poor antibody response after tetanus and pneumococcal vaccination in immunocompromised, hiv-infected...
TRANSCRIPT

ctin. exp. Immunol. 11991) 84, 185-189 AtJONts CK)O99IO49IOOI26N
Poor antibody response after tetanus and pneumococcalvaccination in immunocompromised, HIV-infected patients
M. OPRAVIL. W. FIERZ. L. MATTER*. .1. BLASER & R l .UTHY Department of Medicine. Vnirer.sity Ifcspiial.Zurich, and * Institute of Clinical Microbiology and Immunology, St Gallen, Switzerland
(Acceptedfor publication 19 November 1990)
SUMMARY
Ten patients with symptotnatic HTV infeclion (six with ARC. four with AIDS) received tetanus and23-valent pneumococcal vacctiiiition. Anti-tetanus IgG and IgM. and an(i-pneuniococcal IgGagainst al! 23 capsukir types of the vaccine were measured on days (). II. 17. 30. and 90. Anti-pneumococcal IgG were simultaneously determined in two plasma pools of 100 healthy unimmu-nized blood donors and of 112 healthy adults who had previously received a 14-valent pneumococca!vaccination. Peak IgG responses to both vaccines were observed on day 17: thereafer. Ihe antibodylevels gradually fell again. Anti-tetanus IgG rose from 0-6 U/ml (geomctic mean) to 2'0 U/ml on day17. Anti-tetanus IgM remained unchanged. Anti-pncumoeoccal IgG increased only by l-M-foldcompared with pre-vaccination levels (geometric mean of IgG rises against all 23 polysaccharides in10 patients), and cxeeeded the upper 95'H) limit of unvaccinated blood donors in only 30 out of 230specimens, Prc-vaccinaiion levels for pneumococcal type-specific IgG were significantly higher inHIV-infected patients compared with the pool of unimmuni/cd healthy controls, possibly indicatinga higher rate of previous pneumococcai infections in HIV-seropositivc subjects. However, post-pneumococcal vaccination levels were significantly lower in HIV-infected patients than in the pool ofhealthy controls. The increase in anti-tetanus IgG significantly correlated with the level of CD4lymphocytes and with in riiro lymphocyte proliferation by pokewced mitogen (5 /Jg/ml) andphytohaemagglutinin (2-'i /ig/ml). confirming a particularly low vaccination response in patients whowere severely immunocompromised.
Keywords vaccination tetanus pneumococcal antibodies HIV infection
INTRODUCTIONThe complex effects of HIV on the immune system include bothT cell and B cell immunodeficiency. Polyclonal B cell activationis common in patients with AIDS and leads to excessivespontaneous secretion of immunoglobutin by an increasednumber of fully differentiated B cells. In contrast, the resting Bcells are defective in their ability to develop a proliferativeresponse and to seerete immunoglobulin after appropriatestimulation (Lane et al.. 1983).
When compared with normal subjects, impaired antibodyresponses to pneumococcal and tetanus vaccines have beenreported in various degrees in HI V-infected individuals with andwithout AIDS (Ballet et al.. 1987: Teeuwsen ei al.. 1987; Klein etal.. 1989), but other studies suggested nearly normal responses
L.M.. present address: Institute of Medical Micmbiology, Univer-sity t)f Bern. Switzerland.
Correspondence: Dr Milos Opravil, Division of Infectious Diseases,Department of Medicine, University HospitEil, CH-!<09l Ziirich, Swit-zerland.
(Huang et al., 1987; Janoffc/ al., 1988). No general agreementon the clinical efficacy and on the optimal timing of vaccinationsin the presence of HIV infeclion has emerged so far. In view ofrecent suggestions to immunize adults with asymptomatic orsymptomatic HlV-infection against Sireptocovcm pnemmmiae(ACIP. 1989). more data are needed to characterize theinteractions between the vaccination response and the underly-ing immune defect- We studied the responses to tetanus (T ceildcpcndcnUand pneumococcal (Tcell independent) vaccinationand thcircorrclationsto the severity of the immune dysfunction.
