geographical distribution of tetanus in the world, 1951-60
TRANSCRIPT

Bull. Org. mond. Sante 1966, 34, 71-104Bull. Wid Hith Org.
Geographical Distribution of Tetanusin the World, 1951-60A Review of the Problem
B. BYTCHENKO1
The introduction of tetanus toxoid about three decades ago, which was followed in manyparts ofthe world byprogrammes ofimmunization ofthe population, has contributed greatlyto the control of tetanus in the developed countries. Nevertheless, during the decade1951-60, tetanus remained an unsolved problem in many of the developing countries.
In the present report, it is shown, on the basis of the available literature and WHOstatistics, that tetanus causes more than 50 000 deaths each year all over the world.Indeed, this figure should be regarded as an underestimate, since it only partiallyreflects the actual situation in the developing countries. The paper draws attention to thegeographical distribution of tetanus in the world and indicates that existing "foci " or" zones " of infection may be attributed to environmental conditions as well as to social,economic and cultural factors.
Although tetanus is a disease of high mortality,especially in regions of warm or temperate climate,it usually attracts little attention from the publichealth authorities, rarely being listed among thefirst ten causes of mortality. Such a situation createsthe impression that tetanus need not be consideredvery seriously, perhaps because it is usually nottransmitted from man to man, as are many of themajor communicable diseases. This peculiarity,together with " the quietness of tetanus epidemics "
(Tateno, Suzuki & Kitamoto, 1961), tends to concealits hazards to the population. Each case of thedisease appears to occur separately and un-expectedly, with no trace of contact with other cases.In this respect, cases of tetanus resemble cases ofsnakebite, except that persons bitten by snakesnormally realize their danger immediately.
Despite intensive pharmacological and therapeuticresearch, the prognosis for each case of tetanus isdoubtful; at present, the tetanus case-fatality rateis rather high (30% to 80 %), indicating that at leastthree of every ten, at most four of every five, personsattacked by this disease will succumb to it. It hasbeen said that tetanus is dangerous, not becauseit is large in number, but because it is rare (Schlesin-
1 Bacterial Diseases, Division of Communicable Diseases,World Health Organization, Geneva, Switzerland.
ger, 1960). However, the " rarity " of this diseasecannot be affirmed positively, since compulsoryregistration of tetanus morbidity has not beenestablished in many countries of Africa, Asia, andSouth America. Consequently, data on tetanusfrom these areas are very incomplete and availableonly by extrapolation from reports on causes ofdeath (in particular the epidemiological and vitalstatistics made available to WHO for the years1950 to 1964).
Studies on the epidemiology and area distributionof tetanus have been reported fairly recently inEurope (Conybeare & Logan, 1951; Cimmino,1951; M63e, 1955; Eckmann & Bisaz, 1956; Weller,1956; Matveev, 1960; Kubinyi, Rudnai & Barsy,1962-63); in North America (Axnick & Alexander,1957); and in Japan (Tateno, Suzuki & Kitamoto,1961). Attention to the importance of tetanusthroughout the world was drawn by Matveev &Sergeeva (1959). According to the very approximatecalculation of these authors, there were, during thenine years 1945-53 in the countries in which theincidence of tetanus was recorded, more than350 000 cases, of which 115 000, or nearly one inthree, terminated fatally.
This infection is characterized by the relativestability of its annual rates ofmorbidity and mortality
1701 - 71 -

72 B. BYTCHENKO
in most areas unless there has been interference inthe form of campaigns of mass vaccination.The purpose of the present paper is to draw
attention to the importance of tetanus and the geo-graphical distribution of this disease during thedecade 1951-60. For this purpose, all availabledata were collected from various WHO documentsand from a number of other publications that areincluded in the table of references at the end of thiscommunication. It must be understood that, whilethe information gathered and presented here may beconsidered more or less reliable for Europeancountries, the USA, Canada, Japan, Australia andNew Zealand, it is very incomplete as regardsAfrica, Asia, South America and the countries ofthe WHO Western Pacific Region. It is to be hopedthat further studies of the epidemiology of tetanusin various parts of the world will bring to light newfacts that will help to describe the actual situationmore precisely in the future.
AFRICA
It is known that tetanus is not rare in Africa(Bryant & Fairman, 1940; Lebon, Choussat &Chaussat-Clausse, 1949; Floch, 1949; Sarrouy et al.,1950; Beheyt, 1950; Armengaud, Frament & Biram,1960; Smythe & Bull, 1961) and, although exactmorbidity and mortality data are not available inmany areas, those that have been made available toWHO for the years 1955-64 demonstrate that tetanusconstitutes an important problem throughout thatcontinent.
In the decade 1951-60, from 23 to 39 Africancountries, inhabited by between 105 and 139 millionsof persons, recorded deaths from tetanus. Since thepopulation of that continent in 1960 was reportedto be 242 millions, it is evident that only about onehalf of the African population was covered byofficial records. Furthermore, even the officialrecords must be considered to be incomplete, sincethey reflect only the situation in the towns and thelarger hospitals, whereas tetanus occurs primarilyin rural areas, in most of which tetanus is not anotifiable disease (World Health Organization,1963).The data collected by WHO, if summarized,
indicate that mortality from tetanus appears to beincreasing, the absolute number of cases rangingfrom 2124 in 1951 to 3180 in 1960. However, thistrend can be explained as being due, primarily, toimprovement in the registration of deaths. Thesame figures show that the geographical distribution
of tetanus in Africa was not uniform (see alsoFig. 6, below). During the decade (1951-60) underdiscussion, there were real foci of infection in theCape Verde Islands (mortality rate of 135 per100 000 inhabitants) and some other places (SpanishEquatorial Africa, 13; Angola, 4.4, etc.). On theother hand, according to Bernard, Gallay & Laver-dant (1963), tetanus was not so frequent in Algeria,where the tetanus mortality was only 0.45.On the average, the mortality rate for the 39
African nations that supplied data on tetanus toWHO between 1951 and 1960 was approximately2.0 per 100 000 population. Assuming that thisfigure could be applied to the entire population ofthe African continent (that is, approximately235 000 000 1), this would mean that more than50 000 persons died from tetanus during that decade.However, this figure is probably far too low, sincesome reports on tetanus morbidity indicate that thesituation was even more grave.
Johnstone (1958), for example, calculated that themorbidity rate for tetanus in the area around Ibadan,Nigeria, was about 26.6 per 100 000 inhabitants.In Somalia,2 the number of cases of tetanusreported to the Ministry of Health in 1961 was 1230(843 males and 387 females), which means that themorbidity rate was roughly 49 per 100 000 in-habitants.Armengaud, Louvain & Diop-Mar (1962) have
reported that, in one of the hospitals of Dakar,Senegal, 13 % of all deaths from infectious diseaseswere attributable to tetanus, which killed morepeople than typhoid, pertussis, meningitis, diphtheria,or even malaria. In Nyeri, Kenya, Portsmouth(1963) reported having treated 245 tetanus patientsbetween 1959 and 1961. Tetanus was the third mostimportant cause of death in that area, being ex-ceeded only by bronchopneumonia and gastro-enteritis.
Generally speaking, the mortality from tetanus israther high. For example, Tompkins (1959) hasreported from Nigeria that, among 79 childrenaged from 1 to 7 years with tetanus, there were25 deaths (31.6%). Beheyt (1950), in the Congo(Leopoldville) observed 87 patients with tetanus,51 of whom (58.7%) died. Among 444 tetanuspatients admitted to a hospital in Dakar, Senegal,during two years, 110 (25 %) died (Armengaud et al.,1963). The low average lethality of the disease in
1 Mean figure for 10-year period.2 Somalia, Ministry of Health (1963) Five year plan for
the development of Public Health Services (unpublished).

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60
this group of patients may be explained by the factthat no cases of tetanus neonatorum were included.In the age-group 5-10 years, lethality was only 13%,while for patients aged more than 40 years it was60%. In one Congolese hospital alone, Perin &Van de Voorde (1963) treated 441 tetanus patients,of whom 195 (44.2%) died.The tetanus case-fatality rate found in the Upper
Volta by Pirame (1963) was 74.4%; that is, of 211patients, 157 died. According to Baker (1963),among 430 cases of tetanus admitted to hospital inKenya in 1959, about 211 deaths were reported, fora fatality rate of about 49 %. Somewhat later, Baker& Grounds (1964) conducted a clinical trial of thetreatment of 77 tetanus patients, with and withoutthe use of anti-tetanus serum (ATS). These in-vestigators found that, while 40% of the patientswho received ATS died, 77% of the patients diedwho did not receive it. Portsmouth (1963), inKenya, lost 102 (42 %) of 245 tetanus patients treatedby him; however, the lethality among patients inthis group who were over 45 years of age was ashigh as 75%.The reports of several authors indicate that, in
Africa, the principal characteristics of tetanus arethe same as in other parts of the world; that is, thedisease usually attacks children under 15 years ofage and adults in rural areas. Small-scale studiesconducted in some places revealed that except be-tween the ages of 20 and 40 years, during whichperiod the incidence of tetanus is higher in womenthan in men, there is no appreciable difference inincidence between, the sexes.Most cases of tetanus occur after superficial
wounds and injuries to the legs, arms, head ortrunk, as well as after conditions such as chroniculceration, otitis, dracunculosis and molluscumcontagiosum. In a great number of reported cases,the site of infection could not be traced (Bryant &Fairman, 1940; Thiodet et al., 1956a; Fournier &Cabanel, 1957; Johnstone, 1958; Senecal, 1958;Armengaud, 1959; Tompkins, 1959; Armengaudet al., 1963; Baker, 1963; Pirame, 1963; Pirame &Becquet, 1963; Perin & Van de Voorde, 1963;Portsmouth, 1963; Baker & Grounds, 1964). Somelocal customs, such as piercing of the ears, circum-cision, or the stoppage of ear discharges with pow-dered earth, favour the conditions for contractingtetanus (Senecal, 1958; Armengaud, Louvain &Diop-Mar, 1962).Because its relative frequency is great and its
case-fatality rate is very high, tetanus neonatorum
deserves special attention (Wright, 1960; Wrightet al., 1961; Keet & Murray, 1962; Smythe, 1963).The Lambotte-Legrands (1950) reported that, in theCongo, a quarter of all neonatal deaths were attribu-table to tetanus. Among 441 patients treated byPerin& Van de Voorde (1963) in the Congo (Leopold-ville), there were 261 children under one month ofage (59.2 %). In Dakar, Senegal, approximately1 % of the newborn in 1953 developed tetanus(Senecal & Senghor, 1962). As stated by Gandy(1950), the number of cases of tetanus neonatorumin Morocco is as high as 5000 yearly. Slome (1954)has reported that, among 1019 deaths from tetanusthat were reported in South Africa between 1944 and1950, 60.9% were of children under one year of age,and at least 585 were of newborn children. Whenstudying the causes of death on the Ivory Coast,Guinea, Senegal and Niger, Cantrelle, Etifier &Masse (1960) observed, in some areas, as many as320 neonatal deaths per 1000 live-births, and tetanuswas found to be the fourth most common cause ofdeath.The case-fatality rates for tetanus neonatorum in
Africa, as described by several authorities, aresummarized in Table 1. These data appear to becomparable with those obtained in other parts ofthe world. Wilkinson (1961), for example, hascalculated, from the reports of several authors, thatthe average case-fatality rate for tetanus neonatorumis about 77.9%.The high incidence of tetanus neonatorum in many
parts of Africa is largely due to primitive obstetricalpractices performed by unskilled medicine men orpeasant midwives. Jelliffe (1958) has given thefollowing typical details:
" In some regions the cord may be cut with adirty knife, an unboiled bamboo chip, a spear or apiece of broken glass. Various dressings may beused including different types of vegetable oil, mud,local medicines and animal dung."
Wilkinson (1961) writes that, in some tribes ofSierra Leone, the dirty juice of young banana shootsis applied to the umbilical cord.Some workers have recorded a number of cases
of tetanus that occurred after surgical operations ormedical procedures such as injections and vacci-nations (Senecal, 1958; Pirame, 1963). In a studyconducted at Dakar, Senegal, by Armengaud et al.(1963), among 444 cases of tetanus observed therewere 34 (7.9%) that had resulted from infectionafter vaccination against tuberculosis (BCG) or,
73

B. BYTCHENKO
TABLE ICASE FATALITY OF TETANUS NEONATORUM IN AFRICA,
AS REPORTED BY SEVERAL INVESTIGATORS
No. Case fatalityCountry Author of cases No. a
of deaths
Nigeria Jelliffe (1950) 25 24 (96)
South Africa Klenerman & Scragg (1955) 4 1 (25)
Algeria Sarrouy et al. (1956) 20 4 (80)
Algeria Thiodet et al. (1956b) 4 3 (75)
Algeria Fournier & Cabanel (1957) 20 18 (90)
Nigeria Tompkins (1958) 141 126 89.3
Nigeria Tompkins (1959) 29 24 (82.8)
South Africa Wright (1960) 217 179 82.5
Uganda Musoke (1961) 13 10 (76.9)
Sierra Leone Wilkinson (1961) 114 83 72.8
South Africa Wright et al. (1961) 68 34 (50)
South Africa Keet & Murray (1962) 12 5 (41.7)
Senegal Senecal & Senghor (1962) 120 102 85
Upper Volta Pirame (1963) 56 49 (87.5)
South Africa Smythe (1963) 25 5 (20)
Congo (Leopoldville) Perin & Van de Voorde (1963) 342 171 50
Total 1 210 838 60.9
a The figures in parentheses are percentages of numbers less than 100.
more commonly, against smallpox. In spite oftreatment, eight of these patients died (fatality rateof 23.5 %). It is of interest to note that a mass
vaccination campaign against smallpox had beeninstituted in Dakar in July 1961, immediately afteran outbreak of smallpox in that city in which15 persons had fallen ill but none had died.The seasonal distribution of tetanus in Africa
cannot be established definitely, since the availabledata are inadequate. However, Senecal (1958),Tompkins (1958, 1959) and Baker (1963) considerthat the incidence of this disease is higher during thedry season than during the wet season. Wilkinson(1961), on the contrary, found that most patientswith tetanus were admitted to hospital during thewet season. According to Armengaud et al. (1963),tetanus is observed as an endemic between Decemberand April. These authors could give no explanationfor this phenomenon.
Up to the present, the epidemiology of tetanusin Africa has not been investigated. Also, despitethe alarming morbidity and mortality from thisdisease in some areas, the control of tetanus has notyet been properly organized. As shown in theSecond Report on the World Health Situation, 1957-1960 (World Health Organization, 1963), vaccinationwith tetanus toxoid is practised in some places, butnot widely enough to protect even the populationat greatest risk. In the overwhelming majority ofAfrican countries, active immunization with tetanustoxoid is not compulsory.The obvious approach to the problem seems to be
the organization of routine vaccination of the entirepopulation, beginning with children and pregnantwomen. Immunization of all visitors to hospitalsin areas where tetanus morbidity is very high canprotect many people against this infection (Vervoom,1962). All vaccination campaigns should be ac-
74

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 195S1I-6
companied by large-scale work on health education(Onuigbo, 1963).
THE AMERICAS
When considering tetanus in the Americas, one
should bear in mind the entirely different climatic,geographical, natural and socio-economic conditionsthat exist, for example, in equatorial and polarregions. We shall therefore consider separatelytetanus, first in Canada and the USA, then in MiddleAmerica, and finally in South America.The border that separates the USA and Mexico
also divides the Americas as far as mortality fromtetanus is concerned. Northward of this line, mor-tality from tetanus is relatively low (0.17 per 100 000population); south of it, during the decade 1951-60,the tetanus mortality per 100 000 ranged from 2.6in Guatemala to 63.3 in the Dominican Republic,being on the average 8.50, or nearly 50 times as highas in the northern area.
Canada and the USAThe mortality rates for tetanus in four American
countries that regularly submitted reports before1950 are shown in Table 2, which demonstrates thatin Canada and the USA there has been a consistentdecline in the incidence of this disease, whereas no
such change can be observed in the two Caribbeancountries.
In Canada, the average number of deaths fromtetanus per year has decreased from 48.0 in theperiod 1921-30 to 9.0 for the period 1951-60. In theUSA, the tetanus death-rate, which averaged 330per year in the period 1921-30, had declined to203 annually in the period 1951-60.While tetanus receives but occasional mention
in the Canadian scientific literature (Silverthorne,
1947; Lessard, Potvin & Morin, 1960), this diseaseis still the subject of study and control in the USA.Axnick & Alexander (1957) have shown that themorbidity from tetanus per 100000 population ishighest in the states that have warm climates, suchas Florida (1.5), Alabama (1.3), Georgia (1.0),Mississippi (0.9), Louisiana (0.9) and Arkansas(0.9). According to Long & Sartwell (1947), themortality among the Negro populations of thesestates was more than three times the mortalityamong the whites. The geographical distributionof tetanus by age-groups in the USA during 1962is shown in Fig. 1, while the data on morbidity,mortality and case fatality for that country are
shown in Table 3. From these figures, it can beconcluded that the average case-fatality rate fromtetanus in the USA was as high as 62.26%, andthat, unlike the morbidity rate, this fatality index didnot tend to decrease. Heath, Zusman & Sherman(1964) have stated that, of three tetanus patients inthe USA, two usually die. Previously, Calvin (1930)had noted that, among 183 cases of tetanus observedduring a four-year period in Cook County Hospital,in Chicago, the case-fatality rate ranged, from year
to year, from 27% to 82%.Information gathered from several hospitals by
Huntington, Thompson & Gordon (1937) showedthat, of 72 patients who were not given anti-tetanusserum (ATS), 47 (65%) died, whereas among 228patients who were given ATS intramuscularly andintravenously, the number of deaths was 142 (62 %).In a series of case-histories that was analysed bySpaeth (1941), there were 462 deaths (82%) among570 tetanus patients who were treated without ATS,as compared to 1088 deaths (56.7%) among the1917 patients who had received ATS. Takos (1958)found that, of 170 tetanus patients treated in Miami,
TABLE 2DECENNIAL MORTALITY RATES FROM TETANUS PER 100000 INHABITANTS
OF NORTH AMERICA AND CERTAIN CARIBBEAN COUNTRIES a
Country 1921-1930 1931-1940 [ 1941-1950 1951-1960
Canada 0.49 0.31 0.125 0.06
Jamaica no data 3.29 3.44 3.57
Trinidad and Tobago no data 6.90 7.35 5.57
United States of America 0.20 0.76 0.38 0.18
a Annual Epidemiologkal and Vital Statistks, 1950-1964.
75

