lomaxdosedelivery.pdf - cern indico
TRANSCRIPT
Dose delivery
Tony Lomax :: Head of Medical Physics :: Paul Scherrer Institute
International Conference on Medical Accelerators and Particle Therapy –
4-6th September 2019
Page 2
Overview of presentation
1.Proton therapy and its delivery
2.Improving lateral penumbra
3.Reducing treatment times
4.Protons for FLASH?
5.Summary
Page 3
Overview of presentation
1.Proton therapy and its delivery
2.Improving lateral penumbra
3.Reducing treatment times
4.Protons for FLASH?
5.Summary
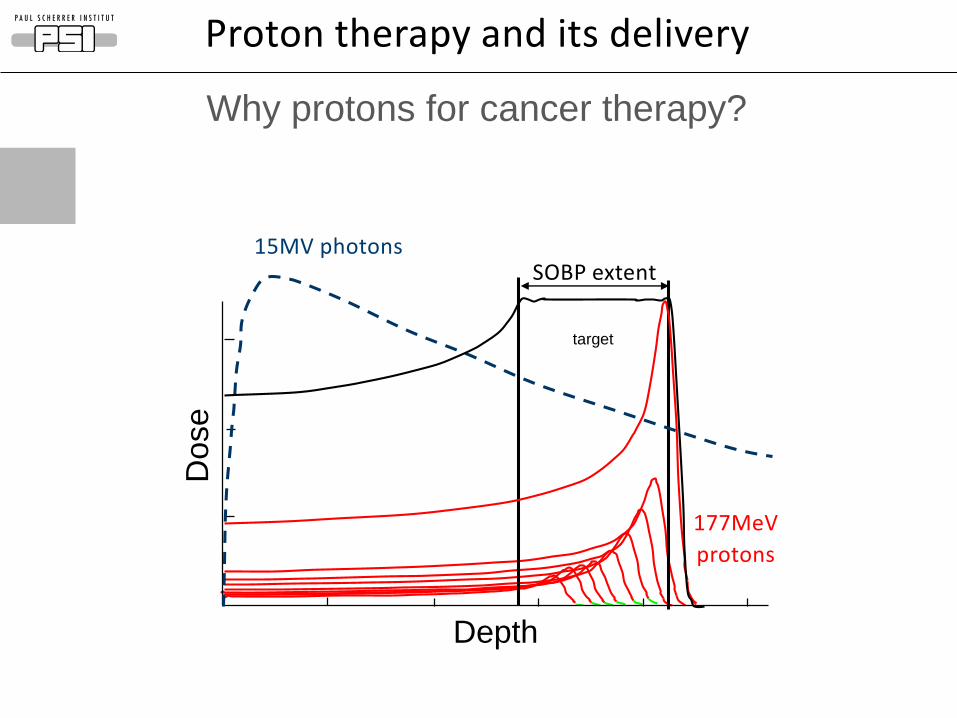
Why protons for cancer therapy?
target
Depth
Dose
15MV photons
177MeV
protons
SOBP extent
Proton therapy and its delivery
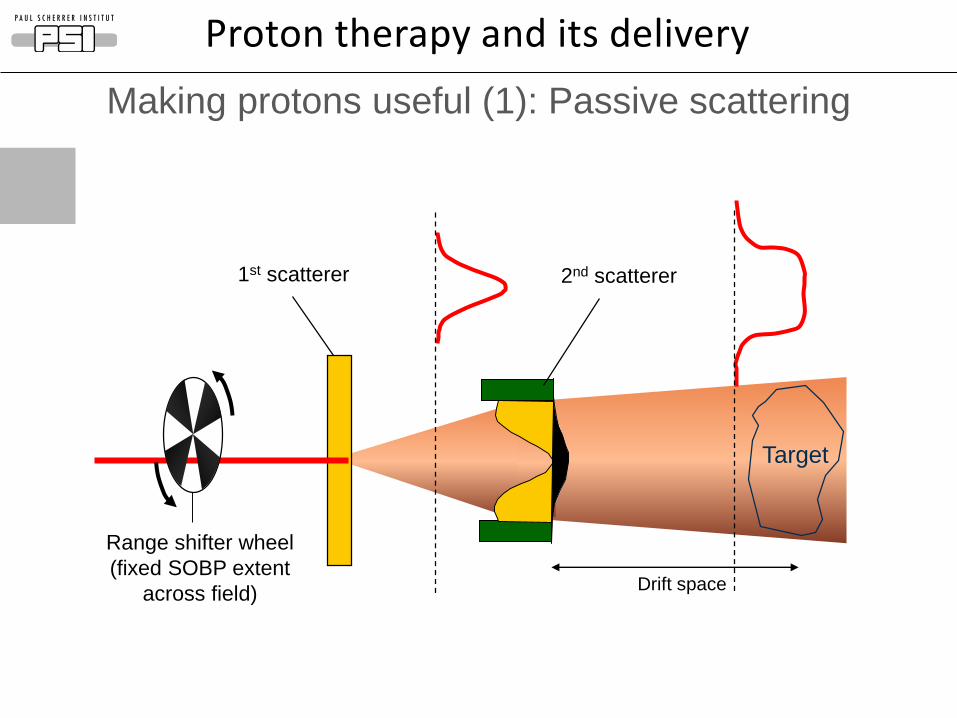
Making protons useful (1): Passive scattering
1st scatterer 2nd scatterer
Target
Drift space
Range shifter wheel
(fixed SOBP extent
across field)
Proton therapy and its delivery
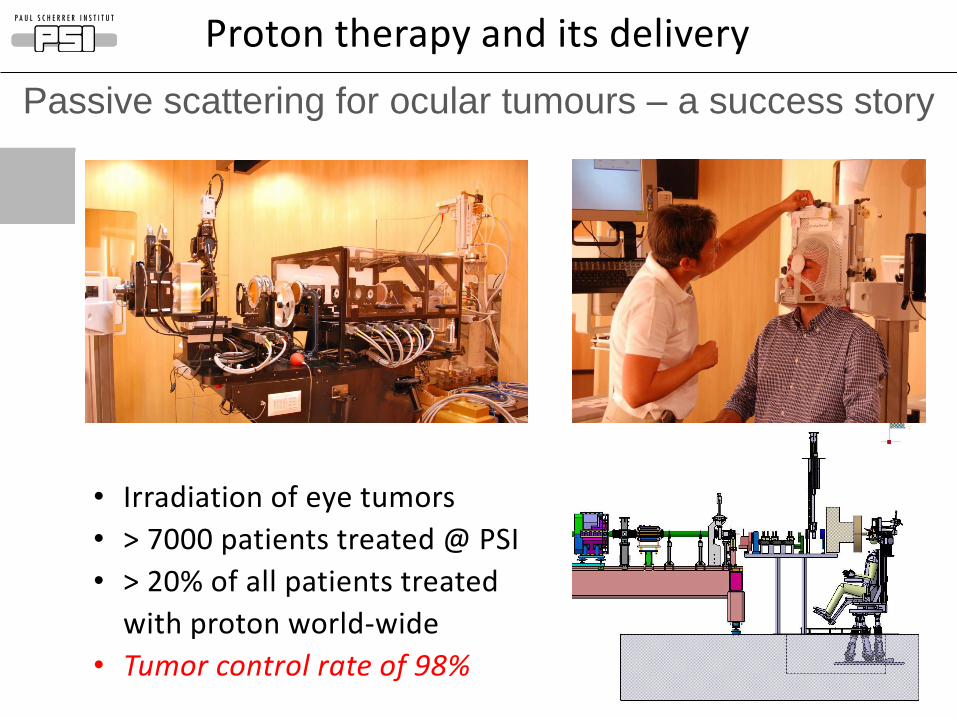
• Irradiation of eye tumors
• > 7000 patients treated @ PSI
• > 20% of all patients treated
with proton world-wide
• Tumor control rate of 98%
Passive scattering for ocular tumours – a success story
Proton therapy and its delivery
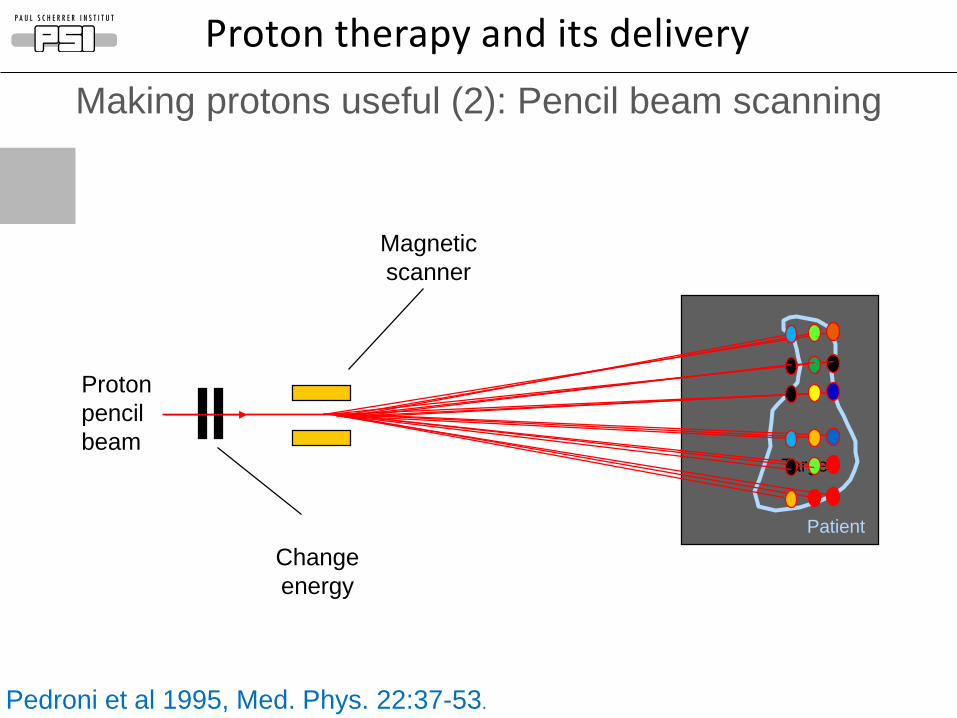
Target
Magnetic
scanner
Change
energy
Patient
Proton
pencil
beam
Pedroni et al 1995, Med. Phys. 22:37-53.
