mri-guided abdominal intervention
TRANSCRIPT

Invited review
MRI-guided abdominal intervention
K. J. Mortele,1 K. Tuncali,1 V. Cantisani,1 S. Shankar,2 E. vanSonnenberg,1,2 C. Tempany,1 S. G. Silverman1
1Section of Abdominal Imaging and Intervention, Department of Radiology, Brigham and Women’s Hospital, 75 Francis Street, Boston, MA02115, USA2Department of Radiology, Dana Farber Cancer Institute, Harvard Medical School, 75 Francis Street, Boston, MA 02115, USA
During the past two decades, interventional radiology hasspawned a new subfield: image-guided therapy. With thisdevelopment, cross-sectional imaging methods such asultrasonography (US), computed tomography (CT), andmagnetic resonance imaging (MRI), formerly reservedexclusively for diagnostic purposes, are now used toguide treatments. At the same time, the introduction ofcross-sectional imaging into the operating room hasprompted the development of new, minimally invasive,surgical procedures. These image-guided therapies,whether performed by interventionists in interventionalsuites or surgeons in operating rooms, result in greaterprecision, less trauma, lower cost, and in some casesimproved efficacy, when compared with open surgery [1,2].
Since the late 1980s, MRI has been added to CT andUS as a cross-sectional imaging tool that can be used toguide the diagnosis and treatment of a variety of disor-ders. Due to its superior soft tissue contrast, multiplanar-ity, lack of ionizing radiation, and, most importantly,ability to image tissue function and temperatures, MRIhas been suggested as the ideal tool to guide minimallyinvasive therapies [1, 3]. However, when the concept ofinterventional MRI was first introduced, restricted patientaccess and slow imaging speed with conventional high-and mid-field MR systems limited its widespread use.Recent technical advances in open-configuration magnetdesign and the development of fast gradient-echo pulsesequences have contributed substantially to an increasinginterest in interventional MRI [1, 4]. As a consequence,minimally invasive diagnostic and therapeutic image-based interventions can now be performed in real timeunder MRI guidance. Many percutaneous interventionalMRI applications have been evaluated in the abdomen
and pelvis: MRI-guided aspiration and biopsy [5, 6],catheter drainage of fluid collections [1], laser ablation ofuterine fibroids [7] and liver tumors [4, 8], MRI-guidedcryotherapy [9–11], radiofrequency ablation (RFA), andfocused ultrasound surgery of abdominal tumors [12].MRI also has been used in animal experiments to guideintravascular procedures such as iliac artery stent [13] andportosystemic shunt placement [14].
We review the history and development of interven-tional MRI, open-configuration MRI systems, interven-tional tools used for MR-guided procedures, and the cur-rent clinical indications for using MRI to guideinterventions in the abdomen.
History and development of interventional MRI
History
When MRI was first postulated as a potential tool to guideinterventions, it was initially thought of solely as anadjunct to guide diagnostic procedures such as biopsy[15, 16]. When it was suggested that MRI could also beused to guide therapy, the field of interventional MRI wasborn [3]. MRI provides a wealth of image-based infor-mation about tissues and tissue function not availablewith other imaging techniques. Therefore, MRI is morethan just a targeting method; it allows monitoring andcontrolling of the changes being actively induced in thetissues during procedures.
Interventional MRI systems
Open systems
In the mid to late 1980s, open-configuration MRI systemswere developed primarily for the purpose of combatingCorrespondence to: K. J. Mortele
Abdom Imaging 28:756–774 (2003)DOI: 10.1007/s00261-003-0048-4 Abdominal
Imaging© Springer-Verlag New York Inc. 2003

claustrophobia and aiding the imaging of pediatric pa-tients. Forward-thinking interventional radiologists, how-ever, used these open MRI systems to gain access topatients to perform a variety of interventions [27]. As aconsequence, interventional MRI systems were devel-oped that provided guidance systems integrated withopen-configuration MRI systems, thereby allowing inter-vention and surgery to occur simultaneously with imaging[17, 18].
Open-configuration MRI scanners are now producedby most major MRI manufacturers. In general, access tothe patient may be via horizontally open (MagnetomOpen System, Siemens Medical Systems, Erlangen, Ger-many) [19–21] or vertically open (Signa SP, GeneralElectric Medical Systems, Milwaukee, WI, USA) systems[5]. Most of these systems are low or middle field inmagnet strength [19–21]. In general, open systems offerimproved patient access during the procedure as com-pared with closed systems. The gradient performance ofthese systems is good and typically ranges between 10and 15 mT/m, thereby providing sufficient image qualityfor targeting and most therapeutic interventions [22].
Closed systems
Interventional MRI-guided procedures also may be per-formed with conventional MRI systems [8]. Closed sys-tems, operating at higher field strengths, provide betterimage quality by means of a higher signal-to-noise ratio.However, patient access is limited, and instrument ma-nipulations are performed when the patient is outside themagnet or, when using a system with a flared opening,with the operator leaning in. Although interventions arefeasible with closed MRI systems, they can be cumber-some because the patient needs to be moved out of themagnet bore to manipulate the instruments, so the proce-dure is only intermittently imaged. As a consequence,targeting may be difficult because most upper abdominalstructures move with respiration. However, some lesionsmay be visualized only with a conventional closed MRIsystem and not with an interventional MRI system oflower field strength. MRI-guided procedures in closedand open systems may not be possible in large patientsbecause the space within the magnet bore typically isrestricted.
Interventional MRI suites
An MR-compatible environment is needed to support aninterventional MRI scanner [2]. Important principles ofinstalling an interventional MRI scanner relate to issuesof siting, patient care, and MR-compatible instrumenta-tion. Siting an interventional MRI scanner must take intoaccount issues related to siting a scanner; these include
magnetic shielding, RF shielding, floor loading, vibration,acoustic damping, and cryogen venting and storage. Fac-tors related to siting the scanner in an interventional suiteor operating room also need to be considered. Theseinclude control of air quality and flow, humidity, temper-ature, zoned lighting, the inclusion of scrub sinks, re-stricted and semi-restricted areas, ports for suction, gases,and therapy devices.
Issues related to patient care include the ability for alloperators and assistants to have access to the patient forthe purpose of performing the procedure, real-time ob-serving and monitoring of the patient, and administeringdrugs and/or anesthesia. Emergency therapy must be ableto be performed. Emergency treatment can be performedinside the procedure room with MR-compatible devices,such as airways and intravenous tubing. Cardiac defibril-lators are not MR compatible. Therefore, to treat ventric-ular fibrillation, the magnet needs to be quenched or thepatient must be brought out of the room.
Another important point is that silent myocardial isch-emia cannot be detected in an MR environment [23, 24].Therefore, before undergoing interventional MRI proce-dures, all patients need to be screened for coronary arterydisease and a risk–benefit assessment should be made todetermine whether the procedure should be performedunder MRI guidance. MRI-guided procedures should beperformed only in patients for whom the benefit of per-forming the procedure under MRI guidance is greaterthan the risk of not detecting silent myocardial ischemia.Just as patients need to be screened before undergoing anMRI examination, physicians need to be screened in thesame fashion. The interventional MRI procedure roomneeds to be surrounded by a checkpoint at the 5 gaussline, which is typically, depending on the field system andparameters of the MRI system, 1 m outside the procedureroom.
MRI-compatible instruments
All instruments used in the interventional MR procedureroom must be MR compatible. A device is MR compat-ible if it can be used safely in the scanner room during theprocedure and without adversely affecting the deviceitself or the procedure for which it is being used [2]. MRcompatibility includes issues related to ferromagnetism,electric interference, image distortion, and device heatingfrom RF energy (Table 1). Interventional and surgicalinstruments may cause artifacts leading to image distor-tion. The size of the artifacts depends mainly on thefollowing factors: the size of the instrument, the orienta-tion of the instrument to the main magnetic field, theimaging sequence used, and the orientation of the fre-quency encoding gradient [25]. The amount of artifact inan MR image increases with instrument size and increas-
K. J. Mortele et al.: MRI-guided abdominal intervention 757

