abdominal compartment syndrome 101 - canadian
TRANSCRIPT
10/22/2015
1
What every Critical Care Nurse Needs to Know:
Abdominal Compartment Syndrome 101
Amanda Di Florio RN. BN. CNCC (c)
Sandra Cook RN. BN. CNCC (c).
Montreal General Hospital Intensive Care Unit
Potential Conflict of Interest
• I Amanda Di Florio have no Conflict of Interest to declare
• I Sandra Cook have no Conflict of Interest to declare

10/22/2015
2
MGH – MUHCLevel 1 trauma
center
• 25-35 cases a year of ACS with a required “open abdomen”
• MVC’s, stabbings, crush injuries, gunshot injuries, sepsis, pancreatitis, falls with pelvic fractures,
Why should we worry?
• Melbrain et al. (2004)– A multicentre ( 13 ICU’s) epidemiological study found a prevalence of IAH (
IAP>12mm/ hg) 58.8%
• Vidal et al. (2008)– In a single site study of 83 critically ill patients found 31% had IAH at time of
admission and another 33% developed the condition after admission.
– ACS developed in 12% (10) of the pt.’s and 80% ( 8/10) of them died.
• Reintam et al ( 2008) – Studied IAP in 257 patients receiving mechanical ventilation. They found 97
patients (37% ) developed IAH . The patients with IAH had a significantly higher mortality than those without.
– Concluded that development of IAH is an independent risk factor for death.
10/22/2015
3
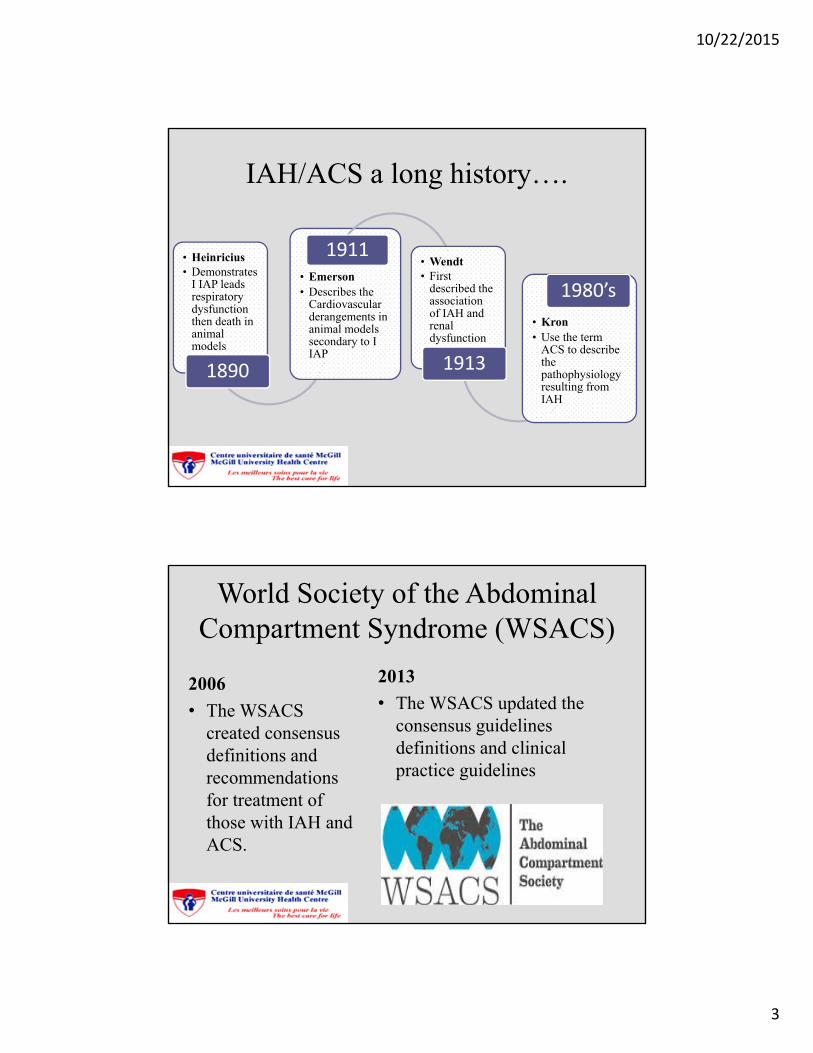
IAH/ACS a long history….
• Heinricius• Demonstrates
I IAP leads respiratory dysfunction then death in animal models
1890
• Emerson • Describes the
Cardiovascular derangements in animal models secondary to I IAP
1911• Wendt• First
described the association of IAH and renal dysfunction
1913
• Kron• Use the term
ACS to describe the pathophysiology resulting from IAH
1980’s
World Society of the Abdominal Compartment Syndrome (WSACS)
2006
• The WSACS created consensus definitions and recommendations for treatment of those with IAH and ACS.
2013
• The WSACS updated the consensus guidelines definitions and clinical practice guidelines
10/22/2015
4
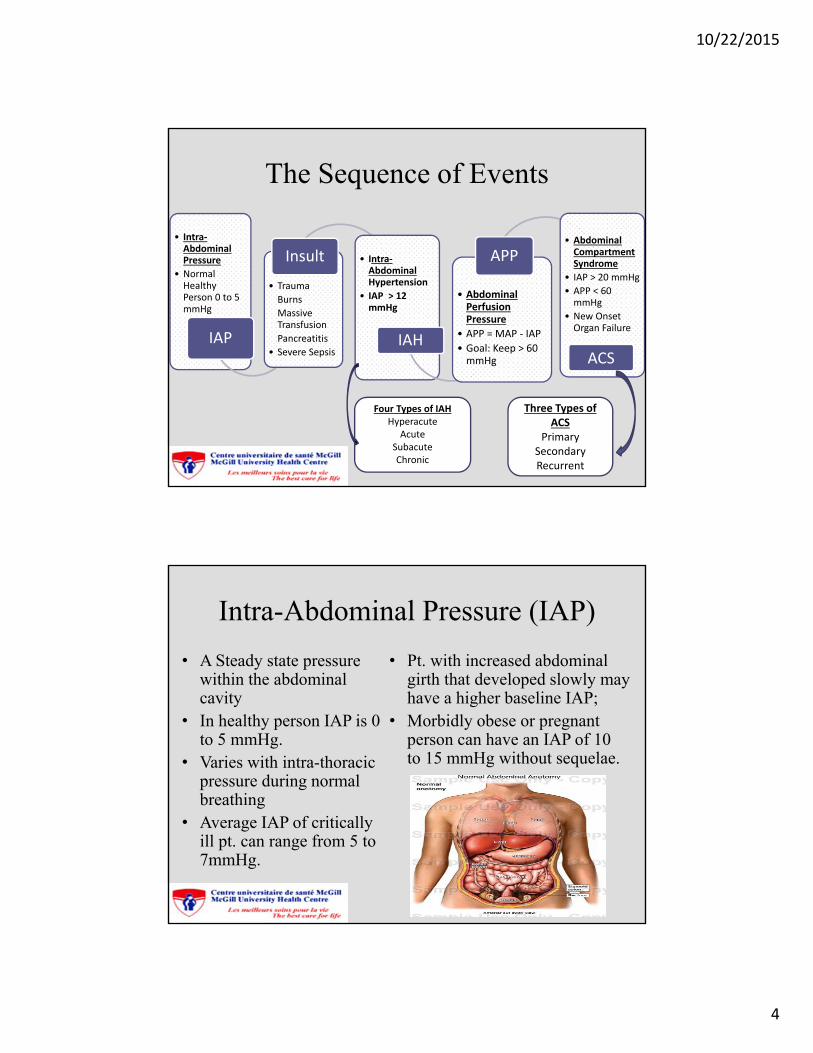
The Sequence of Events
• Intra‐Abdominal Pressure
• Normal Healthy Person 0 to 5 mmHg
IAP
• Trauma
Burns
Massive Transfusion
Pancreatitis
• Severe Sepsis
Insult • Intra‐AbdominalHypertension
• IAP > 12 mmHg
IAH
• Abdominal Perfusion Pressure
• APP = MAP ‐ IAP
• Goal: Keep > 60 mmHg
APP• Abdominal Compartment Syndrome
• IAP > 20 mmHg
• APP < 60 mmHg
• New Onset Organ Failure
ACS
Four Types of IAHHyperacute
AcuteSubacuteChronic
Three Types of ACS
PrimarySecondaryRecurrent
Intra-Abdominal Pressure (IAP)
• A Steady state pressure within the abdominal cavity
• In healthy person IAP is 0 to 5 mmHg.
• Varies with intra-thoracic pressure during normal breathing
• Average IAP of critically ill pt. can range from 5 to 7mmHg.
• Pt. with increased abdominal girth that developed slowly may have a higher baseline IAP;
• Morbidly obese or pregnant person can have an IAP of 10 to 15 mmHg without sequelae.
10/22/2015
5
Abdominal Perfusion Pressure (APP)
• Elevated Intra-abdominal pressure reduces blood flow to the abdominal viscera
• Is calculated by Mean Arterial Pressure (MAP) minus the IAP
• A target APP of at least 60 mmHg correlated with improved survival from IAH and ACS
• APP a better resuscitative endpoint than;
• Arterial pH, • Base deficit• Arterial lactate and• Hourly urine output for
predicting outcomes
APP = MAP – IAP
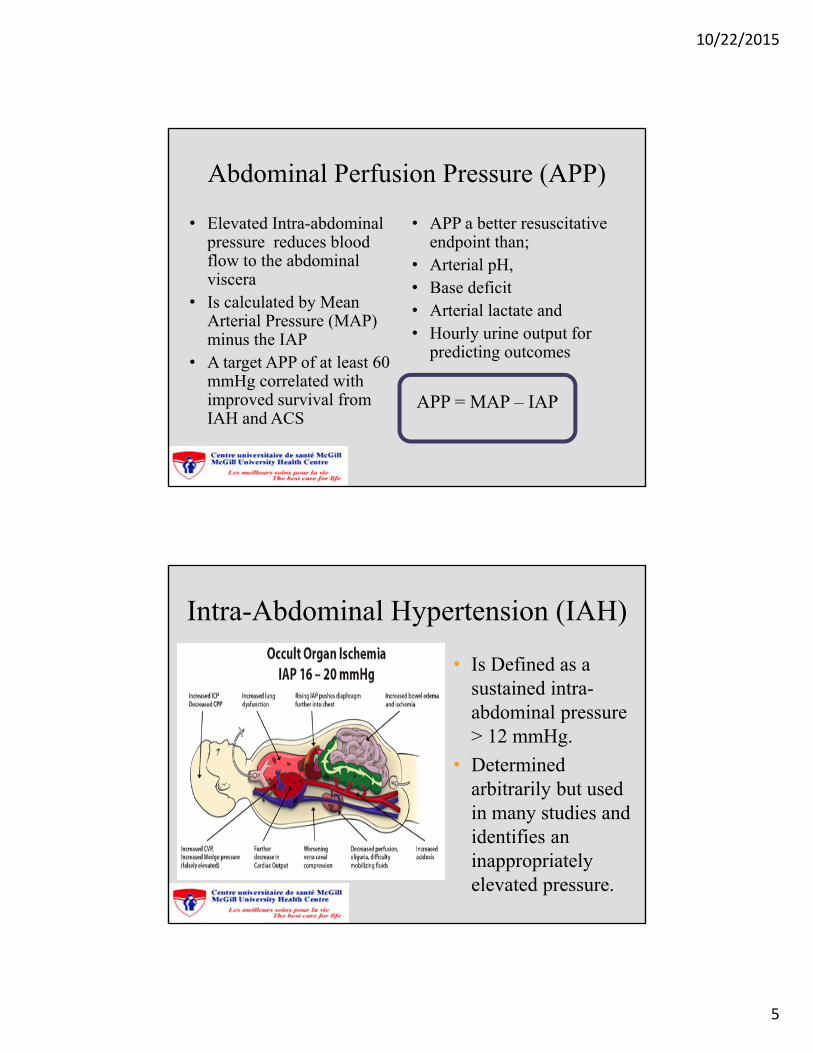
Intra-Abdominal Hypertension (IAH)
• Is Defined as a sustained intra-abdominal pressure > 12 mmHg.
• Determined arbitrarily but used in many studies and identifies an inappropriately elevated pressure.
10/22/2015
6
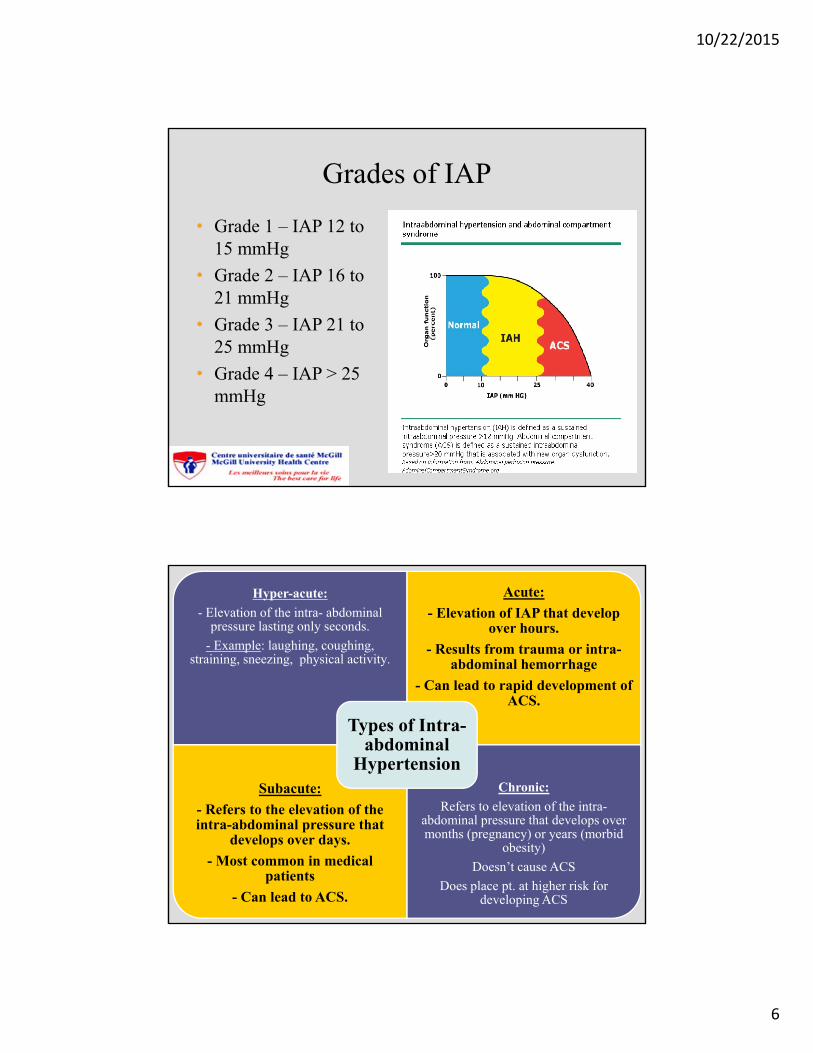
Grades of IAP
• Grade 1 – IAP 12 to 15 mmHg
• Grade 2 – IAP 16 to 21 mmHg
• Grade 3 – IAP 21 to 25 mmHg
• Grade 4 – IAP > 25 mmHg
Hyper-acute:
- Elevation of the intra- abdominal pressure lasting only seconds.