Making protons useful (2): Pencil beam scanning
Proton therapy and its delivery
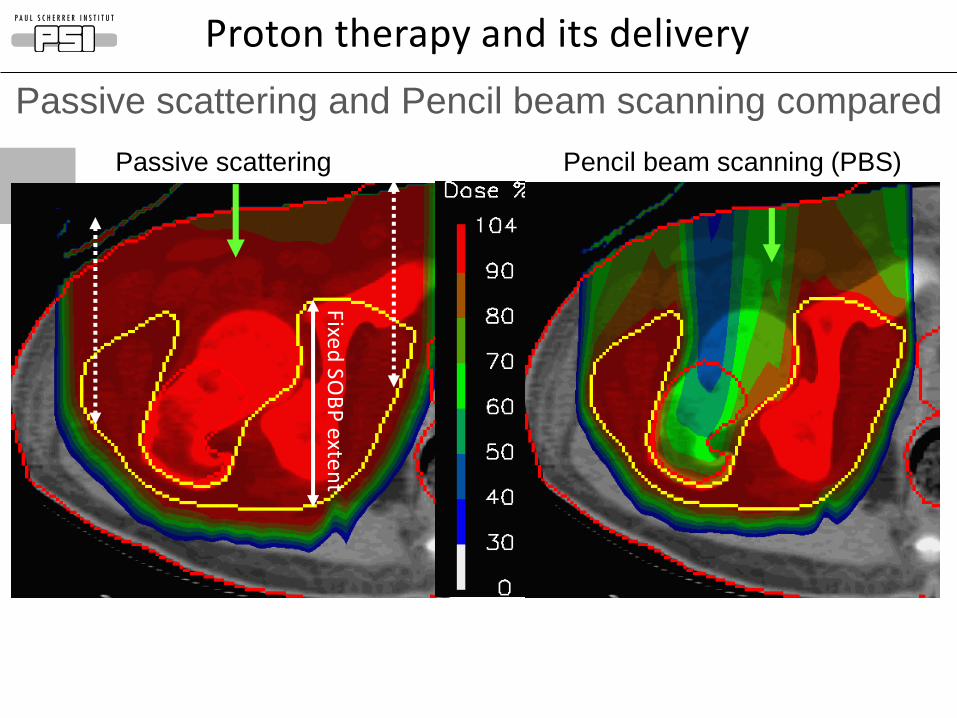
Pencil beam scanning (PBS)Passive scattering
Passive scattering and Pencil beam scanning compared
Proton therapy and its delivery
Fixed
SOB
P e
xten
t
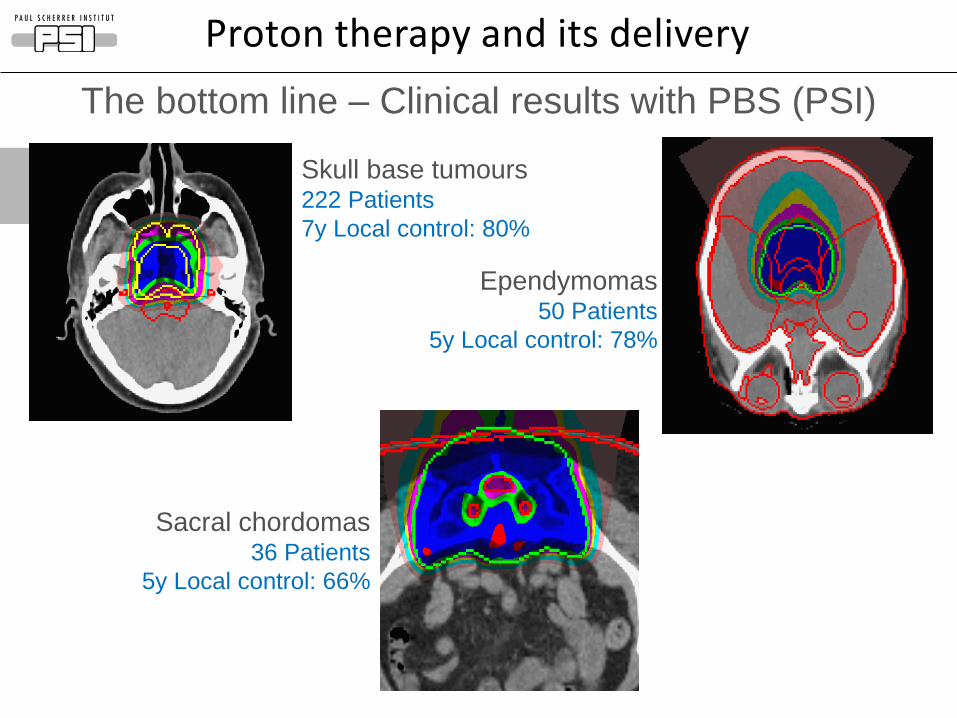
Ependymomas50 Patients
5y Local control: 78%
Skull base tumours222 Patients
7y Local control: 80%
Sacral chordomas36 Patients
5y Local control: 66%
The bottom line – Clinical results with PBS (PSI)
Proton therapy and its delivery
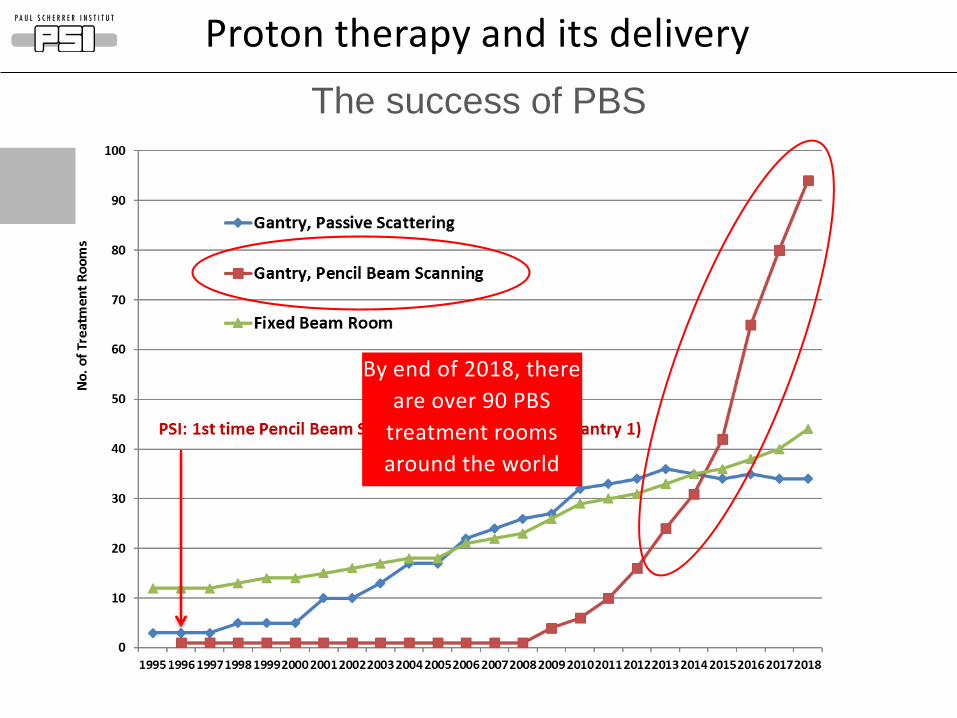
By end of 2018, there
are over 90 PBS
treatment rooms
around the world
The success of PBS
Proton therapy and its delivery
Page 11
Overview of presentation
1.Proton therapy and its delivery
2.Improving lateral penumbra
3.Reducing treatment times
4.Protons for FLASH?
