hernias and abdominal wall defects
TRANSCRIPT
Hernias and AbdominalWall Defects
Daniel J. Scott and Daniel B. Jones
Groin Hernias 1133Abdominal Wall Defects 1161
No disease of the human body, belonging to the province of thesurgeon, requires in its treatment, a better combination of accurate,anatomical knowledge with surgical skill than Hernia in all itsvarieties.
Sir AstleyPaston Cooper, The Anatomy and Surgical Treatmentof Inguinal and Congenital Hernia, Cox, London, 1804
Groin Hernias
Definitions
A hernia is a protrusion of visceral contents through theabdominal wall. There are two key components of a hernia.The first is the defect itself, namely, the size and location ofthe defect. The second component is the hernia sac, which isa protrusion of peritoneum through the defect. The hernia sacmay contain abdominal contents such as small intestine,colon, or bladder, or the sac may be empty.
A sliding hernia exists when a retroperitoneal organ,usually the sigmoid colon, cecum, bladder, or ureter, formspart of the wall of the sac; these organs may be injured duringhernia repair. A Richter's hernia exists when the antimesen-teric portion of intestine (not the complete circumference ofbowel) protrudes into the hernia sac. A Littte's hernia existswhen the sac contains a Meckel's diverticulum. If the sac andits contents can be returned to the abdominal cavity, a herniais termed reducible. If it cannot be returned to the abdominalcavity, as is sometimes the case with a small fascial defectand a large hernia, the hernia is termed irreducible or incar-cerated . If an irreducible hernia contains intestine or otherviscera with blood supply that is compromised, the hernia isstrangulated. This can lead to a life-threatening situation inwhich the hernia sac contains gangrenous bowel and requiresemergent exploration.
Anatomy
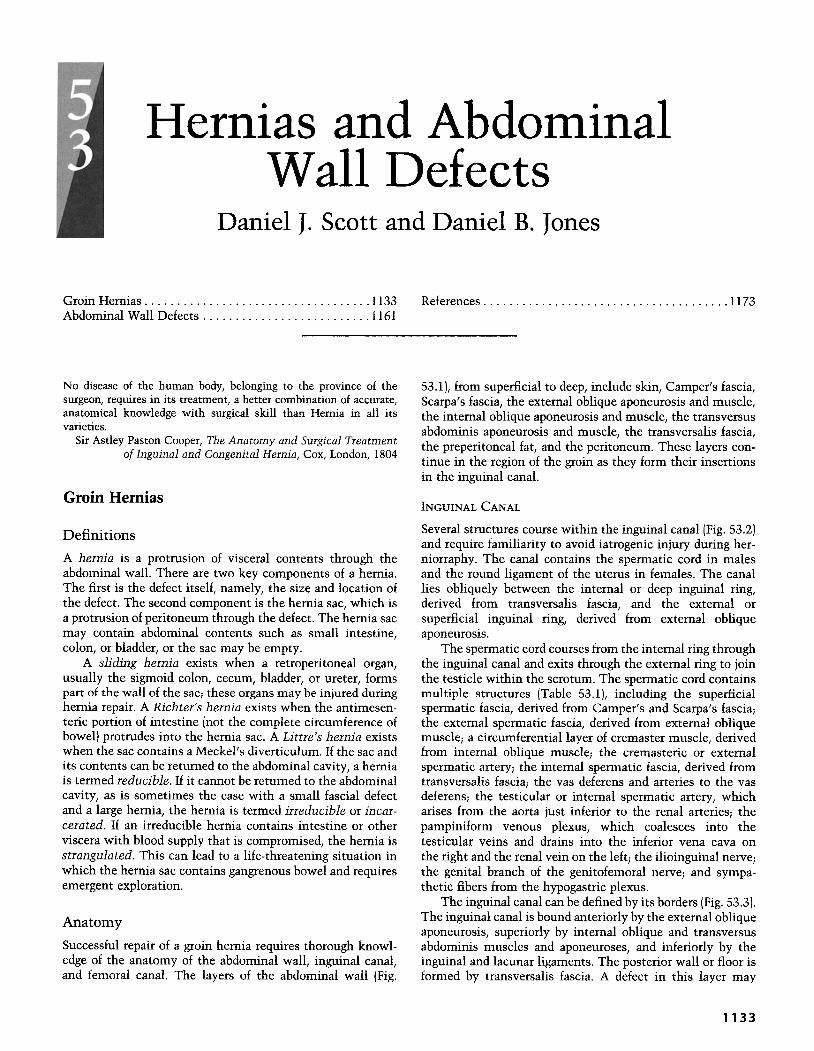
Successful repair of a groin hernia requires thorough knowl-edge of the anatomy of the abdominal wall, inguinal canal,and femoral canal. The layers of the abdominal wall (Fig.
References 1173
53.1), from superficial to deep, include skin, Camper's fascia,Scarpa's fascia, the external oblique aponeurosis and muscle,the internal oblique aponeurosis and muscle, the transversusabdominis aponeurosis and muscle, the transversalis fascia,the preperitoneal fat, and the peritoneum. These layers con-tinue in the region of the groin as they form their insertionsin the inguinal canal.
INGUINAL CANAL
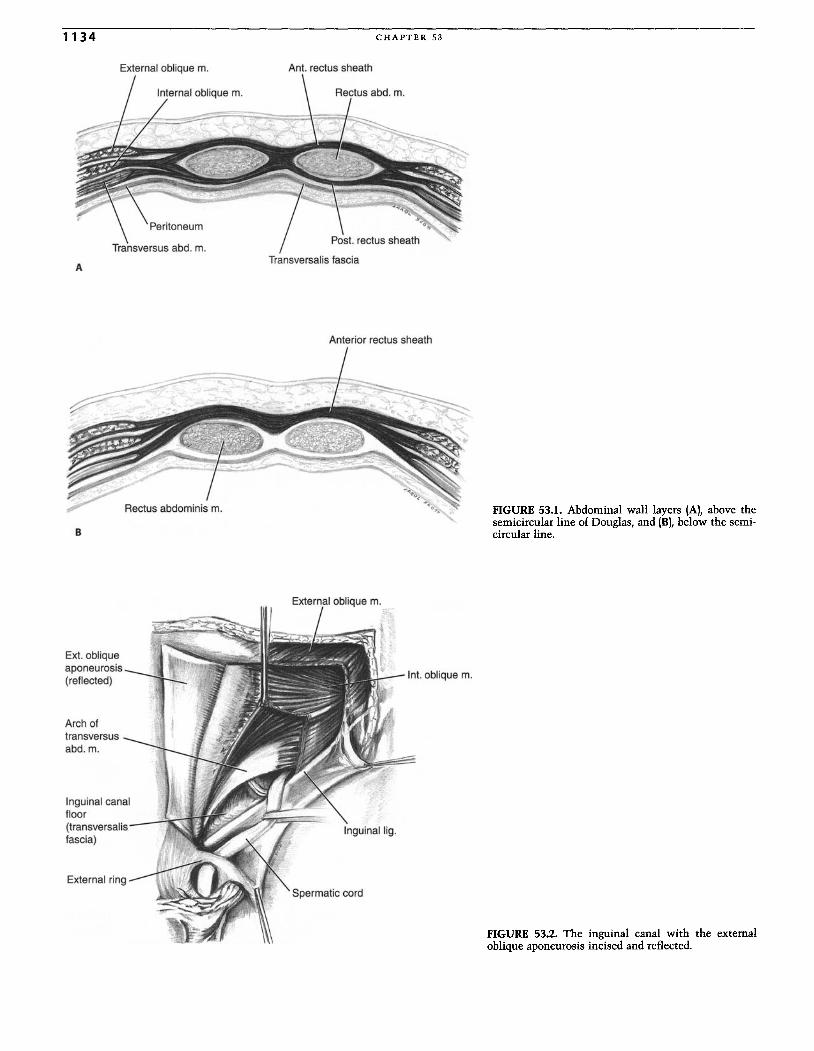
Several structures course within the inguinal canal (Fig. 53.2)and require familiarity to avoid iatrogenic injury during her-niorraphy. The canal contains the spermatic cord in malesand the round ligament of the uterus in females . The canallies obliquely between the internal or deep inguinal ring,derived from transversalis fascia, and the external orsuperficial inguinal ring, derived from external obliqueaponeurosis.
The spermatic cord courses from the internal ring throughthe inguinal canal and exits through the external ring to jointhe testicle within the scrotum. The spermatic cord containsmultiple structures (Table 53.1), including the superficialspermatic fascia, derived from Camper's and Scarpa's fascia;the external spermatic fascia, derived from external obliquemuscle; a circumferential layer of cremaster muscle, derivedfrom internal oblique muscle; the cremasteric or externalspermatic artery; the internal spermatic fascia, derived fromtransversalis fascia; the vas deferens and arteries to the vasdeferens; the testicular or internal spermatic artery, whicharises from the aorta just inferior to the renal arteries; thepampiniform venous plexus, which coalesces into thetesticular veins and drains into the inferior vena cava onthe right and the renal vein on the left; the ilioinguinal nerve;the genital branch of the genitofemoral nerve; and sympa-thetic fibers from the hypogastric plexus.
The inguinal canal can be defined by its borders (Fig. 53.3).The inguinal canal is bound anteriorly by the external obliqueaponeurosis, superiorly by internal oblique and transversusabdominis muscles and aponeuroses, and inferiorly by theinguinal and lacunar ligaments. The posterior wall or floor isformed by transversalis fascia. A defect in this layer may
1 133
1134
Externa l oblique m.
Transversus abd. m.
A
C H A P T E R 53
Ant. rectus sheath
Anterior rectus sheath
B
External oblique m.
FIGURE 53.1. Abdominal wall layers (A), above thesemicircular line of Douglas, and (B), below the semi-circular line.
Ext. obliqueaponeurosis(reflected)
Arch oftransversusabd.m.
Inguinal canalfloor(transversalisfascia)
Spermatic cord
FIGURE 53.2. The inguinal canal with the externaloblique aponeurosis incised and reflected.
HER NIA S A ND ABDOMINAL WALL DEFECTS 1135
TABLE53.1. Spermatic Cord Contents.
NervesIlioinguinal nerveGenital branch of genitofemoral nerveSympathetic fibers
ArteriesCremasteric (external spermatic) arteryTesticular (internal spermatic) arteryArterie s to vas deferens
VeinsPampiniform plexus
MuscleCremaster muscle
FasciaSuperficial spermatic fasciaExternal spermatic fasciaInternal spermatic fascia
Vas deferens
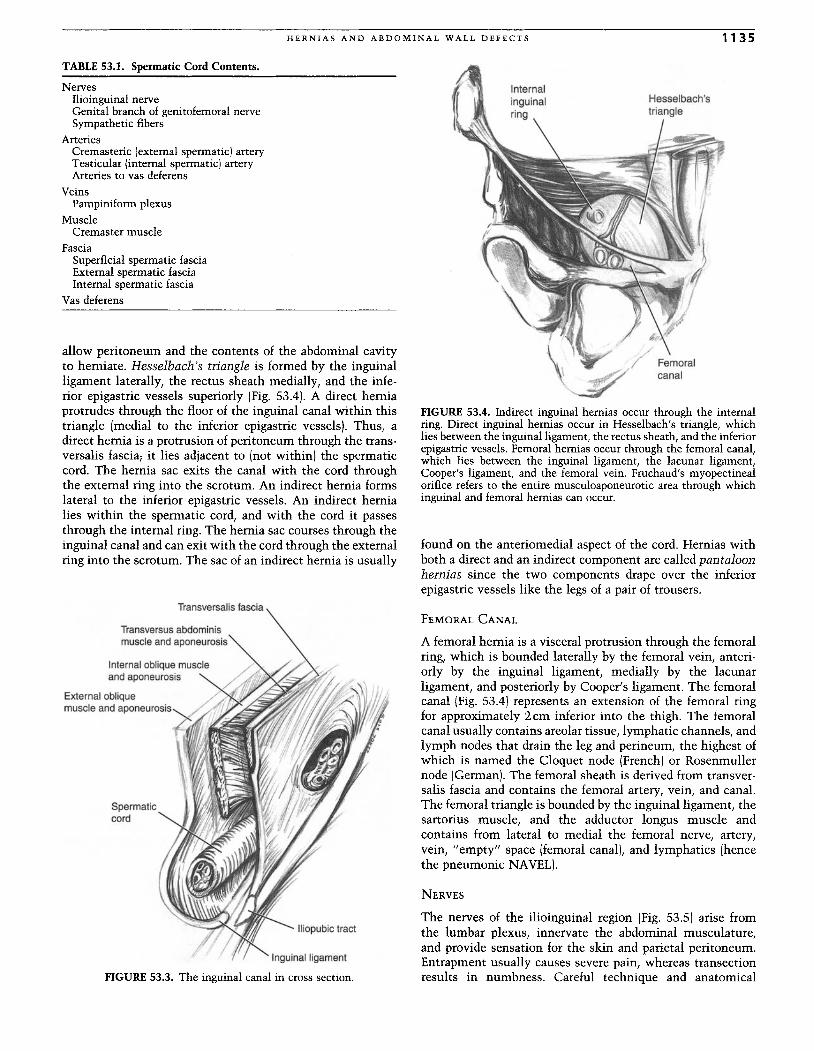
allow peritoneum and the contents of the abdominal cavityto herniate. Hesselbach's triangle is formed by the inguinalligament laterally, the rectus sheath medially, and the infe-rior epigastric vessels superiorly (Fig. 53.4). A direct herniaprotrudes through the floor of the inguinal canal within thistriangle (medial to the inferior epigastric vessels). Thus, adirect hernia is a protrusion of peritoneum through the trans-versalis fascia; it lies adjacent to (not within) the spermaticcord. The hernia sac exits the canal with the cord throughthe external ring into the scrotum. An indirect hernia formslateral to the inferior epigastric vessels . An indirect hernialies within the spermatic cord, and with the cord it passesthrough the internal ring. The hernia sac courses through theinguinal canal and can exit with the cord through the externalring into the scrotum. The sac of an indirect hernia is usually
Transversalisfascia
Transversus abdominismuscle and aponeurosis
Internal oblique muscleand aponeurosis
External obliquemuscleand aponeurosis~
-~
Spermaticcord
Inguinal ligament
FIGURE 53.3. The inguinal canal in cross section.
FIGURE 53.4. Indirect inguinal hernias occur through the internalring. Direct inguinal hernias occur in Hesselbach's triangle, whichlies between the inguinal ligament, the rectus sheath, and the inferiorepigastric vessels . Femoral hernias occur through the femoral canal ,which lies between the inguinal ligament, the lacunar ligament,Cooper's ligament, and the femoral vein. Fruchaud's myopectinealorifice refers to the entire musculoaponeurotic area through whichinguinal and femoral hernias can occur.
found on the anteriomedial aspect of the cord. Hernias withboth a direct and an indirect component are called pantaloonhernias since the two components drape over the inferiorepigastric vessels like the legs of a pair of trousers.
FEMORAL CANAL
A femoral hernia is a visceral protrusion through the femoralring, which is bounded laterally by the femoral vein, anteri-orly by the inguinal ligament, medially by the lacunarligament, and posteriorly by Cooper' s ligament. The femoralcanal (Fig. 53.4) represents an extension of the femoral ringfor approximately 2cm inferior into the thigh. The femoralcanal usually contains areolar tissue, lymphatic channels, andlymph nodes that drain the leg and perineum, the highest ofwhich is named the Cloquet node (French) or Rosenmullernode (German). The femoral sheath is derived from transver-salis fascia and contains the femoral artery, vein, and canal.The femoral triangle is bounded by the inguinal ligament, thesartorius muscle, and the adductor longus muscle andcontains from lateral to medial the femoral nerve, artery,vein, "empty" space (femoral canal), and lymphatics (hencethe pneumonic NAVEL).
NERVES
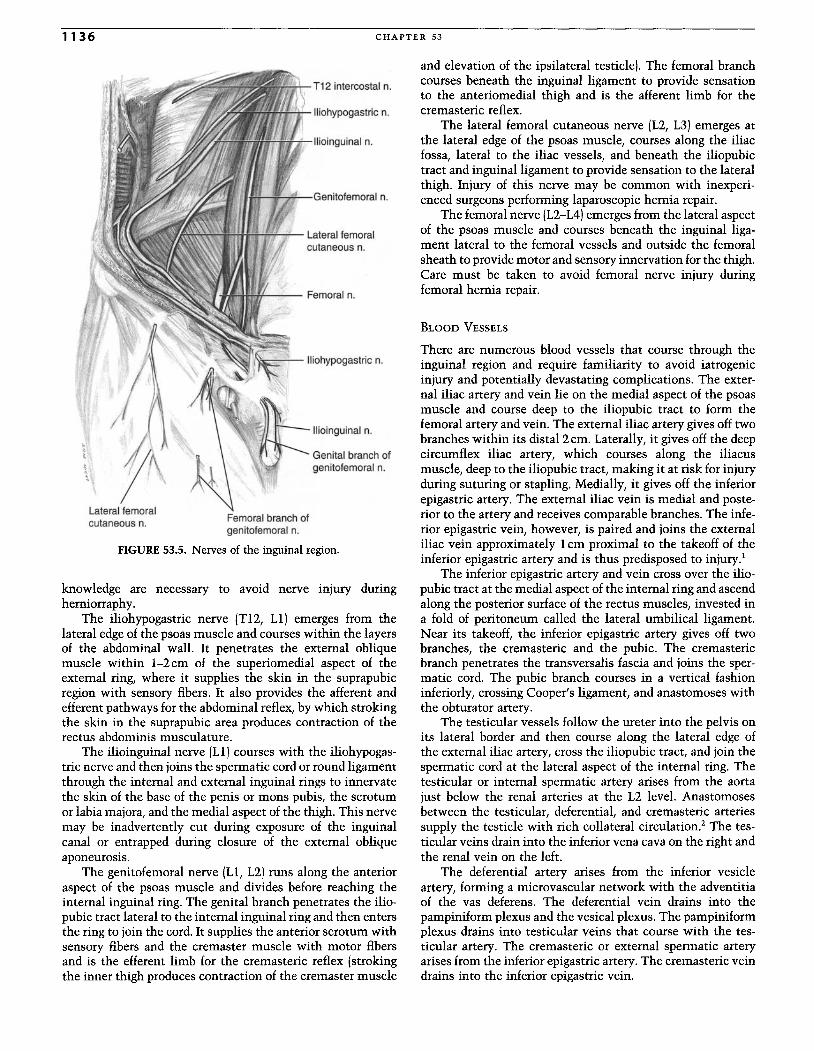
The nerves of the ilioinguinal region (Fig. 53.5) arise fromthe lumbar plexus, innervate the abdominal musculature,and provide sensation for the skin and parietal peritoneum.Entrapment usually causes severe pain, whereas transectionresults in numbness. Careful technique and anatomical
1136 CHAPTER 53
and elevation of the ipsilateral testicle) . The femoral branchcourses beneath the inguinal ligament to provide sensationto the anteriomedial thigh and is the afferent limb for thecremasteric reflex.
The lateral femoral cutaneous nerve (L2, L3) emerges atthe lateral edge of the psoas muscle, courses along the iliacfossa, lateral to the iliac vessels, and beneath the iliopubictract and inguinal ligament to provide sensation to the lateralthigh. Injury of this nerve may be common with inexperi-enced surgeons performing laparoscopic hernia repair.
The femoral nerve (L2-L4) emerges from the lateral aspectof the psoas muscle and courses beneath the inguinal liga-ment lateral to the femoral vessels and outside the femoralsheath to provide motor and sensory innervation for the thigh .Care must be taken to avoid femoral nerve injury duringfemoral hernia repair .
BLOOD VESSELS
There are numerous blood vessels that course through theinguinal region and require familiarity to avoid iatrogenicinjury and potentially devastating complications. The exter-nal iliac artery and vein lie on the medial aspect of the psoasmuscle and course deep to the iliopubic tract to form thefemoral artery and vein . The external iliac artery gives off twobranches within its dista12cm. Laterally, it gives off the deepcircumflex iliac artery, which courses along the iliacusmuscle, deep to the iliopubic tract, making it at risk for injuryduring suturing or stapling. Medially, it gives off the inferiorepigastric artery. The external iliac vein is medial and poste-rior to the artery and receives comparable branches. The infe-rior epigastric vein, however, is paired and joins the externaliliac vein approximately 1em proximal to the takeoff of theinferior epigastric artery and is thus predisposed to injury.'
The inferior epigastric artery and vein cross over the ilio-pubic tract at the medial aspect of the internal ring and ascendalong the posterior surface of the rectus muscles, invested ina fold of peritoneum called the lateral umbilical ligament.Near its takeoff, the inferior epigastric artery gives off twobranches, the cremasteric and the pubic. The cremastericbranch penetrates the transversalis fascia and joins the sper-matic cord. The pubic branch courses in a vertical fashioninferiorly, crossing Cooper's ligament, and anastomoses withthe obturator artery.
The testicular vessels follow the ureter into the pelvis onits lateral border and then course along the lateral edge ofthe external iliac artery, cross the iliopubic tract, and join thespermatic cord at the lateral aspect of the internal ring. Thetesticular or internal spermatic artery arises from the aortajust below the renal arteries at the L2 level. Anastomosesbetween the testicular, deferential, and cremasteric arteriessupply the testicle with rich collateral circulation.' The tes-ticular veins drain into the inferior vena cava on the right andthe renal vein on the left.
The deferential artery arises from the inferior vesicleartery, forming a microvascular network with the adventitiaof the vas deferens. The deferential vein drains into thepampiniform plexus and the vesical plexus. The pampiniformplexus drains into testicular veins that course with the tes-ticular artery. The cremasteric or external spermatic arteryarises from the inferior epigastric artery. The cremasteric veindrains into the inferior epigastric vein.
Iliohypogast ric n.
Genitofemoral n.
T12 intercostal n.
Ilioinguinal n.
Lateral femoralcutaneous n.
Femoral branch ofgenitofemoral n.
FIGURE 53.5. Nerves of the inguinal region.
Lateral femoralcutaneous n.
knowledge are necessary to avoid nerve injury duringherniorraphy.
The iliohypogastric nerve (Tl2, Ll) emerges from thelateral edge of the psoas muscle and courses within the layersof the abdominal wall. It penetrates the external obliquemuscle within 1-2cm of the superiomedial aspect of theexternal ring, where it supplies the skin in the suprapubicregion with sensory fibers. It also provides the afferent andefferent pathways for the abdominal reflex, by which strokingthe skin in the suprapubic area produces contraction of therectus abdominis musculature.
The ilioinguinal nerve [Ll ] courses with the iliohypogas-tric nerve and then joins the spermatic cord or round ligamentthrough the internal and external inguinal rings to innervatethe skin of the base of the penis or mons pubis, the scrotumor labia majora, and the medial aspect of the thigh. This nervemay be inadvertently cut during exposure of the inguinalcanal or entrapped during closure of the external obliqueaponeurosis.
The genitofemoral nerve [Ll, L2) runs along the anterioraspect of the psoas muscle and divides before reaching theinternal inguinal ring. The genital branch penetrates the ilio-pubic tract lateral to the internal inguinal ring and then entersthe ring to join the cord. It supplies the anterior scrotum withsensory fibers and the cremaster muscle with motor fibersand is the efferent limb for the cremasteric reflex (strokingthe inner thigh produces contraction of the cremaster muscle
HERNIA S AND ABDOMINAL WALL DEFECTS 1137
MYOPECTINEAL ORIFICE
Fruchaud published in 1956 the idea that all hernias originatein a single weak area called the myopectineal orifice (Fig.53.4).3This area is bounded superiorly by the internal obliqueand transversus abdominis muscles, inferiorly by the superiorpubic ramus, medially by the rectus muscle and sheath, andlaterally by the iliopsoas muscle. Inguinal and femoral herniasoccur within this area.
INGUINAL LIGAMENT
The inguinal ligament or Poupart's ligament forms from thethickened lateral inferior edge of the external oblique aponeu-rosis (Figs. 53.2 and 53.3). The ligament courses between theanterior superior iliac spine and the pubic tubercle.
ILIOPUBIC TRACT
The iliopubic tract is a thickened lateral extension of thetransversalis fascia that runs from the superior pubic ramusto the iliopectineal arch (Fig. 53.3). It is anterior to Cooper'sligament and posterior to the inguinal ligament. Althoughintimately associated with the inguinal ligament, the iliopu-bic tract is a separate structure and serves a crucial anatomi-cal role in preperitoneal hernia repairs as well as some anteriorrepairs.
LACUNAR LIGAMENT
The lacunar ligament or Gimbernat's ligament is the mostinferior and posterior portion of the inguinal ligament. Theligament is triangular, and its fibers curve to meet Cooper'sligament as it inserts onto the pubic symphysis, forming themedial aspect of the femoral canal.
COOPER'S LIGAMENT
Cooper's ligament or the pectineal ligament is a condensationof transversalis fascia and periosteum of the superior pubic
ramus lateral to the pubic tubercle. It is several millimetersthick, densely adherent to the pubic ramus, and joins theiliopubic tract and lacunar ligaments at their medial inser-tions . Cooper's ligament can be readily palpated as a thickstrong fibrous band, and it is shiny when freed from surround-ing fat and soft tissue.
CONJOINED TENDON
The existence of this structure is debated or at least variable,but it is thought to be a fusion of the lower fibers of theinternal oblique muscle and the aponeurosis of the transver-sus abdominis muscle at their insertions onto the pubictubercle. This structure is largely indistinct from and con-fused with the falx inguinalis or ligament of Henle, which isderived from transversalis fascia as it forms the thickenedlateral aspect of the rectus sheath at its insertion onto thepubic symphysis. Based on work from Hollinshead, Condon,and McVay, Skandalakis et al. concluded that the conjoinedtendon and the falx inguinalis rarely exist and are usuallymistaken for the lateral rectus sheath."
PREPERITONEAL SPACE
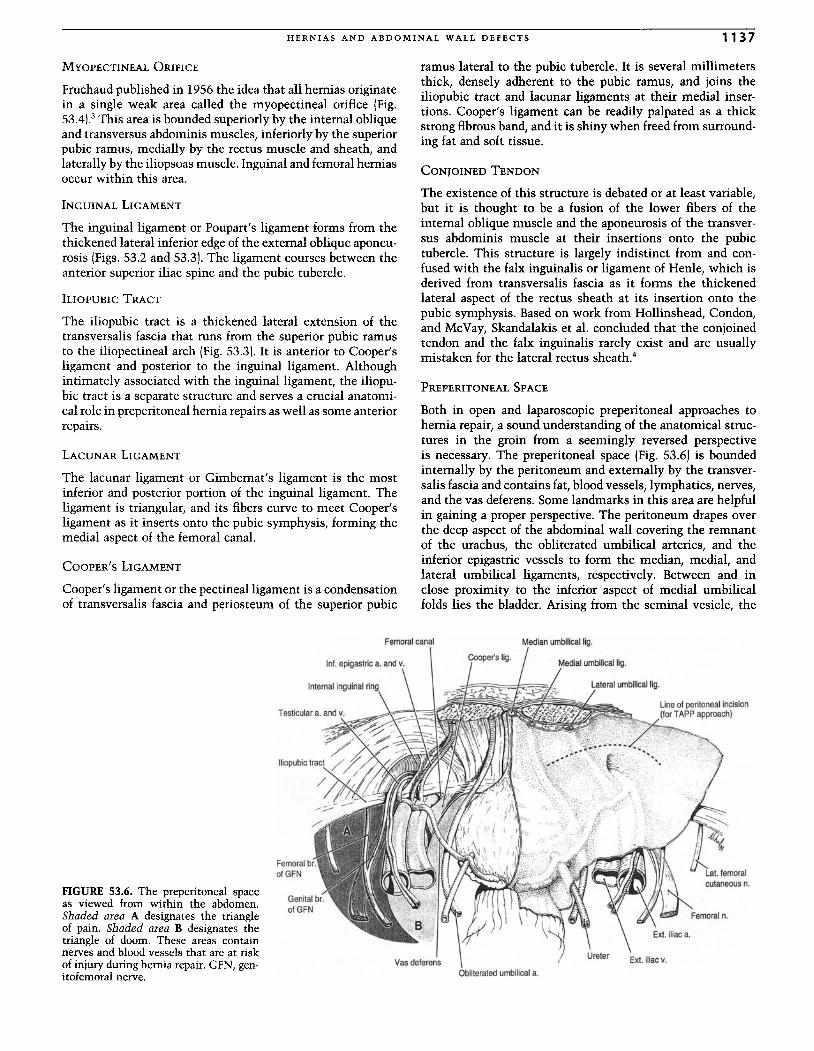
Both in open and laparoscopic preperitoneal approaches tohernia repair, a sound understanding of the anatomical struc-tures in the groin from a seemingly reversed perspectiveis necessary . The preperitoneal space (Fig. 53.6) is boundedinternally by the peritoneum and externally by the transver-salis fascia and contains fat, blood vessels, lymphatics, nerves,and the vas deferens. Some landmarks in this area are helpfulin gaining a proper perspective. The peritoneum drapes overthe deep aspect of the abdominal wall covering the remnantof the urachus, the obliterated umbilical arteries, and theinferior epigastric vessels to form the median, medial, andlateral umbilical ligaments, respectively. Between and inclose proximity to the inferior aspect of medial umbilicalfolds lies the bladder. Arising from the seminal vesicle, the
FIGURE 53.6. The preperitoneal spaceas viewed from within the abdomen.Shaded area A designates the triangleof pain . Shaded area B designates thetriangle of doom. These areas containnerves and blood vessels that are at riskof injury during hernia repair. GFN, gen-itofemoral nerve .
Femoral br.of GFN
Femoral canal
Vasdeferens
Median umbilical lig.
Medial umbilical lig.
Obliteratedumbilicala.
Line of peritoneal incision(forTAPP approach)

1138 CHAPTER 53
vas deferens courses laterally over Cooper's ligament, theexternal iliac vessels, and the iliopubic tract to enter themedial aspect of the internal ring and join the spermatic cord.Entering the internal ring laterally are the testicular vessels.The testicular vessels and the vas deferens at the internal ringform the apex of a theoretical triangle called the triangle ofdoom. Within this triangle lie the external iliac artery andvein, as well as the genital and femoral branches of the geni-tofemoral nerve, hidden under peritoneum and transversalisfascia, placing them at high risk of injury. The triangle of painlies lateral to this, and its apex is formed inferomedially bythe testicular vessels and superolaterally by the iliopubictract. Within this triangle lie the femoral branch of the geni-tofemoral nerve, the femoral nerve, and the lateral cutaneousfemoral nerve. Stapling of these structures during a laparo-scopic hernia repair results in painful neuralgias and shouldbe avoided.
Two eponyms refer to the preperitoneal space in the areaof the bladder. The space of Retzius is retropubic and situatedin front of and to the sides of the bladder. The space of Bogrosis a lateral extension to the space of Retzius, bounded later-ally by the iliac fascia, anteriorly by the transversalis fascia,and medially by the peritoneum.
A significant amount of preperitoneal fat may be present.If this fat herniates through the internal inguinal ring, it isknown as a cord lipoma and may mimic an indirect hernia.
Etiology
There is no doubt that the first appearance of the mammal, with hisunexplained need to push his testicles out of their proper home intothe air, made a mess of the three layered abdominal wall that haddone the reptiles well for 200 million years.
Sir Heneage Ogilvie, Hernia, Edward Arnold, London, 1959
Inguinal hernias may be caused by congenital factors, espe-cially in children.S This necessitates an understanding of theembryology of the inguinal region for proper surgical manage-ment. The ligamentous gubernaculum descends on each sideof the abdomen from the inferior pole of the gonad to theinternal surface of the labial-scrotal swelling. The gubernacu-lum passes through the abdominal wall at the site of thefuture inguinal canal. The processus vaginalis is a diverticularevagination of the peritoneum that forms ventral to thegubernaculum bilaterally and passes through the abdominalwall with the gubernaculum. The testes are initially retro-peritoneal, and with the processus vaginalis they descendthrough the inguinal canal into the scrotum as the guber-naculum contracts. The ovaries descend into the pelvis, andthe inferior aspect of the gubernaculum becomes the roundligament, which passes through the internal ring into thelabia majus. The processus vaginalis normally closes, obliter-ating this extension of the peritoneal cavity through the inter-nal ring. The obliterated remnant attached to the testis isknown as the tunica vaginalis.
If the processus vaginalis remains patent in the male, avariety of hydroceles or an indirect hernia may form. If theprocessus vaginalis remains patent in a female, it extends intothe labia majus and is known as the canal of Nuck. The inci-dence of a patent processus vaginalis is 600/0 at 2 months and400/0 at 2 years of age."However, a patent processus vaginalisdoes not uniformly translate into having an inguinal hernia;the incidence of a patent processus vaginalis in adults without
clinical appearance of a hernia is 200/0 to 30% in autopsyseries."
A variety of connective tissue abnormalities have alsobeen demonstrated as associated with an increased incidenceof hernias. Abnormal collagen structure and composition, aswell as fibroblast dysfunction, have been noted in severalstudies.I:" Related to collagen formation, malnutrition andvitamin deficiencies have been implicated as contributingfactors. Increased elastiolytic enzyme levels found in ciga-rette smokers and in patients with aortic aneurysms havebeen associated with groin hernias." Connective tissuedisorders such as Ehlers-Danlos syndrome and Marfan syn-drome are also associated with an increased incidence ofhernias. 10
Increased intraabdominal pressure has also been associ-ated with hernia formation. This is especially true withperitoneal dialysis and ascites." Obesity and advanced age arealso risk factors. Chronic cough in patients with chronicobstructive pulmonary disease, straining in patients withbenign prostatic hypertrophy or chronic constipation, orstrenuous labor may increase the wear-and-tear effect on theabdominal wall and increase the risk of hernia formation."
Diagnosis
The gold standard for hernia diagnosis is a history and physi-cal exam. Patients will usually complain of a persistent orintermittent bulge in the groin associated with some degreeof discomfort, aggravated by physical exertion. If the herniais reducible, the pain may wax and wane. A more persistentpain is typical of an incarcerated hernia. If fever, tachycardia,exquisite tenderness on palpation, erythema of the overlyingskin, leukocytosis, and obstructive symptoms are present, anirreducible hernia is likely strangulated and warrants imme-diate operative intervention.
To examine a patient for a groin hernia, the physician isseated, and the disrobed patient stands and faces the exam-iner. First, the groin is visually inspected for evidence of abulge and then palpated with the patient straining eitherby coughing or by performing a Valsalva maneuver. Next, thisprocedure is repeated with the examiner's gloved fingerinserted into the redundant scrotal skin, reaching onto theabdominal wall and into the external inguinal ring, just lateralto the pubic tubercle. During the straining exercise, an ingui-nal hernia will be evident as a bulge or mass pushing down-ward onto the examiner's fingertip. The same examinationcan be performed on females by inserting the finger into thelabia majus to gain access to the external ring. Although ithas been claimed by some that it is possible to distinguish adirect hernia from an indirect one by physical exam, this isneither accurate nor necessary since the operative approachfor either is the same.
A femoral hernia will appear as a mass below the inguinalligament in the area medial to the femoral pulse and can beelicited by similar straining techniques. Femoral hernias maybe difficult to diagnose, especially in obese patients, and asecond opinion is frequently reassuring.
After examining the patient for both an inguinal andfemoral hernia with the patient standing, the patient shouldbe reexamined in a similar fashion in the supine position. Itis important to note that both groins should be examined toexclude bilateral hernias. Masses other than hernias in this

HERNIAS AND ABDOMINAL WALL DEFECTS 1139
TABLE53.2. Differential Diagnosis of Groin Masses.
Inguinal hernia
Femoral hernia
Lipoma
Lymphadenitis
Lymphadenopathy
Abscess
Hematoma
Varicocele
Hydrocele
Testicular mass
Testicular torsion
Epididymitis
Ectopic testicle
Femoral aneurysm or pseudoaneurysm
Cyst
Seroma
area must be ruled out, and this can usually be done byphysical exam (Table 53.2).
Herniography, by which a small amount of contrast mate-rial is injected into the peritoneal cavity and radiographs aretaken during a Valsalva maneuver, has been advocated as auseful imaging study in patients with groin pain and no evi-dence of a hernia on physical exam." Computed tomography(CT) and ultrasound scanning may help exclude other causesof groin masses.