ing angle of the instrument to the main magnetic field BO
[1].Once a major obstacle, MR-compatible instrumenta-
tion has been developed to the point that a variety ofprocedures can be performed. An array of basic interven-tional and surgical instruments including needles, scis-sors, elevators, forceps, and blades have been manufac-tured for use during interventions and surgery of theabdomen. MR-compatible monitors and anesthesia deliv-ery systems are used to safely monitor patients [26].Therapy delivery systems such as electrocautery, laser,RF, and cryotherapy, discussed in further detail below,are also available for use during MRI-guided interventions.
MRI-guided abdominopelvic biopsy
All MRI-guided interventions depend on the ability of theinterventional radiologist to position a needle probe underMRI guidance into a relatively small target within thebody. Because nearly all MRI-guided therapies requireneedle or probe placement, research and development ofMRI-guided biopsy techniques have been an importantand fundamental aspect of the beginning of interventionalMRI.
Mueller et al. first described the use of an MR-com-patible needle and showed that, after US-guided place-ment, the liver lesion and the needle could be viewed witha conventional MRI system [15]. Silverman et al. reportedthe first MRI-guided biopsy in which the entire procedurewas performed under MRI guidance [5]. This techniqueused a 0.5-T vertically open-configuration MRI systemspecifically designed to guide radiologic intervention andsurgery (Signa SP, GE Medical Systems). In addition tobeing open, the system contained two important features:(a) images were displayed to the operator inside the roomon two MR-compatible monitors mounted above the field,which allowed ongoing review of images during proce-dures, and (b) the system contained an integrated opticallocalizer and tracker, which allowed interactive control ofthe biopsy needle. Subsequently, Frahm et al. [19] and Luet al. [27] reported MRI-guided biopsy with a 0.2-Thorizontally open-configuration MRI system in whichfreehand techniques using fast gradient echo sequenceswere employed. More recently, fast gradient-echo se-quences were used successfully to guide liver biopsies inclosed magnet systems [21, 28].
There are many ways in which an interventional de-vice can be tracked during a procedure. Most biopsiesreported to date and the ones shown in this review are
Table 1. Overview of MR compatibility
Factor Effect Example Solution
Ferromagneticattraction
Object moves/rotatesto align withmagnet; mayendanger occupants
Most conventionalsurgical instruments
Change instrumentmaterials
Electricalinterference
Device on MRscanner
Low signal-to-noiseratio, stripes,zippers, bright spots
Almost anythingwith electrical plug,ferromagnetic, andan interferencehazard
Provide RF shielding ofdevice; remove theelectronics to remotelocation
MR scanneron device
Magnetic field/RFinterferes withdevice with oftensubtle effects
Computer discs,video displays
Provide remoteelectronics; use liquidcrystal displays
Image distortionby devices
Image artifacts,spatial distortions
Signal void aroundneedle
Move devices out ofimage field of view;match materials totissue susceptibility;break up eddy currentpaths
Device heatingfrom RF energy(in or out ofpatient)
Patient burns fromRF inductive heatingof device and fromcontact with patient
Pulse oximeterwire, ECG wire
Use nonconductivemaerials (e.g.,fiberoptics); keepantennae length to aminimun; inspect forpatient/devicegrounding paths
ECG, electrocardiogram; MR, magnetic resonance; RF, radiofrequency
758 K. J. Mortele et al.: MRI-guided abdominal intervention

performed with passive tracking in which imaging is usedto follow the needle. In passive tracking, the biopsyneedle is visualized by the signal void created by theneedle’s susceptibility artifact. The needle can be seen aslong as the imaging plane includes it. The frequency withwhich the needle is seen is determined by how fast theimages are acquired and reconstructed and shown to theoperator during the procedure [29, 30]. The Signa SP, byusing an optical tracking system, automatically imagesthe device (in this case, a needle) because it is attached toa probe’s position that is sensed by the optical tracker. Asthe probe is moved, its position is sensed, and the scanplane is changed. Other methods of localization includeactive tip tracking, mechanical sensors, and RF localizers[31, 32]. Active tip tracking of needles is achieved byembedding a miniature RF coil in the tip of needle. Thisallows active intraprocedural identification of the spatialposition of the tip. The most important advantages ofactive tracking over passive tracking are the high tempo-ral resolution and the option to use three-dimensionalcoordinates to steer the scan plane [33–36].
In clinical practice, MRI is rarely needed to biopsyabdominal lesions because US and CT are efficient andaccurate guidance modalities. However, MRI-guided bi-opsy may be indicated in patients with lesions that are notvisualized by US and CT or that are visible by CT andMRI but not with US and require angling the needle, suchas a liver lesion beneath the hepatic dome or an adrenalgland mass (Fig. 1). In such cases, using CT guidance, ifthe pleural space and lung are avoided, lesions in theupper abdomen can be reached only by angling the gantryor angling the needle with the triangulation method. Thetriangulation method is limited by the fact that it does notallow direct visualization of the entire needle track in oneimage [27]. US also is problematic because the path of theneedle track may be obscured by bony structures such asthe ribs and by air from interposed bowel loops [27].
In the pelvis, MRI may be helpful in biopsying theprostate gland. Although transrectal ultrasound (TRUS) isused in the vast majority of cases, MRI may be used toguide a biopsy in two groups of patients: (a) men in whomthe serum prostate-specific antigen (PSA) is elevated andrising despite at least one negative TRUS biopsy and thelesion is visualized only with MRI; and (b) men who havehad rectal surgery such as abdomino-perineal resection(APR) and in whom rectal access is not possible. The firstgroup is quite numerous and includes very anxious menwho are facing rising PSA levels and no diagnosis. TheMR-guided biopsy may be done in one or two ways: in aclosed bore system using a transgluteal approach or in theopen horizontal system using a transperineal approach. Inthe latter situation, 1.5-T MR images can be integratedinto the 0.5-T open system to allow targeted biopsiesunder real-time MR guidance. To perform this integra-tion, we use the 3D Slicer, a surgical simulation software,
that allows three-dimensional display of different datasets.
As newer MR techniques are introduced to improvespecificity of MRI, such as spectroscopy, T2 maps, linescan diffusion images, and intravenous gadolinium stud-ies, the ability of MRI to define suspicious targets willincrease and MR-guided biopsies will become more nec-essary.
MRI-guided drainage of fluid collections
A natural extension of MRI-guided biopsy is the use ofMRI guidance to aspirate and drain fluid collections.Although CT and US can be used to guide drainage ofmost abdominal fluid collections, a preliminary report ofMR-guided drainage of fluid collections in a small num-ber of patients demonstrated its feasibility [37]. MRI-guided percutaneous cholecystostomy and nephrostomyalso have been reported (Fig. 2) [30, 31]. These proce-dures require the use of MR-compatible drainage cathe-ters that are placed with the trocar or Seldinger technique.The trocar technique requires MR-compatible stylettesand cannulas. The Seldinger technique requires the use ofMR-compatible guidewires and cannulas. Several MR-compatible nitinol-based guidewires are commerciallyavailable [32]. To perform drainage procedures underMRI-guidance, small catheters need to be visible duringthe procedure. VanSonnenberg et al. used an MR-visiblewire sheath system to localize the puncture site and guidethe drainage in a closed MR system [38].
At this early stage of development, it is not possible topredict the impact of MRI on the guidance of aspirationand drainage procedures. MRI-guided catheter drainagesmay be helpful in pregnant patients or in patients with ahistory of allergy to iodinated contrast agents and inwhom intravenous contrast medium administration isconsidered necessary before drainage. MRI guidance mayalso be useful to drain subdiaphragmatic fluid collectionsbecause a direct approach to them risks contaminating thepleural space. Moreover, an extrapleural access route isoften long, requires caudocranial angulation, and is oftendifficult when using CT or US [1].
MRI-guided vascular interventions
MRI-guided vascular interventions, such as percutaneousdilatation of arterial stenosis, stent and vena cava filterplacement, transjugular intrahepatic portosystemic shunt,and various forms of aneurysm treatment, are beginningto be developed [39, 40]. Catheters and devices can bevisualized actively or passively. Simultaneous active“real-time” tip-tracking MRI is possible, although thereare drawbacks that must be overcome to make this clin-ically feasible. One problem is the increase in the size of
K. J. Mortele et al.: MRI-guided abdominal intervention 759
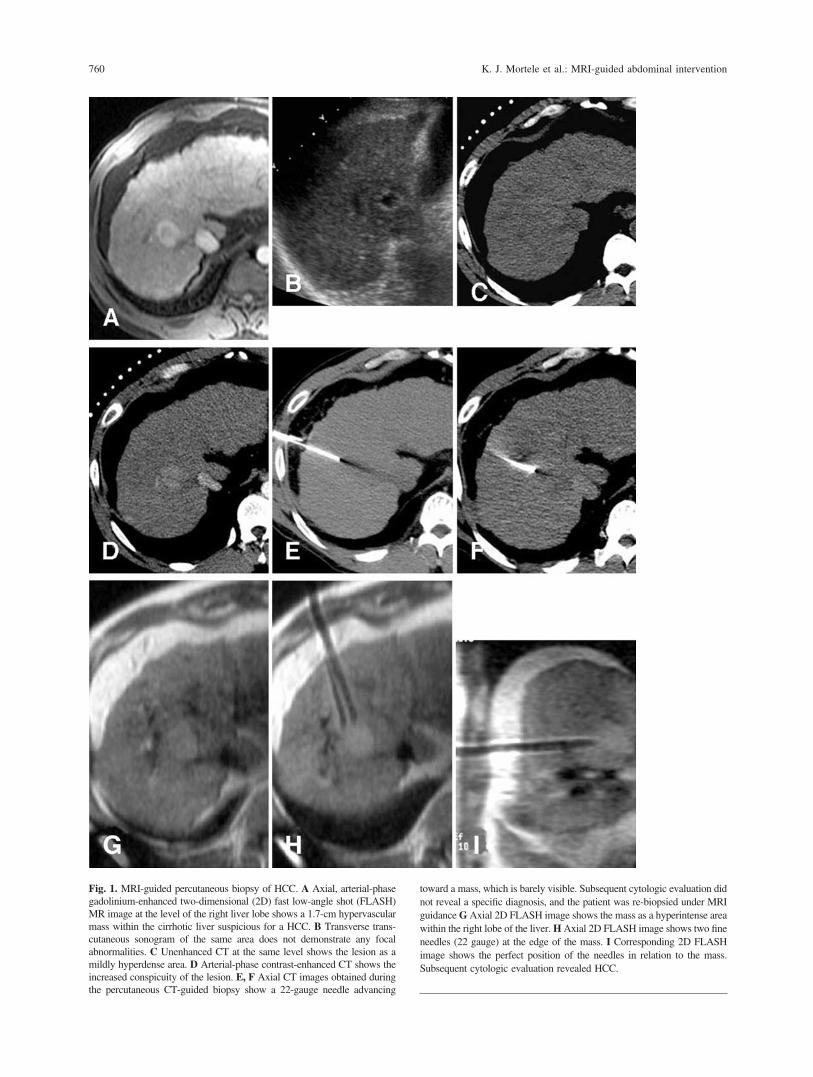
Fig. 1. MRI-guided percutaneous biopsy of HCC. A Axial, arterial-phasegadolinium-enhanced two-dimensional (2D) fast low-angle shot (FLASH)MR image at the level of the right liver lobe shows a 1.7-cm hypervascularmass within the cirrhotic liver suspicious for a HCC. B Transverse trans-cutaneous sonogram of the same area does not demonstrate any focalabnormalities. C Unenhanced CT at the same level shows the lesion as amildly hyperdense area. D Arterial-phase contrast-enhanced CT shows theincreased conspicuity of the lesion. E, F Axial CT images obtained duringthe percutaneous CT-guided biopsy show a 22-gauge needle advancing
toward a mass, which is barely visible. Subsequent cytologic evaluation didnot reveal a specific diagnosis, and the patient was re-biopsied under MRIguidance G Axial 2D FLASH image shows the mass as a hyperintense areawithin the right lobe of the liver. H Axial 2D FLASH image shows two fineneedles (22 gauge) at the edge of the mass. I Corresponding 2D FLASHimage shows the perfect position of the needles in relation to the mass.Subsequent cytologic evaluation revealed HCC.
760 K. J. Mortele et al.: MRI-guided abdominal intervention