5.Summary
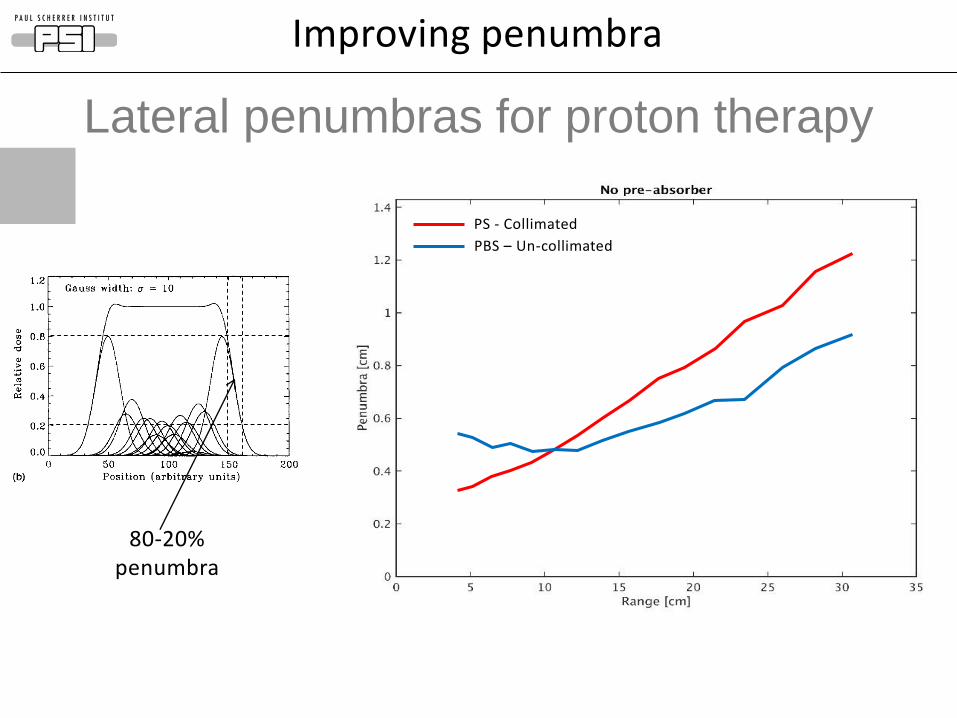
Lateral penumbras for proton therapy
80-20% penumbra
PS - Collimated
PBS – Un-collimated
Improving penumbra
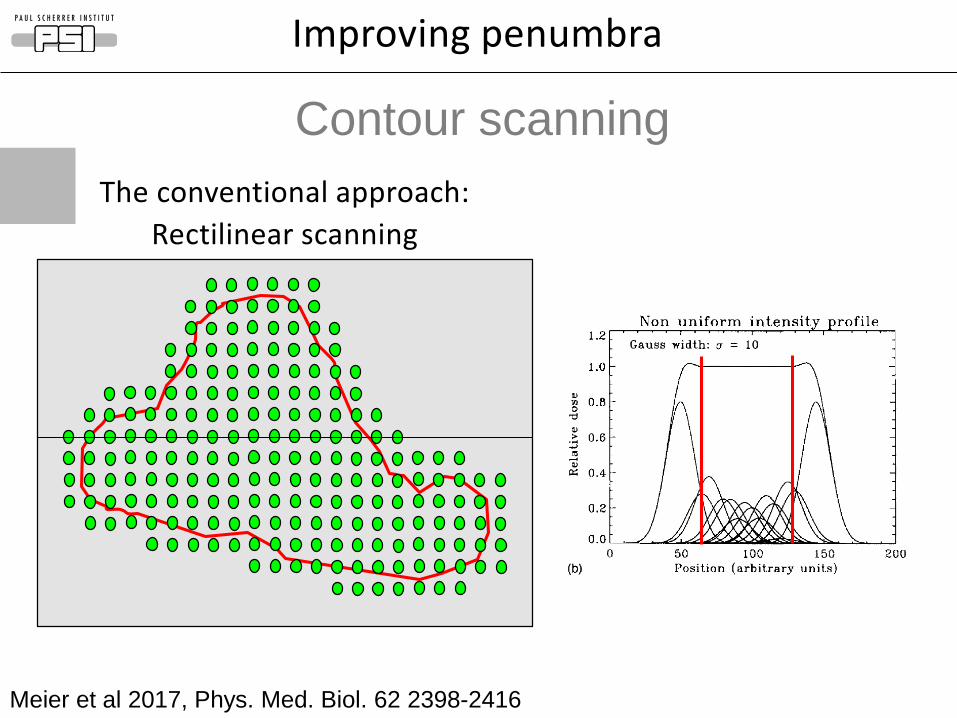
The conventional approach:
Rectilinear scanning
Meier et al 2017, Phys. Med. Biol. 62 2398-2416
Contour scanning
Improving penumbra
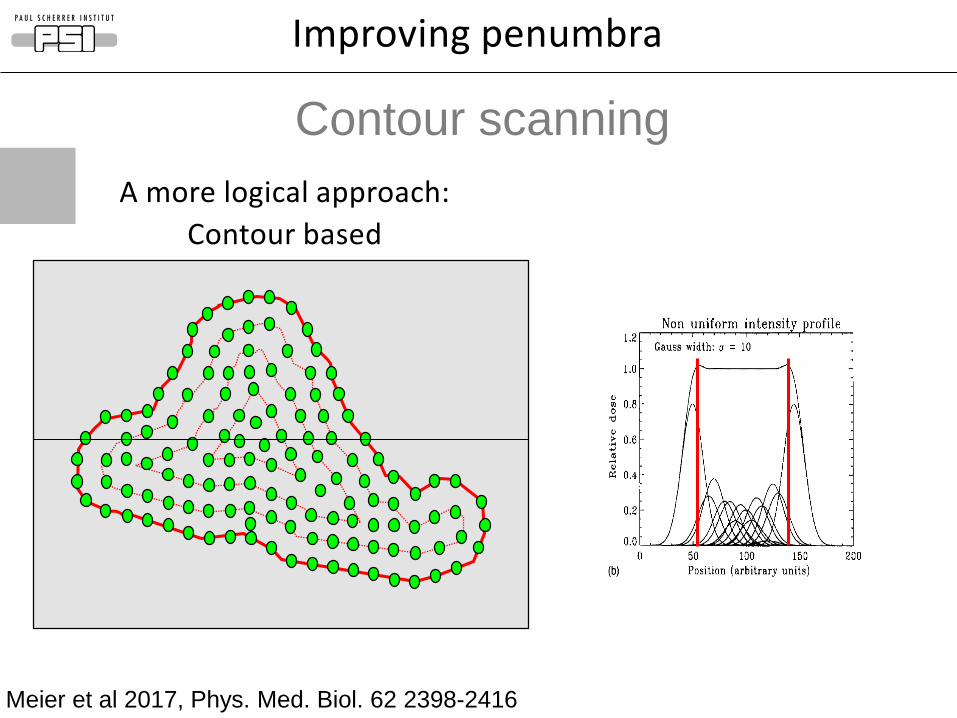
Meier et al 2017, Phys. Med. Biol. 62 2398-2416
Contour scanning
Improving penumbra
A more logical approach:
Contour based
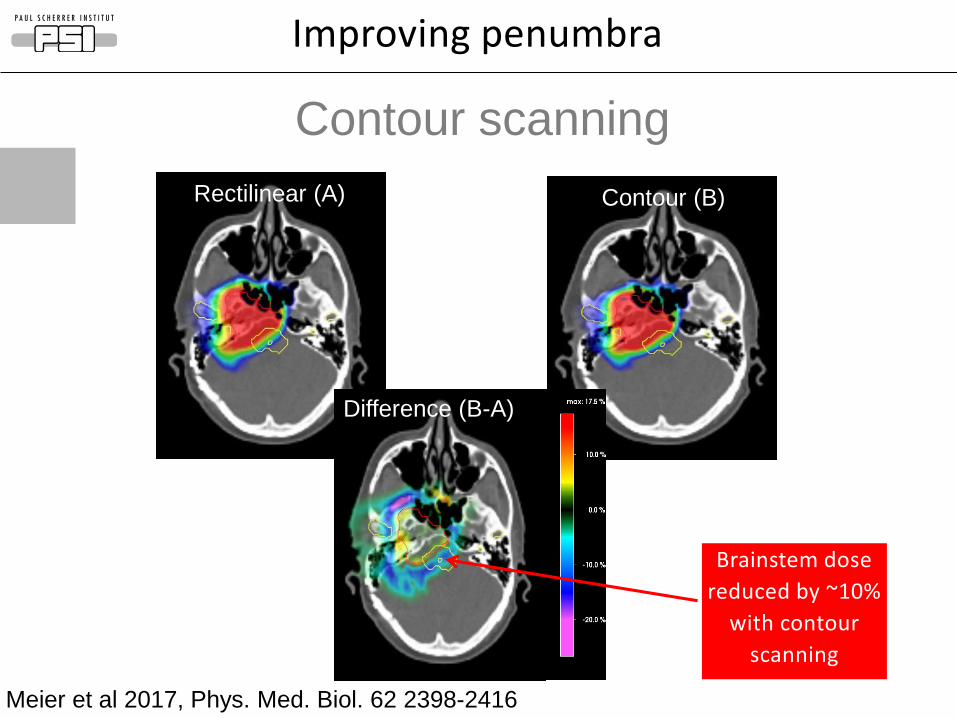
Rectilinear (A) Contour (B)
Difference (B-A)
Brainstem dose
reduced by ~10%
with contour
scanning
Improving penumbra
Contour scanning
Meier et al 2017, Phys. Med. Biol. 62 2398-2416
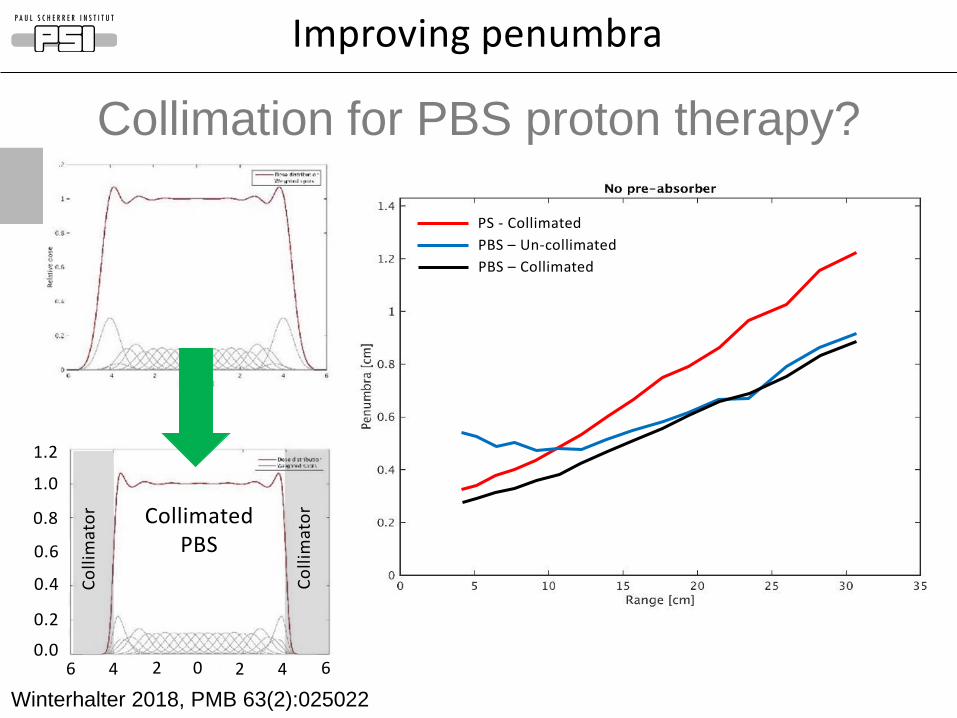
Collimation for PBS proton therapy?
