9241561653_eng.pdf - who | world health organization
TRANSCRIPT
The Work of WHO 1992-1993
Biennial Report of the Director-General
CORRIGENDUM
Page 2, column 1, line 1:
Delete 1993. The increase of$ 105 523 000 or 14.46% in
Insert 1993. The net increase of$ 87 165 000 or 11.86% in

The Work of WHO 1992·1993

The Work of WHO 1992·1993
Biennial Report of the Director-General to the World Health Assembly
and to the United Nations
-~ ~ . 'I .. ~ ~ ~ ~ ~""?~
World Health Organization Geneva 1994
The texts of the World Health Assembly and Executive Board resolutions referred to in this report can be found in the Handbook of Resolutions and Decisions of the World Health Assembly and the Executive Board, Volume I, 1948-1972, Volume II, 1973-1984 and Volume Ill, third edttion (1985-1992).
Throughout this volume the $ sign denotes US dollars.
The abbreviations used in this report include the following:
ACC -Administrative Committee on Coordination ACHR -Advisory Committee on Health Research AGFUND -Arab Gulf Programme for United Nations
Development Organizations ASEAN -Association of South-East Asian Nations CIDA -Canadian International Development
Agency CIOMS -Council for International Organizations of
Medical Sciences DANIDA -Danish International Development Agency ECA -Economic Commission for Africa ECE -Economic Commission for Europe ECLAC -Economic Commission for Latin America
and the Caribbean ESCAP - Economic and Social Commission for Asia
and the Pacific ESCW A - Economic and Social Commission for
Western Asia FAO -Food and Agriculture Organization of the
United Nations FINNIDA -Finnish International Development Agency GTZ -German Technical Cooperation Agency IAEA - International Atomic Energy Agency IARC -International Agency for Research on
ICAO IFAD
ILO
IMO ITU NORAD
Cancer -International Civil Aviation Organization -International Fund for Agricultural Devel-
opment - International Labour Organisation
(Office) - International Maritime Organization -International Telecommunication Union -Norwegian Agency for International
Development
OAU
OECD
PAHO
SAREC
SIDA
-Organization of African Unity
- Organisation for Economic Co-operation and Development
- Pan American Health Organization
- Swedish Agency for Research Cooperation with Developing Countries
- Swedish International Development Authority
UNCTAD -United Nations Conference on Trade and Development
UNDCP -United Nations International Drug Control Programme
UNDP -United Nations Development Programme
UNDRO -Office of the United Nations Disaster Relief Coordinator
UNEP -United Nations Environment Programme
UNESCO -United Nations Educational, Scientific and Cultural Organization
UNFPA -United Nations Population Fund
UNHCR -Office of the United Nations High Commissioner for Refugees
UNICEF -United Nations Children's Fund
UNIDO -United Nations Industrial Development Organization
UNRWA -United Nations Relief and Works Agency for Palestine Refugees in the Near East
USAID -United States Agency for International Development
WFP -World Food Programme
WHO -World Health Organization
WIPO - World Intellectual Property Organization
WMO -World Meteorological Organization
The World Health Organization welcomes requests for permission to reproduce or translate its publications, in part or in full. Applications and enquiries should be addressed to the Office of Publications, World Health Organization, Geneva, Switzerland, which will be glad to provide the latest information on any changes made to the text, plans for new editions, and reprints and translations already available.
ISBN 92 4 156165 3 © World Health Organization 1994
Publications of the World Health Organization enjoy copyright protection in accordance with the provisions of Protocol2 of the Universal Copyright Convention. All rights reserved.
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers' products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
ISSN 0509 2558 PRINTED IN SWITZERLAND
93/9852-At.r-4700
iv
Introduction
1.
2.
3.
4.
5.
6.
Governing bodies
WHO's general programme development and management
Constitutional and legal matters WHO's programme development Informatics management External coordination for health and social development Emergency relief operations
Strategy for health for all
Monitoring and evaluation Regional and national activities and policies Health for all and economic development
Health system development
Assessment of global health situation and future trends Intensified cooperation with countries and peoples in greatest need Technical cooperation among developing countries Health systems research and development Health legislation
Organization of health systems based on primary health care
National health systems and policies District health systems
Development of human resources for health
Policy analysis, planning and management Nursing Educational development Staff development
V
Contents
IX
1
3
3 3 4 4 7
11
11 11 12
13
13 15 16 17 18
21
21 23
27
27 29 30 33
7.
8.
9.
THE WORK OF WHO 1992-1993
Public information and education for health
Public information Education for health
Research promotion and development
General health protection and promotion
Women, health and development Food and nutrition Oral health Injury prevention Tobacco or health
10. Protection and promotion of the health of specific population groups
Maternal and child health and family planning Health of adolescents Human reproduction research Occupational health Health of the elderly
11. Protection and promotion of mental health
Mental health policy, and support to national programmes Psychosocial and behavioural problems and relevant interventions Prevention and control of alcohol and drug abuse Mental and neurological services and treatment
12. Promotion of environmental health
Community water supply and sanitation Environmental health in rural and urban development and housing International Programme on Chemical Safety Control of environmental health hazards
13. Diagnostic, therapeutic and rehabilitative technology
Clinical technology Health laboratory technology and blood safety Radiation medicine Technology development, assessment and transfer Drug management and policies Pharmaceuticals Biologicals Traditional medicine Action Programme on Essential Drugs Rehabilitation
vi
35
35 35
39
43
43 44 47 49 50
53
53 56 58 62 63
65
65 66 66 68
71
71 72 74 75
77
77 77 78 78 78 79 80 80 80 82
14. Disease prevention and control
Immunization Control of tropical diseases Disease vector control Leprosy Tropical disease research Diarrhoeal diseases Acute respiratory infections Tuberculosis Zoonoses
CONTENTS
AIDS and other sexually transmitted diseases Other communicable diseases Research and development in the field of vaccines Blindness and deafness Cancer International Agency for Research on Cancer Cardiovascular diseases Other noncommunicable diseases
15. Health information support
Health literature services WHO publications Technical terminology Distribution and sales
16. Support services
Personnel Office accommodation Budget and finance Equipment and supplies for Member States
Map showing regional offices and the areas they serve
17. African Region
18. Region of the Americas
19. South-East Asia Region
20. European Region
21. Eastern Mediterranean Region
vii
85
85 88 96 97 99
101 103 105 106 108 113 116 117 118 120 121 123
125
125 126 128 128
129
129 129 130 131
132
133
137
141
145
149
THE WORK OF WHO 1992-1993
22. Western Pacific Region
Annex 1. Members and Associate Members of the World Health Organization
Annex 2. Regional distribution of Members and Associate Members of the World Health Organization
Annex 3. Organizational and related meetings, 1992-1993
Annex 4. Intergovernmental organizations that have entered into formal agreements with WHO approved by the World Health Assembly, and nongovernmental organizations in official relations with WHO at 31 December 1993
Annex 5. Structure of the World Health Organization at 31 December 1993 (charts)
Index
viii
153
159
161
163
164
167
171

Introduction
The period 1992-1993 was marked by deep economic and social tensions as well as ethnic, religious and territorial conflicts, on a scale unprecedented since the second world war. In these difficult circumstances WHO continued to deliver its programme of work, to help countries sustain their health achievements, strengthen their human resource capabilities, and enhance their disease prevention and control activities. At the same time WHO initiated a review of its policies, management and structures in order to adapt to the challenges, constraints and opportunities of the changing global environment.
In 1993, within the overall reform process undertaken with the Executive Board and its working group on the WHO response to global change, I introduced a number of mechanisms to enhance coordination throughout WHO's worldwide network. The Global Policy Council, whose membership includes the Regional Directors, and the Management Development Committee will ensure joint participation of headquarters and the regions in all stages of decision-making, from the formulation of strategies and updating of policies to the coordination and tightening of programme budget management procedures, in particular through the development and harmonization of information systems.
During this biennium WHO upheld its commitment to health for all through primary health care, increasing its direct technical support to countries, and coordinating international health work with a view to reducing inequities in access to health care, both between and within countries. WHO's proposed Ninth General Programme of Work (1996-2001) takes the same approach and, to foster cross-sectoral collaboration, suggests a new "clustering" of programmes and activities around four interrelated policy orientations: integration of health and human development in all public policies; equity in access to health services; promotion and protection of health; prevention and control of specific health problems.
In 1992-1993 WHO put much effort into providing countries with workable guidelines and indicators and helping them set measurable goals and targets to achieve cogency in the planning, implementation and evaluation of their health policies and activities nationwide. The establishment and maintenance of a good database have proved essential for identifying health issues, priorities and critical strategies for health development, and for monitoring resources and impact. WHO made a major contribution to the World Bank's World development report 1993: investing in health and seized this opportunity to re-emphasize the close interaction between health, social and economic development.
ix
THE WORK OF WHO 1992-1993
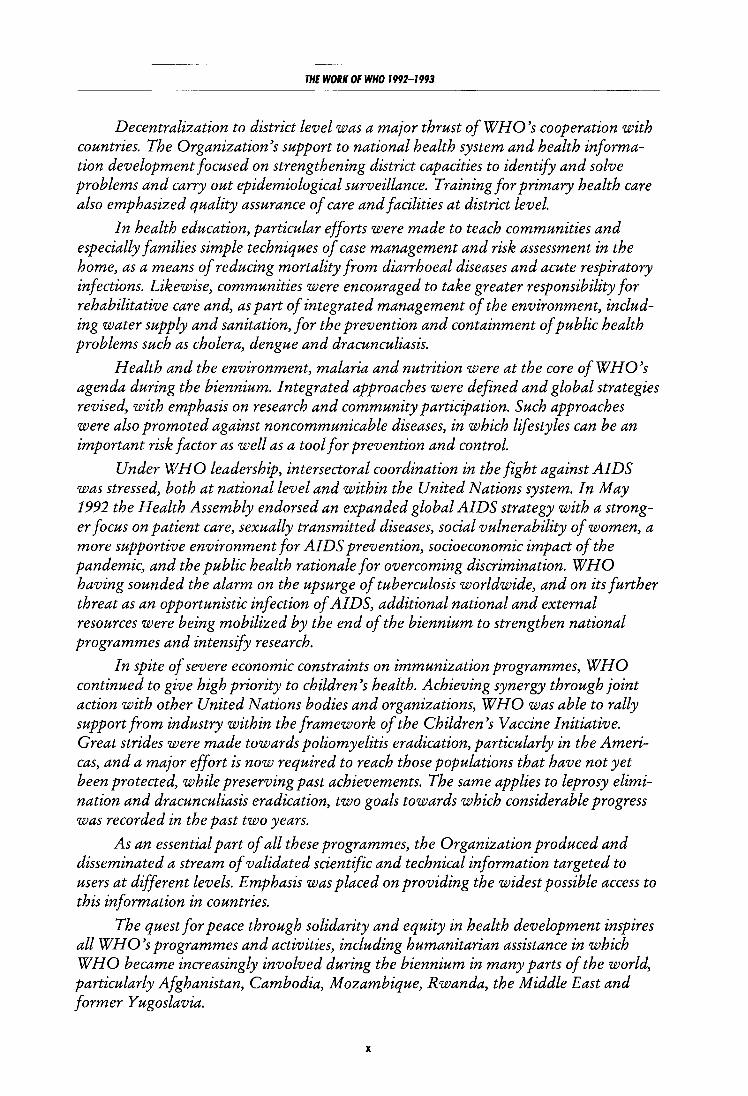
Decentralization to district level was a major thrust of WHO's cooperation with countries. The Organization's support to national health system and health information development focused on strengthening district capacities to identify and solve problems and carry out epidemiological surveillance. Training for primary health care also emphasized quality assurance of care and facilities at district level.
In health education, particular efforts were made to teach communities and especially families simple techniques of case management and risk assessment in the home, as a means of reducing mortality from diarrhoea! diseases and acute respiratory infections. Likewise, communities were encouraged to take greater responsibility for rehabilitative care and, as part of integrated management of the environment, including water supply and sanitation, for the prevention and containment of public health problems such as cholera, dengue and dracunculiasis.
Health and the environment, malaria and nutrition were at the core of WHO's agenda during the biennium. Integrated approaches were defined and global strategies revised, with emphasis on research and community participation. Such approaches were also promoted against noncommunicable diseases, in which lifestyles can be an important risk factor as well as a tool for prevention and control.
Under WHO leadership, intersectoral coordination in the fight against AIDS was stressed, both at national level and within the United Nations system. In May 1992 the Health Assembly endorsed an expanded global AIDS strategy with a stronger focus on patient care, sexually transmitted diseases, social vulnerability of women, a more supportive environment for AIDS prevention, socioeconomic impact of the pandemic, and the public health rationale for overcoming discrimination. WHO having sounded the alarm on the upsurge of tuberculosis worldwide, and on its further threat as an opportunistic infection of AIDS, additional national and external resources were being mobilized by the end of the biennium to strengthen national programmes and intensify research.
In spite of severe economic constraints on immunization programmes, WHO continued to give high priority to children's health. Achieving synergy through joint action with other United Nations bodies and organizations, WHO was able to rally support from industry within the framework of the Children's Vaccine Initiative. Great strides were made towards poliomyelitis eradication, particularly in the Americas, and a major effort is now required to reach those populations that have not yet been protected, while preserving past achievements. The same applies to leprosy elimination and dracunculiasis eradication, two goals towards which considerable progress was recorded in the past two years.
As an essential part of all these programmes, the Organization produced and disseminated a stream of validated scientific and technical information targeted to users at different levels. Emphasis was placed on providing the widest possible access to this information in countries.
The quest for peace through solidarity and equity in health development inspires all WHO's programmes and activities, including humanitarian assistance in which WHO became increasingly involved during the biennium in many parts of the world, particularly Afghanistan, Cambodia, Mozambique, Rwanda, the Middle East and former Yugoslavia.
X
INTRODUCTION
Based on a better appreciation of global interdependence and a reassessment of health within our societies, the "new health partnership" advocated by WHO stresses the need for all countries, sectors, communities and private citizens to share resources and responsibilities, thus making solidarity a deliberate and reasoned policy, at national as well as international level. The reform process which WHO has embarked on will facilitate partnerships with Member States, building both on the diversity of WHO's regions and on their common purpose to achieve health for all in a spirit of justice and mutual respect.
Vf. •
Director-General
xi

1.1 With profound changes sweeping the world, the Organization has undertaken a careful re-examination of its mission and strategies. An important step in this process was the establishment in January 1992 of a working group on the WHO response to global change (decision EB89(19)) with responsibility for drawing up recommendations concerning the Organization's mission, leadership role, preparedness for changes in priorities, and structure; strengthening of WHO's coordinating role within the United Nations system; orientation and preparation of the Ninth General Programme of Work; and enhancement of the technical quality of the Organization's programmes. The group concluded its work during the biennium and submitted detailed recommendations on those points. A number dealt with the Executive Board's own method of work, and one in particular proposed that subgroups or committees of the Board should meet during the Executive Board sessions to review specific programmes. The Programme Committee of the Executive Board met in November 1993 to review planning for the implementation of the Working Group's recommendations prior to their consideration by the Board.
1.2 The interrelation of environment, health and development was highlighted by addresses to the Health Assembly in May 1992. Mr Mario Soares, President of Portugal, spoke of the need, following the ending of the cold war, for renewed efforts to achieve "a new world order founded on law and greater equality of opportunity for all human beings". Dr J aime Paz Zamora, President of Bolivia, referred to the earth as one large ecosystem and life as a phenomenon of global interdependence. Technical Discussions were held on the related theme of "Women, health and development".
1.3 Health Assembly resolutions in 1992 included a request for the establishment of a global
CHAPTER 1
Governing bodies
commissiOn on women's health (resolution WHA45.25), which is to hold its first meeting shortly. In 1993 the Health Assembly called for budgetary reform (resolution WHA46.35), and decided to shorten the duration of the Health Assembly in even-numbered years when programme budgets are not discussed (resolution WHA46.11). Dr Hiroshi Nakajima was reappointed Director-General of the World Health Organization (resolution WHA46.2); he called for a "new partnership in health" to meet the challenge of increasing worldwide change.
1 4 In 1992 the regional committees reviewed the proposed activities to be carried out in each WHO Region1 during the 1994-1995 biennium in the same way that the Executive Board, through its Programme Committee and in accordance with resolution EB79.R9, reviewed the proposed global and interregional activities. These proposals provided the basis for preparation of the Organization's 1994-1995 programme budget, approved by the Health Assembly in May 1993. At the same time the regional committees in 1993, at the request of the Executive Board, studied the implications of recommendations made by the Board's working group on the WHO response to global change, as applicable to regional and country activities, with a view to reporting to the Board in January 1994.
1.5 The Forty-sixth World Health Assembly approved for 1994-1995 an effective working budget level of$ 822 101 000.2 This represents a decrease of 3.5% in real terms when compared with the approved programme budget for 1992-
1 See Annex 2 for d1stnbut1on of Member States and Associate Members 1n the SIX WHO regions: Africa, Americas, South-East Asia, Europe, Eastern Mediterranean, Western Pac1fic.
2 Throughout this book the s1gn $ denotes United States dollars.

THE WORK OF WHO 1992-1993
1993. The increase of$ 105 523 000 or 14.46% in 1994-1995, compared with 1992-1993, is attributable to estimated inflationary cost increases of almost 11% as well as statutory salary and other unavoidable cost increases for which adequate budgetary provision has not been made in recent
2
years. The Health Assembly agreed to reduce assessments on individual Members by their share of the amount of interest earned and available for appropriation($ 12 741 000), credited to them in accordance with the incentive scheme established by resolution WHA41.12.
CHAPTER 2
WHO's general programme development and management
Constitutional and legal matters
2.1 Several changes occurred in the membership of the Organization during the biennium (see Annex 1 ), with the result that there were 187 Members and two Associate Members as at 31 December 1993. Ukraine notified WHO that it wished to reactivate its membership in the Organization.
2 2 During the biennium 34 instruments of acceptance were deposited for the amendment of Articles 24 and 25 of the Constitution to provide for an increase in the membership of the Executive Board from 31 to 32 (resolution WHA39.6); this brought the number of acceptances to 118, the requirement for adoption being two-thirds of the Organization's membership. No instrument of acceptance was deposited for the amendment of Article 7 on suspension of rights and privileges of Members (resolution WHA18.48), so the number of acceptances remained 53. Similarly, no instrument of acceptance was deposited for the amendment of Article 74 to include an Arabic version among the authentic texts of the Constitution (resolution WHA31.18), and the number of acceptances remained 34.
2.3 Cameroon and Bahrain acceded to the Convention on the Privileges and Immunities of the Specialized Agencies with respect to WHO on 30 April and 17 September 1992 respectively. Ukraine and Belarus, which had previously acceded to the Convention with respect to other agencies, submitted notifications of application of the Convention with respect to WHO. Instruments of succession to the Convention were submitted by Bosnia and Herzegovina, Czech Republic, Croatia, Slovakia and Slovenia. As a result, 102 Member States had accepted the Convention with respect to WHO by the end of the biennium.
3
WHO's programme development
Ninth General Programme of Work
2.4 Preparation of WHO's Ninth General Programme of Work covering a specific period (1996-2001), initiated by the Executive Board at its January 1992 session, was pursued by the Board's Programme Committee, the regional committees and staff at all levels of the Organization throughout the biennium; a final draft will be submitted to the Board for review in January 1994. It emphasizes WHO's role in supporting countries and the international health community, and in reducing inequities in the health sector. It provides a global framework for health policy by defining goals and targets. The targets include specific improvements in health, access to care and services of good quality, and policy design and implementation, and are presented as the minimum of what should be achieved by the year 2001. Four related orientations are proposed to reach the goals.
Programme development and management
2 5 To strengthen WHO's policy-making capacity and to ensure effective implementation of programmes and application of the recommendations of the Executive Board's working group on the WHO response to global change (see paragraph 1.1), the Director-General has established a Global Policy Council. The members are the Director-General, the Regional Directors, the Assistant Directors-General and the Director of IARC. The Council's mandate is to restate the mission of WHO in the light of world

THE WORK OF WHO 1992-1993
changes; to review the global and regional strategies for health for all; to ensure the monitoring of the attainment of health-for-all targets and their periodic updating; to ensure that, through the necessary coordination, programme implementation at headquarters, regional and country levels conforms to the global policy, while giving due respect to national priorities; and to adjust WHO's managerial structure to reforms stemming from WHO's response to global change. The Council held its first meeting in November 1993. It will be supported in its work by a Management Development Committee, particularly in matters of management coordination throughout the Organization.
Programme budgeting
2 6 Zero budget growth for six consecutive bienniums has led to a real reduction in the Organization's regular budget and a greater dependence on extrabudgetary resources; this has accentuated the need to be selective in developing WHO's programmes. The Director-General has continued to transfer some resources from existing activities to areas of high priority determined in previous bienniums.
2.7 Resolution WHA46.35 called for profound changes in the way the Organization's programme budget is prepared, starting with the 1996-1997 biennium. It stressed the importance of setting realistic targets and describing "measurable outcomes", and of ensuring the highest standards of accountability and transparency. It expressed concern about the complexity and lack of clarity of the existing budget documents, particularly about the failure to relate financial allocations and staff costs to specific priorities. As a result, the programme budget for the financial period 1996-1997 will be prepared in a simplified form. It will show how strategic and financial priorities are determined within agreed global objectives; how realistic and measurable targets are established in accordance with each health priority; and how a process of regular evaluation tracks progress towards the agreed targets. There will be fewer budgetary tables and more information about sources of financing, both regular and extrabudgetary.
2.8 At regional level several measures were taken to strengthen WHO's programme development and management. In the Americas
4
PAHO/WHO started to assess the effects of "strategic orientations and programme priorities" on policy-making and health development in Member States and on technical cooperation. In the Eastern Mediterranean visits were arranged to enable senior health officials to study WHO's policies and strategies and to exchange views on ways to ensure optimal allocation of resources to priorities.
lnformatics management
2 9 More WHO staff throughout the world were assured of access to a microcomputer connected to a local area network. A new network was commissioned for the Regional Office for South-East Asia in September 1992. WH 0 headquarters became a node of the Internet "network of communications networks" as a first stage in establishing economical and effective communications within and outside the Organization. Central management for both administrative and health databases was updated using new software. PAHO/WHO began replacing its computerized administrative system, and the system in the Regional Office for Europe was also updated. In general, regional offices and certain country offices continued to make more effective use of their administrative and programme management systems. Steps were taken to foster closer interregional cooperation in the use of these systems. WHO supported several Member States in developing their health information systems and improving their reporting systems, including Mexico, Oman, Seychelles, Syrian Arab Republic, United Arab Emirates and six countries in the Western Pacific. The Organization also played an active part in international conferences on health cards (Marseille, France, September 1993) and on health informatics in Africa (Ile-Ife, Nigeria, April 1993).
External coordination for health and social development
2.10 The biennium was marked by the continuing concern of all organizations of the United Nations system to streamline structures and integrate development cooperation programmes with those for humanitarian assistance and peace-keeping. The financial resources of the
WHO'S GENERAL PROGRAMME DEVELOPMENT AND MANAGEMENT
system were stretched as never before, with a vast discrepancy between the tasks assigned and funds available.
2 11 Restructuring of the social and economic sectors of the United Nations system moved ahead. To be able to respond more effectively to the new international situation, the Administrative Committee on Coordination (A CC) carried out a review of its role and functioning. WHO was fully involved in this review process, which began with a meeting in April 1992 at WHO headquarters in Geneva, and was completed at a meeting in April 1993 at FAO headquarters in Rome. WHO is a member of the two consultative bodies reporting to ACC - the Consultative Committee on Administrative Questions (CCAQ) and the Consultative Committee on Programme and Operational Questions (CCPOQ). WHO is one of the nine core members of the ACC Inter-Agency Committee on Sustainable Development which was set up to consider policy relating to follow-up of the 1992 United Nations Conference on Environment and Development and to monitor implementation of Agenda 21 (see paragraph 12.1).
212 The Commission on Sustainable Development was established as a 53-member intergovernmental body by the Economic and Social Council (resolution 1993/207) at the request of the United Nations General Assembly (resolution 471191). At its first meeting in June 1993 this body agreed on a programme of work for the period 1993-1996. WH 0 has been assigned the responsibility for implementation of the health chapter of Agenda 21.
213 WHO provided documentation, technical information and guidance for the discussions with the Economic and Social Council and other organizations of the United Nations system on the prevention and control of HIVIAIDS, leading to a better understanding at political level of the magnitude of the problem and the responsibility of governments. The Council recognized the urgent need to invest in preventive measures and to avoid discrimination against those infected with HIV or suffering from AIDS, approved the activities of the Commission on Human Rights in this respect, endorsed the updated global AIDS strategy and gave its full support to resolution WHA46.37 concerning the feasibility and practicability of establishing a joint, cosponsored United Nations programme on HIV I AIDS. In addition, ACC in October 1993
s
endorsed the WHO policy on non-sponsorship of international conferences on AIDS in countries with HIV I AIDS-specific travel restrictions (resolution WHA45.35) and recommended that all organizations of the United Nations system adopt this policy.
2.14 The Council gave greater prominence to health and social development in its deliberations during 1992 and 1993. WHO, in collaboration with 11 other organizations of the United Nations system, prepared the Secretary-General's report to the 1993 Council's substantive session on preventive action and intensification of the struggle against malaria and diarrhoea! diseases, especially cholera; in 1994 the Secretary-General of the United Nations will submit a report on improved coordination to the Council, specifying goals, workplans, schedules and the resources required to combat these scourges. The Council also adopted a resolution on the subject of tobacco or health (see paragraph 9.53).
2.15 WHO participated in Council discussions on enhancing international cooperation for development, covering the role of the United Nations system, assistance in the eradication of poverty and support to vulnerable groups, the coordination of humanitarian assistance, emergency relief and the "continuum" from relief to rehabilitation and development. WHO was also involved in Council deliberations on the International Year of the Family (1994 ), control of narcotic drugs and psychotropic substances, and strengthening of international cooperation and coordination of efforts to minimize the consequences of the Chernobyl disaster.
216 Together with other agencies, WHO reported to the Council on the implementation of United Nations General Assembly resolution 471199 concerning operational activities of the United Nations system, which called for a substantial increase in multilateral resources for development. WHO emphasized, particularly through CCPOQ, the importance of making action of the United Nations system more responsive to national objectives and more efficient. For instance, WHO supported the establishment of United Nations country offices and confirmed its interest in sharing premises that are being established in Moscow.
217 WHO held discussions and exchanged information with the five United Nations regional commissions: the Economic Commissions for Af-

THE WORK OF WHO 1992-1993
rica, for Europe, and for Latin America and the Caribbean, and the Economic and Social Commissions for Asia and the Pacific, and for Western Asia.
218 The UNICEF/WHO Joint Committee on Health Policy met at WHO headquarters in 1992 and 1993 to discuss, in particular, ways and means to achieve the goals set by the 1990 World Summit for Children, and improved management of district health systems as an essential element of infrastructure.
2.19 From early 1992 WHO joined the World Bank in preparing and launching the Bank's 1993 report, 1 which examines the interplay between health, health policy and economic development. In addition to attending the meeting of the boards of governors of the World Bank and the International Monetary Fund, WHO participated in the annual meetings of the boards of governors of the African Development Bank, the Asian Development Bank, the European Bank for Reconstruction and Development, and the Inter-American Development Bank, all of which are increasingly active in the social sector. In accordance with Executive Board resolution EB92.R4, a draft cooperation agreement is being used as a framework for relations between WHO and the African Development Bank and the African Development Fund prior to submission of this document to the World Health Assembly in May 1994. Opportunities to enhance the collaborative framework and pursue existing and new areas of cooperation were discussed with these multilateral financial institutions on several occasions in 1992 and 1993.
2 20 Joint UNDP/WHO activities were consolidated, and new areas for collaboration determined, particularly at country level.
2 21 WHO coordinated act1v1t1es with UNFPA through that body's technical support services, which include multidisciplinary, interagency country support teams in eight locations throughout the world. The administrative arm of the technical support services is the UNFP A interagency task force, which meets once or twice a year, bringing together organizations within the United Nations system, including WHO. WHO was represented at expert group meetings on population and development and at
1 World Bank. World development report 1993 mvestmg tn health New York, Oxford Unrversity Press, 1993.
6
meetings convened by UNFP A to prepare for the 1994 international conference on population and development.
2 22 WHO expanded collaboration with the Organization of African Unity (OAU) through the WHO Office for OAU and ECA on several subjects including malaria, AIDS, nutrition, humanitarian action and emergency assistance, and on the formulation of a health protocol for the Treaty Establishing the African Economic Community.
2 23 Following the signature of a letter of intent between WHO and the Commission of the European Communities early in 1992, a representative of the Director-General was appointed to facilitate cooperation with the European institutions, concentrating on providing technical expertise for the Commission's regulatory activities and on promoting the health aspects of the European Community's development work. In May 1993 the Council of Ministers invited the Commission to ensure closer cooperation with WHO. Collaboration was also intensified with OECD and other intergovernmental organizations outside the United Nations system.
2 24 During the biennium WHO undertook policy and technical reviews with various governments to strengthen existing collaboration, devise new forms of cooperation, and solicit extrabudgetary support for the Organization's health programmes at global, regional and country levels. The government officials participating in the reviews represented multilateral and bilateral cooperation departments in the appropriate ministries, thus ensuring a comprehensive approach to meeting health needs. Representatives from several countries2 were particularly active in securing support for health programmes coordinated by WHO. Despite the global economic recession affecting official development assistance levels, extrabudgetary support for the Organization's work was maintained. Additional policy consultations organized in 1993 resulted in long-term agreements on financial and other support being offered to WHO so that it can accomplish the work approved by the Member States.
2 25 The work of WHO continued to benefit from the resources made available by the
2 Austrra, Canada, France, Germany, Ireland, Italy, Japan, Netherlands, Norway, Sweden, Swrtzerland, United Krngdom, Unrted States of America.
WHO'S GENERAL PROGRAMME DEVELOPMENT AND MANAGEMENT
nongovernmental community, especially those of the 177 nongovernmental organizations in official relations, a further twelve of which were admitted during the biennium. Examples of this wide-ranging collaboration are humanitarian assistance with the International Federation of Red Cross and Red Crescent Societies and the International Committee of the Red Cross; training of medical personnel with the International Society for Prosthetics and Orthotics and La Leche League International; community mobilization for vaccination programmes with Rotary International; and advocacy in relation to the special needs of women and female children with the International Alliance of Women and Soroptimist International.
2 26 In addition to its work related to the strategy of intensified cooperation with countries and peoples in greatest need, the Organization promoted partnership between governments and cooperating agencies (United Nations, multilateral, bilateral and nongovernmental organizations) so that external resources could be provided for maximum effect in support of overall health development. WHO participated in reviews of bilateral support to certain countries, for instance, support from the Netherlands and Sweden to Zambia. Another example of cooperative work was the fourth population and health project ( 1992-1996) in Bangladesh, costing $ 600 million and managed by the World Bank through a multi-donor consortium in which WHO has an influential voice as well as being executing agency for 21 of the 65 project components. Further examples were a review in Chad carried out in coordination with the African Development Bank, and cooperation in Mozambique in preparing a 12-year development programme for implementation with FINNIDA support.
2.27 The international community's concern about deteriorating health in the former Soviet Union found expression in the convening of a ministerial-level coordinating conference on assistance to the new republics (Washington, January 1992). During the conference a medical working group was set up to meet regularly and conduct missions to assess health needs in the republics. This group agreed on terms of reference for a clearing-house for information on health assistance to the republics; and responsibility for administering it was entrusted to WHO at a second coordinating conference (Lisbon, May 1992). The clearing-house's tasks include collating, analysing and disseminating in-
1
formation on health needs in the republics, and drawing them to the attention of the international community; setting up databases; monitoring the health situation in each republic; and maintaining country information profiles. So far existing WHO information sources have been used to prepare an operational database on the republics, and a health news bulletin issued in English, French and Russian for exchange of information on the health situation, on assistance received and on cooperation established.
Emergency relief operations
2 28 In addition to communicable diseases and other long-standing problems affecting health in many Member States, ecological change, rural-urban migration and severe natural or man-made disasters have posed threats to the very existence of health services in some countries in recent years. WHO has therefore strengthened its mechanisms for emergency preparedness, humanitarian assistance, and relief and rehabilitation in situations of armed conflict. A number of Health Assembly resolutions have endorsed increased involvement by WHO in this field. 1
2.29 Some 20 African countries have benefited from enhanced relief activities. In Eritrea WHO is cooperating in UNHCR efforts to resettle some half a million refugees. In the next phase it is planned to strengthen provincial health services to meet the needs of returning refugees and displaced persons, thus ensuring a continuum of support from relief to rehabilitation. One of several emergency health programmes in Ethiopia provides for the rehabilitation of about 40 provincial hospitals, health centres and health posts. In Mozambique WHO is helping to implement a programme of primary health care for some 100 000 demobilized soldiers, including on-thespot treatment of ailments, health education, collection of epidemiological data, and provision of supplies and equipment.
1 Emergency and humamtarian relief operations (WHA46.6) Health condrtrons of the Arab population rn the occupied Arab terrrtorres, rncluding Polestrne (WHA46 26) Collaboration withrn the United Notrons system health assistance to specrfrc countries - Cuba (WHA46 28) Colloborotron withrn the Unrted Notrons system health assistance to specrfrc countrres (WHA46.29). Health and medrcol servrces in trmes of armed conflict (WHA46.39)

THE WORK OF WHO 1992-1993
2.30 WHO participated in the work of the UNHCR-coordinated interagency task force set up to determine the requirements of republics of the former Soviet Union for humanitarian assistance (see paragraph 2.27), and drew up a health sector plan of action for the consolidated appeal launched for Armenia, Azerbaijan, Georgia and Tajikistan. Activities in the war-afflicted areas of former Yugoslavia included the establishment of programmes for health monitoring, nutritional surveillance, rehabilitation of war victims, provision of medical supplies and additional support in winter.
2.31 WHO is contributing to United Nations programmes for humanitarian assistance to a number of countries in the Eastern Mediterranean; emergency medical supplies and equipment were provided to war-torn regions of Afghani-
stan; considerable quantities of medicines and medical supplies were distributed in Iraq to alleviate extreme shortages resulting from the Gulf conflict; and support was given in setting up a central pharmacy and a reference laboratory and in providing urgent medical assistance in Somalia. WHO is also working closely with local health institutions and experts, as well as Palestinians from the occupied Arab territories, in preparing a master plan for transfer of authority and responsibility for health services and the promotion of broader regional cooperation in health matters. In Egypt a national emergency plan was prepared and a conference organized (Cairo, November 1993) in conjunction with the annual promotion day for the International Decade for Natural Disaster Reduction. Other interventions included support to the Islamic Republic of Iran and to Yemen.
WHO emergency health kits ready for shipment to disaster-stricken areas of the world.
WHO emergency health ki ts me a reliable, standardized, inexpensive, appropriate and quickly available source of the essential drugs (none of them injectable), renewable medical supplies (co tton wool, gloves, etc.) ond health equipment (including o complete steril ization kit) urgently needed in o disaster situation. They ore designed to be used by o primary health core worker with li mited training who treats symptoms rather thon diagnosing diseases. Eoch kit is sufficient for about I 0 000 outpatient consultations ond con serve o population of I 0 000 people for o period of ap proximately three months.
8
WHO'S GENERAL PROGRAMME DEVELOPMENT AND MANAGEMENT
2.32 WHO provided medical kits and other emergency supplies to several countries affected by natural disasters.1 Tuberculosis drugs and technical services were supplied to Cambodia, where WHO is cooperating with UNHCR in the ·repatriation of refugees.
2.33 Workshops were held for training emergency health managers from Asia and the Pacific
1 Albama, Bangladesh, Egypt, Eritrea, Kyrgyzstan, Lebanon, Lesotho, Madagascar, Malawr, Namibia, Pakistan, Phrlrpprnes, Rwanda, Srerra Leone, Swaziland, Unrted Republrc of Tanzania, Yemen, Zambia.
9
(Bangkok, February 1993) and Africa (Tangiers, Morocco, May 1993). Training in emergency relief and humanitarian assistance was organized for WHO Representatives and staff in the Eastern Mediterranean. WHO and the International Committee of the Red Cross cosponsored two emergency preparedness training courses in Geneva and Manila. A consultation convened in October 1992 to discuss a programme on health and development for displaced persons (Hedip) was attended by experts from 16 countries as well as staff of the United Nations and other agencies. A quarterly magazine, Hedip forum, was launched in April 1993, and pilot programmes are under way in several countries.

CHAPTER 3
Strategy for health for all
Monitoring and evaluation
3 1 In May 1992 the Health Assembly approved the report on the second evaluation of the implementation of the Global Strategy for Health for All by theY ear 2000, which is also the eighth report on the world health situation and is based on national and regional evaluation reports. A total of 151 Member States with a population of 5200 million reported their findings concerning advances made and constraints encountered in improving health throughout the world and in providing services on a basis of equity. The global review and reports from the six WHO regions have been published.1
3.2 A common framework was developed for use by Member States in carrying out a third exercise in monitoring progress in the implementation of the health-for-all strategy, from late 1993 to early 1994. It will enable Member States to review achievements in the application of their national health-for-all strategies and report the findings to WHO, using common criteria. Particular importance is attached to the collection and presentation of data broken down according to geographical area, sex, age and priority population groups.
3.3 WHO and UNICEF have agreed on a set of indicators for monitoring progress towards the health goals set by the 1990 World Summit for Children. Joint activities by WHO and UNICEF should prove helpful to both organizations in their efforts to monitor implementation of the health-for-all strategy and attainment
1 Implemental/On of the Global Strategy for Health for All by the Year 2000, second evaluatron. Erghth report on the world health srtuotron, Vols 1-7. Geneva, World Health Organization, 1993
11
of the World Summit goals. At a meeting in October 1993 it was agreed that a joint UNICEF/WHO statement should be issued expressing commitment to the monitoring process agreed to at the Summit, including assessment of mid-decade achievements. It was also agreed to expedite the preparation of comprehensive guidelines on health indicators.
Regional and national activities and policies
3 4 In the Americas the Second Ibero-American Conference of Heads of State and Government and the XXXVI meeting of the Directing Council of PAHO/forty-fourth session of the Regional Committee for the Americas in September 1992 adopted, in pursuance of the regional strategy for health for all, a regional plan for investment in the environment and health. The plan, which specifies investments that will need to be made in Latin America and the Caribbean over the next 12 years, will be useful for guiding countries, institutions financing development, and cooperation agencies in remedying deficiencies in drinking-water supply, wastewater treatment, basic sanitation services and other environmental health measures.
3 5 WHO supported activities to improve the health of the underprivileged in Bangladesh, India, Mongolia, Nepal and Thailand, following a 1991 consultation on this subject which had recommended the adoption of a strategy linking measures for economic and social development that draw upon the energy, inventiveness and capability of the local population. Health ministers from South-East Asia also discussed ways to promote the health of the underprivileged at their ninth meeting (Male, March-April 1993).

THE WORK OF WHO 1992-1993
3 6 Implementation of the health-for-all policy in Europe progressed steadily despite major changes and the diversity of conditions in the Member States, many of which now have national policies based on the European regional policy, an updated version of which was published in 1993\ or have explicitly incorporated elements of it into their legislation and policy documents. Meetings and other activities took place during the biennium in preparation for a 1994 European conference on health policy, at which participants will take stock of developments, explore new avenues for participation with organizations such as the Council of Europe, the Commission of the European Communities and OECD, and consider ways to ensure that health for all is the goal pursued by European Member States for the remainder of the century and beyond.
3.7 In Europe a "regions for health" network was established in 1992, with an initial grouping of 11 regions: 10 in Belgium, France, Germany, Spain, Sweden, Switzerland and the United Kingdom, and a Baltic region comprising Estonia, Latvia and Lithuania. In order to accelerate the implementation of national health policies, it was felt that regions should work together to promote the health-for-all policy according to a strategy that emphasizes dynamic alliances, cooperation to improve health at regional and local levels, transfer of knowledge, the organization of high-quality, effective services without waste or unnecessary duplication, and intersectoral action that makes health for all a common responsibility. A first annual meeting (Barcelona, Spain, October 1993) examined practical examples of ways to orient health professionals towards health promotion.
Health for all and economic development
3 8 In many of the poorest countries, public resources for health have been seriously reduced owing to recent macroeconomic developments,
1 Health for all targets the health polrcy for Europe Copenhagen, World Health Organization, 1993 (Health for All Senes, No 4).
12
and it has therefore become even more necessary than ever for decision-makers to design health policies that take this fact into account. Determining and assessing economically feasible options for the financing, delivery and administration of health services is an important component of WHO's initiative for intensified cooperation with countries and peoples in greatest need, which tackles urgent problems but is also concerned with priorities among human needs (see paragraph 4.11).
3 9 In June 1992 an international conference considered the link in countries in greatest need between the macroeconomic environment and health, examining in detail such issues as health and economic growth, policies for macroeconomic adjustment and for the elimination of poverty, and macroeconomic aspects of health financing. Case studies were presented on Bolivia, Chad, Guinea, Guinea-Bissau, Malawi, Mali and Nepal as well as Latin America and the Caribbean as a whole; they showed how the macroeconomic environment affects health conditions and how it influences the establishment or adjustment of health policies and health financing schemes.
310 WHO contributed to the preparation of the World Bank's 1993 report,2 which examines the interplay between human health, health policy and economic development. This report was used as a point of departure by more than 150 representatives of bilateral and multilateral aid agencies, foundations, international organizations and developing countries at a major conference supported by WHO and the World Bank and hosted by the International Development Research Centre (Ottawa, October 1993 ); this conference provided an opportunity to establish a framework for promoting partnerships so that external aid can be used more effectively for improving health in the developing world. One of the main aims of WHO's contribution will be to reinforce the capacity of countries to formulate and implement effective health policies, thereby facilitating their access to external support.
2 World Bank. World development report 1993 rnvestmg in health. New York, Oxford Unrversity Press, 1993
CHAPTER 4
Health system development
Assessment of global health situation and future trends
4.1 Data collected during the second evaluation of the Global Strategy for Health for All by the Year 2000 have been entered into WHO's health-for-all database. Two documents intended as an aid to ensuring consistency of data disseminated by WHO programmes were updated: one, on global health situation and projections1, provides agreed estimates for many diseases and causes of death, and the other, on demographic data for health assessment and projections2, presents United Nations data in a convenient tabular format. The World health statistics annual provided analyses of the health situation and trends in addition to the latest statistics on causes of death. The World health statistics quarterly dealt with such themes as demographic trends, aging and noncommunicable diseases, diabetes, violence and health, and mortality from cardiovascular diseases in developing countries. A regional bulletin provided information on the health situation, health programmes, demography and socioeconomic conditions in South-East Asia during the period 1988-1990.3
4.2 A network of over 300 experts on health monitoring, evaluation and "futures studies" has proved useful for sharing findings with a view to better management of health systems. In July 1993, a consultation on "health futures" 4 looked at ways to apply futures studies to support health policy formulation and health system reform; many methods, including some from developing countries, were considered promising. It is pro-
1 Document WHO/HST/92 1. 2 Document WHO/HST/GSP /93.2. 3 Document SEA/HS/186 4 Document WHO/HST/93 4.
13
posed to set up an enhanced network for sharing methods, expertise and training opportunities, and WHO will apply some of these techniques in its analysis and formulation of health policy and strategy. A regional consultation (Prague, July 1992) discussed the present environment and future trends of health in Europe, and considered the implications for health action.
Country health information development
4 3 Missions were organized to Cambodia, Guinea-Bissau and Maldives under WHO's intensified cooperation initiative and also to Bangladesh where WHO is responsible for developing the management information system for health and for strengthening the Institute of Epidemiology, Disease Control and Research in Dhaka as part of the World Bank's fourth population and health project. Support, including the organization of workshops, was given for strengthening national health information systems including the improvement of medical records systems in Cambodia, Fiji, Marshall Islands, Micronesia (Federated States of), Samoa and T onga; surveillance of childhood diseases in Cameroon; phased implementation of a health information system in India; strengthening of national epidemiological capacity in Pakistan; health information support at district level in Togo; and cholera surveillance in Zambia. WHO also advised on the establishment of an emergency monitoring system for former Yugoslavia.
4.4 As shown by the dramatic changes in Europe, there is now an unprecedented demand for health information within national information systems. At the same time it is important to make health managers more "information-sensitive". For this purpose projects for training epidemiologists in decision-making and management have
THE WORK OF WHO 1992-1993
been undertaken in the Americas and WHO is providing support for a special course on health data management in the Western Pacific. In the Eastern Mediterranean intercountry activities involving senior national staff were organized to promote the use of epidemiology for disease prevention and control; a regional advisory panel on health information systems was established; and a plan of action for the creation or improvement of a health statistics information system was prepared.
4 5 Progress has been made in developing methods for rapid evaluation and problem-solving procedures for district teams. These have proved effective both for staff training and for planning and improvement of services, and have already been applied in programmes such as that on safe motherhood. Taking into account the new emphasis on public health action at district level, the type of information system required and the means for generating information to support work at this level were discussed by an expert committee in November 1993.
Epidemiological surveillance and statistical services
4 6 WHO continued to support Member States in the implementation of the International health regulations and to disseminate information through the Weekly epidemiological record and an annual update of the International travel and health booklet. A project on epidemiological surveillance systems was developed for the Central American countries. The risk of introduction of cholera in this subregion was assessed and disease outbreaks in Belize and Guyana were investigated by the Caribbean Epidemiology Centre (CAREC).
4.7 An informal WHO/UNICEF consultation in December 19921 made operational recommendations for measuring cause-specific and overall mortality in children, especially in the absence of civil registration systems, in the context of monitoring the health goals set by the 1990 World Summit for Children. A subsequent meeting of experts drafted questionnaires to be used during verbal autopsies as well as a protocol for their evaluation.
1 Document WHO/ESM/UNICEF /CONS/92 5
14
4.8 Epidemiological and statistical support was given to various WHO technical programmes such as those on cardiovascular and tropical diseases. Advice was given on database management for national control programmes, including geographical information systems; development of new health and service indicators; and evaluation of health care systems. Work is also being done on developing methods for the analysis of data from multiple sources as well as new epidemiological methods, including non-conventional procedures and multiple-cause analysis. Countries in Europe are being asked to study and describe the measures they use and report their findings in order to identify cultural differences that may affect measurements of the quality of life.
4 9 The WHO statistical information system (WHOSIS) was upgraded to make it more functional and accessible, and a limited version is now available internationally over Internet, the worldwide computer network. WHO also collaborates within the Consortium for International Earth Science Information Network (CIESIN) to ensure international access to its databases. The Regional Office for the Eastern Mediterranean now has its own health statistics database on its local area network system, thus facilitating the use of health information by programmes and countries. WHO cooperated with the United Nations Statistical Commission, notably by presenting a review of statistical activities related to health at the twenty-sixth session of the ACC Subcommittee on Statistical Activities in April 1992. WHO contributed to the World Bank's 1993 report/ especially in the assessment of the global burden of disease. PAHO/WHO continued to collaborate with the Organization of American States on strategies to improve the coverage and quality of vital statistics in the Americas.
International classification of diseases and other health-related classifications
4.10 Volume 1 (tabular list)3 of the tenth revision of the International Classification of Dis-
2 World Bank. World development report 1993. mvesting in health New York, Oxford Umversrty Press, 1993
l International stat1st1cal classificatiOn of d1seases and related health prob· /ems. Vol. 1 Geneva, World Health Organizatron, 1992

HEALTH SYSTEM DEVELOPMENT
eases (ICD-10) was published in English in 1992 and French in 1993; volume 2 (instruction manual)1 was published in English in 1993, and the French version is in preparation; volume 3 (alphabetical index) is in press in English and in preparation in French. PAHOIWHO is preparing the Spanish versions. National versions and other health-related classifications are being produced in collaboration with WHO technical programmes, scientific associations and nongovernmental organizations. A three-character version of I CD-1 0, containing the rules, definitions, standards and its own index, is being prepared in English and French to meet the needs of developing countries. The mechanism for updating ICD between revisions has been tested and proved to be feasible. A first international computer-based course for reorientation of trained coders in the use of ICD-10 (Southampton, United Kingdom, April 1992) brought together participants from five regions, who will now be able to train other national coders. Regional training courses for early implementation of ICD-10 have been undertaken. A meeting was held to prepare the revision of the International Classification of Impairments, Disabilities and Handicaps2
(Zoetermeer, Netherlands, March 1992), and a reprint incorporating a foreword and a number of corrections to the original version was issued in January 1993. On the occasion of the twentyseventh session of the ACC Subcommittee on Statistical Activities held in Geneva, the centenary of the ICD was commemorated on 7 September 1993 in collaboration with the International Statistical Institute, the Swiss Federal Office of Statistics and the United Nations Statistical Division.
Intensified cooperation with countries and peoples in greatest need
4.11 Health policy and strategy development is a crucial issue for countries undergoing political and economic reforms and/ or transition from emergency to recovery and rehabilitation. It is therefore a major thrust of the WHO initiative
1 International statistical classdlcat/On of d1seases and related health prob· /ems. Vol 2 Geneva, World Health OrganiZatiOn, 1993
1 InternatiOnal classification of lmpalfments, d1sabiilt1es and hand1caps A manual relatmg to the consequences of disease. Geneva, World Health Organization, 1980.
IS
Intensified WHO cooperation
• The chronic global economic recession of the past decade has made it even more difficult for very poor countries to meet the health needs of their populations, and consequently the gap in health service coverage between these countries and the rest of the world has widened. It was against this background that WHO, in 1989, launched the initiative that has come to be known as intensified cooperation with countries and peoples in greatest need. It seeks to coordinate resources and programmes and mobilize international commitment to meet health and development needs on a country-by-country baSIS.
The initiative is country-specific since it is recognized that there are considerable variations not only in the health problems of countries but also in their human and financial resources and the effectiveness of their health systems. The aim is therefore not merely to provide expert advice, but to ensure that staff of both governmental and other agencies are equipped to fulfil their responsibilities. This is a particularly important requirement for ensuring sustainability of health development in very poor countries.
Agreement to launch activities under the WHO initiative in a given country is followed by a joint analysis by WHO and national staff of the different aspects of health development, including the economic and institutional environment for the provision of health care, and an assessment of the form and volume of contributions by donor agencies and the role of private and nongovernmental organizations. The aim is to identify critical strategic issues in health development, areas where resources are most urgently needed, and options for action.
for intensified cooperation with countries and peoples in greatest need (see box).3 Activities in
'The 1n1t1at1ve 1s currently being Implemented in 25 countr1es. Bangladesh, Ben1n, Bol1v1a, Cambod1a, Cape Verde, Central Afr1can Republic, Chad, Dpbouti, Eth1op1a, Guatemala, Guinea, Gu1nea·B1ssau, Ha1t1, Loo People's Democratic Republ1c, Mald1ves, Mongol1a, Mozambique, Myanmar, Nepal, Sao Tome and Pr1ncipe, Uganda, V1et Nom, Yemen, Za1re, Zamb1a
THE WORK OF WHO 1992-1993
this area during the biennium included support to the ministries of health in Mongolia, Mozambique, Yemen and Zambia in reviewing their health policy and implementing health systems reform.
4 12 National policy-making is not the only entry-point for WHO intervention; attention is also given to decentralization and reorganization of health systems. Provincial and district management was in fact the immediate priority in Guinea-Bissau and the Lao People's Democratic Republic. However, strengthening of health management at this level was not an end in itself, and the management teams were subsequently able to play a more active role in national policy development, with a clearer idea of how the other levels should be supported from the centre.
4 13 Developing capacity for economic analySIS 1s another important element of the WHO initiative. In Nepal WHO helped to establish an interministerial task force on health economics, which is now in a position to analyse the health development implications of different scenarios in relation to economic growth and the availability of external financing.
4.14 Partnership with other development agencies (see paragraph 2.26) ensures conformity with national policy, joint project preparation and coordination of funding and is likewise an important feature of the WHO initiative. In Bangladesh donor coordination for the country's fourth population and health project is managed by theW orld Bank through a donor consortium. WHO is the executing agency for 21 of the 65 project components, making it possible to coordinate all the disease control components and giving the Organization an influential voice in the consortium.
415 The WHO initiative is also concerned with supporting governments on aid management. The new national health policy in Mozambique, for instance, forms the basis of a longterm health development plan, which the Government will be able to use to coordinate external cooperation and ensure that it focuses on the country's priority needs. For this purpose, WHO staff introduced Ministry of Health officials to computer software programmes that can be used to keep track of the volume, purpose and disbursement of donor funds.
4.16 Finally, strengthening and integration of disease control is an important thrust of the
16
WHO initiative, as in the Bangladesh project. In Guatemala a training programme on acute communicable diseases control and sanitation surveillance on farms with migrant workers was set up, and has significantly reduced cholera outbreaks. Similarly, an intersectoral approach to cholera control was developed in Zambia.
4.17 Demand for support through the WHO initiative is expected to increase in the future and experience indicates a need to concentrate on the following areas: integration of health into overall socioeconomic development, and poverty alleviation; better use of economic analysis in identifying policy options and guiding health sector reform; improved management of external aid; better coordination of support by different United Nations bodies at country level; and establishment of a stronger link between activities of the WHO initiative and the Organization's overall resource allocation to the countries concerned, so as to focus WHO country budgets on key strategic issues.
Technical cooperation among developing countries (TCDC)
4.18 An interregional consultation on programming of technical cooperation among developing countries in health Qakarta, February 1993) examined country experiences and made recommendations for strengthening this initiative. It considered strategies for promotion and advocacy, recommended the establishment of national focal points for TCDC in health and considered the monitoring, evaluation and financing of activities. The report of the consultation was discussed by the seventeenth meeting of Ministers of Health of Non-Aligned and Other Developing Countries (Geneva, May 1993), who adopted a resolution on this subject.
419 Examples of global and regional activities undertaken during the biennium include support to the Caribbean Cooperation in Health initiative; technical cooperation in pharmaceuticals among ASEAN countries; and TCDC in research, development and research training in human reproduction, including family planning (see paragraphs 10.36-10.41). In the latter activity encouragement is given to efforts such as preparation of research protocols whereby advanced institutions in developing countries support institutions in other developing countries. It is

HEALTH SYSTEM DEVELOPMENT
planned to invest some $ 1 million in these cooperative activities during the next biennium, with the Rockefeller Foundation providing one-half of this sum. WHO actively participates in interagency work in TCDC, including that of the United Nations High-Level Committee on the Review of Technical Cooperation Among Developing Countries and the UNDP Special Unit for TCDC.
Health systems research and development
4 20 Many countries have initiated activities in health systems research, which is now generally recognized as an effective method for acquiring information needed for rational decision-making in health management. WHO has sought to encourage such work, to strengthen national capacities and to ensure sustainability in these efforts. A global working group (Lilongwe, November 1993), bringing together international experts and representatives of nongovernmental organizations, international health research programmes and donor agencies, endorsed this strategy and set long-term priorities for the strengthening of research institutions, cooperation with other institutions and individuals, and consolidation of knowledge in areas of concern to many countries.
4.21 Bridge, the international newsletter on health systems research supported by the International Development Research Centre (Canada), continued to appear three times a year in English and- in collaboration with WHO regional officesArabic and Spanish. It currently covers some ten international health research networks informally organized into a consortium known as the Puebla Group which facilitates cooperation among health researchers in Africa, Latin America and Asia. A first directory of training programmes in health services research, providing practical information on some 150 training programmes, was produced in collaboration with the Foundation for Health Services Research (USA). WHO supported regional meetings in Africa (Kampala, April 1992; Mbabane, May 1993; Lilongwe, November 1993) and theW estern Pacific (Malaysia, 1993) as well as country meetings (Madagascar, Morocco, Namibia, Nigeria, Philippines, Thailand), bringing together decision-makers in governments, nongovernmental organizations, the academic world and research, in order to reinforce commitment to health systems research.
17
4.22 Through the Network of Communityoriented Educational Institutions for Health Sciences, WHO has promoted health systems research in some 15 medical schools in different regions. University task forces to strengthen research capacity were established in the United Republic of Tanzania, Zambia and Zimbabwe. An anthology of health services research was published by PAHO/WH0.1 A separate budgetary allocation for institutional strengthening grants was established in South-East Asia, and response to this scheme has been generally favourable. A workshop was held in collaboration with the European Medical Research Council to support countries of eastern and central Europe in reorganizing their health research administrations and to promote information exchange among European countries. A meeting was convened to devise strategies to improve cooperation between ministries of health and universities in the Eastern Mediterranean (Cairo, June 1992). To increase inputs from social sciences into health systems research, collaborative activities have been pursued with the International Forum for Social Sciences in Health and its regional networks. A third interregional training workshop for senior research managers (Cuernavaca, Mexico, July 1992) was held to promote networking in this field between lead institutions; this was followed in 1993 by regional training courses in Malawi and Thailand.
4.23 WHO, PAHO and the International Development Research Centre (Canada) have produced a five-volume set of training guides2 providing instruction for all levels of health professionals, researchers and managers in the concepts and practice of health systems research; volume 2 contains the core course, volume 1 is intended for decision-makers, volume 3 for researchers and academics, volume 4 for research managers and volume 5 for those who plan to teach.
4.24 The project on health systems research for southern Africa, administered jointly by WHO and the Ministry for Development Cooperation and the Royal Tropical Institute of the Netherlands, has been extended for a second phase of four years (1992-1995) during which infrastruc-
1 White KL et al., eds Health se!VIces research an anthology. Washrngton, Pan American Health Organizatron, 1992 (Screntrfrc Publication, No. 534).
2 Available from. Communications Drvisron, IDRC, PO Box 8500, Ottawa, Ontarro, Canada KIG 3H9.

THE WORK OF WHO 1992-1993
ture and institutional arrangements in the 13 participating countries will be further strengthened and the experience applied to other countries (Cameroon, Ghana, Kenya, Nigeria, Uganda) and other regions. The fourth intercountry workshop on this project (Lilongwe, November 1993) reviewed achievements, identified areas requiring additional efforts, and recommended strategies for consolidating this work. Innovative approaches for further institutionalizing health systems research have been developed through regional task forces and meetings (Teheran, J anuary, 1992; Cuernavaca, Mexico, August 1992; Copenhagen, October, 1993; Y angon, October, 1993). A number of countries (India, Indonesia and Myanmar) have made specific provision for health systems research in their national budgets. Effective partnerships for the application of research in solving priority problems have been established both within the Organization, for instance with the leprosy, human reproduction, tuberculosis, nursing and AIDS programmes, and with other bodies such as the nongovernmental Council on Health Research for Development, UNICEF in respect of the Bamako Initiative, and the Washington-based International Health Policy Programme.
Health legislation
4.25 Major developments in health and environmental legislation occurred in many Member States during the biennium, for example in support of the health reforms in countries of central and eastern Europe. WHO seeks to facilitate such reforms, notably by supplying reliable information but also through direct technical cooperation. Thus consultant services were provided to some 20 countries, and national workshops were organized in several countries, including China, India and Pakistan. WHO also cooperated extensively with the Russian Federation. In an innovative project PAHO/WHO worked directly with legislatures in the Americas, drawing up model health legislation in priority areas and preparing comparative analyses.
4 26 The cornerstone of WHO's work in information transfer at global level remains the quarterly International digest of health legislation, which serves as a clearing-house to give Member States necessary information in userfriendly form. Documentation available to WHO is also communicated in forms such as
18
databases; so far these are available in priority fields of legislation including HIV I AIDS, tobacco or health, and organ transplantation. The LEYES database, containing an index to Latin American and Caribbean health legislation, continues to be produced by PAHOIWHO, and is now available on compact disc. A computerized listing of health legislation enacted or issued in Europe in 1990-1991 was produced in 1992.
4.27 Technical support took diverse forms in the different regions. The Regional Office for Africa has received an unprecedented number of requests for cooperation, and has undertaken an evaluation to measure the impact of legislation at national, district and community levels. A high level of interest in patients' rights in Europe led to a study on this subject, the results of which have been published.1 WHO is working closely with Member States in the Eastern Mediterranean to establish, on the basis of precise legal standards, an appropriate health legislation framework which is perceived as a prerequisite for effective utilization of health resources. In the Western Pacific WH 0 is cooperating with countries in the formulation or revision of legislation, so as to provide a sound foundation for the promotion and implementation of national health policies and strategies. Indeed, in most parts of that Region, health legislation is now seen as a means of promoting beneficial change rather than merely curbing abuses. In China cooperative activities focus on the development of new forms of legislation to deal with priority issues such as health care financing and the registration of health professionals. Throughout theW estern Pacific particular emphasis is placed on using legislation to support action on health priorities such as the effective deployment of human resources, financial viability and quality of care.
4.28 WHO monitors and reports on all significant international, national and subnationallegal instruments dealing with HIV I AIDS, and was closely involved in meetings at which legal, human rights and ethical aspects were discussed. It also monitors laws and other measures for implementation of the International Code of Marketing of Breast-milk Substitutes. Workshops were convened to discuss policy issues relating to application of the Code at national level, and direct
1 See Leenen HJJ, Gevers JKM, Prnet G. The nghts of patients m Europe· a comparative study. Deventer, Kluwer Law and Taxation Publrshers, 1993

HEALTH SYSTEM DEVELOPMENT
support was given to countries in the preparation of implementing legislation.
4 29 An intercountry meeting on health legislation (Cairo, December 1993) provided an opportunity to exchange information and experience and to promote the concept of health legislation as a tool for strengthening health policies and strategies. WHO was involved in preparations for the World Conference on Human Rights (Vienna, June 1993), for which it drew up position papers and commissioned a major re-
19
port on human rights in relation to women's health (see paragraph 9.3). The Organization was also represented at United Nations meetings on human rights issues and cooperates closely with the United Nations Centre for Human Rights. Similarly, close working relations are maintained with other agencies and bodies with an interest in health legislation, within and outside the United Nations system. In the field of bioethics, close links were maintained, in particular with UNESCO, the Council of Europe and CIOMS.

CHAPTER 5
Organization of health systems based on primary health care
National health systems and policies
Health economics and financing
5.1 A guidebook on health insurance for policy-makers was prepared jointly with ILO and used as a basis for appraising insurance options in Ghana. It proved useful in reaching agreement among interest groups concerning the benefit package provided as part of a new social insurance scheme, and showed that partial population coverage would be necessary at first. A Russian version was used as a background document for an intercountry consultation on health financing, attended by m1msters from Kazakhstan, Kyrgyzstan and Uzbekistan (Almaty, December 1993). Further studies on cost recovery mechanisms were supported in several countries. Of particular interest are the effects of charges on service utilization by women and children, and the reactions of communities. Studies in Ghana and Kenya led to reviews of exemptions practice and of banking arrangements for the protection of revenues. Studies of alternative financing options were undertaken in several countries.
5.2 In its report' a WHO study group reviewed recent changes in the methods used in different countries to finance health services. A network was established to provide expert advice on the financing and economics of health services in central and eastern Europe. Similarly, a permanent forum for the exchange of views and experience was established to support European Member States undergoing reforms in health care management and financing. A meeting was held
1 WHO Techn1cal Report Series, No. 829, 1993.
21
to look at ways of coping with the increasing demand for health services with limited resources (Kiel, Germany, November 1992). Health leaders from 12 countries met (Madrid, June 1992) to discuss such issues as contracting of health services, and public and private responsibility for health care. An intercountry consultation of ministers of health (Windhoek, October 1993) reviewed experience of user fees, social insurance innovations, management of private insurance and of the non-profit nongovernmental sector, and identified needs for technical cooperation.
53 In June 1993 a 12-month international master's programme in health economics began at Chulalongkorn University in Bangkok, cosponsored by WHO and the World Bank; some fellowships were reserved for participants from countries such as VietNam that are receiving intensified WHO cooperation. Intercountry seminars and workshops on health economics were organized with WHO and World Bank support at the National Institute of Public Health in Algiers, which now has a health economics unit and resource centre.
Organizational change
5.4 Many countries have expressed the intention to pursue decentralization policies, but have not made significant progress; and in some instances decentralization has led to neglect of social services in favour of directly productive sectors. A series of studies was therefore undertaken with support from NORAD to examine the question of decentralization and health development in the light of experience in countries, particularly Botswana, Kenya and Uganda. Preliminary findings indicate that inadequate capacity at the periphery to take on enlarged responsibilities

THE WORK OF WHO 1992-1993
and to demonstrate results are obstacles to the implementation of sometimes ambitious decentralization policies.
5 5 In Africa the accent was on reorienting health systems towards clear implementation of primary and community health care. Thus the Regional Committee examined the question of restructuring provincial and local hospital networks in 1992, and related activities are in progress. Infrastructure development was the subject of the 1993 Technical Discussions, with emphasis on the formulation of national plans of action.
5.6 Bangladesh, with WHO support, undertook a review of the functions and structure of the Ministry of Health and prepared several programmes for financing by the World Bank and donor agencies. Bhutan reviewed its health development programme in the context of its national plan. A radically revised organizational structure for the Ministry of Health in Ghana was established with WHO support. One innovation was the replacement of vertical programmes by a central coordination and research division with an advisory and standard-setting role; new procedures for resource allocation and financial management were also introduced. Similarly, Mongolia reviewed the structure and functions of its Ministry of Health. A WHO team helped to assess obstacles to integrated service delivery in Namibia, and proposed a restructuring of the Ministry of Health and Social Services on a functional basis rather than according to professional allegiances and interests. The Organization also worked with the Ministry of Health of Zambia in planning sweeping policy reforms in respect of decentralization, public participation, financing and relations with the nongovernmental sector. Joint programme reviews were carried out by WHO and national staff in most Eastern Mediterranean countries.
Management of physical resources for health
57 Studies on health care equipment management were carried out in Botswana in cooperation with GTZ, NORAD, the British Overseas Development Administration and the University of Sussex (United Kingdom), and in Cameroon with support from GTZ, the Rockefeller Foun-
22
dation, and the British Columbia Institute of Technology (Canada). A paper was prepared on the planning and financing of medical equipment.
5.8 Close cooperation continued with training institutions in London, Lyon, Mbabane and Nicosia. Following the closure of WHO projects in Sierra Leone and Togo, agreement was reached for GTZ-supported centres in Mombasa (Kenya) and Diourbel (Senegal) to serve as regional training centres. Training courses for republics of the former Soviet Union and countries of central and eastern Europe and Latin America were organized in Boston (USA) jointly with the American College of Clinical Engineering, the American International Health Alliance, the International Federation for Medical and Biological Engineering, UNICEF and UNIDO. Support was given to workshops on maintenance and repair of health care equipment in Afghanistan, Cyprus, Egypt, Jordan, Syrian Arab Republic, Tunisia and Yemen. The WHO collaborating centre in Cyprus continued to offer training for staff from Africa, South-East Asia and the Eastern Mediterranean. A centre for the maintenance and repair of medical equipment was opened in Damascus in 1992.
5.9 In the area of physical infrastructure and maintenance, PAHO/WHO cooperated directly with 14 engineering and maintenance programmes at health establishments in the Americas, and disseminated technical information, bibliographic material, and information on professional and technical training facilities to all such establishments.
5.10 The role of health facilities planning for quality improvement was discussed at an international public health seminar (Buenos Aires, May 1992) organized by the International Hospital Federation, the public health group of the International Union of Architects and WHO. Guidelines for health facilities planning were discussed at a follow-up meeting. Problems of physical infrastructure faced by countries of central and eastern Europe were examined during the conference of the International Hospital Federation (London, October 1992); and questions of cost-conscious planning, design and maintenance of health care facilities were subsequently explored at a joint conference of WHO and the International Union of Architects (Chicago, USA, June 1993).

