other hand, a licence to practise is first required and then the holder of this licence must be enrolled on a list maintained by the designated authority, usually the registrar of vital statistics. In France it is maintained by the Prefecture and in Viet Nam by the regional health administration. But in both these countries midwives must first be registered by the midwives corporation. In Colombia, Egypt, Japan, and Syria, the register is maintained by the competent ministry.
Registers of midwives may have several subdivisions. In Fiji; for example, one part of the register contains the names of midwives, who are trained abroad, and the other of obstetric nurses, who are trained in Fiji. In New Zealand also, the register comprises two parts; the one contains the names of midwives and the other of maternity nurses. In Syria, the practice is to keep one register for qualified midwives and another for midwives who have not undergone the training prescribed but who have passed an examination which entitles them to practise in villages where there are no trained midwives. In Pakistan (Punjab), the register is divided into four parts, covering dais, trained dais, nurse-dais, and midwives.
In England and Wales, in Kenya, in the Seychelles and in the Union of South Africa, student midwives are enrolled in a special roll.
Lists of midwives are published annually in Cyprus, Seychelles, and Uganda. Although midwives receive a certificate on registration, the publication of their names in these lists also constitutes proof of registration.
The midwifery laws of most of the countries of the British Commonwealth stipulate that registration does not confer on the person registered the right to practise medicine or surgery, to issue medical certificates or certificates of death, or to undertake the charge of cases of abnormality or disease in connexion with parturition.
The minimum age prescribed for admission to the register is 20 years in Cyprus, 21 years in the Union of South Africa and 22 years in New Zealand (20 years for maternity nurses).
455
6. Removal from the register and suspension from practice
A midwife loses the right to exercise her profession if her name is removed from the register of midwives or if she is suspended from practice. In England and Wales and in Uganda, when the midwives board removes the name of a certified midwife from the register, it may also prohibit her from attending women in child-birth in any other capacity.
In general, midwives are not removed from the register or suspended from practice except for reasons of physical or mental health, gross negligence or manifest incompetence. Whether a midwife's name is· removed from the register or she is suspended from practice depends on the nature of the offence committed. A midwife may also be suspended from practice if it appears necessary to do so in order to prevent the spread of infection.
The removal of a midwife's name from the register may be preceded by a warning or censure or suspension from practice. Provision is usually made for a procedure whereby a midwife's name may be restored to the register. The power to withdraw the right to practise is vested in the authority that grants it : in Austria, Denmark, Germany (Federal Republic), Switzerland (Aargau) and the United States of America the health authority; in Syria and Viet Nam the midwives corporation ; in the countries of the British Commonwealth, the midwives board or nursing council.
In England and Wales and in New Zealand a charge preferred against a midwife is first heard by a special committee. In England and Wales this body is known as the Penal Cases Committee and the board may, in the light of the report submitted by this Committee, remove a midwife's name from the register or, as an alternative, suspend her from practice. It may also suspend her during the hearing of a charge of breach of the rules or misconduct. Persons aggrieved by such decisions are entitled to appeal to the courts. The local supervising authorities may suspend a midwife from practice in order to prevent the spread of infection or because they have accused her of malpractice, negligence or misconduct, or have reported her to the board or have taken proceedings against her in a court of law.
In Denmark, where there is reason to believe that a midwife presents a danger to other persons in the course of practice either by reason of physical defects or of mental ill-health caused by a disease or intemperance in the use of alcohol or of narcotics or by reason of manifest gross incompetence, the National Health Service may recommend to the Minister of the Interior and Housing that a midwife's permit to practise be withdrawn. Before making such a recommendation, however, the National Health Service must submit the case to the Council of Forensic Medicine. The midwife concerned may state whether she wishes the case to be decided by the Minister or by the courts. Where, however, the case involves the permanent withdrawal of the midwife's right to practise, the Minister of the Interior must
456
initiate legal proceedings against the person concerned. In cases of urgency, where the continued practice of a midwife would appear to constitute an imminent danger, the National Health Service may suspend any midwife from practice provided they notify the Minister, who may either confirm or abrogate such decision.
In Austria, a midwife's permit to practise may also be withdrawn for refusal to give assistance or for gross negligence in her duties, absence for several weeks from her district without permission of the health authorities, infirmity prejudicial to the exercise of the profession or if she has not practised for a period of two consecutive years or has failed to attend a refresher course.
In Germany (Federal Republic), provision is made for the withdrawal of a midwife's certificate of competence [ Anerkennung] under certain conditions ; when this is done her establishment permit is automatically invalidated. In the Netherlands, a midwife's permit to practise may be withdrawn for serious negligence causing injury to a mother or her infant during or after child-birth and also for misconduct or incompetence.
7. Protection of title, uniform, and insignia
Where unlicensed or unregistered persons are prohibited from practising midwifery, it might be supposed that it would be superfluous to protect a midwife's title, uniform, and insignia. Nevertheless, probably in order to increase the protection given to qualified midwives, a certain number of countries whose laws permit only registered midwives to practise also protect a midwife's title, uniform, and badge. This is the case in England and Wales, Fiji, Germany (Federal Republic), Haiti, Israel, Kenya, New Zealand, Pakistan (Punjab), the Seychelles, Southern Rhodesia, Union of South Africa, United States of America (New York and City of New York) and Viet Nam. In England and Wales, the abbreviation S.C.M. (State Certified Midwife) is also protected.
Professional regulations
The extent of the information given in midwifery laws concerning the acts which a midwife must or is permitted to perform in the discharge of her duties varies from country to country. Such information is often embodied in rules or requirements of practice. Some laws go into great detail on this subject while others, for example that of England and Wales, merely stipulate that a midwife must in all cases abide by what she has been taught. If a midwife fails to abide by these rules, she becomes liable to disciplinary action and, in the event of accident, risks civil or criminal proceedings. In most laws those rules whose non-observation may have serious repercussions on the health of a mother or a child are laid down very strictly.
457
They may be divided into three groups : general rules ; calling in of medical aid ; drugs and instruments which may be employed by a midwife. There are also further rules relating to a midwife's duty to maintain records and to the circumstances under which deliveries may be conducted in the midwife's home.
In England and Wales and in Germany (Federal Republic), there are, in addition to general rules relating to all midwives, special rules relating to midwives practising in institutions. Midwives in institutional practice are subject to the regulations of the establishment in which they are employed-very often under the direct supervision of a physician. In these circumstances she is not necessarily working on her own responsibility, as she is in domiciliary practice, the regulations relating to which are more precise. In Germany (Federal Republic), in addition to technical details, the professional regulations include rules on professional ethics. This is also the case in France, where the regulations include provisions concerning the relations of midwives with their colleagues, the problem of free choice of midwife, sharing of fees (dichotomy), offences against professional honour, etc.
1. Requirements of practice : general rules
Of the general rules, those most frequently given relate to measures for preventing puerperal infection and ophthalmia neonatorum, and the steps to be taken if such infections nevertheless occur. As a corollary to the prophylaxis of puerperal infection, rules are also laid down concerning the making of internal examinations before, during, and after confinement, and the measures of disinfection and asepsis to be adopted by a midwife with respect to herself and her instruments. The interval a midwife must remain with a mother after a birth and the visits to be paid during the lying-in period are also prescribed. In general, precise indications are given concerning the use of anaesthetics and analgesics, the interventions permitted to the midwife and those from which she must abstain, for example version, removal of the adherent placenta, episiotomy and artificial rupture of the fretal membranes.
If a midwife has been in contact with any person, whether or not a patient, suffering from any condition which is or may reasonably be expected to be infectious, or if she herself is liable to be a source of infection, she must without delay notify the competent authorities, and before going to any maternity patient must carry out or allow to be carried out to their satisfaction such measures of disinfection if any as are prescribed. This stipulation exists in Austria, Cyprus, England and Wales, Egypt, Fiji, Federal Republic of Germany, Italy, New Zealand, Seychelles, Sweden and the Union of South Africa. Among the diseases commonly listed in this connexion are scarlet fever, erysipelas, and any diseases of a septic or purulent nature. In the Union of South Africa mention is also made of diphtheria.
In England and Wales, a midwife is required to summon a medical
458
practitioner a if a patient has shown a continuously rapid or rising pulse rate or a rise of temperature to 100.4oF or a rise of temperature above 99.4oF on three successive days. In Germany, a midwife must summon a medical practitioner if a patient's temperature rises above 38oC (100.4°F) during the lying-in period, and she must summon the medical officer of health if the patient's temperature has risen to 39oC (102.2oF) or to 38.5oC (101.3oF) on two consecutive days during the confinement or the lying-in period or during or after a miscarriage. A physician must be summoned in New Zealand if the temperature of a lying-in woman has risen to 100.4oF or over on any two occasions or has been sustained during a period of 24 hours at 100.4 oF. In New York City, a physician must be summoned whenever there is a rise of temperature to 100.4oF at any time after the first day of the lying-in period.
