work of who - who | world health organization
TRANSCRIPT
OFFICIAL RECORDSOF THE
WORLD HEALTH ORGANIZATION
No. 30
WORK OF WHO1950
ANNUAL REPORT OF THE DIRECTOR -GENERALTO THE
WORLD HEALTH ASSEMBLYAND TO THE
UNITED NATIONS
WORLD HEALTH ORGANIZATIONPALAIS DES NATIONS
GENEVA
April 1951
ABBREVIATIONS
The following abbreviations are used in the Official Records of the World Health Organization :
ACC - Administrative Committee on Co- ordination
CCICMS - Council for the Co- ordination of International Congresses of MedicalSciences
CCTA - Commission for Technical Co- operation in Africa South of the Sahara
ECAFE - Economic Commission for Asia and the Far East
ECE - Economic Commission for Europe
FAO - Food and Agriculture Organization
IBE - International Bureau of Education
ICAO - International Civil Aviation Organization
ICITO - Interim Commission of the International Trade Organization
ILO - International Labour Organisation (Office)
IMCO - Intergovernmental Maritime Consultative Organization
IRO - International Refugee Organization
ITU - International Telecommunication Union
OIHP - Office International d'Hygiène Publique
PASB - Pan American Sanitary Bureau
PASO - Pan American Sanitary Organization
TAB - Technical Assistance Board
TAC - Technical Assistance Committee
UNESCO - United Nations Educational, Scientific and Cultural Organization
UNICEF - United Nations International Children's Emergency Fund
UNRPR - United Nations Relief for Palestine Refugees
UNRRA - United Nations Relief and Rehabilitation Administration
UNRWAPRNE - United Nations Relief and Works Agency for Palestine Refugees inthe Near East
WFUNA - World Federation of United Nations Associations
Introduction
TABLE OF CONTENTS
CHAPTER 1 - FIELDS OF ACTIVITY
Page
1
Active Measures in the Control of Malaria, Tuberculosis and Venereal Diseases 5
Research and Related Activities in Other Communicable Diseases 12
Public - Health Administration 18
Healthy Development of the Child 19
Control of the Physical Environment 21
Mental Well -Being 23Social and Occupational Health 25Nutrition 26Health Education of the Public 27Nursing 28Improved Standards of Teaching and Training 30Availability of Essential Drugs and Equipment 37Health Services to Special Groups 38International Conventions, Agreements and Regulations on Health 40Epidemiological Information 43Health Statistics 46International Standards and Pharmacopoeia 48Technical Publications and Reference Services 54Technical Assistance for Economic Development 59Collaboration with Other Organizations 61
Public Information 69General Administration 72
CHAPTER 2 - ACTIVITIES BY REGION AND COUNTRY
African Region 82Region of the Americas 85South -East Asia Region 95European Region 108Eastern Mediterranean Region 121
Western Pacific Region 133
ANNEXES
1. Membership of the World :Health Organization 141
2. Membership of the Executive Board 1423. Expert Committees and Expert Advisory Panels 143
4. Conferences and Meetings called by WHO in 1950 150
5. Seminars, Symposia and Training Centres organized by or in co- operation with the World HealthOrganization in 1950 152
- III -
Page
6. Conferences and Meetings called by the United Nations and Specialized Agencies in 1950 at whichWHO was represented 153
7. Conferences and Meetings of Non - Governmental and Other Organizations in 1950 at which WHOwas represented. 156
8. Tentative Schedule of Meetings to be called by WHO in 1951 159
9. Non- Governmental Organizations in Official Relationship with WHO 160
10. Selected List of Technical Articles and Reports issued by WHO in 1950 161
11. Budgetary Provision for, and Expenditure on, 1950 Programme 169
12. Structure of the Secretariat at Headquarters 171
13. Senior Officials of the World Health Organization 172
14. Geographical Distribution of Staff 173
15. Status of Contributions and Advances to the Working Capital Fund 174
16. Allocations from Technical Assistance Funds to the World Health Organization 180
17. Medical Literature, Teaching Equipment and Supplies for Governmental Programmes . . 181
18. Distribution of Fellowships 184
SUPPLEMENT
Summary Analysis of Reports from Member States 193
-- Iv --
INTRODUCTION
The annual report for 1950 is an attempt to review in concrete terms the work accomplished by the WorldHealth Organization during its second full year of activity as a permanent specialized agency of the UnitedNations. In introducing it I shall not attempt to do more than outline certain important factors which hadeither a decisive or, at least, a substantial influence on lines of action in 1950. A consideration of these factorswill, I believe, not only contribute to a more complete understanding of WHO's development up to the present,but will also indicate some of the many problems which it must solve in the future.
During the year under review, the Organization has had to face up to its role as the co- ordinating agencyin international health work, particularly as a result of the growth -both inside and outside the United Nations-of the various programmes of technical assistance for economic development ; of the progress made indecentralizing its activities and of the different needs of Member countries as expressed in their requests forassistance.
A close study of WHO's work will show that as a result of experience -mainly based on requests fromgovernments -the general policy guiding our operations has inevitably had to move away from what has cometo be known as " the priorities " -in which emphasis was given to a few particular diseases, conditions ortechniques -to a system which can be said to embrace any form of assistance needed by countries for thegeneral promotion and care of health. From the beginning WHO has been regarded as a practical and usefulco- operative medium through which the knowledge, skills and techniques of modern public - health practiceand medical science, now available in some countries, may be made accessible to all nations intent uponstrengthening their public -health services. Governments, by their requests and their co- operation, haveconfirmed this point of view.
WHO has continued to carry out in every possible way the obligations placed upon it by its Constitutionin co- ordinating international health work so that dangers of competition and of harmful or unnecessaryduplication of effort may be avoided as far as possible. In the pages which follow there is ample evidence ofthe closer co- operation with the United Nations and its organs, with the specialized agencies, withnon -governmental organizations (e.g., the World Medical Association, the World Federation for MentalHealth and many others) and also, recently, with inter -governmental organizations outside the framework ofthe United Nations.
The United Nations expanded programme of technical assistance for economic development of under-developed areas, which began in the second half of 1950, has considerably increased WHO's responsibilitiesin co- ordination, as well as in the provision of technical advice and guidance, and has helped to bring about achanged pattern into which the operations of the Organization must fit. As a result of programmes of theUnited Nations, of other intergovernmental organizations concerned with projects of assistance to under-developed countries, and of UNICEF (which is now undertaking large -scale health programmes), resources inthe field of health are available to many governments to an extent never before realized and which it may beyondtheir capacity to absorb. One government is reported to have actually reached the point of stating that it isincapable of accepting programmes in technical assistance beyond those now planned. In effect, WHO,with a limited budget itself, now has the technical responsibility for health programmes amounting to manymillions of dollars. Some of the funds for these programmes come from free contributions and others are
2 WORK OF WHO, 1950
subject to certain political values ; they may have to be disbursed quickly so as to produce speedy results.These considerations must be taken into account. Above all, WHO must assist governments to ascertain thekind of assistance which can be absorbed by their countries and the pace at which they can absorb it, constantlyemphasizing the close relationship of health and disease with economic and social conditions. By taking stockof available resources, governments can assess their requirements over a long period and make plans for meetingthem in an orderly manner. It is most important to avoid a lack of balance in the development of nationalhealth services, as this can so easily react to the detriment of the populations concerned.
The effect of the technical assistance programme on the general standards of living in the under -developedcountries -with the corresponding rise in standards of health -will not be felt for some time. Clearly, however,the health activities made possible by the funds allocated to WHO under this programme and other similarprogrammes will not only contribute immensely to the speed, efficiency and social acceptability of economicdevelopment, but will ultimately demonstrate the truth of one of the cardinal principles of the Organization-namely, that the raising of physical, mental and social health standards will help to establish a happier andmore peaceful world.
The progress made by the Organization in 1950 has been greatly assisted by the rapid decentralizationwhich has taken place during the year. The expansion of the regional network, although it has been a greatstrain on financial resources, has been one of the most significant developments in this process. Because of thegreat amount of responsibility and authority vested in the regional offices, and the contacts established by themwith the countries in the regions, WHO's programmes have been better adapted to local conditions and needsthan was formerly possible. The details of large parts of the programmes have increasingly been planned andcarried out in the regions and in some cases in the countries themselves, and their effectiveness depends toa great extent on the efforts of the regional organs. The Proposed Programme and Budget Estimates for 1952reflect this increased adaptation to the real needs of the countries resulting from the role played in theformulation of the programmes by the regional committees as well as from the decisions of the Third WorldHealth Assembly and the Executive Board.
Besides the three regional offices already in existence and the Special Office for Europe, offices for theWestern Pacific and Africa were established during the year. This will, even if only on a partial basis for thetime being, make it possible for certain areas not responsible for the conduct of their own international affairsto benefit from the services provided by WHO.
These developments are leaving headquarters freer to fulfil its true function of service to the regions. Atthe same time the headquarters office has continued its work on the setting of standards, the provision ofepidemiological and statistical services, the collection and exchange of information and the co- ordination ofresearch.
Increased decentralization has also brought the Organization into closer touch with the most immediateneeds of Member countries and has enabled WHO to begin to assist each country in taking the next appropriatestep towards developing its public- health services, within the limits of its economic, social and cultural circum-stances. The Organization is planning its services to countries to meet the specific needs of individual nations,bearing in mind that these services can achieve lasting success only if they are subordinated to the general aimof building up public- health services which are well balanced and suited to the circumstances.
Surveys made in the regions, consultations with governments, and the exchange of information havethrown into clear relief some of the problems which countries must solve if they are to build strong public -health administrations. The most widespread problem is the lack of well- trained personnel at all levels.Practical evidence of the Organization's interest in the solution of this problem, as well as in the raising ofstandards of training for such personnel, will be found in its increased fellowship programme, and in its sponsor-ship and organization of conferences and seminars, as described in the chapters which follow. In order to solvethis problem, it it will also be necessary in some instances for the administrative structure of public services to
INTRODUCTION 3
be reorganized so that security of tenure can be guaranteed to permanent, adequately paid, full -time public -health officers and auxiliaries who will no longer be affected by the caprice of changing political regimes. Atthe same time it is clear that such reforms must march in step with general fiscal and administrative reformsnot restricted to the health services.
It is not sufficient to provide personnel capable of building up new health services ; adequate conservationand maintenance, which are indispensable for the efficient running of such services, must be ensured. Experiencehas shown that while countries learn the techniques of new construction with comparative ease, the results oftheir work are often nullified by a lack of those habits of conservation and maintenance which are closelylinked with a high degree of individual skill and social responsibility.
Another point which ought to be stressed is the desirability for many countries to use, more widely thanthey have done in the past, certain well- known, tried and proven techniques for preventing or controllingdisease. The efforts of the less -developed countries to catch up as quickly as possible with the skillsand techniques recently evolved by modern science are entirely understandable, and service rendered to thisend is one of the proper functions of WHO. Nevertheless, the question should be raised as to whether someadministrations, in their zeal for using the most modern methods, are really doing everything possible to utilizetechniques which have proved themselves in the past. Some of these techniques -often inexpensive -are theones which have led to the advancement of the more highly developed countries. For instance, it is unfortunatethat smallpox should still remain almost a worldwide problem when the means for controlling it have beenin existence for such a long period, and when all countries could today avail themselves of such methods asthe use of dried vaccines in anti -smallpox campaigns organized according to modern techniques. A re- exami-nation of the tools at our disposal in the worldwide struggle against disease may lead to most useful results.
To help in training the personnel so greatly needed in much of the world, and to make asuccessful programme of technical assistance possible, it will be indispensable for WHO to obtain the servicesof highly qualified experts in the wider field of public- health administration, as well as of those who are morehighly specialized. In fulfilling the increasing number of requests received from governments for both thesetypes of experts for carrying out long -term programmes, the Organization depends -and for a long time mustcontinue to depend -on the relatively few countries which have large numbers of trained personnel.
A development during 1950, the seriousness of which cannot be over -emphasized, was the announcementby six more governments of their intention to withdraw from the Organization. This negative attitude towardsWHO adopted by ten of its Member States cannot fail, if prolonged, to have an adverse effect on the fundamentaltasks pursued by the Organization. It should never be forgotten that full realization of the principle of univer-sality is essential for the attainment of the goals assigned to WHO. Any withdrawal from the Organizationon the part of a Member State is bound to be a loss for the citizens of that State as well as for those of theother States which continue to participate in the Organization.
A most tragic event during 1950 was the conflict in Korea. The part of this report dealingwith our assistance to that war -torn country shows that WHO, acting in accordance with the obligations laidupon it by its Constitution and its agreement with the United Nations, responded promptly to the requestsfor emergency aid to the civilian population which were formulated by the United Nations Security Counciland the Economic and Social Council. This was acknowledged by the Secretary- General in a letter whichexpressed appreciation for the contribution which WHO made to the efforts of the United Nations.
These, then, are some of the developments during 1950 which it has appeared desirable to single out in thisintroduction. For the rest, the various sections of the report will speak for themselves. I only hope that they
4 WORK OF WHO, 1950
will leave all those who are interested in our work with the reassuring impression -a justifiable one, I think-that despite many shortcomings, due at least in part to youth and lack of sufficient experience, despite handicapsresulting from the political divisions which still split the world, and despite financial limitations, the WorldHealth Organization has been moving in the right direction and that its activities in 1950 are a promise forthe future of the world's health.
* *
The report is divided into two chapters. In Chapter 1, the activities of the Organization are arrangedaccording to its Constitutional functions. Chapter 2 points to the specific problems of the different regions,and describes services to governments by region and country. The annexes give, in particular, informationrequested by the United Nations. A summary analysis of reports received from Member States under Article 62of the Constitution appears as a supplement to the report.
BROCK CHISHOLM, M.D.
Director- General
CHAPTER 1
FIELDS OF ACTIVITY
At the International Health Conference in New York in June 1946, those who framed the Constitutionof the World Health Organization agreed that, in order to gain its objective, " the achievement by all peoplesof the highest possible level of health ", the Organization should have twenty -two carefully defined functions.Some of these functions were obviously of greater urgency than others ; some depended, for their implementa-tion, upon factors such as the requests of governments ; a few implied at first only the continuation of certaintasks begun by other organizations. For these reasons, and because of budgetary limitations, WHO has mademore progress in some of the activities required by its Constitution than in others. Close examination, however,would seem to indicate that in all of them a start at least has been made. This chapter is arranged accordingto the Constitutional functions and describes the work which WHO has performed in carrying them out during1950.
The programme for 1950, based upon the budget estimates prepared by the Director -General,' wasestablished by the Second World Health Assembly in June 1949. It has been modified at subsequent sessionsof the Executive Board and at the Third World Health Assembly.' A major reduction was made as the resultof the establishment of an expenditure ceiling based on the amount of income expected to be received for theyear. A comparison of the programme and amounts voted by the Second Health Assembly with the estimatedexpenditure incurred on the 1950 programme is shown in annex 11.
In adopting the 1950 programme the Second Health Assembly accepted a novel proposal that the budgetshould be divided into two parts : the Regular Budget, financed in the normal way through assessed contribu-tions, and the Supplemental Budget for an operating programme of advisory and technical services, to befinanced by added contributions on a voluntary basis. Having adopted this type of budget, WHO was wellequipped to assist, by adapting the supplemental programme, with the technical assistance programme foreconomic development when it was later voted by the United Nations.
Activities in 1950 include those undertaken by WHO's advisory services to governments and its traditionalcentral technical services. Some of the technical aspects of the 1950 programme were greatly influenced bythe recommendations made by the expert committees, for which a more flexible membership was providedduring the year. WHO is now creating large expert advisory panels for each of the subjects on which com-mittees are to be convened. A list of attendances at meetings of expert committees held during 1950, followedby a table showing the geographical distribution of the members of the expert advisory panels establishedby the end of the year, is given in annex 3.
Details of WHO's work in specific fields of activity follow.
ACTIVE MEASURES IN THE CONTROL OF MALARIA, TUBERCULOSISAND VENEREAL DISEASES
WHO shall " stimulate and advance work to eradicate epidemic, endemic andother diseases ".
The main field activities of WHO directed towardsthe eradication of communicable diseases have beenin the control of malaria, tuberculosis and venerealdiseases, as described below.
1 Of Rec. World Huth Org. 182 For reports of sessions of the Health Assembly and
Executive Board held during the year, see Of Rec. World111th Org. 25 ; 26 ; 28 ; 29.
However, governments have also begun to askfor advice and assistance in their campaigns againstother communicable diseases, and in 1950 WHOhas accordingly given this type of assistance toseveral countries. For example, demonstrationteams were sent to three countries to fight epidemicsof poliomyelitis, and a short -term consultant was
- 5 -
6 WORK OF WHO, 1950
sent to a fourth. Consultants were provided forother countries and areas to advise on the preventionand control of endemic communicable diseases -including anthrax, typhus, bilharziasis, trachomaand leprosy ; others have given advice on diphtheriaand whooping cough. Research on some diseaseshas been carried forward to the point where surveysand field demonstrations have become possibleand necessary.
Details of the work on all these communicablediseases are given in the section of the report whichfollows ; this section is limited to a summary ofWHO's continuing efforts in the fight against thethree types of diseases for which large -scale opera-tions have been possible.
Malaria
During 1950, WHO successfully continued andexpanded the antimalaria programme recommendedby the Expert Committee on Malaria at its secondand third sessions and mentioned in the AnnualReport of the Director - General for 1949.3
At the end of the year, nine demonstrationprogrammes in malaria control were in operationin various countries. Four were in different partsof India, and one each in Afghanistan, Pakistan,Thailand, Cambodia and Viet Nam. The projectsin India, Pakistan and Thailand were joint under-takings in which the national governments, WHOand UNICEF collaborated, UNICEF providingthe supplies and equipment ; in Afghanistan thework was carried on by the Government and WHO ;for the projects in Viet Nam and Cambodia,established at the request of the respective nationaladministrations as part of the Economic Co- operationAdministration (ECA) programmes, WHO has pro-vided only the field staff, the cost of which is later tobe paid back by the governments.
The form of the demonstration projects establishedin 1949 remained unchanged during the year. Theseare national undertakings, with WHO givingtechnical guidance in the form of key personnel,and the special projects have been fitted as closelyas possible into the existing national public- healthstructures. The transfer of the full responsibilityfor the programmes to national personnel was, insome cases, considerably advanced during the year.In Iran; the object of the advisory unit is to assistthe Government in establishing a malaria serviceand in developing a national antimalaria programme.
Of Rec. World Huth Org. 24, 4
Of the nine control demonstration teams, three inIndia and the one in Pakistan have completed thesecond season's spraying operations and have enteredinto the final phase of assessment and evaluation.Three teams will complete their operations by theend of 1951.
Owing to the difficult political situation in thearea, the two teams in Cambodia and Viet Namhave not been able to proceed further than thepreliminary phase.
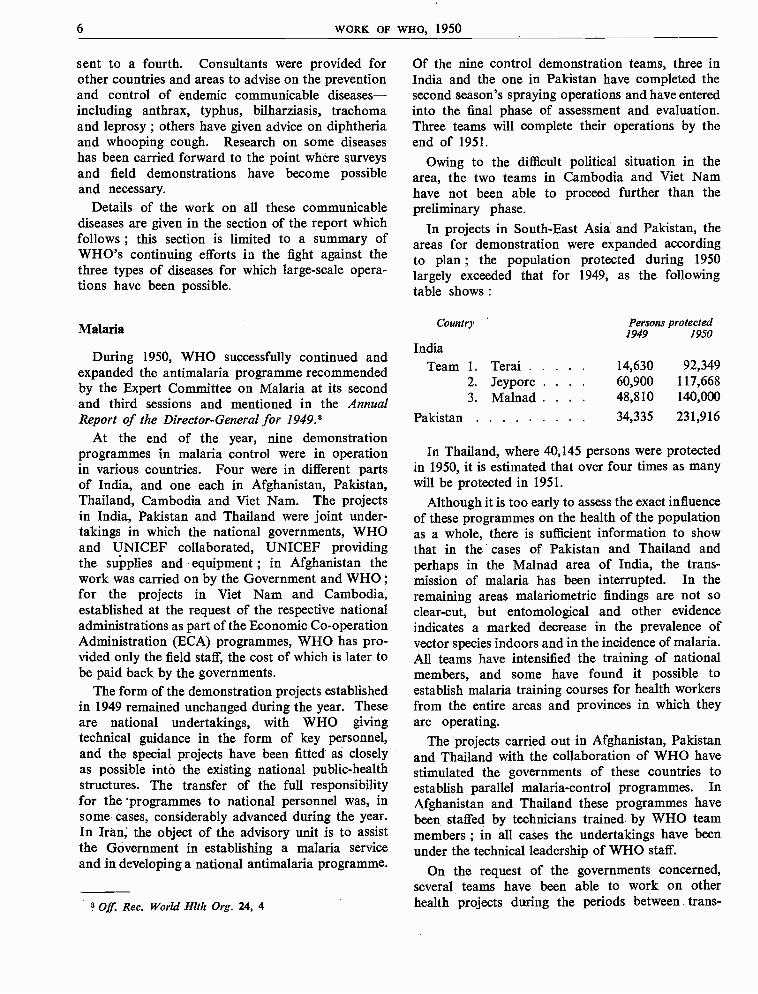
In projects in South -East Asia and Pakistan, theareas for demonstration were expanded accordingto plan ; the population protected during 1950largely exceeded that for 1949, as the followingtable shows :
Country
India
Persons protected1949 1950
Team 1. Terai 14,630 92,3492. Jeypore . 60,900 117,6683. Malnad . 48,810 140,000
Pakistan 34,335 231,916
In Thailand, where 40,145 persons were protectedin 1950, it is estimated that over four times as manywill be protected in 1951.
Although it is too early to assess the exact influenceof these programmes on the health of the populationas a whole, there is sufficient information to showthat in the cases of Pakistan and Thailand andperhaps in the Malnad area of India, the trans-mission of malaria has been interrupted. In theremaining areas malariometric findings are not soclear -cut, but entomological and other evidenceindicates a marked decrease in the prevalence ofvector species indoors and in the incidence of malaria.All teams have intensified the training of nationalmembers, and some have found it possible toestablish malaria training courses for health workersfrom the entire areas and provinces in which theyare operating.
The projects carried out in Afghanistan, Pakistanand Thailand with the collaboration of WHO havestimulated the governments of these countries toestablish parallel malaria -control programmes. InAfghanistan and Thailand these programmes havebeen staffed by technicians trained. by WHO teammembers ; in all cases the undertakings have beenunder the technical leadership of WHO staff.
On the request of the governments concerned,several teams have been able to work on otherhealth projects during the periods between trans-
MALARIA, TUBERCULOSIS, VENEREAL DISEASES 7
mission peaks and after the spraying operationshave been completed. In Pakistan, for example, incollaboration with the Government, a kala -azarsurvey and treatment programme was undertaken,and preliminary evidence indicates that this washighly successful ; also, on numerous occasions theWHO public- health engineer has acted as adviseron environmental sanitation to the government.In Sagar (Bengal), the team undertook ectoparasitesurveys, carried out a small -scale plague -controloperation in a nearby town, and in additionestablished a school sanitation and health pro-gramme. The team leader in Malabar was requestedto draft a plan of filariasis control in Calicut. InThailand, the entomologist of the team advised thenational government on plague control and alsomade recommendations for the control of mosquitonuisance in Bangkok ; in addition, a survey ofother communicable diseases in the area was under-taken, and assistance given in a national ruralsanitation programme. In all demonstration areas,public- health nurses established programmes ofinfant care, and the results in all cases wereencouraging.
Besides the nine demonstration projects beingcarried on by WHO during the year, an advisoryunit was maintained in the Eastern Mediterraneanarea to supervise the malaria programme conductedamongst the Palestine refugees receiving assistanceformerly under UNRPR, now under United NationsRelief and Works Agency for Palestine Refugees inthe Near East (UNRWAPRNE). This programmewas based almost entirely upon residual spraying,and was extended from a purely antimalarialoperation to an insect -control scheme (in particular,the control of flies) by the addition of BHC to theDDT normally used.
During the year, many countries requestedconsultants to assist with malaria problems and tolecture at national malaria institutes. A consultantwas assigned to Ceylon, for example, to advise onthe practicability of attempting vector specieseradication in that country ; another went to theSouth -East Asia Region during the year and lecturedat the Malaria Institute of India.
The regional malaria adviser in New Delhi visiteda number of countries in South -East Asia and also,while assigned for some months to the UNICEFoffice in Bangkok, assisted in the development of
ECA programmes in the Western Pacific Region.A regional adviser was appointed to the RegionalOffice for the Americas for a period of four months,during which he was able to visit almost all countriesof the Americas in which malaria is a problem. InCentral America advice was also given in theestablishment and development of an insect -controlprogramme, which is being undertaken in collabora-tion with UNICEF. A special consultant made anextensive tour of Africa (travelling some 47,800miles) in order to study the problem of malaria inAfrica and to draft the report which served as abasis for discussion at the Malaria Conference inEquatorial Africa, convened in Kampala duringNovember and December. In Europe, WHOcontinued to give advice in UNICEF /WHO pro-grammes in Bulgaria, Poland, and Yugoslavia ; itcarried out a malaria and insect- control programmein Corsica and provided equipment for antimalariacampaigns undertaken by the Government ofPortugal.
No training courses in malariology were under-taken by WHO during the year. The training insti-tutes in India, Pakistan, Israel and Turkey were,however, given assistance in increasing their facilities.In all, ten fellowships in malaria were awarded.
A large number of requests under the expandedprogramme of technical assistance were screenedand registered. Close collaboration was maintainedwith FAO on the proposed joint projects forincreasing food production and raising standardsof health in malarious areas : a joint working partywas held during the latter part of the year toinvestigate suitable areas for such projects. FAOcollaborated by carrying out economic and agri-cultural surveys in most of the areas in which WHOmalaria teams are operating.
Collaboration with other specialized agencies ofthe United Nations was also continued. WHOprovided advice to UNICEF regarding many jointprojects being undertaken by the two organizationsto eradicate malaria and other insect -borne diseases.
A Malaria Conference in Equatorial Africa,sponsored jointly by the Commission for TechnicalCo- operation in Africa South of the Sahara (CCTA)and WHO, was held in Kampala, Uganda from27 November to 9 December. This conference, at
8 WORK OF wxo, 1950
which problems associated with malaria in Africawere considered, was attended by experts from allthe territories in Equatorial and Southern Africawhere malaria is a major public- health problem andby members of the WHO Expert Committee onMalaria.
The recommendations of the conference covereda wide range of subjects (see page 83), and willhave an important bearing on malaria policy inAfrica for many decades to come.4
The fourth session of the Expert Committee onMalaria was held in Kampala between 11 and 16December. The committee considered and approvedall the activities in combating malaria whichWHO has undertaken since its inception, and madea series of recommendations for future developments.It endorsed the findings of the Malaria Conferencein Equatorial Africa, and strongly recommendedthat WHO, with the co- operation of CCTA, shouldassist in implementing these decisions by all themeans at its disposal.
The committee reviewed the progress of malariacontrol by the use of residual insecticides and maderecommendations regarding the possibility of institu-ting experimental control schemes of species eradica-tion absence natural geographical barriers.It fully endorsed the report of the second sessionof the Expert Committee on Insecticides, andreaffirmed its opinion that a free flow of insecticideswithout customs or other restrictions would greatlyfacilitate the control of malaria and other insect -borne diseases.
After considering available information on thespread of anopheline vectors of malaria by inter-national air transport, the committee suggestedthat this might best be prevented by internationalagreement on the designation of internationalairfields according to their degree of, or freedomfrom, infestation.
Recommendations were also made on the establish-ment of a working party to prepare a monographon malaria therapeutics, on further meetings of thedrafting committees on terminology, and theselection of candidates for the award of the DarlingMedal and Prize.
4 The report of this conference will be published, afterapproval by the Executive Board, in the World Health Organi-zation: Technical Report Series.
The report on this session will be published, after approvalby the Executive Board, in the World Health Organization:Technical Report Series.
In close association with its work on malaria,WHO has acted as a clearing house for informationon insecticides, their formulations, and the equip-ment necessary for applying them.
The Expert Committee on Insecticides, at itssecond session, held from 4 to 11 October, establishedspecifications for a number of insecticides and theirformulations as mainly used in malaria control.4The specifications for spraying apparatus, establishedat the first session, were revised in the light ofexperience obtained during the year, and newspecifications for other types of equipment wererecommended. To all countries where malariacontrol is carried out by the modern methods ofresidual spraying these specifications will be valuableas a protection against poor insecticide formulationsand inefficient equipment and as an aid to keepingcosts at a minimum. The committee studied thepresent status of insecticides in the world and thetoxicity of DDT to man and made recommendationsfor disinsectizing ships and aircraft. These recom-mendations were submitted to the Expert Committeeon International Epidemiology and Quarantine ata joint session, as described on page 41.
For a selected list of technical articles and reportsproduced during the year see annex 10.
Tuberculosis
Two major trends have marked WHO's work intuberculosis during 1950. First, there has been thefurther expansion of regional activities. Secondly,the intimation that the Joint Enterprise (the combi-nation of UNICEF and the Scandinavian groupof countries in mass BCG- campaigns) will wind upits field operations by 30 June 1951 has made itnecessary for WHO to plan to continue the servicein some form after that date.
At the end of 1949, only two regions (the EasternMediterranean and the Americas) had advisers intuberculosis. During 1950 two more advisers wereappointed, one to South -East Asia, and the otherto the Western Pacific. The work in Europe wassupervised from headquarters and the Special Officefor Europe as in 1949.
In Chapter 2, in the description of activities in thedifferent regions and countries, it will be seen thatthe year has, on the whole, been a period of solidprogress in building up projects in tuberculosis.Some of them have actually materialized duringthe year ; others will begin to operate in 1951.
MALARIA, TUBERCULOSIS, VENEREAL DISEASES 9
It frequently takes many months for a complete andsatisfactory plan of operation to be prepared withthe governments concerned, but experience has shownthat sound preliminary planning is essential forcarrying out long -term projects.
To summarize field activities in tuberculosis,demonstration and training centres were establishedin 1950 in Turkey and in El Salvador. Detailedplans were made (in most cases in collaboration withUNICEF) for the establishment of others in Burma,Ecuador, India, Iran, Pakistan, the Philippines andThailand. A BCG laboratory was set up in Mexico,with WHO and UNICEF assistance, and othersuch laboratories, BCG campaigns or other typesof assistance in the control of tuberculosis are beingplanned in various other countries of the Americas,in South -East Asia, the Eastern Mediterranean andthe Western Pacific.
A survey of the tuberculosis situation in FrenchSomaliland was also carried out, and assistance intuberculosis nursing was continued during most ofthe year in China.
In Europe, WHO has given advice on the organi-zation of nursing services to Greece, on BCGvaccination to Ireland, and (in collaboration withUNICEF) on streptomycin therapy or the use ofx -ray and laboratory supplies to Austria, Bulgaria,Czechoslovakia, Finland, Greece, Italy, Poland andYugoslavia. X -ray equipment was sent to Monaco.
As will be noted, the area covered has beenextensive, and this in itself is some measure of themagnitude of the problem. Yet there are widestretches in the world still unexplored with regardto needs in tuberculosis control, and in the yearsto come it will be necessary to spread the net widerso that the techniques now being applied to manyunder -developed countries, and the experienceobtained, may be shared by those countries whichhave not yet received assistance.
It is much too early in the history of WHO toestimate the real value of the work alreadyaccomplished, either at headquarters or in the field,but as was mentioned in the Annual Report of theDirector - General for 1949, there is undoubtedevidence that in many places there exists a re-awakening to the great need for raising the standardof methods of tuberculosis control, and for takingadvantage of the relatively limited assistance instaff and equipment which can be offered by inter-national organizations. Workers from all partsof the world now regularly attend internationaland national conferences ; fellowships are beinggranted by many organizations to an extent neverpreviously realized, and documentation is available
in a greater measure than at any other time in thelong history of tuberculosis (for a selected list oftechnical documents produced by WHO, seeannex 10). In all this work WHO has participatedto the limits of its resources, and the daily routineat headquarters provides ample proof that an inter-national centre has an important part to play incampaigns against tuberculosis.
As for BCG vaccination, the Joint Enterprise,with which WHO has been co- operating in anadvisory capacity, has accomplished a vast amountof work in tuberculin- testing and in BCG vaccinationin Europe, North Africa, the Eastern Mediterranean,parts of Asia and, more recently, in Central America.In connexion with this work, WHO has also carriedon research through its special Tuberculosis ResearchOffice in Copenhagen (see page 52).
It has always been the policy to include BCGvaccination as an integral part of the work of thetraining centres which WHO is helping to establishthroughout the world. In addition, there areincreasing demands for vaccination programmes.A special adviser has been appointed at headquartersto deal with this work, and UNICEF has beenasked to continue to supply such funds as cannotbe provided by WHO for the appointment ofstaff to assist governments in carrying out BCGvaccination.
In some ways, the work which WHO is preparingto do is even more responsible than that which wasundertaken by the Joint Enterprise, for it has beenrecognized by the Expert Committee on Tuberculosis,as well as by the Scandinavian partners to the JointEnterprise, that BCG vaccination is merely oneaspect of tuberculosis control ; it will only play apart in the ultimate reduction of morbidity andmortality, and at least equal attention must be givento collateral methods.
During the year the Expert Committee on Tuber-culosis made a number of recommendations to theJoint Enterprise as to dosage, techniques, etc.,which were adopted, and the Expert Committee onBiological Standardization co- operated in grantingapproval, after inspection, to a number of BCGlaboratories in different parts of the world for themanufacture of vaccine which can be used in fielddemonstrations (see page 50).
The Expert Committee on Tuberculosis held itsfifth session in September, and in its report of thissession 6 gave particular attention to the followingitems :
6 To be published, after approval by the Executive Board,in the World Health Organization: Technical Report Sertes.
10 WORK OF WHO, 1950
(1) the training of personnel in tuberculosiscontrol, with emphasis on the uniformity of basiccurricula and the high quality of teachers ;
(2) the use of mass radiography, especiallywhen combined with tuberculin- testing, and theneed for an adequate follow -up ;
(3) the precautions that should be taken bygeneral hospitals in tuberculosis control ;
(4) the desirability of convening a sub -committeeon chemotherapy, in 1951 ;
(5) the importance of continuing BCG vac-cination ;
(6) the compulsory notification of tuberculosis ;
(7) the preparation of a guide for the protectionof nursing personnel serving the tuberculous,and
(8) the organization of committees of medicaland veterinary physicians to direct the controlof bovine tuberculosis. (For work on bovinetuberculosis, see page 16.)
Seventeen fellowships in tuberculosis were grantedduring the year.
Venereal Diseases and Treponematoses
During 1950, WHO continued, consolidated andexpanded its activities in the control of syphilisand other treponematoses, following the broadoutlines laid down by the Expert Committee onVenereal Infections and approved by the ThirdWorld Health Assembly.'
The fact that penicillin is available in absorption -delaying vehicles has made it possible to use a formof treatment that is efficacious, non -toxic and soreadily given as to be administratively feasible formass application. The effectiveness of this formof therapy has been repeatedly demonstrated, in,for example, the significant decreases in the incidenceof syphilis that have followed its use in nationalcontrol campaigns in Finland, Poland and Yugo-slavia.
In India, where the WHO venereal- disease demon-stration team, with headquarters in Simla (HimachalPradesh) is in its second year of operation, the results
Resolution WHA3.37, Of Rec. World Hlth Org. 28, 28
of WHO activities have been especially gratifying.The team has demonstrated that high quality workin venereal- disease control can be conducted in ruralIndia with a minimum of supplies and equipment.Re- surveys of areas in which the team has operated(such as the Ghund valley) indicate a remarkabledecrease in the incidence of new infections. Theimpact of the training aspects of the work has beenevident in higher standards of clinical syphilologyand serology, not only in India, but in other countriesof the region (Afghanistan, Burma, Ceylon,Indonesia, Thailand), which have also sent specialiststo attend the training courses. Efforts are now beingmade to finish the demonstration phase of the workand to include the training programme in the per-manent public- health structure of the country.
The experience of the Simla team has shown thegreat need for supplies for the use of the expertstrained by WHO. Plans have been completed toobtain UNICEF supplies for serologists trained atSimla.
Pending the Egyptian Government's signing ofthe agreement concerning the venereal- diseasedemonstration team at Tanta, the staff attached tothis project performed useful services withUNRWAPRNE following recommendations of aWHO consultant who reviewed the problem ofvenereal -disease control among the Palestine refugees.
In collaboration with UNICEF, large -scale projectsin treponematoses control were started during1950 in Haiti, Indonesia, Iraq and Thailand and itis estimated that some 300,000 persons were treatedduring the year ; a similar project will shortly beginin the Dominican Republic. A control programmewas started in Ecuador, a co- operative project inmaternal and child health and venereal -diseasecontrol in Afghanistan, and detailed plans were madefor control activities in Burma, Ceylon and thePhilippines. The international advisory teams onwhich these activities centre ordinarily consist ofa venereal- disease control officer, a serologist anda public -health nurse.
Because of the scarcity of basic informationregarding bejel, additional experts were appointedto the team in Iraq primarily for the purpose ofstudying the nature of the disease, especially inregard to the frequency of its late complications.
In Europe, national venereal -disease controlcampaigns under the technical supervision of WHOand with supplies furnished by UNICEF werecontinued in Bulgaria, Czechoslovakia, Finland,Poland and Yugoslavia, and at the beginning of the
MALARIA, TUBERCULOSIS, VENEREAL DISEASES 11
year in Hungary. WHO also continued activitiesin Italy and Greece for the suppression of prenataland congenital syphilis and carried out clinical andlaboratory demonstrations on penicillin therapy andthe use of cardiolipin antigens for serodiagnosis inseveral university medical centres in Europe and theEastern Mediterranean Region.
A notable achievement during the year was theestablishment in the United States of America ofthe International Treponematosis Laboratory Centre(in the School of Hygiene and Public Health ofthe Johns Hopkins University, Baltimore). Basicresearch studies on the biology of the varioustreponematoses are being conducted in the laboratorycentre, with the active co- operation of the fieldteams. The recently developed treponema- immobi-lizing test has already made it possible to elucidateseveral fundamental problems in immunity andserological response to therapy.
In the special field of serodiagnosis there have beenseveral important activities. The Organization hascollected information with a view to ascertainingwhich of the many serological tests have gained widestacceptance throughout the world. The exchangeof serum specimens for test performance, evaluationand standardization, arranged in former yearsbetween national laboratories in Bulgaria, Denmark,Ethiopia, Finland, Italy and the United Kingdom,was extended to laboratories in France, Israel,Norway and the United States of America. Planswere made for laboratory training centres in Braziland in Venezuela, and a demonstration of the step -by -step production of cardiolipin antigen wasstaged by a temporary expert consultant at the StatensSeruminstitut in Copenhagen, which has beenselected as a WHO Serological Reference Labo-ratory. These activities have been guided by theSub -Committee on Serology and Laboratory Aspects,which held its second session in Paris duringSeptember.8
Exchange of scientific information regarding recentadvances in the control of venereal diseases has beenfurthered by international symposia held in Helsinki(at which six countries were represented) and in
e The report on this session will be published, after approvalby the Executive Board, in the World Health Organization:Technical Report Series.
Paris (at which 16 countries were represented) ;by the preparation of technical reports and articles(for selected list, see annex 10) ; and by the distri-bution of relevant literature and technical data onclinical, laboratory and public- health aspects ofvenereal- disease control in answer to requestsof national health -administrations. Eighteen fellow-ships for the study of various aspects of venereal-disease control were awarded during 1950.
The recommendation of the Expert Committeeon Venereal Infections' for high priority to be givento the establishment of venereal- disease -controldemonstration projects in major ports led to theproposal to set up a model port- demonstrationproject in Rotterdam, which, it is hoped, will, bytraining courses and study -groups, make an impor-tant contribution to venereal- disease control amongseafarers.
The continued interest of WHO in venereal -diseasecontrol among merchant seamen has also been shownin the preparation of the International List ofVenereal - Disease Treatment Centres at Ports and arevised individual treatment booklet for the use ofseafarers. WHO completed a survey of the serologicallaboratory facilities of the ports along the RhineRiver, and made the information available to theInternational Anti -Venereal- Disease Commissionof the Rhine, which met in the Netherlands duringthe year. The revision of the 1924 Brussels Agree-ment relating to the treatment of venereal diseaseamong merchant seamen has also been furtherconsidered.
WHO was represented at the 1950 Assembly ofthe International Union against Venereal Diseases,held in Zurich in August 1950.
The Expert Committee on Venereal Infections andTreponematoses did not meet during 1950, but ameeting is planned for the autumn of 1951. Fieldadvisers with specialized training in venereal- diseasecontrol have been attached to the Regional Officesin New Delhi, Washington and Alexandria and tothe Special Office for Europe, and the advice ofspecial temporary consultants has been madeavailable to 15 countries in Europe, South -EastAsia and the Western Pacific.
9 World Hlth Org. techa. Rep. Ser. 1950, 13

12 WORK OF WHO, 1950
RESEARCH AND RELATED ACTIVITIES IN OTHER COMMUNICABLE DISEASES
WHO shall " promote and conduct research in the field of health "; " stimulateand advance work to eradicate epidemic, endemic and other diseases ".
The importance of the control of communicablediseases has consistently been emphasized by theHealth Assembly, which has also stressed the factthat, for many of these diseases, more research andscientific knowledge are necessary before field workcan be successfully undertaken. Active research,both in the laboratories and in the field, is necessaryto solve certain problems of the origin of the diseases,the vectors involved, and preventive and therapeuticmeasures to be taken. To promote and conductsuch research WHO has gathered and distributedinformation on a worldwide scale, called togetherexpert groups and committees for advice, andencouraged the co- operation of non -governmentalagencies.
Studies have been undertaken or guided byheadquarters, research centres have been established(see page 16), existing centres and laboratories havebeen aided, field studies have been organized andfellowships have been awarded -nine in epidemio-logy, four in bacteriology and four in immunologyand serology. When requested by governments,consultants have been sent or field activities startedin the control of the various diseases referred to inthis chapter, namely : plague, cholera, typhus andother rickettsioses, yellow fever, parasitic diseases,virus diseases, childhood diseases, trachoma, leprosy,and zoonoses, including brucellosis and rabies.
Plague
At the two sessions of the Joint OIHP /WHO Study -Group on Plague in 1948 and the first session of theWHO Expert Committee on Plague in 1949, severalrecommendations were made as to the orientationof further research.10 Among other things, theexpert committee recommended that a team ofexperts should be sent to work in selected areas withlocal teams provided by the national government.
As a result, the Regional Adviser on plague forSouth -East Asia discussed possibilities for field re-search with the authorities in India, and during 1950areas were selected for research projects. Studieswill be made in these areas on interhuman trans-mission, vectors, plague vaccines, chemotherapy,rodenticidal properties of DDT, and modern rodenti-cides.
Many replies were received to a questionnaire sentto the health administrations of countries in tropicalAfrica, asking for information on the spread of wildrodent plague, and at the end of the year a reportanalysing and summarizing the results was beingprepared. WHO has also collected material for thepublication of a manual on plague, the compilationof which is now far advanced.
The use of rodenticides in ships was referred tothe Expert Committee on Insecticides, which willdiscuss this question fully at its next session.
Cholera
In 1948 and 1949, at three succeeding sessions, theJoint OIHP /WHO Study -Group on Cholera studieddifferent factors in cholera endemicity.11 It alsoadvised on the 1950 programme, which has providedfor preliminary studies of field work to be made.In discussions with the governments and in visits tothe countries concerned, the Regional Adviser forSouth -East Asia has prepared the work of a fieldstudy team, which will investigate practical methodsof cholera control by the use of different techniques,including environmental sanitation measures.
WHO has also stimulated the work of the IndianCouncil of Medical Research by means of a grant(from funds made available by the Office Inter-national d'Hygiène Publique. Active research isbeing carried on by this institute in the retrospectivediagnosis of cholera through agglutinin response
10 Off. Rec. World Hlth Org. 11, 12 ; 19, 18 ; World Hlth 110. Rec. World Hlth Org. 11, 15 ; 19, 24 ; World HlthOrg. techn. Rep. Ser. 1950, 11 Org. techn. Rep. Ser. 1950, 18
OTHER COMMUNICABLE DISEASES 13
following anti -cholera inoculation, the isolation of thecholera vibrio from waters in Calcutta, the mutationof vibrion, diagnosis of cholera by Bandi's Test andthe influence of sulfaguanidine on the excretionof V. cholerae in stools. Methods of discovery ofsubclinical cases in the field have also been studied,and for this some 48,684 stool samples were examinedin the first half -year period. Finally, investigationsare being made on the endemicity of cholera and onthe role of the cholera- carrier.
Typhus and Other Rickettsioses
The Joint OIHP /WHO Study -Group on AfricanRickettsioses held its first session in February 1950in Brazzaville. It reported on the geographicaldistribution of the human rickettsioses in Africa,agreed on their grouping and nomenclature, outlinedtheir characteristics and differential diagnoses, sug-gested preventive measures, and made recommenda-tions on further research to be undertaken."E
In carrying out these recommendations, WHOapproached certain central laboratories, which werefound willing to prepare specific rickettsial suspen-sions. In the manner indicated by the study -groupfive regional laboratories will continue research onthe connexion between classical and murine typhus,the antigenic characteristics of various strains ofclassical virus, reservoirs and agents of murine typhusand the antigenic characteristics of its strains, andthe distribution, vectors and reservoirs of tick -bornerickettsioses.
Studies will also be made on repellents and onproducts to destroy ticks, on transmission by Trom-bididae, on the distribution of Q fever in man, indomestic animals and in ticks, and on the possibleaction of antibiotics.
During the year a summary of the knowledge ofhuman rickettsioses in Africa was prepared,13 andactive help in combating typhus was given to Afghani-stan in the form of consultant services.
Yellow Fever
In December 1949 the Yellow -Fever Panel revisedthe delimitation previously made by UNRRA of theyellow -fever endemic areas in Africa and the Wes-tern Hemisphere, as mentioned in the Annual Reportof the Director -General for 1949. The Committeeon Finance and Transfer of the Office International
d'Hygiène Publique then recommended that OIHPfunds should be made available for a more accuratedelineation of the southernmost limits of the endemicarea in Africa. WHO has accordingly approachedthe governments responsible for the administrationof the various territories in which the necessaryimmunity surveys would have to be carried out, inorder to enlist their active co- operation in thisproject. In launching this scheme, the Chairman ofthe Yellow -Fever Panel has acted as co- ordinatingofficer by visiting Africa (in November and December)and by making preliminary contact with the appro-priate health administrations and serum -testing in-stitutes. In 1951 it is proposed to hold a conferencein South Africa, at which final plans will be discussedwith the medical officers entrusted by their govern-ments with immunity surveys of human populationsin the territories concerned.
During 1950 the following two matters werereferred to the appropriate division of the Yellow -Fever Panel for recommendation : (1) a request bythe United Kingdom, with the concurrence of theGovernment of Tanganyika, for the inclusion ofTanganyika Territory in the African yellow -feverendemic area ; and (2) a request by the BelgianGovernment that the Stanleyville Laboratory bedesignated as an institute for the purposes ofArticle XI (8) of the International Sanitary Con-vention for Aerial Navigation of 1944.
Parasitic Diseases
Bilharziasis
In application of the recommendations of theOIHP /WHO Study -Group on Bilharziasis in Africa,"surveys of bilharziasis were undertaken in Frenchand British Africa, the Belgian Congo, and also incountries in the Eastern Mediterranean region.Experts were appointed to survey these areas with aview to helping the local health services in tracing thedanger zones in their territories and applying thenewer control techniques. A consultant was sent toUNRWAPRNE to advise on the problems ofbilharziasis among Palestine refugees and on pre-ventive measures necessary to prevent the spread ofthis disease when new irrigation projects are under-taken.
WHO has brought to the attention of the UnitedNations, FAO and governments the danger of bil-harziasis inherent in the introduction or extensionof irrigation schemes, as emphasized by the Third
12 World filth Org. techn. Rep. Ser. 1950, 2313 Epidem, vital Stat. Rep. 1950, 3, 161 14 World Hlth Org. techn. Rep. Ser. 1950, 17
14 WORK OF WHO, 1950
World Health Assembly," and the need for controlfrom the earliest stages of these schemes.
In central malacological laboratoires, studies havebeen made on the proper species identification ofsnails collected during the surveys in Africa andWestern Asia. WHO is following closely theseinvestigations, which may result in increased know-ledge of the snail vectors of bilharziasis. New chemicalsdiscovered for use in the destruction of snails, andfield trials of such chemicals carried out in theAmericas and in Africa are also being carefullywatched, and assistance is given wherever possible.
Filariasis, Leishmaniasis, Trypanosomiasis
In response to requests, WHO has furnishedadvice on campaigns against filariasis and on filari-asis skin tests. Consultants on this disease weresent to Ceylon and the Maldive Islands.
Advice was also given on campaigns against kala-azar. When time permitted, the malaria team inIndia worked on filariasis, as well as malaria, andthe team in Pakistan helped in controlling kala -azar.Studies and control work on trypanosomiasis arebeing carefully watched ; and the meeting of theInternational Scientific Committee for Trypano-somiasis Research, held in Brussels in June 1950, wasattended by a representative from WHO.
Virus Diseases
Poliomyelitis
WHO was represented at the European Poliomye-litis Conference in Amsterdam, and assisted in theefforts which were made at this conference to promotethe establishment of an international associationagainst poliomyelitis. Continuous attention is beinggiven to this project, which will be again discussedin 1951 at the International Poliomyelitis Congressin Copenhagen.
Possibilities of making an international study ofpoliomyelitis were explored, and it was recognizedthat the prevalence of this disease in tropical andsub -tropical countries would have to be determined.One of the means of making surveys in these countriesis by serum neutralization tests in mice, using Lansingtype poliomyelitis strains and attempting direct virusisolation.
The Executive Board, at its fifth session, considereda report on a proposal to create a stock of respirators
for international loan,16 but it was decided to post-pone action on this project, because of the diversityof opinion among European health administrationsas to its practicability.
Preliminary work has been done on the establish-ment of an expert advisory panel on poliomyelitis.
WHO began a study on the disquieting possibilityof causal relationship between paralytic poliomyelitisand immunizations, particularly those against diph-theria and pertussis.
In response to requests, poliomyelitis teams wereprovided for India, Chile and Peru, and a consultantwas sent to the United Kingdom.
Influenza
Preliminary work was done on the establishmentof an expert advisory panel on influenza.
The World Influenza Centre, created in 1948 asa joint enterprise of WHO and the Medical ResearchCouncil of Great Britain, is continuing its work inthe collection, evaluation and study of strains fromall over the world, and in the examination of strainsof swine influenza in comparison with human strains.Its work is being extended and supplemented : thenumber of established WHO influenza centres hasbeen increased to 34, and the nomination of centresin Central and South America can be expected verysoon.
A worldwide network of centres will then beestablished, in which observers will watch for out-breaks and be ready to classify the type of influenzawithout loss of time. Specific aid has already beengiven to some of the centres to enable them tofulfil their tasks.
A new type of influenza A virus has been isolatedin Sweden and is under study in the World InfluenzaCentre.
Smallpox
In pursuance of recommendations of the JointOIHP /WHO Study -Group on Smallpox,l" WHO hasgiven further attention to the problem of driedvaccine. An offer of dried calf lymph and of driedchick embryo vaccine has been received, and thepossibility of having field tests carried out in anendemic area is being investigated. It is planned tohold field trials with dried calf lymph in 1951. TheExpert Committee on Biological Standardization islooking into the preparation of standard vaccines.
16 Off. Rec. World Hlth Org. 25, 616 Resolution WHA3.26, Off. Rec. World Hlth Org. 28, 24 " Of Rec. World Hlth Org. 11, 18 ; 19, 22
OTHER COMMUNICABLE DISEASES 15
Childhood Diseases
A questionnaire was sent to governments todetermine the extent to which active immunizationagainst smallpox, diphtheria, whooping cough, scarletfever, measles, tetanus, typhoid, paratyphoid andtuberculosis is advocated or compulsory. Particularswere also requested regarding vaccine production,vaccination programmes and the general public'sresponse to them. When sufficient answers have beenreceived, the results of the inquiry will be summarizedand published.
Technical advice was given on vaccination cam-paigns against diphtheria and whooping cough inColombia and Chile ; a similar campaign wasplanned for Brazil, and a campaign against diphtheriafor the Philippines (see pages 20, 137). Technicaladvice was also given on many UNICEF projects.
In accordance with the decision of the ThirdWorld Health Assembly, the conference on theproduction of diphtheria and whooping cough vac-cines, originally planned for 1950, was postponed.18
Trachoma
A survey based on information received fromgovernments and the study of relevant literature,was published in 1950 on the use of antibiotics andsulfonamides in the treatment of trachoma.19
Information on trachoma was obtained by corre-spondence. A consultant was sent to UNRWAPRNEto advise on an anti -trachoma campaign among thePalestine refugees, and advice was given on an anti -trachoma campaign planned for Formosa and onprojected UNICEF projects.
WHO awarded one fellowship for the study oftrachoma during 1950.
In accordance with a recommendation of theThird World Health Assembly for the establishmentof an expert committee on trachoma,20 an advisorypanel of experts is being created.
Leprosy
The Second and Third World Health Assemblieshaving emphasized the importance of leprosy,preliminary contacts were made with researchworkers, and close co- operation has been established
18 Resolution WHA3.71.3.1, Off. Rec. World Hlth Org.28, 43
19 Bull. World Hlth Org. 1950, 2, 523 -54420 Resolution WHA3.22, Of Rec. World Hlth Org. 28, 23
with the International Leprosy Association. Stepswere also taken to set up a panel of experts on leprosy.
To assist with active measures against the disease,a consultant was sent to Ethiopia, where he is advisingon the use of one of the latest of the sulfone deriva-tives 21 to be used in the treatment of leprosy.
During the year, advice on the building of amodern leper colony was given to the Italian Govern-ment. Advice has also been given on legal measuresfor the sterilization of leprosy patients.
A study on the evaluation of the newer therapeuticmethods in the treatment of leprosy is under con-sideration.
Zoonoses
Of the many diseases common to man and animals,three of the most important- rabies, brucellosis andbovine tuberculosis -were the subject of energeticaction by WHO during the year. In attacking themajor zoonoses, WHO has worked in close co-operation or jointly with FAO, UNICEF and theInternational Office of Epizootics.
In many countries there has been a notable lackof co- operation between health departments anddepartments of agriculture in their work on variousproblems connected with zoonoses. This defect hasbeen overcome in some countries, as, for example, inItaly, Greece, Turkey and Yugoslavia, in which aco- ordinated programme of health and veterinaryservices for the control of brucellosis was arranged.The same principle of promoting a combined efforton the part of the health and veterinary services wasfollowed in Israel in combating rabies and bovinetuberculosis. It is being extended to other countriesand constitutes a basic method of approach by WHOto problems of zoonoses.
A second great difficulty in work on zoonoses hasbeen a lack of adequately trained staff in veterinarypublic health. WHO is meeting this problem byassisting in the organization of veterinary schools,as, for example, in Greece, and in the adaptation ofveterinary courses of instruction in other countriesto meet the need for specially trained graduateveterinarians and lay assistants for field work.
In 1950 the following activities were undertakenby WHO against specific zoonoses
Rabies
In April, at the first session of the WHO ExpertCommittee on Rabies, recommendations were made
21 p, p' - di (y- phenyl -N- propyl -aminophenyl) sulfone sodiumtetrasulfonate.
16 WORK OF WHO, 1950
on necessary measures for controlling this diseasein animals. WHO circulated these recommendationsto governments, and they have been widely acceptedand put into effect. They are also serving as a basisfor a WHO- sponsored demonstration of rabiescontrol in Israel, which is being carried out by thehealth and veterinary services in the country withthe technical guidance of WHO.
In the demonstrations in Israel, a new egg- propa-gated rabies vaccine, which was furnished to WHOwithout cost by a commercial firm in the UnitedStates, is being used for the mass vaccination of dogs.This vaccine gives promise experimentally of beingsuperior to any other vaccine for animals which hasyet been produced.
Besides reducing the immediate problem of rabiesin Israel and providing an example to other countriesof modern methods of control, the Israel campaign,during the next two years, should yield valuable dataon the properties of the vaccine when used in thefield.
Brucellosis
WHO, in collaboration with FAO, has designatedtwelve FAO /WHO centres in different countriesthroughout the world to co- ordinate work onbrucellosis. These brucellosis centres are concernedwith studies on the epidemiology, epizootiology,diagnosis, treatment and prevention of the disease.They serve also as teaching centres for brucellosisworkers in the country in which they are situatedand from countries near by. The centres are alsoserving a very useful purpose in standardizinglaboratory procedures throughout the world, asrecommended by the FAO /WHO Expert Panel onBrucellosis, which was convened in Washington inNovember. Through them the latest advances inbrucellosis research are being rapidly exchanged,and appreciable progress in controlling the ravagesof this disease, both in human beings and in animals,can be expected.
Small financial grants have been made by WHOand UNICEF to many of these centres for thepurchase of needed laboratory equipment and forresearch on problems affecting their particularregion.
Bovine Tuberculosis and other ZoonosesIn December a meeting of a WHO /FAO Expert
Group on Zoonoses was convened. Recommenda-
tions were formulated by this group with referenceto the regional and international control of bovinetuberculosis, anthrax, Q fever, hydatidosis andpsittacosis. The need for international activity onother diseases, such as leptospirosis and thearthropod -borne virus encephalitides, was alsoemphasized.
During the year, in collaboration with FAO, theOrganization made arrangements for long -termstudies in the control of bovine tuberculosis byvaccination of cattle. Surveys on the prevalence ofQ fever in cattle and its relation to human infectionwere begun in England and the Netherlands. Uponthe requests of these countries, WHO supplied theantigens needed to carry out the studies.
Upon the request of the Turkish Government, aconsultant was sent to Turkey for a period of onemonth, to assist in the production of effectivebiological products for the control of anthrax.
Assistance and technical advice were also givento various governments on other zoonoses, includinghydatidosis, tularemia, psittacosis, glanders, lepto-spirosis, salmonellosis, and streptococcal infections.
Research Centres
In efforts to stimulate and co- ordinate research,WHO has continued to assist in the establishment ofresearch centres, as described in this chapter andelsewhere in the report. Among those establishedduring 1950 were an International TreponematosisLaboratory Centre (at Johns Hopkins University,Baltimore) and a WHO Serological Reference Labora-tory (in the Statens Seruminstitut, Copenhagen),(see page 11), an Antibiotics Research and TrainingCentre in Rome (see page 37), and the FAO /WHOBrucellosis Centres mentioned above.
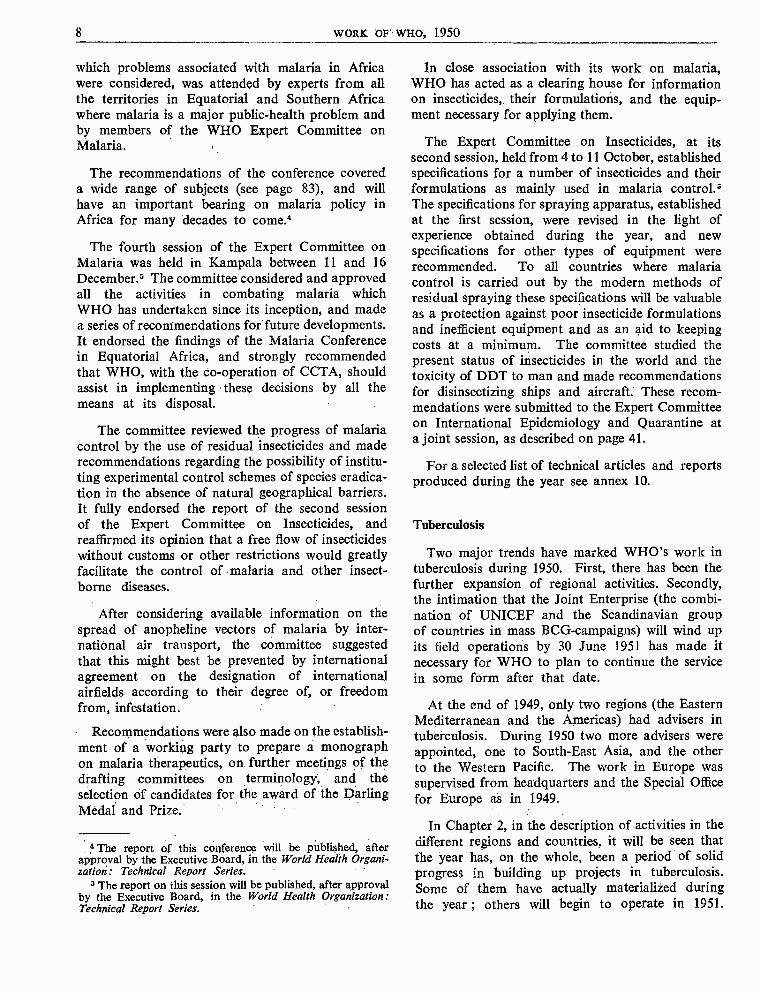
In addition, the International Salmonella Centreand the Worid Influenza Centre have establishednumerous counterparts in many countries, and theTuberculosis Research Office has set up field offices.The Organization has also offered assistance in theform of grants to certain research institutes, such asthe Indian Council of Medical Research, which arecarrying on work essential to WHO projects.
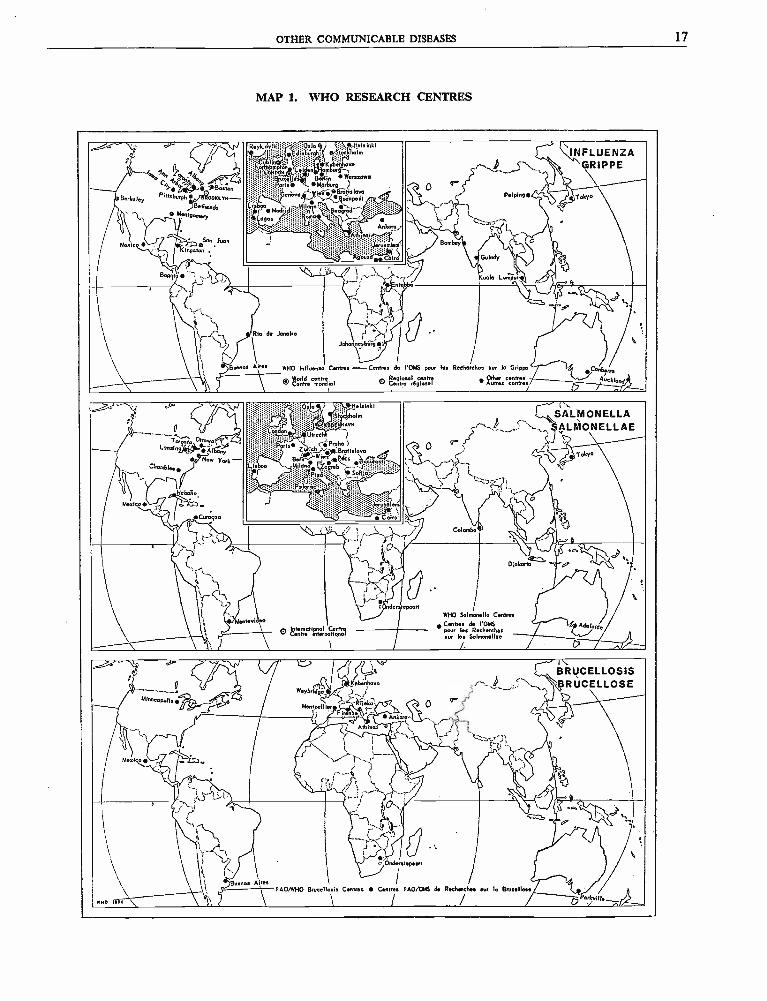
Map 1 shows the network of brucellosis, salmonellaand influenza centres.
OTHER COMMUNICABLE DISEASES 17
MAP 1. WHO RESEARCH CENTRES
.r ^ ¡.1 ___ y/
rJi 0'$B%anBerkeie
Pittsburgh oocaYw-Y
g
Berheado..'..-'... o Monr gama
`
Meaico /£®",JuanKingston .
'Rykis'yikp:p;?"';;E;4alo i 1.bi+ala ink s
qèk4
INFLUENZAnHambw4`-,.L
' Barlin Wánaawe, M«áng.,,;'::;:.: /....::: :ii /`ep t.,,
ude 1.::.. ' . ,+41a>' ._ Miloo:, ` ó_...::i:r::ï::ï;:>:yy!' M^dridli;:':>sn1 %. e gred..,C. ""
^gos . -;.. .
... :.:::::::::...::`!v: .:::U:;: ::: Ankara.>.....'.:..:...:.:e:,.:
....::.ermC`.l:ÿ*9óüïir
l{ ?...
~:::rc::..,
Bombay'
GRIPPE
r' *Peiving tobo
1
_S' E( I, 4
Guindy p
Bog'. +' it
liLj
Kuala umla Lpur
r.
\i9
'; `
,
Buena Aiho
d
Id1\
nr
'`!a
,......±,
\
'
.."
Jdan esbúg et
Centres-Centres de
e
/l'OMS pow lao Reehorehea
1
sw lo Grippe Conbarm
0
W«Id ce h\ Conhe mon1Regioaal tentre ppdh, cenhes Aue
I Cenne rdglonal Aunea contres Auckland
oi
....__ 0.....
.. s{4T«onroLan in'q' nya
s Now Y«k-Chomblee
o
Habciro
Meta co .0 tEZIm
Curogoo
'j. elsinhi..:....:..;:'::'' '»::'t:Er` ESr`kholm
rn.r« : ::: :.::»::.> aen.: : : U ech:.:::.::.. .:.' .... n
..`
..../.:..::.. .
Z`Proh.eh`:'.Brotislavo
.i:? Be á,l°aa B..'o{gari.
tisboo +. µ{Ip: `. reb ' =,.--.f:p :?.::_.._ sü .ps ' Sófü?; ..
., ,,. `Y- :;:!Jd.:dlem
: ::,; ; Cairo'
F°.%,,.,. t
..
r
'
l\SALMONELLAAL ONELLAEp
. Toba
57( ;... 1
Ot 't-, .
-r Colombo 1 '.
'...T
l..;)11 {-
'...Montevi.eo
l
`
fQXaQ`
'.r.Onder tepeprl
WHO 5almanelle1 Centros deCenrre les R
° vaDlak asa ° p
Centresl'OMS Adeloide
hs0 ñmarienal pourl SalmonellaeLé n Inrrmrianol
L11111111111111i `
cu
d a
1!° ;.-'d lc
e\ _p Kobenhavné
° _ . w '..'
li
Minoeopalis d RiManrpeilie.
.
irc;n
'.--.
s;.
'
-
I `BRUCELLOSIS
,. .BRUCELLOSEfJ pi
Mesico od1Je.
!,.t : .¿;a
(..>
Ankm,oe .
Athinai e ....
_.._....'1..' i.......,`
...-é rÎ`.,
y ^.4.-J
`V
, , ^ d.-., ...0' .
}
'';.......
ga
.1
:..
. pe
1
a
ii
.Jç
i \ i Buenos AireaFAOAYHO
f
l T,'
\
c 0
Centres CentrJes
. ,
feveen /I
FAO/OMS de Recherchs
8' \o
le Brucellose\ BrvcaIia1sía saw...,
eno l f / óPoa/«iRa_
18 WORK OF WHO, 1950
PUBLIC- HEALTH ADMINISTRATION
WHO shall " assist governments, upon request, in strengthening health services ".
In view of the fact that the First World HealthAssembly accorded priorities to certain subjects(malaria, tuberculosis, venereal diseases, maternaland child health, nutrition and environmental sanita-tion)," most of the governments which haverequested advisory services during the last two yearshave asked for assistance in these special fields.Recently, however, this type of assistance (oftentaking the form of consultants or teams sent to thecountries) has been considered and used as a spear-head for the stimulation and promotion of generalhealth services.
Early in 1950, in line with this broader policy andfollowing a decision taken at the fifth session of theExecutive Board,83 the general planning and super-vision of activities in the last three subjects mentionedabove, with those in public- health administration,health education of the public, mental health, and,later, social and occupational health, were centralizedin one division of the Secretariat at headquarters -the Organization of Public Health Services. WHO'swork in all of these fields was co- ordinated anddirected towards a common objective -that ofstrengthening the health services of the MemberGovernments. The achievement of this objectiveis conceived as being essential to the improvementof the health of all peoples ; it was stressed as beingof the utmost importance in the general programmeof work covering a specific period, which was adoptedby the Executive Board at its fifth session and by theThird World Health Assembly.24 As " all peoples "obviously includes those of under -developed areas,it follows that it is fundamental to any form ofeconomic development under the technical assistanceprogramme.
Efforts have been made to obtain more informationon the principal health problems of each country andthe organization of national health -administrations.
22 Off Rec. World Hlth Org. 13, 300 -30822 Off. Rec. World Hlth Org. 26, 7624 Off. Rec. World Hlth Org. 25, 30
The replies to questionnaires on this subject, whichwere sent to Member Governments in February 1948,
are incomplete ; more detailed information on a fewcountries is gradually being obtained by the staffsof the regional offices, and an attempt is beingmade to prepare a general outline for the use ofregional advisers in making health surveys.
During 1950, regional advisers and consultants onpublic- health administration visited many countries,including some of the non -self -governing territories.Besides making general health surveys, they discussedproblems with the health and other governmentauthorities. For example, in the Americas, adviceon hospital facilities and projects was given in CostaRica and Surinam ; in the African region, towardsthe end of the year, a three -months consultant wassent to Liberia ; in Europe, a consultant on hospitalconstruction was sent to Luxembourg and anotherconsultant went to Finland at the request of theGovernment to inform the authorities of the workingand results of the first year of the national healthservice in the United Kingdom. Surveys were madeof the public- health services in the Lebanon andSyria, and the regional adviser for the EasternMediterranean also visited other countries in thatregion.
WHO has provided public -health administratorsfor joint projects with other organizations : its teamon public- health administration continued to workwith the UNESCO Pilot Project in Haiti, and itappointed a medical director for the health adminis-tration of the United Nations Relief and WorksAgency for Palestine Refugees in the Near East(UNRWAPRNE) ; WHO offered many other servicesto this agency in 1950. WHO also assigned expertsin public- health administration to missions sent outto countries by the International Bank for Re-construction and Development. A survey of healthconditions was made in Libya at the request of theUnited Nations, and finally, towards the end of theyear, WHO recruited medical officers and public-health workers for the teams sent by the UnitedNations for emergency work in Korea (see page 40).
HEALTHY DEVELOPMENT OF THE CHILD 19
Under the technical assistance programme,additional public - health officers are being providedin each region, as advisers either to the region or toindividual countries where, at the request of govern-ments, they will assist in the preparation of long -range health programmes. In one of the countriesin the African Region such planning began inNovember of 1950.
Great interest has been shown by several countriesin the question of health demonstration areas. Underthe technical assistance programme Ceylon, Chile,Colombia, Egypt, El Salvador, Haiti, Korea, Peruand Venezuela have requested WHO's assistance insuch projects, and plans are being made for surveysof the suggested areas as a preliminary to the actualdemonstration programmes. An exchange of viewswith representatives of the United Nations, FAOand UNESCO on possible co- operation in theestablishment of such areas took place in July. Itwas suggested that when the programmes are readyfor implementation, WHO should organize aworking party, consisting of representatives fromthe United Nations and the specialized agencies, toco- ordinate the work.
At headquarters an advisory panel of experts onpublic -health administration is being formed, anda meeting of a few of the panel members took placein December in Geneva to discuss proposals for aseries of seminars on public -health administrationto be held in 1951 in different regions.
Work also began on special aspects of public -health administration. The hospital consultantsent to Luxembourg, as mentioned above, wasengaged for three months at headquarters, where heprepared designs for three types of hospitals- healthstations, 24 -bed hospitals and 100 -bed hospitals.WHO also began a study of dental health problems,as requested by the Third World Health Assembly :a short -term consultant made a survey of the needsof dental health services in Sweden, Yugoslavia,Egypt and Iran and prepared a report which willbe submitted to the Fourth Health Assembly.
During the year 24 fellowships in public- healthadministration were awarded : one for laboratorywork, two for hospital construction, one for hospitaladministration, two for dentistry and one for portsanitation.
HEALTHY DEVELOPMENT OF THE CHILD
WHO shall " promote maternal and child health and welfare and... foster the abilityto live harmoniously in a changing total environment ".
A broad programme of activity in maternal andchild health was outlined for WHO by its expertcommittee on the subject, which held its first sessionin January 1949.25 In 1950 the work in maternaland child health increased considerably. A reviewof the activities of the past year shows that WHOhas made great progress in carrying out its expressedfunction under the Constitution as referred to in thequotation above.
Increased decentralization to the regional officeshas considerably influenced work in maternal andchild health. Already in 1949, full -time regionaladvisers on maternal and child health had beenappointed to the Special Office for Europe and tothe Regional Office for South -East Asia. In 1950three others were appointed -one to the Regional
25 Off Rec. World Hlth Org. 19, 35
Office for the Eastern Mediterranean, one to theAmericas, and one to the Temporary Office forthe Western Pacific. The surveys and other activitiescarried out by these advisers are doing much tointerest national administrations in setting upmaternal and child health sections as a part of theirpublic- health administrations.
Besides the services given by regional advisers toall countries in their areas, examples of other typesof field projects carried out in 1950 may be cited.The first demonstration team in maternal and childhealth, which went to India in October 1949, hasfinished its " reconnaissance " phase, and has nowbroadened, with UNICEF assistance, into acombined rural and urban health training centre forworkers in maternal and child health. In the Philip-pines, a combined UNICEF /WHO training projecthas just been started to demonstrate maternal and
20 WORK OF WHO, 1950
child health services in a rural area. Similar demon-stration and teaching projects (for which WHO hasprovided a team of international staff and UNICEFthe equipment) are under way in Afghanistan andPakistan ; another team began work in Korea, butwas recalled because of the outbreak of hostilities.
At the end of the year, an Indonesian paediatricianwas beginning a year's fellowship in the study ofsocial and preventive paediatric practices, to enableher to take part in a combined UNICEF /WHOmaternal and child health project to be started inher own country in 1951. Paediatric nurses wereassigned to projects in the Western Pacific (seepages 136, 137). Frequently paediatricians have beenappointed to work with teams on other specializedsubjects, such as those on venereal diseases inIndonesia and Rangoon, and on malaria in Indiaand Thailand.
In some areas advice has been given to govern-ments on specialized aspects of maternal and childhealth. For example, in the United Kingdom aWHO consultant assisted in making a study ofproduction methods for whooping -cough vaccines ;he was then sent by WHO to advise on vaccineproduction and to establish the UNICEF /WHOpertussis- diphtheria immunization campaign in Chile,Colombia and Brazil. Another consultant made anintensive study of the problem of infant diarrhoeain Finland, as a result of which a study of hygieneand sanitation measures was recommended.
The Second Health Assembly approved theconvening of an Expert Group on Prematurity,26which met in April. Among the problems consideredby this group were those of the definition of pre-maturity for statistical purposes, the prevention ofpremature birth and standards of care for prematurebabies. A centre of information on prematurityhas been established at headquarters, on the recom-mendations of the experts,27 and valuable materialis being collected and studied by a special consultant.In several European countries (in Bulgaria, Czecho-slovakia, Finland, France, Poland and Yugoslavia)which sought the advice of the Organization onprojects of premature baby care, programmes havebeen worked out and are being implemented jointlywith UNICEF.
To carry out the recommendation of the ExpertCommittee on Maternal and Child Health thathealth services for children of school age shouldbe extended and reinforced 28 another group of
26 Off. Rec. World Hlth Org. 21, 15227 World Hlth Org. techn. Rep. Ser. 1950, 27, 1128 Off. Rec. World Hlth Org. 19, 39
experts met in August to consider the broad problemof the health of the school -age child. Many requestshave been received for information and advice onimproving school health services, and the report ofthe Expert Committee on School Health Services 29will serve as a valuable guide in this field.
The problem of the handicapped child has alsobeen considered by the Expert Committee onMaternal and Child Health, which recommendedthat WHO should co- operate with other internationalagencies and organizations in studying and planningfor the different categories of handicapped children,especially the homeless and delinquent. In 1950,WHO collaborated in the United Nations studieson juvenile delinquency and homeless children(see page 24), and in February participated ina meeting on the education of physically handicappedchildren, called by the International Union for ChildWelfare under the auspices of UNESCO. A memberof WHO also attended a meeting of representativesof the United Nations Department of Social Affairsand of specialized agencies, to consider internationalco- operative action in the field of rehabilitation. InAugust, a consultant was appointed jointly with theUnited Nations to advise UNICEF on rehabilitationprogrammes for physically handicapped children indifferent European countries, including Austria,Bulgaria, Czechoslovakia, France, Greece, Italy,Poland and Yugoslavia. Plans are now under wayfor a joint meeting on the subject of the crippledchild ; this will be held in 1951 and attended byexperts from the agencies concerned.
In February, IRO requested technical advice onthe health of children in camps for displacedpersons in various countries. A team of five expertsfrom WHO studied the problem and made appro-priate recommendations to IRO.
In April the Expert Committee on the Unificationof Pharmacopoeias considered the subject of aposology table for children and referred a draftof such a table to the Expert Committee on Maternaland Child Health for consideration.30 The subjectis being studied, on the request of members of theMaternal and Child Health Advisory Panel, bythree paediatricians.
For some time, many countries have showngreat interest in the use of films and filmstrips forteaching and demonstration purposes, and in Maya comprehensive international classified film
29 To be published in the World Health Organization:Technical Report Series
30 World Hlth Org. techn. Rep. Ser. 29, 10
CONTROL OF THE PHYSICAL ENVIRONMENT 21
catalogue on the health and welfare of childrenwas published jointly with UNESCO and widelydistributed (for details, see page 71).
In July, Zürich, Switzerland, acted as host tothe Sixth International Congress of Paediatrics, atwhich a co- operative exhibition on " Social Paedia-trics throughout the World " was presented by WHO,UNICEF, the International Red Cross, the Leagueof Red Cross Societies, and the International Unionfor Child Welfare (see page 67). WHO had takenan active part in the organization of this congressever since the first session of the expert committeein January, 1949. After the congress a seminarin social paediatrics was held in Geneva under thejoint auspices of WHO and the International Congressof Paediatrics.
During the last two years, WHO has co- operatedwith UNICEF in over a hundred health projects(in addition to the BCG and feeding programmes)for the benefit of mothers and children. Thesehave been carried out in more than forty countries :approximately 50 % were in Europe, 16 % in South-
East Asia, 14 % in the Americas, and 10 % in boththe Eastern Mediterranean and Western PacificRegions. They have been administered in accordancewith the principles laid down by the Joint Committeeon Health Policy, UNICEF /WHO, at its thirdsession.31
Technical advice has also been given on thedevelopment of the Children's Centre in Paris,which was established by the French Governmentin co- operation with UNICEF and WHO, as de-scribed in the Annual Report of the Director- Generalfor 1949.32
For collaboration with UNICEF, see page 64.Twenty -three fellowships in maternal and child
health were awarded during the year, seven ingynaecology and obstetrics, seven in the organizationof maternal and child health services, eight in paedia-trics and one in school hygiene,
31 Off. Rec. World Hlth Org. 22, 4732 Off. Rec. World HIM Org. 24, 72
CONTROL OF THE PHYSICAL ENVIRONMENT
WHO shall " promote, in co- operation with other specialized agencies where
necessary, the improvement of ... housing, sanitation ... and other aspectsof environmental hygiene ".
In February 1950 a section on environmentalsanitation was established in the Secretariat on apermanent basis, to carry out the sanitation pro-gramme of the Organization. In formulating thisprogramme, WHO has been guided by the recom-mendations made at the first session of the expertcommittee held in 1949 (the report of which wasprinted during 1950 33) and particularly by theprinciple that environmental sanitation is anessential part of any balanced health programme.
33 World HIM Org. techn. Rep. Ser. 1950, 10
Field work has been greatly expanded during theyear.
Work on sanitation has obviously been affectedby many other activities of WHO. As activities inenvironmental sanitation are particularly closelyrelated to those for combating malaria, it has beenthe policy of WHO to include certain experts qualifiedin general sanitation among the members of itsmalaria demonstration teams, and to use theirservices for work in sanitation as well as on malariacontrol, where time has permitted. This policy hasproved to be very useful in certain countries, inwhich governments have called freely upon thesanitary engineers attached to these teams for
22 WORK OF WHO, 1950
assistance in environmental sanitation. This hasbeen particularly true in Afghanistan, the Malnadarea of India, Pakistan and Thailand.
Sanitary engineers were also recruited towardsthe end of the year for each of the five relief teamsattached to the United Nations forces in Korea(see also page 40).
Because much of the success of a sanitation pro-gramme obviously depends on trained personnel,WHO has, where possible, attempted to assistMember States in providing such training. Fellow-ships in environmental sanitation were more widelygranted than before, 12 having been awarded duringthe year. The beneficial results of international semi-nars, in which high -level experts in sanitation parti-cipated, have long been recognized. In 1950 WHO,in co- operation with the Government of the Nether-lands and the International Health Division of theRockefeller Foundation, sponsored a seminar forEuropean sanitary engineers. This seminar, attendedby representatives from 15 countries, was plannedto provide an exchange of knowledge on thefollowing subjects : water purification, sewage andindustrial waste treatment, control of stream pollu-tion, the engineering phases of industrial health,training and education of sanitary engineers, the useof sanitary engineers in health administrations andgeneral sanitation. It is planned to hold additionalseminars of this kind in future years, not only inEurope, but also in the other regions.
In countries which provide training in environ-mental sanitation there is a wide variation in thekinds of training offered. Many of the so- calledeconomically under -developed areas need two typesof sanitary workers -the highly trained and thosepossessing only basic training in the subject. Itis hoped that in 1951, under the technical assistanceprogramme, WHO may help to establish severallocal training centres for comparatively largenumbers of the latter. For the small number ofhighly trained experts which are necessary, as theprovision of local training facilities is often im-practical, training in an environment similar tothat of their own country is clearly desirable. Withthis in mind, WHO took preliminary steps todetermine what assistance might be given instrengthening the teaching faculty of the All -IndiaInstitute of Hygiene and Public Health in Calcuttaso as to enable it to train more sanitary engineersfrom South -East Asia and the Western Pacific.WHO also made a grant to this institute for equip-ment and supplies at the end of the year.
One of the types of assistance which WHO hasbeen able to provide to its Member States is expert
advice both on specific technical problems in environ-mental sanitation and on the organization of adequategovernmental services. Field advisers in environ-mental sanitation will be assigned to each of WHO'sregional offices : three of the offices now have suchadvisers. In some cases, Member States can bestbe assisted by the services of specialists over shortperiods of time, and accordingly, during the yearshort -term consultants were assigned to Liberiaand for special work in Europe.
To provide information on environmental sani-tation by correspondence, an expert advisorypanel, from which members of the expert committeewill in the future also be drawn, has been appointed.In co- operation with the United States PublicHealth Service, WHO arranged for the monthlypublication Public Health Engineering Abstractsto be sent to selected sanitary authorities in variouscountries. On several occasions during the year,the Organization has also, upon request, furnishedinformation on problems of water supply.
The Organization has also devoted a considerableamount of attention to milk sanitation, which, inmany countries of the world, has major healthimplications. It participated in a two -weeks'conference on this subject, sponsored by FAO,UNICEF, the British Council and Reading Uni-versity, and attended by representatives of 21countries. Following a recommendation of theJoint Committee on Health Policy, UNICEF /WHO,for the preparation of a brochure primarily devotedto the health aspects of milk sanitation, includingpasteurization, WHO provided a grant to theNational Institute for Research in Dairying (attachedto Reading University) in England towards the pre-paration of such a brochure.
Although it is recognized that the problem ofhousing has important health implications, it hasnot been possible for WHO to carry on extensivework on this subject. WHO awarded one fellowshipin housing and town planning during the year,and participated in two meetings on this subjectcalled by the United Nations -the latter being aConference on Building Research sponsored bythe United Nations Economic Commission forEurope. A short -term consultant was retained toprepare a paper for this conference and to take partin the discussions. Assistance was also rendered tothe Housing and Town and Country PlanningSection of the United Nations Department of SocialAffairs.
Advice on field work was given during two visitsmade in the year -one to Liberia for discussions withthe public -health authorities on future sanitation pro-

MENTAL WELL -BEING 23
grammes, and the other to Egypt and to refugeecamps in the Hashemite Kingdom of the Jordan,Syria and Lebanon. As a result of these visits, theservices of a full -time sanitary engineer were madeavailable to UNRWAPRNE in the refugee area, on a
reimbursable basis, and a consultant was sent toLiberia, as mentioned above.
Details of activities in environmental sanitationin the various regions will be found in Chapter 2under the regions and countries concerned.
MENTAL WELL -BEING
WHO shall " foster activities in the field of mental health, especially those affectingthe harmony of human relations ".
The publication of the report on the first sessionof the Expert Committee on Mental Health,"marked an important step in the developmentof the mental health programme of the Organization.As the first report of international experts on thissubject, it has aroused widespread interest. Itsrecommendations of principles and priorities toform the basis of the WHO programme, the emphasislaid on the development of postgraduate teachingfacilities for psychiatrists, psychiatric social workers,clinical psychologists and psychiatric nurses, therecognition of the great importance of child psychia-try in the clinical field, and above all its insistenceupon the application of existing knowledge ofmental hygiene to all aspects of general public -health work, have been underlined as being ofparticular importance to governments.
The committee at its second session, held from11 to 16 September 1950 in Geneva, devoted furtherattention to the preventive application of psychiatricknowledge in general public -health practice. It alsodefined the terms " mental health " and " mentalhygiene ".35 It reviewed the opportunities formental hygiene presented by the different servicesin existing public -health practice and outlineddesirable types, principles and methods of training
34 World Hlth Org. techn. Rep. Ser. 1950, 935 Mental health was defined as a condition, subject to
fluctuations due to biological and social factors, which enablesthe individual to achieve a satisfactory synthesis of his ownpotentially conflicting, instinctive drives ; to form and maintainharmonious relations with others ; and to participate inconstructive changes in his social and physical environment.Mental hygiene was interpreted as referring to all the activitiesand techniques which encourage and maintain mental health.
which would enable public- health workers to takeadvantage of these opportunities. It considered,in particular, the mental health problems whichconfront the public -health worker in dealing withprospective parents, pregnant women, infants andchildren of pre -school age, schoolchildren, handi-capped children, the aged, patients segregated bycommunicable diseases, and immigrants, and alsodiscussed the education of the public in mentalhealth and the psychiatric aspects of mass education.
The report on the second session 36 will be presen-ted to the Executive Board early in 1951.
One of the first steps taken by WHO in connexionwith the grave problem of alcoholism, upon whichconsiderables stress was laid at the First WorldHealth Assembly, was the creation of a sub- commit-tee on that subject, depending on the Expert Commit-tee on Mental Health. The report of this AlcoholismSub -Committee, which met in December in Geneva,will be presented to the Executive Board in duecourse. 36
This report sets out principles for developingfacilities for the prevention and early treatment ofalcoholism by public- health services and putsforward recommendations on the way in which theOrganization can assist in this work. Apart fromurging direct assistance to countries in this respect,it recommends that the Organization should publisha comprehensive classified bibliography of studieson alcoholism, and should maintain in its head-quarters library an indexed file of abstracts of suchliterature, since scientific workers engaged in research
36 To be published, after approval by the Executive Board,in the World Health Organization : Technical Report Series.
24 WORK OF WHO, 1950
on and treatment of this condition are much handi-capped by the lack of central reference facilities.In addition, pointing out that at present scientificknowledge on alcoholism is restricted to com-paratively few countries, it strongly advocates thatthe Organization collaborate in regional seminarson the subject.
The current year has also seen the beginnings ofactive collaboration with the United Nations andother specialized agencies in mental health activities.Of note during the year was the contribution madeto the United Nations programme for the welfareof homeless children. For this programme a WHOconsultant made an extensive study of existingknowledge on the nature of psychological damagecaused by the separation of the infant and youngchild from the mother, the methods of mitigatingthis damage where separation is inevitable, and, inaddition, the psychiatric factors contributing to thecause of separation. The full report, which has nowbeen submitted to the United Nations, will bepublished in the Bulletin of the World Health Organi-zation and also in the World Health Organization:Monograph Series, early in 1951.
WHO also contributed to the United Nationsprogramme for the prevention of crime and thetreatment of offenders, by reviewing the existingknowledge and practice on the psychiatric aspectsof the etiology, prevention and treatment of juveniledelinquency. The report on this subject has alsobeen submitted to the United Nations. It waspublished during the year in French in the Bulletinof the World Health Organization 37 and will laterbe issued as a monograph in both languages.
A third contribution to United Nations pro-grammes has been in connexion with rehabilitation ;a study of the current knowledge and practice ofrehabilitation in psychiatry was made by WHOand a report is in the process of preparation.
These three projects mark the beginning of a newtype of activity on the part of the Organization. Apublished review, although not a service to a specificcountry, nevertheless provides valuable assistanceto professional workers and health administratorsin all countries, and could probably not be under-
37 Bull. World Hlth Org. 1950, 3, 63 -162.
taken except by an international organization. Thistype of review is based not only on a thoroughstudy of widely scattered literature, but also onactual discussions in which a consultant, sent byWHO for the purpose of the review to a variety ofcountries to interview experts and visit institutionsconcerned with the problem, has taken part.
Several governments, during the year, requestedexpert advice on such subjects as the role of psychiatryin industry, child guidance and juvenile delinquency,and consultants were sent, notably, to Finland,Ireland, Italy, Norway, the Philippines, Sweden andYugoslavia.
In addition the Organization has been representedat technical meetings called by the United Nationsfor the purpose of planning a co- ordinated pro-gramme in rehabilitation and at meetings of astanding committee composed of representatives ofspecialized agencies and international organizationsconcerned with the prevention of crime and thetreatment of offenders.
WHO has also contributed to developmental workin child psychiatry at the Children's Centre in Parisand has given technical advice on the first UNICEFprogrammes in the fields of juvenile epilepsy, childwelfare and child guidance.
Seven fellowships in mental health and psychiatrywere awarded.
Close relations have been maintained with theWorld Federation for Mental Health, which has con-tinued to expand its activities, and this non- govern-mental organization has proved a valuable link withprofessional organizations in many countries. Duringthe year it has undertaken the collection of technicalinformation on a variety of subjects of interest toWHO. The Organization has been represented at itsannual meeting and also at the meeting of its exe-cutive board.
Representatives of WHO also attended manyinternational scientific meetings concerned withmental health problems, including those of theInternational Congress of Psychiatry, the Inter-national Congress on Criminology, the InternationalCongress on the Education of Maladjusted Children,the International Council of Juvenile Court Judges,and the International Penal and PenitentiaryCongress.
SOCIAL AND OCCUPATIONAL HEALTH 25
SOCIAL AND OCCUPATIONAL HEALTH
WHO shall " promote, in co- operation with other specialized agencies where necessary,the prevention of accidental injuries ; "
" promote, in co- operation with other specialized agencies where necessary,the improvement of ... recreation, economic or working conditions ... "" study and report on, in co- operation with other specialized agencies wherenecessary, administrative and social techniques affecting public health andmedical care from preventive and curative points of view, including hospitalservices and social security ".
On 1 September, a section on social and occupa-tional health was created in the Secretariat at head-quarters, to carry out the activities necessary toimplement the functions quoted above.
As suggested by the Interim Commission andapproved by the First World Health Assembly,SBWHO has set up, in co- operation with ILO, a JointExpert Committee on Occupational Health. This
held its first meeting in August andSeptember 1950. Noting the considerable confusionin the terms used for this field of work (" industrialhygiene ", " industrial health ", " occupationalhealth ", " occupational hygiene ", etc.), the com-mittee proposed the adoption of the term " occupa-tional health " and summarized the scope and aimsof the activities under this heading as " the adapta-tion of work to man and of each man to his job ".It reviewed the common areas of activity of ILO andWHO in occupational health, stressed the importanceof giving special training in occupational medicineto doctors and auxiliary medical personnel, andrecommended close co- operation between industrialmedical services and local public -health services.The committee also gave careful consideration to amemorandum submitted by the American Federationof Labor, suggesting investigations of the effect ofmodern industrial methods on the health and life -expectancy of workers, with a view to proposingpossible preventive measures, and recommendedpreliminary joint investigation of this subject. Thereport of this session of the joint committee willbe submitted to the seventh session of the ExecutiveBoard.
During the past year, the Organization alsocontinued its co- operation with ILO on the hygieneof professional groups and the improvement ofliving conditions of workers ; representatives ofWHO attended several meetings of ILO committeeson these subjects. In particular, WHO and ILOcollaborated in implementing the recommendationsmade by their Joint Committee on the Hygiene ofSeafarers at its first session in December 1949, and inpreparing for the next session of the committee, whichis planned for 1951. The report on the first session ofthe committee 39 was submitted to the Third WorldHealth Assembly, and its publication was authorizedby the Executive Board.
Activities in the regions are just beginning. At therequest of governments, consultants on hospitalconstruction have been sent to several countries,as mentioned on page 18. In general, WHO is, inits preparations for the establishment of healthdemonstration areas and by its participation in thetechnical assistance programme, directing its effortstowards the improvement of health aspects ofeconomic and working conditions.
An expert advisory panel is now being set up,composed of experts competent in the variousaspects of social and occupational health, includingrehabilitation and medico -social welfare.
On the subject of rehabilitation of the physicallyhandicapped, close collaboration has been maintainedwith the Social Affairs Department of the UnitedNations, with ILO, UNESCO, UNICEF and IRO,and also with the non -governmental organizationsconcerned.
"Off. Rec. World Hlth Org. 9, 62 -63 ; 13, 322 se World Huth Org. techn. Rep. Ser. 1950, 20
26 WORK OF WHO, 1950
In 1950 one fellowship in occupational medicineand five in physical rehabilitation were granted.
Some of WHO's work on different aspects ofsocial and occupational health has been carried onas a part of its other activities. In connexion withpublic -health administration, for example, plans weremade to begin studies on physical training and othermedical aspects of recreation, and, at the end of theyear, a list of health qualifications for migrants wasbeing prepared in co- operation with ILO.
In addition, work being undertaken on mentalhealth, alcoholism, and addiction -producing drugs(see pages 23, 42) is helping to implement WHO's
constitutional function regarding the prevention ofaccidental injuries. Relations have been establishedwith the Social Commission of the United Nationson questions of alcoholism and, with the TransportDivision of the Economic Commission for Europe,on alcohol and traffic. Late in the year, the Organi-zation participated in a meeting of a working partyon the prevention of road traffic accidents, convenedby the Sub -Committee on Road Transport of theInland Transport Committee of ECE. Relationswere likewise maintained with various scientificbodies and research workers concerned with theseproblems.
NUTRITION
WHO shall " promote, in co- operation with other specialized agencies where neces-sary, the improvement of nutrition ".
One of the problems studied by WHO during1950 was that of endemic goitre. For the adequatecontrol of this disease in less well - developed partsof the world an effective way must be found ofgiving iodine to the population. In the countrieswhere free - flowing table salt is widely used it ispossible to provide a large number of people withiodine by iodizing this salt. This is the method inpractice in parts of Europe and America where en-demic goitre is prevalent. However, it cannot beapplied to countries where most of the populationstill uses crude salt, which cannot be treated by theprocesses used for iodizing free -flowing salt. WHOhas therefore stimulated research in the iodization ofcrude salt ; this work is progressing, and preliminaryreports indicate that a satisfactory method will beevolved. Once the laboratory stage is passed, it isproposed to conduct field trials, and a number ofcountries have offered facilities for this work. Iffrom these trials a method is obtained which can beused in small factories, then the main obstacle to theprevention and control of endemic goitre in most ofthe world will have been overcome.
WHO supplied a consultant to the Government ofCeylon to report on the incidence of endemic goitrein that island and to indicate any factors other thandeficiency of iodine that might be associated with it.A report has been submitted to the governmentconfirming the fact that there is a high incidence ofthe disease among the population living in the
" wet " part of the island. There does not appearto be any other factor associated with goitre exceptthe deficiency of iodine in the food and waterconsumed by the population in this area.