PATIENTS AND METHODS
PatietilsEight men and two women (median age 35 years, range 23 52)with symptomatic HIV infection and depressed levels of CD4lymphocyles ( < 0 25 x IO''//) were studied. Six patients hadARC (corresponding to CDC stages IV.A or IV.C2). four hadAIDS (CDC stage IV.CI). No active opportunistic infectionswere present. The route of HIV infection was i.v. drug use intwo. heterosexual transmission in one. and homosexual inter-
185

186 A/. Opravil ct al.
course in seven subjects. TTic pulicnts simullancoiisly partici-pated in a phase I study of an immunomodulaling treatment(single intramuscular injection of recombinant HlV-l gp4lpcptidc Louplcd to hicolt al the lime of the vaccinations).Informed consent was obtained from all participants.
ImmuftizutionEach subject was given a 0-5-ml inlratJeltoid injection ofpncumoeoccal vaccine (Pneumovax®-23 Merck Sharp &Dohme, C'hihrct. Switzerland), containing 25 /ig of each of iheIbllowing 23 capsular polysacchandcs (U.S. nomenclature): I.2. 3,4. 5. 8. 9. 12. 14, 17. 19. 20. 22. 23.26. 34.43. 51. 54. 56. 57.68. and 70. Sinnillancously. 0 5 ml of tetanus vaccine wasinjected ( le AnatoxaP\ Herna. Switzerland), conlaiiiiny U) Lf(flocculation units) toxoid. One subject received tetanus vacci-naiion 3 weeks bclorc study entry during a surgical abscessdrainage and was therelbre not included in the evaluation of theanti-ietanus response.
Lahoratorv te.\t.\Blood samples were drawn on days 0 (prc-immuniz:ition). 11.17. 30 and 90 for determinations of haematology. bloodchemistry, and antibodies to the vaccinated antigens. On days 0.30, and 90. lymphtxrytc subsets and lymphiKyte proliferationwere determined. On days 0 and 30. HIV-anligen. and serumIgA. IgM. and IgG were measured.
Anti-tetanus IgG were determined using an filJSA, asdescribed previously (Stifflcr-Roscnberg & hey. 1977). Theassay for anti-tetanus IgM was identical except of using anti-IgM peroxidase (Southern Biotechnology. Birmingham. AL)instead of anti-lgO-phosphatasc. Anti-pncumocuccal IgGagainsl capsular polysaccharides of 23 S. pucumoniae typescontained in the vaccine were determined with a multi-antigenimmunobinding assay on nitrocellulose strips (Matter ct ai.I9K5), hach polysaceharidc was sprayed (Linomat: C'aniag.Mutlen/. Switzerland) onto nitrocellulose sheets, which werecui into strips to be used Tor the immunoassay. Thus 0-2 /jg ofpolysaccharide wore applied per mm of the resulting antigenlines. The results were expressed scmi-quantitati\ely as arbitrar>units based on the reflectometric determination of colour(Camag).
Peripheral blood mononuclear eells were isolated fromheparini/ed samples by separation on a density gradient(l.Niiiphoprep). The cells were ihen stained witli monoclonalantibodies against CD4. CDS (Bccton Dickinson), and CI)2021 (Coulter) and quantified on a flow cytometer(HPlCS Profile.Coulter).
Lymphocyte proliferation tests were performed from per-ipheral blotnl mononuclear cells. The spontaneous proliferationas well as the proliferations induced wiih pokcweed niitogen(PWM; 5/[g/ml; proliferation of Band T lymphocytes) and withphytohaemagglutinin (PHA: 25 /ig.ml; proliferation i.i\' TlymphtK'ytes) were assessed hy 'H-thymidinc tjptakc. A stimula-tion index was calculated as the ratio of the PWM response orthe PHA response to spontaneous proliferation.
Serum p24 HIV antigen was monitored hy an enzymeimmunoassay (Abbott).
Total serum immunoglobulins Ig.A, IgM. and IgG weredetermined by later nephelometry (Bchnng).
