abdominal inflammatory myofibroblastic tumours in children
TRANSCRIPT
www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2011) 46, 2076–2082
Abdominal inflammatory myofibroblastic tumor:a clinicopathologic study with reappraisalof biologic behavior
Ana Catarina Fragoso a,1, Catarina Eloy b,1, José Estevão-Costa a,⁎, Miguel Campos a,Nuno Farinha c, José Manuel Lopes b
aDivision of Pediatric Surgery, Faculty of Medicine, University of Porto, Hospital S. João, 4200-319 Porto, PortugalbDivision of Pathology, Faculty of Medicine, University of Porto, Hospital S. João, 4200-319 Porto, PortugalcUnit of Pediatric Hematology-Oncology, Hospital S. João, 4200-319 Porto, Portugal
Received 9 May 2011; revised 4 July 2011; accepted 4 July 2011
0d
Key words:Inflammatorymyofibroblastic tumor;
Inflammatorypseudotumor;
Abdomen;Children
AbstractBackground and Purpose: Inflammatory myofibroblastic tumor (IMT) is a proliferative lesion ofcontroversial nosology and uncertain prognosis. In an attempt to acquire further understanding ofpathogenesis and biologic behavior, we surveyed abdominal IMTs managed over the last 12 years at asingle institution.Methods: Intra-abdominal IMTs treated between 1995 and 2007 were reviewed concerningdemographic, clinical, and pathologic features as well as therapeutic management and outcome. Allspecimens were reevaluated by histologic examination and immunohistochemistry.Results: There were 7 patients (4 males; age range, 28 days to 14 years). Five lesions were located inalimentary tract: 1 gastric presenting with bleeding, 1 hepatic presenting with a thoracic wall mass, 1pancreatic and 2 colonic presenting with obstructive symptoms. One splenic IMT was foundincidentally. The remaining case arose from the adrenal gland and presented with a palpable mass. Thegastric and adrenal IMTs had evidence of a previous or concomitant infectious setting. Five lesions wereexcised. The pancreatic IMT underwent a drainage procedure followed by steroid administration, andthe hepatic lesion received antibiotics. Histopathology revealed characteristic findings of IMT.Expression of anaplastic lymphoma kinase was negative in all cases. At a median follow-up of 6 years(range, 3-15), all children were asymptomatic with no recurrences. The hepatic and pancreatic IMTdisplayed complete and near total regression, respectively.Conclusion: A benign behavior of abdominal IMTs was observed even in patients not undergoingsurgical excision. Although IMT remains a surgical disease, a conservative approach may be reasonablein select cases.© 2011 Elsevier Inc. All rights reserved.
⁎ Corresponding author. Tel.: +35 1913237460.E-mail address: [email protected] (J. Estevão-Costa).1 Both authors contributed equally for this manuscript.
022-3468/$ – see front matter © 2011 Elsevier Inc. All rights reserved.oi:10.1016/j.jpedsurg.2011.07.009
2077Biological behavior of abdominal IMT
Inflammatory myofibroblastic tumor (IMT) is a rare The procedures followed in the present study were in
condition in children usually mentioned in case reports [1].It is a proliferative lesion composed of spindle cellsaccompanied by inflammatory infiltrate of obscure etio-pathogenesis [1-6]. This issue along with confusingterminology, the wide clinical presentation, and highlyvariable outcome has precluded the establishment of anappropriate therapeutic approach and reliable prognosis[2,7-9]. The present study encompassed abdominal lesionsmanaged over the last 12 years at our institution in aneffort to reappraise the biologic behavior of IMT.1. Material and methods
The charts of all intra-abdominal IMTs consecutivelydiagnosed in children from 1995 to 2007 at the Hospital S.João, University of Porto, were reviewed; 2 instances ofIMT were previously published as individual case reports[10,11]. The files from all patients were reevaluated,including demographic, clinical, and pathologic features aswell as treatment and follow-up data as of December 2010.
The gross specimen description and all histologicmaterial were reevaluated; the tumors were classifiedaccording to the current World Health Organizationcriteria [1]. Immunohistochemical study with vimentin(diluted 1:800; Dako, Glostrup, Denmark), desmin(diluted 1:100; Cell Marque, Rocklin, CA), smoothmuscle actin (diluted 1:200; Neomarkers, Freemont,CA), S-100 protein (diluted 1:1000; Dako), and anaplasticlymphoma tyrosine kinase receptor 1 (ALK-1) (diluted1:20; Dako) was performed in representative tumor areasfrom formalin-fixed, paraffin-embedded blocks, using astandard streptavidin-biotin method and adequate positiveand negative controls.