- Example: laughing, coughing, straining, sneezing, physical activity.
Acute:
- Elevation of IAP that develop over hours.
- Results from trauma or intra-abdominal hemorrhage
- Can lead to rapid development of ACS.
Subacute:
- Refers to the elevation of the intra-abdominal pressure that
develops over days.
- Most common in medical patients
- Can lead to ACS.
Chronic:
Refers to elevation of the intra-abdominal pressure that develops over months (pregnancy) or years (morbid
obesity)
Doesn’t cause ACS
Does place pt. at higher risk for developing ACS
Types of Intra-abdominal
Hypertension
10/22/2015
7
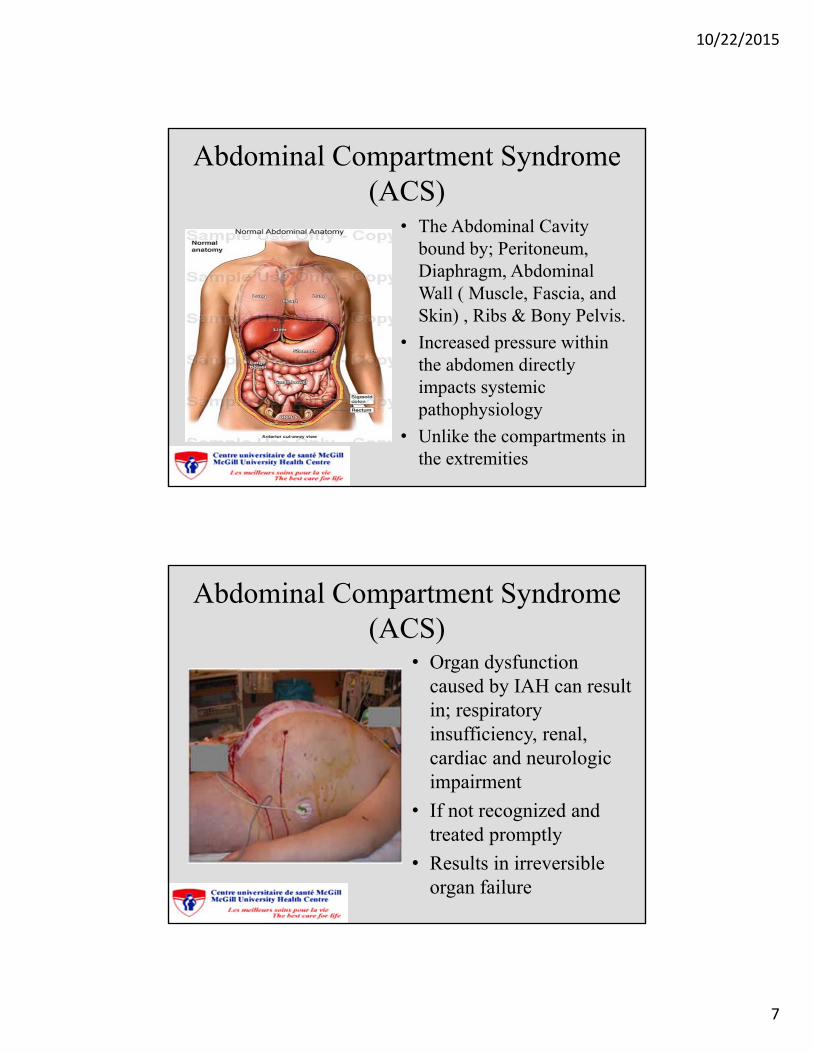
Abdominal Compartment Syndrome (ACS)
• The Abdominal Cavity bound by; Peritoneum, Diaphragm, Abdominal Wall ( Muscle, Fascia, and Skin) , Ribs & Bony Pelvis.
• Increased pressure within the abdomen directly impacts systemic pathophysiology
• Unlike the compartments in the extremities
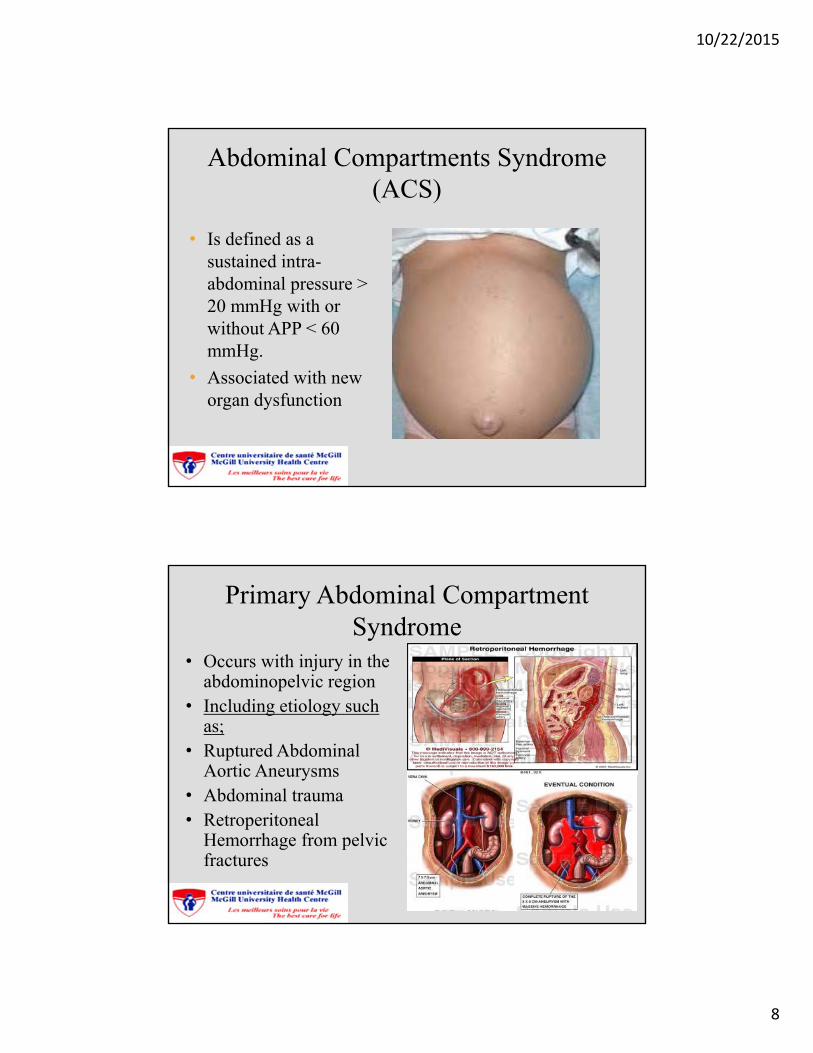
Abdominal Compartment Syndrome (ACS)
• Organ dysfunction caused by IAH can result in; respiratory insufficiency, renal, cardiac and neurologic impairment
• If not recognized and treated promptly
• Results in irreversible organ failure
10/22/2015
8
Abdominal Compartments Syndrome (ACS)
• Is defined as a sustained intra-abdominal pressure > 20 mmHg with or without APP < 60 mmHg.
• Associated with new organ dysfunction
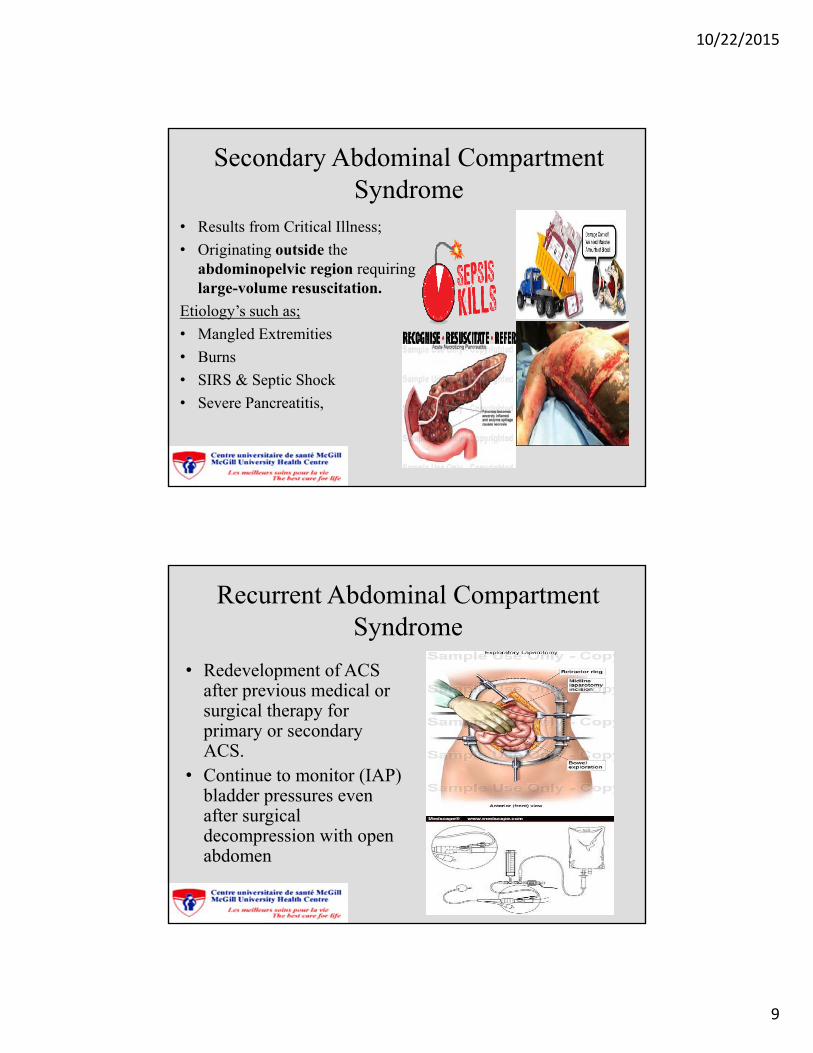
Primary Abdominal Compartment Syndrome
• Occurs with injury in the abdominopelvic region
• Including etiology such as;
• Ruptured Abdominal Aortic Aneurysms
• Abdominal trauma• Retroperitoneal
Hemorrhage from pelvic fractures
10/22/2015
9
Secondary Abdominal Compartment Syndrome
• Results from Critical Illness;
• Originating outside the abdominopelvic region requiring large-volume resuscitation.
Etiology’s such as;
• Mangled Extremities
• Burns
• SIRS & Septic Shock
• Severe Pancreatitis,
Recurrent Abdominal Compartment Syndrome
• Redevelopment of ACS after previous medical or surgical therapy for primary or secondary ACS.
• Continue to monitor (IAP) bladder pressures even after surgical decompression with open abdomen
10/22/2015
10
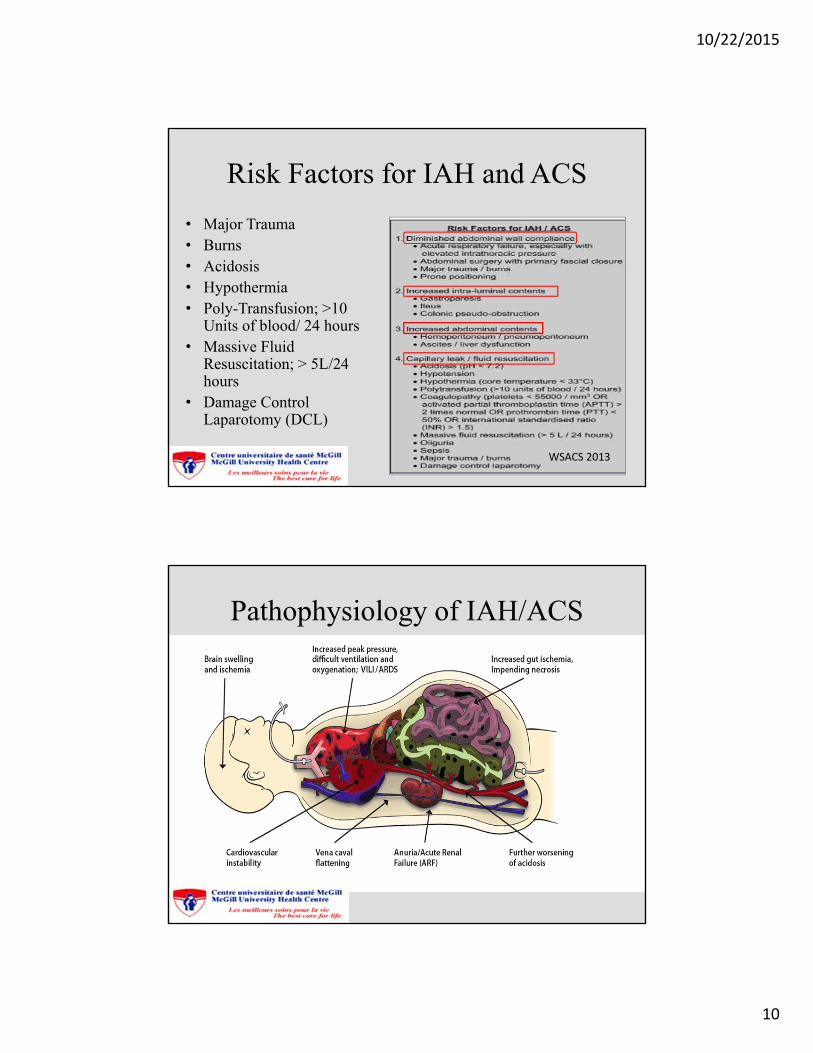
Risk Factors for IAH and ACS
• Major Trauma• Burns• Acidosis• Hypothermia• Poly-Transfusion; >10
Units of blood/ 24 hours• Massive Fluid
Resuscitation; > 5L/24 hours
• Damage Control Laparotomy (DCL)
WSACS 2013
Pathophysiology of IAH/ACS
10/22/2015