Contrnl popuUttinnThe levels of anti-pncumoeoccal IgCi were simultaneouslydetermined in two plasma pools: (i) 1(K) healthy adult unimmu-ni/ed blood donors from Switzerland, sampled during 1988: and(ii) 112 healthy adults whose sera were collected 3 5 weeks afterimmunization with a 14-valent pncumoeoccal vaccine (contain-ing capsular polysaccharide types 1,2.3.4.6.8.9. 12. 14. 19.23,25. 51, and 56), as described elsewhere (Siber et ai. 1984).
Statistical analysisBecause of asymmetrical distribution of the data, the geometricmean was used to describe the average. Comparisons ofconsecutive values and of distributions of" anti-pneumtx-occalIgG were done hy Wilcoxon matched pairs signed rank tcsl.Correlations were calculated by linear regression analysis.
RESt'LTS
Time-course of clinical data, haematology and immunologyDuring the follow up of 3 months. AIDS-defining opportunisticinfections developed in two patients with ARC and in onepatient with pre-existing AIDS. Baseline levels of CD4 lympho-cytes were moderately to severely depressed: geometrie mean0 06 X 10"/. range 0 01 0 21 x 10",/. Laboratory data, mcludmglevels of lymphocyte subsets and lymphocyte proliferations,remained stable during the follow up period, mdicating thatneither the vaccinations nor the concurrent immunomodulatingtreatment affected the immune system adversely (Table I).Levels of total serum immunoglobulins did not change signifi-cantly between day 0 and 30 (geometric mean in g/. day 30 inparenthesis):IgA5 3(5 l):lgM2 9(2 7);andlgG24l(23 5). Inseven patients with detectable HIV antigen, the mean levels ofp24 remained stable. HIV antigen continued to be undeteclablein the remaining three patients. No side-elFeels were observed.
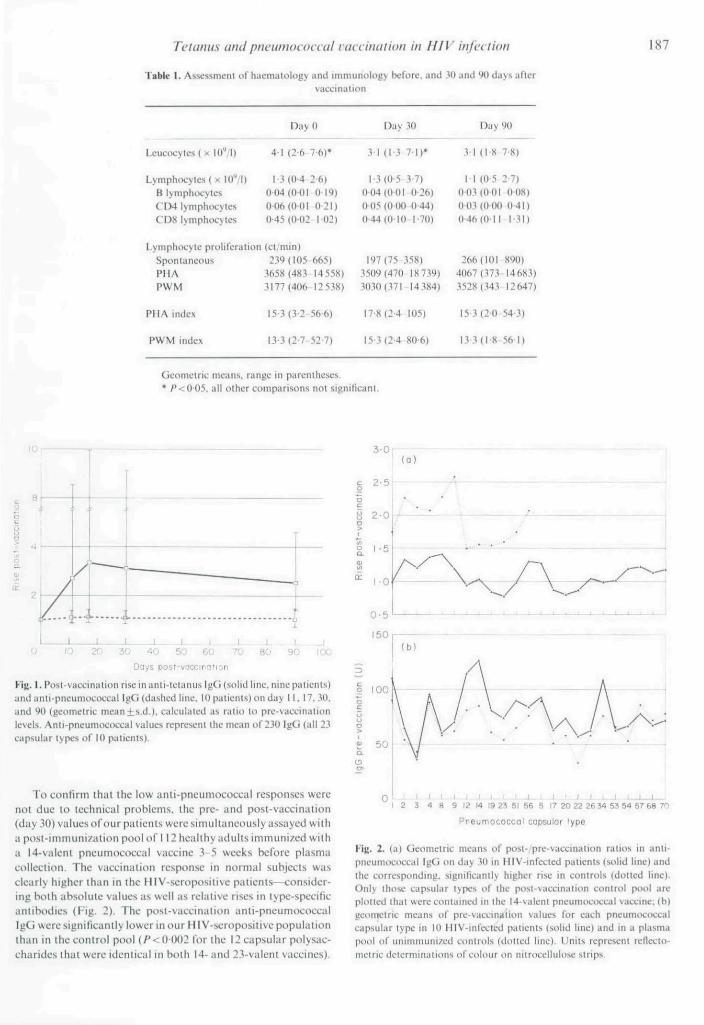
Time-rourse of antibody rheAnti-tetanus IgM remained stable (range 0 34-0-42 U/ml). ascan be expected fora secondary response. IgG response to bothantigens were maximal on day 17 and gradually deereasedthereafter until day 90 (Fig. 1). Anti-tetanus IgG rose 3 34-roldfrom 0 6 U ml to 2 0 U ml on day 17 ( / '<0 02).