The making of internal examinations is in direct relation to the problem of puerperal infection. In most laws explicit restrictions are placed on the making of internal examinations during labour, and especially after birth. In Colombia, such examinations are prohibited whether or not they are made with instruments, and the giving of vaginal douches before or after labour is also strictly forbidden. In Italy, a midwife is recommended not to make any vaginal examination during labour, especially if such an examination was made before the commencement of labour. In the United States of America (New York City), no vaginal examination may be made by a midwife after the birth is complete, and the giving of a vaginal douche before or after labour is strictly prohibited. In Austria, a midwife is prohibited from making an internal examination of a pregnant woman during the first four and a half months of pregnancy ; during the second half of pregnancy, in particular towards its end, a midwife may only make such an examination where absolutely necessary, that is, where a clear diagnosis cannot be established by means of an external or rectal examination. This same proviso applies to women in labour on whom not more than one internal examination may be made. During the lying-in period only rectal examinations may be made. In Germany (Federal Republic), pregnant women or women in labour may likewise only be examined internally where external or rectal examinations do not permit a clear diagnosis to be established. In Germany and in Austria, whenever an internal examination is made a midwife must record the reasons for making such an examination in her register of cases. In Cyprus, it is laid down that midwives shall not make more internal examinations than are absolutely necessary. In New Zealand, maternity nurses may not make any vaginal examination except by the express directions of the medical practi-
a By the Puerperal Pyrexia Regulations, 1951, every medical practitioner attending or called in to visit a person suffering from puerperal pyrexia is required to notify the local medical officer of health, puerperal pyrexia being defined for this purpose as " any febrile condition occurring in a woman in whom a temperature of 100. 4°F (38°C) or more has occurred within fourteen days after child-birth or miscarriage. "
459
tioner responsible for the care of the patient, and midwives may make such an examination only when necessary and on no account during the third stage of labour unless a serious complication has occurred. Internal examinations after a birth is complete are explicitly prohibited in Austria, Germany (Federal Republic) and the United States of America (New York City).
Most laws prescribe that a midwife must not leave a woman in labour until after expulsion of the placenta. In the United States of America (New York City) and in New Zealand, a midwife must not leave a patient who is in the second or third stage of labour and must stay with the patient for at least one hour after the expulsion of the placenta; in Germany (Federal Republic) the interval is two hours, and in Austria and Finland three hours. In Sweden and in the Union of South Africa, the interval which a midwife must remain with a patient is not specified, but it is laid down in general terms that a midwife may not leave a patient until all risk to the mother and child has passed.
Most laws require midwives to visit their patients regularly for a certain number of days during the lying-in period. On the occasion of such visits they must check the temperature and pulse rate, note the state of the lochia, and supervise breast feeding, etc. In Italy, a midwife must visit a mother twice a day during the first five days of the lying-in period, keep a careful record of the patient's temperature and pulse, control the condition of the external genital organs, the lochia, involution of the uterus, and haemorrhage, if any. In Austria, Cyprus, Germany (Federal Republic), Netherlands, New Zealand, Switzerland (Zurich), and the United States of America (New York City), a midwife is required to visit a patient and her infant at least once daily or more frequently during the first part of the lying-in period.
Most laws prohibit the use of anaesthetics and analgesics except in the presence and under the express direction of a medical practitioner. In England and Wales, however, a midwife who has been trained in its use may administer nitrous oxide for the purpose of analgesia under the following conditions: (1) the apparatus used must be of a type approved by the Central Midwives Board ; (2) the patient must have been examined one month before her confinement by a physician who has signed a certificate that he finds no contraindication ; and (3) one other person, being either a State certified midwife or a State registered nurse or a senior medical student or a pupil midwife, is present at the time of the administration in addition to the midwife in charge of the case. The administration by a midwife of any other anaesthetic otherwise than under the personal direction and supervision of a registered medical practitioner is regarded as treatment outside her province. In Sweden also, midwives who have been trained in its use may administer nitrous oxide.
In some countries a midwife is permitted to intervene in certain ways and in special cases. In Austria, it is laid down that the foetal
460
membranes shall be kept intact as long as possible, but may be artificially ruptured in certain cases. In Germany, they may be artificially ruptured only when they present at the vulva, and in Italy only when the cervix is completely dilated, the presentation is cephalic and the head is deeply engaged. In Italy also, when a physician is not available, a midwife may rupture the foetal membranes if the neck of the uterus is not completely dilated in cases of lateral placenta praevia accompanied by haemorrhage when the foetus is in the longitudinal position. Version by internal manamvre is generally prohibited, but is permitted in Austria and in Finland if life is endangered. External version is permitted in England and Wales, in Italy and in the Netherlands under certain conditions. Episiotomy is permitted in England and Wales, as it is in Germany and in Austria, where a midwife may remove the adherent placenta if her patient's life is in danger. In France and in the Netherlands, a midwife may suture superficial lacerations of the perineum.
In the United States of America (New York City) version and removal of the adherent placenta are both prohibited ; midwives are moreover forbidden to attend a woman upon whom a previous Caesarean section has been performed or who has had a pelvic or gynaecological operation, or upon any primiparous woman who is over 35 years of age, or any woman who has given birth to more than ten babies. On being engaged for a delivery, a midwife must refer the patient to a licensed physician or pre-natal clinic for continuous pre-natal care.
In Colombia, midwives may only attend primiparous women if a physician authorizes them to do so after he has examined the patient ; they may only handle multiparous women if the presentation is vertex and there is no history of abnormalities.
In Finland and in Sweden, midwives who have received training in their use may use forceps in emergencies or if a physician is not available. It is recommended that such interventions be performed in the presence of a witness. In other countries the use of forceps is expressly forbidden. All laws require a midwife to take the measures necessary for preventing ophthalmia neonatorum, that is, ocular instillation of silver nitrate (1 % solution) or of protargol or argyrol.
2. Calling in medical aid
A number of laws specify the abnormal conditions occurring during pregnancy, labour or the lying-in period under which medical help must be sought.
In Finland, in Germany (Federal Republic) and in Sweden, it is stipulated that, even in cases of normal child-birth, a midwife shall not oppose the desire of a woman or of her family to call in a physician. In Germany, if the family refuse to call in a physician in any abnormal case in spite of the wish expressed by a midwife, the latter
461
shall obtain a statement in writing to this effect, which she shall forward to the medical officer of health.
Most laws require a midwife to await the arrival of a physician if she calls upon him for aid, and thereafter to follow his instructions. In Colombia, it is stated that no physician shall refuse to assist a midwife if she calls upon him for help.
In Austria, in England and Wales, and in New Zealand, the request for assistance by a physician is made on a special form.
Thus midwives do not usually intervene in abnormal cases. Nevertheless, if the life of a patient or her child is in danger, and when a physician is not readily available, they may undertake certain interventions. In practice, however, the extent of such intervention is very limited since a midwife is prohibited from using instruments and anaesthetics during child-birth. The circumstances under which a midwife is required to call in a physician are explicitly stated in Austria, Belgium, Cyprus, Colombia, Egypt, Fiji, Italy, New Zealand, and the United States of America (New York City, Georgia). In other countries, Sweden for example, it is stated that a midwife shall call in a physician if abnormalities occur during pregnancy or the lyingin period or in cases which are stated in her text book to involve the risk of death to the mother or her child.
It is not possible in this study to list all the abnormal conditions under which midwives are required to call in medical assistance. However, those specified in Colombia, Egypt, New Zealand, and the United States (New York City) are listed below.
Colombia
A midwife is required to call in a physician and not to undertake to attend a woman in child-birth in the following cases :
(a) narrow or deformed pelvis (women with physical defects, patients affected with rickets, deviation of the spinal column or claudication) ;
(b) haemorrhage during pregnancy (placenta praevia); (c) oliguria, oedema (puffiness of the face, hands or feet);
diminution of vision ; vertigo ; persistent cephalia or convulsions ; (d) previous difficult confinements in which medical assistance
was necessary ; (e) presentations other than vertex; (f) prolapse of the cord ; (g) tumours or obstacles which may impede or delay the passage
of the child through the genital canal ; (h) labour of more than 20 hours in primiparous or of more than
12 hours in multiparous women.
A midwife must also call in a physician during the lying-in period in the following cases : convulsions or fits in the mother ; haemorrhage ; shivering ; high temperature and offensive lochia ; retention of urine
462
more than 12 hours after the birth; inflammation of one or both breasts. They must also call in medical aid when the placenta has not been expelled spontaneously two hours after the birth, where the child is premature and there are breast feeding difficulties, where the child is affected with haemorrhage from or suppuration or inflamation about the navel or eyes, with skin eruptions or erysipelas or when the child has not urinated or passed meconium within the first 24 hours.