B. BYTCHENKO
FIG. I
DISTRIBUTION OF REPORTED CASES OF TETANUS IN THE UNITED STATES OF AMERICA,BY STATES AND BY BROAD AGE-GROUPS, IN 1962a
a From US Department of Health, Education, and Welfare, Communicable Disease Center (1963)Morbidity and mortality weekly report, 11, No. 53, p. 3.
MORBIDITY, MORTALITY, AND CASE
TABLE 3
FATALITY FROM TETANUS IN THE UNITED STATES OF AMERICA(1953-1961) a, b
Year 11953 1 1954 [ 1955 1956 1957 1958 1 1959 1960 [1961 T Total
No. of reported cases 506 524 462 468 447 445 445 368 379 4044
Morbidity rate (per 100 000) 0.315 0.321 0.278 0.277 0.260 0.254 0.250 0.203 0.206 0.261
No. of deaths 337 332 265 246 279 303 283 231 242 2518
Mortality rate (per 100000) 0.210 0.203 0.159 0.145 0.162 0.173 0.159 0.127 0.131 0.162
Case fatality (per 100 cases) 66.60 63.35 57.35 52.56 62.41 68.08 63.59 62.77 63.85 62.26
Population (in millions) | 160.2 163.0 165.9 168.8 171.9 1174.7 177.8 180.6 183.6 1 546.90 b
a These figures include Alaska from 1959 and Hawaii from 1960.b Data from: US Department of Health, Education, and Welfare, Communicable Disease Center (1963) Morbidity and mortality
weekly report, 11, No. 53, p. 3.
76
\WHO 4555

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60
TABLE 4CASE FATALITY FROM TETANUS IN CANADA
AND THE UNITED STATES, ACCORDINGTO VARIOUS AUTHORS
No. I DeathsAuthor of
cases No. % a
Gessner & Adiger (1916) 368 258 70.1
Ashhurst (1926) 23 8 (34.7)
Wainwright (1926) 540 305 56.5
Calvin & Goldberg (1930) 183 97 53.0
Graves (1930) 217 113 52.0
Boyce & McFetridge (1935) 185 110 59.4
Huntington, Thompson & Gordon(1937T 642 404 62.9
Moore & Singleton (1939) 102 51 50.0
Spaeth (1941) 2 487 1 550 62.3
Vener & Bower (1941) 100 29 29.0
Vinnard (1945) 352 159 45.1
Silverthorne (1947) 70 47 (67.1)Noel (1950) 105 49 46.6
Takos (1958) 170 91 53.5
Pertstein, Stein & Elam (1960) 300 210 70.0
Greenfield (1963) 36 9 (25.0)
a The figures in parentheses are percentages of numbersless than 100.
Florida, 91 (53.5) died. These findings and those ofsome other investigators are summarized in Table 4.Not shown in this table is the interesting fact that,among tetanus patients, males prevail over femalesin a ratio of 2: 1. According to Heath, Zusman &Sherman (1964), this disproportion was even higherin the non-white population, namely 6 :1.Most of the reported cases in the USA occurred
after minor injuries, operations, abortions, child-birth, frostbite, bums, etc., but in a large numberof cases, the site of the infection was not known(Calvin, 1930; Kirtley, 1940; Vinnard, 1945; Silver-thorne, 1947; Turner & Galloway, 1949; Spivey etal., 1953; Adams & Morton, 1955; Creech, Glover& Ochsner, 1957; Takos, 1958; Perlstein, Stein &Elam, 1960; Botticelli & Waisbren, 1961).During the period 1906 to 1927, 5767 deaths from
tetanus neonatorum were recorded in the USA(Hines, 1930), the incidence of these deaths beinghighest in North Carolina, Louisiana and Penn-sylvania. A study by Vinnard (1945) revealed that,
from a total of 352 cases of tetanus, there were 11(3.1 %) of tetanus neonatorum, with six deaths.In a review (1957), Axnick & Alexander showedthat there was a relative increase of tetanus neo-natorum from 1951 to 1954. The incidence in theage-group 0-1 years exceeded sevenfold to elevenfoldthe number of cases of tetanus in the ages above oneyear in the white population and by fourteenfold toseventeenfold the incidence in the non-white popu-lation. Of 170 tetanus cases treated by Takos(1958), 22 were neonatal, and of these, 21 terminatedfatally. Heath, Zusman & Sherman (1964) havecalculated that tetanus has been responsible for onequarter of the deaths of children before the twenty-eighth day of life.The relatively high number of post-surgical cases
of tetanus that has been found (Bunch & Quattle-baum, 1943; Vinnard, 1945; Takos, 1958) indicatesthe necessity for the improvement of preventivemeasures against infection in all patients whoundergo surgery.A marked variation in the seasonal distribution of
tetanus in the USA has been noted. The incidenceof this disease is highest in July, August, and Septem-ber, and lowest during the winter months (Vinnard,1945; Silverthorne, 1947; Noel, 1950; Heath,Zusman & Sherman, 1964; Top, Huggen & McCul-loch, 1964).The apparent decline in the morbidity and
mortality of tetanus in the USA may be explainedas being due to urbanization, industrialization, themechanization of agriculture and, in particular, asthe result of immunization of the population at risk.At present, the largest group of the population ofthe USA that has been protected against tetanusincludes the veterans of the Second World Warand young people who have been immunizedin childhood. A programme of active immuniza-tion of as many persons as possible is being car-ried out by the American Medical Association,the American College of Surgeons, the AmericanPublic Health Association, the US Public HealthService and the American Academy of Pediatrics.For active-passive prophylaxis in the event ofinjury, adsorbed tetanus toxoid, liquid tetanustoxoid and anti-tetanus human globulin are avail-able commercially everywhere in the USA (Skudder& McCarrol, 1964). The Second Report on theWorld Health Situation, 1957-1960 (World HealthOrganization, 1963) shows that, in 1960 alone,approximately 3 880 000 persons in the UnitedStates received vaccination against tetanus.
6
77

B. BYTCHENKO
Middle AmericaAccording to statistics made available to
for the years 1951-60, the absolute number offrom tetanus in Middle America ranged fronin 1951 to 4757 in 1960 among a populati42 000 000 that was covered by registration (Annual Epidemiological and Vital Statistics,1964). However, these figures must be consvery incomplete, since before 1945 deathstetanus were reported by but 14 countries iregion. Later, however, the number of repcountries was raised, first to 18, then to 22.The highest mortality rate from tetanus the
recorded during the decade 1951-60 was thatDominican Republic (63.3 deaths per 1(population). In 1960, tetanus was listed athe ten principal causes of death in both Cost,and Mexico, in which two countries it accoirespectively, for 2.5% and 0.57% of the total ni
GEOGRAPHICAL DISTRIBUTION OF
of deaths (World Health Organization, 1963). InMexico, tetanus was responsible for more deathsthan leprosy, scarlet fever, meningitis, typhusexanthematicus or rabies (Bol. epidem. (Mix.),1952-63).The decennial mortality rate from tetanus per
100 000 population during the decade 1951-60 washighest in the Dominican Republic (63.33), Nica-ragua (32.8), Costa Rica (21.7), Panama (19.1) andEl Salvador (15.2) and lowest in Guatemala (2.6),as shown by the statistics made available to WHOfor the years 1950-64.Although this difference in recorded mortality
rates is due, largely, to differences in the reliabilityand completeness of the reports, they also reflect,to some extent, actual differences in the distrgbutionof the disease. Such variations may be found evenwithin a single country. Fig. 2 shows that, inMexico, for example (Bol. epidem. (Mix.), 1952-
FIG. 2TETANUS IN MEXICO DURING THE PERIOD 1949-61 a
a Average annual mortality rates per 100000 inhabitants (Amezquita Urias, 1964).
U S A
GULF OF MEXICO
:5 2.0
2.1-5.0
55.1-10.0 0
_10.1-15.0 -
015.1-20.0 0-
> 20.0 0 ,-- GUATEMALA
wHo 556
78

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60 79
63; Silva Martinez, 1964), where the number ofrecorded deaths from tetanus doubled from 1950to 1960, and in 1959 and 1960 reached the totals of2487 and 2570, respectively. Amezquita Urias (1964)observed, during the years 1956-60, real foci oftetanus in several Mexican states. In Nayarit, thetetanus mortality rate per 100 000 population was70.96; in Colima, 35.76; in Sinaloa, 20.2; in Jalisco,20.22; in the territory of Baja California Sur, 16.16;in Tamaulipas, 15.18; in Campeche, 13.26; and inNuevo Leon, 11.28. In Zacatecas, on the other hand,it was but 2.1, approximately, and in the state ofMexico it was 0.5, and in the Federal District itwas 0.9 (Bol. epidem. (Mix.), 1952-53). Malpica(1961) considered that about 60% of all Mexicandeaths from tetanus occurred in the state of Tamau-lipas where, as noted above, the death-rate from thisinfection was found to be 15.18 per 100 000 popu-lation. During the period 1951-60, the tetanusmortality rate per 100 000 for all of Mexico was 6.6.
It should be noted that the number of cases oftetanus that occurred per year in any given area ofMexico was rather consistent. Gomez et al. (1960),for example, have reported that, in the State ofNayarit, there were between 34 and 54 cases oftetanus each year from 1948 to 1958. This obser-vation indicates that, in such foci of infection,conditions must be particularly favourable for itspersistence.Amezquita Urias (1964) noted that, among the
2487 fatal cases of tetanus in Mexico in 1959, therewas a preponderance of males (1389, or 55.87%)over females (1098, or 44.13%).
In the Caribbean area, the incidence of tetanus isapproximately the same as in Mexico. For example,Forde & Williams (1960) have estimated that thetetanus morbidity rates in Barbados in the years1951 through 1954 were, respectively, 13.1, 22.8,12.5 and 22.5. The same investigators report havingtreated 27 patients, of whom eight (29.6%) died.Other studies in Central America and the Caribbeanhave shown tetanus case fatality rates that are evenhigher (Francisco, 1944; Taxay, 1960; Back, 1960;Montgomery, 1961; Miranda & Hempel, 1962).Amezquita Urias (1964) has reported that, of the
2487 patients who died of tetanus in Mexico in1959, 1624 (65.3%) were less than one year of age.Similarly, Miranda & Hempel (1962) have reportedthat, of 190 patients with tetanus admitted to ahospital in Costa Rica in a six-year period, 44(23.1 %) were newborn.
Unlike the situation in the USA, there is no distinctseasonal distribution of tetanus in Mexico,' asshown below:
Season Numberof cases Percentage
December-February 1 773 23.0March-May 1 826 23.7June-August 2 121 27.6September-November 1 969 25.6
For a period of ten years, the highest proportionof admissions to hospital for tetanus in Mexico(9.7%.) occurred in July. In Antigua, on the otherhand, the highest incidence of tetanus has beenobserved during the first and second quarters of theyear, when the sugar crop is harvested (Uttley,1959). The necessity for active immunization againsttetanus has been stressed by many workers in Mexico,Central America and the Caribbean, several ofwhom have proposed definite programmes for thecontrol of tetanus (Gomez et al., 1960; Malpica,1961; Amezquita Urias, 1964; Silva Martinez, 1964).Immunization of the population with tetanus toxoidor diphtheria-pertussis-tetanus (DPT) vaccine hasbeen initiated in Bolivia, Brazil, British Guiana andthe islands of Bermuda, Barbados and Cuba.
South America
Since, prior to 1960, such countries as Argentina,Brazil, Peru and Uruguay reported only thosedeaths from tetanus that occurred in the principalcities, while for Bolivia no data were provided at all,little is known concerning the actual situation oftetanus in South America. Consequently, the mor-tality rates that have been calculated on the basis ofWHO statistics for South America can be consideredas approximations only. The calculated averagemortality rate for tetanus in the entire continent is,of course, greatly influenced by this situation.However, if Argentina and Brazil are excluded fromthe calculations, it becomes apparent that the SouthAmerican rate of mortality from tetanus would beabout as high as that for Middle America-that is,approximately 8.50 per 100 000 population.The apparent increase in tetanus mortality for the
entire South American continent may be attributedto an improvement in registration. According tothe admittedly incomplete data available to WHO,based on an average covered population of 76 000 000,approximately 27 000 deaths from tetanus wererecorded during these 14 years, indicating a death-rate from tetanus of at least 3.5 per 100 000 popula-
' Bol. epidem. (Mix.), 1952-63.

B. BYTCHENKO
tion. If this rate were to be applied to the entirepopulation of South America (that is, about 125 mil-lions), the number of deaths for 10 years wouldexceed 40 000. More recent reports from severalauthors, however, indicate that the true mortalityfigures are even higher. For example, in but fiveyears (1957-61), 4989 cases of tetanus were recordedby principal hospitals in Venezuela. Of this number,2638 (47.46%) terminated fatally (Figueroa & Ro-mero, 1963). In 1960-61, the mortality from tetanusin all of Venezuela, as indicated by these authors,was 12.2 per 100 000 population, being as high as 72in the State of Portuguesa, 28.8 in the State of Co-jedes, and 27.9 in the State of Yaracuy. The lowestmortality rate for tetanus (2.4 per 100 000 popula-tion) was observed in the Federal District.The figures from Venezuela show slight differences
in incidence between the sexes. In the age-groupsfrom 0-1 years to 20-24 years, as well in the age-groups over 45 years, there was a higher incidencein males, while female patients were more numerousin the age-groups from 25 to 44 years.
In the 1200-bed Hospital das Clinicas at the Schoolof Medicine of the University of Sao Paulo, inSao Paulo, Brazil, about 120 tetanus patients havebeen treated each year for the last 16 years (Nenes& Tranchesi, 1948; Bahia, 1953; Pinheiro, 1957,1960, 1962).
Pinheiro (1960) has shown that, in the State ofSao Paulo, with a population of approximately15 000 000, there were 13 299 deaths from tetanusduring the period 1950-58, for an annual mortalityrate per 100 000 of approximately 9.8. Of thesedeaths, 1015 occurred in the capital itself, whereas12 284 (92.36%) occurred in the surrounding State.From the case-histories of 1903 patients with
tetanus admitted to one Sao Paulo hospital duringa 16-year period, 75.7% of the cases occurred inchildren under 14 years of age and in women andmanual workers under 20 years of age. About 78%of the patients were Caucasians. There was a re-markable predominance of males over females(about 2: 1). The disease usually developed afterthe patient had experienced minor injuries, deli-veries, abortions or chronic ulcerations, but manypatients presented no visible site of infection (Pin-heiro, 1957; Veronesi, 1960). Among 148 cases oftetanus treated by Salvaraglio & Ebole (1950),7 (4.73%) were post-surgical. Zubillaga (1952) hasreported that 32 (40%) of 80 patients with tetanuscontracted the disease after infestation with theburrowing flea Sarcopsylla penetrans.
Long ago, von Reuss (1927) stated that, in tropicalareas, tetanus was responsible for from 10% to25% of all child mortality. A study conducted byOropeza (1937) in Venezuela showed that 7% of alldeaths of newborns were due to this infection.Data recently collected by Mattos (1962) reveal
that, from 1957 to 1961, about 5000 cases of tetanusneonatorum were registered in the Brazilian Stateof Sao Paulo. For example, in 1960, there were60.2 cases of this disease per 1000 live-births, andin 1961 this rate rose to 83.7 per 1000. Mattosconsiders that, in Brazil, there are at least 7000 casesof tetanus neonatorum annually, and Oliveira(1958) has reported that, between 1936 and 1945,941 cases of tetanus neonatorum were reported forRio de Janeiro alone, for a yearly average of 94 cases.In Chile, of 141 cases of tetanus in a Santiagohospital, 29 (20.5%) occurred in the newborn(Casorzo & Figueroa, 1951). Later, La Scala (1958)reported that 56 cases of tetanus neonatorum hadbeen admitted to the same hospital during the years1949 to 1957. Figueroa & Romero (1963) stated thatabout 57% of all tetanus patients reported inVenezuela during the years 1957 to 1961 were lessthan one year of age.A number of other reports from South America
show that tetanus is fairly common in Uruguay(Salvaraglio & Ebole, 1950; Fonseca et al., 1961),Venezuela (Zubillaga, 1952), Argentina (Aguileiro,Brahiero & Ghigliazza, 1960), and Chile (Rojas etal., 1960). In Argentina, for example, during 1960,tetanus attacked 469 persons (morbidity rate of2.34 per 100 000 population) and was consideredthe fifteenth most important communicable diseasein that country (World Health Organization,1963).
Kloetzel & Monteiro (1963), who performed aclinical and laboratory study on tetanus in SaoPaulo, Brazil, reported that the cause of death intetanus remains unknown, and that present-daytreatment of this disease is inadequate; almost 60%of untreated patients recovered. In general, the case-fatality rate for tetanus in South America seems torange from 35% (Pinheiro, 1957; Veronesi, 1960;Fonseca et al., 1961; Kloetzel, 1963) to 54%(Salvaraglio & Ebole, 1950).The high case-fatality rate in tetanus neonatorum
has been noted by several authors: Carvalho &Nascimento (1950) set it at 92.5 %; Casorzo &Figueroa (1951) show 79%; Zubillaga (1952) gives65%; Pinheiro (1957) sets it at 84%; La Scala (1958)sets it as high as 89.28%; Veronesi (1960) at 83%;
80