Table 1 Clinicopathologic features of the patients
No. Age/sex Location Presentation Other features
1 10 y/F Stomach Digestive bleeding Anemia. Chronigastritis, H pylo
2 4 y/M Spleen Incidental finding –3 28 d/F Adrenal Palpable mass Anemia; S agal
on aspirate; hempigmentation
4 8 y/F Pancreas Abdominal painand vomiting
–
5 14 y/M Liver Thoracic wall tumor Anemia6 4 y/M Colon Intussusception –7 12 y/M Colon Intestinal obstruction Cerebral palsy
F indicates female; M, male; NED, no evidence of disease; RD, residual diseasea Diffuse involvement of segments VI/VII/VIII.
accordance with the institutional ethical committee. All thesamples enrolled in this study were kept anonymously afterretrieval of follow-up information.
2. Results
The clinicopathologic features of the patients aresummarized in Table 1.
2.1. Demographics and presentation
There were 3 females (43%) and 4 males (57%) with amedian age of 8 years (range, 28 days to 14 years). Thetumors occurred in distinct organs exhibiting differentclinical presentation. Five lesions were located in thealimentary tract: 1 in the stomach, 1 in the liver, 2 in thecolon, and the 2 remaining originated in the spleen and inthe right adrenal gland.
Diagnostic workup of gastric tumor (no. 1) presentingwithgastrointestinal bleeding revealed anemia and an elevatedlesion in the prepyloric region with a large deep ulceration onupper gastrointestinal endoscopy; endoscopic ultrasonogra-phy (US) demonstrated an intramural mass in the muscularispropria with adjacent apparently enlarged “lymph nodes,”which raised the possibility of a leiomyosarcoma.
