chapter 263: abdominal trauma
TRANSCRIPT
Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e
Chapter 263: Abdominal Trauma L. Keith French; Stephanie Gordy; O. John Ma
INTRODUCTION
Abdominal trauma accounts for 15% to 20% of all trauma deaths.1 Although the liver is the most frequently injured abdominal organ, the spleen is the most frequently injured
intra-abdominal organ from sports accidents.2 Death may occur as a consequence of massive hemorrhage and generally results in early demise soon a�er the injury. Patientswho survive the initial traumatic insult are at risk for infection and su�er mortality or morbidity secondary to sepsis.
PATHOPHYSIOLOGY
BLUNT ABDOMINAL TRAUMA
The most common mechanism for blunt abdominal trauma is a motor vehicle collision.1 All abdominal structures are at risk, and ultimately the biomechanics of the traumaticforce determine which organs are a�ected. Compressive, shearing or stretching, and acceleration/deceleration forces impact the abdominal cavity di�erently. This potentiallyleads to abdominal wall, solid organ, or hollow viscous injuries. Abdominal organs may be relatively mobile or fixed. Injury is common in transition areas between thesestructures. The ligament of Treitz and the distal small bowel represent transition areas where mesenteric or small bowel injuries may occur.
Falls from significant heights produce injury as a function of the fall distance, the surface the victim lands on, and the manner of surface impact. Hollow viscous rupture is the
typical intra-abdominal injury.3 Retroperitoneal injury and hemorrhage may occur as force is transmitted along the axial skeleton.
Pedestrians struck by vehicles or motorcyclists and bicyclists who crash generally have no protection to their abdomen and are at high risk for intra-abdominal injuries.
PENETRATING ABDOMINAL TRAUMA
Stab and gunshot wounds produce injury as the foreign object passes through tissue. With gunshot wounds, there may be additional injury from the transmitted energy of theblast. Furthermore, gunshot wounds create secondary missiles such as fragmented bone that may increase the traumatic burden.
The length, trajectory, and fragmentation of the penetrating object will not necessarily be known during the evaluation. Therefore, assume any penetrating injury to the lowerchest, pelvis, flank, or back to have penetrated the abdominal cavity until proven otherwise.
CLINICAL FEATURES
Clinical signs may be obvious (such as evisceration) or occult. Factors making the diagnosis of an abdominal injury challenging include concomitant injuries (particularlysignificant head injuries), referred pain, intoxication with alcohol or other toxicological substances, or language barriers. Young, healthy patients may be able to compensatefor intra-abdominal hemorrhage before clinical signs become overt.
PHYSICAL EXAMINATION
Inspect the abdomen for external signs of trauma (e.g., abrasions, lacerations, contusions, seatbelt marks). A normal-appearing abdomen does not exclude serious intra-abdominal injury. Cullen's sign and Grey Turner's sign (periumbilical and flank ecchymosis) generally represent delayed findings of intraperitoneal bleeding. Followinginspection, palpate the abdomen in all quadrants, making note of tenderness, tympany, or rigidity. For patients who are observed in the ED, serial assessments by the sameprovider are ideal.
Abdominal tenderness, rigidity, distention, or tympany may not be present during the initial examination and may take hours or days to develop. Reliance on physical examalone, particularly with a worrisome mechanism of injury, may result in an unacceptably high misdiagnosis rate. As many as 45% of blunt trauma patients thought to have a
benign abdomen on initial physical exam are later found to have a significant intra-abdominal injury.4
ABDOMINAL WALL INJURIES
Contusions of the abdominal wall musculature may result either from a direct blow or indirectly via a sudden muscular contraction. Symptoms include pain with flexion androtation of the trunk as well as focal tenderness to percussion. Rectus abdominis hematomas may mimic intra-abdominal injury. Rectus hematomas occur from epigastrictrauma or injury to the vessels of the abdominal wall. As a hematoma develops between the rectus sheath, the patient develops pain and o�en a palpable mass inferior to the
umbilicus.2
SOLID ORGAN INJURIES
Signs and symptoms of a solid organ injury are generally due to blood loss. An increase in pulse pressure may be the only clue to loss of ≤15% of total blood volume. As bloodloss continues, heart and respiratory rate increase. Hypotension may not occur until a 30% decrease in circulating volume occurs. At this point, urinary output drops andpatients may become anxious and confused. With some injuries, pain and bleeding may be minimal and overlooked or dismissed. Delayed rupture can occur in splenic andhepatic injuries.
Splenic injuries may cause referred pain into the le� shoulder or arm. Patients with liver injuries may complain of right shoulder pain. Pregnancy and mononucleosis areconditions that may predispose a patient to splenic injuries.
