mustapha jamiu sulayman's projet
TRANSCRIPT
CHAPTER ONE
1.1. GENERAL INTRODUCTION
Hypertension is usually defined by the presence of a chronic
elevation of systemic arterial pressure above a certain threshold
value. However, increasing evidence indicates that the
cardiovascular (CV) risk associated with elevation of blood
pressure (BP) above approximately 115 ⁄ 75 mm Hg increases in a
log-linear fashion. The progressive CV syndrome arising from
complex and interrelated etiologies. Early markers of the
syndrome are often present before BP elevation is sustained;
therefore, hypertension cannot be classified solely by discrete
BP thresholds. Progression is strongly associated with functional
and structural cardiac and vascular abnormalities that damage the
heart, kidneys, brain, vasculature, and other organs and lead to
premature morbidity and death. [1]
1.2. Calcium blockers in relation to fertility
Infertility is defined as the inability to achieve pregnancy
after one year of unprotected intercourse [2]. Conception is
normally achieved within 12 months in 80 to 85% of couples who
are not using contraceptive measures; which mean an estimated 15%
of couples attempting their first pregnancy, may experience
difficulty in conceiving. Some cases of male infertility are due
to anatomical abnormalities such as varicoceles, ductal
obstructions or ejaculatory disorders [3]. Infertility may also be
due to abnormal sperm morphology (tetratozoospermia) and
insufficient sperm motility [4]. A study recently carried out on
the sperm characteristics of infertile males at the University
College Hospital, Ibadan, Nigeria showed that abnormal semen
quality remains a significant contributor to overall infertility
with athenozoospermia being the most common seminal quality
abnormality [5]. A similar study that was done at the Nnamdi
Azikiwe University Teaching Hospital located in South-east
Nigeria showed that oligozoospermia (35.9%) and athenozoospermia
(32.3%) were the most common aetiological factors responsible for
male infertility [6]. There are evidences to show that sperm
counts have been declining over the last 50 years, with a
consequent increase in male infertility. [7]
Primary infertility may result from the use of various drugs.
This phenomenon may be the result of an effect on the
hypothalamic-pituitary-gonadal axis or a direct toxic effect on
the gonads. Some of the drugs are antineoplastic agents
(cyclophosphamide, chlorambucil, busulphan, and methotrexate),
glucocorticosteroids, hormonal steroids (diethylstilbestrol,
medroxyprogesterone acetate, estrogen, and the constituents of
oral contraceptives), antibiotics (sulfasalazine and
cotrimoxazole), thyroid supplements, spironolactone, cimetidine,
colchicine, marijuana, opiates, and neuroleptic agents [8].
Phenothiazines such as chlorpromazine and thioridazine, are
commonly used to treat schizophrenia and are known to cause
hyperprolactinaemia which induces hypospermatogenesis, impotence
and loss of libido in men [9].
1.3. AIMS OF STUDY
The present work is aimed at studying or evaluating the effect of
Nifedipine on the testis.
1.4. SCOPE OF STUDY
The research work is based on the analysis of the effect of the
Nifedipine, giving a group of adult male wistar rats a particular
dose of the Nifedipine to see on the testis. The research work
would be extrapolated towards finding the effect of the
Nifedipine on the following parameters:
1. Morphological changes of the testis (histological changes)
2. Sperm count
3. Sperm motility
4. Endocrine function of the testis (serum testosterone)
Comparative examination of the testes of the group exposed to the
minimum, maximum dose group as well as the control group would
show possible effects on the testes.
1.5. SIGNIFICANCE OF STUDY
The information gathered from the observations and results in
this study would help shed more light on the use of
antihypertensive (Nifedipine) and the effects of the drugs would
help one to make scientific suggestion as to whether the drugs
should be embraced or withdrew as one of the therapeutic drugs in
the management of hypertension.
1.6. STATEMENT OF PROBLEM
Nifedipine is widely used as an antihypertensive drug, effort
would be made, if it should be discourage or encourage among
hypertensive male of reproductive age, Nifedipine affect the male
reproductive system by blocking it functions
1.7. LIMITATION OF STUDY
Available laboratory equipment and facilities did not
favour the study.
Time factor was a constraint on the study.
Electricity was another huge factor on this study.
Lack of proper functioning of the apparatus and equipment
which altered the tissue processing procedure.
2. CHAPTER TWO
2.1. Hypertension
Hypertension is an important worldwide public-health challenge
because of its high frequency and concomitant risks of
cardiovascular and kidney disease. It has been identified as the
leading risk factor for mortality and is ranked third as a cause
of disability-adjusted life-years. [44]
2.2. Incidences
In the year 2001, high blood pressure accounted for “54% of
stroke, 47% of ischaemic heart disease, 75% of hypertensive
disease, and 25% of other cardiovascular disease worldwide” [10].
The negative impact of hypertension on health status is clear,
especially taking into account the disability, decreased quality
of life, and mortality associated with stroke and cardiovascular
disease. In 2001, 7.6 million deaths (13.5% of all deaths) and 92
million disability life-years (6% of total) were attributable to
systolic blood pressure greater than 115 mmHg . [10]
2.3. Drug of study
Name of the drug: Nifedipine
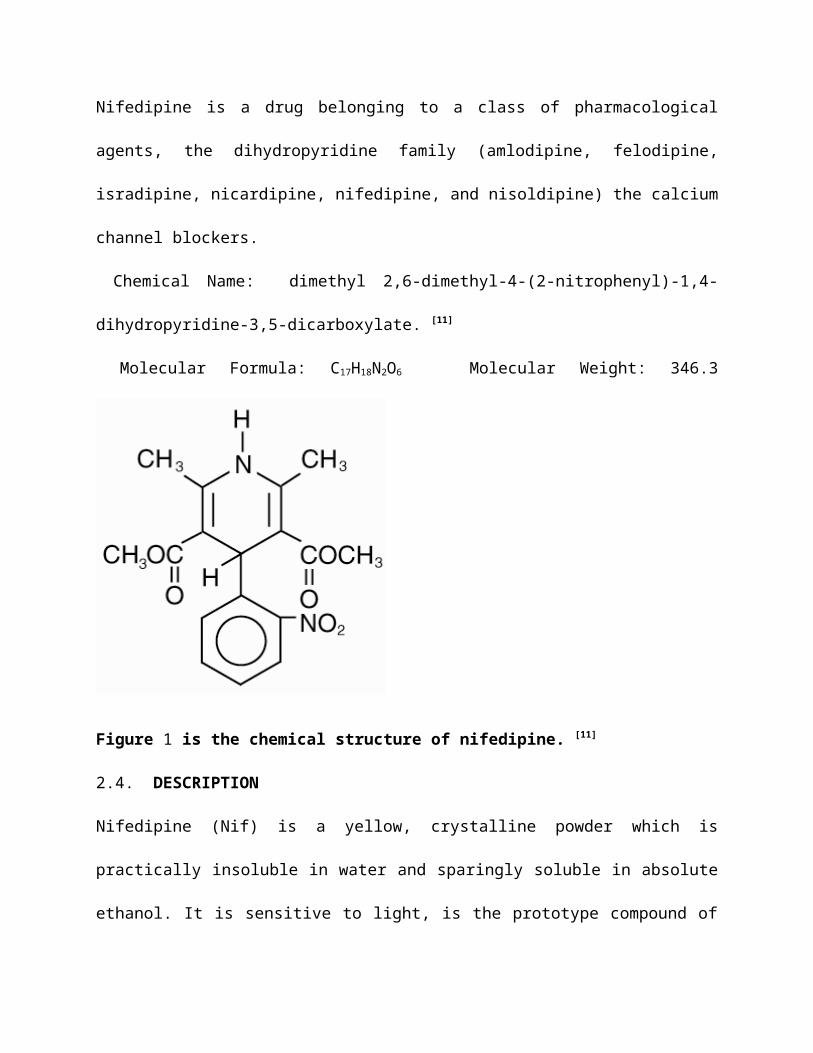
Nifedipine is a drug belonging to a class of pharmacological
agents, the dihydropyridine family (amlodipine, felodipine,
isradipine, nicardipine, nifedipine, and nisoldipine) the calcium
channel blockers.
Chemical Name: dimethyl 2,6-dimethyl-4-(2-nitrophenyl)-1,4-
dihydropyridine-3,5-dicarboxylate. [11]
Molecular Formula: C17H18N2O6 Molecular Weight: 346.3
Figure 1 is the chemical structure of nifedipine. [11]
2.4. DESCRIPTION
Nifedipine (Nif) is a yellow, crystalline powder which is
practically insoluble in water and sparingly soluble in absolute
ethanol. It is sensitive to light, is the prototype compound of
the dihydropyridine class of calcium channel antagonists. Calcium
antagonists inhibit the influx of calcium ion through plasma
membrane channels and thus dilate vascular smooth muscle
contraction. NIF is a selective arterial dilator, and is used for
the treatment of hypertension, angina pectoris, and other
cardiovascular disorders [12].
The exposure of some drugs to light leads to photodecomposition.
These drugs undergo important chemical changes, accompained by
alternation in their activities and in some cases total loss of
their therapeutic activity [13].
NIF is very highly sensitive to photooxidation. NIF exposure to
ultraviolet-visible irradiation produces both aromatization in
the dihydropyridine moiety (turning it into a pyridine ring) and
a reduction of nitro group in to nitroso groups (NDNIF). In
addition, its exposure to ultraviolet light produces
dehydronifedipine (DNIF), NIF photodegradation products have no
pharmacological activity. Several studies related to its
photodecomposition have been reported. [14]
The Manufacturers of NIF products use light resistant coating
and/or packing to minimize their photodegradation. Long term
exposure to sunlight or artificial light may also occur if NIF
formulations are improperly stored by patients. Poor storage
conditions may potentially decrease clinical efficacy of NIF
products [15].
The tablets also contain the following excipients: purified talc,
povidone, lactose, carbomer 934P, hypromellose, silicon dioxide,
magnesium stearate, titanium dioxide, iron oxide red CI77491,
macrogol 4000 and Eudragit E100. The tablets are gluten free.
Furthermore, Nifedipine is a potent vasodilator, which relaxes
vascular smooth muscle probably by its inhibitory effect on the
transmembrane influx of calcium [16].
It has been demonstrated that this drug exerts a prompt and
marked hypotensive effect when administered to hypertensive
patients. [17]
Mechanism of Action
The precise means by which this inhibition relieves angina has
not been fully determined, but includes at least the following
two mechanisms:
1) Relaxation And Prevention Of Coronary Artery Spasm:Nifedipine
dilates the main coronary arteries and coronary arterioles, both
in normal and ischemic regions, and is a potent inhibitor of
coronary artery spasm. This property increases myocardial oxygen
delivery in patients with coronary artery spasm, and is
responsible for the effectiveness of nifedipine in vasospastic
(Prinzmetal’s or variant) angina. Whether this effect plays any
role in classical angina is not clear, but studies of exercise
tolerance have not shown an increase in the maximum exercise
rate-pressure product, a widely accepted measure of oxygen
utilization. This suggests that, in general, relief of spasm or
dilation of coronary arteries is not an important factor in
classical angina.
2) Reduction Of Oxygen Utilization:Nifedipine regularly reduces
arterial pressure at rest and at a given level of exercise by
dilating peripheral arterioles and reducing the total peripheral
resistance (afterload) against which the heart works. This
unloading of the heart reduces myocardial energy consumption and
oxygen requirements and probably accounts for the effectiveness
of nifedipine in chronic stable angina.
Pharmacokinetics
Nifedipine is almost completely absorbed after oral
administration. Plasma drug concentrations rise at a gradual,
controlled rate exhibiting zero order absorption kinetics after
nifedipine long acting tablet administration and reach a plateau
at approximately six hours after the first dose. For subsequent
doses, relatively constant plasma concentrations at this plateau
are maintained with minimal fluctuations over the 24 hour dosing
interval. At steady state, the bioavailability of nifedipine
extended release tablets is 86% relative to an immediate release
dosage form which has a systemic availability of 45 to 68%.
Administration of nifedipine long acting tablets in the presence
of food slightly alters the early rate of drug absorption, but
does not influence the extent of drug bioavailability. Markedly
reduced gastrointestinal retention times over prolonged periods
(i.e. short bowel syndrome) may, however, influence the
pharmacokinetic profile of the drug, which could result in lower
plasma concentrations. The pharmacokinetics of Nifedipine long
acting tablets are linear over the dose range of 30 to 180 mg, in
that plasma concentrations are proportional to dose administered.
There is no evidence of dose dumping in either the presence or
the absence of food. [18]
Distribution
Nifedipine is about 95% bound to plasma protein (albumin). [18]
Biotransformation
The active substance nifedipine is almost completely metabolised
in the liver, primarily by oxidative processes (the cytochrome
P450 enzyme CYP3A4). Some metabolic activity within the gut wall
may also contribute to the presystemic metabolism. These
metabolites show no pharmacodynamic activity. The main metabolite
is the hydroxycarbolic acid derivative (95%); the remaining 5% is
the corresponding lactone. [18]
Excretion/Elimination
Nifedipine is excreted in the form of its metabolites,
predominantly via the kidneys (60 to 80%), and about 5 to 15% is
excreted via the bile in the faeces. The unchanged substance is
recovered only in traces (below 0.1%) in the urine. [18]
Half-life
The terminal elimination half-life is 1.7 to 3.4 hours in an
immediate long acting formulation. In cases of impaired kidney
function, no substantial changes have been detected in comparison
with healthy volunteers. [18]
In cases of impaired liver function, the elimination half-life is
distinctly prolonged and the total clearance is reduced. A dose
reduction may be necessary in severe cases.
Patients on haemodialysis or chronic ambulatory peritoneal
dialysis have not reported significantly altered pharmacokinetics
of nifedipine.
Pharmacodynamics
Nifedipine inhibits the transmembrane influx of calcium ions into
cardiac and vascular smooth muscle. The contractile processes of
these tissues are dependent upon the movement of extracellular
calcium into the muscle cells through specific ion channels.
Nifedipine selectively inhibits the transmembrane influx of
calcium through the slow channel without affecting the
transmembrane influx of sodium through the fast channel to any
significant degree. This results in a reduction of free calcium
ions available within the muscle cells and an inhibition of the
contractile process. Nifedipine does not affect total serum
calcium. The specific mechanisms by which nifedipine relieves
angina and reduces blood pressure have not been fully determined
but are believed to be brought about largely by its vasodilatory
action. [18]
Common side effects
Common side effects of nifedipine include, Headache (7.3-7.9%).
dizziness (456.7%).
Lightheadedness (6.7%), giddiness (6.7%), nausea (6.7%). vomiting
(6.7%). Gastrointestinal distress (6.7%). flushing (5.8- 13.9%).
heat sensation (5.8- 13 -9%). peripheral edema (3.747%),
Hypotension. [19]
SYSTEM OF STUDY
On the male reproductive system
After life itself, fertility is probably the most highly prized
human possession, yet, while medical treatment of the individual
naturally demands priority, relatively little attention is paid
to the effects of treatment on reproductive function.
ANTIHYPERTENSIVE MEDICATIONS
The ultimate goal in treatment of the hypertensive patient is to
achieve the maximum reduction in the long-term total risk of
cardiovascular morbidity and mortality.
Classifications of antihypertensives
Agents useful in the chronic treatment of hypertension may be
classified into one of nine categories. [20]
They are in no particular order: 1) diuretics, 2) beta-blockers,
3) angiotensin converting enzyme inhibitors, 4) angiotensin
receptor antagonists, 5) calcium channel blockers, 6) alpha-
adrenergic blockers, 7) central alpha adrenergic agonists, 8)
direct vasodilators, and 9) peripheral adrenergic neuron
antagonists.
Calcium channel antagonists/blockers
Ca2+ channels allow passage of Ca2+ ions into the cytoplasm
through a selective pore which is opened in response to
depolarization of the cell membrane [21].