ORGANIZATION OF HEALTH SYSTEMS BASED ON PRIMARY HEALTH CARE
District health systems
Improved service delivery
5.11 A community-based development strategy in which components for health, functional literacy and income generation are integrated was tested in an urban slum district of Cairo (see box). A national agency for primary health care promotion was established in Nigeria with WHO support following a review in 1992. The Ministry of Health of Zimbabwe tried out different strategies for linking community health development with the district health system, whereby people in communities have, for instance, been trained by health centre staff to carry out basic preventive and curative procedures. Participants in an interregional consultation (Bandung, Indonesia, 1993) noted that the main lesson to be learned from experience in countries is that a district health system cannot work without simultaneous changes in central administration and regulation.
5.12 As part of efforts to strengthen local health systems, meetings were organized in seven Latin American countries and for the English-speaking Caribbean countries, to analyse local management processes and to introduce managerial and leadership mechanisms. The organization and financing of health services, administration in local health systems, leadership, management information systems, project management and strengthening of training institutions received particular attention in the Americas. Strategies to strengthen local health systems are now being expanded to include work at district (county) level and in urban areas. A study on the implementation of health care models examined local health systems in Bolivia, Dominican Republic and Haiti; the aim is to disseminate a methodology for comprehensive evaluation, with a view to promoting greater efficiency, effectiveness and equity. An intercountry consultation (Lome, September 1992) brought together 14 national experts from five African countries to discuss information support for district management.
5 13 In response to repeated complaints by ministries of health about lack of coordination and wasted time and effort when several training programmes are arranged for the same staff, in 1992 WHO embarked on a project to produce learning materials that concentrate on problemsolving, and to build up the technical and mana-
23
The Ain Shams proiect
• Vulnerable groups exist in all societies: women and children are especially likely to lack access to food, water, shelter and sanitation and consequently to be in poor health. Such was the case in the Ain Shams district of Cairo, which gave its name to a project involving five countries (Egypt, Ghana, Nigeria, Zambia and Zimbabwe) aimed at improving the health of the poorest women. In five districts - one in each country- there was emphasis on functionalliteracy for women, viable economic activities and community-based health services as the key components in improving women's health and that of their families and the community as a whole. The Ain Shams project, now completed, provided lessons in the empowerment of vulnerable groups. It resulted in improved literacy among women with little or no education, and the setting up of community-based health services including a health centre and clinics, 24-hour emergency services, outreach services for maternal and child health, and a referral system. In addition, profit-making economic activities were established and community-managed development projects were organized, such as creating a park, building sanitary facilities and improving roads and lighting.
gerial capacity of health teams at local and district levels, using such materials, combined with supportive supervision and performance monitoring, to enable better integration of health services. The importance of improved management at district level for overall programme coordination was demonstrated in Malaysia and the Philippines in the course of a 1992 review of projects in the Western Pacific.
Health development structures
5.14 A study of the effectiveness of the health committees and boards and other health devel-

THE WORK OF WHO 1992-1993
opment structures that have been established at various levels of district health systems in many countries began after a global framework had been agreed upon at a planning meeting attended by investigators from Colombia, Indonesia, Jamaica, Nigeria, Philippines, Senegal, Sudan and Yemen in February-March 1993. An intercountry workshop on primary health care development (Cairo, April 1993) devised approaches for strengthening local and district planning so as to ensure that each health facility, public and nongovernmental, has clearly defined responsibilities for health care within its specified catchment area.
Urban health
5.15 Following a WHO workshop in March 1993 hosted by the urban health group of Nijmegen Catholic University (Netherlands) with the collaboration of the Swiss Tropical Institute and the London School of Hygiene and Tropical Medicine, proposals on research and development were prepared for the cities of Dar es Salaam, Jakarta, Kingston, Managua and Mirzapur (India) and presented to the Netherlands Government for financing. In Africa a first Healthy Cities meeting was organized (Dakar, July 1992) as part of collaboration with the Healthy Cities network of Quebec (Canada) and the commune of Dakar, and attended by representatives of 14 cities and five nongovernmental organizations from eight countries. A network of African Healthy Cities is being set up, for which preparatory activities were initiated in Accra and Ibadan (Nigeria).
5.16 Approaches to urban health development were discussed at a regional meeting (Harare, November-December 1993) jointly sponsored by WHO and GTZ. Preparations were made for studies of the effects of environmental and housing factors on urban public health, to be carried out in Ibadan (Nigeria) in 1994. Most cities in South-East Asia have launched extensive urban development programmes for slum-dwellers. The European Healthy Cities project expanded to involve over 500 cities. Guidelines for project development were issued. 1 Policies for improving the health of the urban poor were discussed at an interregional meeting (Manila, August 1993 ). The topics covered included ways of extending coverage through health care reform, and approaches for achieving environmentally sustain-
24
able urban development. The World Bank and other agencies support these initiatives, in which WHO plays an important technical role, including the publication of materials.
5.17 One aspect of urban health development is the correct role to be played by each level of health facility. Self-referral to hospital, by-passing the health centre, is a common phenomenon in urban areas where hospitals are the sole providers of complex care. In addition, health services in urban areas are frequently organized in a way that is not conducive to community involvement. However, recent advances in technology have made it possible for specialist health centres with added capacity to carry out fairly complex procedures, such as eye cataract operations, previously requiring hospital admission. Known as "reference health centres" to distinguish them from traditional first-contact health centres, these facilities have been shown to bring appropriate care closer to the population at only 25% of the cost of hospital interventions.2 Following pioneering work in Cali (Colombia) and cities in the United States of America, Europe and Asia, WHO is supporting the establishment of reference health centres in Bangkok, Cairo, Harare, Jakarta and Manila as well as Bombay, Calcutta, Delhi and Madras in India.
Community involvement in health
518 The use of volunteer health workers was reviewed in several countries. The experience of Thailand's self-care programme was shared with other South-East Asian countries. An intercountry study on self-medication was begun in that region. Following a global study showing that traditional healers can be efficient community health workers, investigations were started in Africa, Asia and Latin America to determine the conditions necessary for success. Case studies of community involvement in health in Bolivia, Nepal and Senegal were repeated in 1993; the findings underlined the importance of national political leadership for the success of programmes, although a surprising degree of sustainability was found even without clear
1 Twenty steps for developmg a Healthy City pro1ect. Copenhagen, World Heolth Orgomzotion, 1992.
2 WHO Technrcol Report Serres, No. 827, 1992.
ORGANIZATION OF HEALTH SYSTEMS BASED ON PRIMARY HEALTH CARE
Rgure 5.1 WHO core library
THE WHO CORE LIBRARY FOR DOCTORS
WORKING IN SMALL HOSPITALS
ANAESTHESIA AT THE
DISTRICT HOSPITAL
Moellatl B. Oobsoo
GENERAL SURGERY AT THE
DISTRICT HOSPITAL
John Cook Batu S•nkate"
Ambfose e o. w .,.unna
SURGERY IT THE DISTRICT
HOSPITAL: OBstETRICS,
GYNAECOLOGY, ORTHOPAEDICS,
IMD TRAUMATOLOGY
WHO Basic Radiological System
Manual of Radiographic Interpretation for
General Practitioners
Towards the end of the biennium WHO began promoting a core library for physicians working in small hospitals. This small library consists of seven clinical manuals that are considered indispensable to hospitals at first referral level and could form the nucleus of a hospital library. The three surgery manuals describe life-saving procedures, as does the malaria publication. The book on respiratory infections in children is directly relevant to a major problem in hospitals, and the radiography manual provides a complete set of radiographic images for clinical use. Finally, the book on the relief of cancer pain is included because many cancer patients in developing countries are admitted to hospital on account of intractable pain, and the disease is often so advanced that pain relief is the sole treatment option.
To encourage the widest possible dissemination of these manuals, WHO has made the core library available at a nominal price.
25

THE WORK OF WHO 1992-1993
political support. In conjunction with social security agencies, PAHOIWHO participated in work undertaken at the Inter-American Center for Social Security Studies (Mexico) relating to community participation and setting up management information systems. Globally, the movement towards participatory health development continues to grow slowly but surely, especially at local level.
Hospital performance and quality of core
5 19 Studies indicate that too little attention is paid to the performance of hospitals, a disturbing situation in view of the amount spent on them. An international workshop (Yaounde, November 1992), sponsored by WHO, GTZ and the Prince Leopold Tropical Institute (Belgium), drew attention to the crisis affecting small hospitals that provide services for large rural and urban populations while receiving little support from governments and donors. A seminar on hospital cooperation in Europe was convened jointly with the European Community (Strasbourg, France, November 1992). WHO gave support to Indonesia in testing a medical audit system; to the Islamic Republic of Iran in conducting a national workshop on the role of the hospital in primary health care; to Mongolia in upgrading facilities such as peripheral hospitals; and to Myanmar in producing hospital procedure manuals. PAHO/WHO continued to provide technical support for the strengthening of hospitals in the Americas. Workshops and seminars were held in 10 countries for the purpose of revising hospital accreditation arrangements.
26
5 20 During the biennium WHO issued the report of a study group on the hospital in rural and urban districts/ documents on the hospital of tomorrow2 and on hospital economics and financing,3 and guidelines for the development of district hospitals.4 A limited number of reference works were selected to form a "core library for doctors working in small hospitals" and this package was used in many countries (see Figure 5.1).
5.21 An interregional meeting (Pyongyang, October 1992) stressed the need to incorporate quality assurance in all aspects of a health system.5 WHO encouraged collaboration between institutions active in this field in developing countries, such as DANIDA, USAID, the Nether lands Government and the International Society on Quality Assurance. A joint consultation on quality assurance in developing countries (Maastricht, Netherlands, June 1993) was organized with WHO support through the collaborating centre for hospitals and other health institutions in Utrecht. WHO issued a document on the use of standards, and cooperated with Saudi Arabia in producing a manual.6 A national workshop on quality assurance was held in Zambia jointly with USAID and DANIDA.
1 WHO Techn1cal Report Series, No 819, 1992. 2 Document WHO/SHS/CC/92.1 3 Document WHO/SHS/NHP /92.2 4 D1stnct hosp1tals: gu1delmes for development. Manila, World Health Organ
Ization, 1992 (Western Pac1f1c Ser1es, No 4). 5 Document SEA/HSD/180. 6 Guideline manual on quality of pnmary health care. R1yodh, M1n1stry of
Health of Saud1 Arab1a, 1993

CHAPTER 6
Development of human resources for health
6.1 Optimal performance by health personnel depends on effective training and management as well as proper planning. Rapid socioeconomic, political and technological changes have made planning difficult, yet the demand for cost-effectiveness, efficiency and accountability has rendered it more necessary than ever.
6 2 Against this background, budgetary constraints have obliged WHO to explore new modalities of cooperation in the development of human resources for health. In particular more emphasis has been given to the involvement of collaborating centres, nongovernmental organizations, institutions and individuals in the Organization's work. This experience has mostly been positive and has enabled WHO to maintain the scope of its activities despite the resource constraints.
Policy analysis, planning and management
6 3 Policy analysis for human resources development was given high priority during the biennium, with financial support from Japan. WHO prepared a draft manual on the subject, which was reviewed by an intercountry group (Cairo, June 1993). The group recommended that a revised version of the document should serve as background information for a future meeting of ministers of health in the Eastern Mediterranean. Central American countries and the Dominican Republic have been involved in the development of methods to ensure better integration of health teams and enhance their capability to analyse local health conditions. The Technical Discussions held during the 1992 session of the Regional Committee for South-East Asia (Kathmandu, September) dealt with the balance and relevance of human resources for
27
health, focusing on maldistribution and imbalance of staff, and the appropriateness of training to work requirements. Policy analysis was seen as vital to the solution of specific problems.
6.4 World Bank health sector loans to such countries as Bangladesh, China, Indonesia and Nepal have required the preparation of master plans for health personnel which pay particular attention to numbers, types and distribution. WHO has been involved in this process either directly (Bangladesh, Nepal) or in conjunction with World Bank consultants (China). Existing planning methods were reviewed by an interregional consultation (Bangkok, March 1992) which stressed the importance of decentralizing planning to the implementation level and of involving interest groups. A regional workshop (New Delhi, February 1993) discussed planning and policy development for countries concerned by the WHO intensified support 1mt1at1ve; participants recommended that Member States carry out national reviews of their human resources for health, and draw up guidelines for this purpose. In China WHO organized a workshop (Shanxi, June-July 1992) to identify problems in planning for decentralized health management. Several other national workshops on different aspects of health personnel planning and management were conducted.
Planning tools
6.5 Computerized planning tools were tested and improved with support from Japan. A compendium on planning is now available on diskette, with an operational manual. 1 Computerized supply and requirement projection models
1 Document HRH/93 5.

THE WORK OF WHO 1992-1993
were field-tested in the Caribbean (Barbados, Saint Kitts and Nevis, and Saint Lucia), China and Hong Kong. The work in China included the development of an information system in connection with a World Bank health sector loan, and use of the projection models to determine whether the existing data were adequate for planning and whether the existing infrastructure would be receptive to change; this approach highlighted the multisectoral nature of health workforce planning. In the light of the positive experience, it is expected that these projection models will prove useful in a variety of ways ranging from the creation of scenarios to the monitoring of staffing plans. A revised version of the models, based on the field-test results, will be available in 1994 together with an operating manual. Health workforce planning manuals were also prepared in collaboration with the Western Pacific Regional Training Centre in Sydney, Australia.
6.6 As a basis for planning, it is important for countries to develop their own health workforce norms in accordance with their policies and situation. In this respect WHO is examining two methods: workload indicators of staffing need (WISN) and functional job analysis (FJA). WISN has been tried out in several countries in Africa, South-East Asia and theW estern Pacific, and FJA is seen as having the potential for overcoming traditional professional divisions of labour and thus allowing more efficient deployment of staff.
6.7 An interregional consultation Q akarta, June 1993) reviewed country experiences and identified areas for further study with regard to methodology for multiprofessional policy and planning. It noted that although many models exist for workforce planning and projection, they tend to be complex and try to cover as many events as possible in the planning process. They also tend to concern tertiary care settings in developed countries. The WHO choice therefore reflects a compromise: methods that are relatively simple to use, but capture only significant events. One of the strategies being pursued is to form a core of people to help countries in their own region or outside it to use the methods.
Optimizing human resources for health
6 8 In many countries the problem is no longer one of shortage of health professionals but rather of establishing or maintaining the
28
right balance between them to ensure that the necessary knowledge and skills are available. A year-long experience in Thailand with the RADICAL~ method for optimizing human resources for health provided some information on its strengths and weaknesses, which were reviewed at three meetings (Ayutthaya, Thailand, July 1992 and July 1993; Jakarta/Bandung, Indonesia, July 1993). There are indications that the method might be appropriate for countries without a strong planning tradition, although it clearly needs further refinement.
6.9 The public/private mix of human resources for health was the subject of a meeting (Bangkok, June-July 1992) which examined ways of harmonizing the two sectors, and in particular recommended strengthening the capacity of ministries of health to formulate national policies and plans covering both sectors. A consultation with leading medical practitioners in March 1993 examined political and practical aspects of private practice and public responsibility; it stressed the need to use both public and private services to provide improved access to affordable and high-quality health care. •
6 10 In Seychelles WHO supported a 1992 study on staff requirements and supply projections, as well as management and training issues, and this was expanded in 1993 to cover capacitybuilding for planning and management within the Ministry of Health and strengthening of training programmes. The study gave high priority to review of the responsibilities of nurses. This step-by-step approach may serve as a reference for other countries with similar problems.
Management
6 11 Efforts are being made to create a health workforce information system that will capture data from both public and private sectors. A specific system for nursing/midwifery personnel is also being developed as an integral part of country and global data banks. This professional category poses a particular problem as the designation "nurse" includes a wide range of educational levels and responsibilities. The only corn-
1 RADICAL rs on acronym for Rapid DiagnoSIS, lmmedrote Concern, Action for Lasting Change.

DEVELOPMENT OF HUMAN RESOURCES FOR HEALTH
mon factor is educational level, which it is hoped will be translatable into comparable competencies.
6.12 Participants from Lesotho, Namibia, Swaziland and Zambia attended an intercountry workshop on leadership and management for nurses (Mbabane, April1992) with financial support from the Kellogg Foundation. National meetings were subsequently held on this subject in the United Republic of Tanzania (Morogoro, October 1993) with NORAD support, and in Namibia (Windhoek, November 1993) with support from the Kellogg Foundation. Requests for further support in management and leadership training have been received. To become truly self-sustaining, these activities have to be integrated into national action plans.
6.13 National workshops were organized on use of the WHO manual on human resources management (Colombo, May 1992; Kathmandu, September 1992). Based on the participants' evaluation, the manual was subsequently revised, particularly to make it less culture-specific, and the new version was used in a further workshop (Khartoum, October-November 1993 ). An intercountry workshop (Beirut, June 1993) provided an opportunity for health managers to analyse tasks and work out clear job descriptions, which should help to avoid duplication and strengthen management.
Continuing education
6 14 If there is one area where much has been talked about and consensus reached on its importance, but without this being reflected in action, it is continuing education. Where difficulties exist to provide even basic training, this is not surprising. At the same time not everyone is convinced that continuing education should be an integral part of basic education. Fortunately there are some exceptions. In the Americas work continued on the conceptual and methodological development of continuing education as an alternative approach to training in such fields as management, epidemiology, public health and nursing. Continuing education is being used to support decentralization and strengthening of care at local level. In the Eastern Mediterranean a workshop was held to promote planning of continuing education projects with priority to district health personnel (Rabat, May 1992); it was hoped to extend this approach to other countries, but paradoxically
29
project implementation has not been very successful owing to lack of country support. N evertheless, a first regional meeting (Tunis, June 1992) issued a statement underlining the need for each country to have a continuing education programme for all categories of health personnel as an integral part of its national health system. It recommended the creation of a structure within the ministry of health that would be responsible for the planning, implementation and evaluation of the programmes. A manual on continuing education for health personnel has also been proposed. In Europe WHO is cooperating with the World Federation for Medical Education in a study on how continuing medical education could be implemented and supported. The possibility is being explored of establishing a forum to promote continuing medical education to support health sector reforms in eastern and central Europe.
Nursing
6.15 A global advisory group on nursing and midwifery was established in response to Health Assembly resolution WHA45.5, and a first meeting held in November-December 1992; it recommended that nursing/midwifery be declared a priority area for WHO action, that strategies be developed to ensure its optimal contribution to
health care, and that the necessary resources be made available.' Modest additional funds have since been provided to support research in priority areas identified by the group, and attempts are being made to fill information gaps so as to facilitate monitoring and evaluation as well as planning and deployment. A headquarters coordinating committee streamlines the work of the different technical programmes in strengthening nursing/midwifery services and reviews WHO vacancies to ensure that whenever possible professionals other than physicians can also apply. A WHO study group on nursing beyond the year 2000, convened in July 1993, recognized that a multisectoral and multiprofessional approach would be needed to prepare health care providers to work in a rapidly changing environment. A European regional publication2 provid-
1 Document WHO/HRH/NUR/93 1. 2 Salvage J ed Nursing m actton strengthenmg nursmg and mtdwtfery to
support health for all World Health OrganiZation, Copenhagen, 1993 (European Ser1es, No 48).

THE WORK OF WHO 1992-1993
ed useful background information for the study group, whose conclusions in turn were used as input for the meeting of the global advisory group in November 1993.
6 16 In South-East Asia nursing education has tended to make greater progress than nursing services. An intercountry consultation on reorientation of nursing services in support of health for all (Kathmandu, December 1992) identified and promoted new approaches to collaboration between nursing education and services in order to achieve the goal of providing high-quality nursing care. Both basic and further training of nursing personnel are a priority in all countries in the Eastern Mediterranean. In Egypt teaching modules and training packages have been developed and teacher training promoted. Pakistan has approved a new curriculum with emphasis on community orientation, and Yemen now offers a bachelor of science degree in nursing in addition to a community-oriented programme. In the Western Pacific WHO cooperates with Member States in planning for nursing development. Ministries of health have established nursing units or strengthened nursing expertise at central level. Computerized nursing management information systems have been created to support national planning units in Australia, Papua New Guinea and VietNam.
Educational development
6.17 Although a great deal of innovation has occurred in the education and training of health personnel, there seems as yet little consensus that it should be generally applied. As stressed by a study group on this subject in October 1992,1
problem-based learning must extend beyond limited clinical confines into social and community issues if it is to realize its full potential. Although educational experience can undoubtedly be enhanced if teaching institutions assume new responsibilities in health care organization and service, this is beyond their traditional mandate and they will therefore need to build up new alliances and partnerships with professional associations, service organizations and the community.
618 Although WHO has moved away from the concept of global curricula, attempts are be-
1 WHO Techn1cal Report Series, No 838, 1993
30
ing made to identify those elements which define the quality of educational experience.2 Similarly, efforts are being made to understand the factors which facilitate change, and to establish common criteria so that monitoring of improvements in medical education and practice can be carried out globally. Four issues of a new bulletin, Changing medical education and medical practice, were distributed during the biennium as well as a revised edition of the WHO guide for teachers of primary health care staff.3
6.19 To build on the work of the 1988 World Conference on Medical Education, the World Federation for Medical Education, with support from WHO, UNICEF, UNESCO, UNDP and the World Bank, organized a further major conference in Edinburgh (August 1993) on the theme of societal changes and their implications formedical education. The conference considered such issues as the new skills being demanded of physicians, the economic impact of medical decisions, the importance of better communication with the community and individuals, and the growing consensus that radical reform is required to ensure that the skills of graduates who will practise in the 21st century will be relevant to the needs.
6.20 In Africa support was given in strengthening the College of Medicine in Blantyre (Malawi) and the Faculty of Health Sciences in N'Djamena. Workshops were organized with the aim of adapting medical education to community needs.
6 21 Participants in a regional consultation (New Delhi, February 1993) underlined the need for holistic strategies to achieve meaningful reorientation of medical education, as many activities at country level are still confined to the arena of institutional reform. To accelerate action, it was agreed that more attention must be paid to such issues as organizational development, programme evaluation, the use of health systems research and team approaches. A consortium of medical schools in India continued the second phase of the innovative project on "Inquiry-driven strategies for changing medical education". In Myanmar a twinning initiative was launched with the University of New Mexico in Albuquerque (USA) to test a strategy to reorient medical education using continuing edu-
2 Document WHO/HRH/92.7 3 Abbatt FR. Teachmg for better learnmg. a guide for teachers of p(lmary
health care staff, 2nd ed. Geneva, World Health Organization, 1992.

DEVELOPMENT OF HUMAN RESOURCES FOR HEALTH
cation and the medical association as entry-points. Activities related to training of allied health workers focused on improving staff capacity and curriculum reform. WHO supported Sri Lanka's National Institute of Health Sciences in making a comprehensive evaluation of different programmes for training allied health workers, and the Institute of Health Personnel in Maldives in upgrading the country's training programmes.
6.22 An intercountry workshop on training of trainers of health personnel in Eastern Mediterranean countries (Damascus, November 1992) discussed existing programmes in this region, the role of educational development centres in teacher training and ways to increase trainer capability. Activities to promote the use of national languages in medical education also progressed. WHO sponsored briefing visits of medical professors from Egypt, Sudan, Tunisia and Yemen to faculties in the Syrian Arab Republic for this purpose. Packages containing selected medical texts and reference works in Arabic have been distributed to all medical faculties.
6.23 In the South Pacific a three-point plan was introduced to revitalize the Fiji School of Medicine. A new category of health workers known as primary care practitioners graduated at the end of 1993 and will undergo one year's internship in their countries under the supervision of senior medical officers, for whom a workshop was organized with WHO support (Suva, July 1993). Young health officers were recruited as faculty for the new programme.
6 24 Fellowships still remain an important part of the Organization's work, although there has been a falling trend in recent years and the figure for the 1992-1993 biennium (see Table 6.1) represents a reduction of 875 over 1990-1991. To help ensure relevance of training to country priorities, the application form was revised to provide more details of applicants. A total of 207 new research training grants were processed in the areas of tropical diseases and human reproduction.
Public health training and research
6.25 A meeting of directors of schools of public health (Douala, Cameroon, December 1992), decided to establish a network of African institutions in order to strengthen training and research in this field. In the Americas analysis of current theo-
31
ry and practice of public health has become an important area of work, and two publications were issued.1 2 The seventh and eighth groups taking part in the regional residency programme in international health graduated during the biennium. Learning modules produced in 1991 for a European master of public health course are being revised. Educational policies, basic competencies and learning environments were discussed at a first meeting of the European Dialogue on Training in Public Health (Rome, June 1992) with a view to development of the course. A further meeting was held to review a strategy for training and research in public health (Copenhagen, November-December 1993 ). Following discussion of aspects of public health training by the Regional Committee for the Western Pacific (Manila, September 1993 ), a database was established to promote cooperation between institutions and sharing of resources; this activity is a collaborative undertaking by WHO, the Asia-Pacific Academic Consortium for Public Health and the Regional Training Centre in Sydney (Australia). An intercountry workshop at which ten countries were represented (Sydney, July 1993) considered three aspects of public health training: availability and organization of resources, scope and approaches, and required developments. Participants prepared plans of action for their own countries.
Health learning materials
6.26 Technical support to networks of more than 30 developing countries was increased under the interregional health learning materials programme, which is financed largely from extrabudgetary sources. Meetings were held to plan future strategies and collaboration between projects (Harare, April1992), to examine project evaluation and planning in South-East Asian countries (Colombo, August 1992) and to exchange experience of projects in nine Englishspeaking African countries (Nairobi, December 1993). An intercountry workshop (Damascus, November 1992) provided an opportunity for country coordinators to initiate research on the development of distance learning. Other work-
1 The msis of public health: reflections for the debate Washington, Pan American Health OrganiZation, 1992 (Scientific Publication, No. 540).
2 International health a north south debate. Washmgton, Pan American Health Organization, 1992 (Human Resources Development Series, No. 9 5).
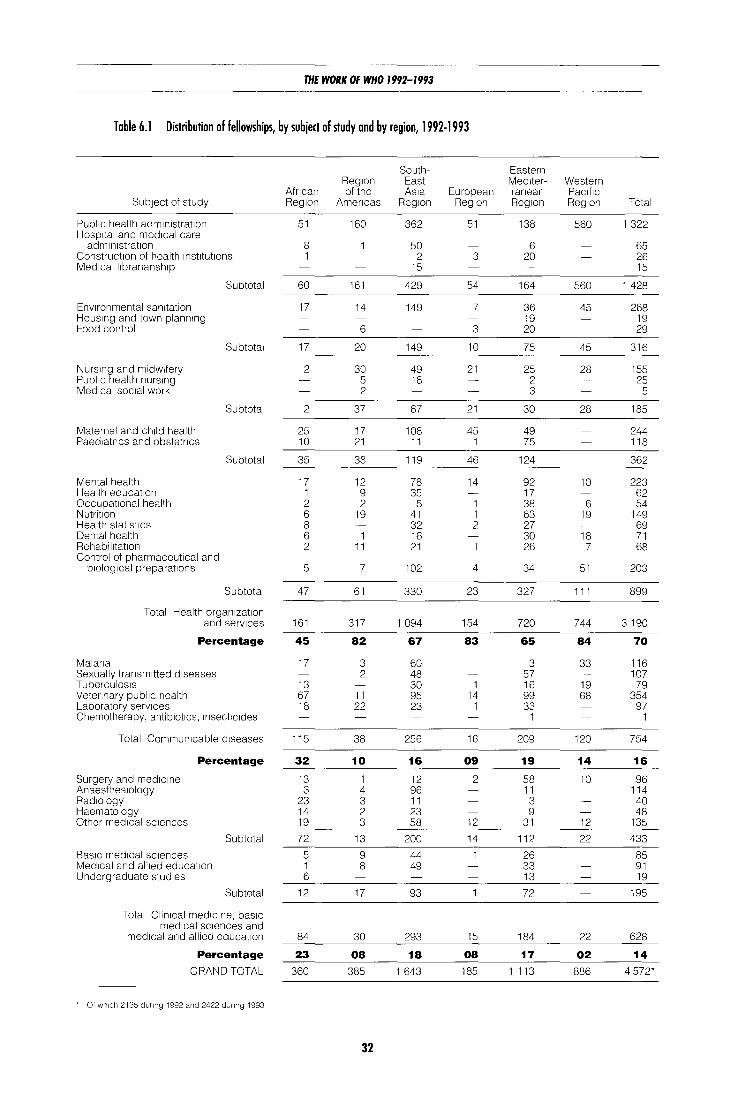
THE WORK OF WHO 1992-1993
Table 6.1 Distribution of fellowships, by subject of study and by region, 1992-1993
South- Eastern Reg1on East Med1ter- Western
Afncan of the As1a European ranean Pac1f1c Subject of study Reg1on Amen cas Reg1on Reg1on Reg1on Reg1on Total
Publ1c health adm1nistrat1on 51 160 362 51 138 560 1 322 Hosp1tal and med1cal care
adm1n1strat1on 8 50 6 65 Construction of health InstitUtions 1 2 3 20 26 Med1call1branansh1p 15 15
Subtotal 60 161 429 54 164 560 1 428
Enwonmental sanitation 17 14 149 7 36 45 268 Hous1ng and town plann1ng 19 19 Food control 6 3 20 29
Subtotal 17 20 149 10 75 45 316
Nurs1ng and midwifery 2 30 49 21 25 28 155 Public health nurs1ng 5 18 2 25 Med1cal soc1al work 2 3 5
Subtotal 2 37 67 21 30 28 185
Maternal and ch1ld health 25 17 108 45 49 244 Paed1atncs and obstetncs 10 21 11 1 75 118
Subtotal 35 38 119 46 124 362
Mental health 17 12 78 14 92 10 223 Health education 1 9 35 17 62 Occupational health 2 2 5 1 38 6 54 Nutrition 6 19 41 1 63 19 149 Health stat1st1cs 8 32 2 27 69 Dental health 6 1 16 30 18 71 Rehabil1tat1on 2 11 21 26 7 68 Control of pharmaceutical and
b1olog1cal preparations 5 7 102 4 34 51 203
Subtotal 47 61 330 23 327 111 899
Total Health organ1zat1on and serv1ces 161 317 1 094 154 720 744 3 190
Percentage 45 82 67 83 65 84 70
Mal ana 17 3 60 3 33 116 Sexually transmitted d1seases 2 48 57 107 TuberculoSIS 13 30 1 16 19 79 Vetennary publ1c health 67 11 95 14 99 68 354 Laboratory serv1ces 18 22 23 1 33 97 Chemotherapy, antibiotics, 1nsect1c1des 1 1
Total Communicable d1seases 115 38 256 16 209 120 754
Percentage 32 10 16 09 19 14 16
Surgery and med1c1ne 13 1 12 2 58 10 96 Anaesthes1ology 3 4 96 11 114 Rad1ology 23 3 11 3 40 Haematology 14 2 23 9 48 Other med1cal sc1ences 19 3 58 12 31 12 135
Subtotal 72 13 200 14 112 22 433
Bas1c med1cal sc1ences 5 9 44 26 85 Med1cal and all1ed education 1 8 49 33 91 Undergraduate stud1es 6 13 19
Subtotal 12 17 93 72 195
Total Clin1cal med1c1ne, bas1c med1cal sc1ences and
med1cal and allied educat1on 84 30 293 15 184 22 628
Percentage 23 08 18 08 17 02 14 GRAND TOTAL 360 385 1 643 185 1 113 886 4 572*
Of wh1ch 2135 dunng 1992 and 2422 dunng 1993
32

DEVELOPMENT OF HUMAN RESOURCES FOR HEALTH
shops, both intercountry and national, were organized on key issues such as project management, writing and editing, distance learning and educational methods, and also on field-testing and evaluation, which was the subject of a meeting (Kigali, September 1993) with participants from nine French-speaking countries. Unfortunately there has been a significant fall in extrabudgetary support in spite of the stated needs.
Staff development
6.27 High priority was again given to the training of WHO Representatives, and three seminars
33
were organized for them during the biennium. A series of workshops on macroeconomics was organized for WHO Representatives and senior staff in Africa. These workshops have enabled WHO Representatives to interact more effectively with members of country support teams responsible for economics. The 1993 seminar for WHO Representatives took into account relevant recommendations of the Executive Board's working group on the WHO response to global change. While training in languages other than English and French has had to be curtailed owing to budget cuts, workshops continued to be held on such topics as report writing, teamwork, time management and crosscultural effectiveness.

CHAPTER 7
Public information and education for health
Public information
7.1 WHO's public information programme enhances awareness of the Organization's work among the general public and transmits important public health messages. Growing general interest in health issues is reflected in the increased time and space now being devoted to health matters in the media. This situation offers more opportunities for WHO to publicize its work and to disseminate authoritative information on health questions. WHO continued to strengthen its contacts with all branches of the news media- wire services, newspapers and magazines, television and radio. Radio programmes were produced and distributed to over 200 radio stations. WHO also worked with international television news and features syndicators of audiovisual material as well as national broadcasters to ensure appropriate distribution through their networks. A large number of briefings, press conferences and interviews were arranged.
7.2 Materials produced to meet requests from the media around the world included some 200 press releases and a range of features, fact sheets and press kits. Efforts were made to improve the technical content of press releases, to simplify their language, and to time their distribution so as to attract maximum attention. Topics dealt with included WHO's global drug policy, immunization of children, tropical diseases, AIDS, cholera, tuberculosis and emergency relief. Press kits in different languages were prepared for the United Nations Conference on Environment and Development (Rio de Janeiro, Brazil, June 1992), the International Conference on Nutrition (Rome, December 1992) and the Ministerial Conference on Malaria (Amsterdam, October 1992).
7.3 A variety of materials were distributed in connection with the special days designated to
35
focus world attention on particular health issues: World Health Day (7 April) on the theme "Heartbeat: the rhythm of health" in 1992 and "Handle life with care: prevent violence and negligence" in 1993; World No-Tobacco Day (31 May) on the theme "Tobacco-free workplaces: safer and healthier" in 1992 and "Health services: our window to a tobacco-free world" in 1993; and World AIDS Day (1 December) on the theme "AIDS: a community commitment" in 1992 and "AIDS: time to act" m 1993.
7 4 WHO continued to provide public information services for a broad range of users through visits and publications and by responding to enquiries. The brochure, Facts about WHO, and the video, The battle for health- a global challenge, produced during the previous biennium, were used for briefing purposes. A large number of enquiries were dealt with and 300 group visits to WHO headquarters were conducted in six languages; by 30 September 1993 there had been about 10 000 visitors from over 60 countries during the biennium.
Education for health
7.5 WHO's three main health education strategies are: advocacy of healthy public policies, "empowerment" of people by increasing their knowledge and skills in health matters, and building social support for health. Within this framework WHO and UNEP cooperated in organizing meetings on supportive environments for health (Nairobi, June 1993; Bangkok, November 1993) for countries in Africa, South-East Asia and theW estern Pacific. Both meetings produced statements that identified important challenges and strategies for action. An outcome of the 1991 conference in Sundsvall (Sweden) has
THE WORK OF WHO 1992-1993
been the preparation of a handbook on promotion of health-supportive environments, to be published in 1994. A joint WHO/World Bank mission assisted in reviewing and strengthening Zambia's national health education infrastructure, with emphasis on health education in schools and on environmental health; a WHO team then visited the country to advise on curriculum development and programme planning.
7 6 Intercountry meetings in Sri Lanka and Costa Rica (Colombo, October 1992; SanJose, November 1993) produced guidelines for introducing comprehensive approaches to school health education for countries in South-East Asia and the Americas. Two national workshops were organized in Argentina and Namibia on the same subject. A health education curriculum for primary schools in Cameroon was designed and reviewed. During two international AIDS conferences (Amsterdam, July 1993; Berlin, June 1993), working groups were organized on strengthening the role of schools in preventing HIV infection. In November 1993 an informal meeting on school-based surveillance of healthrisk behaviour among secondary school students drafted a protocol for such surveillance in developing countries.
7 7 By the end of the biennium 28 countries had formally joined the European Network of Health Promoting Schools, established in 1991. A strategy for action in 1992-1993 was formulated during a first international consultation with national coordinators of the network (Strasbourg, France, May 1992). Two workshops were organized for teachers from eastern European countries (Budapest, September 1992; Prague, April 1993). Prototype action-oriented school health education programmes were introduced in 12 Eastern Mediterranean countries in collaboration with UNICEF and UNESCO. In 1992 a national training course on rural school health education and a national symposium on school health education were held in China with WHO support. Teacher training workshops took place in a number of African countries.
7.8 A WHO intercountry workshop on youth involvement in health promotion was held in Barbados (Bridgetown, November 1992); it formulated a regional youth statement on action for health and helped to initiate a Caribbean youth network. A national workshop on youth and health development took place in India. A brochure entitled "Health facts for youth" was
36
prepared as an aid to youth leaders in promoting action among young people in support of health. In 1993 an informal consultation with workers' organizations proposed ways in which trade unions could be involved in promoting health education at the worksite. A four-year project on health promotion among industrial workers was launched in China.
7 9 During the biennium at least 25 WHO programmes were supported in the production and dissemination of educational materials, exchange of materials and audiovisual coverage of educational events. Sixteen educational video films were produced as were 22 newsreels, which were distributed through television networks worldwide. Similarly, video footage from WHO's image library was made available to external production companies and television networks. An interagency database for the exchange of video materials was established in 1993.
7.10 Radio programmes on priority health issues continued to be provided regularly to over 200 radio stations. On average 13 000 print photographs are distributed each year to the press, publishers, nongovernmental organizations and training institutions. In 1992-1993, 48 exhibitions and displays were prepared for technical meetings, conferences and international health events such as World Health Days, World Health Assemblies, the Ministerial Conference on Malaria (Amsterdam, October 1992), the International Conference on Nutrition (Rome, December 1992), the two international conferences on AIDS mentioned above, and the United Nations Conference on Human Rights (Vienna, June 1993). In South-East Asia information kits on various health issues were prepared and disseminated and a regional newsletter, HF A 2000, is distributed quarterly.
7.11 In November 1992 an interagency meeting on strategies for health advocacy was organized to continue the work of the 1991 third interagency round-table on communication for development. It was concerned particularly with strategies to enlist decision-makers' support for health. The fourth round-table (Lima, February 1993) considered ways to strengthen training in communication for development.
7.12 Health education staff were trained in Botswana, Chad, Congo, Kenya and Namibia with the help of WHO fellowships. In 1993 a

PUBLIC INFORMATION AND EDUCATION FOR HEALTH
manual for training community health workers in human relations, communications and leadership skills was successfully tested during a training session for supervisors and community health workers in Kenya. An intercountry workshop was organized for radio and television health communicators from Cameroon, Central African Republic and Congo (Y aounde, April 1993). A training guide on HIV/AIDS was produced for use by health workers in the Eastern Mediterranean. Four teaching centres in that region are providing training for national health education staff. WHO supported the authorities in Oman in designing a programme to train women health educators for work in health centres. An intercountry workshop was held to discuss ways of integrating health education and promotion into the training of health personnel (Sydney, Australia, July 1992). Technical support for this purpose was provided to Papua New Guinea. A video on the health aspects of household energy use was produced in VietNam with WHO support.
7.13 Support was given to several African countries in strengthening the management of health education programmes and organizing
37
their decentralization to intermediate and district levels. An international conference on community health, with emphasis on community participation and exchange of educational experience, was held in cooperation with the Congolese Government (Brazzaville, September 1992). Following reviews, proposals were made for strengthening national health education programmes in Benin, Guinea and Uganda. Five intercountry working groups were formed and three intercountry workshops organized to strengthen health education programmes and enhance community participation in health in the Americas. Intercountry workshops were conducted in the Eastern Mediterranean to promote the planning of health education programmes (Manama, July 1992) and the production of health education materials for urban health development (Sanaa, July 1993 ). A working group reviewing the health education programme for the Western Pacific (Singapore, March 1993) called for greater emphasis on both community and government action. An international symposium on health education was organized in collaboration with the All China Health Education Association (Shanghai, October 1992).

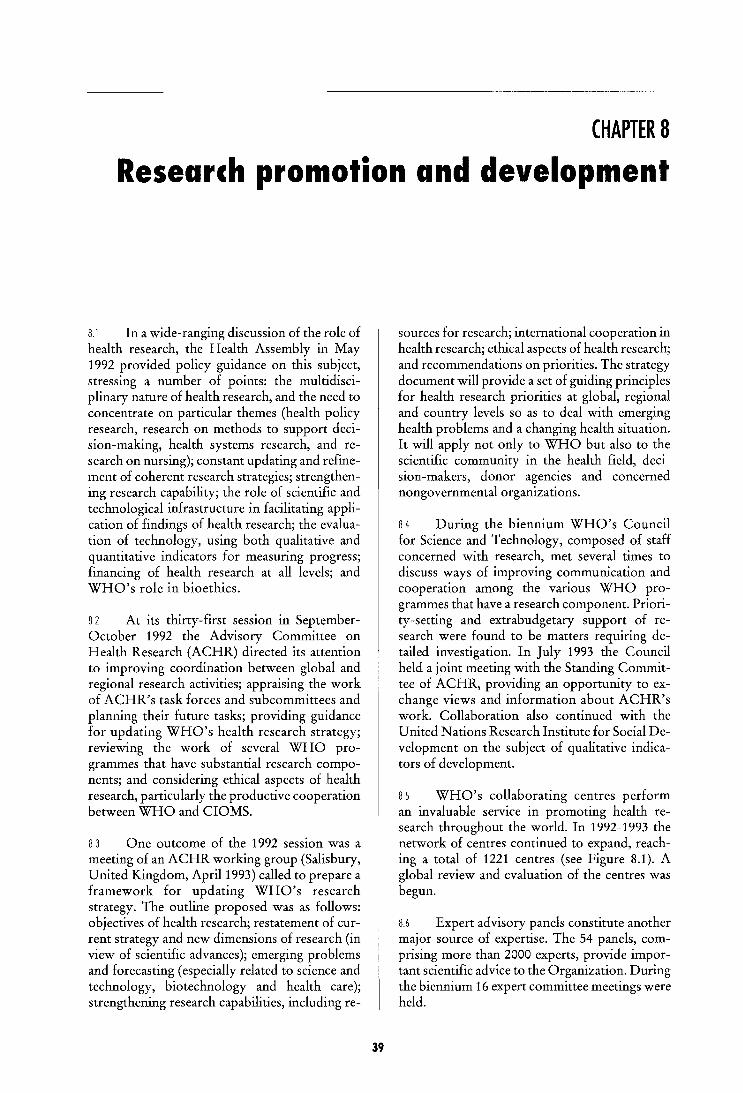
CHAPTER 8
Research promotion and development
8.1 In a wide-ranging discussion of the role of health research, the Health Assembly in May 1992 provided policy guidance on this subject, stressing a number of points: the multidisciplinary nature of health research, and the need to concentrate on particular themes (health policy research, research on methods to support decision-making, health systems research, and research on nursing); constant updating and refinement of coherent research strategies; strengthening research capability; the role of scientific and technological infrastructure in facilitating application of findings of health research; the evaluation of technology, using both qualitative and quantitative indicators for measuring progress; financing of health research at all levels; and WHO's role in bioethics.
8 2 At its thirty-first session in SeptemberOctober 1992 the Advisory Committee on Health Research (ACHR) directed its attention to improving coordination between global and regional research activities; appraising the work of ACHR's task forces and subcommittees and planning their future tasks; providing guidance for updating WHO's health research strategy; reviewing the work of several WHO programmes that have substantial research components; and considering ethical aspects of health research, particularly the productive cooperation between WHO and CIOMS.
8 3 One outcome of the 1992 session was a meeting of an ACHR working group (Salisbury, United Kingdom, April1993) called to prepare a framework for updating WHO's research strategy. The outline proposed was as follows: objectives of health research; restatement of current strategy and new dimensions of research (in view of scientific advances); emerging problems and forecasting (especially related to science and technology, biotechnology and health care); strengthening research capabilities, including re-
39
sources for research; international cooperation in health research; ethical aspects of health research; and recommendations on priorities. The strategy document will provide a set of guiding principles for health research priorities at global, regional and country levels so as to deal with emerging health problems and a changing health situation. It will apply not only to WHO but also to the scientific community in the health field, decision-makers, donor agencies and concerned nongovernmental organizations.
8 4 During the biennium WHO's Council for Science and Technology, composed of staff concerned with research, met several times to discuss ways of improving communication and cooperation among the various WHO programmes that have a research component. Priority-setting and extrabudgetary support of research were found to be matters requiring detailed investigation. In July 1993 the Council held a joint meeting with the Standing Committee of ACHR, providing an opportunity to exchange views and information about ACHR's work. Collaboration also continued with the United Nations Research Institute for Social Development on the subject of qualitative indicators of development.
8 5 WHO's collaborating centres perform an invaluable service in promoting health research throughout the world. In 1992-1993 the network of centres continued to expand, reaching a total of 1221 centres (see Figure 8.1). A global review and evaluation of the centres was begun.
8.6 Expert advisory panels constitute another major source of expertise. The 54 panels, comprising more than 2000 experts, provide important scientific advice to the Organization. During the biennium 16 expert committee meetings were held.
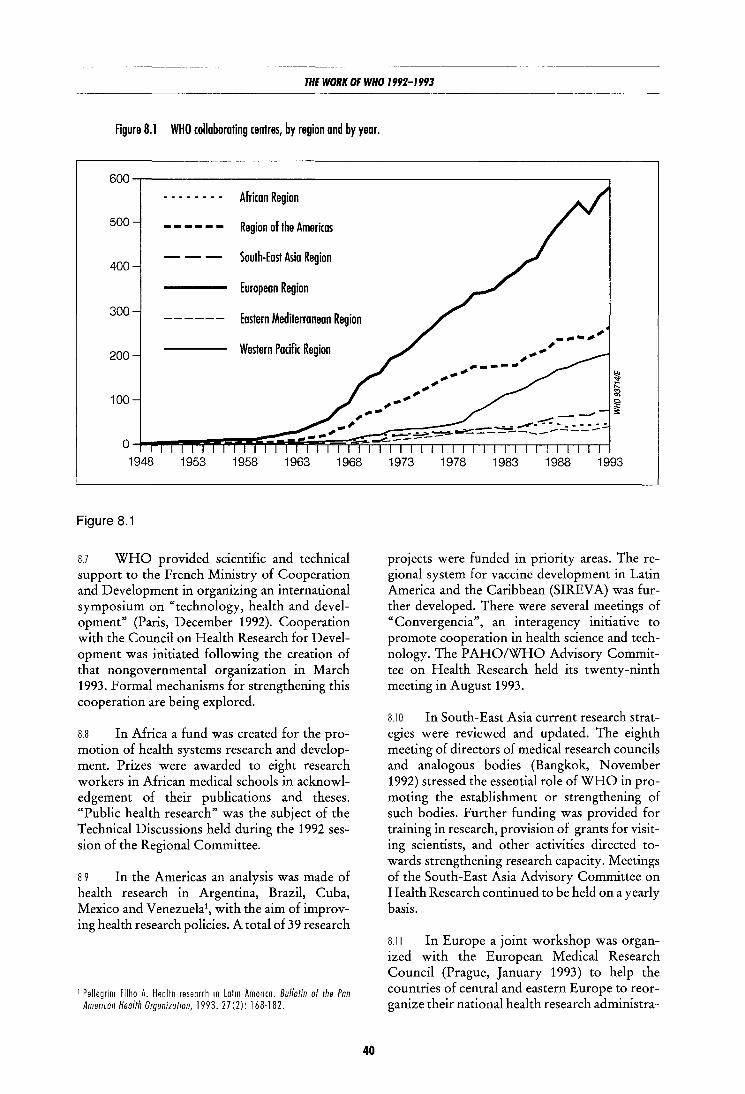
THE WORK OF WHO 1992-1993
Figure 8.1 WHO collaborating centres, by region and by year.
600 . - .. - .... - .. African Region
500 ------ Region of the Americas
--- South-East Asia Region 400
European Region
300 Eastern Mediterranean Region ------
200 Western Pacific Region
100
0 1948 1953 1958 1963 1968
Figure 8.1
8.7 WHO provided scientific and technical support to the French Ministry of Cooperation and Development in organizing an international symposium on "technology, health and development" (Paris, December 1992). Cooperation with the Council on Health Research for Development was initiated following the creation of that nongovernmental organization in March 1993. Formal mechanisms for strengthening this cooperation are being explored.
8.8 In Africa a fund was created for the promotion of health systems research and development. Prizes were awarded to eight research workers in African medical schools in acknowledgement of their publications and theses. "Public health research" was the subject of the Technical Discussions held during the 1992 session of the Regional Committee.
8 9 In the Americas an analysis was made of health research in Argentina, Brazil, Cuba, Mexico and Venezuela', with the aim of improving health research policies. A total of 39 research
1 Pellegrim Filho A. Health research 10 Latm America. Bulletin of the Pan Ameffcan Health Organization, 1993. 27(2): 168-182.
40
1973 1978 1983 1988 1993
projects were funded in priority areas. The regional system for vaccine development in Latin America and the Caribbean (SIREV A) was further developed. There were several meetings of "Convergencia", an interagency initiative to promote cooperation in health science and technology. The PAHO/WHO Advisory Committee on Health Research held its twenty-ninth meeting in August 1993.
8.10 In South-East Asia current research strategies were reviewed and updated. The eighth meeting of directors of medical research councils and analogous bodies (Bangkok, November 1992) stressed the essential role of WHO in promoting the establishment or strengthening of such bodies. Further funding was provided for training in research, provision of grants for visiting scientists, and other activities directed towards strengthening research capacity. Meetings of the South-East Asia Advisory Committee on Health Research continued to be held on a yearly basis.
8.11 In Europe a joint workshop was organized with the European Medical Research Council (Prague, January 1993) to help the countries of central and eastern Europe to reorganize their national health research administra-

RESEARCH PROMOTION AND DEVELOPMENT ----------------------------------------------
tions and to increase the effectiveness of contacts between western and eastern Europe. It was recommended that those countries should consider establishing independent national health research institutions as part of a national science research council.
8.12 In the Eastern Mediterranean support was given to several research projects in priority areas such as nutrition, primary health care, health systems research and assessment of maternal and child health services. Research information was disseminated through a Health services journal.
8.13 In the Western Pacific human resources for health research were promoted by means of training grants, short courses on research design and
41
methods, and the publication of a manual.1 A joint meeting in August 1992 of the regional ACHR and directors of health research councils or analogous bodies stressed the value of networking arrangements between experts and research institutes, and the importance of adequate infrastructure, information exchange and quality control in health research.
8.14 Details of research on particular subjects (for instance, human reproduction, immunization and tropical diseases) may be found in the chapters and sections of this report dealing with the WHO programmes concerned.
1 Health research methodology. a guide for training m research methods. Manila, World Health OrganizatiOn, 1992.

CHAPTER 9
General health protection and
Women, health and development
9.1 WHO is concerned with the way in which the health of women affects and is affected by their social, political, cultural and economic status, and with their contribution to health and overall development. An interdivisional steering committee on women, health and development has been set up with the task of ensuring that WHO's technical programmes and the Ninth General Programme of Work give proper attention to matters affecting women's health in all areas. The committee has prepared a checklist of indicators for programme managers, including indicators relating to differences between the sexes in health and access to and use of health services; the impact of activities on the health of women; and the participation of women and women's organizations in health promotion and disease prevention. It has also indicated areas where research is needed on matters of concern to women. It will work with the Director-General's adviser on health and development policies in preparations for the fourth world conference on women, to be held in Beijing in 1995, and ensure that due importance is given to women's health in the proposed "platform for action".
9.2 The Director-General has appointed an adviser on the employment and participation of women to help achieve WHO's objective of increasing the number of women in professional and higher-graded posts and ensuring their participation in the Organization's activities. Similarly, a multidisciplinary coordination group has been set up to ensure that nurses have access to certain kinds of WHO assignment in which there has been a strong bias towards physicians.
9.3 The United Nations is preparing a report on the subject of women, drug abuse and HIV I
43
• promot1on
AIDS, taking into account the work of a consultation on women and drugs in August 1993. Participants stressed that problems of substance abuse occur among women in all countries, regardless of their cultural, social and economic circumstances, and that priority must therefore be given to public education, treatment and rehabilitation specific to women's needs, and to devising measures and policies that take those needs fully into account. A report on human rights in relation to women's health, which examines the implicit and explicit threats to women's health, was commissioned for the conference on the health of women in central and eastern Europe, to be held in Vienna in 1994. WHO maintains databases on women's health, including bibliographies and lists of indicators.
9 4 The network of multisectoral teams on women's leadership and participation was further strengthened following a fourth UNFPAsupported interregional workshop on leadership and participation of women in maternal and child health and family planning (Washington, November 1992); it now encompasses 42 countries.
9.5 In the context of the 1993 World Health Day on the theme of accident and injury prevention, particular attention was drawn to violence affecting girls and women, including not only physical and mental abuse but also the hidden violence of discrimination or denial of the basic human rights where food, medical care, education and a safe environment are concerned. Resolution WHA46.18 highlighted the importance of eliminating such harmful practices as female genital mutilation and other social and behavioural obstacles affecting the health of women and children. Technical and financial support was provided for national surveys on such practices and for measures to combat them, including training of traditional birth attendants and midwives.

THE WORK OF WHO 1992-1993
9 6 Work continued in the Americas to strengthen national capability for using a method that takes proper account of women's needs in the analysis and evaluation of health policies and programmes. Technical support was provided for subregional training workshops in Costa Rica, Ecuador, Guatemala, Jamaica, Panama, and Trinidad and Tobago. Research focused on violence against women, quality of care in service delivery for women, and women and tropical diseases; the findings on violence were taken into account in formulating policy proposals and reviewed by a Central American seminar on its public health aspects (Managua, March 1992). A publication on gender, women and health1 was prepared by a multidisciplinary group.
9.7 As part of a European initiative, "Investing in women's health", supported by Austria, Norway and Sweden, a preparatory meeting (Copenhagen, March 1993) drew up a plan for a European women's health forum, to be officially inaugurated at the conclusion of the Vienna meeting in 1994. Within the context of the Healthy Cities action plan on women's health, an information network is being established that will link all parts of Europe and provide a specifically urban input for the forum.
9 8 Concerted efforts have been made through intercountry activities in the Eastern Mediterranean to improve quality of life for women and utilize their potential for health promotion and development. For this purpose contributions are being made in several countries to activities outside the health field, such as functional literacy training and income generation. A regional commission for Arab women is being set up, with the participation of interested agencies and influential nongovernmental organizations. The Regional Committee for the Eastern Mediterranean held technical discussions in 1993 on the theme "The role of women in support of health for all". Participants stressed that there should be greater acknowledgement of women's contribution to the health of families and communities, and noted that their involvement in health can be enhanced by using women's networks and community groups to disseminate information on the health risks they face, their right to health care and the
1 Gender, women and health. Washington, Pan American Health OrgamzatiOn, 1993 (Scientrfrc Publicatron, No. 541)
44
options available to them for promoting and protecting their health.
Food and nutrition
9.9 In response to the recommendations in the world declaration and plan of action adopted by the International Conference on Nutrition (Rome, December 1992) the Director-General, reaffirming WHO's continuing commitment to proper food and nutrition for a healthy life, decided in May 1993 to establish a new division to be responsible for all WHO's activities concerned with food aid, food safety and nutrition. It will strengthen the Organization's capacity for action in those areas and support Member States in implementing national plans of action for nutritional improvement, giving priority to the countries that are least developed, have low income or are affected by disasters.
Food aid programmes
9.10 WHO continued to advise on the health aspects of food-assisted development projects supported by the World Food Programme, and is cooperating with WFP to assess the effectiveness of such projects in improving health and to determine whether they should be continued, phased out or modified. The Organization also continued to participate in WFP-financed interagency missions for the design and evaluation of the health aspects of development projects, and to a lesser degree for the design of health-related components of school feeding projects aimed at improving attendance and performance. In such projects particular importance is attached to providing regular treatment for intestinal helminths in areas of high prevalence, and to ensuring a healthy school environment with emphasis on safe water supply and sanitation. Unfortunately, the attention paid to the health aspects of rural development projects supported by food aid is not commensurate with the gravity of the problems encountered and does not suffice to offset the adverse effects associated with some interventions, such as the transmission of malaria and schistosomiasis in rural irrigation schemes. WHO continued its involvement with health and nutrition aspects of emergency operations, particularly in long-term projects for refugees and displaced persons (see paragraphs 2.28 to 2.33).

GENERAL HEALTH PROTECTION AND PROMOTION
Food safety
9.11 Work on the development of internationally agreed food standards continued through WHO's contribution to the Codex Alimentarius Commission. Codex provisions offer adequate health protection and are recognized under the General Agreement on Tariffs and Trade (GATT) as providing sufficient justification for import restrictions. In accordance with the Final Act of the "Uruguay Round" of multilateral trade negotiations launched by GATT, countries could be required to furnish justification for any restrictions based on national regulations that are stricter than the Codex provisions.
9 12 A review article1 and fact-sheet were issued on unsafe food - a common cause of infant diarrhoea. Since cholera and other food-borne diseases may be transmitted by street-vended foods, a document was issued setting out essential safety requirements for such foods. 2 This subject was discussed at an Asian conference on street foods (Beijing, October 1993 ), convened in collaboration with the International Life Sciences Institute. WHO worked with the Industry Council for Development in conducting training courses in Asia and Africa and preparing training materials and a document3 on the use of the system of hazard analysis critical control point evaluations, which should be of value to national authorities and the food industry in improving food safety.
913 WHO cooperated with FAO and UNEP in the food contamination monitoring component of the Global Environmental Monitoring System (GEMS), and with FAO and IAEAin the work of the International Consultative Group on Food Irradiation. In addition, food processing technologies were assessed, workshops were held, and texts were prepared on food irradiation4 and biotechnology.5
1 Motaqem1 Y et al Contaminated weaning food: a major risk factor for d1arrhoea and associated malnutrition Bulletm of the World Health Organ· ization, 71 (l): 79·92 (1993)
2 Document WHO/HPP /FOS/92 3. 3 Document WHO/FNU/FOS/93.3. 4 Safety and nutritional adequacy of 11radwted food. Geneva, World Health
Organization (In press). 5 Document WHO/FNU/FOS/93.6.
4S
Nutrition
914 The International Conference on Nutrition (Rome, December 1992) was the culmination of more than two years' joint effort by WHO and FAO to promote awareness of the extent and seriousness of nutritional and diet-related problems and to achieve consensus on how to deal with them. It was attended by more than 1300 people representing 159 governments and some 160 international and nongovernmental organizations. Initial preparatory work for the conference focused on stimulating effective intersectoral cooperation in countries so as to improve nutritional wellbeing. Regional and subregional meetings were then organized to assess common food and nutrition problems. Information on the resulting country and regional consensus provided background material for a preparatory committee that met in August 1992 to review the main findings and draft a world declaration and plan of action which were subsequently adopted by the conference.6 As they represent a global consensus on the nature and causes of nutritional problems, the declaration and plan now provide a basis for WHO support to national plans of action. In response to requests from governments, WHO has so far provided technical support and funds to 14 least developed countries in Africa, to one each in the Americas, South-East Asia and the Eastern Mediterranean and three in the Western Pacific.
9.15 Accurate assessment of body mass and growth, which is indispensable to interventions aimed at improving physical welfare, remains a much debated topic. In November 1993 WHO convened an expert committee to consider conflicting ideas on this subject and more particularly reference data and guidelines for their use and interpretation at all stages of life.7
916 WHO, UNICEF, Wellstart International (a WHO collaborating centre in San Diego, USA), and the World Alliance for Breastfeeding Action jointly sponsored three lactation management training workshops for 65 Russianspeaking health workers (Saint Petersburg, Russian Federation, August 1993 ). This provided an
6 World declaratiOn and plan af act10n for nutnt10n. Rome, FAO/WHO, 1992.
7 Physical status· the use and interpretation of anthropometry. Report of a WHO Expert Committee. Geneva, World Health Organization (in prepara· lion).
THE WORK OF WHO 1992-1993
opportunity to prepare Russian-language editions of two of WHO's most popular publications: the WHO/UNICEF statement on breastfeeding and the role of maternity services1 and a summary of the latest scientific findings on the physiological basis for infant feeding. 2
9 17 In support of countries implementing the WHO/UNICEF Baby-friendly Hospital Initiative (see box), WHO provided training for health professionals to serve as hospital assessors in China, Egypt, Jordan, Lebanon, Philippines and Russian Federation; prepared guidelines for babyfriendly training workshops; and helped establish lactation management training centres in Manila and in Sao Paulo (Brazil). With financial assistance from USAID, the WHO data bank on breastfeeding was expanded, using a revised set of internationally agreed indicators; it now contains information from more than 2000 surveys or studies carried out in over 170 countries or territories.
9.18 Financial contributions from the Government of the Netherlands and SIDA enabled WHO to provide technical support in translating the International Code of Marketing of Breastmilk Substitutes into appropriate national measures in Guatemala, Iraq, Morocco, Syrian Arab Republic, United Republic of Tanzania, and Viet Nam; to organize a workshop (Cairo, September 1993) on the implementation of the Code for participants from 15 Eastern Mediterranean countries; and to brief 12 consultants (Geneva, September 1993) who can be called upon to help the Organization respond to requests from Member States for technical support on this subject.
9 19 New evidence of the importance of vitamin A nutriture in the broader realm of child health and survival and renewed commitment by national health authorities and international organizations and bodies alike provided the impetus for producing a third revised and expanded edition of WHO's 1978 best-selling field manual for assessing vitamin A deficiency.3 Technical
1 Protectmg, promotmg and supportmg breast-feedmg the speoal role of matern1ty sefVIces. A tomt WHO/UNICEF statement Geneva, World Health Orgamzat1on, 1989 Available or in preparation 1n more than 40 language ed1t1ons
2 Akre J ed. Infant feedmg the physiOlogical baSIS (Supplement to Vol 67 of the Bulletm of the World Health Orgamzat1on), Geneva, 1990 Available or 1n preparation 1n 13 language editions
3 Sommer A V1tamin A defiCiency and 1ts consequences: a f1eld gu1de to thelf detection and control, 3rd ed. Geneva, World Health OrganiZation (in press)
46
The Baby-friendly Hospital Initiative
• The Baby-friendly Hospital Initiative is a global movement, spearheaded by WHO and UNICEF, that aims to give every baby the best start in life by creating a health care environment where breast-feeding is a norm. To become truly baby-friendly, hospitals and maternity wards around the world will want to give practical effect to the principles set out in the joint WHO/ UNICEF statement on breast-feeeding and maternity services.1 WHO and UNICEF are supporting national authorities responsible for designating maternity wards and hospitals as baby-friendly in a variety of ways, including the issue of guidelines and support for training. The initiative is based on the principles described in the joint statement, which are synthesized in "Ten steps to successful breast-feeding":
Every facility providing maternity services and care for newborn infants should:
• have a written breast-feeding policy that is routinely communicated to all health care staff;
• train all health care staff in skills necessary to implement this policy;
• inform all pregnant women about the benefits and management of breastfeeding;
• help mothers initiate breast-feeding within a half-hour of birth;
• show mothers how to breast-feed, and how to maintain lactation even if they should be separated from their infants;
• give newborn infants no food or drink other than breast milk, unless medically indicated;
• practise rooming-in - allow mothers and infants to remain together -24 hours a day;
• encourage breast-feeding on demand; • give no artificial teats or pacifiers (also
called dummies or soothers) to breastfeeding infants;
• foster the establishment of breastfeeding support groups and refer mothers to them on discharge from the hospital or clinic.
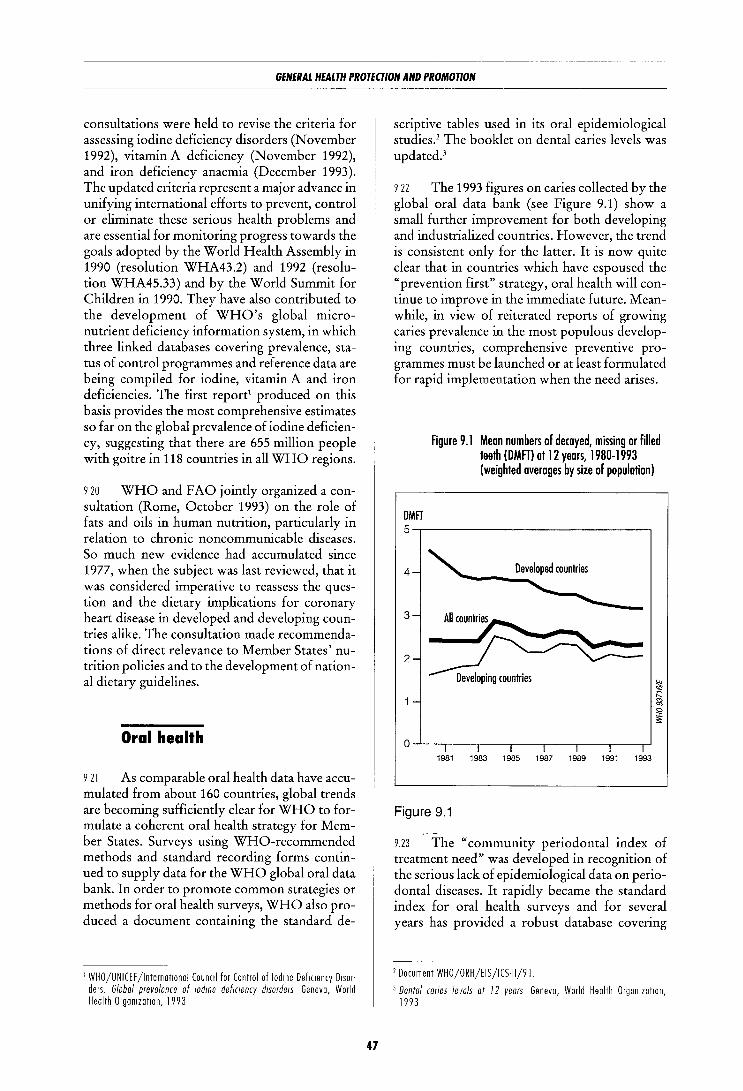
GENERAL HEALTH PROTECTION AND PROMOTION
consultations were held to revise the criteria for assessing iodine deficiency disorders (November 1992), vitamin A deficiency (November 1992), and iron deficiency anaemia (December 1993). The updated criteria represent a major advance in unifying international efforts to prevent, control or eliminate these serious health problems and are essential for monitoring progress towards the goals adopted by the World Health Assembly in 1990 (resolution WHA43.2) and 1992 (resolution WHA45.33) and by the World Summit for Children in 1990. They have also contributed to the development of WHO's global micronutrient deficiency information system, in which three linked databases covering prevalence, status of control programmes and reference data are being compiled for iodine, vitamin A and iron deficiencies. The first report1 produced on this basis provides the most comprehensive estimates so far on the global prevalence of iodine deficiency, suggesting that there are 655 million people with goitre in 118 countries in all WHO regions.
9 20 WHO and FAO jointly organized a consultation (Rome, October 1993) on the role of fats and oils in human nutrition, particularly in relation to chronic noncommunicable diseases. So much new evidence had accumulated since 1977, when the subject was last reviewed, that it was considered imperative to reassess the question and the dietary implications for coronary heart disease in developed and developing countries alike. The consultation made recommendations of direct relevance to Member States' nutrition policies and to the development of national dietary guidelines.
Oral health
9 21 As comparable oral health data have accumulated from about 160 countries, global trends are becoming sufficiently clear for WHO to formulate a coherent oral health strategy for Member States. Surveys using WHO-recommended methods and standard recording forms continued to supply data for the WHO global oral data bank. In order to promote common strategies or methods for oral health surveys, WHO also produced a document containing the standard de-
1 WHO/UNICEF /InternatiOnal Council for Control of lod1ne Def1c1ency Disorders_ Global prevalence of 10dme defiCiency disorders Geneva, World Health Orgamzat1on, 1993
47
scriptive tables used in its oral epidemiological studies.2 The booklet on dental caries levels was updated.3
9 22 The 1993 figures on caries collected by the global oral data bank (see Figure 9.1) show a small further improvement for both developing and industrialized countries. However, the trend is consistent only for the latter. It is now quite clear that in countries which have espoused the "prevention first" strategy, oral health will continue to improve in the immediate future. Meanwhile, in view of reiterated reports of growing caries prevalence in the most populous developing countries, comprehensive preventive programmes must be launched or at least formulated for rapid implementation when the need arises.
DMFT
Figure 9.1 Mean numbers of decoyed, missing or filled teeth (DMFT) ot12 years, 1980-1993 (weighted averages by size of population)
5-.---------------------------.
4
3
2
1981 1983 1985 1987 1989 1991 1993
Figure 9.1
9.23 The "community periodontal index of treatment need" was developed in recognition of the serious lack of epidemiological data on periodontal diseases. It rapidly became the standard index for oral health surveys and for several years has provided a robust database covering
1 Document WHO/ORH/EIS/ICS-11/91. 3 Dental caries levels at 12 years Geneva, World Health OrganiZation,
1993

THE WORK OF WHO 1992-1993
113 countries; a compilation of data for agegroups 15-19 years and 35-44 years, issued in 1992,1 has significantly changed global and national estimations of the need for prevention and treatment of periodontal diseases, and thus provides a basis for goal-setting.
9 24 Eight sites in six countries have reported results from the second international collaborative study of oral health outcomes, in which clinical and sociological data are collected in standard form together with data from care providers and administrators. The information obtained is of value for the preparation of guidelines for improved oral health.
9 25 A new "atraumatic restorative treatment", in which dental cavities are cleaned with hand instruments only and then filled with glass ionomer cement, is being tested in several villages in the province of Khon Kaen in Thailand. Preliminary results indicate that it may prove the most appropriate technology for rural and disadvantaged communities that at present have no access to oral care. Short courses on the technique were given for dental nurses in Cambodia and the Lao People's Democratic Republic.
9.26 Extrabudgetary funds were obtained for a project to provide special curative and preventive services to populations living in zones contaminated as a result of the Chernobyl accident. An international action network on oro-facial mutilations and noma (gangrenous stomatitis) in Africa has been set up; its aim is to combine primary prevention with the availability of moderately complex treatment and with a referral system for very complex care.
9 27 A number of projects have been undertaken as part of the continuing effort to demonstrate the effectiveness of oral disease prevention. With support from the Borrow Dental Milk Foundation (United Kingdom), WHO launched an international milk fluoridation programme; it includes community projects and laboratory and feasibility studies, and is being implemented in nine countries. A five-year community project successfully completed in Bulgaria confirmed that milk can be used like water or salt as a vehicle for fluoride to combat dental caries in children. In other projects, fluoride-containing toothpastes and sealants im-
1 Document WHO/ORH/EIS/CPITN/92.
48
pregnated with prophylactic agents are being used to widen the choice of preventive methods and to convince communities of the prime importance of prevention within the framework of primary health care.
9 28 Intercountry centres for oral health in Nigeria, Syrian Arab Republic and Thailand, together with the WHO collaborating centre for oral health in Europe, recently designated in Minsk, continued to support WHO's strategies. More than 30 WHO collaborating centres in 19 countries have made effective contributions to country activities, for instance by updating situation analyses, formulating national plans of action, and providing training in the planning and management of oral health programmes.
9 29 Considerable work was done in updating existing methods and devising new ones. The fourth edition of Oral health surveys: basic methods is in final draft form as is the third edition of Application of the International Classification of Diseases to dentistry and stomatology. Guidelines on hygiene and infection control in oral care settings, mouth care for severely ill patients, training of examiners for oral health surveys, and hand instruments for community and restricted referral level oral care were completed for distribution. Extensive information material was prepared for World Health Day 1994 on the theme "Oral health for a healthy life".
9.30 Training of oral health personnel remains a major priority for most countries, and in some cases there is a strong focus on situating oral health within the overall context of the health sciences. Methods for training undergraduates and auxiliary personnel using performance simulation have been developed jointly with several collaborating centres, and a manual has been completed. Following a detailed review of current dental education in countries belonging to the Commonwealth of Independent States, proposals were made for radical changes, particularly in orienting the curriculum towards the "health sciences" approach and gearing it to society's health priorities and needs.
9 31 Different aspects of the work were emphasized in the various regions: planning of services and development of human resources and technology (Africa; Americas); application of primary health care principles to the development of services (South-East Asia); quality assurance through information systems, situation

GENERAL HEALTH PROTECTION AND PROMOTION
analysis and implementation of planned services (Eastern Mediterranean; Europe); and surveillance of populations at risk and promotion of preventive measures through the adoption of measurable targets for oral health improvement (Western Pacific).
lniury prevention
9.32 Under the technical coordination of the WHO collaborating centre for community safety promotion at the Karolinska Institute in Stockholm, the network of demonstration projects on community safety expanded to involve ten countries.1
9.33 A WHO-sponsored second international conference on safe communities (Glasgow, United Kingdom, September 1992) included violence prevention in its agenda. The results of case studies were used in an analysis of the concept of safety that took into account the community's views on how it should be protected from a variety of hazards, including natural disasters and willful violence. The conference also examined the inadequacy of political or administrative mechanisms in the area of safety promotion.
9.34 Programme leaders who met on the occasion of a WHO interregional seminar on methods for planning community safety programmes (Toulouse, France, November 1993) decided to produce reference material for health planners and workers in response to the increasing demand for guidance on methodology and information on experience. The group also produced a document on community action for safety in preparation for the 1994 Technical Discussions on the subject of "Community action for health".
9.35 World Health Day 1993 provided an opportunity to present the theme of violence from a public health viewpoint. It was followed by intensive consultation both in the Organization and between WHO and institutes in France and the United States of America with a view to building up a pool of technical expertise and establishing a network of public health experts concerned with the prevention of intentional injury.
1 Argentma, Australia, Denmark, France, lnd10, lndonesta, Sweden, Thatland, Untied Ktngdom, United States of Amertca
49
9.36 A second world conference on injury control (Atlanta, USA, May 1993), organized by the United States National Center for Injury Prevention and Control, a WHO collaborating centre, with support from other WHO collaborating centres, was the occasion for a thorough evaluation of injury control programmes throughout the world. The conference succeeded in its three objectives: to strengthen technical cooperation between research institutes, including WHO collaborating centres; to further the adoption of commonly agreed standards for developing analytical methodology for injury control, including control of violence; and to arouse broad interest in the WHO programme for community safety.
9.37 Using research protocols prepared by WHO in cooperation with nongovernmental organizations and collaborating centres, two epidemiological studies are under way, one (in Toulouse, France; and Albuquerque, USA) dealing with falls in the elderly, and the other with burns, on the basis of a,n epidemiological analysis being carried out in India and several European countries. The International Society for Burn Injuries and WHO are jointly preparing a manual on the epidemiology, prevention and care of burns.
9.38 In connection with the safety helmet initiative carried out under the leadership of the United States National Center for Injury Prevention and Control, WHO convened a symposium on neurotrauma prevention and management (Brussels, December 1993 ). Participants were reminded that brain injuries represent about half of all severe injuries from road accidents and a large proportion of injuries from other causes; they are frequently associated with spinal cord trauma. The symposium initiated an epidemiological analysis based on common protocols, set up a network of research centres to develop protective techniques, formulated strategies to promote the use of such techniques, and established an international forum for improving the medical management of brain-injured persons and for enhancing rehabilitation techniques and services. These activities will be coordinated by WHO collaborating centres.
9.39 WHO collaborated with seven Member States in the Eastern Mediterranean in strengthening measures to promote safety and prevent accidental injury. In 1993 a course on the management of burn injuries was held for nurses, dealing with nursing care, treatment of cases and prevention of sequelae.

