the work of who - who | world health organization
TRANSCRIPT
OFFICIAL RECORDSOF THE
WORLD HEALTH ORGANIZATION
No. 243
THE WORK OF WHO
I)76 I)77Biennial Report of the Director- General
to the LVorld Health Assemblyand to the United Nations
WORLD HEALTH ORGANIZATION
GENEVA
1978
RESOLUTIONS
The texts of the World Health Assembly and Executive Board resolutions referred toin this report can be found in the Handbook of Resolutions and Decisions of the World HealthAssembly and the Executive Board, Volume 1,190-1972 and Volume II, second edition (1973 -1976)Resolutions adopted in 1977 can be found in WHO Official Records Nos. 238 (EB59), 240(wHA3o) and 242 (EB6o), 1977
ABBREVIATIONS
The abbreviations used in this report include the following:
ACC
CIDA
CIOMS
DANIDA
ECAECEECLA
ECWA
ESCAP
FAO
IAEAIARC
IBRD
ILO
OAU
- Administrative Committee on Co-ordination
- Canadian International DevelopmentAgency
- Council for International Organizationsof Medical Sciences
Danish International DevelopmentAgency
- Economic Commission for Africa- Economic Commission for Europe- Economic Commission for Latin
America- Economic Commission for Western
Asia- Economic and Social Commission for
Asia and the PacificFood and Agriculture Organization of
the United Nations- International Atomic Energy Agency- International Agency for Research on
CancerInternational Bank for Reconstruction
and Development- International Labour Organisation
(Office)- Organization of African Unity
PAHOPASBSIDA
- Pan American Health Organization- Pan American Sanitary Bureau- Swedish International Development
AuthorityUNCTAD - United Nations Conference on Trade
and DevelopmentUNDP - United Nations Development Pro..
grammeUNDRO - Office of the Disaster Relief CoordinatorUNEP - United Nations Environment Pro-
grammeUNESCO - United Nations Educational, Scientific
and Cultural OrganizationUNFDAC - United Nations Fund for Drug Abuse
ControlUNFPA - United Nations Fund for Population
ActivitiesUNHCR - Office of the United Nations High
Commissioner for RefugeesUNICEF United Nations Children's FundUNIDO United Nations Industrial Development
OrganizationUSAID United States Agency for International
Development- World Food Programme- World Health Organization
WFPWHO
ISBN 92 4 160243 o© World Health Organization 1978
Publications of the World Health Organization enjoy copyright protection in accordance with the provisions ofProtocol 2 of the Universal Copyright Convention. For rights of reproduction or translation of WHO publications,in part or in tote, application should be made to the Office of Publications, World Health Organization, Geneva,Switzerland. The World Health Organization welcomes such applications.
The designations employed and the presentation of the material in this publication do not imply the expressionof any opinion whatsoever on the part of the Secretariat of the World Health Organization concerning the legal statusof any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries.
Where the designation "country or area" appears in the heading of tables, it covers countries, territories, cities orareas.
The mention of specific companies or of certain manufacturers' products does not imply that they are endorsedor recommended by the World Health Organization in preference to others of a similar nature that are not mentioned.Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
PRINTED IN SWITZERLAND
II
Contents
Page
Preface VII
Introduction Ix
1. Governing bodies : World Health Assembly, Executive Board and regionalcommitteesProgramme budget policyTechnical cooperation 3
Sixth General Programme of Work 6
Programme Committee of the Executive Board 6
Organizational studies of the Executive Board 7
Technical Discussions 8
Programme trends and priorities 9
z. General programme development 14
3
National health programme developmentWHO general programme developmentHealth programme evaluationInformation systems programme
Coordination
T4i6
17
i8
21
Extrabudgetary sources of funds 22
United Nations Children's Fund 23
United Nations Development Programme 23
World Food Programme 24Emergency relief operations 24
4. Research promotion and development z8Global developments 29Ethical aspects of biomedical and health services research 29Safety in the handling of microorganisms and cells 30Research training 30Regional developments 30
5. Strengthening of health servicesPrimary health careHealth service developmentTraditional medicine
III
34
343844
6. Family health
Page
47Maternal and child health 48Nutrition 5zHealth education 55Special Programme of Research, Development and Research Training in Human Reproduction 57
7. Health manpower development 64Production of health manpower 65Deployment of health manpowerExamples of health manpower development activities in other programmes 76
73
8. Communicable disease prevention and control 85
Epidemiological surveillance 85
Malaria and other parasitic diseases 86Smallpox eradication 96Expanded Programme on Immunization IooBacterial and virus diseases 101Veterinary public health 109Vector biology and control 111Special Programme for Research and Training in Tropical Diseases 115Prevention of blindness 118
9. Noncommunicable disease prevention and control 120Mental health 120Cancer 126International Agency for Research on Cancer 129Cardiovascular diseases 132Other chronic noncommunicable diseases 135Oral health 136Radiation medicine 138Human genetics 140Immunology 141Health of working populations 143
Io. Prophylactic, diagnostic and therapeutic substances 145Drug policies and management 145Pharmaceuticals 147Biologicals 148Health laboratory technology 149
11. Promotion of environmental health 151
Provision of basic sanitary measures 151
Pre- investment planning for basic sanitary services 155Control of environmental pollution and hazards 156National environmental health planning 157Food safety 158
12. Health statistics 163
Health statistical methodology 164Dissemination of statistical information 164Development of health statistical services 165International Classification of Diseases 166
13 Health and biomedical information 168
Health literature services 169WHO publications 169
Iv
Page
Public information 171Language services 172Technical terminology 172Distribution and sales 273
14. Constitutional, legal and administrative developments 175
Constitutional and legal matters 275Administration x 76
15. Regional trends 178
African Region 178Region of the Americas s8oSouth -East Asia Region 284European Region 191Eastern Mediterranean Region 198Western Pacific Region 202
Annex 1. Members and Associate Members of the World Health Organizationat 31 December 1977 209
Annex z. Organizational and related meetings zitAnnex 3. Intergovernmental organizations which have entered into formal agree-
ments with WHO approved by the World Health Assembly at31 December 1977, and nongovernmental organizations in officialrelations with WHO at 3i December 1977 212
Annex 4. Structure of WHO at 31 December 1977 215
Index 219
v

Preface
The Twenty- eighth World Health Assembly in 1976 considered it desirable thatthe Director -General should publish in the Official Records in even -numbered years,beginning in 1978, a comprehensive report on the work of WHO during the twopreceding years (resolution wHAZ8.z9). This is the first of the comprehensive reports,covering the years 1976 and 1977.
VII
s


Introduction
1976 and 1977 were exciting years for WHO. New policies were adopted by the governingbodies that are reshaping the activities of the Organization for the next decade, making them morerelevant than ever to the needs of its Member States, and in particular of developing countries.Member States participated as never before in the work of the Organization, charting new policyand programme directions in the World Health Assembly, the Executive Board and regionalcommittees, that reflected the changed world political climate. Gone are the days of donor -recipientrelationships between WHO and its Member States; an era of real partnership has replaced them.
The aspirations of developing countries to improve the lot of their citizens were articulatedin the declaration of the New International Economic Order, and it is in this context that thedynamic developments in WHO over the past two years should be seen. Guided by the principle ofsocial justice, WHO's recently adopted policies reflect a growing concern for the social purpose ofhealth development and for the role of health in promoting social and economic development. To
reduce the gap between the health level of the developed and the developing countries a policy wasadopted aimed at reorienting the work of the Organization to ensure that by 1980 the allocationsof the regular budget will reach the level of at least 6o % in real terms towards technical cooperationwith countries. This policy is in full accord with the Organization's constitutional functions.The strategy for giving effect to this policy is based on the formulation and vigorous implementationof socially relevant technical cooperation programmes, directed towards defined national healthgoals, that foster national self -reliance in health matters and contribute directly and significantlyto the improvement of the health status of the populations concerned. In order to find money forthese additional programmes of technical cooperation with countries, it was necessary to make drasticreductions, particularly in the headquarters establishment but also in regional offices. In this way,a total sum of more than US$ ¢1 million in the regular budget will be made available over the
years Inc? to 1981. Let it not be thought that it was easy to make these reductions far fromit; but if sacrifice there is, it will be more than compensated for if it contributes to providinga fairer share of world health resources to those who need them most.
Justice in the distribution of health resources cannot be achieved through technical coopera-tion between WHO and its Member States alone. Technical cooperation among countries, and par-ticularly among developing countries, is even more important. It is WHO's duty to complement
IX
THE WORK OF WHO
these programmes as part of broader cooperative schemes whenever indicated, making full use ofthe capacities and potentialities of developing countries, including manpower, training and researchfacilities and exchange of technical information. This concept is implicit in our regional structure,but we still have a long way to go in making it an integral part of our programme. To do so weshall have to concentrate still further on fostering national and regional self -reliance in healthmatters, even at the expense of becoming more marginally operational.
Encouraged by one major stride in the direction of international health justice, the Organi-zation quickly took another when it decided that the main social target of governments and WHOin the coming decades should be the attainment by all the citizens of the world by the year z000of a level of health that will permit them to lead a socially and economically productive life. The
full implications of this daring decision are still being assessed, but no time is being lost in initiatingaction for the attainment of the target. Not only will dynamic national health programmeshave to be formulated by governments, but massive international support will be required. Thereare encouraging signs that bilateral and multilateral agencies are aware of this need, partly as aresult of WHO's efforts at placing health more securely on the world economic and social map.For example, growing interest in health development is being shown by such bodies as UNDPand IBRD. The latter has now agreed to provide funds for the health component of economicdevelopment programmes, even if it cannot finance independent health projects as such. Since healthdevelopment and maintenance is an essential component of very many economic development pro-grammes, the potentials of this new policy are tremendous and we must find ways of exploitingit to the full.
Policy directions taken in WHO during 1976 and 1977 laid the foundations for healthdevelopment up to the end of the century. The Sixth General Programme of Work, adopted bythe World Health Assembly in 1976, constitutes a solid policy basis for WHO's activities in theimmediate period ahead. The Organization will use this Programme of Work in a flexible wayto chart its path for the years 1978 to 1983, making the most of the regular budget as well as ofextrabudgetary funds. It will do so by taking defined national health needs as the starting point,then moulding WHO's response to these needs through medium -term programmes followed byprogramme budgets that form two-year portions of these medium -term programmes, finallyclosing the circle through health programme evaluation with the aim of ensuring constant pro-gramme improvement in Member States and in WHO. The evolution of this General Programmeof Work is in itself a remarkable international social achievement. People of all nations workedin harmony in different national and international fora to formulate it. As a result of theseinterlinking efforts within Member States, the governing bodies and the Secretariat, it can confi-dently be claimed that the General Programme of Work is a rightful incarnation of the unityof WHO. However, Member States will accrue benefit from it only if they use it properly.If they go through the Programme methodically, applying what is of relevance to them, they will beable to ensure that the Organization's programmes are true responses to their needs. Through
such collaboration the Programme will come to life.
Another blue print that was formulated during 1977 aims at attaining the main socialtarget mentioned above of "health for all by the year z000 ". An essential feature is the
x

INTRODUCTION
preferential allocation of health resources to the social periphery both within and amongcountries. To attain the target, priority programmes have been identified and the mechan-isms required for health development described, a beginning has been made in assessing theresources needed, and the political support that is essential for success has been highlighted.Of the priority programmes required to reach the target, primary health care must be stressedabove all. It is the key to making essential health care available to the masses of the world'spopulation, irrespective of the social and economic conditions in the countries in which they live.But primary health care has to form part of a broader health system, and the other components ofthat system must be organized in such a way as to support its needs. In the developing countriesmalnutrition is probably the single most important health problem, and we must succeed in makingeffective and realistic nutritional activities a cornerstone o f primary health care. Another essentialfeature for health development is water. WHO is committed to participating in the global effortto attain the target adopted by HABITAT, the United Nations Conference on Human Settle-ments, that is, to have "water for all by zyyo ". Immunization against common diseases of child-hood is another high priority programme, and WHO has resolved to ensure that by rygo all thechildren of the world will be provided with such immunization. The control of communicablediseases will continue to demand major efforts, particularly in the developing countries. Primaryhealth care will have to rely on health technology that is more appropriate than much of what is inuse today, and it is for this reason that the development of such technology is high on the list of priorityprogrammes. For example, experience has shown that it is possible to ensure safe water andsanitary waste disposal through low -cost technology that makes the greatest possible use of localnatural resources, manpower and material. Drugs are inseparable from health technology, andthe formulation of new national policies concerning their manufacture, quality and price control,import and export, will have to be given much greater attention. A breakthrough was recentlyachieved when a WHO Expert Committee came to the conclusion that about zoo essential drugscould meet the vast majority of health care needs. Above all, people to conceive, manage anddeliver these programmes are crucial. Principles for attuning the education and learning of healthworkers to the social needs of populations rather than to the technical dictates of professionalismhave been evolved in WHO ; action for change must now start within countries.
The conversion of policy blue prints into action for health requires energetic planning, andin country health programming we have arrived at a process that is both useful and relativelysimple to apply in widely different national contexts. Country health programming is a continuingnational process for health development that is intimately linked with social and economic devel-opment in general. WHO's function is mainly to ensure the availability of appropriate method-ology and, on request, to collaborate with countries in its practical application. This is an excellentexample of the fulfilment of WHO's dual role of international health coordination and technicalcooperation with its Member States. But to initiate action for health and ensure its dynamiccontinuity, national and international political determination will be required to overcome political,social, economic and professional obstacles. Tremendous challenges lie ahead for WHO and itsMember States, but challenge is the spur to action.
No reflections on the work of WHO for 1976 and r977 would be complete without mentioningsmallpox eradication. We almost reached it, and I am sure we will reach it in the near future.
XI
THE WORK OF WHO
The only area of concern is the Horn of Africa, particularly Somalia, where variola minor hasbeen active. The number of cases in the area has been steadily declining and at the time of writinghas reached zero, but there are still many difficulties which hamper the eradication operations andcontinued support is essential for complete success. When we succeed, the way will be open to a globalabolition of smallpox vaccination, representing an annual saving of rather more thanUS: z000 million to the world community. I can only repeat what I said recently in Bangladeshwhen I signed the death certificate for smallpox in Asia : "Unity -world unity -is the mostpowerful means we possess to break out of the vicious circle of poverty and disease ".
Director- General
XII
I.I
Chapter I
Governing Bodies: lYorid HealthAssemb, Executive Board
and Regional CommitteesAT NO TIME since the very early
days of the Organization havethe governing bodies played
such a vital role in shaping policy and incharting new courses for the years to come.The years 1976 and 1977 witnessed pro-found changes in the orientation of theOrganization as the result of initiativestaken by Member States in the HealthAssembly, the Executive Board and theregional committees. In addition to themajor policy directives of the HealthAssembly, the biennium was marked by aprogressive trend towards a deeper involve-ment of the Executive Board and theregional committees in the work of theOrganization. The following illustratessome of the major issues dealt with duringthe period.
Programme budget policy
I.z Resolutions wHA28.75 andwHAZ8.76, adopted in 1975, presaged thepolicy and programme changes that madethe biennium 1976 -77 so notable in thehistory of WHO. In resolution WHA28.7S,the Health Assembly indicated the mainways in which WHO was giving assistanceto countries, requested the Director -General to continue study of the mosteffective ways and means of providing andaugmenting such assistance, using all pos-
I
sible sources of finance, and called upondeveloping countries to give priority topublic health programmes in the allocationof UNDP funds. In resolution wHA28.76the Assembly decided that the regularprogramme budget should ensure a sub-stantial increase in technical assistance andservices for developing countries from1977 to the end of the Second DevelopmentDecade, and requested the Director -Generalto adjust the proposed programme budgetfor 1977 in compliance with the resolutionand to take it into account in the preparationof the budget proposals for 1978 -79. Acomplete review of the 1977 programmebudget was then undertaken with theobject of releasing additional regular budgetfunds for developing countries and identi-fying activities that could truly be con-sidered to represent technical cooperation,so as to establish a valid base -line againstwhich progress in the implementationof the resolution would be assessed.
1.3 In May 1976 the Health Assemblyadopted an even firmer resolution(wHA29.48) calling upon WHO to reorientits work so that, in real terms, 6o % of theregular budget could be allocated to tech-nical cooperation and the provision ofservices to Member States by 1980. TheAssembly specified the need to cut downall avoidable and non -essential expenditureon establishment and administration, both
THE WORK OF WHO
at headquarters and in the regional offices,to streamline professional and administra-tive cadres, to phase out projects whichhave outlived their utility and to makeoptimum use of the technical and adminis-trative resources available in the individualdeveloping countries. This strategy wasput into effect in the latter half of 1976,making available an additional US $ 41million from the regular budget for tech-nical cooperation programmes over theyears 1978 -81.
1.4 The implementation of resolutionwHA29.48 required drastic reductions inthe WHO establishment, particularly atheadquarters but also in the regions. Re-sponding to the resolution, the RegionalCommittee for Africa set up a workinggroup to assist the Regional Director inexamining the structures of WHO in theAfrican Region, in analysing the activitiesof the Regional Office, in reviewing therole of WHO representatives and per-sonnel at country level, and in reorientingRegional activities and reorganizing thestructure of the Regional Office. It wasalso to study the distinction betweenadministrative services and technical coop-eration (resolution AFR/RC26/R8). In theother regions, resolution wHA29.48 pro-voked a similar searching review of allaspects of the regional programmes andthe introduction of appropriate measuresto give increased emphasis to technicalcooperation wherever possible.
1.5 The Organization's response toresolution WHA29.48 was presented to thefifty -ninth session of the Executive Boardin January 1977 in a report by the Director-
General on policy and strategy for thedevelopment of technical cooperation.1This report gave a comprehensive accountof the policy evolved and the strategyapplied and, after describing the develop-
1 WHO Official Records, No. 238, 1977, p. 181.
2
ment of the role and functions of WHOand the measures envisaged for making theOrganization's work more effective andefficient, outlined the reorientation of theproposed programme budget for 1978 -79and the implications for 1980-8 and thefuture. Compliance with the resolution wassummarized thus:
(s) Cutting down of avoidable and non-essential expenditure on establishmentand administration was being accom-plished through the proposed reduc-tion of 363 posts, representing11.z % of posts under the regularbudget. Proposals were being madefor reducing the cost of meetings,publications, administration, budget,finance and general services.
Streamlining of professional and ad-ministrative cadres was being accom-plished through the post reductionsmentioned, staff development andtraining programmes, and the in-creased use of programme develop-ment teams and task forces.
Phasing out of projects which had out-lived their utility was being accom-plished at all levels of the Organiza-tion to make resources available fornew technical cooperation.
Making use of the technical and adminis-trative resources available in individualdeveloping countries was being accom-plished by increasing the involve-ment of developing countries inWHO activities, strengtheningWHO's collaboration and coopera-tion with Member States, and devel-oping the Organization's coordina-tion and information transfer capa-bilities so that more bilateral andmultilateral resources could be mobi-lized for technical cooperation andso that the results of research andtechnology could be brought to
(z)
(3)
(4)

GOVERNING BODIES
bear on the health needs of popula-tions, particularly in developingcountries, through means whichthey could afford and apply.
Table 1. i shows the net effect in budgetaryand financial terms.'
Technical cooperation
1.7 Of major importance in the reorien-tation of programme budget policy duringthe biennium was the adoption of theconcept of technical cooperation as a guid-ing principle for the Organization's work.
Table 1.1 Proportion of regular programme budget being devoted to technical cooperation (including policyorgans) projected for 1978 -81 within 1977 budget level and on basis of 1977 costs
(expressed in US$)
Year
1977 1978 1979 1980 1981
Technical cooperation 75 208 719 81 848 000 83 726 000 85 689 000 87 820 000Other activities (including policy organs) 71 691 281 65 052 000 63 174 000 61 211 000 59 080 000
Total (including policy organs) 146 900 000 146 900 000 146 900 000 146 900 000 146 900 000Technical cooperation as a proportion of the total
(including policy organs) 51.2% 55.7% 57.0% 58.3% 59.8%
1.6 At its fifty -ninth session, the Execu-tive Board carried out an extensivereview of WHO's future programme bud-get policy and strategy 2 as described in thereport of the Director -General and in thereport of the Programme Committee of theExecutive Board.3 Interpreting the spirit ofresolutions WHA28.75, WHA28.76 andwHA29.48, the Board gave detailed con-sideration to the technical cooperation andcoordination roles of WHO, the identifica-tion and definition of technical cooperation,new trends in programme development andimplementation and the budgetary andfinancial implications, highlighting theseand certain other issues in its report to theAssembly. The Board concluded byendorsing the programme budget strategyproposed by the Director -General, con-sidering that it responded fully to the policydirectives of the Assembly resolutions(resolution EBS9.R9). This strategy wassubsequently approved by the HealthAssembly (resolution wHA30.30).
1 WHO Official Records, No. 238, 1977, p. 199.2 WHO Official Records, No. 238, 1977, p. 114.3 WHO Official Records, No. 238, 1477, p. 165.
3
The term was introduced in the revision ofthe proposed programme budget for 1977,4in preference to that of technical assistance,and reflected recognition of a basic changein WHO's approach that had evolved inrecent years. In the past, this approachtended to be based on the traditional donoragency /recipient country relationship,which was no longer acceptable or appro-priate. In the light of the discussions at theTwenty -ninth Health Assembly in 1976,the Director-General interpreted tech-nical cooperation to mean activities thathad a high degree of social relevance forMember States in the sense that they weredirected towards defined national healthgoals and would contribute directly andsignificantly to the improvement of thehealth status of their populations throughmethods they could apply now and at acost they could afford now. In formulatingthese activities the important principle to bekept in sight over the next decade was theaim of developing national self -reliance in
4 WHO Official Records, No. 231, 1976, pp. 147-149,204-211.
6 WHO Official Records, No. 238, 1977, p. 185.
THE WORK OF WHO
matters of health. The concept of WHOdoing something for countries should beabandoned and replaced by cooperationwith countries and the fostering of coop-eration among countries so that a lastingimpact could be made on health develop-ment.
1.8 This conceptual interpretation wasendorsed by the Executive Board 1 at itsfifty -ninth session in January 1977, whenit confirmed its earlier approval 2 of theterm "technical cooperation" for uniformuse throughout the Organization and in theofficial documentation of WHO. The Boardalso reviewed technical cooperation inrelation to the WHO Constitution.3 TheOrganization's first and pre -eminent func-tion was to act as the directing and coordi-nating authority on international healthwork.4 This coordinating function, whichincluded the two -way international transferof information on health matters, wasintimately connected with the fourth con-stitutional function, namely, to furnishappropriate technical assistance and, inemergencies, necessary aid upon the re-quest or acceptance of governments.3 Inthe past, there had been a tendency to seethese technical assistance and coordinatingroles as if they stood in opposition to eachother. Yet the aim of cooperation amongMember States and through WHO wasembodied in the very spirit of the Constitu-tion of WHO, whose preamble stated thatthe contracting parties agreed to establishthe World Health Organization for thepurpose of cooperation among themselvesand with others to promote and protect the
1 WHO Official Records, No. 238, 1977, p. 117.2 WHO Official Records, No. 231, 5976, p. 128,
para. 13.3 WHO Official Records, No. 238, 1977, p. 116.4 WHO Basic Documents, 28th ed., 1978, p. z,
Article z(a).WHO Basic Documents, 28th ed., 1978, p. 2,
Article z(d).
4
health of all peoples.s The Board agreedthat the catalytic stimulation and coordina-tion of technical cooperation among coun-tries was a fundamental component of theOrganization's coordinating function andwas a promising means of increasing tech-nical cooperation in the spirit of HealthAssembly resolutions WHAZ8.75, wHAZ8.76and wHAZ9.48. Far from standing inopposition to each other, the coordinatingand technical cooperation roles of WHOwere mutually supportive. To reflect thisrelationship, the Board adopted in resolu-tion EB 5 9. R9 the formulation that the pro-posed programme budget strategy wasintended "to enhance the coordinating roleof WHO and within that approach toreorient the working of the Organizationtowards increased, effective technical coop-eration with and services to governments ".This formulation was subsequently ap-proved by the Health Assembly (resolutionwHA3o.3o). The Board considered that theconcept of technical cooperation was anevolving concept and that the interpretationgiven, together with the views of regionalcommittees (for example that of the West-ern Pacific Region 7), should continue to bereviewed, not only by the ProgrammeCommittee of the Board but by the Boardas well.
1.9 The emphasis on technical cooper-ation should be viewed in the context of theinitiatives taken within the United Nationson a system -wide basis during 1976 to helpgive effect to the New International Eco-nomic Order by promoting technical cooper-ation among developing countries. The main gov-erning principles were that these countriesshould devise specific programmes basedon technical cooperation among themselves,which international organizations couldcomplement as part of broader cooperative
WHO Basic Documents, 28th ed., 1978, p. 1,preamble.
Resolution wPR /Rcz7 /R18 (including Annex I).
GOVERNING BODIES
schemes; developing countries should con-tribute to national and regional institutionslocated in other developing countries anduse these for training ; international agenciesshould make full use of the capacities andpotentialities of developing countries, in-cluding manpower, training and researchfacilities and exchange of technical informa-tion; financial priority should be accordedto regional and interregional activitiesemerging under this scheme ; and the leastdeveloped countries, and developing coun-tries with geographical disadvantages,should be given special attention.
1.10 These concepts are not new toWHO: they are implicit in its regionalstructure and have been expressed in manyinterregional activities. Among the meansintroduced in the biennium to promote,accelerate and facilitate national and re-gional self -reliance in health matters were :the strengthening of the role of regionalcommittees themselves ; the establishmentof regional panels of experts to ensure theproper exchange of expertise and experienceamong countries ; and the establishment ofregional advisory committees on biomedicaland health services research to bringexpertise from various countries to bear onresearch requirements and questions ofresearch policy in the regions. Othermeans envisaged for the future include thesetting up of regional centres for opera-tional research, development and trainingin specific programme areas, where coun-tries can work together to solve commonproblems and build up cadres of nationalhealth personnel trained towards self -
reliance in the development of the pro-gramme concerned in their country. Ageneral account of the background, presentstatus and future possibilities of technicalcooperation among developing countries,prepared in response to resolution EB 5 9. R 5 2,was reviewed by the Executive Board at itssixtieth session in May 1977, when it
5
endorsed the proposals of the Director -General for WHO activities in this field and,in resolution EB6o.R4, invited all MemberStates to participate actively in the Tech-nical Discussions on the subject to be heldduring the Thirty- second World HealthAssembly in 1979.
1.I I The profound significance for theOrganization and for Member States of theevolution of the concept of technical co-operation with and among developingcountries may be judged from resolutionWHA30.43, adopted by the Health As-sembly in May 1977, which, because ofits importance as the overriding policydirective for the future, is quoted in full:
The Thirtieth World Health Assembly,
Faced with the magnitude of health problems andthe inadequate and intolerably inequitable distributionof health resources throughout the world today ;
Considering that health is a basic human right anda worldwide social goal, and that it is essential to thesatisfaction of basic human needs and the quality oflife ;
Reaffirming that the ultimate constitutional objectiveof WHO is the attainment by all peoples of the highestpossible level of health ;
Recalling resolutions wHA28.75, wHA28.76 andwHA29.48 on the principles governing technical co-operation with developing countries ;
I. DECIDES that the main social target of governmentsand WHO in the coming decades should be the attain-ment by all the citizens of the world by the year 2000of a level of health that will permit them to lead asocially and economically productive life ;
2. CALLS UPON all countries urgently to collaborate inthe achievement of this goal through the developmentof corresponding health policies and programmes atthe national, regional and interregional level and thegeneration, mobilization and transfer of resources forhealth, so that they become more equitably distributed,particularly among developing countries ;
3. REQUESTS the Executive Board and the Director -General to pursue the reorientation of the work ofWHO for the development of technical cooperationand transfer of resources for health in accordance withone of the Organization's most important functionsas the directing and coordinating authority in inter-national health work.
THE WORK OF WHO
Sixth General Programme of Work
1.12 In accordance with its constitu-tional functions, the Board was deeplyinvolved in the formulation of the SixthGeneral Programme of Work coveringthe specific period 1978 -83, in close con-sultation with Member States and theregional committees.
1.13 The Health Assembly, in approv-ing that Programme (resolution wHAZ9.zo),requested the Board :(s) to carry out annual reviews of the Sixth General
Programme of Work, taking into considerationevents that occur subsequent to its adoption ;
(z) to carry out in -depth studies and evaluation ofparticular programmes, as necessary, to ensure thatthe overall work of the Organization is proceedingin conformity with the Sixth General Programmeof Work ;
(3) to continue the study of long -term trends as
reflected in the Sixth General Programme of Workfor a specific period and their implication for theOrganization's future programmes.
In effect, this resolution, which stated thatthe Sixth General Programme of Workprovided an appropriate policy frameworkfor the formulation of medium -term pro-grammes and programme budgets withinthe period covered, and which recognizedthat there was a continuous evolution ofthe Organization's programme, chargedthe Board with keeping all aspects of pro-gramme development under review.
Programme Committee of the ExecutiveBoard
1.14 In 1976 the Health Assemblyreferred to the more effective role of theExecutive Board in policy -making and inassisting the work of the Assembly (reso-lution wHAZ9.6z). Taking account of itsincreased responsibilities, the Board, inresolution EB58.RI1, decided to establisha programme committee to :
6
(s) advise the Director -General on the policy andstrategy involved in order to respond effectivelyto resolutions wHA28.75, wHAz8.76 and wHA29.48on technical cooperation with developing countriesand on programme budget policy ;
(z) review the general programmes of work coveringa specific period in pursuance of resolutionWHA29.zo and in particular as related to the biennialprogramme budget proposals of the Director -General.
Thus, a mechanism was created that wouldnot only ensure the Board's full partici-pation in programme development butwould also facilitate its work and that ofthe Health Assembly by allowing both toconcentrate on issues of particular import-ance, as identified by the ProgrammeCommittee. The first meeting of theProgramme Committee of the ExecutiveBoard was held in November 1976, whenit considered the policy and strategy forthe development of technical cooperation,reviewed the Sixth General Programmeof Work, examined various proposals forits own future work and submitted a reportto the Executive Board.1 The secondmeeting of the Programme Committee ofthe Board was held in November 1977.It reviewed the implementation of theprogramme budget policy and strategy aswell as the tentative budgetary projectionsfor the biennium 1980-8 s. It also exam-ined the ways in which the Organizationis developing its programme throughcountry health programming, the assess-ment of long -term health trends, medium -term programming for the implementationof the Sixth General Programme of Work,health programme evaluation and theWHO information system. It studiedprocedures for introducing changes intothe Sixth General Programme of Workand made recommendations on all theseissues to the Executive Board.
1.1 5 The method of work of the HealthAssembly and of the Executive Board was
1 WHO Official Records, No. 238, 1977, p. 165.
GOVERNING BODIES
studied by an ad hoc committee of theBoard, established under resolutionEB 5 7. R 5 3. On the basis of this committee'sreport, the Board and the Health Assembly,in resolutions EB59.R8 and WHA30.50respectively, adopted changes in theirproceedings aimed at further rationalizingand improving their work, notably withregard to the review of the programmebudget, the role of the Board's represen-tatives at the Health Assembly, the high-lighting by regional committees of signifi-cant issues in their reports, and the way inwhich the Director- General should respondto requests from the Health Assembly forreports. Finally, the necessary enablingamendments of Articles 34 and 5 5 of theConstitution having come into force uponacceptance by two -thirds of the MemberStates, the Health Assembly decided thatthe programme budget of WHO wouldcover a two -year period beginning with thebiennium 19go -8 z and would be reviewedand approved by the Health Assembly ona two -year basis (resolution WHA30.20).
Organizational studies of the ExecutiveBoard
r.16 The organizational studies of theExecutive Board provide the Board andthe Assembly with a convenient means ofexamining in detail aspects of WHO'swork, policies, procedures and relation-ships that appear to be of special import-ance for the Organization as a whole. Thestudies extend over one or two years,depending on the complexity of the sub-ject, which is selected at least a year inadvance.
z .17 In 1976, the Board, under reso-lution EBS7.R33, transmitted to the HealthAssembly its organizational study on "Theplanning for and impact of extrabudgetaryresources on WHO's programmes andpolicy." The term " extrabudgetary" was
7
used to refer to programme funds from allsources other than contributions to theregular budget by Member States, and inthe widest sense to voluntary contributionsand funds available to the Organizationthrough cooperative programmes in theinternational health field. The report 1posed the question whether it was "thewill of the Member States that their WorldHealth Organization should play a leadingrole, or only a marginal role, in the mobil-ization of resources and development ofhealth programmes to meet the needs ofcountries and peoples throughout theworld." In a narrower sense, the questionwas : How can WHO mobilize additionalexternal resources in support of its ownprogramme budget ? The study analysedthe far -reaching implications of thesequestions. Agreeing that it provided asuitable basis for the fulfilment of WHO'sconstitutional mandate, the Health As-sembly, in resolution WHAZ9.3 z, urged allexisting and potential sources of extra -budgetary funds to provide the Organi-zation with increased support for theexpansion of its efforts in the health field,and requested the Director -General, withinthe established policies of the Organization :(1) to take particularly into account the promotion of
those planned health programmes that couldattract additional resources for the benefit of thedeveloping countries ;
(z) to continue to develop appropriate mechanisms forattracting and coordinating an increased volume ofbilateral and multilateral aid for health purposes ;
(3) to continue his efforts on an interagency basis toharmonize programme budget cycles and planningand operational procedures of the major UnitedNations funding agencies with those applied to theregular programmes of the organizations in theUnited Nations system.
z.z8 In resolution wHAZ9.33, the HealthAssembly, also in 1976, decided that thenext subject of study should be "WHO's
1 WHO Official Records, No. 231, 1976, p. 71,para. 3.1.
THE WORK OF WHO
role at the country level, particularly therole of the WHO representatives." In thecourse of the study, the Board in January1977 identified a number of issues ofspecial significance (resolution EB59.R33)(a) the changes taking place in the relationships be-tween WHO and its Member States ; (b) the strength-ening of countries' capacities to collaborate activelywith WHO in national health development in con-formity with policies and principles established by theWorld Health Assembly, Executive Board and regionalcommittees ; (c) the practical application of newmethods of technical cooperation not only betweenWHO and its Members but also between MemberStates ; and (d) the use of national mechanisms forcollaboration with WHO at country level, such asnational coordinators, coordinating committees, andprogramme managers.
In view of the importance of the subjectfor the future work of the Organization, itwas decided that the study be extended fora further year, the report to be presentedat the Thirty -first World Health Assemblyin 1978 (resolution WHA3o.16).
Technical Discussions
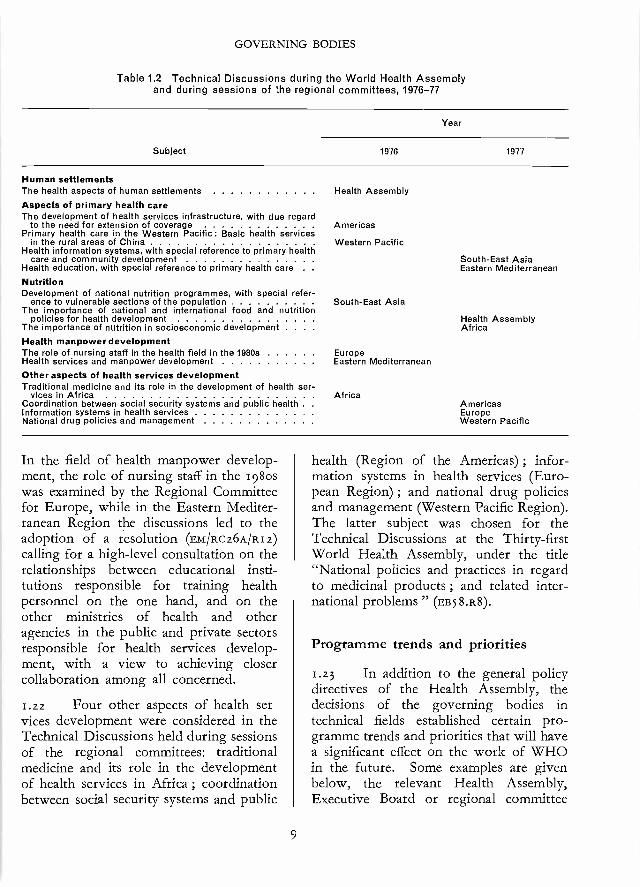
1.19 Technical Discussions were intro-duced at the Fourth World Health As-sembly in 1951 and have been held eachyear, with one exception, since that time.Similar discussions are also a regular featureof regional committee meetings. Thesediscussions give the Health Assembly andthe regional committees an opportunity toreview in some depth subjects of currentglobal or regional public health import-ance. The topics covered in the bienniumare shown in Table r.2, grouped accordingto their main themes.
1.2o The Technical Discussions at theTwenty -ninth World Health Assembly onthe health aspects of human settlementsimmediately preceded the United NationsConference on Human Settlements(HABITAT), and the general policy ex-pressed by the Health Assembly in reso-
8
lution wHA29.46 was brought to theattention of the Conference. The impli-cations of this and related resolutions(WHA29.45, WHA29.47) and the conse-quences of the Conference for MemberStates and WHO are outlined elsewhere inthis report (see page 154). One of the mainsubjects considered by regional committeeswas that of primary health care, whichincludes the concepts of development ofthe health service infrastructure, the ex-tension of coverage of the population andcommunity participation. The discussionson various aspects of this subject duringsessions of the Regional Committees forthe Americas, South -East Asia, the EasternMediterranean and the Western Pacificconstituted a prelude to the InternationalConference on Primary Health Care, to beheld at Alma -Ata, USSR, in September1978. In the case of the Americas, thediscussions led to a decision (resolutionAMR /RC28 /R32) to convene a meeting ofMinisters of Health to adjust the policy andstrategy of the Hemisphere so as to achievethe goals of the Ten -Year Health Plan inthis field as rapidly as possible.
1.21 "The importance of national andinternational food and nutrition policiesfor health development" was the subject ofthe Technical Discussions at the ThirtiethWorld Health Assembly in 1977 and alsoof an agenda item and a draft resolution,included at the request of the Governmentof Sweden. The resolution adopted(wHA3o.5 r) included in its aims the elimi-nation of florid forms of malnutrition aspublic health problems, the intensificationof nutrition programmes, the determinationof groups at risk, the establishment ofpriorities and the development of systemsfor nutritional surveillance and the controlof contamination of foodstuffs. Nutritionwas also highlighted in the discussionsheld during sessions of the Regional Com-mittees for Africa and South -East Asia.
GOVERNING BODIES
Table 1.2 Technical Discussions during the World Health Assemblyand during sessions of the regional committees, 1976 -77
Subject
Year
1976 1977
Human settlementsThe health aspects of human settlements Health Assembly
Aspects of primary health careThe development of health services infrastructure, with due regard
to the need for extension of coverage AmericasPrimary health care in the Western Pacific: Basic health services
in the rural areas of China Western PacificHealth information systems, with special reference to primary health
care and community development South -East AsiaHealth education, with special reference to primary health care . Eastern Mediterranean
NutritionDevelopment of national nutrition programmes, with special refer-
ence to vulnerable sections of the population South -East AsiaThe importance of national and international food and nutrition
policies for health development Health AssemblyThe importance of nutrition in socioeconomic development . . . AfricaHealth manpower developmentThe role of nursing staff in the health field in the 1980s EuropeHealth services and manpower development Eastern Mediterranean
Other aspects of health services developmentTraditional medicine and its role in the development of health ser-
vices in AfricaCoordination between social security systems and public health .
Information systems in health servicesNational drug policies and management
AfricaAmericasEuropeWestern Pacific
In the field of health manpower develop-ment, the role of nursing staff in the 198oswas examined by the Regional Committeefor Europe, while in the Eastern Mediter-ranean Region the discussions led to theadoption of a resolution (EM /Rc26A /RI z)calling for a high -level consultation on therelationships between educational insti-tutions responsible for training healthpersonnel on the one hand, and on theother ministries of health and otheragencies in the public and private sectorsresponsible for health services develop-ment, with a view to achieving closercollaboration among all concerned.
1.22 Four other aspects of health ser-vices development were considered in theTechnical Discussions held during sessionsof the regional committees: traditionalmedicine and its role in the developmentof health services in Africa ; coordinationbetween social security systems and public
9
health (Region of the Americas) ; infor-mation systems in health services (Euro-pean Region) ; and national drug policiesand management (Western Pacific Region).The latter subject was chosen for theTechnical Discussions at the Thirty -firstWorld Health Assembly, under the title"National policies and practices in regardto medicinal products ; and related inter-national problems " (EBS 8.R8).
Programme trends and priorities
1.23 In addition to the general policydirectives of the Health Assembly, thedecisions of the governing bodies intechnical fields established certain pro-gramme trends and priorities that will havea significant effect on the work of WHOin the future. Some examples are givenbelow, the relevant Health Assembly,Executive Board or regional committee
THE WORK OF WHO
resolutions being indicated in each case.A landmark in the history of the Organi-zation was the adoption by the HealthAssembly in 1976 (WHA29.2o) of the SixthGeneral Programme of Work covering thespecific period 1978 -83, which had beenprepared and submitted by the ExecutiveBoard (Es 57.R4S).1 This Programme issubdivided into six major areas of concern :Development of comprehensive healthservices, Disease prevention and control,Promotion of environmental health, Healthmanpower development, Promotion anddevelopment of biomedical and healthservices research, and Programme devel-opment and support. For each area,specific objectives are defined, a varietyof approaches for attaining these objectivesindicated and criteria established for pro-gramme selection, for resource allocationand for determining the organizationallevel for the implementation of programmeactivities. The basic criterion of givingpriority to problems of developing coun-tries is emphasized. The Sixth GeneralProgramme of Work is a solid policy basisfor the more detailed formulation ofWHO's activities in the years to come.By taking defined national health needs asthe starting point, then moulding the WHOresponse to these needs through medium -term programmes, programme budgetsand evaluation, the Organization will usethe Sixth General Programme of Work tochart its path in the years 1978 -83, makingthe best use of regular budget and extra -budgetary funds, and introducing modifi-cations and corrections along the way asnecessary.
1.24 As WHO's activities at countrylevel become increasingly oriented tonational health policies and integratedwith national programmes for health anddevelopment, its planning process must
1 See page 6.
IO
develop accordingly. The approach usedhitherto has been to build the WHO budgetout of an aggregation of individually re-quested projects, each worked out andcosted in detail some two to three yearsprior to the operating period. Such anapproach is unduly rigid and not suited topresent conditions, and it was in thiscontext that proposals concerning thedevelopment of programme budgeting andthe management of WHO's resources atthe country level were submitted to andapproved by four regional committees(AFR /RC26 /R7, SEA/12C29/R4, EM /RC26A /R8and WPR /RC27 /RI). Subsequently, theDirector -General's report on the subjectand the proposals contained therein wereendorsed by the Board (EB59.R5o) andapproved by the Health Assembly(wHA3o.23). This change in procedure,which allows greater flexibility, will facili-tate programming at country level.
1.25 In the light of the evident pro-gress in programme budgeting and themanagement of WHO's resources, theRegional Committee for South -East Asiaviewed with concern recent moves todevelop a central planning and controlauthority for social and economic develop-ment within the United Nations system andthe consequent possibility of the assessedcontributions to WHO being reduced bybeing channelled into such a fund. TheCommittee strongly endorsed the view thatthe Constitutional mandate of the Organi-zation to furnish adequate technical assist-ance had to be safeguarded and requestedthe Regional Director and the Director -General to convey its concern about thesedevelopments to Member States (sEA/RC3o /R7).
1. z6 The need to intensify collabo-ration with Member States for a systematicassessment of the implementation of theOrganization's programme and of itsultimate impact on the health situation of
GOVERNING BODIES
the countries was emphasized in resolutionEB57.R17, on the development of pro-gramme evaluation in WHO, and sub-sequently stressed by regional committees(AFR/Rc26/R4, AMR /RC26 /R28 and AMR/Rc26 /R3z). Provisional guidelines forhealth programme evaluation were devel-oped and distributed for preliminary testingand review at regional and country levels.Reviewing the methods of producing theperiodic reports on the world healthsituation, which provide an analysis andevaluation of the state of health of the worldfor discussion among Member States, theHealth Assembly recommended (wHA29.2z)the implementation of proposals made bythe Director -General for improving theanalytical content, coverage and timingof the reports.
I.27 WHO activities related to disastersand natural catastrophies were highlightedby the Health Assembly (wHA29.39), whichrequested WHO to concentrate on nutri-tion, communicable disease control and theimprovement of health care services inpreparing short- and medium -term plansfor providing aid to the drought- affectedcountries of the Sahel. For emergencyassistance to countries of the Americas, itwas decided (AMR /Rc28 /RIo) that MemberGovernments should make the necessarypreparations and that the Regional Officeshould establish a disaster unit, to be sup-ported by a natural disaster relief voluntaryfund.
I.z8 The need for a comprehensivelong -term programme for the developmentand coordination of biomedical researchand for a reasonable balance betweenstrengthening existing research institutionsand establishing new centres was empha-sized by the Health Assembly, which in1976 requested a comprehensive report(wHA29.64) ; the policy guidelines con-tained in the report were endorsed in 1977
II
(wHA3o.4o). The deep involvement of theregions in the WHO research programmewas ensured by the creation of RegionalAdvisory Committees on Medical Researchand evinced by several resolutions con-cerning : the designation of the NationalInstitute of Dermatology of Venezuela, thePan American Center for Research andTraining in Leprosy and Other TropicalDiseases (AMR /Rc28/R27) ; the increasein regional budgets for biomedical andhealth services research promotion anddevelopment activities (SEA /Rc29 /RI andsEA /Rc3o /R5) ; and the strengthening ofthe Institute for Medical Research, KualaLumpur, Malaysia, with a view to itseventual designation as a WHO regionalcentre for research and training in tropicaldiseases (WPR /RC27 /R9).
I.29 Having considered the reports ofthe Director -General on the promotion ofnational health services and health techno-logy relating to primary health care andrural development, the Health Assembly(WHA29.74) affirmed that WHO's priorityshould be to assist countries to implementsteps that will improve the health of under -served populations. It emphasized theneed for WHO to establish and develop aprogramme of health technology relating toprimary health care and rural development,and to assist Member States to implementtheir programmes of primary health care.Different aspects of the same subject weretaken up by regional committees (AFR/RC26 /R4, AMR /RC28/R32, AMR /RC29 /R14 andEM /Rcz6A /RI I), which, with the HealthAssembly (wHA3o.48), also stressed theneed for appropriate training (AMR /Rc28/RI I, SEA /RC29 /R6, SEA /RC29 /R8, SEA /RC30/RI 2 and WPR /RC27 /RIO). Earlier, theHealth Assembly (wHA29.72) had outlinedthe Organization's role in promoting arational, systematic and well- integratedapproach to health manpower planning,production and management, which was
THE WORK OF WHO
subsequently elaborated by regional com-mittees (AFR /RC26 /R9, AMR /RC29 /R32, SEA/RC29 /R6, SEA /RC29 /R9, SEA /RC29 /RI0, andEM /Rcz6A /RI z). In this context, the HealthAssembly requested the Director -Generalto establish a long -term programme ofhealth manpower development. Otheraspects of general health services develop-ment singled out for special considerationincluded disability prevention and re-habilitation (wHAz9.68), road traffic acci-dents (ES57.R3o and EuR /RC26 /R2), emer-gency medical services (EM /Rc26A /R9), thecontribution of traditional systems ofmedicine to health care (SEA /RC29 /RI I,SEA /RC3o /R13 and wHA3o.49), the healthcare of the elderly (EUR /Rc27 /R6), andhealth and youth (AMR /Rcz9 /RI 5).
1.3o With the dramatic decline in theincidence of smallpox and its eradicationfrom most areas of the world in which itwas previously endemic, attention wasfocused on limiting the retention of variolavirus to certain designated WHO collabo-rating centres and on ensuring that adequatestocks of vaccine would be established tomeet unforeseen emergencies (wHA3o.52).The natural successor to the smallpoxeradication programme was the ExpandedProgramme on Immunization, the policyand strategy of which were approved bythe Health Assembly (wHA3o.53), whichrecommended their implementation andthe identification and the support of centresthat could develop regional vaccine pro-duction capabilities (wHA3o.S4). In thefield of tropical diseases, the Board calledfor a more realistic and flexible approachin the development of the antimalaria pro-gramme, with intensified coordination tomobilize greater resources, emphasis oninstitutional and field training and thedevelopment, production and distributionof antimalarial drugs and insecticides(ESS7.R26). This approach was endorsedby the Health Assembly (wHA29.73) and
I2
reinforced by the Board, which urgedcountries to give high national priority toantimalaria activities on a country basis(ES59.R13). In the Americas, the RegionalCommittee reaffirmed that malaria eradi-cation was the final goal, while recognizingcontrol activities as an intermediate stage(AMR /RC29 /R25). The Committee alsostressed the need for measures to controldengue, yellow fever and the vector Aedesaegypti (AMR /RC29 /R16). Approving theprogress and strategy of the Special Pro-gramme for Research and Training inTropical Diseases as reported by theDirector -General, the Health Assembly(wHA29.71) recommended enlargement ofthe network of collaborating institutionsand the establishment of contacts withuniversities, research institutions and thepharmaceutical sector for the developmentof new methods of disease control andnew preventive and therapeutic substances.
1.31 With regard to noncommunicablediseases, the Executive Board (EB59.R32)established an ad hoc committee to makerecommendations to the Assembly on allWHO's activities relating to cancer, in-cluding those of IARC, with a view todeveloping a rational strategy for inter-national cooperation. The indisputablescientific evidence showing that tobaccosmoking is a major cause of chronicbronchitis, emphysema and lung cancer,as well as a major risk factor for myocardialinfarction and certain pregnancy -relatedand neonatal disorders, was recalled by theHealth Assembly when it urged MemberStates to introduce effective control ofsmoking (wHA29.5 5). In resolutionwHA29.zi, the Director -General was askedto implement his proposals for a multi-disciplinary programme on psychosocialfactors and health. Subsequent resolutionsdrew attention to the need for action inrespect of mental retardation (wHA3o.38and sEA /Rc3o /R4) and for the establishment
GOVERNING BODIES
of a special programme of technical co-operation in mental health (wHA3o.45).The Health Assembly also stressed theimportance of Member States and WHOstrengthening the development of occu-pational health services (wHAz9.57), re-questing a report to the Thirty- secondWorld Health Assembly in 1979 on theprogress achieved. Alarm at the high andincreasing costs of pharmaceutical andbiological substances and medical supplieswas expressed by two regional committeesin resolutions (AFR /Rc26 /RI I, AFR /Rc27 /R8and EM /RC26A /RI r) requesting the improve-ment of facilities for the purchase of theseproducts at reasonable cost and investi-gation of the feasibility of their manu-facture within regions.
r.32. In addition to guiding WHO'soverall human health and environmentprogramme for the future in resolutionwHA29.45, the Health Assembly adoptedresolutions specifically on the health aspectsof human settlements (wHA29.46) and oncommunity water supplies and excretadisposal (wHA29.47). These resolutionsreiterated the importance of improvingenvironmental conditions to contribute tothe prevention not only of communicablediseases but also of noncommunicable anddegenerative diseases, as well as thoseinduced by pollution. Having consideredthe report of the Director -General on theUnited Nations Water Conference, theHealth Assembly (wHA3o.33) urged
Member States to appraise the status oftheir community water supply, sanitationfacilities and services, and to formulate andimplement policies and plans for the Inter-national Drinking Water Supply and Sani-tation Decade 198o -9o, recommended bythe Conference. Concerned at the in-creasing number of accidental releases ofchemicals into the environment, resultingin adverse effects on health of epidemicproportions, and recognizing that so farexisting national or international pro-grammes have been unable to deal ade-quately with the long -term aspects ofhuman exposure to chemicals, the HealthAssembly requested a study of the prob-lem and of the possible options forinternational cooperation (wHA30.47).
1.33 As a final example of the natureand scope of the policy guidance given bythe governing bodies during the biennium,mention may be made of resolutionwHA30.44, in which the Health Assemblystressed the paramount importance ofappropriate and adequate health legislationfor the development of health services,requested the Director -General to streng-then the Organization's programme in thisfield, requested the Executive Board tore- examine the criteria for the InternationalDigest of Health Legislation, and urgedMember States to forward their importanthealth laws and regulations to WHO inaccordance with Article 63 of the Consti-tution.
13
Chapter 2
General Programme
Development
2. z THE ORGANIZATION con-tinued to pursue energeticallyall efforts at programme devel-
opment with a view to collaborating withMember countries in the development ofnational health plans and programmes asan integral part of their overall socio-economic development systems and,through improved programme concepts,to enhancing WHO's own capabilities torespond to countries' needs in a coherentmanner. The biennium saw the furtherevolution of WHO's programme manage-ment system, which includes programmeplanning, budgeting, implementation, evalu-ation and information support. Themost important location for these functionsto take place is the countries themselves.
2.2 Within the WHO Secretariat, co-ordination of programme management iseffected at three levels : regional, head-quarters and global. The functions of theregional programme committees varyaccording to regional circumstances butare mainly concerned with translating theguidance on priorities received from thegoverning bodies, and the expressed wishesof Member States, into practical programmeterms at country and intercountry level.The Headquarters Programme Committeehas an important advisory role in the over-all development of headquarters programmeactivities, including their research compo-
14
nents ; the establishment of criteria andguiding principles for the formulationand implementation of programmes, inaccordance with the policies of theExecutive Board and the World HealthAssembly ; the strengthening of mech-anisms for programme informationsupport ; the review of proposals formedium -term programmes and programmebudgets, giving particular attention tonew technical cooperation programmes ;and the periodic evaluation of selectedaspects of the programmes. Further, witha view to coordinating the developmentand management of the Organization'sprogramme on a global scale, the GlobalProgramme Committee, which is madeup of the Director -General, the DeputyDirector -General, the Regional Directorsand the Assistant Directors -General, wascreated in March 1977. It is a top manage-rial forum for holding round -table reviewsof major issues concerning programmemanagement for the Organization as awhole.
National health programme develop-ment
2.3 The efforts over recent years toevolve a health planning methodologythat could be integrated into the frame-work of total socioeconomic develop-mental planning have borne fruit in the
GENERAL PROGRAMME DEVELOPMENT
form of country health programming -asimple and flexible process that has beenshown to be adaptable to varied socio-economic situations in different countries.As a result, the formulation of health pro-grammes within the context of nationalsocioeconomic plans has tended to replacead hoc, isolated projects. Six countriesinitiated the country health programmingprocess in 1976, and another eight countrieseither started or indicated their interest instarting the process in 1977. These figuresdo not include the Region of the Americas,where a process similar to, but not identicalwith, country health programming hasbeen in operation in many countries in theRegion. WHO's support to country healthprogramming continued to follow thepath of developing national self -reliancein planning for health development. Thissupportive role consists in helping tointerpret the methodology and its appli-cation, while at the same time ensuringthat the essentially national character ofthe process is maintained. Thus, accordingto available figures for 1976 and realisticestimates for 1977, national inputs wereabout 30o man -months, while the WHOinput was around zoo man -months, ofwhich 15o man -months was provided bythe staff of regional offices and 5o man -months by staff from headquarters. In theAmericas, a joint PAHO/WHO project inhealth planning methodology was studying,from late 1976, the determinants andvariables of health planning processes in anumber of developing and developedcountries in all six regions of WHO.
2.4 From the foregoing, it is clear thata great step forward was taken during arelatively short period of time in intro-ducing country health programming as asystematic but pragmatic approach in plan-ning for health development. Guidelineswere updated and are being tested, andtraining activities were in progress in many
I 5
countries in five of the six regions. With theaccumulation of knowledge and experiencein the practical application of countryhealth programming in country situations,it was felt that the time had come for apooling of experiences which would help incharting the future course for the develop-ment of the country health programmingconcept. Accordingly, an interregionalseminar was held in New Delhi in February1977, attended by national health plannersand WHO staff from all six regions, stafffrom WHO headquarters, and high -levelrepresentatives from UNDP, UNFPA,IBRD and USAID. The participants wereunanimous in their conviction that countryhealth programming is a useful tool in theplanning and management of health devel-opment. The seminar also stressed theintersectoral nature of the process. Thefinal recommendations were focused onthe following areas :
(i) the training of national staff inorder to develop national coregroups for country health pro-gramming, and adequate technicalsupport by WHO through thedevelopment and strengthening ofcore groups at regional level and atheadquarters ;
(ii) the development of appropriatemechanisms at regional offices andheadquarters for the collection,analysis and exchange of informationon country health programmingbetween countries and the differentechelons of WHO ;
(iii) the promotion of research oncountry health programming aspart of health services researchwithin the framework of WHO'sresearch programme, with a viewto improving further the countryhealth programming methodology ;and
THE WORK OF WHO
(iv) the need for WHO to promote theinclusion of planning and manage-ment techniques in the trainingcurricula of all categories of healthpersonnel.
WHO general programme development
z.5 The Twenty -ninth World HealthAssembly in May 1976 approved the SixthGeneral Programme of Work covering aspecific period (1978 -83),1 "believing thatthe Programme provides an appropriatepolicy framework for the formulation ofmedium -term programmes" (resolutionwHAZ9.zo). In order to translate this Pro-gramme of Work into operational pro-grammes, the secretariat working groupthat had drafted it was constituted as theMedium -Term Programming WorkingGroup, responsible for developing themethodology for medium -term program-ming for the Organization. This group,made up of the six Regional Directors ofHealth Services and a number of seniorstaff at headquarters, met for the first timein July 1976 and formulated recommend-ations and provisional guidelines formedium -term programming. In January1977 (resolution EB59.R9), the ExecutiveBoard endorsed a summary description ofthe methodology, processes and mechan-isms contained in the guidelines formedium -term programming.2 Oneimportant feature of the methodology isthe emphasis on the country- orientedapproach. The methodology and mechan-isms of medium -term programming haveso far been applied to the global programmearea of health manpower development and,at the regional level (European Region) tothe detailed programme on road trafficaccidents. In addition, an approach similar
1 WHO Official Records, No. 233, 1976, P. 63.2 WHO Official Records, No. 238, 1977, P. 233.
16
to that described in the guidelines formedium -term programming was used inthe development of the mental healthprogramme.
2.6 In July 1977 the Medium -Term Pro-gramming Working Group reviewed theprogress made in the development ofmedium -term programmes and undertook,at country level, in Honduras, a specificstudy of the problems involved in settingtargets for WHO activities based oncountry targets. Advantage was also takenof the visit to Honduras to review criticallythe relevance of the objectives of the SixthGeneral Programme of Work and of WHOprogramming in general to the countrysetting -in terms of local needs andnational planning and programmingschedules. At the same meeting, theWorking Group decided to embark sys-tematically on medium -term programmingto cover all the programme areas of theSixth General Programme of Work before198o (the year in which work on the SeventhGeneral Programme of Work shouldbegin). This preparation of medium -termprogrammes will provide for a completereview and reorientation of the Organi-zation's programmes and will contributeto a more realistic approach in the prepa-ration of the Seventh General Programmeof Work. The current medium -term pro-gramming guidelines will be revisedregularly, and particularly in 1978 in thelight of experience gained in the elabo-ration of the global medium -term pro-gramme for health manpower development.
z.7 The Working Group also formu-lated recommendations to the Head-quarters Programme Committee on a newWHO programme classification structurethat would be in line with the structure ofthe Sixth General Programme of Work.This will be a useful tool for planning andadministrative purposes such as medium-
GENERAL PROGRAMME DEVELOPMENT
term programming, programme budgeting,evaluation, reporting and information sys-tems. The Working Group also stronglyrecommended the progressive elaborationof a methodology for translating medium -term programmes into programme budgets-the latter becoming the basic instrumentsfor programme implementation.
z.8 In January 1977 the ExecutiveBoard requested its Programme Committeeto review the study of long -term healthtrends and their implication for the Organi-zation's future programmes (resolutionEB59.R27). In this respect, a formalanalysis of the answers (over 1 oo) receivedduring a consultation on "Long -term per-spectives concerning WHO's programmes"was carried out and the results presentedto the Programme Committee of theExecutive Board in November 1977.
Health programme evaluation
2.9 The main feature of the work inhealth programme evaluation from January1976 onwards was the development ofguidelines for the Organization's pro-gramme evaluation process and the use of amore systematic approach to evaluation.The long -term objective is to collaboratewith national health authorities in adaptingevaluation methodologies so that theirhealth programmes and services can beevaluated by their own personnel. Under-lying the development of the evaluationprocess is the recognition of the fact thatevaluation is an integral part of the modusoperandi of overall health managementmechanisms -planning, programming,implementation, monitoring and (afterevaluation) reprogramming. Indeed,evaluation should be a continuous process,not merely an ad hoc tool to produce aparticular result. This being so, its success-ful application calls for an objective, criti-
17
cal state of mind at all times. It is essentialthat evaluation should be carried out atall levels, even if at present only inadequateinstruments are available. This means thateveryone involved in the Organization'swork should assume responsibility forevaluation : governments, the WorldHealth Assembly, the Executive Board,regional committees, national health per-sonnel, and WHO staff at country, regionaland headquarters level.
z.io For the development of practicaland flexible evaluation guidelines, an inter-disciplinary team at headquarters workedin close collaboration with the regions,under the auspices of the HeadquartersProgramme Committee. A first set of draftguidelines was elaborated and distributedto regional and headquarters staff for com-ments. This draft was based on a document,Development of evaluation in WHO,' pre-sented to the fifty- seventh session of theExecutive Board in January 1976, onrecommendations contained in the WHOTechnical Report Series, on documents onevaluation in use in the various regions,and on the practical experience of thoseinvolved in evaluation work. The draftguidelines stressed the general principlesand the step -by -step approach involved inthe evaluation process in WHO. Theyalso indicated the linkages between evalu-ation and the planning and programmingprocesses for health, as well as the infor-mation systems support necessary forproper evaluation.
2..11 The discussions at the ThirtiethWorld Health Assembly in May 1977 andin the Programme Committee of theExecutive Board revealed the urgent needto develop evaluation guidelines for useby countries themselves. The formulationof such guidelines was not only in accord-
WHO Official Records, No. 235, 5976, p. 225.
THE WORK OF WHO
ance with resolution EB57.R17 adopted bythe Executive Board in January 1976,recommending all Member States to intro-duce a new approach to evaluating healthprogrammes, but was also consistent withthe policy of concentrating on renderingappropriate services to Member States toimprove their health activities rather thanon improving the Organization's efficiencyand effectiveness in isolation. Accordingly,the revised second draft of the guidelinescontained a section on the process ofevaluation of national health programmesby national health personnel. An additionalreason for developing evaluation guide-lines for national use was that an increasingnumber of countries were embarking oncountry health programming and request-ing a useful methodology for evaluatingtheir health programmes. The seconddraft of the guidelines was prepared fortesting in Member States and in WHObefore the new process of evaluation be-comes fully operational. The testing ofthe national guidelines is foreseen in atleast one country in each region in 1978.
Information systems programme
2.12 Continuing liaison is maintainedamong all the interdependent componentsof programme development to ensure theircoordination. The information require-ments of medium -term programming,country health programming, programmebudgeting and programme evaluation arebeing studied. The nature of the supportto be provided by the new WHO informa-tion system is being determined ; it has tobe appreciated that this is not a one -timeprocess but a continuous cycle of use/refinement /use of the system.
2.13 The coordination of informationmatters within WHO during the bienniumwas effected chiefly by the regional and
18
headquarters focal groups for informationsystems development. This coordinationwas strengthened by the establishment ofa Standing Committee on Information,composed of those persons responsible forthe provision of information services andsystems within WHO. The Committeeadvises on information questions on behalfof the Director -General's Office and theHeadquarters Programme Committee andcoordinates the Organization's technicalcooperation activities that relate to WHOinformation services and information sys-tems development.
2.14 The Organization's programmesrequire information in order to perform,and generate information when performing,the two main functions of technical co-operation with Member States and thepromotion of the international exchangeof health and health- related experienceand information. Equally, rational pro-gramme planning, implementation andevaluation need to be supported by specifictypes of information. To ensure that suchinformation is made available in the rightform and at the right time, and is coordi-nated with the evolving reorientation ofthe Organization's programmes, the devel-opment of a new WHO information sys-tem was proposed by the Director -Generalas part of the programme and budgetestimates for 1974, 1975 and 1976 -77.
2.15 The WHO information systemsdevelopment work stems from a WHOInformation Systems Development Work-ing Group, which was set up in December1973 with a mandate to draw up recom-mendations for the development of a new,user -oriented, WHO information system,serving the requirements of the Secretariat,the Member States, the World HealthAssembly, and the United Nations Eco-nomic and Social Council, and meeting therequirements of coordination within the
GENERAL PROGRAMME DEVELOPMENT
United Nations system. During its two -year mandate, the Working Group carriedout a number of studies culminating inrecommendations on a strategy for WHOinformation systems development, whichwas approved by the Director -Generaland led to the establishment, in April 1976,of a global information systems pro-gramme. In addition to its developmentcomponent, the programme contains aservice component to provide informationservices on all programmes and projects,and support services in administrativemanagement and electronic data processing.
z.16 The WHO information systemcomprises (a) the programme managementinformation system, which provides infor-mation about the Organization's pro-grammes and which includes the revisedreporting system and the administrativeand finance information system, and (b) anumber of special -purpose informationsystems dealing largely with technical andscientific data and information for theOrganization's programmes.
2.17 The WHO information systemsdevelopment strategy aims, first, at devel-oping the framework for the implemen-tation of the WHO programmes manage-ment information system and, when thisgains momentum, at analysing and ration-alizing the special -purpose informationsystems. The work involved is carriedout as a decentralized collaborative respon-sibility of focal groups for informationsystems development in each region and inheadquarters ; thus, coordination is builtinto the mechanism of implementation.
2.18 A concept, known as the "profileconcept ", was developed and introducedthroughout the Organization as a standard-ized method for the storage and continuousupdating of country and programme in-formation (PAHO is examining a slightly
19
different system). Programme and projectprofiles were established in their initial formand their periodic updating provides thebasis of the new reporting system. Regionalprogramme profiles are expected to becomea major source for the regional directors'reports to the regional committees and forthe preparation of global programmeprofiles ; the latter are expected to be amajor source for the Director -General'sreports to the Executive Board and theWorld Health Assembly. In addition,global and regional programme profilesare available for direct reference and useby all regional offices, regional committees,the Executive Board and the HealthAssembly. This system was tested in 1977and will be gradually introduced in 1978.Several complete reporting cycles will berequired before the system stabilizes andis evenly followed in all echelons and pro-grammes of the Organization. Work iswell advanced towards the developmentnot only of programme and project profilesbut also of country profiles ; this work isbeing coordinated with development ofthe methodology for country health pro-gramming.
2.19 In addition to management in-formation, the programmes require othertypes of information such as scientific ortechnical information ; information forprocessing and responding to requestsfrom Member States and organizations ;directories and rosters of persons ororganizations relevant to the programmes ;and bibliographical references. Thesespecial -purpose information systems covera much larger volume of information thandoes the programme management informa-tion system. A survey carried out in 1976identified 290 such systems and highlightedthe need to rationalize existing special-purpose information systems, and todevelop new ones ; a strategy was proposedfor this work. The first practical outcome

THE WORK OF WHO
will be a pilot master directory of personsand organizations of interest to WHOprogrammes, and also information on thenature of this interest -a first step in thereplacement of a large proportion of nearlySo special -purpose directories.
2.20 A new administration and financeinformation system was developed foruniform use throughout the Organization ;accounting, budgeting, personnel, supplyand other subsystems were developed asintegrated parts of the system, whichemploys computers to reduce workloadand increase efficiency in the regions andat headquarters. This system will greatlyfacilitate planning and forecasting, andincludes a warning system to keep bothregular budget spending and extrabudget-ary spending within set limits. Whenfully implemented and operational, thenew system will ensure the direct compar-ability of programme information, main-tained in the profiles mentioned above,with the corresponding administration andfinance information.
2.21 To prepare for the evaluationstage of this new programme, preliminarycriteria were worked out for evaluatingthose components of the WHO informa-tion system that will begin to be opera-tional in 1978. Because the informationsystems programme is primarily a supportprogramme, its evaluation will dependpartly on user satisfaction and partly on anassessment of information -related aspectsof other programmes.
2.22 Experience during the implemen-tation and testing phases of various corn-
ponents of the new system in all echelonsof the Organization provided some indi-cation of the benefits that accrue from thenew WHO information system. Forexample, there was a significant overallreduction in the number and volume ofreports being formally transmitted (withoutdetriment to the substance and quality ofthe information concerned). Again, thenumber of periodical documents andreports reaching the Regional Office forAfrica was reduced from 1 zoo in 1973 toboo in 1974 and 8o in 1976.
z.z3 Programme profiles are alreadybeing used by the Organization's pro-grammes at the country, regional andglobal levels ; their use by Member States,regional committees, the Executive Boardand the World Health Assembly will beprogressively introduced. It is an import-ant part of the strategy that the systemwill gradually be refined on the basis of thevarious users' experience, and this refine-ment process may take several reportingcycles.
2.24 The information system develop-ment described above did not occur inisolation from other information systemactivities within the United Nations. Inaddition to direct consultation with, orcontribution to, other information systemdevelopment activities within the UnitedNations, full collaboration was maintainedthroughout 1976 -77 within the forum ofthe Inter -organization Board for Informa-tion Systems and Related Activities, whereWHO both influences and is influenced byother information systems developmentactivities.
20
Chapter 3
Coordination
3-1COORDINATION
with the UnitedNations system ensures thathealth factors are taken into
account in the policy and programme for-mulation and development of other organi-zations as well as at the broad policylevel ; this coordination contributes to theoverall efforts of the United Nations systemby making available WHO's expertise andknowledge through the work of suchbodies as the ACC, the Economic andSocial Council, the United Nations GeneralAssembly and their subsidiary bodies.
3.2 Resolutions of the thirtieth andthirty -first sessions of the United NationsGeneral Assembly inviting WHO to pre-pare a draft code of medical ethics relatingto the protection of persons against torturewere brought to the attention of the fifty -seventh session of the Executive Board andto the Thirtieth World Health Assembly,which requested the Director -General totransmit the study on this subject, beingundertaken by CIOMS on behalf of WHO,to the Executive Board for considerationbefore it is forwarded to the United NationsGeneral Assembly (resolution wHA3o.32).
3.3 Certain coordination matters whichreceived the Director -General's attentionin 1976 and 1977 were considered withinthe framework of the ACC, the Economic
2I
and Social Council and the United NationsGeneral Assembly. One of these concernedthe United Nations Conference on Scienceand Technology for Development, sched-uled for 1979. An internal WHO com-mittee reviewed the Organization's pre-parations for the Conference and decidedthat the Special Programme for Researchand Training in Tropical Diseases offeredthe best basis for WHO's contribution.Regional offices and country representa-tives were requested to provide all necessaryhelp to national focal points established toreview their countries' needs in the field ofscience and technology.
3.4 The Organization was involvedwith the preparation for and the participa-tion in major conferences of the UnitedNations system, such as the TripartiteWorld Conference on Employment, IncomeDistribution, Social Progress and theInternational Division of Labour, theUnited Nations Conference on HumanSettlements (HABITAT), the UnitedNations Water Conference, the UnitedNations Conference on Desertification andthe World Conference for Action againstApartheid.
3.5 The Director -General contributedto a wide range of reports and documentsprepared by the United Nations for variousintergovernmental bodies. In reply to
THE WORK OF WHO
requests from outside bodies, informationwas provided on such questions as con-sumer protection, human settlements, dis-armament, human rights and apartheid,the role of women in development, ruraldevelopment, the implementation of theDeclaration on the Granting of Inde-pendence to Colonial Peoples and Coun-tries, cooperation with the Organizationof African Unity, the International Devel-opment Strategy of the Second UnitedNations Development Decade, and pro-grammes for the International Year forDisabled Persons, the International Anti -Apartheid Year and the International Yearof the Child.
Extrabudgetary sources of funds
3.6 The Voluntary Fund for HealthPromotion, established by the HealthAssembly in 196o (resolution wHAI3.24)so that voluntary contributions could bereceived from governmental and privatesources for the expansion and accelerationof WHO's activities, has become one of themost important sources of extrabudgetaryfunds. Donations in 1975 and 1976 equalledthe total amount received since the incep-tion of the Fund, as a result of the emphasisgiven by the Executive Board and theWorld Health Assembly to this approachto attaining health for all by the year 2000;receipts in 1977 were also substantial.
3.7 An Extrabudgetary Resources Com-mittee comprising members of the WHOSecretariat was established in 1976 to adviseon strategies for increasing extrabudgetaryresources for the Organization's priorityprogramme areas.
3.8 A central retrieval point was estab-lished in WHO to collect information oncurrent and prospective donors and to
22
keep track of proposed projects and con-tributions. A project catalogue was set up,with descriptions of priority activitiessuitable for extrabudgetary funding, anda compendium of summary descriptionsof these projects is routinely circulated todonors. Such projects, which fall withinWHO's General Programme of Work,range from multimillion- dollar long -termactivities to those where a minimal financialinput can promote national self- reliance ina crucial area.
3.9 Relations were systematically main-tained with all donor countries and co-operation was intensified, particularly withthe Federal Republic of Germany and theNetherlands. A new departure was arequest from the United Kingdom Ministryof Overseas Development for WHO toplan projects for potential financing.
3.10 The Regional Office for the East-ern Mediterranean secured significant con-tributions from Arab countries for usewithin the Region, and the possibility wasexplored of obtaining funds from thissource for use outside the Region.
3.11 Following the substantial contri-bution already made by the Japan Ship-building Industry Foundation (SasakawaHealth Fund), a further US $ r .5 million wasdonated for 1976 and US $ 2.3 million for1 977.
3.12 Efforts continued to secure furtherfunds for urgent health needs in Viet Nam;a special assistance programme was devel-oped in 1976 between the Government andWHO, totalling some US $ 117 million.The main priority areas for internationalassistance are : reconstruction of healthservices, health laboratories, familyplanning, immunization, pharmaceuticalproduction, venereal disease control and,
COORDINATION
above all, malaria. WHO received sizeablecontributions from Australia, Denmark,Malaysia, Netherlands and Switzerland andseveral agencies, including the Japan Ship-building Industry Foundation. In 1977WHO provided US $ 1.5 million from itsregular budget. The Organization con-tinued to collaborate with other UnitedNations bodies, including UNICEF,UNHCR, UNIDO and UNFPA, and withthe Coordinator of International Reha-bilitation Assistance for the Reconstructionof Viet Nam. Responsibility for the specialprogramme was transferred to the RegionalOffice for the Western Pacific and a WHOoffice was established in Hanoi.
3.13 The DANIDA /WHO Joint Pro-gramme continued, with an annual expen-diture of some US $ 600 000. While anumber of training courses were main-tained, a greater share of the Programmewas devoted to projects executed in thedeveloping countries themselves, in linewith the new policy to gear the Programmeclosely to WHO's main areas of activity.Examples in 1977 included support tohealth services development in Guinea-Bissau and to auxiliary training in Sudan.Administrative responsibility for the Pro-gramme was transferred to the RegionalOffice for Europe.
United Nations Children's Fund
3.14 The UNICEF /WHO Joint Com-mittee on Health Policy met in Genevafrom 31 January to z February 1977. Themain item on the agenda was the report onthe UNICEF /WHO joint study on com-munity involvement in primary healthcare, which was endorsed unanimously.The Committee also considered reviewsof the primary health care programme andthe Expanded Programme on Immuniza-
23
tien. Recognizing the vital importance ofa clean and adequate supply of water as afactor for health, the Joint Committeerecommended that WHO and UNICEFshould conduct a study on water supplyand sanitation as components of primaryhealth care.
3.15 The conclusions and recommenda-tions of the Joint Committee were adoptedby the UNICEF Executive Board, whichmet in Manila from 23 May to 3 June 1977.The Board recommended that UNICEFand WHO should increase joint activities innutrition and reiterated its endorsement ofUNICEF's participation, in partnershipwith WHO, in the International Conferenceon Primary Health Care to be held in Alma -Ata, USSR, in September 1978.
3.16 Consultation and cooperation onprogrammes of assistance took place regu-larly in the field and among regional offices.Preparation for the International Year ofthe Child were also being made jointly withUNICEF.
United Nations Development Pro-gramme
3.17 The UNDP Governing Councilat its January and June sessions discussedthe future role and activities of UNDP intechnical cooperation, through the opti-mum use of UNDP country programming.The Council also considered new dimen-sions in technical cooperation and execu-tion of projects by governments, pro-gramme evaluation, and the establishmentof an intergovernmental working groupon overhead costs and an interagencypolicy task force, which was established atUNDP headquarters in October 1977.Another central topic was the laying offoundations for technical cooperationamong developing countries, designed to
THE WORK OF WHO
enhance the self -reliance of developingcountries, which is in line with WHO'sstrategy for technical cooperation. TheOrganization participated in the work ofvarious groups preparing the World Con-ference on Technical Cooperation amongDeveloping Countries which is to takeplace in Buenos Aires, Argentina in 1978.Responsibility for WHO's activities withinthe context of technical cooperation amongdeveloping countries was entrusted to theRegional Office for the Americas.
3.18 Cooperation with China was con-tinued. A Chinese Study Mission onImmunology visited WHO headquartersand institutes in Kenya, Switzerland andthe United Kingdom. Study tours in publichealth and basic health services, two train-ing courses on acupuncture, and an inter-regional study tour on traditional medicinein community health services were arrang-ed in China with UNDP support, for parti-cipants from the developing countries.Responsibility for WHO's activities inChina was delegated to the Regional Officefor the Western Pacific.
World Food Programme
3.19 Table 3.1 shows that assistancegiven by WFP for health supportive activi-ties decreased. On the other hand, WFP'sevaluation processes were strengthenedand collaboration with WHO was rein-forced.
3. zo The vitamin A enrichment ofdried skimmed milk going to xeroph-thalmia -prone areas was regularly imple-mented. A simple field test for the detectionof vitamin A in dried skimmed milk wasdevised with the help of Dutch and Swissindustries ; similarly, the development ofa diagnostic instrument to detect sub -clinical vitamin A deficiency in the fieldwas pursued.
24
3.21 The first project using food aidfor the specific purpose of developing basicrural health services within the WHOprogramme in primary health care wasapproved in late 1977.
Emergency relief operations
3.22 During the biennium WHO parti-cipated fully in the United Nations system'swork in providing emergency relief andrehabilitation assistance to countriesstricken by natural or other disasters. TheOrganization's activities in meeting needsin emergencies and natural disasters werecarried out in close collaboration withUNICEF, UNDRO, UNHCR, FAO, theInternational Committee of the Red Cross,and the International League of Red CrossSocieties. WHO responded to a numberof emergency situations as they arose,maintaining the necessary collaborationwith Member States and with inter-national and other organizations as appro-priate. The following are brief details ofsome of the Organization's activities in thisfield during 1 976 -77.
Angola
3.23 The Organization assigned twopublic health experts to the United Nationsmission that visited Angola in July 1976to assess the emergency situation there,and contributed US $ 5 000 from the Volun-tary Fund for Health Promotion (SpecialAccount for Disasters and Natural Catas-trophes) to provide vaccines and seraurgently needed for the prevention andcontrol of communicable diseases.
Bangladesh
3.24 Following the floods that affectedBangladesh in March -April 1 977, UNDRO
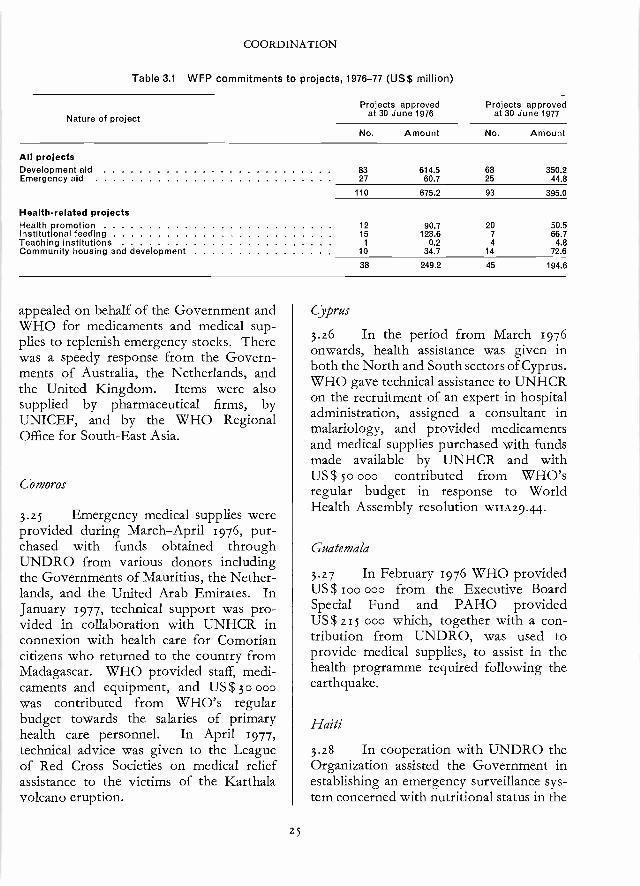
COORDINATION
Table 3.1 WFP commitments to projects, 1976 -77 (US$ million)
Nature of projectProjects approved
at 30 June 1976Projects approved
at 30 June 1977
No. Amount No. Amount
All projectsDevelopment aid 83 614.5 68 350.2Emergency aid 27 60.7 25 44.8
110 675.2 93 395.0
Health- related projectsHealth promotion 12 90.7 20 50.5Institutional feeding 15 123.6 7 66.7Teaching institutions 1 0.2 4 4.8Community housing and development 10 34.7 14 72.6
38 249.2 45 194.6
appealed on behalf of the Government andWHO for medicaments and medical sup-plies to replenish emergency stocks. Therewas a speedy response from the Govern-ments of Australia, the Netherlands, andthe United Kingdom. Items were alsosupplied by pharmaceutical firms, byUNICEF, and by the WHO RegionalOffice for South -East Asia.
Comoros
3.25 Emergency medical supplies wereprovided during March -April 1976, pur-chased with funds obtained throughUNDRO from various donors includingthe Governments of Mauritius, the Nether-lands, and the United Arab Emirates. InJanuary 1977, technical support was pro-vided in collaboration with UNHCR inconnexion with health care for Comoriancitizens who returned to the country fromMadagascar. WHO provided staff, medi-caments and equipment, and US$ 3o 000was contributed from WHO's regularbudget towards the salaries of primaryhealth care personnel. In April 1977,technical advice was given to the Leagueof Red Cross Societies on medical reliefassistance to the victims of the Karthalavolcano eruption.
25
Cyprus
3.26 In the period from March 1976onwards, health assistance was given inboth the North and South sectors of Cyprus.WHO gave technical assistance to UNHCRon the recruitment of an expert in hospitaladministration, assigned a consultant inmalariology, and provided medicamentsand medical supplies purchased with fundsmade available by UNHCR and withUS $ 5o 000 contributed from WHO'sregular budget in response to WorldHealth Assembly resolution wHAZ9.44
Guatemala
3.27 In February 1976 WHO providedUS $ loo 000 from the Executive BoardSpecial Fund and PAHO providedUS $ 215 000 which, together with a con-tribution from UNDRO, was used toprovide medical supplies, to assist in thehealth programme required following theearthquake.
Haiti
3.28 In cooperation with UNDRO theOrganization assisted the Government inestablishing an emergency surveillance sys-tem concerned with nutritional status in the
THE WORK OF WHO
regions affected by a severe drought in1977. Technical cooperation and supplieswere provided from PAHO funds.
Honduras
3.29 Urgently requested medical sup-plies were provided to the Governmentfollowing devastating floods in November1976.
Lebanon
3.3o The Organization allocated inJanuary 1976 the sums of US $ 146 000from the regular budget and US $ 5o 000from the Voluntary Fund for Health Pro-motion (Special Account for Disasters andNatural Catastrophes) to accelerate theprovision of urgently required medica-ments, medical equipment and supplies.In February 1976 short -term consultantsin epidemiology and public health wereassigned. Subsequently, WHO providedfurther supplies and equipment with fundsmade available by UNHCR and the Inter-national Committee of the Red Cross. Inaccordance with Health Assembly resolu-tion wxn29.4o, vaccines and medicamentswere provided, a sanitary engineer and asanitarian were assigned during the lastquarter of 1976, and further supplies weremade available with US $ 13o 000 fromWHO's regular budget and with otherfunds from the United Nations Trust Fundfor Lebanon. In 1977 a senior WHOpublic health administrator assisted theMinistry of Health in its rehabilitationprogramme ; WHO also contributedUS $ 207 000 from the regular budgettowards this programme.
Mexico
3.31 Following the hurricane Liza, theOrganization immediately provided im-portant consignments of medical supplies.
z6
Mocambique
3.32 In collaboration with UNDRO,WHO provided technical advice to poten-tial donors of health assistance followingthe cyclone and floods that occurred inMozambique in February 1977. The costof medical relief assistance was coveredby contributions from governmentsthrough the League of Red Cross Societies,while WHO collaborated with UNICEFto provide medicaments and medical sup-plies, WHO contributing US $ 100 000from the regular budget.
Pakistan
3.33 Assistance to the victims of floodswas provided by means of a donation fromthe Government of Iran to the VoluntaryFund for Health Promotion (Special Ac-count for Disasters and Natural Catas-trophes). At WHO's request, the donationwas in the form of vaccines and sera. Closecooperation was maintained with UNICEF,UNDRO and other agencies involved inassisting the national health authorities intheir efforts to combat the public healthhazards arising from the floods.
Romania
3.34 To provide medical relief assist-ance to the victims of the earthquake inMarch 1977, WHO used funds and suppliesdonated by governments and other sourcesthrough UNDRO and the League of RedCross Societies.
Assistance in epidemics
3.35 WHO, supported by funds ob-tained from governments and other sourcesafter appeals from UNDRO, assisted infield operations to combat an outbreak ofviral haemorrhagic fever in Sudan and
COORDINATION
Zaire in October 1976 and an outbreak ofsmallpox in Somalia in the first half of 1977.
National liberation movements recognized by theOrganization of African Unity
3.36 Following preliminary negotia-tions, UNICEF, UNDP and WHO con-vened a joint meeting in Geneva in June1976 with representatives of the Organi-zation of African Unity and of nationalliberation movements recognized by it.
The meeting resulted in a grant by UNDPof US $ 600 000 for a three -year trainingproject located at Morogoro, UnitedRepublic of Tanzania. WHO is the execu-ting agency for this project, which com-menced in September 1976. The objectivesof the project are to provide training forhealth personnel and fellowships for med-ical and paramedical staff. It will alsoprovide emergency medical supplies andequipment for the populations with whichthe liberation movements are concerned.
27
Chapter 4
Research Promotion and
Development
4ITHE PERIOD 1976 -77 was
characterized by three trends inWHO's research activities :
4.2 First, there was greater emphasison goal- oriented research. Resolutionwxaz8.7o adopted by the World HealthAssembly in May 1975 embodied majorresearch policy directives that influencedchanges in the Organization's technicalactivities, particularly in the fields ofresearch and training in tropical diseases,health services research, the ExpandedProgramme on Immunization, primaryhealth care, and appropriate technologyfor health. All these multidisciplinaryactivities focus on efforts to solve the prob-lems of underprivileged populations.
4.3 Secondly, research became moredecentralized. Advisory Committees onMedical Research (ACMRs) were set upand are functioning in all the regions ;several regions also instituted task forces,study groups and other mechanisms tomobilize human resources at the nationalas well as regional levels. Results achievedso far indicate that much progress can bemade in a short time by strengtheningcooperation among national institutionalbodies (such as medical research councils),regional ACMRs, the global ACMR andthe WHO Secretariat.
28
4.4 Thirdly, the volume of WHO'sresearch efforts increased substantially inspite of the unchanged proportion (approxi-mately 5 %) of regular budget funds usedfor supporting research. This expenditureallows the Organization to play a uniquecatalytic role in the international forumand promote scientific and professionalwork of good quality. For larger, mission-oriented endeavours, WHO has launchedspecial programmes that rely mainly onextrabudgetary funds. Total allocationsfor the Special Programme of Research,Development and Research Training inHuman Reproduction and the SpecialProgramme for Research and Training inTropical Diseases in 1977 were of theorder of US $ zo million. These pro-grammes involve many hundreds ofscientists and institutions around the worldin all regions.
4.5 The volume of research in thefield of general health services, althoughstill low compared with the programme'sneeds, also increased, because a substantialamount of operational research was carriedout in many of the other major pro-grammes. The extrabudgetary fundingspecified for health services research in1977 was just over US $ 1 million. WHO'sresearch activities on health servicesdevelopment are undergoing rapid ex-pansion.
RESEARCH PROMOTION AND DEVELOPMENT
Global developments
4.6 At the global level, the bienniumsaw a more active participation of theACMR in the work of WHO, improvedresearch coordination mechanisms, broadermultisectoral approaches to health problemsand an intensification of research and train-ing efforts in the several special pro-grammes.
4.7 There was greater involvement ofthe global ACMR in WHO's research.The participation of chairmen and mem-bers of all the regional ACMRs in theglobal ACMR underlined its broad func-tions. Group consultations of ACMRmembers with technical programme staffwere initiated. In addition, ACMR mem-bers participated in special committeesexamining problems of worldwide signifi-cance, such as the ethical aspects of medicalresearch and safety in handling micro-organisms and cells, especially in experi-ments on recombinant DNA. IndividualACMR members also devoted periods ofup to a year to assisting WHO in planningand developing its research efforts. ACMRmembers are increasingly acting as focalpoints for contact and coordination withnational medical research councils, acade-mies and analogous bodies.
4.8 New mechanisms were developedto improve coordination : the institutionof Research Development Committees inheadquarters and in the regional offices, aninterregional meeting on coordination ofresearch, held in headquarters after thenineteenth session of the global ACMR,and the use of "task forces ", "scientificworking groups" and "research and train-ing centres" in developing countries.
4.9 Multidisciplinary programme teamswere developed in several areas such ascountry health programming, development
29
of information systems and programmeevaluation, appropriate technology forhealth, research and development in theExpanded Programme on Immunization,research needs in the control of diarrhoealdiseases, health services research, and re-search potentialities of cancer chemotherapyfor developing countries.
4.10 The Special Programme for Re-search and Training in Tropical Diseasesuses technical expertise from many parts ofthe Organization in planning and imple-menting the research activities of itsscientific working groups. The SpecialProgramme of Research, Development andResearch Training in Human Reproduction,in which nearly 7o countries cooperate(including 39 developing countries), is thelargest WHO research effort. Details ofthese two programmes will be foundelsewhere.'
Ethical aspects of biomedical and healthservices research
4.1I In March 1976, an InternationalConference co- sponsored by the WorldMedical Association, the InternationalAssociation of Biological Standardization,CIOMS, the United States Public HealthService and WHO discussed the role of theindividual and the community in the re-search, development and use of biologicals.2
4.12 In March 1977 a WHO ExpertCommittee on the Use of Ionizing Radia-tion and Radionuclides on Human Beingsfor Medical Research, Training and Non-medical Purposes examined the ethicalimplications of this subject, classified re-search projects according to the radiation
1 Pages 115 and 57 respectively.2 Bulletin of the World Health Organization, 54 : 645
(1976).
THE WORK OF WHO
dose delivered to the subject and the risksinvolved, and recommended that all re-search projects involving radiation shouldbe reviewed by ethical review committees.'
4.13 The Organization participated inseveral round -table discussions organizedby CIOMS on ethical problems, in par-ticular those involving research on humansubjects. A member of the ACMR was aparticipant at the loth General Assemblyof CIOMS held in November 1976, atwhich the ethical aspects of biomedicalresearch involving human subjects werediscussed, with special reference to the roleof ethical review committees. In December1977, WHO co- sponsored the 11th CIOMSRound Table Conference on Trends andProspects in Drug Research and Develop-ment, at which the ethical aspects of drugdevelopment were discussed.
Safety in the handling of microorgan-isms and cells
4.14 The ACMR at its 18th and 19thsessions (June 1976 and June 1 977) maderecommendations on a WHO policy ongenetic research and stressed the need formore adequate laboratory safety elements(staff, facilities and equipment) in micro-biological practice since the number ofprofessional disciplines working withpathogenic organisms is increasing, oftenwithout proper training in safety measuresand supervision. Safety services in micro-biology have, in particular, to be developedin line with the promotion of research indeveloping countries. In its initial phasethe special programme on safety measuresin microbiology therefore placed emphasison the development of codes of practice toprevent accidents and infections in micro-
WHO Technical Report Series, No. 611, x977.
30
biological laboratories. The roles of safetyofficers, of the Organization, and of na-tional safety committees were defined andthe preparation of guidelines was begun.
4.15 Work also commenced on a docu-ment to inform public health officers andresearch workers of new technologies ingenetic engineering, the potential benefitsand possible risks of these technologies,and the safety regulations established inMember countries. WHO is cooperatingwith international, regional and nationalbodies in order to complement new tech-nological developments by improvingsafety systems and emergency services.
Research training
4.16 Under the WHO research trainingprogramme, 97 grants were awarded in1976 and 1977 to enable research workersto widen their research experience abroadand thus increase their contribution to theresearch activities of their own countries ontheir return home. In addition, 59 grantswere awarded to promote the exchange ofscientific knowledge by enabling investiga-tors working on subjects of interest toWHO to visit scientists in other countriesworking in similar or related fields.
Regional developments
African Region
4.17 At its first meeting in Brazzavillein November 1976, the Regional ACMRlaid down criteria for choice of prioritiesand the broad guidelines for training re-search workers. It stressed the importanceof the Special Programme for Research andTraining in Tropical Diseases and ofresearch on health services, including tradi-tional medicine. The Committee recom-
RESEARCH PROMOTION AND DEVELOPMENT
mended setting up or strengthening na-tional research councils, bringing thedirectory of existing centres up to date,identifying institutions likely to collaboratein the regional programme and setting upmechanisms for training research workers.
4.18 In Zambia, the Ndola centre wasthe principal focus for promoting theSpecial Programme for Research and Train-ing in Tropical Diseases in Africa.' Anepidemiological survey was carried out ofthe frequency of the six diseases selectedfor the Programme.
4.19 In the Volta River basin area, theintercountry onchocerciasis control pro-ject 2 continued its research programme,devoting particular attention to the filari-cides usable in mass medical treatment andto methods for the biological control ofvectors. At the end of 1976, a chemo-therapy research centre was set up atTamale, Ghana. Cytotaxonomic studies oflarvae established the distribution of thevarious species of the Simulium damnosumcomplex within and outside the programmezone. Considerable research was under-taken on the reinvasion of certain valleysduring the rainy season.
4.2o The second session of the RegionalACMR took place in Brazzaville inNovember -December 1977. The Com-mittee recommended the establishment ofa network of research and training centresin the Region ; reviewed project proposalsin malaria and in health services researchand recommended priorities in these fields ;and recommended the establishment of(i) a Regional research information sys-tem ; (2) task forces on schistosomiasis,onchocerciasis and trypanosomiasis ; (3) anemergency training programme ; and (4) aRegional research grants programme.
1 See also page 116.2 See also page 92.
31
Region of the Americas
4.21 In 1976 -77 many research projectswere in progress in the Region of theAmericas on various aspects of communic-able and noncommunicable diseases. Basicand applied research on maternal and childhealth was also continued. Support wasgiven to immunological research in centresin Brazil and Mexico.
4.22 In 1977 the Organization reviewedthe coordination and promotion of re-search in developing countries in theRegion and carried out trial investigationson this subject in Central America.
4.23 Closer contact was establishedwith bodies responsible for organizinghealth research in Brazil, Colombia, Mexicoand Venezuela. Institutions were identifiedthat could act as collaborating centres forresearch and training. Work was begun onpreparing directories of research institu-tions, investigators and projects.
4.24 Resources were also channelledtowards underserved population groups inthe Region, and research was promoted onsociomedical, organization and administra-tive subjects.
4.25 The Regional ACMR met in Bra-silia in 1976 and in Washington, DC, in1977, when it approved new policies forencouraging the development of researchin the Region.
South -East Asia Region
4.26 The first two sessions of theRegional ACMR were held in New Delhiin January and August 1976, and the thirdwas held in Colombo in April 1977. Itreviewed the recommendations of five re-search study groups that had been workingon malaria, leprosy, alternative strategiesfor delivery of health care, dengue haemor-
THE WORK OF WHO
rhagic fever, and chronic liver diseasesincluding liver cancer. The Region's role inthe Special Programme for Research andTraining in Tropical Diseases was alsoexamined. The Committee considered docu-mentation on facilities for research onprimates and discussed the problems ofdiarrhoeal diseases in children.
4.27 In response to a resolution of theRegional Committee, the Regional ACMRdiscussed the question of traditional medi-cine and reviewed on -going as well asplanned activities in the field.
4.28 Activities carried out in the 27WHO collaborating centres in the Regionwere intensified, and four new centres weredesignated.
4.29 The Regional Committee recom-mended at its twenty -ninth session that2.5 % of the regular regional budget shouldbe allocated to research and that theDirector -General should be requested toprovide a matching grant.
European Region
4.30 The Regional ACMR, composedof 16 experts, held its first meeting inFebruary 1977. Problems and priorities inthe countries were reviewed, as well asfields in which coordination and informa-tion would be mutually beneficial. TheCommittee recommended the establish-ment of planning groups on selected re-search priorities. At the request of theCommittee a planning group on informa-tion systems for medical research met inCopenhagen in June -July 1977 ; its reportwas presented to the second meeting of theRegional ACMR in October 1977 and theCommittee studied its recommendationstogether with other major questions linkedwith the development of this programme.
32
Eastern Mediterranean Region
4.31 The first meeting of the RegionalACMR took place in April 1976. Thesecond was held in March 1977, precededby a great deal of preparatory work,including the compilation of a directory ofresearch institutions in the Region. TheCommittee examined the report of a teamof WHO consultants who visited Egypt,Iran, Iraq and Sudan to survey the researchpotential and needs and who made recom-mendations on research priorities.
4.32 The Committee reviewed a paperoutlining the conceptual framework forhealth services and manpower development,strongly endorsed the priority that hadbeen given to research on these subjects,especially with reference to primary healthcare, and welcomed plans to implement aregion -wide project to undertake relevantstudies in selected areas in collaborationwith the ministries of health and otherinstitutions in the region, as well as todevelop research capabilities in this field.
4.33 The Committee endorsed plansand mechanisms for implementing theregional research programme (includingresearch training awards, grants, contractsand a visiting scientists' programme) andproposed that the programme should befunded initially from WHO's regular bud-get. One recommendation, now beingimplemented by the Regional Office, wasthat a major library in the Region shouldbecome a regional medical library ; anotherconcerned the establishment of a scientificgroup to assist in implementing researchproposals for health services and manpowerdevelopment. This group was establishedand met in July- August 1977 to formulateresearch projects for implementation.
Western Pacific Region
4.34 The Regional ACMR created threetask forces at its first session in June -July
RESEARCH PROMOTION AND DEVELOPMENT
1976, concerned with health services re-search, cardiovascular diseases, and para-sitic and other communicable diseases. Thefirst of these met twice and discussed thedefinition of health services research, itsscope and problem areas, and suggestedsolutions, and considered the progress anddevelopment of the Korean Health Devel-opment Institute, Seoul.
4.35 The Regional ACMR held itssecond session in April 1977, when itreviewed recommendations on ways andmeans of strengthening the Institution forMedical Research in Kuala Lumpur toenable it to provide research and trainingfacilities for the whole Region. The Corn -mittee also approved a multidisciplinaryresearch programme on schistosomiasis.
33
Chapter f
Strengthening of Health Services
5.1THE HEALTH SERVICES in
many countries are not keepingpace with the changing needs
and demands of populations -either inquality or quantity -and it has becomeclear that the present structure and oper-ation of these services do not effectivelymeet the requirements of the majority ofpeople. The World Health Assembly, theExecutive Board and the Regional Com-mittees have discussed this question atlength during the past few years, and thedebate culminated in the adoption ofresolutions WHA28.88 in May 1975, whichstressed the importance of promotingnational health services relating to primaryhealth care, and wHAZ9.74 in May 1976,which dealt with the promotion of nationalhealth services and health technology inrelation to primary health care and ruraldevelopment. In May 1977 the WorldHealth Assembly further adopted resolu-tion wHA30.43, having decided that themain social target of governments andWHO in the coming decades should be"the attainment by all the citizens of theworld by the year z000 of a level of healththat will permit them to lead a sociallyand economically productive life ".
5.2 During 1976 -77 various activitiesin the area of strengthening of healthservices were undertaken in Member coun-tries. These activities were directed
34
towards change, towards adapting to newapproaches, and towards developing newprogrammes that will eventually lead tostrengthening of health infrastructures inorder to meet the fundamental needs ofMember States. In response to the abovemandates, WHO made efforts to preparetechnical guidelines and material for coun-tries to adapt and to use in their nationalprogrammes.
Primary health care
5.3 There is increasing evidence fromall regions that many countries haveaccepted the primary health care approach.So that health care may be provided tounderserved or unserved populations,appropriate health services at local level,supported by a workable referral system,clearly must be developed. This activityis gradually taking place, not in isolationbut within the overall socioeconomicdevelopment process. Integrated ruraldevelopment, of which health is part, isbeing seriously considered by many coun-tries as a solution to constraints arisingfrom sectoral plans drawn up in isolation.Activities that are often considered to beoutside the health sector but have a greatimpact on health, such as the provision ofpotable water, are now being given toppriority, especially among the underserved
STRENGTHENING OF HEALTH SERVICES
populations. In some countries ruraldevelopment schemes with health as anintegral component are being assessed sothat the factors that have contributed totheir success may be taken into accountwhen future programmes are being planned.
5.4 In the African Region, 17 coun-tries have accepted the primary healthcare approach. The South -East AsiaRegion reports that eight countries haveformulated primary health care projects asan integral part of basic health services.Seven countries in the Eastern Mediter-ranean Region have shown interest in thesame approach. In the Sudan, a primaryhealth care programme has been developedin cooperation with several bilateralagencies. In Iran, research on the develop-ment of health services, stressing primaryhealth care delivery, is taking place. ManyMember States in the Western PacificRegion have initiated primary health careprogrammes with particular emphasis onthe development of health care workers.
5.5 The idea is also gaining acceptancein developed countries, where, despiteconstantly rising costs, health services donot necessarily meet the needs of the people.In the European Region, primary healthcare appears to hinge on four main issues :the relationship between social servicesand health services, the rapid increase inthe cost of health services, the role ofoutpatient treatment and health centres,and the function of professionals involvedin primary care. Studies are being carriedout on patterns of health delivery, forinstance on the role of polyclinics in theUSSR and on the outpatient approachin Algeria, Spain and Turkey.
5.6 In the Region of the Americas,Member Governments selected "Com-munity participation in health" as the themefor a public education campaign in 1977 ;
35
17 countries were reported as havingreceived technical assistance in improvingthe operation of community developmentservices. In the South -East Asia Region,several governments were experimentingwith various innovative approaches in-volving community participation throughvoluntary health workers, schoolteachers,practitioners of traditional medicine, healthcooperatives and insurance schemes.
5.7 Each regional office undertookactivities to promote the primary healthcare concept ; meetings were held at whichnationals were invited to share their ex-periences. For instance, the RegionalOffice for Africa convened an expert com-mittee on primary health care in March1977;1 follow -up action has been planned.The Regional Office for the Americas heldthree intercountry working groups onvarious aspects of primary health care :health service coverage (primary healthcare and community participation), techno-logy and administration and organization,subjects that were discussed by the IVthSpecial Meeting of Ministers of Health ofthe Americas in September 1977.
5.8 The Eastern Mediterranean Region,in line with resolution EM /RC25A /R15 andin an effort to promote primary health carein Member countries, formed a RegionalAdvisory Panel on Primary Health Carewith participants from nine countries. AUNICEF /WHO Inter -Agency Consultationon Primary Health Care was held inAlexandria in October 1977 to discussways of promoting and supporting primaryhealth care at country level and to planfuture inter- agency programming efforts.A joint UNICEF /WHO study on com-munity participation in health services
1 World Health Organization. Primary health care.Brazzaville, 1977 (AFRO Technical Report SeriesNo. 3).
THE WORK OF WHO
was completed in 1976 and the reportpublished.'
5.9 WHO, as a member of the ACCTask Force on Rural Development, isparticipating in country studies in inte-grated rural development, initially inBolivia, Lesotho, Liberia, Samoa andSomalia.
5.10 Research is of crucial importancein this field, especially in relation to theappropriateness, effectiveness and efficiencyof technology being developed and used,as well as to other operational aspects suchas training methodologies, organizationand community involvement mechanismsand evaluation. Consultative groups andthe global and regional Advisory Com-mittees on Medical Research formulatedrecommendations regarding priority areasfor research in health services development.
5.11 In the Republic of Korea baselinedata for operations research were collectedand a continuing education programmefor myun (district) health workers wasestablished. In the Philippines the findingsof an operational research study wereapplied in the development of a restructuredrural health service in which midwives withfurther training take charge of primaryhealth care clinics at the periphery.
5.12 In connexion with the acceptanceof the primary health care approach, thefunctions and training of various types ofhealth workers were reviewed in manycountries -the health guardian inHonduras, the sanitary worker in the NewHebrides and the barangay health workerin the Philippines. The guiding principle
1 Report of the 1977 UNICEFIW/HO Joint Com-mittee on Health Policy: Community involvement in primaryhealth care- a study of the processes of community moti-vation and continued participation (document Jczt/UNICEF -WHO /77.z Rev.z).
36
in this review is that all health interventionsshould be undertaken at the most peri-pheral practicable level of the healthservices by a worker suitably trained tofunction at that level. In some countriesseveral cadres of auxiliary workers arebeing developed ; in others nurses arebeing used in primary health care activitiesfor services and as teachers and super-visors. During 1976 -77 there were attemptsin many countries to make medical andnursing education more relevant to localneeds, with greater emphasis on com-munity care. In the Eastern MediterraneanRegion, nursing personnel form the largestsingle category of health personnel andwithout them the health services could notfunction : they are often the only healthworkers in community services, and prob-ably no other health worker has suchready access to the home.
5.13 Traditional medicine 2 was dis-cussed by a regional expert committeemeeting in Brazzaville in February 1976and by the Regional Committee for Africain Kampala in September 1976. The needwas expressed to improve the practice oftraditional medicine and to improve col-laboration between traditional healers,health team personnel, the public andauthorities. In many African countries,research is being carried out in the use ofmedicinal plants. In the South -East AsiaRegion, the Regional Committee in 1976emphasized the need to use traditionalsystems of medicine to complement"modern" medicine, so as to provide thecommunity with the best of both.
5.14 Collaboration with bilateral andnongovernmental agencies continued, notonly in the development of promotional
2 See also page 44.World Health Organization. African traditional
medicine. Brazzaville, 1976 (AFRO Technical ReportSeries No. 1).
STRENGTHENING OF HEALTH SERVICES
materials such as films but also in somecountries (for instance, Cape Verde,Guinea- Bissau, Rwanda and Sudan) in theform of exploratory negotiations, the pro-vision of cost and budget estimates andproject formulation itself. Planning for theInternational Conference on PrimaryHealth Care to be held in Alma -Ata, USSR,in September 1978 continued, and nationaldialogues and regional conferences tookplace, in close cooperation with UNICEF.Other organizations also expressed interestin the Conference and have organizedpreparatory conferences with WHO, suchas the WHO /New York Academy ofSciences Symposium on Primary HealthCare for the Industrialized Nations, heldin New York in December 1977.
5.15 WHO's technical programmes arebeing reoriented ; coordination at all levelsof the various programmes is vital to ensurethat wherever primary health care pro-grammes are being implemented the variousactivities are not developed in isolation.Much remains to be done, especially re-garding the development of suitableindices that Member States can use toassess the progress made in the develop-ment of health care and the overall improve-ment of the health status of their popu-lations.
Appropriate technology for health
5.16 The new programme of appro-priate technology for health, establishedfollowing the adoption by the WorldHealth Assembly of resolution wHAz9.74in May 1976, was launched in January 1977with a consultation to initiate a series ofprocedures in preparation for a longer -term programme. The ultimate goal is topromote national self -reliance in problem -solving in primary health care delivery.1977 was an extremely active year, withthe focus on the promotion of the concept,
37
planning and programming for the future,the development of an information system,research, and the initiation of countryactivities. An illustrated brochure definingand explaining the programme content wasprepared, articles appeared in WHO publi-cations, a photographic library was startedand an illustrated panel prepared forexhibition in the regions. The RegionalOffice for the Eastern Mediterranean organ-ized a meeting in November 1977 forWHO staff at country level.
5.17 As the first priority should be thedevelopment of technologies of directbenefit to local communities, a provisionallist of recognized needs for appropriatetechnology was sent as a checklist to coun-tries in all regions, and they were requestedto state their own requirements and prior-ities. Based on an analysis of countrystatements, a consultation in December19-77 established priorities for researchactivities and field projects and formulateda global plan of action relating to outputtargets, defining the four main functionsof the programme as : direct assistance tocountries, collaboration with selected insti-tutions, evaluation of progress, and thecollection and dissemination of informationon existing and new technologies. Asimplified health technology literature bankwas set up in the Regional Office for Africaand a contract was made with the Appro-priate Health Resources and TechnologiesAction Group in London, United King-dom, to establish a clearing -house toexplore the range of needs for informationservices and to identify groups capable oftaking responsibility for meeting theseneeds.
5.18 There are numerous researchactivities covering, for instance, villageobstetrics, oral electrolytes for rehydration,anaemia and vitamin A deficiency screening,and certain immunization technologies, in