Egypt
A midwife must call in an authorized physician in the following cases:
(a) when a woman is in danger because of abnormal pregnancy or pregnancy accompanied by complications such as deformation or contraction of the pelvis, abundant uterine haemorrhage or risk of miscarriage, or when she is suffering from a serious illness, from oedema of the hands and feet or of the face, convulsions (eclampsia) or severe nervous crises, offensive vaginal discharges, ulceration of the genital organs ;
(b) in cases of abnormal or complicated delivery, whether before or at term, where there is a possibility of uterine inertia (eclampsia), severe nervous crises or offensive vaginal discharges, ulceration of the genital organs, abundant haemorrhage or when the placenta has not been expelled spontaneously within two hours after birth or when the perineum or vagina has been lacerated ;
(c) in cases of abnormal or complicated delivery where accidents arise such as convulsions (eclampsia), severe nervous crises, abdominal distension, offensive lochia, shivering accompanied by a rise of temperature, rise of temperature above 38oC with an increasing pulse rate for more than 24 hours, breast congestion accompanied by rise of temperature or by pain, post-partum haemorrhage or oedema of the thighs;
(d) in cases of an abnormal infant or an infant suffering from complications following on birth or any other accident or malformation endangering the infant's life, such as ano-rectal obstruction, extreme debility of a premature or a full-term infant, inflammation about or discharge from the eyes, however slight, serious skin eruptions, especially those marked by watery blisters, inflammation about the navel or of the navel itself or haemorrhage from the navel.
New Zealand
A midwife shall use and continue to use all reasonable endeavours to obtain the assistance of a registered medical practitioner under the following circumstances :
(a) in the case of a woman in labour:
(i) in all presentations other than the uncomplicated vertex;
463
(ii) if the midwife cannot recognize the presentation; (iii) if an hour after birth of the infant the placenta has not been expelled and cannot be expressed ; (iv) whenever there appears to be insufficient room in the pelvis or vagina for the infant to be born, or when an abnormal swelling is felt in these regions or in the abdomen ; (v) in all cases of abnormal haemorrhage or convulsions; (vi) in cases of serious rupture of the perineum, or other serious injury of the soft parts;
(b) in the case of a lying-in woman :
(i) who after delivery does not make satisfactory progress ; (ii) who shows abdominal swelling and signs of insufficient contraction of the uterus ; (iii) who has foul-smelling discharges; (iv) who has secondary post-partum haemorrhage; (v) whose temperature has risen to 100.4°F or over on any two occasions or has been sustained during a period of twentyfour hours at 100.4oF or over; (vi) who has unusual swelling of the breasts with local tenderness or pain ; (vii) where the infant is suffering from ophthalmia neonatorum.
United States of America (New York City)
If any of the following conditions develop or are suspected, a midwife shall seek medical aid :
(a) during pregnancy:
( 1) whenever the patient is known to have or have had syphilis or is suspected of having or having had syphilis ; (2) whenever there is vaginal bleeding, including staining; (3) whenever there is swelling or puffiness of the face, eyes or hands; (4) whenever there is excessive vomiting early in pregnancy or any vomiting in the last trimester of pregnancy ; (5) whenever there is persistent headache ; (6) whenever there is dimness of vision; (7) whenever there are fits or convulsions ; (8) whenever there is a purulent discharge; (9) whenever there are sores or warts of the genitals ; (10) whenever there is a history of or signs or symptoms of diabetes; (11) whenever there is a history of high blood pressure, kidney condition or toxaemia ;
464
(12) whenever there is a sudden rapid gain in weight; (13) whenever the foetal heart cannot be heard at any time during pregnancy ; (14) whenever these is a history of or signs or symptoms of heart disease, rheumatic fever or tuberculosis ; (15) whenever the midwife is called for an emergency delivery of a patient who has had no pre-natal care or blood test ;
(b) during delivery:
(1) the presenting part is other than uncomplicated vertex (head); (2) fits or convulsions ; (3) excessive bleeding; (4) prolapse of the cord; (5) a swelling or tumour that obstructs the birth of the child; (6) signs of exhaustion or collapse of the mother; (7) labour prolonged over 24 hours or ruptured membranes over 12 hours ; (8) when foetal heart has been heard and ceases to be heard or when the foetal heart has not been heard ; (9) vagina has been lacerated during delivery ;
(c) during the lying-in period :
( 1) whenever there are convulsions ; (2) whenever there is excessive bleeding ; (3) whenever there is a rise of temperature to 100.4oF any time after the first day ; (4) whenever there is swelling and redness of the breasts; (5) whenever there is a severe chill (rigor) with rise of temperature; (6) whenever there is inability to nurse the child; (7) whenever one or both legs become swollen ; (8) when there is inability to void urine for 12 hours or whenever there are frequent small voidings of urine ;
(d) in the case of a newborn infant:
( 1) whenever there is any deformity or malformation or injury ; (2) whenever there is inability to suckle or nurse ; (3) whenever there is inflammation around, or discharge from the navel; (4) whenever there is swelling and redness of the eyelids with a discharge from the eyes ; (5) whenever there is bleeding from the mouth, navel or bowels or in the skin ;
465
(6) whenever there is any rash, sore or nasal discharge or whenever the mother has had a history of syphilis or a positive serological test for syphilis ; (7) whenever there is difficulty in feeding, persisting vomiting or diarrhoea ; (8) whenever there is evidence of general feebleness or of a premature birth (the baby weighing less than five pounds, seeming unusually small or feeble, having a constant low temperature); (9) if a baby is not breast fed, a physician shall be called to prescribe a formula for the child ; (10) whenever a baby displays jaundice (yellow skin) at birth; (11) should the child not breathe at birth.
3. Drugs and instruments
In order to prevent midwives from employing drugs or instruments which would enable them to perform prohibited acts, the contents of a midwife's obstetric kit, as well as the conditions under which she may employ such drugs and instruments, are given in certain laws. In Denmark, England and Wales, and Sweden, however, the regulations merely state that a midwife shall employ only those drugs and instruments she has been taught to use in the course of her training.
It is not possible in this study to give an exhaustive list of the drugs and the equipment a midwife must have at her disposal in each country.a
The most commonly mentioned drug is silver nitrate (or a solution of protargol or argyrol) to be used for the prevention of ophthalmia neonatorum. Most laws prohibit the use of ergot or other ecbolic drugs before or during delivery. Thus in Fiji and in New Zealand, midwives are forbidden to administer ergot, pituitrin or any other ecbolic drug before or during labour or any sedative drugs or any anaesthetic other than chloroform, except by the express direction of a physician given in each individual case. Chloroform may only be administered in the presence of and by the express direction of a medical practitioner. Midwives who infringe these rules are deemed to have been guilty of malpractice in respect of their calling and are liable to have their names removed from the register, as are midwives who use any instrument to aid delivery unless directed to do so by a physician. In Belgium, a midwife may administer ergot or ergotine but only after the birth is complete.
In Germany, a midwife is entitled to carry with her 10 tablets of quinine (lg each), as well as two ampoules of femergin or neofemergin and two ampoules of orasthin or myopituigan. If a mid-
a Details of the drugs and instruments a midwife may employ are given in the legislation of Austria,* Belgium,* Colombia,* Egypt, France,* Germany (Federal Republic), Haiti (drugs only), Italy, New Zealand,* Seychelles, Syria (drugs only), and the United States of America (New York City) *. Appendix 2 contains the relevant provisions of the countries marked with an asterisk.
466
wife misuses these drugs, the local medical officer of health may forbid her to have them in her possession.
In Japan, no instruments or drugs may be used by midwives except under the direction of a physician. In United States of America (New York City) a midwife is permitted to use only an extremely limited range of equipment and drugs. She may not use instruments of any kind nor assist labour by any artificial, forcible, or mechanical means, nor administer, prescribe, advise or employ any poisonous or dangerous drug, herb or medicine, including anaesthesia, analgesia, ergot or pituitrin in any case of labour. In Connecticut, midwives may prescribe a teaspoonful of liquid ergot of rye but only after expulsion of the placenta.
In many countries, Cyprus for example, a midwife is required to have two obstetrical kits, one for the actual delivery, the other for use during the lying-in period.
4. Supervision of midwives
In general, midwives are under the direct supervision of physicians attached to the public-health services. In Denmark, in Finland and in Sweden for example, the local medical officers of health supervise midwives in their respective areas, general control being in the hands of the public-health department.