Epidemiology and Classification
Approximately 680,000 inguinal hernia repairs are performedannually." Greater than 900/0 are performed on males. Femalepatients undergo three times as many femoral repairs asmales, although females undergo three times as many ingui-nal repairs as femoral repairs. In Rutledge's report of 1437primary groin hernias, 600/0 were indirect, 360/0 direct, and 40/0femoral." In the Lichtenstein group's report of 4000 primaryinguinal hernias, 44.40/0 were indirect, 43.1 % direct, 12.50/0pantaloon, 11.40/0 sliding, and 250/0 bilateral." Indirect ingui-nal hernias are more common on the right side, possiblyrelated to the later descent of the right testicle and delayedclosure of the processus vaginalis. The true overall incidenceof sliding hernias is only about 2% but rises with age. Mul-tiple classification schemes have been developed; the mostwidely accepted is the Nyhus classification (Table 53.3).16
Management
Traditionally, hernias are electively repaired since the naturalhistory of hernias dictates that they only become larger, donot resolve spontaneously, and can lead to intestinal obstruc-tion or strangulation. However, several investigators haverecently questioned the need to repair asymptomatic hernias,and a multicenter prospective randomized trial is underwaycomparing "watchful waiting" versus a Lichtenstein repair inthis population of patients. Meanwhile, most surgeons agreethat all symptomatic hernias should be repaired. The onlyexception to this dictum is in patients too debilitated toundergo repair or in patients whose operative risks are exces-
sively high. In this instance, a truss, a device worn tocompress the hernia, may offer some relief of symptoms.Otherwise, trusses are of little benefit and should not beoffered as a treatment option. Trusses are contraindicated infemoral hernias due to a high risk of strangulation. I? With theadvent of highly successful local anesthetic techniques forhernia repair, most patients can undergo operative repair.
Generally, it is safe to attempt reduction of an incarcer-ated hernia in the absence of evidence of strangulation. Anal-gesics may be required, and Trendelenberg positioning maybe helpful. In a chronically incarcerated hernia, a very smallbut real risk of en masse reduction exists, in which the herniamay be successfully reduced into the abdominal cavity butthe contents of the sac remain incarcerated within a con-stricting fibrous band at the neck of the sac. This is usuallymanifested as continued obstructive symptoms and can leadto strangulation, bowel necrosis, and even patient death, war-ranting close follow-up after hernia reduction and immediateexploration if an en masse reduction is thought to haveoccurred." Any hernia that is unable to be successfullyreduced requires prompt operative intervention.
Repairs
ANTERIOR ApPROACHES
The goal of all repairs is to close the myofascial defect throughwhich the hernia protrudes. This can be done from a numberof approaches with or without placement of a prostheticmesh. The classic tissue repairs use permanent suture toreinforce the internal inguinal ring and the floor of the ingui-nal canal and do not employ the use of a prosthesis. Theseinclude the Marcy, Bassini, Shouldice, and McVay repairs.The Lichtenstein repair employs prosthetic mesh, as does theplug technique. Common to all of these methods is the ante-rior dissection of the inguinal canal and hernia sac, followedby a myofascial repair, and closure of the canal. The basictechnique of inguinal canal and sac dissection is the same forall anterior approaches, while the repair of the myofascialdefect differs.
In an anterior repair, the groin is explored through anoblique incision parallel to the inguinal ligament in the linesof Langer and is carried down through Camper's and Scarpa'sfascias to the external oblique aponeurosis. This aponeurosisis incised parallel to the axis of its fibers perpendicular to andthrough the external ring, taking care to preserve, if possible,
TABLE 53.3. Nyhus Classification of Groin Hernias.
Type 1. Indirect inguinal hernia-normal internal inguinal ring
Type 2. Indirect inguinal hernia-enlarged internal inguinal ringbut intact inguinal canal floor
Type 3. Posterior wall defectA. Direct inguinal herniaB. Indirect inguinal hernia-enlarged internal inguinal
ring with destruction of adjacent inguinal canal floor(e.g., massive scrotal, sliding, or pantaloon hernias)
C. Femoral hernias
Type 4. Recurrent herniaA. DirectB. IndirectC. FemoralD. Combined
1140 CHAPTER 53
External oblique aponeurosis
External inguinal ring Ilioinguinal n.(overlying spermatic cord)
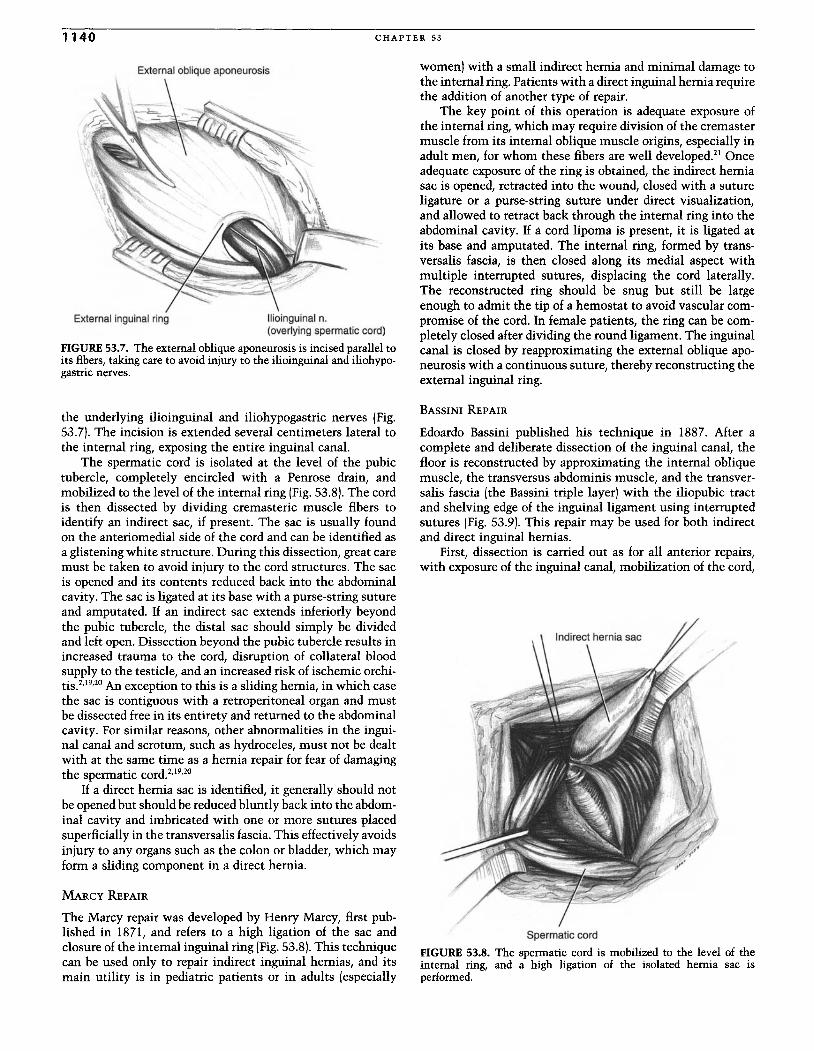
FIGURE 53.7. The external oblique aponeurosis is incised parallel toits fibers, taking care to avoid injury to the ilioinguinal and iliohypo-gastric nerves.
the underlying ilioinguinal and iliohypogastric nerves (Fig.53.7). The incision is extended several centimeters lateral tothe internal ring, exposing the entire inguinal canal.
The spermatic cord is isolated at the level of the pubictubercle, completely encircled with a Penrose drain, andmobilized to the level of the internal ring (Fig. 53.8).The cordis then dissected by dividing cremasteric muscle fibers toidentify an indirect sac, if present. The sac is usually foundon the anteriomedial side of the cord and can be identified asa glistening white structure. During this dissection, great caremust be taken to avoid injury to the cord structures. The sacis opened and its contents reduced back into the abdominalcavity. The sac is ligated at its base with a purse-string sutureand amputated. If an indirect sac extends inferiorly beyondthe pubic tubercle, the distal sac should simply be dividedand left open. Dissection beyond the pubic tubercle results inincreased trauma to the cord, disruption of collateral bloodsupply to the testicle, and an increased risk of ischemic orchi-tiS.2,19,20 An exception to this is a sliding hernia, in which casethe sac is contiguous with a retroperitoneal organ and mustbe dissected free in its entirety and returned to the abdominalcavity. For similar reasons, other abnormalities in the ingui-nal canal and scrotum, such as hydroceles, must not be dealtwith at the same time as a hernia repair for fear of damagingthe spermatic cord.2,19,20
If a direct hernia sac is identified, it generally should notbe opened but should be reduced bluntly back into the abdom-inal cavity and imbricated with one or more sutures placedsuperficially in the transversalis fascia. This effectively avoidsinjury to any organs such as the colon or bladder, which mayform a sliding component in a direct hernia.
MARCY REPAIR
The Marcy repair was developed by Henry Marcy, first pub-lished in 1871, and refers to a high ligation of the sac andclosure of the internal inguinal ring (Fig. 53.8).This techniquecan be used only to repair indirect inguinal hernias, and itsmain utility is in pediatric patients or in adults (especially
women) with a small indirect hernia and minimal damage tothe internal ring. Patients with a direct inguinal hernia requirethe addition of another type of repair.
The key point of this operation is adequate exposure ofthe internal ring, which may require division of the cremastermuscle from its internal oblique muscle origins, especially inadult men, for whom these fibers are well developed." Onceadequate exposure of the ring is obtained, the indirect herniasac is opened, retracted into the wound, closed with a sutureligature or a purse-string suture under direct visualization,and allowed to retract back through the internal ring into theabdominal cavity. If a cord lipoma is present, it is ligated atits base and amputated. The internal ring, formed by trans-versalis fascia, is then closed along its medial aspect withmultiple interrupted sutures, displacing the cord laterally.The reconstructed ring should be snug but still be largeenough to admit the tip of a hemostat to avoid vascular com-promise of the cord. In female patients, the ring can be com-pletely closed after dividing the round ligament. The inguinalcanal is closed by reapproximating the external oblique apo-neurosis with a continuous suture, thereby reconstructing theexternal inguinal ring.
BASSINI REPAIR
Edoardo Bassini published his technique in 1887. After acomplete and deliberate dissection of the inguinal canal, thefloor is reconstructed by approximating the internal obliquemuscle, the transversus abdominis muscle, and the transver-salis fascia (the Bassini triple layer) with the iliopubic tractand shelving edge of the inguinal ligament using interruptedsutures (Fig. 53.9). This repair may be used for both indirectand direct inguinal hernias.
First, dissection is carried out as for all anterior repairs,with exposure of the inguinal canal, mobilization of the cord,
Spermatic cord
FIGURE 53.8. The spermatic cord is mobilized to the level of theinternal ring, and a high ligation of the isolated hernia sac isperformed.
HERNIA S AND ABD OMIN AL WALL DEFE CTS 1141
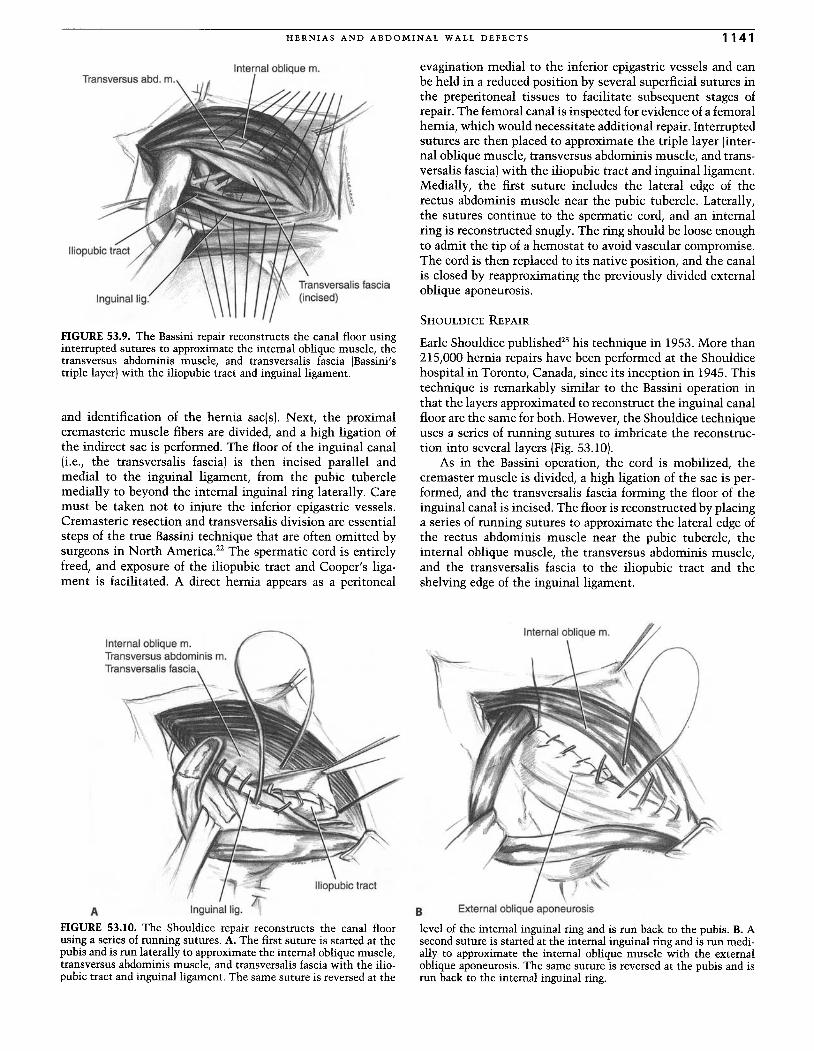
Internal oblique m.
FIGURE 53.9. The Bassini repair reconstructs the canal floor usinginterrupted sutures to approximate the internal oblique muscle, thetransversus abdominis muscle, and transversalis fascia (Bassini'striple layer)with the iliopubic tract and inguinal ligament.
and identification of the hernia sacls] . Next, the proximalcremasteric muscle fibers are divided, and a high ligation ofthe indirect sac is performed. Th e floor of the inguinal canal[i.e., the transversalis fascia ) is then incised parallel andmedial to the inguinal ligament, from th e pubic tuberclemedially to beyond the internal inguinal ring laterally. Caremust be taken not to injure th e inferior epigastric vessels.Cremasteric resection and transversalis division are essentialsteps of the true Bassini technique that are often omitted bysurgeons in North America." Th e spermatic cord is entirelyfreed, and exposure of the iliopubic tract and Cooper's liga-ment is facilitated. A direct hernia appears as a peritoneal
evagination medial to the inferior epigastric vessels and canbe held in a reduced position by several superficial sutures inthe preperitoneal tissues to facilitate subsequent stages ofrepair. The femoral canal is inspected for evidence of a femoralhernia, which would necessitat e additional repair. Interruptedsutures are then placed to approximate the triple layer (inter-nal oblique muscle, transversus abdominis muscle, and trans-versalis fascia )with the iliopubic tract and inguinal ligament.Medially, the first suture includes the lateral edge of th erectus abdominis muscle near the pubic tubercle. Laterally,the sutures continue to the spermatic cord, and an internalring is reconstructed snugly. The ring should be loose enoughto admit the tip of a hemostat to avoid vascular compromise.The cord is then replaced to its native position, and the canalis closed by reapproximating the previously divided externaloblique aponeurosis.
SHOULDICE REPAIR
Earle Shouldice published'" his technique in 1953. More than215,000 hernia repairs have been performed at the Shouldicehospital in Toronto, Canada, since its inception in 1945. Thistechnique is remarkably similar to the Bassini operation inthat the layers approximated to recon struct the inguinal canalfloor are the same for both. However, the Shouldice techniqueuses a series of running sutures to imbricate the reconstruc-tion into several layers (Fig. 53.10).
As in the Bassini operation, the cord is mobilized, thecremaster muscle is divided, a high ligation of the sac is per-formed, and the transversalis fascia forming the floor of theinguinal canal is incised. Th e floor is reconstructed by placinga series of running sutures to approximate the lateral edge ofthe rectus abdominis muscle near the pubic tubercle, theinternal oblique muscle, th e transversus abdominis muscle,and the transversalis fascia to the iliopubic tract and theshelving edge of the inguinal ligament.
B External oblique aponeurosis
level of the internal inguinal ring and is run back to the pubis. B. Asecondsuture is started at the internal inguinal ring and is run medi-ally to approximate the internal oblique muscle with the externalobliqueaponeurosis. The same suture is reversed at the pubis and isrun back to the internal inguinal ring.
Internal oblique m.Transversus abdominis m.Transversalis fascia
A Inguinal lig. l'FIGURE 53.10. The Shouldice repair reconstructs the canal floorusinga series of running sutures. A. The first suture is started at thepubisand is run laterally to approximate the internal obliquemuscle,transversus abdominismuscle, and transversalis fascia with the ilio-pubic tract and inguinal ligament. The same suture is reversed at the
l~\.
Internal ObUq", : p--,:t{ I
""
1142 CHAPTER 53
The Bassini and the Shouldice repairs are criticized for notaddressing the femoral canal and for approximating tissuelayers that are not normally in juxtaposition, yielding a non-anatomic reconstruction. However, proponents of both oper-ations point out that postoperative femoral hernias occur veryrarely (in 0.14% of cases]," and that a wealth of data supportsthe efficacy of these techniques.
Glassow published the largest series of Shouldice repairsin 1986 with outstanding results." In 12,548 first-time repairsperformed between 1954 and 1974, the recurrence rate was1.1% over a lO-year follow-up period. In 1874 repairs of recur-rent hernias, the recurrence rate was 3.3%. Likewise, Wantzpublished results of 5120 repairs with a recurrence rate of1.3% for first-time hernias and 6.7% for recurrent hernias,with an overall complication rate of 1.9%.26
A multicenter prospective randomized controlled trialin France subsequently compared 1706 nonrecurrent herniarepairs in 1578 adult men using Bassini, Cooper's ligament,Shouldice with polypropylene suture, and Shouldice withstainless steel suture techniques." Recurrence rates over5.75-year median follow-up were 8.6% for Bassini, 11.2% forCooper's ligament, 6.5% for Shouldice with polypropylene,and 5.9% for Shouldice with stainless steel. The difference inrecurrence rates using different suture in the Shouldice groupswas not statistically significant. Postoperative morbidity wascomparable for all groups except for delayed ambulation inpatients undergoing Cooper's ligament repairs. The authorsconcluded that the Shouldice repair should be the gold stan-dard for inguinal hernia repair .
McGillicuddy reported the results of a prospective ran-domized trial comparing Shouldice and Lichtenstein repairsin 717 hernias in 672 patients." Recurrence rates over 5-yearmean follow-up were 2% for Shouldice and 0.5% for Lichten-stein repairs (not statistically different). Complications werecomparable, and the author reported both procedures werecomparable and effective, although he personally favored theLichtenstein approach for its relative simplicity.
MCVAY (COOPER'S LIGAMENT) REPAIR
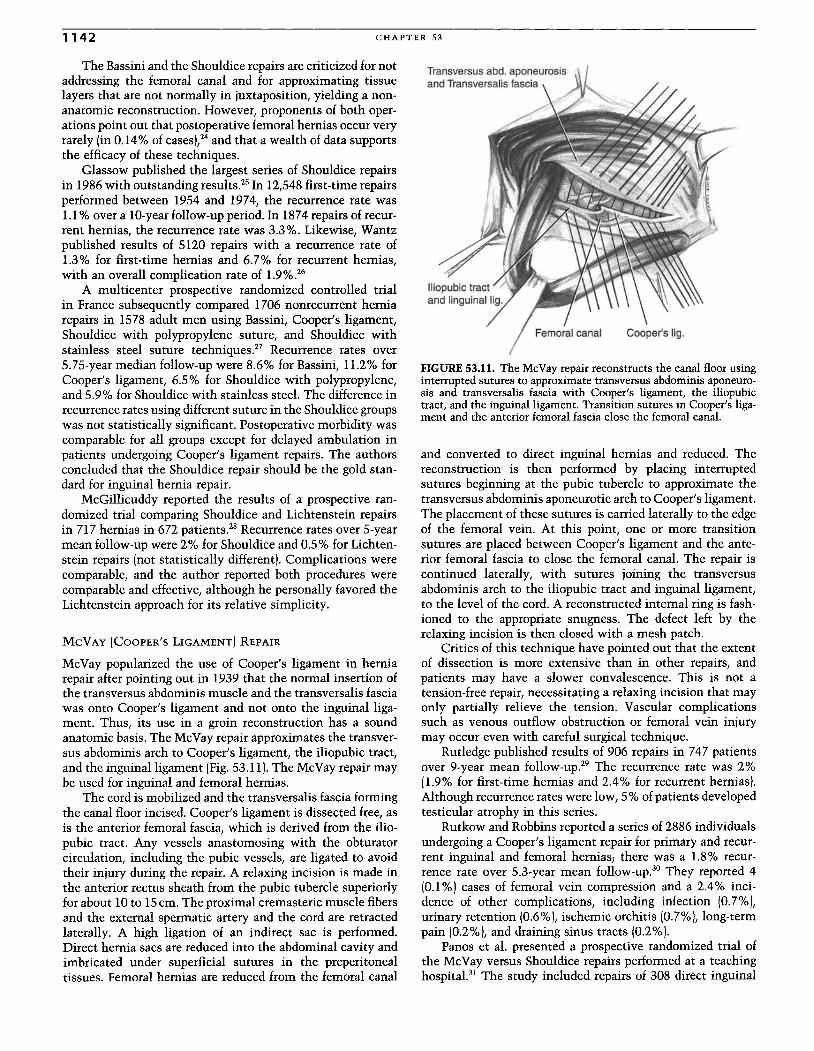
McVay popularized the use of Cooper's ligament in herniarepair after pointing out in 1939 that the normal insertion ofthe transversus abdominis muscle and the transversalis fasciawas onto Cooper's ligament and not onto the inguinal liga-ment. Thus, its use in a groin reconstruction has a soundanatomic basis. The McVay repair approximates the transver-sus abdominis arch to Cooper 's ligament, the iliopubic tract,and the inguinal ligament (Fig. 53.11). The McVay repair maybe used for inguinal and femoral hernias.
The cord is mobilized and the transversalis fascia formingthe canal floor incised. Cooper's ligament is dissected free, asis the anterior femoral fascia, which is derived from the ilio-pubic tract. Any vessels anastomosing with the obturatorcirculation, including the pubic vessels, are ligated to avoidtheir injury during the repair. A relaxing incision is made inthe anterior rectus sheath from the pubic tubercle superiorlyfor about 10 to 15em. The proximal cremasteric muscle fibersand the external spermatic artery and the cord are retractedlaterally. A high ligation of an indirect sac is performed.Direct hernia sacs are reduced into the abdominal cavity andimbricated under superficial sutures in the preperitonealtissues. Femoral hernias are reduced from the femoral canal
FIGURE 53.11. The McVay repair reconstructs the canal floor usinginterrupted sutures to approximate transversus abdominis aponeuro-sis and transversalis fascia with Cooper's ligament, the iliopubictract , and the inguinal ligament. Transition sutures in Cooper's liga-ment and the anterior femoral fascia close the femoral canal.
and converted to direct inguinal hernias and reduced . Thereconstruction is then performed by placing interruptedsutures beginning at the pubic tubercle to approximate thetransversus abdominis aponeurotic arch to Cooper's ligament.The placement of these sutures is carried laterally to the edgeof the femoral vein. At this point, one or more transitionsutures are placed between Cooper 's ligament and the ante-rior femoral fascia to close the femoral canal. The repair iscontinued laterally, with sutures joining the transversusabdominis arch to the iliopubic tract and inguinal ligament,to the level of the cord. A reconstructed internal ring is fash-ioned to the appropriate snugness. The defect left by therelaxing incision is then closed with a mesh patch.
Critics of this technique have pointed out that the extentof dissection is more extensive than in other repairs, andpatients may have a slower convalescence. This is not atension-free repair, necessitating a relaxing incision that mayonly partially relieve the tension. Vascular complicationssuch as venous outflow obstruction or femoral vein injurymay occur even with careful surgical technique.
Rutledge published results of 906 repairs in 747 patientsover 9-year mean follow-up." The recurrence rate was 2%(1.9% for first -time hernias and 2.4% for recurrent hernias).Although recurrence rates were low,S % of patients developedtesticular atrophy in this series.
Rutkow and Robbins reported a series of 2886 individualsundergoing a Cooper's ligament repair for primary and recur-rent inguinal and femoral hernias; there was a 1.8% recur-rence rate over 5.3-year mean follow-up ." They reported 4(0.1 %) cases of femoral vein compression and a 2.4% inci-dence of other complications, including infection (0.7%),urinary retention (0.6%1, ischemic orchitis (0.7%), long-termpain (0.2%1, and draining sinus tracts (0.2%).
Panos et al. presented a prospective randomized trial ofthe McVay versus Shouldice repairs performed at a teachinghospital." The study included repairs of 308 direct inguinal
HERNIA S AND ABD OMINAL WALL DEFECT S 1143
hernias in 269 patients. Recurrence rates were 6.6% forMcVay versus 8.8% for Shouldice (not statistically signifi-cant) over 36.4-month mean follow-up . Of note, bilateralhernias repaired simultaneously with either of these tension-creating methods produced a recurrence rate of 12.8% versus5.6% for unilateral repairs (P:O; .05).
LICHTENSTEIN REPAIR
Irving Lichtenstein has championed the tension-free approachto groin hernia repair since its introduction in 1986.32
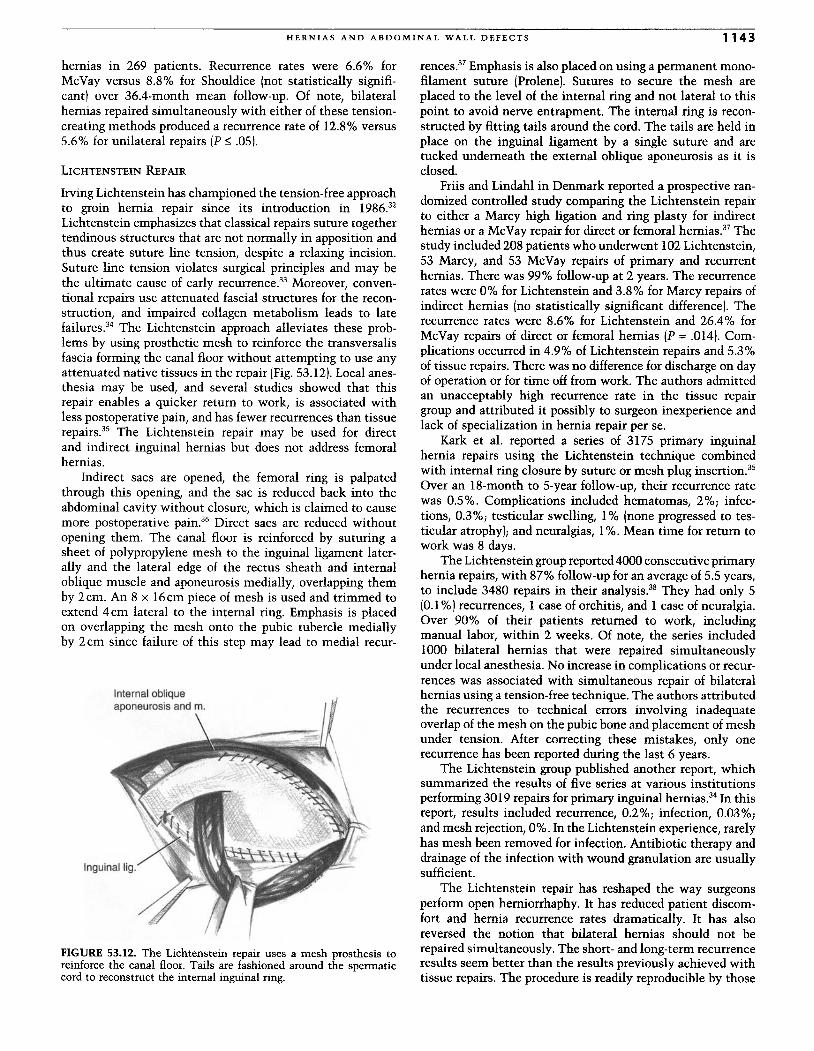
Lichtenstein emphasizes that classical repairs suture togethertendinous structures that are not normally in apposition andthus create suture line tension, despite a relaxing incision.Suture line tension violates surgical principles and may bethe ultimate cause of early recurrence." Moreover, conven-tional repairs use attenuated fascial structures for the recon-struction, and impaired collagen metabolism leads to latefailures." The Lichtenstein approach alleviates these prob-lems by using prosthetic mesh to reinforce the transversalisfascia forming the canal floor without attempting to use anyattenuated native tissues in the repair (Fig. 53.12). Local anes-thesia may be used, and several studies showed that thisrepair enables a quicker return to work, is associated withless postoperative pain, and has fewer recurrences than tissuerepairs." The Lichtenstein repair may be used for directand indirect inguinal hernias but does not address femoralhernias.
Indirect sacs are opened, the femoral ring is palpatedthrough this opening, and the sac is reduced back into theabdominal cavity without closure, which is claimed to causemore postoperative pain ." Direct sacs are reduced withoutopening them. The canal floor is reinforced by suturing asheet of polypropylene mesh to the inguinal ligament later-ally and the lateral edge of the rectus sheath and internaloblique muscle and aponeurosis medially, overlapping themby 2cm. An 8 x 16cm piece of mesh is used and trimmed toextend 4cm lateral to the internal ring. Emphasis is placedon overlapping the mesh onto the pubic tubercle mediallyby 2cm since failure of this step may lead to medial recur-
Internal obliqueaponeurosis and m.
FIGURE 53.12. The Lichtenstein repair uses a mesh prosthesis toreinforce the canal floor. Tails are fashioned around the spermaticcord to reconstruct the internal inguinal ring.
rences ." Emphasis is also placed on using a permanent mono-filament suture [Prolene]. Sutures to secure the mesh areplaced to the level of the internal ring and not lateral to thispoint to avoid nerve entrapment. The internal ring is recon-structed by fitting tails around the cord. The tails are held inplace on the inguinal ligament by a single suture and aretucked underneath the external oblique aponeurosis as it isclosed.
Friis and Lindahl in Denmark reported a prospective ran-domized controlled study comparing the Lichtenstein repairto either a Marcy high ligation and ring plasty for indirecthernias or a McVay repair for direct or femoral hernias." Thestudy included 208 patients who underwent 102 Lichtenstein,53 Marcy, and 53 McVay repairs of primary and recurrenthernias. There was 99% follow-up at 2 years. The recurrencerates were 0% for Lichtenstein and 3.8% for Marcy repairs ofindirect hernias (no statistically significant difference). Therecurrence rates were 8.6% for Lichtenstein and 26.4% forMcVay repairs of direct or femoral hernias (p =.014). Com-plications occurred in 4.9% of Lichtenstein repairs and 5.3%of tissue repairs . There was no difference for discharge on dayof operation or for time off from work. The authors admittedan unacceptably high recurrence rate in the tissue repairgroup and attributed it possibly to surgeon inexperience andlack of specialization in hernia repair per se.
Kark et al. reported a series of 3175 primary inguinalhernia repairs using the Lichtenstein technique combinedwith internal ring closure by suture or mesh plug insertion."Over an 18-month to 5-year follow-up, their recurrence ratewas 0.5% . Complications included hematomas, 2%; infec-tions, 0.3%; testicular swelling, 1% (none progressed to tes-ticular atrophy); and neuralgias, 1%. Mean time for return towork was 8 days.
The Lichtenstein group reported 4000 consecutive primaryhernia repairs, with 87% follow-up for an average of 5.5 years,to include 3480 repairs in their analysis." They had only 5(0.1%) recurrences, 1 case of orchitis, and 1 case of neuralgia.Over 90% of their patients returned to work, includingmanual labor, within 2 weeks. Of note, the series included1000 bilateral hernias that were repaired simultaneouslyunder local anesthesia. No increase in complications or recur-rences was associated with simultaneous repair of bilateralhernias using a tension-free technique. The authors attributedthe recurrences to technical errors involving inadequateoverlap of the mesh on the pubic bone and placement of meshunder tension. After correcting these mistakes, only onerecurrence has been reported during the last 6 years .
The Lichtenstein group published another report, whichsummarized the results of five series at various institutionsperforming 3019 repairs for primary inguinal hernias." In thisreport, results included recurrence, 0.2%; infection, 0.03%;and mesh rejection, 0%. In the Lichtenstein experience, rarelyhas mesh been removed for infection. Antibiotic therapy anddrainage of the infection with wound granulation are usuallysufficient.
The Lichtenstein repair has reshaped the way surgeonsperform open herniorrhaphy. It has reduced patient discom-fort and hernia recurrence rates dramatically. It has alsoreversed the notion that bilateral hernias should not berepaired simultaneously. The short- and long-term recurrenceresults seem better than the results previously achieved withtissue repairs . The procedure is readily reproducible by those
1144 CHAPTER 53
who do not specialize in hernia repair, with comparable excel-lent results."
MESH PLUG REPAIR
Various techniques have been developed that use a polypro-pylene mesh plug to fill the hernia defect and effect a repair .These techniques are championed as tension free and arebecoming popular in combination with a mesh patch repair .
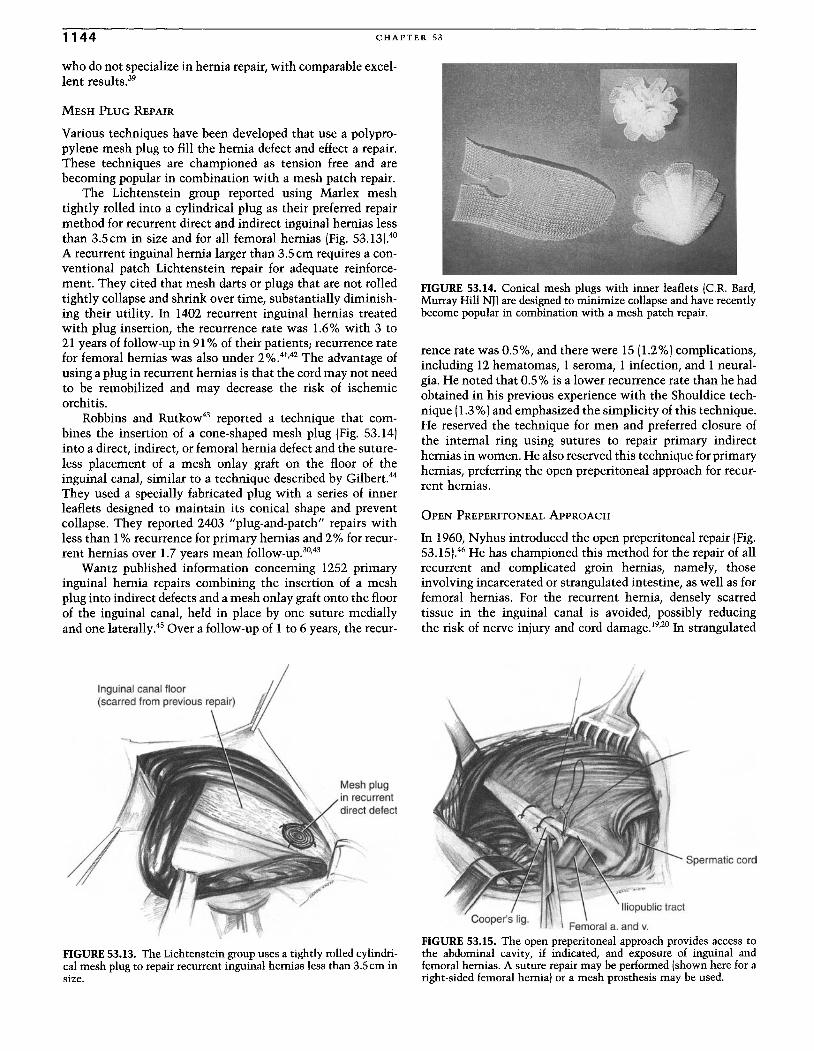
The Lichtenstein group reported using Marlex meshtightly rolled into a cylindrical plug as their preferred repairmethod for recurrent direct and indirect inguinal hernias lessthan 3.5cm in size and for all femoral hernias (Fig. 53.13).40A recurrent inguinal hernia larger than 3.5em requires a con-ventional patch Lichtenstein repair for adequate reinforce-ment. They cited that mesh darts or plugs that are not rolledtightly collapse and shrink over time, substantially diminish-ing their utility. In 1402 recurrent inguinal hernias treatedwith plug insertion, the recurrence rate was 1.6% with 3 to21 years of follow-up in 91% of their patients; recurrence ratefor femoral hernias was also under 2%.41,42 The advantage ofusing a plug in recurrent hernias is that the cord may not needto be remobilized and may decrease the risk of ischemicorchitis.