The splenic lesion (no. 2) was incidentally found onpathologic examination of a ruptured organ excised becauseof blunt abdominal trauma.
The adrenal lesion (no. 3) presented as an abdominal massin a pale and febrile 28-day-old patient with a history ofdystocia during labor and delivery. The laboratory evaluationrevealed severe anemia (Hb, 6.7 g/dL), leukocytosis, andelevated serum C-reactive protein (122 mg/dL) level. An
Treatment Size (cm) Follow-up
Duration Status
cri+
Partial gastrectomy 3 15 y NED
Not lesion oriented 2 14 y NEDactiaeossideric
Nephroadrenalectomy 7 13 y NED
Drainage procedure,oral corticoids
2.2 6 y RD
Antibiotics (!) a 6 y NEDSegmental colectomy 3 5 y NEDRight colectomy 13 3 y NED
.
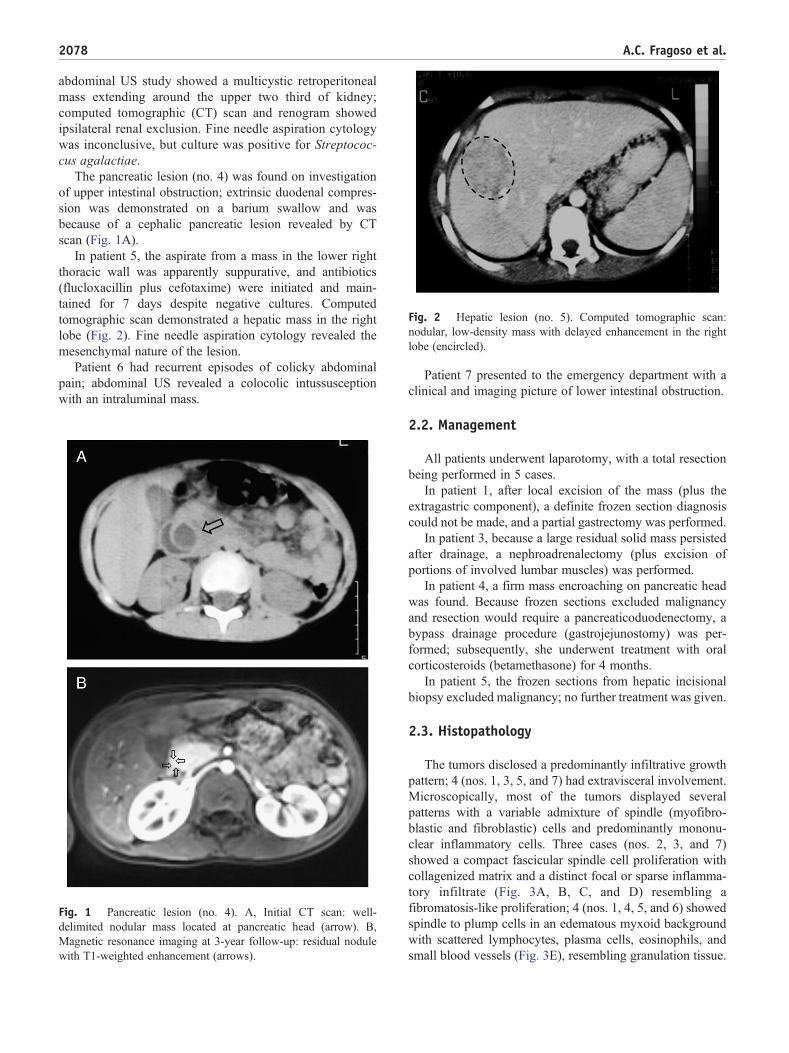
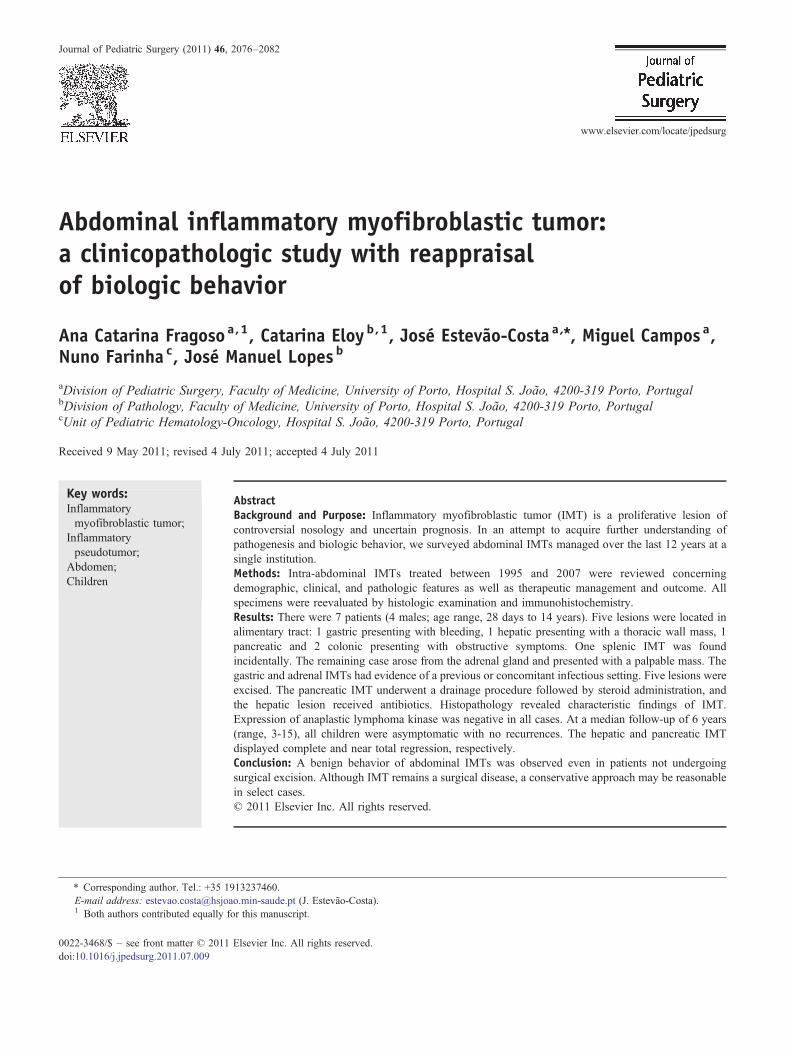
Fig. 2 Hepatic lesion (no. 5). Computed tomographic scan:nodular, low-density mass with delayed enhancement in the rightlobe (encircled).
2078 A.C. Fragoso et al.
abdominal US study showed a multicystic retroperitonealmass extending around the upper two third of kidney;computed tomographic (CT) scan and renogram showedipsilateral renal exclusion. Fine needle aspiration cytologywas inconclusive, but culture was positive for Streptococ-cus agalactiae.
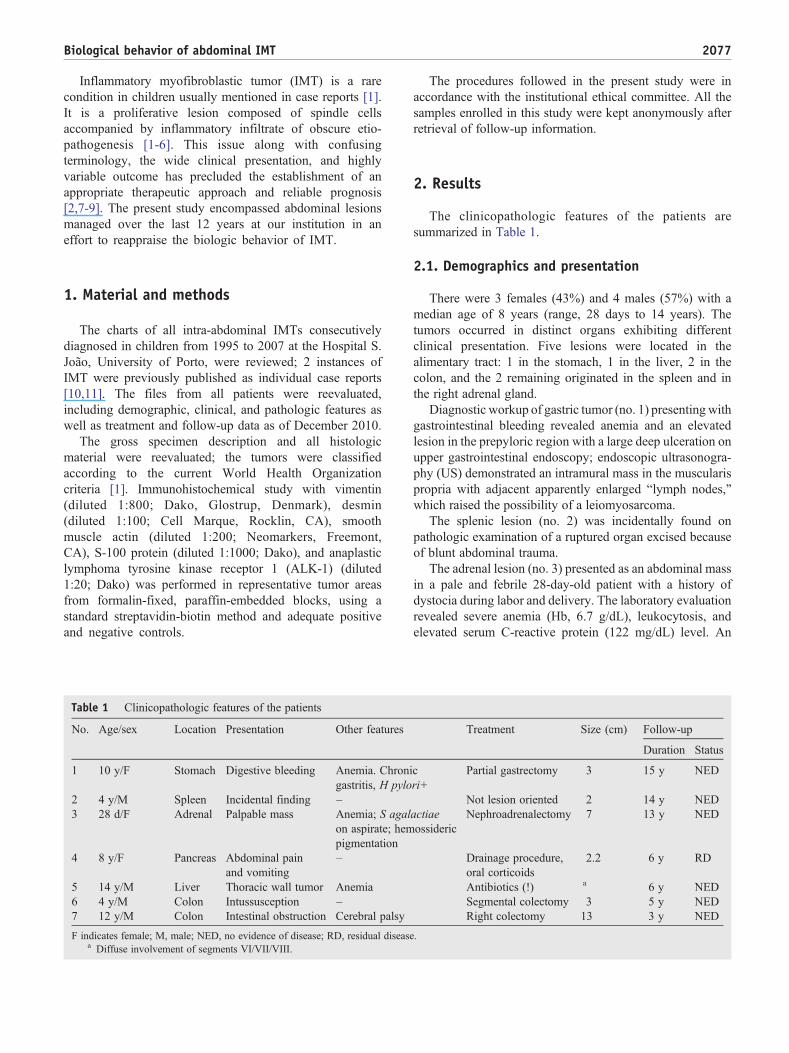
The pancreatic lesion (no. 4) was found on investigationof upper intestinal obstruction; extrinsic duodenal compres-sion was demonstrated on a barium swallow and wasbecause of a cephalic pancreatic lesion revealed by CTscan (Fig. 1A).