The Ca2+ flux creates a net inward, depolarizing current and the
resulting accumulation of Ca2+ in the cytoplasm can act as a
chemical trigger for secretion of hormones and neurotransmitters,
contraction of muscle and a variety of other Ca2+-sensitive
events. Thus, upon sensing membrane potential changes, Ca2+
channels simultaneously generate an electrical signal while
directly creating an intracellular chemical messenger. This dual
ability is unique among the family of ion channels and allows the
Ca2+ channel to play a variety of roles in excitation-secretion
and excitation-contraction coupling. It has now become clear that
versatility of function is reflected by diversity of the types of
Ca2+ channels on the membrane of individual cells. [22]
The term ‘‘calcium channel antagonists’’ refers to a chemically,
pharmacologically and therapeutically heterogeneous group of
drugs prominent both as cardiovascular therapeutic agents and as
molecular tools. The calcium antagonist consist of at least three
distinct classes of drugs as follows: 1,4-dihydropyridines
(prototype: Nifedipine ), phenylalkylamines :prototype
verapamil), and benzothiazepines (prototype:diltiazem). [23]
The cardiovascular activities of these drugs as
antihypertensive, anti-anginal and selective antiarrhythmic
agents are due to their interaction at one particular calcium
mobilization process—calcium entry through a voltage-gated
calcium channel of the L-type. Many studies have demonstrated
that in accord with their chemical heterogeneity these agents
interact at discrete receptor sites associated with a major
subunit of the channel. [24]
Iranloye et al, reported that Nifedipine appears to have a
deleterious effect on sperm functions in rats which is not
mediated by a change in testosterone secretion, Group 1 (control)
received distilled water; Group 2, received nifedipine 0.57
mg/kg; and Group 3, received 0.57 mg/kg and serve as a recovery
group and the treatment was done orally for 30 days. [25]
Amlodipine (as besylate, mesylate or maleate) is a long-acting
calcium channel blocker (dihydropyridine class) used as an anti-
hypertensive and in the treatment of angina [26].
Like other calcium channel blockers, amlodipine acts by relaxing
the smooth muscle in the arterial wall, decreasing peripheral
resistance and hence reducing blood pressure; in angina it
increases blood flow to the heart muscle.
The preliminary observations showed that administration of
Amlodipine lead to an abnormal morphology of the testis in that,
it had a deleterious effect on the seminiferous tubules in a dose
related fashion. By these preliminary observations, alteration in
the testis histology may have implication for infertility in man.
It could be observed from the result obtained in this study that
a high dose of 0.056mg/g/bodyweight of amlodipine gradually
produced an abnormal morphology of the testis while a higher dose
of 0.114mg/g/bodyweight led to a complete destruction of the
histological architecture of the testis when administered daily
for 8 weeks. The high doses were designed to represent human
exposure to high levels of amlodipine. Therefore, one can
conclude that high doses of amlodipine could lead to infertility
in man. [27]
Clinical nifedipine-associated infertility has been reported to
have negative effect on the acrosome. The acrosomal reaction is a
complex calcium-dependent process [28].
Premature spontaneous acrosome reaction prior to reaching the
oocyte, may lead to early sperm cell death. On the other hand,
the inability of sperm to undergo stimulated acrosome reaction in
response to oocyte investments and/or follicular fluid may lead
to the failure of sperm to fertilize the ovum. It has recently
been demonstrated that nifedipine, a calcium channel blocker, has
the capability of blocking acrosome reaction [29].
Benoff et al., reported a group of men taking nifedipine for
hypertension were found to have reversible disordered expression
of head-directed mannose-ligand receptors and low rates of
acrosome reaction during capacitating conditions. [30]
Following cessation of the drug, the acrosome reaction status
returned to normal and subsequently, pregnancy was achieved. [31]
Calcium ion has been shown to be a primary determinant of sperm
cell function, including progressive motility, hyper activated
motility, capacitation, and acrosome reaction; accordingly, a
number of Ca2+ - permeable channels and transporters have been
reported [32].
The therapeutic administrations of calcium antagonist for
hypertension control causes reversible male infertility
associated with an IVF Failure. A mechanism of inhibition of
sperm fertilizing potential through insertion of lipophilic
calcium ion antagonists into the bilayer of the sperm plasma
membrane. [33]
The possibility exists that the nifedipine used by the majority
of men in the control of hypertension has more of an adverse
effect on sperm function than verapamil, however, verapamil may
increase sperm motility and accelerate acrosome reaction [34].
However, a fundamental question is whether drugs blocking calcium
channel have any side effect that reduces male fertility as
available reports suggested that calcium ion mediates sperm
functions and fertilization process [35].
Furthermore, there are concerns about the induction of
infertility by CCB in males [36].
Recently, a particular study group reported that CCB appear to
have a reversible anti-fertility effect on male rats. Following
the exposure of male rats to CCB, a significant reduction in the
epididymal sperm count and motility was observed; which did not
occur through inhibition of the pituitary gonadal axis as
testosterone, follicle stimulating hormone and luteinizing
hormone levels remained unchanged [37].
Previously, many drugs have been shown to have adverse effect on
male fertility.
There is substantial evidence that CCB induces significant
oxidative stress in the testes, which appears to be responsible
for the adverse effects of decreased sperm count and motility
ultimately leading to reduced fertility in rats. [38]
Furthermore it was also reported by Olivari et al, that the
weight would be significantly less after chronic Nifedipine
therapy. [39]
ORGAN OF STUDY (TESTIS)
GROSS ANATOMY OF THE TESTIS
Introduction
The testes (testicles) are the male gonads—paired ovoid
reproductive glands that produce sperms (spermatozoa) and male
hormones, primarily testosterone. [40]
Shape: The testes (singular, testis) are paired, whitish, ovoid
organs.
Measurement: each measures about 4 cm (1.5 in.) long and 2.5 cm
(1 in.) in diameter, each testis weighs between 10 and 14 g. [41]
The testes are suspended in the scrotum by the spermatic cords,
with the left testis usually suspended (hanging) more inferiorly
than the right testis. [40]
Coverings: Two tissue layers, or tunics, cover the testes, the
outer tunica vaginalis is a thin serous sac derived from the
peritoneum during the descent of the testes. The tunica albuginea
(al''byoo-jin'e-a˘) is a tough fibrous membrane that directly
encapsulates each testis. [41]
The surface of each testis is covered by the visceral layer of
the tunica vaginalis, except where the testis attaches to the
epididymis and spermatic cord. The tunica vaginalis is a closed
peritoneal sac partially surrounding the testis, which represents
the closed-off distal part of the embryonic processus vaginalis.
The visceral layer of the tunica vaginalis is closely applied to
the testis, epididymis, and inferior part of the ductus deferens.
The slit-like recess of the tunica vaginalis, the sinus of the
epididymis, is between the body of the epididymis and the
posterolateral surface of the testis. [40]
The parietal layer of the tunica vaginalis, adjacent to the
internal spermatic fascia, is more extensive than the visceral
layer and extends superiorly for a short distance onto the distal
part of the spermatic cord. The small amount of fluid in the
cavity of the tunica vaginalis separates the visceral and
parietal layers, allowing the testis to move freely in the
scrotum. [40]
Fibrous inward extensions of the tunica albuginea partition the
testis into 250 to 300 wedge-shaped testicular lobules. Each
lobule of the testis contains tightly convoluted seminiferous
tubules that may exceed 70 cm (28 in.) in length if uncoiled. The
seminiferous tubules are the functional units of the testis
because it is here that spermatogenesis, the production of
spermatozoa, occurs. Spermatozoa are produced at the rate of
thousands per second—more than 100 million per day— throughout
the life of a healthy, sexually mature male. [41]
EPIDIDYMIS
The epididymis is an elongated structure on the posterior surface
of the testis.
Efferent ductules of the testis transport newly developed sperms
to the epididymis from the rete testis. The epididymis is formed
by minute convolutions of the duct of the epididymis, so tightly
compacted that they appear solid, the duct becomes progressively
smaller as it passes from the head of the epididymis on the
superior part of the testis to its tail. At the tail of the
epididymis, the ductus deferens begins as the continuation of the
epididymal duct. In the lengthy course of this duct, the sperms
are stored and continue to mature. The epididymis consists of:
Head of the epididymis: the superior expanded part that is
composed of lobules formed by the coiled ends of 12-14
efferent ductules.
Body of the epididymis: consists of the convoluted duct of
the epididymis.
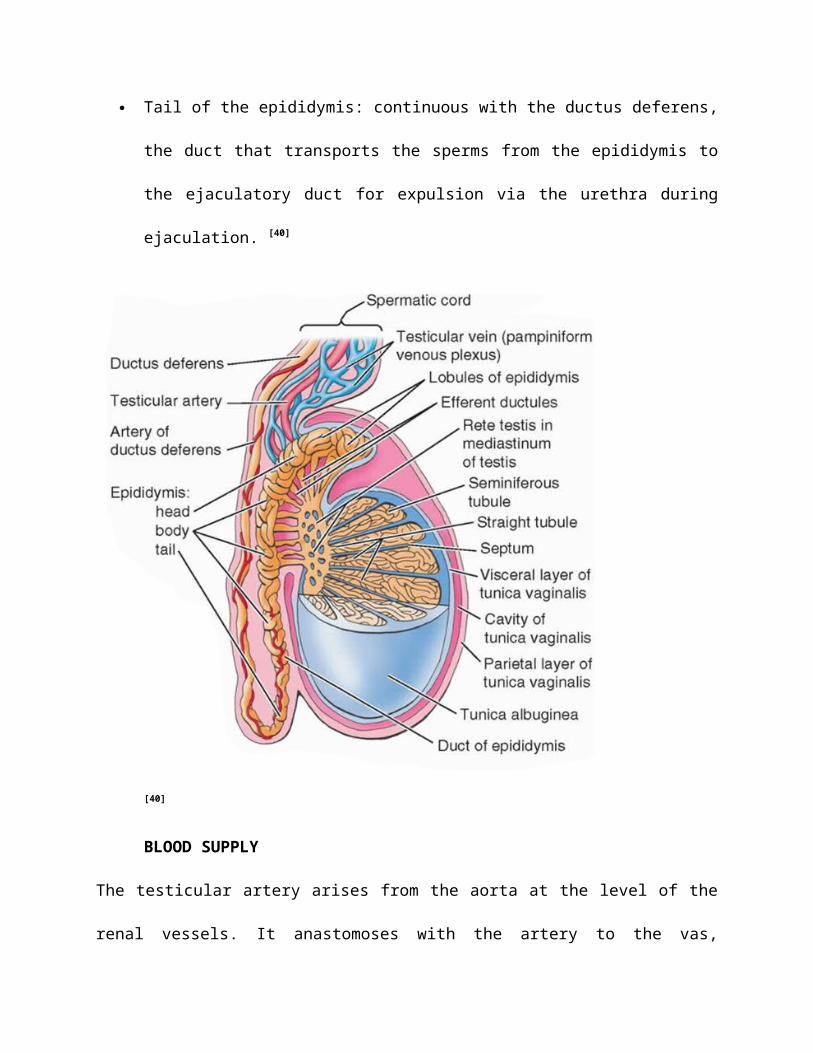
Tail of the epididymis: continuous with the ductus deferens,
the duct that transports the sperms from the epididymis to
the ejaculatory duct for expulsion via the urethra during
ejaculation. [40]
[40]
BLOOD SUPPLY
The testicular artery arises from the aorta at the level of the
renal vessels. It anastomoses with the artery to the vas,
supplying the vas deferens and epididymis, which arises from the
inferior vesical branch of the internal iliac artery. This cross-
connection means that ligation of the testicular artery is not
necessarily followed by testicular atrophy. The pampiniform
plexus of veins becomes a single vessel, the testicular vein, in
the region of the internal ring. On the right this drains into
the inferior vena cava, on the left into the renal vein. [42]
LYMPH DRAINAGE
The lymphatic drainage of the testis obeys the usual rule; it
accompanies the venous drainage and thus passes to the para-
aortic lymph nodes at the level of the renal vessels. Free
communication occurs between the lymphatics on either side; there
is also a plentiful anastomosis with the para-aortic
intrathoracic nodes and, in turn, with the cervical nodes, so
that spread of malignant disease from the testis to the nodes at
the root of the neck is not rare. [42]
NERVE SUPPLY
The testis is supplied tenth thoracic (T10) sympathetic fibres
via the renal and aortic plexus. These convey afferent (pain)
fibres—hence referred pain from the testis to the loin. [42]
Histologically each testis is surrounded by a thick capsule of
dense connective tissue, the tunica albuginea. The tunica
albuginea is thickened on the posterior surface of the testis to
form the mediastinum testis, from which fibrous septa penetrate
the gland, dividing it into about 250 pyramidal compartments
called the testicular lobules. These septa are incomplete, and
there is frequent intercommunication between the lobules. Each
lobule is occupied by one to four seminiferous tubules enmeshed
in a web of loose connective tissue that is rich in blood and
lymphatic vessels, nerves, and interstitial cells, also known as
Leydig cells. Seminiferous tubules produce male reproductive
cells, the spermatozoa, whereas interstitial cells secrete
testicular androgens. During embryonic development the testes
develop retroperitoneally in the dorsal wall of the abdominal
cavity. They migrate during fetal development and become
positioned within the scrotum, at the ends of the spermatic
cords. Because of this migration, each testis carries with it a
serous sac, the tunica vaginalis, derived from the peritoneum.
The tunic consists of an outer parietal layer and an inner
visceral layer, covering the tunica albuginea on the anterior and
lateral sides of the testis.
SPERMATOGENESIS
Spermatogenesis is the process of formation of spermatozoids.
That is- the sequence of events in the seminiferous tubules of
the testes that leads to the production of spermatozoa.The
process begins with a primitive germ cell, the spermatogonium,
situated next to the basal lamina of the epithelium. At sexual
maturity, spermatogonia begin to divide by mitosis, producing
successive generations of cells. The newly formed cells can
follow one of two paths: they can continue dividing as stem
cells, also called type-A spermatogonia, if they differentiate
during progressive mitotic cycles to become type-B spermatogonia.
Type-B spermatogonia are progenitor cells that will differentiate
into primary spermatocytes. Soon after their formation, these
cells enter the prophase of the first meiotic division. Since the
prophase of this division takes about 22 days, the majority of
spermatocytes seen in sections will be in this phase. The primary
spermatocytes are the largest cells of the spermatogenic lineage
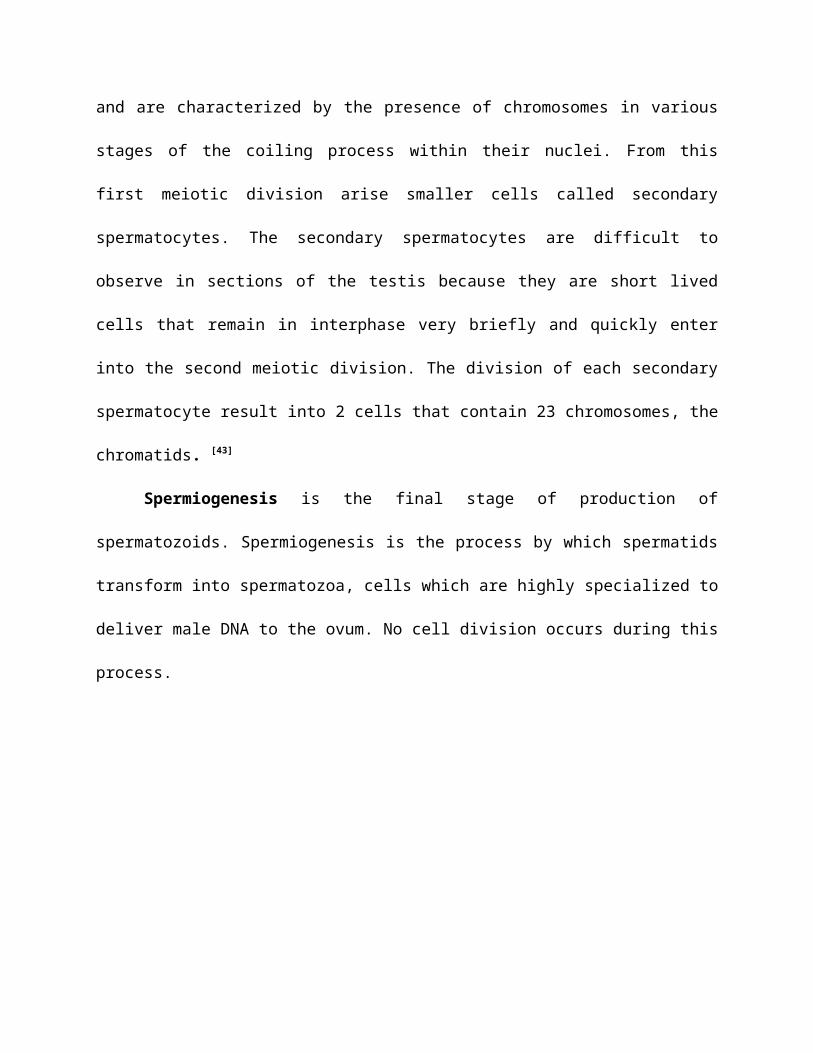
and are characterized by the presence of chromosomes in various
stages of the coiling process within their nuclei. From this
first meiotic division arise smaller cells called secondary
spermatocytes. The secondary spermatocytes are difficult to
observe in sections of the testis because they are short lived
cells that remain in interphase very briefly and quickly enter
into the second meiotic division. The division of each secondary
spermatocyte result into 2 cells that contain 23 chromosomes, the
chromatids. [43]
Spermiogenesis is the final stage of production of
spermatozoids. Spermiogenesis is the process by which spermatids
transform into spermatozoa, cells which are highly specialized to
deliver male DNA to the ovum. No cell division occurs during this
process.