Robbins and Rutkow" reported a technique that com-bines the insertion of a cone-shaped mesh plug (Fig. 53.14)into a direct, indirect, or femoral hernia defect and the suture-less placement of a mesh onlay graft on the floor of theinguinal canal, similar to a technique described by Gilbert."They used a specially fabricated plug with a series of innerleaflets designed to maintain its conical shape and preventcollapse. They reported 2403 "plug-and-patch" repairs withless than 1% recurrence for primary hernias and 2% for recur-rent hernias over 1.7 years mean follow-up.P'"
Wantz published information concerning 1252 primaryinguinal hernia repairs combining the insertion of a meshplug into indirect defects and a mesh onlay graft onto the floorof the inguinal canal, held in place by one suture mediallyand one laterally." Over a follow-up of 1 to 6 years, the recur-
Mesh plugin recurrentdirect defect
\\', '"',
FIGURE 53.13. The Lichtenstein group uses a tightly rolled cylindri-cal mesh plug to repair recurrent inguinal hernias less than 3.5 em insize.
FIGURE 53.14. Conical mesh plugs with inner leaflets (C.R. Bard,Murray Hill NTI are designed to minimize collapse and have recentlybecome popular in combination with a mesh patch repair.
renee rate was 0.5%, and there were 15 (1.2%)complications,including 12 hematomas, 1 seroma, 1 infection, and 1 neural-gia. He noted that 0.5% is a lower recurrence rate than he hadobtained in his previous experience with the Shouldice tech-nique (1.3%)and emphasized the simplicity of this technique.He reserved the technique for men and preferred closure ofthe internal ring using sutures to repair primary indirecthernias in women. He also reserved this technique for primaryhernias, preferring the open preperitoneal approach for recur-rent hernias.
OPEN PREPERITONEAL ApPROACH
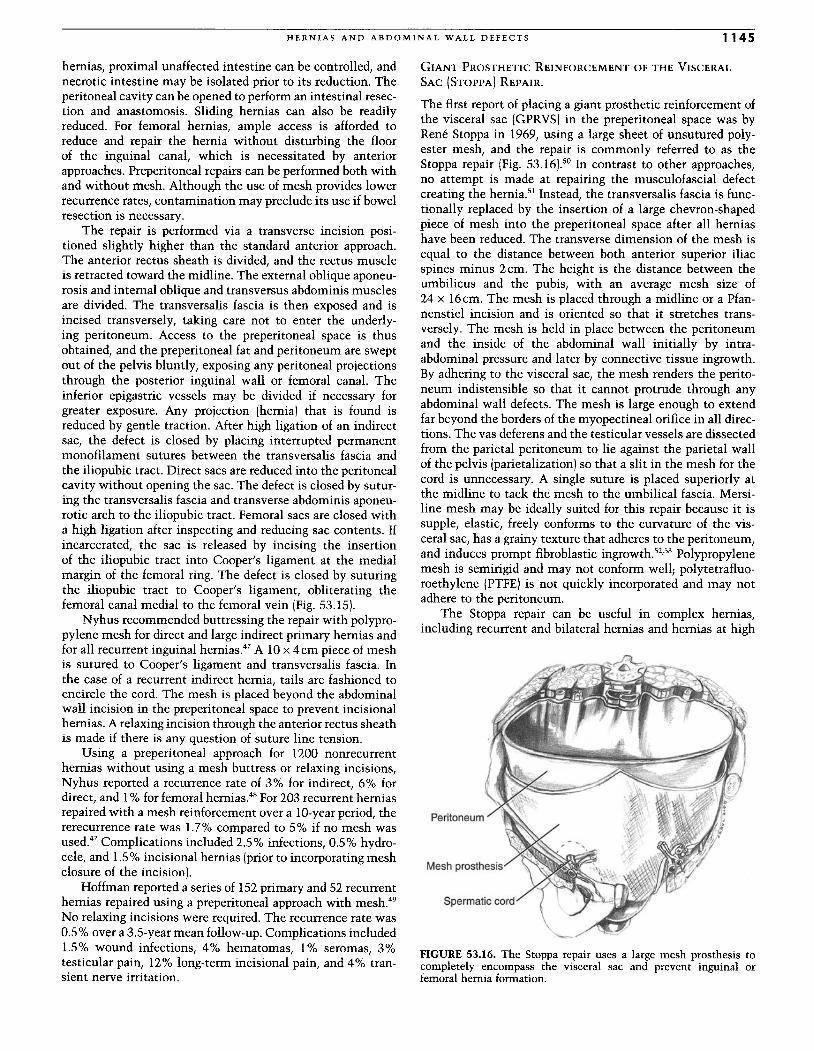
In 1960, Nyhus introduced the open preperitoneal repair (Fig.53.15).46 He has championed this method for the repair of allrecurrent and complicated groin hernias, namely, thoseinvolving incarcerated or strangulated intestine, as well as forfemoral hernias. For the recurrent hernia, densely scarredtissue in the inguinal canal is avoided, possibly reducingthe risk of nerve injury and cord damage.V" In strangulated
Sperma tic cord
Femoral a. and v.
FIGURE 53.15. The open preperitoneal approach provides access tothe abdominal cavity, if indicated, and exposure of inguinal andfemoral hernias. A suture repair may be performed (shown here for aright-sided femoral hernia) or a mesh prosthesis may be used.
H ERNIA S AND AB DOMINAL WALL D E F E C T S 1145
hernias, proximal unaffected intestine can be controlled andnecrotic intestine may be isolated prior to its reduction: Theperitoneal cavity can be opened to perform an intestinal resec-tion and anastomosis. Sliding hernias can also be readilyreduced . For femoral hernias, ample access is afforded toreduce and repair the hernia without disturbing the floorof the inguinal canal , which is necessitated by anteriorapproaches . Preperitoneal repairs can be performed both withand without mesh. Although the use of mesh provides lowerrecurrence rates, contamination may preclude its use if bowelresection is necessary.
The repair is performed via a transverse incision posi-tioned slightly higher than the standard anterior approach .The anterior rectus sheath is divided, and the rectus muscleis retracted toward the midline. The external oblique aponeu-rosis and internal oblique and transversus abdominis musclesare divided . The transversalis fascia is then exposed and isincised transversely, taking care not to enter the underly-ing peritoneum. Access to the preperitoneal space is thusobtained, and the preperitoneal fat and peritoneum are sweptout of the pelvis bluntly, exposing any peritoneal projectionsthrough the posterior inguinal wall or femoral canal. Theinferior epigastric vessels may be divided if necessary forgreater exposure . Any projection (hernia) that is found isreduced by gentle traction. After high ligation of an indirectsac, the defect is closed by placing interrupted permanentmonofilament sutures between the transversalis fascia andthe iliopubic tract. Direct sacs are reduced into the peritonealcavity without opening the sac. The defect is closed by sutur-ing the transversalis fascia and transverse abdominis aponeu-rotic arch to the iliopubic tract. Femoral sacs are closed witha high ligation after inspecting and reducing sac contents. Ifincarcerated, the sac is released by incising the insertionof the iliopubic tract into Cooper 's ligament at the medialmargin of the femoral ring. The defect is closed by suturingthe iliopubic tract to Cooper's ligament, obliterating thefemoral canal medial to the femoral vein (Fig. 53.15).
Nyhus recommended buttressing the repair with polypro-pylene mesh for direct and large indirect primary hernias andfor all recurrent inguinal hernias." A 10 x 4cm piece of meshis sutured to Cooper 's ligament and transversalis fascia. Inthe case of a recurrent indirect hernia, tails are fashioned toencircle the cord. The mesh is placed beyond the abdominalwall incision in the preperitoneal space to prevent incisionalhernias. A relaxing incision through the anterior rectus sheathis made if there is any question of suture line tension.
Using a preperitoneal approach for 1200 nonrecurrenthernias without using a mesh buttress or relaxing incisions,Nyhus reported a recurrence rate of 3% for indirect 6% fordirect, and 1% for femoral hernias." For 203 recurren~ herniasrepaired with a mesh reinforcement over a lO-year period, thererecurrence rate was 1.7% compared to 5% if no mesh wasused ." Complications included 2.5% infections, 0.5% hydro-cele, and 1.5% incisional hernias (prior to incorporating meshclosure of the incision) .
Hoffman reported a series of 152 primary and 52 recurrenthernias repaired using a preperitoneal approach with mesh."No relaxing incisions were required. The recurrence rate was0.5% over a 3.5-year mean follow-up . Complications included1.5% wound infections, 4% hematomas, 1% seromas, 3%testicular pain, 12% long-term incisional pain, and 4% tran-sient nerve irritation.
GIANT PROSTHETIC REINFORCEMENT OF THE VISCERAL
SAC (STOPPA) REPAIR.
The first report of placing a giant prosthetic reinforcement ofthe visceral sac (GPRVS) in the preperitoneal space was byRene Stoppa in 1969, using a large sheet of unsutured poly-ester mesh, and the repair is commonly referred to as theStoppa repair (Fig. 53.16).50 In contrast to other approaches,no attempt is made at repairing the musculofascial defectcreating the hernia." Instead, the transversalis fascia is func-tionally replaced by the insertion of a large chevron-shapedpiece of mesh into the preperitoneal space after all herniashave been reduced . The transverse dimension of the mesh isequal to the distance between both anterior superior iliacspines minus 2cm. The height is the distance between theumbilicus and the pubis, with an average mesh size of24 x 16cm. The mesh is placed through a midline or a Pfan-nenstiel incision and is oriented so that it stretches trans -versely . The mesh is held in place between the peritoneumand the inside of the abdominal wall initially by intra-abdominal pressure and later by connective tissue ingrowth.By adhering to the visceral sac, the mesh renders the perito-neum indistensible so that it cannot protrude through anyabdominal wall defects . The mesh is large enough to extendfar beyond the borders of the myopectineal orifice in all direc-tions . The vas deferens and the testicular vessels are dissectedfrom the parietal peritoneum to lie against the parietal wallof the pelvis (parietalization) so that a slit in the mesh for thecord is unnecessary. A single suture is placed superiorly atthe midline to tack the mesh to the umbilical fascia. Mersi -line mesh may be ideally suited for this repair because it issupple , elastic, freely conforms to the curvature of the vis-ceral sac, has a grainy texture that adheres to the peritoneumand induces prompt fibroblastic ingrowth.P'" Polypropylen~mesh is semirigid and may not conform well; polytetrafluo-roethylene (PTFE) is not quickly incorporated and may notadhere to the peritoneum.
The Stoppa repair can be useful in complex herniasincluding recurrent and bilateral hernias and hernias at high
Peritoneum
Spermatic cord
FIGURE 53.16. The Stoppa repair uses a large mesh prosthesis tocompletely encompass the visceral sac and prevent inguinal orfemoral hernia formation.

1146 CHAPTER 53
risk for recurrence, such as in patients with connective tissuedisorders, ascites, obesity, or advanced age. The Stoppa repairis contraindicated if contamination is present since risk ofprosthetic infection is high.
In 1984, Stoppa published a series of 1223 GPRVS repairswith a recurrence rate of 1.4% and an incidence of complica-tions comparable to conventional repairs." In a subsequentreport, the recurrence rate was less than 1% for primaryhernias and 1.1% for recurrent hernias, with an overall com-plication rate of 3.3% for recurrent hernias."
In 1997, Mathonnet reported 1048 GPRVS repairs of bilat-eral hernias using Dacron mesh with a 1.6% recurrence rateand an overall complication rate of 8.5%, including 2% hema-toma, 1.6% infection (none required mesh removal), 9% pain,and 0.7% seroma."
Wantz described a unilateral GPRVS repair using a 12 x15em diamond-shaped piece of mesh inserted into a singlegroin through a transverse incision above the internal ring.Wantz reported in 1989 a series of 237 unilateral and bilateralGPRVS repairs using a variety of prosthetic materials forrecurrent hernias and in patients at high risk for recurrences.fIn 85 unilateral repairs, there were no recurrences. In 152bilateral repairs, there were 9 (5.90/0) recurrences. The overallrecurrence rate was 3.7. More recently, Wantz published aseries of GPRVSrepairs of 15 primary and 54 recurrent femoralhernias with no recurrences.f
LAPAROSCOPIC ApPROACHES
Considering all that is written about the radical treatment of theinguinal hernia up until now, it can be somewhat risky to try topublish more about this subject.
Edoardo Bassini, 1890
Since its introduction by Cer" in 1982 into the armamen-tarium of hernia repairs, laparoscopic repairs have undergoneconsiderable evolution and have been the source of muchcontroversy.58 It was not until the 1990s with the tremendoussuccess of laparoscopic cholecystectomies that the laparo-scopic hernia repair received much attention. Early reportsused a wide variety of techniques, initially met with highrecurrence rates and numerous complications. Three tech-niques proved more effective and emerged as the most popular.These techniques are the transabdominal preperitoneal(TAPP), the intraperitoneal onlay mesh (IPOM), and thetotally extraperitoneal (TEP).
These repairs approach the myopectineal orifice posteri-orly, similar in anatomical perspective to the open preperito-neal approaches. A clear understanding of the anatomy fromthis perspective (Fig. 53.6) is crucial to avoid a number ofcomplications, mainly vascular and nerve injuries. Laparos-copy provides a clear view of the entire myopectineal orifice,and repairs of both inguinal and femoral hernias can be per-formed.
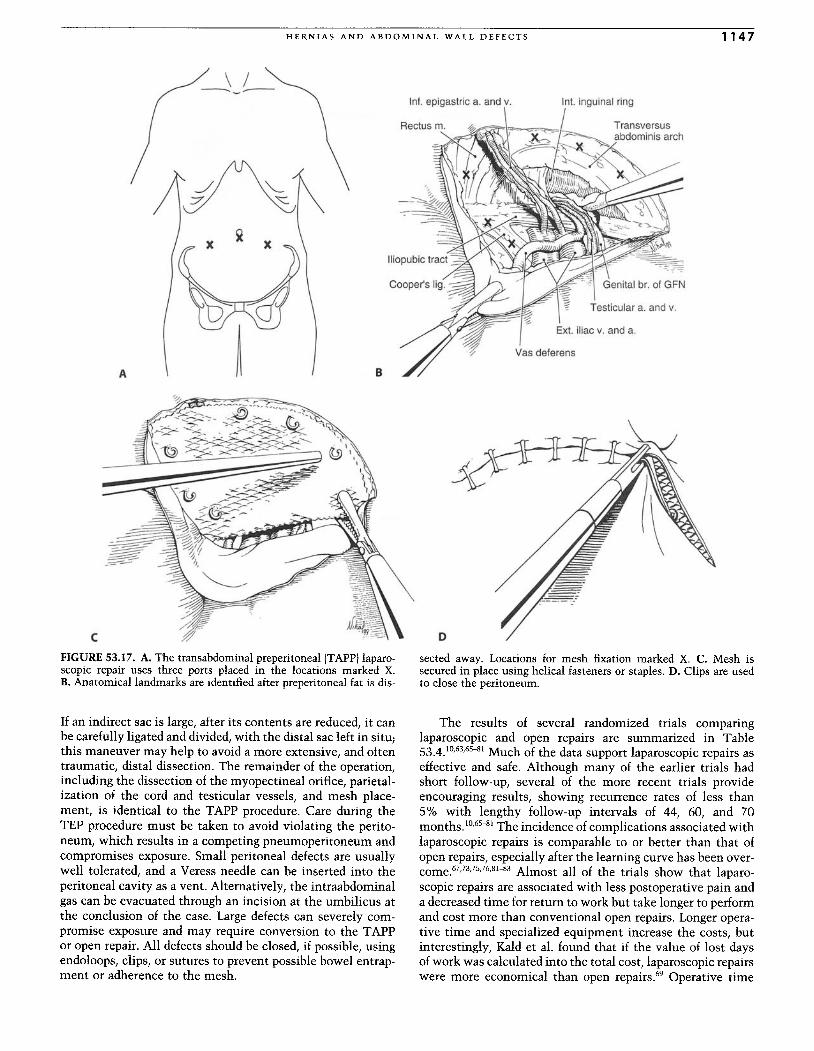
In the TAPP procedure (Fig. 53.17), three trocars are placedthrough the abdominal wall into the peritoneal cavity after apneumoperitoneum has been created. The peritoneum cepha-lad to the groin is then transversely incised from the medianumbilical fold to several centimeters lateral to the internalring, taking care not to injure the underlying inferior epigas-tric vessels.
The hernias are reduced using blunt dissection and gentletraction. Large indirect sacs can be divided after the contents
are reduced, leaving the distal sac in situ. The preperitonealtissues are broadly dissected beyond the midline and lateralto the internal ring, from below Cooper's ligament to abovethe transversus abdominis arch. The vas deferens and testicu-lar vessels are parietalized by carefully freeing them fromtheir proximal and lateral peritoneal attachments. The infe-rior epigastric vessels are defined but not completely skele-tonized, which can lead to bleeding. Clear identification ofHesselbach's triangle, the femoral canal and vessels, and allanatomic landmarks is achieved.
A large piece of polypropylene mesh (12 x 15cm) is thenplaced over the entire myopectineal orifice, with generousoverlap of its borders, and secured in place with helical fasten-ers or staples. The fasteners are applied medially into therectus muscle, superiorly to the transversus abdominis arch,inferiorly to Cooper's ligament up to the medial aspect of theexternal iliac vein, and laterally to the iliopubic tract. Alter-natively, if a sufficiently large prosthesis is used, meshfixation may not be required as excellent results can beobtained.
Some authors described placing a slit in the mesh, passingthe cord through the slit, and tacking the tails in place withstaples. Passing the cord through a slit and encircling the cordwith mesh has been associated with chronic pain and seromasand may be unnecessary.i"?'
The peritoneum is reapproximated using staples orsutures. Care must be taken to completely close the perito-neum without leaving gaps that can allow small-bowelentrapment or adherence to the mesh. Trocars are removedand the trocar fascial defects are closed to prevent incisionalhemias.f
The IPOM repair uses an intraabdominal approach andplaces a large piece of mesh against the peritoneum afterhernia contents have been reduced. The mesh is securedwith staples placed into the same anatomic structures as inthe TAPP repair but is placed in an intraperitoneal positioninstead of a preperitoneal position. Some authors described aminimal dissection of the peritoneum and clearly identifyingCooper's ligament to adequately secure the mesh and mini-mize recurrence." To minimize the potential for adhesivecomplications, including bowel obstruction and fistulas,PTFE is favored over polypropylene mesh.63
,64
The TEP technique (Fig. 53.18)65 is now considered theideallaparoscopic approach by many surgeons. The TEP oper-ation avoids potential intraabdominal injuries by gainingaccess to the groin via a completely extraperitoneal approach.A small infraumbilical incision is made and carried downthrough the anterior rectus sheath. The rectus muscle isretracted away from the midline, and the anterior surfaceof the posterior rectus sheath is clearly visualized. A balloondissector is placed along this surface, advanced inferiorly tothe pubic bone, and is inflated with air or saline, creating aworking space between the peritoneum and the abdominalwall. The balloon dissector is deflated and removed. Alterna-tively, the preperitoneal space can be dissected bluntly usingan operating laparoscope or digitally; this technique may beslower and more tedious but can be more cost-effective.
After the preperitoneal working space has been developed,a cannula is inserted, and the preperitoneal space is insuf-flated. Two additional trocars are placed in the midline underdirect visualization without violation of the peritoneum. Thehernia is reduced using blunt dissection and gentle traction.
A
\ /--..... ----
HERNIA S AND ABD OMINAL WALL DEFE CTS
In!. epigastr ic a. and v.
B
lnt , inguinal ring
Testicular a. and v.
1147
C
FIGURE 53.17. A. The transabdominal preperitoneal (TAPP) laparo-scopic repair uses three ports placed in the locations marked X.B. Anatomical landmarks are identified after preperitoneal fat is dis-
If an indirect sac is large, after its contents are reduced, it canbe carefully ligated and divided, with the distal sac left in situ,this maneuver may help to avoid a more extensive, and oftentraumatic, distal dissection. The remainder of the operation,including the dissection of the myopectineal orifice, parietal-ization of the cord and testicular vessels, and mesh place-ment, is identical to th e TAPP procedure. Care during th eTEP procedure must be tak en to avoid violating the perito-neum, which results in a competing pneumoperitoneum andcompromises exposure. Small peritoneal defects are usuallywell tol erated, and a Veress needle can be inserted into th eperitoneal cavity as a vent. Alternatively, the intraabdominalgas can be evacuated through an incis ion at the umbilicus atthe conclusion of the case. Large defects can severely com -promise exposure and may require conversion to the TAPPor open repair. All defects should be closed, if possible, usingendoloops, clips, or sutures to prevent possible bowel entrap-ment or adherence to the mesh.
osected away. Locations for mesh fixation marked X. C. Mesh issecured in place using helical fasteners or staples. D. Clips are usedto close the peritoneum.
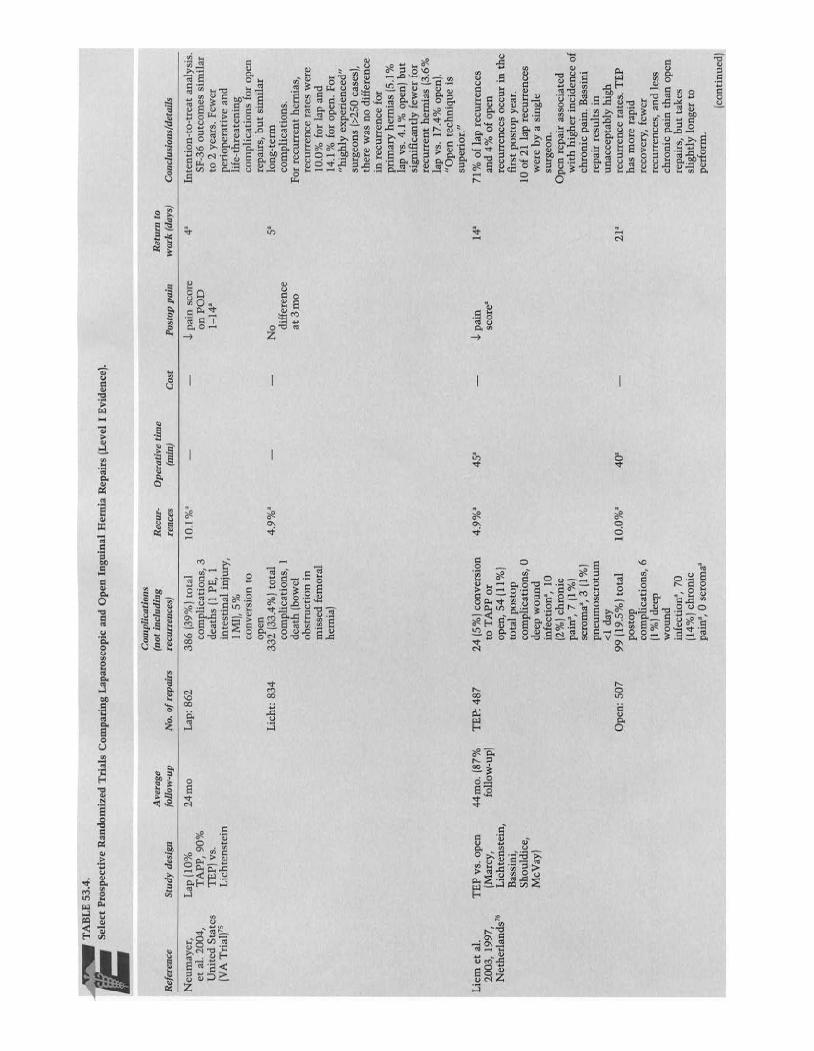
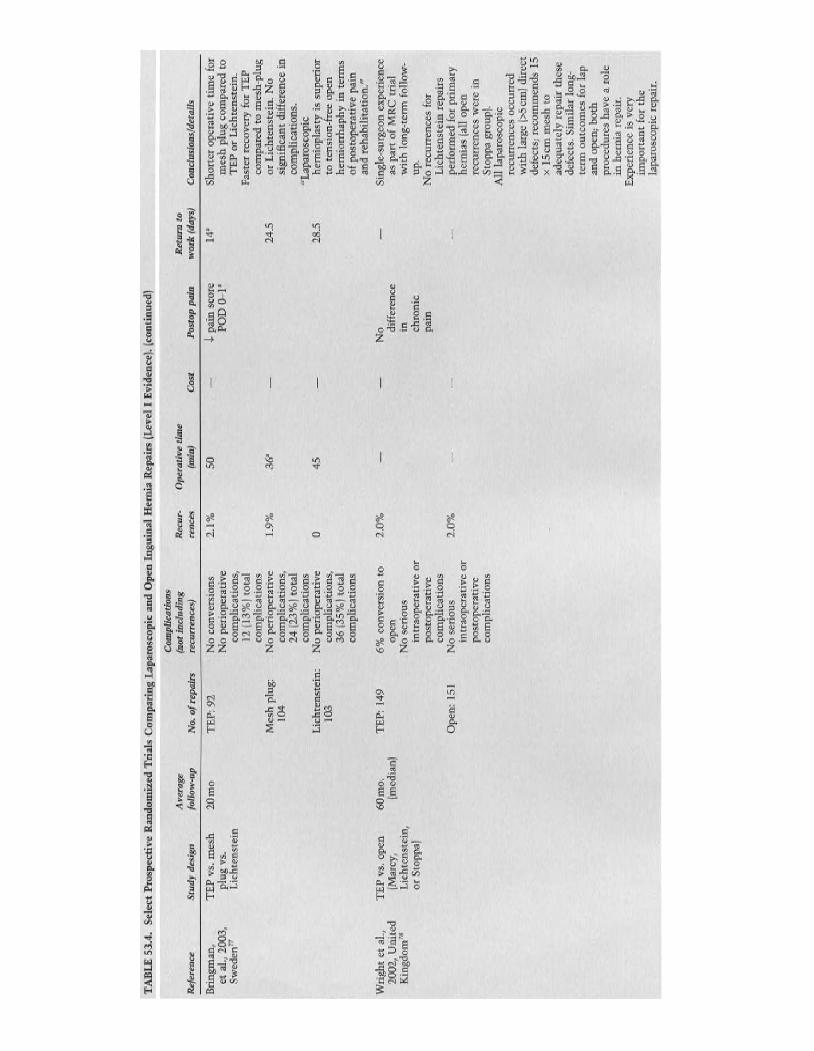
The results of several randomized trials comparinglaparoscopic and open repairs are summarized in Table53.4.10,63,65-8 1 Much of the data support laparoscopic repairs aseffective and safe. Although many of th e earlier trial s hadshort follow-up, several of the more recent trials provideencouraging results, showing recurrence rate s of less than5% with lengthy follow-up intervals of 44, 60, and 70months.IO
,6S-8 1 The incidence of complications associated withlaparoscopic repairs is comparable to or better than that ofopen repairs , especially after the learning curve has been over-come .67,73,75,76,81-83 Almost all of th e trials show that laparo-scopic repairs are associated with less postoperative pain anda decreased time for return to work but take longer to performand cost more than conventional open repairs . Longer opera-tive time and specialized equipment increase the costs, butinterestingly, Kald et a1. found that if the value of lost daysof work was calculated into the total cost , laparoscopic repairswere more economical than open repairs.f Operative time
c
"•••
B
o
A
E
F
G
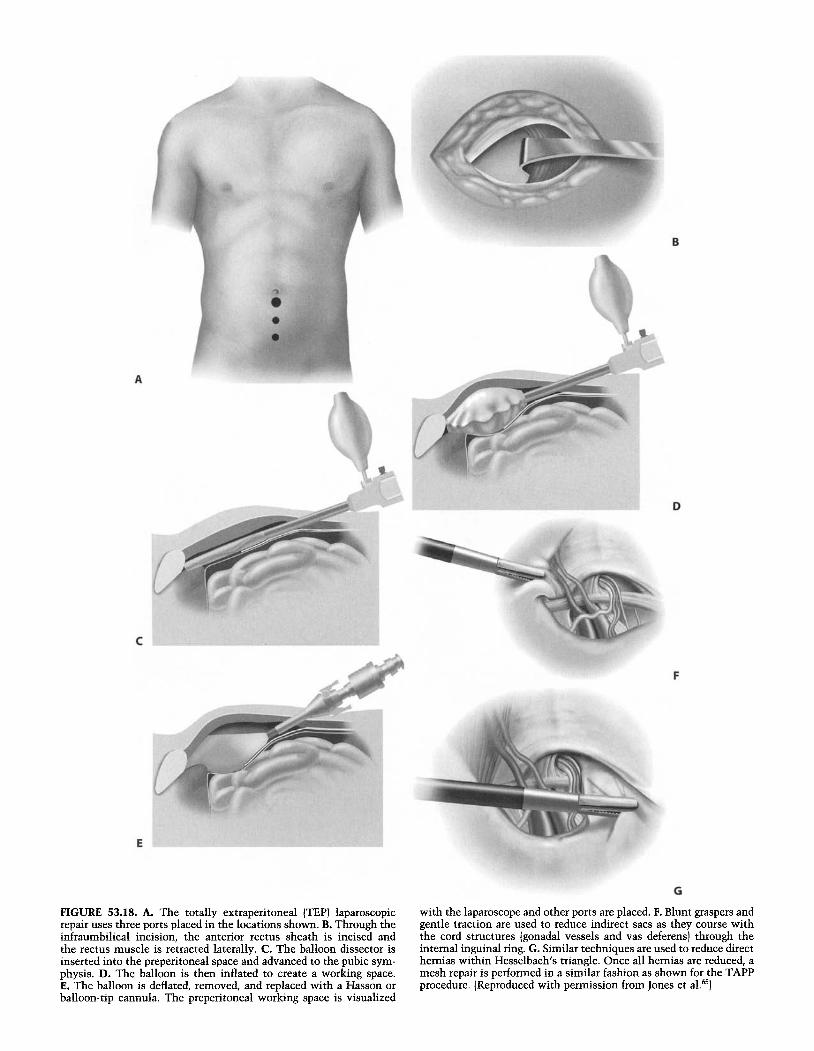
FIGURE 53.18. A. The totally extraperitoneal (TEP) laparoscopicrepair uses three ports placed in the locations shown. B. Through theinfraumbilical incision, the anterior rectus sheath is incised andthe rectus muscle is retracted laterally. C. The balloon dissector isinserted into the preperitoneal space and advanced to the pubic sym-physis. D. The balloon is then inflated to create a working space.E. The balloon is deflated, removed, and replaced with a Hasson orballoon-tip cannula. The preperitoneal working space is visualized
with the laparoscope and other ports are placed. F. Blunt graspers andgentle traction are used to reduce indirect sacs as they course withthe cord structures (gonadal vessels and vas deferens] through theinternal inguinal ring. G. Similar techniques are used to reduce directhernias within Hesselbach's triangle. Once all hernias are reduced, amesh repair is performed in a similar fashion as shown for the TAPPprocedure. (Reproduced with permission from Jones et a1.65
)
~~~_
TA
BL
E53
.4.
Sel
ect
Pro
spec
tive
Ran
dom
ized
Tri
als
Com
pari
ngL
apar
osco
pic
and
Ope
nIn
guin
alH
erni
aR
epai
rs(L
evel
IE
vide
nce)
.
Com
plic
atio
nsA
vera
ge( n
oti
nclu
ding
Rec
ur-
Ope
rati
veti
me
Ret
urn
toR
efer
ence
Stu
dy
desi
gnfo
llow
-up
No
.of
repa
irs
recu
rren
ces)
renc
es(m
in)
Cos
tP
osto
ppa
inw
ork
(day
s)C
oncl
usio
ns/d
etai
ls
Neu
may
er,
Lap
110%
24m
oL
ap:
862
386
139%
Jto
tal
10.1
%'
J.pa
insc
ore
4'In
tent
ion-
to-t
reat
anal
ysis
.et
al.
2004
,T
APP
,90
%co
mp
lica
tion
s,3
onP
OD
SF-3
6o u
tcom
essi
mil
arU
nit
edSt
ates
TE
P)v
s.de
aths
/lPE
,1
1-1
4'to
2ye
ars.
Few
er(V
AT
rial
f5L
ich
tens
tein
inte
stin
alin
jury
,p
erio
pera
tiv
ean
d1
MI)
,5%
life
-th
reat
enin
gco
nver
sion
toco
mpl
icat
ions
for
open
open
repa
irs,
but
sim
ilar
Lic
ht:
834
332
(33.
4%
)tot
al4.
9%
'N
o5
'lo
ng-
term
com
plic
atio
ns,
1di
ffer
ence
com
plic
atio
ns.
deat
h[b
owel
at3
mo
For
recu
rren
th
erni
as,
obs t
ruct
ion
inre
curr
ence
rate
sw
ere
mis
sed
fem
oral
10.0
%fo
rla
pan
dh
erni
a)14
.1%
for
open
.Fo
r"h
ighl
yex
per
ien
ced
"su
rgeo
ns(>
250
case
s),
ther
ew
asno
diff
eren
cein
recu
rren
cefo
rpr
imar
yhe
rnia
s(5
.1%
lap
vs.
4.1
%op
en)b
ut
sign
ific
antl
yfe
wer
for
recu
rren
th
erni
as13
.6%
lap
vs.
17.4
%op
en).
"Ope
nte
chni
que
issu
peri
or."
L iem
etal
.T
EP
vs.o
pen
44
mo.
(87%
TE
P:4
8724
(5%
)co
nver
sion
4.9
%'
45'
J.pa
in14
'71
%of
lap
recu
rren
ces
2003
,19
97,
(Mar
cy,
follo
w-u
p)to
TA
PP
orsc
ore'
and
4%
ofop
enN
ethe
rlan
ds"
Lic
hten
stei
n,op
en,
54(1
1%)
recu
rren
ces
occu
rin
the
Bas
sini
,to
tal
post
opfi
rst
post
opye
ar.
Shou
ldic
e,co
mpl
icat
ions
,0
10of
21la
pre
curr
ence
sM
cVay
)de
epw
ou
nd
wer
eby
asi
ngle
infe
ctio
n',
10su
rgeo
n.
12%
)ch
roni
cO
pen
repa
iras
soci
ated
pain
',7u%
)w
ith
high
erin
cide
nce
ofse
rom
a",3
(1%
)ch
roni
cpa
in.B
assi
nip
neu
mo
scro
tum
repa
irre
sult
sin
<1
day
un
acce
ptab
lyhi
ghO
pen
:50
799
(19.
5%
)to
tal
10.0
%'
40'
21
're
curr
ence
rate
s.T
EP
post
opha
sm
ore
rapi
dco
mpl
icat
ions
,6
reco
very
,fe
wer
(1%
)dee
pre
curr
ence
s,an
dle
ssw
oun
dch
ron
icpa
inth
anop
enin
fect
ion'
,70
repa
irs,
bu
tta
kes
(14%
)ch
roni
csl
igh
tly
long
erto
pain
',0
sero
rna"
per
form
.
(con
tinu
ed)
TA
BL
E53
.4.
Sele
ctPr
osp
ecti
veR
ando
miz
edT
rial
sC
om
pari
ngL
apar
osco
pic
and
Ope
nIn
gui
nal
Her
nia
Rep
airs
(Lev
elI
Evid
ence
).(c
onti
nued
)
Rec
ur-
Ope
rati
veti
me
Ret
urn
tore
nces
(min
)C
ost
Pos
top
pain
wo
rk(d
ays)
2.1
%50
J..pa
insc
ore
14"
PO
D0
-1'
1.9%
36"
24.5
045
28.5
Ref
eren
ce
Bri
ngm
an,
etaI
.,20
03,
Swe
den
"
Wri
ght
etal
.,20
02,
Un
ited
Kin
gdom
?"
Stu
dy
desi
gn
TE
Pvs
.m
esh
plu
gv
s.L
ich
ten
stei
n
TE
Pvs
.op
en(M
arcy
,L
icht
enst
ein,
orSt
oppa
]
Ave
rage
foll
ow-u
p
20m
o
60
mo
.(m
edia
n)
No.
ofre
pair
s
TE
P:92
Mes
hpl
ug:
104
Lic
hte
nste
in:
103
TE
P:
149
Op
en:
151
Com
plic
atio
ns(n
otin
clud
ing
recu
rren
ces)
No
conv
ersi
ons
No
peri
oper
ativ
eco
mpl
icat
ions
,12
(13
%)
tota
lco
mpl
icat
ions
No
peri
oper
ativ
eco
mpl
icat
ions
,24
(23
%)t
ota
lco
mpl
icat
ions
No
per
iop
erat
ive
com
plic
atio
ns,
36
(35
%)
tota
lco
mpl
icat
ions
6%
conv
ersi
on
toop
enN
ose
riou
sin
trao
pera
tive
orpo
stop
erat
ive
com
plic
atio
nsN
ose
riou
sin
trao
pera
tive
orpo
stop
erat
ive
com
plic
atio
ns
2.0
%
2.0
%
No di
ffer
ence
in chro
nic
pain
Con
clu
sion
s/d
etai
ls
Sho
rter
oper
ativ
eti
me
for
me
shpl
ugco
mpa
red
toT
EP
orL
ich
tens
tein
.F
aste
rre
cov
ery
for
TE
Pco
mpa
red
tom
esh
-plu
gor
Lic
hten
stei
n.