11
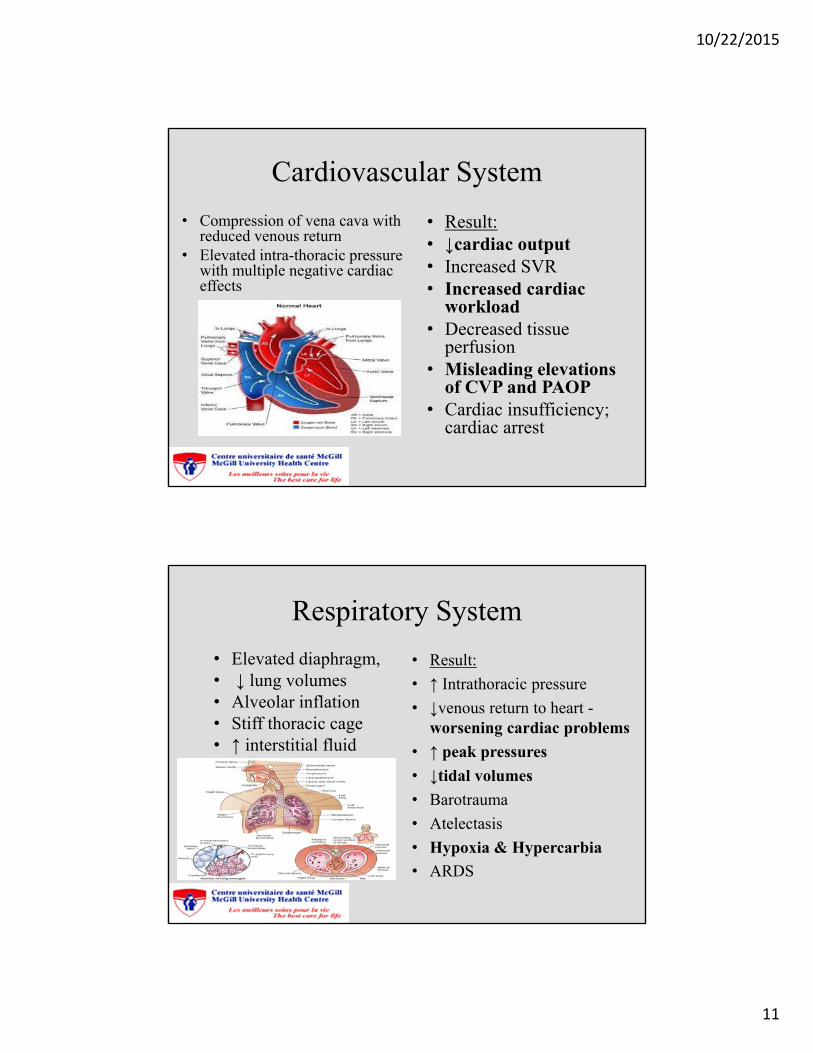
Cardiovascular System
• Compression of vena cava with reduced venous return
• Elevated intra-thoracic pressure with multiple negative cardiac effects
• Result:• ↓cardiac output• Increased SVR• Increased cardiac
workload• Decreased tissue
perfusion• Misleading elevations
of CVP and PAOP• Cardiac insufficiency;
cardiac arrest
Respiratory System
• Elevated diaphragm,• ↓ lung volumes• Alveolar inflation• Stiff thoracic cage• ↑ interstitial fluid
• Result:
• ↑ Intrathoracic pressure
• ↓venous return to heart -worsening cardiac problems
• ↑ peak pressures
• ↓tidal volumes
• Barotrauma
• Atelectasis
• Hypoxia & Hypercarbia
• ARDS
10/22/2015
12
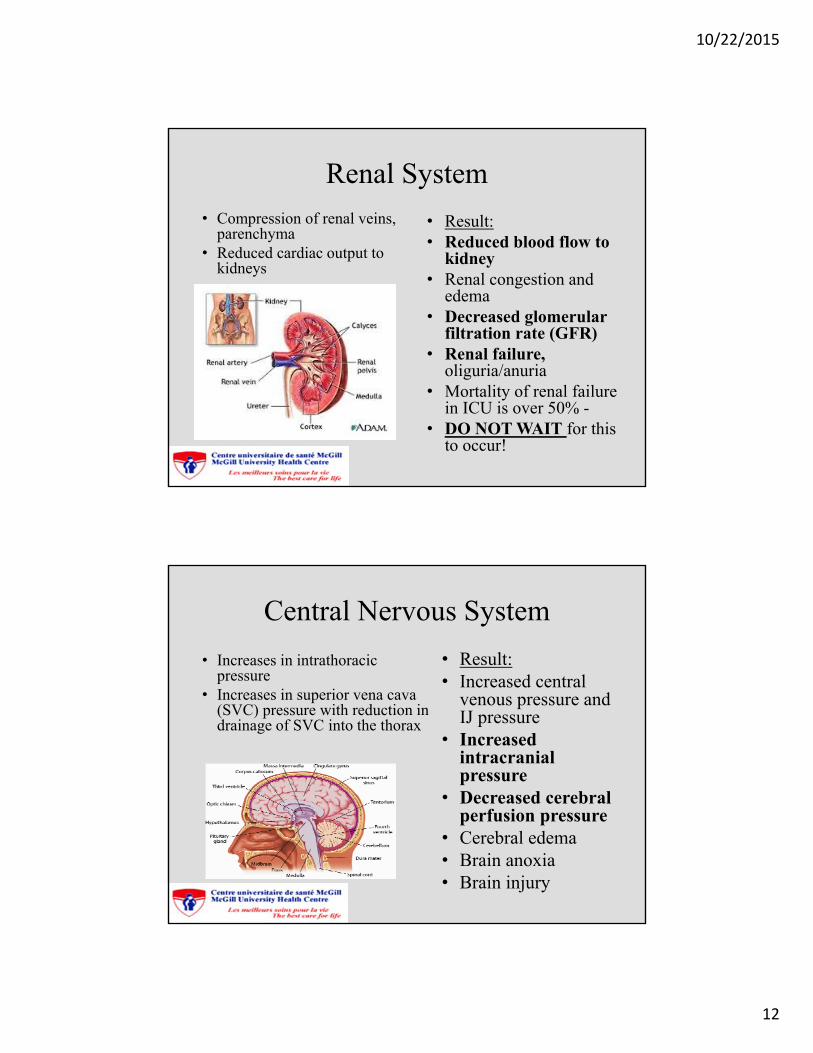
Renal System
• Compression of renal veins, parenchyma
• Reduced cardiac output to kidneys
• Result:• Reduced blood flow to
kidney• Renal congestion and
edema• Decreased glomerular
filtration rate (GFR) • Renal failure,
oliguria/anuria • Mortality of renal failure
in ICU is over 50% -• DO NOT WAIT for this
to occur!
Central Nervous System
• Increases in intrathoracic pressure
• Increases in superior vena cava (SVC) pressure with reduction in drainage of SVC into the thorax
• Result:• Increased central
venous pressure and IJ pressure
• Increased intracranial pressure
• Decreased cerebral perfusion pressure
• Cerebral edema• Brain anoxia• Brain injury
10/22/2015
13
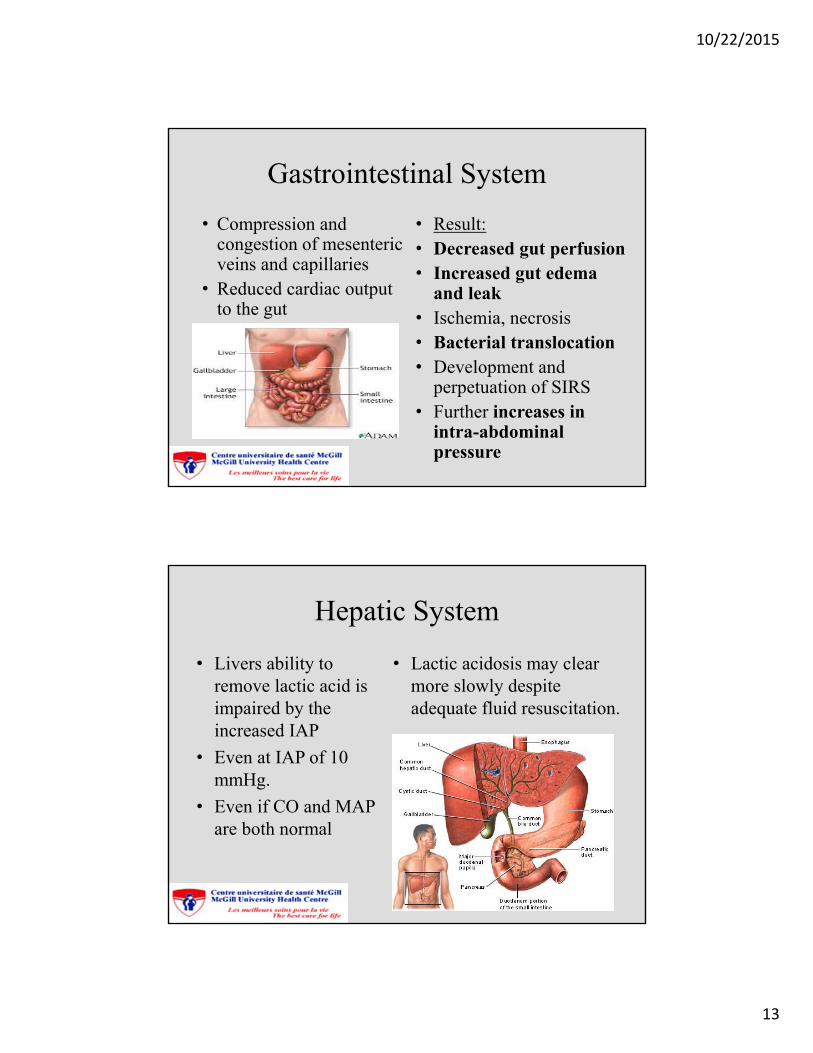
Gastrointestinal System
• Compression and congestion of mesenteric veins and capillaries
• Reduced cardiac output to the gut
• Result:• Decreased gut perfusion• Increased gut edema
and leak• Ischemia, necrosis• Bacterial translocation• Development and
perpetuation of SIRS• Further increases in
intra-abdominal pressure
Hepatic System
• Livers ability to remove lactic acid is impaired by the increased IAP
• Even at IAP of 10 mmHg.
• Even if CO and MAP are both normal
• Lactic acidosis may clear more slowly despite adequate fluid resuscitation.
10/22/2015
14
Clinical Presentation
• Recognize IAH early so it can be treated before progressing to ACS
• Challenge to communicate with intubated patient
• If they can convey symptoms they may complain of;
• Malaise & weakness
• Light-headedness
• Dyspnea
• Abdominal bloating
• Abdominal pain
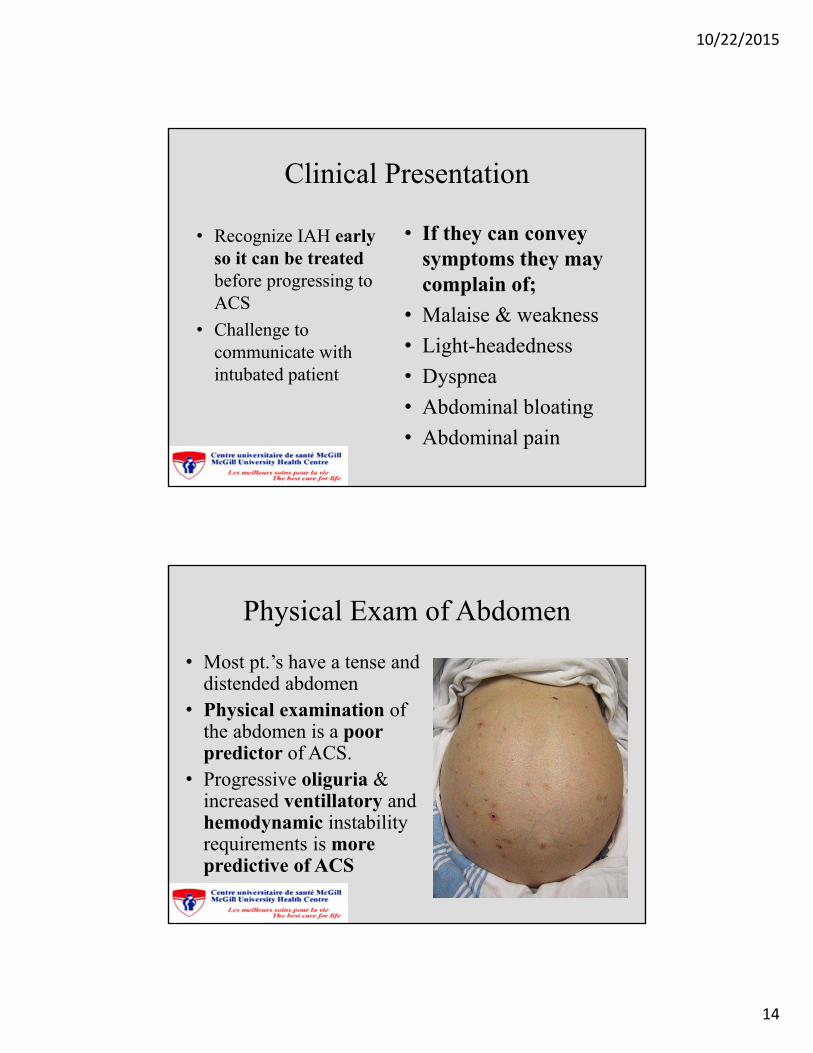
Physical Exam of Abdomen
• Most pt.’s have a tense and distended abdomen
• Physical examination of the abdomen is a poor predictor of ACS.