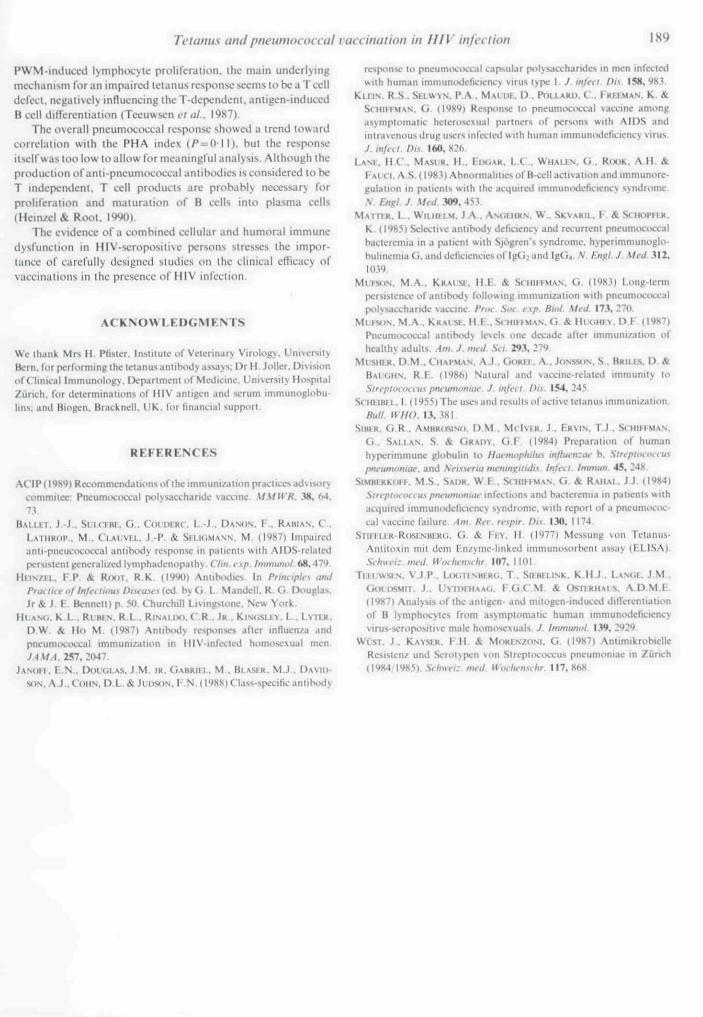
The response in anti-pneunu>coccal IgG was minimal; if allcapsular types were considered, only a I M-fold overall rise wasobserved on day 17 (/>< OOO1. geometric mean ofall 23 capsulartypes vaccinated, 10 patients); if type-specific responses werecalculated, the changes varied between maximally I 4I-f\)ld forcapsular type H and minimally ()• 78-fold for capsular type 23(Fig. 2). If the absolute values of anti-pneumococcal IgG wereconsidered, only 30 out of a tota! of 230 sfwcimens (all 23eapsular types. 10 patients) exceeded the upper 95".. limit ofunvaccinated normal blood donors between day 17 and .11). andonly 20 out of 2.3() specimens still remained above this upperlimit on day 90.
Compuri.son t>f anti-pncumococciil igG with Iwalthy lontrttlsA pool of 100 healthy unimmunized blood donors was analysedsimultaneously as control. The type-speei(ic mean pre-vaccina-tion values of our HIV-infected patients were significantlyhigher ( / '<002). possibly indicating a higher rate of previouspneumocoeeal infccUons (Fig. 2).
Ti'titnus and pneumococcal i (laination in I III' injvciion 187
Tab)« I. Assessment of haemalology antl imnuinology befnre. and 30 and 90 days aRervaccinalinn
Leucocyle.s ( x lO**/!)