In Germany (Federal Republic}, midwives are under the direct control of the local medical officer, to whom they must report on their establishment, together with their diplomas, register of cases and equipment ; they must also submit an annual report on their activities to this officer. In Austria, Cyprus, Israel and New Zealand also, the local medical officers supervise the midwives within their districts. In England and Wales, Southern Rhodesia, Uganda and the Union of South Africa, supervision is exercised by the local authority. In England and Wales, the local health authorities may suspend a midwife from practice to prevent the spread of infection. They may also suspend from practice until the case is decided, a certified midwife against whom they have instituted proceedings, or on whose part malpractice, negligence or misconduct has been reported by them to the Central Midwives Board. It is to this authority that a midwife is required to send notification of: (a) intention to practise ; (b) sending for medical aid ; (c) liability to be a source of infection; (d) artificial feeding of infants; (e) death or stillbirth (whether a medical practitioner is in attendance or not); (f) layingout of a dead body for burial ; (g) intention of acting or having acted as a maternity nurse.
5. Records
All the laws studied require midwives to keep a register of cases and, in some instances, also records of pregnancy, labour and lying-in, in which they keep notes of their observations and treatment. The form of such records and registers is usually prescribed.
467
Provision is usually made for the submission of these registers to the health authorities at specified intervals, usually annually, or these records must be made available for inspection by the health authorities on request.
These records are of a confidential nature and must be returned to the health authorities when the midwife retires or dies, or leaves the district under the jurisdiction of the authorities concerned.
In Italy, midwives are required to keep a register of births, as well as of abortions. Both these registers must be submitted every month to the local health authorities for inspection. They must also be submitted quarterly to the same authorities, who retain the register of births and forward the register of abortions to the provincial medical officer.
6. Deliveries at a midwife's home
Most laws prohibit midwives from receiving women into their own home for the purpose of delivery. In Austria, a midwife may not receive a women into her own home for delivery other than in an emergency, unless she has obtained a permit to this end from the competent authorities. However, such permits are only granted if there is a lack of transport facilities in the district or similar difficulties, and the midwife's home satisfies the requirements of hygiene. But even then pregnant women may only be accepted fairly shortly before the presumed date of confinement. In Denmark, a midwife may not receive women into her house for the purpose of delivery unless the medical officer health has recognized her house as suitable for this purpose. In Finland, permission is only given in cases of distress or extreme urgency. In Germany, if a woman wishes to be delivered in the midwife's home, the midwife must inform the medical officer of health in good time. In Sweden, a midwife may receive women into her own home for delivery in exceptional cases, provided she informs her superior officer in each particular case. In Switzerland (Zurich), a midwife is forbidden to deliver women in her own home or in any other person's home, unless she holds a general permit to that effect issued by the public-health department or a special permit issued in each particular case by the district medical officer. In New York City (United States of America), it is unlawful for a midwife to use her home as a place of delivery unless the woman received is a member,of her own immediate family.
Conclusion
The aim of this study has been to indicate the main tendencies in the midwifery legislation of thirty countries with respect to training, administrative regulations and requirements of practice.
The provisions relating to the period and nature of midwifery training varies considerably from country to country. There is
468
a very marked tendency in countries with well-organized health services to co-ordinate the training of midwives with that of nurses, either by providing midwives with a basic training in nursing or by encouraging nurses to specialize in obstetrics. This study also shows that certain countries have only been able gradually to restrict the practice of midwifery to qualified midwives. It would thus appear that this historical factor should be taken into consideration when new midwifery laws are framed and that while the principle of restricting the practice of midwifery to qualified midwives should be retained, provisions should also be included which allow midwives who have not yet received the prescribed training to continue to practise in areas where there are insufficient qualified persons.
Most laws enumerate the acts which a midwife must perform in the discharge of her duties and those from which she must abstain, as well as the circumstances under which she must call in medical aid, and the drugs and equipment she may have at her disposal. In certain countries a more liberal attitude is being taken towards the use of certain drugs and of certain methods of anaesthesia.
The care which legislators have taken to delimit the extent of a midwife's practice is but a reflection of the responsibility which a midwife is required to bear, for "it must be borne in mind that at each confinement she is responsible for at least two lives ". 4
APPENDICES
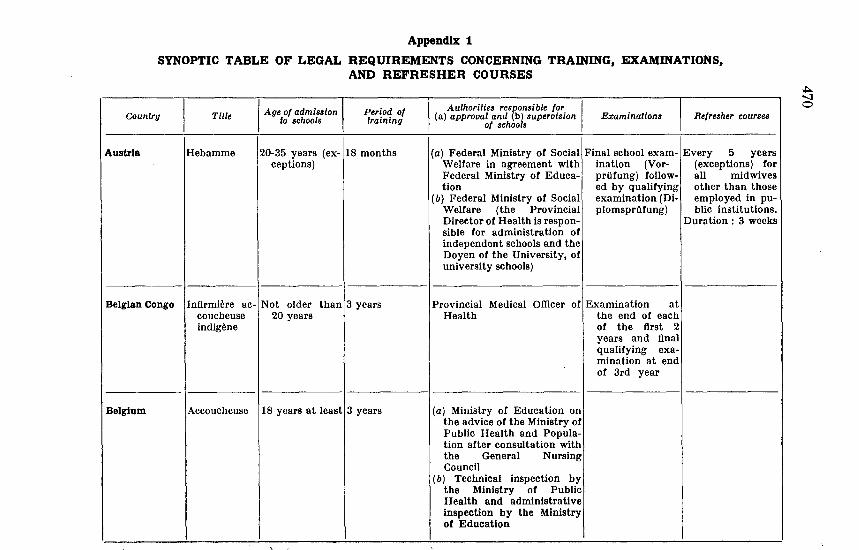
Appendix 1
SYNOPTIC TABLE OF LEGAL REQUIREMENTS CONCERNING TRAINING, EXAMINATIONS, AND REFRESHER COURSES
Country Title
Austria Hebamme
I Age of admission
to schools Period of training
20-35 years (ex-118 months ceptions)
Belgian Congo I Infirmiere ac-~ Not older than 13 years coucheuse 20 years indigene
Belgium Accoucheuse 118 years at leastj3 years
Authorities res(Jonsible for I (a) approval and (b) supervision
of schools Examinations Refresher courses
(a) Federal Ministry of Social Final school exam- Every 5 years Welfare in agreement with ination (Vor- (exceptions) for Federal Ministry of Educa- prOfung) follow- all midwives tion ed by qualifying other than those
(b) Federal Ministry of Social examination (Di- employed in pu-Welfare (the Provincial plomsprofung) blic institutions. Director of Health is respon- Duration : 3 weeks sible for administration of independent schools and the Doyen of the University, of university schools)
Provincial Medical Officer ofiExamination at Health the end of each
of the first 2 years and final qualifying examination at end of 3rd year
(a) Ministry of Education on the advice of the Ministry of Public Health and Population after consultation with the General Nursing Council
(b) Technical inspection by the Ministry of Public Health and administrative inspection by the Ministry of Education
.+:>.. -...J 0
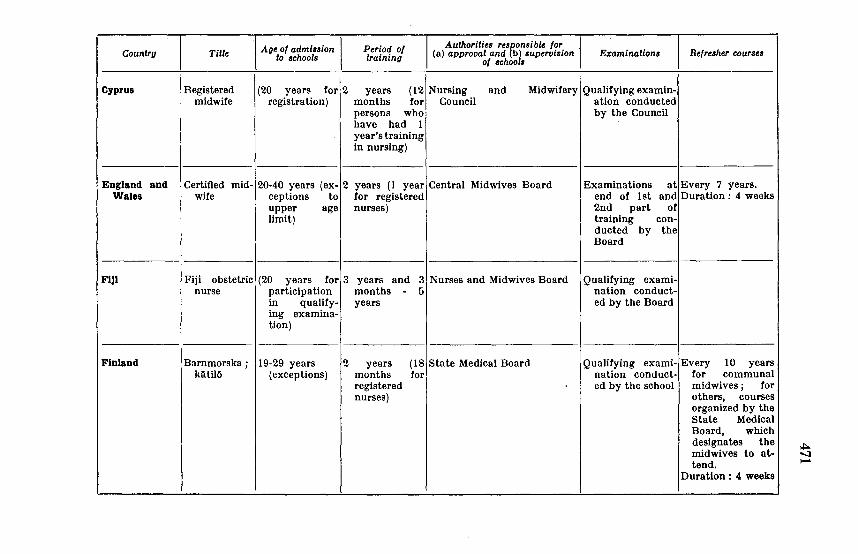
Age of admi~aion I Period of Authorities resnonsible for Country Title (a) approval and b) supervision Examinations Refresher courses to schools training of school&
Cyprus Registered (20 years for 2 years (12 Nursing and Midwifery Qualifying examin-midwife registration) months for Council ation conducted
persons who by the Council have had 1 year's training in nursing)
England and Certified mid- 20-40 years (ex- 2 years (I year Central Midwives Board Examinations at Every 7 years. Wales wife ceptions to for registered end of lst and Duration: 4 weeks
upper age nurses) 2nd part of limit) training con-
ducted by the Board
FIJI Fiji obstetric (20 years for 3 years and 3 Nurses and Midwives Board Qualifying exami-nurse participation months - 5 nation conduct-
in qualify- years ed by the Board ing examina-tion)
Finland Barnmorska ; 19-29 years 2 years (18 State Medical Board Qualifying exami- Every 10 years klitilll (exceptions) months for nation conduct- for communal
registered ed by the school midwives; for nurses) others, courses
organized by the State Medical Board, which designates the midwives to at-tend.