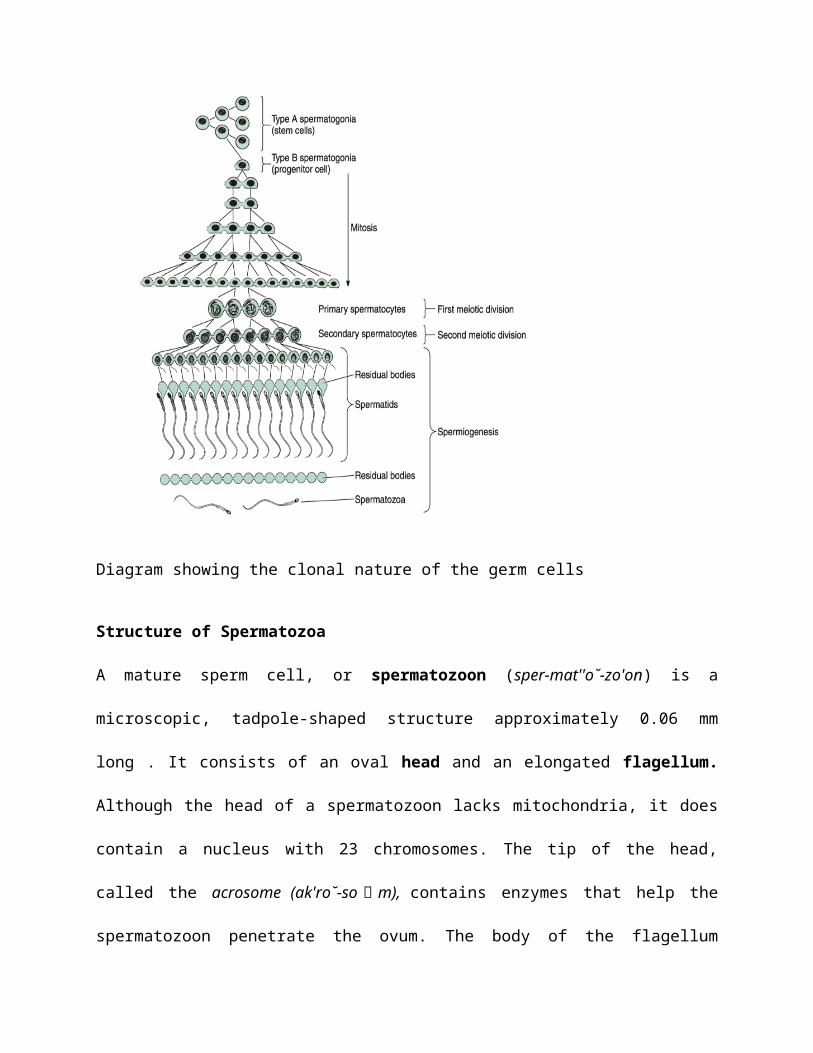
Diagram showing the clonal nature of the germ cells
Structure of Spermatozoa
A mature sperm cell, or spermatozoon (sper-mat''o˘-zo'on) is a
microscopic, tadpole-shaped structure approximately 0.06 mm
long . It consists of an oval head and an elongated flagellum.
Although the head of a spermatozoon lacks mitochondria, it does
contain a nucleus with 23 chromosomes. The tip of the head,
called the acrosome (ak'ro˘-so  ̄ m), contains enzymes that help the
spermatozoon penetrate the ovum. The body of the flagellum
contains numerous mitochondria spiraled around a filamentous
core. The mitochondria provide the energy necessary for
locomotion. The flagellum propels the spermatozoon with a lashing
movement. The maximum unassisted rate of spermatozoa movement is
about 3 mm per hour.
Semen
Semen, also called seminal fluid, is the substance discharged during
ejaculation (table 20.4). Generally, between 1.5 and 5.0 ml of
semen are ejected during ejaculation. The bulk of the fluid
(about 60%) is produced by the seminal vesicles, and the rest
(about 40%) is contributed by the prostate. Spermatozoa account
for less than 1% of the volume. There are usually between 60 and
150 million sperm cells per milliliter of ejaculate. In the
condition of oligospermia (ol''ı˘-go-sper'me-a˘), the male ejaculates fewer
than 10 million sperm cells per milliliter and is likely to have
fertility problems. [41]
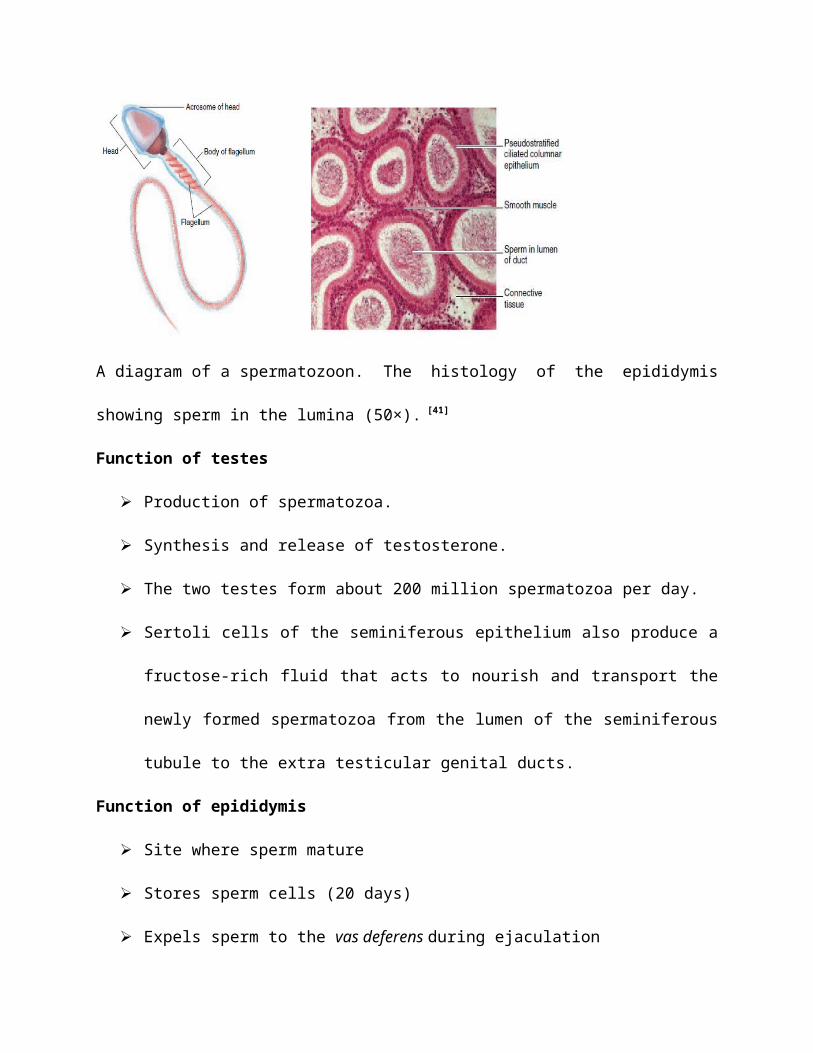
A diagram of a spermatozoon. The histology of the epididymis
showing sperm in the lumina (50×). [41]
Function of testes
Production of spermatozoa.
Synthesis and release of testosterone.
The two testes form about 200 million spermatozoa per day.
Sertoli cells of the seminiferous epithelium also produce a
fructose-rich fluid that acts to nourish and transport the
newly formed spermatozoa from the lumen of the seminiferous
tubule to the extra testicular genital ducts.
Function of epididymis
Site where sperm mature
Stores sperm cells (20 days)
Expels sperm to the vas deferens during ejaculation

CHAPTER THREE
3.0 MATERIALS AND METHODS
The materials used in the accomplishment of this project
includes Nifedipine, Petri dish, Wistar rats (17),microtome, Water
bowl, Beaker, Calibrated syringe, Basket, Cannula, Animal cage,
Dissecting set, Condensation, Cotton wool, Oven, Water bath,
Plastic mould, Paraffin wax, Filter paper, Wooden block, Wash
hand basin, Measuring cylinder, weighing balance, Stationeries,
Light Microscope, Conical flask, Industrial salt (NaCl), Spatula,
Absolute alcohol, Dissecting kits, Xylene solution,
paraformaldehyde solution, formalin solution, specimen bottles,
Haematoxylin stain, Eosin stain, Slides.
3.1 BREEDING OF ANIMALS
Seventeen adult albino rats comprising of males only were
obtained with an average weight of 140 g. The rats after
procurement were subsequently housed in cages under light and
dark cycle at room temperature in the experimental animal house
of the department of anatomy, university of Ilorin. Proper
aeration was maintained and ensuring cross ventilation throughout
the animal house. They were fed with rat pelletized feed and
water was given. The feeds were obtained from Bendel feeds
Nigeria limited, Yoruba road, Ilorin. The rats were left to
acclimatize before treatment was carried out.
3.2 GROUPING OF ANIMALS
The rats were divided into three groups using a simple random
sampling as follows: two experimental groups and one control
group.
Control group (n=5), they were neither treated with 2ml of
distilled water.
Low dose group: (n=6), they were treated with 0.3mg/kg body
weight.
Higher dose group: (n=6), they were treated with 0.6mg/kg body
weight
3.3 PREPARATION OF NIFEDIPINE SOLUTION AND DOSAGE
Nifedipine tablets, each weighing 60mg, produced by Bayer
Schering Pharma AG 51368 Leverkusen, Germany, Nigeria Reg No: A4-
2373, manufacture date: 10-11-2010, Expiration: 10-11-2004.
5 tablets was slightly crushed and dissolved in distilled water
for about 4dyas for achieve total dissolution.
Calculation of dosage: since the therapeutic use of
Nifedipine is between 20mg to 90mg and since normal physiological
man weighs 70kg, therefore: 20mg70kg=0.3mgkg -1 therefore the
minimal dose given was 0.3mg/kg while the maximal dose group was
multiply by 2 therefore 2*0.3mg/kg ¿0.6mgkg -1
3.4 TREATMENT OF ANIMALS
Treatment was done orally using oral cannula and it lasted for 25
days.
Control group: 2ml of distilled water.
Low dose group: 0.3mg/kg body weight.
Higher dose group: 0.6mg/kg body weight.
Termination of treatment
After 25th day the rats were sacrificed to remove the male
reproductive system (testis and epididymis.
3.5 BODY AND ORGAN WEIGHT
The body weights were taken every 72 hours using weighing
balance.
3.6 SACRIFICE
At the end of the 25th day of treatment, the animals were
anaesthetized by giving katamine hydrochloride 25mg
interperitoneally (IP), then thoracolaparactomy was performed to
open the thorax and the abdomen, the epididymis was collected,
blood was taken from the heart through the right ventricle, total
body perfusion was done by using normal saline firstly to remove
the blood from vascular space followed by the introduction of 4%
paraformaldehyde for general body fixation which is then followed
by the removal of necessary organs.
3.7 TISSUE HOMOGENIZATION
The epididymis was homogenized in 1ml of normal saline mixed and
counted, and the collected blood was centrifuged at 2000 rpm for
20 min. The supernatant was subsequently collected and analysed
for hormonal bioassay (testosterone, LH, FSH).
HAEMATOLOGICAL ANALYSIS
The full blood count analysis include, packed cell volume (PCV),
white blood cell (WBC) count, red blood cell(RBC) count, and
blood film morphology, which may include differential count and
others.
The blood samples collected from the animals were stored in EDTA
bottles from which they were collected in time to run the
analysis.
PACKED CELL VOLUME PROCEDURE
The plain capillary tube was filled to 2/3 of its volume with the
blood and sealed at one end with plasticine. They were then
placed on the microhaematocrit centrifuge and centrifuged for 5
minutes at 10,000 rpm. After the centrifugation, the spun blood
was placed in the groove column of the microhaematocrit reader.
The packed cell volume was read as follows;
1. Allow the bottom level of the packed cells to stay at the
zero mark
2. Allow the top plasma level to stay at 100 mark.
3. Use the adjustable slanting mover to stay at the meniscus
level of the plasma/blood cells.
4. The reading of the pack can now be recorded.
WHITE BLOOD CELL COUNT PROCEDURE
0.02m/s of the blood sample of each rat was added to 0.38m/s of
diluting fluid (Turk’s solution) and allowed to mix well. The
counting chamber to be used is then cleaned and the cover slip
fixed. A few drops of the mixed blood sample and Turk’s solution
were charged into the counting chamber. The cells were allowed to
settle by placing on a firm bench for few minutes; four (4) big
squares of sixteen (16) smaller squares were counted.
The WBC count was calculated with the formula below
WBC = (number of cells counted ÷ depth of the counting
chamber) ×dilution ratio
Dilution ration for WBC count is 1:20
RED BLOOD CELL COUNT PROCEDURE
0.02ml of the blood sample of each rat was added to 4ml of
diluting fluid (formal citrate) and allowed to mix well for 2
minutes by tilting for proper reaction. After few drops had been
charged into the counting chamber as explained above, it is left
for 2 minutes before counting. The cells in 80 or 160 smaller
squares, including the cells that touch the bottom and left-hand
margins of the small square are counted.
The RBC count was calculated using the formula below:
RBC = (number of cells counted/volume counted) ×dilution
ratio×106
Dilution ratio is 1:200
LEISHMAN STAINING PROCEDURE
The slides were placed in a staining rack and the Leish-man stain
was applied for 2 minutes, few drops of 6.8pH was added and
allowed to act for 7 minutes. The slides where washed with 6.8pH
buffer solution and allow to air dry. The slides were then
examined and counting was done under the microscope at an (oil
immersion) objective magnification (×100).
SEMINAL ANALYSIS PROCEDURE
The semen analysis was done to determine the sperm count,
progressivity, motility and morphology.
In this study, epididymal sperm count, motility, morphology,
sperm motility was done immediately after semen collection,
whereby a rubber pipette was used to take small quantity of the
semen mixed with normal saline and drop it on a glass slide for
viewing under microscope, using an x40 objective magnification
with reduced light. Sperm counts were carried out using the
Neubeurs Haemocytometer counting chamber.
Progressivity was graded as follows:
A – Excellent forward directional movement (EFDM)
B – Good forward directional movement (GFDM)
C – Fair forward directional movement (FFDM)
D – Poor forward directional movement (PFDM)
(W.H.O, 1976).
HORMONAL ASSAY PROCEDURES
Similar procedure is required for all the hormones tested for,
which is analysed bellow
Immunoenzymometric assay: the essential reagents required for an
Immunoenzymometric assay include high affinity and specificity
antibodies (enzyme and immobilized), with different and distinct
epitope recognition, in excess, and in native antigen. In this
procedure, the immobilization takes place during the assay at the
surface of a microplate well through the interaction of
streptavidin coated on the well and exogenously added
biotinylated monocional anti-hormone assay for (LH, progesterone,
FSH) antibody.
upon mixing monoclonal biotinylated antibody, the enzyme label
antibody and a serum containing the native antigen, reaction
results between the native antigen and antibodies without
competition or steric hindrance to form a soluble sandwich
complex. The interaction is illustrated by the following
equation:
EnzAb(p) +AgLH +BtnAb(m) EnzAb(p).AgLH.BtnAb(m)
BtnAb(m)= Biotinylated Monoclonal Antibody (Excess Quality)
AgLH= Native Antigen (Variable Quantity)
EnzAb(p)= Enzyme labelled Antibody (Excess Quantity)
EnzAb(p)-AgLH-BtnAb(m) = Antigen-Antibodies Sandwich Complex
Ka = Rate Constant of Association
K-a = Rate Constant of Dissociation
Simultaneously, the complex is deposited to the well through the
high affinity reaction of streptavidinn and biotinylated
antibody.