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60 81
Pinheiro (1962) at 76.9%, and Figueroa & Romero(1963) at 60%.The geographical distribution of tetanus in South
America remains to be investigated. However, thereis evidence that, in Venezuela, the States of Portu-guesa, Cojedes, Yaracuy, Barinas, Amazonas, Sucre,Trujillo, and Apure are foci of infection (Figueroa& Romero, 1963), as are the provinces of Sao Pauloand Maceio in Brazil (Mattos, 1962).As one moves southward from the equator, the
seasonal distribution of tetanus is found to be moreand more distinct (Veronesi, 1960), with thehighest incidence of the disease falling in Septemberto November (spring) and the lowest in April-June(autumn).
Public awareness of tetanus as a public healthproblem in South America has been growing steadilyduring the past 20 years (Veronesi, 1960; Figueroa& Romero, 1963). Immunization with tetanus toxoidor with diphtheria-pertussis-tetanus (DPT) vaccinehas been initiated in some parts of Argentina andBrazil. In view of the high morbidity from tetanusneonatorum, recommendations for the vaccinationof pregnant women in Brazil were made by Lacazet al. in 1955.As may be concluded from the Second Report on
the World Health Situation, 1957-1960 (WorldHealth Organization, 1963), the progress of thecontrol of tetanus in the Americas during the period1951-60 has been rather slow, except in the USAand Canada.
ASIA
In Asia, the existence of tetanus has been knownfor centuries, and the Indian Clinical ResearchAdvisory Committee (Indian Research Fund Associ-ation, 1946) suggested that there was urgent need tostudy the problem. More recently, Tateno, Suzuki& Kitamoto (1961) have reviewed the situationregarding tetanus in Japan, and the first InternationalConference on Tetanus was held in Bombay, India,in November 1963.
Before 1950, only five countries in Asia recordeddeaths from tetanus and reported them to WHO:Ceylon, Hong Kong, Israel, Japan and Thailand.During the decade 1951-60, the number of Statesthat reported tetanus to WHO never exceeded 32,covering not more than 40% of the population ofAsia. During this entire period, no data wereavailable for Afghanistan, Burma, China (mainland),Iran, Mongolia, or Viet-Nam, while Ceylon, India,Indonesia, Laos and Cambodia supplied only in-
complete figures that had been collected fromhospitals in the principal cities. Consequently, thefigures shown in WHO statistics from 1960 to 1964represent but a relatively small proportion of thetetanus cases that actually occurred in Asia duringthat period.The highest mortality rates from tetanus per
100 000 population for the indicated period were 61(Macao, 1952), 44 (Goa, Damao, Diu, 1952), 26(Taiwan, 1954), 9 (Philippines, 1960), 6 (Federationof Malaya, 1961), and so on. The lowest tetanusmortality rates for Asian countries in the periodspecified were those of Israel (0.37, 1960) and Japan(0.64, 1960). The average tetanus mortality rateper 100 000 population for the entire covered Asianpopulation for the decade 1951-60 was 2.7, rangingfrom 2.4 in 1958 to 3.8 in 1952. The minimummortality rate for tetanus cases in the 32 countrieslisted in the Annual Epidemiological and Vital Sta-tistics published by WHO covering the period underreview was 2.3 per 100 000 population, with ap-proximately 14 000 deaths; the highest morbidityrate was 3.0, with approximately 19 000 deaths.The number of deaths from tetanus in the Asiancountries that reported to WHO, excluding India,was 6700 in 1954 and 4800 in 1960. However, if thedeaths reported in India for 1958 are included(Vital Statistics ofIndia, 1960) the figure for 21 Statesis 15 500, yielding a mortality rate per 100 000population of 2.4. Despite the incompleteness of thedata, it can be assumed that, from a population of645 000 000, there were at least 155 800 deaths fromtetanus in 21 Asian countries during the decade1951-60. Moreover, if a mortality rate of 2.3 to 2.8holds true for all of Asia, which has an estimatedpopulation of 1 532 000 000, there must have beenabout 350 000 to 420 000 deaths from this diseaseduring the decade in question.As noted above, however, these calculations are
based on very incomplete data. Indeed, the mortalityrate from tetanus in many Asian countries willexceed 2.8.The following figures 1 show that there has been a
constant increase in admissions to hospital fortetanus in both the Punjab and Rajasthan during theyears 1956-62, the numbers for 1961 being almost2.5 times those for 1956.
1 From the annual reports (1962-63) on the public healthadministration for the Punjab and from a statement issuedby the National Institute of Communicable Diseases, NewDelhi, showing the number of patients treated for tetanusin the 25 State Public Hospitals in Rajasthan during theyears 1950-61.

82 B. BYTCHENKO
TABLE 5TETANUS ADMISSIONS IN SOME HOSPITALS OF INDIA
No. of IPercentageAuthor Town Hospital Year(s) tetanus of all
patients admissions
Patel, Mehta & Nanavati (1963) Bombay King Edward Memorial Hospital 1954-1962 4733 1.9
Vakil et al. (1963) Bombay J.J. Group of Hospitals 1954-1962 1 852 1.4
Vaishnava et al. (1964) Delhi Irwin Hospital 1960-1963 2 030 -
Ayyar, Ramakrishnan & Singh (1963) Delhi Safdarjang Hospital 1961 249 1.2
Srivastava & Chatterji (1961) Agra S.N. Hospital 1952-1959 702 0.6
Mathur & Singh (1963) Lucknow Gandhi Memorial Hospital 1951-1958 974 -
Bhatt & Anwikar (1962) Nagpur Medical College 1951-1956 8881958-1959
Kochhar (1960) Amritsar Medical College 1955-1958 200 2.2
Barua (1961) WestBengal Hooghly Sadar A.G. Hospital 1957-1960 280 1.8
Laha & Vaishya (1963) Gwalior G.R. Medical College and J.A. Groupof Hospitals 1954-1961 1 024 4.8
Year Punjab Rajasthan
1956 1 062 1 1071957 1 501 9411958 1 794 1 2421959 2001 13871960 2 470 2 0801961 2 681 2 7561962 2 984
The tetanus morbidity rate in the Punjab hasgradually increased from 6.2 per 100 000 in 1956 to16.5 in 1961. With regard to Rajasthan, it is ofinterest to note that, in 1951, only 319 tetanus caseswere reported from the State Public Hospitals,"whereas the corresponding number for 1961 was2756, or 8.6 times as high.However, this phenomenal increase may be more
apparent than real, quite probably being attribut-able to factors such as the improvement of publichealth records, the compulsory hospitalization ofsevere cases of this disease, and the gradual improve-ment in the health consciousness of the populationand in its attitude toward the public health services.The situation is very much the same in other parts
of India. For example, in Goa, Damao and Diu, theaverage mortality per 100 000 population during
1 From the annual reports (1962-63) on the public healthadministration for the Punjab and from a statement issuedby the National Institute of Communicable Diseases, NewDelhi, showing the number of patients treated for tetanusin the 25 State Public Hospitals in Rajasthan during theyears 1950-61
the period 1951-58 was estimated to be 14.8, witha peak of 44.06 in 1952. However, in some ruralareas, there are foci in which tetanus is the fourth-ranking cause of death, with a mortality rate of90.8 per 100000 (Gordon, Singh & Wyon, 1961;Parikh, 1963) or even more than 100 per 100000(Pai, 1963). Many Indian hospitals have an ex-tremely high number of tetanus patients (Table 5).
All of these data suggest that India should beincluded in the zone in which the tetanus mortalityrate is between 5 and 10 per 100000 population.This estimate has been substantiated by surveysconducted recently in some rural and urban areasof India by Joag (1963), who found that the tetanusmortality rate per 100000 was approximately 9.7.The role of tetanus as one of the leading causes
of death in Asia was stressed by Silva (1960), whoestimated that, in Ceylon, this infection strikes morethan 1500 persons each year, and that the mortalityrate from this disease is not less than 5 per 100 000inhabitants.
In Abadan, Iran, tetanus has been listed as thetwelfth most important cause of all deaths and asthe sixth most important cause of all infant deaths,the gross mortality rate from this disease beingapproximately 9.9 per 100 000 population.2 Reports
' Pakdel (1961), The main causes of death in Abadanamong company employees and their dependants. Seventhmeeting, Persian Gulf Medical Society. (Unpublished.)
GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60
on tetanus appear from time to time in the Iranianmedical literature (Yazdani, 1954; Binechvar &Ghavampour, 1954).
In Singapore, data collected from the GeneralHospital for three years by Gwee & Nadarajah in1960 showed that 77 to 87 patients with tetanus hadbeen admitted during each year. The tetanus mor-bidity rate per 100 000 population in that cityincreased from 5.2 in 1957 to 6.4 in 1959. Theseauthors also observed a rise in the tetanus case-fatality rate during the years 1957-59, particularlyin the newborn.
In Indonesia, also, tetanus is one of the principalcauses of death (Indonesia, 1957, 1958). Duringthe period 1957-58, of every 1000 patients deceasedin the principal hospitals, 38 died from tetanus(3.8%). Altogether, in only these two years, 1565deaths from tetanus were recorded, 703 (44.9%)of which were from tetanus neonatorum. Accord-ing to Poesponegoro & Ranti (1959), during a periodof only nine years (1949-57), 1062 children withtetanus were admitted to the Paediatric Departmentof the General Hospital of Djakarta, of whom573 (53.9%) died. These hospitalized childrenincluded 578 newborns. De Reus (1963) has reportedseeing, in three hospitals on the island of Deli,Indonesia, between 1956 and 1961, 257 tetanuspatients, of whom 102 were newborn.Very little is known concerning tetanus in main-
land China. According to Young-En Kao (1948),however, among the specific infectious diseases thatwere registered in the National Kweyang MedicalCollege and Hospital between 1939 and 1945, therewere 51 cases of tetanus neonatorum, representing1.14% of all admissions, thus exceeding the incidenceof smallpox, scarlet fever, mumps, erysipelas, rheu-matic fever, rabies, cholera and septicaemia. Thesame author (1951) has observed tetanus neonato-rum in Nanking.The rank of tetanus among other important
causes of death in Asia has not yet been determined,but in Japan, where Tateno, Suzuki & Kitamoto(1961) have recently investigated this disease, it wasfound that, in 1958, tetanus killed more people thandid Japanese encephalitis, poliomyelitis, epidemicmeningitis, pertussis, scarlet fever, typhoid fever,or rabies; indeed, the number of deaths from tetanuswas almost tenfold greater than that from typhoidfever. Similarly, the Second Report on the WorldHealih Situation (World Health Organization, 1963)shows that, in Ceylon, tetanus kills more peoplethan either poliomyelitis or rabies.
While no reliable data on the actual incidence oftetanus in Burma are available, some observers(unpublished report to WHO) have noted that,during 1963, the Rangoon General Hospital ad-mitted 217 cases of tetanus, 81 of which terminatedfatally; neonatal tetanus accounted for 63 admissionsand 40 deaths in this series. A report from Turkey(World Health Organization, 1963) shows that, in1960, there were 445 deaths from tetanus, asagainst 442 from typhoid fever and 50 from rabies.There is no country in which the distribution of
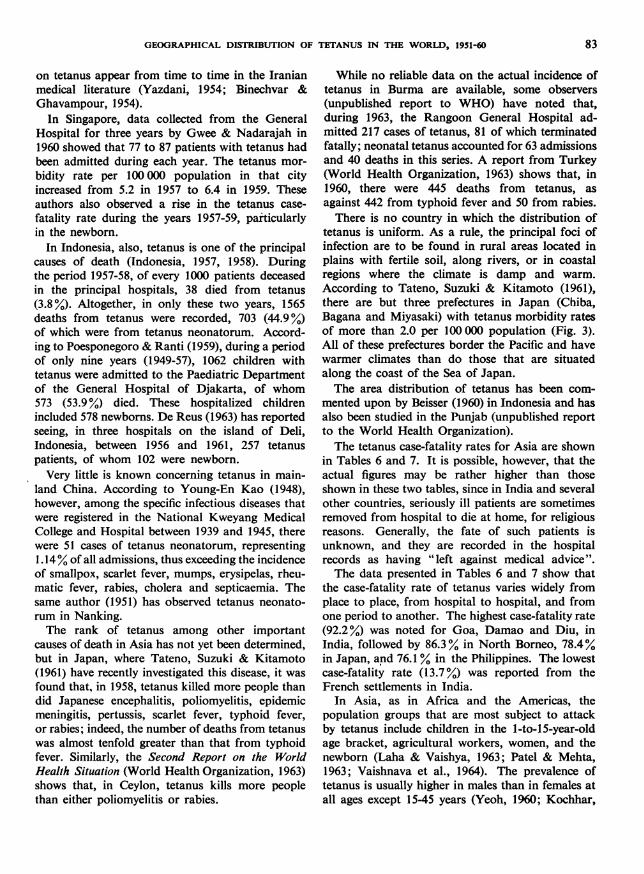
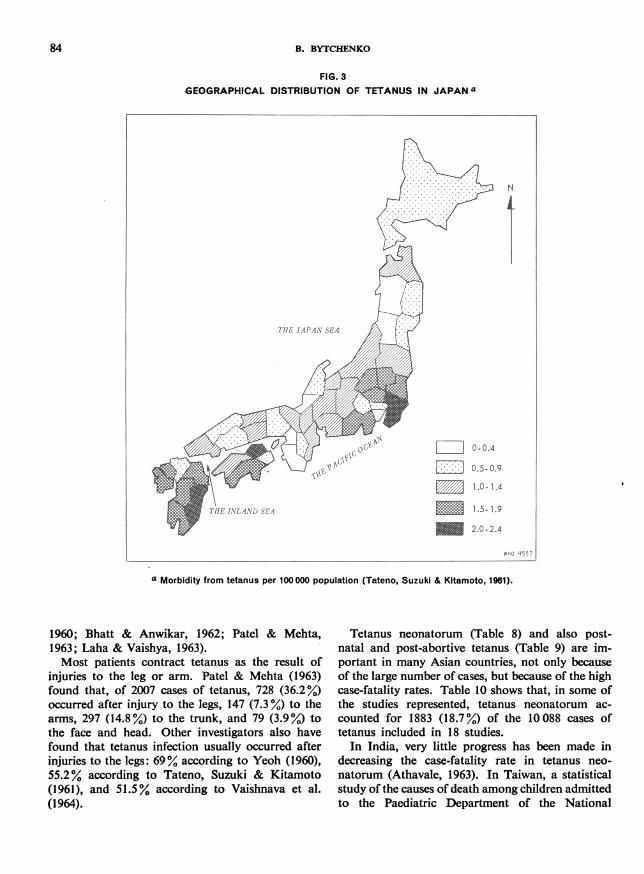
tetanus is uniform. As a rule, the principal foci ofinfection are to be found in rural areas located inplains with fertile soil, along rivers, or in coastalregions where the climate is damp and warm.According to Tateno, Suzuki & Kitamoto (1961),there are but three prefectures in Japan (Chiba,Bagana and Miyasaki) with tetanus morbidity ratesof more than 2.0 per 100 000 population (Fig. 3).All of these prefectures border the Pacific and havewarmer climates than do those that are situatedalong the coast of the Sea of Japan.The area distribution of tetanus has been com-
mented upon by Beisser (1960) in Indonesia and hasalso been studied in the Punjab (unpublished reportto the World Health Organization).The tetanus case-fatality rates for Asia are shown
in Tables 6 and 7. It is possible, however, that theactual figures may be rather higher than thoseshown in these two tables, since in India and severalother countries, seriously ill patients are sometimesremoved from hospital to die at home, for religiousreasons. Generally, the fate of such patients isunknown, and they are recorded in the hospitalrecords as having "left against medical advice".The data presented in Tables 6 and 7 show that
the case-fatality rate of tetanus varies widely fromplace to place, from hospital to hospital, and fromone period to another. The highest case-fatality rate(92.2%) was noted for Goa, Damao and Diu, inIndia, followed by 86.3% in North Borneo, 78.4%in Japan, and 76.1 % in the Philippines. The lowestcase-fatality rate (13.7%.) was reported from theFrench settlements in India.
In Asia, as in Africa and the Americas, thepopulation groups that are most subject to attackby tetanus include children in the 1-to-15-year-oldage bracket, agricultural workers, women, and thenewborn (Laha & Vaishya, 1963; Patel & Mehta,1963; Vaishnava et al., 1964). The prevalence oftetanus is usually higher in males than in females atall ages except 15-45 years (Yeoh, 1960; Kochhar,
83
B. BYTCHENKO
FIG. 3GEOGRAPHICAL DISTRIBUTION OF TETANUS IN JAPAN a
THE JAPAN SEA
THE INLAND SEA
a Morbidity from tetanus per 100000 population (Tateno, Suzuki & Kitamoto, 1961).
1960; Bhatt & Anwikar, 1962; Patel & Mehta,1963; Laha & Vaishya, 1963).Most patients contract tetanus as the result of
injuries to the leg or arm. Patel & Mehta (1963)found that, of 2007 cases of tetanus, 728 (36.2%)occurred after injury to the legs, 147 (7.3%) to thearms, 297 (14.8%) to the trunk, and 79 (3.9%) tothe face and head. Other investigators also havefound that tetanus infection usually occurred afterinjuries to the legs: 69% according to Yeoh (1960),55.2% according to Tateno, Suzuki & Kitamoto(1961), and 51.5% according to Vaishnava et al.(1964).
Tetanus neonatorum (Table 8) and also post-natal and post-abortive tetanus (Table 9) are im-portant in many Asian countries, not only becauseof the large number of cases, but because of the highcase-fatality rates. Table 10 shows that, in some ofthe studies represented, tetanus neonatorum ac-
counted for 1883 (18.7%,) of the 10088 cases oftetanus included in 18 studies.
In India, very little progress has been made indecreasing the case-fatality rate in tetanus neo-
natorum (Athavale, 1963). In Taiwan, a statisticalstudy of the causes of death among children admittedto the Paediatric Department of the National
N
0.5.0.9
1.0-1.4
1.5- 1.9
2.0-2.4
WHO '557
84
r.r'"'ffissw w-c0so
,ICv
et-to