the catheter, because this requires a microcoil to be placedwithin the catheter tip that can be accomplished only ifthe catheter is of sufficient diameter. Another disadvan-tage of the active tip-tracking technique is that the guide-wire in the MR environment can act potentially as anantenna and cause considerable heating of adjacent tis-sues [41]. This is also true for the applied connectionsbetween the system and the microcoil. Thus far, materialsto overcome this limitation have not been sufficientlyminiaturized to be incorporated into a small catheter [42].However, recent developments using optical fibers as analternative for conducting leads have shown promisingresults [43]. Passive visualization depicts the device di-rectly in the MR image. Because the image quality of fastimaging sequences is not sufficient to allow the visual-ization of small plastic catheters, local markers may beused along the instrument [35].
MRI-guided abdominal and pelvic tumor ablation
MRI is one of the cross-sectional imaging techniques thatcan be used to guide a variety of minimally invasivetherapies. One of these minimally invasive therapies isthe use of thermal-based energies to ablate tumors non-surgically. Concomitant with the development of open-configuration MRI systems and interventional MRI, therehas been worldwide interest in the use of imaging to guidepercutaneous ablation of abdominal tumors by using vas-cular and direct percutaneous approaches [44]. Improvingfocal therapy methods for hepatocellular carcinoma(HCC) and metastatic colorectal cancer to the liver hasbeen the major driving force in developing image-guidedpercutaneous tumor ablation of liver tumors. In 1986,surgical resection was considered the only potentiallycurative treatment for HCC. However, only 20% of pa-tients with HCC are eligible for subtotal hepatectomy(reserved for patients with Child-Pugh’s classes A and Band with disease limited to one lobe) or orthotopic livertransplantation (reserved for patients with unifocal orlimited multifocal disease who are not good candidatesfor partial resection) [45, 46]. Similarly, in patients withcolorectal cancer, it is estimated that at least 50% ofpatients will die of metastatic disease, and, for many,progressive involvement of the liver is the major deter-minant of survival [45, 46]. Surgical resection, the onlypotentially curative option for liver metastases from coloncancer, is possible in only 5% to 10% of patients. Ofthose, only a minority of patients actually have surgery.Nevertheless, the 5-year survival rate improves from vir-tually 0% without surgery to 23% to 49% with surgery.Although surgery is the only known cure for hepaticmetastases, morbidity rates from surgery have been re-ported to range from 15% to 43%. Therefore, the rationalefor percutaneous tumor ablation research is to develop aless invasive, repeatable, and effective method that willallow more patients, including nonsurgical candidates, tobe treated.
Many ablative agents have been investigated [47]. Ingeneral, these agents result in tumor cell death whenusing thermal-based energy (e.g., heat or cold) or chem-ical agents such as ethanol. Thermal agents include lasers,RF, microwaves, all of which heat tissue, and cryotherapythat freezes tissue [45, 47]. Increasing interest in intersti-tial therapies as part of cancer treatment has intensifiedinterest in noninvasive methods of monitoring tempera-ture distributions in vivo because the biological efficacyof thermal-ablation techniques is strongly dependent onachieving desired temperatures in all parts of the tumor[48]. MRI is the ideal imaging technique to guide thermalablations because of its ability to guide probe placementand monitor thermal changes in tissue [3]. Through MRmonitoring, thermal lesion size and configuration can bedirectly controlled by the interventionist and adjustedduring the procedure. Temperature-sensitive MRI se-
Fig. 2. MRI-guided percutaneous nephrostomy tube placement. Intra-procedural gradient-echo T1-weighted MR image shows a nephrostomytube within the left kidney.
K. J. Mortele et al.: MRI-guided abdominal intervention 761
quences have been developed to enable accurate onlinemonitoring of heat deposition [8, 49, 50] (Fig. 3). Three-dimensional mapping of temperature changes with MRImay be based on the relaxation time, T1, the diffusioncoefficient (D), or proton resonance frequency (PRF) oftissue water. Temperature-sensitive contrast agents alsomay be used [51, 52]. Among these methods of MRItemperature mapping, the PRF-based method has beenconsidered the preferred choice for many applications atmiddle and high fields (�1 Tesla) because of its sensi-tivity and linear relation with temperature and near inde-pendence with respect to tissue type. PRF methods useRF-spoiled gradient-echo imaging methods to measurethe phase change in resonance resulting from the temper-
ature-dependent change in resonance frequency. Whenfield homogeneity is poor due to small ferromagneticparts in the needle or at low field strengths (�0.5 T),diffusion and T1-based methods may provide better re-sults. Temperature-sensitive contrast agents may be par-ticularly suitable when absolute thermoregulation is de-sired, e.g., when a precise indication exists for passing acertain temperature threshold [52].
Ethanol ablation
Ethanol was one of the first ablative agents used percu-taneously. It is relatively easy, inexpensive, and effective
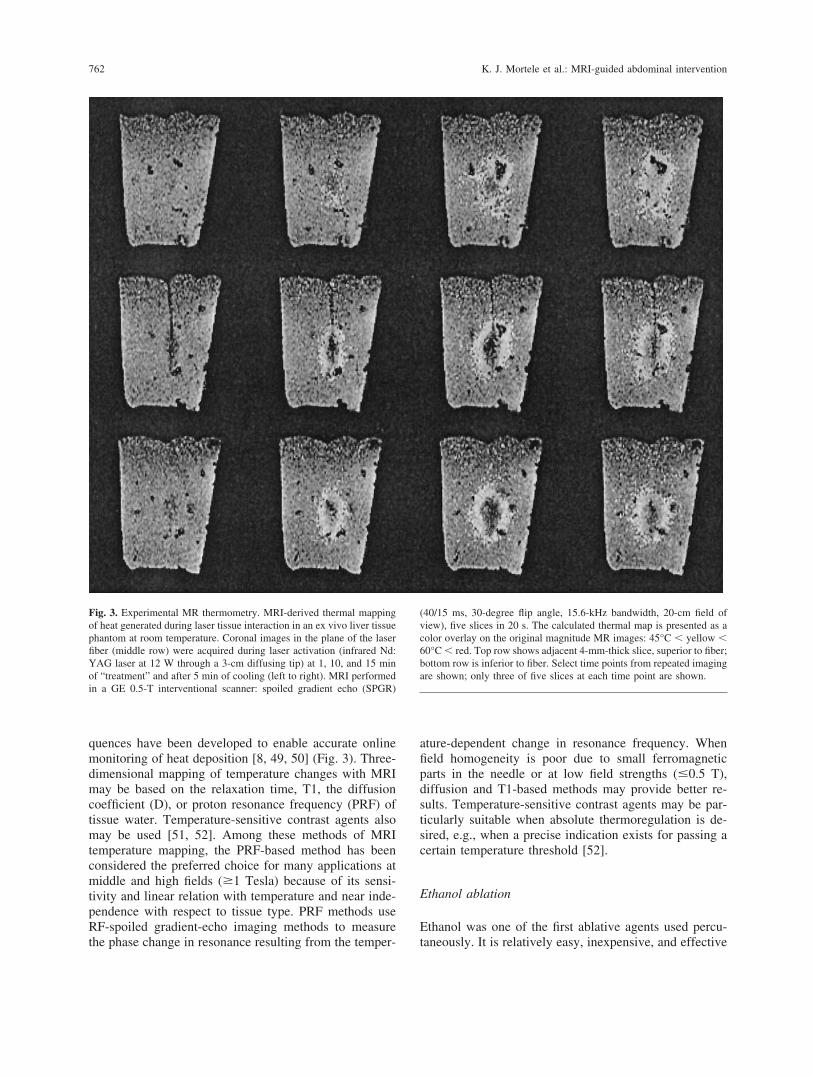
Fig. 3. Experimental MR thermometry. MRI-derived thermal mappingof heat generated during laser tissue interaction in an ex vivo liver tissuephantom at room temperature. Coronal images in the plane of the laserfiber (middle row) were acquired during laser activation (infrared Nd:YAG laser at 12 W through a 3-cm diffusing tip) at 1, 10, and 15 minof “treatment” and after 5 min of cooling (left to right). MRI performedin a GE 0.5-T interventional scanner: spoiled gradient echo (SPGR)
(40/15 ms, 30-degree flip angle, 15.6-kHz bandwidth, 20-cm field ofview), five slices in 20 s. The calculated thermal map is presented as acolor overlay on the original magnitude MR images: 45°C � yellow �60°C � red. Top row shows adjacent 4-mm-thick slice, superior to fiber;bottom row is inferior to fiber. Select time points from repeated imagingare shown; only three of five slices at each time point are shown.
762 K. J. Mortele et al.: MRI-guided abdominal intervention