THE WORK OF WHO 1992-1993
Tobacco or health
Strengthening notional programmes
9.40 WHO's direct support to Member States included involvement in establishing and strengthening comprehensive national tobacco control programmes in all regions.
9 41 WHO cosponsored an all-Africa conference on tobacco control (Harare, November 1993 ). Tobacco-producing countries in Africa took initial steps towards harmonizing their national tobacco control programmes and considered possible ways of reducing their economic dependence on this product. There was general realization of the need for greater efforts in all countries to counter the growing presence of tobacco advertising, mainly by transnational tobacco companies; in Senegal, for example, expenditure on tobacco advertising exceeds 1000 million CFA francs annually.
942 In the Americas PAHO/WHO participated actively in a meeting of the Latin American Committee against Tobacco Use (San Jose, June 1993) and collaborated with the United States National Institutes of Health in setting up tobacco control projects in Chile and Mexico.
9 43 In South-East Asia WHO cooperated with Bangladesh, India, Mongolia, Nepal and Thailand in strengthening national action plans to combat tobacco use.
9 44 Missions were sent to eight countries of central and eastern Europe to assist in implementing national tobacco control programmes. Among other regional and national meetings in Europe, the Organization supported the second and third European seminars on tobacco or health for national policy advisers and programme managers (Budapest, January 1992; Vienna, March 1993 ), which brought together participants from 35 countries.
9 45 In the Eastern Mediterranean a consultation (Alexandria, May 1992) reviewed national tobacco control policies and programmes and formulated guidelines. A joint consultation between WHO and the International Union against Cancer (Cairo, February 1993) discussed the political manipulation of tobacco control and the role of physicians in antismoking activities.
50
9 46 In the Western Pacific WHO participated in a variety of activities undertaken by Member States and supported the work of nongovernmental organizations concerned with tobacco control, including regional and national conferences, meetings and workshops. By the end of the biennium nine countries and areas had established tobacco control policies backed by at least some legislative measures, and most Member States had designated national focal points. The majority of countries and areas had taken steps towards implementing the Western Pacific regional action plan on tobacco or health for 1990-1994 but, as the Regional Committee noted in 1992, more vigorous action is needed.
Health promotion, advocacy and public information
9 47 The 1992 and 1993 World No-Tobacco Days were widely observed throughout the world and were well reported in the news media. WHO issued information and recommendations on tobacco-free workplaces and on the role of health services and health personnel in attaining a tobacco-free society, and awarded medals to anti-tobacco campaigners from all regions. Worldwide distribution of the quarterly newsletter Tobacco alert continued.
9.48 WHO promoted tobacco control measures at several international conferences including a world conference on tobacco or health (Buenos Aires, March-April 1992). The agreements reached to hold smoke-free Olympic Games in 1992 at Albertville (France) and Barcelona (Spain) and in 1994 at Lillehammer (Norway) were of great publicity value. Throughout the world action was stepped up to encourage Member States to adopt comprehensive tobacco control policies.
Data collection and research
9 49 Research findings were published in the form of monographs on women and tobacco1
and on tobacco controllegislation2 and a techni-
1 Women and tobacco Geneva, World Health Orgamat1on, 1992 1 Roemer R Legtsfative actton to combat the world tobacco epidemtc, 2nd
ed1t1on. Geneva, World Health Orgamzation, 1993.

GENERAL HEALTH PROTEUION AND PROMOTION
cal document on the interaction of smoking and workplace hazards.1
9 50 In conjunction with the University of Oxford (United Kingdom), WHO initiated and supported a series of prospective epidemiological studies to monitor the health effects of tobacco use in several countries.2
9 51 PAHO/WHO published a report on tobacco use, tobacco-related diseases and prevention and control measures in the Americas.3 The Organization also collaborated with the Office of the Surgeon General of the United States of America in preparing a wide-ranging report on the problems posed by tobacco consumption in the Americas4 and stressing the need for regional coordination and cooperation to create a smokefree society.
1 Document WHO/OCH/TOH/92 1 2 Argentrna, Chrna, Cuba, Egypt, India, Mexrco, Poland, Unrted Kingdom,
Unrted States of America 3 Tobacco or health. status 1n the Amencas. Washrngton, Pan Amerrcon
Health Orgonrzotron, 1992 (Scientific Publrcot10n, No 536). 4 Unrted States Deportment of Health and Human Servrces Smoking and
health 1n the Amencas· a 1992 report of the Surgeon General, in collabora· t10n with the Pan Amencan Health Organization. Atlanta, 1992 (OHHS Publrcotion, No. (CD() 92-8420)
SI
lnteragency collaboration
9.52 WHO worked closely with ICAO and participated in the twenty-ninth session of its Assembly (Montreal, September 1992), which decided to urge all contracting States to take measures to restrict smoking progressively on all international passenger flights, with the objective of completely banning smoking by July 1996.
9.53 In response to Health Assembly resolution WHA45.20, the Director-General submitted a report on tobacco or health to the Economic and Social Council of the United Nations, which in July 1993 adopted a resolution requesting the Secretary-General of the United Nations to set up a focal point for multisectoral collaboration on the economic and social aspects of tobacco production and consumption, taking into account the serious health consequences of tobacco use.
9.54 In pursuance of the further Health Assembly resolution WHA46.8, the DirectorGeneral has urged the Secretary-General of the United Nations to ban the sale and use of tobacco products in all workplaces and public areas in buildings owned, operated or controlled by organizations of the United Nations system.
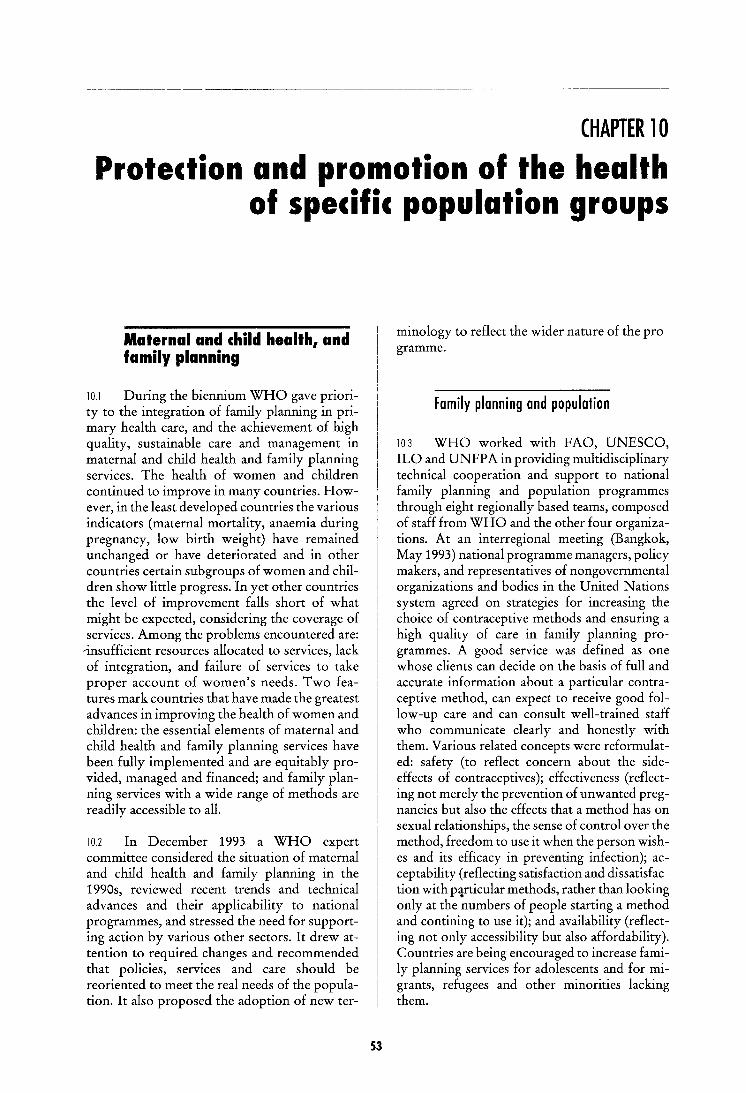
CHAPTER 10
Protection and promotion of the health of specific population groups
Maternal and child health, and family planning
10.1 During the biennium WHO gave priority to the integration of family planning in primary health care, and the achievement of high quality, sustainable care and management in maternal and child health and family planning services. The health of women and children continued to improve in many countries. However, in the least developed countries the various indicators (maternal mortality, anaemia during pregnancy, low birth weight) have remained unchanged or have deteriorated and in other countries certain subgroups of women and children show little progress. In yet other countries the level of improvement falls short of what might be expected, considering the coverage of services. Among the problems encountered are:
-insufficient resources allocated to services, lack of integration, and failure of services to take proper account of women's needs. Two features mark countries that have made the greatest advances in improving the health of women and children: the essential elements of maternal and child health and family planning services have been fully implemented and are equitably provided, managed and financed; and family planning services with a wide range of methods are readily accessible to all.
10.2 In December 1993 a WHO expert committee considered the situation of maternal and child health and family planning in the 1990s, reviewed recent trends and technical advances and their applicability to national programmes, and stressed the need for supporting action by various other sectors. It drew attention to required changes and recommended that policies, services and care should be reoriented to meet the real needs of the population. It also proposed the adoption of new ter-
53
minology to reflect the wider nature of the programme.
Family planning and population
103 WHO worked with FAO, UNESCO, ILO and UNFP A in providing multidisciplinary technical cooperation and support to national family planning and population programmes through eight regionally based teams, composed of staff from WHO and the other four organizations. At an interregional meeting (Bangkok, May 1993) national programme managers, policy makers, and representatives of nongovernmental organizations and bodies in the United Nations system agreed on strategies for increasing the choice of contraceptive methods and ensuring a high quality of care in family planning programmes. A good service was defined as one whose clients can decide on the basis of full and accurate information about a particular contraceptive method, can expect to receive good follow-up care and can consult well-trained staff who communicate clearly and honestly with them. Various related concepts were reformulated: safety (to reflect concern about the sideeffects of contraceptives); effectiveness (reflecting not merely the prevention of unwanted pregnancies but also the effects that a method has on sexual relationships, the sense of control over the method, freedom to use it when the person wishes and its efficacy in preventing infection); acceptability (reflecting satisfaction and dissatisfaction with p~rticular methods, rather than looking only at the numbers of people starting a method and contining to use it); and availability (reflecting not only accessibility but also affordability). Countries are being encouraged to increase family planning services for adolescents and for migrants, refugees and other minorities lacking them.
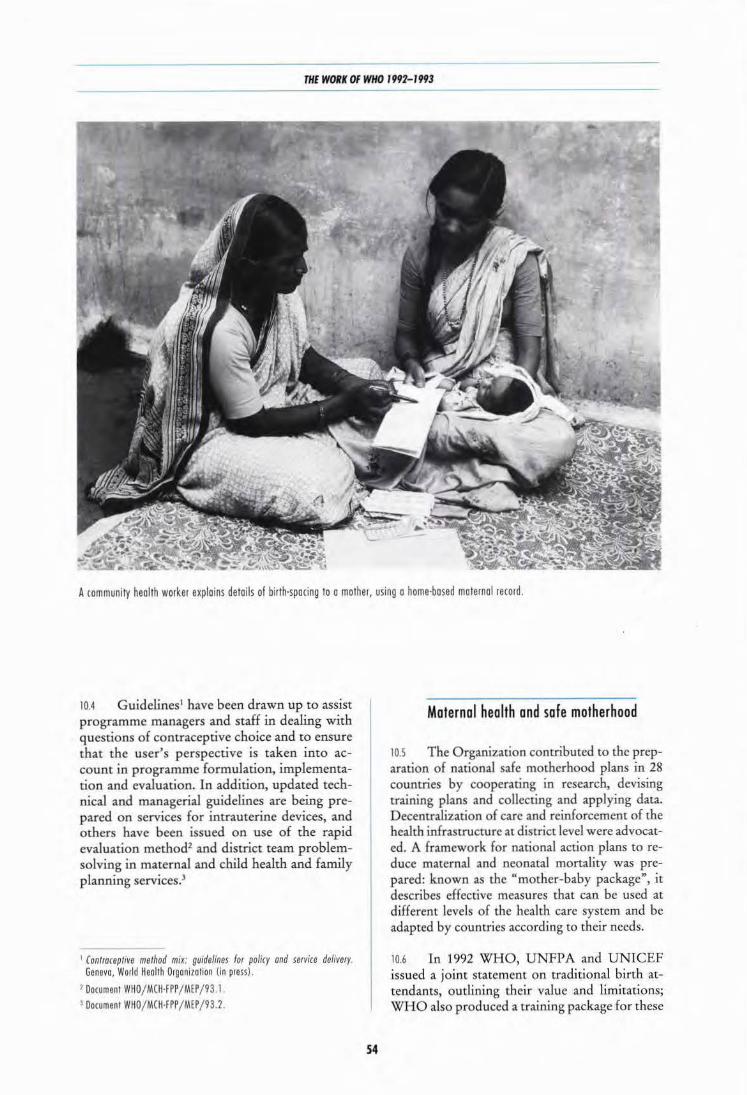
THE WORK OF WHO 1992-1993
A community health worker explains details of birth·spacing to a mother, using a home·based maternal record.
10.4 Guidelines1 have been drawn up to assist programme managers and staff in dealing with questions of contraceptive choice and to ensure that the user's perspective is taken into account in programme formulation, implementation and evaluation. In addition, updated technical and managerial guidelines are being prepared on services for intrauterine devices, and others have been issued on use of the rapid evaluation method2 and district team problemsolving in maternal and child health and family planning services.3
1 (ontwceptive method mix: guidelines for policy and service delivery. Geneva, World Heollh Organization (in press).
1 Document WHO/MCH·FPP /MEP / 931 . 3 Document WHO/ MCH·FPP / MEP / 93.2.
54
Maternal health and safe motherhood
10.5 The Organization contributed to the preparation of national safe motherhood plans in 28 countries by cooperating in research, devising training plans and collecting and applying data. Decentralization of care and reinforcement of the health infrastructure at district level were advocated. A framework for national action plans to reduce maternal and neonatal mortality was prepared: known as the "mother-baby package", it describes effective measures that can be used at different levels of the health care system and be adapted by countries according to their needs.
10.6 In 1992 WHO, UNFPA and UNICEF issued a joint statement on traditional birth attendants, outlining their value and limitations; WHO also produced a training package for these

PROTECTION AND PROMOTION OF THE HEALTH OF SPECIFIC POPULATION GROUPS
practitioners. In 1993 WHO and UNDP initiated a project to strengthen national capacity to reduce maternal mortality and disabilities. In collaboration with the International Confederation of Midwives and UNICEF, the Organization convened an international workshop (V ancouver, Canada, May 1993) to examine ways of improving the quality of maternal health care.
Child health and development
10 7 The Organization concentrated its efforts in this area on the promotion of perinatal and neonatal health; breast-feeding; growth, development and care of children in difficult social circumstances; application of the Convention on the Rights of the Child; and action following the 1990 World Summit for Children. Health Assembly resolution WHA45.22 served as a basis for adapting and applying an integrated strategy for maternal care and care of the newborn in district-based programmes. Findings of earlier studies on locallyproduced kits were applied in national programmes to promote clean delivery practices (for instance, in China, Philippines and VietNam) as a complement to administration of tetanus toxoid to eliminate neonatal tetanus and reduce maternal and neonatal sepsis. Guidelines and training materials for the management of hypothermia, an important and often unrecognized underlying cause of neonatal mortality and morbidity, were fieldtested. Methods and materials were devised for the successful management of birth asphyxia, another major cause of early neonatal mortality, and protocols and training materials were tested for the management of sick newborn infants. A simple method for assessment of gestational age was developed to identify newborns requiring special care or possible referral. On the basis of earlier research, the home-based growth and development record was widely used in China in primary health care and day-care centres in collaboration with UNESCO and UNICEF; this type of record was also used in Kiribati, Papua New Guinea, Philippines and Viet N am, and enables both pregnant women and health workers to recognize risks and take appropriate action.
Regional activities
10 8 In Africa particular attention was paid to extending the coverage of services, improving the
ss
quality of care and reducing maternal and neonatal mortality and morbidity. Following a regional consultation on prevention of maternal mortality and on infertility in sub-Saharan Africa (Kigali, January 1992), a regional task force was created to plan a centre for training and research on safe motherhood and the status of women. Workshops on problem-solving for district teams were organized in Senegal and United Republic of Tanzania and a regional support project, "Accelerated action for safe motherhood in the African Region", was launched. WHO assisted in the design of a national maternal health and safe motherhood programme in Lesotho and participated in programme evaluation in Gambia. As part of efforts to strengthen national capacity, an intercountry workshop (Brazzaville, February 1993) was held to brief representatives from 37 countries, UNICEF and the International Children's Centre on a number of topics including data collection for the regional family health data bank, which was started during the biennium. Collaboration with UNICEF was strengthened through the merging of existing interagency task forces into a single joint UNICEF/WHO technical advisory group.
10 9 Activities in the Americas focused on perinatal conditions and low birth weight as leading causes of neonatal deaths. Development of specific perinatal care was supported and training in aspects of maternal and child health services and research was strengthened. Member States made particular efforts to integrate maternal and child health programmes. The Organization undertook joint activities with national and nongovernmental organizations including Family Health International, International Project Assistance Services (USA), Family Care International, the Population Council and the United States Centers for Disease Control. Financial support was received from Italy, Netherlands, the Kellogg Foundation, UNICEF and UNFP A. Work continued on perinatal health projects in Bolivia, Honduras, Nicaragua and Peru, together with the promotion of maternal and child health education in nursing schools in eight countries.
1010 Further progress was made in South-East Asia in developing well-integrated maternal and child health and family planning services as part of primary health care. The safe motherhood initiative was successfully promoted at country level: for example, the Ministry of Health of Indonesia drew up a strategy and plan of action for

THE WORK OF WHO 1992-1993
1992-1996 in close cooperation with WHO and UNDP, a multisectoral task force in Nepal drafted a national plan of action for 1993-1997, and Bangladesh adopted the long-term objective of building up an effective, realistic and comprehensive programme of care to reduce maternal and neonatal mortality and morbidity. The Organization took an active part in a ministerial conference on children organized by the South Asian Association for Regional Cooperation (Colombo, September 1992), which outlined challenges, opportunities and future tasks and drew up strategies for achieving the goals of the 1990 World Summit for Children as part of overall development strategy.
10.11 In countries of central and eastern Europe emphasis was given to assisting specific groups such as teenagers and socially deprived women in overcoming barriers to family planning. Reducing the high rate of abortion in those countries, accounting for a sizeable proportion of maternal deaths, is a key goal of the programme "From abortion to contraception", resulting from the 1990 Tbilisi conference on this subject. WHO cooperated with Estonia, Romania and Russian Federation in improving maternal and child health care and family planning, and with Albania in upgrading family planning and gynaecological services.
1012 In the Eastern Mediterranean activities focused on strengthening national capacity for planning and implementing effective maternal and child health and family planning programmes. Support was provided to countries in setting up safe motherhood programmes and in reducing maternal and infant mortality rates. In a number of countries the prevalence of low birth weight remains high, even though maternal and child health programmes have been in operation for decades. An intercountry consultation on ways to reduce the frequency of low birth weight (Rabat, June 1992) reviewed past efforts, identified reasons for failures, and drew up an improved strategy for combating this problem.
1013 Activities in the Western Pacific were largely devoted to strengthening the management of national maternal and child health programmes. WHO's "rapid evaluation method", which combines various epidemiological and service research procedures, was used for collecting information on the performance, strengths and weaknesses of maternal and child health and family planning services in China, Papua New
S6
Guinea and VietNam as a guide to improving the services. An integrated management information system for maternal and child health and family planning services was used experimentally in some areas of China after training of all health workers involved. In most Member States family planning has become an integral part of family health services, including the introduction of new contraceptive methods such as subdermal implants and long-acting injectable contraceptive hormones. The family planning acceptance rate is generally low, varying between 2% (Papua New Guinea) and 35% (Tuvalu) of women of reproductive age; the low rate is attributable to such factors as religious beliefs, lack of awareness, misconceptions, poor logistics, insufficient managerial skills, and financial problems.
Health of adolescents
1014 WHO, with support from UNFPA and UNICEF, launched a new initiative to promote the healthy development of young people, including strengthening of the information base, a review of the current health status of young people in developing countries, and technical support to countries. This initiative has also strengthened WHO's collaboration with nongovernmental organizations at country level. In the Americas activities accelerated following the approval in 1991 of a regional plan of action to promote the health of adolescents; and a network of institutions in this field in 10 countries was set up with support from the Kellogg Foundation.
10.15 Materials issued during the biennium included a publication on the health of young people1
; two documents prepared jointly with the International Youth Foundation, one on principles of success in programming for young people2 and the other containing summaries of more than 400 exemplary programmes or projects3
; and a module for training in counselling skills in adolescent sexuality and reproductive health.4 In the Americas documentation centres were established in Brazil and Colombia,
1 The health of young people a challenge and a promrse. Geneva, World Health OrganiZatiOn, 1993.
2 Document WHO/ADH/92 3. 3 Document WHO/ADH/92.4. 4 Document WHO/ADH/93.3
PROTEaiON AND PROMOTION OF THE HEALTH OF SPECIFIC POPULATION GROUPS ~~~~--------~~--~- ----------~----~-~---~~-
and PAHOIWHO developed instruments for service evaluation, care of adolescents, and clinical history-taking. A manual on health in adolescence was widely disseminated, and an information system to provide data on adolescents was designed in Brazil in cooperation with UNFPA and the Kellogg Foundation.
10.16 Research on the interaction of adolescents, adults and health providers was expanded. The "narrative research method" 1 (see box) was used in Africa, and a meeting was held (Dakar, April 1993) to bring young people together with representatives of ministries of health to decide on future action. The method was also used in Brazil, Chile, Switzerland and Thailand. A survey in Indonesia, Nigeria and Philippines explored the extent to which services for maternal and child health, for family planning and for the control of sexually transmitted diseases are meeting the needs of young people. In Nigeria a review of law and policy on adolescent health was completed. The research instruments from these studies are being elaborated for wider use.
10.17 A number of countries formulated national policies for adolescent health, including Brazil, Chile, Colombia, Costa Rica and Indonesia. An intercountry consultation involving representatives of governments and nongovernmental organizations in the Eastern Mediterranean (Beirut, June 1993) prepared a social profile of adolescent girls, including adverse lifestyle factors that may impair their reproductive health, and suggested action at country level to provide special services for this group. An intersectoral meeting on the health of young people was held in Morocco (Rabat, June 1992), and a school sentinel service for adolescent health was set up in Tunisia. A joint project with the Council of Europe and the Commission of the European Communities was undertaken on health promotion for children and adolescents in schools. Health education courses and workshops on adolescent health were held in countries of the Western Pacific.
10.18 Training in counselling on adolescent sexuality and reproductive health was carried out with national affiliates of the International Planned Parenthood Federation in 10 countries in South-East Asia, the Eastern Mediterranean
1 Document WHO/ADH/93.4.
57
The narrative research method
• Today the health of young people is of growing concern in most parts of tli.e world as changing behaviour patterns confront them with new health hazards. This is especially true of sexual and reproductive health. WHO together with UNFPA, the World
Assembly of Youth and the World Organization of the Scout Movement and their affiliates undertook a study of the sexual behaviour of young people in 11 countries of sub-Saharan Africa, with over 12 000 respondents. It was carried out using a technique known as the "narrative research method", which was designed for this purpose but can be used for any research that lends itself to a storyline. In the present study selected young people from the youth organizations used role play to develop a story which they regarded as most typical of the way in which a relationship between two young people in their communities leads to an unwanted pregnancy. This story was then presented to representative samples of young people in each of their countries for modification. The resulting aggregated story, as well as differences among adolescents of different sex, age and residence, were reviewed by the youth organizations to plan future action. The intention of the study was to capitalize on those who know most about young people's behaviour- young people themselves. It emerged from the study that there was substantial agreement on the choice of story in all the countries, suggesting the existence of a common adolescent culture that crosses national and cultural boundaries. Moreover, the predominant story tended to be shared by respondents of both sexes. It was also clear that there is a great need to prepare young people for dealing with relationships and sexual encounters, and also to prepare families and responsible adults such as teachers, so that they can give the necessary support. Health services too must be adapted so that young people are able and willing to use them for prevention, care and treatment. This method will be of value in designing programmes for adolescents throughout the world, spearheaded by youth leaders who, because of their age, motivation and experience, are in the best position to learn about the realities of young people's lives and provide that information to those who make policy and implement programmes for adolescent health and development, including youth organizations.

THE WORK OF WHO 11JIJ2-11JIJ3
and the Western Pacific, using the WHO module. PAHO/WHO supported 11 regional meetings for training and sensitization on adolescent health for multidisciplinary teams. A core curriculum for professional training in adolescent health and development is being prepared.
Human reproduction research
1019 1992 marked the twentieth anniversary of the Special Programme of Research, Development and Research Training in Human Reproduction, which is funded almost exclusively from extra budgetary contributions and is cosponsored by UNDP, UNFPA, WHO and the World Bank. To mark this occasion, a special report on the global status of reproductive health was issued as part of the Programme's 1990-1991 biennial report. 1
Contraceptive safety
10.20 In May 1993 a group of experts met to review available data on the use of depotmedroxyprogesterone acetate (DMP A) and the risk of cancers of the breast, cervix, endometrium and ovary, including data from the large WHO collaborative study of neoplasia and steroidal contraceptives. The experts concluded that there was no evidence for an overall increase in the risk of cancer at any of the four sites reviewed, associated with the use of DMPA, and therefore did not recommend restricting its use as a contraceptive on the grounds of risk of neoplasia. Although an increased risk of breast cancer was observed in certain subgroups of women using DMPA, the findings were difficult to interpret. It was considered unlikely that the growths observed represented new tumours caused by DMP A. On the other hand there was good evidence of protection against endometrial cancer. It was also recommended that further studies should be conducted to collect data on long-term DMPA use by young women and the effect of its use in combination with estrogen. In 1992, following the publication of results of the WHO study of DMPA and breast cancer, the United
1 Khanna J, Van look PFA, Gr1ff1n PO, eds Reproducttve health· a key to a bnghter future Geneva, World Health Organ1zat1on, 1992.
ss
States Food and Drug Administration approved its use as a contraceptive.
New monthly injectable contraceptive preparations
10.21 In 1992 major phase Ill clinical trials were completed on two once-a-month injectable preparations, Mesigyna (50 mg of norethisterone enantate plus 5 mg of estradiol valerate) and Cyclofem (25 mg of medroxyprogesterone acetate and 5 mg of estradiol cypionate), developed by WHO. One of the trials, conducted in 12 centres in Egypt, evaluated the two preparations and the results will be taken into account in deciding whether to approve them for the national family planning programme. The second trial, in China, compared the same preparations and Chinese Injectable No. 1. Preliminary analyses confirmed the high efficacy and superior clinical efficacy of Mesigyna and Cyclofem; and this may lead to a shift to use of these preparations in China. In June 1993 a consultation of experts reviewed the available data on the new preparations and confirmed that they were safe and effective in preventing pregnancy. They also offer significant advances over progestogen-only injectables owing to the relatively high frequency of predictable menstrual patterns. Preliminary data suggest that return to ovulation occurs within a reasonable time, but further work is required to confirm return to fertility. The experts recommended these methods for routine use in family planning clinics, bearing in mind that they have contraindications similar to those applicable to oral contraceptives.
Intrauterine devices
10 22 Until recently many of the copper-bearing intrauterine devices (IUDs) were approved by national drug regulatory authorities for up to only four years of continuous use as there was little information on their efficacy beyond that period. Long-term studies by WHO on two copper-bearing IUDs- the TCu220C and TCu380A - have now provided data on up to nine years of continuous use. The pregnancy rates for the devices at nine years of use represented an annual risk of accidental pregnancy of less than 1% with one device and less than 0.5% with the other. Comparative trials of these devices are continu-

PROTEatON AND PROMOTION OF THE HEALTH OF SPECIFIC POPULATION GROUPS
ing and will provide information on their safety and efficacy up to and beyond ten years of use. In the light of these studies, the United States Food and Drug Administration decided in August 1991 to extend the approved duration of use of the TCu380A from six to eight years.
10.23 An important issue in recent years has been whether use of the IUD is related to pelvic inflammatory disease (PID) and whether longterm use is associated with severe forms of the disease. A study of the large database on IUDs maintained by WHO has shown that in a total of 22 908 insertions in 12 trials, the overall rate of PID was 1.6 cases per 1000 woman-years of use, i.e. only three cases of PID could be expected in two thousand women using an IUD for one year. The study also showed that the risk of PID was seven times higher than the above rate in the 20 days following insertion of the device, but thereafter was low and remained constant for at least eight years of use. There was no evidence of an increase in the severity of PID with increasing duration of use. Because of the greater risk of PID associated with insertion, IUDs should be left in place up to their maximum lifespan and not be routinely replaced earlier, if there are no contraindications to continued use and the woman wishes to continue with the method.
Mifepristone for emergency contraception
10.24 Antiprogestogens have been shown to have potential for use in emergency contraception. These compounds neutralize the action of the hormone progesterone and can block ovulation or retard the preparation of the uterus for implantation, depending on whether they are administered before or after ovulation. WHO funded two randomized trials to compare the efficacy and side-effects of a single dose of 600 mg of mifepristone with those of the standard Yuzpe regimen ("morning-after" pill), which is the currently used method in emergency contraception. In these trials none of the 597 women given mifepristone became pregnant as compared to nine pregnancies among the 589 treated with the Yuzpe regimen. The women treated with mifepristone reported less nausea and vomiting, as well as lower rates of other sideeffects, than the women treated with the Yuzpe regimen; but the onset of their next menstrual period was more likely to be delayed. In view of the encouraging results, it is now planned to con-
59
duct a multicentre trial to determine the lowest effective dose of mifepristone for emergency contraception.
Methods for the regulation of male fertility
10.25 Work continued in evaluating hormonal contraceptive options for men and assessing the safety and efficacy of various methods for occlusion of the vas deferens. A five-centre study in Indonesia on sperm suppression induced by combined androgen-progestogen administration was completed in 1992, and the results submitted for publication. It was found that testosterone enantate or 19-nortestosterone ester plus DMPA resulted in much higher rates of azoospermia in Indonesian men (97%) than previously observed with such drug combinations in Caucasian men. The multicentre study on the contraceptive reliability of testosterone-induced severe oligozoospermia continued in 15 centres in nine countries. Previous studies had revealed variations in the responsiveness of men of different ethnic origins to contraceptive steroids, and the underlying mechanisms are being explored further in investigations supported by WHO and collaborating agencies.
10.26 A study is under way in China on the safety and efficacy of three different methods of vas occlusion, the "no-scalpel method", percutaneous injection of a sclerosing agent, and injection of a polyurethane plug into the lumen of the vas deferens. A consultation was held in September 1992 to review progress in research on Tripterygium wilfordii, which is used in traditional Chinese medicine for the treatment of psoriasis; it recommended setting up a programme of limited duration to determine whether an antifertility drug could be developed from the active compounds identified in extracts of this plant.
Vaccines for fertility regulation
10.27 It is proposed to develop a birth-spacing vaccine that will be effective for a period of up to 18 months, since this is perceived to be a useful interval for users at practically all stages in their reproductive lives. A prototype anti-hCG vaccine was developed solely to demonstrate the
THE WORK OF WHO 1992-1993
safety and feasibility of the approach and not as a final product. It had therefore been envisaged that this vaccine would not be used beyond the phase I clinical trial stage, and that an improved anti-hCG vaccine would be prepared for further clinical testing and product development. However, the results of the phase I trial were considered sufficiently encouraging to proceed with a phase II trial to determine whether the level of anti-hCG antibodies produced in response to the vaccine does in fact provide protection against pregnancy in fertile women.
10.28 Studies to develop an anti-trophoblast vaccine continued. This research concentrated on the use of monoclonal antibodies and molecular genetics techniques in order to identify and characterize tissue-specific antigens, with particular emphasis on antigens that may be suitable for the development of a vaccine which will have an effect prior to the completion of implantation.
Methods for the natural regulation of fertility
10.29 The highest research priority for WHO in this area continued to be lactation and its role in the suppression of ovulation. In addition, research was conducted on indicators of the fertile period, including new possibilities for the measurement of urinary steroid glucuronides, and on natural family planning. The prospective multicentre study of the relation of breast-feeding practices to the duration of lactational amenorrhoea continued. The purpose of this study, which involves 3850 mother-infant pairs, is to elucidate the factors that determine lactational infertility. Other current research included studies on the effects of supplementary nutrition to nursing mothers on the return of ovulation, studies on the immunoactivity and bioactivity of luteinizing hormone and prolactin, and studies on the interface between breast-feeding and the adoption of other methods of contraception.
10 30 Accurate estimation of the fertile interval in women is vital to the efficacy of family planning methods based on periodic abstinence. Research concentrated on inexpensive and simple methods or devices that can be used in the home to measure biochemical or biophysical markers of the fertile period. The measurement of cervico-vaginal fluid volume using a simple de-
60
vice was tested in a multicentre trial, as was the measurement of guaiacol peroxidase, an enzyme with a concentration in cervical mucus that is inversely related to blood estrogen levels during the follicular phase of the cycle. WHO also provided support for the development of assays of urinary steroid glucuronides that require only the collection of urine on to filter paper, thus avoiding the problems of storage and transport of liquid urine.
Prevention and management of infertility
10.31 Research has focused on the prevention of infertility caused by sexually transmitted diseases and the management of infertility, especially in developing countries. This work includes standardizing the investigation of infertile couples, evaluating certain treatments of infertility in the male and the female, developing and evaluating kits for simplified diagnosis of sexually transmitted diseases, and estimating their prevalence through seroprevalence studies in developing countries. Also under way are the development of a vaccine against genital infection with Chlamydia trachomatis and the evaluation of barrier methods for the prevention of sexually transmitted diseases. In 1992 WHO was instrumental in introducing polymerase chain reaction (PCR) methodology for chlamydial antigen detection in tertiary health care centres in six de~eloping countries.
Introduction and transfer of technology
10 32 A strategy for the introduction of new and underutilized methods of fertility regulation was drawn up during the biennium. The strategy shifts the emphasis in the introduction of methods from the product itself to users' needs and programme capabilities, and also provides background information for decisions by national family planning programmes concerning additional methods. It takes into account not only the potential demand for a method but also the capability of services to cope with the demand and to back up the method with the appropriate care. The strategy will be implemented initially in selected countries in Latin America and sub-Saharan Africa.
10 33 Studies on the introduction of the once-amonth injectable contraceptive, Cyclofem, into

-------------------- -----
PROTECTION AND PROMOTION OF THE HEALTH OF SPECIFIC POPULATION GROUPS
national family planning programmes in Indonesia, Jamaica, Mexico, Thailand and Tunisia have been completed or are being assessed. They examine such factors as use-effectiveness, reasons for discontinuation of methods and service delivery constraints in each of these countries, based on the experience of 7700 women, and the findings are now being written up. After completion of the pilot phase, the study in Chile was extended to additional clinics at the end of 1992. New studies were begun in Brazil, Colombia and Peru in 1993.
10_34 Following a 1991 meeting on women's perspectives in the selection and introduction of fertility regulation methods, representatives of women's health groups, researchers and policymakers from Bangladesh, India, Indonesia and Philippines met for further discussion of this topic (Manila, October 1992).
Social science research
10J5 Work continued in the major research initiative on the determinants of induced abortion, launched in 1991. Of 27 projects supported by WHO, about half were completed by the end of 1993. In the area of male fertility and contraception, studies supported thus far under the condom acceptability initiative were completed by the end of 1992, and new studies continue to be accepted. Research was begun on the role of men in determining family size and in making decisions about contraceptives. Acceptability studies of contraceptive methods including vasectomy, female sterilization, the diaphragm, IUDs and monthly injectable preparations are under way. Several studies concerned with gender roles are proceeding. Factors affecting contraceptive use continue to be of major interest to researchers in the developing world, and remain a priority subject for research supported by WHO.
Resources for research
10.36 WHO seeks to strengthen the capabilities of developing countries to plan and carry out priority research in reproductive health. It also maintains contacts with a network of research centres that participate in global research activities.
10_37 A total of 105 institutions in 56 countries were working with WHO during the biennium;
61
of these, 50 (in 30 countries) were designated as WHO collaborating centres for research in human reproduction, while the remainder were involved in research capability strengthening. Efforts were made to encourage and support technical cooperation among developing countries. A special fund has been set aside for this purpose, to which the Rockefeller Foundation contributes.
10.38 In Africa emphasis continued to be given to the least developed countries and to the promotion of "South-South" collaboration for research capability strengthening. A task force on the prevention of maternal mortality and infertility was established following a regional consultation on this subject (Kigali, January 1992). A research management workshop (Harare, March 1992) brought together scientists from eight countries.
10.39 Assessments of research needs in reproductive health were supported in Chile, Panama, Peru and English-speaking countries of the Caribbean. These were followed by interagency coordination and fund-raising to meet the research challenges identified. Promotion of training capabilities in the Americas included support for a master's degree course in reproductive epidemiology and a one-year course in the organization of clinical trials. Much of the responsibility for the award of short-term training grants has been delegated to regional research and training organizations. This policy improves coordination, reduces costs and administrative time spent, and encourages involvement of researchers themselves in decisionmaking. A regional network for epidemiological research is now fully operational and a regional programme on social science research is under way. Reproductive health research will benefit from strengthening of non-human primate facilities in Chile, research on molecular biology in Mexico, and reproductive immunology research in Cuba and Peru. Technical cooperation among developing countries is an important part of the strategy, as is the encouragement of links with leading research institutions in developed countries. Workshops on scientific writing were conducted in Argentina, Brazil, Chile and Venezuela.
10.40 Two intercountry meetings organized in Cairo to assess research needs, one dealing with maternal and child health (November 1991) and the other with reproductive health (December 1992), provided a basis for formulating an Eastern Mediterranean regional strategy to promote

THE WORK OF WHO 1992-1993
research and strengthen national research capacity in these fields.
10 41 A shift of emphasis in support in SouthEast Asia and the Western Pacific led to a substantial increase in collaboration with least developed countries, which now receive about 50% of the available funds. Following the signature of a memorandum of understanding, it is expected that collaboration will be strengthened with India in the development of research capacity and the promotion of research in human reproduction.
Occupational health
10 42 In April1992 the Joint ILO/WHO Committee on Occupational Health reviewed programmes on occupational health and safety, discussed aspects of occupational health in Member States, drew up general policies and designated areas for collaboration between the two agencies.
10.43 A first meeting of WHO collaborating centres in occupational health (Moscow, September 1992) discussed ways of strengthening "networking" of institutions in this field, at national and international level. In support of this aim, WHO issued a directory of its collaborating centres in occupational health1 and launched a quarterly newsletter. A planning group was set up to coordinate the international activities of the collaborating centres and advise on the programme; at its first two meetings, in December 1992 and June 1993, it surveyed global needs and determined priorities.
10 44 In May 1993 the Joint ILO/WHO Committee on the Health of Seafarers reviewed the occupational health problems of seafarers and formulated recommendations and guidance in the following areas: injury prevention; prevention of blood-borne and sexually transmitted infections; education of seafarers on the dangers to their health and careers from abuse of drugs and alcohol; prevention and control of mental diseases and psychosocial disturbances; procedures for periodic updating of the International medical
1 leht1nen S Collaborotmg centres in occupational health· directoty, net· working, pnonties and future perspecttves Geneva, World Health Orgon1· zot1on, 1992
62
guide for ships; and harmonization of medical examination requirements for seafarers. The Committee appealed to all the parties concerned to collect comparable statistics concerning accidents and other health problems of seafarers.
10.45 Work continued on reference methods and quality assurance in the evaluation of exposure to airborne fibres at work, with the support of the International Fibre Safety Group and Commission of the European Communities. Following a comparative analysis in 1992, the methods were refined at two expert meetings (Sheffield, United Kingdom, February 1993; New Orleans, USA, May 1993).
10.46 The importance is now recognized of obtaining data on doses and health risks for biological monitoring of exposure to chemicals at work. Meetings organized in collaboration with the International Programme on Chemical Safety worked out strategies (Kyoto, Japan, October 1992), identified chemicals requiring priority attention (Geneva, December 1992) and drew up guidelines for data collection (Geneva, November 1993).
10 47 A workshop on medical surveillance of workers exposed to dusts inducing pneumoconiosis, organized in collaboration with ILO and in association with an international conference on occupational lung diseases (Prague, September 1992), outlined requirements for improving the prevention of occupational respiratory diseases. Subsequently, technical guidelines on the medical screening of workers exposed to mineral dusts were prepared for use in training programmes to improve medical surveillance in Member States. In addition, the interaction between smoking and workplace hazards was reviewed.2
10.48 A J01llt WHO/ILO interregional task group on health protection of workers in smallscale undertakings (Bangkok, November 1993) reviewed the global situation and worked out acceptable, low-cost but effective measures.
10 49 In collaboration with the International Commission on Occupational Health, an international directory of occupational health databases and data banks was issued in loose-leaf
'Document WHO/OCH/TOH/92 1

PROTECTION AND PROMOTION OF THE HEALTH OF SPECIFIC POPULATION GROUPS
format and on computer diskette. 1 The reports of a WHO expert committee on health promotion in the workplace in relation to alcohol and drug abuse,2 and a WHO study group on aging and working capacity3 were published. Activities dealing with safe use of pesticides included the publication of guidelines4 and sponsorship of an international symposium on health and ergonomic aspects of the safe use of chemicals in agriculture and forestry (Kiev, June 1993 ).
10.50 The wide range of activities to promote the health of working populations at regional level included education and training in occupational health in Africa, promotion of interagency and intersectoral cooperation in the Americas through the initiative "1992: Year of Workers' Health", integration of health care for workers in national health systems using the primary health care approach in South-East Asia, strengthening of occupational health services with particular attention to countries of central and eastern Europe, framing of appropriate legislation in the Eastern Mediterranean, and safety promotion in small-scale undertakings in the Western Pacific.
Health of the elderly
10.51 During the biennium, as part of the international research programme on aging requested by the World Health Assembly in 1987, the Organization proceeded with the development and implementation of three studies on osteoporosis, age-associated dementias, and determinants of healthy aging, as described below, while detailed planning was begun for a fourth (on immunology and aging) following receipt of funding. An international study to assess home care needs was also launched. The United States National Institute on Aging continued its technical and financial support to research activities and additional funds became available for the implementation of research projects in countries.
1 Sevdla JM InternatiOnal d11ectory of databases and data banks tn occupational health. Palma de Mallorca, World Health OrganiZation/International Commission on Occupational Health, 1993
2 WHO Techmcal Report Series, No. 833, 1993 3 WHO Techmcal Report Se11es, No. 835, 1993 4 Control technology for the formulatron and packrng of pestiCides Geneva,
World Health Orgamzat1on, 1992.
63
10.52 In the osteoporosis study, the hospital discharge data survey and case-control study proposal were finalized in collaboration with the coordinating centre at Stanford University (USA). The selection of instruments for the casecontrol study was completed and approved by the principal investigators from the participating centres (Brazil, China, Hong Kong, Hungary, Iceland, Nigeria, Trinidad and Tobago) and from parallel study centres (Chile, Italy, Poland) during their first meeting in March 1993. Translation of the study proposal and instruments and their adaptation to each culture then began. A survey on the prevalence of osteoporosis in the population of part of Beijing was started in 1992 under contract with the University of California (USA).
10 53 In the project on age-associated dementias, the pilot studies already carried out in 1991 in Nigeria and the United States of America by participating centres were followed by studies in Chile, Malta and Spain in 1992. The project coordinating centre located in the office of the Studio Multicentrico Italiano sulla Demenza in Florence (Italy) made an analysis of the pilot studies, following which the study instruments were finalized, translated, printed and distributed to all participating centres. Data collection for the field study began in each centre in August 1993 and data on the prevalence of dementia conditions should be available by the end of 1994. The results of standardization of the clinical diagnosis of dementia carried out in 1991-1992 are now in press. The results of the pilot study were submitted for publication at the end of 1993.
10.54 In 1992 a group of experts met to initiate the project on determinants of healthy aging. The Centre for Ageing Studies of Flinders University of South Australia was designated as coordinating centre and Costa Rica, Israel, Italy, Jamaica, Thailand and Zimbabwe were selected as participating countries. During 1993 the coordinating centre, in collaboration with Yale University (USA) and Duke University (USA), drew up a proposal for a pilot study and prepared instruments for assessing physical, mental and social functioning in the aged population. In March 1993 WHO hosted a meeting of the research network on successful aging of the MacArthur Foundation (USA). The subsequent selection of the assessment instruments mentioned above was based on recommendations made by the network. Harmonization of these instruments and the feasibility and validation study in three of the

THE WORK OF WHO 1992-1993
participating countries (Costa Rica, Italy, Thailand) were completed.
10.55 In Europe another project on healthy aging, established jointly with the European Community, focuses on health promotion for the elderly. A meeting (Heidelberg, Germany, October 1992) examined the contribution of prevention and rehabilitation to healthy aging, and urged life-long preparation for healthy aging through health promotion and the creation of environments allowing elderly people to realize their potential and to remain in their own homes for as long as possible.
10.56 A major home care initiative was launched during the biennium, recognizing that such care is given in many countries, affords the best quality of life for most people and is often less expensive than many kinds of acute and chronic care in institutions. It was stimulated by the recognition in all WHO regions that well-planned home care may contribute appreciably to the containment of costs in providing good quality health services for the elderly. Preliminary steps were taken to determine the need for home care from existing data from three developed and nine developing countries, analysed with the assistance of the United States National Institutes of Health, Duke University (USA) and the United States Bureau of the Census, as a basis for advice to be given to individual countries on the needs of their elderly populations. WHO also participated in a project to design a valid and reliable survey instrument in various languages which would allow for both the assessment of needs of
64
individuals in the home setting and for intercountry comparison. The home care initiative was strengthened at international level by the creation of a World Organization for Care in the Home and Hospice, with which WHO forged close links. One aspect of home care -family support - was highlighted in a book published in 1992 on WHO's behal£.1
10.57 WHO convened an interregional consultation (Alexandria, October 1992) to prepare a strategy for health care of the elderly, which in due course will be incorporated into the United Nations strategy for aging populations. Following the consultation, efforts have been made in several regions to encourage Member States to pay more attention to national policies and strategies for care of the rapidly expanding population group of the elderly. In Africa, for example, an average of 5. 9% of the population in Member States is aged 60 years and over, while only 7% of the countries have policies for the care and welfare of this age group. Thus much technical collaboration at regional level has been aimed at raising awareness and improving assessment of the health needs of the elderly; strengthening geriatric and gerontological services within the framework of primary health care; and encouraging health protection and promotion for the elderly with particular emphasis on involvement of the elderly themselves in these activities.
1 Kend1g Hl, Hashimoto A, Coppard LC, eds. Family support for the elderly the international expenence. Oxford, Oxford University Press, 1992.
CHAPTER 11
Protection and promotion of mental health
Mental health policy, and support to national programmes
11.1 In its work to ensure that psychosocial and behavioural factors are fully taken into account in the whole range of health care, and in its specific activities related to mental and neurological disorders, WHO received support from the Carnegie Corporation (USA), Delagrange International!Synthelabo Recherche (France), Digital Equipment Corporation (USA), Johann Jacobs Foundation (Switzerland), the Laureate Foundation (USA), the United States National Institute of Mental Health, Ravizza Farmaceutici (Italy) and the Upjohn Company (USA), as well as UNICEF and the World Bank. Work in the Western Pacific was supported by the Sasakawa Foundation Qapan).
Development of national mental health programmes
11.2 Guidelines on formulating national mental health programmes and instruments for assessing mental health policies and programmes were produced in 1992 and are being field-tested. WHO collaborated with countries of central and eastern Europe in strengthening their mental health programmes.
11.3 To increase public and professional awareness of the burden of neurological disorders, WHO organized meetings on neurology and public health: the first in May 1993 supported by the International School of Neurological Sciences in Venice (Italy); the second in October 1993, for French-speaking countries, supported by the Institute of Neurological Epidemiology and Tropical Neurology in Limoges (France); and a third in Berlin in December 1993, for countries of central
6S
and eastern Europe, supported by the European Federation of Neurological Societies. The three groups contributed substantially to a forthcoming publication on neurology and public health.
11 4 Methods were devised for assessing costeffectiveness in mental health programmes, information systems were established in support of national mental health programmes, a national workshop on computer-assisted mental health recording and reporting was held in China, and national workshops were organized to share information about programme development in some 40 countries. To facilitate national planning, WHO has started a new series of monographs on the epidemiology of mental disorders and psychosocial problems; and the first three, dealing with personality disorders, with dementia and with schizophrenia, are being published1 in addition to a paper on the epidemiology of suicidal behaviour. A fourth edition of an annotated directory of mental health training manuals2 and a report on WHO's research activities in mental health were issued.
Classification and assessment
11 5 Building on the chapter of mental and behavioural disorders in the tenth revision of the International Classification of Diseases (ICD-10), diagnostic guidelines3 (so far issued in
1 de Girolama G, Reich JH. Personality disorders. Geneva, World Health OrganiZation, 1993. Warner, R, de Grrolamo G. Schizophrenia. Geneva, World Health Orgama· lion (in press). Henderson, AS, Dementw Geneva, World Health OrganizatiOn (rn press)
2 Document WHO/MNH/MND/92 15. 3 The /CD· I 0 classificatiOn of mental and behavioural d1sorders. Cltnical
desmptions and diagnostic gu1delmes Geneva, World Health Organrzation, 1992.

THE WORK OF WHO 1992-1993
10 languages), diagnostic criteria for research, and tables for conversion between ICD-8, ICD-9 and ICD-10 were published. 1 A primary health care version of the chapter for field trials was produced2 and a lexicon of alcohol and drug terms and another of psychiatric mental health terms used in ICD-10 and related publications are in print. Several standardized assessment instruments were produced and are now widely used by mental health workers. Experts and institutions in some 50 countries participated in the field work that led to the compilation of these texts, and a network of WHO collaborating centres was set up to provide training, compare experience and conduct further research.
11 6 A study was begun in five countries to investigate the somatic presentation of psychological disorders in different cultural circumstances and develop diagnostic instruments for their assessment. An adaptation of the International Classification of Diseases for neurology was prepared in collaboration with a network of centres and with major nongovernmental organizations. In September-October 1992 a meeting was held to discuss diagnostic criteria for acute onset of flaccid paralysis. Three meetings took place as part of a new WHO study aimed at producing an instrument for assessing changes in quality of life due to health care interventions (Geneva, February and June 1992; Paris, June 1993).
Psychosocial and behavioural problems and relevant interventions
11 7 A set of 25 papers was produced on behavioural approaches to medical problems and on the teaching of communication and interaction skills, for incorporation into teaching modules for medical schools. Preliminary studies were undertaken in Belarus, Egypt, India and Zimbabwe on measures to improve communication skills in health workers. A booklet on the management of psychosocial consequences of disasters was prepared/ as well as a draft manual on refugee mental health, for use by nonprofes-
1 Document WHO/MNH/92.16 2 Document WHO/MNH/MND/93.1 3 Document WHO/MNH/PSF/91 3
66
sionals working in camps. WHO helped to assess needs and provided mental health consultant services in former Yugoslavia and in Somalia. The Organization also collaborated with psychiatrists in the Philippines to produce a manual on psychosocial care for victims of natural disasters and provided training and education on psychosocial aspects of health as part of medical education in China. A study in India classified ways in which adolescents adopt risk-taking behaviour.
11 8 A document was issued on the psychosocial and mental health aspects of women's health.4 In collaboration with UNICEF, a network of centres linked by a newsletter, Skills for life, was set up to promote communication or other psychosocial skills as a means of helping children and adolescents to avoid behaviour deleterious to health. A WHO life-skills resource package is being tested in Colombia, Nigeria, Thailand and Zimbabwe, to meet the needs of school-age children, particularly those actually in school. Training guidelines were produced for health workers on ways to improve parent-infant interaction, and training workshops on this topic were held in Brazil, Norway and Portugal.
Prevention and control of alcohol and drug abuse
11 9 Evaluations of drug prevention and control programmes were undertaken or continued in several countries and areas5 and prevention of psychoactive substance abuse was widely promoted. Following a feasibility study, an abuse trends linkage alerting system (ATLAS) was set up; it is compatible with other data reporting systems of the United Nations and provides a framework for revising existing WHO epidemiological instruments on drug abuse. This activity was supplemented by a number of regional initiatives, especially in the Americas, South-East Asia and Europe, which should enhance WHO's capacity to provide accurate information on patterns of substance abuse. Rapid assessment procedures, involving qualitative re-
4 Document WHO/FHE/MNH/92 1. 1 Afghanistan, BoliVIa, Brazil, Chile, Ch1na, Estonia, Hong Kong, Latv1a,
L1thuan1a, Macao, Maur1t1us, Myanmar, Nepal, Sri Lanka, and some mem· bers of the Commonwealth of Independent States (Kazakhstan, Kyrgyzstan, Tapk1stan, Turkmemstan, Uzbek1stan)

PROTECTION AND PROMOTION OF MENTAL HEALTH
search, were developed and applied in various settings, including Central Africa and selected small island countries. A similar approach was used for reviewing health aspects of drug use in relation to sports and for gathering information on drug use by women in 25 countries. As part of its contribution to the 1994 International Year of the Family, WHO prepared a position paper on preventing substance abuse in families. It also collaborated with theW orld Bank in incorporating global data on substance abuse into the Bank's 1993 report.'
11 10 An expert committee report was issued dealing with the prevention of alcohol- and drugrelated problems in the workplace;2 it recommended in particular that their solution should combine comprehensive prevention policies and health promotion programmes. A joint UNDCP/ ILO/WHO project on prevention of drug and alcohol use among workers and their families is being implemented in Egypt, Mexico, Namibia, Poland and Sri Lanka. WHO has started a dialogue with representatives of the alcoholic beverage industry in order to alert them to the public health consequences of trends in alcohol consumption, including alcohol-related traffic accidents and violence. In 1992 the Regional Committee for Europe strongly endorsed a European alcohol action plan, after which several technical meetings were held to decide on how the plan should be implemented in countries. Following earlier work on this subject, WHO began a review of the health policy and legal aspects of treatment and rehabilitation of persons dependent on or suffering from abuse of drugs and alcohol.
11.11 Qualitative and quantitative assessment techniques were designed to support studies on the WHO initiative on cocaine, including such topics as the natural history of the substance and factors causing cocaine abuse and harm; drug use among street children and indigenous populations; the impact of intentional inhalation of volatile organic substances; and the health consequences of cannabis use.
11.12 Cost-effective community-based approaches to treatment and rehabilitation, and
1 World Bank World development report 1993 tnvestmg tn health. New York, Oxford Unrversrty Press, 1993.
2 WHO Technical Report Serres, No. 833, 1993
67
their integration with primary health care, are being evaluated with a view to using them in areas with high rates of substance abuse. Work was completed on a simple procedure for assessing the quality of care in the treatment of substance abuse; this, together with other training materials produced by WHO for use in the primary health care setting, formed the basis for training focusing on the needs of developing countries.
11 13 A matter of particular concern in Asia has been the rapid increase in HIV -infection caused by drug injection. Descriptive and epidemiological data on drug injection practices have been collected in Bangkok, with a view to designing and testing cost-effective interventions.
11.14 In September-October 1992 a WHO expert committee updated the definition of drug dependence, linking it closely to the ICD-10 diagnostic criteria for the dependence syndrome, and made a number of recommendations on the prevention and management of drug dependence and other drug-related problems.3
11 15 Several participating centres received support from the international drug monitoring programme in strengthening their capability for collecting data on abuse-related adverse drug reactions and recognizing early warning signs of non-medical use of newly marketed psychoactive drugs. As part of efforts to rationalize the prescribing of psychotropic drugs in the Americas, a seminar was organized (Montevideo, October 1993) to make government officials, prescribers and journalists more aware of the problem of inappropriate use of drugs. Collaboration was strengthened with professional bodies such as the World Psychiatric Association, which has set up an educational task force on the use of benzodiazepines.
11 16 The difficulties faced by small regulatory agencies in controlling unofficial drug distribution systems were examined at a consultation (Vienna, June 1993) organized jointly with UNDCP, and guidelines for effective import control and inspection are being drawn up. Field-testing of a software package for computer-assisted regulatory procedures is in progress. WHO cooperated with Benin and Nigeria in
3 WHO Technrcol Report Seties, No 836, 1993

THE WORK OF WHO 1992-1993
strengthening their national regulatory agencies. Human resources development for regulatory control was supported through a series of international training seminars (Beijing, June 1992; Shanghai, June 1993; Abidjan, December 1992; Tokyo, July 1992 and July 1993).
Mental and neurological services
11.17 A major international review of laws on promotion of mental health and support to the mentally ill, covering 45 countries in all regions, was started with funding from the United States National Institute of Mental Health. Technical advice was provided in drafting mental health legislation in China and Fiji, and updating legislation in Argentina, Brazil, Colombia, Panama and Venezuela. Training for mental health leaders as well as courses on psychosocial rehabilitation, focusing on family training and patient edu-
Creotive educolion for the mentolly hondicopped in finlond.
68
cation, were organized in several countries in 1992. Field-testing of instruments for quality assurance in mental health care began in 16 countries in all regions. Instruments for the assessment of mental health services are now available in eight languages.
11.18 Guidelines on treatment of epilepsy, on family care of schizophrenic patients (currently available in six languages) and on case management of and housing for the mentally ill were produced, and a computer-based multi-media information system on epilepsy is being established.
11.19 Strategy reviews and implementation guidelines on the prevention of mental retardation, epilepsy, suicidal behaviour and staff "burn-out" syndrome were produced. In addition, WHO supported a number of studies of such topics as lithium prophylaxis in manic depressive disorders (eight countries); depression in old age (one country); eye movements in pa-

PROTECTION AND PROMOTION OF MENTAL HEALTH
tients with schizophrenia (seven countries); and combined utilization of antidepressants and antioxidants in the treatment of therapy-resistant depression (19 countries).
Epidemiological studies
11.20 Several studies involving the differential diagnosis of dementia (six countries), the epidemiology of cognitive impairment and dementia (seven countries), and psychological problems in general health care (14 countries) were completed with WHO support. The preparatory phase was completed and data collection started for several other studies and projects, including a major study on the effects of radiation on brain development in utero that is being carried out as part of the international programme on the health effects of the Chernobyl accident (see paragraph 12.31).
11.21 The results of a WHO-coordinated study on the determinants of outcome of severe mental
69
disorders in 10 countries were published.1 A follow-up study on the long-term course and outcome of schizophrenia in 15 countries is under way. A study was initiated on the psychopathology of obsessive and compulsive disorders of indigenous populations in six countries.
11.22 A study was carried out in nine countries on cultural differences relevant to the diagnosis and classification of mental disorders, especially in respect of substance abuse, and on this basis to develop culturally relevant diagnostic instruments. A further study to evaluate the accuracy of epidemiological data obtained with the diagnostic instruments began in 12 countries. A review of the effectiveness of treatment of mental disorders has been published.2
1 Jablensky A et al. Schizophrenia: manifestations, inCidence and course in different cultures A World Health Organization study. Cambridge, Cambridge University Press, 1992 (Psychological medicine monograph supplement 20).
2 Sartorrus, N et al. Treatment of mental disorders· a review of effectiveness. Washington, American Psychiatric Press Inc., 1993.
CHAPTER 12
Promotion of environmental health
12 1 The WHO Commission on Health and Environment completed its work, and its report was issued, 1 together with the reports of its panels on energy, food and agriculture, industry, and urbanization.2 The series served as the basis for determining the health aspects of Agenda 21, the action programme for the 1990s and beyond, adopted by 172 countries at the United Nations Conference on Environment and Development (UNCED), commonly referred to as the "Earth Summit" and held at Rio de Janeiro, Brazil, in June 1992.
12.2 A new global strategy for health and environment based on the recommendations of the WHO Commission and prepared in response to Agenda 21 was endorsed by the Health Assembly in May 1993. An interregional consultation (October 1993) was convened to coordinate the development of global and regional action plans for implementing the strategy, and a WHO council on the Earth Summit action programme for health and environment first met in January 1993 to advise on the institutional, financial and coordination aspects. In pursuance of the council's recommendations, WHO, in collaboration with UNDP, provided support to countries incorporating health and environment considerations in national plans for sustainable development.
Community water supply and sanitation
12.3 Meanwhile WHO directed its efforts towards ensuring that the development of water supply and sanitation services proceeded in a manner consistent with the intersectoral approach
1 Our planet, our health. Genevo, World Heolth Orgon1zot1on, 1992. 1 Documents WHO/EHE/92 2; WHO/EHE/92 3; WHO/EHE/92.4; WHO/
EHE/92.5.
71
to the environment as defined by UNCED and WHO's global strategy for health and environment. Special attention was given to capacitybuilding at the national level, a major initiative being the WHO/UNICEF joint water supply and sanitation monitoring programme for the 1990s. In 1992 subregional workshops in Africa (Mbabane,June; Cotonou, Benin, September) and the Caribbean (Kingston, February) introduced monitoring procedures to almost 100 countries. Following these workshops, several countries,3
supported by WHO and UNICEF, started activities or established programmes to strengthen their monitoring capability. These procedures are being modified in collaboration with UNR W A to respond to needs in Gaza. As part of the WHO/ UNICEF joint programme, information was collected on the status of water supply and sanitation for 1990 and 1991, and annual reporting was continued for advocacy purposes.
12.4 During the biennium particular emphasis was given to hygiene education associated with water supply and sanitation. WHO collaborated with theW orld Bank in producing training tools and manuals, and with UNICEF in familiarizing regional and country sanitary engineers of both agencies with the latest hygiene education and community participation principles under a joint training programme.
12 5 School sanitation and hygiene education were the subject of a consultation (Cali, Colombia, March 1993) and a round-table (Hanoi, June 1993). Hygiene education activities were sponsored in Benin and Burkina Faso through a nongovernmental organization (EAST4
), and field
3 Ben1n, Bronl, Cope Verde, Egypt, lnd1o, Jomo1co, Popuo New Gu1neo, Phil1pp1nes, Sri lonko, Togo, Vonuotu
4 Acronym of "Eou, Agmultu1e et Sonte en Mil1eu trop1col" (Woter, AgTICulture ond Heolth 1n the Trop1cs).
THE WORK OF WHO 1992-1993
demonstration projects were initiated in Zimbabwe. Closer ties were established with UNESCO in promoting school health and with UNICEF in formulating a joint strategy on hygiene education.
12.6 Water resource management for the control of disease vectors continued to receive emphasis, largely through activities of the joint WHO/FAO/UNEP/United Nations Centre for Human Settlements (UNCHS) panel of experts on environmental management.
12 7 An interregional workshop considered ways to use agricultural extension programmes to promote environmental management for disease vector control (Tegucigalpa, October 1992). In 1992 a national training course on health opportunities in water resources development was organized in Zimbabwe in collaboration with the Danish Bilharziasis Laboratory; follow-up activities included a joint FAO/WHO mission to the country and a national policy review by the Liverpool School of Hygiene and Tropical Medicine and the Blair Research Institute (Harare, October 1993 ).
12.8 At the first meeting of the Water Supply and Sanitation Collaborative Council (Oslo, September 1991), an operation and maintenance working group was constituted under WHO's leadership, resulting in the organization of a national workshop in the Philippines (Manila, August 1992), an intercountry workshop on leakage detection and reduction in Pakistan (Lahore, October 1992), and a conference on sustainability of rural and urban water supplies in Ghana (Accra, April 1993). The working group also drew up guidelines for the formulation of technical and institutional development strategies and prepared training packages on leakage control and the management of rural water supply and sanitation facilities. The September 1993 meeting of the Collaborative Council endorsed the working group's activities and requested WHO to convene a new working group on the promotion of education in sanitation and hygiene.
12 9 In response to the global cholera epidemic (see paragraph 14.79), WHO prepared a series of fact sheets illustrating simple techniques in environmental sanitation and cholera prevention. The Organization installed 450 water supply chlorinators in countries affected by cholera. In Africa WHO organized cholera preparedness workshops and conducted rapid assessments of water and sanitation needs.
72
12.10 Member countries received support in installing or improving systems for use of wastewater. Guidelines on the chemical and viral aspects of wastewater use were completed during the biennium. WHO held a regional workshop on wastewater (Amman, February 1992) and initiated follow-up action in Bahrain, Cyprus, Egypt, Oman and Tunisia.
12.11 Work in pursuance of the policy of in tensified cooperation with countries and peoples in greatest need took place in Benin (monitoring, hygiene education and vector control), Guatemala (management and health education), Mozambique (information systems and cholera control), Yemen (management and hygiene education) and Zambia (cholera control and school sanitation).
12 12 In September 1993 the Regional Committee for Africa endorsed the establishment of Africa 2000, a programme to accelerate water-supply and sanitation development.
12.13 WHO continued to participate in the ACC Intersecretariat Group for Water Resources, which in 1993 became the ACC Subcommittee on Water Resources, and to act as secretariat for the Interagency Steering Committee for Water Supply and Sanitation and host to the secretariat of the Water Supply and Sanitation Collaborative Council.
Environmental health in rural and urban development and housing
1214 Pursuant to resolution WHA44.27 on urban health, the Organization accorded high priority to urban environmental health activities in view of the continued rapid growth and deteriorating environmental conditions in many of the world's cities. Comprehensive and integrated urban health development activities took place in an increasing number of cities in all regions. In Africa three major meetings were convened during the biennium: the first and second meetings for French-speaking African countries under the Healthy Cities project (Dakar, July 1992; Tunis, September 1993) and a regional workshop on urban health (Harare, November 1993 ). Other regional activities included an intercountry workshop on the improvement of health and environmental conditions in urban slum areas
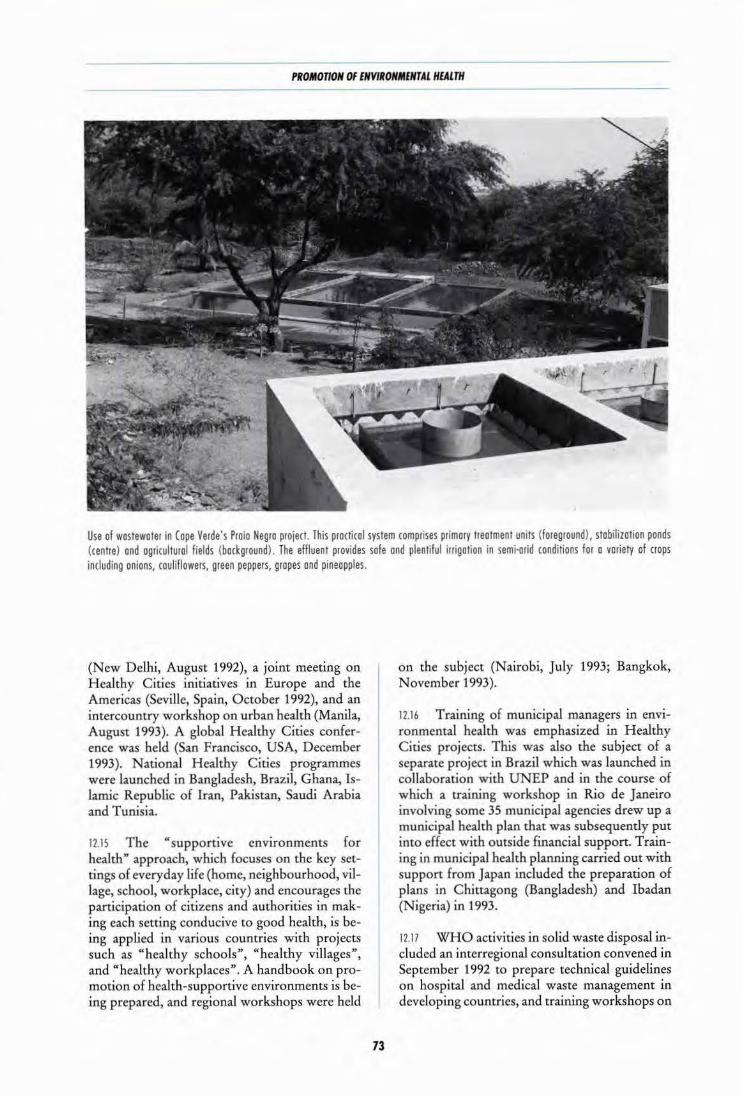
I'ROMOnON OF ENVIRONMENTAL HEALTH
Use of wostewoter in Cope Verde's Proio Negro project. This practical system comprises primary treatment units (foreground), stobilizotion ponds (centre) and agricultural fields (background). The effluent provides sole ond plentiful irrigation in semi·arid conditions for o variety of crops including onions, couliflowers, green peppers, gropes and pineapples.
(New Delhi, August 1992), a joint meeting on Healthy Cities initiatives in Europe and the Americas (Seville, Spain, October 1992), and an intercountry workshop on urban health (Manila, August 1993). A global Healthy Cities conference was held (San Francisco, USA, December 1993). National Healthy Cities programmes were launched in Bangladesh, Brazil, Ghana, Islamic Republic of Iran, Pakistan, Saudi Arabia and Tunisia.
12.15 The "supportive environments for health" approach, which focuses on the key settings of everyday life (home, neighbourhood, village, school, workplace, city) and encourages the participation of citizens and authorities in making each setting conducive to good health, is being applied in various countries with projects such as "healthy schools", "healthy villages", and "healthy workplaces". A handbook on promotion of health-supportive environments is being prepared, and regional workshops were held
73
on the subject (Nairobi, July 1993; Bangkok, November 1993).
12.16 Training of municipal managers in environmental health was emphasized in Healthy Cities projects. This was also the subject of a separate project in Brazil which was launched in collaboration with UNEP and in the course of which a training workshop in Rio de Janeiro involving some 35 municipal agencies drew up a municipal health plan that was subsequently put into effect with outside financial support. Training in municipal health planning carried out with support from Japan included the preparation of plans in Chittagong (Bangladesh) and Ibadan (Nigeria) in 1993.
12.17 WHO activities in solid waste disposal included an interregional consultation convened in September 1992 to prepare technical guidelines on hospital and medical waste management in developing countries, and training workshops on