• Progressive oliguria & increased ventillatory and hemodynamic instability requirements is more predictive of ACS
10/22/2015
15
Chest X-ray
• Shows decreased lung volumes
• Atelectasis
• Elevated hemi-diaphragms
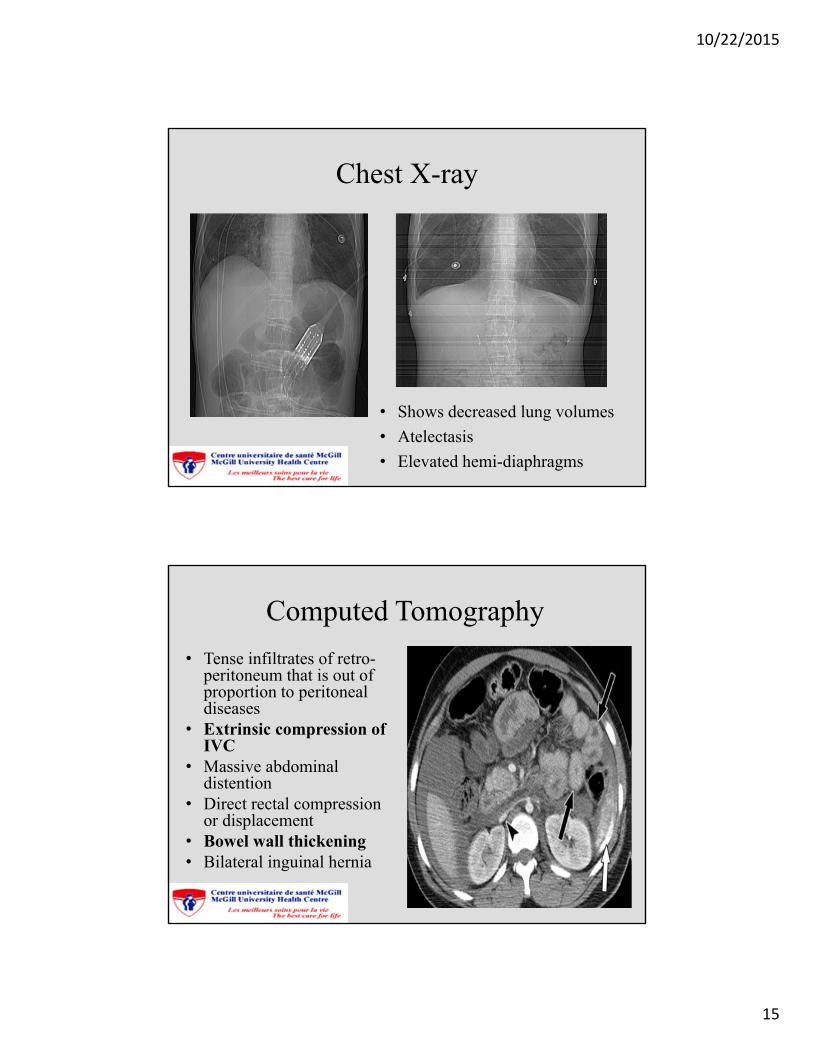
Computed Tomography
• Tense infiltrates of retro-peritoneum that is out of proportion to peritoneal diseases
• Extrinsic compression of IVC
• Massive abdominal distention
• Direct rectal compression or displacement
• Bowel wall thickening• Bilateral inguinal hernia
10/22/2015
16
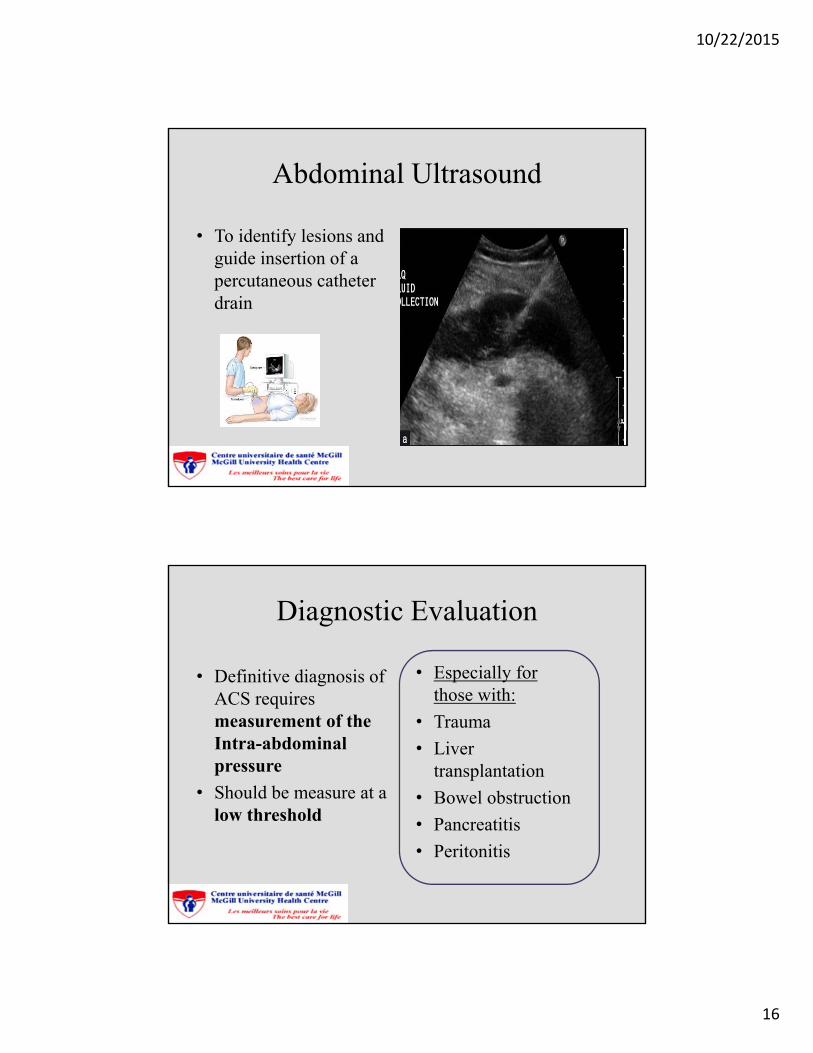
Abdominal Ultrasound
• To identify lesions and guide insertion of a percutaneous catheter drain
Diagnostic Evaluation
• Definitive diagnosis of ACS requires measurement of the Intra-abdominal pressure
• Should be measure at a low threshold
• Especially for those with:
• Trauma
• Liver transplantation
• Bowel obstruction
• Pancreatitis
• Peritonitis
10/22/2015
17
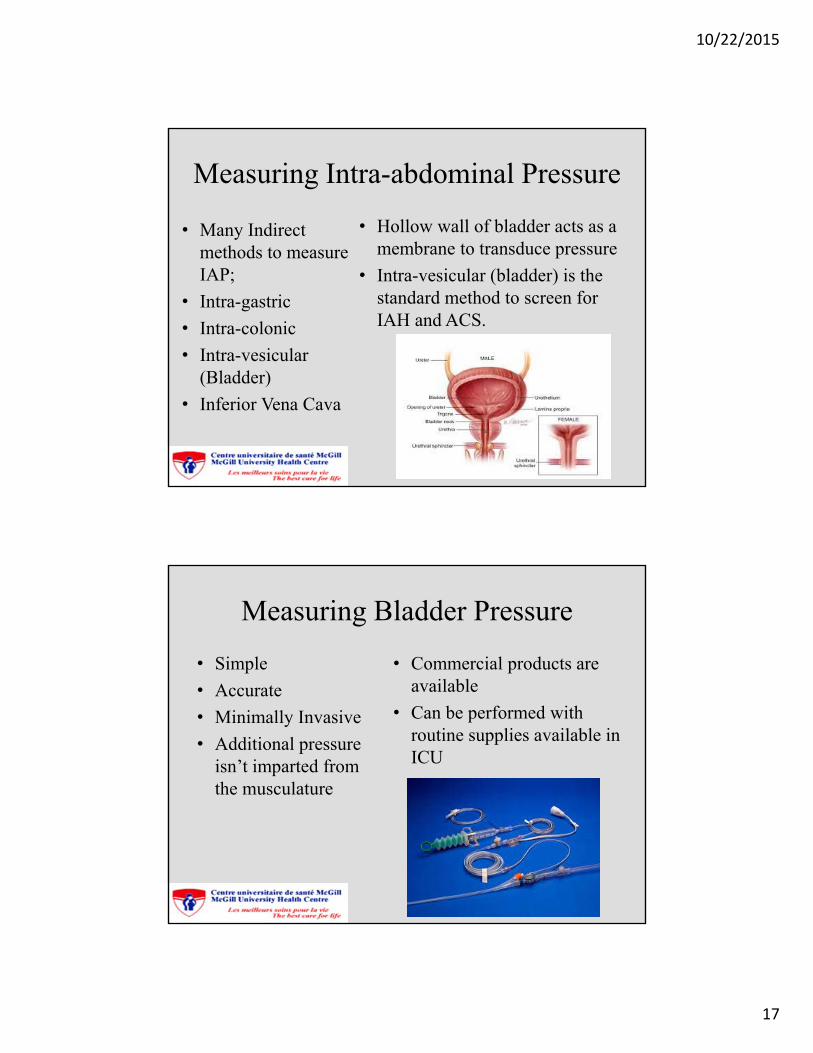
Measuring Intra-abdominal Pressure
• Many Indirect methods to measure IAP;
• Intra-gastric
• Intra-colonic
• Intra-vesicular (Bladder)
• Inferior Vena Cava
• Hollow wall of bladder acts as a membrane to transduce pressure
• Intra-vesicular (bladder) is the standard method to screen for IAH and ACS.
Measuring Bladder Pressure
• Simple
• Accurate
• Minimally Invasive
• Additional pressure isn’t imparted from the musculature
• Commercial products are available
• Can be performed with routine supplies available in ICU
10/22/2015
18
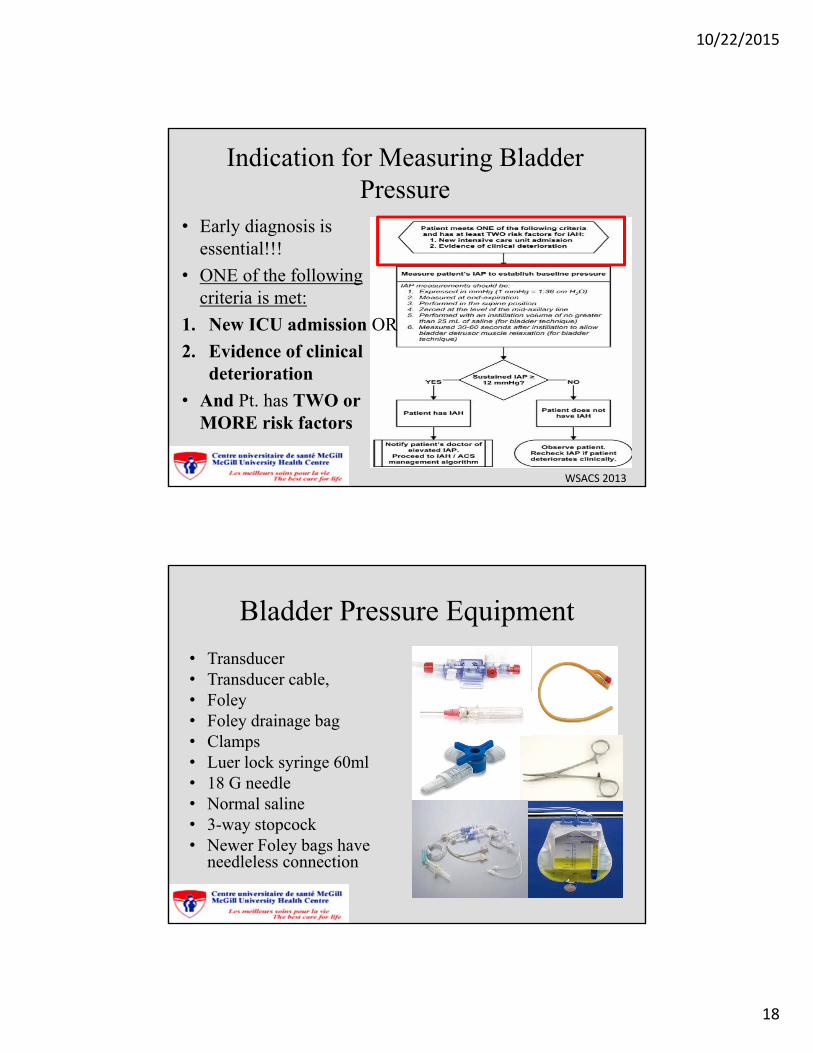
Indication for Measuring Bladder Pressure
• Early diagnosis is essential!!!
• ONE of the following criteria is met:
1. New ICU admission OR
2. Evidence of clinical deterioration
• And Pt. has TWO or MORE risk factors
WSACS 2013
Bladder Pressure Equipment
• Transducer• Transducer cable,• Foley• Foley drainage bag• Clamps• Luer lock syringe 60ml• 18 G needle• Normal saline• 3-way stopcock• Newer Foley bags have
needleless connection
10/22/2015
19
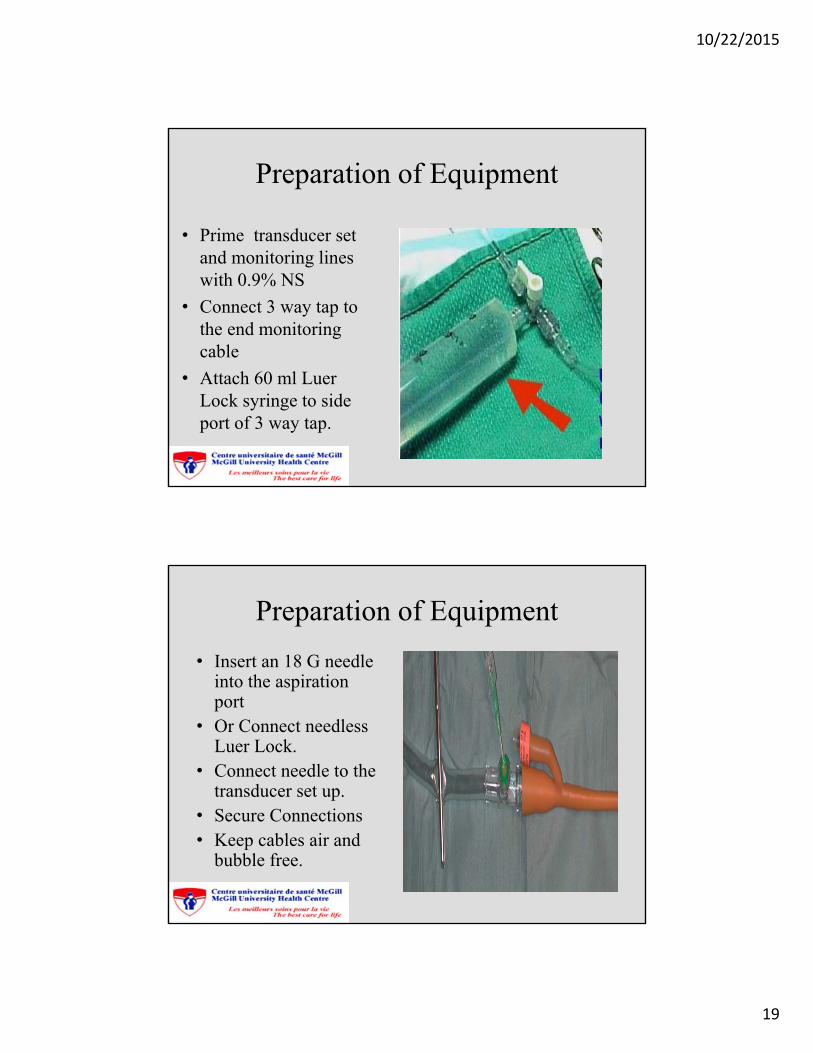
Preparation of Equipment
• Prime transducer set and monitoring lines with 0.9% NS
• Connect 3 way tap to the end monitoring cable
• Attach 60 ml LuerLock syringe to side port of 3 way tap.
Preparation of Equipment
• Insert an 18 G needle into the aspiration port
• Or Connect needless Luer Lock.
• Connect needle to the transducer set up.
• Secure Connections• Keep cables air and
bubble free.
10/22/2015
20
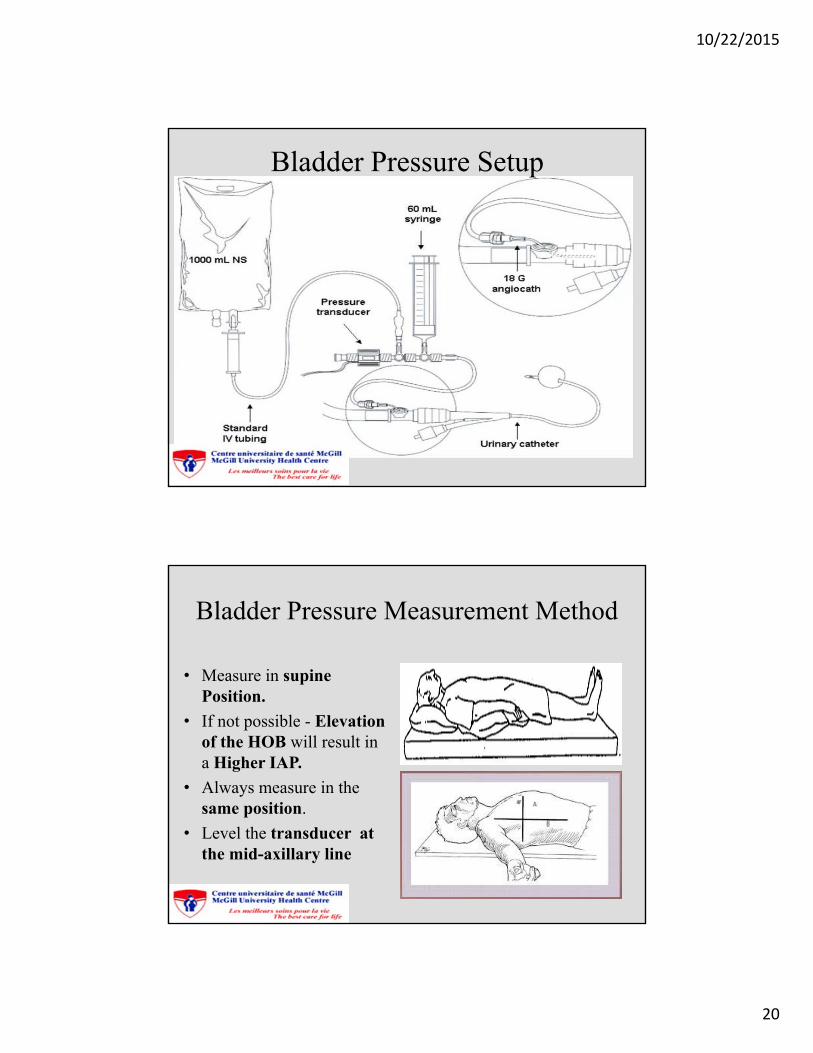
Bladder Pressure Setup
Bladder Pressure Measurement Method
• Measure in supine Position.