in ablating tissues. Percutaneous injection of absoluteethanol is an established form of therapy for treatment ofsmall HCC in many parts of the world [53, 54]. Alcoholcauses tissue necrosis predominantly by cellular dehydra-tion and vascular thrombosis. Two characteristics of HCCmake it amenable to alcohol injection therapy [53, 54]: (a)it is a well-vascularized, soft tumor so that ethanol easilydiffuses within it; and (b) it is frequently encapsulated,which prevents ethanol from escaping. Metastatic tumorstypically are not soft or encapsulated; therefore, alcohol isnot as useful in the treatment of metastatic liver disease.
US and CT have been used successfully in the depo-sition of alcohol and, as such, MRI has not been usedwidely. MRI may be helpful in the guidance of percuta-neous injection of alcohol into lesions that are not viewedby US or CT. In addition, MRI monitoring of ethanoldiffusion may be useful. Lu et al. reported on the use ofMRI in the treatment of hepatic lesions in anesthetizedpigs [20]. Their study showed that ethanol appears hy-pointense on T2-weighted images. They postulated that, ifethanol were injected into HCC under MRI guidance, itcould be easily distinguished from T2 hyperintense tumorduring treatment. Shinmoto et al. showed that a water-suppressed T2 weighted rapid acquisition with relaxationenhancement sequence could be used to differentiate al-cohol from long T2 water components of tumor andedema [54]. The future of MRI-guided alcohol ablation isuncertain and likely will be dictated by the relative ben-efits of alcohol as an ablative agent in the treatment ofliver tumors.
Laser ablation
Bown in 1983 described interstitial hyperthermia via lasertechnology with the insertion of a light-conducting quartzfiber into a tumor [55]. In 1989, Steger et al. describedinterstitial laser photocoagulation for metastatic liver le-sions in two patients [56]. Since then, lasers have beenused to deliver localized, controlled heat deposition tomultiple organs. Laser energy can be delivered by usingdifferent materials such as a neodymium yttrium alumi-num garnet (Nd:YAG), carbon dioxide, and argon viasmall fiber optics that are small enough to be insertedcoaxially through an 18-gauge needle [57]. Laser light isconverted into heat in the target area, resulting in coag-ulative necrosis, secondary degeneration and atrophy, andtumor shrinkage with minimal damage to surroundingstructures [57].
Early clinical trials using US and CT guidance wereencouraging, with up to 82% of treated lesions achievinggreater than 50% tumor necrosis [58–61]. However, the“zone of kill” achieved with a single fiberoptic was lim-ited, requiring multiple fibers and multiple sessions totreat most liver tumors [62] (Fig. 4). Diffusing tip fibers,
loaded into small catheters, produce larger kill zones. Todate, the largest experience with MRI-guided laser abla-tion of the tumors has been reported by Vogl et al. [4] Byusing an Nd-YAG laser, 932 liver tumors were treated in335 patients. CT was used to guide the placement of thecatheters. Then patients were moved to a closed MRIsystem to observe the thermal changes during laser dep-osition. Local tumor control rate was 71% in the first 100patients, 79% in the following 75 patients, and 97% at 6months in the remaining patients who were treated with acooled power laser-ablation system. The study demon-strated the feasibility and utility of monitoring tissuedestruction with MRI. It also showed that CT could beused to place laser fibers and MRI to monitor the treat-ment.
Law et al. [7] reported their experience with MRI-guided laser ablations of symptomatic uterine fibroids in30 outpatients. The procedure was well tolerated by allbut one patient. That patient experienced abdominal dis-comfort and the procedure was terminated after 12 min.At 6 months, all patients were asymptomatic; none re-quired further medical or surgical treatments for the fi-broids. Three months after laser ablation, the treatedfibroid volume had decreased by a mean of 37.5% (range,25–49%).
Fig. 4. MRI-guided laser ablation. MRI shows the acute irreversibleeffects of the thermal ablation. T1-weighted FSE (300/18 ms, 8-cm fieldof view, 1.5 T) of in vivo interstitial Nd:YAG laser coagulation at 3 Wfor 2.5 min from a 0.6-mm bare fiber in normal rabbit liver. The thermallesion appears on the right as a target-like ellipse. The T1 bright rim isa region of red blood cell breakdown and hepatocellular coagulation; thecentral region is more severely denatured and desiccated.
K. J. Mortele et al.: MRI-guided abdominal intervention 763