THE WORK OF WHO
particular the "cold chain ". The aim isthat developing countries should parti-cipate fully by developing local solutions,drawing upon local traditions and re-sources and, where possible, setting up thelocal or intercountry production of toolsand techniques.5.19 The main activities will be atcountry level. Programmes were proposedby the regions (for the Lao People'sDemocratic Republic and the Philippines,for instance), their content discussed andfinancing explored ; preliminary steps weretaken to organize workshops and seminarsin 1978 ; discussions took place with allregions to establish, in certain countries,study areas for exploring the process ofproblem identification, design and fieldtesting of technologies and problemsrelating to acceptance, production, market-ing and evaluation.5.zo In the Region of the Americas,countries were encouraged to formulateappropriate technology policies and toassess new technologies in terms of theirimpact on existing national health facilitiesand maintenance programmes, their adapt-ability to special conditions in the country,their cost and their potential hazards.
5.21 The important question of main-tenance and repair of equipment has tendedto be neglected in the past. Special effortsin this connexion were made in the EasternMediterranean Region, where, in additionto cooperation in several national projects,it is planned to set up a regional trainingcentre in Iraq. All the other regionsacknowledged the need to help countriesto develop programmes in the main-tenance of health care facilities.
Health service development
Health care facilities
5.22 In 1974 a comprehensive study ofthe planning, programming, design and
38
architecture of hospitals and other healthcare facilities in developing countries wasundertaken by WHO. The study attemptedto bridge the gap between existing knowl-edge and experience and their practicalapplication. Its final outcome will be theimplementation of technology appropriateto the development of health care facilities,and practical advice on all phases of devel-opment, from area -wide planning to equip-ment, maintenance, operation and adminis-tration. In November 1976 a meeting ofinvestigators identified the difficulties metin the planning, design and operation ofhealth care facilities in developing areas ;examined ways of solving problems; andreviewed the relevance of the WHO studyand advised on its content, its furtherdevelopment and the application of itsresults.
5.23 Reactions to the first volume ofApproaches to Planning and Design of HealthCare Facilities in Developing Areas,' publish-ed in 1976, demonstrated the timeliness ofthe study. It fills a gap not only for devel-oping countries but also for professionalsfrom developed countries, who often donot realize to what extent their trainingand experience are out of phase with theconditions and needs of developing coun-tries. A case study project will be under-taken in this connexion, with the followingobjectives : to identify the range of existingoptions, together with constraints andproblems; to verify in practice the use-fulness of various standards and criteria;and to provide the basis for linking testedtechnologies relating to the planning,design and functioning of health carefacilities with relevant national and WHOprogrammes and projects.
5.24 An interregional seminar on theorganization and management of out-
World Health Organization. Approaches to planningand design of health care facilities in developing areas, Vol. I.Geneva, 1976 (WHO Offset Publication No. 29).
STRENGTHENING OF HEALTH SERVICES
patient health care and ambulatory healthservices took place in Sofia, Bulgaria, inOctober 1977, and was attended by parti-cipants from French -speaking countries.
5.25 In the African Region, most coun-tries have embarked on structural reor-ganization of their health networks toimprove coordination; zo countries haveregionalized their services. Concern forrationalization is also reflected in effortsto strengthen hospital administration, asin the Comoros, Mali, Mozambique andTogo.
5.26 In the Region of the Americas, theincreased demand for medical care innational and regional hospitals stimulatedefforts to strengthen the role of localhospitals and to relate them more effectivelyto the primary care service network. Theintroduction of progressive patient careschemes at the hospital level providesanother important means of tailoring theuse of resources and technologies to themedical requirements of the individual andthe community. Experience gained inBrazil, Chile, Colombia, Peru and Uruguaycan be applied in programmes aimed at amore efficient and effective utilization ofthe present capacity of the 13 000 hospitalsin Latin America.
5.27 At the current stage of develop-ment of health services, ambulatory carehas become very important in rural andurban areas as it facilitates the channellingof medical technologies concentrated inhospitals towards the peripheral healthcare network. An important project forthe development of ambulatory serviceswas undertaken in Managua, Nicaragua.
5.28 In the South -East Asia Region,governments, with WHO collaboration,are operating a number of national projectsto develop a well -organized referral system
39
in support of primary health care as part ofthe national health services. A nationalhealth programming exercise in Thailandidentified the provincial care project as oneof its most important projects, the mainobjective being to provide integrated,preventive, promotive, curative, and re-habilitative medical care to the under -served rural population. Particular atten-tion is being paid to increasing the provi-sion of primary health care and the two -wayreferral services - health centre to districthospital to provincial hospital, and viceversa.
5.29 In many countries of the EuropeanRegion, the provision of medical carerequires the more active participation ofgovernment (central and local), insurance,welfare and other organizations. For thisreason, during 1976-77 special stress wasplaced on planning for medical institutions,the study of economic aspects of medicalcare and its impact on health, the improve-ment of management standards and the useof experimental models and operationalresearch.
5.30 With the socioeconomic changesin the Eastern Mediterranean Region, therehas been an upsurge in the building of newhospitals, accompanied by increased effortsto modernize and expand hospital servicesin almost all countries of the Region.Improved planning, design and manage-ment, and the integration and regionaliza-tion of services are recognized needs.During the past few years, notable improve-ments in hospital architecture, design andadministration have been effected in Iran,Jordan, Pakistan, Syrian Arab Republicand Yemen. A national course in trainingin hospital administration, sponsored byWHO in collaboration with the NationalInstitute of Public Administration, wasorganized in Lahore, Pakistan, in Decem-ber 1976.
THE WORK OF WHO
5.31 In the Western Pacific Region, anumber of operations research studies andmedical care administration projects werefurther developed in order to improvehealth service design and operation. In thePhilippines the second phase of the opera-tions research study of the rural healthservices was completed. The purpose wasto develop an effective management systemwith components of supervision, supplyand information monitoring to support therestructured health service delivery system.In the Republic of Korea, a study wasundertaken in collaboration with UNICEFto develop and improve health servicedesign for use in the delivery of health careto the rural population.
Utilization of medical care
5.32 The results of the WHO /Inter-national Collaborative Study on MedicalCare Utilization were published in 1976.1In order to provide a guide for policy -makers, a practice- oriented version waspublished in 1977.2
Emergency care
5.33 Recognizing that preparation fornatural or man -made disasters can greatlyreduce the toll in lives and human misery,a growing number of countries are pre-paring emergency health plans. A steadyincrease in the number of medical emer-gencies in countries of the Eastern Medi-terranean Region was noted by Sub -Committee A of the Regional Committeein 1976, which urged the Regional Directorto continue WHO collaboration in devel-
1 Kohn, R. & White, K. L., ed. Health care : Aninternational study. London, Oxford University Press,1976.
2 White, K. L., Anderson, D. O., Kalimo, E.,Kleczkowski, B. M., Purola, T. & Vukmanovie, C.Health Services : Concepts and information for nationalplanning and managements. Geneva, World HealthOrganization, 1977 (Public Health Papers, No. 67).
40
oping emergency medical services and toconsider establishing a Regional AdvisoryCommittee on this subject (resolutionEM /RC26A /R9).
5.34 To give persons responsible fororganizing emergency medical services anopportunity to study experience in othercountries, in 1976 WHO organized aninterregional travelling seminar in Iranand the USSR. Officials from seven coun-tries of the Eastern Mediterranean Region(Egypt, Iran, Iraq, Kuwait, Libyan ArabJamahiriya, Pakistan and Sudan) took part.
Financing of health services
5.35 As part of the overall effort tostrengthen national health services, methodsof financing the health sector, includingthe non -public part, were studied. Indeveloped countries the rising costs ofhealth services were a major cause ofconcern; in developing countries lack offunds, lack of coordination between dif-ferent sources funding health activities, andthe considerable difference between healthexpenditure in practice and the declaredpolicies of equitable distribution of fundsand services were identified as majorproblems.
5.36 Problems of rising costs of medicalcare under social security and possible costcontainment measures were extensivelydiscussed at an expert meeting organizedby ILO in May 1977 with the activeparticipation of WHO.
5.37 A WHO study group in November1977, attended by representatives of severalbilateral and multilateral aid agencies andtechnical organizations, examined data col-lected in a worldwide survey of methodsof financing health services. Major problemareas were identified, mainly in developingcountries, such as lack of funds, lack of
STRENGTHENING OF HEALTH SERVICES
coordination of resources, inequitable dis-tribution of available funds, and inade-quate attention to cost aspects. Case studieswere provided from three Latin Americancountries and three European countries, aswell as from Bangladesh, Republic ofKorea and Senegal. The group consideredsome approaches to solving the mainproblems, such as the mobilization ofnew sources of financing, and the suitabilityof social security and health insuranceschemes in developing countries. Low -cost methods for surveying a country'shealth sector financing were identified thatcould be used to assess the possible discre-pancies between intended health policiesand reality and to stimulate correctiveaction.
Disability prevention and rehabilitation
5.38 There are probably some 400million disabled persons in the world, mostof whom do not receive attention fromrehabilitation or other services. Healthservices have always been geared to mor-tality- related problems rather than todisability, and governments have givenlow priority to the promotion of servicesfor the disabled. Such services are notlacking : on the contrary, some US $ zoomillion is contributed annually to servicesin developing countries by voluntary andnongovernmental organizations. They are,however, unevenly distributed, giving a fewpatients, mainly in capital cities, long -term,high -cost institutional care, often by expa-triate staff using sophisticated equipment.
5.39 1976 saw a major step forward inattempts to create change. A totally newpolicy and programme was discussed bythe Governing Bodies, and the WorldHealth Assembly recommended reorienta-tion towards the introduction of effectivemeasures for disability prevention, with theapplication of rehabilitation at the primary
41
health care level (resolution wHAz9.68).The first step must be a survey of thepopulation's needs ; in 1976 -77 surveysbegan in five countries with SIDA support.New policies on manpower were developed,involving the use of simply but adequatelytrained multipurpose community -basedworkers rather than specialized rehabilita-tion teams to provide therapy. Projectsrelated to the prevention of disability in theproductive age are planned for threecountries. Since 1975 cooperation withorganizations within and outside the UnitedNations system has increased, and jointdiscussion and action for planning coopera-tion in the field is now the rule rather thanthe exception.
5.40 In the Region of the Americas,cooperation in rehabilitation activities wascontinued. A prosthetics school in Argen-tina was reorganized. A plan was preparedto consolidate rehabilitation services on anational basis in Bolivia. Collaboration wasestablished with the Sarah KubitschekCenter, Brasilia, for training rehabilitationstaff at all levels. In Chile a fellowship wasprovided in speech therapy. In Colombiatraining courses in rehabilitation werestarted for doctors, and special courseswere included in a seminar in Medellín.Consultations were held in Guatemala onthe possibility of integrating rehabilitationactivities into existing basic health services.Cooperation was strengthened between theschool of physical therapy in Jamaica andinstitutions in other English- speaking coun-tries and territories in the Caribbean.Assistance was likewise provided to Mexicoin postgraduate courses for physiotherapistsand occupational and speech therapists.A course in respiratory rehabilitation wasgiven for doctors, and the Organizationparticipated in a national study group onsocial rehabilitation. In Uruguay rehabili-tation services were promoted in ruralareas. In Venezuela a course for doctors
THE WORK OF WHO
in cardiopulmonary rehabilitation wasgiven, and research was begun on theidentification of patients needing rehabilita-tion services at the primary health care level.
5.41 In the South -East Asia Region, aseminar on medical rehabilitation wasorganized in August 1977. In Burma ateam of specialists in occupational therapy,orthopaedics and rehabilitation and physio-therapy assisted in the planning, organiza-tion and establishment of a school foroccupational therapists and advised onteaching. Problems in orthopaedics andrehabilitation were reviewed and advice wasgiven on the planning and development ofthe Kemmendine Orthopaedic Hospital.A four -week national intensive course ofpractical exercise therapy in rehabilitationfor physiotherapists was also held. In India,WHO collaborated in the organization of anational workshop on disability preventionand medical rehabilitation, psychology,physiotherapy, prosthetics and orthotics,health education and social welfare.
5.42 The European Region was closelyinvolved in a study carried out in Yugo-slavia on disability in the productive age,and a national symposium on the subjecttook place in February 1 977. The increasedmortality and morbidity resulting fromroad traffic accidents in Europe led theRegional Office to develop a Europeanprogramme on prevention which nowforms the nucleus of a WHO globalprogramme. Another programme beingdeveloped as a result of concern voiced byMember States relates to the phenomenonof an aging population, with all its econ-omic, social and health implications. Thisconcern motivated the Regional Com-mittee meeting in Algiers in 1976 to invitethe Regional Director to develop a com-prehensive programme on the health careof the elderly.
42
5.43 In the Eastern MediterraneanRegion, which has fairly extensive rehabili-tation programmes, WHO mainly sup-ported the training of relevant personnelbut also helped in organizing and strength-ening rehabilitation departments, in settingup prosthetic and orthopaedic workshopsand by providing supplies for the produc-tion of prosthetic aids. An important partof the programme is the work of theRegional Training Centre for TechnicalOrthopaedics in Teheran, Iran, which ° hascontinued to train orthotist /prosthetistsfrom countries within and outside theRegion. In Afghanistan, WHO activitiesare now focused on providing supplies andequipment for the production of prosthe-tic aids. In Jordan, Lebanon, Pakistan,Saudi Arabia and the Syrian Arab Republic,the training of prosthetic and orthotictechnicians or of physiotherapists andoccupational therapists was supported.
Health planning
5.44 WHO cooperated with countriesin developing their capabilities to formulate,implement and evaluate their health poli-cies, plans and programmes in a wayconducive to social promotion and econ-omic development. Country healthprogramming, with WHO collaborationin national efforts, took place in Burma,Guinea- Bissau, Nigeria and Sudan, as wellas in related training workshops in Burma,Mozambique and Nigeria.
5.45 In the Region of the Americas,countries concentrated on redefining na-tional health plans with the aim of extendinghealth care coverage in rural areas. Brazil,Colombia, Costa Rica, Guatemala, Haiti,Honduras, Mexico, Nicaragua and Para-guay were involved in this process ; Bolivia,Ecuador and El Salvador completed it.The Pan American Health Planning Pro-gramme ended in December 1976 after a
STRENGTHENING OF HEALTH SERVICES
five -year period of UNDP assistance. Theinterregional project on ComprehensiveHealth Planning in Colombia, which under-took research in the development of severalhealth subsystems, ended in December1 977.
5.46 In the South -East Asia Region,country health programming projects wereformulated : in Burma, which now has 6service programmes ; in Nepal, where theHealth Planning Unit received assistancein developing the information base neededfor implementing and evaluating 12
health projects ; and in Thailand, where19 health projects were established. InIndonesia, national health planning wasevaluated at a meeting of the Joint WHO/Indonesia Coordinating Committee inNovember 1976.
5.47 In the European Region, effortswere concentrated on information onhealth planning systems and on relatedtraining. Activities are increasingly beingdevoted to evaluation and research, includ-ing studies comparing several countries'planning approaches. A planning meetingand a workshop were held in Copenhagenin December 1976 and June 1977 respectivelyon behalf of the Regional Office for theAmericas and PAHO. Case studies fromseveral European countries were finalizedas part of a worldwide review of healthplanning methodologies.
5.48 A first Coordination Meeting onEconomics and Health was held inCopenhagen in July 1976 at the sug-gestion of the European Medical ResearchCouncil. It was recommended that theRegional Office for Europe should assumeresponsibility for coordinating activities inthe field of health economics. A workinggroup on the role of health economics andplanning in the development of nationalhealth policy was organized in Cologne,
43
Federal Republic of Germany, by theRegional Office in June 1977.
5.49 In Eastern Mediterranean coun-tries, health services have developed tosuch a degree that many governments havebeen able to formulate long -term nationalhealth plans. Three countries (Pakistan,Sudan and Yemen) have initiated or arecontinuing country health programming.
5.5o In the Western Pacific Regioncountry health programming was begunin Fiji and Samoa in 1976. Health planningand management activities were expandedthrough an intercountry project providingtraining and advisory services in planningand programming, project formulation andmanagement, operations research, infor-mation systems development and economicanalysis.
Health service information
5.51 The continuous improvement ofan information base for the management ofhealth delivery systems in Member coun-tries is an important aspect of WHO'stechnical cooperation programme. Thissubject was discussed in regional AdvisoryCommittees on Medical Research andRegional Committees (during the TechnicalDiscussions in the case of the South -EastAsia and European Regions).
5.52 Regions oriented their health sta-tistical activities to promote the establish-ment at country level of informationservices in line with the needs for manage-ment of health delivery systems. In coun-tries where health planning is in progressor the reorganization of specific healthprogrammes had been undertaken, theinformation base received great attention.Country health programming proved to bean important entry point and a catalyst forthe development of management informa-tion systems.
THE WORK OF WHO
5-53 In the African Region, WHOcontributed to the development of healthinformation systems in six countries(Burundi, Lesotho, Nigeria, Rwanda, Zaireand Zambia).
5.54 In the Region of the Americas,Bolivia, Colombia, Costa Rica, El Salvador,Honduras and Peru were designing andimplementing information systems as partof their health management processes, withemphasis on incorporating such systemsinto programmes for extending healthservices coverage to rural populations andmarginal periurban areas.
5.55 In the South -East Asia Region thedevelopment of health information systemsis considered a priority for effective planningand management. As a result of countryhealth programming, projects for establish-ing such systems were developed inBurma, Nepal and Thailand. Indonesiainstituted a number of experimental projectsaimed at improving the management ofhealth centres, and Mongolia was devel-oping a national health information system.
5.56 In the European Region the mea-surement of levels of health as a basis forassessing the need for and the outcome ofhealth service interventions was debated bya working group in Nieberow, Poland, inMarch 1977. A meeting in Copenhagen inDecember i 976 focused on information onthe health of the elderly, the use of thehealth services by the elderly and the pre-diction of demographic changes in thepopulation's age structure. The SecondJoint ECE/WHO meeting in Geneva inOctober i 976 considered the integration ofvarious components of health informationsystems with other (e.g., social and demo-graphic) systems, and a Joint InternationalFederation for Information Processing/WHO Working Group in Prague, Czecho-slovakia in August 1976 examined the
44
development of health data banks and theiruse in health service management. WHOcollaborated with Algeria, Iceland andMorocco in developing components oftheir health information systems.
5.57 In the Eastern MediterraneanRegion a number of countries were devel-oping health information systems or sub-systems in collaboration with WHO.Projects were formulated in Kuwait, LibyanArab Jamahiriya, Qatar, Saudi Arabia andthe United Arab Emirates. In Sudan thedevelopment of a management informationsystem was an important element in theformulation of a primary health care pro-gramme.
5.58 In the Western Pacific Regionactivities to strengthen information systemsat country level included cooperation withMalaysia in developing a comprehensiveinformation system to support planningand management; a similar effort is under-way in the Philippines.
5.59 Research continues to be focusedon the development of better indicators,lay reporting, primary health care and theneed to evaluate different aspects of healthservices, with special emphasis on coverage.
Traditional medicine
W7HO's action programme
5.6o Following the publication of thereport of a joint UNICEF /WHO study 1recommending the mobilization and train-ing of practitioners of traditional medicine,including traditional birth attendants, forprimary health care services, several Mem-ber States enquired about follow -up action
1 Djukanovie, V. & Mach, E. P., ed. Alternativeapproaches to meeting basic health needs in developing coun-tries. Geneva, World Health Organization, 1975.
STRENGTHENING OF HEALTH SERVICES
by the Organization, particularly regardingthe promotion and development of theirrespective traditional and indigenous sys-tems of medicine. A small group consulta-tion was held and in January 1976 thesubject was considered by the ExecutiveBoard. The following action was proposed :
(I)
(2)
(3)
(4)
(s)
Collecting all available data on tradi-tional healers and indigenous sys-tems of medicine -the results ofsurvey and research findings, of stu-dies of traditional practices, and oftraining programmes for traditionalhealers and indigenous practitioners.Analysing the available informationin order to determine the relevanceof traditional healing to the primaryhealth care needs of the variouspopulations.Studying, in the field, existing sys-tems of traditional or indigenousmedicine in each Region.Suggesting the main directions foraction, with special regard to thetraining of traditional healers andtheir utilization in the health system.Suggesting further action in thisfield by Member States, and by theWHO Secretariat.
5.61 An interdivisional working groupwas formed at headquarters to coordinatethe various activities. The regions initiatedtraining programmes for practitioners oftraditional medicine, including traditionalbirth attendants, and orientation coursesfor physicians, nurses, midwives and otherhealth workers. Studies and research wereundertaken to ensure the further develop-ment of services and the application ofsimple technology in the work of thesepractitioners. In October 1976 regionaloffice representatives concerned with tradi-tional medicine met in New Delhi andproposed the following programme objec-tives : (I) to foster a realistic approach to
45
traditional medicine, in order to promoteand further contribute to health care;(2) to explore the merits of traditionalmedicine in the light of modern science, inorder to maximize useful and effectivepractices and discourage harmful ones ;and (3) to promote the integration of provenvaluable knowledge and skills in tradi-tional and scientific medicine.
5.62 High priority would be given tothe developing countries, particularly asregards primary health care within thecontext of each country's political struc-ture, economic resources and developmentplans. The programme would be carriedout in close collaboration with the regionaloffices and primarily at the country leveland with active community participation.The suggested approaches included theformulation of national health policies thatwould contain provisions concerning tradi-tional medicine and mechanisms for the
and utilization theuseful elements of traditional medicine inthe country's health care system. Theadministrative machinery needed to ensureeffective planning, utilization and super-vision of practitioners of traditional medi-cine would be reviewed within the contextof the national health care delivery system.
5.63 Multidisciplinary investigations onsystems of traditional medicine would beencouraged, and special attention given tolaboratory and clinical investigations identi-fying effective remedies comprising medi-cinal plants, animal products, and mineralsubstances. Investigations would also beconducted on psychosocial and anthropo-logical aspects of traditional medicine,as well as on acupuncture, moxibustionand other healing methods. Whereverpossible priority would be given to thedevelopment of useful local resources suchas herbs for the production of medicinalsubstances.
THE WORK OF WHO
Research and studies
5.64 Many claims are made concerningthe control and cure of diseases by healersand practitioners of traditional medicine.Recently, reports have been received thatherbs are being used in several tropicalcountries for the control of diabetes mellitusand the management of rheumatoid arthri-tis. Such claims need to be investigatedscientifically; efforts are therefore beingmade to locate collaborating centres withthe facilities to undertake such work.
5.6 5 In May 1977 the World HealthAssembly urged interested governments togive adequate importance to the utilizationof their traditional systems of medicinewith appropriate regulations as suited totheir national health systems ; requested theDirector -General to assist Member Statesto organize educational and research activi-ties and to award fellowships for trainingin research techniques, for studies ofhealth care systems and for investigatingthe technological procedures related totraditional /indigenous systems of medicine ;and further requested the Director -Generaland the Regional Directors to give highpriority to technical cooperation for theseactivities and to consider their appropriatefinancing (resolution WHn30.49).
5.66 As a follow -up to this resolutiona study tour on traditional medicine in
community health services was organizedin China in August 1977, with 29 partici-pants from the same number of developingcountries. The main purpose was to studythe manner in which China has harnessedits legacy of traditional medicine to theneeds of its vast rural population and hascombined the traditional Chinese systemwith western medicine. The group studiedthe training of health personnel, includingpractitioners of traditional Chinese medi-cine and barefoot doctors. The group alsoexamined the preparation and use of medi-cinal herbs, the production of pharmaceu-ticals and the use of special methods suchas acupuncture. Agricultural practices,irrigation projects, housing schemes andrural development were also studied.
5.67 A consultation held in Geneva inNovember -December 1977 reviewed andendorsed the Organization's programme ontraditional medicine, and made recommen-dations on future action regarding thecollection and analysis of informationrelating especially to the role and functionsof the various practitioners of traditionalmedicine, including birth attendants, andtheir training ; the integration of traditionalsystems with modern medicine ; and variousresearch activities and studies to be pursued,with particular reference to primary healthcare.
46
Chapter 6
Farni'y flea it/i
6.,THE ORGANIZATION is now
facing the challenge of promotingfamily health care, in particular
as an integral part of primary health careand rural development. There is a need toidentify more clearly the problems andneeds of the family as a whole, as well as toimprove and reorient health care on thebasis of the family as a unit of care. Familyhealth care ultimately depends upon theeducation of family members about theirresponsibilities for their own health care,and upon health workers, who must, seebeyond the individual to the family andcommunity.
6.2 The health sector is not the onlysector involved in meeting the basic healthneeds of the family ; many family healthactivities are part of broader, intersectoralprogrammes. In 1976 -77, special activitiesfor the promotion of integrated develop-ment were carried out in connexion withthe status of women, with population andwith nutrition as they relate to health anddevelopment. During i 976 both the Exec-utive Board and the World Health Assem-bly discussed women's health, womenas health care providers, and womenin health and development in general. Inaccordance with resolution wxn29.43adopted in 1976, working groups reviewedissues relating to women in WHO's pro-grammes, highlighting the specific health
47
needs of women and the contribution ofwomen in the health sector. During1976 -77 WHO worked closely with theUnited Nations and organizations withinthe United Nations system to develop aninterorganizational programme for theWomen's Decade of Equality, Peace andDevelopment, following the adoption bythe United Nations General Assembly ofResolution 35 20 (xxx) in December 1975.
6.3 Population issues are regarded asan integral part of overall development,including health development. WHOworks through the ACC subcommittee onpopulation to harmonize the activities ofthe United Nations agencies in this field,and participates in the interagency taskforce that is developing a common con-ceptual framework, with models. Suchmodels can serve not only as a basis fornational coordination of programmesamong the development sectors but alsofor facilitating technical cooperation. TheOrganization also contributes to the moni-toring, review and appraisal of follow -upactions to the World Population Plan ofAction, which contains major sectionsdirectly related to WHO's programme ofwork. The Plan includes various resolu-tions on fertility and health and on thereduction of maternal and infant mortalityand morbidity. The data compiled andanalysed for this exercise will therefore

THE WORK OF WHO
provide a valuable basis for the evaluationof health programmes, especially those inmaternal and child health and familyplanning.
Maternal and child health
6.4 The years 1976 and 1977 weremarked by increased technical cooperationat the country level, with its emphasis ondeveloping local strategies to providematernal and child health care that meetsthe specific needs of given communitiesand suits the life -style of the populationsconcerned. This approach was in line withrecommendations by the WHO ExpertCommittee on Maternal and Child Healthand endorsed in national and internationalmeetings and seminars.
6.5 The Organization worked withalmost all the developing countries instrengthening the maternal and child healthcare component of health services, usuallywith family planning as an integral part.Specific country projects emphasizing ser-vice organization, administration, or train-ing were implemented in more than 7ocountries. Table 6.1 lists 6z countries andareas where there were projects, existingor planned in 1976 -77, in which WHO, asexecuting agency, collaborated withUNFPA ; the projects were supported byWHO intercountry family health teams andby 32 WHO staff members at the countrylevel. These activities at country levelaccounted for 75% of the total funds pro-vided by UNFPA in 1977. During 1976-77the number of new country projects in-creased by about 5o% in the African andEastern Mediterranean Regions. Thecountry projects reflect the diversity in thetypes of new or expanded national pro-
WHO Technical Report Series, No. Goo, 1976.
48
grammes being developed. In parts ofAfrica, for example, in addition to commonmaternal and child health problems, in-fertility is a major concern ; the Organi-zation worked with the Central AfricanEmpire, Congo, Gabon, Sudan and theUnited Republic of Cameroon in analysingthe problem. In Mexico and Thailand, theemphasis was on the extension of familyplanning to provide nationwide coverage ;in Morocco, Nepal and Viet Nam, on thepromotion of maternal and child health,with child spacing or family planning ; inIraq, on the reorientation of maternal andchild health care, to reach rural populations.
Table 6.1 Countries and areas with family health/family planning projects, 1976 -77 a
TotalAfrican RegionBotswana, Burundi, Central African Empire, Congo,
Gambia,' Guinea, Guinea -Bissau,° Kenya, Lesotho,Liberia, Mali, Mauritius, Nigeria, Seychelles,°Sierra Leone, Swaziland, Togo, United Republicof Tanzania 18
Region of the AmericasBolivia, Brazil, Chile, Colombia, Cuba, Dominican
Republic, Ecuador, Haiti, Honduras, Mexico, Peru,St Kitts -Nevis, St Vincent 13
South -East Asia RegionBangladesh, Indonesia, Mongolia, Nepal, Sri Lanka,
Thailand 6
European RegionAlgeria, Morocco, Turkey 3
Eastern Mediterranean RegionAfghanistan, Democratic Yemen, Egypt, Iran, Jordan,
Pakistan, Somalia,° Sudan, Syrian Arab Republic,Yemen 10
Western Pacific RegionCook Islands, Fiji, Gilbert Islands, Malaysia, New
Hebrides, Papua New Guinea, Philippines, Samoa,Solomon Islands, Tonga, Tuvalu, Viet Nam 12
62
With UNFPA funding.° Project request submitted but approval not yet received
at the end of 1977.
6.6 Most of these country projects hadbeen in progress for several years, andduring 1976 -77 attention was given to theseries of tripartite reviews and annualprogramme reviews that form part of theregular project monitoring system. Inaddition,1WHO was involved in eleven
FAMILY HEALTH
national programme evaluations. Certainevaluations led to concrete changes. In Chileand Haiti, for example, the evaluation pin-pointed areas where service extension wasdeficient, and changes were made to ensurewider coverage. In Malaysia, the evalua-tion led to a revision of the informationsystem, with emphasis on maternal mortality,which was found to be relatively high incomparison with infant and childhoodmortality. In Sri Lanka, the evaluationindicated the need to change to a simplermethod for treating gastroenteritis (e.g.,oral rehydration).
6.7 WHO and Member countriessought ways to reorientate maternal andchild health programmes within the pri-mary health care approach. This reorien-tation was the subject of seminars in theSouth -East Asia and Western PacificRegions in 1976 ; it requires the develop-ment of new strategies, better approachesto management, appropriate technology,and human resource development. Onemanagerial strategy being developed andpromoted by WHO is the risk approach,which uses health problem indicators toidentify levels of risk and to set prioritiesaccording to local circumstances and re-sources. The aim is to give special attentionto those in greatest need -and at greatestrisk -within a framework of basic healthcare for all mothers and children, achievedby maximum utilization of existing re-sources, including nonconventional com-munity resources such as teachers, tradi-tional birth attendants, and women'sgroups. Studies on the application of therisk approach were started in 1977 inMalaysia and Turkey. Based on the dataof the PAHO study on patterns of mortalityin childhood,' a new strategy of care was
1 Puffer, R. R. & Serrano, C. V. Patterns of mortalityin childhood : Report of the Inter- American Investigationof Mortality in Childhood. Washington, DC, Pan Ameri-can Health Organization, 1973 (Scientific PublicationNo. z6z).
49
being applied and evaluated in a few statesin Brazil.
6.8 A programme was initiated withthe International Planned ParenthoodFederation to re- examine the technologiescurrently being used in maternal and childhealth and family planning care, to identifythose technologies which require modifi-cation for use in the home or by auxiliariesand to identify areas where new techno-logies need to be developed. The develop-ment of appropriate technology for theperinatal period began in 1977, throughthe PAHO Latin American Center forPerinatology and Human Development,which has an on -going programme ofresearch on the simplification, cost reduc-tion and qualitative improvement of tech-niques for maternal care.
6.9 Other activities for the promotionof appropriate maternal and child healthcare technologies being applied at thecountry level included the distribution in1976 of a guide for use at the primary levelon the treatment and prevention of dehy-dration in diarrhoeal diseases, and in 1977operational research on the application ofthe oral rehydration technique describedin the guide was carried out in a few coun-tries in each Region.'
6.io The better utilization of local andtraditional human resources is fundamentalto primary health care. In four regions(Africa, the Americas, Eastern Mediter-ranean and Western Pacific), action wastaken to improve the utilization, trainingand supervision of traditional birth atten-dants in broader maternal and child healthcare. In the Region of the Americas,teaching materials for traditional birthattendants were prepared.
' See also page 101.
THE WORK OF WHO
6.1 i A strategy based on buildingnational self -reliance was evolved in 1976-77 in the field of human resources devel-opment. It emphasizes the systematicstrengthening of national institutionalcapacities to meet the maternal and childhealth and family planning service needsof the country, within the country. Thisstrategy is the basis of a programme ofteacher -training in fertility managementand maternal and child health care initiatedin 1977. Courses and other types of trainingactivity are supported only as part of amore comprehensive programme of man-power planning, adaptation of educationalmethods, and management skills develop-ment, carried out within the context oflocal situations. A multidisciplinary coregroup of persons involved in the trainingof all levels of health personnel in thecountry is made responsible for the devel-opment of the national programme. Theapproach is flexible and the nature of WHOinvolvement and support differs from coun-try to country. This type of programme be-gan in 1977 in the Sudan, as a complementto the national primary health care pro-gramme, and in Mexico, as part of thenewly inaugurated national family planningprogramme, which emphasizes the inte-gration of maternal and child health andfamily planning in rural areas. PAHO alsodeveloped a diagnostic and evaluativemethod for national human resources devel-opment in the area of maternal and childhealth and family planning ;, the methodwas applied experimentally in Brazil during1976 -77.
6.1 z In the field of management, PAHOcollaborated with the School of PublicHealth of Mexico and the University of theWest Indies in carrying out a programmeto improve the administration of familyplanning programmes ; it included thetraining of national administrators of familyplanning programmes from thirteen
50
countries in regional courses. PAHO alsoformulated guidelines on the use of indi-cators and service statistics for improvingprogramme management in this field. Thedevelopment of management _ skills alsoformed part of a course given by WHO incollaboration with the Government ofBulgaria for French -speaking senior ma-ternal and child health administrators fromdeveloping countries.
6.13 The systems approach proveduseful in the formulation and implemen-tation of projects. In Nigeria, for example,the management techniques and projectdesign developed with the project systemsanalysis method in Sokoto and NigerStates in 1973 were used as examples forprogramme development in the rest of thecountry during 1976 -77. The ` systemsapproach was used in Algeria to improvethe process of selection of appropriatetechnologies, based on the systematicanalysis of what actions were possible ateach level of the services, and on the pro-gramme objectives set.
6.14 Data on the physical and psycho-logical growth and development of childrenare important for national policy formu-lation and programme planning. WHO,through its collaborating centres on growthand development in Romania, Senegal, theUnited Kingdom and the USSR, is collect-ing such data and has also developed a fieldmanual on standardized procedures. Thestudies in Dakar are unique : they involvecollecting data on the growth and develop-ment of two generations.
6.15 The Regional Office for South -East Asia initiated a series of studies onthe main causes of high levels of peri-natal mortality and morbidity occurringin Burma, India and Sri Lanka. The datacollected will serve as the basis for orientingthe training of health workers and for
FAMILY HEALTH
effective intervention. The problem ofperinatal care in developing countries wasalso discussed in a workshop held inGimo, Sweden, with participants from allregions ; practical recommendations weremade on perinatal care in out -of- hospitalenvironments.
6.16 Low birthweight, a problem ofmajor public health significance, was re-viewed at a workshop organized jointlyby the Swedish Agency for Research andCooperation with Developing Countriesand WHO in Uppsala in June 1977, withparticipants from various disciplines in-cluding economics, sociology, paediatricsand obstetrics. Birthweight distributionand percentage of low birthweight wereconsidered to be a yardstick of development.An estimated 2z million low -birthweightinfants are born each year. This problemhas serious implications as regards notonly immediate survival but also the sub-sequent ability of the child to achieve itsfull potential. WHO set up a task force tostudy the extent and nature of low birth -weight, the contributing factors before andduring pregnancy and the practical inter-vention measures for prevention.
6.17 Infant feeding practices are criticalfor infant survival and health. Because ofthe importance of breast -feeding and therole of lactation in prolonging post-partum amenorrhoea, and thus birthspacing, WHO developed a multinationalresearch and education programme, work-ing closely with UNICEF and FAO, andin collaboration with SIDA and UNFPA.The countries involved are Chile, Ethiopia,Guatemala, Hungary, India, Nigeria,Philippines, Sweden and Zaire. During1976 -77, extensive epidemiological datawere collected on breast -feeding, and com-plementary social surveys were made onthis subject. On the basis of the data col-lected, a series of measures are now beingplanned and implemented. Many additional
51
countries and agencies have expressedinterest in the WHO collaborative pro-gramme and wish to participate.
6.18 A WHO Expert Committee onHealth Needs of Adolescents, meeting inGeneva in 1976, highlighted the need fora deeper understanding of adolescents intoday's rapidly changing societies and theneed for greater compassion and insightduring this transitional period.' A seriesof meetings arranged by the RegionalOffice for Europe during 1976 -77 reviewedthe problems of children in the 10 -13 and14 -18 age groups and the role of the family,school and community in preventing andtreating these problems. A survey oneducation and services meeting repro-ductive health needs of adolescents wasstarted, and physiologically orientedresearch on the effects of contraception onthe maturation process in adolescence wasalso begun.
6.19 A major cause of maternal andperinatal mortality is hypertensive diseaseof pregnancy (pre -eclamptic toxaemia),which is seen in most parts of the world.Its etiology remains unknown. It can occurin 0.5-35% of pregnant women and isresponsible for one -fifth to one -third ofall maternal deaths. In 1977, a meetingreviewed existing knowledge on the epi-demiology, clinical course, prevention andmanagement of this syndrome. Whilemore work is required on detection andprevention, the group emphasized that thewidely used treatment with diuretics is noteffective, and may even be harmful ; theyconfirmed the value of adequate antenatalcare, with appropriate diet and bed rest.
6.zo A number of countries, especiallyAsian countries, are now incorporatingsuch services as medical termination ofpregnancy and sterilization into their
' WHO Technical Report Series, No. 609, 1977.
THE WORK OF WHO
national maternal and child health andfamily planning programmes. WHOtherefore prepared guidelines for femalesterilization to provide up -to -date, accurateinformation on the technical and organi-zational aspects of introducing this type ofservice.' In India, the Organization alsosupported teacher -training for healthprofessionals in the medical termination ofpregnancy.
6.21 WHO's activities in maternal andchild health are carried out in close col-laboration with many nongovernmentalorganizations and United Nations bodiesin various fields related to health and devel-opment (role and status of women, socialproductivity of youth, social services andlegislation for women and children) :UNICEF, the International Federation ofGynecology and Obstetrics, the Inter-national Children's Centre, the InternationalPaediatric Association, the InternationalPlanned Parenthood Federation and manyothers. During 1976-77, a review wasmade of the legislative and service aspectsof day care approaches, and a project wasstarted with UNICEF in Bangladesh.Activities were carried out with the Inter-national Federation of Gynecology andObstetrics and the International PaediatricAssociation, to strengthen the contributionof the professional organizations to socialpaediatrics and social obstetrics. Prepara-tory work began for the International Yearof the Child, proclaimed for 1979 by theUnited Nations General Assembly.
Nutrition
Multisectoral approach
6.2z Although the health sector hasdefinite and important responsibilities in
' World Health Organization. Female sterilization :Guidelines for the development of services. Geneva, 1976(WHO Offset Publication No. z6).
52
preventing and alleviating the effects ofmalnutrition, the multisectoral causalfactors involved can only be correctedin cooperation with other sectors. WHOhas therefore made special efforts to co-ordinate its work in nutrition with that ofother agencies concerned with food,nutrition and related fields. During 1976-77 working relations were strengthenedwith UNICEF, FAO, IBRD, and bilateralagencies interested in nutrition. Collabo-ration began with the new United NationsUniversity. Cooperation with these andother agencies included the organizationof joint expert committee meetings, con-sultations, workshops and other scientificmeetings, the establishment of interagencyworking groups on specific subjects, andthe organization of joint missions fortechnical collaboration with countries.Collaboration also extended beyond theUnited Nations system to bring expertisefrom many scientific disciplines into inter-national work. New institutional arrange-ments included the creation of an ACCSub -Committee on Nutrition with a per-manent secretariat and an advisory group,which will replace the former Protein -Calorie Advisory Group.
6.23 In any country, nutrition of thepopulation has to be considered withinnational development strategies. Eachaspect of planning and programming fornutrition improvement is a component ofsocioeconomic development plans, andapproaches must vary according to theparticular national conditions, resourcesand opportunities. The ninth report of ajoint FAO /WHO Expert Committee onNutrition, dealing with food and nutritionstrategies in national development, waspublished in 1976.2 This subject wasfurther debated in the Technical Discussions
2 WHO Technical Report Series, No. 584, 2976.
FAMILY HEALTH
held during the sessions of the RegionalCommittee for South -East Asia held in1976 (" Development of national nutritionprogrammes, with special attention to thevulnerable sectors of the population"),the Regional Committee for Africa in1977 (" The importance of nutrition insocioeconomic development "), and theWorld Health Assembly in 1977 (" Theimportance of national and internationalfood and nutrition policies for healthdevelopment "). The Health Assemblyadopted a resolution (wHA3o.51) whichrequested that a higher priority be givento nutrition -oriented programmes inMember States and in the Organization,and that WHO take specific actions tostrengthen the programme of cooperationin this field with its Member States.
6.24 In the Region of the Americas,the Interagency Project on National Foodand Nutrition Policy, the institute of Nutri-tion of Central America and Panama, andthe Caribbean Food and Nutrition Institutecooperated with Barbados, Bolivia, Brazil,Chile, Colombia, Cuba, Guatemala, Hon-duras, Jamaica, Nicaragua, Paraguay andTrinidad and Tobago in developing foodand nutrition policies. In other regions,coordination for technical cooperation withcountries in this field is arranged on anad hoc basis ; for example, WHO workswith UNICEF and FAO in Senegal andMalaysia, and with IBRD in Indonesia.
Nutritional surveillance
6.25 The need to establish a nutritionalsurveillance system is felt by many coun-tries ; such a system is seen as providingan early warning of disasters or as a basisfor planning and evaluating programmes.A nutritional surveillance system is animportant component of any action pro-gramme and WHO is making efforts to
53
cooperate with countries in extending itsuse.
6.26 The report of a joint FAO/UNICEF /WHO Expert Committee on themethodology of nutritional surveillancewas published in 1976,1 and a workinggroup of the three organizations wasestablished to coordinate technical co-operation with countries. Guidelines forthe presentation and use of height andweight data of children, as well as anthropo-metric reference data for international use,were developed in collaboration with othersworking in this field. The significance andvalidity of certain indicators are being testedin WHO -supported field studies in India,Israel, Italy and Yugoslavia. Develop-mental work on national systems of nutri-tional surveillance was undertaken in thePhilippines and Sri Lanka. In Africa,nutritional status assessments were madein Angola, Botswana, Cape Verde, Congo,Kenya, Mauritania, Mozambique, Nigeria,Rwanda, Senegal, Uganda, United Republicof Tanzania, Upper Volta and Zaire. InColombia, the Organization cooperatedin developing a model national food andnutritional surveillance system using exist-ing information being collected in differentsectors for other purposes.
Nutrition in health services
6.27 Nutrition is not an independentactivity within the health sector but mustbe closely linked or integrated with otherrelated programmes such as maternal andchild health, family planning, preventionand treatment of diarrhoeal diseases, con-trol of infectious diseases, and other ele-ments of basic health services ; this isparticularly true at the primary level ofhealth care. During 1976 -77 the Organi-
1 WHO Technical Report Series, No. 593, 1976.
THE WORK OF WHO
zation ..stressed the importance of inte-grating nutrition with health services.Three consultations were held, to reviewnational experience or develop guidelinesin this respect : in Teheran, Iran, on strate-gies in nutrition through local health ser-vices ; in New Delhi, India, on the opera-tional integration of nutrition with familyplanning programmes ; and in KualaLumpur, Malaysia, on nutrition in familyhealth. Operational methodology in thedelivery of nutrition and nutrition -relatedactivities such as family planning wasstudied in India, Somalia, Thailand andthe United Republic of Tanzania with thesupport of UNFPA and the InternationalPlanned Parenthood Federation. Thetechnical discussions in the South -EastAsia Region mentioned above were fol-lowed up in 1977 by a regional meeting onnutrition in health services. With the shiftof priority to effective intervention as partof the primary health care approach, theOrganization began a reassessment oftechnologies and approaches used in nutri-tion ; many will need to be revised andadapted for use in the home and at theperiphery, while new ones will have to becreated. One aspect on which work startedin 1976 -77 was the home preparation ofweaning foods from locally available foods ;WHO supported field studies on this pos-sibility in India and Sudan. A more sys-tematic approach is required to the wholearea of appropriate technologies in nutri-tion and will be developed in the comingyears.
6.z8 For many years, nutrition edu-cation has been recognized as a majorfunction of the health services in pre-venting malnutrition. However, the expe-rience of national services in this respecthas often been unsatisfactory and theeffectiveness of the activity has not beencarefully evaluated, particularly in relationto primary health care. In 1977 WHO,
54
in collaboration with UNICEF and FAO,undertook a comprehensive review andanalysis of experience in this field. Also,the directors of major international trainingcourses in public health nutrition met inGeneva in 1976 to identify the requirementsfor specialized personnel, in terms ofnumbers and capabilities.
6.29 The horrors of natural or man-made disasters are frequently compoundedby the consequences of malnutrition ;WHO, in collaboration with other agencies,prepared a guide 1 for field workers pro-viding nutritional assistance during disas-ter conditions.
6.3o In most industrialized countries,nutritional problems are not related toprimary undernutrition, but they are ofpublic health significance ; studies werecarried out on nutritional problems of theelderly in six countries of the EuropeanRegion, and on problems related to theincreasing use of "ready -made foods ".
Measures against specific nutritional deficiencies
6.3 i Special attention was given toprotein -energy malnutrition, nutritionalanaemia, vitamin A deficiency and endemicgoitre. There is still a very high casefatality rate among children with protein -energy malnutrition ; this rate could besubstantially reduced with appropriatemanagement. A manual on the treatmentand management of severe protein- energymalnutrition was prepared in 1976 and wasbeing tested in different areas in 1977.Support was provided to countries inter-ested in the development of low -costmixtures for use in programmes for the
1 Ville de Goyet, C. de et al. Guide to the managementof nutritional emergencies in large populations. Geneva,World Health Organization, 1978.

FAMILY HEALTH
prevention of protein -energy malnutrition.Also in 1977, an Expert Consultation wasconvened jointly with FAO on the use offats and oils in human nutrition.' Anothertopic of special importance- meeting thenutritional needs of lactating and pregnantwomen -was considered in the TechnicalDiscussions during the Thirtieth WorldHealth Assembly, mentioned above.
6.3z The control of protein- energymalnutrition, particularly in children, is acomplex problem requiring sustained multi-disciplinary efforts in the health and othersectors ; in contrast, for the control of somespecific nutritional deficiencies there aretechniques of proved efficacity that can beapplied in the health sector alone. Forinstance, some countries in Central Americawere already, with the technical cooperationof the Institute of Nutrition of CentralAmerica and Panama, combating vitaminA deficiency by means of sugar fortification.The possibility of using other food vehicleswas explored elsewhere. The feasibilityand effectiveness of periodic distribution oflarge doses of vitamin A was examined inIndonesia and the Philippines. With thetechnical cooperation of WHO, both theWorld Food Programme and the EuropeanEconomic Community decided to fortifywith vitamin A the skim milk donated forsupplementary feeding programmes tocountries where deficiency of this vitaminoccurs. Applied research to test thefeasibility and effectiveness of differentapproaches in the control of nutritionalanaemias was carried out in Burma, Guate-mala, India and Thailand ; food fortifi-cation and iron supplement distributionwere compared. Adequate techniques arealready available for the prevention ofgoitre ; a joint report is being prepared in
' Food and Agriculture Organization of the UnitedNations. Role of dietary fats and oils in human nutrition.Rome, 1978.
55
collaboration with UNICEF, reviewingthe latest information on prevalence andon recommended measures for control.
Health education
6.33 One of the major objectives ofhealth education is to stimulate people toassume responsibility for their own healthcare and thereby to promote individual,family, community and national self -reliance in the health field. During 1976 -77,as part of their series of joint studies onalternative approaches to meeting basichealth needs, WHO and UNICEF carriedout a study, "Community involvement inprimary health care : a study of the processof community motivation and continuedparticipation ". The study sought topresent examples of community involve-ment, to identify elements of individualand community motivation and organi-zation that led to the initiation and main-tenance of community -based health acti-vities, and to describe the characteristics ofthe mobilization and education processesacting from within and from outside thecommunity. Case studies were carried outin nine communities in Botswana, CostaRica, Indonesia, Mexico, Samoa, Senegal,Sri Lanka, Viet Nam and Yugoslavia. Theconclusions justified the renewed interestin the community development approachcentred on community participation, andindicated that increased access to educa-tion, both informal and formal, has led togreater involvement of people in com-munity activities. The important roleplayed by women in this process washighlighted. The readiness of communitiesto accept change appeared to have in-creased greatly since the 19 5 os, mainlyon account of better communications(roads, radio, television, newspapers).Nevertheless, more needs to be knownabout certain aspects of the process : corn-
THE WORK OF WHO
munity involvement in the totality of theplanning process, the importance of tradi-tional decision -making structures, and thenature and extent of both national andinternational external support.
6.34 With the wider adoption of theprimary health care approach, healthauthorities are calling for stronger andmore effective educational activities as partof health development programmes. Manycountries are far from being able to meetthis need. Also, many policy- makers,planners and programmers regard healtheducation as involving only films, posters,booklets, or other media. This viewignores the fact that health programmes,like other development programmes, aimnot only to provide information but alsoto change behaviour. The technical dis-cussions during the 1977 session of Sub -Committee A of the Regional Committeefor the Eastern Mediterranean, on thesubject of "Health education with particularreference to the primary health care ap-proach", reviewed many of the lessonslearned. A paper entitled "WHO's col-laborative research in health education forthe promotion of health delivery ", pre-pared for the 18th session of the AdvisoryCommittee on Medical Research in 1976,challenged the universality of the premisesupon which everyday practice of healtheducation is based. Similarly, WHO'sresearch activities in health educationduring the biennium stressed the opera-tional aspects rather than theoretical issues.The research was specific to local situationsand therefore ensured the development ofthe most relevant messages and methodsof health education.
6.35 WHO collaborated with countriesin all regions to build national capabilitiesfor health education activities. In Afgha-nistan, Indonesia, Malaysia, Pakistan,Philippines and Sri Lanka, existing ser-
56
vices in health education were strengthened,while in Antigua, Qatar, St Lucia andSt Vincent, WHO worked on developingsuch services.
6.36 Health education provides a linkbetween the health system and other sectors.One example is health education in schools,where in recent years the emphasis hasbeen on preparation for future family life.During the biennium, WHO joined withILO, FAO and UNESCO to develop,with collaboration from UNICEF, UNDP,UNFPA and the International PlannedParenthood Federation, educational com-ponents that are completely integrated inrural development programmes, with parti-cular emphasis on family health. An inter-regional meeting was held in Afghanistanin 1976, and follow -up workshops are tobe held at the national level. In 1977 aninterdisciplinary meeting was held inUganda.
6.37 Health education does not workin isolation but as a component of the otherhealth programmes. In the Philippines, astudy was begun in collaboration with theoral rehydration project. It aims to identifythe factors that influence the community'sresponse to the programme, to ascertainpeople's perception of diarrhoeal problems,to assess the public image and acceptabilityof rehydration and to review the natureand scope of health education and its impacton community participation in the healthactivity. A manual on health education forimmunization was prepared and is beingtested in several countries. In addition tothe work developed in the educationalaspects of family planning and maternal andchild health, studies were begun on child-bearing and child- rearing practices andtheir implications for health education inmaternal and child health activities. Otherwork was started on health educationalaspects of rural water supply.
FAMILY HEALTH
Special Programme of Research, Devel-opment and Research Training inHuman Reproduction
6.38 Although a number of MemberStates report progress in their familyplanning programmes, the predominanttone remains one of disquiet. The "pill ",the most widely used modern method ofcontraception, has received wide publicitybecause of its association with thrombo-embolism. Nearly as often, questions havebeen raised to which at present there areno answers (Do hormonal contraceptivescause cancer ? Can intrauterine deviceslead to infection and sterility ? What arethe risks to subsequent pregnancies fromabortion used as a method of birth control ?What is the likelihood that sterilization, inmen or women, will lead to psychologicaldisturbances ?). Providing family planningcare, particularly in the rural areas ofdeveloping countries, is proving verydifficult. Even where it is available, accept-ance rates are low and discontinuationrates disappointingly high.
6.39 These are genuine problems, mostof which cannot be resolved merely byincreasing inputs of services or funds ;they require research. The total worldeffort in research on the biomedical andservice aspects of fertility regulation is,however, pitifully small: governmentalallocations for this field represent onlyabout one per cent of their expenditures onhealth research, even though family plan-ning is potentially of concern to all couplesof reproductive age. The WHO SpecialProgramme of Research in Human Repro-duction 1 is acting as a focus for the scant
1 A fuller description of the Programme can be foundin Special programme of research, development and researchtraining in human reproduction, Fifth Annual Report,November 1976 (WHO document HRP 76.1R Rev. 1)and Sixth Annual Report, November 1977 (WHOdocument HRP 77.3).
57
resources available, both technical andfinancial. It responds to Member States'demands to intensify and internationalizeresearch in this field and to strengthennational capabilities for such research. Itsstrategy is programme- oriented and aimsat providing technologies appropriate toconditions in developing countries."Technology" is used here to refer notonly to methods of fertility regulation butalso to their acceptability and service pro-vision, principally at the primary healthcare level. While placing greatest emphasison research in fertility regulation, theProgramme also includes research in in-fertility and pregnancy wastage.
Technology for fertility regulation
6.4o The research on technology forfertility regulation has two main aspects :assessing in developing countries the safety,efficacy and acceptability of currentlyavailable methods, and conducting researchto improve these methods and developentirely new ones.
6.41 Safety and effectiveness of existingmethods. Assessment in developing coun-tries of existing methods is needed becauseon the whole, careful studies of the safetyand effectiveness of methods such as thepill, intrauterine devices (IUDs), injectables,periodic abstinence, surgical sterilizationand abortion techniques have only beenconducted on women in developed coun-tries. The authorities in developing coun-tries are asking to what extent the findingsare applicable to healthy women there,given differences in body size, nutritionalhabits, and reproductive patterns, and whathappens when, for instance, the pill, theIUD, or injectables are provided to mal-nourished women or those with parasiticinfestation.
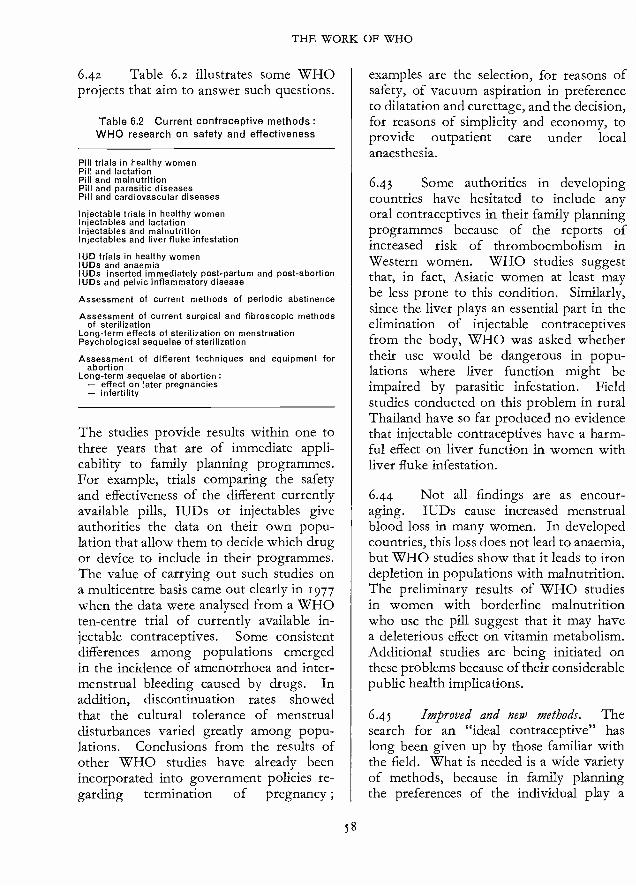
THE WORK OF WHO
6.42 Table 6.2 illustrates some WHOprojects that aim to answer such questions.
Table 6.2 Current contraceptive methods :WHO research on safety and effectiveness
Pill trials in healthy womenPill and lactationPill and malnutritionPill and parasitic diseasesPill and cardiovascular diseases
Injectable trials in healthy womenInjectables and lactationInjectables and malnutritionInjectables and liver fluke infestation
IUD trials in healthy womenIUDs and anaemiaIUDs inserted immediately post -partum and post- abortionIUDs and pelvic inflammatory disease
Assessment of current methods of periodic abstinence
Assessment of current surgical and fibroscopic methodsof sterilization
Long -term effects of sterilization on menstruationPsychological sequelae of sterilization
Assessment of different techniques and equipment forabortion
Long -term sequelae of abortion :- effect on later pregnancies- infertility
The studies provide results within one tothree years that are of immediate appli-cability to family planning programmes.For example, trials comparing the safetyand effectiveness of the different currentlyavailable pills, IUDs or injectables giveauthorities the data on their own popu-lation that allow them to decide which drugor device to include in their programmes.The value of carrying out such studies ona multicentre basis came out clearly in 1977when the data were analysed from a WHOten -centre trial of currently available in-jectable contraceptives. Some consistentdifferences among populations emergedin the incidence of amenorrhoea and inter -menstrual bleeding caused by drugs. Inaddition, discontinuation rates showedthat the cultural tolerance of menstrualdisturbances varied greatly among popu-lations. Conclusions from the results ofother WHO studies have already beenincorporated into government policies re-garding termination of pregnancy ;
58
examples are the selection, for reasons ofsafety, of vacuum aspiration in preferenceto dilatation and curettage, and the decision,for reasons of simplicity and economy, toprovide outpatient care under localanaesthesia.
6.43 Some authorities in developingcountries have hesitated to include anyoral contraceptives in their family planningprogrammes because of the reports ofincreased risk of thromboembolism inWestern women. WHO studies suggestthat, in fact, Asiatic women at least maybe less prone to this condition. Similarly,since the liver plays an essential part in theelimination of injectable contraceptivesfrom the body, WHO was asked whethertheir use would be dangerous in popu-lations where liver function might beimpaired by parasitic infestation. Fieldstudies conducted on this problem in ruralThailand have so far produced no evidencethat injectable contraceptives have a harm-ful effect on liver function in women withliver fluke infestation.
6.44 Not all findings are as encour-aging. IUDs cause increased menstrualblood loss in many women. In developedcountries, this loss does not lead to anaemia,but WHO studies show that it leads to irondepletion in populations with malnutrition.The preliminary results of WHO studiesin women with borderline malnutritionwho use the pill suggest that it may havea deleterious effect on vitamin metabolism.Additional studies are being initiated onthese problems because of their considerablepublic health implications.
6.45 Improved and new methods. Thesearch for an "ideal contraceptive" haslong been given up by those familiar withthe field. What is needed is a wide varietyof methods, because in family planningthe preferences of the individual play a

FAMILY HEALTH
vital role. Moreover, the ease with which agiven method can be provided depends onthe prevailing health service conditions, thelevel of education, and other local factors.There are also health -related reasons whynot just one but a range of methods mustbe available : some methods lead to sideeffects in a proportion of cases ; some arecontraindicated in women with certaindiseases or conditions ; some appear suit-able for women in developed countries butinadvisable, for nutritional or other reasons,for women in the developing world.
6.46 The Programme's approach tomeeting these requirements follows threemain lines, aiming (I) to make currentmethods and techniques of fertility regu-lation safer, more effective, simpler to useand to provide, and more acceptable ;(z) to make available to family planningprogrammes entirely new birth controlmodalities that, in the opinion of thoseresponsible for running the programmes,would considerably extend acceptance anduse, e.g., drugs for men, vaccines, post -coital preparations and abortifacient drugs ;and (3) to strengthen in developing coun-tries national capabilities for research inhuman reproduction and family planning.
6.47 These research and developmentefforts (see Table 6.3) are longer -termendeavours than the assessment of existingmethods, since the development of familyplanning methods inevitably involves alengthy step -by -step demonstration ofefficacy and safety. The time needed isusually between io and 15 years fromthe identification of a compound to themarketing of a birth control drug.
6.48 These methods are at differentstages of development. Some very positiveresults are already emerging. For example,for long -acting injectable contraceptives,in great demand in many developing coun-tries because of their ease of administration,
59
Table 6.3 WHO research on improvedand new methods of contraception
Paper pill
Longer- acting injectablesBiodegradable implants
Hormone -loaded IUDsPost -placental devices
Intra -cervical devices
Vaginal rings
Kits and devices for determination of the fertile period
Chemical sterilization for women
Drugs for abortion (e.g., prostaglandins, plant products)
Post -coital drugs
Pills and injectables for men
Vaccines against pregnancyVaccines against sperm and ova
the Programme has developed a drugdelivery system that releases steroids at alow and constant rate ; this should helpovercome some of the major side effectscaused by currently available preparations.
studies have shown that menstrualblood loss can be considerably reduced ascompared with pre- insertion levels by theuse of entirely new IUDs that releasehormones ; clinical studies are now startingon hormone -releasing IUDs with a poten-tial ten- to twenty -year life -span. Themedicated vaginal rings under develop-ment in the Programme can be inserted orremoved at will by the user after elementaryinstruction by an auxiliary health worker.Women who have used them expresssatisfaction, and if clinical testing con-tinues to give good results, the ringsshould be available to the public in threeto four years.
6.49 The development of simple andaccurate "do -it- yourself" kits for deter-mination of the fertile period by womenwishing to use methods based on periodicabstinence has required a great deal ofcomplex research. Several substances havebeen identified in the urine that display a
THE WORK OF WHO
distinct pattern during the menstrual cycleand upon which simplified techniques forpredicting ovulation could be based. Thevalue of prostaglandins as a non -surgicaland safer method of second -trimestertermination of pregnancy has been shownby the Programme, and this research isalmost completed. A prostaglandin sup-pository was developed and is being testedfor use as an outpatient self -administeredmethod for termination of first- trimesterpregnancy. This method should greatlylighten the burden on health services whereabortion is provided in family planningprogrammes.
6.5o Other methods such as birthcontrol vaccines and fertility- regulatingdrugs for men are at an earlier stage ofdevelopment. The uncertainties are great,but the Programme has nevertheless in-cluded some high -risk lines of researchwhere it was felt that a successful outcomewould have a very great impact. Planningemphasizes the use of cut -off points, atwhich decisions are taken on continuation ;a number of unpromising lines havealready been discontinued.
Infertility
6.51 Much of the Programme's re-search concerned with the development offertility -regulating methods has directapplication to the diagnosis and treatmentof infertility. For example, in the researchon immunological methods, sera frominfertile couples are being studied for thedetection of antibodies that may accountfor their infertility. Various diagnosticprocedures, such as semen analysis, usedin the clinical management of infertilityhave been standardized. Simple means ofdetermining the fertile period are relevantto the treatment of infertility. Otherresearch that relates to infertility includeswork on the regulation of male fertility,
6o
sequelae of induced abortion, and post -coital methods.
6.52 In addition, during 1976-77 epi-demiological research on infertility wasconducted, at the request of the Govern-ments, in areas of Sudan and the UnitedRepublic of Cameroon, where the incidenceof infertility presents a major public healthproblem. A WHO Collaborating Centrefor Research on Fertility Promoting Agentsformulated guidelines for the assessmentof drugs used in the treatment of infertility.
The health rationale for family planning
6.53 Many studies in developed coun-tries have shown that the best age to havebabies is between 20 and 30 years, for bothmother and offspring ; the child's healthand development is best in small familiesand mothers are at greater risk at high pari-ties. The effects of short pregnancy inter-vals are less well documented. Authoritiesin developing countries have askedwhether the same relationships are to befound in their own populations wheremalnutrition prevails, infections are rifeand health care is inadequate. Or does thehostile environment exacerbate these asso-ciations ? If so, the rationale for theirfamily planning programmes would befurther strengthened and the women atgreatest risk, and hence in greatest need offamily planning care, could be identified.
6.54 The results from centres in fiveof the nine countries involved in a WHOcollaborative study aiming to answer thesequestions (India, Iran, Lebanon, Philip-pines and Turkey) were published. I.2
1 Omran, A. R. & Standley, C. C., ed. Family for-mation pattern: and health. Geneva, World HealthOrganization, 1976.
2 Standley, C. C. & Kessler, A. Impact of fertilityregulation on the health and nutrition of mother andchild. In: Symposium on the Motber/Child Dyad -Nutritional Aspects, Uppsala, June 1977 (in press).
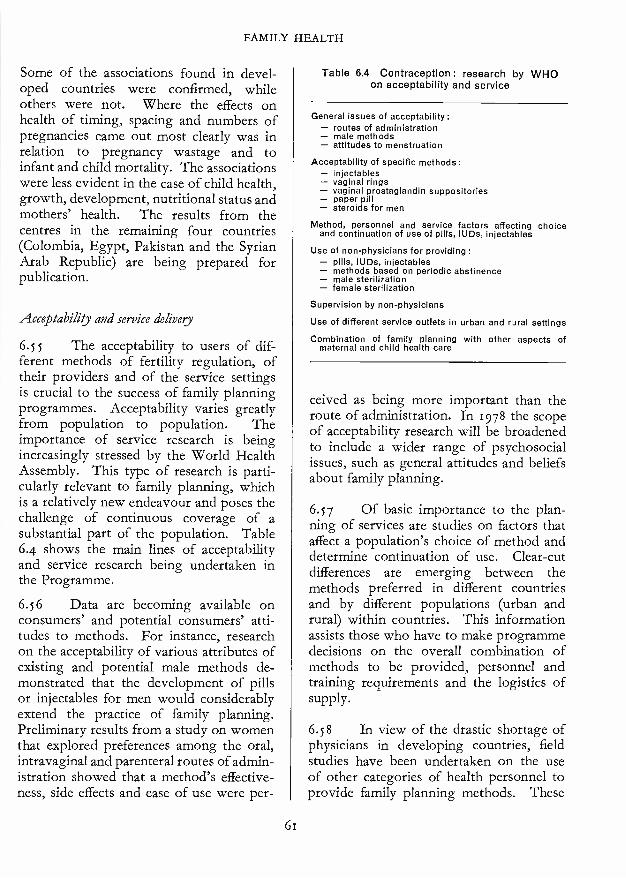
FAMILY HEALTH
Some of the associations found in devel-oped countries were confirmed, whileothers were not. Where the effects onhealth of timing, spacing and numbers ofpregnancies came out most clearly was inrelation to pregnancy wastage and toinfant and child mortality. The associationswere less evident in the case of child health,growth, development, nutritional status andmothers' health. The results from thecentres in the remaining four countries(Colombia, Egypt, Pakistan and the SyrianArab Republic) are being prepared forpublication.
Acceptability and service delivery
6.S5 The acceptability to users of dif-ferent methods of fertility regulation, oftheir providers and of the service settingsis crucial to the success of family planningprogrammes. Acceptability varies greatlyfrom population to population. Theimportance of service research is beingincreasingly stressed by the World HealthAssembly. This type of research is parti-cularly relevant to family planning, whichis a relatively new endeavour and poses thechallenge of continuous coverage of asubstantial part of the population. Table6.4 shows the main lines of acceptabilityand service research being undertaken inthe Programme.
6.56 Data are becoming available onconsumers' and potential consumers' atti-tudes to methods. For instance, researchon the acceptability of various attributes ofexisting and potential male methods de-monstrated that the development of pillsor injectables for men would considerablyextend the practice of family planning.Preliminary results from a study on womenthat explored preferences among the oral,intravaginal and parenteral routes of admin-istration showed that a method's effective-ness, side effects and ease of use were per-
61
Table 6.4 Contraception : research by WHOon acceptability and service
General issues of acceptability:- routes of administration- male methods- attitudes to menstruation
Acceptability of specific methods:- injectables- vaginal rings- vaginal prostaglandin suppositories- paper pill- steroids for men
Method, personnel and service factors affecting choiceand continuation of use of pills, IUDs, injectables
Use of non -physicians for providing :- pills, IUDs, injectables- methods based on periodic abstinence- male sterilization- female sterilization
Supervision by non -physicians
Use of different service outlets in urban and rural settings
Combination of family planning with other aspects ofmaternal and child health care
ceived as being more important than theroute of administration. In 1978 the scopeof acceptability research will be broadenedto include a wider range of psychosocialissues, such as general attitudes and beliefsabout family planning.
6.57 Of basic importance to the plan-ning of services are studies on factors thataffect a population's choice of method anddetermine continuation of use. Clear -cutdifferences are emerging between themethods preferred in different countriesand by different populations (urban andrural) within countries. This informationassists those who have to make programmedecisions on the overall combination ofmethods to be provided, personnel andtraining requirements and the logistics ofsupply.
6.58 In view of the drastic shortage ofphysicians in developing countries, fieldstudies have been undertaken on the useof other categories of health personnel toprovide family planning methods. These