• If not possible - Elevation of the HOB will result in a Higher IAP.
• Always measure in the same position.
• Level the transducer at the mid-axillary line
10/22/2015
21
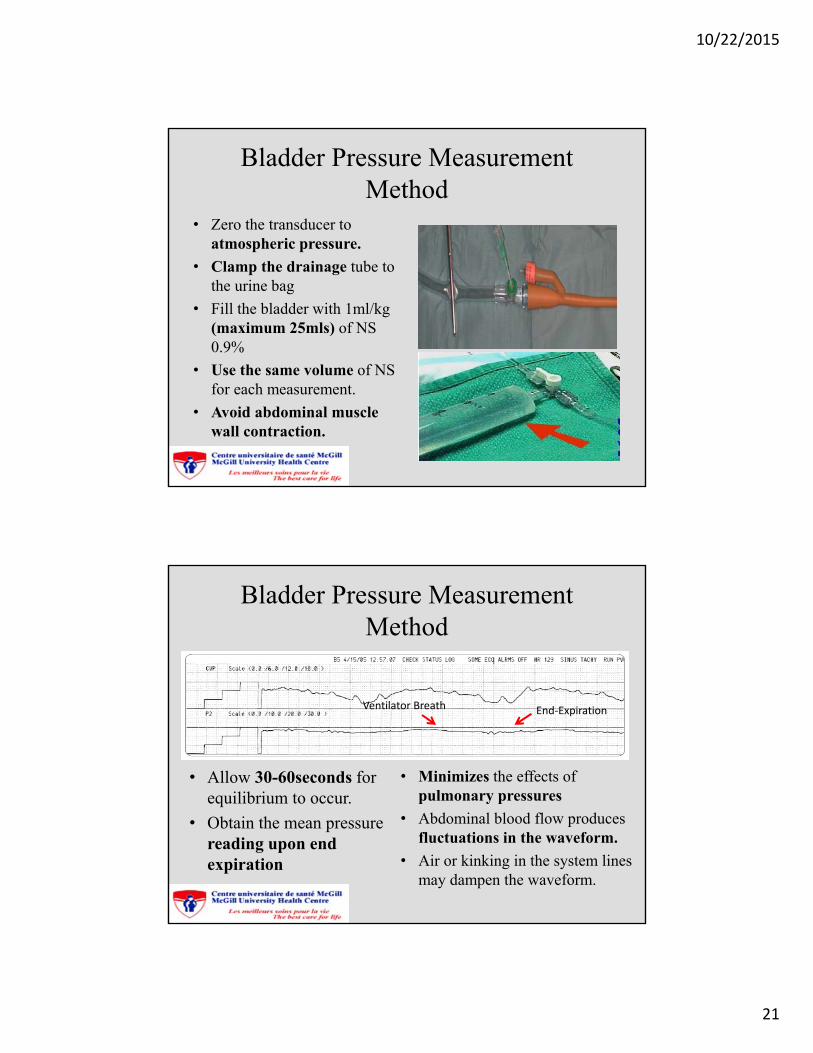
Bladder Pressure Measurement Method
• Zero the transducer to atmospheric pressure.
• Clamp the drainage tube to the urine bag
• Fill the bladder with 1ml/kg (maximum 25mls) of NS 0.9%
• Use the same volume of NSfor each measurement.
• Avoid abdominal muscle wall contraction.
Bladder Pressure Measurement Method
• Minimizes the effects of pulmonary pressures
• Abdominal blood flow produces fluctuations in the waveform.
• Air or kinking in the system lines may dampen the waveform.
• Allow 30-60seconds for equilibrium to occur.
• Obtain the mean pressure reading upon end expiration
Ventilator Breath End‐Expiration
10/22/2015
22
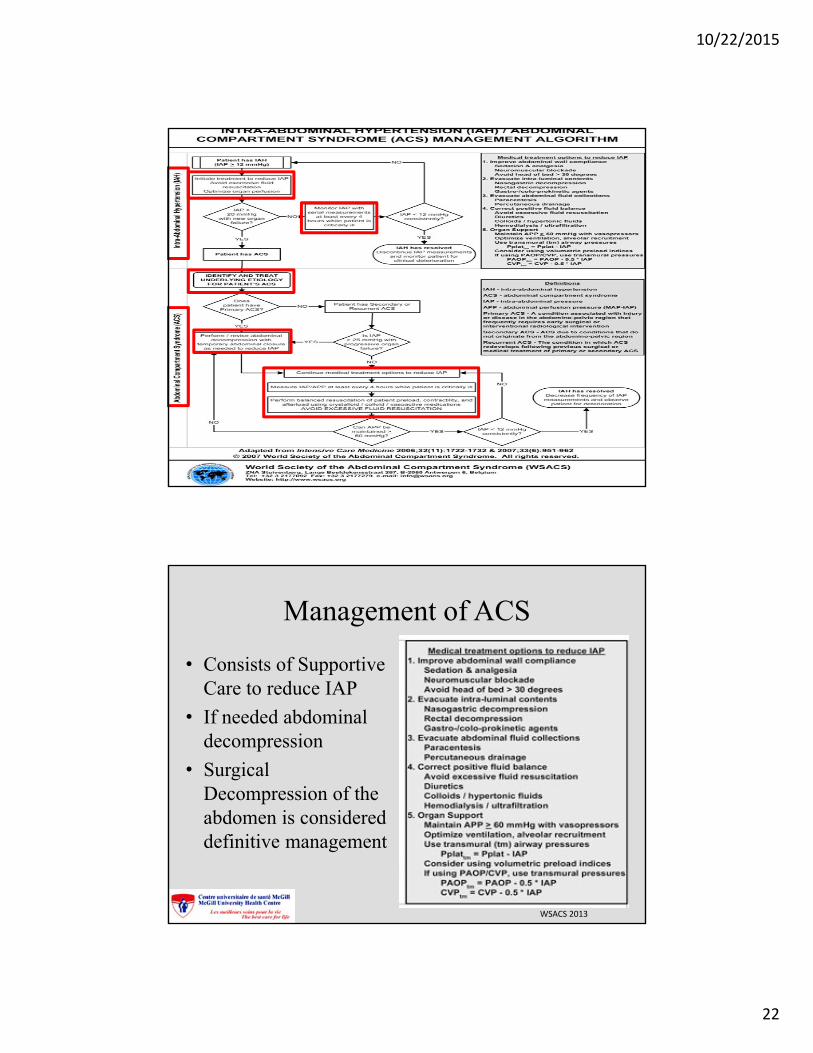
Management of ACS
• Consists of Supportive Care to reduce IAP
• If needed abdominal decompression
• Surgical Decompression of the abdomen is considered definitive management
WSACS 2013
10/22/2015
23
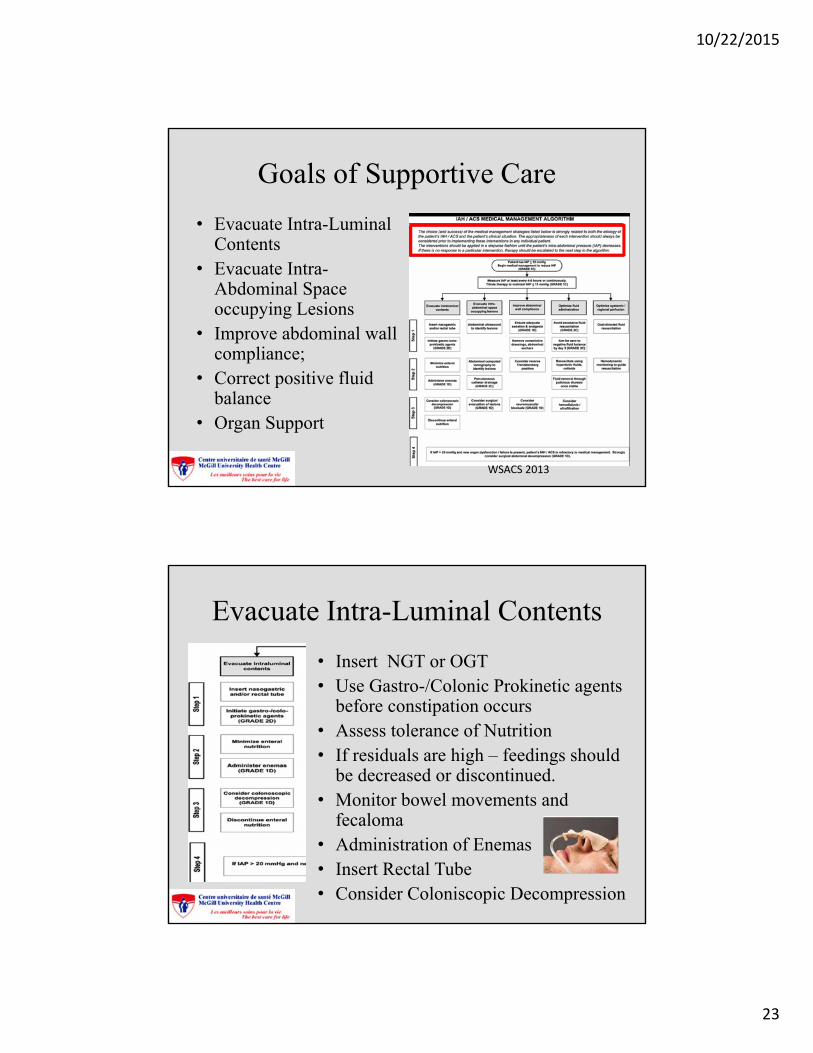
Goals of Supportive Care
• Evacuate Intra-Luminal Contents
• Evacuate Intra-Abdominal Space occupying Lesions
• Improve abdominal wall compliance;
• Correct positive fluid balance
• Organ Support
WSACS 2013
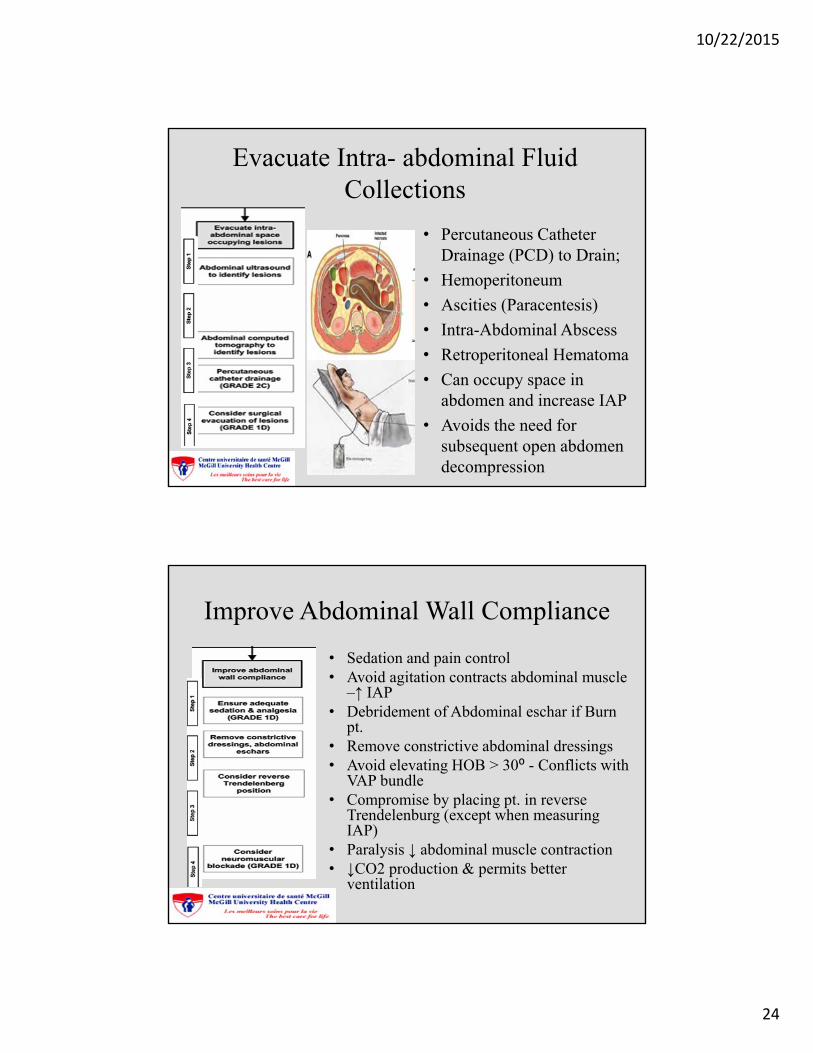
Evacuate Intra-Luminal Contents
• Insert NGT or OGT• Use Gastro-/Colonic Prokinetic agents
before constipation occurs• Assess tolerance of Nutrition• If residuals are high – feedings should
be decreased or discontinued.• Monitor bowel movements and
fecaloma • Administration of Enemas• Insert Rectal Tube • Consider Coloniscopic Decompression
10/22/2015
24
Evacuate Intra- abdominal Fluid Collections
• Percutaneous Catheter Drainage (PCD) to Drain;
• Hemoperitoneum
• Ascities (Paracentesis)
• Intra-Abdominal Abscess
• Retroperitoneal Hematoma
• Can occupy space in abdomen and increase IAP
• Avoids the need for subsequent open abdomen decompression
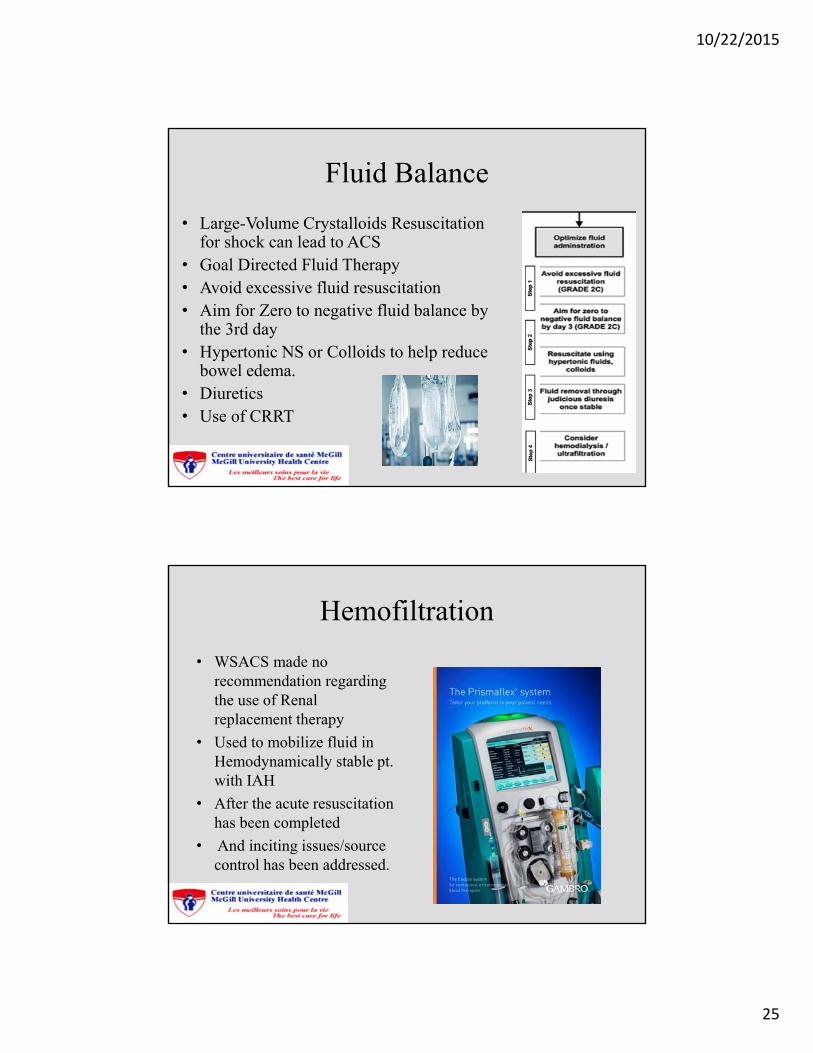
Improve Abdominal Wall Compliance
• Sedation and pain control• Avoid agitation contracts abdominal muscle
–↑ IAP• Debridement of Abdominal eschar if Burn
pt.• Remove constrictive abdominal dressings• Avoid elevating HOB > 30⁰ - Conflicts with
VAP bundle• Compromise by placing pt. in reverse
Trendelenburg (except when measuring IAP)
• Paralysis ↓ abdominal muscle contraction• ↓CO2 production & permits better
ventilation
10/22/2015
25
Fluid Balance
• Large-Volume Crystalloids Resuscitation for shock can lead to ACS
• Goal Directed Fluid Therapy• Avoid excessive fluid resuscitation• Aim for Zero to negative fluid balance by
the 3rd day• Hypertonic NS or Colloids to help reduce
bowel edema.• Diuretics • Use of CRRT
Hemofiltration
• WSACS made no recommendation regarding the use of Renal replacement therapy
• Used to mobilize fluid in Hemodynamically stable pt. with IAH
• After the acute resuscitation has been completed
• And inciting issues/source control has been addressed.