A survey of endemic goitre was also made inBrazil, Colombia, Ecuador, Guatemala and Mexico.This survey and the visiting consultant had the effectof stimulating wide interest in the countriesconcerned : a report was presented at the NutritionConference organized by FAO in Rio de Janeiroin June, in which WHO took an active part.
During the year assistance on nutrition was alsogiven to several national health -administrations. TheGovernment of Egypt invited WHO to collaboratewith FAO in making a report on the possibilityof extending the nutrition services of the governmentin keeping with the requirements of the country.An expert from WHO and one from FAO visitedEgypt, made extensive surveys and furnished thejoint report requested, with certain recommendations.Again with FAO, WHO helped the government toconduct a three -months' course in nutrition for thecountries of the Eastern Mediterranean Region ;several lectures were conducted and fellowships madeavailable to the countries concerned. A nutritioncourse given in Cairo was attended by 36 traineesfrom these countries.
At the request of the Government of YugoslaviaWHO agreed to assist in creating a nutrition instituteat Zagreb. A consultant on nutrition spent some
HEALTH EDUCATION OF THE PUBLIC 27
time in the country studying existing facilities andassessing requirements, and teaching equipment hasbeen supplied for the institutes at Zagreb andSarajevo. It is now planned that WHO will collabor-ate with the government in conducting a seminar onnutrition in 1951.
The Government of India asked for help inestablishing a training course for hospital dietitians,and in particular the services of an experiencedhospital dietitian who worked with the dietitian atthe Calcutta Medical College Hospital in organizingthis course.
WHO is also prepared to lend its services tointer -governmental nutrition institutes. It providedtwo short -term lecturers to the Institute of Nutritionof Central America and Panama, who assisted thecountries associated with the Institute (Costa Rica,El Salvador, Guatemala and Honduras) by givinglectures and demonstrations on modern methodsof conducting studies in nutrition.
A survey was made in the Eastern Mediterraneanarea, when, at the suggestion of the Chief MedicalOfficer of UNRWAPRNE, WHO sent an expertto areas in Arab Palestine and the Lebanon, to studythe nutritional status of the Arab refugees. It wasfound that in general the state of nutrition of these
refugees was considerably better than had been anti-cipated.
One of the most widespread nutritional disordersin tropical and sub -tropical areas is a syndrome atpresent ill- defined and known by various names,such as kwashiorkor, malignant malnutrition,polydeficiency disease, m'buaki, syndrome dépig-mentation- cedère, infantile pellegra, etc. It appearsthat the highest incidence of the disease occurs ininfants and young children and that the mortalityrates in some parts of Africa are disturbingly high.Following the recommendation of the Joint FAO/WHO Expert Committee on Nutrition that WHOshould stimulate inquiries into the epidemiology ofthis disease, WHO recruited a consultant, who, witha member of the staff of FAO from Washington,made a survey of the incidence, clinical character-istics, and the various ecological factors of this con-dition. The report includes recommendations of thepreventive measures that might be taken.
Of great importance during the year were theInfant Metabolism Seminars organized by WHOand held in the autumn in the Netherlands andSweden (see page 116, 118).
WHO awarded eight fellowships during 1950for nutrition and dietetics, and four for food control.
HEALTH EDUCATION OF THE PUBLIC
WHO shall " assist in developing an informed public opinion among all peopleson matters of health ".
During 1950 WHO gradually extended its healtheducation activities, in implementation of the con-stitutional function quoted above.
Health authorities in various countries are givingincreasing attention to the need for developing healtheducation as an integral part of organized healthservices, for experience has shown that more effectiveresults are obtained by these services when the activeparticipation of the people they benefit is obtained.During the year, therefore, WHO was called uponto play an active role in facilitating the exchangebetween countries of information on various aspectsof health education. Information was supplied on :trends in school and college programmes and in
courses in adult education ; the planning, organi-zation and administration of such programmes andcourses ; opportunities for training in public- healtheducation ; organization of school- community pro-jects ; and methods of health education, includingthe use of such illustrative media as films, filmstrips,posters and pamphlets.
WHO assisted in a survey of health education inSweden, at the request of the Government, and planswere made for giving similar assistance to othercountries in 1951. Full -time health educators wereassigned to the demonstration project in venereal -disease control in Simla, India, and to the joint WHO/UNICEF teacher -training demonstration in Sarawak.
28 WORK OP WHO, 1950
Jointly with UNESCO and the governmentsconcerned, WHO carried out the planning for alarge number of projects and continued to assumethe responsibility for providing technical guidanceand staff to help with the general health and health -education aspects of these projects. During 1950WHO added a full -time health educator to the teamassigned to the UNESCO /WHO Project in Fun-damental Education in Haiti. The Organization alsoassigned a short -term consultant in health educationto a UNESCO team conducting a survey of fun-damental education needs in the Arab States (par-ticularly in Egypt and Iraq). At the end of the year,this survey was being carried on by the UNESCOteam of four specialists in fundamental education,the WHO consultant, and a matching team providedby the participating governments in the region.
Most of the above- mentioned surveys have includeda study of the present level of health education invarious community groups, such as school -agechildren, teachers and parents. Teaching methodshave been reviewed and the needs of the differentgroups investigated with a view to intensifying, wherepossible, future health education work among them.
The surveys have served to emphasize once againthat, in any attempt to improve health education,it is of great importance to obtain the active par-ticipation of the people themselves and to take fullyinto account their problems and interests and theresources and social and cultural background of theareas in which they live.
Other joint activities of WHO included participa-tion in the International Seminar on Methods andTechniques of Adult Education held in Austria duringJune and July and representation at the InternationalConference on Public Education sponsored by theInternational Bureau of Education in co- operationwith UNESCO.
During 1950 WHO had the services of a consultantin the social sciences who advised on the social andcultural aspects of the health education programmeand assisted in formulating the social science aspectsof WHO's general programme, particularly asregards nursing and mental health. This consultantmade a study of conditions in the South -East Asiaand Western Pacific regions and assisted in thebriefing of staff engaged in field projects in thoseregions. She also appraised general needs forbriefing international health staff and worked withthe library in building up collections of literaturegiving information on social conditions in thedifferent countries and in preparing annotatedbibliographies.
Because of the increasing number of requestsreceived from governments for assistance in healtheducation, two health education specialists havebeen engaged for the Regional Office for the Americasand one for the Special Office for Europe.
WHO awarded one fellowship in health educationduring the year.
NURSING
WHO shall " act as the directing and co- ordinating authority on internationalhealth work ; "
" promote improved standards of teaching and training in the health, medicaland related professions ".
The wide variety of skills which are impliedin the term " nursing " tends to complicate theproblem of establishing nursing services adequatein quantity and quality for inclusion in nationalhealth services. Through international co- operation,it is thought that governments will be better ableto define the type of nursing services they wish toincorporate in their administrations.
The Second World Health Assembly recognizedthe value of such co- operation in meeting the growingneed for more nurses and for higher standards oftraining, by authorizing the creation of an expertcommittee on nursing during 1950.40
40 Resolution WHA2.77, Off. Rec. World Hlth Org. 21, 46
NURSING 29
In the report of the first session of this committee,held in February in Geneva, 41 special stress waslaid on the necessity for studying the real healthneeds of people in various communities and thenursing services required to meet them. In somecountries, primary nursing education is beingreoriented as a basic preparation for all nursingservices, including those concerned with positivehealth, the development of specialist skills beingplaced later, in supervised practice and post -basicnursing education. The Expert Committee onNursing made a study of the problems of nursingeducation and, pointing out that many functionsnow performed by nurses could be safely entrustedto workers with a less comprehensive training,recommended that nurses should undertake thetraining and subsequent supervision of such workers.It also recommended that " the programme ofevery basic school of nursing should include theintegration of the principles of mental health,public health, and prevention of disease, to preparethe nurse for her functions in teaching patientsand families about positive health. "42 It recom-mended that national health -administrations shouldmake a study of their total nursing 'resources witha view to developing national policies and pro-grammes for their nursing services.
During 1950 WHO began its nursing activitiesboth at headquarters and in the field, along thelines laid down by the expert committee andapproved in principles by the Third World HealthAssembly in resolution WHA3.38.43
In the latter part of the year a consultant wasemployed for six weeks at headquarters to assistin preparing a guide to help national health- admin-istrations in making the study of their resourcesand needs which was recommended by the committee.This guide will be available on request, and nursingadvisers attached to headquarters or the regionaloffices will be at the disposal of governments toassist them with this study.
In co- operation with the Rockefeller Foundationand the United Nations Department of SocialAffairs, plans were made to begin a pilot study ofthe types of community workers employed in the
41 World Hlth Org. techo. Rep. Ser. 1950, 2442 World Hlth Org. techo. Rep. Ser. 1950, 24, 1243 Off. Rec. World Hlth Org. 28, 28
health services of two European countries. Atthe end of the year WHO called a meeting of atechnical advisory committee consisting of repre-sentatives of France, the United Kingdom and theagencies concerned. At this meeting techniqueswere developed and objectives defined for thepilot study, which will begin early in 1951 in Franceand the United Kingdom and will be used as amodel for further studies in other communities.
In the control of communicable diseases, public-health nurses have continued to work with themalaria -control demonstration teams in India,Pakistan and Thailand, giving particular attentionto work with women and children and to theteaching of understudies. In most of the teamsthey have been able to extend their activities toundertake work in maternal and child health inthe villages and to assist local staff employed inthis work. One public -health nurse has been attachedto the tuberculosis demonstration centre in Istanbul,where she has helped to set up nursing activitiesand to organize teaching programmes for trainednurses and nurse aides. Another, working withthe Simla demonstration team in venereal- diseasecontrol in India, has taken charge of the nursingaspects of the demonstration and the teaching ofunderstudies.
Teams of paediatric nurses and public -healthnurses experienced in maternal and child healthwere assigned to teaching centres and hospitals inthe Western Pacific region in connexion with projectssponsored by WHO and UNICEF in Brunei,Sarawak, Malaya and North Borneo, where theyhelped to establish facilities for training nurses,midwives and other auxiliary workers.
WHO assisted the Netherlands Government andthe Institute of Preventive Medicine at Leydenin the organization of a two -weeks' working con-ference for public -health nurses. This conferencewas held at Noordwyck in October and was attendedby 43 public- health nurses from ten countries.Methods and techniques in health education used bypublic -health nurses in the course of their workformed the main subject of study. During the pre-paration for this meeting, as well as in the conferenceitself, emphasis was laid on the active participationof the delegates, and continued activity will beencouraged through correspondence and visitingconsultants.

30 WORK OF WHO, 1950
Twelve fellowships in nursing were awardedduring the year - seven in general nursing, one innursing education and four in public- healthnursing.
In addition, 27 nurses were granted short -term
fellowships to enable them to attend the workingconference mentioned above and six received short -term fellowships for a conference on the psychologyof hospitalization organized at the Cassel Hospitalin London.
IMPROVED STANDARDS OF TEACHING AND TRAINING
WHO shall " promote improved standards of teaching and training in the health,medical and related professions ".
The growing interest of international organizations,agencies and governments in the education andtraining of public -health workers, as being one ofthe basic conditions for the improvement of healthservices and the health of the population generally,has had great influence on the work of theOrganization in 1950.
After the Third World Health Assembly haddrawn attention to the need for the adequate pre-paration of medical workers and other personnelessential to health care,44 the. Executive Boardproposed that a thorough technical discussion ofthe subject should take place at the Fourth WorldHealth Assembly.4J This proposal was receivedfavourably by many governments, and the necessarypreparations for the discussion were made.
The Third World Health Assembly also stressedthe importance of the sociological and preventiveaspects of the education of health personnel 44 and,at its sixth session, the Executive Board emphasizedthe desirability of making studies of the types ofmedical education -particularly in public health andsocial medicine -current in various countries.46Information on this subject has accordingly beencollected. Part of it is expected to serve as a basisfor the technical discussions mentioned above.
The action of the Third World Health Assemblyand Executive Board followed recommendations
44 Resolution WHA3.2, Off. Rec. World Hlth Org. 28, 1545 Resolution EB6.R37, Off. Rec. World HIM Org. 29, 1546 Resolution EB6.R35, Of Rec. World Hlth Org. 29, 15
made by the Expert Committee on Professional andTechnical Education of Medical and AuxiliaryPersonnel at its first session held in Geneva inFebruary.47 The committee also formulated pro-posals for the orientation of training programmes andother aspects of the Organization's work, and madea series of recommendations on the training ofdoctors and other health workers. It listed specificactivities which, in its view, WHO should undertake,and outlined a long -term programme in professionaland technical education to serve as a guide in thepreparation of the Organization's annual programmes.
The Regional Committees for South -East Asiaand for the Eastern Mediterranean encouraged thecountries in their respective regions to give attentionto problems arising in the education and training ofhealth workers, and to the importance of collabora-tion in solving them. Emphasis was placed onspecific needs in the training of auxiliary healthworkers. The Regional Office for the Americasfurther strengthened its educational branch by estab-lishing a division of education, training and generaltechnical services to serve both WHO and the PanAmerican Sanitary Bureau. In some regional officesthe expansion of regional and national health pro-grammes justified the appointment of regional ad-visers in professional and technical education ofmedical and auxiliary personnel. These advisers willalso help with technical assistance programmes,which, in many instances cannot be carried out with-out the prior training of local health workers.
47 World Hlth Org. techn. Rep. Ser. 1950, 22
IMPROVED STANDARDS OF TEACHING AND TRAINING 31
The gradual collection of information on problemsof medical education in various countries was con-tinued. A register of medical and public -healthschools, being compiled for reference purposes, isstill incomplete because of the difficulty of obtaininginformation on some countries. Data on scientificinstitutions and on trends in research was distributedto various governments on request. The WorldMedical Association supplied the Organization withthe results of an inquiry into medical education, andarrangements are being made with organizationssuch as this association and the International Uni-versities Bureau to co- ordinate studies now beingmade on various aspects of the subject.
WHO also helped to increase the training facilitiesfor health workers in non -self -governing territoriesby such services as fellowships, by co- operating withthe United Nations in collecting relevant data, and byproviding information on teaching institutions tothe appropriate organs of the United Nations.
WHO studied trends in nursing education in manycountries and is building up an information centreon existing programmes and methods. Currentliterature on the subject and contacts with advisersand consultants show that there is a tendencythroughout the world for the education of nurses tobe re- examined in the light of the many and varieddemands of modern health services. The ExpertCommittee on Nursing studied this situation andmade detailed recommendations on nursing education(see page 29).
Besides undertaking the studies and endeavouringto stimulate international interest in medical andrelated training WHO provided direct assistance toindividual countries for the improvement of teachingand training. Wherever possible, attention was givento the training of local personnel. Three fellowshipsin medical education were awarded in 1950.
Information on teaching facilities in the regionswas supplied by the regional offices, and consult-ants have conferred with the health authorities ofcountries (Egypt, France, Greece, India, Lebanon,the Netherlands, the Scandinavian countries andSwitzerland) on public- health schools, public -healthdepartments and field- training facilities. Trainingresources also received special attention in surveysmade in connexion with technical assistance andUNICEF programmes.
WHO has helped to strengthen facilities forteaching and training by (1) providing direct assistance
in organizing training courses and seminars andstressing the training aspects of other WHO activi-ties ; (2) awarding and administering an increasingnumber of fellowships, and (3) providing medicalliterature and teaching equipment.
Training Courses
In services to governments, training was empha-sized by the following types of activities : 48
1. The holding of short discussion groups andsymposia, jointly sponsored by WHO and thegovernments concerned, e.g., on child health (India),on nutrition (Egypt), on syphilis (Finland andFrance), on infant metabolism (Leyden and Stock-holm), on environmental sanitation and public -
health nursing (the Netherlands). The latter,attended by 43 public- health nurses from 10European countries, deserves special mention.
2. The provision of long courses at specialdemonstration centres, such as those in tuberculosis(Turkey) and in anaesthesiology (Copenhagen).In the last two years several countries (Czechoslo-vakia, Denmark, France, Greece, Israel, Swedenand Yugoslavia) have asked for help from WHOin setting up training centres in anaesthesiology.Teaching equipment was provided and teacherswere on their way to such a centre at Prague,when the announcement of Czechoslovakia'sdecision to end its participation in WHO inter-rupted the plans.
3. The sending of demonstration teams in specialsubjects, e.g. on congenital heart diseases (toAustria and Yugoslavia) and on thoracic surgery(to Israel and Turkey). These teams introducednew methods, and their visits led to many suc-cessful operations by local surgeons in countrieswhere such operations had not been performedbefore. The visits to Austria, Israel and Yugoslavialasted two weeks each, and that to Turkey, onemonth.
4. The establishment, with UNICEF, of de-monstration and training projects with chiefemphasis on maternal and child health, e.g. inAfghanistan (combined with the control of
48 Details of these activities are given under individualsubjects and regions.
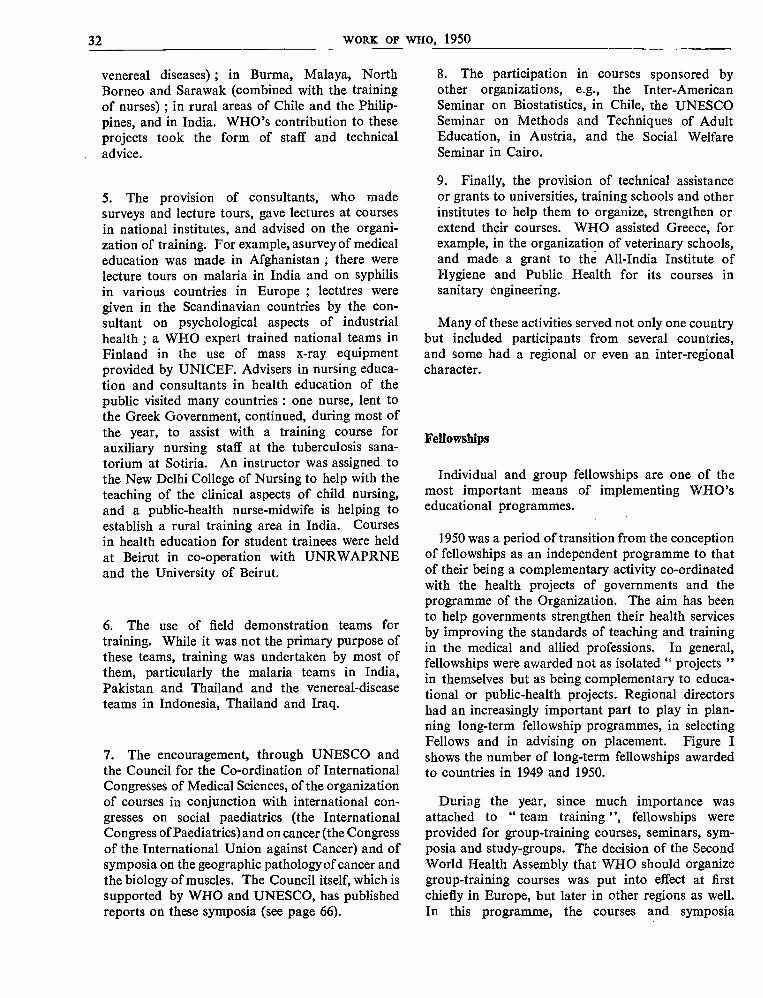
32 WORK OF WHO, 1950
venereal diseases) ; in Burma, Malaya, NorthBorneo and Sarawak (combined with the trainingof nurses) ; in rural areas of Chile and the Philip-pines, and in India. WHO's contribution to theseprojects took the form of staff and technicaladvice.
5. The provision of consultants, who madesurveys and lecture tours, gave lectures at coursesin national institutes, and advised on the organi-zation of training. For example, asurvey of medicaleducation was made in Afghanistan ; there werelecture tours on malaria in India and on syphilisin various countries in Europe ; lectúres weregiven in the Scandinavian countries by the con-sultant on psychological aspects of industrialhealth ; a WHO expert trained national teams inFinland in the use of mass x -ray equipmentprovided by UNICEF. Advisers in nursing educa-tion and consultants in health education of thepublic visited many countries : one nurse, lent tothe Greek Government, continued, during most ofthe year, to assist with a training course forauxiliary nursing staff at the tuberculosis sana-torium at Sotiria. An instructor was assigned tothe New Delhi College of Nursing to help with theteaching of the clinical aspects of child nursing,and a public -health nurse - midwife is helping toestablish a rural training area in India. Coursesin health education for student trainees were heldat Beirut in co- operation with UNRWAPRNEand the University of Beirut.
6. The use of field demonstration teams fortraining. While it was not the primary purpose ofthese teams, training was undertaken by most ofthem, particularly the malaria teams in India,Pakistan and Thailand and the venereal- diseaseteams in Indonesia, Thailand and Iraq.
7. The encouragement, through UNESCO andthe Council for the Co- ordination of InternationalCongresses of Medical Sciences, of the organizationof courses in conjunction with international con-gresses on social paediatrics (the InternationalCongress of Paediatrics) and on cancer (the Congressof the International Union against Cancer) and ofsymposia on the geographic pathology of cancer andthe biology of muscles. The Council itself, which issupported by WHO and UNESCO, has publishedreports on these symposia (see page 66).
8. The participation in courses sponsored byother organizations, e.g., the Inter -AmericanSeminar on Biostatistics, in Chile, the UNESCOSeminar on Methods and Techniques of AdultEducation, in Austria, and the Social WelfareSeminar in Cairo.
9. Finally, the provision of technical assistanceor grants to universities, training schools and otherinstitutes to help them to organize, strengthen orextend their courses. WHO assisted Greece, forexample, in the organization of veterinary schools,and made a grant to the All -India Institute ofHygiene and Public Health for its courses insanitary engineering.
Many of these activities served not only one countrybut included participants from several countries,and some had a regional or even an inter -regionalcharacter.
Fellowships
Individual and group fellowships are one of themost important means of implementing WHO'seducational programmes.
1950 was a period of transition from the conceptionof fellowships as an independent programme to thatof their being a complementary activity co- ordinatedwith the health projects of governments and theprogramme of the Organization. The aim has beento help governments strengthen their health servicesby improving the standards of teaching and trainingin the medical and allied professions. In general,fellowships were awarded not as isolated " projects "in themselves but as being complementary to educa-tional or public -health projects. Regional directorshad an increasingly important part to play in plan-ning long -term fellowship programmes, in selectingFellows and in advising on placement. Figure Ishows the number of long -term fellowships awardedto countries in 1949 and 1950.
During the year, since much importance wasattached to " team training ", fellowships wereprovided for group- training courses, seminars, sym-posia and study -groups. The decision of the SecondWorld Health Assembly that WHO should organizegroup -training courses was put into effect at firstchiefly in Europe, but later in other regions as well.In this programme, the courses and symposia
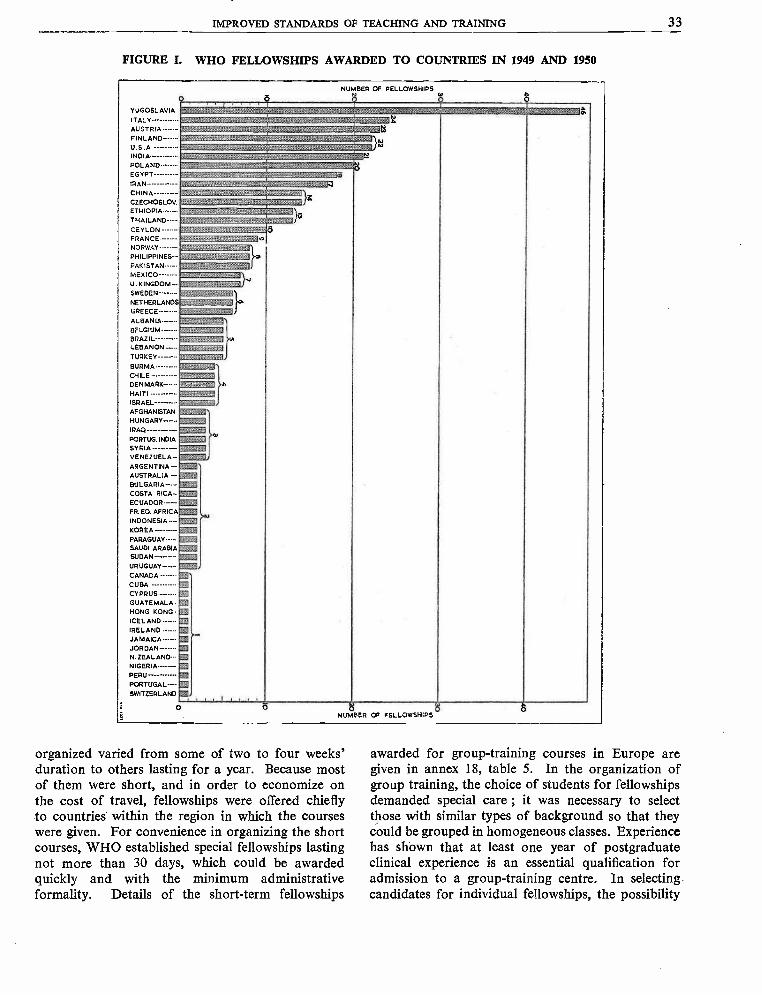
IMPROVED STANDARDS OF TEACHING AND TRAINING 33
FIGURE I. WHO FELLOWSHIPS AWARDED TO COUNTRIES IN 1949 AND 1950
NUMBER OF FELLOWSHIPS
ó ó.YUGOSLAVIA
ITALYAUSTRIAFINLAND
o,
r.
INU.S.A N
INDIA A.,
POLAND- - - - -.EGYPT___._.._
IRAN._.___._
NO-gym
iv
CHINA- - '- - -'CZECHOSLOV
t:.hoiF., .;:.. :
. 3° /ETHIOPIA - - - --THAILAND ----
;r+.. :.,....... ..1
.. O. JOpCEYLON
FRANCE... - -....
NORWAY -----
?s::::'oaT::n',...îrof.o
PHILIPPINES--PAKISTANMEXICO ----- -.U. KINGDOM- -SWEDEN ------NETHERLANDS
GREECE
ALBANIA----- -BELGIUMBRAZIL ----- ---LEBANONTURKEY
BURMACHILEDENMARK - - - -
HAITIISRAEL------- -AFGHANISTANHUNGARY - - - -
IRAQ
PORTUG. INDIA
SYRIAVENEZUELA --ARGENT INA- --d:AUSTRALIA ---BULGARIA - -COSTA RICAECUADOR
FR. EO. AFRICA
INDONESIA - - --KOREA.PARAGUAY
SAUDI ARABIA:'SUDAN___ -__ -.
URUGUAYCANADACUBACYPRUS - - - - -GUATEMALA -HONG KONG ICELANDIRELANDJAMAICA ------JORDANN. ZEALAND--NIGERIA
PORTUGAL--- -
SWITZERLAND
!,:ye :.:E-;',`'::q jo.
,, LOPLOOPLOM
u.
FoORSOLLOO
`POLOLIWALR.
:' - to
co
WO :,..n..., °..ex:
%... 359-- -
WOPOO
MOELOOP
->s%',
WOMWS
PLL
HE
xEVre
LO
pp2 o O 18 O
NUMBER OF FELLOWSHIPS
organized varied from some of two to four weeks'duration to others lasting for a year. Because mostof them were short, and in order to economize onthe cost of travel, fellowships were offered chieflyto countries within the region in which the courseswere given. For convenience in organizing the shortcourses, WHO established special fellowships lastingnot more than 30 days, which could be awardedquickly and with the minimum administrativeformality. Details of the short -term fellowships
awarded for group- training courses in Europe aregiven in annex 18, table 5. In the organization ofgroup training, the choice of students for fellowshipsdemanded special care ; it was necessary to selectthose with similar types of background so that theycould be grouped in homogeneous classes. Experiencehas shown that at least one year of postgraduateclinical experience is an essential qualification foradmission to a group- training centre. In selectingcandidates for individual fellowships, the possibility
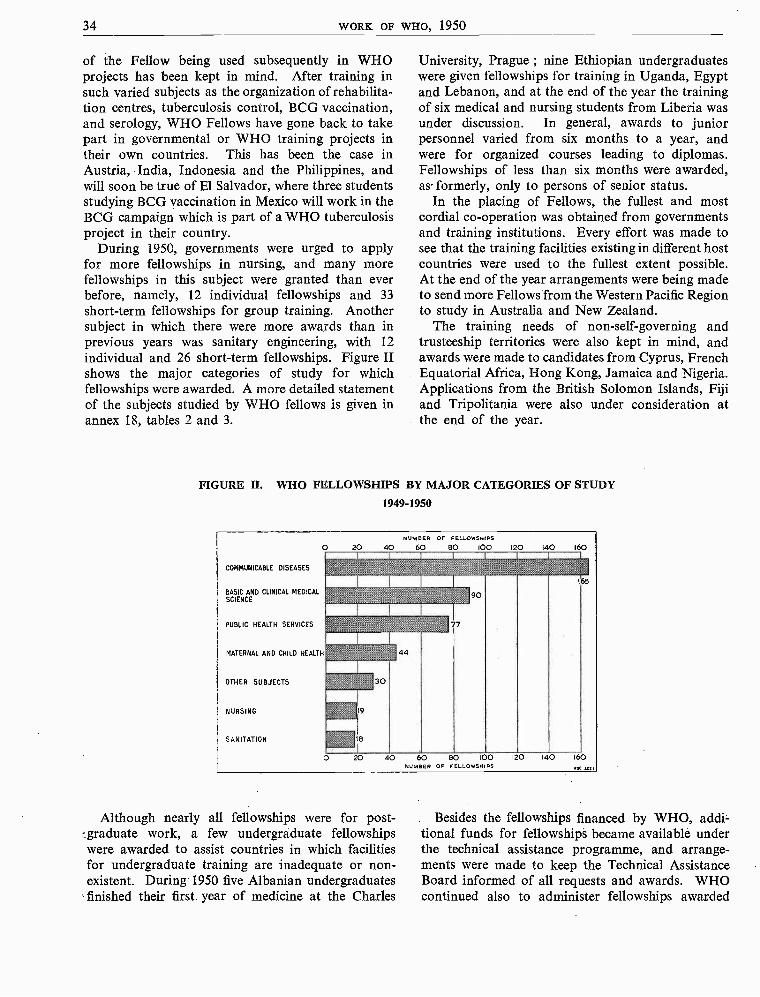
34 WORK OF WHO, 1950
of the Fellow being used subsequently in WHOprojects has been kept in mind. After training insuch varied subjects as the organization of rehabilita-tion centres, tuberculosis control, BCG vaccination,and serology, WHO Fellows have gone back to takepart in governmental or WHO training projects intheir own countries. This has been the case inAustria, India, Indonesia and the Philippines, andwill soon be true of El Salvador, where three studentsstudying BCG vaccination in Mexico will work in theBCG campaign which is part of a WHO tuberculosisproject in their country.
During 1950, governments were urged to applyfor more fellowships in nursing, and many morefellowships in this subject were granted than everbefore, namely, 12 individual fellowships and 33short -term fellowships for group training. Anothersubject in which there were more awards than inprevious years was sanitary engineering, with 12individual and 26 short -term fellowships. Figure IIshows the major categories of study for whichfellowships were awarded. A more detailed statementof the subjects studied by WHO fellows is given inannex 18, tables 2 and 3.
University, Prague ; nine Ethiopian undergraduateswere given fellowships for training in Uganda, Egyptand Lebanon, and at the end of the year the trainingof six medical and nursing students from Liberia wasunder discussion. In general, awards to juniorpersonnel varied from six months to a year, andwere for organized courses leading to diplomas.Fellowships of less than six months were awarded,as formerly, only to persons of senior status.
In the placing of Fellows, the fullest and mostcordial co- operation was obtained from governmentsand training institutions. Every effort was made tosee that the training facilities existing in different hostcountries were used to the fullest extent possible.At the end of the year arrangements were being madeto send more Fellows from the Western Pacific Regionto study in Australia and New Zealand.
The training needs of non -self -governing andtrusteeship territories were also kept in mind, andawards were made to candidates from Cyprus, FrenchEquatorial Africa, Hong Kong, Jamaica and Nigeria.Applications from the British Solomon Islands, Fijiand Tripolitania were also under consideration atthe end of the year.
FIGURE II. WHO FELLOWSHIPS BY MAJOR CATEGORIES OF STUDY
1949 -1950
O
COMMUNICABLE DISEASES
BASIC AND CLINICAL MEDICALSCIENCE
PUBLIC HEALTH SERVICES
MATERNAL AND CHILD HEALTH
OTHER SUBJECTS
NURSING
SANITATION
NUMBER OF FELLOWSHIPS
20 40 60 BO 100 120 140 160
" ' 'p,% "AIM
165
m,ft `f'-`;+` 90_aÿÿ'S.'.Ssu' 'à''hax'a.'ros
.
",._ 77
ZÁ44f "'%' %'30
19
O 20 40 60 BO IOO 120 140 160NUMBER OF FELLOWSHIPS 1x01021
Although nearly all fellowships were for post-graduate work, a few undergraduate fellowshipswere awarded to assist countries in which facilitiesfor undergraduate training are inadequate or non -existent. During 1950 five Albanian undergraduatesfinished their first year of medicine at the Charles
Besides the fellowships financed by WHO, addi-tional funds for fellowships became available underthe technical assistance programme, and arrange-ments were made to keep the Technical AssistanceBoard informed of all requests and awards. WHOcontinued also to administer fellowships awarded
IMPROVED STANDARDS OF TEACHING AND TRAINING 35
by UNICEF. As in 1949, most of these fellowshipswere awarded for joint projects in South -East Asiaand the Western Pacific, but in 1950 one Europeancountry and three countries in the Western Hemi-sphere also benefited. A more detailed statement ofthe beneficiary countries of UNICEF fellowshipsadministered by WHO appears in annex 18, table 6,while Figure III shows the regional distribution ofthe fellowships awarded by WHO and of UNICEFfellowships administered by WHO.
by the regional offices, which report regularly toheadquarters, so that complete information may beavailable and uniformity of policy assured. (Acomparative statement of the fellowships awardedfor study within and outside the region is given inannex 18, table 4.)
To keep pace with these new developments, andin accordance with the new orientation of policy inawarding fellowships, the Fellowships Manual, deal-ing with policy, responsibilities and procedures for
FIGURE III. FELLOWSHIPS AWARDED TO REGIONS1947 -1950
(WHO fellowships and UNICEF fellowships- administered by WHO)
AFRICA AMERICAS SOUTH-EAST ASIA EUROPE E. MEDITERRANEAN WESTERN PACIFIC160
140
120
VI
°-100IIna3
-JJLL 80LLO¢m
60z
40
20
151
160
140
120
100ÿmmA0T
80 mrrOExtn60 al
40
20
O
136
-Miii V! HO
',%O/; UNICEFIAOUIx15TEFE0
BY .01-
_ .;..
114
100
:2%
:<?
__ _ _ _ ,;
-
94
_
irV.
- - -.v
:z
`ï:Ai:::.,..
s:k
':'?, _
:$
- -
.
:':if<to: -4;..:.
::
- _ _
44_ _ _
: .;
_ - 47 _
- - - '<' -:
4'
-
35
-
21-
0
E:'ÿ
i c
E< 0
1
I.,
35,3
ï20 19
-
00 010 j 0f'1301 r rr rr'=i
-
r00 00,rr".} 0
t5 -
...
_
0 0 r00r l i .... /?' 5"i
% 010 0r irOl i.
vï
';_0 r
.{
.';, 5;::
:`::.:, 0Y> 0,
;;; e %
:::/1947 1948 1949 1950 1947 1948 1949 1950 1947 1948 1949 1950 947 1942 1949 1950 1947 1948 1949 1950 1947 1948 1949 1950
. . . .Wh0 1025
* In 1947 and 1948 fellowships were awarded to UNRRA -aided countries only.
Collaboration with the United Nations and otherspecialized agencies continued in the form of ex-changes of views and sharing of information. Thesection on WHO Fellowships in the United NationsHandbook of International Fellowships (1949) wasrevised ; advice was given to UNESCO in revisingits publication, Study Abroad, and documentationwas prepared for the fourth session of the TechnicalWorking Group on Fellowships of the ACC, inwhich the Organization took an active part.
Much progress was made during 1950 in decen-tralizing the responsibility for fellowships fromheadquarters to the regions. Fellowships organizedwithin the region are now awarded and administered
the administration of fellowships, was revised duringthe year.
The Organization has kept in close touch withfellowship holders, both during and after theirtraining. Monthly reports, comprehensive reportsand follow -up reports are received from the Fellowsthemselves, and in addition, governments are askedto report, two years after . the end of the fellowship,on the manner in which the services of each ex-Fellow are being used. Study of the follow -upreports from governments has shown that nearly allex- Fellows are employed in government or govern-ment-sponsored services, and that many of them areholding more responsible and influential posts than
36 WORK OF WHO, 1950
before their fellowships. There can, of course, beno method for evaluating with scientific accuracythe usefulness of fellowships. A good criterion,however, is the answer to the question " Is there ahealth service or a teaching facility in the countrywhich has come into being, or which is functioningmore effectively, because of WHO fellowships ? " Thereports show that, young as the Organization's fel-lowships programme is, there are few countries inthe world for which an affirmative answer could notbe given. For example :
1. The recipient of a fellowship for the study ofindustrial hygiene was, on return to his country,appointed head of the laboratory for industrialair analysis at the institute of industrial hygiene,a post involving research work, direction of fieldwork and teaching.2. A nurse whose fellowship enabled her toattend a course in industrial nursing was, immedi-ately after her return home, made supervisor andconsultant in industrial nursing for her country,and later chairman of the industrial nurses'section of the national public- health nurses'association. She has also organized and conductedcourses for public -health nurses in industry.3. A psychiatrist who studied psychiatric socialwork in a country where this type of service ishighly developed, is now taking a prominent partin the establishment of training for psychiatricsocial workers in his own country.4. Two physicians who used their fellowships tostudy chest diseases have set up special depart-ments for these diseases at their own hospitals,have published articles on the technique of bron-choscopy and have organized postgraduate teach-ing in the subject : a third has been appointedregional adviser in tuberculosis in a WHO regionaloffice.
5. A research worker on cancer was given animportant appointment in the cancer researchdepartment of a radio -therapy institute within onemonth of his return from his fellowship. Anothersuch worker, taking up her previous appoint-ment as chief of the clinical laboratory of a Statecancer institute, has been put in charge of a cancerprophylaxis centre, where many new methodslearned during her fellowship have been put intopractice.
Measures have been taken towards carrying outa suggestion made at the Third World Health
Assembly that candidates for fellowships should beencouraged to prepare reports on problems in theirown country related to the subjects for which theirfellowships are to be used.49 This has not beenenforced as a routine procedure, but in the selectionof Fellows it is being applied when appropriate andpracticable.
The total number of WHO fellowships awardedduring 1950 was 345, of which 107 were of the short -term type. The distribution by beneficiary country,between 1947, when the fellowship programme began,and the end of 1950, is shown in annex 18 table 1.
Medical Literature, Supplies and Teaching Equipment
In 1950 WHO continued to provide governmentswith medical literature and teaching equipment.Because budgetary provisions for this service weresmaller than for previous years ($75,000 against$115,000 in 1949), only the most essential materialwas furnished, all of which went to assist medical andhealth institutions, especially educational and trainingcentres and related hospitals and laboratories whichtrain professional, technical and other public- healthpersonnel. For a list of countries to which thesesupplies were furnished see annex 17.
Through the regional offices, an agreement,sponsored by UNESCO, on the importation ofeducational, scientific and cultural materials, wasbrought to the attention of Member Governmentswith the suggestion that they ratify it as soon aspossible. This agreement would facilitate the freerflow of many items essential for professional andtechnical education. WHO also collaborated withUNESCO by furnishing advice on apparatus andmaterials for the teaching of science in primary andsecondary schools, information on the health aspectsof the teaching of biology, and names of dentallibraries which would benefit from assistance in theform of dental literature. The two organizationsbegan work on inventories of supplies for medicalschools and schools for auxiliary health personnel,to be provided under the technical assistance pro-gramme.
(For medical supplies furnished by WHO, seepage 38).
49 Off. Rec. World Hlth Org. 28, 206
AVAILABILITY OF ESSENTIAL DRUGS AND EQUIPMENT 37
AVAILABILITY OF ESSENTIAL DRUGS AND EQUIPMENT
WHO shall " assist governments, upon request, in strengthening health services; "" promote and conduct research in the field of health ".
Antibiotics
The enormous value of penicillin in fightingdisease and the discovery of other important anti-biotics have made Member States, since the days ofthe Interim Commission, emphasize the need forassisting governments in obtaining these therapeuticsubstances. Various steps were taken by UNRRAand WHO but they did not entirely meet the require-ments of Member States, and the Executive Boardat its third session directed that an expert committeeshould be established on the subject.so
Accordingly, an Expert Committee on Antibioticswas convened in Geneva from 11 to 15 April. 51 Thiscommittee considered the difficulties experienced bygovernments in obtaining antibiotics and studiedrequirements, which differ from country to countryaccording to the magnitude of the health problems,the level of economic development and industrialactivity and the ability to apply scientific discoveries.The committee recommended that in the case ofcountries needing assistance, WHO should arrangefor the extension of training facilities for scientificand technical personnel in methods of productionand research on antibiotics.
To this end a number of national research institutessuggested by the committee are being formed intoan international group for the purpose of con-ducting research on antibiotics. These instituteswill share their problems and their knowledge,will exchange personnel, and will provide train-ing for the scientists of Member States. TheIstituto Superiore di Sanità, Rome, with its Depart-ment of Fermentation Chemistry and Antibiotics,has already agreed to join this group, and has beenapproved as a training centre.
WHO also plans to set up centres for the study ofproduction methods of antibiotics in South -EastAsia, Europe, the Eastern Mediterranean and SouthAmerica, in collaboration with interested govern-ments. The first centre for Asia will probably be
set up in India. It will provide facilities for theapplication of the knowledge emanating from theinternational research group and will also be usedfor training technical staff for other centres.
WHO has also asked a number of institutionsresponsible for culture collections to serve as deposi-tories of official cultures for the production andtesting of antibiotics of approved quality, and tomake them available to governments and researchcentres on request.
Two fellowships in antibiotics were awardedduring the year.
Insecticides
During the year WHO provided countries onrequest with advice on insecticides and took actionto implement the resolution of the Third WorldHealth Assembly regarding the free flow of insecti-cides and the waiving of customs duties." It isvery gratifying to be able to report that Iran hasrecently abolished customs duties on insecticidesand a number of essential drugs such as quinine,mepacrine, proguanil, all antibiotics and certainheavy metal compounds. Afghanistan levies nocustoms duty on insecticides. Ceylon waives dutyon insecticides imported for its national healthprogrammes, and India has recently extended thesuspension of tariffs on insecticides. The health admi-nistrations in these countries may now be able toexpand some of their activities, since smaller partsof their budgets are reverted to the treasury inthe form of customs revenues. (See also page 66).
Details of the work of the Expert Committee onInsecticides are given on page 8.
In the Secretariat at headquarters a new sectionhas been set up, under the direction of an expertwith extensive experience in chemicals and antibiotics.This section will advise governments and givethem any necessary technical assistance in theproduction of antibiotics and insecticides.
°° Off. Rec. World Hlth Org. 17, 13el World Hlth Org. techo. Rep. Ser. 1950, 26 °° Resolution WHA3.43, Off Rec. World HIM Org. 28, 30
38 WORK OF WHO, 1950
Medical Supplies and Equipment
A hundred thousand dollars' worth of medicalsupplies were furnished to governments for specificprojects (which had been approved, after detailedexamination, by the Executive Board) 53 either tohelp governments to continue programmes afterWHO demonstration teams have finished theirtask, or to further health projects carried out bygovernmental administrations. Some difficultiesencountered in obtaining supplies available onlyagainst hard or other foreign currency had to besolved. WHO helped, by these supplies, in thecarrying out of a wide variety of projects andcampaigns, including an antileprosy campaign,a project for training of nurses, a mass chest -survey, antimalaria campaigns in four MemberStates, and in the establishment of a health servicefor nomadic tribes and of a cardiac clinic.Details are given in annex 17. In many casesthe Member States concerned reimbursed WHO forthese supplies in local currency. Following thedecision of the Third World Health Assembly, theprovision of supplies for government programmes willnot be continued in 1951.54
Information regarding medical literature andteaching equipment supplied to governments is
given on page 36. WHO continued during the year
J3 Resolution EB6.R15, Off. Rec. World filth Org. 29, 754 Resolution WHA3.71, Off. Rec. World Hlth Org. 28, 41
to provide medical supplies, literature and equip-ment for consultants and teams in the field.
For the earthquake disaster in Assam, India,$4,000 was allotted for emergency services andsupplies such as sulfa drugs and chloride of lime.Each medical officer detailed for duty under theUnified Command in Korea was supplied with akit for all minor medical and surgical emergencies.The Regional Office for the Americas co- operated inWHO's supply programme by furnishing suppliesfor many Member States both inside and outside theregion.
Services were also continued to governmentsneeding assistance in solving their problems ofobtaining medical supplies. At WHO's request, theEconomic Commission for Europe circulated aquestionnaire to European countries on the availa-bility of supplies and various items of equipment.Moreover, at the sixth session of the EconomicCommission for Asia and the Far East, attendedby a WHO observer from the South -East AsiaRegional Office, the commission was urged toconsider the manufacture of essential materials suchas insecticides, antimalarial drugs, penicillin andstreptomycin. ECAFE has agreed to co- operate inevery way possible. Information on sources ofsupply and cost of essential items not manufacturedlocally, as well as availability of technical details ofpenicillin production and the processing of penicillinto be imported in bulk were furnished upon requestto certain Member States in the South -East AsiaRegion.
HEALTH SERVICES TO SPECIAL GROUPS
WHO shall " provide or assist in providing, upon the request of the United Nations,health services and facilities to special groups, such as the peoples of trustterritories ".
WHO not only served specific governments on theirrequest, but, in fulfilment of the function quotedabove and in co- operation with the United Nations,gave assistance to two special groups of people -the Palestine refugees and the civilians in Korea -andmade a survey of health conditions in Libya.
Palestine Refugees
The help given in maintaining a health programmefor some 800,000 refugees now living in areas ofLebanon, Syria, Jordan (including Arab Palestine)and the Gaza area was continued during 1950.
HEALTH SERVICES TO SPECIAL GROUPS 39
In 1949 this aid was given to UNRPR, the emergencyrelief organization for the refugees set up by theUnited Nations and three non -governmental organi-zations -the American Friends Service Committee,the International Committee of the Red Crossand the League of Red Cross Societies.55 On 1 May1950 the United Nations took over the entire projectin order to unify operations, and as the new pro-gramme called for the gradual termination of directrelief in favour of " works projects ", its namewas changed to " United Nations Relief and WorksAgency for Palestine Refugees in the Near East "(UNRWAPRNE). In the administration of thisproject the Agency has had the co- operation of thegovernments concerned - those of Egypt, theHashemite Kingdom of the Jordan, Iraq, Israel,the Lebanon, Saudi Arabia and Syria -and hasbeen assisted by several of the specialized agenciesand other organs of the United Nations.
During 1950 WHO's main contributions were theprovision of (a) staff specially assigned toUNRWAPRNE ; (b) technical advice from visitingexperts and (c) a grant of US $50,000.
In UNRWAPRNE, medical, health and sanitationactivities are centred in a medical branch, one ofseveral functional branches located at the head-
in Beirut. At the head is the Chief MedicalOfficer provided by WHO, and there are, in addition,a deputy chief, a malariologist (also from WHO),a sanitary engineer (loaned by WHO on a re-imbursable basis), a chief nurse and a supply officer.The health services in each district are headed by adistrict medical officer, who has a district nurse andsometimes another nurse and a sanitary officer onhis staff. Where there are sub- depots or laboratories,further appropriate staff is provided. This inter-national personnel, which WHO helped to recruit,numbers 30 for all districts ; the rest of the medicalbranch, comprising approximately 1,300 persons,were recruited locally and with a few exceptions arePalestine refugees.
In . addition to assigning permanent officers toUNRWAPRNE, WHO sent technical experts fromeither headquarters or the regional office in Alexan-dria to visit the area in which the Agency is operating,to survey the situation and make appropriaterecommendations. Among those sent in 1950 werea malaria sanitary engineer, a malariologist, anutrition expert, consultants in venereal diseases,
55 Off; Rec. World Hlth Org. 24, 24
bilharziasis, trachoma and nursing, public -healthadministrators, a planning officer, a specialist inhealth education, sanitary engineers and a publicinformation officer. Malaria -control and fly- controloperations were continued (see page 7) ; classesin health education were organized. The PublicInformation section of the Regional Office providednews coverage of some aspects of the health pro-gramme.
The grant of $50,000, which was voted by theSecond World Health Assembly for hygiene andsanitation purposes,56 was used to purchase all thematerials and equipment needed in the campaignsfor insect control.
The aim of the health work among the refugeeshas been to maintain the highest possible standardsof health until their problems have been settledand they are able to take care of themselves. Inspite of the abnormal conditions, both physicaland moral, under which the refugees are living(overcrowding, inferior housing, limited diet, home-lessness and lack of economic opportunity) the healthprogramme was showing positive results by the endof 1950, and a reasonable standard of health had beenattained.
In view of the limited funds available, emphasiswas placed on the prevention of communicablediseases through immunization, sanitation andinsecticide campaigns. No epidemics occurred, andthe incidence of preventable endemic diseases wasgenerally low. Sanitation, while elementary, seemedto be adequate for controlling filth and water -bornediseases in general : many improvements were beingplanned. With regard to the " works projects " putinto operation during the year, WHO was given theopportunity of surveying areas before these projectswere begun and of assessing possible health hazards,such as the danger of malaria and bilharziasis con-nected with plans for new schemes of housing,irrigation, etc.
Medical care, both in out -patient departments andin hospitals, was provided ; preventive dentistry,elective surgery and physical rehabilitation wereundertaken to a certain extent, but only after themore urgent problems had been met. The nutritionalstatus was found to be reasonably satisfactory, withonly minor dietary deficiencies and no cases of
56 Off. Rec. World Hlth Org. 21, 45
40 WORK OF WHO, 1950
starvation or semi -starvation. Medical supplieswere adequate.
Possibilities for training were not neglected. InNovember a symposium on the prophylactic andtherapeutic aspects of tropical diseases was arrangedjointly by the Department of Internal Medicine ofthe American University of Beirut, UNRWAPRNEand WHO. About 650 doctors from all parts of theregion attended this symposium, and twenty -onepapers were read by specialists in tropical medicine.The subjects reviewed included the control of malaria,tuberculosis, venereal diseases, typhoid fever, bru-cellosis and amoebiasis ; the treatment of diarrhoealand enteric diseases ; maternal and child care ;sanitation, and health education. The majority ofthe UNRWAPRNE doctors had the opportunityof participating in this symposium.
The future of the health programme among thePalestine refugees is dependent upon many otherfactors. Reports received suggest that it should becontinued even after the United Nations has stoppedgiving direct relief, but that greater emphasis shouldprobably be placed on public health. With thedevelopment of the " works projects ", and as therefugees become self -supporting, it is expected thatthey, individually or through their governments,will provide their own clinical medical services andwill ultimately take over the health programmeitself.
Aid to Korea
On 31 July the Security Council called upon organsof the United Nations, its specialized agencies andappropriate non -governmental organizations toprovide assistance to the Unified Command inKorea for the relief and support of the civilianpopulation.
WHO immediately complied by offering anyassistance which it could provide, and was askedto furnish medical and sanitary personnel to servein Korea under the Unified Command : a director
to co- ordinate health and welfare services and to actas adviser to the government ; a public -health officerto assist the Ministry of Health ; an administrativeofficer, and five teams, each composed of one medicalofficer (primarily trained in public health) and onesanitary engineer, to help to organize health servicesand relief programmes.
At the end of the year all this medical staffwas on duty in Korea, and a second administrativeofficer, requested in November, was being recruited.WHO, on the request of the United Nations, hadalso promised to supply five more teams.
In addition to responding to the call of the SecurityCouncil, the Organization, along with the UnitedNations and other agencies, has made plans toimplement the resolutions on aid to Korea which wereadopted by the Economic and Social Council andthe General Assembly."
Health Conditions in Libya
At the request of the United Nations High Com-missioner for Libya and in conjunction with thestudy carried out by a United Nations preparatorymission on technical assistance, a representativeof WHO made a survey of the health conditions inthis territory in the middle of the year. His reportswere sent to the United Nations. As a result of hisrecommendations and those of the head of theUnited Nations Mission to Libya, a consultant inpublic -health administration is to be sent in January1951 on a year's assignment. This consultant willadvise on the implementation of the public- healthaspects of a technical assistance survey which isbeing made, and will help to draw up a plan for theeconomic, social and cultural development of Libya,as recommended by the General Assembly of theUnited Nations.b8
" UN document A.159568 UN document A.1533
INTERNATIONAL CONVENTIONS, AGREEMENTS AND REGULATIONS ON HEALTH
WHO shall " propose conventions, agreements and regulations ... with respectto international health matters and ... perform such duties as may beassigned thereby to the Organization and are consistent with its objective ".
In 1950 WHO's main contribution to new inter-national legislation on health matters was theconsiderable amount of work carried out in connexionwith the preparation of the draft International
Sanitary Regulations. Other action in this sphereincluded advice given to the United Nations regardingadministration of the Paris Protocol of 19 November1948 and preparation of a new unified convention
INTERNATIONAL CONVENTIONS, AGREEMENTS AND REGULATIONS ON HEALTH 41
on narcotic drugs, and the information supplied togovernments on the status of WHO RegulationsNo. 1 regarding nomenclature.
Nomenclature of Diseases and Causes of Death
For the vast majority of Member States, WHORegulations No. 1 regarding Nomenclature (includingthe Compilation and Publication of Statistics) withrespect to Diseases and Causes of Death 69 cameinto force on 1 January 1950. The SupplementaryRegulations adopted in 1949 80 provide for them tobecome applicable at a later date to countriesjoining the Organization after their adoption by theFirst World Health Assembly. In 1950 the Regula-tions and the Supplementary Regulations weresent to the Office of the Secretary - General of theUnited Nations, where they were registered underNo. 847 of 8 June. They were also notified to thenew Member States and the new Associate Member.By the end of the year no notification of rejectionhad been received although reservations or sugges-tions concerning them had been made by certaincountries, namely, in 1949, by Australia, Burma,Ceylon, China, Iceland, India, Israel, New Zealand,Sweden, the Union of South Africa and the UnitedKingdom and, in 1950, by Pakistan, SouthernRhodesia, Switzerland, Viet Nam and Yugoslavia.Hungary, in 1949, reserved the right to send inreservations, but has not done so. The full text ofthe comments made by the various countries wasbrought to the attention of all Members of WHO.
Details of work done during the year on theManual of the International Statistical Classificationof Diseases, Injuries and Causes of Death, 81 on whichthe Regulations are based, are given on page 47.
Preparation of International Sanitary Regulations
The Fourth World Health Assembly will have theimportant responsibility of adopting InternationalSanitary Regulations to replace the existing Inter-national Sanitary Conventions. Work on theseregulations has been going on for several years.After a set of principles to govern the SanitaryRegulations had been approved by the SecondWorld Health Assembly, draft regulations wereprepared in December 1949 by the Expert Committeeon International Epidemiology and Quarantine.At the fifth session of the Executive Board it wasdecided that the draft regulations should be sub-
69 Off. Rec. World Hlth Org. 13, 34980 Off. Rec. World Hlth Org. 21, 38361 The Manual was published in English as Supplement I
(1948) to the Bulletin of the World Health Organization.
mitted to a legal sub -committee and that the text, asamended, should then be sent to governments andappropriate international bodies for comment.88A legal sub -committee was therefore created ; itmet twice in the spring, first between 3 and 6 Februaryand then between 13 and 21 March, to revise thetexts, which were completed and forwarded togovernments early in April. In October, the expertcommittee held its third session : it examined andincorporated, where practicable, suggestionsforwarded by some 30 governments and inter-national bodies and recommendations for thedisinsection of ships and aircraft submitted by theExpert Committee on Insecticides. The text thusamended was again revised by the Legal Sub-Committee, which held a third session early inNovember. The draft regulations will be consideredin April 1951 by a special committee of the HealthAssembly, composed of delegations from MemberStates and comprising epidemiologists, legal experts,and experts in quarantine and transportation.During or immediately after the session of thespecial committee, final texts of the regulations willbe prepared for adoption by the Fourth WorldHealth Assembly.
The draft regulations cover the " pestilential "diseases (cholera, plague, yellow fever, smallpoxand typhus) and relapsing fever, and include inannexes special clauses relating to the Pilgrimageto Mecca (the sanitary control of pilgrim traffic,and standards of hygiene and welfare on pilgrimships and aircraft carrying pilgrims).
Attention may be called to the fact that althoughthe regulations do not differ in essentials from theSanitary Conventions which preceded them, theirlegal status is entirely different and will greatlyfacilitate their adaptation to new scientific ortechnical developments. The Sanitary Conventions,being international treaties, required formal ratifica-tion by the parliaments of all the countries whichadopted them. The procedure was a cumbersomeone and could be resorted to only when changesbecame absolutely imperative. The regulations, onthe other hand, can be amended by decision of theWorld Health Assembly, which has also the powerto adopt " Recommended Practices " to help healthadministrations fulfil their obligations under theregulations. In addition, the Assembly can alsoadopt additional regulations covering diseases otherthan those covered by the text now underconsideration.
The protocolary clauses of the regulations areworded so that a government which does not wish
62 Off. Rec. World Hlth Org. 25, 4
42 WORK OF WHO, 1950
to accept any particular article of the regulations isstill bound by the corresponding article of theSanitary Conventions. This has been done to facili-tate the transfer from the conventions to the regula-tions and the acceptance of the regulations withoutreservations.
Details of the administration of the existingSanitary Conventions are given on page 43.
Addiction -Producing Drugs
It will be recalled that, when the activities of theLeague of Nations were taken over by the UnitedNations, the international control of addiction -producing drugs, under the 1925 and 1931 conven-tions, was also automatically transferred andentrusted to the Commission on Narcotic Drugs ofthe Economic and Social Council. In the same way,the technical and advisory obligations in the enforce-ment of these conventions, which had been theresponsibility of the League of Nations HealthOrganization, devolved upon WHO.
A new single convention is to be prepared by theUnited Nations, embodying the various conventionsand protocols now in force. In the meantime,by the Paris Protocol of 1948, which came intoeffect on 1 December 1949, as described in theAnnual Report of the Director- General for 1949,drugs outside the scope of the 1931 Conventionwere brought under international control, and ameans was provided of controlling new syntheticdrugs which are found to be addiction -producing.
It was expected that, soon after the Protocolhad become effective, governments would sendnotifications of new synthetic substances to theSecretary - General of the United Nations, whowould request WHO to give its opinion on theiraddictive or non- addictive character. Therefore, asearly as January 1949, the Expert Committee onDrugs Liable to Produce Addiction (then knownas the Expert Committee on Habit- Forming Drugs)considered at its first session the substances concernedand made recommendations regarding them. 63
However, up to January 1950 very few such notifica-tions had been received and the expert committee,therefore, at its second session,s" confirmed itsprevious recommendations in general terms. Itparticularly stressed the danger in the use of thesubstance known as keto- bemidone and referred tofurther research work done on acetyl- methadoneand the addiction liability of 3- hydroxy -N- methyl-morphinan.
ea Off Rec. World Hlth Org. 19, 2964 World Hlth Org. techn. Rep. Ser. 1950, 21
One of the main tasks confronting the committeeat this session was to provide definitions, on therequest of the Commission on Narcotic Drugs, for" drug addiction ", " addiction -forming drugs "," habit -forming drugs " and the " fundamentalstructure of addiction- producing drugs ". As aresult of the definitions it established, the expertcommittee proposed that its name be changed from" Expert Committee on Habit -Forming Drugs " to" Expert Committee on Drugs Liable to ProduceAddiction ", as better corresponding to the scientificaspect of the subject.65 This change of title was laterconfirmed by the Executive Board.66 The committeerecommended that in the future as sharp a distinctionas possible should be drawn between addiction -producing drugs and substances which might giverise to a certain habit.
With regard to a request from the SwissGovernment for the exemption of the preparation" Ipecopan " from the provisions of the 1925Convention, the expert committee was of the opinionthat this exemption should not be granted. Thisopinion was notified to the Economic and SocialCouncil for transmission to the Swiss Government.As for a request from France for the classificationof a new product, morpholylethylmorphine, inGroup II of Article 1 of the 1931 Convention, it wasdecided that as an ether of morphine (other thanmethylmorphine and ethylmorphine), this substancebelonged by definition to sub -group b of Group Iof the 1931 Convention ; it was considered that theavailable evidence did not permit a decision to bemade on its addiction -producing properties and,in the absence of specific evidence to the contrary,that it was probably convertible to morphine. Thisopinion was communicated to the Secretary -Generalof the United Nations.
Diacetylmorphine (heroin) was given specialconsideration in the light of the information whichhad been obtained on its use in various countries.Although some countries had submitted smaller
G5 The distinction made between these two types of drugswas as follows : " Drug addiction is a state of periodic orchronic intoxication, detrimental to the individual and tosociety, produced by the repeated consumption of a drug(natural or synthetic). Its characteristics include : (1) an over-powering desire or need (compulsion) to continue taking thedrug and to obtain it by any means ; (2) a tendency to increasethe dose ; (3) a psychic (psychological) and sometimes aphysical dependence on the effects of the drug. An addiction -producing drug is one which produces addiction as defined." A habit-forming drug is one which is or may be takenrepeatedly without the production of all of the characteristicsoutlined in the definition of addiction and which is notgenerally considered to be detrimental to the individual andto society."
66 Off. Rec. World Hlth Org. 25, 8
EPIDEMIOLOGICAL INFORMATION 43
estimates of the use of diacetylmorphine for 1950,there existed information that in others the pro-duction of the drug was still on the increase. Severalimportant countries continued to maintain that theirphysicians considered it indispensable for certainmedical uses. On the proposal of the expert com-mittee, the Executive Board requested the Director -General to take steps to secure further informationfrom Member States on the use or dispensabilityof diacetylmorphine throughout their countries. s'To the inquiry which was accordingly made on thissubject, 32 answers were received by the end ofthe year : 19 governments expressed themselves asbeing in favour of the dispensability of diacetyl-morphine ; five as wishing to retain its use ; otherspromised to communicate further.
Among other subjects which came before thecommittee were the present status of drug addictionin India and chronic barbiturate intoxication.
The committee recommended the convening ofmeetings of experts on drug addiction and alcoholismplanned by the Expert Committee on Mental Health,which it considered to be of great importance (seepage 23).
67 Off. Rec. World lilth Org. 25, 8
During the year, WHO, through contact withresearch workers and producers and the generalchecking of literature, has kept abreast of develop-ments in the new synthetic substances of the pethidineand methadone types, some of which have effectson which there is not yet general agreement. Specialtechnical advice on these substances was given toGreece, at the request of the Government.
WHO has also given advice to other bodies of theUnited Nations, particularly the Permanent CentralOpium Board and the Supervisory Body. It hasalso maintained close relations with the ECOSOCCommission on Narcotic Drugs and the NarcoticsDivision of the United Nations.
As to problems of alcohol, pharmacologicalquestions regarding its effect, as well as the etiological,therapeutic and social aspects of alcoholism, havebeen under consideration. Special attention wasgiven to tetraethylthiuram disulphide (known underthe names of antabuse, abstinyl, refusal and others)and to the results and side reactions of its use as anauxiliary aid in the treatment of alcoholics. WHOcarried out investigations on this drug in Denmarkand Sweden- countries with wide experience in itsuse. The question of alcohol and traffic was consi-dered to be of special importance in the " preventionof accidental injuries " (see page 26).
EPII)ENiIOLOGICAL INFORMATION
WHO shall " establish and maintain such ... technical services as may be required,including epidemiological... services ".
Work on international epidemiology proceeded inthe following two main directions : (1) the administra-tion of existing International Sanitary Conventions,including the operation of epidemiological intelligenceservices and the settlement of quarantine disputes,and (2) research on communicable diseases, withthe furnishing of technical advice to health adminis-trations in the form of expert committees' reports(see page 12). In addition, technical advice was given,on request, to a number of countries on methodsfor the control of a series of communicable diseases.Activities carried out in the preparation of theSanitary Regulations to replace the InternationalSanitary Conventions, are described on page 41.
Administration of International Sanitary ConventionsEpidemiological Intelligence
One of the most important fields of application ofthe International Sanitary Conventions in force is
the collection by WHO of information on thepresence or movement of the pestilential diseases,i.e., of cholera, plague, smallpox, typhus and yellowfever, in the various territories of the world, andmore particularly in seaports and airports. Notifica-tion of these diseases to WHO is one of the essentialobligations laid on countries by the InternationalSanitary Conventions. WHO, in turn, again inaccordance with the Conventions, makes everyeffort to provide national and local health- administra-tions with the information thus collected, in orderto enable them to take immediate measures for theirprotection, or conversely, to withdraw quarantinemeasures when they became unnecessary.
WHO continued to make full use of the mostmodern means of distributing this information, notonly by the dispatch of telegrams to countries inclose relationship with infected areas, but by regular
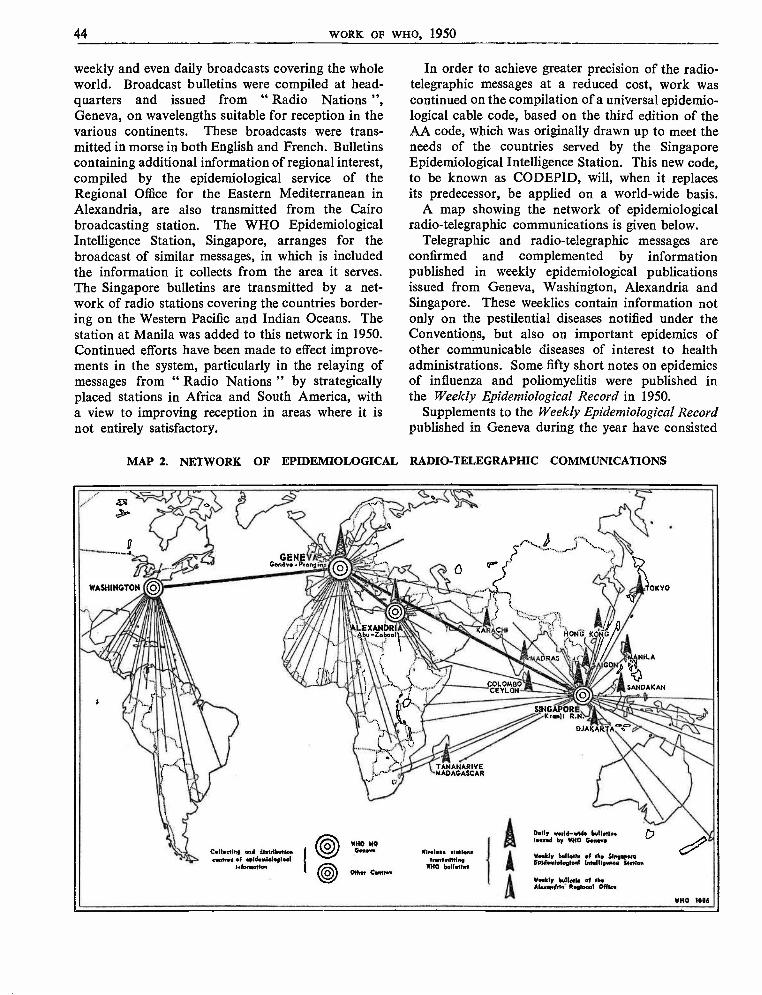
44 WORK OF WHO, 1950
weekly and even daily broadcasts covering the wholeworld. Broadcast bulletins were compiled at head-quarters and issued from " Radio Nations ",Geneva, on wavelengths suitable for reception in thevarious continents. These broadcasts were trans-mitted in morse in both English and French. Bulletinscontaining additional information of regional interest,compiled by the epidemiological service of theRegional Office for the Eastern Mediterranean inAlexandria, are also transmitted from the Cairobroadcasting station. The WHO EpidemiologicalIntelligence Station, Singapore, arranges for thebroadcast of similar messages, in which is includedthe information it collects from the area it serves.The Singapore bulletins are transmitted by a net-work of radio stations covering the countries border-ing on the Western Pacific and Indian Oceans. Thestation at Manila was added to this network in 1950.Continued efforts have been made to effect improve-ments in the system, particularly in the relaying ofmessages from " Radio Nations " by strategicallyplaced stations in Africa and South America, witha view to improving reception in areas where it isnot entirely satisfactory.
In order to achieve greater precision of the radio-telegraphic messages at a reduced cost, work wascontinued on the compilation of a universal epidemio-logical cable code, based on the third edition of theAA code, which was originally drawn up to meet theneeds of the countries served by the SingaporeEpidemiological Intelligence Station. This new code,to be known as CODEPID, will, when it replacesits predecessor, be applied on a world -wide basis.
A map showing the network of epidemiologicalradio -telegraphic communications is given below.
Telegraphic and radio -telegraphic messages areconfirmed and complemented by informationpublished in weekly epidemiological publicationsissued from Geneva, Washington, Alexandria andSingapore. These weeklies contain information notonly on the pestilential diseases notified under theConventions, but also on important epidemics ofother communicable diseases of interest to healthadministrations. Some fifty short notes on epidemicsof influenza and poliomyelitis were published inthe Weekly Epidemiological Record in 1950.
Supplements to the Weekly Epidemiological Recordpublished in Geneva during the year have consisted
MAP 2. NETWORK OF EPIDEMIOLOGICAL RADIO -TELEGRAPHIC COMMUNICATIONS
SINGAPORE `t 'K ranii R.N.
DJAKARTA
C.tleetiny and distributioncentres el pideataleyleel
tnkmetten
Weekly Iwll.tie of the 5lnyeponEyid.eleleptevl Intellip.nev Nolen
EPIDEMIOLOGICAL INFORMATION 45
of a list of the inoculation and vaccination certificaterequirements of countries, a list of ports qualifiedto carry out deratting of ships and to issue derattingor deratting exemption certificates, and an addendumto the first list of ports accepting internationalquarantine messages by wireless. Maps showing theyellow -fever endemic areas as delineated by theWHO Yellow -Fever Panel have also been included.
Similarly, supplements to the Weekly Fasciculusof the Singapore Epidemiological Station containedcumulative data on pestilential and other com-municable diseases occurring during 1949 in theterritories of the area served by that station.
About thirty requests from health administrationsfor technical advice on the control of communicablediseases and quarantine matters generally wereanswered during the year.
Settlement of International Quarantine DisputesDuring the same period WHO dealt with 28 inter-
national disputes arising out of the application of theSanitary Conventions ; of that number 25 weresettled by the Secretariat, one is in the course ofsettlement, and two were placed on the agenda of thethird session of the Expert Committee on Inter-national Epidemiology and Quarantine (9 -18 Octo-ber), since the efforts of WHO, which included inone case, discussions at the Third World HealthAssembly,68 were ineffective in reaching a solution.These two disputes were considered by the expertcommittee in plenary session, and not, as is usual, byits Section on Quarantine.
The first case before the committee related tocomplaints made by the Governments of India andPakistan against the anti- cholera measures imposedby the Government of Saudi Arabia on pilgrimsdesiring to proceed from India or Eastern Pakistanto the Hedjaz. After having heard statements byrepresentatives of the Governments concerned, andhaving taken all available evidence into account,the committee decided that the requirement of theSaudi Arabian Government for stool examinationsof pilgrims before departure, with appropriatecertifications, was in excess of the provisions of theexisting International Sanitary Conventions. Thecommittee also decided that present epidemiologicalevidence did not justify this requirement.
The second case was a protest by the UnitedKingdom against regulations recently introduced bythe Egyptian Government which required healthypassengers disembarking in Egypt, after passingthrough or embarking in cholera -infected areas, toundergo stool examinations. In this connexion the
68 Resolution WHA3.56, Of. Rec. World Hlth Org. 28, 35
committee took the view that such examinations arepermitted under Article 33 of the InternationalSanitary Convention of 1926 and under Article 30,read with Article 26 of the International SanitaryConvention for Aerial Navigation of 1933. Thecommittee nevertheless considered that such examina-tions should be confined strictly to persons comingfrom infected local areas and should be employedwith discretion.
During 1950, the Singapore Station and theRegional Office in Alexandria also negotiatedseveral complaints and appeals on the applicationof quarantine measures in territories lying withintheir spheres of competence.
Epidemiological Information on CommunicableDiseases
In addition to receiving and distributing notifica-cations relating to pestilential diseases, WHO hascollected, studied and published information on themore important communicable diseases. An epidemicwatch unit carefully goes through the 105 epidemio-logical reports covering weekly or ten -day periods,the 100 monthly reports and the quarterly and annualreports received by the Division of EpidemiologicalServices. In all, some 6,500 documents covering170 countries or territories and relating to 12 to15 diseases each are thus examined and abstractedin the course of a year. Graphs relating to 16 diseasesin 44 countries make it possible to check up rapidlyon any abnormality in their trend.
Watch is also kept over selected daily newspapersin a number of countries for information on theprevalence of disease. This information, however, isnever used without official confirmation.
The numerical data extracted from the manynational reports mentioned above are tabulated andpublished from time to time in the monthly Epidemio-logical and Vital Statistics Report. This periodicalalso includes tables on births, infant deaths andgeneral mortality (see page 47) and articles concerningthe geographical distribution and trend of com-municable diseases as well as demographic facts.In 1950 there appeared articles on poliomyelitis from1947 to 1949, human rickettsioses in Africa, entericfevers in 1949 and 1950, the evolution of mortalityin Europe during the twentieth century, births,general mortality and infantile mortality in 1949 andtuberculosis mortality. (A selected list of technicalarticles published during the year is given inannex 10.)
Work was continued on the preparation of theAnnual Epidemiological and Vital Statistics, coveringthe war and post -war periods.
46 WORK OF WHO, 1950
HEALTH STATISTICS
WHO shall " establish and maintain such ... technical services as may be required,including... statistical services ";" establish and revise as necessary international nomenclatures of diseases, ofcauses of death and of public- health practices ".
WHO's programme of health statistics wasexpanded during the year, in accordance with reso-lutions WHA2.38, WHA2.39 and WHA2.40 of theSecond World Health Assembly.
The Expert Committee on Health Statistics heldits second session in Geneva from 18 to 21 April.This session was immediately preceded by meetingsof the three sub- committees established by theExecutive Board at its fourth session : 69 the Sub -Committee on the Definition of Stillbirth andAbortion met in Paris from 27 February to 3 March ;the Sub -Committee on the Registration of Casesof Cancer as well as their Statistical Presentationmet, also in Paris, from 6 to 10 March ; and theSub -Committee on Hospital Statistics met in Genevafrom 11 to 14 April.
After reviewing the work of the three sub-committees, the expert committee adopted theirreports with minor amendments and some commentswhich appear as footnotes to the printed reports.'°One of the most important recommendations of theexpert committee was for the adoption of thesuggested definitions of " live birth " 71 and " foetaldeath ", 72 of a directive for the registration and
69 Off Rec. World Hlth Org. 22, 370 World Hlth Org. techn. Rep. Ser. 1950, 2571 " Live birth is the complete expulsion or extraction from
its mother of a product of conception, irrespective of theduration of pregnancy, which, after such separation, breathesor shows any other evidence of life, such as beating of theheart, pulsation of the umbilical cord, or definite movementof voluntary muscles, whether or not the umbilical cord hasbeen cut or the placenta is attached ; each product of such abirth is considered live- born." (World Hlth Org. techn. Rep.Ser. 1950, 25, 12
72 " Foetal death is death prior to the complete expulsionor extraction from its mother of a product of conception,irrespective of the duration of pregnancy ; the death is indicatedby the fact that after such separation the foetus does notbreathe or show any other evidence of life, such as beatingof the heart, pulsation of the umbilical cord, or definite move-ment of voluntary muscles." (World HIM Org. techn. Rep.Ser. 1950, 25, 12)
tabulation of live births and infant deaths,73 and of astatistical definition of cancer. 74 All these wereadopted by the Third Health Assembly (in resolutionWHA3.6) as recommendations under Article 23of the Constitution and Article 17 of WHO Regula-tions No. 1, and were transmitted to governments.
The definitions of " live birth " and " foetaldeath " are of the utmost importance to vitalstatistics, particularly in the international compara-bility of data and the establishment of some of themost important indices in health work. Efforts toreach international agreement on these definitionshave been made from the time of the League ofNations Health Organization. However, as nowformulated, they appear to meet the objectionsraised to those formerly proposed. Their adoptionby as many governments as possible in the statisticalcollection and presentation of data at least, if notin the legal sense, should be encouraged, and willmark a definite step forward.
On the recommendations of the sub -committeesthe expert committee also decided upon problems tobe suggested for study to national committees onvital and health statistics (or their equivalents).75Because of the great variety and complexity of these
73 " All live -born infants should be registered and countedas such irrespective of the period of gestation, and if they dieat any time following birth they should also be registeredand counted as deaths." (World Hlth Org. techn. Rep. Ser.1950, 25, 12)
74 " (a) Total cancer deaths should be based uponnos. 140 -205 of the International Statistical Classification(1948).
(b) For comparability with the past, the following sub-groups should also be shown :
(i) Cancer excluding Hodgkin's disease, leukaemia andaleukaemia -nos. 140 -205, except 201 and 204.
(ii) Hodgkin's disease -no. 201.(iii) Leukaemia and aleukaemia -no. 204." (World filth
Org. techn. Rep. Ser. 1950, 25, 19)75 World Hlth Org. techn. Rep. Ser. 1950, 25
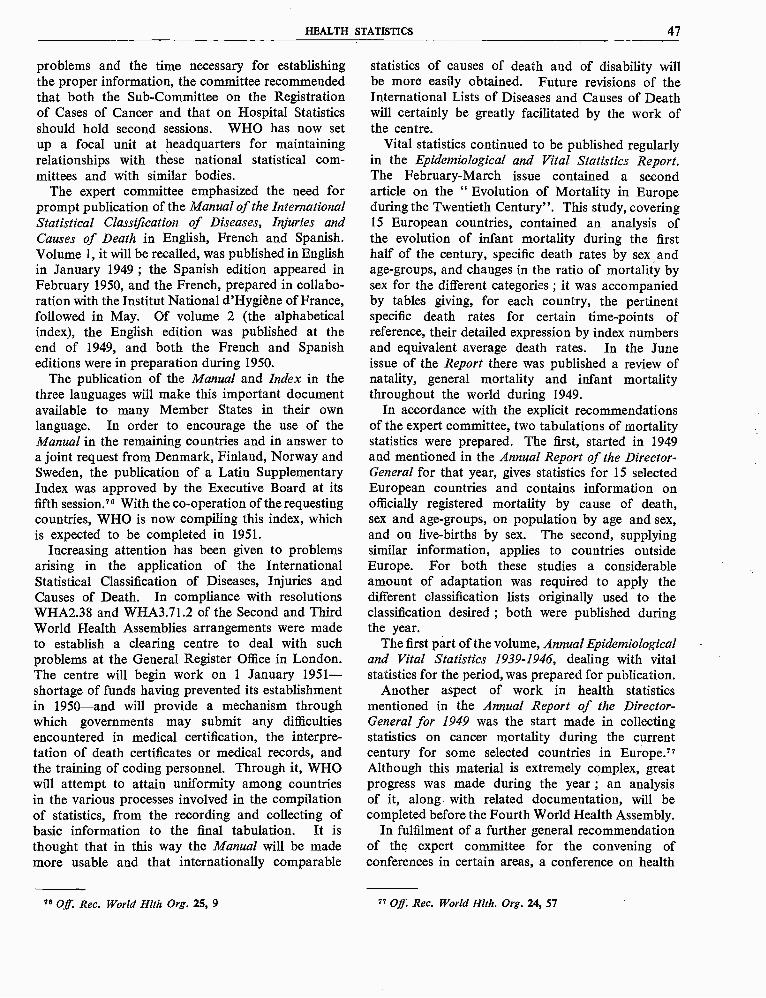
HEALTH STATISTICS 47
problems and the time necessary for establishingthe proper information, the committee recommendedthat both the Sub -Committee on the Registrationof Cases of Cancer and that on Hospital Statisticsshould hold second sessions. WHO has now setup a focal unit at headquarters for maintainingrelationships with these national statistical com-mittees and with similar bodies.
The expert committee emphasized the need forprompt publication of the Manual of the InternationalStatistical Classification of Diseases, Injuries andCauses of Death in English, French and Spanish.Volume 1, it will be recalled, was published in Englishin January 1949 ; the Spanish edition appeared inFebruary 1950, and the French, prepared in collabo-ration with the Institut National d'Hygiène of France,followed in May. Of volume 2 (the alphabeticalindex), the English edition was published at theend of 1949, and both the French and Spanisheditions were in preparation during 1950.
The publication of the Manual and Index in thethree languages will make this important documentavailable to many Member States in their ownlanguage. In order to encourage the use of theManual in the remaining countries and in answer toa joint request from Denmark, Finland, Norway andSweden, the publication of a Latin SupplementaryIndex was approved by the Executive Board at itsfifth session.76 With the co- operation of the requestingcountries, WHO is now compiling this index, whichis expected to be completed in 1951.
Increasing attention has been given to problemsarising in the application of the InternationalStatistical Classification of Diseases, Injuries andCauses of Death. In compliance with resolutionsWHA2.38 and WHA3.71.2 of the Second and ThirdWorld Health Assemblies arrangements were madeto establish a clearing centre to deal with suchproblems at the General Register Office in London.The centre will begin work on 1 January 1951 -shortage of funds having prevented its establishmentin 1950 -and will provide a mechanism throughwhich governments may submit any difficultiesencountered in medical certification, the interpre-tation of death certificates or medical records, andthe training of coding personnel. Through it, WHOwill attempt to attain uniformity among countriesin the various processes involved in the compilationof statistics, from the recording and collecting ofbasic information to the final tabulation. It isthought that in this way the Manual will be mademore usable and that internationally comparable
76 Off. Rec. World Hlth Org. 25, 9
statistics of causes of death and of disability willbe more easily obtained. Future revisions of theInternational Lists of Diseases and Causes of Deathwill certainly be greatly facilitated by the work ofthe centre.
Vital statistics continued to be published regularlyin the Epidemiological and Vital Statistics Report.The February -March issue contained a secondarticle on the " Evolution of Mortality in Europeduring the Twentieth Century ". This study, covering15 European countries, contained an analysis ofthe evolution of infant mortality during the firsthalf of the century, specific death rates by sex andage -groups, and changes in the ratio of mortality bysex for the different categories ; it was accompaniedby tables giving, for each country, the pertinentspecific death rates for certain time -points ofreference, their detailed expression by index numbersand equivalent average death rates. In the Juneissue of the Report there was published a review ofnatality, general mortality and infant mortalitythroughout the world during 1949.
In accordance with the explicit recommendationsof the expert committee, two tabulations of mortalitystatistics were prepared. The first, started in 1949and mentioned in the Annual Report of the Director -General for that year, gives statistics for 15 selectedEuropean countries and contains information onofficially registered mortality by cause of death,sex and age -groups, on population by age and sex,and on live- births by sex. The second, supplyingsimilar information, applies to countries outsideEurope. For both these studies a considerableamount of adaptation was required to apply thedifferent classification lists originally used to theclassification desired ; both were published duringthe year.
The first part of the volume, Annual Epidemiologicaland Vital Statistics 1939 -1946, dealing with vitalstatistics for the period, was prepared for publication.
Another aspect of work in health statisticsmentioned in the Annual Report of the Director -General for 1949 was the start made in collectingstatistics on cancer mortality during the currentcentury for some selected countries in Europe."Although this material is extremely complex, greatprogress was made during the year ; an analysisof it, along with related documentation, will becompleted before the Fourth World Health Assembly.
In fulfilment of a further general recommendationof the expert committee for the convening ofconferences in certain areas, a conference on health
77 Off. Rec. World Hlth. Org. 24, 57
48 WORK OF WHO, 1950
statistics was held at Istanbul in September, followingthe meeting of the Regional Committee for theEastern Mediterranean. This conference, organizedby the Regional Director and attended by delegatesfrom countries in the region, recommended theestablishment of national committees and trainingcourses. The possibility of setting up a trainingcentre under the technical assistance programme isnow being considered with the United Nations.
Before the conference, a preliminary survey of vitaland health statistics was made in several countriesof the region ; consultations were held withresponsible central health and statistical authorities,and suitable measures of collaboration with WHO
were discussed, with a view to helping to improve thecollection of national vital and health statistics.Some of the possible means of assistance mentioned,such as fellowships and training courses, will beprovided by WHO in 1951 and 1952, if the budgetpermits.
During the year, the Organization was able toanswer many requests for information on morbidityand mortality statistics from governmental or semi-official agencies, responsible institutions and indivi-duals. The register of demographic informationwhich was built up during the year, greatly facilitatedthis task of giving information and advice.
Three fellowships in vital statistics were awarded.
INTERNATIONAL STANDARDS AND PHARMACOPOEIA
WHO shall " develop, establish and promote international standards with respectto food, biological, pharmaceutical and similar products "; " standardizediagnostic procedures as necessary ".
It is principally in biological standardization, theunification of pharmacopoeias and the very importantwork being carried on by the Tuberculosis ResearchOffice that WHO has continued to carry outthese functions.
Biological Standardization
The recommendations made by the Expert Com-mittee on Biological Standardization at its thirdsession (May 1949) entailed a considerable amountof work, which had to be completed before thecommittee could usefully meet again. For thisreason it was not possible to hold the fourth sessionearlier than November 1950, and during the yearthe main activities in biological standardization weredirected towards the carrying out of the programmerecommended by the expert committee at its thirdsession. The following are of special note :
Cholera VaccineFrom further work performed on the antigenic
analysis of cholera vibrios, it seems that there is
no evidence that freeze -dried 0 antigens to be usedfor rabbit immunization in the production ofdiagnostic antisera lack the factors necessary foridentitifying true cholera vibrios. The expertcommittee, therefore, at its fourth session, authorizedthe establishment of these dried standard preparationsof the Ogawa and Inaba types of cholera vibrios,and arranged for the Haffkine Institute in Bombayto distribute freeze -dried cultures of its challengestrains (of Vibrio cholerae) to interested workers.
The monospecific antisera were prepared by theKasauli Institute and dispatched to Copenhagen,and a further 200 ml is being held at the dispositionof the committee. Using the three freeze -driedcholera vaccines of known potency, which wereprepared in the Haffkine Institute, the StatensSeruminstitut at Copenhagen was authorized tobegin a collaborative assay of the provisionalreference vaccine, in order to determine whether itshould be adopted as the international referencepreparation. Participants in the collaborative testswill be asked to carry out assays by using (1) aspecified method and (2) any other method whichthey may chose.
INTERNATIONAL STANDARDS AND PHARMACOPOEIA 49
MAP 3. BIOLOGICAL STANDARDS
', Addl-ALt
.. ,L.' Co. tshoCiJ
Cape Town
ati World centre.Centres ma thous '
e Notional centres related ro world centresCentre. nationaux rand. nun centres mondiaux
® Other national centre.Autres centres nationaux
:::I Countries receiving standards from the world entre.Paye centresdo. entree mondiaux
Dunedin
Pertussis Vaccine
A follow -up study has been undertaken to establishthe usefulness of the National Institutes of Health(NIH) turbidity standard in the enumeration oforganisms present in a pertussis vaccine. Lettersinviting comments were sent to the laboratoryworkers who applied to WHO for the NIH referencepertussis vaccine and turbidity standard. In thelight of information obtained, it was decided thatthe Statens Seruminstitut, Copenhagen, shouldestablish an opacity standard for the direct visualcharacterization of bacterial suspensions, using theNIH opacity standard suspension. A unitage is tobe assigned to it as the opacity of 10 provisionalunits per ml.
Diphtheria Toxoid
It has long been recognized that diphtheria toxoidpresents a very difficult problem for biologicalstandardization, and a considerable amount ofresearch on the subject has been carried out atCopenhagen and elsewhere. The committee con-sidered that it was not possible at this stage to
WHO 1087
establish a single international reference preparationwhich could be used for the standardization of alltoxoids, whether plain or adsorbed. It thereforerecommended the establishment of one internationalreference preparation of a plain diphtheria toxoidand a second of an aluminium phosphate adsorbedtoxoid. Further research will be carried out by theStatens Seruminstitut, Copenhagen, with a view todetermining the unitage of immunizing power tobe assigned to the two reference preparations.
Hormones
In view of the recent clinical importance of adreno-corticotrophic hormone (ACTH) in the treatmentof rheumatoid arthritis, a quantity from the ArmourLaboratories (which, according to the decision ofthe expert committee, is to constitute the inter-national standard) was obtained. It is proposed thatthe unit should be the activity contained in 1 mg.In the choice of such a relatively large weight ofmaterial, the convenience of the clinician is beingplaced before that of the assayist.
Reference preparations were established for twoother hormones, thyrotrophin and growth hormones.
50 WORK OF WHO, 1950
Streptomycin
For the international standard of streptomycin itis proposed that the NIH working standard beadopted instead of the NIH master standard, ashad been decided at the last session of the expertcommittee. The reasons which have led to thisdecision are that the working standard, which is thestreptomycin sulphate, is a purer preparation thanthe other ; it is also easier to handle, and furthermoreis available in greater quantities to the committee.It is proposed to fix the potency at 780 internationalunits (or microgram equivalents) per mg.
Smallpox Vaccine
The committee was requested by the Third WorldHealth Assembly to examine the question ofestablishing a centre for testing and standardizingsmallpox vaccines, with particular reference to driedvaccines. It considered that the keeping powers andpotency of dried vaccine lymph under tropicalconditions had not yet been proved superior tothose of glycerinated vaccine lymph. It suggestedan investigation of dried vaccines and indicated thelines along which such a study should be made.
BCG Vaccine and Tubercle BacilliAfter examining a request of the Expert Committee
on Tuberculosis, the committee agreed to investigatethe relative potency of freeze -dried and liquid BCGvaccines. It drew up a set of minimum standards forlaboratories engaged in the detection of tuberclebacilli.
UNICEF had asked the committee to undertakeperiodic activity- testing of BCG vaccine and toexamine possibilities of using the Paris BCG PilotStation, as mentioned in the Annual Report of theDirector- General for 1949. It was learned that thispilot station had been reorganized and that adjust-ments had been made in the personnel and financialprovisions. To comply with the proposal that thetask of testing the activity of the BCG vaccinesshould not remain with a single BCG pilot station,possibilities of establishing at least one other stationwere examined, and the committee recommendedthat the test centres of both Paris and Copenhagenshould be recognized as suitable for this purpose.
The expert committee was also requested to giveits approval of laboratories producing BCG vaccinesfor the UNICEF vaccination campaign. Accordingly,the BCG -producing laboratory in Mexico wasvisited in January, the laboratories of the InstitutPasteur Hellénique in Athens in April, those of theInstitut Pasteur in Tunis and Casablanca in July ;and those of Melbourne, Saigon and Formosa in
September and October. The vaccines prepared inMexico, Tunis and Casablanca were approved forgeneral use.
Blood -Grouping Reference Laboratory
The committee agreed to a proposal made by theCouncil of the International Society of Haematologyfor the establishment of an international blood -grouping reference laboratory, to be recognizedby WHO. It considered that international work inhaematology would be facilitated by the provisionof certain international standards of the commonerRh blood -grouping sera.
With regard to facilities for checking, providingand distributing the rarer blood -grouping sera, thecommittee suggested that WHO, after consultingwith the International Society of Haematology,should serve as a co- ordinating centre and shouldadvertise research laboratories willing to place theirfacilities at the disposal of interested research workers.
Other Recommendations of the Expert Committee
Following the recommendations of the Sub -Committee on Serology and Laboratory Aspects ofthe Expert Committee on Venereal Infections,possibilities of making cardiolipin (at presentprotected by patents) internationally available werediscussed, and the committee agreed to set upinternational standards for both cardiolipin andlecithin.
The Expert Committee on Antibiotics havingendorsed the opinion that the committee shouldestablish international reference preparations of newantibiotics as early as possible, the establishment ofan international standard for aureomycin and terra -mycin, and international reference preparations forchloramphenicol and bacitracin, was accordinglyrecommended. Furthermore, it was decided thatresearch workers who had isolated specimens ofcertain important antibiotics and had describedthem in scientific journals would be invited to depositthese specimens in a collection of " authors' pre-parations " for the benefit of all research workers.
Advice was given to the Expert Committee on theUnification of Pharmacopoeias in its work on thePharmacopoea Internationalis - in particular on thebiological assays contained in the appendices ofmonographs dealing with preparations for whichthere are international biological standards. Sincethe specifications for these assays have pointed tothe desirability of establishing certain referencepreparations, international standards are to be setup for oxophenarsine, dimercaprol and dextro-tubocurarine.
INTERNATIONAL STANDARDS AND PHARMACOPOEIA 51
International Salmonella CentreBy the end of the year, the International Salmonella
Centre in Copenhagen, maintained by WHO, hadestablished 37 salmonella centres all over the world(see map, p. 17).
Laboratories were supplied with 780 salmonellatest strains and 248 ampoules of salmonella testsera ; 459 strains were received from other labora-tories for diagnosis, mostly strains of the salmonellagroup. Among these strains were several new typeswhich were analysed, and the results were published.
The centre has also devoted part of its time to theEscherichia - Klebsiella group of micro -organisms.1146 Escherichia test strains and 68 ampoules ofEscherichia test sera were distributed to variouslaboratories during 1950.
Unification of Pharmacopoeias
The Third Health Assembly, in resolutionWHA3.10, approved the publication of the Pharma-copoea Internationalis and recommended that afterits provisions had been adopted by the appropriateauthorities of Member Governments, they should beincluded in the national pharmacopoeias.
In order to prepare definitive texts of the 245
monographs and appendices to be published inVolume I of the first edition, considerable work wasdone during the year. Special attention was givento the unification of symbols, nomenclature, expressions, structural formulae and general arrangementsthroughout. With the collaboration of all membersof the Expert Committee on the Unification ofPharmacopoeias, and after consultation with severalorganizations, it was possible to have second galleyproofs of the English text printed in time to beexamined at the sixth session of the expert committeein April.
During the revision of these texts, it was foundnecessary to include a number of additional mono-graphs and appendices. In accordance with newdevelopments, changes in the existing texts weremade, particularly in those concerning the antitoxicsera and their assays, which were modified on thebasis of advice from the Expert Committee onBiological Standardization. The final text of theTable of Usual and Maximal Doses for Adults wasalso prepared in collaboration with the WorldMedical Association.
As the expert committee can meet only twice ayear, final approval of a large part of the Englishand French texts was obtained through correspon-dence with the experts.
It had been recommended by the expert committeeand by the Executive Board that the French edition
should be published simultaneously with the English,unless too much time elapsed before the completionof the final French text. With the help of the expertfrom France and his assistants, it was found possibleto have French galley proofs revised by October,and both the English and French texts wereaccordingly in page proofs in the last month ofthe year. The two editions will therefore be issuedtogether, and will be available for sale and distribu-tion in 1951.
Arrangements were made for the translation of thePharmacopoea Internationalis into Spanish at theRegional Office for the Americas. It is expected topublish this first Spanish edition in the course of1951, and Spanish editions of supplements to thePharmacopoea Internationalis will appear shortlyafter those in English and French.
Preparatory work was also carried out by corre-spondence with members of the expert committeeon (a) the draft monographs and appendices forVolume II of the first edition of the PharmacopoeaInternationalis, and (b) questions to be studied duringthe two sessions of the expert committee held inApril and November, and at the one session of theSub- Committee on Non -Proprietary Names, inNovember.
On the invitation of the Board of Trustees of theUnited States Pharmacopoeia) Convention, theexpert committee held its sixth session in New Yorkfrom 20 to 29 April. For the most part, this sessionwas devoted to the consideration of 151 monographsand appendices which had been submitted by themembers for inclusion in Volume II of the firstedition. Comments obtained from other expertcommittees and organizations were also considered,and reports on injections, methods of sterilization,pyrogen tests and assays were amended or referredto the Chairman and Secretary of the committeefor revision.