No
sign
ific
ant
diff
eren
cein
com
plic
atio
ns.
"Lap
aros
copi
che
rnio
plas
tyis
supe
rior
tote
nsio
n-fr
eeop
enhe
rnio
rrh
aph
yin
term
sof
post
oper
ativ
epa
inan
dre
habi
lita
tion
."
Sin
gle-
surg
eon
expe
rien
ceas
part
ofM
RC
tria
lw
ith
long
-ter
mfo
llow
-up
.N
ore
curr
ence
sfo
rL
ich
ten
stei
nre
pai
rspe
rfor
med
for
prim
ary
hern
ias
(all
open
recu
rren
ces
wer
ein
Sto
ppa
grou
p).
All
lapa
rosc
opic
recu
rren
ces
occu
rred
wit
hla
rge
(>5
cm)
dire
ctde
fect
s;re
com
men
ds15
x15
emm
esh
toad
equ
atel
yre
pai
rth
ese
defe
cts.
Sim
ilar
long
-te
rmou
tco
mes
for
lap
and
open
;bo
thpr
oced
ures
hav
ea
role
inh
ern
iare
pair
.E
xper
ienc
eis
very
imp
orta
nt
for
the
lapa
rosc
opic
rep
air.
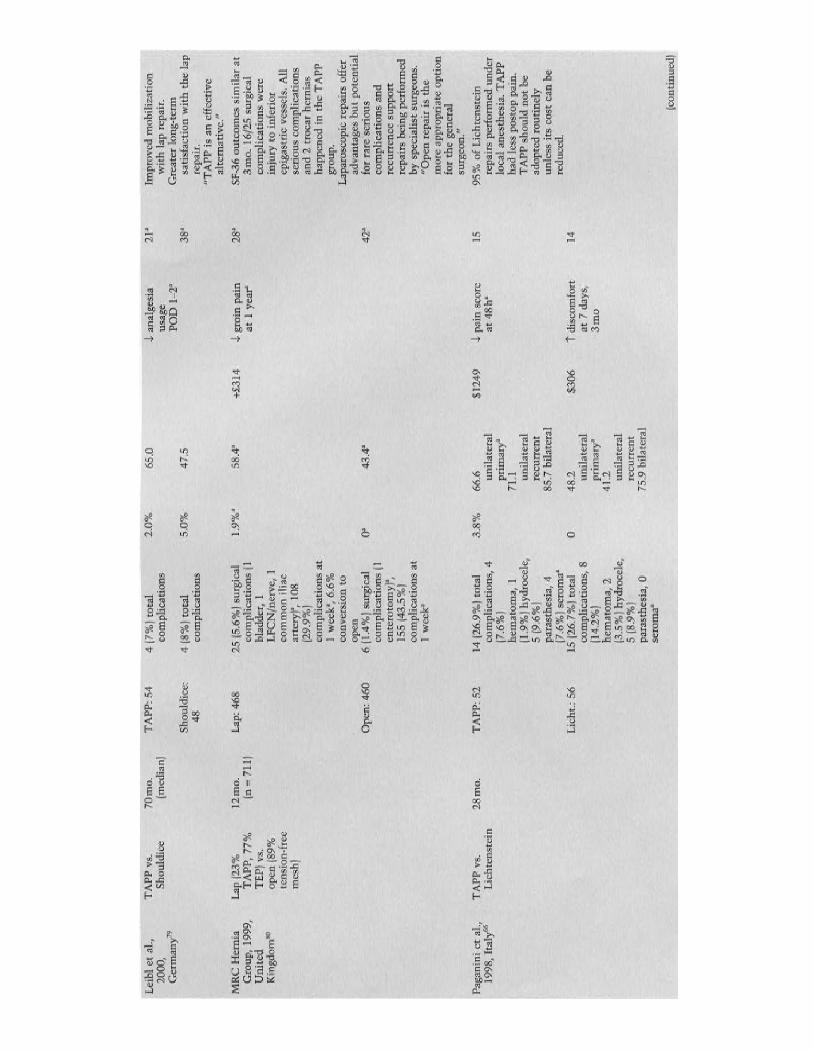
Lei
blet
al.,
TA
PPvs
.7
0m
o.
TA
PP:5
44
(7%
)to
tal
2.0%
65.0
J.an
alge
sia
21"
Impr
oved
mob
iliz
atio
n20
00,
Sho
uldi
ce(m
edia
n)co
mpl
icat
ions
usag
ew
ith
lap
repa
ir.
Ger
man
y"PO
D1_
2"G
reat
erlo
ng-t
erm
Sho
uldi
ce:
4(8
%)
tota
l5.
0%47
.538
asa
tisf
acti
onw
ith
the
lap
48co
mpl
icat
ions
repa
ir.
"TA
PPis
anef
fect
ive
alte
rnat
ive.
"
MR
CH
erni
aL
ap(2
3%12
mo.
Lap
:46
825
(5.6
%)
surg
ical
1.9%
a58
.4a
+£3
14J.
groi
npa
in28
aSF
-36
outc
omes
sim
ilar
atG
roup
,19
99,
TA
PP
,77
%(n
=71
1)co
mpl
icat
ions
(1at
1y
ear
3m
o.
16/2
5su
rgic
alU
nite
dT
EP)
vs.
blad
der,
1co
mpl
icat
ions
wer
eK
ingd
om'"
open
(89%
LF
CN
/ner
ve,
1in
jury
toin
feri
orte
nsio
n-fr
eeco
mm
on
ilia
cep
igas
tric
vess
els.
All
mes
h)ar
tery
]',
108
seri
ous
com
plic
atio
ns(2
9.9%
)an
d2
troc
arhe
rnia
sco
mpl
icat
ions
atha
ppen
edin
the
TA
PP1
wee
k',
6.6%
grou
p.
conv
ersi
onto
Lap
aros
copi
cre
pair
sof
fer
open
adva
ntag
esb
ut
pote
ntia
lO
pen:
460
6(1
.4%
)su
rgic
al0'
43.4
'42
'fo
rra
rese
riou
sco
mpl
icat
ions
(1co
mpl
icat
ions
and
ente
roto
my)
',re
curr
ence
supp
ort
155
(43.
5%)
repa
irs
bein
gpe
rfor
med
com
plic
atio
nsat
bysp
ecia
list
surg
eons
.1
wee
k'
"Op
enre
pair
isth
em
ore
appr
opri
ate
opti
onfo
rth
ege
nera
lsu
rgeo
n."
Pag
anin
iet
a!.,
TA
PPvs
.28
mo.
TA
PP:
5214
(26.
9%)
tota
l3
.8%
66.6
$124
9J.
pain
scor
e15
95%
ofL
icht
enst
ein
1998
,It
aly6
6L
ich
ten
stei
nco
mpl
icat
ions
,4
unil
ater
alat
48
h're
pair
spe
rfor
med
unde
r(7
.6%
)pr
imar
y'lo
cal
anes
thes
ia.T
APP
hem
atom
a,1
71.1
had
less
post
oppa
in.
(1.9
%)
hydr
ocel
e,un
ilat
eral
TA
PPsh
ould
no
tbe
5(9
.6%
)re
curr
ent
adop
ted
rout
inel
ypa
rast
hesi
a,4
85.7
bila
tera
lun
less
itsco
stca
nbe
(7.6
%)
sero
ma"
redu
ced.
Lic
ht.:
5615
(26.
7%)
tota
l0
48.2
$306
tdi
scom
fort
14co
mpl
icat
ions
,8
unil
ater
alat
7da
ys,
(14.
2%)
prim
ary'
3m
ohe
mat
oma,
241
.2(3
.5%
)hy
droc
ele,
unil
ater
al5
(8.9
%)
recu
rren
tpa
rast
hesi
a,0
75.9
bila
tera
lse
rom
a"
(con
tinu
ed)
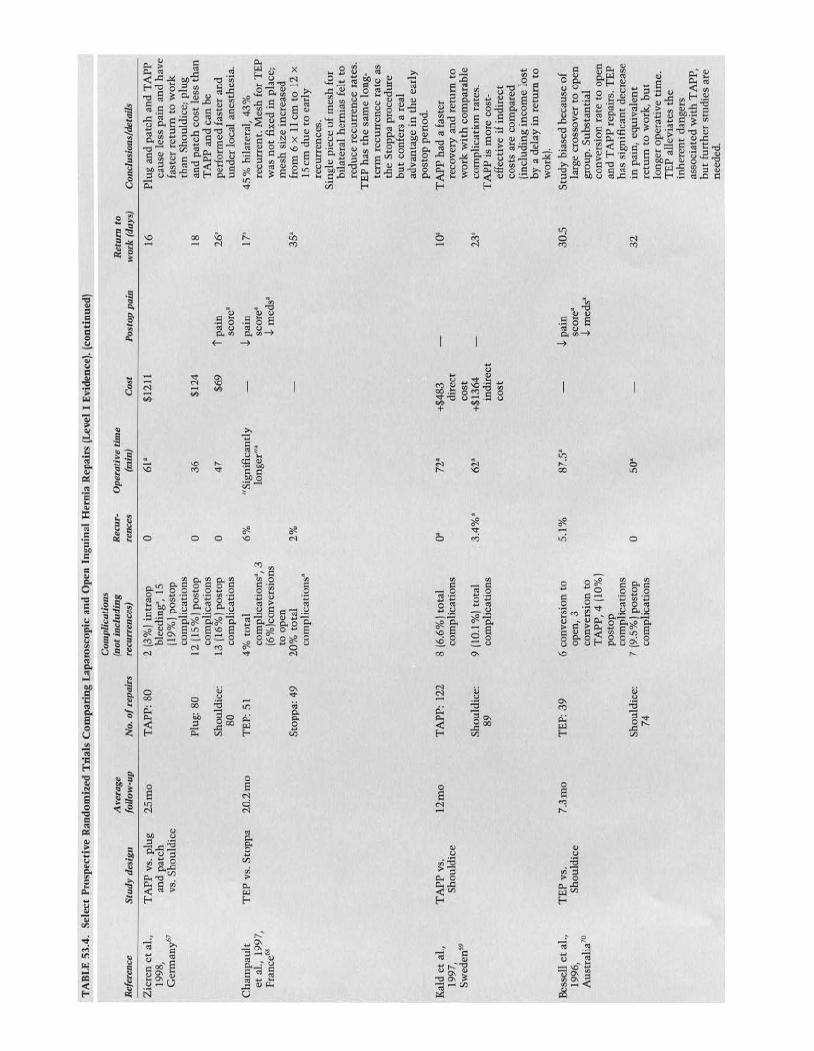
TA
BL
E53
.4.
Sele
ctP
rosp
ecti
veR
ando
miz
edT
rial
sC
ompa
rin
gL
apar
osc
opic
and
Ope
nIn
guin
alH
erni
aR
epai
rs(L
evel
IE
vide
nce)
.(c
onti
nued
)
Com
plic
atio
nsA
vera
ge(n
otin
clu
din
gR
ecur
-O
pera
tive
tim
eR
etur
nto
Ref
eren
ceS t
ud
yde
sign
foll
ow-u
pN
o.o
frep
airs
recu
rren
ces)
renc
es
(min
)C
ost
Pos
top
pain
wor
k(d
ays)
Con
clus
ion
s/de
tail
s
Zie
ren
etal
.,T
APP
vs.
plug
25
mo
TA
PP:8
02
(3%
)in
trao
pa
61"
$121
116
Plug
and
pat
chan
dT
AP
P19
98,
and
patc
hbl
eedi
ng',
15ca
use
less
pain
and
hav
eC
erm
any'
"vs
.Sh
ould
ice
(19%
)po
stop
fast
erre
turn
tow
ork
com
plic
atio
nsth
anSh
ould
ice,
plug
Plug
:80
12(1
5%1
post
opa
36
$124
18an
dpa
tch
cost
less
than
com
plic
atio
nsT
APP
and
can
beSh
ould
ice:
13(1
6%)
post
opa
47$6
9t
pain
26'
perf
orm
edfa
ster
and
80co
mpl
icat
ions
scor
e"un
der
loca
lan
esth
esia
.
Ch
ampa
ult
TE
Pvs
.St
oppa
20.2
mo
TE
P:5
14
%to
tal
6%
"Sig
nif
ican
tly
J..pa
in17
'45
%bi
late
ral,
43%
etal
.,19
97,
com
plic
atio
ns",
3lo
nger
:"sc
ore"
recu
rren
t.M
esh
for
TE
PFr
anc
e"(6
%)c
onve
rsio
nsJ..
med
s"w
asn
ot
fixe
din
plac
e;to
open
mes
hsi
zein
crea
sed
Sto
ppa:
4920
%to
tal
2%
35"
from
6x
11em
to12
xco
mpl
icat
ions
"15
emdu
eto
earl
yre
curr
ence
s.Si
ngle
piec
eof
mes
hfo
rb i
late
ral
her
nia
sfe
ltto
redu
cere
curr
ence
rate
s.T
EP
has
the
sam
elo
ng-
term
recu
rren
cera
teas
the
Sto
ppa
proc
edur
eb
ut
conf
ers
are
alad
vant
age
inth
eea
rly
post
oppe
riod
.
Kal
det
al.,
TA
PPvs
.1
2m
oT
APP
:12
28
(6.6
%)
tota
la"
72"
+$4
8310
"T
APP
had
afa
ster
1997
,S
houl
dice
com
plic
atio
nsdi
rect
reco
very
and
retu
rnto
Sw
eden
"co
stw
ork
wit
hco
mpa
rabl
eS
houl
dice
:9
(10
.1%
)to
tal
3.4
%"
62"
+$1
364
23"
com
plic
atio
nra
tes.
89co
mpl
icat
ions
indi
rect
TA
PPis
mor
eco
st-
cost
effe
ctiv
eif
indi
rect
cost
sar
eco
mpa
red
(inc
ludi
ngin
com
elo
stby
ade
lay
inre
turn
tow
ork)
.
Bes
sell
etal
.,T
EP
vs.
7 .3
mo
TE
P:3
96
conv
ersi
onto
5.1
%87
SJ..
pain
30.5
Stu
dybi
ased
beca
use
of19
96,
Shou
ldic
eop
en,
3sc
ore"
larg
ecr
osso
ver
toop
enA
ust
ralia
'?co
nver
sion
toJ..
med
s"gr
oup
.Sub
stan
tial
TA
PP,
4(1
0%)
conv
ersi
onra
teto
open
post
opan
dT
APP
repa
irs.
TE
Pco
mpl
icat
ions
has
sign
ific
ant
decr
ease
Sho
uldi
ce:
7(9
.5%
)po
stop
a50
"32
inpa
in,
equ
ival
e nt
74co
mpl
icat
ions
r etu
rnto
wor
k,b
ut
long
erop
erat
ive
tim
e.T
EP
alle
viat
esth
ein
here
nt
dang
ers
asso
ciat
edw
ith
TA
PP,
bu
tfu
rthe
rst
udie
sar
ene
eded
.
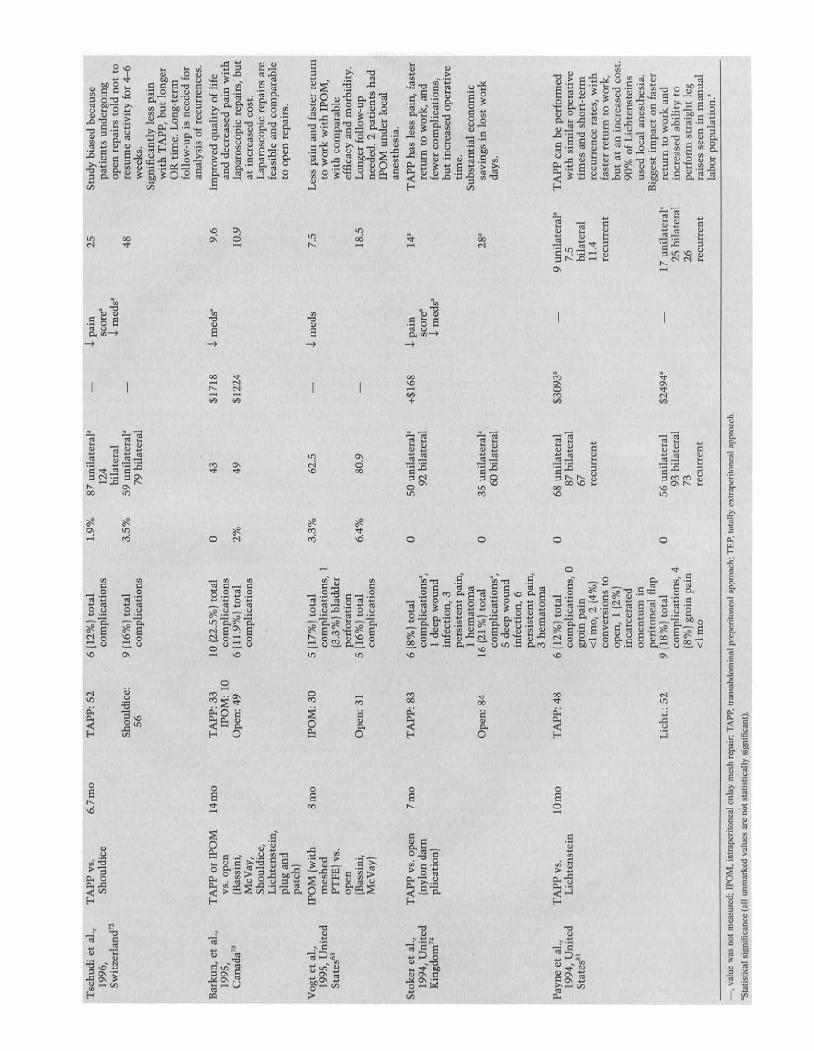
Tsc
hu
diet
al.,
TA
PPvs
.6.
7m
oT
APP
:52
6(1
2%)
tota
l1.
9%87
unil
ater
al'
J.pa
in25
Stud
ybi
ased
beca
use
1996
,Sh
ould
ice
com
plic
atio
ns12
4sc
ore
'pa
tien
tsun
derg
oing
Swit
zerl
and
"bi
late
ral
J.m
eds"
open
repa
irs
told
no
tto
Shou
ldic
e:9
(16%
)to
tal
3.5
%59
un
ilat
eral
'48
resu
me
acti
vity
for
4-6
56co
mp
lica
tion
s79
bila
tera
lw
eeks
.Si
gnif
ican
tly
less
pain
wit
hT
APP
,b
ut
long
erO
Rti
me.
Lon
g-t e
rmfo
llow
-up
isn
eede
dfo
ran
alys
isof
recu
rren
ces.
Bar
kun,
etal
.,T
APP
orIP
OM
14
mo
TA
PP:3
310
(22.
5%)
tota
l0
43$1
718
J.rn
eds"
9.6
Impr
oved
qual
ity
oflif
e19
95,
vs.o
pen
IPO
M:
10co
mpl
icat
ions
and
decr
ease
dpa
inw
ith
Can
ada?
(Bas
sini
,O
pen
:49
6(1
1.9
%)
tota
l2
%49
$122
410
.9la
par
osc
opic
repa
irs,
bu
tM
cVay
,co
mpl
icat
ions
atin
crea
sed
cost
.S
houl
dice
,L
apar
osco
pic
repa
irs
are
Lic
hten
stei
n,fe
asib
lean
dco
mpa
rabl
epl
ugan
dto
open
rep
airs
.pa
tch)
Vog
tet
aI.,
IPO
M(w
ith
8m
oIP
OM
:30
5(1
7%)
tota
l3.
3%62
.5J.
med
s7.
5L
ess
pain
and
fast
erre
turn
1995
,U
nit
edm
eshe
dco
mpl
icat
ions
,1
tow
ork
wit
hIP
OM
,S
tate
s'"
PTFE
jvs
.(3
.3%
)bl
adde
rw
ith
com
para
ble
open
perf
orat
ion
effi
cacy
and
mor
bidi
ty.
[Bas
sin
i,O
pen:
315
(16%
)to
tal
6.4
%80
.918
.5L
onge
rfo
llow
-up
McV
ay)
com
plic
atio
nsne
eded
.2
pati
ents
had
IPO
Mun
der
loca
lan
esth
esia
.
Sto
ker
etal
.,T
APP
vs.o
pen
7m
oT
AP
P:8
36
(8%
)to
tal
050
unil
ater
al'
+$1
68J.
pain
14'
TA
PPha
sle
sspa
in,
fast
er19
94,
Uni
ted
(nyl
ond
amco
mpl
icat
ions
',92
bila
tera
lsc
ore'
retu
rnto
wor
k,an
dK
ingd
om"
plic
atio
n)1
deep
wo
un
dJ.
med
s"fe
wer
com
plic
atio
ns,
infe
ctio
n,3
bu
tin
crea
sed
oper
ativ
epe
rsis
tent
pain
,ti
me.
1h
emat
om
aSu
bsta
ntia
lec
onom
icO
pen
:84
16(2
1%)
tota
l0
35un
ilat
eral
'28
'sa
ving
sin
lost
wor
kco
mpl
icat
ion
s',
60bi
late
ral
days
.5
deep
wo
un
din
fect
ion,
6pe
rsis
t en
tpa
in,
3h
emat
om
a
Pay
neet
al.,
TA
PP
vs.
lOm
oT
AP
P:48
6(1
2%)t
otal
068
unil
ater
al$3
093'
9un
ilat
eral
'T
APP
can
bepe
rfor
med
1994
,U
nit
edL
ich
tens
tein
com
plic
atio
ns,
087
bila
tera
l7.
5w
ith
sim
ilar
oper
ati
ve
Stat
es"
groi
npa
in67
bila
tera
lti
mes
and
shor
t-te
rm<
lmo,
2(4
%)
recu
rren
t11
.4re
curr
ence
rate
s,w
ith
con
vers
ions
tore
curr
ent
fast
erre
turn
tow
ork,
open
,1
(2%
)bu
tat
anin
crea
sed
cost
.in
carc
era
ted
90%
ofL
ich
tens
tein
som
en
tum
inu
sed
loca
lan
esth
esia
.pe
rito
neal
flap
Big
gest
imp
act
onfa
ster
Lic
ht.:
529
(18%
)to
tal
056
un
ilat
eral
$249
4'17
un
ilat
eral
're
turn
tow
ork
and
com
plic
atio
ns,
493
bila
tera
l25
bila
tera
lin
crea
sed
abil
ity
to(8
%)g
roin
pain
7326
perf
orm
stra
ight
leg
<lm
ore
curr
ent
recu
rren
tra
ises
seen
inm
anua
lla
bor
popu
lati
on.'
-,v
alue
was
not
mea
sure
d;lP
OM
,in
trap
erit
onea
lon
lay
mes
hre
pair
;T
AP
P,tr
ansa
bdom
inal
prep
erit
onea
lap
proa
ch;T
EP,
tota
lly
extr
aper
itone
alap
proa
ch.
'Sta
tisti
cal
sign
ific
ance
(all
unm
arke
dva
lues
are
not
stat
istic
ally
sign
ific
ant)
.

1154 CHAPTER 53
decreases with surgeon experience and the costs decrease aswell. 84,85 In our own series comparing the cost of TEP versusLichtenstein repairs (n = 60), TEP costs on average $778 morethan Lichtenstein repairs."
A steep learning curve for laparoscopic repairs exists andmust be overcome to achieve reliably good outcomes in termsof both complications and recurrence rates. 76- 78,80 The learningcurve for TEP procedures has been estimated to be 30 casesor more." Rare but serious complications such as visceral andvascular injury have been reported and highlight the needfor adequate training. Fortunately, additional training outsidethe operating room using surgical simulators may shortenthe learning curve and improve operative performance."Nonetheless, the learning curve effect may account, to alarge extent, for the great variability of reported results. Forexample, although surgeons enrolling patients in the recentlyreported Veterans Administration (VA) trial were required tohave performed 25 laparoscopic procedures, the breakpointfor outcomes in this setting was over 250 cases. For these"highly experienced" surgeons, recurrences were similar forprimary hernias (5.1 % laparoscopic, 4.1% open) and improvedfor recurrent hernias (3.6% laparoscopic, 17.40/0 open) com-pared to the "less-experienced" surgeons, who had inferiorresults (100/0 recurrence) for laparoscopic but not open repairs.The learning curve for laparoscopic repairs in the VA trialseems much higher than that reported in other series, andsome surgeons have questioned these results." In any case,these data suggest that surgeon experience plays a major rolein outcomes for laparoscopic hernia repairs. In the hands ofexperts, laparoscopic repairs may be performed faster thanopen repairs and with fewer complications.P'" Importantly,long-term data now support efficacy of laparoscopic repairswith acceptably low recurrence rates. 76,78,79
Several studies have compared the various types of lapa-roscopic repairs and are summarized in Table 53.5.78
,90-92 TheTEP approach avoids intraperitoneal dissection and the asso-ciated potential for visceral injury and postoperative adhesionformation." In theory, it may avoid the cardiorespiratoryalterations associated with creating a pneumoperitoneum,but there have been reports of respiratory acidosis associatedwith a pneumopreperitoneum." It appears that TEP has thefewest complications, making it the preferred method. 78,90,91,94
Although rarely done, TEP repairs may be successfully per-formed using regional anesthesia."
The disadvantage of the TEP approach is that it is techni-cally more difficult since the working space is smaller, andthe anatomic perspective is confusing until considerableexperience is gained.7o,9o,91 Moreover, previous lower abdomi-nal surgery or irradiation is a relative contraindication to TEPsince scars and peritoneal adhesions make this proceduredangerous and difficult, with a high rate of conversion toTAPP or open and a high rate of visceral injuries. 81
,90,91 It is adifficult approach with incarcerated or large scrotal hernias,and some authors have recommended using the TAPPapproach for these." Others, however, have met with successusing the TEP repair in large scrotal hernias, modifyingtheir technique by routinely dividing the inferior epigastricvessels." Although small peritoneal tears are usually welltolerated and can be sutured closed, large peritoneal breachesnecessitate conversion to a TAPP procedure. The conversionrate in Liem's prospective trial of 487 TEP repairs was 50/0,
which is comparable to most large series.'? Surgeons who usethe TEP approach should therefore be proficient in the TAPPapproach as well. 85
The TAPP approach has several inherent dangers due tothe violation of the peritoneal cavity. Abdominal organs andvasculature can be injured by trocar insertion." The inferiorepigastric vessels are especially at risk when lateral trocarsare inserted medial to the edge of the rectus sheath. Injury ofdeeper structures can usually be avoided by placing trocarsunder direct visualization. Intraabdominal adhesions fromprior abdominal operations can increase the risk of injury.The TAPP approach creates peritoneal flaps that must becompletely closed. If a gap remains, bowel can be exposed tothe mesh, allowing adhesions, erosions, or obstruction."Bowel can also herniate through a peritoneal opening andbecome incarcerated.t':" Incisional hernias at trocar sites aremore common after TAPP repairs, occurring in up to 1% ofpatients, necessitating fascial closure of all ports larger than5mm.62 The advantage of the TAPP approach is a largeworking space, improved visualization, and an easier learningcurve.61
,81 The approach facilitates easier reduction and repairof incarcerated and large scrotal hernias." and it also allowsother laparoscopic procedures to be performed simultane-ously, which has been supported as a safe practice by limiteddata."
Conceptually similar to laparoscopic ventral hernia repair,IPOM has appeal because of its simplicity and the lack ofextensive preperitoneal dissection." Although several trialshave shown the efficacy and safety of this technique, manyare skeptical of leaving a prosthetic in direct contact with theviscera, citing reports of bowel erosion and obstruction." Theprosthetic of choice in this circumstance has become PTFE,but structures under the peritoneum can also be obscured byplacement of an opaque prosthesis, placing them at riskduring mesh stapling. To overcome this problem, Vogt et al.meshed the PTFE graft with a skin graft mesher and reportedfavorable results." Still, mesh cannot be fixated in the areasoverlying the iliac vessels or the adjacent nerves. Althoughinitial enthusiasm for this technique was fueled by its rela-tively simple nature, use of the IPOM repair has never becomewidespread.
As highlighted above, the optimal type of approachremains controversial. There is still some hesitancy in thesurgical community to replace conventional hernia repairswith the laparoscopic approach. Multiple types of open repairshave long-standing and well-proven results, are associatedwith low morbidity and disability, and can be more easilyperformed under local anesthesia. It is difficult to endorse anew approach that is more difficult to learn, requires generalanesthesia, costs more, and has the potential, althoughrare, of causing serious abdominal complications. There iscurrently a consensus that laparoscopic approaches areindicated in bilateral and recurrent hernias.61,91,97,98 The lapa-roscopic approach provides access to both groins from thesame approach with no additional incisions. The laparoscopicapproach shares the same benefits as the open preperitonealapproach in recurrent hernia repair by avoiding scarred ante-rior tissue planes and potential cord injury." Many surgeonsalso use the laparoscopic approach for unilateral nonrecurrenthernias, especially in individuals requiring a more rapidconvalescence.
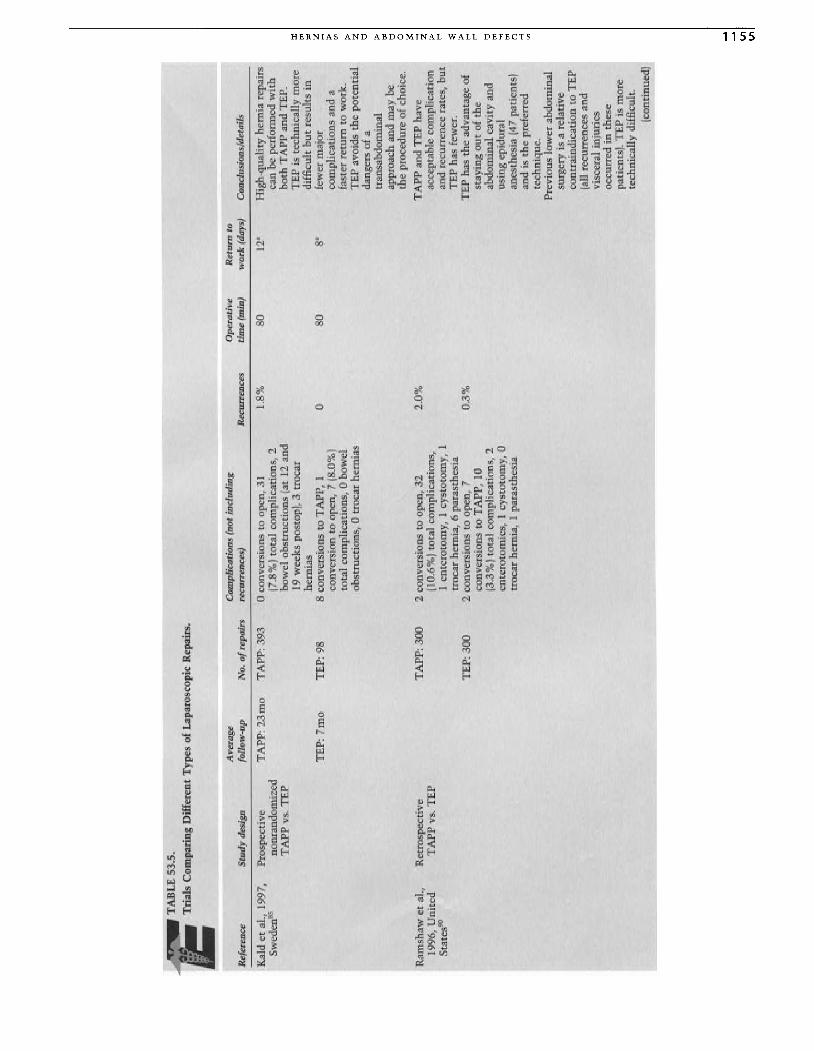
~~
TA
BL
E53
.5.
Tri
als
Com
pari
ngD
iffe
rent
Typ
esof
Lap
aros
copi
cR
epai
rs.
Ref
eren
ceS
tud
yde
sign
Ave
rage
foll
ow-u
pC
ompl
icat
ions
(not
incl
udin
gN
o.of
repa
irs
recu
rren
ces)
Rec
urre
nces
Ope
rati
veti
me
(min
)R
etu
rnto
wo
rk(d
ays)
Con
clus
ions
/det
ails
Kal
det
aI.,
1997
,S
wed
en"
Ram
shaw
etal
.,19
96,
Un
ited
Sta
res'
?
Pro
spec
tive
TA
PP:
23m
ono
nran
dom
ized
TA
PP
vs.
TE
P
TE
P:7
mo
Ret
rosp
ecti
veT
AP
Pvs
.TE
P
TA
PP:
393
TE
P:
9S
TA
PP:
30
0
TE
P:3
00
oco
nver
sion
sto
open
,31
(7.S
%)
tota
lco
mpl
icat
ions
,2
bow
elo
bst
mct
ion
s(a
t12
and
19w
eek
spo
stop
],3
troc
arhe
rnia
sS
conv
ersi
ons
toT
APP
,1
conv
ersi
onto
open
,7
(S.O
%I
tota
lco
mpl
icat
ions
,0
bow
elob
stru
ctio
ns,
0tr
ocar
hern
ias
2co
nver
sion
sto
open
,32
(10.
6%
)to
tal
com
plic
atio
ns,
1en
tero
tom
y,1
cyst
otom
y,1
troc
arhe
rnia
,6
para
sthe
sia
2co
nver
sion
sto
open
,7
conv
ersi
ons
toT
APP
,10
(3.3
%)t
otal
com
plic
atio
ns,
2en
tero
tom
ies,
1cy
stot
omy,
0tr
ocar
hern
ia,
1pa
rast
hesi
a
I.S% o 2.0
%
0.3%
so so
12' S'
Hig
h-qu
alit
yhe
rnia
repa
irs
can
bepe
rfor
med
wit
hb
oth
TA
PP
and
TE
P.T
EP
iste
chni
call
ym
ore
diff
icul
tb
ut
resu
lts
infe
wer
maj
orco
mpl
icat
ions
and
afa
ster
retu
rnto
wor
k.T
EP
avoi
dsth
ep
ote
nti
alda
nger
sof
atr
ansa
bdom
inal
appr
oach
and
may
beth
epr
oced
ure
ofch
oice
.
TA
PPan
dT
EP
have
acce
ptab
leco
mpl
icat
ion
and
recu
rren
cera
tes,
bu
tT
EP
has
few
er.
TE
Pha
sth
ead
vant
age
ofst
ayin
go
ut
ofth
eab
dom
inal
cavi
tyan
dus
ing
epid
ural
anes
thes
ia(4
7pa
tien
ts]
and
isth
epr
efer
red
tech
niq
ue.
Pre
viou
slo
wer
abdo
min
alsu
rger
yis
are
lati
veco
ntra
indi
cati
onto
TE
P(a
llre
curr
ence
san
dvi
scer
alin
juri
esoc
curr
edin
thes
epa
tien
ts).
TE
Pis
mor
ete
chni
call
ydi
ffic
ult.