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60
TABLE 6CASE FATALITY FROM TETANUS IN SOME COUNTRIES OF ASIA
Country 1 Year(s) | No. of cases | No. of deaths [ Cas(e)atality
North Borneo a 1951 23 20 (86.3)Cambodia a 1951 23 5 (21.7)Ceylon a 1951 1150 346 30.0Ceylon 1955-1957 2817 1100 39.0India
Punjab b 1956-1962 14 493 3 972 27.4
Rajasthan c 1960 2 080 808 38.8
West Bengal c 1960 1 024 574 56.0
French Settlements a 1951-1952 167 23 13.7
Goa, Damao and Diu a 1951 284 262 92.2Iraq a 1951-1953 1 004 266 26.5
Israel a 1951-1953 116 39 33.6
Japan a 1951-1953 4 394 3 447 78.4
Jordan a 1951 37 15 (40.5)Macao a 1951 183 95 51.9
Philippines a 1951 1 697 1 292 76.1
Ryukyu Islands a 1951 200 42 21.0
Singapore a 1951-1952 159 73 45.9
Viet-Nam a 1951 213 41 19.2
Viet-Nam a 1960 472 112 23.7
a Epidem. Vital Statisf. Rep., 1954, 7, 263-265.b Annual reports on the public health administration for the Punjab, 1960-62.c Vital Statistks of India, 1960.d The figures in parentheses are percentages of numbers less than 100.
Taiwan University Hospital showed tetanus to beamong the most important (Lue, Hung-Chi, 1960).In Thailand, although tetanus is not yet a notifiabledisease, an epidemiological sampling study con-ducted by Stahlie (1960) showed that, among 2344children studied, 37 died from various causes, and ofthese 37 patients, 19 had presented the symptoms oftetanus. Stahlie considers tetanus to be definitelyone of the leading causes of infant mortality andhas appealed that it be made notifiable. In India,in the rural Punjab, Gordon, Singh & Wyon (1961)found that, of 33 patients who died of tetanus,30 were apparently newborn infants.
Situations of this sort exist in many other placesin Asia in which health services, especially maternaland child health institutions, are lacking, and in
which there is an absence of health education butwidespread poverty, religious prejudices, and tra-ditional unhygienic customs and habits (Yodh &Shah, 1956; Menon, 1960; Harper, 1961; Gwee &Lee, 1962). Most mothers in the rural parts of Asiaare delivered of their infants with the help of localmidwives such as the dais of India, the dukun ofIndonesia, and the monthamyae of Thailand, or withthat of elderly relatives who are frequently ignorantof infection and who use unsterilized scissors, knives,or other sharp instruments to sever the umbilicalcord. In some places, wounds are treated with dust,the ashes of cow dung, or even with earth (Silva,1960; Gordon, Singh & Wyon, 1961).De Reus (1963) has stated that the high incidence
of tetanus neonatorum in Indonesia is principally
85

B. BYTCHENKO
TABLE 7CASE FATALITY FROM TETANUS IN ASIA ACCORDING TO VARIOUS AUTHORS
[No. Cs' deathso fatalityCountry Author of cases of No.hs %Casobserved(%a
Natkunam (1960)
Silva (1960)
Lewis et al. (1954)
Hanna (1958)
Kochhar (1960)
Ghosh & Soni (1961)
Sinha (1961)
Srivastava & Chatterji (1961)
Shah et al. (1962)
Jain (1962)
Bhatt & Anwikar (1962)
Limaye (1962)
Arora, Desai & Kazi (1963)
Ayyar, Ramakrishnan & Birenda Singh(1963)
Barua (1963)
Basu (1963)
Mahadevan (1963)
Modi (1963)
Sharma (1963)
Vaishnava et al. (1964)
Vakil et al. (1963a)
K.E.M. Hospital Group (1963a)
Poesponegoro & Ranti (1959)
Tateno, Suzuki & Kitamoto (1961)
Yeoh (1960)
Gwee & Nadarajah (1960)
Tran Van Bang &Nguyen Duy San (1960)
89
384
40
77
200
248
91
702
214
63
888
144
170
249
383
114
2 021
554
510
2 030
293
4 839
1 062
945
130
272
265
36
110
29
36
92
151
35
329
95
19
408
61
68
121
108
41
747
243
229
954
114
2 216
573
i55
63
109
115
(40.4)
28.6
(72.5)
(51.9)
46.0
60.8
(38.4)46.8
44.4
(30.1)
45.9
42.3
40.0
48.6
28.2
35.9
37.0
43.8
44.9
47.0
39.0
45.8
53.9
79.9
48.4
40.0
43.4
a The figures in parentheses are percentages from numbers less than 100.
attributable to local customs and rituals associatedwith childbirth. In many places, the cord is cutwith a bamboo sliver and then dressed with a mixtureof lemon juice, coconut oil and salt or with somesimilar preparation. De Reus thinks that this customwill not disappear in the near future and thereforebelieves that the active immunization of motherswith tetanus toxoid is indispensable if tetanus neo-
natorum is to be controlled.
Some studies have shown that post-natal and post-abortive tetanus account for from 3.3% (Patel et al.,1960) to 22.2% (Jain, 1962) of all cases of tetanus(Table 9). The case-fatality rate in this case isreported as ranging from 64.2% (Patel, 1960) to72.4% (Bhatt & Anwikar, 1962).A relatively large number of cases of this disease
occurring after injections, vaccinations, and ope-rations have been reported from Asia by many
Ceylon
Ceylon
India
India
India
India
India
India
India
India
India
India
India
India
India
India
India
India
India
India
India
India
Indonesia
Japan
Singapore
Singapore
Viet-Nam
86

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60
TABLE 8CASE FATALITY IN TETANUS NEONATORUM IN ASIA,
AS REPORTED BY VARIOUS INVESTIGATORS
No.of tetanus N Case
Country Author neo- fatalitynatorum of eahs acases
Ceylon Silva (1960) 21 15 (71.4)Ceylon Natkunam (1960) 9 9 (100)India Lewis et al. (1954) 12 3 (25.0)India Matveyev & Paul (1959) 47 41 (87.2)India Nazareth & Edibam (1959) 16 9 (56.2)India Kochhar (1960) 42 39 (92.8)India Patel et al. (1960) 308 272 88.3
India Barua (1961) 54 39 (72.2)India Ghosh & Soni (1961) 88 76 (86.3)India Srivastava & Chatterji (1961) 108 79 73.1
India Syngal (1961) 18 14 (77.8)India Shah et al. (1962) 9 8 (88.9)India Jain (1962) 23 17 (73.9)India Bhatt & Anwikar (1962) 71 61 (85.9)India Basu (1963) 29 20 (68.9)India Ayyar, Ramakrishman &
Birenda Singh (1963) 81 50 (61.7)Indonesia Poesponegoro & Ranti (1959) 578 447 77.3
Iraq Critchley (1958) 364 263 72.2
Japan Tateno, Suzuki & Kitamoto (1961) 7 4 (57.1)
Singapore Loh Slew Gek (1951) 174 159 91.3
Singapore Gwee & Nadarajah (1960) 27 20 (74.0)Viet-Nam Tran Van Bang &
Nguyen Duy San (1960) 1 1 (100)
Total 2087 1 646 78.9
a The figures shown in parentheses are percentages of numbers less than 100.
authors, among them Tran Van Bang & Nguyen DuySan (1960), Murti, Bhaskran & Rajyalakshmi (1961),Tateno, Suzuki& Kitamoto (1961), Bhatt & Anwikar(1962), Patel & Mehta (1963) and Heredia (1963).This circumstance bears unhappy witness to thefact that many practitioners, and even some clini-cians, underestimate the risk of tetanus.
Special attention should be given here to otogenoustetanus, a condition that is often observed in India(Kochhar, 1960; Natkunam, 1960; Barua, 1961;Bhatt & Anwikar, 1962; Wagle, 1963). Ghosh
(1950), for example, has stated that 70% of childrenwith tetanus also suffered from otitis. Toxigenicstrains of Clostridium tetani have been isolated bysome workers from the ear discharges of somechildren with tetanus (Hazra & Agnihotri, 1960;K.E.M. Hospital Group, 1963b; Sen, Vaishnava& Passey, 1963). In a series of tetanus patientstreated by Srivastava & Chatterji (1961), the pro-portion of otogenous tetanus was 11.6%; whereasthe corresponding figure given by Patel & Mehta(1963) was 20.2%.
87

B. BYTCHENKO
TABLE 9POST-NATAL AND POST-ABORTIVE TETANUS IN ASIA, AS REPORTED
BY VARIOUS INVESTIGATORS
Total No. Post-natal andCountry Author of cases post-abortive cases
observed No. %a
India Kochhar (1960) 200 14 7.0
India Patel et al. (1960) 2 007 67 3.3
India Barua (1961) 280 20 7.1
India Srivastava & Chatterji (1961) 702 61 8.7
India Shah et al. (1962) 214 26 12.1
India Jain (1962) 63 14 (22.2)
India Bhatt & Anwikar (1962) 888 113 12.7
Japan Tateno, Suzuki & Kitamoto (1961) 183 17 9.3
Singapore Yeoh (1960) 130 3 2.3
Viet-Nam Tran Van Bang &Nguyen Duy San (1960) 265 14 5.3
a The figures shown in parentheses are percentages of numbers less than 100.
The seasonal distribution of tetanus in Asia varieswith the area. The seasons of peak incidence of thisdisease are usually closely connected with the warm,damp season and the time of the most intensivework in the fields. In Japan (Tateno, Suzuki &Kitamoto, 1961), where the winters are cold, ad-missions to hospital for tetanus are highest duringsummer (June and July), while in India (Barua,1961; Vaishnava et al., 1964), the greatest numberof tetanus patients is registered during the monsoonperiod (July and August). On the other hand, Laha& Vaishya (1963) report that the highest number oftetanus patients in Gwalior, India, came to hospitalduring December. In Indonesia, Poesponegoro &Ranti (1959) found that most of the children sufferingfrom tetanus in Djakarta were admitted to hospitalduring April and May.A tendency toward an increase in the incidence of
tetanus has been observed in India, the Philippines,Indonesia, and some other Asian countries. On theother hand, Cyprus, Israel, and Taiwan have recentlyinitiated the mass immunization of children' withtetanus toxoid and have achieved good results. InTaiwan, the mortality rate from tetanus per 100 000population has decreased from the 1954 level of25.8 to 3.7 in 1960. In Israel, the 1953 level of 1.9had been reduced to 0.4 by 1960. In this connexion,it is of interest that, strangely enough, the incidence
of tetanus in Japan has been decreasing constantlyfrom 1947 through 1960, without any specificmeasures of immunization being applied (Tateno,Suzuki & Kitamoto, 1961). These authors suggestthat this decline could be a consequence of the massuse of antibiotics and chemotherapeutic agents bythe Japanese population.Campaigns of immunization with diphtheria-
pertussis-tetanus (DPT) or diphtheria-tetanus (DT)vaccines have been launched in Singapore, HongKong, Iran and Jordan, and similar campaigns arebeing planned for Thailand, Viet-Nam, Indonesiaand Burma (World Health Organization, 1963).
EUROPE
Although the epidemiology of tetanus has beenstudied more intensively in Europe than elsewhere(Eckmann, 1960; Matveev, 1960), even on that con-tinent there are some countries that became awareof the problem only within the last 10 or 20 years.Table 11, which has been prepared on the basis ofthe data available to WHO, shows the changingtrends of tetanus infection in some European coun-tries during the last four decades. Inspection of thistable reveals that the mortality rate from tetanus hasbeen decreasing gradually; even the Second WorldWar made no significant change in this process.
88

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60
TABLE 10TETANUS NEONATORUM IN SOME COUNTRIES OF ASIA
No. of Percentage ofTotal No. tetanus tetanusCountry Author of cases neonatorum neonatorum
observed cases cases a
Ceylon Natkunam (1960) 89 9 (10.1)
Ceylon Silva (1960) 2 738 298 10.9
India Sheth (1956) 105 19 18.1
India Kochhar (1960) 200 42 21.0
India Patel et al. (1960) 2 007 308 15.3
India Barua (1961) 280 54 19.3
India Ghosh & Soni (1961) 248 88 35.5
India Srivastava & Chatterji (1961) 702 110 15.6
India Shah, Shah & Damany (1962) 214 9 4.2
India Jain (1962) 63 23 (36.5)
India Bhatt & Anwikar (1962) 888 71 8.0
India Ayyar, Ramakrishnan & BirendaSingh (1963) 249 81 32.5
India Basu (1963) 114 29 25.4
India Vakil et al. (1963) 293 17 5.8
Japan Tateno et al. (1961) 183 7 3.8
Singapore Yeoh (1960) 130 1 0.8
Iran Pakdel (1961) 18 14 (77.8)
Indonesia Vital Statistics (1957-1958) 1 567 703 44.8
1 10088 1883 18.7
a The figures in parentheses are percentages from numbers less than 100.
Indeed, the only countries in which the number ofcases of tetanus increased between 1941 and 1950were Italy, Finland, the Netherlands and Switzer-land. In the last-named country, this apparentincrease may have occurred because the notificationof cases of tetanus occurring after minor injurieswas initiated only in 1942; prior to that year, onlypost-partum, post-abortive, and neonatal caseswere notifiable.A remarkable fall in the number of deaths from
tetanus was observed in most countries of Europeduring the decade 1951-60. The principal causes forthis decline are rapid urbanization, industrialization,the mechanization of agriculture, improvement ofpublic health services, and especially the massimmunization of children with the DPT or DTvaccines.
Nevertheless, despite the progress that has beenmade in anti-tetanus vaccination during the decade1951-60, approximately 26220 persons died fromthis disease in 22 countries of Europe with a popula-tion of 340 123 000 in the decade 1951-60. To thisnumber could be added 1290 deaths in Bulgaria,where Denchev (1962) gives a mortality rate fortetanus of 1.5 per 100 000 population and 2267deaths in Romania, where Bacila et al. (1961) havereported a rate of 1.3. The inclusion of these latterfigures brings the total numbers of deaths fromtetanus in Europe during the 10-year period to29 779 in a covered population of 365 108 000, for amean mortality rate of 0.81. If this rate is correctfor the entire population (411 000 000) of Europe(excluding the USSR), it would mean that, in the10-year period under consideration, 33 000 Euro-
89