In patient 5, the aspirate from a mass in the lower rightthoracic wall was apparently suppurative, and antibiotics(flucloxacillin plus cefotaxime) were initiated and main-tained for 7 days despite negative cultures. Computedtomographic scan demonstrated a hepatic mass in the rightlobe (Fig. 2). Fine needle aspiration cytology revealed themesenchymal nature of the lesion.
Patient 6 had recurrent episodes of colicky abdominalpain; abdominal US revealed a colocolic intussusceptionwith an intraluminal mass.
Fig. 1 Pancreatic lesion (no. 4). A, Initial CT scan: well-delimited nodular mass located at pancreatic head (arrow). B,Magnetic resonance imaging at 3-year follow-up: residual nodulewith T1-weighted enhancement (arrows).
Patient 7 presented to the emergency department with aclinical and imaging picture of lower intestinal obstruction.
2.2. Management
All patients underwent laparotomy, with a total resectionbeing performed in 5 cases.
In patient 1, after local excision of the mass (plus theextragastric component), a definite frozen section diagnosiscould not be made, and a partial gastrectomy was performed.
In patient 3, because a large residual solid mass persistedafter drainage, a nephroadrenalectomy (plus excision ofportions of involved lumbar muscles) was performed.
In patient 4, a firm mass encroaching on pancreatic headwas found. Because frozen sections excluded malignancyand resection would require a pancreaticoduodenectomy, abypass drainage procedure (gastrojejunostomy) was per-formed; subsequently, she underwent treatment with oralcorticosteroids (betamethasone) for 4 months.
In patient 5, the frozen sections from hepatic incisionalbiopsy excluded malignancy; no further treatment was given.
2.3. Histopathology
The tumors disclosed a predominantly infiltrative growthpattern; 4 (nos. 1, 3, 5, and 7) had extravisceral involvement.Microscopically, most of the tumors displayed severalpatterns with a variable admixture of spindle (myofibro-blastic and fibroblastic) cells and predominantly mononu-clear inflammatory cells. Three cases (nos. 2, 3, and 7)showed a compact fascicular spindle cell proliferation withcollagenized matrix and a distinct focal or sparse inflamma-tory infiltrate (Fig. 3A, B, C, and D) resembling afibromatosis-like proliferation; 4 (nos. 1, 4, 5, and 6) showedspindle to plump cells in an edematous myxoid backgroundwith scattered lymphocytes, plasma cells, eosinophils, andsmall blood vessels (Fig. 3E), resembling granulation tissue.
Fig. 3 Morphological features. A, Macroscopy of case 7 (colonic). B to D, Respective microscopy showing an infiltrative growth withinmuscularis propria (B, H&E, original magnification ×4; ⁎ inset, desmin, original magnification ×200), with variable areas of fasciculate pattern(C, H&E original magnification ×100) and mixed inflammatory infiltrate (D, H&E original magnification ×200). E, Microscopy of case 6(colonic) disclosing myxoid stroma and few spindle cells (H&E, original magnification ×200).
2079Biological behavior of abdominal IMT
Foci of necrosis were present in 4 cases (nos. 1, 4, 5, and 6).Atypical tumor cells were rarely found, and the mitotic indexof all tumors was low (b1/10 high-power fields). None of thetumors disclosed ganglion-like cells, Reed-Sternberg–likecells, or calcification/ossification foci. Strong diffusevimentin and focal to diffuse smooth muscle actin wereobserved in the spindle cell cytoplasm of all tumors, andfocal desmin was observed in one (no. 3). None of the lesionsdisclosed S-100 protein and anaplastic lymphoma tyrosinekinase receptor (ALK) expression in the spindle tumor cells.The mucosa overlying the gastric tumor (no. 1) showed signsof chronic gastritis associated with the presence of Helico-bacter pylori. In case 3 (adrenal), there was extensivehemosideric pigmentation, positive with Perls staining, inand around the tumor.