LymphiKvtes ( x lO''/!)B IvniphocvtesC'D4 lymphiKvtesCD8 lymphocytes
DayO
4-1 (2-6 7 6)*
I-.M0 4 2-6)0()4(0-OI 0 19)0-06(001 0-21)045(0-02 102)
Day 30
3 1 { 1 - 3 7 - 1 ) *
1-3(0-5 3-7)0 04(0 01 0 26)0()5(0(K) 0 44)044(0 10 1-70)
Day 90
3-1 (18 7-8)
I I (0-5 27)0 03(001 008)0()3(0(KI 0 41)0-46(0 11 131)
Lymphocyte proliferation (ct;min)Spontaneous 239(105 665)P I I A .1658(483 14 558)PWM 3177(406 12538)
197(75 358) 26f. (HH XyO)3509(470 18739) 4067(373 14683)3030 (.371-14384) 3528 (.343 12 647)
PHA nulcx
PWM Index
15-3(3-2 56-6)
13-3(2-7-52-7)
17 8(2-4 105)
l.V3(2 4 80 6)
15 3(2 0 54 3)
!33( l 8 56 I)
Geometric means, range in parentheses.• /*<0-05, all other comparisons not significant.
10, 3-0
i.0 10 20 30 40 50 60 7& 80 90 tOO
Days post-uocctii(]fion
Kiy. I. Post-vacci nation rise in anti-tetanus IgG (solid line, nine patients)and anti-pneumoccMTcal IgG (dashed line. 10 patients) on day II, 17,30,and W (geometric mean + s.d.). calculated as ratio to pre-vaccinalionlevels. Antl-pneumococcal values represent the mean of 230 IgG (all 23capsular types of 10 patients).
T(i confirm thai Ihc low anii-pnciimococcal responses werenot due to icchnicLil problems, (he prc- und post-vaccination(day 30) values ofour patients were simultaneously assayed withapost-immuni/ation pool of I I2liciilthy adults immunized witha I4-v;itcnt pneumococcal vaccine 3 5 weeks before plasmacollection. The vaccination response in normal subjects wasclearly higher than in the HlV-seropositive patients—consider-ing both absolute values as well as relative rises in type-specificantibodies (Fig. 2). The post-vaccination anti-pneumix'occalIgO were signilicantly lower in our HI V-scroposilivc populationthan in the control pool (/*<()()()2 lor the 12 capsular polysac-eharides that were identical in both 14- and 23-valenl vaccines).
12 14 19 23 Bl 56 S 17 2O 22 26 34 53 54 S7 68 70Pneumococcol capsulor lype
Kis- 2. (a) Geometric means of post-/pre-vaccination ratios in anti-pneumococcal igG on day 30 in HIV-infected patients (solid line) andthe corresponding, signilicantly higher rise in controls (doited line).Only ihose capsular types nf the post-vaccinaiion control pool areplolied Ihal were contained in Ihe t4-valeni pneumococeal vaccine; (b)geometric means of pre-vaccinalion values for each pneumiKoccalcapsular type in 10 HlV-inleeled patients (solid line) and in a plasmapool of unimtmini/ed coritiols (dotted line). Units represent rcflecto-metric determinations of colour on nitrocellulose strips.

188 M. Opravil Qi al.
e h (a)
^ 6%wt
c 4a
eh (bl
£110 20 30 40 50 60
PHA indeic
0 50 100 150 200 250CD4 lymphocytes
Fig. 3. The change in ;inti tctiinus IgG in nine HlV-inlccicd palionts isdisplayed its arrows from Iho biisclint lo the posi-vaccinalion value onday 17. The antibody increase correlated significantly with phytohaem-aggluiinin (PHA) index (a) (/'<0-001,/- = 0-91) and with baseline levelsof Cn4 lymphocytes per mm' {P<0Q2. r = 0 78).
Correlation of vaccination responsesThe increase in anti-tetanus IgG correlated with In vitmlymphocyte proliferation by I'M A and PWM (r< 0 00!. r - 0 91for PHA index; P<{)mZ.r = {)m for PWM index) and with UK-baseline values orCD4 lymphocytes (P<0-02. r = 07H). Thusthe antibody production was significantly diminished in patientswith severe immune deficiency (Fig. 3).