THE WORK OF WHO 1992-1993
solid waste management in Fiji in 1992 and the Philippines in January 1993.
International Programme on Chemical Safety
1218 Programme development. The International Programme on Chemical Safety (IPCS), established in 1980 as a joint activity of ILO, WHO and UNEP, was designated by UNCED as the nucleus for international cooperation on environmentally sound management of toxic chemicals. Resolution WHA45.32 of the World Health Assembly, adopted in 1992, has established mechanisms to coordinate WHO's contribution to IPCS. To strengthen interagency coordination in this area, ILO, WHO and UNEP developed a strategy in collaboration with other potentially interested international institutions such as FAO, OECD, UNIDO and the Commission of the European Communities.
1219 International conference on chemical safety. UNCED requested the executive heads of ILO, WHO and UNEP to arrange for further consideration to be given to the recommendations made by a group of experts in 1991 1 for increased coordination between United Nations bodies and other international organizations involved in chemical risk assessment and management. The government-designated experts called for appropriate measures to enhance the role of IPCS and for an intergovernmental forum on chemical risk assessment and management to give policy guidance, develop strategies in a coordinated manner, provide the required political support and foster understanding of the issues by governments. Accordingly, all Member States and intergovernmental and nongovernmental organizations concerned have been invited to participate in an international conference on chemical safety to be held in Stockholm in 1994. The Government of Sweden is acting as host to the conference and several governments have offered human and financial resources for its organization.
12 20 Risk evaluation. Evaluation by IPCS of the risks to health and the environment from certain priority chemicals provides a basis for chemical risk management and the findings are
1 Document UNEP/IPCS/IMCRAM/exp/4
74
widely disseminated in all Member States through various publications meeting the needs of specific professional groups. During the biennium 28 volumes of the Environmental Health Criteria series were published to review present knowledge and evaluate risks associated with exposure to specific chemicals; 10 Health and Safety Guides were produced, providing concisely evaluated information on priority chemicals in non-technical language for decision-makers and managers, including advice on protective measures and emergency response action; and 179 International Chemical Safety Cards were issued in several languages, each summarizing essential product identity data and health and safety information on one page for use at workplaces.
1221 During three meetings of the Joint FAO/ WHO Expert Committee on Food Additives certain additives, contaminants, naturally occurring toxicants and veterinary drug residues in food were considered,2 and at the annual Joint FAO/WHO Meetings on Pesticide Residues acceptable daily intakes were established.3 IPCS also worked on questions concerning assessment and safe use of pesticides with various organizations, whose activities are not always well coordinated. At a consultation held in July 1992 on consolidation of work on pesticides, a proposal was made for core groups to assess toxicological and ecotoxicological data and for panels to draw up practical recommendations on pesticide levels in food, drinking-water, the workplace and the environment.
12 22 Methodology for health risk assessment. IPCS continued to prepare monographs on principles for evaluating the toxicity of chemicals for various organs and organ systems and is devising methods for quantitative risk assessment and for setting exposure limits for chemicals in air, water and food. The monographs enable scientists and others to understand the process of risk evaluation for chemicals, and assist countries in undertaking their own national risk evaluations and management. One of the earliest published was Principles for evaluating health risks to progeny associated with exposure to chemicals during pregnancy (Environmental Health Criteria 30); and in view of recent scientific developments in
1 The reports were publ1shed 1n the WHO Techn1col Report Ser1es, No. 828 (1992), No 832 (1993) ond No 837 (1993)
3 The report of the f1rst wos publ1shed 1n FAO Plant Production and Protection Papers, No. 116 (1992) and the second 1s 1n preparation

PROMOTION OF ENVIRONMENTAL HEALTH
reproductive and developmental toxicology, it is currently under review for updating and expansion. Several other monographs and reports were issued during the biennium, including Quality management for chemical safety testing (Environmental Health Criteria 141) and Principles for evaluating the effects of chemicals on the aged population (Environmental Health Criteria 144).
12.23 Prevention and treatment of chemical poisoning. Guidelines on how to set up and operate poison control facilities, a manual to help laboratories in developing countries provide a basic analytical toxicology service using a minimum of complex apparatus, and a handbook containing basic information on diagnosis and treatment of poisoning were prepared in 1993. Several monographs on antidotes were also in preparation. Work on the INTO X software package for poison information centres continued and a first version of the global database on chemical substances, pharmaceuticals, poisonous plants and animals was made available in 1992. Several Poison Information Monographs were produced on CD-ROM, containing evaluated information concerning the toxic properties of chemicals, on how to diagnose and treat affected persons, and on how to prevent poisoning. lntercountry training workshops were held in Canada, Islamic Republic of Iran, Uruguay and Venezuela to strengthen national capabilities for the prevention and management of poisoning.
12 24 Human resource development. Training materials were produced on: the effect of metabolism on toxicity; chemical safety; safe use of pesticides; and environmental epidemiology. lntercountry workshops and training courses were organized on all aspects of chemical safety, including environmental epidemiology, in Costa Rica, Philippines, Venezuela, Viet N am and Zimbabwe. Capacity-building is being promoted through expansion of IPCS's network of national institutions concerned with chemical safety, for example in Africa, and IPCS news is increasing public awareness of chemical risks among the public at large.
Control of environmental health hazards
12.25 Monitoring and assessment of pollution. The WHO/UNEP global network for monitoring water quality expanded to include new coun-
75
tries in Africa and in central and eastern Europe. A comprehensive guide for assessing water quality through sampling and analysis of biota, sediments and water was published in collaboration with UNEP and UNESC0.1 Training courses on monitoring methods were organized in support of programmes concerned with international river basins (Mekong, Nile, Plate). National and regional workshops on various aspects of water quality monitoring were organized in Colombia, Fiji, and Trinidad and Tobago in 1993.
12.26 Additional parameters were included in the WHO/UNEP air quality monitoring project and the data were made more easily accessible. A major WHO/UNEP assessment of air pollution and its effects on health in 20 cities was completed and the findings published.2 The WHO/ UNEP human exposure assessment location (HEAL) project continued to provide guidance on exposure assessment and support for quality assurance in monitoring several pollutants, including lead and nitrogen oxides. Twenty countries were represented at a meeting which reviewed work on assessment of exposure to lead (Bangkok, November 1992).
12.27 Education, training and research in environmental health were promoted through the WHO global environmental epidemiology network, whose membership now includes about 2000 institutions and individuals in all regions. One-week training workshops for national staff were held in several countries.3 A variety of training materials were developed, including a textbook on basic epidemiology.4 An extensive review of the potential public health impact of global climate change began in collaboration with WMO, UNEP and the Intergovernmental Panel on Climate Change. The health effects of ultraviolet radiation were assessed and an international collaborative epidemiological research project on the health impact of solar ultraviolet radiation and ozone layer depletion was started jointly with WMO, UNEP and IARC.
1 Chopmon D, ed. Water quality assessments London, Chopmon and Hall, 1992
2 World Health Organization. Urban an pollution m megaot1es of the world. Oxford, Blockwell, 1992.
3 Argentmo, Ch1no, Eth10p1o, Gabon, Hungary, Nicaragua, Philippines, Poland, Thailand, Venezuela, Viet Nom.
4 Beoglehole R, Bonito R, Kjellstrom T. Bas1c ep1dem1ology. Geneva, World Health Organization, 1993

THE WORK OF WHO 1992-1993
12.28 Control of environmental pollution. The revision of WHO's guidelines for drinkingwater quality, last issued in 1984, was completed during the biennium; volume 1 was published in 1993/ and volumes 2 and 3 will appear in 1994. An interregional workshop in May 1993 considered the application of the WHO guidelines for air quality in Europe to different climates and under different conditions. Research on epidemiological, social and technical aspects of the domestic use of biomass fuel and coal were undertaken in Ethiopia (indoor air pollution and safety aspects) and VietNam (health education aspects).
12 29 As a contribution to capacity-building in environmental health risk monitoring and management, guidelines were issued on the assessment of sources of air, water and land pollution.2
The WHO global environmental technology network (GETNET), set up in 1991 to link specialists in environmental management technology, expanded to include 340 members in 87 countries. Three workshops on different aspects of environmental management and control were held (Bangkok, August 1992; Amman, October 1992; Bucharest, September 1993).
12.30 Member States in all regions were supported in their efforts to control air and water pollution. For example, the health effects of air
1 Guidelines for d11nking·water quality, Vol I. Recommendations. World Health Organization, Geneva, 1993.
2 Documents WHO/PEP /GETNET/93. l-A and B
76
pollution from motor vehicles were studied in Manila and expertise was provided in drawing up an air quality management plan for the Philippines. In the Americas surveys on hazardous waste were carried out in more than 15 countries. In Europe support was given in preparing guidelines for land-based pollution control and for control of microbiological and chemical pollutants in the Mediterranean.
12 31 Radiation protection. Implementation of the international programme on the health effects of the Chernobyl accident, endorsed by the Health Assembly in 1991, continued during the biennium through five pilot projects concerned with haematology, thyroid effects, brain damage in utero, epidemiological registration, and oral health (samples of tooth enamel being used for individual dosimetry determination). WHO supported work in Belarus, Russian Federation and Ukraine through the supply of medical, computer and auxiliary equipment and diagnostic kits. Over 100 specialists were trained, either in their own countries or abroad. Two meetings were held to strengthen coordination between health-related projects concerned with the consequences of the Chernobyl accident (Kiev, November 1992; Geneva, May 1993). A consultation was organized on coordination of studies of health damage in workers responsible for cleanup following the Chernobyl accident and their offspring in the Baltic countries (Helsinki, May 1992). A fourth coordination meeting of participants in the WHO radiation emergency medical preparedness and assistance network (REMPAN) endorsed a WHO plan for emergency assistance and the establishment of an international database on radiation exposure.
CHAPTER 13
Diagnostic, therapeutic and rehabilitative technology
Clinical technology
13.1 During the biennium WHO paid particular attention to improving surgical and anaesthetic services at district hospitals in developing countries. Health Volunteers Overseas (USA), a non-profit organization, financed the preparation of videotapes based on the orthopaedics sections of WHO handbooks. The scope, limitations and implications of providing day care surgery in developing countries were examined in collaboration with the International Society of Surgery. Jointly with the International Society of Orthopaedic Surgery and Traumatology, WHO assessed the suitability of a simplified modern technology for treating fractures in small hospitals. A handbook describing simple surgical procedures for correcting deformities in poliomyelitis was published.1 N ongovernmental organizations concerned with improving care of patients in district hospitals cooperated with WHO in the assessment of training needs and the organization of refresher courses in a number of developing countries.
13.2 The Organization evaluated the impact on Cameroon's health services of practical procedures introduced into the undergraduate curriculum in medical schools and during internship so as to prepare young doctors for district hospital work. It continued to support Cameroon, Mozambique and Niger in introducing appropriate technology for anaesthesiology and surgery in peripheral areas. Training of clinical staff of provincial and district hospitals in Mozambique has shown very encouraging results. A Portuguese version of the WHO handbook on surgery at the
1 Krol J, ed. Rehabilitation surgery for deformities due to poliomyelitiS. Techniques for the district hosp1tal. Geneva, World Health Organization, 1993.
77
district hospital has been distributed. A meeting on the integration of basic surgery into primary health care (Irbid, Jordan, November 1992) resulted in the modification of programmes in Egypt and Sudan.
Health laboratory technology and blood safety
13.3 Regional and interregional meetings were held on strengthening public health laboratories at primary health care level, quality assurance, standardization and quality assessment, production of basic laboratory reagents, and blood safety. A total of 320 laboratories in 111 countries are registered in five WHO international external quality assessment schemes (see box); and two additional schemes were established in 1992.
13.4 WHO collaborated with FINNIDA, the Finnish Red Cross and the French Red Cross in organizing courses on transfusion medicine and transfusion services. Training courses on blood safety were held in five African countries. Regional training centres for blood transfusion were established in Amman and Tunis. Two major publications were issued on this subject.2
13 5 Studies were in progress during the biennium on the incidence of HIV transmission through blood transfusion (in collaboration with the United States Centres for Disease Control); transfusion requirements for anaemic pregnant women; the prevalence of markers of transfusion-transmissible infectious agents in seven
2 Guidelines for quality assurance programmes for blood transfusion serv1ces. Geneva, World Health Organization, 1993; G1bbs WN, Britten AFH, eds. Gu1delmes for the organization of a blood transfusion service. Geneva, World Health Orgamzation, 1992.

THE WORK OF WHO 1992-1993
WHO improves the performance of laboratories
• By establishing international external quality assessment schemes (IEQAS) WHO aims to improve the performance and reliability of the participating laboratories (for instance, those dealing with clinical chemistry, haematology, microbiology, coagulation and parasitology) and to encourage their staff to establish national or regional schemes. Laboratories enrolled in the schemes perform tests on specimens received from the organizers and return the results to the organizers, who analyse them statistically, assess performance and send back confidential reports and educational material. This procedure provides a basis for comparing laboratories' performance and also for assessing kits, equipment and methods. However, participation in an IEQAS is only part of a laboratory's quality assurance procedures: each laboratory will have established an internal quality control programme (I QC), and poor performance in an IEQAS will prompt examination of that programme to determine and correct the shortcoming. The ultimate goal is to arrange for those laboratories that perform satisfactorily in an IEQAS to start national or regional schemes.
countries; virus inactivation of fresh frozen plasma and cryoprecipitate; production of coldchain equipment for blood and blood products; development of a cost-effective screening technique for schistosomiasis detection in urine; and assessment of a rapid diagnostic test for Plasmodium falciparum.
Radiation medicine
13.6 Diagnostic imaging technology. New technical specifications were drawn up for an improved "WHO radiographic unit" as a part of the WHO Imaging System. Training seminars in diagnostic ultrasound and in nuclear medicine were held in cooperation with IAEA. Support
78
was provided to China, Cyprus, Mali and United Republic of Tanzania in the rational planning and use of radiological diagnostic services.
13 7 Radiotherapy. WHO continued to collaborate with IAEA in improving radiation dose measurement and promoting technology transfer through the secondary standard dosimetry laboratories network, comprising 71laboratories in 50 countries, 36 of them developing. A consultation on the design requirements for a new kind of high voltage X-ray machine for use in developing countries was organized jointly with IAEA and UNIDO (Washington, December 1993).
13.8 Radiation protection. In collaboration with other international organizations, WHO continued to revise the basic safety standards for radiation protection, and the five-volume Manual on radiation protection in hospitals and general practice published between 197 4 and 1980.
Technology development, assessment and transfer
13.9 Significant progress in interagency collaboration was made through the convening of a meeting to establish an international network of agencies for health technology assessment (Paris, September 1993). A second meeting on technology development, assessment and transfer (Alexandria, October 1993) brought together representatives of several international agencies as well as senior health officials. A cohesive collaborative programme was planned, leaving each region latitude to decide its own priorities and pace of implementation while all involved work together to promote the programme at country level, sharing experiences and developing core activities such as training, exchange of information and collaboration with nongovernmental organizations.
Drug management and policies
13.10 The Organization collaborates with national drug regulatory authorities in harmonizing approaches to drug registration and surveillance, establishing international standards for quality assurance, and exchanging information on national regulatory decisions. The rational use of drugs can be ensured only within a well-

DIAGNOSTIC, THERAPEUTIC AND REHABILITATIVE TECHNOLOGY
defined framework of regulation. Through its model lists of essential drugs and related prescribing information, WHO helps countries to foster cost-effective drug use and procurement.
Pharmaceuticals
13.11 The Organization continued to produce a wide range of information, primarily for drug regulatory authorities, which is made available in the quarterly subscription periodical WHO drug information, the monthly WHO pharmaceuticals newsletter, the United Nations Consolidated List of Products whose Consumption and/ or Sale have been Banned, Withdrawn, Severely Restricted or Not Approved by Governments, WHO's Model Prescribing Information series and the cumulative lists of international nonproprietary names (INN).
13.12 To complement established normative instruments such as The International Pharmacopoeia, WHO's Good Practices in the Manufacture and Quality Control of Pharmaceutical Products, the WHO Certification Scheme on the Quality of Pharmaceutical Products moving in International Commerce, and WHO's Guiding Principles for Small National Regulatory Authorities, the Organization has developed, with financial support from Germany and Italy, a computer package on drug registration for national drug regulatory authorities, now available in English, French and Spanish and being used in some 20 countries.
1313 New normative texts being prepared under WHO's aegis include international standards for good clinical practice and for good laboratory practice in the field of drug development, and criteria for interchangeable products from several sources. Collaboration continued with the International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use, which brings together representatives of regulatory bodies from Europe, North America and Japan.
13.14 A comprehensive set of recommendations on measures needed to deal with the alarming prevalence in some countries of spurious and substandard medicines was drawn up at a workshop convened in April 1992 by WHO and the International Federation of Pharmaceutical Manufacturers Associations.
79
13.15 In April 1993 a meeting of interested parties was held in collaboration with CIOMS to discuss means of advancing the principles embodied in WHO's Ethical Criteria for Medicinal Drug Promotion. Broad consensus was reached by industry representatives, consumers and other parties on the approaches required to attain this objective.
13 16 The participants in a meeting organized jointly in September 1993 with CIOMS and the WHO collaborating centre for international drug monitoring in Uppsala (Sweden) stressed the need for wider monitoring of the action of drugs in routine use and more reliable comparative information on the risk/benefit ratio and cost-effectiveness of drug use in both developed and developing countries.
13.17 The databases that WHO maintains to serve national drug regulatory authorities were broadened to include information not only on suspected adverse drug reactions, but also on spurious products, and on newly adopted national regulations to control the labelling and advertising of medicinal plants.
13.18 An eighth revision of the Model List of Essential Drugs was produced at a WHO expert committee meeting in November 1993.
13.19 A second international meeting on the role of the pharmacist (Tokyo, August-September 1993 ), organized in collaboration with the International Pharmaceutical Federation and the Commonwealth Pharmaceutical Association with financial support from Japan, made recommendations for improving the quality of pharmaceutical services and resultant benefits for governments and the public and propounded a concept of pharmaceutical care.
13.20 Collaboration was maintained with the International Federation of Pharmaceutical Manufacturers Associations and the World Federation of Proprietary Medicine Manufacturers and with a number of national funding agencies, including in particular the German Foundation for International Development, in training key staff in the various aspects of national regulatory and enforcement activities.
13.21 Training of staff for drug regulatory authorities in developing countries continued. Following satisfactory evaluation in June 1992 of seven courses sponsored by the German Foun-

THE WORK OF WHO 1992-1993
dation for International Development, regional courses were organized in Benin and in Tunisia and Zimbabwe at the end of 1993. The model software package for handling drug regulatory data (see paragraph 13.12) was introduced in Africa, the Americas and the Eastern Mediterranean with financial support from Italy and Germany. WHO cooperated with UNDCP in organizing a technical workshop on parallel distribution systems for narcotic and psychoactive substances at national level (Vienna, June 1993).
Biologicals
13 22 The Organization continued to work closely with national regulatory authorities, providing guidance on the production and licensing procedures necessary to ensure the quality of biological products used in health care programmes.
13.23 Guidelines were issued for national authorities on good manufacturing practices, quality assurance and regulations. Several developing countries participating in the Children's Vaccine Initiative invited a team of experts to evaluate the manufacture and regulation of locally produced vaccines; in all cases significant changes in administrative procedures were recommended.
13.24 In pursuance of WHO's constitutional functions in regard to the standardization of biological products, 19 new or replacement international reference materials were established: six for the diagnosis or therapy of blood disorders and one for quantifying an antigen of HIV. Some 27 000 ampoules of international reference materials, prepared principally in national collaborating laboratories in Denmark, Nether lands and United Kingdom, were made available for standardizing product dosage and diagnostic procedures. New or revised production and quality control requirements were issued for six products, including human plasma fractions and an improved typhoid vaccine.
Traditional medicine
13 25 Work continued in drawing up guidelines on the standardization, assessment for efficacy, and utilization of traditional medicines, including herbal preparations. The Organiza-
80
tion collaborated with the World Conservation Union and the World Wide Fund for Nature in preparing guidelines on the conservation of medicinal plants; helped to draft a document on the integration of traditional and modern medicines in a project conducted under the aegis of the Cooperation Council for Arab Gulf States; and participated in a UNIDO consultation on the industrial utilization of medicinal and aromatic plants in Asia and the Pacific (Vienna, July 1993), which stressed the need for the development of coherent national policies and effective regulation to control the quality and use of the final products.
·---··----~~-» •~•-H--~>~ ,,_
Action Programme on Essential Drugs
13 26 Because of the global economic crisis and the shift from centrally planned to free market economies in various countries, new thinking and strategic planning were needed in the area of essential drugs. Many developing countries, some eastern European countries and the Commonwealth of Independent States requested WHO's cooperation in assessing new situations. The technical support provided focused on setting priorities and determining strategies to increase access to and appropriate use of essential drugs. This often meant redefining the responsibilities of the ministry of health and its relations with other ministries.
13 27 No ready-made solutions were available; emphasis was placed on finding innovative and rapid answers to various questions: how drugs were to be financed; how public health goals, including equity, could be maintained in a changing combination of public and private sectors; and how national regulatory authorities could control an increasingly complex pharmaceutical sector, with particular regard to drug quality, safety and the provision of accurate information for both prescribers and consumers alike.
13 28 In face of the growing global disparity between needs and accessibility, WHO intensified its direct and operational country support activities, particularly in Africa and the Americas, but also in Asia, where Maldives and Mongolia joined the list of more than 80 developing countries that are receiving technical and/or financial support. National capacity-building continued to be a major aim. At over 20 national

DIAGNOSTIC, THERAPEUTIC AND REHABILITATIVE TECHNOLOGY
workshops in four WHO regions, and at three intercountry strategic planning workshops in Africa, policy-makers from some 30 countries met to develop or review their own national drug policies and to exchange experience. In Benin, Bolivia, Guinea and Nepal, ways of improving technical and managerial methods used in the pharmaceutical supply system were tested.
13.29 To stimulate technical cooperation among developing countries, staff members from some national essential drugs programmes in participating countries acted as advisers or trainers in others; thus materials and procedures, such as standard treatment guidelines or procurement specifications, developed in one country could be used and sometimes further developed by others.
13.30 More resources were devoted to training and to the preparation of practical manuals and materials, in collaboration with national and international partners. Subjects covered included the technical and managerial aspects of financing, rational use, procurement, quality assurance and registration of drugs, and information, education and communication strategies. A successful field test at medical schools in seven countries of a problem-based method of teaching the principles of rational prescribing, 1 designed in collaboration with University of Groningen (Netherlands), aroused widespread academic interest.
13.31 With WHO's technical and financial support, a three-month course in drug management and rational drug use, designed to meet the needs of developing countries, was successfully launched at Robert Gordon University in Aberdeen (United Kingdom). Practical drug procurement guidelines, developed and used at workshops attended by over 120 people from 14 developing countries with the support of the Preferential Trade Area of Eastern and Southern African States, were further improved. In the Eastern Mediterranean a series of seminars on teaching rational drug use and the essential drugs concept were held for schools of medicine and pharmacy in 11 countries. Altogether, thousands of health workers in over 40 countries attended WHO-supported training courses and workshops on drug management and use.
1 Document DAP /91/12.
81
13 32 WHO continued its vigorous information and advocacy strategy exemplified by the MarchApril 1992 issue of World health on essential drugs, with a strong focus on national drug policy and rational use, and the brochure "Essential drugs, action for equity", produced in English, French and Spanish. The expanded Essential drugs monitor, published in English, French and Spanish, reached an estimated 200 000 policymakers, administrators, health workers, nongovernmental organizations, and industry and consumer organizations in 150 Member States with news of policy developments, essential drug programmes, research, and strategies for rational use. Many copies of the Monitor, and particularly of one issue on the theme of national drug policy, were also provided as instructional material on the subject of pharmaceuticals in primary health care for workshops and universities. The Organization developed a database consisting of important but unpublished technical reports and guidelines, which provides rapid access to material relating to a given technical or geographical area and is proving an invaluable tool. WHO's documentation centre on essential drugs continued to respond to the information needs of developing countries, distributing an average of 3000 documents per month to individuals, universities, and nongovernmental and other organizations.
13.33 More than 20 global and national operational research projects were carried out during the biennium, covering such topics as public attitudes to and use of drugs, injection practices, the stability of drugs during international transport, and monitoring of price and availability. Of particular interest were the development and fieldtesting of indicators for monitoring national drug policy implementation and, in collaboration with the International Network for the Rational Use of Drugs, of standardized indicators to measure the impact of interventions designed to influence drug use. A 15-country study on the application of the WHO Certification Scheme on the Quality of Pharmaceutical Products moving in International Commerce revealed shortcomings in its functioning in both importing and exporting countries. Nine reports on WHOsupported research were issued during the biennium, and a new database providing standardized information on research completed or in progress was established.
13.34 The goal of formulating national drug policies and launching essential drugs programmes in

THE WORK OF WHO 1992- 1993
at least 70 countries by 1995 is likely to be reached before the target date, but it is important to increase the number of countries involved and to improve their policies and programmes. The need for close coordination of all the elements of a na6onal drug policy, based on WHO guiding principles, has become increasingly evident as large-scale financial support has become available from other organizations, such as the World Bank, the European Community, the African Development Bank, non governmental organizations and the bilateral agencies. The concept of a standard policy framework to be developed with WHO support is therefore being energetically promoted among Member States and donors.
Rehabilitation
13.35 On completion of the United Nations Decade of Disabled Persons (1983-1992) WHO carried out a review of the progress made. It showed that preventive measures had significantly reduced the incidence of some diseases that cause disabilities; that public awareness about disability had increased during the decade, leading to modest improvements in the social integration of people with mild to moderate disabilities in some countries; and that in most developing countries there had been no significant increase in rehabilitation services. In the light of these findings, the Health Assembly adopted resolution WHA45.10 which outlined actions to
strengthen disability prevention and rehabilitation and provided a framework for the programme's work during the biennium.
A mother helps her child, with the support of o community rehobilito· lion worker.
82
13.36 Three intercounrry workshops (Harare, July 1992; Saly Mbour, Senegal, October 1992; Lima, May 1993), with participants from 46 countries, recommended ways to promote the incorporation of community-based rehabilitation into national primary health care programmes and to strengthen referral services for people with disabilities. WHO cooperated with IMPACT, the international initiative against avoidable disability, in setting up a pilot project in India for inclusion of disability prevention in primary health care. Egypt, Islamic Republic of Iran and Lebanon have incorporated community-based rehabilitation into primary health care, with appropriate referral services, and several other countries in the Eastern Mediterranean are establishing programmes. National seminars on community-based rehabilitation were organized in several countries' and served as forums for the preparation of intcrsectoral plans for rehabilitation involving health, education, social and vocational services. In a number of countries2 WHO participated in planning or evaluation of community-based rehabilitation programmes.
13.37 The existing methodology for cost analysis in primary health care1 was adapted for use in determining the cost of rehabilitation services in Mauritius and Zimbabwe, as a first step in the preparation of general guidelines for cost analysis of community-based services and referral for rehabilitation.
13.38 A variety of training activities were carried out to promote community-based rehabilitation. In 1992 physicians, nurses, therapists and middlelevel rehabilitation personnel were trained for community-based rehabilitation through national programmes in Ben in, China and Mongolia. In the Americas several workshops were organized to strengthen intersectoral action for rehabilitation. In 1993 WHO, in collaboration with the International Leprosy Association, provided training in the United States of America for professional staff of government and nongovernmentalleprosy programmes, with emphasis on integration of people with leprosy into community-based rehabilitation programmes.
' Benin, Burkino Foso, Czech Republ ic, COte d' lvoire, fquutoriol Guinea, Gohon, Indo nesia, lesotho. Swo1ilond.
' Eritreo, Glrono, Guyana, Indonesia, Konya, Mongolia, Thollond, Zimbabwe. a Datument WHO/SHS/ NHP /90.S.

DIAGNOSTIC, THERAPEUTIC AND REHABILITATIVE TECHNOLOGY
13.39 Training materials produced during the biennium included recommendations for middle-level rehabilitation workers, based on country experience, 1 a manual on promoting the development of young children with cerebral palsy2 and guidelines for preventing deformities in poliomyelitis3
•
1340 In November 1993 WHO hosted two meetings with representatives of 32 international nongovernmental organizations that support rehabilitation programmes in developing countries in order to discuss ways in which they can apply WHO guidelines in this effort. One outcome of the discussions was a broad outline of action for improving prosthetic and orthotic services in developing countries.
13.41 Collaboration with UNDP, ILO, UNESCO, UNICEF and the United Nations Of-
1 Document WHO/RHB/92.1 2 Document WHO/RHB/93.1 3 Document WHO/EPI/POLIO/RHB/91.1.
83
fice at Vienna continued, for instance, in the implementation of a UNDP-supported project in Ghana, the setting-up of a task force on disabled children and women, the preparation of recommendations to countries for intersectoral rehabilitation programmes, and the drafting of uniform guidelines for programme evaluation. WHO is collaborating with the Economic and Social Cornmission for Asia and the Pacific to promote the Asia and Pacific Decade of Disabled Persons (1993-2002). A joint review was carried out with UNHCR of disabilities among refugees at 11 sites in Africa; and plans were made to organize community-based rehabilitation in two of the areas in early 1994. A plan for emergency rehabilitation of people injured in war in former Yugoslavia was prepared, with emphasis on provision of prostheses and other procedures to deal with physical trauma. Together with the United Nations Statistical Office, WHO reviewed databases on disability in four countries, including data from community-based rehabilitation programmes and national census and survey data, with a view to preparing guidelines on data collection for national planning and for programme monitoring and evaluation.

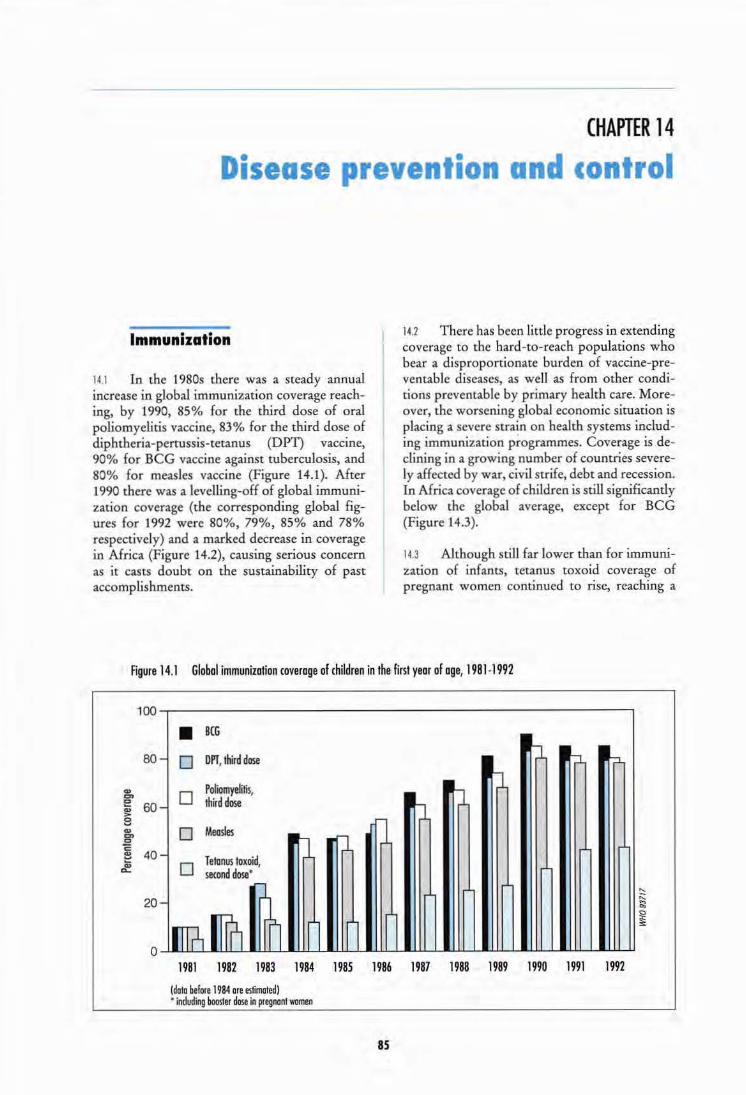
Disease -e e I o n CHAPTER 14
ontrol
Immunization
14.1 In the 1980s there was a steady annual increase in global immunization coverage reaching, by 1990, 85% for the third dose of oral poliomyelitis vaccine, 83% for the third dose of diphtheria-pertussis-tetanus (DP'I) vaccine, 90% for BCG vaccine against tuberculosis, and 80% for measles vaccine (Figure 14.1). After 1990 there was a levelling-off of global immunization coverage (the corresponding global figures for 1992 were 80%, 79%, 85% and 78% respectively) and a marked decrease in coverage in Africa (Figure 14.2), causing serious concern as it casts doubt on the sustainability of past accomplishments.
14.2 There has been little progress in extending coverage to the bard-to-reach populations who bear a disproportionate burden of vaccine-preventable diseases, as well as from other conditions preventable by primary health care. Moreover, the worsening global economic situation is placing a severe strain on health systems including immunization programmes. Coverage is declining in a growing number of countries severely affected by war, civil strife, debt and recession. In Africa coverage of children is still significantly below the global average, except for BCG (Figure 14.3).
14.3 Although still far lower than for immunization of infants, tetanus toxoid coverage of pregnant wornen continued to rise, reaching a
Figure 14.1 Global immunization coverage of children in the first year of age, 1981-1992
100
• BCG
80
Q) en e 60 Q) > 8 "' en c:> E ~ 40 ~
- 0 orr, third dose b b b
Poliomyelitis, b tJ
- 0 third dose b rJ 0 Meosles
IJ rJ - Tetanus toxoid, 0 second dose •
20
0 -l rn?, llln ~ lrl lrl lrl
1981 1982 1983 1984 1985 1986 1987 1988 1989 1990 1991 1992
(data before 1984 are estimated) • induding booster dose in pregnant women
as
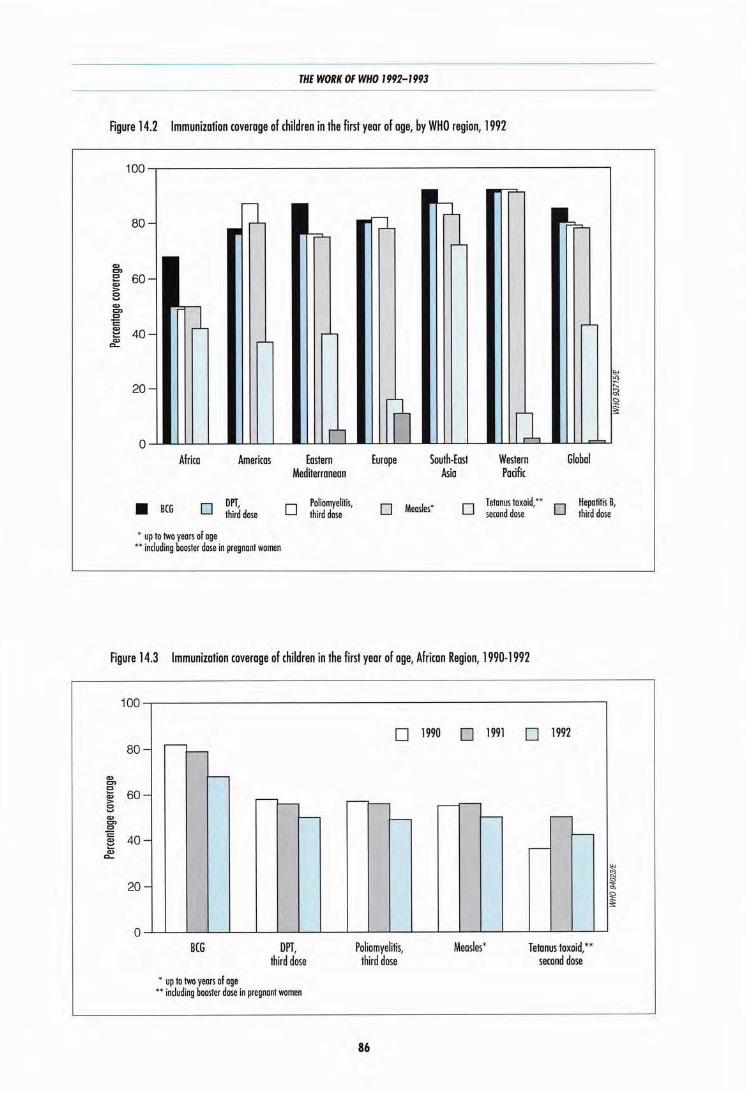
THE WORK OF WHO 1992- 1993
Figure 14.2 Immunization coverage of children in the first year of age, by WHO region, 1992
80
Q) en E 60 Q)
> 8 Q)
en .E! c: Q)
40 ::: Q)
c...
20
Africa Americas
• BCG 0 DPT, third dose
• up to two years of age •• including booster dose in pregnant women
Eastern Mediterranean
0 Poliomyelitis, third dose
Europe South· East Asia
Western Pacific
Global
O Measles• 0 Tetanus toxoid;• O Hepam~ 8, second dose third dose
Figure 14.3 Immunization coverage of children in the first year of age, African Region, 1990·1992
100
80 -
Q) en E 60 Q)
> 8
-Q)
= 0 "E 40 Q)
::: -Q)
c...
20 -
0
.---1--
f--
BCG
• up to two yeors of age
.---,__ f--
OPT, third dose
•• including booster dose in pregnant women
0
1--
Poliomyelitis, third dose
86
1990 0 1991
1--
Measles*
0 1992
...---I--
~
Tetanus toxoid,** second dose

DISEASE PREVENTION AND CONTROL
reported 4 3% for pregnant women in developing countries in 1992, compared with 39% in 1990 (Figure 14.1); the highest coverage was achieved in South-East Asia (Figure 14.2).
14.4 During the biennium many countries added yellow fever and hepatitis B vaccines to their immunization programmes. Of the 33 African countries at risk from yellow fever, 17 have policies for provision of the vaccine; and in 1992 their coverage reached 10% for children under one year of age. Forty-eight countries in the world established policies for routine hepatitis B immunization, and a system for monitoring the coverage in children under one year was developed.
14.5 On the basis of reported coverage and estimated vaccine efficacy and morbidity rates, WHO calculated that in 1992 immunization prevented 2. 9 million deaths from measles, neonatal tetanus and pertussis in developing countries, and an estimated 4 36 000 cases of paralytic poliomyelitis. Nevertheless, an estimated 2.1 million deaths from measles, neonatal tetanus and pertussis, and over 140 000 cases of poliomyelitis occurred in developing countries in 1992, indicating clearly a need to sustain and if possible increase the immunization coverage.
14.6 The greatest success in disease control has been achieved in the Americas, where the last case of poliomyelitis due to wild virus was reported in August 1991. Other regions also showed improvements: 131 countries reported no poliomyelitis, as compared with 80 in 1985.
14 7 Efforts have been made to improve systems for routine disease surveillance. Guidelines on bringing about such improvements as a necessary step towards poliomyelitis eradication, neonatal tetanus elimination and measles control have been distributed. Numerous workshops on disease surveillance for control were conducted in all regions, and the quality of surveillance data has markedly improved in many countries. Assessments of surveillance were conducted in 19 countries in two regions. They will be continued so that eventually countries can certify the eradication of poliomyelitis and elimination of neonatal tetanus.
14 8 Large outbreaks of measles, diphtheria and yellow fever continued to affect children who could have been protected if immunization programmes had been given sufficiently high pri-
87
ority. Measles remains one of the greatest killers of children, causing an estimated 1.1 million child deaths a year in developing countries. Declining or stationary immunization coverage and continued high case-fatality rates in many areas are clear warnings that efforts must be stepped up to reach the 1995 measles reduction goals. Crucial to the attainment of those goals are ensuring coverage of over 90% in all districts and intensified measures in urban areas. Outbreaks of the disease raise awareness of the importance of universal child immunization and the need for prevention and treatment of potentially lethal complications.
14.9 Diphtheria has been spreading in the Russian Federation and Ukraine over the last two years; it is currently out of control and is affecting other republics of the former Soviet Union. Growing numbers of cases have also been imported to countries in central and western Europe. In the first 10 months of 1993 approximately 12 000 cases of diphtheria were reported to the Regional Office for Europe, double the number for the whole of 1992.
14 10 Kenya experienced an outbreak of yellow fever for the first time in more than 40 years. Mass immunization was undertaken in response to the emergency in and around the area of the outbreak, which has since been brought under control.
14.11 A global poliomyelitis diagnostic laboratory network of 41 national laboratories, 17 regional reference laboratories and five special reference laboratories was established. Initially, each of the national laboratories has been working on poliovirus isolation and poliomyelitis serotyping. Meanwhile, an immunofluorescent test has been developed in a WHO-funded study that may prove to be a short cut in poliovirus detection; this and other methods for diagnosing poliomyelitis are undergoing further study. Finally, one of the product development groups of the Children's Vaccine Initiative has made progress in preparing a more heat-stable poliomyelitis vaccine that could be used in immunization programmes in the future.
14.12 1992-1993 saw a stronger focus on managerial considerations than in the previous biennium, when emphasis was on the introduction of new technology for the logistics of immunization services. Computer software was developed to improve the forecasting of needs for vaccines and equipment. Following surveys that
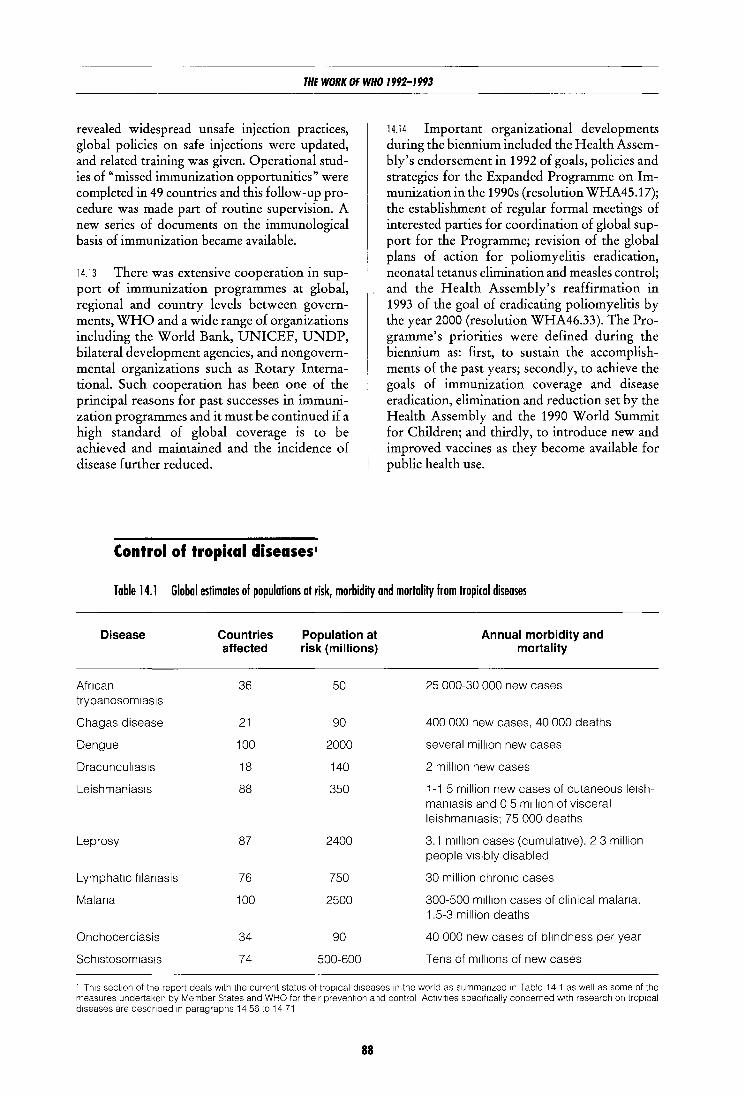
THE WORK OF WHO 1992-1993
revealed widespread unsafe injection practices, global policies on safe injections were updated, and related training was given. Operational studies of "missed immunization opportunities" were completed in 49 countries and this follow-up procedure was made part of routine supervision. A new series of documents on the immunological basis of immunization became available.
14.13 There was extensive cooperation in support of immunization programmes at global, regional and country levels between governments, WHO and a wide range of organizations including the World Bank, UNICEF, UNDP, bilateral development agencies, and nongovernmental organizations such as Rotary International. Such cooperation has been one of the principal reasons for past successes in immunization programmes and it must be continued if a high standard of global coverage is to be achieved and maintained and the incidence of disease further reduced.
Control of tropical diseases1
14.14 Important organizational developments during the biennium included the Health Assembly's endorsement in 1992 of goals, policies and strategies for the Expanded Programme on Immunization in the 1990s (resolution WHA45.17); the establishment of regular formal meetings of interested parties for coordination of global support for the Programme; revision of the global plans of action for poliomyelitis eradication, neonatal tetanus elimination and measles control; and the Health Assembly's reaffirmation in 1993 of the goal of eradicating poliomyelitis by the year 2000 (resolution WHA46.33). The Programme's priorities were defined during the biennium as: first, to sustain the accomplishments of the past years; secondly, to achieve the goals of immunization coverage and disease eradication, elimination and reduction set by the Health Assembly and the 1990 World Summit for Children; and thirdly, to introduce new and improved vaccines as they become available for public health use.
Table 14.1 Global estimates of populations at risk, morbidity and mortality from tropical diseases
Disease Countries Population at Annual morbidity and affected risk (millions) mortality
Afncan 36 50 25 000-30 000 new cases trypanosom1as1s
Chagas disease 21 90 400 000 new cases, 40 000 deaths
Dengue 100 2000 several mill1on new cases
Dracuncul1as1s 18 140 2 million new cases
Leishmaniasis 88 350 1-1 5 million new cases of cutaneous le1sh-man1asis and 0 5 m1lllon of visceral leishmaniasis; 75 000 deaths
Leprosy 87 2400 3.1 m1ll1on cases (cumulative), 2 3 million people VISibly disabled
Lymphatic f1lanasis 76 750 30 million chronic cases
Malana 100 2500 300-500 m1ll1on cases of clinical malana, 1.5-3 million deaths
Onchocerciasis 34 90 40 000 new cases of blmdness per year
Sch1stosom1as1s 74 500-600 Tens of m1ll1ons of new cases
' Th1s sect1on of the report deals w1th the current status of trop1cal d1seases 1n the world as summanzed 1n Table 14 1 as well as some of the measures undertaken by Member States and WHO for the1r prevention and control Act1v1t1es spec1f1cally concerned w1th research on trop1cal d1seases are descnbed 1n paragraphs 14 56 to 14 71
88
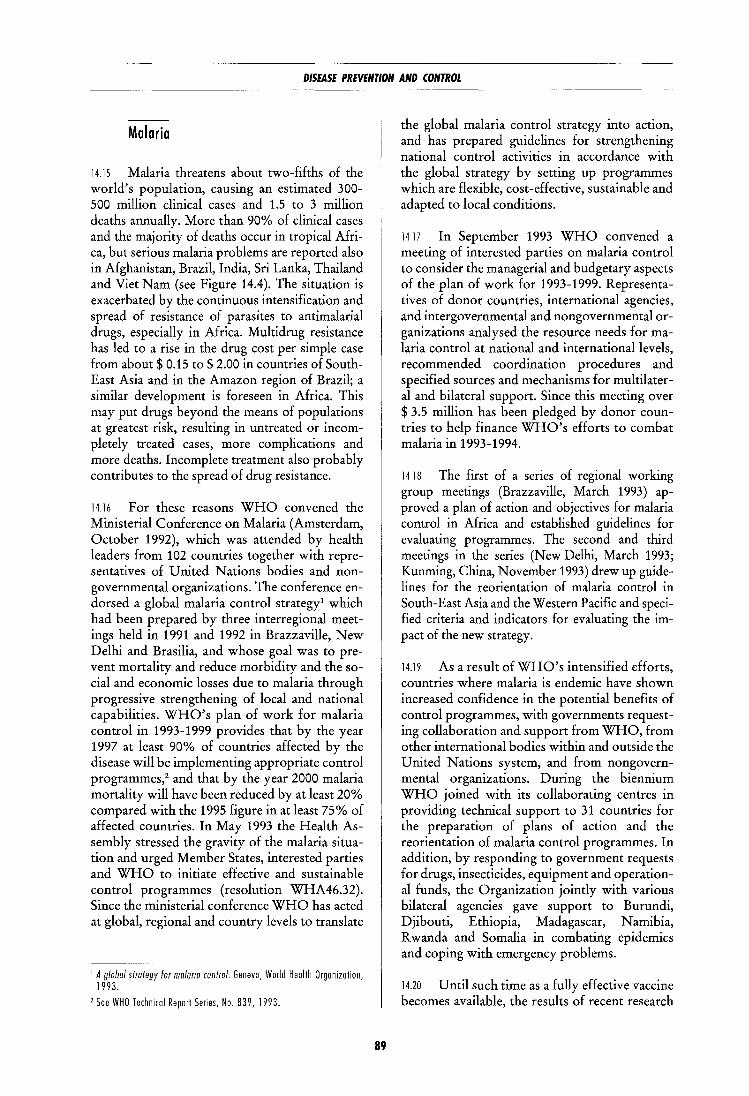
DISEASE PREVENTION AND CONTROL
Malaria
14.15 Malaria threatens about two-fifths of the world's population, causing an estimated 300-500 million clinical cases and 1.5 to 3 million deaths annually. More than 90% of clinical cases and the majority of deaths occur in tropical Africa, but serious malaria problems are reported also in Afghanistan, Brazil, India, Sri Lanka, Thailand and VietNam (see Figure 14.4). The situation is exacerbated by the continuous intensification and spread of resistance of parasites to antimalarial drugs, especially in Africa. Multidrug resistance has led to a rise in the drug cost per simple case from about$ 0.15 to$ 2.00 in countries of SouthEast Asia and in the Amazon region of Brazil; a similar development is foreseen in Africa. This may put drugs beyond the means of populations at greatest risk, resulting in untreated or incompletely treated cases, more complications and more deaths. Incomplete treatment also probably contributes to the spread of drug resistance.
14.16 For these reasons WHO convened the Ministerial Conference on Malaria (Amsterdam, October 1992), which was attended by health leaders from 102 countries together with representatives of United Nations bodies and nongovernmental organizations. The conference endorsed a global malaria control strategy! which had been prepared by three interregional meetings held in 1991 and 1992 in Brazzaville, New Delhi and Brasilia, and whose goal was to prevent mortality and reduce morbidity and the social and economic losses due to malaria through progressive strengthening of local and national capabilities. WHO's plan of work for malaria control in 1993-1999 provides that by the year 1997 at least 90% of countries affected by the disease will be implementing appropriate control programmes,2 and that by the year 2000 malaria mortality will have been reduced by at least 20% compared with the 1995 figure in at least 75% of affected countries. In May 1993 the Health Assembly stressed the gravity of the malaria situation and urged Member States, interested parties and WHO to initiate effective and sustainable control programmes (resolution WHA46.32). Since the ministerial conference WHO has acted at global, regional and country levels to translate
1 A global strategy for malarta control. Geneva, World Health Organization, 1993.
2 See WHO Technical Report Series, No. 839, 1993.
89
the global malaria control strategy into action, and has prepared guidelines for strengthening national control activities in accordance with the global strategy by setting up programmes which are flexible, cost-effective, sustainable and adapted to local conditions.
1417 In September 1993 WHO convened a meeting of interested parties on malaria control to consider the managerial and budgetary aspects of the plan of work for 1993-1999. Representatives of donor countries, international agencies, and intergovernmental and nongovernmental organizations analysed the resource needs formalaria control at national and international levels, recommended coordination procedures and specified sources and mechanisms for multilateral and bilateral support. Since this meeting over $ 3.5 million has been pledged by donor countries to help finance WHO's efforts to combat malaria in 1993-1994.
14 18 The first of a series of regional working group meetings (Brazzaville, March 1993) approved a plan of action and objectives for malaria control in Africa and established guidelines for evaluating programmes. The second and third meetings in the series (New Delhi, March 1993; Kunming, China, November 1993) drew up guidelines for the reorientation of malaria control in South-East Asia and the Western Pacific and specified criteria and indicators for evaluating the impact of the new strategy.
14.19 As a result of WHO's intensified efforts, countries where malaria is endemic have shown increased confidence in the potential benefits of control programmes, with governments requesting collaboration and support from WHO, from other international bodies within and outside the United Nations system, and from nongovernmental organizations. During the biennium WHO joined with its collaborating centres in providing technical support to 31 countries for the preparation of plans of action and the reorientation of malaria control programmes. In addition, by responding to government requests for drugs, insecticides, equipment and operational funds, the Organization jointly with various bilateral agencies gave support to Burundi, Djibouti, Ethiopia, Madagascar, Namibia, R wanda and Somalia in combating epidemics and coping with emergency problems.
14.20 Until such time as a fully effective vaccine becomes available, the results of recent research
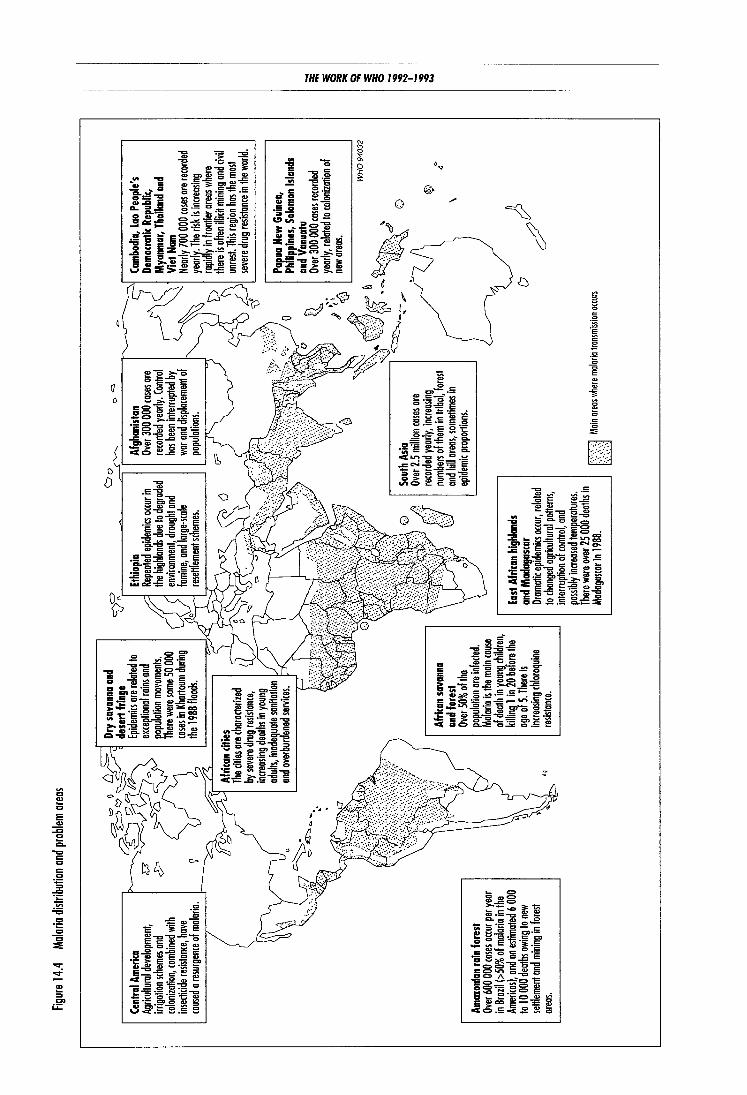
Figure
14.4
M
alaria
dist
ributi
on a
nd p
roble
m ar
eas
Cent
ral A
meri
ca
Agric
ultura
l dev
elopm
ent,
irriga
tion
schem
es an
d co
loniza
tion,
comb
ined w
ith
insect
icide
resis
tance
, hov
e ca
used
a re
surge
nce o
f mala
ria.
Amaz
onian
rain
fore
st Ov
er 60
0 000
cases
occu
r per
year
in Br
azil (
>50%
of m
alaria
in th
e Am
ericas
), an
d on
estim
ated
6 00
0 to
1 0 00
0 dea
ths ow
ing to
new
settle
ment
and
minin
g in f
orest
areas
.
Dry
sava
nna
and
dese
rt fri
nge
Epide
mics
ore r
elated
to
exce
ption
al rai
ns an
d po
pulat
ion m
ovem
ents.
Th
ere w
ere so
me 50
000
cases
in K
harto
um d
uring
the
198
8 floo
ds.
Afric
an c
ities
Th
e citie
s ore
chara
cteriz
ed
by se
vere
drug
resis
tance
, inc
reasin
g de
aths i
n you
ng
adult
s, ino
degu
ate sa
nitati
on
and
overb
urde
ned s
ervice
s.
Afric
an s
avan
na
and
fore
st Ov
er 50
% of
the
popu
lation
ore
infec
ted.
Mala
ria is
the m
ain ca
use
of de
ath in
youn
g_ ch
ildren
, kil
ling_
1 in 2
0 befo
re the
ag
e of
5. Th
ere is
inc
reasin
g ch
loroq
uine
resist
ance
.
<::::
>=
<::J
o lj 0
0
c::::
l
Ethio
pia
Repe
ated
epide
mics
occu
r in
the hi
ghlan
ds du
e to d
egrad
ed
envir
onme
nt, d
rough
t and
fam
ine, a
nd la
rge·sc
ole
resett
lemen
t sch
emes.
Afg
hani
stan
Over
300 0
00 ca
ses or
e rec
orded
yea
rly. C
ontro
l ha
s bee
n int
errup
ted by
wa
r and
disp
lacem
ent o
f po
pulot
ions.
Sout
h As
ia Ov
er 2.5
milli
on co
ses o
re rec
orded
yea
rly, i
ncrea
sing
numb
ers of
them
in tr
ibal,
forest
an
d hil
l area
s, so
metim
es in
epide
mic p
roport
ions.
East
Afric
an h
ighl
ands
I
and
Mad
agas
car
()
Dram
atic e
pidem
ics oc
cur,
relate
d to
chan
ged
agric
ultura
l patt
erns,
interr
uptio
n of c
ontro
l, an
d po
ssibly
incre
ased t
empe
ratur
es.
There
were
ove
r 25 0
00 d
eaths
in
Mad
agasc
ar in
1988
. j j
/ri>j M
ain a
reas w
here
malar
ia tra
nsmi
ssion
occu
rs
Cam
bodi
a, La
o Pe
ople
's De
moc
ratic
Repu
blic,
Mya
nmar
, Tha
iland
and
Vi
et No
m Ne
arly
700 0
00 ca
ses or
e rec
orded
ye
arly.
The r
isk is
incre
asing
rap
idly i
n fro
ntier
areas
whe
re the
re is
often
illici
t mini
ng an
d civi
l un
rest. T
his re
gion
has t
he m
ost
seve
re dru
g res
istan
ce in
the w
orld.
Papu
a Ne
w Gu
inea
, Ph
ilipp
ines
, Solo
mon
Islan
ds
and
Van
uatu
Ov
er 30
0 000
cases
reco
rded
yearl
y, rel
ated t
o colo
nizati
on of
ne
w are
as.
WH
09
40
32
0
~
~ ~
\
o?J
~ ~ =
~ ~ C
) -'0 ~ .!..
'0
~

DISEASE PREVENTION AND CONTROL
Preventing malaria: health education for young children in Cambodia.
on insecticide- impregnated bednets, the potent artemisinin derivatives and new diagnostic tools are now being applied in malaria control (see paragraph 14.45). In 1992 WHO collaborated with Thailand in establishing a surveillance system to monitor adverse reactions to artemisinin derivatives and drew up methodological guidelines that can be used by neighbouring countries for the next few years.
14.21 Few of the countries affected have enough well-trained, motivated personnel tO
achieve and maintain a satisfactory level of malaria control. During the biennium some 170 nationals were trained in planning, implementing and evaluating malaria control programmes in seven international courses for health personnel of various levels. New manuals, visual aids and other teaching materials were prepared on basic epidemiology, entomology, treatment of severe malaria and training of trainers for the control of tropical diseases. The increase in instructional activities has not, however, been matched by the availability of human and financial resources. Training is pointless without the necessary supplies, equipment and infrastruc-
91
ture to enable the trainees to do the work for which they have been prepared. Steps have therefore been taken to ensure that the development of national programmes and of the necessary human resources both move forward in a coordinated manner. Progress was made in meeting the enormous demand for suitable training materials in English and French.
Dracunculiasis (guinea-worm disease)
14.22 If the present momentum can be maintained for the control of dracunculiasis, the disease can be eradicated. In early 1980 the global annual incidence was estimated at 5-10 million; the present estimate is less than 2 million. A significant decrease in incidence has been observed in some endemic countries where active surveillance and notification have been carried out. During 1991 -1992 the incidence decreased by 68% in Cameroon, 50% in Ghana, 43% in India, and 35% in Nigeria. Pakistan is on the verge of eradicating the disease, with 23 cases in 1992 compared with 160 in 1991.