Improving penumbra
PS - Collimated
PBS – Un-collimated
PBS – Collimated
6 4 2 0 2 4 60.0
0.2
0.4
0.6
0.8
1.0
1.2
Co
llim
ato
r
Co
llim
ato
rCollimated PBS
Winterhalter 2018, PMB 63(2):025022
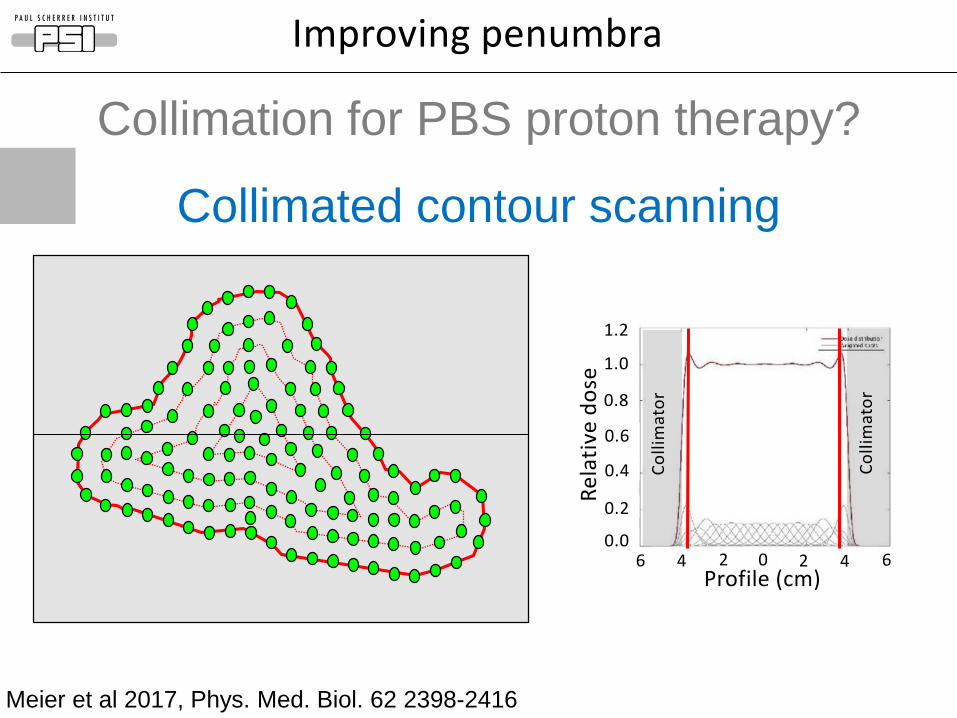
Collimated contour scanning
Meier et al 2017, Phys. Med. Biol. 62 2398-2416
6 4 2 0 2 4 60.0
0.2
0.4
0.6
0.8
1.0
1.2
Profile (cm)R
ela
tive
do
se
Co
llim
ato
r
Co
llim
ato
r
Improving penumbra
Collimation for PBS proton therapy?
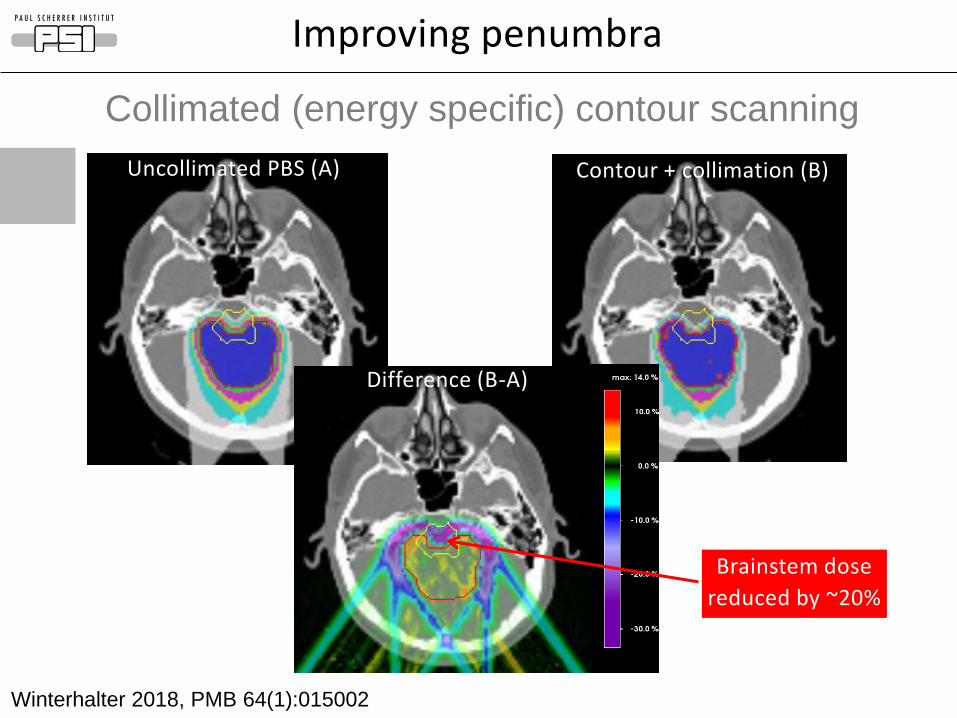
Uncollimated PBS (A) Contour + collimation (B)
Difference (B-A)
Winterhalter 2018, PMB 64(1):015002
Brainstem dose
reduced by ~20%
Collimated (energy specific) contour scanning
Improving penumbra
Page 19
Overview of presentation
1.Proton therapy and its delivery
2.Improving lateral penumbra
3.Reducing treatment times
4.Protons for FLASH?
5.Summary
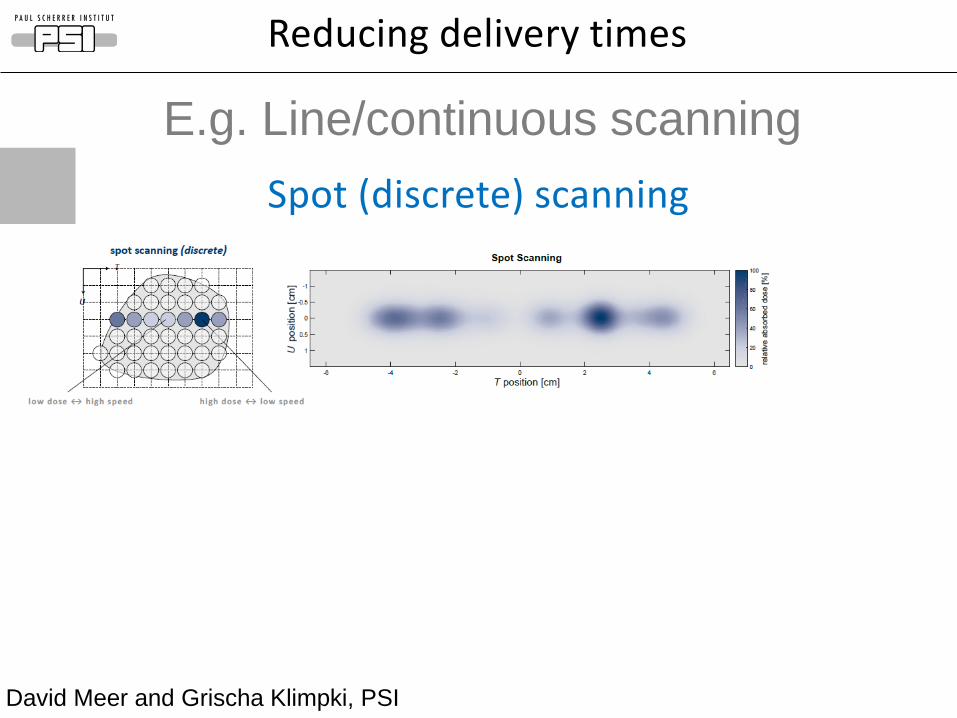
David Meer and Grischa Klimpki, PSI
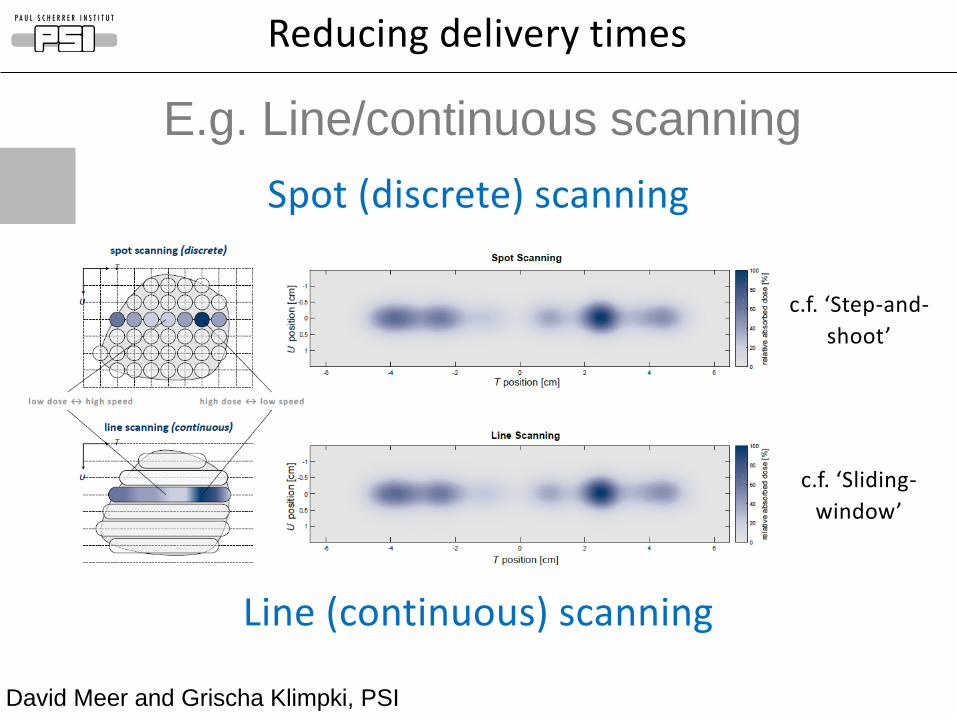
E.g. Line/continuous scanning
Spot (discrete) scanning
Reducing delivery times
E.g. Line/continuous scanning
David Meer and Grischa Klimpki, PSI
Spot (discrete) scanning
Line (continuous) scanning
c.f. ‘Step-and-
shoot’
c.f. ‘Sliding-
window’