Duration : 4 weeks
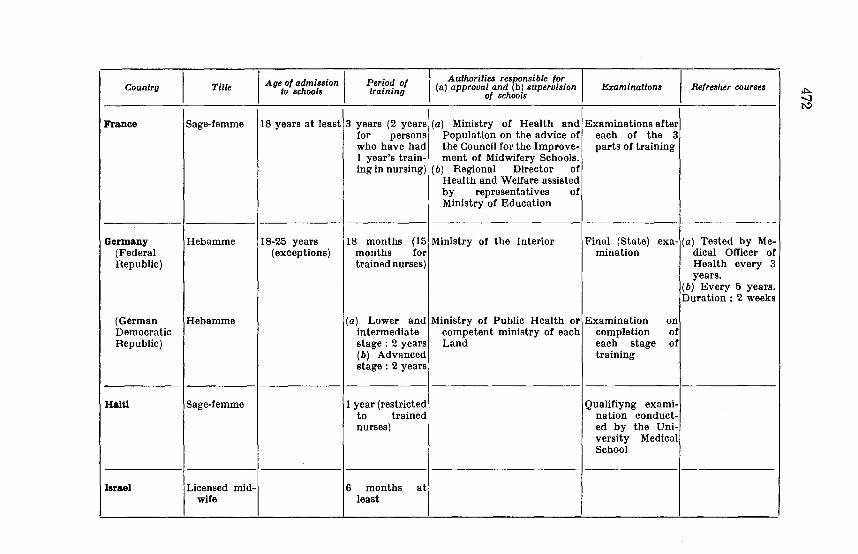
Counlru Title I Age of admission I to schools
Period of !raining
Authorities responsible tor (a) approval and (b) supervision
of schools Examinations I Refresher courses
France Sage-femme 18 years at least 3 years (2 years (a) Ministry of Health and Examinations after for persons Population on the advice of each of the 3 who have had the Council for the Improve- parts of training 1 year's train- ment of Midwifery Schools. ing in nursing) (b) Regional Director of
Health and Welfare assisted by representatives of Ministry of Education
Germany Hebamme 18-25 years 18 months (15 Ministry of the Interior Final {State) ex a- (a) Tested by Me-(Federal (exceptions) months for mination dical Officer of Republic) trained nurses) Health every 3
years. (b) Every 5 years. Duration : 2 weeks
(German Hebamme (a) Lower and Ministry of Public Health or Examination on Democratic intermediate competent ministry of each completion of Republic) stage : 2 years Land each stage of
(b) Advanced training stage : 2 years
Haiti Sage-femme I year (restricted Qualifiyng ex ami-to trained nation conduct-nurses) ed by the Uni-
versity Medical School
Israel Licensed mid- 6 months at wife least
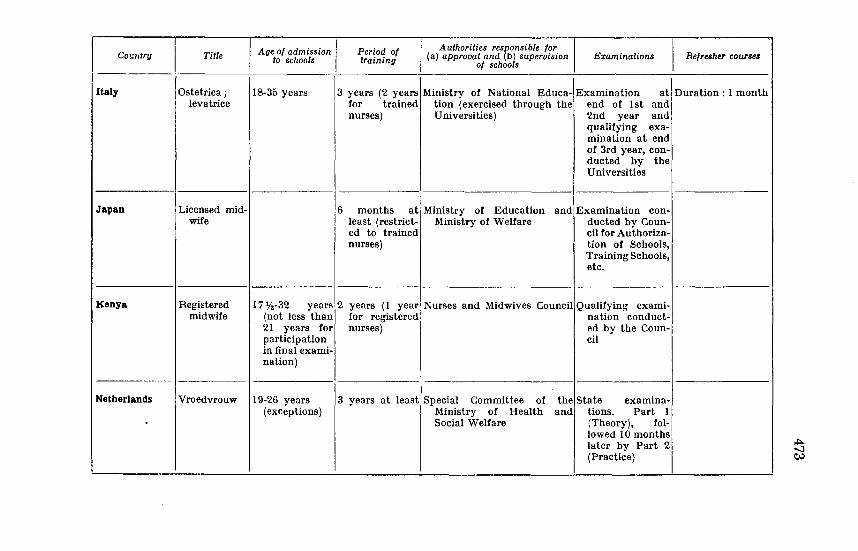
I i Age of admission I Period of I Authorities resoonsible for
Refresher courses Country Tille (a) approval and b) supervision Examinations to schools training of schools
13 years (2 years Italy Ostetrica; 18-35 years Ministry of National Educa- Examination at Duration : 1 month leva trice for trained tion (exercised through the end of 1st and
nurses) Universities) 2nd year and qualifying exa-mination at end of 3rd year, con-ducted by the Universities
Japan Licensed mid- 6 months at Ministry of Education and Examination con-wife least (restrict- Ministry of Welfare ducted by Coun-
ed to trained cil for Authoriza-nurses) tion of Schools,
Training Schools, etc.
Kenya Registered 17 7'2-32 years 2 years ( 1 year Nurses and Midwives Council Qualifying ex ami-midwife (not less than for registered nation conduct-
21 years for nurses) ed by the Coun-participation cil in final exami-nation)
Netherlands Vroedvrouw 19-26 years 3 years at least Special Committee of the State examina-(exceptions) Ministry of Health and tions. Part 1
Social Welfare (Theory), fol-lowed 10 months later by Part 2 (Practice)
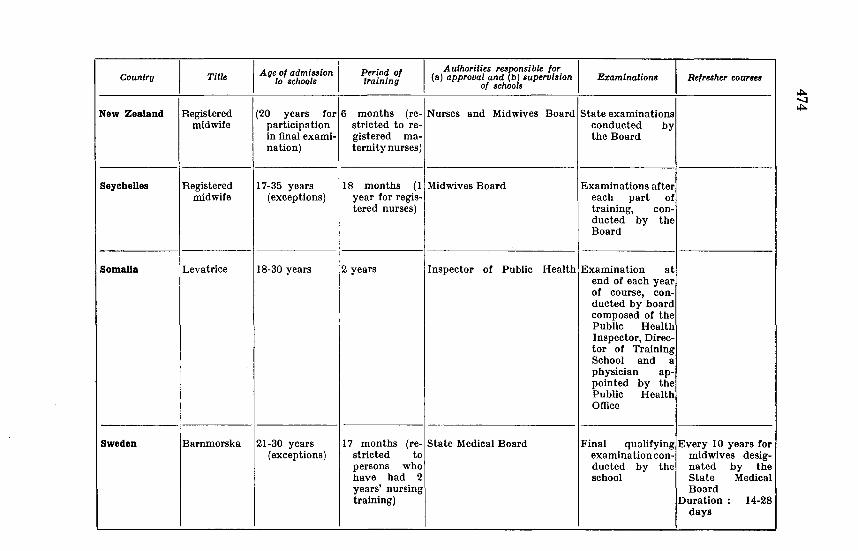
Country
New Zealand
Seychelles
Somalia
Sweden
I Title I Age of admission I
to schools Period of training
Authorities responsible for I (a) approval and (b) supervision
of schools Examinations Refresher cour1es
Registered midwife
(20 years for 6 months (re- Nurses participation stricted to re-
and Midwives Board State examinations
Registered midwife
in final exami- gistered rna-nation) ternitynurses)
17-35 years (exceptions)
18 months (1 Midwives Board year for regis-tered nurses)
conducted by the Board
Examinations after each part of training, conducted by the Board
Leva trice 18-30 years 2 years Inspector of Public Health Examination at
Barnmorska 21-30 years (exceptions)
17 months (re- State Medical Board stricted to persons who have had 2 years' nursing training)
end of each year of course, conducted by board composed of the Public Health Inspector, Director of Training School and a physician appointed by the Public Health Office
Final qualifying Every 10 years for examinationcon- midwives desigducted by the nated by the school State Medical
Board Duration : 14-28
days
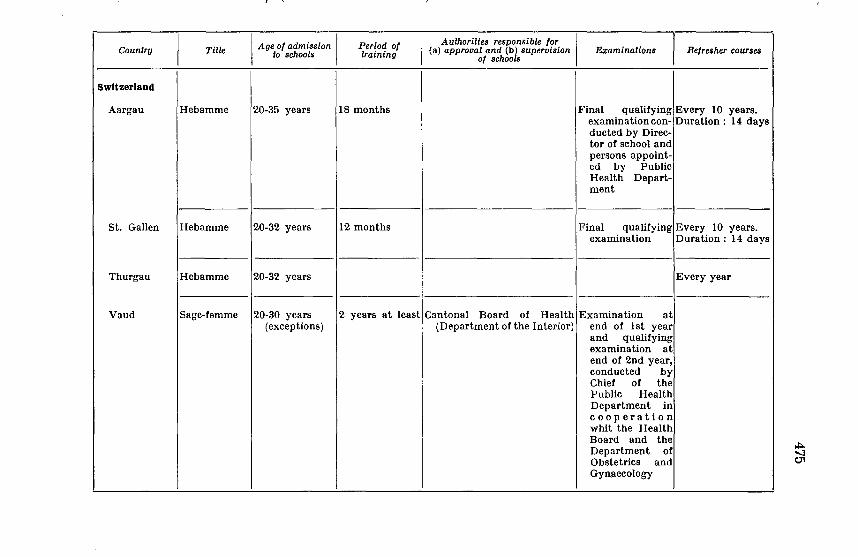
Country Title I Age of admission I to schools
Period of training
Authorities responsible for {a) approval and {b) supervision
of schools I Examinations Refresher courses
Switzerland
Aargau Hebamme 20-35 years 18 months Final qualifying Every 10 years. examination con- Duration : 14 days ducted by Direc-tor of school and persons appoint-ed by Public Health Depart-ment