(con
tinu
ed)
:t m "Z > '" > Z o > '" o o ~ z > r- :;: > r- r- o m ." m o .., '" ... ... VI
VI
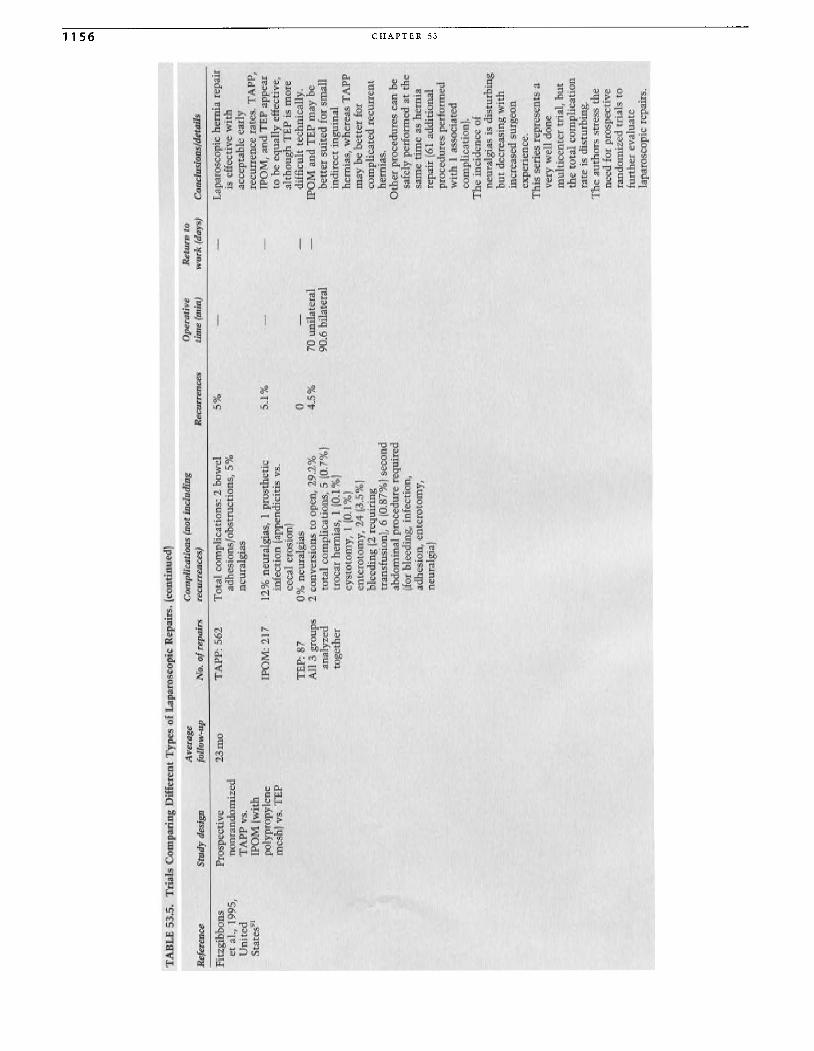
TA
BL
E53
.5.
Tri
als
Com
pari
ngD
iffe
rent
Typ
esof
Lap
aros
copi
cR
epai
rs.
(con
tin
ued
)
U1
0\
Ref
eren
ceS
tud
yde
sign
Ave
rage
foll
ow-u
pC
ompl
icat
ions
(not
incl
ud
ing
No.
ofre
pair
sre
curr
ence
s)R
ecur
renc
esO
pera
tive
tim
e(m
in)
Ret
urn
tow
ork
(day
s)C
oncl
usio
ns/d
etai
ls
Fit
zgib
bons
etal
.,19
95,
Un
ited
Stat
es"
Pro
spec
tive
23m
ono
nran
dom
ized
TA
PP
vs.
IPO
M(w
ith
poly
prop
ylen
em
esh)
vs.
TE
P
TA
PP
:56
2
IPO
M:
217
TE
P:8
7A
ll3
gro
ups
anal
yzed
toge
ther
Tot
alco
mpl
icat
ions
:2
bow
elad
hesi
ons/
obst
ruct
ions
,5
%ne
ural
gias
12%
neur
algi
as,
1pr
ost
het
icin
fect
ion
(app
endi
citi
svs
.ce
cal
eros
ionI
0%
neu
ralg
ias
2co
nver
sion
sto
open
,29
.2%
tota
lco
mpl
icat
ions
,5
(0.7
%)
troc
arh
ern
ias,
1(0
.1%
)cy
sto
tom
y,1
(0.1
%)
ente
roto
my,
24(3
.5%
)b
leed
ing
(2re
quir
ing
tran
sfus
ion)
,6
(0.8
7%)
seco
ndab
dom
inal
proc
edur
ere
quir
ed(f
orbl
eedi
ng,
infe
ctio
n,
adhe
sion
,en
tero
tom
y,ne
ura
lgia
]
5% 5.1
%
o 4.5
%70
un
ilat
eral
90.6
bila
tera
l
Lap
aros
copi
che
rnia
repa
iris
effe
ctiv
ew
ith
acce
pta
ble
earl
yre
curr
ence
rate
s.T
APP
,IP
OM
,an
dT
EP
appe
arto
beeq
uall
yef
fect
ive,
alth
ough
TE
Pis
mor
edi
ffic
ult
tec
hn
ical
ly.
IPO
Man
dT
EP
may
be
bett
ersu
ited
for
sma
llin
dire
ctin
guin
alh
ern
ias,
whe
reas
TA
PPm
aybe
bet
ter
for
com
plic
ated
recu
rren
th
erni
as.
Oth
erpr
oced
ures
can
besa
fely
perf
orm
edat
the
sam
eti
me
ashe
rnia
repa
ir(6
1ad
diti
onal
proc
edur
espe
rfor
med
wit
h1
asso
ciat
edco
mpl
icat
ion)
.T
hein
cide
nce
ofne
ural
gias
isdi
stur
bin
gb
utde
crea
sin
gw
ith
incr
ease
dsu
rgeo
nex
peri
ence
.T
his
seri
esre
pres
ents
ave
ryw
ell
done
mu
ltic
ente
rtr
ial,
bu
tth
eto
tal
com
plic
atio
nra
teis
dist
urbi
ng.
Th
eau
tho
rsst
ress
the
need
for
pros
pect
ive
rand
omiz
edtr
ials
tofu
rthe
rev
alu
ate
lapa
rosc
opic
repa
irs.
n ::I: :>- '">-i tn " <J> '"
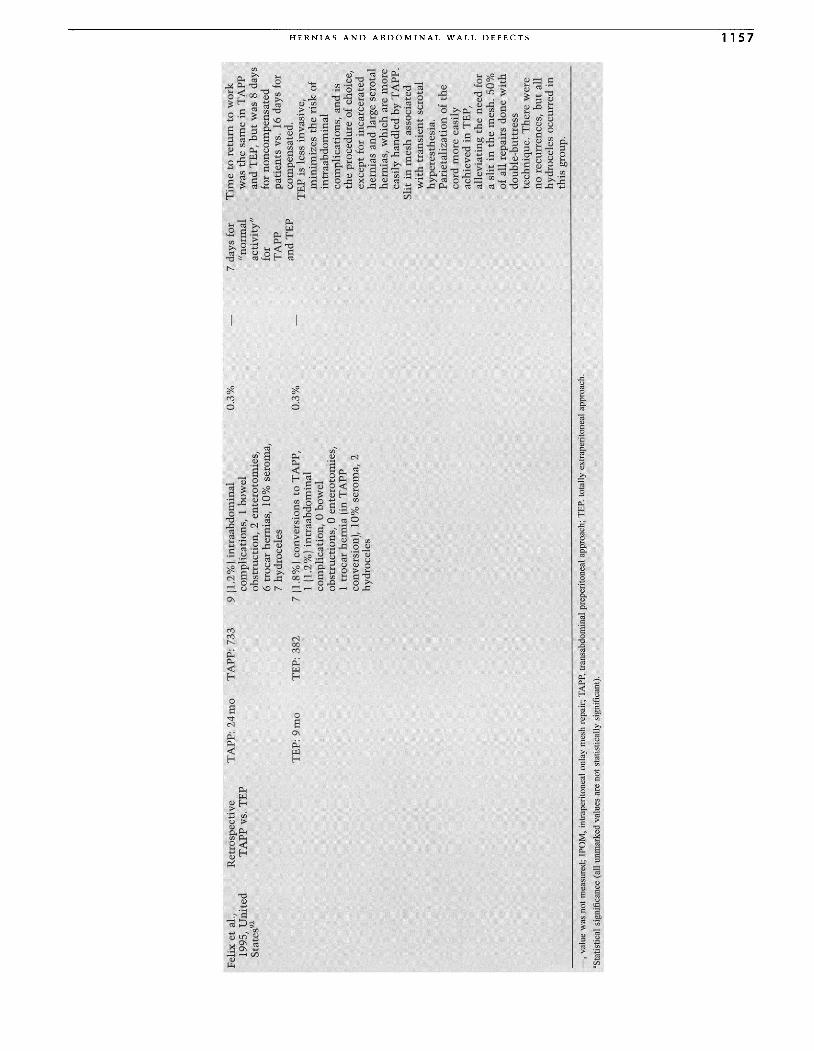
Felix
etal
.,19
95,
Un
ited
Sta
tes'
?
Ret
rosp
ecti
veT
AP
Pvs
.TE
PT
APP
:2
4m
o
TE
P:
9m
o
TA
PP
:73
3
TE
P:3
82
9(1
.2%
)in
traa
bd
om
inal
com
plic
atio
ns,
1bo
wel
obst
ruct
ion,
2en
tero
tom
ies,
6tr
ocar
hern
ias,
10%
sero
ma,
7hy
droc
eles
7(1
.8%
)co
nver
sion
sto
TA
PP
,1
(1.2
%)
intr
aabd
omin
alco
mpl
icat
ion,
0bo
wel
obst
ruct
ions
,0
ente
roto
mie
s,1
troc
arhe
rnia
(in
TA
PP
conv
ersi
on),
10%
sero
ma,
2hy
droc
eles
0.3
%
0.3
%
7da
ysfo
r"n
orm
alac
tiv
ity
"fo
rT
AP
Pan
dT
EP
Tim
eto
retu
rnto
wo
rkw
asth
esa
me
inT
APP
and
TE
P,b
ut
was
8da
ys
for
no
nco
mp
ensa
ted
pat
ien
tsvs
,16
days
for
com
pens
ated
.T
EP
isle
ssin
vasi
ve,
min
imiz
esth
eri
skof
intr
aab
do
min
alco
mpl
icat
ions
,an
dis
the
proc
edur
eof
choi
ce,
exce
ptfo
rin
carc
erat
edhe
rnia
san
dla
rge
scro
tal
hern
ias,
wh
ich
are
mo
reea
sily
hand
led
byT
AP
P.
Sli
tin
mes
has
soci
ated
wit
htr
ansi
ent
scro
tal
hype
rest
hesi
a.P
arie
tali
zati
on
ofth
eco
rdm
ore
easi
lyac
hiev
edin
TE
P,al
levi
atin
gth
ene
edfo
ra
slit
inth
em
esh
.50
%of
all
repa
irs
done
wit
hdo
uble
-bu
ttre
sste
chni
que.
Th
ere
wer
eno
recu
rren
ces,
bu
tal
lhy
droc
eles
occu
rred
inth
isgr
oup
.
:I: '" "Z > '" > Z o > t:O o o =: z > t'" ~ > t'" r- o '" ." '"o -i '"
-,
valu
ew
asno
tm
easu
red
;IP
OM
,in
trap
erito
neal
onla
ym
esh
repa
ir;
TA
PP.
tran
sabd
omin
alpr
eper
itone
alap
proa
ch;T
EP.
tota
llyex
trap
crit
onea
lapp
roac
h.
'Sta
tist
ical
sign
ific
ance
(all
unm
arke
dva
lues
are
not
stat
isti
cally
sign
ific
ant)
.
... ... U1 ......

1158 CHAPTER 53
Complications
There exists great variety in the methods and completenessby which complication rates are reported, and caution mustbe used not to draw premature conclusions from inadequatedata. Generally complication rates decrease with increasedsurgeon experience, but a thorough knowledge of anatomyand of potential hazards is essential to hernia repair.Complication rates following open inguinal hernia repairsaverage 70/0 to 12%.99 Reports on laparoscopic approaches arewidely variable, but the rates of complications for both con-ventional and laparoscopic repairs is now thought to becomparable.r'-":100,101
RECURRENCE
Ten percent is reported as the average recurrence rate forgroin hernias, although most surgeons boast to have rateswell below the average." Lichtenstein, for example, reportsrates of less than 10/0, with similar results reproduced byothers using the same technique.P:" Recurrence rates follow-ing conventional repairs vary from 1% to 7% for indirectinguinal hernias, from 4% to 100/0 for direct inguinal hernias,from 1% to 70/0 for femoral hernias, and from 50/0 to 350/0 forrecurrent hernia repair. 13,102 Lichtenstein noted that 500/00frecurrences after anterior repairs first appear 5 years or moreafter the initial operation, and 750/0 of recurrences becomeevident within 10 years of the original operation.l'" In con-trast, Stoppa noted that recurrences after a preperitonealrepair usually occur within the first postoperative year andare due to technical errors." Failure to diagnose multiplehernias at the time of initial operation, failure to close anenlarged internal ring, and breakdown of the repair undertension have all been implicated in the causes of recur-rences.P:'?' Elkberg showed an incidence of 60/0 for multipleipsilateral hernias and 170/0 for bilateral hernias using her-niography, suggesting missed hernias may account forrecurrence. 105
For laparoscopic repairs, the reasons for recurrence aresurgeon inexperience, inadequate dissection, insufficientprosthesis size, insufficient prosthesis overlap of herniadefects, inadequate fixation, prosthesis folding or twisting,missed hernias or lipomas, and mesh dislodgment secondaryto hematoma formation. 10,85,106-108 Recurrence is directlyrelated to surgeon experience, with failures occurring muchmore frequently early in the surgeon's learning curve. 1O,84,8S
Incomplete dissection can result in missed indirect herniasand missed cord lipomas, especially in the TEP procedure andespecially with inexperienced surgeons.106,108,109 Inadequatedissection can also limit the size of mesh that can be used orresult in incomplete fixation or folding. At least a 12 x 15cmpiece of mesh should be used to ensure a 2- to 3-cm overlapof all hernia defects and prevent technical causes for recur-rence. Several investigators advocated that mesh fixation isunnecessary if the mesh is large enough, and the impressiveresults of Champault's series supports this practice.6B,84,107,110
For laparoscopic repair of bilateral hernias, some advocatethe use of a single piece of mesh to alleviate medial recur-rence. 68,111 Using a slit to allow passage of the cord mayincrease recurrence. 109 Parietalization of the cord withalleviation of the need for a slit, or a slitted piece of meshreinforced by a second nonslitted piece, the so-called double-buttress technique'P may be used. Historically, Stoppa rec-
ommended not using a slit in the GPRVS to alleviate thepossibility of recurrence through this defect. 52
In contrast to conventional repairs, recurrences usinglaparoscopic repairs usually appear within the first postop-erative year. 1O,73,106 Tetik et al. published a multicenter retro-spective analysis of 1514laparoscopic repairs with a recurrencerate of 2.2% over an average follow-up of 13 months.!" Recur-rence rates were 22% for the plug and patch, 3% for simplering closure, 2.20/0 for IPOM, 0.7% for TAPP, and 0.40/0 forTEP. Phillips et al. published a multicenter review of 3229repairs with a recurrence rate of 1.60/0 over a mean follow-upof 22 months.!" Felix et al. published a multicenter retrospec-tive analysis of 10,053 TAPP and TEP repairs in 7661 patients;repairs were performed only by surgeons experienced in lapa-roscopic repairs. The recurrence rate was 0.4% over a meanfollow-up of 36 months.l'" The rates in prospective random-ized trials with up to 70-month follow-up vary widely, withmost studies reporting less than 5%, but some documentingrates as high as 100/0 (Table 53.5).10,63,66-73,81,85,90-92
NERVE ENTRAPMENT
Nerve injury results in numbness, pain, and parasthesias inthe distribution of the nerve; these results can be mild orincapacitating.115 Complete nerve transection is likely tocause only numbness and little long-term morbidity, whereaspartial transection or entrapment with a staple, suture, orsubsequent encroachment by scar tissue is likely to causeneuroma formation and pain. 2o,116 Symptoms usually appearimmediately postoperatively and intensify over the first 2weeks; most resolve within 8 weeks.117Treatment consists ofrest and injections with local anesthetic and corticosteroidsuntil symptoms resolve.l'" In a minority of patients, symp-toms persist, necessitating exploration and entrapment releaseor neurectomy.!"
The incidence of nerve injuries following conventionalopen repairs is less than 20/0.2,115,118 Cunningham et al. noteda disturbingly high incidence of postoperative pain in a pro-spective randomized trial comparing McVay, Bassini, andShouldice repairs.!" In 276 patients with 315 repairs per-formed, 62.9 % had pain (11.9% moderate to severe) at 1 year,and 53.60/0 had pain (10.60/0 moderate to severe) at 2 years.The incidence of pain was not affected by the type of repairperformed. Most often, the pain was associated with a liga-mentous somatic etiology attributed to undue tightness of theinguinal ligament at its insertion on the pubic tubercle createdby the repair. Only a minority of patients suffered from painsecondary to a neurologic etiology. The excellent results fol-lowing tension-free repairs such as the Lichtenstein proce-dure support the conclusion that postoperative pain is due totension created, with neuralgias occurring only rarely (wellless than 1% in Lichtenstein's series]." The ilioinguinal, ilio-hypogastric, and genital branch of the genitofemoral nerve aremost at risk during open repairs. The nerves are generallyvisible and can be avoided. If a nerve must be divided toperform the repair, complete nerve division is usually associ-ated with minimal morbidity.2o,29,116,1l9
Nerve entrapment can occur with any of the laparoscopicapproaches but may be lowest with the TEP repair." Tetik etal. reported nerve injury in less than 20/0 of 1514 repairs, withover 900/0 of these resolving with conservative therapy andonly 2 patients requiring reexploration and staple removal.l"

HERNIAS AND ABDOMINAL WALL DEFECTS 1159
Phillips et al. reported a 1.6% incidence of neuralgias in 3229repairs.'!" Other investigators have reported rates as high as12%, with an increased incidence associated with the IPOMtechnique and with surgeon inexperience."
Nerve injury typically occurs during laparoscopic repairswhen staples are placed inferior to the iliopubic tract in thearea lateral to the testicular vessels. The lateral femoral cuta-neous nerve, femoral nerve, and femoral branch of the geni-tofemoral nerve are at risk. These nerves lie superficial to theinternal oblique muscle and cannot be visualized. Carefulattention to anatomical danger zones during mesh fixation isnecessary to avoid entrapment. The triangle of pain and thetriangle of doom (Fig. 53.6) designate areas that are anatomi-cal danger zones that require avoidance. Seid combined thetwo triangles and extended their boundaries to the anteriorsuperior iliac spine laterally, labeling this area the trapezoidof disaster. 117 MacFadyen noted that stapling or suturing thatcauses nerve entrapment will cause pain lasting 6 months orlonger." Some advocate not securing the mesh in place at all,which effectively alleviates this complication. 76
Entrapment of the lateral femoral cutaneous nerve is themost common nerve injury encountered in laparoscopicrepairs. It results in pain and numbness in the upper lateralthigh and is called meralgia pataestheticaP" Broin et a1. care-fully detailed its course in cadavers and found that it was amean distance of 6.6cm from the inferior epigastric vesselsand 5.6cm from the internal inguinal ring as it passes belowthe iliopubic tract."! They recommended avoiding entrap-ment of this nerve by staying above the iliopubic tract andnot straying too far lateral to the internal inguinal ring whenstaples are placed.
Entrapment of the ilioinguinal, iliohypogastric, and genitalbranches of the genitofemoral nerve can occur during laparo-scopic repairs if excessive pressure is applied externally duringmesh fixation, compressing the muscles enough to allow thestaples to reach the nerves.!"
ISCHEMIC ORCHITIS/TESTICULAR ATROPHy/VAS
DEFERENS INJURY
Wantz has extensively studied ischemic orchitis and itssequela testicular atrophy.2o,122 Ischemic orchitis is a poten-tially devastating but rare complication of hernia repair andis caused by surgical trauma to the veins of the spermaticcord. Anterior approaches are more apt to cause testicularatrophy than posterior approaches since they require moredissection and handling of the cord. It was once thought thatthe cause was insufficient arterial supply to the testicle sec-ondary to overzealous tightening of the reconstructed internalinguinal ring. It is now known that the cause is venousthrombosis of the injured pampiniform plexus and disruptionof collateral arterial and venous circulation by distal corddissection. 19,20,122 This is more likely to occur in recurrenthernias, which involve scar tissue and a difficult dissection,or when the distal sac is dissected. The result is a swollen,hard cord, testicle, and epididymis. Fever and leukocytosismay occur, but infection is not part of the natural history ofthis phenomenon. The symptoms become apparent 2 to 5days postoperatively. The pain usually lasts several weeks,but the swelling and induration may last 4 to 5 months.
Ischemic orchitis may resolve without sequelae or maycause the testicle to shrink, resulting in a completely atrophic
testicle. There is no known treatment of ischemic orchitisthat prevents progression to testicular atrophy. Only rarelydoes the testicle become necrotic or require removal. Anatrophic testicle is painless, not prone to malignantdegeneration, and does not diminish serum testosterone orfertility .20
Wantz made several recommendations to avoid ischemicorchitis: avoid dissection of the distal hernia sac except insliding hernias, avoid dissection beyond the pubic tubercle,use a preperitoneal approach for all recurrent hernias or inpatients with prior inguinal or scrotal surgery, and delay therepair of a contralateral hernia for at least 1 year in patientswith ischemic orchitis." Using this approach in over 6000repairs, Wantz reduced the incidence of ischemic orchitisfrom 0.65% to 0.03% in primary hernias and from 2.25% to0.97% in recurrent hernias when compared to his priorseries.!" Skandalakis et al. reported an incidence of testicularatrophy of 0.1% after 3010 cases of open hernia repairs?
The incidence of ischemic orchitis following laparoscopicrepair is not well documented but is thought to be sufficientlylow since a minimum of cord handling and dissection arerequired, similar to the open preperitoneal approach.'
Direct injury to the vas deferens itself can result in infer-tility if the contralateral side is abnormal. Injury usuallymanifests as a painful spermatic granuloma, formed by highlyantigenic spermatozoa once they have escaped the vas. Exci-sion of the granuloma and microsurgical repair of the vas istreatment of choice."
BOWEL OBSTRUCTION AND INTRAABDOMINAL
ADHESIVE COMPLICATIONS
Unique to the laparoscopic approach is the potential for intra-abdominal adhesions and intestinal obstruction. There havebeen multiple case reports of such occurrences, most of whichfollowed TAPP repairs, but the overall incidence remainssmall, on the order of less than 10/0.60,81,96,98,123-125 The TAPPapproach creates peritoneal flaps, which must be closed com-pletely. If a gap remains, bowel can be exposed to the mesh,allowing adhesions, obstruction, erosions, and fistulas.6o,126-128
Bowel can herniate through a peritoneal opening and becomeincarcerated.":"
The IPOM procedure places mesh in an intraperitonealposition with no protection between the mesh and bowel.Both polypropylene mesh and PTFE have been used, but pro-ponents of PTFE cite its inertness and decreased adhesionformation as an advantage.Y" A porcine study comparedmeshed and unmeshed PTFE with Marlex placed by the TAPPand IPOM methods and noted equal rates of adhesion forma-tion with both PTFE and Marlex but significantly fewer adhe-sions with the TAPP method.!"
Others have also found a higher incidence of adhesionformation following the IPOM procedure in animalmodels.P'v"! Although several series support the efficacy andsafety of the IPOM approach, many feel that a peritonealcovering over the prosthesis decreases the risk of complica-tions." Even though the TEP procedure avoids intraperitonealdissection, there have been reports of intestinal obstructionfollowing TEP repairs when bowel has herniated throughperitoneal rents that were either not seen or not adequatelyrepaired at the time of operation.P':':"

1160 CHAPTER 53
Incisional hernias at trocar sites can occur after laparo-scopic repairs and cause intestinal obstruction and strangula-tion." They are more common after TAPP repairs, occurringin up to 1% of patients, necessitating fascial closure of allports larger than 5mm.6o
,85 Alternatively, nonbladed and radi-ally dilating trocars may obviate the need for fascial closure. 134
Preexisting umbilical hernias can substantially increase therisk of postoperative umbilical hernias, despite routineclosure, and require additional attention.r"
Some authors feel that the mere possibility of intestinalobstruction as a complication of hernia surgery is reasonenough to completely abandon the laparoscopic approach.Others point out that the risk is minimal, especially with theTEP procedure, by following strict technical guidelines.
VASCULAR INJURIES
In laparoscopic repairs, the inferior epigastric, external iliac,femoral, and testicular vessels are at risk. Injuries may resultin intraoperative hemorrhage or may present as postoperativehematomas. The inferior epigastric vessels can be injured iftrocars are placed medial to the lateral border of the rectussheath. The pressure of insufflation during laparoscopic pro-cedures can tamponade small venous injuries. After comple-tion of the procedure, hemostasis should be verified with theinsufflation pressure minimized. Injuries caused during trocarinsertion may not be evident until trocars are removed, man-dating careful inspection of these sites under camera visual-ization as trocars are removed.'?' The reported incidence ofpostoperative hematoma formation is 1% to 8%.100 Laparo-scopic repairs should be avoided in patients with uncorrectedcoagulopathies or in cirrhotics (especially with a history ofvarices) to minimize the risk of retroperitoneal bleeding,which has the potential to fill a very large volume prior totamponading.
In open repairs, bleeding is not a common intraoperativeproblem, but the incidence of hematoma formation may beas high as 31 0/0. 71 Meticulous efforts to achieve completehemostasis should be made. Hematomas may be self-limitedor may necessitate evacuation.
VISCERAL INJURIES
At risk are the small intestine, colon, and bladder, andalthough rare, injuries to these structures can be the sourceof considerable morbidity, especially if their diagnosis andtreatment are delayed.'?' Many of these injuries can occur ifan attempt is made to open the sac of a direct sliding hernia.If direct sacs are not opened but are simply reduced andinverted, the risk of injury may be minimized.
In laparoscopic repairs, risk of injury may be minimizedby bladder decompression with a Foley catheter, use of anopen Hasson cannula technique, insertion of trocars underdirect visualization, and thorough anatomical knowledgewith cautious dissection.!" Confining dissection to the arealateral to the medial umbilical ligament is helpful in avoidingbladder iniury.l'" Entering the peritoneal cavity with theTAPP and IPOM techniques increases the potential for vis-ceral injury.
WOUND INFECTIONS
Hernia repair is regarded as a clean operation and as suchshould have an infection rate of less than 2%.136 Antibiotic
prophylaxis has been the area of controversy. For clean cases,prophylaxis is normally not indicated. However, implanta-tion of a mesh prosthesis has been used as an indication, andsome surgeons routinely give prophylactic antibiotics to allhernia repairs. Platt published a landmark study in 1990 thatshowed significant benefit to patients undergoing open herniarepairs who received antibiotics.!" On the other hand, Taylorpresented a randomized double-blinded prospective study of619 open hernia repairs comparing antibiotic prophylaxis andno prophylaxis.r" The study showed no benefit from antibi-otic prophylaxis, but a high rate (8.90/0) of wound infectionsoccurred in both groups. Gilbert's prospective study compar-ing prophylaxis versus no prophylaxis and mesh versus nomesh in 2493 repairs confirmed these flndings.!" There wasno difference in wound infections between patients whounderwent repairs with mesh versus those without mesh,regardless of whether they had received antibiotics. Theoverall incidence for infection was less than 10/0. There wasa threefold increase in wound infections in patients over 60years of age. The results of these studies continue to makeantibiotic prophylaxis a controversial subject, and eitherpoint of view can be justified.
Of note, in repairs performed using mesh, deep woundinfections very rarely, if ever, require removal of the prosthe-sis.34
,139 They can usually be managed with drainage and anti-biotics, allowing the wound to granulate.
Special Considerations
FEMORAL REPAIRS
Femoral hernias are much less common than inguinal herniasbut are more often associated with complicated presenta-tions, with a 200/0 incidence of incarceration." Some authorshave suggested that the ideal way to repair femoral hernias isvia a preperitoneal approach, either open or laparoscopic.""This facilitates control of hernia contents and avoids disrup-tion of the inguinal floor mandated by an anterior approachand avoids the difficulty associated with approaching afemoral hernia through a thigh incision. The McVay repairhas been used, however, with successful results." Strangu-lated femoral hernias require proximal control, resection, andanastomosis of intestine and may best be approached througha preperitoneal incision or a midline laparotomy.
COMPLICATED GROIN HERNIAS
Approximately 100/0 of inguinal hernias and 20% of femoralhernias present incarcerated." Incarcerated hernias can causeintestinal obstruction or strangulation and infarction, result-ing in a high incidence of infection, hernia recurrence, andoperative mortality, especially in elderly patients. The pos-sibility of such complications has prompted the recommenda-tion that all hernias be repaired electively and promptly assoon as the diagnosis is made.!"
The laparoscopic approach in the repair of incarceratedhernias is controversial and may be contraindicated,100
although successful reduction and repair have been reported. 142
The data on this indication are limited, and caution must beexercised, especially if there is any question of bowel viabil-ity, in which situation a resection would be required, and amesh repair would be contraindicated for fear of infectious

HERNIAS AND ABDOMINAL WALL DEFECTS 1161
complications. The laparoscopic approach is, however, wellsuited for the repair of recurrent hernias.61,75,91,97,98
Many authors have advocated the open preperitonealapproach as the procedure of choice for recurrent and incar-cerated hernias. 19,20 For recurrent hernias, dense scar tissue inthe inguinal canal can be avoided, reducing the risk of nerveinjury and cord damage. In strangulated hernias, proximalunaffected intestine can be controlled prior to the release ofnecrotic intestine. The peritoneal cavity can be openedwithout an additional incision, and an intestinal resectionand anastomosis may be performed.
PEDIATRIC HERNIAS
The incidence of inguinal hernias in children is between 10and 20 per 1000 live births, with a 4: 1 male-to-female ratio.The overall incidence, incidence of bilaterality, male pre-dominance, and incidence of incarceration are higher in pre-mature infants. The incidence of bilaterality is at least 10%in full-term infants and as high as 55% in premature infants.The incidence of inguinal hernia in cryptorchid infantsapproaches 650/0. Approximately 55% to 700/0 of inguinalhernias in children are on the right side, and 1% have a directcomponent.' The higher incidence of right-sided hernias isthought to be due to the later descent of the right testicle andpotentially delayed closure of the processus vaginalis. Incar-ceration occurs in 9% to 200/0 of cases, is more frequent inchildren younger than 6 months of age, and in the absence ofsigns of strangulation, can usually be managed by manualreduction followed by prompt elective repair. Elective repairis associated with a much lower incidence of complicationscompared to emergent operations, especially in low birthweight infants. Elective repair should be performed as soonas possible to avoid reincarceration, which occurs in up to160/0 of cases.':"
The most widely accepted repair of pediatric inguinalhernias is a high ligation of the sac (Fig. 53.8). This techniquealone is usually sufficient since the vast majority of pediatrichernias are indirect with no laxity of the internal ring. If ringlaxity exists, a few sutures can be placed in the transversalisfascia to approximate the tissues. Recurrence rates of lessthan 1% are reported."
Considerable debate exists concerning routine contralat-eral groin exploration. Historically, this has been advocated,given the high incidence of bilaterality. The incidence of apatent contralateral processus vaginalis is higher in girls thanin boys who present with a unilateral hernia. Developmentof a contralateral hernia following unilateral repair is alsohigher in infants presenting at less than 1 year of age andin infants who present initially with a left-sided unilateralhernia.
Surana and Puri reported the development of a contralat-eral hernia in only 100/0 of 116 patients following a unilateralrepair and testicular damage in up to 100/0 of their patients;consequently, they viewed contralateral exploration as un-necessary and hazardous.!" Iona prospectively analyzed 354patients undergoing bilateral repairs or unilateral repairs withcontralateral exploration and found bilateral involvement in68% of patients younger than 1 year of age and 41% of patients1 to 6 years of age, with no increased risk of cornplications.v"Iona advocated routine contralateral exploration of all patientsyounger than 6 years old. Selective contralateral exploration
on the basis of a laparoscopic evaluation for a patent proces-sus vaginalis performed through the opened hernia sacdecreases the number of negative explorations and may be thebest option. 146
Abdominal Wall Defects
Ventral Hernias
Approximately 90,000 ventral hernias are repaired in theUnited States each year.!" Important to remember is theanatomical structure of the anterior abdominal wall, whichabove the semilunar line of Douglas consists of skin, subcu-taneous fat, anterior rectus sheath, rectus muscle, posteriorrectus sheath, and peritoneum. Below the semilunar line, thelayers are the same except that there is no posterior rectussheath. Laterally, the layers are skin, subcutaneous fat, exter-nal oblique aponeurosis and muscle, internal oblique aponeu-rosis and muscle, transversus abdominis aponeurosis andmuscle, transversalis fascia, and peritoneum.
A ventral hernia is a defect in the abdominal wall. Ventralhernias present as a protrusion or bulge and may containpreperitoneal fat or intestinal contents. The size may rangefrom very small to massive. Patients mayor may not besymptomatic. The fascial edge along the circumference of thedefect is usually palpable on exam. In obese patients, a CTscan or ultrasound examination may help confirm the diag-nosis. As with groin hernias, ventral hernias may presentwith incarceration, strangulation, or bowel obstruction; elec-tive repair is preferred to emergent repair.
Umbilical hernias are due to an error in the embryologicdevelopment of the abdominal wall. Umbilical hernias occurin 10% to 300/0 of live births but frequently close during thefirst few years of life. If larger than 2cm, the likelihood ofthe defect spontaneously closing is much less, and repair isnot delayed. Otherwise, repair is usually postponed until thechild reaches 4 years of age to allow time for spontaneousclosure. Most infants are asymptomatic, and incarceration orstrangulation is extremely rare.' Repair consists of simplefascial closure. Defects may persist, become evident in adult-hood, and should be repaired. In cirrhotic patients withuncontrolled ascites, umbilical hernias may rupture, requir-ing emergent repair. In such instances, a herniorraphycombined with a peritoneal-venous shunt is effective, butmortality rates are high.
Epigastric hernias arise in the upper abdomen alongthe linea alba, and usually appear in adulthood, often inassociation with obesity or pregnancy. Epigastric herniasfrequently present as small defects with incarceratedpreperitoneal fat or omentum, causing pain and warrantingrepair. Diastasis recti is a condition in which the medialborders of the rectus muscles slowly spread apart, with thin-ning and stretching of the rectus sheath, resulting in a diffusebulge in the upper midline abdomen. In contrast to epigastrichernias, diastasis recti is not a fascial defect or hernia per seand consequently presents no threat of complication. Diasta-sis recti is merely a cosmetic deformity. Excision of thethinned fascia and placement of a mesh prosthesis alleviatethe deformity.
Incisional hernias occur in at least 2% to 11% of abdom-inal wound closures. 148-150 In a 10-year prospective trial of 337

1162 CHAPTER 53
laparotomy patients, Mudge showed that in 62 patients whodeveloped hernias, 56% did so after the first postoperativeyear, and 350/0 did so after 5 years, demonstrating the widevariety in intervals between operation and hernia forma-tion."! Approximately 17% present with incarceration 152 andmortality rates for repair of complicated hernias is three timeshigher than for elective repairs.v"
Many risk factors for developing an incisional hernia havebeen cited,. including obesity, wound infection, advanced age,postoperative pulmonary complications, jaundice, abdominaldistension, emergency operation, reuse of a previous incision,p.regnan~y, postoperative chemotherapy, steroids, malnutri-non, ascites, and peritoneal dialysis. Most of these risk factorsare associated with excessive strain on the incision or poorwound healing. Wound infection is the most important riskfactor, with hernias four times more likely to occur after awound infection.l'" Obesity has also been clearly establishedas a risk factor. 150,155
Carlson showed that reuse of a previous midline incisionin combination with a wound infection was associated witha 10-fold increase in risk of hernia formation.':" Reuse of anincision has been shown to double the incidence of subse-quent incisional hernias.!" Incisional hernias occur more fre-quently after a vertical midline incision than after a transversesubcostal, or paramedian incision. 149
,157 This may be due t~the fact that emergency operations are more likely to be per-formed through a midline incision for more complete andrapid exposure; the emergent nature of the operation, and notthe type of incision, may be associated with a higher rate ofpostoperative hernias. This theory was supported by a trialconducted by Ellis, who found no difference in hernia inci-dence for different types of incisions in patients undergoingelective abdominal procedures.!"
Suture technique has been extensively studied with nodifference in hernia incidence shown between continuous andinterrupted suture techniques or layered versus mass woundclosure.148
,159 The advantages of using a continuous sutureare more rapid closure and decreased material costs with noincrease in hernia or dehiscence rates. 154,160 Continuoussutures, at least theoretically, evenly distribute the tensionand cause less tissue necrosis.'?' Permanent suture may beassociated with suture sinus formation.l'" infection.l'" or latehernia formation due to gradual sawing of the suture throughthe fascia, resulting in a "buttonhole" hernia. 152
,162
Absorbable suture alleviates these problems, but mustdeg~ade slowly enough to provide sufficient tensile strengthuntil adequate wound healing has occurred. Monofilamentsuture is preferred over braided suture, which has intersticesthat can harbor bacteria.l" Polydioxanone (PDS) and polygly-conate (Maxon) are monofilament absorbable sutures thatretain 700/0 to 750/0 of their tensile strength at 14 days, arecompletely absorbed by 180 to 210 days, and may be ideal forf . 1 1 159 162 S h .aSCIa c osure.' utures t at are more rapidly absorbed,such as polyglactin (Vicryl), may be associated with a higherincidence of incisional hernias.!" Sutures should be placed atleast 1em back from the fascial edge and no more than 1emapart to provide an adequate closure.l'" A suture-to-wound-length ratio of less than 4 is associated with an increasedh . incid 150 herma mci ence, emp asizing the need to incorporate anadequate amount of tissue in the closure. Overtighteningshould be avoided, as tissue ischemia and necrosis can occurpredisposing to wound breakdown, dehiscence, and herniaformation.