Reducing delivery times
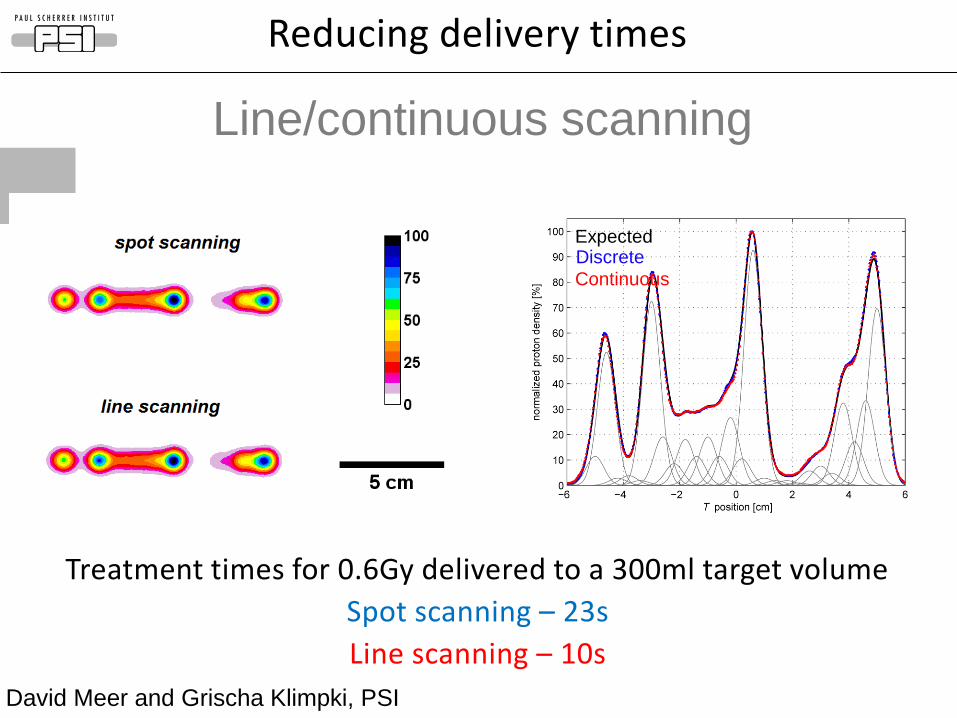
ExpectedDiscrete
Continuous
Line/continuous scanning
Reducing delivery times
Treatment times for 0.6Gy delivered to a 300ml target volume
Spot scanning – 23s
Line scanning – 10s
David Meer and Grischa Klimpki, PSI
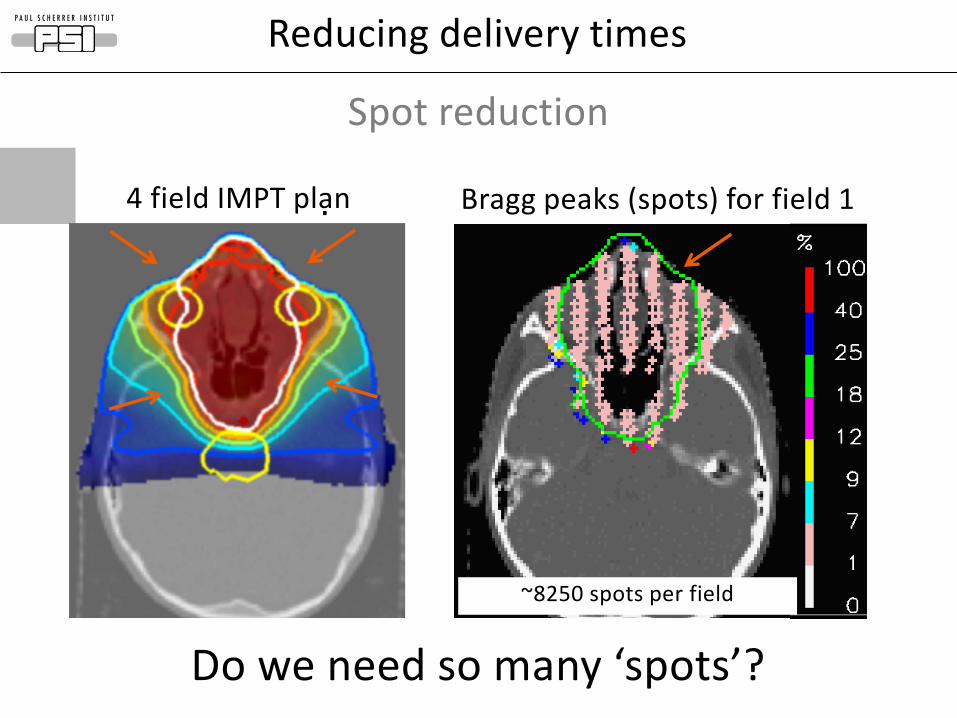
Bragg peaks (spots) for field 14 field IMPT plan
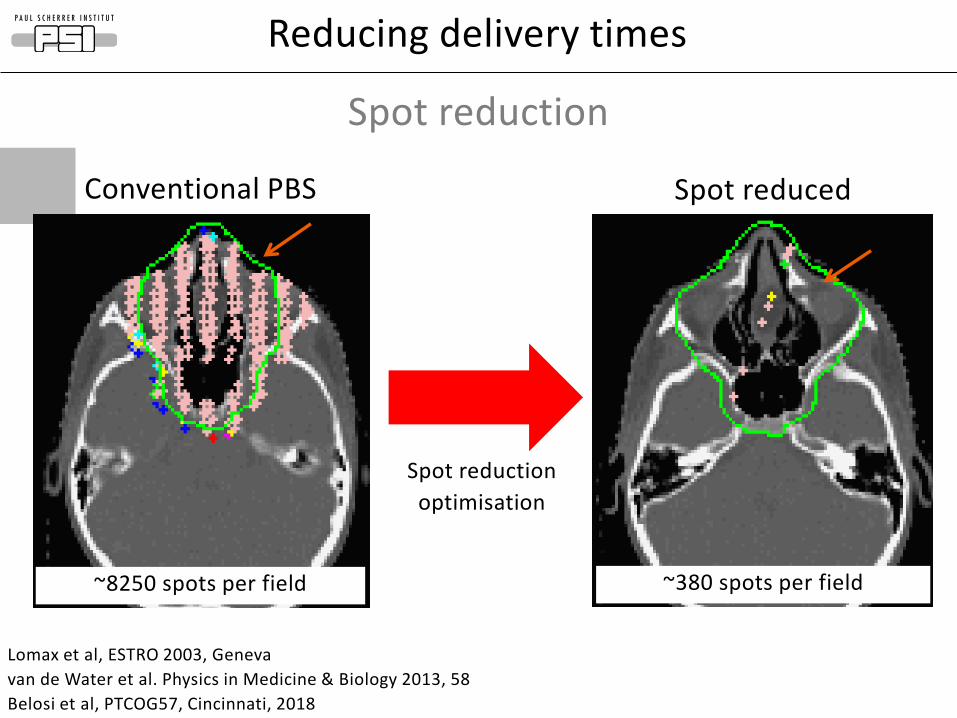
~8250 spots per field
Spot reduction
Do we need so many ‘spots’?
Reducing delivery times
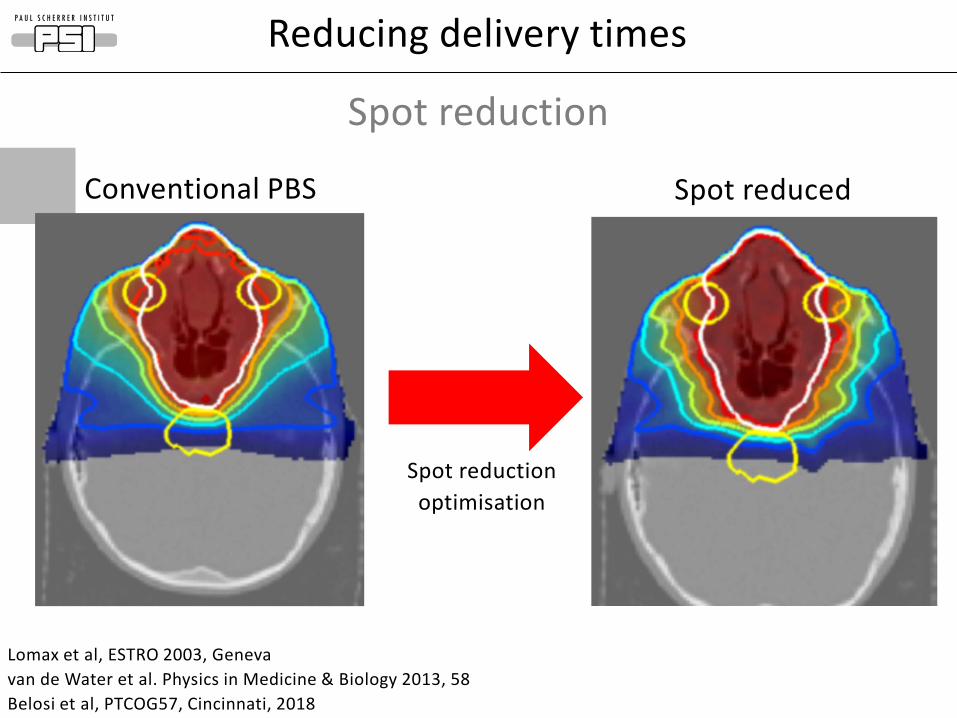
Conventional PBS Spot reduced
Spot reduction
optimisation
Reducing delivery times
Spot reduction
Lomax et al, ESTRO 2003, Geneva
van de Water et al. Physics in Medicine & Biology 2013, 58
Belosi et al, PTCOG57, Cincinnati, 2018
Lomax et al, ESTRO 2003, Geneva
van de Water et al. Physics in Medicine & Biology 2013, 58
Belosi et al, PTCOG57, Cincinnati, 2018
~8250 spots per field ~380 spots per field
Conventional PBS Spot reduced
Spot reduction
optimisation
Reducing delivery times
Spot reduction
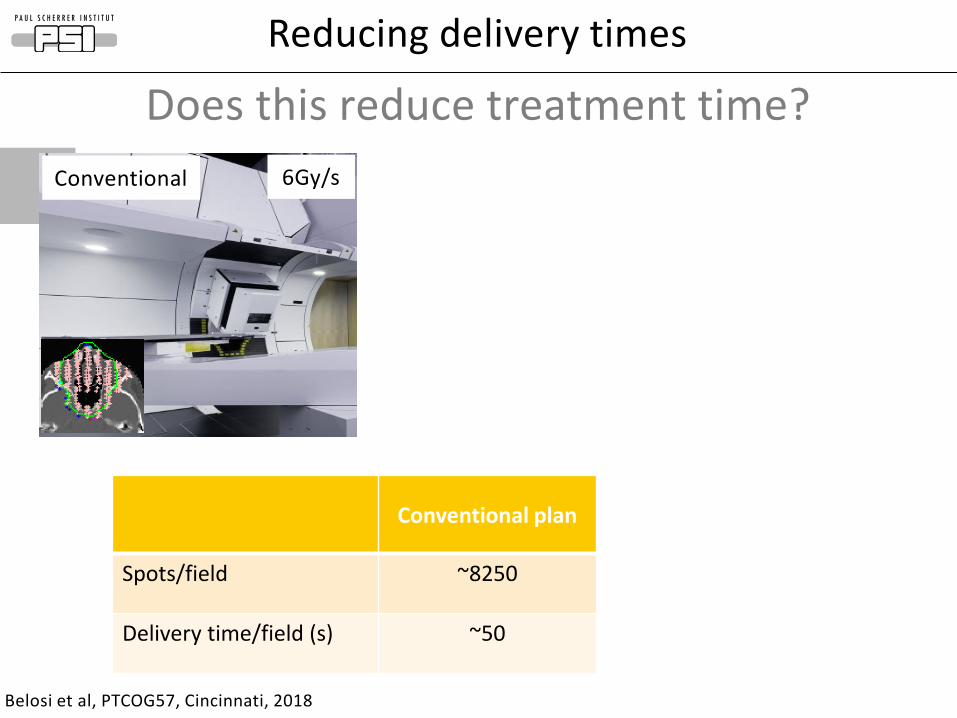
Belosi et al, PTCOG57, Cincinnati, 2018
Conventional plan
Spots/field ~8250
Delivery time/field (s) ~50
Conventional
Does this reduce treatment time?