The rise in anti-pneumococcal IgG (geometric mean ofpost-/pre-vaccination ratio for all 23 capsular types on day 17)showed a trend toward eorrelation with PHA inde.x (/' = 0-l I.r = 054).
No significant correlation was ob.served between the re-sponses to both vaccinations and CDC stage of HIV inleciion.risk groups, levels of leucocytes, total lymphocytes, CDX. or Blymphocytes.
DISCUSSION
The immunization response in our HIV-infecied patients wasmore pronounced alter tetanus than after pneumocoeeal vacci-nation. Although the laboratory methods used to determine theantibody rise may contribute to this difference, a generally lowerimmunogenicity oi the pneumocoeeal vaccine must be consi-dered.
Comparative studies on tetanus vaccination demonstratedIgG rises in HIV-infected patients similar lo those in ourpopulation, hut lower than in normal individuals (Teeuwsen tvai. 1987; Ballet el ai. 1987). Since all patients had beenpreviously immunized against tetanus, the observed responserepresented a booster effect, consisting predominantly of asignificant IgG elevation. The mean pre-vaccination IgG werehigher than the known protective level of 0 01 IJ ml (Scheibel.1955). Thus, humoral itnmunity against tetanus in HIV patientsseems to be sufficient several years after previous vaccinationand can increase substantially after a booster injection.
In contrast, pneumocoeeal vaccination results in an onlylimited IgG response in these patients. The antibody levelsvaried eonsiderably between different capsular polysaccharideantigens; the stongest rises were seen for capsular types 8. 4. 2.56, and 5. However, even the maximal type-specific antibodyresponse did not e.\cced a 1 4-[\)ld rise, confirming previouslydemonstrated itnpairment of pneumocoeeal vaccination re-sponse in HIV-infectcd individuals (Ballet ct ai. 1987).
After pneumocoeeal vaccination ofhealthy adults, antibodylevels remain elevated during at least 5 years, but may fall to pre-vaeeination levels within IOyears(Mufsonf'f i//.. 1983. 1987). Inasymptomatic HIV-seropositive homosexual men, elevatedantibodies could be still detected I year after pneumocoeealvaccination, but the elevation was considerably lower thanduring the peak response (JanofT vt ul.. 1988). Significantlylower antibody responses were delected 7 months after pneumo-coeeal vaccination in asymptomatic HIV-seropositive indi-viduals compared with HlV-seronegativeeontrols (Klein et ai.1989)., suggesting that not only the antibody rise but also thetime period after the vaccination must be considered when IgGlevels are compared. In our symptomatic HIV-infected patients,we observed a peak antibody response during the .second tothird week after the vaccination and a subsequent declinestarting thereafter. Although the protective levels of pneumo-coeeal antibodies have not been clearly established (Musher etai. I9S6)andour laboratory method did not permit an absoluteantibody quantification, the long-term effieacy of pneumoeoc-cal immunization in patients with advanced HIV infectionremains questionable in view of the low and temporary nature ofthe vaccination response.
The results ol anli-pneumocoeeal IgG were obtained semi-quantitatively using a multi-antigen immunobinding assay onnitrocellulose strips. As different capsular polysaccharides havevariable binding affinities on nitrocellulose, only relative differ-ences in optical density were used for comparisons. Thesimultaneous determination of anti-pneumoeoccal IgG in twoplasma pools of healthy unmatched HIV-seronegative controlsenabled us to approximately assess the influence of HIVinfection on the production of pneumocoeeal antibodies. Meanpre-vaccinatiiin IgG levels in our patients exceeded in 18 out of23 capsular types the corresponding values of the controlplasma pool (P<0-02). possibly as a result of a higher rate ofprevious pneumocoeeal infections among the HIV-infectedsubjects (SimberkofT ct ai. 1984) or consequence of increasedspontaneous secretion of immunoglobulins (Lane et ai. 1983).