THE WORK OF WHO
studies indicate, for example, that mid-wives, given proper training, encounterlittle difficulty in acquiring the knowledgeand skills required to insert IUDs. Thetraining manuals, checklists and recordforms developed for this research havealready been requested by family planningauthorities. More innovative studiessuggest that theatre nurses can be trainedto perform female sterilization, and medi-cal students to carry out vasectomy. Inaddition, the scope of service research wasbroadened in 1977 at the request of govern-ments to cover more general service issues,such as integration of family planningwith other services in primary health care.
National self -reliance in research
6.59 A major effort by the Programme,in cooperation with national authorities,is devoted to building up self -reliance indeveloping countries for research on fer-tility regulation, through the strengtheningof their institutions and through a researchtraining effort that is now the largest in thefield (Table 6.5). The aim is to developresources for national family planning pro-grammes to carry out research, adapttechnology, interpret advances made else-where, and permit the full contribution tothe field of scientists from developingcountries. This institution -strengtheninginvolves much more than technical andfinancial inputs by WHO : it is a "learningby doing" process in which the developingcountries' institutions are actively parti-cipating in and contributing to the inter-national research effort.
6.6o Core support (for equipment, sup-plies and salaries) to help build up or rein-force a research nucleus assured of somecontinuity of support was given to a net-work of collaborating centres in Argentina,Brazil, Chile, Cuba, Egypt, India (3 centres),
62
Table 6.5 Strengthening research capabilities
Core and other support to nuclei for research
WHO Collaborating Centres in Human Reproduction:salaries
- network of centres for clinical and equipmentfield research supplies
- research and training centres consultantstraining
Project -related strengthening of capabilities as above)Research training grantsResearch training coursesQuality control and standardization of laboratory methodsSmall supplies and spare partsJournal subscriptions and booksTechnical meetingsPublications °
° Proceedings of meetings supported by the Programme :Cinader, B. & de Weck, A., ed. Immunological response of
the female reproductive tract. Copenhagen, Scriptor, 1976.Harper, M. J. K. et al. Development of vaccines for
fertility regulation. Copenhagen, Scriptor, 1976.Harper, M. J. K. et al., ed. Ovum transport and fertility
regulation. Copenhagen, Scriptor, 1976.Boettcher, B. et al., ed. Auto- and iso- antibodies to antigens
of the human reproductive system, Acta. pathol.microbiol. scand., suppl. 258 (1977).
Diczfalusy, E., ed. Regulation of human fertility. Copen-hagen, Scriptor, 1977.
Mexico (2), Nigeria, Pakistan, Philippines,Republic of Korea, Singapore, Thailand (z),Tunisia, Yugoslavia and Zambia. Thecentres, as well as many other institutionsin developing countries, participate inTask Force projects, for which they alsoreceive support in the form of equipment,supplies and salaries. The Task Forces areone of the main mechanisms for researchand development in the Programme andbring together into teams scientists fromdifferent institutions, countries and disci-plines to plan and implement research ondifferent approaches to fertility regulationand on their acceptability and servicedelivery.
6.61 Manpower resources werestrengthened in several ways. In additionto funding posts, the Programme providedthe assistance of consultants, particularlyin the training of laboratory personnel.In 1976 -77, about i oo research training
FAMILY HEALTH
grants for training abroad, mostly of ayear's duration, were awarded and severaltraining courses were organized, for ex-ample on clinical trial methodology and onthe standardization of laboratory methods.'A special effort was made to extend to thecentres expertise in social science andepidemiology.
6.6z Laboratory facilities for the radio -immunoassay of sex hormones and clinicalchemistry were strengthened in centres inCuba, Egypt, India (3 centres), Republicof Korea and Thailand to enable them toconduct the pharmacological and metabolicstudies needed in the assessment of fertility -regulating methods. A similar build -upis planned for the centre in Tunisia. Pri-mate facilities were strengthened in Argen-tina and India. To ensure the comparabilityof results in multicentre trials and to helpcentres monitor their own assay perform-ance, all centres with laboratory facilitiesparticipate in the programme of standard-ization and quality control of laboratorymethodology, which now covers 143laboratories in 44 countries.
6.63 A few institutions in developedcountries were strengthened, primarily toincrease their capacity for research training
See also page 8z.
and for collaborative research with develop-ing countries, including the multicentreassessment of fertility -regulating methods.These centres are in Australia, Canada,Hungary, Sweden, the United Kingdom, theUSA, the USSR and Berlin (West).
International scope of the Programme
6.64 Scientists from 69 countries, ofwhich 45 are developing countries, areinvolved in the Programme, either asinvestigators, advisers, trainees, or in othercapacities. The Programme was mainlysupported in 1977 by contributions to theVoluntary Fund for Health Promotionfrom Canada, Denmark, Finland, Norway,the United Kingdom and UNFPA.
6.65 Coordination with a large numberof other agencies is achieved through avariety of mechanisms, ranging from jointplanning and conduct of projects toconsultation on technical issues. Fifteengovernmental and nongovernmental agen-cies with active programmes of research infertility regulation were invited to a meetingconvened by WHO in September 1977.They represented almost the entire publicsector investment in research on the bio-medical and service aspects of family plan-ning. The meeting reviewed the agencies'priorities, strategies, and current and plan-ned activities.
63
Chapter 7
lieu/i/i Manpower Development
7.1DECISIONS taken by the World
Health Assembly in 1976 con-firmed the preparatory work of
many years and heralded a new role forWHO in its relationship with its MemberStates in the field of health manpower devel-opment (resolution wHAz9.7z). The mainthrust of the new programme is to bringtogether the planning, training ( "produc-tion") and management aspects of man-power into an administrativeand functional whole geared entirely to thedevelopment of health services, the latterbeing structured to meet the real healthneeds and demands of entire populations.The concept of integrated development ofhealth services and manpower developmentwas well received in countries, and steps arebeing taken in several of them to reformthe administrative structure of healthservices and health manpower develop-ment and break down barriers betweeneducation and service.
7. z Within the Organization this policybrought about important changes, pro-moting cooperation among all sectors con-cerned with the development of healthservices and health manpower. The resultis that when WHO meets countries' re-quests for cooperation in their nationalhealth planning, the preparation of man-power is an integral part of the plan.
64
7.3 The concept of integration wasembodied in the Sixth General Programmeof Work and endorsed by the Health As-sembly in resolution wHA29.7z. However,despite their general acceptance of theprinciple of giving priority to universalhealth coverage, most governments do notyet appear to be in a position to take thepolitical decision to initiate the changes intheir health service orientation and expen-diture which such a priority requires.
7.4 A significant step during the bien-nium was the formulation of a global WHOmedium -term programme for health man-power development (1978 -83) on the basisof the Sixth General Programme of Work.This programme clarifies the main prob-lems that countries face in relation tohealth manpower planning, production andmanagement, and proposes a step -by -stepprocess whereby WHO can collaboratewith Member States in their efforts totackle these problems systematically andto achieve well- defined, and wheneverpossible quantified, targets.
7.5 Some aspects of the medium -termprogramme are already starting to becomeoperational in several countries -for ex-ample, the fundamental task of trainingand retraining teachers of all categories ofhealth worker. In 1971 WHO providedfellowships for a limited number of experi-
HEALTH MANPOWER DEVELOPMENT
enced health teachers to study new ap-proaches to education in the health sciencesat a WHO collaborating centre in the USA(Center for Educational Development,Illinois University Medical College,Chicago). The fellows and other highlytrained personnel concerned subsequentlytook responsibility for inaugurating eightregional centres in five WHO regions.Students from the regional centres are nowreturning to their countries and the firstnational teacher training centres have al-ready been established in India, the Philip-pines and the Republic of Korea. In carry-ing out this programme WHO has givenparticular attention to developing newmaterials to assist learning, to preparingnew approaches to evaluation, includingthe instruments required for its accom-plishment, and to promoting research in newmethods of education and communication.The programme provides an opportunityfor teachers to learn in their own countrieshow to facilitate students' learning and howto prepare learning programmes that aremore relevant to local health needs anddemands.
7.6 During 1976 -77 the Organizationmade progress in promoting courses inmodern principles and processes of edu-cation and awarded many fellowships forthe study of education in the health sciencesfor nurses, doctors, and environmental andother health workers, particularly thoseconcerned with the training of auxiliariesand indigenous practitioners. It supportedinstitutions experimenting with new cur-ricula and organized courses in manage-ment and workshops on the productionand use of low -cost educational materials,and established a centre in Geneva foreducational technology
7.7 The Organization prepared a long-term international programme of trainingin health management and held a meetingof national managers in Geneva in October
65
1977 which discussed a plan of action tocooperate with Member States in trainingtheir own health managers.
7.8 The study on the internationalmigration of physicians and nurses wascompleted ;1 it provides a description ofthis complex and changing problem andsuggests a useful range of options for actionon the different situations in which Membercountries find themselves.
7.9 A detailed proposal was elaboratedin cooperation with ILO on the work andliving conditions of nurses, which formedthe basis of an international convention onthis subject adopted by the ILO Conferencein 1977.
Production of health manpower
Health services and manpower development
7.10 Health services and health man-power development suffer from the rela-tively low status accorded to health innational plans for socioeconomic develop-ment. The frequent absence or inadequacyof national health manpower policies resultsin the absence of well- conceived nationalhealth manpower systems forming anintegral part of existing health systems.Recognizing this problem, the WorldHealth Assembly noted in 1976 that theremedy "requires a new and vigorouseffort involving the concept of the unity ofmedical science and health activities and asystematic and integrated approach tohealth manpower planning, production andmanagement directly related to the assessedneeds of populations" (resolutionWHAZ9.7z). A consultation of experts in
1 The results of this study are to be published byWHO. See also page 76.
2International Labour Organisation. Employmentand conditions of work and life of nursing personnel. Geneva,1976.
THE WORK OF WHO
1976 reviewed experience with severalforms of coordination between develop-ment of health services and development ofhealth manpower. A strategy for nationalaction is being promoted, and steps arebeing taken to share country experiences.
7.11 In the African Region, activitiesin the field of health services and man-power development took the form of con-sultation among Member countries on thedevelopment and application of mechan-isms that put the concept into practice.
7.12. In 1976 PAHO /WHO launchedthe Latin American Programme of Edu-cational Development for Health, fundedby the Kellogg Foundation, which aims atexpediting the experimental use of teaching -service integration in Latin American coun-tries by enlisting the support of nationalcoordination groups (known as HealthEducation Research and DevelopmentNuclei). These latter serve as the initialfocal points for coordination between ser-vice and training institutions ; during 1976-77 support was given in their developmentin Bolivia, Brazil, Costa Rica, the Domin-ican Republic, Ecuador, Honduras, Mexico,Nicaragua, Paraguay, Peru and Venezuela.
7.13 In the South -East Asia Region,representatives of the health and educationfields met in 1977 to discuss the Region'smedium -term programme for health man-power development.
7.14 In the European Region, an inter -country working group on country healthprogramming as a determinant of healthmanpower development was convened inBerne, Switzerland, in April 1977.
7.15 At the loth CIOMS Round TableConference in Ulm, Federal Republic ofGermany, in July 1976 on health needs ofsociety, organized in cooperation withWHO, participants stressed the need for
66
cooperative planning and integrated devel-opment of health services and health man-power, and drew attention to the reformsneeded in aligning the medical curriculumwith the needs of the health services.'
Health manpower planning
7.16 As a result of poor coordinationbetween planning for health manpowerand planning for other sectors, there hasbeen (a) little direct relationship betweenthose planning for and managing the healthservices and those responsible for thetraining of health manpower, (b) a lackof planning for the training of new cat-egories of health personnel required to meetrecognized health care needs, and (c) a lackof clear definition of the functions andinterrelations of the various categories ofpersonnel engaged in the delivery of healthcare.
7.17 A publication completed on theprinciples and methods of health manpowerplanning 2 describes the experience accu-mulated during the last decade, the diffi-culties most frequently encountered in theconduct of the health manpower planningprocess, and the most relevant techniquesthat can be used, with their benefits andlimitations.
7.18 In the Region of the Americas, theOrganization cooperated with severalhealth ministries on theoretical and prac-tical aspects of manpower planning ; orga-nization of manpower units, preparationof their staff, and management of the co-ordination process ; and the participation
1 Gellhorn, A., Fülóp, T. & Bankowski, Z., ed.Health needs of society : A challenge for medical education.Geneva, 5977 (published by WHO on behalf of CIOMS).
2 Hall, T. L. & Mejía, A., ed. Health manpowerplanning: Principles, methods and issues. Geneva, WorldHealth Organization, 5978.
HEALTH MANPOWER DEVELOPMENT
of various agencies in policy formulationand development plans.
7.19 In the Western Pacific Region,WHO cooperated with the Lao People'sDemocratic Republic to draw up plans forthe period up to 1986 to provide manpowerto fill gaps in the remodelled health services.
Health manpower management
7.2o The problems experienced inhealth manpower management include :the uneconomic utilization of health staff,the imbalance between different disciplines,categories and levels, and the inequities ingeographical distribution, aggravated bythe migration of qualified staff; and in-adequate management training for top -level and middle -level health administratorswho are responsible for the planning,management and evaluation of health pro-grammes. Health manpower managementin the context of health services and man-power development covers such questionsas options for policies to attract and retainhealth manpower in deprived areas, careerschemes, moral and financial incentives, andthe continuous evaluation (monitoring) ofindividual and health team performance,both in relation to community needs andas a basis for planning continuingeducation.
7.21 A programme to improve themanagement skills of health workers at alllevels was initiated, consisting of the devel-opment and strengthening of a network ofinstitutions. In order to plan concertedglobal action to meet the problems of healthmanpower management, a consultationwas held in Geneva in October 1977 ontraining in health management. This wasfollowed by a workshop on internationalcollaboration in training and research inhealth administration, to identify and con-sider various operational issues impinging
67
on the development of international col-laboration, technical cooperation andmutual support systems for training andresearch in health administration.
7.22 The European Region took actionin this field by organizing two workinggroups on the education of managers inhealth services, one in Lysebu, Norway,in 1976, and one in Dusseldorf, FederalRepublic of Germany, in 1977.
7.23 The English -language and Rus-sian- language training programme forpublic health administrators continued atthe Central Institute for Advanced MedicalStudies, Moscow, USSR, in collaborationwith WHO ; during the academic years1975 -76 and 1976 -77, 71 participantsattended the courses and received theEnglish -language diploma of Master ofSocial Medicine or its Russian -languageequivalent. In May 1977 the fourth scien-tific meeting for teachers and alumni ofthese courses, attended by zo8 participantsfrom 15 countries, was organized in Praguein collaboration with WHO.
7.24 In the Eastern Mediterranean Re-gion an itinerant workshop on managementwas organized for deans of medical schoolsas part of a strategy aimed at makingmedical education more relevant to theneeds of populations.
7.25 Progress was made, in collabora-tion with UNESCO, in achieving inter-national recognition of qualifications and ofwork experience. Following the conventionof Caribbean countries on this subject,similar conventions were proposed forArab and European countries.
Health coverage and new categories of healthpersonnel
7.26 Inadequate numbers and quality ofhealth manpower continue to be the most
THE WORK OF WHO
serious impediment to a satisfactory healthcoverage of the world's population. Thissituation is aggravated by undue emphasison the conventional training of certaincategories of health personnel (particularlyphysicians and nurses) at the expense ofother categories; hesitation in furthering the"health team" concept, both in training andin service ; and a failure to make use of thebest elements of traditional medicine. As aconsequence, very large population groupsin the developing countries have negligibleaccess to health services.
7.27 During 1976-77 the Organizationgave high priority to a rapid, balancedincrease in numbers of health personneland to strengthening the facilities requiredfor this purpose. In particular, it promotedthe development of health personnel whoare likely to provide primary health services,particularly in underserved communities.A health team approach was formulated,with emphasis on the training and use ofauxiliaries and community health workers,including, where appropriate, those prac-tising traditional medicine, in addition tothe existing categories of health profes-sionals.
7.28 An expert committee on the train-ing and utilization of auxiliary personnelfor rural health teams in developing coun-tries was convened in 1977 to analyse thesituation and make recommendations onthis subject.
7.29 A working guide entitled ThePrimary Health Worker 1 was published inEnglish and French ; it contains guidelinesfor training and for adaptation to localcircumstances. Adaptations of the guidemade in Ghana, Iran, the Lao People'sDemocratic Republic, Mozambique, Peru
1 World Health Organization. The primary healthworker: Working guide, guidelines for training, guidelinesfor adaptation (experimental edition). Geneva, 1977.
68
and Sudan were translated into locallanguages. Also published were directoriesof schools for medical assistants, dentalauxiliaries and medical laboratory techni-cians.2
7.3o Many countries of the AfricanRegion have decided to use the services oftraditional health practitioners in ruralareas, after suitable training. In addition,eight countries have now institutionalizedthe retraining of traditional birth attend-ants ; a study group on their training andsupervision was convened by the RegionalOffice. This training, together with thetraining of village health workers andmaternal and child health auxiliaries, willcontribute to the primary health careapproach.
7.31 In some countries in the WesternPacific Region, such as Fiji and the LaoPeople's Democratic Republic, medicalassistants are now trained and used asintermediate -level health workers. This isalso the case in other regions (Africa,South -East Asia, Eastern Mediterranean)-in Bangladesh, for instance, where medicalassistants were recently introduced. InPapua New Guinea, the functions of theaid -post orderly are being reviewed withthe aim of making him a more effectiveprimary health care worker.
7.32 Nursing /midwifery personnel wereincreasingly involved in the training ofcommunity health workers in many coun-tries, for instance, in Honduras, India,Indonesia and Upper Volta. In the LaoPeople's Democratic Republic and in thePhilippines, they were engaged in thetraining of primary health care workers and
2 World Health Organization. World directory ofschools for medical assistants, 1973, Geneva 1976 ; Worlddirectory of schools for dental auxiliaries, 1973, Geneva,1977 ; World directory of schools for medical laboratorytechnicians and assistants, 1973, Geneva, 1977.
HEALTH MANPOWER DEVELOPMENT
traditional birth attendants while at thesame time fulfilling some supervisoryfunctions.
Curricular reform
7.33 Curricula and teaching methodsare often not suited to the effective teamtraining of health workers to meet com-munity health needs. Educational pro-grammes are primarily directed towardsinstitutional curative care rather than tohealth promotion, prevention and rehabili-tation for the entire population. Alternativeapproaches being used in training healthmanpower of different types and in dif-ferent settings, particularly with communityorientation, were embodied in a publicationwhich describes, and offers comments on,several educational programmes aimed atensuring relevant, effective and efficienteducational processes.'
7.34 A start was made on studyingways in which basic curricula in nursingeducation could be reshaped to becomemore relevant to local conditions andproduce staff oriented towards work in thefield of primary health care. In accordancewith the World Health Assembly's decisionin May 1977 on the strengthening of thetraining of nurses in primary health care(resolution wHA3o.48), strategies and ap-proaches were formulated, and coordinativeaction was undertaken with regional officesto promote collaboration with countrieswishing to effect the required changes.
7-35 In the African Region, pro-grammes are being designed on the basis ofwell -defined duties and taking into consid-eration available supervisory structures andthe composition of health teams. As a
Katz, F. M. Personnel for health care : Case studies foreducational programmes. Geneva, World Health Orga-nization, 1978 (Public Health Papers, No. 68).
69
result, about 3o categories of health auxi-liaries have so far been trained. A meetingof regional experts on the problems ofhealth teams was convened in 1977.Training in environmental health sciencesfor sanitary engineers and sanitarians wasalso supported in five country and threeintercountry programmes.
7.36 In the Region of the Americas,efforts to promote the training of technicaland auxiliary health personnel were inten-sified, and auxiliary training centres inBolivia and Ecuador were provided withteaching materials and equipment. ASpanish version of a short WHO guide forteachers of health auxiliaries was published.'Cooperation with Member countries in thefield of medical education consisted mainlyof supporting individual medical schools inimproving their academic programmes.These activities took the form of participa-tion in curriculum revision and the designof interdisciplinary research programmes.In January 1976, in collaboration with thePan American Federation of Associationsof Medical Schools, the Organizationarranged a meeting of Latin Americanspecialists at Caracas, Venezuela, to estab-lish principles for developing medicaleducation in Latin America and the Carib-bean area.' Efforts were made to strengthenteaching methods by introducing the inte-gration of teaching specialties. Examplesof this approach are the programme forthe strategic training of health personnel inBrazil and three projects for manpowerdevelopment in the Dominican Republic,Honduras and Nicaragua. In the Latin
2 Wakeford, R. E. Métodos didácticos para un apren-dizaje eficaz : Guía breve para profesores de auxiliares desalud. Washington, DC, Organización Panamericana de laSalud, 3976 (Publicación Científica No. 327).
3 Pan American Health Organization. First meetingon basic principles for the development of medical educationin Latin America and the Caribbean area : Final report.Washington, DC, 1977 (Scientific Publication No. 34i).
THE WORK OF WHO
American countries the training of staffespecially equipped to participate in cover-age extension and primary care activities isbeing reinforced by a reformulation offunctions and a better utilization of thevarious categories of existing health per-sonnel. Emphasis is being placed onexpanding the role of nurses, with the aimof using them in primary health care ser-vices. Some countries now include trainingfor these functions in the basic curricula oftheir nursing schools. In other countriesthere are plans to revise curricula to includethe training of nurses in family health care.
7.37 In the South -East Asia Region thereview of curricula for various categories ofnurses continued, particularly in Bangla-desh, Burma and Thailand. An inter -country workshop on community- orientednursing education programmes was heldwith the participation of senior educators,followed by a meeting of decision -makerswho could implement the changes in thevarious countries of the Region. In addi-tion, teaching /learning materials were beingplanned that would be useful in such arevised educational programme. The trendtowards making medical education com-munity- oriented continued in almost allcountries of the Region, and the attentionof governments was drawn to a suggestedcurriculum for strengthening the teachingof community medicine, based on a studyof the teaching of this subject in five coun-tries. WHO also cooperated in developingnew curricula for sanitary engineers inBurma, India, Indonesia, Sri Lanka andThailand.
7.38 In the European Region, technicalcooperation in projects on medical andallied health education was provided inAlgeria, Poland and Spain. Projects werecontinued in Belgium, Iceland, Italy andTurkey, and started in Portugal.
70
7.39 In the Western Pacific Region,WHO cooperated with the Gilbert Islands,New Hebrides, Samoa and Tonga in thedevelopment of their nursing curriculumprogrammes. Almost all countries of theRegion now have a basic nursing educationprogramme.
Teacher training
7.40 At present there is a shortage ofteachers of health personnel who are com-petent both in educational planning andprocesses and in their own specialty.Moreover, professional groups often op-pose radical changes in the education andtraining of health staff, even though suchchanges are based on established serviceneeds.
7.41 In October 1976, the directors ofseven regional teacher training centres metin Shiraz, Iran, with outstanding experts inthe field to discuss the implications of thefuture expanded role of the regional andnational centres (which will undertakemultiprofessional instead of single- profes-sional programme activities) and theirpotential function in the mechanisms forhealth services and manpower development.Agreement was reached on continuingcollaboration, communication, the ex-change of educational materials, and col-laborative efforts in the organization oftraining and research programmes.
7.42 The African Region paid particularattention to the training of teachers ofauxiliaries by experimenting in the use andapplication of new teaching methods inKenya and the United Republic of Tanza-nia.
7.43 The Latin American Centres forEducational Technology in Health in Riode Janeiro, Brazil, and Mexico City con-centrated on the training of instructors inpedagogy.
HEALTH MANPOWER DEVELOPMENT
7.44 In the South -East Asia Region, theRegional Teacher Training Centres inPeradenya, Sri Lanka, and Bangkok, Thai-land, continued to conduct training courses.Several intercountry training courses havenow resulted in the introduction of newteaching methods and educational pro-grammes in various countries. For example,two medical institutions in Bangladeshstarted units of medical education, and anational teacher- training centre was estab-lished at the Jawaharlal Institute of Post-graduate Medical Education and Research,Pondicherry, India.
7.45 In the European Region, twostudies were initiated -one on the specificproblems of teacher -training and the otheron educational measurement for teachers ofhealth professionals.
7.46 In the Eastern Mediterranean Re-gion, several medical schools in Egypt,Pakistan and Sudan established medicaleducation departments or units, which arenow becoming self -reliant in planning andconducting teacher -training activities.
7.47 In the Western Pacific Region, theRegional Teacher -Training Centre in Syd-ney, Australia, expanded its activities, anda total of 25o persons from izo institutionsin the Region have attended courses andworkshops organized by the Centre sinceits inception in 197z.
7.48 A revision of the EducationalHandbook for Health Personnel) was issuedin English and French and was translatedinto eight other languages by interestedMember States. This publication also incor-porated a guide for teachers on the organi-zation of short educational workshops thathas been field- tested and translated intofour languages.
1 Guilbert, J. -J. Educational handbook for healthpersonnel. Geneva, World Health Organization, 1977(WHO Offset Publication No. 35).
71
7.49 Efforts were made to strengthenteacher competencies in midwifery edu-cation programmes and a monograph fornurse /midwife teachers was published by aWHO collaborating centre in 1977 ; itdescribes the process of designing modulesand gives 5 9 examples of modules in mid-wifery and child care, including familyplanning.2 The use of the modular ap-proach enhances self -directed learning andcould solve problems associated with short-age of qualified teachers. The Organizationsupported teacher -training workshops ona modular midwifery curriculum, one in theEastern Mediterranean Region and anotherin the Western Pacific Region, and also aDANIDA- sponsored intercountry courseon modern methods of teaching nursing inthe Eastern Mediterranean Region.
Teaching /learning materials
7.5o There is an overall and seriousshortage of teaching and learning materialsfor all categories of health workers, includ-ing textbooks and manuals, audiovisualmedia, self -instructional packages and otherinnovative ways of facilitating learning.During the biennium WHO producedresource materials for learners, teachers, andthose responsible for educational pro-grammes. A list of reference materials forhealth auxiliaries and their teachers waspublished in 1976.3 Work proceeded on therevision of an experimental manual of basicmedical laboratory techniques, with theincorporation of comments received fromregional offices and some 7o schools.
2 British Life Assurance Trust Centre for Healthand Medical Education. Facilitating teaching- learningwith modules : An approach for nurse/midwife teachers.London, 1977.
3 World Health Organization. Reference material forhealth auxiliaries and their teachers. Geneva, 1976 (WHO(Offset Publication No. z8).
THE WORK OF WHO
7.51 The African, South -East Asia andEastern Mediterranean Regions began tocarry out national needs and resourcessurveys on teaching /learning materials.A meeting of deans and directors of univer-sity centres for health sciences was con-vened to assess the relevance of availableteaching materials. In the Eastern Mediter-ranean Region, a survey revealed theextreme shortage of suitable teaching/learning materials in Jordan and Sudan,particularly for non- physician education ;this finding stimulated a major effort in theRegion to improve the availability ofresources for students and teachers.
7.5z In the Americas, a regional pro-gramme of continuing education was drawnup for the purposes of evaluating needs forteaching /learning materials and resources,and establishing action plans in eightLatin American and Caribbean countries.The medical and nursing textbooks pro-grammes continued to provide sources oflow -cost learning materials for studentsin the Region ; there are plans to extend thisprogramme to cover dentistry, veterinarymedicine and sanitary engineering.
7.53 In accordance with the WorldHealth Assembly's decision to give specialemphasis to the research and training pro-grammes in tropical and parasitic diseases,a start was made on the production of slidesets with texts on parasites, and a slide bankon tropical medicine was established. Thefirst sets on schistosomiasis and malariawere made available for distribution, inslide or microfiche format and with accom-panying texts.
7.54 In the quest for newer and moreeffective learning tools, an improved patientmanagement process using the flow -chartapproach was developed ; the intentionis to provide intermediate -level health staffand peripheral health workers, such as
72
traditional birth attendants and primaryhealth care workers, with the skills toundertake essential promotive, preventiveand curative primary care services. The flow-charts are simple guidelines covering spe-cific diagnostic and management tech-niques. For the midwife, a set of flow -chartsfor obstetric emergencies and antenatalcare will be tested for adaptation to coun-tries with different cultures and languages.The flow -chart system will help auxiliaryhealth and midwifery personnel to effectsafe and rational patient management inthe absence of supervision and in spite ofthe many constraints in primary healthcare work.
7.55 In the African Region cooperationwith Guinea -Bissau in providing primaryhealth care in villages took the form ofsupplying posters depicting seven majorhealth problems, for the training of illiteratevillage health workers. The same imageswere printed on labels for identifyingmedicaments supplied in "village pharma-cies". In addition, eight manuals weretranslated into Portuguese for use by thehealth team as training and reference works.
7.56 In the field of educational techno-logy, the Latin American Centre for Educa-tional Technology in Health in Rio deJaneiro, Brazil continued the developmentof educational research and trainingsystems. An audiovisual production unitwas installed in 1976. During the year,projects on the development of self -instructional techniques and large -scaletraining of health personnel were com-pleted. In 1977, activities were concentra-ted on the adaptation of technology to localconditions, and on the development ofalternative training systems, including thedevelopment of instruction programmes inthe educational and health sectors, usingsmall computers. Thus, the Centre's presentactivities are concentrating on research and
HEALTH MANPOWER DEVELOPMENT
development projects and the setting up ofmechanisms for transferring knowledgeacquired to other training institutions.
7.S7 The project on the use of non-verbal communication in disseminatinghealth messages in developing countrieswith different languages and cultures pro-gressed to the implementation phase. Astory -board on immunization in a slide -tape version was prepared and tested inthree countries. Based on the results ofthese trials, an animated film was producedand tested in Egypt in both urban and ruralareas, prior to extensive use as a healtheducation instrument in the ExpandedProgramme on Immunization. A biblio-graphy of extracts from the literature onnonverbal communication media was pre-pared in a limited number of copies forfield testing.
7.58 The European Region compiled aworkbook on the nursing process andcollected the data for another on the organi-zation and management of nursing/mid-wifery services.
7.59 In the Western Pacific Regionequipment, reference books and biblio-graphical tools were provided for expand-ing the capacity of the Central MedicalLibrary in Viet Nam to produce documentsand abstracts in Vietnamese.
Deployment of health manpower
Continuing education and fellowships
7.6o There is a general lack of provisionfor the continuing education of all cate-gories of staff as an integral part of thehealth care and educational systems. Thereis also little provision for retraining per-sonnel already in service. WHO developedpost -graduate training programmes in va-rious disciplines. The first post -graduate
73
course in public health in French wasorganized by the African Region, wherepost -basic nursing courses also continuedto be offered in Luanda.
7.61 In the European Region, threestudies were initiated -one on specializedtraining in relation to community healthneeds, excluding hospitals, another ontraining patterns for public health medicalofficers, and a third on principles andmethods of quality control in health care asa basis for planning continuing educationprogrammes relevant to service needs.
7.62 During the seventh meeting ofdirectors of schools of public health fromthe African, South -East Asia, EasternMediterranean and Western Pacific Regions,which took place in Teheran, Iran, in 1 977,postgraduate programmes and schools ofpublic health were re- examined, in partic-ular as regards their contribution to therealization of the integrated health servicesand manpower development approach andthe development of primary health careservices. A new curriculum was preparedfor the course in English for a Master'sdegree in public health offered at the Schoolof Public Health in Teheran.
7.63 An important part of WHO'sactivities in continuing education is thefellowship programme, most of the func-tions of which have been decentralized tothe regional offices for some years. Thisarrangement ensures that awards are adap-ted to countries' needs and that fellowshipsare efficiently and economically adminis-tered. During the period January 1976 -June 1977 the Organization awarded 4247fellowships for study (Table 7.1) and duringthe period January- December 1976 2540fellowships were awarded for participationin meetings or other educational activities(courses, seminars or workshops) organizedby WHO.
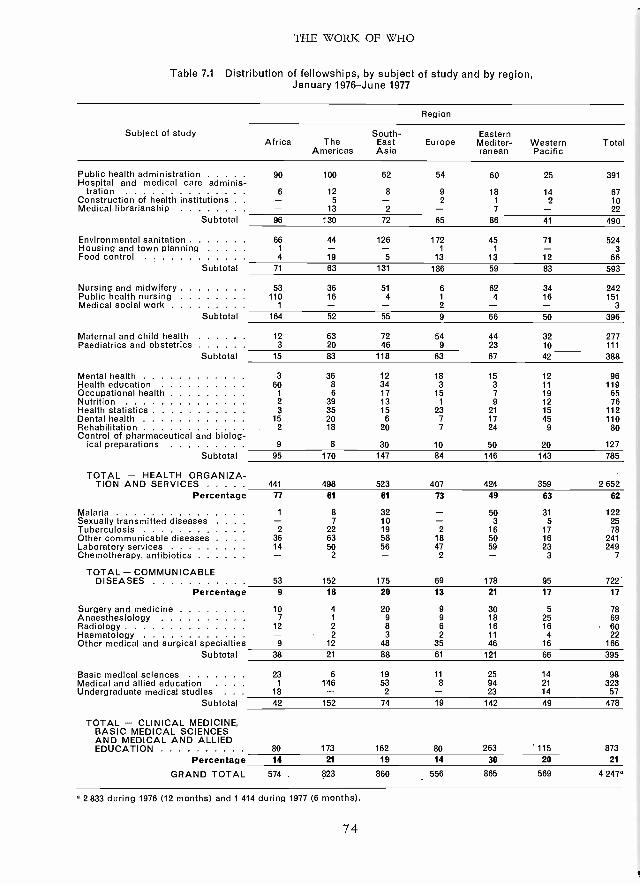
THE WORK OF WHO
Table 7.1 Distribution of fellowships, by subject of study and by region,January 1976 -June 1977
Subject of study
Region
South- EasternAfrica The East Europe Mediter- Western Total
Americas Asia ranean Pacific
Public health administration 90 100 62 54 60 25 391Hospital and medical care adminis-
tration 6 12 8 9 18 14 67Construction of health institutions . . - 5 - 2 1 2 10Medical librarianship - 13 2 - 7 - 22
Subtotal 96 130 72 65 86 41 490
Environmental sanitation 66 44 126 172 45 71 524Housing and town planning 1 - - 1 1 - 3Food control 4 19 5 13 13 12 66
Subtotal 71 63 131 186 59 83 593
Nursing and midwifery 53 36 51 6 62 34 242Public health nursing 110 16 4 1 4 16 151Medical social work 1 - - 2 3
Subtotal 164 52 55 9 66 50 396
Maternal and child health 12 63 72 54 44 32 277Paediatrics and obstetrics 3 20 46 9 23 10 111
Subtotal 15 83 118 63 67 42 388
Mental health 3 36 12 18 15 12 96Health education 60 8 34 3 3 11 119Occupational health 1 6 17 15 7 19 65Nutrition 2 39 13 1 9 12 76Health statistics 3 35 15 23 21 15 112Dental health 15 20 6 7 17 45 110Rehabilitation 2 18 20 7 24 9 80Control of pharmaceutical and biolog-
ical preparations 9 8 30 10 50 20 127
Subtotal 95 170 147 84 146 143 785
TOTAL - HEALTH ORGANIZA-TION AND SERVICES 441 498 523 407 424 359 2652
Percentage 77 61 61 73 49 63 62
Malaria 1 8 32 - 50 31 122Sexually transmitted diseases . . . . - 7 10 3 5 25Tuberculosis 2 22 19 2 16 17 78Other communicable diseases . . . 36 63 58 18 50 16 241Laboratory services 14 50 56 47 59 23 249Chemotherapy, antibiotics - 2 2 - 3 7
TOTAL - COMMUNICABLEDISEASES 53 152 175 69 178 95 722
Percentage 9 18 20 13 21 17 17
Surgery and medicine 10 4 20 9 30 5 78Anaesthesiology 7 1 9 9 18 25 69Radiology 12 2 8 6 16 16 60Haematology - 2 3 2 11 4 22Other medical and surgical specialties 9 12 48 35 46 16 166
Subtotal 38 21 88 61 121 66 395
Basic medical sciences 23 6 19 11 25 14 98Medical and allied education . . . . 1 146 53 8 94 21 323Undergraduate medical studies . . . 18 - 2 - 23 14 57
Subtotal 42 152 74 19 142 49 478
TOTAL - CLINICAL MEDICINE,BASIC MEDICAL SCIENCESAND MEDICAL AND ALLIEDEDUCATION 80 173 162 80 263 115 873
Percentage 14 21 19 14 30 20 21
GRAND TOTAL 574 823 860 556 865 569 4 2474
2 833 during 1976 (12 months) and 1 414 during 1977 (6 months).
74
HEALTH MANPOWER DEVELOPMENT
7.64 In the African Region, the fellow-ships programme gave priority to thetraining of teachers and officers responsiblefor management and services. Wherepossible, the training of fellows in institu-tions within the Region was emphasized.
7.65 As in the African Region, theemphasis in the fellowship programme ofthe South -East Asia Region was on train-ing within the Region. The RegionalOffice continued to collaborate with head-quarters in reviewing the fellowships pro-gramme and in identifying the interrelation-ship between fellowships and other com-ponents of WHO assistance. Althoughthere was progressive regionalization of thefellowship programme, i.e., placement offellows in institutions within the Regionwherever possible, the Regional Officecontinued to receive requests from Mem-ber States for fellowships to be awardedoutside the Region, even in subjects ofstudy for which facilities were availablewithin the Region.
7.66 In the European Region, theintercountry exchange of information onthe placement, supervision and follow -upof WHO fellows allowed closer collabora-tion between the Regional Office and thenational fellowships officers of MemberStates. The courses at the Universities ofOslo, Norway, and Leeds, United King-dom, on national health services aim tostimulate the exchange of information be-tween staff and trainees ; fellows may attendeither or both courses, which are heldconsecutively with a view to encouragingan exchange of ideas. The EuropeanRegional Office organized 23 trainingcourses in 1976, attended by a total of 169participants from 4o countries. As fromJanuary 1977, the Regional Office assumedresponsibility for administrative and tech-nical matters concerning undergraduatefellows from the African and Eastern
75
Mediterranean Regions studying in Bel-gium, France and Italy. Assistance in theform of fellowships and foreign lecturerswas provided for the English- and Russian -language courses for public health adminis-trators given in Moscow, USSR.
Evaluation and research
7.67 The lack of systematic monitoringof health workers' activities and subsequentadjustment of the planning and trainingprocesses is an obstacle to the efficientplanning and implementation of the healthservices. A first effort to develop evaluationprocesses was undertaken by the RegionalOffice for the Eastern Mediterranean, wherea study was undertaken that attempts todescribe the major activities of the healthmanpower development programme, toidentify the major issues or problems to beresolved, and to outline some possiblealternative strategies to deal with thoseproblems and issues.
7.68 The meaning, purpose and use oflearning objectives were discussed in 1976by a study group,' which proposed guide-lines for the evaluation and constructionof educational objectives that would makethem relevant to health service needs and tothe health needs and demands of the popu-lation.
7.69 Research activities on the tasks ofthe various members of the health teamwere completed in Brazil, Egypt andHungary.
7.7o Research aimed at defining thescientific basis for the profile of specialistphysicians was carried out by the WHOCollaborating Centre for Postgraduate Edu-cation at the Central Institute for AdvancedMedical Studies, Moscow, USSR.
' WHO Technical Report Series, No. 6o8, 1977.
THE WORK OF WHO
7.71 A feasibility study on the develop-ment of new approaches to trainingprimary health care workers was carriedout in Sudan to gather the data necessaryfor a two -year study. The resulting com-munication transfer project aims at develop-ing an improved system of communicationat village level in the Sudan, which willform a basis for adaptation to the needs ofother countries. Traditional concepts andpractices are being identified in selectedvillage communities. On the basis of thedata collected, scientific health informationwill be translated into educational conceptsand methods suitable to the villagers' frameof reference.
Migration of health personnel
7.72 The emigration of trained healthpersonnel is a costly drain on the healthservices of some countries least able toafford the loss. The WHO multinationalstudy on the international migration ofphysicians and nurses was completed andthe results submitted to the sponsoringagencies.' The findings showed that themigration of physicians and nurses, partic-ularly from developing countries to devel-oped countries, has increased significantlyduring the past few years. Unattractiveworking, service and living conditions forhealth workers, particularly in rural areas,poor career prospects and job satisfaction,and irrelevant training programmes andlack of health manpower planning wereidentified among the reasons.
Health manpower development informationservice
7.73 The Sixth General Programme ofWork covering a specific period (1978 -83)
1 See footnote i on page 65.
76
stressed the need to create services withinspecific programme areas to ensure theadequate provision and use of information.A health manpower development informa-tion service was created in July 1977 toserve as the focal point for (a) promotingthe exchange among Member States ofinformation on health manpower develop-ment, and (b) coordinating the developmentand operation of appropriate mechanisms,whether existing or new, for this purpose.
7.74 The service issued Health Man -power News on a trial basis to regionaloffices in September 1977 ; it aims toprovide educators, health workers andWHO field staff with information aboutnew trends and developments in healthmanpower development throughout theworld.
7.75 In Central America, an informationsystem was inaugurated for the collectionand distribution of basic information onavailable health personnel.
Examples of health manpower develop-ment activities in other programmes
Health services manpower development, healthmanpower planning and management
7.76 In the programme of strength-ening of health services various workshopsaimed at increased effectiveness in healthservice delivery. Other workshops con-centrated on country health programmingapproaches and their management andadministrative aspects.
7.77 The WHO -supported African In-stitute of Health Planning in Dakar, Sene-gal, provided French -language and English -language courses on health planning forhealth workers from many countries of theAfrican region. A workshop on project
HEALTH MANPOWER DEVELOPMENT
formulation, held in 1976, was attended bynationals and staff from some UnitedNations bodies. With the cooperation ofUNICEF, a multisectoral workshop onpublic health practice research, focusing onprimary health care, was held in 1976 inMbabane, Swaziland, for nationals fromBotswana, Lesotho and Swaziland. Aworkshop on country health programmingand project formulation was organized in1976 in Kano, Nigeria, with the participa-tion of national representatives from theNigerian Federal and State Governments,universities and international agencies.Similar workshops took place in 1977 inAngola, Ghana, Madagascar and Mozam-bique ; all of them emphasized the import-ance of the multisectoral approach toplanning and programming of countries'health systems.
7.78 National workshops were alsoorganized in 1976 in Bangladesh andMongolia, and in 1977 similar workshopswere organized in Bangladesh, Nepal andSri Lanka. The Regional Office for South -East Asia held a training course on theconcepts of country health programming,emphasizing programming and manage-ment aspects of maternal and child health.
7.79 A course on operational researchin public health was held in Bratislava,Czechoslovakia, in 1976. WHO alsocontributed in 1977 to a course in Lisbon,Portugal on the application of systemsanalysis to health management. In Thailandin 1976 a national workshop concentratedon implementation and management.
7.8o In the Western Pacific Region,training courses on management wereconducted in the Philippines in 1976 and1977 with WHO's collaboration. A nationalcourse on country health programming wassponsored in Papua New Guinea in 1977.A series of three courses in health manage-
77
ment was organized in the Philippinesduring 1977 with support from severalagencies.
7.81 A programme of manpower devel-opment in fertility management and mater-nal and child health care is being developedrelating to the training of all levels of healthworkers. A programme of this type wasinitiated in the Sudan in 1977 to comple-ment the national primary health careprogramme ; planning was also carried outfor the Mexican national family planningprogramme.
7.82 A Regional Programme of Con-tinuing Education in the administrationof family planning programmes was carriedout in the Region of the Americas, incollaboration with the School of PublicHealth in Mexico and with the Universityof the West Indies.
7.83 Under the programme of collabo-ration between the Government of Bulgariaand WHO, a training course on methods ofplanning, organization and management ofmaternal and child health services tookplace in Bulgaria in July 1977, for leadersand directors of maternal and child healthservices from French -speaking developingcountries (1 z participants from 9 countries).
7.84 The European Regional Office, incollaboration with the International Chil-dren's Centre, Paris, France, conducted atraining course on family health and familyplanning in Paris in October 1976, con-tinued in Algiers in October -November1976. Another course was conducted inIzmir, Turkey, in October -November 1977.
7.8 5 In the planning of mental healthservices, manpower planning aspects wereexamined at country level in three work-shops on psychiatric epidemiology or-ganized jointly with national healthadministrations (in Brussels, Belgium, in
THE WORK OF WHO
March 1977 ; Teheran, Iran, in April 1977 ;and Jakarta, Indonesia, in July 1977).These workshops made recommendationson the integration of mental health pro-grammes in general health planning. Tostrengthen expertise in modern techniquesfor planning, implementation, evaluationand research among the cadre of mentalhealth planners in developing countries, afour -month training programme was estab-lished in Geneva and in WHO collaboratingcentres in Czechoslovakia, Denmark, Indiaand the United Kingdom. The EuropeanRegional Office established a series ofcourses on the planning and evaluation ofmental health services. Three courses onmental health for public health adminis-trators from developing countries wereconducted in collaboration with schools ofpublic health in Belgium (in March 1977)and the United Kingdom (in May 1976 andMay 1977).
7.86 An international one -month courseon the organization of occupational healthservices was held in Bulgaria in 1976 totrain senior health planners from develop-ing countries (17 participants from 12
countries in all regions) in the integration ofoccupational health into public healthservices ; a second, similar course wasconducted in 1977.
7.87 As regards requirements for na-tional environmental health personnel,during 1976 -77 much emphasis was placedon the development of manpower studiesin accordance with Health Assembly resolu-tion WHAz6.59 adopted in 1973. In theEuropean Region a consultation was heldin December 1976 to review the results ofa study initiated in 1973 concerningregional manpower requirements in envi-ronmental health. A similar study isunderway in the South -East Asia Region,while a suitable methodology is beingdeveloped in cooperation with all Regional
78
Offices. Arrangements were made forcooperation with UNESCO in the educa-tion and training of environmental en-gineers and technicians.
Health coverage and new categories of healthpersonnel (including speciali <ed training)
7.88 In accordance with World HealthAssembly resolution wHAz8.88 of 1973 onthe promotion of national health servicerelated to primary health care, the pro-gramme of strengthening of health servicesdeveloped strategies for the training ofprimary health care workers. In 1976,training workshops were conducted in theSouth -East Asia Region for communityhealth workers ; the objectives of theseworkshops included : (a) defining educa-tional objectives for the retraining of healthworkers to enable them to adopt anappropriate approach to communities, andto train and support community healthworkers at the peripheral level ; (b) for-mulating . educational objectives for thetraining of community health workers onthe basis of tasks as defined by the commu-nities involved ; and (c) proposing train-ing requirements and the range of activitiesthat should be undertaken by communityhealth workers at the peripheral level,including team work.
7.89 At the University of Zaire, athree -year course for dietitian- nutritionistswas organized. In the Americas, specialefforts were made to strengthen and stan-dardize training programmes for non-medical nutritionists, while in the EasternMediterranean Region courses in publichealth nutrition were given at the Schoolof Public Health in Teheran, Iran.
7.90 Progress in building nationalcapabilities to train qualified health educa-tion specialists has been hindered by thelack of training facilities and the paucity of
HEALTH MANPOWER DEVELOPMENT
training personnel. WHO worked in allthe regions to establish national or regionalcourses to meet the needs of the countries.For example, the Organization contributedto the development of the African RegionalTraining Centre at the University of Ibadan,Nigeria, which offers a diploma course anda Master's degree in public health, withhealth education as a specialty ; the firstgroup of health education specialists gra-duated from the Centre in 1976. University -level training in health education was alsodeveloped at the Department of HealthEducation in Kenya, the Institute of PublicHealth in Kuala Lumpur, Malaysia, and theInstitute of Health Education in PapuaNew Guinea. Training as health educationauxiliaries was developed for students inthe National School for Social Action inGabon, and in Guinea -Bissau health educa-tion courses were organized for socialauxiliaries, members of the youth move-ment and first -aid workers.
7.91 The Organization's Special Pro-gramme of Research, Development andResearch Training in Human Reproductionis now the world's largest programme onthe training of scientists and techniciansfor research in human reproduction andfamily planning. Lack of expertise in epi-demiology and statistics is a major impedi-ment to service research in family planning,including field studies and clinical trials offertility -regulating methods. A course onthe application of epidemiology to suchresearch was organized by the SpecialProgramme in 1976 -77 at the LondonSchool of Hygiene and Tropical Medicine,United Kingdom, attended by trainees fromWHO collaborating centres in Hungary,India, Nigeria and Thailand. An under-standing of the cultural factors affectingfamily planning attitudes and practice isessential in the planning of appropriateprogrammes and selection of methods offertility regulation ; in both 1976 and 1977
79
a one -year training programme on researchinto acceptability was organized at theUniversity of Exeter, United Kingdom, forsocial scientists from developing countries.The highest priority for health serviceresearch in the Special Programme has beenthe use of different categories of non-physician health personnel to perform dif-ferent tasks in family planning care.Strengthening of laboratory capability wasalso a major objective of the Programme;three courses were held in Costa Rica,Thailand and the United Kingdom onlaboratory management, quality control,and the use of specialized equipment andstandardized procedures, respectively, at-tended by a total of 73 participants from47 developing countries.
7.9z WHO -sponsored English- languageand French -language courses in the epi-demiology and control of communicablediseases, which have been conducted since1966, were continued in collaboration withinstitutes in Czechoslovakia (Prague), Egypt(Alexandria), France (Paris), Ivory Coast(Abidjan), USSR (Moscow) and UpperVolta (Bobo -Dioulasso). The courses werestrengthened by special emphasis on evalu-ation procedures and on modern teachingmethods. Since 1966 over 30o persons from79 countries have attended the courses.
7.93 A travelling seminar on antimalariameasures for sanitary engineers was organi-zed in 1976 ; it started in Berkeley, USA,and was completed in El Salvador ; in 1977a similar seminar was conducted in Bombay,India. In collaboration with the Ministryof Health of Algeria, a seminar on environ-mental health project formulations in vectorcontrol was held at the Institut national dela Santé publique, Algiers ; its mainobjective was to assist in the planning andprogramming of a national plan for envi-ronmental health in Algeria. At the requestof the Bulgarian Government, lectures on
THE WORK OF WHO
vector biology and control were given inOctober 1977 at the Institute of Hygieneand Epidemiology, Varna, Bulgaria, as partof the training of entomologists in epide-miological surveillance and control ofcommunicable diseases. Supported by agrant from DANIDA, a course on theecology and control of rodents was givenin 1976 at the Danish Pest InfestationLaboratory, Lyngby, Denmark, and at thePest Infestation Control Laboratory, Tol-worth, United Kingdom, attended by15 participants from 11 developing coun-tries ; particular emphasis was laid on thedetection of resistance to rodenticides andthe counter -measures to be taken should itappear. In the Western Pacific Region, thefirst regional seminar on the safe use ofpesticides was organized in Manila in 1976 ;it was followed, also in 1976, by an inter-regional seminar on epidemiologicalmethodology for the study of pesticidepoisoning and of potential long -term effectsof exposure to pesticides, arranged inGeneva for senior health administrators incharge of emergency services.
7.94 In the South -East Asia Region,training in mental health for all categoriesof health personnel was supported in fourcountries. Mental health training for nursesreceived special attention in several re-gions ; to improve the exchange of informa-tion and the coordination of these activities,a cooperative network consisting of nursingschools in all parts of the world is beingestablished.
7.95 The Organization sponsored atraining course in the Federal Republic ofGermany and the United Kingdom inJanuary -April 1976 to familiarize X -rayengineers and engineering technicians withthe different types of radiological equip-ment and routine maintenance and repairof such equipment ; the course was attendedby participants from countries in all WHOregions except the European Region.
8o
7.96 WHO conducted training coursesin collaboration with its network of im-munology research and training centres (inSao Paulo, Brazil ; New Delhi, India ;Teheran, Iran ; Nairobi, Kenya ; Ibadan,Nigeria ; and Lausanne, Switzerland), vary-ing in duration from two weeks to threemonths and attended by approximately140 participants from at least 4o developingcountries ; the major aims of the courses,which are a regular feature of WHO's im-munology programme, were to teachmodern concepts and techniques in im-munology as applied to diseases of localpublic health importance.
7.97 Manpower development in thehealth laboratory field was promotedthrough the participation of WHO fieldstaff in several national training courses,support to training centres and the provi-sion of teaching aids. For instance, aNational Quality Control Seminar washeld in New Delhi, organized by theDirectorate of Health Services of theGovernment of India. With the support ofDANIDA, WHO organized interregionaltraining courses for the improvement ofquality analysis in clinical chemistry, inGhana (Accra), Iraq (Baghdad), IvoryCoast (Abidjan) and Malaysia (Kuala Lum-pur), for 56 participants from 42 countries ;as a follow -up to these courses, all parti-cipants were included in a proficiencytesting programme based on WHO col-laborating centres. An interregional train-ing course on simple techniques used forlaboratory diagnosis in haematology washeld in Thailand for 15 participants from1z countries ; the diagnosis of anaemias ofpublic health importance and methods ofcontrol were stressed.
7.98 There is a great shortage of trainedmanpower for environmental hazards con-trol, particularly in developing countries.Under an agreement with the Government
HEALTH MANPOWER DEVELOPMENT
of Bulgaria and WHO, three trainingcourses in environmental pollution controlwere organized in Sofia during 1976 and1977. These courses were attended by4S participants from developing countries.Other training activities included an inter-regional course on coastal water pollutioncontrol in 1976, organized in Copenhagen,Denmark, under the sponsorship of DA-NIDA ; regional courses on solid wastemanagement in 1976 and water pollutioncontrol in 1977, organized by the RegionalOffice for the Western Pacific ; and severalregional training courses in air pollutionmonitoring and control in 1977 (in allregions except Europe).
7.99 WHO continued its work toupgrade the training of food hygienists.Courses in food microbiology were held in1977 at the FAO /WHO CollaboratingCentre for Research and Training in FoodHygiene at the Robert von OstertagInstitute of Veterinary Medicine, Berlin ;at the University of Surrey, Guildford,United Kingdom ; and at the CentralInstitute for Nutrition and Food Research,Zeist, Netherlands. In addition, a courseon food control was held in Sofia, Bulgaria.
Curricular reform
7.100 The Organization cooperatedwith various countries in the revision anddevelopment of suitable curricula for theundergraduate teaching of physicians andother health workers in maternal and childhealth, family planning, paediatrics andobstetrics. There was a need to orientcurricula more towards the specific mater-nal and child health tasks that healthworkers have to perform at various levelsin each country, depending on national andlocal priorities. In India, a new curriculumdevised by the WHO ad hoc committee onpaediatrics education was demonstrated intwo medical colleges in order to propagate
óI
new concepts of teaching child health at theundergraduate level, and arrangementswere made for heads of departments inother medical colleges to visit these twocentres.
7.101 The mental health programmepromoted new curricula in mental healthfor nurses, with emphasis on the manage-ment of mental disorders (where increasingstress is placed on community and out-patient experience) and on the psychologicalaspects of nursing. Training programmesin the area of drug dependence and alcohol -related problems were carried out in coun-tries in three Regions (the Americas,Europe, and South -East Asia). Activitiesto strengthen the teaching of psychiatry inmedical education were undertaken in theSouth -East Asia and Eastern MediterraneanRegions. The establishment of psychiatryin the medical curriculum and a betterundergraduate orientation in mental healthhas now been achieved in all countries ofthe South -East Asia Region.
7.1o2 The Organization initiated a jointtraining programme with the InternationalFederation of Health Records Organiza-tions, with the objective of increasing andimproving training facilities in the healthrecords field. Within the framework ofthis programme, a technical service agree-ment was concluded with the New SouthWales Training School for Medical RecordsAdministration, Australia, for a two -yearstudy on : (a) setting learning objectivesbased on a systematic analysis of thestudents' future professional functions, and(b) evaluating the teaching programme andmethods to ascertain whether the objectiveshave been achieved.
Teacher training
7.103 As part of WHO's family healthprogramme, courses were organized for

THE WORK OF WHO
teachers in paediatrics and administratorsin maternal and, child health. In 1976 -77 aUNICEF /WHO course for senior teacherstrained 24 potential professors of childhealth and paediatrics ; this collaborativetraining effort is now being shifted fromthe interregional to the country level in theSouth -East Asia Region, with the participa-don of a team of paediatricians trained inIndia, Peru, Philippines, Sudan and Thai-land.
7.104 A manual on health statistics forteachers of medical students was publishedin 1977, jointly sponsored by the Inter-national Epidemiological Association andWHO ;1 its purpose is to help teachers torelate their teaching of statistics to therealities of human biology, medical practiceand research and the management of healthservices. A workshop on educationalaspects of teaching health statistics washeld in Cardiff, United Kingdom, in 1977,with the collaboration of the Department ofEducation, University College, Cardiff ; theparticipants -experienced teachers of me-dical undergraduate and postgraduatestudents, medical records personnel, inter-mediate level statistical staff and teachers ofstatistics in international training courses -learned how to assist their students toattain learning objectives more effectively.
Teaching /learning materials
7.105 To improve the teaching offertility- regulating methods based on per-iodic abstinence, the Organization devel-oped a curriculum outline in the form of amanual for teachers, including supportiveteaching /learning materials ; this manualis about to be field- tested in different coun-tries. WHO supplied much -needed teach-
Lowe, C. R. & Lwanga, S. K., ed. Health statistics :A manual for teachers of medical students. Oxford, OxfordUniversity Press, 1977.
ing materials and teaching aids on malariaand parasitic diseases, including self- instruc-tional packages, to various institutions inall regions. Work was begun in 1977 on thepreparation of teaching -aid packagesdealing with various aspects of environ-mental hazards control. Training material,in the form of instructors' notes andparticipants' notes, was prepared for thereorientation of trained coders to the useof the Ninth Revision of the InternationalClassification of Diseases.
Continuing education /fellowships
7.106 The Organization's programmein family health emphasized the need topromote post -graduate training in fertilitymanagement and maternal and child healthcare. During 1976 -77 three courses weregiven at the University of Singapore,attended by 39 participants from developingcountries, covering the multidisciplinaryteam -work approach and the developmentof skills of service management for inte-grated maternal and child health and familyplanning care and instructional techniques.
7.107 Through its network of collabo-rating centres (in Buenos Aires, Argentina ;Santiago, Chile ; New Delhi, India ; Stock-holm, Sweden ; and Moscow, USSR) theSpecial Programme of Research, Develop-ment and Research Training in HumanReproduction sponsored courses on ad-vanced laboratory methodology and re-productive biology. In addition, two col-laborating centres for clinical research inhuman reproduction provided advancedresearch training : in Ibadan, Nigeria, inthe form of a three -year course for Africanscientists on reproductive biology, and inBangkok, Thailand, on laboratory metho-dology. About 100 research training grantswere awarded by the Special Programmeduring the biennium, primarily to trainees
HEALTH MANPOWER DEVELOPMENT
from developing countries, and mainly insuch areas as laboratory and clinicalresearch methods, male reproduction, im-munology and infertility. During theperiod of training, trainees are encouragedto formulate a research project that theywill conduct, with WHO support, onreturn to their home institutions.
7.108 The malaria and other parasiticdiseases programme helped to organizeshort -term and long -term courses for healthworkers wishing to follow a career intropical public health. The objectives ofthe long -term courses are to enable theparticipants (a) to select priorities in publichealth activities in terms of feasibility underthe local socioeconomic conditions, (b) toplan, implement, and manage eradicationor control programmes for malaria andother parasitic diseases, and (c) to provideor secure required training for subordinatestaff. The first course of this kind (inEnglish) was organized at the School ofPublic Health, University of Teheran, Iran,during September 1975- December 1976 ;a second course is extending over theperiod August 1977- December 1978.Similar ten -month courses in Spanish areorganized regularly at the School ofPublic Health, Mexico City. The RegionalOffice for Africa, in collaboration with theNational University of Benin, has organizeda French -language post -graduate publichealth course in Cotonou, Benin, fromSeptember 1977 to June 1978.
7.109 During 1976 -77 the ExpandedProgramme on Immunization sponsoredone interregional and six regional trainingseminars attended by more than zoo par-ticipants from over 6o countries. Theinterregional seminar served the dual pur-pose of field -testing a newly developedExpanded Programme training course fornational programme managers, and train-ing international staff to be trainers of pro-
83
gramme manager -level national staff fromcountries participating in the ExpandedProgramme. The six regional seminarswere attended by senior health officials andby representatives of potential donoragencies ; they discussed the strategies andobjectives of the Expanded Programme.
7.1 i0 In September 1977, the SpecialProgramme for Research and Training inTropical Diseases organized a joint FAO /WHO /OAU leadership training seminaron trypanosomiasis in Nairobi, Kenya. Theoverall objective of the seminar, which wasattended by approximately 5o young scien-tists from 34 countries in the African andEastern Mediterranean Regions, was totrain graduates who were not yet expe-rienced in trypanosomiasis but who wishedto take up a career in the field control ofthe disease ; emphasis was placed on theinterrelationships between the entomo-logical and veterinary disciplines.
7.111 In collaboration with the Natio-nal Institute of Neurological and Com-municative Disorders and Stroke, USA,the Organization sponsored courses forsenior public health workers and neuro-logists on the use of anti -epileptic drugsand on genetic metabolic diseases of thenervous system. A fellowships programmefor advanced post -doctoral training in theneurosciences, financed by the NationalInstitute, was designed which during itsinitial phase will place emphasis on con-vulsive and cerebrovascular disorders. Incollaboration with the Menarini Founda-tion, Florence, Italy, an international sym-posium was organized on perspectives inpsychopharmacotherapy, to review prob-lems in the treatment of common mentaland neurological disorders, both in devel-oped and developing countries. TheOrganization collaborated with the Natio-nal Institute of Mental Health, USA, to
THE-,WORK OFiWHO
arrange a workshop on psychopharmaco-therapy, attended by specialists from deve-loping countries. Post -graduate trainingcourses in psychiatry were supported in sixcountries in the South -East Asia, EasternMediterranean and Western PacificRegions ; for instance, WHO cooperatedwith Saudi Arabia in developing localpost -graduate courses in psychologicalmedicine.
7.112 Fifteen senior pathologists fromEgypt, Iran, Iraq, Libyan Arab Jamahiriya,Saudi Arabia, Sudan and Tunisia and about20 observers from the University ofBaghdad attended a WHO seminar on thehistological classification of tumours, heldin 1 976 at the College of Medicine, Uni-versity of Baghdad, Iraq, in collaborationwith the Regional Office for the EasternMediterranean. The seminar concentratednot only on correct diagnosis but also onthe problem of standardization in recordingand reporting diagnostic information ; theneed for uniformity to promote interna-tional communication was stressed. Incollaboration with the International Societyand Federation of Cardiology, WHO spon-sored ten -day teaching seminars in MexicoCity in 1976 and Accra, Ghana in 1977 onthe epidemiology and prevention of cardio-vascular diseases. Forty fellows attendedeach seminar. Candidates for the scholar-ships programme sponsored by the Swedish
National Association against Heart andChest Diseases were selected.
7.113 In collaboration with the Insti-tute of Occupational and RadiologicalHealth in Belgrade, Yugoslavia, WHOsponsored a one -month course on occu-pational toxicology. The course providedtraining for occupational health personnelin the methodology of evaluating toxiceffects of industrial chemicals and theconduct of epidemiological studies, parti-cularly monitoring occupational health.Twenty -four participants from 15 countriesin all WHO regions attended the course.
7.114 Under the auspices of the inter-agency Ad Hoc Working Group on RuralPotable Water Supply and Sanitation,WHO organized a French- language work-shop on rural water supply and sanitationin Ouagadougou, Upper Volta, inDecember 1976 ; the workshop broughttogether 3o senior planners and watersupply personnel from 15 countries in theAfrican and European Regions. TheGovernments of France, Switzerland,Upper Volta and USA provided financialand material support for the workshop,which emphasized the problems of watersupply and sanitation in rural areas andencouraged the allocation of higher priorityto programmes in the sector. The work-shop was followed by sector studies underthe WHO /IBRD Cooperative Programme.
84
Chapter 8
Communicable Disease Prevention
and Control
8.1 C TUDIES of mortality and morbid-) ity continue to reflect and
highlight the epidemiologicalimportance of the interrelationship betweencommunicable diseases, malnutrition andunhealthy environment. While techniquesof communicable diseases control have un-doubtedly improved, and new ones arebeing devised, their application should beseen in the context of national socioeco-nomic development and the utilization ofoverall resources. Problems resulting fromweakness of epidemiological surveillancesystems, health infrastructure and support-ing services continue to demand specialattention. Within such a context, thecommunicable diseases programme focusedon (i) improving epidemiological andcontrol services as an integral part ofnational health services at all levels ;(z) collaborating in the investigation andassessment of specific diseases of publichealth importance, to identify the mostpromising epidemiological and controlmeasures ; (3) the training of professionaland auxiliary staff at planning, operationaland research levels ; and (4) promotingand coordinating basic and applied re-search, particularly on diseases for whichcontrol measures are more difficult toapply or about which more knowledge isrequired.
85
Epidemiological surveillance
8.z During its nineteenth session inNovember 1976, the Committee on Inter-national Surveillance of CommunicableDiseases undertook a broad review ofthe basic concepts underlying the Inter-national Health Regulations. The Com-mittee felt that the Regulations wouldcontinue to be of value despite changingepidemiological circumstances. Since theRegulations represented the maximum mea-sures that should be taken, Member Statescould reduce their requirements relatingto international travel at any time inaccordance with the current epidemio-logical situation. The Committee expressedconcern that the vaccination certificaterequirements notified to WHO by manyStates did not agree with the actual practiceat points of entry to those countries ; thissituation often resulted in unnecessarydifficulties for travellers.
8.3 An outbreak of viral haemorrhagicfever in southern Sudan and northernZaire in the latter half of 1976 led theCommittee to consider whether such dis-eases should be included in the existing listof diseases under surveillance. Theirinclusion was not recommended because ofthe difficulty of excluding other diseasescausing greater morbidity and mortalityand because the prompt reporting of
THE WORK OF WHO
significant outbreaks of communicable dis-eases is the best foundation for theirinternational control, irrespective of theirinclusion in any particular list.
8.4 Between the Committee's meetingand the Thirtieth World Health Assemblyin May 1977, which approved the Com-mittee's recommendations and views 1(resolution wHA30.19), a previously un-suspected focus of smallpox in Somaliahad become evident. This outbreak,which subsequently gave rise to some3000 cases, caused concern that wasapparent in the Assembly's discussion onthe modification, on sound epidemio-logical grounds, of smallpox vaccinationcertificate requirements by Member States.In general, however, the absence of majordifficulties in administering the Inter-national Health Regulations during 1976-77 reflected a relatively tranquil period asregards communicable diseases relating tointernational travel.
8.5 The surveillance and control ofsalmonella and food -borne outbreaks werereoriented within the framework of sur-veillance and control of acute infections ofthe intestinal tract and the promotion ofenvironmental health (in particular, jointFAO/WHO monitoring of food contami-nation and food -borne diseases to ensurefood safety and the control of thesediseases). This activity will increasinglydevolve on regional offices ; those for theAmericas and Europe, in particular, arealready developing it. Interregional co-ordination and dissemination of informa-tion to assist these regional activities is theresponsibility of WHO headquarters.
8.6 Although the laboratory plays anessential role in the surveillance of influenza,epidemiological indices need to be used in
1 WHO Official Records, No. 240, 1977, Annex ,.
86
systems designed to provide an earlywarning of developments in the diseasesituation and to evaluate the impact of thedisease. To assist in the promotion ofnational systems monitoring epidemio-logical indices, a study was carried out ofefficient systems used in the Netherlandsand the United Kingdom. Informationon the organization and epidemiologicaleffectiveness of these systems was madeavailable to health administrations, inparticular through the Weekly Epidemio-logical Record.
Malaria and other parasitic diseases
Malaria
8.7 Malaria continues to be a majorpublic health problem in the majority oftropical countries. The recent past has seena return of malaria to wide areas that hadbeen largely freed from the disease(Fig. 8.i). The number of microscopicallydiagnosed malaria cases reported has in-creased from 3.z million in 197z to 7.5million in r 976. In the epicentre of malaria,i.e., tropical Africa, the malaria situationhas remained practically unchanged, withbolo- and hyper -endemicity prevailing inmost African countries south of the Sahara.In South -East Asia, reported cases haveincreased from 1.9 million in 197z to 6.5million in 1976. Malaria has re- establisheditself at the former endemic levels in severalareas of Bangladesh, India and Sri Lanka,and the situation has worsened in Thailand.
8.8 Technical problems in the form ofvector resistance to insecticides, drugresistance of parasites, and factors asso-ciated with human ecology are still un-solved ; administrative and financial con-straints remain important obstacles to theimplementation of effective control pro-grammes, especially in the rural areas of
COMMUNICABLE DISEASE PREVENTION AND CONTROL
the tropics. Resistant falciparum malariahas established itself in areas with a popu-lation of nearly 45 million, and areas witha population of 90 million are at graverisk of invasion by resistant strains of thisparasite.
8.9 In pursuance of the revised strategyof the antimalaria programme called forby the World Health Assembly in 1968(resolution WHAZ1.22), a thorough reviewwas made of the programme at all levels.A Health Assembly resolution of 1976(wHA29.73) provided the basis for theOrganization's present policy.
8.10 In the African Region a pro-gramme covering the period 1978 -83 wasprepared with the principal objective ofreducing mortality and morbidity. Feasi-bility studies will be conducted and eradi-cation programmes undertaken in areaswith adequate technical and financial re-sources.
8.11 In the Region of the Americas themajority of countries reviewed their pro-grammes in order to (I) include the appli-cation of combined control methods usinginsecticides, antimalarial drugs and engi-neering schemes such as drainage, land-fill and cleaning of canals to eliminate orreduce mosquito breeding places, and (z)assign a high priority to the training ofprofessionals who work in malaria. Thusa Master in Public Health course withemphasis on malaria and other parasiticdiseases has been held in Mexico since1976, a postgraduate entomological coursestressing epidemiology was conducted inSao Paulo in both 1976 and 1977, anda seminar for engineers on mosquitocontrol, with emphasis on bio- environ-mental methods, was held in California,USA, and in El Salvador in 1976. Assess-ments were conducted of the programmesin Brazil, Haiti and Nicaragua, and periodic
87
coordination border meetings were heldby the malaria programmes of neighbour-ing countries. Thus the rigid criteria of thetraditional methodologies are evolvingtowards operational flexibility on a sounderepidemiological, socioeconomic, health andresources basis, in each country.
8.1z In the South -East Asia Region,assessments of the Bangladesh and Indo-nesia programmes were made and stepstaken to institute a malaria containmentprogramme in areas of India with a popu-lation of 7o million people where Plas-modium falciparum is prevalent. Greatefforts were made to reorganize the malariaservice in India by decentralizing andredistributing technical staff, strengtheningsurveillance activities, and concentratingefforts in areas of great socioeconomicimportance.
8.13 In the European Region advicewas given to the Governments of Algeriaand Turkey in making plans to control thetransmission of malaria and in assessing theprogramme. WHO also contributed staffand funds during the malaria epidemic inthe Adana area of south -eastern Turkey,where 103 000 cases were reported up tothe beginning of October 1977 and wherethe local vector shows resistance to mostof the classical insecticides.
8.14 In the Eastern MediterraneanRegion, time -limited eradication pro-grammes were converted into non -time-limited malaria control programmes inAfghanistan, Ethiopia 1 and Pakistan. Thecoordinated malaria programme in theArabian peninsula was being organizedand will be carried out simultaneously inDemocratic Yemen, Oman, the United
1 In May 1977 the World Health Assembly agreed toEthiopia's request to be included in the African Region(resolution wHA3o35)
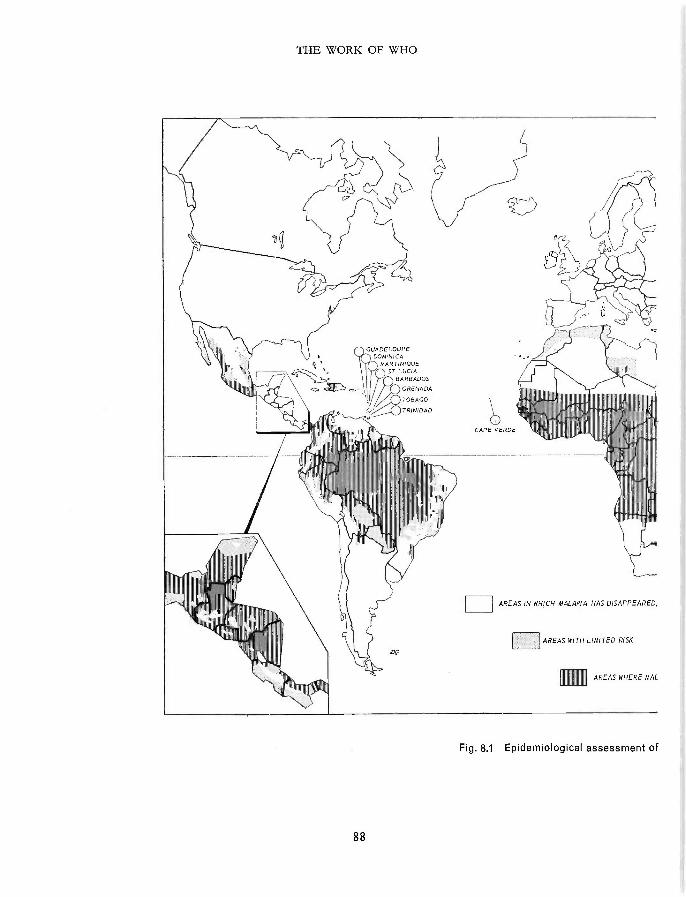
THE WORK OF WHO
GUADELOUPEDOMINICA
MARTINIQUEST LUCIA
BARBADOS
GRENADA//XTRBADO_ TRINIDAD
DQ
CAPE VERDE
AREAS IN WHICH MALARIA HAS DISAPPEARED,
AREAS WITH LIMITED RISK
AREAS WHERE MAL
Fig. 8.1 Epidemiological assessment of
88
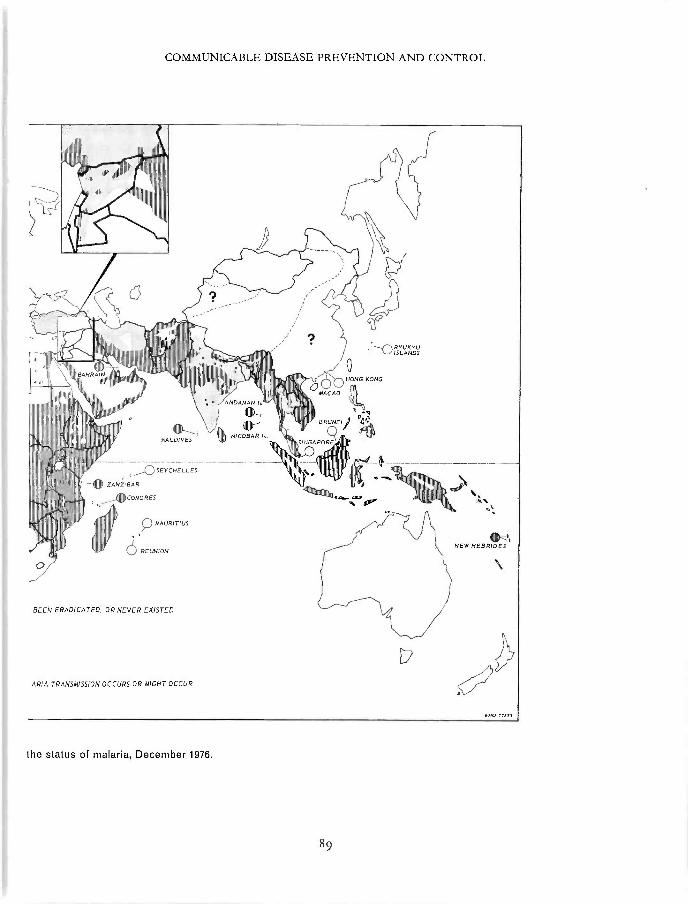
COMMUNICABLE DISEASE PREVENTION AND CONTROL
ANDA MAN I
,'Jl RYUKVUll_JJ ISLANDS
HONG KONG
°MACAO
BRUNE /MALDIVES
111111'
Iq NICOBAR Is.
SEYCHELLES
ZANZIBAR
COMORES
pMAURITIUS
REUNION
BEEN ERADICATED, OR NEVER EXISTED
WY\S/NEW HEBRIDES
ARIA TRANSMISSION OCCURS OR MIGHT OCCUR
the status of malaria, December 1976.
89
THE WORK OF WHO
Arab Emirates and Yemen. In order topromote self -reliance and self -help, theRegional Office encouraged countryschemes aimed at the direct participation ofcommunities in antimalaria operations andsupported intercountry coordination andcooperation to develop common policiesand strategies.
8.15 Coordination activities took placebetween countries in the South -East Asiaand Western Pacific Regions (Malaysia,Singapore and Thailand). Courses andseminars were organized with WHO co-operation in the Lao People's Demo-cratic Republic, Malaysia, Papua NewGuinea and the Philippines. A regionalcourse for professional staff on the opera-tion and assessment of antimalaria pro-grammes was organized in Kuala Lumpurin July 1976.
8.i6 Priority areas of applied malariaresearch include : base -line assessment andmonitoring of drug sensitivity in P. falci-parum, evaluation of community partici-pation in antimalarial activities, chemo-prophylaxis in children of malaria- endemicareas, approaches towards malaria controlin problem areas, impact of pattern appli-cation of insecticides, and strain distributionof P. falciparum. Efforts were made,within the framework of the Special Pro-gramme for Research and Training inTropical Diseases, to assist the regions inthe implementation of these programmes.Work on strain differentiation and on drugsusceptibility testing and monitoring (invitro) relating to P. falciparum infection wasalready being implemented in the South -East Asia Region, and a project was under-way on chemoprophylaxis in malaria -endemic areas of Africa.
8.17 An applied research project thatwas in progress in Bendel State, Nigeria,should assist in answering the following
90
question, with special reference to tropicalAfrica : What malaria control strategy,using presently available methods, is to berecommended and where, when, and howshould it be applied ? Given the variety ofsituations available for study in BendelState, extrapolation of the results to otherparts of Nigeria and tropical Africa will bepossible. Antimalaria strategies will beevaluated not only in terms of their effect onthe transmission of infection but also interms of their effect on the health ofpopulations.
8.18 A review of research activitieswithin the framework of the Special Pro-gramme for Research and Training inTropical Diseases was carried out inDecember 1977 with the participation ofmalariologists, scientists, public healthadministrators, and representatives fromtropical countries, WHO regions, andinternational and bilateral agencies.
8.19 In chemotherapy, emphasis wasgiven to clinical trials of mefloquine, tothe formulation of sustained -release systemsof highly potent drugs such as 8- amino-quinolines and triazines, to comparativetrials of existing drugs and their combi-nations, and to the screening of selectedcompounds for tissue schizontocidal andsporontocidal activity. Promising candidatecompounds (e.g., menoctone -type drugs,related naphthoquinones, diamino- quina-zolines and 8- aminoquinolines) were fol-lowed up and investigations conducted onsuch factors as parasite -drug interaction,the mechanism of drug resistance, andlead -directed synthesis of compounds.
8.2o The successful establishment ofthe continuous in vitro cultivation of P.falciparum, which renders the parasitematerial available to laboratories outsidemalaria- endemic areas, opened up newhorizons for the mass production of mero-
COMMUNICABLE DISEASE PREVENTION AND CONTROL
zoites, while the successful immunizationof humans against P. vivax and P. falciparuminfections, using irradiated sporozoites, andrecent advances in the area of gametevaccines will greatly facilitate work onvaccine development. In the short term,studies in the immunoserological researcharea are likely to produce simple andreliable immunodiagnostic test systems,which are urgently required for epidemio-logical purposes in the field.
Schistosomiasis
8. z 1 In 1976 -77, WHO staff visited thefollowing countries : Brazil (where possibly6 million people are infected), to advise onthe implementation of control measuresagainst Schistosoma mansoni infections ; CapeVerde, to advise on the strategy, tactics andimplementation of a national plan to controlintestinal helminthiases ; Jordan, to evalu-ate the threat of schistosomiasis ; Mexico,to give instruction on epidemiology andcontrol and to advise an internationalmeeting on the chemotherapy of cesto-diases ; Saudi Arabia, to advise on thechemotherapy of schistosomiasis and onthe projected national control scheme ; andTunisia, to assess the schistosomiasis con-trol programme. Visits were made to theWHO Tropical Disease Research Centre,Ndola, Zambia, in connexion with trials ofa new schistosomicide. Liaison was estab-lished with IARC on the subject of drugtoxicology.
8.2 z The aim of the UNDP /WHOproject "Research on the epidemiology andmethodology of the control of schisto-somiasis in man -made lakes" in Accra,Ghana, supported by the Edna McConnellClark Foundation and the Governments ofCanada, the Netherlands and the UnitedKingdom, is to provide a feasible andacceptable methodology for the controlof schistosomiasis in Lake Volta and otherman -made lakes by the end of 1978, when
91
the Government of Ghana assumes re-sponsibility for activities. Acceptable curerates were obtained in the three chemo-therapeutic campaigns implemented from1975 to 1977, and age- specific intensities ofinfection were markedly diminished. Focalchemical control of snails in human watercontact sites drastically reduced the num-bers of infected intermediate hosts. Theintroduction of water supplies in lakesidevillages greatly reduced human contactwith lake water.
8.23 In the Philippines, WHO col-laborated in FAO /IBRD /Asian Develop-ment Bank missions on the planning ofland development schemes with a schisto-somiasis control component.
8.24 Activities in the programme onman -made lakes, in response to HealthAssembly resolutions in 1975 (wHAZ8.53),and 1976 (wHA29.58), included : continuedwork on elaborating guidelines for theprevention of schistosomiasis and otherhealth hazards in water developmentschemes, a mission to South America toassess present and future health problemsin all types of existing and planned waterdevelopment projects, and sending a ques-tionnaire on schistosomiasis control to anumber of Member States.
8.z5 In 1 977 a Scientific WorkingGroup on Schistosomiasis, held within theframework of the WHO Special Pro-gramme for Research and Training inTropical Diseases, elaborated strategy forfuture research.
Filarial infections (including onchocerciasis)
8.z6 Work on the control of bancroftianfilariasis included the WHO interregionalproject located in the United Republic ofTanzania, the object of which is to developsimple methods of controlling the diseasethat can be applied on a community basis.A longitudinal study of the transmission
THE WORK OF WHO
of lVuchereria bancrofti was underway toassess the effects of different controlmeasures (large -scale diethylcarbamazinetreatment, vector control, house modifi-cation). In Egypt, a survey conducted inthe Qalyubia area in connexion with con-trol operations received WHO support.As part of the intercountry epidemio-logical and surveillance services project,cooperation was provided in the SouthPacific to the New Hebrides in revising thereporting system, to Niue in planning apost -control survey, and to Tonga inanalysing the results of the entomologicalblood survey of 1976 and in organizing anationwide control programme and train-ing newly recruited staff.
8.27 Particular problems that arose inconnexion with the onchocerciasis con-trol programme in the Volta River basinarea in West Africa (see below) concernedthe methods used for epidemiological sur-veillance, the early detection of personswho are at special risk of blindness, theanalysis of data, the possibility of intro-ducing nodulectomy or chemotherapy intothe programme, the reinvasion of parts ofthe controlled area by Simulium damnosummigrating over great distances, and thedefinition of criteria by which areas pre-viously deserted, largely on account ofonchocerciasis, may be judged safe forresettlement. Advice was given to theGovernment of Sudan in making plans tocontrol the transmission of onchocerciasisand to treat infected persons who are atrisk of blindness or have acute skin lesions.
8.z8 The advent of funds for the SpecialProgramme for Research and Training inTropical Diseases enabled the researchprogramme on filarial diseases to be greatlyexpanded and coordinated with the researchactivities of the onchocerciasis controlprogramme. The Scientific WorkingGroup on Filariasis concentrated on the
92
field of chemotherapy, where there is adire need for improved macrofilaricides(especially those effective against Onchocercavolvulus), for slow- acting microfilaricides,and for chemoprophylactic drugs. Severalresearch projects were started in Africadesigned to determine the most effectiveand acceptable ways of using the drugs thatare at present available for treating oncho-cerciasis. The search for new filaricidesinvolves a long -term programme consistingof basic lead -directed chemical synthesis,followed by screening in animal models,and finally toxicity studies and clinicaltrials. Research was sponsored to study(a) the feasibility of vaccine development,(b) the mechanism and means of preventingthe production of immuno -pathologicallesions in infected persons, (c) in vitromaintenance and culture methods forfilarial parasites, and (d) a programme ofepidemiological research to developmethods of detecting persons at specialrisk and to improve methods of controllingtransmission, particularly by the use ofrelatively simple measures of the "self -help" kind.
Onchocerciasis control programme
8.29 During 1976 and 1977 phases IIand III of the control programme in theVolta River basin area were implementedaccording to schedule. This means that,as planned, operations now cover an areaof 700 00o km' in seven countries of WestAfrica -Benin, Ghana, Ivory Coast, Mali,Niger, Togo and Upper Volta -and ap-proximately i z o0o km of river are beingsurveyed and treated weekly in the rainyseason. The biodegradable insecticideABATE (temephos 1) formulated specificallyfor the programme is being applied byhelicopters and fixed -wing aircraft based
1 Proposed international common name.
COMMUNICABLE DISEASE PREVENTION AND CONTROL
at Tamale in northern Ghana and Bobo -Dioulasso in Upper Volta.
8.3o The data collected continuouslyby mobile entomological teams workingfrom 7 sector and zz subsector offices con-firmed that the vector is being successfullycontrolled throughout the area. Modi-fication of the spraying technique resultedin a substantial improvement in the controlof difficult breeding sites such as Bui on theBlack Volta.
8.31 Epidemiological base -line datawere collected from over 3 0o villagesthroughout the programme area and willbe used in the assessment of vector controlmeasures. At the same time, detailedophthalmological examinations of patientsin a smaller number of villages led to abetter understanding of how blindnessdevelops as a result of onchocerciasis
8.3 z While the control of onchocerciasisis essential to improve the wellbeing of theafflicted population, the programme wasplanned to open up the area for economicdevelopment. During the biennium, donorcountries and international agencies wereengaged in carrying out preinvestmentstudies. The programme's economic devel-opment unit was strengthened in 1977 sothat it can play a more active role in thecollection, analysis and dissemination ofdevelopment data in the area covered bythe programme. While some resettlementschemes and agricultural and industrialprojects were already underway, the pro-gramme was requested to provide criteriathat would indicate when a river valleyshould be considered safe for settlement.A working group of the programme'sScientific Advisory Panel set as criteria anannual biting rate for S. damnosum sensulato of loon flies and an annual transmissionpotential of ioo infective -stage larvae,levels that have already been reached inmany river valleys.
93
8.33 The overall administrative respon-sibility for the programme was transferredfrom WHO headquarters to the RegionalOffice for Africa at the beginning of 1977.At the same time a new programme directorwas appointed with full responsibility for allactivities. All functions are now controlledfrom programme headquarters in Ouaga-dougou. In addition, a liaison officer wasappointed at the Regional Office.
8.34 The programme is financedthrough a special Onchocerciasis Fund re-ceiving donations to date from 14 countriesand agencies. The budget requirementfor the first six -year period (1974 -79)is now estimated at US $ 57 3 zo 000, i.e.,about US $ 4 million less than estimatedearlier. The programme established anumber of contracts with institutions andscientists to carry out applied research in(a) vector ecology, including studies on thevarious species of the S. damnosum complexand on the development of samplingdevices ; (b) vector control -mainly testingalternative insecticides and formulations,(c) epidemiological, clinical and parasito-logical aspects of the disease and (d) chemo-therapy. With the establishment of thelarvicide operations, chemotherapy researchis being intensified in collaboration with theSpecial Programme for Research andTraining in Tropical Diseases.
8.35 An aquatic monitoring programmeshowed that the non -target riverine faunais remaining healthy despite the weeklyapplication of insecticide.
8.36 The programme's Scientific andTechnical Advisory Committee, EcologicalPanel, and Economic Development Advis-ory Committee met regularly to reviewthe operational, research and environmentalaspects of the programme. These bodiesreported to the Joint Coordinating Com-mittee, which met in December 1976 andDecember 1977 to consider progress and