10/22/2015
26
Diuretics
• WSACS made no recommendation regarding the use of Diuretics
• To aid mobilize fluids in Hemodynamically stable pt. with IAH
• After Acute resuscitation has been completed and inciting issues/sources have been controlled.
Albumin
• WSACS made no recommendation regarding the administration of albumin versus not
• To help mobilize fluids in Hemodynamically stable pt. with IAH after the acute resuscitation has been done.
• And inciting issues and sources have been controlled.
10/22/2015
27
Organ Support
• Keep APP> 60 mmHg or greater with fluids
• Inotropes & Vasopressors can be used
• IAH can falsely elevated CVP and PAWP
• WSACS recommends using formula to correct for this
CVP corrected = CVP measured ‐ IAP/2PCOP corrected = PCOP measured ‐ IAP/2
Ventilation & Oxygenation
• High Peak Pressure and Higher Mean Airway Pressures can be problematic
• Decrease Tidal Volumes
• Pressure –limited Mode
• Permissive Hypercapnia may be necessary
• PEEP – may reduce ventilation perfusion mismatch and Improve Hypoxia
10/22/2015
28
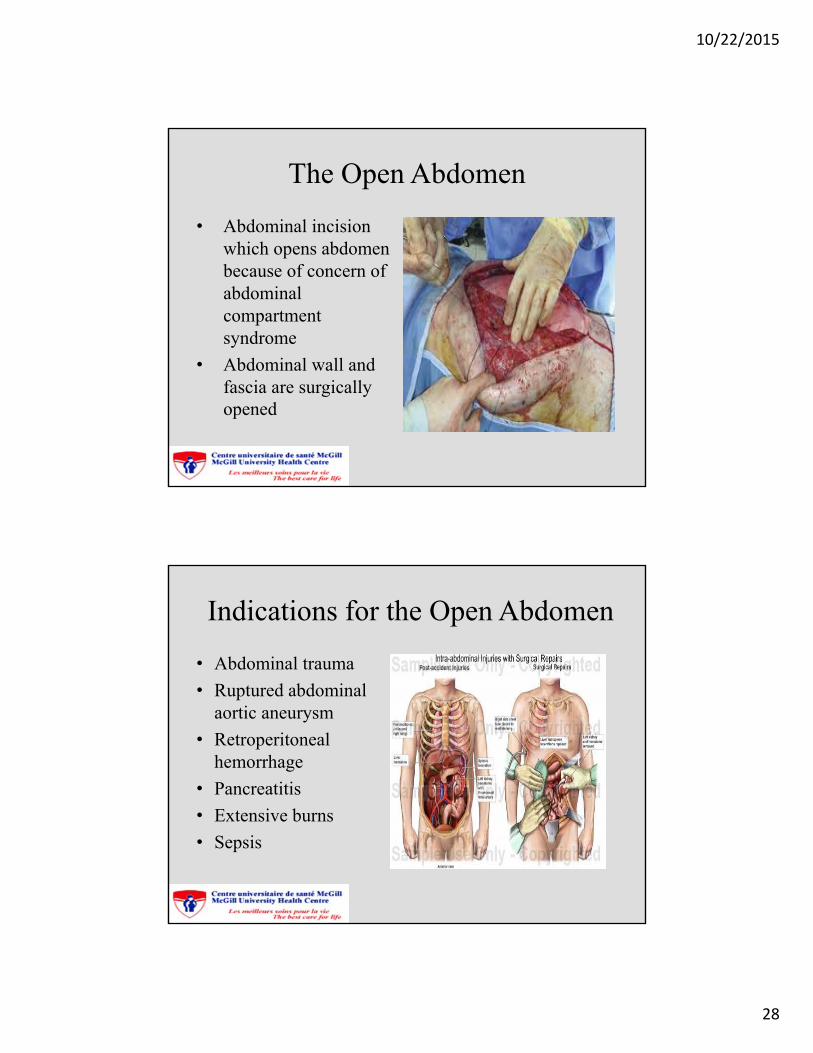
The Open Abdomen
• Abdominal incision which opens abdomen because of concern of abdominal compartment syndrome
• Abdominal wall and fascia are surgically opened
Indications for the Open Abdomen
• Abdominal trauma
• Ruptured abdominal aortic aneurysm
• Retroperitoneal hemorrhage
• Pancreatitis
• Extensive burns
• Sepsis
10/22/2015
29
Pathophysiology of the Abdomen
• Intestine is highly vascularized• Rich network of arteries, veins,
capillaries and lymphatic vessels
• In pathologic states there is a decrease in clearance of fluid from extracellular space.
• Resulting in swelling of the intestinal wall, interfering with perfusion of bowel
Pathophysiology of the Abdomen
• Peritoneal surface is highly vascularized
• Colonized with inflammatory cells
• Trauma results in excretion of pro-inflammatory substances
• That increase the local inflammatory response
• Leading to SIRS and potentially MODS.
10/22/2015
30
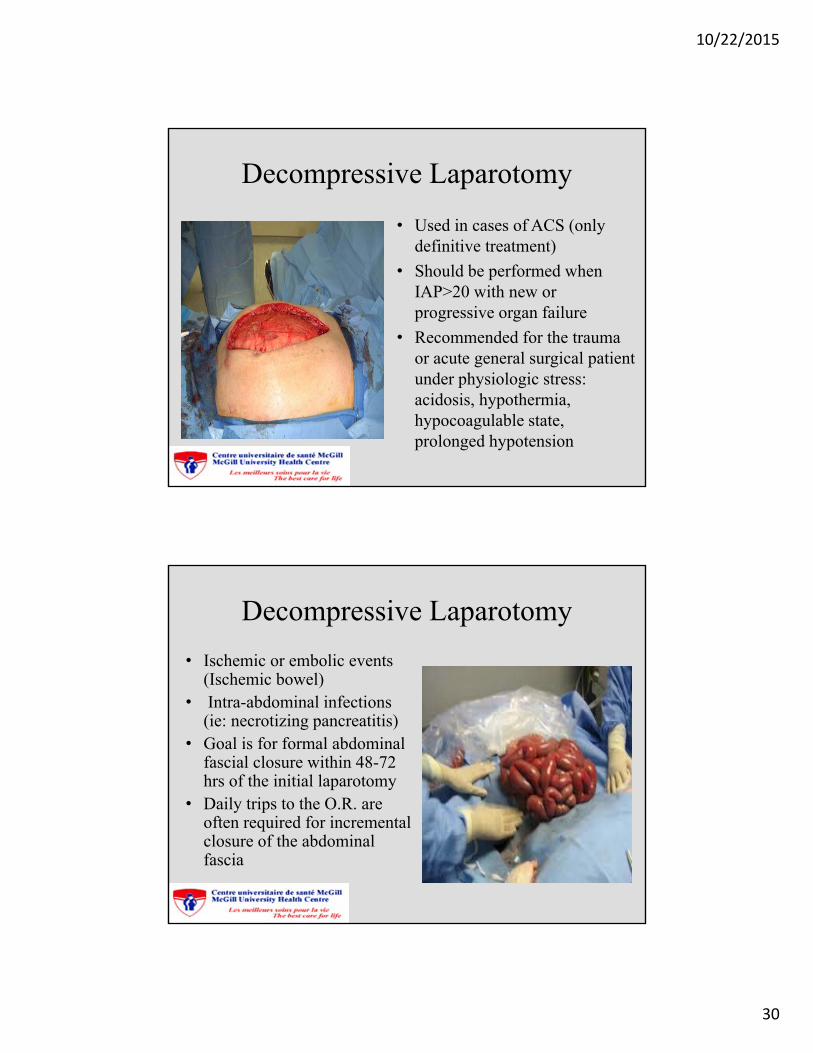
Decompressive Laparotomy
• Used in cases of ACS (only definitive treatment)
• Should be performed when IAP>20 with new or progressive organ failure
• Recommended for the trauma or acute general surgical patient under physiologic stress: acidosis, hypothermia, hypocoagulable state, prolonged hypotension
Decompressive Laparotomy
• Ischemic or embolic events (Ischemic bowel)
• Intra-abdominal infections (ie: necrotizing pancreatitis)
• Goal is for formal abdominal fascial closure within 48-72 hrs of the initial laparotomy
• Daily trips to the O.R. are often required for incremental closure of the abdominal fascia
10/22/2015
31
Benefits of Decompressive Laparotomy
• Decrease in intrathoracic pressure
• Improved oxygenation/ventilation
• Increased cardiac output
• Increased urine output
• Ease of re-exploration (2nd look)
• Control of abdominal contents
• Decrease in risk of IAH and ACS
• Fascial preservation for closure of the abdominal wall
Complications: Fluid Loss
• Significant amount of fluid can be lost through an open abdomen
• Requires close monitoring of negative pressure wound system suction output/overall pt. Intake and output
• Risk of hypovolemia
10/22/2015
32
Complications: Fluid Loss
• Loss of hypotonic fluid from the wound and peritoneal cavity can result in hypovolemic hypernatremia
• Serum Na+ levels need to be closely monitored
• In these cases, isotonic fluids should be used in the hypovolemic pt.
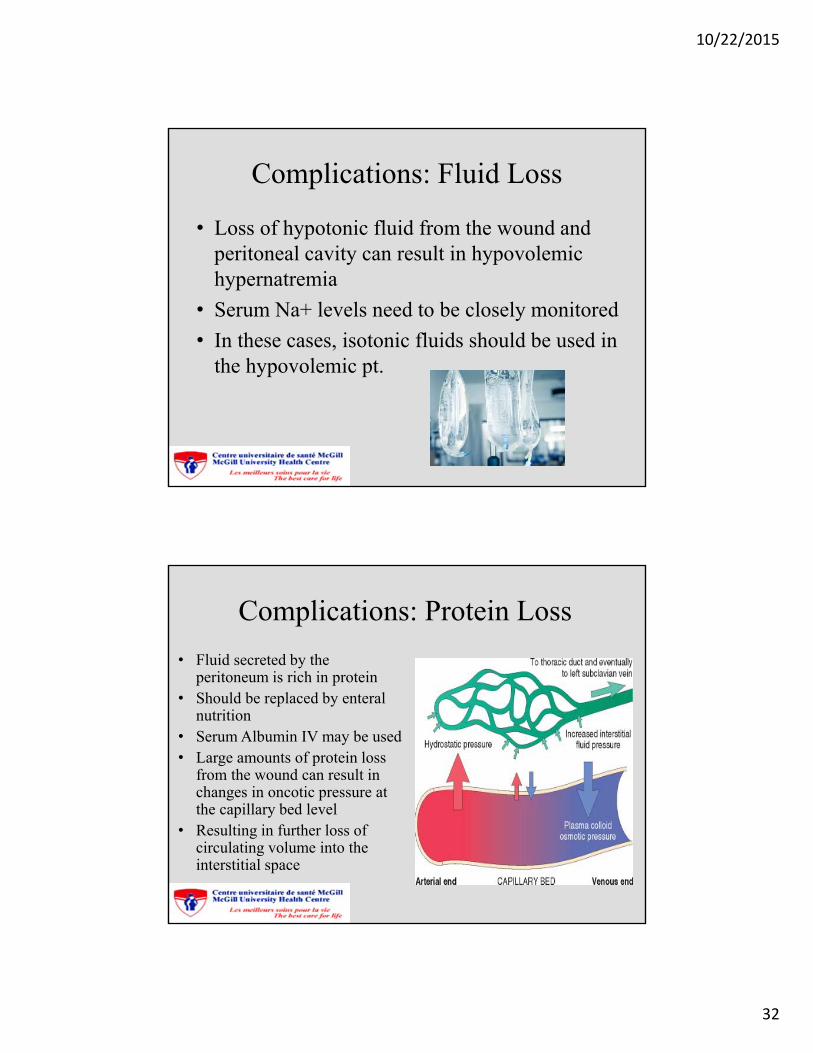
Complications: Protein Loss
• Fluid secreted by the peritoneum is rich in protein
• Should be replaced by enteral nutrition
• Serum Albumin IV may be used • Large amounts of protein loss
from the wound can result in changes in oncotic pressure at the capillary bed level
• Resulting in further loss of circulating volume into the interstitial space
10/22/2015
33
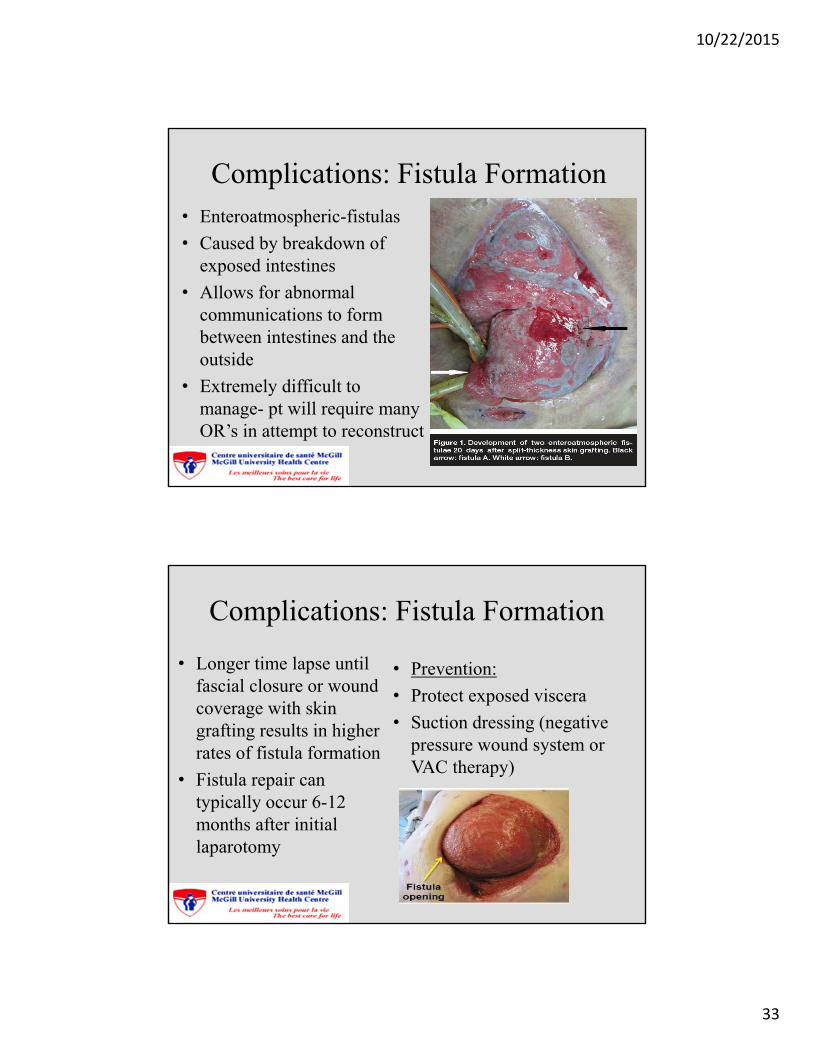
Complications: Fistula Formation• Enteroatmospheric-fistulas
• Caused by breakdown of exposed intestines
• Allows for abnormal communications to form between intestines and the outside
• Extremely difficult to manage- pt will require many OR’s in attempt to reconstruct
Complications: Fistula Formation
• Longer time lapse until fascial closure or wound coverage with skin grafting results in higher rates of fistula formation
• Fistula repair can typically occur 6-12 months after initial laparotomy
• Prevention:
• Protect exposed viscera
• Suction dressing (negative pressure wound system or VAC therapy)
10/22/2015
34
Complications: Fistula Formation
• Minimization of fistula output: nasogastric drainage diverts gastric secretions from entering the proximal small bowel
• PPI’s or H2 – receptor antagonists will decrease the volume and acidity of gastric secretions resulting in decreased fistula output
Complications: Fistula Formation
• Subcutaneous Octreotide : somatostatin analogue
• Octreotide inhibits the secretion of many GI hormones; gastrin, glucagon, cholecystokinin, secretin, insulin, and vasoactive intestinal peptide.