At the seventh session, held at headquarters from30 October to 4 November, the committee considered178 new or revised drafts of monographs andappendices for Volume II of the first edition, as wellas a Table of Usual Doses of Drugs for Children.Many of these draft monographs and appendiceswere finished at the session, but, owing to lack of timeand in some cases, complete information, otherswere left for revision by correspondence. Manyof the drafts were submitted to specialists, and muchlaboratory work was done by the members of thecommittee.
Besides covering the new important drugs, parti-cularly antibiotics, Volume II will include mono-graphs and appendices on injections, tablets and
52 WORK OF WHO, 1950
tinctures, as well as on cardiolipin and purifiedlecithin, used for the serological test of syphilis.
For the purpose of supplying practical informationto the medical and pharmaceutical professions, alist of synonyms of drugs included in the first editionof the Pharmacopoea Internationalis, Volume I, hasbeen drafted. This list is to be issued as a supplementto the Bulletin of the World Health Organization.
The Third World Health Assembly and theExecutive Board recommended (in resolutionsWHA3.11 and EB6.R29) establishing a mechanismfor giving international non -proprietary names tothe new important drugs which might be includedin the Pharmacopoea Internationalis and its Supple-ments to avoid the difficulties caused by the multi-plication of non -proprietary names for new drugsmoving in international commerce, and the resultingconfusion in prescribing, dispensing and controllingthem. Member States were asked for their opinions.Replies received from 31 Member States andexamined by the Sub -Committee on Non -ProprietaryNames indicated approval of the scheme. Althoughthe large number of already- existing trade markswould not make it possible to devise names univer-sally acceptable, in all cases, those selected are tobe communicated to Member States with a recom-mendation that they be adopted for national andinternational use, and that adequate protectionbe granted to them on the national level. A numberof these international pharmacopoeial names wereselected at the session of the Sub -Committee onNon -Proprietary Names held on 6 and 7 November.
One of WHO's functions is to co- ordinate regula-tions and methods used by health administrationsin the control of drugs for the purposes of publichealth and international commerce. In implemen-tation of a recommendation of the Executive Board(in resolution EB6.R29). Member States were askedto furnish information on this subject which mightbe of use to national health -authorities of othercountries and the pharmacopoeial commissions.By the end of the year, 30 replies had been received,and it was planned to use this information inpreparing a conference on the control of drugs, tobe convened by WHO in 1952 or 1953 and attendedby representatives of national drug administrations.
The Organization also made arrangements togrant fellowships to pharmaceutical and pharma-copoeial workers in under- developed countries forperiods of two months to a year. Students who,under these fellowships will study problems in theestablishment of pharmacopoeial standards and inthe control of drugs, will be so selected that theirresearch and studies may be of general benefit to
the public- health authorities of their respectivecountries.
During the year, negotiations were continued withthe Belgian Government, and as a result thePermanent International Pharmacopoeia Secretariatwas placed under the aegis of WHO. Relations weremaintained with other WHO expert committees andwith international organizations, e.g., the WorldMedical Association, the International Union ofChemistry, and the International PharmaceuticalFederation, on subjects of mutual interest.
Tuberculosis Research Office
The scientific and investigative work of theTuberculosis Research Office has been furtherextended and the staff consequently increased. Theoffice itself, situated in Copenhagen, has administereda number of pilot stations -usually established inco- operation with local governments or tuberculosisoffices -in Austria, Egypt, Finland, Iceland andIndia.
On 28 December the office was moved to newquarters, which are very well suited to its needs.The Danish Government bought the premises andoffered them to the Research Office rent free as apermanent office.
During the year work proceeded with the JointEnterprise, and the compilation of the BCG campaignstatistics received from many countries was keptup to date as far as possible. Visits were made toseveral countries in Europe and to Africa, Americaand Asia to attend meetings, discuss plans andinspect or supervise the work. The Director andDeputy -Director visited headquarters in Decemberto discuss the work of the office and the 1951 and1952 budgets, and the WHO Assistant Director -General for Administration and Finance paid a visitto the Research Office to advise on negotiationswith the Danish Government.
A report on " Mass BCG Vaccination in Czecho-slovakia 1948 -1949 ", consisting of results obtainedfrom 3,328,810 persons tested and 2,118,562 vac-cinated, was published in September. The materialfrom Beirut (41,744 tests and 27,872 vaccinated)and from the Palestine refugee camps (208,374 testedand 149,013 vaccinated), together with tuberculinsensitivity curves by age for twelve countries parti-cipating in the campaign, was incorporated in a
Report of the Statistical Work in connexion withMass BCG Vaccination 1949 -1950 ", prepared at therequest at the Joint Enterprise.
As of 31 October preliminary data received fromcountries where the campaign had been completedor was still in progress indicated that a total of
INTERNATIONAL STANDARDS AND PHARMACOPOEIA 53
31,362,299 persons had been tested and 14,182,207vaccinated. Approximately 55 % of the detailed stati-stics on testing and 61 % of those on vaccination duringthe campaign were received by the end of the year.
A sampling survey of post- vaccination allergyhas been set up in Greece. Re- testing by speciallytrained teams was first begun in the school in Athens,where emphasis has been placed on determining theduration of tuberculin allergy and variations whichmay have resulted from different lots of BCG used.
The training of statisticians to do the field workfor the campaign was also continued. During theperiod under review, statisticians or statistical clerkssupervised field statistical offices in Austria, Ecuador,Egypt, Finland, Greece, India, Israel, Lebanon,Malta, Mexico, Syria and Yugoslavia.
While it is recognized that the only strictly scientificmethod for evaluating BCG is by a controlled studyin which one group is vaccinated and a comparablegroup is not, long -range projects based on the massBCG campaign should also be of great value inproviding information on the effectiveness ofvaccination. Such projects are under way in Finlandand Denmark.
As described in the Annual Report of the Director-
General for 1949, a programme, of a pilot nature,for the evaluation of the effect of the mass BCGvaccinations was set up last year in Finland, and anoffice was established in Helsinki to make a nationalroster of the tuberculin- tested and vaccinated duringthe Finnish campaign (which was completed during1948 -49). This roster covers the age group 1 -25
years ; punch card copies of about one million fieldrecords have now been made for a central file, topermit direct matching of current death certificatesfrom the Finnish Vital Statistics Office. A detailedanalysis of Finnish mortality statistics in tuber-culosis was made for the purpose of working outtuberculosis mortality trends based on pre- vaccina-tion experience. Thus, the observed tuberculosismortality of the vaccinated may be compared withthat of the natural reactors to tuberculin and withthe expected trends.
In Denmark, in the spring of 1950, the DanishTuberculosis Mass Campaign was begun, with aprogramme of tuberculin testing and BCG vaccina-tion of all persons in the country (except in Copen-hagen), between the ages of 1 and 6, and 15 and 34.An estimated .1,400,000 people will be tested withinthe three years planned for this work, and mobilemicro- photofluorographic units are being used toexamine adolescents and adults. Because of theexcellent diagnostic facilities in Denmark, thecampaign will provide an unusually fine opportunity
for studying tuberculosis morbidity in conjunctionwith data on tuberculin testing and vaccination.The Research Office has selected a tuberculosisspecialist to take charge of the research project andhas detailed one trained statistician as his assistant.It has also agreed to help finance and assist in thesetting up of a national roster for the collection andanalysis of statistical data from the campaign and forfollow -up evaluation in terms of morbidity andmortality. Detailed analytical study of Danish mor-tality statistics in tuberculosis has also begun.
The remaining pilot stations have been concernedmostly with epidemiological studies. In Vienna, thestatistical office was created in February and isengaged in the collection of data from the BCGcampaign. In South India a co- operative researchproject was started in March with the Union MissionTuberculosis Sanatorium in Arogyavaran (Madana-palle), where a field station for epidemiologicalresearch in tuberculosis in rural areas was set up.
The special research team that went to India inSeptember 1949 moved to Egypt in April 1950 tocontinue its studies on the variations and possiblecauses of differences in tuberculin sensitivity and non-specific reactions in widely separated areas and racialgroups.
Studies on reactions to various types of tuberculinhave been conducted in the office in Reykjavik,Iceland, in an endeavour to obtain a picture of thespectrum of sensitivity to these antigens. Plans havebeen worked out for a co- operative project betweenthe Research Office and the Tuberculosis Service ofIceland, for the establishment of a national roster,which will permit observations to be made on epidem-iological factors influencing the rapid decline in theincidence of the disease.
The Research Office has also carried out a seriesof studies on BCG vaccine with the Joint Enterpriseand the Statens Seruminstitut, Copenhagen. Thesestudies were made for the purpose of developing apractical method for field evaluation of BCG vaccine,of determining the effects of a wide variety of factorson the efficacy of the vaccine, of comparing vaccinesfrom various production centres, and, finally, ofcorrelating the findings on human populations in thefield with the results of simultaneous laboratory work.
As a result of these studies, two papers, the firstentitled Effect of Age of Vaccine and Variationsin Storage Temperature and Dosage on AllergyProduction and Vaccination Lesions Ten Weeks afterVaccination ", and the second " Effect of Variationin Dosage. of BCG Vaccine on Allergy Productionand Vaccination Lesions Nine Weeks after Vaccina-tion " were published in 1950 in the Bulletin of the
54 WORK OF WHO, 1950
World Health Organization.During the studies 78 a total of 13,301 Danish
schoolchildren were tuberculin -tested and 11,623non -reactors were vaccinated. Approximately 9.3of those vaccinated were re- tested with tuberculineight to eleven weeks after vaccination.
A proposal has recently been made to the DanishGovernment to make a special fund available forco- ordinated laboratory and field research ontuberculosis immunization. The project is conceivedas an all -out effort, for a period of at least five years,to find an ideal vaccine against tuberculosis.
Many other field studies have been made : amongthem, (1) a study to determine whether there arefamilial peculiarities in response to tuberculin(agreement in post -vaccinal reactions was foundamong sibling groups) ; (2) a statistical comparison
78 Bull, World Hltle Org. 1950, 3, 1 -24, 279 -300
of the effectiveness of different methods of vaccinationin terms of post -vaccination tuberculin sensitivity(in which the intracutaneous method appeared to bemore effective than the percutaneous) ; (3) a study todetermine the variations between duplicate tubercul-osis tests on the same person (observations now beinganalysed) ; (4) a study to determine the reaction tograded doses of PPD tuberculin given to patientsknown to have active tuberculosis (in this connexiona paper entitled " Tuberculin sensitivity : a study on245 tuberculous patients " was prepared for publica-tion by Acta Tuberculosea Scandinavica) ; (5) pilotstudies to standardize a new batch of tuberculinby duplicate testing with varying doses and compara-tive testing of the old and new tuberculins (resultsbeing analysed), and (6) a comparison between theMantoux and Trambusti tests (carried out by testing1,500 children in Finland).
TECHNICAL PUBLICATIONS AND REFERENCE SERVICES
WHO shall " provide information, counsel and assistance in the field of health"
PublicationsThe publications of WHO constitute an important
means of advancing the work of the Organizationand serve as an essential link between it and themedical and public- health professions. During thepast year the growing interest in these publicationshas been reflected in a substantial rise in sales andrequests for copies and in the increased attentionwhich has been paid to WHO in the medical andscientific press.
The Third Health Assembly, in recognizing, in itsresolution WHA3.63, " the fundamental importanceof the programme of publications of the Organi-zation, considered not only as a statutory obligationinherited from previous international organizations,but also as an activity particularly favourable to theeffectiveness and prestige of WHO ", indicatedgeneral lines of action for the guidance of theDirector - General, while referring certain specificpoints to the Executive Board for further study anddecision.
In addition to the continuing publication ofalready established periodicals, two new series wereinitiated in 1950 : the World Health Organization:Technical Report Series and the World HealthOrganization: Monograph Series. A list of the
publications printed in 1950 is given in the table atthe end of this section.
Bulletin of the World Health OrganizationIt was emphasized by the Third Health Assembly,
in resolution WHA3.63, that the Bulletin of theWorld Health Organization is the fundamentalpublication of the Organization, that it shouldcontain only papers of high technical and scientificquality, and that, starting in 1952, it should bepublished monthly. Then, in addition, the ExecutiveBoard at its sixth session in June decided, in reso-lution EB6.R9, that the separate editions in Englishand French which had been published up to thattime should be replaced by a single edition contain-ing articles either in English or in French, accordingto the language in which they were submitted, withsummaries in both languages. Volume 3, number 1,published in November 1950, was the first of themixed -language edition.
The contents of the Bulletin have covered a widerange of subjects reflecting the interests of theOrganization. BCG vaccination was the subject ofa special number (volume 2, number 3), whichcontained, in addition to a paper by the head of theBCG Service of the Institut Pasteur, Paris, three
TECHNICAL PUBLICATIONS AND REFERENCE SERVICES 55
studies dealing with the preliminary findings of themass BCG- vaccination programme of the JointEnterprise. The first of a series of research studieson BCG vaccination from the WHO TuberculosisResearch Office in Copenhagen also appeared duringthe year, and arrangements were made to hold thetype for possible reprinting of the whole series inmonograph form.
The Bulletin also included articles, covering awide geographical area, on the epidemiologicalaspects of certain communicable diseases, such asplague, bilharziasis, malaria, sandfly fever, venerealdiseases, Q fever and brucellosis. Of the papersreporting laboratory work, most have reflected theOrganization's special interest in biological stan-dardization and have dealt with digitalis, liverextracts, blood- typing sera, and cholera vaccine.Finally there were published a number of articleson various subjects of international significance -insecticides and insect control, communicable dis-eases, and mental health. Many of these articlespublished in the Bulletin resulted from studies andreports by WHO field workers and consultants.
For publication during the forthcoming yearWHO invited contributions on different subjects,and made arrangements with the Pan AmericanSanitary Bureau for some of the articles in theBulletin to be published simultaneously in Spanishin the Boletín de la Oficina Sanitaria Panamericana.
Supplements to the Bulletin of the World HealthOrganization
During the year, French and Spanish editions ofvolume 1 of the Manual of the International StatisticalClassification of Diseases, Injuries and Causes ofDeath were published. At the end of the year, theEnglish and French editions of the PharmacopoeaInternationalis were in press and arrangements hadbeen made with the Pan American Sanitary Bureaufor the preparation of the Spanish edition in Wash-ington. The number of requests for the Manualand the many inquiries about the PharmacopoeaInternationalis gave evidence of a considerableinterest in these two publications.
World Health Organization: Monograph SeriesA new series entitled the World Health Organi-
zation: Monograph Series was introduced towardsthe end of the year. This series was designed toinclude reprints and, where necessary, completetranslations of important studies initially publishedin the Bulletin, as well as occasional specializedmonographs on the treatment and control of disease.The first number was a reprint in French (from
volume 3, number 1 of the Bulletin) of a studyon the psychiatric aspects of juvenile delinquency,prepared on behalf of WHO as a contribution tothe United Nations programme on the preventionof crime and the treatment of offenders (see page 24).Arrangements were made for the publication of anEnglish translation in the same series. Other mono-graphs were under consideration at the end of theyear.
International Digest of Health Legislation
The International Digest of Health Legislation isunique in that it is the only periodical in existencewhich is devoted solely to the publication of healthlegislation of international significance. A reporton methods to be used in the selection and publicationof material for the Digest was considered andapproved by the Third Health Assembly.
With the first number of volume 2, the Digest wasrestyled typographically, and the opportunity wastaken to introduce editorial improvements andto add a bibliographical section. Although thecoverage of the Digest has been considerably extended,it is still not entirely comprehensive ; it cannot beuntil all governments, in fulfilment of their consti-tutional obligations, supply the Organization regularlywith information on their health legislation.
Arrangements have been made with other organi-zations which publish legislation (the United Nationsand ILO) to define the subjects covered by each so asto avoid unnecessary duplication. During 1950, theDigest published information from six States andterritories of the African region, from eleven in theAmerican region, one in South -East Asia, five inthe Eastern Mediterranean, four in the WesternPacific, eighteen countries in Europe, and from oneterritory not yet included within any definite region.
To supplement the information contained in theDigest, WHO arranged to make available to govern-ments, on request, photostat copies of the completetexts of those laws and regulations which were notreproduced in full.
Chronicle of the World Health Organization
The Chronicle of the World Health Organization,a monthly record of the work of the Organizationand of its chief technical publications, continued tobe published regularly in English, French andSpanish. Late in the year the Temporary Officefor the Western Pacific Region made plans to resumethe publication of the Chinese edition, which hadbeen virtually suspended because of conditions inChina, and it is hoped that this work may again be
56 WORK OF WHO, 1950
undertaken in 1951. The Russian edition remains inarrears.
Articles from the Chronicle have been reproducedin whole or in part in medical journals in a numberof countries. WHO has assisted by regularly supply-ing the medical press with advance copies of theEnglish and French editions on special airmailpaper.
World Health Organization: Technical Report SeriesThe first of the World Health Organization:
Technical Report Series was published in January1950, and by the end of the year 29 numbers hadbeen issued in English and French. This seriesincludes the reports of WHO expert committees ;joint committees with other specialized agencies,and other study and advisory groups. Such reportswere previously printed in special numbers of theOfficial Records of the World Health Organization.
The publication of these reports separately andin a more convenient and attractive style has resultedin a striking increase in sales and requests and in theattention given to them in the technical press.
Official Records of the World Health Organization
Seven numbers of the Official Records of theWorld Health Organization were published during1950. They included the Annual Report of theDirector - General for 1949, the Proposed Programmeand Budget Estimates for 1951, the Proceedings ofthe Third World Health Assembly, the Reports ofthe Fifth and Sixth Sessions of the Executive Board,and a report of the Board's Standing Committee onAdministration and Finance, containing commentsand recommendations on the programme and budgetestimates and a review of the organizational structureand administrative efficiency of the Organization.
During the year, the format of the Official Recordswas changed to the new size adopted for similarUnited Nations volumes, and the general appearancewas improved by the adoption of a new type -faceand cover page.
Before the Third World Health Assembly, asecond edition of the Handbook of Basic Documentswas published in an improved format, with thecontents brought up to date
Other Publications
In addition to the regular publications, a newedition of the International List of Venereal -DiseaseTreatment Centres, which had previously been issuedby the Office International d'Hygiène Publique,
was in press by the beginning of 1951. WHO alsopublished, jointly with UNESCO, Child WelfareFilms, an index of films and filmstrips (see page 71) ;another joint publication with UNESCO is PeriodicaMedica Mundi, an alphabetical list of current medicaland medico -biological periodicals with abbreviatedtitles and a country and subject index. This listwas prepared on the recommendation of the Co-ordinating Committee on Abstracting and Indexingin the Medical and the Biological Sciences, a com-mittee sponsored jointly by UNESCO and WHO,and was in proof form by the end of the year.
Much of the text of the Annual Epidemiologicaland Vital Statistics, 1939 -1946 was also in proof form.This volume and the Weekly Epidemiological Record,the Epidemiological and Vital Statistics Report andthe Weekly Fasciculus of the Singapore Epidemiologi-cal Intelligence Station are referred to under " Epi-demiological Information " (page 43) and " HealthStatistics " (page 46).
Distribution and Sales
Because of WHO's obligation to make the tech-nical information which it publishes available togovernments and certain non -governmental insti-tutions, and also in response to the needs for spread-ing information about the Organization, a largenumber of its publications are distributed free ofcharge.
Institutions which receive these publicationswithout cost fall into two groups : (1) WHO deposi-tory libraries and (2) libraries of scientific andmedical institutions whose activities fall within thepurview of WHO. In addition, many free copies aresent in exchange for other medical periodicals,of which approximately 900 are now received byWHO (usually in exchange for the Bulletin and theChronicle).
Different criteria for free distribution havecontinued to be adopted for the various publications :the Chronicle, which publicizes the work of theOrganization and its technical publications, hasthe widest free distribution ; the Bulletin and theDigest have been sent free only to governmentdepartments, to a limited number of scientific insti-tutions and libraries, and to a_very few specialists ;the Epidemiological. and Vital Statistics Report hasbeen sent free to a number of statistical institu-tions, to some libraries, and to a certain number ofspecialists. In considering requests for free copies ofpublications, WHO has had to take into considera-tion the special currency difficulties existing in somecountries, especially in under- developed areas.
TECHNICAL PUBLICATIONS AND REFERENCE SERVICES 57
MAP 4. WHO DEPOSITORY LIBRARIES
Further progress was made towards establishinga network of depository libraries at which all WHOpublications are accessible (see map 4 above).It is believed that this system will ultimately leadto a reduction in the free distribution of all publi-cations except the Chronicle, which may with advan-tage continue to be distributed rather widely.
Limited attempts at sales promotion have beenmade with encouraging results. Sales of backnumbers have in certain cases more than doubledthe figures reported in the Annual Report of theDirector - General for 1949.79
The receipts from sales of WHO publications in1950 amounted to $28,436.20, this sum representingonly monies actually received by the Organization.To this sum, however, may be added the value -estimated at over $5,000 -of the 900 medicalperiodicals received in exchange for WHO publi-cations.
79 Of Rec. World Hlth Org. 24, 64
Library and Reference Services
The functions of the WHO Library are twofold :first, to assist in the implementation of the pro-gramme of the Organization and, secondly, toprovide members of the Secretariat with essentialtechnical literature. Both aspects of the work haveshown a marked increase during the year.
The increase in the use of the Library is shownby the loan figures : 5,783 books were lent in 1950as compared with 2,466 in 1949 : 23,583 issuesof current periodicals were circulated, comparedwith 10,832 in 1949. Over 1,100 current periodicals(an increase of over 300) are now received regularly,900 being in exchange for WHO publications. Gapsin the literature of special subjects of interest havebeen filled, and the transfer of the books of theLibrary of the Office International d'Hygiène Publi-que has considerably enriched the collection in itshistorical aspects.
The supply of medical literature to governmentsand to field teams continues and, while there is adecrease in the number of subscriptions to periodicals,
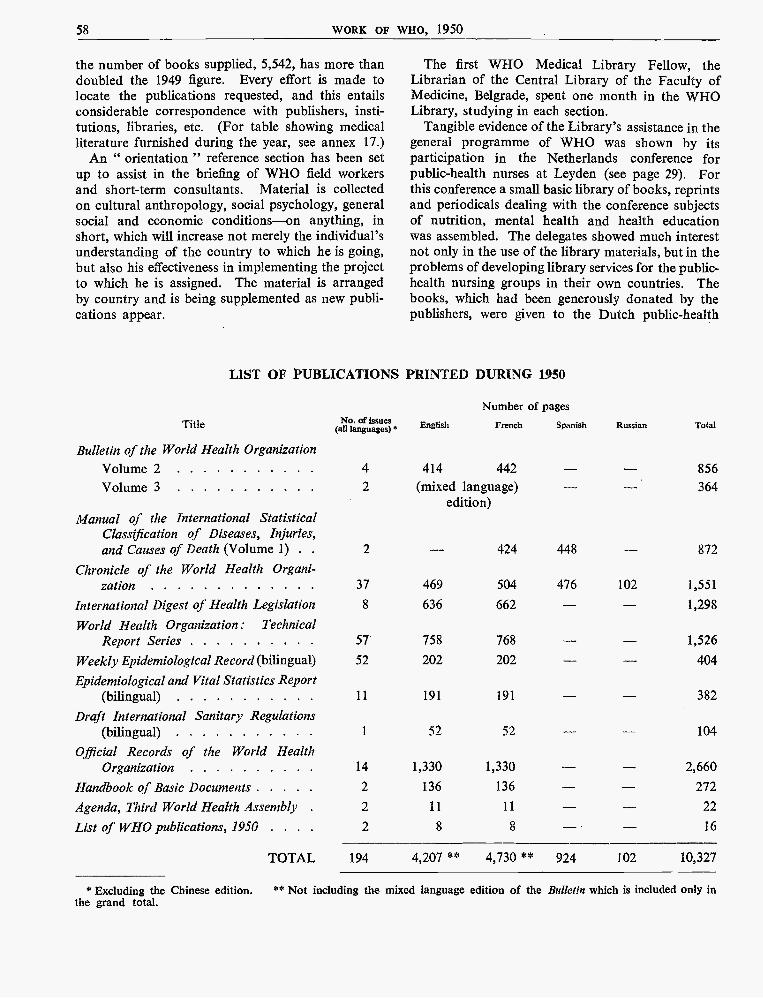
58 WORK OF WHO, 1950
the number of books supplied, 5,542, has more thandoubled the 1949 figure. Every effort is made tolocate the publications requested, and this entailsconsiderable correspondence with publishers, insti-tutions, libraries, etc. (For table showing medicalliterature furnished during the year, see annex 17.)
An " orientation " reference section has been setup to assist in the briefing of WHO field workersand short -term consultants. Material is collectedon cultural anthropology, social psychology, generalsocial and economic conditions -on anything, inshort, which will increase not merely the individual'sunderstanding of the country to which he is going,but also his effectiveness in implementing the projectto which he is assigned. The material is arrangedby country and is being supplemented as new publi-cations appear.
The first WHO Medical Library Fellow, theLibrarian of the Central Library of the Faculty ofMedicine, Belgrade, spent one month in the WHOLibrary, studying in each section.
Tangible evidence of the Library's assistance in thegeneral programme of WHO was shown by itsparticipation in the Netherlands conference forpublic -health nurses at Leyden (see page 29). Forthis conference a small basic library of books, reprintsand periodicals dealing with the conference subjectsof nutrition, mental health and health educationwas assembled. The delegates showed much interestnot only in the use of the library materials, but in theproblems of developing library services for the public -
health nursing groups in their own countries. Thebooks, which had been generously donated by thepublishers, were given to the Dutch public -health
LIST OF PUBLICATIONS PRINTED DURING 1950
Title
Bulletin of the World Health Organization
No. of issues(all languages)*
Number of pages
English French Spanish Russian Total
Volume 2 4 414 442 856
Volume 3 2 (mixed language) 364edition)
Manual of the International StatisticalClassification of Diseases, Injuries,and Causes of Death (Volume 1) . . 2 - 424 448 872
Chronicle of the World Health Organi-zation 37 469 504 476 102 1,551
International Digest of Health Legislation 8 636 662 - - 1,298
World Health Organization : TechnicalReport Series 57 758 768 1,526
Weekly Epidemiological Record (bilingual) 52 202 202 404
Epidemiological and Vital Statistics Report(bilingual) 11 191 191 382
Draft International Sanitary Regulations(bilingual) 1 52 52 - - 104
Official Records of the World HealthOrganization 14 1,330 1,330 2,660
Handbook of Basic Documents 2 136 136 272
Agenda, Third World Health Assembly . 2 11 11 22
List of WHO publications, 195D . . . . 2 8 8 16
TOTAL 194 4,207 ** 4,730 ** 924 102 10,327
* Excluding the Chinese edition. ** Not including the mixed language edition of the Bulletin which is included only inthe grand total.
TECHNICAL ASSISTANCE FOR ECONOMIC DEVELOPMENT 59
nurses as a collection, and will be made available forloan.
Because of delays in the publication of indexes tocurrent medical literature, the indexing of currentperiodicals continues to be an activity of the utmostimportance -one which, by keeping members of theSecretariat informed of the most recent developmentsin their technical fields, more than justifies the labourinvolved. During the year 16,189 articles were indexedas compared with 2,377 in 1949. The Library hasalso continued the indexing of health legislationreceived from over fifty governments in preparationfor the International Digest of Health Legislation.
Translations
The total volume of translations completed in 1950was : into French : 11,958 pages ; into English :
3,164 pages ; into Russian : 597 pages, and intoSpanish : 513 pages.
The unit used for estimating the volume of materialtranslated is a foolscap page of normal typescript indouble spacing.
The output for 1950 again represents an increase-this time of 18.8 % over the preceding year. Thegrowing number of WHO expert committees, thedevelopment of technical publications and, inparticular, the holding of seminars and symposia,have caused a further increase in the number ofhighly technical texts requiring translation. Arrange-ments have continued to be made for some of themto be translated outside the Organization. A total of1,046 pages were commissioned outside the sectionduring 1950 and this has proved a useful auxiliarymethod, but careful revision of such translations isalways necessary.
TECHNICAL ASSISTANCE FOR ECONOMIC DEVELOPMENT
WHO shall " furnish appropriate technical assistance ... upon the request oracceptance of governments; " "provide, or assist in providing, upon therequest of the United Nations, health services and facilities to specialgroups..."
The Third World Health Assembly noted withinterest and approval the resolution of the UnitedNations General Assembly concerning the expandedprogramme of technical assistance for economicdevelopment of under- developed areas,80 and theguiding principles for this programme establishedby the Economic and Social Council.81 It authorizedthe Director - General to participate in the delibera-tions of the Technical Assistance Board, to representWHO at meetings on technical assistance of interestto WHO, and to implement the expanded programmeof technical assistance as approved, subject to con-ditions established by the Health Assembly and theExecutive Board.82
BO Resolution 304(IV) of the General Assembly of theUnited Nations
81 Resolutions 222(IX) adopted by the Economic and Socialon 14 and 15 August 1949. Reproduced in Off. Rec. Worldfilth Org. 23, 26
82 Resolution WHA3.116, Off. Rec. World Hlth Org. 28, 68
Technical Assistance Conference
In June 1950 the Secretary -General of the UnitedNations called a conference of all governments whichare Members of the United Nations or of the special-ized agencies co- operating in the technical assistanceprogramme. This conference, which was attended byrepresentatives of more than 50 nations, pledged asum equivalent to $20,012,500 to the United Nations'Special Account for financing the technical assistanceprogramme for the first financial period, whichextends until 31 December 1951. Thereafter thefinancial period will correspond with the calendaryear.
In accordance with the decision of ECOSOC andthe Technical Assistance Conference, WHO willautomatically receive 22% of the first ten milliondollars or its equivalents and 22% of 70% of thesecond ten million. WHO's allocation of the pro-mised contribution for the first period would there-fore be just over $3,740,000. The remainder will be
60 WORK OF WHO, 1950
distributed among the participating organizations bythe Technical Assistance Board. Up to the end of1950, the allccation which could be made availableto WHO out of contributions received by the Secre-tary- General was $1,481,231.04. (For details of thesecontributions, see annex 16.)
It should be noted that parts of the contributionspromised and received are either non -convertible orhave a limited convertibility ; this fact obviouslyaffects the use of the funds to some extent.
Technical Assistance Board
The Technical Assistance Board consists of theexecutive heads, or their representatives, of theUnited Nations, ILO, FAO, UNESCO, ICAO andWHO, called the " participating organizations ".The Secretary- General, or his representative, is theChairman of the Board. The International Bank forReconstruction and Development and the Inter-national Monetary Fund are also represented on theBoard : these two organizations, although notparticipating in the technical assistance funds, havepledged their fullest co- operation in carrying out theprogramme. The Board also maintains liaison witha large number of international organizations notconnected with the United Nations which are operat-ing in the field of technical assistance.S3
The Technical Assistance Board is notified of allrequests for technical assistance received from govern-ments by the partipating organizations, whetherunder this programme or any other. It reviews theseprogrammes, arranges where necessary for jointaction between organizations, approves major pro-jects, allocates some of the funds and, in general,co- ordinates the activities of and maintains liaisonwith all the agencies engaged in technical assistance.During 1950 it held seven meetings, in all of whichWHO participated. As an experiment in internationaladministration, the Board is proving to be verysuccessful and will undoubtedly become even moreeffective as time goes on.
At the end of the year WHO was collaboratingwith FAO in joint surveys of areas for foodproduction and malaria control, and with UNESCOin fundamental education projects.
83 These include the United States Technical Co- operationAdministration, the Co- ordinating Committee on TechnicalAssistance of the Inter -American Economic and SocialCouncil of the Organization of American States, the EconomicCo- operation Administration, the Commonwealth Consul-tative Committee on South and South -East Asia and the Inter -American Institute for American Affairs.
Requests for Technical Assistance
When a request for technical assistance is sent toone of the participating organizations by a govern-ment, all the others are immediately informed so
that they may consider whether or not they are inter-ested in the project. If no interest is declared withinthree weeks the request is automatically free foraction by the organization receiving the request ; ifinterest is shown, it becomes a joint project and isimplemented by the interested organizations. Onlyrequests which are declared " important " (thosewhich involve expenditure of large sums, long -termcommitments or which are regional rather thannational in character) are co- ordinated by theTechnical Assistance Board. A consultative missionmay then be sent to the country or, as was done inHaiti, Indonesia, Iran and Pakistan, resident repre-sentatives may be appointed in order to assist thegovernments in the planning.
At 31 December 1950, 32 countries had requestedtechnical assistance from WHO under the expandedprogramme. These were : Afghanistan, Burma,Ceylon, China, Chile, Colombia, Costa Rica, theDominican Republic, Ecuador, Egypt, El Salvador,Ethiopia, Guatemala, Haiti, India, Indonesia, Iran,Iraq, Israel, Lebanon, Liberia, Libya, Norway,Pakistan, Peru, Saudi Arabia, Sweden, Syria, Thai-land, Turkey, Venezuela Yugoslavia. addition,one request was received for a training centre in vitaland health statistics for a region -the EasternMediterranean -with Egypt as the host government.This centre would benefit Egypt, Ethiopia, Iran,Iraq, Israel, Lebanon, Pakistan, Saudi Arabia, Syriaand Turkey.
WHO participated in a consultative mission toIndonesia, consisting of representatives of theUnited Nations, FAO, UNESCO and WHO ; in amission to Turkey, sent by the International Bankfor Reconstruction and Development ; in an FAO/WHO survey in El Salvador, and in surveys inLiberia, Libya and Egypt.
The requests received by WHO are for a varietyof types of assistance, but mostly in the fields recom-mended at the sixth session of the Executive Boardin resolution EB6.R1, namely : (1) stimulation ofcampaigns against communicable diseases ; (2) pro-fessional and technical education, including fellow-ships ; and (3) public -health administration.
WHO's Approach to Technical Assistance
As the relation between a people's health andeconomic development has long been recognized,WHO is directing its efforts in the technical assistance
COLLABORATION WITH OTHER ORGANIZATIONS 61
programme towards strengthening the health servicesin under -developed countries so that they may beable adequately to use funds which become availablefor health purposes and deal with the problems aris-ing from general economic development. The Organi-zation, because of its decentralized structure, is in agood position to take over its share of technicalassistance projects, which are administered for themost part by the regional offices. Through itsregional directors and regional committees, it hasinformed all Member Governments of the types ofservices available in technical assistance. Thetechnical competence of the regional staffs and theirknowledge of local health conditions were drawnupon : these staffs were available to assist govern-ments to formulate requests for health projects, topoint out health aspects of requests for other pro-jects and, afterwards, to advise on the plans arisingfrom these requests.
In conformity with the recommendation of theExecutive Board (in resolution EB6.R1) that in
implementing the programme of technical assistance,the possibility of utilizing existing personnel should,as far as possible, be considered, it is the policy ofWHO to keep expenditure for the administration ofthis programme to the minimum. Therefore, insteadof establishing a new division to deal with technicalassistance activities, as was done in some of the otherparticipating organizations, WHO set up a smallunit of three at headquarters to ensure co- ordination,both within and outside the Organization. Some ofthis work is also carried on by the New York LiaisonOffice.
In so far as is necessary, the staff at headquartersand in the regional offices will be increased, but onlyin direct proportion to the extra work required. Theprogramme to be carried out in 1951 is so extensivethat much more field staff will be necessary. If WHOis to fulfil its function adequately, governments mustcontribute some of their best specialists, particularlyin public -health administration, so that the availablefunds may be used in the most effective way.
COLLABORATION WITH OTHER ORGANIZATIONS
WHO shall " establish and maintain effective collaboration with the United Nations,specialized agencies, governmental health administrations, professionalgroups and such other organizations as may be deemed appropriate ; "" promote co- operation among scientific and professional groups whichcontribute to the advancement of health ".
The United Nations, its specialized agencies,other inter -governmental organizations and the inter-national non -governmental organizations (includingin each case their component and regional bodies)present a complex picture of interrelationships andcomplementary responsibilities. The objective ofWHO has always been to achieve effective liaison,joint planning of programmes and satisfactory inter-change of information and ideas within this frame-work. The attainment of this objective calls for avariety of techniques, ranging from formal representa-tion at meetings of other organizations, throughinter -secretariat consultation and planning, to theroutine exchange of reports and individual personalcontacts. The efforts being made in all these waysare leading slowly to the establishment of an integratedand co- ordinated international programme, particu-larly in the economic and social field.
Before the actual establishment of the Organizationitself, the Interim Commission did much useful workto this end. Later the First World Health Assemblyset the key -note for WHO's efforts by drawing theattention of Members to the desirability of ensuringthat each national delegation pursued a co- ordinatednational policy at all meetings of the United Nationsand its specialized agencies. It also requested theDirector - General, in consultation with the UnitedNations and its specialized agencies, to give constantattention to the relative priority of programmeprojects and to the steps to be taken to ensure theco- ordination of the programmes of WHO withthose of the other organizations. 64
WHO, both at headquarters and in its New YorkLiaison Office, has established and maintained
84 Of Rec. World Hlth Org. 13, 329
62 WORK OF WHO, 1950
relations with other organizations, and has tried toensure that its officials understand the need fordeveloping these relations.
The policy of insisting upon inter -agency consulta-tion before entering into commitments has, as far aspossible, always been followed by the Organization.In this connexion, quite recently, when consideringpriorities in projects for international action, theEconomic and Social Council not only adoptedcriteria 85 markedly similar to those contained inWHO's long -term programme of work as pro-visionally adopted by the Third World HealthAssembly, in resolution WHA3.1, but also affirmedthis principle of inter -agency consultation beforecommitment. B6
Under the Charter and the agreements with thespecialized agencies, the Economic and SocialCouncil has the responsibility of co- ordinating inter-national work in the economic and social field. Tothis end, it examines the reports and proposed pro-grammes of the specialized agencies and makesrecommendations which are taken into account bythe various governing bodies in their approval of pro-grammes, and by the Directors - General in day -to -dayoperation. In this task of co- ordination, the Councilis assisted by the Administrative Committee onCo- ordination (ACC) -consisting of the Secretary -General of the United Nations and the Directors -General of the agencies concerned -and by itsPreparatory Committee. The ACC is serviced bycommittees or working parties on special subjects towhich the Directors - General of the specializedagencies appoint officers with particular competencein the subjects under consideration. Such bodiesinclude the Consultative Committee on Admin-istrative Questions, the Consultative Committee onPublic Information, the Working Group on Publica-tions, the Technical Working Group on Fellowshipsand the United Nations Film Board.
This mechanism is working with increasing effec-tiveness, as was pointed out by the Economic andSocial Council at its eleventh session 87 which, more-over, asked the ACC to indicate to it -on the basisof the aforementioned criteria for the choice of pro-jects for international action -fields of work whichit considers deserve special discussion.88 The Councilhas thus recognized that the ACC is more than an
85 ECOSOC resolution 324(IX)A, UN document E/1849,pp. 63, 68
88 ECOSOC resolution 324(IX)B, UN document E/1849,p. 63
87 UN document .E/1849, p. 7288 UN document E/1849, p. 67
inter -secretariat body. It is a mechanism for bringingtogether in one place the technical policies establishedby the governing bodies of all the specialized agencies,and as such should be used to the full. It offers thegreatest possible prospect of achieving, between theorgans and specialized agencies of the United Nations,the co- ordination of aims without which any co-ordination of 'individual programmes or policies isrendered difficult.
It should not, however, be imagined that all co-ordination is achieved through the ACC. As soon asany joint arrangements are made, either through theACC, through recommendations of the Economicand Social Council, or through the activities of thespecialized agencies, the planning and operation ofjoint programmes are carried out between the officersentrusted with the technical responsibility for theseprogrammes in their respective organizations. A goodexample of the results of this direct liaison may beseen in the establishment of the Joint FAO /WHOExpert Committee on Nutrition, and of joint ILO/WHO committees on the Hygiene of Seafarers andon Occupational Health. The pattern followed inthese cases will no doubt be used more extensively inthe future.
If co- ordination within the United Nations familycan be achieved, its relations with other inter-governmental bodies and with non -governmentalorganizations will also be simplified. As a result ofthe expanded programme of technical assistance foreconomic development, WHO has come into rela-tions with a much greater number of these inter-governmental and " bilateral " international organi-zations than ever before, and problems of co-ordination are thus increased. As for the non-governmental organizations, the Executive Board atits sixth session, in resolution EB6.R8, requested theDirector - General to adopt a policy of closer collabora-tion with those with which WHO is in relation, inorder to encourage them to implement certain partsof the WHO programme. This policy is beingfollowed, as described below, and, in addition, otherinternational non- governmental organizations activein the field of health are being encouraged to amal-gamate, reorganize or otherwise prepare themselvesfor full co- operation with WHO. This is a long -termoperation designed to establish a strong and effectivenetwork of voluntary organizations co- operating.with WHO throughout the world.
Complete co- ordination with organizations of suchcomplex structure can of course never be achieved,it will be at best a continuous process demanding
COLLABORATION WITH OTHER ORGANIZATIONS 63
from each organization concerned the greatest degreeof awareness of the aims and methods of the others.
The representation of WHO at assemblies andconferences of other organizations has been plannedso as to ensure maximum efficiency and the properpresentation of any technical points which mightarise. Recently WHO was represented at some ofthese meetings by officers of other agencies, wherethere was some coincidence of interest. (For lists ofmeetings at which WHO was represented during theyear, see annexes 6 and 7.)
Another means of contact has been by reciprocalreporting ; a system for exchanging internal progressreports with other agencies has been fostered, andcordial personal relations are growing, with theresult that misunderstandings and ambiguities aretending to disappear.
Co- operation with the United Nations
Special Projects
At the request of the United Nations, WHO assistedwith three special projects, which are describedin detail in the section beginning on page 38.
They are :
(1) the work of the United Nations Relief andWorks Agency for Palestine Refugees in theNear East ;
(2) relief and rehabilitation of the civilian popula-tion in Korea ;
a general investigation of conditions in Libya.(3)
As in the past close liaison has been maintainedwith the United Nations Department of Trusteeshipand Information from Non -Self -Governing Terri-tories and with other organs concerned with thoseterritories. The Special Committee on InformationTransmitted under Article 73e of the Charter hassuggested that in trust territories WHO should giveparticular attention to the problems of preventableblindness and to methods of compiling vital statistics.
InsecticidesThe Annual Report of the Director - General for 1949
referred to the resolution on the availability ofinsecticides, which was adopted by the Economic andSocial Council.89 In accordance with this resolution,
99 Of Rec. World Hlth Org. 24, 71
the Secretary - General presented a further report tothe eleventh session of the Council. The question wasalso referred, through the Interim Commission of theInternational Trade Organization, to the fifth sessionof the Contracting Parties to the General Agreementon Tariffs and Trade, along with a draft agreementon the importation of insecticides, on which theywere asked to comment. These comments havebeen received. Although some representatives ofthe Contracting Parties felt that the scope of theagreement should be broadened, it was neverthelessagreed to be a feasible and workable instrument ofinternational trade which would be useful to WHO.It will be presented to the Executive Board at itsseventh session.
Long -Range Activities for Children
At the end of 1949 a meeting to plan a co- ordinatedlong -term programme for children was held by theUnited Nations and interested specialized agencies.In April and again in October of 1950, the matter wasdiscussed by the ACC, which wished to make surethat all of these organizations were in a position tofulfil their technical responsibilities in long -term pro-grammes for children, and that no new internationalagency would be created whose work would overlapthat of existing organizations.
The ACC included these considerations in itsreport to the Economic and Social Council, which,at its eleventh session, recommended to the GeneralAssembly the establishment of a " United NationsInternational Children's Endowment Fund " tocarry out programmes on behalf of children, withthe technical co- operation of the competent special-ized agencies.80
The General Assembly, in December, did notaccept the recommendation to establish an endow-ment fund, but, briefly, requested the Economic andSocial Council, in consultation with the appropriatespecialized agencies, to give more support to nationalprogrammes designed to aid children ; it decided ona reconstitution of the UNICEF Executive Board,re- defined the functions of the Board especially withregard to long -term programmes for children, andprovided for close collaboration with specializedagencies. It also decided to reconsider the future ofUNICEF at the end of three years.91
90 ECOSOC resolution 310(XI) of 11 August 195091 UN document A/1597
64 WORK OF WHO, 1950
United Nations International Children's EmergencyFund
The year 1950 marked further progress in relationswith UNICEF. The number of joint health -projectsfor which, basically, WHO carried the technicalresponsibility and UNICEF provided supplies (andoften funds for the personnel involved) increasedfurther in 1950. Details are given elsewhere in theappropriate chapters of this report.
At the fourth session of the Joint Committee onHealth Policy, UNICEF /WHO, held in Geneva on30 and 31 May, the range of subjects in which jointprojects could be established was enlarged to includeBCG vaccination, a scheme for the training of child -health workers in India, and the establishment ofplants for the production of insecticides andantibiotics.
In spite of a clear dividing line between the respon-sibilities of UNICEF and those of WHO, a need forclose co- ordination was felt in both the planning andthe implementation of joint projects. A number ofarrangements were therefore concluded outliningprinciples and procedures for this co-ordination.'Negotiations were required, also, to determine therespective responsibilities of the two organizations inthe anti- tuberculosis campaign carried out up to nowby the Joint Enterprise (see page 9).
Close co- operation with UNICEF has continued inthe regional offices and the appointment of a WHOrepresentative to the Far Eastern Headquarters ofUNICEF in Bangkok has greatly contributed to themaintenance of.; effective relations between the twoorganizations in that area.
Co- operation in Other United Nations Programmes
WHO has been asked to prepare detailed studies inmental health in connexion with different UnitedNations programmes. Of the two already completed,one is on the psychiatric aspects of juvenile delin-quency ; the other on the psychological damage causedby the separation of the young child from its mother.A third, on psychiatric rehabilitation, is in course ofpreparation (see page 24).
WHO also participated in a series of consultationswith the United Nations, other specialized agenciesand non -governmental organizations in order to out-line a well co- ordinated international programme onthe rehabilitation of the physically handicapped, asrequested by the Economic and Social Council. AnACC technical working group on this subject,meeting in Geneva on 17 and 18 December, agreedthat the organizations concerned should exchange,through the Technical Assistance Board and by
correspondence, information on current and proposedaction. The group also agreed to meet from time totime in order to review current activities and planfuture stages of the long -range programme.
Reference is made on page 42 to the opinions ex-pressed -by the Expert Committee on Drugs Liable toProduce Addiction regarding the exemption of certaindrugs from the provisions of the 1925 Convention andthe 1948 Protocol, and to the definitions provided bythis expert committee at the request of the UnitedNations Commission on Narcotic Drugs. During theyear, technical advice was given to the PermanentCentral Opium Board of the United Nations andliaison established with the United Nations Depart-ment of Social Affairs on questions of alcoholism.
Co- operation with the Statistical Office of theUnited Nations Population Division continued alongthe lines described in the Annual Report of theDirector -General for 1949. The study on wastageof human life (particularly as regards pregnancy andinfant mortality) on which the two organizationsare collaborating is progressing according to thetime schedule. Preliminary conversations were alsoheld on possible co- operation in statistical aspectsof the expanded programme of technical assistance.
The area of collaboration between WHO and theDepartment of Social Affairs of the United Nationswas widened in 1950. Working together, both areassisting, along with other organizations, in theproject for the training of nurses, at Soissons,France. WHO contributed to the work of the secondUnited Nations Social Welfare Seminar for ArabStates, and, through the Regional Office for South -East Asia, participated in the Conference of Expertson Handicapped Children, organized jointly by theUnited Nations Social Activities Division and certainspecialized agencies, on the occasion of the IndianConference of Social Work. Arrangements weremade for the WHO consultant on the medicalaspects of the problem of handicapped children toserve as consultant to the United Nations and toUNICEF. " -
Inter -agency arrangements for establishing stan-dards for the granting and administration of fellow-ships and for referring requests from one agency toanother proved most valuable. The various agenciesare now working together, both in the administrationof fellowships and in consultations with governmentson arrangements for foreign study (see page 34).
COLLABORATION WITH OTHER ORGANIZATIONS 65
WHO collaborated closely with the United Nationsin drawing up uniform Financial Regulations, infollowing a similar scale of assessment and in sup-plying information on salary, allowance and leavesystems, budgetary procedure etc. (see page 74).The Organization also participated in meetings . ofthe Joint Staff Pension Board and the Panel ofAuditors, and in meetings called by United Nationsorgans dealing with publications and public informa-tion.
Regional Economic Problems
Close relations have been maintained with theEconomic Commission for Europe on the questionsof supplies (see page 38) and housing (see page 22).Through the Regional Office for South -East Asia,WHO co- operated with the Economic Commissionfor Asia and the Far East in the public -health aspectsof proposed projects for flood control and, throughthe Regional Office for the Americas, with the Eco-nomic Commission for Latin America, which invitedthe Organization to send a representative to a meetingon economic development and immigration which itis convening early in 1951.
Co- operation with Specialized Agencies
International Labour Organisation
The mechanism for co- operation between ILO andWHO in promoting the health of workers is nowcomplete. At the end of 1950, the two organizationswere working together on the implementation ofrecommendations made at the first session of theJoint ILO /WHO Expert Committee on OccupationalHealth, held in December, 1949, and at the secondsession of the Joint ILO /WHO Committee on theHygiene of Seafarers, held in May 1950 (see page 25).In addition, WHO took part in the. ILO SpecialTripartite Conference concerning Rhine Boatmen,at which questions of social security and conditionsof employment were considered.
In May and June the ILO held a 'preparatoryconference on migration, in which the representativesof the United Nations and interested specializedagencies, including WHO, participated as workingmembers. WHO helped ILO to draw up standardsfor the medical examination of migrants and co-operated in the planning of technical assistanceprogrammes by advising on the health aspects ofmigration.
There is also constant interchange of informationbetween the two organizations on the protection ofthe health of women and children and on conditionsof employment for nurses.
Food and Agriculture Organization
Since the first session of the Joint FAO /WHOExpert Committee on Nutrition, held in November1949, the two organizations have established, foractivities relating to nutrition, a working arrangement
_providing for full co- operation in planning and forco- ordination of effort. In preparation for the LatinAmerican nutrition conference organized by FAOin Rio de Janeiro in June, a WHO consultant carriedout surveys of infant nutrition and endemic goitrein some of the countries of the Americas. Moreover,three members of the WHO staff took an active partin the Conference. A joint survey of nutrition inEgypt was made during 1950, and during the lastthree months of the year, FAO and WHO helpedthe Egyptian Government to organize a nutritioncourse in Cairo (see page 26).
Preliminary work for joint programmes to controlmalaria and increase food production, as describedin the Annual Report of the Director - General for1949 92 continued in 1950. A meeting to discussrequests received from governments for assistancein such projects was held in Washington, in October,when it was recommended that á programme bestarted in Latin America in 1951, and that preliminarysurveys be made for other projects`in the EasternMediterranean and South -East Asia 'Regions (seepage 7).
In 1950, FAO and WHO started to co- operate onprogrammes for the control of animal diseases trans-missible to man. This work is shared between thetwo organizations, each acting on behalf of the otherin areas where it has qualified representatives.Efforts will be mainly directed towards the control ofrabies, brucellosis, anthrax and bovine tuberculosis(see pages 15, 16). WHO is also collaborating inthis work with the International Office of Epizootics.
United Nations Educational, Scientific and CulturalOrganization
Reference was made in the Annual Report of theDirector- General for 1949 to three important under-takings in which WHO and UNESCO co- operate :the Pilot Project for Fundamental Education in Haiti,the Council for the Co- ordination of InternationalCongresses of Medical Sciences, and the compilation
92 Off. Rec. World Hlth Org. 24, 4, 72
66 WORK OF WHO, 1950
of a catalogue of films dealing with the health andwelfare of children.93
Each of these activities continued within the year.The Haiti project was expanded ; through theCCICMS, UNESCO and WHO assisted in theorganization of several international conferences inmedical sciences, and the English edition of the filmcatalogue was issued in 1950 (see also belowand page 71). In addition, new programmes infundamental education were planned : a regionaltraining and production centre for Latin America tobe established in Mexico, and a similar project inthe Arab States, in preparation for which WHOprovided an expert to a UNESCO survey team.WHO was consulted by UNESCO in connexionwith the survey being prepared by that organizationat the request of the Economic and Social Councilon the need for, and possibility of, establishingUnited Nations Research Laboratories.
WHO also gave technical advice on the programmefor the Interim International Arid Zone ResearchCouncil, which was established by UNESCO in ful-filment of a further request made by the Economicand Social Council and which met in Paris during theyear.
The whole range of joint activities between WHOand UNESCO was discussed at a meeting in October,which proved so fruitful that it is intended to havesimilar meetings periodically in the future.
Other Specialized Agencies
During 1950, as in previous years, close liaison wasmaintained with the International Civil AviationOrganization in the preparation of the InternationalSanitary Regulations. ICAO has been invited to sendrepresentatives to the special committee which willmeet in April 1951 to consider the draft WHOSanitary Regulations before their submission to theFourth World Health Assembly.
WHO continued to co- operate with the Inter-national Refugee Organization in matters relating tothe health of refugees, and provided a team of fiveexperts to give advice on the health of refugeechildren in various countries in Europe.
The Interim Commission of the InternationalTrade Organization assisted WHO by giving itscomments on a draft agreement on the importationof insecticides, as described above.
93 Off Rec. World Hlth Org. 24, 12, 13, 73, 76
Co- operation with the International Bank forReconstruction and Development was most satis-factory : towards the end of the year a WHO expertwas included in a mission sent by the Bank to Turkeyin connexion with a technical assistance project (seepage 60), and a request was received for anotherexpert for a mission to Iraq.
The programmes of technical assistance for eco-nomic development have, generally speaking, broughtabout an intensification of liaison work betweenWHO and the other specialized agencies.
Non -Governmental Organizations
Council for the Co- ordination of InternationalCongresses of Medical Sciences
1950 was the first year of operation of the Councilfor the Co- ordination of International Congresses ofMedical Sciences as a fully self -governing institution,linked by special arrangements with WHO andUNESCO. Practically all of WHO's activitiesdirected towards the co- ordination of congresseswere entrusted to the Council, and the Organizationmade budgetary provision for an allocation to theCouncil for this purpose. WHO co- operated withUNESCO on matters of policy regarding the Council,and was represented at all meetings of its executivecommittee during the year.
During the year, 30 organizations ratified thestatutes of the Council, and more are expected to doso. Some congresses (e.g. the congress on radiologyand the one on cancer) adjusted the dates and placesof their meetings in order to make it easier for personsinterested to attend more than one congress. Twentycongresses received financial assistance for the im-provement of their technical services (interpretation,scientific publication and organization of scientificmeetings), in accordance with conditions stipulatedby WHO and UNESCO. The initiative of some ofthem in organizing international advanced coursesand symposia in selected subjects has been referredto on page 32. The Council published three copiesof its Bulletin giving model statutes of internationalunions and the procedure for registering them, a listof existing organizations, reports on the symposiaand other relevant information on congresses.
Relations with Other Non -Governmental Organizations
Good relations were maintained with the inter-national non -governmental organizations in officialrelationship with WHO. A list of the meetings of these
COLLABORATION WITH OTHER ORGANIZATIONS 67
organizations at which WHO was represented duringthe year is given in annex 7. The Executive Board,at its sixth session, in resolution EB6.R17, approvedcontinued co- operation with 18 non -governmentalorganizations after the biennial review required underthe adopted procedure. B4 Principles drawn up by theBoard to govern the admission of non -governmentalorganizations into relation with WHO, on the onehand, and relations between WHO and regional andnational non -governmental organizations on theother, were adopted -the former with an amendment-by the Third Health Assembly in resolutionsWHA3.113 and WHA3.114.
The list of organizations admitted to officialrelationship with WHO was extended to includethe International Conference of Social Work ; theInternational Pharmaceutical Federation ; the Inter-national Federation for Housing and Town Planning,and the International League against Rheumatism.A list of the 22 non- governmental organizationsnow in official relations with WHO is given inannex 9.
In compliance with resolution EB6.R8 of theExecutive Board, non -governmental organizationswere encouraged to promote world -wide applicationof WHO's principles and, particularly, to organizeinternational federations of their affiliated nationalbodies. WHO made the fullest possible use of theresources of these organizations, and instances ofco- operation on particular subjects are given undervarious sections of this report. The following details,however, may be of particular interest.
WHO and UNICEF were associated during theearly part of the year with the International Com-mittee of the Red Cross, the League of Red CrossSocieties and the International Union for ChildWelfare, in organizing the Sixth InternationalCongress of Paediatrics held at Zürich in July and inplanning an exhibition for the congress. This exhibit," Social Paediatrics throughout the World ", wasshown for 12 days with an average daily attendance of800 persons, and was followed by a Post -CongressSeminar on Social Paediatrics in which WHO alsoparticipated. The Organization was represented atvarious meetings of the above -mentioned organiza-tions and, in February, at a congress on the Educa-tional Problems of Physically Handicapped Childrencalled by the International Union for Child Welfareunder the auspices of UNESCO. WHO also co-operated with both Red Cross organizations, as wellas the American Friends Service Committee, in the
94 Off. Rec. World Hlth Org. 25, 65
United Nations Relief for Palestine Refugees untilApril, when the work was taken over by anotheragency (see page 39).
Close collaboration with the International Unionagainst Tuberculosis continues. The participation ofits Secretary - General in the work of the WHO ExpertCommittee on Tuberculosis provided a link betweenthe union and WHO, and helped to keep bothorganizations informed of common activities.
WHO was in continuous contact with the Inter-national Pharmaceutical Federation, whose vice -president is a member of the Expert Committee on theUnification of Pharmacopoeias. The two organiza-tions exchanged information on the labelling ofpharmaceutical products, on international non-proprietary names for drugs which might be describedin the Pharmacopoea Internationalis and in the co-ordination of national regulations on the control ofdrugs.
On behalf of the Organization, the World Federa-tion for Mental Health collected information on thefacilities in different countries for training psych-iatrists, clinical psychologists, psychiatric socialworkers and nurses. It also provided information onexperts in the treatment of alcoholism, and on theuse of group and individual psychotherapy in prisons.During the year the Organization was representedat meetings of the Federation, whose AssistantDirector attended the second session of the WHOExpert Committee on Mental Health.
Close co- operation was also maintained with theWorld Medical Association, particularly in con-nexion with the preparation of the Table of Usualand Maximal Doses for Adults, and as regards namesof drugs for inclusion in the Pharmacopoea Inter -nationalis. Both organizations are working on studieson medical education. Representatives of theassociation attended meetings of the WHO ExpertCommittee on Professional and Technical Educationof Medical and Auxiliary Personnel, and WHO inturn sent observers to those of the WMA's Committeeon Medical Education.
The International Union against Venereal Diseasescontributed to the public's understanding of theWHO programme, especially in the control ofvenereal diseases. The Union, which is now attempt-ing to extend the area of its activities, intends to openregional offices which will work in close co- operationwith those of WHO. Such an office may soon beestablished in New Delhi.
A special joint inquiry into existing types of educa-tion for public- health nurses was started with the
68 WORK OF WHO, 1950
International Council of Nurses. This Council,through its associated organization, the FlorenceNightingale International Foundation, is prepared toundertake studies in nursing education and in post -basic nursing education at WHO's request. Co-operation with the Council was also maintainedthrough its Executive Secretary, who has served onWHO's Expert Committee on Nursing.
Effective liaison was achieved with the InternationalDental Federation, through reciprocal representationat meetings and the exchange of information. TheFederation helped to select a temporary consultantin dental health, who was attached to WHO, toformulate (in consultation with the Federation) adental health programme for the consideration of theFourth World Health Assembly.
A second Seminar on World Health was organizedby the World Federation of United Nations Associa-tions at the time of the Third World Health Assemblyin Geneva. This seminar was attended by 25 youngphysicians and medical students from nine countries.The national United Nations associations also helpedto spread knowledge of the aims of the Organizationthroughout the world : in many countries theycontributed greatly to the celebration of WorldHealth Day, and the Association of Great Britainand Northern Ireland organized a lecture tour in theUnited Kingdom for the Director -General in con-nexion with United Nations Week (see page 69).
The usefulness of certain non -governmental organi-zations has not yet been fully explored. As WHO'sactivities increase, however, in such subjects asenvironmental sanitation, housing and social andoccupational health, and in diseases such as cancerand rheumatism, and as new activities are started,more help will be needed from the appropriate non-governmental organizations with which the Organiza-tion is in official relation. The following may serve asexamples. In planning WHO's work on leprosy,which has scarcely begun, the International Leprosy,Association will be consulted regularly ; until nowcontact has been maintained through correspondence.Relations with the International Association for thePrevention of Blindness have so far been confinedto the exchange of printed information, as no special-ized service of WHO deals with this important subject.The Biometric Society could undoubtedly provideuseful advice in connexion with several questionsconcerning biological standardization.
Besides the organizations which have been broughtinto official relations with WHO, other bodies associ-
ated with it formally co- operated in many ways. Forexample, WHO maintained liaison with the InterimCommittee of the International Universities Associa-tion, which carried on its activities under the sponsor-ship of UNESCO in 1950 : an observer from WHOattended several meetings of the committee, whichoffered its full co- operation, particularly in the co-ordination of research and the collection of informa-tion on medical and other education. As additionalexamples mention may be made of the InternationalUnion of Chemistry and of the Council on Pharmacyand Chemistry of the American Medical Association.The former advised WHO on internationally accept-able symbols, graphic formulae and standards ofreagents, the latter on the subject of non -proprietarynames for drugs.
In conclusion, it may be added that reports fromregional offices give a most satisfactory picture of theclose and co- operative work done in conjunction withnon -governmental and other organizations in theregions.
Intergovernmental Organizations
During 1950, as mentioned above, mostly becauseof the technical assistance programme, WHO co-operated with a much greater number of inter-governmental organizations outside the frameworkof the United Nations than ever before. Suchorganizations included the Caribbean Commission,the Inter -American Institute for American Affairs, theOrganization of American States (including itseconomic and social council and its consultativecommittee for technical assistance), the Common-wealth Scheme for Technical Assistance of SouthAsia and South -East Asia, the Commission forTechnical Co- operation in Africa South of the Sahara,the Central Commission for Navigation on the Rhine,the Council for Europe, the International Office ofEpizootics, the Organization of European EconomicCo- operation, the Pacific Science Council, the SouthPacific Commission and the Economic Co- operationAdministration.
At Suva, in the Fiji Islands, the Organization wasrepresented at the fifth session of the South PacificCommission, which has undertaken an independenthealth programme and is seeking to co- ordinate itsactivities with those of the agencies in the UnitedNations system. Consultations were held, particularlywith regard to epidemiological reporting. Before the

PUBLIC INFORMATION 69
meeting of the commission, the Director -Generalvisited some of its officers and its research council.
At the end of the year a conference on malaria inEquatorial Africa was held in Uganda under the
joint sponsorship of WHO and the Commission forTechnical Co- operation in Africa South of theSahara. The work of this conference is described inthe section on malaria.
PUBLIC INFORMATION
WHO shall " generally... take all necessary action to attain the objective of theOrganization ".
" Informed opinion and active co- operation on the part of the public are ofthe utmost importance in the improvement of the health of the people B°,
Experiences of the past year have demonstratedconclusively that the interest of the general publicin the work of the Organization is almost everywheregreater than are the possibilities of supplying informa-tion about it. Many organizations are obliged to lookfor appropriate outlets for the large amount ofinformational material which they produce, whereasWHO, because of its small budget and the emphasison its essential technical work, is in the almostunique position of being unable to respond adequatelyto the requests for general information which itreceives. For example, during 1950, as describedbelow, there was such a demand for the folder,WHO... What It Is... What It Does... How It Works,that two unscheduled re- printings had to be under-taken ; it was estimated that about twice as manycopies of the first WHO poster would be required ascould be printed ; and a large number of requests forspecially prepared articles and exhibit material had toremain unfulfilled.
It was expected that the appointment of publicinformation officers at the regional offices for South -East Asia and the Eastern Mediterranean during thesecond half of 1949, and at the Regional Office forthe Americas early in 1950, would help to meet notonly the special needs of the regions but also thegrowing demand for general information. Theseappointments have, in fact, led to improvements inthe situation, but, in spite of everything, the gapbetween the demand for informational material andthe possibilities of meeting it seems to be steadilywidening : in some countries, the local and nationalhealth authorities, as well as the usual public -infor-
es Preamble to the Constitution of the World HealthOrganization.
mation channels (press, periodicals, radio, cinema,etc.), are asking for general information on theOrganization in larger quantities and in greatervariety than can be supplied.
In an attempt to offset these various difficulties,the already existing co- operation with the UnitedNations, on the one hand, and with several of thespecialized agencies (particularly UNESCO), onthe other, has been considerably increased. A largeamount of material has regularly been channelledto these other agencies, through which it has beenpossible to achieve relatively wide distribution forcertain limited types of information. Similar fruitfulco- operation has been maintained with individualUnited Nations Information Centres in all parts ofthe world and with the World Federation of UnitedNations Associations and its national and localaffiliates.
With regard to World Health Day, celebrated on7 April on the theme " Know your own HealthServices ", the excellent work done by a large numberof governmental and non -governmental agencies re-sulted in a more effective and widespread obser-vance of the event than was the case in 1949. However,WHO and its Member Governments have yet toexplore other possibilities for the effective use of thisday as a means of focusing attention on the needfor people everywhere to participate in raising levelsof health.
In October the Director - General gave a seriesof lectures in England on the United Nations, theWorld Health Organization and international affairs.He addressed town meetings in Nottingham, Bir-mingham, Oxford and Reading, the Rotary Club inNottingham, and senior pupils at Eton College andWolverhampton High School. He also spoke at
70 WORK OF WHO, 1950
Chatham House in London. Earlier in the yearhe gave addresses in Australia, New Zealand, Austria,France, Sweden, Switzerland and the United Statesof America. He broadcast in Australia, New Zealand,Singapore and Calcutta and, on behalf of the UnitedNations, in Geneva and New York.
Press and Publications
In 1950, at headquarters and in the regionaloffices, WHO issued a total of approximately 250press releases and press notices. These releases,which covered the current activities of the Organiza-tion, were prepared in English and French (andsometimes in the other major languages of theregions) and were made available to local andforeign correspondents, newspapers and magazineeditors, science -writers, and representatives of govern-ments and non -governmental organizations. In mostcases they were also cabled to Lake Success forfurther distribution in all parts of the world.
Apart from carrying on routine activities, such assending out press releases, holding press conferencesand helping in the preparation of articles on WHO,the Organization distributed 5,000 copies of special" information -folders " for the Third World HealthAssembly, and for World Health Day. These folderscomprised, in all, some twenty -five feature -lengtharticles representing nearly a hundred pages of text.
In addition, the four -page WHO Newslettercontinued to be sent out monthly (in English andFrench from Geneva, and in English, Spanish andPortuguese from Washington). Its format wasenlarged and improved during the year, and thenumber of photographic plates more than trebled.Regular world -wide distribution of the Newsletter,which has steadily increased during the past twoyears, now amounts to over 30,000 copies of eachissue in the four languages. Further, approximately3,000 copies of certain special issues were distributedfor World Health Day, for the Third World HealthAssembly, and on other occasions.
The basic information leaflet, WHO... WhatIt Is... What It Does... How It Works, was muchin demand. Although a third revised edition waspublished late in 1949, the initial supply of 50,000copies in English and 40,000 in French was exhaustedbefore the end of the first half of 1950. A secondprinting of 45,000 copies was also used much morequickly than was foreseen and, pending the publi-cation of a new revised text in 1951, another and stilllarger printing had therefore to be ordered in thethird quarter of the year. Besides the English andFrench texts, smaller editions of the leaflet were
published (either by WHO or by various govern-mental and non -governmental agencies) in a numberof other languages, including Arabic, Chinese,German, Italian, Portuguese, Russian and Spanish,and publication in additional languages is plannedtentatively for the future.
As an up -to -date supplement to the more generalinformation contained in the leaflet, a brief roneo-graphed summary of essential facts on the structureand activities of the Organization, arranged in a formsuitable for quick reference, was published atfrequent intervals during the year. Moreover, at theclose of 1950, final arrangements were being madefor the publication of a 32 -page illustrated booklet,which will contain detailed and concrete informationon some major aspects of the Organization's work.The text of this booklet was prepared by an inter-nationally known writer on science who was undercontract to WHO ; it is designed for the general publicand will be published in English and French.
Requests for special articles for popular sciencemagazines, general health and paramedical publi-cations, yearbooks, encyclopaedias, and handbookson international organizations have increased steadilyduring the year to such a point that it has becomenecessary to place strict limitations on the numberto be fulfilled. Many invitations to give talks andlectures on WHO had also to be declined at head-quarters, at the regional offices, and at the New YorkLiaison Office.
Radio
Radio activities were increased during 1950 toprovide for the regular dispatch of news items onWHO to radio stations and networks in over thirtycountries and for the recording of scripts for the useof various radio centres. Some of this materialwas subsequently published in magazines and news-papers.
In radio work, co- operation with the UnitedNations has been particularly close. Both head-quarters and the regions regularly sent news itemsand scripts, recorded or in the form of copy, tonational broadcasting stations, and, for furtherdistribution, to Lake Success ; UNESCO alsodistributed radio news and feature items for WHO.
During the year, delegates, committee membersand field, regional and headquarters staff membersmade approximately 200 recordings on WHO in32 languages, and over 300 copies of talks were sentto radio stations in 45 countries. Other materialwas provided to radio reporters and directors of
PUBLIC INFORMATION 71
feature programmes, who, when visiting head-quarters, are also afforded studio facilities forrecording commentaries on WHO.
Twice a week, via the United Nations Short -Wave Service, direct broadcasts were made on variousaspects of the work of the Organization. Reportson these broadcasts have now been received frommany countries of Europe, reception being good asfar north as the Scandinavian countries ; lettersconcerning them have also come from listeners inSouth Africa and the United States of America.
The regional and other offices have been active inradio work. In the regional offices at New Delhi,Alexandria and Washington scripts were writtenand recordings made for broadcast over the nationalradio systems of the countries within the regions, aswell as over the United Nations system, and aweekly series of programmes on WHO was broad-cast in Spanish by the New York Liaison Office forrelay to South America.
During the Third World Health Assembly theUnited Nations Radio Division (Geneva) allottedto WHO a special nightly period for the transmissionof Assembly news. Commentaries were recordedin a number of languages and airmailed to Europeanand overseas stations for national broadcasts, anddispatches on the work of the Assembly were alsosent to Lake Success by radio circuit for immediatebroadcast throughout the American continent.
Visual Media
For the first time it became possible during theyear to begin real work in the " visual media " -toundertake the dissemination of information throughstill -photos, films, filmstrips and exhibits, and toattempt to meet the widespread demand for thistype of material from all the regions and from manyindividuals, publications, and governmental andnon -governmental agencies.
Beginning on 1 May, WHO assigned to its staff anexpert on this subject, who found it necessary toarrange for the photographing of major activities ofWHO throughout the world, since the existing filescontained relatively few photographs of professionalquality. Photographic assignments were thereforemade in every region, and as the material thusobtained becomes available, it is being assembled fordifferent types of presentation in exhibits, filmstrips
and publications, and for transmission to news-papers and magazines. Meanwhile, a limited distri-bution of the photographs already available from theearlier files has been continued.
Another urgent task was to meet the immediatedemand for exhibit materials for special meetings andcongresses. This called for the preparation of alarge -scale exhibit for the Third World Health Assem-bly and one on maternal and child health for theSixth International Congress of Paediatrics inZürich ; the revision of the latter for display at theWhite House Conference in Washington ; thesupplying of material for a meeting of the AmericanPublic Health Association in St. Louis ; the compila-tion of a small exhibit on certain aspects of theOrganization's work in treponematoses ; a seriesof panels on the structure, activities and services ofWHO for use by WHO offices at New Dehli, Alexan-dria and New York ; a small photographic exhibitfor a series of lectures given by the Director -General ;and finally, travelling exhibits for permanent usethroughout the various regional offices. Thesetravelling exhibits were made possible through thegenerous co- operation of the UNESCO Departmentof Mass Communications, and are expected to beavailable in several languages early in 1951.
WHO prepared special material on its epidemio-logical services for a United Nations " ScreenMagazine ", and also co- operated closely with theUnited Nations on plans for a film on health workin India, which is being produced jointly by theUnited Nations and the Indian Government. Anumber of ideas for the production of films to besponsored by outside commercial and philanthropicagencies were outlined or prepared in script formfor presentation to prospective sponsors ; amongthese scripts was one for a feature -length docu-mentary film on international co- operation in thesolution of health problems, which was written bytwo outside consultants. Towards the end of theyear, an outstanding specialist in the production ofdocumentary films and other visual media wasengaged for one month to assist in planning a com-prehensive long -term programme in this field.
During the first half of 1950, WHO producedjointly with UNESCO a 200 -page illustrated indexof films on the health and welfare of children, entitledChild Welfare Films. This catalogue (in one editionof 4,000 copies) was placed on sale at $1.00 per copythrough the United Nations sales distributionagencies.
A prominent artist was commissioned to designthe first WHO poster ; this poster was officially
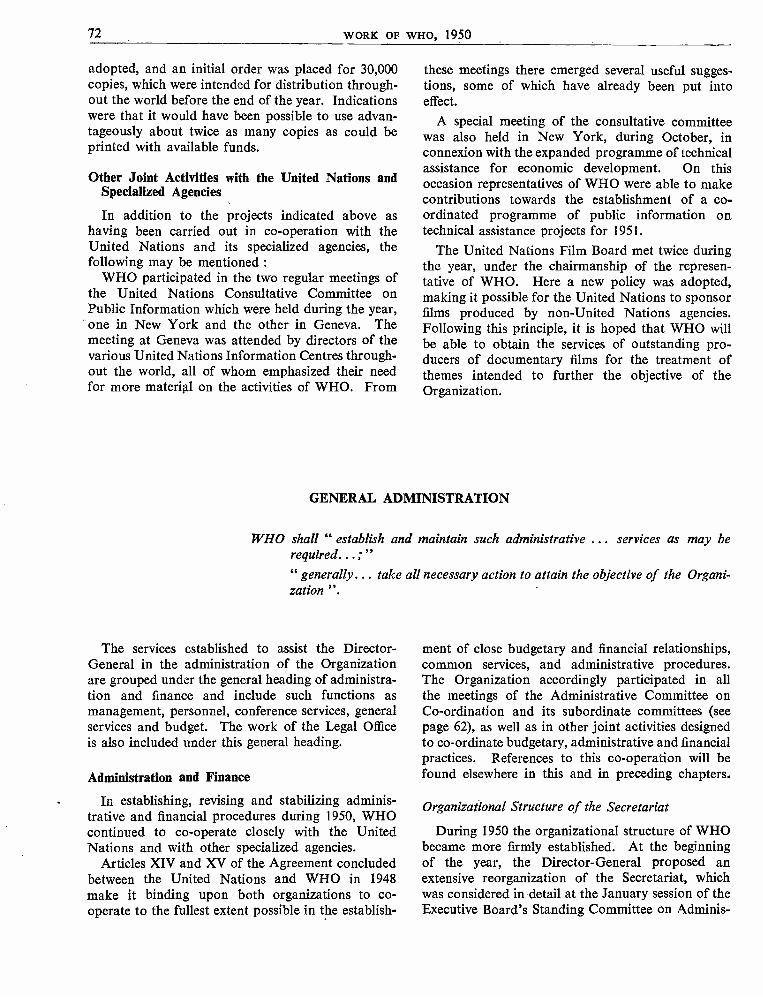
72 WORK OF WHO, 1950
adopted, and an initial order was placed for 30,000copies, which were intended for distribution through-out the world before the end of the year. Indicationswere that it would have been possible to use advan-tageously about twice as many copies as could beprinted with available funds.
Other Joint Activities with the United Nations andSpecialized Agencies
In addition to the projects indicated above ashaving been carried out in co- operation with theUnited Nations and its specialized agencies, thefollowing may be mentioned :
WHO participated in the two regular meetings ofthe United Nations Consultative Committee onPublic Information which were held during the year,one in New York and the other in Geneva. Themeeting at Geneva was attended by directors of thevarious United Nations Information Centres through-out the world, all of whom emphasized their needfor more material on the activities of WHO. From
these meetings there emerged several useful sugges-tions, some of which have already been put intoeffect.
A special meeting of the consultative committeewas also held in New York, during October, inconnexion with the expanded programme of technicalassistance for economic development. On thisoccasion representatives of WHO were able to makecontributions towards the establishment of a co-ordinated programme of public information ontechnical assistance projects for 1951.
The United Nations Film Board met twice duringthe year, under the chairmanship of the represen-tative of WHO. Here a new policy was adopted,making it possible for the United Nations to sponsorfilms produced by non -United Nations agencies.Following this principle, it is hoped that WHO willbe able to obtain the services of outstanding pro-ducers of documentary films for the treatment ofthemes intended to further the objective of theOrganization.
GENERAL ADMINISTRATION
WHO shall " establish and maintain such administrative ... services as may berequired... ; "" generally... take all necessary action to attain the objective of the Organi-zation ".
The services established to assist the Director -General in the administration of the Organizationare grouped under the general heading of administra-tion and finance and include such functions asmanagement, personnel, conference services, generalservices and budget. The work of the Legal Officeis also included under this general heading.
Administration and Finance
In establishing, revising and stabilizing adminis-trative and financial procedures during 1950, WHOcontinued to co- operate closely with the UnitedNations and with other specialized agencies.
Articles XIV and XV of the Agreement concludedbetween the United Nations and WHO in 1948make it binding upon both organizations to co-operate to the fullest extent possible in the establish-
ment of close budgetary and financial relationships,common services, and administrative procedures.The Organization accordingly participated in allthe meetings of the Administrative Committee onCo- ordination and its subordinate committees (seepage 62), as well as in other joint activities designedto co- ordinate budgetary, administrative and financialpractices. References to this co- operation will befound elsewhere in this and in preceding chapters.
Organizational Structure of the Secretariat
During 1950 the organizational structure of WHObecame more firmly established. At the beginningof the year, the Director - General proposed anextensive reorganization of the Secretariat, whichwas considered in detail at the January session of theExecutive Board's Standing Committee on Adminis-
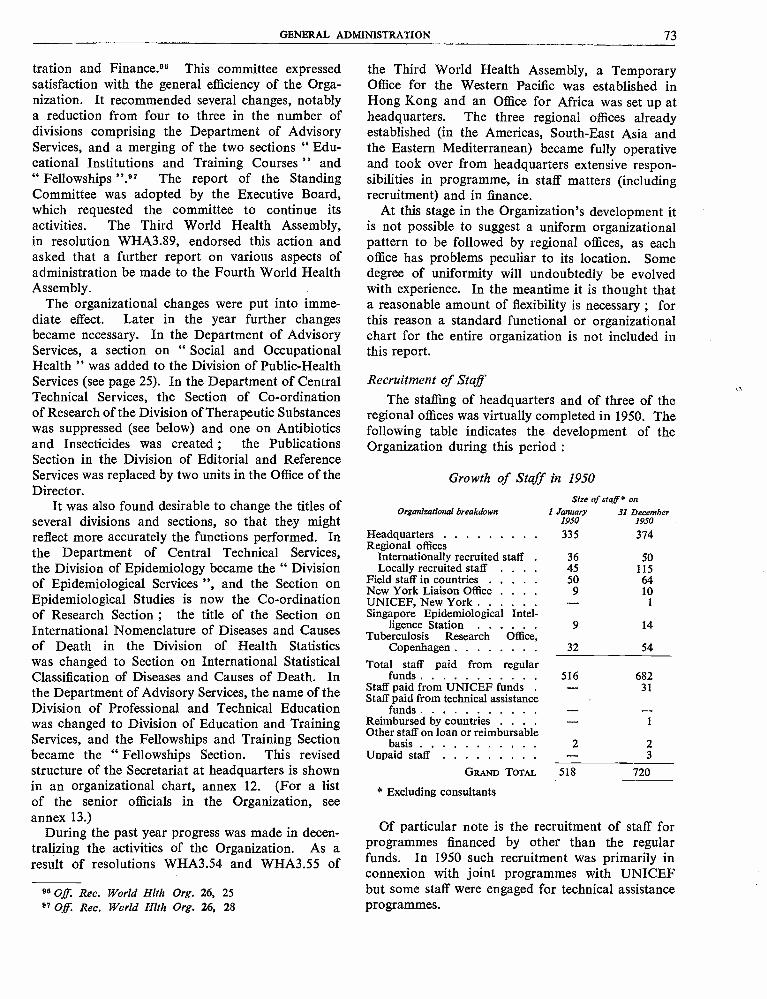
GENERAL ADMINISTRATION 73
tration and Finance.99 This committee expressedsatisfaction with the general efficiency of the Orga-nization. It recommended several changes, notablya reduction from four to three in the number ofdivisions comprising the Department of AdvisoryServices, and a merging of the two sections " Edu-cational Institutions and Training Courses " and" Fellowships ".97 The report of the StandingCommittee was adopted by the Executive Board,which requested the committee to continue itsactivities. The Third World Health Assembly,in resolution WHA3.89, endorsed this action andasked that a further report on various aspects ofadministration be made to the Fourth World HealthAssembly.
The organizational changes were put into imme-diate effect. Later in the year further changesbecame necessary. In the Department of AdvisoryServices, a section on " Social and OccupationalHealth " was added to the Division of Public- HealthServices (see page 25). In the Department of CentralTechnical Services, the Section of Co- ordinationof Research of the Division of Therapeutic Substanceswas suppressed (see below) and one on Antibioticsand Insecticides was created ; the PublicationsSection in the Division of Editorial and ReferenceServices was replaced by two units in the Office of theDirector.
It was also found desirable to change the titles ofseveral divisions and sections, so that they mightreflect more accurately the functions performed. Inthe Department of Central Technical Services,the Division of Epidemiology became the " Divisionof Epidemiological Services ", and the Section onEpidemiological Studies is now the Co- ordinationof Research Section ; the title of the Section onInternational Nomenclature of Diseases and Causesof Death in the Division of Health Statisticswas changed to Section on International StatisticalClassification of Diseases and Causes of Death. Inthe Department of Advisory Services, the name of theDivision of Professional and Technical Educationwas changed to Division of Education and TrainingServices, and the Fellowships and Training Sectionbecame the " Fellowships Section. This revisedstructure of the Secretariat at headquarters is shownin an organizational chart, annex 12. (For a listof the senior officials in the Organization, seeannex 13.)
During the past year progress was made in decen-tralizing the activities of the Organization. As aresult of resolutions WHA3.54 and WHA3.55 of
96 Off. Rec. World Hlth Org. 26, 2597 OJf. Rec. World Hlth Org. 26, 28
the Third World Health Assembly, a TemporaryOffice for the Western Pacific was established inHong Kong and an Office for Africa was set up atheadquarters. The three regional offices alreadyestablished (in the Americas, South -East Asia andthe Eastern Mediterranean) became fully operativeand took over from headquarters extensive respon-sibilities in programme, in staff matters (includingrecruitment) and in finance.
At this stage in the Organization's development itis not possible to suggest a uniform organizationalpattern to be followed by regional offices, as eachoffice has problems peculiar to its location. Somedegree of uniformity will undoubtedly be evolvedwith experience. In the meantime it is thought thata reasonable amount of flexibility is necessary ; forthis reason a standard functional or organizationalchart for the entire organization is not included inthis report.
Recruitment of Staff
The staffing of headquarters and of three of theregional offices was virtually completed in 1950. Thefollowing table indicates the development of theOrganization during this period :
Growth of Staff in 1950
Organizational breakdown
HeadquartersRegional offices
Internationally recruited staffLocally recruited staff .
Field staff in countriesNew York Liaison Office .
UNICEF, New YorkSingapore Epidemiological Intel-
ligence StationTuberculosis Research Office,
CopenhagenTotal staff paid from regular
fundsStaff paid from UNICEF fundsStaff paid from technical assistance
fundsReimbursed by countries .
Other staff on loan or reimbursablebasis
Unpaid staffGRAND TOTAL
* Excluding consultants
Size of sta ff O on
1 January 31 December1950 1950
335 374
36 5045 11550 64
9 10- 1
9 14
32 54
516 682- 31
- -- 1
2 2- 3
518 720
Of particular note is the recruitment of staff forprogrammes financed by other than the regularfunds. In 1950 such recruitment was primarily inconnexion with joint programmes with UNICEFbut some staff were engaged for technical assistanceprogrammes.
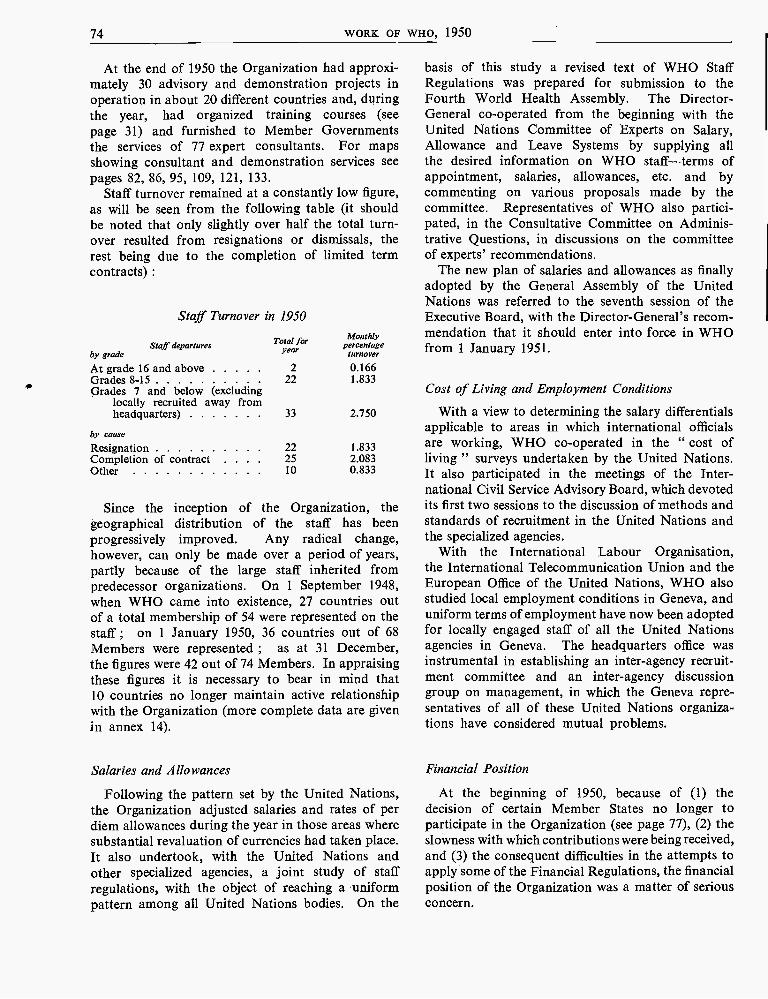
74 WORK OF WHO, 1950
At the end of 1950 the Organization had approxi-mately 30 advisory and demonstration projects inoperation in about 20 different countries and, duringthe year, had organized training courses (seepage 31) and furnished to Member Governmentsthe services of 77 expert consultants. For mapsshowing consultant and demonstration services seepages 82, 86, 95, 109, 121, 133.
Staff turnover remained at a constantly low figure,as will be seen from the following table (it shouldbe noted that only slightly over half the total turn-over resulted from resignations or dismissals, therest being due to the completion of limited termcontracts) :
Staff Turnover in 1950
Staff departuresby grade
Total foryear
Monthlypercentage
turnover
At grade 16 and above 2 0.166Grades 8 -15 22 1.833Grades 7 and below (excluding
locally recruited away fromheadquarters)
by cause
33 2.750
Resignation 22 1.833Completion of contract 25 2.083Other 10 0.833
Since the inception of the Organization, thegeographical distribution of the staff has beenprogressively improved. Any radical change,however, can only be made over a period of years,partly because of the large staff inherited frompredecessor organizations. On 1 September 1948,when WHO came into existence, 27 countries outof a total membership of 54 were represented on thestaff ; on 1 January 1950, 36 countries out of 68Members were represented ; as at 31 December,the figures were 42 out of 74 Members. In appraisingthese figures it is necessary to bear in mind that10 countries no longer maintain active relationshipwith the Organization (more complete data are givenin annex 14).
Salaries and Allowances
Following the pattern set by the United Nations,the Organization adjusted salaries and rates of perdiem allowances during the year in those areas wheresubstantial revaluation of currencies had taken place.It also undertook, with the United Nations andother specialized agencies, a joint study of staffregulations, with the object of reaching a uniformpattern among all United Nations bodies. On the
basis of this study a revised text of WHO StaffRegulations was prepared for submission to theFourth World Health Assembly. The Director -General co- operated from the beginning with theUnited Nations Committee of Experts on Salary,Allowance and Leave Systems by supplying allthe desired information on WHO staff -terms ofappointment, salaries, allowances, etc. and bycommenting on various proposals made by thecommittee. Representatives of WHO also partici-pated, in the Consultative Committee on Adminis-trative Questions, in discussions on the committeeof experts' recommendations.
The new plan of salaries and allowances as finallyadopted by the General Assembly of the UnitedNations was referred to the seventh session of theExecutive Board, with the Director -General's recom-mendation that it should enter into force in WHOfrom 1 January 1951.
Cost of Living and Employment Conditions
With a view to determining the salary differentialsapplicable to areas in which international officialsare working, WHO co- operated in the " cost ofliving " surveys undertaken by the United Nations.It also participated in the meetings of the Inter-national Civil Service Advisory Board, which devotedits first two sessions to the discussion of methods andstandards of recruitment in the United Nations andthe specialized agencies.
With the International Labour Organisation,the International Telecommunication Union and theEuropean Office of the United Nations, WHO alsostudied local employment conditions in Geneva, anduniform terms of employment have now been adoptedfor locally engaged staff of all the United Nationsagencies in Geneva. The headquarters office wasinstrumental in establishing an inter -agency recruit-ment committee and an inter -agency discussiongroup on management, in which the Geneva repre-sentatives of all of these United Nations organiza-tions have considered mutual problems.
Financial Position
At the beginning of 1950, because of (1) thedecision of certain Member States no longer toparticipate in the Organization (see page 77), (2) theslowness with which contributions were being received,and (3) the consequent difficulties in the attempts toapply some of the Financial Regulations, the financialposition of the Organization was a matter of seriousconcern.
GENERAL ADMINISTRATION 75
As many of the non -participating Member Stateshad not paid their contributions to the 1948 and 1949budgets in fu11,98 and as it appeared that thesecontributions might not be forthcoming, the Organi-zation, although not having used up the totalappropriations for either year, found that it hadspent more than it had collected. In accordancewith the Financial Regulations the working capitalfund was drawn upon to meet this excess of expen-diture, the amounts withdrawn being repayableinto the fund, in normal circumstances, on receiptof contributions. The fund was therefore seriouslydepleted. Furthermore, according to FinancialRegulations 13 and 16 (e), the unobligated balanceof appropriations at the end of the year should havebeen surrendered and used to adjust the assessmentsof Member States in future years. Since, however,many of the contributions had not been paidpromptly, and some not at all, these balances werenot in cash and could have been appropriated in thismanner only by further depleting the workingcapital fund.
The Director -General reported this situation tothe Executive Board at its fifth session. The Boardtook two important decisions, later confirmed bythe Health Assembly. The first was to establish,after careful examination of the funds expected tobe available for 1950, an expenditure ceiling of$6,300,000 for the 1950 budget of $7,501,500. Thesecond was to set aside the provisions of the FinancialRegulations with regard to the unused budget sur-pluses of the 1949 fiscal year (this decision was ex-tended by the Third World Health Assembly to applyto surpluses of 1950 and 1951 as well), and to placethese balances in a suspense account representingthe unpaid contibutions of various Member States.The Health Assembly reserved the right to examinethe status of this suspense account from to time, and,if any of the account should become cash by thepayment of overdue contributions, to appropriatethis cash in the manner provided for in the FinancialRegulations.
The result of these actions has been to place theOrganization in a more satisfactory financial position.The Director - General has further studied the situa-tion and will propose additional measures forimproving it to the Executive Board and the FourthWorld Health Assembly.
98 Of these States, contributions to the 1948 budget werepaid in full by Albania, Czechoslovakia, Poland andRoumania ; Bulgaria paid half and Hungary about a third.Czechoslovakia and Roumania made small payments to the1949 budget.
Form of Presentation of Programme and Budget
In conformity with instructions of the ThirdWorld Health Assembly in resolution WHA3.107and based on certain guiding principles established bythe Executive Board, in resolution EB6.R20, theProposed Programme and Budget Estimates for 1952reflect a new method of planning and budgeting. Forthe first time, they were prepared at regional levelsand discussed by regional committees before beingco- ordinated at headquarters. These estimates forthe regions were made to show all the regionalactivities, grouped by countries and projects, and,together with the estimates for headquarters, wereconsolidated into proposals for an integrated pro-gramme and budget for 1952.
The General Assembly of the United Nationspassed a resolution requesting the specialized agenciesto provide expenditure estimates for technicalassistance and other extra -budgetary funds, as wellas for those coming from the regular budget.99Accordingly, in the description of activities proposedfor 1952, the Proposed Programme and BudgetEstimates for 1952 also indicate the source of fundsfrom which these activities are to be financed (whetherfrom regular, UNICEF or technical assistance funds).
These estimates should give the Health Assemblya comprehensive picture of the total programmeproposed for 1952.
Assessments and Contributions
Member States of the Organization have consis-tently been assessed in accordance with principlessimilar to those governing the assessments to thebudget of the United Nations ; the WHO scale ofassessment was computed on that basis. In consider-ing a resolution of the General Assembly calling fora closer relationship between the assessments of theUnited Nations and those of the specialized agencies,the Third World Health Assembly pointed out thatthe Organization had in fact been following theUnited Nations scale of assessments. On the basis ofdata provided by the United Nations, it then estab-lished the assessments of those countries which hadjoined the Organization during 1950 ; finally, in ful-filment of the principle that no one Member Stateshould contribute more than one -third of the regularexpenses for any year -a principle to be put intoeffect gradually, starting in 1950 -it fixed (in resolu-tion WHA3.91) the contribution of the United Statesof America for the year 1951 at 35 % of the total,
99 UN document A.1587
76 WORK OF WHO, 1950
this being a reduction of 1 % from the assessmentsfor 1950.
During 1950 special emphasis was given to variousmethods of facilitating the collection of contributions.Early in the year cables were dispatched to allMember States which had not paid their contribu-tions for 1948 and 1949. Then a new system wasintroduced : all Members were sent regular monthlystatements of the status of contributions, andseparate letters were written each month to thosewhose contributions remained unpaid. Althoughthese measures have produced some improvement inpayments, the unpaid contributions for the year 1948and 1949 still represent an unsatisfactory situation.
There is attached as annex 15 a statement showingthe status of contributions to the budgets for theyears 1948, 1949 and 1950 and the assessments to theworking capital fund. It should be noted that on31 December 1950, 58.86 % of the 1950 budget hadbeen collected, as compared with 73.29 % of thebudget at the end of 1949. This was primarily due,however, to the difficulties which the United Statesof America experienced in making its paymentbecause of the ceiling placed on its contributions bythe United States Congress. This ceiling has nowbeen lifted, and when the United States pays thebalance of its contributions, the percentage will showan improvement of some 2 % over that of 1949.
Working Capital Fund
At the Third World Health Assembly, after a care-ful study had been made of the status of the workingcapital fund, it was decided that the fund as estab-lished by the Second World Health Assembly shouldbe maintained for 1951. Also the Director -Generalwas authorized (in resolution WHA3.105) to takefrom the fund a sum of one million Swiss francs($233,645), for the purpose of constituting a buildingfund, and provision was then made for the repaymentof this sum to the fund. These decisions are beingput into effect.
Repayment of the United Nations Loan
The balance of the loan from the United Nations,amounting to $1,300,000 as at 1 January 1950, wasrepaid in full during the early part of the year, wellin advance of the date on which it was due. Of thisamount $900,000 represented the balance of the loanto the Interim Commission.
Financial Regulations
At meetings of the Consultative Committee onAdministrative Questions it became apparent that thebest way to achieve uniformity of financial practicesamong the United Nations and its specialized agencieswas by the adoption of uniform financial regulations.Uniform regulations were therefore agreed upon bythat committee in February. They were approvedby the Administrative Committee on Co- ordinationin May, too late to allow of their being studied ade-quately by the Third World Health Assembly, whichtherefore decided to continue with WHO's presentProvisional Financial Regulations for one more year.The Director - General circulated copies of the uniformregulations to all Member States, and will submitthem to the seventh session of the Executive Boardand to the Fourth World Health Assembly for furtherconsideration.