THE WORK OF WHO 1992-1993 -------------------------------
A housewife's flour sieve con fil ter wo ter ond prevent transmission of drocunculiosis.
14.23 WHO convened a fourth regional conference on dracunculiasis in Africa (Enugu, Nigeria, March 1992) and, as in previous years, joined with UNDP and UNICEF in organizing reviews of national dracunculiasis eradication programmes. A total of 16 national programmes were analysed, including assessment of current epidemiological trends and control activities; and in each case recommendations were made for continuation of the programmes. The WHO/UNICEF interagency technical team for the dracunculiasis eradication programme in Africa, set up in Ouagadougou in 1992, provides direct support to national programmes in French-speaking Africa. In 1992 WHO held a first formal consultation, in the Islamic Republic of Iran, to initiate the process of certification of eradication. The following year WHO experts discovered that transmission of dracunculiasis probably still occurs in Yemen. Updated criteria for the certification of dracunculiasis eradication were issued in 1993}
1 Documen1 WHO/Fil/93. 187 .
92
Schistosomiasis
14.24 The WHO Expert Committee on the Control of Schistosomiasis2 recognized that schistosomiasis is increasingly becoming an urban health problem in Africa and Brazil and affects thousands of refugees, especially in Cambodia. SchistOsomiasis is also causing increasing concern in water resources development schemes, as emphasized in a new WHO publication.3 A Swahili version of the 1990 WHO publication Health education in the control of schistosomiasis was issued and distributed in Kenya and the United Republic of Tanzania. WHO supported Mali, Morocco and Yemen in long-term planning for control of the disease.
14.25 The high price of praziquantel is the single major impediment tO the implementation of national control programmes in all the countries concerned, although discussions with the manufacturers during the biennium have resulted in some price reductions. With support from Italy, WHO is collaborating with ministries of health tO improve the delivery of antischistosomal drugs.
1426 With the help of USAID, a geographical information system was developed to strengthen the management and control of schistosomiasis, and WHO joined with the International Development Research Centre (Canada) in introducing it in Botswana and Senegal.
14.27 A WHO study group (Manila, October 1993) reviewed the current status of the epidemiology and control of food borne trematode infections (see Figure 14.5). An estimated 40 million people are infected, although the pattern of morbidity is changing along with the environment and people's habits. The study group recommended a coordinated control strategy emphasizing health education, food safety in domestic and commercial food processing, proper sanitation to reduce faecal contamination of food production through use of wastewater, and systematic case detection and treatment within the health care system.
7 WHO Technical Re por1 Selies, No. 830, 1993. 1 Hu nter JM et ol. Porositic dlseoses in woler resources development. Geneva, World Health Orgonizo1ion, 1993.
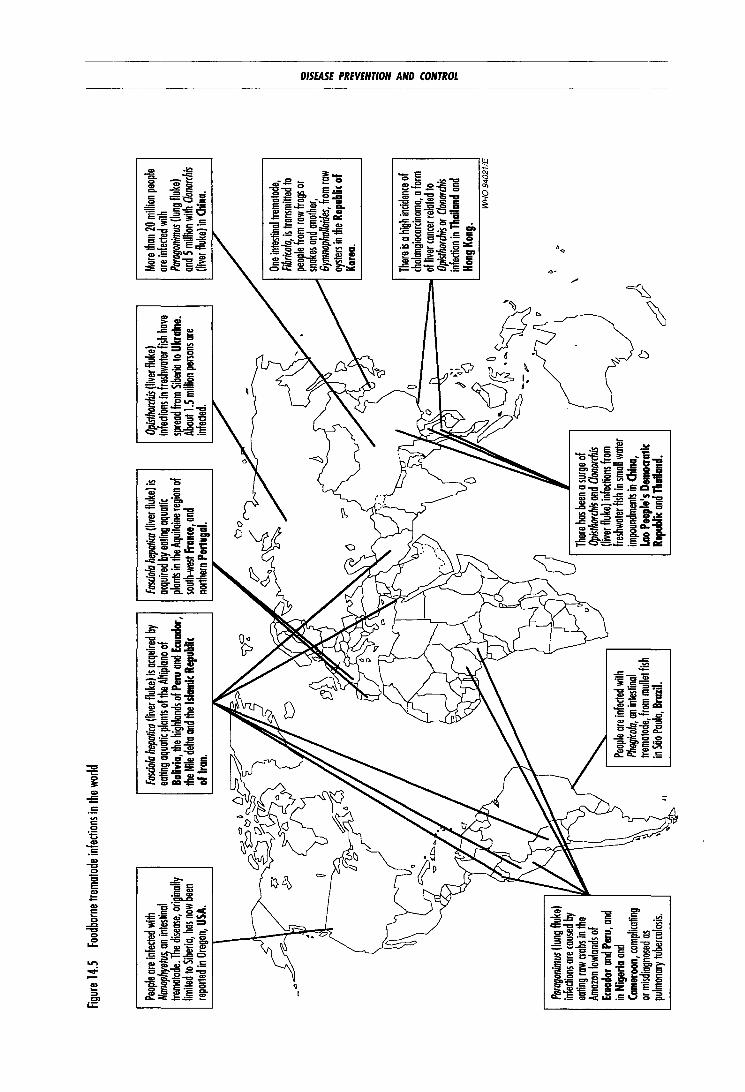
Figure
14.5
Fo
od bo
rne t
rem
atode
infec
tions
in th
e wo
rld
Peop
le are
infec
ted w
ith
Nano
phyet
us, an
intes
tinal
trema
tode.
The d
isease
, orig
inally
lim
ited t
o Sibe
ria, h
as no
w be
en
report
ed in
Oreg
on, U
SA.
.. ~
1'1/
Parag
onim
us (lu
ng fl
uke)
infec
tions
are c
aused
by
eatin
g row
crab
s in t
he
Amazo
n low
lands
of
Ecua
dor a
nd P
eru,
and
in Ni
geria
and
Cam
eroon
, com
plicat
ing
or mi
sdiag
nosed
as
pulm
onary
tube
rculos
is.
/ I
'-..
..,
Fasci
ola he
patic
a {liv
er flu
ke) i
s acq
uired
by
eatin
g aq
uatic
plan
ts of
the A
lliplon
o of
Boliv
ia, th
e high
lands
of P
eru an
d Ecu
ador
, the
Nile
delta
and t
he Is
lamic
Repu
blic
of Ir
an.
\ 1
1
I ~
AI/-\
Peop
le ore
infec
ted w
ith
Phag
icola,
an in
testin
al tre
matod
e, fro
m mu
llet fi
sh in
Sfio P
aulo,
Braz
il.
Fasci
ola he
patic
a (liv
er flu
ke l is
ac
quire
d by e
ating
aqua
tic
plants
in th
e Aqu
itaine
regio
n of
south
-west
Fran
ce, a
nd
north
ern P
ortu
gal.
There
has b
een a
surge
of
Opisth
orchis
and
Clono
rchis
!liver
fluke
) infe
dions
from
fre
shwa
ter fi
sh in
small
wate
r im
poun
dmen
ts in
China
, La
o Pe
ople'
s D
emoa
atic
Repu
blic a
nd T
haila
nd.
Opisth
orchis
(live
r fluk
e) inf
edion
s in f
reshw
ater f
ish h
ave
sprea
d from
Sibe
ria to
Ukr
aine.
Abou
tl.5 m
illion
perso
ns or
e inf
eded
. I '\
.""'\
,/
?
() ~~ Mo
re tha
n 20
milli
on pe
ople
are in
feded
with
Pa
ragon
imus
!lung
fluke
) an
d 5 m
illion
with
Clon
orchis
!liv
er flu
ke) i
n Chin
a.
One i
ntesti
nal t
remato
de,
Fibric
ola, is
tron
smiH
ed to
1
peo~le fr
om ro
w fro
gs or
sno e
s and
anoth
er,
Gymn
opha
lloide
s, fro
m row
oy
sters
in the
Rep
ublic
of
Korea
.
There
is a h
igh in
ciden
ce of
chola
ngioc
orcino
ma, a
form
of liv
er can
cer re
lated
to
Opisth
orchis
or C
lonorc
his
infed
ion in
Tha
iland
and
Hong
Kon
g. W
H0
94
02
1/E
t \
~ ~
5:.: .... ... ;;: ... ~ a:
::::! ~ ~
~ s a:
:iil ~
THE WORK OF WHO 1992-1993
lymphatic filariasis
14.28 In 1991 the WHO Expert Committee on Filariasis' estimated that 78 million persons are infected throughout the world and that 750 million persons are at risk. It stressed the importance of establishing the precise social, psychological and economic consequences of the disease in endemic countries.
14.29 Strategies to reduce clinical disease in endemic areas through chemotherapy and vector control were initiated during the biennium. In clinical trials it was found that single doses of ivermectin as well as diethylcarbamazine citrate (DEC) were highly effective in suppressing parasitaemia (see paragraph 14.60). Further, experience in China has shown that the use of DEC-medicated salt can effectively reduce prev-
1 WHO Technical Repo11 Series. No. 821 , 1992.
Sofe woter: the ideol woy to prevent filoriosis.
94
alence rates in infected populations. WHO is actively encouraging the manufacture and distribution of this salt through the private sector.
Onchocerciasis
14.30 The last decade has seen a decline in the prevalence of onchocerciasis infection, mainly due to the remarkable success of vector control in the Onchocerciasis Control Programme in West Africa. A symposium was organized (New York, September 1993) to mark the fifth anniversary of the donation of ivermectin by the manufacturer Merck & Co. Supply of this drug has enabled a major breakthrough in onchocerciasis control, and so far six million treatments have been distributed. Rapid assessment indicators and drug supply processes were tested in operational research projects in endemic countries. It can now be concluded that annual treatment of endemic communities suffices to reduce the par-

DISEASE PREVENTION AND CONTROL
asite load, prevent new cases of blindness and improve anterior segment eye lesions. In the Americas a strategic planning council coordinated by PAHO/WHO has been promoting a regional initiative to eliminate onchocerciasis.
14 31 Of the 34 countries where onchocerciasis is endemic, 29 have implemented or prepared plans to conduct regional or national programmes for distributing ivermectin based on the 1993 guidelines and recommendations of the WHO Expert Committee on Onchocerciasis Control. Effective cooperation has grown as a result not only of political commitment by ministries of health but also of increasing interest among national and international agencies concerned with health and blindness. Currently 21 such agencies are involved in this cooperation, more than twice as many as two years ago, with WHO playing a coordinating role.
American trypanosomiasis (Chagas disease)
14.32 The ministers of health of the countries of the Southern Cone1 have launched an initiative to eliminate Chagas disease in the coming decade through control of vectors and blood banks. Technical representatives of each ministry have been designated to form an intergovernmental commission overseeing the implementation and evaluation of national control programmes. Field activities have been planned and budgeted and common indicators to assess impact and costs agreed upon. At their last meeting (Santa Cruz, Bolivia, October 1993) the representatives reiterated their commitment to continue financing the activities in 1994-1995.
14.33 A study carried out in Argentina, Chile, Honduras and Paraguay showed that rates of house reinfestation by triatomines 18 months after the application of insecticide paints are 1.5 to 3 times lower than those observed after traditional spraying. The paints, manufactured in Brazil, have already been applied routinely by the control programme in the state of Ceara and operational costs have decreased, while vector control has become more efficient.
1 Argentina, Bolivia, Brazil, Chile, Paraguay, Uruguay
95
Leishmaniasis
14.34 A WHO imtlatlve for research on leishmaniasis control led to the mobilization of funds for nine new projects aimed at validating new vector and/ or reservoir control methods. In a hyperendemic area of central Tunisia a technique to control zoonotic cutaneous leishmaniasis, based on large-scale deep ploughing of rodent burrows around a city, proved to be feasible and efficient; the project was strongly backed by the national authorities and by regional and local institutions.
14.35 In the Indian state of Bihar the use of pyrethroid-impregnated bednets led to a dramatic reduction in the density of the vector Phlebotomus argentipes in dwellings over a fivemonth period, suggesting that it could be analternative to classical house spraying with residual insecticide. The method was well accepted by local communities.
14.36 With the spread of the AIDS pandemic, the incidence of visceral leishmaniasis is expected to rise because of the increasing frequency of HIV I Leishmania eo-infections. WH 0 has established an international registry in Geneva to centralize and diffuse worldwide epidemiological data on these eo-infections. A case report form was prepared and widely diffused to facilitate and standardize the collection of baseline data for evaluating the severity of the problem and its geographical extent.
African trypanosomiasis (sleeping sickness)
14.37 With the recrudescence of sleeping sickness, a number of countries called for intercountry coordination of surveillance and control activities, and various approaches have been devised: in central Africa national control projects are being implemented under an initiative involving 10 countries; in west Africa projects are being launched within the framework of the onchocerciasis control programme; and in south-east Africa surveillance and control involving eight countries has been promoted through a regional tsetse control programme supported by the European Community.
14.38 A joint FAO/WHO project for training in trypanosomiasis control to support sustainable
THE WORK OF WHO 1992-1993
agricultural development should provide an institutional framework for training in this field, complementing the training dispensed by WHO at national level. Training materials such as films, manuals and modules have been prepared for use in Chad, Congo, Uganda and other countries.
14.39 To strengthen surveillance and control, WHO has set up a sleeping sickness epidemiological "observatory" which will assess disease prevalence, the extent of foci, patient status, drug availability and use, vector occurrence and distribution, and current methods for and progress in vector control. Geographical information systems greatly facilitate analysis of epidemiological and managerial data collected in the field and allow effective programme management.
14.40 As in past years a JOlllt FAO/OAU/ WHO training seminar was held (Kampala, October 1993 ), fostering an exchange of views and maintaining a high level of national consciousness about the risk of sleeping sickness epidemics as experienced recently by Sudan, Uganda and Zaire.
14 41 The establishment of a WHO revolving fund with support from the Netherlands has allowed rapid provision of standardized equipment, material, reagents, test kits and drugs to national programmes. The annual donation by RhonePoulenc (France) of 85 000 ampoules of pentamidine for the treatment of early stage sleeping sickness was a major contribution from the private sector. Other contributions have been made by nongovernmental organizations, such as Medecins sans Frontieres in northern Uganda, and Fometro of Belgium which supplied 10 000 ampoules of eflornithine for the treatment of late stage sleeping sickness cases resistant to melarsoprol.
Dengue
14 42 The frequency of dengue epidemics has increased significantly in the past decade, and dengue and dengue haemorrhagic fever epidemics now threaten two-fifths of the world's population, or approximately 2000 million people living in urban areas in 100 countries in Africa, the Americas, Asia and the Pacific, causing millions of cases annually with thousands of deaths. An unknown number of people are also at risk in rural areas of China, India, Indonesia, Myanmar and Thailand. In May 1993 the Health Assembly
96
adopted resolution WHA46.31 recognizing that dengue, dengue haemorrhagic fever and dengue shock syndrome are threatening lives and wellbeing in a large proportion of populations in tropical regions and confirming that the prevention and control of these conditions should be among the priorities of WHO. The resolution called for the establishment of strategies to contain the spread and increasing incidence of the diseases in a manner sustainable by countries.
Disease vector control
14.43 As from May 1993 the University Sains Malaysia undertook, on WHO's behalf, the preparation of insecticide-impregnated papers and solutions and the storage and dispatch of material for monitoring the insecticide susceptibility of disease vectors, while WHO continued to coordinate the activities and to maintain a global database on this subject.
14 44 The WHO pesticides evaluation scheme (WHOPES), in operation since 1982, initiated new procedures to facilitate contributions by the national authorities and by industry in the evaluation of pesticide products and formulations for use in tropical disease vector control. Under the scheme, the Organization, through its collaborating centres in Gembloux (Belgium) and Atlanta (USA), promoted research on pesticide formulations and the setting of specifications, particularly by means of collaborative studies with industry to design methods for analysis of insecticides in conjunction with the Collaborative International Pesticide Analytical Council; routine analysis of samples of pesticides intended for national disease control programmes to ensure compliance with WHO specifications; and development of standardized chemical, physical and biological assays for the analysis of selected insecticides used in impregnation of nets and traps, including bednets. During the biennium WHO PES field trials on 11 chemicals, produced by seven pesticide manufacturers, were conducted in 14 countries of Africa, South-East Asia and the Western Pacific. Different formulations and types of application were evaluated, including impregnation of nets and traps, indoor residual spraying and ultra-low-volume application, against the vectors of African trypanosomiasis, arboviral diseases and malaria. WHO's 1985 specifications for public health pesticides were revised and produced in a new format suitable

DISEASE PREVENTION AND CONTROL
for frequent updating. Following extensive review by FAO and experts from industry, guideline specifications for household pesticides were prepared for joint publication by FAO and WHO.
14.45 The Organization promoted personal protection measures, particularly the use of insecticide-impregnated materials for bednets and curtains. Pre-impregnated bednets are now commercially available, and WHO tested their efficacy in 1993 under field conditions in collaboration with regional organizations. Developed with the assistance of WHO, insecticide-treated bednets are now being used in national malaria control programmes in Benin, Burundi, Cameroon, Cote d'Ivoire and other countries. To contain malaria epidemics, large-scale vector control operations were carried out in refugee camps in Rwanda in 1993, and WHO provided guidance on the use of insecticide-treated bednets in refugee camps in Bangladesh, Kenya and Mauritania. In Ethiopia WHO was involved in the reorientation and decentralization of national vector control programmes to suit local epidemiological conditions.
14.46 A study group on the technical, operational and managerial aspects of vector control for malaria and other diseases, including dengue, was organized in November 1993.
14.47 Molluscicide use has continued to decline owing to the rising cost of purchasing and delivering chemical molluscicides and training personnel to use them. In 1992 WHO issued a document on mollusciciding in schistosomiasis control, 1 emphasizing that the selective and appropriate use of molluscicides has a role in control, and providing practical guidelines for their application and for monitoring of their effects.
14 48 Large-scale control of the tsetse fly by trapping vectors of trypanosomiasis was successfully carried out in Uganda. In the case of sandflies, the diversity of ecological and epidemiological entities means that vector control measures have to be very specific. Insecticide-spraying was applied in termite hills in Kenya against Phlebotomus martini, and in acacia woodlands in Sudan against P. orientalis. As regards leishmaniasis, control of the vector was frequently a
1 Document WHO/SCHIST0/92.107.
97
by-product of antimalaria operations; for indoor residual spraying, several insecticides were used.
Leprosy
14.49 Good progress was again made against leprosy during the biennium. The disease burden was reduced by more than 40%; estimated cases decreased from 5.5 million to 3.1 million and registered cases from 3.2 million to 1.9 million. In all, over the last eight years, 4.3 million patients have been cured through multidrug therapy, with a cumulative coverage of 85% (see Table 14.2). However, progress in introducing this therapy in the WHO regions has been rather uneven (see Figure 14.6 ), the highest levels of coverage being achieved in the Western Pacific (97%) and South-East Asia (88%), and the lowest in the Americas (46%).
14 50 Health Assembly resolution WHA44.9 calling for the elimination of leprosy as a public health problem by the year 2000 generated a wholehearted response from the main countries where the disease is endemic, which pledged increased political commitment and priority for leprosy control. With support from WHO, countries have been able to formulate national elimination strategies and plans of action. The international donor community, particularly the member associations of the International Federation of Anti-Leprosy Associations as well as the
Table 14.2 leprosy situation, 1985 and 1993
1985 1993
Number of affected countries 124 87
Estimated cases 10-12 million 3 I mill1on
Reg1stered cases 54 m1ll1on I 9 m1ll1on
New cases per year na 650 000
Cumulative total of pat1ents cured through mult1drug therapy 9 000 4.3 m1ll1on
Cumulative coverage of multidrug therapy I 6% 85%
Global reduction in prevalence over the last eight years 64%
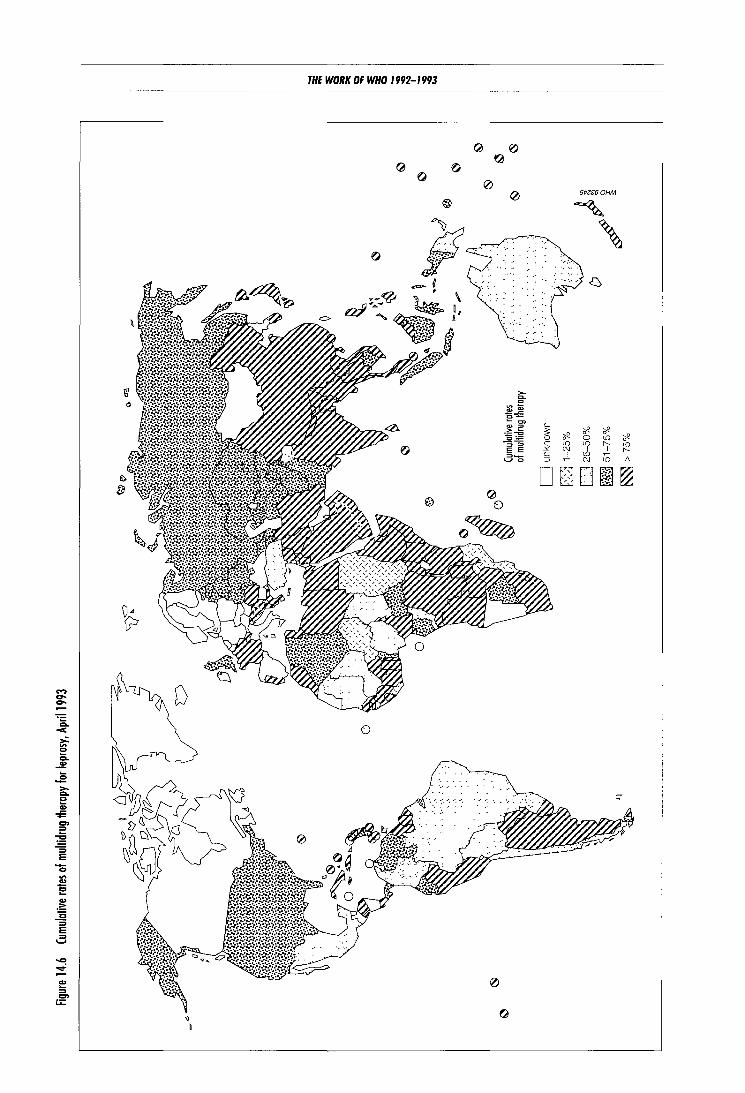
<)
b
THE WORK OF WHO 1992-1993
QJ 0
0
0
@
QJ Ql(')
0 e; St>6S60HM
' ' D

DISEASE PREVENTION AND CONTROL
Sasakawa Foundation, continued to provide substantial support to countries amounting to more than$ 80 million per year. WHO is closely collaborating with nongovernmental and other organizations particularly at country level, so that the goal of elimination can be attained.
14.51 WHO's working group on leprosy control, established in 1991, continued to oversee activities, in which nongovernmental organizations increased their participation. The strategy of targeting high-priority countries is most appropriate for leprosy in view of the very uneven distribution of the disease; in fact, one country (India) contributes 52% of all estimated cases in the world and five others (Bangladesh, Brazil, Indonesia, Myanmar, Nigeria) a further 27%. The working group endorsed the global strategy in July 1993 and countries are already preparing revised action plans based on it. WHO continued to assist in preparing plans of action for applying multidrug therapy (Indonesia, Madagascar, Nigeria, Sudan) and in carrying out independent evaluations of programmes (China, India, Myanmar, VietNam). Coordination of activities between ministries of health, nongovernmental organizations and WHO is steadily improving in a number of countries, sometimes through formal tripartite agreements (Papua New Guinea, T ogo ).
14 52 Improved monitoring and evaluation has made it possible to produce half-yearly statistics on the leprosy situation and coverage with multidrug therapy, to update case estimates for countries annually, and to identify unrealistic data on registered cases. In some countries case registers were reviewed in order to remove inactive and non-existent cases (Brazil, Nigeria). WHO promoted national conferences on leprosy to increase awareness of the disease and promote control strategies (Brazil, Egypt, Islamic Republic of Iran).
14 53 While the number of leprosy sufferers (i.e., patients in need of chemotherapy) is steadily declining, the number of people disabled as a result of the disease is not showing a similar decline because multidrug therapy has no direct impact on disability. WHO therefore promotes the prevention and management of disabilities within leprosy control; and a manual for health workers on this subject was published.1
1 Srinivasan H. Prevention of dtsabthttes in patients with leprosy: a practtcal guide. Geneva, World Health Orgamzation, 1993.
99
14 54 WHO continued to support the training of managers in leprosy control through the provision of training modules and the organization of national workshops. The modules were revised in 1993, based on experience over a twoyear period. Workshops were conducted in 14 countries in 1992-1993 for a total of 322 participants.
14.55 WHO continued to promote health systems research in leprosy to facilitate problemsolving at local level. For this purpose two workshops were held in Brazil and Thailand, and these activities demonstrated the value of the WHO training modules. A task force for health systems research in leprosy met in 1992 and 1993 to review proposals emanating from the workshops.
Tropical disease research
14 56 The prime responsibility of the UNDP/ World Bank/WHO Special Programme for Research and Training in Tropical Diseases is for research, whereas that of the WHO Division of Control of Tropical Diseases is for control. During the biennium the Special Programme gave particular emphasis to product development and applied field research. It also undertook applied field research on the subject of women and tropical diseases, for example, dealing with factors affecting women's use of community health services, self-medication practices, and sex differences in the clinical manifestations and impact of the diseases; this activity will be jointly managed with the Division of Control of Tropical Diseases. The Special Programme's dual roles of developing better tools against six groups of tropical diseases, and of improving endemic countries' capacity for relevant research, were increasingly combined.
14 57 Malaria. Three steps were taken to improve treatment of cerebral malaria: phase Ill clinical trials of the drug artemether were begun in six centres; a clinical trial of an anti-TNF (tumour necrosis factor) monoclonal antibody was undertaken in Gambia; and studies of the toxicology of artemether injection were completed. Phase I studies in healthy volunteers with the related compound arteether showed injections to be safe and well tolerated. A randomized, placebo-controlled double-blind field trial of the Colombian SPf66 malaria candidate vaccine was begun in children in the United Republic of Tanzania.

THE WORk OF WHO 1992-1993
14 58 Studies of insecticide-treated bednets, which have proved very successful in reducing child mortality in Gambia, were extended to three other African countries; and research to devise methods for genetic manipulation of mosquito vectors was undertaken, with the longterm aim of reducing their ability to transmit malaria parasites.
14.59 Schistosomiasis. Phase I studies of combinations of praziquantel and albendazole (an antihelminthic) were completed in Sudan, and phase 11/111 studies begun in China, Kenya and Philippines. Preliminary indications were that the combination is safe and effective. In vaccine development, negotiations with manufacturers on extending and improving the production of several antigens neared completion. An independent standard testing facility was set up, and preparations began for phase I trials of some promising schistosome antigens.
14.60 Lymphatic filariasis and onchocerciasis. lvermectin, which has been successfully used in treating onchocerciasis, was tested against lymphatic filariasis. Clinical trials in nine endemic countries/territories1 showed that a single dose of 400 micrograms of ivermectin/kg of body weight suppressed microfilarial production in lymphatic filariasis for over a year, with equal efficacy at one year to a 6 mg/kg dose of the traditional drug diethylcarbamazine citrate (DEC). But a combination of low-dose ivermectin (20 micrograms/kg) with a 6 mg/kg dose of DEC gave the best overall results at one year. At the same time, ivermectin was shown to produce fewer side-effects.
14 61 Operational studies on the use of Bacillus sphaericus for control of the mosquito vector Culex quinquefasciatus were launched in Brazil, Cameroon, India, Sri Lanka and United Republic ofT anzania.
14.62 Yearly mass treatments for onchocerciasis with ivermectin were shown to improve anterior segment eye lesions and to reduce the incidence of posterior segment lesions (and thus optic nerve disease). Moreover, no evidence was found that ivermectin induced any life-threatening reactions or had adverse effects when used in preg-
1 Brazil, French Polynesia, Ha1t1, lnd1a, lndones1a, Kenya, Malaysia, Papua New Gumea, Sn Lanka.
100
nancy. The drug also improved lichenform skin lesions. Annual mass treatment was found to be acceptable to affected communities. Large-scale use of six-monthly treatment with ivermectin in Guatemala showed that the drug on its own was capable of interrupting transmission in the study area, and data from Ghana indicated that repeated treatment might help reduce transmission in parts of Africa.
14.63 DNA probes were developed to detect and differentiate between forest (less blinding) and savanna (more blinding) Onchocerca, and between human and animal parasites, and are now in routine use in the Onchocerciasis Control Programme in West Africa.
14.64 Operational research in Nigeria demonstrated the effectiveness and accuracy of simple visual assessment of skin nodules to identify high-risk communities in need of broad-based ivermectin treatment, thus reducing reliance on painful and risky skin-snipping.
1465 Leprosy. Follow-up of 14 000 personyears of multidrug therapy revealed only four cases of relapse with skin lesions. Tests of potentially more rapid treatments including ofloxacin were begun in 15 centres. A comparative study was started in India of BCG, BCG with heat-killed Mycobacterium leprae, the Indian Cancer Research Centre bacillus, and the Indian bacterium M. w. Preliminary results of a vaccine trial in Venezuela showed no substantial difference between the protection offered by BCG and BCG with heat-killed M. leprae. Cloning and sequencing of the M. leprae genome began.
14.66 African trypanosomiasis. In 1993 Uganda became the first African country to register eflornithine, the new drug for the gambiense form of African trypanosomiasis which had previously been registered in the United States of America and the European Community. The antigen-ELISA test was modified as a "Card indirect agglutination test for trypanosomiasis" (CIA TT). Preliminary field trials showed this test to be highly specific and sensitive for both the gambiense and the rhodesiense forms of African trypanosomiasis.
14.67 Chagas disease. A joint initiative for the elimination of Chagas disease transmission by Triatoma infestans was launched in late 1993 by Argentina, Brazil, Bolivia, Chile, Paraguay and

DISEASE PREVENTION AND CONTROL
Uruguay. Two types of blood screening kit were manufactured in Buenos Aires using molecularly defined antigens, and field trials were begun for screening blood bank products infected by Trypanosoma cruzi.
14.68 Leishmaniasis. A field trial in Venezuela of killed Leishmania (L. braziliensis and L. mexicana ), both separate and combined with BCG vaccine, was undertaken in cooperation with the United States National Institutes of Health, and is due to be completed in 1994. Clinical phase I-II studies of killed L. major with BCG were begun in the Islamic Republic of Iran, and of a single-strain "Mayrinck vaccine" (L. amazonensis) in Brazil.
14.69 Clinical trials started of lipid-associated amphotericin B against visceral and mucosal leishmaniasis, and a randomized, double-blind controlled trial of allopurinol began m Colombia.
Social research
14.70 Studies in Ghana and Nigeria showed that pregnant adolescent girls in whom the malaria mortality risk is particularly high did not attend malaria clinics for treatment because their parents were ashamed of public recognition of their pregnancy. In Colombia a study showed that women with malaria wait longer than other members of their families before seeking treatment, and suffer worse consequences from the disease. A multi-country study in Africa showed that school questionnaires could be used for the rapid identification of communities suffering high levels of urinary schistosomiasis, at one-thirtieth of the cost of egg examination by mobile teams. Several studies also showed significant gender differences in reporting of urinary schistosomiasis - because among girls it was wrongly viewed as a sexually transmitted disease. A study was launched in seven countries in Africa and Asia to determine the social and economic importance of lymphatic filariasis. An important component of these studies will be the clinical investigation of genital manifestations of the disease in women. In one area of Nigeria communities considered the skin manifestations of onchocerciasis to be more important than blindness, because of their effect on relationships and marriage prospects.
101
Research capability strengthening
14.71 Nine new grants were awarded for strengthening the capacity of institutions in operational research on malaria, and for research training in social sciences and economics. Research training grants were awarded to 111 young scientists including 34 women. Fourteen institutions submitted final reports on their use of institution-strengthening grants, while 45 others continued to receive grants. The award of small grants proved very successful in supporting short-term research projects. In the Eastern Mediterranean nine grants were awarded for research on leishmaniasis and 14 for research on schistosomiasis in 1993.
Diarrhoeal diseases
14.72 In 1990, the latest year for which data are readily available, 12.9 million children under the age of five died in developing countries, and nearly a quarter of them from diarrhoea; preventing these deaths is a task of high priority for WHO.
14 73 Training activities emphasized case management and better programme management. In 1992 WHO's revised guidelines for conducting clinical training courses at health centres and small hospitals' were widely used by national programmes for the first time, reflecting a trend towards decentralizing case management training. Over 1000 courses - more than triple the number in the previous biennium - were held, mainly in the upwards of 400 diarrhoea training units in 80 countries throughout the world. The Organization supported 38 national training courses for programme managers in the largest countries (bringing the total since 1987 to 122), and nearly 150 courses for first-level supervisors were held (a total of about 630 courses since their revision in 1987).
14 74 In an attempt to complement in-service training of physicians and eventually reduce the need for it, WHO has for some time been involved in compiling instructional material on diarrhoea! diseases for use in medical schools.
1 Document CDD/SER/90.2 Rev.1 1992.

THE WOilK OF WHO 1992- 1993
After successful field trials, the full series appeared in 1992 in the form of a manual' and four guides.2 Materials for distance learning, training at nursing and paramedical schools, and training of pharmacists and other purveyors of pharmaceutical products were also prepared.
14.75 In 1992 WHO devised a new, more databased and problem-specific method for reviewing progress in national programmes, known as "focused programme review". The aim is to identify constraints o.n progress and then design specific activities to deal with them. During 1992 and 1993 th.is method was successfully applied in 13 countries, while six carried out other types of programme reVlew.
14.76 WHO's 1990 monograph on the rational use of drugs in the management of acute diarrhoea in children was well received by responsible national authorities, and was translated into Bengali, Chinese, French, Spanish and Viemamese; since its publication a number of countries have banned or restricted the use of antidiarrhoeal drugs. The provision of oral rehydration salts (ORS) remained a key clement in the control of diarrhoea in children; at the end of 1992, the global access rate (the proportion of the population with a regular supply of ORS in their community) was estimated to be 73%, 5% higher than at the end of 1991.
14.77 Despite effective case management training in many countries, the essential function of advising a mother on how to care for her child at home during an episode of diarrhoea remains one of the least practised features of case management. To help resolve this problem, WHO .issued a guide for health workers on counselling mothers;3 it will be used in clinical management training courses. The O rganization also completed a guide for national programme managers on the effective use of radio, which is vital for communication in developing countries.
14.78 There is now conclusive evidence that breast-feeding gives significant protection against illness and death associated with diar-
' Readings on diarrhoea: student manual. Geneva. World Health Orgonizo· lion, 1992.
7 Uocuments COD/SER/93.1; COO/SfR/93.2; CDO/SER/93.3; COD/SER/ 93.4
>Document C00/93.1.
102
rhoea in infants, and also minimizes its adverse nutritional effects. Epidemiological studies have shown that exdusive breast-feeding in the first four to six months of life and continued breastfeeding until the end of the first year are associated with milder forms and lower incidence of diarrhoea and with lower mortality. To ensure appropriate support from health workers - often the main source of advice to breast-feeding mothers - WHO and UNICEF produced a training package on lactation management.~
14.79 The global task force on cholera control continued to coordinate WHO support to affected countr ies. Guidelines were issued5 and control efforts were pursued in all the countries concerned, particularly in Africa, where there were many more deaths than in South America. In 1993 the Organization planned a series of steps to support governments in improving the situation in southern Africa, notably by increasing health workers' case management skills; raising the capacity of district health teams to prepare for, detect and respond to outbreaks; strengthening the capacity of laboratories to confirm suspected cases; developing policies to reduce the disruptive aspects of cholera epidemics on trade and tourism; and determining long-term infrastructural needs for food safety, water and sanitation systems, the lack of which is the main cause of cholera. A resurgence of the disease in the Eastern Mediterranean elicited increased technical and financial support to the countries concerned. In South-East Asia a new strain of cholera, designated Vibrio cholerae 0139,
A demonstration of how to chlorinate woler during o cholera out· break in Peru.
• Documents WHO/CDR/ 93.4; WHO/ CDR/93. 5; WHO/ CDR/ 93.6. 1 Guidelines for cltolora control. Geneva, Wo1ld Health 01ganizotion, 1993.

DISEASE PREVENTION AND CONTROL
emerged during the biennium to cause major epidemics and largely replaced Vibrio cholerae 01 as the predominant strain in several countries.
14.80 WHO continued to support research for the development and evaluation of new or improved methods of treatment and prevention of diarrhoea; 35 new projects received support during the biennium, bringing the total number of WHO-sponsored projects to 453. Half of these new projects related to breast-feeding practices and nutrition. The search for better ORS formulations continued: an outpatient study was conducted in Bangladesh to compare treatment of outpatients with rice-based and glucose-based ORS solutions; and two large studies in Egypt and Pakistan showed that standard WHO ORS solution is as efficacious as rice-based solution for treating diarrhoea in infants and children. Other research included a study among outpatients of the impact of zinc supplementation on persistent diarrhoea and the testing in six countries of a model for clinical management of the condition. A WHO-supported study in Bangladesh demonstrated that breast-feeding is of particular importance in the prevention of shigellosis among young and malnourished children. Other studies showed that for infants with diarrhoea under six months of age fed exclusively on animal milk or formula, these foods do not normally need to be diluted and should be given in full strength as soon as dehydration has been corrected. In Brazil the use of dummies was found to be associated with increased risk of early termination of breast-feeding.
14.81 The Organization continued to support research to evaluate candidate vaccines for the most important causes of acute diarrhoea, including rotavirus infection, cholera, shigellosis and disease caused by enterotoxigenic Escherichia coli. An evaluation of the efficacy of tetravalent rhesus-human rotavirus vaccine was completed in Brazil, and a large trial involving a higher dose of the vaccine was initiated in Venezuela. A trial of the live oral cholera vaccine CVD-1 03 HgR was begun in Indonesia.
14.82 It is generally recognized that WHO's recommendations on diarrhoea case management are much better understood when they are formulated using local terms and concepts. A protocol was therefore developed for the compilation of descriptive data on beliefs and practices regarding diarrhoea to be used in the implementation of national programmes.
103
Acute respiratory infections
14.83 Acute respiratory infections, especially pneumonia, either directly caused or contributed to about one-third of the 12.9 million deaths in children under five in developing countries in 1990. The central strategy for reducing this death rate is case management using a simple standard protocol for the diagnosis and treatment of pneumonia.
14.84 Training is one of the main channels through which standard case management can be introduced into primary health care. A new training module on outpatient case management was used for the first time in English at an interregional course in Thailand in 1992, and was subsequently translated into French and Spanish. After two successful tests in Kenya in 1992, a course for training community health workers was made available to national programmes; it includes a guide for cultural and technical adaptation of case management methods. Preparation of training materials for inpatient care was started.
14.85 In courses using materials produced in previous years, 27 4 officers were trained in programme management and about 32 000 physicians and other health workers in case management. By the end of 1993, 192 acute respiratory infection training units had been established in 28 countries.
14.86 Childhood immunization against measles and pertussis makes an important contribution to the reduction of deaths associated with acute respiratory infections. In order to enlarge the arsenal of preventive measures, WHO, in association with the London School of Hygiene and Tropical Medicine, commissioned a series of reviews to determine effective and feasible interventions for reducing morbidity from pneumonia in children in developing countries. The impact of vitamin A supplementation on childhood pneumonia was one of the subjects investigated; and data from 12 studies were analysed at a meeting in March 1992.1 Groups of experts also met in March 1992 to analyse the first round of intervention reviews and in March 1993 to analyse the second round.2 They concluded that some threequarters of all pneumonia deaths result from bacterial infection; that vitamin A supplementation
1 Document WHO/CDR/93.2. 2 Prevention of pneumonia 1n children. Lancet, 1993,341:821-822.

THE WORK OF WHO 1992-1993
has no beneficial impact on the mortality of pneumonia not associated with measles; that antibiotic treatment of upper respiratory infection plays no role in the prevention of acute lower respiratory tract infections; and that pneumococcal conjugate vaccine, if it proves effective, could have a substantial impact in preventing pneumoma.
14.87 One important target is the establishment by 1995 of acute respiratory disease control programmes in all countries with an infant mortality rate greater than 40 per 1000 live births. Among the 88 countries falling into this category, 56 ( 64 %) had control programmes in at least one major administrative division by the end of 1993. Since progress is relatively slow in sub-Saharan Africa because of other priorities, more extrabudgetary funds were provided in that region. WHO organized a meeting with representatives of UNICEF and 15 nongovernmental organizations to plan joint action for the control of acute respiratory infections in Africa (Trieste, Italy, December 1992) and a workshop to train African consultants in planning, evaluation and problem-solving (Cotonou, Benin, November 1993). These activities were part of WHO's strategy of giving more direct technical support to national programmes.
14 88 During the biennium WHO developed a prototype home-care card to assist health workers to improve communication with families. The results obtained by applying WHO's recently completed "focused ethnographic study protocol" are used to adapt messages contained in the home-care card and to choose appropriate terminology for use at local level. As recommended at a meeting in May 1992, new guidelines are being developed to assist programme managers in applying the results of ethnographic studies in programme planning and implementation. A workshop was organized for ethnographers from several African countries in 1993.
14.89 WHO developed a survey instrument for evaluating case management practices, including communication with families, at first-level health facilities; it was field-tested in 1992 in India, Papua New Guinea, Philippines and Swaziland, and completed in 1993. To obtain information on home management of children with acute respiratory infections, including care-seeking practices, the Organization devised a procedure for household surveys that also collect information on diarrhoea! diseases and breast-feeding.
104
14.90 Review papers on overlap in the clinical presentation and treatment of malaria and pneumonia in children, 1 the use of bronchodilators,Z and the management of fever in young children with acute respiratory infections3 were issued, as was the first volume of an annotated bibliography of selected articles on pneumonia and related infections in young children.4 Six issues of ARI news were published by the Appropriate Health Resources and Technologies Action Group (United Kingdom) in collaboration with WHO.
14 91 On completion of a multicentre study on the clinical signs and etiological agents of pneumonia, sepsis and meningitis in infants under three months of age, conducted in Ethiopia, Gambia, Papua New Guinea and Philippines, a meeting of the principal investigators and consultants was held to analyse the results (Beijing, November 1993). The etiology of pneumonia in malnourished children was studied in Gambia, and the clinical significance of in vitro resistance of pneumonia-causing bacteria to cotrimoxazole or amoxycillin in Pakistan. WHO collaborated with other agencies in organizing a field trial of Haemophilus influenzae type b vaccine in Gambia. A manual on the monitoring of antimicrobial resistance of Streptococcus pneumoniae and H. influenzae was field-tested in Egypt, Pakistan, Thailand and Viet N am. In Guatemala support was given in working out procedures for monitoring indoor air pollution from burning biomass fuels and for using behavioural methods to measure the duration of exposure of mothers and their infants to smoke.
14.92 In 1992 WHO and UNICEF began cooperating in the design of an integrated approach to the management of the lethal scourges- pneumonia, diarrhoea, malaria, measles and malnutrition -which cause almost three-quarters of deaths among children under five years in developing countries. The integrated approach is summarized in a set of case management charts for the health worker, entitled: "Assess the child and classify the illness", "Treat the child" and "Advise the mother". A separate chart deals with infants under two months of age. The new ap-
1 Document WHO/ARI/92 23- WHO/MAL/92.1 065. 2 Document WHO/ARI/93.29. 3 Document WHO/ARI/93.30. 4 Document WHO/ARI/93 27.

DISEASE PREVENTION AND CONTROL
proach facilitates case management of these dangerous conditions in children in outpatient settings, increases efficiency in training and the organization of services, and stresses the importance of "clinical encounters" to promote immunization and improve infant feeding.
Tuberculosis
14.93 One-third of the world's population is infected with the bacillus Mycobacterium tuberculosis, and approximately one in ten of those infected people will develop active tuberculosis at some time. In 1992 there were over eight million new cases of the disease; the number of sufferers will continue to increase and nearly 90 million new cases are likely to occur in the period 1990-1999. Most cases and more than 98% of deaths occur in the developing world, but the incidence of the disease is also increasing for the first time in many decades in some countries in Europe and North America.
14.94 Tuberculosis is now the world's leading cause of death from a single infectious agent and accounts for over a quarter of avoidable deaths among adults. An estimated 2.9 million persons died of it in 1992: 1.2 million in South-East Asia, 679 000 in the Western Pacific, 493 000 in Africa and over half a million in the rest of the world. Deaths from the disease are expected to increase to over 3.5 million per annum by the year 2000. Moreover, the epidemic has become more difficult to control because of the emergence of multidrug-resistant strains of the bacillus and because of the HIV pandemic. For instance, between 1985 and 1991 the annual number of tuberculosis cases more than doubled in Malawi and nearly tripled in Zambia as a consequence of HIV infection.
14.95 In 1993 the Health Assembly, recognizing the seriousness of the situation, called upon Member States to take rapid action regarding case detection and registration, short-course therapy, and supplies of antituberculosis drugs (resolution WHA46.36). By the end of the biennium recognition by Member States of the magnitude of the problem was beginning to result in the mobilization of additional national and external resources to improve national programmes and intensify research. WHO's objectives for global control of tuberculosis are to treat successfully 85% of detected smear-posi-
105
tive cases and to detect 70% of infectious cases by the year 2000. This can be achieved by the use of WHO recommended short-course chemotherapy, with supervision of drug consumption and use of recording and reporting systems which meet WHO's criteria. As districts achieve high cure rates, case detection activities can be intensified to find remaining cases.
14.96 During the biennium WHO issued guidelines on tuberculosis treatment1 and provided technical support to national control programmes in over 30 of the most seriously-affected countries. In China detailed monitoring was carried out in a large project supported by the World Bank. A combined tuberculosis and leprosy control project was initiated in Bangladesh in 1993, also with World Bank support. Reviews of national tuberculosis programmes in India and Zimbabwe in 1992 resulted in revision of national policies and preparation of projects for external finance by the World Bank and other institutions. One outcome of technical support to Guinea was the compilation of a national tuberculosis control manual applicable to many countries. Six countries in the Americas and one in the Western Pacific carried out evaluations of their programmes with WHO support. New methods of programme review and evaluation were devised in the light of experience gained in these countries.
14.97 Training materials for middle-level programme managers and treatment guidelines for national programmes were prepared, tested, refined, issued in various languages, and used in workshops at global, regional or national level in several countries.2 Guidelines were produced for setting up national control programmes and international reference laboratories to monitor drug-resistant tuberculosis.
14.98 A WHO information base was established to monitor the status of national tuberculosis programmes. Based on information from 139 countries and territories surveyed, it was found that less than 40% routinely used short-course chemotherapy in sputum-positive cases of pulmonary tuberculosis. Half reported drug shortages in 1991, over half were partially or fully
1 Treatment of tuberculosis. guidelines for natiOnal programmes. Geneva, World Health Organization, 1993
2 Bangladesh, Egypt, Guinea, lnd1a, N1caragua, Philippines, Un1ted Republic of Tanzania, Z1mbabwe.

THE WORK OF WHO 1992-1993
dependent on donors to meet needs for drugs, and more than a third were uncertain whether funding would be sufficient to meet their current year's needs. Following this survey, case studies have been undertaken in eight sub-Saharan African countries to determine ways of improving their supply systems.
14 99 Research begun or under way during the biennium included studies on diagnostic methods, testing of new drugs, and trials of the operational feasibility of using isoniazid for preventive therapy in persons with HIV infection. Operational research conducted in collaboration with control programmes in Malawi, Mozambique and United Republic of Tanzania demonstrated the remarkable cost-effectiveness of short-course chemotherapy for pulmonary tuberculosis. A further study in Botswana suggests that these results are valid for middle-income developing countries.
14 lOO Research to quantify the impact of HIV infection on tuberculosis continued in the United Republic of Tanzania. Further work began in Malawi to determine the effect of HIV infection on the results of tuberculosis treatment, and also to assess the efficacy of new treatment and supervision regimens aimed at mitigating the enormous increase in workload brought about by the epidemic of combined HIV and tuberculosis infection.
14 101 The main obstacle to tuberculosis control is not lack of medical knowledge but inadequate political will. An effective and relatively inexpensive cure already exists, but it is not being widely used. In 1993 WHO therefore initiated a vigorous publicity campaign to bring the tuberculosis crisis to the attention of governments, journalists, nongovernmental organizations, and health and public interest groups. In furtherance of this campaign, an information package presenting basic facts about the disease to a non-scientific audience was widely disseminated, and the JulyAugust 1993 issue of the magazine World health was devoted entirely to tuberculosis.
Zoonoses
14.102 Rabies was a growing health problem and economic burden in many parts of Africa, the Americas and Asia, and was reported in more than 90 countries. Dog rabies was present in about 65% of infected countries and was the
106
main cause of human deaths from rabies. In Africa and Asia WHO concentrated on research on canine biology and oral immunization techniques for dogs and the promotion of appropriate strategies for the control and elimination of canine rabies. A national rabies coordinating committee was established in Nigeria, and an informal group was set up for training and research on rabies in southern and eastern Africa. Fourteen Asian countries endorsed a common strategy primarily based on parenteral vaccination of dogs.
14 103 Significant progress was made in oral vaccination of dogs and safety requirements were framed in order to reduce the risk of contact between candidate vaccines and human beings during mass vaccination campaigns. A field study was carried out to evaluate several vaccinebait delivery techniques. Discussions on requirements for the release of live rabies vaccines for oral immunization of dogs were held with a number of Asian and north African countries.
14 104 Very encouraging results were reported in those western European countries which conduct regular campaigns for oral vaccination of foxes against rabies. With the exception of a few foci, the rabies front at the end of 1993 followed approximately a line from W olin on the Baltic Sea to Trieste on the Adriatic Sea (see Figure 14.7). A meeting on rabies control in Europe (Piestany, Slovakia, October 1993) helped to strengthen scientific and field collaboration on wildlife rabies, especially between members of the Commonwealth of Independent States and other European countries.
14 105 WHO coordinated studies on canine biology in Turkey, Yemen and Zambia during 1992-1993. In the first two countries a large proportion of the dog population, whether owned or unowned, could not be captured for parenteral vaccination. In such cases oral vaccination may prove to be the only means of achieving sufficient coverage to eliminate the animal reservoir of the disease.
14106 In South-East Asia WHO provided consultants, supplies, equipment and training of health personnel and helped to organize national and regional workshops on rabies control. Support was given in particular to India, Indonesia, Nepal and Sri Lanka. In the Americas cooperation focused on strengthening national programmes for the elimination of canine rabies.
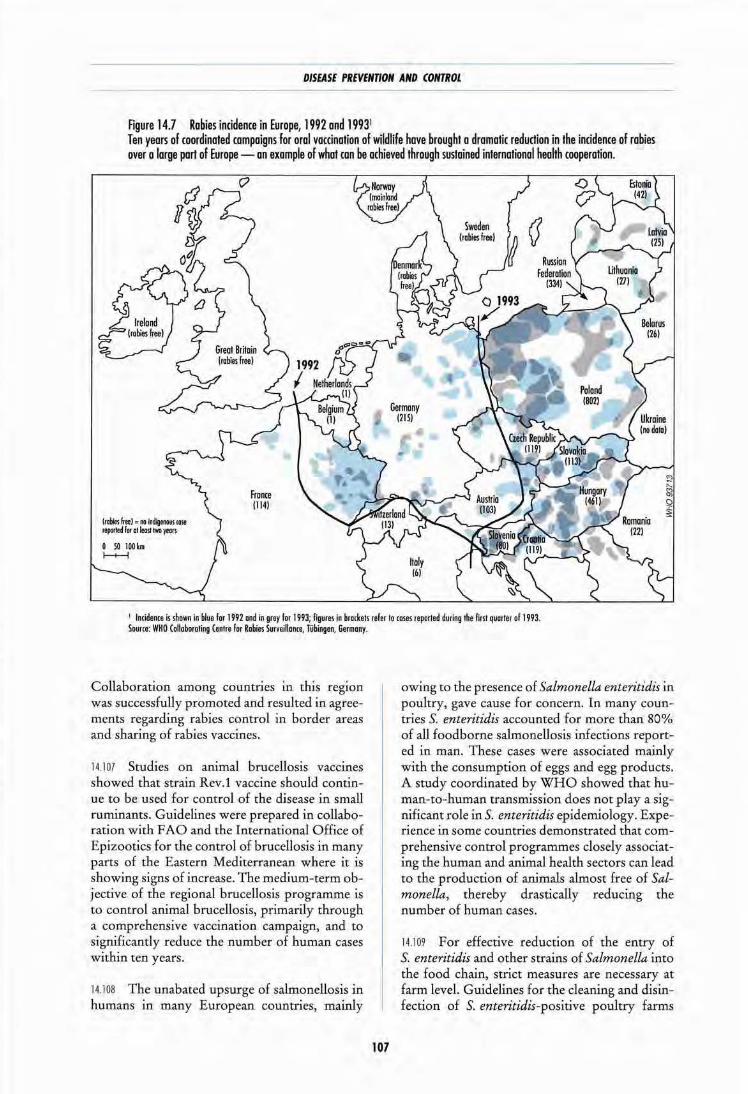
DISEASE PREVENTION AND CONTROL
Figure 14.7 Rabies incidence in Europe, 1992 and 19931
Ten years of coordinated campaigns for oral vaccination of wildlife hove brought a dramatic reduction in the incidence of rabies over a large part of Europe - on example of what can be achieved through sustained international health cooperation.
(robie! heel c 110 fcldigfi>OIIt case teporled r .. at least two )'till•
Fro nee (114)
1 Incidence is shown in blue lor 1992 and in grey I or 1993; figures in brodcets refer to coses reported during the first quorler of 1993. Source: WHO Collaboroting Centre for Robies Surveillance, Tubingen, Germany.
Collaboration among countries in this region was successfully promoted and resulted in agreements regarding rabies control in border areas and sharing of rabies vaccines.
14.107 Studies on animal brucellosis vaccines showed that strain Rev.l vaccine should continue to be used for control of the disease in small ruminants. Guidelines were prepared in collaboration with FAO and the International Office of Epizootics for the control of brucellosis in many parts of the Eastern Mediterranean where it is showing signs of increase. The medium-term objective of the regional brucellosis programme is to control animal brucellosis, primarily through a comprehensive vaccination campaign, and to significantly reduce the number of human cases within ten years.
14.108 The unabated upsurge of salmonellosis in humans in many European countries, mainly
107
owing to the presence of Salmonella enteritidis .in poultry, gave cause for concern. In many countries S. enteritidis accounted for more than 80% of all foodborne salmonellosis infections reported in man. These cases were associated mainly with the consumption of eggs and egg products. A study coordinated by WHO showed that human.-to-human transmission does not play a significant role inS. enteritidis epidemiology. Experience in some countries demonstrated that comprehensive control programmes closely associating the human and animal health sectors can lead to the production of animals almost free of Salmonella, thereby drastically reducing the number of human cases.
14.109 For effective reduction of the entry of S. enteritidis and other strains of Salmonella into the food chain, strict measures are necessary at farm level. Guidelines for the cleaning and disinfection of S. enteritidis-positive poultry farms
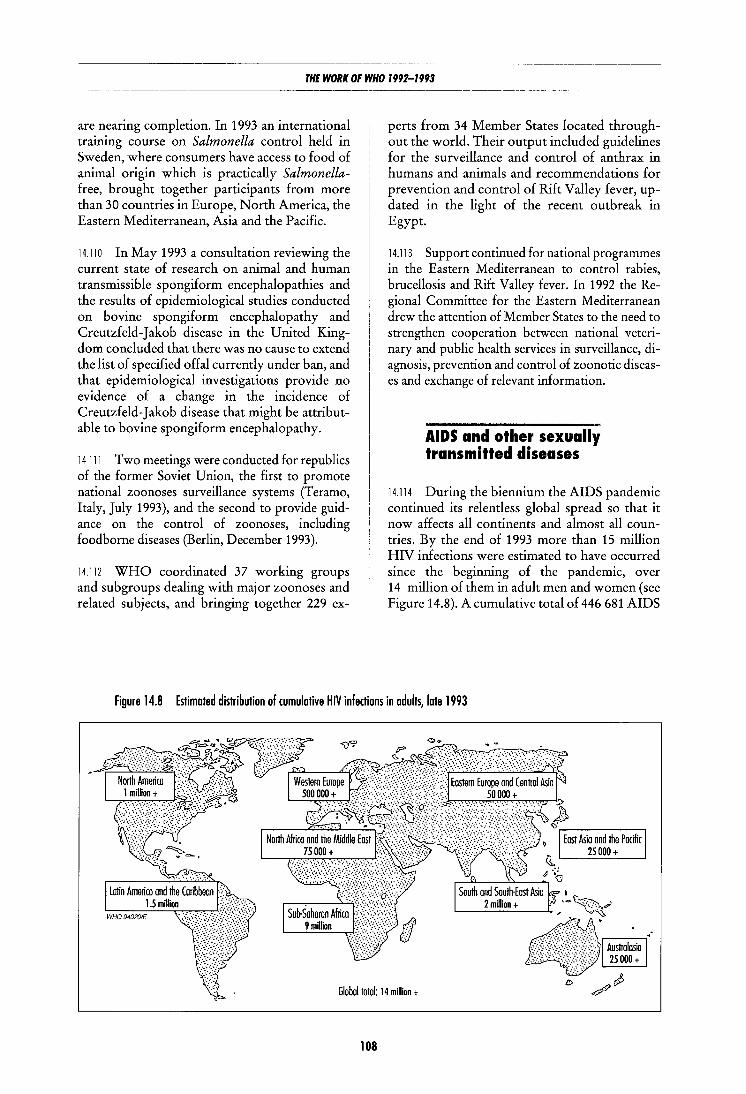
THE WORK OF WHO 1992-1993
are nearing completion. In 1993 an international training course on Salmonella control held in Sweden, where consumers have access to food of animal origin which is practically Salmonellafree, brought together participants from more than 30 countries in Europe, North America, the Eastern Mediterranean, Asia and the Pacific.
14.110 In May 1993 a consultation reviewing the current state of research on animal and human transmissible spongiform encephalopathies and the results of epidemiological studies conducted on bovine spongiform encephalopathy and Creutzfeld-Jakob disease in the United Kingdom concluded that there was no cause to extend the list of specified offal currently under ban, and that epidemiological investigations provide no evidence of a change in the incidence of Creutzfeld-Jakob disease that might be attributable to bovine spongiform encephalopathy.
14 111 Two meetings were conducted for republics of the former Soviet Union, the first to promote national zoonoses surveillance systems (T eramo, Italy, July 1993), and the second to provide guidance on the control of zoonoses, including food borne diseases (Berlin, December 1993 ).
14.112 WHO coordinated 37 working groups and subgroups dealing with major zoonoses and related subjects, and bringing together 229 ex-
perts from 34 Member States located throughout the world. Their output included guidelines for the surveillance and control of anthrax in humans and animals and recommendations for prevention and control of Rift Valley fever, updated in the light of the recent outbreak in Egypt.
14.113 Support continued for national programmes in the Eastern Mediterranean to control rabies, brucellosis and Rift Valley fever. In 1992 the Regional Committee for the Eastern Mediterranean drew the attention of Member States to the need to strengthen cooperation between national veterinary and public health services in surveillance, diagnosis, prevention and control of zoonotic diseases and exchange of relevant information.
AIDS and other sexually transmitted diseases
14.114 During the biennium the AIDS pandemic continued its relentless global spread so that it now affects all continents and almost all countries. By the end of 1993 more than 15 million HIV infections were estimated to have occurred since the beginning of the pandemic, over 14 million of them in adult men and women (see Figure 14.8). A cumulative total of 446 681 AIDS
Figure 14.8 Estimated distribution of cumulative HIV infections in adults, late 1993
Global total: 14 million +
108
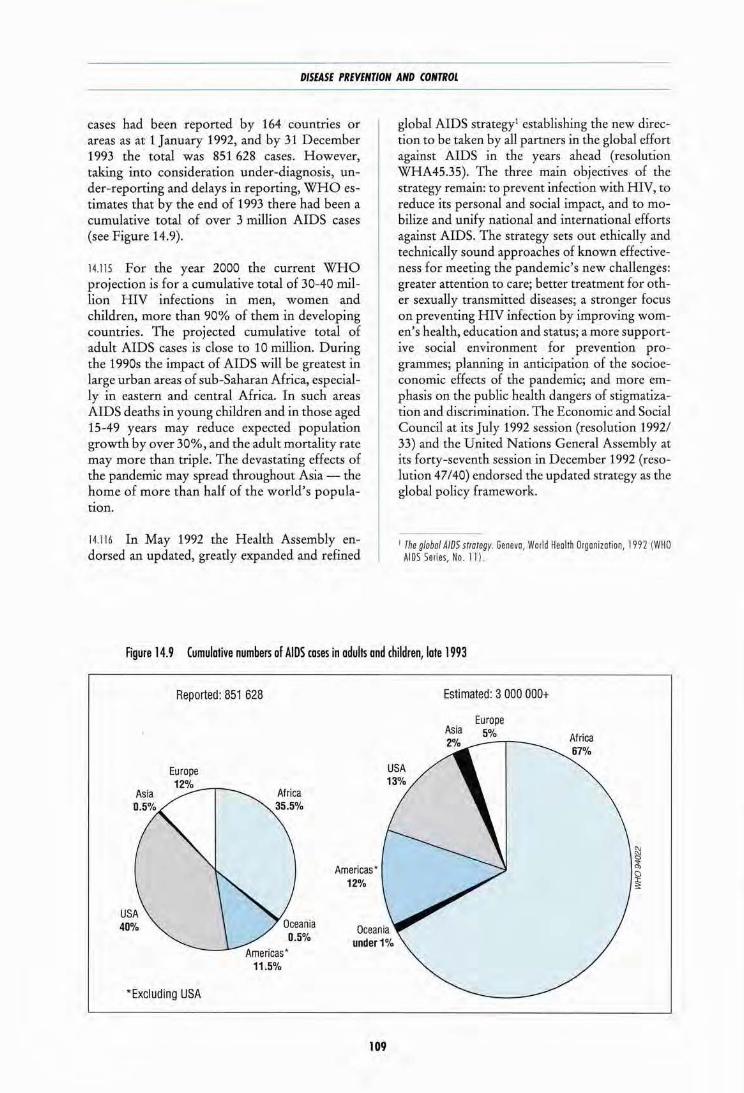
DISEASE PREVENTION AND CONTROL
cases had been reported by 164 countries or areas as at 1 January 1992, and by 31 December 1993 the total was 851 628 cases. However, taking into consideration under-diagnosis, under-reporting and delays in reporting, WHO estimates that by the end of 1993 there had been a cumulative total of over 3 million AIDS cases (see Figure 14.9).
14.115 For the year 2000 the current WHO projection is for a cumulative total of 30-40 million HIV infections in men, women and children, more than 90% of them in developing countries. The projected cumulative total of adult AIDS cases is close to 10 million. During the 1990s the impact of AIDS will be greatest in large urban areas of sub-Saharan Africa, especially in eastern and central Africa. In such areas AIDS deaths in young children and in those aged 15-49 years may reduce expected population growth by over 30%, and the adult mortality rate may more than triple. The devastating effects of the pandemic may spread throughout Asia- the home of more than half of the world's population.
14.116 In May 1992 the Health Assembly endorsed an updated, greatly expanded and refined
global AIDS strategy1 establishing the new direction to be taken by all partners in the global effort against AIDS in the years ahead (resolution WHA45.35). The three main objectives of the strategy remain: to prevent infection with HIV, to reduce its personal and social impact, and to mobilize and unify national and international efforts against AIDS. The strategy sets out ethically and technically sound approaches of known effectiveness for meeting the pandemic's new challenges: greater attention to care; better treatment for other sexually transmitted diseases; a stronger focus on preventing HIV infection by improving women's health, education and status; a more supportive social environment for prevention programmes; planning in anticipation of the socioeconomic effects of the pandemic; and more emphasis on the public health dangers of stigmatization and discrimination. The Economic and Social Council at its July 1992 session (resolution 1992/ 33) and the United Nations General Assembly at its forty-seventh session in December 1992 (resolution 47 /40) endorsed the updated strategy as the global policy framework.
I rhe global A/OS strategy. Genevo, Wodd Health Organization, 1992 (WHO AIDS Series, No. l ll
Figure 14.9 Cumulative numbers af AIDS cases in adults and children, late 1993
Reported: 851 628
"Excluding USA
Americas• 12%
109
Estimated: 3 000 000+
Europe Asia 5%

THE WORK OF WHO 1992-1993
14.117 At an extraordinary meeting in November 1992 the Management Committee of the Global Programme on AIDS recommended the establishment of a task force on HIV I AIDS coordination and proposed terms of reference and a membership of twelve divided equally among developing countries, donor countries, bodies within the United Nations system, and nongovernmental organizations. In May 1993 the Health Assembly requested the Director-General to study the feasibility and practicability of establishing a joint and cosponsored United Nations programme on HIV and AIDS, in close consultation with the executive heads ofUNDP, UNICEF, UNFPA, UNESCO and the World Bank (resolution WHA46.37). In July 1993 the Economic and Social Council expressed its full support of that resolution and called upon the executive heads to cooperate fully in the consultative process.
14.118 In order to strengthen multisectoral action with other bodies in the United Nations system, the Organization collaborated with UNDP in mobilizing external resources for country programmes within the framework of the WHO/UNDP alliance to combat AIDS; with UNFP A through participation in studies on condom requirements and logistics management for the 1990s; with the World Bank in the preparation of its 1993 report, 1 through the provision of estimates and projections of HIV and AIDS incidence and prevalence, global estimates of the cost of prevention and care, and estimates of the possible impact on HIV transmission of preventive activities worldwide; with UNESCO in issuing a guide for health education in schools, for use by policy-makers and education planners;2 and with UNICEF in the joint publication of the booklet "Living with AIDS in the community", which was adapted for general use from the original produced for Uganda by the AIDS Support Organisation, the national AIDS programme, UNICEF and WHO.
14.119 WHO continued to strengthen national AIDS programmes by providing technical support through its regional offices. Steps were taken to formulate second-generation medium-term plans for national AIDS programmes that call for a multisectoral approach, bearing in mind the in-
1 World Bank World development report 1993. investmg m health New York, Oxford University Press, 1993.
2 School health educatiOn to prevent AIDS and sexually transmitted d1seas· es Geneva, World Health OrganiZatiOn, 1992 (WHO AIDS Ser1es, No. 10).
110
creasing numbers of interested parties involved in AIDS activities in countries. It is of particular concern that while the number of countries having a medium-term plan financially supported by WHO increased approximately five-fold between early 1988 and the end of 1992, the amount of resources allocated to national AIDS programmes during that time (including multibilateral contributions) has remained about the same. With the involvement of a growing number of donors from different sectors in national AIDS programmes, coordination has become an important requirement at country level and globally. One step towards improving coordination at country level was the development in 1993 of a computerized database to facilitate monitoring of AIDS programmes.
14.120 A national AIDS programme management course was successfully field-tested in Zimbabwe in 1993. It is designed to help countries in planning, implementing and evaluating their programmes and, above all, in setting priorities. A set of priority indicators of progress in prevention was selected and a methodology devised for their use in national programmes. Protocols were prepared for application of the indicators and field-tests completed in Cote d'Ivoire, Honduras, India, Sri Lanka and United Republic of Tanzania. The population survey originally concerned with measurement of prevention indicators was expanded to include measurement of care and support indicators. These evaluation activities took longer than anticipated, but the real progress made will result in the establishment of a global framework for reporting on national AIDS prevention and care activities.
14.121 Approximately 60 million condoms were procured for national AIDS programmes during the biennium. Attention was focused on supply policy, quality assurance, logistics management training and social marketing. The WHO condom specifications were revised with respect to lubrication, elasticity and size in response to feedback from users. A training course on logistics was established and a project survey completed with support from major donors and nongovernmental organizations.
14122 With regard to safe blood, distance learning materials were produced for training blood transfusion staff with the minimum disruption of daily routine and at minimal cost. Guidelines to assist countries in more cost-effective methods of screening blood for HIV were also drafted (see also paragraphs 13.3-13.5).
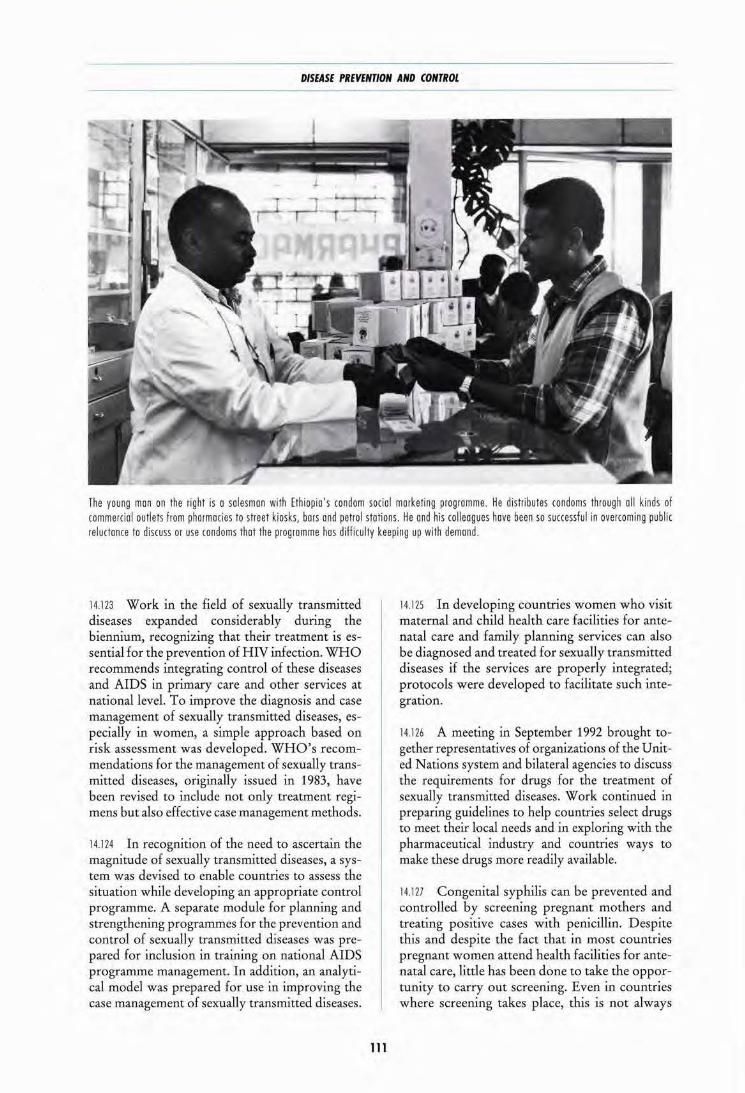
DISEASE PREVENTION AND CONTROL
The young man on the right is a salesman with Ethiopia 's condom social marketing programme. He distributes condoms through oil kinds of commercial outlets from pharmacies to street kiosks, bors ond petrol stations. He and his colleagues hove been so successful in overcoming public reluctance to discuss or use condoms that the programme hos diffi culty keeping up with demand.
14.123 Work in the field of sexually transmitted diseases expanded considerably during the biennium, recognizing that their treatment is essential for the prevention of HIV infection. WHO recommends integrating control of these diseases and AIDS in primary care and other services at national level. To improve the diagnosis and case management of sexually transmitted diseases, especially in women, a simple approach based on risk assessment was developed. WHO's recommendations for the management of sexually transmitted diseases, originally issued in 1983, have been revised to include not only treatment t:egimens but also effective case management methods.
14.124 In recognition of the need to ascertain the magnitude of sexually transmitted diseases, a system was devised to enable countries to assess the situation while developing an appropriate control programme. A separate module for planning and strengthening programmes for the prevention and control of sexually transmitted diseases was prepared for inclusion in training on national AIDS programme management. In addition, an analytical model was prepared for use in improving the case management of sexually transmitted diseases.
111
14.125 In developing countries women who visit maternal and child health care facilities fot: antenatal care and family planning services can also be diagnosed and treated for sexually transmitted diseases if the services are properly integrated; protocols were developed to facilitate such integration.
14.126 A meeting in September 1992 brought to
gether representatives of organizations of the United Nations system and bilateral agencies to discuss the requirements for drugs for the treatment of sexually transmitted diseases. Work continued in preparing guidelines to help countries select drugs to meet their local needs and in exploring with the pharmaceutical industry and countries ways to make these drugs more readily available.
14.127 Congenital syphilis can be prevented and controlled by screening pregnant mothers and treating positive cases with penicillin. Despite this and despite the fact that in most countries pregnant women attend health facilities for antenatal care, little has been done to take the opportunity to carry out screening. Even in countries where screening takes place, this is not always

THE WORK OF WHO 1992-1993 ---------------
followed by treatment. WHO therefore developed operational guidelines for programme managers and health workers for the prevention and control of congenital syphilis, and supported operational research on this subject in Brazil.
14.128 Responsibility for AIDS prevention and care does not rest entirely with the government authorities in a country. A large number of nongovernmental organizations at community and national level provide essential and appropriate support to individuals and communities. From 1990 to 1992 WHO supported 92 community projects undertaken by nongovernmental organizations in 35 countries with a total allocation of$ 3.1 million. However, in order to use its limited resources more effectively, WHO has gradually reduced this form of support and instead now concentrates on helping nongovernmental organizations to obtain the financial, material and technical resources they need, and to build working relations amongst themselves and with national AIDS programmes.
14.129 At a meeting in May 1992 to consider effective approaches to AIDS prevention, 15 types of measures aimed at enabling people to change risky sexual behaviour were presented by those involved in their design and implementation; discussion centred on factors which contributed to the success of the interventions, constraints encountered and lessons learned. A project to provide sex workers and their clients in six districts of Abidjan with treatment for sexually transmitted diseases, condoms and education on HIV prevention led to greater use of health services and increased condom sales. Technical support was provided for similar projects in the Dominican Republic, India and Mexico. The findings of two technical working groups held in November and December 1992 to review recent experience of outreach work with high-risk behaviour groups are being incorporated into a guide for the planning of interventions.
14.130 Research was initiated in four countries on the conditions under which peer education on HIV is effective in schools; and a guide for setting up health promotion projects for AIDS prevention among young people not in school was finalized following field-testing in seven countries. A major review of data from developed and developing countries has provided convincing evidence that sex education in schools does not encourage or lead to increased levels of sexual activity; rather, it results in safer sexual practices
112
and fewer unwanted pregnancies, and may even delay the onset of sexual activity.
14.131 As increasing numbers of HIV infections develop into AIDS cases, the need for care and support for patients and their families is growing fast. WHO therefore continued to support governments in planning and strengthening health care services, for instance by preparing guidelines for clinical diagnosis and treatment of HIV infection in adults and young children; updating modules for basic HIV education for nurses and midwives that emphasizes prevention and care; and issuing an AIDS home care handbook' which had been assessed in Uganda and Zambia. Following a regional workshop on communitybased care in Uganda in 1991, similar workshops were held in R wanda in 1992 and Thailand in 1993. A feasibility study on including communitybased care in existing urban health centres was started in Nairobi in 1993. A study was undertaken in Uganda to assess the additional costs of providing preventive tuberculosis therapy to HIV -seropositive persons.
14 132 Protocols were drawn up for three priority areas of social and behavioural research: sexual behaviour, particularly among young people; household and community response to HIV and AIDS in developing countries; and negotiation of safer sex by women. Following site assessment visits, proposals were made for conducting research in 10 developing countries.
14.133 WHO provided support in implementing national plans for infrastructure strengthening, training and vaccine-related research at four sites in Brazil, Rwanda, Thailand and Uganda. Laboratories in those countries collected specimens from 222 recent seroconverters in study populations; specimens from 63 of these patients were then examined by the WHO network for HIV isolation and characterization (comprising 12laboratories in North America and Europe). Initial results suggest that the distribution of HIV -1 anti genic subtypes is constantly changing, with different subtypes rapidly replacing others in a given population- a situation that poses a considerable challenge for the development of an HIV vaccine.
14134 In November 1993 the Advisory Council on HIV I AIDS recommended that priority areas
1 Document WHO/GPA/IDS/HCS/93 2.