THE WORK OF WHO
to approve the budget for the followingyear. At its third meeting, held in Ouaga-dougou in December 1976, five partici-pating countries requested an extension ofoperations beyond the present boundaries ;this possibility is now under consideration.
African trypanosomiasis
8.37 During the biennium the Organ-ization provided assistance to Angola,United Republic of Cameroon and Sudanin serious outbreaks of trypanosomiasis.The situation in Mozambique caused con-cern, and systematic reinvestigation of theendemic areas in this country is indicated.
8.3 8 Continuous surveillance of thepopulation at risk is the essential safeguardagainst serious outbreaks of the disease.The joint FAO /WHO Expert Committeeon African Trypanosomiasis, meeting inRome in November 1976, concluded thatsuch surveillance costs approximatelyUS $ 0.44 per inhabitant per year. It is clearthat at such cost surveillance activities insome countries are bound to be inadequateas regards frequency and coverage. Thedevelopment of cheap, simple diagnosticand control methods is required and variouslaboratories in Africa, America and Europeare jointly involved in research on thesesubjects.
8.39 The UNDP /WHO Applied Re-search Programme centred at Bobo -Diou-lasso, Upper Volta, was already providingsatisfactory technical results in the field oflow- dosage application of insecticidesagainst Glossina and in the evaluation ofthe indirect haemagglutination test incapillary tubes under field conditions. Incollaboration with the Organization forCoordination and Cooperation in the Con-trol of Major Endemic Diseases in WestAfrica, and government services, a thou-sand of these tests were carried out in
94
Ivory Coast and Upper Volta. Since theresults showed that the test is less reliableunder field conditions than in the lab-oratory, it is now under further study.
8.40 Investigations were begun in col-laboration with the Bernhard Nocht In-stitute, Hamburg, Federal Republic ofGermany, and the London School ofHygiene and Tropical Medicine, Englandon the possibility of an animal reservoiroccurring for Trypanosomagambiense. Shouldthis possibility be confirmed in furtherstudies, it would have important conse-quences for the control strategy of sleepingsickness due to T. gambienne infection. Forinstance, elimination of the human reser-voirs would no longer provide a permanentsolution to the problem of T. gambienneinfections. Furthermore, vaccination, iftechnically feasible, would have to beregarded as only a temporary solution.
8.41 The current and proposed re-search programmes in Africa were drawnup during two meetings of the SpecialProgramme for Research and Training inTropical Diseases in Arusha, United Re-public of Tanzania, in September 1976 andBobo -Dioulasso, Upper Volta, in April1977. As a result, one group of laboratoriesin East Africa initiated integrated pro-grammes on immunology, pathology andclinical medicine. The chemotherapycomponent is covered by some zo researchagreements. Radio- labelled antitrypano-somal compounds will be made availableand used in drug distribution experimentsand mode of action studies in variouslaboratories. A network of medical centresin Africa is being created within thecontext of the Special Programme for thepurpose of providing facilities for clinicaltrials of new compounds and joint studieson histopathology and pathogenesis, inaccordance with standard protocols de-signed by Scientific Working Groups.
COMMUNICABLE DISEASE PREVENTION AND CONTROL
American trypanosomiasis
8.42 The prevalence of the Americantrypanosomiasis remains uncertain becauseof incompleteness of the base -line data, noris it known what proportion of T. crudinfections are followed by manifest disease.An increase in periurban spread of Chagas'disease has caused concern in recent years.Applied research on simple methods ofhousing improvement as a means of con-trolling the disease will be carried out aspart of the programme of the WHOChagas' Disease Vector Research Unit inVenezuela.
8.43 A meeting of the Special Pro-gramme Scientific Working Group onAmerican trypanosomiasis was held inBuenos Aires in 1977. The programmefor research on the development of newcontrol methods will include work onmethods for longitudinal studies of epi-demiology, new chemotherapeutic agentsand research on immunology and vectorcontrol. A new collaborating laboratoryfor diagnostic tests for Chagas' disease wasdesignated in Sao Paulo, Brazil, with thereference task of comparing existing andnewly developed serodiagnostic tests.
Leishmaniases
8.44 Although no concrete data areavailable on the incidence of leishmanialdiseases, mucocutaneous leishmaniasisseems frequent during development pro-jects in the forest areas of South America.South -East Asia experienced a resurgenceof epidemics of visceral leishmaniasis. InAfrica an epidemic of visceral leishmaniasisrapidly developed during 1977 inMachakos, Kenya. The Organization pro-vided technical assistance and contributeddrugs during an outbreak in Bihar State,India, in 1977. A WHO consultant assisted
95
in epidemiological studies and in thetraining of national health personnel inIraq.
8.45 The leishmaniasis research pro-gramme, as part of the Special Programmefor Research and Training in TropicalDiseases, was reviewed by a ScientificWorking Group meeting in Geneva inDecember 1977. The Working Groupconcluded that the public health importanceof the leishmaniases had been under-estimated in the past, and decided to initiateprogrammes to obtain better informationon their distribution and prevalence. More-over, leishmaniasis was considered to bea valuable model for study of the principlesof host defence mechanisms, particularlymacrophage action.
Research coordination
8.46 Work in this field was carried outin close collaboration with the SpecialProgramme for Research and Training inTropical Diseases. An ad hoc team visitedJapan, Malaysia, the Philippines, the Repub-lic of Korea and Singapore in connexionwith coordination of research programmesand projects. As a result the RegionalAdvisory Committee on Medical Researchof the Western Pacific Region recom-mended that research in the field of parasiticand other communicable diseases shouldbe concerned with malaria, schistosomiasis,filariasis, leprosy, dengue haemorrhagicfever and enteric diseases. Also, theRegional Committee adopted a resolution(wPRJRcz7 /R9) requesting the RegionalDirector to take steps in order to (1)
strengthen the Institute of Medical Re-search in Kuala Lumpur, Malaysia, (z)develop cooperation with the Multidisci-plinary Programme of OperationalResearch in the Republic of Korea, and(3) establish three task forces to advise on
THE WORK OF WHO
the development of regional research pro-grammes in health services, in parasitic andcommunicable diseases and in cardio-vascular diseases.
8.47 At its first plenary session inGeneva in June 1977, the Special Pro-gramme Scientific Working Group onEpidemiology made recommendations con-cerning its future structure and functionsand on the implementation of the epi-demiological research and training pro-gramme at the WHO Tropical DiseaseResearch Centre, Ndola, Zambia.
Smallpox eradication
8.48 During 1976 and 1977 smallpoxwas limited to the nomadic population ofthe Ogaden, which includes part of north-ern Kenya, southern Ethiopia and Somalia(Fig. 8.z). Elsewhere in the world, con-tinuing surveillance failed to reveal anycases of smallpox. During the biennium,6000 diagnostic specimens from 6o coun-tries were tested by WHO diagnostic labo-ratories (collaborating centres) in Moscowand Atlanta. Except for specimens fromEthiopia, Kenya and Somalia, none waspositive for smallpox.
8.49 During the first half of 1976 thelast smallpox foci were localized in south-ern Ethiopia. During the summer of thesame year, when these foci were aboutto be eliminated, smallpox occurred insouthern Somalia. Subsequently, at theend of 1976, there was an outbreak innorthern Kenya, where the index case wasbelieved to have come from southernSomalia.
8.5o Since the chains of transmissionlinking these outbreaks could not be
96
documented, despite intensive investiga-tions carried out by national /WHO teams,WHO sponsored a coordination meetingin Nairobi in March 1977. The situationwas appraised by national and WHOepidemiologists from Ethiopia, Kenya,Somalia and Sudan. Operations in theOgaden area were recognized as beingcrucial to the ultimate success of theglobal smallpox eradication effort ; it wastherefore decided that a special joint sur-veillance containment operation should beconducted by Ethiopia, Kenya and Somalia.
8.51 In southern Somalia, the searchoperation revealed widespread smallpoxepidemics in April -June 1977, and WHOcollaborated in organizing emergency mea-sures. UNDRO provided a number ofvehicles, spare parts and supplies, whichwere airlifted to Mogadishu. In June, atthe height of the epidemic, 24 WHOepidemiologists and 3500 national fieldworkers were engaged in the campaign.Somalia recorded 3400 cases in 1977, butintensive containment activities rapidlybrought the outbreaks under control, andthe last known case (as of January 1978) wasnotified in October 1977 (Fig. 8.3).
8.5z Ethiopian smallpox search opera-tions in the Ogaden were virtually inter-rupted from July 1976. In September,with the collaboration of the InternationalCommittee of the Red Cross, new out-breaks were detected, but these werequickly contained. The last known caseswere recorded in November 1976. How-ever, months of continuing search willbe needed in order to ensure that foci arecompletely eliminated.
8.53 In 1976 and 1977, internationalcommissions set up by the Organizationfor the certification of smallpox eradicationvisited 7 countries in Asia, 15 countries in
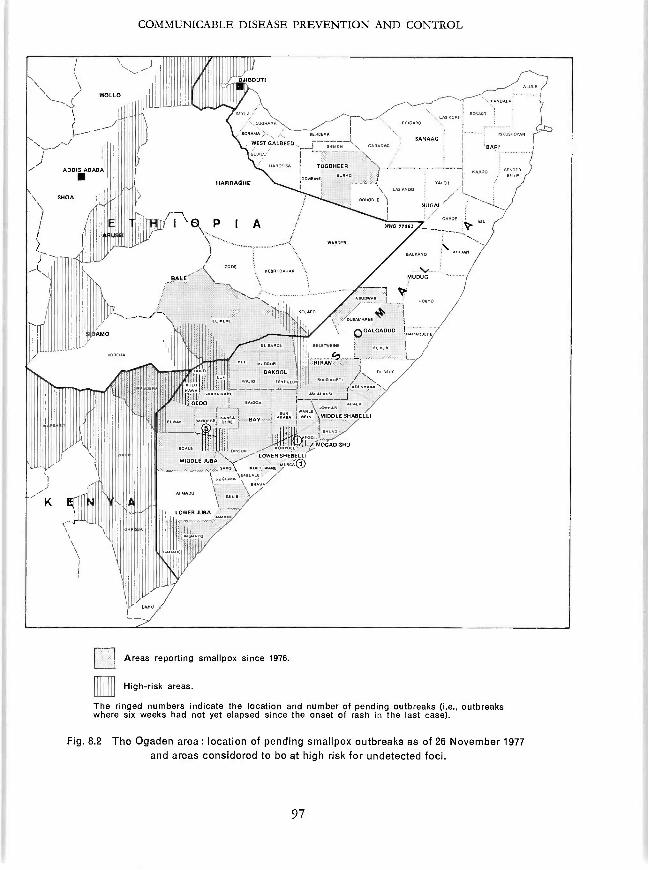
COMMUNICABLE DISEASE PREVENTION AND CONTROL
WOLLO
ADDIS ABABA
SHOA
\
AMO
DJIBOUTI
11
HARRAGHE
I
ERiDARD
I
WEST GALBEED,
eERRExA
EAx \ ARRDAGSANAAG :'
. JI \ \
RARGEiSA i TOGDHEER \I .
IODWEI I
I `-0. P I A
CODE
BALE \
'TY--~\ 11
J
K
KERRI DAKAR
uBAKOOL
Ili I GEDO J.
^uti
\ LAS MOO
eoRODLE \I
WO MU
PLULA
ISKLVIOPAN
BART
BARDOREiLE
NELREO
Iri1
i
WARDER
MUDUG
LL=A.,AaER,11
'--0 IRARARD/1
I
C9i_l
_ED RAN
ELDER
.
4\ A, ALA
Ad IN \ti MIDDLE SHABELLI
n^TLi IÿMOGADISMU/
"- LOWERSHEBELLI
u U. AL'iDA /\ R`Rv
Areas reporting smallpox since 1976.
High -risk areas.
The ringed numbers indicate the location and number of pending outbreaks (i.e., outbreakswhere six weeks had not yet elapsed since the onset of rash in the last case).
Fig. 8.2 The Ogaden area: location of pending smallpox outbreaks as of 26 November 1977and areas considered to be at high risk for undetected foci.
97
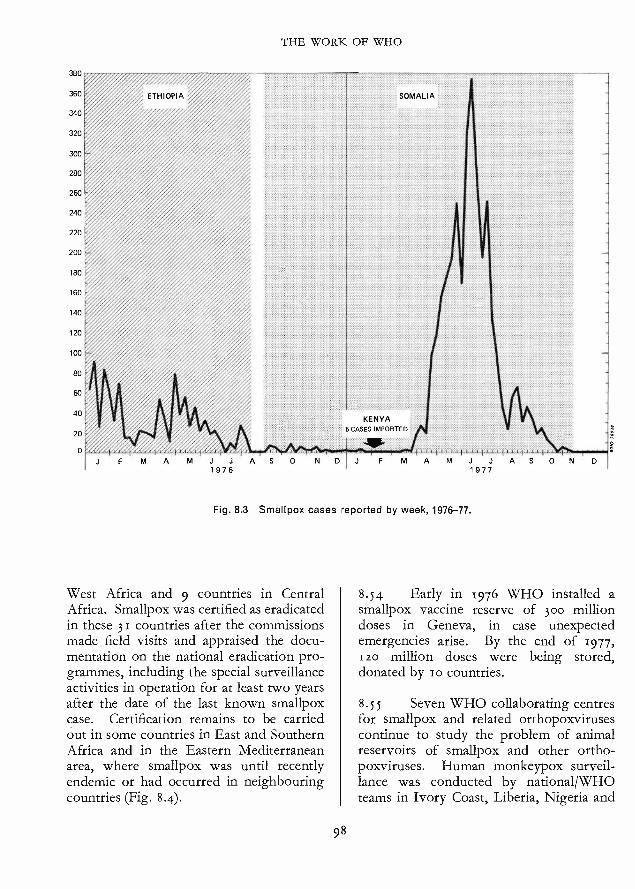
380
360
340
320
300
280
260
240
220
200
180
160
140
120
100
80
40
20
0
THE WORK OF WHO
ETHIOPIA SOMALIA
..................................................................
KENYACASES IMPORTED
1976A N D J J J AS
1977
Fig. 8.3 Smallpox cases reported by week, 1976 -77.
West Africa and 9 countries in CentralAfrica. Smallpox was certified as eradicatedin these 31 countries after the commissionsmade field visits and appraised the docu-mentation on the national eradication pro-grammes, including the special surveillanceactivities in operation for at least two yearsafter the date of the last known smallpoxcase. Certification remains to be carriedout in some countries in East and SouthernAfrica and in the Eastern Mediterraneanarea, where smallpox was until recentlyendemic or had occurred in neighbouringcountries (Fig. 8.4).
98
N D
8.54 Early in 1976 WHO installed asmallpox vaccine reserve of 30o milliondoses in Geneva, in case unexpectedemergencies arise. By the end of 1977,Izo million doses were being stored,donated by io countries.
8.55 Seven WHO collaborating centresfor smallpox and related orthopoxvirusescontinue to study the problem of animalreservoirs of smallpox and other ortho-poxviruses. Human monkeypox surveil-lance was conducted by national/WHOteams in Ivory Coast, Liberia, Nigeria and
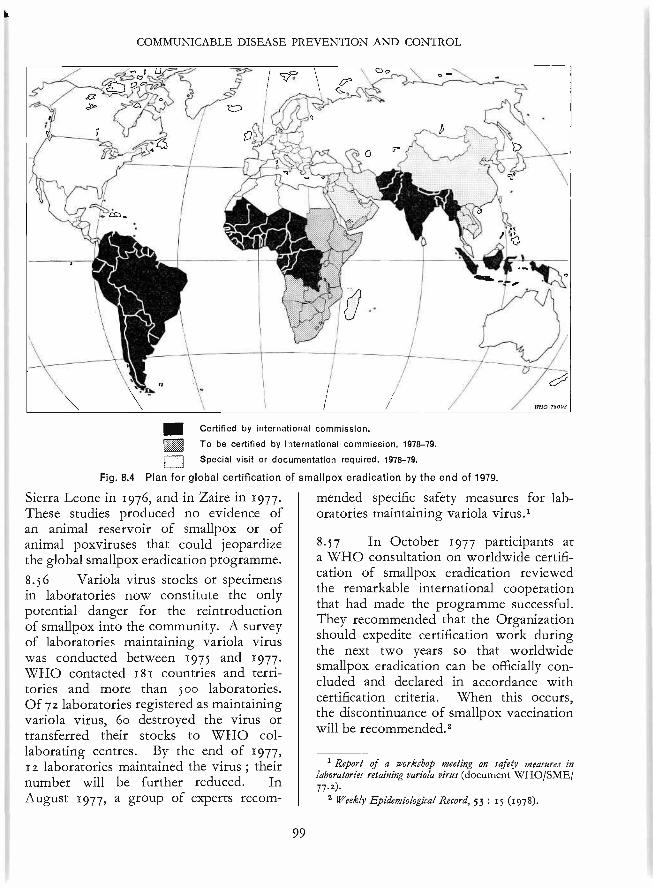
COMMUNICABLE DISEASE PREVENTION AND CONTROL
1Certified by international commission.
To be certified by international commission, 1978 -79.
Special visit or documentation required, 1978 -79.
Fig. 8.4 Plan for global certification of smallpox eradication by the end of 1979.
Sierra Leone in 1976, and in Zaire in 1977.These studies produced no evidence ofan animal reservoir of smallpox or ofanimal poxviruses that could jeopardizethe global smallpox eradication programme.8.56 Variola virus stocks or specimensin laboratories now constitute the onlypotential danger for the reintroductionof smallpox into the community. A surveyof laboratories maintaining variola viruswas conducted between 1975 and 1977.WHO contacted 181 countries and terri-tories and more than Soo laboratories.Of 72 laboratories registered as maintainingvariola virus, 6o destroyed the virus ortransferred their stocks to WHO col-laborating centres. By the end of 1977,I z laboratories maintained the virus ; theirnumber will be further reduced. InAugust 1977, a group of experts recom-
99
mended specific safety measures for lab-oratories maintaining variola virus.'
8-57 In October 1977 participants ata WHO consultation on worldwide certifi-cation of smallpox eradication reviewedthe remarkable international cooperationthat had made the programme successful.They recommended that the Organizationshould expedite certification work duringthe next two years so that worldwidesmallpox eradication can be officially con-cluded and declared in accordance withcertification criteria. When this occurs,the discontinuance of smallpox vaccinationwill be recommended.2
1 Report of a workshop meeting on safety measures inlaboratories retaining variola virus (document WHO/SME/77.2).
2 lVeekly Epidemiological Record, 53 : 15 (1978).
THE WORK OF WHO
Expanded Programme on Immunization
8.58 The Expanded Programme onImmunization has its basis in resolutionsadopted by the World Health Assembly in1974 (wHA27.57), 1976 (WHA29.62) and1977 (wHA3o.53, WHA30.S4). It is a world-wide collaborative programme of MemberStates, with the objective of (1) providingimmunizations for all children of the worldby 199o, concentrating particularly onimmunizations against diphtheria, pertussis,tetanus, measles, poliomyelitis and tuber-culosis ; and (2) reducing morbidity andmortality from other selected diseases ofpublic health importance for which safeand effective vaccines currently exist orbecome available.
Planning, training and operations
8.59 The policies established in resol-ution wHA3 o. 5 3 served as a basis fordeveloping in 1977 a draft manual ofoperations for use as a guide in the pre-paration of detailed regional and countryplans and as a resource for staff training atall levels.
8.6o During 1976 -77 regional advisersresponsible for the programme were desig-nated and a full -time programme managerwas appointed at WHO headquarters,where there is now a staff of 12. A WHOworking group on the programme, at-tended by government representatives andregional and headquarters staff, met inDecember 1976. Regional advisers met inMay and November 1977 to discuss jointproblems and coordinate global policies.By the end of 1977, one interregional andsix regional training seminars had beenheld, attended by participants from over6o countries, as well as representatives ofinternational, voluntary and national devel-opment agencies. Activities were initiatedin many of those countries. During 1977,
I00
three films dealing with various aspects ofthe programme were completed with directWHO participation, and a fourth film wasin preparation.
Research and development
8.61 Highest priority was accorded tooperational rather than basic research.
8.6z Vaccines. Support from UNDPpermitted WHO to investigate the pos-sibility of increasing the stability of measlesand poliomyelitis vaccines as well as thepertussis component of diphtheria / pertussis/tetanus vaccines. The possibility of de-creasing the reactogenicity of the pertussiscomponent was also being investigated.In addition, the stability of BCG vaccinewas being evaluated.
8.63 Immunization schedules. Studieswere underway to determine the optimumage for measles vaccination. The possibilityof completing diphtheria /pertussis /tetanusimmunizations with two doses rather thanthe usual three doses was being investigated.
8.64 Improving the cold chain. Prototypeswere being developed for (i) a refrigeratorand freezer capable of being operated onmultifuel sources, (z) a cold box suitablefor transporting vaccines by vehicle indeveloping countries, and (3) a vaccinecontainer suitable for use by primary healthworkers in developing countries. Threecommercially available chemical and bio-logical enzyme -based indicators were beingtested for their suitability as indicators ofvaccine potency during storage. Theperformance characteristics of a wide rangeof existing refrigerators, freezers, ice -makers, and cold boxes in tropical condi-tions were also being tested.
8.65 Improving techniques of vaccine ad-ministration. Arrangements were made for
COMMUNICABLE DISEASE PREVENTION AND CONTROL
extensive comparative testing of five com-mercially available jet injectors. During1976 -77, additional studies were completedon the feasibility of giving BCG vaccina-tions with a bifurcated needle. In 1977, astudy was also planned for 1978 -79 todetermine the feasibility of administeringa concentrated tetanus toxoid with abifurcated needle.
8.66 Improving immunization coverage
rates. In two developing countries, WHOsupported field studies to examine coveragerates, seroconversion rates and operationalcosts ; the use of mobile health teams wasalso compared with the use of fixed healthcentres. In addition, a project was formu-lated that will analyse the major motiva-tional opportunities available at the villagelevel for promoting childhood immuniza-tions.
8.67 Programme management. Studieswere planned for evaluating the full rangeof managerial tasks required to provide animmunization programme with adequatesupplies of potent vaccine ; knowledgegained from the study will be incorporatedin the training of national staff responsiblefor vaccine supplies. Studies were alsoplanned to evaluate the feasibility of train-ing selected villagers to be the primaryreporting sources in disease surveillanceschemes at the village level.
8.68 Vaccine production. A projectsupported by UNDP permitted WHO toincrease the quality control of vaccines bothin countries already producing vaccinesand in countries about to start vaccineproduction. The project, which is stillcontinuing, provides for (I) the preparationof manuals for the production and qualitycontrol of diphtheria /pertussis /tetanus vac-cines, (z) the designing and selection ofequipment for both production and controllaboratories, (3) the training of laboratoryworkers in the quality control of vaccines,
r
IOI
and (4) the support of research on morestable vaccines (see above). During 1977,the manuals were written, advice wasprovided on laboratory design and equip-ment, a seminar on vaccine production andquality control was conducted in Geneva,a training course for quality control of virusvaccines was held in London, a meeting ofexperts in production and quality controlwas convened in Geneva to discuss prob-lems concerning pertussis vaccine, andprogress was achieved in several areas ofvaccine research.
Financial support from outside WHO
8.69 Outside support provides themajor basis for extending the activities ofthe Expanded Programme on Immuniza-tion. Table 8.1 summarizes extrabudgetaryassistance received by the programme up tothe end of 1977.
Bacterial and virus diseases
Cholera and other bacterial enteric infections
8.7o Both the recrudescence of cholerain the Eastern Mediterranean area on theeve of the Mecca pilgrimage and theoccurrence of cholera in the Gilbert Islandsin the Pacific caused serious concern, andthe countries affected received technicaland material aid from WHO.
8.71 A major activity was the creationin headquarters and in regional offices ofinterdisciplinary working groups on diar-rhoeal diseases. While recognizing theimportance of a multidisciplinary approachto the control of diarrhoeas, these groupsgave priority to the promotion of oralrehydration as an element of primary healthcare in the management of dehydrationassociated with diarrhoeas. The use of oral
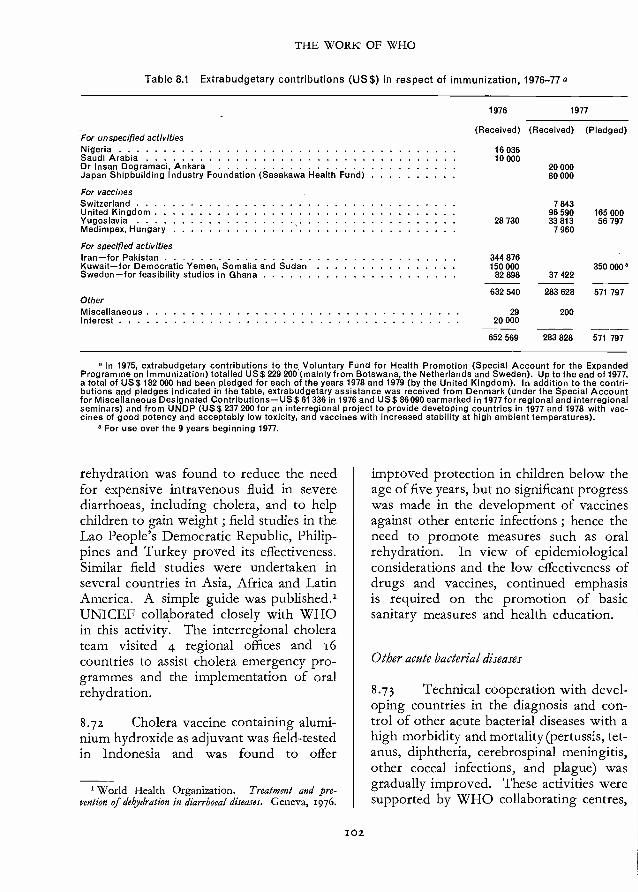
THE WORK OF WHO
Table 8.1 Extrabudgetary contributions (US$) in respect of immunization, 1976 -77 a
For unspecified activities
1976
(Received)
1977
(Received) (Pledged)
Nigeria 16 036Saudi Arabia 10 000Dr Insan Dogramaci, Ankara 20 000Japan Shipbuilding Industry Foundation (Sasakawa Health Fund) 80000
For vaccinesSwitzerland 7 843United Kingdom 96 590 165 000Yugoslavia 28 730 33 813 56 797Medimpex, Hungary 7 960
For specified activitiesIran -for Pakistan 344 876Kuwait -for Democratic Yemen, Somalia and Sudan 150 000 350 000 °Sweden -for feasibility studies in Ghana 82 898 37 422
632 540 283 628 571 797OtherMiscellaneous 29 200Interest 20 000
652 569 283 828 571 797
In 1975, extrabudgetary contributions to the Voluntary Fund for Health Promotion (Special Account for the ExpandedProgramme on Immunization) totalled US$ 229 200 (mainly from Botswana, the Netherlands and Sweden). Up to the end of 1977,a total of US$ 182 000 had been pledged for each of the years 1978 and 1979 (by the United Kingdom). In addition to the contri-butions and pledges indicated in the table, extrabudgetary assistance was received from Denmark (under the Special Accountfor Miscellaneous Designated Contributions -US$ 61336 in 1976 and US$ 86090 earmarked in 1977 for regional and interregionalseminars) and from UNDP (US$ 237 200 for an interregional project to provide developing countries in 1977 and 1978 with vac-cines of good potency and acceptably low toxicity, and vaccines with increased stability at high ambient temperatures).
b For use over the 9 years beginning 1977.
rehydration was found to reduce the needfor expensive intravenous fluid in severediarrhoeas, including cholera, and to helpchildren to gain weight ; field studies in theLao People's Democratic Republic, Philip-pines and Turkey proved its effectiveness.Similar field studies were undertaken inseveral countries in Asia, Africa and LatinAmerica. A simple guide was published.'UNICEF collaborated closely with WHOin this activity. The interregional cholerateam visited 4 regional offices and 16countries to assist cholera emergency pro-grammes and the implementation of oralrehydration.
8.72 Cholera vaccine containing alumi-nium hydroxide as adjuvant was field- testedin Indonesia and was found to offer
' World Health Organization. Treatment and pre-vention of dehydration in diarrhoea) diseases. Geneva, 1976.
IO2
improved protection in children below theage of five years, but no significant progresswas made in the development of vaccinesagainst other enteric infections ; hence theneed to promote measures such as oralrehydration. In view of epidemiologicalconsiderations and the low effectiveness ofdrugs and vaccines, continued emphasisis required on the promotion of basicsanitary measures and health education.
Other acute bacterial diseases
8.73 Technical cooperation with devel-oping countries in the diagnosis and con-trol of other acute bacterial diseases with ahigh morbidity and mortality (pertussis, tet-anus, diphtheria, cerebrospinal meningitis,other coccal infections, and plague) wasgradually improved. These activities weresupported by WHO collaborating centres,
COMMUNICABLE DISEASE PREVENTION AND CONTROL
which continued to assist in the preparationof simplified guidelines for the diagnosisand treatment of these diseases, as well asin research and reference work.
8.74 There was considerable publicconcern regarding severe reactions arisingfrom vaccination against pertussis, and aWHO cooperative study on the toxicityand reactogenicity of diphtheria /pertussis/tetanus vaccines was carried out with theparticipation of 13 national laboratories.Its results indicated an urgent need to stan-dardize laboratory tests currently used forcontrolling the toxic properties and poten-cy of such vaccines. Research on new orimproved pertussis vaccines of low toxicitywas undertaken. Dried stable diphtheria/pertussis /tetanus vaccine was developedand tested successfully both in the labora-tory and the field.
8.75 The stability of polysaccharidemeningococcal vaccines of serogroups Aand C was increased and a new proteinvaccine of serogroup B was ready for trialin human subjects. New vaccines againstpneumococcal infections and diseasescaused by Haemophilus influentae were understudy.
8.76 A WHO cooperative study in-volving zz national laboratories evaluatedreference activity in the field of strepto-coccal infection at national and internationallevels.
Leprosy
8.77 Action taken in accordance withWorld Health Assembly resolutions adop-ted in 1974 (wHA27.58), 1975 (wHAZ8.56),1976 (wHA29.7o), and 1977 (wHA3o.36)resulted in three main developments in1976 -77: the convening of the ExpertCommittee on Leprosy, a review of direct
103
technical cooperation in leprosy control,and intensification of leprosy research acti-vities.
8.78 WHO Expert Committee on Le-prosy.' At its fifth meeting, in Geneva inOctober 1976, the Committee recommend-ed guidelines for the formulation and man-agement of leprosy control programmes asan integrated element of community healthcare. Specific recommendations were alsomade on manpower development. Second-ary dapsone resistance of Mycobacteriumleprae in multibacillary cases was identifiedas being a serious problem ; the use ofcombined therapeutic regimens in suchcases was recommended. The Committeealso stressed the need for adequate informa-tion support.
8.79 In line with the Committee's rec-ommendations, WHO participated in threeother meetings : the First InternationalWorkshop on the Training of LeprosyWorkers in Asia, held in Bangkok inNovember 1976, jointly sponsored by theGovernment of Thailand and the JapanShipbuilding Industry Foundation (Sasa-kawa Health Fund) ; the First InternationalWorkshop on the Chemotherapy of Leprosyin Asia, held in Manila in January- February1977, jointly sponsored by the Govern-ment of the Philippines and the Japan Ship-building Industry Foundation (SasakawaHealth Fund) ; and a joint meeting ofrepresentatives of the International Federa-tion of Anti -Leprosy Associations andLEPRA, United Kingdom, held in Londonin August 1977. The Bangkok meetingreviewed the need for training in leprosyin the South -East Asia and WesternPacific Regions ; WHO subsequently co-operated in identifying institutions in thetwo regions that could increase their train-ing capacity. The Manila and London
1 WHO Technical Report Series, No. 607, 1977.
THE WORK OF WHO
meetings prepared guidelines for the fieldapplication of therapeutic regimens.
8.8o Technical cooperation in lepro y con-trol. The period 1976 -77 saw increasingacceptance of leprosy project formulationas a component of country health pro-gramming. WHO's tasks for the future inthe strengthening of leprosy control weredefined. Recommendations were made onimproved coordination at country levelthrough the use of advisory groups.
8.81 Cooperation with UNICEF andthe International Leprosy Association con-tinued. The International Union againstTuberculosis also began cooperating withvoluntary agencies in the field of leprosy.Important financial contributions werereceived from a number of voluntaryagencies, including the Danish Save theChildren Fund, the Deutsches AussitzigenHilfswerk, Emmaus- Suisse, the Japan Ship-building Industry Foundation (SasakawaHealth Fund), and the Lepers' Trust Board,New Zealand, and from the Order of Malta.
8.82 In the African Region, a combinedtuberculosis and leprosy population survey(1974 -March 1977) completed in UpperVolta confirmed the considerable reduction(75%) in the prevalence of leprosy achievedby mobile units in recent years. In theRegion of the Americas, as part of the10 -year health plan for 1971 -8o, countrieswith a leprosy problem set targets for 198oin the reduction of prevalence. In theSouth -East Asia Region the mass -scalerifampicin drug trial was continued in theMandalay area of Burma ; significant epi-demiological results, reproducible in othercountries, are expected. In the WesternPacific Region, a regional leprosy advisoryteam began operations in 1977. In VietNam, the strengthening of the leprosycontrol programme received priority ; sub-stantial extrabudgetary resources were madeavailable through WHO.
104
8.83 Research. During 1976 -77 WHOsupported collaborative research in 52
projects in 24 countries.
8.84 In October 1976 a workshop heldin Baltimore, USA, identified researchpriorities for the Region of the Americas.A second workshop, "The armadillo : amodel for leprosy research ", took place inMay 1977 in Caracas, Venezuela. Therecommendations of both meetings wereendorsed by the Regional Advisory Com-mittee on Medical Research.
8.85 The National Institute of Derma-tology of Venezuela was established as thePan American Center for Research andTraining in Leprosy and Other TropicalDiseases. In October -November 1977 theCenter's Director and the Regional Adviserin Leprosy visited countries to explain theservices available through the Center andto encourage the development of nationalprogrammes.
8.86 The twelfth USA -Japan LeprosyResearch Conference, held in Boston, USA,in September 1977, devoted particularattention to problems relating to thebiology of M. leprae and immunologicalmechanisms in the host -organism relation-ship.
8.87 There are two aspects to theleprosy component of the Special Pro-gramme for Research and Training inTropical Diseases -a programme on re-search in the immunology of leprosy andone on research in the chemotherapy ofleprosy ; in 1977 the Special Programmefunded 24 immunology projects in i t coun-tries and 21 chemotherapy projects in 9countries.
8.88 In immunology, the observationthat killed Mycobacterium leprae can inducecell- mediated immunity in experimental

COMMUNICABLE DISEASE PREVENTION AND CONTROL
animals and protect mice from M. lepraeinfection gives further hope of vaccinedevelopment ; additional studies, includ-ing vaccine tests in armadillos, are planned.Work has also continued on the develop-ment of a skin -test for the detection of sub -clinical leprosy infection ; studies are beingcarried out on the purification of twodifferent M. leprae antigens in an attempt toobtain more specific preparations.
8.89 The planning committee on thechemotherapy programme met in April1976 and identified four major objectives :(I) assessment of the prevalence of dapsoneresistance by means of field surveys ;(z) controlled trials of combinations ofexisting drugs in lepromatous leprosy ;(3) laboratory studies designed to provideinformation on the tools necessary toattain the first two objectives ; and (4) thedevelopment of new effective drugs. Therelevant Scientific Working Group first metin April 1977 and adopted a standard pro-tocol for chemotherapy trials ; trials inpreviously untreated patients with lepro-matous leprosy are now in the preparatorystage at two treatment centres in leprosy -endemic countries, in collaboration withthree specialized laboratories. In addition,three drug -development projects were be-gun -two on the synthesis of new clofazi-mine analogues, and the third on themechanism of action of chaulmoogric acid.Eighteen projects relevant to the otherobjectives were also undertaken.
8.90 In addition, new studies on epide-miology and M. leprae cultivation areunder consideration ; in this connexion,preliminary steps and pilot studies arecurrently being undertaken, partly in con-junction with the trans -disease ScientificWorking Group on subjects relevant toepidemiology.
8.91 Within the framework of theSpecial Programme's leprosy component,
IOf
and in close liaison with the RegionalAdvisory Committees on Medical Research,efforts were made to strengthen researchcapabilities in the affected countries. Agood example of this policy is the initiativetaken by the Regional Office for South -East Asia, which convened a study groupon leprosy research in February 1977. Thegroup made recommendations forming theoutline of a Regional plan for research inleprosy, subsequently endorsed by theRegional Advisory Committee on MedicalResearch. In the other regions also, coun-tries are being increasingly involved inthe preparation of research plans, in co-operation with the Special Programme'sglobal Scientific Working Groups.
Tuberculosis and other respiratory infections
8.92 Tuberculosis remains a problem ofconsiderable public health importance inmany parts of the world. Programmeevaluation projects revealed the organiza-tional weakness of the treatment compo-nent of national programmes resulting inserious shortcomings regarding the all -
important regularity of drug ingestion,motivation of patients, and follow -up. Atthe global level, this situation is reflectedin the slow decline that has occurred inmortality rates despite the therapeuticefficacy of modern drug regimens. Thenumber of deaths from tuberculosis isestimated to exceed half a million each year,the bulk (74 %) of this heavy toll occurringin Asian countries.
8.93 The need for continued epidemio-logical surveillance of tuberculosis at thenational and international levels was thesubject of a Symposium on TuberculosisSurveillance, organized in Brno, Czechoslo-vakia, by the WHO Regional Office forEurope, with the active participation of theInternational Union against Tuberculosis.