Cryotherapy
Cryotherapy is defined as therapeutic tissue destruction insitu by freezing. Once administered predominantlythrough “open” surgical means, it was known mostly by
the term cryosurgery. Now, cryotherapy can be per-formed percutaneously, without the use of surgical tech-niques, so the term cryotherapy is more appropriate.Cryoablation and cryodestruction refer to processes thatoccur during cryotherapy. Cryotherapy is one of the old-
Fig. 5. MRI-guided cryoablation of liver metastasis. A Axial SPGRT1-weighted MR image at the level of segment 7 shows a 2-cmhypointense mass within the liver in this patient with renal cell carci-noma. B Axial FSE T2-weighted MR image shows hyperintense ap-pearance of the mass. C Axial, arterial phase gadolinium-enhancedfat-suppressed T1-weighted MR image shows rim enhancement of thelesion suspicious for metastasis. D, E Intraprocedural axial and coronalSPGR images show one cryoprobe within the lesion. F, G Axial FSET2-weighted MR images obtained during cryotherapy with five cryo-
probes show enlargement of the ice ball. H Axial SPGR T1-weightedMR image obtained 12 h after ablation shows a 5-cm hypointense masswithin the liver covering the lesion. I Axial FSE T2-weighted MR imageshows hyperintense appearance of the ablated area. Note the ablatedmetastasis within the ablation area. J Axial, arterial phase gadolinium-enhanced fat-suppressed T1-weighted MR image shows rim enhance-ment of the ablated metastasis and the ablation area. Note a surgicalmargin of at least 1 cm surrounding the ablated metastasis. (Continuedon page 765.)
764 K. J. Mortele et al.: MRI-guided abdominal intervention

est methods of tissue destruction known to mankind. Itwas used even during the times of Hippocrates to controlhemorrhage. It was initially used as an anesthetic in 1845to treat cancer, when a solution of ice and brine was usedto treat melanoma. In this century, cryotherapy has beenused for a variety of cancer treatments in the brain, headand neck, breast, and, more recently, the liver and prostategland. Cryotherapy destroys tissue mainly by cellulardehydration, cell membrane rupture, and vascular stasis.Cell death occurs typically at �30°C to �40°C and isdependent on several factors including tissue type, rate,duration, depth of freezing, and thawing. Cryotherapy is a“time-tested,” effective ablation technique. It is not doselimited, blood loss is minimal, and, perhaps more impor-
tantly, it is amenable to imaging. Tissue effects can beseen with US, CT, and MRI. Further, lesions produced bycryotherapy are sharply marginated and depict the zone oftissue necrosis accurately.
In the abdomen and pelvis, the liver and prostategland have been the most common sites in which cryo-therapy has been used. In the liver, it has been used inpatients with HCC or metastases who are unable to un-dergo hepatic resection [45, 62]. In the operating room,US is used for lesion detection, guidance of cryosurgicalprobe placement, and monitoring of the freezing process[63]. US depicts the effects of freezing in real time andaccurately demonstrates the zone of necrosis that is sub-sequently produced [64]. However, US is limited by its
Fig. 5. Continued.
K. J. Mortele et al.: MRI-guided abdominal intervention 765

Fig. 6. MRI-guided cryoablation of renal cell carcinoma (RCC). AAxial FSE T2-weighted MR image shows hyperintense appearance ofthe renal mass in the interpolar region of the right kidney. B Axial,arterial phase gadolinium-enhanced fat-suppressed T1-weightedFAME MR image shows strong and homogeneous enhancement ofthe lesion suspicious for RCC. C, D Intraprocedural oblique sagittalSPGR images show three cryoprobes within the lesion andenlargement of the ice ball. E Axial SPGR T1-weighted MR imageobtained 12 h after ablation shows a 5-cm triangular hypointense areawithin the kidney covering the lesion. Note an ablation margin of atleast 1 cm surrounding the ablated metastasis.
766 K. J. Mortele et al.: MRI-guided abdominal intervention

inability to image beyond the proximal edge of the iceball because the energy is reflected at this front edge. Asa result, the tumor may not be completely visualizedduring the treatment and may be incompletely treated.The relatively small surgical incisions used during mini-mally invasive liver surgery also may limit the ability toimage lesions completely with US [65]. Although livercryosurgery with intraoperative US guidance has beenused in many centers for over a decade, the overallsurvival in patients with metastatic colorectal carcinomahas not been significantly different from that achievedusing conventional surgical techniques [66]. Neverthe-less, cryotherapy is used because more normal liver canbe preserved than with surgical resection.
Although cryotherapy has been recognized as a usefulablative agent in the treatment of malignant liver lesions,it was considered a “surgical only” option because of thenecessity for large probes. Recently, there has been thedevelopment of cryoneedles (as small as 18-gauge nee-dles) that can be placed percutaneously. MRI-guidedcryotherapy holds significant promise for several reasons.First, the short T2 relaxation time of ice results in excel-lent depiction of the ice ball or cryolesion, which, withT1- or T2-weighted sequences, is represented as a signalvoid [67, 68] (Fig. 5). Second, by using a variety of pulsesequences, excellent contrast between the ice ball and the
tumor can be achieved in a multiplanar or a three-dimen-sional format. This results in the accurate depiction of theentire ice ball and its relation in all dimensions to thetreated tumor [67, 68].
The concept of percutaneous MRI-guided cryotherapywas introduced in vitro and in vivo [3]. Tacke et al. [10]recently reported on the use of a novel MRI-compatibleprobe in animals with a 1.5-T magnet in the rabbit liver.As with US, the size of the ice ball or cryolesion visual-ized with MRI correlated closely with necrosis. Silver-man et al. described a new method for cryoablating tu-mors percutaneously under MRI guidance [11]. By usingan optical tracking system, cryoneedles were placed, andliver tumors were ablated during two freeze cycles. Byusing repetitive multiplanar T1-weighted fast spin echo(FSE) or T1-weighted spin echo images, MRI was used tomonitor progress of the treatment, whether the lesion wasadequately covered, and to be sure vital structures wereavoided. Consistent with the results of animal studies,intraprocedural depiction of ice balls correlated well withpostprocedural estimates of necrosis [10].
Cryotherapy of renal tumors has been performed suc-cessfully with open, laparoscopic, and percutaneous ap-proaches [69]. Indications for minimally invasive therapyof renal tumors are solitary kidneys, multiple tumors, or
Fig. 7. MRI of irreversible effects in tissue due to RFA (12 min, 130 W,�98°C). T1-weighted FSE (400/18 ms, 16-cm field of view, 0.5 T)image shows target-like appearance of the thermal lesion. The T1 brightrim is a region of red blood cell breakdown and hepatocellular coagu-
lation; the central region is more severely denatured and desiccated.T2-weighted FSE (3000/88 ms, 16-cm field of view, 0.5 T) shows abright rim emphasizing edema and hyperemia surrounding the lesion.
K. J. Mortele et al.: MRI-guided abdominal intervention 767

renal insufficiency, when it is necessary to achieve com-plete tumor ablation with sparing of as much normalparenchyma as possible (Fig. 6). In addition, only 2- to3.5-mm incisions are required for probe placement, re-sulting in morbidity reduction.
The rationale for MRI-guided cryotherapy is summa-rized as follows: (a) freezing is an effective ablativetechnique and can be monitored well with MRI; (b) MRI,like US, is near real time and multiplanar; (c) unlike US,it can depict the entire ice ball and surrounding structures,
Fig. 8. MRI-guided focused US. A Coronal T2-weighted MR image atthe level of the uterus shows a 7.1- � 7.3-cm heterogeneous hypointensemass consistent with a fibroid. B Axial, delayed phase gadolinium-enhanced fat-suppressed T1-weighted SGR MR image shows homoge-neous enhancement of the lesion. C Intraprocedural axial SPGR imageshows the external US generator (arrow) with the patient lying on top ofit. Note the absence of any interfering vital structures between thefibroid and the external US generator. D Gadolinium-enhanced coronal
fat-saturated SPGR T1-weighted MR image obtained after the procedureshows a 3- � 3.8-cm hypovascular area within the fibroid. E CoronalFSE T2-weighted MR image obtained 3 months after the procedureshows hyperintense appearance of the ablated area. F Gadolinium-enhanced axial fat-saturated SPGR T1-weighted MR image obtained atthe same time point shows persistence of the hypovascular area withinthe fibroid. (Continued on page 769.)
768 K. J. Mortele et al.: MRI-guided abdominal intervention