St. Gallen Hebamme 20-32 years 12 months Final qualifying Every 10 years. examination Duration : 14 days
Thurgau Hebamme 20-32 years Every year
Vaud Sage-femme 20-30 years 2 years at least Cantonal Board of Health Examination at (exceptions) (Department of the Interior) end of I st year
and qualifying examination at end of 2nd year, conducted by Chief of the Public Health Department in cooperation whit the Health Board and the Department of Obstetrics and Gynaecology
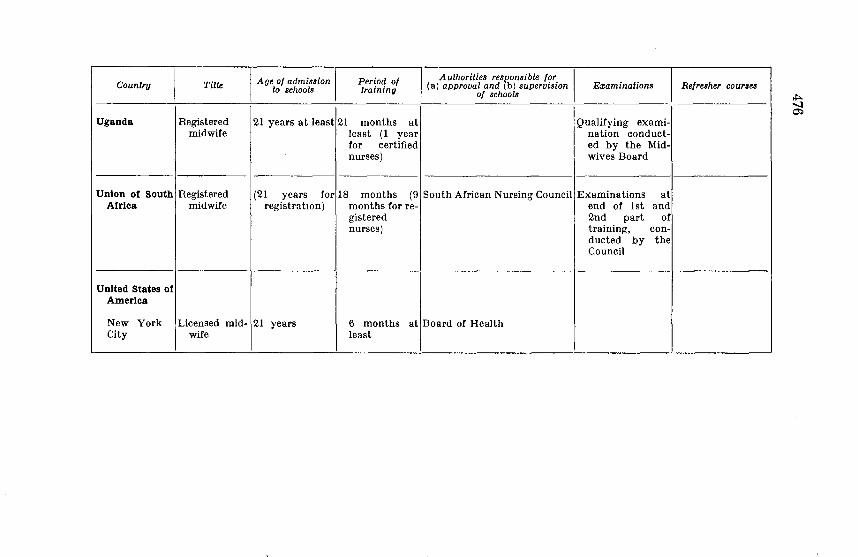
I Age of admission Period of Authorities responsible for
I Country Title (a) approval and (b) supervision Examinations Refresher course& to schools training of schools
Uganda Registered 21 years at least 21 months at Qualifying exami-midwife least (1 year nation conduct-
for certified ed by the Mid-nurses) wives Board
Union of South Registered (21 years for 18 months (9 South African Nursing Council Examinations at Africa midwife registratwn) months for re- end of 1st and
gistered 2nd part of nurses) training, con-
ducted by the Council
-
United States of America
New York Licensed mid- 21 years 6 months at Board of Health City wife least
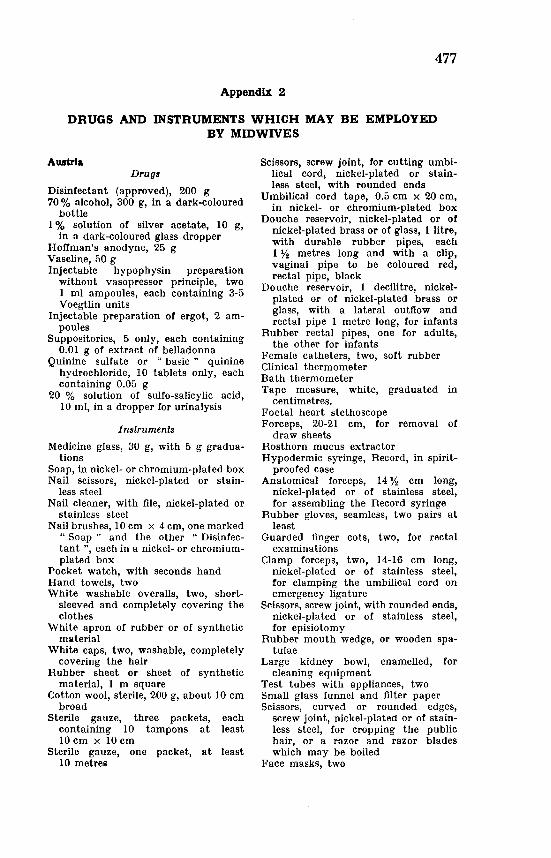
477
Appendix 2
DRUGS AND INSTRUMENTS WHICH MAY BE EMPLOYED BY MIDWIVES
Austria Drugs
Disinfectant (approved), 200 g 70% alcohol, 300 g, in a dark-coloured
bottle 1 % solution of silver acetate, 10 g,
in a dark-coloured glass dropper Hoffman's anodyne, 25 g Vaseline, 50 g Injectable hypophysin preparation
without vasopressor principle, two I ml ampoules, each containing 3-5 Voegtlin units
Injectable preparation of ergot, 2 ampoules
Suppositories, 5 only, each containing 0.01 g of extract of belladonna
Quinine sulfate or " basic " quinine hydrochloride, 10 tablets only, each containing 0.05 g
20 % solution of sulfo-salicylic acid, 10 ml, in a dropper for urinalysis
Instruments
Medicine glass, 30 g, with 5 g graduations
Soap, in nickel- or chromium-plated box Nail scissors, nickel-plated or stain
less steel Nail cleaner, with file, nickel-plated or
stainless steel Nail brushes, 10 em x 4 em, one marked
" Soap " and the other " Disinfectant ", each in a nickel- or chromiumplated box
Pocket watch, with seconds hand Hand towels, two White washable overalls, two, short
sleeved and completely covering the clothes
White apron of rubber or of synthetic material
White caps, two, washable, completely covering the hair
Rubber sheet or sheet of synthetic material, 1 m square
Cotton wool, sterile, 200 g, about 10 em broad
Sterile gauze, three packets, each containing 10 tampons at least 10 em x 10 em
Sterile gauze, one packet, at least 10 metres
Scissors, screw joint, for cutting umbilical cord, nickel-plated or stainless steel, with rounded ends
Umbilical cord tape, 0.5 em x 20 em, in nickel- or chromium-plated box
Douche reservoir, nickel-plated or of nickel-plated brass or of glass, 1 litre, with durable rubber pipes, each 1 % metres long and with a clip, vaginal pipe to be coloured red, rectal pipe, black
Douche reservoir, 1 decilitre, nickelplated or of nickel-plated brass or glass, with a lateral outflow and rectal pipe 1 metre long, for infants
Rubber rectal pipes, one for adults, the other for infants
Female catheters, two, soft rubber Clinical thermometer Bath thermometer Tape measure, white, graduated in
centimetres. Foetal heart stethoscope Forceps, 20-21 em, for removal of
draw sheets Rosthorn mucus extractor Hypodermic syringe, Record, in spirit
proofed case Anatomical forceps, 14% em long,
nickel-plated or of stainless steel, for assembling the Record syringe
Rubber gloves, seamless, two pairs at least
Guarded finger cots, two, for rectal examinations
Clamp forceps, two, 14-16 em long, nickel-plated or of stainless steel, for clamping the umbilical cord on emergency ligature
Scissors, screw joint, with rounded ends, nickel-plated or of stainless steel, for episiotomy
Rubber mouth wedge, or wooden spatulae