B. BYTCHENKO
TABLE 11DECENNIAL MORTALITY RATES FROM TETANUS
IN SOME COUNTRIES OF EUROPE
Country
Austria
Denmark
Finland
France
Germany
Greece
Ireland
Italy
Malta
Netherlands
Norway
Spain
Sweden
Switzerland
United Kingdom
England and Wales
Northern Ireland
Scotland
1921-30
2.49
2.41
0.80
1.88
9.29
0.60
0.46
2.06
0.48
0.73
0.38
0.71
0.31
193140
2.69
1.30
0.36
0.64
2.44
0.64
1.52
7.03
0.44
0.33
1.82
0.28
0.30
0.26
0.26
PER 100000 INHABITANTS(1921460) a
1941-50
1.97
1.14
0.43
2.25
0.56
0.47
0.55
2.00
5.67
0.53
0.33
1.63
0.24
1.03
0.18
0.31
0.24
a Data from Ann. epidem. vital Stat., 1951 40.
peans died from tetanus. However, if we were toinclude the USSR, where, according to Matveev(1960), about 960 to 1000 persons yearly die oftetanus (mortality rate of 0.5), the total number ofdeaths from tetanus in Europe during the decade1951-60 must have been more than 40 000, or almosttwice as many as during the period 1945-53 (Matveev& Sergeeva, 1959).
In many European countries, tetanus is the cause
of more deaths than diphtheria, typhoid fever,scarlet fever and rabies combined (Mose, 1955;Matveev, 1960; Bacila et al., 1961; Schuch &Windorfer, 1963).
In 1960, the morbidity rate for tetanus per 100 000population remained high in the following countries;Yugoslavia, 8.20; Hungary, 5.30; Romania, 5.10;Portugal, 4.66; and Bulgaria, 4.10 (Cayolla daMotta, 1957; Bacila et al., 1961; Denchev, 1962).The southern part of Europe (aside from Portugal,where the mortality rate from tetanus exceeds3.5 per 100 000 population) must therefore be includ-
ed in the zone of tetanus with mortality rates between1.0 and 2.0 (Matveev, 1960). A second zone, witha tetanus mortality rate of less than 1.0, covers theareas above 50° north latitude; consequently, one
finds a distinct increase in tetanus as one moves
from north to south.The distribution of tetanus cases in any given
country is not uniform. In general, most cases
occur in rural areas with fertile soil and extensiveagriculture. In Yugoslavia, for example, Kacharevic(1952) has noted that a rural population (82%) ismore prone to tetanus infection than is an urbanpopulation (18 %). Usually, in any country, a
disproportionally large number of all reportedcases of tetanus will be found within a few circum-scribed areas. Such foci of infection have beenoutlined, for example, by Cimmino (1951) in Italy,by Kacharevic (1952) in Yugoslavia, by M6se (1955)in Austria, by Eckmann & Bisaz (1956) in Switzer-land, by Weller (1956) in Germany, by Cayolla daMotta (1957) in Portugal, by Zavazal (1957) in
1951-60
1.02
0.34
0.11
1.11
0.32
1.16
0.32
1.17
1.19
0.20
0.08
1.22
0.11
0.52
0.09
0.24
0.11
r -
90

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60
Czechoslovakia, by Matveev (1960) in the USSR,as shown in Fig. 4, by Bacila et al. (1961) in Roma-nia, by Neyman & Wejdan (1958), Kukiz & Mikulski(1960), Lutynski (1961) and Sawicki (1964) inPoland, by Kubinyi, Rudnai & Barsy (1962-63) inHungary, as shown in Fig. 5, by Denchev (1962)in Bulgaria, and by Melnotte, Senault & Manciaux(1961) and by Gerbaut et al. (1963) in France. InEngland and Wales, the highest rates of tetanusmorbidity and mortality were observed in theeastern and southern regions (Conybeare & Logan,1951; Fulford, 1960).Throughout Europe, with the exception of France,
children aged from 2 to 15 years and adults agedfrom 26 to 30 years, especially in rural areas,suffered from tetanus more frequently than didother portions of the population. In Portugal, forexample, 70% of those who died from tetanus during1955 and 1956 were aged less than 19 years, and66% were below 14 years of age (Cayolla da Motta,1957). The predominance of persons in the age-group 2-15 years in the over-all number of tetanuspatients also has been reported from Yugoslavia(Kacharevic, 1952), Germany (Hubner & Freuden-berg, 1954), Italy (Caruso, 1960; Zonchello, 1961),Bulgaria (Denchev, 1962), Hungary (Petrilla, 1960;Kubinyi, Rudnai & Barsy, 1962-63), from Romania(Bacila et al., 1961), the USSR (Matveev, 1960;Rossichin, 1962; Nesterenko, 1962), and Englandand Wales (Cox, Knowelden & Sharrard, 1963).Also, Fulford (1960), in England and Wales,indicated that the number of deaths from tetanusthere was highest in boys between the agesof 5 and 15 years. On the other hand, Torres-Gost &Figueroa-Egea (1963a) have indicated that, in Spain,the highest incidence of tetanus was reported inpersons aged from 26 to 30 years.An interesting point that should be stressed here
is that most authors who have studied the epide-miology of tetanus in Europe (for example, Matveev,1960; Denchev, 1962; Torres-Gost & Figueroa-Egea, 1963a) have noticed that the ratio of tetanusin males and females was 2: 1, save for the age-group 20-49 years. This ratio has been observedclearly in tetanus neonatorum as well (Kacharevic,1952).Because of active immunization programmes, the
sex and age distribution of tetanus has shown amarked decrease in children and adult males and arelative increase for women and the elderly in somecountries of Europe. This tendency has been noticedin France (Jeune, Vincent & Numbert, 1962; Rapin
& Amstutz, 1963; Gerbaut et al., 1963; Chassagne& Gaigneux, 1964), where the active immunizationof soldiers and children against tetanus was initiatedabout 1936-40 (Ramon, 1962), as well as in someareas of Italy (Chignoli 1961), Germany (Schuch& Windorfer, 1963); Hungary (Kubinyi, Rudnai& Barsy, 1962-63) and the USSR (Nesterenko, 1962).
It can be seen from Table 12 that, during thedecade 1951-60, the tetanus case fatality in Europewas almost as high as in Asia, which indicates thatthe latest modes of treatment of this disease, in-cluding the use of drugs such as the muscle relaxantsand of artificial respiration, either were not verysuccessful or were not available to most tetanuspatients.
Supposedly negligible untreated injuries were themain causes of tetanus in Europe. For example,among 2712 cases of this disease reported by Den-chev (1962) from Bulgaria, 1763 (65%) were attribu-table to " trivial injuries ". Matveev (1960) reportedthat, in the Ukraine, about 78% of all cases oftetanus followed such trauma. Approximately thesame picture has been drawn by many other in-vestigators, among them Kacharevic (1952), Hubner& Freudenberg (1954), Mincsev (1957), Jeune,Vincent & Numbert (1962), Freudenberg (1963),Rapin & Amstutz (1963), and Cox, Knowelden &Sharrard (1963). A tetanus infection that developedafter bee stings has been described by Hulbner &Freudenberg (1954), and one that occurred after afinger prick with a sewing needle by Hay (1953).As a rule, tetanus neonatorum was observed after
delivery at home in rural areas. A number of suchcases were reported from Yugoslavia (Kacharevic,1952; Simovi6, 1958, 1960), from Portugal (Ramal-hao, 1956), from Italy (Caruso, 1960; Figueiredo,1961; Bolletti & Pujatti, 1963), from France (Bayeret al., 1953; Dordain, Jeanne & Evreux, 1963;Gerbaut et al., 1963), from Germany (Hubner &Freudenberg, 1954; Morl, 1956; Weller, 1956), fromCzechoslovakia (Zavazal, 1957; Masar, 1960),from Bulgaria (Denchev, 1962), from Romania(Corneleac & Filimon, 1960; Bacila et al., 1961),from Hungary (Kubinyi, Rudnai & Barsy, 1962-63),and from Poland (Kukiz & Mikulski, 1960; Sawicki,1964).Table 13 shows the case-fatality experience re-
ported by several investigators in Europe. Com-parison of this table with Table 1 shows that casefatality from tetanus neonatorum is apparentlyhigher in Europe than in Africa, and comparisonwith Table 8 indicates that the case-fatality rates
91

B. BYTCHENKO
FIG. 4GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE USSR a
a Morbidity rates per 100000 population (Matveev, 1960).
FIG. 5GEOGRAPHICAL DISTRIBUTION OF TETANUS IN HUNGARYa
a Incidence per 100000 population (Kubinyl, Rudnai & Barsy, 1962.63).
A-
Zone 1 0.02,0.3
Zone 11 0.5-0.7
Zone III 0.8- 1.1
Zone IV 1.3-5.7
W 0.5.1.4
1.5t2.4
2.5-3.4
- 3.5-4.4
4.55.54
5.5-6.4
- 6.5-7.4
WHO 4559
92

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60
TABLE 12CASE FATALITY FROM TETANUS IN SEVERAL COUNTRIES OF EUROPE,
AS REPORTED BY VARIOUS INVESTIGATORS
No.of tetanus No. of Case
Country Author cases deaths fatalityobserved a
Austria Kaiser (1954) 233 88 37.7M6se (1955) 135 51 37.8
Belgium Lafontaine & Koopmansch (1954) 135 92 68.1
Bulgaria Denchev (1962) 3 250 1 290 39.7
Czechoslovakia Masar (1960) 976 412 42.2
Denmark Perdrup (1949) 527 197 37.4Uldall (1961) 63 31 (49.2)
Finland Savolainen (1951) 13 10 (76.9)
France Bayer et al. (1953) 279 202 72.4Hollender & Schvingt (1955) 21 13 (62.0)Jeune, Vincent & Numbert (1962) 172 118 68.6Dordain, Jeanne & Evreux (1963) 88 60 68.2Gerbaut et al. (1963) 558 246 44.1Melnotte & Foliquet (1963) 885 644 76.7Rapin & Amstutz (1963) 448 154 34.4
Germany Hoppe (1952) 85 41 (48.2)Mohlenbruch (1952) 197 114 57.8Linneweh (1953) 85 51 60.0Hubner & Freudenberg (1954) 1 894 930 49.1Weller (1956) 507 208 41.0Gerster & Moeschlin (1961) 7 2 (28.6)B6ttger (1962) 100 34 34.0Schuch & Windorfer (1963) 23 2 (8.7)
Greece Katsilabros (1963) 100 18 18.0
Hungary Kubinyl, Rudnal & Barsy (1962-63) 4 010 1 735 43.2
Italy Bozzi (1932) 320 164 51.2Fiandaca (1946) 70 39 55.7Recchia (1956) 631 300 47.5Caruso (1960) 349 114 32.6Petrone (1960) 2131 1 486 69.7Zauli Naldi & Gasparroni (1961) 28 10 (33.7)Zonchello (1961) 120 50 41.6
Poland Neyman & Wejdan (1958) 317 146 46.0Lewandowski (1960) 13 4 (30.7)Lissner (1960) 35 15 (42.8)Kaniak, Cywicki & Smolenska (1960) 230 79 34.3Kukiz & Mikulski (1960) 627 288 45.9
Portugal Ramalhao (1956) 160 48 30.0
Romania B&cil& et al. (1961) 376 96 25.5
Spain Torres-Gost & Figueroa-Egea (1963a) 372 216 58.0
Sweden Nilsson & Nordstr0m (1962) 32 5 (15.6)Eriksson & Ullberg-Oisson (1963) 162 62 38.3
Switzerland Eckmann & Bisaz (1956) 534 231 43.2Stirnemann (1963) 149 82 55.0
United Kingdom Fulford (1960) 2000 540 27.0
USSR Matveev (1960) 2 500 930 37.4Nesterenko (1962) 540 181 33.5
a The figures shown in parentheses are percentages of numbers less than 100.
93

94 B. BYTCHENKO
TABLE 13
CASE FATALITY IN TETANUS NEONATORUM IN EUROPE,AS REPORTED BY VARIOUS INVESTIGATORS
No. N o. of CaseAuthor of cases fata ity
observed deaths (%) a
Casorzo & Figueroa (1951) 14 6 (42.8)
Bayer et al. (1953) 5 5 (100.0)
RamalhAo (1956) 6 5 (83.3)
Weller (1956) 52 39 (75.0)
Simovit (1958) 14 6 (42.8)
Caruso (1960) 11 8 (72.7)
Corneleac& Filimon (1960) 27 16 (59.2)
Masar (1960) 141 112 79.4
Uldall (1961) 8 6 (75.0)
Figueiredo (1961) 21 15 (71.4)
Zauli Nald! &Gasparroni (1961) 7 5 (71.4)
Denchev (1962) 510 430 81.1
Dordain, Jeanne &Evreux (1963) 5 5 (100.0)Gerbaut et al. (1963) 24 21 (87.5)
Kubinyl, Rudnai &Barsy (1962-63) 311 229 73.6
Total 1156 908 78.5
a The figures In parentheses are percentages of numberssmaller than 100.
for tetanus neonatorum in Europe (78.5 %) andAsia (78.9 %) appear to be nearly identical.Among other injuries that are followed by tetanus
in Europe, especial note should be made of traumato the uterus, chronic ulcerations, injections, burnsand frostbite (Savolainen, 1951; Bourns, 1953;Henrion, 1954; Huibner & Freudenberg, 1954;Gabele, 1954; Triebold, 1956; Ramsay, France &Dampsey, 1956; Nissen & Enderlin, 1957; Riis,1958; Garland, 1959; Boyd, Mackay-Scollay &Conybeare, 1959; Matveev, 1960; Deparis, Mani-gand & Bataillard, 1960; Petrilla, 1960; Woodward,1960; J0rgensen & Lou, 1961; Denchev, 1962;Jeune, Vincent & Numbert, 1962; and Dordain,Jeanne & Evreux, 1963).The morbidity of tetanus in the northern and
central parts of Europe is closely related to summerwork in the fields, being highest in June, July andAugust (Matveev, 1960; Masar, 1960; Kukiz &
Mikulski, 1960; Denchev, 1962; Kubinyi, Rudnai& Barsy, 1962-63; Torres-Gost & Figueroa-Egea,1963b). The seasonal distribution of this disease isless pronounced in the southern parts of Europe,where a considerable number of cases of tetanus issometimes registered during the first and secondquarters of the year (Cayolla da Motta, 1957).Notification of this disease, as well as the immuni-zation of children and some other population groupsunder greatest risk has been made compulsory inBulgaria, Czechoslovakia, France, Hungary, Poland,Romania, and the USSR. More recently, Portugal 1and Italy 2 have been added to this list.To summarize the tetanus situation in Europe, it
should be said that the incidence of this disease inthat continent during the decade 1951-60 was de-creasing slowly because of the active immunizationof the population but that many persons, especiallyadults, remained without protection against thisinfection.
AUSTRALIA AND OCEANIA
On the basis of occasional reports, it may beassumed that tetanus is common in Australia andOceania (Lancaster, 1953; Hunter, 1959; Alhadyet al., 1960; Alhady, 1961; Kennedy, 1960; Clifton,1961; Forbes, 1961; Maddocks & Dawborn, 1961;Ryan, 1961).
Before 1950, only Australia and New Zealandregularly reported tetanus; the following decennialmortality rates per 100 000 population were re-ported to WHO:
Years Australia New Zealand
1921-30 1.51 0.871931-40 1.10 0.501941-50 0.89 0.551951-60 0.53 0.45
During the decade 1951-60, however, the datareceived show that the mortality rate from tetanusper 100 000 population was high on Niue Island(26.6), the Cook Islands (23.1), and in FrenchPolynesia (8.8). In 1960, tetanus was listed amongthe principal causes of death in the Fiji Islands andon Niue Island (World Health Organization, 1963).Altogether, it appears that there were 960 deathsfrom this cause in Australia and Oceania during thedecade in question. However, if the mean mortality
1 Decree No. 44198 of 20 February 1962 (Int. Dig. HlthLegis., 1963, 14, 468).
' Law No. 292 of 5 March 1963 (Int. Dig. Hith Legis.,1963, 14, 654).