DISEASE PREVENTION AND CONTROL
for research relating to women and AIDS should include the development of female controlled methods for preventing HIV transmission, including virucides, microbicides and mechanical barrier methods; effective preventive approaches for women sex workers; and rapid cost-effective diagnostic tests for sexually transmitted diseases. Protocols for research on a safe and effective vaginal microbicide were drawn up following strong endorsement of this approach at a major meeting in November 1993.
14 135 A double-blind placebo controlled trial of the use of low-dose oral interferon alpha in symptomatic HIV -infected patients in Uganda revealed that it conferred no benefit as regards survival, progress of the disease or subjective symptoms. Other studies were carried out with WHO support on short-course chemotherapy for tuberculosis in HIV -infected people in Haiti and on the efficacy and optimal duration of tuberculosis chemoprophylaxis in tuberculin-positive, HIVinfected persons in Thailand, United Republic of Tanzania and Zambia. Reduction of the use of the Western blot technique for HIV testing permitted a significant decrease in the cost of testing. The initial results of a study on the risk of nosocomial transmission of HIV in children admitted to paediatric wards in four African cities were reassuring and suggested that the various skin piercing procedures that they experienced accounted for little if any HIV transmission.
14.136 At a meeting in June 1993 attended by representatives of regulatory agencies and pharmaceutical companies, it was agreed that efforts to develop and approve drugs and vaccines for HIV I AIDS should be accelerated in developed countries and extended to developing countries. A joint WHO/International Federation of Pharmaceutical Manufacturers Associations statement on HIV I AIDS was drawn up, representing a major commitment to making drugs and vaccines of assured quality and efficacy available for both prevention and treatment.
14 137 In 1993 the Organization confirmed that it would not sponsor, cosponsor or financially support international conferences or meetings on AIDS in countries with entry requirements that discriminate solely on the basis of a person's HIV status, nor would representatives of WHO attend such conferences unless attendance is deemed essential for promoting WHO's programme. In April 1993 the Inter-Agency Advisory Group on AIDS requested that WHO's
113
policy should be submitted to the Administrative Committee on Coordination, which approved it as the formal policy for the whole of the United Nations system at its October 1993 meeting. In 1993 WHO issued guidelines on HIV infection and AIDS in prisons, 1 providing standards - from a public health perspective -which prison authorities should strive to achieve in their efforts to prevent HIV transmission and to provide care to those affected by HIV I AIDS.
14 138 In April-May 1992 a WHO/UNICEF consultation on HIV transmission and breastfeeding issued a consensus statement recommending that breast-feeding should continue in all populations, irrespective of HIV infection rates. In November 1992 a further consultation on HIV testing and counselling emphasized that mandatory testing has no place in AIDS control programmes, and that no benefits to the individual or for public health derive from such testing that cannot be achieved by less intrusive means such as voluntary testing and counselling.
14.139 The Organization promoted the worldwide observance of the fifth and sixth World AIDS Days on 1 December 1992 and 1993 respectively by disseminating information packages and issuing press releases on the chosen themes. World AIDS Day is now an annual event in most countries and provides an opportunity to stimulate awareness of AIDS and of the efforts being made to fight the pandemic. The theme "AIDS: a community commitment" was chosen for 1992 in order to highlight the importance of local communities combining their strengths in the global fight. In 1993 the theme was "AIDS: time to act", which underlined the need for urgent action and served as a rallying call for the world to join in ensuring a multisectoral response to the HIV I AIDS pandemic.
Other communicable diseases
Viral and bacterial diseases
14.140 Influenza. With a view to strengthening surveillance and increasing the chances of early detection of new variants of the influenza virus, WHO started a collaborative study on the origin of
1 Document WHO/GPA/DIR/93.3

THE WORK OF WHO 1992-1993 ------------------------------------------------------------------------------------
pandemic strains in southern China. Studies comparing the traditional inactivated influenza vaccine with the less commonly used live virus vaccine showed the latter to be slightly more effective in children. Recommendations regarding the influenza virus strains to be included in vaccines in 1992 and 1993 were made on the basis of information and virus isolates obtained in WHO's network of national and international laboratories.
14.141 Viral hepatitis. Hepatitis B vaccine is now being more widely included in national immunization programmes: nearly 50 countries have a national policy of universal administration of the vaccine to infants. :Crogress is also being made in immunizing health care workers. During the biennium WHO continued to support laboratory research on the production of plasma-derived hepatitis B vaccine in the Democratic People's Republic of Korea, Mongolia and Myanmar, and nationals of those countries and of Indonesia were awarded WHO fellowships to train in the production of the vaccine. Safe and highly effective vaccines to prevent hepatitis A are now licensed in many countries and WHO prepared guidelines for their use in immunizing travellers and other groups at risk.
14.142 Arthropod-borne viruses and viral haemorrhagic fevers are major causes of morbidity and mortality. Dengue viruses appear in new areas as the mosquito vector Aedes aegypti invades additional urban habitats. This spread is most notable in the Americas, where nearly all countries in Central and South America and the Caribbean are now at risk of epidemic dengue. An outbreak of dengue fever in Comoros showed that dengue is also a threat in Africa. WHO continues actively supporting vaccine development, surveillance of infection, control of outbreaks, and vector control (see paragraph 14.42).
14.143 Viral haemorrhagic fevers are an important group of emerging infectious diseases. WHO was active in the investigations that revealed the etiological role of the hantaviruses in an outbreak of fatal adult respiratory distress syndrome in south-western United States of America. In recent years other emerging viral haemorrhagic fevers have been recognized as major causes of fatal human infection (for instance, in Brazil and Venezuela). Rift Valley fever virus remains an important pathogen affecting man and domestic animals in much of Africa; during 1993 cases were diagnosed in Upper Egypt, and WHO responded to requests for technical sup-
114
port. The Organization was also involved in combating an outbreak of Lassa fever in Nigeria.
14.144 Yellow fever remains a major threat in Africa and South America. In 1992 it occurred for the first time in Kenya, and WHO assembled field teams to assist in investigating the outbreak, providing diagnostic reagents and equipment, and starting an emergency vaccination campaign.
14145 Japanese encephalitis is increasingly recognized as an important disease that can be prevented by immunization. WHO has sponsored efforts in several Asian countries to improve methods for production of the vaccine and make it more readily available.
14.146 Plague. Sporadic cases and periodic outbreaks of bubonic plague were reported in 12 countries during the biennium; natural foci of the disease exist in Africa, the Americas and Asia.
14.147 Meningitis. Epidemic cerebrospinal meningitis remained a problem, particularly in Africa (see Figure 14.10). Surveillance of Neisseria meningitidis strains continued, including monitoring of susceptibility to antibiotics. WHO prepared practi~al guidelines on the control of epidemic meningococcal disease.
14 148 Legionellosis. A surveillance system in 22 European countries for Legionella infections in travellers was devised in cooperation with the WHO collaborating centre in Stockholm, and recommendations for further work on the control of these infections were made during two WHO consultations (Haniotis-Halkidiki, Greece, May 1992; Vienna, May 1993 ).
14.149 Streptococcal infections and their suppurative and non-suppurative sequelae remain an important health concern. A WHO collaborative study on the production of group A streptococcal M and OF typing sera resulted in the establishment of a standard set of typing sera for use in regional and national programmes for the prevention and control of rheumatic fever and rheumatic heart disease.
Antimicrobial resistance and hospital infections
14.150 WHONET computer software was used in monitoring resistance to antimicrobials in a
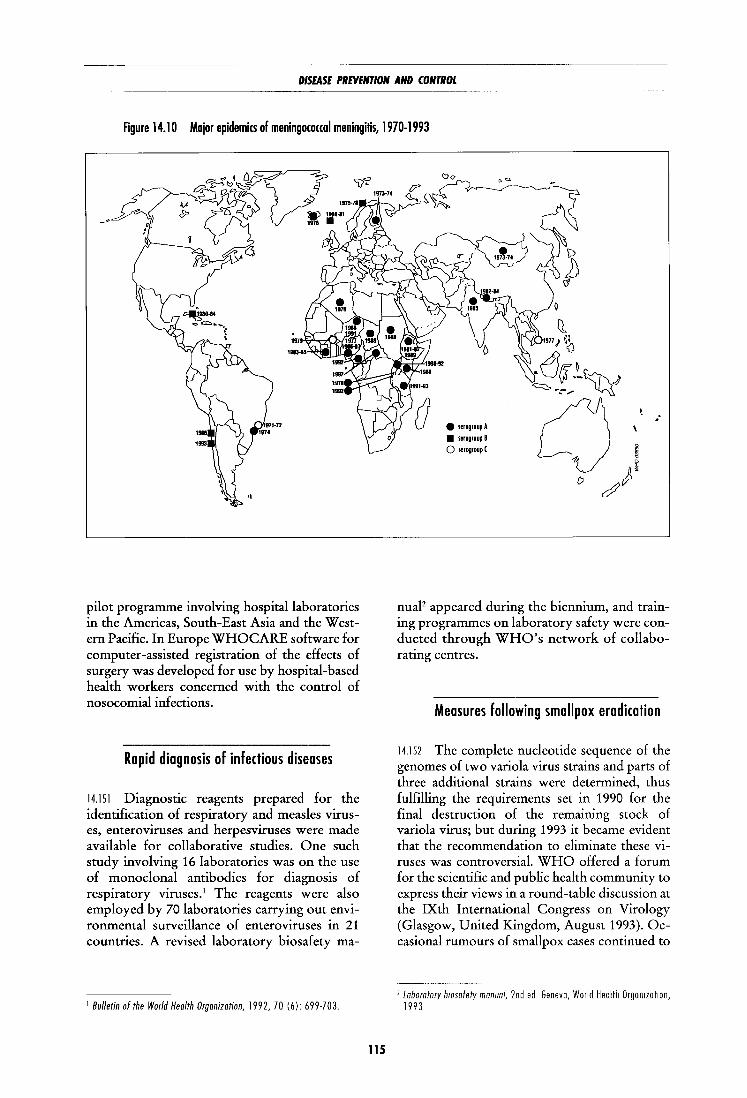
DISEASE PREVENTION AND CONTROL
Figure 14.10 Major epidemi(s of meningo(O((OI meningitis, 1970-1993
pilot programme involving hospital laboratories in the Americas, South-East Asia and the Western Pacific. In Europe WHOCARE software for computer-assisted registration of the effects of surgery was developed for use by hospital-based health workers concerned with the control of nosocomial infections.
Rapid diagnosis of infectious diseases
14.151 Diagnostic reagents prepared for the identification of respiratory and measles viruses, enteroviruses and herpesviruses were made available for collaborative studies. One such study involving 16 laboratories was on the use of monoclonal antibodies for diagnosis of respiratory viruses.1 The reagents were also employed by 70 laboratories carrying out environmental surveillance of enteroviruses in 21 countries. A revised laboratory biosafety ma-
1 Bulletin of the World Health Organization, 1992, 70 (6): 699·703.
115
e serogroupA
• serogroupB 0 serogroup(
.-
nuaP appeared during the biennium, and training programmes on laboratory safety were conducted through WHO's network of collaborating centres.
Measures following smallpox eradication
14.152 The complete nucleotide sequence of the genomes of two variola virus strains and parts of three additional strains were determined, thus fulfilling the requirements set in 1990 for the final destruction of the remaining stock of variola virus; but during 1993 it became evident that the recommendation to eliminate these viruses was controversial. WHO offered a forum for the scientific and public health community to express their views in a round-table discussion at the IXth International Congress on Virology (Glasgow, United Kingdom, August 1993). Occasional rumours of smallpox cases continued to
1 Laboratory b10safety manual, 2nd ed Geneva, World Health Orgon1ZOI1on, 1993

THE WORK OF WHO 1992-1993
circulate, particularly in areas of political unrest. A few were true cases of poxvirus infections, including monkeypox in Africa, but none was due to variola virus; the WHO collaborating centres on smallpox and other poxvirus infections provided the laboratory diagnosis.
Intestinal parasitic infections
14.153 Major collaborative projects for the control of intestinal parasitic infections were launched in Addis Ababa, Rodrigues (Mauritius), and Dhofar Governorate (Oman), and two national control programmes were in progress in Seychelles and in Zanzibar (United Republic of Tanzania). Collaboration to combat these infections began in China, Maldives, Mexico and Myanmar. A set of bench aids for the diagnosis of intestinal protozoa was under development following successful trials of such aids for the identification of intestinal helminths. A software package for field evaluation of the impact of helminth control programmes was devised and field-tested.
Research and development in the field of vaccines
Children's Vaccine Initiative
14 154 This initiative provides a strategic framework for work on vaccines undertaken within WHO and elsewhere, including institutions in the public and private sectors. It is sponsored jointly by UNICEF, UNDP, the World Bank and the Rockefeller Foundation, and its secretariat is provided by WHO. It has two main working components: product development groups, which promote, facilitate and manage projects leading to the development of vaccines and related preparations, each group focusing on a particular vaccine; and task forces, which examine strategic, logistic and policy questions, such as priority-setting, demand and supply, and collaboration with industry, relevant to the development and introduction of vaccines. In addition, there is a management advisory group which reviews budgetary matters and progress of activities, and a consultative group which provides an international forum for information exchange and consultation on priority activities.
116
New vaccines against bacterial diseases
14.155 There was substantial progress in the development of new, more effective vaccines against cholera and other diarrhoea! diseases. Several promising cholera vaccines are now at the clinical trial stage, and urgent work is in progress to produce a vaccine against cholera following the appearance of the 0139 strain of Vibrio cholerae which is beginning to cause epidemics in South-East Asia. New Shigella vaccines are now being tested on human beings.
14.156 Vaccines suitable for inclusion in infant immunization schedules have been developed against group A and C meningococcal meningitis and are being tested in Gambia and other endemic areas, while vaccines against group B meningococcal meningitis produced in Cuba and Norway are being compared in clinical trials.
14 157 The search for vaccines against pneumococcal species is complicated by the variability of pathogenic polysaccharide serotypes and by the absence of immunogenicity of polysaccharide vaccines in children under two years of age; but several vaccines have been developed to overcome these difficulties and will soon be in production.
14158 The effectiveness of BCG against tuberculosis varies considerably in different countries but, owing to important advances, this vaccine can now be engineered to improve the expression of potentially protective antigens. Alternatively, site-directed mutagenesis of Mycobacterium tuberculosis can make the bacterium harmless by deleting selected virulence factors.
New vaccines against viral diseases
14 159 Dengue virus infection is spreading throughout the tropical zone and vaccines are urgently needed; a candidate tetravalent live attenuated vaccine was developed in Thailand with the support of WHO and may be produced commercially in the near future. Substantial progress was also made in characterizing the genomes of the dengue and Japanese encephalitis virus, facilitating the development of a suitable vaccine.
14 160 Many cases of measles occur before the usual immunization age and there is a need for a vaccine that can be given three to four months

DISEASE PREVENTION AND CONTROL
after birth; several candidate preparations are now undergoing preclinical tests. Two other viral pathogens, respiratory syncytial virus and parainfluenza virus type 3, contribute to many of the serious respiratory infections of infancy; excellent progress has been made towards defining antigenic formulations which may offer protection against the first, and initial live vaccine studies with bovine and attenuated human strains of the second have produced vaccines that are both safe and immunogenic in seronegative infants.
14 161 An inactivated hepatitis A vaccine is now available, but the present cost of production limits its use in the developing world. Combination vaccines in which hepatitis B vaccines will be added to new immunization formulations for infants are now in prospect. Hepatitis C is emerging as a major cause of liver cirrhosis and cancer, especially in industrial countries, and studies are in progress to define important antigens for vaccine development; a WHO collaborating centre announced success in growing the virus in tissue culture, a critical step in vaccine research. Hepatitis E poses a risk particularly in the developing countries; however, substantial progress was made in the application of recombinant DNA technology to the production of protective immunogens.
Improvement of existing voccines
14 162 It would be preferable to find animal models other than non-human primates for assessing the neurovirulence of new vaccine lots. An advance in this area was the production, under WHO auspices, of transgenic mice expressing the human poliomyelitis virus receptor; the Organization issued guidelines for the handling of such mice. Other approaches based on genetic engineering showed encouraging progress and trials of a new genetically stable candidate replacement vaccine for the existing type 3 Sabin poliomyelitis strain began in man, inspiring hope that the dangers of reversion to virulence in attenuated strains may soon be minimized. In regard to tetanus, work proceeded on the elaboration of a single-dose vaccine that would provide phased release of antigens and replace the current three-dose immunization. There are difficulties regarding the stability of the preparation, but it is hoped that a single-dose tetanus vaccine may be available by 1996.
117
Training
14.163 In 1992-1993 64 scientists from developing countries were trained at the WHO Immunology Research and Training Centre located in Geneva and Lausanne (Switzerland) in areas of immunology and biotechnology related to the evaluation of vaccine immunogenicity and efficacy. In 1992 a further 39 scientists from SouthEast Asia participated in a refresher course in Semarang (Indonesia); and a similar course was organized in Teheran with the support of the Islamic Republic of Iran.
Blindness and deafness
14.164 Further progress was made towards the target of the establishment of national blindness prevention programmes in all countries where sight loss is a public health problem. In 1993 WHO drew up an inventory of national plans, committees and programmes in 93 countries out of an estimated 116 in need. 1 Thanks to the help of a contribution from the International Association of Lions Clubs, WHO was able to coordinate its work in this area more effectively. The Organization has also cooperated closely with a consortium of six nongovernmental organizations which is providing funds for distribution of ivermectin against onchocerciasis, and is promoting common strategies and methods for control operations in 12 African and four Latin American countries. Through this initiative about 2.5 million people were treated in 1993 (see also paragraphs 14.30 and 14.62). Recommendations on management of severe visual disability in children2 were formulated at a meeting held jointly with the International Council for Education of the Visually Handicapped (Bangkok, July 1992).
14.165 Continued support from the Edna McConnell Clark Foundation enabled the Organization to produce two manuals on the management of trachoma within primary health care systems/ and training courses on simplified as-
1 Document WHO/PBL/93.30. 2 Document WHO/PBL/93 27 3 Documents WHO/PBL/93 29 and WHO/PBL/93 33.
THE WORK OF WHO 1992-1993
sessment of this condition were conducted in Mali in 1992 and Kenya in 1993. Applied research on cost-effective cataract surgery was carried out in India and Mali. In September 1993 a WHO consultation considered the effects of solar ultraviolet radiation on the eye and called for a major international study on this subject.
14 166 Training of personnel in blindness prevention remained a priority in Africa. Strategies for national programme development were planned at a workshop for Portuguese-speaking countries (Maputo, October 1993 ), supported by the Consultative Group of N ongovernmental Organizations.
14 167 In the Americas further progress was made in setting up national programmes, and AGFUND made contributions to nine countries for this purpose. WHO responded to an appeal for emergency relief to deal with an epidemic of neuropathy in Cuba.
14.168 In South-East Asia aspects of programme management were examined in 1993 during a course in Thailand supported by the International Association of Lions Clubs. WHO gave technical advice on the preparation of a proposal to the World Bank for strengthening the Indian national programme.
14 169 Several countries in eastern Europe revised their programmes for blindness prevention. A national seminar on this subject was organized in Romania in 1993 with support from Orbis International (USA).
14 170 In the Eastern Mediterranean, Sudan and Tunisia revised their national programmes; Tunisia also proceeded with a nationwide assessment of sight loss and its causes, as did Morocco. An intercountry meeting on national blindness prevention programmes (Cairo, April 1993) called for a fuller evaluation of the programmes in most countries
14.171 WHO support was provided to China in 1992 for a course on management of cataract and in 1993 for a national seminar on prevention of sensory impairments in the elderly. A Western Pacific regional workshop on evaluation of national blindness prevention programmes (Sydney, Australia, October 1992) was held with support from the Consultative Group of Nongovernmental Organizations.
118
• One problem in setting up national programmes to prevent hearing impairment is the lack of epidemiological data on this condition. WHO has therefore designed a standardized examination form which makes it possible for a field survey team with portable audiometers and lowcost instruments to carry out a simple hearing assessment on as many as two hundred people per day, using trained auxiliary staff for part of the procedure.
14.172 With regard to the prevention of deafness and hearing impairment, a working group in March 1992 devised a uniform ear examination record which was subsequently field-tested in Thailand in 1992 and India in 1993. The Foundation for Advanced Studies on International Development Qapan), Kansai Medical University Qapan) and the Tokyo-based Asian Interactive Association on the Hearing Impaired provided financial support for WHO's work in this field from March 1992 onwards. A task force on the prevention of deafness (Alexandria, October 1992) reviewed the situation in the Eastern Mediterranean and called for urgent epidemiological assessment of hearing impairment and its causes in different populations.
Cancer
• WHO estimates that 9 million cases of cancer occur in the world every year. By the year 2015 the annual figure is expected to reach 15 million cases, two-thirds of them in developing countries, which have only 5% of the resources available for cancer control in the world.
14173 WHO's act1v1t1es in cancer control are based on the fact that enough is now known about cancer for effective action to be taken that will significantly reduce morbidity and mortality worldwide and that, given the right priorities and approaches, even the limited resources available can be used in such a way as to have a real impact on the problem.

DISEASE PREVENTION AND CONTROL
Primary prevention
14 174 Policies on healthy lifestyles and optimal diet were worked out together with the WHO cardiovascular diseases and nutrition programmes. Various WHO programmes also contribute to the primary prevention of cancer. Examples are the programmes on tobacco or health and immunization against hepatitis B. Other contributions are made by WHO collaborating centres. For instance, during the biennium a WHO collaborating centre in Regensburg (Germany) began work on tumours associated with the EpsteinBarr virus, that are found in countries with a high incidence of nasopharyngeal cancer. The melanoma programme, carried out by the Italian National Institute for Cancer Treatment and Research on behalf of WHO, devised strategies to prevent this disorder by informing the public about the dangers of excessive exposure to sunshine, particularly in childhood; individuals at high risk can now be identified and offered preventive advice.
Early detection
14 175 Managerial guidelines for the control of cervical cancer were issued' and innovative methods of early detection introduced and coordinated. Cost-benefit evaluation of early detection programmes for cancers of the breast, cervix, mouth and skin was promoted in countries in Africa, the Americas, South-East Asia and the Eastern Mediterranean. A trial on self-examination of the breast is under way in the Russian Federation.
14.176 A new project was launched to promote simple methods for the early detection of cancer of the mouth and cervix in developing countries. WHO collaborated with the Indian Ministry of Health and Family Welfare in studies to detect cases at an earlier stage by visual inspection. Similar studies were begun in southern Africa and the Western Pacific in collaboration with the World Bank. Once the results of these investigations are available, it will be possible to decide whether the approach can be recommended and applied widely in developing countries.
1 Miller AB. Cervical cancer screemng programmes Geneva, Warld Health OrganiZatiOn, 1992.
119
Treatment
14.177 Mortality from cervical, breast, mouth and skin cancers, if they are detected early, can be significantly reduced by standard therapies. WHO encourages the provision of adequate services, especially radiotherapy. Six radiotherapists/ oncologists were trained in a radiotherapy and oncology project carried out in Zimbabwe in 1989-1993 with Swiss support; and 14 others have been trained in Sri Lanka. WHO initiated the preparation of a manual on basic radiotherapy, together with IAEA.
14178 During the biennium WHO prepared, from among over 100 drugs, a model list of 22 essential drugs for cancer chemotherapy, selected for their cost-effectiveness and efficacy and designed to satisfy the needs of most patients in national programmes.
Palliative care
14 179 Palliative treatment and care, including symptom control and pain relief, will be important for years to come for the large numbers of patients for whom curative therapy is not possible. More than 40 countries have established government policies on cancer pain and terminal care; and pain relief or palliative care is included in several national cancer control programmes. WHO recommends the use of a number of non-opioid and opioid analgesics and adjuvants for relieving cancer pain. Oral morphine consumption in the world has increased five-fold in recent years, bringing a great improvement in quality of life for many cancer patients. A WHO working group (Banff, Canada, September 1993) approved a manual on palliative care for those providing home care. Joint meetings organized by WHO and the International Association for the Study of Pain (Arezzo, Italy, June 1993; Paris, August 1993) prepared guidelines on cancer pain relief and supportive care for children. Eight WHO collaborating centres have been carrying out research and training and applying methods for cancer pain relief and palliative care.
National cancer control programmes
14 180 The cornerstone of WHO's approach to cancer control is the development of national

THE WORK OF WHO 1992-1993
programmes. WHO issued a handbook1 summarizing ways to apply scientific knowledge in cancer control, based on the experience of 12 countries. Requests have subsequently been received from 40 other countries to help them to set up such programmes. So far, WHO has provided guidance to over 40 countries, each of which is establishing a programme in accordance with its existing cancer care structure and resources. Arrangements were discussed with 14 countries in the Eastern Mediterranean at an intercountry workshop (Cairo, November 1993) and six committed themselves to set up national programmes. The target is that at least half of the Member States will have formulated strategies and programmes for cancer control by the year 2000.
14 181 Six district cancer control demonstration projects are being established in India, making use of existing health infrastructure to cover a large population for the control of oral, cervical and breast cancers through primary prevention, early detection and referral for curative treatment as well as palliative care; it is expected that they will become models for the whole country and possibly for other developing countries.
International Agency for Research on Cancer2
Descriptive epidemiology
14 182 In 1992 IARC published data on the incidence of cancer in 46 countries ( 170 populations) for the period 1983-1987.3 An estimated 7.62 million new cases of cancer occurred in 1985 (3.85 million males and 3.77 million females), the lung being the commonest site (nearly 900 000 cases). Data on time trends~ show a decrease in stomach cancer, an increase in malignant melanoma of the skin, and mixed patterns,
1 Document WHO/CAN/92.1. 2 For a more detailed description of IARC's activities 1n the b1enn1um, see
International Agency for Research on Cancer, B1ennwl report, 1992-1993. Lyon, 1993.
3 Park1n OM et al. Cancer modence m five contments, Vol VI. Lyon, International Agency for Research on Cancer, 1992 (IARC Scientific Publications, No 120)
4 Coleman M et al Trends m cancer modence and mortality. Lyon, International Agency for Research on Cancer, 1993 (IARC SCJent1f1c Publications, No 121)
120
linked to known trends in smoking habits, for lung cancer. IARC gave extensive support for setting up and running cancer registries in developing countries in Africa, Asia and Latin America.
Etiological studies
14 183 Cancer related to occupational exposure was studied with respect to phenoxy acid herbicides, styrene, man-made mineral fibres, the pulp and paper industry, biological laboratory work, lead, the wood and leather industries, asphalt vapours, mercury, textile manufacture, the nuclear industry, steel works and the rubber industry. Special attention was paid to the high levels of occupational exposure often prevailing in developing countries.
14.184 In a European prospective investigation into cancer and nutrition, pilot studies were completed on food composition and methods for dietary assessment, and recruitment of an estimated 420 000 participants in seven countries was well advanced. Each participant's diet is being recorded, and blood samples are taken for biological measurements.
14.185 Lymphomas in patients suffering from AIDS were studied to characterize interactions between HIV and Epstein-Barr virus. Various cancers in relation to HIV infection were the subject of an epidemiological study in central Africa.
14 186 It was found that induction of the enzyme nitric oxide synthase in infected tissues may be involved in the endogenous formation of carcinogenic nitrosamines, implicated in cancer of vanous organs.
14 187 A range of epidemiological studies in Gambia and Thailand, including the development of methods in !ARC's laboratories to measure exposures, yielded detailed information on the interaction between hepatitis virus infection and aflatoxin exposure in the etiology of liver cancer.
14.188 Epidemiological results from investigations in Colombia and Spain, using sensitive methods for detecting human papillomavirus, showed a close association between this agent and cervical cancer. The combined in vivo and in vitro evidence for the carcinogenicity of at least

DISEASE PREVENTION AND CONTROL
some types of the virus has been assessed as being consistent enough for the relationship to be considered causal.1
Genetics and cancer
14.189 It has become clear that genetic differences in enzymes that convert many substances into active carcinogens influence individual susceptibility to certain forms of cancer. Thus smokers may react differently to the carcinogens in tobacco smoke, and aflatoxins ingested in foods may be converted more or less efficiently into DNA-binding agents. Differences in the enzymes that repair DNA damage can also affect individual susceptibility to carcinogens.
14.190 Attemps to map the breast cancer gene located on chromosome 17q continued. Counselling is being provided to women in families identified as being at high risk. Studies have suggested that other genes predisposing to breast cancer also seem to exist.
Mechanisms of carcinogenesis
14.191 Mutations in oncogenes are being measured at frequencies as low as one in 10-s DNA bases, as a method for detecting the very earliest molecular lesions in the pathway to cancer. Similarly, specific forms of damage caused by ultraviolet radiation in the p53 tumour-suppressor gene in skin cells are being detected and quantified. Mutations detected in these genes in oral, oesophageal and stomach tumours throw light on the ways in which loss of control of cell proliferation can lead to cancer. Methods are also being refined for the detection of very low levels of carcinogen-DNA adducts as early markers of carcmogemc processes.
14 192 Studies have shown that genes for connexon proteins that form communicational junctions between cells may act as tumour-suppressor genes by improving the control of cellular growth and proliferation that results from such communication.
1 Muiioz N. et al. The epidemiology of cefV!ca! cancer and human papillomavtrus lyon, International Agency for Research on Cancer, 1992 (IARC Sctenttftc Publications, No 119)
121
Cancer prevention research
14.193 In the hepatitis intervention study in Gambia, a good level of protection among vaccinated children continued to be observed. In parallel, appropriate measures to reduce exposure to aflatoxin were investigated. Cancer registration was set up in order to document the incidence of cancer, particularly of the liver, over the forthcoming decades.
14.194 In a chemoprevention trial in Venezuela, over 1000 subjects were recruited and received antioxidant vitamins. Precancerous lesions of the stomach are being monitored by immunochemical and histological methods. A pilot study showed that treatment to eradicate infection with H elicobacter pylori was much less efficacious than had been seen in developed countries and this treatment was therefore not included in the trial.
Information and training
14.195 Four new volumes were published in the IARC Monographs series. They dealt with strong acid mists, solar and ultraviolet radiation, food constituents and contaminants, and a range of colouring matters and their use in hairdressing. Factors evaluated as carcinogenic to humans were occupational exposure to strong inorganic acid mists containing sulfuric acid, solar radiation, Chinese-style salted fish, naturally occurring mixtures of aflatoxins, and the manufacture of the dyestuff magenta. Among other factors, 1,3-butadiene and occupational exposures in hairdressers and barbers were categorized as probably carcinogenic. In addition, work started on the publication of a series of fascicles on the classification of rodent tumours.
14.196 During the biennium 23 fellowships were awarded to young scientists from 12 countries, and 10 training courses on various aspects of cancer research were attended by a total of 426 participants.
Cardiovascular diseases
14.197 Activities under the WHO programme for the prevention of rheumatic fever and rheumatic heart disease continued in close collabora-
THE WORK OF WHO 1992-1993
tion with the International Society and Federation of Cardiology. Phase I (assessment) was completed in 16 countries, with support from AGFUND, and phase II (community control) was begun. A further nine countries joined the programme during the biennium, bringing the total to 25.
14198 The WHO project for multinational monitoring of trends and determinants of cardiovascular diseases (MONICA), the largest collaborative epidemiological study of these diseases ever carried out, continued in 25 countries and entered the final stage of data collection. The first analyses of trends in risk factors, based on two population surveys, were prepared. A first cross-sectional comparison of morbidity data in stroke cases was prepared and a similar analysis for coronary events was submitted for publication in the journal Circulation. The third and final population survey was prepared and a special training workshop organized (Gargano, Italy, March 1993). The steering committee for MONICA met twice during the biennium and the principal investigators reviewed progress and took decisions on policy, publications and quality control at a meeting supported by the regional authorities of Catalonia and the Hospital Sant Pau (Barcelona, Spain, August 1992). At the same time coordination meetings were held on MONICA optional studies relating to vitamins and polyunsaturated acids, dietary monitoring, drugs, physical activity and psychosocial factors. The main results from MONICA to date concern: cross-sectional comparisons of risk factor levels; relations between various risk factors; five-year trends in risk factors; acute coronary care; medical services; cross-sectional comparisons of incidence rates for stroke; and management of stroke around the world. These results were presented at a number of conferences and congresses during the biennium.
14199 A meeting between WHO and the United States Institute of Medicine (Washington, October 1992) worked out details of a joint study to review the current status of the epidemiology, prevention and control of cardiovascular diseases in developing countries and agreed upon a strategy for intervention based on needs and priorities. A plan of action was drawn up covering health statistics and epidemiology, prevention and case management, and an implementation committee was established to carry the work forward.
14.200 As part of an international conference on preventive cardiology (Oslo, June-July 1993) workshops were held on: prevention of cardia-
122
vascular diseases in countries of the Eastern Mediterranean; cardiovascular diseases in developing countries; and the establishment of a global database.
14.201 The data collection phase of the project for cardiovascular diseases and alimentary comparison (CARDIAC), a multicentre study launched in 1985 to assess the relation between food intake and cardiovascular diseases, was completed in 1992 and the WHO collaborating centre in Izumo Qapan) began an analysis of the results.
14.202 Collection of specimens and data for the WHO/International Society and Federation of Cardiology study on pathobiological determinants of atherosclerosis in youth was also completed. The data are now being analysed and special investigations are in progress at reference centres in Budapest, Geneva, Havana, Heidelberg (Germany), Malmo (Sweden), Sienna (Italy) and St Louis (USA).
14 203 An education programme for patients with hypertension was started in 1990 by WHO and the World Hypertension League in Canada, China, Cuba, Ghana, Hungary, India and the Russian Federation. The aim is to assess whether educating patients influences compliance with treatment regimens and consequently management of the disease. Each centre prepared a local protocol and completed the data collection phase at the end of 1993.
14 204 In November 1992 a WHO scientific group assessed the influence of specific nutritional, metabolic and haemostatic factors, alcohol, physical activity, sex hormones and psychosocial and economic factors on cardiovascular disease risk, and recommended areas for future research by WHO and other bodies.
14205 In October 1993 a WHO study group reviewed global demographic changes in relation to the epidemiology of cardiovascular diseases in the elderly, assessed the effectiveness and cost of preventive strategies, and indicated policy options and research priorities for prevention.
14.206 World Health Day 1992 was devoted to cardiovascular diseases under the slogan "Heartbeat - the rhythm of health", and was marked by activities all over the world, in developed and developing countries alike. WHO's concerns include physical activity and sport, as demonstrated by a new technical cooperation

DISEASE PREVENTION AND CONTROL
agreement with the International Olympic Committee concluded in June 1993.
14 207 WHO's publications on cardiovascular diseases during the biennium included a special edition of World health statistics quarterly! and an expert committee report on rehabilitation after cardiovascular diseases.2
Other noncommunicable diseases
14.208 Diabetes mellitus. Global estimates of the prevalence of diabetes in adults were published.3
WHO cosponsored World Diabetes Days (14 November 1992 and 1993) when many countries, both developed and developing, tried to increase local awareness of the growing problem of diabetes. In November 1992 a WHO study group meeting on the prevention of diabetes reviewed existing knowledge and recommended preventive strategies that could be relevant to the prevention of other noncommunicable diseases sharing common risk factors with diabetes. WHO's guidelines on the development of national diabetes programmes4 were translated into French, Spanish and Russian.
14 209 The International Diabetes Federation and WHO convened a joint meeting (Budapest, March 1992) concerned with the implementation of the 1989 St Vincent declaration on diabetes care and research in Europe, which called on Member States to establish national diabetes task forces. A meeting of the Eastern Mediterranean regional advisory panel for diabetes (Karachi, December 1992) prepared guidelines for diabetes care and programme implementation. A subsequent meeting (Alexandria, November 1993) prepared materials for educating diabetes patients.
14 210 Protocols were received from centres in 52 countries for participation in the WHO multinational project on childhood diabetes, and 30 participating centres were recruited for a diabetes atherosclerosis intervention study. An interna-
1 World health statrstics quarterly, 1993, 46 (2). 1 WHO Technical Report Series, No. 831, 1993 3 World health statrstics quarterly, 1992, 45 (4). 4 Document WHO/DBO/DM/91 1
123
tional workshop on clinical epidemiology training in diabetes (Omiya, Japan, July-August 1993), cosponsored by WHO, drew up guidelines for future international training courses in this field.
14.211 Chronic rheumatic diseases. The protocol was elaborated for the WHO multinational collaborative study on the predictors of osteoarthritis, with the aim of designing a scientifically based approach to primary prevention of osteoarthritis in the community. WHO cosponsored an international conference (Maastricht, Netherlands, April-May 1992) which defined methods for measuring the results of treatment in clinical trials concerned with rheumatoid arthritis.
14.212 A working group on Kashin-Bek disease was organized in conjunction with the WHO collaborating centre for the epidemiology of rheumatic conditions (Stockholm, May 1992), in which experts in clinical rheumatology, biochemistry and epidemiology from China, Germany, New Zealand, Sweden, United Kingdom and United States of America participated.
14.213 A WHO study group on assessment of the risk of osteoporotic fracture and its role in screening (Rome, June 1992) reviewed the extent of the problem of osteoporosis, evaluated the risk and benefit of different screening techniques and their impact on various target populations, and proposed strategies for preventing the condition. In June-July the fifth meeting of the joint WHO/International League of Associations for Rheumatology task force examined the classification of antirheumatic drugs and refined the existing guidelines for their use.
14 214 Chronic nonspecific pulmonary diseases. These diseases, particularly asthma, are increasingly posing a problem in both developed and developing countries; in 1992 a number of consultations were held, leading to a meeting on asthma (Chicago, USA, March 1993) convened jointly by WHO and the United States National Heart, Lung and Blood Institute. The convening of a WH 0 scientific group on asthma in N ovemher 1993 was the first step in the formulation of a global strategy for asthma management.
14 215 Integrated programmes. WHO continued to promote its integrated programme for community health in noncommunicable diseases (INTERHEALTH) with 16 demonstration projects in developed and developing countries in all regions. The European programme of

THE WORK OF WHO 1992-1993
countrywide integrated noncommunicable disease intervention (CINDI) has 14 demonstration projects. During the biennium meetings took place of the INTERHEALTH steering committee Goensuu, Finland, April 1992) and programme directors (Beijing, April 1993). A teleconference on the prevention of chronic lifestyle diseases was organized during the latter meeting. First results achieved at the national level are very encouraging. One example is Mauritius, a country with a high prevalence of noncommunicable diseases, especially diabetes and arterial hypertension, where a comprehensive preventive strategy has reduced the prevalence of hypertension, lowered the cholesterol levels of the population, and reduced tobacco and alcohol consumption as well as promoting physical activity. In other INTERHEAL TH demonstration projects, comprehensive community-based intervention programmes are being undertaken following baseline surveys.
14.216 Hereditary diseases. In November 1993 a WHO scientific group recommended further use of genetic technology in the prevention and control of hereditary diseases in view of results achieved by national genetics services. WHO policy and recommendations concerning selected hereditary diseases were reviewed at WHO meetings on haemophilia (Geneva, February 1992), neurofibromatosis (Vienna, June 1992), cystic fibrosis (Washington, October 1992), haemoglobinopathies (Nicosia, April 1993) and haemochromatosis (Kiryat Anavim, Israel, April 1993). Several countries1 have developed control
1 Australia, Brazil, China, Cyprus, India, Italy, Jamaica, Myanmar, Nrgerra, Pakistan, Saudi Arabra, Thailand, Tunrsia.
124
programmes based on WHO approaches and recommendations.
14 217 A WHO working group on haemoglobinopathies with members from 15 countries in Europe and the Eastern Mediterranean evaluated and monitored national programme activities (Nicosia, March 1993). Subsequently a regional advisory working group on hereditary disorders was set up in the Eastern Mediterranean.
14 218 In view of the increasing awareness in many countries of problems connected with hereditary diseases, WHO prepared and issued educational materials on haemophilia and the haemoglobinopathies as well as guidelines on general principles involved in setting up national programmes for the control of congenital malformations and the haemoglobinopathies. In 1992 support was given in organizing a training course in Cuba for personnel from Latin American countries on the use of modern techniques in the control of hereditary diseases.
14 219 To assist in assessing the role of modern technology in the control of hereditary diseases, WHO cosponsored a sixth international conference on early prenatal diagnosis of genetic diseases (Milan, Italy, May 1992) at which the feasibility was considered of establishing a WHO international register on this subject. An international multicentre study was initiated on the predictive value of individual genetic and environmental risk factors for familial hypercholesterolaemia. Ethical questions relating to clinical applications of genetics were reviewed at the second and third international bioethics seminars (Fukui, Japan, March 1992 and November 1993 ).

CHAPTER 15
Health information support
Health literature services
15.1 During the biennium expanded information services were provided over the headquarters local area network, backed by intensified training of technical staff throughout the Organization, in order to improve access to scientific and technical information for Member States. Particular emphasis was given to health economics. Guidance was given to users in Member States, including ministries of health, in reorganizing their information systems.
15.2 WHOLIS, the computerized WHO library information system, was enhanced by the addition of abstracts and was included in the Latin American health sciences literature database (LILACS) CD-ROM, which is distributed by BIREME, the Latin American and Caribbean Center on Health Sciences Information. WHOLIS has become available on Internet. WHODOC, the regular listing of new WHO publications and documents, continued to be disseminated on diskette and through Internet as well as in print.
15.3 "Essential information kits" were produced in cooperation with technical programmes; these are subject packages that combine essential information sources with explanations for using them correctly. They fill a need in countries that have few information resources, and in others where it may be difficult to make the appropriate choice and use of information for specific applications.
15.4 Relevant information is distributed through a monthly WHO Library Digest for Africa, either electronically via satellite to groundstations or in printed form to WHO Representatives. In addition, 16 documentation centres were set up in the WHO Representatives' offices using a common computer-based proce-
125
dure. A major initiative was the launching of a project for an African Index Medicus by the Association for Health Information and Libraries in Africa, sponsored by WHO with support from bilateral agencies. The aim is to create local databases in countries using a common procedure, and merge them into a regional product.
15 5 In October 1992 BIREME organized a first regional congress on health sciences information (Sao Paulo, Brazil, October 1992) to review and upgrade cooperative information activities in Latin America and the Caribbean. Professional workshops and interdisciplinary seminars were held during this meeting.
15.6 The health literature, library and information services network (HELLIS) for South-East Asia was strengthened by the introduction of new procedures for the development and provision of computerized databases, training of library staff and continued compilation of an Index Medicus for South-East Asia.
15.7 WHO's European network of documentation centres was enlarged and now consists of 25 centres in central and eastern Europe; a newsletter, Ex libris, was issued to improve communication between the centres. WHO also provided documentation modules to liaison and information offices in countries of central and eastern Europe and in republics of the former Soviet Union.
15.8 In the Eastern Mediterranean a project entitled "ExtraMED" was set up to allow access on CD-ROM to full texts of selected health science periodicals issued in the developing countries. A health and biomedical information plan for the Islamic Republic of Iran was drawn up and reviewed at an intercountry meeting (Alexandria, February 1993); the intention is to produce guidelines for the formulation of similar national plans in other Member States.

THE WORK OF WHO 1992-1993
15 9 MED LINE on CD-ROM was acquired by most Member States in the Western Pacific. The Chinese biomedical literature analysis and retrieval system (CBLARS) came into operation; through collaboration between WHO and the Chinese Academy of Medical Sciences, 13 Chinese medical schools gained online access to this database as well as to MEDLINE. Workshops and training courses were conducted in Cambodia, China, Malaysia, Philippines and VietNam to upgrade the knowledge and skills of medical and health librarians and information providers, with emphasis on the application of new information technology.
WHO publications
15.10 Among the most important of the some 120 books published during the biennium were the first two volumes of the tenth revision of The international statistical classification of diseases and related health problems (ICD-10), containing the tabular list of diseases and the instruction manual; the third volume, containing the alphabetical index, is in press. Two key extensions of ICD-10, Chapter V, were also published as The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines and Diagnostic criteria for research. The second editions of three successful WHO handbooks appeared - On being in charge, Teaching for better learning and the Laboratory biosafety manual - as well as new guidelines for cholera control, treatment of tuberculosis, and quality assurance in blood transfusion services. Our planet, our health, the report of the WHO Commission on Health and Environment, served as the Organization's published contribution to the 1992 United Nations Conference on Environment and Development. On the AIDS pandemic, WHO published a progress report, a guide for epidemiological studies of oral manifestations of HIV infection, a physicians' manual on AIDS in Africa, and texts in the WHO AIDS Series on school health education and the global AIDS strategy. A textbook on Basic epidemiology made a promising start. Many of the 24 reports of expert committees, study groups and scientific groups published in the WHO Technical Report Series contained further studies on biological standardization, specifications for pharmaceutical preparations, drug dependence, food additives, essential drugs, and the like. Others addressed key topics such as
126
the control of schistosomiasis and lymphatic filariasis, changing trends in the financing of health services, and rehabilitation after cardiovascular diseases.
15 11 In the peer-reviewed research and review articles published in English or French in the bimonthly Bulletin of the World Health Organization, tropical diseases and health conditions in developing countries took pride of place. Regular features included reports on WHO meetings, publications and activities, and updates on timely topics. The quarterly World health forum focused on the following "round-table" themes: nurses, doctors and patients; substance abuse; screening for breast cancer; humanitarian or pragmatic approaches to medical practice; and changes in medical education. The illustrated bimonthly magazine World health sought to inform and instruct on a variety of subjects of public health importance. 1 WHO drug information, the quarterly journal with reports on major drug regulatory action in different countries, and information on medicinal products and selected essential drugs from WHO's Model List, also ensured a wide circulation of the latest lists of international nonproprietary names (INN) for pharmaceutical substances.
15.12 To enable health information from WHO to reach targeted readers in countries through national channels, 35 low-cost reprints of WHO publications were licensed in India; and 362 agreements were prepared for translations of WHO books into 48 national or regional languages by publishers, academic presses, ministries and aid organizations, among others. Copies of over 200 published translations of WHO texts were received in WHO during 1992 and 1993. A much-translated title remained the joint WHO/UNICEF statement on breast-feeding, which has appeared or is in preparation in more than 40 languages, on a par with the 1986 classic Cancer pain relief The core classification ICD-1 0, and the mental health extensions, were also being translated for publication and use in numerous language versions.
1 The themes of 1ssues were, in 1992, Heart health (World Health Day issue), Essential drugs, Commun1ty health; Water; Nursmg care; Health and econom1c development, and, 1n 1993, Accidents and violence (World Health Day issue); Children's Vacc1ne Initiative, World health situation, T uberculos1s; Chem1cal safety; Family health
HEALTH INFORMATION SUPPORT
Figure 15.1 Publications programme
Malaria: books as weapons in the fight against disease
WHO publications are produced in various languages, cover numerous aspects of the Organization's work, and are designed for a wide range of readers. For instance, in the field of malaria, WHO publications include: details of a global strategy for controlling the disease, of interest to decision-makers and administrators; training manuals on laboratory methods and microscopy and illustrations of various stages in the life cycle of the malaria parasite, invaluable to technicians involved in the laboratory diagnosis of the disease; books for the clinician on how to treat malaria of various degrees of severity; and health information for travellers, with details of measures to be taken to avoid suffering from malaria.
PLANCHESPOUR LE DIAGNOSTIC DU -PAWDISME
PLANCHES N° 1-8
Basic malaria .
m1croscopy
Part I. Learner's Guide
-----
127
VOYA(;ES IN'IF.RNA110~AUX
E'I'SAN'm
Parasitic diseases in water resources
development "k k'\.\)1,1 IIUt'f'ol.\.hlf: fk~--: 'U
THE WORK OF WHO 1992-1993
15.13 In the regions PAHO focused on disseminating health-related information of particular interest in the Americas through scientific publications and periodicals. Major publications included Pro salute novi mundi: a history of the Pan American Health Organization, a substantial volume on Reproductive health in the Americas, and a collection of papers on Gender, women and health in the Americas. In South-East Asia nine new titles were published in the regional series, together with the regional volume (Vol. 4) of the Eighth Report on the World Health Situation. Among the books published in Europe were an updated edition of Health for all targets: the health policy for Europe and the collected papers from a symposium on Health promotion and chronic illness. In the Eastern Mediterranean a number of textbooks and dictionaries were produced in connection with the arabization of medical education in the Arabic-speaking countries; and translation of WHO publications into other national languages of the Region was promoted. New publications in the Western Pacific included Medicinal plants in Viet Nam, produced in collaboration with the Institute of Materia Medica in Hanoi, as well as works on Health research methodology and District hospitals: guidelines for development.
Technical terminology
1514 A major step in the development of WHO's terminology information system (WHOTERM) was taken with the release during the biennium of the first terminology database management system, for distribution to users in the Organization and to national and international institutions. Preparation of a multilingual terminology database started with work on spe-
128
cific subjects, including food and nutrition and environmental health, with support from national research institutions and WHO collaborating centres. Progress was made in the compilation of a WHO dictionary intended to facilitate exchange of information on the Organization's programmes and activities through harmonization and standardization of technical terminology.
Distribution and sales
1515 WHO publications were made more accessible in developing countries by strengthening the networks of health-related establishments and libraries receiving comprehensive or selective groups of publications. By the end of the biennium 1008 libraries that receive WHO publications free of charge or on subscription had expressed willingness to make their collections accessible to the public without restriction. During 1992-1993 six new depository libraries were officially designated, bringing the total to 146 now open to readers throughout the world for consultation.
15.16 Annotated catalogues of publications were issued in English, French and Spanish. Numerous subject catalogues were produced on different topics. Displays of WHO publications were arranged for over 200 specialized meetings and congresses. The momentum of sales of publications achieved in the previous biennium was maintained. In 1992-1993 the income from sales reached a record level of $ 7.2 million; in fact, 1993 was the eighth consecutive year showing a growth in income. New strategies were introduced to enhance sales in developing countries and improve the performance of sales agents in developed countries.
Personnel
16.1 On 30 November 1993 the total number of staff (excluding PAHO) was 4448, compared with 4657 on 30 November 1992 and 4693 on 30 November 1991 - a decrease of some 5.22% during the biennium November 1991 toN ovember 1993. The number of professional staff rose from 1568 in November 1991 to 1587 in November 1993, and that of general service staff decreased from 3125 to 2861 in the same period.
16.2 Although the proportion of women in established offices1 was still below the target of 30% set by the Health Assembly, steady progress was made. The proportion of professional and higher-graded posts in established offices filled by women increased from 23.2% in October 1990 to 25.1% in September 1992 (mid-biennium). During the same period the number of posts in established offices at grades P.S and above filled by women increased from 11.2% to 13.5%. The percentage of women employed as associate professional officers rose from 40% to 47.6%. The percentage of women employed as consultants in all locations rose from 23.3% in 1990 to 25.2% in 1992; at headquarters 29.2% of all consultants and 38% of short-term professionals employed between October 1990 and September 1992 were women. There was a small increase in the proportion of women members of WHO's 54 expert advisory panels.
16.3 Although the target of 40% for appointments of nationals from unrepresented and under-represented countries was not met, 22%
1 Established offices include headquarters, regronal offices, offrces of the WHO Representatives and IARC, but not projects.
129
CHAPTER 16
Support services
of the appointments made in the period were of nationals of those countries. The number of unrepresented countries increased from 27 to 42 by mid-biennium (mainly owing to the addition of 13 newly independent countries, of which two were previously inactive, and four other new Member States), that of under-represented countries remained at 11, and that of over-represented countries increased from 24 to 26. The number of adequately represented countries - the ultimate criterion for evaluating geographical representation- increased from 101 to 103. The number of staff in excess of the upper limits of desirable ranges fell by 2.2%.
Office accommodation
16.4 The telephone exchange in the Regional Office for Africa, which dated from the construction of the building, was replaced and the new facility should greatly improve external communications.
16.5 Because of the expansion of programmes supported by extra budgetary funds, the Regional Office for South-East Asia plans to add a floor to one of its buildings, which will provide 13 extra offices; the construction should be completed in 1994.
16.6 Certain legal difficulties, arising from negotiations with the Host Government, prevented the implementation of plans for the extension to the Regional Office for the Eastern Mediterranean. Discussions are still under way between the Regional Office and the local authorities to find an acceptable solution.
16 7 The extension to the Regional Office for the Western Pacific was completed and the premises are now occupied.
THE WORK OF WHO 1992-1993
Budget and finance
16 8 The programme budget proposals for 1994-1995, covering the third and last period of the Eighth General Programme of Work, were prepared and submitted to the Programme Committee of the Executive Board for review of the global and interregional component in accordance with resolution EB79.R9. In parallel, the regional components were reviewed by the regional committees. After these reviews the Director-General consolidated the programme budget proposals and submitted them to the Executive Board at its ninety-first session in January 1993. The proposals were then modified to take into account favourable exchange rate movements and to meet concerns expressed by the Executive Board during its review. The modified programme budget proposals for 1994-1995 were subsequently approved by the Forty-sixth World Health Assembly in May 1993. The effective working budget for 1994-1995 was established at $ 822 101 000, providing for a net decrease in real terms of $ 24 112 200, or 3.28%. The overall cost increase in the approved budget for 1994-1995 was $111277 200, or 15.14%, an amount which incorporated considerable cost increases that had occurred before the 1994-1995 biennium but had not been included in the approved budget for 1992-1993. No provision was made in the 1994-1995 budget for exchange rate fluctuations.
16 9 In 1993 an interim financial report covering the first year of the biennium 1992-1993 was reviewed by the Committee of the Executive Board to Consider Certain Financial Matters prior to the Forty-sixth World Health Assembly, and was subsequently accepted by the Health Assembly.
16 10 Because of adverse exchange rate fluctuations during the biennium in respect of the Swiss franc, the Danish krone, the CF A franc, the Egyptian pound and the Philippine peso, it was necessary for the Organization to use $ 8 840 500 against the exchange rate facility approved by the Health Assembly for 1992-1993, namely $ 31 million. The reduced use of this facility resulted from improved exchange rates from the latter part of 1992 to the end of 1993.
16 11 In 1992-1993 obligations totalling $ 688 816 477 were incurred under the regular budget and $ 756 715 939 under funds from
130
other sources. As at 31 December 1993 arrears of contributions in respect of 1992 and 1993 amounted to$ 106 168 561. The obligations in respect of the regular budget for 1992-1993, shown as percentages under the main categories of the Eighth General Programme of Work, were as follows:
% Direction, coordination and management 11.02
Health systems infrastructure 32.39
Health science and technology 28.76
Programme support (including health information support) 27.83
100.00
1612 Obligations incurred under the 1992-1993 regular budget were considerably lower than the approved budget level of$ 734 936 000. This was due to an expected under-collection of assessed contributions, particularly from one of the largest contributors, which obliged the DirectorGeneral to reduce the implementation of the approved programme for the biennium. Nonetheless, the Director-General endeavoured to implement the planned programme to the maximum extent possible. In spite of this programme reduction and the application of various economy measures, it was still necessary to use the internal borrowing facility granted to the DirectorGeneral under Financial Regulation 5.1. The Director-General expressed to the Member States his concern over the weakened financial position of the Organization and its impact on programmes. Financial data for all sources of funds, and financial statements at 31 December 1993, with supporting schedules and tables, are presented in the Director-General's financial report for the biennium to the Forty-seventh World Health Assembly.
1613 The integrated computer-based system for administration and finance information (AFI) system is established on a large common central database and provides information support for budget preparation, budget control, expenditure and general ledger accounting, payments, treasury operations, supplies, personnel, payroll and the master mailing list. The records of expenditure accounting from the regions are integrated in the headquarters database each month for information purposes. The system also allows technical programmes to query their allot-

SUPPORT SERVICES
ments, earmark their funds, link obligations to programme activities and transfer data to "local" microcomputers for further analysis.
16.14 During the biennium the administration and finance information system was expanded to include data required for management of the investment portfolio and shipping of supplies to their destinations. The component for processing travel claims was redesigned. Studies were begun to devise system components to handle data on temporary staff and consultants, and to process staff health insurance claims so as to allow a finer analysis for cost-containment purposes. A project is under way to redesign the regional office administration and finance information system, which supports budget control, expenditure accounting and general ledger accounting. The new system will allow links to programme and project activities and provide all the budgetary and expenditure information required for their management.
Equipment and supplies for Member States
1615 The total value of supplies and equipment purchased by WHO (including PAHO) during the 1992-1993 biennium reached $255 511335. Compared with 1990-1991, this represents an increase of 3% in monetary terms. The staff working in the supply services at headquarters was reduced by approximately 15%.
1616 In 1992-1993 the Global Programme on AIDS continued to be the largest user, in dollar terms, of the WHO procurement and supply services. Whereas procurement from regular budget sources decreased by approximately 20%, activities in respect of emergency relief operations increased substantially; countries benefiting included Afghanistan, Iraq, Somalia and republics of former Yugoslavia. Pharmaceutical products and hospital supplies and equipment constituted the major part of all commodities. The cost of supplies and equipment for republics of former Yugoslavia amounted to more than $ 10 million.
1617 Member States continued to avail themselves of the services offered by WHO in the purchase of medical supplies and equipment for their health programmes, either through the WHO Revolving Fund or against reimbursement in convertible and nonconvertible currencies. There was a considerable increase in the
131
number of requests received from nongovernmental organizations. In particular, those organizations, and also other bodies within the United Nations system, made more use of WHO's services in procuring condoms and test kits for AIDS control programmes, thus benefiting from the advantageous prices that WHO has negotiated with manufacturers worldwide.
16.18 Many urgent requests for supplies were received in Africa as a result of outbreaks of meningitis, cholera and yellow fever, and national emergencies related to civil unrest in some countries. Additional urgent procurement requirements had to be met following the regionalization of most of the AIDS control programmes.
1619 PAHO/WHO continued to purchase supplies, equipment and services in the Americas in support of its own projects and on behalf of Member States against reimbursement or through established revolving fund arrangements for the Expanded Programme on Immunization. The procurement value during the biennium 1992-1993 was$ 93 662 011. A greatly increased demand for supplies was met during the peak of the cholera outbreak in Peru.
16 20 Additional work arose in South-East Asia in connection with the purchase of supplies on behalf of India for its national AIDS control programme. Also, staff had to be increased in order to meet the extra demand from the fourth population and health project in Bangladesh.
16.21 Most requests for supplies in Europe were in respect of republics of former Yugoslavia. At the same time larger numbers of requests were received from the Commonwealth of Independent States.
16.22 There was a heavy demand for medical supplies and equipment to cope with natural disasters and other emergencies in the Eastern Mediterranean. The transfer to that region of responsibility for much of the Global Programme on AIDS and also of Operation Salam for humanitarian assistance to Afghanistan widened the scope of traditional supply work.
16 23 In the Western Pacific local purchases for projects and reimbursable procurement on behalf of Member States increased. Project supplies for all Member States remained at the same level as during the previous biennium.
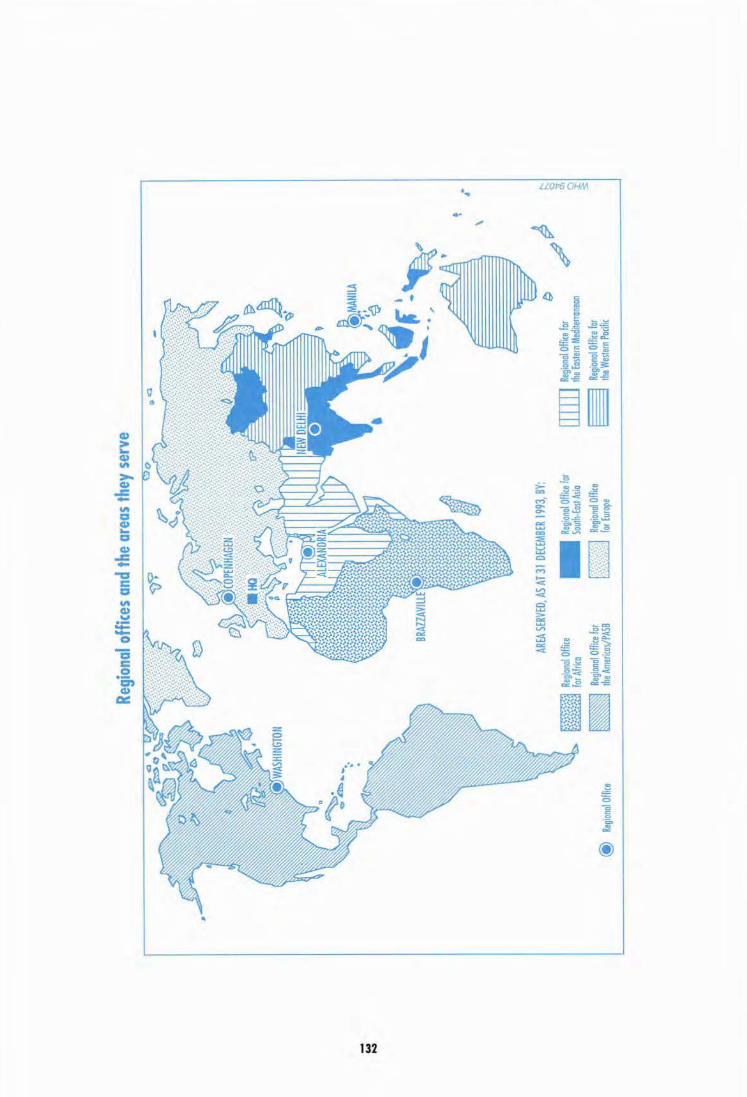
- w ....,
~
@
Regio
nal O
flice
Regio
nal o
ffice
s an
d th
e ar
eas
they
ser
ve
AREA
SERV
ED, A
S AT
31 D
ECEM
BER
1993
, BY:
Regio
nal O
ffice
for A
frica
~
Regio
nal O
ffice f
or ~
the A
meric
as/PA
SB
-
hgion
ol Of
fice f
or So
uth-E
ast A
sia
Regio
nal O
ffice
for E
urope
t JtfM
NilA
~~
4r~"
~
[]]] Re
giona
l Olfi<
e for
the E
astern
Med~erranean
~
Regio
nal O
ffice
for
~
the W
estern
Paci
fic
t
\
/~ t
4. ·~:::
: ~ ~

17.1 The sociopolitical upheavals concomitant with the establishment of democratic institutions have ushered in a new period of hope and challenge for Africa, mirrored in the health sector by the adoption at the forty-third session of the Regional Committee in Gaborone in September 1993 of the minimum district health-for-all package - "the final common path" - for the achievement of health for all through primary health care in accordance with the African Health Development Framework.
17.2 Despite progress in some areas, the health situation in countries of the African Region is still of great concern. The high prevalence of parasitic and infectious diseases, the spread of the AIDS pandemic, and the disturbing increase in noncommunicable diseases continue to be formidable impediments to progress. Massive population drifts and the settlement of displaced persons and refugees in camps lacking adequate water supply and sanitation are the legacy of conflicts in certain countries of the Region. Inaccessibility of basic health care services, precarious nutrition and the consequences of drought have added to the difficulties.
17.3 Within this context of social, political and health crises, WHO pursued efforts to reduce immediate suffering and to strengthen the capacity of countries to cope with the multiple challenges impeding their development. In the same spirit, an unprecedented initiative for widespread social mobilization in favour of community health in Africa was launched by African ministers of health at the International Conference on Community Health in Africa (Brazzaville, September 1992).
17.4 Given the considerable deterioration in national capacities for financing health systems, the African ministers of health decided to make health care financing one of the priority areas for
133
CHAPTER 17
African Region
intervention by WHO. A situation analysis of health care financing mechanisms and problems was consequently undertaken in Member States, and some innovative community health financing schemes were reported. National experts were recruited as economists on WHO country teams, and workshops were organized, stressing the relation between economics and health. Contacts were established with donors and development banks to solicit funding for programme activities on health care financing at country level. Technical support was given to some countries for necessary health care financing reforms.
17.5 WH 0 provided support to 10 countries in the elaboration of their national health development plans and policies. A framework for the reorientation and restructuring of hospitals was prepared, in pursuance of directives of the fortysecond session of the Regional Committee in 1992, to promote integration of hospital networks into health systems. Efforts were also made to develop effective coordination mechanisms to assist Member States of the Region in emergency and humanitarian relief.
17.6 With regard to health information and epidemiological surveillance systems, WHO supported training and development activities in five countries. Close collaboration with the Association for Health Information and Libraries in Africa reactivated a long-dormant project for an African Index Medicus. By the end of 1993 centres in Ghana, Malawi, Mozambique, United Republic of Tanzania, Zambia and Zimbabwe were participating in the project, and the inaugural issue had been widely distributed.
17.7 The regionalization of technical and administrative support under the Global Programme on AIDS to the African Region reached an advanced stage. The programmes of 43 countries have been regionalized. Although the re-

THE WORK OF WHO 1992-1993
duction in financial support to countries and WHO from donors for AIDS control was a major concern, national AIDS programmes made significant progress in implementing appropriate strategies. Youth groups and clubs have been formed in many countries. Communities have set up associations, and over 1000 local nongovernmental organizations are engaged in the provision of care to AIDS patients and support to their families. Field-testing of indicators for assessing the impact of interventions at country level was completed. A guide to national AIDS programmes was issued, emphasizing the desirability of implementing programmes within the national health development framework, with decentralization to district and community levels in order to ensure sustainability of measures, accelerate the dissemination of knowledge about AIDS, and promote changes in behaviour and the adoption of a healthy lifestyle by all, particularly young people and children.
17 8 In preparation for the 1992 International Conference on Nutrition (see paragraph 9.14), 39 Member States made a comprehensive review of their nutrition situation and two meetings were held (Dakar, February 1992; Nairobi, March 1992) bringing together representatives of all countries of the Region. One outcome of these meetings was the adoption, in principle, of an International Decade on Food and Nutrition for Africa. To follow up the recommendations of the international conference, steps were taken to establish national plans for each country by the end of 1994. Technical and financial support was provided to several Member States1 under the initiative for intensified cooperation with countries and peoples in greatest need.
17 9 Particular attention was directed to control of iodine deficiency diseases in 1992. Preventive activities were undertaken in 23 countries, of which 17 had national control programmes. Emphasis was put on iodized salt consumption, and workshops on this subject were organized in Botswana and Senegal in 1992. A survey on micronutrient deficiency in the Region, completed in 1993, showed that 16 out of the 34 countries where vitamin A deficiency is prevalent had already initiated preventive activities.
1 Benrn, Central Afrrcan Republic, Chad, Guinea, Gurnea-Brssau, Madagascar, Mozambrque, Sao Tome and Principe, Uganda, Zambia
134
17.10 Efforts were made to strengthen the management of national maternal and child health/ family planning programmes, with emphasis on service coverage, improved quality of care and rapid reduction of morbidity and mortality among mothers and neonates. Management support activities included collaboration in workshops on district team problem-solving methods in Senegal and United Republic of Tanzania, as well as the finalization of a project on accelerated action for safe motherhood in the African Region. A regional joint consultation on the prevention of maternal mortality and on infertility in sub-Saharan Africa was organized at the Regional Centre for Training and Research in Family Health (Kigali, January 1992). The first of a series of regional training courses in family health research methods was successfully conducted by the regional centre for 12 trainees from Burkina Faso, Cameroon, Cote d'Ivoire, Madagascar and R wanda. A regional data bank on selected maternal and child health/family planning indicators was established in the Regional Office, based on the global database at headquarters. Collaboration with UNFP A and UNICEF was strengthened.
17 11 The final evaluation report on the International Drinking Water Supply and Sanitation Decade ( 1981-1990) was presented to the Regional Committee in 1992. In the course of the Decade approximately 223 million people had access to an adequate and safe water supply and 156 million access to appropriate sanitation in the African Region. During the same period approximately 226 million people remained without satisfactory water supply and 333 million without appropriate sanitation. WHO provided technical and financial support to 32 Member States for institutional and human resources development, and for construction and rehabilitation of low-cost water supply and sanitation systems in rural areas. Member States affected by cholera were given special financial and technical support to prepare short- and long-term plans for the prevention and control of outbreaks. National experts were recruited in 15 countries to work as sanitary engineers in the country support team, and they were included among the experts participating in the second regional environmental health coordination meeting (Nairobi, March 1992). Collaboration continued with UNEP, FAO, UNESCO/ Intergovernmental Oceanographic Commission and IAEA in implementing the programme on assessment and control of pollution in coast-

AFRICAN REGION
al and marine environments in west, central and east Africa.
17.12 Following activities to promote Healthy Cities throughout the Region, a first meeting for French-speaking African countries was organized within the framework of collaboration between the Healthy Cities network of Quebec (Canada) and Dakar commune (Dakar, July 1992). An outcome of the meeting was support for the preparation of action plans in five of the 14 cities participating in the meeting. A WHO/ GTZ workshop (Harare, November 1993) brought together participants from 16 countries to launch a regional Healthy Cities network.
17.13 Immunization rates in the Region reached 82% for BCG, 57% for a third dose of poliomyelitis vaccine and 50% for a second dose of tetanus toxoid. Efforts to improve disease surveillance and control in countries focused on training of programme managers and district health teams in the use of indicators for monitoring progress. A number of Member States, mainly in southern Africa, reported no cases of poliomyelitis and a very low incidence of neonatal tetanus. Assessments in some of these countries confirmed a virtual absence of poliovirus transmission, a very low incidence of neonatal tetanus, and a significant reduction in measles cases and deaths.
17 14 The malaria control programme was accorded the highest priority. Following the 1992 Ministerial Conference on Malaria (see paragraph 14.16), tremendous progress was made in the African Region. More than 20 countries established or reformulated malaria control programmes with the technical support of WHO, and some 25 organized training on control strategies for district health workers. A regional plan of action for the period 1994-1997 was adopted.
13S
17.15 Following a review of the status of national dracunculiasis eradication programmes at a fourth African regional conference (Enugu, Nigeria, March 1992), all endemic countries began implementing their workplans. The efficacy of the regional eradication strategy was evident from the progress made in two of the most heavily endemic countries, Ghana and Nigeria, as well as in other less endemic countries.
17 16 Considerable strides were made in leprosy control in Africa. Prevalence dropped as a result of better coverage of multidrug therapy from 27% in 1990 to 45.5% in 1993, with several countries attaining 100% coverage. Support was provided to countries with severe leprosy problems and inadequate multidrug therapy through consultant services for management training and expansion of coverage. Outbreaks of type A meningococcal meningitis, cholera and plague were of particular concern. Support included consultant services, information exchange, provision of vaccines and drugs, and organization of training workshops. Training materials were elaborated and tested as part of an effort to promote integrated disease control in countries, especially at district level.
1717 Human resource and material support for health science training institutions continued, with efforts centring on the revision of medical training. A programme was set up to strengthen continuing education, and steps were taken to enhance the role of nurses and midwives in safe motherhood, research and epidemiological surveillance. Incidents affecting security in several countries caused disruption of technical programmes and required special efforts by WHO staff. Responses were made, under emergency arrangements, to health-related problems caused by extensive population movements resulting from such incidents.