This reaction is illustrated bellow:
EnzAb(p)-AgLH-BtnAb(m) + streptavidinnc.w. =immobilized complex
Streptavindinc.w. = streptavidin immobilized on well
Immobilized complex = Antibodies-Antigen sandwich bound.
After equilibrium is attained, the antibody-bound fraction is
separated from unbound antigen by decantation or aspiration. The
activity in the antibody-bound fraction is directly proportional
to the native antigen concentration. By utilizing several
different serum reference of known antigen values, a dose
response curve can be generated from which the antigen
concentration of an unknown can be ascertained.
REAGENT PREPARATION
1. Wash buffer
Dilute contents of wash concentrate to 100ml with distilled or
deionized water in a suitable storage container. Stored at 2-30C
for up to 60days.
2. Working Substrate Solution.
Pour the contents of the amber vial labelled Solution ‘A’ into
the clear vial labelled Solution ‘B’. Place the yellow cap on the
clear vial for easy identification. Mix and labelled accordingly.
TEST PROCEDURE
1. Format the microplate wells for each serum reference,
control and patient specimen to be assayed in duplicate.
Replace any unused microwell strips into the aluminium bag,
seal and stored at 2-8oC.
2. Pipette 0.050ml (50µl) of the appropriate serum reference,
control or specimen into the assigned well.
3. Add 0.100ml (100µl) of the assay hormone-Enzyme Reagent to
all wells.
4. Swirl the microplate gently for 20-30 seconds to mix and
cover.
5. Incubate 60 minutes at room temperature.
6. Discard the contents of the microplate by decantation or
aspiration. If decanting blot the plate dry with absorbent
paper.
7. Add 350ul of wash buffer decant or aspirate. Repeat two (2)
additional times for a total of three (3) washes. An
automatic or manual plate washer can be used.
8. Add 0.100ml (100µl) of working substrate solution to all
wells; always add reagents in the same order to minimize
reaction time differences between wells.
9. Incubate room temperature for fifteen (15) times.
10. Add 0.050ml (50µl) of stop solution to each well and
gently mix for 15-20 seconds.
11. Read the absorbance in each well at 450nm (using a
reference wavelength of 620-630nm to minimize well
imperfections) in a microplate reader. And the result should
be read within 30 minutes of adding the stop solution.
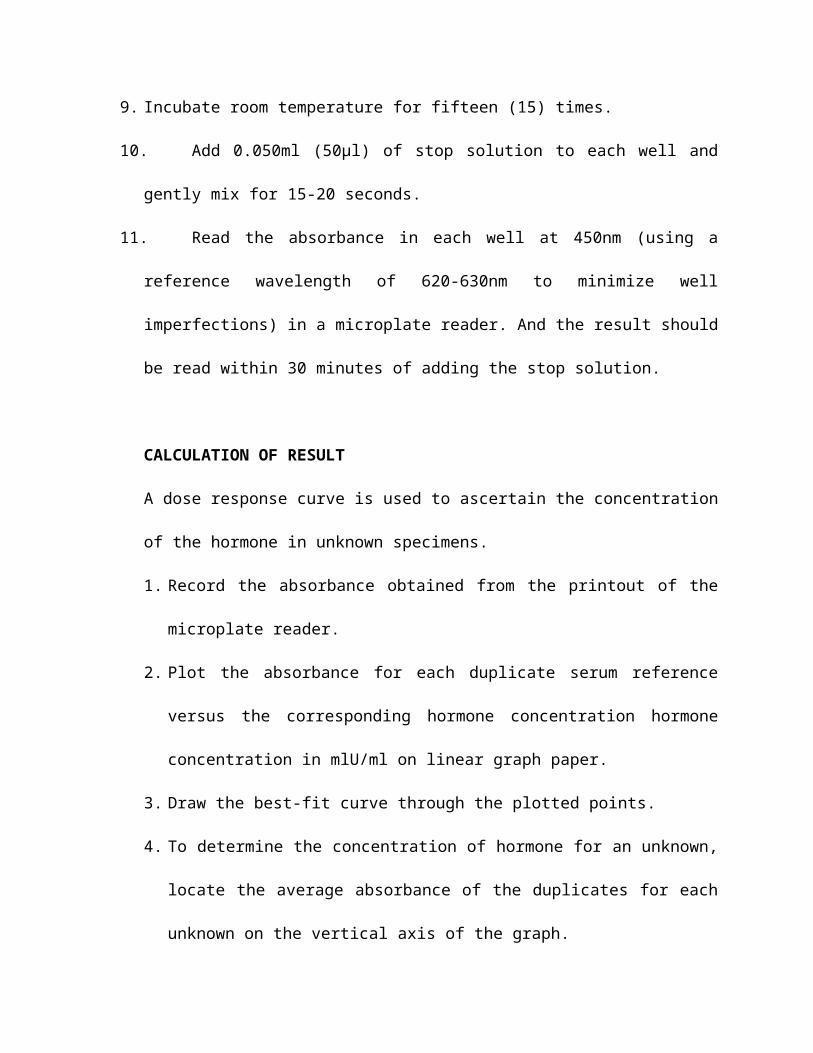
CALCULATION OF RESULT
A dose response curve is used to ascertain the concentration
of the hormone in unknown specimens.
1. Record the absorbance obtained from the printout of the
microplate reader.
2. Plot the absorbance for each duplicate serum reference
versus the corresponding hormone concentration hormone
concentration in mlU/ml on linear graph paper.
3. Draw the best-fit curve through the plotted points.
4. To determine the concentration of hormone for an unknown,
locate the average absorbance of the duplicates for each
unknown on the vertical axis of the graph.
0 1 2 3 4 5 6 7 8 9 10 11 120
0.51
1.52
2.5
Serum Testosterone
Conc. ng/ml
Absorbance
Graph 1: showing the standard curve used for the calculation of
the serum testosterone.
0 5 10 15 20 25 30 35 40 45 50 55 600
0.51
1.52
Serum Progesterone
Conc. ng/ml
Absorbance
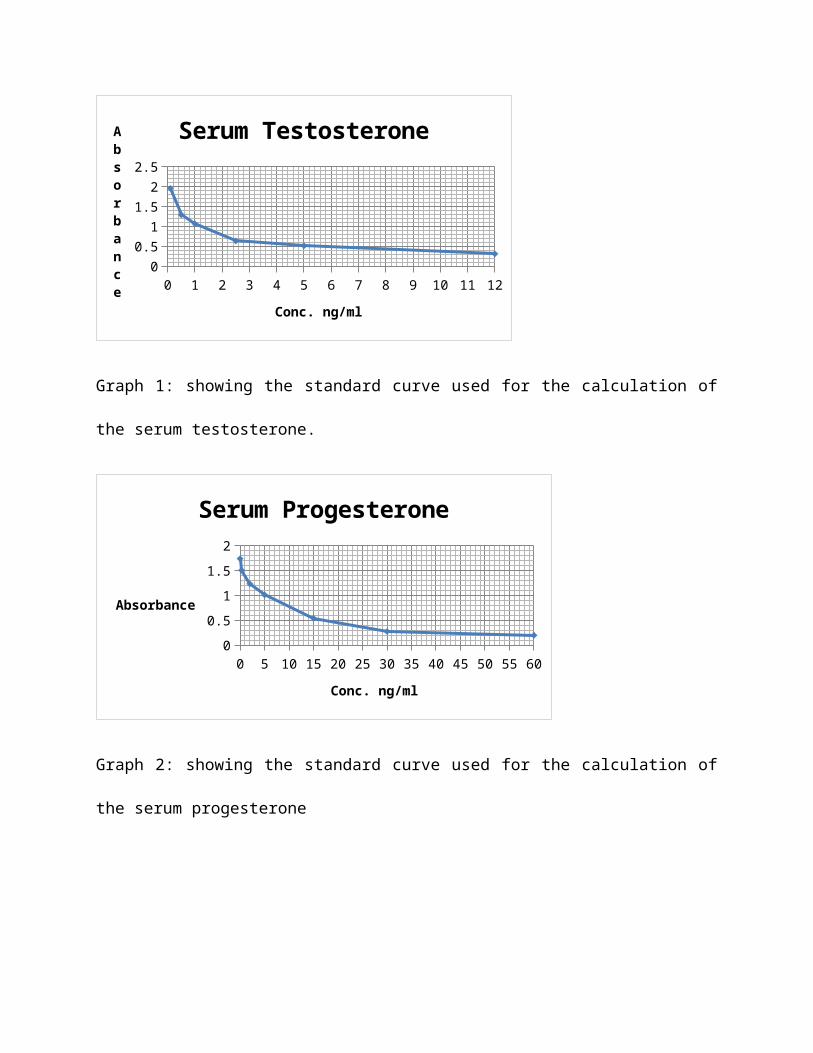
Graph 2: showing the standard curve used for the calculation of
the serum progesterone
0250
500
7501000
1250
1500
1750
2000
2250
2500
2750
3000
0
1
2
Serum Estradiol
Conc. pg/ml
Absorbance
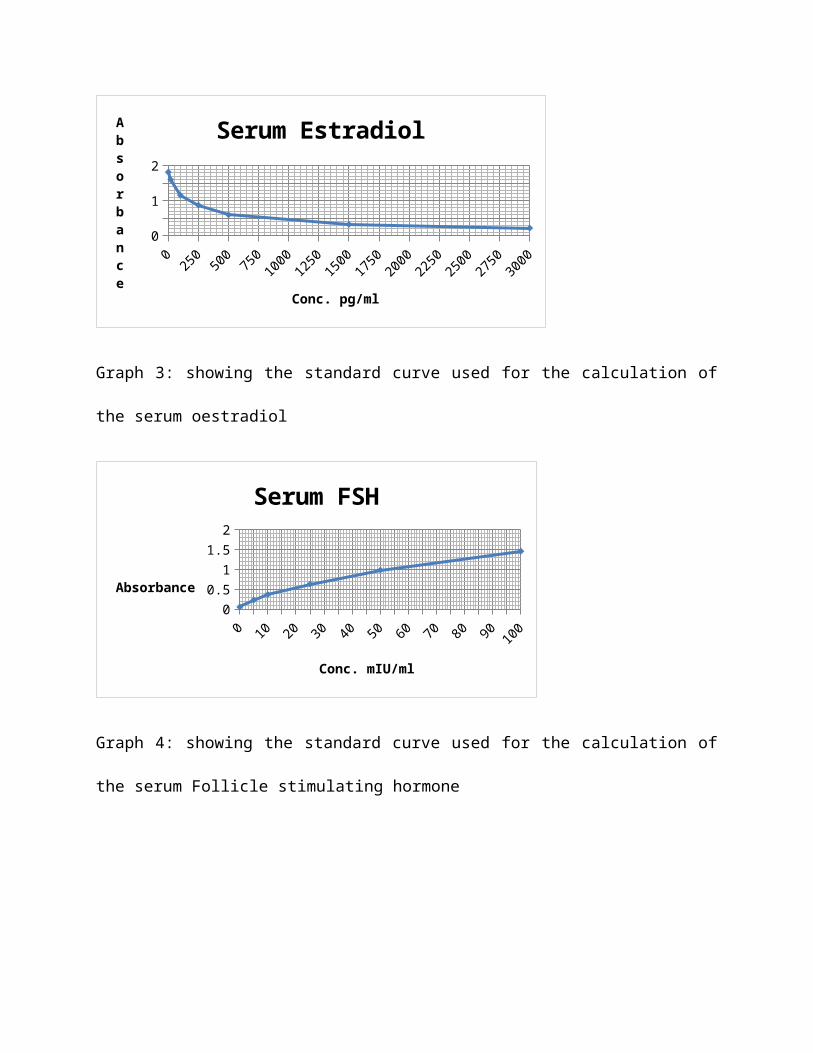
Graph 3: showing the standard curve used for the calculation of
the serum oestradiol
0 10 20 30 40 50 60 70 80 90 100
00.51
1.52
Serum FSH
Conc. mIU/ml
Absorbance
Graph 4: showing the standard curve used for the calculation of
the serum Follicle stimulating hormone
0 25 50 75 100 125 150 175 2000
1
2
Serum LH
Conc. mIU/ml
Absorbance
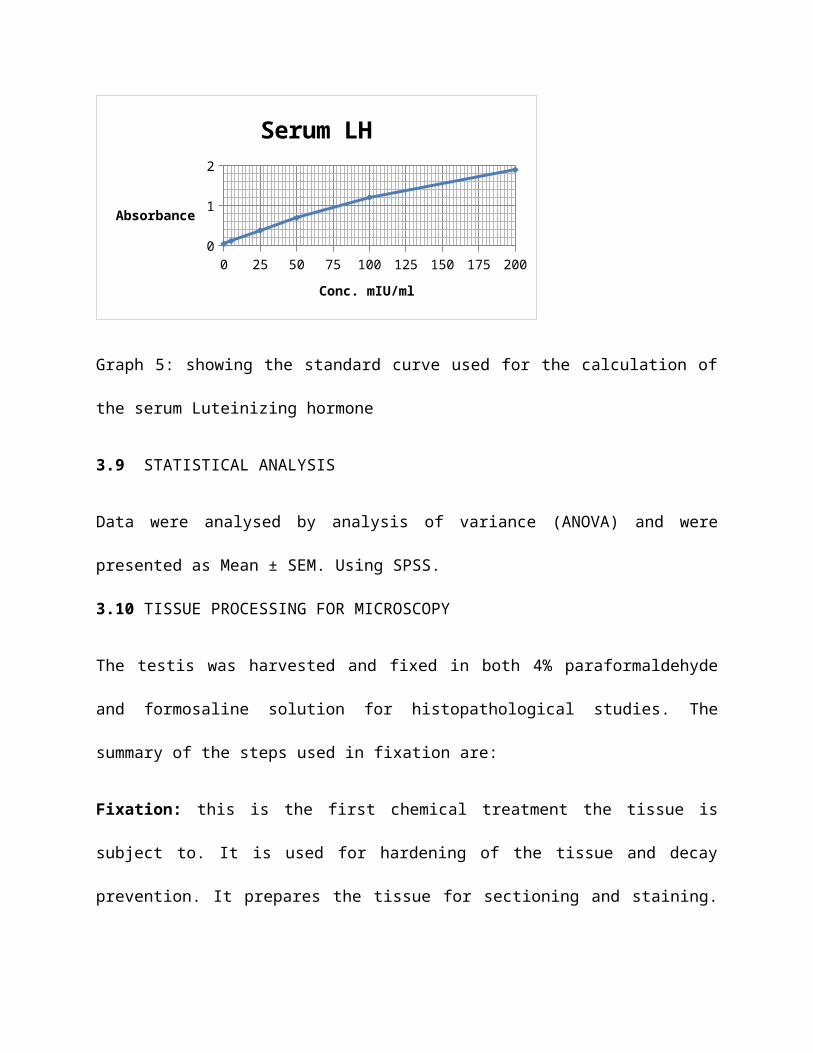
Graph 5: showing the standard curve used for the calculation of
the serum Luteinizing hormone
3.9 STATISTICAL ANALYSIS
Data were analysed by analysis of variance (ANOVA) and were
presented as Mean ± SEM. Using SPSS.
3.10 TISSUE PROCESSING FOR MICROSCOPY
The testis was harvested and fixed in both 4% paraformaldehyde
and formosaline solution for histopathological studies. The
summary of the steps used in fixation are:
Fixation: this is the first chemical treatment the tissue is
subject to. It is used for hardening of the tissue and decay
prevention. It prepares the tissue for sectioning and staining.
The testis tissue was fixed in 4% paraformaldehyde and some in
formosaline solution.
Dehydration: this is the removal of water from tissue during its
preparation for microscopical study, by placing it successively
in strong solutions of alcohol i.e. from 70%, 90%, and absolute
alcohol.
Clearing: this is the process of removing the cloudiness from
microscopical specimens after dehydration by means of two changes
in xylene. The xylene increases the transparency of the testis
tissue.
Infiltration/Impregnation: the tissues were transferred into two
changes of molten paraffin wax in an oven which was maintained at
about 55 °C for removal of the xylene. Each infiltration step was
left for about 1 hour each.