THE WORK OF WHO
The meeting emphasized the importanceof agreeing on appropriate and practicalcriteria for the epidemiological, social andeconomic evaluation of the impact madeby tuberculosis control programmes, and ofuniform, complete recording and reporting.A reporting system based on the bacterio-logical diagnosis was recommended.
8.94 The demand for wider, moreintensive distribution of current technicalknowledge and guidance on the planning,implementation, management and evalua-tion of integrated national tuberculosiscontrol programmes was met as follows :(i) by training various categories of keyworkers at the international, regional andnational levels, (z) by the participation, inclose collaboration with the InternationalUnion against Tuberculosis, in seminars(in Egypt, Kuwait, Peru and Syrian ArabRepublic), workshops and conferences (Fin-land, Republic of Korea and Turkey), andscientific committees (on diagnostic meth-ods, bacteriology and immunology, treat-ment, prevention, epidemiology, and ani-mal tuberculosis) ; and (3) through coopera-tion in national programmes (for instance,in Afghanistan, Algeria, Argentina, Ban-gladesh, Bolivia, Brazil, Burma, Indonesia,Maldives and Venezuela). At the requestof the Government of the United Republicof Tanzania, WHO and the InternationalUnion against Tuberculosis cooperated inconducting a national seminar and, sub-sequently, in reformulating the nationaltuberculosis control programme. A tech-nical guide for sputum examination wasdeveloped jointly by the InternationalUnion against Tuberculosis and WHO.'
8.95 As regards the prevention of tuber-culosis, preparations were made to deliver
S International Union against Tuberculosis. Tech-nical guide for collection, storage and transport of sputumspecimens and for examinations for tuberculosis by directmicroscopy. Paris, 5977.
1o6
BCG vaccination as part of the ExpandedProgramme on Immunization. A consulta-tion was held on "The choice of a BCGstrain" for the production of freeze -driedvaccine, and technical guides on the WHO -sponsored international quality control ofBCG vaccine were drawn up.2 Investiga-tions into various BCG vaccination tech-niques and their operational implicationswere completed, and trials continued regard-ing the protection afforded in differentethnic and age groups, its duration, dose -dependence, and possible interference withecological factors such as mycobacteriaother than tuberculosis. The Organizationcooperated with the Indian Council ofMedical Research in a consultation on themethodology and implementation of theCouncil's tuberculosis prevention trial.Research projects continued also in thefields of epidemiology, surveillance, im-munology, bacteriology, short -course che-motherapy, and the operational aspects ofprogramme delivery.
8.96 Acute respiratory infections areone of the principal causes of morbidityand mortality in many countries. A studywas made of the magnitude of this prob-blem ; 88 countries were found to reportmore than 66o 000 deaths from acuterespiratory infections each year, i.e., 6.3%of the total deaths and over zo% of deathsin children. In an endeavour to assess thesituation, visits were made to a number ofcountries in the African, American, Euro-pean and Eastern Mediterranean Regionsand investigations were begun to identifypossible control measures, curative andpreventive. In 1978 acute respiratoryinfections will be the subject of a newprogramme.
2 W/HO- sponsored international quality control of BCGvaccine (document WHO /TB /TECHNICAL GUIDE/77.8); In vitro assays of BCG products (document WHO/TB /TECHNICAL GUIDE /77.9).
COMMUNICABLE DISEASE PREVENTION AND CONTROL
Sexually transmitted diseases and endemictreponematoses
8.97 The results of studies indicatedthat sexually transmitted diseases mayaffect Io -2o% of the population in somecountries and may lead to severe complica-tions, particularly in countries where healthservices are not well developed. The prob-lem is aggravated by the increasing resist-ance of the gonococcus to antimicrobialtreatment ; in certain areas, for example, theproportion of strains fully sensitive topenicillin is known to have decreased byan average of 6 -7 % annually in recent years.Moreover, gonococcal strains have emerg-ed that are completely resistant to penicillin.A system was developed to monitor thespread of these strains. Health administra-tions were kept informed on the globalsituation and on methods for the identifi-cation and control of resistant strains. Inaddition, administrations were encouragedto establish treatment schedules based onthe local gonococcal sensitivity pattern andcost /effectiveness considerations. Reportsfrom many countries indicate that non -gonococcal urethritis and vaginitis are nowmore frequently seen than gonorrhoea.
8.98 Diagnostic facilities and curativeand control services remain inadequate insome areas, and cooperative research wasdirected primarily towards developingsimplified, low -cost diagnostic and controltechnologies. For instance, field evaluationwas begun of a gonococcal culture mediumthat is considerably cheaper than theconventional medium. In one country,assessment was begun of the impact of asimplified control approach that can beapplied in health care units not yet sup-ported by a laboratory diagnostic service.Support was provided to some researchgroups in developing countries to obtaindata essential for formulating a nationalcontrol programme. A WHO Scientific
I07
Group in 1976 reviewed recent advances ingonococcal research and outlined promisingareas of basic and applied research that maylead to improved techniques of diagnosis,treatment, prevention and control.' Theprogramme for the control of sexuallytransmitted diseases in Viet Nam wassupported by a voluntary contributionfrom the Government of Australia, WHOacting as intermediary.
8.99 In the course of a WHO sympo-sium, representatives from countries in theEuropean Region agreed on the technolo-gies to be applied in the surveillance andcontrol of sexually transmitted diseases ;the importance was stressed of providinggeneral practitioners with guidance on thediagnosis and treatment of these diseases(a manual is in preparation). As part ofthe European Region's programme oneconomic aspects of communicable diseases,a start was made on developing workingprotocols that can be used in multinationalstudies aimed at assessing the economicburden imposed by sexually transmitteddiseases.
8.1 oo Training and refresher pro-grammes were established on the subjectof laboratory diagnostic, clinical and epi-demiological aspects of the control ofsexually transmitted diseases. Workshopswere held for the Philippines and for theAndean area. In addition, consultativeservices were provided for six countries.
8.I0 1 Yaws and bejel, the prevalenceof which diminished substantially followingWHO /UNICEF mass campaigns, againbecame rampant in some areas. WHOdevised procedures for the evaluation andactive surveillance of these diseases andassisted, in collaboration with other agen-
' WHO Technical Report Series, No. 616, 1978.
THE WORK OF WHO
cies, in establishing programmes for system-atic control in some countries.
Virus, chlamydial, rickettsial and related diseases
8.ioz The WHO virus diseases pro-gramme consists of surveillance activities,support to laboratory development forviral diagnosis, support to prevention andcontrol measures and encouragement ofapplied research. A meeting of directors ofcollaborating centres in 1977 made tech-nical recommendations on future activitiesin this field, and in particular the develop-ment of laboratory surveillance of viraldiseases in subtropical and tropical coun-tries. Following an informal consultationheld at the Pasteur Institute, Paris, in1976,' a study was undertaken, togetherwith national laboratories and WHO col-laborating centres, of rapid techniques foridentifying virus infections, in order toevaluate their potential usefulness and thetechnological problems involved.
8.103 Influenza. In January 1976, thevirus A /New Jersey /76 isolated during anepidemic in a military camp in the USAwas found to resemble the virus of swineinfluenza which caused the 1918 pandemic.In less than two months an attenuated re-combinant strain was made available tovaccine producers. In April, an informalconsultation held in Geneva advised publichealth services on appropriate measures.'The virus fortunately did not spread andin 1976 and 1977 the variant A/Victoria/3/75 remained the prevalent strain, togetherwith B /Hong Kong /5/7z, and both causedonly moderate outbreaks. WHO intensifiedthe surveillance carried out by the networkof national influenza centres and organizedthree training workshops on new tech-
1 Bulletin of the World Health Organization, 55 : 33(1977).
2 Bulletin of the World Health Organization, S3 : 1
(1976).
I o8
niques for directors of these centres. InDecember 1977 the national influenzacentres in Moscow and Hong Kongisolated strains of a new influenza virus,A /USSR /9o/77, found to be related to thevirus A /FM /1/47 (HINT) which was pre-valent all over the world from 1947 to1957. In less than two weeks all nationalinfluenza centres were alerted and providedwith the necessary reagents to carry outadequate surveillance, and the appropriatestrain was made available to vaccine pro-ducers.
8.104 Measles. There is some un-certainty about the best age for immuniza-tion of children in Africa, where the diseaseis particularly severe. A collaborative studywith the Ministry of Health of Kenyashowed that 9o% of children no longer havematernal antibodies at 7 -8 months of age,when the incidence of measles begins to risesharply. Almost all children vaccinated atthis age showed a satisfactory serocon-version.'
8.105 Poliomyelitis. The epidemiologyof poliomyelitis is now changing. Activesurveillance of the disease necessitatesserological surveys and laboratory identifi-cation of "wild" type and attenuated strainsof poliovirus. Increased laboratory supportfor surveillance was established and pro-vided satisfactory results in countries in theEastern Mediterranean Region.
8.1o6 Infantile viral gastroenteritis. Rota -viruses were characterized in faeces bymeans of immune electron microscopy andfound associated with 50-75% of acutegastroenteritis in infants in temperateclimates. Collaborative studies were under-taken to ascertain their possible publichealth importance in various parts of theworld, particularly in tropical climates.
8 Bulletin of the World Health Organization, S5 : zr(1977).
COMMUNICABLE DISEASE PREVENTION AND CONTROL
8.107 Viral hepatitis. An Expert Com-mittee in 1976 reviewed important advancesin the field of hepatitis A and B.' A seminarheld jointly by WHO headquarters andfour. Regional Offices (Africa, South -EastAsia, Eastern Mediterranean, and WesternPacific) in Kuala Lumpur in 1977 examinedthe basis on which appropriate surveillanceof hepatitis A and B could be establishedin the countries and considered the pros-pects of vaccination in warm - climate coun-tries with a high incidence of hepatitis B.
8.1o8 Arbovirus and Ebola virus infections.During 1976 -77 limited outbreaks of yellowfever occurred in South America, and a veryfew cases were notified in Africa. Denguehaemorrhagic fever became endemic inIndonesia and Burma in addition to Thai-land, where a Collaborating Centre on theImmunopathology of Dengue Haemor-rhagic Fever was created in 1976. Theappearance in 1977 of dengue virus type 1in the Caribbean area, where types z and 3already existed, gave rise to a continuingthreat of outbreaks of haemorrhagic fever.In 1976, WHO was requested to helpidentify and circumscribe two dramaticoutbreaks of viral haemorrhagic feverwhich occurred simultaneously insouthern Sudan and northern Zaire. Anew virus, Ebola virus, resembling Mar-burg virus, was characterized in high -security laboratories. WHO staff membersand consultants were sent to the sites of theoutbreaks as part of the activities of WHOEmergency Aid in Epidemics. A reserve ofdisposable protective clothing was con-stituted. To assist countries in the manage-ment of these and other viral infections,two publications were issued by theOrganization.2, 3 In 1976 an international
1 WHO Technical Report Series, No. 6oz, 1977.2 Madeley, C. R. Guide to the collection and transport of
virological specimens. Geneva, World Health Organi-zation, 1977.
109
symposium on haemorrhagic fevers washeld in Argentina, where a national centrefor their study was established, and in 1977WHO co- sponsored a colloquium on viralhaemorrhagic fevers, organized by thePrince Leopold Institute of Tropical Medi-cine in Antwerp, Belgium.
8.109 Chlamydial infections. Chlamy-diae are now increasingly recognized asagents of sexually transmitted diseases. Anoutline of recommended criteria for theirlaboratory diagnosis was published.4
8.110 Rickettsia/ infections. Recent devel-opments and trends in rickettsial infectionswere reviewed at an international sympo-sium organized in Bratislava, Czechoslova-kia, in 1976. Special attention was given tothe laboratory diagnosis of louse -bornetyphus in areas where the disease continuesto be endemic and is an important cause ofmorbidity and mortality. Five leadingrickettsial laboratories agreed to developsimplified standard methods and to makeavailable the necessary reagents.
Veterinary public health
Zoonoses centres
8.111 Experience with the Pan Amer -can Zoonoses Center showed that suchinstitutions at regional or interregionallevel, with their coordinating and catalysingfunctions, serve countries best in theirefforts to mobilize resources and mutualassistance. A coordinating centre was
a Simpson, D. I. H. Marburg and Ebola virus in-fections: A guide for their diagnosis, management and con-trol. Geneva, World Health Organization, 1977 (WHOOffset Publication No. 36).
Bulletin of the IVorld Health Organization, 54: 245(1976).
6 For veterinary public health activities relating tofood hygiene and food safety, see page 161.
THE WORK OF WHO
established in Athens to promote inter-national cooperation in the control ofrabies and hydatidosis in Mediterraneancountries. The control of other diseases(brucellosis, leptospirosis and cysticercosis)will be incorporated in subsequent phasesof the centre's programme. Similar centresare being planned for East Africa, Westand Central Africa and some South -EastAsian and Eastern Mediterranean coun-tries. The establishment of centres for thecontrol of zoonoses constitutes an import-ant development in the prevention andcontrol of these diseases.
Control of rabies and other zoonoses
8.11z The spread of rabies gave riseto emergency situations in some countries.WHO assisted in such cases, particularlyin Africa. Some successes in rabies controlwere reported from South American coun-tries. Comparative studies on potency testsfor rabies vaccines and field trials on diffe-rent tissue culture vaccines were initiatedto improve the protective measures.
8.113 In November 1977 the SecondEuropean Conference on Surveillance andControl of Rabies, held in Frankfurt amMain, Federal Republic of Germany, en-dorsed proposals for improved methods ofwildlife rabies control, which were a majorachievement of the FAO/WHO Coordina-ted Research Programme on Wildlife Rabiesin Europe. In order to provide the epide-miological services required for thisrational control procedure, a EuropeanRabies Surveillance System was established.
8.114 WHO promoted internationalcooperation in the control of cysticercosisand echinococcosis (hydatidosis) (a jointFAO /UNEP /WHO meeting), brucellosis(WHO consultations held in Spain forMediterranean countries), mycotic zoonosesand leptospirosis (planning meetings heldin Geneva).
IIO
Prevention and control of zoonoses and environ-mental pollution from animal sources
8.115 Animal environmental factors ashuman health hazards were the majorconcern of a meeting of experts held inRome. Particular attention was paid to thehealth risks associated with large -scaleanimal production and intensive farming.Recommendations for a WHO policy andinternational collaboration were elaboratedwhich should lead to codes of practice forthe prevention of human disease at all stagesof farm management, production of food ofanimal origin, and disposal and recycling ofanimal wastes. There is an urgent need tocope with the health risks associated withanimals in urban areas ; the Rome meetingrecommended action aimed at preventingor minimizing such risks.
Comparative medicine
8.116 In the field of comparative medi-cine, the advancement of knowledge ofhuman diseases is furthered through studyof comparable conditions in animals. Re-search using animal models for humandisease continued to receive WHO support.A WHO meeting of investigators dealtwith studies on animal models to determinethe cause and prevention of non -geneticdevelopmental defects where some environ-mental factors are considered to be ofincreasing importance.'
8.117 The programme on the ecologyof influenza viruses in animals and theirrelation to human influenza was expanded.A number of new strains of influenza viruswith new properties were isolated from alarge number of bird species. In someareas up to 5% of apparently normalmigrating birds were found to be carrying
' Bulletin of the World Health Organization, 55 : 475( =977).
COMMUNICABLE DISEASE PREVENTION AND CONTROL
virus. Some strains isolated from thesebirds were indistinguishable from humanstrains of Victoria /75 (H3Nz).
Vector biology and control
8.118 The function of WHO's vectorbiology and control programme is todevelop materials, methods and strategiesfor the control of arthropod vectors, rodentreservoirs and snail intermediate hosts ofdisease. Investigations in all fields relatingto vector control and the safe use ofpesticides are being carried out in collabo-ration with Member States and certainUnited Nations bodies. In recent yearsvector control has been achieved mainlythrough the use of chemicals. This ap-proach has given rise to problems such aspesticide resistance, hazards to non -targetorganisms including man, and environ-mental contamination. A programme ofresearch is now underway to develop betterchemical and non -chemical methods ofcontrol. The Organization carried out areview of the situation and prepared adocument on pest /vector management sys-tems 1 in collaboration with UNEP andFAO.
Ecology and chemical control
8.119 Vector resistance. The WHOExpert Committee on Insecticides statedthat resistance to pesticides is probably thebiggest single obstacle to vector controland is one of the main reasons why malariaeradication has been unsuccessful in manycountries.2 About one -third of all malariaprogrammes face a vector resistance prob-lem. During the past two years this prob-lem was studied in Central and South
1 United Nations Environment Programme. Over-view in the priority subject area: Health of people and of theenvironment (UNEP Report No. z), 1977.
2 WHO Technical Report Series, No. 585, 1976, p. 7.
III
America (Anopheles albimanus), in the East-ern Mediterranean area and the Indo-Pakistan subcontinent (An. culicifacies andAn. stephensi), and in Turkey (An. sacharovi).
8.1 zo Additional standardized resist-ance test methods were being developed forblackflies, snails and fish, a major non -target organism.
8.121 WHO collaborating centres inEurope and the USA continued to carryout research on cross -resistance and speedof development of resistance, with specialemphasis on insecticides showing opera-tional promise.
8.122 Testing and evaluation of new insec-ticides. The number of new candidatepesticides from industry has diminishedconsiderably in the last few years. TheWHO programme for the testing andevaluation of insecticides was reorganizedso that the few new chemicals producedcan be evaluated more rapidly. Compoundsalready in the scheme were being re- evalua-ted in new types of formulations for bothmalaria control and for the control ofother vectors, especially Simulium andGlossina. Some synthetic pyrethroidsappeared to be promising ; relevant safetyaspects were being investigated in coopera-tion with WHO collaborating centres inFrance, the United Kingdom, the USA andYugoslavia.
8.123 Vectors of malaria. Several pyre -throids were tested in but 3 trials by theWHO collaborating centre in Upper Voltaand two were subjected to small village -scale trials against An. gambiae and An.funestus at the WHO Anopheles ControlResearch Unit in Nigeria. In large -scale
3 Huts are specially constructed with traps forestimating the number of mosquitos entering andleaving.
THE WORK OF WHO
trials organized by this unit, chlorphoximand pirimiphos- methyl proved effective incontrolling An. gambiae and An. funestus forthree months and were found safe for use.
8.124 A large -scale epidemiological trialof fenitrothion was concluded at Kisumu,Kenya, in an area inhabited by about5o 000 people.' Excellent control of An.gambiae and An. funestus was achievedthroughout the trial and a marked andrapid decrease in the numbers of malariacases was observed. The last spray roundwas effective for almost one year.
8.125 Two field trials of mosquitoadulticides were carried out in Indonesia atthe USAID- supported Semarang Sub -Unitof the Vector and Rodent Control ResearchUnit against DDT -dieldrin- resistant An.aconitus, the main vector of malaria inIndonesia (Java). One residual applicationof fenitrothion provided good control ofAn. aconitus during the whole breedingseason of this species. However, ultra -low- volume application produced onlytransitory results. Residual application ofmalathion controlled the vector for only ashort period after application.
8.126 The Organization cooperatedwith Indonesia, Pakistan and Turkey inevaluating their antimalaria activities andin preparing detailed plans for future action,and with Burma in analysing the vectorcontrol component of vector -borne diseasecontrol departments.
8.127 Vectors of filariasis. Studies on thedynamics of filariasis transmission werecarried out in Indonesia (Java), Samoaand the United Republic of Tanzania.
8.1 z8 Large -scale field trials using larvi-cides for Culex pipiens fatigans control, sup-
1 WHO Chronicle, 3i : 102 (1977).
I12
ported by the Government of the Nether-lands, were conducted by the WHO Vectorand Rodent Control Research Unit in theJakarta area. An organophosphorus insec-ticide (pirimiphos -methyl) and three insectgrowth regulators (diflubenzuron, metho-prene and OMS 139o) gave satisfactorycontrol for two to five weeks. These com-pounds could be considered for use in areaswhere fenthion and chlorpyrifos 2 cannot beused.
8.129 Vectors of yellow fever and denguehaemorrhagic fever. In southern Nigeria, theWHO Arbovirus Vector Research Unitcontinued to study the bionomics of yellowfever vectors. Dengue virus was isolatedat the University of Ibadan from materialprovided by the Unit. Aedes africanus,usually considered a sylvatic vector, wasfound to be peridomestic in certain situa-tions. Preliminary trials using hand -heldultra -low- volume equipment were initiatedfor the control of Ae. aegypti and Ae.africanus.
8.13o WHO -supported investigationsundertaken in Bangui, Central AfricanEmpire, and Dakar, Senegal, on the longe-vity of Ae. africanus, Ae. opok, and one of theAe. taylori group showed that these speciesmay serve as yellow fever reservoirs as wellas vectors in savanna areas.
8.131 The PAHO Advisory Committeeon Yellow Fever, Dengue and Ae. aegyptimet in Panama in March 1976 to study theRegional policy for the prevention of thedisease transmitted by this vector.
8.132 Vectors of onchocerciasis. In co-operation with the WHO onchocerciasiscontrol programme 8 and a collaboratinglaboratory on the Ivory Coast, 8 com-
2 Proposed international common name.3 For details of this programme, see page 9z.
COMMUNICABLE DISEASE PREVENTION AND CONTROL
pounds in zz formulations were tested forSimulium control in small -scale river trialsand 4 compounds in 5 formulations inlarge -scale trials, with special emphasis onthe side effects on non -target organisms.Promising results in this search for environ-mentally acceptable larvicides were obtain-ed with a micro- encapsulated formulationof an organophosphorus compound, chlor-pyrifos- methyl.'
8.133 Chemical monitoring of insecti-cide residues following application wascarried out for the onchocerciasis controlprogramme during operational use of thelarvicide temephos ;' information was ob-tained on the movement of this larvicidein the river water and on its fate in non -target organisms and in the mud.
8.134 Vectors of trypanosomiasis. Withinthe framework of a joint UNDP /FAO /WHO project, and with the financial sup-port of of Germanyand the technical assistance of a Nether-lands institute, several insecticides appliedby helicopter at low or ultra -low volumewere evaluated against riverine tsetse fliesin Upper Volta. Endosulfan and one pyre -throid were particularly effective and couldbe applied as aerosols for curbing out-breaks of sleeping sickness. The effects onthe non -target organisms were minimal inmost cases.
8.135 Studies on the vectors of Chagas'Disease carried out at the WHO Chagas'Disease Research Unit in Venezuela showedthat reinfestation of insecticide -treatedhouses was relatively rapid, occurring with-in a few weeks when insecticides of shortpersistence were used. New insecticidesthat might be used to replace organochlo-rines as an adjunct to housing improve-ments were evaluated.
1 Proposed international common names.
I13
8.136 Vectors of plague and murine typhusand rodent reservoirs. Following the 1976epidemic of African haemorrhagic fever inSudan and Zaire, a search was made inSudan for a possible rodent reservoir ofthe newly described Ebola virus ; thecollected material is being studied in theUnited Kingdom.2
8.137 In Nigeria, studies were carriedout on rodents of the Mastomys natalensisgroup, the only proven reservoir of Lassafever virus, to clarify the epidemiology ofthis disease. The different species of theM. natalensis complex are at present recog-nizable only by the number of chromo-somes.
8.138 In Indonesia, the Vector andRodent Control Research Unit beganstudying the ecology of potential reservoirsand vectors of plague in the Bogor -Cilotoarea of Western Java ; some investigationswere also carried out in the city of Jakarta.Flea resistance to DDT was found to bewidespread in these areas and control trialswith alternative insecticides were com-menced.
8.139 The WHO Rodent Control De-monstration Unit in Rangoon, Burma, sup-ported by DANIDA and the UnitedKingdom through the Colombo plan,completed an 18 -month study on theecology, distribution and disease reservoirimportance of the small -mammal popula-tion of Rangoon. Six species of rodentsand one species of shrew were found to bepresent in the city in high densities. Asignificant percentage of animals trappedin surveys were seropositive for plague andmurine typhus. Studies on rodent and fleacontrol were pursued.
8.140 Snail intermediate hosts. WHOcollaborating centres carried out a variety
2 See also page 109.
THE WORK OF WHO
of investigations on the screening of newmolluscicides in Japan and the UnitedKingdom, on the biology and identificationof snails in Denmark, and on the biologicalcontrol of snails in Brazil and the UnitedKingdom. Close liaison was maintainedwith UNEP in developing environmentallysound snail control strategies.
Pesticide production, formulation and safe use
8.141 In collaboration with UNIDO,the Organization carried out a feasibilitystudy for establishing a DDT plant in VietNam. WHO also participated in a sympo-sium on pesticides organized by UNIDOin collaboration with ES CAP in Bangkok.
8.142 In a number of countries wheremalathion is now used for malaria controloperations, the odour of currently availablewater -dispersible powders has created prob-lems. An improved formulation of thisinsecticide was evaluated and found to bemore acceptable.
8.143 In mid -1976 some malathionwater -dispersible powders used in Pakistanand Iran caused outbreaks of poisoning.Intoxication occurred among several hun-dred spraymen who took little or nosafety precautions, and five died. Aninvestigation carried out by three WHOcollaborating centres in Belgium, theUnited Kingdom and the USA in coop-eration with manufacturers of malathiondemonstrated that the poisoning resultedfrom potentiation of malathion by animpurity formed in the powder duringshipping and field storage. A new set ofmalathion specifications, including specificanalytical methods, that will prevent theprocurement of such unstable water -dis-persible powders was adopted by the WHOExpert Committee on Chemistry and Speci-
114
fications of Insecticides which met in1977.1
8.144 In collaboration with IARC,WHO extended the toxicological investi-gation of newly developed pesticides toinclude testing for possible mutagenicityand carcinogenicity potential.
Biological control
8.145 At the WHO Anopheles ControlResearch Unit, Kaduna, Nigeria, z8 patho-genic microorganisms associated withmalaria vectors were isolated fromAnopheles gambiae and An. funestus. Lab-oratory trials with several of these agentswere encouraging, as they induced highlarval mortality.
8.146 The first Scientific WorkingGroup on Biological Control of InsectVectors of Disease was held in 1 977 aspart of the Special Programme for Researchand Training in Tropical Diseases. TheGroup reviewed the scheme for isolationand characterization of biological controlagents, protocols for safety tests and thedesign of field trials.
8.147 A meeting was convened inKaduna for investigations on the bio-logical control of vectors in Nigeria.
8.148 The operational use of larvi-vorous fish was pursued in several countriesin the Eastern Mediterranean area.
Vector genetics and genetic control
8.149 A feasibility study on the geneticcontrol of An. gambiae was carried out inSenegal. Liaison was maintained with
1 The report of the Expert Committee will be pub-lished in the WHO Technical Report Series during1978.
COMMUNICABLE DISEASE PREVENTION AND CONTROL
USAID teams working on the geneticcontrol of An. albimanus in El Salvadorand Glossina morsitans in the United Repub-lic of Tanzania, and a Franco - Germanteam working on the genetic control ofG. p. gambiensis in Upper Volta.
8.15o WHO convened an informal con-sultation on species complexes in insectvectors of disease. The report stressed thepractical significance of complexes ofclosely related species of vectors andparasites in relation to the epidemiologyof vector -borne diseases and the develop-ment of control methods.' Recommen-dations of the group are being imple-mented.
Equipment for pesticides
8.151 The WHO Expert Committee onVector Biology and Control met in 1976to consider engineering aspects of vectorcontrol operations.2 In accordance withits recommendations, WHO collaboratingcentres are being established for the evalu-ation and testing of pesticide applicationequipment in cooperation with manu-facturers and national programmes. TheCommittee also updated specifications forspraying equipment. WHO intensifiedits cooperation with FAO in the jointevaluation of equipment.
Vector control in international health
8.15z A WHO collaborating laboratoryin Washington, DC (Agricultural Environ-mental Quality Institute, United StatesDepartment of Agriculture), carried outtests both in the laboratory and in operatingaircraft on the efficacy of a new pyrethroid,
For species complexes in the Simuliidae, see Bulletinof the World Health Organization, 56, No. i (1978).
2 WHO Technical Report Series, No. 603, 1977.
I15
(+)- phenothrin (d- phenothrin, S 2539Forte), for the disinsection of aircraft. In1977 the Thirtieth World Health Assemblyapproved the use of this compound for thedisinsection of aircraft (resolutionwHA3o.1 9).
Special Programme for Research andTraining in Tropical Diseases
8.153 The period 1976 -77 saw thecompletion of the planning phase of theSpecial Programme for Research andTraining in Tropical Diseases and thetransition to a preparatory phase of organi-zation and pilot activities leading to thefull operation of projects. Detailed tech-nical proposals for research and trainingwere endorsed by a meeting in December1 976 of representatives of 35 participatinggovernments, agencies and foundationsrepresenting both the affected tropicaltries and the developed world. Adminis-trative, financial and organizational planswere developed at the meeting, and it wasagreed that the Programme was set on asound technical foundation and that itshould begin large -scale operations in1977.
8.154 The Special Programme has twointerdependent objectives : (a) to developimproved tools for the control of tropicaldiseases, and (b) to strengthen the relevantbiomedical research capability in tropicalcountries. The Programme is based on ananalysis carried out in consultation withnumerous experts on (i) the six selecteddiseases (malaria, schistosomiasis, filariasis,trypanosomiasis, leprosy and leishmaniasis),current problems of their control andpotential research approaches ; (z) ap-proaches to disease control that combinemeasures against several diseases -in thefields of epidemiology, biomedical research
THE WORK OF WHO
and biological control of vectors ; (3) train-ing and institution- strengthening ; (4) socio-economic aspects ; and (5) programmemanagement.
Research and development
8.155 Research in the Special Pro-gramme is planned, implemented andevaluated by scientific working groupscomprising scientists selected on a world-wide basis according to their knowledgeand skills. Scientific working groups arebeing established to cover all fields whereresearch development is needed. By theend of 1977 scientific working groups hadbeen established for the chemotherapy ofmalaria, the immunology of malaria,schistosomiasis, filariasis, African trypano-somiasis, the immunology of leprosy, thechemotherapy of leprosy, epidemiology,and the biological control of diseasevectors. A scientific working group onbiomedical research will be established in1978.
8.156 In each case, a disease- orientedparent Scientific Working Group meetsinitially to provide an overview of thedisease problems and is convened periodi-cally to review the status of the programme.The parent group may later divide intotarget -oriented groups (for instance, onchemotherapy, immunology or operationalresearch). The parent groups for filariasis,schistosomiasis, African trypanosomiasis,Chagas' diseases and leishmaniasis all metin 1 977.
8.157 In addition, an Informal WorkingGroup, meeting in Washington, DC, inMarch 1977, agreed on areas of highpriority for socioeconomic research, in-cluding the sociocultural acceptance oftechnologies, and social, cultural and econ-omic adaptations to disease.
I16
Training and institution- strengthening
8.158 The emphasis on the strengthen-ing of the research capability, initiallyon the African continent, is beingextended to cover other endemic areas.Pilot activities were begun or will shortlybegin, based on four centres in Ndola(Zambia), Nairobi (Kenya), Kuala Lumpur(Malaysia), and Cotonou (Benin). Thefirst meeting of the Research StrengtheningGroup was held in October 1977. Inaddition, six workshops, symposia orseminars were conducted during 1977 fortraining scientists, and a number of researchtraining grants were awarded.
8.159 An official agreement was signedbetween the Government of Zambia andWHO for the formal establishment of theTropical Diseases Research Centre inNdola, Zambia, which is the base for thefirst phase of the Special Programme'sepidemiological studies, as well as for drugtrials.
8.16o The Research StrengtheningGroup at its first meeting in Geneva inOctober 1977 established main policyguidelines covering this component of theProgramme : (1) to strengthen researchand training institutions, so as to assisttropical countries in developing the infra-structure necessary to cope with problemsrelated to disease control ; (z) to supportthe training of persons from tropical coun-tries, so as to develop scientists and otherresearch personnel of the highest qualityto help meet manpower needs ; (3) toencourage and assist in the diffusion,interpretation and integration of newknowledge so as favourably to influencehealth policies and their implementation ;and (4) to contribute to the rapid transferto the affected countries of the knowledge,technology and skills that are relevant totheir health objectives and within thesphere of the Special Programme.
COMMUNICABLE DISEASE PREVENTION AND CONTROL
8.161 The research -strengthening activ-ities are by definition long -term com-mitments with explicit government in-volvement, in contrast to the scientificworking group projects, which are limitedin time and scope to a specific task. Theseactivities will therefore be developed inclose consultation with governments,regional Advisory Committees on MedicalResearch and other appropriate regionalbodies.
8.16z Institutions strengthened by theProgramme will be designated as centreswithin a network. Networks will bebalanced on a regional basis to include asmany as possible of the facilities forresearch and training that are required inthe region.
8.163 Institution -strengthening is lim-ited to centres in tropical countries. Asmuch training as possible should takeplace in the tropical countries, makingmaximum use of Special Programme net-work centres. However, in some casestraining in nontropical countries will benecessary.
Technical review
8.164 A Technical Review Group con-vened in September 1 976 considered thetechnical and scientific aspects of the Pro-gramme, strongly endorsed the generaldevelopment of the Programme and itsobjectives, examined and in general ap-proved the balance of the various activitiesand recommended a number of adjust-ments in specific aspects of the Programme.
8.165 Major funds to support the Pro-gramme became available in 1977, and asecond Technical Review Group convenedin September 1977 felt that significant pro-gress had already been made in moving theProgramme into the phase of implement-
I17
ation. The Group reviewed the plans andpilot operations of the Special Programme,endorsed its objectives and proposed linesof development, and made certain modi-fications and recommendations for imple-mentation, which were accepted by theDirector- General. The Group stressed theneed to continue to strengthen the manage-ment of the Programme by the incorpor-ation of efficient and effective scientific andfinancial control systems ; the importanceof developing Special Programme activitiesin active consultation with the global andregional Advisory Committees on MedicalResearch, regional offices, and national andother bodies planning and funding researchon the six diseases ; and the importance ofthe Programme's training and institution -strengthening activities.
Financing
8.166 At the December 1 976 meetingof cooperating parties a total of approxi-mately US $ 7.5 million was pledged foractivities in 1977 and a number of parti-cipants indicated their intention to providelong -term financial support. For theperiod 1 January to 3o September 1977,voluntary contributions totalling overUS $ 6 300 000 were received to supportthe activities of the Special Programme,including contributions from the Govern-ments of Cyprus, Denmark, the Netherlands,Norway, Sweden, the United Kingdom andthe USA, and from UNDP (co- sponsor ofthe Programme), the International LeprosyAssociation, and the Japan ShipbuildingIndustry Foundation (Sasakawa HealthFund). For the full year 1977, financialsupport from the regular budget of WHOtotalled approximately US $ 903 000. Thesefunds, plus additional pledges from theGovernments of Austria, Belgium, Fin-land, Nigeria and Switzerland, and theInternational Development Research
THE WORK OF WHO
Centre, brought the total financial supportfor the Special Programme to approximatelyUS $ 11.5 million for 1977.
8.167 The parties cooperating in theSpecial Programme realize that 5 -2o yearsof scientific and financial support will berequired to attain its objectives, and somegovernments and agencies have alreadyindicated 3 -5 -year support during theinitial period of rapid implementation.Such longer -term support enables WHOto build up and maintain the participationand confidence of the scientific communityand to begin strengthening research capa-bilities within the endemic countries.
Information transfer
8.168 The Special Programme News-letter was distributed periodically to indi-viduals and institutions in developingcountries presently or potentially concernedwith or interested in the areas of researchwithin the Programme. Reports of scienti-fic working groups were distributed tointerested persons. Contact was madewith relevant scientific and public healthjournals, and information displays wereprepared for use at scientific meetings. Ahandbook was compiled for use by allpersons involved in the research of theSpecial Programme, and invitations tosubmit research proposals were widelydistributed.
Prevention of blindness
8.169 The technical cooperation pro-gramme for the prevention of blindnesswas established at the end of 1976 in accord-ance with World Health Assembly resolu-tions, and in particular resolution wHAz8.54adopted in 1975. However, specific activi-ties began early in 1976.
I18
8.17o The programme will deal initiallywith the most urgent priorities identifiedfor WHO action -trachoma, xerophthalmiaand onchocerciasis. Other recognizedpriorities are cataract, eye injuries andglaucoma. The long -term objective is tointroduce adequate eye care and to pro-mote eye health at the peripheral level, themain emphasis being on health education,intersectoral coordination of activities, pro-motion of national programmes and mobi-lization of extrabudgetary resources, inclose collaboration with other organiza-tions in this field, notably the InternationalAgency for the Prevention of Blindness.
8.171 In 1976, "Foresight preventsblindness" was the theme for World HealthDay. This activity, together with parallelaction taken by the International Agencyfor the Prevention of Blindness, resultedin the setting up of national committeesfor the prevention of blindness in 47 coun-tries. Information material was widelydistributed in many languages and specialevents marked the day in a number ofcountries. Meetings held in New Delhiand Baghdad outlined strategies for blind-ness prevention and advocated the devel-opment of programmes in various coun-tries. An example of interagency collabor-ation was the endorsement by the WorldFood Programme of a WHO recommen-dation for the enrichment of dry skimmedmilk with vitamin A.1
8.172 In 1977, activities were especiallyaimed at further developing regional andnational policies, programmes and projects.In Africa, as initial steps in the promotionof national programmes, surveys werecarried out in Chad, Ghana and Nigeriaand planned in other countries. Attentionwas given to the eye care component of theonchocerciasis control programme in the
1 See page 55.
COMMUNICABLE DISEASE PREVENTION AND CONTROL
Volta River basin area ; experience gainedthere will benefit other countries affectedby onchocerciasis. In the Americas, pre-liminary contacts were made to prepare awork plan for a regional prevention ofblindness programme. Prevalence andmorbidity studies of trachoma, xerophthal-mia and onchocerciasis and pilot projectsfor glaucoma prevention and control wereundertaken. Several countries in theRegion explored the possibility of initiatingcomprehensive programmes.
8.173 In the South -East Asia Region,programmes were already well establishedfor the prevention and treatment ofxerophthalmia in Bangladesh and Indo-nesia and the control of trachoma in Burma.A further example of activities at thenational level is the problem- oriented pro-gramme for the prevention and control ofblindness planned by the Government ofIndia, which includes the promotion ofhealth education in eye care, the provisionof comprehensive eye care through mobileunits, and the establishment of a permanentinfrastructure for eye health at differentlevels. Other activities included a surveyof blindness, the management of eyeinjuries and glaucoma screening in Burma.Throughout the Region special attention
was given to training and health educationprogrammes and to mobilizing additionalinputs from multilateral, bilateral and non-governmental organizations.
8.174 In the Eastern MediterraneanRegion, WHO continued to cooperate inthe control of trachoma and other com-municable eye diseases in Iraq, LibyanArab Jamahiriya, Oman, Sudan, SyrianArab Republic and Yemen. In addition,a committee including some Ministers ofHealth from the Region was set up tostudy promotive measures for the pre-vention of blindness, including a feasibilitystudy with regard to the setting up of aRegional centre.
8.175 In the Western Pacific Region,WHO cooperated in the formulation of anational programme in Fiji.
8.176 Data on blindness in a numberof countries were collected in collaborationwith the International Agency for thePrevention of Blindness and with theWorld Council for the Welfare of theBlind. Guidelines and visual aids fortraining personnel, especially auxiliaryhealth workers, were being prepared, aswell as guidelines for defining the methodsused in field assessment.
I19
Chapter 9
Noncommunicable Disease
Prevention and Control
Mental health
Overall programme developments
9.1 A MEDIUM -TERM mental healthprogramme for the period 1975-8 z was developed in 1974-75
and initiated in 1975. It involves the useof a new mechanism : the CoordinatingGroup for the WHO Mental Health Pro-gramme. This broadly -based Group,which meets every two years, consists ofWHO staff members and representativesfrom a wide range of disciplines concernedwith mental health, including heads of WHOcollaborating centres, representatives ofUnited Nations agencies and govern-mental and nongovernmental organizationsand public health administrators.
9.2 At its first meeting in 1976 theGroup agreed on the content of themedium -term programme, the focal pointsfor each activity, and methods for co-ordinating work so as to ensure thatnational, regional and global activitiescomplement and strengthen each other.Shortly afterwards coordinating mechan-isms at regional and national levels wereestablished. In 1976 the WHO RegionalOffice for Europe convened its AdvisoryCommittee on the European Mental HealthProgramme (1970 -83) in Copenhagen, andthe Regional Office for the Eastern Mediter-
I20
ranean Region held a Group Meeting onMental Health in Cairo ; in 1977 theRegional Office for South -East Asia heldthe first meeting of its Mental HealthAdvisory Group. Similar mechanisms arebeing developed in the Region of theAmericas and the Western Pacific Region.In the African Region a workshop onMental Health Services and ResearchStrategies in Africa, organized jointly byWHO and the African Psychiatric Associa-tion, reviewed priority mental health needsand strategies for meeting them ; recom-mendations were forwarded to all govern-ments in Africa. In response to resolutionwHA3o.45 adopted by the World HealthAssembly in May 1977, requesting actionto deal with the urgent problems arisingfrom the severe psychosocial stresses facingpopulations of developing countries andparticularly the high -risk populations insouthern Africa, proposals for a mentalhealth programme were developed jointlywith appropriate governments and authori-ties and steps were taken to obtain thenecessary extrabudgetary support.
9.3 At the national level various typesof coordinating mechanisms evolved. Forexample, multidisciplinary resource centreswere established in Colombia and Indiato coordinate work in those countries, assistthe work of the regional coordinatinggroup and cooperate with other countries
NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
and WHO in developing appropriate men-tal health technologies and training pro-grammes. In another country the mainchannel for cooperation with WHO is aspecially formed liaison group consisting ofpublic health officials, a representative ofthe national mental health professionalassociation and other mental health experts.In yet another country collaboration withWHO is coordinated through the advisoryboard of an association of universitiesbrought together by WHO's programme.
9.4 In August 1977 the second meetingof the Coordinating Group took place inManila. Progress in the programme wasevaluated in the context of Health Assemblyresolutions adopted since the first meeting.In particular, discussion centred upon thedevelopment of effective cooperationamong countries and with WHO in theintegration of mental health into nationalhealth and social policies.
Development of community health services
9.5 WHO is cooperating with a num-ber of developing countries in the effort todevelop and test new approaches to mentalhealth care, characterized by the use ofsimple interventions of proven efficacy, ahighly selective approach to the definitionof mental health priorities and the locationof activities within the existing healthservices, in particular at the peripheral level.
9.6 By the end of 1977, the secondphase of a collaborative study to establishthe feasibility of this approach was wellunderway in communities in Colombia,India, Senegal and Sudan. Simple screeningmethods for mental disorders in bothadults and children were developed in thisstudy, and it was shown in all four countriesthat approximately 15% of all patientsseeking health care at the primary levelsuffer from definite mental disorders, in
I21
many cases in combination with physicaldisorders. It was also shown that evenbrief exposure to mental health traininghas a strikingly beneficial effect on attitudesof health staff towards mental health, allowshealth workers to detect the majority ofmental disorders, and leads to the provi-sion of effective treatment at health centres.This work was facilitated by the definitionof a limited range of "essential psycho -
tropic drugs" sufficient for the effectivemanagement of neuropsychiatric disorders.Similar projects were initiated in Brazil andPhilippines in 1977.
9.7 Development of appropriate mentalhealth inputs into national health policieswas the main line of action in all regions.Regional offices cooperated closely withcountries, including in particular Gambia,Mauritius, Nigeria, Seychelles, Togo, Zam-bia (African Region) ; Colombia, Domi-nican Republic, El Salvador, Honduras,Jamaica, Peru, Uruguay, Venezuela (Regionof the Americas) ; Bangladesh, India,Indonesia, Mongolia, Sri Lanka, Thailand(South -East Asia Region) ; Portugal (Euro-pean Region) ; Ethiopia,' Iran, Iraq, Kuwait,Libyan Arab Jamahiriya, Oman, SaudiArabia, Sudan, Syrian Arab Republic,United Arab Emirates (Eastern Mediter-ranean Region) ; Philippines, Republic ofKorea (Western Pacific Region).
9.8 An important mechanism of co-operation with countries in the EuropeanRegion was collaboration with nationalmental health service pilot areas in tencountries. Through the study of mentalhealth services and their staffing, patientcensus and cohort studies, and cost -efficiency studies, it is hoped to develop andextend the range and quality of mental
1 In May 1977 the World Health Assembly agreed toEthiopia's request to be included in the African Region(resolution W1- 1A3o.35).
THE WORK OF WHO
health services and to improve their co-ordination with general health care and withother social services.' Meetings were heldto review constraints to development andmake recommendations for comprehensivecommunity mental health services in thelight of the most recent trends in Europeancountries.
9.9 Regional and interregional activitieswere undertaken to develop mental healthservices for specified population groups. Areview of previous work in the field ofmental retardation was carried out and astrategy for future action developed inwhich work on mental retardation is anintegral part of several existing programmes-for example, mental health, maternal andchild health, and disability prevention.Priority was given to action within existingservices and to interventions concernedwith children. Work was started on simplemethods of detection for use by health staffproviding care for young children and onsimple methods for training parents ofretarded children. The Thirtieth WorldHealth Assembly endorsed this new stra-tegy (resolution WHA ;o. ;8).
9.10 The WHO Regional Office forEurope, as the focal point for the Organiza-tion's programme on health care ofthe elderly, convened a working groupon the prevention of mental disorders inthe elderly. A review was undertaken ofexisting emergency mental admission unitsfor the elderly.
9.11 In the area of child and adolescentmental health, information on mentalhealth education programmes relating tothe use and abuse of alcohol, tobacco anddrugs was being collected in Europeancountries with a view to assessing the short-
1 May, A. R. Mental health services in Europe. Geneva,World Health Organization, 1976 (WHO OffsetPublication No. 23).
1 22
term and long -term effects of such pro-grammes. The role of youth advisoryservices and other community services inthe prevention and early detection ofmental problems in young people was thesubject of a meeting held in 1977 and acomparative epidemiological study wasundertaken to explore reasons for recenttrends in suicide rates among youngpeople in European countries.
9.12 Child and adolescent mental healthwas also an important concern in the Regionof the Americas, as was indicated by theadoption in 1976 of Regional Committeeresolution AMR /RC28 /R33 on health andyouth. Most countries in this Region weredeveloping mental health programmes asan integral part of their family health pro-grammes, with particular emphasis onactivities at the community level.
9.1; A study group on the applicationof advances in neurosciences for the controlof neurological disorders was convened inMarch 1977. Recommendations were madewith regard to education of the community,and training of professional and non-professional workers ; epidemiological re-search concerning neurological disordersand in particular epilepsy ; and otherresearch, for example, on the developmentof new drugs and vaccines, and on therelationship between neurological disordersand physiological and social factors inmalnutrition.
9.14 Many countries are seeking a moreeffective legislative framework for mentalhealth care. In 1975 -76 the WHO RegionalOffice for the Eastern Mediterranean car-ried out a detailed study of mental healthlegislation in countries in that region, andin 1976 -77 an international survey of men-tal health legislation was undertaken.2 A
2 International Digest of Health Legislation, 28, No. 4(1978).
NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
new project begun in 1977 in the field offorensic psychiatry was concerned with thestudy of legal provisions for the assessmentof dangerousness in the mentally ill.
9.15 In response to a request by theUnited Nations Special Committee AgainstApartheid, a report was prepared based onthe available published information con-cerning mental health care in the Republicof South Africa. The report stressed theexistence of racial inequality and discrimin-atory practices within the mental healthservices of that country and concluded thatsuch policies are the direct effect of apartheidin the health field.
9.16 Two projects concerned with al-cohol consumption were launched in 1976with extrabudgetary support. The firstaims at ascertaining and commenting uponthe response to problems created by alcoholconsumption in communities in Mexico,the United Kingdom and Zambia. For thesecond project, on the prevention ofalcohol- related disabilities, international re-views of the types and effectiveness ofrelevant measures, policies and programmeswere prepared for discussion at a first meet-ing in October 1977, and a publication wasprepared on the identification and classifica-tion of these disabilities.'
9.17 A report on WHO's approach andunderlying policy in dealing with drugdependence problems was submitted to thetwenty- seventh session of the UnitedNations Commission on Narcotic Drugs.The major emphasis of current work is onthe development of effective managementsystems and treatment programmes, inte-grated into general health and social welfareefforts. Support from UNFDAC greatly
Edwards, G., Gross, M., Keller, M., Moser, J. &Room, R. Alcohol- related disabilities. Geneva, WorldHealth Organization, 1977 (WHO Offset PublicationNo. 32).
1 23
facilitated WHO's collaboration with gov-ernments in this field. Focusing ondeveloping countries, the approach in-volves the training of key personnelthrough fellowships, and epidemiologicalsurveys in rural and urban target com-munities, followed by the introduction andsystematic evaluation of treatment pro-grammes. Projects using this approachwere underway in Burma, Egypt, Iran,Pakistan and Thailand, and being plannedin Afghanistan, Malaysia and Peru.
9.18 In response to resolution wPRo/Rc27 /R5 of the WHO Regional Committeefor the Western Pacific, a working groupon early intervention programmes in drugabuse was held in late 1976 and made rec-ommendations for setting up such pro-grammes. Cooperation was pursued withMalaysia in developing a national systemfor the treatment and rehabilitation of drug -dependent persons and with Viet Nam inestablishing a comprehensive programmefor drug dependence.
9.19 In October 1976 a meeting ofexperts was convened to advise WHO onits functions and responsibilities under theConvention on Psychotropic Substances.An Expert Committee on Drug Depen-dence met in late 1977 to review the instru-ments for scheduling drugs under theConvention and to consider necessarynotifications.2 Particular attention waspaid to the development of new methodsfor assessing dependence -liability, abusepotential, therapeutic usefulness, and publichealth and social problems. All MemberStates were requested to provide informa-tion on their experience relative to Articles 3and 1 o of the Convention concerningcombined substances and labelling of drugs.WHO designated two collaborating centresin the area of drug dependence ; four other
2 WHO Technical Report Series, No. 618, 1978.
THE_WORK OF WHO
centres were in the process of designation.Extrabudgetary resources were obtained tosupport two intercountry workshops fordecision- makers.
P ychosocial aspects of the human environment
9.zo In May 1976 the World HealthAssembly adopted resolution wHnz9.z1,requesting the Director - General to initiatea programme in the area of psychosocialfactors and their influence on health and thefunctioning of health services. In pursuanceof this resolution three types of work werecarried out.
9.21 First, a series of workshops wasplanned in which top -level health adminis-trators from developing and developedcountries, together with experts in thesocial sciences and related disciplines,would critically examine health programmesand identify needs for psychosocial inputs.The first of these workshops, in English,was held in late 1976, organized jointlywith the Swedish Government and theWHO collaborating centre in Stockholm.The second, in French, organized jointlywith the Belgian Government, takes placein January 1978.
9.22 Secondly, activities were under-taken to facilitate the application of existingknowledge in improving the provision ofhealth and psychosocial care. Psychosocialdevelopment and mental health in child-hood was reviewed by an Expert Commit-tee in November 1976.1 Interventionsaiming to prevent adverse health and psy-chosocial effects of uprooting occurring asa result of rapid social change, migrationand resettlement were reviewed and abibliography prepared. A collaborativestudy in six countries on the prevention
1 WHO Technical Report Series, No. 613, 1977.
124
and reduction of social disabilities in peoplesuffering from mental disorders was initia-ted, as well as a project aimed at assessingthe adverse psychosocial effects of masshealth campaigns such as fertility regula-tion programmes.
9.23 Thirdly, to obtain new knowledgein key areas of psychosocial functioning, amajor cross -cultural study, supported byextrabudgetary resources and involvingcentres in nine developing countries, wasbegun in 1976. This study focuses onfactors in family life protecting mentalhealth and on the way in which stressfullife events affect vulnerable individuals indifferent sociocultural settings. In thisconnexion a review was made of theavailable evidence on factors and interven-tions promoting healthy family functioning.
Health manpower development
9.24 A radical change of emphasis wasintroduced in regional and interregionaltraining activities, which now focus onimparting mental health skills to a varietyof health and social service personnel andon imparting public health skills to mentalhealth workers. Details of mental healthtraining and education activities are report-ed in chapter 7.
Promotion of biomedical and health practiceresearch
9.25 The Organization developed abroad strategy for improving existingtreatment methods, particularly in develop-ing countries ; comprehensive informationon effective treatment methods and funda-mental research is being made available toall Member States through a network ofcollaborating centres and publications.$ A
2 World Health Organization. Advances in the drugtherapy of mental illness. Geneva, 1976.
NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
WHO project designed to evaluate the dif-ferences in effectiveness of psychotropicsubstances that occur in different popula-dons depending, for example, on climate,nutrition, endemic diseases, genetic poly-morphism in drug metabolism or organsensitivity was initiated, with extrabudget-ary support, in seven countries. With theassistance of funds from UNFDAC, anotherstudy was begun in four countries on theabuse potential and usefulness in therapyof thebaine derivatives.
9.26 In an effort to increase under-standing and cooperation in research on thebiological basis of mental disorders, col-laborative studies were carried out on theassociation between colour blindness andthe presence of affective disorder, on therelationship between plasma amitriptylinelevel and therapeutic response in affectivedisorder, and on the antithymic immunefactor in schizophrenia.
9.27 In view of the major public healthimportance of neurological disorders aseries of studies was started on epilepsy,cerebrovascular disorders, and parasitic andinfective disorders of the nervous systemand on the pharmacokinetics of anti -convulsant drugs. This research is beingcarried out through the network of eightWHO collaborating centres.
9.28 Following the demonstration in aprevious WHO study that important dif-ferences exist in the prognosis of severemental disorders in developing and devel-oped countries, a new study supported fromextrabudgetary sources was undertaken innine countries to identify possible dif-ferences in morbidity risks associated withsuch disorders in different cultures, and toexplore the role of the family, the com-munity and different biological factors indetermining the course and outcome ofsevere mental illness.
125
9.29 Since patients with psychologicaldisorders, and in particular various formsof depression, represent a sizeable propor-tion of all patients attending general healthservices, a study was initiated in five coun-tries (Canada, India, Iran, Japan and Swit-zerland) to determine the frequency andtypes of such conditions and to developmethods for improving the capacity of non-specialist health workers to deal with them.
9.3o Collaborative work on the epide-miology of drug abuse was continued, withsupport from UNFDAC. A case -reportingform for collecting "minimum essential"data on drug users in contact with treat-ment and other institutions was tested inseven countries and the results reviewed inlate 1977. A general methodology forevaluating drug dependence treatment pro-grammes was developed and the instru-ments and methods will be tested inevaluation studies in these same sevencountries. Testing on students of a self -administered drug use survey instrumentwas begun in nine countries. Plans weremade for the pilot testing of previouslydeveloped WHO guidelines for reportingavailable information on nonmedical druguse.
Mechanisms for programme development andsupport
9.31 In addition to the coordinativeactivities described above, methods ofassessment and classification, and alsoinformation systems, were being developedto facilitate the identification of areas ofimmediate concern at the national level.
9.32 A trial of the multi -axial classifi-cation of psychiatric disorders in child-hood 1 was initiated in several European
1 Rutter, M., Schaffer, D. & Shepherd, M. A multi-axial classification of child psychiatric disorders. Geneva,World Health Organization, 1975.
THE WORK OF WHO
countries in 1976. A consultation convenedin Geneva in July 1976 reviewed thecurrent state of casefinding and assessmentmethods in psychiatry and formulatedproposals for a study of this topic, to beinitiated in 1978. To facilitate collabora-tion in the prevention and treatment ofcerebrovascular disorders, a draft outlineof a classification and glossary of thesedisorders was prepared.
9.33 A project on monitoring mentalhealth needs was launched in seven coun-tries to develop and test methods for thecreation, maintenance and evaluation of themental health component of national healthinformation systems. The WHO RegionalOffice for Europe assumed global responsi-bility for efforts in the area of comparativeassessment of costs of mental health care.The project was implemented in a numberof European countries and is now beingextended to other parts of the world.Routinely collected national statistical infor-mation is used to identify a basic set ofpsychosocial and economic indicators de-scribing countries' mental health problemsand the resources available for theirresolution. In another project, so farimplemented in three countries, methodswere being developed to make possiblemental health projections on the basis ofanticipated social, economic and demo-graphic development of a country. Amanual was drafted for use in the collection,processing, analysis and application ofmorbidity and health services statistics inmental health.
Cancer
9.i4 After reviewing the Organization'slong -term cancer programme, the ThirtiethWorld Health Assembly requested in May1977 (resolution wHA30.41) that the pro-gramme be continued, including the devel-
126
opment of health services, cancer controland research, the training of qualifiedoncologists, and the establishment offavourable conditions for exchange ofexperience on all aspects of the problem, atinternational and country level.
9.35 The Executive Board, in January1977 (resolution EB59.R3z), established anAd Hoc Committee to make recommenda-tions on all WHO's activities in the fieldof cancer, including those of IARC, and tobase such recommendations on the Organi-zation's medium -term programme on can-cer, as described in the Sixth General Pro-gramme of Work. These recommendationsshould also cover the distribution ofactivities in the field of cancer research be-tween WHO headquarters and IARC, aswell as measures to ensure the best possiblecoordination of these activities. The reportof the Ad Hoc Committee was presentedto the Executive Board in January 1978.
9.36 A report on the importance andresearch potentialities of cancer chemo-therapy for developing countries was sub-mitted to the Advisory Committee onMedical Research for discussion. The re-port stressed that drug- sensitive tumoursare more common in developing than indeveloped countries. Another significantconclusion concerned the numerous poten-tialities existing in developing countries,primarily related to the expertise gainedfrom the use of natural products in tradi-tional medicine. This expertise mayprovide a rational approach to the isolationof biologically active substances.
9.37 In connexion with assisting coun-tries in the formulation of national policieson cancer control and research, a consulta-tion of the Joint Working Group onStrengthening Cancer Control Activities atthe Country Level was held in June 1977in Geneva. The countries selected for
NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
development of cancer control activitieswere Sri Lanka and Thailand (South -EastAsia Region) and Iraq, Kuwait andSudan (Eastern Mediterranean Region). Aplan of action for 1978 was elaborated.
9.38 Advances in knowledge of cancertherapy can only come from trying newtreatments, and clinical trials are generallyacknowledged as being the most efficientmechanisms for this purpose. However,results of trials can be misinterpreted, andit may be difficult to incorporate the resultsinto the practice of oncology. A meetingon standardization of the reporting ofresults of cancer treatment was thereforeheld in Italy in June 1977. Several stan-dards and terms were formulated. Repre-sentatives of the International Unionagainst Cancer and the European Organi-zation for Research on Treatment of Canceragreed that the recommendations of theWHO meeting could be readily adoptedby their own organizations.
9.39 In 1976 standardization of hospital -based cancer registries was completed andan instruction manual published.' A systemof hospital registration of cancer cases isbeing proposed that both developed anddeveloping countries should find acceptableand practicable. Implementation of theWHO programme on standardized hospital -based cancer registries was begun in anumber of countries including Italy, Kenya,Liberia, Pakistan, Poland, Uganda, UnitedRepublic of Cameroon and the USSR. Thethree main aims of standardization ofhospital -based cancer registries are : (a) toprovide more reliable data for population -based registries, (b) to serve as a base -linefor collaborative studies between institu-tions, and (c) to evaluate cancer healthservices in particular areas.
1 World Health Organization. IVHO handbook forstandardized cancer registries (hospital -based). Geneva,1976 (WHO Offset Publication No. 25).
I27
9.40 In continuation of the compre-hensive programme on the InternationalHistological Classification of Tumours,WHO published classifications in 1976 -77of haematopoietic and lymphoid tissues,'intestinal tumours,' testis tumours,4 andgastric and oesophageal tumours.' Revi-sions and updating were started on the firstclassification of lung cancer, published in1967.
9.41 Further work was undertaken onthe definition of precancerous lesions ofvarious sites ; these efforts are directedtowards early detection.
9.42 Guidelines on the definition, no-menclature and classification of cirrhosis,hepatic fibrosis, and chronic hepatitis andtheir relation to cancer were published in1977.6
9.43 The programme of standardizationof the cytological terminology in cancerwas finalized in 1977 by the publication onthe cytology of non -gynaecological sites.'Thus comprehensive classifications are nowavailable covering the entire field of cytolo-gical diagnosis of cancer.
2 Mathé, G., Rappaport, H., O'Conor, G. T. &Torloni, H. Histological and cytological typing of neo-plastic diseases of haematopoietic and lymphoid tissues.Geneva, World Health Organization, 1976 (Inter-national Histological Classification of Tumours, No. 14).
6 Morson, B. C. & Sobin, L. H. Histological typingof intestinal tumours. Geneva, World Health Organi-zation, 1976 (International Histological Classificationof Tumours, No. 15).
4 Mostofi, F. K. & Sobin, L. H. Histological typingof testis tumours. Geneva, World Health Organization,1977 (International Histological Classification ofTumours, No. 16).
Oota, K. & Sobin, L. H. Histological typing ofgastric and oesophageal tumours. Geneva, World HealthOrganization, 1977 (International Histological Classi-fication of Tumours, No. 18).
6 Bulletin of the [Vorld Health Organization, 55: 521
(1977)' Riotton, G., Christopherson, W. M. & Lunt, R.
Cytology of non - gynaecological sites. Geneva, WorldHealth Organization, 1977 (International HistologicalClassification of Tumours, No. 17).
THE WORK OF WHO
9.44 WHO collaborating centres forthe evaluation of methods of diagnosis andtreatment of melanoma, stomach and ova-rian cancers continued their activities :reappraisal of the different aspects of theproblems, clinical trials, registration, andabstracting of current literature. New col-laborating centres were established forcervical cancer (Sofia, Bulgaria), bladderand prostate cancers (Stockholm, Sweden),lung (Miami, USA) and colon (Glasgow,United Kingdom).
9.45 The principal interest of WHO inthe field of biology of cancer lies in thepractical application of some of the resultsof basic research. In connexion with thisaim, meetings were held in 1976 on theimmunotherapy of solid tumours, in Vien-na, and on the biological behaviour oftumours and chronobiological aspects oftreatment, in Oslo. An international sym-posium on cell proliferation and differentia-tion in normal and neoplastic systems washeld in October x 977, in Essen, FederalRepublic of Germany.
9.46 In order to review and coordinateWHO's activities in the field of cancer,interregional meetings were held in Wash-ington, DC, in 1976 and Tunisia in 1977.Particular attention was paid to the poten-tial of existing informational systems oncancer, community approaches and screen-ing techniques.
9.47 The Expert Committee on Chemo-therapy of Solid Tumours met in November1976 and elaborated guidelines on thismajor modality for the treatment of com-mon cancers. Among the subjects discussedwere basic concepts in cancer therapy,approaches to specific tumours, drug devel-opment and clinical trial strategies, andinternational cooperation.1
1 WHO Technical Report Series, No. boy, 1977.
i28
g.48 In the Region of the Americas,Argentina, Brazil, Chile, Colombia, CostaRica, Mexico, Peru, Uruguay and Vene-zuela are participating in a system forproviding information on existing re-search and resources in cancer, in order toidentify programme areas, priorities andcooperative projects. This programme, inwhich the PAHO /WHO Regional Libraryof Medicine and the Health Sciences andthe National Cancer Institute, USA, areparticipating, is in line with the recom-mendation of the XXIIIrd Meeting of theDirecting Council of PAHO and with therecommendations contained in resolutionsof the World Health Assembly (wHAZ6.6i,wxA27.63, and WHAZ8.85) on long -termplanning of international cooperation incancer research.
9.49 In the South -East Asia Region,WHO provided consultancy services in theformulation of national cancer control plansin Bangladesh, India, Indonesia and SriLanka.
9-5° The European Regional Officesponsored a working group on child cancercontrol in Prague in 1977. This groupreviewed the efficacy of treatment andmanagement methods, the possible role ofenvironmental factors, the consequences oftreatment, and options as regards rehabilita-tion. Other matters considered includedgenetic, physical and chemical preventionapproaches, including screening, as well asthe structure of cancer control services andthe training of personnel manning them.The results of the working group wereused for the later conference on compre-hensive cancer control mentioned belowand are to be incorporated in a proposedstudy on child cancer. The Region'sconference on comprehensive cancer con-trol was held in Copenhagen in July 1977 ;its deliberations will be of great importancein planning future activities in the Region
NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
in the field of cancer, particularly withreference to the possible creation of amedium -term programme.
9.51 In the Eastern Mediterranean Re-gion, WHO seminars on bone turnouts andfemale genital tract tumours were held inPakistan, and a Regional seminar on theinternational histological classification oftumours was held in Iraq. The Organiza-tion collaborated in the First Middle EastCancer Conference held in Cairo in 1977.Regional centres continued their work onbladder cancer and cancer of the head andneck (in Egypt), oesophageal cancer andlymphoma (in Iran), and breast and uterinecancer (in Tunisia). A Regional AdvisoryPanel on Cancer was constituted and acancer programme for the Region wasdefined.
9.52 In the Western Pacific Region,WHO co- sponsored the Third Asian CancerCongress in 1977.
International Agency for Research onCancer 1
9.53 IARC's programme utilizes re-cent advances in fundamental research andnew techniques in the study of humancancer, and includes research into theextrapolation to man of carcinogenic risksas determined in animal experiments, fieldstudies on putative oncogenic viruses, andthe standardization of methods for measur-ing environmental carcinogens.
9.54 In view of the worldwide shortageof personnel competent in cancer epidemio-logy and environmental oncology, who are
1 For more detailed descriptions of IARC's activities,see International Agency for Research on Cancer,Annual Report, 1976, Lyon, 1976 ; Annual Report, 1977,Lyon, 2977.
I29
necessary for the effective direction ofpreventive measures at the national level,fellowships were awarded for researchtraining, and specialized courses aimed atprimary prevention were organized bothin Lyon and in the regions, with particularemphasis on environmental carcinogenesis.
9.55 The Research Centres in Nairobi,Singapore and Teheran were activelyinvolved in the programme, and up to theend of 1977 more than 7o research agree-ments were in operation with nationallaboratories in z8 countries.
Cancer registries
9.56 Volume 3 of Cancer Incidence inFive Continents,2 containing computerizedand standardized morbidity data on 8opopulations, was published, and a start wasmade on annotating and comparing thedata contained in this and the two earliervolumes.
9.57 The Agency, together with WHOheadquarters, continued to collaborate withthe International Association of CancerRegistries in preparing a monograph on thepurposes and techniques of cancer registra-tion, which is intended to improve the inter-national comparability of registry data.
9.58 Collaboration was also continuedwith the cancer registry in Dakar andadvice was given on improving the record-ing system for cancer data in the MustaphaHospital, Algiers. The cancer registrylinked with the Research Centre in Singa-pore maintained its highly efficient per-formance and, under the direction of theResearch Centre in Teheran, the cancer
2 Muir, C. S., Waterhouse, J. A. H., Correa, P. &Powell, J. Cancer Incidence in Five Continents, vol. 3,Lyon, 1976, International Agency for Research onCancer (IARC Scientific Publications, No. 15).
THE WORK OF WHO
registry in Babol, which is linked with thecancer study on the Caspian littoral, nowcovers almost the entire population in thearea.
9-59 The clearing -house for on -goingresearch in cancer epidemiology publishedits second annual directory and has accu-mulated a total of 908 entries for 71 coun-tries.'
Carcinogens
9.60 In an effort to coordinate carcino-genicity testing at the international level,the Agency continued its survey of labora-tories carrying out tests and of the sub-stances that they are testing. The reports ofchemicals being tested are cross -checkedwith studies reported in the Directory ofOn -going Research in Cancer Epidemio-logy in order to identify the gaps that needto be filled by further research. Workcontinued to bring the carcinogenicitysurvey up to date.
9.61 The working groups convened bythe Agency continued their evaluation ofpublished data on chemicals for which thereis evidence of human exposure and six vol-umes of the monographs on the evaluationof carcinogenic risk of chemicals to man,covering 116 chemicals, were completedduring 1976 -77.
9.6z In collaboration with WHO head-quarters, IARC contributed to WHO'sprogramme on screening for adverse biolo-gical effects by carrying out assays ofmutagenicity on several pesticides and onan antischistosomal drug.
9.63 New technology was used for thedetection and measurement of volatilenitrosamines in beverages and foods col-
Muir, C. S., Wagner, G. & Davis, W. Directory ofon-going research in cancer epidemiology, Lyon, InternationalAgency for Research on Cancer, 1977 (IARC ScientificPublications, No. 17).
130
lected in the oesophageal cancer studies inFrance and Iran. A technique was devel-oped and standardized that may providean indirect measure of potential nitro -samine exposure. Nitrite determinationsin saliva were carried out in the oesopha-geal cancer study area in Iran.
9.64 The Agency supported a col-laborative study on the biological effects ofexposure to asbestos and participated inan epidemiological study on the possiblecarcinogenic hazards in the mineral fibresindustry.
9.65 A meeting was organized of scien-tists involved in research on carcinogenesis,epidemiologists, public and environmentalhealth officials and jurists to discuss carcino-genic risks and strategies for intervention,with the aim of establishing objectiveguidelines for rational decision -makingwhere there is a carcinogenic hazard.
Role of viruses in cancer
9.66 The study in Uganda of thepossible role of Epstein -Barr virus in theetiology of Burkitt's lymphoma was con-tinued. In addition, advantage was takenof a governmental malaria suppressiontrial in the United Republic of Tanzania, incollaboration with WHO headquarters, toobserve whether the incidence of Burkitt'slymphoma will also decline, in order to testthe hypothesis that malaria plays a role inpromoting Burkitt's lymphoma.
9.67 An international symposium onthe etiology and control of nasopharyngealcarcinoma was organized in Kyoto, Japan,in April 1977. The study of nasopharyngealcarcinoma continued and in the WHOImmunology Research and Training Centre,Singapore, an immunogenetic profile spe-cific for nasopharyngeal carcinoma wasidentified and interpreted as a risk marker
NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
or indicator of the prognosis in patientswith that condition.
9.68 Evidence is accumulating thathepatitis B virus is involved in the etiologyof liver cancer and prospective studies wereinitiated. The relationship between viralinfection and exposure to environmentalchemicals -mycotoxins -has yet to be elu-cidated, but it is hoped that these studieswill lead to the possibility of prevention.
Respiratory cancer
9.69 The effects of different types oftobacco and alcohol consumption on theincidence of a variety of forms of cancerwere studied. The smoking and drinkinghabits of a rural population in northernThailand were shown to be associated withan increased risk of cancer of the larynx orlung that varies according to the acidityor alkalinity of the smoke from differenttypes of local cigars. The study of lungcancer among Singapore Chinese womenwas continued ; the high rates found inthis population are apparently not related tosmoking. A case -control study was begunin collaboration with the National Instituteof Oncology, Havana, to determine thecauses of lung cancer mortality in Cubanwomen.
Oesophageal cancer
9.7o In Iran, the association of oesopha-geal cancer with poor socioeconomic statusof long duration was confirmed. Foodsamples taken in the high and low incidenceareas were analysed for volatile N- nitrosocompounds, polycyclic aromatic hydro-carbons and aflatoxins, but no significantdifferences were found. Wheat samplesfrom the high incidence area wereexamined for contaminants, in particularfungi and their associated toxins, and
131
extraneous seeds, but here too no signifi-cant contaminants were found.
9.71 Also in Iran, the possible impli-cation of opium smoking in the causationof oesophageal cancer was investigated.Opium samples and the dottle scraped fromopium smokers' pipes were found to bemutagenic. The opium dottle is apparentlyeaten, and even administered to youngchildren as a medicine.
9.72 The high incidence and distribu-tion of oesophageal cancer in Ille- et- Vilaine,France can be convincingly explained interms of the level of consumption ofalcoholic beverages and tobacco. Anutritional study comparing the dietaryintake of some zoo oesophageal cancerpatients with that of nearly Boo controlsrevealed no important differences. In asearch for the carcinogen involved, samplesof apple brandy were tested for mutageni-city ; a small number of fractions showedmutagenic activity that was not correlatedwith nitrosamine concentration.
Alcohol consumption and cancer
9.73 The causes of death of a cohort ofDanish brewery workers were being fol-lowed and compared with the general malepopulation ; by the end of 1977, over3000 deaths had been recorded in thecohort. No significant difference was foundbetween observed and expected numbers ofdeaths from cancers of the colon and of therectum, but a significant excess risk in thecohort was observed for cancer of theoesophagus and pharynx. Observed morta-lity from liver cirrhosis, gastroduodenalulcer, and motor vehicle accidents washigher than expected.
IARC's role in non participating states
9.74 Although the details of the cancerproblem vary from country to country, the
THE WORK OF WHO
results of research in industrialized statesmay be relevant to non -industrializedstates -and vice versa. The Agency partici-pates in the transfer of knowledge amongcountries by ensuring that in the executionof its programmes there is full involvementof local scientists and laboratories, as wellas a build -up of local scientific expertise ;this has been the case, for example, inIran and Uganda.
9.75 The Agency's epidemiological stu-dies have direct relevance for public healthauthorities in developing countries, enab-ling them to
- evaluate the importance of local cancerproblems relative to other diseasesidentify tumours of exceptional localimportanceascertain the absolute number of cancercases and the consequent demands onhealth services
- determine the relative importance ofcancers associated with particularlife- styles, and the feasibility of theirprimary prevention.
Cardiovascular diseases
9.76 Prevention and control at com-munity level are the ultimate objectives ofthe long -term programme on cardiovascu-lar diseases, formulated in response toWorld Health Assembly resolutionwnAz9.49 of May 1976. This programmeis being increasingly oriented towards thedeveloping world.
9.77 A major milestone was the estab-lishment of pilot programmes for thecomprehensive prevention and control ofcardiovascular diseases relevant to thecommunities under study. If comprehen-sive programmes prove to be feasible andeffective, they will be extended and, ulti-
132
mately, integrated with other chronicdisease control programmes.
9.78 Rheumatic heart disease is themajor cardiovascular problem of publichealth importance in many developingcountries. A multicentre project using acommunity approach to the prevention ofrheumatic heart disease is in progress infour regions (Africa, the Americas, South-
East Asia, Eastern Mediterranean). Thisapproach is based on the identification ofsubjects with rheumatic fever and rheumaticheart disease, especially among school-children. Prevention of recurrences is thenensured by means of the regular adminis-tration of prophylactic measures againststreptococcal reinfections, including regularinjections of benzathine penicillin. Anexpansion of the programme took placein 1976 -77 with the involvement of 7centres in Latin American countries and inthe Philippines. There are now 15 centres
A consultationin September 1977 identified researchpriorities and recent advances requiringimplementation in the control of rheumaticheart disease.
9.79 The project on the communitycontrol of hypertension, which started in197z, now includes 18 communities invarious parts of the developed and develop-ing world and covers all WHO regions.Approximately 3o 00o hypertensive sub-jects had been registered up to the end of1977 ; they will be followed up and treatedas necessary. An interim analysis of thedata obtained was carried out at the annualmeetings of investigators in 1976 and 1977.The project was planned for a period of fiveyears, and in 1977 evaluation of the projectwas begun. The expected long -term effectsare a decrease in the prevalence of hyper-tension, in the incidence of stroke and othercomplications of hypertension and, pos-sibly, in the incidence of ischaemic heart
NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
disease. The results will be published in1980.
9.8o The double -blind randomized trialto determine whether the incidence ofischaemic heart disease can be reduced bylowering high blood lipid levels in 15 000healthy men by using the drug clofibratewas completed in 1977. The results of thisten -year trial, which was conducted infour centres in European countries, provideinformation on both positive and negativeaspects of using hypolipidaemic drugs inthe prevention of ischaemic heart disease.A report on the trial is in preparation.
9.81 A consultation was held in October1977 on the prevention of atherosclerosisin childhood and adolescence. At presentfive collaborating centres are involved.WHO is promoting investigations in thisfield and acts as a clearing -house of informa-tion obtained, with a view to facilitating theprevention of ischaemic heart disease indeveloping countries which are still freeof this health problem.
9.82 The results of a collaborativeproject begun in the i96os on atherosclero-sis of the aorta and coronary arteries in fivetowns in Czechoslovakia, Sweden andthe USSR (3) were published,' providinginformation on autopsy findings in 17 z87subjects over the age of to years in fivedemographically defined populations ; someform of atherosclerotic lesion was presentin nearly all cases.
9.83 In collaboration with the Inter-national Society and Federation of Cardio-logy (ISFC), work was carried out in1976-77 on preparing internationallyacceptable nomenclatures in different areasof cardiovascular disease. Several joint
1 Bulletin of the World Health Organization, 53 : 485(1976).
133
WHO /ISFC meetings of the Task Forceon Classification of Arrhythmias were held.The Task Force on Nomenclature of Ischae-mic Heart Disease also finalized its report.A WHO /ISFC Task Force on Cardio-myopathies was established to review theclassification and nomenclature in thisarea.
9.84 An international study on normalvalues in pulmonary circulation was com-pleted, haemodynamic data having beenobtained by catheterization from more thanboo persons free from cardiovascular dis-eases. Recommendations were made onranges of findings that can be accepted asnormal and on methods to be applied inhaemodynamic examinations of the pul-monary circulation.
9.85 The trace element research projectis carried out in collaboration with IAEAto find out whether trace element imbal-ances play a role in the etiology and patho-genesis of myocardial infarction, andwhether arterial hypertension is causallyrelated to such factors as the accumulationof the pollutant cadmium in kidneys. Someresults of the project were evaluated at anIAEA /WHO consultation in September1977. Higher zinc and lower copperconcentrations were found in blood andtissues of cardiac patients than in controls.Whether these changes are causally relatedto myocardial infarction is not yet known.No support was found for the hypothesisthat higher kidney cadmium by itself isrelated to hypertension, but an excess ofcadmium together with a deficit in zincseems likely to be related.
9.86 Many studies have shown thatmortality from cardiovascular diseases ishigher in areas served by soft demineralizedwater than in those served by hard water.The nature and biomedical significance ofthis statistical association are still unknown,
THE WORK OF WHO
and internationally coordinated studies arebeing carried out in an attempt to identifythe factors in water that may influencecardiovascular health. Under the coordina-tion of a WHO Collaborating Centre forReference on Studies of CardiovascularDiseases in Relation to Drinking -WaterQuality, located in Ottawa, institutions inCanada, Finland, Hungary, Italy, the UnitedKingdom and Yugoslavia are collectingand analysing drinking -water in areas wherethere is good information on cardiovasculardiseases. In addition, information on watercomposition was collected in the WHOnetwork of myocardial infarction registersin Europe. Results consistently show thepresence of higher myocardial infarctionrates in soft water areas.
9.87 The coordination of activities onsmoking and health on a worldwide basiswas further developed during 1976 -77, inparticular following the adoption by theWorld Health Assembly in 1976 of resolu-tion wHA29. S 5 . In collaboration with otheragencies within the United Nations systemand with nongovernmental and otherorganizations, WHO was active in suchareas as antismoking legislation, antismok-ing education, and disseminating informa-tion on the harmful effects of smoking. AWHO Expert Advisory Panel on Smokingand Health was established, and plans weremade for the Expert Committee on Smok-ing Control to meet in 1978. Work alsoproceeded on establishing a network ofWHO collaborating centres on smokingand health.
9.88 To strengthen the role of theWHO Regional Office for Africa andenable more flexible utilization of theavailable expertise in this Region, an inter-regional team stationed in Accra, Ghana,was transferred in January 1977 to thesupervision of the Regional Office inBrazzaville. Epidemiological studies
134
carried out by the team among school-children and adults provided informationon the prevalence and incidence of differentcardiovascular diseases among the popu-lations studied. New projects on the pre-vention of rheumatic fever and rheumaticheart disease and control of hypertensionwere started in pilot areas in Abidjan,Ivory Coast and in Dakar, Senegal.
9.89 In countries of South and CentralAmerica the WHO Regional Office forthe Americas supported projects on theprevention of rheumatic fever and rheu-matic heart disease in seven pilot areas andon the control of hypertension in nineareas.
9.90 The main problems in the South -East Asia Region in the field of cardio-vascular diseases are rheumatic fever,hypertension, ischaemic heart disease andcongenital heart diseases. In several areaswhere the basic epidemiological informa-tion and resources and organization areavailable, projects on the prevention ofrheumatic fever and rheumatic heart diseaseand the control of hypertension and strokewere continued on a pilot basis. The areasconcerned also provide data on the geo-graphical distribution of cardiovasculardiseases and on experience in the organi-zation of preventive and control pro-grammes in cardiovascular and other non -communicable diseases.
9.91 During the biennium the long-term programme on cardiovascular diseasesof the European Region concentrated uponestablishing pilot areas for the compre-hensive community control of cardio-vascular diseases. Methodologies forintervention and evaluation were devel-oped at working groups on this topic,held in Koli, Finland, in 1976 and inGeneva in 1977.
NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
9.92 Environmental and life -style fac-tors are important in the development ofchronic diseases in general and cardio-vascular diseases in particular, but thereare good prospects that their effects can bemodified. This approach is reflected inthe European collaborative multifactorpreventive trial, and in the North Kareliaproject in Finland, and was discussedduring the Commission for EuropeanCommunities /WHO Workshop on the Roleof Physical Activity in Prevention ofCardiovascular Diseases, held in Luxem-bourg in 1977.
9.93 With the aim of helping govern-ments to evaluate the impact of the coro-nary bypass surgery, the demand for whichhas increased substantially in Europe duringrecent years, the WHO Regional Office forEurope held a meeting jointly with theNetherlands Government in The Haguein 1977 on this subject.
9.94 Pilot programmes for preventiveactivities specifically directed at rheumaticfever and rheumatic heart disease wereestablished in three countries of the EasternMediterranean Region (Cyprus, Egypt andIran).
9.95 Control of hypertension and pre-vention of rheumatic fever and rheumaticheart disease are priorities of the long -termcardiovascular disease programme in theWestern Pacific Region. A CardiovascularDisease Task Force was established andattached to the Regional Advisory Com-mittee on Medical Research. A systematictraining programme for WHO fellows inepidemiology and methods of preventionof cardiovascular diseases was prepared.The establishment of a regional trainingand research centre in the field of cardio-vascular diseases was initiated in collab-oration with the governments of severalMember States in the Region.
135
Other chronic noncommunicablediseases
9.96 The main task of the programmeson other chronic noncommunicable diseasesis to achieve uniformity of terminologyused, to elaborate classification and agreeddiagnostic criteria, and to develop andcoordinate training and control pro-grammes through the network of collab-orating centres and countries involved.
9.97 The WHO programme ondiabetes mellitus and its vascular compli-cations was extended, and information onapproximately 5 000 patients in i 1 coun-tries was discussed at the WHO Meetingof Investigators on the Multinational Studyof Vascular Disease in Diabetics, held inGeneva in October 1977 ; special attentionwas given to the frequency of large -vesseland small -vessel diseases in the diabeticpopulation investigated during the study.
9.98 Since the main cause of death in thediabetic population is often associated withlarge -vessel disease, the pathogenesis ofthis condition was investigated in relationto various environmental risk factorsinvolved. Small -vessel disease in thediabetic population is another socio-medical problem and is responsible formuch morbidity and invalidity ; preventivemeasures against the development of suchcomplications were considered and dis-cussed and will be reported upon later.
9.99 WHO, in close collaboration withthe International Diabetes Federation,established an organizing committee during1977 for a postgraduate course on diabetesmellitus and elaborated a preliminary pro-gramme for the course, which will takeplace in 1978.
9.100 A group of experts met in Genevain July 1976 to discuss the formulation of
THE WORK OF WHO
a definition and classification of chroniclung diseases. The proposals were dis-tributed to various pathologists aroundthe world for consideration and comments.A preliminary programme and plan for theepidemiological investigation of chroniclung diseases in various population groupsin 1978 was drawn up.
9.101 A Working Group on IntensiveCare for Respiratory Insufficiency washeld in 1976 in the European RegionalOffice, which led to a multinational studyon patients suffering from respiratoryinsufficiency, with the support of theResearch Unit for Respiratory Physio-pathology, Institut National de la Santé etde la Recherche médicale, Nancy, France.
9.1oz A progress report on rheumaticdiseases was submitted in 1976 to the WorldHealth Assembly, which adopted resolutionwHAz9.66, aimed at promoting nationaland international efforts in the preventionand control of rheumatic diseases.
9.103 A WHO collaborating centrewas designated in Mainz, Federal Republicof Germany, in 1976 for the developmentof a standardized methodology for thehistopathological definition and classifica-tion of rheumatoid arthritis and allieddiseases.
9.104 With a view to supporting theinitiative of the International Leagueagainst Rheumatism to make 1977 WorldRheumatism Year, WHO published aspecial issue of World Health (June 1977),which included reviews of some aspectsof rheumatic diseases by leading specialistsin this field. Also in connexion withWorld Rheumatism Year, WHO sponsoredand supported an advanced course oninvestigative rheumatology in London in1977.
136
9.105 The European League againstRheumatism, sponsored by the EuropeanRegional Office, organized a Workshop onChronic Rheumatic Diseases in Childhoodin March 1977.
9.106 The WHO Meeting of Investi-gators on Chronic Liver Diseases inNovember 1977 considered various epi-demiological aspects of chronic liver diseasesin an attempt to define what should bethe main area of future investigations indifferent population groups.
Oral health
9.107 The oral disease problems facinghealth administrators in nearly all coun-tries are as follows. First, a very highproportion of the population is affected byone or both of the two main oral diseases.Secondly, one of the diseases, caries, ifleft untreated, causes intense pain andcreates an insistent demand for immediateservices ; both caries and periodontaldisease lead to loss of teeth and subsequentdemand for prosthetic services. Thirdly,in no country are adequate oral health careservices available to the entire population.
9.108 Information available in theWHO global oral data bank indicates thata rapid increase in dental caries is nowoccurring in developing countries. Inresponse to this trend, a new programmeof prevention of oral diseases, financedalmost entirely by extrabudgetary funds,was launched in January 1976 in accordancewith resolution wHAZ8.64 adopted by theWorld Health Assembly in 1975. Thecomplementary and supporting pro-grammes that have both direct technicalcooperation and methods developmentand testing components are manpower andservices development, global epidemiology,and research.
NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
9.109 The main activity in the pre-vention programme is the provision ofdirect technical cooperation in the fieldof planning and implementing preventiveprogrammes as integral parts of oral healthservices. Technical cooperation was estab-lished with 24 countries in 4 WHOregions, as part of the prevention andmanpower and services development pro-grammes.
9.110 Subsidiary activities included thecoordination of research in the develop-ment and application of new preventiveagents, and field demonstration projectsin Thailand and French Polynesia to testand evaluate the effectiveness of variouspreventive methods and at the same timeprovide oral disease prevention for up tozo 00o children for 3 years.
9.111 As part of the manpower andservices development programme, a com-prehensive manual was completed givingguidance to administrators on choosingdental equipment and materials suitablefor different service and staffing situations.It was circulated to 5o dental equipmentmanufacturers in order to promote theproduction of robust, easily maintainedequipment for all environments. TheWorld Directory of Schools for DentalAuxiliaries, giving details of courses, entryqualifications and numbers of places avail-able, was published.' In the EuropeanRegion a study on the training and use ofdental auxiliary personnel was completed,and detailed information was collectedon the patterns of organization of dentalhealth services in z8 countries.
9.1I2 In the epidemiology programme,the standard methods for assessing andmonitoring oral diseases in populations
' World Health Organization. World directory ofschools for dental auxiliaries, 1973. Geneva, 1977.
137
were updated. A second edition of themanual on oral health surveys was pub-lished ; it includes a section on the assess-ment of specific treatment needs as anaid to more precise manpower planning.2In cooperation with the InternationalDental Federation, further developmentand field testing were carried out of newmethods for detecting oral cancer andassessing dentofacial anomalies and perio-dontal diseases. Twenty -two countriesrequested technical cooperation in theplanning of epidemiological surveys andin the analyses of data collected, and 16data sets were analysed by WHO.
9.113 The research programme in-cluded a project on the basic etiology ofcaries and a project on health care servicesdelivery. A further stage was completedin the study of caries etiology in PapuaNew Guinea. Major findings, some ofwhich have been confirmed in a highlyindustrialized community, include theidentification of lithium as a factor in theetiology of caries ; its exact role has yet tobe clarified.3 The other research projectincluded the development of a compre-hensive methodology for the assessmentand evaluation of oral care delivery systems.This procedure was successfully applied insix countries - Australia, Federal Republicof Germany, Japan, New Zealand, Norwayand Poland. Results clearly indicate thedesirability and feasibility of oral diseasepreventive programmes ; in one countryone of the highest caries levels was reducedby one -third over I0-15 years. The projectis supported by the United States PublicHealth Service and by the participatingcountries. The results provide, for the
2 World Health Organization. Oral health surveys,basic methods, znd ed. Geneva, 1977.
3 Schamschula, R. G. et al. WHO study of dentalcaries etiology in Papua New Guinea. Geneva, WorldHealth Organization, 1978 (WHO Offset PublicationNo. 40).
THE WORK OF WHO
first time, a valid basis for planning neworal care services and improving existingservices.
Radiation medicine
9.114 The radiation medicine pro-gramme in 1976 -77 was aimed at thepromotion, improvement and optimizationof radiation medicine services in the con-text of national health service programmes,with special emphasis on basic radiologicalservices in developing countries.
Radiodiagnosis
9.115 Country health planning in thisfield is mostly inadequate. The require-ments of diagnostic radiological servicesvary considerably with the clinical patternand level of health care. It is therefore
the diagnosticradiology in the perspective of the wholeprocess of the investigation, diagnosis,prevention and treatment of communicableand noncommunicable diseases. To thisend, a project was started jointly with theInternational Society of Radiology in 1976
on the efficacy of radiodiagnosis and cost -benefit relations with respect to planninghealth services. A first consultation withthe Society was held in Montreux, Switzer-land, in 1976 which produced a plan ofoperation to obtain updated informationon existing radiological services. Followingthis consultation, pilot studies were startedin Kenya, in collaboration with the Minis-try of Health, and in the United Kingdom.A group of investigators met in Brussels,with the support of the Belgian Govern-ment, in November 1977 to evaluate thedata so far obtained from the pilot studies.Conclusions and recommendations wereobtained on how to organize relevant,internationally coordinated studies, and a
138
detailed plan of operation for the projectwas agreed upon.
Radiotherapy
9.116 The ever -increasing importanceof cancer in the developing world neces-sitates the establishment of appropriateradiotherapy services in the context ofcancer control programmes. When suchservices are being planned, it must be bornein mind that they may take 5 -10 years tobecome fully operational ; the needs ofcancer control in ten years' time must there-fore be considered during the planningstage. In order to investigate the presentstage of development of radiotherapythroughout the world, to define the needsin relation to the stage of development ofhealth care and to provide the basis forhealth planning, information is collectedin a similar way as for radiodiagnosis, incollaboration with the International Societyof Radiology and radiotherapy centres.
9.117 An atlas of typical treatment plansfor cobalt-6o teletherapy, prepared by WHOjointly with IAEA, was finalized in 1977
and will be published in the IAEA seriesof atlases on dose distributions. Designedmainly for radiotherapists in developingcountries who do not have easy access toliterature, the atlas contains examples oftreatment strategies and individual treat-ment plans for over zo of the most commoncancer sites, and includes contributionsfrom more than 3o radiotherapy centresthroughout the world.
9.118 One of the prerequisites forsuccessful radiotherapy is the applicationof the correct dose to the tumour. In orderto improve clinical dosimetry, the IAEA/WHO postal dose intercomparison servicewas continued in 1976 -77. Small thermo-luminescent dosimeters are mailed toradiotherapy institutes in all WHO regions,
NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
where they are irradiated with a prescribeddose and returned for measurement.Advice on how to improve dosimetry isthen given to the centres where this isnecessary. A total of 140 centres in 5 WHOregions participated in the service in 1976,and 17o centres in all 6 regions took partin the programme in 1977. Anotherapproach to the improvement of dosi-metry was made by the establishment, in1976, of the joint IAEA /WHO networkof secondary standard dosimetry lab-oratories, with the aim of providing regularcalibration of dosimetric equipment incountries without primary standard lab-oratories and providing training in medicalphysics and radiation protection. AllMember Governments were invited tojoin ; 4z have so far responded to theinvitation and either have designated lab-oratories as members or receive advice andassistance in building up calibration faci-lities in their countries. Two dosimetricintercomparisons were carried out in 1976-77 between primary standard laboratoriesand WHO collaborating centres for second-ary standard dosimetry in order to checkthe compatibility of dosimetry throughoutthe world.
Nuclear medicine
9.119 A meeting on the organizationof services and routine procedures innuclear medicine was held, with thefinancial support of the Government ofBelgium, in Brussels in November 1977.The meeting discussed primarily the organi-zation of basic nuclear medicine servicesand of the procedures to be applied, therelation of nuclear medicine to a particulardisease pattern in a given country and therequirements as regards premises, equip-ment, staff and radiopharmaceuticals. FiveWHO collaborating centres for nuclearmedicine were designated in 1976 and there
139
are now eight such centres, in Denmark, theFederal Republic of Germany, India, Iran,Japan, Mexico, the USA and the USSR. Astudy of the feasibility of, and cost -benefitrelation for, nuclear medicine applicationswas started jointly by IAEA and WHO in1976 and a pilot study was carried out inIndia in 1976 -77.
Radiobiology
9.120 A Scientific Group on the Long -Term Effects of Radium and Thorium inMan was convened in Geneva in September1977. Several groups of investigators areengaged in studies of the biomedical effectsof thorium dioxide, which was used as aradiological contrast medium in the 193osand 194os, and which has caused differenttypes of cancer as a late effect. During thelast 25 years, a number of surveys andepidemiological studies on the effects onman of natural alpha- emitters have beencarried out in several countries, e.g.,Denmark, Federal Republic of Germany,German Democratic Republic, Japan, Por-tugal, the United Kingdom, the USA andthe USSR. The Scientific Group compiledupdated information on these studies andconcluded that this unique material onexperience gained is essential for any fore-cast of the potential dangers from trans-uranic isotopes, the public health implica-tions of which are of the highest importancein view of the growing uses of atomicenergy.
9.121 An Expert Committee on theUse of Ionizing Radiation and Radionuc-lides on Human Beings for Medical Re-search, Training and Nonmedical Purposeswas convened in Geneva in March 1977 toconsider deliberate irradiation of humans,to evaluate the health risks involved and torecommend measures for keeping theseirradiations under appropriate control.'
1 WHO Technical Report Series, No. 611, 1977.
THE WORK OF WHO
Radiation protection
9.122 The fourth volume of the manualon radiation protection in hospitals andgeneral practice, Radiation Protection inDentistry, was published.' During 1976 -77,as in previous years, films for personnelmonitoring of radiation workers in medicalestablishments were provided ; about 450films per month were supplied by theService central de Protection contre lesRayonnements ionisants, Le Vesinet,France, to 7 countries in the Eastern Medi-terranean Region, and about boo films permonth were supplied by the Institute forRadiation Protection and EnvironmentalResearch, Neuherberg, Federal Republicof Germany, to 4 countries in the South -East Asia Region and 4 countries in theWestern Pacific Region.
9.123 A 10 -week training course in themaintenance and repair of X -ray equipmentwas organized with manufacturers of radio-logical equipment in the Federal Republicof Germany, the Netherlands and theUnited Kingdom in 1976, attended by8 engineers and engineering techniciansfrom 5 WHO regions.
9.124 The Division of Training andMedical Applications at the Bureau ofRadiological Health, United States Depart-ment of Health, Education and Welfare,Rockville, MD, USA was designated in1977 as a WHO collaborating centre fortraining and general tasks in radiationmedicine. The Centre assists WHO in thecollection and distribution of informationand teaching material for radiation medicinestaff and in the preparation of guidelines fortraining in the medical applications ofionizing radiations.
' Koren, K. & Wuerhmann, A. H. Manual onradiation protection in horpitalr and general practice, vol. 4Radiation protection in dentistry. Geneva, World HealthOrganization, 1977.
140
Human genetics
Population genetics
9.125 Data on the genetic structure ofhuman populations provide fundamentalknowledge that can be used in solving somepublic health problems. Studies wereinitiated in Guatemala, in collaborationwith the University of Geneva, on genealo-gical analysis, assortative mating, and fre-quency of mortality -antenatal, perinataland infant -among different popula-tion groups ; in Bulgaria (Department ofMedical Genetics, Medical Academy, Sofia),where approximately 3000 blood donorsfrom four districts were studied for haemo-globinopathies, glucose-6- phosphate -dehy-drogenase, and some white and red cellantigens ; and in Italy (Institute of Zoology,University of Ferrara), where the level ofhomozygosity and heterozygosity on ABOand Rh systems was estimated by testing8244 blood donors from 26 communes.
9.126 Different individuals and differentpopulations vary in their susceptibility todisease in areas highly endemic for diseasessuch as malaria, schistosomiasis and leprosy,one reason being the modified effect of thehuman genotype. To promote work onthis subject, mainly in connexion withmalaria, financial support was given to theDepartment of Anthropology, Universityof Delhi, India, to the Iranian NationalBlood Transfusion Service, Teheran, Iran,and to the Tissue Typing Laboratory,Addenbrooke's Hospital, Cambridge, Uni-ted Kingdom.
Clinical genetics
9.127 Cooperation was continued withthe University of Ibadan, Nigeria, with theInstitut Pasteur, Dakar, Senegal, and with
NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
the Institute of Medical Genetics, Moscow,USSR, in respect of research into haemo-globinopathies and allied disorders.
9.128 Haemoglobinopathies constitutean important public health problem incountries where malaria eradication hasrecently been achieved or is likely to beachieved in the near future. In certain partsof the world, it is necessary to improve themedical services in outpatient clinics andhospitals, with special emphasis on theseconditions. A manual on haemoglobinvariants 1 was prepared by the Departmentof Clinical Biochemistry, University ofCambridge, United Kingdom, which is theWHO collaborating centre for haemo-globinopathies.
9.129 Support was given to two insti-tutes in respect of studies on human leuco-cyte antigens, in order to stimulate the useof this system in connexion with the im-mune response to some non -infectious andinfectious diseases -the Laboratoire d'Im-muno- Hématologie, Hôpital Saint -Louis,Paris, France, and the Centre for Immuno-genetics and Histocompatibility of theNational Research Council of Italy, Instituteof Medical Genetics, University of Turin,Italy.
Biochemical genetics
9.130 Continued support was given tothe Institute for Experimental Medicine,Leningrad, USSR, for the study of mole-cular mechanisms of some inborn errors ofmetabolism and their possible treatment,and to the Institute of Genetics and Bio-physics, Naples, Italy, for research onglucose -6- phosphate -dehydrogenase defi-ciency.
1 Lehmann, H. & Kynoch, P. A. M. Human haemo-globin variants and their characteristics. Amsterdam,New York & Oxford, North Holland, x976.
141
Cytogenetics
9.131 With the assistance of WHO, anInternational Registry for Abnormal Karyo-types in Man was established in the JohnsHopkins University, Baltimore, MD, USA.About 3o countries were involved in thiswork. The different types of chromo-somal abnormalities in man have been sum-marized and three books 2 have so far beenprepared on this subject and are beingwidely used as manuals ; they list approxi-mately 25 000 cases of different chromo-somal abnormalities and variants in man.
WHO collaborating centres
9.132 The following WHO collabora-ting centres received support : UniversityCollege Hospital, Ibadan, Nigeria (glucose -6- phosphate -dehydrogenase) ; Zoology De-partment, University of Texas, Austin,USA (serum protein groups) ; PopulationGenetics Laboratory, University of Hawaii,Honolulu, USA (processing of humangenetics data) ; Department of ClinicalBiochemistry, University of Cambridge,United Kingdom (abnormal haemoglobins).A new WHO collaborating centre wasestablished in the Institute of Genetics andBiophysics, Naples, Italy (glucose -6 -phos-phate- dehydrogenase).
Immunology
9.133 The immunology programme wasreorientated to give the required support tothe WHO Special Programme for Researchand Training in Tropical Diseases. Tech-nical help was provided for the variousscientific working groups, and training
2 Repository of chromosomal variants and anomalies inman. Second listing, April 1976 ; Third listing,November 1976 ; Fourth listing, April 1977. Baltimore,MD, Johns Hopkins University.
THE WORK OF WHO
activities were increased at the WHO Im-munology Research and Training Centresin operation in all regions. Courses onfundamental and applied immunology wereorganized in Brazil (Sao Paulo), India(New Delhi), Iran (Teheran), Kenya (Nai-robi), Nigeria (Ibadan) and Switzerland(Lausanne/Geneva). The courses in Nairobiwere supported by funds from the Govern-ment of the Federal Republic of Germany,and those in Lausanne /Geneva were sup-ported by the Swiss Government. TheSwiss Government also agreed to supportthe further extension of the training pro-gramme of the Lausanne /Geneva centre byproviding funds for a course in French,mainly intended for candidates fromFrench -speaking Africa, from 1978.
9.134 A programme for establishingclinical immunology laboratories in theCaribbean area was started with the finan-cial support of the Government of theNetherlands. The programme has twophases ; during the first, scientists fromdifferent countries in the area are trained inAmsterdam and during the second phasethe trainees will be helped to establishlaboratories on their return home. In 1977students from Cuba, Jamaica and Surinamattended the first course in Amsterdam.
9.135 In cooperation with the RegionalOffices for South -East Asia, the EasternMediterranean and the Western Pacific, acollaborating centre for the study of theimmunopathology of dengue haemorrhagicfever was established in Bangkok. Its firstactivity was a meeting to identify researchpriorities in this field. The centre will bethe focal point for coordination of researchon this subject to be conducted in severalcountries. The programme has beenorganized along similar lines to the WHOSpecial Programme for Research and Train-ing in Tropical Diseases.
142
9.136 The programme on the standardi-zation of reagents and methodology usefulin the field of clinical immunology wassupported by extra contributions providedby Canada, the Federal Republic of Ger-many and Sweden, and was carried out incooperation with the International Unionof Immunological Societies. A standardfluorescein -labelled sheep anti -human Ig,a fluorescein- labelled sheep anti -humanIgM and a standard for six serum proteinswere prepared and accepted as WHOInternational Standards. As regards thestandardization of methodology, 18 meth-ods used for the detection of immunecomplexes were evaluated by 13 labora-tories in different countries. A collaborativeassay of the standardization of methods fordetecting antiglobulin was also started.
9.137 The effects of pathological con-ditions such as parasitic and virus diseaseon the immune response were reviewed bya scientific group held in Geneva in Novem-ber 1977. The field of primary immuno-deficiency was also reviewed and a classifi-cation of this condition updated. A meetingwas organized on the standardization ofmethodology and reagents for the diag-nosis of leukaemias and lymphomas. Astudy was also made of allergic diseases, aserious public health problem whose im-portance is likely to increase wherever thereis increased industrialization.
9.138 Research at the WHO Immuno-logy Research and Training Centres focusedon problems of public health importancesuch as trypanosomiasis and schistosomiasis(Nairobi), trypanosomiasis and leprosy(Geneva), leishmaniasis (Lausanne) andChagas' disease (Sao Paulo). It was shownin Nairobi that the eosinophil, a type of cellwhose function is unclear, plays a majorrole in immunity against schistosoma. Thecentre in Geneva showed that immuno-pathological mechanisms are an important
NONCOMMUNICABLE DISEASE PREVENTION AND CONTROL
contributory factor in the development ofthe lesions found in experimental trypano-somiasis.
Health of working populations
9.139 The Twenty -ninth World HealthAssembly, in adopting resolution wHA29. 5 7in May 1976, endorsed a new orientationfor the occupational health programme ofWHO, recognizing the impact of occupa-tional health services on both the health andeconomic status of developing countries.The main features of the new orientationare that health is considered in its totality,and that occupational health services shouldbe an integral part of public health services.
9.140 A new occupational health in-formation system was designed, based onthe completion of inventories at the coun-try level, to identify the health problems ofworkers. Such inventories were preparedby the governments of 76 countriesthroughout the world. Inventories formedthe background for a discussion at theWHO Regional Committee for Africa inSeptember 1977, which proposed an inter -country and regional programme aimed atproviding improved health services forworkers and their families and the develop-ment of research and training centres inAfrica, pooling the resources available tohelp individual countries. Similar discus-sions will be held later at other RegionalCommittees.
9.141 WHO's work during 1976 -77reflected the new orientation of the pro-gramme. The Organization collaboratedin the development of model occupationalhealth services extending from the ruralareas to the central level in a number ofcountries, including Burma, Egypt, Malay-sia and Sudan. In addition, WHO
143
participated in establishing an occupationalhealth centre in Guinea, a department ofoccupational health in the Ministry ofPublic Health in Bahrain and a similarproject in Qatar, and the development of anational coordinating committee for oc-cupational health services under the leader-ship of public health planners in Iraq.Consultants were provided for the Philip-pines, Sri Lanka and several Latin Ameri-can countries.
9.142 Together with ILO and theAfrican -American Labor Center, WHOorganized in 1976 a conference on the healthof African miners. One of the conclusionsof the conference was that there is an urgentneed to train personnel, to develop guide-lines, and to enact regulations to combatthe high incidence of diseases and accidentsamong miners. In addition, WHO beganresearch programmes to explore miners'health problems in the Republic of Koreaand in Zambia.
9.143 Migrant workers all over theworld are subject to a complex of poten-tially serious health problems. Following arecommendation of the seventh session ofthe Joint ILO /WHO Committee on Occu-pational Health, a Standing ILO /WHOCommittee on the Health of MigrantWorkers was established. Information wascollected on the state of health of migrantworkers in different parts of the world, andguidelines were prepared on measures forthe health protection of migrant workers,both in their countries of origin and in thehost countries. These guidelines wereexamined at a symposium organized jointlyby the Yugoslav Government, ILO andWHO in Dubrovnik in November 1977.
9.144 A priority in WHO's programmeis the development of measures to combatthe health problems of workers in smallindustries, defined as workplaces employing
THE WORK OF WHO
up to ioo persons. A major challenge liesin providing adequate occupational healthservices for these workers, who are widelyscattered. Trials of different models forservices are currently taking place in eightdeveloping countries. Field investigationson the health problems of this vulnerablesector of the working population werecarried out together with WHO collabora-ting centres in iz countries.
9.145 More than 7o % of the world'seconomically active population is engagedin agriculture, where there are hazardsarising from mechanization. WHO col-laborating centres in 1976 -77 studied theapplication of ergonomics to the design ofagricultural machinery in relation to work-ers' health and safety, and documents werecirculated for testing recommendations indifferent countries.
9.146 The programme cannot be effec-tive without the development of criteriaand standards and the coordination ofresearch programmes. In 1976 -77 WHOassisted in the coordination of research onsimultaneous exposure to multiple hazardsat work, with the assistance of collaboratingcentres in Bulgaria, Egypt, Japan and theUSA. An international meeting in Sofia,Bulgaria, reviewed knowledge in this areain November 1976 and reported on theinteraction of extrinsic occupational en-vironmental factors with intrinsic suscep-tibility to occupational exposure.
9.147 In August 1976 the WHO Ex-pert Committee on methods used in estab-lishing permissible levels in occupationalexposure to harmful agents met inGeneva with the participation of ILOand achieved a considerable measure of
agreement among countries that had hither-to differed widely in their approach to thisactivity.1 In accordance with the recom-mendations of this Committee, theExecutive Board requested the Director -General to develop, as soon as possible,internationally recommended health -basedpermissible levels for occupational exposureto chemical agents (resolution EB6o.R2).
9.148 Following an Executive Boardresolution of 1974 (EBS 3.R23) concerningthe development of criteria for the earlydetection of health impairment resultingfrom occupational exposure to healthhazards, a start was made in 1976 on workto produce criteria in respect of exposure toindustrial solvents. A further consultationin 1977 identified parameters indicatingearly biological changes resulting fromoccupational exposure to heavy metals(cadmium, lead, manganese and mercury).The task is formidable, since workers areexposed to thousands of potentially harm-ful agents. For this reason priority is beinggiven to commonly encountered toxic sub-stances in workplaces.
9.149 Attempts were made to produceguidelines for monitoring the work environ-ment by means of simplified techniques,and WHO achieved some success withmethods relating to heat stress, gases andvapours and to the preliminary survey ofthe occupational environment as a whole.However, simplification and standardiza-tion have not yet been achieved, althoughcollaborating institutions are working onthese problems in different parts of theworld.
1 WHO Technical Report Series, No. 6or, rm.
144
Chapter l
Prophylactic, Diagnostic and Therapeutic
Substances
Drug policies and management
i o. i TN 1976 A NEW PROGRAMME1 on drug policies and management
was initiated with major emphasison collaborating directly with countries inthe formulation of national drug policieswithin the framework of their health andsocial development policies, and in settingpriorities within the drug sector as a wholeso as to ensure that safe, efficacious andeconomic drugs are accessible to all whoneed them.
10. z Global, regional and country stu-dies on drug policies and management wereundertaken by means of on- the -spot investi-gations, information exchange and consul-tation. The following major problems wereidentified :
(1) Inadequate availability of essentialdrugs, especially in rural areas of develop-ing countries -often So % of the populationdoes not receive adequate preventive andcurative care including essential drugs andvaccines.
(z) Uneven distribution of pharmaceu-tical production between developed anddeveloping countries (90 % is located indeveloped countries), causing a seriouseconomic deficit in developing countries.
(3) Excessive, inadequate or inappro-priate use of drugs by health workers.
145
The major obstacles in the formulationof national drug policies are :
(a) lack of multisectoral approaches andidentification of the needs for drugs-governments often place lowpriority on drug policies ;
(b) lack of resources for identifyingproblems relating to the formulationof policies, planning and implemen-tation ;
economic conditions -lower incomeand purchasing power, limited bud-get for health action and limitedhard currency reserves;
free market policies, especially in theprivate sector, based on the recogni-tion of drugs as ordinary commodi-ties ;
(e) the intensive marketing powers ofindustries, mainly expatriate indus-tries of transnational origin ;
the passive and uncritical acceptanceof drugs, information, pricing andtechnology.
(c)
(d)
(f)
10.3 In response to governments' con-cern about drug expenditures, the RegionalOffice for the Americas began studies invarious countries to identify factors affect-ing costs and to provide recommendationsfor reducing expenditures.
THE WORK OF WHO
Strategies in formulating drug policies
10.4 Different strategies in formulatingnational drug policies and implementingthe programme for improving the nationalmanagement capabilities in the pharma-ceutical supply system were elaborated.These strategies, which were drawn up inconsultation with experts from both devel-oped and developing countries and withrepresentatives of United Nations bodies(UNDP, UNICEF, UNIDO and UNCTAD)and nongovernmental organizations, tookinto account discussions during the Execu-tive Board, the World Health Assemblyand, in particular, the Technical Presenta-tion during the twenty- eighth session of theRegional Committee for the Western Paci-fic. The strategies, which are also in accord-ance with resolutions of the RegionalCommittees for Africa (AFR /RC26 /RI I) andthe Eastern Mediterranean (EM /RC26A /RI I),comprise the following technical com-ponents : (I) drug research and devel-opment to meet the needs of developingcountries ; (z) drug legislation and regula-tory control for ensuring the provision ofsafe, efficacious and economical products ;(3) selection of essential drugs ; (4) qualitycontrol of drugs and vaccines ; (5) collectiveand bulk procurement from multisourcesupply ; (6) local production ; (7) establish-ment of appropriate distribution systems ;(8) transfer procedures and control of drugprices ; (9) drug information, utilizationsurveillance and education and training ofhealth workers ; (io) better utilization oflocally available natural resources, especial-ly medicinal plants, for health care ; and(1 1) self- medication and use of drugs atcommunity level.
I o. 5 These global strategies will bereviewed at regional and country levels,in particular through technical cooperationamong developing countries ; in this con-nexion, a programme on technical coopera-
146
Lion among developing countries in drugpolicies and management was initiated inthe South -East Asia Region.
Selection of essential drugs
10.6 A group of consultants consideredthe selection of essential drugs to meet theneeds of primary and secondary healthservices, and drew up an example of anannotated list of about zoo essential activesubstances for use in primary and secondaryhealth care. Their report was circulated toscientists, government officials and phar-maceutical industries, whose commentswere reviewed by the WHO Expert Com-mittee on the Selection of Essential Drugsin October 1977. The Expert Committeedrew up a model list of nearly zoo essentialactive substances.'
10.7 WHO is ready to collaborate withcountries, when required, in the procure-ment and production of essential drugs, byproviding technical cooperation in thefollowing fields : product selection ; qualitycontrol ; marketing intelligence ; transfer ofappropriate technology for production,storage and distribution ; and improvedutilization through information provision,education and training.
Use of medicinal plants
Io.8 The use of medicinal plants, whichare abundant in developing countries, toge-ther with Western medicines in health careis one of the most appropriate approaches tosocial and economic development linked tothe health sector. The WHO Seminar onthe Use of Medicinal Plants in Health Care,held in Tokyo in September 1977 andsponsored by the Japanese Governmentthrough contributions to the VoluntaryFund for Health Promotion, discussed the
' WHO Technical Report Series, No. 615, 5977.
PROPHYLACTIC, DIAGNOSTIC AND THERAPEUTIC SUBSTANCES
alternative policies for the effective utiliza-tion of medicinal plants, the identificationof the most useful medicinal plants in theWestern Pacific and South -East Asia Re-gions and the required specifications forquality, and appropriate technology forefficient delivery and use.
Multisectoral approaches within the UnitedNations system
10.9 A UNIDO/UNCTAD /WHO in-tersectoral task force was formed to promoteand assist cooperation among developingcountries. In this connexion, a global pro-ject for cooperation among the developingcountries in the pharmaceutical sector wassubmitted to UNDP in 1977 and approved.For the implementation of this project,WHO will act as executive agency in asso-ciation with the other agencies.
Pharmaceuticals
10.10 The Organization continued itsefforts to improve the quality of drugsimported and distributed in developingcountries that lack their own drug controllaboratory facilities.
I0.11 A revised certification scheme onthe quality of pharmaceutical productsmoving in international commerce, adoptedin 1975 by the Twenty- eighth World HealthAssembly (resolution WHAZ 8.6 5) providesthat the health authorities of exportingcountries should supply a certificate statingthat the product is authorized for sale inthe exporting country and that the manu-facturer is subject to regular inspection.By the end of 1977, 25 Member countrieshad agreed to participate in the scheme andhad designated responsible national autho-rities.'
1 Supplement to W/HO Chronicle, 31, No. 1z (1977).
147
10.12 The development of basic testsfor drugs- simplified laboratory proceduresprimarily designed to confirm the identityof pharmaceutical substances and to ensurethat gross degradation has not occurred -is another approach designed to ensure thequality of drugs, both at the port of entryand along the distribution chain in situationswhere laboratory facilities do not exist. InApril 1977 the Expert Committee on Spe-cifications for Pharmaceutical Preparationsrecommended that work should be con-tinued on the development of such testsand on their validation by collaboratinglaboratories in countries with extremeclimatic conditions.'
1 0.13 The revision of drug quality spe-cifications contained in the InternationalPharmacopoeia continued. With the helpof experts, revised drafts of over 4o generalmethods of analysis were prepared on thebasis of comments obtained from nationalpharmacopoeia commissions and otherinterested parties. The process of revisingmonographs for a number of substanceswas initiated, principally in respect of pro-ducts essential for primary health needs.
10.14 In 1976, for the first time, a cumu-lative list of the 3500 international nonpro-prietary names for pharmaceutical sub-stances was published from a computerprintout.' An updated version 4 was pub-lished in 1977. The use of electronic dataprocessing made it possible to include,besides the international nonproprietarynames for pharmaceutical substances inLatin, English, French, Russian and Spa-nish, references to national nonproprietary
a WHO Technical Report Series, No. 6,4, 1977.' World Health Organization. International nonpro-
prietary names (INN) for pharmaceutical substances, cumu-lative list No. 4, 1976. Geneva, 1976.
4 World Health Organization. International nonpro-prietary names (INN) for pharmaceutical substances, cumu-lative list No. J, 1977. Geneva, 1977.
THE WORK OF WHO
names, pharmacopoeia monographs andthe lists of narcotic drugs under interna-tional control and schedules mentionedunder the Convention on PsychotropicSubstances. This new type of cumulativelist will greatly assist national authorities,particularly those with limited access torecent reference literature.
to. t 5 During 1976 -77 four lists of pro-posed international nonproprietary namesfor pharmaceutical substances were pub-lished in the WHO Chronicle and circulatedto all Member States.'
1 0.16 With the rapid development ofdrug epidemiology and the demand formany national drug regulatory authoritiesto review all currently available drugswithin their jurisdiction, the safety andefficacy of many established drugs is underre- examination. As a result, the terms underwhich many of these drugs are registeredin various countries have been modifiedand other drugs have been withdrawn fromuse. Since different national authorities donot always take the same action with regardto the same drugs, the World Health Assem-bly in 1975 requested the Director -Generalto disseminate to Member States evaluatedinformation on drugs (resolution wHn28.66). A three -monthly bulletin provid-ing background information on thesedecisions is now circulated ; it also includesother topical information on drug regula-tory control and new drug registration.
10.17 During the biennium France andBelgium joined the group of 22 countriesactively participating in the internationalmonitoring system for adverse reactionsto drugs. Work is in progress to transferthe operational aspects of the programmeto a WHO collaborating centre in Uppsala,
1 WHO Chronicle, 3o, No. 3 (Suppl.), No. 9 (Suppl.)(1976) ; 31, No. 3 (Suppl.), No. 9 (Suppl.) (1977)
148
Sweden ; the current processing procedureswill remain unchanged, and WHO head-quarters will retain full responsibility forthe programme as regards policy, coordina-tion, participation of national and othercentres, and dissemination of information.
1o.18 The series of annual symposia onthe clinical pharmacological evaluation indrug control, organized by the RegionalOffice for Europe in collaboration withthe Government of the Federal Republicof Germany, continued in 1976 and 1977.
Biologicals
10.19 As in previous years, existinginternational reference materials were exam-ined and replaced where necessary andnew ones were established. During 1976 -77,however, the demand was greatest forblood products and related substances.New technology, especially in the moresensitive measurement of concentrationand activity of blood substances, particu-larly those relating to blood coagulation,highlighted the need for such referencematerials. A long- needed, comprehensiveset of requirements for the production andquality control of blood products andrelated substances was reviewed by anExpert Committee in December 1977. TheOrganization continued to promote theestablishment of national policies for theprovision of blood and blood derivatives.
10.20 An interregional training coursein quality control of vaccines in 1976 andan interregional training seminar on bio-logical standardization in 1977 were attend-ed by participants from developing coun-tries.
1 0.21 Many international societies withexpertise in haematology, allergy and immu-nology provided invaluable assistance to
PROPHYLACTIC, DIAGNOSTIC AND THERAPEUTIC SUBSTANCES
WHO in carrying out work leading to theestablishment of international referencematerials. To ensure that the proposedreference materials will satisfy the rigidcriteria demanded of them, guidelines fortheir procurement and handling wereadopted.
10.22 With the financial support ofUNDP, the following types of work werecarried out on behalf of the ExpandedProgramme on Immunization : (i) researchon the production and testing of morestable measles, poliomyelitis and diph-theria /pertussis/tetanus vaccines -the initialwork showed that the stability of all thesevaccines can be improved ; (z) the comple-tion of manuals on the production andcontrol of diphtheria, tetanus and pertussisvaccines ; and (3) training staff from thedeveloping countries in the productionand control of vaccines.
10.23 A reference centre for the produc-tion and control of biological productswas established in Mexico to provideservices to all the countries of the Regionof the Americas, thereby contributing tothe success of the Expanded Programmeon Immunization.
10.24 The Organization cooperated withcountries and UNICEF in ensuring thatvaccines used in immunization programmesmeet WHO requirements with respect tosafety and potency, either by reading proto-cols of the tests on the vaccines or by sub-mitting batches of vaccines to externalcontrol. Eleven government laboratoriesassisted WHO in this work.
10.25 The quality control of oral polio-myelitis vaccine continued on new seedviruses prepared from the original Sabinstrains.
10.26 WHO staff visited productionunits in the developing countries to advise
149
on increasing vaccine production andimproving quality. A working group onbacterial vaccine production and controlwas convened in Zagreb, Yugoslavia, inMay 1977, an interregional seminar on thesetting up of quality control facilities washeld in Geneva in September 1977, and atraining course on this subject was held inLondon in October 1977.
Health laboratory technology
10.27 The most important problem thatcountries face today in the area of healthlaboratory technology is the inadequatedevelopment or even absence of laboratoryservices at intermediate and peripherallevels ; these services are also largely unre-lated to the priority health needs of commu-nities in rural areas and the technologyemployed is not appropriate to the diag-nostic materials and reagents available andthe existing trained manpower.
10.28 During visits of WHO staff toseveral countries (Chad, Lao People'sDemocratic Republic, Malaysia, Papua NewGuinea, Sri Lanka and United Republic ofCameroon) to study how the Organizationcould better cooperate with them in solvingthese problems, it became clear that WHOshould reorientate its programme with theaims of (1) providing simple and appro-priate technology for laboratory supportfor the control of the most important healthproblems, (z) improving the availability ofessential diagnostic reagents and equipmentat a reasonable cost, and (3) expanding thetransfer of laboratory technology throughthe organization of training activities.
10.29 Accordingly, details of methodsfor essential laboratory tests in clinicalchemistry that can be used in intermediatelaboratories were circulated, including amanual with details of procedures ; similar

THE WORK OF WHO
lists for haematology and bacteriology arealso under preparation. On behalf of WHO,the International Federation of ClinicalChemistry is drawing up simple guidelinesfor the preparation and evaluation of lab-oratory reagents, including diagnostic kits.The development of simple laboratoryequipment was also pursued ; field trials of asimple photoelectric colorimeter were underway in Fiji, India, Indonesia, Iran, Malaysiaand Sudan.
10.30 Work on the preparation of inter-national control sera with assigned valuesfor a number of constituents for use inclinical biochemistry was nearing comple-tion. The purpose of these sera is to enablecountries to evaluate their own control
material and improve laboratory perform-ance through national quality controlprogrammes. Simple guidelines were beingprepared on the practice of such qualitycontrol at the intermediate level.
10.31 The development and extensionof blood transfusion services was promoted;in many countries there is a serious shortageof blood for transfusion, particularly outsidethe large towns. A seminar on bloodtransfusion was organized in Kuala Lumpur,Malaysia, for countries in the WesternPacific Region. Guidelines were preparedfor the development of a countrywide ser-vice and WHO sponsored the First AfricanCongress on Blood Transfusion held inYamoussoukro, Ivory Coast, in April 1977.
150
Chapter II
Promotion of Environmental
health
Provision of basic sanitary measures
Assessment of community water supply andexcreta disposal in developing countries
II.I FOLLOWING the report on statusas of 1970, a mid -decade (1975)status survey enabled the World
Health Assembly in 1976 to review progressand adopt specific regional targets for theremaining half of the Second UnitedNations Development Decade (resolutionWHA29.47).
II.2 The country -by- country and re-gional information on coverage of com-munity water supply and excreta disposalservices and on the investment made during1971 -75, published in the World HealthStatistics Report, Vol. 29, No. Io, 1976, andused widely by countries and by organiza-tions within the United Nations system,enabled WHO to prepare a strategy andplan of action for consideration by theUnited Nations Water Conference.
11.3 The Regional Committee forAfrica approved the evaluation activity ofthe long -term programme in environmentalhealth (resolution AFR/RC27/RIo), and theRegional Office convened a meeting ofexperts on environmental health in Octo-ber 1976 to consider the waste disposalsector.
ISI
11.4 A considerable number of com-munity water supply and sewerage projectswere initiated in some countries in theEastern Mediterranean Region ; however,shortage of trained manpower posed aproblem. WHO assigned sanitary engineers-for instance, in Libyan Arab Jamahiriyaand Saudi Arabia -to fill the manpowergap. In other countries, technical support,through the assignment of staff, was usedto assist national counterparts in formulat-ing projects that would be acceptable forfunding -for instance, in Afghanistan, De-mocratic Yemen, Sudan and Yemen. Thecurrent emphasis on training courses forwater and sewerage systems operators willneed to be continued in future years toensure the operation and maintenance ofcompleted installations.
11.5 Many countries of the WesternPacific Region have given lower priorityto sewerage construction and services thanto water supplies. However, the progressmade in water supply and sewerage in thisRegion has been quite creditable consider-ing the urgent demand on regional re-sources from many sectors. In the SouthPacific, rural sanitation continued withtechnical cooperation from WHO andmaterial assistance from UNICEF ; heretoo, efforts are being made to improve levelsof training and management.
THE WORK OF WHO
United Nations Water Conference, z977
II.6 WHO participated fully in theUnited Nations Water Conference held inMar del Plata, Argentina, in March 1977.In addition to making written contributionsto the background papers for the Confer-ence, WHO regional offices participated inthe preparatory meetings organized by theregional economic commissions of theUnited Nations. Strategies and a Plan ofAction to enable countries to achieve thetargets set by the United Nations Con-ference on Human Settlements (HABITAT)were prepared by WHO in collaborationwith IBRD and were adopted in toto by theWater Conference.
11.7 The Conference called upon coun-tries to adopt specific and detailed plans forwater supply and sanitation services suitedto their individual and specific conditions,and recommended that the internationalcommunity should adopt a more effectiveapproach in supporting, financially and inother ways, the increased national commit-ments of developing countries. Thedecade 198o -90 was designated Inter-national Drinking -Water Supply and Sani-tation Decade, for implementation of thePlan of Action.
11.8 Considering the recommendationsof the Conference, the World HealthAssembly in May 1977 urged MemberStates to act upon Resolution II of theConference immediately by proceedingwith a rapid assessment of their on -goingprogrammes and the extent to which theycould usefully be expanded. The HealthAssembly also requested the Director -General to collaborate actively with Mem-ber States in these activities, in closecooperation with all the relevant organi-zations within the United Nations system(resolution wHA3o.33). The regional officestook follow -up action in 1977.
1 f2
11.9 In the Region of the Americas,special attention was given to strengthen-ing and further developing water supplyand sewerage institutions to facilitate theextension of coverage and to improveoperational, financial and managementcapacity. With economic support from thegovernments, UNDP, IBRD, CIDA, andthe Inter -American Development Bank,WHO provided technical cooperation forinstitutional development in most of thecountries of the Region.
II.I0 Water -borne diseases are stillamong the most important health problemsin South -East Asia, and the countries ofthat Region gave high priority to basicsanitary measures. Country reports onwater supply and sanitation were up -datedwith a view to enabling countries to reviewtheir targets in accordance with the recom-mendations of the United Nations WaterConference. In some countries WHOacted as the coordinating agency in evaluat-ing the impact of basic sanitary measures,with the object of improving project for-mulations and securing additional externalresources.
I I.I I In consultation with the govern-ments concerned, the Regional Office forEurope prepared an intercountry medium -term programme on basic sanitation, inpursuance of the World Health Assemblyresolutions wHA29.46 and wHA3o.33.
II.I2 The 63rd Session of the UnitedNations Economic and Social Council inJuly- August 1977 approved the report ofthe United Nations Water Conferencecontaining the Plan of Action, and request-ed the Secretary- General of the UnitedNations to make the necessary arrange-ments for an in -depth study of the implica-tions of Resolution II of the Conference,"Community Water Supply ", and forlaunching the International Drinking -Water
PROMOTION OF ENVIRONMENTAL HEALTH
Supply and Sanitation Decade recom-mended in the Plan of Action. The studywill be reviewed at a special session of theCommittee on Natural Resources in 1978during which WHO will present a situationanalysis and other information required forplanning the Drinking -Water Supply andSanitation Decade.
Transfer and adaptation of technology
11.13 Developing countries must drawup their own criteria for the nationalplanning and installation of communitywater supplies, adopting appropriate tech-nology with maximum utilization of localresources. To this end, the Organizationcontinued the preparation of guides andmanuals for the use of health and regulatoryauthorities, 1, 2, S
11.14 The International ReferenceCentre for Community Water Supply, inVoorburg, Netherlands, expanded its workas a WHO collaborating centre in supportof the WHO water supply programme.The Centre hosted seven major inter-national seminars during 1976 -77 and alsomoved into phase II of a collaborativeresearch project on slow sand filtration.This research project brings together re-search institutes and government watersupply departments in six developing coun-tries. Phase II provides for the constructionof at least 15 village water supplies thatutilize slow sand filtration technology andincludes social, economic and technicalresearch as well as extensive training oftreatment plant operators and other water-works personnel. In addition, the Centre
1 Salvato, J. A. Guide to sanitation in tourist establish-ments. Geneva, World Health Organization, 1976.
2 World Health Organization. Surveillance of drinking-water quality. Geneva, 1976 (WHO Monograph Series,No. 63).
2 World Health Organization. Typical designs for engi-neering components. New Delhi, 1977 (WHO RegionalPublications, South -East Asia Series, No. 3).
153
published a manual on hand pumps underthe joint sponsorship of WHO and UNEPin 1977, the first comprehensive accountof the subject.4
II,15 The Pan American Center forSanitary Engineering and EnvironmentalSciences, Lima, Peru, continued its investi-gations to develop and adapt technologyappropriate to the needs of the countries ofthe Region, including lower -cost methodsfor water treatment and simple technologyfor the disposal of waste- water. The Center,in collaboration with the InternationalDevelopment Research Centre, enlarged itscapacity for information systems relating totransfer of technology and manpowerdevelopment.
II.16 The need to improve waterquality was the basis for convening thePan American Conference on Drinking -Water Quality Improvement sponsoredjointly by CIDA, the Water and SewerageAuthority of Trinidad and Tobago, andPAHO. Also as part of the programmefor operation and maintenance, a regionalprogramme was established for the analy-tical control of water and waste -waterlaboratories, involving collaboration with73 laboratories in 25 countries in theexchange of information on laboratorymethods, procedures and equipment andfacilities.
11.17 The Organization cooperatedwith several Member countries in thepreparation of national or regional plansfor solid wastes management, the solutionof specific problems, and the training ofstaff. Two regional courses on the manage-ment of solid waste were held in BuenosAires.
International Reference Centre for CommunityWater Supply. Hand Pumps. The Hague, 1977(Technical Paper Series, No. so).