and the ice ball can be discriminated from tumor duringthe procedure; and (d) unlike heating, the margins ofnecrosis after cryoablation are sharp and unambiguous,and the MR assessments correlate well with necrosis.Visualizing ablative changes intraprocedurally obviates24-h follow-up MRI or CT. MRI is the only imagingmethod that monitors thermal ablations. Although tumorablation with ethanol injection, RF, and interstitial lasertherapy also can be performed with imaging guidance, theamount of tissue change demonstrated at US and CTduring these therapies is limited and variable and does notaccurately reflect the zone of necrosis [70].
Radiofrequency ablation
Percutaneous RF electrocautery is a thermal ablationtechnique that causes local tissue destruction by inducingionic agitation. This results in heat deposition within thetissue secondary to the increased resistivity of the inter-vening tissue to the passage of rapidly alternating current(400–500 kHz). Nearly immediate coagulation necrosis isinduced at temperatures between 60°C and 100°C. Athigher temperatures, tissue vaporizes and carbonizes.Thus, an essential objective of RFA is to achieve andmaintain temperatures between 50°C and 100°C through-out the entire target volume for at least 4 to 6 min [71].
Used neurosurgically for over three decades, Rossi etal. reported its first use in the liver after treating 13patients with small HCC with US-guided percutaneousRFA [72]. Subsequently, Livraghi et al. reported its use in
metastatic liver disease [73]. At least one 18- to 21-gaugeRF probe is placed under image guidance into the lesion.Complete ablation of lesions, measuring 2 to 4 cm, hasbeen achieved [74]. New RF probe designs are nowavailable, which include multipronged arrays, internallycooled electrodes, clustered electrodes, and saline-cooledelectrodes. These advances increase the lesion diameterthat can be treated [47].
Because of the interference of RFA with MRI, mul-tiple strategies have been attempted to allow MRI tomonitor RFAs in real time. Lewin et al. reported on thefirst human clinical series of MRI-guided RFA of abdom-inal masses [12, 25]. Although RF needle electrodes wereplaced under MR guidance, MRI was performed and thegenerator was turned off during imaging, and ablatedregions were re-imaged after each session. By using anopen-configuration MRI system (Magnetom Open, Sie-mens Medical Systems), a 50- to 200-W RF generator(Radionics, Inc. Burlington, MA, USA), and a prototypeMRI-compatible 17- � 2-mm shielded electrode with a 1-to 3-cm exposed tip, 11 tumors were treated in sevenpatients with a total of 13 ablations. There was no signif-icant morbidity. Four patients showed stable or decreas-ing tumor on average follow-up of 152 days. Short tauinversion recovery T2-weighted sequences were used be-tween sessions for monitoring tissue ablation with RF.This study showed that MRI-guided RFA of abdominalmasses was feasible (Fig. 7).
By using a standard RF electrode, thermal ablationcan be performed with electrode tip temperatures of 85°C
Fig. 8. Continued.
K. J. Mortele et al.: MRI-guided abdominal intervention 769

to 90°C for 6 to 20 min at each electrode location.Intraprocedural monitoring with MRI, in which imagingoccurs during the treatment, may be possible with arecently developed switching mechanism that briefly in-terrupts RF deposition during the sampling for imagingpulse sequences. Ablation duration of a particular lesionis then determined by MRI [25].
Focused ultrasound surgery
Focused US surgery (FUS) is the therapeutic heat destruc-tion of tissues using US energy that is focused on atarget deep in the body [75–77]. US beams can befocused and controlled for energy delivery deep intothe body without affecting superficial structures. TheUS beam interacts with tissue at the target volumethrough two mechanisms. First, the temperature is el-evated due to energy absorption from the sonic waves,resulting in different degrees of thermal damage. Sec-ond, there is the phenomenon of transient or inertialcavitation. FUS has two major advantages: it is com-pletely noninvasive because it requires no skin punc-ture (i.e., it is transcutaneous), and the ablative effect isnot limited by the geometry of a probe. FUS can betargeted to more complicated lesion geometries byarranging that the multiple sonications will conform tothe target shape and configuration, thus creating mul-tiple “hot spots” that fit precisely to the contour of thelesion (Fig. 8). Recently, Wu et al. [78] reported theirexperience in the investigation of the pathologicchanges of HCC after FUS treatment. They examinedthe surgical specimens of six patients previouslytreated with FUS 5 to 18 days previously and con-firmed that complete necrosis of the tumors wasachieved.
FUS is limited in that it can be applied only in areaswhere there is no intervening bone or air between the USprobe and target lesion; however, techniques are currentlybeing developed to traverse bone [79]. Also, current FUSsystems are designed for fixed targets; therefore, applica-tions in the upper abdomen in which the targets movewith respiration are difficult. However, just as US is usedcurrently to image the liver, FUS may be used to treatliver tumors in the future.
Uterine fibroids have been one of the first major areasof clinical application of FUS using MR guidance andmonitoring; other areas are the treatment of breast fibro-adenomas and breast cancer [79, 80]. Preliminary expe-rience with MRI-guided US surgery has shown that MRI-guided FUS is feasible for local treatment of leiomyomas[81]. The advantage of using MRI to guide this form oftherapy is that it is not only excellent for defining thetarget but also allows direct, continuous real-time mea-surement of temperature changes. It allows for directdosimetry and ensures that a therapeutic thermal dose has
been delivered to the target. For example, if those changesare not achieved, repeated sonications in the same areamay occur.
Brachytherapy
Prostate cancer is the second leading cause of cancerdeath in American men [82]. Treatment options for lo-calized prostate cancer include radical prostatectomy,cryotherapy, external beam radiation therapy, and inter-stitial radiation therapy (brachytherapy). Brachytherapyinvolves the trans-perirenal placement of radiation tissue-killing seeds. When performed under US guidance, it is adesirable treatment because it is an outpatient procedurewith low morbidity rates and low cost relative to othertreatments [83]. Outcomes compare favorably with othertreatments for localized prostate cancer. However, US islimited in its ability to define the margins of the prostategland, urethra, and rectum and to guide the delivery of theintended radiation dose to selected portions of the gland.
Because MRI defines prostate gland anatomy and theextent of prostate cancer better than US [84], it is used toimprove radiation dosimetry planning and radiation seedplacement. The feasibility and safety of MRI-guidedprostate brachytherapy has been demonstrated previously[85]. In that initial report, all nine patients were success-fully implanted without complication. No aberrant seedswere found in the bladder at cystoscopy. All patientsreceived 95% or greater of the ideal radiation dose to thetarget tissues. This is a significant improvement over the85% reported with US-guided methods. In a more recentupdate, of 43 patients [86], a minimum of 89% coverageof the tumor volume was achieved, in addition to main-taining the prostatic urethra and most of the anterior rectalwall below tolerance levels. Whether MRI-guided pros-tate brachytherapy improves survival and cancer controlmeasures (e.g., PSA measurements) remains to be estab-lished.
With the patient under general anesthesia, in the litho-tomy position, and the bladder catheterized, MRI is firstperformed with a surface coil. The prostate, urethra, andrectum are manually contoured on axial T2-weightedimages. By using special computer software, prostategland volumes and the desired radiation dose to eachportion of the gland are calculated. These dosimetriccalculations determine the number of needles and numberof radiation seeds required to ablate the peripheral glandthat contains the cancer. Then, iodine-125 radiation seedsloaded into 18-gauge needles are placed into the prostategland at predetermined depths at locations defined by thedosimetric plan. The ability to place the seeds precisely isaided by real-time MRI that views the advancing needlesand a Plexiglas template that contains rows and columnsof holes at 5-mm intervals. This template is attached to arectal obturator, which keeps the template at a fixed
770 K. J. Mortele et al.: MRI-guided abdominal intervention

position abutting the perineum. It also serves to straightenthe anorectal junction and to delineate the rectal wall.Multiplanar MRI is used to confirm accurate placement ofeach needle before each seed is deposited (Fig. 9).
Conclusion
MRI-guided abdominopelvic intervention, although stillin its early stages of development, is now gaining accep-
tance, and early experience points to advantages in treat-ing abdominal and pelvic cancers. In the liver, the abilityof MRI to monitor real-time changes in tissue temperaturepoints to MRI as the optimal imaging method for moni-toring abdominal tumor ablation using thermal-based en-ergies. The advantages of diagnostic MRI in the liver andthe prostate gland, with its superior ability to detect andcharacterize lesions and depict anatomy, have allowedMRI to become a useful modality to guide biopsy andsubsequent treatment.
Fig. 9. MRI-guided brachytherapy. A Axial FSE T2-weighted MRimage obtained with the endorectal coil shows diffuse hypointenseappearance of the peripheral zone of the prostate gland compatible withprostate carcinoma. B Intraprocedural axial SPGR image shows suscep-tibility artifacts of the radiation seeds deployed within the prostate
gland. C Conventional anteroposterior radiograph of the pelvis obtainedafter the procedure shows anatomic distribution of the seeds. D Gado-linium-enhanced axial SPGR T1-weighted MR image after brachyther-apy shows multiple seeds within the peripheral zone of the prostategland.
K. J. Mortele et al.: MRI-guided abdominal intervention 771