2.4. Outcome
After a median period of 6 years (range, 3-15) of follow-up, all patients are asymptomatic without any evidence of
progression or metastatic disease. Patients submitted toexcision have no evidence of recurrence. The pancreatic IMT(no. 4) shrunk progressively with near total regression at3-year follow-up on imaging assessment (Fig. 1B) andremained stable. The hepatic lesion (no. 5) displayed totalregression on a magnetic resonance imaging study per-formed at 3-month follow-up examination.
3. Discussion
Inflammatory myofibroblastic tumor is an entity withdistinctive histopathologic characteristics but interchange-ably designated with a vast array of terms (eg, inflammatorypseudotumor, plasma cell granuloma, inflammatory fibro-sarcoma, fibrous histiocytoma, inflammatory fibroid polyp,inflammatory myofibrohistiocytic proliferation, inflammato-ry myofibroblastic proliferation, omental mesenteric myxoidhamartoma, xanthoma, fibroxanthoma, and xanthogranu-loma) [8,9]. Additional features such as wide clinical
2080 A.C. Fragoso et al.
presentation, variable course, scarce series reports, andabsence of controlled studies have not allowed a definitiveetiopathogenesis, an appropriate therapeutic approach, andan accurate prognosis to be established [2,7-9].
Epidemiology and sites of involvement have not beenuniformly described. Inflammatory myofibroblastic tumor isprimarily a visceral and soft tissue tumor of children andyoung adults; it is most frequently seen in the first 2 decadesof life and occurs more commonly in the lung, mesentery,and omentum [9,12-19]. The present series is in accordancewith the IMT predilection for children and adolescents and,to the best of our knowledge, includes the youngest intra-abdominal case (28-day-old) reported to date. Concerningthe anatomical distribution of intra-abdominal IMTs, all thelesions in the current series originated from visceral organsdespite adjacent involvement of omentum/mesentery (nos. 1and 7), retroperitoneum (no. 3), or soft tissue (no. 5). This isin contrast with aforementioned demographics; however,accurate data regarding location are difficult to collect.
The present series illustrates the unspecific and widespectrum of clinical presentation of IMTs, from asymptom-atic (no. 2) to severe malaise with systemic manifestations(no. 3). Anemia was a frequent finding (3 cases). As occurredin patients 1, 4, 5, and 7, the symptoms and imaging studiesof IMT masses may mimic malignancy; clinical awarenessis, therefore, crucial to establish the correct diagnosis throughadequate histopathologic examination.
The etiopathogenesis of IMT is still poorly understood[1-4]. Although IMT is now classified with intermediateneoplasms in the current World Health Organizationhistologic typing of tumors of soft tissue and bone, it is notclear whether IMT is a reactive proliferation or a trueneoplasm and whether it is benign or malignant [1,5,6].Some authors sustain that an aberrant or exaggeratedresponse to tissue injury is at the root of this condition;infective, inflammatory, reparative, and immunologic pro-cesses have been postulated, and approximately 20% to 25%of patients have history of antecedent trauma or surgicalinstrumentation [20-23]. Interestingly, 2 cases in the presentseries occurred in a postinfectious/inflammatory setting. Theassociation of chronic gastritis and H pylori along with thepresence of ulceration in gastric IMT (no. 1) favors that itmay evolve from an inflammatory/infectious driven etiology.A similar explanation may be plausible for patient 3 whoseinfection was probably secondary to neonatal adrenalhemorrhage suggested by the clinical picture (dystociaduring labor and delivery and anemia) and hemosidericpigmentation on pathologic examination.
As a cause or consequence of the obscure and confusingaforementioned issues, the outcome of IMTs is stilluncertain, and a high degree of evidence to support atherapeutic modality is also lacking. Inflammatory myofi-broblastic tumors present a wide spectrum of biologicbehavior; some lesions exhibit aggressiveness associatedwith local spread and recurrence after successful excision,and a few may perhaps metastasize [2,24-26]. Because the
reported series are not uniform or are limited to subsets ofIMT, wide ranges of rates of local recurrence have beenrecorded from 2% to 37% and distant metastasis from 0% to11% [14,27].
Search for predictive features affecting outcome has beenfocused on clinical, pathologic, and cytogenetic findings.