THE WORK OF WHO
i i .18 In 1976 the Regional Office forSouth -East Asia published a manual on themanagement of solid wastes.'
Institutional development
II.19 The establishment of a WesternPacific Regional Centre for Promotion ofEnvironmental Planning and AppliedStudies was authorized (Regional Commit-tee resolution wPR /RC28 /R13). Its objectivesare (1) to promote and facilitate effectivecollaboration among institutions and scien-tific and technical personnel of MemberStates in the Region, and (2) to supportefforts in developing national self -reliancein the field of environmental health andenvironmental protection.
Human settlements and health
11.20 The Technical Discussions at theTwenty -ninth World Health Assembly inMay 1976 dealt with the subject of "Healthaspects of human settlements ".2 A generalobjective agreed by the participants was toensure that health is accepted as an integralpart of the planning and development ofhuman settlements at the local, national andinternational levels. Priority health needsin human settlements were identified as(a) adequate nutrition, (b) adequate and safewater and hygienic means of wastes dis-posal, and (c) the provision of health care.The Health Assembly took further actionin adopting resolution wHA29.46 on thissubject.
I 1.21 The report of the TechnicalDiscussions and the Assembly's resolutionwere presented at the United Nations
' Flintoff, F. Management of solid Wastes in developingcountries. New Delhi, World Health Organization, 1976(WHO Regional Publications, South -East Asia Series,No. 1).
2 Martin, A. E., ed. Health aspects of human settle-ments. Geneva, World Health Organization, 1977(Public Health Papers, No. 66).
154
Conference on Human Settlements (HABI-TAT), held in Vancouver, Canada, inMay June 1976. These and other inputs ofthe Organization, including contributionsfrom the regional offices, ensured thathealth was prominently mentioned in theDeclaration of Principles of the Conference.They also influenced the adoption of threeRecommendations for National Action thatrelate particularly to health : one calls forpriority action to establish targets for theprovision of safe water and hygienic wastesdisposal for all the population (by 1990 ifpossible), the second relates to the controlof pollution and the third recommends thathealth, nutrition and other social servicesshould receive priority in national develop-ment planning and in the allocation ofresources.
I1.22 The Regional Committee forAfrica urged Member States to give highpriority to health aspects when planninghuman settlements and requested the Direc-tor- General (I) to study the recommenda-tions of HABITAT in respect to increasedtechnical collaboration with countries, and(2) to collaborate with the organizationalarrangements within the United Nationssystem for human settlements (resolutionAFR /RC26 /R3).
11.23 At the request of the Govern-ment of the Philippines, consultation wasprovided in the assessment of the healthaspects of housing and human settlementsdevelopment, and in the preparation ofrecommendations whereby the Departmentof Health can exert a greater influence onthese development activities.
I1.24 The Regional Office for Europeconvened two consultations closely asso-ciated with the objectives of the HABITATConference -"Environmental health as-pects of human settlements in Europe" and"Basic sanitation problems of European
PROMOTION OF ENVIRONMENTAL HEALTH
communities ". A programme of activitieswas recommended as a result of bothconsultations.
11.25 During 1977, an assessment wasbegun of the role of the Organization inthe field of human settlements. The assess-ment, based on views of regional offices,is a preliminary step in identifying WHO'sfuture policy and role in the evolving workof national and international bodies in thefield of human settlements.
UNICEF /IWHO joint study on the watersupply and sanitation components of primaryhealth care
11.26 In response to a decision of thetwenty -first session of the UNICEF /WHOJoint Committee on Health Policy inJanuary 1977, a joint study was startedwhich will focus on issues involved incoordinated approaches for the planningand implementation of accelerated pro-grammes of community water supply andsanitation within the context of overalldevelopment plans and policies of whichprimary health care is a part. These issuesinclude political will and national commit-ment, community motivation and partici-pation, manpower development, appro-priate technology, financial requirementsand issues relating to the planning, and theoperation and maintenance of these servicesand facilities. The findings will be used asa basis for recommendations on policyformulation aimed at accelerating the pro-vision of community water supply andsanitation as components of primary healthcare and as a part of general nationaldevelopment efforts.
Pre -investment planning for basicsanitary services
11.27 An important objective of WHOis the improvement of health through better
15
drinking -water supplies and better arrange-ments for wastes disposal. The pre -investment planning programme isdesigned to stimulate and enhance policyformulation and planning efforts in thisfield. WHO collaboration is aimed bothat upgrading national planning capabilitiesand at providing advisory expertise whererequired.
11.z8 During 1976 -77 field work onnationwide water supply and sanitationsector studies was completed in Afgha-nistan, Congo, Egypt, Malawi, Malaysia,Peru, Philippines, Portugal, Somalia, SriLanka, Sudan, Thailand and United Repub-lic of Tanzania, bringing to 4o the totalnumber of studies so far undertaken. In thesame period, pre -investment projects werecompleted in 17 countries, bringing to 38the total number carried out to date underWHO supervision. Pre -investment projectswere still in operation or had been startedin Afghanistan, Gabon, Gambia, Guinea,Indonesia, Ivory Coast, Lesotho, Malta,Morocco, Portugal, Rwanda, Senegal, So-malia, Sudan, Turkey and Zaire.
I I.z9 The increasing recognition of theimportance of national planning in thissector is evidenced by the following : (a) fiveyears ago, sector studies were being under-taken only at the suggestion of internationalagencies, whereas numerous requests arenow being received from governments ;(b) several governments have incorporatedsector study recommendations into nationalpolicy documents ; (c) several governmentshave requested WHO to collaborate indetailed national planning exercises as afollow -up to sector studies ; (d) the method-ology developed for national studies of thewater supply sector is now being con-sidered for use in other fields of environ-mental health.
11.3o National sector developmentcomprises endeavours and activities in
THE WORK OF WHO
various ministries (planning, interior, publicworks, public health, finance), at both cen-tral and peripheral levels, undertaken in arational time sequence. WHO and otherexternal specialized organizations are in-creasingly being requested to participatenot only in overall planning exercises butalso in many diversified sector developmentactivities, such as carrying out studies of"subsectors" (e.g., rural water supply,urban sewerage), investigating water lossesand instituting measures for leakage con-trol, improving the operation and main-tenance of facilities, undertaking tariffstudies, improving financial and overallorganizational management, and identifyingand preparing investment projects.
I1.31 To date, WHO's major inter-national partners in sector developmentwork have been UNDP, which has financedmost of the project studies undertaken byWHO, and IBRD, with which WHO hashad a cooperative programme since 1971.During 1976 -77, a cooperative programmewith the African Development Bank was inforce, and cooperative activities were under-taken or planned with several bilateral aidorganizations. Contacts were establishedwith one national and two multinationaldevelopment funds in the Eastern Mediter-ranean Region. The growth of these col-laborative activities is evidence of the widerecognition of WHO's expertise in theplanning of community water supply andsanitation.
Control of environmental pollution andhazards
11.32 Concerned at the acute, chronicand delayed toxic effects that may resultfrom exposure to chemicals in air, water,food and consumer products and at theplace of work, particularly if combinedwith exposure to other chemicals, infectious
156
agents and physical factors, the WorldHealth Assembly in May 1977 requested theDirector -General to study the problem andlong -term strategies in this field and toexamine the possible options for inter-national cooperation that would result inmore effective arrangements for the evalua-tion of health risks from chemicals, theprovision of rapid and effective response inemergencies, and the development of man-power (resolution wHA3o.47)
11.33 The programme on environ-mental health criteria initiated in 1973 inclose collaboration with some 25 nationalfocal points and UNEP, aiming at provid-ing information on environmental healthrisks as a basis for formulating nationalenvironmental health standards and otheraction to control and improve the qualityof the human environment, made substan-tial progress in 1976 and 1977. Fourenvironmental health criteria documentswere published in collaboration withUNEP.1 A scientific group met in late1976 to review advances made and tosuggest improvements in the programme.Several new collaborating centres on en-vironmental health effects were designatedto provide continued support to the pro-gramme, for example, in Japan, Nether-lands, Sweden and the USSR. The WHOCollaborating Centre on EnvironmentalHealth Effects at the National Institute ofEnvironmental Health Sciences, USA, notonly provided expert advice but also madea substantial financial contribution to theprogramme.
II.34 In connexion with the UNEPConference on the Ozone Layer, convenedin early 1977, a preliminary evaluation wasmade of the health effects of ultraviolet
1 World Health Organization. Environmental HealthCriteria. z : Mercury, Geneva, 1976. 2 : Polychlorinatedbiphenyl: and terphenyls, Geneva, 1976. 9 : Lead, Geneva,1977. ¢ : Oxides of nitrogen, Geneva, 1977.
PROMOTION OF ENVIRONMENTAL HEALTH
radiation. The revision of basic safetystandards for ionizing radiation was ini-tiated in 1977 jointly with ILO, IAEA andthe Nuclear Energy Agency of the Organi-sation for Economic Cooperation andDevelopment. An agreement was reachedwith the International Radiation ProtectionAssociation with a view to the joint pre-paration of environmental health criteriadocuments on non -ionizing radiations. TheRegional Office for Europe was particu-larly active in this field.
1 1.3 5 Environmental health standardsremain an important management tool inenvironmental hazards control. Theyshould be based primarily on health riskassessments, and a number of activitiesfacilitating the application of WHOenvironmental health criteria documents tostandard -setting and other activities relatedto control were initiated in 1977 with theWHO Collaborating Centre on Environ-mental Health Effects in Bilthoven, Nether-lands.
11.36 Health aspects of the productionof synthetic rubber and plastics were thesubject of a symposium jointly organizedwith the WHO Collaborating Centre onEnvironmental Health Effects at the Na-tional Institute of Environmental HealthSciences, USA, in 1976. WHO alsoactively participated in UNEP's Industryand Environment Programme. At therequest of the Environment CoordinationBoard, a joint study was undertaken withUNDP, UNIDO, ILO and IBRD on theimpact of industrialization on environ-mental health.
11.37 The Regional Office for Europeissued a report on the health implicationsof nuclear power production, including acomparative assessment of health risksassociated with alternative energy conver-sion cycles ; the report was presented at the
157
International Conference on Nuclear Powerand its Fuel Cycles, held in Salzburg,Austria, in May 1977. The Regional Officefor Europe also studied the potential healthhazards of drinking -water technology(chlorination, ozonization, use of desalina-tion and demineralization).
11.38 The Pan American Center forHuman Ecology and Health established in1975 in Mexico City began implementingits five -year programme. It gave highpriority to the assessment of the impact andeffects of development projects on healthand the environment.
11.39 As part of UNEP's Global En-vironmental Monitoring System, WHO,together with other relevant internationalorganizations, initiated global projects onair and water quality monitoring. Theobjectives of these projects are to strengthennational environmental quality monitoringprogrammes for the protection of humanhealth and to collect data for the globalassessment of the environment. SixtyMember States participated in the extendedair quality monitoring project, based onnational centres and involving all WHOregional offices.1, 2 The preparatory phaseof a similar global water quality monitoringproject was completed by the end of 1977and sampling locations were selected inabout 7o Member States. Technicalcooperation under these projects includesthe provision of equipment, training, andtechnical advisory services and the organi-zation of inter -laboratory data qualitycontrol studies.
I1.40 Monitoring of environmentalradio -activity was continued with the
1 World Health Organization. Air quality in selectedurban areas 1973 -1974. Geneva, 1976 (WHO OffsetPublication No. 3o).
' World Health Organization. Air monitoring pro-gramme design for urban and industrial areas. Geneva, 1977(WHO Offset Publication No. 33).
THE WORK OF WHO
participation of 27 collaborating labora-tories in 19 countries. In cooperation withIAEA, a code of practice on basic re-quirements for personnel monitoring wasrevised.11.41 In order to assess the exposure ofhuman populations to environmental agentsan integrated approach to monitoring isrequired, including biological surveillance.This field was discussed by a joint UNEP/WHO Government Expert meeting, whichrecommended a programme of monitoringselected pollutants (several metals andchlorinated hydrocarbons) in tissues andbody fluids. Methods for such monitoringwere discussed at a workshop jointlyorganized in Luxembourg in April 1977 bythe Commission of European Communities,the United States Environmental ProtectionAgency and WHO. A group reviewed aWHO collaborative programme in anothertype of biological monitoring -the studyof chromosome aberrations -in July 1976and again in 1977.11.42 A scientific group in December1976 reviewed the possibility of using theexisting health information systems, includ-ing morbidity and mortality statistics, in theassessment of health effects related tochanges in environmental conditions. Thegroup concluded that it was premature toundertake routine monitoring of healtheffects before health information systemshad been improved. Such monitoringcould be successfully undertaken, however,on specific population segments such asinfants and children. Epidemiologicalstudies on the effects of air pollution onchild health, carried out for several yearsby the Regional Office for Europe incollaboration with six Member States, werereviewed in 1977 and recommendationswere made for further similar studies inother countries of the Region.11.43 Technology transfer is an import-ant component of technical cooperation
158
in the field of environmental pollutioncontrol. An example of such activitiesundertaken by the Regional Office forEurope in 1976 and 1977 was the prepara-tion of manuals on the control of air pollu-tion from industrial sources (with thesupport of the Federal Republic of Ger-many), on air and water pollution monitor-ing control, and on non -ionizing radiationprotection. In the South -East Asia Region,WHO assisted in the development ofnational legislation, particularly in India,and in the preparation of an inventory ofpollution sources in the Region. Amongthe pollution control activities in the East-ern Mediterranean Region were projects onindustrial and agricultural pollution in Iran,on air pollution control in Israel, and onstrengthening of an environmental centrein Pakistan. In the Western Pacific Region,WHO participated in various pollutioncontrol activities, including a water qualitymanagement project for Laguna de Bay inthe Philippines.
11.44 WHO participated in the UNEPAction Plan for the Mediterranean andassumed a leading role in the project onland -based sources of marine pollution inthe Mediterranean, which was carried out incollaboration with ECE, UNEP, UNIDO,FAO, UNESCO and IAEA. Two WHORegional Offices (Europe and EasternMediterranean) were involved in the imple-mentation of this as well as of anotherproject on the assessment of coastal pollu-tion in the Mediterranean. WHO alsoparticipated in a broader project initiatedby UNEP in 1977 on the assessment andcontrol of pollution in other regional seaareas.
National environmental health planning
11.45 The role and functions of healthadministrations in the field of environ-

PROMOTION OF ENVIRONMENTAL HEALTH
mental health are evolving as many coun-tries are adopting new strategies forplanning, implementing, controlling andcoordinating environmental quality andprotection programmes.
I1.46 WHO has confronted the prob-lems involved by examining the methodsthrough which environmental health maybe incorporated into the policy and plan-ning of developing nations for environ-mental protection. This activity is a part ofthe Organization's long -term programmeon human health and environment and iscarried out in support of the cooperativeprogrammes of the regional offices withMember States interested in initiating orimproving the effectiveness of environ-mental health planning and its coordinationwith other national developmental efforts.
11.47 In the Western Pacific Region,institutional development and sanitationprogrammes werePeople's Democratic Republic, Malaysia,Papua New Guinea, Samoa, SolomonIslands and Tonga. Cooperation in envi-ronmental sanitation services was providedin connexion with projects for the develop-ment of basic health services in the NewHebrides, Philippines, Republic of Koreaand Solomon Islands. Some countries inthe Western Pacific and Eastern Mediter-ranean Regions created new institutions orseparate pollution control commissionswith functions that overlap with those ofthe health authorities ; much effort will beneeded to harmonize the work of theseagencies in order to achieve common goals.
11.48 An interregional symposium wasconvened in Geneva in July 1977 to reviewand discuss the problems and the factorsinvolved in environmental quality planningand policy in developing countries. It wasattended by nationals from zo countriesand by representatives from United Nations
159
economic commissions and specializedagencies. The symposium proposed astrategy for the development of a nationalenvironmental quality programme as wellas directions for improvement covering theenactment of legislation, organizationalarrangements, changes in the planningprocess, information and education. Italso suggested that each country shouldestablish a high -level national coordinatingbody for overall environmental policy andplanning and for approval of standards ; thetraditional approach involving uncoordina-ted actions taken by separate ministries is nolonger sufficient.
Food safety
Food safety evaluation
I1.49 Food safety evaluation consistsof the elaboration of reports, mainlythrough deliberations of committees ofexperts, to provide advice to Membercountries on the health hazards that mayarise from biological or chemical con-tamination of food.
11.50 The task of the Joint FAO /WHOExpert Committee on Food Additives in1976 was to provide toxicological evalua-tion of intentional food additives and ofcontaminants.' Toxicological assessmentsof a number of substances belonging to theclass of artificial sweeteners, antioxidants,thickening agents and antimicrobials werecarried out. In 1977 the Committee under-took evaluations and re- evaluations ofsubstances in the general classes of acidsand salts, antioxidants, food colours, sweet-eners and thickening agents, as well asmiscellaneous food additives. The Com-mittee felt that annual meetings wereinadequate for evaluating the increasing
' WHO Technical Report Series, No. 599. 1976.
THE WORK OF WHO
amount of toxicological data and the largenumber of food additives, flavours, proces-sing aids, packaging materials and con-taminants. In May 1977 the World HealthAssembly asked the Director -General toconsider ways and means of overcomingthis problem (resolution wHn3o.47).
I1.51 The two sessions of the JointFAO /WHO Meeting on Pesticide Residuesin 1976 ' and 1977 provided toxicologicalevaluations and established maximumresidue limits for pesticide chemicals be-longing to the classes of organophos-phorous pesticides and carbamates, as wellas for other miscellaneous pest controlchemicals. Acceptable daily intake figuresfor man were allocated to several substancesand further work was recommended forthose chemicals on which the existinginformation was inadequate for assessingpotential hazards to man.
11.52 In 1976 Joint FAO/IAEA/WHO Expert Committee on the Whole-someness of Irradiated Food establishedunconditional acceptances for irradiatedwheat, potatoes, chicken, papaya and straw-berries, as well as provisional acceptancesfor cod and red fish, onions and rice.'
11.53 A guide to shellfish hygiene 'was published in 1976. It covers diseasestransmitted by shellfish, marine environ-mental factors (physical and biological)affecting the quality of shellfish and admi-nistrative measures, including legislation,establishment of a control service, pro-vision of facilities for the treatment andhandling of polluted shellfish and improve-ment of sanitary conditions in growingareas.
' WHO Technical Report Series, No. 6rz, 1977.' WHO Technical Report Series, No. 604, 1977.' Wood, P. C. Guide to shellfish hygiene. Geneva,
World Health Organization, 1976 (WHO OffsetPublication No. 31).
16o
II.54 The WHO Expert Committeeon Microbiological Aspects of FoodHygiene met in 1976 to consider therelative public health importance of variousfood -borne disease agents and the meansfor prevention and control of food -bornediseases, with particular reference to typesof food processing, local food habits, andpopulation movements and tourism.*Microbiological specifications for foods,cost /benefit aspects of microbiologicaltesting of foods and laboratory qualityassurance were also discussed.
11.55 The second Joint FAO /WHOExpert Consultation on MicrobiologicalSpecifications for Foods, sponsored byUNEP, finalized guidelines for the estab-lishment of microbiological criteria, setmicrobiological specifications for frozenshrimps and prawns and recommended aroutine method for the detection of sal-monella on the surface of frogs' legs.
1 1.5 6 A working group on aviationcatering problems was convened in 1976because outbreaks of food -borne diseasehad shown that the organization andsurveillance of aviation catering servicesneeded strengthening. The group madea number of recommendations for theimprovement of hygiene control and betterimplementation of existing regulations inorder to provide safe food and water forair -crews and passengers. A new editionof the guide to hygiene and sanitation inaviation was published.'
Elaboration of food standards and codes ofpractice
11.57 The purpose of the work of theCodex Alimentarius Commission, whose
' WHO Technical Report Series, No. 598, 1976.' Bailey, J. Guide to hygiene and sanitation in aviation
(znd ed.), Geneva, World Health Organization, 1977.
PROMOTION OF ENVIRONMENTAL HEALTH
membership now stands at 115, is toprotect consumers against health hazardsin food and against fraud, to ensure fairpractices in the food trade, and to facilitateinternational trade in foods.
11.58 The eleventh session of theCodex Alimentarius Commission, held inApril 1976, adopted z 1 international foodstandards, including standards for infantformulas, canned baby foods, cereal -basedfoods for infants and children, grape juice,pineapple juice, frozen shrimps, cannedluncheon meat, citrus marmalade, cocoabutter and chocolate. The Commissionhas now established a total of 13o foodstandards. In addition, new codes ofpractice were adopted for the inspectionof slaughtered animals, for the processingof fresh meat, egg products and poultry,for the handling of fish and for the proces-sing and handling of frozen foods. Aworking group drafted a revision of theCommission's General Principles of FoodHygiene. To date, 53 countries haveindicated, according to one of the methodsof accepting the Codex Standards, theiracceptance of several of these standards.
1 1.5 9 During 1976 -77 the Commissionreappraised its programme of work andpriorities, giving more attention to theneeds of developing countries. CodexCoordinating Committees were establishedin Africa, Latin America and Asia withthe aim of developing a concerted approachto instituting modern food law and regu-lations and other aspects of food controlinfrastructure.
Food control
11.6o The Organization continued tostimulate the establishment in MemberStates of the infrastructures required forthe maintenance of the safety, nutritionalvalue and quality of foods and to promote
161
national food control programmes, espe-cially with regard to training. A foodcontrol strategy was developed by aworking group convened late in 1977.
I1.61 In collaboration with UNEP,FAO and IARC, a mycotoxin controlproject, combined with a follow -up studyon its effect on liver cancer, was initiatedin Swaziland with the aim of elaboratingpractical measures for mycotoxin pre-vention that will serve as a model for usein other African countries.
11.6z WHO collaborated in epidemio-logical studies on an outbreak of foodpoisoning in Kayes, Mali, in 1976 due tothe consumption of rice contaminatedwith a chlorinated pesticide.
11.63 Of z7 African countries replyingto a questionnaire, z3 indicated that theyhave legislation for food hygiene ; 9
considered that livestock was slaughteredconditions conforming
WHO cooperated with a number of coun-tries in updating food control legislation.
11.64 A consultation on food infor-mation problems was held in 1976. As afollow -up, a survey of the organization offood control administration in Europewas started in 1977, for the purpose ofpreparing a concise document briefly de-scribing the measures taken in each Membercountry to promote food safety and hygieneand the different ways in which this workis organized.
11.65 A conference held in October1977 reviewed the organization and meth-odology of food control laboratories atcentral, regional and local levels.
11.66 The Organization continued tocollaborate with FAO, the Arab Organi-zation for Standardization and Metrologyand other interested international agenciesin carrying out food control and hygiene
THE WORK OF WHO
activities on an intercountry basis. Col-laborative programmes were discussed ata joint meeting in Alexandria in July 1977.
Joint FAO /W/HO Food and Animal FeedContamination Monitoring Programme
11.67 The Joint FAO /WHO Food andAnimal Feed Contamination MonitoringProgramme, funded by UNEP, was con-tinued. Its objectives are (1) to collect,evaluate and disseminate information onthe levels of certain contaminants inspecific foods on a worldwide basis, and(z) to provide assistance to countrieswishing to initiate or strengthen their foodcontamination monitoring activities.
I1.6ó Up to the end of 1977, 14 insti-tutes had been designated as Joint FAO/WHO Collaborating Centres for Food
Contamination Monitoring. During 1977they provided WHO with informationrelating to the period 1971 -75 on levels of(i) organochlorine pesticides and poly-chlorinated biphenyls in whole fluid milk,whole dried milk, butter and human milk ;and (z) lead in canned fruit, canned fruitjuice including concentrates, canned vege-tables and canned milk.
11.69 During the latter part of 1977,information was obtained from 16 devel-oping countries on their food contami-nation monitoring activities or their poten-tial for such activity. At the same time,information was obtained on the needs ofdeveloping countries for facilities, equip-ment and personnel in order to strengthentheir food contamination monitoring pro-grammes.
16z
Chapter- 12
flea 1M Statistics
I2.xTHE
MAIN OBJECTIVE ofthe Organization's health sta-tistics programme is to co-
operate with Member States in the devel-opment of information support requiredfor the planning, management and evalu-ation of their health programmes.
12.2 National policies on health sta-tistics have undergone considerable changesduring need forclose link between the health managers andthe health statistical services is now clearlyrecognized. In the past, national healthstatistics services tended to be orientedtowards an undefined audience includinghealth managers, research workers, teachersand students, and the general public.While statistical information is indeedused for various purposes, statistical ser-vices cannot meet their priorities if theyattempt to satisfy a wide range of usersevenly. The health manager has graduallyemerged as the primary and most import-ant user of health statistics, and statisticalservices in many countries have beenmodified accordingly.
12.3 Secondly, recognition of health asan essential component of socioeconomicdevelopment has led to a review and re-orientation of health statistical serviceswithin the framework of the total sta-tistics information system. What is re-
163
quired, therefore, is the establishment ofa cohesive national statistical policy andthe development of health statistical ser-vices within this context.
12.4 Thirdly, the interrelationshipbetween statistics and other types of in-formation supporting national health pro-grammes is under critical review. Healthmanagers require a variety of quantitativeand non -quantitative information, and sta-tistical data constitute an integral part ofthe total information needed. Thus anoverall approach to health information isconsidered desirable, although countriesvary in the extent to which they adopt anintegrated approach.
12.5 WHO's health statistics pro-gramme was reoriented in line with thesetrends in national policy, as well as in thelight of resolution WHA29.48 calling forincreased technical cooperation with devel-oping countries. The programme is nowmore directly involved in comprehensiveand specific health programmes than pre-viously, when separate statistical projectswere more frequent. The developmentand application of methodology appro-priate for conditions in developing coun-tries are emphasized in all the programme'sstatistical activities.
I2.6 Resolution WHA3o.46 adopted bythe Health Assembly in 1977 emphasized
THE WORK OF WHO
that WHO's activities in the field of sta-tistical and other information systems andservices should continue to have the neces-sary priority at headquarters and in theregions. WHO's central services for dis-seminating world health statistics to Mem-ber States and for establishing internationalstatistical standards, particularly the Inter-national Classification of Diseases andrelated classifications, were maintained andimproved.
Health statistical methodology
12.7 Activities in health statisticalmethodology were expanded to providesupport services to WHO -assisted pro-grammes, comprising (I) a sound statis-tical and mathematical basis for planningand executing projects and for analysingand evaluating field data ; (2) a valid me-thodological basis for applying operationalresearch, systems analysis and modellingto epidemiological investigations and tothe development and improvement ofhealth delivery systems ; and (3) a relevantmethodological basis for the use of scientificcomputing facilities in medical, epidemio-logical and health service applications.Advice was also given on the policy impli-cations of these three aspects.
12.8 Increasing emphasis was givento the needs of developing countries,especially in respect of transferring to them,in an appropriate form, the technologicaladvances in applied statistics, operationalresearch, systems analysis and medicalcomputing that have already been estab-lished elsewhere.
12.9 Special attention was given to theoperational problems of health deliverysystems, the optimal allocation of re-sources and the selection of intervention
164
strategies by decision -makers. These activi-ties included work on the methodologyof public health forecasting, in accordancewith the Sixth General Programme ofWork, and were promoted by collaborationwith the International Institute of AppliedSystems Analysis.
I2.Io In Europe, close contact wasmaintained with several intergovernmentaland nongovernmental organizations in thefield of informatics and medical computing.
Dissemination of statistical information
I2.11 Following the adoption of resolu-tion WHA29.22 by the World Health As-sembly, groundwork was undertakenduring 1976 -77 for the preparation of thesixth report on the world health situation,to be issued in 1979. Coordinated withthis work, progress was made in the pre-paration of the third edition of HealthServices in Europe, also scheduled for publi-cation in 1979.
12.12 The latest statistics available fromthe Member States were included in theWorld Health Statistics Annual, 1973-76,published in three volumes,' and theWorld Health Statistics Annual, 1977, alsopublished in three volumes.2
12.13 The World Health StatisticsReport, another vehicle for transmittinginformation of current international publicinterest, appeared quarterly instead of
1 World Health Organization. 'World Health StatisticsAnnual, 1973-76. Volume I: Vital statistics and causes ofdeath, Volume II: Infectious diseases: Cases, deaths andvaccinations, and Volume III: Health personnel and hospitalestablishments. Geneva, 1976.
2 World Health Organization. IVorld Health StatisticsAnnual, 1977. Volume I: Vital statistics and causes ofdeath, Volume II: Infectious Diseases: Cases and deaths,and Volume III: Health personnel and hospital establishments.Geneva, 1977.
HEALTH STATISTICS
monthly as from 1977. Accent was put onanalytical studies on special subjects. Inview of the priority given by MemberStates to the reduction of fetal, infant andchildhood mortality and cancer mortality,revealed by an opinion survey of users ofWHO's statistical publications, variousaspects of these topics were featured inseveral issues of the Report. In addition,a special issue was devoted to water andsanitation.
12.14 A project on cancer statisticsinformation systems was commenced jointlywith IARC, with the aim of improvingstatistics on cancer at both the national andinternational levels ; an initial meeting todiscuss procedures was held in Minsk,USSR, in December 1976. A pilotproject was also begun on monitoringmental health needs ; procedures werediscussed at a meeting held in Geneva inMarch 1976 and at a second meeting, heldjointly with the United States NationalInstitute of Mental Health in Washington,DC, in 1977, and attended by collaboratorsfrom participating countries.
12.15 Among the UNFPA -supportedactivities, international collaboration byexperts on the basic methods of analysisresulted in the publication of a manual ofmortality analysis in 1977.1 The firstvolume of the results of another UNFPA-funded undertaking, a comparative studyof the effects of social and biological factorson perinatal mortality, was completed in1977. Data from an ad hoc survey on fetal,infant and early childhood mortality andfertility, carried out in Afghanistan, Algeriaand Sierra Leone, also funded by UNFPA,were extensively analysed.
12.16 The fourth survey on the healthdemography of the African Region was
World Health Organization. Manual on mortalityanalysis. Geneva, 1977.
i
165
completed, on the subject of three aspectsof health services -personnel, traininginstitutions and infrastructure. Seventeencountries were covered in this survey.
Development of health statisticalservices
12.17 Technical cooperation withMember countries continued with a viewto promoting and strengthening nationalhealth information systems, and particularlytheir statistical component. The pro-gramme covered about 5o developingcountries and is designed to improveinformation services for decision -makingin health. The Regional Committees forSouth -East Asia and Europe devoted theirTechnical Discussions to the topic of in-formation systems in the health services.
12.18 In addition to the activities underthe regular budget, the following activitieswere financed from the Voluntary Fundfor Health Promotion : a project for devel-oping a health statistical information sys-tem in Pakistan, a workshop on the devel-opment and improvement of a nationalhealth information system in Tunisia, andsystems analyses of vital statistics servicesconducted in Honduras, Jamaica, Mexico,Philippines and Thailand.
12.19 Other major activities under-taken included : a regional working groupon the measurement of levels of health,held jointly with the International Epi-demiological Association, in Nieborow,Poland, in March 1977 and the preparationof a publication on the measurement oflevels of health ;2 a joint working groupwith the International Federation for In-formation Processing on health data banks,
2 World Health Organization. The measurement oflevels of health. Copenhagen (WHO RegionalPublications, European Series, in preparation).
THE WORK OF WHO
held in Prague in August 1976 ; a regionalseminar on civil registration, in Wash-ington, DC, in October 1977 ; a workinggroup on primary health records and theiruse in developing countries, organizedjointly with the Faculty of Medicine andHealth Centre, Rijeka, Yugoslavia, inOctober 1977 ; a regional seminar onmedical records, in Montevideo, Uruguay,in November 1977 ; and the preparationof an outline for an information system foranalysing national health expenditures andcost.
i z.2o The activities for developingand improving medical records systemscontinued in four Regions (the Americas,South -East Asia, Eastern Mediterraneanand Western Pacific). Education andtraining programmes for health statisticspersonnel and teachers were carried out inall regions.
International Classification of Disease
12.21 The biennium 1976 -77 saw theculmination of the programme for thedecennial revision of the InternationalClassification of Diseases. The draft pro-posals for the Ninth Revision (ICD -9)recommended by the International RevisionConference in 1975 were adopted by theWorld Health Assembly in 1976 (resolutionwHA29.34). The new revision, to comeinto use on i January 1979, is intendedto be much more useful to the clinicianthan previous revisions, which wereoriented more towards the medical statis-tician. It includes new definitions andrecommendations concerning maternal andperinatal morbidity and mortality, and aproposed form of certificate of cause ofperinatal death.
12.22 The Health Assembly alsoapproved the publication of supplementaryclassifications, for trial purposes, of Impair-
166
ments and Handicaps and of Procedures inMedicine, endorsed recommendations ofthe Revision Conference supporting thecollection of morbidity and mortality sta-tistics by lay personnel in developingcountries and proposed the preparation ofthe International Nomenclature of Diseasesas an improvement to the Tenth Revisionof the International Classification ofDiseases (resolution wHAz9.3 5).
12.23 By the end of 1977, ICD -9 hadbeen published in English,' French andSpanish, and the Russian edition was inpreparation. Of the supplementary clas-sifications, the provisional InternationalClassification of Procedures in Medicineand the Classification of Impairments andHandicaps are being published in 1978.An adaptation of ICD to oncology(ICD -O) 2 was prepared in collaborationwith IARC and with assistance from theUS National Cancer Institute. The Englishversion was published at the end of 1976and brought into immediate use in manycancer registries, including that of the USA.Versions in other languages were in pre-paration.
12.24 In collaboration with theRegional Office for South -East Asia, aclassification suitable for use with layreports of morbidity and mortality wasdrafted ; field trials were in progress in anumber of countries of the Region by theend of 1977. Work on medical nomen-clature was started in cooperation withCIOMS, and drafts on respiratory diseasesand neurological disorders were preparedand circulated to competent bodies forcomment.
12.25 In 1977 courses intended tofamiliarize coders with the provisions of
' World Health Organization. Manual of the inter-national statistical classification of diseases, injuries, andcauses of death, 1975 revision. Geneva, 1977.
2 World Health Organization. ICD -O : Internationalclassification of diseases for oncology. Geneva, 1976.
HEALTH STATISTICS
ICD -9 were organized by the RegionalOffices for Africa (in Accra), Europe (inLondon, Moscow and Paris) and theWestern Pacific (in Kuala Lumpur, Singa-pore and Sydney).
iz.z6 Two new International Centresfor the ICD were established in Wash-ington, DC (for North America), and inSao Paulo, Brazil (for the Portugueselanguage).
167
Chapter 13
Health and Biomedical
Information
13.1 THE BIENNIUM 1976 -77 was aperiod of challenge and changefor the information services of
WHO. Already charged with primaryresponsibility for implementing the partof resolution \HA25.26 of 1972 that calledupon the Organization to assume a leadingrole in developing biomedical communica-tions, these services suffered substantialcuts in funds and manpower in the realloca-tion of the regular budget funds towardsincreased technical cooperation during1977 -80 required by resolution wHA29.48.
13.2 In 1976 the health and biomedicalinformation programme was formed, link-ing the WHO publications programme,which maintains a flow of biomedical infor-mation from the Organization to the out-side world, with the library and healthliterature services, which are concernedwith the flow of biomedical informationfrom the outside world into the Organiza-tion. A third component of the overallprogramme was concerned with transmit-ting health information to the public. Thisreorganization was an attempt to enableWHO to deal more responsively and coher-ently with its widely varied target audien-ces, which include, for instance, researchworkers in collaborating centres, publichealth administrators in both developingand developed countries, and the interestedpublic.
168
13.3 The content of certain periodicalsand publications produced at headquartershas been or is being modified so as toreflect the emphasis throughout the Orga-nization on meeting the problems and needsof the developing world. To tap the resour-ces of knowledge and expertise in theregions and make these available, regionalpublications programmes are being devel-oped or expanded. The concept of regionalmedical libraries and related health literatureservices, already established in severalregions, is in the process of being expanded.With the agreement of the Member Statesconcerned, two new working languages,Arabic and Chinese, are being introducedselectively in the documentation for theWorld Health Assembly and the ExecutiveBoard, and in the case of Arabic in publi-cations, so as to provide a service to personsusing these languages with minimum diver-sion of funds from technical cooperation.Similarly, the transfer of the Spanish trans-lation facilities for technical publicationsto the Region of the Americas from head-quarters should maintain the flow of essen-tial information in Spanish at lower cost.
13.4 In the light of resolutions WHA29.25 and wHA29.48, an examination wasmade of technical documents productionat headquarters, with a view to improvingquality and reducing costs, and in 1977 astart was made with the control of technical
HEALTH AND BIOMEDICAL INFORMATION
documents. By making distribution moreselective it was possible to reduce the num-ber of printed pages by some 34 %(5 millionpages) compared with 1976. The policyof restricting the output of technical docu-ments will be maintained in 1978, when it isexpected that a further reduction in volumewill be achieved, with consequent econo-mies in staffing, printing, translation anddistribution costs.
Health literature services
13.5 The library and health literatureservices activities of WHO during the bien-nium were focused primarily on respond-ing to resolution wHAz9.48, i.e., reorient-ing the work to make additional fundsavailable for technical cooperation withMember States. Certain existing operationswere re- examined and several new initia-tives were proposed.
13.6 One important change was thephasing out of the WHO MEDLINECentre. Despite the abundant informationon research and clinical medicine that theCentre made available, a review in the lightof the new emphasis on technical coopera-tion with developing countries revealedthat the MEDLARS/MEDLINE data basewas not sufficiently oriented to publichealth problems in developing countriesto justify the continuance of a WHO centre.In cooperation with the regional offices,other arrangements were made for MemberStates in need of the MEDLINE serviceto gain access to it.
13.7 In furtherance of the idea of a net-work of regional medical and public healthlibraries and documentation centres thatwould bring health literature much closerto users in Member States, arrangementswere made by the Regional Office for theEastern Mediterranean and by the PahlaviLibrary of Medicine and Biomedical Com-
169
munications Centre in Teheran, Iran, forthe facilities of this library to be availableon a regional basis as from January 1978.
13.8 To make current medical literatureavailable to developing countries at mini-mum cost, work continued on the pro-gramme of arranging shipments of journalsand other literature from libraries in devel-oped countries to countries more acutelyin need of this material, the cost of shipmentbeing borne wherever possible by donorinstitutions. This programme is beingextended to assist in building up the stocksof the WHO Tropical Diseases ResearchCentre Library at Ndola, Zambia, and inreplenishing the depleted medical librariesof Viet Nam.
13.9 In an effort to determine whatadditional steps WHO can and should takein assuming a leading role in developingbiomedical communications in responseto resolution WHAZ5.z6, tentative planswere made for the convening during 1978of a meeting of experts in this field fromboth developed and developing countries,as called for in this resolution.
13.10 Also in progress was the compre-hensive reclassification of much of thematerial in the WHO library to arrange itin accordance with priority programmesand projects.
WHO publications
13.11 Two interrelated trends emergedin the WHO publications programmeduring the biennium -a reduction in thenumber and volume of some headquarterspublications, particularly the Official Records,in compliance with resolutions wHA29.25and wHA29.48, to release funds for tech-nical cooperation in developing countries,and further development of the regionalpublications programme.
THE WORK OF WHO
13.1 z As a consequence of much closercooperation between headquarters and theregional offices, the Regional Office for theAmericas (which has had its own technicalpublications programme for 5o years)agreed to issue Spanish translations of someheadquarters publications in its ScientificPublication series. The first volume of theWHO Regional Publications, European Serieswas published in 1976 and several othersappeared in 1977. The South -East AsiaRegional Office also began publishing itsregional series in 1976.
13.13 The Health Assembly examinedthe high cost of conference documentationand recognized that the main costs arosefrom (1) the sheer volume of documen-tation, and (z) the number of languagesinto which the documentation had to betranslated. To reduce the volume, theHealth Assembly agreed to a 5o % cutin the Director -General's comprehensivereport to the Health Assembly and theUnited Nations on the work of WHO andthe proposed programme budget, presentedto it biennially, and the financial report,presented annually (resolution WHA30.3o).The Executive Board approved recommen-dations of its ad hoc committee appointed tostudy the whole question of conferencedocumentation and of official and workinglanguages (resolution EB6o.R7). Theimplementation of these recommendationswould drastically reduce the extent towhich the Board's summary records aretranslated from the original English ;similar recommendations were made forboth the verbatim records and the summaryrecords of the Health Assembly's meetings.The net result of the reductions alreadyapproved and those to be submitted to theThirty -first World Health Assembly wouldallow a reallocation of some US $ 900 00o ayear for other programmes.13.14 Among the periodicals issued byheadquarters, three volumes (18 issues) of
170
the Bulletin of the World Health Organizationwere published during the biennium in abilingual (English and French) edition andalso in Russian. In addition the necessarygroundwork was laid for a complete reorien-tation of the Bulletin, beginning with thefirst issue of 1978, to enable it to respondmore closely to technical cooperation needsof Member States ; in particular, this reorien-tation reduces the proportion of narrowlyspecialized scientific articles and replacesthem with review articles providing autho-ritative accounts of the current state ofscientific knowledge so that readers, parti-cularly those in developing countries with-out access to such information, can keepabreast of new developments in fields ofconcern to WHO.
13.15 Two volumes (24 issues) of theWHO Chronicle were published in separateEnglish, French, Russian and Spanish edi-tions during the biennium. While its overallgeneral form remained unchanged, effortswere made to improve the effectiveness ofthe Chronicle as a vehicle of informationtransfer by the inclusion of livelier andmore topical articles, greater use of illus-trations and added stress on regional acti-vities.
13.16 During the same period two vol-umes (8 issues) of the International Digest ofHealth Legislation were issued in separateEnglish and French editions. In January1977 responsibility for the publication ofthe Digest passed from the Legal Divisionto the Health and Biomedical InformationProgramme. With the Health Assemblyreflecting renewed interest in health legisla-tion as a tool of technical cooperation inits adoption of resolution wNA3o.44, thefuture role of the Digest and other healthlegislation activities is now under study.One possibility being explored is that ofencouraging existing institutions aroundthe world to become WHO collaboratingcentres in health legislation ; these would
HEALTH AND BIOMEDICAL INFORMATION
act as repositories of information on variousaspects of the subject and would assist inproviding an information service for Mem-ber States.
13.17 In the case of the non -periodicaltechnical publications, the emphasis wason limiting publication to material that is ofdirect value to Member States, and in par-ticular to developing countries. One resultof this policy is that information aboutspecialized activities of interest to only alimited audience is increasingly beingoffered for publication in non -WHO media.Another is that duplicate publication of thesame material by two or more internationalagencies has been discouraged, and theprinciple of one agency being the solepublisher has been introduced.
13.18 Simpler and less costly publica-tion processes have, whenever possible,been brought into use. Publication in theWHO Offset Publications series, using type-script instead of letterpress reproduction, isbeing increasingly chosen. The TechnicalReport Series, the Monograph Series, and thePublic Health Papers were continued, aswere non -serial publications. The WHOFood Additive Series and Pesticide ResiduesSeries were discontinued, but a new seriesentitled Environmental Health Criteria wasintroduced in collaboration with UNEP.
Public information
13.19 Reflecting the more problem -oriented approach being taken by WHO indeveloping new programmes to combatthe major illnesses of the world, the themesof the two World Health Days during thebiennium were : prevention of blindness ;and immunization against the six prevent-able diseases of childhood -diphtheria,whooping cough, tetanus, poliomyelitis,measles and tuberculosis. In addition tothe extensive press publicity generated by
171
the World Health Days, 1 yo radio networksin over yo countries broadcast special pro-grammes. In the South -East Asia andWestern Pacific Regions, special recordedmessages from the Regional Directors werebroadcast by over 30 national networks.In the European Region a series of fivetelevision spots produced for WHO by theInternational Green Cross and emphasizingthe importance of immunization was shownon seven national networks.
13.20 As part of the considerable publicinterest stimulated by the themes of thetwo World Health Days, a number ofAfrican countries set up special organiza-tions to deal with the problems of prevent-ing blindness. In 1977, President Carter ofthe United States launched a major nation-wide campaign to reach millions of childrennot already immunized against the six pre-ventable childhood diseases. Similar stresswas given to immunization in Malaysia andSingapore, where hospitals, maternal andchild health clinics and local health centresjoined forces to promote immunization.The immunization programmes in Ghanawere the subject of a 2o- minute colourfilm, jointly produced by WHO andUNICEF in collaboration with the GhanaFilm Industry Corporation ; 1 oo copies ofthis film were sold, an indication of theinterest it aroused.
13.21 Apart from the World HealthDays, the major public health news storyof the biennium was smallpox eradication,which was the subject of a number of pressreleases and features. Interest in this storywas especially high in the African andSouth -East Asia Regions because eradica-tion was certified in parts of central andsouthern Africa and in Bangladesh, Bhutan,Burma, India and Nepal.
13.22 World Health further improved itscirculation with the resumption of a guar-
THE WORK OF WHO
terly Italian -language edition, bringing itsaggregate circulation in all languages -Arabic, English, French, German, Italian,Persian, Portuguese, Russian and Spanish -to about 23o 00o copies per issue. Thefrequency of WHO's feature radio pro-gramme was increased from 10 to 1z timesa year and it was broadcast by about 250stations around the world. Rural radio as ameans of promoting health was the subjectof a seminar sponsored by the RegionalOffice for Africa, attended by radio repre-sentatives of the seven countries coveredby the onchocerciasis control programmein the Volta River basin area.
13.23 In addition to the World HealthFilm Day films -Focus on Sight in 1 976 andProtect Them Now in 1977 -film productionincluded Did You Take Your Tablets ?, pro-duced with the assistance of the RoyalDutch Tuberculosis Association ; Seeds ofHealth, dealing with primary health carein Guatemala, produced with the assistanceof the World Council of Churches ; andThe Powerful Protector, showing how vaccinesare manufactured, produced with the assist-ance of the Green Cross of the FederalRepublic of Germany. The South -EastAsia Regional Office produced three films :one on smallpox in 1976 entitled IndiaRemains Alert, and Food for Sight and Outof the Ivory Tower in 1977, dealing with theprevention of blindness and the role ofmedical students in primary health care,respectively. With the financial support ofthe New Zealand Government, the RegionalOffice for the Western Pacific is completinga film on filariasis. The Regional Officefor Africa is working in close cooperationwith the National Film Office of Canada(Office national du Film du Canada) to helpin the production of 32 educational filmsfor use in training auxiliary health workersin Africa. Work began on several films dur-ing 1977 as part of this US $ 1.2 million pro-gramme, which extends over three years.
172
Language services
13.24 The scope of the functions of thelanguage services was broadened by theadoption of Arabic and Chinese as workinglanguages (World Health Assembly resolu-tions wHA28.33 and WHA28.34.) It wasagreed that implementation would beselective, and limited programmes wereestablished in close cooperation with theRegional Office for the Eastern Mediterra-nean and the Council of Arab Ministers ofHealth in the case of Arabic, and with theappropriate national authorities in the caseof Chinese. A staff of three Arabic andfour Chinese translators was recruited.13.25 The overall shift from centralizedactivities towards more technical coopera-tion with Member States in response toresolution wHA29.48 involved heavy cutsin the translation staff as projected in therevised 1978 -79 programme budget.
13.26 Another move towards decentra-is up /WHO
Publications and Documentation Centerto be located in Mexico City. It is plannedthat this Center will be run by PAHO andit will be responsible for technical publica-tions in the Spanish language. Preparationsare well advanced and the Center is expectedto become operational in 1978.
Technical terminology
13.27 The progressive expansion ofWHO activities has emphasized the needfor standardized technical terminology thatwill permit clear and unimpeded communi-cation between different disciplines andbetween the Organization and its MemberStates. Accordingly, the technical termi-nology service was strengthened duringthe biennium. One example of its work isthe major effort, now underway, to stan-dardize definitions of often -used but fre-quently misunderstood terms in the fieldof basic health care. The Regional Office
HEALTH AND BIOMEDICAL INFORMATION
for Europe prepared a glossary on air pollu-tion 1 that brings together, for the firsttime in a single volume, recommendedterminology in this multidisciplinary field.All such glossaries are developed in closecoordination with interested intergovern-mental and nongovernmental organizationsand headquarters, regional and projectstaff.
13.28 Acting on a report on the use ofunits of the Système international d'Unités(SI) in medicine prepared in response toresolution wHA29.65, the Thirtieth WorldHealth Assembly recommended their use"by the entire scientific community, andparticularly the medical communitythroughout the world" (resolution WHA30.39). The only exception was therecommendation that instruments for mea-suring pressure within the body be tem-porarily graduated in both kilopascals andmillimetres of mercury. In the same resolu-tion the World Health Assembly requestedthe preparation of a booklet to assist thechange to SI units that would be broughtto the attention of all Member States of theOrganization. This booklet,2 describingSI units, discussing factors involved intheir practical application, and giving fac-tors for converting values in old units tovalues in SI units, was prepared in co-operation with another intergovernmentalorganization (the Bureau international desPoids et Mesures) and with nongovern-mental organizations responsible for clinicalchemistry, haematology, nutrition, andradiology, and was published with theirapproval.
1 World Health Organization. Glossary on air pollu-tion. Copenhagen (WHO Regional Publications, Euro-pean Series, in press).
2 World Health Organization. The SI for the healthprofessions. Geneva, 1977.
173
Distribution and sales13.29 New sales promotion measuresaimed at bringing WHO publications tothe attention of widely varied groups ofpotential readers throughout the worldwere intensified during the biennium. In1976, for example, WHO publications wereshown at 87 international and national con-ferences and book fairs covering about 3odifferent subject areas, were advertised inscientific and technical journals and weresupplied to a large and growing networkof such journals for review purposes. Cata-logues and leaflets listing publications bysubject were distributed to interested groupsof scientists and health workers, and mail-ing lists were established to enable theOrganization to keep addressees regularlyinformed of new publications in their fieldsof interest.13.3o Systematic polling of certain cate-gories of readers who receive publicationsfree of charge eliminated inactive recipientsand permitted the reorientation of freedistribution to new recipients. The com-puterization of the distribution and salesactivities, particularly the mailing lists,progressed satisfactorily, and when com-pleted will not only substantially increasethe distribution and sales network but alsoenable the whole distribution process torespond more flexibly and effectively tothe needs of Member States, regionaloffices, WHO Representatives and theSecretariat.13.31 Indicative of the success of thesepromotional activities is the fact that saleshave reached record levels despite theworldwide recession that has seriouslyreduced library acquisition budgets incertain countries. Fig. 13.1 shows thedistribution of sales of WHO publications inthe regions and in certain countries in 1976.The total revenue from the sale of WHOpublications amounted to US $ i 494 000in 1976 and US $ 1 857 000 in 1977.
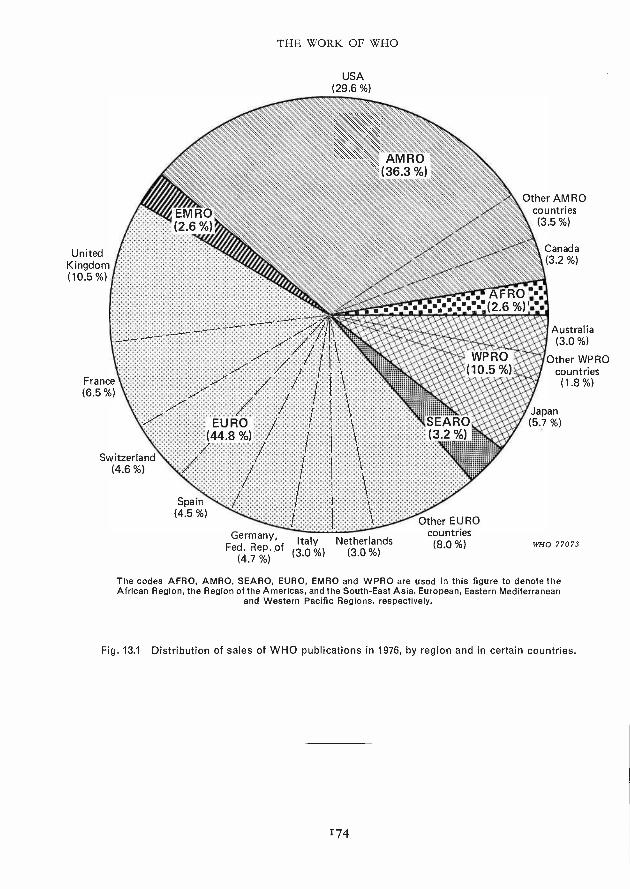
UnitedKingdom(10.5 %)
THE WORK OF WHO
USA(29.6 %)
Other AM ROcountries(3.5 %)
Australia(3.0 %)
Other WPROcountries(1.8 %)
Switzerland(4.6 %)
Germany, Italy NetherlandsFed. Rep. of (3.0%) (3.0 %)
(4.7 %)
Other EUROcountries(8.0 %) WHO 77073
The codes AFRO, AMRO, SEARO, EURO, EMRO and WPRO are used in this figure to denote theAfrican Region, the Region of the Americas, and the South -East Asia, European, Eastern Mediterranean
and Western Pacific Regions, respectively.
Fig. 13.1 Distribution of sales of WHO publications in 1976, by region and in certain countries.
174
Chapter 14
Constitutional, Legal and Administrative
Developments
Constitutional and legal matters
14.1 DURING THE BIENNIUM 1976-77 five new Members joinedthe Organization : Angola, Cape
Verde, Papua New Guinea (formerly anAssociate Member), Sao Tome and Principe,and Surinam. On 12 July 1976 the SocialistRepublic of Viet Nam notified the Director -General of the unification of the formerDemocratic Republic of Viet -Nam and ofthe Republic of South Viet -Nam (bothWHO Members) and stated that it wouldcontinue to exercise the official member-ship ; this notification was circulated toMembers and Associate Members andbrought to the attention of the ThirtiethWorld Health Assembly. As a result ofthese changes the Organization had, at theend of 1977, 15o Members and two Asso-ciate Members.' A list of Members andAssociate Members is given in Annex 1.
14.2 The Twenty -ninth World HealthAssembly adopted on 17 May 1976 a furtheramendment to Articles 24 and 25 of theConstitution, increasing to 31 the number ofseats on the Executive Board, last broughtup to 3o by an amendment which had beenadopted in 1967 and which had entered
' The associate membership of one of these, SouthernRhodesia, is regarded as being in suspense.
175
into force in 1975. The new amendmentwill similarly enter into force upon thedeposit of instruments of acceptance byat least two -thirds of the Members. A totalof 18 such instruments had been depositedby the end of 1977.
14.3 The amendments to Articles 34and 55 of the Constitution which had beenadopted in 1973 and which permit a transi-tion to biennial budgeting came into forceon 3 February 1977 upon the deposit of thetooth instrument of acceptance. TheThirtieth World Health Assembly thereuponintroduced biennial budgeting with effectfrom the biennium 1980 -81.
14.4 In October 1977, following aresolution of Sub -Committee A of the Re-gional Committee for the Eastern Medi-terranean, the Government of Kuwaitproposed an amendment to Article 74 ofthe Constitution which would provide foran authentic Arabic text (in addition to theChinese, English, French, Russian andSpanish texts) and submitted such a text foradoption by the World Health Assembly.The Director -General communicated thisproposal to Members, informing them thatthe necessary steps would be taken toenable the Executive Board to put thisitem on the provisional agenda of theThirty -first World Health Assembly to beheld in May 1978.
THE WORK OF WHO
14.5 During the biennium 1976 -77,five Members (Bahamas, Greece, Republicof Korea, Tonga and Uruguay, becamebound, through instruments of accessionor declarations of succession, by the Con-vention on the Privileges and Immunitiesof the Specialized Agencies together withits Annex VII, which relates specificallyto the World Health Organization.
14.6 Under a project agreement withthe United Nations Environment Pro-gramme, WHO prepared a series of studiesserving as the basis for the drafting of aProtocol for the Protection of the Medi-terranean Sea against Pollution from Land -based Sources. Drafts for this Protocol,which is to supplement the Conventionsigned in Barcelona on 16 February 1976,were considered at intergovernmental meet-ings held with WHO participation inFebruary 1977 in Athens and in October1977 in Venice. It is expected that the Pro-tocol will be signed before the end of 1979.
Administration
Establishment
14.7 On 3o November 1977, the totalstaff (excluding staff of the Pan AmericanHealth Organization) was 4226 as comparedwith 4338 on 3o November 1975 and 4236on 3o November 1976, a decrease ofapproxi-mately z.3 5 % between 1975 and 1976,and a 2.6 % decrease at the end of 1977.
Staff development and training
14.8 The staff development and trainingprogramme established in 1975 became fullyoperational in the regions. Committeeswere established in the regional offices toadvise on training needs and to collaborate
1 Budgetary and financial data are presented separ-ately in the annual financial reports.
176
in the design and conduct of specificcourses for regional staff members.
14.9 Two four -week training coursesin management for senior regional andsenior national health staff were conducted,in Manila in 1976 and New Delhi in 1977,with participants from i z developingcountries. These courses were followed upby WHO -supported national courses inthe Philippines and Papua New Guinea in1977, and others are planned elsewhere.Training courses in management for fieldand regional office professional staff inthe Region of the Americas were conduc-ted in Brasilia and Washington in 1976 andin Bogotá, Panama City and Washingtonin 1977. The number of professional staffinvolved in programmes covering variousaspects of management training in head-quarters and the regions totalled 178.
14.10 Courses for locally recruitedregional office staff covering the topic ofteamwork in office management, attendedby a total of 135 general service staff, wereconducted in the Regional Offices for theAmericas, South -East Asia and the EasternMediterranean.
14.11 At headquarters the programmefor general service staff concentrated onmanagement training, and 91 staff membersparticipated in management training pro-grammes and workshops. Also at head-quarters, new on -entry briefing coursesfor general service staff were put intooperation. Skills training was providedat headquarters and at several regionaloffices.
14.12 A total of 53 staff were grantedstudy leave, mostly for refresher training.
14.13 A plan of action was formulatedto implement World Health Assemblyresolutions WHA28.4o and wHA29.43
CONSTITUTIONAL, LEGAL AND ADMINISTRATIVE DEVELOPMENTS
on the recruitment, promotion and train-ing of women in WHO.
Office accommodation
14.14 Construction of a new prefabrica-ted building for WHO headquarters, con-taining 132 offices and 3 small meetingrooms, authorized by World Health Assem-bly resolution wI1A28.24, was completedand the building was occupied in thesummer of 1976. This move made itpossible to terminate the rental agreementfor office space in the ILO building somethree months earlier than planned.
Supply services
14.15 The problems that affected supplyoperations after the energy crisis continuedin 1976 -77, albeit somewhat lessened.Commodity prices and shipping costscontinued to rise, deliveries were slow,
lesssuppliers were unwilling to accept smallorders.
14.16 Despite these constraints, the valueof supplies and equipment providedthrough headquarters purchasing opera-tions during the period 1976 -77 reachedthe record level of 90 I 19 line items, witha total value of US $ 46 5 5 i 526. This figureincludes US $ 13 526 089 for reimbursablepurchases made on behalf of MemberGovernments, the United Nations andspecialized agencies within the United
Nations system, and governmental andnongovernmental organizations. Purchasesfrom research grants awarded to investi-gators or institutions amounted toUS $ 2 126 732 and represent 4.57% oftotal purchases.
14.17 A large portion of the purchaseswere financed from extrabudgetary funds.Some of the important operations duringthe biennium were : assistance to the mostseriously affected countries through theSecretary -General's Special Account forthe United Nations Emergency Operation(US $ 7 389 272), rehabilitation of healthservices in the Lebanon, through theUnited Nations Trust Fund for Lebanon(US$ i 895 172), and major assistance inthe form of medical supplies and equipmentto the Lao People's Democratic Republicand to Viet Nam from the VoluntaryFund for Health Promotion, from thespecial account for Indochina Humanita-
and from regular funds(total US $ z 478 855 for both countries).Purchases were continued in support ofthe long -term programme of United NationsHumanitarian Assistance to Cyprus, fundedby UNHCR and amounting to US $I 113 725 for the two -year period.
14.18 WHO continued to participatein the studies of the Working Group onInter -Agency Procurement Services, whosegoal is to identify common user itemsand obtain better terms from majorsuppliers through bulk buying.
177
Chapter z f
Regional Trends'
African Region
15.1 DURING 1976 -77 the RegionalDURINGwas adapted to
meet the new aims of the worldprogramme, and there was a consequentoverhaul of structures to enable the prob-lems of the Region to be tackled without anincrease in staff. Seven new MemberStates that have recently become inde-pendent have joined the African Regionand one State has been transferred to theRegion at its own request. The MemberStates of the Region include the majorityof the least developed and most severelyaffected countries listed by the UnitedNations -countries that are very oftenafflicted by natural disasters -and it includesmost of the national liberation movementsrecognized by the Organization of AfricanUnity.
15.2 In the reorganization of the Re-gional Office, units have been replaced bymultidisciplinary groups and steps havebeen taken to increase decentralization anddelegate decision -making, as far as possible,to the level at which the problem has to besolved. WHO Representatives' offices havebeen strengthened by the addition of admin-istrative officers or administrative assist-ants. Staff has been cut by i o %, in spite of
Fig. 15.1 on page 181 shows the location of theWHO regional offices and the areas they serve.
178
the fact that the Region has recently be-come administratively responsible for theonchocerciasis control programme in theVolta River basin area.2
15.3 Epidemiological surveillance dataare now centralized and processed at theRegional Office, thus allowing the staff ofthe three epidemiological centres in Nai-robi, Brazzaville and Abidjan to be re-located in five strategically sited advancedunits for the promotion and support of theExpanded Programme on Immunization.
15.4 All WHO teams collaborating onprojects for the development of healthservices or for the training of health per-sonnel try to introduce the primary healthcare approach, and in most countriesprimary health care has now begun or isat the planning stage. A meeting of regionalexperts held in 1977 reviewed the status ofthe situation in this field, where activecommunity participation is being given themain emphasis.
15.5 Most countries of the Regioninclude a health plan in their national plansfor social and economic development.Fourteen have used or are preparing to usethe health programming method proposedby WHO and so introduce strategic plan-ning into such plans and follow it bypractical planning to produce projects thatcan be efficiently managed.
2 See also page 92.
REGIONAL TRENDS
15.6 After a short trial period, WHO'snew information system has been extendedto cover the whole Region since it ties inwith the two management methods rec-ommended by the Regional Committee :management by objectives and managementby exception. Only the information essen-tial for decision -making is passed on toa higher level, thus cutting down paperwork at regional level and strengtheningtechnical cooperation at country levelwithout having to increase staff. TheWHO information system in the AfricanRegion is closely linked to the nationalinformation systems that provide the basisfor long -term planning, medium -termprogramming and periodic evaluation ofthe world health situation.
15.7 The training of health personnelremains the cornerstone of health develop-ment but it is changing rapidly with a viewto producing the type of manpower thathealth teams need if they are to attain thesocial and health objectives defined by theWorld Health Assembly in resolutionwHA30.43.
15.8 The situation as regards environ-mental health has somewhat improved.Much has been done but much still remainsto be done. New approaches and newtechniques making use of local materialsand local personnel are being examinedinstead of resorting as is usual to importedproducts that are difficult to service and,owing to shipping charges, cost twice asmuch as in their country of origin.
15.9 Studies are underway to look intothe possibility of local manufacture ofpharmaceutical products, biologicals andtherapeutic substances and vaccines with aview to cutting down costs and facilitatingthe supply of products essential for protect-ing the health of the least privileged popula-tion groups. Traditional African medicineand medicinal substances come under this
179
heading. The African Development Bankis taking a special interest in this type ofwork and ECA, UNIDO, UNICEF andWHO are all contributing to it.
15.10 Research activities are expandingas the number of research workers andinstitutes increases. The two main topics ofinterest are the control of communicablediseases and the development of health caresystems to help solve problems in priorityfields, as far as available resources allow.
15.11 As regards international coor-dination, at country level national authori-ties are increasingly taking a greater shareof responsibility in their relations withexternal sources of cooperation. At thesubregional level, one area in whichcooperation between various countries isbeing strengthened is the development ofmajor lakes and river basins. At theregional level, the Conference on HealthCoordination and Cooperation in Africaprovides a meeting -place every two yearsfor the countries of the Region and forother WHO Member States from outsidethe Region that are concerned with devel-opment in Africa. The distinction madebetween donor and recipient countries isbecoming obsolete and is giving way to theconcept of collaboration among WHOMember States.
2 Collaboration among the countriesof the Region continues to expand. Evencountries like Niger that have limitedresources and have suffered natural disastershave contributed funds both to WHOprogrammes for research and to technicalcooperation. Guinea has sent a largenumber of technical staff to Mozambique,which in turn has passed on new findings inpublic health and planning to the otherPortuguese -speaking countries of the Re-gion. Mutual assistance has in any casealways been a feature of the African tradi-tion.
THE WORK OF WHO
15.13 In order to channel and controlall the new trends that are appearing at anever faster pace, it has been necessary toestablish and improve the machinery forconsultation and collaboration with theRegional Committee, Member States andnational technical staff. The subcom-mittees and working groups set up at theRegional level -the Regional AdvisoryCommittee on Medical Research and theRegional panels of experts and expertcommittees -are engaged on this task. Theincrease in the number of nationals ap-pointed as project leaders or projectdirectors in their own countries is anindication of the extent to which nationalsare becoming involved in collaborationwith WHO. In two countries, nationalcoordinators for WHO activities havereplaced the WHO Representatives.
Region of the Americas
15.14 The rate of population increasein Latin America is about 2.9% per annum.Even though no rise in the rate of increaseis expected in the coming years (a predictionbased on projected decreases in generalbirth and death rates), by the year z000
Latin America will have a population ofapproximately 650 million inhabitants, ordouble the present number. With thistrend, it is to be assumed that in the comingyears rural urban migration will continue toincrease periurban marginality, thus alsoincreasing the health risks- unless, ofcourse, there is a marked change in thesocioeconomic and cultural situation at therural level.
15.15 Countries are increasingly defin-ing the existing situation and are becomingaware of the fact that, in order to findimmediate solutions to their present andfuture health problems, it is necessary toimprove coordination of all resources of
18o
the health sector ; increase the participationof related social and economic sectors ; andfind a unified and balanced approach tointernational cooperation. This awarenessis being reflected in a series of structuraland functional changes both at the decision-making levels of the countries and in theadministrative and executive organs ofPAHO /WHO.
Extension of health service coverage
15.16 One essential activity in theoverall programme is to extend healthservice coverage to the most deprivedsectors in rural and periurban areas inorder to provide health care to all. To thisend, the approach of primary health careand community participation has beenadopted. However, in order to acceleratethe attainment of the desired goal, govern-ments must acquire a better knowledge ofthe nature of problems of each specificnational process and must adopt newstrategies. The IV Special Meeting ofMinisters of Health of the Americas (Sep-tember 1977) was held to evaluate pro-grammes and redefine strategies.
15.17 To strengthen community -basedcomprehensive health services, people needto be educated and motivated to utilize theservices, and countries need to developinnovative approaches to bring about theeffective participation and involvement ofthe community in the solution of its ownproblems. Strengthening of the healthsector by the better use of available andpotential resources, as well as propercoordination of the various institutionsinvolved in health care, is another relevantaction being taken by the governments ofthe Region.
15.18 As part of the community partici-pation process, emphasis is being placed on
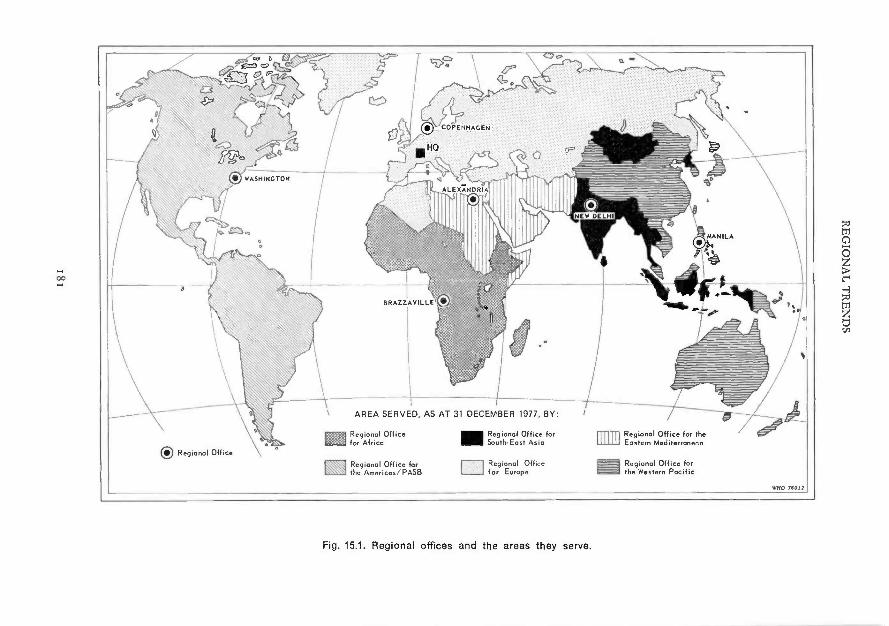
BRAZZAVILLE
ORegional Office
AREA SERVED, AS AT 31 DECEMBER 1977, BY:
Regional Officefor Africa
Regional Office forthe Americas /PASB
-Regional Office forSouth -East Asia DE Regional Office for the
Eastern Mediterranean
Regional Office M. Regional Office forfor Europe the Western Pacific
N910 )boA]
Fig. 15.1. Regional offices and the areas they serve.
THE WORK OF WHO
the leadership role of adolescents and youngpeople not only in achieving individualhealth and welfare but also in protectingcommunity health. The role of women inhealth services is also being emphasized.Traditionally, women have played a strong-er role in health programmes than in otherdevelopment programmes, but generallyat lower echelons of the health services.Their status and participation at decision -making levels should be improved.
Maternal and child health services
15.19 As the most vulnerable groupsof the population, mothers and childrenshould be given high priority in theformulation of national health plans andthe PAHO /WHO technical cooperationprogramme.
15.zo Activities designed to control therisks associated with the processes ofhuman reproduction, with the physical andpsychosocial growth and development ofchildren and young people and with theirenvironment are urgently needed in orderto protect the family group against adverseconditions that could lead to deteriorationof the mental health of the family as awhole. At the same time, other social sup-port activities - including those concernedwith providing food, housing, recreation,vocational counselling and employment -must go hand in hand with health educa-tion, promotion of responsible parenthood,and a general family health counselling.
15.21 The activities the countries havebeen undertaking in this area, as well as thetechnical cooperation the Organization hasgiven to them, should be intensified.Guidance is required on the use of appro-priate technology, education, training ofhuman resources and promotion of re-search, preferably applied research, in the
18z
field of family health. In this regard, therole of the multinational centres (theLatin American Center for Perinatologyand Human Development, the Institute ofNutrition of Central America and Panama,and the Caribbean Food and NutritionInstitute) is crucial.
Disease prevention and control
15.22 The distribution and dynamicsof the most prevalent diseases of the Regionare wide and varied. The rate of infantmortality ranges from 15 to over loo per1 000 live births, with the higher ratesreflecting a higher frequency of preventablehealth problems. The proportion of deathsfrom cardiovascular diseases shows a rangeof 3.3- 48.5 %.
15.23 Enteric diseases, as a group,represent a serious health problem in LatinAmerica and the Caribbean area. Of thatgroup, the Region is increasingly concernedwith infant gastroenteritis, which, togetherwith respiratory tract diseases and mal-nutrition, continues to be one of the prin-cipal causes of death in the Americas. Eventhough it is clearly established that poorenvironmental conditions -such as lack ofsewerage systems, inadequate water supply,proliferation of flies and other vectors,and poor personal and food hygiene-contribute to the spread and severity of theenteric diseases, a large research project isbeing undertaken to identify etiologies andthe mechanism of transmission in infantgastroenteritis in the Caribbean, underthe sponsorship of PAHO and the Inter-national Development Research Centre.
15.24 Within the context of extensionof health service coverage to underservedpopulations, and as part of the Region'scontinued efforts to reduce morbidity and
REGIONAL TRENDS
mortality caused by diseases, especially inyoung children, the Organization willcontinue to implement the Expanded Pro-gramme on Immunization in the Americas(against poliomyelitis, diphtheria, whoop-ing cough, tetanus, tuberculosis, andmeasles) on a permanent and systematicbasis, with complete coverage at the com-munity and family levels of all susceptiblepopulations. The Organization, recog-nizing the importance of providing enoughvaccine for the susceptible children, yearafter year, has developed a proposal for arevolving fund to assist countries in pur-chasing vaccines and vaccine -related mate-rial.
15.25 Because of the increased morbid-ity and mortality caused by cardiovascular,malignant and metabolic diseases, theRegion continues to give particular attentionto the risk factors that contribute to thepathogenicity of these diseases.
15.26 The Organization also worksclosely with health authorities in theMember countries in an effort to expandlaboratory services and improve theirefficiency.
15.27 Experience has shown that thereis a need to continue introducing changesin the malaria control programme. Aftersome success in the control of this disease,the programmes have stagnated in somecountries and the epidemiological situationhas deteriorated in some areas. Accord-ingly, the Organization must continuecooperating with countries in the testingof new strategies and methodologies anddetermining the most effective measuresto be adopted in each particular circum-stance.
Environmental health
15.28 PAHO's technical cooperationprogramme in environmental health con-
183
tinues to give priority attention to assistingcountries of the Region to modernize andexpand water supply and sanitation services,particularly in rural and marginal urbanareas, and to creating or strengtheningnational institutions to manage the services.The resources of the Organization will beutilized to support the efforts of Membercountries in framing national plans to meetthe goals established at the United Nationsconferences on human settlements (HABI-TAT) and on water ; specifically, toprovide water and sanitation facilities toas many people as possible during thedecade 198o -9o.
15.29 One of the strategies for attainingthis goal is to integrate water supply andsanitation development projects as a com-ponent of primary health care. Another isfor the countries and the Organization todevelop new approaches to assure anincreasing flow of national and internationalbilateral funds and better intergovernmentalcooperation.
15.3o Large -scale river basin develop-ment projects planned in the Region of theAmericas are expected to have a profoundimpact on human health. To assess anyadverse impact on human health resultingfrom changing environmental conditions,the Pan American Center for HumanEcology and Health is playing an increasingrole in cooperation with Member countrieson these and other development projects.
15.31 Industrialization and urbanizationare on the increase in the Region and so areair, water, and solid waste disposal prob-lems. Member Governments are lookingfor guidance to enable them to developrealistic environmental health criteria andstandards which are compatible with theirplans for socioeconomic development, tostrengthen existing monitoring systems
THE WORK OF WHO
and to establish additional systems tomeasure pollution of the environment.
15.32 The Pan American Center forSanitary Engineering and EnvironmentalSciences is intensifying its research activi-ties to develop new technologies, as wellas adapting and transferring appropriatetechnology, working closely with technicalinstitutions at national, subregional, andregional levels. An integral part of thiseffort will be to assist countries in estab-lishing their own information facilities aspart of a regional network of collaboratingcentres for the exchange of information.
15.33 There are serious occupationalhealth problems in the Region associatedwith injuries caused by industrial work andexposures to toxic substances, particularlyamong agricultural workers. Unfortunately,with present levels of funding, the Organi-zation can only continue to provide limitedassistance to governments in developingprevention and control programmes.
Development of human resources
15.34 The development of humanresources is of fundamental importanceto all parts of the health programme.Although work continues on all aspects ofeducation and training in the healthsciences, efforts must be especially directedtowards the planning required if the goalof extension of coverage to all the popula-tions that today do not benefit from healthservices is to become a reality.
15.35 In the course of providing tech-nical cooperation to increase human re-sources for health, a new strategy wasintroduced which facilitates action at countrylevel, comparison of the various projects,and ultimately a regional consensus basedon experience. In line with this strategy,
184
"project networks ", involving institutionsin several countries, whose work pro-gramme is adapted in each case to localconditions, have been taking shape. Ineach network, specific funds are availableand mechanisms are set up for adequatecoordination and periodic exchanges amongthose directly responsible for each project,thus facilitating cross -fertilization and in-creasing the potential for results.
15.36 Policy changes in the develop-ment and utilization of health manpowerare prerequisites for the successful imple-mentation of community -based health ser-vices. The health team approach must beused and the functions of each membermust be clearly defined. The team leader,a physician in most cases, must understandthe new concepts of patient and family care.In view of the shortage of professionalhealth manpower, new categories of healthworkers may need to be introduced into thehealth as nurse practitioners,physicians' assistants, community healthaides, dental auxiliaries. Even the roles ofthe existing health workers may need tobe expanded or changed. These changeswill necessitate the development of inno-vative education and in- service trainingprogrammes as well as appropriate per-sonnel management, supervision, and legis-lation policies. The first steps have beentaken to expand the textbook programmeto cover all health professions and alsointermediate and auxiliary personnel.
15.37 In summary, the Region'sstrategy in the development of humanresources is based on the comprehensiverationalization of the process of planning,training and utilization of human resources.Among the most important aspects are thepromotion and development of mechanismsfor coordination between service and teach-ing institutions; improvement of planningmethodology ; support of institutional and
REGIONAL TRENDS
programme development for the trainingof all levels of personnel ; establishment ofa regional network of biomedical informa-tion ; production and provision of instruc-tional material ; and teacher training andeducational research. Special emphasis isbeing given to the consolidation of nationalunits linked to the Regional Library ofMedicine and Health Sciences and the LatinAmerican Centres for Educational Techno-logy in Health, dealing with programmes inthe area of medicine, nursing, and dentistry,and the training of technicians in all healthfields.
Technical cooperation among developing countries
15.38 The increased emphasis on tech-nical cooperation among developing coun-tries constitutes a highlight in the work ofthe Organization. This approach is asignificant step towards furthering thecapabilities and skills of developing coun-tries, and enhancing their individual andcollective self -reliance. More and morethe countries of Latin America and theCaribbean are coming to depend on eachother. In view of the experience of tech-nical cooperation among developing coun-tries in the Region of the Americas, theDirector - General chose the Regional Officefor the Americas as the "focal point" withinWHO for this activity.
Programming and evaluating PAHO f WHOtechnical cooperation
15.39 The new system for programmingand evaluating PAHO /WHO technicalcooperation exemplifies how the Organi-zation is trying to meet the challengespresented by the rapidly increasing andchanging demands in the field of health.This new system emphasizes the importanceof the full participation of the governmentsat all stages of programming and evaluating
185
PAHO technical cooperation in nationalprogrammes. It calls for an integrated pro-gramme of cooperation rather than frag-mented projects of isolated activities ;coordinates the components of the pro-gramming, budgeting, information, con-trol, and evaluation processes ; and issufficiently flexible to adapt to the individualcircumstances of each country while re-maining compatible with the systems ofWHO, the United Nations, and otherexternal cooperation agencies.
15.40 When the Pan American HealthOrganization celebrated its 75th anniversaryon z December 1977, it reaffirmed itsbelief that health is a " . . . universal right,and not a privilege to be enjoyed by thefew ".1 With the strongest spirit of coopera-tion, it will continue to strive towards thegoal of bringing to every man, woman, andchild the benefits of basic health services.
South -East Asia Region
15.41 A remarkable achievement duringthe period 1976 -77 was the eradication ofsmallpox from three countries in theRegion. With the expected declarationof a similar status in respect of two morecountries, it is hoped that the curtain can bepulled down on this disease, which haskilled or maimed hundreds of thousands ofpeople in the Region over the centuries.
15.42 The conquest of smallpox sym-bolizes a new upsurge of hope and aspira-tion among the people for better health,and a renewed resolve and manifest willon the part of the governments to provideit.
1 Pan American Health Organization. Ten-yearhealth plan for the Americas. Washington, DC, 1973(Official Document No. 1 i8), p. 4.

THE WORK OF WHO
15.43 Health is now accepted bygovernments in the Region as an inter -sectoral concern that depends on overallsocioeconomic development. Conversely,there can be little economic productivity ina population with a low state of health.In this context, the development of countryhealth programming is of great relevance.Wherever it has been undertaken in theRegion, such programming has not onlyresulted in a better mobilization of resourcesto meet priority health problems but hasalso provided a more purposeful directionto the coordinating and collaborative effortsof WHO.
Strengthening of health services
15.44 The concept of primary healthcare has been widely accepted in the Regionand the programmes in this field have beenmaking headway in all countries. Burma,Nepal and Thailand have formulated pro-jects as an outcome of country health pro-gramming ; in Indonesia the primary healthcare programme has been developed incollaboration with UNICEF as an inter -sectoral activity. The potential role ofvoluntary health workers, including tradi-tional medical practitioners, in this import-ant area is being examined in some coun-tries. The crucial issue of the preparationof voluntary health workers, as well as theformulation of manuals and handbooks, isbeing pursued. Programmes for the promo-tion of traditional medicine are beingtaken up, including the research, trainingand service aspects as a composite package.One important development in primaryhealth care is the close attention given tohealth service research, which has beenidentified as a priority area by the RegionalAdvisory Committee on Medical Research.
15.45 All the countries in the Regionare giving priority to the integrated devel-
186
opment of the infrastructure of healthservices with stress on base- institutionssuch as district or township hospitals assupporting units for primary health care.The base -institutions are being used notonly for providing professional leadershipin planning the programme but also as atraining base and for logistic support to theprimary health care worker.
15.46 In the field of medical care, thegeneral trend is to train the health workerso that he can render basic, primary medicalcare adequately and safely. In some coun-tries, for example in the DemocraticPeople's Republic of Korea and in Mongo-lia, the institution of specialized medicalcare services at the community level isnoteworthy. An important Regional pro-gramme concerns rehabilitation, in whichthe emphasis is on preventing disability andinvolving the community. This programmehas been accepted in many countries as anintegral part of the general health services.
15.47 Countries with national policiesin family planning continued their effortsto reduce the problem of uncontrolledfertility with a view to improving thehealth of mothers and children. WHO'scollaborative programme, mainly fundedby UNFPA, supported these efforts.
15.48 Support has also been given forbuilding up the national training base andservice facilities for the medical terminationof pregnancy programme in India ; for thebasic and in- service training and educationof various categories of health workers,including traditional practitioners, in SriLanka ; and to research on family planningthrough the WHO Special Programme ofResearch, Development and ResearchTraining in Human Reproduction, inIndia, Indonesia and Thailand.
15.49 Collaborative studies on perinatalmortality and morbidity and the incidence
REGIONAL TRENDS
of low birthweight have continued in threecountries of the Region, the intention beingto produce accurate information on thepattern of pregnancy and its outcome andon the extent of the problem. During theperiod under review, an interdisciplinarygroup evaluated the work done on neo-natology in the Region in recent years andfinalized guidelines for the future.
15.5o Recognizing the fact that a reduc-tion in infant and child mortality andmorbidity rates is absolutely necessary forimproving the quality of life of the people,the Regional Committee recommended thatspecial attention be given to the problemsof child health. Accordingly, a Regionalprogramme on child health has beenprepared and is under consideration bygovernments.
15.51 With governments now includingschool health in their health plans, pro-grammes in this field have received agreater impetus. Collaborative efforts weredirected towards expanding the training ofelementary schoolteachers, strengtheningschool health teams and providing in-service training for all categories of workersinvolved in the school health programme.
15.5 z An essential element in the pro-motion of maternal and child care in theRegion has been WHO's collaboration inproviding proper training and educationin this field. The most significant develop-ments in this regard have been in the com-munity- oriented undergraduate teachingprogrammes in child health for medicalcolleges in Bangladesh and India.
15.53 In nutrition, even though thedirect input from WHO has been limited,the Organization's technical leadership inthis field is being recognized by the coun-tries of the Region as well as by the UnitedNations and other agencies. It is encourag-
187
ing to report that WHO's support to andparticipation in various missions, studiesand project formulations concerning nu-trition undertaken by UNICEF, WFP, FAOand IBRD have been on the increase. Asa follow -up of the recommendations of theTechnical Discussions held during thetwenty -ninth session of the Regional Com-mittee, an intercountry meeting on theorganization and delivery of nutritionactivities in the health sector was organizedat the Regional Office in November 1977.
15.54 The Regional Advisory Com-mittee on Medical Research, set up inJanuary 1976, has held three meetings andhas identified the priority areas for researchin the Region as being communicablediseases, nutrition, control of human fer-tility, environmental health, delivery ofhealth services, and a miscellaneous groupwhich includes chronic liver diseases andliver cancer. Study groups have been setup to develop detailed research protocolsin these fields.
'5.55 In order that more realistic priori-ties for research could be set and a stillbetter organization of research in Membercountries instituted, a regional researchprogramme was being formulated, based onreviews of national research which couldbenefit from the WHO Special Programmefor Research and Training in TropicalDiseases.
1 5.5 6 The regionalization of WHO'sresearch programme has created a greaterawareness of the need to solve urgentproblems, both among Member States andamong their scientists.
Health manpower development
15.57 A crucial factor in improving thecoverage and quality of health services is
THE WORK OF WHO
the availability of enough health personnelwith community- oriented training. TheRegional Office has therefore given highpriority to collaboration with Membercountries in order to encourage them toreorient the training of health manpowerso as to respond to the community's needs.Need -based and task -oriented training pro-grammes have been undertaken to develophealth teams consisting of appropriatehealth personnel, including new categoriesof basic health workers, in order to providecommunity- oriented primary health care.A three -tier system of manpower, withemphasis on local and intermediate levels,has been evolved by most countries. TheOrganization has collaborated in develop-ing suitable curricula, teaching and learn-ing materials, manuals and procedures, andhas also provided subsidies for organizingthe training programmes.
15.58 The Regional Office surveyedtraining programmes in various countriesand the job descriptions of various multi-purpose primary health care workers ; italso developed guidelines for evaluatingthese programmes. In addition, the Organi-zation collaborated with some countries inthe training and use of voluntary /commu-nity health workers and organized a meetingto discuss the functions and utilization ofsuch workers. Information on traditionalsystems of medicine and the practitionersof such systems was collected, and an inter -country seminar discussed their utilizationin primary health care.
15.59 With the aim of providing super-visory links between multipurpose andvoluntary health workers and primaryhealth centres, countries have been assistedin the training of middle -level workers(health assistants or medical assistants). Anintercountry seminar was organized todefine the roles of such personnel.
188
15.6o An intercountry seminar onmedical education suitable for developingcountries led to the development of asuggested curriculum for training in com-munity medicine. Various steps have alsobeen taken towards attaining regional self -sufficiency in postgraduate and specializedtraining programmes, and governmentshave been encouraged to determine care-fully the areas and disciplines in which suchtraining should be developed. In the awardof fellowships emphasis is being laid ontraining within the Region ; in 1977, 37%of the fellowships awarded by the RegionalOffice were for studies within the Region.
15.61 In health statistics, three elementscan be identified as contributing to a shiftin emphasis in the assistance providedto countries in the Region. These are(i) the increasing participation of statisti-cians as members of multidisciplinaryprojects rather than in projects of vital andhealth statistics per se ; (ii) a conscious effortto clarify, in relation to practical applica-tion, the concept of health informationsystems vis -à -vis traditional health statisticalactivities, and (iii) attempts to bring anelement of realism to the collection ofinformation in situations where medicallyqualified personnel are not available inadequate numbers.
15.62 Thus statisticians have helped insuch projects as country health program-ming, research on communicable diseaseepidemiology, development of protocolsfor surveying selected health problems inrural areas, and the development of fieldprojects for the study of infant and earlychildhood mortalities.
15.63 A working group on lay reportingof morbidity and mortality statistics drewup, for use by nonmedical personnel, adetailed list of "symptom associations andconditions ", and two minimal lists, one for
REGIONAL TRENDS
reporting causes of death and the second forreporting "reasons for contact with healthservices ". Field trials to test these lists arein progress in Burma, Sri Lanka and Thai-land and some initial steps have also beentaken in India.
Disease prevention and control
15.64 Communicable diseases continueto cause major public health problems inthe Region. The main constraints in con-trolling these diseases are poor environ-mental conditions and low coverage by thehealth services. Most of the disease controlprogrammes were organized as verticalcampaigns, but the present trend is tointegrate these programmes. First, suchprogrammes as those against leprosy andtuberculosis can be combined into oneprogramme for the control of mycobacterialdiseases. Similarly programmes for thecontrol of vector -borne diseases can becombined according to their modes oftransmission. Secondly the ultimate goal isto have an integrated health service takingcare of all these diseases.
15.65 The interregional WHO Vectorand Rodent Control Research Unit inJakarta and Semarang has its own researchprogramme, and collaborates in field activi-ties for the control of malaria, filariasis,dengue, and Japanese encephalitis.
15.66 The Rodent Control Demonstra-tion Unit in Rangoon is engaged, in coop-eration with the national authorities, in thecontrol of flea -bearing rodents in Burma,in relation to endemic plague.
15.67 Countries of the Region havebeen trying to strengthen their epidemio-logical surveillance for more than a decade.Epidemiological units and divisions havebeen established in ministries of health butthe number of diseases under surveillance
189
and the accuracy of the data are not yetsatisfactory. By making epidemiologicalsurveillance a responsibility of the healthinformation system governments hope toimprove surveillance. WHO is assistingin the training of personnel and in pro-viding the necessary technical inputs.
15.68 Programmes against leprosy andtuberculosis, which are both major publichealth problems in most of the countries,have not yet been effective, mainly onaccount of the low coverage of the popu-lation by immunization in the case oftuberculosis and case -finding and case -holding in the case of both diseases. Thereis also the emerging problem of resistanceof Mycobacterium leprae to drugs. Researchinto the chemotherapy and epidemiologyof these diseases is planned or is underwayin some countries.
15.69 In regard to gastroenteritis,which is a major killer of children, thecountries of the Region are increasing theavailability of oral rehydration therapy inthe rural areas. Some operational researchis planned to find out the most effectivemeans of distribution of oral rehydrationelectrolytes.
15.7o Cholera has been reported fromBangladesh, Nepal and Sri Lanka, whileBurma is the only country in the Regionwhich is still reporting human plague. Inother countries such as India and Indonesiasylvatic plague foci exist.
15.71 The problem of sexually trans-mitted diseases appears to be increasing.In places where surveillance has been good,such as Sri Lanka, this trend has beenevident. In recent years there has beenincreasing awareness among governmentsof the seriousness of the problem, and somecountries have developed control pro-grammes in collaboration with WHO.
THE WORK OF WHO
15.72 The extent and effectiveness ofimmunization programmes in the differentcountries of the Region is varied. In onecountry there is an efficient national immu-nization programme covering tuberculosis,diphtheria, pertussis, tetanus, poliomyelitis,measles and meningococcal meningitis, andits results have been very good. But inother countries, immunization against onlythree or four of these diseases has beenintroduced and the coverage is not yetsatisfactory, often reaching, except in thecase of smallpox, only a relatively smallproportion of children in limited urbanareas.
15.73 The Expanded Programme onImmunization was accorded high priorityin the Region after the successful conclu-sion of the smallpox eradication programmein almost all countries.
15.74 Intensive smallpox surveillancewas carried out during 1976 in Bangladesh,Bhutan, India and Nepal. In April 1977 aninternational commission certified thesmallpox -free status of Bhutan, India andNepal. Bangladesh continued country-wide surveillance throughout 1977. Burmahad its last smallpox case in 1969. Aninternational commission assessed the pro-gramme in Bangladesh and Burma inNovember- December 1977 and certifiedboth countries as smallpox -free. So as tobe prepared for any unforeseen recurrenceof smallpox, 5o million doses of freeze -dried vaccine will be preserved at theRegional Office cold store, as from 1978.
15.75 The overall malaria situation inthe Region continues to be serious, but theincreased national commitments to con-trolling the disease have generated sub-stantial additional assistance from bilateralsources, improving the medium -term pros-pects of antimalaria programmes. Therewas a further reduction in the number of
1 q0
microscopically diagnosed cases in Indo-nesia (Java and Bali), Maldives, Nepal andSri Lanka. Though the relative prevalenceof Plasmodium falciparum has decreased insome countries, chloroquine- resistant fal-ciparum malaria spread to areas withpopulations totalling nearly 45 million,and further areas with populations totallingabout 90 million are at risk. The problemof vector resistance to DDT is also in-creasing, so that regular and carefulmonitoring of the susceptibility of vectorsto insecticides assumes greater importance.Efforts are being continued to retrain per-sonnel and to promote the local productionof antimalaria drugs.
15.76 Filariasis remains a public healthproblem in many countries, and controlactivities have not produced any noticeableimpact. The difficulty has been in under-standing the epidemiology of the disease.India is studying the impact on the epi-demiology of the disease of filaricidal drugsadministered to a whole communitythrough their salt supplies. Kala azar(visceral leishmaniasis) has re- emerged inIndia in the northern districts of BiharState after a lapse of some ten years. WHOis collaborating with the Government ofIndia in ensuring supplies of appropriatedrugs. There is a possibility that neigh-bouring countries which have similarecological conditions, such as Bangladeshand Nepal, might also become affected.
15.77 The training of public healthveterinarians continues but otherwise theprogramme has not been very effective inthe Region. Only a few countries havefollowed recommendations to establishveterinary public health units in theirministries of health.
15.78 In the programme for the devel-opment of health laboratory services themain emphasis is on the training of lab-
REGIONAL TRENDS
oratory manpower, the establishment ofcertain specialized laboratories, quality con-trol, and standardization of procedures.In Thailand, work on the construction ofthe National Breeding Centre for Lab-oratory Animals began at Mahidol Uni-versity, Bangkok. The Centre is expectedto be ready in 1979. In India, the VirusResearch Centre has started a two -weekcourse on the breeding of mice, and acolony of Chinese hamsters is now estab-lished at the animal facility of the CentralDrug Research Institute, Lucknow.
15.79 The prevention of blindness isbeing dealt with in several Member Statesthrough national committees which areformulating eye health policies and plan-ning national strategies. This has resultedin better coordination at the national leveland greater collaboration with interna-tional and nongovernmental agencies.WHO is providing direct technical co-operation in these programmes, in whichhealth education receives priority attention.
15.8o Cancer is an emerging problemin the countries of the Region, in some ofwhich a comprehensive cancer control pro-gramme has been formulated as an integralpart of the existing public health services,with WHO collaboration.
15.81 Chronic liver diseases (includingliver cancer) have been identified by theRegional Advisory Committee on MedicalResearch as a public health problem in theRegion and a project of retrospective andprospective research on these conditionshas been formulated in which almost allthe countries are collaborating.
15.82 Cardiovascular diseases are alsobecoming a problem of major public healthimportance in the Region. Some countriesare planning institutes for training spe-cialists and developing cardiovascularservices. Sri Lanka is beginning to study
191
the epidemiology of cardiovascular diseases.A collaborative investigation on peripheralocclusive vascular disorders in India andNepal is planned.
15.83 In the field of radiation health,WHO has continued to assist with nationalpersonnel film badge services in mostcountries, and in planning radiology, radio-therapy, radiological physics and nuclearmedicine services in India. In collaborationwith IAEA, the possibilities for usingnuclear techniques in epidemiological in-vestigations were explored. Self -reliancein the repair and maintenance of nuclearand electro- medical equipment in hospitalsis also being promoted jointly with IAEA.
15.84 Countries of the South -EastAsia Region are becoming more interestedin the integration of mental health activi-ties with the general health services.Orientation and training in mental healthfor all categories of health personnel con-tinued in projects in Bangladesh, India,Indonesia and Thailand. Psychiatry hasnow been included in the medical curricu-lum in all countries of the Region ;nevertheless there remains a paucity oftrained psychiatrists and teaching personnel.The Department of Psychiatry at the Post-graduate Institute of Medical Educationand Research, Chandigarh (India), wasdesignated as a WHO Collaborating Centrefor Research and Training in Mental Healthin 1977. UNFDAC projects in Thailandand Burma are paying increasing attentionto the epidemiology of drug addiction andthe evaluation of treatment regimes andmethods.
Environmental health
15.85 In the field of environmentalhealth, water supply and excreta disposalhave remained the main areas of activityand will continue to be so for years to
THE WORK OF WHO
come, since water and filth -borne diseasesare still major public health problems inSouth -East Asia. Interest among govern-ments is growing and they are making allpossible efforts, with the available nationaland international and bilateral resources,to extend their programmes in order toachieve the national targets recommendedby the World Health Assembly for theSecond United Nations DevelopmentDecade, 1971 -80. WHO is increasinglycooperating in the planning and imple-mentation of these programmes.
15.86 WHO's collaboration withMember States in attracting investmentfunds is being intensified, through projectfeasibility studies and pre- investment plan-ning as well as through sector studies underthe IBRD /WHO Cooperative Programme.
15.87 The Organization's activities arealso increasing in areas such as environ-mental pollution control, environmentalplanning, pre- investment studies and envi-ronmental health information systems, tosupport the important recommendationsof HABITAT, the United Nations Con-ference on Human Settlements.
15.88 Current studies on the use ofappropriate technology in environmentalhealth at the village level, especially forwater supply and wastes disposal, areexpected to make these environmentalhealth efforts more relevant to the social,cultural, economic and environmental con-ditions of the communities in the Region.
15.89 In the South -East Asia Region,extrabudgetary resources for health andrelated sectors come mainly from bodieswithin the United Nations system,particularly UNDP and UNFPA. Althoughthe financial crisis in UNDP continued toaffect programmes and projects, it has beenpossible in 1977 to provide more funds
192
from UNDP sources than in the previousyears.
15.90 The multisectoral and integratedapproach to the solution of health prob-lems, coupled with judicious forwardplanning and closer coordination at countrylevel, has led to the formulation of pro-jects effective enough to attract more fundsand also to improved utilization of bud-getary provisions.
European Region
General programme development
15.91 In accordance with the generalWHO policy of Member States ultimatelybecoming self -reliant, the EuropeanRegional Office withdrew the WHORepresentative in Algeria at the end of1976, while 1977 saw the closure of theoffice of the last WHO Representative inthe Region -in Turkey. With the gradualphasing out of this type of WHO repre-sentation in the countries of the Region,the direct dialogue with the governmentsof the Member countries has been inten-sified through meetings in the countryinvolved or at the Regional Office. Thissystem ensures fruitful discussions withgovernment officials on the developmentof programmes in the individual countries.
15.92 Another new feature in theimplementation of the Region's programmeis the increased involvement of membersof the Regional Committee in the develop-ment of the intercountry programme. In1976, no fewer than seven groups of suchmembers met to advise on programmeplanning in their specific fields. In March1977, a consultative group on programmedevelopment reviewed trends and policiesin the European Region as a basis for thedevelopment of the future programme and