Audit Procedures
The Second World Health Assembly (in resolutionWHA2.52) endorsed principles to govern audit pro-cedures, as recommended by the AdministrativeCommittee on Co- ordination, and agreed with theestablishment of a panel of external auditors of theUnited Nations and the specialized agencies. TheWHO external auditor was placed on the panel,which held its first meeting in New York in October.
Technical Assistance Programme
A large number of administrative and financialproblems arose with the beginning of the expandedprogramme of technical assistance for economicdevelopment (see page 59). The fact that contributionsare received in different currencies, some of which havea limited convertibility, and the restrictions placedupon their use, will create practical difficulties incarrying out the projects envisaged. It is apparentthat the administration of this programme will be adifficult task, and will require a considerable amountof time and attention.
For the first period (ending 31 December 1951)WHO shares in the contributions to the SpecialAccount to the extent of 22 % of the first ten milliondollars and 22 % of 70 % of the second ten millioncontributed (see page 59). There is attached asannex 16 a list of the contributions which have beennotified to WHO as at 31 December 1950 and theamounts allocated to the Organization.
RAJKUMARI AMRIT KAUR, India, President ofthe Third World Health Assembly.
Dr. H. S. GEAR, Chairman of the ExecutiveBoard.
PLENARY MEETING of the Third World Health Assembly, held in May 1950at the Palais des Nations, Geneva.
First session of the Expert Committee onProfessional and Technical Education of Medi-cal and Auxiliary Personnel, held in Genevafrom 6 to 10 February 1950. Left to right(seated round table) : Dr. M. S. Akalin ; MissM. Andrei! ; Dr. G. W. Anderson (Vice- Chair-man) ; Dr. R. Sand (Chairman) ; Dr. E. Grzegor-zewski (WHO) ; Dr. J. M. Macintosh (Rappor-teur) ; Dr. H. Romero ; Dr. G. H. de PaulaSouza ; Dr. J. Parisot ; Dr. A. Stampar ;Dr. J. B. Grant.
The Malaria Conference in EquatorialAfrica was held at Kampala, Uganda,from 27 November to 9 December 1950and was attended by experts from theterritories of Equatorial and SouthernAfrica and by members of the WHOExpert Committee on Malaria.
First session of the Expert Committee onAntibiotics, held in Geneva from 11 to 15April 1950. Left to right (seated round table) :
Professor S. A. Waksman ; Professor M. -M.Janot (Vice- Chairman) ; Professor R. V. Christie(Rapporteur) ; Dr. S. S. Sokhey (AssistantDirector -General, WHO) ; Professor E. B. Chain(Chairman) ; Dr Mélanie Craipeau (WHO) ;Professor H. Theorell ; Mme Y. Bezoari (WHO).
GENERAL ADMINISTRATION 77
Accommodation for the Headquarters Office
In February, WHO signed an agreement with theUnited Nations concerning the premises of WHO'sheadquarters office in Geneva. By this agreement theUnited Nations undertook to add to the Palais desNations, at WHO's expense, by raising the presenttwo -floor annex to the Palais by three floors, and byconstructing a six -floor annex on the opposite sideof the courtyard. These constructions will provideapproximately 170 offices, and 40 additional officeswill be obtained by transformations within the Palaisitself. In consideration of the amount which WHOwill spend on the new constructions, the UnitedNations is leasing approximately 285 offices toWHO for 99 years. These offices will form a blockin the existing Palais and will be rented at thenominal charge of 1 Swiss franc per year. The leaseis renewable on terms to be fixed at the time whenit expires, and WHO also has an option on anyadditional space which might become available.
Both the Executive Board at its fifth session and theThird World Health Assembly approved this agree-ment, considering that it was economical and wouldgive WHO sufficient security of tenure for a longperiod.
The necessary construction and internal trans-formation will cost approximately 4,000,000 Swissfrancs. The Swiss Government, to help the Organi-zation in establishing its headquarters in Geneva,donated the sum of 3,000,000 Swiss francs. For thebalance of the expenditure the Third World HealthAssembly established a separate building fund of1,000,000 Swiss francs (see page 76).
By the end of the year the new constructions, whichwere begun in April 1950, were well advanced andexpected to be ready for occupation by July 1951.
Furniture for the offices which WHO has occupiedin the Palais was originally loaned by the UnitedNations. As, however, the United Nations found thatit needed this furniture for its own use, WHO hasbeen obliged to buy new furniture, not only for itstemporary offices, but also for the additional oneswhich will be at its disposal when the new constructionhas been completed. This process of acquiringfurniture and equipment was started in 1949 andwas practically completed during 1950, within theregular funds available.
In this manner, during 1950, thanks to the gener-osity of the Swiss Government and to the co- operationof the United Nations, and with substantial economiesto the Organization, arrangements were completed
for the physical requirements of headquarters formany years to come. The next step will be to provideadequate accommodation for the regional offices.
Legal and Constitutional Questions
The following important legal and constitutionalquestions arose during the year (see also InternationalConventions, Agreements and Regulations on Health,page 40) :
Membership of the Organization 100
The total number of Member States of the WorldHealth Organization is now 74, including six newMembers who joined the Organization in 1950. Twoof these, Nicaragua and Cuba, joined on 24 April and9 May respectively, when they deposited their instru-ments of acceptance with the Secretary - General ofthe United Nations. Viet Nam and the Kingdomsof Cambodia and Laos became Members on 17 May,and the Republic of the United States of Indonesiaon 23 May, after a favourable vote by the ThirdWorld Health Assembly (resolutions WHA3.75 andWHA3.76). In addition, on 16 May, the ThirdWorld Health Assembly (in resolution WHA3.77)admitted its first Associate Member, SouthernRhodesia.
During 1950 six Governments notified WHO thatthey no longer considered themselves as Members :Roumania (20 February), Albania (25 February),Czechoslovakia (14 April), Hungary (19 May), Poland(15 August) and China (7 May). Following thecommunication from China a protest was receivedfrom the Government of the People's Republic ofChina, challenging the right of the Government inTaipeh to represent the country. By the end of theyear in all ten countries had sent such notificationsto the Director -General ; 101 since, however, theConstitution contains no provision for withdrawalfrom WHO, these countries are still considered to beMembers of the Organization. The texts of thenotifications were forwarded to governments, andthose which had been received in time were broughtto the attention of the Third World Health Assembly,which (in resolutions WHA3.84 and WHA3.90)declared that WHO would always welcome therenewed collaboration of these States in the work ofthe Organization.
100 For complete list of Members see annex 1.101 The others were Bulgaria, the Byelorussian SSR, the
Ukrainian SSR and the USSR.
78 WORK OF WHO, 1950
Absences from the Executive Board
In application of Article 87 of its Rules of Pro-cedure, the Third World Health Assembly was in-formed that the members of the Executive Boarddesignated by the Byelorussian SSR, China and theUSSR had failed to attend two consecutive sessionsof the Board. The terms of office of the membersdesignated by China and the USSR were in any casedue to expire at that time, but that of the memberdesignated by the Byelorussian SSR extended untilMay 1951. After some discussion, the HealthAssembly decided (in resolution WHA3.78) thatrepeated and consecutive absences from sessions ofthe Board by the person designated by any Membermade it justifiable to presume that the Member hadwithdrawn from the Board. It consequently elected(resolution WHA3.120) another State, Brazil, todesignate a person to serve on the Board for theremainder of the term of the member from theByelorussian SSR.
If the Fourth World Health Assembly accepts aproposal made by the Executive Board at its sixthsession (in resolution EB6.R34) the Rules of Pro-cedure will be amended so that the procedure referredto above will become statutory.
Representation of the Board at the Health Assembly
The Executive Board, at its fifth session, appointedthree of its members to act as its personal represen-tatives at the Third World Health Assembly. Thisprocedure proved a success. In their report to thesixth session of the Executive Board these threerepresentatives suggested that future representationof the Board at the Health Assembly should beundertaken by two members only. The proposal willbe considered by the Board at its sixth session.
Status of the Executive Board
At the beginning of 1950, the Australian Govern-ment proposed the amendment of Articles 24 and55 of the WHO Constitution. The proposed modifica-tion to Article 24 was to the effect that a person desig-nated by a government to serve on the Executive Boardwould no longer act in an individual capacity but asa representative of the State designating him ; thatto Article 55 aimed at broadening the powers of theExecutive Board and formulating them more specifi-cally. These proposals were not accepted by the ThirdWorld Health Assembly, which, however, decided(in resolution WHA3.96) that the Executive Boardmight recommend modifications in the Director -General's budget estimates when submitting these tothe Health Assembly.
Biennial Health Assemblies
A further amendment to the Constitution was pro-posed by the Governments of Denmark, Norwayand Sweden, namely that Article 13 should bemodified so as to provide for regular sessions of theHealth Assembly to be convened once in every twoyears instead of annually. In principle, this proposalwas approved by the Health Assembly (in resolutionWHA3.96), which requested the Director- Generalto make a careful study of the new arrangements andfurther changes in the Constitution which thisamendment would necessitate. The matter will bereconsidered by the Fourth World Health Assembly.
Agreements with Governments
During 1950, discussions were continued with theEgyptian Government on the final text of an agree-ment which would grant to the Organization theprivileges, immunities and facilities necessary forcarrying out its functions in Egypt. On the basis of astatement by the State Adviser to the Ministries ofForeign Affairs and Justice that the Egyptian Govern-ment was in agreement with the draft proposed,the Third World Health Assembly passed resolutionWHA3.83 adopting the text of the agreement andauthorizing the Director - General to exchange noteswith the Egyptian Government concerning the inter-pretation of two points previously raised by thatGovernment. These were (1) the judicial immunityof Egyptian citizens in respect of Egyptian penaljurisdiction, and (2) the application of measures,applied in accordance with international sanitaryconventions, to persons entering the country.
After this resolution had been adopted, theEgyptian Government was invited to sign the agree-ment. However, in September, the Director - Generalwas informed that an Egyptian inter -ministerialcommittee had re- examined it and had suggestedsubstantial amendments to the text approved by theHealth Assembly. At the end of the year the EgyptianMinister of Foreign Affairs and the Director - Generalhad agreed on a revised text for the agreement andan exchange of letters which, it was thought, wouldovercome the difficulties which had arisen. Thesetexts will be submitted to the Fourth World HealthAssembly for approval.
Other agreements with governments were concludedduring the year on regional programmes and oncertain aspects of the general administration of theOrganization. No statement of the objects of theseagreements is given here, as they were concluded forthe purpose of determining the mode of implementa-tion of the various projects of WHO as set out inother parts of this report.
GENERAL ADMINISTRATION 79
Privileges and Immunities.
Consequent upon resolutions of previous sessionsof the Health Assembly and Executive Board con-cerning the rights of Associate Members 102 and uponresolution WHA3.47 establishing expert advisorypanels, the Third World Health Assembly adopted(in resolution WHA3.102) a revision of Annex VIIof the Convention on the Privileges and Immunitiesof the Specialized Agencies. The revised text,which was communicated to governments during theyear, provides that : (1) the provisions of Article Vand of Section 25, paragraphs 1 and 2(I) of Article VIIof the Convention (i.e., the privileges, immunitiesand facilities granted to delegates of Member States)shall be extended to representatives of AssociateMembers ; (2) the provisions of Article 2 ofAnnex VII, granting in certain cases immunity fromlegal process and privileges in respect of communica-tions to experts serving on committees, shall beextended to experts serving on advisory panels.
Up to 31 December 1949 three Members hadacceded to this Convention : the Netherlands(2 December 1948), the United Kingdom (withreservations) (16 August 1949), and India (10 Feb-ruary 1949).103 The following countries acceded to itduring 1950: Denmark (25 January), Norway(25 January), the Republic of the Philippines (20March), and Luxembourg (20 September). Twoadditional countries, the Hashemite Kingdom of theJordan and Turkey, informed the Organization thatthey had approved the Convention and had takenthe necessary steps for depositing an instrument of
102 Resolution WHA2.105, Off. Rec. World Hlth Org. 21, 56 ;Of Rec. World Hlth Org. 22, 8
103 For list of other Members who agreed during 1949 toapply the provisions of the convention, see Of Rec. WorldHlth Org. 24, 79
acceptance with the Secretary - General of the UnitedNations. Four Members- Haiti, Ireland, Viet Namand Yugoslavia- stated that pending formal ratifica-tion of the Convention they were prepared to applyin their territories its provisions with respect to theUnited Nations laissez -passer.
Office International d'Hygiène Publique
It will be recalled that, although most of thefunctions of the Office International d'HygiènePublique had been assumed by WHO, the Officecould not be legally dissolved until the Rome Agree-ment of 1907 (setting up the Office) had been abro-gated by the consent of all the parties concerned. Asit became evident that some of the governments,signatories to the Rome Agreement, were unable totake action, the Permanent Committee of the Officemet in Geneva on 5 and 6 May, some days before theopening of the Third World Health Assembly, andunanimously decided that, without waiting for thelegal dissolution, the activities of the Office should beterminated de facto as from 15 November and itsassets turned over to WHO. The Third WorldHealth Assembly thereupon adopted resolutionsWHA3.53 and WHA3.98 agreeing to continue toassume the functions and duties imposed upon it bythe Office and accepting this transfer. Accordingly,the Committee of Finance and Transfer of the Officemet in Paris on 14 November. At this meeting, towhich WHO was invited to send representatives, thefinal arrangements for the disposal of the assets andliabilities of the Office were made. The whole of thelibrary and archives, part of which had been lent toWHO, were prepared for transfer ; a sum was setset aside to cover the cost of liquidation, and a resolu-tion was taken for the transfer of all remaining assetsto WHO.
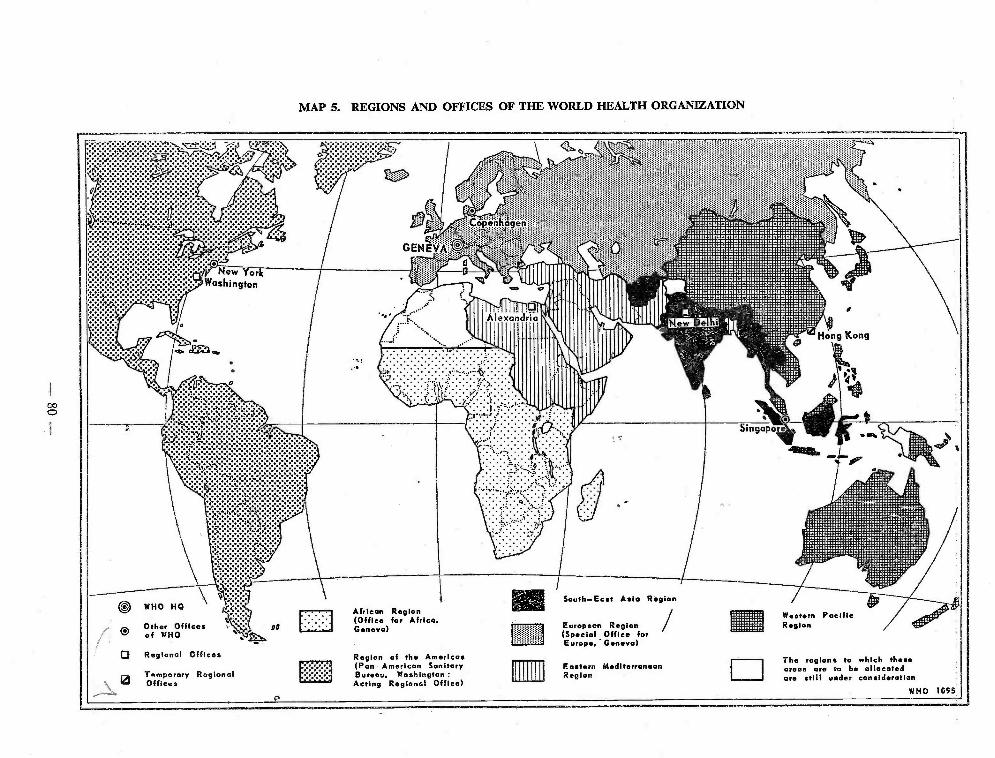
MAP 5. REGIONS AND OFFICES OF THE WORLD HEALTH ORGANIZATION
Other Officesof WHO
African Region(Office for Africa.G
Eur Region(Special Office forEurope, Geneva)
Regional Offices Region of the Americas(Pan American SanitaryBureau, Washington:Acting Regional Office)
The regions to which thoseareas are to be allocatedare still under consideration
CHAPTER 2
ACTIVITIES BY REGION AND COUNTRY
With the gradual decentralization of activities from headquarters to the regions and the establishmentof a temporary regional office for the Western Pacific and an office for Africa (for map showing WHO regionsand offices, see page 81), the ground was prepared for health projects to be initiated, planned and carriedout by the regional offices. The final step will be for the countries and then the peoples themselves to assumethis responsibility. This charter describes the health activities stimulated, and in some cases guided, by WHOin regions and in countries.
These activities have varied greatly according to the region, and consequently the reports on these regionsare not really comparable. In South -East Asia, for example, where a WHO regional office was first established,efforts have been directed mostly towards training and demonstration by the use of teams and consultants.Activities have been carried on, particularly in the fields of malaria, venereal diseases, and maternal and childhealth, with parallel teams provided by the governments, which will continue the work after the withdrawalof WHO Staff. The training of nurses has also been stressed, and extensive plans have been drawn up forassistance in tuberculosis control. As this office has been functioning longer than any of the other WHOregional offices, it has had an opportunity to make a careful study of the problems and needs of the countriesin the region, which are described somewhat in detail in this chapter of the report.
The second regional office which came into existence was the office for the Eastern Mediterranean Region,at Alexandria. In this region WHO has helped to establish demonstration and training projects, includingmalaria teams and a tuberculosis centre, and has given assistance to special groups, such as the Palestinerefugees. Surveys of public -health administration, sanitation and tuberculosis have been made, and manyprojects have been planned to begin in the region in 1951.
With the Pan American Sanitary Bureau, serving as WHO's Regional Office for the Americas, a highdegree of co- ordination and co- operation was established during 1950, particularly in administrative arrange-ments. The planning and development of programmes has proceeded. Work with UNICEF on tuberculosiscontrol, insect control and maternal and child health has particularly characterized WHO's activities in theAmericas ; malaria surveys and investigations into endemic goitre have also been made, and technical advicehas been given on such subjects as diphtheria and whooping cough, and poliomyelitis.
Europe, where the Special Office continued to function, has requested an entirely different type ofassistance -the organization of study -groups and training courses to which many European countries havesent representatives, and the furnishing of teams in highly specialized subjects such as anaesthesiology, juvenileepilepsy and congenital heart diseases. As was to be expected, countries in which medical knowledge andpublic- health services are highly advanced were the first to avail themselves of services facilitating the exchangeof scientific information. Those countries, with no lack of information themselves, have recognized thatconstant interchange of knowledge is a condition of continuing progress. Many joint programmes with otherorganizations have also been carried out in Europe.
In the Western Pacific, the temporary regional office was established late in the year. Here most of theactivities carried on by WHO have been undertaken jointly with UNICEF. Surveys were started in the countriesin this region ; the Philippines were assisted with a number of improvements in health services, and underthe auspices of WHO and UNICEF, nursing teams have begun or continued to work in several other countries.Events in China, Korea and other countries have, however, interrupted important projects in this region.
In the African Region, from which so far few requests have been received, work is just beginning. TheOffice for Africa was established at headquarters in October ; extensive surveys were undertaken ; an importantconference was held, and consultants have been sent to Liberia.
A description of WHO's activities in its six regions -the African area, the Americas, South -East Asia,Europe, the Eastern Mediterranean and the Western Pacific in that order, is set out below.
- 81 -
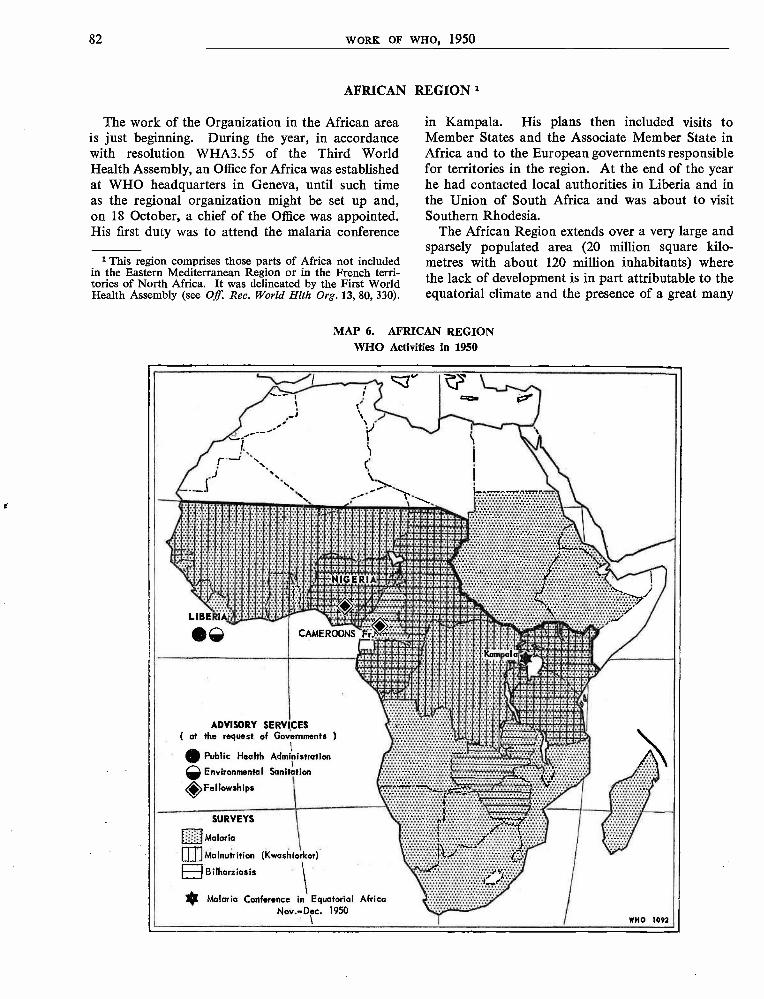
82 WORK OF WHO, 1950
AFRICAN REGION 1
The work of the Organization in the African areais just beginning. During the year, in accordancewith resolution WHA3.55 of the Third WorldHealth Assembly, an Office for Africa was establishedat WHO headquarters in Geneva, until such timeas the regional organization might be set up and,on 18 October, a chief of the Office was appointed.His first duty was to attend the malaria conference
1 This region comprises those parts of Africa not includedin the Eastern Mediterranean Region or in the French terri-tories of North Africa. It was delineated by the First WorldHealth Assembly (see Off. Rec. World Hlth Org.13, 80, 330).
in Kampala. His plans then included visits toMember States and the Associate Member State inAfrica and to the European governments responsiblefor territories in the region. At the end of the yearhe had contacted local authorities in Liberia and inthe Union of South Africa and was about to visitSouthern Rhodesia.
The African Region extends over a very large andsparsely populated area (20 million square kilo-metres with about 120 million inhabitants) wherethe lack of development is in part attributable to theequatorial climate and the presence of a great many
MAP 6. AFRICAN REGIONWHO Activities in 1950
LIBERIA
®®
11111111111
awoloaaaa . ;.Mk. Oldlófaaa004'aammle caaç
iawww881a1¢4iwwF 4iglagSaieñi>b lFilfapXCCCItIlS16100hJ10. '' iq/JV7!7.WW207Pfi1RS4@.
.88EEESS®88' glB@88®ggaaww faaqatlaaaaaww107assw O am mE$$wwwEmm;..'"esd AWéEEOEfytOE OOIOfdldaaa0000w,a w9. aw°iaw>ag$gwwag4c444i Meta M,"
+aalaEY'. . .
7laaaw;vwY . .
MEESiBBi4faaaoozXt>pla:®ESae8888'. .'tmse>deiaa'888E4ig4"IM
am70..
A .. ... ..
CAMEROONS F
Kampa
xC0á:_:AakwegMsiamaixEEa'fox.-.7 aaaawwwi
1NEEE8808i:4ww70iaiaal.
88Q$SVEE 'dg;0t00Ofb3iY8B8eEmB
Waaawaaww5VáEEM555>dWfatCww107pialaaKO 88EEEismiI**axiom=
*Sei48880
i
ayagáa0o.
1"
ADVISORY SERV CES( at the request of Governments )
Public Health Administration
Environmental Sanitation< Fellowships
SURVEYS
Malaria
rmMalnutrition (Kwashiorkor)
lI B i lhariiasis
* Malaria Conference in Equatorial AfricaNov.-Dee. 1950
WHO 1092
AFRICAN REGION 83
tropical and semi- tropical diseases. Here, with theknowledge and means now available, two AfricanMember States, one Associate Member and fourEuropean Member States responsible for the inter-national affairs of territories within the region, areengaged in the common task (though in somerespects with widely different methods of approach)of breaking the vicious circle of disease and poverty.In creating the Office for Africa the Organizationhopes to find ways to assist in this work.
At the Second World Health Assembly it wasagreed to hold a malaria conference in EquatorialAfrica.2 During 1950 a malaria consultant made acomprehensive survey in Africa and his report wasconsidered at the conference, which took place inKampala, Uganda, from 27 November to 9 De-cember. This conference, convened by WHO andthe Commission for Technical Co- operation inAfrica South of the Sahara (CCTA), was attendedby some forty experts, most of whom had longexperience of malaria in Africa.
The two main questions before the conferencewere (1) whether malaria control was possible evenin regions where the adult population has developeda high degree of immunity to the disease, and (2)whether the application of insecticides with residualaction could control malaria carried by such vectorsas Anopheles gambiae. To both questions, theconference replied in the affirmative and consequentlyrecommended to the governments concerned thatmalaria should be controlled by modern methods assoon as this was economically possible, whatever theoriginal degree of endemicity.
The conference emphasized the economic im-portance of malaria even in Tropical Africa andrecognized the necessity for making available facilitiesfor training in malariology. It would be impossibleto control malaria on a large scale in Africa to -day,because trained professional personnel is scarce.Moreover, no programme of malaria control willbe feasible until a proper malaria -control serviceis established, with trained personnel, in the countriesconcerned.
The conference discussed methods by which WHOcould assist governments to undertake malariacontrol, and it put forward a series of recommenda-tions which have been communicated to the ExecutiveBoard, on the one hand, and to the Commissionfor Technical Co- operation in Africa South of theSahara, on the other. The report and recommenda-tions of the conference were also considered by theExpert Committee on Malaria at its fourth session,which was held in Kampala following the conference.
2 Off. Rec. World Hlth Org. 18, 63 ; 21, 47, 190, 193
In 1950, the following surveys were made. InAugust, at the request of the Liberian Government,experts from headquarters, in public -health admi-nistration and in environmental sanitation, visitedLiberia, as described below. During the last quarterof the year, a consultant on nutrition made a surveyof the epidemiological features of malignant mal-nutrition (kwashiorkor) amongst infants, on a tripacross Africa from East to West. Also, during thelast three months of the year, two consultants madea survey of bilharziasis in Central Africa, inaccordance with the recommendations of the JointOIHP /WHO Study -Group on Bilharziasis in Africa,to help the local health services to delimitate the dangerzones in their territories and to apply the newertechniques of control where possible. The reportsof these surveys will be available at the beginning of1951.
The Deputy Director - General, during his visitto Kampala, arranged for the Organization to sendmedical literature to nurses' training schools inUganda. It is expected that WHO will supplyliterature to these schools after an official requesthas been received.
It is too early to draw up exact details of futureplans. It is fully realized that these must evolve outof the deliberations with the authorities in countriesconnected with the Office for Africa. It can be said,however, that the provisional schedule is :
(1) to establish close contact with all governmentsand the CCTA ;
(2) to gain their confidence by studying tho-roughly the many plans that have been drawn upand are being actively carried out in the area ;
(3) to offer, as WHO services, projects fitting inwith these plans wherever they may be needed andrequested, especially as regards training ;
(4) to make an intensive study of the problemsand, only afterwards,
(5) to recruit staff and draw up programmes inclose co- operation with the governments.
Special studies may be undertaken in co- operationwith FAO, UNESCO and ICAO in an endeavour todetermine :
(1) how to stimulate well -balanced developmentof resources (from the economic, educational,cultural and medical aspects) ;
84 WORK OF WHO, 1950
(2) how to prevent the disadvantages consequenton an industrial revolution, which undoubtedlywill gradually take place in Africa, and
(3) why countries that were relatively highlydeveloped centuries ago have not kept pace eco-nomically with the evolution of those parts
of the world which are now technically moreadvanced.
Plans for determining the southernmost limit ofthe area of yellow fever endemicity in Africa arereferred to under the chapter " Research andRelated Activities in Other Communicable Diseases ".
Activities undertaken by Individual Governments with Help from WHO
French Equatorial AfricaOn application from the French Government, two
fellowships in malaria were awarded to students forstudy in Portugal, Italy and Saudi Arabia.
Gold Coast
An application for a fellowship for the Gold Coastwas received from the Government of the UnitedKingdom.
Liberia
At the request of the Liberian Government,experts from headquarters in public -health admi-nistration and in environmental sanitation visitedLiberia in August. As a result of their recommenda-tions for the provision of advice and the grantingof fellowships, two consultants, experts in public -health administration and sanitary engineeringrespectively, were engaged for a three months'assignment in Liberia. A programme of technicalassistance was also considered.
Medical literature and teaching material were senttowards the end of the year for the Nursing Schoolin Liberia, and five to six fellowships were underconsideration.
Nigeria
On .application from the Government of the UnitedKingdom, one fellowship in tuberculosis was awardedto a Nigerian student for study in the UnitedKingdom.
Southern Rhodesia
WHO made a grant during the year to the Govern-ment Research Laboratory in Salisbury, SouthernRhodesia, for work on the unification of the classifi-cation of snail vectors of disease.
Two applications for fellowships were receivedfrom Southern Rhodesia, and were under considera-tion at the end of the year.
Union of South Africa
A grant was made to the South African Institutefor Medical Research, Johannesburg, for the pre-paration and distribution of standard suspensionsof rickettsiae, as recommended by the Joint OIHP/WHO Study -Group on African Rickettsioses.
A FAO /WHO brucellosis centre was establishedin the Onderstepoort Veterinary Laboratory.
REGION OF THE AMERICAS 85
REGION OF THE AMERICAS 1
At the end of 1950 the Pan American SanitaryBureau had served its first full year as the WHORegional Office for the Americas. During the year,two more American Republics, Members of thePan American Sanitary Organization, Cuba andNicaragua, joined WHO. In the Region of theAmericas, therefore, the following countries are nowMembers of WHO : Argentina, Bolivia, Brazil,Canada, Chile, Costa Rica, Cuba, the DominicanRepublic, Ecuador, El Salvador, Guatemala, Haiti,Honduras, Mexico, Nicaragua, Paraguay, Peru,the United States of America, Uruguay andVenezuela. France, the Netherlands and the UnitedKingdom, responsible for the international relationsof certain territories in the Americas, also participateas members of the Regional Committee.
The Pan American Sanitary Conference, directlyor through its Directing Council, serves as theWHO Regional Committee for the Americas. Con-sequently, a part of the Thirteenth Pan AmericanSanitary Conference and the Fourth Meeting of theDirecting Council, held at Ciudad Trujillo in theDominican Republic in September and October,corresponded to the second session of the RegionalCommittee.
The Regional Committee unanimously agreed topropose to the Executive Board the appointment ofDr. Fred L. Soper (who was re- elected Directorof the Pan American Sanitary Bureau), as RegionalDirector for the Americas for a four -year periodbeginning 1 February 1951. It expressed satisfactionwith the 1951 regional budget of $637,063, recom-mended an additional $9,875 for the meeting of theRegional Committee, authorized the technical assist-ance programme and budget proposed for the regionin 1951, and noted the 1952 programme and budgetestimates for the Regional Office. The committeealso accepted the principle of maintaining uniformconditions of service for WHO and PASB staffworking together. After considering the require-ment that governments pay field service allowancesto WHO staff members, it recommended that thissubject should be placed on the agenda of the FourthWorld Health Assembly and that the Director-
1 This region comprises all of the Americas, in accordancewith a decision of the first World Health Assembly. (See Off.Rec. World Hlth Org. 13, 81, 331.)
General should arrange to have it reconsidered bythe Technical Assistance Board.
During 1950, the Pan American Sanitary Bureaucontinued to provide to the American Republicsstaff and services for which funds are available underthe terms of the Pan American Sanitary Code(Havana 1924). However, only the activities inwhich assistance was given by WHO and for whichthe field work was largely carried on by staff of thePan American Sanitary Bureau are reported here.
The Regional Office served not only the countrieswithin the Region of the Americas, but also manyMember States outside the region, particularly inrelation to fellowships and supplies. The RegionalOffice was concerned with 139 fellowship awardsduring the year -63 to students in the Americas and76 given to students from outside the region forstudy in the United States of America. During thefirst eleven months of 1950, 1,316 supply contracts,to a value of $263,226.55, were placed for WHOby the Regional Office, while supply estimates weregiven, specifications prepared and other procurementservices undertaken to a value of $1,269,500 ; some330 supply services, which cannot be assessed on adollar basis, were also carried out. Supplies wereprocured for 35 countries outside the Americas insupport of WHO projects. Under a WHO specialallotment, medical literature and teaching equipmentwere purchased for 11 countries of the region (Argen-tina, Brazil, Chile, Costa Rica, Ecuador, El Salvador,Haiti, Mexico, Paraguay, Uruguay and Venezuela).The Regional Office also arranged for the inspectionand testing of insecticides as well as for their purchaseand delivery.
At the request of the United Nations, evaluationswere made of medical supplies required by theUnified Command in Korea. The cost of supplieslisted was estimated at nineteen and a half milliondollars, and a further list of supplies, composed ofdonations from Member Governments, at threeand half million dollars. These evaluations wereforwarded to the United Nations.
In connexion with reconstruction following UnitedNations action in Korea, the Regional Office recruitedpersonnel (three medical officers from Canada,
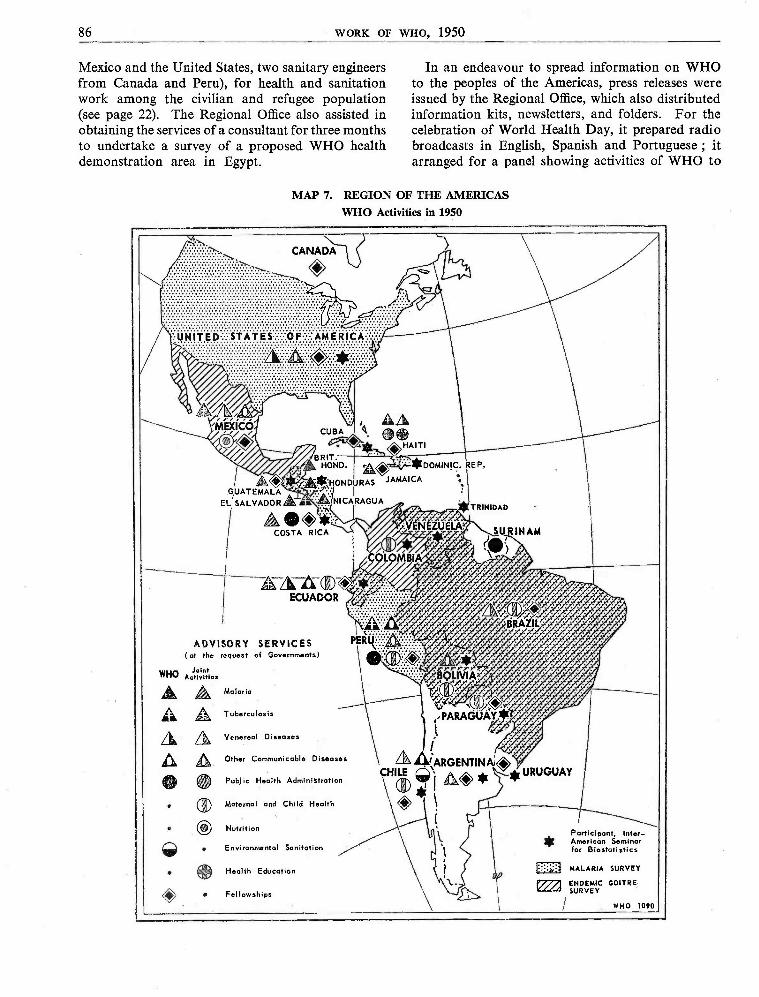
86 WORK OF WHO, 1950
Mexico and the United States, two sanitary engineersfrom Canada and Peru), for health and sanitationwork among the civilian and refugee population(see page 22). The Regional Office also assisted inobtaining the services of a consultant for three monthsto undertake a survey of a proposed WHO healthdemonstration area in Egypt.
In an endeavour to spread information on WHOto the peoples of the Americas, press releases wereissued by the Regional Office, which also distributedinformation kits, newsletters, and folders. For thecelebration of World Health Day, it prepared radiobroadcasts in English, Spanish and Portuguese ; itarranged for a panel showing activities of WHO to
MAP 7. REGION OF THE AMERICASWHO Activities in 1950
CANADA
HAITI
A 40 *HONDURASGUATEMALA fr.
EL SALVADOR AK ®'M: NICARAGUAG' /.
TRINIDAD
COSTA RICA SURINAM
A-4TCECUADOR
ADVISORY SERVICES(at the request of Governments)
WHO faintActiviti es
Malaria
Tuberculosis
Venereal Diseases
Other Communicable Diseases
Public Health Administration
Maternal and Child Health
Nutrition
Environmental Sanitation
Health Education
Fellowships
Participant, Inter_American Seminarfor Biostatistics
MALARIA SURVEY
WHO 1090
REGION OF THE AMERICAS 87
be included in the exhibit of the United States PublicHealth Service, and it supplied material in variouslanguages to local broadcasting stations and tonewspapers and news agencies throughout theAmericas.
As regional centre for epidemiological statisticsand information, the Regional Office maintainedtelegraphic exchange of epidemiological informationwith headquarters in Geneva, and with Singaporeand Manila, and regularly issued weekly and monthlyepidemiological reports. The office distributedto the Latin American republics Volume 1 of theSpanish version of the International StatisticalClassification of Diseases, Injuries and Causes ofDeath and the provisional alphabetical index.
During the year, the Regional Office acted on thefollowing quarantine matters affecting countriesof the Americas : (1) the withdrawal of quarantinemeasures applied against Tumbes, Peru, on accountof plague ; (2) the declaration by Egypt thatVenezuela was free from plague for quarantinepurposes ; and (3) Portugal's agreement to relaxthe requirement for yellow -fever vaccination certi-ficates for passengers from South America touchingin Dakar, French West Africa, on the basis of con-tinued assurances from the French authorities thatDakar was free from Aedes aegypti.
To assist its professional staff called upon to planWHO programmes in the Americas and to negotiatewith Member Governments regarding such pro-
grammes, the Regional Office prepared an officemanual giving information on policies, proceduresand services involved.
The office also made arrangements for the JointFAO /WHO Expert Panel on Brucellosis, which heldits first session in Washington in November.
All field programmes in the region were supportedby the technical and administrative services of theRegional Office. The Library of the Office, with itsextensive reference service, furnished informationalmaterial to field staff, and, in co- operation with theUnited States Department of Agriculture, suppliedmicrofilms and photostatic copies of needed informa-tion to doctors and public -health workers in theAmericas. The PASB Bulletin was issued regularlyeach month with original articles, and special publica-tions, nos. 242 -251, also appeared during 1950.Travel arrangements were made for WHO consul-tants and members of the staff of the RegionalOffice, as well as for the Fellows arriving in theregion from all parts of the world, travelling fromone part of the region to another, or leaving tostudy outside the Americas.
Many of WHO's regional activities have been inoperation for part of the year only and thereforehave not developed to a stage where any evaluationof them can be made. However, the programmesare progressing satisfactorily, and it is expected thatin the report for next year more in the nature ofevaluation will be possible.
Regional Activities involving Several Countries
Biostatistics. The Inter -American Seminar forBiostatistics, held in Chile from September toDecember, was organized and financed by theUnited Nations, the Pan American Sanitary Bureau,the Inter -American Statistical Institute, the NationalOffice of Vital Statistics of the United States PublicHealth Service, WHO and the Government of Chile.There were approximately 25 participants, comingfrom Argentina, Bolivia, Colombia, Costa Rica,Cuba, the Dominican Republic, Ecuador, Guate-mala, Honduras, Paraguay, Trinidad, the UnitedStates of America, Uruguay and Venezuela.
Malaria. The WHO regional consultant in malariasurveyed the current malaria situation in Bolivia,
Brazil, Costa Rica, Cuba, the Dominican Republic,Ecuador, El Salvador, Guatemala, Haiti, Honduras,Nicaragua, Paraguay, Peru, the United States ofAmerica and Venezuela. At the same time hediscussed with health authorities the latest advancesin insecticides, the techniques of applying them andresults obtained. A report on this survey wasprepared for the Regional Committee.
Maternal and Child Health. The regional consul-tant in maternal and child health studied the workbeing done and examined available facilities inBolivia, Brazil, Colombia, Guatemala, Mexico,Paraguay and Uruguay.
88 WORK OF WHO, 1950
Endemic Goitre. Health authorities in eightCentral and South American countries (BoliviaBrazil, Colombia, Ecuador, Guatemala, Mexico,Paraguay and Venezuela) were interviewed by aWHO consultant on the problem of endemic goitre.The information thus obtained was compiled andsubmitted to Member States and, with additionaldata from other sources, served as authority forthe recommendations on endemic goitre approvedat the second conference on nutrition problems ofLatin America, held in Rio de Janeiro in June.
Joint Programmes with UNICEF
As a result of negotiations with UNICEF, jointprogrammes, as described below, were implementedin Bolivia, Brazil, British Honduras, Chile, Colom-bia, Costa Rica, El Salvador, Guatemala, Haiti,Honduras, Nicaragua and Peru. The RegionalOffice helped the countries concerned by givingtechnical advice on the plans of operation for theseprogrammes, UNICEF furnishing the supplies andequipment. Besides the special programmes inBrazil, El Salvador, Haiti and Peru described inthe paragraphs devoted to those countries, a numberof programmes involving more than one countrywere undertaken.
WHO and UNICEF co- operated in preparingin Chile and Colombia for immunization campaignsagainst diphtheria and pertussis, designed to minimizethe effects of these diseases and reduce mortalityfrom them, particularly in children under five.A WHO consultant visited the countries early inthe year to assist in the local production of diphtheria -pertussis vaccine. In Colombia the head of theprogramme took charge on 1 May. At the end ofthe year, a Chilean doctor with a fellowship in theUnited States was studying methods for the produc-tion of vaccine.
In co- operation with UNICEF the insect -controlprogramme in Central America was started inBritish Honduras, Costa Rica, El Salvador, Gua-temala, Honduras and Nicaragua, with a view toreducing the incidence of insect -borne diseases andchild mortality. Supplies were furnished for thisprogramme, and an intensive training programmein insect control for personnel from the participatingcountries was completed during the year.
The BCG programme in Mexico, for whichassistance was given by WHO and UNICEF, isunder the direction of a member of the staff of theJoint Enterprise. Arrangements were completedin that country for BCG vaccine to be producedand distributed to other Latin American countries.An important phase of the programme is the trainingof teams from other countries in the techniques ofBCG production and vaccination.
In June the Executive Board of UNICEF allocatedover $400,000 for additional activities, chiefly inmaternal and child health. These activities includeprogrammes in maternal and child health (forChile, Paraguay and Peru), in insect -control andhealth education (for Peru) and in tuberculosiscontrol (for Chile and Peru) ; the construction ofa 200 -bed children's hospital in Bolivia, and thesupply of laboratory equipment to Chile and Peru.
In November the UNICEF Executive Boardapproved recommendations of the ProgrammeCommittee of UNICEF for projects in Latin Ame-rica. These include programmes in maternal andchild health (for Colombia and El Salvador), inmalaria control (for the Dominican Republic andParaguay) and in tuberculosis control (for Ecuador),as well as a milk conservation project for Chile. Anadditional sum of $840,000 was voted by theUNICEF Executive Board to the Latin Americanarea reserve, bringing it up to $1,265,000.
Activities undertaken by Individual Governments with Help from WHO
AlaskaA fellowship in sanitary engineering was awarded
to a student from Alaska to study for three monthsin Europe.
ArgentinaA WHO /FAO brucellosis centre was established
in Buenos Aires.
Fellowships were awarded to two doctors fromArgentina for study in the United States -one inepidemiology at Johns Hopkins University andthe other in nutrition at Harvard University, bothfor a period of ten months.
Under a special allotment, medical literature waspurchased for Argentina.
REGION OF THE AMERICAS 9
Bolivia
Construction plans and lists of equipment fora 200 -bed children's hospital at La Paz were com-pleted, with the assistance of WHO and UNICEF.Plans in connexion with this project were also madefor the training of personnel and for a feedingp ogramme.
A national campaign against typhus, based onthe use of insecticides with residual action, was under-taken by the Ministry of Health of Bolivia in co-operation with WHO and UNICEF. This campaignis an expansion of a small -scale programme carriedout by the Government with the help of the Rocke-feller Foundation and aims to control typhus in themountain areas adjoining Peru by the use of moderninsecticides. The number of inhabitants included inthe areas represents more than half of the populationof the country, or approximately 2,000,000 people.
A malaria survey was made in Bolivia by theregional consultant.
Brazil
A consultant on endemic goitre made a study ofthat disease in Brazil, showing that one -fourth ofthe population of Brazil living in the mountainsand highlands away from the coast needed goitreprophylaxis.
A survey of the antimalaria work being carriedon in Brazil was made by the regional consultanton malaria.
A maternal and child health programme wasplanned by WHO, in co- operation with UNICEF,to include training of personnel and a diphtheria -pertussis immunization campaign. Funds providedby UNICEF were used for the training of personnel,the improvement of vaccine production, purchaseof vaccine where necessary, equipment for maternaland child health centres, and supplies of powderedwhole and skimmed milk.
Four fellowships were awarded to studentsfrom Brazil for study in the United States : twofor study of communicable diseases, one each forbacteriology and public -health administration.
Under a special allotment, teaching equipmentwas purchased for Brazil.
British Honduras
The insect -control programme in British Honduraswas started by WHO in co- operation with UNICEF,which supplied DDT and equipment. The Pan
American Sanitary Bureau assisted in trainingpersonnel and initiating the programme. The firstcycle of DDT spraying was completed in Belize,and the second cycle was started in the rural areassurrounding Corozal and Toledo. Towards the endof the year an inspection trip to all districts of BritishHonduras revealed that, in common with the CentralAmerican countries, British Honduras had no com-plete record of malaria incidence before the DDTspraying started. However, although neither spleennor parasite rates, nor data on mosquito prevalence,were available, each district medical officer kept arecord of all the patients he saw at the hospital. Acomparison of these records with those kept afterspraying should give a fairly good indication of thedifference in the number of cases before and afterspraying -especially among children and amongpatients treated for the first time.
Canada
Canada was awarded one fellowship during 1950.
Chile
A WHO team consisting of a physician, nurse andphysiotherapist conducted training courses in techni-ques of treatment and rehabilitation of victims ofpoliomyelitis in Chile.
A study of diphtheria and pertussis was made inthe country, where whooping cough is said to havethe second highest mortality rate of any infectiousdisease, and a vaccination programme is being carriedout by the national department of health, withWHO and UNICEF assistance. The programme isfor children within the age -group of four monthsto five years and the immunization of 40% of thepopulation in this group is contemplated. A WHOconsultant advised health authorities of Chile onthe preparation of the combined diphtheria -pertussisvaccine and the general planning of the programme.UNICEF is contributing the material and equipmentnecessary for the preparation and use of the vaccine.The Regional Office was informed by the MichiganState Laboratories that tests of combined diph-theria- pertussis vaccine prepared by the BacteriologyInstitute of Chile gave satisfactory results.
During the year the regional adviser on tuber-culosis visited Chile to discuss possible WHO/UNICEF programmes with the authorities.
90 WORK OF WHO, 1950
The regional consultant in venereal diseasesvisited the Chilean venereal- disease services. Acomparative study of the specificity of serologicallipoidal antigens and the cardiolipin- lecithin -choles-terol antigen is being carried out with the technicalassistance of the Regional Office.
At the end of the year a consultant was providedto advise on garbage and waste disposal in the cityof Santiago.
Chile, with WHO and UNICEF assistance, iscarrying out a programme to enlarge and strengthenmaternal and child health services. UNICEF isproviding maternal and child health centres, hospitalsand mobile units with clinical equipment, vehiclesand ambulances, and x -ray and dental equipment.The Regional Office provides technical assistancefor planning and operating the programme.
Four fellowships were awarded.
Under a special allotment, medical literature andteaching equipment were purchased for Chile.
Colombia
A nation -wide programme of diphtheria -pertussisimmunization is being carried out by Colombia withWHO and UNICEF assistance, as already describedin the section on joint programmes with UNICEF.In preparation for the campaign, a WHO consultantin diphtheria and pertussis immunization visitedthe country early in the year to assist in the localproduction of a combined vaccine. In June WHOmade a consultant available in Bogotá to assist theGovernment. The detailed plan of operations calledfor close co- ordination of activities connected withvaccination, health education and statistical infor-mation, the latter including a study on post- vaccina-tion reactions. UNICEF is providing vaccine andequipment for its production and use. The pro-gramme was initiated in the city of Cucuta in Sep-tember. During the first two months of operation,4,225 children were given the first inoculation and1,002 the second. The Government allocated fundsto extend the programme to other parts of the coun-try and appointed additional personnel for itsimplementation. The health -education aspects of thecampaign were intensified, and a manual of pro-cedures for the local health educators was completed.The Inter -American Co- operative Health Services
agreed to provide the services of a Colombianpublic -health nurse trained in Chile.
The regional consultant in maternal and childhealth collaborated with health authorities inColombia in the preparation of a maternal and childhealth programme to be carried out with UNICEFfinancial assistance. This programme provides forequipping a department of midwifery in the Schoolof Public Health in Bogotá, organizing three demon-stration courses in midwifery, and developing faci-lities in schools of public health for training physi-cians in maternal and child health. The programmeis to be carried out in co- operation with the Ministryof Hygiene, schools of public health, the nationalschool of nursing, the San José Hospital and theRegional Office, which is providing technical assis-tance.
The consultant in endemic goitre, who visitedColombia during the year, reported that iodizedsalt was available only in a few localities. However,a good grade of iodized salt should be obtainablein all parts of the country as a result of the modernmethod of iodizing.
Costa Rica
The insect -control programme began on 1 Julyin Guanacaste Province under the direction of theDepartment of Sanitary Engineering of Costa Rica,with help from WHO and UNICEF, and 30,000 lb.of DDT were distributed.
A preliminary survey of hospital facilities wascompleted during the year. Costa Rica requestedassistance in the construction of buildings for cancerand maternity services in the San Juan de DiosHospital, the establishment of a school of medicine,and the integration of rural and district hospitaland health- centre units. An architect was appointedas consultant, to prepare preliminary drawings forthe buildings for cancer and maternity services.
Assistance was also furnished in the preparationof a programme for mass BCG -vaccination.
Two fellowships were awarded for study in theUnited States -one for nine months in hospitaladministration at Columbia University and theother for eight months in hospital construction withthe United States Public Health Service. Anotherwas granted for attendance at the seminar on bio-statistics in Chile.
WHO provided medical literature and teachingequipment to Costa Rica under a special allotment.
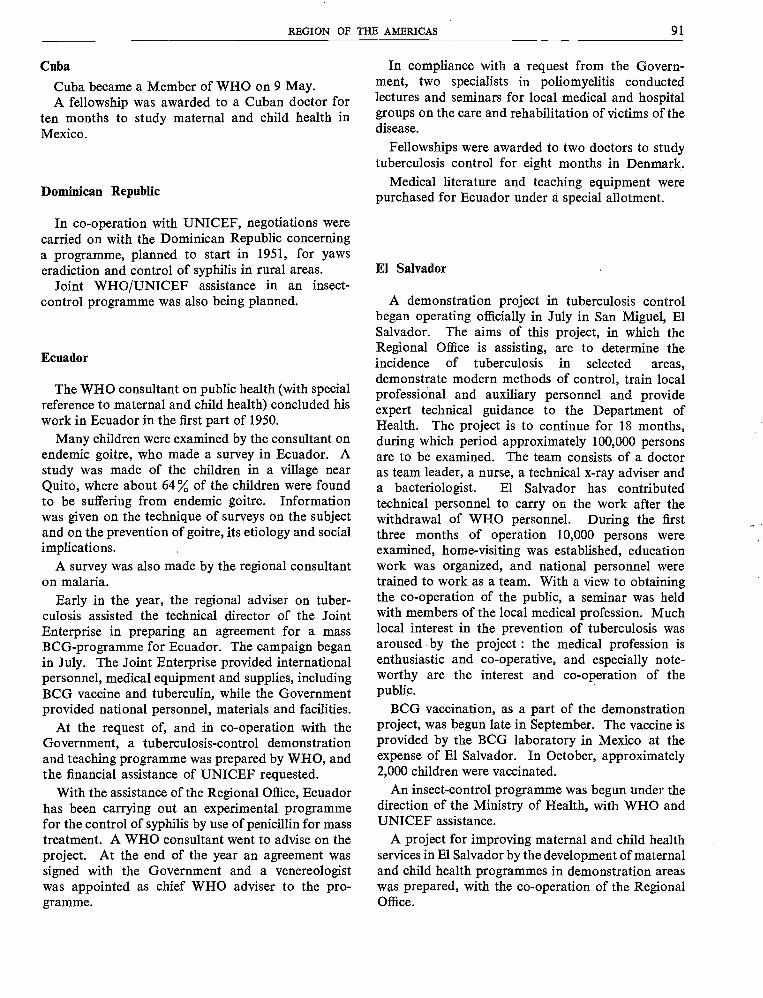
REGION OF THE AMERICAS 91
Cuba
Cuba became a Member of WHO on 9 May.A fellowship was awarded to a Cuban doctor for
ten months to study maternal and child health inMexico.
Dominican Republic
In co- operation with UNICEF, negotiations werecarried on with the Dominican Republic concerninga programme, planned to start in 1951, for yawseradiction and control of syphilis in rural areas.
Joint WHO /UNICEF assistance in an insect -control programme was also being planned.
Ecuador
The WHO consultant on public health (with specialreference to maternal and child health) concluded hiswork in Ecuador in the first part of 1950.
Many children were examined by the consultant onendemic goitre, who made a survey in Ecuador. Astudy was made of the children in a village nearQuito, where about 64 % of the children were foundto be suffering from endemic goitre. Informationwas given on the technique of surveys on the subjectand on the prevention of goitre, its etiology and socialimplications.
A survey was also made by the regional consultanton malaria.
Early in the year, the regional adviser on tuber-culosis assisted the technical director of the JointEnterprise in preparing an agreement for a massBCG- programme for Ecuador. The campaign beganin July. The Joint Enterprise provided internationalpersonnel, medical equipment and supplies, includingBCG vaccine and tuberculin, while the Governmentprovided national personnel, materials and facilities.
At the request of, and in co- operation with theGovernment, a tuberculosis -control demonstrationand teaching programme was prepared by WHO, andthe financial assistance of UNICEF requested.
With the assistance of the Regional Office, Ecuadorhas been carrying out an experimental programmefor the control of syphilis by use of penicillin for masstreatment. A WHO consultant went to advise on theproject. At the end of the year an agreement wassigned with the Government and a venereologistwas appointed as chief WHO adviser to the pro-gramme.
In compliance with a request from the Govern-ment, two specialists in poliomyelitis conductedlectures and seminars for local medical and hospitalgroups on the care and rehabilitation of victims of thedisease.
Fellowships were awarded to two doctors to studytuberculosis control for eight months in Denmark.
Medical literature and teaching equipment werepurchased for Ecuador under a special allotment.
El Salvador
A demonstration project in tuberculosis controlbegan operating officially in July in San Miguel, ElSalvador. The aims of this project, in which theRegional Office is assisting, are to determine theincidence of tuberculosis in selected areas,demonstrate modern methods of control, train localprofessional and auxiliary personnel and provideexpert technical guidance to the Department ofHealth. The project is to continue for 18 months,during which period approximately 100,000 personsare to be examined. The team consists of a doctoras team leader, a nurse, a technical x -ray adviser anda bacteriologist. El Salvador has contributedtechnical personnel to carry on the work after thewithdrawal of WHO personnel. During the firstthree months of operation 10,000 persons wereexamined, home -visiting was established, educationwork was organized, and national personnel weretrained to work as a team. With a view to obtainingthe co- operation of the public, a seminar was heldwith members of the local medical profession. Muchlocal interest in the prevention of tuberculosis wasaroused by the project : the medical profession isenthusiastic and co- operative, and especially note-worthy are the interest and co- operation of thepublic.
BCG vaccination, as a part of the demonstrationproject, was begun late in September. The vaccine isprovided by the BCG laboratory in Mexico at theexpense of El Salvador. In October, approximately2,000 children were vaccinated.
An insect -control programme was begun under thedirection of the Ministry of Health, with WHO andUNICEF assistance.
A project for improving maternal and child healthservices in El Salvador by the development of maternaland child health programmes in demonstration areaswas prepared, with the co- operation of the RegionalOffice.
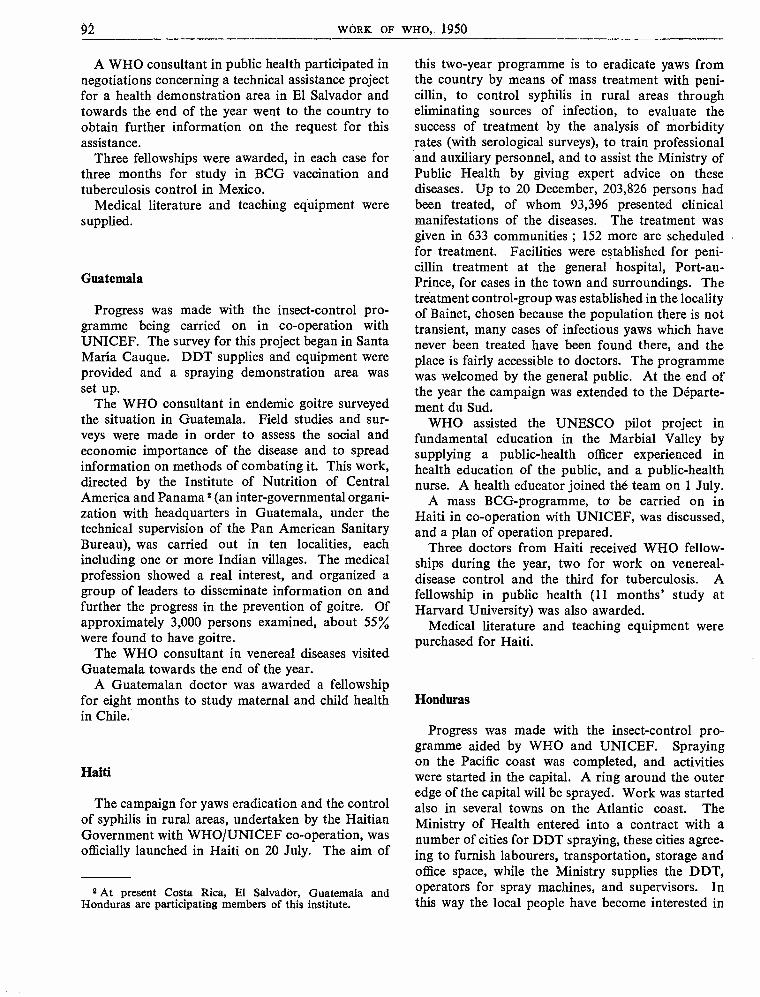
92 WORK OF WHO, 1950
A WHO consultant in public health participated innegotiations concerning a technical assistance projectfor a health demonstration area in El Salvador andtowards the end of the year went to the country toobtain further information on the request for thisassistance.
Three fellowships were awarded, in each case forthree months for study in BCG vaccination andtuberculosis control in Mexico.
Medical literature and teaching equipment weresupplied.
Guatemala
Progress was made with the insect -control pro-gramme being carried on in co- operation withUNICEF. The survey for this project began in SantaMaría Cauque. DDT supplies and equipment wereprovided and a spraying demonstration area wasset up.
The WHO consultant in endemic goitre surveyedthe situation in Guatemala. Field studies and sur-veys were made in order to assess the social andeconomic importance of the disease and to spreadinformation on methods of combating it. This work,directed by the Institute of Nutrition of CentralAmerica and Panama 2 (an inter -governmental organi-zation with headquarters in Guatemala, under thetechnical supervision of the Pan American SanitaryBureau), was carried out in ten localities, eachincluding one or more Indian villages. The medicalprofession showed a real interest, and organized agroup of leaders to disseminate information on andfurther the progress in the prevention of goitre. Ofapproximately 3,000 persons examined, about 55%were found to have goitre.
The WHO consultant in venereal diseases visitedGuatemala towards the end of the year.
A Guatemalan doctor was awarded a fellowshipfor eight months to study maternal and child healthin Chile.
Haiti
The campaign for yaws eradication and the controlof syphilis in rural areas, undertaken by the HaitianGovernment with WHO /UNICEF co- operation, wasofficially launched in Haiti on 20 July. The aim of
2 At present Costa Rica, El Salvador, Guatemala andHonduras are participating members of this institute.
this two -year programme is to eradicate yaws fromthe country by means of mass treatment with peni-cillin, to control syphilis in rural areas througheliminating sources of infection, to evaluate thesuccess of treatment by the analysis of morbidityrates (with serological surveys), to train professionaland auxiliary personnel, and to assist the Ministry ofPublic Health by giving expert advice on thesediseases. Up to 20 December, 203,826 persons hadbeen treated, of whom 93,396 presented clinicalmanifestations of the diseases. The treatment wasgiven in 633 communities ; 152 more are scheduledfor treatment. Facilities were established for peni-cillin treatment at the general hospital, Port -au-Prince, for cases in the town and surroundings. Thetreatment control -group was established in the localityof Bainet, chosen because the population there is nottransient, many cases of infectious yaws which havenever been treated have been found there, and theplace is fairly accessible to doctors. The programmewas welcomed by the general public. At the end ofthe year the campaign was extended to the Départe-ment du Sud.
WHO assisted the UNESCO pilot project infundamental education in the Marbial Valley bysupplying a public- health officer experienced inhealth education of the public, and a public -healthnurse. A health educator joined thé team on 1 July.
A mass BCG- programme, to be carried on inHaiti in co- operation with UNICEF, was discussed,and a plan of operation prepared.
Three doctors from Haiti received WHO fellow-ships during the year, two for work on venereal -disease control and the third for tuberculosis. Afellowship in public health (11 months' study atHarvard University) was also awarded.
Medical literature and teaching equipment werepurchased for Haiti.
Honduras
Progress was made with the insect -control pro-gramme aided by WHO and UNICEF. Sprayingon the Pacific coast was completed, and activitieswere started in the capital. A ring around the outeredge of the capital will be sprayed. Work was startedalso in several towns on the Atlantic coast. TheMinistry of Health entered into a contract with anumber of cities for DDT spraying, these cities agree-ing to furnish labourers, transportation, storage andoffice space, while the Ministry supplies the DDT,operators for spray machines, and supervisors. Inthis way the local people have become interested in
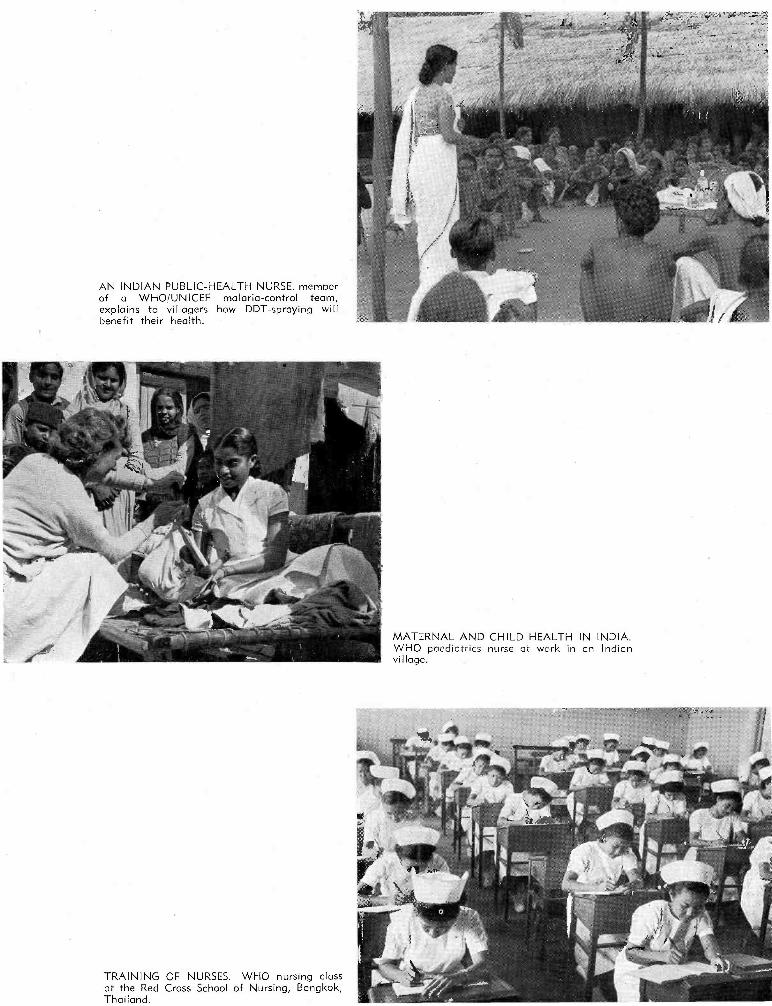
AN INDIAN PUBLIC -HEALTH NURSE, memberof a WHO/UNICEF malaria- control team,explains to villagers how DDT -spraying willbenefit their health.
TRAINING OF NURSES. WHO nursing classat the Red Cross School of Nursing, Bangkok,Thailand.
MATERNAL AND CHILD HEALTH IN INDIA.WHO paediatrics nurse at work in an Indianvillage.
TUBERCULIN TESTS in Shanghai TuberculosisCentre. The children on the left are registering,the small boy on the right is being tested.
BCG WORK IN MEXICO. The chief nurse ofthe BCG Institute of Mexico inoculates a
youngster at a Government nursery home.
MENTAL HEALTHCONSULTANT in thePhilippines, lecturing tothe Philippine PublicHealth Association.
SHANGHAI TUBERCULOSIS CENTRE. Childrenreceiving BCG vaccination from a WHO tuber-culosis adviser, while a local doctor watches.
YAWS CAMPAIGN,HAITI. Patients'names are inscribedand their case -his-tories recorded bythe nurse.
REGION OF THE AMERICAS 93
the spraying programme and have learned about theorganization and technique of insect control and itsbenefits to the public.
A survey was made in Honduras by the regionalconsultant in malaria.
Jamaica
An island -wide BCG- programme, to be carried onin co- operation with WHO and UNICEF, was pre-pared by the health authorities, with the assistanceof the WHO regional adviser in tuberculosis. It willprobably be started in 1951.
A fellowship was awarded to a doctor from Jamaicafor ten months to study tuberculosis control in theUnited Kingdom.
Mexico
The regional consultant in venereal disease assistedthe Government by giving advice in the Tijuanaprophylaxis project for venereal diseases and in asimilar project in Agua Prieta near the border betweenMexico and the United States of America.
Early in the year the Regional Office assisted thetechnical director of the Joint Enterprise in preparingan agreement for a mass BCG- programme in Mexico.This campaign began in July. The BCG laboratoryin Mexico, with WHO technical advice, was set up asa large -scale producing unit for other Latin Americancountries. Vaccine was sent from this laboratory toEcuador, El Salvador and Trinidad.
In Mexico City a pilot study was carried out toassist the WHO Tuberculosis Research Office inCopenhagen to evaluate different vaccines, tech-niques and procedures employed in tuberculintesting, and to provide information on other pointsconnected with the establishment of standards forBCG and tuberculin.
The Regional Office assisted in the proposed ILOpilot study of conditions of work of nurses by obtain-ing further information on the present status ofnursing and special problems involved.
The consultant in endemic goitre made a survey inMexico. The work was confined to a critical analysisof data already collected on the endemic -goitreproblem and the formulating of a practical procedurefor prevention. The consultant visited several villages,which had been previously inspected and where theincidence of goitre was known to be high. Incidenceis particularly high in the mountainous areas, andespecially in the foothills and highlands. The dataanalysed by the consultant indicated that in theeight States studied where goitre exists, the average
incidence is about 34 %. This study has apparentlyaroused interest in preventive measures.
Detailed plans were made for joint WHO /UNICEFassistance in a hospital project for Oaxaca.
Preliminary discussions took place with UNESCOon a scheme for a production and training centre(to be located probably in Mexico) in fundamentaleducation for Latin American States.
A request was received from the Mexican Govern-ment for assistance in brucellosis control.
Five Mexican doctors were awarded fellowships-one in child psychiatry for one year ; one in public-health veterinary medicine for eight months ; one inpublic -health administration for six months, and twoin communicable diseases for two weeks.
Medical literature and teaching equipment werepurchased for Mexico.
Nicaragua
Nicaragua became a Member of WHO on 24 April.An insect -control programme, carried out in co-
operation with WHO and UNICEF, was started.Managua, the capital, with a population of about110,000, was completely sprayed, and DDT squadsbegan work in the rural areas. A request for fundsfor additional material was prepared for presentationto UNICEF, and discussions took place with theNicaraguan authorities regarding the amount ofDDT necessary for completing the programme.
A survey was made by the regional consultant inmalaria.
Paraguay
A programme for the improvement of maternaland child health services in Paraguay, to be carriedout with the technical guidance of the Regional Officeand the financial assistance of UNICEF, was inpreparation at the end of the year. A WHO con-sultant went to Paraguay to assist health authoritiesin planning this programme, which may include theprovision of skimmed milk for mothers and children.
In connexion with the survey on endemic goitre,another WHO consultant visited Paraguay, wherethis disease constitutes an important public- healthproblem. A survey made earlier in 35 cities and townsshowed that about 30 % of the population had goitre.
A survey was made by the regional consultant inmalaria.
Fellowships were awarded to two Paraguayandoctors, one in venereal- disease control, for sixmonths, and the other for a three months' course inserology.
94 WORK OF WHO, 1950
Medical literature and teaching equipment werepurchased.
Peru
Work began at the end of May on the typhus-control programme in the Department of Cuzco. Theprogramme is being carried out by the Division ofCommunicable Diseases of the Ministry of Healthof Peru, with WHO and UNICEF assistance, and isdesigned to control the disease on a national scaleand to train national and foreign personnel in controltechniques. Activities were accelerated because of theearthquake on 21 May in the Cuzco -Puno area. APeruvian physician was placed in charge of thiscontrol project for the Department of Cuzco andwas aided by an epidemiologist. UNICEF suppliesand equipment, including DDT and jeep station -wagons, were delivered and put to immediate use.This emergency work, which lasted from 29: May to5 June, was followed by a DDT campaign in ruralareas. By 27 June, 158,170 persons and 21,918
habitations had been treated with DDT.The Regional Office assisted Peru in preparing
plans for a maternal and child health project to becarried out with UNICEF financial assistance. Thisprogramme is intended to assist mothers and childrenin the rural areas Lima, Pativilca,Huaras and Cajacay, which were visited by a WHOconsultant in December, and is to include skimmed -milk feeding.
WHO sent a team to assist in combating an out-break of poliomyelitis. Physiotherapists gave technicaladvice and conducted training courses for doctors andnurses.
At the request of the national health- authorities, atuberculosis project was prepared to supplement theprogramme in maternal and child health.
A preliminary survey was conducted in July todetermine the assistance necessary for three largehospitals in Lima : the children's hospital with 500
beds, the Loaiza Hospital with 700 beds, and theDos de Mayo Hospital with 800 beds.
A survey was made by the regional consultant onmalaria.
The WHO consultant in endemic goitre completeda survey of that disease in Peru. Information wascollected and children examined.
A Peruvian doctor was awarded a fellowship tostudy venereal -disease control in the United States ofAmerica for eight months.
Surinam
A survey for hospital projects was carried out inSurinam.
Trinidad
Trinidad was visited by the regional adviser ontuberculosis.
United States of America
In January a WHO consultant on malaria completeda lecture tour in the United States on malaria control.
The regional adviser on venereal disease held aseminar at the Johns Hopkins School of Hygiene andPublic Health where an International Treponema-toses Laboratory Centre was set up.
A WHO consultant on mental health met withpsychiatrists working on psychiatric aspects ofjuvenile delinquency in the United States.
A FAO /WHO brucellosis centre was established inMinneapolis.
Fellowships for two or three months' study inEurope were awarded to 15 persons in the UnitedStates. The subjects of study were communicablediseases, sanitation and maternal and child health.
Uruguay
During the year, two Uruguayan students wereawarded fellowships : one in psychiatry for ten monthsat the University of Cincinnati, United States ofAmerica ; the second in bacteriology for six monthswith the United States Public Health Service. Athird attended the seminar on biostatistics in Chile.
Medical literature and teaching equipment werepurchased for Uruguay under a special allotment.
Venezuela
The WHO consultant in endemic goitre visitedVenezuela in connexion with a survey on the subject.
During the year three Venezuelan doctors wereawarded fellowships for periods ranging from threeto six months.
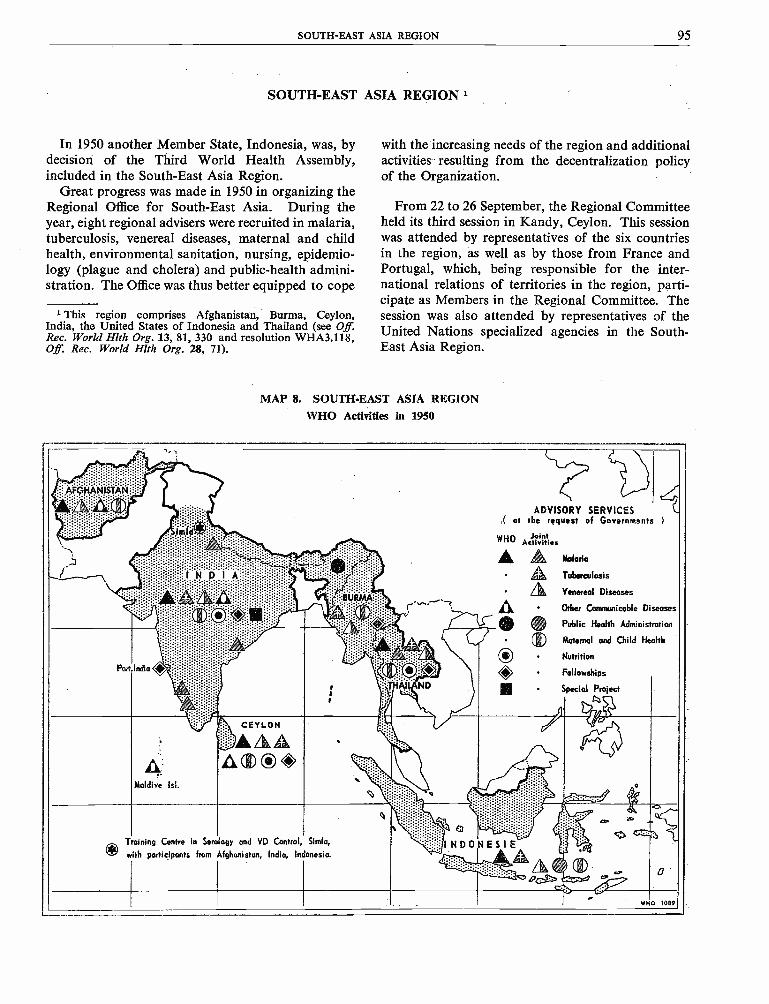
SOUTH -EAST ASIA REGION 95
SOUTH -EAST ASIA REGION 1
In 1950 another Member State, Indonesia, was, bydecision of the Third World Health Assembly,included in the South -East Asia Region.
Great progress was made in 1950 in organizing theRegional Office for South -East Asia. During theyear, eight regional advisers were recruited in malaria,tuberculosis, venereal diseases, maternal and childhealth, environmental sanitation, nursing, epidemio-logy (plague and cholera) and public- health admini-stration. The Office was thus better equipped to cope
1 This region comprises Afghanistan, Burma, Ceylon,India, the United States of Indonesia and Thailand (see Off.Rec. World Hlth Org. 13, 81, 330 and resolution WHA3.118,Off. Rec. World Hlth Org. 28, 71).
with the increasing needs of the region and additionalactivities resulting from the decentralization policyof the Organization.
From 22 to 26 September, the Regional Committeeheld its third session in Kandy, Ceylon. This sessionwas attended by representatives of the six countriesin the region, as well as by those from France andPortugal, which, being responsible for the inter-national relations of territories in the region, parti-cipate as Members in the Regional Committee. Thesession was also attended by representatives of theUnited Nations specialized agencies in the South -
East Asia Region.
MAP 8. SOUTH -EAST ASIA REGIONWHO Activities in 1950
AFGHANiii.'
- 1
imfá',./ .i ;; {;,,
i <' :::.:i 1idD111''::i:::::.:
i''aO
ADVISORY SERVICES( at the request of Governments
WHO JointAetiviti.s
:...t . ® Malaria, Tuberculosis
,: ??: °' "'''' .. 4 Venereal Diseases::BURAAA::r -
r A Other Communicable Diseases
Public Health Administration
`-1J)
Part
i''si E : i :i:i í i :`:'. . .: '':: :-'::
India `'ii is
.::::::::::::
.K
V
9/í.Y / /v/,:-::° ;:;:
: o:t?. HA9LAND
Ill()®
Special
Maternal and Child Health
Nutrition
Fellowships
Project
AMaldive Isl.
CEYLON
A O,O ®,P0
Training
with
9 Centre in Serology
participants from
gY and VD Control
Afghanistan, India, Indonesia.
Simla
cl
INDONESIE
.
. a8®h11 d
WHO 1089
96 WORK OF WHO, 1950
Holding five plenary meetings, the Regional Com-mittee, for the first time, discussed and decidedupon a detailed health programme. Programmesand budgets for 1951 and 1952 were examined andapproved, and the committee also discussed generallyand endorsed programmes proposed for individualcountries for the specific period 1952 -1955. Amongthe subjects discussed were the establishment ofseparate sections in national health directorates fordealing with international health matters, the employ-ment of international staff in field projects, the train-ing of health personnel, population problems, anincrease in the budget for 1952 and accommodationfor the regional office and its staff. Great emphasiswas placed on the acute need for assistance in obtain-
ing medical supplies and for their manufacture withinthe region.
This session of the Regional Committee wasfollowed by a study -group, attended by 28 directorsof public - health services of the countries of the region,in implementation of a resolution passed by theRegional Committee at its second session. During afour -day deliberation, this study -group discussed, andin some cases made recommendations on, public -
health administration, the general promotion ofhealth, health education of the public, training ofhealth personnel, environmental sanitation, thecontrol of communicable diseases, health statisticsand related topics.
General Statement of Activities in the Region
Tuberculosis Training Centres
Tuberculosis demonstration and training areas arebeing planned in the region on the recommendationof the Expert Committee on Tuberculosis. Whileeach of these centres will undoubtedly provide im-portant direct services to the community, theiressential function will be to initiate training schemesat the highest level in order that such training may beprogressively extended and diffused throughout thecountries with the ultimate aim of creating fullyintegrated and efficient national services.
At present the largest cities of India, and some ofthe provinces, have some clinical services for tuber-culosis, but for most of the country such services arelacking or are elementary in the extreme. Preventivecontrol is, on the whole, still more elementary.Throughout India laboratory facilities for the special-ized diagnosis of tuberculosis and personnel trainedin such work are almost entirely lacking.
The position in other countries of the region, withthe exception of Ceylon, is even less favourable thanin India. In Ceylon the nucleus of an effective tuber-culosis service has been established, but it requiresconsiderable strengthening and expansion.
Governments have taken steps to improve thetraining of medical and auxiliary personnel : post-
graduate training of doctors in antituberculosistechniques, which has been going on in India for anumber of years, has recently been extended and isprogressing. Tuberculous Diseases Diploma courses,for example, were started at Delhi University in 1947and at Amritsar in 1949, following the lead set byMadras University, which initiated a diploma coursein 1939. It seems probable that similar diplomacourses will shortly be started at Calcutta. Theuniversities are subsidized by the Government.Free refresher courses in tuberculosis work, whichwere organized long ago by the Tuberculosis Asso-ciation of India and are offered yearly or oftener forgeneral practitioners at different university centres,are being continued or expanded. Courses for labo-ratory and x -ray technicians are available in severalplaces. With few exceptions, however, the traininggiven to doctors and auxiliary workers is not up tomodern standards.
In Ceylon, training courses for nurses and sanitaryinspectors in environmental work have been going onfor at least twelve months in connexion with theRural Tuberculosis Control Project at Kotte, whichwas started by the Government but for which inter-national assistance will now be given.
The governments concerned have undertaken tocontinue all antituberculosis projects set up or to be

SOUTH -EAST ASIA REGION 97
set up in the region, after the withdrawal of inter-national staff. For BCG vaccination, the technicaldirection of which will become WHO's responsibilityin the near future (if requested by governments andassisted by international funds), the Government ofIndia is appointing a BCG adviser to serve on theDirectorate -General of Health Services, which willgenerally supervise the work of the 90 teams trainedby the Joint Enterprise. Immediate supervision ofthese teams will continue to be exercised by thegovernments of the States and provinces in which theyare operating.
Very little work in small -scale tuberculin surveyshas hitherto been undertaken in India. Probably themost complete survey project by tuberculin test withx -ray follow -up has been that at Madanapalle inSouth India, conducted by Dr. Frimodt - Moller in1948, 1949 and 1950. This project is now beingextended and assisted by funds furnished by theWHO Tuberculosis Research Office, and byUNICEF.
It produced the following figures calculated for anestimated population of 14,000 :
Tuberculosis morbidity 1.16
Proved bacillary cases 0.7
Tuberculosis mortality rate 253.5
per 100,000
The tuberculosis mortality rate for Madanapallethus corresponds with the estimate of a number ofexperts that the rate for India is about 250 per100,000.
An indication of a possible change in the healthadministration of a country as the result of a WHOproject is to be found in Thailand, where, in requestingthe establishment of a tuberculosis demonstration andtraining area, the Government has undertaken toplace the national tuberculosis service on a soundadministrative basis by bringing the clinical, pre-ventive and institutional services under centralcontrol.
Malaria Projects
The Government of Afghanistan is continuing themalaria- control project at Laghman, which was
undertaken by WHO during 1949. It has also agreedto take over the present malaria- control project in theKhanabad -Kunduz area after the withdrawal of theWHO team at the end of 1951. The four malariacontrol projects in India and the one in Thailandwill also be continued by the respective Governmentsafter the withdrawal of the WHO teams.
Surveys have preceded and followed the demonstra-tions in malaria control. Excellent examples of theway in which other branches of public health may beinfluenced by work on a special project are found inthe outstanding activities in maternal and child healthwhich have been carried on by the public -healthnurses and the nursing staff of the parallel teams.Also, the presence of malaria teams in India and inThailand has enabled demonstrations to be made ofthe use of DDT in plague control and for the eradica-tion of bedbugs. Malaria operations in Afghanistanhave given rise to a general desire for the extensionof malaria control activities to different parts of thecountry. Generally speaking, the health of peoplein many of the areas in which these demonstrationteams have been working seems already to be defi-nitely improved.
Nursing
Nursing activities have been carried out by sevenpublic -health nurses attached to different field teams(six of these nurses are working in India and one inThailand), by one paediatric nurse assigned to achildren's ward at Irwin Hospital in India and by onesister tutor in Burma. The activities of the public -health nurses vary from team to team, but their firstand foremost task has been to plan nursing duties andprocedures for the specialized projects in which theyare working. Their main activities have thereforebeen the collection of information, the taking of bloodand other laboratory samples, and the treatment ofmalaria, syphilis, gonorrhoea and minor ailments.
The opportunity has also been taken to establishante- natal, post -natal and infant and child -welfareclinics, to make school inspections and to develophealth teaching programmes in schools, villages andhomes. School health work has been much appreci-ated by teachers, pupils and parents, who, in someareas, gather together to hear the health stories toldby the nurses and who are proud, in turn, to showthat they have carried out previous instructions.
98 WORK OF WHO, 1950
In some areas home visiting; covering all houses ina particular area, is undertaken, and advice is givenon such problems as personal hygiene, diet, domesticsanitation, the care of infants and small children andthe treatment of minor ailments. The nurses alsoparticipate in teaching programmes for teams sent bygovernments for definite courses of instruction, andalso in short refresher courses for health visitors,midwives and dhais.
Achievements in nursing have demonstrated boththe acute need for an improved nursing service and thereadiness of the rural population to take advantageof the help given them by WHO nurses and thoseworking with them. In one area, where even seniorpublic- health officials were apprehensive about theprospect of home visiting being undertaken in ruralcommunities, the nurses on this team were able todemonstrate that they could carry out this functionjust as in more highly developed countries.
The teaching duties of the two nurses attached tohospitals should have a widespread effect. Nursingstudents from the outside, as well as pupil nursesfrom the Irwin Hospital in New Delhi, are beinggiven both practical and theoretical training inpaediatric nursing. It is expected that further groupswill be sent to this hospital for similar courses ofinstruction.
In Burma an appointment of a sister tutor hasrecently been made, and a teaching programme hasbeen started.
Demonstration Project in the Control of VenerealDisease
The demonstration and training project for thecontrol of venereal disease in India has resulted in awider dissemination of the use of penicillin and theinstitution of simplified serological tests all over thecountry. The results of preliminary surveys made bythe team have brought to light the prevalence of thedisease in areas where, because of their inaccessibilityand . the lack of any organized. medical . services,morbidity statistics were unknown. Visits of WHOconsultants to the main cities have in several casesStimulated the health authorities to undertake controlprojects, as, for example, in Bombay. The use of the
team's headquarters as a training ground for workersfrom other areas in the region has also facilitated theinitiation of similar projects.
Because of the lack of advisers on venereal diseaseon the staffs of the national health services of all thecountries in the region, the presence of an expert onthis subject in the Regional Office has been parti-cularly useful.
The Regional Office has maintained close collabora-tion with the countries in the region in order to assistthem in their plans for the production of penicillin,larger amounts of which are needed. Requests foraid from UNICEF in this project have beenstimulated.
Maternal and Child Health
In the governmental health services of India,Ceylon, Burma and Thailand, there are separateadvisers on maternal and child health. In Afghanistan,a separate society sponsored by the Government existsand is responsible for activities in this field. Becauseof difficulties in the collection of statistics, the mater-nal and infant morbidity and mortality figures areunreliable, and the present projects have been in exis-tence for too short a period to permit of any evalua-tion. These projects, however, are mainly connectedwith existing facilities for training nurses and doctors,and there has been a noticeable improvement in thequality of training offered to students.
In those countries where facilities for maternal andchild health services exist, it has been observed thatthere is not enough emphasis on paediatric care.Infant mortality in the countries of this region com-pares very .unfavourably with that in Westerncountries and is estimated to be ten times higher thanin New Zealand, the United Kingdom, and the UnitedStates of America. Lack of care of the mother duringdelivery, together with ignorance of the basic prin-ciples of the care and feeding of infants are apparenteverywhere.
Infant mortality is highest within the first monthafter birth. As in many cases no registration takesplace, the actual mortality cannot be estimated. InIndonesia, for example, infants are recorded as being .born only after they have been officially received bythe priest for baptism, which usually occurs around thetenth to twelfth day after birth ; there are no records
SOUTH -EAST ASIA REGION 99
of infants who die before this occasion. InAfghanistan a random questioning of women hasrevealed that although a large number of pregnanciesoccur, there are only one to two children per family.Abortions and miscarriages are frequent in womenwho have pregnancies following on obvious mal-nutrition. This has caused an acceptance of theinevitable loss of infant lives which can be overcomeonly by much work and education. It may well besaid that paediatric care in this region is in its infancy.The results of the schemes at present being plannedwill not be obvious for some time to come, but in thoseareas where public- health workers have establishedthemselves, the fact that they have been accepted bythe rural population is indicative of future success andof the urgent necessity for their work.
Co- operation with Other Organizations
In the Regional Office, co- operation has been main-tained with the United Nations Information Centreand with specialized agencies having offices in Delhi,by mutual representation at meetings, planning andthe exchange of reports and documents.
Daily working relationships have been establishedwith the UNICEF office in Delhi, particularly withregard to the implementation of joint WHO /UNICEFprogrammes and the planning of joint activitieswithin the region. Close collaboration was also main-tained with the UNICEF Far Eastern Headquartersin Bangkok, to which a WHO Senior Medical
Afghanistan
Officer was appointed to represent the OrganizationVisits have been exchanged frequently betweenWHO and UNICEF officials, and detailed procedureshave been worked out between the two offices forWHO's participation in. UNICEF -assisted healthprojects.
A representative of the Regional Office attended the110th Session of the Governing Body of ILO inMysore in January, and the ILO Asian Conference inCeylon, which also took place at the beginning of theyear.
A representative of the United Nations StatisticalOffice discussed with the Regional Office possibilitiesof holding a joint course in health statistics in 1951;the Regional Office sent a representative to theECAFE meeting in Bangkok in May ; it was repre-sented by a Medical Officer in the joint mission set upby the Technical Assistance Board to survey theneeds of Indonesia, and it participated in the meetingsof the joint committee on co- ordination in Burma,Thailand and Indonesia, together with the EconomicCo- operation Administration of the United Statesof America, UNICEF and governmental organiza-tions interested in medical aid.
The representative of UNESCO in the region iscollaborating with WHO in the drawing up of aschool -health- education scheme. FAO has collabor-ated in the agricultural and economic survey in theChiengmai area in Thailand, and has undertakento provide a nutritionist for Thailand to replace oneappointed by WHO.
Activities undertaken by Individual Governments with Help from WHO
In Afghanistan, where the national health- organi-zational structure still needs to be developed, atten-tion has been concentrated on two acute health prob-lems : malaria and maternal and child health. It ishoped gradually to expand the general health servicesaround projects in these subjects, and to provide atthe same time an experienced adviser in public -healthadministration to guide this work.
After a three months' survey of the malariasituation in Afghanistan, followed by a pilot demon-stration project, had been carried out in 1949, theteam operating this project selected an area foroperations in 1950, which were to be carried out bya full team. Impressed by the success of the pilot
project, the Afghan Government extended the opera-tions over the entire Laghman District, at its owncost ; WHO assisted by procuring DDT and equip-ment to the extent of $11,000 on a partly reimbursablebasis.
In 1950, at the request of the Government, WHOprovided a complete malaria demonstration teamconsisting of an entomologist (leader), a malario-logist, a public -health engineer, and a malariainspector, with the requisite equipment and supplies.This team is at present operating around Khanabad,an area with agricultural and industrial potentialitiesin the Northern Province. Local personnel has beentrained. Spraying operations commenced on 20 June ;50,324 premises were sprayed and a population of45,000 directly protected.
100 WOaK OF WHO, 1950
It is hoped that the area of operations will beextended in 1951 and additional national stafftrained to work in the malaria organization of thecountry. The Government has agreed to continue thepresent malaria- control project in the Khanabad-Kunduz area after the withdrawal of the WHO teamat the end of 1951. WHO operations in Afghanistanhave given rise to a general desire for the extensionof malaria control all over the country.
Following the 1949 epidemic of louse -borne typhusduring which WHO suppplied vaccine, DDT and dust -guns, an experienced medical officer of health wasprovided by the Organization to help the Govern-ment in control operations. These were speciallydevised to cover the winter months when the incidenceof the disease is at its peak. Mass delousing opera-tions were carried out in schools, police stations,military barracks and jails. This helped to keep theincidence of typhus under control. WHO also helpedthe Afghan Government in the procurement of therequisite supplies of DDT and antityphus vaccine.Organization is needed in systematic delousing byDDT dusting, etc., if this disease is to be controlledand eventually eradicated. In view of the shorttransmission period for malaria, national experts inmalaria should be trained in delousing operationsand should be available during the winter months forthe control of typhus. Work in the control of malariaand typhus could then be entrusted to one unit, andeconomy in personnel and equipment thereby effec-ted.
Following the survey on venereal disease made in1949, it was decided to integrate the programme forthe control of venereal disease with the maternaland child health project. The senior adviser of theproject, a clinical pathologist with experience inserology, went to Kabul in September, taking withhim supplies and equipment, and made the necessaryarrangements with the Government. The plan ofoperations provides for the carrying out of a pilotproject in maternal and child health and control ofvenereal disease by a professional team of threeforeign staff members -a clinical pathologist, anobstetrician and a public- health nurse, all of whomhave been recruited.
During the year, a student with a fellowship invenereal disease proceeded with his studies in theUnited States of America. Medical literature andteaching equipment were sent to Afghanistan.
Burma
In Burma, because of disturbed internal conditions,very little field work has been done during the year.The two most acute needs are for work on the controlof tuberculosis and on maternal and child health,and plans for international assistance in bothsubjects are now ready. The work in maternal andchild health, to be carried out with the assistance ofUNICEF, will actually result in the reorganizationof a large part of the health services of the country.
A survey and evaluation schedule of tuberculosishave been completed. In response to a request fromthe Government of Burma, WHO and UNICEF areassisting in the establishment of a tuberculosis controland training centre in Rangoon. Procurement ofsupplies is going forward ; premises are being adaptedfor a laboratory, and the clinic is being renovated andimproved.
Burma was visited in December 1949 by a WHOadviser on maternal and child health and, at the endof 1950, by the adviser on venereal disease. As aresult of these visits a programme on maternal andchild health and the control of venereal disease isbeing prepared jointly by WHO and UNICEF. Thisproject provides for equipment and supplies forcentres in maternal and child health and for children'swards and maternity wards, medical literature andteaching equipment for the training of nurses andmidwives, equipment for school dental work and forhealth education, and laboratory equipment andsupplies for the treatment of venereal disease. Inaddition, a project for control of venereal diseasesis being evolved for the Kachin State. The servicesof a paediatrician, a serologist, three sister tutors andfour public- health nurses are being provided atRangoon. One sister tutor began institutional workat the Rangoon General Hospital in September.
Four fellowships were awarded in Burma during1950, three of them in communicable diseases andone in the basic medical sciences. Medical literatureand teaching equipment were also supplied.
Ceylon
In Ceylon, a fairly good national health service hasalready been built up by the Government. There are,however, some weak points, and WHO is assistingthe Government in the reorganization of the
SOUTH -EAST ASIA REGION 101
tuberculosis services, the improvement and reorienta-tion of services in maternal and child health and thecontrol of venereal disease.
For some years past Ceylon has organized and verysuccessfully operated a country -wide DDT sprayingprogramme without international assistance. In 1949technical advice on the advisability of undertaking aspecies eradication programme was requested and inthe early part of 1950 a WHO malaria consultantmade. a survey of this subject. After a careful studyhe advised against undertaking the programme.
Following discussions in Colombo between theGovernment and WHO and UNICEF representativesin June, the Government requested assistance fromUNICEF in setting up a rural centre for tuberculosiscontrol at Kotte and a diagnostic laboratory inColombo. WHO and UNICEF will assist with thisproject, but the grant of laboratory equipment wasdeferred pending the provision of a suitable buildingin Colombo. In September the Government promisedto provide the requisite premises before the end of1952, and it is hoped to set up a temporary tubercu-losis laboratory at Welisara Sanatorium.
A " Joint Enterprise " team began BCG vaccina-tion in Ceylon at the request of the Government andtrained three local teams, which are now continuingthe campaign. One of these teams is working withthe rural tuberculosis -control project at Kotte, whichwas started without international assistance and willbe extended by the provision of a mobile mass -radiography unit and an x -ray technician.
The Government of Ceylon requested assistancefrom UNICEF and WHO in connexion with maternaland child health, and it is planned to provide twosister tutors in paediatrics and two in midwifery fortwo years, four fellowships, and equipment and sup-plies for the new Children's Hospital, the De SoysaMaternity Hospital and the Nurses' Training Schoolin Colombo, and for the Kalutarai Health Unit.