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60
rate of 0.7 were correct for the entire populationof Oceania during that period, the actual number ofdeaths would exceed 1000. Indeed, since registrationin this area is far from complete, even this latterfigure must be considered underestimated.According to Lancaster (1953), tetanus has caused
twice as many deaths as diphtheria in some parts ofAustralia. During the period 1944-56, Johnson(1956) encountered 195 cases of tetanus in Queens-land, and he showed that children between 2 and15 years of age predominated (88 cases, or 46.3 %).Of these 190 cases of tetanus, 89 terminated fatally,thus indicating that the over-all case-fatality rate fortetanus in that area was about 46.8 %.Tetanus neonatorum is important in New Guinea
and the adjacent islands (Jones, 1946; Johnson,1956; Earle & Mellon, 1958). According to Scho-field, Tucker & Westbrook (1961), direct obser-vations among the Abelam people of the SepikDistrict of New Guinea revealed that the incidenceof tetanus neonatorum was approximately 80 per1000 live-births. Immunization of children bymeans of the DPT vaccine is carried out routinelyin Australia, New Zealand, French Polynesia,Papua, and several other places. In order to combattetanus neonatorum in New Guinea, the immuni-zation of pregnant women has been proposed andinitiated quite recently (Schofield, Tucker & West-brook, 1961).
DISCUSSION
Although the tetanus problem is not a new one-indeed, its history is long-it cannot be deniedthat, to the present time, very little has been learnedabout the epidemiology of this disease in the worldas a whole. For example, only recently was itrealized that tetanus is as prevalent in peacetimeas it is during wars. Even in the more advancedcountries of Europe and North America, detailedstudies on the geographical distribution of tetanuswere begun no more than 10 to 20 years ago, andmany parts of Africa, Asia, and South Americaremain unexplored in this respect. This neglect oftetanus has occurred largely because there are manyother urgent problems with respect to other com-municable diseases, such as plague, smallpox, cholera,enteric infections and tuberculosis, which are eitherresponsible for high general morbidity and mortalityrates or represent considerable hazards with respectto the possibility of serious outbreaks or epidemics.On the basis of the available statistics and on the
literature, the world-wide distribution of tetanus hasbeen calculated and is presented in Fig. 6.
Since tetanus is so closely related to such an in-exhaustible "source " as the soil itself, it is anendemic infection that causes more deaths in theworld than rabies, smallpox, plague, anthrax, lepto-spirosis, poliomyelitis, or many other infectious orparasitic diseases. The present report has demon-strated that tetanus exists in most countries through-out the world, but with considerable differences inmorbidity and mortality rates according to variousgeographical and socio-economic conditions. Theexistence of various regions that may be describedas tetanus "zones " or " foci " proves that thenatural distribution of Clostridium tetani is notuniform and depends, to a great extent, on certainconditions. The studies conducted in the USA byDubovsky & Meyer (1922), in France by Lavergne,Helluy & Faivre (1949), in the USSR by Illutovic& Tarasov (1957) and by Matveev (1960), in Polandby Lutynski (1961), and in Bulgaria by Denchev(1962) have indicated that a hot, damp climate,together with a fertile soil rich in organic matter arefavourite environments for this organism. Mishustin& Perzovskaya (1954) observed the ability ofCl. tetani to persist and multiply in black soil andthat the presence of the rhizospheres of wheatstimulates this process. Similar phenomena havebeen observed by Matveev (1960) in experiments onthe behaviour of Cl. tetani in dry and wet sand andsoil.There is little doubt that Cl. tetani, like many other
clostridia, inhabits the soil. However, the nutritionalrequirements of this organism, as well as its toxi-genicity and its ecological relationships with thethousands of other bacteria, fungi, protozoa, algaeand plants under natural conditions are practicallyunknown. As a rule, however, there is a relationshipbetween the frequency of isolations of Cl. tetanifrom the soil of certain areas and the level of mor-bidity from tetanus (Matveev, Solov'ev & Volkova,1957; Denchev, 1962; Orzuev & Matveev, 1964).
Consequently, areas in which the incidence oftetanus is very high may be considered to be foci ofthe disease. Such natural foci of other clostridialdiseases have been described elsewhere by Prevot(1955), by Smith (1955), by Matveev (1959, 1960),and by Dolman & Murakami (1961), but the" dynamics " of tetanus foci (that is, the changesthat occur in the distribution of Cl. tetani in the soiland in the number of cases of tetanus in the samearea) have not yet been properly investigated.
95

96 B. BYTCHENKO
02
...........~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~(
rb
LU~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~(
o (U~~.. . .. . . o 1
w ~~~~~~~~~~~~~~~~~~~~~~~0
LU~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~(
z
C I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~1
La-~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~r0~~~~~~~~~~~~~~~~~~~~~~~~~
z~~~~~~~~~~~~~mJE~~~~~~~~~~~
0~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~c13 ~ ~ ~ .....Z (U~..... .

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60
In both cultivated and uncultivated areas, an
important role in the dissemination of certain toxi-genic strains of Cl. tetani may be ascribable tocertain domesticated animals, such as cattle, horses,sheep and goats. It is very probable, also, that thecultivation of certain plants may influence theCl. tetani population of the soil.A feature of tetanus foci is their stability, which is
obvious from the consistency of the reports on theyearly number of tetanus cases in the same places(Veronesi, 1960; Mattos, 1962; Patel & Mehta,1963) unless and until there is interference from thepublic health services.
Social and economic factors such as poverty,ignorance, religious prejudices, unhygienic customsand habits, together with the lack of health servicesin regions with warm climate and fertile soil, are
largely responsible for the high incidence of thisdisease in some places.
Urbanization, industrialization, and the mechani-zation of agriculture can interfere with the normalprocess of distribution of Cl. tetani and reduce themorbidity rate, as has occurred, for example, inthe USA, the United Kingdom, Germany, and theNetherlands during the last 40 years, even beforeactive immunization against this disease was initiated.A possible explanation for this phenomenon is
that, on the one hand, people in towns and citieshave less contact with the soil than do rural popu-
lations; on the other hand, the population ofCl. tetani in the soil of industrial towns may declinegradually because of the lack of fertilizers. This lastspeculation has been challenged, however, by thefindings of Orzuev & Matveev (1964), who haveshown that, in the soil of Tashkent, the capital ofthe Uzbek SSR, Cl. tetani is to be found more oftenthan in the soils of nearby farms. Similarly, thelarge numbers of tetanus patients that are recordedfrom some towns in India indicate the possibilitythat there may be heavy contamination of the soilin those towns with Cl. tetani.
Also, the relatively low incidence of tetanus intowns could well be due to the intensive use ofantibiotics and other antibacterial agents by urbanpopulations, which may result, indirectly, in theprotection of the populace against tetanus (Tateno,Suzuki & Kitamoto, 1961). It is reasonable tosuppose, of course, that there may be differentreasons in different places for changes in the be-haviour of tetanus, and that each such differenceshould be studied, but the fact does remain that theincidence of tetanus is much lower in urban than in
rural areas (Kacharevic, 1952; Matveev, 1960;Pinheiro, 1960; Barua, 1961; Vaishnava et al., 1964).The highest rates of morbidity from tetanus continueto exist in the developing countries that are situatednear the equator. The number of tetanus victimsin the world during the decade 1951-60 quiteprobably exceeded 1 000 000 persons, of whomapproximately half died. These figures are severaltimes greater than those calculated by Matveev &Sergeeva (1959), but they should nevertheless beregarded as underestimates of the actual situation.During the decade under investigation, tetanus
proved to be fatal to approximately one half of thepatients who contracted it, despite the recent intro-duction of new modes of treatment. It is note-worthy that case-fatality rates differed betweendifferent areas. In Japan, the Philippines and theUSA, case fatality was high (60 %-78 %), in com-parison with only 40 %-50% in Africa, Asia andEurope. Apart from factors such as differences inpublic health services, hospital facilities, the periodof incubation, the severity of the individual case,methods of treatment, and case distribution by age,sex, profession or season, there may be significantdifferences in the area distribution of strains ofCl. tetani with differing abilities to multiply and toproduce toxins in the human body. Also, as hasbeen shown by Illutovic (1961, 1962), strains ofthis organism that have been isolated from the soilsof different areas differed from each other, not onlyin their toxigenicity, but even in the antigenicstructures of the toxins that were produced. Un-fortunately, studies of this kind are quite limited innumber (Fildes, 1927; Lavergne, Helluy & Faivre,1949; Orzuev & Matveev, 1964).During the decade in question, children between
the ages of 2 and 15 years, and adults aged between26 and 30 years, all over the world (except in France)suffered from this disease more than did the membersof other age-groups. In some areas, tetanus neonato-rum accounted for from 10% to 30% of all casesof tetanus; nevertheless, tetanus is an infection towhich persons of all ages are subject, since a largeproportion of the persons who suffered from it wereadults (Yodh & Shah, 1956; Veronesi, 1960; Patel& Mehta, 1963; Matveev, 1960).An interesting fact that has been noted by many
investigators but that still requires investigation andexplanation, is the relatively high incidence of thisdisease in males, especially newborns, in manycountries of Europe and Asia. Kacharevic (1952)was the first author to suggest that males may be
97
B. BYTCHENKO
more sensitive to the tetanus toxin than are females,and his experiments with pigs and other animalsappear to offer some proofofthis thesis. The same ideawas put forward independently by Denchev (1962).The frequent occurrence of tetanus after otherwise
trivial injuries, chronic ulcerations, and variouskinds of operations, injections and vaccinations hasbeen reported from various countries, indicatingthat there is a necessity for increased attention topreventive measures against tetanus in all personswho are subject to this type of risk. Because of thestrong connexion between tetanus and the soil, thereis, at present, no possibility of controlling thisinfection other than the active immunization of thepopulation at risk. The efficacy of active immuniza-tion was proved during the Second World War,during which the American and British armies,whose members had been vaccinated against tetanus,suffered almost no casualties from this disease, insharp contrast to thr experience of the Germanarmy, the members of which had not received thisprotection (Boyd, 1946; Long & Sartwell, 1947).Because of active immunization, success in
combating tetanus has been scored in some countriesof Europe, North America, Asia, Australia andOceania. For the prevention of tetanus after injuries,projects for active-passive prophylaxis against thedisease have been reviewed and developed furtherby Matveev (1960), Eckmann (1960), Filler & Eller-beck (1960), Laurent & Parish (1960), Tasman &Huygen (1962), Smith et al. (1963), Jannes (1964)and Kremlev (1964).
Experience indicates that the active immunizationof pregnant women may help to eradicate tetanusneonatorum (Katitch, 1960; Vuksanovic, Kolbas &Sucic, 1960; Bacila et al., 1961; Schofield, Tucker& Westbrook, 1961; Kubinyi, Rudnai & Barsy,1962-63; Kril, Prasilava & Neubertova, 1964;Newell et al., 1964).
Nevertheless, during the decade 1951-60, only asmall proportion of the world's population wasprotected against tetanus, despite the fact that teta-nus toxoid, which can provide excellent prophylaxisagainst this disease, was discovered nearly 40 yearsago (Ramon & Zoeller, 1926; Ramon, 1962, 1963).
SUMMARY
Tetanus, since it is an almost ubiquitous infection,constitutes an important problem in most develop-ing countries. In a major portion of the world, thisdisease is still not notifiable. Nevertheless, on thebasis of available information, it would appear to
be possible to construct a tentative outline of thegeographical distribution of tetanus in the world.As one moves from the polar areas toward the
equator, one can see clearly the changes in the mor-bidity and mortality rates from tetanus, which reachtheir highest levels in the tropical countries. Thedistinct seasonal distribution of this infection incountries with cold or moderate climates is foundto be less distinct in areas with subtropical or tro-pical climates. Even within a given country, if itcontains a variety of landscapes and climatic con-ditions, the population that inhabits the areas withwarm, damp climates and fertile soil are, as a rule,more prone to tetanus than people who inhabitmountains or deserts, provided that there are noappreciable differences in socio-economic and cul-tural conditions between these areas.
Factors such as industrialization, urbanization,mechanization of agriculture, the widespread use ofchemical fertilizers rather than animal dung, andimprovements in education, the standard of living,and public health services, reduced the incidence oftetanus in many European countries, Canada, theUSA, Japan and Australia even before the inceptionof programmes of mass immunization againsttetanus. However, the most effective means of com-bating tetanus within a short period hMs proved tobe the active immunization of the entire population.
In non-immunized populations, children belowthe age of 15 years suffer from tetanus more oftenthan do persons of greater age. In populations inwhich immunization programmes have been initi-ated, one can observe the relative increase in theincidence of tetanus among non-immunized personsas against the gradual over-all decline of the disease.As it has been general practice to protect childrenand soldiers against tetanus, the disease has becomeboth " younger " and " older ", continuing to affectunprotected newborns, women, and the elderly.
In many areas, a difference in incidence betweenthe sexes has been observed, with the predominanceof males among the newborn, the age-group 2 to15 years, and in persons over 50 years of age. Thesefindings suggest that males are more sensitive totetanus toxin than are females in these age ranges.The overwhelming majority of cases of tetanus
in the world were due to the infection of otherwisenegligible injuries to the extremities, particularlythe legs. The higher proportions of tetanus neonato-rum, post-abortive and post-partum tetanus as wellas tetanus after injections, vaccinations, chroniculcerations, otitis, parasitic and infectious diseases
98

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN T1HE WORLD, 1951-60 99
of the skin, and so on, were common in areas wherethere is poverty, religious prejudice and unhygieniccustoms, and where education and public healthservices are absent or deficient.The over-all case fatality from tetanus varied
widely from place to place, being as high as 60% to
78% in Japan, the Philippines, and the USA andabout 40% to 50% in Africa, India, and someEuropean countries, indicating that, during thedecade 1951-60, more than 500 000 persons mayhave died from this disease, which can be easilyprevented by vaccination.
RtSUMI
Le tetanos, infection presque universellement repandue,revet une grande importance dans la plupart des pays endeveloppement. Bien que dans la plus grande partie dumonde la declaration de cette maladie ne soit pas obliga-toire, les informations dont on dispose permettent cepen-dant de dresser a grands traits une carte provisoire de sarepartition geographique.A mesure que l'on s'avance des regions polaires vers
l'equateur, on constate de nettes variations des taux demorbidite et de mortalite par infection tetanique. Ces tauxatteignent leur niveau le plus eleve dans les zones tropi-cales. L'influence des saisons sur la repartition de lamaladie, evidente dans les pays a climat froid ou tempere,s'estompe en revanche dans les contrees a climat tropicalou subtropical. A l'interieur d'un meme pays offrant unecertaine variete du sol et des conditions climatiques, lespopulations des endroits ou le climat est chaud et humideet le sol fertile sont habituellement plus exposees autetanos que les habitants vivant en regions montagneusesou desertiques.Dds avant la mise en aeuvre des programmes de vaccina-
tion antit6tanique de masse, certains facteurs ont contribueA reduire l'incidence de la maladie dans beaucoup de payseuropeens, au Canada, aux Etats-Unis d'Amerique, auJapon et en Australie. Ce sont notamment l'industriali-sation et l'urbanisation, la mecanisation de l'agriculture,l'utilisation de produits chimiques au lieu d'engrais d'ori-gine animale, 1'elevation du niveau de l'enseignement etdu standard de vie, ainsi que l'amelioration des servicesde sante publique. A court terme, l'immunisation activede l'ensemble de la population reste cependant l'arme laplus efficace.Dans une population non immunisee, les enfants de
moins de 15 ans sont plus frequemment victimes dutetanos que les personnes plus agees. Lorsque des vacci-
nations ont eu lieu, on assiste a une augmentation relativedes cas de t6tanos chez les personnes non immunise-es,contrastant avec le declin progressif et g6neralise de lin-fection. La vaccination antit6tanique, qui s'adresse g6ne-ralement aux enfants et aux soldats, modifie les donn6esepidemiologiques de l'affection qui frappera surtout lesgroupes d'age extremes, nouveau-nes non immunises,femmes, personnes agees.On a observe en maints endroits que l'incidence du
tetanos n'etait pas la meme dans les deux sexes. Le sexemasculin, dans les categories des nouveau-nes, des enfantsde 2 a 15 ans et des personnes de plus de 50 ans, est plusfrequemment victime de la maladie. II semble donc quedans ces groupes d'age, le sexe masculin soit davantagesensible a la toxine tetanique.Dans la tres grande majorite des cas, le t6tanos resulte
de l'infection de blessures, par ailleurs anodines, desextremites, et surtout des jambes. Le tetanos du nouveau-ne, le tetanos post-partum ou post-abortum, ainsi que let6tanos resultant d'injections, de vaccinations, d'ulce-rations chroniques, d'otites, d'affections cutanees para-sitaires ou infectieuses, s'observent principalement dansdes regions pauvres, ou rfgnent aes prejug6s religieux etdes habitudes antihygieniques, aggraves par l'absence oules lacunes des services d'enseignement et de sant6publique.Le nombre des d6c6s dus au tetanos est tres variable
suivant les endroits: au Japon, aux Philippines et auxEtats-Unis d'Amerique, la mort survient dans 60-78%des cas, cependant qu'en Afrique, en Inde et dans certainspays europeens, la proportion des d&c&s n'est que de 40-50%. On peut estimer a plus de 500 000 le nombre despersonnes qui, au cours de la decennie 1951-1960, ontsuccomb6 a cette affection qu'il est aise de prevenir parla vaccination.
REFERENCES
Adams, J. Q. & Morton, R. J. (1955) Amer. J. Obstet.Gynec., 69, 169-173
Aguileiro, M. J. M., Brahiero, R. L. & Ghigliazza, H. M.(1960) Sem. m6d. Mex., 117, 969-976
Alhady, S. M. A. (1961) med. J. Aust., 2,219-220
Alhady, S. M. A., Bowler, D. P., Reid, H. A. & Scott,L. T. (1960) Brit. med. J., 1, 540-545
Amezquita Urias, G. (1964) Higiene, 16, 123Armengaud, M. (1959) Bull. et Mem. Fac. mixte Med.Pharm. Dakar, 7, 296