HOLLOW VISCOUS AND MESENTERIC INJURIES
In blunt abdominal trauma, the incidence of blunt bowel and mesenteric injuries varies (1% to 12%) but occurs in about 5% of patients.5,6 Hollow viscus injuries producesymptoms from the combination of blood loss and peritoneal contamination by GI contents. Hemorrhage from a mesenteric injury may be minimal and not be obvious onphysical exam. Chemical irritation of the peritoneum from gastric acid contents may produce immediate pain, although bacterial contamination of the abdominal cavity may
result in delayed signs and symptoms. Delays in diagnosis and operative management are associated with an increase in mortality.6
RETROPERITONEAL INJURIES
The retroperitoneal structures discussed in this chapter include the pancreas (excluding the tail) and duodenum. See "Genitourinary Injuries" for a discussion of kidney,ureter, and bladder injuries.
Pancreatic injuries are present in approximately 4% of patients with abdominal trauma and are associated with significant morbidity and mortality.7 There are no specificsigns and symptoms of pancreatic injury, but mechanism of injury provides some clues to diagnosis. Pancreatic trauma o�en occurs from rapid deceleration. Unrestraineddrivers who hit the steering column or bicyclists who fall against a handlebar are at risk for pancreatic injuries. Initial symptoms may be delayed if the injury is minor.
Duodenal injuries may be relatively asymptomatic on presentation, and a small hematoma of the duodenum may go undiagnosed. As a duodenal hematoma expands,however, signs and symptoms of gastric outlet obstruction develop (abdominal pain, distention, and vomiting). Duodenal rupture generally occurs following high-velocitydeceleration events where the intraluminal pressure of the pylorus and proximal small bowel rapidly increases. The ruptured contents are generally contained within theretroperitoneum and may be missed with studies that investigate the peritoneum exclusively. For patients with a delayed presentation, fever and leukocytosis herald thedevelopment of an abscess or sepsis.
DIAPHRAGMATIC INJURIES