The Government also requested the services of aconsultant to study the problem of endemic goitre.A WHO expert visited Ceylon from 16 February to23 March, investigated the problem and made recom-mendations.
Medical literature and teaching equipment weresupplied, and four fellowships, in paediatric nursing,venereal diseases and nutrition, were awarded. Eight
UNICEF fellowships administered by WHO werealso awarded.
In 1949 the Government requested a demonstrationteam in the control of venereal diseases. Followinga preliminary survey by a consultant, recommenda-tions for a control scheme were drawn up, and a planof operations is now under consideration by theGovernment. This scheme provides for a demonstra-tion team to work in Colombo and in a provincialhospital, within the existing framework of the organ-ized venereal- disease control in the city. The teachingof undergraduate and postgraduate students will beone of the main functions of the team, which will alsowork with the teams on maternal and child healthand assist in the detection and treatment of syphilisamong pregnant women and among children.
Agreement was reached by the Regional Committeein September that a port project in venereal- diseasecontrol for seafarers should be started, with a modelclinic at Colombo. Preparations are being made forimplementing this project and integrating it with themain venereal -disease team.
In December 1949, the Government of Ceylonrequested that the expert who had carried out afilariasis survey should conduct a course of intensivetraining in filariasis control. He was sent to Ceylonon a two months' assignment, after which his serviceswere extended by the Government of Ceylon for afurther period of two and a half months. The trainingwas concluded about the end of January, and he wasthen engaged by the Government of Ceylon onactivities in connexion with the filariasis- controlschemes of various municipalities.
India
India is a vast sub -continent, and although a fairlyextensive substratum of health services exists, thereare big gaps both in quality and quantity. A nationalcommission (the Bhore Committee) made an ex-tensive survey of the health needs of the country andrecommended elaborate improvements. Unfortu-nately, because of acute financial stringency, theseplans have not been implemented to any extent, andit is doubtful whether, during the immediate future,much can be attempted.. The general policy seems tobe to maintain the status quo for the present. WHOhas therefore concentrated on helping to fill some ofthe larger gaps in the national health services byintroducing modern methods of malaria control in
102 WORK OF WHO. 1950
areas where this has not been attempted previously,and by giving assistance in large -scale trainingschemes for the control of tuberculosis and venerealdisease. One of WHO's most useful contributions willbe the strengthening of national teaching institutionsto train various categories of health workers whoare badly needed. This will be a slow process, how-ever, on account of the extremely limited financialresources which are available for making use of suchtrained personnel.
During 1950, besides providing supplies for amalaria -control programme in Bombay State andsending a lecturer to the Malaria Institute of India,WHO supervised four malaria -control teams workingin India in joint projects with UNICEF.
The following work has been carried out by theseteams :
Team No. 1, Terai, United Provinces
This project was begun in May 1949. The area ofoperations was the Western Terai, situated in theNaini Tal District of the United Provinces. Itextends for -about 300 square miles and has a popu-lation of approximately 15,000, living in 257 villages.
The international staff consists of the team leaderand a public -health nurse. Spraying operations werebegun on 27 May, and the total number of premisessprayed was 12,090, with a directly protected popula-tion of 14,631.
In 1950 the field of operations was enlarged toinclude East Terai and the Bhabar area. This in-creased the area to 1,500 square miles and the totalpopulation to about 100,000. For the whole areathe team carried out a malariometric survey, whichincluded a post- operational survey of the areasprayed in 1949.
The team has trained " matching personnel " inmalaria control, health officers, compounders (a typeof pharmacist who assists qualified medical men) anda forest officer.
Team No. 2, Jeypore Hill Tracts, Orissa
This team was in the field by the end of May 1949.The area of operations is situated in the eastern partof Jeypore Hills in Orissa. The demonstration andcheck areas, divided into approximately equal parts,covered about 660 square miles, and the populationof the demonstration area was estimated at about
61,000. The international staff consisted of a teamleader and a public -health nurse.
Spraying operations, which started in July andended in December, were carried out in two phases(the pre- and post -monsoon). The total number ofpremises sprayed in 1949 was 46,856 and the popula-tion protected 60,900.
In 1950 operations were enlarged by the addition ofthe check area, and the total area dealt with was660 square miles with a population of 120,000.Malariometric surveys were carried out from Januaryto March.
Lack of adequate accommodation for WHO staff,particularly of suitable premises for the laboratory,and frequent changes in the staff of the parallel teamadversely affected the operation of this project.
In 1950 the team gave training in malaria controlto six WHO Fellows who were studying at the MalariaInstitute of India.
Team No. 3, Malnad, Mysore
The Malnad team was in the field in June 1949. Thearea of operations is Sagar Taluk, Shimoga District,Mysore State. The demonstration and check areascovered about 482 and 400 square miles with anestimated population of 48,800 and 25,000 respec-tively. The international staff consists of a teamleader and a public -health nurse.
Spraying operations were started on 12 August1949. The total number of premises sprayed was34,137, and the population directly protected, 48,810.In 1950 the demonstration area was enlarged toinclude Hasangar Taluk and portions of SorabTaluk, with an area of about 720 square miles and anestimated population of 69,000. The total areacovered during 1950 was 1,600 square miles with apopulation of about 140,000.
During the absence of the team leader, who wasaway on sick leave, the work was competently super-vised and directed by the leader of the parallel team.
Efforts made by the team to develop school -healtheducation met with great success. In health education,the " roadside " clinics, which were held by the WHOnurse and are now a regular feature of the team'swork, were greatly appreciated by the rural popula-tion of this sparsely populated area. Local healthcommittees have been formed and are enthusiasticallyco- operating in the work.
A survey of the records of three dispensaries whichdraw their patients from the sprayed areas showed a
SOUTH -EAST ASIA REGION 103
decrease of over 80 % for new patients treated formalaria, as compared to figures for the precedingyear, six months after the completion of the firstspraying. Governmental co- operation has been verygood.
Team No. 4, Ernad, Madras
This team was in the field on 12 December 1949.The area of operation is in the Ernad and WalluvanadTaluks of the Malabar District in Madras State. Thedemonstration area covers about 93 square miles andhas a population of approximately 49,000 ; the checkarea is about 46 square miles. International staffconsists of a team leader and a public -health nurse.
Spraying operations commenced on 17 January.The total number of premises sprayed was 38,110and the population directly protected, 51,238. Theleader of this team was also requested to draft a planfor filariasis control in Calicut.
A reconnaissance team in maternal and child health,consisting of a paediatrician and a paediatric nurse,arrived in Delhi in September 1949. This teammade a survey of needs and facilities in paediatrics,and observed paediatric work in other parts of India.The paediatrician assisted in the teaching in DelhiCollege of Nursing.
The draft plan of operations for the team, preparedby the paediatrician and forwarded as a guide to theGovernment, envisaged the establishment of twoareas, one urban, the other rural, which would servenot only for demonstrating modern techniques, butalso as training areas for schools such as the DelhiCollege. of Nursing, the Lady Hardinge MedicalCollege and the Lady Reading Health Visitors'School. In January 1950, with the approval of theGovernment of India, the WHO team started workat Najafgarh, the rural -health project area. TheWHO staff also worked in Chowla village in theNajafgarh health unit.
A matching team has been appointed, and workwill be begun on a health centre area, comprising 26villages, with a population of 21,000, and a ruraltraining area. Already 20 nursing students havepassed through the area. The paediatric nurse hascompleted a course of lectures at the nursing college,and the children's ward of the Irwin Hospital will beused for practical training.
Plans for expanding this work include the organiza-tion of paediatric work and teaching in the Irwinand the Lady Hardinge Hospitals, and the provisionof more teaching facilities at the College of Nursing,equipment for 100 maternal and child health centresand facilities for school dental work.
In collaboration with the Government of India, afour -day symposium on maternal and child healthwas held at the WHO Regional Office beginning on30 December, 1949. Representatives from all overIndia -doctors, nurses, health visitors, social workersand representatives of voluntary agencies- attended.A series of resolutions were passed to serve as a guidein the development of this type of work in India. Thegeneral conclusions were that, although during thelast 30 years progress had been made in midwiferyservices and the control of epidemic diseases, work onpaediatrics left a great deal to be desired.
WHO and UNICEF have agreed to help theGovernment in establishing a maternal and childhealth department at the All -India Institute ofHygiene and Public Health, Calcutta. When com-pleted, this department should provide high -gradetraining in maternal and child health for India andsurrounding countries.
It is proposed to set up three tuberculosis demon-stration and training are as in India -one in Delhi,another in Patna and the third in Trivandrum -withjoint assistance from WHO and UNICEF. Opera-tions in Delhi and Trivandrum will probably startat the beginning of 1951, and in Patna when thebuildings are completed (about April 1951).
The Government requested assistance in furtherprojects : (1) in increasing facilities for teachingthoracic surgery in Vellore and Delhi, and im-proving those for postgraduate teaching in tuber-culosis at Delhi University, and (2) in expanding atuberculosis -control project which has been inoperation for some time at Madanapalle. Theseprojects were approved by WHO, but for the former,which was not approved by UNICEF, it is hoped tosecure financial support from the Technical AssistanceBoard.
BCG vaccination, begun by WHO in 1949, wascontinued by six teams of the Joint Enterprise during1950.. The number of teams was later in the yearreduced to three. The work has been introducedinto all States in India except Madhya Pradesh,
104 WORK OF WHO, 1950
and about 90 local teams have been trained tocontinue it. On the whole the response to propagandain favour of vaccination has not been encouraging.
A demonstration team in the control of venerealdisease started operations in India in April at Simla(Himachal Pradesh). It spent some time arrangingfor alterations to buildings and the fitting up of thelaboratory, and established clinics in conjunctionwith existing hospitals. In the first months, theteam's main concern was the establishment ofsuitable working conditions ; it also made a studyof the local situation, especially the incidence andprevalence of the disease in the area. Materialwas obtained from many sources, and the teammoved frequently into rural areas, gaining knowledgeof field conditions and valuable data on mass treat-ment methods. In Ghund Valley, an isolated ruralarea, 1,600 out of a population of 2,000 were surveyedand treated, and 37 % of the treated population wereresurveyed after six months. A one -year follow -upwill shortly be undertaken. As a result of the masstreatment, the number of cases of treatment forgenital lesions at the dispensary dropped from 20per month to two in five months. The inhabitantsof the neighbouring State of Balsan and Baghirequested a visit by the team, and through it they wereable to obtain their first experience of modern medicalservice.
Training of satellite teams was started in December1949. Sixteen teams, composed of serologists,clinicians and nurses from 11 States, worked withthe team for varying periods up to three monthsand returned to their States, to apply the methodslearned. In many instances they have experienceddifficulty in applying these methods, as they havelacked equipment and drugs. UNICEF is consider-ing the possibility of supplying such teams with aminimum of laboratory equipment and drugs on thecompletion of their courses of training, to enablethem to start working immediately.
In addition, on request from the Bombayauthorities a one -week course for laboratory workersand technicians was given by the team serologist,and was attended by 17 trainees from the State.The demonstration has succeeded in popularizingsimple serological techniques with the use of thenew antigens. It has also shown the value of newantibiotics in the treatment of venereal disease, andthe possibility of completing treatment on an ambu-latory basis in a short time, as well as of providingfor mass therapy, in rural areas.
In addition to a high incidence of syphilis, thearea of Himachal Pradesh has cases of granulomainguinale, a disease which responds to treatmentwith streptomycin and other new antibiotics such asaureomycin. This treatment is now used in manyof the subsidiary hospitals for which drugs havebeen supplied by WHO. It has resulted in con-siderably shortening the stay in hospital.
The Government has recognized the desirabilityof standardizing serological tests for syphilis ina country as large as India, especially as conditionsexist there which are responsible for reactions ofa " false " nature -the prevalence of leprosy andmalaria, for instance, and chronic malnutrition,all of which are liable to cause a " false positive "reaction. A plan for the local manufacture ofcardiolipin antigen, and its distribution on a non-profit basis, is being considered by UNICEF. TheGovernment of India is also contemplating revivingthe Technique Standardization Committee, under theauspices of the Indian Council of Medical Research.It has requested assistance in establishing an All -India Postgraduate Training Centre at the MadrasGeneral Hospital.
By a resolution of the Third World HealthAssembly, field operations in connexion with controlof cholera were included in the regular programmefor 1951, and the Regional Committee, at its thirdsession, also recommended WHO assistance to theIndian Council of Medical Research to continueinvestigations on the epidemiology of the disease.One national worker was given a fellowship to studycertain aspects of such investigations and plans arebeing made for further collaboration.
At the request of the Government, the servicesof a poliomyelitis advisory and demonstration team,consisting of an orthopaedic surgeon, a nursespecialist and a physiotherapist, were provided toIndia for a period of two months. The team arrivedon 13 January and visited Bombay, Calcutta,Madras, Poona and Delhi to study the incidenceof poliomyelitis, the availability of facilities fordealing with it and the possibility of giving lecturesand demonstrations. Lecture- demonstrations wereheld at Calcutta and Madras and short courses atBombay and Delhi. The medical and nurse specialistsleft on 20 March, but the physiotherapist, at therequest and expense of the Government, remaineduntil 15 July to conduct a physiotherapy- trainingprogramme in Bombay. On 17 July she was
SOUTH-EAST AS REGION 105
unfortunately killed in an air crash when going toKashmir on holiday.
The cases of poliomyelitis reported from someof the countries of the region during 1949 and forsix months of 1950 are as follows : for Afghanistan,Burma and Thailand, none in 1949, none in 1950 ;for Ceylon, 85 in 1949, 49 in 1950 ; for India, 1,011in 1949, 312 in 1950.
At the request of the Government WHO sent ahospital dietitian to India in July as consultant tohelp in the establishment of a diet kitchen at theMedical College Hospital, Calcutta, and to assistin a course in dietitics at the All -India Institute ofHygiene and Public Health.
The Government of India is participating in theWorld Influenza Centre set up by the Interim Com-mission of WHO, and has delegated an observerfrom the Pasteur Institute, Coonoor, to serve withthe Centre. Two national centres are now beingestablished, and two others are planned.
Medical literature and teaching equipment weresent to the Lady Hardinge Medical College and tothe Malaria Institute in New Delhi.
Three fellowships were awarded to India duringthe year, in leprosy, public- health administrationand in the bacteriology of cholera, as mentionedabove.
In Assam, emergency supplies were sent to theMedical College to assist in alleviating conditionscaused by an earthquake.
India, Portuguese
Three fellowships in communicable diseases wereawarded to Portuguese India.
Indonesia
Indonesia is a new Member country, where anextensive rebuilding of national health services,made necessary by the long period of political unrest,is in progress. The aims of the Organization areto help the Government in its planning of thisvery important work, and at the same time to givespecial assistance in tackling one or two very acuteproblems -the control of yaws, for instance, aproject in which WHO and UNICEF are assistingand which is already in operation.
Yaws has been considered by the Government asone of the major scourges of the country. It hasmainly afflicted the rural population, and has resultedin much preventable crippling. For many years a
campaign against this disease had been conductedby the Government, through the use of rural clinics,mobile teams, etc. Aid in combating this diseasewas requested in 1949, and a scheme was preparedfor renewing the campaign, which had stoppedbecause of the war.
Yaws control and the diagnosis and treatmentof syphilis in pregnant women and of congenitalsyphilis are now being undertaken with financialassistance from UNICEF and the technical guidanceof WHO. Two areas with a population of threeand a half million were chosen as the primary sitesfor the first phase of the campaign ; an internationalconsultant has acted as adviser to the Governmenton the project, and a serologist is working in thelaboratory with one experienced Indonesianbacteriologist.
The campaign, which started in May and is tolast two years, is being conducted by mobile teamsunder the supervision of doctors or public- healthworkers, who are being trained at the central traininginstitute which has been established. Six teamshave been, and others are being, trained. Planshave been made for the work to be expanded toother areas of the Island of Java, and to the restof Indonesia. Research in a selected area is alsoplanned. In connexion with these projects, theadviser on venereal diseases visited the country inDecember.
As a result of the recommendations of the Tech-nical Assistance Exploratory Mission to Indonesia,a request was made for the services of a consultantfor two or three months to make a preliminarysurvey of tuberculosis in the country. This requestis being acceded to.
A malaria survey was carried out by the regionaladviser in malaria in September. As a result theGovernment of Indonesia has accepted a recom-mendation that a team of two malariologists and amalaria inspector should be given travel fellowshipsto visit the WHO demonstration teams at Chiengmai(Thailand) and Dacca (Pakistan). A WHO malariateam, consisting of a malariologist or entomologist,sanitary engineer or sanitarian, and a public -healthnurse, will start a malaria demonstration project in1951, to be established at Tjillatjap, in the presidencyof Banjumas. This demonstration will cover apopulation of 83,000 people in an area of 100 squarekilometres, with a check area covering 20,000 peopleand extending over 35 square kilometres. Thespleen index in both areas is over 90 %.
106 WORK OF WHO, 1950
Indonesia was visited by the WHO adviser inmaternal and child health attached to the UNICEFFar Eastern Headquarters, Bangkok, and the Govern-ment has since requested assistance in a maternaland child health demonstration project which isexpected to start early in 1951 and for which WHOwill provide a public- health nurse and a paediatrician.
During the year three UNICEF fellowships wereawarded to Indonesia and administered by WHO.
Maldive Islands
A consultant in filariasis control was sent to theMaldive Islands in the last part of the year.
Thailand
In Thailand WHO's objective has been to con-centrate on the control of malaria on an extensivescale with the help of other international organiza-tions, to assist in the reorganization of services innursing and maternal and child health and to tacklethe acute problem of yaws.
The initial work of the malaria -control demon-stration project, set up in the Sarapee district closeto Chiengmai, was described in last year's report.3After surveys had been made, personnel trained andexperimental spraying programmes completed, themain spraying operations were started on 18 April.In these operations, 31,397 premises were sprayedand a population of 40,145 was directly protected.Full results are not available. The Government ofThailand set up parallel teams for malaria control,one in the Hangdong District and the other in thePhrabhudabad District, and agreed to continue theproject after the withdrawal of WHO personnel. Byresolution of the Executive Board, WHO providedsupplies of DDT, sprayers and other equipment forthe governmental malaria campaign.
The entomologist attached to the team advisedon plague control and mosquito nuisance in Bangkok,assisted in a rural sanitation programme and madea survey of other communicable diseases.
3 Of Rec. World Hlth Org. 24, 36
An urban demonstration unit in maternal andchild health was also planned with WHO andUNICEF assistance during the year. This workwill be carried on by a paediatrician, a public -healthnurse, a district midwifery supervisor and a super-visor of sanitary inspectors. Teaching and otherequipment, and supplies, will be provided. TheGovernment has undertaken to establish a divisionof nursing in its Ministry of Health, and a nurse -consultant will be recruited to assist with this division.The Government has also agreed to appoint areturned UNICEF /WHO Fellow to the maternal andchild health section of the Department of Health,and an additional medical officer and two public -health nurses to the parallel team.
The Government asked for assistance in investigat-ing the endemic goitre problem, and also requestedthe services of a general nutritionist, who is expectedto be provided by FAO.
A plan of operations for the setting -up of a tuber-culosis demonstration and training area at Bangkokwas drawn up by the regional adviser on tuberculosisin May, in consultation with officers of the ThaiMinistry of Health and of UNICEF Far EasternHeadquarters. This plan involved help from WHOand UNICEF in enlarging and improving the tuber-culosis clinic. The planning of the laboratory isnow going forward, and equipment and internationalpersonnel for this project should arrive early in1951.
In 1950 a treponematoses- control programme wasformulated and will soon be implemented by WHOand UNICEF. The programme is directed againstyaws, which is prevalent in rural areas, and includesthe diagnosis and treatment of syphilis in pregnantwomen and in children. A site for the team'swork has been selected at Rajburi, about 60 kilo-metres from Bangkok, with a population of 250,000.This area is sufficiently close to Bangkok to permitstudents to come for training. In addition, teamsof workers for other areas will be trained at thecentre to carry on the programme in areas of highincidence. A consultant and serologist are alreadyin Thailand for this project, and a public- healthnurse has been selected.
In the first phase of operation five teams will betrained and research work will be undertaken, asin similar programmes in other countries in the
SOUTH -EAST ASIA REGION 107
region. Five -year plans have already been madefor an expanded programme to cover the entirecountry.
In connexion with this project, the adviser onvenereal diseases visited the country in December.
Seven fellowships were alloted to Thailand duringthe year, in such subjects as malaria, venerealdiseases and nutrition. Four others, awarded byUNICEF, were administered by WHO. Medicalliterature and teaching equipment were supplied.
108 WORK OF WHO, 1950
EUROPEAN REGION 1
The Special Office for Europe was establishedon 1 January 1949 at headquarters in Geneva.During the first year of its existence, its work inadministering advisory services in Europe wascarried out by an Acting Director and a secretary.With the development of European programmes in1950, the staff was strengthened by the engagementof two field advisers, and further additions to thetechnical advisory staff have been approved. Eco-nomies in staffing continued to be effected by theuse of headquarters staff either as short -term con-sultants on specific problems or as permanentadvisers in subjects such as mental hygiene, nutrition,etc., for which field advisers were not available tothe Special Office. Pending the establishment of aRegional Organization for Europe, and as long asthe Special Office is situated at headquarters, it willbe possible to administer this region with a nuclearstaff, since specialists are normally available on loanfrom headquarters, but the staff of the office shouldinclude officers experienced in public- health admi-nistration.
The fairly rapid development of programmes inEurope and the interest shown by countries whichhad not previously participated in them emphasizedthe need for establishing a co- ordinating grouprepresenting the countries of the region. A con-siderable degree of co- ordination was achieved in1950 through activities such as the group- trainingprogrammes, but it has been suggested that the SpecialOffice would be much assisted by a regular annualmeeting of a consultative committee on programmerepresenting all the Member States in the region.Governments were consulted on this proposaltowards the end of the year.
The pattern of activities in 1950 was determinedby two important factors : (1) the need for technicalsupervision of existing programmes, such as thosefor which UNICEF furnished supplies, and (2) asurvey of the programme needs of Member States,as expressed in the European Conference of October
1 The region comprises the whole of Europe, includingGreece, but excluding Turkey, according to decisions of theFirst and Second World Health Assemblies (Off. Rec. WorldHlth Org. 13, 80, 330 ; 21, 53).
1948 and in consultations with individual govern-ments in 1949.
Europe is an area of high technical development,which presents a suitable field for study and experi-ment on programmes which may subsequently beof importance to other areas of the world. MemberStates in the region have crystallized their needs byrequesting two main types of services : (1) assistancein improving professional and technical educationand training and (2) the provision of consultants onspecific problems.
UNICEF Supply Programmes
There is little doubt that the emergency characterof UNICEF's work in Europe in its initial phasesmade it difficult and sometimes impossible for WHOto give adequate technical advice. There were, ofcourse, important exceptions to this generalization,as in the prenatal and infantile syphilis programmes.In 1949 and 1950 the situation had somewhat changed.Supplies were being delivered in increasing quantititesto certain countries for a fairly wide variety of medicalprogrammes, the effect of which may be measuredby the fact that over four million dollars was spentby UNICEF for medical supplies in Europe. Fre-quent consultations with UNICEF, a definition ofthe responsibilities of its European headquartersand of those of the Special Office for Europe, andreadiness on the part of WHO to provide advisersand consultants for supply programmes withoutdelay all contributed to the smoother operation ofjoint programmes in 1950. WHO is increasinglyplaying the role designed for it in these programmes,which, however, need further co- ordination in orderto be of the utmost help in forwarding the objectivesof the Organization in Europe. To give a singleexample, the UNICEF $250,000 supply programmefor handicapped children has provided a stimulusfor a whole new and important field of activity forWHO and other interested agencies. Without earlyco- operative planning and follow -up the supplyprogramme would lose much of its value.
SYMPOSIUM ON SYPHILIS, PARIS. Dr. Mary Pangborn,discoverer of cardiolipin, illustrating steps in thepreparation of cardiolipin and lecithin.
SYMPOSIUM ON SYPHILIS, PARIS. Professor C. R. Reinof New York University, who explained the Rein- Bossackserodiagnostic test at the symposium, in informaldiscussion.
ANAESTHESIOLOGY TRAINING CENTRE, COPENHAGEN.A demonstration of anaesthesia by Dr. Stuart C. Cullen(United States).
ANAESTHESIOLOGY IN TURKEY. Dr. E. Waino Andersenof Denmark, who was trained at the Copenhagen Centre(see above), demonstrating to Turkish doctors the newmethods of anaesthesia.
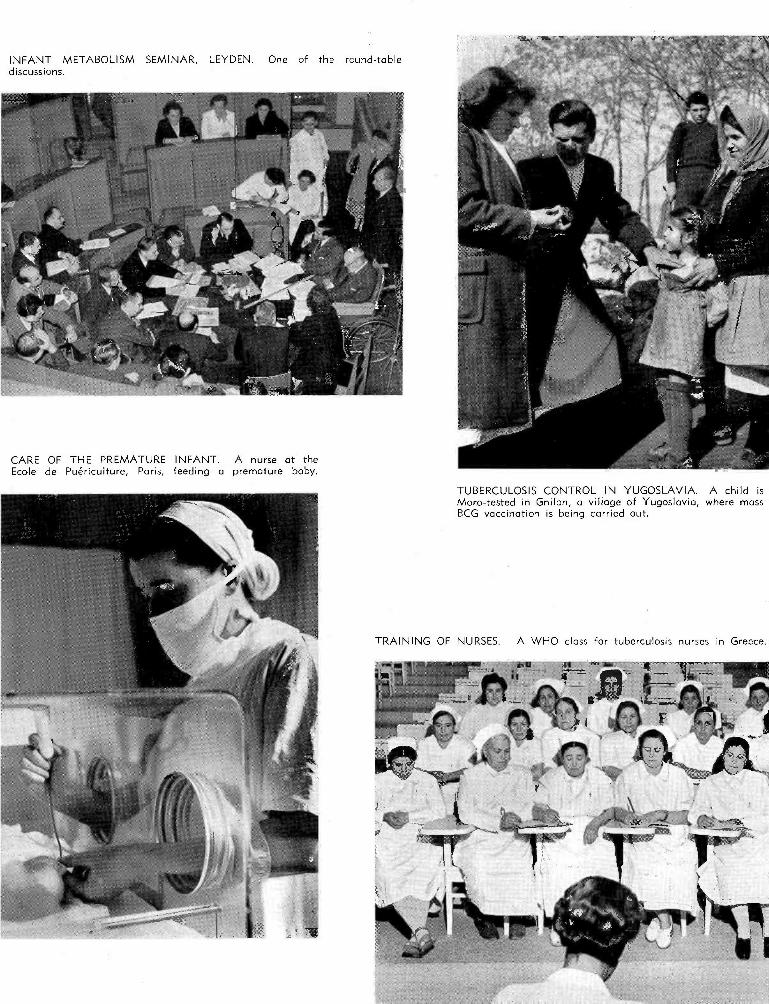
INFANT METABOLISM SEMINAR, LEYDEN. One of the round -tablediscussions.
CARE OF THE PREMATURE INFANT. A nurse at theEcole de Puériculture, Paris, feeding a premature baby.
TUBERCULOSIS CONTROL IN YUGOSLAVIA. A child isMoro -tested in Gnilan, a village of Yugoslavia, where massBCG vaccination is being carried out.
TRAINING OF NURSES. A WHO class for tuberculosis nurses in Greece.
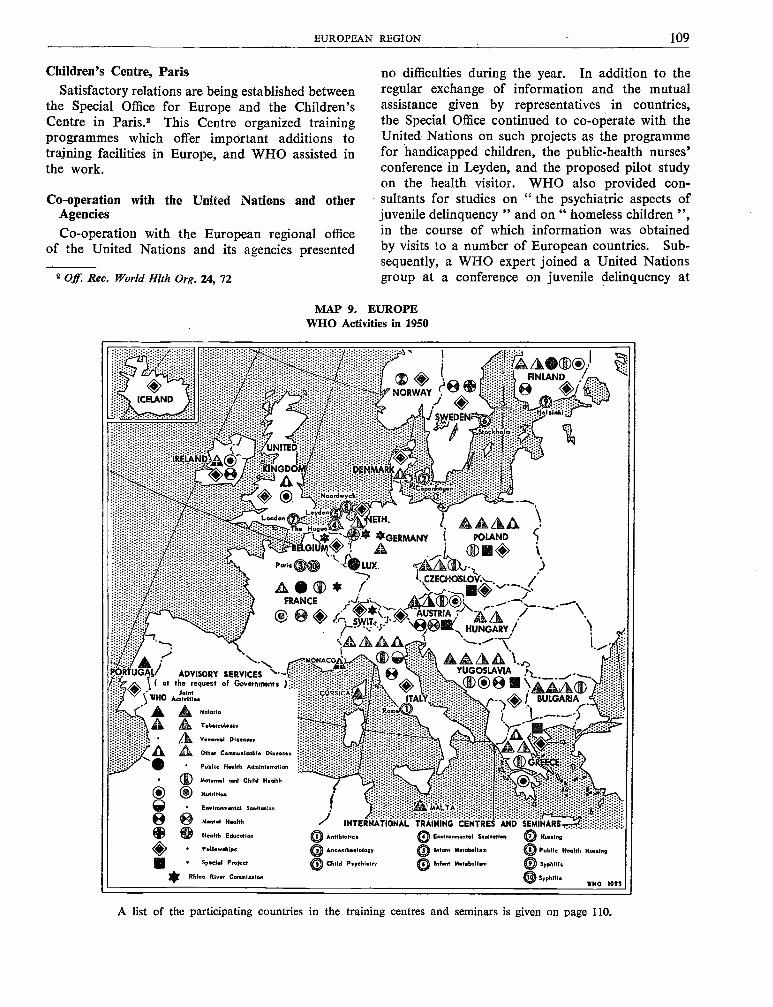
EUROPEAN REGION 109
Children's Centre, ParisSatisfactory relations are being established between
the Special Office for Europe and the Children'sCentre in Paris.2 This Centre organized trainingprogrammes which offer important additions totraining facilities in Europe, and WHO assisted inthe work.
Co- operation with the United Nations and otherAgencies
Co- operation with the European regional officeof the United Nations and its agencies presented
2 Off. Rec. World Hlth Org. 24, 72
no difficulties during the year. In addition to theregular exchange of information and the mutualassistance given by representatives in countries,the Special Office continued to co- operate with theUnited Nations on such projects as the programmefor handicapped children, the public- health nurses'conference in Leyden, and the proposed pilot studyon the health visitor. WHO also provided con-sultants for studies on " the psychiatric aspects ofjuvenile delinquency " and on " homeless children ",in the course of which information was obtainedby visits to a number of European countries. Sub-sequently, a WHO expert joined a United Nationsgroup at a conference on juvenile delinquency at
MAP 9. EUROPEWHO Activities in 1950
elslnki:1
OU/
ADVISORY SERVICES( at the request of Governments )
WHO AerlJvai itl..
(, A A Malaria
© ® Tubereuiosis
® Venereal Diseases
AA other Communicable Diseases
; %u.` e d.tJETH.....'! ® 1 ®®®Th. ¡fr.- ¡t
...GERMANY Í POLAND 1LGwn+t ® 1 A ¡ 41® Q 1
Paris ?IP; .140 LUX. e®-tiZA ® * / .CZECHOSLOV:,
1 `,®O v -FRANCE c ® ®Q' - -,`-
® r ® 'O` AUSTRIA / \+ ®HUNGARY/
Public Health Administration
® Mat.mal and Child Hedth
OO NutritionEnvionmental Sanitation
® 0 Mental Health
Health Education
Fellowships
Special Protect
Rhine River Commiselen
?MONACO AAAA -jYUGOSLAVIA h..® ® ®U \ ®V
¡ BULGARIA
1
J,
INTERNÁTIONAL1® Anribioriea
Anossthesiolopy
®j Child Psychiatry
,::TRAINING CENTRES AND SEMINARS T7 q:
0 Environmental Sanitation 7® Nursing
Infant Metabolism
Infant Metabolism
Public Health Nurslny
9® Syphilis
® SyphilisWHO 1097
A list of the participating countries in the training centres and seminars is given on page 110.
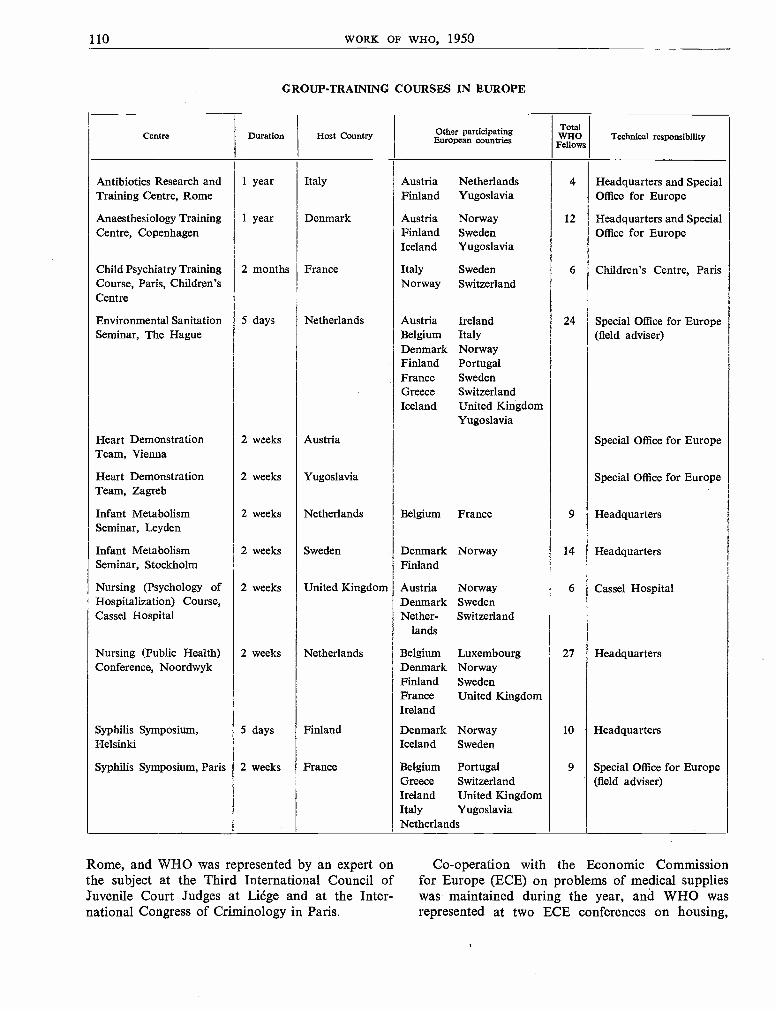
110 WORK OF WHO, 1950
GROUP -TRAINING COURSES IN EUROPE
Centre Duration Host Country Other participatingEuropean countries
TotalWHO
FellowsTechnical responsibility
Antibiotics Research and 1 year Italy Austria Netherlands 4 Headquarters and SpecialTraining Centre, Rome Finland Yugoslavia Office for Europe
Anaesthesiology Training 1 year Denmark Austria Norway 12 Headquarters and SpecialCentre, Copenhagen Finland Sweden Office for Europe
Iceland Yugoslavia
Child Psychiatry Training 2 months France Italy Sweden 6 Children's Centre, ParisCourse, Paris, Children's Norway SwitzerlandCentre
Environmental Sanitation 5 days Netherlands Austria Ireland 24 Special Office for EuropeSeminar, The Hague Belgium Italy (field adviser)
Denmark NorwayFinland PortugalFrance SwedenGreece SwitzerlandIceland United Kingdom
Yugoslavia
Heart Demonstration 2 weeks Austria Special Office for EuropeTeam, Vienna
Heart Demonstration 2 weeks Yugoslavia Special Office for EuropeTeam, Zagreb
Infant Metabolism 2 weeks Netherlands Belgium France 9 HeadquartersSeminar, Leyden
Infant Metabolism 2 weeks Sweden Denmark Norway 14 HeadquartersSeminar, Stockholm Finland
Nursing (Psychology of 2 weeks United Kingdom Austria Norway 6 Cassel HospitalHospitalization) Course,Cassel Hospital
Denmark SwedenNether- Switzerland
lands
Nursing (Public Health) 2 weeks Netherlands Belgium Luxembourg 27 HeadquartersConference, Noordwyk Denmark Norway
Finland SwedenFrance United KingdomIreland
Syphilis Symposium,Helsinki
5 days Finland Denmark NorwayIceland Sweden
10 Headquarters
Syphilis Symposium, Paris 2 weeks France Belgium Portugal 9 Special Office for EuropeGreece Switzerland (field adviser)Ireland United KingdomItaly YugoslaviaNetherlands
Rome, and WHO was represented by an expert onthe subject at the Third International Council ofJuvenile Court Judges at Liége and at the Inter-national Congress of Criminology in Paris.
Co- operation with the Economic Commissionfor Europe (ECE) on problems of medical supplieswas maintained during the year, and WHO wasrepresented at two ECE conferences on housing,
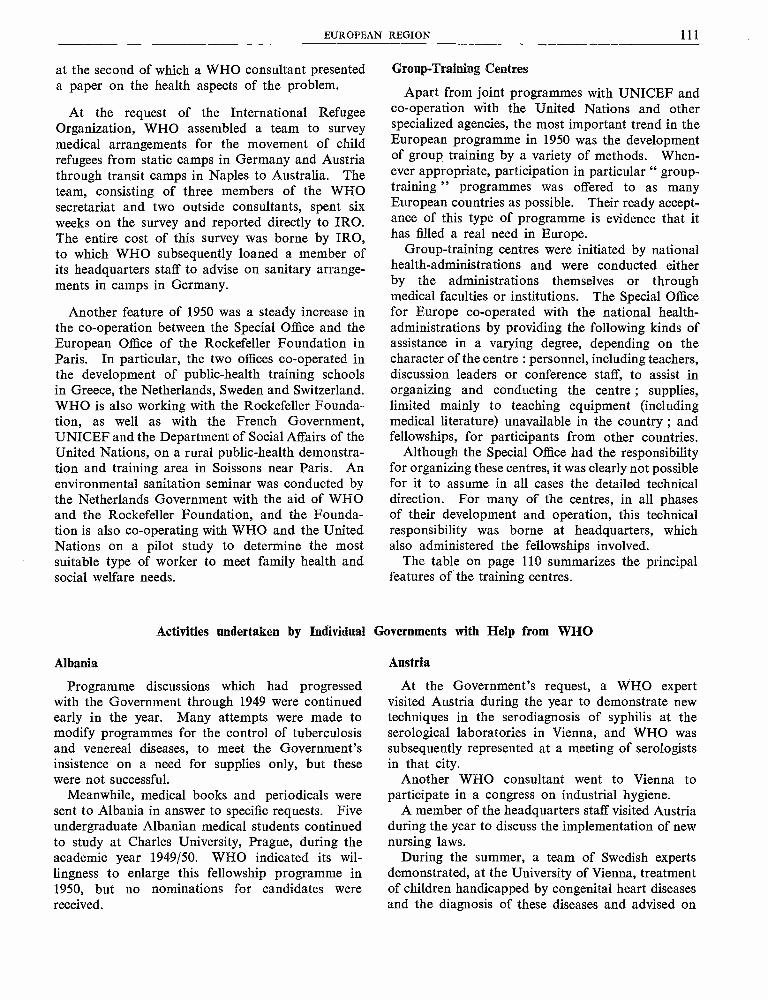
EUROPEAN REGION 111
at the second of which a WHO consultant presenteda paper on the health aspects of the problem.
At the request of the International RefugeeOrganization, WHO assembled a team to surveymedical arrangements for the movement of childrefugees from static camps in Germany and Austriathrough transit camps in Naples to Australia. Theteam, consisting of three members of the WHOsecretariat and two outside consultants, spent sixweeks on the survey and reported directly to IRO.The entire cost of this survey was borne by IRO,to which WHO subsequently loaned a member ofits headquarters staff to advise on sanitary arrange-ments in camps in Germany.
Another feature of 1950 was a steady increase inthe co- operation between the Special Office and theEuropean Office of the Rockefeller Foundation inParis. In particular, the two offices co- operated inthe development of public- health training schoolsin Greece, the Netherlands, Sweden and Switzerland.WHO is also working with the Rockefeller Founda-tion, as well as with the French Government,UNICEF and the Department of Social Affairs of theUnited Nations, on a rural public -health demonstra-tion and training area in Soissons near Paris. Anenvironmental sanitation seminar was conducted bythe Netherlands Government with the aid of WHOand the Rockefeller Foundation, and the Founda-tion is also co- operating with WHO and the UnitedNations on a pilot study to determine the mostsuitable type of worker to meet family health andsocial welfare needs.
Albania
Group -Training Centres
Apart from joint programmes with UNICEF andco- operation with the United Nations and otherspecialized agencies, the most important trend in theEuropean programme in 1950 was the developmentof group training by a variety of methods. When-ever appropriate, participation in particular " group -training " programmes was offered to as manyEuropean countries as possible. Their ready accept-ance of this type of programme is evidence that ithas filled a real need in Europe.
Group -training centres were initiated by nationalhealth- administrations and were conducted eitherby the administrations themselves or throughmedical faculties or institutions. The Special Officefor Europe co- operated with the national health -administrations by providing the following kinds ofassistance in a varying degree, depending on thecharacter of the centre : personnel, including teachers,discussion leaders or conference staff, to assist inorganizing and conducting the centre ; supplies,limited mainly to teaching equipment (includingmedical literature) unavailable in the country ; andfellowships, for participants from other countries.
Although the Special Office had the responsibilityfor organizing these centres, it was clearly not possiblefor it to assume in all cases the detailed technicaldirection. For many of the centres, in all phasesof their development and operation, this technicalresponsibility was borne at headquarters, whichalso administered the fellowships involved.
The table on page 110 summarizes the principalfeatures of the training centres.
Activities undertaken by Individual Governments with Help from WHO
Programme discussions which had progressedwith the Government through 1949 were continuedearly in the year. Many attempts were made tomodify programmes for the control of tuberculosisand venereal diseases, to meet the Government'sinsistence on a need for supplies only, but thesewere not successful.
Meanwhile, medical books and periodicals weresent to Albania in answer to specific requests. Fiveundergraduate Albanian medical students continuedto study at Charles University, Prague, during theacademic year 1949/50. WHO indicated its wil-lingness to enlarge this fellowship programme in1950, but no nominations for candidates werereceived.
Austria
At the Government's request, a WHO expertvisited Austria during the year to demonstrate newtechniques in the serodiagnosis of syphilis at theserological laboratories in Vienna, and WHO wassubsequently represented at a meeting of serologistsin that city.
Another WHO consultant went to Vienna toparticipate in a congress on industrial hygiene.
A member of the headquarters staff visited Austriaduring the year to discuss the implementation of newnursing laws.
During the summer, a team of Swedish expertsdemonstrated, at the University of Vienna, treatmentof children handicapped by congenital heart diseasesand the diagnosis of these diseases and advised on
112 WORK OF WHO, 1950
the establishment of a heart clinic, for whichUNICEF provided supplies.
In connexion with other UNICEF supply -pro-grammes, WHO provided an expert on the use ofstreptomycin, and a member of the headquartersstaff visited Austria to assist with a juvenileepilepsy clinic in Vienna. This programme, whichwas being implemented at the end of the year,includes fellowships to be administered by WHOand the provision of a consultant on the use ofelectro- encephalography apparatus provided byUNICEF. WHO also advised on the strengtheningof tuberculosis diagnostic services, supplies beingfurnished by UNICEF. Finally a WHO consultantvisited Austria to advise on the programme forhandicapped children, for which the Governmenthad requested UNICEF assistance.
Medical books and periodicals and a film fordemonstration purposes were supplied by WHO,and 16 fellowships were awarded, which includedparticipation in the group- training programmereferred to previously. Austria also nominated acandidate to the antibiotics research and trainingcentre in Rome.
Belgium
Belgium was represented at a preparatory meeting,held in Rotterdam in December 1950, for constitutingthe International Anti -Venereal- Disease Commissionof the Rhine.
Belgium also participated actively in the public -health nurses' conference, the infant metabolismseminar and the seminar on environmental sanita-tion. Fourteen fellowships were awarded, ten ofthem being short -term fellowships for training pro-grammes organized in Europe.
The Deputy Director- General, accompanied bythe Chief of the Special Office for Europe, visitedBelgium towards the end of the year to confer withthe health administration on regional activities,including programmes planned for 1951.
Bulgaria
Although the Bulgarian Government had indicated,by the end of 1949, that it was no longer interestedin the work of the Organization, funds continuedto remain available for medical literature andfellowships in accordance with previous requests.
WHO also continued to advise on the UNICEFsupply programmes designed principally to streng-
then maternal and child health services (a ruralmaternal and child health project and a programmefor premature infants) and to extend x -ray diagnosticfacilities for tuberculosis control.
The WHO liaison officer attached to the Europeanheadquarters of UNICEF visited Bulgaria early in1950 to survey the medical programmes, and afollow -up visit was planned for later in the year.
Advice was also given on the WHO /UNICEFmalaria programmes, and a WHO expert advisedon the content of the programme for handicappedchildren for which the Government had requestedassistance from UNICEF.
Byelorussian SSR
The delivery of medical books and periodicalspreviously requested by the Government was con-tinued during 1950 to the limit of available funds.
Czechoslovakia
Early in the year the Government's requests forseveral specific projects were being actively imple-mented by WHO: (1) Assistance was given inestablishing a State Medical Library with a docu-mentation centre designed to service libraries inCzechoslovakia and other European countries. AWHO expert on documentation made an initialsurvey, books, periodicals and microfilm -duplicatingequipment were ordered, and it was agreed that theexpert should return early in the summer. (2) Assist-ance was also given in establishing an anaesthesiologytraining centre, open also to fellowship candidatesfrom other European countries. Essential equip-ment was provided for this centre, and a seniorteacher in anaesthesiology was recruited by WHOwith a view to starting a training course on 1 May1950. (3) Plans were also made for a Swedishteam to demonstrate diagnosis and treatment ofcongenital heart disease in children.
While these and other WHO services, includingassistance in starting penicillin production, werebeing given, the Government announced in Aprilthat it no longer considered itself a Member of WHOand subsequently failed to affirm its desire for theservices to be continued.
Excellent progress was achieved in the BCGprogramme in Czechoslovakia which was carriedon by the Joint Enterprise, about three -and -a -half
EUROPEAN REGION 113
million children having been tested by mid -1950.UNICEF supplies enabled the Government toextend programmes for premature children and forthe control of tuberculosis and syphilis. Arrange-ments for a follow -up visit by a WHO expert onvenereal- disease control, which had been agreedon, were not implemented. The WHO liaisonofficer attached to the European Office of UNICEFvisited Czechoslovakia during the year, at the requestof the Government, to evaluate the impact ofUNICEF supplies on these medical programmes.A WHO expert also advised on the content of aprogramme for handicapped children for which theGovernment had requested UNICEF assistance.
Over and above the assistance to the State MedicalLibrary, medical books and periodicals were suppliedto Czechoslovakia during the year, and one fellowshipwas awarded.
Denmark
The Danish Government, assisted by WHO,established an anaesthesiology training centreattached to the University of Copenhagen. Thiscentre opened its first full year of postgraduatetraining in anaesthesiology in May with the parti-cipation of Danish nationals and WHO fellowshipcandidates from other European countries. Inaddition to providing anaesthesiological apparatusfor teaching purposes, WHO sent a series of instruc-tors to this training centre with the aim of providinga foreign staff of one senior and two juniorinstructors. Although, owing to recruitment diffi-culties, it was impossible to maintain this level,WHO continuously provided teachers to the centre,which is conducting training in anaesthesiology onthe most modern lines. Towards the end of theyear consideration was being given to beginning asecond training course in 1951. WHO is fullyprepared to continue to co- operate with the Govern-ment in this centre, and it is anticipated that someof the staffing problems in 1951 will be solved byhaving recourse to the services of Danish juniorinstructors trained during the first year.
The Government, besides assisting the variousEuropean countries which sent students to thetraining centre, provided places for fellowships inCopenhagen for the study of brucellosis, and madeDanish experts available to demonstrate diagnosisof congenital heart diseases in children and treatmentof cases in the Eastern Mediterranean region.
A WHO expert presented a paper on the controlof syphilis to the Danish Dermatological Societyin Copenhagen, and other WHO syphilis specialistshad an interesting series of conferences with theirDanish colleagues en route from the syphilis sympo-sium in Helsinki to the one held in Paris. WHO alsomade a grant to the Statens Seruminstitut at Copen-hagen, selected as a WHO serological referencelaboratory.
A FAO /WHO brucellosis centre was establishedat Copenhagen.
Denmark participated actively in the group -training programme and was awarded, in addition,18 fellowships, 14 of which were short -term fellow-ships for group -training courses in Europe. Anumber of medical books were also provided.
Finland
At the request of the Government, a WHO expert,accompanied by the European regional adviser,surveyed the maternal and child health programmein Finland, paying particular attention to the highincidence of infantile diarrhoea. This survey wasco- ordinated with a visit from a UNICEF expertin connexion with the supply of milk- processingequipment. At the end of the year the report onthe survey was being studied by the Governmentwith a view to implementing its recommendations in1951. The regional adviser again visited Finland,together with an expert, to advise on UNICEFprogrammes on the rehabilitation of physicallyhandicapped children. Similarly, a WHO consultantfrom Sweden went to Finland early in the year, tofollow up on the joint WHO /UNICEF venereal -disease- control programme, and an expert onstreptomycin examined and approved treatmentcentres in the country. WHO also provided anexpert to train national teams in the use of the massx -ray equipment supplied by UNICEF.
The Government's request for an expert to giveinformation on the results of the first year of opera-tion of the national health service in the UnitedKingdom was met by providing a British expert todiscuss the matter with interested professionalgroups.
After a preliminary visit by a member of theSecretariat to discuss a programme in the psychiatricaspects of industrial medicine, a WHO consultant
114 WORK OF WHO, 1950
went to Finland to advise on the role of psychiatryin industry, and in particular on the establishmentof group training courses.
During the year, the Government, in co- operationwith WHO, conducted, in Helsinki, a highly success-ful symposium on syphilis to which WHO contributedfour discussion leaders and participants from otherScandinavian countries. Finland also took part inother group- training programmes, and nominated acandidate to the antibiotics research and trainingcentre in Rome. Twenty -one fellowships wereawarded, nine of them being short -term fellowshipsfor group- training programmes.
Supplies of medical books and periodicals wereprovided. The Executive Board approved an alloca-tion to strengthen public -health nursing schools inFinland, and by the end of the year, WHO hadprovided teaching equipment to a value of $12,000.
France
Among the most successful courses of the yearwas the symposium on syphilis, organized in Parisby the French Government with the assistance ofWHO. The discussions, which were on a highscientific level, brought to bear on the post -warproblem of syphilis the combined experience ofthe traditional European schools and those of theWestern World.
Regional advisers and experts from headquarterscontinued to work closely with the Governmenton the development of joint programmes withUNICEF, particularly in maternal and child health(the care of premature children and the rehabilitationof the physically handicapped) and mental hygiene.WHO also provided a nurse consultant to the Ecolede Puériculture in Paris. A joint WHO /UNICEFprogramme in malaria and insect control was begunin Corsica.
Similar close co- operation was established onprogrammes now being conducted by the Children'sCentre in Paris. During 1950 WHO gave technicaladvice on the content of the training programmesof the Children's Centre and provided fellowships.
France was represented at the preparatory meetingof the International Anti -Venereal- Disease Com-mission of the Rhine, held in Rotterdam in December1950.
The Government indicated its willingness toco- operate with WHO, the United Nations and theRockefeller Foundation in a study designed todetermine the type of " health visitors " required tomeet family health and social welfare needs. Pre-liminary consideration was given to conducting apilot study of this problem in 1951 in France andthe United Kingdom, and the Government thereforeparticipated in a technical advisory group which metin Geneva in December.
An expert from France was also invited to discusswith other European experts specific programmes inpublic -health administration in 1951. This meetingwas convened in Geneva late in 1950.
A number of discussions took place jointlybetween the Government, WHO, the Children'sCentre and the Rockefeller Foundation on theestablishment of a demonstration and training areain rural public- health in Soissons, near Paris. WHOindicated its willingness to co- operate in this projectand gave technical approval of certain essentialsupplies to be provided by UNICEF.
Assistance was requested in combating brucellosis.
France participated in the infant metabolismseminar, the environmental sanitation seminar andthe conference for public- health nurses in theNetherlands. Medical books and periodicals wereprovided and 14 fellowships were awarded, ten ofwhich were short -term fellowships for group- trainingcourses ; one was for Morocco.
Germany
Germany participated in the preparatory meetingof the International Anti -Venereal- Disease Com-mission of the Rhine.
A WHO consultant visited Germany to advise onthe use of streptomycin supplied by UNICEF.During a lecture tour of Europe another consultantfrom WHO presented a paper on syphilis controlin the city of Hamburg.
At the request of the International RefugeeOrganization, WHO assembled a small team tosurvey arrangements for the transport of childrefugees from camps in. Germany to embarkationpoints in Italy. The cost of this survey was borneby IRO. A member of the WHO Secretariatsubsequently visited Germany to advise on environ-mental sanitation problems in connexion with IROcamps.
EUROPEAN REGION 115
Greece
At the request of the Government and in co-operation with the Rockefeller Foundation, amember of the Secretariat visited Greece to adviseon the reorganization of the School of Hygiene inAthens. A WHO nurse- consultant continued anassignment to assist in developing a nurses' trainingschool in one of the largest sanatoria in Greece.On the successful completion of the first trainingyear and after plans for continuing the training hadbeen drawn up, this consultant was withdrawn.Another member of the WHO Secretariat visitedGreece on general problems connected with thetraining of nurses.
A tuberculosis consultant advised on laboratorysupplies furnished by UNICEF, and plans weremade for WHO and UNICEF to assist in theestablishment of tuberculosis centres.
The regional adviser in venereal disease visitedGreece to follow up on joint WHO /UNICEFprogrammes in the control of venereal disease andspecifically to implement programmes on the treat-ment of syphilis at selected centres. Similarly, theregional adviser in maternal and child health visitedthe country to advise on mobile clinics for children,which the Government had requested from UNICEF,and to assist with a UNICEF programme for physi-cally handicapped children.
WHO was asked to assist in establishing ananaesthesiology training centre in Greece.
Advice was given, with FAO, in the establishmentof a brucellosis study and training centre.
Medical books, periodicals, films and other teach-ing materials were provided to the school of hygieneand to the university medical clinics in Athens.Five fellowships were awarded, two of them beingshort -term fellowships for group- training courses.
Hungary
A request from the Government for supplies fora virus institute was considered by the ExecutiveBoard. As these supplies were to be used principallyfor research purposes, the Board felt that this requestcould not be met by WHO. Joint programmeswith UNICEF in the control of malaria, tuberculosisand venereal diseases did not advance in 1950because of the termination of working arrangementsbetween the Government and UNICEF.
WHO fellowship money was available to Hungaryduring the year, but was not utilized. However,in response to previous requests, WHO providedto many institutions in Hungary medical periodicalsto a total value of over $5,000. This service wascontinued through 1950, although the Governmentindicated in May that it no longer considered itselfa Member of the Organization.
Iceland
The Government of Iceland participated activelyin group- training programmes and was one of thefirst European countries to nominate Fellows to theanaesthesiology training centre in Copenhagen, thesyphilis symposium in Helsinki and the seminar onenvironmental sanitation in the Netherlands. Threefellowships (two of them short -term) were thereforeawarded to Iceland during the year.
Ireland
At the request of the Government, a WHO experton mental health visited Ireland to advise on servicesin child guidance.
A consultant was sent to Ireland to discuss thenutrition programme with the Government. It isplanned to continue assistance with this programmein 1951 by providing the services of a short -termconsultant.
A member of the Secretariat went to Dublin todiscuss the possible expansion of the Government'sBCG programme.
Ireland took part in the environmental sanitationseminar, the syphilis symposium in Paris and thepublic -health nurses' conference. One individualfellowship and six short -term fellowships for group -training were awarded.
Italy
The field office in Rome, which had been main-tained in the previous year in connexion with thegovernmental survey of health services, was closedearly in 1950. Implementation of the recom-mendations resulting from this survey, in whichWHO and the Rockefeller Foundation had assisted,proceeded during the year.
The adviser in maternal and child health twicevisited Italy for programme discussions, and assistedin planning a programme for premature infants,for which supplies will be provided by UNICEF.
116 WORK OF WHO, 1950
Two visits were also made by the regional adviseron venereal disease to help to plan the continuationof the Joint WHO /UNICEF programme on thecontrol of syphilis.
Technical advice was given in connexion with theexperimental use of antibiotics in trachoma controlin a village in Sicily which has a high incidence ofthat disease.
A WHO expert advised the Government on aprogramme for handicapped children, in the imple-meñtation of which WHO will co- operate with theUnited Nations Department of Social Affairs andwith UNICEF.
WHO sent a consultant in environmental sanita-tion to Milan for technical discussions on water -supply problems. It gave advice on the use ofstreptomycin supplies furnished by UNICEF anda consultant visited centres receiving these supplies.Plans were made for setting up tuberculosis trainingcentres in 1951.
WHO reached agreement during the year withthe Department of Biochemistry in the IstitutoSuperiore di Sanity in Rome, which will provideinternational research and training facilities in anti-biotics. This centre will meet the need felt bymany countries, in and outside of Europe, whichlack facilities for basic research on antibiotics,particularly as regards problems of production.
In 1950 Italy requested advisory services in mentalhygiene and nutrition, which will probably be givenin 1951.
Assistance in combating brucellosis was requested.Medical books were supplied to Italy and 20
fellowships were awarded, six of them short -termfellowships for group training. Italy participatedin the environmental sanitation seminar in theNetherlands, the syphilis symposium in Paris and thetraining course in child psychiatry conducted by theChildren's Centre in Paris.
Luxembourg
As the request of the Government, WHO sent aconsultant to Luxembourg to advise on the construc-tion of a general hospital in the city of Luxembourg.
Monaco
The Executive Board agreed to furnish the sumof $6,000 to Monaco, as part of the cost of a massx -ray unit, which the Government subsequentlypurchased. A member of the Secretariat visitedMonaco to discuss the use of this unit in the controlof tuberculosis..
Netherlands
During the year, the Netherlands Governmentput forward plans for the creation of an internationalhealth exhibit. A WHO expert from headquarterson health education of the public gave technicaladvice on this project, in co- operation with anexpert from the Netherlands, who subsequently cameto Geneva for consultations.
The Government of the Netherlands offeredfacilities for four conferences, which constituted anextremely important contribution to the Europeanprogramme. The first was a working conferencefor public -health nurses, at which European countrieswere widely represented ; the results of this confer-ence gave evidence of the careful and detailedplanning which had gone into its preparation. Thesecond, organized in Leyden, was on the specialtopic of infant metabolism, and attracted leadingpaediatric specialists from the Netherlands, France,Belgium and the United States. The third, a seminaron environmental sanitation, had the widest Euro-pean representation of any conference held duringthe year and provided a solid basis for further co-operation among this important group of Europeanexperts. Finally, in December, and as a participatinggovernment, the Netherlands acted as host to thepreparatory meeting of the International Anti -Venereal- Disease Commission of the Rhine, heldin Rotterdam ; this commission should be establishedin 1951.
At the request of the Government, WHO sub-mitted a draft plan for a demonstration and trainingproject in the control of venereal disease in the portof Rotterdam. This project, which should be ofinterest to many countries, was being carefullyconsidered, and it is hoped to start operations in1951.
Assistance in combating brucellosis was alsorequested.
Medical books and periodicals were supplied tothe Netherlands and during the year five fellowshipswere awarded, two for short training- courses. TheGovernment also suggested a candidate for a fellow-ship at the antibiotics research and training centrein Rome.
Norway
Individual discussion- leaders provided by WHOto the syphilis symposium in Helsinki subsequentlyvisited Norway as consultants on national questionsof venereal- disease control.
EUROPEAN REGION 117
After a preparatory visit had been made by anexpert from headquarters, WHO sent a consultantto Norway in the psychiatric problems of industry.This was in response to a governmental request fora visiting lecturer who was also to discuss the organi-zation of group- training programmes.
The Government's interest in developing workin mental hygiene was shown by discussions on thepossibility of organizing a seminar on this subjectin Norway during 1951.
Medical books and periodicals were providedduring the year, and 20 fellowships were awarded,13 being short -term fellowships in group training.Norway participated in the infant metabolismseminar in Stockholm, the syphilis symposium inHelsinki, the environmental sanitation seminar, andthe conference for public -health nurses in theNetherlands, the specialized nursing- course in theUnited Kingdom and the course in child psychiatryconducted by the Children's Centre in Paris. Inaddition, four Norwegians were sent to the anaesthe-siology training centre in Copenhagen. This re-presented the most active participation in group -training of any European country.
Poland
Agreement was reached with the Polish Govern-ment early in the year on the establishment of avenereal- disease training- centre in Warsaw and abiochemistry training- centre in Wroclaw. The train-ing centre in venereal diseases was planned forPoland because of the great experience of thatcountry in mass control ; the biochemistry centrewas to fill a gap in the development of this sciencein many European countries during the war andpost -war years. The procurement of essential teach-ing supplies was under way and the Government wasbeing consulted on the selection of foreign lecturerswhen Poland's decision to stop its participation inthe Organization was communicated to WHO.Assistance in brucellosis control was also beinggiven. On its subsequent failure to reaffirm itsdesire for WHO's services, these important projectshad to be abandoned.
Supplies of medical books and periodicals weresent to Poland during the year. Funds were madeavailable for fellowships, but were not utilized in1950.
The volume of the UNICEF supply -programme toPoland was considerably increased in 1950. Largequantities of x -ray apparatus technically approvedby a WHO expert were sent to equip a whole networkof tuberculosis dispensaries. Much assistance hasbeen given in developing urban and rural servicesin maternal and child health, including specificassistance to the Child Institute in Warsaw and to" well -baby stations " throughout the country.New programmes were started in the control ofcommunicable diseases, and those already established(such as the one on the control of syphilis and theproject for malaria and insect control, on whichgovernmental co- operation with WHO had alwaysbeen on the highest level) were continued. TheWHO liaison officer to the UNICEF Europeanheadquarters visited Poland during the year andstated that UNICEF supplies were being used totheir best advantage in national medical programmes.A WHO consultant advised on the content of aprogramme for handicapped children, for whichthe Government had requested UNICEF assistance.Advice was also given on UNICEF supplies fordiphtheria and pertussis vaccine production andimmunization.
Portugal
The Executive Board approved an expenditure of$4,500 for supplies designed to extend the malariacontrol programme in Portugal. A member ofthe headquarters staff subsequently visited thecountry in connexion with this programme. Theregional adviser in maternal and child health wasinvited by the Government to visit Portugal andwill probably go there at the beginningof 1951.
During the year a programme for WHO assistancein leprosy research was under discussion.
Portugal participated in the syphilis symposium inParis and the environmental sanitation seminar inthe Netherlands. Three fellowships were awarded,two of them being short -term fellowships for trainingcourses.
The use of funds available to Portugal for medicalliterature and teaching equipment was being discussedat the end of the year.
118 WORK OF WHO, 1950
Roumania
Funds available to Roumania for fellowships andfor medical literature were not used during the year.The Government's decision to withdraw from WHO,communicated in February, was followed by failureto reaffirm its desire for WHO's services.
Sweden
One of the most important developments in Europeduring the year was the proposal to establish aScandinavian training school in public health. Thisproject is now being discussed with a number ofinterested agencies, and WHO has indicated wil-lingness to co- operate in every possible way. Amember of the headquarters staff visited Stockholmto advise on methods of health education, particularlyin relation to public -health training.
Following a preliminary planning visit by anexpert on mental health from headquarters, WHOsent a consultant to Sweden to discuss the psychiatricproblems of industry and new training methods.
The visit of a consultant in environmental sanita-tion was planned, but subsequently had to be post-poned until 1951.
During 1950 the Swedish Government madeimportant contributions to the work of WHO in anumber of ways. In addition to providing the entirecongenital- heart -disease team which visited Austriaand Yugoslavia, it assisted, with its highly- developedservices, in many of the studies mentioned in thisreport. The Government also acted as host tothe seminar on infant metabolism, which was soably organized. For this seminar, as for the similarinfant -metabolism seminar in Leyden, WHO pro-vided five of the discussion leaders, fellowshipsfor participants from neighbouring countries andpart of the servicing staff.
Sweden participated widely in other seminarsand group- training activities in Europe. In 1950it was awarded 16 fellowships, 12 for short group -training courses.
A WHO consultant in dentistry made a survey inSweden towards the end of the year.
Switzerland
Switzerland participated in the preparatory meetingof the International Anti -Venereal- Disease Com-mission of the Rhine.
The Government co- operated with WHO andUNICEF in organizing a seminar on social paedia-trics, which was held during the year immediatelyafter the Sixth International Congress of Paediatricsin Zürich. Switzerland also participated in thesyphilis symposium in Paris and the seminar on en-vironmental sanitation in the Netherlands, and sentcandidates to the training course at the CasselHospital in London and the child psychiatry courseconducted at the Children's Centre in Paris. Sixfellowships were awarded, five of them being forshort training courses.
Ukrainian SSR
Funds originally made available to the Ukrainein 1948 were used during 1950 to continue fulfillinga previous request for a large number of medicalbooks and periodicals. Later in the year the Govern-ment failed to affirm its desire for this service, whichwas therefore discontinued.
United Kingdom
A WHO venereal -disease consultant visitedEngland and Scotland during the year and deliveredthe Malcolm Morris lecture in London on the subjectof syphilis control.
At the request of the Government, WHO providedthree experts, who visited the United Kingdom duringthe year. These experts were concerned with ratherspecialized aspects of current problems in thecountry : poliomyelitis control, the control of thecommon cold virus, and questions of nutrition.The United Kingdom also requested technicaladvice in connexion with crippling rheumatoiddiseases and assistance in brucellosis control.
WHO received much assistance from the UnitedKingdom during the year. As well as providingfacilities for the studies mentioned on page 119 ofthis report, the United Kingdom supplied a numberof the consultants for other European countries. Italso provided facilities, particularly for work onenvironmental sanitation and venereal diseases.Members of the headquarters staff paid a numberof visits to the United Kingdom to gather informa-tion of importance to WHO programmes.
A short course, conducted at the Cassel Hospitalnear London on the psychological problems ofhospitalization, was attended by nursing represen-tatives of six other European countries. The Govern-ment agreed to organize, early in 1951, a group -training course for persons engaged in the treatment
EUROPEAN REGION 119
of physically handicapped children. This is essentialfor following up programmes in certain Europeancountries, for which UNICEF has furnished supplies,and WHO, technical advice. For this technicalguidance, WHO engaged a consultant, who willsubsequently be responsible for organizing thetraining course. The United Nations Department ofSocial Affairs, and other bodies, including ILO,UNESCO and UNICEF, have expressed interestin this training course for handicapped children.
The Government agreed to co- operate with WHO,the United Nations and the Rockefeller Foundationin a study to be made in 1951 on the work of the" health visitor ". This is designed as a pilot studyof the well -developed but somewhat different dutiesof " health visitors " in the United Kingdom andFrance. The United Kingdom participated in atechnical advisory group for this pilot study, whichmet in Geneva in December.
The United Kingdom participated in the sympo-sium on syphilis in Paris, and in the public- healthnurses' conference and environmental sanitationseminar in the Netherlands. Thirteen fellowshipswere awarded, six of them for short training courses.
Yugoslavia
At the request of the Government, WHO provideda team to Austria and Yugoslavia to demonstratethe diagnosis of heart diseases in children and theirtreatment. The team, which was entirely Swedishin composition, first visited Vienna and then spenttwo very active weeks in Zagreb demonstrating newtechniques of investigation and surgery. It includeda cardiologist, a surgeon, an anaesthesiologist anda theatre nurse. The successful results of this shortvisit were due, in the estimation of team members,to the high degree of specialist skills previouslyacquired by their Yugoslav colleagues throughfellowships and other means. Within a few weeksof the team's departure, the elements of a new heartclinic had been established in Zagreb, and successful" blue -baby " operations were being performed byYugoslav specialists. The Executive Board sub-sequently approved an allocation of $10,080 forsupplies for this heart clinic. These supplies, togetherwith those provided during the visit of the team,afforded definite assistance to the Government inestablishing this clinic. Proposals for the furthertraining of Yugoslav specialists in the particular
techniques required for this work for children arenow being discussed.
WHO provided a consultant to advise on the im-provement of institutes of nutrition. Immediatesupport was recommended for institutes in Sarajevoand Zagreb, to which WHO provided teachingequipment. Further implementation of the consul-tant's recommendations, including fellowship grantsand the organization of a national training- centre,are being discussed with the Government. FAO hasexpressed an interest in this project.
A further member of WHO's staff visited Yugo-slavia to advise on the development of mental -hygiene programmes. Arrangements were made toprovide a consultant on the subject, who will visitYugoslavia in 1951.
WHO continued to participate actively in jointprogrammes with UNICEF in Yugoslavia. At therequest of the Government, a consultant surveyedthe endemic syphilis areas of Bosnia and Herzegovinaand strongly recommended continued support tothe programme for syphilis control, in view of theexcellent results achieved.
After visiting the country, a member of the Secre-tariat recommended UNICEF support for a brucel-losis research and study centre. WHO gave technicalapproval for supplies for continued work on themalaria programme on which a WHO team hadbeen engaged in Yugoslavia during 1949. The WHOliaison officer to the European headquarters ofUNICEF also visited Yugoslavia, where he studiedquestions of vaccine and sera production, the sendingof laboratory supplies to sanitary epidemiologicalstations, tuberculosis control, and health programmesfor children. Advice was given on a rural programmefor child welfare and on the control of communicablediseases of children. Towards the end of the yeara further WHO consultant advised on a new pro-gramme for handicapped children for which theGovernment had requested UNICEF supplies.Advice was also given on supplies for antituber-culosis campaigns. In December, a consultant wentto Yugoslavia to advise the Government on themodernization of an existing penicillin -plant and onproduction of crystalline penicillin. A WHO consul-tant in dentistry made a survey in Yugoslavia towardsthe end of the year.
Yugoslavia participated in the environmentalsanitation seminar in the Netherlands, the symposium
120 WORK OF WHO, 1950
on syphilis in Paris and the anaesthesiology trainingcentre in Copenhagen. A candidate was also nomi-nated for the antibiotics research and training centrein Rome.
Twenty -five fellowships were awarded, three ofthem for short -term training courses. An interesting
development was the nomination of a candidate tostudy library techniques in the WHO Library atGeneva headquarters. Medical literature, mostlyin the form of medical periodicals, was suppliedto various training centres and institutions in Yugo-slavia.
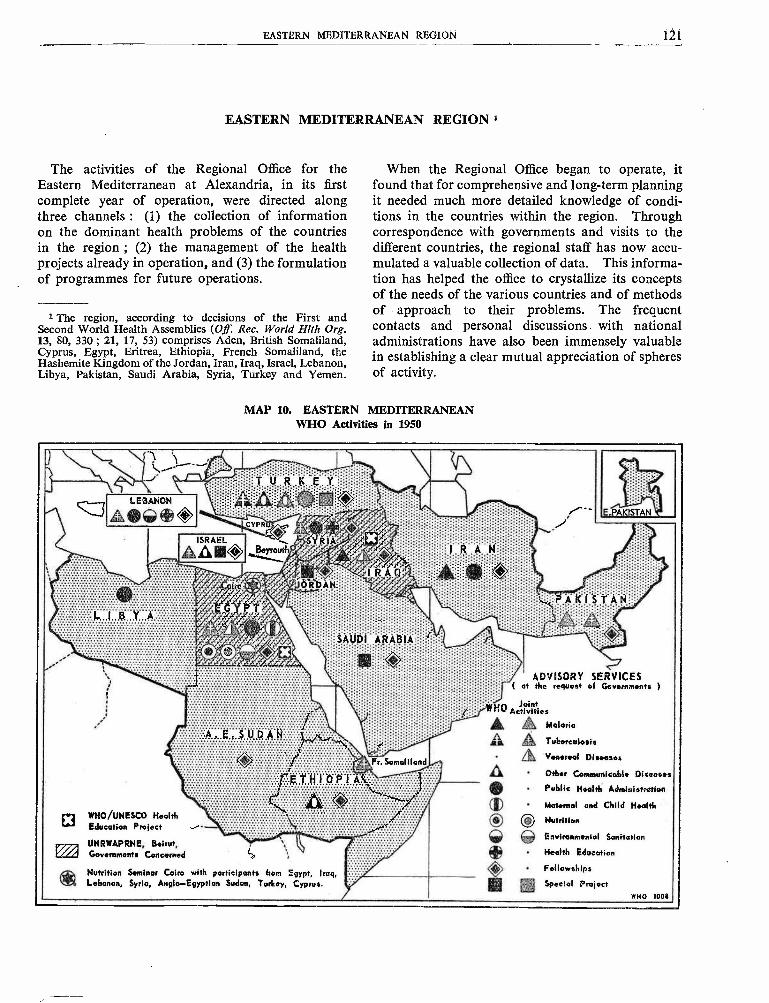
EASTERN MEDITERRANEAN REGION 121
EASTERN MEDITERRANEAN REGION 1
The activities of the Regional Office for theEastern Mediterranean at Alexandria, in its firstcomplete year of operation, were directed alongthree channels : (1) the collection of informationon the dominant health problems of the countriesin the region ; (2) the management of the healthprojects already in operation, and (3) the formulationof programmes for future operations.
1 The region, according to decisions of the First andSecond World Health Assemblies (Off Rec. World filth Org.13, 80, 330 ; 21, 17, 53) comprises Aden, British Somaliland,Cyprus, Egypt, Eritrea, Ethiopia, French Somaliland, theHashemite Kingdom of the Jordan, Iran, Iraq, Israel, Lebanon,Libya, Pakistan, Saudi Arabia, Syria, Turkey and Yemen.
When the Regional Office began to operate, itfound that for comprehensive and long -term planningit needed much more detailed knowledge of condi-tions in the countries within the region. Throughcorrespondence with governments and visits to thedifferent countries, the regional staff has now accu-mulated a valuable collection of data. This informa-tion has helped the office to crystallize its conceptsof the needs of the various countries and of methodsof - approach to their problems. The frequentcontacts and personal discussions with nationaladministrations have also been immensely valuablein establishing a clear mutual appreciation of spheresof activity.
MAP 10. EASTERN MEDITERRANEANWHO Activities in 1950
LEBANON
A®G)~O::
JÓRDÀ
EGYPTA
Á,Ü®Î, .iR,4Blli
ADVISORY SERVICES( at the request of Governments
WHO Ac Fvhistiies
D WHO /UNESCO HealthEducation Project .iUNRWAPRNE, Beirut,Governments Concerned l.'
Nutrition Seminar Cairo with participants from Egypt, Iraq,Lebanon, Syria, Anglo- Egyptian Sudan, Turkey, Cyprus.
Malaria
Tuberculosis
Venereal Diseases
Other Communicable Diseases
Public Health Administration
Maternal and Child Health
® O NutritionEnvironmental Sanitation
Health Education
Fellowships
Special ProjectWHO 10011
122 WORK OF WHO, 1950
From a review of the information collected, itcan be said that, on the whole, steady progress isbeing made in the public -health services of mostcountries in the region. There is, however, a relativelack of balance among the divisions of these services,some being very small and others overgrown. Thecurative side of medicine is as a rule given greaterweight than the preventive side -a natural tendency,especially in the present state of development ofmost of the countries, which lack funds and trainedpersonnel. There is also a tendency towards over -centralization and not enough emphasis on theprovision of active field services.
In specific diseases the principal scourges of theEastern Mediterranean Region, as of much of therest of the world, are malaria, tuberculosis andvenereal diseases. Trachoma and leishmaniasis alsopresent particular problems because of their wide-spread incidence in the region ; bilharziasis and bejelexist in more localized areas, but are neverthelessof considerable importance, and certain States areespecially concerned with leprosy.
There is room for improvement in environmentalsanitation even in cities and towns, and in ruralareas sanitation, where it exists at all, is still in arudimentary stage.
These and other regional questions were con-sidered, and the programmes for 1951 and 1952were discussed and approved, at the third sessionof the Regional Committee, held at Yildiz Palace,Istanbul, from 4 to 7 September. Until govern-ments have studied the proposals and have agreedto accept the commitments involved, however, theprogrammes cannot be regarded as final. In otherwords, the proceedings at Istanbul marked no morethan the first steps of a process which will be com-pleted when the specific projects have been negotiatedwith governments and agreements have been signedby the responsible national authorities.
In the programmes for each country planned for1951, in consideration of the problems mentionedabove, emphasis was necessarily placed on environ-mental sanitation and on the control of communi-cable diseases of special regional importance. Twoother factors, however, played a part in determiningthese programmes : the ability of individual govern-ments to provide personnel and services (and on thisbasis scales of expenditure had to be adjusted toensure that projects would be continued after thewithdrawal of international aid), and the necessityfor adjusting the projects, not only to the needs andcapacities of the countries, but also to the kindsof assistance which each of the three budgetarysources (namely, the regular budget, UNICEF and
the technical assistance programme) could appro-priately render.
This task was made more difficult by the factthat even approximate information on the availabilityof funds from the different sources was not forth-coming until shortly before the meeting of theRegional Committee. A further difficulty was thatprogrammes which have to be based on monetaryapproximations varying with the financial responseof Member States cannot be forecast with certainty.In these circumstances, the full pattern of the pro-gramme proposed for each country could not bediscussed in advance with governments. However,governments will have the opportunity of studyingfor a longer period the programmes planned for1952.
The third session of the Regional Committee wasattended by delegates from 10 out of 11 MemberStates, with representatives from France and theUnited Kingdom, responsible for the internationalaffairs of territories within the region, participatingas Members. The Hashemite Kingdom of theJordan was not represented, but its report waspresented in the form of a document. Delegateswho, for the most part, represented the leadingpublic- health authorities in their countries, stressedthe need for increasing allocations for communicablediseases and professional and technical education.Serious doubts about the value of the work of short -term consultants were expressed, and it was urgedthat appointments of this type of staff be limitedto special purposes. Among other important actionstaken by the committee were the following :
(1) governments were urged to hasten action inwaiving customs duties on insecticides and phar-maceutical products required for the welfare ofthe people ;(2) Member States were called upon to remedythe defects in public -health administration broughtout in the survey undertaken by the RegionalOffice ;
(3) governments were requested to review andimprove their existing smallpox vaccination ser-vices ;
(4) it was recommended that bilateral or multi-lateral sanitary agreements should be made betweenneighbouring countries on diseases of commonconcern ;
(5) the setting -up of national inter -departmentalcommittees to co- ordinate plans for the technicalassistance programme for economic developmentwas recommended and countries were urged toco- operate closely with the Regional Office.
EASTERN MEDITERRANEAN REGÍON 113
Recognizing the importance of establishing orimproving vital and health statistics, the RegionalOffice organized a conference on this subject, whichtook place immediately after the Regional Com-mittee had concluded its work. This regional con-ference was attended by delegates from the countrieswhich had been represented at the Regional Com-mittee ; it made several recommendations, amongwhich was a proposal for the establishment ofnational committees on statistics and trainingcourses for statisticians.
At Istanbul, the opportunity was taken to exhibita large variety of material for the health education
Malaria
of the public, which was furnished by the EgyptianDelegation and supplemented by a noteworthycontribution from the Turkish Ministry of Health.
The final day of the session was devoted to aseminar on WHO and its relations with nationaladministrations. The fact that the seminar lastedmuch longer than was planned was evidence of theneed for such an activity, and of the keen interesttaken in it.
During the year, the Regional Office administered21 allotments for advisory and demonstrationservices, and 23 for fellowships, medical literatureand teaching equipment.
Regional Activities involving several Countries
Antimalaria activities in the region have rangedover a wide field. In Pakistan, where UNICEFprovided supplies and WHO technical assistance,the malaria demonstration team is nearing the com-pletion of two years of its programme, and one ofthe most significant results is that the Governmenthas undertaken extensive antimalaria operations intwo other centres in the province where the team isoperating. In Iran, the method of collaborationhas been on different lines : the Government itselfhas provided stores and equipment for a nation-wide campaign, and WHO has furnished an advisoryteam of experts. A comparative study of the twomethods of assistance given to Iran and Pakistanrespectively should be invaluable in framing futureregional policy. Advisory services in malaria controlhave also been provided in Iraq, to assist the Govern-ment in residual insecticide spraying in areasinundated by abnormal floods.
Projects in the other countries in the region arenot so well advanced : malaria demonstration teamsare planned for Iraq, Lebanon and Saudi Arabia,and a malaria control plan is envisaged for Syriain conjunction with a FAO /WHO project for theraising of food production.
For equipment, special allocations were made tothe Malaria Institute of Pakistan and the RoshPinna Malaria Research Station in Israel. Aresearch programme for field and laboratory observa-tions on the effectiveness of DDT against variousspecies of local anopheline vectors was under wayat the Rosh Pinna Station. Unfortunately, a
regional course in malariology at the MalariaInstitute of Pakistan planned for 1950 could notbe held, but at the end of the year alternative arrange-ments were being studied.
Venereal Diseases
In Iraq, a project for the clinical and serologicalinvestigation and the mass treatment of bejel wasformulated, approved by UNICEF and WHO, andstarted in the last quarter of 1950. This programmewill be extended to Syria at a later date. In Egypt,arrangements were completed for the demonstrationproject in the control of venereal diseases, whichwill be started on 1 February 1951.
Tuberculosis
The regional adviser and a consultant surveyedtuberculosis problems in the region and assisted thehealth authorities in planning an antituberculosiscampaign in French Somaliland, Iran, Iraq, Israel,Pakistan and Turkey.
In May a tuberculosis demonstration training -centre was inaugurated at Istanbul. Activities under-taken there have been centred on training coursesfor medical officers, nurses and x -ray technicians.A programme for setting up further demonstrationcentres in Turkey, to be operated entirely by localstaff, has also been prepared.
Plans for other projects in tuberculosis controlinclude a tuberculosis training- centre at Karachi,sponsored jointly by WHO and UNICEF andscheduled to start work early in 1951, a similar
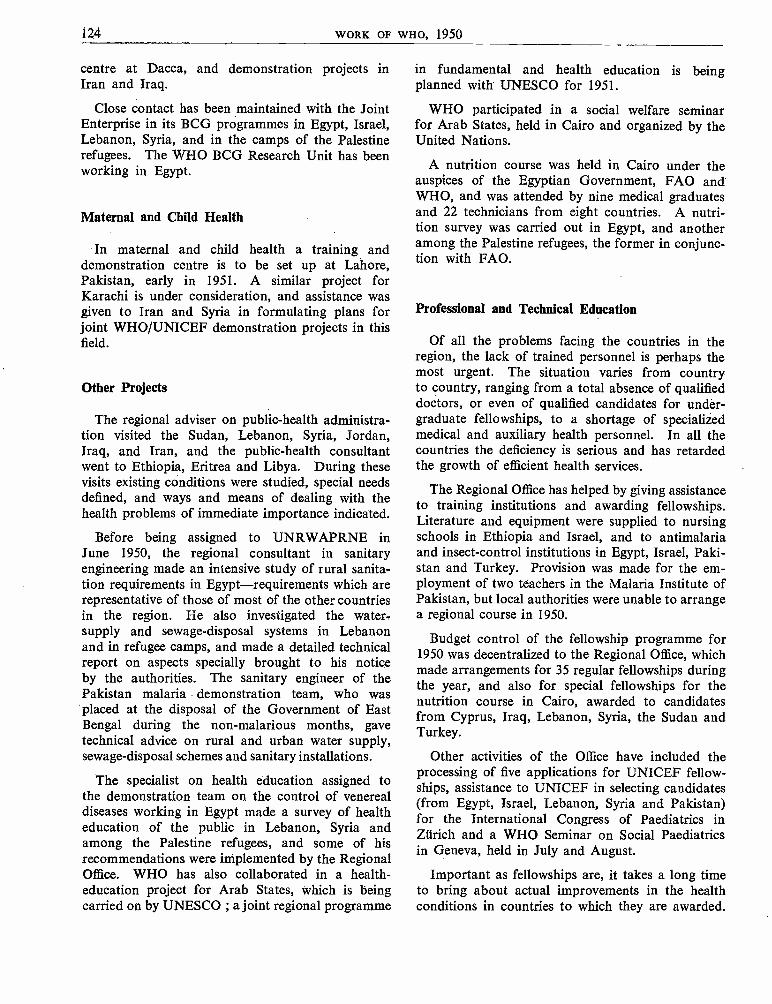
124 WORK OF WHO, 1950
centre at Dacca, and demonstration projects inIran and Iraq.
Close contact has been maintained with the JointEnterprise in its BCG programmes in Egypt, Israel,Lebanon, Syria, and in the camps of the Palestinerefugees. The WHO BCG Research Unit has beenworking in Egypt.
Maternal and Child Health
In maternal and child health a training anddemonstration centre is to be set up at Lahore,Pakistan, early in 1951. A similar project forKarachi is under consideration, and assistance wasgiven to Iran and Syria in formulating plans forjoint WHO /UNICEF demonstration projects in thisfield.
Other Projects
The regional adviser on public -health administra-tion visited the Sudan, Lebanon, Syria, Jordan,Iraq, and Iran, and the public -health consultantwent to Ethiopia, Eritrea and Libya. During thesevisits existing conditions were studied, special needsdefined, and ways and means of dealing with thehealth problems of immediate importance indicated.
Before being assigned to UNRWAPRNE inJune 1950, the regional consultant in sanitaryengineering made an intensive study of rural sanita-tion requirements in Egypt- requirements which arerepresentative of those of most of the other countriesin the region. He also investigated the water-supply and sewage- disposal systems in Lebanonand in refugee camps, and made a detailed technicalreport on aspects specially brought to his noticeby the authorities. The sanitary engineer of thePakistan malaria demonstration team, who wasplaced at the disposal of the Government of EastBengal during the non- malarious months, gavetechnical advice on rural and urban water supply,sewage -disposal schemes and sanitary installations.
The specialist on health education assigned tothe demonstration team on the control of venerealdiseases working in Egypt made a survey of healtheducation of the public in Lebanon, Syria andamong the Palestine refugees, and some of hisrecommendations were implemented by the RegionalOffice. WHO has also collaborated in a health -education project for Arab States, which is beingcarried on by UNESCO ; a joint regional programme
in fundamental and health education is beingplanned with UNESCO for 1951.
WHO participated in a social welfare seminarfor Arab States, held in Cairo and organized by theUnited Nations.
A nutrition course was held in Cairo under theauspices of the Egyptian Government, FAO andWHO, and was attended by nine medical graduatesand 22 technicians from eight countries. A nutri-tion survey was carried out in Egypt, and anotheramong the Palestine refugees, the former in conjunc-tion with FAO.
Professional and Technical Education
Of all the problems facing the countries in theregion, the lack of trained personnel is perhaps themost urgent. The situation varies from countryto country, ranging from a total absence of qualifieddoctors, or even of qualified candidates for under-graduate fellowships, to a shortage of specializedmedical and auxiliary health personnel. In all thecountries the deficiency is serious and has retardedthe growth of efficient health services.
The Regional Office has helped by giving assistanceto training institutions and awarding fellowships.Literature and equipment were supplied to nursingschools in Ethiopia and Israel, and to antimalariaand insect -control institutions in Egypt, Israel, Paki-stan and Turkey. Provision was made for the em-ployment of two teachers in the Malaria Institute ofPakistan, but local authorities were unable to arrangea regional course in 1950.
Budget control of the fellowship programme for1950 was decentralized to the Regional Office, whichmade arrangements for 35 regular fellowships duringthe year, and also for special fellowships for thenutrition course in Cairo, awarded to candidatesfrom Cyprus, Iraq, Lebanon, Syria, the Sudan andTurkey.
Other activities of the Office have included theprocessing of five applications for UNICEF fellow-ships, assistance to UNICEF in selecting candidates(from Egypt, Israel, Lebanon, Syria and Pakistan)for the International Congress of Paediatrics inZürich and a WHO Seminar on Social Paediatricsin Geneva, held in July and August.
Important as fellowships are, it takes a long timeto bring about actual improvements in the healthconditions in countries to which they are awarded.
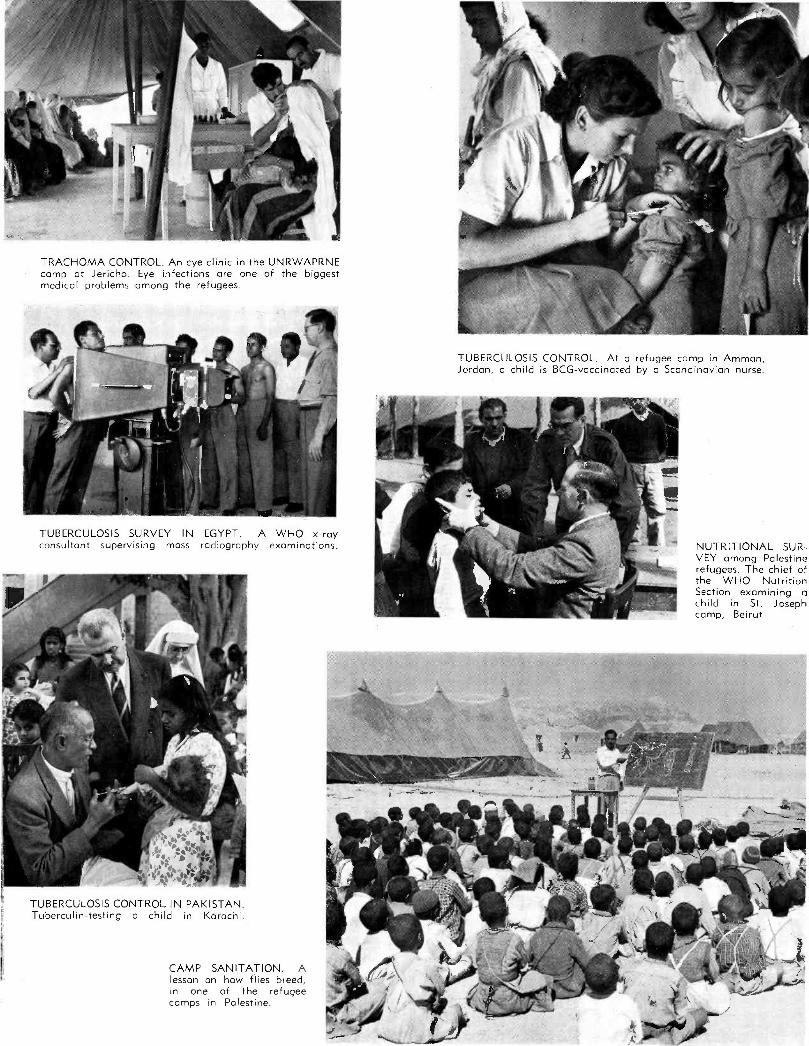
TRACHOMA CONTROL. An eye clinic in the UNRWAPRNEcamp at Jericho. Eye infections are one of the biggestmedical problems among the refugees.
TUBERCULOSIS SURVEY IN EGYPT. A WHO x -rayconsultant supervising mass radiography examinations.
TUBERCULOSIS CONTROL IN PAKISTAN.Tuberculin- testing a child in Karachi.
CAMP SANITATION. Alesson on how flies breed,in one of the refugeecamps in Palestine.
TUBERCULOSIS CONTROL. At a refugee camp in Amman,Jordan, a child is BCG -vaccinated by a Scandinavian nurse.
NUTRITIONAL SUR-VEY among Palestinerefugees. The chief ofthe WHO NutritionSection examining ochild in St. Josephcamp, Beirut
MALARIA CONTROL. A spraying squad in Orissa, India,receives instruction from the leader of a WHO /UNICEFmalaria- control team in the proper method of mixing DDTsolution and in the use of spraying equipment.
VENEREAL -DISEASE CONTROL. The leader of a controlteam takes blood samples for analysis from patients at arural hospital near Simla.
TUBERCULOSIS CONTROL. In a district of Patiala, India, thelocal language text of a BCG campaign poster is translated forthe benefit of the Danish doctor.
TUBERCULIN -TESTING at Victoria Girls' College, Patiala. Theleader of the WHO tuberculosis research team watched by Indianmedical officers and the Director of the WHO TuberculosisResearch Office.
EASTERN MEDITERRANEAN REGION 125
In the careful planning which is necessary for thefellowship programme of each country, the followingpoints have been noted by the Regional Office asdeserving special consideration : (1) fellowshipsshould not only cover applied health activities,but should provide for advanced studies for thestaff of national teaching institutions ; (2) allocationsmade to each country should be supplemented bythat country in the form of contributions in localcurrency to the international travel expenses of theFellows ; (3) the duplication of subjects of studyshould not be permitted in cases where collateralfellowships are available from several sources -theGovernment, UNICEF, or other international bodies,such as the Rockefeller Foundation, and (4) can-didates for fellowships should not only be well-
Aden
qualified, but should also be assured of definite postsin their country's health services on their return.
Health Services to Palestine RefugeesIn addition to continuing to furnish a public -
health administrator to supervise the health pro-grammes for the refugees from Palestine, WHOhas led campaigns in malaria and sanitation amongthe refugees, has provided the services of a specialistin health education, and has made surveys in nutri-tion, nursing and maternal and child health. Thehealth conditions of the refugees remain satisfactory.
Details of this project, in which the Regional Officehas co- operated with headquarters in giving assist-ance to UNRWAPRNE (the United Nations agencyresponsible) are given on page 38.
Activities undertaken by Individual Governments with Help from WHO
A request received from Aden for a BCG teamwas being considered at the end of the year, andanother for health posters in Arabic and an epidia-scope was being fulfilled.
British Somaliland
Teaching equipment was sent to British Somali-land during 1950.
Cyprus
Medical literature was furnished to Cyprus, andan order was placed for an epidiascope. A fellow-ship in nutrition was awarded to a candidate fromCyprus for the training centre in Cairo, and anotherin public- health administration is being applied foron behalf of the island by the Government of theUnited Kingdom.
Egypt
On 20 December the Host Agreement with theEgyptian Government was initialled by Egyptiangovernmental authorities and the Director -General.
The negotiations for the establishment at Tantaof the demonstration team on the control of venerealdisease were finally completed in October. In themeantime, the members of the team were engagedin preliminary arrangements for the selection of
understudies ; they collected information on localconditions and developed a detailed training pro-gramme in collaboration with the Ministries ofHealth and Social Affairs. They also assistedUNRPR, its successor agency UNRWAPRNE,and the governments concerned, in improving thehealth conditions of the Palestine refugees. At theend of the year the Egyptian Government, havingdealt with the legislative aspects of the project,was proceeding with the physical preparations, andit is expected that operations will begin early inFebruary 1951. In the meantime the necessaryequipment and supplies (including a serologicallaboratory unit, procaine penicillin, etc.) and lite-rature were procured and have been stored in theRegional Office.
WHO consultants in maternal and child healthand in nursing made a survey in Egypt which lastedfrom December 1949 to the end of January 1950.
They prepared comprehensive reports with recom-mendations which are receiving the serious considera-tion of the Government in its future plans fordeveloping these services. In October the pro-gramme and curriculum of the School of Nursingin Alexandria were examined, and at the end ofthe year suitable recommendations were beingstudied. The greatest need appears to be forfellowships for the training of experienced nursesas instructors.
The problem of establishing a tuberculosis train-ing- centre was being examined by the Ministry of
126 WORK OF WHO, 1950
Health and the regional adviser on tuberculosis.This project will probably be started in 1951 withthe assistance of WHO and UNICEF.
The BCG- vaccination campaign carried on by theJoint Enterprise, which was planned to last oneyear, has been extended until June 1951. At thebeginning of this campaign some opposition wasencountered in the large cities, particularly amongthe medical profession, chiefly because of inadequatepreparatory propaganda and information. Thecampaign had therefore to be undertaken cautiouslyand among selected groups in rural districts. Thesituation has improved, and operations are graduallybeing resumed in the large towns. Up to July297,499 persons had been tested, of whom 118,714showed positive reactions and 82,129 were vaccinated.The relatively low proportion of those vaccinatedis due to the reluctance of the people to return forthe reading of the test and vaccination in case ofnegative reaction. A WHO BCG- research teamhas been working on the technical aspects of testingand vaccination in a large industrial town, Mahallael Kobra, since the month of April.