Recurrence has been associated with abdominopelviclocation, large size, older age, multinodular mass, andincomplete resection [28,29]. In our series, despite the intra-abdominal location, the presence of 2 large lesions, and theextravisceral involvement in most of the patients, there wereno recurrences at a median follow-up of 6 years, an event thatusually develops within 24 months after diagnosis [14].Those findings corroborate the absence of individualprognostic indicators. In fact, an extrapulmonary primarysite accounts for the major number of relapses (2/3), but therecurrence rate is similar to pulmonary IMTs. In addition,occasional IMTs that are only biopsied or excised withpositive margins sometimes neither recur nor progress[14,29,30]. In the present series, none of the patientsdeveloped distant metastasis, an event that is almost alwaysidentified at presentation or within the first year afterdiagnosis [16]. Metastases have been associated withyounger age and large size, but the 2 dozen cases ofmetastatic IMTs recorded in literature affected patients over abroad range of ages and of anatomical primary sites [16,28].
Onmicroscopic examination, as we observed in the presentseries, IMTs consist of a proliferation of spindle- to stellate-shaped cells usually lacking cytologic atypia and a myxoidstromawith variable amounts of intercellular collagen; mitoticindex is usually 1 to 2 mitosis/10 high-power field [1,6].Histologic variability is part of the morphological spectrum ofIMTs, so it is not surprising that current investigation onpossible predictors such as cellularity, mitotic activity,necrosis, nuclear atypia, and ganglion-like cells is too limitedto draw conclusions regarding prognosis [28,30-32].
On immunohistochemistry, IMT cells typically expressvimentin diffusely, variable smooth muscle actin anddesmin, and are negative for c-Kit [14]. Up to 71% arepositive for ALK-1, and approximately 50% have clonerearrangement involving the ALK locus on chromosome2p23 that provides support for the neoplastic nature of IMT[21,28,33-37]. However, as a predictor, ALK expression hasnot demonstrated a clear relationship with prognosis. On onehand, ALK-1–negative tumors occur in older patients anddisplay greater nuclear pleomorphism and atypical mitoses;in 2 recent series, metastatic IMTs were confined to ALK-1–negative lesions [5,28]. On the other hand, positive ALK-1status may be more frequent in younger males and associatedwith a higher recurrence rate [38,39]. None of these features(cytologic atypia, ALK-1 positivity, local recurrence, anddistant metastasis) were observed in any of the cases in thepresent series that disclosed bonafide features of IMTs.Despite morphologically undistinguishable, ALK-1–nega-tive IMTs remain controversial lesions with a wide-rangingbiologic behavior, from aggressive sarcomatous tumors

2081Biological behavior of abdominal IMT
doing poorly after surgery and chemotherapy to inflamma-tory-type pseudotumors with a probable reactive relatedetiopathogenesis [38]. The patients in our series appear to bepart of the latter group of this large spectrum because some ofthem occurred in association with a postinfectious/inflam-matory setting, and all disclosed a favorable outcome after afairly long follow-up despite the fact that no resection wasperformed in 2 cases.
The question of appropriate treatment for IMTs is notsettled. Surgical excision has been the cornerstone of therapybecause of the uncertainty in diagnosis, risk of diseaseprogression, and lack of reliable alternative options [40].Radiotherapy and chemotherapy have unclear roles asadjunctive modalities, but there are increasing reports ofsuccessful resolution with antibiotics, steroids, imatinib, ornonsteroidal anti-inflammatory drugs [41-48]. In our series,because tumor resection was considered mutilating and/orextensive, 2 patients (nos. 4 and 5) were effectively managedwith corticosteroids and antibiotics, respectively; whetherthese lesions responded to treatment or spontaneouslyregressed, a well-known event that may occur even inrecurrent cases, remains to be elucidated [49,50].
There are no definitive clinical, histopathologic, orcytogenetic features to predict IMT outcome [14,30,31]. Ourseries of abdominal ALK-negative IMTs showed a benignbehavior even in patients not undergoing surgical resection.Despite the fact that IMT remains a surgical disease, aconservative approach may be an alternative to consider inselected cases where the surgeon debates the risks andbenefits of resection associated with substantial morbidity.
4. Note added in proof
Since the submission of this article, an additional patientwith a hepatic IMT was successfully managed withconservative approach.
References
[1] Coffin CM, Fletcher JA. Inflammatory myofibroblastic tumour. In:Fletcher CDM, Unni KK, Mertens F, editors. World HealthOrganization classification of tumours. Pathology and genetics oftumours of soft tissue and bone. Lyon: IARC Press; 2002. p. 91-3.
[2] Makhlouf HR, Sobin LH. Inflammatory myofibroblastic tumors(inflammatory pseudotumors) of the gastrointestinal tract: how closelyare they related to inflammatory fibroid polyps? Hum Pathol 2002;23:307-15.
[3] Nonaka D, Birbe R, Rosai J. So-called inflammatory myofibroblastictumor: a proliferative lesion of fibroblastic reticulum cells? Histopa-thology 2005;46:604-13.
[4] Treissman SP, Gillis A, Lee CLY, et al. Omental-mesentericinflammatory pseudotumor. Cancer 1994;73:1433-7.