REGIONAL TRENDS
for increased collaboration with nationalinstitutes and agencies. The group stressedthat, although it is agreed that the greatesthealth needs are in the developing world,health authorities in Europe also faceurgent health -related problems ; that solu-tions to these will eventually benefit thedeveloping world as well ; that in settingpriorities for the European Region, therelevance to developing countries of thesolution to a problem, actual or potential,should be carefully considered. The groupendorsed the continuation of the medium -term programmes being implemented bythe Regional Office. Based on its discus-sions, the areas proposed for funding in1978 -79 from the Regional Director'sDevelopment Programme are : researchpromotion and development ; the pre-vention of road traffic accidents and thehealth care of the elderly (programmes forwhich the Regional Office has globalresponsibility) ; appropriate technology forhealth ; national drug policies and manage-ment ; and urgent and unpredictable healthproblems.
15.93 The Regional Advisory Com-mittee for Medical Research met inFebruary 1977 and established five mainpriority areas for study, and planninggroups have been established on theresearch priorities as well as on informationsystems for medical research.
15.94 With the advent of German asthe fourth working language in the Euro-pean Region, it proved necessary to con-vene a meeting to establish a basic termi-nology list with German equivalents forpublic health and administrative termi-nology in use in WHO.
Strengthening of health services
15.95 In Europe, a variety of types ofsystem for the delivery of medical care have
193
emerged and are developing : nationalhealth services, sickness insurance schemes,and private medical practice. Througheach of these systems efforts are made toformulate criteria for assessing the healthstatus of a population and the impact onhealth of medical institutions, to raisemanagement standards and to make useof experimental models, systems analysisand operational research.
15.96 There is now widespread accept-ance of the strategy of using pilot areasfor research purposes and encouragingdifferent institutions to collaborate withWHO in carrying out international re-search. A study has been made of healthplanning in eight European countries withdifferent systems of health care, in orderto provide insight into the various ap-proaches used, and a separate study wasmade of the system applied in the Gabrovodistrict in Bulgaria.
15.97 The training programmes forsenior health planners in the EuropeanRegion have been revised so as to stressactive student participation. The newmodel was used with success for the coursesin 1976 and 1977. The need for improvingmanagement (planning and evaluation in-cluded) at all levels of the health servicesis becoming increasingly evident in thecountries of the Region. A working groupstudied the educational needs of managersin the health services ; emphasis was placedon the need to give such training to middle -level medical and nursing managementstaff.
15.98 There is general concern aboutthe rising cost of health care without acommensurate rise in health benefits, andit is necessary to strengthen the capacity ofnational health administrations in healtheconomics. A recent working group con-tributed to a better understanding of the
THE WORK OF WHO
role of health economics in national healthplanning and policy- making. A study hasbeen undertaken on consumers' respon-sibility for, and participation in, the plan-ning of medical care delivery.
Health care of the elderly
1 5.99 Following the Director -General'sdecision in 1976 to transfer to the EuropeanRegion the responsibility for developinga global programme for the health care ofthe elderly, the Regional Committee forEurope in 1977 accepted the detailed pro-gramme and agreed to the establishmentof a Regional consultative group, toregular liaison meetings not only withgovernmental and nongovernmental organi-zations but also with interregionalliaison groups, and to regular meetings ofdirectors of national institutes of geronto-logy, two of which have already been held,in Copenhagen and in Bethesda, USA.Further, a research planning group hasbeen established as part of the Europeanprogramme in biomedical and health ser-vices research.
15.100 By the end of 1977, a detailedsearch of population -based epidemiologicalstudies for Europe had been completed ;it will be expanded to cover the globalsituation. Related activities within otherRegional programmes have included thepreparation of a detailed protocol for anepidemiological study to be undertaken bya series of national institutes ; a workinggroup on nursing aspects of the care of theelderly ; and study of the nutritional needsof the elderly.
Road traffic accidents
15.101 Special consideration is alsobeing given to the development of another
194
worldwide programme for which theDirector -General transferred the responsi-bility to the Regional Office in June 1976,the programme on the prevention of roadtraffic accidents. The Regional Committeefor Europe, at its twenty -sixth session,approved the establishment of a Regionalconsultative group, which met to adviseon the development of the medium -termprogramme ; a liaison meeting was held,in December 1976, with representatives ofa large number of intergovernmental andnongovernmental organizations. The needto increase collaboration and improve co-ordination at the international level wasstrongly felt ; a meeting with represen-tatives from other regional offices was alsoconvened, and a plan of action was estab-lished which identified the responsibilityof each WHO region. The project managerof the programme visited three of the otherregional offices.
15.102 A technical advisorywas convened at which participating ex-perts and representatives from road safetyinstitutes discussed the activities to beimplemented within the programme andthe designation of ad hoc technical groupsfor specific problems. Close contact andcollaboration have been maintained withother intergovernmental organizations,especially the Organisation for EconomicCooperation and Development and theECE.
Health laboratory services
15.103 The role of the laboratory inthe prevention and control of hospital-acquired infections was discussed by aworking group in 1976 which developedguidelines to fill the gap existing in thefield of hospital infections, by outlining therole of laboratory services as the commonlink between the hospital administrations,
REGIONAL TRENDS
the surveillance and control programmesand the continuing education of the staff.
Family health
15.104 The relationship between chil-dren and the environment in which theygrow up (including the social dimension)forms the theme of a series of meetings onproblems of children of school age, whichwill culminate in 1978 in the Conference onthe Child and Adolescent in Society.
15.105 A contractual agreement hasbeen drawn up with the InternationalChildren's Centre for the preparation ofdocumentation on family health and familyplanning for use in developing countriesin the Region, especially those where pro-jects are supported by UNFPA.
15.106 In such countries, primaryhealth care became the national entry pointfor the development of family planningprogrammes. To overcome the scarcity ofhuman resources in the field, there havebeen extensive training activities for multi-disciplinary teams of health and social per-sonnel working in family health /familyplanning programmes and the decentral-ization of such training from intercountryto country level has been achieved.
15.107 During a meeting on the role ofnutrition in public health, convened in1976, it became clear that the main charac-teristics in the field of nutrition in mostcountries in Europe are : an increase in thedeleterious effects on health and on physicaland mental development of overnutrition ;an increase in the use of ready -made foodsand collective feeding ; and the realizationthat social, medical and psychologicalfactors have much more influence in pro-ducing unfavourable nutrition habits inthe elderly than purely financial factors orthe availability of food.
195
15.108 The problem areas in healtheducation remain the inadequate integra-tion of health education in public healthservices ; the absence of a scientific evalu-ation of health education measures ; andthe lack of training facilities in healtheducation. To tackle these problems anadvisory committee on health educationand social sciences was convened in 1976and working groups were organized in1976 and 1977 to consider, respectively,the place of health education in healthadministrations and the principles andmethods of health education.
Health manpower development
15.109 The Region's medium -termhealth manpower development programmewas reviewed by a steering committee inApril 1976. The programme was modifiedand now has three subprogrammes -forcontinuing education, for teacher training,and for strengthening communication andcollaboration between health and edu-cation authorities and among various typesof health worker. Within each of the threesubprogrammes a number of activities,including several studies and workinggroups, took place in 1976 -77.
15.110 The impact of such activitiesat national level depends largely on theeducational policies and commitments ofMember States. A flexible approach withinthe framework of the medium -term pro-gramme might best respond to the needsexpressed by countries in the Region. Ifthe programme is to remain realistic andcountry- oriented, information on healthmanpower development will play an in-creasingly important role. Much of theinformation needed is already available inthe capacity study on graduate medicaleducation in the European Region, and inthe inventory of teacher training centres,
THE WORK OF WHO
both of which are on -going activities.These, together with the assessment ofcare patterns, and of examination patterns,assumed even greater significance when,on i July 1976, the Commission of theEuropean Communities agreed that thereshould be free movement of physicianswithin the Communities as from 1 January1 977.
Nursing
15.111 The renewed interest in nursing/midwifery confirms the timeliness of theintroduction in 1976 of the Europeanmedium -term programme in nursing /mid-wifery and of the Regional Committee'sTechnical Discussions in September 1976on the role of nursing staff in the healthfield in the 198os. The programme, whichis scheduled to run until the end of 1983,has gathered momentum over the first twoyears in collaboration with national groupsand individual experts. It is composed offour major components -the nursing pro-cess, organization and management ofnursing /midwifery services, education ofnursing /midwifery personnel, and resourceplanning. Participating centres will bedesignated throughout the Region ; elevencountries have already formally expressedtheir interest in providing such centres.Management and technical advisory groupsof nationals have been organized and closeliaison has been developed with profes-sional nursing organizations in Europe.Preliminary studies and the collection ofessential information have been carriedout and a workbook on the nursing processhas been prepared.
15.112 The nursing component of otherprogrammes in the Region, e.g., mentalhealth, community health, health man-power development, has been enlarged andstrengthened through greater use of nurse
196
consultants and the inclusion of nurses inworking groups and other types ofmeetings.
Communicable disease prevention and control
15.113 Though communicable diseasesare not a major public health problem inthe European Region, international traveland the trade in food and animal feedscontinued to cause a fairly large number ofminor outbreaks, mostly of enteric in-fections of bacterial and viral origin. Therecommendations of the 1976 workinggroup on aviation catering have been verywell accepted and some European air -service companies have already includedthem in the instructions to their cateringpersonnel. Sexually transmitted diseaseswere discussed at a symposium in 1976,which resulted in the preparation of amanual for general practitioners on themanagement of these diseases. The eco-nomic aspects of communicable diseaseswere considered at two meetings duringthe period, those of viral hepatitis at ameeting in 1976, and sexually transmitteddiseases in 1977.
15.114 In 1977, the malaria epidemicin the south -eastern part of Turkey hadbecome so serious as to justify emergencyrelief operations, with financial supportfrom the Director -General's developmentprogramme and other sources.
Noncommunicable disease prevention and control
15.'15 The second phase of theRegion's long -term programme on cardio-vascular diseases culminated in the estab-lishment of a number of pilot areas forcomprehensive community control. Al-though it is far from being a breakthroughin the community- oriented approach forthe control of cardiovascular diseases -in
REGIONAL TRENDS
contrast to the individual or selected -group- oriented approach -this develop-ment does nevertheless indicate the grow-ing involvement of cardiologists and publichealth administrators in such activities.
15.116 In the field of primary pre-vention of cardiovascular diseases, theresults of a number of studies corrobor-ated the theory of preventability. Evidenceis slowly accumulating on the intricateinterrelation of environmental, genetic andbehavioural factors in the causation ofvarious chronic diseases, smoking beingthe best example.
15.117 Mortality due to cardiovasculardiseases, and especially ischaemic heartdisease, continued to decrease or level offin the countries with the highest mortalityrates. Of special interest is the project inNorth Karelia, Finland, where systematichealth education has led to changes in life-style, with a considerable resultant de-crease in mortality due to cardiovasculardiseases.
15.118 The trend in most EuropeanMember States towards community -oriented delivery of mental health carecontinues ; it is agreed that there is a needto develop and extend the range andquality of mental health care, social wel-fare and other community services.
15.119 Information collected on mentalhealth services in pilot areas in someEuropean countries would indicate thatabout 2o% of the population may haverecourse to mental health services in thecourse of a lifetime and that every thirdhospital bed in the European Region isused for a patient suffering from a mentaldisorder. Yet many European countries donot adequately formulate the mental healthcomponent in their national health policyand there is still a lack of adequate tools for
197
the monitoring and management of mentalhealth care.
15.120 There is general recognitionthat increased efforts in primary preventionare needed ; emphasis is being placed onmental health education, particularly in theyounger age groups, taking into accountthe psychosocial factors and paying specialattention to the abuse of drugs and alcohol.
Promotion of environmental health
15.121 Pre- investment studies have beencarried out in several countries of theRegion, in order to attract externalfinancing for water supply and wastes dis-posal projects. These activities haveresulted in IBRD investment in watersupply projects in Algeria, Morocco andPortugal.
15.122 A consultation in 1976 onenvironmental health aspects of humansettlements in Europe recommended aprogramme of activities for housinghygiene and public health aspects of townand regional planning ; another, on basicsanitation problems of European com-munities, recommended a programme forwater supply and community wastes dis-posal, and for the training of sanitariansand operators. A proposal for a medium -term intercountry programme on basicsanitation in Europe has now beendesigned.
15.123 In 1976, a consultation reviewedthe results of a survey of regional man-power requirements in environmentalhealth as a basis for evaluating currenttraining programmes and preparing newones. The group recommended the pre-paration of a guide for environmentalhealth manpower planners, to assistMember States in designing their training
THE WORK OF WHO
programmes at various levels in order toproduce the required type and number ofpersonnel to meet their manpower needs.
15.124 As part of the Europeanmedium -term programme on environ-mental pollution control a Manual onUrban Air Quality Management was pub-lished in 1976 as No. 1 in the new WHORegional Publications, European Series. Mean-while, preparations have started for thepublication of a complementary volumedealing with air pollutants from industrialsources. Glossaries of air pollution, waterpollution and solid waste managementterms will be published in 1978 -79.
15.125 In 1976 a working group dis-cussed the intake by man of minute con-taminants from water and food. Fol-lowing its recommendations, studies andmeetings in 1977 concentrated on thehealth hazards from chlorination andozonation derivatives in the treatment ofdrinking -water and the possible health -related problems from the use of desalinatedand demineralized drinking- water.
15.126 Interlaboratory comparisons ofwater pollution analyses were continuedwith the collaboration of over 3o nationallaboratories in about 20 European coun-tries, and of IAEA (for radiochemicalwater samples). The results of a study onthe eutrophication of natural lakes wereissued in 1976.
15.127 As part of the comprehensiveUNEP- supported activities in the Mediter-ranean, two projects, executed by theRegional Office for Europe in cooperationwith the Regional Office for the EasternMediterranean, started in 1976, one dealingwith sanitary surveillance of beaches andcoastal water, the other with an inventoryof land -based sources of pollution.Eighteen Mediterranean countries, and
198
also other international organizations, aretaking part in this programme.
15.128 Two European projects forUNEP's Global Environmental MonitoringSystem, in the fields of air pollution andwater pollution respectively, were estab-lished in 1976, and a preliminary survey ofthe networks in the European Membercountries was prepared in 1977.
15.129 The environmental pollutioncontrol programme was analysed at a con-sultation in September 1977 with a view toemphasizing the problems and future trendsand proposing priorities for future activitiesin the industrial and urbanized EuropeanRegion with its special and growing prob-lems, among which are the increasingnumber of toxic chemical substances beingintroduced in industrial production andcontributing to pollution of air and waterand of the products used by the generalpopulation.
Prophylactic, diagnostic and therapeutic sub-stances
15.13o The series of annual symposia onclinical pharmacological evaluation in drugcontrol, which began in 1972, continued.Two symposia were arranged during thebiennium to evaluate individual drugcategories such as antihypertensives, anti -rheumatics, antidepressants, contraceptivesand drugs used to combat coronary heartdisease.
15.131 So far, the development ofclinical pharmacological units has mostlybeen limited to large university hospitals,with a resulting selective coverage of thepopulation. A working group convenedin April 1977 defined the functions ofclinical pharmacological services in a muchwider context and highlighted the role of
REGIONAL TRENDS
clinical pharmacologists in the develop-ment of drug monitoring programmes,drug use studies and special teaching pro-grammes for the hospital team and thegeneral practitioner.
15.132 A working group on bacterialvaccine production and control, convenedin 1977, dealt with new and more rationalmethods of vaccine production and withcollaboration in control procedures.
Eastern Mediterranean Region
15.133 The expansion of compre-hensive national health services is one ofWHO's main areas of collaboration withgovernments, and it is normally a verylengthy process. In substantial parts ofthe Eastern Mediterranean Region, how-ever, economic events have taken a for-tunate turn in the past few years, and eco-nomic development has raced along at anunparalleled pace. This has given impetusto the development of health services inthe Region.
15.134 Iran, Kuwait, Libyan ArabJamahiriya, Qatar, Saudi Arabia and theUnited Arab Emirates have, over andabove their normal contributions to WHO,curtailed their own demands on the WHObudget so that activities in other countriesof the Region can be expanded. Thegenerous financial support given by themore economically favoured to the lessfortunate of the Region's Member coun-tries is an indication of the prevailingspirit of collaboration. Mutual assistanceand technical cooperation continue tocharacterize intercountry relations in theRegion.
15.135 In each of the countries, richand poor alike, there has been rapid socialdevelopment, as well as substantial changes
199
in the patterns of diseases, and a majorimprovement in the resources available forhealth. In addition, coordination of thework of the United Nations and inter-governmental, nongovernmental and bi-lateral agencies has notably increased andthere is a definite trend for these agenciesto combine forces in a multidisciplinaryapproach to the solution of healthproblems.
15.136 Most of the countries of theRegion have now prepared national healthplans which aim at extending health ser-vices to all sections of the population.Consequently, there is a greater desire todevelop intersectoral activities and planningfor socioeconomic development, while thisin turn will benefit from the developmentand strengthening of health services andadministration with WHO's collaborationover the past twenty -eight years.
Primary health care
15.137 The concepts of country healthprogramming and primary health care havebeen accepted by many countries in theRegion, and WHO has assisted the Govern-ments of Afghanistan, Pakistan, Sudan andYemen in preparing country health pro-grammes which lean strongly towardspromotion of primary health care. Countryhealth programming is planned for 1978in Democratic Yemen, Iraq and Somalia,while in Afghanistan and Yemen it wasused as a basis for the preparation ofnational health plans. It was also useful inthe structural and functional reorganiza-tion of the Ministry of Health in Yemen.
15.138 In order to promote the con-cept of primary health care in the countriesof the Region and the development ofintersectoral coordination so that govern-ments are able to provide, with the re-sources available, better health services
THE WORK OF WHO
for all people, an inter- agency consultationwas held at the Regional Office in October1977 and a seminar is planned to takeplace early in 1978. These meetings shouldmake useful contributions to the Inter-national Conference on Primary HealthCare which will be held in Alma -Ata,USSR, in September 1978.
15.139 The concept of appropriatehealth technology is also being promoted,in order to assist governments further indeveloping self -reliance and to reduce thecost of health services. Countries are beingencouraged to use simpler technologies tomeet their health and other social develop-ment needs, particularly for rural areas.
15.140 The task of providing fullhealth care to rural peoples is an enormousone, and the importance of the propertraining and utilization of nursing per-sonnel in this regard is paramount. In thecountries of the Eastern MediterraneanRegion, nurses form the largest singlecategory of health personnel. They areindispensable to the successful functioningof the health services system.
Health manpower development
15.141 WHO maintains its belief thatone of the best investments for its fundsand effort in this Region is in the trainingof health workers. This training shouldbe such as to ensure that those trained willmerge effectively into the evolving healthservices system. To this end, the Regionalfellowships programme is making animportant contribution (in 1976 over boofellowships were awarded). Since this pro-gramme began in 1949, almost 10 000individuals working in the health field atprofessional and other levels have beenexposed to new ideas and new knowledge.They have returned from neighbouringcountries, from countries outside the
200
Region, and more recently from recognizedpost -basic and postgraduate training insti-tutions within the Region, to dedicatethemselves to meeting the health needs oftheir own people.
15.142 The overall thrust of the pro-gramme in health manpower developmenthas always been and remains in the directionof institutional development in general, andteacher training_has constituted an im-portant element. As a result, not only hasthe Region witnessed a remarkable increasein the actual number of professionalschools, but to an increasing extent theseschools are now preparing the types ofhealth personnel which the countries mostneed. The Regional Office has found itpossible to provide fewer long -term fieldstaff and to make greater use of well-trained national talent in WHO -assistedprojects. It is probable that within a fewyears the only international staff to beassigned to countries will be short -termexperts in highly specialized fields in whichthe countries may not yet have developedthe necessary expertise.
15.143 The Organization continues topromote the concept of integrated healthservices and manpower development. Inresponse to a decision of the 1976 sessionof Sub -Committee A of the Regional Com-mittee, a Ministerial Consultation on HealthServices and Manpower Development isdue to be held in Teheran early in 1978. TheConsultation will represent an importantstep in the preparation of a comprehensivepolicy for the integrated promotion ofhealth services and manpower developmentfor each of the Region's Member States.
Family health
15.144 Closely related to the develop-ment of primary health care services is the
REGIONAL TRENDS
family health programme, with specialemphasis on remote rural areas. The activeinvolvement of the population requires thatactivities in maternal and child health,family planning, nutrition and health edu-cation should be integrated into this pro-gramme. Specific objectives are set inaccordance with national policies, usingthe criteria of maternal, child, and familyhealth and sometimes including social,economic and demographic criteria as well.In planning the health component of multi -sectoral food and nutrition policies andprogrammes, the aim is to attack the rootcauses of malnutrition and improve nutri-tional standards. Food supply problemsrequire the formulation and implementationof national food and nutrition policies ; incooperation with UNICEF and FAO,advisory assistance is being provided byWHO in several countries to develop suchpolicies.
15.145 Children make up a very highproportion of the underserved populationsof the Region. More than two millionchildren under the age of three years diein the Region each year, and of these deathsabout a quarter of a million are caused bysix diseases preventable by immunization,while at least half a million are caused bydiarrhoeal diseases. In 1976 and 1977,intensified immunization programmes werelaunched ; and since 1973, WHO andUNICEF have joined in the developmentand testing of a new technique for oralrehydration for infantile diarrhoea. Thisformula has proved highly successful inthe treatment of cholera in Bangladesh,and it is hoped that the results of con-trolled field trials, in which WHO is col-laborating with Egypt, Iran and Somalia,will serve as a springboard for a vigorouscampaign of education and promotion tomake this treatment available as widely aspossible throughout the Region.
20I
Disease prevention and control
15.146 Communicable diseases still con-stitute a considerable hazard, especially tothe rural population. Malaria and schisto-somiasis are increasing in prevalence incertain parts of the Region, particularly inrelation to the irrigation schemes that arebeing rapidly expanded in many countries.In spite of efforts by the governments andWHO to improve the situation, many prob-lems remain : for example, the lack ofreliable data on prevalence and geographicaldistribution, inadequate diagnostic capabili-ties, and unknown aspects of the relationbetween host, agent and environment.With the tools available, however, well -conducted control programmes can contrib-ute substantially to a reduction in the levelof transmission and in the prevalence,incidence and intensity of infection.
15.147 In collaboration with govern-ments of the Region and with increasedWHO assistance, the fight continues againstthree other parasitic infections- leishma-niasis, trypanosomiasis and filariasis. Activi-ties to combat leprosy are also beingstrengthened ; the progress being made inimmunological research has advanced to astage which gives hope of a real break-through.
15.148 In the global smallpox eradica-tion campaign, notwithstanding the out-standing achievements of Afghanistan andPakistan, which are now smallpox -free, therecent outbreak in Somalia was a serioussetback. This episode should inducebordering countries, as recommended byWHO, to use the greatest vigilance andrepeated searches, adopting the most mod-ern and efficient means, and to instituteeducational campaigns.
15.149 Although the health laboratoryprogramme in the Region is a substantial

THE WORK OF WHO
one in which training courses in the dif-ferent laboratory disciplines are beinggiven high priority, laboratories still tendtowards serving the individual rather thanthe community. A much greater effort mustbe made to increase and improve the labora-tory contribution to epidemiological activi-ties, and plans have been made to designatecertain laboratories as Regional labora-tories, where the control of vaccines andother activities which require special skillscan be carried out.
15.15o Efforts to stimulate countries ofthe Region to develop their psychiatricresources are continuing, with specialemphasis on the training of personnel tomeet the various mental health needs. Newideas emanating from WHO- assisted studieson the monitoring of mental health needs inKuwait and on strategies for extendingmental health care in Sudan should beparticularly helpful in the future planningand programming of mental health care.
15.151 Of the noncommunicable dis-eases prevalent in the Region, cancer hasreceived most attention. Progress is beingmade towards a better understanding of themagnitude, distribution and specific natureof cancer in the Eastern Mediterranean,following the guidelines set in the Region'scancer programme adopted in 1975 andelaborated further by the Regional AdvisoryPanel on Cancer, which met for the secondtime in Tunis in November 1976.
Environmental health
15.152 In several Member States wherefinancial means are available, much is beingdone by the respective governments toaccelerate the development of communitywater supplies. This is an encouragingdevelopment, but only marginal progresshas been made in many other countries.
202
Notable achievements during 1977 haveincluded the near completion of the finaldesign of a water supply system for Kabul,Afghanistan, and the accelerated develop-ment of rural water supplies in Yemen.The more industrialized countries of theRegion are now facing the problems ofenvironmental pollution, and the Organi-zation is stressing the economic and publichealth benefits to be derived from earlyattention to these problems. The monitor-ing of air and sea water pollution is nowclaiming long overdue attention.
Medical services
15.153 Socioeconomic change in theRegion has also meant the growth of newhospitals, new efforts to modernize andexpand hospital services, and the devotionof more attention to emergency medicalservices and associated intensive care. Inresponse to a request by Sub -Committee Aof the Regional Committee in 1976, stepsare being taken to establish a regionaladvisory committee on emergency medicalservices to advise on future WHO coopera-tion with countries during emergencies.Because of the rapid development andextension of health and hospital services,the whole pattern of supply and use of drugsin countries of the Region needs urgentreview. Studies are continuing to deter-mine drug requirements and utilization inhospitals and in primary health care, inorder to provide basic data for the estab-lishment of national drug policies.
Research
15.154 Biomedical research continuesto receive active attention. The RegionalAdvisory Committee on Biomedical Re-search, which has held two sessions (April1976 and March 1977), is guiding the pro-gramme ; in addition, two consultant
REGIONAL TRENDS
teams have visited various countries tostudy the potential resources for researchin the Region. A directory of institutionsinvolved in biomedical research was com-piled and is being further developed. Oneof the major libraries in the Region isbeing designated as a Regional MedicalLibrary. Following a proposal of theRegional Advisory Committee, a smallscientific group was established to assist inthe implementation of project proposals forresearch in the priority areas of healthservices and manpower development. Itmet for the first time in July- August 1977.
Administrative matters
15.155 With regard to administrativepolicy, the Regional Office continues tomaintain a small staff, so that more fundscan be made available for country pro-grammes. In the past five years the staff hasactually decreased, and further reductionsare planned in the future, to the extentpossible without impairing the efficiency ofthe Office, in line with overall WHOpolicy and as reflected in the programmebudget proposals for the years 1978 -79.
15.156 Finally, the official use of theArabic language is being further increasedin the Regional Office in accordance withresolution wHAZ8.34 adopted in 1975 bythe Twenty- eighth World Health Assembly.
Western Pacific Region
15.157 Country health programming isbeing developed and will continue in severalcountries of the Region. In correlationwith this the Regional Office will concentratemuch of its efforts on organizing, orparticipating in, national courses on man-agement of health services.
203
15.158 Efficient information systemsare needed to support managerial functionsat the national and international levels. Inthe Western Pacific Region WHO has beencollaborating with Member States in thedesign and development of dynamic andresponsive, totally integrated, health man-agement information systems aimed atsatisfying the information needs for plan-ning and management in ministries anddepartments of health. It has also beenfurther improving its own internal infor-mation system in order to provide adequateand appropriate support to the managementfunctions associated with collaborativeactivities.
15.159 Research promotion and devel-opment will be mainly directed towardsstrengthening national research capabilities,particularly in the developing countries,through the establishment of nationalresearch councils, the development ofcareer structures in research, the trainingof research workers and the provision ofsupport to research institutions. Animportant aim is to strengthen certaininstitutions sufficiently to enable themeventually to become part of a network ofcollaborating centres in the Region, thusfacilitating coordination of research, par-ticularly on Regional problems, and theexchange of scientific workers. Theexchange of scientific information andstimulation of research through researchgrants is being continued. More attentionis being given to health services research,to the application of existing knowledgeand to the elucidation of the natural historyof diseases, particularly the parasitic andother infections common in the Region.
15.16o The Western Pacific Region hasfocused its activities on promoting theprimary health care concept, particularlyin the developing countries, to achieve thegeneral goal of "Health for all by the year
THE WORK OF WHO
z000 ". Developing or strengthening con-ventional health services in rural areas is notan absolutely satisfactory way of meetingthe needs and expectations of the popula-tion. Dialogues on the subject, establishedwith WHO cooperation, have contributedtowards the clarification of some politicaland socioeconomic issues related to healthdevelopment in underserved areas. Anumber of governments are already awareof the crucial issues that should be bornein mind or studied further once they haveaccepted the challenge offered by the goalof total coverage.
15.16 x The trend in the Region now isto continue research and developmentactivities in areas of new relevant tech-nology, the promotion in the communityof self -reliance in managing and financingits share of health -related activities, theinterrelationship between the develop-ment of health manpower and primaryhealth care, and the involvement of sectorsother than health in total rural develop-ment. An intersectoral approach is anessential prerequisite for progress at boththe national and international levels andcan be achieved through technical coopera-tion among developing countries, as re-commended by the United Nations system.Existing country or intercountry projectsin which WHO cooperates in the develop-ment of comprehensive health services willbe reoriented to take into account theconcept of technical cooperation amongdeveloping countries, and new approacheswill be devised with the participation ofUNDP and other bodies of the UnitedNations.
15.162 In the prophylactic, diagnosticand therapeutic substances programme,WHO is working with governments onpolicy, legislation, management, produc-tion, procurement and distribution, withthe aim of promoting the rationalizationof
zoo
existing systems, particularly in developingcountries. Self -reliance is being engenderedthrough exploration of the efficacy ofmedicinal plants, and the development ofa closer relationship between traditionaland western medicine than has existed inthe past is being encouraged. The WesternPacific Region is ideally suited for thedevelopment of an intercountry programmebecause of the considerable experienceaccumulated in some countries of theRegion in the field of traditional medicine.
15.163 Emphasis in family health willcontinue to be on the expansion of servicesand improved coverage, in particular ofthose at high risk. A promising trendtowards the delegation of wider respon-sibilities to various categories of healthworker, particularly health auxiliaries, isemerging in the Region. For instance,newer categories of frontline health workerare being trained and programmes for thepreparation of nursing /midwifery person-nel are being oriented to include com-munity health practice with stress on healthpromotion, disease prevention and com-munication skills.
15.164 Innovative approaches are undertrial to introduce the concept of primaryhealth care in the delivery of services forthe promotion of family health. Such effortshave been manifested through the organiza-tion of national and regional seminars onthe delivery of maternal and child healthand family planning within primary healthcare, and through efforts to develop anintegrated approach to family health, asexemplified in Bohol Province, Philippines.
15.165 A trend showing a significantdecline in fertility and crude birth rates isalready discernible in a number of countriesand areas in the Region. The determinantsof reduction in fertility are varied andcomplex, and the effect of family planning

REGIONAL TRENDS
programmes appears to be greatest wherethey are carried out as part of multidiscipli-nary and intersectoral programmes forrural development. The approach ofintegrating family planning into maternaland child health and other health anddevelopment activities is now widely ap-plied ; the Regional Office has collaboratedin planning and implementing such inte-grated family health projects in twelvecountries or areas. The expansion of theseactivities has highlighted the need toevaluate them and the first round of evalu-ation of the projects has been completed inthree countries or areas.
15.166 Progress has also been made inintegrating nutrition activities into maternaland child health services, and as a conse-quence nutrition surveillance in severalcountries has improved. As governmentsstrive to provide improved coveragethrough primary health care, prospects forfurther progress are bright, providedadequate training and support can be givento frontline workers. National training innutrition has been enhanced, particularly inMalaysia, Papua New Guinea and thePhilippines. However, difficulty has beenexperienced in developing national foodand nutrition policies, partly because of lackof an adequate data base but also becauseof the complexities of coordinating thework of the various agencies and profes-sional disciplines concerned with nutritionand food supply.
15.167 Emphasis on the community -supported primary health care approach hasbrought into sharp focus the importance ofhealth education and community involve-ment in health action. Consequently, amajor thrust in health education has beenthe promotion of close collaboration be-tween health and other agencies concernedwith community efforts for development,and expansion of the concept of community
205
participation from mere acceptance ofhealth services to the sharing of responsi-bility in their management and delivery. Thishas been illustrated in a number of inter-agency seminars held at national level toencourage intersectoral collaboration andpromote teamwork among those workingat community level. Capabilities for provid-ing media support to health programmesare gradually being strengthened in manyparts of the Region. Facilities for the train-ing of professional leaders in health educa-tion have also expanded substantially.However, further efforts are needed todevise practical ways of training field -levelhealth workers to motivate and enlistcommunity support, to combine the teach-ing of health education theory with practicalexperience, and to encourage a comprehen-sive approach in health education with apooling of person -to- person, mass -mediaand community organization activities.
15.168 Member States of the Regionhave become increasingly aware of the needto optimize their investment in health man-power through active collaboration amongall agencies concerned with its develop-ment. A close functional relationship isgradually emerging between service andplanning agencies, teaching institutions andministries of education and health. System-atic planning of manpower needs will befacilitated as greater predictive accuracyis developed within planning method-ologies and also when country healthprogramming is undertaken.
15.169 Interest in the training and use offrontline and middle -level health personnelcontinues to grow, with recognition of theneed to prepare them for their expandedroles. A number of countries or areas havealready started to provide auxiliaries withadditional training in clinical diagnosis andtreatment and in preventive and promotivework, to enable them to play a wider role
THE WORK OF WHO
in health care delivery. Curricula are alsobeing developed and programmes initiatedfor the training of new categories of village-level health worker in many parts of theRegion.
15.170 A major challenge is to examinethe relevance of existing curricula to theneeds and job requirements of variouscategories of health worker. This is expect-ed to be a long process requiring close col-laboration between governments andWHO.
15.171 Continuing education is be-coming a routine requirement for all healthworkers, in order to meet changing needsin health care and to promote professionalgrowth, career development and job satis-faction. However, the concept needs to bebetter understood so that national systemsof continuing education can emerge for allcategories of health personnel.
15.17z A major development has beenrecognition of the need for training toimprove the management capabilities ofhealth personnel. A beginning has beenmade and training in management will begiven greater emphasis in the years to come.
15.173 The main thrust of futureactivities will be in the area of educationaltechnology, with a view to developingcost -effective training methods, such astask -oriented training, improved screeningfor student enrolment and more meaningfulevaluation of student performance. It isenvisaged that national teacher trainingcentres will play a major role in thisendeavour.
15.174 The fellowships programme ofWHO is expected to become increasinglyimportant for the training of teachers ascountries acquire the ability to developtraining facilities suited to their own needs.Fellowships will be better utilized, with
zo6
training needs more explicitly defined andevaluated.
15.175 Member Governments, espe-cially in the developing countries, haveshown great interest in the Expanded Pro-gramme on Immunization, and more re-quests are being received for WHO col-laboration in the development and expan-sion of programmes not only to cover agreater proportion of the susceptible popu-lation but also to include other diseasesagainst which immunizing agents alreadyexist. There will be need for more researchon logistics, the cold chain, the productionof better vaccines, the utilization of healthmanpower and other aspects of the deliveryof immunization programmes at the locallevel.
15.176 This development also calls forstrengthening of local laboratory servicesin order to test the quality of vaccines, andfor the designation of a Regional testingcentre for areas where local laboratoryservices are not available. The idea ofstrengthening vaccine -producing capabili-ties in certain developing countries, so thatthey may ultimately meet the needs of otherdeveloping countries in the Region, will bepursued.
15.177 The lack of adequate epidemio-logical services and epidemiological sur-veillance, so essential for disease intelligenceand control, remains a problem which hasto be solved. Efforts are being made totrain health manpower to meet the criticalshortage of epidemiologists. The develop-ment of adequate statistical and laboratorysupport, particularly at the intermediate andperipheral levels, needs to continue.
15.178 Attention continues to be givento the diarrhoeal diseases, sexually trans-mitted diseases, arbovirus infections anddiseases included under the Special Pro-
REGIONAL TRENDS
gramme for Research and Training inTropical Diseases, notably schistosomiasis,filariasis, malaria and leprosy, which afflicta large proportion of the population ofmany of the developing countries in theRegion. Research towards a better under-standing of the epidemiological and otherfeatures of these diseases, so that adequatepreventive and control measures can bedevised, remains a priority.
15.179 The intensification of BCG im-munization as part of the ExpandedProgramme on Immunization is expectedto have a significant effect on tuberculosiscontrol in the Region, although case -finding, domiciliary treatment and trainingof health personnel will need to becontinued.
i 5 . r 8o As regards malaria, there is someroom for cautious optimism about theimmediate future, since organized anti -malaria measures were introduced ratherlate in a number of countries of the Regionor have recently been reorganized or revital-ized. It is obvious, nevertheless, that astage without marked progress is slowlybeing reached, during which, at least inparts of some countries, malaria willcontinue to constitute a public health prob-lem unless radical changes are introduced.Malaria manpower development and newapproaches in the implementation of proj-ects at the periphery will be vital elementsin surmounting some of the operationaland administrative difficulties encounteredin remote areas ; at the same time, solutionsto some of the technical problems, particu-larly in relation to the occurrence ofmulti- drug -resistant strains of Plasmodiumfalciparum and to the elusive vectors Ano-pheles balabacensis and An. farauti, demandthe active promotion of immediate re-search into the development of alternativeantimalarial drugs and of supplementary oralternative measures of vector control.
207
15.181 Even developing countries in theRegion are becoming concerned about theincreasing prevalence of chronic and de-generative diseases such as cancer andcardiovascular diseases. The developmentof cancer registries, studies on causationfactors and the establishment of com-munity -based control programmes againstcancer, cardiovascular diseases and otherchronic diseases show a rising trend.
15.18 z Collaboration with MemberStates in the Region in the field of environ-mental health encompasses a broad rangeof activities, with emphasis on advisory andconsultant services aimed at strengtheningnational institutions and programmes forproviding environmental health services,promoting and planning water supply andsewerage development, elaborating poli-cies and implementing programmes forcontrolling all forms of pollution and healthhazards, setting up surveillance and moni-toring systems for the early detection andcontrol of pollution, and training man-power through individual and group edu-cational activities.
15.183 In relative terms, technical co-operation activities in most aspects ofenvironmental pollution control are on theincrease, including the training of specialistmanpower. Although water supply andsewerage development has accelerated,WHO cooperation in this field has notneeded to be increased to the same extentbecause there are many sources other thanWHO providing cooperation and coun-tries are developing some technical capacityof their own to undertake such pro-grammes ; nevertheless, various planningand programme management aspects con-tinue to need technical cooperation fromWHO.
15.184 It is expected that, because ofthe paucity of trained national staff, WHO
THE WORK OF WHO
will become more involved in trainingprogrammes for various categories ofenvironmental health and pollution controlstaff as national programmes are developed.
15.185 Broad environmental planningstudies to develop policy options and toguide control strategies have not beeninitiated in most countries or areas in theRegion. These complex activities, whichare multidisciplinary in nature, will requireincreasing support from WHO in futureyears.
15.186 WHO cooperation in the area ofhealth statistics continues. It is concernedwith the development of simple and system-
atic procedures for the collection, proces-sing, analysis and compilation of healthstatistical data, primarily related to theperipheral health and medical care services ;with the improvement of records systems,particularly those of health centres andhospitals ; and with the training of nationalhealth statistical personnel. The NinthRevision of the International Classificationof Diseases is being introduced in theWestern Pacific Region and its use stronglyencouraged. The use by lay or nonmedicalhealth personnel of the classification whichis being developed for mortality andmorbidity data is being encouraged as anessential tool in the efficient operation of theprimary health care system.
zo8
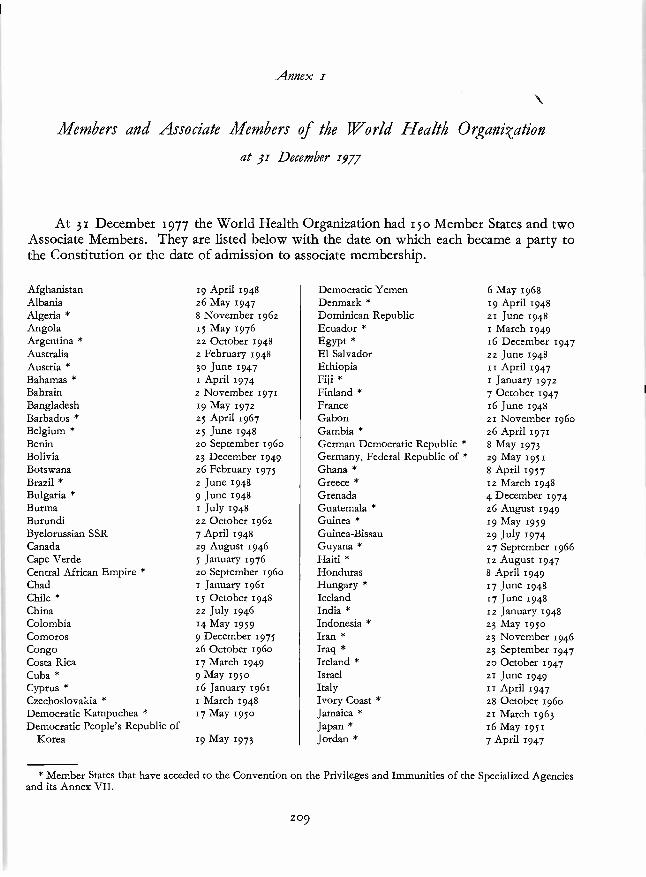
Annex z
Members and Associate Members of the World Health Organisation
at 31 December 1977
At 31 December 1977 the World Health Organization had 150 Member States and twoAssociate Members. They are listed below with the date on which each became a party tothe Constitution or the date of admission to associate membership.
AfghanistanAlbaniaAlgeria *AngolaArgentina *AustraliaAustria *Bahamas *BahrainBangladeshBarbados *Belgium *BeninBoliviaBotswanaBrazil *Bulgaria *BurmaBurundiByelorussian SSRCanadaCape VerdeCentral African Empire *ChadChile *ChinaColombiaComorosCongoCosta RicaCuba *Cyprus *CzechoslovakiaDemocratic Kampuchea *Democratic People's Republic of
Korea
19 April 1948z6 May 19478 November 196215 May 197622 October 1948z February 194830 June 19471 April 19742 November 197119 May 197225 April 196725 June 1948zo September 196o23 December 1949z6 February 1975z June 19489 June 19481 July 194822 October 19627 April 194829 August 19465 January 1976zo September 196o1 January 196115 October 194822 July 194614 May 19599 December 197526 October 196o17 March 19499 May 19So16 January 1961r March 194817 May 195o
19 May 1973
Democratic YemenDenmark *Dominican RepublicEcuador *Egypt *El SalvadorEthiopiaFiji *Finland *FranceGabonGambia *German Democratic Republic *Germany, Federal Republic of *Ghana *GreeceGrenadaGuatemala *Guinea *Guinea- BissauGuyana *Haiti *HondurasHungary *IcelandIndia *Indonesia *Iran *Iraq *Ireland *IsraelItalyIvory Coast *JamaicaJapanJordan *
6 May 196819 April 194821 June 1948, March 194916 December 194722 June 194811 April 19471 January 19727 October 1947x6 June 194821 November 196oz6 April 19718 May 1973z9 May 19518 April 195712 March 19484 December 197426 August 194919 May 195929 July 197427 September 196612 August 19478 April 194917 June 194817 June 194812 January 194823 May 195o23 November 194623 September 1947zo October 194721 June 1949II April 194728 October 196o21 March 196316 May 19517 April 1947
* Member States that have acceded to the Convention on the Privileges and Immunities of the Specialized Agenciesand its Annex VII.
209
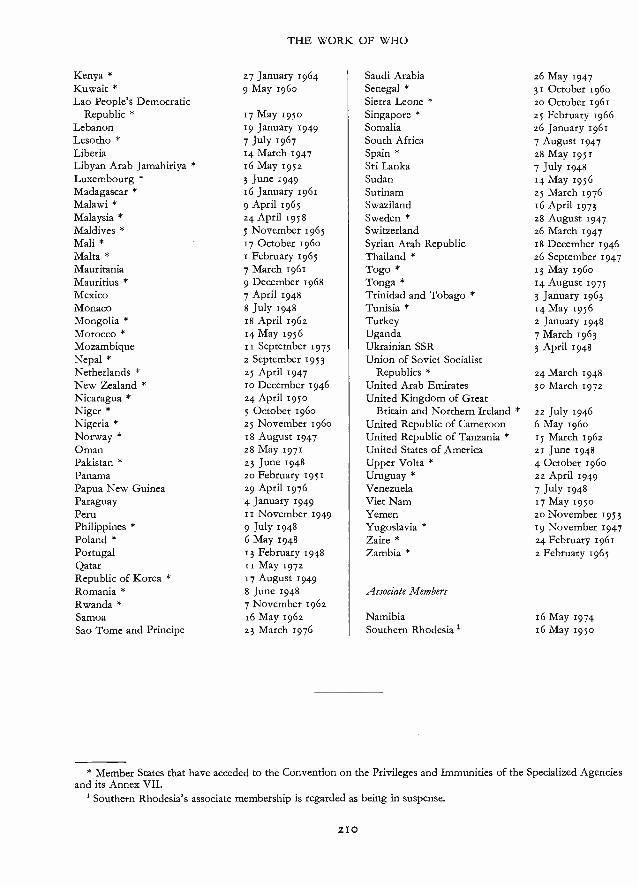
THE WORK OF WHO
Kenya * 27 January 1964Kuwait * 9 May 1960Lao People's Democratic
Republic * 17 May 1950Lebanon 19 January 1949Lesotho * 7 July 1967Liberia 14 March 1947Libyan Arab Jamahiriya * 16 May 1952Luxembourg * 3 June 1949Madagascar * 16 January 1961Malawi * 9 April 1965Malaysia * 24 April 5958Maldives * 5 November 1965Mali * 17 October 1960Malta * 1 February 1965Mauritania 7 March 1961Mauritius * 9 December 1968Mexico 7 April 1948Monaco 8 July 1948Mongolia * 18 April 1962Morocco * 14 May 1956Mozambique 11 September 1975Nepal * z September 1953Netherlands * 25 April 1947New Zealand * 10 December 1946Nicaragua * 24 April 1950Niger * 5 October 1960Nigeria * 25 November 1960Norway * 18 August 1947Oman 28 May 1971Pakistan * 23 June 1948Panama 20 February 1951Papua New Guinea 29 April 1976Paraguay 4 January 1949Peru 11 November 1949Philippines * 9 July 1948Poland * 6 May 1948Portugal 13 February 1948Qatar si May 1972Republic of Korea * 17 August 1949Romania * 8 June 1948Rwanda * 7 November 1962Samoa x6 May 1962Sao Tome and Principe z3 March 1976
Saudi ArabiaSenegal *Sierra Leone *Singapore *SomaliaSouth AfricaSpain *Sri LankaSudanSurinamSwazilandSweden *SwitzerlandSyrian Arab RepublicThailand *Togo *Tonga *Trinidad and Tobago *Tunisia *TurkeyUgandaUkrainian SSRUnion of Soviet Socialist
Republics *United Arab EmiratesUnited Kingdom of Great
Britain and Northern Ireland *United Republic of CameroonUnited Republic of Tanzania *United States of AmericaUpper Volta *Uruguay *VenezuelaViet NamYemenYugoslavia *Zaire *Zambia *
Associate Members
NamibiaSouthern Rhodesia
26 May 194731 October 196020 October 1961z5 February 1966z6 January 19617 August 194728 May 1951
7 July 194814 May 195625 March 197616 April 197328 August 194726 March 194718 December 1946z6 September 194713 May 196014 August 19753 January 196314 May 19562 January 19487 March 19633 April 1948
24 March 194830 March 1972
22 July 19466 May 196015 March 196221 June 19484 October 196022 April 19497 July 194817 May 195020 November 195319 November 194724 February 1961z February 1965
16 May 197416 May 1950
* Member States that have acceded to the Convention on the Privileges and Immunities of the Specialized Agenciesand its Annex VII.
1 Southern Rhodesia's associate membership is regarded as being in suspense.
2I0
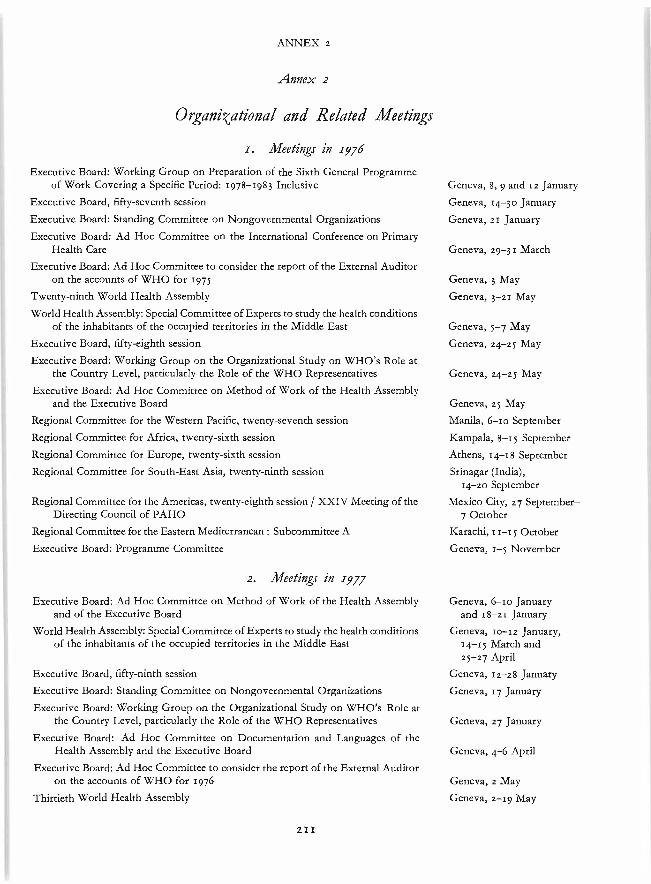
ANNEX z
Annex 2
Organizational and Related Meetings
r. Meetings in 1976
Executive Board: Working Group on Preparation of the Sixth General Programmeof Work Covering a Specific Period: 1978 -1983 Inclusive
Executive Board, fifty- seventh session
Executive Board: Standing Committee on Nongovernmental Organizations
Executive Board: Ad Hoc Committee on the International Conference on PrimaryHealth Care
Executive Board: Ad Hoc Committee to consider the report of the External Auditoron the accounts of WHO for 1975
Twenty -ninth World Health Assembly
World Health Assembly: Special Committee of Experts to study the health conditionsof the inhabitants of the occupied territories in the Middle East
Executive Board, fifty- eighth session
Executive Board: Working Group on the Organizational Study on WHO's Role atthe Country Level, particularly the Role of the WHO Representatives
Executive Board: Ad Hoc Committee on Method of Work of the Health Assemblyand the Executive Board
Regional Committee for the Western Pacific, twenty- seventh session
Regional Committee for Africa, twenty -sixth session
Regional Committee for Europe, twenty -sixth session
Regional Committee for South -East Asia, twenty-ninth session
Regional Committee for the Americas, twenty- eighth session / XXIV Meeting of theDirecting Council of PAHO
Regional Committee for the Eastern Mediterranean : Subcommittee A
Executive Board: Programme Committee
2. Meetings in 1977
Executive Board: Ad Hoc Committee on Method of Work of the Health Assemblyand of the Executive Board
World Health Assembly: Special Committee of Experts to study the health conditionsof the inhabitants of the occupied territories in the Middle East
Executive Board, fifty-ninth session
Executive Board: Standing Committee on Nongovernmental Organizations
Executive Board: Working Group on the Organizational Study on WHO's Role atthe Country Level, particularly the Role of the WHO Representatives
Executive Board: Ad Hoc Committee on Documentation and Languages of theHealth Assembly and the Executive Board
Executive Board: Ad Hoc Committee to consider the report of the External Auditoron the accounts of WHO for 1976
Thirtieth World Health Assembly
2 I I
Geneva, 8, 9 and iz January
Geneva, 14 -30 January
Geneva, 21 January
Geneva, 29 -31 March
Geneva, 3 May
Geneva, 3 -21 May
Geneva, 5 -7 May
Geneva, 24 -25 May
Geneva, 24 -25 May
Geneva, 25 May
Manila, 6-10 September
Kampala, September
Athens, 14 -18 September
Srinagar (India),14 -20 September
Mexico City, 27 September-7 October
Karachi, 11 -15 October
Geneva, 1 -5 November
Geneva, 6 -10 Januaryand 18 -21 January
Geneva, 10-12 January,14 -15 March and25 -27 April
Geneva, i2-28 January
Geneva, 17 January
Geneva, z7 January
Geneva, 4 -6 April
Geneva, z May
Geneva, 2 -19 May
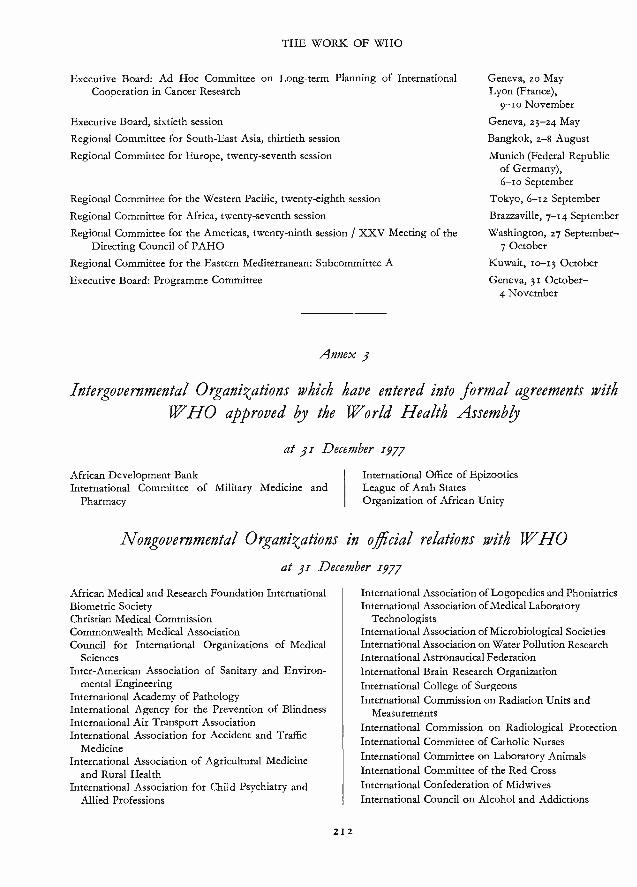
THE WORK OF WHO
Executive Board: Ad Hoc Committee on Long -term Planning of InternationalCooperation in Cancer Research
Executive Board, sixtieth session
Regional Committee for South -East Asia, thirtieth session
Regional Committee for Europe, twenty- seventh session
Regional Committee for the Western Pacific, twenty- eighth session
Regional Committee for Africa, twenty- seventh session
Regional Committee for the Americas, twenty-ninth session / XXV Meeting of theDirecting Council of PAHO
Regional Committee for the Eastern Mediterranean: Subcommittee A
Executive Board: Programme Committee
Annex 3
Geneva, zo MayLyon (France),
9 -10 November
Geneva, 23 -24 May
Bangkok, 2-8 August
Munich (Federal Republicof Germany),6 -10 September
Tokyo, 6 -1 z September
Brazzaville, 7 -14 September
Washington, 27 September-7 October
Kuwait, 10-13 October
Geneva, 31 October -4 November
Intergovernmental Organizations which have entered into formal agreements withIF HO approved by the World Health Assembly
at 31 December 1977
African Development BankInternational Committee of Military Medicine and
Pharmacy
International Office of EpizooticsLeague of Arab StatesOrganization of African Unity
Nongovernmental Organi <ations in official relations with WHO
at 31 December 1977
African Medical and Research Foundation InternationalBiometric SocietyChristian Medical CommissionCommonwealth Medical AssociationCouncil for International Organizations of Medical
SciencesInter -American Association of Sanitary and Environ-
mental EngineeringInternational Academy of PathologyInternational Agency for the Prevention of BlindnessInternational Air Transport AssociationInternational Association for Accident and Traffic
MedicineInternational Association of Agricultural Medicine
and Rural HealthInternational Association for Child Psychiatry and
Allied Professions
21 2
International Association of Logopedics and PhoniatricsInternational Association of Medical Laboratory
TechnologistsInternational Association of Microbiological SocietiesInternational Association on Water Pollution ResearchInternational Astronautical FederationInternational Brain Research OrganizationInternational College of SurgeonsInternational Commission on Radiation Units and
MeasurementsInternational Commission on Radiological ProtectionInternational Committee of Catholic NursesInternational Committee on Laboratory AnimalsInternational Committee of the Red CrossInternational Confederation of MidwivesInternational Council on Alcohol and Addictions
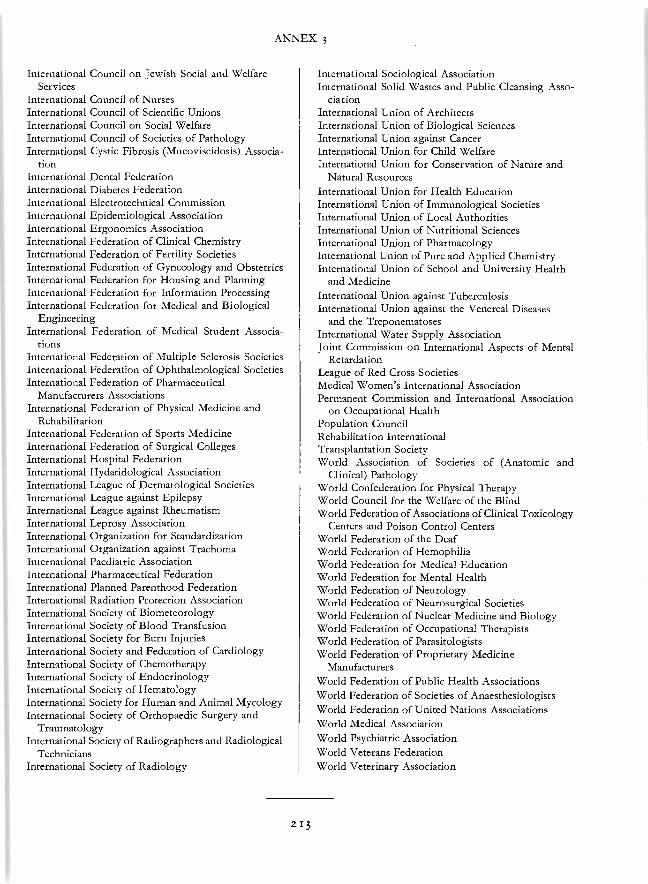
ANNEX 3
International Council on Jewish Social and WelfareServices
International Council of NursesInternational Council of Scientific UnionsInternational Council on Social WelfareInternational Council of Societies of PathologyInternational Cystic Fibrosis (Mucoviscidosis) Associa-
tionInternational Dental FederationInternational Diabetes FederationInternational Electrotechnical CommissionInternational Epidemiological AssociationInternational Ergonomics AssociationInternational Federation of Clinical ChemistryInternational Federation of Fertility SocietiesInternational Federation of Gynecology and ObstetricsInternational Federation for Housing and PlanningInternational Federation for Information ProcessingInternational Federation for Medical and Biological
EngineeringInternational Federation of Medical Student Associa-
tionsInternational Federation of Multiple Sclerosis SocietiesInternational Federation of Ophthalmological SocietiesInternational Federation of Pharmaceutical
Manufacturers AssociationsInternational Federation of Physical Medicine and
RehabilitationInternational Federation of Sports MedicineInternational Federation of Surgical CollegesInternational Hospital FederationInternational Hydatidological AssociationInternational League of Dermatological SocietiesInternational League against EpilepsyInternational League against RheumatismInternational Leprosy AssociationInternational Organization for StandardizationInternational Organization against TrachomaInternational Paediatric AssociationInternational Pharmaceutical FederationInternational Planned Parenthood FederationInternational Radiation Protection AssociationInternational Society of BiometeorologyInternational Society of Blood TransfusionInternational Society for Burn InjuriesInternational Society and Federation of CardiologyInternational Society of ChemotherapyInternational Society of EndocrinologyInternational Society of HematologyInternational Society for Human and Animal MycologyInternational Society of Orthopaedic Surgery and
TraumatologyInternational Society of Radiographers and Radiological
TechniciansInternational Society of Radiology
International Sociological AssociationInternational Solid Wastes and Public Cleansing Asso-
ciationInternational Union of ArchitectsInternational Union of Biological SciencesInternational Union against CancerInternational Union for Child WelfareInternational Union for Conservation of Nature and
Natural ResourcesInternational Union for Health EducationInternational Union of Immunological SocietiesInternational Union of Local AuthoritiesInternational Union of Nutritional SciencesInternational Union of PharmacologyInternational Union of Pure and Applied ChemistryInternational Union of School and University Health
and MedicineInternational Union against TuberculosisInternational Union against the Venereal Diseases
and the TreponematosesInternational Water Supply AssociationJoint Commission on International Aspects of Mental
RetardationLeague of Red Cross SocietiesMedical Women's International AssociationPermanent Commission and International Association
on Occupational HealthPopulation CouncilRehabilitation InternationalTransplantation SocietyWorld Association of Societies of (Anatomic and
Clinical) PathologyWorld Confederation for Physical TherapyWorld Council for the Welfare of the BlindWorld Federation of Associations of Clinical Toxicology
Centers and Poison Control CentersWorld Federation of the DeafWorld Federation of HemophiliaWorld Federation for Medical EducationWorld Federation for Mental HealthWorld Federation of NeurologyWorld Federation of Neurosurgical SocietiesWorld Federation of Nuclear Medicine and BiologyWorld Federation of Occupational TherapistsWorld Federation of ParasitologistsWorld Federation of Proprietary Medicine
ManufacturersWorld Federation of Public Health AssociationsWorld Federation of Societies of AnaesthesiologistsWorld Federation of United Nations AssociationsWorld Medical AssociationWorld Psychiatric AssociationWorld Veterans FederationWorld Veterinary Association
213

HEADQUARTERS
Annex 4
Structure of the World Health Organizationat 31 December 1977
WHO Secretariat as a Whole
DIRECTOR-GENERAL'SOFFICE
INTERNATIONAL AGENCYREGIONAL OFFICES FOR RESEARCH ON CANCER
Office of Research Promotionend Development
Health and BiomedicalInformation Programme
Legal DivisionInternal AuditEmergency Relief Operations
ASSISTANTDIRECTOR -GENERAL
Division of Coordination'Division of Health StatisticsSpecial Programme for
Research and Trainingin Tropical Diseases
Information SystemsProgramme
Division of Malaria and otherParasitic Diseases
Division of CommunicableDiseases
Division of Vector Biologyand Control
Expanded Programme on
Division of EnvironmentalHealth
Division of Family HealthDivision of Health Manpower
DevelopmentDivision of Strengthening
of Health ServicesSpecial Programme of
Research, Developmentand Research Trainingin Human Reproduction
Division of NoncommunicableDiseases
Division of Prophylactic,Diagnostic andTherapeutic Substances
Division of Mental Health
Division of Personnel andGeneral Services
Division of Budget andFinance
'The Liaison Office with the United Nations and the WHO medical advisers to UNICEF (who are also responsible for liaison with UNFPA)report to the Division of Coordination.
AFRICA\\\\\\\\\\\\\\\\\
REGIONALDIRECTOR
Health Services
THE AMERICAS2
\\\\ÑÉ6ÎÓÑÁ\L\ \ \ \ \ \ \ \ \\\ \ \\\ \\\\\ \\ \\\
Administrationand Finance
Assistant Director
WHORepresentatives
TechnicalServices
SOUTH -EAST AS /A
\ \ \RIERGI
TNQARL\\
EUROPE
Deputy Director
Health Services
Administration
EASTERN MEDITERRANEAN
REGIONALDIRECTOR
WESTERN PACIFIC
REGIONALDIRECTOR
H Administrationand Finance
Health Services
Administrationand Finance
Health Services
Administrationand Finance
Health Services
Administrationand Finance
WHORepresentatives
WHORepresentatives
WHORepresentatives
WHORepresentatives
Area Offices
2Regional Office for the Americas/Pan American Sanitary Bureau.
'The responsibilities of this Assistant Director -General include the chairmanship of the HeadquartersProgramme Committee.
wxo >)aYl
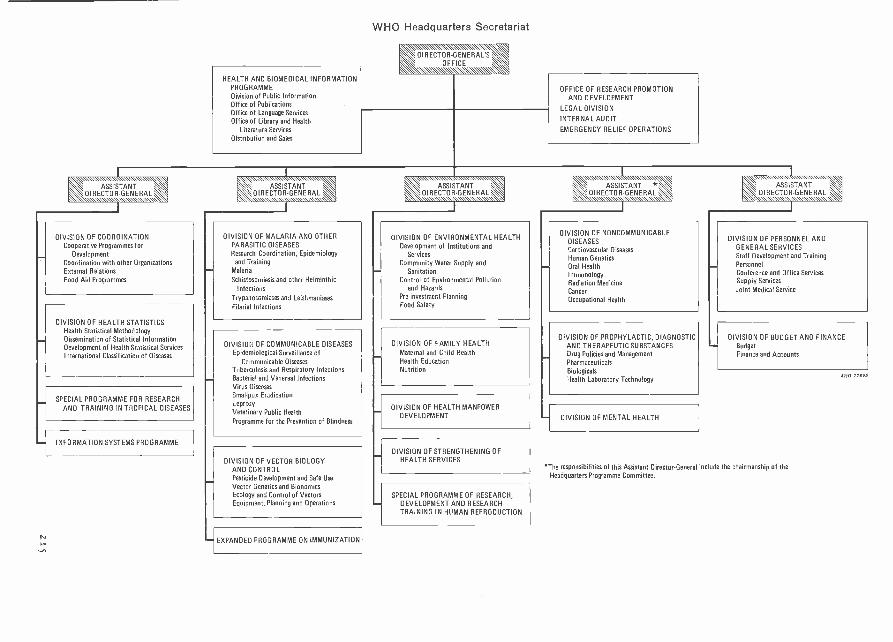
HEALTH AND BIOMEDICAL INFORMATIONPROGRAMMEDivision of Public InformationOffice of PublicationsOffice of Language ServicesOffice of Library and Health
Literature ServicesDistribution and Sales
WHO Headquarters Secretariat
OFFICE OF RESEARCH PROMOTIONAND DEVELOPMENT
LEGAL DIVISION
INTERNAL AUDIT
EMERGENCY RELIEF OPERATIONS
ASSISTANTDIRECTOR-GENERA
DIVISION OF COORDINATIONCooperative Programmes for
DevelopmentCoordination with other OrganizationsExternal RelationsFood Aid Programmes
DIVISION OF HEALTH STATISTICSHealth Statistical MethodologyDissemination of Statistical InformationDevelopment of Health Statistical ServicesInternational Classification of Diseases
SPECIAL PROGRAMME FOR RESEARCHAND TRAINING IN TROPICAL DISEASES
INFORMATION SYSTEMS PROGRAMME
DIVISION OF MALARIA AND OTHERPARASITIC DISEASESResearch Coordination, Epidemiology
and TrainingMalaria
Schistosomiasis and other Helminthic
InfectionsTrypanosomiases and Leishmaniases
Filarial Infections
DIVISION OF COMMUNICABLE DISEASESEpidemiological Surveillance of
Communicable DiseasesTuberculosis and Respiratory InfectionsBacterial and Venereal InfectionsVirus DiseasesSmallpox EradicationLeprosyVeterinary Public Health
Programme for the Prevention of Blindness
DIVISION OF VECTOR BIOLOGYAND CONTROLPesticide Development and Safe UseVector Genetics and BionomicsEcology and Control of VectorsEquipment, Planning and Operations
EXPANDED PROGRAMME ON IMMUNIZATION
DIVISION OF ENVIRONMENTAL HEALTHDevelopment of Institutions and
ServicesCommunity Water Supply and
SanitationControl of Environmental Pollution
and HazardsPo- investment PlanningFood Safety
DIVISION OF FAMILY HEALTHMaternal and Child HealthHealth EducationNutrition
DIVISION OF HEALTH MANPOWERDEVELOPMENT
DIVISION OF STRENGTHENING OFHEALTH SERVICES
SPECIAL PROGRAMME OF RESEARCH,DEVELOPMENT AND RESEARCHTRAINING IN HUMAN REPRODUCTION
DIVISION OF NONCOMMUNICABLEDISEASESCardiovascular DiseasesHuman GeneticsOral HealthImmunologyRadiation MedicineCancerOccupational Health
DIVISION OF PROPHYLACTIC, DIAGNOSTICAND THERAPEUTIC SUBSTANCESDrug Policies and ManagementPharmaceuticalsBiologicalsHealth Laboratory Technology
- DIVISION OF MENTAL HEALTH
DIVISION OF PERSONNEL ANDGENERAL SERVICESStaff Development and TrainingPersonnelConference and Office ServicesSupply Services
Joint Medical Service
DIVISION OF BUDGET AND FINANCEBudgetFinance and Accounts
The responsibilities of this Assistant Director-General include the chairmanship of theHeadquarters Programme Committee.
0 7789