100 B. BYTCHENKO
Armengaud, M., Frament, V. & Biram, D. (1960) Mid.Afr. noire, 7, 264
Armengaud, M., Louvain, M. & Diop-Mar, I. (1962)Bull. et Mem. Fac. mixte Med. Pharm. Dakar, 10,172-179
Armengaud, M., Louvain, M., Diop-Mar, T. & Sanokho,A. (1963) Bull. Soc. Me'd. Afr. noire Langue franc., 8,75-101
Arora, V. D., Desai, A. V. & Kazi, S. (1963) Tetanus inchildren in a general hospital. In: Study Group ofTetanus, International conference on tetanus, Bombay,Birla Matushri Sabhaghar, p. 39
Ashhurst, A. P. C. (1926) J. Amer. med. Ass., 87, 2089Athavale, V. B. (1963) Clinical manifestations of tetanus
neonatorum. In: Study Group of Tetanus, Inter-national conference on tetanus, Bombay, Birla MatushriSabhaghar, p. 39
Axnick, M. W. & Alexander, E. R. (1957) Amer. J. publ.Hlth, 47, 1493
Ayyar, R. D., Ramakrishnan, S. P. & Birenda Singh(1963) Antiseptic, 60, 371-379
Bacila, E., Ciocirlie, C., Javorovsci, V., Teodorescu, G.& Margineanu, T. (1961) Microbiologia (Buc.), 6,425-430
Back, E. H. (1960) Lancet, 2, 601Bahia, A. (1953) Matern. e Inf. (S. Paulo), 12, 189-200Baker, W. (1963) E. Afr. med. J., 40, 127-131Baker, W. & Grounds, J. G. (1964) E. Afr. med. J., 41,
93-96Barua, A. R. (1961) J. Indian med. Ass., 37, 270-274Barua, A. R. (1963) Study of 383 consecutive cases of
tetanus. In: Study Group of Tetanus, Internationalconference on tetanus, Bombay, Birla Matushri Sab-haghar, p. 38
Basu, K. S. (1963) Indian med. J., 57, 124-125Bayer, J., Corre-Hurst, L., Sapin-Jaleustre, H. & Tissier,M. (1953) Presse mid., 61, 701-703
Beheyt, P. (1950) Ann. Soc. belge Mid. trop, 30, 341-348Beisser, 0. (1960) Berita Departemen Kesehatan Republic
Indonesia, 2, 5-12Bernard, J. G., Gallay, C. & Laverdant, C. (1963)
Rev. Immunol. (Paris), 27, 145-161Bhatt- A. N. & Anwikar, A. K. (1962) J. Indian med. Ass.,
38, 71-75Binechvar & Ghavampour, M. (1954) Rev. Fac. Med.
(Tehhran), 11, 681-686Bolletti, M. & Pujatti, G. (1963) Acta paediat. lat. (Reggio
Emilia), 14, 225-256Bottger, G. (1962) Munch. med. Wschr., 104, 853Botticelli, J. T. & Waisbren, B. A. (1961) Amer. J. med.
Sci., 242, 44-50Boums, N. K. (1953) Brit. med. J., 1, 491Boyce, F. F. & McFetridge, E. M. (1935) New Orleans
med. surg. J., 87, 825Boyd, J. S. (1946) Lancet, 1, 113-119Boyd, J., Mackay-Scollay, E. M. & Conybeare, E. T.
(1959) Proc. roy. Soc. Med., 52, 109-114Bozzi, E. (1932) Osped. maggiore Novara, 20, 213
Bryant, J. & Fairman, N. E. (1940), Lancet, 2, 263Bunch, G. H. & Quattlebaum, J. (1943) Amer. J. Surg.,
61, 180-185Calvin, J. K. (1930) Amer. J. Dis. Child., 39, 674-675Calvin, J. K. & Goldberg, A. H. (1930) J. Amer. Med.
Ass., 94, 1977-1981Cantrelle, P. A., Etifier, J. & Masse, N. (1960) MortalitJ
et morbidite' de l'enfance en Afrique. In: Universitede Dakar et Centre international de l'Enfance, Journeesafricaines de Pediatrie (Dakar, 16-17 avril), pp. 66-79
Caruso, G. (1960) Acta med. ital. Mal. infett., 15, 249-254Carvalho, A. A. & Nascimento, C. A. (1950) Arch. Hig.
(S. Paulo), 28, 199-209Casorzo, L. & Figueroa, L. (1951) Arch. Soc. Ciruj.
Chile, 3, 73-93Cayolla da Motta, L. (1957) Bol. Serv. Sauide piubl.
(Lisboa), 4, 477-501Chassagne, P. & Gaigneux, Y. (1964) Bull. Inst. nat. Hyg.,
19, 489-510Chignoli, V. (1961) Acta med. ital. Mal. infett., 16, 280Cimmino, A. (1951) Nuovi Ann. Ig., 2, 241-257Clifton, B. S. (1961) Med. J. Aust., 1, 618-624Conybeare, E. & Logan, W. (1951) Brit. med. J., 1, 504-508Corneleac, V. & Filimon, E. (1960) Microbiologia (Buc.),
5, 273-276Cox, C. A., Knowelden, J. & Sharrard, W. J. W. (1963)
Brit. med. J., 2, 1360-1366Creech, 0. Jr, Glover, A. & Ochsner, A. (1957) Ann.
Surg., 146, 369Critchley, A. (1958) Publ. Hlth (Lond.), 71, 459-469Denchev, V. (1962) [Trans. Res. Inst. Epidem. Microbiol.
(Sofia)], 8, 73-82Deparis, M., Manigand, C. & Bataillard, J. (1960) Rev.
Prat. (Paris), 10, 463-465De Reus, T. (1963) Ned. T. Geneesk., 107, 1265-1267Dolman, C. E. & Murakami, L. (1961) J. infect. Dis.,
109, 107-128Dordain, M., Jeanne, C. & Evreux, R. (1963) Rev. Hyg.
Meid. soc., 11, 69-79Dubovsky, J. & Meyer, K. (1922) J. infect. Dis., 31,
614-616Earle, A. M. & Mellon, W. L. (1958) Amer. J. trop. Med.
Hyg., 7, 315-316Eckmann, L. (1960) Tetanus: Prophylaxe und Therapie,
Schwabe, Basel & StuttgartEckmann, L. & Bisaz, E. (1956) Schweiz. med. Wschr., 86,
641-645Eriksson, E. & Ullberg-Olsson, K. (1963) Comparison
between modern intensive therapy and ordinary treat-ment of tetanus. A review of the Swedish tetanus cases1950-1960. In: Study Group of Tetanus, Internationalconference on tetanus, Bombay, Birla Matushri Sab-haghar, p. 65
Fiandaca, R. (1946) Riv. PolicL inf., 6, 326Figueiredo, I. (1961) Rev. med. Aero. (Rio de J.), 13,
40-53Figueroa, P. E. R. & Romero, H. R. (1963) Rev. venez.
Sanid., 28, 104-112

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60 101
Fildes, P. (1927) Brit. J. exp. Path., 8, 219-226Filler, R. M. & Ellerbeck, W. (1960) J. Amer. med. Ass.,
174, 1-4Floch, H. (1949) Bull. Acad. nat. Mid. (Paris), 133,419-422
Fonseca, D., Irastorza, J. F., Ferreira, R. M., Ferreira, E.& Roncaglio, A. (1961) An. Fac. Med. Montevideo, 46,108-123
Forbes, J. A. (1961) Med. J. Aust., 2, 72-73Forde, H. M. & Williams, H. M. (1960) W. Indian med.
J., 9, 9-13Fournier, A. & Cabanel, G. (1957) Algerie Mid., 5, 577Francisco, R. (1944) Clinics, 3, 373-414Freudenberg, E. (1963) Schweiz. med. Wschr., 93, 1319-
1326Fulford, G. E. (1960) Lancet, 1, 1121-1123Gabele, A. (1954) Zbl. Gyndk., 76, 1604-1617Gandy, J. (1950) Bull. Inst. Hyg. Maroc, 10, 319-322Garland, H. (1959) Proc. roy. Soc. Med., 52, 877-880Garza Brito, A. (1955) Bol. Epidem. (Mix.), 19, 36-38Gerbaut, P., Lorrain, J., Weber, M. & Canton, P.
(1963) Ann. Med. Nancy, 2, 1086-1096Gerster, P. & Moeschlin, S. (1961) Dtsch. med. Wschr.,
86, 890-897, 927-928Gessner, H. B. & Adiger, D. (1916) New Orleans med.
surg. J., 69, 91Ghosh, S. M. (1950) J. Indian med. Ass., 19, 328Ghosh, S. & Soni, S. (1961) Indian J. Child Hlth, 10,
440-449Gomez, J. J. O., Barrios, I. C., Guerrero, L. M., Guevara,A. G. & Parra, M. G. (1960) Higiene, 12, 199-208
Gordon, J. E., Singh, S. & Wyon, J. B. (1961) J. Indianmed. Ass., 37, 157-161
Graves, A. M. (1930) Ann. Surg., 92, 1075Greenfield, I. (1963) Etiology, pathogenesis and clinicalfeatures of tetanus. In: Study Group of Tetanus,International conference on tetanus, Bombay, BirlaMatushri Sabhaghar, p. 36
Grounds, J. G. (1964) J. trop. Med. Hyg., 67, 257-259Gwee, A. L. & Lee, Y. K. (1962) Singapore med. J., 3,
174-177Gwee, A. L. & Nadarajah, I. (1960) Singapore med. J.,
1, 164-166Hanna, W. A. (1958) Brit. med. J., 1, 460-461Harper, J. (1961) Med. J. Malaya, 16, 32-45Hay, K. M. (1953) Brit. med. J., 1, 733Hazra, A. K. & Agnihotri, S. R. (1960) Indian J. med. Sci.
14, 197-200Heath, C. W., Zusman, J. & Sherman, T. L. (1964) Amer.
J. publ. Hlth, 54, 769-779Henrion, C. (1954) Brux.-mJd., 34, 232, 238Heredia, A. F. (1963) Prevention of surgical tetanus in the
tropics. In: Study Group of Tetanus, Internationalconference on tetanus, Bombay, Birla Matushri Sab-haghar, p. 66
Hines, E. A. (1930) Amer. J. Dis. Child., 39, 560-572Hollender, L. & Schvingt, E. (1955) Acta chir. belg., 3,
251-266
Hoppe, J. (1952) Chirurg., 23, 353Hubner, A., & Freudenberg, K. (1954) Rev. Immunol.
(Paris), 18, 344Hunter, W. J. (1959) Med. J. Aust., 2, 98-99Huntington, R. W., Thompson, W. R. & Gordon, N. H.
(1937) Ann. Surg., 105, 93Ikram-Ul-Haq (1964) Medicus (Karachi), 29, 97-108Illutovic, A. U. (1961) i. Mikrobiol. (Mosk.), No. 3,
pp. 76-80Illutovic, A. U. (1962) 2. Mikrobiol. (Mosk.), No. 11,
pp. 123-126Illutovic, A. U. & Tarasov, J. D. (1957) Sborn. nau6nie
trudov Stavropolsk naudnoissledovatelskogo InstitutaVakein i Syvorotok, 4, 243-273
Indian Research Fund Association (1946) Report of thefourth meeting of the Indian Clinical Research AdvisoryCommittee, Bombay, India
Indonesia, Ministry of Health, Division of Statistics(1957) Causes of deaths in hospitals, 1957, Djakarta
Indonesia, Ministry of Health, Division of Statistics(1958) Causes of deaths in hospitals, 1958, Djakarta
Int. Dig. Hith Legis., 1963, 14, 468, 654Jain, R. C. (1962) J. Indian med. Ass., 38, 405-409Jannes, L. (1964) Brit. J. exp. Path., 14, 498-501Jelliffe, D. B. (1950) Arch. Dis. Childh., 25, 190Jelliffe, D. B. (1958) Diseases of children in the sub-tropicsand tropics. Arnold, London, pp. 1-28
Jeune, M. M., Vincent, P. & Numbert, G. (1962) Rev.lyon. Med., 11, 1331-1338
Joag, J. G. (1963) Incidence of tetanus in the Sholapurdistrict during 1961 and 1962. In: Study Group ofTetanus, International conference on tetanus, Bombay.Birla Matushri Sabhaghar, p. 62
Johnson, D. W. (1956) Med. J. Aust., 2, 710-715Johnstone, D. D. (1958) Brit. med. J., 1, 12-16Jones, R. (1946) N.Z. med. J., 45,423J0rgensen, K. R. & Lou, H. (1961) Ugeskr. Lag., 123/8,
264-268Kacharevic, D. Z. (1952) Glas. Khig. Inst., 24, 1-21Kaiser, M. (1954) Wien. klin. Wschr., 66, 727-730Kaniak, R. V., Cywicki, J. & Smolenska, W. (1960)
Przegl. epidem., 14, 177-181Katitch, R. V. (1960) Rev. Immunol., 24, 521-524Katsilabros, L. (1963) High doses of adrenaline in the
treatment of tetanus. In: Study Group of Tetanus,International conference on tetanus, Bombay, BirlaMatushri Sabhaghar, p. 59
Keet, M. P. & Murray, A. B. (1962) S. Afr. med. J., 37,401-404
K.E.M. Hospital Group (1963a) Analysis of variousaspects in 4839 patients with tetanus. In: Study Groupof Tetanus, International conference on tetanus, Bom-bay, Birla Matushri Sabhaghar, p. 35
K.E.M. Hospital Group (1963b) Presence of Cl. tetanion various parts of the body. In: Study Group ofTetanus, International conference on tetanus, Bombay,Birla Matushri Sabhaghar, p. 43
Kennedy, D. P. (1960) N.Z. med. J., 59, 551