Embedding: this is the fixing of a specimen within a mass of firm
material in order to facilitate the cutting of thin sections for
microscopy. An embedding mould was used to keep the specimen
intact.
Sectioning: cutting of excess wax to expose the embedded tissues
preceded this part. The rotator microtome was adjusted to 4 µ and
the microtome knife was placed at an angle of about 45 °C to the
block. The ribbon obtained was placed on albumenized slide. Water
was added to spread the section, thereafter the slides were
placed on hot plate to dry off the water on the slide and melt
the wax leaving the section.
Staining and Mounting: the slides were stained with haematoxylin
and eosin (H & E) and mounted with DPX (Dextrin-tricresol
phthalate xylene), and cover slip is used.
CHAPTER FOUR
MORPHOLOGICAL OBSERVATIONS
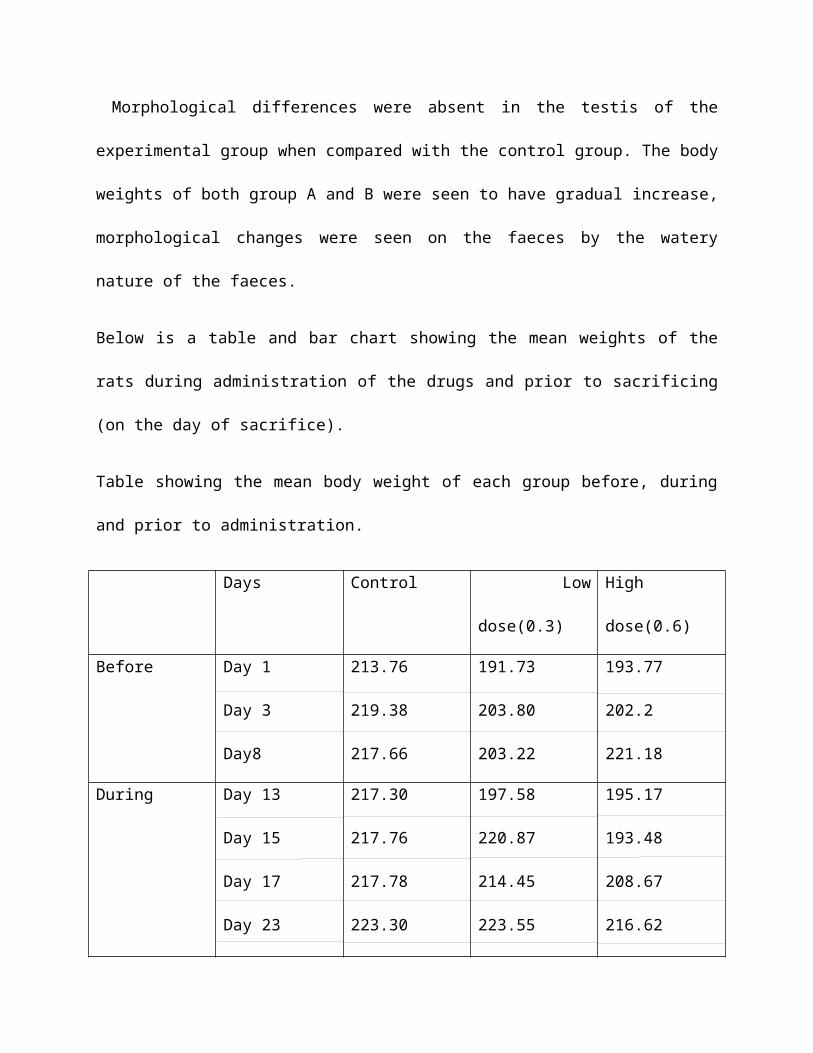
Morphological differences were absent in the testis of the
experimental group when compared with the control group. The body
weights of both group A and B were seen to have gradual increase,
morphological changes were seen on the faeces by the watery
nature of the faeces.
Below is a table and bar chart showing the mean weights of the
rats during administration of the drugs and prior to sacrificing
(on the day of sacrifice).
Table showing the mean body weight of each group before, during
and prior to administration.
Days Control Low
dose(0.3)
High
dose(0.6)
Before Day 1
Day 3
Day8
213.76
219.38
217.66
191.73
203.80
203.22
193.77
202.2
221.18
During Day 13
Day 15
Day 17
Day 23
217.30
217.76
217.78
223.30
197.58
220.87
214.45
223.55
195.17
193.48
208.67
216.62
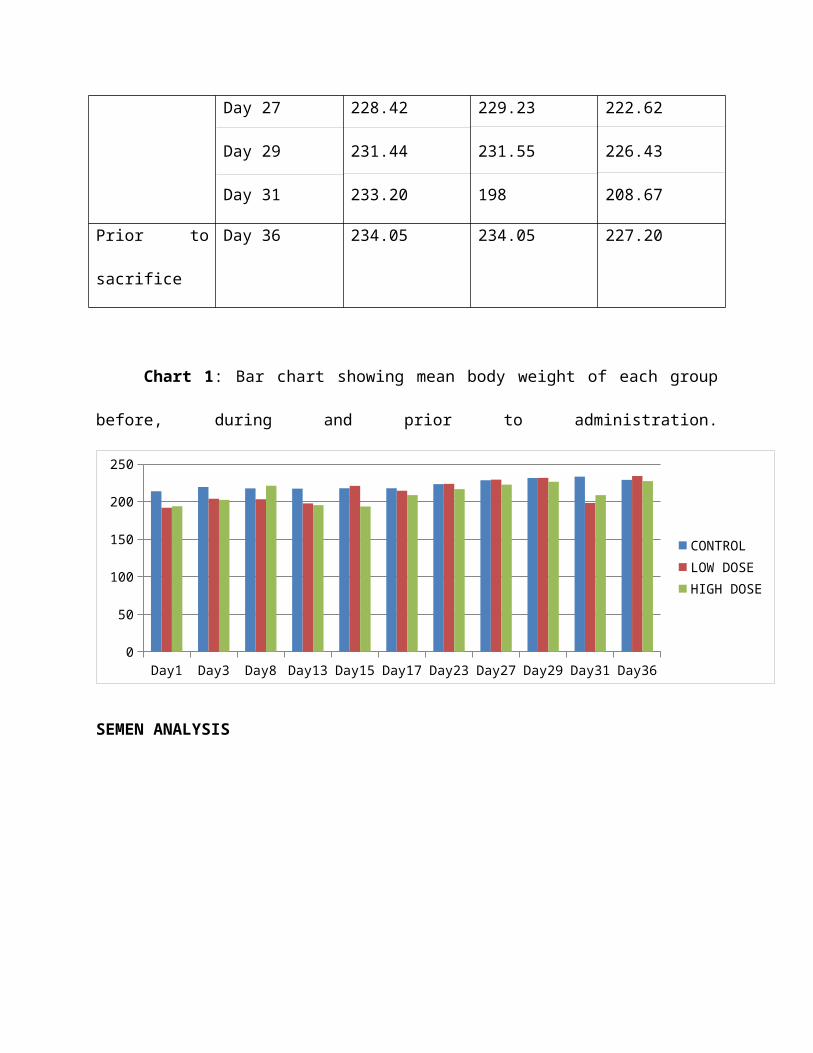
Day 27
Day 29
Day 31
228.42
231.44
233.20
229.23
231.55
198
222.62
226.43
208.67
Prior to
sacrifice
Day 36 234.05 234.05 227.20
Chart 1: Bar chart showing mean body weight of each group
before, during and prior to administration.
Day1 Day3 Day8 Day13 Day15 Day17 Day23 Day27 Day29 Day31 Day360
50
100
150
200
250
CONTROLLOW DOSEHIGH DOSE
SEMEN ANALYSIS
CONTROL LOW DOSE HIGH DOSE52
54
56
58
60
62
64
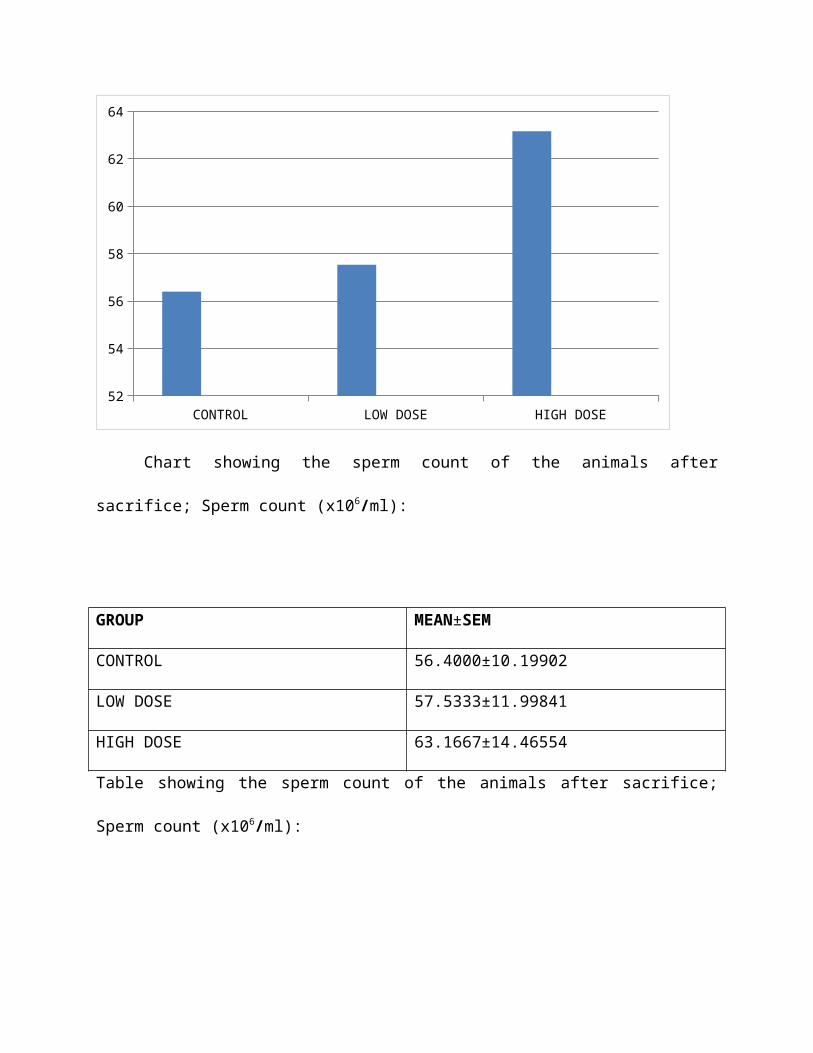
Chart showing the sperm count of the animals after
sacrifice; Sperm count (x106/ml):
GROUP MEAN±SEM
CONTROL 56.4000±10.19902
LOW DOSE 57.5333±11.99841
HIGH DOSE 63.1667±14.46554
Table showing the sperm count of the animals after sacrifice;
Sperm count (x106/ml):
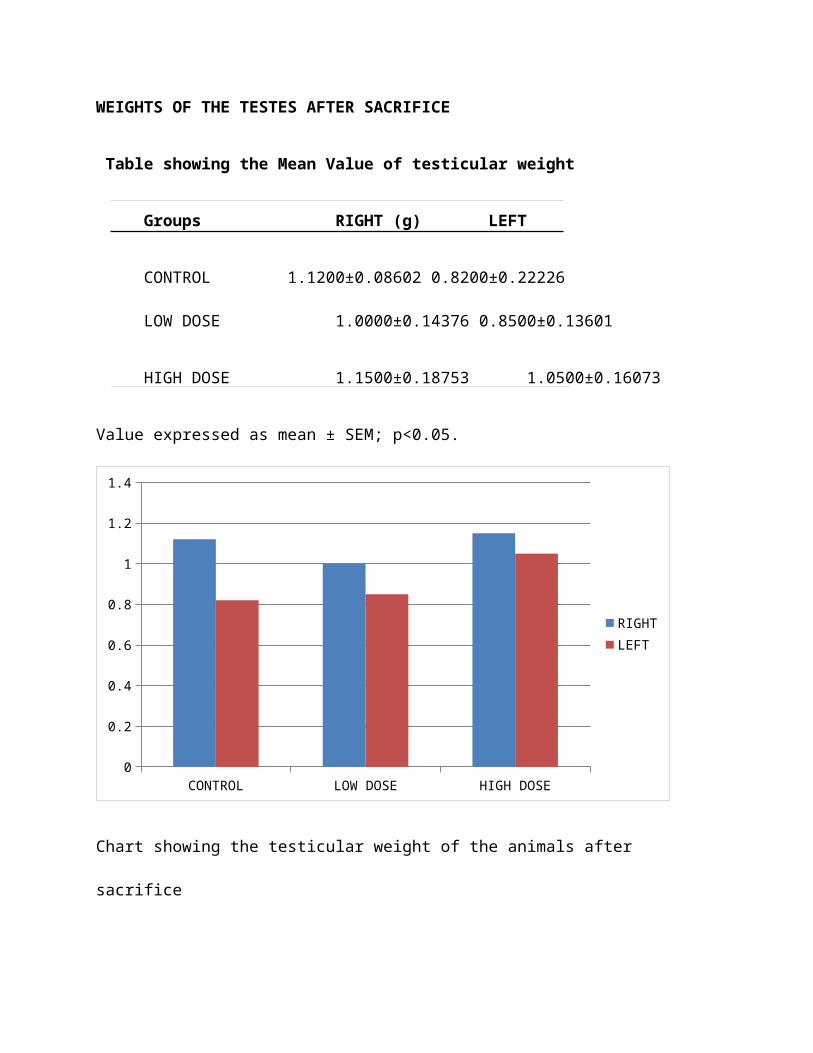
WEIGHTS OF THE TESTES AFTER SACRIFICE
Table showing the Mean Value of testicular weight
Groups RIGHT (g) LEFT
CONTROL 1.1200±0.08602 0.8200±0.22226
LOW DOSE 1.0000±0.14376 0.8500±0.13601
HIGH DOSE 1.1500±0.18753 1.0500±0.16073
Value expressed as mean ± SEM; p<0.05.