Although the feasibility of MRI-guided procedures inthe abdomen and pelvis has been demonstrated, futureclinical trials should expand on their usefulness [87].Undoubtedly, as the field evolves, more applications willbe introduced. For the next generation of MR interven-tionists, the task of achieving real-time imaging guidanceof therapies with high temporal and spatial resolution willbe of the utmost importance to progress in the field. Theprospects are promising enough to warrant intensive ef-forts to explore and expand the scope of MRI-guidedprocedures in the future.
Acknowledgments. We thank Ferenc Jolesz, M.D., Paul Morrison, Pai-rash Saiviroonporn, Vince Colucci, and Dan Kacher.
References
1. Adam G, Bucker A, Nolte-Ernsting C, et al. Interventional MRimaging: percutaneous abdominal and skeletal biopsies and drain-ages of the abdomen. Eur Radiol 1999;9:1471–1478
2. Silverman SG, Jolesz FA, Newman RW, et al. Design and imple-mentation of an interventional MR imaging suite. AJR 1997;168:1465–1471
3. Jolesz F, Silverman SG. Interventional magnetic resonance therapy.Semin Interv Radiol 1995;12:20–27
4. Vogl TJ, Mack MG, Muller PK, et al. Interventional MR: interstitialtherapy. Eur Radiol 1999;9:1479–1487
5. Silverman SG, Collick BD, Figueira MR, et al. Interactive biopsy inan open configuration MRI system. Radiology 1995;197:175–181
6. Lewin JS, Petersilge CA, Hatem S, et al. Interactive MR imaging-guided biopsy and aspiration with a modified clinical C-arm system.AJR 1998;170:1593–1601
7. Law P, Regan L. Interstitial thermo-ablation under MRI guidancefor the treatment of fibroids. Curr Opin Obstet Gynecol 2000;12:277–282
8. Vogl TJ, Mack MG, Straub R, et al. Magnetic resonance imaging–guided abdominal interventional radiology: laser induced thermo-therapy of liver metastasis. Endoscopy 1997;29:577–583
9. Silverman SG, Tuncali K, Adams DF, et al. MR imaging-guidedpercutaneous cryotherapy of liver tumors: initial experience. Radi-ology 2000;217:657–664
10. Tacke J, Adam G, Speetzen R, et al. MR -guided Interstitial cryo-therapy of the liver with a novel, nitrogen-cooled cryoprobe. MagnReson Med 1998;39:354–360
11. Silverman SG, Tuncali K, Adams DF, et al. Percutaneous MRimaging-guided cryotherapy of liver metastases. Radiology 1999;213(suppl):122
12. Lewin JS, Connell CF, Duerek JL, et al. Interactive MRI-guidedradiofrequency interstitial thermal ablation of abdominal tumors:clinical trial for evaluation of safety and feasibility. J Magn ResonImaging 1998;8:40–47
13. Buecker A, Neuerburg JM, Adam G, et al. Stent placement with realtime MRI guidance: initial animal experiment experiences. RofoFortschr Geb Roentgenstr 1998;169:655–657
14. Wildermuth S, Debatin JF, Leung DA, et al. MR-guided intravas-cular procedures: initial demonstration in a pig model. Radiology1997;202:578–583
15. Mueller PR, Stark DD, Simeone JF, et al. MR-guided aspirationbiopsy: needle design and clinical trials. Radiology 1986;161:605–609
16. Mueller PR, Stark DD, Simeone JF, et al. Clinical use of a nonfer-romagnetic needle for magnetic resonance-guided biopsy. Gastro-intest Radiol 1989;14:61–64
17. Schenck JF, Jolesz FA, Roemer PB, et al. Superconducting openconfiguration MR imaging system for image-guided therapy. Radi-ology 1995;195:805–814
18. Gronemeyer DH, Kaufman L, Rothschild P, et al. New possibilitiesand aspects of low-field magnetic resonance tomography. RadiolDiagn 1989;30:519–527
19. Frahm VC, Gehl HB, Robberg WA. Technique or MR-guided corebiopsy of abdominal masses using an open low-field scanner: fea-sibility and first clinical results. Fortschr Rontgenstr 1996;164:1:62–67
20. Lu DSK, Sinha S, Lucas J, et al. MR-guided percutaneous ethanolablation of liver tissue in a .2-T open MR system: preliminary studyin porcine model. J Magn Reson Imaging 1997;7:303–308
21. Mahfouz AE, Rahmouni A, Zylbersztejn C, Mathieu D. MR-guidedbiopsy using ultrafast T1- and T2-weighted reordered turbo fastlow-angle shot sequences: feasibility and preliminary clinical ap-plications. AJR 1996;167:167–169
22. Duerk JL, Lewin JS, Wendt M, Petersilge C. Remember true-FISP?A high SNR, near 1-second imaging method for T2-like contrastinterventional MRI at 0.2 T. J Magn Reson Imaging 1998;8:203–208
23. Shellock FG, Kanal E. Magnetic resonance: bioeffects, safety, andpatient management. New York: Raven, 1994:61–69
24. Hughes CW, Bell C. Anesthesia equipment in remote hospitallocations. In: Ehrenwerth J, Eisenkraft JB, eds. Anesthesia equip-ment: principles and applications. St Louis: Mosby, 1993:565–587
25. Lewin JS, Duerk JL, Jain JR, et al. Needle localization in MRguided biopsy and aspiration: effect of field strength, sequencedesign, and magnetic field orientation. AJR 1996;166:1337–1345
26. Gunther RW, Bucher A, Adam G. Interventional magnetic reso-nance: realistic prospect or wishful thinking? Cardiovasc IntervRadiol 1999;22:187–195
27. Lu DSK, Lee H, Farahani K, et al. Biopsy of hepatic dome lesions:semi-real-time coronal MR guidance technique. AJR 1997;168:737–739
28. Rofsky NM, Yang BM, Scholssberg P, et al. MR-Guided needleaspiration biopsies of hepatic masses using a closed bore magnet.J Comput Assist Tomogr 1998;22:633–637
29. Dumoulin CL, Souza P, Darrow RD. Real time position monitoringof invasive devices using magnetic resonance imaging. Magn ResonMed 1993;29:411–415
30. Gohnde SC, Pfammatter T, Steiner P, et al. MR-guided cholecys-tectomy: assessment of biplanar, real-time needle tracking in threepigs. Cardiovasc Interv Radiol 1997;20:295–299
31. Hagspiel KD, Kandarpa K, Silverman SG. Interactive MR-guidedpercutaneous nephrostomy. J Mag Res Imaging 1998;8:1319–1322
32. Keyvan F, Lu DS, Neguyen K, Ong KC, Sinha S, Lufkin RB. MRIguided aspiration and drainage: feasibility studies. Proc RSNA1998, p 564
33. Leung DA, Debatin JF, Wildermuth S, et al. Intravascular MRtracking catheter: preliminary experimental evaluation. AJR 1995;164:1265–1270
34. Wendt M, Busch M, Wetzler R, et al. Shifted rotated keyholeimaging and active tip-tracking for interventional procedure guid-ance. J Magn Reson Imaging 1998;8:251–258
35. Glovinski A, Adam G, Buecker A, et al. Catheter visualizationsuing locally induced actively controlled field inhomogeneities.Magn Reson Med 1997;38:251–258
36. Glowinski A, Kursch J, Adam G, et al. Device visualization forinterventional MRI using local magnetic fields: basic theory and itsapplication to catheter visualization. IEEE Trans Med Imaging1998;17:786–793
37. Gehl HB, Frahm C et al. A technique of MRI guided drainage withan open low field magnet. Fortschr Rontgenstr 1996;165:70–73
38. vanSonnenberg E, Hajek P, Gylys-Morin V, et al. A wire-sheathsystem for MR-guided biopsy and drainage: laboratory studies andexperience in 10 patients. AJR 1988;151:815–817
772 K. J. Mortele et al.: MRI-guided abdominal intervention