Methods of controlling bilharziasis and theproblem of rural sanitation were subjected tointensive study by WHO in collaboration with theGovernment and the Rockefeller Foundation, intheir joint project at Sindibis. Similar studies wereundertaken in the sugar -growing region at KomOmbo in Upper Egypt and in the Sudan (seepage 130.)
Repeated discussions were held with the Ministryof Health and the Rockefeller Foundation on theexpansion of the pilot project at Sindibis into alarge -scale demonstration area. This project receivedthe approval of the Regional Committee and is nowon the technical assistance programme for 1951.Discussions have also taken place with the FAORegional Office in Cairo on the manner in whichthat organization could usefully participate. Atthe end of the year a WHO consultant in public -health administration began a three months' assign-ment in Egypt, to make a survey of the proposedarea. A specialist in health education has alsostudied possibilities for a programme in healtheducation in that area, in collaboration withUNESCO.
In November and December a social welfareseminar for Arab States of the Middle East wasconvened by the United Nations in Cairo. TheDirector of the Regional Office and the expert onnutrition from headquarters participated in thismeeting.
An expert from WHO and one from FAO carriedout a joint survey of nutritional problems in repre-
sentative localities and population groups. Theirfindings were reported to the Government, and WHOhas offered assistance in drawing up a programme,as outlined in the report. No request for thisprogramme, however, has yet been received. Anutrition training- centre was organized jointly bythe Egyptian Government, WHO and FAO, andit began to function on 1 October in Cairo. Atthis centre, a three months' course in nutrition wascompleted at the end of the year under the directionof an expert from FAO.
Fellowships were made available by WHO, andthe course, designed to introduce the latest techniquesand knowledge on nutrition, was attended by ninemedical graduates and 22 technicians from eightcountries in the region.
Seven fellowship awards were made, six to twomissions of three engineers each to study watersupply and pipe- manufacturing plants in the UnitedStates of America for a period of one month, andone for the study of venereal diseases, also in theUnited States. Placement arrangements were pro-ceeding for two Fellows to study tuberculosis andindustrial hygiene. Arrangements were completedfor a fellowship for the study of obstetrics andgynaecology in Cairo, and another in maternal andchild health in the United Kingdom.
Teaching equipment and medical literature weresupplied to the insect eradication centre during theyear.
A consultant on dentistry made a survey in Egypt.
Eritrea
Eritrea was visited in April by the consultant inpublic -health administration, who found that themain problem was the lack of trained personnel.
Ethiopia
In Ethiopia the approved policy of placing specialemphasis on fellowship programmes, supplementedby periodical visits of experts in public- healthadministration, was continued during 1950. AddisAbaba was accordingly visited by the RegionalDirector and members of the staff. The fellowshipprogramme was revised and brought up to dateby providing for a larger number of doctors thanin the earlier programmes. The Government onits part undertook to match the WHO programmeby reserving 25 % of all its educational missionsabroad for medical subjects. The Government alsocontinued local training of its medical auxiliarypersonnel.
EASTERN MEDITERRANEAN REGION 127
A request from the Government for assistance inattacking a problem of immediate importan ce-leprosy-was complied with by the provision of drugs(particularly the new sulfone derivatives) and theservices of a consultant, and at the end of the yeara leprosy -control programme was being initiated.
Eleven fellowships were awarded during the year.One, in public health with special reference to hospitaladministration, in the United Kingdom, Sudan andUganda, was awarded for a period of six months ;one for a nurse tutor was arranged, but could notbe taken up owing to sudden illness of the Fellow.Awards were made to five women for training innursing and midwifery in Uganda, and to fourmedical students, two in Alexandria, and two inBeirut. Placements were also arranged for twomedical students and two sanitary inspectors inUganda for courses in 1951.
Teaching equipment and literature were procuredfor two schools for nurses in Ethiopia.
French Somaliland
The tuberculosis problem was surveyed in April1950, and recommendations were made to theauthorities in Djibouti, who have arranged to under-take BCG vaccination and to set up an isolationand treatment centre. The local training of auxiliarymedical personnel has been begun, but no qualifiedstudents are as yet available for WHO fellowships.
Iran
Following the malaria survey made in 1949,arrangements were completed for the Governmentto supply equipment, stores and personnel for anation -wide campaign of malaria control and forWHO to provide a team consisting of a malariologist,an entomologist and a sanitary engineer to furnishexpert advice on the organization and techniquesof the antimalarial measures. The first member ofthe advisory team, the entomologist, arrived inTeheran in February and was followed by themalariologist and sanitary engineer. Apart fromstandardizing the presentation of spraying andepidemiological data, the team has tried to developan efficient central organization for malaria controlbased on modern administrative procedures. Atthe same time, the national teams which proceededto various centres in the provinces had, by the endof July, sprayed 404,690 structures, and protected
a population of 700,000. For 1951 a considerableexpansion of this programme is being planned.The national effort in malaria control has also beenfacilitated by the work of former WHO Fellows, whoattended courses in malaria in Italy during 1949and 1950.
The nursing problem in Iran was studied inJanuary, and the maternal and child health situationin July. In maternal and child health, emphasiswas placed on the planning of a WHO /UNICEFdemonstration project.
In tuberculosis the regional adviser synchronizedhis visit with that of the head of the Joint Enterpriseand of a member of the League of Red CrossSocieties. . A joint plan for tuberculosis control inIran was drawn up and was later revised to givegreater prominence to BCG vaccination and thework and composition of the epidemiological units.It will probably be implemented early in 1951.In response to a request from the Government foradvice in public -health administration, the regionaladviser visited Teheran in August.
A field survey in fundamental and health educationis being undertaken with UNESCO.
A request for a DDT plant and a plant for theproduction of powdered milk was transmitted toUNICEF.
Towards the end of the year a WHO consultantmade a survey of dentistry in Iran.
Nine fellowships were awarded to Iran duringthe year : in public -health administration, venerealdiseases, maternal and child health, paediatrics,trachoma and malaria. Medical books and perio-dicals on nursing and general hygiene have beenprovided, as well as cinema projectors and projectionscreens for teaching purposes.
On the invitation of the Government of Iran, thefourth session of the Regional Committee will beheld in Teheran in September 1951.
Iraq
The principal WHO activity in Iraq is the setting -up of a joint WHO /UNICEF demonstration ofbejel control. Last year, a regional survey wascarried out by a consultant to determine the spreadof bejel -a non -venereally transmitted form ofsyphilis. His findings were that the disease, whilefound in parts of Syria and Jordan, is most prevalentin Iraq. The Iraqi Government is constructing acentral clinic and laboratory in Baghdad which
128 WORK OF WHO, 1950
will serve as headquarters for a mass attack on bejel,under which it is expected that 70,000 patientswill be treated in the first year. The clinic shouldbe ready by February 1951. Mobile clinics andlaboratories will seek out the desert Bedouin tribessuffering from the disease, and all infectious caseswill be treated with penicillin. On the researchside, cultures will be made of strains of locallyencountered bejel, and sent to the United States ofAmerica, for comparison with similar strains ofyaws and pinta from countries in Latin Americaand the Western Pacific. The anti -bejel demonstra-tion will further serve as a training- centre for Fellowsfrom other countries in the region and, it is hoped,will ultimately be extended to the other countrieswhere bejel has been found.
At the end of the year operations were practicallyready to begin. By the end of December supplieshad been sent by UNICEF, and the chief medicaladviser, the serologist and the venereologist hadarrived in the country and where making preliminaryarrangements. In the meantime, temporary officeand laboratory accommodation had been providedby the Government. Surveys were made, and thetown of Hit on the Euphrates was suggested as abase for field operations. Two representative areasmay be selected for the work.
The Iraqi Government asked for WHO assistancein combating the increased malaria transmissionwhich resulted from the abnormal floods in theBaghdad area last spring. A consultant was sentto advise the Government, and supplies of DDTwere made available for an emergency spraying -programme. The malaria situation and controlprogramme were studied and, under a joint WHO/UNICEF programme, a malaria -control demonstra-tion is envisaged for 1951.
A short survey on health education was made,and a rural -health survey, which might developinto a rural -health demonstration area, was discussedwith authorities in December, on the occasion of avisit by the Regional Director.
The regional adviser in tuberculosis paid a visitto Baghdad in April and assisted the Government indrawing up a plan for a co- ordinated antituberculosisproject to be carried out with the assistance of WHOand UNICEF. A request for aid on this subjecthas been received. It is planned to establish anantituberculosis centre in Iraq early in 1951 andalso to send a team for BCG vaccination.
Two fellowships were awarded.
Iraq has been supplied with medical literatureand teaching equipment, including a microscope,serological apparatus and nursing equipment.
Israel
The control of tuberculosis, particularly amongimmigrants, has been emphasized in the govern-mental health programme, and requests for aidwere addressed to the Joint Enterprise and to WHO.The BCG -vaccination campaign initiated in 1949was concluded in July 1950. Since, a control pro-gramme has been continued by the national advisoryboard for tuberculosis, which is implementing therecommendations made by the WHO expert withparticular reference to the co- ordination of theprogramme and the establishment of a clearingcentre for infected immigrants.
The Government offered facilities for regionalmalaria research at the Rosh Pinna Malaria Station,and WHO accordingly prepared an outline forresearch on insecticides. A detailed scheme ofinvestigations for the malaria season of 1950 wasworked out.
The problems of rabies and brucellosis controlwere investigated, and plans have been made forassistance in these fields (see page 16).
WHO has also supplied medical literature andhas sent teaching equipment and stores to themalaria research station, to nursing schools and tothe influenza centre. It has awarded three fellowshipsto Israel : in public -health administration, sanitaryengineering and malaria, and negotiations areproceeding for a further award in maternal and childhealth.
A team of Danish specialists in thoracic surgerywas also sent to Israel towards the end of the year,and demonstrated the latest methods of surgery onpatients with congenital heart diseases. WHO alsofurnished the equipment for these demonstrations.
Jordan, Hashemite Kingdom of the
After a survey had been made by the planningofficer of the Regional Office at the end of 1949, itwas recommended that the public -health administra-tion in Jordan should be strengthened by extendingthe work of mobile medical units, and WHO pro-vided a mobile clinic, fitted with drugs and equip-ment, for use in desert and semi -desert areas, par-ticularly among the nomadic population.
EASTERN MEDITERRANEAN REGION 129
In June the regional adviser in public- healthadministration carried out surveys. Plans weremade for further advisory services to be renderedduring 1951 by specialists in maternal and childhealth and malaria.
A health- education programme in the refugeecamps located in Jordan was carried out by employ-ing local personnel which will later be utilized bythe Government. Medical literature on generalpublic -health subjects has been supplied, and provi-sion has been made for equipment to be sent tothe State Laboratory.
WHO awarded one fellowship in sanitary engineer-ing to Jordan, and negotiations are proceedingfor others in public -health administration andepidemiology.
Lebanon
After the Lebanese Government had requestedthe Eastern Mediterranean Regional Office to arrangefor an antituberculosis vaccination campaign in thecountry, UNICEF was approached and a campaignwas started in October 1949 in the Beirut urbanarea, under the auspices of the Joint Enterprise.This campaign was completed in March 1950, with28,311 persons vaccinated out of 43,463 tested.During 1951 and 1952 the services of a BCG -adviserwill be made available to the Government, to con-tinue BCG vaccination under a joint WHO /UNICEFprogramme.
The sanitary engineer attached to the RegionalOffice made a survey in 1950 and gave technicaladvice to the Government on methods of improvingwater supplies and dealing with the problem ofsewage disposal near the bathing- beaches of Beirut.
In public- health administration the regionaladviser carried out a detailed investigation of theadministration of health services in the country.Under the technical assistance programme, provisionhas been made for the establishment of a public -health central laboratory and the launching of ajoint FAO /WHO rural health programme in theBekaa settlement area. In addition, a malaria -control demonstration team will be established inLebanon, under the technical assistance programme,in 1951.
The nursing adviser made a survey of the nursingsituation in November, visiting schools of theAmerican and French Universities and the LebaneseRed Cross. She made suggestions for the improve-ment of nursing education and defined proposalsfor the use of the services of a lecturer requestedfor the schools. It was planned to give further
assistance in nursing as well as in maternal andchild health in 1951.
On the request of the Government, WHO alsoagreed to assist in the establishment of a school ofhygiene. The Government decided on the forma-tion of a special committee to prepare a plan for atraining institution for doctors, nurses and sanitaryinspectors, with the full co- operation of the twouniversities in Beirut. The Regional Office hasbeen closely following developments with theintention of giving assistance when the programmeis sufficiently advanced.
A study was made of the health education of thepublic, and it was arranged for students to workon a health- education programme in the refugeecamps during their summer vacations. A mobilehealth education unit was supplied to the Govern-ment, which has agreed to maintain and utilize itin rural areas. A request from the Lebanon for apublic -health film in Arabic was passed to the UnitedNations for its consideration. Provision was alsomade for the partial fulfilment of a request forequipment for the State Laboratory.
A survey of dentistry was made by a consultanttowards the end of the year.
Four fellowships were awarded to the Lebanonduring 1950: one in biostatistics, one in serology,one in sanitary engineering and one in biochemistry.Medical literature was also supplied.
Libya
At the request of the United Nations and inconnexion with a technical assistance programme,the consultant on public -health administration visitedLibya in June (see page 18). The main problemseemed to be the lack of trained health personnel.A long -term fellowship programme is advocated forimplementation over a period of from three to fiveyears, when qualified candidates from secondaryschools become available. In the meantime, afurther consultant is being sent to Libya to adviseon the technical assistance programme.
Pakistan
The malaria demonstration -team in Pakistancompleted its second spraying operation in August,having covered an area (193 square miles, with apopulation of 231,916) substantially larger than thatcovered in 1949, when about 35,000 people wereprotected. It encountered considerable difficultiesbecause of excessive rainfall and lack of motor -roads. It has been demonstrated that, with sound
130 WORK OF WHO, 1950
organization and detailed operational planning, ahigh standard of performance is feasible even on adifficult terrain such as that in East Bengal. Sincethe completion of the operational phase, the teamhas devoted its efforts to collecting data for the finalappreciation of the work. The analysis is stillincomplete, but available information shows amarked reduction of spleen and parasite rates inthe sprayed area.
The team also carried out a preliminary surveyof the incidence of kala -azar from January to July,with the examination of 6,108 children in 82 villages.Of these, 2,718 with enlarged spleens had positivekala -azar reactions and received treatment. Entomo-logical searches show that sandflies have completelydisappeared from the sprayed area, but the efficacyof DDT in checking transmission of the diseasewill be brought out conclusively by the re- examina-tion of the negative cases which was going on towardsthe end of the year.
The cost of operation was about 16 US centsper capita, which is considered to be a satisfactoryfigure.
As a direct result of the demonstration, the HealthMinistry has undertaken DDT- spraying in twoother districts, utilizing the local staff trained bythe WHO team. The railway administration ofthe Ministry of Communications has also assignedhealth workers to be trained by the demonstrationteam before undertaking malaria control in the areaunder its jurisdiction.
The public- health nurse attached to the team hastrained midwives and has assisted in improvingconditions in maternal and child health. It wasfound difficult to popularize these activities, but inthe latter half of the year there began to be a markedincrease in confidence on the part of the peopleconcerned.
An agricultural survey was also made.WHO forwarded to the Government a report of
a preliminary survey of venereal disease in Karachi,Lahore and Dacca. This report stressed the needfor establishing additional venereal- disease clinicsand for modernizing those used for the teachingof medical undergraduates, and suggested a surveyto secure adequate statistics, by the use of variousmethods, such as the routine serological testing ofexpectant mothers.
Two projects for assisting with tuberculosistraining- centres at Karachi and at Dacca have beenstudied by WHO and UNICEF. The Karachiproject received final approval in May, and pre-parations are under way to commence operationsearly in January 1951, The Dacca scheme has also
been approved by WHO, but is awaiting the approvalof UNICEF.
A further plan for joint WHO /UNICEF assis-tance in a maternal and child health training anddemonstration centre at Lahore has been studied,and this project will also begin in January 1951.Assistance in establishing similar centres at Karachiand in the Northwest Frontier Province is also beingplanned.
WHO has supplied medical literature on malariafor Pakistan and has made arrangements for pro-curing periodicals and books on tuberculosis. Alarge proportion of the equipment and storesrequested for the Malaria Institute of Pakistanhave been supplied, and orders for the remainingitems are being processed. Specimens of anophelinesprevalent in North Africa and in Mediterraneancountries were obtained from various sources andsupplied to the Malaria Institute.
One fellowship was awarded in malariology andfive UNICEF fellowships were also administeredby WHO.
Saudi Arabia
In 1950, on the request of the Saudi Arabianpublic- health service, the Regional Office madearrangements for a supply of smallpox vaccine tobe shipped in instalments from Egypt. Plans weremade for assistance to Saudi Arabia in 1951 and1952 in public- health administration, environmentalsanitation, maternal and child health, and control ofmalaria, venereal disease and tuberculosis. Underthe technical assistance programme, a quarantinestation for pilgrims is to be established ; advisoryservices are to be given in environmental sanitationand in rural public -health administration, and acourse for auxiliary medical personnel will be held.
Two fellowships in communicable diseases wereawarded to candidates from Saudi Arabia.
Sudan, Anglo- Egyptian
The local medical installations in the Sudan werevisited in January. It was found that some of theteaching institutions, in particular those for thetraining of sanitary inspectors, were eminentlysuitable for the regional training of auxiliary healthpersonnel, but for the present full to capacity withlocal students.
Studies on methods of controlling bilharziasisand problems of rural sanitation were made in theGezira Cotton Estate in the Sudan by the Egyptian
EASTERN MEDITERRANEAN REGION 131
Government, WHO and the Rockefeller Foundation.Two fellowships were awarded to the Sudan in
1950: one for the study of public -health admini-stration in the United Kingdom and one for nutri-tion at the training centre in Cairo. Placementarrangements have also been completed for a fellow-ship in the study of obstetrics and gynaecology inCairo, and another in maternal and child healthin the United Kingdom.
Syria
The regional adviser in public -health administra-tion made a survey and discussed the major healthproblems of Syria with the public- health authoritiesearly in 1950. Plans for assistance to Syria for1951 and 1952 were based on these discussions anda visit by the regional adviser in tuberculosis.
During the year the WHO malaria consultantwith UNRWAPRNE carried out a malaria survey oftwo valleys in the Jezireh area. A high incidenceof the disease was reported in both districts, par-ticularly in rice cultivation lands, where it wasobserved to cause serious depopulation and economiclosses. Malaria control by spraying with residualaction insecticides is considered feasible.
WHO has received a request from Syria for acountry -wide malaria survey. This will be under-taken as soon as a regional adviser is appointed,and plans for a malaria demonstration -team havealso been formulated.
Governmental malaria -control operations in 1950covered 175 villages in areas inhabited by 173,703persons.
A joint WHO /FAO programme for raising foodproduction and improving standards of health in theJezireh area will also be started in 1951.
The bilharziasis problem in Syria was studied,and the disease found to be strictly confined to afew tributaries of the Balkish river in North -EastJezireh. It is considered that this localized problemshould be readily susceptible to control by a pro-gramme of snail eradication. A WHO expert hassince been assigned to make a further survey and toplan action against bilharziasis in Syria.
The regional adviser in tuberculosis visitedDamascus in March and aided in the planning of aBCG programme. At the end of the year opera-tions were proceeding satisfactorily and werescheduled to last until March 1951. The response of
the population has been most encouraging : up to1 July, 166,676 persons were tested, 75,386 of whomwere vaccinated.
The specialist in health education visited thecountry in May and suggested that the subject ofhealth education should be introduced into thecurriculum of the teachers' college of the Universityof Syria. A request for a mobile health- educationunit is being fulfilled.
In November the nursing adviser from the RegionalOffice made a survey of nursing conditions in Syriaand discussed with the Government possibilitiesof improving nursing education and using fellow-ships in this subject.
Three fellowships have been awarded to Syria inpublic- health administration and the control oftuberculosis and venereal diseases. Negotiations areproceeding for others in maternal and child health,sanitary engineering and ophthalmology.
Turkey
The third session of the Regional Committee washeld in Istanbul in September, and this session wasfollowed by a conference on health statistics (seepage 123).
After several visits by the regional adviser andconsultant in tuberculosis, plans were completedfor the tuberculosis demonstration and trainingproject at Istanbul. The agreement entailed thebuilding of a model tuberculosis -control centre bythe Government and by the Tuberculosis ControlLeague of Istanbul. In May, the chief adviser, anx -ray technician, an officer from the WHO Tuber-culosis Research Office and a chief nurse arrived,together with sufficient equipment to begin theprogramme. The Government co- operated byplacing two junior and one senior phthisiologist atthe disposal of the WHO team.
At this centre three courses of instruction havebeen held. The first, from 15 May to 2 June, wasattended by 29 doctors selected by the Ministry ofHealth from those employed on tuberculosis controlin the country. The second, from 24 July to 12August, was for trained nurses and the third, from13 November to 30 December, was for public -health officers whose duties covered the organi-zation and administration of antituberculosiswork in the governmental services. For the lastcourse some 20 doctors were nominated and givenfellowships by the Government. A report on the
132 WORK OF WHO, 1950
first six months showed that BCG vaccinations,technical demonstrations and epidemiological surveyshad also been started.
In the meantime the demonstration centre con-tinued its regular work on approved lines ; it held aseminar on phthisiology every month at the Uni-versity of Istanbul, at which both medical andmedico -social aspects of tuberculosis were discussed.
Teaching equipment is also being sent to Turkey.A motor and miscroscopes requested for use in theMalaria Institute at Adana were supplied, a refri-gerator centrifuge and deep -freeze refrigerator wererequested for the Central Institute of Hygiene,Ankara. One fellowship has been awarded inpublic- health administration and another is beingnegotiated.
A consultant on anthrax was sent to Turkey inNovember at the request of the Government, toassist in the production of biological products foranthrax control. At the end of the year his reporthad just been received.
Plans were also made for assistance in brucellosiscontrol.
Towards the end of the year, a WHO team ofDanish experts in thoracic surgery spent a monthin Turkey, where they demonstrated the latestmethods of surgery on patients with congenitalheart diseases. This was done by carrying outactual operations with the assistance of local staff.The medical and surgical equipment for theseoperations was also provided by WHO.
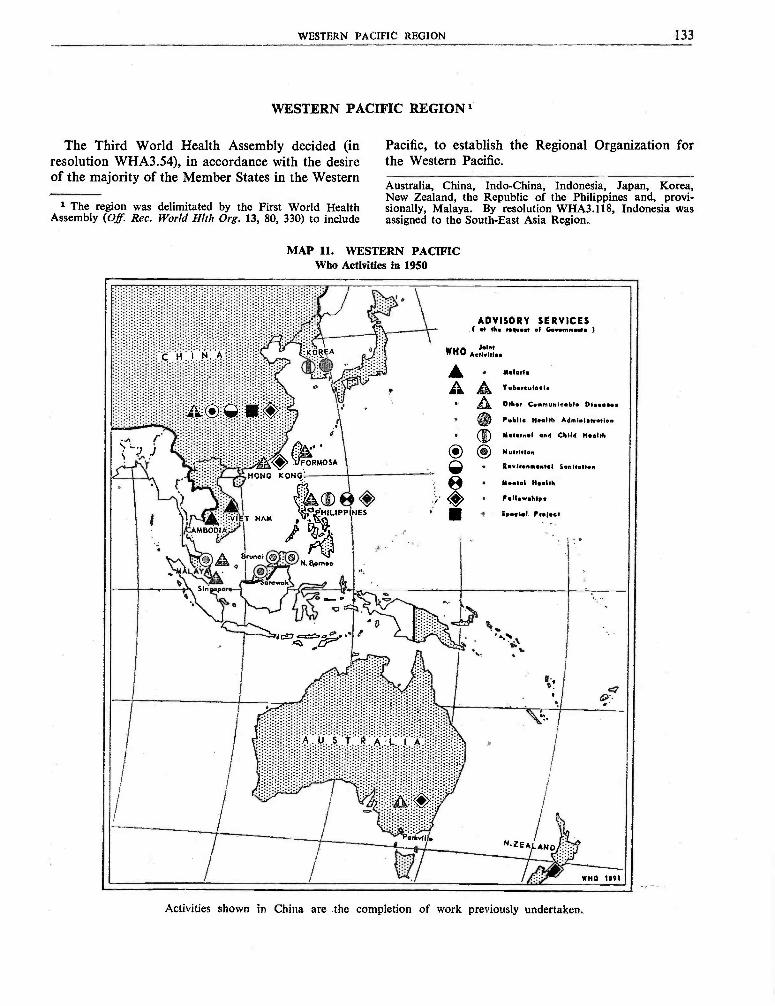
WESTERN PACIFIC REGION 133
WESTERN PACIFIC REGION 1
The Third World Health Assembly decided (in Pacific, to establish the Regional Organization forresolution WHA3.54), in accordance with the desire the Western Pacific.of the majority of the Member States in the Western
Australia, China, Indo- China, Indonesia, Japan, Korea,New Zealand, the Republic of the Philippines and, provi-
i The region was delimitated by the First World Health sionally, Malaya. By resolution WHA3.118, Indonesia wasAssembly (Of. Rec. World Hlth Org. 13, 80, 330) to include assigned to the South -East Asia Region.
MAP 11. WESTERN PACIFICWho Activities in 1950
ADVISORY SERVICESt .r eh. request al G..emm.m 1
WHO Aol 17lee
Malaria
Tubveulele
Other Communicable 01
Public Health Administration
Yet.rn.l end Child Health
Nutrition
Environmental Sonitette
M.nt.l Health
F.ile.r.h 1ps
Sp.aiei Proles,
/CAM BOD1,4j.
Brunei
Sin. pore
Párk.11le
MHO 1091
Activities shown in China are the completion of work previously undertaken.
134 WORK OF WHO,: 1950
The need for setting up an office in this regionbecame urgent during 1950 because of the closecontact necessary between Member Governmentsand WHO, especially in implementing joint projectswith UNICEF in the region. Accordingly, early inthe year a representative of WHO made a recon-naissance tour in order to examine possible placesfor the location of the office.
In the meantime, during July and August, activitiesin the region were directed. from Geneva. Thedirection was then taken over by a small emergencyoffice in Bangkok. On 1 September, the TemporaryOffice for the Western Pacific was established inHong Kong, pending a final decision on the locationby the Regional Committee, which it was planned toconvene some time in March 1951.2
At the first session of the Regional Committee aRegional Director will be selected and a permanentsite chosen for the Office. Representatives of MemberStates will have the opportunity of exchanging ideasfor group planning, for co- ordinating and integratingfuture proposals, and for discussing various prob-lems which have arisen during the year.
The Temporary Office for the Western Pacific isstill very small and has not functioned long enoughto have undertaken extensive services to the countrieswithin the region. It has maintained the closest co-operation with the Singapore Epidemiological Intel-ligence Station. While no epidemiological studieshave been started, plans for future studies of thegeography of diseases affecting the region are beingdrawn up, and research on various health problemsis also planned on an intra- regional basis, as economyand expediency permit.
WHO has provided services to governments in theregion through direct assistance to governmentalprogrammes, through joint programmes withUNICEF, and through participation in the enlargedprogramme of technical assistance for economicdevelopment of under -developed areas.
Direct assistance took the form of fellowships,projects for which technical advice and equipmenthave been supplied by WHO (the equipment some-times being provided on a reimbursable basis), sur-veys, the dissemination of information, and the provi-sion of medical literature and teaching equipment.
Co- operation with UNICEF in health projectsto be developed by the governments constituted amajor activity of the Temporary Office during the
2 A decision of the Executive Board in January 1951 post-poned this meeting.
year. Surveys were conducted by WHO regionaladvisers to guide governments in formulatingrequests for supplies from UNICEF ; further surveyswere made to examine the possibilities of the specificprojects proposed. When these projects have beenapproved by both WHO and UNICEF, WHO willhave the responsibility of technical supervision ofactivities.
Under the programme for technical assistance,WHO helped to plan the Keelung Port Project invenereal diseases in Formosa (Taiwan), and projectsfor the control of tuberculosis and leprosy whichwere requested by South Korea but had to be laidaside on account of the conflict in that country.
To provide information in the field of health,the Office is translating the Chronicle of the WorldHealth Organization into Chinese, for diffusion tothe Chinese- speaking people, and it has also pre-pared a brochure which will give Member Stateswithin the region the fullest information on thetechnical assistance programme and the manner inwhich they can take advantage of the facilitiesavailable.
Collaboration has been maintained with specializedagencies of the United Nations, such as FAO, aswell as with government health -administrations ofall the countries mentioned in the report. Futureplans call for co- operation with the many scientificand professional groups which contribute in oneway or another to the advancement of health incountries within the region. The signing of agree-ments with Member States has not been as promptas had been expected, because of certain provisionswhich have required clarification and also becauseof the financial responsibilities entailed. Some ofthe countries perhaps do not yet sufficiently realizethe value of investing in the health of their peoples ;others understand their health problems, but needoutside assistance in solving them because of lackof financial resources and of technically trainedpersonnel ; and there are others, economically under-developed, in which health facilities have not keptpace with the progress of modern trends in publichealth.
All the States concerned have, however, showna keen desire to avail themselves to the utmostof WHO or WHO /UNICEF assistance. A closerstudy of the health problems in the region is greatlyneeded, and as soon as initial organizational problemsare solved and adequate staff is obtained, theRegional Office will begin to work on such a study.
WESTERN PACIFIC REGION 135
Assistance to Countries in the Region
Australia
WHO awarded two fellowships to Australia forphysicians to study social paediatrics in Canada,the United States of America, Finland, Sweden, andNorway. The Australian Government has askedfor two more fellowships for 1951.
An expert consultant visited Melbourne to lookinto the production of BCG vaccine with a viewto having it approved by WHO for future use intuberculosis projects in the region. WHO is alsomaking inquiries into the possibility of using thetraining facilities of the country for the training ofpersonnel from other countries in the region.
An FAO /WHO brucellosis centre was establishedat Parkville.
Brunei
On account of the ravages of the last war, Bruneiis greatly in need of assistance in improving itspublic -health conditions. WHO activities were begunearly in February in the form of a WHO /UNICEFnursing project, designed to improve the nursingstandards in the country. Working against heavyodds, the WHO /UNICEF team has been able toestablish ante -natal and pre -school clinics, makehome and school visits and undertake health educa-tion. The two principal problems which it hasencountered are the lack of suitable understudiesand the inadequacy of space in the clinics, resultingfrom increasing attendance. The activities of theteam aroused interest and enthusiasm in the typeof work in which it is engaged, and the Govern-ment requested that the project be extended from12 to 18 months. At the end of the year, thetuberculosis adviser visited Brunei to discuss possi-bilities of starting a control project for tuberculosis,including BCG vaccination.
Cambodia
To obtain a general picture of the health situationin Cambodia, two members of the advisory staffof the Temporary Office visited this country duringthe year. Their survey revealed that the greatestproblem is the scarcity of trained personnel, andassistance in organizing courses at the nurses'training school and " health officer " school atPnom -Penh is planned for 1951.
In compliance with a request from the Govern-ment for the provision of a malaria and insect -control team, on a reimbursable basis, a team leaderwas sent to the country, and a sanitary engineerhad been recruited by the end of the year. TheKing of Cambodia is taking an active interest inthis activity, and the project will probably be inoperation early in 1951. Assistance in public -health administration was also planned.
China
In line with the policy of regionalization andalso because the Temporary Office for the WesternPacific was to be established in Hong Kong, WHO'sShanghai Office was closed on 31 July. Of the threemembers of its staff, the nurse was reassigned toNew Delhi ; the sanitary engineer returned to Geneva;the third, a surgeon, was unable to obtain an exitpermit and remained in Canton on work not con-nected with WHO.
There was some disruption in the fellowshipprogramme for China. Fellowships previouslyawarded were not taken up because of the inabilityof the recipients to obtain passports and permissionto leave the country. Of those who were usingtheir fellowships, three were still in the UnitedStates of America at the end of the year.
Medical literature was sent to China for theShanghai Medical College and has been orderedfor institutions such as the Chinese Medical Associa-tion and the Canton Central Hospital.
Formosa (Taiwan)
In Formosa two projects are being worked outin collaboration with UNICEF -a tuberculosis -BCG programme and a maternal and child health -trachoma project. Visits were made by regionaladvisers in BCG and in tuberculosis, and plans ofoperation for the proposed projects drawn up.With the agreement of the authorities to all therecommendations made on the tuberculosis project,technical approval for this project has been givenby WHO, and it was being started at the end of theyear.
A report on BCG protection was submitted to theExpert Committee on Biological Standardization.Official WHO recognition of the laboratory at
136 WORK OF WHO, 1950
Taipeh is being withheld pending its compliancewith certain recommendations made by the regionaladviser.
At Keelung a port -project in venereal diseases,which was proposed under the technical assistanceprogramme, was being revised in line with WHOrecommendations.
One fellowship was awarded and used duringthe year. Other applications submitted by Formosawere being considered in connexion with UNICEFprojects or under the technical assistance programme.
Hong Kong
The regional adviser in tuberculosis visitedHong Kong, and a joint WHO /UNICEF project intuberculosis was being started at the end of theyear. Supplies from UNICEF had already beendelivered, and a mobile x -ray unit was underprocurement. WHO has also included in its 1951budget a programme in health education proposedby the Hong Kong Government in September.
Six fellowships -in such subjects as nutrition,tuberculosis and paediatrics -were awarded byUNICEF and administered by WHO during theyear. One WHO fellowship in port sanitation wasalso awarded.
Japan
Japan is not a Member of WHO. In view, how-ever, of the extensive BCG campaign which has beencarried out in that country in the last two decades,is has been proposed that the regional advisers intuberculosis and BCG should visit Japan in orderto obtain information on the results of the massimmunization programme This possibility wasbeing considered at the end of the year.
Korea
The present war conditions in Korea necessitatedthe withdrawal from this country of the WHOteam on maternal and child health, after it hadmade a survey and had begun its work. Firstevacuated to Tokyo, one member of the team hassince resigned, and the other, a public -health nurse,was reassigned to the Philippines. A survey oftuberculosis was also made by one of the experts,before the team was withdrawn.
On account of the conflict, a fellowship whichhad been awarded was not utilized.
On 31 July, in compliance with a request of theSecurity Council, WHO recruited experts andassigned them to handle health aspects of a reliefprogramme for civilians in the devastated area underthe Unified Command in Korea (see page 40).
Malaya
A joint WHO /UNICEF project for the improve-ment of standards of nursing in Malaya was startedearly in June. This is being carried out by a teamof three nurses -an instructor in nursing arts, apublic -health nurse, and a midwife. These nursesarrived during the summer and began work in theschools, by teaching and training nurses and orga-nizing postgraduate courses. At the end of theyear, the school of nursing was in full operation ;nursing of the sick had been improved, a prenatalclinic had been set up, and a premature baby unitwas functioning satisfactorily. A paediatric nursewas expected to join the team in January 1951.
In connexion with a BCG campaign againsttuberculosis, also being undertaken jointly by WHOand UNICEF, the regional adviser in tuberculosisvisited the country, investigated the situation andmade recommendations. Subsequently, supplies weresent by UNICEF, and a team of a doctor and twonurses, assisted by a local team of seven, startedactivities.
A WHO /UNICEF treponematoses project wasbeing negotiated at the end of 1950 and was expectedto begin early in 1951. Assistance in dentistry wasalso being planned by WHO and UNICEF.
In answer to a further request from the Govern-ment, a joint WHO /FAO project for rabies controlwas being considered.
Four UNICEF fellowships for health visitorswere awarded to students in Malaya by UNICEFand were administered by WHO. Three of theFellows were studying in the United Kingdom andone of them in Ireland, and all four are expectedto assist in the local training of nurses in Malayain 1951. Two UNICEF fellowships in dentalnursing were also awarded for study in New Zealand.
New Zealand
New Zealand has so far taken advantage of WHO'sassistance only by requesting and being awarded afellowship in public- health nursing. On the occa-sion of a visit paid to the country by the Director -General, the Government, however, requested
WESTERN PACIFIC REGION 137
medical literature on behalf of the library of theMedical School of Dunedin. At the end of theyear some of the books had already been suppliedand the rest were being procured by the WHOLibrary.
North Borneo
A programme in nursing and maternal and childhealth was undertaken in North Borneo with assis-tance from WHO and UNICEF. A team of three-a sister tutor, a public -health nurse and a mid-wife- arrived in the country on 9 March and hassince been doing paediatric nursing and conductingtraining courses. A small maternity ward had beenopened in the hospital by the end of the year.
A joint WHO /UNICEF project in public -healtheducation was also approved and a health educatorwas being recruited for North Borneo and Sarawak.Such a project is thought to be essential if activitiesto improve health are to be effectively carried out.
Surveys on malaria and tuberculosis were plannedfor 1951.
Republic of the Philippines
In 1950 the Philippine Republic was assisted byWHO, in collaboration with UNICEF, in a numberof projects.
At the end of the year a WHO specialist in BCGproduction had finished his work in Alabang afterhaving observed conditions in various institutionsin the country and having helped the Governmentto put into effect certain changes which will leadto WHO's official recognition of the diagnostic andBCG--production laboratory located there. Thisrecognition has been recommended, and the firstbatch of BCG vaccine for clinical use was sentout from this laboratory on 1 November. In fullproduction, the laboratory will be one of the largestof its kind in the world and could be a source ofBCG vaccine not only for countries within the regionbut for others.
The regional adviser in tuberculosis went toManila to consult with the Government, withUNICEF, and the BCG -production expert aboutthe new five -year plan for tuberculosis control beingprepared by the Government. Preliminary draftproposals for assistance in this project have alreadybeen made.
WHO and UNICEF were planning to giveassistance in diphtheria immunization, and, as anemergency measure, the necessary toxoid to begin
the campaign was procured and shipped. Planswere also made for establishing a toxoid -productionlaboratory, and for offering a fellowship for studyat the Haffkine Institute in India to the Director -elect of this laboratory.
A WHO /UNICEF rural -health demonstrationprogramme and teaching centre was in operation,with a team of two -a WHO paediatrician andpublic -health nurse -helping a selected local staffto deal with problems in health and social welfare,with emphasis on maternal and child health. Sup-plies and equipment were being furnished byUNICEF. Another project, directed towards theequipping of child -care centres all over the country,was being planned and may be integrated later withthe rural demonstration programme mentionedabove.
A joint WHO /UNICEF treponematoses pro-gramme and a school health programme were alsobeing planned jointly with UNICEF.
A survey was completed by a WHO consultantin mental health early in the year, and a Filipinonational was being recruited as psychiatrist for ajoint WHO /UNICEF project for assistance inmental health work.
Three WHO fellowships were awarded during1950, two in public- health administration and one inthe control of venereal disease. Four other fellow-ships were awarded by UNICEF and administeredby WHO.
From information furnished by WHO andUNICEF staff members who visited or were assignedto the various joint projects in the Philippines, itappears that the assistance offered to this countryis being used to the best possible advantage.
Sarawak
For a nurse -training project in Sarawak, WHOhas furnished a team of two -a paediatric nurse anda midwife. This project was begun during the year.Equipment was sent by UNICEF ; courses in mid-wifery and paediatric nursing were conducted in theschool of nursing, and improvements effected in thechildren's ward of Kuching Hospital. The teaching ofunderstudies was reported to be highly successful.The team responsible for this programme also helpedwith a UNICEF feeding -programme. It is believedthat these projects will furnish a suitable backgroundand to some extent a foundation for future projectswhich WHO may undertake in the country.
138 WORK OF WHO, 1950
For an exchange of views on the various problemswhich arose in connexion with the nursing projectsin North Borneo, Brunei, and Sarawak, a con-ference of all nurses working on these projects washeld in Kuching from 14 to 17 November. Amongthe important points brought out at the conferencewere (1) the desirability of training personnel todeal with problems within the locality in whichthey were to work ; (2) the importance of personnelengaged in training activities knowing the languagesof the countries to which they were assigned -andhence the need for Chinese -speaking tutors -and(3) the need for increasing the training of localmidwives in home deliveries. The conference further-more offered an excellent opportunity for the variouspublic- health workers in the three countries toclarify certain administrative relationships.
Assistance to Sarawak in a malaria -control pro-gramme and in a tuberculosis survey was planned for1951.
Singapore
In Singapore WHO collaborated with UNICEFin various projects primarily designed to improvethe health of mothers and children. At the end ofthe year, a feeding programme had been in progressfor some time.
Plans were made for the BCG -team workingin Malaya to carry out a similar programme inSingapore.
During the year three fellowships were awardedby UNICEF and administered by WHO -one for
a BCG statistician who will later be made availableto the BCG team, another for a health visitor, anda third for a midwife.
Viet Nam
On the occasion of visits to Viet Nam, the Chiefof the Temporary Office and three regional advisers-on maternal and child health, BCG and tuberculosis- investigated the general public -health situation inthe country in order to determine how WHO couldhelp to improve the existing activities. The adviseron BCG observed BCG production at the PasteurInstitute at Saigon and suggested certain changes tobring the laboratory up to the standard required forofficial recognition by WHO. WHO planned to pro-vide two teams for a country -wide BCG project, butthe personnel has not as yet been recruited.
For a project in malaria and insect control inViet Nam, in which WHO is assisting on a reim-bursable basis, WHO recruited a malariologist andsanitary engineer. The sanitary engineer arrived inDecember and began to organize a spraying pro-gramme and to assist in the training of personnel.
A survey in public -health administration wasplanned for 1951, and a public -health expert recruitedfor this project.
Because of certain difficulties, in particular, thescarcity of suitable candidates, Viet Nam made norequests for fellowships during the year until Decem-ber, when a request for one in paediatrics wasreceived.
ANNEXES
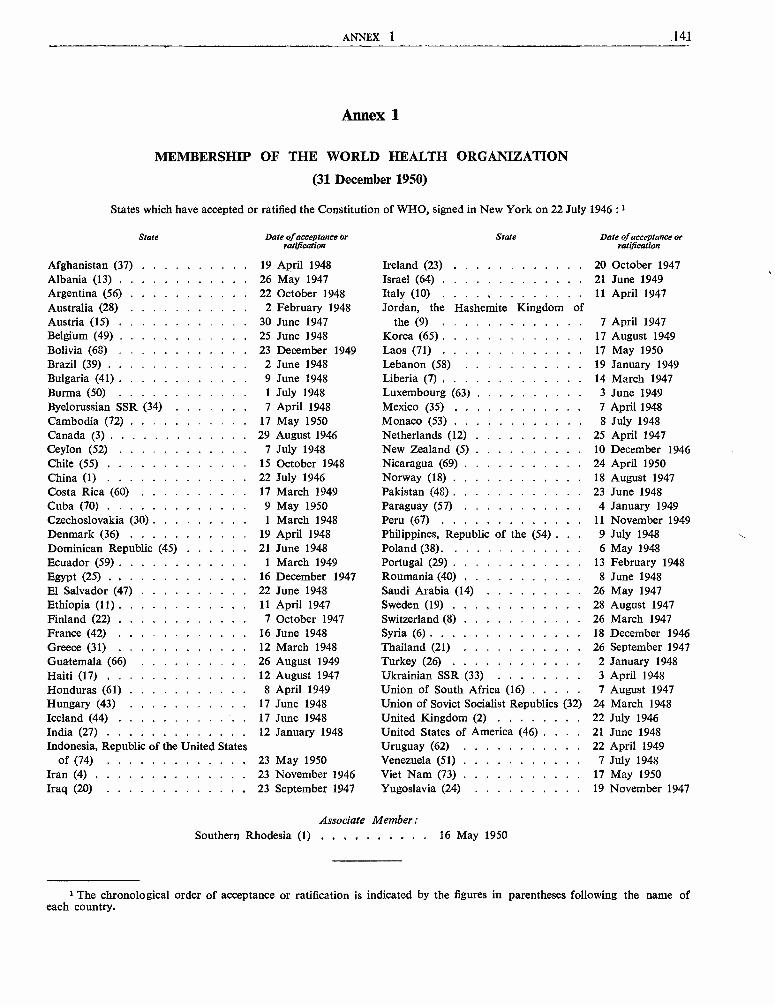
ANNEX 1 .141
Annex 1
MEMBERSHIP OF THE WORLD HEALTH ORGANIZATION
(31 December 1950)
States which have accepted or ratified the Constitution of WHO, signed in New York on 22 July 1946 :1
State
Afghanistan (37)Albania (13)Argentina (56)
Date of acceptance orratification
19 April 194826 May 194722 October 1948
State
Ireland (23)Israel (64)Italy (10)
Date of acceptance orratification
20 October 194721 June 194911 April 1947
Australia (28) 2 February 1948 Jordan, the Hashemite Kingdom ofAustria (15) 30 June 1947 the (9) 7 April 1947Belgium (49) 25 June 1948 Korea (65) 17 August 1949Bolivia (68) 23 December 1949 Laos (71) 17 May 1950Brazil (39) 2 June 1948 Lebanon (58) 19 January 1949Bulgaria (41) 9 June 1948 Liberia (7) 14 March 1947Burma (50) 1 July 1948 Luxembourg (63) 3 June 1949Byelorussian SSR (34) 7 April 1948 Mexico (35) 7 April 1948Cambodia (72) 17 May 1950 Monaco (53) 8 July 1948Canada (3) 29 August 1946 Netherlands (12) 25 April 1947Ceylon (52) 7 July 1948 New Zealand (5) 10 December 1946Chile (55) 15 October 1948 Nicaragua (69) 24 April 1950China (1) 22 July 1946 Norway (18) 18 August 1947Costa Rica (60) 17 March 1949 Pakistan (48) 23 June 1948Cuba (70) 9 May 1950 Paraguay (57) 4 January 1949Czechoslovakia (30) 1 March 1948 Peru (67) 11 November 1949Denmark (36) 19 April 1948 Philippines, Republic of the (54) . . . 9 July 1948Dominican Republic (45) 21 June 1948 Poland (38). 6 May 1948Ecuador (59) 1 March 1949 Portugal (29) 13 February 1948Egypt (25) 16 December 1947 Roumania (40) 8 June 1948El Salvador (47) 22 June 1948 Saudi Arabia (14) 26 May 1947Ethiopia (11) 11 April 1947 Sweden (19) 28 August 1947Finland (22) 7 October 1947 Switzerland (8) 26 March 1947France (42) 16 June 1948 Syria (6) 18 December 1946Greece (31) 12 March 1948 Thailand (21) 26 September 1947Guatemala (66) 26 August 1949 Turkey (26) 2 January 1948Haiti (1 7) 12 August 1947 Ukrainian SSR (33) 3 April 1948Honduras (61) 8 April 1949 Union of South Africa (16) 7 August 1947Hungary (43) 17 June 1948 Union of Soviet Socialist Republics (32) 24 March 1948Iceland (44) 17 June 1948 United Kingdom (2) 22 July 1946India (27) 12 January 1948 United States of America (46) . 21 June 1948Indonesia, Republic of the United States Uruguay (62) 22 April 1949
of (74) 23 May 1950 Venezuela (51) 7 July 1948Iran (4) 23 November 1946 Viet Nam (73) 17 May 1950Iraq (20) 23 September 1947 Yugoslavia (24) 19 November 1947
Associate Member:Southern Rhodesia (1) 16 May 1950
1 The chronological order of acceptance or ratification is indicated by the figures in parentheses following the name ofeach country.
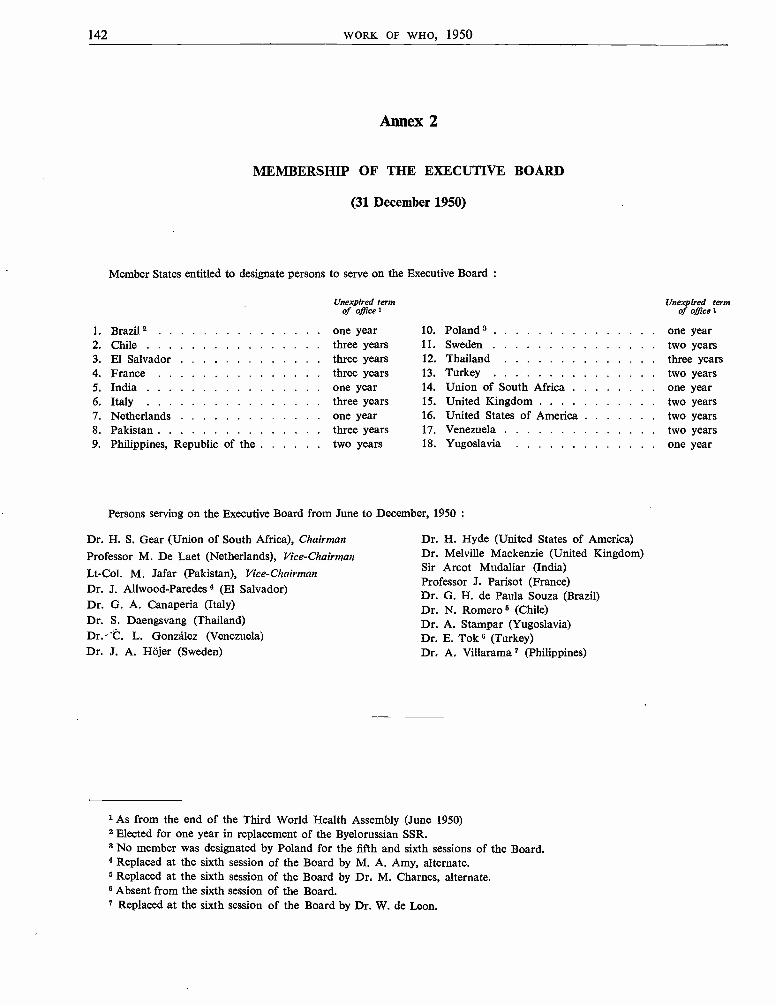
142 WORK OF WHO, 1950
Annex 2
MEMBERSHIP OF THE EXECUTIVE BOARD
(31 December 1950)
Member States entitled to designate persons to serve on the Executive Board :
Unexpired termof office 1
1. Brazil one year2. Chile three years3. El Salvador three years4. France three years5. India one year6. Italy three years7. Netherlands one year8. Pakistan three years9. Philippines, Republic of the two years
Unexpired termof office 1
10. Poland 3 one year11. Sweden two years12. Thailand three years13. Turkey two years14. Union of South Africa one year15. United Kingdom two years16. United States of America two years17. Venezuela two years18. Yugoslavia one year
Persons serving on the Executive Board from June to December, 1950 :
Dr. H. S. Gear (Union of South Africa), ChairmanProfessor M. De Laet (Netherlands), Vice - ChairmanLt -Col. M. Jafar (Pakistan), Vice - Chairman
Dr. J. Allwood- Paredes 4 (El Salvador)Dr. G. A. Canaperia (Italy)Dr. S. Daengsvang (Thailand)Dr.- C. L. González (Venezuela)Dr. J. A. HSjer (Sweden)
Dr. H. Hyde (United States of America)Dr. Melville Mackenzie (United Kingdom)Sir Arcot Mudaliar (India)Professor J. Parisot (France)Dr. G. H. de Paula Souza (Brazil)Dr. N. Romero 5 (Chile)Dr. A. Stampar (Yugoslavia)Dr. E. Tok 6 (Turkey)Dr. A. Villarama 7 (Philippines)
1 As from the end of the Third World Health Assembly (June 1950)Elected for one year in replacement of the Byelorussian SSR.
3 No member was designated by Poland for the fifth and sixth sessions of the Board.4 Replaced at the sixth session of the Board by M. A. Amy, alternate.s Replaced at the sixth session of the Board by Dr, M. Chames, alternate.6 Absent from the sixth session of the Board.7 Replaced at the sixth session of the Board by Dr. W. de Leon.
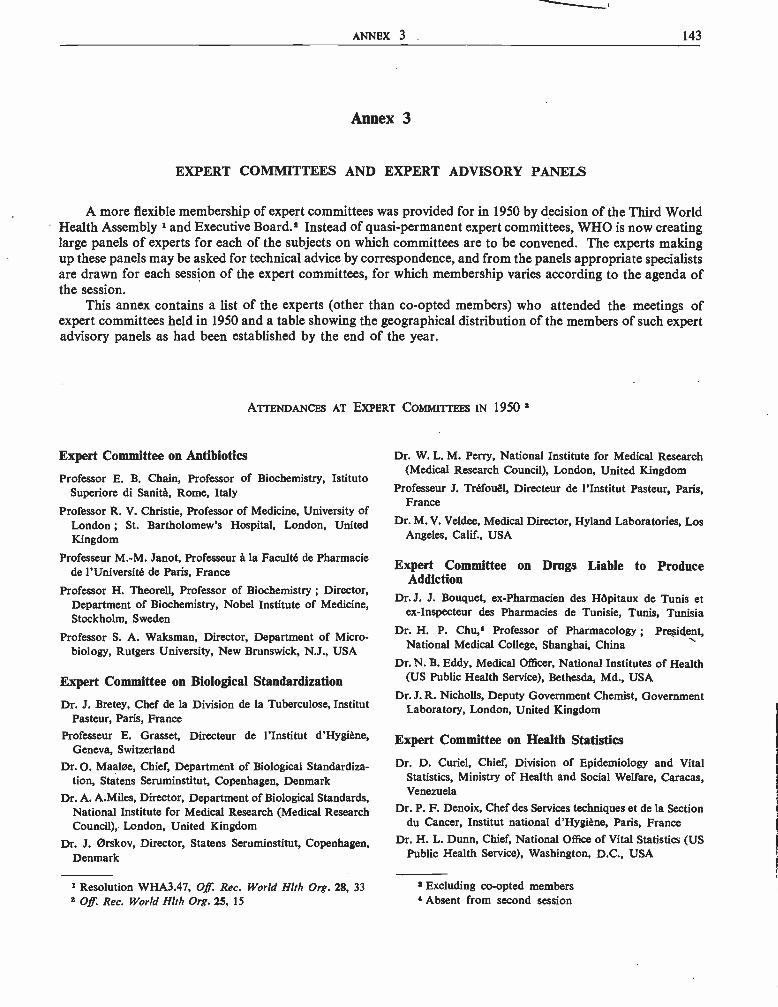
ANNEX 3 143
Annex 3
EXPERT COMMITTEES AND EXPERT ADVISORY PANELS
A more flexible membership of expert committees was provided for in 1950 by decision of the Third WorldHealth Assembly 1 and Executive Board.' Instead of quasi -permanent expert committees, WHO is now creatinglarge panels of experts for each of the subjects on which committees are to be convened. The experts makingup these panels may be asked for technical advice by correspondence, and from the panels appropriate specialistsare drawn for each session of the expert committees, for which membership varies according to the agenda ofthe session.
This annex contains a list of the experts (other than co -opted members) who attended the meetings ofexpert committees held in 1950 and a table showing the geographical distribution of the members of such expertadvisory panels as had been established by the end of the year.
ATTENDANCES AT EXPERT COMMITTEES IN 1950 3
Expert Committee on Antibiotics
Professor E. B. Chain, Professor of Biochemistry, IstitutoSuperiore di Sanità, Rome, Italy
Professor R. V. Christie, Professor of Medicine, University ofLondon ; St. Bartholomew's Hospital, London, UnitedKingdom
Professeur M.-M. Janot, Professeur à la Faculté de Pharmaciede l'Université de Paris, France
Professor H. Theorell, Professor of Biochemistry ; Director,Department of Biochemistry, Nobel Institute of Medicine,Stockholm, Sweden
Professor S. A. Waksman, Director, Department of Micro-biology, Rutgers University, New Brunswick, N.J., USA
Expert Committee on Biological Standardization
Dr. J. Bretey, Chef de la Division de la Tuberculose, InstitutPasteur, Paris, France
Professeur E. Grasset, Directeur de l'Institut d'Hygiéne,Geneva, Switzerland
Dr. O. Maala e, Chief, Department of Biological Standardiza-tion, Statens Seruminstitut, Copenhagen, Denmark
Dr. A. A.Miles, Director, Department of Biological Standards,National Institute for Medical Research (Medical ResearchCouncil), London, United Kingdom
Dr. J. Orskov, Director, Statens Seruminstitut, Copenhagen,Denmark
1 Resolution WHA3.47, Off. Rec. World Hlth Org. 28, 332 Off Rec. World Hlth Org. 25, 15
Dr. W. L. M. Perry, National Institute for Medical Research(Medical Research Council), London, United Kingdom
Professeur J. Tréfouél, Directeur de l'Institut Pasteur, Paris,France
Dr. M. V. Veldee, Medical Director, Hyland Laboratories, LosAngeles, Calif., USA
Expert Committee on Drugs Liable to ProduceAddiction
Dr. J. J. Bouquet, ex- Pharmacien des Hôpitaux de Tunis etex- Inspecteur des Pharmacies de Tunisie, Tunis, Tunisia
Dr. H. P. Chu,* Professor of Pharmacology ; President,National Medical College, Shanghai, China
Dr. N. B. Eddy, Medical Officer, National Institutes of Health(US Public Health Service), Bethesda, Md., USA
Dr. J. R. Nicholls, Deputy Government Chemist, GovernmentLaboratory, London, United Kingdom
Expert Committee on Health Statistics
Dr. D. Curiel, Chief, Division of Epidemiology and VitalStatistics, Ministry of Health and Social Welfare, Caracas,Venezuela
Dr. P. F. Denoix, Chef des Services techniques et de la Sectiondu Cancer, Institut national d'Hygiène, Paris, France
Dr. H. L. Dunn, Chief, National Office of Vital Statistics (USPublic Health Service), Washington, D.C., USA
3 Excluding co -opted members4 Absent from second session

144 WORK OF WHO, 1950
Dr. M. Kacprzak,s Professor of Hygiene ; Director, StateSchool of Hygiene ; President, National Health Council,Warsaw, Poland
Dr. P. Stocks, Chief Medical Statistician, General RegisterOffice of England and Wales, London, United Kingdom
Sub -Committee on the Definition of Stillbirth and Abortion
Dr. D. Baird, Regius Professor of Midwifery, University ofAberdeen, United Kingdom
Dr. M. A. van Bouwdijk Bastiaanse, Professor of Obstetricsand Gynaecology, University of Amsterdam, Netherlands
Dr. E. F. Daily, Director of Health Services, US Children'sBureau, Federal Security Agency, Washington, D.C., USA
Dr. L. Dérobert, Professeur agrégé a la Faculté de Médecinede l'Université de Paris, France
F. Fraser Harris, Director, Health and Welfare Division,Dominion Bureau of Statistics, Ottawa, Canada
Member of Expert Committee on Health Statistics present:
Dr. P. Stocks, Chief Medical Statistician, General RegisterOffice of England and Wales, London, United Kingdom
Sub- Committee ou Hospital Statistics
Dr. E. L. Crosby, Director, Johns Hopkins Hospital, Balti-more, Md., USA
Dr. P. Foltz,6 Director, Ospedale Maggiore di San GiovanniBattista e della Citta di Torino, Turin, Italy
Dr. Marie Lindhardt, Head, Statistical Section, NationalHealth Service, Copenhagen, Denmark
Professor J. Rasuhin, Professor of Social Medicine, Universityof Zagreb, Yugoslavia
Member of Expert Committee on Health Statistics present :
Dr. P. Stocks, Chief Medical Statistician, General RegisterOffice of England and Wales, London, United Kingdom
Sub- Committee on the Registration of Cases of Cancer as wellas their Statistical Presentation
Dr. J. Clemmesen, Chief, Danish Cancer Registry, Copenhagen,Denmark
Dr. H. F. Dom, Chief, Office of Biometry, National CancerInstitute, National Institutes of Health (US Public HealthService), Washington, D.C., USA
Members of Expert Committee on Health Statistics present:
Dr. P. F. Denoix, Chef des Services techniques et de la Sectiondu Cancer, Institut national d'Hygiène, Paris, France
Dr. P. Stocks, Chief Medical Statistician, General RegisterOffice of England and Wales, London, United Kingdom
8 Absent from second session6 Absent from first session
Expert Committee on InsecticidesFor Insecticides and Spraying Equipment:
Dr. R. A. E. Galley, Secretary, Inter -departmental InsecticideCommittees, Agricultural Research Council, London,United Kingdom
Professor G. G. Mer, Chief Adviser, Antimalaria Service ofthe Government of Israel ; Director, Malaria ResearchStation, Rosh Pinna, Israel
Professor A. Missiroli, Chief, Parasitological Laboratory,Istituto Superiore di Sanita, Rome, Italy
Dr. S. W. Simmons, Scientist Director, Chief, TechnicalDevelopment Services, Communicable Disease Center,(US Public Health Service), Savannah, Ga., USA
Dr. J. Treboux, Laboratoire de Recherches J. R. Geigy S.A.,Basle, Switzerland
For Disinsectization of Ships and Aircraft:
M. Aziz Bey, Chief Health Inspector, Medical and HealthDepartment, Nicosia, Cyprus
Dr. J. H. Hughes, Scientist, Chief, Entomology Section,Division of Foreign Quarantine (US Public Health Service),Washington, D.C., USA
Médecin Inspecteur Divisionnaire J. Lembrez, Directeur duService de Contrôle sanitaire aux Frontières maritimeset aériennes, Marseilles, France
Dr. J. A. Logan, Superintendent, Ente Regionale per laLotta Anti Anofelica in Sardegna (ERLAAS), Cagliari,Sardinia
Advisers on Shipping:
Amiral R. Boris, Paris, FranceG. Holt, United Kingdom Shipping Expert, London, United
Kingdom
Expert Committee on International Epidemiology andQuarantine
Dr. R. Dujarric de la Rivière, Sous -Directeur de l'InstitutPasteur, Paris, France
Dr. G. L. Dunnahoo, Medical Director, Chief, ForeignQuarantine Division (US Public Health Service), Washington,D.C., USA
Dr. H. S. Gear, Deputy Chief Health Officer, Union HealthDepartment, Cape Town, Union of South Africa
Prof. A. Halawani, Director, Fouad I Institute of Researchand Hospital for Tropical Diseases, Cairo, Egypt
Dr. L. J. M. Lentjes, Medical Director, " Stoomvaartmaat-schappij Nederland ", Amsterdam, Netherlands
Dr. Melville Mackenzie, Principal Medical Officer, Ministryof Health, London, United Kingdom
Dr. K. C. K. E. Raja, Director -General of Health Services,New Delhi, India
Dr. G. H. de Paula Souza, Director and Professor, Faculty ofHygiene and Public Health, University of São Paulo, Brazil

ANNEX 3 145
Ex Officio Member:
Dr. M. T. Morgan, Chairman, Comité permanent de l'OfficeInternational d'Hygiène Publique ; Port of London HealthAuthority, London, United Kingdom
Quarantine Section
Dr. G. L. Dunnahoo, Medical Director, Chief, ForeignQuarantine Division, US Public Health Service, Wash-ington, D.C., USA
Dr. H. S. Gear, Deputy Chief Health Officer, Union HealthDepartment, Cape Town, Union of South Africa
Dr. Melville Mackenzie, Principal Medical Officer, Ministryof Health, London, United Kingdom
Dr. K. C. K. E. Raja, Director -General of Health Services,New Delhi, India
Dr. G. H. de Paula Souza, Director and Professor, Facultyof Hygiene and Public Health, University of Sao Paulo,Brazil
Legal Sub -Committee
H. B. Calderwood,7 Expert, International OrganizationAffairs, Office of UN Economic and Social Affairs, Depart-ment of State, Washington, D.C., USA
Miss J. A. C. Gutteridge, Assistant Legal Adviser, ForeignOffice, London, United Kingdom
Me J. Secretan,7 Professeur à la Faculté de Droit de l'Universitéde Lausanne, Switzerland
Expert Committee on Malaria
Dr. S. Annecke, Deputy Chief Health Officer, Union Depart-ment of Health, Tzaneen, Transvaal, Union of SouthAfrica
Professor F. J. C. Cambournac, Professor, Institute of TropicalMedicine, Lisbon ; Director, Malaria Institute, Aguas deMoura, Portugal
Major -General Sir Gordon Covell, Adviser on Malaria,Ministry of Health ; Director, Malaria Laboratory, HortonHospital, Epsom, Surrey, United Kingdom
Dr. A. Gabaldón,8 Director, Malaria Division, Ministry ofHealth and Social Welfare, Maracay, Venezuela
Professor G. Macdonald, Director, Ross Institute, LondonSchool of Hygiene and Tropical Medicine, London, UnitedKingdom
Dr. P. F. Russell, Malaria Adviser, International HealthDivision, Rockefeller Foundation, New York, USA
Lt -Col. J. Singh, Director, Malaria Institute of India ;Additional Deputy Director - General of Health Services,New Delhi, India
Professor N. H. Swellengrebel, Director, Institute for TropicalHygiene, Amsterdam, Netherlands
7 Absent from second session.8 Absent from fourth session.
Médecin- Général M. A. Vaucel, Inspecteur, Pathologietropicale, Paris, France
Dr. D. Bagster Wilson, Director, East African Malaria Unit,Muheza, Tanganyika
Expert Committee on Mental Health
Dr. W. C. Menninger, The Menninger Foundation, Topeka,Kans., USA
Dr. Elsa B. Nordlund, Director, Child Guidance Department,Nortulls Hospital, Stockholm, Sweden
Dr. A. C. Pacheco e Silva, Professor of Clinical Psychiatry,University of São Paulo, Brazil
Professor T. Ferguson Rodger, Department of PsychologicalMedicine, University of Glasgow, United Kingdom
Dr. J. Roudinesco, Médecin de l'Hôpital Ambroise Paré(Service de Psychiatrie infantile), Paris, France
Dr. Th. Hart de Ruyter, Director, Department of MentalHealth, City Medical Service, Amsterdam, Netherlands
Dr. K. Soddy, Assistant Director, World Federation forMental Health, London, United Kingdom
Dr. K. Zimmerman, Chief, Mental Health Service, CaliforniaState Department of Public Health, San Francisco, Calif.,USA
Alcoholism Sub- Committee
Dr. S. Betlheim, University Neuro -Psychiatric Clinic,Zagreb, Yugoslavia
Dr. E. Dérobert, Professeur agrégé à la Faculté de Médecinede l'Université de Paris, France
Dr. R. Fleming, Director, Alcoholic Clinic, Peter Bent BrighamHospital, Boston, Mass., USA
Dr. G. A. R. Lundquist, Assistant Professor of Psychiatry,Chief Physician, Langbro Hospital, Stockholm, Sweden.
Professeur M. Muller, Professeur de Psychiatrie, Médecin -Directeur de l'Hôpital psychiatrique de Münsingen, Berne,Switzerland
Dr. M. Schmidt, Chief Psychiatrist, Institute of ForensicPsychiatry, Department of Police, Copenhagen, Denmark.
Expert Committee on Nursing
Miss T. K. Adranvala, Chief Nursing Superintendent, Direct-orate- General of Health Services, New Delhi, India
Mlle M. L. David, Directrice- adjointe de l'Ecole d'Assistanceaux Malades, Ecole d'Infirmières, Montrouge (Seine),France
Miss M. I. Lambie, formerly Director, Division of Nursing,Department of Health, Wellington, New Zealand
Miss G. Peake, Director, School of Nursing of " La Benefi-cencia ", Concepción, Chile
Miss L. Petry, Chief Nurse Officer, US Public Health ServiceWashington, D.C., USA

146 WORK OF WHO, 1950
Miss V. Snellman, Inspector of Nursing Education, StateBoard of Health, Helsinki, Finland
Miss F. N. Udell, Chief Nursing Officer, Colonial Office,London, United Kingdom
Expert Group on Prematurity
Dr. L. Camacho, Chief, Maternal and Child Health Centre,Public Health Department, Quito, Ecuador
Dr. V. Mary Crosse, Paediatrician, Birmingham RegionalHospital Board, Birmingham, United Kingdom
Professeur M. Lelong, Clinique de Puériculture de la Facultéde Médecine de l'Université de Paris, France
Dr. S. Z. Levine, Professor of Paediatrics and Paediatrician -in- Chief, New York Hospital, Cornell Medical Center,New York City, N.Y., USA
Miss E. Magnussen, Director, Nursing Division, NationalHealth Service, Copenhagen, Denmark
Dr. A. Ylppó, Professor of Paediatrics, University of Helsinki ;Chief, Children's Clinic, Helsinki, Finland
Expert Committee on Professional and TechnicalEducation of Medical and Auxiliary Personnel
Dr. M. S. Akalin, Director, School of Public Health, Ankara,Turkey
Dr. G. W. Anderson, Mayo Professor and Director, School ofPublic Health, University of Minnesota, Minneapolis,Minn., USA
Miss M. Andrell, Instructor of Nursing, Royal SwedishBoard of Health, Stockholm, Sweden
Dr. C. K. Lakshmanan, Director, All -India Institute of Hygieneand Public Health, Calcutta, India
Dr. J. M. Mackintosh, Dean, London School of Hygiene andTropical Medicine, London, United Kingdom
Dr. H. Romero, Professor of Hygiene and Preventive Medicine ;Director, School of Hygiene, University of Chile, Santiago,Chile
Dr. R. Sand, Professeur de Médecine sociale à l'Universitélibre de Bruxelles, Brussels, Belgium
Preparatory Working Group on a Public Health AdministrationSeminar
Dr. R. F. Bridgman, Inspecteur de la Santé, Direction dépar-tementale de la Santé de la Seine, Paris, France
Dr. G. A. Canaperia, Chief Medical Officer, Office of theHigh Commissioner for Hygiene and Public Health, Rome,Italy
Sir Andrew. Davidson Medical Adviser, Department ofHealth, Edinburgh, United Kingdom
Dr. K. Evang, Director- General of Public Health, Oslo,Norway
Dr. J. Goossens, Directeur général, Ministère de la Santépublique et de la Famille, Brussels, Belgium
Dr. J. A. Wier, Director -General of Public Health, Stockholm,Sweden
Dr. J. M. Mackintosh, Dean, London School of Hygiene andTropical Medicine, London, United Kingdom
Professor A. Stampar, President of the Yugoslav Academy ofSciences and Arts ; Professor of Public Health and SocialMedicine, University of Zagreb, Yugoslavia
Expert Committee on Rabies
Dr. M. L. Ahuja, Director, Central Research Institute,Kasauli, East Punjab, India
Dr. I. A. Galloway, Director, Virus Research Institute,Pirbright, Surrey, United Kingdom
Dr. K. Habel, Director, Laboratory of Infectious Diseases,Microbiological Institute, National Institutes of Health(US Public Health Service), Bethesda, Md., USA
Dr. H. N. Johnson, Laboratories of the International HealthDivision, Rockefeller Foundation, New York N.Y., USA
Dr. H. Koprowski, Assistant Director, Department of Viraland Rickettsial Research, Lederle Laboratories Division,Pearl River, N.Y., USA
Dr. P. Lépine, Chef du Service des Ultra- Virus, Institut Pasteur,Paris, France
Expert Committee on School Health Services
Dr. C. Fraser Brockington, County Medical Officer of Health,West Riding of Yorkshire, United Kingdom
Dr. E. C. de Castro, School Physician, Municipality of theFederal District, Rio de Janeiro, Brazil
Professor J. H. de Haas, Maternal and Child Health Section,Public Health Department, The Hague, Netherlands
Miss H. Lindquist, School Nurse, Stockholm, Sweden
Dr. Dorothy B. Nyswander, Professor of Health Education,University of California, School of Public Health, Berkeley,Calif., USA
Dr. M. E. Wegman, Professor of Paediatrics, Louisiana StateUniversity, New Orleans, La., USA
Expert Committee on Tuberculosis
Dr. M. S. Abaza Bey, Adviser, Misr Weaving and SpinningCo., Cairo, Egypt
Dr. J. I. Baldó, Chief, Tuberculosis Division, Ministry of Healthand Social Welfare, Caracas, Venezuela
Dr. P. V. Benjamin, Tuberculosis Adviser, Directorate - Generalof Health Services, New Delhi, India
Dr. E. Bernard, Professeur à la Faculté de Médecine de l'Uni-versité de Paris, France
Dr. I. Gonda,9 Chief, Tuberculosis Control Division, Depart-ment of Public Health for Slovakia, Bratislava, Czecho-slovakia
9 Absent from fifth session.

ANNEX 3 147
Dr. P. M. D'Arcy Hart, Director, Tuberculosis Research Unit,National Institute for Medical Research (Medical ResearchCouncil), London, United Kingdom
Dr. H. E. Hilleboe, Commissioner of Health, New YorkState Department of Health, Albany, N.Y., USA
Dr. J. H. Holm, Chief, Tuberculosis Division, Statens Serum -institut, Copenhagen, Denmark
Expert Committee on the Unification of Pharmaco-poeias
Dr. H. Baggesgaard- Rasmussen, Professor of Organic Chemi-stry, Royal Danish School of Pharmacy ; Member ofthe Danish Pharmacopoeia Commission, Copenhagen,Denmark
Professor E. Fullerton Cook, formerly Chairman, Committeeof Revision of the Pharmacopoeia of the United States ofAmerica, New York, N.Y., USA
Dr. I. R. Fahmy, Professor of Pharmacognosy, Faculty ofMedicine, Fouad I University ; Secretary, Egyptian Pharma-copoeia Commission, Cairo, Egypt
Dr. H. Flück, Professeur de Pharmacognosie à l'Ecole poly-technique fédérale ; Membre de la Commission fédérale dela Pharmacopée, Zürich, Switzerland
Dr. C. H. Hampshire, formerly Secretary, British Pharma-copoeia Commission, London, United Kingdom
Dr. R. Hazard, Professeur de Pharmacologie et de Matièremédicale à la Faculté de Médecine de l'Université de Paris ;Membre de la Commission de la Pharmacopée française,Paris, France
Dr. C. Heymans, Professor of Pharmacology and Toxicology,University of Ghent, Belgium
Professor D. van Os, Professor of Pharmacy and Toxicology,University of Groningen ; Chairman of the NetherlandsPharmacopoeia Commission, Groningen, Netherlands
Sub -Committee on Non- Proprietary Names
Professor H. Baggesgaard- Rasmussen, Professor of OrganicChemistry, Royal Danish School of Pharmacy ; Memberof the Danish Pharmacopoeia Commission, Copenhagen,Denmark
Dr. C. H. Hampshire, formerly Secretary, British Pharma-copoeia Commission, London, United Kingdom
Dr. R. Hazard, Professeur de Pharmacologie et de Matièremédicale à la Faculté de Médecine de l'Université de Paris ;Membre de la Commission de la Pharmacopée française,Paris, France
Expert Committee on Venereal Infections and Tre-ponematoses
Dr. W. E. Coutts, Professor of Venereology ; Chief, Depart-ment of Social Hygiene, Public Health Administration,Santiago, Chile
Dr. R. Degos, Professeur agrégé à la Faculté de Médecine del'Université de Paris, France
Dr. S. Hellerstrom, Professor of Dermato- syphilology, Uni-versity of Stockholm, Sweden
Dr. E. H. Hermans, Medical Director, Anti -Venereal DiseaseAssociation, Rotterdam, Netherlands
Dr. J. F. Mahoney, Commissioner of Health, City of NewYork, N.Y., USA
Dr. G. L. McElligott, Director, Venereal Diseases Department,St. Mary's Hospital ; Venereal Disease Adviser, Ministry ofHealth, London, United Kingdom
Dr. I. H. Nagi, Director, Venereal Disease Section, Ministryof Public Health, Cairo, Egypt
Dr. R. V. Najam, Professor of Venereology, GovernmentGeneral Hospital, Madras, India
Sub -Committee on Serology and Laboratory Aspects
A. Harris, Chief, Serology Section, Venereal Disease ResearchLaboratory, (US Public Health Service), Staten Island, N.Y.,USA
Dr. R. Laporte, Chef du Service de Sérologie, Institut Pasteur,Paris, France
Dr. I. N. Orpwood Price, Director, Venereal Diseases Refe-rence Laboratory (Public Health Laboratory Service),St. Peter's Hospital, London, United Kingdom
Dr. F. Rappaport, Chief of Laboratories, Municipal andBeilinson Hospitals, Tel Aviv, Israel
Dr. K. V. Venkatraman, Serologist to the Government ofIndia, School of Tropical Medicine, Calcutta, India
Dr. T. M. Vogelsang, Professor of Bacteriology, Gade'sInstitute, University of Bergen, Norway
Joint ILO /WHO Expert Committee on OccupationalHealth
Sir Joseph Blore, formerly Member of the Viceroy's ExecutiveCouncil for Labour Questions, Delhi, India
Professeur L. Carozzi, Secretary -General of the PermanentInternational Commission on Industrial Medicine ; Pro-fesseur honoraire d'Hygiène industrielle à l'Université deGenève ; Directeur du Centre de Médecine du Travail,Geneva, Switzerland
Dr. L. Greenburg, Executive Director, Division of IndustrialHygiene and Safety Standards, Department of Labor,New York State, New York, USA
Dr. B. Kesic, Chief, Institute of Industrial Hygiene, Zagreb,Yugoslavia
Professeur P. Mazel, Directeur de l'Institut de Médecine duTravail de l'Université de Lyon, Lyons, France
Dr. E. R. A. Merewether, H.M. Senior Medical Inspector ofFactories, London, United Kingdom
Dr. L. Noro, Director, Industrial Medical Institute, Helsinki,Finland
Dr. I. Urbandt, Technical Adviser on Industrial Medicine tothe Ministry of Public Health, Buenos Aires, Argentina
Dr. A. Uytdenhoef, Inspecteur médical en chef des Industries,Ministère du Travail et de la Prévoyance sociale, Brussels,Belgium
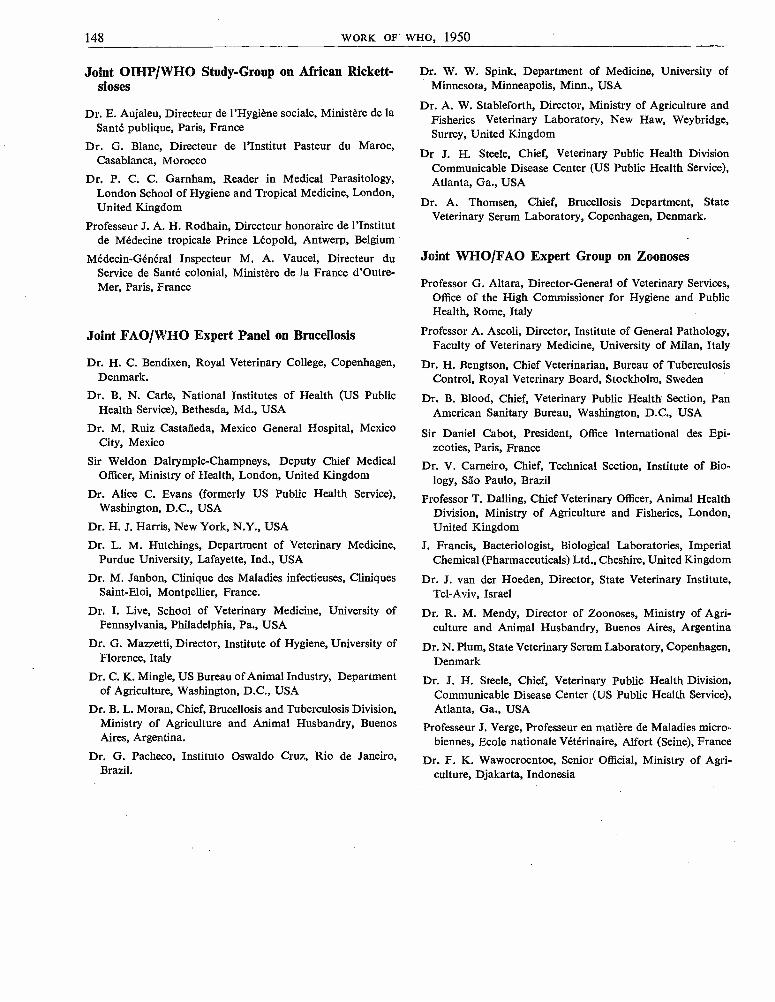
148 WORK OF WHO, 1950
Joint OIHP /WHO Study -Group on African Rickett-sioses
Dr. E. Aujaleu, Directeur de l'Hygiène sociale, Ministère de laSanté publique, Paris, France
Dr. G. Blanc, Directeur de l'Institut Pasteur du Maroc,Casablanca, Morocco
Dr. P. C. C. Garnham, Reader in Medical Parasitology,London School of Hygiene and Tropical Medicine, London,United Kingdom
Professeur J. A. H. Rodhain, Directeur honoraire de l'Institutde Médecine tropicale Prince Léopold, Antwerp, Belgium
Médecin -Général Inspecteur M. A. Vaucel, Directeur duService de Santé colonial, Ministère de la France d'Outre -Mer, Paris, France
Joint FAO /WHO Expert Panel on Brucellosis
Dr. H. C. Bendixen, Royal Veterinary College, Copenhagen,Denmark.
Dr. B. N. Carle, National Institutes of Health (US PublicHealth Service), Bethesda, Md., USA
Dr. M. Ruiz Castañeda, Mexico General Hospital, MexicoCity, Mexico
Sir Weldon Dalrymple-Champneys, Deputy Chief MedicalOfficer, Ministry of Health, London, United Kingdom
Dr. Alice C. Evans (formerly US Public Health Service),Washington, D.C., USA
Dr. H. J. Harris, New York, N.Y., USA
Dr. L. M. Hutchings, Department of Veterinary Medicine,Purdue University, Lafayette, Ind., USA
Dr. M. Janbon, Clinique des Maladies infectieuses, CliniquesSaint -Eloi, Montpellier, France.
Dr. L Live, School of Veterinary Medicine, University ofPennsylvania, Philadelphia, Pa., USA
Dr. G. Mazzetti, Director, Institute of Hygiene, University ofFlorence, Italy
Dr. C. K. Mingle, US Bureau of Animal Industry, Departmentof Agriculture, Washington, D.C., USA
Dr. B. L. Moran, Chief, Brucellosis and Tuberculosis Division,Ministry of Agriculture and Animal Husbandry, BuenosAires, Argentina.
Dr. G. Pacheco, Instituto Oswaldo Cruz, Rio de Janeiro,Brazil.
Dr. W. W. Spink, Department of Medicine, University ofMinnesota, Minneapolis, Minn., USA
Dr. A. W. Stableforth, Director, Ministry of Agriculture andFisheries Veterinary Laboratory, New Haw, Weybridge,Surrey, United Kingdom
Dr J. H. Steele, Chief, Veterinary Public Health DivisionCommunicable Disease Center (US Public Health Service),Atlanta, Ga., USA
Dr. A. Thomsen, Chief, Brucellosis Department, StateVeterinary Serum Laboratory, Copenhagen, Denmark.
Joint WHO /FAO Expert Group on Zoonoses
Professor G. Altara, Director -General of Veterinary Services,Office of the High Commissioner for Hygiene and PublicHealth, Rome, Italy
Professor A. Ascoli, Director, Institute of General Pathology,Faculty of Veterinary Medicine, University of Milan, Italy
Dr. H. Bengtson, Chief Veterinarian, Bureau of TuberculosisControl, Royal Veterinary Board, Stockholm, Sweden
Dr. B. Blood, Chief, Veterinary Public Health Section, PanAmerican Sanitary Bureau, Washington, D.C., USA
Sir Daniel Cabot, President, Office International des Epi-zooties, Paris, France
Dr. V. Carneiro, Chief, Technical Section, Institute of Bio-logy, Sáo Paulo, Brazil
Professor T. Dalling, Chief Veterinary Officer, Animal HealthDivision, Ministry of Agriculture and Fisheries, London,United Kingdom
J. Francis, Bacteriologist, Biological Laboratories, ImperialChemical (Pharmaceuticals) Ltd., Cheshire, United Kingdom
Dr. J. van der Hoeden, Director, State Veterinary Institute,Tel -Aviv, Israel
Dr. R. M. Mendy, Director of Zoonoses, Ministry of Agri-culture and Animal Husbandry, Buenos Aires, Argentina
Dr. N. Plum, State Veterinary Serum Laboratory, Copenhagen,Denmark
Dr. J. H. Steele, Chief, Veterinary Public Health Division,Communicable Disease Center (US Public Health Service),Atlanta, Ga., USA
Professeur J. Verge, Professeur en matière de Maladies micro-biennes, Ecole nationale Vétérinaire, Alfort (Seine), France
Dr. F. K. Wawoeroentoe, Senior Official, Ministry of Agri-culture, Djakarta, Indonesia
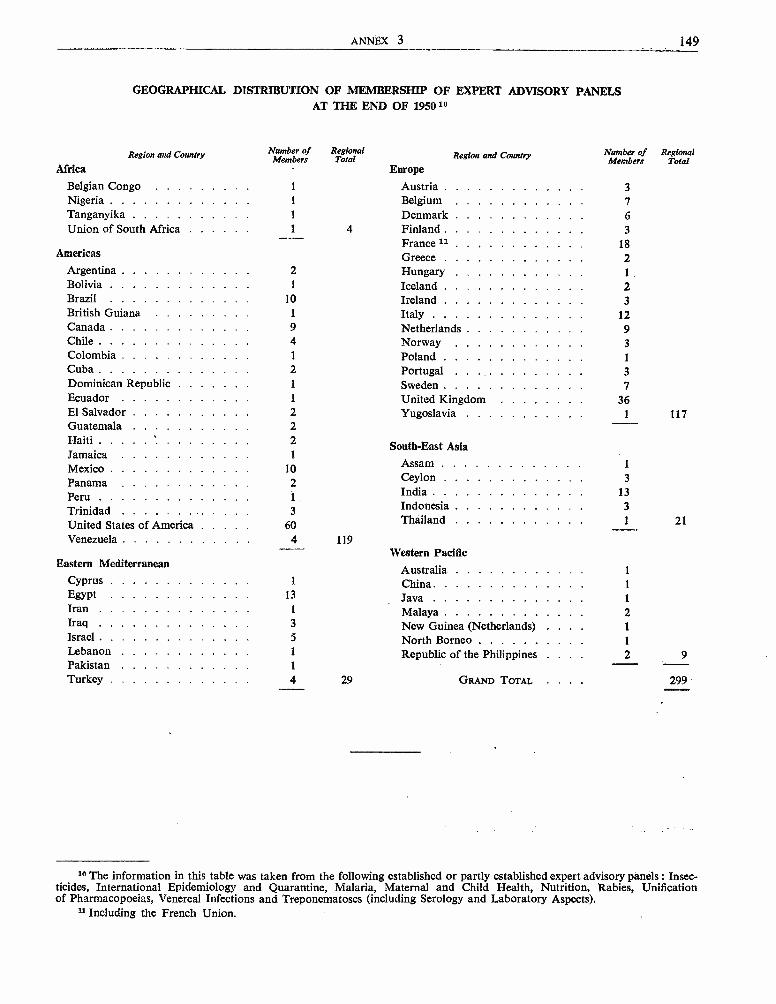
ANNEX 3 149
GEOGRAPHICAL DISTRIBUTION OF MEMBERSHIP OF EXPERT ADVISORY PANELSAT THE END OF 195010
Region and Country
Africa
Number ofMembers
RegionalTotal Region and Country
Europe
Number ofMembers
RegionalTotal
Belgian Congo 1 Austria 3
Nigeria 1 Belgium 7Tanganyika l Denmark 6Union of South Africa 1 4 Finland 3- - France 11 18
Americas Greece 2Argentina 2 Hungary 1
Bolivia 1 Iceland 2Brazil 10 Ireland 3British Guiana 1 Italy 12Canada 9 Netherlands 9Chile 4 Norway 3Colombia 1 Poland 1
Cuba 2 Portugal 3Dominican Republic 1 Sweden 7Ecuador 1 United Kingdom 36El Salvador 2 Yugoslavia 1 117Guatemala 2Haiti 2 South -East AsiaJamaica 1
Mexico 10Assam 1
Panama 2 Ceylon 3
Peru 1India 13
Trinidad 3 Indonesia 3
United States of America 60 Thailand 1 21
Venezuela 4 119Western Pacific
Eastern Mediterranean Australia 1
Cyprus 1 China 1
Egypt 13 Java 1
Iran 1 Malaya 2Iraq 3 New Guinea (Netherlands) 1
Israel 5 North Borneo 1
Lebanon 1 Republic of the Philippines 2 9Pakistan 1
Turkey 4 29 GRAND TOTAL 299
10 The information in this table was taken from the following established or partly established expert advisory panels : Insec-ticides, International Epidemiology and Quarantine, Malaria, Maternal and Child Health, Nutrition, Rabies, Unificationof Pharmacopoeias, Venereal Infections and Treponematoses (including Serology and Laboratory Aspects).
u Including the French Union.
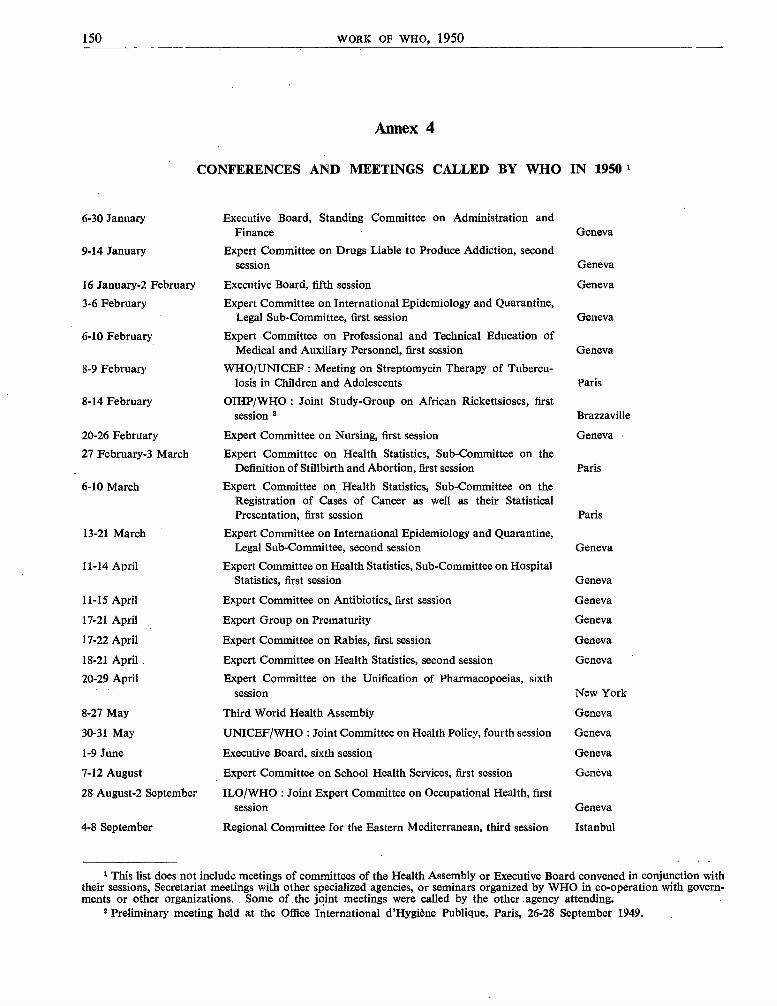
150 WORK OF WHO, 1950
6 -30 January
9 -14 January
16 January -2 February
3 -6 February
6 -10 February
8 -9 February
8 -14 February
Annex 4
CONFERENCES AND MEETINGS CALLED BY WHO IN 19501
Executive Board, Standing Committee on Administration andFinance Geneva
Expert Committee on Drugs Liable to Produce Addiction, secondsession Geneva
Executive Board, fifth session Geneva
Expert Committee on International Epidemiology and Quarantine,Legal Sub -Committee, first session Geneva
Expert Committee on Professional and Technical Education ofMedical and Auxiliary Personnel, first session Geneva
WHO /UNICEF : Meeting on Streptomycin Therapy of Tubercu-losis in Children and Adolescents Paris
OIHP /WHO : Joint Study -Group on African Rickettsioses, firstsession 2 Brazzaville
20 -26 February Expert Committee on Nursing, first session Geneva
27 February -3 March Expert Committee on Health Statistics, Sub -Committee on theDefinition of Stillbirth and Abortion, first session Paris
6 -10 March Expert Committee on Health Statistics, Sub -Committee on theRegistration of Cases of Cancer as well as their StatisticalPresentation, first session Paris
13 -21 March Expert Committee on International Epidemiology and Quarantine,Legal Sub- Committee, second session Geneva
11 -14 April Expert Committee on Health Statistics, Sub -Committee on HospitalStatistics, first session Geneva
11 -15 April Expert Committee on Antibiotics, first session Geneva
17 -21 April Expert Group on Prematurity Geneva
17 -22 April Expert Committee on Rabies, first session Geneva
18 -21 April Expert Committee on Health Statistics, second session Geneva
20 -29 April Expert Committee on the Unification of Pharmacopoeias, sixthsession New York
8 -27 May Third World Health Assembly Geneva
30 -31 May UNICEF /WHO : Joint Committee on Health Policy, fourth session Geneva
1 -9 June Executive Board, sixth session Geneva
7 -12 August Expert Committee on School Health Services, first session Geneva
28 August -2 September ILO /WHO : Joint Expert Committee on Occupational Health, firstsession Geneva
4 -8 September Regional Committee for the Eastern Mediterranean, third session Istanbul
1 This list does not include meetings of committees of the Health Assembly or Executive Board convened in conjunction withtheir sessions, Secretariat meetings with other specialized agencies, or seminars organized by WHO in co- operation with govern-ments or other organizations. Some of the joint meetings were called by the other agency attending.