CONTROL LOW DOSE HIGH DOSE0
0.2
0.4
0.6
0.8
1
1.2
1.4
RIGHTLEFT
Chart showing the testicular weight of the animals after
sacrifice
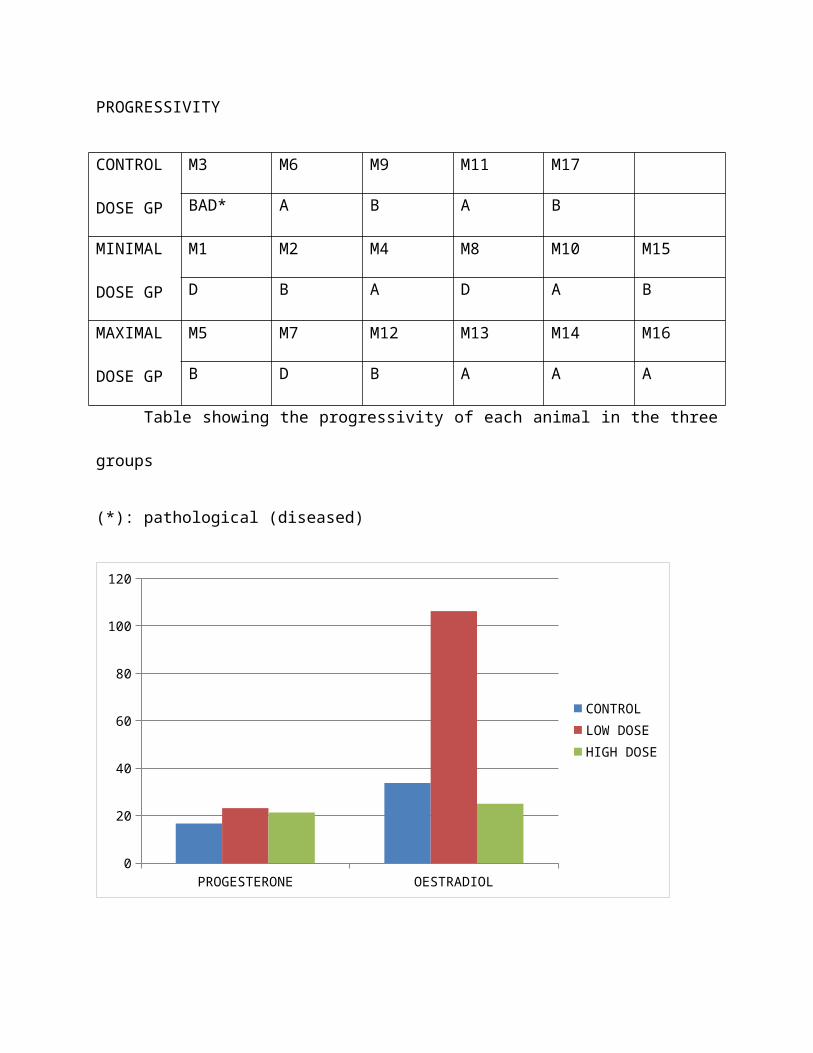
PROGRESSIVITY
CONTROL
DOSE GP
M3 M6 M9 M11 M17
BAD* A B A B
MINIMAL
DOSE GP
M1 M2 M4 M8 M10 M15
D B A D A B
MAXIMAL
DOSE GP
M5 M7 M12 M13 M14 M16
B D B A A A
Table showing the progressivity of each animal in the three
groups
(*): pathological (diseased)
PROGESTERONE OESTRADIOL0
20
40
60
80
100
120
CONTROLLOW DOSEHIGH DOSE
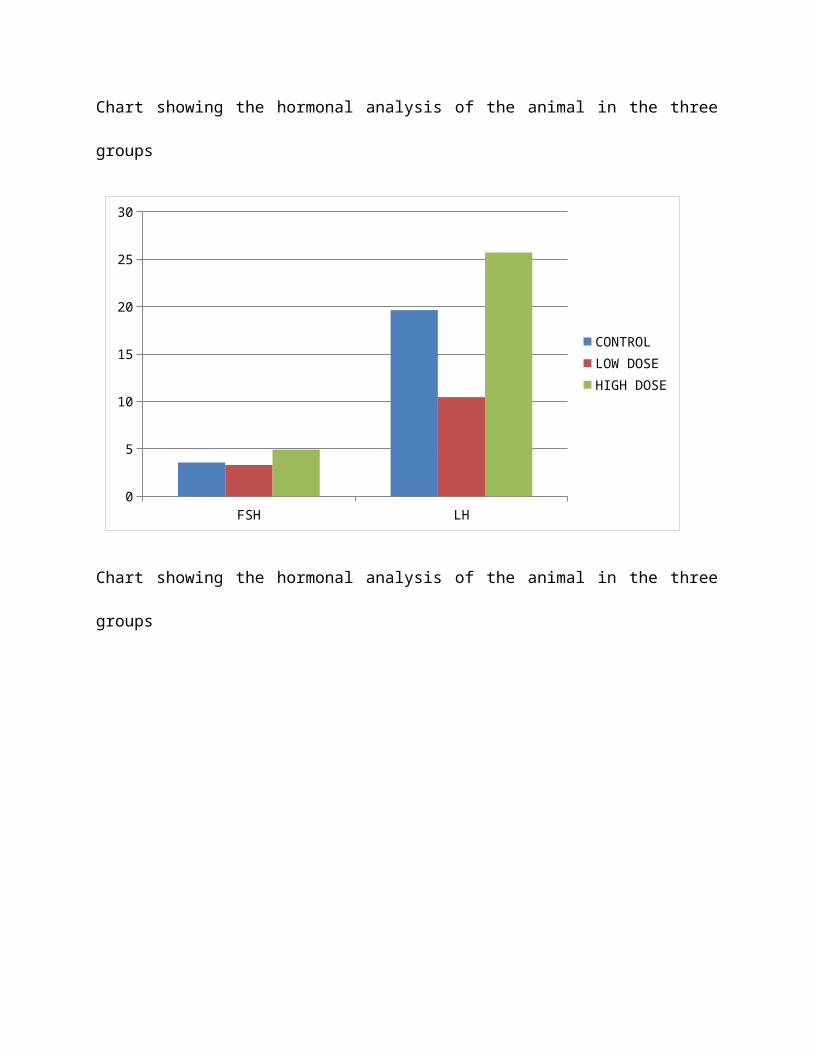
Chart showing the hormonal analysis of the animal in the three
groups
FSH LH0
5
10
15
20
25
30
CONTROLLOW DOSEHIGH DOSE
Chart showing the hormonal analysis of the animal in the three
groups
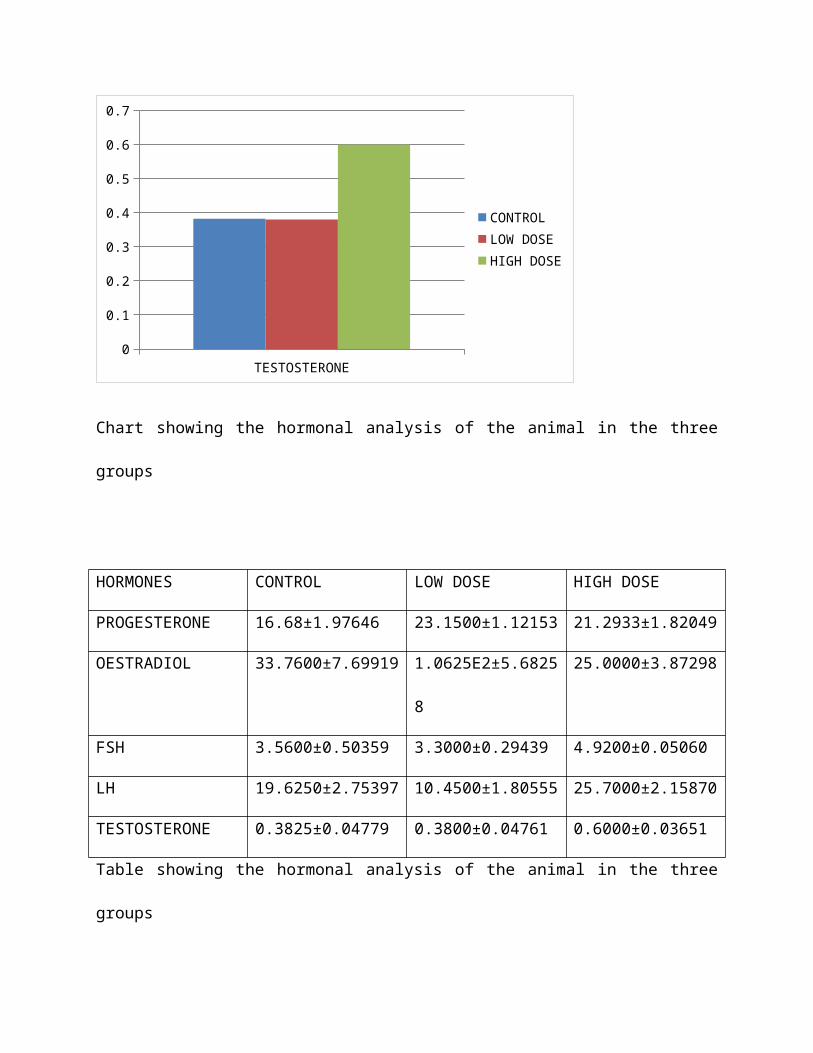
TESTOSTERONE0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
CONTROLLOW DOSEHIGH DOSE
Chart showing the hormonal analysis of the animal in the three
groups
HORMONES CONTROL LOW DOSE HIGH DOSE
PROGESTERONE 16.68±1.97646 23.1500±1.12153 21.2933±1.82049
OESTRADIOL 33.7600±7.69919 1.0625E2±5.6825
8
25.0000±3.87298
FSH 3.5600±0.50359 3.3000±0.29439 4.9200±0.05060
LH 19.6250±2.75397 10.4500±1.80555 25.7000±2.15870
TESTOSTERONE 0.3825±0.04779 0.3800±0.04761 0.6000±0.03651
Table showing the hormonal analysis of the animal in the three
groups
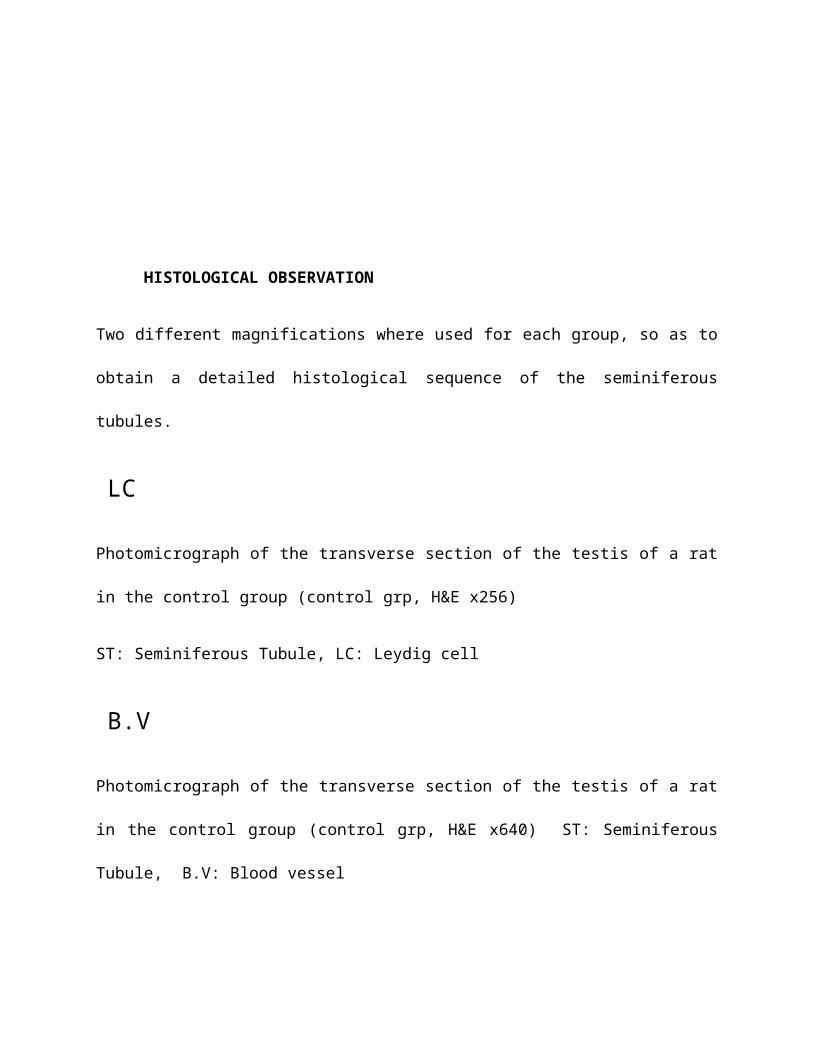
HISTOLOGICAL OBSERVATION
Two different magnifications where used for each group, so as to
obtain a detailed histological sequence of the seminiferous
tubules.
Photomicrograph of the transverse section of the testis of a rat
in the control group (control grp, H&E x256)
ST: Seminiferous Tubule, LC: Leydig cell
Photomicrograph of the transverse section of the testis of a rat
in the control group (control grp, H&E x640) ST: Seminiferous
Tubule, B.V: Blood vessel
LC
B.V
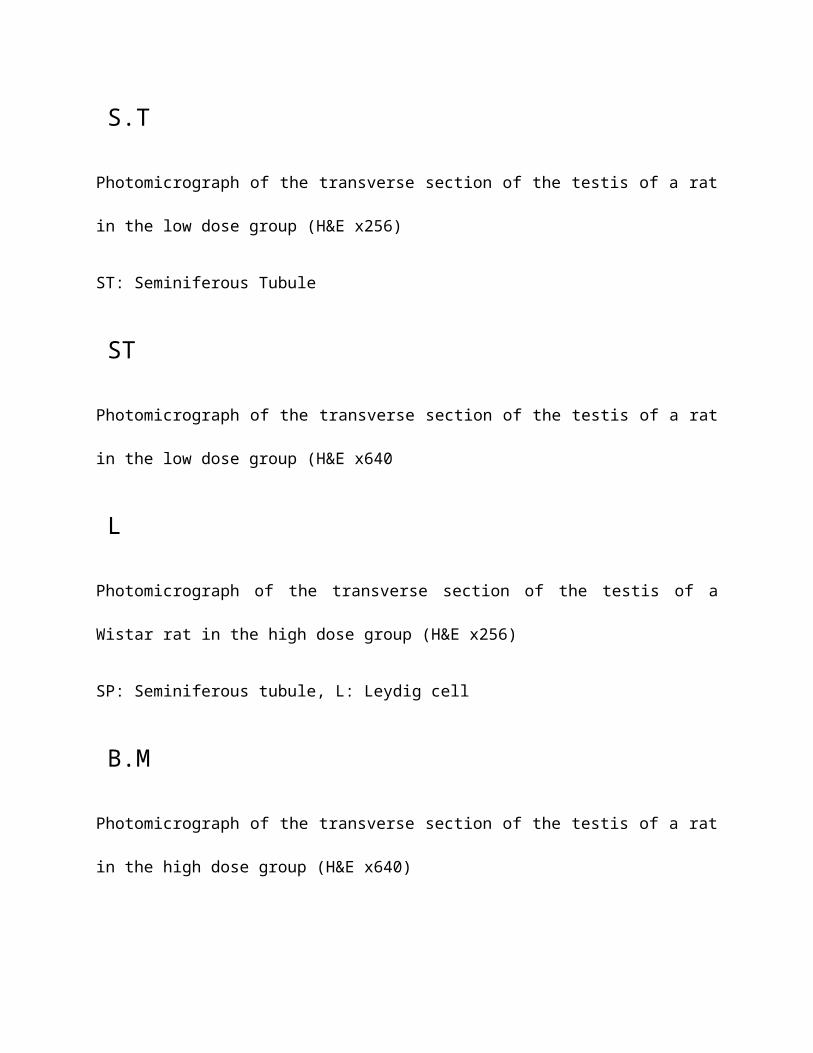
Photomicrograph of the transverse section of the testis of a rat
in the low dose group (H&E x256)
ST: Seminiferous Tubule
Photomicrograph of the transverse section of the testis of a rat
in the low dose group (H&E x640
Photomicrograph of the transverse section of the testis of a
Wistar rat in the high dose group (H&E x256)
SP: Seminiferous tubule, L: Leydig cell
Photomicrograph of the transverse section of the testis of a rat
in the high dose group (H&E x640)
S.T
ST
L
B.M
ST: Spermatids, SC: Spermatocytes, SG: Spermatogonium, M: Myoid
cells
B.M: Basement Membrane
HAEMATOLOGICAL OBSERVATIONS
The tables below show the mean results of haematological analysis
of the blood samples of in the three groups.