6Gy/s
Reducing delivery times
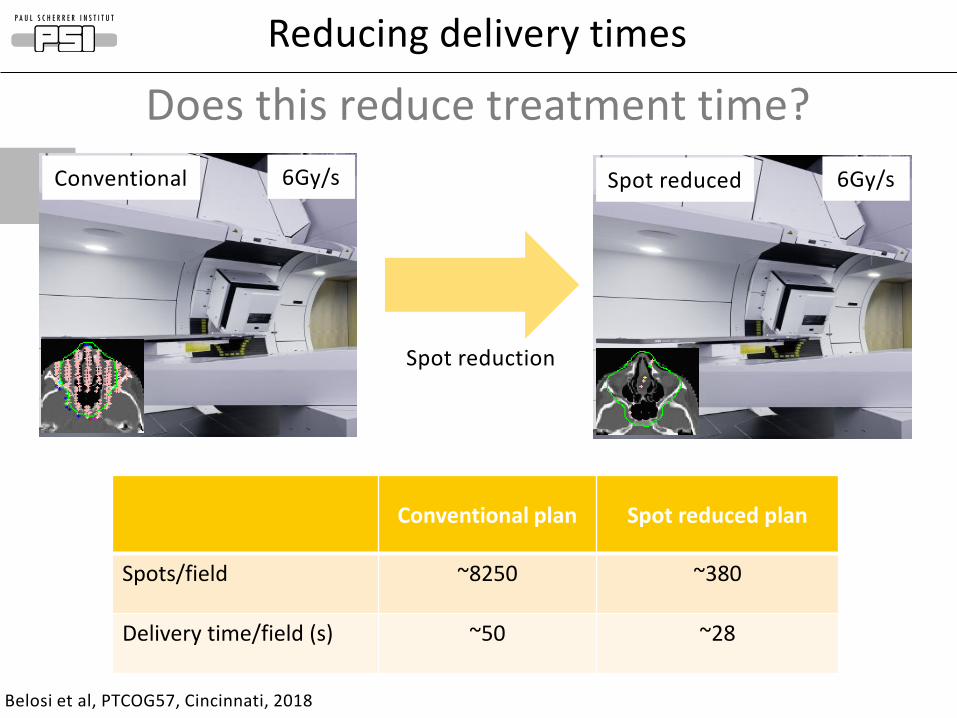
Belosi et al, PTCOG57, Cincinnati, 2018
Conventional plan Spot reduced plan
Spots/field ~8250 ~380
Delivery time/field (s) ~50 ~28
Spot reduction
Conventional Spot reduced6Gy/s 6Gy/s
Reducing delivery times
Does this reduce treatment time?
Page 28
Overview of presentation
1.Proton therapy and its delivery
2.Improving lateral penumbra
3.Reducing treatment times
4.Protons for FLASH?
5.Summary
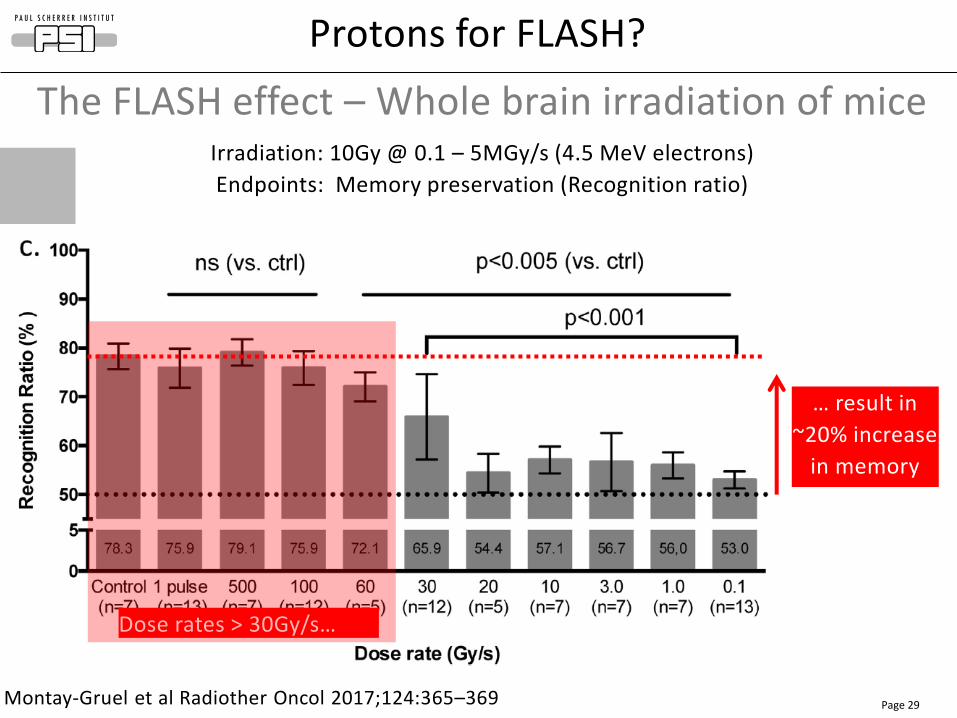
Page 29Montay-Gruel et al Radiother Oncol 2017;124:365–369
Protons for FLASH?
The FLASH effect – Whole brain irradiation of miceIrradiation: 10Gy @ 0.1 – 5MGy/s (4.5 MeV electrons)
Endpoints: Memory preservation (Recognition ratio)
… result in
~20% increase
in memory
preservation…
Dose rates > 30Gy/s…
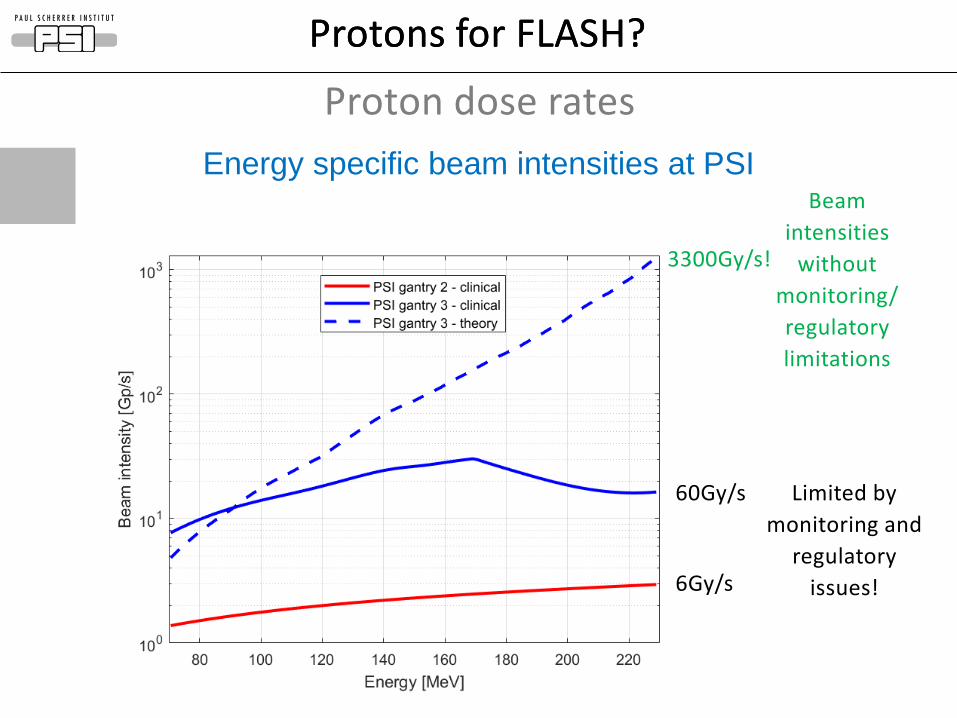
Protons for FLASH?Protons for FLASH?
Proton dose rates
6Gy/s
60Gy/s
3300Gy/s!
Limited by
monitoring and
regulatory
issues!