Large kidney bowl, enamelled, for cleaning equipment
Test tubes with appliances, two Small glass funnel and filter paper Scissors, curved or rounded edges,
screw joint, nickel-plated or of stainless steel, for cropping the public hair, or a razor and razor blades which may be boiled
Face masks, two
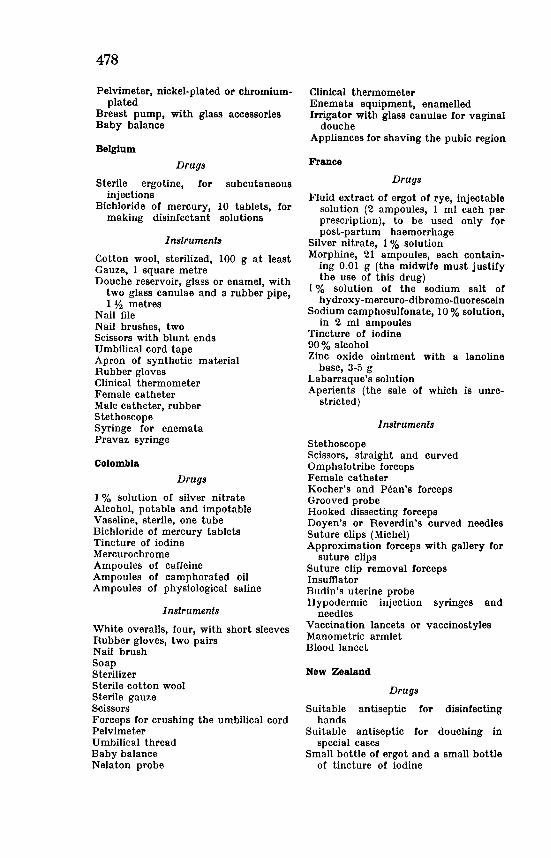
478
Pelvimeter, nickel-plated or chromiumplated
Breast pump, with glass accessories Baby balance
Belgium
Drugs
Sterile ergotine, for subcutaneous injections
Bichloride of mercury, 10 tablets, for making disinfectant solutions
Instruments
Cotton wool, sterilized, 100 g at least Gauze, 1 square metre Douche reservoir, glass or enamel, with
two glass canulae and a rubber pipe, 1% metres
Nail file Nail brushes, two Scissors with blunt ends Umbilical cord tape Apron of synthetic material Rubber gloves Clinical thermometer Female catheter Male catheter, rubber Stethoscope Syringe for enemata Pravaz syringe
Colombia
Drugs
1 % solution of silver nitrate Alcohol, potable and impotable Vaseline, sterile, one tube Bichloride of mercury tablets Tincture of iodine Mercurochrome Ampoules of caffeine Ampoules of camphorated oil Ampoules of physiological saline
Instruments
White overalls, four, with short sleeves Rubber gloves, two pairs Nail brush Soap Sterilizer Sterile cotton wool Sterile gauze Scissors Forceps for crushing the umbilical cord Pelvimeter Umbilical thread Baby balance Nelaton probe
Clinical thermometer Enemata equipment, enamelled Irrigator with glass canulae for vaginal
douche Appliances for shaving the pubic region
France
Drugs
Fluid extract of ergot of rye, injectable solution (2 ampoules, 1 ml each per prescription), to be used only for post-partum haemorrhage
Silver nitrate, 1% solution Morphine, 21 ampoules, each contain
ing 0.01 g (the midwife must justify the use of this drug)
1 % solution of the sodium salt of hydroxy-mercuro-dibromo-fluorescein
Sodium camphosulfonate, 10% solution, in 2 ml ampoules
Tincture of iodine 90% alcohol Zinc oxide ointment with a lanoline
base, 3-5 g Labarraque's solution Aperients (the sale of which is unre
stricted)
Instruments
Stethoscope Scissors, straight and curved Omphalotribe forceps Female catheter Kocher's and Pean's forceps Grooved probe Hooked dissecting forceps Doyen's or Reverdin's curved needles Suture clips (Michel) Approximation forceps with gallery for
suture clips Suture clip removal forceps Insumator Budin's uterine probe Hypodermic injection syringes and
needles Vaccination lancets or vaccinostyles Manometric armlet Blood lancet
New Zealand
Drugs
Suitable antiseptic for disinfecting hands
Suitable antiseptic for douching in special cases
Small bottle of ergot and a small bottle of tincture of iodine
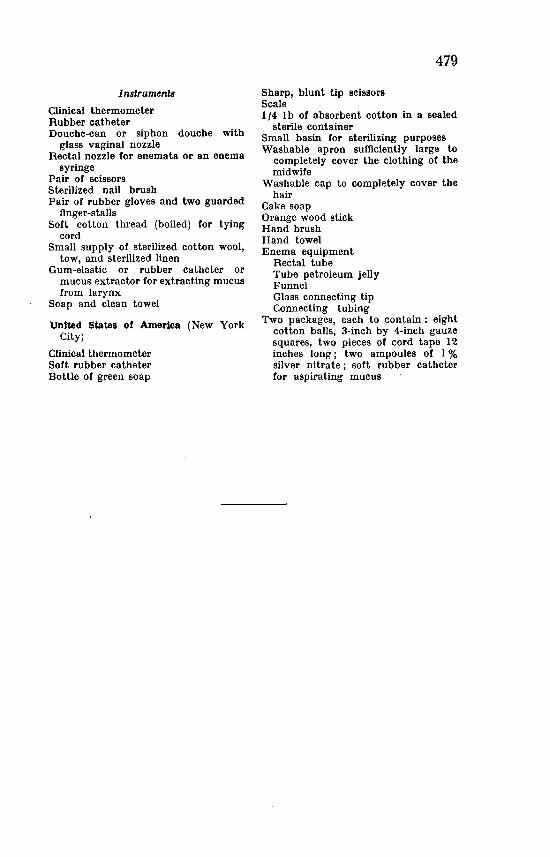
Inslrumenls
Clinical thermometer Rubber catheter Douche-can or siphon douche with
glass vaginal nozzle Rectal nozzle for enemata or an enema
syringe Pair of scissors Sterilized nail brush Pair of rubber gloves and two guarded
finger-stalls Soft cotton thread (boiled) for tying
cord Small supply of sterilized cotton wool,
tow, and sterilized linen Gum-elastic or rubber catheter or
mucus extractor for extracting mucus from larynx
Soap and clean towel
United States of America (New York City)
Clinical thermometer Soft rubber catheter Bottle of green soap
Sharp, blunt tip scissors Scale
479
1/4 lb of absorbent cotton in a sealed sterile container
Small basin for sterilizing purposes Washable apron sufficiently large to
completely cover the clothing of the midwife
Washable cap to completely cover the hair
Cake soap Orange wood stick Hand brush Hand towel Enema equipment
Rectal tube Tube petroleum jelly Funnel Glass connecting tip Connecting tubing
Two packages, each to contain : eight cotton balls, 3-inch by 4-inch gauze squares two pieces of cord tape 12 inches iong; two ampoules of 1% silver nitrate; soft rubber catheter for aspirating mucus