[5] Mergan F, Jaubert F, Sauvat F, et al. Inflammatory myofibroblastictumor children: clinical review with anaplastic lymphoma kinase,Epstein-Barr virus, and human herpesvirus 8 detection analysis.J Pediatr Surg 2005;40:1581-6.
[6] Weiss SW, Goldblum JR. Enzinger and Weiss's soft tissue tumors.5th ed. Philadelphia: Mosby Elsevier; 2008.
[7] Lazure T, Ferlicot S, Gauthier F, et al. Gastric inflammatorymyofibroblastic tumors in children: an unpredictable course. J PediatrGastroenterol Nutr 2002;34:319-22.
[8] Saleem MH, Ben-Hamida MA, Barrett AM, et al. Lower abdominalinflammatory myofibroblastic tumor—an unusual presentation—acase report and brief literature review. Eur J Pediatr 2007;166:679-83.
[9] Vaughan KG, Aziz A, Meza MP, et al. Mesenteric inflammatorypseudotumor as a cause of abdominal pain in teenager: presentationand literature review. Pediatr Surg Int 2005;21:497-9.
[10] Estevão-Costa J, Correia-Pinto J, Rodrigues FC, et al. Gastricinflammatory myofibroblastic proliferation in children. Pediatr SurgInt 1998;13:95-8.
[11] Soares-Oliveira M, Carvalho JL, Estevão-Costa J, et al. Inflammatorypseudotumor of the spleen in a child. Med Pediatr Oncol 2001;37:77-8.
[12] Ciftci AO, Akçoren Z, Tanyel FC, et al. Inflammatory pseudotumorcausing intestinal obstruction: diagnostic and therapeutic aspects.J Pediatr Surg 1998;33:1843-5.
[13] Coffin CM, Humphrey PA, Dehner LP. Extrapulmonary inflammatorymyofibroblastic tumor: a clinical and pathological survey. SeminDiagn Pathol 1998;15:85-101.
[14] Coffin CM, Watterson J, Priest J, et al. Extrapulmonary inflammatorymyofibroblastic tumor (inflammatory pseudotumor). A clinicopatho-logic and immunohistochemical study of 84 cases. Am J Surg Pathol1995;19:859-72.
[15] Fisher C. Soft tissue sarcomas with non-EWS translocations:molecular genetics features and pathologic and clinical correlations.Virchows Arch 2010;456:153-66.
[16] Gleason BC, Hornick JL. Inflammatory myofibroblastic tumours:where are we now? J Clin Pathol 2008;61:428-37.
[17] Huang CC, Lien HH, Chen DF, et al. Paediatric intra-abdominalinflammatory myofibroblastic tumour. Asian J Surg 2006;29:58-61.
[18] Mali VP, Tan HC, Loh D, et al. Inflammatory tumour of theretroperitoneum- a case report. AnnAcadMedSingapore 2005;34:632-5.
[19] Stringer MD, Ramani P, Yeung CK, et al. Abdominal inflammatorymyofibroblastic tumours in children. Br J Surg 1992;79:1357-60.
[20] Alfieri R, Alaggio R, Ruol A, et al. Hepatogastric inflammatorypseudotumor presumably deriving from prior amebic infection.Tumori 2008;94:584-8.
[21] Harik LR, Merino C, Coindre JM, et al. Pseudosarcomatousmyofibroblastic proliferations of the bladder: a clinicopathologicstudy of 42 cases. Am J Surg Pathol 2006;30:787-94.
[22] Sing Y, Ramdial PK. Cryptococcal inflammatory pseudotumors. Am JPathol 2007;31:1521-7.
[23] Yu JS, Park C, Kim JH, et al. Inflammatory myofibroblastic tumors inthe liver: MRI of two immunohistochemically-verified cases. J MagnReson Imaging 2007;26:418-21.
[24] Coffin CM, Dehner LP, Meis-Kindblom JM. Inflammatory myofibro-blastic tumors, inflammatory fibrosarcoma and related lesions. Anhistorical review with differential diagnostic considerations. SeminDiagn Pathol 1998;15:102-10.
[25] Karnak I, Senocak ME, Ciftci AO, et al. Inflammatory myofibroblastictumor in children: diagnosis and treatment. J Pediatr Surg 2001;36:908-12.
[26] Meis-Kindblom JM, Kjellstrom C, Kindblom IJ. Inflammatoryfibrosarcoma: update, reappraisal and perspective on its place in thespectrum of inflammatory myofibroblastic tumors. Semin DiagnPathol 1998;15:133-43.
[27] Meis JM, Enzinger FM. Inflammatory fibrosarcoma of the mesenteryand retroperitoneum. A tumor closely simulating inflammatorypseudotumor. Am J Surg Pathol 1991;15:1146-56.
[28] Coffin CM, Hornick JL, Fletcher CD. Inflammatory myofibroblastictumor: comparison of clinicopathologic, histologic, and immunohis-tochemical features including ALK expression in atypical andaggressive cases. Am J Surg Pathol 2007;31:509-20.