• Inhibits gastric acid secretion, pancreatic exocrine secretion, intestinal and gallbladder contractility
10/22/2015
35
Complications: Loss of Domain
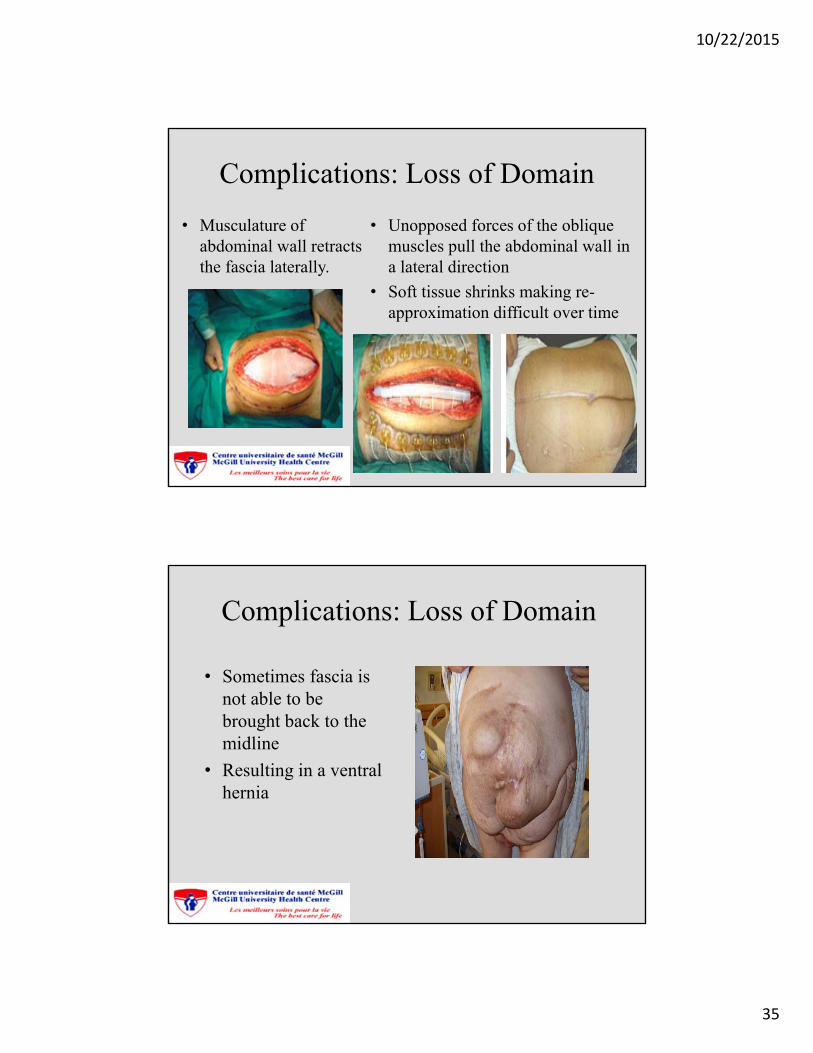
• Musculature of abdominal wall retracts the fascia laterally.
• Unopposed forces of the oblique muscles pull the abdominal wall in a lateral direction
• Soft tissue shrinks making re-approximation difficult over time
Complications: Loss of Domain
• Sometimes fascia is not able to be brought back to the midline
• Resulting in a ventral hernia
10/22/2015
36
Complications: Hernia
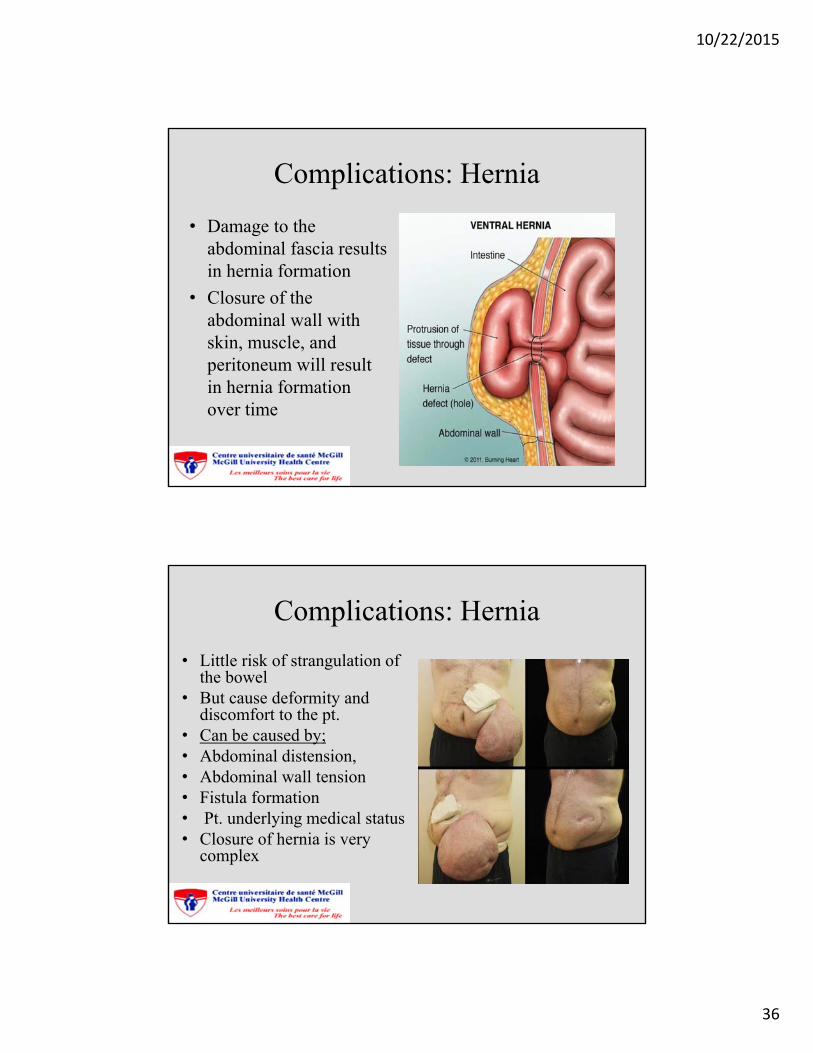
• Damage to the abdominal fascia results in hernia formation
• Closure of the abdominal wall with skin, muscle, and peritoneum will result in hernia formation over time
Complications: Hernia
• Little risk of strangulation of the bowel
• But cause deformity and discomfort to the pt.
• Can be caused by;• Abdominal distension,• Abdominal wall tension• Fistula formation • Pt. underlying medical status• Closure of hernia is very
complex
10/22/2015
37
Complications: Infection
• Large open surface area provides a venue for bacterial colonization
• Abdominal cavity infections
• Large potential for abscess formation
• Use of prophylactic antibiotics
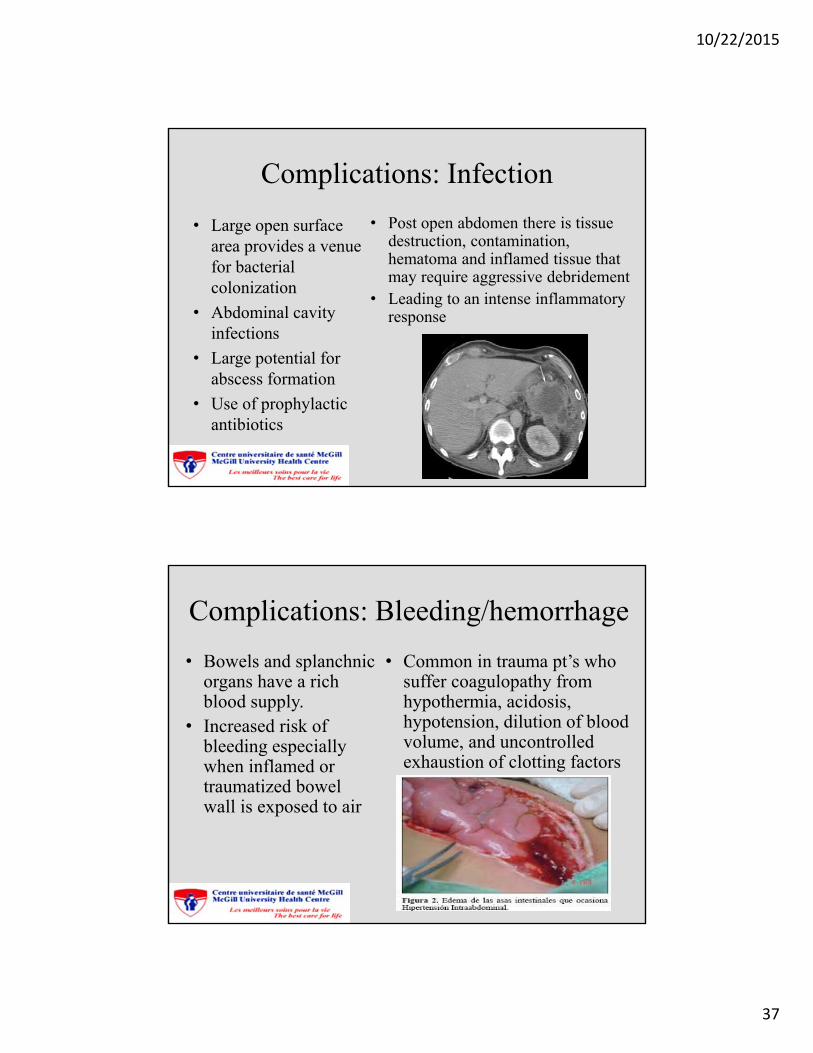
• Post open abdomen there is tissue destruction, contamination, hematoma and inflamed tissue that may require aggressive debridement
• Leading to an intense inflammatory response
Complications: Bleeding/hemorrhage
• Bowels and splanchnic organs have a rich blood supply.