39. Buecker A, Neuerburg JM, Adam G, et al. Real-time MR guidancefor inferior vena cava filter placement. J Vasc Interv Radiol 2001;12:753–756
40. Buecker A, Neuerburg JM, Adam GB, et al. Real-time MR fluo-roscopy for MR-guided iliac artery stent placement. J Magn ResonImaging 2000;12:616–622
41. Yeung CJ, Ataslar E. RF transmit power limit for the barewireloopless catheter antenna. J Magn Reson Imaging 2000;12:86–91
42. Ladd ME, Quick HH. Reduction of resonant RF heating in intra-vascular catheters using coaxial chokes. Magn Reson Med 2000;43:615–619
43. Konings MK, Bartels LW, van Swol CF, Bakker CJ. Developmentof an MR-safe tracking with a laser-driven tip coil. J Magn ResonImaging 2001;13:131–1345
44. D’Agostino HB, Solinas A. Percutaneous ablation therapy for hep-atocellular carcinomas. AJR 1995;164:1165–1167
45. Crews KA, Kuhn JA, McCarty TM, et al. Cryosurgical ablation ofhepatic tumors. Am J Surg 1997;114:614–618
46. Steele G Jr, Ravikumar TS. Resection of hepatic metastases fromcolorectal cancer: biologic perspectives. Ann Surg 1989;210:127–138
47. Gazelle GS, Goldberg SN, Solbiati L, Livraghi T. Tumor ablationwith radio-frequency energy. Radiology 2000;217:633–646
48. Dickinson RJ, Hall AS, Hind AJ, Young IR. Measurement ofchanges in tissue temperature using MR imaging. J Comput AssistTomogr 1986;10:468–472
49. Sinha S, Oshiro T, Sinha U, Lufkin R. Phase imaging on a 0.2T MRscanner: applications to temperature monitoring during ablationprocedures. J Magn Reson Imaging 1997;7:918–928
50. Kettenbach J, Silverman SG, Hata N, et al. Monitoring and visual-ization for MR-guided laser ablations in an open MR system. JMagn Reson Imaging 1998;8:933–943
51. Fosshelm S, Ilyasov K, Wiggen U, et al. Paramagnetic liposomes asthermosensitive probes for MRI in vitro feasibility studies. In:Proceedings of the ISMRM. KnowledgeAccess International, To-ronto, 1999:725
52. Bartholet A, Goudemant J, Laurent S, et al. Spin transition molec-ular materials: intelligent contrast agents for magnetic resonancethermometry. In: Proceedings of the ISMRM. KnowledgeAccessInternational, Toronto, 2000
53. Livraghi T, Vettori C, Lazzaroni S, et al. Liver metastases: resultsof percutaneous ethanol injection in 14 patients. Radiology 1991;179:709–712
54. Shinmoto H, Mulkern RV, Oshio SG, et al. MR appearance andspectral features of injected ethanol in the liver: implication for fastMR-guided percutaneous ethanol injection therapy. J Comput AssistTomogr 1997;21:82–88
55. Bown SG. Phototherapy of tumors. World J Surg 1983;7:700–70956. Steger AC, Lees WR, Walmsley K, Brown SG. Interstitial laser
hyperthermia: a new approach to local destruction of tumours. BMJ1989;299:362–365
57. Vogl TJ, Muller PK, Hammerrstingl R, et al. Malignant liver tumorstreated with imaging guided laser induced thermotherapy, techniqueand prospective results. Radiology 1995;196:257–265
58. Amin Z, Bown SG, Lees WR. Liver tumor ablation by interstitiallaser photocoagulation review of experimental and clinical studies.Semin Interv Radiol 1993;10:88–100
59. Amin Z, Bown SG, Lees WR. Local treatment of colorectal livermetastases: a comparison of interstitial laser photocoagulation (ILP)and percutaneous alcohol injection (PAI). Clin Radiol 1993;48:166–171
60. Amin Z, Buonaccorsi G, Mills T, et al. Interstitial laser photoco-agulation: evaluation of a 1320nm Nd-Yag and an 805nm diodelaser: the significance of charring the fibre tip. Lasers Med Sci1993;8:113–120
61. Amin Z, Donald J, Masters A, et al. Hepatic metastases: interstitiallaser photocoagulation with real-time US monitoring and dynamicCT evaluation treatment. Radiology 1993;187:339–347
62. Wong WS, Patel SC, Cruz FS, et al. Cryosurgery as a treatment foradvanced stage hepatocellular carcinoma. Cancer 1998;82:1268–1278
63. Brewer WH, Austin RS, Capps GW, et al. Intraoperative monitor-ing and postoperative imaging of hepatic cryosurgery. Semin SurgOncol 1998;14:129–155
64. Weber SM, Lee FT, Warner TF, et al. Hepatic cryoablation: USmonitoring of extent of necrosis in normal pig liver. Radiology1998;207:73–77
65. Lee FT, Mahve DM, Chosy SG et al. Hepatic cryosurgery withintraoperative US guidance. Radiology 1997;202:624–632
66. Steele G Jr. Cryoablation in hepatic surgery. Semin Liver Dis1994;14:120–125
67. Gilbert JC, Rubinsky B, Roos MS, et al. MR-monitored cryosurgeryin rabbit brain. Magn Reson Imaging 1993;11:1155–1164
68. Matsumoto R, Oshio K, Jolesz FA. Monitoring of laser and freez-ing-induced ablation in the liver with T1-weighted MR imaging. JMagn Reson Imaging 1993;3:770–776
69. Shingleton BW, Sewell PE. Percutaneous tumor ablation with mag-netic resonance imaging guidance. J Urol 2001;165:773–776
70. Goldberg SN, Gazelle GS, Mueller PR. Thermal ablation therapyfor focal malignancy: a unified approach to underlying principles,techniques, and diagnostic imaging guidance. AJR 2000;174:323–331
71. Goldberg S, Gazelle G, Dawson S, et al. Tissue ablation withradiofrequency: effect of probe size, gauge, duration, and temper-ature on lesion volume. Acad Radiol 1995;2:399–404
72. Rossi S, Fornari F, Buscarini L. Percutaneous ultrasound-guidedradiofrequency electrocautery for the treatment of small hepatocel-lular carcinoma. J Interv Radiol 1993;8:97–103
73. Livraghi T, Goldberg S, Monti F, et al. Saline-enhanced radiofre-quency tissue ablation in the treatment of liver metastases. Radiol-ogy 1997;202:205–210
74. Goldberg S, Gazelle S, Dawson S, et al. Tissue ablation withradiofrequency: effect of probe size, gauge, and temperature onlesion volume. Acad Radiol 1995;2:399–404
75. Hynynen K, Damainou CA, Colucci Y, et al. MR monitoring offocused ultrasonic surgery of renal cortex: experimental and simu-lation studies. J Magn Reson Imaging 1995;5:259–266
76. Yang R, Reilly CR, Rescoria FJ, et al. High-intensity focusedultrasound in the treatment of experimental liver cancer. Arch Surg1991;126:1002–1010
77. Yang R, Sanghvi NT, Rescorla FJ, et al. Extracorporeal liverablation using sonography-guided high-intensity focused ultra-sound. Invest Radiol 1992;27:796–803
78. Wu F, Wang Z, Chen W. Pathological study of extracorporeallyablated hepatocellular carcinoma with high-intensity focused ultra-sound. Zhonghua Zhong Liu Za Zhi 2001;23:237–239
79. Hynynen K, Darkazanli A, Unger E, Schenck JF. MRI-guidednoninvasive ultrasound surgery. Med Phys 1992;20:107–116
80. Vessey MP, Villard-Mackintosh L, McPherson K, et al. The epi-demiology of hysterectomy: findings in a large cohort study. Br JObstet Gynaecol 1992;5:402–407
81. Tempany CM, Stewart EA, McDannold N, Quade BJ, Jolesz FA,Hynynen K. MR imaging-guided focused ultrasound surgery ofuterine leiomyomas: a feasibility study. Radiology 2003;226:897–905
82. Wingo PA, Landio S, Reis LAG. An adjustment to the 1997estimate for new prostate cancer cases. CA Cancer J Clin 1997;47:239–242
83. Prestidge BR, Prete JJ, Bucholtz TA, et al. A survey of currentclinical practice of permanent prostate brachytherapy in the UnitedStates. Int J Radiat Oncol Biol Phys 1998;40:461–465
K. J. Mortele et al.: MRI-guided abdominal intervention 773

84. Seltzer SE, Getty DJ, Tempany CMC, et al. Staging prostate cancerwith MR imaging: a combined radiologist–computer system. Ra-diology 1997;202:219–226
85. D’Amico AV, Cormack R, Tempany CMC, et al. Real time mag-netic resonance image guided interstitial brachytherapy in the treat-ment of selected patients with clinically localized prostate cancer.Int J Radiat Oncol Biol Phys 1998;42:507–515
86. D’Amico A, Cormack R, Kumar S, Tempany CM. Real-time mag-netic resonance imaging-guided brachytherapy in the treatment ofselected patients with clinically localized prostate cancer. J En-dourol 2000;14:367–370
87. Silverman SG, Duerk JL, Lu DSK, Jolesz FA. Research in inter-ventional MRI: where do we go from here? Acad Radiol 1999;6:368–369
774 K. J. Mortele et al.: MRI-guided abdominal intervention