Beam
intensities
without
monitoring/
regulatory
limitations
Energy specific beam intensities at PSI
20
40
60
80
95
107
[%]
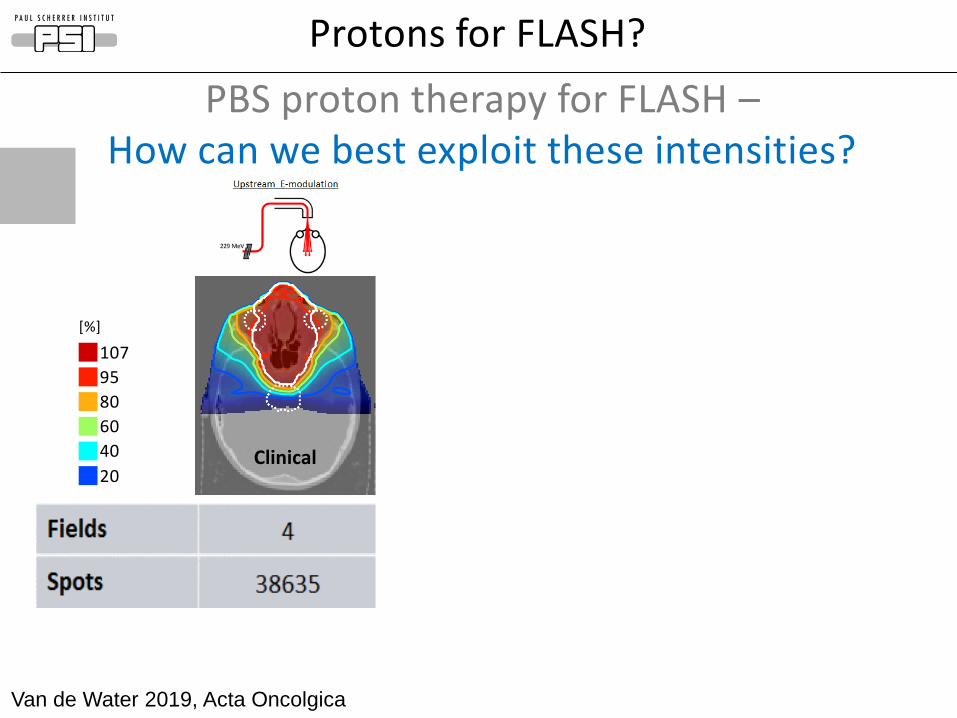
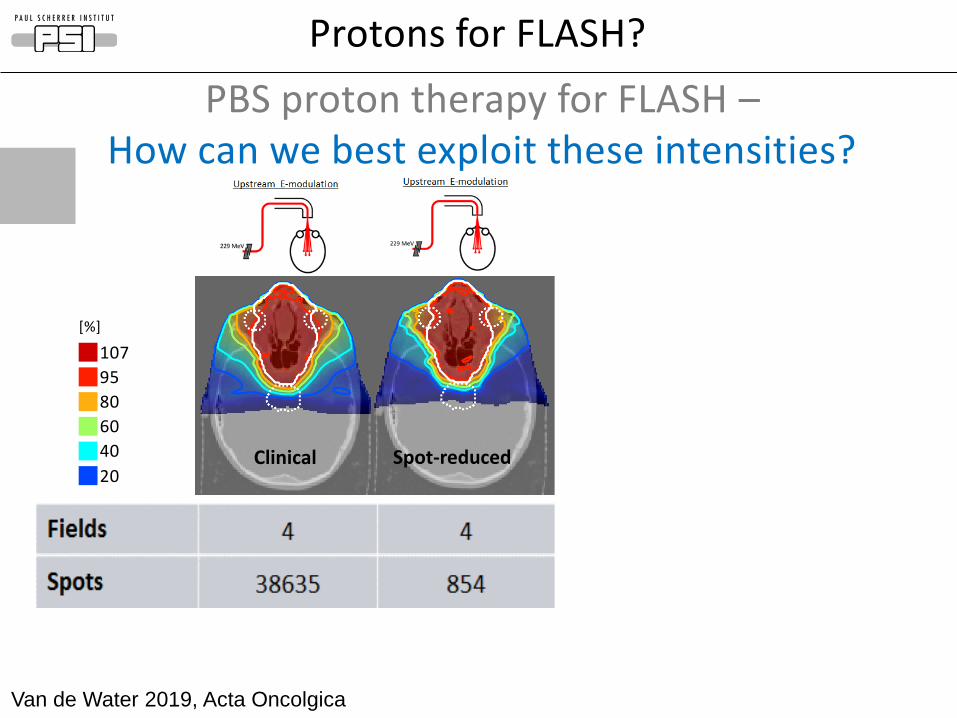
Range compensated/ spot reduction
Protons for FLASH?
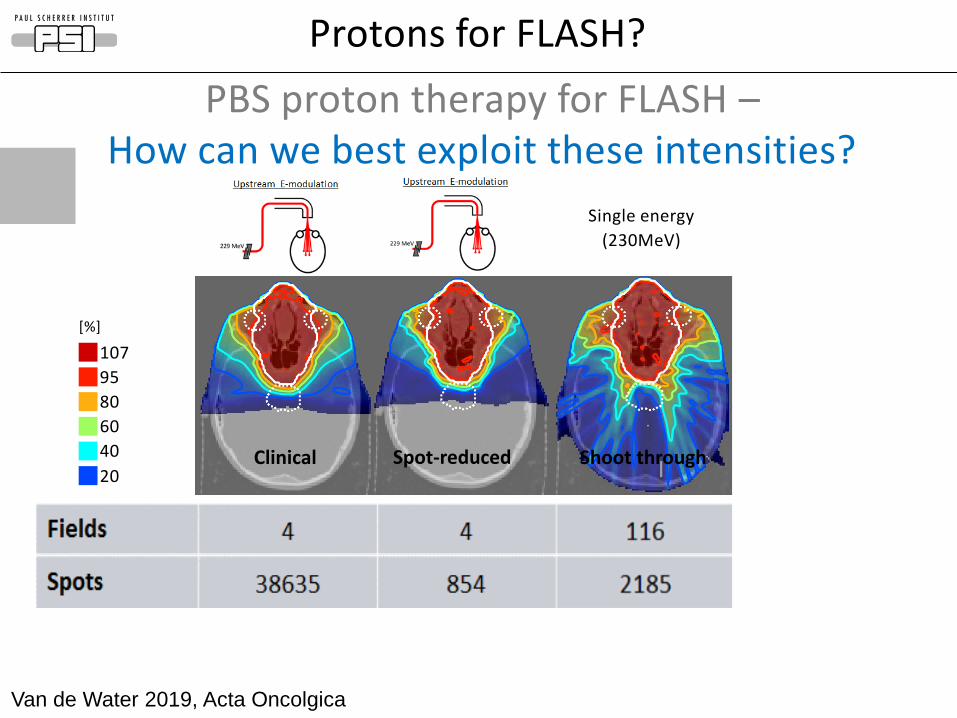
Van de Water 2019, Acta Oncolgica
Single energy
(230MeV)
Clinical Spot-reduced Shoot through
PBS proton therapy for FLASH –How can we best exploit these intensities?
20
40
60
80
95
107
[%]
Range compensated/ spot reduction
Protons for FLASH?
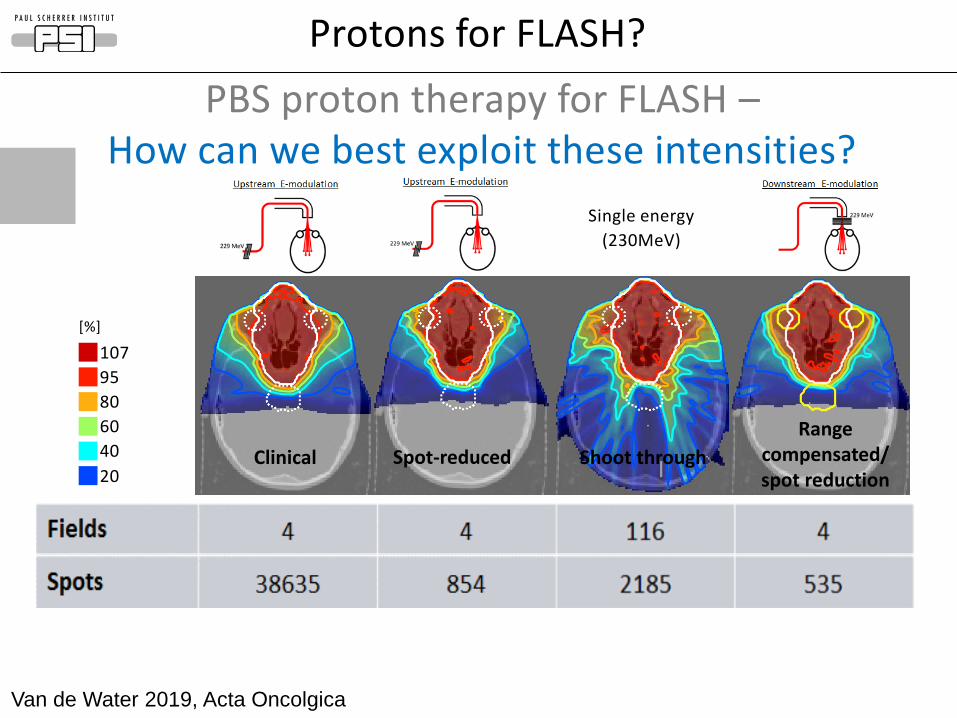
Van de Water 2019, Acta Oncolgica
Single energy
(230MeV)
Clinical Spot-reduced Shoot through
PBS proton therapy for FLASH –How can we best exploit these intensities?
20
40
60
80
95
107
[%]
Range compensated/ spot reduction
Protons for FLASH?
Van de Water 2019, Acta Oncolgica
Single energy
(230MeV)
Clinical Spot-reduced Shoot through
PBS proton therapy for FLASH –How can we best exploit these intensities?
20
40
60
80
95
107
[%]
Range compensated/ spot reduction
Protons for FLASH?
Van de Water 2019, Acta Oncolgica
Single energy
(230MeV)
Clinical Spot-reduced Shoot through
PBS proton therapy for FLASH –How can we best exploit these intensities?
20
40
60
80
95
107
[%]
Range compensated/ spot reduction
Protons for FLASH?