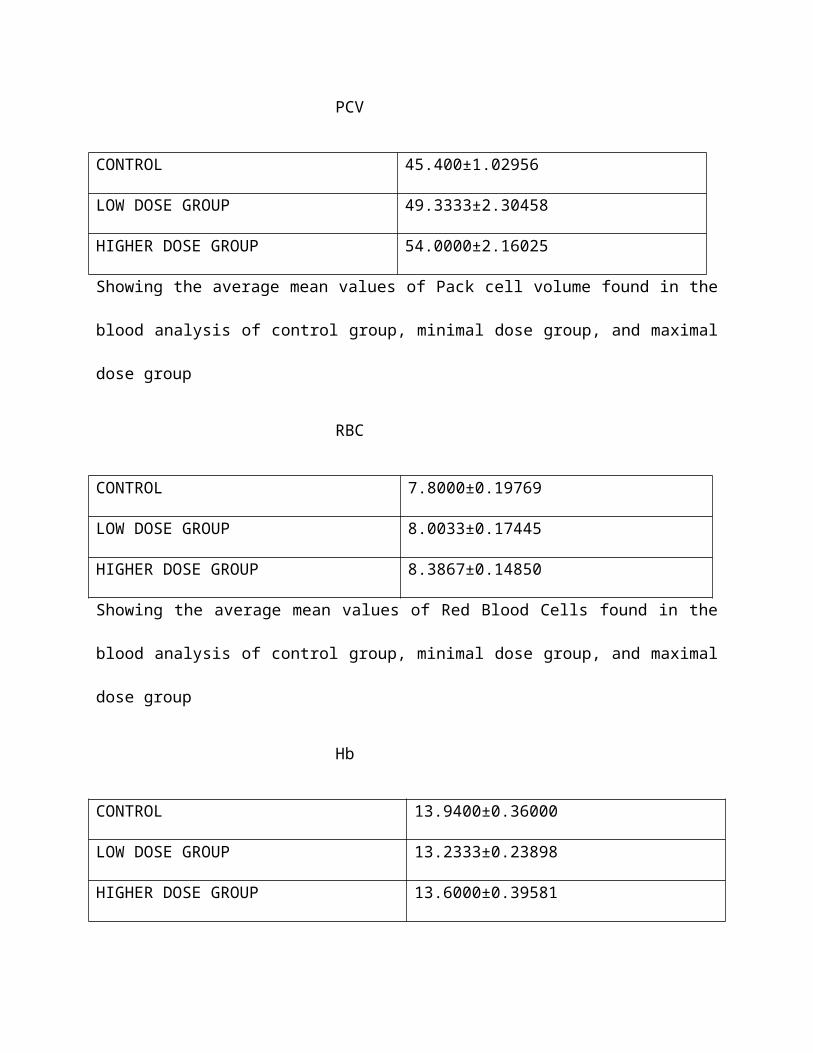
PCV
CONTROL 45.400±1.02956
LOW DOSE GROUP 49.3333±2.30458
HIGHER DOSE GROUP 54.0000±2.16025
Showing the average mean values of Pack cell volume found in the
blood analysis of control group, minimal dose group, and maximal
dose group
RBC
CONTROL 7.8000±0.19769
LOW DOSE GROUP 8.0033±0.17445
HIGHER DOSE GROUP 8.3867±0.14850
Showing the average mean values of Red Blood Cells found in the
blood analysis of control group, minimal dose group, and maximal
dose group
Hb
CONTROL 13.9400±0.36000
LOW DOSE GROUP 13.2333±0.23898
HIGHER DOSE GROUP 13.6000±0.39581
Showing the average mean values of Haemoglobin found in the blood
analysis of control group, minimal dose group, and maximal dose
group
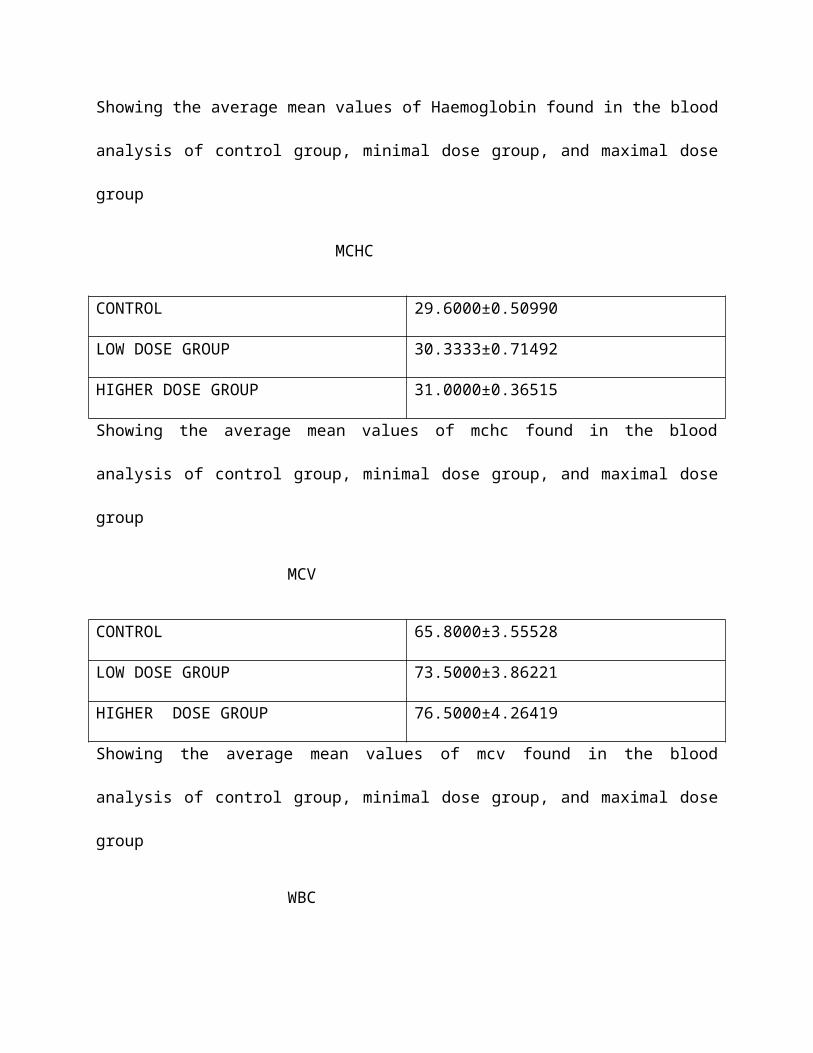
MCHC
CONTROL 29.6000±0.50990
LOW DOSE GROUP 30.3333±0.71492
HIGHER DOSE GROUP 31.0000±0.36515
Showing the average mean values of mchc found in the blood
analysis of control group, minimal dose group, and maximal dose
group
MCV
CONTROL 65.8000±3.55528
LOW DOSE GROUP 73.5000±3.86221
HIGHER DOSE GROUP 76.5000±4.26419
Showing the average mean values of mcv found in the blood
analysis of control group, minimal dose group, and maximal dose
group
WBC
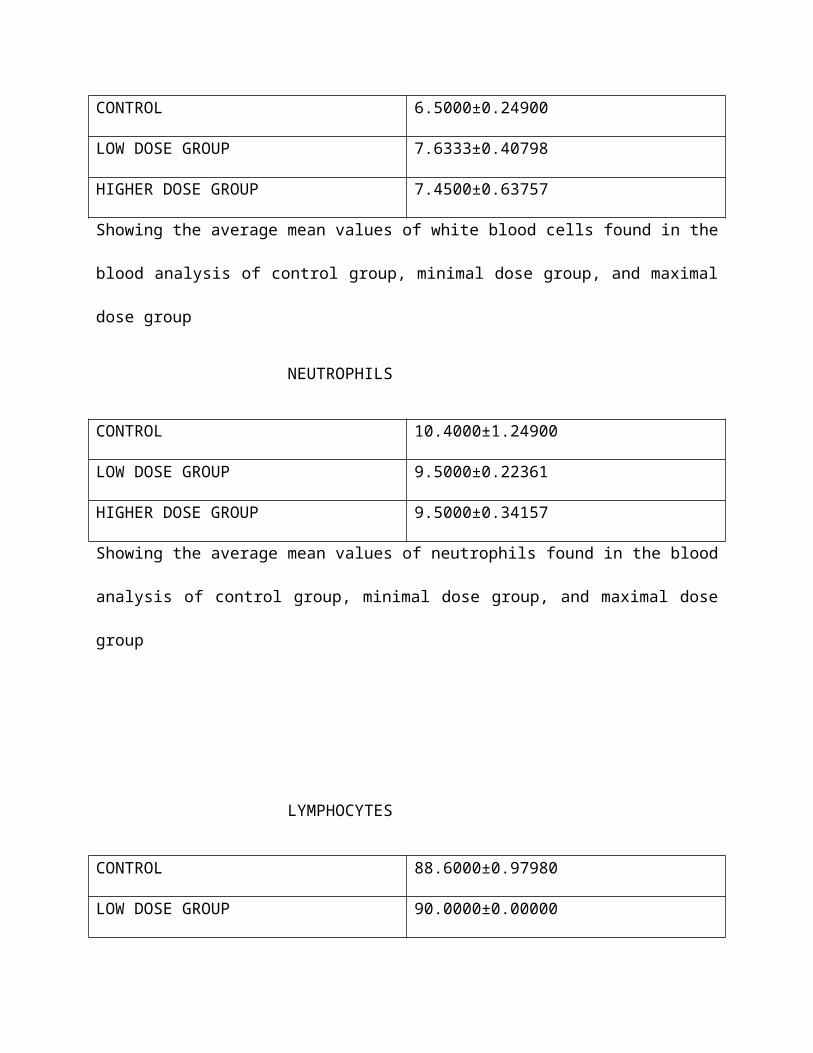
CONTROL 6.5000±0.24900
LOW DOSE GROUP 7.6333±0.40798
HIGHER DOSE GROUP 7.4500±0.63757
Showing the average mean values of white blood cells found in the
blood analysis of control group, minimal dose group, and maximal
dose group
NEUTROPHILS
CONTROL 10.4000±1.24900
LOW DOSE GROUP 9.5000±0.22361
HIGHER DOSE GROUP 9.5000±0.34157
Showing the average mean values of neutrophils found in the blood
analysis of control group, minimal dose group, and maximal dose
group
LYMPHOCYTES
CONTROL 88.6000±0.97980
LOW DOSE GROUP 90.0000±0.00000
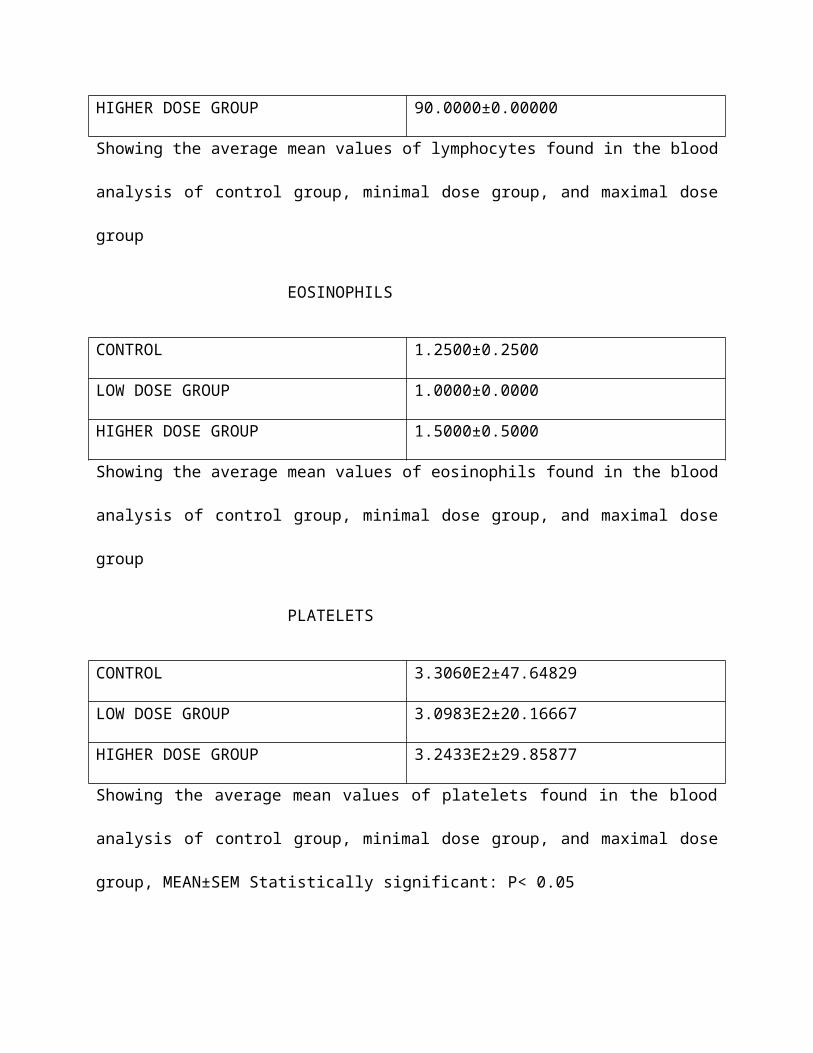
HIGHER DOSE GROUP 90.0000±0.00000
Showing the average mean values of lymphocytes found in the blood
analysis of control group, minimal dose group, and maximal dose
group
EOSINOPHILS
CONTROL 1.2500±0.2500
LOW DOSE GROUP 1.0000±0.0000
HIGHER DOSE GROUP 1.5000±0.5000
Showing the average mean values of eosinophils found in the blood
analysis of control group, minimal dose group, and maximal dose
group
PLATELETS
CONTROL 3.3060E2±47.64829
LOW DOSE GROUP 3.0983E2±20.16667
HIGHER DOSE GROUP 3.2433E2±29.85877
Showing the average mean values of platelets found in the blood
analysis of control group, minimal dose group, and maximal dose
group, MEAN±SEM Statistically significant: P< 0.05
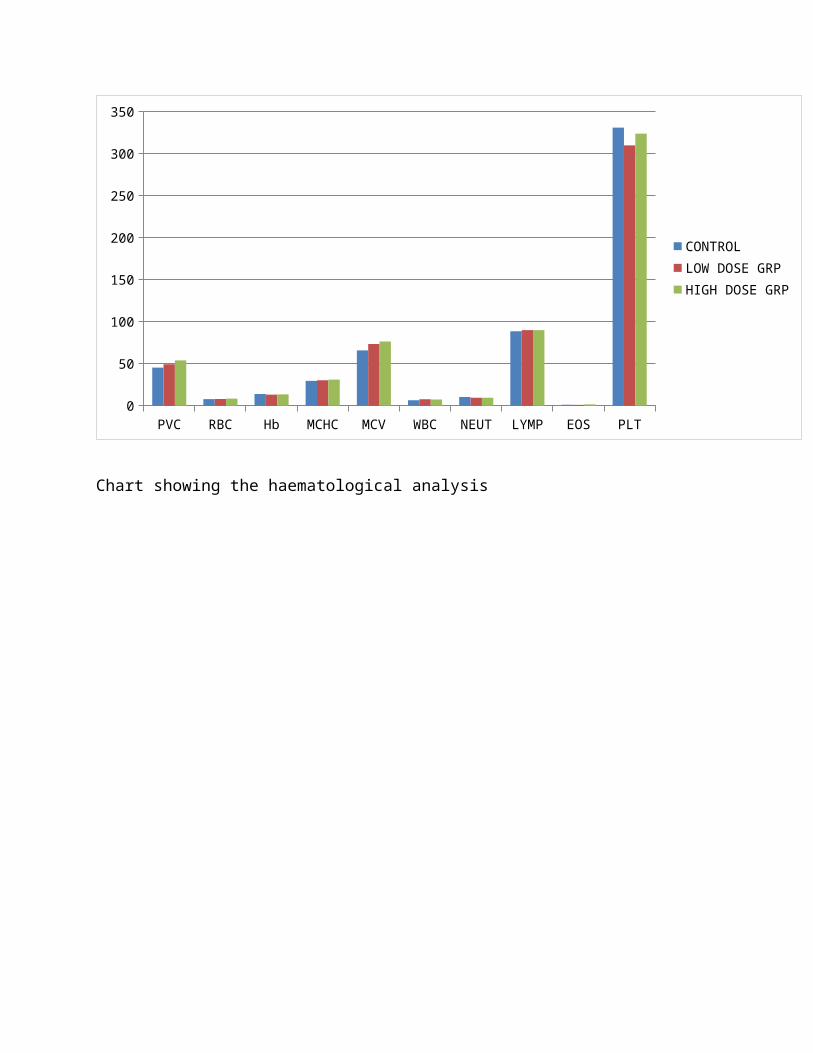
PVC RBC Hb MCHC MCV WBC NEUT LYMP EOS PLT0
50
100
150
200
250
300
350
CONTROLLOW DOSE GRPHIGH DOSE GRP
Chart showing the haematological analysis
CHAPTER FIVE
Male wistar rats were randomly selected to three groups, one of
which served as a control group and the other groups were treated
with Nifedipine at different dose (0.3 for low dose and 0.6 for
high dose mg/kg respectively.
There was no significant difference (p<0.05) in body weight
between the control group and the treated groups of rats where
weight change is concerned. However, this is not in correlation
with the report of Olivari et al, which reported that the weight
would be significantly less after chronic Nifedipine therapy. [39]
Even the comparison of right and left testicular weight between
the control and treated groups showed insignificant effect of
Nifedipine (p=0.528 and 0.375), respectively.
Weight changes may indicate physiological abnormalities in the
function of certain organs or systems, which could further
develop into serious health complications. Decrease in testicular
mass is an index of reproductive toxicity and could indicate
atrophic and degeneration of tissue. [45] It was thus important
that proper weight monitoring was done as one of the steps to
ensure that the rats were in good health. This served to show
also that patient undergoing Nifedipine therapy will very
unlikely experience drastic and unhealthy weight changes.
Sperm count was important to analyze the toxicity of the drug in
study on the spermatozoa production in the gonads of the rats.