2 Preliminary meeting held at the Office International d'Hygiène Publique, Paris, 26 -28 September 1949.
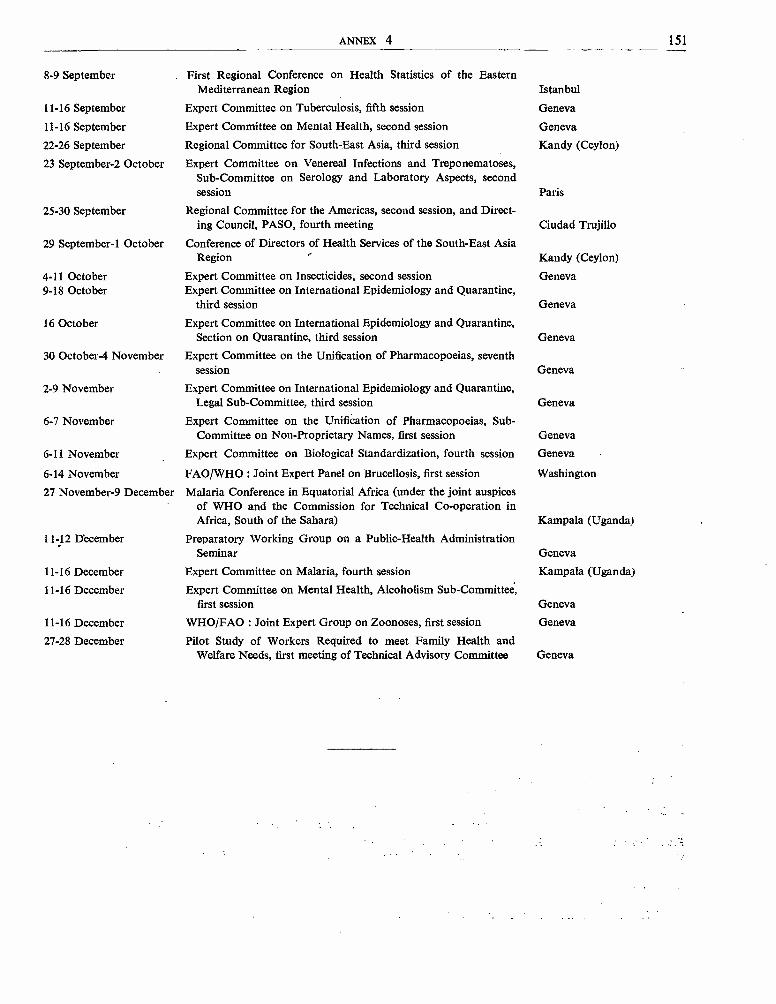
ANNEX 4 151
8 -9 September
11 -16 September
11 -16 September
22 -26 September
23 September -2 October
25 -30 September
29 September -1 October
4 -11 October9 -18 October
16 October
30 October -4 November
2 -9 November
6 -7 November
6 -11 November
6 -14 November
27 November -9 December
11-12 December
11 -16 December
11 -16 December
11 -16 December
27 -28 December
First Regional Conference on Health Statistics of the EasternMediterranean Region
Expert Committee on Tuberculosis, fifth session
Expert Committee on Mental Health, second session
Regional Committee for South -East Asia, third session
Expert Committee on Venereal Infections and Treponematoses,Sub -Committee on Serology and Laboratory Aspects, secondsession
Regional Committee for the Americas, second session, and Direct-ing Council, PASO, fourth meeting
Conference of Directors of Health Services of the South -East AsiaRegion
Expert Committee on Insecticides, second sessionExpert Committee on International Epidemiology and Quarantine,
third session
Expert Committee on International Epidemiology and Quarantine,Section on Quarantine, third session
Expert Committee on the Unification of Pharmacopoeias, seventhsession
Expert Committee on International Epidemiology and Quarantine,Legal Sub -Committee, third session
Expert Committee on the Unification of Pharmacopoeias, Sub -Committee on Non -Proprietary Names, first session
Expert Committee on Biological Standardization, fourth session
FAO /WHO : Joint Expert Panel on Brucellosis, first session
Malaria Conference in Equatorial Africa (under the joint auspicesof WHO and the Commission for Technical Co- operation inAfrica, South of the Sahara)
Preparatory Working Group on a Public -Health AdministrationSeminar
Expert Committee on Malaria, fourth session
Expert Committee on Mental Health, Alcoholism Sub -Committee,first session
WHO /FAO : Joint Expert Group on Zoonoses, first session
Pilot Study of Workers Required to meet Family Health andWelfare Needs, first meeting of Technical Advisory Committee
Istanbul
Geneva
Geneva
Kandy (Ceylon)
Paris
Ciudad Trujillo
Kandy (Ceylon)
Geneva
Geneva
Geneva
Geneva
Geneva
Geneva
Geneva
Washington
Kampala (Uganda)
Geneva
Kampala (Uganda)
Geneva
Geneva
Geneva
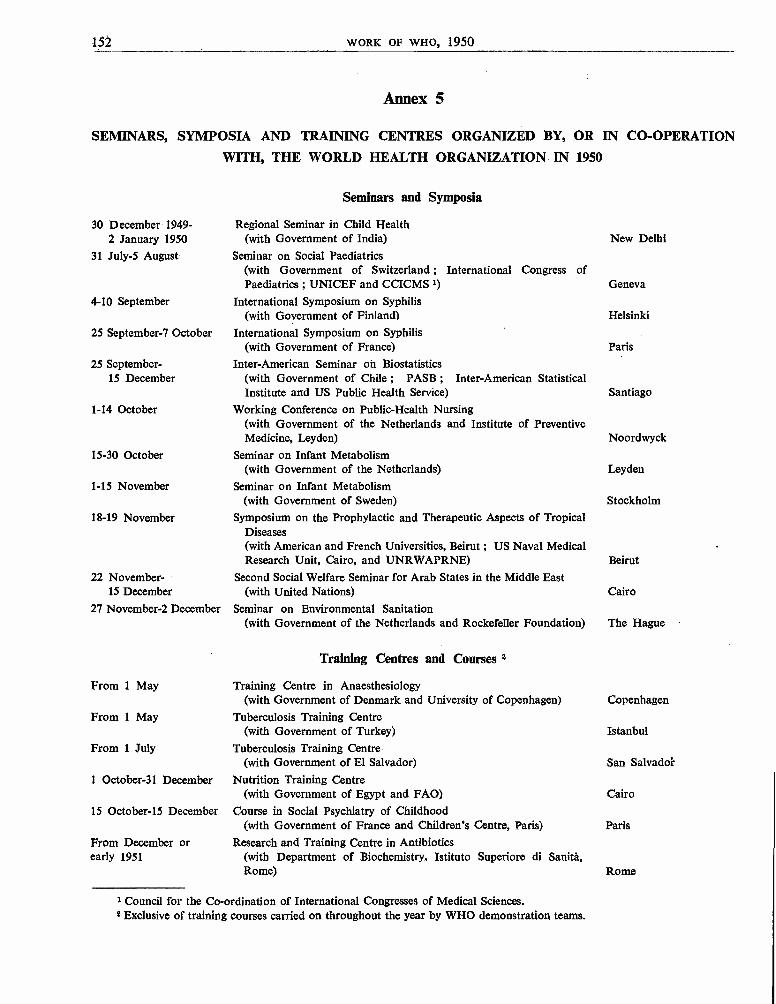
152 WORK OF WHO, 1950
Annex 5
SEMINARS, SYMPOSIA AND TRAINING CENTRES ORGANIZED BY, OR IN CO- OPERATIONWITH, THE WORLD HEALTH ORGANIZATION IN 1950
30 December 1949-2 January 1950
31 July -5 August
4 -10 September
25 September -7 October
25 September -15 December
1 -14 October
15 -30 October
1 -15 November
18 -19 November
22 November -15 December
27 November -2 December
From 1 May
From 1 May
From 1 July
1 October -31 December
15 October -15 December
From December orearly 1951
Seminars and Symposia
Regional Seminar in Child Health(with Government of India)
Seminar on Social Paediatrics(with Government of Switzerland ; International Congress ofPaediatrics ; UNICEF and CCICMS 1)
International Symposium on Syphilis(with Government of Finland)
International Symposium on Syphilis(with Government of France)
Inter -American Seminar on Biostatistics(with Government of Chile ; PASB ; Inter -American StatisticalInstitute and US Public Health Service)
Working Conference on Public -Health Nursing(with Government of the Netherlands and Institute of PreventiveMedicine, Leyden)
Seminar on Infant Metabolism(with Government of the Netherlands)
Seminar on Infant Metabolism(with Government of Sweden)
Symposium on the Prophylactic and Therapeutic Aspects of TropicalDiseases(with American and French Universities, Beirut ; US Naval MedicalResearch Unit, Cairo, and UNRWAPRNE)
Second Social Welfare Seminar for Arab States in the Middle East(with United Nations)
Seminar on Environmental Sanitation(with Government of the Netherlands and Rockefeller Foundation)
Training Centres and Courses 2
Training Centre in Anaesthesiology(with Government of Denmark and University of Copenhagen)
Tuberculosis Training Centre(with Government of Turkey)
Tuberculosis Training Centre(with Government of El Salvador)
Nutrition Training Centre(with Government of Egypt and FAO)
Course in Social Psychiatry of Childhood(with Government of France and Children's Centre, Paris)
Research and Training Centre in Antibiotics(with Department of Biochemistry. Istituto Superiore di Sanitá,Rome)
1 Council for the Co- ordination of International Congresses of Medical Sciences.$ Exclusive of training courses carried on throughout the year by WHO demonstration teams.
New Delhi
Geneva
Helsinki
Paris
Santiago
Noordwyck
Leyden
Stockholm
Beirut
Cairo
The Hague
Copenhagen
Istanbul
San Salvador
Cairo
Paris
Rome
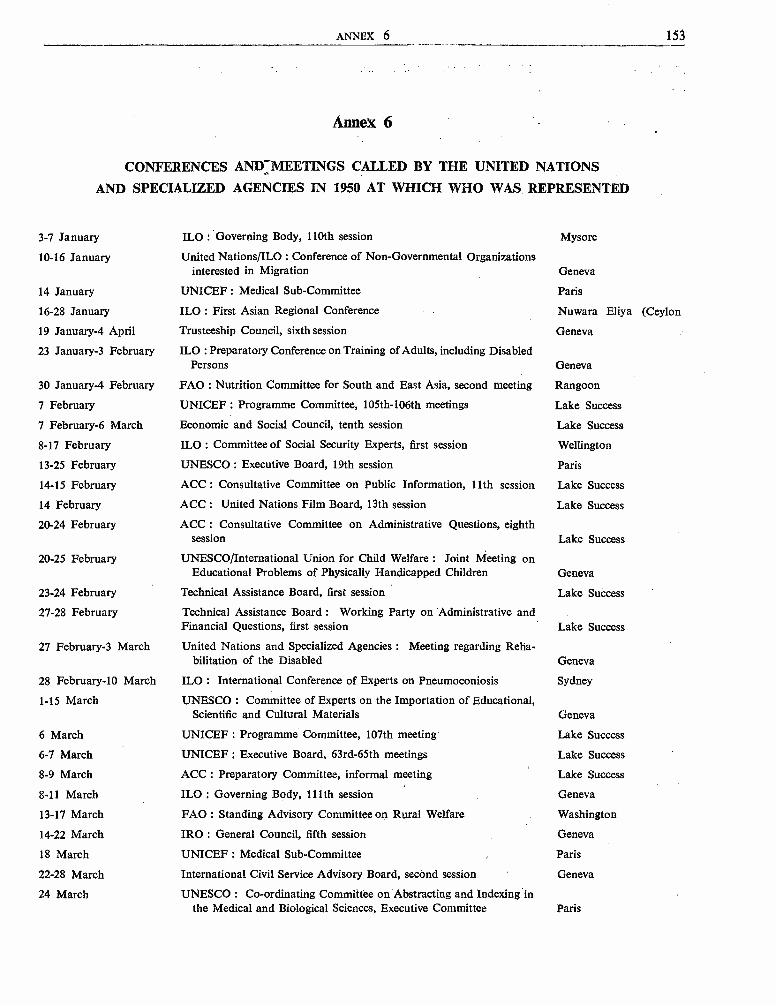
ANNEX 6 153
Annex 6
CONFERENCES AND:MEETINGS CALLED BY THE UNITED NATIONS
AND SPECIALIZED AGENCIES IN 1950 AT WHICH WHO WAS REPRESENTED
3 -7 January
10 -16 January
14 January
16 -28 January
19 January -4 April
23 January-3 February
30 January-4 February
7 February
7 February -6 March
8 -17 February
13 -25 February
14 -15 February
14 February
20 -24 February
20 -25 February
23 -24 February
27 -28 February
27 February-3 March
28 February -10 March
1 -15 March
6 March
6 -7 March
8 -9 March
8 -11 March
13 -17 March
14 -22 March
18 March
22 -28 March
24 March
ILO : Governing Body, 110th session
United Nations /ILO : Conference of Non -Governmental Organizationsinterested in Migration
UNICEF : Medical Sub -Committee
ILO : First Asian Regional Conference
Trusteeship Council, sixth session
ILO : Preparatory Conference on Training of Adults, including DisabledPersons
FAO : Nutrition Committee for South and East Asia, second meeting
UNICEF : Programme Committee, 105th -106th meetings
Economic and Social Council, tenth session
ILO : Committee of Social Security Experts, first session
UNESCO : Executive Board, 19th session
ACC : Consultative Committee on Public Information, 11th session
ACC : United Nations Film Board, 13th session
ACC : Consultative Committee on Administrative Questions, eighthsession
UNESCO /International Union for Child Welfare : Joint Meeting onEducational Problems of Physically Handicapped Children
Technical Assistance Board, first session
Technical Assistance Board : Working Party on Administrative andFinancial Questions, first session
United Nations and Specialized Agencies : Meeting regarding Reha-bilitation of the Disabled
ILO : International Conference of Experts on Pneumoconiosis
UNESCO Committee of Experts on the Importation of Educational,Scientific and Cultural Materials
UNICEF : Programme Committee, 107th meeting
UNICEF : Executive Board, 63rd -65th meetings
ACC : Preparatory Committee, informal meeting
ILO : Governing Body, 111th session
FAO : Standing Advisory Committee on Rural Welfare
IRO : General Council, fifth session
UNICEF : Medical Sub -Committee
International Civil Service Advisory Board, second session
UNESCO : Co- ordinating Committee on Abstracting and Indexing inthe Medical and Biological Sciences, Executive Committee
Mysore
Geneva
Paris
Nuwara Eliya (Ceylon
Geneva
Geneva
Rangoon
Lake Success
Lake Success
Wellington
Paris
Lake Success
Lake Success
Lake Success
Geneva
Lake Success
Lake Success
Geneva
Sydney
Geneva
Lake Success
Lake Success
Lake Success
Geneva
Washington
Geneva
Paris
Geneva
Paris
154 WORK OF WHO, 1950
27 March -4 April
27 -30 March
27 March -19 May
3 -4 April
3 April -5 May
13 -15 April
20 -21 April
20 -21 April
25 April -9 May
28 -29 April
2 -3 May
6 May
8 -17 May
9 May
10 -12 May
15 -16 May
16 -18 May
16 -20 May
19 -20 May
22 May
22 May -2 June
22 May -17 June
2 -30 June
31 May -15 June
1 June -21 July
7 June -1 July
5 -6 June
5 -13 June
8 -9 June
8 -9 June
12 -13 June
12 -16 June
14 -24 June
18 June -29 July
19 -20 June
27 -28 June
27 June
ECOSOC : Transport and Communications Commission, fourth session
FAO: European Committee on Agricultural Technology, secondmeeting
ECOSOC : Commission on Human Rights, sixth session
Technical Assistance Board : Working Party on Administrative andFinancial Questions, second session
ECOSOC : Social Commission, sixth session
UNESCO : National United States Commission, eighth meeting
Technical Assistance Board, second session
UNESCO : Third Conference of Organizers of International VoluntaryWork Camps
ILO : Preliminary Migration Conference
ACC : Preparatory Committee, 12th session
Administrative Committee on Co- ordination, ninth session
UNICEF : Medical Sub -Committee
FAO : Council, ninth session
UNICEF : Committee on Administrative Budget, special meeting
ACC : Technical Working Group on Fellowships, fourth session
UNESCO : Executive Board, 21st session
Meeting of Specialized Agencies and International Organizationsconcerned with the Prevention of Crime and the Treatment ofOffenders
ECOSOC : ECAFE, sixth session
UNESCO /International Universities' Bureau /Interim Committee ofUniversities, fourth session
UNICEF : Committee on Administrative Budget, special meeting
ECOSOC : Population Commission, fifth session
UNESCO : General Conference, fifth session
ILO : Governing Body, 112th session
ECOSOC : ECE, fifth session
Trusteeship Council, seventh session
ILO : 33rd International Labour Conference
UNICEF : Programme Committee, 108th -110th meetings
FAO : Nutrition Conference on Problems in Latin America, secondsession
United Nations : Scientific Conference on the Conservation andUtilization of Resources, Preparatory Committee
UNICEF : Committee on Administrative Budget, ninth session
First Technical Assistance Conference
Technical Assistance Board, third session
United Nations : Permanent Central Opium Board, 55th session, andthird joint session with the Narcotic Drugs Supervisory Body
UNESCO : International Seminar on Methods and Techniques ofAdult Education
UNICEF : Executive Board, 66th -69th meetings
ACC : Consultative Committee on Public Information, 12th session
ACC : United Nations Film Board, 14th session
Lake Success
Geneva
Lake Success
Lake Success
Lake Success
Washington
Lake Success
Paris
Geneva
Paris
Paris
Paris
Rome
Lake Success
Lake Success
Florence
Geneva
Bangkok
Florence
Lake Success
Lake Success
Florence
Geneva
Geneva
Lake Success
Geneva
Lake Success
Rio de Janeiro
Lake Success
Lake Success
Lake Success
Lake Success
Geneva
Salzburg
Lake Success
Geneva
Geneva
ANNEX 6 155
3 July Technical Assistance Board, Working Party on Administrative andFinancial Questions, third session Lake Success
3 July -19 August Economic and Social Council, i 1 t session Geneva
4 -5 July UNESCO : Meeting of Experts on the International Interchange ofTeachers Geneva
5 -7 July ACC : Consultative Committee on Administrative Questions, ninthsession Lake Success
6 -14 July UNESCO /International Bureau of Education : 13th InternationalConference on Public Education Geneva
6 July Technical Assistance Board, fourth session Geneva
10 -22 July FAO /University of Reading /British Council : First InternationalMeeting on Dairy Technology Reading
18, 31 July -3, 16 August Technical Assistance Board, fifth session Geneva
2 August United Nations and Specialized Agencies : meeting to discuss proposedConference on Rehabilitation of Handicapped Children New Delhi
12 August ACC : Preparatory Committee, informal session Geneva
18 August -12 September Special Committee on Information transmitted under Article 73 a ofthe Charter Lake Success
25 -26 August UNICEF : Medical Sub- Committee Paris
26 August -2 September UNESCO : Executive Board, 23rd session Paris
28 -29 August UNESCO /Organization of American States : Co- ordinationCommittee of Mexico Fundamental Education Centre Washington
4 -6 September ACC : Consultative Committee on Administrative Questions, tenthsession Paris
5 -15 September ECOSOC : Sub -Commission on Statistical Sampling, fourth session Lake Success
6 -20 September BANK : Board of Governors, fifth annual meeting Paris
6 -20 September FUND : Board of Governors, fifth annual meeting Paris
12 September Advisory Committee on Administrative and Budgetary Questions Lake Success
19 September-I 5 December United Nations : General Assembly, fifth session Lake Success
20 -22 September Technical Assistance Board, sixth session Lake Success
6 -27 October ACC Preparatory Committee, 13th session Lake Success
16 -25 October United Nations : Joint Staff Pension Fund, first session Lake Success
17 October ACC : Consultative Committee on Public Information, special session New York
17 October Administrative Committee on Co- ordination, tenth session Lake Success
24 October -3 November ILO : Petroleum Committee, Sub -Committee on Health Services,third session Geneva
25 October -1 November FAO : Council, tenth session Washington
29 October UNESCO : International Advisory Committee on the Study of theTechnique of International Conferences, second session New York
29 October -3 November UNESCO /Organization of American States : Co- ordinatingCommittee of Mexico Fundamental Education Centre Montevideo
31 October -18 November United Nations : Permanent Central Opium Board, 56th session ;Narcotic Drugs Supervisory Body, 34th session ; fourth joint sessionof the two organizations Geneva
2 -10 November UNESCO : Executive Board, 24th session Paris
9 -10 November UNICEF : Programme Committee, 111th -114th meetings Lake Success
156
13 -22 November
16 November
16 -17 November
20 -23 November
20 -24 November
21 November
21 -25 November
27 -28 November
1 -14 December
1 -2 December
4 -8 December
5 -12 December
8 -20 December
18 -19 December
19 -21 December
20 -22 December
WORK OF WHO, 1950
United Nations : Conference on Building Research (under the auspicesof Housing Sub -Committee of ECE) Geneva
UNICEF : Committee on Administrative Budget, tenth session Lake Success
UNESCO : Inter- Agency Working Party on Technical Assistance andFundamental Education for Social and Economic Development Paris
UNESCO : Interim International Arid Zone Research Council Paris
Technical Assistance Board, seventh session Lake Success
UNICEF : Programme Committee, 115th meeting New York
ILO : Governing Body, 113th session Brussels
UNICEF : Executive Board, 70th -73rd meetings Lake Success
FAO : Latin American Meeting on Food and Agricultural Programmesand Outlook (held in conjunction with the Fourth Inter -AmericanConference on Agriculture) Montevideo
UNESCO : Meeting on United Nations Research Laboratories Paris
ECOSOC : ECE, Inland Transport Committee, ad hoc Working Partyon Prevention of Road Accidents, first session Geneva
ICITO: General Agreement on Tariffs and Trade, ContractingParties, fifth session (Working Party to consider a Draft Agreementon the Importation of Insecticides) Torquay
UNESCO : First Regional Conference of National Commissions for theWestern Hemisphere Havana
United Nations : Meeting of Technical Working Group on SocialRehabilitation of the Disabled Geneva
United Nations : Conference on Handicapped Children
Joint ECAFE /UNESCO Working Party on Educational and ScientificMaterials, second session Bangkok
Jamshedpur (India)
Annex 7
CONFERENCES AND MEETINGS OF NON -GOVERNMENTAL AND OTHER ORGANIZATIONS
IN 1950 AT WHICH WHO WAS REPRESENTED
6 -7 January
6 -7 January
18 -19 January
16 -21 February
20 -25 February
23 February
Sixth All -India Conference of Obstetricians and Gynaecologists Madras
Council for the Co- ordination of International Congresses of MedicalSciences, Executive Committee, fourth session Paris
Sixth International Congress of Paediatrics, Organizing Committee,fourth meeting Zürich
World Federation for Mental Health, Executive Committee, fifthsession London
International Union for Child Welfare : Conference of Experts on theEducational Problems of Orthopaedically Handicapped Children Geneva
Sixth International Congress of Paediatrics : Organizing Committee,fifth meeting Zürich
ANNEX 7 157
1 -3 March
20 March -10 April
30-31 March
16 -28 April
22 -23 April
24 -28 April
24 -28 April
24 -28 April
25 April -5 May2 -3 May
4-7 May
5 -6 May
8 -13 May
8 -19 May
14 -19 May
17 -24 May
25 -26 May
29 May -2 June3 June20 June
20 -23 June
29 June -1 July
2 -6 July
6 -12 July
15 -22 July
17 -19 July
17 -20 July
23 -28 July
24 -29 July
24 -28 July
28 -30 July
28 July -2 August
7 -18 August
14 -19 August
14 -21 August
International Council of Nurses, Florence Nightingale InternationalFoundation Council, first meeting
Organization of American States, Inter -American Economic and SocialCouncil, first special meeting
Council for the Co- ordination of International Congresses of MedicalSciences : Executive Committee, fifth session
Pan American Sanitary Organization, Executive Committee, tenthsession
Meeting of Society of Swiss Physiologists and PharmacologistsWorld Medical Association, Council MeetingRoyal Sanitary Institute, Annual Health CongressNational Conference of Social WorkSouth Pacific Commission, First South Pacific ConferenceLeague of Red Cross Societies, Nursing Advisory Committee, tenth
session
Third Central American Congress of Venereal Diseases
Office International d'Hygiène Publique, Permanent Committee, fifthsession
International Office of Epizootics, eighteenth annual meetingWorld Federation of United Nations Associations, International
Seminar on World Health Problems
International and Fourth American Congress on Obstetrics andGynaecology
International American Institute for Child Protection, DirectingCouncil
Journées Nationales de Prophylaxie Antivénérienne
Third European Poliomyelitis ConferenceSwiss Academy of Medical Sciences, Annual MeetingOrganization of American States, Inter -American Economic and Social
Council, Co- ordinating Committee on Technical Assistance, firstmeeting
International Scientific Committee for Research on TrypanosomiasisThird General Conference of Consultative Non -Governmental
Organizations
Northern Nurses' Association, Quadrennial CongressInternational Union for Child Welfare, General CouncilInternational Union against Cancer, Fifth International CongressCouncil for the Co- ordination of International Congresses of Medical
Sciences, Executive Committee, sixth sessionThird International Council of Juvenile Court JudgesFifth International Conference of Social WorkInternational Dental Federation, 50th Anniversary ConferenceSixth International Congress of PaediatricsFifth International Congress of Schools of Social WorkInternational Union against Venereal Diseases, Joint Conference of
Syphilologists and Paediatricians, and 27th Annual GeneralAssembly
South Pacific Commission, South Pacific Research Council, secondsession
Twelfth International Penal and Penitentiary CongressThird Assembly of the World Organization for Early Childhood
Education
London
Washington, D.C.
Paris
Washington, D.C.Geneva
Copenhagen
EastbourneAtlantic City, N.J.Nasinu, Fiji
Geneva
San Salvador(El Salvador)
GenevaParis
Geneva
New York
Montevideo
Bordeaux
Amsterdam
Geneva
Washington, D.C.Antwerp
Geneva
GothenburgLondonParis
Paris
Liége
Paris
Paris
ZürichParis
Zürich
Sydney
The Hague
Vienna
158 WORK OF WHO, 1950
15 -18 August
17 -24 August
19 -20 August
21 -27 August
25 -26 August
27 August -9 September
Eighteenth International Physiological Congress
Fifth International Congress on Microbiology
Meeting of the Scandinavian Pharmacological Society
CARE European Conference
First Congress of the Scandinavian Association of Anaesthesiologists
World Federation for Mental Health, third annual meeting ; ExecutiveBoard, sixth session ; Inter -Professional Advisory Committee
28 -31 August International Conference of Family Life Organizations
30 August -2 September First International Conference on Alcohol and Traffic
3 -6 September International Union against Tuberculosis, twelfth conference
3 -9 September
5 -8 September
9 -18 September
10 -19 September
17 -20 September
20 -23 September
18 -27 September
2 -10 October
10 October
12 October
13 -14 October
13 -18 October
16 -21 October
17 -18 October
17 -19 October
20 -22 October
23 -25 October
23 -27 October
6 -9 November
10 -12 November
26 -28 November
3 -7 December
3 -9 December
6 -9 December
First International Congress of Cardiology
Eleventh Conference on Science, Philosophy and Religion
Sixth Triennial Conference of the Associated Country Women of theWorld
Second International Congress of Criminology
American College of Chest Physicians, First International Congress onDiseases of the Chest
Pan -American Sanitary Organization, Executive Committee, eleventhsession
International Congress of Psychiatry
Thirteenth Pan American Sanitary Conference
World Medical Association, Committee on Education
Pan American Sanitary Organization, Executive Committee, twelfthsession
League of Red Cross Societies, Health Advisory Committee, fourthsession
World Medical Association, Council Meeting
World Medical Association, Fourth General Assembly
Journées Thérapeutiques
Austrian Congress on Industrial Hygiene
World Medical Association, Conference of Medical Editors
Thirtieth Congress of Hygiene (organized by the Société de Médecinepublique et de Génie sanitaire)
American College of Surgeons, 29th Annual Hospital StandardizationConference
Conjoint meeting of the National Malaria Society, American Societyof Tropical Medicine and the American Academy of TropicalMedicine
Council for the Co- ordination of International Congresses of MedicalSciences, Executive Committee, seventh session
Indian Council of Medical Research, Scientific Advisory Board andScientific Advisory Committees
Mid -Century White House Conference
International Universities' Bureau, General Conference of Universities
Conference for Serologists from Austria and from Foreign Countriesin Vienna
Copenhagen
Rio de Janeiro
Copenhagen
Oslo
Oslo
Paris
Helsinki
Stockholm
Copenhagen
Paris
New York
Copenhagen
Paris
Rome
Ciudad Trujillo
Paris
Ciudad Trujillo
New York
Ciudad Trujillo
Monte Carlo
New York
New York
Paris
Vienna
New York
Paris
Boston, Mass.
Savannah, Ga. (USA)
Paris
Agra
Washington, D.C.
Nice
Vienna
ANNEX 8 159
8 -10 December
22 -26 December
26 -28 December
Harvard School of Public Health, Conference on health problems ofindustries operating in tropical and subtropical areas of the world Boston, Mass.
Indian Conference of Social Work, Fourth Annual Session Jamshedpur
First Council of the Nutrition Institute of Central America and Panama San José (Costa Rica)
Annex 8
TENTATIVE SCHEDULE OF MEETINGS TO BE CALLED BY WHO IN 1951
8 January Executive Board, Standing Committee on Administration and Finance Geneva
22 January Executive Board, seventh session Geneva
January Léon Bernard Foundation Committee Geneva
March Expert Committee on Environmental Sanitation, second session Geneva
March Regional Committee for the Western Pacific, first session
9 April Special Committee to consider the Draft International SanitaryRegulations Geneva
16 -25 April Expert Committee on the Unification of Pharmacopoeias, eighthsession Geneva
April Expert Committee on International Epidemiology and Quarantine,Legal Sub -Committee, fourth session Geneva
April FAO /WHO : Joint Expert Committee on Nutrition, second session Rome
7 May Fourth World Health Assembly Geneva
May Léon Bernard Foundation Committee Geneva
May Expert Committee on Venereal Infections and Treponematoses, Sub -Committee on Serology and Laboratory Aspects, third session Paris
1 June Executive Board, eighth session Geneva
June Expert Committee on Insecticides, third session Savannah, Ga. (USA)
June Consultative Committee for Europe on Programmes, first session Geneva
July Expert Committee on Nursing, second session Geneva
July Expert Committee on Public -Health Administration, first session Geneva
20 -27 August Regional Committee for the Americas, third session, and DirectingCouncil, PASO, fifth meeting Washington
September Regional Committee for the Eastern Mediterranean, fourth session Teheran
September Regional Committee for South -East Asia, fourth session Rangoon
15 -20 October Expert Committee on the Unification of Pharmacopoeias, ninth session Geneva
22 -24 October Expert Committee on the Unification of Pharmacopoeias, Sub -Committee on Non -Proprietary Names, second session Geneva
October Expert Committee on Venereal Infections and Treponematoses, fourthsession Alexandria
October Expert Committee on Health Statistics, Sub -Committee on HospitalStatistics, second session Paris
October Expert Committee on Health Statistics, Sub -Committee on theRegistration of Cases of Cancer as well as their StatisticalPresentation, second session London
160 WORK OF WHO, 1950
November
November
November -December
Month not yet decided:
Spring
Summer
Summer
Autumn
Autumn
Autumn
Autumn
Autumn
Autumn
Late 1951 or early 1952:
Expert Committee on Health Statistics, third session
International Serodiagnostic Laboratory Conference
Expert Committee on Insecticides, fourth session
Expert Committee on Trachoma, first session
Expert Committee on Maternity Care, first session
Expert Committee on Professional and Technical Education of Medicaland Auxiliary Personnel, second session
Expert Committee on Mental Health, Sub -Committee on DrugAddiction, first session
Expert Committee on Cholera, first session
Expert Committee on Drugs Liable to Produce Addiction, thirdsession
Expert Committee on Tuberculosis, sixth session
ILO /WHO : Joint Committee on the Hygiene of Seafarers, secondsession
Joint Expert Committee with United Nations and Specialized Agencieson the Crippled Child, first session
Expert Committee on Biological Standardization, fifth session
Expert Meeting on Psychiatric Examination of Offenders
Expert Committee on Health Education of the Public, first session
ILO /WHO : Joint Expert Committee on Occupational Health, secondsession
Annex 9
Geneva
Paris
Geneva or Marseille
Alexandria
Geneva
Geneva
India
Geneva
Geneva
Geneva
Copenhagen
Geneva
NON -GOVERNMENTAL ORGANIZATIONS IN OFFICIAL RELATIONSHIP WITH WHO
Biometric Society,New Haven, Connecticut, USA
Council for the Co- ordination of International Congressesof Medical Sciences,Paris, France
Inter -American Association of Sanitary Engineering,Washington, D.C., USA
International Academy of Forensic and Social Medicine,Brussels, Belgium
International Association for the Prevention of Blindness,Paris, France
International Committee of the Red Cross,Geneva, Switzerland
International Conference of Social Work,Columbus, Ohio, USA
International Council of Nurses,London, England
International Dental Federation,Brussels, Belgium
International Federation for Housing and Town Planning,Amsterdam, Netherlands
International Hospital Federation,London, England
ANNEX 10 161
International League against Rheumatism,London, England
International Leprosy Association,London, England
International Pharmaceutical Federation,Overschie, Netherlands
International Union against Cancer,Paris, France
International Union for Child Welfare,Geneva, Switzerland
International Union against Tuberculosis,Paris, France
International Union against Venereal Diseases,Paris, France
League of Red Cross Societies,Geneva, Switzerland
World Federation for Mental Health,London, England
World Federation of United Nations Associations,Geneva, Switzerland
World Medical Association,New York, USA
Annex 10
SELECTED LIST OF TECHNICAL ARTICLES AND REPORTS ISSUED BY WHO IN 1950
The articles and reports listed exist, unless otherwise indicated, in English and in French, inmimeograph or printed form. Those marked with an asterisk are in English only, with a summaryin French in the case of articles in the Bulletin of the World Health Organization. Referencenumbers in brackets apply to working documents (mimeographed) which are not normally availablefor distribution. The list does not include short articles on technical subjects published in theChronicle of the World Health Organization.
Antibiotics 1
EXPERT COMMITTEE ON ANTIBIOTICS. Report on first session.World Hlth Org. techn. Rep. Ser. 1950, 26
WAKSMAN, S. A. Plan of organization of an antibioticsprogramme (WHO /Antib /1, March 1950)
Biological Standardization
BONNEFOI, A., GRABAR, J., LE MINOR, L. & LE MINOR, S. Pre-paration of agglutinating sera (WHO /BS1104, November1950)
CHU, C. M., ANDREWES, C. H. & GLEDHILL, A. W. Influenzain 1948 -1949.* Bull. World Hlth Org. 1950, 3, 187 -214
CUMMINGS, M. M. Detection of the tubercle bacillus : surveyof current laboratory procedure. Bull. World Hltiz Org.1950, 2, 705 -721
DAVIES, M. G., MILES, A. A. & PERRY, W. L. M. The collaborativeassay of the proposed third international standardsulpharsphenamine (WHO /BS /110, November 1950)
EDWARDS, Lydia B. & GELTING, Anna S. BCG- vaccinestudies : I. Effect of age of vaccine and variation in storagetemperature and dosage on allergy production and vaccina-tion lesions ten weeks after vaccination.* Bull. WorldHlth Org. 1950, 3, 1 -24
1 See also under Epidemiology.
EDWARDS, Lydia B. & GELTING, Anna S. BCG- vaccinestudies : 2. Effect of variation in dosage of BCG vaccineallergy production and vaccination lesions nine weeksafter vaccination.* Bull. World Hlth Org. 1950, 3, 279 -300
EXPERT COMMITTEE ON BIOLOGICAL STANDARDIZATION. Reporton the third session. World Hlth Org. techn. Rep. Ser.1950, 2
EXPERT COMMITTEE ON BIOLOGICAL STANDARDIZATION. Reportof the Sub -Committee on Fat -Soluble Vitamins. WorldHlth Org. techn. Rep. Ser. 1950, 3
EXPERT COMMITTEE ON BIOLOGICAL STANDARDIZATION. Reporton the fourth session (WHO /BS/112, November 1950) 8
FASQUELLE, R. & FASQUELLE, J. Desiccation of vacciniavirus and smallpox vaccination (WHO /BS/105, November1950)
FELIX, A. Standardization of diagnostic agglutination tests :typhoid and paratyphoid A and B fevers.3 Bull. WorldHlth Org. 1950, 2, 643 -649
FELIX, A. Standardization of serological tests for the diagnosisof the typhus group of fevers.3 Bull. World Hlth Org.1950, 2, 637 -642
2 To be printed in 1951 after approval by the ExecutiveBoard.
3 Issued in mimeograph form in 1949.
162 WORK OF WHO, 1950
FRANCIS, A. E. & BLANCHARD, Dorothy M. Enumeration ofHaemophilus Pertussis in suspensions in relation to theUnited States National Institute of Health turbidity refer-ence standard for pertussis vaccine (WHO /BS /88, October1950)
GAUTIER, R. The BCG Pilot Station in Paris (WHO /BS /75,October 1950)
GIROUD, P. Pasteur Institute Typhus Service (WHO /BS /103'November 1950)
GRASSET, E. Detection of tubercle bacillus (WHO /BS /99,November 1950)
GREENBERG, L. A standard preparation for the assay ofdiphtheria toxoid (WHO /BS /86, October 1950)
HUMPHREY, J. H. A note of the assay of streptokinase (WHO/BS /95, October 1950)
HUMPHREY, J. H. A note on hyaluronidase and the Britishhyaluronidase standard (WHO /BS /78, October 1950)
HUMPHREY, J. H. & PERRY, W. L. M. A proposal for the col-laborative assay of the proposed second internationalstandard for penicillin (WHO /BS194, October 1950)
IRWIN, J. O. & STANDFAST, A. F. B. The Kendrick test forpertussis vaccine (WHO /BS /96, October 1950)
KAUFFMANN, F. On the serology of the Vibrio cholerae(WHO /BS /98, October 1950)
KAUFFMANN, F. International Salmonella Centre.* Bull.World Hlth Org. 1950, 3, 171 -175
MCCLEAN, D. Memorandum on dried material for smallpoxvaccination (WHO /BS /73, October 1950)
MILES, A. A. Interim report on the proposed internationalstandard scarlet fever antitoxin (WHO /BS184, October1950)
MILES, A. A. Note on the provisional international standardfor adrenocorticotrophic hormone ( WHO/BS/85 & Corr. 1,October 1950)
MILES, A. A. Proposals for the establishment of an inter-national standard for streptomycin (WHO /BS /76, October1950)
MILES, A. A. International standards for anti -A and anti -Bblood -grouping sera.* Bull. World Hlth Org. 1950, 3,301 -308
MILES, A. A. & PERRY, W. L. M. Third international digitalisstandard. Bull. World Hlth Org. 1950, 2, 655 -672
MURRAY, R. Diphtheria and tetanus toxoids (WHO /BS /83,October 1950)
MURRAY, R. Dried cholera vaccines (WHO /BS /82, October1950)
4 Issued in mimeograph form in 1949.
NATIONAL INSTITUTE FOR MEDICAL RESEARCH, London. Theproposed international standard diphtheria toxoid com-pared with the Hold toxoid (WHO IBS1102, November1950)
PATON, W. D. M. The standardization of pyrogens (WHO/BS /90, October 1950)
PERRY, W. L. M. A proposal for the collaborative assay ofthe proposed third international soluble insulin standard(WHO /BS /89, October 1950)
PERRY, W. L. M. Note on methods of assay for chorionicgonadotrophin (WHO /BS /93, October 1950)
PITTMAN, M. Comments on biological standardization ofpertussis vaccine (WHO /BS /81, October 1950)
SMITH, E. L. Standardization of liver extracts.4 Bull. WorldHlth Org. 1950, 2, 651 -654
SOKHEY, sir s. s. & HABBU, M. K. Antigenic structure of thecholera vibrio and protective power of the vaccine.* Bull.World Hlth Org. 1950, 3, 55 -61
SOKHEY, sir s. s. & HABBU, M. K. Biological assay of choleravaccine.* Bull. World Hlth Org. 1950, 3, 43 -53
SOKHEY, sir s. s. & HABBU, M. K. Casein hydrolysate choleravaccine.* Bull. World HIM Org. 1950, 3, 33 -42
SOKHEY, sir S. S., HABBU, M. K. & BHARUCHA, K. H. Hydro -lysate of casein for the preparation of plague and choleravaccines.* Bull. World Hlth Org. 1950, 3, 25 -31
STATENS SERUMINSTITUT, Copenhagen. Memorandum on thepotency evaluation of tetanus toxoid (WHOIBS/92, October1950)
STATENS SERUMINSTITUT, Copenhagen. Preliminary reporton the proposed new international standard histolyticusantitoxin (WHO/BS /91, October 1950)
STATENS SERUMINSTITUT, Copenhagen. Second memorandumon the potency evaluation of antitoxins (WHO /BS /77,October 1950)
STATENS SERUMINSTITUT, Copenhagen. Second memorandumon the potency evaluation of diphtheria toxoid (WHOIBSI79, October 1950)
TRÉFOUËL, J. Experiments on the standardization of diph-theria toxoid (WHO /BS /108, November 1950)
VAN DEINSE, F. & SÉNÉCHAL, Françoise. BCG on Sauton'smedium : effect of a long series of subcultures on themorphological and biological properties of BCG cultures.Bull. World Hlth Org. 1950, 2, 347 -354
WIENER, A. s. Heredity and nomenclature of the Rh -Hrblood types.* Bull. World Hlth Org. 1950, 3, 265 -278
WILSON, G. s. Minimum requirements for a tuberculosisdiagnostic laboratory (WHO /BS 1100, November 1950)
WHO Tuberculosis Research Office, Copenhagen. Presentstatus of field comparison of BCG vaccines in Copenhagenand available facilities in 1951 (WHO /BS /109, November1950)
ANNEX 10 163
Drugs Liable to produce Addiction
CORDEIRO DE PARIAS, PERNAMBUCO, P. Filho & PARREIRAS, D.
Report regarding experiments on persons smoking mari-huana cigarettes * (WHO /APD /21, April 1950) 5
EXPERT COMMITTEE ON DRUGS LIABLE TO PRODUCE ADDICTION.
Report on the second session. World Hlth Org. techn.Rep. Ser. 1950, 21
Epidemiology
Bilharziasis:
JOINT OIHP /WHO STUDY -GROUP ON BILHARZIASIS IN AFRICA.
Report on the first session.° World Hlth Org. techn. Rep.Ser. 1950, 17
WRIGHT, W. H. Bilharziasis as a public -health problem inthe Pacific. Bull. World Hlth Org. 1950, 2, 581 -595
Brucellosis:
BENDTSEN, H. A new method for staining living bacteria,spermia, etc., particularly serviceable for the preparationof brucella ring -test antigen (preliminary report) (Brucel-losis Information Series No. 3, June 1950)
BENDTSEN, H. Sensitivity of tetrazolium- stained ring testantigens (WHO /Bruc. /10, September 1950)
BOSGRA, O. Brucella abortus strain 19 vaccine dried fromthe frozen state (WHO /Bruc /22, October 1950)
CARRÈRE, L. & RENOUX, G. Trial of Copenhagen antigenfor intradermal tests on goats (WHO /Bruc /15, October1950)
CARRÈRE, L. & RENOUX, G. Trial of the ring test with goat'smilk (WHO /Bruc116, October 1950)
CASTANEDA, R. Present position regarding treatment ofhuman brucellosis (Brucellosis Information Series No. 1,June 1950)
DALRYMPLE -CHAMPNEYS, sir weldon, Results of treatingundulant fever cases in England with aureomycin andchloromycetin (WHO / Bruclll, September 1950)
JANBON, M. Considerations on the general development ofhuman brucellosis (WHO /Bruc /14, October 1950)
JOINT FAO /WHO EXPERT PANEL ON BRUCELLOSIS. Report Onthe first session (WHO /Bruc /33, December 1950)'
KAPLAN, M. M. Present knowledge of brucellosis : a sum-mary.* Bull. World Hlth Org. 1950, 3, 309 -322
KAPLAN, M. M. The preparation, standardization and useof hermatoxylin stained antigen of the Brucella abortusring test (ABR) (Brucellosis Information Series No. 4,June 1950)
b This document continues the series previously groupedunder the symbol WHO /HFD / -. Future documents in theseries will bear the symbol WHO /APD, the continuity of thenumbering remaining uninterrupted.
Issued in mimeograph form in 1949.' To be printed in 1951 after approval by the Executive
Board.
KAPLAN, M. M. The use of the Brucella abortus ring test(ABR) in the control of brucellosis in dairy cattle(Brucellosis Information Series No. 2, June 1950)
MOLINELLI, E. A. Recent developments in the therapy ofhuman brucellosis : IV. Aureomycin therapy (WHO / Brucl6,August 1950)
MORAN, B. L. Some observations on caprine brucellosis *(WHO /Bruc /12, October 1950)
RENOUX, G. Blocking antibodies in the serum of subjectsinfected with brucellosis (WHO /Bruc /13, October 1950)
Standardized Brucella abortus agglutination suspension andstandardized Brucella abortus agglutination concentrate(WHO /Bruc /20 & WHO /Bruc 121, October 1950)
Cholera:
ABDEL -AZIZ, A. Observations on the effect of anti -choleravaccination upon cholera -carriers (WHOIEpid149, October1950)
JOINT OIHP /WHO STUDY -GROUP ON CHOLERA. Report On thethird session.$ World Hlth Org. techn. Rep. Ser. 1950, 18
PANDIT, C. G. The role of the carriers in the spread of cholera(WHO /Epid /48, October 1950)
POLLITZER, R. A note on the incidence and epidemiologicalimportance of cholera carriers (WHOIEpid /50, October1950)
Communicable Diseases of Childhood:
Active immunization against common communicable diseasesof childhood : report of a group of consultants convenedby the Director -Generals World Hlth Org. techn. Rep.Ser. 1950, 6
International Epidemiology and Quarantine:
EXPERT COMMITTEE ON INTERNATIONAL EPIDEMIOLOGY AND
QUARANTINE : LEGAL SUB -COMMITTEE. Report On the firstsession (WHO /Epid /33, February 1950)
EXPERT COMMITTEE ON INTERNATIONAL EPIDEMIOLOGY AND
QUARANTINE : LEGAL SUB -COMMITTEE. Report on thesecond session (WHOIEpid/34, April 1950)
Draft International Sanitary Regulations (WHOIEpid/35,April 1950)
Annex A to Draft International Sanitary Regulations -Provisions for the sanitary control of pilgrim traffic ap-proaching or leaving the Hedjaz during the season of thepilgrimage (WHOIEpid136, April 1950)
Annex B to Draft International Sanitary Regulations -Provisions on safety and sanitary standards for pilgrimships and for aircraft carrying pilgrims (WHO /Epid /37,April 1950)
Table of comparison between the two texts of the DraftInternational Sanitary Regulations (WHO /Epid /41, Sep-tember 1950)
8 Issued in mimeograph form in 1949.
164 WORK OF WHO, 1950
Comparative table of the provisions of the InternationalSanitary Conventions and of the Draft InternationalSanitary Regulations (WHO /Epid/42, September 1950)
Draft International Sanitary Regulations - Comments andsuggestions concerning the draft drawn up by the ExpertCommittee, from governments and interested internationalorganizations (WHO /Epid /44 & Add. 1, Add. 2, Add. 3,September 1950 ; WHO /Epid /47, October 1950)
Legality of quarantine measures directed against non- pesti-lential communicable diseases in international traffic(WHO /Epid /45, September 1950)
EXPERT COMMITTEE ON INTERNATIONAL EPIDEMIOLOGY AND
QUARANTINE : LEGAL SUB -COMMITTEE. Third report 9 (WHO/
Epid /39, August 1950)
EXPERT COMMITTEE ON INTERNATIONAL EPIDEMIOLOGY AND
QUARANTINE. Report on the third session (WHO /Epid 151Rev. 1 & Corr. 1, October 1950)
EXPERT COMMITTEE ON INTERNATIONAL EPIDEMIOLOGY AND
QUARANTINE : SECTION ON QUARANTINE. Report On thethird session (WHO /Q/38 Rev. 1, October 1950)
Draft WHO Regulation No. 2 - International SanitaryRegulations 10 (WHO /Epid 153 & Corr. 1, November 1950)
Draft WHO Regulation No. 2 - International SanitaryRegulations Annex A10 (WHOIEpid154, November 1950)
Draft WHO Regulation No. 2 - International SanitaryRegulations Annex B 10 (WHOIEpid/55, November 1950)
EXPERT COMMITTEE ON INTERNATIONAL EPIDEMIOLOGY AND
QUARANTINE : LEGAL SUB -COMMITTEE. Fourth report (thirdsession) (WHO /Epid /56, November 1950)
Plague:
A note on the possibility of using DDT as a rodenticide(WHO /Epid /43, September 1950)
Deratization of ships with the aid of rodenticides (WHO /Q/33 & Add. 1, October 1950)
EXPERT COMMITTEE ON PLAGUE. Report on the first session."World Hlth Org. techn. Rep. Ser. 1950, 11
JORDAN, K. Notes on a collection of fleas from Peru. Bull.World Hlth Org. 1950, 2, 597 -609
POLLITZER, R. A note on the use of anti -coagulants for ratextermination.* Bull. World Hlth Org. 1950, 3, 343 -345
POLLITZER, R. The behaviour of plague bacilli in glycerineand rhamnose media * ( WHO/Plague/15, November 1950)
ScHuLZ, K. H. Control of plague in Taranto, Italy, 1945 /1946: An account of a successful programme of rodentextermination. Bull. World Hlth Org. 1950, 2, 675 -685
9 Agreement on the points mentioned in this report wasreached by correspondence.
I° Printed and distributed to governments as a workingpaper for the special committee of the Health Assembly dueto meet in April 1951.
"Issued in mimeograph form in 1949.
Poliomyelitis:
The incidence of poliomyelitis in the world 1947 -1949. Epidem.vital. Stat. Rep. 1950, 1, 3 -26
Q Fever:
SIDKY, M. M. Epidemiology of Q Fever. Bull. World HlthOrg. 1950, 2, 563 -579
Q fever (WHO /loon /6, November 1950)
Rabies:
AHUJA, M. L. The incidence of rabies virus in embryonatedduck eggs * (WHO /Rabies /7, March 1950)
BLACK, J. & KOPROWSKI, H. Street rabies virus one yearafter vaccination with either avianized chick embryovaccine or phenolized veterinary vaccine * (WHO /Rabies 15,March 1950)
EXPERT COMMITTEE ON RABIES. Report on the first session.World Hlth Org. techn. Rep. Ser. 1950, 28
Guide to the preventive treatment of rabies * (WHO /Rabies /4,March 1950)
HABEL, K. Progress in the development of new types ofrabies vaccines for use in humans * (WHO /Rabies /9, March1950)
RABEL, K. Ten years experience with mouse potency testsfor rabies vaccines * (WHO /Rabies /8, March 1950)
JOHNSON, H. N. Incidence of rabies in the United Statesof America * (WHO /Rabies /12, April 1950)
KAPLAN, M. M. Considerations with regard to a WHO -sponsored field demonstration for the control of rabies indogs, utilizing the Flury vaccine (WHO /Rabies/14 Rev. 1,April 1950)
KLIMT, C. R. & GRAB, B. Note on the planning of a fieldtrial of antirabies hyperimmune serum (WHO /Rabies/13& Corr. 1, April 1950)
KOPROWSKI, H., VAN DER SCHEER, J., BLACK, Ch. E. & BLACK, J.
Antiserum in rabies - use of hyperimmune antirabiesserum -concentrates in experimental rabies and indicationsfor its use after exposure of humans to rabies * (WHO/Rabies /2, March 1950)
KOPROWSKI, H. & BLACK, J. Studies on chick -embryo adaptedrabies virus - II. Pathogenicity for dogs and use of egg -adapted strains for vaccination purposes * (WHO /Rabies /3,March 1950)
Notes on the incidence of rabies in Latin America * (WHO/Rabies/16, April 1950)
POWELL, H. M. & CULBERTSON, C. G. Cultivation of fixedrabies virus in embryonated duck eggs * (WHO /Rabies /6,March 1950)
Statistics of rabies in man (WHO /Rabies /15, April 1950)
Summary of replies to questionnaire on rabies - part Iand part II (WHO /Rabies/l1 Part I & Part II, April 1950 ;WHO /Rabies /11 Add. 1 ; WHO /Rabies /11 Add. 1 Erratum,June 1950)
ANNEX 10 165
ZEISSIG, A. Control of rabies in foxes in New York State ''(WHO /Rabies /10, March 1950)
Rickettsioses:
FREYCHE, M. J. & DEUTSCHMAN, Z. Human rickettsioses inAfrica. Epidem. vital Stat. Rep. 1950, 7 -8, 160 -195
JOINT OIHP /WHO STUDY -GROUP ON AFRICAN RICKETTSIOSES.Report on the first session.'a World Hlth Org. techn.Rep. Ser. 1950, 23
Smallpox: 's
KRISHNAMURTHY, V. N. Studies on the effects of penicillin,and streptomycin on vaccine lymph (calf lymph) underdifferent conditions * (WHO /Smallpox /2, March 1950)
Trachoma:
FREYCHE, M. J. Antibiotics and sulfonamides in the treatmentof trachoma. Bull. World Hlth Org. 1950, 2, 523 -544
Yellow fever:
YELLOW -FEVER PANEL. Report on the first session.14 WorldHIM Org. techa. Rep. Ser. 1950, 19
Zoonoses:
BENGSTON, H. The control of tuberculosis in cattle (WHO!Zoon /3, November 1950)
BLOOD, B. D. The control of hydatidosis (WHO /Zoon /7,December 1950)
JOINT WHO /FAO EXPERT GROUP ON ZOONOSES. Report Onthe first session l' (WHO /Zoon /15 Rev. 1, December 1950)
KAPLAN, M. M. Reduction of anthrax in agriculture andindustry (WHO /Zoon /8, December 1950)
KAPLAN, M. M. The control of tuberculosis in cattle (WHO!Zoon /10, December 1950)
KAPLAN, M. M. The control of tuberculosis in cattle (WHO!Zoon /11, December 1950)
MENDY, R. M. Animal tuberculosis in Argentina 18 (WHO!Zoon /14, December 1950)
STEELE, J. H. The control of bovine tuberculosis - Bovinetuberculosis in the United States (WHO /Zoon/4, November1950)
YOUNG, J. A. & STUART PATERSON, J. The control of tuber-culosis in cattle (WHO /Zoon /12, December 1950)
12 Document WHO /Typhus /2, listed in the Annual Report ofthe Director -General for 1949 (Off. Rec. World Hlth Org. 24,96) is the report on a preparatory meeting of the study -group,held in Paris, 26 -28 September 1949. The technical contentof that report is included in the report of the study -group onits first session.
18 See also under Biological Standardization.14 Issued in mimeograph form in 1949.16 To be printed in 1951 after approval by the Executive
Board.16 Exists only in English and in Spanish.
Health Statistics
Application of International Statistical Classification ofDiseases, Injuries and Causes of Death to hospital mor-bidity statistics (WHO /HS /Hosp.Stat /6, April 1950)
CLEMMESEN, s. Essentials of cancer sociology (WHO /HS/CANC /11, February 1950)
DENOIx, P. F. Statistical survey of the therapeutic resultsachieved in cancerology (WHO /HS /CANC /S, February1950)
DUNHAM, Ethel c. Problems relating to collection of vitalstatistics on prematurity (WHO /HS /STDEF /5, February1950)
DUNN, H. L. United States' experience with the Sixth Revi-sion of the International Statistical Classification of Diseases,Injuries and Causes of Death (WHO /HS124, April 1950)
EXPERT COMMITTEE ON HEALTH STATISTICS. Report On thefirst session.'' World Hlth Org. techn. Rep. Ser. 1950, 5
EXPERT COMMITTEE ON HEALTH STATISTICS. Report On thesecond session, including reports on the first sessions ofthe sub -committees on Definition of Stillbirth, Registra-tion of Cases of Cancer, Hospital Statistics. World HlthOrg. techn. Rep. Ser. 1950, 25
PASCUA, M. Deaths by cause, sex and age in some non -European countries. Epidem. vital Stat. Rep. 1950, 11,272 -274
PASCUA, M. Evolution of mortality in Europe during thetwentieth century. Epidem. vital Stat. Rep. 1950, 2 -3,30 -62
PASCUA, M. Natality, mortality, infant mortality in 1949.Epidem. vital Stat. Rep. 1950, 6, 126 -134
Questions regarding the International Statistical Classifica-tion of Diseases, Injuries and Causes of Death (WHO /HS/23, April 1950)
SIGURJÓNSSON, J. Trend of infant mortality in Iceland.Bull. World Hlth Org. 1950, 2, 723 -730
STOCKS, P. Contributions of statistics to world health.Bull. World Hlth Org. 1950, 2, 731 -741
STOCKS, P. Interpretation of rules for death coding (WHO/HS /22, March 1950)
STOCKS, P. Report on the definition of stillbirth and abortion(WHO /HS /STDEF /4, February 1950)
US NATIONAL COMMITTEE ON VITAL AND HEALTH STATISTICS,
Proposed definitions of live birth and fetal death (WHO/HS /STDEF /3, February 1950)
17 Issued in mimeograph form in 1949.
166 WORK OF WHO, 1950
Malaria and Insecticides 18
ALESSANDRINI, Maria E. Residual DDT content : A rapidmethod for the detection and determination of smallquantities of DDT on sprayed surfaces. Bull. WorldHlth Org. 1950, 2, 629 -636
ANNECKE, s. Economic importance of malaria (WHOIMall57, October 1950)
ANNECKE, s. Report on malaria control in Transvaal (WHO/Ma1/58, October 1950)
BERNARD, P. Malaria control in Madagascar (WHO /Mal /52'October 1950)
BLAIR, D. M. Report on malaria control in Southern Rhodesia(WHO /Ma1/49, October 1950)
BRUCE -CHWATT, L. J. Malaria in pregnancy and infancyin the African population of Southern Nigeria (WHO!Ma1/62, November 1950)
BRUCE -CHWATT, L. J. Summary on malaria in Nigeria (WHO!Ma1/43, August 1950)
BRUCE -CHWATT, L. J. The Ilaro experimental vector specieseradication scheme by residual insecticide spraying *(WHO /Ma1/40, May 1950)
BRUCE -CHWATT, L. J. & KEE HOOK COI. Report On trials onaircraft disinsectization in West Africa * (WHO ¡Insecti-cides 16, May 1950)
CAMBOURNAC, F. J. C. Le paludisme au Portugal 19 (WHO!Ma1/35, February 1950)
CAMBOURNAC, F. J. c. Report on malaria in EquatorialAfrica (WHO /Mal /58, October 1950 & WHO /Mal /58Annexes,E° November 1950)
COVELL, sir G. The therapeutics of malaria in Africa (WHO!Mal/53, October 1950)
DAVIDOVICI, S., LEVINSON, Z. & REUTER, S. The toxicity ofDDT -Lanoline residues to flies and mosquitos * (WHO/Ma1/37, March 1950)
DOWLING, M. A. c. Report on programme of malaria eradica-tion scheme - Colony of Mauritius (WHO /Mal134,February 1950)
ELLIOTT, R. Some observations tending to suggest a recentdecrease in immunity to malaria in the population ofFreetown (WHO /Ma1/55, October 1950)
EXPERT COMMITTEE ON INSECTICIDES. Report on the firstsession.21 World HIM Org. techn. Rep. Ser. 1950, 4
EXPERT COMMITTEE ON INSECTICIDES. Report on the secondsession 22 (WHO /Insecticides /11, November 1950)
18 See also under Epidemiology -Plague.19 Exists only in French.20 Annexes exist only in French.21 Issued in mimeograph form in 1949.
EXPERT COMMITTEE ON MALARIA. Report on the third ses -sion.21 World Hlth Org. techn. Rep. Ser. 1950, 8
EXPERT COMMITEE ON MALARIA. Report on the fourth Ses-sion 22 (WHO /Mal /70, December 1950)
FARINAUD, M. E. & CHOUMARA, R. Le paludisme dans les Popu-lations Montagnardes du Sud- Indochinois 23 (WHO /Mal/44 & Add. 1, August, 1950)
GARNHAM, P. C. c. Note on some residual insecticide trialsfor malaria control in East Africa (WHO/Mal156, October1950)
HERTIG, M. Observations on the density of phlebotomuspopulations following DDT campaigns. Bull. WorldHlth Org. 1950, 2, 621 -628
HOLSTEIN, M. M. Note on malaria epidemiology in FrenchWest Africa (WHO /Ma1/50, October 1950)
MACDONALD, G. Malaria transmission rates and infantparasite rates (WHO /Mal /59, October 1950)
MACDONALD, G. The economic importance of malaria inAfrica (WHO!Mal /60, October 1950)
MAD WAR, S. & EL SHAWARBY. A short report on the eradica-tion of Anopheles sergenti from the cases in Egypt, 1946-1948 * (WHO/Mal139, April 1950)
MASTBAUM, o. Field experiments with DDT emulsion andwettable DDT, with special reference to malaria incidencein Swaziland during the transmission season 1949/50(WHOIMal/51, October 1950)
MEILLON, E. de. Species and subspecies of vectors and theirbionomics (WHOIMal 154, October 1950)
PAMPANA, E. Large -scale malaria control campaigns usingresidual insecticides (WHO /Mal /46, October 1950 ; WHO!Mal /46 Add. 1, November 1950)
Summary review of literature on camoquin * (WHO /Ma1/38& Corr. 1, April 1950)
VARGAS, L. Malaria along the Mexico - United States Border.Bull. World Hlth, Org. 1950, 2, 611 -620
VINCE, I. H. Malaria control by means of DDT in Katanga(1947 -1950) (WHO /Mal /47, October 1950)
Maternal and Child Health 24
DOWNS, Elinor F. Cyanosis of infants caused by highnitrate concentrations in rural water- supplies.25 Bull.World Hlth Org. 1950, 3, 165 -169 *
EXPERT COMMITTEE ON SCHOOL HEALTH SERVICES. Reporton the first session 26 (WHO /MCH /23, December 1950)
22 To be printed in 1951 after approval by the ExecutiveBoard.
23 Exists only in French.24 See also under Epidemiology- Communicable Diseases
of Childhood.25 Issued in mimeograph form in 1949.26 To be printed in 1951 after approval by the Executive
Board.
ANNEX 10 167
EXPERT GROUP ON PREMATURITY. Final report. World HlthOrg. techn. Rep. Ser. 1950, 27
Is a birth weight of 2,500 gm. or less a satisfactory criterionor prematurity ? (WHO /MCH /17, March 1950)
Problems relating to collection of vital statistics on pre-maturity (WHO /MCH/I8, February 1950)
The health of the school age child (WHO /MCHl22, July 1950)
What information is available on the incidence of prema-turity ? (WHO /MCH /16, March 1950)
Mental Health
BOVET, L. Les aspects psychiatriques de la délinquancejuvénile.s7 Bull. World Hlth Org. 1950, 3, 63 -162
EXPERT COMMITTEE ON MENTAL HEALTH. Report on the firstsession." World Hlth Org. techn. Rep. Ser. 1950, 9
EXPERT COMMITTEE ON MENTAL HEALTH. Report on the secondsession 29 (WHO /Ment /17, October 1950)
GUTTMACHER, M. S. Psychiatric examination of offenders.30Bull. World Hlth Org. 1950, 2, 743 -749
JELLINEK, E. M. Classification of the drinkers (WHO /Meat/20, December 1950)
JELLINEK, E. M. Estimates of number of " alcoholics " andrates of alcoholics per 100,000 adult population (20 yearsand older) for certain countries (WHO /Mentl21, December1950)
Nursing
EXPERT COMMITTEE ON NURSING. Report On the first session.World Hlth Org. techn. Rep. Ser. 1950, 24
Workers required to meet family health and welfare needs :Pilot study (INTINurs /2, December 1950)
Nutrition
JOINT FAO /WHO EXPERT COMMITTEE ON NUTRITION. Reporton the first session.30 World Hlth Org. techn. Rep. Ser.1950, 16
Occupational Health
JOINT ILO /WHO COMMITTEE ON THE HYGIENE OF SEAFARER:Report on the first session. World HIM Org. techn. Rep.Ser. 1950, 20
JOINT ILO /WHO EXPERT COMMITTEE ON OCCUPATIONAL HEALTH.
Report on the first session (WHO /Occ.Health /2, Sep-tember 1950)
27 Published in French and in English as World Health Orga-nization: Monograph Series No. 1.
S8 Issued in mimeograph form in 1949.29 To be printed in 1951 after approval by the Executive
Board.30 Issued in mimeograph form in 1949.
Organization of Public -Health Services
EXPERT COMMITTEE ON ENVIRONMENTAL SANITATION. Reporton the first session.31 World Hlth Org. techn. Rep. Ser.1950, 10
Professional and Technical Education
EXPERT COMMITTEE ON PROFESSIONAL AND TECHNICAL EDUCA-
TION OF MEDICAL AND AUXILIARY PERSONNEL. Reporton the first session. World Hlth Org. techn. Rep, Ser.1950, 22
Tuberculosis 32
COCCHI, C. & PASQUINUCCI, G. Treatment of tuberculousmeningitis : a summary of three years' experience atFlorence.* Bull. World Hlth Org. 1950, 3, 215 -264
EXPERT COMMITTEE ON TUBERCULOSIS. Report on the fourthsession. S3 World Hlth Org. techa. Rep. Ser. 1950, 7
EXPERT COMMITTEE ON TUBERCULOSIS. Report On the fifthsession 84 (WHO /TBC/37, October 1950)
Le programme de lutte antituberculose en Tunisie 36 (WHO/TBC/41, December 1950)
MCDOUGALL, J. B. Inexpensive buildings in the treatment oftuberculosis.* Bull. World Hlth Org. 1950, 3, 337 -342
MCDOUGALL, J. B. Role and responsibilities of the generalhospital in the treatment of tuberculosis.* Bull. WorldHlth Org. 1950, 3, 325 -335
MCDOUGALL, J. B. Tuberculosis mortality, 1937 to 1949.Epidenz. vital Stat. Rep. 1950, 10, 241 -250
The tuberculosis control problem in Luxembourg (WHOITBC /40, December 1950)
The tuberculosis control programme in Sweden * (WHO/TBCJ30 & Corr. I, December 1950)
Tuberculosis in South Korea * (WHOITBC/29, May 1950)
USTVEDT, H. J. Local reaction in BCG vaccination. Bull.World Hlth Org. 1950, 2, 441 -468
USTVEDT, H. J. Technique of tuberculin- testing : A compar-ative study. Bull. World Hlth Org. 1950, 2, 355 -440
USTVEDT, H. J. Tuberculosis disease in BCG -vaccinatedindividuals. Bull. World Hlth Org. 1950, 2, 469 -514
31 Issued in mimeograph form in 1949.32 See also under Biological Standardization.33 Issued in mimeograph form in 1949.34 To be printed in 1951 after approval by the Executive
Board.35 Exists only in French.
168 WORK OF WHO, 1950
Unification of Pharmacopoeias
EXPERT COMMITTEE ON THE UNIFICATION OF PHARMACOPOEIAS.
Report on the fourth session.38 World Hlth Org. techn.Rep. Ser. 1950, 1
EXPERT COMMITTEE ON THE UNIFICATION OF PHARMACOPOEIAS.
Report on the fifth session.88 World Hlth Org. techn.Rep. Ser. 1950, 12
EXPERT COMMITTEE ON THE UNIFICATION OF PHARMACOPOEIAS.
Report on the sixth session.88 World Huth Org. techn.Rep. Ser. 1950, 29
EXPERT COMMITTEE ON THE UNIFICATION OF PHARMACOPOEIAS.
Report on the seventh session 37 (WHOfPharm /125,November 1950)
EXPERT COMMITTEE ON THE UNIFICATION OF PHARMACOPOEIAS :
SUB -COMMITTEE ON NON -PROPRIETARY NAMES. Report Onthe first session 37 (WHO /Pharm /126, November 1950)
Veneral Diseases and Treponematoses
Applications for the proposed International SerodiagnosticLaboratory Conference 1951 -1952 ( WHO/ VD /SERO /9,August 1950 & WHO!VD /SERO /9 Add. 1, September1950)
BEKIERKUNST, A. & MILGROM, F. Complement fixation re-actions with cardiolipin antigen compared with Kahnreactions.38 Bull. World Hlth Org. 1950, 2, 687 -688
Cardiolipin antigens (WHO /VD /SERO /10, October 1950)
COUTTS, W. E. Lymphogranuloma venereum: A generalreview. Bull. World HIM Org. 1950, 2, 545 -562
COUTTS, W. E., DEGOS, R., HELLESTROM, S., HERMANS, E. H.MCELLIGOTT, G. L. M., MAHONEY, J. F., NAGI, I. H. & RAJAM,R. V. Minimum penicillin therapy in the treatment oftreponemai infections by WHO /UNICEF field teams(WHO /VD /72, December 1950)
CUTLER, J. C. Survey of venereal diseases in Afghanistan 3°Bull. World Hlth Org. 1950, 2, 689 -703
EXPERT COMMITTEE ON VENEREAL INFECTIONS. Report on thethird session.89 World Huth Org. techn. Rep. Ser. 1950, 13
EXPERT COMMITTEE ON VENEREAL INFECTIONS : SUB -COMMITTEE
ON SEROLOGY AND LABORATORY ASPECTS. Report on thefirst session." World Hlth Org. techn. Rep. Ser. 1950, 14
EXPERT COMMITTEE ON VENEREAL INFECTIONS AND TREPO-NEMATOSES : SUB -COMMITTEE ON SEROLOGY AND LABORATORY
ASPECTS. Report on the second session 4° (WHO!VD /73,November 1950)
36 Issued in mimeograph form in 1949.S7 To be printed in 1951 after approval by the Executive
Board.38 Issued in mimeograph form in 1949.39 Issued in mimeograph form in 1949.
Information on early sero -laboratory conferences (WHO!VD /SERO /2, August 1950 & WHO /VD /SERO 12 Add. 1& Add. 2, September 1950)
International Serodiagnostic Laboratory Conference : Reporton preliminary survey (WHO!VDISERO 14, August 1950)
International symposium on syphilis : Section I. Earlysyphilis (WHO!VD167, October 1950)
International symposium on syphilis : Section II. Prenataland infantile syphilis (WHO!VD168, October 1950)
International symposium on syphilis : Section III. Neuro-syphilis (WHO/ VDl69, October 1950)
International symposium on syphilis : Section IV. Serologyin syphilis (WHO!VD /70, October 1950)
Laboratory activities in a serologic testing phase of the WHOprogramme (WHO /VD /SERO /3, August 1950 & WHO!VD /SERO13 Add. 1, September 1950)
Preliminary report on serologic methods in the world labora-tories in Member States and their serological methods(WHO!VD,SERO /7, August 1950 & WHO /VD /SERO /7Add. 1, September 1950)
Preliminary serological report of the WHO venereal- diseasedemonstration team, Simla (India) (WHO! VD /SEROl6,August 1950 & WHO /VD /SERO /6 Add. 1, September 1950)
Production and control of cardiolipin lecithin (WHO!VD/SERO 11, July 1950)
Reference list : BAL (British anti- lewisite), 2,3- dimercapto-propanol in toxic manifestations resulting from usage ofmetallic compounds (arsenicals, gold, mercury etc.) *( WHO/VD /58, February 1950)
Reference list : Non- specific urethritis, including Reiter'sdisease (WHO!VD165, May 1950)
Reference list : Penicillin in early syphilis (WHO /VD160,February 1950)
Reference list : Penicillin in latent and late syphilis, includingcardiovascular syphilis (WHO!VD /63. February 1950)
Reference list : Penicillin in neurosyphilis (WHO!VD /61,February 1950)
Reference list : Penicillin in syphilis - general (WHO /VD/59, February 1950)
Reference list : Penicillin in the treatment of yaws (WHO!VD /56, February 1950)
40 To be printed in 1951 after approval by the ExecutiveBoard.
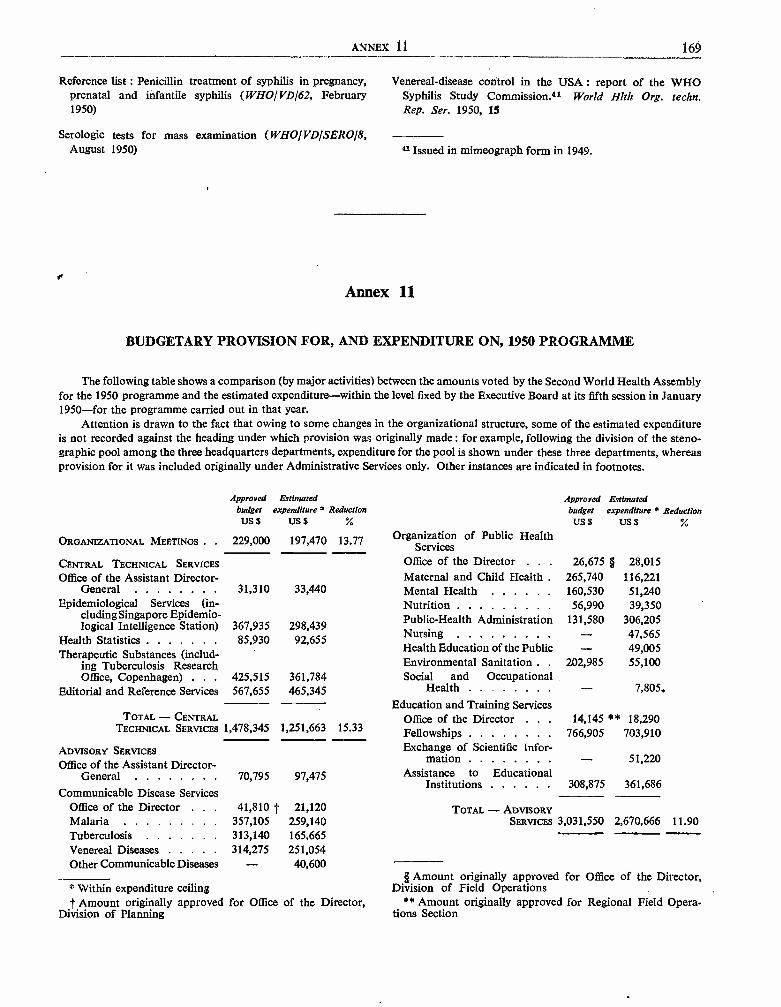
ANNEX 11 169
Reference list : Penicillin treatment of syphilis in pregnancy, Venereal- disease control in the USA : report of the WHOprenatal and infantile syphilis (WHO /VD /62, February Syphilis Study Commission.41 World Hlth Org. techn.1950) Rep. Ser. 1950, 15
Serologic tests for mass examination (WHO /VD /SERO 18,August 1950) 91 Issued in mimeograph form in 1949.
Annex 11
BUDGETARY PROVISION FOR, AND EXPENDITURE ON, 1950 PROGRAMME
The following table shows a comparison (by major activities) between the amounts voted by the Second World Health Assemblyfor the 1950 programme and the estimated expenditure -within the level fixed by the Executive Board at its fifth session in January1950 -for the programme carried out in that year.
Attention is drawn to the fact that owing to some changes in the organizational structure, some of the estimated expenditureis not recorded against the heading under which provision was originally made : for example, following the division of the steno-graphic pool among the three headquarters departments, expenditure for the pool is shown under these three departments, whereasprovision for it was included originally under Administrative Services only. Other instances are indicated in footnotes.
Approved Estimatedbudget expenditure' ReductionUS$ US$ %
ORGANIZATIONAL MEETINGS . . 229,000 197,470 13.77
ApprovedbudgetUS$
Organization of Public HealthServices
Estimatedexpenditure a Reduction
US$
CENTRAL TECHNICAL SERVICES Office of the Director . . 26,675 § 28,015
Office of the Assistant Director - Maternal and Child Health . 265,740 116,221General 31,310 33,440 Mental Health 160,530 51,240
Epidemiological Services (in- Nutrition 56,990 39,350cluding Singapore Epidemio-logical Intelligence Station) 367,935 298,439
Public- Health Administration 131,580 306,205
Health Statistics 85,930 92,655 Nursing - 47,565
Therapeutic Substances (includ- Health Education of the Public - 49,005
ing Tuberculosis Research Environmental Sanitation . . 202,985 55,100Office, Copenhagen) . . . 425,515 361,784 Social and Occupational
Editorial and Reference Services 567,655 465,345 Health -Education and Training Services
7,805,
TOTAL - CENTRAL Office of the Director . . . 14,145 ** 18,290TECHNICAL SERVICES 1,478,345 1,251,663 15.33 Fellowships 766,905 703,910
ADVISORY SERVICES Exchange of Scientific Infor-Office of the Assistant Director - mation - 51,220
General 70,795 97,475 Assistance to EducationalInstitutions 308,875 361,686
Communicable Disease ServicesOffice of the Director 41,810 t 21,120 TOTAL - ADVISORYMalaria 357,105 259,140 SERVICES 3,031,550 2,670,666 11.90Tuberculosis 313,140 165,665Venereal Diseases 314,275 251,054Other Communicable Diseases 40,600
* Within expenditure ceilingt Amount originally approved for Office of the Director,
Division of Planning
§ Amount originally approved for Office of the Director,Division of Field Operations
** Amount originally approved for Regional Field Opera-tions Section
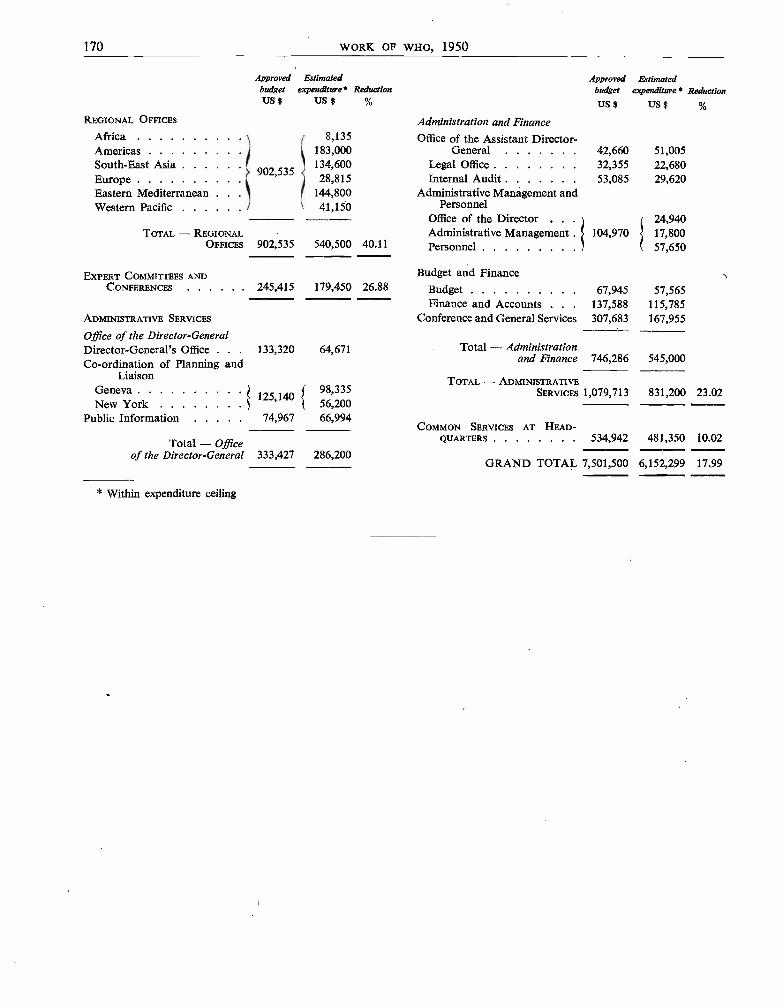
170 WORK OF WHO, 1950
REGIONAL OFFICES
ApprovedbudgetUS $
Estimatedexpenditure*
US $Reduction
Approvedbudget
US$
Administration and Finance
Estimatedexpenditure* Reduction
US$
Africa 8,135 Office of the Assistant Director -Americas 183,000 General 42,660 51,005South -East AsiaEurope
902,535134,60028,815
Legal Office 32,355Internal Audit 53,085
22,68029,620
Eastern Mediterranean 144,800 Administrative Management andWestern Pacific 41,150 Personnel
Office of the Director . . . 24,940TOTAL - REGIONAL Administrative Management . 104,970 17,800
OFFICES 902,535 540,500 40.11 Personnel 57,650
EXPERT COMMITTEES AND Budget and FinanceCONFERENCES 245,415 179,450 26.88 Budget 67,945 57,565
Finance and Accounts . . . 137,588 115,785ADMINISTRATIVE SERVICES Conference and General Services 307,683 167,955
Office of the Director - GeneralDirector -General's Office . . . 133,320 64,671 Total - AdministrationCo- ordination of Planning and and Finance 746,286 545,000
Liaison TOTAL - ADMINISTRATIVEGeneva
125,14098,335 SERVICES 1,079,713 831,200 23.02
New York 56,200Public Information 74,967 66,994
COMMON SERVICES AT HEAD-
Total - Office QUARTERS 534,942 481,350 10.02
of the Director- General 333,427 286,200GRAND TOTAL 7,501,500 6,152,299 17.99
* Within expenditure ceiling
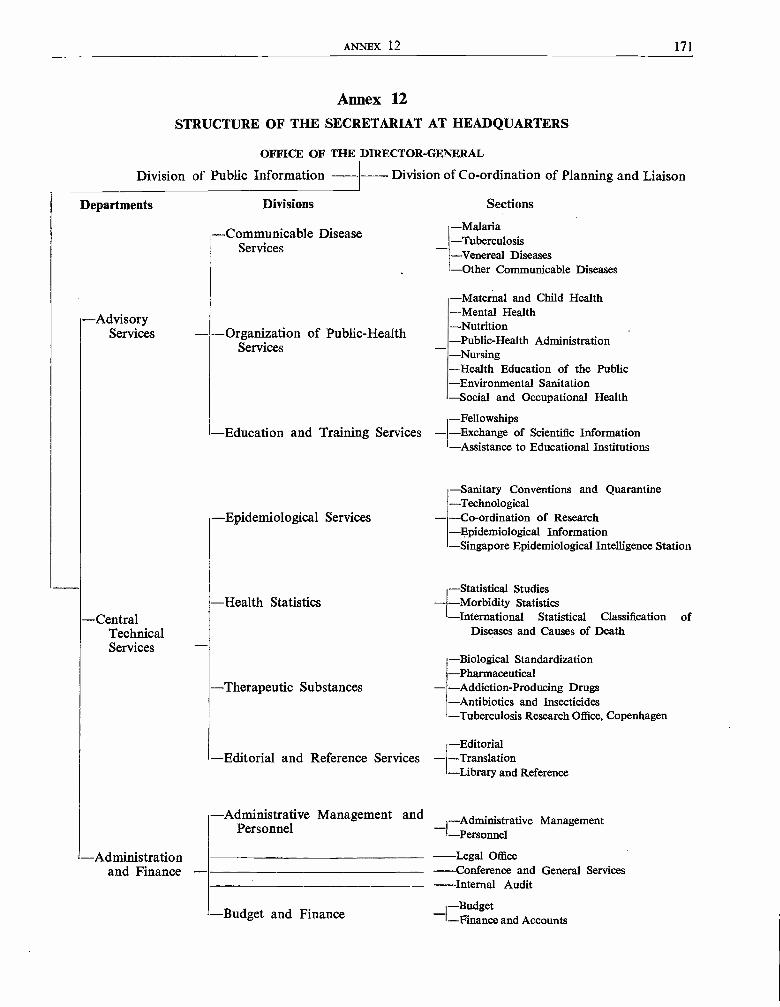
ANNEX 12 171
Annex 12STRUCTURE OF THE SECRETARIAT AT HEADQUARTERS
OFFICE OF THE DIRECTOR -GENERAL
Division of Public Information
Departments
-AdvisoryServices
-CentralTechnicalServices
-Administrationand Finance
-- Division of Co- ordination of Planning and Liaison
Divisions Sections
-Communicable DiseaseServices
- Organization of Public- HealthServices
-Education and Training Services -
-Epidemiological Services
-Health Statistics
-Therapeutic Substances
-Editorial and Reference Services -
-Administrative Management andPersonnel
-Budget and Finance
-Malaria-Tuberculosis-Venereal Diseases-Other Communicable Diseases
-Maternal and Child Health-Mental Health-Nutrition-Public -Health Administration-Nursing-Health Education of the Public-Environmental Sanitation-Social and Occupational Health
-Fellowships-Exchange of Scientific Information- Assistance to Educational Institutions
-Sanitary Conventions and Quarantine-Technological-Co- ordination of Research-Epidemiological Information-Singapore Epidemiological Intelligence Station
-Statistical Studies-Morbidity Statistics-International Statistical Classification of
Diseases and Causes of Death
-Biological Standardization-Pharmaceutical- Addiction- Producing Drugs-Antibiotics and Insecticides-Tuberculosis Research Office, Copenhagen
-Editorial-Translation-Library and Reference
Administrative Management_1-Administrative
-Legal Office-Conference and General Services-- Internal Audit
-Budget-I-Finance and Accounts
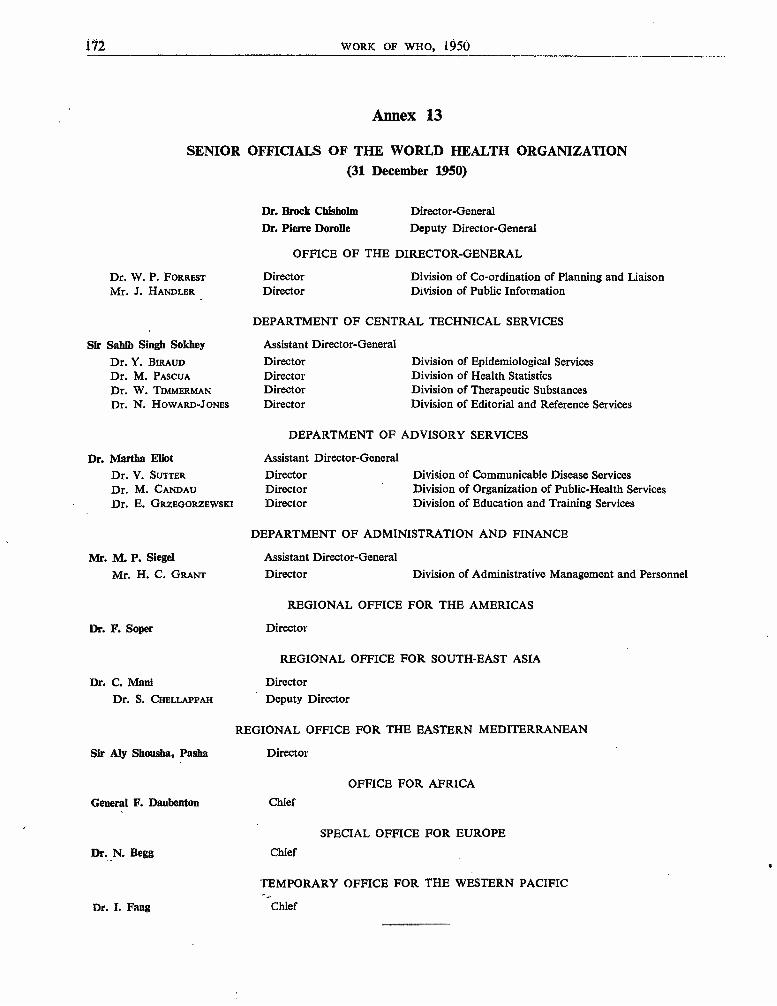
172 WORK OF WHO, 1950
Annex 13
SENIOR OFFICIALS OF THE WORLD HEALTH ORGANIZATION(31 December 1950)
Dr. W. P. FORRESTMr. J. HANDLER
Sir Sahib Singh SokheyDr. Y. BIRAUDDr. M. PASCUADr. W. TIMMERMANDr. N. HOWARD -JONES
Dr. Martha EliotDr. V. SUTTERDr. M. CANDAUDr. E. GRZEGORZEWSKI
Mr. M. P. SiegelMr. H. C. GRANT
Dr. F. Soper
Dr. C. ManiDr. S. CHELLAPPAH
Sir My Shousba, Pasha
General F. Daubenton
Dr. N. Begg
Dr. I. Fang
Dr. Brock Chisholm
Dr. Pierre Dorolle
Director -General
Deputy Director - General
OFFICE OF THE DIRECTOR -GENERAL
DirectorDirector
Division of Co- ordination of Planning and LiaisonDivision of Public Information
DEPARTMENT OF CENTRAL TECHNICAL SERVICES
Assistant Director - General
DirectorDirectorDirectorDirector
Division of Epidemiological ServicesDivision of Health StatisticsDivision of Therapeutic SubstancesDivision of Editorial and Reference Services
DEPARTMENT OF ADVISORY SERVICES
Assistant Director- GeneralDirectorDirectorDirector
Division of Communicable Disease ServicesDivision of Organization of Public -Health ServicesDivision of Education and Training Services
DEPARTMENT OF ADMINISTRATION AND FINANCE
Assistant Director- General
Director Division of Administrative Management and Personnel
REGIONAL OFFICE FOR THE AMERICAS
Director
REGIONAL OFFICE FOR SOUTH -EAST ASIA
Director
Deputy Director
REGIONAL OFFICE FOR THE EASTERN MEDITERRANEAN
Director
OFFICE FOR AFRICA
Chief
SPECIAL OFFICE FOR EUROPE
Chief
TEMPORARY OFFICE FOR THE WESTERN PACIFIC
Chief
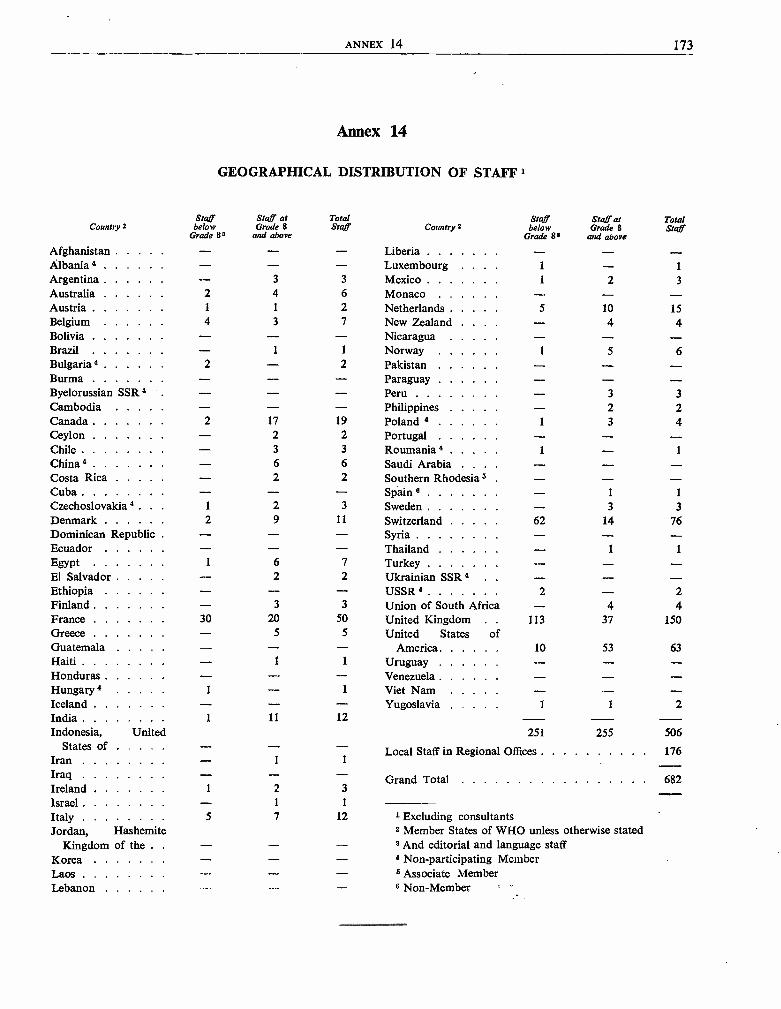
ANNEX 14 173
Annex 14
GEOGRAPHICAL DISTRIBUTION OF STAFF 1
Staff Staff at Total Staff Staff at TotalCountry 2 below Grade 8 Staff Country 2 below Grade B Staff
Grade 8a and above Grade 8= and above
Afghanistan - - - Liberia - - -Albania 4 - - Luxembourg 1 - 1
Argentina - 3 3 Mexico 1 2 3
Australia 2 4 6 Monaco - - -Austria 1 1 2 Netherlands 5 10 15Belgium 4 3 7 New Zealand - 4 4Bolivia - - - Nicaragua - - -Brazil - 1 1 Norway 1 5 6Bulgaria 4 2 - 2 Pakistan - -- -Burma - - - Paraguay - - -Byelorussian SSR 4 . - - Peru - 3 3Cambodia - - - Philippines - 2 2Canada . 2 17 19 Poland 4 1 3 4Ceylon - 2 2 Portugal - - -Chile - 3 3 Roumania 4 1 - 1
China 4 - 6 6 Saudi Arabia . . . - - -Costa Rica - 2 2 Southern Rhodesia s - -Cuba . . . . . . - - - Spain e - 1 1
Czechoslovakia 4. 1 2 3 Sweden - 3 3Denmark 2 9 11 Switzerland 62 14 76Dominican Republic - - - Syria - - -Ecuador - - - Thailand - 1 1
Egypt 1 6 7 Turkey - - -El Salvador - 2 2 Ukrainian SSR 4 - - -Ethiopia - - - USSR 4 2 - 2Finland - 3 3 Union of South Africa - 4 4France 30 20 50 United Kingdom 113 37 150Greece - 5 5 United States ofGuatemala - - - America 10 53 63Haiti . . 1 1 Uruguay - - -Honduras - - - Venezuela - - -Hungary 4 1 - 1 Viet Nam - - -Iceland - - - Yugoslavia 1 1 2India 1 11 12 -Indonesia, United 251 255 506
States of - "- - Local Staff in Regional Offices 176Iran - 1 1
Iraq - - - Grand Total 682Ireland 1 2 3
Israel - 1 1
Italy 5 7 12 1 Excluding consultantsJordan, Hashemite 2 Member States of WHO unless otherwise stated
Kingdom of the . . - - - 8 And editorial and language staffKorea - 4 Non -participating MemberLaos - - - 5 Associate MemberLebanon 6 Non -Member
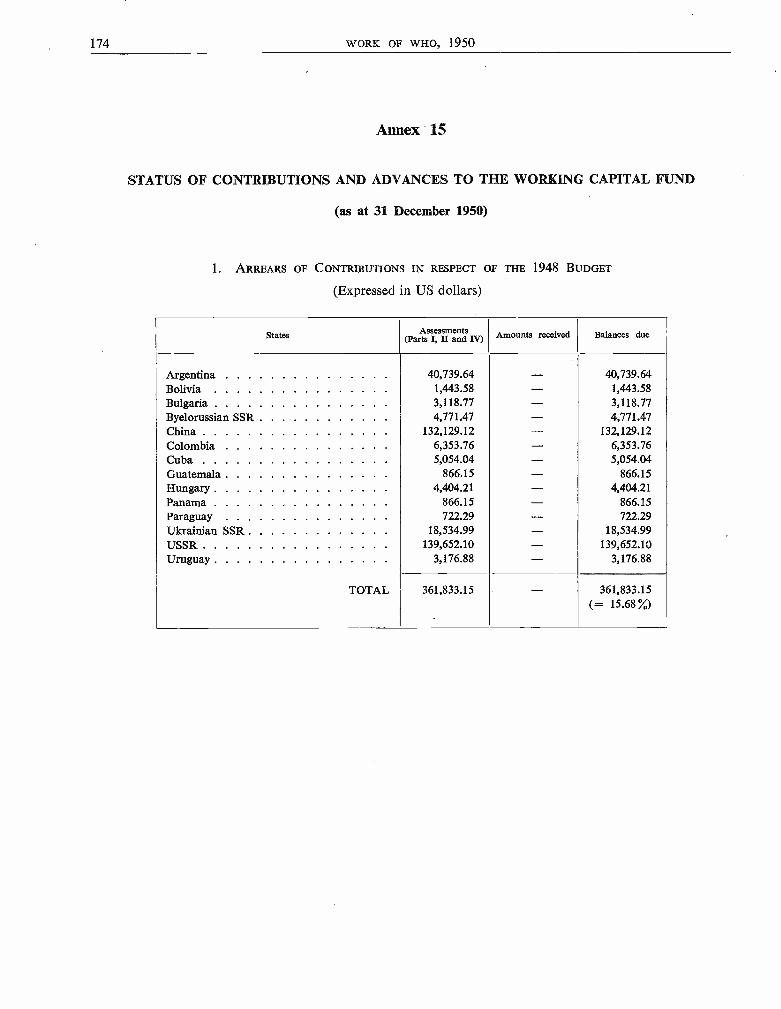
174 WORK OF WHO, 1950
Annex 15
STATUS OF CONTRIBUTIONS AND ADVANCES TO THE WORKING CAPITAL FUND
(as at 31 December 1950)
1. ARREARS OF CONTRIBUTIONS IN RESPECT OF THE 1948 BUDGET
(Expressed in US dollars)
States Assessments(Parts I, II and Iv) Amounts received Balances due
Argentina 40,739.64 - 40,739.64Bolivia 1,443.58 - 1,443.58Bulgaria 3,118.77 - 3,118.77Byelorussian SSR 4,771.47 - 4,771.47China 132,129.12 - 132,129.12Colombia 6,353.76 - 6,353.76Cuba 5,054.04 - 5,054.04Guatemala 866.15 - 866.15Hungary 4,404.21 - 4,404.21Panama 866.15 - 866.15Paraguay 722.29 - 722.29Ukrainian SSR 18,534.99 - 18,534.99USSR 139,652.10 - 139,652.10Uruguay 3,176.88 - 3,176.88
TOTAL 361,833.15 - 361,833.15(= 15.68 %)
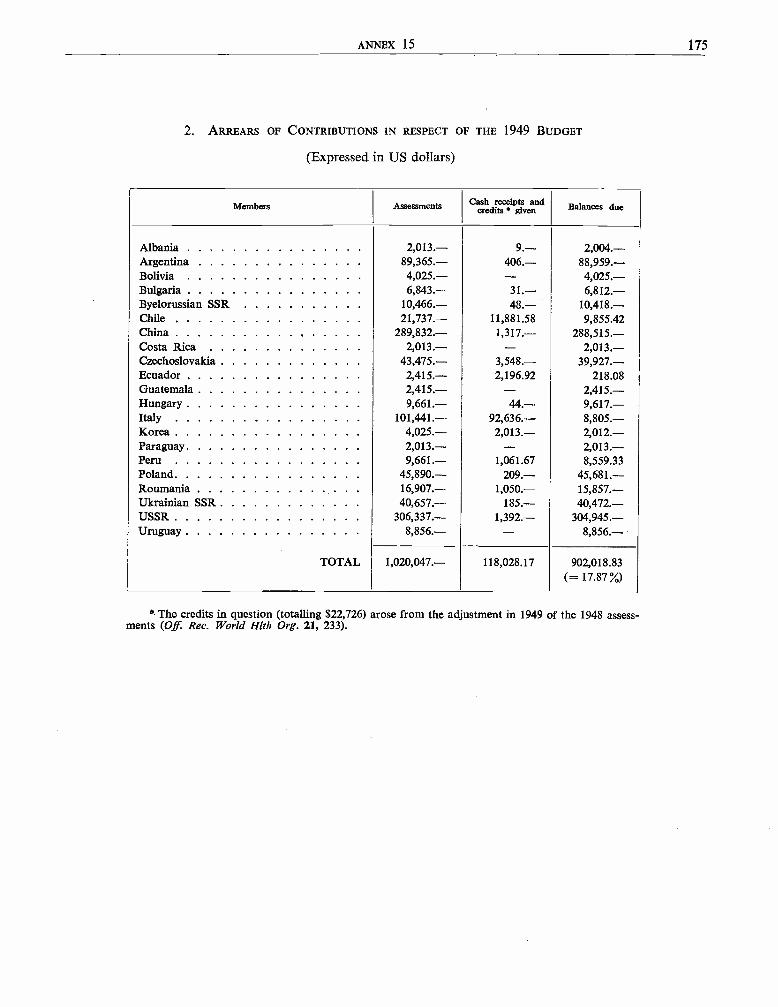
ANNEX 15 175
2. ARREARS OF CONTRIBUTIONS IN RESPECT OF THE 1949 BUDGET
(Expressed in US dollars)
Members Assessments Cash receipts andcredits given Balances due
Albania 2,013.- 9.- 2,004. -Argentina 89,365.- 406.- 88,959. -Bolivia 4,025.- - 4,025. -Bulgaria 6,843.- 31.- 6,812. -Byelorussian SSR 10,466.- 48.- 10,418. -Chile 21,737.- 11,881.58 9,855.42China 289,832.- 1,317.- 288,515. -Costa Rica 2,013.- - 2,013. -Czechoslovakia 43,475.- 3,548.- 39,927. -Ecuador 2,415.- 2,196.92 218.08Guatemala 2,415.- - 2,415. -Hungary 9,661. - 44.- 9,617. -Italy 101,441.- 92,636.- 8,805. -Korea 4,025.- 2,013.- 2,012. -Paraguay 2,013.- - 2,013. -Peru 9,661.- 1,061.67 8,559.33Poland 45,890.- 209.- 45,681. -Roumania 16,907.- 1,050.- 15,857. -Ukrainian SSR 40,657.- 185.- 40,472. -USSR 306,337.- 1,392.- 304,945. -Uruguay 8,856.- - 8,856. -
TOTAL 1,020,047.- 118,028.17 902,018.83(= 17.87 %)
* The credits in question (totalling $22,726) arose from the adjustment in 1949 of the 1948 assess-ments (Off. Rec. World Hlth Org. 21, 233).