Van de Water 2019, Acta Oncolgica
Single energy
(230MeV)
Clinical Spot-reduced Shoot through
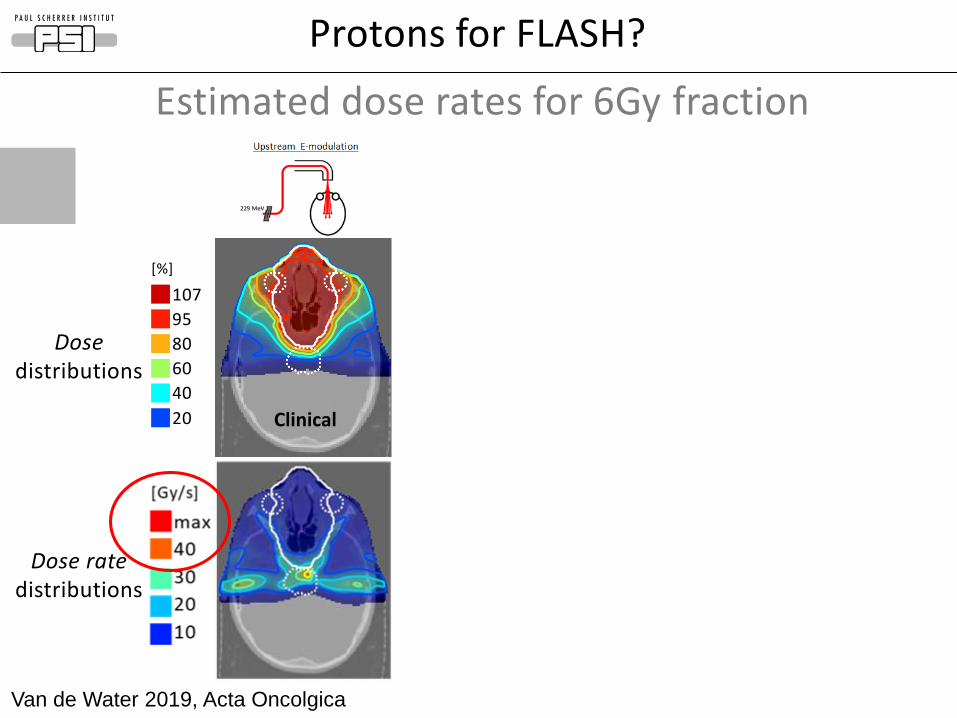
Dose distributions
Dose rate distributions
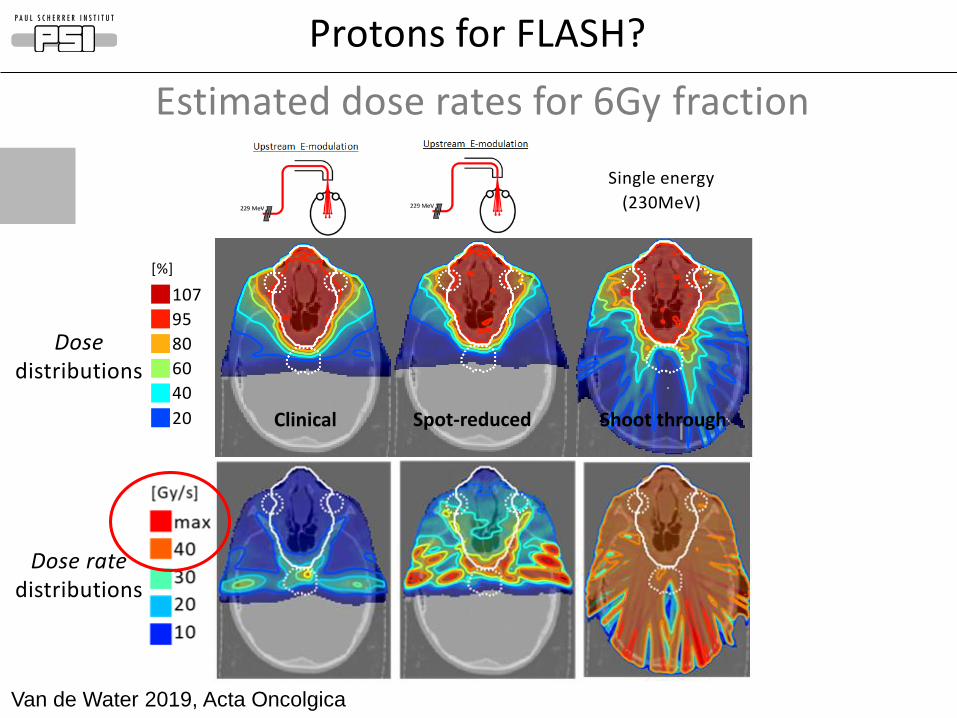
Estimated dose rates for 6Gy fraction
20
40
60
80
95
107
[%]
Range compensated/ spot reduction
Protons for FLASH?
Van de Water 2019, Acta Oncolgica
Single energy
(230MeV)
Clinical Spot-reduced Shoot through
Dose distributions
Dose rate distributions
Estimated dose rates for 6Gy fraction
20
40
60
80
95
107
[%]
Range compensated/ spot reduction
Protons for FLASH?
Van de Water 2019, Acta Oncolgica
Single energy
(230MeV)
Clinical Spot-reduced Shoot through
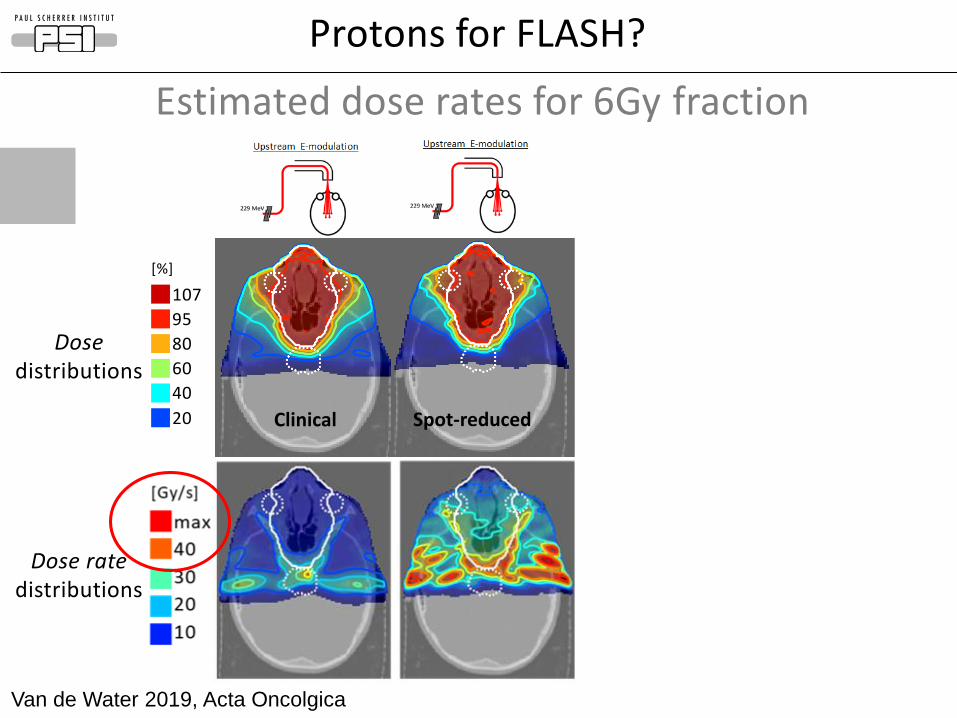
Dose distributions
Dose rate distributions
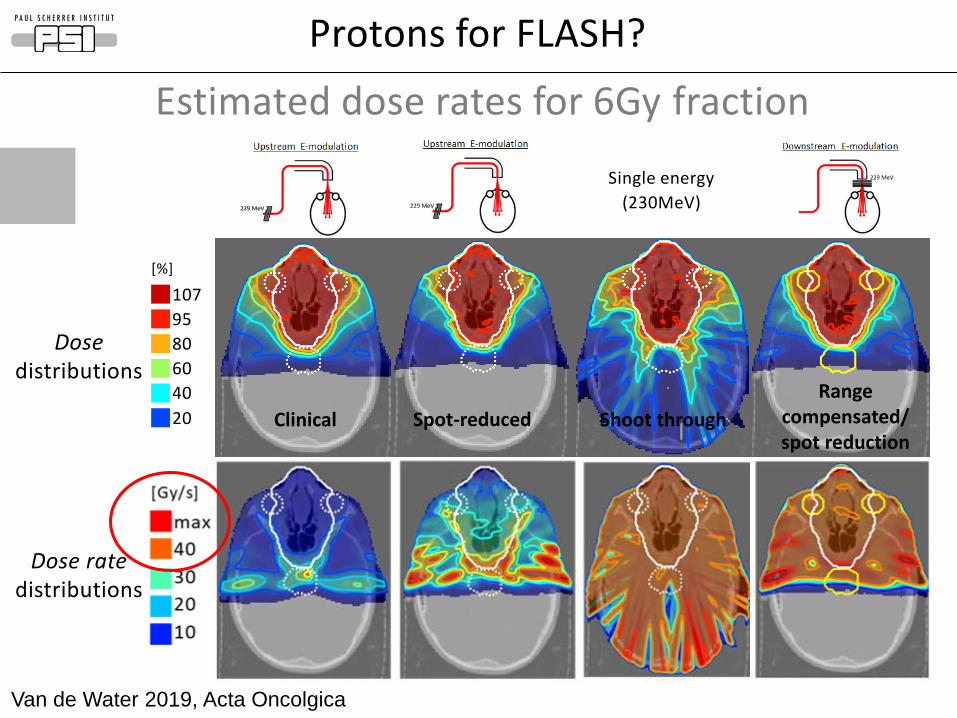
Estimated dose rates for 6Gy fraction
20
40
60
80
95
107
[%]
Range compensated/ spot reduction
Protons for FLASH?
Van de Water 2019, Acta Oncolgica
Single energy
(230MeV)
Clinical Spot-reduced Shoot through
Dose distributions
Dose rate distributions
Estimated dose rates for 6Gy fraction
Summary
• The 3D localization of the Bragg peak allows for high degrees of modulation, leading to exquisite levels of dose conformation
• PBS is currently the most flexible and (now) most widely used delivery modality
• But improvements are still necessary…• Reducing treatment times• Improving lateral penumbra• FLASH compatible PBS• …
• Whatever, there are still lots of interesting developments to be done in accelerators, beam delivery, medical physics, biology and clinics…
Thanks for your attention.