Of note, the tremendous surge in laparoscopic procedureshas spurred the birth of a new type of incisional hernia the~rocar ~ernia. M~ltiple reports.of ~uch hernias have app~aredIn the literature. The overall incidence of trocar hernias fol-lowing laparoscopic procedures is less than 10/0. 164 All fascialdefects larger than 5mm should be closed with a fascialclosure device to prevent this complication/" Recently,trocars that do not use traditional cutting obturators havebeen introduced to decrease the risk of hernia formation.some level I evidence suggests that these nonbladed and radi-ally dilating trocars do not require closure.F"
REPAIR TECHNIQUES
Various repair methods exist, and a prosthetic mesh mayormay not be used. In open repairs, the hernia is approachedthrough a skin incision placed directly over the fascial defectusually incorporating the scar from the previous incision. Th~sac is dissected free from subcutaneous tissues and the fascialedges. The sac may be opened to facilitate lysis of adhesionsand ~nspection and reduction of sac contents. If possible, thesac IS not completely excised, so that there is a sufficientamount of sac to close over the intestinal contents. Thisprovides protection against adhesive complications if mesh isto be used in the repair. The superficial and deep surfaces ofthe fascia are exposed several centimeters back from thehernia defect. Attenuated fascia is excised. A thorough searchfor con~omita?t hernias is performed. Depending on the typeof repair, fascia may then be closed with or without placinga mesh buttress. Fascia should only be closed when it can be~one so without tension. Closed suction drains may be placedIn the dead space superficial to the fascia to minimize seromaformation.
~n the case of very large hernias existing for a long periodof time, most of the intestines and omentum reside in thehernia sac instead of the abdominal cavity. As a result, theabdominal cavity may no longer be large enough to accom-modate the viscera when hernia repair is attempted. This canresult i~ diaphragmatic dysfunction and intestinal circulatorycongestion after contents are reduced." In this case, theabdominal cavity can be enlarged preoperatively by creatinga pneumoperitoneum.l" The abdominal wall stretches asseveral liters of air are insufflated into the abdominal cavityover the course of 2 to 3 weeks. Because tension-free repairscan be performed using a mesh prosthesis, this technique isnot routinely required.
Hernias recur on average 1.7 years after repair, accordingto a retrospective review by Leber of 200 hernias repaired withmesh followed for an average of 6.7 years.!" Recurrence ratesafter incisional hernia repair vary widely but are disappoint-ing at best, ranging from 200/0 to 630/0, and are notably higherafter primary repair than after mesh repairs. 148,157,166 Infectionafter hernia repair is a feared complication since infection isassociated with a markedly higher rate of recurrence. Mostinfections can usually be managed with antibiotics anddebridement and rarely necessitate mesh removal. Simultane-ously performed intraabdominal procedures may increase therisk of infection and should be avoided.l'" Several repair tech-niques are worthy of detailed discussion.
PRIMARY REPAIR
Ventral hernias may be repaired by primary closure as longas the repair can be performed in a tension-free fashion. The
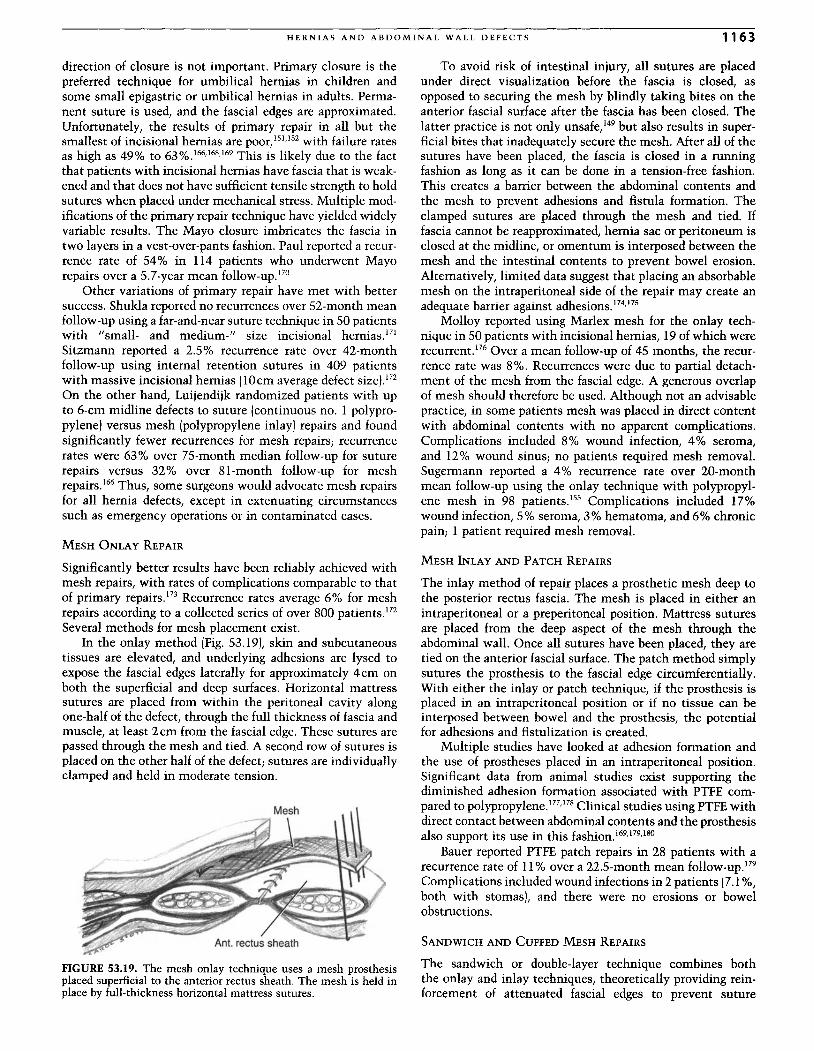
HERNIAS AND ABDOMINAL WALL DEFECTS 1163
direction of closure is not important. Primary closure is thepreferred technique for umbilical hernias in children andsome small epigastric or umbilical hernias in adults. Perma-nent suture is used, and the fascial edges are approximated.Unfortunately, the results of primary repair in all but thesmallest of incisional hernias are poor,1 51,152with failure ratesas high as 49% to 63%.166,168,169 This is likely due to the factthat patients with incisional hernias have fascia that is weak-ened and that does not have sufficient tensile strength to holdsutures when placed under mechanical stress. Multiple mod-ifications of the primary repair technique have yielded widelyvariable results. The Mayo closure imbricates the fascia intwo layers in a vest-over-pants fashion. Paul reported a recur-rence rate of 54% in 114 patients who underwent Mayorepairs over a 5.7-year mean follow-up ."?
Other variations of primary repair have met with bettersuccess. Shukla reported no recurrences over 52-month meanfollow-up using a far-and-near suture technique in 50 patientswith "small- and medium-" size incisional hernias.' ?'Sitzmann reported a 2.5% recurrence rate over 42-monthfollow-up using internal retention sutures in 409 patientswith massive incisional hernias (lOcm average defect size).172On the other hand, Luijendijk randomized patients with upto 6-cm midline defects to suture (continuous no. 1 polypro-pylene) versus mesh (polypropylene inlay) repairs and foundsignificantly fewer recurrences for mesh repairs ; recurrencerates were 63% over 75-month median follow-up for suturerepairs versus 32% over 81-month follow-up for meshrepairs .l" Thus, some surgeons would advocate mesh repairsfor all hernia defects, except in extenuating circumstancessuch as emergency operations or in contaminated cases .
MESH ONLAY REPAIR
Significantly better results have been reliably achieved withmesh repairs, with rates of complications comparable to thatof primary repairs.! " Recurrence rates average 6% for meshrepairs according to a collected series of over 800 patients.!"Several methods for mesh placement exist.
In the onlay method (Fig. 53.19), skin and subcutaneoustissues are elevated, and underlying adhesions are lysed toexpose the fascial edges laterally for approximately 4cm onboth the superficial and deep surfaces . Horizontal mattresssutures are placed from within the peritoneal cavity alongone-half of the defect, through the full thickness of fascia andmuscle, at least 2 em from the fascial edge. These sutures arepassed through the mesh and tied. A second row of sutures isplaced on the other half of the defect; sutures are individuallyclamped and held in moderate tension.
FIGURE 53.19. The mesh onlay technique uses a mesh prosthesisplaced superficial to the anterior rectus sheath. The mesh is held inplace by full-thickness horizontal mattress sutures.
To avoid risk of intestinal injury, all sutures are placedunder direct visualization before the fascia is closed, asopposed to securing the mesh by blindly taking bites on theanterior fascial surface after the fascia has been closed. Thelatter practice is not only unsafe.!" but also results in super-ficial bites that inadequately secure the mesh. After all of thesutures have been placed, the fascia is closed in a runningfashion as long as it can be done in a tension-free fashion.This creates a barrier between the abdominal contents andthe mesh to prevent adhesions and fistula formation. Theclamped sutures are placed through the mesh and tied . Iffascia cannot be reapproximated, hernia sac or peritoneum isclosed at the midline, or omentum is interposed between themesh and the intestinal contents to prevent bowel erosion.Alternatively, limited data suggest that placing an absorbablemesh on the intraperitoneal side of the repair may create anadequate barrier against adhesions.P''!"
Molloy reported using Marlex mesh for the onlay tech -nique in 50 patients with incisional hernias, 19 of which wererecurrent.I" Over a mean follow-up of 45 months, the recur-rence rate was 8%. Recurrences were due to partial detach-ment of the mesh from the fascial edge. A generous overlapof mesh should therefore be used. Although not an advisablepractice, in some patients mesh was placed in direct contentwith abdominal contents with no apparent complications.Complications included 8% wound infection, 4% seroma,and 12% wound sinus; no patients required mesh removal.Sugermann reported a 4% recurrence rate over 20-monthmean follow-up using the onlay technique with polypropyl-ene mesh in 98 patients.!" Complications included 17%wound infection, 5% seroma, 3% hematoma, and 6% chronicpain; 1 patient required mesh removal.
MESH INLAY AND PATCH REPAIRS
The inlay method of repair places a prosthetic mesh deep tothe posterior rectus fascia. The mesh is placed in either anintraperitoneal or a preperitoneal position. Mattress suturesare placed from the deep aspect of the mesh through theabdominal wall. Once all sutures have been placed, they aretied on the anterior fascial surface. The patch method simplysutures the prosthesis to the fascial edge circumferentially.With either the inlay or patch technique, if the prosthesis isplaced in an intraperitoneal position or if no tissue can beinterposed between bowel and the prosthesis, the potentialfor adhesions and fistulization is created.
Multiple studies have looked at adhesion formation andthe use of prostheses placed in an intraperitoneal position.Significant data from animal studies exist supporting thediminished adhesion formation associated with PTFE com-pared to polypropylene.F' '!" Clinical studies using PTFE withdirect contact between abdominal contents and the prosthesisalso support its use in this fashion.169,1 79,1 8o
Bauer reported PTFE patch repairs in 28 patients with arecurrence rate of 11% over a 22.5-month mean follow-up.!"Complications included wound infections in 2 patients (7.1%,both with stomas), and there were no erosions or bowelobstructions.
SANDWICH AND CUFFED MESH REPAIRS
The sandwich or double-layer technique combines boththe onlay and inlay techniques, theoretically providing rein-forcement of attenuated fascial edges to prevent suture
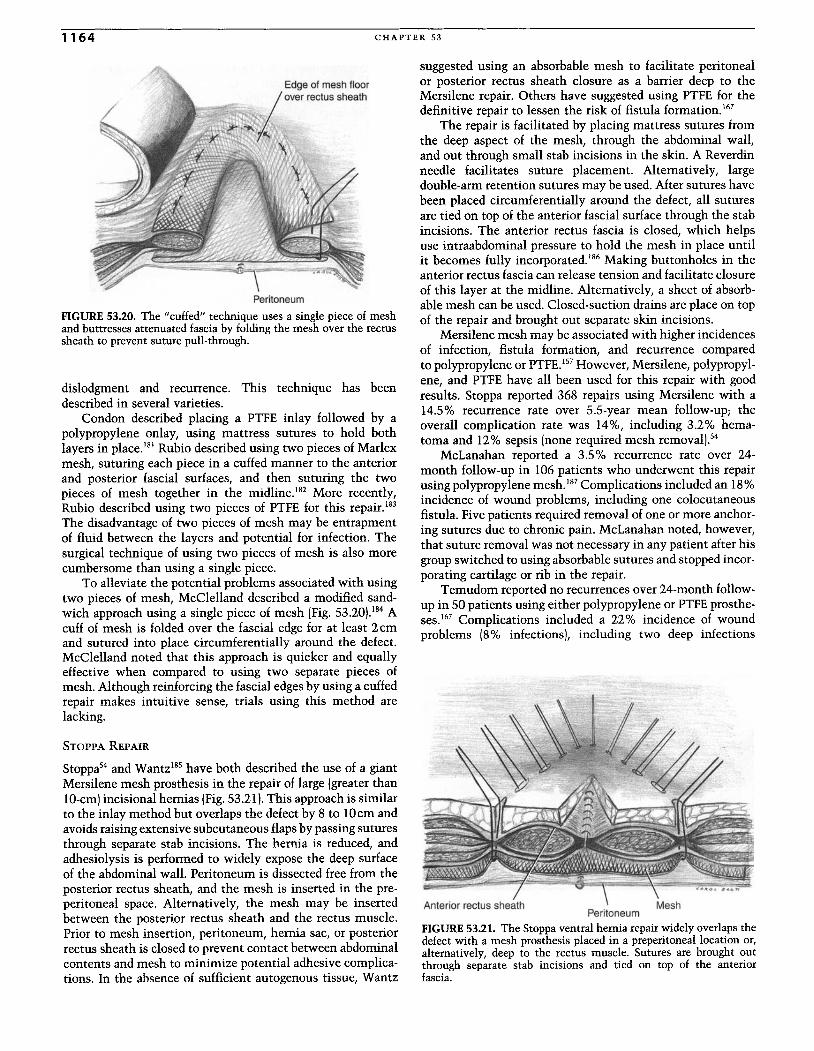
1164 CHAPTER 53
Peritoneum
FIGURE 53.20. The "cuffed" technique uses a single piece of meshand buttresses attenuated fascia by folding the mesh over the rectussheath to prevent suture pull-through.
dislodgment and recurrence. This technique has beendescribed in several varieties.
Condon described placing a PTFE inlay followed by apolypropylene onlay, using mattress sutures to hold bothlayers in place. "! Rubio described using two pieces of Marlexmesh, suturing each piece in a cuffed manner to the anteriorand post erior fascial surfaces, and then suturing the twopieces of mesh together in the midline.F' More recently,Rubio described using two pieces of PTFE for this repair. 183
The disadvantage of two pieces of mesh may be entrapmentof fluid between the layers and potential for infection. Thesurgical technique of using two pieces of mesh is also morecumbersome than using a single piece.
To alleviate the potential problems associated with usingtwo pieces of mesh, McClelland described a modified sand-wich approach using a single piece of mesh (Fig. 53.20).184 Acuff of mesh is folded over the fascial edge for at least 2 emand sutured into place circumferentially around the defect.McClelland noted that this approach is quicker and equallyeffective when compared to using two separate pieces ofmesh. Although reinforcing the fascial edges by using a cuffedrepair makes intuitive sense, trials using this method arelacking.
STOPPA REPAIR
Stoppa" and Wantzl85 have both described the use of a giantMersilene mesh prosthesis in the repair of large (greater thanlO-cm)incisional hernias (Fig. 53.211. This approach is similarto the inlay method but overlaps the defect by 8 to lOcm andavoids raising extensive subcutaneous flaps by passing suturesthrough separate stab incisions. The hernia is reduced andadhesiolysis is performed to widely expose the deep surfaceof the abdominal wall . Peritoneum is dissected free from theposterior rectus sheath, and the mesh is inserted in the pre-peritoneal space. Alternatively, the mesh may be insertedbetween the posterior rectus sheath and the rectus muscle.Prior to mesh insertion, peritoneum, hernia sac, or posteriorrectus sheath is closed to prevent contact between abdominalcontents and mesh to minimize potential adhesive complica-tions. In the absence of sufficient autogenous tissue, Wantz
suggested using an absorbable mesh to facilitate peritonealor posterior rectus sheath closure as a barrier deep to theMersilene repair. Others have suggested using PTFE for th edefinitive repair to lessen the risk of fistula formation. !"
The repair is facilitated by placing mattress sutures fromthe deep aspect of the mesh, through the abdominal wall ,and out through small stab incisions in the skin. A Reverdinneedle facilitates suture placement. Alternatively, largedouble-arm retention sutures may be used. After sutures havebeen placed circumferentially around the defect all suturesare tied on top of the anterior fascial surface through the stabincisions. The anterior rectus fascia is closed, which helpsuse intraabdominal pressure to hold the mesh in place untilit becomes fully incorporated.l'" Making buttonholes in theanterior rectus fascia can release tension and facilitate closureof this layer at the midline. Alternatively, a sheet of absorb-able mesh can be used. Closed-suction drains are place on topof the repair and brought out separate skin incisions.
Mersilene mesh may be associated with higher incidencesof infection, fistula formation, and recurrence comparedto polypropylene or PTFE.157However, Mersilene, polypropyl-ene, and PTFE have all been used for this repair with goodresults. Stoppa reported 368 repairs using Mersilene with a14.5% recurrence rate over 5.5-year mean follow-up; theoverall complication rate was 14%, including 3.2% hema-toma and 12% sepsis (none required mesh removal' ."
McLanahan reported a 3.5% recurrence rate over 24-month follow-up in 106 patients who underwent this repairusing polypropylene mesh. !" Complications included an 18%incidence of wound problems, including one colocutaneousfistula. Five patients required removal of one or more anchor-ing sutures due to chronic pain . McLanahan noted, however,that suture removal was not necessary in any patient after hisgroup switched to using absorbable sutures and stopped incor-porating cartilage or rib in the repair.
Temudom reported no recurrences over 24-month follow-up in 50 patients using either polypropylene or PTFE prosthe-ses.!" Complications included a 22% incidence of woundproblems (8% infections], including two deep infections
Peritoneum
FIGURE .53.21. The Stoppa ventral hern ia repair widely overlaps thedefect WIth a mesh prosthesis placed in a preperitoneallocation oralt ernatively, deep to the rectus muscle. Sutures are brought ou tthrough separate stab incisions and tied on top of the anteriorfascia.

HERNIAS AND ABDOMINAL WALL DEFECTS 1165
requmng mesh removal (one patient who had undergonesimultaneous gastric bypass, one who had an undetectedenterotomy). Seven patients had chronic pain, which resolvedwithout the need for suture removal.
Amid reported no recurrences in 54 patients (no follow-upinterval specified) using polypropylene mesh, with the onlycomplication being a seroma in 1 patient.l'" In 25 patients,mesh was secured with staples as opposed to anchoringsutures. Amid claimed that the stapling technique adequatelyholds the mesh in place until it is incorporated, is faster thansuturing, and alleviates the cosmetically unappealing skinretractions at the stab incisions.
LAPAROSCOPIC REPAIR
Laparoscopy has gained considerable momentum in the areaof ventral hernias, with standardized techniques becomingwell established. Most often, a transabdominal approach isused by placing several trocars in an intraperitoneal position,reducing the hernia through sharp adhesiolysis and bluntmanipulation, leaving the hernia sac in situ, and using a meshprosthesis to close the defect. Mesh is sized externally toprovide at least 3 em of overlap on all sides of the defect. Asuture is placed through each comer and tied, with tails leftlong. The skin is marked at the sites where the four cornersutures will exit, and small stab incisions are made. Mesh isthen rolled and passed intraabdominally through a port,unfolded, and positioned over the defect.
A fascial closure device is passed through the skin stabincision and used to individually retrieve the tails of eachcomer suture. The tails are tied superficial to fascia in a sub-cutaneous position. Additional transfascial sutures are placedat 4- to 5-cm intervals. Helical fasteners or other similarfixation devices are used to secure the mesh to peritoneumand fascia at l-cm intervals between the comer sutures, pre-venting herniation of bowel or omentum between the meshand the abdominal wall.
The laparoscopic approach facilitates adhesiolysis andhernia repair with minimal access and without the needfor a large subcutaneous dissection. Intraperitoneal meshplacement uses intraabdominal pressure to help hold theprosthesis in place. Intraperitoneal mesh placement does,however, create the potential for bowel adhesions and fistulaformation. Polypropylene has been used successfully forthis repair.!" but most authors recommend PTFE147,189,190 orseveral other newly available composite meshes to decreasethe risks of adhesive complications. Recurrences are usuallydue to inadequate mesh overlap or fixation. Mesh securityrelies primarily on the transfascial sutures, and using onlytacks for mesh fixation may be inadequate.':" While someseries have documented good results with tacks only.'?' mostsurgeons advocate routine use of sutures to prevent meshmigration.
With appropriate techniques, recurrence rates followinglaparoscopic repairs are generally about 40/0 with 4-yearfollow-up; conversion rates are about 40/0. Although random-ized controlled trials are still lacking, available data verifythat this approach is safe and effective. 147,188,189 As shown inTable 53.6, numerous comparative trials suggest that thelaparoscopic approach results in decreased overall complica-tions, fewer wound infections, fewer recurrences, fasterrecovery, decreased overall cost, and less pain but is associ-
ated with an increased rate of seroma formation, more fre-quent bowel injuries, and longer operative times compared tothe conventional open approaches (Table 53.6).192-201 With I-to 54-month (2years on average) follow-up, these comparativetrials documented recurrence rates of 0%-61 % (130/0 average)for open repairs and 0%-13% (4% average) for laparoscopicrepairs.
Several large cohort trials supported these results, asshown in Table 53.7. With up to 47-month follow-up, thesetrials documented an average conversion rate of 4.50/0 and, instudies that used both tacks and suture fixation, a recurrentrate of 3.90/0.147,191,202-210
Importantly, there is a learning curve for the laparoscopicapproach. Good surgical judgment, knowledge of the proce-dure, and great care must be taken to perform the repair cor-rectly and safely. Special attention must be paid to identifyingand repairing (laparoscopically or via a conversion to an openapproach) enterotomies or other visceral injuries as theyoccur, such that missed injuries and postoperative abdominalsepsis may be avoided. Byfar, this is the most troubling pitfallregarding laparoscopic hernia procedures as missed injuriesmay lead to mortalities.194,195,203,208 Whether to proceed withmesh placement in the setting of an adequately repairedenterotomy is controversial. Viable options include notplacing mesh and performing a tissue repair or returning tothe operating room after several days of antibiotic therapy.r'"Alternatively, if there is no spillage of enteric contents,several authors have successfully placed mesh during theinitial operation, as planned, with good results.203,204
Since no effort is made to remove the hernia sac, seromaformation is a common occurrence following laparoscopicrepairs. Depending on the definition used, seroma formationmay occur as frequently as 43%,197 but is self-limited in thevast majority of patients. While aspirating such seromasmay be tempting, only the few (30/0-18%) patients with per-sistent (>6 weeks) seromas should be decompressed sinceneedle aspiration may be associated with subsequent meshinfection.197,204 In addition, compression bandages or abdomi-nal binders worn for 7-14 days following surgery may helpminimize seromas."?
As previously mentioned, transfascial suture fixationseems important for repair durability. On the other hand,significant persistent pain may develop at these fixation sitesin 10/0-260/0 of cases. Some authors have suggested avoidingoverzealous tightening of these sutures to avoid pain. Suturesites can be injected using a combination of steroid and localanesthetic, or sutures can be removed via a cut-down proce-dure if pain persists. Studies are currently underway investi-gating the use of absorbable sutures and the efficacy of repairsusing nonsuture fixation strategies with a variety of pros-thetic types.
Because of the advantages of fewer wound infections andrecurrences and a faster recovery, laparoscopic approacheswill likely continue playing a major role for ventral herniarepair.
COMPLEX ABDOMINAL WALL CLOSURES
AND BIOMATERIALS
Abdominal wall closure can be difficult and morbid in theemergency setting. Emergency closures are often required inthe face of vigorous resuscitation with massive tissue edema
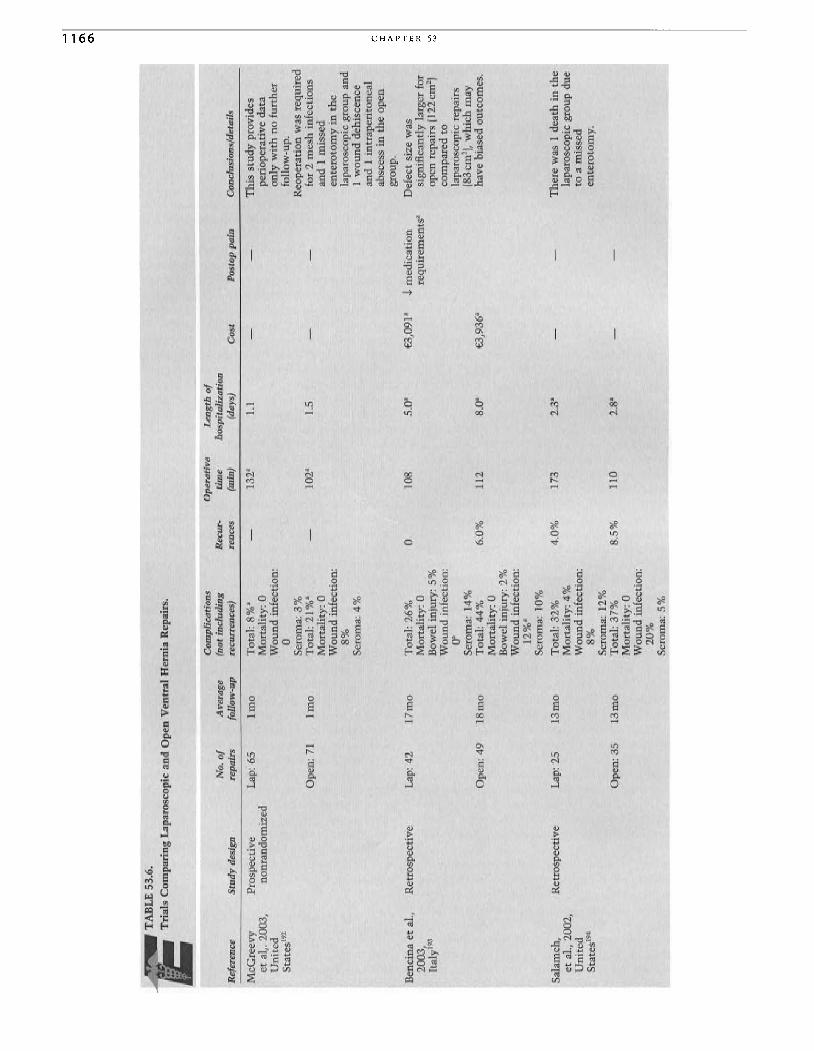
.... 0\
0\
TA
BL
E53
.6.
Tri
als
Com
pari
ngL
apar
osco
pic
and
Op
enV
entr
alH
ern
iaR
epai
rs.
-.
Com
plic
atio
nsO
pera
tive
Len
gth
of
No
.o
fA
vera
ge(n
otin
clu
din
gR
ecur
-ti
me
hosp
ital
izat
ion
Ref
eren
ceS
tud
yde
sign
repa
irs
foll
ow-u
pre
curr
ence
s)re
nces
(min
)(d
ays)
Cos
tP
osto
pp
ain
Con
clus
ions
/det
ails
McG
reev
yP
rosp
ecti
veL
ap:6
5I
mo
Tot
al:
8%"
-13
2"1.
1-
-T
his
stu
dy
prov
ides
etal
,.20
03,
no
nra
nd
om
ized
Mo
rtal
ity:
0pe
riop
erat
ive
data
Un
ited
Wo
un
din
fect
ion:
on
lyw
ith
nofu
rth
erS
tate
s"?
0fo
llow
-up.
Ser
oma:
3%
Reo
pera
tio
nw
asre
quir
edO
pen
:71
lm
oT
ota
l:21
%"
-10
2"l.
5-
-fo
r2
mes
hin
fect
ions
Mor
tali
ty:
0an
d1
mis
sed
Wo
un
din
fect
ion:
ente
roto
my
inth
e8%
lapa
rosc
opic
grou
pan
dS
erom
a:4%
1w
ou
nd
dehi
scen
cean
d1
intr
aper
iton
eal
oab
sces
sin
the
op
en::c
grou
p.
> ""B
enci
naet
al.,
Ret
rosp
ecti
veL
ap:
421
7m
oT
otal
:26
%0
108
5.0"
€3,0
9l"
J.m
edic
atio
nD
efec
tsi
zew
as.., m
2003
,M
ort
alit
y:0
req
uir
emen
ts"
sign
ific
antl
yla
rger
for
"It
aly"
?B
owel
inju
ry:5
%o
pen
repa
irs
(12
2cm
2)
'" '"W
ou
nd
infe
ctio
n:co
mpa
red
to0"
lapa
rosc
opic
repa
irs
Ser
oma:
14%
(83
crrr
'[, w
hic
hm
ayO
pen:
491
8m
oT
ota
l:44
%6.
0%11
28.
0"€3
,936
"ha
vebi
ased
outc
omes
.M
ort
alit
y:0
Bow
elin
jury
:2
%W
ou
nd
infe
ctio
n:
12%
"S
erom
a:10
%
Sal
ameh
,R
etro
spec
tive
Lap
:25
13
mo
Tot
al:
32
%4.
0%17
32.
3"-
-T
her
ew
as1
dea
thin
the
etaI
.,20
02,
Mor
tali
ty:
4%
lapa
rosc
opic
grou
pdu
eU
nit
edW
ou
nd
infe
ctio
n:to
am
isse
dS
tate
s!"
8%en
tero
tom
y.
Ser
oma:
12%
Op
en:3
51
3m
oT
otal
:3
7%
8.5%
110
2.8"
Mor
tali
ty:
0W
ou
nd
infe
ctio
n:20
%S
erom
a:5%
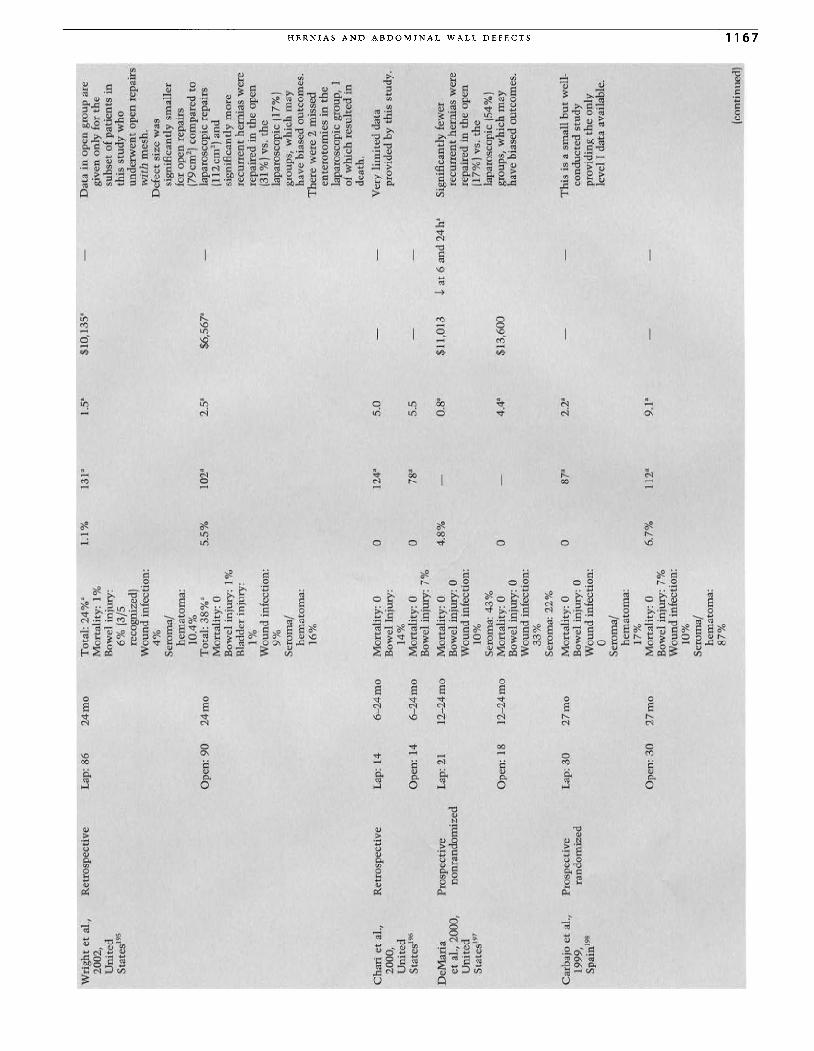
Wri
ght
etal
.,R
etro
spec
tive
Lap
:86
24
mo
Tot
al:
24%
a1.
1%13
1"1.
5a$l
O,1
35a
-D
ata
inop
engr
oup
are
2002
,M
orta
lity
:1%
give
non
lyfo
rth
eU
nit
edB
owel
inju
ry:
sub
set
ofp
atie
nts
inS
tate
s!"
6%(3
/5th
isst
ud
yw
ho
reco
gniz
ed)
un
der
wen
to
pen
repa
irs
Wo
un
din
fect
ion
:w
ith
mes
h.
4%D
efec
tsi
zew
asS
ero
ma/
sign
ific
antl
ysm
alle
rh
emat
om
a:fo
rop
enre
pair
s10
.4%
(79c
m2
)co
mpa
red
toO
pen
:90
24
mo
To
tal:
38%
"5.
5%10
2a2.
5a$6
,567
a-
lapa
rosc
opic
repa
irs
Mor
tali
ty:
0(1
12
cm2
)an
dB
owel
inju
ry:
1%si
gnif
ican
tly
mo
reB
ladd
erin
jury
:re
curr
ent
her
nia
sw
ere
1%re
pair
edin
the
op
enW
ou
nd
infe
ctio
n:(3
1%
)vs
.th
e9
%la
par
osc
opic
(17%
)S
ero
ma/
grou
ps,
wh
ich
may
:J:h
emat
om
a:ha
vebi
ased
outc
omes
.'"
16%
Th
ere
wer
e2
mis
sed
"zen
tero
tom
ies
inth
e:>-
lapa
rosc
opic
grou
p,1
'"of
wh
ich
resu
lted
in:>- z
dea
th.
0
Ch
ari
etal
.,R
etro
spec
tive
Lap
:14
6-2
4m
oM
orta
lity
:0
012
4a5.
0-
Ver
yli
mit
edda
ta:>-
2000
,B
owel
Inju
ry:
prov
ided
byth
isst
ud
y.
til 0
Un
ited
14%
0
Sta
tes'
l"O
pen:
146-
24
mo
Mor
tali
ty:
00
78a
5.5
--
Is::
Bow
elin
jury
:7%
z :>-D
eMar
iaP
rosp
ecti
veL
ap:
211
2-2
4m
oM
orta
lity
:0
4.8
%-
0.8
a$1
1,01
3.j,
at6
and
24
haS
igni
fica
ntly
few
err-
etal
.,20
00,
no
nra
nd
om
ized
Bow
elin
jury
:0re
curr
ent
her
nia
sw
ere
::;:
Un
ited
Wo
un
din
fect
ion:
repa
ired
inth
eo
pen
:>- e-S
tate
s"?
10%
(17%
)vs
.th
er-
Ser
oma:
43%
lap
aro
scop
ic(5
4%
)0 '"
Op
en:
181
2-2
4m
oM
ort
alit
y:0
0-
4.4a
$13,
600
grou
ps,
wh
ich
may
."
Bow
elin
jury
:0
have
bias
edou
tcom
es.
'"(JW
ou
nd
infe
ctio
n:.., '"
33
%S
erom
a:2
2%
Car
bajo
etal
.,P
rosp
ecti
veL
ap:
302
7m
oM
ort
alit
y:0
087
a2.
2a-
-T
his
isa
smal
lb
ut
wel
l-19
99,
rand
omiz
edB
owel
inju
ry:
0co
nd
uct
edst
ud
ySp
ain!