2082 A.C. Fragoso et al.
[29] Janik JS, Janik JP, Lovell MA, et al. Recurrent inflammatorypseudotumors in children. J Pediatr Surg 2003;38:1491-5.
[30] Hussong JW, BrownM, Perkins SL, et al. Comparison of DNA ploidy,histologic and immunohistochemical findings with clinical outcome ininflammatory myofibroblastic tumors. Mod Pathol 1999;12:279-86.
[31] Sebire NJ, Malone M, Ashworth M, et al. Diagnostic pediatric surgicalpathology. London: Churchill Livingstone Elsevier; 2010.
[32] Yamamoto H, Oda Y, Saito T, et al. p53 mutation and MDM2amplification in inflammatory myofibroblastic tumours. Histopathol-ogy 2003;42:431-9.
[33] Cessna MH, Zhou H, Sanger WG, et al. Expression of ALK1 and p80in inflammatory myofibroblastic tumor and its mesenchymal mimics: astudy of 135 cases. Mod Pathol 2002;15:931-8.
[34] Cook JR, Dehner LP, Collins MH, et al. Anaplastic lymphoma kinase(ALK) expression in the inflammatory myofibroblastic tumor: acomparative immunohistochemical study. Am J Surg Pathol 2001;25:1364-71.
[35] Ma Z, Hill DA, Collins MH, et al. Fusion of ALK to the Ran-bindingprotein 2 (RANBP2) gene in inflammatory myofibroblastic tumor.Genes Chromosomes Cancer 2003;37:98-105.
[36] Montgomery EA, Shuster DD, Burkart AL, et al. Inflammatorymyofibroblastic tumors of the urinary tract: a clinicopathologic studyof 46 cases, including a malignant example inflammatory fibrosarcomaand a subset associated with high-grade urothelial carcinoma. Am JSurg Pathol 2006;30:1502-12.
[37] Su LD, Atayde-Perez A, Sheldon S, et al. Inflammatory myofibro-blastic tumor: cytogenetic evidence supporting clonal origin. ModPathol 1998;11:364-8.
[38] Alaggio R, Cecchetto G, Bisogno G, et al. Inflammatory myofibro-blastic tumors in childhood. Cancer 2010;116:216-26.
[39] Coffin CM, Patel A, Perkins S, et al. ALK1 and p80 expression andchromosomal rearrangements involving 2p23 in inflammatory myofi-broblastic tumor. Mod Pathol 2001;14:569-76.
[40] Yamamoto H, Watanabe K, Nagata M, et al. Inflammatorymyofibroblastic tumor (IMT) of the pancreas. J Hepatobiliary PancreatSurg 2002;9:116-9.
[41] Applebaum H, Kieran MW, Cripe TP, et al. The rationale fornonsteroidal anti-inflammatory drug therapy for inflammatory tumors:a Children's Oncology Group study. J Pediatr Surg 2005;40:999-1003.
[42] Colakoglu O, Unsal B, Hasiyanli M, et al. A successfully managedinflammatory pseudotumor of liver without surgery: report of a case.Act Gastro Belg 2005;68:382-4.
[43] Czauderna P, Schaarschmidt K, Komasara L, et al. Abdominalinflammatory masses mimicking neoplasia in children—experience oftwo centers. Pediatr Surg Int 2005;21:346-50.
[44] Germanidis G, Xanthakis I, Tsitouridis I, et al. Regression ofinflammatory myofibroblastic tumor of the gastrointestinal tractunder infliximab treatment. Dig Dis Sci 2005;50:262-5.
[45] Jimenez JM, Poustchi-Amin M, Leonidas JC, et al. Extraperitonealabdominopelvic inflammatory pseudotumor: report of four cases.Pediatr Radiol 1997;27:170-4.
[46] Przkora R, Bolder U, Schwarz S, et al. Regression of nonresectableinflammatory myofibroblastic tumours after treatment with nonsteroi-dal anti-inflammatory drugs. Eur J Clin Invest 2004;34:320-1.
[47] Su W, Ko A, O'Connell TX, et al. Treatment of pseudotumors withnonsteroidal anti-inflammatory drugs. J Pediatr Surg 2000;35:1635-7.
[48] Williams ME, Longmaid HE, Trey G, et al. Renal failure resultingfrom infiltration by inflammatory myofibroblastic tumor responsive tocorticosteroid therapy. Am J Kidney Dis 1998;31:E5.
[49] Brage-Varela A, Estévez-Boullosa P, Pombo-Otero J, et al. Multifocalhepatic pseudotumor: spontaneous regression in a diabetic patient. RevEsp Enferm Dig 2010;102:507-9.
[50] Sanders BM, West KW, Gingalewski C, et al. Inflammatorypseudotumor of the alimentary tract: clinical and surgical experience.J Pediatr Surg 2001;36:169-73.