102 B. BYTCHENKO
Kirtley, J. A. Jr. (1940) Amer. J. Surg., 49, 480484Klenerman, P. & Scragg, J. (1955) S. Afr. med. J., 29,
853-854Kloetzel, K. (1963) J. Amer. med. Ass., 185, 559-567Kloetzel, K. & Monteiro, D. M. (1963) Rev. Inst. Med.
trop. S. Paulo, 5, 111-117Kochhar, K. S. (1960) Indian J. Surg., 21, 29-34Kremlev, G. I. (1964) it. Mikrobiol. (Mosk.), No. 12,
pp. 39-43Kril, R., Prasilava, F. & Neubertova, E. (1964) Clin.
Pediat. (Pologna), 46, 509-517Kubinyi, L., Rudnai, 0. & Barsy, G. (1962-63) Acta
microbiol. Acad. Sci. hung., 9, 133-143Kukiz, T. & Mikulski, Z. (1960) Przegl. epidem., 14,
117-126Lacaz, C. S., Mattos, A. G., Galvao, A. L. A. & Souto,A. B. (1955) J. Pediat. (Rio de J.), 20, 120
Lafontaine, A. & Koopmansch, W. (1954) Brux.-med., 34,411-414
Laha, P. J. & Vaishya, P. D. (1963) A study of the inci-dence of 1000 cases of tetanus in Gwalior and its neigh-bouring districts. In: Study Group of Tetanus, Inter-national conference on tetanus, Bombay, Birla MatushriSabhaghar, p. 63
Lambotte-Legrand, J. & Lambotte-Legrand, C. (1950)Ann. Soc. belge Med. trop., 30, 541-546
Lancaster, H. (1953) Med. J. Aust., 2, 417-418La Scala, F. (1958) J. Pediat. (Rio de J.), 23, 383-392Laurent, L. J. M. & Parish, N. J. (1960). Lancet, 2, 494Lavergne, V., Helluy & Faivre, G. (1949) Rev. Immunol.
(Paris), 13, 315-324Leal, G. (1945) Arch. venez. Pueric., 7, 1353Lebon, J., Choussat, N. & Chaussat-Clausse, J. (1949)
Bull. Acad. nat. Med. (Paris), 133, 4245Lepine, P. (1960). In: Proceedings of the Symposium on
Immunization in Childhood. Edinburgh & London,Livingstone, p. 89
Lessard, R., Potvin, A. & Morin, Y. (1960) Canad. med.Ass. J., 83, 1199-1202
Levandowski, A. (1960) Przegl. epidem., 14, 163-169Lewis, R. A., Satoskar, R. S., Joag, G. G., Dave, B. T.& Patel, J. C. (1954) J. Amer. med. Ass., 39, 630-634
Limaye, M. R. (1962) J. Indian med. Ass., 39, 630-634Linneweh, F. (1953) Med. Klin., 48, 195Lissner, M. (1960) Przegel. epidem., 14, 171-173Loh Siew Gek (1951) Med. J. Malaya, 5, 181-194Long, A. P. & Sartwell, P. E. (1947) Bull. U.S. Army med.
Dep., 7, 371-385Lue, Hung-Chi (1960) Mem. Col. Med. Taiwan Univ., 6,
57-69Lutynski, R. (1961) Przegl. epidem., 15, 285-288Maddocks, J. & Dawbom, J. K. (1961) Med. J. Aust., 1,
625-626Mahadevan, B. (1963) Incidence and prevention oj
tetanus, with particular reference to the armed forces.In: Study Group of Tetanus, International conferenceon tetanus, Bombay, Birla Matushri Sabhaghar, p. 71
Malpica, M. (1961) Higiene, 13, 61-62
Masar, J. (1960) Cs. Epidem., 9, 156-162Mathur, H. H. & Singh, R. V. (1963) Tetanus, a clinical
study. In: Study Group of Tetanus, Internationalconference on tetanus, Bombay, Birla Matushri Sab-haghar, p. 37
Mattos, A. G. (1962) Pediat. prat. (S. Paulo), 33, 269-276Matveev, K. J. (1959) [Botulism], Moscow, Medgiz,
pp. 147-153Matveev, K. J. (1960) [Epidemiology and prophylaxisof tetanus], Moscow, Medgiz, vol. 3, pp. 12-25, 59-60
Matveev, K. J. & Sergeeva, T. U. (1959) 2. Mikrobiol.(Mosk.), 2, 134-142
Matveev, K. J., Solov'ev, S. V. & Volkova, Z. M. (1957)i. Mikrobiol. (Mosk.), 3, 54-58
Matveyev, M. P. & Paul, S. S. (1959) Indian J. ChildHlth, 8, 181-194
Melnotte, P. & Foliguet, J. M. (1963) Rev. Hyg. Mid.soc., 11, 51-64
Melnotte, P., Senault, R. & Manciaux, M. (1961) Con-cours med., 83, 2733-2742
Menon, K. A. (1960) Med. J. Malaya, 14, 184-186Mincsev, M. (1957) Zbl. Chir., 82, 1-26, 17-27Miranda, G. G. & Hempel, Y. B. (1962) Rev. med. C.
Rica, 29, 297-304Mishustin, E. N. & Perzovskaya, M. J. (1954) [Micro-
organisms and the self-purification of the soil], Moscow,Publishing House of the Academy of Sciences of theUSSR
Modi, N. J. (1963) Some observations on 554 cases oftetanus. In: Study Group of Tetanus, Internationalconference on tetanus, Bombay, Birla Matushri Sab-haghar, p. 38
Mohlenbruch, A. (1952) Chirurg, 8, 357Montgomery, R. D. (1961) W. Indian med. J., 10, 84-101Moore, R. M. & Singleton, A. 0. (1939) Surg. Gynec.
Obstet., 69, 146Morl, F. (1956) Z. artzl. Fortbild., 50, 535-538Mose, J. R. (1955) Arch. Hyg. (Berl.), 139B, 137-147Moynihan, N. H. (1956) Brit. med. J., 1, 260-264Murray, K. D. (1959) Med. J. Aust., 2, 659Murti, B. R., Bhaskaran, C. S. & Rajyalakshmi, K. (1961)
J. Indian med. ass., 37, 187-189Musoke, L. K. (1961) Arch. Dis. Childh., 36, 305-315Natkunam, R. (1960) Ceylon med. J., 5, No. 3, 123-124Nazareth, F. A. & Edibam, B. C. (1959) Indian J. Child
Hlth, 8, 349-356Nenes, D. P. & Tranchesi, J. (1948) Rev. Hosp. Clin.
Fac. Med. S. Paulo, 3, 99-106Nesterenko, L. P. (1962) J. Microbiol. Epidem. Immuno-
biol., 12, 65-70Newell, K. W., Lehmann, A. D., LeBlanc, D. R. & Oso-
rio, N. G. (1964) Bull. Wld Hlth Org., 30, 439-444Neyman, K. & Wejdan, H. (1958) Przegl. epidem., 12,
135-145Nilsson, E. & Nordstr0m, L. (1962) Nord. Med., 67,
122-124Nissen, R. & Enderlin, F. (1957) Dtsch. med. Wschr., 82,
539-543

GEOGRAPHICAL DISTRIBUTION OF TETANUS IN THE WORLD, 1951-60 103
Noel, 0. F. (1950) 5th. med. J. (Bgham, Ala.), 43, 53-56Oliveira, N. (1958) J. Pediat. (Rio de J.), 23, 80-96Onuigbo, W. J. B. (1963) J. trop. Pediat., 9, 85-87Oropeza, P. (1937) El tetanos infantil en Venezuela,
Caracas, Tipografia Americana (Thesis)Orzuev, M. I. & Matveev, K. I. (1964) i. Mikrobiol.
(Mosk.), No. 12, pp. 11, 94-99Pai, D. N. (1963) Tetanus mortality in India. In: StudyGroup of Tetanus, International conference on tetanus,Bombay, Birla Matushri Sabhaghar, p. 63
Parikh, V. V. (1963) The incidence of tetanus: a survey inKheralu Taluka. In: Study Group of Tetanus, Inter-national conference on tetanus, Bombay, Birla MatushriSabhaghar, p. 62
Patel, J. C. (1960) J. Obstet. Gynaec. India, 11/12,188-192
Patel, J. C., Dhirawani, M. K. & Trivedi, R. R. (1960)Indian J. Child Hlth 9, 459-468
Patel, J. C. & Mehta, B. C. (1963) Indian J. med. Sci.,17, 791-811
Patel, J. C., Mehta, B. C. & Nanavati, B. H. (1963)J. Indian med. Ass., 40, 443-447
Perdrup, A. (1949) Acta chir. scand., 97, 495-502Perin, F. & Van de Voorde, R. R. (1963) Ann. Soc. belgeMid. trop., 43, 225-240
Perlstein, M. A., Stein, M. D. & Elam, H. (1960) J. Amer.med. Ass., 173, 1536-1541
Petrilla, A. (1960) Acta microbiol. Acad. Sci. hung., 7,65-70
Petrone, P. (1960) Ann. Sclavo, 2, 684-691Pinheiro, D. (1957) J. Pediat. (Rio de J.), 51, 171-180Pinheiro, D. (1960) J. bras. Med., 3, 729-746Pinheiro, D. (1962) Pediat. prdt. (S. Paulo), 33, 263-268Pirame, Y. (1963) Presse med., 71, 1045-1046Pirame, Y. & Becquet, R. (1963) Bull. Soc. Path. exot.,
56, 469-474Poesponegoro, S. D. & Ranti, J. S. F. (1959) J. Indones.
med. Ass., 9, 1-11Portsmouth, 0. H. D. (1963) E. Afr. med. J. 40, 643-648
Prevot, A. R. (1955) Biologie des maladies dues auxanaerobies, Paris, Flammarion
Ramalhao, J. (1956) Portugal med., 40, 96-111Ramon, G. (1962) Rev. Immunol. (Paris), 26, 185-284Ramon, G. (1963) Rev. Hyg. Med. soc., 11, 47-49Ramon, G. & Zoeller, M. (1926) C.R. Soc. Biol. (Paris),
94, 106Ramsay, A. M., France, E. M. & Dampsey, B. M.
(1956) Lancet, 2, 548-550Rapin, M. & Amstutz, P. (1963) Rev. Hyg. MMd. soc.,
11, 47-49Recchia, F. (1956) Mal. Infez., 2, 355-416Riis, P. (1958) Nord. Med., 60, 1048-1049Rojas, M., Weitman, J., Moya, H., Segovia, M., Jimenez,
L., Villalobos, M., Tello, A. & Rodo, F. (1960) Rev.med. Chile, 88, 349-358
Rossichin, V. V. (1962) J. Microbiol. Epidemiol. Immuno-biol., 4, 120-121
Ryan, B. (1961) Papua N. Guinea med. J., 5, 27-29Salvaraglio, F. & Ebole, 0. (1950) Ann. Inst. Hyg. Monte-
video, 4, 59-71Sarrouy, C., Gillot, F., Clausse, J., Peretti, E. & Gatto, L.
(1956) Algerie med., 60, 277-290Sarrouy, C., Gillot, F. & Pantin (1950) Pediatrie, 5,
777-778Savolainen, T. (1951) Acta path. microbiol. scand., 91,
177-180Sawicki, F. (1964) Przegl. epidem., 18, 71-76Schlesinger, B. E. (1960) In: Proceedings of a symposium
on immunization in childhood, London, Livingstone,p. 73
Schofield, F. D., Tucker, V. M. & Westbrook, G. R.(1961) Brit. med. J., 2, 785-789
Schuch, P. & Windorfer, A. (1963) Dtsch. med. Wschr.,88, 2181-2188
Sen, R., Vaishnava, H. & Passey, M. N. (1963) Bacterio-logical investigations in clinical cases of tetanus in Delhi.In: Study Group of Tetanus, International conferenceon tetanus, Bombay, Birla Matushri Sabhaghar, p. 44
Senecal, J. (1958) Tetanus. In: Diseases of children in thesubtropics and tropics, Jelliffe, D. B., ed., London,Arnold, pp. 594-600
S6n6cal, J. & Senghor, G. (1962) Turk. J. Pediat., 4,98-102
Shah, R. M., Shah, L. J. & Damany, S. I. (1962) IndianJ. med. Sci., 16, 867-872
Sharma, D. P. (1963) Study of 510 cases of tetanusadmitted in P.L.S. Hospital, Meerut in last 3 years.In: Study Group of Tetanus, International conferenceon tetanus, Bombay, Birla Matushri Sabhaghar, p. 38
Sheth, S. (1956) Indian J. Pediat., 23, 197-199Silva, C. C. (1960) J. Ceylon publ. Hlth Ass., 1, 61-67Silva Martinez, M. (1964) Higiene, 16, 110-122Silverthorne, N. (1947) J. Pediat., 30, 195-198Simovic, N. (1958) Ann. paediat. (Basel), 190, 237-251Simovic, N. (1960) Jugosl. Pediat., 3, 1-4, 53-58Sinha, B. N. (1961) J. Indian med. Ass., 36, 286-288Skudder, P. A. & McCarroll, J. R. (1964) J. Amer. med.
Ass., 188, 625-627Slome, R. (1954) S. Afr. med. 1., 28, 473-475Smith, J. W. G., Evans, D. G., Jones, D. A., Gear,M. W. L., Cunliffe, A. C. & Barr, M. (1963) Brit. med.J., 1, 237-238
Smith, L. D. (1955) Introduction to the pathogenicanaerobes, Chicago, University of Chicago Press,pp. 48-49, 77-79, 88-107, 126-129
Smythe, P. M. (1963) Brit. med. J., 1, 565-571Smythe, P. M. & Bull, A. B. (1961) Brit. med. J., 1, 732-
736Spaeth, R. (1941) Arch. intern. Med., 68, 1133-1160Spivey, 0. S., Grulee, C. G., Hickman, B. T. & Stewart,
S. E. (1953) J. Pediat, 42, 345Srivastava, S. P. & Chatterji, G. G. (1961) J. Indian med.
Ass., 36, 289-295Stahlie, T. D. (1960) J. trop. Pediat., 6, 15-18Stirnemann, U. (1963) Schweiz. med. Wschr., 16, 601-607

104 B. BYTCHENKO
Syngal, K. L. (1961) Indian J. Child Hlth, 10, 190-194Takos, M. J. (1958) Industr. Med. Surg., 27, 518-519Tasman, A. & Huygen, F. J. A. (1962) Bull. Wld Hlth
Org., 26, 397-407Tateno, I., Suzuki, S. & Kitamoto, 0. (1961) Jap. J. exp.Med., 31, 365-380
Taxay, E. P. (1960) W. Ind. med. J., 9, 14-16Thiodet, J., Fourrier, A., Massonat, J. & Deyme, H.
(1956a) Algerie med., 60, 41-43Thiodet, J., Fourrier, J., Massonat, J. & Deyme, H.
(1956b) Alg&rie med., 60, 45-47Tompkins, A. B. (1958) Brit. med. J., 1, 1382-1385Tompkins, A. B. (1959) Arch. Dis. Childh., 34, 398-405Top, F. H., Huggen, D. W. & McCulloch, W. F. (1964)An epidemiological study of tetanus in Iowa, Iowa City,State University of Iowa
Torres-Gost, J. & Figueroa-Egea, J. (1963a) Determina-tive factors of tetanus. In: Study Group of Tetanus,International conference on tetanus, Bombay, BirlaMatushri Sabhaghar, p. 37
Torres-Gost, J. & Figueroa-Egea, J. (1963b) Mortalityin tetanus. In: Study Group of Tetanus, Internationalconference on tetanus, Bombay, Birla Matushri Sab-haghar, p. 37
Tran Van Bang & Nguyen Duy San (1960) Acta med.vietnam., 4, 1239-1241
Triebold, H. (1956) Gynaecologia (Basel), 142, 129Turner, V. C. & Galloway, T. C. (1949) Arch. Surg., 58,478-483
Uldall, T. (1961) Ugeskr. Log., 123/26, 907-911Uttley, K. H. (1959) W. Indian med. J., 8, 41Vaishnava, H., Neogy, C. N., Dixit, N. S., Passey,M. N., Gupta, S. C. & Laurence, D. R. (1964) J. Ass.Phycns India, 12, 691-701
Vakil, B. J., Aiyer, S. N., Tulpule, A., Mehta, A. J. &Tulpule, T. H. (1964) J. Indian, med. Ass., 42, 203-212
Vakil, B. J., Tulpule, T. H., Armitage, P. & Laurence,D. R. (1963) Clin. Pharmacol. Ther., 4, 182-187
Vener, H. J. & Bower, A. G. (1941) J. Amer. med. Ass.,116, 1627
Veronesi, R. (1956) Amer. J. med. Sci., 232, 629-647Veronesi, R. (1960) Contribua_Vdo para o estudo clinico e
experimental do tetano, Sao Paulo (Thesis)Vervoorn, J. D. (1962) Trop. geogr. Med., 14, 284-286Vinnard, R. T. (1945) Surgery, 18, 482-492Von Reuss, A. R. (1927) Diseases of the newborn, NewYork, Word & Co.
Vuksanovic, V., Kolbas, V. & Sucic, V. (1960) Jugosl.Pediat., 3, 98-106
Wagle, C. S. (1963) Indian J. med. Sci., 17, 157-159Wainwright, J. M. (1926) Arch. Surg., 12, 1062Weller, E. (1956) Dtsch. med. Wschr., 81, 267-272Wilkinson, J. L. (1961) Brit. med. J., 1, 1721-1724Woodward, W. W. (1960) Brit. med. J., 2, 916World Health Organization (1963) Second report on the
world health situation, 1957-1960, Geneva (Off. Rec.Wld Hlth Org., 122)
Wright, R. (1960) S. Afr. med. J., 34, 111-113Wright, R., Symes, M. K., Jackson, B. G., Mann,N. M. & Adams, E. B. (1961) Lancet, 1, 678-680
Yazdani, 1. (1954) Rev. Fac. Med. (Teheran), 11, 513-522Yeoh, G. S. (1960) Singapore med. J., 1, 59-62Yodh, B. B. & Shah, S. N. (1956) J. Ass. Physcns India, 4,
337-341Young-En Kao (1948) Chin. med. J., 66, 487-493Young-En Kao (1951) Chlin. med. J., 69, 512-517Zauli Naldi, G. & Gasparroni, L. (1961) Clin. Pediat.
(Bologna), 43, 550-558Zavazal, V. (1957) Z. arztl. Fortbild., 57, 133-136Zonchello, S. A. (1961) Arch. ital. Sci. med. trop., 17,
198-208Zubillaga, R. A. (1952) Arch. venez. Pueric., 15, 180-204