"W
ou
nd
infe
ctio
n:pr
ovid
ing
the
on
ly0
leve
lI
data
avai
labl
e.S
eror
na/
hem
ato
ma:
17%
Op
en:3
02
7m
oM
orta
lity
:0
6.7
%11
2a9.
1"B
owel
inju
ry:
7%W
ou
nd
infe
ctio
n:10
%S
erom
a/h
emat
om
a:87
%...
(con
tinu
ed)
..... 0\ '"
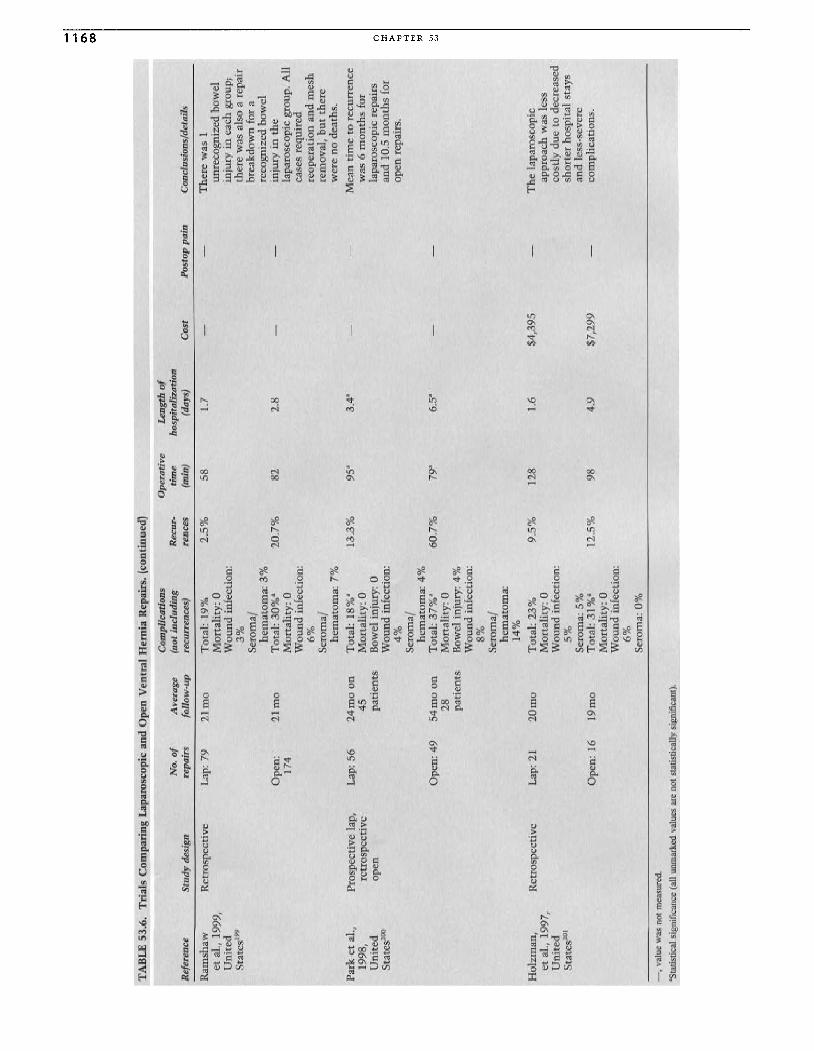
0\ co
TA
BL
E53
.6.
Tri
als
Com
pari
ngL
apar
osco
pic
and
Op
enV
entr
alH
ern
iaR
epai
rs.
(con
tinu
ed)
Com
plic
atio
ns
Op
erat
ive
Len
gth
ofN
o.o
fA
vera
ge(n
otin
clu
din
gR
ecur
-ti
me
hos
pita
liza
tion
Ref
eren
ce
Stu d
yd
esig
nre
pair
sfo
llo
w-u
pre
curr
enc
es)
ren
ces
(min
)(d
ays
)C
ost
Pos
top
pai
nC
oncl
usio
ns/d
eta
ils
Ram
shaw
Ret
rosp
ecti
veL
ap:
792
1m
oT
ota
l:19
%2.
5%
581.
7-
-T
her
ew
as1
etal
.,19
99,
Mor
tali
ty:
0u
nre
cogn
ized
bow
el
Un
ited
Wo
un
din
fect
ion:
inju
ryin
each
gro
up;
Stat
es'?
"3
%th
ere
was
also
are
pai
rSe
rom
ajbr
eakd
own
for
ah
emat
om
a:3
%re
cogn
ized
bow
elO
pen
:2
1m
oT
ota
l:30
%'
20.7
%82
2.8
--
inju
ryin
the
174
Mo
rtal
ity:
0la
paro
scop
icgr
ou
p.A
llW
ou
nd
infe
ctio
n:
case
sre
quir
ed6
%re
oper
atio
nan
dm
esh
Ser
omaj
rem
oval
,b
ut
ther
eh
emat
om
a:7%
wer
en
ode
aths
.P
ark
etal
.,P
rosp
e cti
ve
lap
,L
ap:5
62
4m
oon
To
tal:
18%
'13
.3%
95'
3.4
'-
-M
ean
tim
eto
recu
rren
ce19
98,
retr
osp
e cti
ve
45M
ort
alit
y:0
was
6m
on
ths
for
Un
ited
open
pati
ents
Bow
elin
jury
:0
lapa
rosc
opic
repa
irs
oS
tate
s200
Wo
un
din
fect
ion:
and
10.5
mo
nth
sfo
r:z:
4%
open
rep
airs
.:> ';
j
Sero
maj
.; '"h
emat
om
a:4
%'"
Ope
n:
4954
mo
onT
otal
:37
%'
60.7
%79
'6
.5'
--
'" '"28
Mo
rtal
ity
:0pa
t ien
tsB
owel
inju
ry:
4%
Wo
un
din
fect
ion
:8%
Sero
maj
hem
ato
ma:
14%
Ho
lzm
an,
Ret
rosp
ecti
ve
Lap
:2
120
mo
Tot
al:
23%
9.5
%12
81.
6$4
,395
-T
he
lap
aros
cop
icet
al.,
199
7,M
ort
alit
y:0
appr
oach
was
less
Un
ited
Wo
un
din
fect
ion
:co
stly
due
tode
crea
sed
Stat
esW
I5%
sho
rter
hos
pita
lst
ays
Sero
ma:
5%an
dle
ss-s
ever
eO
pen
:16
19m
oT
ota
l:3
1%'
12.5
%98
4.9
$7,
299
-co
mpl
icat
ions
.M
ort
alit
y:0
Wou
nd
infe
ctio
n:6%
Sero
ma:
0%
-,
valu
ew
asno
tm
easu
red
.
'Sta
tist
ical
sign
ific
ance
(all
unm
arke
dva
lues
are
not
stat
isti
cally
sign
ific
ant)
.
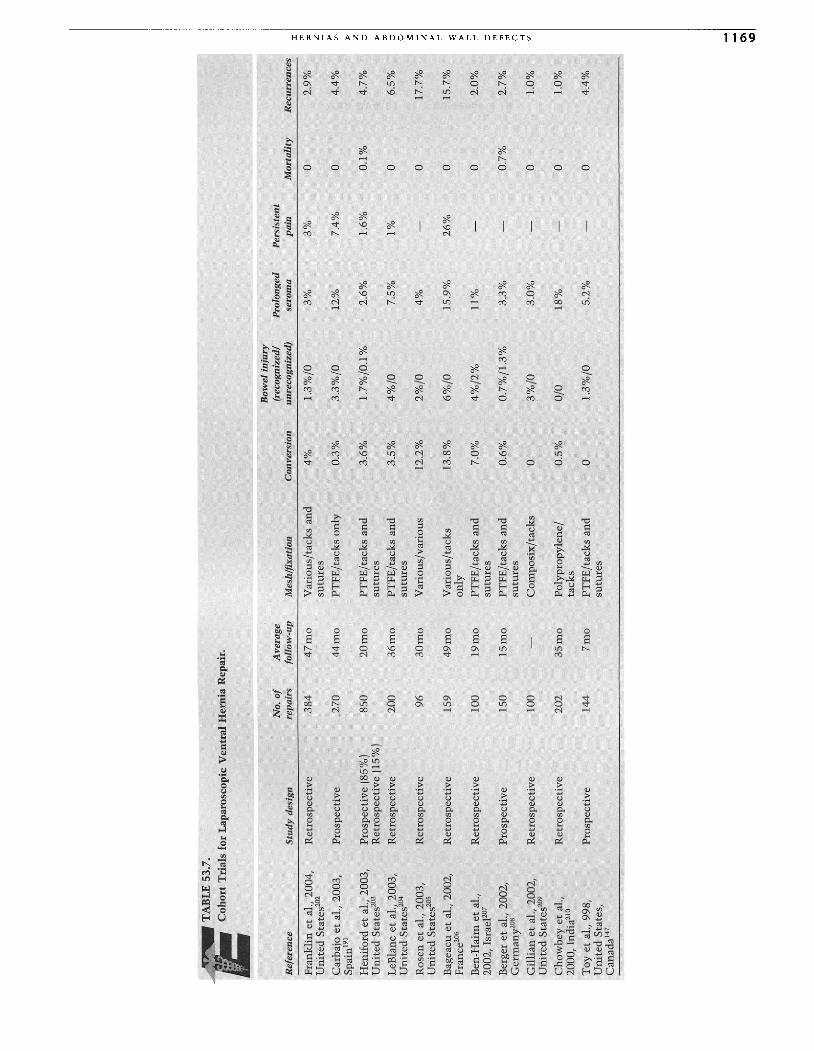
TA
BL
E53
.7.
Co
ho
rtT
rial
sfo
rL
apar
osco
pic
Ven
tral
Her
nia
Rep
air.
Bow
elin
jury
No.
of
Ave
rag
e(r
ecog
nize
d/P
rolo
nged
Per
sist
ent
Ref
eren
ceS
tud
yde
sign
repa
irs
foll
ow-u
pM
esh
/fix
atio
nC
onve
rsio
nun
reco
gniz
ed)
sero
ma
pain
Mor
tali
tyR
ecur
renc
es:t
Fra
nk
lin
etal
.,20
04,
Ret
rosp
ecti
ve
38
44
7m
oV
ario
us/
tack
san
d4
%1.
3%
/03
%3
%0
2.9
%'" "
Un
ited
Sta
tes20
2su
ture
sZ
Car
bajo
etal
.,20
03,
Pro
spec
tive
270
44
mo
PT
FE
/tac
kson
ly0
.3%
3.3
%/0
12%
7.4%
04
.4%
;,- CJ>
Spai
n'?
';,-
Hen
ifo
rdet
al.,
2003
,P
rosp
ecti
ve
185
%)
850
20
mo
PT
FE
/tac
ks
and
3.6
%1
.7%
/0.1
%2.
6%1.
6%0
.1%
4.7
%z tl
Un
ited
Sta
tes20
3R
etro
spec
tive
(15
%)
sutu
res
;,-
LeB
lanc
etal
.,20
03,
Re t
rosp
ecti
ve
200
36
mo
PT
FE
/tac
ks
and
3.5
%4
%/0
7.5%
1%0
6.5
%tll tl
Un
ited
Sta
tes'
?'su
ture
s0
Ros
enet
al.,
2003
,V
ario
us/
var
ious
2%
/0~
Ret
rosp
ecti
ve
963
0m
o12
.2%
4%
-0
17.7
%z
Un
ited
Sta
tes20
S;,-
Bag
eacu
etal
.,20
02,
Var
ious
/tac
ks
6%
/0r-
Ret
rosp
ecti
ve15
94
9m
o13
.8%
15.9
%26
%0
15.7
%:;;
Pra
nce
r"on
ly;,-
Ben
-Hai
met
al.,
Ret
rosp
ecti
ve
100
19m
oP
TF
E/t
acks
and
7.0%
4%
/2%
11%
02.
0%r-
-,...
2002
,Is
rael
207
sutu
res
oB
erge
ret
al.,
2002
,P
TF
E/t
ack
san
d0
.7%
/1.3
%'"
Pro
spec
tive
150
15
mo
0.6
%3
.3%
-0
.7%
2.7
%'" '"
Ger
man
y'?"
sutu
res
(1
Gil
lian
etal
.,20
02,
..,R
etro
spec
tive
100
-C
om
po
six
/tac
ks0
3%
/03
.0%
-0
1.0%
CJ>
Un
ited
Sta
tes'
?"
Ch
ow
bey
etal
.,R
etro
spec
tive
202
35
mo
Pol
ypro
py
len
e/0
.5%
0/0
18%
-0
1.0%
2000
,In
dia"
?ta
cks
To
yet
al.,
998,
Pro
spec
tive
144
7m
oP
TF
E/t
acks
and
01.
3%
/05.
2%-
04.
4%U
nit
edS
tate
s,su
ture
sC
anad
a!"
-'
-'
0\
10

1170 CHAPTER 53
or, in the case of tissue loss secondary to trauma, surgicaldebridement for necrotizing infections, or resection of tumors.Such wounds may be heavily contaminated, and postopera-tive wound sepsis is common. Primary fascial approximationmay create a closure under tension and result in abdominalcompartment syndrome, dehiscence, evisceration, or fistulaformation.211
,212 A prosthetic repair provides tension-freeclosure and is effective in alleviating evisceration and restor-ing abdominal wall continuity in the acute phase.i"
Prosthetic repairs, however, can be fraught with long-termcomplications. Voyles reported nine of nine patients withMarlex mesh closures of contaminated abdominal wall defectsfollowed by split-thickness skin grafting who either extrudedtheir mesh or developed enteric flstulas.i" Six of nine patientswho underwent Marlex closures followed by wound healingby secondary intention without skin grafting developed fistu-las or mesh extrusion. Voyles reported decreased complica-tions if the Marlex closure was covered with full-thicknessskin or tissue flaps.
In a review of 14 studies on polypropylene mesh closureemergency abdominal wall defects, Jones reported an overallcomplication rate of 55% in 128 patients, with enteric fistu-lization in 23 0/0.214 No fistulization or mesh extrusion occurredin wounds covered with full-thickness skin or muscle flaps.After polypropylene mesh closure followed by split-thicknessskin grafting, Stone reported a mortality of 23% related toprogressive wound sepsis.r"
The use of absorbable mesh provides a lower incidence offistulization and wound complications but universally leadsto ventral hernias, which must be dealt with at a later date.The proponents of absorbable mesh note that it is effectivein closing acute abdominal wall defects that are contami-nated. Unlike permanent mesh, absorbable mesh does notchronically harbor infection. This allows complete clearanceof infection prior to definitive ventral hernia repair, providinga better chance of a successful repair. It also provides noresidual foreign body to complicate wound managementshould a fistula form.
Buck reported using polyglycolic acid (Dexon) mesh in 26patients with no dehiscence or mesh infection and a fistularate of 8% .215 Greene reported a fistula rate of 120/0 usingDexon in 59 patients.i" He noted that when polyglactin(Vicryl) was used as a substitute, it ripped with suturing andwas too rapidly absorbed.
In 166 patients, Fabian reported an overall fistula rate of80/0 and no wound-related deaths using a protocol that calledfor absorbable mesh repair of emergency defects, followed bymesh removal prior to wound coverage and planned repair ofthe ventral hernia at a later date. 211
,217 Mesh was removed 2to 3 weeks postinsertion (after granulation tissue developed)and split- or full-thickness skin grafts were placed 2 to 3 dayslater after wounds were packed to minimize bacterial con-tamination. Definitive hernia repairs were then performed 6to 12 months later, after adhesions had matured to a filmystage. Using this method, Fabian reported being able toperform primary fascial closure at the time of mesh removalin 22% of patients who originally received mesh closures formassive edema. These patients were spared a subsequentplanned ventral hernia repair. Over a mean 24-month follow-up, only 50/0 of 73 patients who underwent planned delayedrepair using a modified components separation (withoutmesh) developed recurrent hernias.
Complex cases, including intraabdominal abscesses, fis-tulas, mesh infections, abdomens originally closed by second-ary intention, or recurrent hernias in the setting of hostileabdomens or previous skin grafts may be well suited for repairusing autogenous tissue, namely, through methods of fascialpartitioning. The so-called components separation technique,as described by Ramirez in 1990, involves adhesiolysis, reduc-tion of the hernia (usually midline), and reconstruction of theabdominal wall using relaxing incisions that allow medialtransposition of the muscular layers.i" After widely under-mining the subcutaneous tissue, parasagittal relaxing inci-sions are made in the external oblique aponeurosis and muscleabout 2 em lateral to its insertion into the rectus sheath start-ing at the groin and continuing 5 to 7em cephalad to thecostal margin; the external oblique muscle is separated fromthe internal oblique muscle as far laterally as possible, andthe linea alba is closed primarily. If tension exists, additionallength can be gained by incising the rectus sheath and reflect-ing the fascia off the muscle toward the midline; alterna-tively, the transversus abdominis muscle may be incised viaa transperitoneal approach to provide further medial mobili-zation. Defects as large as 20 em at the umbilical level can beclosed using these maneuvers.i"
Mesh may also be used in conjunction with componentsseparation, either for reinforcement of emaciated tissues orwhen inadequate autogenous tissue exists.F" As an alterna-tive to wide subcutaneous undermining, separate skinincisions can be used to mobilize the external oblique myo-aponeurosis.
Recently, endoscopic techniques using balloon dissectionand muscular transection under videoscopic control havebeen developed.l" For massive hernias in patients with lossof domain, components separation may be combined with theuse of tissue expanders to gain additional skin, muscle, andfascia laterally for subsequent midline mobilization.i"
Shestak repaired 22 midline hernias up to 14cm wide and24cm long using components separation (with mesh in only1 patient) and reported a recurrence rate of 50/0 over 52-monthmean follow-up.F" De Vries Reilingh used components sepa-ration (primary running fascial closure without mesh) torepair complex midline hernias in 43 patients having a meandefect size of 18em long x 13cm wide; the recurrence ratewas 300/0 over 15.6-month mean follow-up.!" While therecurrence rate in the latter series may seem high, 15 patientshad simultaneous intestinal surgery (3 Hartmann's reversal,2 ileostomy reversal, 4 enterocutaneous fistula repairs, 5ostomy relocations, 2 other), and 35 % of reconstructions weredone under contaminated conditions. Thus, component sepa-ration may be quite useful in these settings with acceptableresults; large series or comparative trials, however, are not yetavailable.
New biomaterials are now available that facilitate herniarepair through remodeling of native tissues and may be espe-cially useful in the setting of contamination. Through tissueengineering, human or porcine specimens can be decellular-ized with maintenance of the architectural integrity, thusserving as a collagen matrix. Currently available materialsmade from porcine small intestine submucosa, porcinedermis, and human cadaveric dermis, when implanted, allowfibroblast ingrowth with subsequent collagen deposition andremodeling. The lack of a true foreign body has proven espe-cially useful in complex abdominal wall reconstructions in

HERNIAS AND ABDOMINAL WALL DEFECTS 1171
the setting of contamination, but long-term documentationof efficacy for routine hernia repair is lacking. These prosthe-ses are currently very expensive; are often available in onlysmall sizes, requiring tedious suturing for creation of largercomposite pieces; and some have difficult handling character-istics (very flimsy). Nonetheless, the recent introduction ofthese materials has fueled significant enthusiasm fortheir use.
Ueno repaired 18 ventral and 2 inguinal hernias in thesetting of bacterial contamination using small intestinal sub-mucosa (SIS; Surgisis, Cook Surgical, Bloomington, IN) anddocumented a 300/0 recurrence rate over 15.7-month meanfollow-up.F" Franklin repaired 58 hernias in 53 patients usingSIS, including 34% with potential contamination and 220/0with gross contamination, and reported no mesh-related com-plications and no recurrences over 19-month median follow-Up.224 Eid laparoscopically repaired 12 ventral hernias usingSIS at the time of Roux-en-Y gastric bypass operations formorbid obesity and found no recurrences over 13-monthmean follow-up.i" These series documented no mesh reac-tions and good compatibility between the porcine-derivedprosthetic and the human host. Moreover, SIS seems to with-stand bacterial contamination relatively well. Porcine dermis(Permacol, Tissue Science Laboratories, Covington, GA) andhuman cadaveric dermis (Alloderm, LifeCell Corp., Branch-burg, NT) have recently been introduced, and although dataare lacking, early reports suggest good utility of thesebiomaterials.P'v'"
Other Abdominal Hernias
SPIGELIAN
The Spigelian or semilunar line marks the transition frommuscle to aponeurosis of the transversus abdominis muscle.The Spigelian fascia lies between this line and the lateralborder of the rectus sheath. A defect in this fascia results ina Spigelian hernia. Up to 900/0 are located 0 to 6cm cranial tothe interspinal plane (the horizontal plane through both ante-rior iliac spinesl.i" The defect originates in the transversusabdominis muscle and mayor may not involve the moresuperficial layers; hernia sac and contents often lie in anintramural location between the abdominal wall layers andmay not be palpable. Consequently, patients often presentwith vague complaints of pain and nonspecific tenderness onexam. Computed tomography or ultrasound scanning may aidin the diagnosis. Ultimate diagnosis may not be made untilthe time of surgical exploration.
Exploration may be undertaken via an incision directlyover the defect if palpable. If it is nonpalpable, explorationvia a preperitoneal approach through a midline or parame-dian incision avoids an extensive subcutaneous dissection.The defect is usually small and can be repaired primarily.Recently, success has been reported using laparoscopicapproaches.F'<"
LUMBAR
Lumbar hernias occur spontaneously, posttraumatically, or asincisional hernias (such as following nephrectomy). They rep-resent defects through the transversalis fascia and transversusabdominis muscle aponeurosis. Retroperitoneal fat or a
peritoneum-lined sac may herniate through the defect.Patients present with a symptomatic posterior bulge butrarely with a strangulated hernia.
There are two lumbar triangles. The inferior or Petit'striangle is bordered by the latissimus dorsi muscle, the exter-nal oblique muscle, and the iliac crest; it is covered only bysuperficial fascia. The superior or Grynfeltt's triangle is bor-dered by the 12th rib, internal oblique muscle, and sacrospi-nalis muscle; it is covered by the lattissimus dorsi muscle.
Repair can be performed primarily if the defect is small,but a myofascial flap, such as a gluteus maximus fascial flapfor inferior triangle hernias, or repair with mesh is necessaryfor larger defects. An oblique incision from the 12th rib medi-ally to the iliac crest laterally provides adequate exposure.Recent reports documented success with laparoscopic repairsusing mesh.r"
PELVIC FLOOR HERNIAS
Pelvic floor hernias include (in decreasing frequency) obtura-tor, perineal, and sciatic hernias. Obturator hernias occurwhen abdominal contents herniate through the obturatorcanal along the course of the obturator neurovascular bundle.The obturator membrane, which covers the obturator foramenand forms the canal, is indistensible, and herniated boweloften becomes incarcerated and strangulated. These herniasare most often seen in emaciated females in their eighthdecade, almost always occurring on the right side. A preop-erative diagnosis is difficult and infrequently made.
Patients usually present with partial or complete acutesmall-bowel obstruction without a palpable hernia. Rarelya mass may be palpable on the anteriomedial aspect ofthe thigh or on pelvic and rectal examinations. A Howship-Romberg sign (obturator neuralgia produced by compressionof the obturator nerve by the hernia on extension and adduc-tion followed by medial rotation of the ipsilateral thigh)may be present in up to 500/0 of cases. Computed tomographyor abdominopelvic ultrasound scanning can confirm thediagnosis.
Exploration may be carried out via a number of incisions,but a lower midline provides the best exposure for resectingcompromised bowel and adequate repair of the hernia defect.r"The defect may be closed primarily, with mesh, or by advanc-ing adductor longus muscle flap. Recently, success has alsobeen reported using laparoscopic approaches.r" Mortalityrates may be as high as 750/0, secondary to the advanced ageand debilitated states of most patients and to delays in diag-nosis. Therefore, prompt treatment should be rendered.P"
Perineal hernias may occur spontaneously or as incisionalhernias after procedures such as abdominoperineal resectionsor pelvic exenterations. These hernias occur anteriorly inwomen, involving the urogenital diaphragm and passing intothe labia majora. Posterior perineal hernias are defects in thelevator ani muscles and occur in the ischiorectal fossa betweenthe bladder and the rectum. Patients present with softreducible masses. A primary repair or a repair with meshmay be performed through either a perineal or an abdominalapproach.r"
Sciatic hernias are the rarest of all hernias and occur inthe greater or lesser sciatic foramen through a defect in thepiriformis muscle. Patients may be symptomatic with sciaticnerve palsy and a palpable mass or may simply present with

1172 CHAPTER 53
intestinal obstruction. Repair can be performed via a glutealapproach or a transabdominal approach. 236
PARAST0 MAL
Parastomal hernias occur through defects adjacent to ostomysites. The incidence of paracolostomy hernias is 12% to 320/0and for paraileostomy hernias is less than 10%.237 Construc-tion of the ostomy through an appropriately small fascialdefect in the rectus sheath and not maturing the ostomythrough the laparotomy incision decrease the risk of subse-quent hernia formation. The majority of patients are asymp-tomatic. Patients may present with obstruction, incarceration,a poor-fitting appliance, or local pain and warrant repair.Options include primary fascial repair, prosthetic fascialrepair, or stomal relocation. Local procedures can be techni-cally demanding and pose infection risk if a prosthetic is usedbut avoid laparotomy and potentially extensive adhesiolysis.Formal laparotomy alleviates ostomy contamination of pros-thetic material and provides access for repair or relocation.
No prospective randomized trials have been performed;Rubin published the largest study comparing repair tech-niques, which included a retrospective analysis of 68 repairsin 55 patients.r" Hernias recurred in 63% of the 68 repairs,and complications occurred in 63% of the patients. Incisionalhernias at the laparotomy site or at the old ostomy siteoccurred in 21 0/0. In primary parastomal hernias, 76% ofprimary fascial repairs, 50% of prosthetic repairs, and 330/0 ofstoma relocations failed. For recurrent parastomal hernias,1000/0 of primary fascial repairs, 330/0 of prosthetic repairs, and71% of stomal relocations failed. Because parastomal herniasare generally well tolerated and all types of repair are associ-ated with significant morbidity and high recurrence rates,repair should be avoided if possible.
INTERNAL HERNIAS
Internal hernias occur when intraperitoneal contents prolapsethrough a normal or abnormal orifice. Normally existing ori-fices include the foramen of Winslow (known as the herniaof Blandin). Abnormally existing orifices are congenital peri-toneal fossae and include left and right paraduodenal, perice-cal, intersigmoid, paravascular, and supravesiclar and herniasinside the broad ligament of the uterus. These hernias accountfor up to 2% of all abdominal hernias.r" Patients present witha closed-loop intestinal obstruction, and diagnosis is usuallymade at the time of operation.
The operation involves reduction of incarcerated bowel,resection of nonviable segments, and primary closure ofthe hernia orifice. In the case of left and right paraduodenalhernias, the orifices are intimately associated with the infe-rior and superior mesenteric vessels, respectively, and greatcare must be taken during reduction and repair to preservethese vessels.
Internal hernias may also be iatrogenic, occurring after aprevious operation in which a defect in mesentery or omentumwas not adequately closed. Frequently, these defects occurafter loop or Roux-en-Y gastrojejunostomy formation eitherbehind the afferent (known as a Petersen hernia) or efferentlimbs. Retroanastomotic hernias are best avoided by closureof all mesenteric defects at the time of initial operation. If
such a hernia occurs, reduction and closure are necessary atlaparotomy.
CONGENITAL ABDOMINAL WALL DEFECTS
Gastroschisis refers to herniation of the abdominal viscerawithout a sac and in the presence of an intact umbilical cord.It is now thought to be a separate entity from omphalocele.It is twice as common as omphalocele but associatedwith half as many anomalies. The most common associatedanomaly is intestinal atresia, which is present in 100/0 ofcases. The eviscerated intestine is edematous, matted withfibrinous adhesions, and shortened, resulting in intestinalabsorptive and motility dysfunction.r"
Repair can be performed by primary fascial closure or astaged procedure with closure of skin followed by subsequentfascial closure. Gentle stretching of the abdominal wallcan enlarge the abdominal cavity and help facilitate repair.If visceroabdominal disproportion is severe, the evisceratedintestine is enclosed within a prosthetic silo attached at itsbase to the abdominal wall. As the edema diminishes, sequen-tial compression of the top of the silo returns the herniatedcontents into the abdomen and allows fascial closure. Mortal-ity is less than 100/0.
Omphalocele refers to herniation of the abdominal viscerainto the umbilical cord, resulting in a sac lined internally byperitoneum and externally by amnion. The size of the defectmay range from small to massive. Pelvic involvement canresult in cloacal extrophy. Structural and chromosomalanomalies are present in up to 500/0 of cases. Repair of theabdominal defect can be performed similar to the methodsused for gastroschisis. The severity of associated anomalieslargely determines long-term survival.
CONGENITAL DIAPHRAGMATIC HERNIAS
Congenital diaphragmatic hernias occur in 1 of every 2100pregnancies (including spontaneously aborted pregnancies)and 1 of every 4800 live births.i" They can be characterizedby their location. Bochdalek hernias are located posteriolater-ally, and Morgagni hernias are located anteriorly.
Bochdalek hernias occur between the costal and spinaldiaphragmatic attachments and account for the majority ofcongenital diaphragmatic hernias. The defect is the result ofembryological failure of the pleuroperitoneal canal to close asthe pleuroperitoneal membranes (laterally), the dorsal mesen-tery (posteriorly), and the septum transversum (anteriorly)fuse to form the diaphragm. The left side closes after the right;there is thus a 4: 1 preponderance for left-sided hernias. Non-rotation of the intestine is usually associated with the defect.Hernia contents are enclosed within a sac in only 10% to 200/0of cases. Because abdominal contents occupy the thoraciccavity during fetal development, pulmonary hypoplasia canbe severe. Mortality rates are as high as 800/0 in the firstmonth of life, despite advances in ionotropic therapy, ventila-tory support, and extracorporeal membrane oxygenation(ECMO).242
Immediate repair at birth results in higher mortality ratesand delaying repair to the first few days to weeks of life afterpulmonary function has stabilized is advantageous.r" Repairis via an abdominal approach and consists of reduction ofhernia contents, sac excision, primary or prosthetic (usuallyPTFE) diaphragm repair, and a Ladd procedure. Occasionally,
HERNIAS AND ABDOMINAL WALL DEFECTS 1173
Bochdalek hernias may be diagnosed in older children exhib-iting only mild symptoms. Elective repair is indicated toavoid potential complications.
Morgagni hernias occur between the sternal and costaldiaphragmatic attachments in a retrosternal or parasternalposition. They result from failure of the septum transversumto fuse with the thoracic wall and account for 2% of con-genital diaphragmatic hernias. Associated cardiac anomaliesare frequent, and the defect may be part of the Cantrell pen-talogy (defects in the abdominal wall, sternum, diaphragm,pericardium, and heart). Contents are usually enclosed withina sac, and 90% of hernias are right-sided. In infants, respira-tory distress is usually present. When discovered in adults,symptoms are often mild or absent.
Repair is indicated in all cases to prevent incarceration.The repair can be performed via an abdominal or thoracicapproach, similar to the repair of Bochdalek hernias. Recently,success in adult patients has been reported using laparoscopicapproaches.e"
References
1. Condon RE, Carilli S. The biology and anatomy of inguino-femoral hernia. Semin Laparosc Surg 1994;1:75-85.
2. Skandalakis TE, Skandalakis LT, Colborn GL. Testicular atrophyand neuropathy in herniorrhaphy. Am Surg 1996;62:775-782.
3. Fruchaud H. Anatomie Chirurgicale des Hernies de l'Aine. Paris:Doin; 1956.
4. Skandalakis TE, Colborn GL, Androulakis TA, et al. Embryologicand anatomic basis of inguinal hernorrhaphy. Surg Clin NorthAm 1993;73:799-836.
5. Skinner MA, Grosfeld TL. Inguinal and umbilical hernia repairin infants and children. Surg Clin North Am 1993;73:439-449.
6. Rowe MI, Copelson LW, Clatworthy HW. The patent processusvaginalis and the inguinal hernia. J Pediatr Surg 1969;4:102-107.
7. Peacock EE, Madden JW. Studies on the biology and treatmentof recurrent inguinal hernias: II. Morphologic changes. Ann Surg1974;179:567-571.
8. Read RC. Attenuation of rectus sheath in inguinal herniation.Am TSurg 1970;120:610-614.
9. Read RC. A review: the role of protease-antiprotease imbalancein the pathogenesis of herniation and abdominal aortic aneu-rysm in certain smokers. Post Gen Surg 1992;4:161-165.
10. Liem MSL, Van Der Graff Y, Van Steensel CJ, et al. Comparisonof conventional anterior surgery and laparoscopic surgery foringuinal-hernia repair. N Engl J Med 1997;336:1541-1547.
11. Hurst RD, Butler BN, Soybel 01, et al. Management of groinhernias in patients with ascites. Ann Surg 1992;216:696-700.
12. MacAthur DC, Grieve DC, Thompson AM, et al. Herniographyfor groin pain of uncertain origin. Br J Surg 1997;84:684-685.
13. Rutkow 1M, Robbins AW. Demographic, classificatory, andsocioeconomic aspects of hernia repair in the United States. SurgClin North Am 1993;73:413-426.
14. Rutledge RH. Cooper's ligament repair. In: Nyhus LM, Baker RJ,Fischer TE, eds. Mastery of Surgery. Boston: Little Brown;1997:1817-1825.
15. Amid PK, Shulman AG, Lichtenstein IL. Open "tension-free"repair of inguinal hernias: the Lichtenstein technique. Eur J Surg1996;162:447-453.
16. Nyhus LM. Individualization of hernia repair: a new era. Surg1993;114:1-2.
17. Cheek CM, Williams MH, Farndon JR. Trusses in the manage-ment of hernia today. Br J Surg 1995;82:1611-1613.
18. Sohrabi AK, Wille G, Guernsey 1, et al. En masse reduction ofhernia. Contemp Surg 1997;50:100-104.
19. Reid I, Devlin HB. Testicular atrophy as a consequence of ingui-nal hernia repair. Brit J Surg 1994;81:91-93.
20. Wantz GE. Testicular atrophy and chronic residual neuralgia asrisks of inguinal hernioplasty. Surg Clin North Am 1993;73:571-582.
21. Griffith CA. The Marcy repair revisited. Surg Clin North Am1984;64:215-227.
22. Wantz GE. The operation of Bassini as described by AttilioCatterina. Surg Gynecol Obstet 1989;168:67-80.
23. Shouldice EE. The treatment of hernia. Ontario Med Rev1953;20:670-684.
24. Wantz GE. The Canadian repair: personal observations. World JSurg 1989;13:516-521.
25. Glassow F. The Shouldice hospital technique. Int Surg 1986;71:148-153.
26. Wantz GE. Shouldice repair. Contemp Surg 1988;33:15-21.27. Hay J, Boudet M, Fingerhut A, et al. Shouldice inguinal hernia
repair in the male adult: the gold standard? A multicenter con-trolled trial in 1578 patients. Ann Surg 1995;222:719-727.
28. McGillicuddy JE. Prospective randomized comparison of theShouldice and Lichtenstein hernia repair procedures. Arch Surg1998;133:974-978.
29. Rutledge RH. A 25 year experience with a single technique forall groin hernias in adults. Surg 1988;103:1-10.
30. Rutkow 1M, Robbins AW. "Tension-free" inguinal herniorrha-phy: a preliminary report on the mesh plug technique. Surg1993;114:3-8.
31. Panos RG, Beck DE, Maresh TE, et al. Preliminary results ofa prospective randomized study of Cooper's ligament versusShouldice herniorrhaphy technique. Surg Gynecol Obstet 1992;175:315-319.
32. Lichtenstein IL, Shulman AG. Ambulatory outpatient herniasurgery, including a new concept, introducing tension-freerepair. Int Surg 1986;71:1-4.
33. Lichtenstein IL, Shulman AG, Amid PK, et al. The tension-freehernioplasty. Am TSurg 1989;157:188-193.
34. Shulman AG, Amid PK, Lichtenstein IL. The safety of meshrepair for primary inguinal hernias: results of 3019 operationfrom five diverse surgical sources. Am Surg 1992;58:255-257.
35. Kark AE, Kurzer MN, Belsham PA. Three thousand one hundredseventy-five primary inguinal hernia repairs: advantages ofambulatory open mesh repair using local anesthesia. J Am ColISurg 1998;186:447-456.
36. Shulman AG, Amid PK, Lichtenstein IL. Ligation of hernia saca needless step in adult hernioplasty. Int Surg 1993;78:152-153.