A plasma pool of 112 previously vaccinated healthy blooddonors (Siber ct ai. 1984) served as a post-immunizationcontrol, demonstrating higher levels of pneumocoeeal vaccina-tion response in normal individuals than in our patients. Thecomparison of the type-specific antibodies involved only thosecapsular polysaccharides that were simultaneously present inboth 14- and 23-valent vaccines. The ability of symptomaticHIV-intected patients to develop a pneumoct^cal vaccinationresponse was clearly decreased in comparison with this post-vaccination pool and illustrates the funetional humoral defi-ciency. Although the two plasma pools were not matched, therelative distribution of the typ>e-specific antibodies parallel eachother. The prevalences of pneumocoeeal serotypes remainedsimilar between 1978 and 1984 in Zurich, as well as betweenZurich and Montreal. Canada, in 1984 (Wust.. Kayser &Morenzoni, 1987).
A significant correlation could be detected between theincrease in anti-tetanus IgG and the severity of the immunedefect based on the pre-vaccination levels of CD4 lymphocytesand ihe lymphocyte proliferation. e.xpressed as PHA and PWMindices. The results suggest that a satisfactory antibody responseis only achievable in the presence of adequate proliferativeresponses and CD4 lymphocyte levels over 150-200/mm'. Asthe anti-tetanus IgG production correlated both with PHA- and
Tetanus and pneumococcal vaccination in / / / I ' infection 189
i*WM-induced lymphtKyte proliferation, the main underlyingmechiinism for an impaired telanus response seems to be a T celldefect, ncgiiiivcly inlluencing the T-dependent, antigen-inducedB cell dilTercntiation (Teeuwsen vt al,. 1^87).
The overall pncunuKOccal response showed a trend tow;irdcorrelation with the PHA index (/* = 01l ) . bui the responseitself was too low to allow (nr mcaningliil analysis. Alihouyli ihcproduction ofanii-pneumococcal antibodies is considered lo heT independent. T cell products are prohabl> neces.sar> forprotiferution and maturation of B cells into plasma cells(nein/cl& Rtxit. l*J90).
The evidence of a combined ceHukir and humoral immunedysfunction in HIV-scroposiiive persons stresses the impor-tance of carefully designed studies on the clinical efficacy ofvaccinations in the presence of HIV infcctUm.
.\CKNOWI.KI)GMI'.NTS
We ihank Mrs II. Pfister. Instiiutc of Veterinary Virolog>\ UniversilyBern, t'orpcrriirminpthc lelanus;iniitiody iiNsuys; Dr M. Jollcr. Divisionof^'linical Immunology. Department of Medicine. University HospitulZflrich. for dctcrminations of HIV aniigcn and scrum immunoglohu-lins; anil Biogen. BracJcncil. I 'K. for ItnanLiiil support.
REFERENCES
ACIP( 19X9) Recommendations of ihc immuni/atiori practices advisorycommiiec: PneumiKoccal poKsacchandc vaccme. MMWR. 38. M.
lUii.i.r. J .J . . Sii-tKBi-. G.. CoiuLRt. L.J.. OASON. F . . RAIHAN. C .LATHRof.. M.. CLAUVEL. J . -P . & SliLKiMANS. M. (I9K7) Impairediinti-pncucococcal antibody response in patients wilh .MDS-rcl;itcdporsislcnl genfr;ilized lymphadeiiopiithy. Clm.ixp. tmmunol. 68.479,
Hii\7iL, r P . & R<K«. R-K (I9W) AntiVxHiics In PrimtpU-\ mdPrat tiiT of Iftfi tiou.\ Di.uii.sf\ icti by G I. Mandell. R. G. Dougljs.ir & J F. Bcnnctu p. 5(1 Churchill Livinjjstonc. New York.
lh AN(i. K L . RiBiis. R.L . RiNAiixi. ( \R . J« . KiNtiSLtv. L.. LrrtR.D W & Ho M, (1987) .Antibodv rfsponsi-s after influen/a anilpneumiKDccal immuni7.iilion in HlV-mfeclod homosexual menJAMA.2Srj,2O41
JANOH . F..N., Dcnxjijss. J.M. JR. CIABRIII . M.. BIASFR. M.J.. DAVI»-
sos. A.J..O)HN. D.L.&JuiwjiN. l-.N.(I9«H)Class-.specifieantib<jdy
response lo pneumococcal capsular polysaocharides in men infectedwith human immumxleficiency virus lype I. J. infect. />i.v, 158, 98.1.