CHAPTER 18
Region of the Americas
18.1 In 1992 the Pan American Sanitary Bureau celebrated 90 years as the oldest continuously functioning international health agency in the world. The organizational structure of the Pan American Health Organization's secretariat, the Pan American Sanitary Bureau/WHO Regional Office for the Americas, was adjusted in early 1993 to better enable it to meet its constitutional obligations to assist Member States in achieving health for the people of the Americas. One of the purposes of this adjustment was to strengthen the secretariat for improved implementation of the regional strategic orientations and programme priorities in line with WHO's Ninth General Programme of Work.
18.2 In 1993 PAHO/WHO started to assess the impact of its strategic orientations and programme priorities on national health development, particularly on policy-making and health activities in the Member States, and its technical cooperation. This evaluation is part of a biennial review to determine the progress made towards the achievement of the Organization's quadrennial goals in 1 991-1994.
18.3 In 1992 the Regional Committee for the Americas reviewed and approved several plans of action for the Region, including programmes on adolescent health, elimination of leprosy, and elimination of vitamin A deficiency. Of particular importance was the Committee's approval of a regional plan of action for investment in the environment and health which will marshal national and international resources. The Committee also approved the promotion of activities to link the health and tourism sectors in the Region and, in its capacity as the Directing Council of PAHO, admitted Puerto Rico as an Associate Member.
18.4 In 1993 the forty-fifth session of the Regional Committee/XXXVII Directing Coun-
137
cil of PAHO reviewed the proposed programme budget for 1994-1995. Some of the most noteworthy resolutions adopted at this session were those urging Member States to comply with guidelines established for certifying eradication of poliomyelitis caused by indigenous wild poliovirus, to implement measures to eliminate measles, to step up vaccination against all diseases under the Expanded Programme on Immunization, and to ensure the sustainability of all these efforts. The Regional Committee also approved resolutions aimed at strengthening HIV I AIDS prevention and control programmes, adopting measures to reduce maternal mortality, and establishing a regional programme of bioethics. A new health initiative on behalf of the indigenous peoples of the Americas was approved, as was the formulation of a regional plan of action on violence and health, including violence against women and all risk groups.
185 During 1992-1993,16 joint evaluations of technical cooperation were carried out with Member States. Almost all the Member States participated in the PAHO/WHO programme for technical cooperation among countries. Training and the development of human resources were particularly emphasized; and the subregional health initiatives in the Caribbean, Central America, the Andean Area and the Southern Cone1 continued to serve as an important mechanism for implementing projects envisaged under the technical cooperation programme. A strategic plan was prepared to strengthen the Andean Cooperation in Health initiative and several national technical working groups prepared action plans in the priority areas of maternal and child health, essential drugs, sub-
1 Argentrna, Bolrvra, Brazil, Chile, Paraguay, Uruguay

THE WORK OF WHO 1992-1993
stance abuse, environmental health and disaster preparedness. A draft health promotion charter for Latin American countries was prepared at the International Conference on Health Promotion (Santafe de Bogota, November 1992); and a similar document was produced the following year under the aegis of the Caribbean Cooperation in Health initiative. Significant progress was achieved in the Central American Health Initiative's four priority areas of health infrastructure, health promotion and disease control, health care for special groups, and the environment and health. The Southern Cone Health Initiative was instrumental in the control of Chagas disease and cholera.
18.6 During the biennium the Region continued a movement towards democracy which incorporated constitutional reforms, free and open electoral processes, and formal acceptance of the obligation to protect human rights. The economic recovery that began in 1991 has reached a phase of moderate expansion, gradual price stabilization, alleviation of the debt burden, and a favourable net transfer of resources. The process of market integration continued to intensify in the Region - for instance, within the framework of the Southern Cone Common Market (MERCOSUR), the Caribbean Community (CARICOM) and the North American Free Trade Agreement (NAFTA). However, there was no significant reduction in unemployment levels as compared to previous years. Declining family income left some 60 million people in poverty during the 1980s, a figure that reached a very high level in 1991.
18.7 Efforts were made to increase the capability of the Organization's programmes and country offices, as well as ministries of health, to enhance project preparation skills, strengthen project monitoring, successfully negotiate external financing for priority health areas, and expand resource mobilization for health by encouraging the full participation of ministries, other bodies within the United Nations system and nongovernmental organizations. The Organization participated in the second and third Ibero-American conferences of Heads of State and Government (Madrid, July 1992; Salvador, Brazil, July 1993), which approved several proposals relating to health. Discussions continued with the United Nations system in preparation for the 1995 world summit on social development. The Organization is collaborating with the Economic Commission for Latin America and the Caribbean in preparing
138
a document on health with equity, which reviews health aspects of the economic transformation currently under way in the Americas.
18 8 The Organization participated in the first meeting of the commission on health, labour and social security of the Latin American Parliament (PARLATINO) held in Havana in March 1993, and over the next few years its technical cooperation will focus on the five health priorities identified during the meeting. A cooperation agreement was reached with the Central American Parliament, and progress was made in formalizing similar agreements with the Andean Parliament. The Organization is also participating in a network of agencies that supports the formulation of integrated social policies by governments.
18 9 The epidemiological profile of the Region continued to change, especially regarding mortality. The relative importance of chronic and degenerative causes of disease is increasing, particularly in countries where total mortality and fertility have already declined. The ever-growing urban concentration and the increased life expectancy of the populations have resulted in the simultaneous presence of "old" health problems such as malaria, dengue, cholera, diarrhoea! diseases and acute respiratory infections and "new" problems such as cardiovascular diseases, violence, cancer and AIDS.
18.10 Several innovations in the health sector during the biennium stand out clearly. In the wake of the victories over smallpox, a series of regional, subregional and national plans and programmes have been launched for the purpose of eradicating, eliminating or controlling a wide variety of infectious diseases. In August 1993 the Region celebrated its second year free of confirmed cases of poliomyelitis caused by indigenous wild poliovirus, and countries have now entered the certification phase. As a result of mass immunization campaigns, better surveillance of illnesses with rash and fever, and weekly "negative reporting", there have been no confirmed cases of measles in the English-speaking Caribbean in nearly two years. Argentina, Brazil, Chile, Colombia, Cuba, Dominican Republic, Peru and the Central American countries have launched similar campaigns aimed at eliminating or controlling measles. The goal set at the 1990 World Summit for Children of reducing the incidence of neonatal tetanus to no more than one case per 1000 live births has practically been reached in the Region. With surveillance and vac-

REGION OF THE AMERICAS
cination of all women of childbearing age in high-risk areas as the principal strategies, there is confidence that the commitment to eliminate this disease by 1995 will be fulfilled.
18.11 The countries of the Southern Cone are committed to an initiative to eliminate the vectorial transmissiOn and interrupt the transfusional transmission of Trypanosoma cruzi. This initiative has stimulated cooperation among other countries with similar problems regarding Chagas disease. Similarly, the countries of the Andean subregion have begun to implement a plan for the control of iodine deficiency disorders.
18.12 Despite reductions in their regular budgets, health ministries, in close collaboration with the Organization, have managed to stem the cholera epidemic. National efforts for consciousness-raising and emergency preparedness and relief, coupled with efforts to disinfect water systems, improve basic hygiene and monitor food handling, have kept cholera at bay and resulted in a near-30% reduction in all deaths from diarrhoea! diseases.
18 13 Technical cooperation with national AIDS programmes in preparation for "second cycle" multisectoral medium-term plans continued through 1993; national plans were completed and technical reviews carried out in several countries. Technical cooperation activities included workshops on applied epidemiology and strategic planning.
1814 PAHO/WHO provided emergency technical support to control Cuba's epidemic of neuropathy with predominantly optic clinical manifestations, which has produced over 50 000 cases since it was first detected in 1992 and is now under control.
18.15 The declaration adopted at the 1992 International Conference on Health Promotion (see paragraph 18.5) set targets and advocated approaches to encourage healthy behaviour. Member governments were urged to adopt public policies aimed to strengthen health promotion and address emerging health problems. The Organization promoted the first and second meetings of Central American ministers of environment and of health (El Salvador, September 1992; Hondu-
139
ras, September 1993), convened to agree on national plans for implementing the resolutions of the 1992 United Nations Conference on Environment and Development (see paragraph 12.1).
18.16 PAHO/WHO continued to support efforts to reorganize the health sector on the basis of decentralization and to cooperate with all Member States in setting up and evaluating local health systems; it worked out approaches for applying the local health system strategy at district or county level, and for supporting the establishment of "healthy counties". Progress was also made in applying the local health system strategy in urban areas.
1817 With the advent of the United Nations International Decade for Natural Disaster Reduction, emphasis has shifted from preparedness and relief to prevention and mitigation. PAHO/ WHO has broadened its objectives to include a wider range of disaster prevention and mitigation activities in the health sector, including the delivery of emergency humanitarian assistance. The crisis in Haiti has been attended to within this framework and in accordance with a plan for humanitarian action launched by the Organization of American States and the United Nations. PAHO/WHO has been designated as coordinating body for the design and delivery of basic health services under this plan and, since December 1993, has managed the supply of fuel for all humanitarian activities. The terms of the Central American development programme for refugees and displaced persons (PRODERE) were modified to include mental health and physical rehabilitation of war-related disabilities in several countries. Many important lessons about integrated health care for special groups, interagency collaboration and promotion of peace have been learned from PRODERE, which completed its third and final year in 1993. By the same token, health has continued to serve as a "bridge for peace" in Central America. In El Salvador the Chapultepec Peace Agreement resulted in a request from all parties to find ways to provide basic services to the demobilizing military forces under the aegis of the United Nations. PAHO/ WHO responded by organizing and delivering services to the former combatants and their dependents, with financial support from the international community.


CHAPTER 19
South·East Asia Region
19.1 With growing social awareness and consciousness among the people of the Region and the operation of free market forces, health development has received a new impetus. The ministers of health of the countries of the Region met twice during the biennium and considered AIDS control, trends in communicable diseases, technical cooperation among developing countries, the combination of public and private provision of health care, and primary health care in a changing socioeconomic and epidemiological situation. They renewed their commitment to improve the quality of services in their countries. The health-for-all leadership initiative begun in 1985 continued to make progress in sensitizing decision-makers to critical aspects of health development. An intercountry consultation was held on the subject of strengthening women's leadership for health for all (New Delhi, February 1992).
19.2 The results of the second evaluation of the implementation of the health-for-all strategy, published in 1993,1 showed that significant achievements have been made in reducing mortality among infants, children and mothers. Substantial progress has also been made in immunizing children against childhood diseases and introducing family planning programmes in many countries. However, there remain wide variations in health status among and within countries.
19 3 WHO provided technical support to Bangladesh, Bhutan, Indonesia, Nepal, Sri Lanka and Thailand in formulating national health policies and plans. Other areas covered were health economics, health care financing and management. There is a dearth of skilled health planners
1 Implementation of the global strategy for health for all by the year 2000, second evaluation: Eighth report on the world health situation. Vol. 4: South·Eost Asia Regron. Geneva, World Health Organrzat10n, 1993.
141
in most of the Member States, partly owing to
the "brain drain" to more developed countries. WHO therefore collaborated in organizing meetings, courses, fellowships and local training in health management. Bangladesh, Bhutan, Maldives, Mongolia, Myanmar and Nepal benefited from intensified WHO cooperation with countries and peoples in greatest need to improve national capability in these fields.
19 4 Support was given to India, Indonesia, Nepal and Thailand in reviewing existing public health laws as well as draft legislation on AIDS. Study tours were organized for officials to study health legislation abroad.
19.5 Health infrastructure was expanded and service coverage improved in all the Member States through training and deployment of vast numbers of community health volunteers and the involvement of the community in planning and management of local health activities.
19.6 Bangladesh, Bhutan, Nepal, Maldives, Mongolia, Myanmar and Sri Lanka are reviewing current patterns of resource allocation and utilization in the health sector and revising their health policies and strategies. Indonesia has been analysing trends in the health system as a basis for studying the implications of its policies and strategies. Mongolia is reviewing the structure and functions of its ministry of health. WHO will continue to support such reviews. In the coming decade, further efforts must be made to reach the underserved or underprivileged in both rural and urban areas, using primary health care approaches based on community involvement, leadership development for health for all, quality assurance, self-care, integration of services, and intersectoral collaboration.
19.7 At its forty-fifth session the Regional Committee for South-East Asia discussed the

THE WORK OF WHO 1992-1993
subject of "Balance and relevance in human resources for health" and urged Member countries to carry out a thorough analysis of the present situation, with particular attention to imbalances. To improve methods for analysing policy on human resources for health and strengthen national capabilities in this area, WHO has developed tools, strengthened its information base, and promoted research. It has also continued to support the development of nursing and medical education systems.
19.8 There is increasing recognition in the Region of the importance of information and education for health, as reflected in the inclusion of these activities in most health programmes. Health matters are being given better coverage in the press, radio and television. School health education has come into sharper focus, as has the role of women in health development.
19.9 A review was made of the current strategies for health research in the Region and a publication on this subject is under preparation.
19.10 Emphasis was given to health protection and promotion and their practical applications, particularly in respect of oral health and injury prevention, the creation of a supportive and safe work environment and the provision of health and social services to disabled persons and groups such as women, children, adolescents and the elderly. Prevention of dental caries and oral diseases and promotion of oral health are not yet integrated in many health services. Collection of data on road and agricultural injuries was intensified with the aim of strengthening measures to check the continuing rise in mortality from injuries. In many countries comprehensive tobacco control programmes have been established, including epidemiological surveillance, public education, legislative and administrative measures, and early detection and treatment of the consequences of tobacco use such as oral cancer.
19.11 All the Member States recognize the advantages of a holistic approach to child survival and development. WHO, together with UNICEF, UNDP, UNFPA and other professional and nongovernmental organizations, plays a leading role in establishing integrated systems for providing maternal and child health and family planning services as a part of primary health care. However, maternal mortality remains unacceptably high with considerable variations within countries. A number of training activities
142
in this field took place during the biennium. Family planning and birth-spacing have been accepted as a means of achieving better health for mothers and children, and WHO pays particular attention to improving the quality of family planning services.
1912 The socioeconomic and health implications of the changing demographic situation in some countries with large populations make it imperative to take timely decisions on introducing short- and long-term measures to protect and promote the health of the elderly. Development of policies and the design of services for the elderly based on community approaches supported by appropriate institutional care have become an important feature of WHO's technical collaboration with countries.
1913 Concern about drug abuse has been growing in several countries as a result of the epidemics of HIV infection among drug injectors, who now form substantial reservoirs of the virus in Myanmar, Thailand and some Indian states and cities. However, some approaches to the containment of these epidemics have not been found acceptable because they have been seen as condoning drug use. In a number of countries problems of alcohol use are more serious, although they have less visibility from a political point of view. A community approach, developed with centres in India, Myanmar and Sri Lanka, has proved very effective in curtailing urban heroin abuse and rural opium and alcohol abuse.
19 14 A number of countries experiencing rapid urbanization and industrialization have given high priority to community water supply and sanitation, and initiated other environmental health activities. Training within countries and abroad was given on computer-based project management and water and sanitation project implementation for engineers in Bangladesh, India, Maldives, Nepal and Sri Lanka. WHO continued to promote intersectoral community approaches to solve problems of rapid population growth and unplanned urbanization. Regional consultations on sanitation, solid waste management, surface water drainage and urban health have highlighted some of the strategies and actions that countries could adopt.
19 15 Collaborative efforts in the management of environmental health hazards focused on technical support in capacity-building for preparing national action plans on health and envi-

SOUTH-EAST ASIA REGION
ronment. WHO collaborated in studies on groundwater pollution, industrial water consumption, and pollution monitoring systems and on environmental epidemiology in critically polluted areas in India. Air and water quality monitoring activities continued in India, Indonesia and Thailand.
19 16 A document was prepared giving an overview of the current situation and future perspectives for strengthening national food safety programmes. Support to institutional development included the surveillance, prevention and control of food adulteration in India, training of food safety staff at district and provincial levels in Indonesia and Sri Lanka, and the establishment of a computerized information network on food analysis and quality control in Thailand. Studies on street-vended foods, pesticide residues and plastic food containers, and on dietary intake of heavy metals were conducted in various countries. Selected Codex Alimentarius texts and guidelines were translated and published in Indonesia, and national food standards were reviewed and harmonized with the Codex standards in India.
19.17 Support for strengthening health laboratories as part of primary health care included the formulation of national policies, introduction of simple diagnostic tests at peripheral level, and establishment of a quality assessment network. Guidelines were issued on the organization of health laboratory service networks, including appropriate technology and quality assurance.
19.18 National essential drug programmes have been developed in Member countries, sometimes with extra budgetary support. Although essential drugs have generally become more readily available, there have been acute shortages in some countries owing to political disturbances. WHO has complied with requests for procurement of drugs to ameliorate the situation. Strengthening of drug regulatory and quality control systems, improvement of good manufacturing practices, studies on the bioavailability and stability of pharmaceutical preparations, and drug evaluation were some of the areas in which WHO collaborated with countries in 1992-1993.
19.19 Assessments of the operation of the WHO Certification Scheme on the Quality of Pharmaceutical Products moving in International Commerce were undertaken in Myanmar and Sri Lanka. Other activities in this field included the development of standard treatment regimens,
143
strengthening of technical and managerial capabilities in the area of drug information, organization of training courses and convening of a WHO intercountry consultative meeting on the rational use of essential drugs in 1993.
19.20 The wealth of expertise in the well-accepted systems of traditional medicine in the Region has facilitated their development in various ways: establishment of herbal gardens; production and quality control of traditional medicines using modern machinery and applying good manufacturing practices; improvement of traditional medical services in the public sector; and training of traditional medicine practitioners for delivery of primary health care.
19 21 High immunization coverage has been achieved in most of the Member States, but many deaths still occur from measles, neonatal tetanus and poliomyelitis. Surveillance has improved but remains the weakest component of most national programmes. Vaccine supply is a matter of concern in several countries; and WHO, donor agencies and governments are seeking ways to improve self-sufficiency in this area. Local production of cold chain equipment (including complete solar systems) is progressing well.
19 22 While the overall incidence of malaria in the Region has remained unchanged over the last ten years, the situation in forest areas has become more serious. WHO has formulated technical and operational guidelines, indicators and criteria to implement the new global strategy formalaria control, and all the malarious countries are preparing plans of operation.
19.23 WHO continued to cooperate in all aspects of prevention and control of intestinal parasitic infections, visceral leishmaniasis, filariasis, schistosomiasis and dracunculiasis. Intestinal parasitic infections are widespread in the Region. Visceral leishmaniasis is still a problem in parts of India, as well as Bangladesh and Nepal, as is lymphatic filariasis in Bangladesh, India, Indonesia, Maldives, Myanmar, Nepal, Sri Lanka and Thailand. Schistosomiasis is endemic in parts of Indonesia and in limited areas of Thailand. Dracunculiasis is now a problem in India only, but has shown a downward trend in recent years.
19.24 All the Member States now have well developed programmes for the control of diarrhoea! diseases, implemented through primary health care. Training receives the highest priority

THE WORK OF WHO 1992-1993
and 10 countries have established some 55 units giving health workers practical training in diarrhoea case management. Nine countries produce their own oral rehydration salts. A new strain of cholera, designated Vibrio cholerae 0139, was first isolated in an outbreak in V ell ore (India) in October 1992. It then spread rapidly to West Bengal and some other states in India. Large outbreaks have since been reported from Bangladesh. A few cases have also been reported from Thailand and Nepal. Because there is very little resistance to this new strain, it has the potential for pandemic spread. All countries have been alerted and advised to intensify surveillance activities.
19.25 Early diagnosis and treatment is a key strategy for reducing mortality from acute respiratory infections in children. Ten Member States have started control programmes, and substantial progress has been made in several of them. More than 9000 doctors, 18 000 health workers and 30 000 health volunteers have received training in standard case management, facilitated by the translation of training materials in local languages. Health facility, household and mortality surveys have been carried out in some countries for evaluation purposes.
19 26 Tuberculosis continues to be a serious public health problem. In 1991 about two million cases were reported in the Region, almost half the world total, and nearly one million deaths annually. However, there is renewed interest in control of the disease because of its relationship with HIV infection and AIDS. WHO is providing support for the reorganization of control programmes through evaluation and planning activities or the initiation of pilot projects, with emphasis on management at district level. Many nongovernmental organizations, the World Bank and bilateral agencies are involved in control programmes in some countries.
19.27 Despite the significant progress made in leprosy control during the past decade, SouthEast Asia, with a registered case-load of 1 347 000 in 1993, accounts for 70% of all registered cases in the world. Control activities were intensified in endemic countries and multidrug
144
therapy helped to reduce the disease burden. WHO collaborated in reviewing and modifying national plans for leprosy control, including provision for resource mobilization and coordination. In 1992 the Regional Committee adopted a regional strategy for leprosy elimination, which provides a framework for the development of control programmes.
19 28 Some Member States continue to be plagued by rabies. WHO provided support in the form of consultant services, supplies and equipment, training for health personnel and the organization of workshops on rabies control. Courses were conducted for provincial staff in Indonesia. Nepal intensified its control measures and human deaths from the disease were reduced in Sri Lanka through a project supported by WHO and AGFUND. In Mongolia the main emphasis was on eradication of plague and control of brucellosis. WHO supported several countries in the development of new vaccines and in transfer of technology for the production of vaccine and sera, including plasma-derived hepatitis B vaccine in Mongolia and Myanmar, and tetanus toxoid and snake venom antisera in Bangladesh. Efforts were made in Thailand to improve the efficacy of vaccines used in the Expanded Programme on Immunization as well as vaccines against dengue haemorrhagic fever and Japanese encephalitis.
19 29 HIV infection did not begin to spread extensively in South-East Asia until the mid-1980s, but the impact is already severe. More than 1.5 million people are estimated to have been infected and about 20 000 have already developed AIDS. In response to this threat, governments have set up national control programmes with WHO support. Political commitment is growing and multisectoral action, including the involvement of nongovernmental organizations and the private sector, is being undertaken. The aim is to interrupt transmission by promoting safer sexual behaviour including condom use, and to ensure early diagnosis and treatment of sexually transmitted diseases. Emphasis is also being given to safe and rational use of blood and blood products and to prevention of transmission through contaminated injecting equipment.
20.1 The dramatic changes sweeping through the European Region in 1990-1991 continued in 1992-1993. Nineteen new Member States emerged from the democratization process in countries of central and eastern Europe and republics of the former Soviet Union. In western Europe the 1992 Maastricht Treaty on European Union was finally ratified and came into force on 1 November 1993.
20.2 The economic recession and resulting unemployment in many countries is having an impact on health care. Although the situation in several countries of central and eastern Europe has started to return to normal after their political transition, they still face serious socioeconomic problems. Conditions in republics of the former Soviet Union are generally more difficult, particularly as a result of the collapse of industrial enterprises and the rise in unemployment and inflation. The disturbing increase in the gap between "haves" and "have nots" is causing concern and has grave implications for the health of vulnerable people.
20 3 Communicable diseases have reappeared in a number of newly independent States. The statistics on diphtheria are alarming and reflect insufficient immunization coverage. Progress is being made, however, in reducing the incidence of poliomyelitis, measles, mumps and rubella. A small number of cholera cases have occurred in a few Member States, but most seem to be imported. AIDS is spreading at a slower pace than in other regions, but the potential impact of this disease in central and eastern Europe is worrying. The tobacco industry has continued to expand in that part of the Region, where countries have not had time to establish appropriate legislation and health promotion programmes.
20.4 Some interesting developments have taken place with regard to health service reforms.
145
CHAPTER 20
European Region
In the United Kingdom reform of health care financing has allowed general practitioners to become independent fund holders; Germany has introduced diagnosis-related groupings for the remuneration of hospital services through the health insurance system; Finland has introduced a model for subsidizing municipal services, including health, through a global budget with less central control; and several countries of central and eastern Europe and newly independent States are well on the way to implementing reforms. In 1992, for example, Hungary enacted legislation on health insurance, government primary health care for outpatients, and public health; there were similar examples in Albania, Kazakhstan, Poland and Romania.
20 5 Armed conflicts in Europe continue to cause suffering and loss of life. In the conflict in former Yugoslavia, more than 150 000 people have reportedly been killed and hundreds of thousands wounded, close to four million people have been made refugees, probably as many as 20 000 women have been raped, thousands of people have been tortured, and around 3000 have been amputated. The consequences of the conflicts affecting Armenia, Azerbaijan, Georgia and Tajikistan are receiving less attention from the outside world, yet the toll of human suffering is considerable.
20.6 In collaboration with other bodies of the United Nations system, intergovernmental and nongovernmental organizations and donors, WHO carried out an intensive programme of humanitarian assistance in republics of former Yugoslavia, focusing on public health and nutrition, equipment, supplies and logistic support and help to war victims. The policy of providing a broad range of standardized "kits" ensured that the supply of pharmaceuticals and equipment closely matched needs. These kits are now being widely used by other organizations. A

THE WORK OF WHO 1992-1993
WHO Special Representative in Tajikistan helped to coordinate humanitarian assistance.
20.7 Close cooperation continued with the Commission of the European Communities and the Council of Europe. One joint venture was the establishment in 1993 of a European Network of Health-promoting Schools, with a secretariat located at the Regional Office. Its aim is to make schools a healthy setting for living, learning and working. A joint two-year health care telecommunications project known as the "European Nervous System" was launched with the Commission. Its purpose is to demonstrate, through selected pilot areas and in collaboration with national health administrations and industry, ways of applying communications technology to meet selected information needs. It is regarded as a first step towards the realization of a collaborative, trans-European health information network.
20.8 Many countries now have their own national policies based on the European health-forall policy. England is the most recent in that regard, with its "Health of the nation" policy document and rigorous implementation process. Both the full text of the updated health policy for Europe and summary were published and widely distributed during 1992-1993.1
20 9 The number of networks of key partners concerned with health for all, whether institutions, groups or individuals, continued to grow. Some comprise general practitioners, diabetes specialists, health care financing experts and consumer organizations. Twenty countries have joined the countrywide integrated noncommunicable disease intervention (CINDI) programme, 11 of them countries of central and eastern Europe or newly independent States. A European Forum of Pharmaceutical Associations and WHO was established in early 1992 to improve contacts and collaboration and to upgrade the role of the pharmacist in Europe through joint activities. A European Forum of National Medical Associations and WHO was constituted in 1991. At its first meeting in 1992 it issued a declaration on tobacco which, among other points, urged physicians to stop smoking. At its meeting in 1993 it adopted recommendations for
1 Health for all targets: the health policy for Europe. Copenhagen, World Health Organization, 1993 (Health for All Senes, No. 4).
146
national medical associations calling for measures to ensure the quality of care.
20.10 The European Healthy Cities network was expanded in central and eastern Europe. More than 600 cities are now linked through some 20 national networks to this successful movement, which requires participants to draw up and implement local health-for-all policies and plans. Policies have also been promoted through a newly created network of "regions for health", grouping 11 regions in 10 European countries. This network has considerable potential, given that there are some 1500 regions in Europe.
20.11 Two European action plans on alcohol and on tobacco, endorsed by the Regional Committee in 1992, were actively implemented. A task force was set up for execution of the Action Plan for a Tobacco-free Europe, especially in central and eastern Europe. The European Alcohol Action Plan was translated into nine languages, and a European network of national counterparts in alcohol research centres and advocacy groups established.
20.12 A conference of ministers of health and ministers of finance and planning on investment in health (Riga, 1-2 April 1993 ), organized with the help of voluntary donations, endorsed a Riga statement on principles for action to invest in health, and adopted a Riga initiative outlining activities for implementation of AIDS programmes in central and eastern Europe. High priority has been given to following up this conference.
20.13 During 1992 the Rome and Bilthoven (Netherlands) divisions of the European Environment and Health Centre became fully operational, and in 1993 a project office was established in Nancy (France). Preparation continued of a comprehensive report on the current environmental situation entitled "Concern for Europe's tomorrow". It will be Europe's contribution to the second European conference on environment and health, to be convened in Helsinki in 1994 jointly with the Commission of the European Communities. WHO was actively involved in preparations for a ministerial conference on environment for Europe (Lucerne, Switzerland, April1993), which endorsed a special action programme for central and eastern Europe.
2014 Major changes have taken place in health services. In central and eastern Europe there is strong public pressure for privatization and the

EUROPEAN REGION
introduction of new financing mechanisms and health insurance systems. A permanent working group was set up within the project on health care reform (EUROCARE) in order to monitor and stimulate regional developments. As part of the project, a series of overviews of health care in transition and health care reforms in central and eastern Europe are being produced, and will be regularly updated.
20.15 A "Second Declaration of Alma-Ata" was made by nursing and midwifery leaders attending a first WHO meeting of government chief nurses of newly independent States (Almaty, September 1993). It states that training of nurses, midwives and other middle-level personnel should be a priority for all countries, and highlights the advantages of preparing national action plans for nursing, endorsed by ministries of health. A special effort was made to distribute teaching/learning materials in central and eastern Europe and to newly independent States, and a fund-raising project (LEMON) was launched to ensure their translation into as many languages as possible.
147
20 16 After analysing vaccine needs in countries, WHO collaborated with UNICEF and other major donors in meeting the most acute requirements. Steps were also taken to supply necessary pharmaceuticals in central and eastern Europe. The European diabetes action plan endorsed by the Regional Committee in 1991 has been progressing on schedule: 46 Member States have established active national programmes related to the St Vincent Declaration on diabetes, and particular emphasis has been given to central and eastern Europe and newly independent States. EUROHEALTH, the special programme for intensified cooperation with those countries, remained a top priority; and the network of WHO "liaison offices" in the countries was expanded to 16.
20.17 During the biennium the Regional Office operated with a 10% freeze on its regular budget allocation, a situation that had serious implications for programme delivery given the increased number of European Member States. Particular efforts were made to improve management procedures and to introduce new management tools.

CHAPTER 21
Eastern Mediterranean Region
21.1 At its thirty-ninth session in 1992 the Regional Committee for the Eastern Mediterranean adopted 12 resolutions on topics including membership of Palestine in the Committee, advocacy of health for all among medical practitioners, zoonotic diseases, promotion of healthy lifestyles, and reduction of maternal and infant mortality. Technical Discussions were held on "The impact of rapid urbanization on health". At its fortieth session in 1993 Palestine was welcomed as a member in the Committee in accordance with Article 47 of the Constitution. Technical papers were presented on leishmaniasis and abuse of narcotic and psychoactive drugs, as were progress reports on malaria control, AIDS prevention and control, poliomyelitis eradication and WHO-sponsored research. The subject of the Technical Discussions was "The role of women in support of health for all".
21 2 In the field of information systems support, the local area network in the Regional Office was expanded, and plans were made for implementing WHO's revised administration and finance information system. The regional advisory panel on health information systems undertook the preparation of a manual on the establishment of national health information systems. Training in management techniques and planning was carried out in most countries. A regional advisory panel on health care financing was established.
21 3 The development of health systems based on primary health care progressed in all countries. Access to health care services exceeded 80% in the Region as a whole. A number of Member States started to decentralize their health services. Management of care through district health systems was encouraged and a problem-solving approach using district teams was widely accepted. T earns were formed for training and supervisory tasks in several countries includingYemen.
149
21.4 Different approaches were used during the biennium to maintain and improve quality of care. Consideration was also given to solutions such as cost-sharing and insurance schemes to meet ever-rising costs. Two important meetings were held to further interest in health systems research and development, bringing together managers, directors and researchers: one to promote cooperation between universities and ministries of health in this field (Cairo, June 1992) and the other to discuss health systems research at the periphery (Damascus, October 1992).
21 5 Health care promotion gained momentum through the encouragement of multisectoral cooperation. A special feature in the Region is the basic minimum needs/quality-of-life approach to health promotion and disease prevention, which has proved its value in many countries including Egypt, Jordan, Somalia and Sudan.
21.6 Health legislation was drawn up to meet the needs of national health-for-all strategies. Financial support was provided for the establishment of emergency medical services in Qatar, with support from AGFUND, and in certain other areas, including Gaza, through UNR W A. In Afghanistan, Egypt, Syrian Arab Republic, Tunisia and Yemen medical equipment maintenance programmes were strengthened, following situation surveys, through the issue of new manuals and training of staff. Guidelines on management of medical, surgical and accident emergencies for physicians were prepared.
21.7 With the establishment of a reliable health information system, efforts were directed to the formulation of coordinated policies and plans for the production and management of human resources for health. Most Member States no longer face serious shortages of health personnel; consequently, the emphasis is now on improvement of quality. WHO promoted continuing ed-

THE WORK OF WHO 1992-1993
ucation programmes for all categories of personnel within national health systems. In June 1993 the regional advisory panel on nursing drew up strategies to strengthen managerial capabilities and improve services, including the production of teaching/learning materials in national languages. An intercountry workshop on training for trainers of health personnel (Damascus, November 1992) reviewed recent approaches in this field and considered the use of national languages for teaching/learning materials. It was decided to decentralize the health leadership development programme, the first course being held in English in Islamabad, starting in August 1993.
21.8 As part of continued cooperation in national health education programmes, a "prototype action-oriented school health curriculum for primary schools", developed by WHO and UNICEF in collaboration with UNESCO and the Islamic Educational, Scientific and Cultural Organization, has so far been introduced in 12 countries. Intercountry activities focused on improving the quality of life of women in the Region and increasing their potential for health promotion.
21 9 WHO cooperated with Member States in measures to prevent malnutrition due to insufficient, excessive or unbalanced intake; proteinenergy and micronutrient malnutrition, especially iodine deficiency disorders; and anaemia and vitamin A deficiency. A manual on rapid nutritional assessment in emergencies is in preparation.
21.10 The Regional Training and Research Centre for Oral Health in Damascus conducted several training courses in the planning and management of preventive oral health programmes.
21 11 Accident prevention programmes focused on safety promotion and accident injury control, including advocacy of coordinated multisectoral action. National occupational health programmes have grown as the awareness and commitment of governments increase.
2112 Programmes on tobacco or health were established or strengthened in the Region. All countries produced education materials on the hazards of smoking.
2113 National capacity to implement maternal and child health and family planning programmes was strengthened. A consultation (Beirut, June 1993) was held to consider the health
150
and socioeconomic status of adolescent girls. Safe motherhood programmes aimed at reducing maternal and infant mortality were established in several countries. Many were supported in efforts to reduce the frequency of low birth weight, which can affect 30% of babies. The Baby-friendly Hospital Initiative was promoted.
2114 Several countries sought cooperation in formulating multisectoral plans on health of the elderly following the preparation, through regional or intercountry activities, of a strategy for 1992-2001 and of regional and national plans to promote health and psychosocial care for the elderly.
21 15 The main task of the mental health programme during the biennium was to integrate mental health into primary health care, with emphasis on mental health promotion and the prevention of mental and neurological disorders. Drug abuse, however, remained a serious health and social problem in the Region.
21 16 All countries were supported in implementing essential drugs programmes focused on the development of national drug policies, in reviewing national lists of essential drugs, and in improving drug quality assurance systems through measures to strengthen quality control laboratories and train staff in drug inspection.
2117 Health laboratory services were extended; efforts to improve their performance included the preparation of a manual on quality assurance for peripheral and intermediate laboratories, and guidelines on the facilities needed to cope with emergencies as part of a national contingency plan. Local production of reagents received high priority, and progress was made in developing blood transfusion services.
21.18 A regional strategy on health and environment was drawn up at an intercountry meeting (Amman, June 1993) and adopted by the Regional Committee in October 1993.
21.19 As arid conditions and lack of water resources pose considerable problems in the Eastern Mediterranean, activities concerned with water quality control and wastewater use were intensified in many areas. The high cost of city sewerage is a major constraint, but several governments have succeeded in providing a reasonable level of financial support for water supply and sanitation.
EASTERN MEDITERRANEAN REGION
21 20 Rapid urbanization and urban population growth are causing severe health and environmental problems. In some rural areas settlements have grown up which have the character of small urban communities, accommodating large numbers of people who commute to nearby cities. An integrated approach to the growing difficulties experienced by these settlements has been promoted through "healthy villages" programmes.
21 21 Industrialization and the use of pesticides, herbicides and artificial fertilizers in agriculture increase hazards due to toxic chemicals, and there has been little action to ensure their safe use. A number of countries, however, are showing a keen interest in national chemical safety programmes. WHO continued to promote training in this field, as in other aspects of environmental health such as monitoring and control of air and water pollution, including bacterial pollution of the sea. Support was also given for food safety programmes, for instance, in the preparation of guidelines on integrating food safety into primary health care and the strengthening of food laboratory services.
21.22 The Centre for Environmental Health Activities in Amman conducted 40 national and 10 intercountry training and research courses, and strengthened its network for disseminating environmental health information.
21.23 The regional health and biomedical information programme provided services and advice to countries as well as maintaining its traditional role of support for Regional Office programmes. A number of countries have been preparing national plans in this field in cooperation with WHO. A collaborating centre for health and biomedical information was designated in the Islamic Republic of Iran in February 1993. Other activities included involvement in ExtraMED, a global project in which the full text of over 200 health journals not contained in the main databases such as MEDLINE will be placed on CD-ROM monthly.
21 24 The battle against communicable and noncommunicable diseases is still the main area of collaboration between WHO and the Member States, in respect of both emergency measures
151
during outbreaks of disease or epidemics, and continuing disease prevention and control programmes.
21.25 Cholera epidemics affected seven Member States, and malaria, leishmaniasis and Rift V alley fever reached epidemic proportions in some areas. WHO's role has been to mobilize specialist consultant services, prepare guidelines and training aids, and provide emergency supplies. The Organization has also fostered collaboration between neighbouring countries, as in the case of poliomyelitis eradication in the Gulf States and the Maghreb; the same approach is being tried for malaria control.
21 26 The Eastern Mediterranean Region has been relatively less affected by the rapid spread of HIV infection than some other regions. Efforts in national programme planning, in training, and particularly in promoting the social and cultural values of the Region that inculcate selfrespect and morality in individual relationships, have contributed to its prevention.
21.27 The use of scientific methods for the prevention and control of cardiovascular diseases, cancer, diabetes and other noncommunicable disorders is being promoted, along with initiatives to inform and motivate national authorities, nongovernmental organizations and communities.
21 28 The WHO standards for recruitment of international staff were applied in the Regional Office. However, there were difficulties in meeting the target of 40% in the appointment of nationals from under-represented countries and in recruiting a greater proportion of women. The plans to extend the Regional Office building were delayed pending the solution of problems concerning the title to the land made available by the Host Government. Steps were taken to improve accountability in regard to supplies and equipment ordered for Member States.
21.29 A 10% reduction in programme implementation, imposed by the expected deficit in contributions, made it difficult to respond to critical situations in times of unprecedented need, including emergencies, in the Region.


CHAPTER 22
Western Pacific Region
22.1 Socioeconomic and political change in the Region has been swift and widespread. Positive and welcome developments included renewed optimism in Cambodia for peaceful economic growth. At the forty-fourth session of the Regional Committee, held in Manila in 1993, further changes were recognized, for example, in the presence ofT uvalu as a full member of the Cornmittee. The participation of Macao on its own behalf, though without voting rights, in future sessions of the Committee was also announced.
22.2 Demographic, environmental and economic developments have also been changing the patterns of disease in theW estern Pacific. Diseases such as diabetes, heart disease and cancer that are associated with unhealthy lifestyles have increased generally. This is also true of the developing countries where traditional communicable diseases such as tuberculosis remained undiminished. These developments have made it necessary to review the way health services are organized. Health promotion as an extension of the primary health care strategy is now emphasized as the main approach to the solution of health problems, and the training of health personnel at all levels has had to be adjusted accordingly. Other key approaches are surveillance to monitor the changing health status of the Region, the collection and dissemination of accurate and timely health information from a broad geographical base and greater attention to management issues such as financing and quality of care.
22 3 The availability of adequate and appropriate human resources is a critical component of the infrastructure needed for health development. The orientation of training towards community-based primary health care services continued during the biennium. Sharing of the Region's health training resources was encouraged. A first group of primary care practitioners graduated from the Fiji School of Medicine in
153
December 1993, products of a new academic strategy and curriculum that promises to be well suited to the needs of Pacific island nations. New approaches to medical education were reviewed and changes were made in the basic training of health workers such as nurses and dental health practitioners. Distance learning was promoted, as was postgraduate and continuing medical education in various countries.
22 4 In the important area of disease prevention and control, coverage of infants with the six antigens of the Expanded Programme on Immunization was over 90% during the biennium. Remaining pockets of low coverage are the target of future action. Tuberculosis incidence remained high, but the rates for poliomyelitis, diphtheria and pertussis declined significantly. Measles incidence has fallen significantly during the last decade as a result of immunization, but outbreaks still occur in most countries.
22.5 In 1992 there was a 21% reduction in cases of poliomyelitis compared with the previous year, and the lowest annual total ever reported: 2087 cases. Given sufficient vaccine and funding, it is expected that the regional goal of eradication of the disease by 1995 can be attained. Efforts were directed to improving surveillance, even in countries reporting no cases of the disease, and to increasing supplementary immunization. China, Lao People's Democratic Republic, Philippines and Vi et N am conducted national immunization days, during which 120 million children under the age of five years were protected with oral poliovirus vaccine. In 1993 the Regional Committee recognized the need to ensure the potency, safety and efficacy of the vaccine, and adopted a resolution to that effect.
22 6 Immunization against hepatitis B was increased. Technical support was given for local production of plasma-derived vaccine in China

THE WORK OF WHO 1992-1993
and Vi et N am. By 1992, 27 countries had incorporated the vaccine into their immunization schedules, although only on a limited scale in some cases. Where vitamin A is deficient it is also given during immunization sessions, as in the Philippines.
22.7 The goal has been adopted of eliminating leprosy as a public health problem (less than one case per 10 000 population) in all parts of the Region by the year 2000. 1992 data indicated a reduction of about 10% in the number of reported cases compared with the previous year. Overall prevalence in the Region is 0.44 per 10 000. Coverage of multidrug therapy was 70% in 1992. Extrabudgetary funding has been essential for this purpose and for other activities such as training and programme evaluation.
22 8 Malaria control has been a focus of attention. The nine malarious countries in the Region reported nearly 800 000 microscopically confirmed cases in 1991, a total that was expected to fall in subsequent years. All the malarious countries are currently implementing intensive control strategies, or plan to do so in the near future. More than two million cases are believed to be unreported or incompletely treated. However, following a reorientation of the malaria control programmes, data are now collected and analysed with greater emphasis on numbers of clinically diagnosed cases and amounts of drugs used. Impressive reductions in the numbers of microscopically confirmed cases have been achieved in parts of the Solomon Islands and also in Viet N am where two million adult curative doses of artemisinin, a derivative of Artemisia annua, are being produced annually for use in areas with high levels of multidrug resistance. Two meetings were held in Kunming (China) in November 1993 for countries of the Western Pacific and South-East Asia sharing at least one national border with another malarious country. The meetings made recommendations for strengthening a variety of malaria control measures within countries, across common borders and between regions, including the establishment of networks for information exchange, monitoring of drug resistance, operational research and training.
22 9 The number of cases of tuberculosis reported in the Region possibly represents as little as one-third of the real total, estimated at 1. 9
million. There was no decline in the numbers of new cases during the biennium and, given the disease's close link with HIV infection and the
154
spread of drug resistant strains, an increasing trend can be expected in the future. Measures such as short-course chemotherapy, appropriate care management and surveillance are being intensified.
2210 It is conservatively estimated that between 50 000 and 100 000 people are already infected with HIV in the Region and the numbers are growing rapidly. However, all Member States now have national AIDS committees as well as laboratory facilities to test for HIV antibody, and high priority is given to management and control of sexually transmitted diseases. The means of transmission have been evolving as information, education and other health promotive activities help to alter behaviour patterns. In Australia, for example, the epidemic seems to be reaching a plateau. An evaluation of the national five-year strategy concluded that the most effective interventions in the early days of the epidemic were funding of sex worker groups and the establishment of needle and syringe exchange schemes in major cities. In 1993 the Regional Committee called for the drafting of guidelines for national authorities, greater involvement of other government departments and nongovernmental organizations in the planning of activities, better surveillance and more intensive exchange of information, particularly the results of scientific studies.
22.11 At its 1993 session the Regional Committee endorsed the regional programme for health promotion which stresses, on the one hand, action by individuals to adopt healthy lifestyles and, on the other, the creation of supportive environments for health and the mobilization of communities and governments to achieve health goals. The programme identifies and addresses health issues in relation to different age groups, recognizing that the dominant diseases are those influenced by changes in lifestyle as well as factors external to the individual such as urbanization, industrialization, migration and environmental change. Moreover, chronic illness and degenerative changes will affect the Region's aging populations. Strategies for health promotion therefore form a significant element of many programmes in the Region.
22.12 Demographic changes in the Region have continued to require new strategies to prevent environmental degradation and safeguard environmental health. Following the 1992 United Nations Conference on Environment and Devel-

WESTERN PACIFIC REGION
opment (see paragraph 12.1), an international symposium on improving environmental management in north-east Asia was convened in the Republic of Korea in 1992. Similarly, national workshops were organized in Malaysia and Philippines to draw up plans for follow-up activities. The integration of environmental management in rural and urban development programmes has become a priority concern. Regional workshops have proved very helpful in dealing with specific issues; for instance, one held in Fiji (Suva, May 1992) reviewed solid waste management options for small island nations constrained by geographical limitations and shortages of financial and human resources. National training programmes, such as the series of environmental planning and management courses conducted in collaboration with the Government of Malaysia,
ISS
have given good results. Urban health development activities, closely linked with health promotion and primary health care, are under way in several countries.1
22.13 Directions for the future will be determined by the Region's main concerns as described above. Priority setting will be a crucial exercise, and the first steps in this respect were taken in 1992-1993. The coordinated and concerted efforts of the Member States will, however, be the key to accomplishing the many and ambitious goals of health for all in the Western Pacific.
1 Austrolio, Chrno, Jopon, Moloysro, Popuo New Gurneo, Philippines, Repub· lie of Koreo, Vie! Nom.

Annexes
157
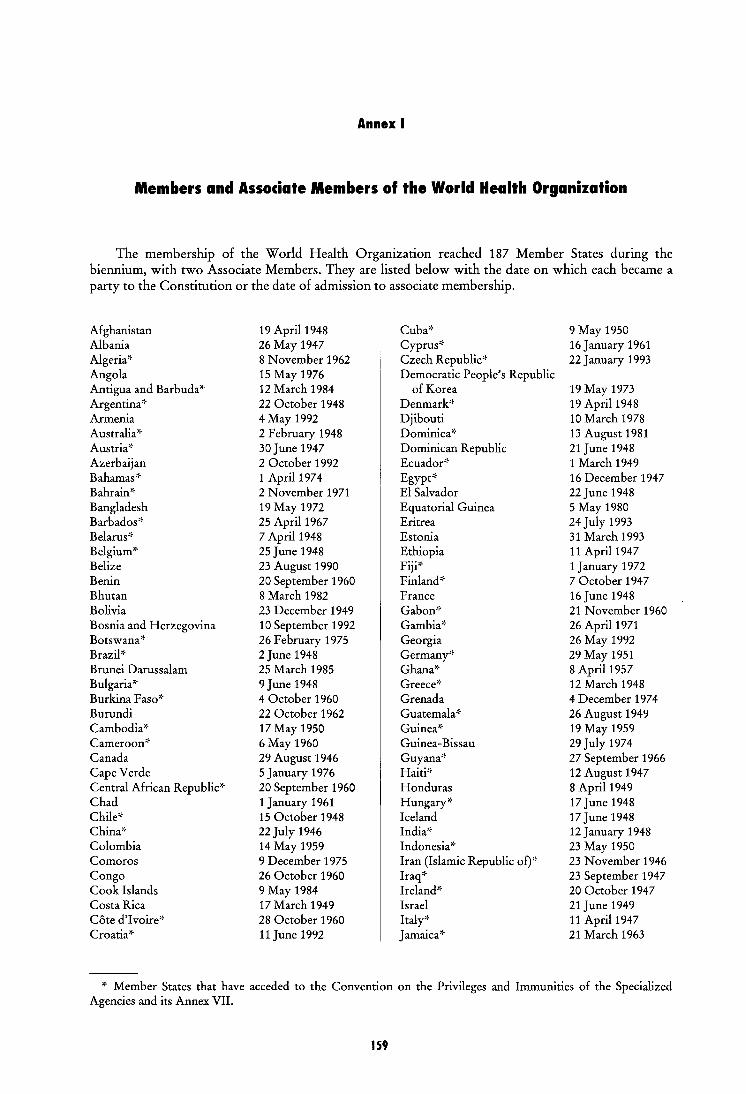
Annex I
Members and Associate Members of the World Health Organization
The membership of the World Health Organization reached 187 Member States during the biennium, with two Associate Members. They are listed below with the date on which each became a party to the Constitution or the date of admission to associate membership.
Afghanistan 19 April 1948 Cuba* 9 May 1950 Albania 26 May 1947 Cyprus* 16 January 1961 Algeria'f 8 November 1962 Czech Republic* 22 January 1993 Angola 15 May 1976 Democratic People's Republic Antigua and Barbuda* 12 March 1984 of Korea 19 May 1973 Argentina'' 22 October 1948 Denmark* 19 April1948 Armenia 4 May 1992 Djibouti 10 March 1978 Australia* 2 February 1948 Dominica* 13 August 1981 Austria~· 30 June 1947 Dominican Republic 21 June 1948 Azerbaijan 2 October 1992 Ecuador'f 1 March 1949 Bahamas'f 1 April1974 Egypt* 16 December 1947 Bahrain* 2 November 1971 El Salvador 22June 1948 Bangladesh 19 May 1972 Equatorial Guinea 5 May 1980 Barbados'f 25 April1967 Eritrea 24 July 1993 Belarus~· 7 April1948 Estonia 31 March 1 993 Belgium'f 25June 1948 Ethiopia 11 April1947 Belize 23 August 1990 Fiji'f 1 January 1972 Benin 20 September 1 960 Finland'f 7 October 1947 Bhutan 8 March 1982 France 16June1948 Bolivia 23 December 1949 Gabon'f 21 November 1960 Bosnia and Herzegovina 10 September 1992 Gambia* 26 April 1971 Botswana'' 26 February 1975 Georgia 26 May 1992 Brazil'f 2June 1948 Germany'f 29 May 1951 Brunei Darussalam 25 March 1985 Ghana'f 8 April1957 Bulgaria'f 9 June 1948 Greece* 12 March 1948 Burkina Faso'' 4 October 1960 Grenada 4 December 1974 Burundi 22 October 1962 Guatemala* 26 August 1949 Cambodia'' 17 May 1950 Guinea'' 19 May 1959 Cameroon* 6 May 1960 Guinea-Bissau 29 July 1974 Canada 29 August 1946 Guyana* 27 September 1966 Cape Verde 5 January 1976 Haiti* 12 August 1947 Central African Republic'' 20 September 1960 Honduras 8 April1949 Chad 1 January 1961 Hungary* 17 June 1948 Chile* 15 October 1948 Iceland 17 June 1948 China'f 22July 1946 India'f 12 January 1948 Colombia 14 May 1959 Indonesia'' 23 May 1950 Comoros 9 December 1975 Iran (Islamic Republic of)'f 23 November 1946 Congo 26 October 1960 Iraq'f 23 September 1947 Cook Islands 9 May 1984 Ireland* 20 October 1947 Costa Rica 17 March 1949 Israel 21 June 1949 Cote d'I voire'f 28 October 1960 Italy'' 11 April1947 Croatia* 11 June 1992 Jamaica'f 21 March 1963
* Member States that have acceded to the Convention on the Privileges and Immunities of the Specialized Agencies and its Annex VII.
1S9
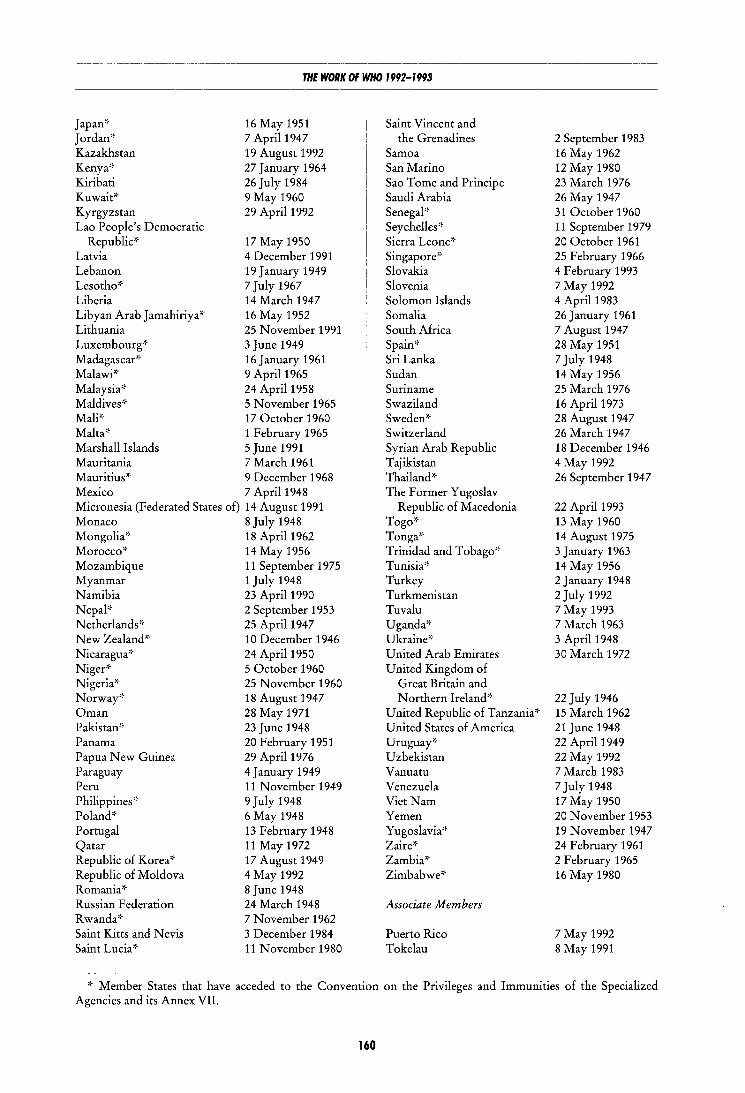
THE WORK OF WHO 1992-1993
Japan':· Jordan* Kazakhstan Kenya* Kiribati Kuwait'~
Kyrgyzstan Lao People's Democratic
16 May 1951 7 April1947 19 August 1992 27 January 1964 26 July 1984 9 May 1960 29 April1992
Republic'~ 17 May 1950 Latvia 4 December 1991 Lebanon 19 January 1949 Lesotho'~ 7 July 1967 Liberia 14 March 1947 Libyan Arab J amahiriya'~ 16 May 1952 Lithuania 25 November 1991 Luxembourg'~ 3 June 1949 Madagascar'~ 16 January 1961 Malawi'~ 9 April1965 Malaysia'-· 24 April1958 Maldives'~ 5 November 1965 Mali':· 17 October 1960 Malta'~ 1 February 1965 Marshall Islands 5 June 1991 Mauritania 7 March 1961 Mauritius'~ 9 December 1968 Mexico 7 April1948 Micronesia (Federated States of) 14 August 1991 Monaco 8 July 1948 Mongolia'-· 18 April1962 Morocco'~ 14 May 1956 Mozambique 11 September 1975 Myanmar 1 July 1948 Namibia 23 April1990 Nepal'~ 2 September 1953 Netherlands'-· 25 April1947 New Zealand'~ 10 December 1946 Nicaragua'~ 24 April1950 Niger'-· 5 October 1960 Nigeria'-· 25 November 1960 Norway'-· 18 August 1947 Oman 28 May 1971 Pakistan'~ 23 June 1948 Panama 20 February 1951 Papua New Guinea 29 April1976 Paraguay 4 January 1949 Peru 11 November 1949 Philippines'~ 9 July 1948 Poland'~ 6 May 1948 Portugal 13 February 1948 Qatar 11 May 1972 Republic of Korea* 17 August 1949 Republic of Moldova 4 May 1992 Romania'-· 8 June 1948 Russian Federation 24 March 1948 R wanda'-· 7 November 1962 Saint Kitts and Nevis 3 December 1984 Saint Lucia'' 11 November 1980
Saint Vincent and the Grenadines
Samoa San Marino Sao Tome and Principe Saudi Arabia Senegal'~
Seychelles'~ Sierra Leone':· Singapore'~
Slovakia Slovenia Solomon Islands Somalia South Africa Spain'-· Sri Lanka Sudan Suriname Swaziland Sweden* Switzerland Syrian Arab Republic Tajikistan Thailand* The Former Yugoslav
Republic of Macedonia Togo'~
Tonga* Trinidad and Tobago'~ Tunisia'~
Turkey Turkmenistan Tuvalu Uganda'' Ukraine'-· United Arab Emirates United Kingdom of
Great Britain and Northern Ireland'-·
United Republic of Tanzania'~ United States of America Uruguay* Uzbekistan Vanuatu Venezuela VietNam Yemen Yugoslavia'-· Zaire'~
Zambia'~
Zimbabwe'~
Associate M embers
Puerto Rico Tokelau
2 September 1983 16 May 1962 12 May 1980 23 March 1976 26 May 1947 31 October 1960 11 September 1979 20 October 1961 25 February 1966 4 February 1993 7 May 1992 4 April1983 26January 1961 7 August 1947 28 May 1951 7 July 1948 14 May 1956 25 March 1976 16 April1973 28 August 1947 26 March 1947 18 December 1946 4 May 1992 26 September 1947
22 April1993 13 May 1960 14 August 1975 3 January 1 963 14 May 1956 2 January 1948 2July 1992 7 May 1993 7 March 1963 3 April1948 30 March 1972
22July 1946 15 March 1962 21 June 1948 22 April 1949 22 May 1992 7 March 1983 7 July 1948 17 May 1950 20 November 1953 19 November 1947 24 February 1961 2 February 1965 16 May 1980
7 May 1992 8 May 1991
'~ Member States that have acceded to the Convention on the Privileges and Immunities of the Specialized Agencies and its Annex VII.
160
ANNEXES
Annex 2
Regional Distribution of Members
and Associate Members of the World Health Organization
Algeria Angola Benin Botswana Burkina Faso Burundi Cameroon Cape Verde Central African Republic Chad Comoros Congo
Antigua and Barbuda Argentina Bahamas Barbados Belize Bolivia Brazil Canada Chile Colombia Costa Rica
Bangladesh Bhutan Democratic People's
Republic of Korea
African Region
Cote d'Ivoire Madagascar Equatorial Guinea Malawi Eritrea Mali Ethiopia Mauritania Gabon Mauritius Gambia Mozambique Ghana Namibia Guinea Niger Guinea-Bissau Nigeria Kenya Rwanda Lesotho Sao Tome and Principe Liberia Senegal
Region of the Americas
Cuba Mexico Dominica Nicaragua Dominican Republic Panama Ecuador El Salvador Grenada Guatemala Guyana Haiti Honduras Jamaica
India Indonesia Mal dives Mongolia
Paraguay Peru Saint Kitts and Nevis Saint Lucia Saint Vincent
and the Grenadines Suriname Trinidad and Tobago
South-East Asia Region
161
Myanmar Nepal
Seychelles Sierra Leone South Africa Swaziland Togo Uganda United Republic
of Tanzania Zaire Zambia Zimbabwe
United States of America Uruguay Venezuela
Associate M ember:
Puerto Rico
Sri Lanka Thailand
Albania Armenia Austria Azerbaijan Belarus Belgium Bosnia and
Herzegovina Bulgaria Croatia Czech Republic Denmark Estonia Finland
Afghanistan Bahrain Cyprus Djibouti Egypt Iran
(Islamic Republic of)
Australia Brunei Darussalam Cambodia China Cook Islands Fiji Japan
THE WORK OF WHO 1992-1993
European Region
France Malta Georgia Monaco Germany Netherlands Greece Norway Hungary Poland Iceland Portugal Ireland Republic of Moldova Israel Romania Italy Russian Federation Kazakhstan San Marino Kyrgyzstan Slovakia Latvia Slovenia Lithuania Spain Luxembourg Sweden
Eastern Mediterranean Region
Iraq
Jordan
Kuwait
Lebanon
Libyan Arab Jamahiriya
Morocco
Oman
Pakistan
Qatar
Saudi Arabia
Somalia
Western Pacifi( Region
Kiribati Lao People's
Democratic Republic Malaysia Marshall Islands Micronesia (Federated
States of)
162
New Zealand Papua New Guinea Philippines Republic of Korea Samoa Singapore Solomon Islands
Switzerland Tajikistan The Former Yugoslav
Republic of Macedonia
Turkey Turkmenistan Ukraine United Kingdom of
Great Britain and Northern Ireland
Uzbekistan Yugoslavia
Sudan
Syrian Arab Republic
Tunisia
United Arab Emirates
Yemen
Tonga Tuvalu Vanuatu VietNam
Associate M ember Tokelau
ANNEXES
Annex 3
Organizational and related meetings
1. Meetings in 1992
Executive Board: Committee on Drug Policies Executive Board, eighty-ninth session Executive Board: Standing Committee on Nongovernmental Organizations Executive Board: Committee to Consider Certain Financial Matters prior
to the Forty-fifth World Health Assembly Forty-fifth World Health Assembly Executive Board, ninetieth session Executive Board: Programme Committee Regional Committee for Africa, forty-second session Regional Committee for the Western Pacific, forty-third session Regional Committee for South-East Asia, forty-fifth session Regional Committee for Europe, forty-second session Regional Committee for the Americas, forty-fourth session/
XXXVI Meeting of the Directing Council of P AHO Regional Committee for the Eastern Mediterranean, thirty-ninth session
2. Meetings in 1993
Executive Board, ninety-first session Executive Board: Standing Committee on Nongovernmental Organizations Executive Board: Committee to Consider Certain Financial Matters
prior to the Forty-sixth World Health Assembly Forty-sixth World Health Assembly Executive Board, ninety-second session Executive Board: Programme Committee Executive Board: Programmee Committee
Regional Committee for Africa, forty-third session Regional Committee for Europe, forty-third session Regional Committee for the Western Pacific, forty-fourth session Regional Committee for South-East Asia, forty-sixth session Regional Committee for the Americas, forty-fifth session/XXXVII meeting
of the Directing Council of P AHO Regional Committee for the Eastern Mediterranean, fortieth session
163
Geneva, 17-18 January Geneva, 20-28 January Geneva, 21 January
Geneva, 4 May Geneva, 4-14 May Geneva, 18-19 May Geneva, 24-28 August Brazzaville, 2-9 September Hong Kong, 7-11 September Kathmandu, 7-13 September Copenhagen, 14-19 September Washington, D.C.,
21-26 September Alexandria, 3-7 October
Geneva, 18-29 January Geneva, 19 January
Geneva, 3 May Geneva, 3-14 May Geneva, 17-18 May Geneva, 5-9 July Geneva, 29 November-
1 December Gaborone, 1-8 September Athens, 6-1 0 September Manila, 13-17 September New Delhi, 21-27 September Washington, D.C.,
27 September - 2 October Alexandria, 2-5 October
THE WORK OF WHO 1992-1993
Annex 4
Intergovernmental Organizations that have entered into Formal Agreements with WHO approved by the World Health Assembly,
and Nongovernmental Organizations in Official Relations with WHO at 31 December 1993
I. Intergovernmental organizations
African Development Bank International Committee of Military Medicine
and Pharmacy International Office of Epizootics
Islamic Development Bank League of Arab States Organization of African Unity
2. Nongovernmental organizations
African Medical and Research Foundation International
Aga Khan Foundation Association of the Institutes and Schools of Tropical
Medicine in Europe CMC- Churches' Action for Health Christoffel-Blindenmission Collegium lnternationale N euro-
Psychopharmacologicum Commonwealth Association for Mental
Handicap and Developmental Disabilities Commonwealth Medical Association Commonwealth Pharmaceutical Association Council for International Organizations of Medical
Sciences Helen Keller International, Incorporated Industry Council for Development Inter-American Association of Sanitary
and Environmental Engineering International Academy of Legal Medicine
and Social Medicine International Academy of Pathology International Agency for the Prevention of Blindness International Air Transport Association International Alliance of Women International Association for Accident
and Traffic Medicine International Association for Adolescent Health International Association of Agricultural Medicine
and Rural Health International Association of Cancer Registries International Association for Child and Adolescent
Psychiatry and Allied Professions International Association of Hydatid Disease International Association of Lions Clubs
164
International Association of Logopedics and Phoniatrics
International Association of Medical Laboratory Technologists
International Association for the Study of the Liver International Association for the Study of Pain International Association for Suicide Prevention International Association on Water Quality International Astronautical Federation International Bureau for Epilepsy International Catholic Committee of Nurses
and Medico-Social Assistants International Clearinghouse for Birth Defects
Monitoring Systems International College of Surgeons International Commission on Occupational Health International Commission on Radiation Units
and Measurements International Commission on Radiological
Protection International Committee of the Red Cross International Confederation of Midwives International Conference of Deans of French-
language Faculties of Medicine International Council on Alcohol and Addictions International Council on Jewish Social and
Welfare Services International Council for Laboratory Animal
Science International Council of Nurses International Council of Scientific Unions International Council on Social Welfare International Council of Societies of Pathology International Council for Standardization in
Haematology
ANNEXES
International Council of Women International Cystic Fibrosis (Mucoviscidosis)
Association International Dental Federation International Diabetes Federation International Electrotechnical Commission International Epidemiological Association International Ergonomics Association International Eye Foundation International Federation on Ageing International Federation of Business and
Professional Women International Federation of Chemical, Energy
and General Workers' Unions International Federation of Clinical Chemistry International Federation for Family Life
Promotion International Federation of Fertility Societies International Federation of Gynecology and
Obstetrics International Federation of Health Records
Organizations International Federation of Hospital Engineering International Federation for Housing and Planning International Federation of Hydrotherapy and
Climatotherapy International Federation for Information Processing International Federation for Medical and Biological
Engineering International Federation of Medical Student
Associations International Federation of Multiple Sclerosis
Societies International Federation of Ophthalmological
Societies International Federation of Oto-Rhino
Laryngological Societies International Federation of Pharmaceutical
Manufacturers Associations International Federation of Physical Medicine
and Rehabilitation International Federation for Preventive and
Social Medicine International Federation of Red Cross and
Red Crescent Societies International Federation of Sports Medicine International Federation of Surgical Colleges International Group of National Associations of
Manufacturers of Agrochemical Products International Hospital Federation International Lactation Consultant Association International League of Dermatological Societies International League of Associations for Rheumatology International League against Epilepsy International Leprosy Association International Leprosy Union International Life Sciences Institute International Medical Informatics Association International Medical Society of Paraplegia International Organization of Consumers Unions
165
International Organization for Standardization International Organization against Trachoma International Pediatric Association International Pharmaceutical Federation International Physicians for the Preventiof\ of
Nuclear War International Planned Parenthood Federation International Radiation Protection Association International Society for Biomedical Research on
Alcoholism International Society of Biometeorology International Society of Blood Transfusion International Society for Burn Injuries International Society of Chemotherapy International Society and Federation of Cardiology International Society of Haematology International Society for Human and Animal
Mycology International Society of Orthopaedic Surgery
and Traumatology International Society of Nurses in Cancer Care International Society for Prosthetics and Orthotics International Society of Radiographers and
Radiological Technologists International Society of Radiology International Society for the Study of Behavioural
Development International Sociological Association International Solid Wastes and Public Cleansing
Association International Special Dietary Foods Industries International Union of Architects International Union of Biological Sciences International Union against Cancer International Union for Conservation of Nature
and Natural Resources International Union of Family Organizations International Union for Health Promotion
and Education International Union of Immunological Societies International Union of Local Authorities International Union of Microbiological Societies International Union of Nutritional Sciences International Union of Pharmacology International Union of Pure and Applied Chemistry International Union of Toxicology International Union against Tuberculosis and Lung
Disease International Union against the Venereal Diseases
and the Treponematoses International Water Supply Association Inter-Parliamentary Union Joint Commission on International Aspects of
Mental Retardation La Leche League International Medical Women's International Association Medicus Mundi Internationalis (International
Organization for Cooperation in Health Care) Mother and Child International National Council for International Health
THE WORK OF WHO 1992-1993
Network of Community-Oriented Educational Institutions for Health Sciences
OXFAM (Oxford Committee for Famine Relief) Population Council Rehabilitation International Rotary International Royal Commonwealth Society for the Blind Save the Children Fund (UK) Soroptimist International W odd Assembly of Youth W odd Association of Girl Guides and Girl Scouts W odd Association of the Major Metropolises W odd Association for Psychosocial Rehabilitation World Association of Societies of (Anatomic and
Clinical) Pathology World Blind Union W odd Confederation for Physical Therapy World Federation of Associations of Poisons Centres
and Clinical Toxicology Centres W odd Federation of the Deaf W odd Federation of Hemophilia W odd Federation for Medical Education
166
W odd Federation for Mental Health W odd Federation of Neurology W odd Federation of Neurosurgical Societies W odd Federation of Nuclear Medicine and Biology W odd Federation of Occupational Therapists W odd Federation of Parasitologists W odd Federation of Proprietary Medicine
Manufacturers W odd Federation of Public Health Associations W odd Federation of Societies of Anaesthesiologists World Federation of United Nations Associations W odd Hypertension League W odd Organization of National Colleges,
Academies and Academic Associations of General Practitioners/Family Physicians
W odd Organization of the Scout Movement W odd Psychiatric Association W odd Rehabilitation Fund W odd Veterans Federation W odd Veterinary Association W odd Vision International