37. Friis E, Lindahl F. The tension-free hernioplasty in a randomizedtrial. Am J Surg 1996;172:315-319.
38. Burger JW, Luijendijk RW, Hop WC, et al. Long-term follow-upof a randomized controlled trial of suture versus mesh repair ofincisional hernia. Ann Surg 2004;240:578-583.
39. Beecherl EE, Jones DB, Carrico CJ. McVay to Lichtenstein: evo-lution of inguinal herniorrhaphy at a teaching institution. Paperresented at: North Texas Chapter of American College ofSurgeons; 1997.
40. Shulman AG, Amid PK, Lichtenstein IL. Patch or plug for groinhernia-which? Am J Surg 1994;167:331-336.
41. Shulman AG, Amid PK, Lichtenstein IL. The "plug" repair of1402 recurrent inguinal hernias. Arch Surg 1990;125:265-267.
42. Shulman AG, Amid PK, Lichtenstein IL. Prosthetic mesh plugrepair of femoral and recurrent inguinal hernias: the Americanexperience. Ann R ColI Surg EngI1992;74:97-99.
43. Rutkow IR, Robbins AW. Mesh plug hernia repair: a follow-upreport. Surg 1995;117:597-598.
44. Gilbert AI. Sutureless repair of inguinal hernia. Am T Surg1992;163:331-335.
1174 CHAPTER 53
45. Wantz GE. Experience with the tension-free hernioplasty forprimary inguinal hernias in men. J Am Coll Surg 1996;183:351-356.
46. Nyhus LM, Condon RE, Harkins HN. Clinical experiences withthe preperitoneal hernia repair for all types of hernia of the groin:with particular reference to the importance of transversalisfascia analogues. Am J Surg 1960;100:234-244.
47. Nyhus LM, Pollak R, Bombeck CT. The preperitoneal approachand prosthetic buttress repair for recurrent hernia: the evolutionof a technique. Ann Surg 1988;208:733-737.
48. Nyhus LM. Iliopubic tract repair of inguinal and femoral hernia:the posterior (preperitoneal) approach. Surg Clin North Am1993;73:487-499.
49. Hoffman HC, Traverso ALV. Preperitoneal prosthetic hernior-rhaphy: one surgeon's successful technique. Arch Surg 1993;128:964-970.
50. Stoppa RE, Quintyn M. Les deficiences de la paroi abdominalechez Ie suget age: colloque avec Ie praticien. Semin Hop Paris1969;45:2182-2184.
51. Stoppa RE, Rives JL, Warlaumont CR, et al. The use of Dacronin the repair of hernias of the groin. Surg Clin North Am1984;64:269-285.
52. Stoppa RE. The giant prosthesis for the reinforcement of thevisceral sac in the repair of groin and incisional hernias. In:Nyhus LM, Baker RJ, Fischer JE, eds. Mastery of Surgery. Boston:Little Brown; 1997:1859-1869.
53. Wantz GE. Giant prosthetic reinforcement of the visceral sac.Surg Gynecol Obstet 1989;169:408-417.
54. Stoppa RE. The treatment of complicated groin and incisionalhernias. World J Surg 1989;13:545-554.
55. Mathonnet M, Cubertafond, Gainant A. Bilateral inguinalhernias: giant prosthetic reinforcement of the visceral sac.Hernia 1997;1:93-95.
56. Munshi lA, Wantz GE. Management of recurrent and perivascu-lar femoral hernias by the giant prosthetic reinforcement of thevisceral sac. J Am CoIl Surg 1996;182:417-422.
57. Ger R. The management of certain abdominal hernia by intra-abdominal closure of the neck of the sac. Ann R CoIl Engl1982:64:342-344.
58. Molmenti EP, Soper NJ. Inguinal hernias. In: Jones DB, Wu JS,Soper NJ, ed. Laparoscopic Surgery: Principles and Procedures.St. Louis: Quality Medical; 1997:233-246.
59. Korman JE, Hiatt JR, Feldmar D, et al. Mesh configurations inlaparoscopic extraperitoneal herniorrhaphy. Surg Endosc 1997;11:1102-1105.
60. Felix EL, Michas CA, Gonzalez MH. Laparoscopic hernioplasty:TAPP versus TEP. Surg Endosc 1995;9:984-989.
61. Swanstrom LL. Laparoscopic herniorraphy. Surg Clin North Am1996;76:483-491.
62. Jones DB, Callery MP, Soper NJ. Strangulated incisional herniaat trocar site. Surg Laparosc Endosc 1996;6:152-154.
63. Vogt DM, Curet MJ, Pitcher DE, et al. Preliminary results ofa prospective randomized trial of laparoscopic onlay versusconventional inguinal herniorrhaphy. Am J Surg 1995;169:84-90.
64. Toy FK, Moskowitz M, Smoot RT, et al. Results of a prospectivemulticenter trial evaluating the ePTFE peritoneal onlay laparo-scopic inguinal hernioplasty. J Laparoendosc Surg 1996;6:375-385.
65. Jones DB, Maithel SK, Schneider BE, eds. Atlas of MinimallyInvasive Surgery. Cine-Med, Woodbury, CT, 2006.
66. Paganini AM, Lezoche E, Carle F, et al. A randomized, con-trolled, clinical study of laparoscopic versus open tension-freeinguinal hernia repair. Surg Endosc 1998;12:979-986.
67. Zieren J, Zieren H, Jacobe CA, et al. Prospective randomizedstudy comparing laparoscopic and open tension-free inguinalhernia repairwith Shouldice's operation. Am JSurg 1998;175:330-333.
68. Champault G, Rizk N, Catheline JM, et al. Inguinal herniarepair: totally pre-peritoneal laparoscopic approach versusStoppa operation, randomized trial: 100 cases. Hernia 1997;1:31-36.
69. Kald A, Anderberg, Carlsson P, Park PO, et al. Surgical outcomeand cost-minimization-analyses of laparoscopic and open herniarepair: a randomized prospective trial with 1 year follow-up. EurJ Surg 1997;163:505-510.
70. Bessell JR, Baxter P, Riddell P, et al. A randomized controlledtrial of laparoscopic extraperitoneal hernia repair as a day surgi-cal procedure. Surg Endosc 1996;10:495-500.
71. Wright DM, Kennedy A, Baxter IN, et al. Early outcome afteropen versus extraperitoneal endoscopic tension-free hernio-plasty: a randomized clinical trial. Surg 1996;119:552-557.
72. Tschudi 1, Wagner M, Klaiber C, et al. Controlled multicentertrial of laparoscopic transabdominal preperitoneal hernioplastyversus Shouldice herniorrhaphy. Surg Endosc 1996;10:845-847.
73. Barkun JS, Wexler MJ, Hinchey EJ, et al. Laparoscopic versusopen inguinal herniorrhaphy: preliminary results of a random-ized controlled trial. Surg 1995;118:703-710.
74. Stoker DL, Spiegelhalter DJ, Singh R, Wellwood JM. Laparo-scopic versus open inguinal hernia repair: randomized prospec-tive trial. Lancet 1994;343:1243-1245.
75. Neumayer L, Giobbie-Hurder A, Jonasson 0, et al. Open meshversus laparoscopic mesh repair of inguinal hernia. N Engl J Med2004;350: 1819-1827.
76. Liem MSL, Van Duyn EB, Van Der Graaf Y, Van VroonhovenTJMV. Recurrences after conventional anterior and laparoscopicinguinal hernia repair: a randomized comparison. Ann Surg2003;237:136-141.
77. Bringman S, Ramel S, Heikkinen T, et al. Tension-free inguinalhernia repair: TEP versus mesh-plug versus Lichtenstein: a pro-spective randomized controlled trial. Ann Surg 2003;237:142-147.
78. Wright D, Paterson C, Scott N, et al. Five-year follow-up ofpatients undergoing laparoscopic or open groin hernia repair: arandomized controlled trial. Ann Surg 2002;235:333-337.
79. Leibl BJ, Daubler P, Schmedt CG, et al. Long-term results of arandomized clinical trial between laparoscopic hernioplasty andShouldice repair. Br J Surg 2000;87:780-783.
80. The MRC Laparoscopic Groin Hernia Trial Group. Laparoscopicversus open repair of groin hernia: a randomised comparison.Lancet 1999;354:183-188.
81. Payne JH, Grininger LM, Izawa MT, et al. Laparoscopic or openinguinal herniorrhaphy? A randomized prospective trial. ArchSurg 1994;129:973-981.
82. Schmedt CG, Sauerland S, Bittner R. Comparison of endoscopicprocedures versus Lichtenstein and other open mesh techniquesfor inguinal hernia repair: a meta-analysis of randomized con-trolled trials. Surg Endosc 2005;19:188-199.
83. Memon MA, Cooper N1, Memon B, et al. Meta-analysis ofrandomized clinical trials comparing open and laparoscopicinguinal hernia repair. Br J Surg 2003;90:1479-1492.
84. Liem MSL, Van Steensel C1,Boelhouwer RU, et al. The learningcurve for totally extraperitoneal laparoscopic inguinal herniarepair. Am J Surg 1996;171:281-285.
85. Kald A, Anderberg B, Smedh K, Karlsson M. Transperitoneal ortotally extraperitoneal approach in laparoscopic hernia repair:results of 491 consecutive herniorrhaphies. Surg Laparosc Endosc1997;7:86-89.
86. Schneider BE, Castillo JM, Villegas L, Scott DJ, Jones DB. Lapa-roscopic totally extraperitoneal versus Lichtenstein herniorrha-phy: cost comparison at teaching hospitals. Surg Laparosc EndoscPercutan Tech 2003;13:261-267.
87. Hamilton EC, Scott DJ, Kapoor A, et al. Improving operativeperformance using a laparoscopic hernia simulator. Am J Surg2001;182:725-728.
HERNIAS AND ABDOMINAL WALL DEFECTS 1175
88. Grunwaldt LJ, Schwaitzberg SD, Rattner DW, Jones DB. Is lapa-roscopic inguinal hernia repair an operation of the past? J AmColI Surg 2005;200:616-620.
89. Winslow ER, Quasebarth M, Brunt LM. Perioperative outcomesand complications of open versus laparoscopic extraperitonealinguinal hernia repair in a mature surgical practice. Surg Endosc2004;18:211-217.
90. Ramshaw BJ, Tucker JG, Conner T, et al. A comparison of theapproaches to laparoscopic herniorrhaphy. Surg Endosc 1996;10:29-32.
91. Fitzgibbons R1, Camps 1, Comet D, et al. Laparoscopic inguinalherniorrhaphy: results of a multicenter trial. Ann Surg1995;221:3-13.
92. Felix EL, Michas CA, Gonzalez MH. Laparoscopic hernioplasty:TAPP versus TEP. Surg Endosc 1995;9:984-989.
93. Waisbren SJ,Herz BL,Ducheine Y, et al. Iatrogenic "respiratoryacidosis" during laparoscopic preperi toneal hernia repair. JLaparoendosc Surg 1996;6:181-183.
94. Scott DJ, Jones DB.Hernia. In: McClelland RN, ed. Selected Read-ings in General Surgery. Vol. 26, No.4, Issues 1 2, 1999.
95. Ferzli GS, Kiel T. The role of the endoscopic extraperitonealapproach in large inguinal scrotal hernias. Surg Endosc 1997;11:299-302.
96. Hendrickse CW, Ewans DS. Intestinal obstruction followinglaparoscopic inguinal hernia repair. Br J Surg 1993;80:1432.
97. Neugebauer E, Troidl H, Kum Ck, et al. The EAES consensusdevelopment conferences on laparoscopic cholecystectomy,appendectomy, and hernia repair. Surg Endosc 1995;9:550-563.
98. Phillips EH, Arregui M, Carrol B1, et al. Incidence of complica-tions following laparoscopic hernioplasty. Surg Endosc 1995;9:16-21.
99. MacFadyen BV, Mathis CR. Inguinal herniorraphy: complica-tions and recurrences. Semin Laparosc Surg 1994:1:128-140.
100. Payne JH Jr. Complications of laparoscopic inguinal hernior-rhaphy. Semin Laparosc Surg 1997;4:166-181.
101. Sayad P, Hallak A, Ferzli G. Laparoscopic herniorrhaphy: reviewof complications and recurrence. J Laparoendosc Surg 1998;8:3-10.
102. Condon RE, Nyhus LM. Complications of groin hernias. In:Nyhus LM, Condon RE, eds. Hernia. Philadelphia: Lippincott;1995:269-282.
103. Lichtenstein IL, Shore JM. Exploding the myths of hernia repair.Am J Surg 1976;132:307.
104. LeBlanc KA, Booth WV. Avoiding complications with laparo-scopic herniorrhaphy. Surg Laparosc Endosc 1993;3:420-424.
105. Elkberg 0, Lasson A, Kesek P, et al. Ipsilateral multiple groinhernias. Surgery 1994;115:557-562.
106. Lowham AS, Filipi C1, Fitzgibbons, et al. Mechanisms of herniarecurrence after preperitoneal mesh repair: traditional and lapa-roscopic. Ann Surg 1997;225:422-431.
107. Deans GT, Wilson MS, Royston CMS, et al. Recurrent inguinalhernia after laparoscopic repair: possible cause and prevention.Br J Surg 1995;82:539-541.
108. Phillips EP, Rosenthal R, Fallas M1, et al. Reasons of earlyrecurrences following laparoscopic hernioplasty. Surg Endosc1995;9:140-145.
109. Felix E, Scott S, Crafton B, et al. Causes of recurrence afterlaparoscopic hernioplasty: a multicenter study. Surg Endosc1998;12:226-231.
110. Van Steensel C1, Weidema WF. Laparoscopic inguinal herniarepair without fixation of the prosthesis. In: Arregui MF, NaganRF, eds. Inguinal Hernia, Advances or Controversies. Oxford:Radcliffe Medical Press; 1994:435-436.
111. Deans GT, Wilson MS, Royston CMS. Laparoscopic "bikinimesh" repair of bilateral inguinal hernia. Br J Surg 1995;82:1383-1385.
112. Felix EL, Michas C. Double-buttress laparoscopic herniorrha-phy. J Laparoendosc Surg 1993;3:1-8.
113. Tetik C, Arregui ME, Dulucq JL, et al. Complications and recur-rences associated with laparoscopic repair of groin hernias. Amulti-institutional retrospective analysis. Surg Endosc 1994;8:1316-1323.
114. Phillips EH, Arregui M, Carrol B1, et al. Incidence of complica-tions following laparoscopic hernioplasty. Surg Endosc 1995;9:16-21.
115. Cunningham 1,Temple WJ, Mitchell P, et al. Cooperative herniastudy: pain in the postrepair patient. Ann Surg 1996;224:598-602.
116. Sampath P, Yeo C, Campbell IN. Nerve injury associated withlaparoscopic inguinal herniorrhaphy. Surg 1995;118:829-833.
117. Seid AS, Amos E. Entrapment neuropathy in laparoscopicherniorrhaphy. Surg Endosc 1994;8:1050-1053.
118. Choi PD, Nath R, Mackinnon SEe Iatrogenic injury to the ilio-inguinal and iliohypogastric nerves in the groin: a case report,diagnosis, and management. Ann Plast Surg 1996;37:60-65.
119. Dittrick GW, Ridl K, Kuhn JA, McCarty TM. Routine ilioingui-nal nerve excision in inguinal hernia repairs. Am J Surg 2004;188:736-740.
120. Eubanks SE, Newman L, Goehring L, et al. Meralgia paraes-thetica: a complication of laparoscopic herniorrhaphy. SurgLaparosc Endosc 1993;3:381-385.
121. Broin EO, Homer C, Mealy K, et al. Meralgia paraestheticafollowing laparoscopic inguinal hernia repair, an anatomicalanalysis. Surg Endosc 1995;9:76-78.
122. Fong Y, Wantz GE. Prevention of ischemic orchitis during ingui-nal hernioplasty. Surg Gynecol Obstet 1992;174:399-402.
123. Milkins R, Wedgwood K. Intestinal obstruction following lapa-roscopic inguinal hernia repair. Br J Surg 1994;81:471.
124. Spier LN, Lazzaro RS, Procaccino A, et al. Entrapment of smallbowel after laparoscopic herniorrhaphy. Surg Endosc 1993;7:535-536.
125. Petersen TI, Qvist N, Wara P. Intestinal obstruction-a proce-dure-related complication of laparoscopic inguinal hernia repair.Surg Laparosc Endosc 1995;5:214-216.
126. Miller K, Junger W. Ileocutaneous fistula formation followinglaparoscopic polypropylene mesh hernia repair. Surg Endosc1997;11:772-773.
127. Gray MR, Curtis JM, Elkington JS. Colovesical fistula afterlaparoscopic inguinal hernia repair. Br J Surg 1994;81:1213-1214.
128. Hume RH, Bour J. Mesh migration following laparoscopic ingui-nal hernia repair. J Laparoendosc Surg 1996;6:333-335.
129. Vader VL, Vogt DM, Zucker KA, et al. Adhesion formation inlaparoscopic inguinal hernia repair. Surg Enclose 1997;11:825-829.
130. Rasim SM, Alzahrani MA, Sigman HH, et al. Comparisonof adhesion formation and tensile strength after three laparo-scopic herniorraphy techniques. Surg Lapar Endosc 1997;7:133-136.
131. Schlechter B, Marks J, Shillings tad RB, et al. Intra-abdominalmesh prosthesis in a canine model. Surg Endosc 1994;8:127-129.
132. Azurin D1, Schuricht AL, Stoldt HS, et al. Small bowel obstruc-tion following endoscopic extraperitoneal-preperitoneal hernior-rhaphy. J Laparoendosc Surg 1995;5:263-266.
133. Lodha K, Deans A, Bhattacharya P, et al. Obstructing internalhernia complication totally extraperitoneal inguinal herniarepair. J Laparoendosc Surg 1998;8:167-168.
134. Bhoyrul S, Payne 1,Steffes B, Swanstrom L, Way LW. A random-ized prospective study of radially expanding trocars in laparo-scopic surgery. J Gastrointest Surg 2000;4:392-397.
135. Carter Sl, Jones DB. Complications of laparoscopic surgery. In:Jones DB, Wu JS, Soper NT, eds. Laparoscopic Surgery: Principlesand Procedures. St. Louis: Quality Medical; 1997:89-96.
136. Cruse PJE, Foard R. The epidemiology of wound infection. SurgClin North Am 1980;60:27-40.
1176 CHAPTER 53
137. Platt R, Zaleznik DF, Hopkins CC, et al. Perioperative antibioticprophylaxis for hernia and breast surgery. N Engl J Med1990;322:153-160.
138. Taylor EW, Byrne DJ, Leaper DJ, et al. Antibiotic prophylaxisand open groin hernia repair. World J Surg 1997;21:811-815.
139. Gilbert AI, Felton LL. Infection in inguinal hernia repair con-sidering biomaterials and antibiotics. Surg Gynecol Obstet1993;177:126-130.
140. Condon RE. Surgical treatment of inguinal hernia, 1997 [edito-rial]. J Gastrointest Surg 1997;1:299-300.
141. Oishi SN, Page CP, Sxhwesinger WH. Complicated presentationof groin hernias. Am J Surg 1991;162:568-571.
142. Ishihara T, Kubota, Eda N, et al. Laparoscopic approach to incar-cerated inguinal hernia. Surg Endosc 1996;10:1111-1113.
143. Gahukamble DB, Khamage AS. Early versus delayed repair ofreduced incarcerated inguinal hernias in the pediatric popula-tion. J Ped Surg 1996;31:1218-1220.
144. Surana R, Puri P. Is contralateral exploration necessary in infantswith unilateral inguinal hernia? J Pediatr Surg 1993;28:1026-1027.
145. [ona J. The incidence of positive contralateral inguinal explora-tion among preschool children-a retrospective and prospectivestudy. J Pediatr Surg 1996;31:656-660.
146. Wulkan ML, Wiener ES, VanBalen N, et al. Laparoscopy throughthe open ipsilateral sac to evaluate presence of contralateralhernia. J Pediatr Surg 1996;31:1174-1177.
147. Toy FK, Bailey RW, Carey S, et al. Prospective, multicenterstudy of laparoscopic ventral hernioplasty: preliminary results.Surg Endosc 1998 12:955-959.
148. Santora TA, Roslyn JJ. Incisional hernia. Surg Clin North Am1993;73:557-570.
149. Carlson MA, Ludqig KA, Condon RE. Ventral hernia and othercomplications of 1000 midline incisions. South Med J 1995;88:450-453.
150. Israelsson LA, Jonsson T, Knutsson A. Suture technique andwound healing in midline laparotomy incisions. Eur J Surg1996;162:605-609.
151. Mudge M, Hughes LE. Incisional hernia: a 10 year prospectivestudy of incidence and attitudes. Br J Surg 1985;72:70-71.
152. Read RC, Yonder G. Recent trends in the management of inci-sional herniation. Arch Surg 1989;124:485-488.
153. Heydorn Wh, Velanovich V. A 5 year US army experience with36,250 abdominal hernia repairs. Am Surg 1990;56:596-600.
154. Gislason H, Gronbech JE, Soreide 0. Burst abdomen andincisional hernia after major gastrointestinal operations-comparison of three closure techniques. Eur JSurg 1995;161:349-354.
155. Sugerman HJ, Kellum JM, Reines D, et al. Greater risk of inci-sional hernia with morbidly obese than steroid-dependentpatients and low recurrence with prefascial polypropylene mesh.Am J Surg 1996;171:80-84.
156. Lamont PM, Ellis H. Incisional hernia in re-opened abdominalincisions: an overlooked risk factor. Br J Surg 1988;75:374-376.
157. Leber GE, Garb JL,Alexander AI, et al. Long-term complicationsassociated with prosthetic repair of incisional hernias. Arch Surg1998;133:378-382.
158. Ellis H, Coleridge-Smith PD, Joyce AD. Abdominal incisions-vertical or transverse? Postgrad Med J 1984;60:407-410.
159. Trimbos JB, Smit IB, Holm JP, et al. A randomized clinical trialcomparing two methods of fascia closure following midlinelaparotomy. Arch Surg 1992;127:1232-1234.
160. Sahlin S, Ahlberg J, Granstrom L, et al. Monofilament versusmultifilament absorbable sutures for abdominal closure. Br JSurg 1993;80:322-324.
161. Wissing J, Van Vroonhoven TJMV, Schattenkerk ME, et al.Fascia closure after midline laparotomy: results of a randomizedtrial. Br J Surg 1987;74:738-741.
162. Krukowski ZH, Cusick EL, Engeset J, et al. Polydioxanone orpolypropylene for closure of midline abdominal incisions: a pro-spective comparative clinical trial. Br JSurg 1987;74:828-830.
163. Chu CC, Williams DF. Effects of physical configuration andchemical structure of suture materials on bacterial adhesion.Am J Surg 1984;147:197-204.
164. Nezhat C, Nezhat F, Seidman DS, et al. Incisional hernias afteroperative laparoscopy. JLaparoendosc Surg 1997;7:111-115.
165. Caldizoni MW, Romano M, Bozza F, et al. Progressive pneumo-peritoneum in the management of giant incisional hernias: astudy of 41 patients. Br J Surg 1990;77:306-308.
166. Luijendijk RW, Hop WCJ, Van Den Tol P, et al. A comparisonof suture repair with mesh repair for incisional hernia. N Engl JMed 2000;343:392-398.
167. Temudom T, Siadati M, Sarr MG. Repair of complex giant orrecurrent ventral hernias by using tension-free intraparietalprosthetic mesh (Stoppa technique): lessons learned from initialexperience (50 patients). Surg 1996;120:738-744.
168. Van Der Linden FTPM, Van Vroonhoven THJMV. Long-termresults after correction of incisional hernia. Neth J Surg 1988;40:127-129.
169. Koller R, Miholic J, Iakl RJ. Repair of incisional hernias withexpanded polytetrafluoroethylene. Eur J Surg 1997;163:261-266.
170. Paul A, Korenkov M, Peters S, et al. Unacceptable results of theMayo procedure for repair of abdominal incisional hernias. EurJ Surg 1998;164:361-367.
171. Shukla VK, Gupta A, Singh H, et al. Cardiff repair of incisionalhernia: a university hospital experience. Eur I Surg 1998;164:271-274.
172. Sitzmann TV, McFadden DW. The internal retention repair ofmassive ventral hernia. Am Surg 1989;55:719-723.
173. George CD, Ellis H. The results of incisional hernia repair: a 12year review. Ann R Coll Surg 1986;68:185-187.
174. Porter JM. A combination of Vicryl and Marlex mesh: a tech-nique for abdominal wall closure in difficult cases. J Trauma1995;39:1178-1180.
175. Naim JO, Pulley D, Scanlan K, et al. Reduction of postoperativeadhesions to Marlex mesh using experimental adhesion barriersin rats. J Laparoendosc Surg 1993;3:187.
176. Molloy RG, Moran KT, Waldron RP, et al. Massive incisionalhernia: abdominal wall replacement with Marlex mesh. Br J Surg1991;78:242-244.
177. Brown LB, Richardson JD, Malangoni MA, et al. Comparison ofprosthetic materials for abdominal wall reconstruction in thepresence of contamination and infection. Ann Surg 1985;201:705-711.
178. Cristoforoni PM, Kim YB, Preys Z, et al. Adhesion formationafter incisional hernia repair: a randomized porcine trial. AmSurg 1996;62:935-938.
179. Bauer JJ, Salky BA, Gelernt 1M, et al. Repair of large abdominalwall defects with expanded polytetrafluoroethylene (PTFE). AnnSurg 1987;206:765-769.
180. Gillion JF, Begin GF, Marecos C, et al. Expanded polytetrafluo-roethylene patches used in the intraperitoneal or extraperitonealposition for repair of incisional hernias of the anterolateralabdominal wall. Am J Surg 1997;174:16-19.
181. Condon RE. Incisional hernia. In: Nyhus LM, Condon RE, eds.Hernia. Philadelphia: Lippincott; 1995:319-336.
182. Rubio PA. New technique for repairing large ventral incisionalhernias with Marlex mesh. Surg Gynecol Obstet 1986;162:275-276.
183. Rubio PA. Giant ventral hernias: a technical challenge. Int Surg1994;79:166-168.
184. McClelland RN. Ventral hernia repair. Sel Readings Gen Surg1993;20:38-47.
185. Wantz GE. Incisional hernioplasty with Mersiline. Surg GynecolObstet 1991;172:129-137.
HERNIAS AND ABDOMINAL WALL DEFECTS 1177
186. Amid PK, Shulman AG, Lichtenstein IL. A simple stapling tech-nique for prosthetic repair of massive incisional hernias. AmSurg 1994;60:934-937.
187. McLanahan D, King LT, Weems C, et al. Retrorectus prostheticmesh repair of midline abdominal hernia. Am J Surg 1997;173:445-449.
188. Holzman MD, Purut CM, Reintgen K, et al. Laparoscopic ventraland incisional hernioplasty. Surg Endosc 1997;11:32-35.
189. Park A, Gagner M, Pomp A. Laparoscopic repair of large inci-sional hernias. Surg Laparosc Endosc 1996;6:123-128.
190. LeBlanc KA, Booth WV, Whitaker JM. Laparoscopic repair ofventral hernias using an intraperitoneal onlay patch: report ofcurrent results. Contemp Surg 1994;45:211-214.
191. Carbajo MA, Martin del Olmo JC, Blanco JI, et al. Laparoscopicapproach to incisional hernia: lessons learned from 270 patientsover 8 years. Surg Endosc 2003;17:118-122.
192. McGreevy JM, Goodney PP, Birkmeyer CM, et al. A prospectivestudy comparing the complication rates between laparoscopicand open ventral hernia repairs. Surg Endosc 2003;17:1778-1780.
193. Bencini L, Sanchez LJ, Boffi B, et al. Incisional hernia repair:retrospective comparison of laparoscopic and open techniques.Surg Endosc 2003;17:1546-1551.
194. Salameh JR, Sweeney JF, Graviss EA, et al. Laparoscopic ventralhernia repair during the learning curve. Hernia 2002;6: 182-187.
195. Wright BE,Niskanen BD, Peterson DJ, et al. Laparoscopic ventralhernia repair: are there comparative advantages over traditionalmethods of repair? Am Surg 2002;68:291-296.
196. Chari R, Chari V, Eisenstat M, Chung R. A case controlled studyof laparoscopic incisional hernia repair. Surg Endosc 2000; 14:117-119.
197. DeMaria EJ, Moss JM, Sugerman HJ. Laparoscopic intraperito-neal polytetraflouroethylene (PTFE) prosthetic patch repair ofventral hernia: prospective comparison to open prefascial poly-propylene mesh repair. Surg Endosc 2000;14:326-329.
198. Carbajo MA, Martin del Olmo JC, Blanco JI, et al. Laparoscopictreatment versus open surgery in the solution of major incisionaland abdominal wall hernias with mesh. SurgEndosc 1999;13:250-252.
199. Ramshaw BJ, Esartia P, Schwab J, et al. Comparison of laparo-scopic and open ventral herniorrhaphy. Am Surg 1999;65:827-832.
200. Park A, Birch DW, Lovrics P. Laparoscopic and open incisionalhernia repair: a comparison study. Surgery 1998;124:816-822.
201. Holzman MD, Purut CM, Reintgen K, et al. Laparoscopic ventraland incisional hernioplasty. Surg Endosc 1997;11:32-35.
202. Franklin ME, Gonzalez H, Glass JL, Manjarrez A. Laparoscopicventral and incisional hernia repair: an l l-year experience.Hernia 2004;8:23-27.
203. Heniford BT, Park AE, Ramshaw BJ, Voeller G. Laparoscopicrepair of ventral hernias: 9 years' experience with 850 consecu-tive hernias. Ann Surg 2003;238:391-400.
204. LeBlanc KA, Whitaker JM, Bellanger DE, Rhynes VK. Laparo-scopic incisional and ventral hernioplasty: lessns learned from200 patients. Hernia 2003;7:118-124.
205. Rosen M, Brody F, Ponsky J, et al. Recurrence after laparoscopicventral hernia repair: a 5-year experience. Surg Endosc 2003; 17:123-128.
206. Bageacu S, Blanc P, Breton C, et al. Laparoscopic repair of inci-sional hernia: a retrospective study of 159 patients. Surg Endosc2002;16:345-348.
207. Ben-Haim M, Kuriansky J, Tal R, et al. Pitfalls and complica-tions with laparoscopic intraperitoneal expanded polytetrafluo-roethylene patch repair of postoperative ventral hernia: lessonsfrom the first 100 consecutive cases. Surg Endosc 2002;16:785-788.
208. Berger D, Bientzle M, Muller A. Postoperative complicationsafter laparoscopic incisional hernia repair: incidence and treat-ment. Surg Endosc 2002;16:1720-1723.
209. Gillian GK, Geis WP, Grover G. Laparoscopic incisional andventral hernia repair (LIVH): an evolving outpatient technique.JSLS 2002;6:315-322.
210. Chowbey PK, Sharma A, Khullar R, et al. A. laparoscopic ventralhernia repair. J Laparoendosc Adv Surg Tech A 2000;10:79-84.
211. Fabian TC, Croce MA, Pritchard FE, et al. Planned ventralhernia: staged management for acute abdominal wall defects.Ann Surg 1994;219:643-653.
212. Stone HH, Fabian TC, Turkleson ML, et al. Management ofacute full-thickness losses of the abdominal wall. Ann Surg1981;193:612-618.
213. Voyles CR, Richardson JD, Bland KI,et al. Emergency abdominalwall reconstruction with polypropylene mesh: short-term ben-efits versus long-term complications. Ann Surg 1981;194:219-223.
214. Jones JW, Jurkovich GJ. Polypropylene mesh closure of infectedabdominal wounds. Am Surg 1989;55:73-76.
215. Buck JR, Fath H, Chung SK, et al. Use of absorbable mesh as anaid in abdominal wall closure in the emergent setting. Am Surg1995;61:655-658.
216. Greene MA, Mullins RJ, Malangoni MA, et al. Laparotomywound closure with absorbable polyglycolic acid mesh. SurgGynecolObstet 1993;176:213-218.
217. Jernigan TW, Fabian TC, Croce MA, et al. Staged managementof giant abdominal wall defects: acute and long-term results.Ann Surg 2003;238:349-357.
218. Ramirez OM, Ruas E, Dellon AL. "Components separation"method for closure of abdominal-wall defects: an anatomic andclinical study. Plast Recontr Surg 1990;86:519-526.
219. De Vries Reilingh TS, Van Goor H, Rosman C, et al. "Compo-nents separation technique" for the repair of large abdominalwall hernias. J Am ColI Surg 2003;196:32-37.
220. Hultman CS, Pratt B,Cairns BA,et al. Multidisciplinary approachto abdominal wall reconstruction after decompressive laparot-omy for abdominal compartment syndrome. Ann Plast Surg2005;54:269-275.
221. Admire AA, Dolich MO, Sisley AC, Samimi KJ.Massive ventralhernias: role of tissue expansion in abdominal wall restorationfollowing abdominal compartment syndrome. Am Surg 2002;68:491-496.
222. Shestak KC, Edington HJ, Johnson RR. The separation of ana-tomic components technique for the reconstruction of massivemidline abdominal wall defects: anatomy, surgical technique,applications, and limitations revisited. Plast Reconstr Surg2000;105:731-738.
223. Ueno T, Pickett LC, De La Fuente SG, et al. Clinical applicationof porcine small intestinal submucosa in the management ofinfected or potentially contaminated abdominal defects. JGastrointest Surg 2004;8:109-112.
224. Franklin ME Jr, Gonzalez H Jr, Glass JL. Use of porcine smallintestinal submucosa as a prosthetic device for laparoscopicrepair of hernias in contaminated fields: 2-year follow-up. Hernia2004;8: 186-189.
225. Eid GM, Mattar SG, Hamad G, et al. Repair of ventral herniasin morbidly obese patients undergoing laparoscopic gastricbypass should not be deferred. Surg Endosc 2004;18:207-210.
226. Adedeji OA, Bailey CA. Varma JS. Porcine dermal collagen graftin abdominal-wall reconstruction. Br J Plast Surg 2002;55:85-86.
227. Buinewicz B, Rosen B. Acellular cadaveric dermis (AlloDerm): anew alternative for abdominal hernia repair. Ann Plast Surg2004;52: 188-194.
228. Spangen L. Spigelian hernia. Surg Clin N Am 1984;64:351-366.229. Felix EL, Michas C. Laparoscopic repair of spigelian hernias.
Surg Laparosc Endosc 1994;4:308-310.

1178 CHAPTER 53
230. Amendolara M. Videolaparoscopic treatment of spigelianhernias. Surg Laparosc Endosc 1998;8:136-139.
231. Heniford BT, Iannitti DA, Gagner M. Laparoscopic inferior andsuperior lumbar hernia repair. Arch Surg 1997;132:1141-1144.
232. Marchal F, Parent S, Tortuyaux JM, et al. Obturator hemias-report of seven cases. Hernia 1997;1:23-26.
233. Bryant TL, Umstot RK. Laparoscopic repair of an incarceratedobturator hernia. Surg Endosc 1996;10:437-438.
234. Ziegler D, Rhoads JE. Obturator hernia needs a laparotomy, nota diagnosis. Am J Surg 1995;170:67-68.
235. SO JB, Palmer MT, Shellito PC. Postoperative perineal hernia.Dis Colon Rectum 1997;40:953-957.
236. Cali RL, Pitsch Rm, Blatchford GJ, et al. Rare pelvic floorhernias: report of a case and review of the literature. Dis ColonRectum 1992;35:604-612.
237. Martin L, Foster G. Parasomal hernia. Ann R Coll Surg Engl1996;78:81-84.
238. Rubin MS, Schoetz DJ, Matthews JB. Parastomal hernia: isrelocation superior to fascial repair? Arch Surg 1994;129:413-419.
239. Armstrong 0, Letessier E, Genier F, et al. Internal hernia: reportof nine cases. Hernia 1997;1:143-145.
240. Langer JC. Gastroschisis and ophalocele. Semin Ped Surg1996;5:124-128.
241. Heiss KF. Congenital diaphragmatic hernia in 1994: a hard lookat the need for "emergency surgery." Semin Thor CardiovascSurg 1994;6:221-227.
242. West KWW, Bengston K, Rescorla FJ, et al. Delayed surgicalrepair and ECMO improves survival in congenital diaphragmatichernia. Ann Surg 1992;216:454.
243. Orita M, Okino M, Yamashita K, et al. Laparoscopic repair of adiaphragmatic hernia through the foramen of Morgagni. SurgEndosc 1997;11:668-670.