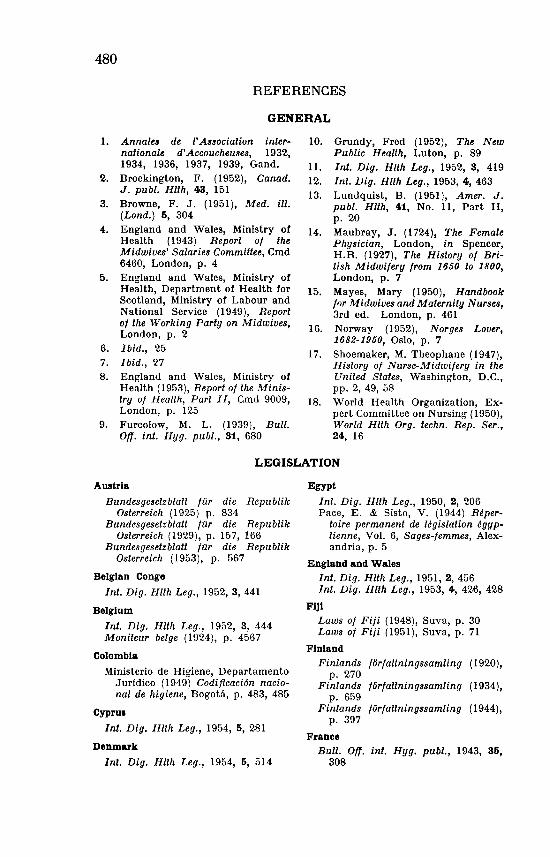
480
REFERENCES
GENERAL
1. Annalu de ['Association internationale d' Accoucheuses, 1932, 1934, 1936, 1937, 1939, Gand.
2. Brockington, F. (1952), Canad. J. publ. Hlth, 43, 151
3. Browne, F. J. (1951), Med. ill. (Lond.) 5, 304
4. England and Wales, Ministry of Health (1943) Report of the Midwives' Salaries Committee, Cmd 6460, London, p. 4
5. England and Wales, Ministry of Health, Department of Health for Scotland, Ministry of Labour and National Service (1949), Report of the Working Party on Midwives, London, p. 2
6. Ibid., 25 7. Ibid., 27 8. England and Wales, Ministry of
Health (1953), Report of the Ministry of Health, Part II, Cmd 9009, London, p. 125
9. Furcolow, M. L. ( 1939), Bull. on. int. Hyg. publ., 31, 680
10. Grundy, Fred (1952), The New Public Health, Luton, p. 89
11. Int. Dig. Hlth Leg., 1952, 3, 419 12. Int. Dig. Hlth Leg., 1953, 4, 463 13. Lundquist, B. (1951), Amer. J.
publ. Hlth, 41, No. 11, Part II, p. 20
14. Maubray, J. (1724), The Female Physician, London, in Spencer, H.R. (1927), The History of British Midwifery from 1650 to 1800, London, p. 7
15. Mayes, Mary (1950), Handbook for Midwives and Maternity Nurses, 3rd ed. London, p. 461
16. Norway (1952), Norges Lover, 1682-1950, Oslo, p. 7
17. Shoemaker, M. Theophane (1947), History of Nurse-Midwifery in the United States, Washington, D.C., pp. 2, 49, 58
18. World Health Organization, Expert Committee on Nursing (1950), World Hlth Org. techn. Rep. Ser., 24, 16
LEGISLATION
Austria
Bundesgesetzblatt fur die Republik Osterreich ( 1925) p. 834
Bundesgesetzblatt fur die Republik Osterreich (1929), p. 157, 166
Bundesgesetzblatt fur die Republik Osterreich (1953), p. 567
Belgian Congo
Int. Dig. Hlth Leg., 1952, 3, 441
Belgium
Int. Dig. Hlth Leg., 1952, 3, 444 Moniteur beige (1924), p. 4567
Colombia
Ministerio de Higiene, Departamento Jurldico (1949) Codificaci6n nacional de higiene, Bogota, p. 483, 485
Cypru1
Int. Dig. Hlth Leg., 1954, 5, 281
Denmark
Int. Dig. Hlth Leg., 1954, 5, 514
Egypt
Int. Dig. Hlth Leg., 1950, 2, 206 Pace, E. & Sisto, V. (1944) Reper
toire permanent de Legislation egyptienne, Vol. 6, Sages-femmes, Alexandria, p. 5
England and Wales Int. Dig. Hlth Leg., 1951, 2, 456 Int. Dig. Hlth Leg., 1953, 4, 426, 42.8
Fiji Laws of Fiji (1948), Suva, p. 30 Laws of Fiji (1951), Suva, p. 71
Finland
Finlands forfaltningssamling ( 1920), p. 270
Finlands forfaltningssamling (1934), p. 659
Finlands forfattningssamling ( 1944), p. 397
France Bull. on. int. Hyg. pub/., 1943, 35,
308
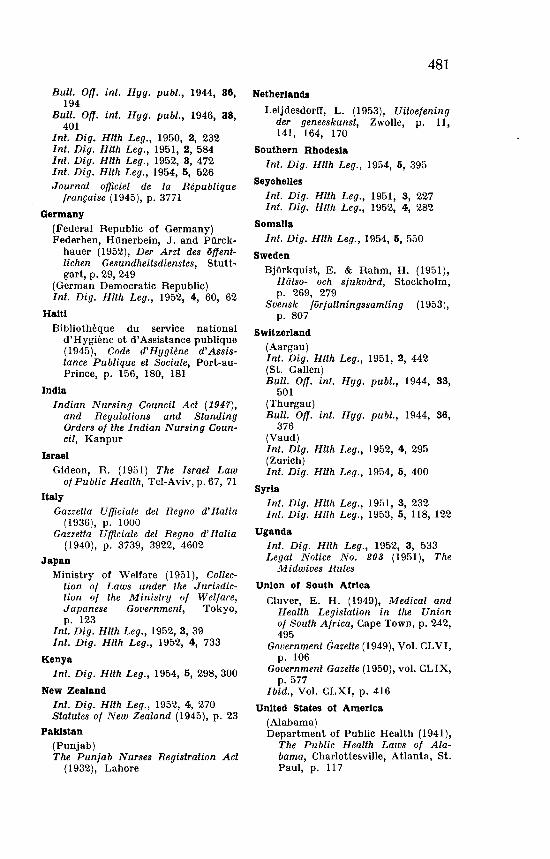
Bull. Off. int. Hyg. publ., 1944, 36, 194
Bull. Off. int. Hyg. publ., 1946, 38, 401
Int. Dig. Hlth Leg., 1950, 2, 232 Int. Dig. Hlth Leg., 1951, 2, 584 Int. Dig. Hlth Leg., 1952, 3, 472 Int. Dig. Hlth Leg., 1954, 5, 526 Journal officiel de Ia Republique
franr;aise (1945), p. 3771
Germany
(Federal Republic of Germany) Federhen, Hiinerbein, J. and Piirck
hauer (1952), Der Arzt des offentlichen Gesundheitsdienstes, Stuttgart, p. 29, 249
(German Democratic Republic) Int. Dig. Hlth Leg., 1952, 4, 60, 62
Haiti
Bibliothllque du service national d'Hygiime et d'Assistance publique (1945), Code d'Hygiene d'Assistance Publique et Sociale, Port-auPrince, p. 156, 180, 181
India
Indian Nursing Council Act (1947), and Regulations and Standing Orders of the Indian Nursing Council, Kanpur
Israel Gideon, R. (1951) The Israel Law
of Public Health, Tel-Aviv, p. 67, 71
Italy Gazzetta U fficiale del Regno d' It alia
(1936), p. 1000 Gazzetta Ufficiale del Regno d' ltalia
(1940), p. 3739, 3922, 4602
Japan Ministry of Welfare ( 1951 ), Collec
tion of Laws under the Jurisdiction of the Ministry of Welfare, Japanese Gouernment, Tokyo, p. 123
Int. Dig. Hlth Leg., 1952, 3, 39 Int. Dig. Hlth Leg., 1952, 4, 733
Kenya Int. Dig. Hlth Leg., 1954, 5, 298, 300
New Zealand Int. Dig. Hlth Leg., 1952, 4, 270 Statutes of New Zealand (1945), p. 23
Pakistan (Punjab) The Punjab Nurses Registration Act
(1932), Lahore
481
Netherlands
LeijdesdorfT, L. (1953), Uitoefening der geneeskunst, Zwolle, p. 11, 141, 164, 170
Southern Rhodesia
Int. Dig. Hlth Leg., 1954, 5, 395
Seychelles
Int. Dig. Hlth Leg., 1951, 3, 227 Int. Dig. Hlth Leg., 1952, 4, 282
Somalia
Int. Dig. Hlth Leg., 1954, 5, 550
Sweden
Bj6rkquist, E. & Rahm, H. (1951), Hiilso- och sjukviird, Stockholm, p. 269, 279
Svensk forfattningssamling (1953), p. 807
Switzerland (Aargau) Int. Dig. Hlth Leg., 1951, 2, 442 (St. Gallen) Bull. Off. int. Hyg. pub/., 1944, 33,
501 (Thurgau) Bull. Off. int. Hyg. publ., 1944, 36,
376 (Vaud) Int. Dig. Hlth Leg., 1952, 4, 295 (Zurich) Int. Dig. Hlth Leg., 1954, 5, 400
Syria Int. Dig. Hlth Leg., 1951, 3, 232 Int. Dig. Hlth Leg., 1953, 5, 118, 122
Uganda Int. Dig. Hlth Leg., 1952, 3, 533 Legal Notice No. 203 ( 1951 ), The
Midwives Rules
Union of South Africa
Cluver, E. H. (1949), Medical and Health Legislation in the Union of South Africa, Cape Town, p. 242, 495
Government Gazette (1949), Vol. CLVI, p. 106
Government Gazette (1950), vol. CLIX, p. 577
Ibid., Vol. CLXI, p. 416
United States of America (Alabama) Department of Public Health (1941),
The Public Health Laws of Alabama, Charlottesville, Atlanta, St. Paul, p. 117
482
(Arkansas) State Board of Health (1947), Rules
and Regulations pertaining to the practice of midwives in Arkansas, Little Rock
(Connecticut)
State Department of Health (1950), Statutes of Connecticut relating to Public Health, Hartford, p. 432
(Georgia)
Department of Public Health (1949), Health Laws and Rules and Regulations of State Board of Health, Atlanta, p. 112
(New York)
State Department of Health (1950), The Public Health Law, p. 99, 164
(New York City) Department of Health of the City
of New York (1949), The Sanitary Code of the City of New York, p. 196
(North Carolina) State Board of Health (1951), Public
Health Laws of North Carolina, Raleigh, p. 33
(South Carolina) State Health Department ( 1944),
Public Health Laws of South Carolina, Columbia, p. 38
(West Virginia) Department of Health (1950), The
Public Health Laws of West Virginia and a Manual of Regulations of the West Virginia Board of Health, Charleston, p. 185
VietNam Int. Dig. Hlth Leg., 1954, 5, 582