Annex 5
Structure of the World Health Organization at 31 December 1993

Division of Emergency and Humanitarian Action (EHA) ' Office of Legal Counsel (LEG) Off1ce of Internal Audit (OIA)
' Includes the Representative of the Director-General of WHO to the Umted Nat1ons system and other intergovernmental bod1es at New York: the WHO Senior Health Adviser to UNICEF, New York; the Representative of the Director-General of WHO to the European Community at Brussels, and the WHO Office for the Orgamzation of African Unity and the Economic Commission for Afnca, Addis Ababa
' Includes the WHO Pan Afncan Centre for Emergency Preparedness and Response, AddiS Ababa
'Regional Office for the Americas/ Pan Amencan Samtary Bureau
Headquarters
Structure of the Secretariat of the World Health Organization
Cabinet ol the Director-General (CDG) AdVISer on POlicy CooperatiOn (DGP)
Adv1ser on Health and Development Policies (DGH)
Act1on Programme on Essential Drugs (DAP) D1vis1on of Drug Management and Pollc1es
(DMP) DIVISIOn of Food and Nutntlon (FNU) Programme on Health Technology (PHn
Division of Diarrhoea! and Acute Respiratory D1sease Control (GDR)
D1v1sion of Commumcable Diseases (CDS) DIViSIOn of Control of TrOPICal Diseases (CTD) Expanded Programme on lmmumzat1on (EPI) Special Programme for Research and Trammg
in Tropical Diseases (TOR)
Division of Family Health (FHE) Division of Health Education (HED) Division of Development of Human Resources
for Health (HRH) Spec1al Programme of Research. Development
and Research Trammg m Human Reproduction (HRP)
Health and Biomedical Information Programme (HBI)
Division of Epidemiological Surveillance and Health S1tuation and Trend Assessment (HSn
Division of Strengthening of Health Serv1ces (SHS)
DiviSIOn of Health ProtectiOn and Promotion (HPP)
Division of Mental Health (MNH) Division of Noncommunicable Diseases (NCD) Programme on Substance Abuse (PSA) Office of Research Promotion and
Development (RPD)
Division of Budget and Fmance (BFI) DiviSIOn of Conference and General Serv1ces
(CGS) Division of lnteragency Affairs (INA) Division of Personnel (PER) Adviser on lnformatics (AOI) Information Technology Off1ce (ITO) Management Development Off1ce (MOO) Programme for Resource Mobilization (RMB)
DIVISion of Environmental Health (EHE) Programme for the Promotion of Chemical
Safety (PCS)
South-East Asia
-
Regional Offices
Programme Coordination,
Promotion and Information
Programme Management
Support Programme
Assistant Director
Deputy Director
Programme Management
Support Programme -
-Programme Management
Support Programme -
-Programme Management
Support Programme -
-Programme Management
Support Programme
I
I
WHO lntercountry Health Development Teams
WHO Representatives OnchocerciaSIS Control
Programme in West Africa
Health Systems Infrastructure
Health Programmes Development
WHO Representallves
WHO Representatives
WHO Representatives Director of Health, UNRWA
WHO Representatives WHO Country Liaison Off1cers
International Agency for Research on Cancer
DIRECTOR
Secretariat
PAHOIWHO Representatives Programme Coordmat1on
Offices Caribbean Programme
Coordmation
WH094034/E
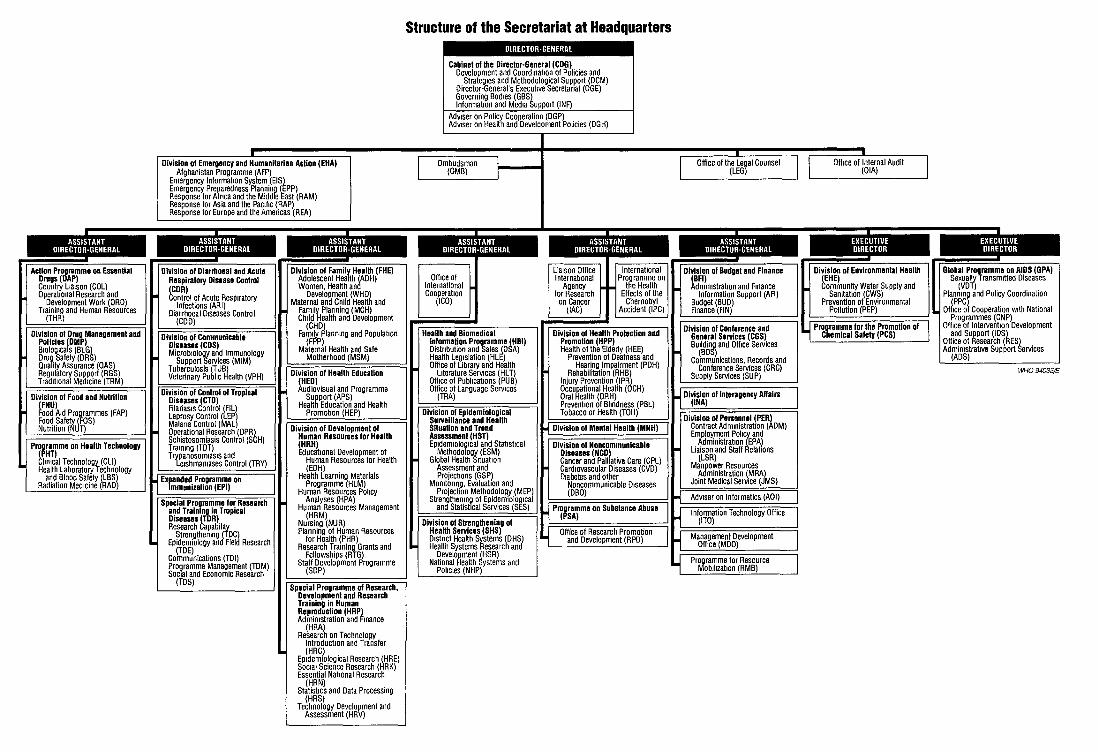
ASSISTANT DIRECTOR-GENERAL
Action Programme on Essential Drugs (OAP} Country LiaiSOn (COL} Operational Research and
Development Work (ORD) Training and Human Resources
(THR)
Division of Drug Management and Policies jDMP} BIOIOQICa S (BLG) Drug Safety (DRS) Quality Assurance (QAS) Regulatory Support (RGS) Traditional Medicine (TRM)
Division of Food and Nutrition (FNU} Food Aid Programmes (FAP) Food Safety (FOS) Nutrition (NUT)
Programme on Health Technology (PHT) Clm1cal Technology (CLI) Health Laboratory Technology
and Blood Safety (LBS) Radiation Med1cine (RAD)
Division of Emergency and Humanitarian Action (EHA) Afghanistan Programme (AFP)
Emergency information System (EIS) Emergency Preparedness Planning (EPP) Response for Afnca and the Middle East (RAM} Response for Asia and the Pac1f1c (RAP) Response for Europe and the Americas (REA)
Di~~~:n Resources for Health IHRH} Educalianal Development of
Human Resources for Health (EDH}
Health Learning Materials Programme (HLM)
Human Resources Policy Analyses (HPA)
Human Resources Management (HRM)
Nursing (NUR) Planning of Human Resources
for Health (PHR) Research Traming Grants and
Fellowships (RTG) Staff Development Programme
(SDP}
on Technology lntroduclian and Transfer (HRC)
Epidemiological Research (HRE) Soc1al Science Research (HRK) Essential NatiOnal Research
(HRN) StatistiCS and Data Processing
(HRS} Technology Development and
Assessment (HRV)
Structure of the Secretariat at Headquarters
Ombudsman (OMB)
ASSISTANT DIRECTOR· GENERAL
OffiCe of International CooperatiOn
(I CO)
Health and Biomedical Information Programme IHBI} Distnbution and Sales (DSA) Health Legislation (HLE) Office of Library and Health
Literature Serv1ces (HLT) Off1ce of Publications (PUB} Office of Language Serv1ces
(TRA)
Division of Epidemiological Surveillance and Health Situation and Trend Assessmenf (HST} Epidemiological and Stat1st1cal
Methodology (ESM) Global Health S1tuat1on
Assessment and Projections (GSP)
Momtonng, Evaluation and Projection Methodology (MEP/
Strengthenmg of Epidemiolog1ca and Statistical Services (SES)
Division of Strengthening of Health Services (SHS} D1stnct Health Systems (OHS) Health Systems Research and
Development (HSR) National Health Systems and
Policies (NHP)
(DGH)
Division of Health Profection and Promotion (HPP} Health of the Elderly (HEE)
Prevention of Deafness and Hearing Impairment (PDH)
Rehabilitation (RHB) Injury Prevention (IPRJ Occupational Health (OCH) Oral Health (ORH) Prevention of Blindness (PBL) Tobacco or Health (TOH)
Office of the Legal Counsel (LEG)
Off1ce of Internal Audit (OIA)
EXECUTIVE DIRECTOR
Division of Environmental Health (EHE} Community Water Supply and
Sanitation (CWS) Prevention of Environmental
Pollution (PEP)
Programme for the Promotion of Chemical Safety (PCS)
EXECUTIVE , DIRECTOR
Global Programme on AIDS (GPA) Sexually Transm1tted Diseases
(VDT) Planmng and Policy Coordination
(PPG) Office of Cooperation w1th National
Programmes (GNP) Off1ce oflntervent1on Development
and Support (lDS) Office of Research (RES) Admimstrat1ve Support Services
(ADS)
Wf-1094033/E

Index
References are by paragraph. Main references are in heavy type.
Abortion, 10.11, 10.35 ACC, see Administrative Committee on Coordina-
tion Accidents, see Injury prevention ACHR, see Advisory committees on health research Administration and finance information system
(AFI), 16.13-16.14 Administrative Committee on Coordination (ACC),
2.11, 2.13, 14.137 Inter-Agency Committee on Sustainable Develop-
ment, 2.11 lntersecretariat Group for Water Resources, 12.13 Subcommittee on Statistical Activities, 4.9, 4.10 Subcommittee on Water Resources, 12.13
Adolescent health, see Youth and adolescence Advisory committees on health research (ACHR),
global, 8.2-8.4 regional, 8.9, 8.10, 8.13
Afghanistan, 2.31, 5.8, 14.15, 16.16, 21.6 Operation Salam, 16.22
African Development Bank, 2.19, 2.26, 13.34 African Development Fund, 2.19 African Economic Community, treaty, 2.22 African health development framework, 17.1 African Region, 17.1-17.17, Annex 2
see also individual activities African trypanosomiasis (sleeping sickness), 14.37-
14.41, 14.44, 14.48 research, 14.66
AGFUND, see Arab Gulf Programme for United Nations Development Organizations
Aging, see Elderly, health of AIDS (acquired immunodeficiency syndrome), 2.13,
2.22, 7.6, 9.3, 11.13, 14.36, 14.94, 14.99, 14.100, 14.114-14.124, 14.128-14.139, 14.185, 17.2, 17.7, 18.12, 19.13, 19.26, 19.29, 21.26, 22.9, 22.10
blood and blood products, safety and screening, 13.5, 14.122
discrimination, avoidance of, 2.13, 14.116 global programme and strategy, 2.13, 14.116,
14.117, 17.7 health education and information, 7.10, 7.12, 14.130 inter-agency advisory group, 14.137 legal and ethical aspects, 4.26, 4.28, 14.116 research, 4.24 Riga initiative, 20.12 supplies, 16.16-16.18, 16.20, 16.22
171
training, 7.12 United Nations joint programme, 2.13, 14.117 WHO/UNDP alliance, 14.118 World AIDS days, 7.3, 14.139 see also Sexually transmitted diseases
Albania, 10.11 Alcohol abuse, 11.10, 19.13
European action plan, 20.11 Algeria, 5.3 American College of Clinical Engineering, 5.8 American International Health Alliance, 5.8 American trypanosomiasis (Chagas disease), 14.32-
14.33, 18.11 research, 14.67
Americas, Region of the, 18.1-18.17, Annex 2 see also Pan American Health Organization and
individual activities Anaesthesiology, 13.2 Andean Area, 18.8, 18.11
Andean Parliament, 18.8 Cooperation in Health initiative, 18.5
Anthrax, 14.112 Appropriate Health Resources and Technologies Ac
tion Group, 14.90 Arab Gulf Programme for United Nations Develop
ment Organizations (AGFUND), 14.167, 14.197, 19.28, 21.6
Arabic, use of, 6.22, 15.13 Argentina, 8.9, 11.17, 14.33, 14.67,18.10 ARI news, 14.90 Armenia, 2.30 Arthritis, 14.211 Arthropod-borne viral diseases, 14.142 ASEAN, see Association of South-East Asian Na-
tions Asia and Pacific Decade of Disabled Persons, 13.41 Asian Development Bank, 2.19 Asian Interactive Association on the Hearing Im
paired, 14.172 Asia-Pacific Academic Consortium for Public Health,
6.25 Assessments on Member States, 1.5 Associate Members of WHO, 2.1, Annexes 1 and 2 Association for Health Information and Libraries in
Africa, 15.4, 17.6
THE WORK OF WHO 1992-1993 -----------------------~----
Association of South-East Asian Nations (ASEAN), 4.19
Asthma, 14.214 Atherosclerosis, 14.202, 14.210 Australia, 6.16, 22.10 Austria, 9.7 Auxiliary health personnel, see Community health
workers and the various categories of health personnel
Azerbaijan, 2.30
Baby-friendly Hospital Initiative, 9.17, 21.13 Bacterial diseases, 14.140-14.149
see also individual diseases Bahrain, 2.3, 12.10 Bamako initiative, essential drugs, 4.24 Bangladesh, 3.5, 9.43, 10.10, 12.14, 12.16, 14.45, 14.51,
14.80, 14.96, 19.3, 19.6, 19.14, 19.23, 19.24,19.28 fourth population and health project, 2.26, 4.3, 4.14,
4.16, 5.6, 6.4, 16.20 Barbados, 6.5 Belarus, 2.3, 11.7, 12.31 Belize, 4.6 Benin, 7.13, 11.16, 12.5, 13.21, 13.28, 13.38, 14.45 Bhutan, 5.6, 19.3, 19.6 Bilharziasis, see Schistosomiasis Bioethics, 4.29, 14.219 Biologicals, 13.22-13.24 Birth control, see Fertility regulation Blindness prevention, 14.164-14.171
see also Onchocerciasis Blood and blood products, screening and safety, 13.3-
13.5, 14.122 external quality assessment scheme, 13.3
Bolivia, 3.9, 5.12, 5.18, 10.9, 13.28, 14.67 Borrow Dental Milk Foundation, 9.27 Bosnia and Herzegovina, 2.3 Botswana, 5.4, 5.7, 7.12, 14.26, 14.99 Brazil, 8.9, 9.17, 10.15, 10.16, 10.17, 10.33, 11.8, 11.17,
12.14, 12.16, 14.15, 14.24, 14.33, 14.51, 14.52, 14.55, 14.61, 14.67, 14.68, 14.80, 14.81, 14.127, 14.133, 14.143, 18.10
Breast-feeding, 9.16, 9.17, 10.29, 14.78, 14.80, 14.89, 14.138,21.13
Bridge, 4.21 Brucellosis, 14.107, 14.113,19.28 Budget, see Programme budget (WHO) Bulgaria, 9.27 Bulletin of the World Health Organization, 15.11 Burkina Faso, 12.5 Burn injuries, 9.37, 9.39 Burundi, 14.19, 14.45 Byelorussian SSR, see Belarus
Cambodia, 2.32, 4.3, 9.25, 14.24, 15.9 Cameroon, 2.3, 4.3, 4.24, 5.7, 7.6, 7.12, 13.2, 14.22,
14.45, 14.61 Canada, 5.7, 14.203
172
Cancer, 10.20, 14.161, 14.173-14.181,21.27 see also International Agency for Research on Can
cer Cardiovascular diseases, 14.197-14.207, 21.27
cardiovascular diseases and alimentary comparison project (CARDIAC), 14.201
multinational monitoring project (MONICA), 14.198
Caribbean Area, 3.9, 4.26, 7.8, 8.9, 10.39, 15.2, 15.5, 18.5, 18.10, 18.15
Cooperation in Health initiative, 4.19, 18.5 Community (CARICOM), 18.6 Epidemiology Centre (CAREC), 4.6
Carnegie Corporation (USA), 11.1 CCAQ, see Consultative Committee on Administra
tive Questions CCPOQ, see Consultative Committee on Pro
gramme and Operational Questions Central African Republic, 7.12 Central America, 4.6, 18.5, 18.8, 18.10, 18.17
Chapultepec peace agreement, 18.17 development programme for refugees and displaced
persons (PRODERE), 18.17 health initiative, 18.5
Central and eastern Europe, 9.3, 9.44, 10.11, 11.2, 11.3, 13.26, 15.7, 20.2, 20.10, 20.12, 20.14, 20.15, 20.16
European cooperative health programme (EUROHEALTH), 20.16
Cerebral palsy, 13.39 Chad, 2.26, 3.9, 6.20, 7.12, 14.38 Chagas disease, see American trypanosomiasis Changing medical education and medical practice,
6.18 Chemical safety, 10.49, 12.18-12.24,21.21
health and safety guides, 12.20 international cards, 12.20 international programme (IPCS), 10.46 management, 12.18, 12.19, 12.20 occupational exposure, 10.46 poisons control and information, 12.23 risk evaluation, 12.19, 12.20, 12.22 see also Drugs
Chernobyl accident, 2.15, 9.26, 11.20 international programme, 11.20, 12.31
Children, 2.25, 10.7-10.13, 11.8, 14.90-14.92, 14.164, 19.25
AIDS/HIV infection, 7.6, 14.131, 14.135 Baby-friendly Hospital Initiative, 9.17, 21.13 convention, rights of the child, 10.7 diarrhoea! diseases, 9.12, 14.72, 14.76, 14.78, 14.80 immunization, 14.1-14.14, 14.86, 14.156, 14.160,
14.161, 14.193,22.4 vaccine initiative, 13.23, 14.11, 14.154 world summit (1990), 2.18, 3.3, 4.7, 9.19, 10.7, 10.10,
14.14, 18.10 see also Maternal and child health; Youth and ado
lescence Chile, 9.42, 10.16, 10.17, 10.33, 10.39, 10.53, 14.33,
14.67, 18.10
China, 4.25, 4.27, 6.4, 6.5, 7.7, 7.8, 7.13, 9.17, 10.7, 10.13, 10.21, 10.26, 10.52, 11.4, 11.7, 11.17, 12.27, 13.6, 13.38, 14.29, 14.42, 14.51, 14.59, 14.96, 14.140, 14.153, 14.171, 14.203, 15.9, 22.5, 22.6
Cholera, 2.14, 4.6, 9.12, 12.9, 12.11, 14.79, 14.155, 16.18, 16.19, 17.11, 17.16, 18.12, 19.24, 21.25
global task force, 14.79 CIOMS, see Council for International Organizations
of Medical Sciences Circulation, 14.198 Clinical technology, 13.1-13.2 Codex Alimentarius, FAO/WHO, 9.11, 19.16 Collaborating centres (WHO), 8.5, 14.151
accident and injury prevention, 9.36, 9.37, 9.38 cancer, 14.174, 14.179 cardiovascular diseases, 14.201 community safety promotion, 9.32 drug monitoring, 13.16 equipment maintenance and repair, 5.8 health and biomedical information, 21.23 hepatitis, 14.161 hospitals and other health institutions, 5.21 human reproduction research, 10.37 legionellosis, 14.148 malaria, 14.19 mental health, 11.5 occupational health, 10.43 oral health, 9.28, 9.30 pesticides, 14.44 rheumatic conditions, 14.212 smallpox and other poxvirus infections, 14.152
Collaborative International Pesticide Analytical Council, 14.44
Colombia, 5.17, 10.15, 10.17, 10.33, 11.8, 11.17, 14.69, 14.70, 14.188, 18.10
Commission of the European Communities, see European Communities
Commission on Health and Environment (WHO), 12.1-12.2, 15.10
Commission on Sustainable Development (United Nations), 2.12
Committee of the Executive Board to Consider Certain Financial Matters, 16.9
Commonwealth of Independent States, 9.30, 13.26, 14.104, 16.21
Commonwealth Pharmaceutical Association, 13.19 Communicable diseases, see individual diseases Community health workers, 5.18, 6.23 Community safety and health, 3.5, 5.11, 5.18, 7.13,
9.32-9.34, 14.215, 17.3 Comoros, 14.142 Conferences, see individual topics Congo, 7.12, 7.13, 14.38 Consortium for International Earth Science Informa
tion Network (CIESIN), 4.9 Constitutional and legal matters, 2.1-2.3 Consultative Committee on Administrative Ques
tions (CCAQ), 2.11 Consultative Committee on Programme and Opera
tional Questions (CCPOQ), 2.11, 2.16
INDEX
173
Consultative Group of Nongovernmental Organiza-tions, 14.166, 14.171
Continuing education, 6.14 Contraceptives, see Fertility regulation Contributions of Member States to WHO, incentive
scheme, 1.5 Conventions,
privileges and immunities, specialized agencies, 2.3 rights of the child, 10.7
Convergencia initiative, health science and technology, 8.9
Cooperation Council for Arab Gulf States, 13.25 Coordination and collaboration, 1.1, 2.10-2.27, 18.7-
18.8 see also individual organizations and activities
Coronary heart disease, 9.20 Costa Rica, 9.6, 10.17, 10.54 Cote d'Ivoire, 14.40, 14.45, 14.120, 14.129 Council of Europe, 3.6, 4.29, 10.17, 20.7 Council on Health Research for Development, 4.24,
8.7 Council for International Organizations of Medical
Sciences (CIOMS), 4.29, 8.2, 13.15, 13.16 Council for Science and Technology (WHO), 8.4 Country health information development, 4.3-4.5 Creutzfeld-Jakob disease, 14.110 Croatia, 2.3 Cuba, 8.9, 10.39, 14.156, 14.167, 14.202, 14.203, 18.10,
18.14 Cyprus, 5.8, 12.10, 13.6 Cystic fibrosis (mucoviscidosis), 14.216 Czech Republic, 2.3
Danish International Development Agency (DANI-DA), 5.21
Data processing, see Information systems Deafness, 14.172 Delagrange lnternational!Synthelabo Recherche
(France), 11.1 Dementias, 10.51, 10.53, 11.20 Democratic People's Republic of Korea, 14.141 Demography, see Population Dengue and dengue haemorrhagic fever, 14.42, 14.46,
14.142, 14.159,19.28 Denmark, 13.24 Dental health, see Oral health Diabetes, 14.208-14.210, 14.215, 20.16, 21.27
European action plan, 20.16 St Vincent declaration, 14.209, 20.16
Diarrhoea! diseases, 2.14, 9.12, 14.72-14.82, 14.89, 14.92, 14.155, 18.12,19.24
see also Cholera Digital Equipment Corporation (USA), 11.1 Diphtheria, 14.1, 14.8, 14.9, 22.4 Director-General, reappointment, 1.3 Disability prevention and rehabilitation, 2.15, 2.29,
13.35-13.41 Disaster relief, see Emergency relief and supplies Disease vector control, see Vector control
THE WORK OF WHO 1992-1993
Displaced persons, see Refugees and displaced per-sons
District health systems, 5.11-5.21 Djibouti, 14.19 Documents (WHO), see Health literature services Dominican Republic, 5.12, 6.3, 14.129, 18.10 Dracunculiasis (guinea-worm disease), 14.22-14.23,
17.15, 19.23 Drugs,
abuse, 9.3, 11.9-11.16, 11.22, 19.13 alerting system (ATLAS), 11.9 control of narcotic drugs and psychotropic
substances, 2.15 essential, 13.10, 19.18, 19.19, 21.16
action programme, 13.26-13.34 Bamako initiative, 4.24 model list, 13.18, 14.178
management and policies, 13.10 pharmaceuticals, 13.11-13.21, 13.33, 19.18, 19.19 rational use, 13.33, 14.76,19.19
international network, 13.33
EAST organization (water, agriculture and health in the tropics), 12.5
Eastern Mediterranean Region, 21.1-21.29, Annex 2 see also individual activities
ECA, see Economic Commission for Africa Economic Commission for Africa, 2.17 Economic Commission for Europe, 2.17 Economic Commission for Latin America and the
Caribbean, 2.17 Economic development, health aspects, 3.8-3.10 Economic and Social Commission for Asia and the
Pacific, 2.17, 13.41 Economic and Social Commission for West ern Asia,
2.17 Economic and Social Council of the United Nations,
2.12-2-16, 9.53, 14.116, 14.117 Commission on Sustainable Development, 2.12
Ecuador, 9.6 · Edna McConnell Clark Foundation, 14.165 Education, see Health education; Medical education Egypt, 2.31, 5.8, 5.11, 5.17, 6.16, 6.22, 9.17, 10.21, 11.7,
11.10, 12.10, 13.2, 13.36, 14.52, 14.80, 14.91, 14.143, 21.5, 21.6
El Salvador, 18.17 Elderly, health of, 9.37, 10.51-10.57, 14.171, 19.12,
21.14 international research programme, 10.51
Emergency relief and supplies, 2.15, 2.22, 2.28-2.33, 9.10, 11.7, 16.16, 16.18, 16.22, 17.5, 18.17, 20.6, 21.6, 21.25
international decade, natural disasters, 2.31, 18.17 Encephalitis, Japanese, 14.145, 14.159,19.28 Environment and development, United Nations con
ference (1992), 2.11, 7.2, 12.1-12.3, 12.18, 12.19, 15.10, 18.15, 22.12
Agenda 21, 2.11, 2.12, 12.1, 12.2
174
Environment and health, Americas, investment plan, 3.4 Central America, national plans, 18.15 Eastern Mediterranean, regional strategy, 21.18 Europe, regional centre, 20.13
Environmental health, 1.2, 3.4, 7.5, 9.13, 12.1-12.31, 18.15, 19.15, 20.13, 21.21, 21.22, 22.12
global network, technology (GETNET), 12.29 WHO commission, 12.1-12.2, 15.10 see also Chemical safety; Environmental pollution;
Environment and development; Water supply and sanitation
Environmental Health Criteria, 12.20, 12.22 Environmental health hazards, control, 12.25-12.31
human exposure assessment location (HEAL) project, 12.26
Environmental management, panel of experts (PEEM), 12.6
Environmental pollution, 12.25-12.30, 14.91, 19.15, 21.21
see also Chemical safety; Water supply and sanitation
Epidemiology and statistical services, 4.6-4.9, 12.27, 12.31
WHO statistical information system (WHOSIS), 4.9
Epilepsy, 11.18, 11.19 Equipment management, 5.7-5.10 Eritrea, 2.29 ESCAP, see Economic and Social Commission for
Asia and the Pacific Essential drugs, see Drugs Essential drugs monitor, 13.32 Estonia, 10.11 Ethiopia, 2.29, 12.28, 14.19, 14.45, 14.91, 14.153 European Bank for Reconstruction and Develop-
ment, 2.19 European Communities (Commission), 2.23, 3.6,
5.19, 10.17, 10.45, 10.55, 12.18, 13.34, 14.37, 14.66, 20.7, 20.13
Treaty on European Union, 20.1 European cooperative health programme (EURO-
HEALTH), 20.16 European Dialogue on Training in Public Health, 6.25 European Federation of Neurological Societies, 11.3 European Forum of National Medical Associations
and WHO, 20.9 European Forum of Pharmaceutical Associations and
WH0,20.9 European Medical Research Council, 4.22, 8.11 European Network of Health-promoting Schools,
7.7, 20.7 European Region, 20.1-20.17, Annex 2
see also individual activities European Union, see European Communities (Com
mission) Evaluation and monitoring of programmes, see under
Health for all by the year 2000 and Health situation and trend assessment
Executive Board, 1.1, 1.4, 2.4, 16.8 Committee to Consider Certain Financial Matters,
16.9 membership, 2.2 Programme Committee, 1.1, 1.4, 2.4, 16.8 sessions, Annex 3 resolutions, 1.1, 1.4, 2.19, 16.8 working group, WHO response to global change,
1.1, 2.5 Ex libris, 15.7 Expanded Programme on Immunization, see Immu
nization Expert advisory panels (WHO), 8.6 Expert committees (WHO),
alcohol- and drug-related problems in the work-place, 11.1 0
anthropometry, 9.15 cardiovascular diseases, 14.207 drug dependence, 11.14 essential drugs, 13.18 filariasis, 14.28 health promotion in the workplace, 10.49 information systems, district level, 4.5 maternal and child health and family planning, 10.2 onchocerciasis, 14.31 schistosomiasis, 14.2 4
Eye diseases, see Blindness prevention
Family Care International, 10.9 Family Health International, 10.9 Family planning, 9.4, 10.1-10.13, 10.32-10.33, 17.10,
19.11, 21.13 see also Fertility regulation
FAO, see Food and Agricultural Organization of the United Nations
Fellowships, 6.24, 7.12, 14.141,14.196 Fertility regulation, 10.25-10.30, 10.35
contraceptives, 10.4, 10.13, 10.20-10.24, 10.35 emergency contraception, 10.24 human reproduction research, 4.24, 10.19-10-41 infertility, 10.31, 10.38 intrauterine devices, 10.22-10.23 natural methods, 10.29-10.30 regulation of male fertility, 10.25-10.26 resources for research, 10.36-10.41 social science research, 10.35 technology transfer, 10.32-10.34 vaccine development, 10.27-10.28
Fiji, 4.3, 6.23, 11.17 Filariasis, 14.28-14.29, 19.23
research, 14.60, 14.70 see also Onchocerciasis
Finnish International Development Agency (FINNIDA), 2.26, 13.4
Finnish Red Cross, 13.4 Fluoridation of milk, 9.27 Fometro, 14.41 Food and nutrition, 2.22, 9.9-9.20, 14.80, 14.92,
14.184, 14.201, 17.2, 17.9, 21.9
INDEX
11S
food aid programmes, 9.10 food safety, 12.21,14.108-14.111, 19.16, 21.21 international conference (1992), 7.2, 7.10, 9.9, 9.14,
17.8 international decade, Africa, 17.8 world declaration and plan of action, 9.14 see also Micronutrient deficiencies
Food and Agriculture Organization of the United Nations (FAO), 9.13, 9.14, 9.20, 10.3, 12.6, 12.7, 12.18, 12.21, 14.38, 14.40, 14.44, 14.107, 17.11
Foundation for Advanced Studies on International Development, 14.172
Foundation for Health Services Research, 4.21 France, 8.7, 9.35 French Red Cross, 13.4
Gambia, 10.8, 14.57, 14.58, 14.91, 14.156, 14.187, 14.193
General Agreement on Tariffs and Trade (GATT), 9.11
General Programme of Work of WHO, eighth, 16.8, 16.11 ninth, 1.1, 2.4, 9.1, 18.1
Genetics, 14.216, 14.219, 14.189-14-190, 14.191, 14.192
Geriatrics and gerontology, see Elderly, health of German Foundation for International Development,
13.20, 13.21 German Technical Cooperation Agency (GTZ), 5.7,
5.8, 5.16, 5.19 Germany, 13.12, 13.21, 14.202 Ghana, 4.24, 5.1, 5.6, 12.14, 13.41, 14.22, 14.62, 14.70,
14.203, 17.6, 17.15 Global change, WHO response to, 1.1, 2.5 Global environmental epidemiology network, 12.27 Global Environmental Monitoring System (GEMS),
9.13 Global Policy Council (WHO), 2.5 Governing bodies, see Executive Board; Regional
committees; World Health Assembly Grants, research training, 6.24, 8.10, 8.13, 10.39, 14.71 GTZ, see German Technical Cooperation Agency Guatemala, 4.16, 9.6, 9.18, 12.11, 14.62, 14.91 Guidelines for drinking-water quality, 12.28 Guinea, 3.9, 7.13, 13.28, 14.96 Guinea-Bissau, 3.9, 4.3, 4.12 Guinea-worm disease, see Dracunculiasis Guyana, 4.6
Haemoglobinopathies, 14.216, 14.217, 14.218 Haemophilia, 14.216, 14.218 Haemorrhagic fevers, viral, 14.143
see also Dengue and dengue haemorrhagic fever Haiti, 5.12, 14.135, 18.17 Health education, 7.5-7.13, 14.130, 14.203, 19.8, 21.8
environmental health and sanitation, 12.4, 12.5, 12.8, 12.11
THE WORK OF WHO 1992-1993
Health for all by the year 2000, 3.1-3.10, 20.8, 20.9 economic development and, 3.8-3.10 monitoring and evaluation, 3.1-3.3, 4.1, 19.2 see also Primary health care
Health information support, 4.9, 15.1-15.16, 17.6 see also Health literature services; Information sys
tems; Publications Health laboratory technology, 13.3-13.5 Health legislation, 4.25-4.29, 21.6
documentation system, Latin America and the Caribbean (LEYES), 4.26
Health literature services, 15.1-15.9 Africa (library digest, Index Medicus), 15.4 Eastern Mediterranean (ExtraMED), 15.8, 21.23 Latin America and the Caribbean (LILACS,
BIREME), 15.2, 15.5 medical literature retrieval system (MEDLINE),
15.9 South-East Asia (HELLIS, Index Medicus), 15.6 WHO database (WHOLIS), 15.2
Health promotion, Eastern Mediterranean, 21.5 Europe, 7.7 Latin America and the Caribbean, 18.5 Western Pacific, 22.11
Health policy, 3.4-3.7, 3.9, 3.10 Health research, see Research Health services journal, 8.12 Health situation and trend assessment, 4.1-4.2 Health systems/services,
based on primary health care, 5.1-5.21, 21.3, 22.2 community participation, 5.11, 5.18 costs and financing, 3.8, 3.9, 5.1-5.3, 17.4, 20.4,
20.12, 20.14, 21.2 development, 4.1-4.29 district and peripheral levels, 5.11-5.18
Ain Shams project, 5.11 European project on health care reform (EURO-
CARE), 20.14 European "regions for health" network, 3.7, 20.10 management, 4.2, 5.7-5.10 national health systems and policies, 5.1-5.10, 21.3 organizational change, 5.4-5.6 research, 4.20-4.24, 6.25, 21.4 structural aspects, 5.14 see also Primary health care
Health Volunteers Overseas, 13.1 Healthy cities and villages, 5.15-5.16, 9.7, 12.14, 12.15,
12.16, 17.12, 20.10, 21.20, 22.12 Hearing impairment, 14.172 Hedip forum, 2.33 Helminth infections, 9.10 Hepatitis, viral, 14.4, 14.141, 14.161, 14.187, 14.193,
19.28, 22.6 Hereditary diseases, 14.216-14.219 HFA 2000,7.10 HIV infection, see AIDS Honduras, 10.9, 14.33, 14.120 Hong Kong, 6.5
176
Hospitals, 5.5, 5.19-5.21, 13.1, 13.2, 17.5 baby-friendly initiative, 9.17, 21.13 core library for doctors, 5.20 waste management, 12.17
Housing, 12.14-12.15 Human immunodeficiency virus (HIV), see AIDS Human reproduction research, 4.24, 10.19-10.41 Human resources for health, 6.1-6.27, 19.7, 21.7, 22.3
continuing education, 6.14 management, 6.3-6.4, 6.11-6.13 network of community-oriented educational insti-
tutions, 4.22 planning tools, 6.5-6.7 policy analysis, 6.3-6.4 see also Fellowships; Grants; Medical education;
Teaching/learning materials and the various categories of health personnel
Human rights, 4.29, 9.3, 9.5 United Nations centre, 4.29 United Nations conference (1993), 7.10
Humanitarian assistance, 2.15, 2.22, 2.25, 2.28, 2.30, 2.31, 2.33, 20.6
Hungary, 14.202, 14.203 Hypercholesterolaemia, 14.219 Hypertension, 14.215
IAEA, see International Atomic Energy Agency IARC, see International Agency for Research on Can
cer IARC Monographs, 14.195 Ibero-American conferences of Heads of State and
Government, 3.4, 18.7 ICAO, see International Civil Aviation Organization ICD, see International Classification of Diseases ILO, see International Labour Organisation Immunization, 2.25, 14.1-14.14, 14.86, 14.174, 16.19,
17.13, 18.10, 19.21, 19.28, 22.4 see also individual diseases
IMPACT (international initiative against avoidable disability), 13.36
Index Medicus, 15.4, 15.6, 17.6 India, 3.5, 4.3, 4.24, 4.25, 5.17, 6.21, 7.8, 9.37, 9.43,
10.41, 11.7, 13.36, 14.15, 14.22, 14.35, 14.42, 14.51, 14.61, 14.65, 14.89, 14.96, 14.106, 14.120, 14.129, 14.165, 14.168, 14.172, 14.181, 14.203, 15.12, 16.20, 19.4, 19.13, 19.14, 19.15, 19.16, 19.23,19.24
Indonesia, 4.24, 5.17, 5.19, 6.4, 10.10, 10.16, 10.17, 10.25, 10.33, 14.42, 14.51, 14.81, 14.106, 19.3, 19.4, 19.6, 19.15, 19.16, 19.23
Industrial health, see Occupational health Industry Council for Development, 9.12 Infectious diseases, rapid diagnosis, 14.151 Infertility, 10.31, 10.38, 17.10 Influenza, 14.140 Information systems, 2.9, 4.4, 6.11, 6.16, 12.23, 14.12,
14.150, 14.153, 20.7 computer software (WHONET), 14.150 "European Nervous System", 20.7
Information systems (continued) health sciences information, Latin America and the
Caribbean, 15.2, 15.5 WHO statistics (WHOSIS), 4.9 WHO terminology (WHOTERM), 15.14
Injury prevention, 9.5, 9.32-9.39, 11.10, 12.31, 21.11 Intensified cooperation with countries and peoples in
greatest need, 2.26, 3.8, 4.3, 4.11-4.17, 5.3, 6.4, 12.11, 17.8, 19.3
lnteragency Steering Committee for Water Supply and Sanitation, 12.13
lnter-American Center for Social Security Studies, 5.18
Inter-American Development Bank, 2.19 Intergovernmental Oceanographic Commission,
17.11 Intergovernmental organizations, Annex 4
see also Coordination and collaboration and individual organizations
Intergovernmental Panel on Climate Change, 12.27 International Agency for Research on Cancer
(IARC), 2.5, 12.27, 14.182-14.196 International Alliance of Women, 2.5 International Association of Lions Clubs, 14.164,
14.168 International Association for the Study of Pain,
14.179 International Atomic Energy Agency (IAEA), 9.13,
13.6, 13.7, 14.177, 17.11 International Children's Centre, .1 0.8 International Civil Aviation Organization (ICAO),
9.52 International Classification of Diseases (ICD), 4.10,
11.5, 11.6, 11.14 application to dentistry and stomatology, 9.29
International Classification of Impairments, Disabilities and Handicaps, 4.10
International Code of Marketing of Breast-milk Substitutes, 4.28, 9.18
International Commission on Occupational Health, 10.49
International Committee of the Red Cross, 2.25, 2.33 International Confederation of Midwives, 10.6 International Consultative Group on Food Irradia-
tion, 9.13 International Council for Education of the Visually
Handicapped, 14.164 International Decade on Food and Nutrition for Afri
ca, 17.8 International Decade for Natural Disaster Reduction,
2.31, 18.17 International Development Research Centre (Cana-
da), 3.10, 4.21, 4.23, 14.26 International Diabetes Federation, 14.209 International digest of health legislation, 4.26 International Drinking Water Supply and Sanitation
Decade, 17.11 International Federation of Anti-Leprosy Associa
tions, 14.50 International Federation for Medical and Biological
Engineering, 5.8
INDEX
177
International Federation of Pharmaceutical Manufacturers Associations, 13.14, 13.20, 14.136
International Federation of Red Cross and Red Crescent Societies, 2.25
International Fibre Safety Group, 10.45 International Forum for Social Sciences in Health,
4.22 International Health Policy Programme, 4.24 International Hospital Federation, 5.10 International Labour Organisation (ILO), 5.1, 10.3,
10.42, 10.44, 10.47, 10.48, 11.10, 12.18, 12.19, 13.41
International League of Associations for Rheumatol-ogy, 14.213
International Leprosy Association, 13.38 International Life Sciences Institute, 9.12 International Monetary Fund, 2.19 International Office of Epizootics, 14.107 International Olympic Committee, 9.48, 14.206 International Pharmaceutical Federation, 13.19 International Planned Parenthood Federation, 10.18 International Programme on Chemical Safety, 10.46,
12.18-12.24 International Project Assistance Services, 10.9 International Society for Burn Injuries, 9.37 International Society and Federation of Cardiology,
14.197,14.202 International Society of Orthopaedic Surgery and
Traumatology, 13.1 International Society of Prosthetics and Orthotics,
2.25 International Society on Quality Assurance, 5.21 International Society of Surgery, 13.1 International Statistical Institute, 4.10 International Union of Architects, 5.10 International Union against Cancer, 9.45 International Year of the Family, 2.15, 11.9 International Youth Foundation, 10.15 Internet, international computer network, 4.9 Intestinal parasitic infections, 14.153 Investing in health,
Riga statement, 20.12 women's health, 9.7
Iodine deficiency disorders, 9.19, 17.9, 21.9 IPCS, see International Programme on Chemical
Safety IPCS news, 12.24 Iran, Islamic Republic of, 2.31, 5.19, 12.14, 13.36,
14.23, 14.52, 14.68, 15.8 Iraq, 2.31, 9.18, 16.16 Islamic Educational, Scientific and Cultural Organi-
zation, 21.8 Israel, 10.54 Italy, 10.9, 10.54, 13.12, 13.21, 14.25, 14.202 lvermectin, 14.29, 14.30, 14.31, 14.60, 14.62, 14.164
Jamaica, 9.6, 10.33, 10.54 Japan, 6.3, 6.5, 12.16, 13.19 Japanese encephalitis, 14.145, 14.159,19.28
THE WORK OF WHO 1992-1993
JohannJacobs Foundation, 11.1 Joint Committee on Health Policy, UNICEF/WHO,
2.18 Joint Committee on the Health of Seafarers, ILO/
WHO, 10.44 Joint Committee on Occupational Health, ILO/
WHO, 1Q.42 Joint Expert Committee on Food Additives, FAO/
WHO, 12.21 Joint Meetings on Pesticide Residues, FAO/WHO,
12.21 Jordan, 5.8, 9.17, 21.5
Kazakhstan, 5.1 Kellogg Foundation, 6.12, 10.9, 10.14, 10.15 Kenya, 4.24, 5.1, 5.4, 5.8, 7.12, 14.10, 14.24, 14.45,
14.48, 14.59, 14.84, 14.131, 14.144, 14.165 Kiribati, 10.7 Kyrgyzstan, 5.1
Laboratory technology and blood safety, 13.3-13.5, 14.151, 19.17, 21.17
La Leche League International, 2.25 Lao People's Democratic Republic, 4.12, 9.25, 22.5 Lassa fever, 14.143 Latin America, 2.17, 3.9, 4.26, 8.9, 10.32, 18.5, 18.15 Latin American and Caribbean Center on Health Sci-
ences Information (BIREME), 15.2, 15.5 Latin American Committee against Tobacco Use, 9.42 Latin American Parliament (PARLATINO), 18.8 Laureate Foundation, 11.1 Learning materials, see Teaching/learning materials Lebanon, 9.17, 13.36 Legionellosis (Legionnaires' disease), 14.148 Leishmaniases, 14.34-14.36, 14.48, 19.23, 21.25
research 14.68-14.69, 14.71 Leprosy, 14.49-14.55, 17.16, 19.27, 22.7
research, 4.24, 14.55, 14.65 Lesotho, 10.8 Libraries, see Health literature services
Macao, 22.1 MacArthur Foundation, 10.54 Madagascar, 4.21, 14.19, 14.51 Malaria, 2.14, 9.10, 14.15-14.21, 14.44, 14.45, 14.46,
14.48, 14.90, 14.92, 17.14, 19.22, 21.25, 22.8 ministerial conference (1992), 7.2, 7.10, 14.16, 17.14 research, 14.20, 14.57-14.58, 14.70, 14.71
Malawi, 3.9, 6.20, 14.94, 14.99, 14.100, 17.6 Malaysia, 5.13, 15.9, 22.12 Maldives, 4.3, 6.21, 13.28, 14.153, 19.3, 19.6, 19.14,
19.23 Mali, 3.9, 13.6, 14.24, 14.165 Malnutrition, see Food and nutrition Malta, 10.53
178
Management Development Committee (WHO), 2.5 Manpower, see Human resources for health Marshall Islands, 4.3 Maternal and child health, 9.4, 10.1-10.13, 17.10,
19.11, 21.13 Maternal mortality, 10.38 Mauritania, 14.45 Mauritius, 13.37, 14.153, 14.215 Measles, 14.1, 14.5, 14.7, 14.8, 14.14, 14.86, 14.92,
14.151, 14.160, 17.13, 18.10, 19.21, 22.4 Medecins sans Frontieres, 14.41 Medical education, 2.25, 6.14, 6.17-6.25, 9.30, 11.7,
13.2, 14.74, 17.17, 22.3 Meetings, see individual topics Member States, 2.1, 20.1, Annexes 1 and 2
assessments, 1.5 contributions, incentive scheme, 1.5 voting privileges and services, suspension, 2.2
Meningitis, 14.91, 14.147, 14.156, 16.18, 17.16 Mental health, 11.1-11.22, 21.15
see also Alcohol abuse; Drugs, abuse Merck & Co. (USA), 14.30 Mexico, 2.9, 8.9, 9.42, 10.33, 11.10, 14.129,14.153 Micronesia, Federated States of, 4.3 Micronutrient deficiencies, 9.19, 17.9, 21.9, 22.6 Midwifery, see Nursing and midwifery Mifepristone, 10.24 Milk fluoridation, 9.27 Ministers of Health of Non-Aligned and Other De
veloping Countries, 4.18 Mongolia, 3.5, 4.11, 5.6, 5.19, 9.43, 13.28, 13.38,
14.141, 19.3, 19.6, 19.28 Morocco, 4.21, 9.18, 10.17, 14.24, 14.170 Mozambique, 2.26, 2.29, 4.11, 4.15, 12.11, 13.2, 14.99,
17.6 Myanmar, 4.24, 5.19, 6.21, 14.42, 14.51, 14.141,
14.153, 19.3, 19.6, 19.13, 19.19, 19.23,19.28
Namibia, 4.21, 5.6, 6.12, 7.12, 11.10,14.19 Nepal, 3.5, 3.9, 4.13, 5.18, 6.4, 9.43, 10.10, 13.28,
14.106, 19.3, 19.4, 19.6, 19.14, 19.23, 19.24,19.28 Netherlands, 2.26, 4.24, 5.21, 9.18, 10.9, 13.24, 14.41 Network of Community-oriented Educational Insti-
tutions for Health Sciences, 4.22 Neurological disorders, see Mental health Neuropathy, 18.14 Nicaragua, 10.9, 12.27 Niger, 13.2 Nigeria, 4.21, 4.24, 5.11, 5.14, 5.16, 9.28, 10.16, 10.53,
11.8, 11.16, 12.16, 14.22, 14.51, 14.52, 14.64, 14.70, 14.102, 14.143, 17.15
Noncommunicable diseases, 9.20, 17.2 country-wide intervention programme (CINDI),
14.215,20.9 integrated programme (INTERHEAL TH), 14.215 see also individual diseases
N ongovernmental organizations in official relations with WHO, 2.25, Annex 4
North American Free Trade Agreement (NAFTA), 18.6
Norway, 9.7, 11.8,14.156 Norwegian Agency for International Development
(NORAD), 5.4, 5.7, 6.12 Nosocomial infections, 14.150 Nursing and midwifery, 4.24, 6.11, 6.12, 6.15-6.16,
9.39, 10.6, 14.131, 17.17, 20.15 Nutrition, see Food and nutrition
OAU, see Organization of African Unity Occupational health, 7.8, 10.42-10.50, 14.183, 14.195 Occupied Arab territories, 2.31 OECD, see Organisation for Economic Co-operation
and Development OIE, see International Office of Epizootics Oman, 2.9, 7.12, 12.10, 14.153 Onchocerciasis, 14.30-14.31, 14.164
research, 14.30, 14.60-14.64, 14.70 Oncology, see Cancer Operation Salam for humanitarian assistance to Af-
ghanistan, 16.22 Oral health, 9.21-9.31, 12.31, 21.10 Oral rehydration, 14.76, 14.80, 19.24 Orbis International, 14.169 Organ transplantation, 4.26 Organisation for Economic Co-operation and Devel-
opment (OECD), 2.23, 3.6, 12.18 Organization of African Unity (OAU), 2.22, 14.40 Organization of American States, 4.9, 18.17 Organizational and related meetings, Annex 3 Organizational structure of WHO, Annex 5 Orthopaedics, 13.1 Osteoarthritis, 14.211 Osteoporosis, 10.51, 10.52, 14.213
Paediatrics, see Children P AHO, see Pan American Health Organization Pakistan, 4.3, 4.25, 6.16, 12.14, 14.22, 14.80, 14.91 Palestine, 21.1 Pan American Health Organization (PAHO), 2.9,
9.42, 9.51, 10.15, 10.18, 14.30, 16.19, 18.1, 18.2, 18.5, 18.14, 18.16, 18.17
Directing Council, 3.4, 18.3, 18.4 see also Americas, Region of the
Pan American Sanitary Bureau, see Regional Office for the Americas
Panama, 9.6, 10.39,11.17 Panel of Experts on Environmental Management for
Vector Control (PEEM), 12.6 Papua New Guinea, 6.16, 7.12, 10.7, 10.13, 14.51,
14.89, 14.91 Paraguay, 14.33, 14.67 Parasitic diseases, 14.153, 17.2, 19.23
see also Tropical diseases; Vector control and individual diseases
Pelvic inflammatory disease, 10.23
INDEX
179
Periodontal disease, 9.23 Pertussis, 14.1, 14.5, 14.86, 22.4 Peru, 10.9, 10.33, 10.39, 16.19,18.10 Pesticides, see Vector control Pharmaceuticals, see Drugs Philippines, 4.21, 5.13, 5.17, 9.17, 10.7, 10.16, 11.7,
12.30, 14.59, 14.89, 14.91, 15.9, 22.5, 22.6, 22.12 Physical resources for health, management, 5.7-5.10 Plague, 14.146, 17.16,19.28 Pneumococcosis, 14.157 Pneumoconiosis, 10.47 Pneumonia, 14.83, 14.86, 14.90, 14.91, 14.92 Poison Information Monographs, 12.23 Poland, 11.10 Poliomyelitis, 13.1, 13.39, 17.13, 18.10, 19.21, 21.25,
22.4, 22.5 immunization and vaccine development, 14.1, 14.5,
14.6, 14.7, 14.11, 14.14,14.162 Pollution, see Environmental pollution Population, health and development, 2.21, 2.26 Population Council, 10.9 Portugal, 11.8 Preferential Trade Area of Eastern and Southern
African States, 13.31 Primary health care, 2.29, 5.1-5.21, 22.2, 22.3
see also Community health workers; Health for all by the year 2000; Health systems/services
Programme budgets (WHO), 2.6-2.8, 16.8-16.14 for 1992-1993, 16.8 for 1994-1995, 1.4, 1.5, 16.8
Programme Committee of the Executive Board, 1.1, 1.4, 2.4, 16.8
Programme of WHO, development and management, 2.1-2.33
see also General Programme of Work of WHO Prosthetic and orthotic services, 13.40 Psychosocial and behavioural problems, see Mental
health Public health training and research, 6.25 Public information, 7.1-7.4, 7.9, 7.10
see also Health education Publications (WHO), 14.195,15.10-15.13
distribution and sales, 15.15-15.16 listing of publications and documents
(WHODOC), 15.2 Puebla Group, 4.21 Puerto Rico, 18.3 Pulmonary diseases, chronic, 14.214
Qatar, 21.6
Rabies, 14.102-14.106, 14.113, 19.28 Radiation accidents and radiological emergenCles,
11.20, 12.31 emergency network (REMP AN), 12.31 see also Chernobyl accident
Radiation medicine, 12.27, 12.31, 13.6-13.8
THE WORK OF WHO 1992-1993
Ravizza Farmaceutici (Italy), 11.1 Refugees and displaced persons, 2.29, 2.32, 2.33, 11.7,
14.45, 17.2, 18.17 Central American programme (PRODERE), 18.17
Regional Committee for Africa, 5.5, 8.8, 17.1, 17.5, 17.11
Regional Committee for the Americas, 3.4, 18.3, 18.4 Regional Committee for the Eastern Mediterranean,
9.8, 14.113,21.1 Regional Committee for Europe, 11.10, 20.11, 20.16 Regional Committee for South-East Asia, 19.7, 19.27 Regional Committee for the Western Pacific, 9.46,
22.1, 22.5, 22.10, 22.11 Regional committees, 1.4, 16.8
sessions, Annex 3 Regional Office for Africa, 16.4, 17.10 Regional Office for the Americas, 18.1 Regional Office for the Eastern Mediterranean, 16.6,
21.23, 21.28 Regional Office for Europe, 2.9, 20.7, 20.17 Regional Office for South-East Asia, 2.9, 16.5 Regional Office for the Western Pacific, 16.7 Rehabilitation, 2.15, 2.29, 13.35-13.41 Rehydration, 14.76, 14.80, 19.24 Representatives (WHO), 2.33, 6.27 Research, 8.1-8.14, 19.9
Advisory committees on health research (ACHR), 8.2-8.4, 8.9, 8.10, 8.13
Council on Health Research for Development, 4.24, 8.7
ethical aspects, 8.2, 8.3 grants, 6.24, 8.10, 8.13, 10.39, 14.71 networking, 4.21, 4.22 prizes, 8.8, see also Health systems/ services, research and indi
vidual subjects of research Respiratory infections, acute, 10.47, 14.83-14.92,
14.151, 14.160,19.25 Rheumatic diseases, chronic, 14.211-14.213 Rheumatic fever and rheumatic heart disease, 14.149,
14.197 RhOne-Poulenc (France), 14.41 Rift Valley fever, 14.113, 14.143, 21.25 Road accidents, 9.38, 11.10 Rockefeller Foundation, 4.19, 5.7, 10.37, 14.154 Romania, 10.11, 14.169 Rotary International, 2.25, 14.13 Rural development and housing, 12.14-12.17 Russian Federation, 4.25, 9.17, 10.11, 12.31, 14.9,
14.175, 14.203 Rwanda, 14.19, 14.45, 14.131,14.133
Safe motherhood, 10.5-10.6, 10.8, 10.12, 17.10, 21.13 initiative, 10.10
Saint Kitts and Nevis, 6.5 Saint Lucia, 6.5 Salmonellosis, 14.108-14.109 Samoa, 4.3 Sanitation, see Water Supply and Sanitation
180
Sasakawa Foundation, 11.1, 14.50 Saudi Arabia, 5.21, 12.14 Schistosomiasis, 9.10, 12.7, 14.24-14.27, 19.23
research, 14.59, 14.70, 14.71 Schizophrenia, 11.18, 11.19, 11.21 Scientific groups (WHO):
asthma, 14.214 cardiovascular diseases, 14.204 hereditary diseases, 14.216
Senegal, 5.8, 5.15, 5.18, 9.41, 10.8, 12.14, 14.26, 17.12 Sexually transmitted diseases, 10.31, 14.123-14.127,
22.10 see also AIDS and individual diseases
Seychelles, 2.9, 6.10, 14.153 Shigellosis, 14.155 SIDA, see Swedish International Development
Authority Sierra Leone, 5.8 Skills for life, 11.8 Sleeping sickness, see African trypanosomiasis Slovakia, 2.3 Smallpox, 14.152, 18.10 Smoking, see Tobacco Solomon Islands, 22.8 Somalia,2.31, 11.7, 14.19, 16.16,21.5 South Asian Association for Regional Cooperation,
10.10 South-East Asia Region, 19.1-19.29, Annex 2
see also individual activities Southern Cone, 14.32, 18.5, 18.11
common market (MERCOSUR), 18.6 health initiative, 18.5
Soviet Union, former, 2.27, 2.30, 14.9, 14.111, 15.7, 20.2
Spain, 10.53, 14.188,14.198 Special Programme of Research, Development and
Research Training in Human Reproduction, 10.19-10.41
Special Programme for Research and Training in Tropical Diseases, 14.56-14.71
Spongiform encephalopathies, 14.110 Sri Lanka, 6.21, 11.10, 14.15, 14.61, 14.106, 14.120,
14.177, 19.3, 19.6, 19.13, 19.14, 19.16, 19.19, 19.23,19.28
Staff of WHO, 6.27, 9.2, 16.1-16.3, 21.28 Statistics, see Epidemiology and statistical services Sterility, see Infertility Streptococcal infections, 14.149 Structure of WHO, Annex 5 Study groups (WHO):
aging and working capacity, 10.49 cardiovascular diseases in the elderly, 14.205 diabetes, 14.208 foodborne trematode infections, 14.27 osteoporotic fracture risk, 14.213 vector control, 14.46
Substance abuse, 11.11, 11.12, 11.22 see also Drugs, abuse
Sudan, 6.22, 13.2, 14.40, 14.48, 14.51, 14.59, 14.170, 21.5
Support services (WHO), 16.1-16.23
Supportive environments for health, 7.5, 12.15 Surgery, 13.1, 13.2
computerized registration system (WHOCARE), 14.150
Sustainable development, 2.11, 2.12 Swaziland, 14.89 Sweden, 2.26, 9.7, 12.19, 14.109,14.202 Swedish International Development Authority
(SIDA), 9.18 Switzerland, 4.10, 10.16, 14.177, 14.202 Syphilis, 14.127 Syrian Arab Republic, 2.9, 5.8, 6.22, 9.18, 9.28, 21.6
Tajikistan, 2.30, 20.6 Tanzania, see United Republic of Tanzania Teaching/learning materials, 5.13, 6.26, 12.24, 14.21,
14.38, 14.84, 14.209, 17.16, 20.15, 21.7 Technical cooperation among developing countries
(TCDC), 4.18-4.19 United Nations committee, 4.19 UNDP special unit, 4.19
Technical Discussions, Health Assembly, 1.2, 9.34 regional committees, 5.5, 6.3, 21.1
Technology development, assessment and transfer, 8.9, 13.9
Terminology, WHO information system (WHOTERM), 15.14
Tetanus, 14.1, 14.3, 14.5, 14.7, 14.14, 14.162, 17.13, 18.10, 19.21, 19.28
Thailand, 3.5, 4.21, 5.3, 5.17, 6.8, 9.28, 9.43, 10.16, 10.33, 10.54, 11.8, 11.13, 14.15, 14.20, 14.42, 14.55, 14.84, 14.91, 14.131, 14.133, 14.135, 14.159, 14.168, 14.172, 14.187, 19.3, 19.4, 19.13, 19.15, 19.16, 19.23, 19.24,19.28
Tobacco, 2.14, 4.26, 9.40-9.54, 10.47, 14.174, 20.11, 21.12
European action plan, 20.11 Latin American committee, 9.42 world no-tobacco days, 7.3, 9.47
Tobacco alert, 9.47 Togo, 4.3, 5.8, 14.51 Tonga, 4.3 Toxicology, see Chemical safety; Drugs Traditional birth attendants, 10.6 Traditional medicine, 5.18, 13.25, 19.20 Trinidad and Tobago, 9.6 Tropical diseases,
control, 14.15-14.42 research and training, 14.56-14.71 see also Vector control and individual diseases
Trypanosomiasis, see African Trypanosomiasis; American trypanosomiasis
Tuberculosis, 14.1, 14.93-14.101, 14.131, 14.135, 14.158, 19.26, 22.4, 22.9
research, 4.24 Tunisia, 5.8, 6.22, 10.17, 10.33, 12.10, 12.14, 13.21,
14.34, 14.170,21.6
INDEX
181
Turkey, 14.105 Tuvalu, 10.13, 22.1
Uganda, 4.24, 5.4, 7.13, 14.38, 14.40, 14.41, 14.48, 14.66, 14.118, 14.131, 14.133, 14.135
Ukraine, 2.3, 12.31, 14.9 UNDCP, see United Nations International Drug
Control Programme UNDP, see United Nations Development Pro
gramme UNEP, see United Nations Environment Programme UNESCO, see United Nations Educational, Scientific
and Cultural Organization UNFPA, see United Nations Population Fund UNHCR, see United Nations High Commissioner
for Refugees UNICEF, see United Nations Children's Fund UNIDO, see United Nations Industrial Development
Organization United Arab Emirates, 2.9 United Kingdom of Great Britain and Northern Ire
land, 13.24, 14.90, 14.110, 20.8 Overseas Development Administration, 5.7
United Nations, 2.15, 2.16, 9.54, 13.41, 14.126, 14.137 General Assembly resolutions, 2.12, 2.16 statistical activities, 4.9, 4.10, 13.41 see also Coordination and collaboration, individual
organizations and bodies United Nations Centre for Human Rights, 4.29 United Nations Centre for Human Settlements
(UNCHS), 12.6 United Nations Children's Fund (UNICEF), 3.3,
4.7, 5.8, 6.19, 7.7, 9.16, 9.17, 10.6, 10.7, 10.8, 10.9, 10.14, 11.1, 11.8, 12.3, 12.4, 12.5, 13.41, 14.13, 14.23, 14.78, 14.87, 14.92, 14.117, 14.118, 14.138, 14.154, 17.10, 19.11, 20.16, 21.8
United Nations Decade of Disabled Persons, 13.35 United Nations Development Programme (UNDP),
2.20, 4.19, 6.19, 10.6, 10.10, 10.19, 12.2, 13.41, 14.13, 14.23, 14.56, 14.117, 14.118, 14.154,19.11
United Nations Educational, Scientific and Cultural Organization (UNESCO), 4.29, 6.19, 7.7, 1 0.3, 10.7, 12.5, 12.25, 13.41, 14.117, 14.118, 17.11,21.8
United Nations Environment Programme (UNEP), 7.5, 9.13, 12.6, 12.16, 12.18, 12.19, 12.25, 12.26, 12.27, 17.11
United Nations General Assembly, 2.12, 2.16, 14.116 United Nations High Commissioner for Refugees,
Office of the (UNHCR), 2.29, 2.30, 2.32, 13.41 United Nations High-Level Committee on the Re
view ofT echnical Cooperation Among Developing Countries, 4.19
United Nations Industrial Development Organization (UNIDO), 5.8, 12.18, 13.7, 13.25
United Nations International Drug Control Programme (UNDCP), 11.10, 11.16, 13.21
United Nations Population Fund (UNFPA), 2.21, 9.4, 10.3, 10.6, 10.9, 10.14, 10.15, 10.16, 10.19, 14.117, 14.118, 17.10,19.11
THE WORK OF WHO 1992-1993
United Nations Relief and Works Agency for Palestine Refugees in the Near East (UNRWA), 12.3, 21.6
United Nations Research Institute for Social Development, 8.4
United Republic of Tanzania, 4.22, 6.12, 9.18, 10.8, 13.6, 14.24, 14.57, 14.61, 14.99, 14.100, 14.120, 14.135, 14.153, 17.6
United States of America, 5.8, 5.17, 6.21, 9.35, 9.36, 9.38, 9.42, 9.51, 10.9, 10.20, 10.22, 10.51, 10.53, 10.56, 11.1, 11.17, 13.5, 14.66, 14.68. 14.143, 14.199, 14.202,14.214
Agency for International Development (USAID), 5.21, 9.17, 14.26
UNRWA, see United Nations Relief and Works Agency for Palestine Refugees in the Near East
Upjohn Company (USA), 11.1 Urban development and housing, 12.14-12.17
see also Healthy cities Uruguay, 14.67 USAID, see under United States of America Uzbekistan, 5.1
Vaccine research and development, 14.154-14.163 Latin American and Caribbean initiative
(SIREVA), 8.9 see also Children, vaccine initiative; Immunization
and individual diseases Vector control, 10.49, 12.6, 12.7, 12.21, 14.43-14.48
Collaborative International Pesticide Analytical Council, 14.44
panel of experts (PEEM), 12.6 pesticides evaluation scheme (WHOPES), 14.44
Venereal diseases, see Sexually transmitted diseases Venezuela, 8.9, 11.17, 14.65, 14.68, 14.81, 14.143,
14.194 Veterinary public health, 14.102-14.113 Viet Nam, 5.3, 6.16, 7.12, 9.18, 10.7, 10.13, 12.28,
14.15, 14.51, 14.91, 15.9, 15.13, 22.5, 22.6, 22.8 Violence, 9.33, 9.35, 9.36, 11.10
against women, 9.5, 9.6 Viral diseases, 14.140-14.149
see also individual diseases and viruses Vitamin A deficiency, 9.19, 17.9, 21.9 Voting privileges and services, suspension, 2.2
Waste disposal and management, see Environmental pollution; Water supply and sanitation
Water supply and sanitation, 3.4, 9.10, 12.3-12.13, 12.25, 12.28, 12.29, 14.24, 17.2, 17.11, 19.14, 21.19
ACC subcommittee, 12.13 Africa 2000 programme, 12.12 collaborative council, 12.8, 12.13 interagency committee, 12.13 international decade, 17.11 joint monitoring programme, 12.3
Weekly epidemiological record, 4.6 Wells tart International, 9.16 Western Pacific Region, 22.1-22.13, Annex 2
see also individual activities
182
WFP, see World Food Programme WHO drug information, 13.11, 15.11 WHO pharmaceuticals newsletter, 13.11 WHO Representatives, 2.33, 6.27 WHO staff development, 6.27 Women, health and development, 1.2, 1.3, 2.25, 9.1-
9.8, 11.8, 14.56, 21.1, 21.8 see also Family planning; Maternal and child health
Workers' health, see Occupational health World AIDS Day, 7.3, 14.139 World Alliance for Breastfeeding Action, 9.16 World Assembly of Youth, 10.16 World Bank, 2.19, 2.26, 3.10, 4.3, 4.9, 4.14, 5.3, 5.6,
5.16, 6.4, 6.5, 6.19, 7.5, 10.19, 11.1, 11.9, 12.4, 13.34, 14.13, 14.56, 14.96, 14.117, 14.118, 14.154, 14.168, 14.176,19.26
World development report 1993, 4.9 World Conservation Union, 13.25 World Diabetes Day, 14.208 World Federation for Medical Education, 6.14, 6.19 World Federation of Proprietary Medicine Manufac-
turers, 13.20 World Food Programme (WFP), 9.10 World health, 13.32, 14.101,15.11 World Health Assembly, 1.2, 1.4, 1.5, 2.19, 3.1, 7.10,
8.1, 10.51, 12.2, 12.31, 16.8, 16.9, 16.10, 16.12 meetings, Annex 3 resolutions, 1.3, 1.5, 2.7, 2.13, 2.28, 9.5, 9.19, 9.53,
9.54, 10.7, 12.14, 12.18, 13.35, 14.14, 14.16, 14.42, 14.50, 14.95, 14.116
Technical Discussions, 1.2, 9.34 World Health Day, 7.3, 7.10, 9.5, 9.29, 9.35, 14.206 World health forum, 15.11 World health situation, eighth report, 3.1 World health statistics annual, 4.1 World health statistics quarterly, 4.1, 14.207 World Hypertension League, 14.203 World Meteorological Organization, 12.27 World No-Tobacco Day, 7.3, 9.47 World Organization for Care in the Home and
Hospice, 10.56 World Organization of the Scout Movement, 10.16 World Psychiatric Association, 11.15 World Wide Fund for Nature, 13.25
Yellow fever, 14.4, 14.8, 14.10, 14.144,16.18 Yemen, 2.31, 4.11, 5.8, 6.16, 6.22, 12.11, 14.23, 14.24,
14.105, 21.3, 21.6 Youth and adolescence, 7.6, 7.8, 10.14-10.18, 11.8,
21.13 behaviour, narrative research method, 10.16
Yugoslavia, former, 2.30, 4.3, 11.7, 13.41, 16.16, 16.21, 20.6
Zaire, 14.40 Zambia, 2.26, 4.3, 4.11, 4.16, 4.22, 5.6, 5.21, 7.5, 12.11,
14.94, 14.105, 14.131, 14.135, 17.6 Zimbabwe, 4.22, 5.11, 5.17, 10.54, 11.7, 11.8, 12.5,
12.7, 13.21, 13.37, 14.96, 14.120, 14.177, 17.6 Zoonoses, 14.102-14.113