INDEX
Index
References are by paragraph. Main references by subject are in bold type.
Abortifacient drugs, 6.46, 6.49Abstinence, periodic, 6.41, 6.49, 7.105ACC, see Administrative Committee on CoordinationAccidents, agricultural and industrial, 9.142, 9.145,
15.33road traffic, 1.29, 2.5, 5.42,
15.I0I- 15.102Acupuncture, 3.18, 5.63, 5.66Administration and finance information system, z.,6,
2.20Administrative Committee on Co- ordination (ACC),
3.1, 3.3, 6.22
Sub -Committee on Nutrition, 6.22Sub -Committee on Population, 6.3task force on rural development, 5.9
Administrative costs, reduction, 1.3, 1.5Administrative matters, 14.7-14.18Adolescence, see Youth and adolescenceAdvisory committees on medical research, regional,
I.I0, 1.28, 4.3, 4.7, 5.10, 5.51, 8.91,8.161, 8.165
Africa, 4.17, 4.20, 15.13
Americas, 4.25, 8.84Eastern Mediterranean, 4.31 -4.33, 15.154Europe, 4.30, 15.93South -East Asia, 4.26, 4.27, 8.91,
15.81
Western Pacific, 4.34, 4.35, 8.46,Aedes aegypti, 1.3o, 8.129, 8.131
Afghanistan, 5.43, 6.35, 8.14, 8.94, 9.17,11.28, 12.15, 15.137, 15.148, 15.152
Africa, Conference on Health Coordination and Co-operation in, 15.11
African Congress on Blood Transfusion, First, Yamous-soukro, Ivory Coast (1977), 10.31
African Development Bank, 11.31, 15.9African Institute of Health Planning, 7.77African Psychiatric Association, 9.2African Region, 4.17-4.20, 15.1-15.13African -American Labor Center, 9.142
9.73, 15.92,
15.44,
9.95
15.54,
11.4,
219
Agricultural workers, accidents and exposure to toxicsubstances, 9.145, 15.33
Air pollution, 7,98, 11.42, 11.43, 13.27, 15.31,15.124, 15.128, 15.129, 15.152
Air quality management, 15.124Air quality monitoring, 11.39Aircraft, disinsection, 8.152
food, catering, 11.5 6, 15.113
Alcohol and alcoholism, 7.101, 9.11, 9.16, 15.120cancer studies, 9.69, 9.72, 9.73
Algeria, 5.5, 5.56, 6.13, 7.38,8.94, 9.58, 12.15, 15.121
Allergic diseases, 9.137Ambulatory care, 5.5, 5.24, 5.27Amenorrhoea and intermenstrual bleeding, 6.17,
6.42
Americas, meetings of ministers of health, I.zo,15.16
Americas, Region of the, 1.27,15.14-15.40
Americas, Regional Library of Medicine and theHealth Sciences, 9.48, 15.37
Americas, Ten -year Health Plan, I.zoAnaemias, 5.18, 6.44, 7.97
nutritional, 6.31, 6.3zAngola, 3.23, 6.26, 7.77, 8.37, 14.1Animal diseases, 8.94, 8.103, 8.111 -8.117Animal wastes, 8.115
Anopheles Control Research Unit (Kaduna, Nigeria),8.123, 8.145
Anticonvulsant drugs, 7.111, 9.27Antidepressant drugs, 15.130Antigua, 6.35Apartheid, 3.4, 3.5, 9.15Approaches to planning and design of health care facilities
in developing areas, 5.23
"Appropriate technology ", 1.5, 1.29, 5.1,5.16 -5.21, 5.2z, 6.7, 6.8, 6.27, 6.39, 10.7,I0.28, I1.13- 1I.18, I1.26, 12.5, I2.8, 15.21,15.88, 15.92, 15.139, 15.161
7.93, 8.13,
4.21-4.25,
5.7,
THE WORK OF WHO
research, 1.5, 4.9, 5.10, 5.16, 5.61, 15.32,15.161
transfer, 10.4, 10.7, 10.18, 11.15, 11.43Arab Organization for Standardization and Metrology,
11.66Arabic language, 13.3, 13.24, 14.4, 15.156Arbovirus Vector Research Unit, 8.129Arboviruses, 8.108, 8.129, 15.178
see also Dengue and dengue haemorrhagic fever;Encephalitis; Yellow fever
Argentina, 5.40, 8.94, 8.108, 9.48Arthritis, rheumatoid, 5.64Arthropods, 8.118Asbestos, 9.64Asian Development Bank, 8.23Associate Members of WHO, 14.1, (Annex 1)Atherosclerosis, 9.81, 9.8zAudiovisual materials, 7.5o,
8.176see also Films; Teaching learning materials
Australia, 3.12, 3.24, 7.102, 8.98, 9.113Austria, 8.166
7.53, 7.56, 7.57,
Auxiliary health personnel, 3.13, 5.12, 5.39, 7.6,7.16, 7.26 -7.32, 7.35, 7.36, 7.50, 7.54,7.88, 8.176, 9.111, 13.23, 15.36, 15.57,15.58, 15.163, 15.169
teacher training, 7.6, 7.36, 7.42, 7.5osee also Medical assistants and auxiliaries; Primary
health care workers; Community health workers;Voluntary health workers, and under the variouscategories of health personnel
Bacterial diseases, 8.70 -8.101Bahamas, 14.5
Bahrain, 9.141Bangladesh, 3.24, 5.37, 6.21, 7.31, 7.37, 7.44,
7.78, 8.7, 8. x z, 8.94, 8.173, 9.7, 9.49,15.52, 15.70, 15.74, 15.76, 15.84, 15.145
Barbados, 6.24Barefoot doctors, 5.66BCG vaccination and vaccine, 8.58, 8.62, 8.65,
8.95, 15.72, 15.179Bejel, 8.1orBelgium, 7.38, 7.85, 8.Io8, 8.166, 9.21, 9.115,
9.119, 10.17Benin, 8.29Bhutan, 15.74Biennial budgeting, 1.15,Biologicals, 10.19 -10.26,
cost, 1.31, 15.9development and use, international conference (1976),
4.11regional and local production, 1.3x,standardization, 9.136, 9.137
international reference materials, 10.19, I0.21interregional seminar (1977), to.zo
14.310.28 -10.30
15.9
220
Biomedical information, 13.1-13.31Biomedical research, see ResearchBirth control, see Fertility regulationBirthweight, low, 6.16, 15.49Blindness and visual impairment, 8.27, 8.31,
8.169 -8.176, 13.19, 13.20, 13.23, 15.79training, 8.173, 8.176
Blood products and substances, 10.19Blood transfusion services, Io.31Bolivia, 5.9, 5.40, 5.45, 5.54, 6.24,
7.36, 8.94Botswana, 6.26, 6.33"Brain drain ", see Migration of health personnelBrazil, 4.23, 5.26, 5.40, 5.45, 6.7, 6.I I, 6.24,
7.12, 7.36, 7.69, 8.11, 8.21, 8.94, 9.6,9.48
Breast -feeding, 6.17Brucellosis, 8.,,,, 8.114Budget, see Programme budgetsBulgaria, 6.12, 7.83, 7.93, 7.98, 15.96Bulletin of the World Health Organization, 13.14Bureau international des Poids et Mesures, 13.28Burkitt's lymphoma, 9.66Burma, 5.41, 5.44, 5.46, 5.55, 6.15, 6.32, 7.37,
8.82, 8.94, 8.108, 8.126, 8.173, 9.17,9.141, 15.44, 15.63, 15.66, 15.70, 15.74,15.84
Burundi, 5.53
7.12,
Cameroon, see United Republic of CameroonCanada, 6.64, 8.22, 9.29, 9.136, 13.23Canadian International Development Agency (CIDA),
11.9, 1x.16Cancer, 1.31, 4.26, 9.34-9.75, 9.112, 9.12o,
1I.61, 12.23, 15.25, 15.80- 15.81, 15.15x,15.181
Ad Hoc Committee of the Executive Board, 1.31,
9.35chemotherapy, 4.9, 9.36, 9.47classification (histology and cytology), 7.112,
9.40 -9.43, 9.51, 12.23epidemiological research, directories, 9.59, 9.6oinformation systems, 9.46, 12.14radiotherapy, 9.115 -9.118regional advisory panel (Eastern Mediterranean),
9.51, 15.151registries, 9.39, 9.56-9.59, 12.23, I5.181rehabilitation, 9.5oresearch, 4.9, 9.34, 9.35, 9.36,
9.53-9.75, 15.54, 15.81standardization of reporting of results of treatment,
meeting, Italy (1977), 9.38statistics, 12.13, I2.14, 12.23training, 9.34, 9.5o
Cape Verde, 5.14, 6.26, 8.21, 14.1
9.45, 9.48,
Carcinogens, environmental, 8.144,9.6o -9.65, 9.68
Cardiomyopathies, 9.83Cardiovascular diseases, 9.76 -9.95, 9.97, 15.22,
15.25, 15.82, 15.I15- 15.117, 15.181classification, 9.83community control, long -term programmes (Euro
pean and Western Pacific Regions), 9.76, 9.919.95, 15.115 -15.116
drug evaluation trials, 9.8o, 15.13ointerregional team, 9.88rehabilitation, 5.40research, 4.34, 8.46, 9.78
multifactor preventive studies, North Kareliproject (Finland), 9.92, 15.117
regional research and training centre, WesterPacific, 9.95
training, 7.112, 9.95, 15.82workshop on the role of physical activity in preven
tion, Luxembourg (1977), 9.92
Caribbean Food and Nutrition Institute, 6.24, 15.21Caries, 9.107, 9.108, 9.113Cataract, 8.170Causes of death, see DeathCentral African Empire, 6.5, 8.130Cerebrospinal meningitis, 8.73
vaccination and vaccine, 8.75, 15.72Cerebrovascular diseases, 7.111, 9.27, 9.32Chad, 8.172, Io.z8Chagas' disease, 8.42-8.43
research, 8.42, 8.43, 8.135, 8.156, 9.138Chagas' Disease Vector Research Unit, Venezuela,
8.42, 8.135Chemicals, carcinogenicity and toxicity, 1.32, 8.143,
8.144, 9.60 -9.63, 9.68, 11.32, 11.49- 11.51,15.129
occupational exposure, 7.113, 9.64, 15.33permissible levels, 9.147
Children, 6.18, 8.16, 15.50-15.51, 15.52, 15.104cancer, 9.5o, 9.71cardiovascular diseases, 9.78, 9.81, 9.88diarrhoeal diseases and gastroenteritis, 4.26, 8.71,
8.106, 15.23, 15.69, 15.145effects of air pollution, 11.42growth and development, 6.z6, 6.37, 6.54,
8.I16, 15.20, 15.I07psychosocial development, 6.14, 9.22, 15.20
mental health, 9.6, 9.9, 9.11 -9.12, 9.22, 9.32mortality, 6.3, 6.31, 6.54, 12.13, 12.15,
15.22, 15.50, 15.62, 15.145inter -American investigation, 6.7nutrition, 6.17, 6.31, 6.32, 6.54oral health, 9.110rheumatism, 9.105see also Immunization; Maternal and child health;
Paediatrics; School healthChile, 5.26, 5.40, 6.6, 6.17, 6.24, 9.48
9.53, 9.54,
INDEX
a
n
22I
China, 3.18, 5.66Chinese language, 13.3, 13.24Chlamydial infections, 8.109
see also TrachomaCholera, 8.70 -8.72, 15.7o, 15.145
interregional team, 8.71vaccine, 8.72
Chromosomal aberrations, 11.41international registry, 9.531
Chronic and degenerative diseases, 9.34- 9.106,15.116- 15.I20, 15.181
training, 9.96
Chronicle (WHO), 13.15CIOMS, see Council for International Organizations
of Medical SciencesCirrhosis, 9.42, 9.73Clark, Edna McConnell, Foundation, 8.22
Classification of diseases, 7.11z, 9.31-9.32,9.51, 9.83, 12.6, 12.21 -12.26
Clinical chemistry, 6.62, 7.97, 10.29, Io.3oClinical pharmacology, 10.18, 15.130, 15.131
see also Drugs, safety and efficacyCoastal water pollution, 7.98, 11.44, 14.6, 15.127Codex Alimentarius Commission, 11.57-11.59"Cold chain ", 5.18, 8.64, 15.175
Collaborating centres, 4.23, 4.28,9.96, 13.16, 15.159
cancer, 9.44cardiovascular diseases, 9.78, 9.81, 9.86drug dependence, 9.19education, 7.5, 7.49, 7.7oenvironmental pollution and hazards, 11.33, 11.35,
11.36, 15.32food contaminants, joint FAO/WHO, 11.68food hygiene, joint FAO/WHO, 7.99human genetics, 9.128, 9.132human reproduction, 6.52, 6.54,
6.63, 7.91, 7.107immunology, 4.25, 8. o8, 9.55, 9.58, 9.135mental health, 6.14, 7.85, 9.21, 9.25, 9.27,
15.84occupational health, 9.144, 9.145, 9146, 9.149pharmaceuticals, 10.17radiation, 9.118, 9.119, 9.124,reagents, 7.97rheumatic diseases, 9.103smallpox, 8.48, 8-55trypanosomiasis, 8.40, 8.43vector biology and control, 8.121, 8.,zz, 8.123,
8.132, 8.140, 8.143, 8.151, 8.152virus diseases, 8.I0zwater supply, 11.14
Colombia, 4.23, 5.26, 5.40, 5.45, 5.54, 6.24, 6.26,9.3, 9.6, 9.7, 9.48
Colombo Plan, 8.139Colour blindness, 9.26
9.40 -9.43,
8.73, 9.87,
6.6o, 6.6z,
11.40
THE WORK OF WHO
Commission of European Communities, 9.92, 11.41,15.I IO
Committee on International Surveillance of Communi-cable Diseases, 8.2 -8.4
Committee on Occupational Health, Joint ILO /WHO,9.143
Communicable diseases, 3.23, 6.27, 8.1- 8.168,15.64 -15.76, 15.113- 15.114, 15.146- 15.148,15.178-15.180
courses on epidemiology and control, 7.92research, 4.34, 8.1, 8.46-8.47, 15.10, 15.54,
15.62Communicable eye diseases, see Blindness and visual
impairment; TrachomaCommunications sciences, 7.5, 7.71, 15.163
see also Nonverbal communicationCommunity development, 5.6, 6.33Community health services, training, 7.27, 7.32,
7.33, 7.61, 7.88, 15.36, 15.58, 15.163medical education, 7.37, 15.6omental health, 9.5 -9.19, 15.118nursing, 15.112, 15.163see also Health services
Community health workers, 5.39, 7.27, 7.29, 7.30,7.32, 7.55, 7.88, 8.67, 15.36, 15.44, 15.169
Community participation in health programmes, 5.6,
5.7, 5.10, 6.37, 8.14, 8.16, 11.26, 15.4,15.16, 15.17, 15.18, 15.46, 15.144, 15.161,15.167
joint study, UNICEF /WHO, 3.14, 5.8, 6.33Community water supplies, see Water suppliesComoros, 3.25, 5.25Comparative medicine, 8.116 -8.117Computing, medical, 12.7, 12.8, 1 2.10
see also Electronic data processingCongenital defects, 9.90Congo, 6.5, 6.26, 11.z8Constitutional and legal matters, 1.8, 14.1 -14.6
amendments to the WHO Constitution, 1.15,14.2 -14.4
Consumer protection, 3.5Contraception, 6.38
in adolescence, 6.18Contraceptives, injectable, 6.41, 6.42, 6.43, 6.48,
6.56oral, for men,
for women,6.56,
6.46,6.38,
15.130
6.5o,6.41,
6.51,6.42,
6.566.43, 6.44,
postcoital preparations, 6.46, 6.51vaccines, trials, 6.46, 6.5osee also Abortifacient drugs; Fertility regulation;
Intrauterine devicesContributions to WHO, voluntary, see Extrabudgetary
sources of fundsConvention on the Privileges and Immunities of the
Specialized Agencies, 14.5
Convention on Psychotropic Substances, 9.19, 10.14
222
Coordination with the United Nations system oforganizations, 3.1-3.36, 5.39, 6.2, 6.3, 6.21,6.22., 9.87, 11.22, 15.39, 15.53, 15.135,15.161
development of central planning and control auth-ority, 1.25
harmonization of programme budget cycles, 1.17information systems development, 2.15, 2.24see also under names of individual organizations
Coordinator of International Rehabilitation Assistancefor the Reconstruction of Viet -Nam, 3.12
Costa Rica, 5.45, 5.54, 6.33, 7.12, 9.48Council for International Organizations of Medical
Sciences (CIOMS), 3.2, 4.11, 4.13, 7.15,12.24
Country health programming, 1.14, 2.3 -2.4, 2.I I,2.12, 2.18, 5.28, 5.44, 5.46, 5.49, 5.50,5.52, 5.55, 15.5, 15.43, 15.44, 15.62,15.137, 15.157, 15.168
interregional seminar, New Delhi (1977), 2.4methodology, 2.4, 2.18research, 2.4, 4.9training, 2.4, 5.44, 7.76, 7.77, 7.78, 7.80working group, Europe (1977), 7.14
Cuba, 6.24Cyprus, 3.26, 8.166, 14.17Cysticercosis, 8.III, 8.114Cytogenetics, 9.131Cytology, 9.43Czechoslovakia, 7.92
Danish International Development Agency (DANIDA),3.13, 7.49, 7.93, 7.97, 7.98, 8.139
Danish "Save the Children" Fund, 8.81Data banks, 5.56, 9.108, 12.19Death, non -medical reporting of causes of, 15.63
see also International Classification of Diseases;Mortality
Declaration on the Granting of Independence to Col-onial Peoples and Countries, 3.5
Democratic People's Republic of Korea, 15.46Democratic Yemen, 8.14, 11.4, 15.137Dengue and dengue haemorrhagic fever, 1.30, 8.108,
8.129, 8.131, 15.65research, 4.26, 8.46, 9.135
Denmark, 3.12, 6.64, 8.166Dental auxiliaries, 7.29, 9.111, 15.36Dental equipment, 9.I I IDental health, see Oral healthDentofacial anomalies, 9.112Depression, treatment, 9.29, 15.130Desertification, 3.4Deutsches Auss £ tzigen -Hilfswerk, 8.81Developing countries, basic health needs, joint UNICEF/
WHO study, 5.6o
INDEX
environmental quality planning and policy, inter-regional symposium, Geneva (1977), 11.48
mental health, special programme, 1.31, 9.2, 9.5,
9.6, 9.25water supplies and excreta disposal, assessment,
I I.I-I I.5see also Least developed countries; Technical co-
operationDevelopment projects, see Rural development; Socio-
economic development and health; United NationsDevelopment Programme; Water resources andriver basin development projects
Diabetes, 5.64, 9.97-9.99Diagnostic procedures, 7.97,
8.99, 8.100, 8.102, 8.109,standardization, 6.5 I, 7.112,
8.38,8.II0,9.137,
8.94, 8.98,9.115, 10.29
15.78Diagnostic substances, 9.137, 10.1 -10.31, 15.162Diarrhoeal diseases, 6.9, 6.27, 6.37, 8.71,
15.545, 15.178research, 4.9, 4.26see also Enteric infections
Diphtheria, 8.73vaccination, 8.58, 15.72see also DPT vaccine
Director -General's development programme, 15.114Director -General's report to the Health Assembly and
UN on the work of WHO, biennial, reduction,13.13
Disability prevention and rehabilitation, 1.29,
5.38-5.43, 9.9, 9.50, 15.46training, 5.40, 5.43
Disarmament, 3.5
Disaster relief, see Emergency assistanceDisasters and Natural Catastrophes, Special Account,
3.23, 3.30, 3.33DNA (Deoxyribonucleic acid), 4.7Documentation, 13.2, 13.3, 13.13
reduction, 2.22, 13.4PAHO centre, establishment, 13.26see also Health literature services
Dominican Republic, 7.1z, 7.36,DPT vaccine, 8.62, 8.63, 8.68, 10.22Drinking- water, 5.3, 11.27
cardiovascular disease studies, 9.86quality control, 11.16, I1.56supply, inter -agency ad hoc working group,
international decade (1980 -1990), 1.32, 11.7,Î1.I2
treatment, hazards, 9.86, 11.3 7, 15.125Drought relief, 1.27, 3.28Drugs, 7.55, 1o.i -10.18
availability and use, 50.2, 10.4, 10.7, 15.131,15.153
cost, 1.31, 10.2, 10.3, 10.4dependence and abuse, 7.101, 9.11, 9.17 -9.19,
9.25, 9.30, 15.84, 15.120rehabilitation, 9.18
9.7
7.114
223
training, 7.101, 9.17working group on early intervention programmes,
Western Pacific (1976), 9.18listing of essential substances, 9.6, 10.4,
10.6 -10.7monitoring system for adverse reactions, 10.17national policies and management, 1.22, Io.I -10.5,
15.9z, 15.153, 15.162nonproprietary names, 10.14 -10.15quality control, 10.4, 10.7, 10.8, I0.10 -10.13
certification scheme, 1 0.11
research and development, 4.13, 8.159, 10.4safety and efficacy, evaluation and monitoring, 10.4,
Io.16, 15.130- 15.131symposia, Europe (1976 and 1977), Io.18, 15.130
see also Abortifacient drugs; Anticonvulsant drugs;Contraceptives, oral; Filaricides; Pharmaceuticalproduction
Eastern Mediterranean Region, 4.31-4.33,15.133- 15.156
Ebola virus, 8.108, 8.136ECA, see Economic Commission for AfricaECE, see Economic Commission for EuropeEchinococcosis, 8.114
see also HydatidosisEconometrics, see Health economicsEconomic Commission for Africa (ECA), 15.9Economic Commission for Europe (ECE), 5.56,
II.44, 15.IO2Economic Order, New International, 1.9Economic and Social Commission for Asia and the
Pacific (ESCAP), 8.141Ecuador, 5.45, 7.12, 7.36Education, see Health education; Medical educationEducational handbook for health personnel, 7.48Educational technology, 7.5, 7.33, 7.68, 15.173
centres, establishment, Geneva, 7.6Latin America, 7.43, 7.56, 15.37
see also Teaching learning materialsEgypt, 4.31, 7.46, 7.57, 7.69, 7.92, 8.26,
8.94, 9.17, 9.141, 11.28, 15.145El Salvador, 5.45, 5.54, 8.149, 9.7Elderly, care of, 1.29, 5.42, 5.56, 15.92,
15.99 -15.100mental disorders, prevention, 9.10nutrition, 6.30, 15.100, 15.107
Electronic data processing, 10.14, I2.I0Emergency assistance, I.8, 1.27, 3.22 -3.35, 6.29,
8.51, 8.54, 8.108, 15.1, 15.114see also Health care, emergencies
Emmaüs- Suisse, 8.81Encephalitis, Japanese, 15.65Enteric infections, 6.6, 8.5, 8.46, 8.70 -8.72, 8.106,
15.23, 15.69, 15.113vaccines, 8.72
THE WORK OF WHO
Environmental health, 1.32, 8.5, II.I- 11.69,15.8, 15.28 -15.33, 15.85- 15.88, 15.121- 15.129,15.152, 15.182-15.185
criteria, 11.33, 11.34, 11.35, 15.31information systems, 1 1.42, 15.32, 15.87management, 11.5, 15.28monitoring and surveillance, 11.39-11.42, 15.31,
15.128, 15.182planning, 7.93, 11.45-II.48, 15.185
regional centre, Western Pacific, 11.19research, 11.14, 11.15, 15.23, 15.54symposium on environmental quality planning and
policy in developing countries (1977), 11.48training, 7.35, 7.37, 7.87, 7.98, 11.5, 11.14,
11.15, 11.17, I1.26, 11.32, 11.39, 15.122,15.123, 15.182 -15.184
see also Environmental pollution and hazards; Sanitaryand public health engineering; Sanitation;Sewerage; Wastes disposal; Water supplies
Environmental health criteria, 11.33, 13.18Environmental pollution and hazards, 7.98, 7.105,
8.118, 9.85, 11.21, 11.32- 11.44, 11.47,15.31, 15.87, 15.124-15.I29, 15.152, 15.182,15.183, 15.184
from agricultural sources, 11-43from animal sources, 8. x I 5
from industrial sources, 11.43, 15.124, 15.129symposium on synthetic rubber and plastics, USA
(1976), 11.36relation to infection, 8.1see also Air pollution; Coastal water pollution;
Marine pollution; Water pollutionEpidemiology and epidemiological surveillance, 8.1,
8.2 -8.6, 8.27, 8.5o, 8.53, 8.67, 8.93, 8.99,8.101, 8.102, 8.103, 8.105, 8.107, 8.113,
15.67, 15.74, 15.177centres, Africa, 15.3research, 8.95, 8.155, 8.159, 9.11, 9.13,
9.60, 9.64, 9.75, 9.88, 9.106, 9.112,12.7, 15.62, 15.76, 15.82, 15.83, 15.I00
training, 7.92, 7.93, 9.95, 15.67, 15.177Epilepsy, 7.111, 9.13, 9.27Equipment, dental, 9.111
electromedical, repair and maintenance, 5.21, 15.83radiological, 7.95, 9.118, 9.123, 15.83see also Supplies and equipment
Ergonomics, 9.145ESCAP, see Economic and Social Commission for
Asia and the PacificEthics, medical, 3.2, 4.7, 4.11-4.13Ethiopia, 6.17, 8.14, 8.48, 8.49, 8.5o, 8.5z,
9.7European Economic Community, 6.32, 9.92European League against Rheumatism, 9.105European Medical Research Council, 5.48European Organization for Research on Treatment of
Cancer, 9.38
224
European Region, 4.3o, 15.91 -15.132programme development, 15.91-15.92publications, 13.12Regional Director's Development Programme,
15.92Evaluation of programmes, 1.13, 1.14, 2.2, 2.7,
2.12, 4.9, 7.67, 15.39development of guidelines, 1.26, 2.9-2.11, 8.94,
15.58Excreta disposal,Executive Board,
1.14, 1.24,
1.32,lc .1,
1.26,
1I.1 -11.5,1.6, 1.8,
1.30, 1.31
15.85x.10, 1.12,
Ad Hoc Committee on Documentation and Lan-guages, x3.13
Ad Hoc Committee on Methods of Work of theHealth Assembly and of the Executive Board,1.15
Ad Hoc Committee on WHO Activities in the Fieldof Cancer, 1.31, 9.35
membership, 14.2methods of work, 1.15organizational studies, 1., 6 -, ., 8Programme Committee, 1.6, 1.8, 1.14, z.8,
2.11review of programme budget policy and strategy,
1.6summary records, 13.13
Executive Board Special Fund, 3.27Expert Advisory Panel on Smoking and Health,
establishment, 9.87Expert advisory panels, regional, establishment, x.1o,
5.8, 9.51, 15.13, 15.151Expert Committee on African Trypanosomiasis, Joint
FAO/WHO (1976), 8.38Expert Committee on Biological Standardization
(1977), 10.19
Expert Committee on Chemistry and Specificationsof Insecticides (1977), 8.143
Expert Committee on Chemotherapy of Solid Tumours(1976), 9.47
Expert Committee on Child Mental Health and Psy-chosocial Development (1976), 9.22
Expert Committee on Drug Dependence (1977), 9.19Expert Committee on Food Additives, Joint FAO/
WHO (1976 and 1977), 11.50Expert Committee on Health Needs of Adolescents
(1976), 6.18Expert Committee on Insecticides (1975), 8.119Expert Committee on Leprosy (1976), 8.78 -8.79Expert Committee on Maternal and Child Health
(1975), 6.4Expert Committee on the Methodology of Nutritional
Surveillance, Joint FAO/UNICEF/WHO (1975),6.26
Expert Committee on Methods Used in EstablishingPermissible Levels in Occupational Exposure toHarmful Agents (1976), 9.147
INDEX
Expert Committee on Microbiological Aspects of FoodHygiene (1976), 11.54
Expert Committee on Nutrition, Joint FAO/WHO(1974), 6.23
Expert Committee on the Selection of Essential Drugs(1977), 10.6
Expert Committee on Specifications for PharmaceuticalPreparations (1977), 10.I2
Expert Committee on the Training and Utilization ofAuxiliary Personnel for Rural Health Teams inDeveloping Countries (1977), 7.28
Expert Committee on the Use of Ionizing Radiationand Radionuclides on Human Beings for MedicalResearch, Training and Nonmedical Purposes(1977), 4.12, 9.121
Expert Committee on Vector Biology and Control(1976), 8.151
Expert Committee on Viral Hepatitis (1976), 8.107Expert Committee on the Wholesomeness of Irradiated
Food, Joint FAO/IAEA/WHO (1976), 11.52Expert committees, African Region, 5.7, 5.13, 15.13Expert Consultation on Microbiological Specifications
for Foods, Joint FAO/WHO, 11.55
Extrabudgetary sources of funds, 1.17, 3.6 -3.13,8.69, 15.89 -15.90
mobilization, 4.4, 8.170, 8.173, 9.2, 15.90use, 4.4, 4.5, 9.16, 9.19, 9.23, 9.25, 9.28, 9.108,
14.17WHO Secretariat committee, 3.7
Eye diseases and injuries, see BIindness and visualimpairment; Communicable eye diseases
Family health, 6.2 -6.64, 9.12, 15.20, 15.21,15.104 -15.108, 15.144 -15.145, 15.163 -15.167
training, 7.36, 7.84, 15.21see also Maternal and child health
Family planning, 3.12, 6.3, 6.5, 6.8, 6.1 t, 6.20,6.27, 6.37, 6.38, 6.39, 6.42, 6.43, 6.45,6.47, 6.49, 6.53 -6.54, 6.58, 6.65, 7.49,7.81, 15.47, 15.105, 15.165
attitudes and beliefs, 6.56, 7.91projects, by Region, 6.5, (table 6.1)research, 6.39, 6.46, 6.65, 7.91, 15.48services, 6.55 -6.56, 6.6o, 7.91
staff for, 6.5 7, 6.5 8, 7.91role of nurses and midwives, 6.58, 7.91
training, 6.I1, 6.12, 6.57, 6.58, 7.81, 7.82,
7.84 7.91, 7.100, 7.106, 15.48, 15.106,15.164
see also Fertility regulationFAO, see Food and Agriculture Organization of the
United NationsFats and oils, 6.31Fellowships, 3.36, 5.40, 5.65, 7.5, 7.6,
7.63 -7.66, 7.111, 7.112, 9.17, 15.174
225
distribution, by subject and region, 7.63, (table 7.1)programme regionalization, 7.63 -7.65, 15.60,
15.141Fertility, 6.3, 12.15Fertility regulation, 6.39, 6.40, 6.6o, 6.65,
15.47, 15.54, 15.165current methods, acceptability, 6.55-6.58,
(table 6.4), 6.6o, 7.91mental health aspects, 9.22safety and efficacy, 6.41 -6.44, (table 6.2),
6.63new and improved methods, 6.45 -6.5o, (table 6.3)training aspects, 6.II, 7.81, 7.91, 7.105, 7.106see also Infertility
Fetal mortality, 6.39, 6.54, 9.125, 12.13, 12.15Fibrosis, hepatic, 9.42Fiji, 5.5o, 7.31, 8.175, 10.29, 11.47Filarial infections, 8.26 -8.36, 13.23, 15.65, 15.76,
15.147, 15.178chemotherapy and chemoprophylaxis, 8.z6,
8.28, 15.76insecticides, 8.127 -8.128research, 8.26, 8.28, 8.46, 8.155, 8.156, 15.76training, 8.26vaccine development, feasibility studies, 8.28see also Onchocerciasis
Filaricides, 4.19, 8.28, 15.76Films, 5.14, 7.57, 8.6o, 13.20, 13.23Financial report, reduction, 13.13Finland, 6.64, 8.166Fish, larvivorous, 8.148Fleas, 8.139, 15.66
resistance to DDT, 8.138Food additives, evaluation, 11.5o
see also Food safety and hygieneFood Additives Series (WHO), 13.18
Food and Agriculture Organization of the UnitedNations (FAO), 3.22, 6.17, 6.36, 11.44
joint activities, communicable diseases, 7.110, 8.23,8.113, 8.114, 8.118, 8.134, 8.151
food safety and hygiene, II.5o, 11.55, 11.61,'1.66
nutrition, 6.22, 6.23, 6.24, 6.26, 6.28,6.31, 15.53, 15.144
pesticides, II.51, II.68Food and foodstuffs, 11.57, 15.113
irradiated foods, 11.52"ready- made" foods, 6.3o, 15.107weaning foods, 6.27
Food contamination and hazards, 1.21, 9.63, 9.7o,11.49, I1.50, 1I.51, I1.53, 11.57, 11.62,11.67, 11.69, 15.125
monitoring programme, joint FAO/WHO, 8.5,11.67 -11.69
Food safety and hygiene, 11.49- 11.56, 11.60 -11.69microbiological aspects, 7.99, 11.54, 11.55training, 7.99, ,I.6o
6.6z,
Food standards, 11.57-11.59Food supplements, 3.20, 6.32, 8.171Food -borne diseases, 8.5, 11.53, 11.54,
11.56, 15.113France, 7.92, 7.114, 9.10I, 10.17French Polynesia, 9.110
THE WORK OF WHO
11.55,
Gabon, 6.5, 7.90, 11.28Gambia, 9.7, I. 28Gastroenteritis, 6.6, 8.106, 15.23, 15.69General Programme of Work of WHO, Sixth,
1.I2 -1.13, 1.14, 1.23, 2.5, 2.7, 7.3, 7.4,7.73, 9.35
review, z.6Seventh, preparation, z.6
Genetic engineering, 4.15Genetics, see Human geneticsGeriatrics, see Elderly, care ofGerman, introduction as working language in the
European Region, 15.94Germany, Federal Republic of, 3.9, 8.134, 9.113,
9.133, 9.136, 10.18, 11.43, 13.23Ghana, 7.29, 7.77, 8.22, 8.29, 8.172, 13.zoGilbert Islands, 7.39, 8.70Glaucoma, 8.170, 8.172, 8.173Glossaries, 9.32, 13.27, 15.94, 15.124Goitre, 6.31, 6.32Gonococcal infections, 8.97, 8.98Gonorrhoea, 8.97Governing bodies, see Executive Board; Regional
committees; World Health AssemblyGreece, 14.5Green Cross, 13.19, 13.23Guatemala, 3.27, 5.40, 5.45, 6.17,
13.23
6.24, 6.32,
Guide to hygiene and sanitation in aviation, 11.56Guide to shellfish hygiene, 11.53Guides, technical, 6.9, 6.z9, 7.29,
7.50, 8.71, 8.94, 8.95, 8.108,7.36,I1.13,
7.48,11.53,
I1.56, 15.123see also Glossaries ; Manpower development, manage-
ment and planning, guides, manuals and text-books ; Manuals, technical; Textbooks
Guinea, 9.141, 11.28, 15.12Guinea -Bissau, 3.13, 5.14, 5.44, 7.55, 7.90
HABITAT (1976), 1.20,51.24, 15.28, 15.87
Haematology, 7.97Haemoglobinopathies and allied disorders, 9.125,
9.127 -9.128Haemorrhagic fevers, viral, 3.35, 8.3, 8.108,
8.136see also Dengue and dengue haemorrhagic fever
Haiti, 3.28, 5.45, 6.6, 8.II
3.4, 11.6, II.2I-II.22,
226
Handicaps, classification, 12.22, 12.23see also Disability prevention and rehabilitation
Headquarters accommodation, 14.14
Headquarters Programme Committee, 2.2, 2.7,2.10, 2.13
Headquarters staff, 14.11reduction of establishment, 1.3 -1.4
Health care, delivery, 4.26, 3.22 -5.32, 11.20, 12.9,15.45-15.46
costs, 5.5, 5.35,15.139
information system, 12.19emergencies, services in, 1.29,
15.153seminar, Iran and USSR (1976),
intensive care, 9.101, 15.153for respiratory insufficiency, working group,
Europe (1976), 9.101outpatient and ambulatory services,
seminar, Sofia (1977), 5.24systems, 5.5, 5.31, 5.52, 12.7, 12.9, 15.10,
15.95use, 5.32see also Primary health care
Health economics, 5.29, 5.48, 5.50, 5.56, 8.93,8.99, 9.33, 15.98, 15.113
Health education, 5.41, 6.18, 6.33 -6.37,8.72, 15.108, 15.167
in cardiovascular diseases, 15.117in communicable diseases, 15.145, 15.148in family health, 6.1, 6.36, 6.37, 15.20in mental health, 9.13, 15.120in nutrition, 6.28in prevention of blindness, 8.170- 8.171, 8.173,
15.79on tobacco and alcohol, 9.11, 9.87training, 7.90, 15.167
Health laboratory services, see Laboratory technologyand services
Health legislation, 1.33, 13.16, 15.36environmental quality and pollution control,
11.48family health, 6.21food control, 11.53, 11.59, 11.63mental health, 9.54prophylactic, diagnostic and therapeutic substances,
10.4, 15.162smoking, 9.87
Health literature services, 13.5 -13.10see also Guides; Manuals; Medical libraries; Teaching/
learning materials; TextbooksHealth management, 5.29, 5.50, 5.56, 5.58, 6.7,
6.13, 7.79, 15.95, 15.97information systems, 5.5 2,
12.4, 15.158research, 7.21
5,36, 5.38, 9.33, 15.98,
4.15, 5.33-5.34,
5.34
5.5, 5.27
7.57,
11.43,
5.54, 5.55, 5.57,
INDEX
statistical support, 6.12, 7.104, 12.1, 12.2,12.4, 15.61 -15.62
training, 2.4, 6.11, 6.12, 7.21 -7.24, 7.64,7.80, 15.97, 15.157, 15.172
long -term programming, 7.7Health manpower, see Manpower development man-
agement and planningHealth manpower news, 7.74Health planning, national, 2..1, 2.3-2.4, 5.44-5.50,
7.2, 7.85, 15.5, 15.96, 15.98, 15.136methodology, 2.3, 2.4, 5.47, 15.168Pan American programme, 5.45research, 5.47training, 5.47, 7.77, 15.97see also Country health programming; General Pro-
gramme of WorkHealth records, see Medical recordsHealth sciences, training, 7.5, 7.6,
15.37centres, meeting of deans and directors, 7.51
Health services, development, 1.21, 1.29, 3.12,3.13, 3.18, 5.1 -5.67, 15.4, 15.16- 15.18,
15.44-15.56, 15.95-15.98, 15.133, 15.153,15.157-15.161
African survey, 12.16financing, 5.35-5.37
study group (1977), 5.37information systems, 1.22, 5.16, 5.50,
5.51-5.59integration of nutrition, 6.27 -6.30see also Health management; Health planning; Man-
power development, management and planning;Public health administration
Health services in Europe, 12.11Health services research, 1.Io, 1.28, 2.4, 4.2, 4.5,
4.9, 4.17, 4.20, 4.24, 4.32, 4.33, 4.34, 5.4,5.10, 5.59, 6.55, 7.91, 8.46, 15.44, 15.54,15.95- 15.96, 15.99, 15.154,
ethical aspects, 4.11-4.13Health statistics, see StatisticsHealth teams, 7.20, 7.26, 7.27, 7.28, 7.33,
7.35, 7.69, 15.7, 15.36, 15.57Helminthiases, 8.21Hepatitis, viral, 8.107, 9.68, 15.113
see also Liver cancer and other chronic liver diseasesHistological classification of tumours, 7.112, 9.40,
9.51Honduras, 2.6, 3.29, 5.Z2, 5.45, 5.54, 6.24,
7.12, 7.32, 7.36, 9.7, 12.18Hospital infections, 15.103Hospitals, planning, administration and maintenance,
7.38, 15.34,
15.159
3.26, 5.22, 5.25, 5.26, 5.28, 5.30, 15.45,15.153
Housing, 8.42, 8.135, 11.23, 15.20, 15.122see also Human settlements
Human ecology, 8.8centre, Mexico City, 11.3 8, 15.30
227
Human genetics, 4.14, 9.125-9.132
Human reproduction, 6.37, 15.20development of institutions for research, 6.46,
6.59 -6.63, (table 6.5)special programme (formerly expanded programme),
4.4, 4.10, 6.38 -6.65, 7.91, 7.107, 15.48see also Family planning; Fertility; Population dy-
namics; SterilizationHuman rights, 3.5Human settlements, I.zo, 1.32, 3.4, 3.5, 11.6,
11.20- 11.25, 15.28, 15.87, 15.122Hungary, 6.17, 7.69Hydatidosis, 8.1,1Hypertension, arterial,
9.90, 9.95in pregnancy, 6.19
9.79, 9.85, 9.88, 9.89,
IAEA, see International Atomic Energy AgencyIARC, see International Agency for Research on CancerIBRD, see International Bank for Reconstruction and
DevelopmentIceland, 5.56, 7.38ILO, see International Labour OrganisationImmunization, 3.12, 6.37, 7.57, 13.19-13.20,
15.72, 15.145Expanded Programme on, 1.30, 3.14, 4.2, 4.9,
7.57, 7.109, 8.95, 10.23,
15.3, 15.24, 15.73, 15.175, 15.179financing, 8.69, (table 8.1)planning and management of services, 8.6o, 8.67research, 8.61, 8.63, 8.65 -8.67, 8.95,seminars, 7.109, 8.6otechniques, 8.65, 8.95training and use of staff, 8.59, 15.175
Immunology, 7.107, 8.41, 8.43, 8.87, 8.88,8.94, 8.95, 8.155, 9.126, 9.129, 9.133-9.138,15.147
centres for research and training, 7.96, 9.67, 9.133,9.138
Chinese study mission, 3.18Impairments and handicaps, classification, 12.22, 22.23India, 5.41, 6.15, 6.17, 6.zo, 6.26, 6.27, 6.32,
15.175
7.5, 7.32, 7.37, 7.44, 7.97, 7.100, 7.103,8.7, 8.12, 8.44, 8.95, 8.119, 8.173, 9.3, 9.6,9.7, 9.29, 9.49, 10.29, 11.43, 15.48, 15.52,15.63, 15.70, 15.74, 15.76, 15.78, 15.82,15.83, 15.84
Indochina, Special Account (UN) for HumanitarianAssistance, 14.17
Indonesia, 5.46, 5.55, 6.24, 6 32, 6.33, 6.35,7.32, 7.37, 7.85, 8.12, 8.72, 8.94, 8.108,8.125, 8.126, 8.127, 8.138, 8.173, 9.7,9.49, 10.29, 11.28, 15.44, 15.48, 15.70,15.75, 15.84
Industrial development, health aspects, 11.36, 15.31
THE WORK OF WHO
Industrial hygiene and safety, 9.64, 9.142-9.148,
9.149see also Occupational health
Infarction, myocardial, 9.85, 9.86
Infertility, 6.5, 6.51 -6.52research, 6.39, 7.107
Influenza, 8.6, 8.203, 8.117vaccines, 8.75, 8.103
Information systems, I.zz, 2.7, 2.10, 5.50,
5.51 -5.59, 6.6, 12.6, 12.17, 15.61, 15.67,15.158
joint meeting, ECE/WHO (1976), 5.56WHO programme, 1.14, 2.12 -2.24, 5.16,
15.6, 15.158working group, 2.15
see also under subjects
Insecticides, application, evaluation and testing, 8.16,8.29, 8.34, 8.39, 8.122- 8.125, 8.128, 8.129,8.232- 8.235, 8.142
production, 1.30, 8.141resistance to, 8.8, 8.13, 8.119 -8.121, 15.75see also Pesticides
Institute of Nutrition of Central America and Panama(INCAP), 6.24, 6.3 2, 15.21
Insurance, health, 5.6, 5.37, 15.95Inter -Agency Ad Hoc Working Group on Rural
Potable Water Supply and Sanitation, 7.114
Inter -Agency Consultation on Primary Health Care,WHO/UNICEF, Alexandria, Egypt (1977), 5.8
Inter -American Development Bank, 12.9Intergovernmental organizations, (Annex 3)International Agency for the Prevention of Blindness,
8.170, 8.171, 8.176International Agency for Research on Cancer (IARC),
1.31, 8.21, 8.144, 9.35, 9.53-9.75, 11.61,12.14, 12.23
International Anti -Apartheid Year, 3.5International Association of Biological Standardiza-
tion, 4.52International Association of Cancer Registries, 9.57International Atomic Energy Agency (IAEA), 9.85,
9.117, 9.118, 9.119, 11.34, 21.40, 11.44,1I.52, 15.83, 15.126
International Bank for Reconstruction and Develop-ment (IBRD), 2.4, 6.22, 6.24, 7.114, 8.23,I1.6, 11.9, 11.31, 11.36, 15.53, 15.86,15.121
International Children's Centre, 6.21, 7.84, 15.105International Classification of Diseases, ,z.6,
I2.21 -I2.26centres, 22.26Ninth Revision, 7.505, I2.21, 12.23, 12.25,
15.186Tenth Revision, 12.22
International Committee of the Red Cross, 3.22, 3.30,8.5z
228
International Conference on Nuclear Power and itsFuel Cycles, 11.37
International Conference on Primary Health Care (1978),1.20, 3.15, 5.14, 15.138
International Conference on the Role of the Individualand the Community in the Research, Developmentand Use of Biologicals, 4.11
International Dental Federation, 9.11 zInternational Development Research Centre, 8.166,
11.15, 15.23International Diabetes Federation, 9.99International Digest of Health Legislation, 1.33, 13.16International Drinking -Water Supply and Sanitation
Decade (1980 -1990), 1.32, 11.7, 11.12International Epidemiological Association, 7.104,
12.19International Federation of Anti -Leprosy Associations,
8.79International. Federation of Clinical Chemistry, 20.29International Federation of Gynecology and Obstetrics,
6.zrInternational Federation of Health Records Organiza-
tions, 7.1ozInternational Federation for Information Processing,
5.56, 12.19International Green Cross, 13.19International Health Regulations, 8.2, 8.4International Histological Classification of Tumours,
9.40, 9.52International Institute of Applied Systems Analysis,
12.9International Labour Organization (ILO), 5.36, 6.36,
7.9, 9.142, 9.143, 9.147, 11.34, 11.36International League against Rheumatism, 9.104International Leprosy Association, 8.81, 8.166International nomenclature of diseases, proposed, 12.22International nonproprietary names for pharmaceutical
substances, 10.14 -10.15International Paediatric Association, 6.21International Pharmacopoeia, 1 0.13
International Planned Parenthood Federation, 6.8,6.21, 6.27, 6.36
International Radiation Protection Association, 11.34International Society and Federation of Cardiology,
7.112, 9.83International Society of Radiology, 9.115, 9.116International Union against Cancer, 9.38International Union of Immunological Societies, 9.136International Union against Tuberculosis, 8.81,
8.93-8.94International Year of the Child (1979), 3.5, 3.16,
6.21International Year for Disabled Persons, 3.5Inter- organization Board for Information Systems and
Related Activities, 2.24Intrauterine devices, 6.38, 6.41, 6.42, 6.44, 6.58
hormone -releasing, 6.48
Iran, 3.33, 4.31, 5.4, 5.30, 7.29, 7.85, 8.143,9.7, 9.17, 9.29, 9.71, 9.74, 10.29,15.134, 15.145
Iraq, 4.31, 6.5, 8.44, 8.174, 9.7, 9.37, 9.141,15.137
Iron, dietary supplement, 6.32Ischaemic heart disease, 9.79 -9.80, 9.81, 9.83,
15.117Israel, 6.z6, 11.43Italy, 6.26, 7.38, 9.39Ivory Coast, 7.92, 8.29, 8.39, 8.55, I1.28
11.43,
INDEX
9.90,
Jamaica, 5.40, 6.12, 6.24, 7.82, 9.7, 12.18Japan, 8.46, 9.29, 9.113Japan Shipbuilding Industry Foundation (Sasakawa
Memorial Health Foundation), 3.11, 3.12,8.79, 8.81, 8.166
Joint Committee on Health Policy, UNICEF/ WHO,(1976), 3.14 -3.15, 1126
Joint FAO/IAEA/WHO Expert Committee on theWholesomeness of Irradiated Food (1976), 11.52
Joint FAO/UNICEF/WHO Expert Committee on theMethodology of Nutritional Surveillance (1975),6.26
Joint FAO/WHO Expert Committee on AfricanTrypanosomiasis (1976), 8.38
Joint FAO/WHO Expert Committee on Food Additives(1976, 1977), 1150
Joint FAO/WHO Expert Committee on Nutrition(1974), 6.23
Joint FAO/WHO Expert Consultation on Micro-biological Specifications for Food, 11.55
Joint FAO/WHO food contamination monitoringprogramme, 8.5, 11.67 -11.69
Joint FAO/WHO meetings on pesticide residues(1976-1977), 11.51
Joint ILO/WHO Committee on Occupational Health,9.143
Jordan, 5.30, 5.43, 7.51, 8.21
Kala -azar, 15.76Kellogg Foundation,Kenya, 6.26, 7.42,
8.124, 9.39Kuwait, 5.57, 8.94,
7.I27.90, 8.44, 8.48, 8.49, 8.5o,
9.7, 9.37, 15.134, 15.150
Laboratory animals, 25.78see also Primates
Laboratory technology and services, 3.12, 6.6z,8.74, 8.ioo, 8.102, 8.105, 8.109, 8.1,o,9.134, 10.27 -10.31, 11.16, 11.39, 11.65,15.26, 15.78, 15.103, 15.149, 15.176, 15.177
training of personnel, 6.61, 7.29, 7.50, 7.91,
7.97, 7.207, 10.28, 15.78see also Collaborating centres;'_Diagnosticprocedures;
Microbiological laboratories
229
Lactation, 6.17Lakes, man -made, 8.22, 8.2.4
natural, eutrophication, 15.126Land reclamation and development, 8.23Languages, 13.3, 13.13, 13.24-13.26, 14.4,
15.94, 15.156
Lao People's Democratic Republic, 5.19, 7.19,
7.29, 7.31, 7.32, 8.15, 8.71, 10.28, 11.47,14.17
Larvicides, 8.34, 8.132, 8.133Lassa fever, 8.137Latin American Centre for Perinatology and Human
Development, 6.8, 15.21Latin American centres for educational technology
in health, 7.43, 7.56, 15.37Latin American Programme of Educational Develop-
ment for Health, 7.12League of Red Cross Societies, 3.22, 3.25,
3.34Least developed countries, 1.9, 15.1Lebanon, 3.30, 5.43, 14.17Legal matters, 14.1 -14.6
see also Health legislationLeishmaniasis, 8.44-8.45, 15.147
research, 8.45, 8.156, 9.138Lepers' Trust Board (New Zealand), 8.81LEPRA (United Kingdom), 8.79Leprosy, 8.77 -8.91, 15.68, 15.147,
chemotherapy, 8.78, 8.82, 8.87,15.68
drug resistance, 8.89, 15.68combined leprosy and tuberculosis activities, 8.82,
15.64immunology, 8.86, 8.87, 8.88, 8.155, 9.126,
3.32,
15.1788.89, 8.155,
9.138, 15.147research, 1.28, 4.26, 8.46, 8.83 -8.91training, 1.28, 8.78, 8.79, 8.85
Leptospirosis, 8.111, 8.114Lesotho, 5.9, 5.53, 11.28Leukaemias, 9.137Liberation movements recognized by OAU, 3.36,
15.1
Liberia, 5.9,Libraries, see Health literature services; Medical
librariesLibyan Arab Jamahiriya, 5.5 7, 8.174, 9.7, 11.4,
15.134Liver cancer and other chronic liver diseases,
9.42, 9.68, 9.106, 11.61, 15.54, 15.81Long -term planning, 1.14, 2.8, 9.34, 9.76,
11.46, 15.6
Lymphomas, 9.66, 9.137
8.55, 9.39
4.26,
Madagascar, 7.77Malaria, 1.30, 3.12, 3.26, 8.7 -8.20, 8.,z6, 9.66,
15.75, 15.114, 15.146, 15.178
THE WORK OF WHO
chemotherapy and chemoprophylaxis, 8.16, 8.155coordination between countries, 8.14, 8.15
intercountry border meetings, 8.11
drugs, production and distribution, 1.30,15.180
resistance of parasites,15.18o
trials, 8.16, 8.19
immunology, 8.155, 9.126, 9.128research, 4.20, 4.26, 8.16 -8.20, 8.46, 15./8o
review, 8.18revised strategy, 8.9-8.15, 15.27, 15.180seminars for sanitary engineers (1976 and 1977), 7.93training, 1.30, 7.53, 7.105, 7.108, 8.11, 8.15,
15.75vaccine, trials, 8.2ovector control, 15.65, 15.18o
biological, 8.145, 8.149insecticides, 1.3o, 8.16, 8.122, 8.123-8.125,
8.142 -8.143resistance of vectors, 8.8, 8.13, 8.119,
15.75, 15.18oMalawi, /1.28Malaysia, 1.28, 3.12, 4.35, 5.58, 6.6, 6.7, 6.24,
6.35, 7.90, 8.15, 8.46, 9.17, 9.18, 9.141,10.28, 10.29, 11.28, 11.47, 13.20, 15.166
Maldives, 8.94, 15.75Mali, 5.25, 8.29, 11.62Malnutrition, I.2I, 6.22, 6.z8, 6.41, 6.44,
6.53, 8.1, 9.13, 15.23, 15.144Malta, 11.28
Management, see Health management ; Programme ofWHO, management
Manpower development, management and planning,2.4, 3.13, 3.36, 7.1- 7.114, 12.16, 15.4,
15.7, 15.34- 15.37, 15.57-15.60, 15.I09- 15.I12,15.141- 15.143, 15.168 -15.174
continuing education, 5.II, 7.20, 7.52,7.60 -7.66, 7.82, 7.106- 7.114, 15.36, 15.48,15.51, 15.I09, 15.171
curricula, 7.15, 7. 33-7.39, 7.44,7.100- 7.102, 7.105, 15.57, 15.17o
evaluation, 7.5, 7.67 -7.68guides, manuals and textbooks, 7.36, 7.48, 7.5o, 7.52,
7.104, 7.105, 15.36, 15.44, 15.57, 15.123information service, 7.73-7.75, 15.110integration with health services development, 1.21,
7.1-7.3, 7.10-7.15, 7.62, 7.67, 7.68, 15.37,15.109, 15.143, /5.161, 15.168
international migration of health personnel, 7.8,7.20, 7.72
international recognition of qualifications, 7.25,15.110
Latin America programme,
8.8, 8.19, 15.75,
15.75,
7.62,
7.12long- and medium -term programmes of WHO, 1.29,
2.5, 2.6, 7.4, 7.5, 7.13, 15.109
230
research, 4.32, 4.33, 7.5, 7.36, 7.41,7.67-7.72, 15.37, 15.154
see also Auxiliary health personnel; Educationaltechnology ; Teacher training
Manual of the international statistical classification of diseases,injuries, and causes of death, 12.23
Manuals, technical, 6.14, 6.31, 6.37, 7.50, 7.55,7.58, 7.104, 7.105, 8.59, 8.68, 8.99,8.168, 9.33, 9.11/, 9.112, 9.128, 9.131,I0.22, 10.29, 11.13, 11.14, 11.18, 11.43,12.15, 15.44, 15.11/, 15.113, 15.124
see also Glossaries; Guides, technical; Manpowerdevelopment, management and planning, guides,manuals and textbooks ; Textbooks
Marine pollution, 7.98, 11.44, 11.53, 14.6,15.152
Maternal and child health, 6.3, 6.4 -6.21, 6.27,6.31, 6.37, 6.53, 6.54, 9.9, 15.19 -15.21,15.47- 15.52, 15.164, 15.165, 15.166
planning and management of services, training,7.78, 7.83, 7.103, 7.106, 15.164
research, 4.21, 6.8risk approach, 6.7, 15./63training, 6.7, 6.11, 6.15, 6.z0, 7.30, 7.54,
7.81, 7.100, 15.52Mauritania, 6.26Mauritius, 3.25, 9.7Measles, 8.104
vaccination and vaccine, 8.58, 8.6z, 8.63,8.104, 10.22, 15.72
Mecca pilgrimage, 8.7oMedical assistants and auxiliaries,
15.39Medical care, see Health careMedical education, 5.1 z, 7.24,
7.44, 7.46, 7.104, 15.37,curricula, 7.15, 7.36, 7.37,
15.60, 15.84international recognition of qualifications, 7.25,
15.II0medical textbooks, provision of, 7.5zpsychiatric training, 7.101, 7.1II, 15.84
Medical libraries, 7.59, 13.8regional, 4.33, 9.48, 13.3, 13.7, 15.37,
15.154WHO library, 13.2, 13.5, 13.10
Medical physics, 9.118Medical records, 7.102, 7.104, 12.19, 12.20,
15.186Medicinal plants, 5.13, 5.63, 5.64, 5.66, 10.4,
Io.8, 15.162seminar, Tokyo (1977), 10.8
Mediterranean, pollution, 11.44, 14.6, 15.127Medium -term programming, 1.13, 1.14, 1.23,
2.2, 2.5, 2.6, 2.7, 2.12, 7.4, 7.5, 7.13,II.II, 15.6, 15.92, 15.I01, 15.I09, 15.I11,15.122, 15.124
7.29, 7.31, 15.36,
7.26, 7.38,15.52, 15.I107.44, 7.100,
INDEX
WHO Secretariat working group, 2.5, 2.6, 2.7MEDLINE, discontinuation, 13.6Meetings, organizational and related, (Annex z)Membership of WHO, 14.1, 15.1, (Annex 1)Menarini Foundation, 7.111Meningitis, see Cerebrospinal meningitisMenstrual disturbances, 6.42, 6.44, 6.48Mental health, 9.1 -9.33, 15.zo, 15.I12,
15.118 -15.120classification of disorders, 9.31-9.32community services, 9.5-9.19
15.119
information systems, 9.3 I, 9.33integration into general health services, 7.85,
9.4 -9.8, 15.84medium -term programme of WHO, 2.5, 9.1 -9.2monitoring of needs, 9.33, 12.14planning, management and evaluation of services,
7.85, 9.2-9.4, 9.6, 15.150research, 9.2, 9.25 -9.30special programme of technical cooperation with
pilot studies, Europe, 9.8, 9.12, 15.118-drug treatment, 7.111, 9.6, 9.25, 9.27
developing countries, 1.31, 9.2, 9.5, 9.6,
9.25training, 7.94, 7.101, 7.'11, 9.3, 9.6, 9.24,
15.84, 15.150working group on prevention of mental disorders
in the elderly, Europe, 9.10Mental retardation, 1.31, 9.9Metabolism, disorders, 15.25
inborn errors, 7.111, 9.130Mexico, 3.31, 4.23, 5.40, 5.45, 6.5, 6.11,
6.12, 6.33, 7.12, 7.82, 8.21, 9.16, 9.48,I2.18
Microbiological laboratories, prevention of accidentsand infections, 4.7, 4.14-4.15
Midwifery, 5.I I, 6.58, 7.32, 7.54,15.163
management of services, training, 7.58, 15.111teacher training, 7.49see also Nursing; Traditional birth attendants
Migration of health personnel, 7.8, 7.20, 7.72Milk, hygiene, 11.68
vitamin A enrichment, 3.19, 6.32, 8.171Miners, African Conference on Health of (1976), 9.142Molluscicides, 8.zz, 8.140
vector resistance, 8.120Mongolia, 5.55, 7.78, 9.7, 15.46Monkeypox, 8.55Monograph Series, 13.18Morocco, 5.56, 6.5, x1.28, 15.121Mortality, analysis and classification, 9.125, 12.24,
15.63, 15.186manuals, 12.15
infant and childhood, 6.3, 6.31, 6.54, 12.13,I2.15, 15.22, 15.50, 15.6z, 15.145
inter -American investigation, 6.7
23 I
maternal, 6.3, 6.6, 6.19, 12.21perinatal, 6.15, 6.19, 12.15, 12.21,
certificate, 12.21Moxibustion, 5.63Mozambique, 3.32, 5.25,
7.77, 8.37, 15.12Mycotic zoonoses, 8.114Mycotoxins, 9.68, 11.61Myocardial infarction, 9.85, 9.86
5.44, 6.z6,
15.49
7.29,
Narcotic drugs, 10.14National coordinators, 1.18, 15.13National health planning, see Country health pro-
gramming ; Health planningNational staff, employment in WHO programmes,
1.18, 15.13, 15.142Neonatology, 15.49Nepal, 5.46, 5.55, 6.5, 7.78, 15.44,
15.74, 15.75, 15.76, 15.82Netherlands, 3.9, 3.12, 3.20, 3.24, 3.25, 8.6,
8.zz, 8.128, 8.134, 8.166, 9.93, 9.134Neurological disorders, 7.111, 9.13, 9.27, 12.24
parasitic and infective, 9.27
15.70,
Neurosciences,New Hebrides,New Zealand,
9.6,5.12,
9.113,
7.111,7.39,13.23
9.138.z6, 11.47
Nicaragua, 5.27, 5.45, 6.24,Niger, 8.29, 15.12Nigeria, 5.44, 5.53, 6.13, 6.17, 6.z6, 7.77,
8.17, 8.55, 8.129, 8.137, 8.147, 8.166,8.172, 9.7
Niue, 8.26Nomenclatures, 9.42, 9.83, 12.22, 12.24Noncommunicable diseases, 1.31, 9.1- 9.149,
15.I15- 15.120, 15.150 -15.151Nongovernmental organizations in official relations
with WHO, (Annex 3)Nonverbal communication, 7.57Norway, 6.64, 8.166, 9.113Nuclear energy, 9.120, 11.37Nuclear medicine, 9.119, 15.83Nursing, 1.21, 15.100, 15.II1- 15.112,
auxiliaries, 15.36education and training, 5.12, 6.5 8, 7.26,
7.34, 7.36, 7.37, 7.39, 7.60, 7.72,15.37, 15.II1, 15.140, 15.163
management of services, training,15.II1
medium -term programme (Europe), 15.111mental health, training, 7.94, 7.101teacher training, 7.49textbooks and other educational materials,
7.52, 7.58, 15.II1work and living conditions, 7.9
Nutrition, 1.21, 3.15, 6.z, 6.22 -6.32, 11.20,11.21, 15.20, 15.53, 15.107, 15.144, 15.166
7.12, 7.36, 8.11
15.'40
7.32,
7.58, 15.97,
7.37,
THE WORK OF WHO
consultation on the use of fats and oils, joint FAO/WHO (1977), 6.31
interrelationship between nutritional status andimmunological function, 8.1
national policy development, 6.23-6.24, 15.144,15.166
inter- agency project, Americas, 6.24research, 6.32, 15.54surveillance, 1.21, 3.28, 6.25 -6.26, 15.166training, 7.89, 15.166
meeting of directors of international courses,Geneva (1976), 6.z8
OAU, see Organization of African UnityObstetrics, 5.18, 6.21, 7.100Occupational health, 1.31, 9.139,
criteria and standards, 9.146information systems, 9.140integration into general health services, 7.86,
9.139monitoring, 7.113, 9.149research and training, 7.113, 9.142
centres, Africa, 9.140, 9.242see also Working populations, health of
Occupational therapy, training, 5.40,Official languages, 13.13, 25.156OJfrcial Records, reduction, 13.11, 13.13
Offset publications (WHO), 13.18Oman, 8.24, 8.174, 9.7Onchocerciasis, 8.170, 8.172
chemotherapy, 8.27, 8.34research, 4.19, 4.20, 8.z8vector biology and control, 8.27, 8.29, 8.31,
8.34, 8.132-8.133Volta River basin area, control programme, 4.19,
8.27, 8.29 -8.36, 8.172, 15.2financing, 8.34
Oncology, see Cancer, researchOperational research, 1.10,
5.31, 5.50, 6.9, 7.79,22.8, 15.69, 15.95
Opium, 9.71
Oral health, 9.107 -9.113training, 9.108, 9.209, 9.'11, 15.37
Organization of African Unity, 3.5, 7.110Organization for Coordination and Cooperation in the
Control of Major Endemic Diseases in WestAfrica, 8.39
Organisation for Economic Cooperation and Develop-ment, 15.102
Nuclear Energy Agency, 12.34
Organizational and related meetings, (Annex 2)Organizational studies by the Executive Board,
1.16 -1.18
9.141, 1533
5.41, 5.43
4.5,8.46,
5.11, 5.29,8.61, 12.7,
232
Orthopedic and orthotic services, see Disability preven-tion and rehabilitation
Orthopaedics, 5.43"Overnutrition" (overfeeding and overeating), 15.107
Paediatrics, 6.21, 7.100, 7.103, 15.52PAHO, see Pan American Health OrganizationPakistan, 3.33, 5.30, 5.43, 5.49, 6.35, 7.46,
8.14, 8.119, 8.126, 8.143, 9.17, 9.39, 9.51,11.43, 12.18, 15.137, 15.148
Pan American Centre for Human Ecology and Health,11.38, 15.30
Pan American Centre for Research and Training inLeprosy and other Tropical Diseases, 1.28, 8.85
Pan American Centre for Sanitary Engineering andEnvironmental Sciences, 11.15, 15.32
Pan American Conference on Drinking -Water QualityImprovement, 11.16
Pan American Federation of Associations of MedicalSchools, 7.36
Pan American Health Organization (PAHO),15.24-15.40
anniversary, seventy -fifth, 15.40publications, 13.12, 13.26
Pan American Health Planning Programme, 5.45Pan American Zoonoses Centre,Papua New Guinea, 7.31, 7.8o,
9.I13, I0.28, 11.47, 14.1,Paraguay, 5.45, 6.24, 7.12
Parasitic diseases, 6.41, 6.43,
8.1117.9o, 8.15,15.166
8.7-8.47, 9.137,15.147
research, 4.34, 8.46 -8.47, 15.159training, 7.53, 7.105, 7.108, 8.11
Perinatal care, 6.8, 6.15Periodontal diseases, 9.207, 9.112Personnel, see Manpower development, management
and planning; Staff of WHOPertussis, 8.73
vaccination and vaccines, 8.58, 8.62,25.72
see also DPT vaccine
8.68, 8.74,
Peru, 5.26, 5.54, 7.12, 7.29, 7.103,9.17, 9.48, 11.28
8.94, 9.7,
Pesticide Residues Series (1VHO), 23.28
Pesticides, 8.118, 8.141, 8.142equipment for application, 8.151health hazards, 7.93, 8.118, 8.143-8.144, 9.62,
11.51, 11.62residues, 8.133, 11.51, 11.62, 11.68resistance, 8.118, 8.119 -8.121, 8.238see also Insecticides; Molluscicides; Rodent control
and rodenticidesPharmaceutical production, 10.2, 20.7
regional and national, 1.31, 3.12, I0.4, 15.9,
15.75, 15.162
INDEX
Pharmaceutical, see DrugsPharmacology, clinical,
psychopharmacology,traditional substances,
so.,8,7.111
5.63,
15.130,
5.66,
15.131
9.36, 15.9see also Medicinal plants ; Traditional medicine
Philippines, 5.11, 5.12, 5.19, 5 31, 5.58, 6.17,6.z6, 6.32, 6.35, 6.37, 7.5, 7.32, 7.103, 8.15,8.23, 8.46, 8.71, 8.79, 9.6, 9.7, 9.141,11.23, 11.28, 11.43, 11.47, 12.18, 15.164,15.166
Physicians, free movement (European Communities),15.I IO
Physics, medical, 9.118Physiotherapy, training, 5.40, 5.41, 5.43Plague, 8.73, 8.138, 8.139, 15.66, 15.70
Planning, see Health planning; Manpower development,management and planning
Pneumococcal infections, vaccines, 8.75Poisoning, by pesticides, 8.143
see also ToxicologyPoland, 7.38, 9.39, 9.113Poliomyelitis, 8.505
vaccination and vaccines, 8.58, 8.62, 10.22,10.25, 15.72
Pollution, see Air pollution; Coastal water pollution;Environmental pollution ; Marine pollution ; Waterpollution
Population, World Plan of Action, 6.3Population dynamics, 6.2, 6.3, 15.14Portugal, 7.38, 9.7, 11.28, 15.121Postgraduate training, 5.40, 7.60, 7.62, 7.104,
7.111, 9.99, 15.60, 15.141
Poxviruses, research, 8.55Pregnancy, and its outcome, 15.49
spacing, 6.17, 6.53, 6.54termination, 6.zo, 6.38, 6.41, 6.42, 6.49,
6.51, 15.48wastage, 6.39, 6.54, 12.13, 12.15
Preventive and social medicine, 7.23
Primary health care, 1.20, 1.29, 3.14, 3.21, 4.2,5.2, 5.3-5.25, 5.16, 5.28, 5.40, 5.57, 5.67,6.1, 6.7, 6.10, 6.11, 6.27, 6.z8, 6.34,6.39, 6.58, 7.27, 7.30, 7.54, 7.62, 13.23,15.4, 15.16, 15.29, 15.44-15.45, 15.57,15.137-15.140, 15.160, 15.161, 15.164,15.166, 15.167, 15.186
expert advisory panel, Eastern Mediterranean Region,5.8
inter- agency consultation, UNICEF/WHO,Alexandria, Egypt (1977), 5.8
international conference (1978), 1.20, 3.15,15.138
joint study on community involvement, UNICEFWHO, 3.14, 5.8, 6.33
joint study on water supply and sanitation com-ponents, UNICEF/WHO, 11.26
5.14,
233
records, 12.19research, 4.32 5.67, 7.77role of nurses and midwives, 5.11,
7.34, 7.36, 7.54, 15.140symposium, New York (1977), 5.14use of traditional health workers, 5.60,
7.27, 7.54, 15.44, 15.58
5.12,
5.62,
7.32,
5.67,
Primary health care workers, training, 6.9, 7.27,
7.31, 7.32, 7.36, 7.54, 7.55, 7.71, 7.81,7.88, 15.45, 15.57, 15.58
Primates, for biomedical research, 4.26, 6.6zProcedures in medicine, classification, 12.22, 12.23Profiles, programme and project, 2.18, 2.20, 2.23Programme budgets, 1.23, 2.2, 2.7, 2.12
for 1977, 1.2, I.7for 1978 and 1979, 1.2, 1.5
for 1980 and 1981, 1.5, 1.14form of presentation, 13.13harmonization of cycles in UN system, 1.17policy, I.z -I.6, 1.7, 1.14, 124regional, 1.28, 15.39strategy, 1.8, 1.13see also under Regional committees
Programme committees,Global Programme Committee, 2.2Headquarters Programme Committee, 2.2, 2.7,
2.10, 2.13Programme Committee of the Executive Board, 1.6,
I.8, I.14, 2.8, 2.11regional programme committees, 2.2
Programme of WHO, general development, 1.6,1.13, 1.14, 1.24, 2.1, 2.5 -2.8
management, 2.1, 2.2information system, 2.16, 2.17, 15.6, 15.15 8
new classification structure, 2.7trends and priorities, 1.23-1.33, 15.92
Project systems analysis, see Systems analysisProphylactic substances, 1.30, I0.1- 10.31,
15.130- 15.132, 15.162see also Immunization
Proposed programme budget, reduction in volumeof publication, 13.13
Prostaglandins, 6.49Prosthetics, 5.40, 5.42, 5.43Protein -Calorie Advisory Group of the United Nations,
see Administrative Committee on Coordination,Sub -Committee on Nutrition
Protein -energy malnutrition, 6.31, 6.32Protocol for the Protection of the Mediterranean Sea
against Pollution from Land -based Sources, 14.6Psychiatry, forensic, 9.14
training, 7.101, 7.111, 15.84, 15.150Psychopharmacology and psychopharmacotherapy,
7.111, 9.6, 9.25, 9.27Psychosocial factors and health, 1.31, 6.56,
9.20 -9.23, 15.120Psychotropic substances, 9.6, 9.19, 9.25, 10.14
THE WORK OF WHO
Public health administration, research and training,7.21, 7.23, 7.66
see also Health managementPublic Health Papers, 13.18Public health research, 7.77, 7.79Public health services, see Health servicesPublic health training, 7.60 -7.62, 7.90, 7.108,
8.11African centre, 7.90schools, meeting of directors, Teheran (1977), 7.62
Public information, 13.19-13.23Publications, WHO programme, 13.2-13.4,
13.11 -13.18distribution and sales, 13.29-13.31reduction, 1.5, 13.17regional publications, 13.3, 13.12, 13.26
Qatar, 5.57, 6.35, 9.141, 15.134
Rabies, 8.111, 8.112 -8.113surveillance and control, second European conference
Frankfort -am -Main, Federal Republic of Germany
(1977), 8.113vaccines, 8.112wildlife rabies, joint FAO/WHO programme, 8.113
Racial discrimination, see ApartheidRadiation health and protection, 4.12, 9.120,
9.122- 9.I24, I1.52, 15.83ionizing radiation, 4.12, 9.12I, 11.34monitoring, 9.122, 11.40, 15.83non -ionizing radiation, 11.34, 11.43training, 9.118, 9.123
Radiation medicine, 9.114-9.124, 15.83training of radiographers, 9.124
Radio, promotion of rural health by, 13.22Radiobiology, 9.120Radiological equipment, maintenance and repair, 7.95,
9.123, 15.83calibration of dosimeters, 9.118see also X -ray equipment
Radiological technicians, training, 7.95, 9.118Radiotherapy, 9.116 -9.119
dosimetry, 9.118Reagents, laboratory, 8.110,
1o.28, 10.29Regional Committee for Africa, 1.24, 1.26, 1.29,
1.31, 10.4, 15.13working group on administrative structures, 1.4
Regional Committee for the Americas, 1.26, 1.27,x.28, 1.29, 1.30
Regional Committee for the Eastern Mediterranean,1.24, 1.29, 1.31, 15.143
Regional Committee for Europe, 1.29, 15.92,15.99, 15.101
Regional Committee for South -East Asia, 1.24,1.28, 1.29, 1.31, 15.50
9.136, 9.137,
1.25,
234
Regional Committee for the Western Pacific, 1.24,1.28, 1.29
Regional committees, 1.1
strengthening of role, I.Iotechnical discussions, 1.19
Regional Office for Africa, 1.4, 5.17,15.2 -15.3
Regional Office for the Americas, 3.17, 8.5,14.10, 15.38
disaster unit, establishment, x.27
Regional Office for the Eastern Mediterranean, 14.10,15.142, 15.155- 15.156
Regional Office for Europe, 3.13, 5.48, 7.66, 8.5,9.10, 9.33, 15.92, 15.99, 15.101
Regional Office for South -East Asia, 14.10Regional Office for the Western Pacific, 3.12, 3.18Regional offices, review and reorganization of adminis-
trative structures, 1.3
staff, reduction of establishment, 1.3 -1.4, 15.2,15.155
staff training, 14.8 -14.10, 14.11Rehabilitation, see Disability prevention and rehabilita-
don, and under individual diseases and conditionsRehydration, 5.18, 6.6, 6.9, 6.37, 8.71, 8.72,
15.69, 15.145Reproduction, see Human reproductionRepublic of Korea, 4.34, 5.11, 5.3,,
8.46, 9.7, 9.142, 11.47, 14.5Research, 4.1-4.35, 15.10, 15.159
ethical aspects, 4.7, 4.11-4.13financing, 1.28, 4.4, 4.29, 4.33, 15.12, 15.92information systems, 4.9, 4.20, 4.30, 15.93regional developments, 4.17-4.35, 15.54- 15.55,
15.93, 15.99, 15.154, 15.159regionalization and establishment of regional advisory
8.33, 9.88,
14.9,
5.37, 7.5,
committees, 1.10, 1.28,training, 4.16, 4.17, 4.18,
centres, 1.x0, 1.28, 1.30,4.20
directories, 4.17, 4.23,grants and awards, 4.16,
4.3,4.35
4.8,
4.31,4.20,
15.56
4.18
15.1544.33, 6.61,
7.107, 8.158, 15.519IARC programme, 9.54
see also Health services research ; Human reproduc-tion, research ; Operational research ; Tropicaldiseases, research
Research coordination, 1.28,8.46 -8.47, 15.159
ad hoc team, 8.46Respiratory diseases, 8.92 -8.96, 12.24, 15.23
chronic, 9.I00 -9.101Respiratory insufficiency, intensive care, working
group, Europe (1976) 9.101rehabilitation, 5.40
Rheumatic diseases, 9.102 -9.105Rheumatic fever, 9.78, 9.88, 9.89,
9.95
4.6, 4.7, 4.8, 4.22,
9.90, 9.94,
INDEX
Rheumatic heart diseases, 9.78, 9.88, 9.89, 9.90,
9.94, 9.95Rheumatoid arthritis, 5.64, 9.103Rickettsial diseases, 8.110Rodent control and rodenticides, 7.93, 8.'18,
8.136 -8.139, 15.66Rodent Control Demonstration Unit (Rangoon),
8.139, 15.66Romania, 3.34Royal Dutch Tuberculosis Association, 13.23Rural development, 2.29, 3.5, 5.1, 5.3, 5.9,
5.66, 6.1, 6.36, 7.71, 15,88, 15.139,15.161, 15.165
water supply and sanitation, 6.37, 7.114, 8.22,1I.5, 1I.14, I1.30, 15.28, 15.152
inter -agency ad hoc working group, 7.114Rural health, 3.21, 5.11, 5.28,
6.5, 6.11, 6.36, 7.28, 7.30,15.16, 15.62, 15.69, 15.139-
5.31,7.55,
15.140
5.40, 5.54,13.22,
Rwanda, 5.14, 5.53, 6.26, 11.28
Sahel, 1.27St Lucia, 6.35St Vincent, 6.35Salmonella, 8.5, 11.55Samoa, 5.9, 5.50, 6.33, 7.39, 8.127, 11.47Sanitary and public health engineering, training, 7.35,
7.37, 7.87, 15.122Sanitation, 1.32, 3.14, 7.114, 8.11, 8.72,
II.I- II.12, II.24, 11.26, 11.47, 15.28,15.29, 15.85, 15.I22
inter- agency ad hoc working group, 7.114international decade (1980 -1990), 1.32, 11.7,
1I.I2medium -term programme, Europe, 15.122pre -investment planning, 11.27 -11.31, 15.86,
15.121statistics, II.2, 12.13see also Environmental health ; Sanitary and public
health engineering ; Sewerage and sewagedisposal ; Wastes disposal ; Water supplies
Sao Tome and Principe, 14.1Saudi Arabia, 5.43, 5.57, 7.112, 8.z,, 9.7,
11.4, 15.134Schistosomiasis, 8.21 -8.25, 15.146, 15.178
chemotherapy, 8.21, 8.22drug toxicology, 8.21research, 4.20, 4.35, 8.21, 8.25, 8.46, 8.155,
8.156, 9.126, 9.138training, 7.53
Schistosomicides, 8.21, 9.62Schizophrenia, 9.26School health, 9.78, 15.51Scientific Group on Environmental Health Criteria
(1976), 11.33Scientific Group on Immunodeficiency (1977), 9.137
235
Scientific Group on the Long -term Effects of Radiumand Thorium in Man (1977), 9.120
Scientific Group on Monitoring of Health Effects ofEnvironmental Agents (1976), 11.42
Scientific Group on Neisseria and Gonococcal Infections(1976), 8.98
Self- medication, 10.4
Senegal, 5.37, 6.14, 6.24, 6.z6, 6.33, 8130,8.149, 9.6, 9.58, 11.28
Sewerage, II.4, 11.5, 11.9, 11.30, 15.182,15.183
Sex hormones, radioimmunoassay, 6.62
Sexually transmitted diseases, 3.12, 8.97- 8.200,8.109, 15.71, 15.113, 15.178
Seychelles, 9.7Shellfish, hygiene, 11.53SIDA, see Swedish International Development AuthoritySierra Leone, 8.55, 12.15Singapore, 8.15, 8.46, 13.20
Smallpox, 3.35, 8.4, 13.23, 15.74eradication, 1.30, 8.48-8.57, 13.21, 15.41- 15.42,
15.73, 15.148certification of, 8.53, 8.57, 15.74
vaccination and vaccine, 15.72discontinuation of vaccination, 8.57stocks of variola virus, 1.30, 8.54,vaccination certificate, 8.4
Smoking and health, 1.31, 9.11, 9.69, 9.72,9.87, 15.116
expert advisory panel, establishment, 9.87Snail control, see MolluscicidesSocial medicine, 7.23Social security, 1.22, 5.36, 5.37Socioeconomic development and health, interrelation-
ship, 1.25, 2.1, 2.3, 5.3, 5.44, 6.23, 7.10,8.32, 10.8, 15.5, 15.31, 15.43, 15.135,15.136
Solomon Islands, 11.47Somalia, 3.35, 5.9, 6.27, 8.4, 8.48, 8.49,
8.5o, 8.51, 1/.28, 15.137, 15.145, 15.148
South Africa, 9.15South -East Asia Region, 4.26-4.29, 15.42-25.90Southern Africa, psychosocial problems, 9.2Spain, 5.5, 7.38Spanish, translation of technical publications, 13.3,
13.12, 13.26Speech therapy, 5.40Sri Lanka, 6.6, 6.15, 6.26, 6.33, 6.35, 7.37,
7.78, 8.7, 9.7, 9.37, 9.49, 9.141, 10.28,11.28, 15.48, 15.63, 15.70, 15.71, 15.75,15.82
Staff of WHO, 14.7-14.13, 15.142reduction of posts, 1.3 -1.5, 13.25, 14.7, 15.2,
15.155training, 5.5, 14.8-14.13women, 14.13
8.56, 15.74
THE WORK OF WHO
Standing Committee on the Health of Migrant Workers,establishment, 9.143
Standing Committee on Information, 2.13Statistics, 5.5z, 6.12, 9.33, 11.42, 12.1- 12.26,
15.61 -15.63, 15.177, 15.186development of services, 12.3, 12.17 -12.20dissemination by WHO's central services, 12.6,
Iz.11 -12.16information systems, 12.3, 12.14, 12.17,
12.18, 12.19methodology, 12.5, 12.7 -12.10mortality and morbidity data classification, use by
lay (nonmedical) health perrsonnel, 12.22,12.24, 15.63, 15.186
training, 7.204, 7.105, 12.20, 12.25, 15.186working group on measurement of levels of health
(Europe, 1977), 5.56, 12.19see also International Classification of Diseases
Sterility, see InfertilitySterilization, 6.2o, 6.38, 6.41, 6.58Steroids, 6.48Streptococcal infections, 8.76, 9.78Stress, heat, 9.49
psychosocial, 9.z, 9.23Stroke, 9.79, 9.90Structure of WHO, (Annex 4)Study Group on the Application of Advances in
Neurosciences (1977), 9.13Study Group on Criteria for the Evaluation of Learning
Objectives in the Education of Health Personnel(1976), 7.68
Study Group on Financing of Health Services (1977),5.37
Sudan, 3.13, 3.35, 4.31, 5.4, 5.14, 5.44,5.49, 5.57, 6.5, 6.11, 6.27, 6.52, 7.29,7.46, 7.51, 7.71, 7.81, 7.103, 8.3, 8.27,8.37, 8.108, 8.136, 8.174, 9.6, 9.7, 9.37,9.141, 10.29, 11.4, 11.28, 15.137, 15.150
Sugar, vitamin A enrichment, 6.32Suicide, 9.11Supplies and equipment, provision of, 14.15 -14.18
cost, 131for emergency and relief operations, 3.23-3.34,
3.36, 8.44working group on inter -agency procurement services,
14.18see also Equipment
Surgery, coronary, 9.93Surinam, 14.ISurveillance, see Epidemiology and epidemiological
surveillanceSwaziland, 11.61Sweden, 6.17, 8.166, 9.2x, 9.136Swedish Agency for Research and Cooperation with
Developing Countries, 6.16Swedish International Development Authority (SIDA),
5.39, 6.17
236
Swedish National Association against Heart and ChestDiseases, 7.112
Switzerland, 3.12, 3.20, 7.114, 8.166, 9.29,
9.133Syrian Arab Republic, 5.30,
9.7Système international d'Unités (SI), 13.28Systems analysis, 6.13, 7.79, 12.7, 12.8, 12.9,
12.18, 15.95
5.43, 8.94, 8.174,
Tanzania, see United Republic of TanzaniaTeacher training, 6.ií, 6.20, 7.5, 7.40-7.49,
7.64, 7.103 -7.104, 12.20, 15.37, 15.109,15.142, 15.174
centres, 7.5, 7.44, 7.47, 15.110, 15.173meeting of directors, Shiraz (Iran) (1976), 7.41
Teaching/learning materials, 6.1o, 7.5, 7.6, 7.36,
7.37, 7.41, 7.50-7.59, 7.105, 8.176, 9.124,
15.37, 15.57Teams, see Health teamsTechnical cooperation, 1.z, 1.3, 1.4, 1.5, 1.6,
1.7 -1.11, 1.14, 1.18, 2.14, 12.5, 15.12,
15.39among developing countries, 1.7, 1.8, 1.9,
1.10, 1.11, 1.18, 3.17, 50.5, 15.11- 15.12,15.38, 15.161
task force (UNIDO/UNCTAD/WHO), 10.9world conference (1978), 3.17
Technical discussions, at Health Assembly, I.I0,1.19 -1.22, 6.23, 6.31, 11.20 -I1.21
at regional committees, 1.19Africa, 1.2I, 1.22, 6.23Americas, 1.zo, 1.22Eastern Mediterranean, 1.20, 1.21, 6.34Europe, 1.21, 1.22, 5.51, 12.17, 15.111South -East Asia, 1.20, 1.21, 5.52, 6.23,
12.17, 15.53Western Pacific, 1.20, 1.22
Technical Report Series, 13.18
Terminology, 9.38, 9.43, 9.96, 13.27 -13.28,
15.94Tetanus, 8.73
vaccination and vaccine, 5.58, 8.65, 15.72see also DPT vaccine
Textbooks (medical and nursing), 7.50, 7.52, 15.36
Thailand, 5.28, 5.46, 5.55, 6.5, 6.27, 6.32, 6.43,
7.37, 7.79, 7.103, 8.7, 8.15, 8.79, 8.108,
9.7, 9.17, 9.37, 9.I10, I1.28, 12.18, 15.44,15.48, 15.63, 15.78, 15.84
Therapeutic substances, 1.30, Io.1- 10.31, 15.9,15.130, 15.132, 15.16z,
Tobacco (smoking), 1.31, 9.11,15.116
Togo, 5.25, 8.29, 9.7Tonga, 7.39, 8.26, .11.47, 14.5
9.69, 9.72, 9.87,
INDEX
Torture, 3.zTown planning, 15.122
see also Human settlementsToxaemia, 6.19
Toxicology, 7.93, 7.113, 8.z,, 8.28, 8.144see also Chemicals, carcinogenicity and toxicity ; Drugs,
safety and efficacy; Food safety and hygiene;Pesticides, health hazards
Trace elements, in cardiovascular diseases, 9.85Trachoma, 8.170, 8.172, 8.173, 8.174Traditional birth attendants, 5.6o, 5.61, 5.67, 6.7,
6.,o, 7.30, 7.32, 7.54Traditional health workers, 5.6, 5.13, 5.6z, 5.66,
5.67, 7.30, 15.44, 1558joint study, UNICEF /WHO, 5.6otraining, 5.60, 5.61, 5.66, 7.6, 7.27, 15.48
Traditional medicine, 1.22, 1.29, 3.18, 5.13,5.60 -5.67, 7.26, 15.9, 15.44, 15.58, 15.162
consultation, Geneva (1977), 5.67education, 5.65, 5.67research, 4.17, 4.27, 5.63, 5.64-5.67study tour, China (1977), 5.66
Traffic accidents (road), 1.29, 2.5,15.92, 15.101- 15.1oz
Training, see Manpower development, management andplanning; Medical education
Translation, reduction in staff, 13.25Spanish, technical publications, 13.3, 13.12, 13.26
Treponematoses, endemic, 8., 01Trinidad and Tobago, 6.24, 11.16Tropical diseases, 1.28, 1.30
drugs, 1.30, 8.159research and training, 7.53, 7.110
centres, national, 4.19, 8.41regional, 1.28, 4.18, 4.35, 8.21, 8.46,
8.47, 8.85, 8.158, 8.159, 8.163special programme, 1.30, 3.3, 4.2, 4.10,
4.17, 4.26, 7.53, 7.110, 8.16, 8.18, 8.25,8.z8, 8.34, 8.41, 8.43, 8.45, 8.46, 8.47,8.87, 8.91, 8.146, 8.153-8.168, 9.133,9.135, 15.55, 15.178
financing, 4.4, 8.166 -8.167strengthening of institutions, 8.91, 8.154,
8.158 -8.163Tropical Diseases Research Centre, Ndola (Zambia),
4.18, 8.21, 8.47, 8.159, 13.8Trypanosomiasis, 8.37 -8.41, 15.147
chemotherapy, 8.41research, 4.20, 8.38, 8.39 -8.41, 8.155, 8.156,
9.138seminar, FAO /WHO /OAU, Nairobi (1977), 7.110vector control, genetic, 8.149
insecticides, 8.39, 8.122, 8.134-8.135see also Chagas' disease
Tuberculosis, 8.92 -8.95, 15.68, 15.179BCG vaccination and vaccine, 8.58, 8.62, 8.65,
8.95, 15.72, 15.179
5.42, 9.73,
237
chemotherapy, 8.92, 8.95, 15.68combined leprosy and tuberculosis activities, 8.82,
15.64training, 8.94, 15.179
Tumours, classification, 7.112, 9.40, 9.43, 9.51,12.23
Tunisia, 8.21, 12.18Turkey, 5.5, 6.7, 7.38, 8.13, 8.71, 8.119,
8.126, 11.28, 15.114Typhus, 8.1,0, 8.139
Uganda, 6.26, 9.39, 9.74Ulcer, gastroduodenal, 9.73UNCTAD, see United Nations Conference on Trade
and DevelopmentUNDP, see United Nations Development ProgrammeUNDRO, see United Nations Disaster Relief CoordinatorUNEP, see United Nations Environment ProgrammeUNESCO, see United Nations Educational, Scientific
and Cultural OrganizationUNFDAC, see United Nations Fund for Drug Abuse
ControlUNFPA, see United Nations Fund for Population
ActivitiesUNHCR, see United Nations High Commissioner for
RefugeesUNICEF, see United Nations Children's FundUNIDO, see United Nations Industrial Development
OrganizationUnion of Soviet Socialist Republics, 5.5, 7.92, 9.39United Arab Emirates, 3.25, 5.57, 8.14, 9.7,
15.134United Kingdom of Great Britain and Northern
Ireland, 3.9, 3.24, 5.17, 6.64, 7.85, 8.6,8.22, 8.139, 8.166, 9.16
United Nations, 3.1, 3.2, 3.3, 3.23, 6.2, 11.12Committee on Natural Resources, 11.12see also Coordination with the United Nations system
of organizationsUnited Nations Children's Fund (UNICEF), 3.12,
3.14 -3.16, 3.36, 10.4, 10.24, 13.20, 15.9joint activities, communicable diseases, 8.71, 8.81,
8.101, 15.145emergency assistance, 3.22, 3.24, 3.32,family health, 6.17, 6.21, 6.36, 7.103nutrition, 6.22, 6.24, 6.z6, 6.28, 6.32,
15.53, 15.144primary health care, 5.8, 5.14, 5.31, 5.6o,
6.33, 7.77, 15.44water supplies and waste water disposal, 11.5,
11.26United Nations Commission on Narcotic Drugs, 9.17United Nations Conference on Desertification, 3.4United Nations Conference on Human Settlements
(HABITAT), Vancouver (1976), 1.20, 3.4,11.6, 11.21 -11.22, 11.24, 15.28, 15.87
3.33
THE WORK OF WHO
United Nations Conference on Science and Technologyfor Development (1979), 3.3
United Nations Conference on Trade and Development(UNCTAD), 10.4, 10.9
United Nations Development Decade, Second, 1.2,11.x, 15.85
international development strategy, 3.5United Nations Development Programme (UNDP),
1.2, 2.4, 3.17-3.18, 3.36, 5.45, 6.36, 8.22,8.39, 8.62, 8.68, 8.134, 8.166, 10.4, 10.9,10.22, 11.9, 11.31, II.36, 15.89, 15.161
United Nations Disaster Relief Coordinator (UNDRO),3.22, 3.24, 3.25, 3.27, 3.28, 3.32, 3.33,3.34, 3.35, 8.51
United Nations Educational, Scientific and CulturalOrganization (UNESCO), 6.36, 7.25, 7.87,11.44
United Nations Emergency Operation (UNEO), 14.17United Nations Environment Programme (UNEP),
8.114, 8.118, 8.140, 11.14, 11.33, 11.36,1I.41, 11.44, 11.55, II.61, 12.67, 13.18,14.6, 15.127
Conference on the Ozone Layer (1977), 11.34Environmental Coordination Board, 11.36Global Montoring System, 51.39, 15.128
United Nations Fund for Drug Abuse Control(UNFDAC), 9.17, 9.25, 9.30, 15.84
United Nations Fund for Population Activities(UNFPA), 2.4, 3.22, 6.5, 6.17, 6.27, 6.36,6.64, 12.15, 15.47, 15.89, 15.105
United Nations High Commissioner for Refugees,Office of the (UNHCR), 3.12, 3.22, 3.25,3.26, 3.30, 14.17
United Nations Industrial Development Organization(UNIDO), 3.12, 8.141, 10.4, 10.9, 11.36,11.44, 15.9
United Nations Special Committee against Apartheid,9.15
United Nations Special Coordinator for RehabilitationAssistance to Viet Nam, 3.12
United Nations system, see Coordination with theUnited Nations system of organizations
United Nations Trust Fund for Lebanon, 3.30, 14.17United Nations University, 6.22United Nations Water Conference (1977), 1.32, 3.4,
11.2, I1.6- II.52, 15.28United Republic of Cameroon, 6.5, 6.52, 8.37,
9.39, 20.28United Republic of Tanzania, 3.36, 6.26, 6.27,
7.42, 8.94, 8.127, 8.149, 9.66, 11.28United States Agency for International Development
(USAID), 2.4, 8.125, 8.149United States of America, 4.11, 7.111,
8.103, 8.166, 9.48, 9.113, 11.41, 12.14,12.23, 13.20
Upper Volta, 6.z6, 7.32, 7.92, 7.114,8.39, 8.82, 8.134, 8.149
7.114,
8.29,
238
Urbanization, 15.14, 15.31Urethritis, 8.97Uruguay, 5.26, 5.40, 9.7, 9.48, 14.5USAID, see United States Agency for International
Development
Vaccination, see Immunization, and under individualdiseases
Vaccination certificates, 8.2smallpox, 8.4
Vaccines, production and quality control, 8.68, 8.95,I0.4, 10.24 -10.26, 15.132, 15.175
training, 8.68, 10.20, 10.22, Io.z6working group, Zagreb, Yugoslavia (1977),
50.26regional and local production, 1.31, 15.9, 55.549,
15.176research, 8.62, 8.68, 8.74 -8.75, 10.22, 15.175storage and transportation, 5.18, 8.64, 15.175supplies, management, 8.67, 10.2
revolving fund, Americas, 15.24see also BCG ; DPT and under individual diseases
Vaginitis, 8.97Variola virus, 1.30, 8.54, 15.74
survey of laboratory stocks, 8.56Vascular diseases in diabetics, meeting of investigators
on the multinational study, Geneva (1977),9.97-9.98
Vasectomy, 6.58Vector biology and control, 8.8, 8.11, 8.13, 8.26,
8.29, 8.30, 8.31, 8.34, 8.43, 8.118 -8.152,15.64, 15.180
biological control, 4.19, 8.15, 8.540,8.545- 8.148, 8.554, 8.155
genetic control, 8.149-8.15oresearch units, 4.19, 8.34seminars and courses (1976 and 1977), 7.93, 8.IIsee also Insecticides; Pesticides
Vector and Rodent Control Research Unit (Jakarta),8.125, 8.128, 8.138, 15.65
Venereal diseases, see Sexually transmitted diseasesVenezuela, 1.28, 4.23, 5.40, 7.12, 8.94, 9.7,
9.48Veterinary public health, 8.222- 8.157, 15.77Viet Nam, 6.5, 6.33, 7.59, 8.82, 8.98, 8.141,
9.18, 13.8, 14.1special assistance, 3.12, 14.17
Village health workers, see Community health workersVirus diseases, 8.102- 8.108, 9.137
research, 8.102, 15.78Virus- associated cancers, 9.53, 9.66 -9.68Visceral leishmaniasis, see Kala -azarVitamin A deficiency, 3.zo, 5.28, 6.35, 6.32Volta River basin area, onchocerciasis control pro-
gramme, 4.29, 8.27, 8.28, 8.29 -8.36,8.172, 15.2
INDEX
financing, 8.34Voluntary Fund for Health Promotion, 3.6, 6.64,
10.8, 12.18, 14.17Voluntary health workers, 15.44, 15.5 8, 15.59
Wastes disposal, 11.3, 11.20, 11.21, 11.27,15.88, 15.121, 15.122
animal wastes, 8.115management of solid wastes, 7.98, 11.17, 11.18,
15.31, 15.124waste water disposal, 11.4, 11.5, 11.9, 11.15,
11.30, 15.183Water pollution, 7.98,
15.I28, 15.I29research, 15.126see also Coastal water pollution ; Marine pollution
Water quality control, 11.16, 11.37, 11.39, 11.43see also Drinking -water
Water resources and river basin development projectshealth aspects, 8.22, 8.24, 8.32, 15.11,15.30, 15.146
see also Volta River basin area, onchocerciasis controprogramme
Water supplies, 1.32, 3.14, 7.114, 8.22,II.I -I Z.16, II.13- II.14, 11.20, II.2I, I1.26,1I.30, 15.28, 15.29, 15.85, 15.88, 15.122,15.152, 15.182, 15.183
pre- investment planning, Z1.27- 1I.31, 15.86,15.I21
statistics, II.2, I2.13Water -borne diseases, 11.10, 15.85Weaning foods, 6.27Weekly epidemiological record, 8.6Western Pacific Region, 4.34-4.35,WHO representatives, 1.4, 1.18,
15.91see also National coordinators
Whooping cough, see PertussisWomen in health and development, 3.5, 6.2, 6.7,
6.21, 6.33, 15.18,Women's Decade of Equality, Peace and Development,
6.2Working languages, 13.13, 13.24, 15.94Working populations, health of, 1.31, 9.139 -9.149
agricultural workers, 9.145, 15.33industrial workers, 7.113, 9.64, 9.146-9.149
in small industries, 9.114migrant workers, 9.143miners, 9.142
World Bank, see International Bank for Reconstructionand Development
World Conference for Action against Apartheid, 3.4World Conference (Tripartite) on Employment, Income
11.43, 15.31, 15.124,
15.157- 15.18615.2, 15.13,
Distribution, Social Progress and InternationalDivision of Labour (1976), 3.4
World Conference on Technical Cooperation amongDeveloping Countries, Buenos Aires (1978), 3.17
World Council of Churches, 13.23World Council for Welfare of the Blind, 8.176World directory of schools for dental auxiliaries, 7.29,
9.II1World directory of schools for medical assistants, 7.29World directory of schools for medical laboratory technicians,
7.29World Food Programme (WFP), 3.19 -3.21, 6.32,
8.171, 15.53World Health, 9.104, 13.22World Health Assembly, 1.1 -1.3, 1.6, 1.8, 1.11,
1.13, 1.17, ,.18, 1.23,1.28, 1.29, 1.30, 1.31,
1.24,1.32,
1.26,
1.33
1.27,
methods of work, 1.15
summary and verbatim records, 13.13World Health Days (1976 and 1977), 8.171,
13.19 -13.20World health situation reports, 1.26
sixth, preparation, 12.IIWorld Health Statistics Annuals, 12.12World Health Statistics Report, 11.2, 12.13World Medical Association, 4.11World Population Plan of Action, 6.3World Rheumatism Year (1977), 9.104
X -ray equipment, maintenance and repair, 7.95,9.123, 15.83
training, 7.95, 9.123Xerophthalmia, 3.20, 8.170, 8.172, 8.173
Yaws, 8.,o,Yellow fever, 1.30, 8.108
vector biology and control, 8.129 -8.131Yemen, 5.30, 5.49, 8.14, 8.174, 11.4,
15.152Youth and adolescence, 1.29, 9.12, 15.20, 15.104
cardiovascular diseases, 9.81health education, contraception, 6.18drugs and alcohol, 9.11, 15.120mental health, 9.11 -9.12, 15.120role in health and development, 6.21,
Yugoslavia, 5.4z, 6.z6, 6.33, 7.113,
15.137,
r5.18I2.19
Zaire, 3.35, 5.53, 6.17, 6.z6, 8.3, 8.55, 8.108,8.136, 11.28
Zambia, 5.5 3, 8.159, 9.7, 9.16, 9.142Zoonoses, 8.1II -8.115
239
WHO publications may be obtained, direct or through bCU,.3t rs, from :
ALGERIA : Société Nationale d'Edition et de Diffusion, 3 bd ZiroutYoucef, ALGIERS
ARGENTINA : Carlos Hirsch SRI,. Florida 165. Galerías Güemes,Escritorio 453/465, BUENOS AIRES
AUSTRALIA : Mall Order Sales : Australian Government Pub-lishing Service Bookshops. P.O. Box 84, CANBERRA A.C.T.2600 ; or over the counter from Australian Government Publica-tions and Inquiry Centres at: 113 -115 London Circuit, CAN-BERRA CITY A.C.T. 2600; Shop 42, The Valley Centre, BRISBANE,Queensland 4000; 347 Swanston Street, MELBOURNE VIC 3000;309 Pitt Street, SYDNEY N.S.W. 2000; Mt Newman House,200 St. George's Terrace, PERTH WA 6000 ; Industry House,12 Pirie Street, ADELAIDE SA 5000 ; 156 -162 Macquarie Street,HOBART TAS 7000 - Hunter Publications, 58A Gipps Street,COLLINGWOOD VIC 3066
AUSTRIA: Gerold & Co., Graben 31, 1011 VIENNA IBANGLADESH : WHO Representative, G.P.O. Box 250, DACCA 5
- The Association of Voluntary Agencies, P.O. Box 5045,DACCA 5
BELGIUM : Office international de Librairie, 30 avenue Marnix,1050 BRUSSELS - Subscriptions to World Health only : Jean deLannoy. 112 rue du Trône, 1050 BRUSSELS
BRAZIL: Biblioteca Regional de Medicina OMS /OPS, Unidadede Venda de Publicacôes. Caixa Postal 20.381, Vila Ciemen-tino, 04023 SXo PAULO, S.P.
BURMA : see India, WHO Regional OfficeCANADA : Single and bulk copies of individual publications (not
subscriptions) : Canadian Public Health Association, 1335Carling Avenue, Suite 210, OTTAWA. Ont. K1Z 8N8. Sub-scriptions : Subscription orders, accompanied by cheque made outto the Royal Bank of Canada, OTTAWA, Account World HealthOrganization, should be sent to the World Health Organization,P.O. Box 1800. Postal Station B, OTTAWA, Ont. KIP SRS. Cor-respondence concerning subscriptions should be forwarded to theWorld Health Organization, Distribution and Sales, 1211 GENEVA27, Switzerland
CHINA : China National Publications Import Corporation, P.O.Box 88, PEKING
COLOMBIA: Distrilibros Ltd, Pío Alfonso Garcia, Carrera 4a,Nos 36-119, CARTAGENA
CZECHOSLOVAKIA: Artia, Ve Smeckach 30, 111 27 PRAGUE 1DENMARK : Einar Munksgaard, Ltd, Nerregade, 6 1164 COPEN-
HAGEN KECUADOR : Librería Científica S.A., P.O. Box 362, Luque 223,
GUAYAQUILEGYPT : Nabaa El Fikr Bookshop, 55 Saad Zaghloul Street,
ALEXANDRIAEL SALVADOR : Librería Estudiantil, Edificio Comercial B No 3,
Avenida Libertad, SAN SALVADORFIJI: The WHO Representative, P.O. Box 113, SUVAFINLAND : Akateetninen Kiriakauppa, Keskuskatu 2, 00101
HELSINKI 10FRANCE : Librairie Arnette. 2 rue Casimir -Delavigne, 75006 PARISGERMAN DEMOCRATIC REPUBLIC : Buchhaus Leipzig. Post -
fach 140. 701 LEIPZIGGERMANY, FEDERAL REPUBLIC OF : Govi- Verlag GmbH,
Ginnheimerstrasse 20, Postfach 5360. 6236 ESCHBORN - W. E.Saarbach, Postfach 101610, Follerstrasse 2, 5 COLOGNE 1 - Alex.Horn, Spiegelgasse 9, Postfach 3340, 6200 WIESBADEN
GREECE : G. C. Eleftheroudakis S.A., Librairie internationale.rue Nikis 4, ATHENS (T. 126)
HAITI : Max Bouchereau, Librairie "Ala Caravelle ", Boite postale111 -B. PORT -AU- PRINCE
HONG KONG : Hong Kong Government Information Services,Beaconsfield House. 6th Floor, Queen's Road, Central, VICTORIA
HUNGARY: Kultura, P.O.B. 149. BUDAPEST 62 - AkadémiaiKônyvesbolt. Váci utca 22, BUDAPEST V
ICELAND : Snaebjern Jonsson & Co., P.O. Box 1131, Hafnar-straeti 9, REYKJAVIK
INDIA : WHO Regional Office for South -East Asia, World HealthHouse, Indraprastha Estate, Ring Road, NEW DELHI 110002 -Oxford Book & Stationery Co., Scindia House, NEW DELHI110000; 17 Park Street, CALCUrrA 700016 (Sub -Agent)
INDONESIA : M/s Kalman Book Service Ltd, 31n. Cikini RayaNo. 63, P.O. Box 3105 /Jkt., JAKARTA
IRAN: Iranian Amalgamated Distribution Agency, 151 KhiabanSoraya, TEHERAN
IRELAND : The Stationery Office, DUBLIN 4ISRAEL : Heiliger & Co., 3 Nathan Strauss Street, JERUSALEMITALY : Edizioni Minerva Medica, Corso Bramante 83-85, 10126
TURIN; Via Lamarmora 3, 20100 MILANJAPAN : Mariam Co. Ltd, P.O. Box 5050, TOKYO International
100-31KENYA : The Caxton Press Ltd, Gathani House, Homa. Bay Road,
P.O. Box 41742, NAIROBIKUWAIT : The Kuwait Bookshops Co. Ltd, Thunayan AI -Ghanem
Bldg. P.O. Box 2942, KUwAIT
LAO PEOPLE'S DEMOCRATIC REPUBLIC: The WHORepresentative, P.O. Box 343, VIENTIANE
LEBANON : Documenta Scientifica /Redico, P.O. Box 5641, BEIRUTLUXEMBOURG: Librairie du Centre, 49 bd Royal, LUXEMBOURGMALAYSIA: The WHO Representative, Room 1004, Fitzpatrick
Building, Jalan Raja Chulan, KUALA LUMPUR 05 -02 - Jubilee(Book) Store Ltd. 97 Jalan Tuanku Abdul Rahman, P.O. Box 629,KUALA LUMPUR 01 -08 - Parry's Book Center ,K .L. HiltonHotel, J1n. Treacher, P.O. Box 960, KUALA LUMPUR
MEXICO: La Prensa Médica Mexican, Ediciones Cientificas,Paseo de las Facultades 26, Apt. Postal 20-413. MEXICO CITY 20,D.F.
MONGOLIA : see India, WHO Regional OfficeMOROCCO : Editions La Porte. 281 avenue Mohammed V, RABATMOZAMBIQUE : INLD, Caixa Postal 4030, MAPUTONEPAL: see India, WHO Regional OfficeNETHERLANDS : N. V. Martinus Niihoff's Boekhandel en
Uitgevers Maatschappii, Lange Voorhout 9, THE HAGUE 2000NEW ZEALAND : Government Printing Office, Mulgrave Street,
Private Bag, WELLINGTON 1, Government Bookshops at :Rutland Street, P.O. Box 5344, AUCKLAND ; 130 Oxford Terrace,P.O. Box 1721, CHRISTCHURCH; Alma Street, P.O. Box 857.HAMILTON ; Princes Street. P.O. Box 1104, DUNEDIN - R. Hill& Son, Ltd, Ideal House, Cnr Gillies Avenue & Eden St., New-market, AUCKLAND 1
NIGERIA : University Bookshop Nigeria Ltd, University ofIbadan, IBADAN
NORWAY : Johan Grundt Tanum Bokhandel, Karl Johansgt. 43,1010 OSLO 1
PAKISTAN : Mirza Book Agency, 65 Shahrah Quaid -E. Azam,P.O. Box 729, LAHORE 3
PHILIPPINES : World Health Organization, Regional Office forthe Western Pacific, P.O. Box 2932, MANILA - The Modern BookCompany Inc., P.O. Box 632, 926 Rizal Avenue, MANILA
POLAND: Skladnica Ksiegarska. ul Mazowiecka 9, 00052 WARSAW(except periodicals) - BKWZ Ruch, ul Wronia 23, 00840WARSAW (periodicals only)
PORTUGAL: Livraria Rodrigues, 186 Rua do Ouro, LISBON 2REPUBLIC OF KOREA: The WHO Representative, Central
P.O. Box 540, SEOULSINGAPORE: The WHO Representative, 144 Moulmein Road,
G.P.O. Box 3457, SINGAPORE 11 - Select Books (Pte) Ltd,215 Tanglin Shopping Centre. 2 /F, 19 Tanglin Road, SINGA-PORE 10
SOUTH AFRICA : Van Schaik's Bookstore (Pty) Ltd, P.O. Box724, PRETORIA 0001
SPAIN : Comercial Atheneum S.A., Consejo de Ciento 130 -136,BARCELONA 15 ; General Moscardó 29, MADRID 20 - LibreriaDiaz de Santos, Lagasca 95, MADRID 6; Balmes 417 y 419,BARCELONA 6
SRI LANKA: see India, WHO Regional OfficeSWEDEN: Aktiebolaget C. E. Frizzes Kungl. Hovbokhandel,
Regeringsgatan 12, 10327 STOCKHOLMSWITZERLAND: Medizinischet Verlag Hans Huber, Lünggass
Strasse 76, 3012 BERNE 9THAILAND: see India, WHO Regional OfficeTUNISIA : Société Tunisienne de Diffusion, 5 avenue de Carthage,
TUNISTURKEY : Librairie Hachette, 469 ay. de l'Indépendance, ISTANBULUNITED KINGDOM : H. M. Stationery Office : 49 High Holborn.
LONDON WC1V 6HB; 13a Castle Street, EDINBURGH EH2 3AR;41 The Hayes, CARDIFF CF1 1JW ; 80 Chichester Street. BELFASTBT1 4JY ; Brazennose Street, MANCHESTER M60 8AS ; 258 BroadStreet, BIRMINGHAM Bl 2HE; Southey House, Wine Street.BRISTOL BSI 2BQ. All mail orders should be sent to P.O. Box 569,LONDON SEl 9NH
UNITED STATES OF AMERICA : Single and bulk copies ofindividual publications (not subscriptions) : WHO PublicationsCentre USA, 49 Sheridan Avenue, ALBANY, NY 12210. Sub-scriptions : Subscription orders, accompanied by check made outto the Chemical Bank, New York, Account World HealthOrganization, should be sent to the World Health Organization,P.O. Box 5284, Church Street Station, NEw YORK, NY 10249.Correspondence concerning subscriptions should be forwarded tothe World Heath Organization, Distribution and Sales, 1211GENEVA 27. Switzerland. Publications are also available from theUnited Nations Bookshop, NEW YORK, NY 10017 (retail only)
USSR : For readers in the USSR requiring Russian editions : Kom-somolskij prospekt 18, Medicinskaja Kniga, Moscow - Forreaders outside the USSR requiring Russian editions : Kuzneckijmost 18, Mefdunarodnaja Kniga, Moscow G -200
VENEZUELA : Editorial Interamericana de Venezuela C.A., Apar-tado 50785, CARACAS 105 - Librería del Este, Apartado 60337,CARACAS 106
YUGOSLAVIA : Jugoslovenska Kniiga, Terazile 27 /II, 11000BELGRADE
Special terms for developing countries are obtainable on application to the WHO Representatives or WHO Regional Officeslisted above or to the World Health Organization, Distribution and Sales Service, 1211 Geneva 27, Switzerland. Ordersfrom countries where sales agents have not yet been appointed may also be sent to the Geneva address, but must bepaid for in pounds sterling, US dollars or Swiss francs.
Price: Sw. fr.18.- Prices are subject to change without notice. C /1/78