• Increased risk of bleeding especially when inflamed or traumatized bowel wall is exposed to air
• Common in trauma pt’s who suffer coagulopathy from hypothermia, acidosis, hypotension, dilution of blood volume, and uncontrolled exhaustion of clotting factors
10/22/2015
38
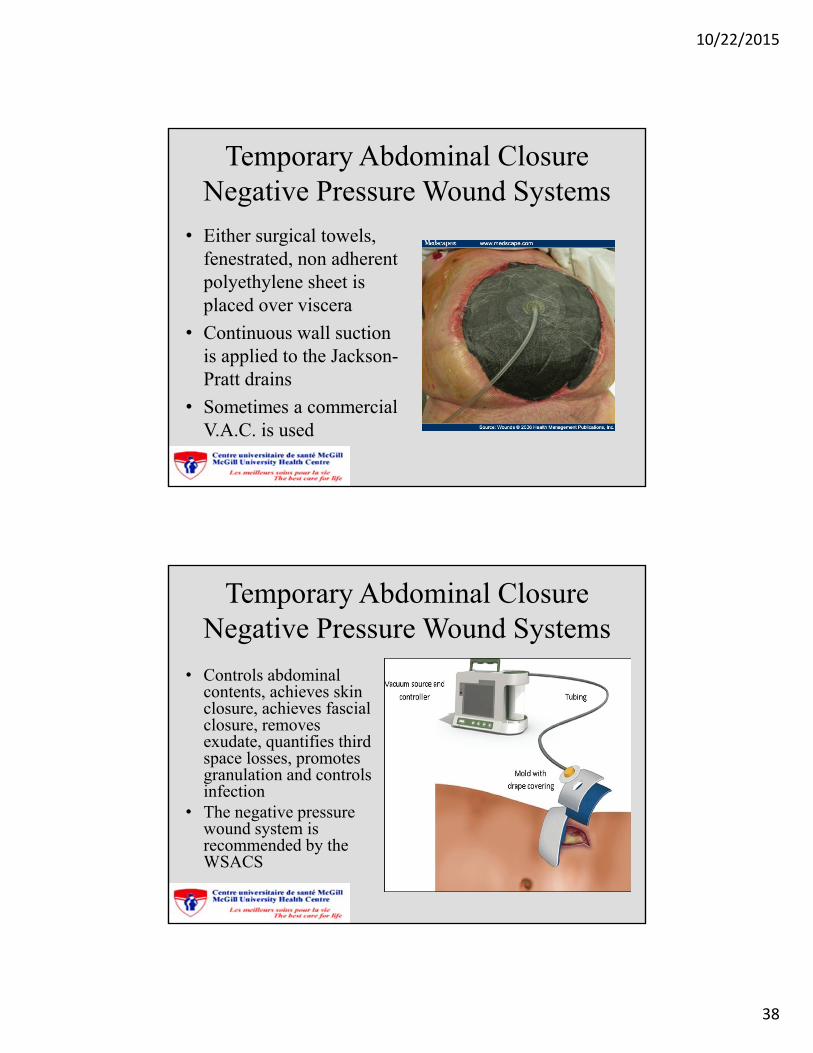
Temporary Abdominal ClosureNegative Pressure Wound Systems
• Either surgical towels, fenestrated, non adherent polyethylene sheet is placed over viscera
• Continuous wall suction is applied to the Jackson-Pratt drains
• Sometimes a commercial V.A.C. is used
Temporary Abdominal ClosureNegative Pressure Wound Systems
• Controls abdominal contents, achieves skin closure, achieves fascial closure, removes exudate, quantifies third space losses, promotes granulation and controls infection
• The negative pressure wound system is recommended by the WSACS
10/22/2015
39
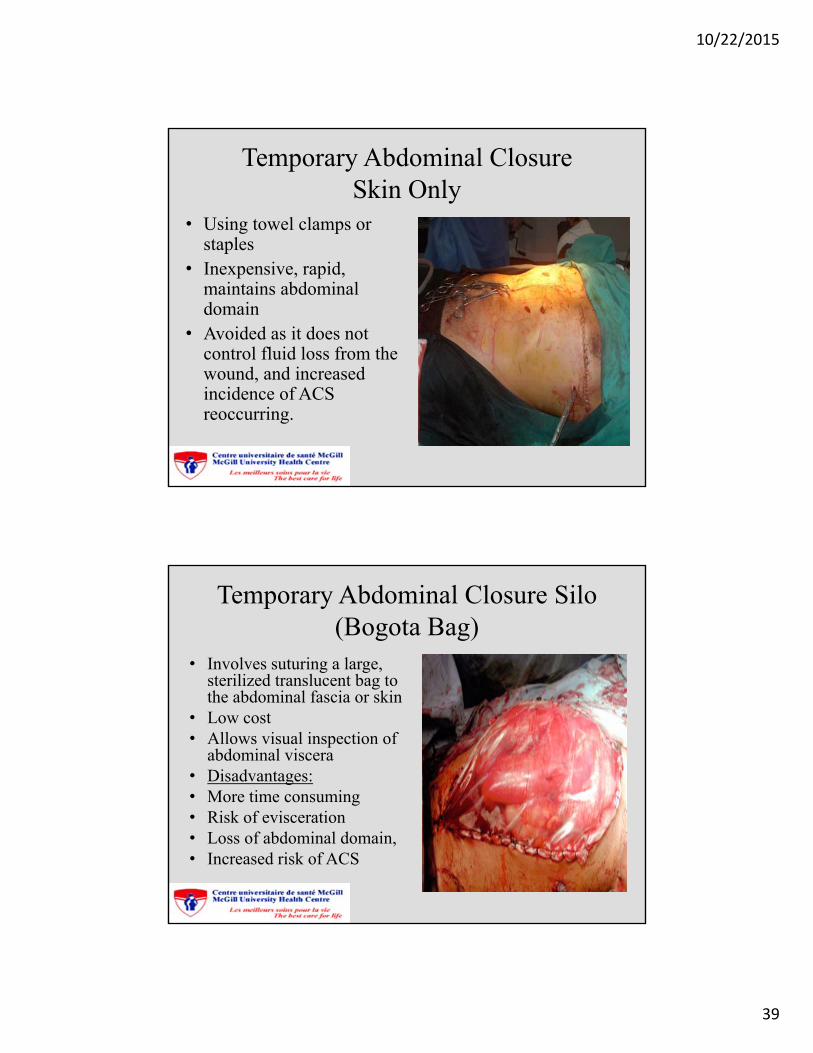
Temporary Abdominal ClosureSkin Only
• Using towel clamps or staples
• Inexpensive, rapid, maintains abdominal domain
• Avoided as it does not control fluid loss from the wound, and increased incidence of ACS reoccurring.
Temporary Abdominal Closure Silo (Bogota Bag)
• Involves suturing a large, sterilized translucent bag to the abdominal fascia or skin
• Low cost• Allows visual inspection of
abdominal viscera• Disadvantages:• More time consuming• Risk of evisceration• Loss of abdominal domain,• Increased risk of ACS
10/22/2015
40
Temporary Abdominal ClosureZipper (Wittmann Patch)
• Velcro like prosthetic is placed over the abdomen
• Allows for easy entrance into the abdomen for re-exploration
• Facilitates closure of the abdomen with serial narrowing and trimming of the mesh until the abdomen is closed
• Risk of fascial necrosis
10/22/2015
41
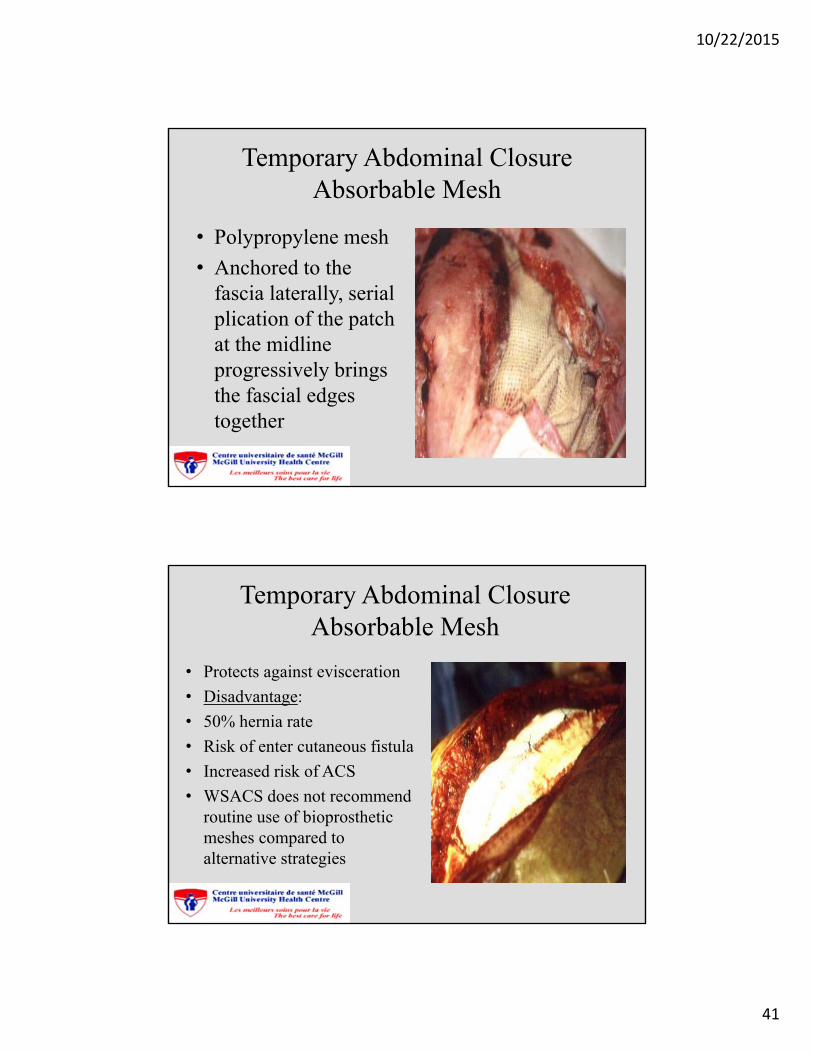
Temporary Abdominal ClosureAbsorbable Mesh
• Polypropylene mesh
• Anchored to the fascia laterally, serial plication of the patch at the midline progressively brings the fascial edges together
Temporary Abdominal ClosureAbsorbable Mesh
• Protects against evisceration
• Disadvantage:
• 50% hernia rate
• Risk of enter cutaneous fistula
• Increased risk of ACS
• WSACS does not recommend routine use of bioprosthetic meshes compared to alternative strategies
10/22/2015
42
Nutrition Support Considerations
• Early administration of enteral nutrition;
• Improves wound healing
• Reduces hospital and ICU lengths of stay
• Decreases infection rates
• May improve survival after critical illness and injury
• Helps decrease gut edema,
• Helps earlier fascial closure
• Either nasogastric tube or post pyloric tube placement
Nutrition Support Considerations
• Sometimes TPN may need to be used (depending on extent of bowel resection/damage)
• In case of TPN central line or PICC line placement
10/22/2015
43
Nursing Care
• Monitor the dressing for any signs of leakage
• Notify surgical team if so - dressing will need to be changed
• Abdominal contents should be inspected for; colour, warmth, capillary refill
• Importance of always maintaining a good seal in dressing and drains
• Drains and Jackson-Pratt’s need to be hooked up to suction immediately post-op
Nursing Care
• Sedation and pain control
• Pt. needs to remain sedated due to risk of evisceration if pt too agitated.
• Monitoring CVP’s- negative balance is preferred (aggressive diuresis)
• Pt should remain intubated due to frequent trips to OR for attempts at fascial closure or dressing changes
10/22/2015
44
Nursing Care
• Enteral feeding-recommended and safe in open abdomen
• Post-op monitoring for bleeding (check the canister, serial Hgb’s, hemodynamics)
• Psychosocial aspects: Body image issues, especially with younger trauma patient population
• Post-op monitoring of bladder pressures for IAH
• Patient positioning: minimal turning, pt cannot be sat up at 90 degrees, risk of evisceration
• Risk of skin breakdown and VAP
• In case of evisceration: cover with moistened sterile dressing and contact stat surgical service
Conclusion
• ACS is extremely common in the critical care patient population
• Unfortunately overlooked or missed
• Increased mortality and morbidity
• ICU nurses play an extremely important role in assessing and caring for these patients
• Should a bladder pressure be considered like a CVP measurement?

10/22/2015
45
10/22/2015
46
Special Thank You..
• Dr. Andrew Beckett, Trauma staff MGH
• Dr. Kosar Khwaja, Trauma staff MGH
• Ms. Julie Kinnon, Nurse Educator, MGH ICU
• Ms. Cathy Becker, Nurse Educator, MGH ICU
• Ms. Colleen Stone, Head Nurse, MGH ICU
References• Demetriades. D. (2012). Total management of the open abdomen. International Wound Journal, 9(Suppl.1), 17-24.
• Emergency Nurses Association “Trauma Nursing Core Course” Sixth Edition, 2007.
• Fernandez, Luis. G., & Geibel, John. (2013). Temporary Abdominal Closure Techniques. Medscape References, 1-16.
• Friese, R. (2012). The Open Abdomen: Definitions, management principles, and nutrition support considerations. Nutrition in Clinical Practice XX(X). 1-7.
• Gestering, M., Sanfey, H., Frankel, H., L. & Collins, K. A. (2014). Abdominal Compartment Syndrome. Up To Date: 1- 17.
• Godat, L., Kobayashi, L., Costantini, T., & Coimbra, R. (2013). Abdominal damage control surgery and reconstruction: World Society of Emergency Surgery position paper. World Journal of Emergency Surgery, 8:53, 1-7.
• Harrell, Bradeley, R. & Melander, Sheila. (2012). Identifying the Association Among Risk Factors and Mortality in Trauma patients with Intra-Abdominal Hypertension and Abdominal Compartment Syndrome. Journal of Trauma Nursing, 19, 3. 182 – 189.
• Kausen, T., Otto, J., Steinau, G. Hoer, J., Srinivasan, P. K., & Schachtrupp, A.(2012). Recognition and Management of Abdominal Compartment Syndrome among German anesthetists and surgeons: a national survey. Annals of Intensive Care, 2, (1). 57.
• Kaplan, M., Banwell, P., Orgill, D.P., Ivatury, R.R., Demetriades, D., Moore, F.A.,...Henry, S. (2005). Guidelines for the management of the open abdomen: Recommendations from a multidisciplinary expert advisory panel. Supplement To Wounds: A Compendium Of Clinical Research and Practice, 1-24.
• Kirkpatrick, A.W., Roberts, D.J., De Waele, J., Jaeschke, R., Malbrain, M.L.N.G., De Keulenaer, B.,... Olvera, C. (2013). Intra-abdominal hypertension and the abdominal compartment syndrome: Updated consensus definitions and clinical practice guidelines from the World Society of the Abdominal Compartment Syndrome. Intensive Care Medicine, 39, 1190-1206.

10/22/2015
47
References• Leppaniemi, Ari. (2009). Surgical management of abdominal compartment syndrome; indications and techniques.
Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 17:17. 1 -5.
• Luckianov, G. M., Ellis, M., Governale, D. & Kaplan, L. J. (2012). Abdominal Compartment Syndrome: Risk Factors, Diagnosis, and Current Therapy. Hindawi Publishing Corporation Critical Care Research and Practice 2012, 8. doi: 10.1155/2012/908 169.
• Lee, Rosemary Khoelh. (2012). Intra-Abdominal Hypertension and Abdominal Compartment Syndrome: A Comprehensive Overview. Critical Care Nurse, 2012, 32, 1, 1- 32.
• Mazzei, M. A., Guerrini, S., Squitieri, N. C., Cagini, L., Macarini, L., Coppolino, F., Giganti, M., Volterrani, L.. .(2013). The Role of US examination in the management of acute abdomen. Critical Ultrasound Journal, 5(1): 56.
• MacLean, A.A., O’Keeffe, T., & Augenstein, J. (2008). Management strategies for the open abdomen: Survey of the American Association for the Surgery of Trauma Membership. Acta Chirurgical Belgica, 108, 212-222.
• Martin, N., & Sarani, B. (2014). Management of the open abdomen in adults. UpToDate, 1-21.
• Navsaria, P., Nicol, A., Hudson, D., Cockwill, J. & Smith, J. (2013). Negative pressure wound therapy management of the “open abdomen” following trauma: a Prospective study and systematic review. World Journal of Emergency Surgery,4: 1- 8.
• Saggi, B. H., Ivatory, R., & Sugerman, H. J. (2001). Abdominal Compartment Syndrome. Surgical Therapy NCBI, 1 – 17.
• Sucher, Joseph, F., Balogh, Zsolt, J. & Moore, Frederick, A. (2006). Abdominal Compartment Syndrome and Management of the Open Abdomen. Intensive Care Med. 32(11): 1722 – 1732
• Urden, L.D., Stacey, K.M., Lough, M.E., Thelan’s Critical Care Nursing Diagnosis and Management, 5th Edition, 2006.
• Yuan, Y., Ren, J., & He, Y. (2013). Current status of the open abdomen treatment for intra-abdominal infection. Gastroenterology Research and Practice, (article ID 532013). 1-7.
• Walker, Jeffery, & Criddle, Laura M.(2013). Pathophysiology and Management of Abdominal Compartments Syndrome. American Journal of Critical Care, 2013, 12: 367 – 371.
• Wagner, K. D., Johnson, K. L., and Hardin-Pierce, M. G., High- Acuity Nursing, 5th Edition, 2010.