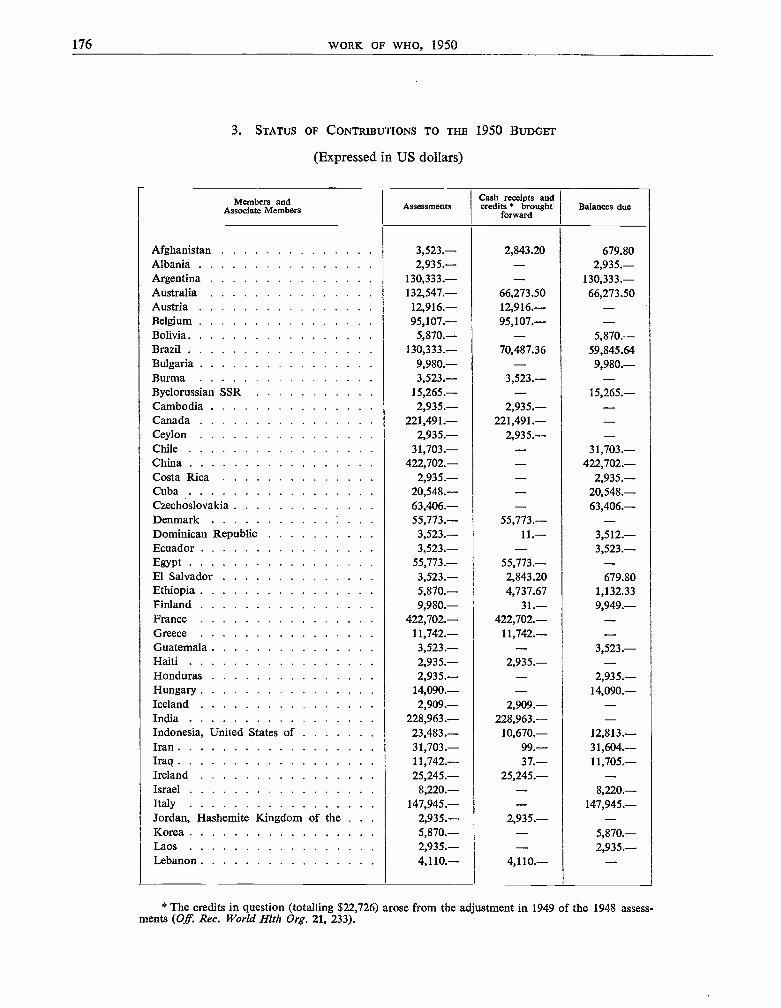
176 WORK OF WHO, 1950
3. STATUS OF CONTRIBUTIONS TO THE 1950 BUDGET
(Expressed in US dollars)
Members andAssociate Members Assessments
Cash receipts andcredits brought
forwardBalances due
Afghanistan 3,523.- 2,843.20 679.80Albania 2,935.- - 2,935. -Argentina 130,333.- - 130,333.-Australia 132,547.- 66,273.50 66,273.50Austria 12,916.- 12,916.- -Belgium 95,107.- 95,107.- -Bolivia 5,870.- - 5,870.- -Brazil 130,333.- 70,487.36 59,845.64Bulgaria 9,980.- - 9,980. -Burma 3,523.- 3,523.- -Byelorussian SSR 15,265.- - 15,265. -Cambodia 2,935.- 2,935.- -Canada 221,491.- 221,491.- -Ceylon 2,935.- 2,935.- -Chile 31,703.- - 31,703. -China 422,702.- - 422,702. -Costa Rica 2,935.- - 2,935. -Cuba 20,548.- - 20,548. -Czechoslovakia 63,406.- - 63,406. -Denmark 55,773.- 55,773.- -Dominican Republic 3,523.- 11.- 3,512. -Ecuador 3,523.- - 3,523. -Egypt 55,773.- 55,773.- -El Salvador 3,523.- 2,843.20 679.80Ethiopia 5,870.- 4,737.67 1,132.33Finland 9,980.- 31.- 9,949. -France 422,702.- 422,702.- -Greece 11,742.- 11,742.- -Guatemala 3,523.- - 3,523. -Haiti 2,935.- 2,935.- -Honduras 2,935.- - 2,935. -Hungary 14,090.- - 14,090. -Iceland 2,909.- 2,909.- -India 228,963.- 228,963.- -Indonesia, United States of 23,483.- 10,670.- 12,813. -Iran 31,703.- 99.- 31,604. -Iraq 11,742.- 37.- 11,705. -Ireland 25,245.- 25,245.- -Israel 8,220.- - 8,220. -Italy 147,945.- - 147,945. -Jordan, Hashemite Kingdom of the . . . 2,935.- 2,935.- -Korea 5,870.- - 5,870. -Laos 2,935.- - 2,935. -Lebanon 4,110.- 4,110.- -
* The credits in question (totalling $22,726) arose from the adjustment in 1949 of the 1948 assess-ments (Off. Rec. World Hlth Org. 21, 233).
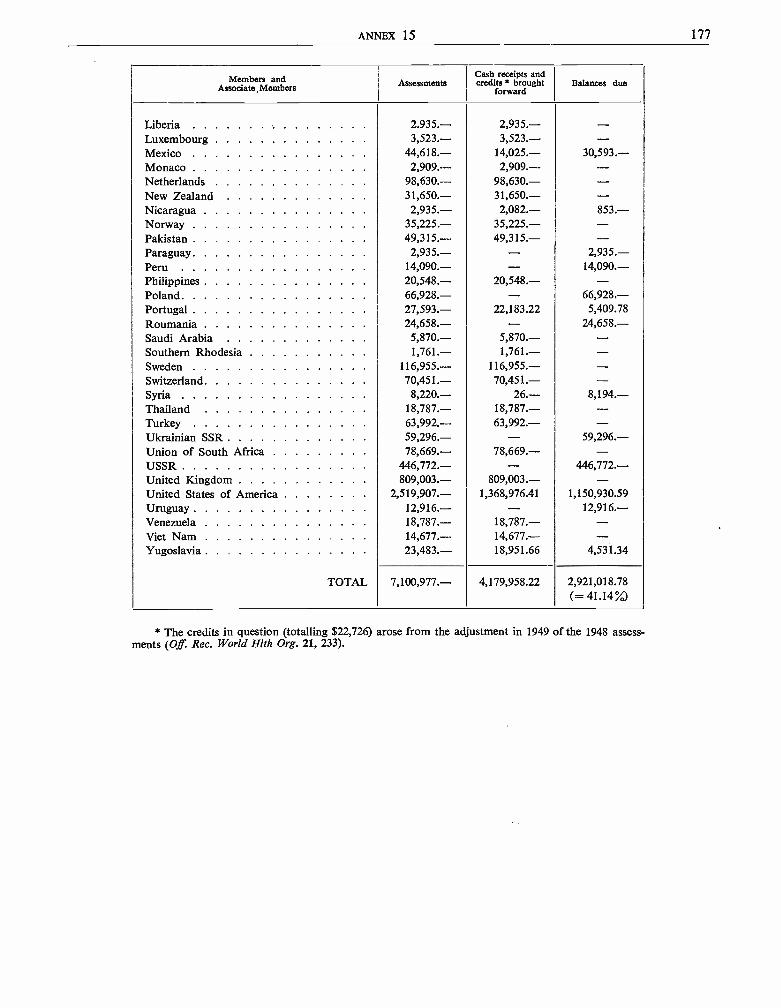
ANNEX 15 177
Associate Members AssessmentsCash receipts andcredits' brought
forwardBalances duo
Liberia 2.935.- 2,935.- -Luxembourg 3,523.- 3,523.- -Mexico 44,618. -- 14,025.- 30,593. -Monaco 2,909.- 2,909.- -Netherlands 98,630.- 98,630.- -New Zealand 31,650.- 31,650.- -Nicaragua 2,935.- 2,082.- 853. -Norway 35,225.- 35,225.- -Pakistan 49,315.- 49,315.- -Paraguay 2,935.- - 2,935. -Peru 14,090.- - 14,090. -Philippines 20,548.- 20,548.- -Poland 66,928.- - 66,928. -Portugal 27,593.- 22,183.22 5,409.78Roumania 24,658.- - 24,658. -Saudi Arabia 5,870.- 5,870.- -Southern Rhodesia 1,761.- 1,761.- -Sweden 116,955.- 116,955.- -Switzerland 70,451.- 70,451.- -Syria 8,220.- 26.- 8,194. -Thailand 18,787.- 18,787.- -Turkey 63,992.- 63,992.- -Ukrainian SSR 59,296.- - 59,296. -Union of South Africa 78,669.- 78,669.- -USSR 446,772.- - 446,772. -United Kingdom 809,003.- 809,003.- -United States of America 2,519,907.- 1,368,976.41 1,150,930.59Uruguay 12,916.- - 12,916. -Venezuela 18,787.- 18,787.- -Viet Nam 14,677.- 14,677.- -Yugoslavia 23,483.- 18,951.66 4,531.34
TOTAL 7,100,977.- 4,179,958.22 2,921,018.78(= 41.14 %)
* The credits in question (totalling $22,726) arose from the adjustment in 1949 of the 1948 assess-ments (Of Rec. World Hlth Org. 21, 233).
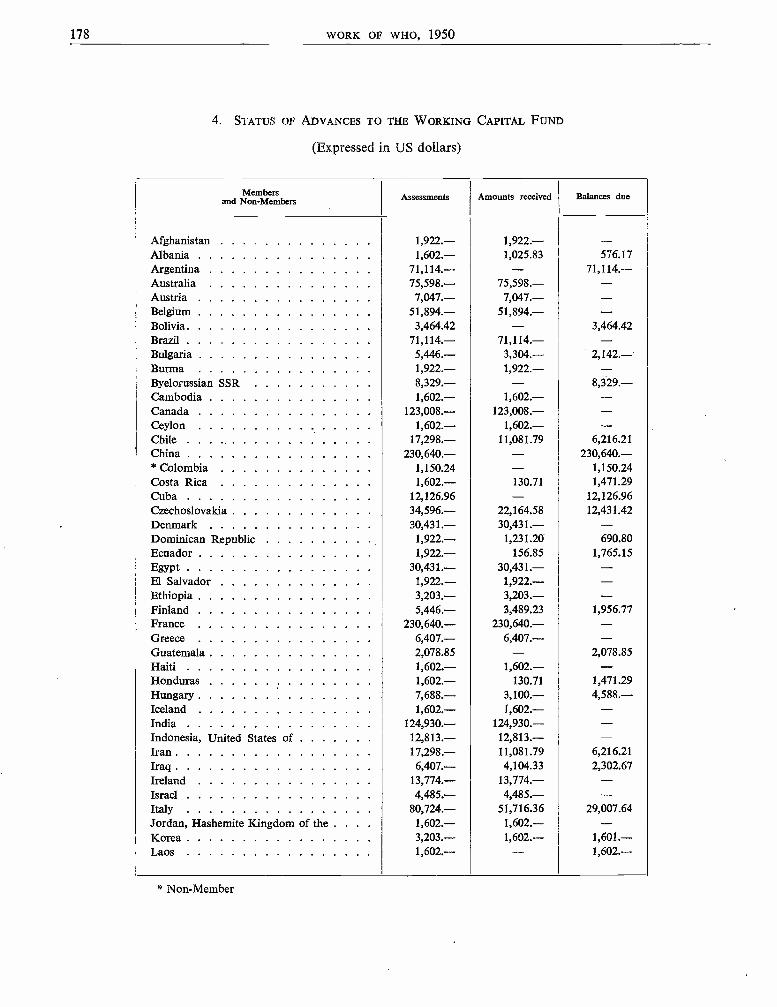
178 WORK OF WHO, 1950
4. STATUS OF ADVANCES TO THE WORKING CAPITAL FUND
(Expressed in US dollars
and Assessments Amounts received Balances due
Afghanistan 1,922.- 1,922.-- --Albania 1'602.- 1,025.83 576.17Argentina 71'114.-- -- 71,114.--Australia 75,598.- 75.598.-- --Austria 7,047.- 7,047.- -Belgium 51.894.- 51.894.- -Bolivia 3.464.42 - 3'464.42Brazil 71.114.-- 71.114.-- --Bulgaria 5.446.- 3,304.- 2,142.-Burma 1.922.-- 1,922.- --Byelorussian SSR 8,32*-- -- 8,329.--Cambodia 1,002.-- 1.002.-- --Canada 123^008.-- 123.008.-- --Ceylon 1.602.-- 1,*02.-- --Chile 17,298.- 11/81.79 6,216.27China 230,640.- - 230,640.-* Colombia 1.150.24 -- 1,150.24Costa Rica 1,602.- 130.71 1^471.29
Cuba 12.120.96 -- 12,126.96Czechoslovakia 34,596.-- 22,164.0 12,43142Denmark 30,431.- 30,431.- -Dominican Republic 1,922.- 1,231.20 6*0.80Ecuador 1.922.-- 150.85 1.705.15Egypt 30,431.- 30,431.- -El Salvador 1,922.- 1,922.-- --Ethiopia 3,203.-- 3.203.-- --Finland 5^440.-- 3^489.23 1.956.77France 230,640.- 230,640.- -Greece 6.407.-- 6,407.- --Guatemala 2.078.85 -- 2,078.85Haiti 1.002'- 1.002.- -Honduras 1,602.-- 130.71 1,471.29Hungary 7,688.-- 3'100.-- 4,588.--Iceland 1.602.-- 1.002.-- --India 124,930.- 124,930.- -Indonesia, United States of 12,813.-- 12,813,- --Iran 17`298.-- 11,081.79 6,210.21Iraq 6,407.-- 4.104.33 I\302.67Ireland 13,774.-- 13.774.-- -_Israel 4,485,- 4,485.- --Italy 80,724-- 51,716.30 2e.007.64Jordan, Hashemite Kingdom of the . . . . 1,602.- 1,602.-- --Korea 3^203.- 1,602.- 1'601.--
* Non-Membe
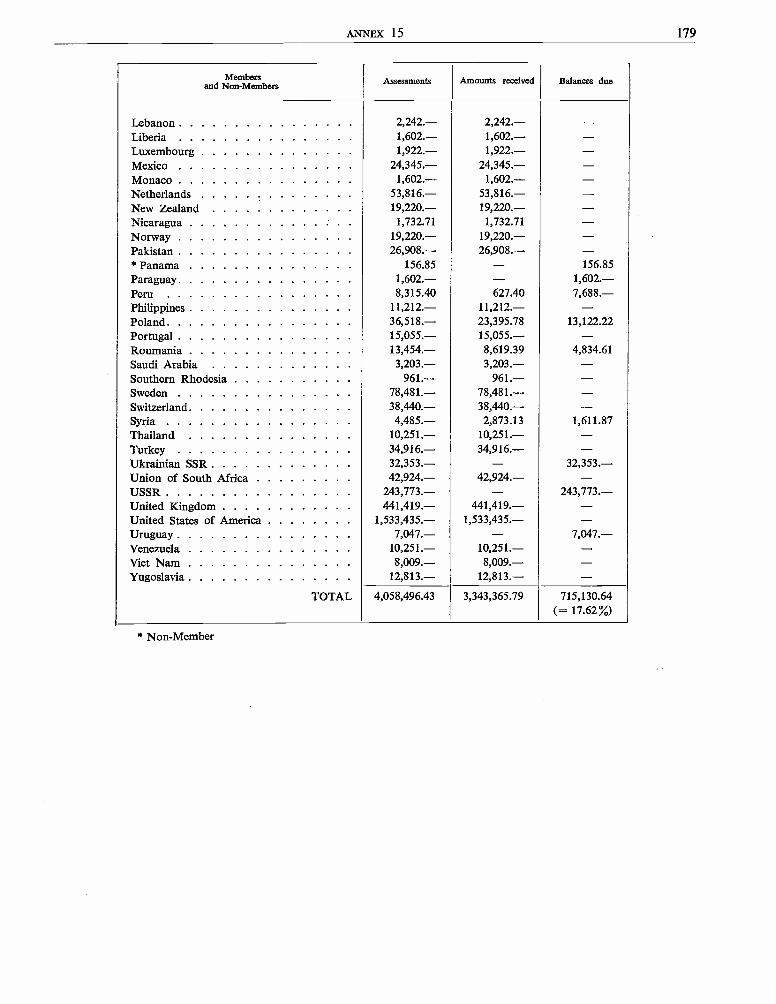
ANNEX 15 179
Membersand Non -Members Assessments Amounts received Balances due
Lebanon 2,242.- 2,242.- -Liberia 1,602.- 1,602.- -Luxembourg 1,922.- 1,922.- -Mexico 24,345.- 24,345.- -Monaco 1,602.- 1,602.- -Netherlands 53,816.- 53,816.- -New Zealand 19,220.- 19,220.- -Nicaragua 1,732.71 1,732.71 -Norway 19,220.- 19,220.- -Pakistan 26,908.- 26,908.- -* Panama 156.85 - 156.85Paraguay 1,602.- - 1,602. -Peru 8,315.40 627.40 7,688. -Philippines 11,212.- 11,212.- -Poland 36,518.- 23,395.78 13,122.22Portugal 15,055.- 15,055.- -Roumania 13,454.- 8,619.39 4,834.61Saudi Arabia 3,203.- 3,203.- -Southern Rhodesia 961.- 961.- -Sweden 78,481.- 78,481.- -Switzerland 38,440.- 38,440.- -Syria 4,485.- 2,873.13 1,611.87Thailand 10,251.- 10,251.- -Turkey 34,916.- 34,916.- -Ukrainian SSR 32,353.- - 32,353. -Union of South Africa 42,924.- 42,924.- -USSR 243,773.- - 243,773. -United Kingdom 441,419.- 441,419.- -United States of America 1,533,435.- 1,533,435.- -Uruguay 7,047.- - 7,047. -Venezuela 10,251.- 10,251.- -Viet Nam 8,009.- 8,009.- -Yugoslavia 12,813.- 12,813.- -
TOTAL 4,058,496.43 3,343,365.79 715,130.64(= 17.62%)
* Non -Member
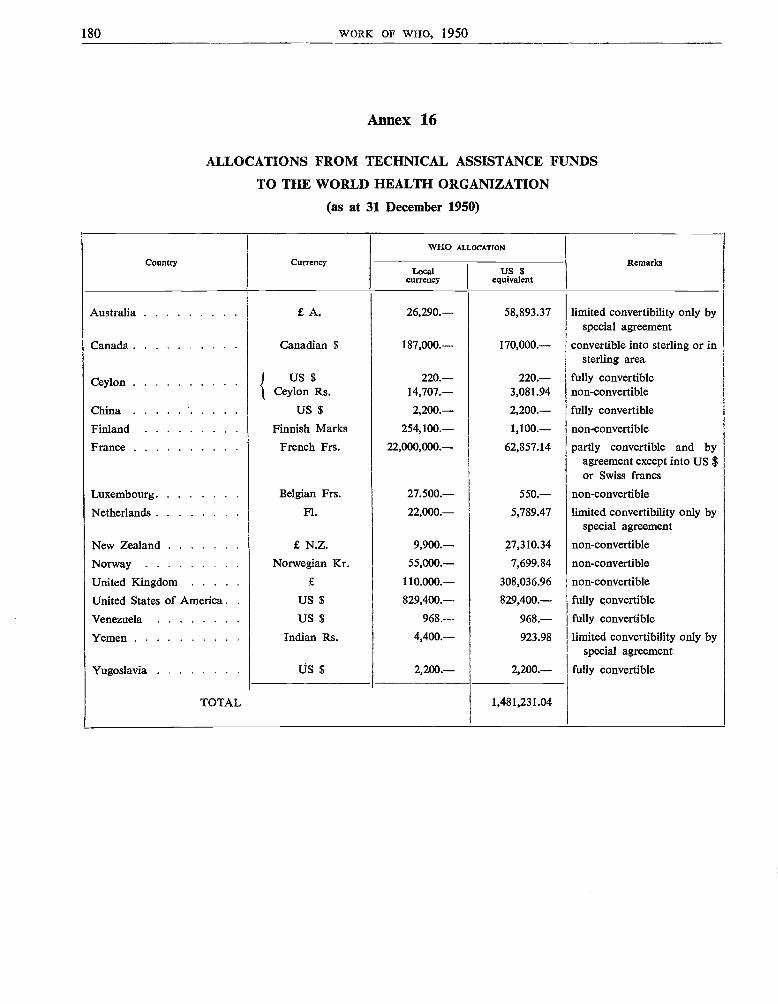
180 WORK OF WHO, 1950
Annex 16
ALLOCATIONS FROM TECHNICAL ASSISTANCE FUNDS
TO THE WORLD HEALTH ORGANIZATION
(as at 31 December 1950)
Country Currency
WHO ALLOCATION
RemarksLocal
currencyUS $
equivalent
Australia £ A. 26,290.- 58,893.37 limited convertibility only byspecial agreement
Canada Canadian $ 187,000.- 170,000.- convertible into sterling or insterling area
Ceylon US $ 220.- 220.- fully convertibleCeylon Rs. 14,707.- 3,081.94 non- convertible
China US $ 2,200.- 2,200.- fully convertible
Finland Finnish Marks 254,100.- 1,100.- non -convertible
France French Frs. 22,000,000.- 62,857.14 partly convertible and byagreement except into US $or Swiss francs
Luxembourg Belgian Frs. 27.500.- 550.- non- convertible
Netherlands Fl. 22,000.- 5,789.47 limited convertibility only byspecial agreement
New Zealand £ N.Z. 9,900.- 27,310.34 non -convertible
Norway Norwegian Kr. 55,000.- 7,699.84 non -convertible
United Kingdom £ 110.000.- 308,036.96 non -convertible
United States of America . . US $ 829,400.- 829,400.- fully convertible
Venezuela US $ 968.- 968.- fully convertible
Yemen Indian Rs. 4,400.- 923.98 limited convertibility only byspecial agreement
Yugoslavia US $ 2,200.- 2,200.- fully convertible
TOTAL 1,481,231.04
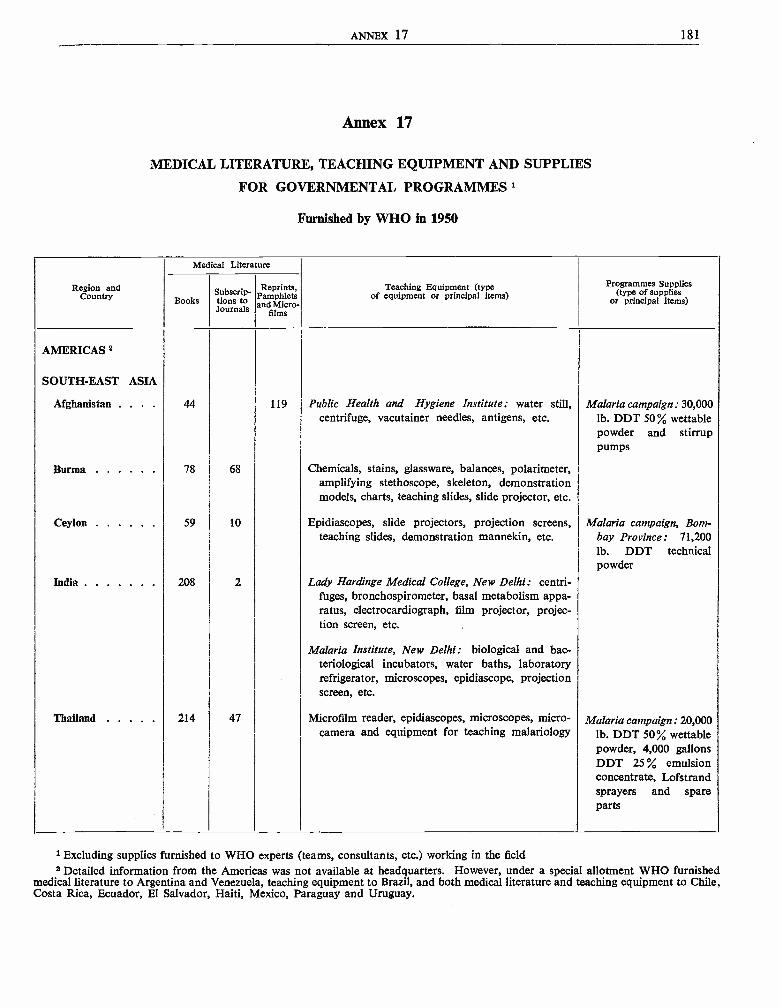
ANNEX 17 181
Annex 17
MEDICAL LITERATURE, TEACHING EQUIPMENT AND SUPPLIES
FOR GOVERNMENTAL PROGRAMMES
Furnished by WHO in 1950
Region andCountry
Medical Literature
Teaching Equipment (typeof equipment or principal items)
Programmes Supplies(type of supplies
or principal items)BooksSubscrip-fions toJournals
Reprints,Pamphletsand Micro-
films
AMERICAS 2
SOUTH -EAST ASIA
Afghanistan . . . . 44 119 Public Health and Hygiene Institute: water still,centrifuge, vacutainer needles, antigens, etc.
Malaria campaign: 30,000lb. DDT 50%, wettablepowder and stirruppumps
Burma 78 68 Chemicals, stains, glassware, balances, polarimeter,amplifying stethoscope, skeleton, demonstrationmodels, charts, teaching slides, slide projector, etc.
Ceylon 59 10 Epidiascopes, slide projectors, projection screens,teaching slides, demonstration mannekin, etc.
Malaria campaign, Bom-bay Province: 71,200lb. DDT technicalpowder
India 208 2 Lady Hardinge Medical College, New Delhi: centri-fuges, bronchospirometer, basal metabolism appa-ratus, electrocardiograph, film projector, projec-tion screen, etc. .
Malaria Institute, New Delhi: biological and bac-teriological incubators, water baths, laboratoryrefrigerator, microscopes, epidiascope, projectionscreen, etc.
Thailand 214 47 Microfilm reader, epidiascopes, microscopes, micro-camera and equipment for teaching malariology
Malaria campaign: 20,000lb. DDT 50% wettablepowder, 4,000 gallonsDDT 25 % emulsionconcentrate, Lofstrandsprayers and spareparts
1 Excluding supplies furnished to WHO experts (teams, consultants, etc.) working in the field2 Detailed information from the Americas was not available at headquarters. However, under a special allotment WHO furnished
medical literature to Argentina and Venezuela, teaching equipment to Brazil, and both medical literature and teaching equipment to Chile,Costa Rica, Ecuador, El Salvador, Haiti, Mexico, Paraguay and Uruguay.
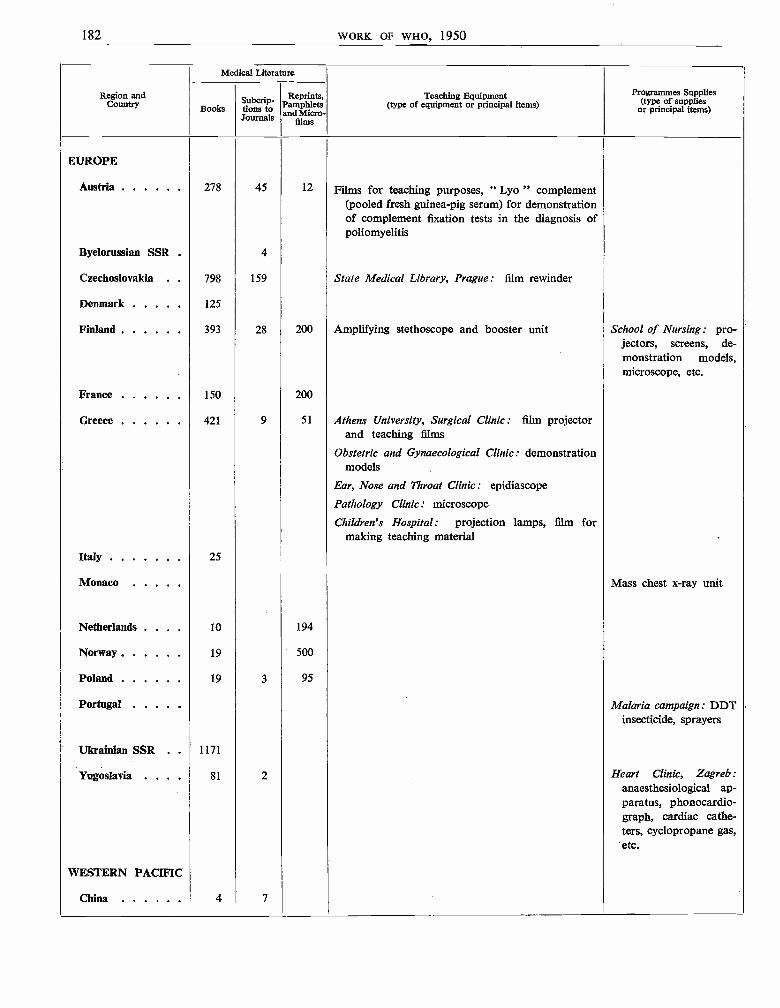
182 WORK OF WHO, 1950
Region andCountry
Medical Literature
Teaching Equipment(type of equipment or principal items)
Programmes Supplies(type of supplies
or principal items)Books tions toJournals
Reprints,Pamphletsdo
films
EUROPE
Austria 278 45 12 Films for teaching purposes, " Lyo " complement(pooled fresh guinea -pig serum) for demonstrationof complement fixation tests in the diagnosis ofpoliomyelitis
Byelorussian SSR . 4
Czechoslovakia . 798 159 State Medical Library, Prague: film rewinder
Denmark 125
Finland 393 28 200 Amplifying stethoscope and booster unit School of Nursing: pro-jectors, screens, de-monstration models,microscope, etc.
France 150 200
Greece 421 9 51 Athens University, Surgical Clinic: film projectorand teaching films
Obstetric and Gynaecological Clinic: demonstrationmodels
Ear, Nose and Throat Clinic: epidiascope
Pathology Clinic: microscope
Children's Hospital: projection lamps, film formaking teaching material
Italy 25
Monaco Mass chest x -ray unit
Netherlands . . . 10 194
Norway 19 500
Poland 19 3 95
Portugal Malaria campaign: DDTinsecticide, sprayers
Ukrainian SSR . . 1171
Yugoslavia . . . . 81 2 Heart Clinic, Zagreb:anaesthesiological ap-paratus, phonocardio-graph, cardiac cathe-ters, cyclopropane gas,etc.
WESTERN PACIFIC
China 4 7
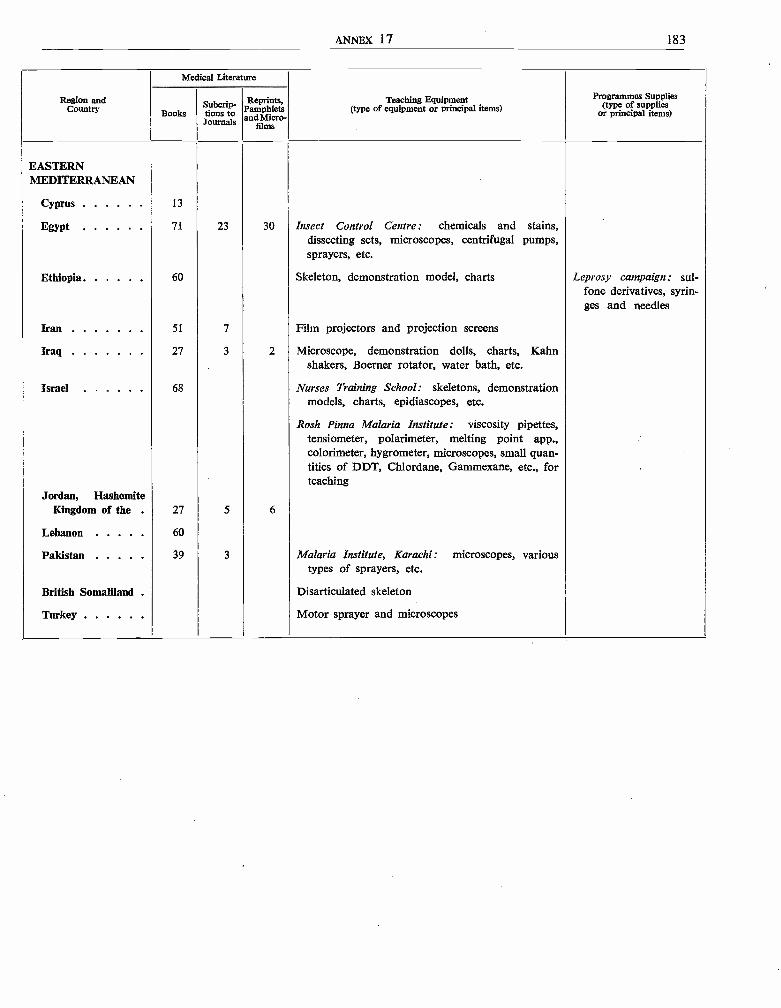
ANNEX 17 183
Region andCountry
Medical Literature
Teaching Equipment(type of equipment or principal items)
Programmes Supplies
or principal items)BooksSubcriptions to
JJournals
Reprints,Pamphletsand Micro-
Sims
EASTERNMEDITERRANEAN
Cyprus 13
Egypt 71 23 30 Insect Control Centre: chemicals and stains,dissecting sets, microscopes, centrifugal pumps,sprayers, etc.
Ethiopia 60 Skeleton, demonstration model, charts Leprosy campaign: sul-fone derivatives, syrin-ges and needles
Iran 51 7 Film projectors and projection screens
Iraq 27 3 2 Microscope, demonstration dolls, charts, Kahnshakers, Boerner rotator, water bath, etc.
Israel 68 Nurses Training School: skeletons, demonstrationmodels, charts, epidiascopes, etc.
Rosh Pinna Malaria Institute: viscosity pipettes,tensiometer, polarimeter, melting point app.,colorimeter, hygrometer, microscopes, small quan-tities of DDT, Chlordane, Gammexane, etc., forteaching
Jordan, HashemiteKingdom of the 27 5 6
Lebanon 60
Pakistan 39 3 Malaria Institute, Karachi: microscopes, varioustypes of sprayers, etc.
British Somaliland Disarticulated skeleton
Turkey Motor sprayer and microscopes
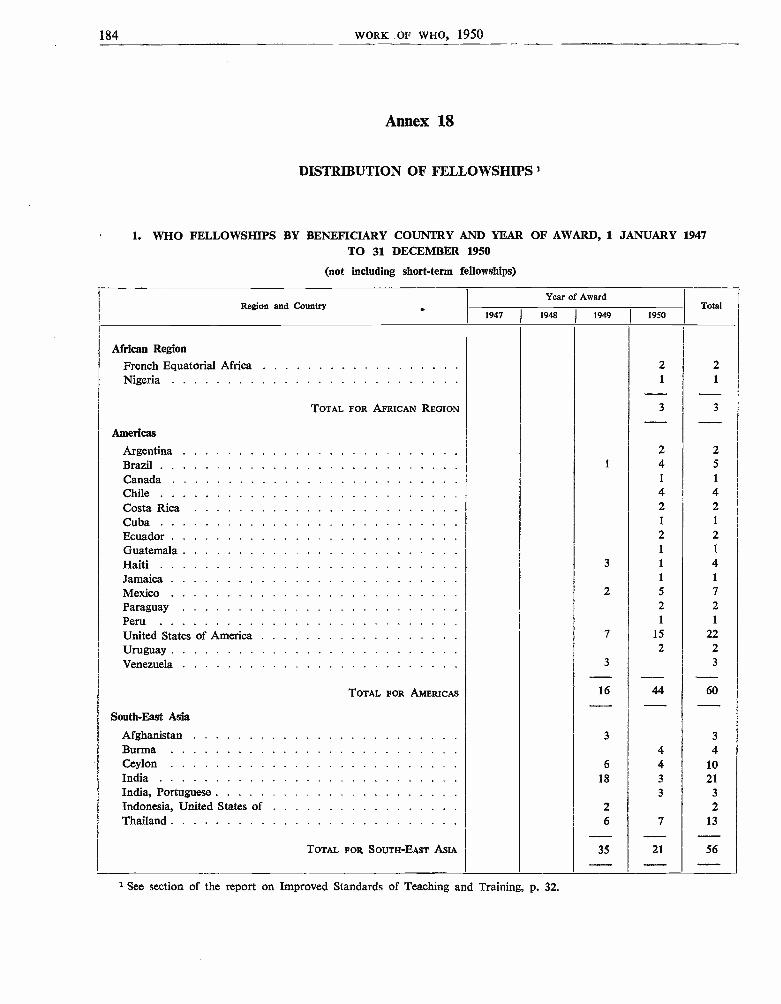
184 WORK OF WHO, 1950
Annex 18
DISTRIBUTION OF FELLOWSHIPS I
1. WHO FELLOWSHIPS BY BENEFICIARY COUNTRY AND YEAR OF AWARD, 1 JANUARY 1947TO 31 DECEMBER 1950
(not including short -term fellowships)
Region and Country .Year of Award
Total1947 1948 I 1949 I 1950
African Region
French Equatorial Africa 2 2Nigeria 1 1
TOTAL FOR AFRICAN REGION 3 3
____Americas
Argentina 2 2
Brazil 1 4 5
Canada 1 1
Chile 4 4Costa Rica 2 2Cuba 1 1
Ecuador 2 2
Guatemala 1 1
Haiti 3 1 4
Jamaica 1 1
Mexico 2 5 7
Paraguay 2 2Peru 1 1
United States of America 7 15 22
Uruguay 2 2Venezuela 3 3
TOTAL FOR AMERICAS 16 44 60
South -East Asia_
Afghanistan 3 3
Burma 4 4Ceylon 6 4 10India 18 3 21India, Portuguese 3 3
Indonesia, United States of 2 2Thailand 6 7 13
TOTAL FOR SOUTH -EAST ASIA 35 21 56
1 See section of the report on Improved Standards of Teaching and Training, p. 32.
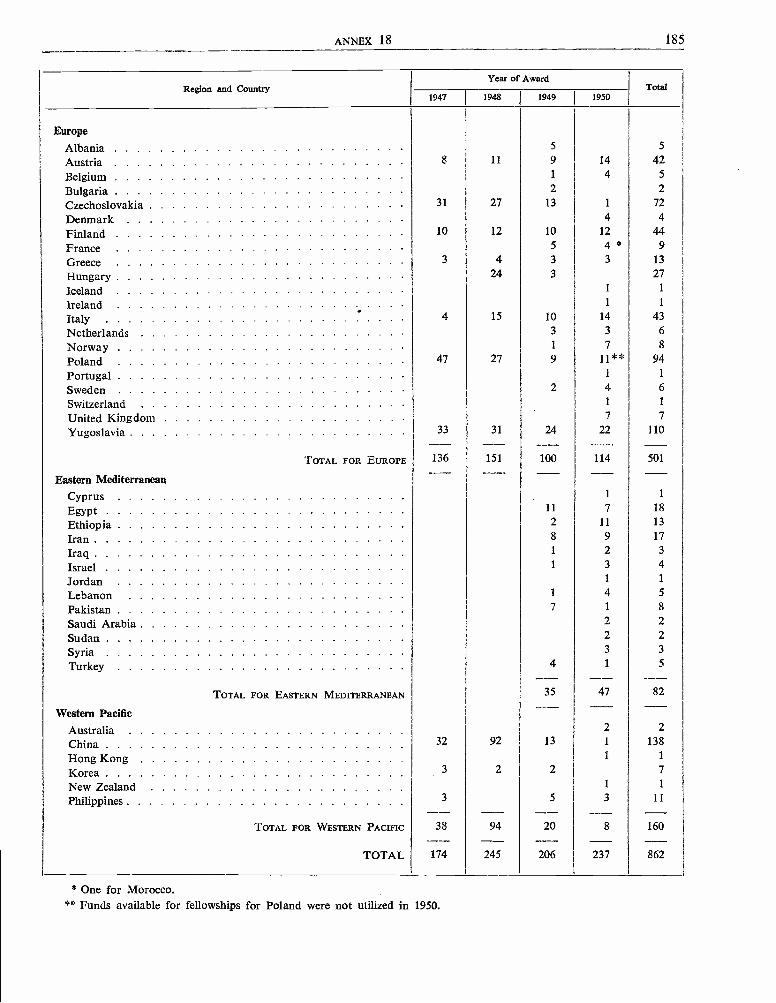
ANNEX 18 185
Region and CountryYear of Award
Total1947 1948 1949 1950
Europe
Albania 5 5
Austria 8 11 9 14 42
Belgium 1 4 5
Bulgaria 2 2
Czechoslovakia 31 27 13 1 72
Denmark 4 4
Finland 10 12 10 12 44
France 5 4 a 9
Greece 3 4 3 3 13
Hungary 24 3 27
Iceland 1 1
Ireland 1 1
Italy 4 15 10 14 43
Netherlands 3 3 6
Norway 1 7 8
Poland 47 27 9 11** 94
Portugal 1 1
Sweden 2 4 6
Switzerland 1 1
United Kingdom 7 7
Yugoslavia 33 31 24 22 110
TOTAL FOR EUROPE 136 151 100 114 501
Eastern Mediterranean
Cyprus 1 1
Egypt 11 7 18
Ethiopia 2 11 13
Iran 8 9 17
Iraq 1 2 3
Israel 1 3 4
Jordan 1 1
Lebanon 1 4 5
Pakistan 7 1 8
Saudi Arabia 2 2
Sudan 2 2
Syria 3 3
Turkey 4 1 5
TOTAL FOR EASTERN MEDITERRANEAN 35 47 82
Western Pacific
Australia 2 2
China 32 92 13 1 138
Hong Kong 1 1
Korea 3 2 2 7
New Zealand 1 1
Philippines 3 5 3 11
TOTAL FOR WESTERN PACIFIC 38 94 20 8 160
TOTAL 174 245 206 237 862
* One for Morocco.** Funds available for fellowships for Poland were not utilized in 1950.
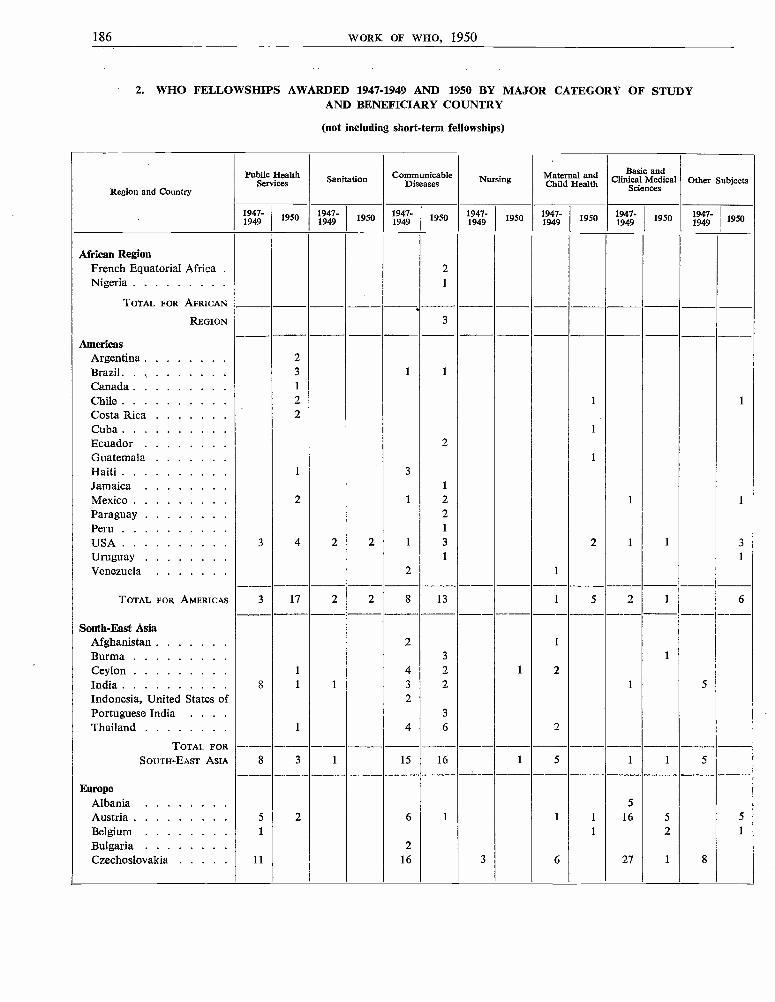
186 WORK OF WHO, 1950
2. WHO FELLOWSHIPS AWARDED 1947 -1949 AND 1950 BY MAJOR CATEGORY OF STUDYAND BENEFICIARY COUNTRY
(not including short -term fellowships)
Region and Country
Public Health Sanitation CommunicableDiseases Nursingg Maternal and
Child HealthBasic and
Clinical MedicalSciences
Other Subjects
1947-1949 1950 1947-
1949 1950 1947-1949 1950 1947-
1949 1950 1947-1949 1950 1947-
1949 1950 1947- 1
1949 1
1950
African RegionFrench Equatorial Africa 2Nigeria I
TOTAL FOR AFRICAN
REGION 3
AmericasArgentina 2Brazil 3 1 1
Canada 1
Chile 2 1 1
Costa Rica 2
Cuba 1
Ecuador 2
Guatemala 1
Haiti 1 3
Jamaica 1
Mexico 2 1 2 1 1
Paraguay 2Peru 1
USA 3 4 2 2 1 3 2 1 1 3
Uruguay 1 1
Venezuela 2 1
TOTAL FOR AMERICAS 3 17 2 2 8 13 1 5 2 1 6
South -Fast AsiaAfghanistan 2 1
Burma 3 1
Ceylon 1 4 2 1 2India 8 1 1 3 2 1 5
Indonesia, United States of 2
Portuguese India . . . 3
Thailand 1 4 6 2
TOTAL FORSOUTH -EAST ASIA 8 3 1 15 16 1 5 1 1 5
EuropeAlbania 5
Austria 5 2 6 1 1 1 16 5 5
Belgium 1 1 2 1
Bulgaria 2Czechoslovakia 11 16 3 6 27 1 8
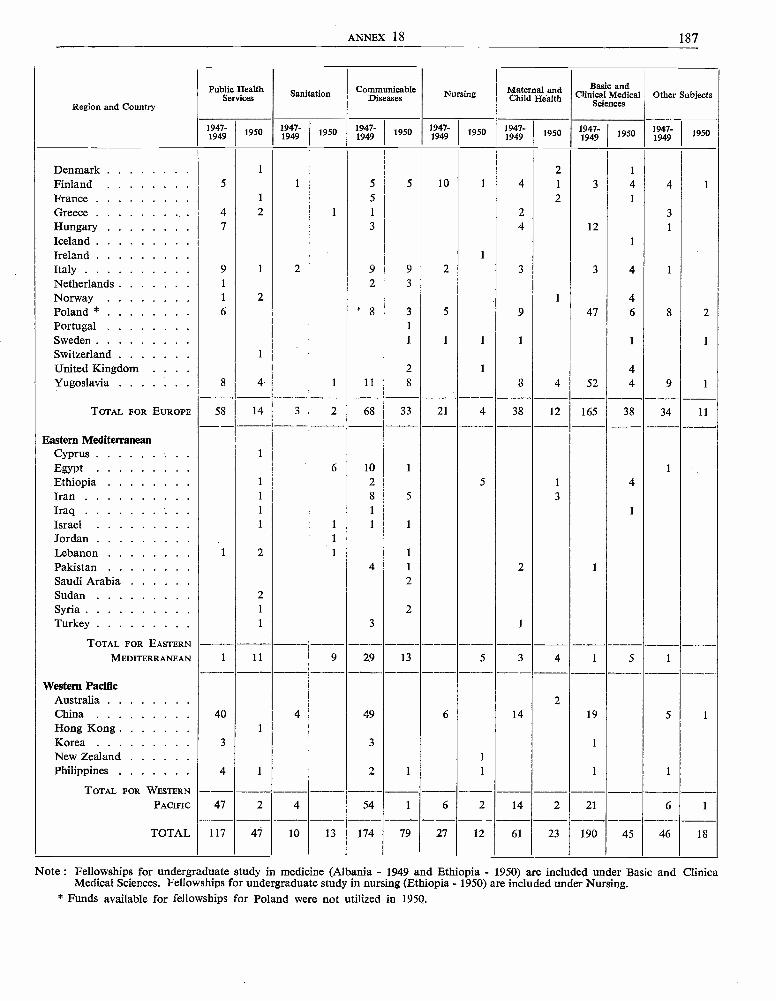
ANNEX 18 187
Region and Country
Public HealthServices Sanitation Communicable
Diseases Nursing Maternal andChild Health
Basic andClinical Medical
SciencesOther Subjects
1947-1949
1950 1947-1949 1950 1947-
1949 1950 1947-1949 1950 1947-
1949 1950 1947-1949 1950 1947-
1949 1950
Denmark 1 2 1
Finland 5 1 5 5 10 1 4 1 3 4 4France 1 5 2 1
Greece 4 2 1 1 2 3
Hungary 7 3 4 12 1
IcelandIreland 1
Italy 9 1 2 9 9 2 3 3 4 1
Netherlands 1 2 3
Norway 1 2 1 4Poland * 6 ° 8 3 5 9 47 6 8 2Portugal 1
Sweden 1 1 1 1 1 1
Switzerland 1
United Kingdom . . . 2 1 4Yugoslavia 8 4 1 11 8 8 4 52 4 9 1
TOTAL FOR EUROPE 58 14 3 2 68 33 21 4 38 12 165 38 34 11
Eastern MediterraneanCyprus 1
Egypt 6 10 1 1
Ethiopia 1 2 5 1 4Iran 1 8 5 3
Iraq 1 1 1
Israel 1 1 1 1
Jordan 1
Lebanon 1 2 1 1
Pakistan 4 1 2 1
Saudi Arabia 2Sudan 2
Syria 1 2
Turkey 1 3 1
TOTAL FOR EASTERN
MEDITERRANEAN 1 11 9 29 13 5 3 4 1 5 1
Western PacificAustralia 2China 40 4 49 6 14 19 5 1
Hong Kong 1
Korea 3 3 1
New Zealand 1
Philippines 4 1 2 1 1 1 1
TOTAL FOR WESTERN
47 2 4 54 1 6 2 14 2 21 6 1PACIFIC
TOTAL 117 47 10 13 174 79 27 12 61 23 190 45 46 18
Note : Fellowships for undergraduate study in medicine (Albania - 1949 and Ethiopia - 1950) are included under Basic and ClinicaMedical Sciences. Fellowships for undergraduate study in nursing (Ethiopia - 1950) are included under Nursing.
* Funds available for fellowships for Poland were not utilized in 1950.
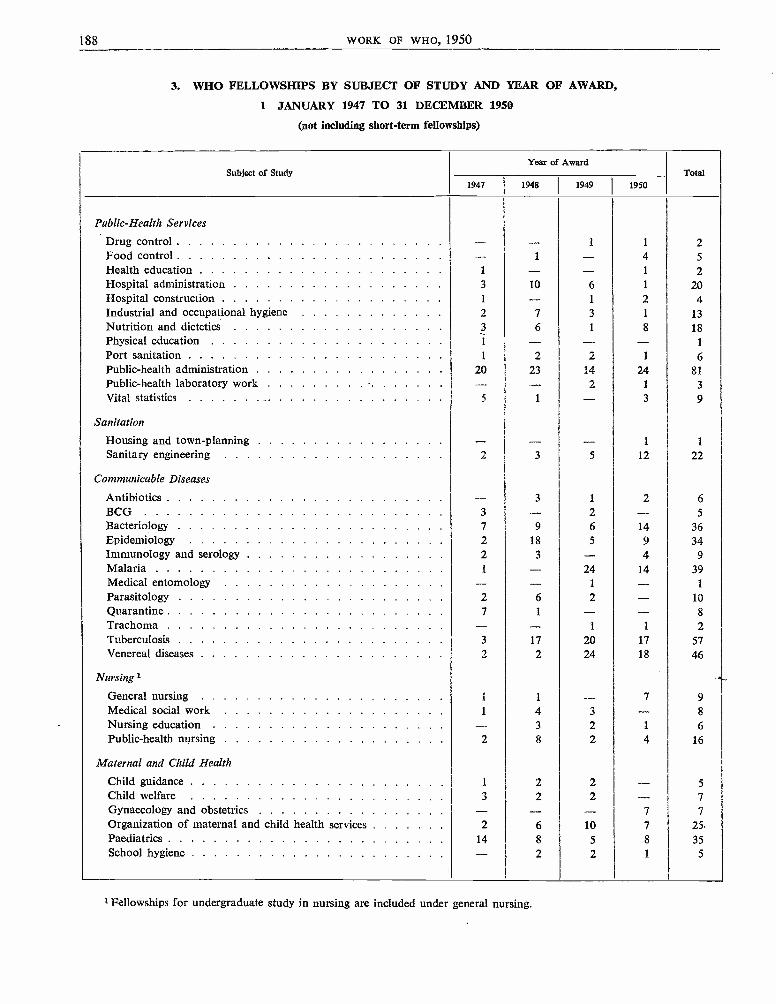
188 WORK OF WHO, 1950
3. WHO FELLOWSHIPS BY SUBJECT OF STUDY AND YEAR OF AWARD,
1 JANUARY 1947 TO 31 DECEMBER 1950
(not including short-term fellowships)
Subject of StudyYear of Award
Total1947 1948 1949 1950
Public-Health Services
Drug control - - 1 1 2Food control - 1 4 5
Health education 1 - 1 2Hospital administration 3 10 6 1 20Hospital construction 1 - 1 2 4Industrial and occupational hygiene 2 7 3 1 13Nutrition and dietetics 3 6 1 8 18Physical education 1 - - - 1
Port sanitation 1 2 2 1 6Public-health administration 20 23 14 24 81Public-health laboratory work - - - 2 1 3
Vital statistics 5 1 3 9
Sanitation
Housing and town-planning - - 1 1
Sanitary engineering 2 3 5 12 22
Communicable Diseases
Antibiotics -- 3 1 2 6
BCG 3 - 2 - 5
Bacteriology 7 9 6 14 36Epidemiology 2 18 5 9 34Immunology and serology 2 3 - 4 9
Malaria 1 - 24 14 39Medical entomology - - 1 - 1
Parasitology 2 6 2 - 10Quarantine 7 1 - - 8
Trachoma - - 1 1 2Tuberculosis 3 17 20 17 57Venereal diseases 2 2 24 18 46
Nursing 1
General nursing 1 1 -- 7 9
Medical social work 1 4 3 - 8
Nursing education - 3 2 1 6Public-health nursing 2 8 2 4 16
Maternal and Child Health
Child guidance 1 2 2 - 5
Child welfare 3 2 2 7
Gynaecology and obstetrics - - - 7 7
Organization of maternal and child health services 2 6 10 7 25Paediatrics 14 8 5 8 35School hygiene - 2 2 1 5
Fellowships for undergraduate study in nursing are included under general nursing.
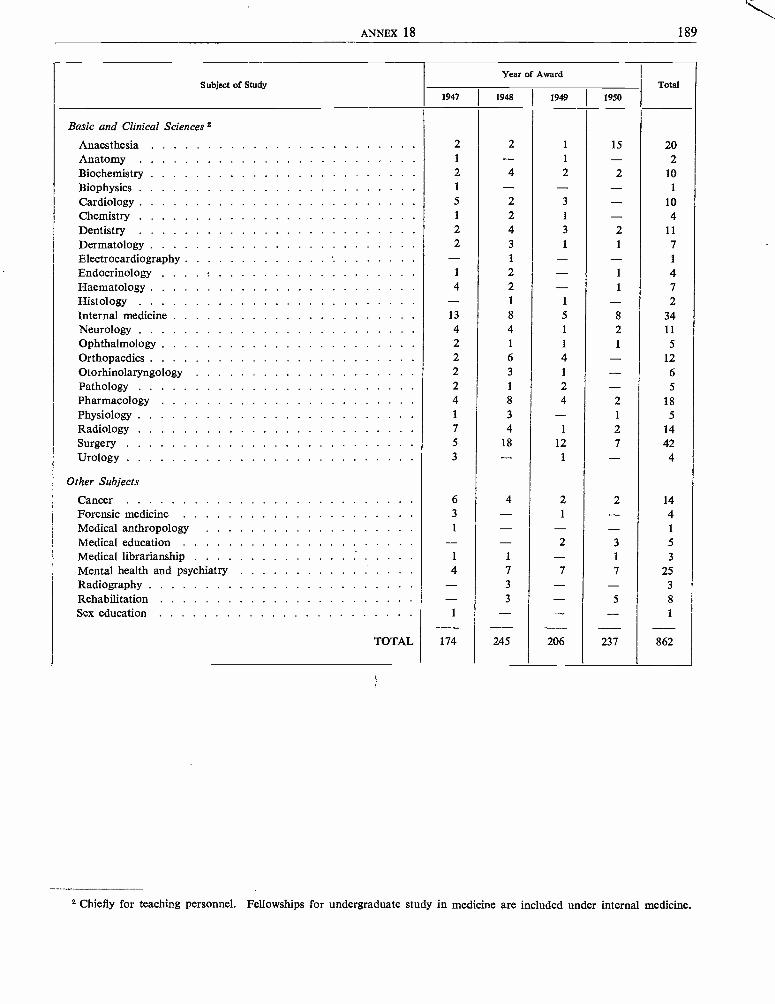
ANNEX 18 189
Subject of StudyYear of Award
Total1947 1948 1949 1950
Basic and Clinical Sciences 2
Anaesthesia 2 2 1 15 20Anatomy 1 - 1 - 2Biochemistry 2 4 2 2 10
Biophysics 1 - - - 1
Cardiology 5 2 3 - 10
Chemistry 1 2 1 - 4Dentistry 2 4 3 2 11
Dermatology 2 3 1 1 7
Electrocardiography - 1 - - 1
Endocrinology 1 2 - 1 4Haematology 4 2 - 1 7Histology - 1 1 - 2Internal medicine 13 8 5 8 34Neurology 4 4 1 2 11
Ophthalmology 2 1 1 1 5
Orthopaedics 2 6 4 - 12
Otorhinolaryngology 2 3 1 - 6
Pathology 2 1 2 - 5
Pharmacology 4 8 4 2 18
Physiology 1 3 - 1 5
Radiology 7 4 1 2 14
Surgery 5 18 12 7 42Urology 3 - 1 - 4
Other Subjects
Cancer 6 4 2 2 14Forensic medicine 3 - 1 - 4Medical anthropology 1 - - - 1
Medical education - - 2 3 5
Medical librarianship 1 1 - 1 3
Mental health and psychiatry 4 7 7 7 25Radiography - 3 - - 3
Rehabilitation - 3 - 5 8
Sex education 1 - - - 1
TOTAL 174 245 206 237 862
2 Chiefly for teaching personnel. Fellowships for undergraduate study in medicine are included under internal medicine.
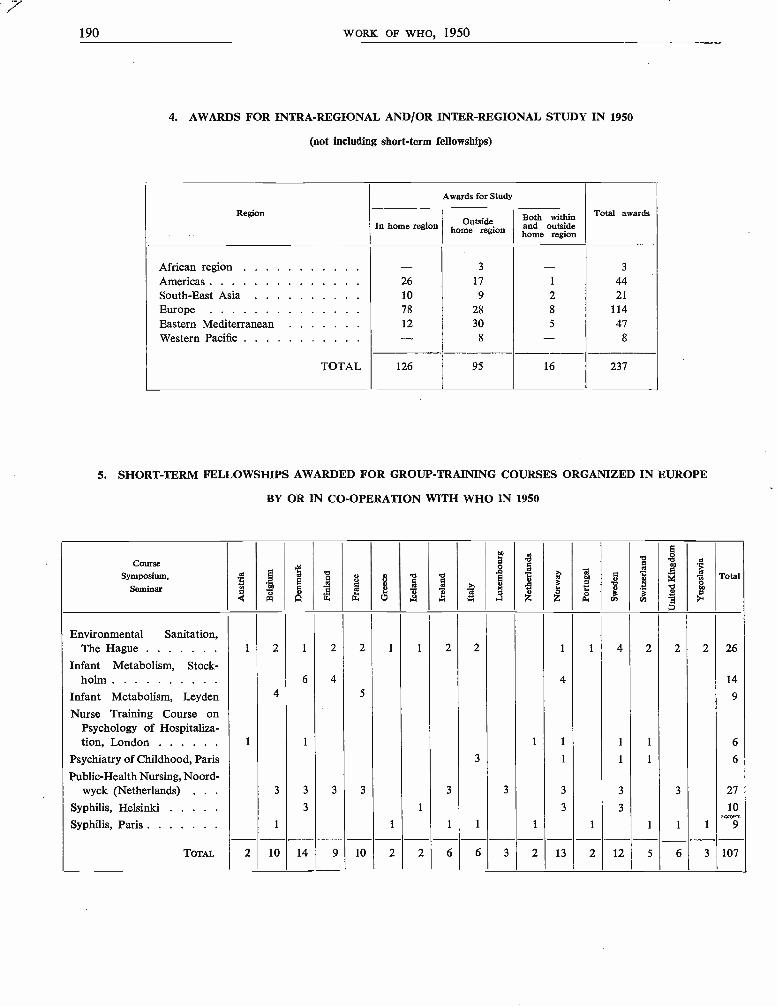
190 WORK OF WHO, 1950
4. AWARDS FOR INTRA -REGIONAL AND /OR INTER- REGIONAL STUDY IN 1950
(not including short -term fellowships)
Region
Awards for Study
Total awardsIn home region Outside
home regionBoth withinand outsidehome region
African region . . . . . . . . . - 3 - 3
Americas 26 17 1 44South -East Asia 10 9 2 21
Europe 78 28 8 114Eastern Mediterranean 12 30 5 47Western Pacific - 8 - 8
TOTAL 126 95 16 237
5. SHORT -TERM FELLOWSHIPS AWARDED FOR GROUP -TRAINING COURSES ORGANIZED IN EUROPE
BY OR IN CO- OPERATION WITH WHO IN 1950
Course
Symposium,
Seminarr°ÿ.a Ñ
w
il
pNA
q.oi7
w"
gyw
3HO
vm1
vp
ed
a-
a,
m
e
K1a
N
g
.%az
3mf.Oz
eo
oa
da
b
c'"áti
o
aI1N
2
^°
a'Total
Environmental Sanitation,The Hague 1 2 1 2 2 1 1 2 2 1 1 4 2 2 2 26
Infant Metabolism, Stock-holm 6 4 4 14
Infant Metabolism, Leyden 4 5 9
Nurse Training Course onPsychology of Hospitaliza-tion, London 1 1 1 1 1 1 6
Psychiatry of Childhood, Paris 3 1 1 1 6
Public -Health Nursing, Noord-wyck (Netherlands) 3 3 3 3 3 3 3 3 3 27
Syphilis, Helsinki 3 1 3 3 10
Syphilis, Paris 1 1 1 1 1 1 1 1 1
TOTAL. 2 10 14 9 10 2 2 6 6 3 2 13 2 12 5 6 3 107
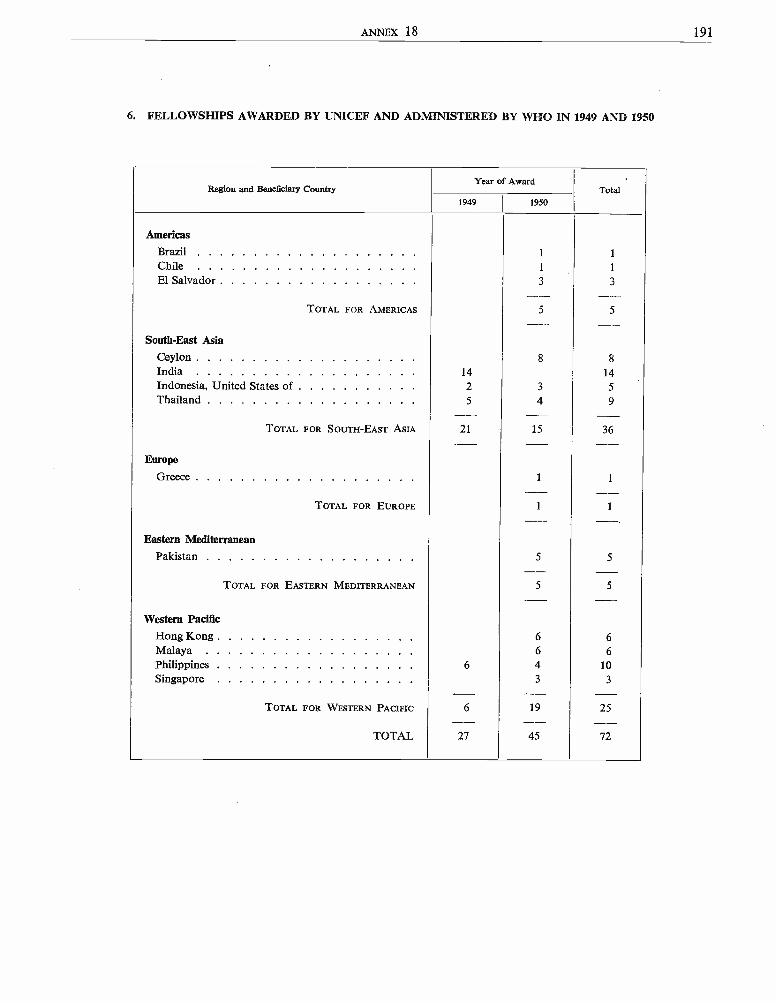
ANNEX 18 191
6. FELLOWSHIPS AWARDED BY UNICEF AND ADMINISTERED BY WHO IN 1949 AND 1950
Region and Beneficiary CountryYear of Award
Total1949 1950
Americas
Brazil 1 1
Chile 1 1
El Salvador 3 3
TOTAL FOR AMERICAS 5 5
South -East Asia
Ceylon 8 8
India 14 14Indonesia, United States of 2 3 5
Thailand 5 4 9
TOTAL FOR SOUTH -EAST ASIA 21 15 36
Europe
Greece 1 1
TOTAL FOR EUROPE 1 1
Eastern MediterraneanPakistan 5 5
TOTAL FOR EASTERN MEDITERRANEAN 5 5
Western Pacific
Hong Kong 6 6Malaya 6 6
Philippines 6 4 10
Singapore 3 3
TOTAL FOR WESTERN PACIFIC 6 19 25
TOTAL 27 45 72


SUPPLEMENT
SUMMARY ANALYSIS OF REPORTS FROM MEMBER STATES
SUMMARY ANALYSIS OF REPORTS FROM MEMBER STATES
Article 62 of the Constitution of the World Health Organization requires that " each Member shallreport annually on the action taken with respect to recommendations made to it by the Organization and withrespect to conventions, agreements and regulations ".
Rule 5(a) of the Rules of Procedure of the Health Assembly requires that the annual report of the Director -General shall include " a summary analysis of annual reports from Members under Articles 61 and 62 ofthe Constitution ".
A summary analysis of annual reports under Article 61 is not included in the present report pending furtherconsideration of the form of such reports by the Executive Board.
As a basis for the first summary analysis of reports under Article 62, a list of certain main recommendationsmade to governments by the Organization since its inception was circulated to Member States in August 1950with the request that the actions taken thereon up to 30 September 1950 be reported by 30 November 1950.1No doubt, because governments were thus given only a very short period in which to prepare the necessarymaterial, reports were received from only 13 Member States in time to be included.2
The brief statements in this supplement summarize the information contained in reports received fromGreece, Iceland, India, Iran, Ireland, Lebanon, New Zealand, Norway, Portugal, Syria, Thailand, Union ofSouth Africa and Venezuela.
Summaries are not strictly limited to actions taken up to 30 September 1950 since the reports receivedmade no clear distinction in many instances between procedures already in effect and actions taken in implementa-tion of WHO recommendations.
Establishment of National Committees on Vital andHealth Statistics
Five countries, Iceland, Norway, Portugal, Thai-land and Venezuela have established national com-mittees to deal with the recommendations of the Con-ference on the Sixth Decennial Revision of the Inter-national Lists of Diseases and Causes of Death,Paris, April 1948.3 The national committee inIceland has also undertaken statistical studiesof special public- health problems ; the nationalcommittee in Portugal has organized the compi-lation of statistical returns of notifiable diseases,the number of which has been increased from14 to 27. Five sub -committees have been formedin Venezuela to deal with problems arising fromthe application of the procedure laid down in theManual of the International Statistical Classificationof Diseases, Injuries and Causes of Death.
l Circular Letter 53, 19502 Reports received after 1 January 1951 will be included in
a summary in the annual report of the Director- General for1951.
3 Endorsed by the First World Health Assembly, Off. Rec.World Hlth Org. 13, 304, item 6(4)
Implementation of the recommendations is inprocess in India and under consideration by theGovernment of the Union of South Africa where theproposal has received the endorsement of the NationalHealth Council. A health statistics office, to beattached to the Ministry of Health in Greece has beenconsidered but postponed owing to a reorganizationof the general statistical services. The collection andevaluation of vital statistics, a function of the Depart-ment of Health in Ireland, is being transferred to anewly founded central statistics office which will beconcerned with application of the new nomenclatureof diseases and causes of death.
Although Iran has no specific national committee,questions relating to vital and health statistics aretaken care of by the national health statistics com-mission of the Ministry of Health.
Lebanon has established a national commission forvital and health statistics.
Registration, Compilation and Transmission of HealthStatistics
Resolution WHA2.39 of the Second World HealthAssembly, drawing attention to the importance of theregistration, compilation and transmission of health
- 195 -
196 SUPPLEMENT
statistics, has been given due consideration in Iceland,India, Ireland, Norway, Portugal and Thailand.4
In Iceland, comprehensive reports on public health,published annually, include vital and health statistics.Infant mortality statistics are based on definitions for" ° live births " and " stillbirths " (foetal deaths -group III) which are practically the same as thoserecommended by the Expert Committee on HealthStatistics, but reliable data are available only on still-births (foetal deaths -group III).
In India, a single organization under the " RegistrarGeneral and ex-officio Census Commissioner " dealswith population statistics, including vital statistics,and is concerned with developing and improvingtheir systematic collection.
Ireland has established a central statistics office tocentralize and further improve the quality of itsstatistics.
The Division of Vital Statistics attached to theDepartment of Public Health in Thailand has intro-duced some of the recommendations of the ExpertCommittee on Health Statistics. These recommenda-tions will also be taken into consideration in Portugalin due course, and in Norway in connexion with theplanned revision of an annual report on sanitaryand medical conditions (Sunnhetstilstanden og Medi-sinalforholdene), one of a series of official statisticsissued by the Central Bureau of Statistics. Therevision will be undertaken in consultation with theNational Committee on Health Statistics, and a sub-committee has been established as a first step towardsrealization of the plan.
Statistics on Mortality and Notifiable Diseases
Iceland, New Zealand and the Union of SouthAfrica reported that reliable statistics on mortalityand information on the proportion of deaths fromcertified causes are available in their published annualreports or official yearbooks.
An enumeration of the population is carried outeach year in Iceland where practically all deaths arereported, and where the proportion of deaths ade-quately certified is increasing, 86 % of the total deathsin 1946 -1948 having been certified as to cause byphysicians. Under a new act, passed in May 1950,death certificates by a qualified physician will becompulsory for all cases from 1 January 1951.
4 See also summaries on national committees on vital andhealth statistics, mortality and notifiable diseases, and WHORegulations No. 1.
The report from New Zealand stated that alldeaths are certified by physicians except for aproportion of Maori deaths. In Venezuelamedical certificates of death are compulsory inareas where there are physicians and death certi-ficates by the Civil Registrars are required in allother areas.
Venezuela also reported the creation of an area of" organized notification " from which the Ministryof Health and Social Welfare receives data of definitestatistical value on morbidity and mortality fromnotifiable communicable diseases. Tabulations ofdeaths from communicable diseases appear in threeseries of official publications ; a Weekly Epidemiologi-cal Bulletin for internal circulation, monthly tabula-tions, and a Yearbook of Epidemiology and VitalStatistics.
The reporting of the principal communicable dis-eases in Iceland is considered practically complete,that for milder infectious diseases complete only inthe smaller districts. New Zealand also reported thatits notification of the principal communicable diseasesis considered to be substantially accurate.
Weekly reporting of notifiable diseases is requiredin the Union of South Africa and Venezuela, and. inIceland from Reykjavik.
The recommendations of the Expert Committee onHealth Statistics regarding mortality statistics andnotifiable diseases s will receive due consideration inNorway in connexion with the revision of an annualreport on sanitary and medical conditions (Sunnhet-stilstanden og Medisinalforholdene), in Ireland andThailand, and to the extent possible in Iran wheremany areas have few if any physicians and no properadministrative machinery for registration and certifi-cation of causes of death.
Teaching and Training of Personnel in HealthStatistics
Courses of study in this particular field are availableto medical students and medical personnel in Iceland,India, New Zealand, Norway, Portugal, Thailandand Venezuela. In Thailand an introductory courseon health statistics is given to students of sanitationand general nursing ; a course on medical recordingprocedure and elementary statistical methodologyis given to all third year medical students ; and acourse in advanced statistical methodology andvital statistics is given at the School of Hygiene and
5 World Hlth Org. techn. Rep. Ser. 1950, 5
ANALYSIS OF REPORTS FROM MEMBER STATES 197
Public Health. In addition to courses for medicaldirectors of hospitals and physicians specializingin public -health work in Venezuela, training in thefundamental principles of statistics as applied tohealth is given to fifth year medical students. Clericalofficers employed by hospital boards in New Zea-land also receive instruction in methods of compilingand reporting for medical records.
Ireland, Iran and the Union of South Africa aregiving consideration to the resolution of the ExpertCommittee on Health Statistics in this connexion.6
WHO Regulations No. 1 Regarding Nomenclature(including the Compilation and Publication ofStatistics) with respect to Diseases and Causes ofDeath
Eight countries reported action on WHO Regu-lations No. 1. Iceland, India, New Zealand and theUnion of South Africa indicated that effect is beinggiven to application of the Regulations subject tocertain reservations and observations.' Icelandpostponed application until 1951 in order to avoiddisrupting the continuity of its statistics for the fiveyear period 1946 -1950. In Ireland, Norway, Portugaland Venezuela (considered as having adopted theWHO Regulations without reservations by virtueof Article 20) arrangements are being made to incor-porate the Regulations into their procedure forcompiling statistics of causes of death and includerevision of the certificate of cause of death in adher-ence to the international model, issuing of directivesto registrars, preparation of instructions to certifyingphysicians, etc.8
Indiscriminate Use and Unrestricted Distributionof Streptomycin 9
Warnings against the indiscriminate use andunrestricted distribution of streptomycin have beenofficially drawn to the attention of health authoritiesand medical practitioners in Greece, India, Ireland,Iran, Norway, Thailand, the Union of South Africaand Venezuela.
6 World Hlth Org. techn. Rep. Ser. 1950, 5Reservations made regarding individual articles of the
Regulations have been reported to Member States.See also summary on comparability of mortality statistics
and notifiable diseases.9 Of Rec. World Hlth Org. 17, 11, item 2.2.3
Although not subject to medical control in Greece,streptomycin may be obtained only with a doctor'scertificate. State -owned streptomycin is used prin-cipally for the free treatment of tubercular meningitisand miliary tuberculosis, for very exceptional casesin other forms of the disease such as tubercularlaryngitis, tubercular enteritis, etc. only on the adviceof a special commission, which determines the formof the disease to be so treated and examines all suchcases.
In Iceland, streptomycin is made available todoctors only by the state medicine import, the onlydistribution centre. Standard treatment regimenshave not been adopted and streptomycin therapyis carried out mainly in sanatoria and hospitals andonly occasionally in private practice.
The drug is issued in India only against certificatesby government medical officers and medical practi-tioners of high professional competence called" assessors ", who are specifically appointed for thepurpose by the Government on the recommendationof the State governments.
Supplies of the drug in New Zealand are limitedand are available to hospitals only.
One hospital in each of 15 provinces in Norway isofficially authorized to treat tubercular meningitisand miliary tuberculosis with streptomycin whichis furnished by the Government. Notification oftuberculosis cases so treated, and investigations ofstreptomycin resistance of tubercular bacilli inpulmonary patients is obligatory. Informationregarding the measures to be taken in order to limitthe spread of such bacilli has been outlined inofficial circular letters.
Indirect control over issues of streptomycin isexercised in the Union of South Africa by restrictingrefunds on expenditures for the drugs to dulyapproved cases only. Active research in its use inconjunction with sulfone derivatives and para-aminosalicylic acid has been carried out for someyears in tuberculosis hospitals under the controlof the Department of Health. In Venezuela thedrug is sold only on presentation of a medicalprescription.
Malaria Control
Only seven countries (Greece, India, Iran, Portu-gal, Thailand, the Union of South Africa and
198 SUPPLEMENT
Syria) reported on action taken for the control ofmalaria."
In Greece, after an experimental phase (1945)during which the effectiveness of modern methods ofmalaria control was proved and the techniquesadapted to local conditions, a national programmewas started in 1946 which has been continuedwithout interruption. Larval control, no longerapplied in rural areas has, for purely economicreasons, been adopted for the protection of urbancentres, with the substitution of DDT for the oldlarvicides, and this has considerably increased itseffectiveness. Although the initial objective of eradi-cating malaria has not been accomplished owing tothe fact that during 1946 -1949 guerilla activitiesand military operations prevented the nationalmalaria- control service from extending its controlprogramme to all the malarious areas in the country,the overall results have been more than satisfactory.Mass chemotherapy or chemoprophylaxis has notbeen adopted, and the demand for antimalariadrugs has been extremely small during the past fewyears.
In accordance with other measures recommendedby the Executive Board, efforts are being made by theMinistry of Agriculture to improve methods ofirrigation, cultivation and animal husbandry. TheMinistry of Reconstruction also gives duetion to the malaria factor when planning villagesfor repatriated persons, etc. Research on malariacontrol methods is encouraged. The results of exten-sive epidemiological surveys, carried out each yearto ascertain the malaria incidence and to provide aguide in the preparation of control programmes, arepublished regularly. Strict measures have beenadopted by the Athens Sanitary Airport to preventthe exportation or importation of living anophelesor other arthropods. These measures includeresidual spraying of constructions or habitationswithin a radius of 1 km., and disinsectization ofaircraft, etc. Close surveillance is maintained inorder that action may be taken if necessary.
The Malaria Institute of India, a central organiza-tion, provides technical advice on malaria controlin that country and training courses for medicalstudents and engineers ; conducts a wide programmeof research in the various aspects of the malariaproblems (including chemotherapeutic research) bothin the laboratory and in the field ; and also conductssuccessful demonstrations of control measures. Localorganizations, established in most of the malarious.
to For recommendations to governments on malaria control,see Off. Rec. World Hith Org. 25, 9, item 3.2.
States, have adopted the policy of malaria controlby residual spraying with DDT and other newinsecticides. Concurrent entomological and epide-miological investigations are undertaken wherevercontrol programmes are introduced. Due attentionis given to the possibilities of creating malariogenicconditions by new multipurpose projects includingirrigation and road construction, and antimalariaorganizations are associated with such projects fromtheir inception. Antimalaria legislation has beenenacted in a number of States.
The Government in Iran has devoted a largeproportion of its budget to malaria -control projectsand has established a malaria -control department.Abundant supplies of DDT have been made availablefor residual spraying. Steps have also been taken tosecure the services of an expert to explore the practi-cability of establishing plants for the local productionof insecticides in sufficient quantities for localconsumption and for export to other countries inthe Eastern Mediterranean region. DDT sprayers,entirely locally produced, are being tested. AllIranian Fellows, trained in the field of malaria underWHO fellowships, have been assigned to malaria -control projects on their return to Iran.
Potential malaria cases in Portugal may be esti-mated to be approximately 300,000. During 1949and 1950 a total of 142,465 individuals were pro-tected, mainly through the use of insecticides forresidual spraying. Mass treatment of infectedpersons was, however, continued in the 55 dispen-saries located throughout the country, and larvalcontrol was employed in certain urban centres andsome rice fields.
During a demonstration control programme inKarabu, Syria, DDT was applied to a total of 265,122square metres. In the light of the experience gained,the Health Ministry extended its campaign in 1950,with favourable results, to Hauram and to severalsummer resorts.
Waiving of Customs Duties on Insecticides
Insecticides have been exempt from customsduties 11 in Lebanon for the past year, and also inIran where a bill has been enacted requiring thewaiving of duties not only on DDT but also on allother antimalarial products such as aralen, palu-
11 The Third World Health Assembly, in resolutionWHA3.43, urged Member States to take action to ensure thefreer flow of insecticides.
ANALYSIS OF REPORTS FROM MEMBER STATES 199
drine, camoquin, quinine, atabrine etc. Measuresto this effect are under consideration in Ireland,Norway and the Union of South Africa, and willbe given due consideration in Thailand when themanufacture of formulated DDT is undertaken bythe Government.
Correct Labelling of Insecticides by Manufacturers
The issue of regulations requiring correct labellingof insecticidal products as regards their content inactive ingredients is under consideration in Iceland,India and Ireland. The recommendation of theSecond World Health Assembly to this effect (resolu-tion WHA2.18) has been drawn to the attentionof the proper authorities in Norway.
The Food, Drugs and Disinfectants Act, No. 13,passed by the Government of the Union of SouthAfrica in 1929 provides that such products, in so faras they may also be germicides, must be labelled soas to indicate, inter alia, their active ingredients.Machinery has also been set up for approval ofinsecticides intended for agricultural purposes.
No action has been taken in New Zealand wherethere are no insect -borne diseases apart from thosecaused by the common housefly, or in Thailand,since insecticides are not manufactured in thatcountry.
Maritime Aspects of Venereal -Disease Control
Five countries, Greece, Iceland, Ireland, NewZealand and Norway, reported that they werealready parties to the Brussels Agreement in 1950,that facilities for free treatment of seamen hadalready been established, and that therefore noaction was required.12 Greece is, however, consider-ing the establishment of additional dispensaries inports, other than Piraeus and Salonika, where theforeign traffic is considerable. The law in force inNorway on venereal diseases provides for examina-tion, treatment, free hospitalization, where necessary,and after- control free of charge, to all persons suf-fering from venereal disease, irrespective of natio-nality, place of residence or economic status.
India, Portugal, Thailand, Venezuela and theUnion of South Africa, though not yet parties to theAgreement, have nevertheless established treatmentfacilities in their respective countries. Regulations
12 The Executive Board at its fifth session approved therecommendations of the Expert Committee on VenerealInfections ( World Hlth Org. techn. Rep. Ser. 1950, 13), and drewthe attention of Member States to the importance of morecountries adhering to the Brussels Agreement. (Off. Rec. WorldHlth Org. 25, 11, item 3.2.4)
in force in the Union of South Africa provide for thelevying of charges upon ships using its ports todefray, in whole or in part, the expenses of hospitalsestablished for the care and treatment of seamen.
Adherence to the Agreement is under considera-tion in Thailand, and also in Iran.
National Laboratory Centres for Serodiagnosis ofSyphilis 13
India is planning the establishment of a centralvenereal- diseases organization in collaboration witha maternal and child care centre at the All -IndiaInstitute of Hygiene and Public Health, Calcutta,which will serve as a national reference laboratorycentre for serodiagnostic procedures in syphilis inthat country. Action on the designation of suchreference laboratories in the other countries underreview had either not been taken or was not reportedon.
Control of Bilharziasis
Due consideration is given to safety measures forcontrol of bilharziasis 14 in Venezuela where canalsand other waterworks of colonial origin constructedfor sugar -cane plantations are found to be infected.New irrigation canals, particularly in populatedareas and wherever contamination may arise, areplanned to prevent its development. Campaignshave been introduced for the construction and useof latrines, baths and wash -houses for public use,and notices are issued, wherever necessary, warningthe public not to enter contaminated waters. Periodicinspections are carried out by the Ministry of Healthand Social Welfare.
Safety measures for effective control are underconsideration in both Iran and the Union of SouthAfrica. Greece has taken no action since cases ofbilharziasis in that country are extremely rare andare imported from abroad.
Administrative Divisions for Maternal and ChildHealth
The recommendation of the Expert Committee onMaternal and Child Health that administrativedivisions be established in national health- adminis-
13 Recommended by the Sub- Committee on Serologyand Laboratory Aspects. World Hlth Org. techn. Rep. Ser.1950, 14, 13
14 Recommended by the Executive Board at its fifth session ;Off. Rec. World Hlth Org. 25, 6, item 2.1.6.3 ; and by the JointOIHP /WHO Study -Group on Bilharziasis in Africa, WorldHlth Org. techn. Rep. Ser. 1950, 17
200 SUPPLEMENT
trations 18 was implemented in 1950 in both Iranand Lebanon.
Iran created a special department within theframework of the Ministry of Health which isactively functioning under the direction of a well -qualified and experienced doctor. Steps are beingtaken to ensure its development and also the develop-ment of the maternal and child health programmes.Although the department works in close co- operationwith voluntary agencies it is considered as a depart-ment of the Ministry of Health.
The administrative division created in Lebanon issupervised by a hygienist who has just completed ayear's study at Harvard University, United States ofAmerica.
In Syria an encouraging beginning has been madeby the Ministry of Health in setting up a demonstra-tion centre of maternity and child welfare. Furtheradvances are being planned within the availablebudget.
Proposals to bring all questions relating to mater-nal and child health under the full jurisdiction of theMinistry of Health in Greece are under consideration.The recommendation was also given due considera-tion in both Iceland and Norway but changes in theorganization already established were not consideredwarranted or feasible.
Maternal and child health services in India,Ireland, Portugal, Thailand, Venezuela and theUnion of South Africa have been administeredin conformity with the recommendation of theexpert committee for some time. All maternityhospitals in New Zealand are under the close super-vision of the Department of Health and a service forinfant welfare is maintained by the New ZealandSociety for the Health of Women and Children.
Endemic Goitre and Use of Iodized Salt in GoitrousRegions 16
In response to the request for information concern-ing the incidence of endemic goitre and the preventivemeasures followed, Norway reported in 1949 that theincidence in that country had fallen to a point wherethe disease was no longer considered a major healthproblem. The fall in incidence might be attributedto the use of iodized table salt over a number ofyears and a considerable increase in the consumption
16 See Of Rec. World Hlth Org. 19, 4316 See recommendation of the FAO /WHO Expert Com-
mittee on Nutrition, World Hlth Org. techn. Rep. Ser. 1950,16, 14.
of salt -water fish. Intensive propaganda has resultedin the almost exclusive use of iodized salt which issold in goitrous areas at a price equivalent to thatof ordinary table salt. Children in a few of theelementary schools have been supplied with tabletscontaining iodine.
New Zealand also reported a reduction in incidenceof the disease in schoolchildren. The use of iodizedsalt, freely available for many years, is advocated ineducational propaganda.
Thailand, with a total of 25,972 cases reported in1950 following a survey of its various provinces, hasalso carried out a publicity campaign urging the useof foodstuffs containing iodine and has distributediodized salt in goitrous regions. Surveys have alsobeen conducted in Ireland, by the Medical ResearchCouncil, and iodized salt is available for those whowish to use it. Consideration is being given to thebest methods of promoting its use in areas wherethe disease is endemic.
The practicability of iodization of salt for humanconsumption is under consideration in India andVenezuela and also in South Africa where coarse rawsalt is consumed by a vast majority of the population.
Investigations on incidence and methods ofprevention are being made by the authorities inPortugal where the disease is endemic in certainareas.
Development of Psychiatric Treatment Facilities 17
Portugal has established three psychiatric welfarecentres responsible for the orientation, co- ordinationand supervision of psychiatric welfare in theirrespective zones, for the registration of patientsadmitted to official and private establishments, forgrants to patients' dependents and for compilation ofstatistics, etc. Apart from its own facilities and thoseof a central dispensary, each centre may call onregional dispensaries, psychiatric clinics, homes andhospitals within its zone. In addition to these psy-chiatric welfare centres, Portugal has 17 hospitalsand 30 mental -health dispensaries. Preventiveaction, observation and treatment of patients,supervision of those given domiciliary treatment, andmental -health consultations are carried out by thedispensaries. Acute and new cases are treatedin the out -patients' sections of clinics. Chronic
17 See recommendation of the Expert Committee on MentalHealth World Hlth Org. techn. Rep. Ser. 1950, 9, 32 (d).
ANALYSIS OP REPORTS FROM MEMBER STATES 201
diseases, for which in- patient treatment is advised, aretreated in homes where ergotherapy is available, i.e.,agricultural colonies, establishments for abnormalchildren, dangerous patients and for alcoholics anddrug addicts.
Venezuela reported that its psychiatric treatmentfacilities and trained personnel are far from adequate.National and state institutions provide approximately2,000 beds against an estimated need for approxi-mately 10,000. The training of social workers in psy-chiatry has been intensified and specialized training -courses are given to doctors, nurses and assistants.
Courses in psychiatry are also available for medicalstudents in Iceland at the State Psychiatric Hospital,where treatment and research facilities are wellprovided for. Treatment facilities available in themental hospitals in Ireland are free to those whoare unable to pay. Mental hospitals are providedand maintained by the Government in New Zealandwhere development of preventive measures is underconsideration. Norway's national programme alsoincludes provision for work in this field. A divisionof mental diseases in the Department of MedicalServices in Thailand is responsible for all mentalinstitutes and psychiatric treatment facilities in thatcountry.
Establishment of Preventive Mental -Health Sectionsin National Ministries of Health and of MentalHygiene Sections in Public- Health Institutes 18
Three countries, Ireland, Norway and Venezuela,have established mental -health divisions in theirnational health services. In addition to its maindivision, Norway has various clinics on the locallevel operated by the Mental Health Association, avoluntary organization. Venezuela has set up acentral mental -health dispensary which operatesin liaison with health units, is planning other dis-pensaries, and has also set up mental health sectionsin its Division for School Health, its Maternal andChild Health Division, and in the Venezuela Councilfor Children which works in co- operation with theMaternal and Child Health Division. Psychiatricclinics are also attached to the out -patients' depart-ments in hospitals.
Hospitals for mental diseases in New Zealand areadministered by the Department of Health. AlthoughIceland has no special mental health section in itsMinistry of Health, its psychiatric hospital servesas a consultative body on problems in this field. The
establishment of a section for mental health in thePublic Health Centre for Reykjavik is, however,being planned. Iran and Thailand are also consideringsetting up mental -health centres and the latter hasasked for a survey to be made of the mental-hygiene problems in the country.
Development of Mental Health Services for Children
According to the report submitted, progress hasbeen made in the development of mental- healthservices for children in Venezuela. Consultativeservices for children are available in a central dis-pensary and in a centre for children of pre -schoolage which will be attached to the division for maternaland child health. Services for abandoned childrenare available through the Venezuela Council forChildren, and there are observation facilities in arehabilitation institute attached to the federaldistrict. Plans are being made for the establishmentof institutes for child psychiatry in two zones whereall classes of abnormal children will receive in- andout -patient treatment, and which will providefacilities for training polyvalent personnel.
Mental -health services for children have also beenestablished in Greece, at a clinic attached to theAthens Psychiatric Hospital ; in Iceland, on a smallscale, in connexion with the public schools inReykjavik ; and in Norway in connexion with theschool- health services in the larger cities. Therecommendation of the Expert Committee on MentalHealth regarding such services 19 is under considera-tion in Iran, Ireland and Thailand.
International Biological Standards
The International Standard Preparations recom-mended for official recognition by the Third WorldHealth Assembly in resolution WHA3.8 have beenaccepted in Norway, Portugal and Thailand, and areunder consideration in Iceland. These standards willbe applied, in both Norway and Thailand, to prepa-rations to be included in the national pharmacopoeiasand also, in Norway, to all other products, outsidethe scope of the pharmacopoeia, which are labelled.
Amendments are being considered to regulationsin force in the Union of South Africa governing thecontrol of therapeutic substances, with a view toincluding those preparations recommended by the
19 Recommended by the Expert Committee on Mental 19 World Hlth Org. techa. Rep. Ser. 1950, 9, 35, sectionHealth, World Hlth Org. techa, Rep. Ser. 1950, 9, 32 (e). 14(e).

202 SUPPLEMENT
World Health Assembly but not already coveredby the existing regulations. India is examiningways of enforcing the application of the InternationalStandards under the provisions of its national DrugsAct, 1940.
World Health Day
In Iceland, India, Lebanon, New Zealand, Thai-land and the Union of South Africa, World HealthDay was observed on the official date, when publicitywas given in the press and on the radio to nationalpublic -health services and the work of WHO. InGreece, Iran and Portugal, however, observance ofWorld Health Day was postponed to other conve-nient dates due to the fact that 7 April conflictedwith important religious festivals or other occasions.Ireland and Norway reported that very little couldbe done in 1950 as the official date fell on GoodFriday.
The publicity campaigns, organized and conductedby national health services, emphasized the theme" Learn to know your own Health Services "
(particularly in Iran and Portugal) and outlinedthe aims and functions of WHO and its role in thenational health programmes. In Greece, attentionwas also drawn to the importance and responsibilityof the individual and to his role in the improvementof public health. In Iran, the material containedin the WHO Information Kit was translated intoPersian and was distributed to provincial and ruralhealth centres.
Official ceremonies were organized in Greece andIran at which lectures, following the line of the pressand radio publicity, were given to medical and hospi-tal personnel, government officials, students intraining institutes and in schools.
The ceremonies in Greece were spectacular. Aflame was carried from the Temple of Health inNauplia to the theatre of Epidaurus where repre-sentatives of the local authorities and more than5,000 persons were gathered. Various recitationsand addresses were given, school children formed theword Hygeia in the theatre and some, in costumeand accompanied by school choirs and a municipalband, performed national dances.