Ki.tiN. R.S.. SELWYN. P.A.. MAI !»;. D.. POLI^ARD. C . FREEMAN. K. &
StHii-TMAN. CJ. (1989) Response to pneumociKxal vaceine amongasynipt omit lie hcterosexiiiil piirlners of persons with AIDS andintravetiousdrut' user\ infeck-d Milh humun immunodeticiency virus.J. inftit. Dis. 160. H2ft
I.ANt. w e . MASI;R. H.. FtMMR. L.C . WHAU;N, G . , R(XJK. AH. &
F A K I. A.S. (1983) Abnormulitiesof B-cell actuation .ind imniunore-gulation in patients wiih the acquired immunodeficiency syndrome.S.Engl.J. l/t-J, 309.45.1.
MAirfR, I , . WiLi«tM. J.A.. AstirHRN. W.. SKVARIL. K A STHOPRJI,K. (1985) SclfciiveanliKxJy deficiency and recurreni pneumociKX"albaetereinia in a patient wilh Sjogren's syndrome, hyperimmunoglivbulmemia G. and delkienLics ol" IgG; and igG... N. Enftl J. Mi'd. 312,lO.V).
Min«iN. M.A.. KRAII^:, H .E . & SrHlFfMAS. G. (19H3) Long-termpersistence of antibody following immuniziition with pneumucoccHlpulysaccharidc vaeeinc. Prm Sot i'\p. Biol. Mfd. 173, 270.
MLhS»)N. M.A . KRAI St. H C . SrHihJMAS.G & Hu.Htv. D F (1987)PneunuKTOccal antiKxly levels one decade dWet immuni/ation ofhealthy adults. Am, J, nttd. .Set. 293. 279.
Mt;sniR. D.M-. CHAPMAN. A.J . GORI;I. A,. JONS.S«IS. S . BRILIS. D &
BAitiHN. R.F. (1986) Natural and vaccine-related immunity tctStrt-ptiHiHiWi pnvumoniiif J. in/iTt l)i.\ 154. 245
ScHKiHi:t,. I. (19551 The uses and results nf active tetanus immunization.Bidl HHO. 13. lSl
SiHtR. G.R.. A.MMiiasiNo. DM.. Mclvf.R. J.. F,RVIS. T J.. SrniJfMAS.G.. SALLAN. S, & GRAHV. G . F . (1984) Preparation of humanhypcrimmune globulin to Hiwmophilus inftuenzat- h, StrrptotiMXUSpnt-unumiui'. and .Veiswna mfnin^itidi.\. Infect Inmiun 45. 248.
SiMBJRKohK M.S. SAIJR. W F . Stmn^MAN. G & RAIIAI . J J (1984)StuptiHuicu.\ pntiimonitif infections and baclcremia in patients wiihacquired immunoddiciency >yndrome. wiih report of a pncumococ-eal %aceine failure .-tni. Rvi. rr.tptr. l)i\. 130, 1174
SnriutH RC)SKNBI:HU. G . & I'lY. 11 (U)77l Mi.-ssung von Tetanus-Aniitotin mil dem Hn/ynie-linked immuno.sorbcnt assay IF.LISA).Schwci:. nwd. Wnchvnsthr 107. 1101.
TI:F;I wsiN, V.J.P.. UxniNBtRti. T.. SiKBELtNK. K.MJ.. I.ANGE. J.M..Got iWMiT. J.. UvnWHAAd. F.G.C.M. & OsnuHAi s, A.D.M.E.(1987) Analysis of the antigen- and mitogen-ind need diflcrentialionof B lymphtx-ytes from asymptomatic human immuniMleficiencyvirus-iicropOMlive male homosexuals J Immunol. 139. 2929
WCST. J . KAVSLR. F H & MoKENZoNi. G. (1987) AniimikrobiellcResislcn/ und Seroiypcn von SirepKKtKxus pneumoniae in Zurieh(1984,1985). Schwviz, med. M'ochvnsthr. 117, 868.