Damage to cells involved in spermatogenesis or lowered sex
hormones could be reasons behind changes in sperm production. [46]
Rats in the control and treated groups (low dose and high dose)
had a mean sperm count of 56.4000±10.19902 x106/ml,
57.5333±11.99841 x106/ml and 63.1667±14.46554 x106/ml.
respectively, Despite a higher sperm count in the treated groups,
the difference between the three groups was insignificant
(p=0.726) to draw a conclusion that the drug affects sperm
numbers, by increasing the quantity of sperms based on the dose
given, thus, low dose increase slightly and at a higher dose,
increases highly.
Motility between rats of control and treated groups were similar
to each group. Clearly, sperm motility was not affected by the
treatment of nifedipine.
Sperm quality is dependent on variables of the sperm, the count,
motility, progressivity and morphology. While the increase in
sperm numbers will essentially increase the chances of a sperm
fertilizing an oocyte, this relation will not be of importance if
sperm motility was low. It is important that the sperm is motile
in a progressive manner to be able to move up the cervix and
along the fallopian tube to eventually encounter and fuse with an
oocyte. Low sperm motility is often attributed to chemical-
induced testicular toxicity. [45]
The three groups showed the same order in the number of abnormal
sperm according to types of abnormality – sperm with banana-like
form, folded on itself, without a hook, amorphous and lastly
double-tailed. No sperm of the last category was observed.
Sperm morphology influences the degree of its motility. The
energy required for the sperm to be motile is generated in the
axoneme, whereas the tail is required for the progressive
movement of the sperm. Hence, abnormalities in the anatomy of the
sperm will largely impair its movements. An individual’s sperm
morphology may also reveal the overall health of the testes since
its production is within the testis.[47]
The close-level of normality in the treated and control groups
showed that nifedipine does not affect the morphology of sperm,
rather it slightly increases the quantity of sperm, the overall
sperm analysis showed that Nifedipine did not adversely affect,
if at all, the quality of sperm.
The testosterone level was significantly increased (p=0.012) in
the high dose group when compare with the control. As
testosterone is required in the later stages of spermatogenesis,
this could possibly be one of the factors behind a slightly high
mean sperm count in the treated group. The comparative mean
concentration of testosterone between the control and treated
(higher dose group) also indicates that Leydig cells were not
damaged or adversely affected by Nifedipine.
The Follicle Stimulating Hormone level (FSH) was statistically
significantly (p=0.028) increased in the higher dose group when
compared with the control group, and would require a larger
sample size to test its accuracy. It has been proposed that FSH
levels increase as a result of seminiferous tissue damage due to
higher inhibin secretion.[48] FSH is inversely proportional to
spermatogonia population but the concentration of FSH is higher
in the treated group, which also had a higher sperm count than
the control group. Which value was statistically significant,
this could be due to a higher incidence of spermatogonia which do
not mature to become spermatozoa in the treated group. Elevated
FSH concentration could also point to germinal epithelial damage
and can be linked severe oligospermia or azoospermia of bad
prognosis. [48]
The Luteinizing Hormone (LH) level was significantly increased
(p=0.037) in the higher treated dose group compare with the
control group LH is an important hormone as it stimulates Leydig
cells to produce testosterone. The higher testosterone level in
the treated group (higher dose) might have indicated that LH
levels in the treated group were higher than the control too.
This is, however, not the case. First of all, LH concentration of
an individual cannot be determined with just a single test.
Instead, it has to be done several times over a period of time as
LH is secreted in bursts which vary from 30 minutes to 480
minutes. Secondly, it has a short half-life. Therefore, a single
determination of LH can only be 50% accurate. [48]
High levels of LH may indicate hyperthyroidism or androgen
resistance syndrome.[48] Despite some fluctuations with the
treated groups in sperm count, testis weight and hormone levels,
the difference could be used to draw a conclusion on such effects
as they were statistically significant. And above hormone results
were against the experiment carried out by Almaida et al, which
reported that calcium channel blockers had effect on the
testicular weight in that calcium channel blockers suppress
spermatogenesis [49]. Also discovered was that calcium antagonist
(amlodipine) used in the treatment of hypertension decreased the
plasma follicle-stimulating hormone (FSH) and testosterone but
not luteinizing hormone (LH) [50]
The results of my findings was also against Iranloye et al, that
reported, that Nifedipine appears to have a deleterious effect on
sperm functions in rats which is not mediated by a change in
testosterone secretion. [25]
Progesterone level is significantly increased (p=0.049) in the
treated group (higher dose) compared with the control group.
The oestradiol level was highly significant (p=0.049) in the
treated group (low dose) compared with the control.
Histologically, the results showed that the drug Nifedipine had a
destructive effect on the seminiferous tubule in a the low dose
related manner for the result showed a progressive destruction of
the seminiferous tubules which was against the high sperm count.
Haematologically the PCV was significantly increased (p=0.049) in
the treated group (higher dose) while the level all other
haematological parameters were statistically insignificant.
CONCLUSION
Many literatures had reported that antihypertensives especially
calcium blockers have deleterious effects on the reproductive
functions but with my extensive findings i realized that
Nifedipine which is the leading drug among the group of calcium
blockers do not have adverse effects on the testicular functions
based on the sperm count, testicular weight, and the hormonal
analysis.
But histologically speaking findings appears to be limited;
Nifedipine appears to have showed damage on the testicular
architecture in the lower dose group as this not certain because
the appeared damage might be artefacts as there was no
disorganization, degeneration or destruction of the testicular
histo-architecture.
However, the present study shows with substantial evidence that
CCB does not induces antifertility effects in the males.
Although, this study was unable to provide a substantial answer
to the microstructure of the testis.
After treating rats with 0.3 and 0.6mg/kg per dose of Nifedipine
for 28 days, statistical significant difference were seen between
the control and treated rat groups in major parameters it is
therefore concluded that Nifedipine did not adversely affect the
male reproductive health of treated rats. However, further
studies are warranted to draw a definite conclusion.
RECOMENDATION
It is recommended that further work should be done to elucidate
the toxicity effects of Nifedipine on the testis morphology of
male adult Wistar rats.
1. Thomas D. Giles, MD; Barry J. Materson, MD; Jay N. Cohn,
MD; John B. Kostis, MD Definition and Classification of
Hypertension: An Update THE JOURNAL OF CLINICAL HYPERTENSION
VOL. 11 NO. 11 NOVEMBER 2009 pg 611-614.)
2. Purvis K, Christiansen E (1992). Male infertility: Current
concepts. Ann. Med. 24: 259-272.
3. Sinclair S (2000). Male infertility: Nutritional and
environmental consideration. Alt. Med. Rev. 5: 28-38.
4. Feng HL (2003). Molecular biology of male infertility. Arch.
Androl. 49: 19-27.)
5. Adeniji et al., 2003(Adeniji RA, Olayemi O, Okunlola MA,
Aimakhu CO (2003). Pattern of semen analysis of male
partners of infertile couples at the University College
Hospital, Ibadan. W. Afr. J. Med. Med. 22: 243-245.
6. Ikechebelu JI, Adinma JI, Orie EF, Ikegwuonu SO (2003), High
prevalence of male infertility in southeastern. Niger. J.
Obstet. Gynaecol. 23: 657-659.
7. Carlsen E, Giwercman AJ, Keiding N, Skakkebaek NE (1993).
Decline in semen quality from 1930 to 1991. Ugeskr Laeger,
155: 2230-2235.
8. Buchanan and Davis, 1984
9. Petty RG (1999), Prolactin and anti psychotic medications:
Mechanism of action. Schizophrenia Res. 35: 67-73.
10. Lawes, C. M., Hoorn, S. V., & Rodgers, A. (2008).
Global burden of blood-pressure-related disease, 2001.
Lancet, 371(9623). 1513-1518.
11. 0893 5206 CCDS 11 Update 24 Aug 2010 reference ID: 2
910908.
12. Katayoun Javidnia, Ramin Miria,, Ladan Movahed, Shohreh
Golrangi Photostability Determination of Commercially
Available Nifedipine Oral Dosage Forms in Iran Iranian
Journal of Pharmaceutical Research (2003) 111-115
13. Albini A and Fasani E. Photochemistry of Drug: an
Overview and Practical Problems. In: Albini A and Fasani E.
(Eds.) Drug Photochemistry and Photostability. 1st ed. The Royal
Society of Chemistry, Cambridge (1998) 1-65.
14. Graham-Clarke EM and Herborn BS. Hypertention.In:
Walker R and Edwards C. (Eds.) Clinical Pharmacy and Ttherapeutics.
2nd ed. Churchill Livingestone, Edinburg (1999) 247-260.
15. Grundy JS, Kherani R and Foster RT. Photostability
determination of commercially available Nifedipine oral
dosage formulations. J. Pharm. Biomed. Anal.(1994) 12: 1529-
1553).
16. Fleckenstein, A., Tritthart, H., Doring, H.J. & Byon,
KY. (1972) Bay a 1040-emn hoch-aktiver Ca++-antagonistisher
Inhibitor der electromechanishen Kopplungsprozesse im
Warmbluter-Myokad. Arzneimittel-Forsch., 22, 22-33
17. Guazzi, M., Olivari, MT., Polese, A., Fiorentini, C.,
Magrini, F. & Moruzzi, P. (1977), Nifedipine, a new
antihypertensive with rapid action. Olin. Pharmacol. Ther.,
22, 528-532.)
18. Arrow Pharmaceuticals (NZ) Limited Mount Eden Central
Business Park, 33a Normanby Road, Mt. Eden, Auckland, New
Zealand, 20 August 2010
19. Banzet OC. SN: Thibomier. M; Singlas, E: Alexandre. M;
Corvol. P. Acute antihypertensive effect and
pharmacokinetics of a tablet preparation of nifedipine.
European Journal of Clinicai Pharmacology 1983: 24: 145- 1
50.
20. Drugs for hypertension. The Medical Letter 1999; 41:23-
28.
21. Hagiwara & Byerly, 1981, 1983; Tsien, 1983; Reuter,
1983
22. DIFFERENT TYPES OF CALCIUM CHANNELS BY E. W. MCCLESKEY,
A. P. FOX, D. FELDMAN1 AND R. W. TSIEN J. exp. Biol. 124, 177-190
(1986
23. Vaghy PL, Williams JS, Schwartz A. Receptor
pharmacology of calcium entry blocking agents. Am J Cardiol
1987; 59:9A-17A).
24. Calcium channel antagonists: Clinical uses—Past,
present and future David J. Triggle b i o c h e m i cal
pharmacology 7 4 ( 2 0 07 ) 1– 9.
25. (Iranloye BO, Morakinyo AO, Uwah J, Bello O, Daramola
OA effects of nifedipine on functions of the testis, Nig Q J Hosp Med. 2009
Jul-Sep;19(3):165-8.)
26. (U.S. National Library of Medicine: Drug Information
Portal – Amlodipine)
27. Adefule Adebayo1, Adesanya Olamide1, Akpan Helen1,
Huthman Ibrahim Oluwaseun1, Soyebo Olusegun1, Huthman
Adebukola Selimot: Toxicity Effects of Amlodipine on the
Testis Histology in Adult Wistar Rats American Journal of
Medicine and Medical Sciences 2012, 2(3): 36-40)
28. Fraser LR (1993). Calcium channels play a pivotal role
in the sequence of ionic changes involved in initiation of
mouse sperm acrosomal exocytosis. Mol. Reprod. Dev. 36: 368-
376.
29. Fraser LR, McIntyre K (1989). Calcium channel
antagonists modulate the acrosome reaction but not
capacitation in mouse spermatozoa. J. Reprod. Fert. 86: 223-
233.
30. Benoff S, Cooper GW, Hurley I, Mandel FS, Rosenfeld DL,
Scholl GM, Gilbert BR, Hershlag A (1994). The effect of
calcium ion channel blockers on sperm fertilization
potential. Fertil. Steril. 62: 606-617.
31. Hershlag G, Cooper W, Benoff S (1995). Pregnancy
following discontinuation of a calcium channel blocker in
the male partner. Hum. Reprod. 10: 599-606.
32. Westenbroek RE and Babcock DF. Discrete regional
distributions suggest diverse functional roles of calcium
channel alpha 1 subunits in sperm. Dev Biol. 1999 Mar 15;
207(2):457-69.
33. Susan Benoff, George W. Cooper, Ian Hurley, Francine S.
Mandel, Daviv L. Rosenfeld, Gerald M. Scholl, Bruce
R.Gilbert, Avner Hershlag; the effect of calcium ion channel
blockers on sperm fertilizationpotential: fertility and
sterility vol 62, No. 3, September 1994
34. Roldan, E.R., Wramsby, H. and Yanagimachi, R. (1987)
Verapamil, a Ca21 channel antagonist, accelerates the in vitro
penetration of zona-free hamster eggs by human spermatozoa.
Clin. Reprod. Fertil., 5, 1–4.
35. Adeoya-Osiguwa S, Fraser LR. A biphasic pattern of
45Ca2+ uptake by mouse spermatozoa in vitro correlates with
changing functional potential. J Reprod Fertil. 1993 Sep;
99(1):187-94.
36. Almeida SA, Teófilo JM, Anselmo Franci JA, Brentegani
LG, Lamano-Carvalho TL. Antireproductive effect of the
calcium channel blocker amlodipine in male rats. Exp Toxicol
Pathol. 2000 Aug;52(4):353-6.
37. Morakinyo AO, Iranloye BO, Adegoke OA. Antireproductive
effect of calcium channel blockers on male rats. Reprod Med
Biol. 2009; 8(3):97-102.
38. Morakinyo AO, Iranloye BO, Daramola AO, Adegoke OA,
Antifertility effect of calcium channel blockers on male
rats: association with oxidative stress Advances in Medical
Sciences · Vol. 56(1) · 2011 · pp 95-105
39. Olivari MT, Bartorelli C, Polese A, Fiorentini C,
Moruzzi P, Guazzi MD: Treatment of hypertension with
nifedipine, a calcium antagonist. Circulation 59: 1056,
1979.
40. Moore KL, Dalley AF and Agur AMR: “Clinically Oriented
Anatomy”, 6th Ed., Lippincott, Williams & Wilkins, Baltimore,
2010;
41. Van De Graaff : Female reproductive system, Human
Anatomy, 6th edition The McGraw−Hill Companies, 2001; chpt
21, pp726-752.
42. Harold Ellis: “The male genital organs” , In: Clinical
Anatomy: Applied anatomy for junior doctors. 11th Edition.
Massachusetts, Black Well Publishing Inc. 2006;
43. (Junqueira L C and Carneiro J: “The Male Reproductive
System”,In:Basic Histology. 10th Edition. USA,McGraw-Hill
Companies 2003; 10/22/page-10/22/page.
44. Manimunda SP, Sugunan AP, Benegal V, Balakrishna N, Rao
MV, Pesala KS.. Association of hypertension with risk
factors & hypertension related behaviour among the
aboriginal Nicobarese tribe living in Car Nicobar Island,
India. Indian J Med Res 2011;133:287-93.
45. Metwally SA, Hekma AA, Fawzy HM, Hamdy A. The
Protective Effect of Linseed Oil Against Carbendazim Induced
Testicular Toxicity in Rats. Eur J Sci Res 2011;49:208-24.
46. Possible toxic effect of antihypertensive drug
olmesartan on male reproductive system of rat Srinivasa
Jayachandraa, AnnGie Ng, International Journal of Basic &
Clinical Pharmacology | January-February 2013 | Vol 2 |
Issue 1 pg 83-88.
47. Carreira JT, Mingoti GZ, Rodrigues LH, Silva C, Perri
SH, Koivisto MB. Impact of proximal cytoplasmic droplets on
quality traits and in-vitro embryo production efficiency of
cryopreserved bull spermatozoa. Acta Vet Scand 2012;54:1-7.
48. Martin-du Pan R. Endocrine pathology: Effects on male
fertility, 2003. Available at
http://www.gfmer.ch/Books/Reproductive_health/Endocrine_
pathology.html. Accessed 27 August 2011.
49. Almaida SA, Teofilo JM, Anselmo Franci JA, Brentegani
LG, Lamano-Carvalho TL (2000). Antireproductive Effect of
Calcium Channel Blocker Amilodipine in Male Rats: Exp
Toxicol Pathol; 52:353-6
50. Rabia Latif, Ghulam Mustafa Lodhi, Muhammad Aslam,
2008. Effect of Amlodipine on Serum Testosterone, testicular
weight and gonado-somatic index in adult rats: J ayyaub med
coll abbottabad; 20 (4)
51.
52.