The diaphragm may spasm secondary to a direct blow to the epigastrium. The patient will experience di�iculty breathing as the diaphragm loses its ability to relax and allowthe lungs to expand. This process is sometimes referred to as "getting the wind knocked out." As the diaphragm relaxes, symptoms abate.
Diaphragmatic rupture may result from a penetrating injury or blunt force mechanism. The condition is uncommon (0.8% to 5% of patients with thoracoabdominal injury) and
is almost exclusively a le�-sided phenomenon.8 Signs and symptoms are nonspecific and may be attributed to associated injuries. Failure to diagnose and treat diaphragmaticrupture may lead to delayed herniation or strangulation of abdominal contents through the diaphragmatic defect.
DIAGNOSIS
Although multiple diagnostic modalities exist to detect intra-abdominal injuries, no study is fail proof. Therefore, a combination of careful physical exam, attention to themechanisms and circumstances of injury, and judicious selection of diagnostic studies is used for diagnosis. Hemodynamic instability may limit the utilization of somediagnostic testing before definitive treatment is initiated (such as laparotomy or transfer to a trauma center).
Not every patient with multisystem or isolated abdominal trauma will need a diagnostic evaluation beyond a physical exam. However, because the consequences of a missedintra-abdominal injury may be significant, augment an initial exam with laboratory analysis, imaging study, or repeat examination in several conditions (Table 263-1).
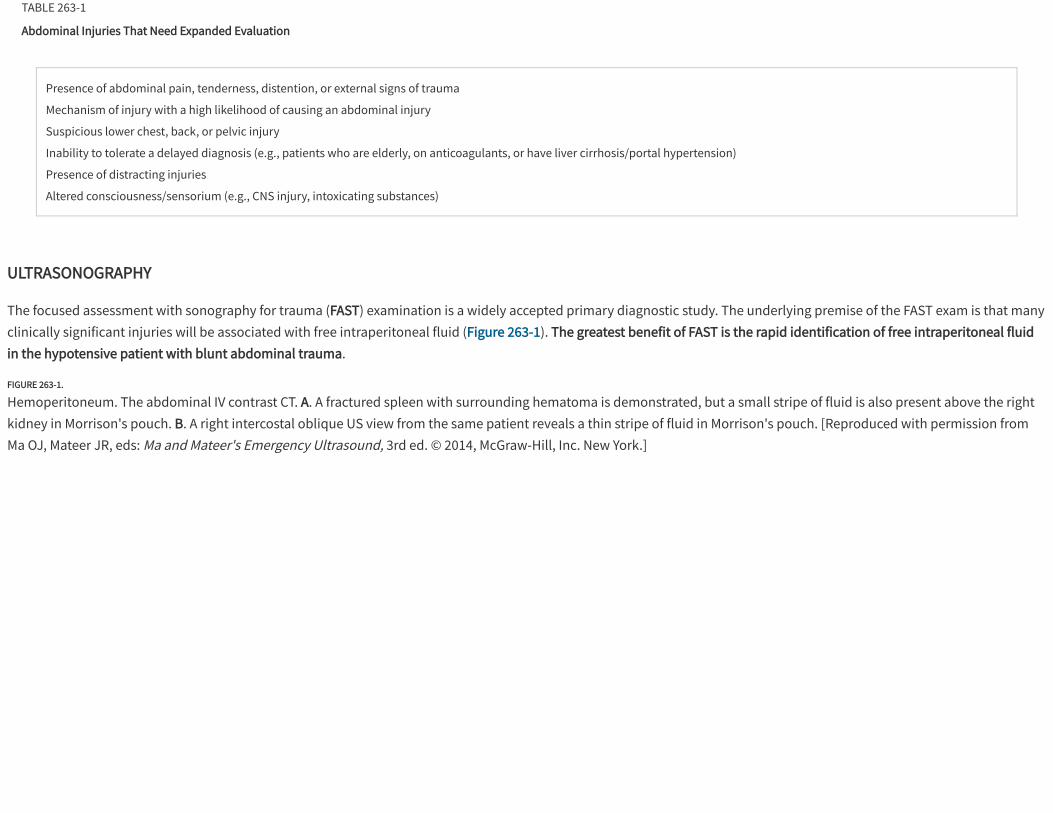
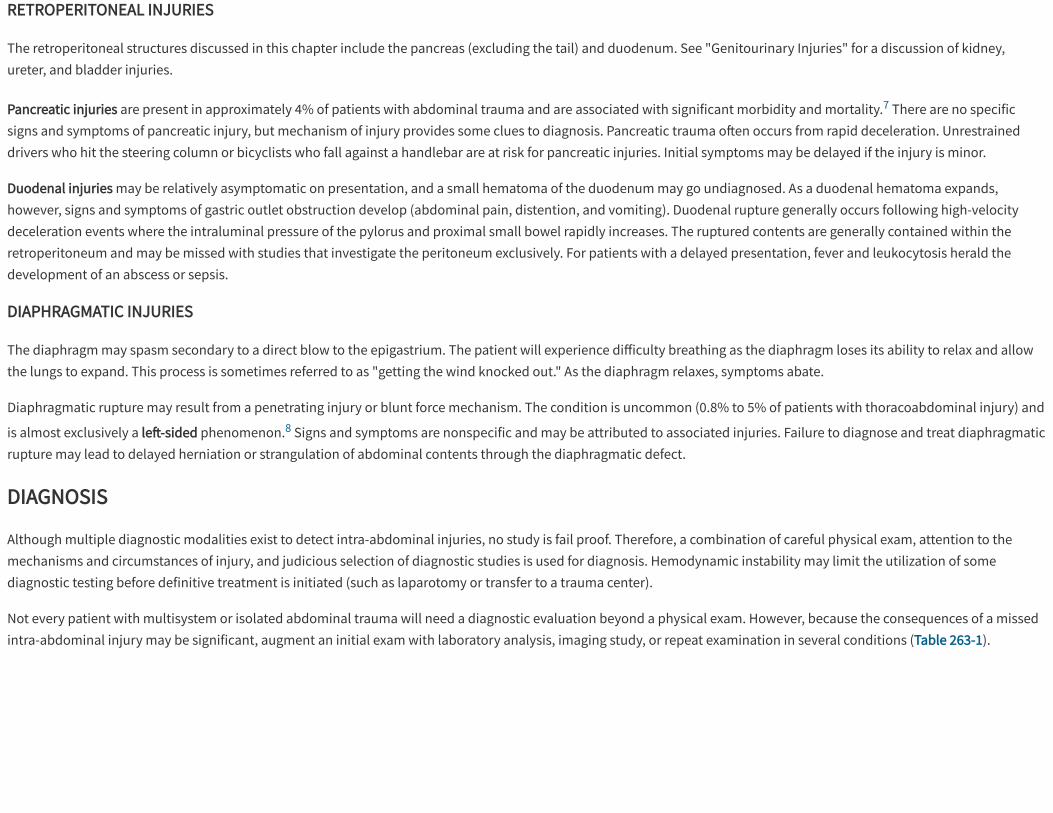
TABLE 263-1
Abdominal Injuries That Need Expanded Evaluation
Presence of abdominal pain, tenderness, distention, or external signs of trauma
Mechanism of injury with a high likelihood of causing an abdominal injury
Suspicious lower chest, back, or pelvic injury
Inability to tolerate a delayed diagnosis (e.g., patients who are elderly, on anticoagulants, or have liver cirrhosis/portal hypertension)
Presence of distracting injuries
Altered consciousness/sensorium (e.g., CNS injury, intoxicating substances)
ULTRASONOGRAPHY
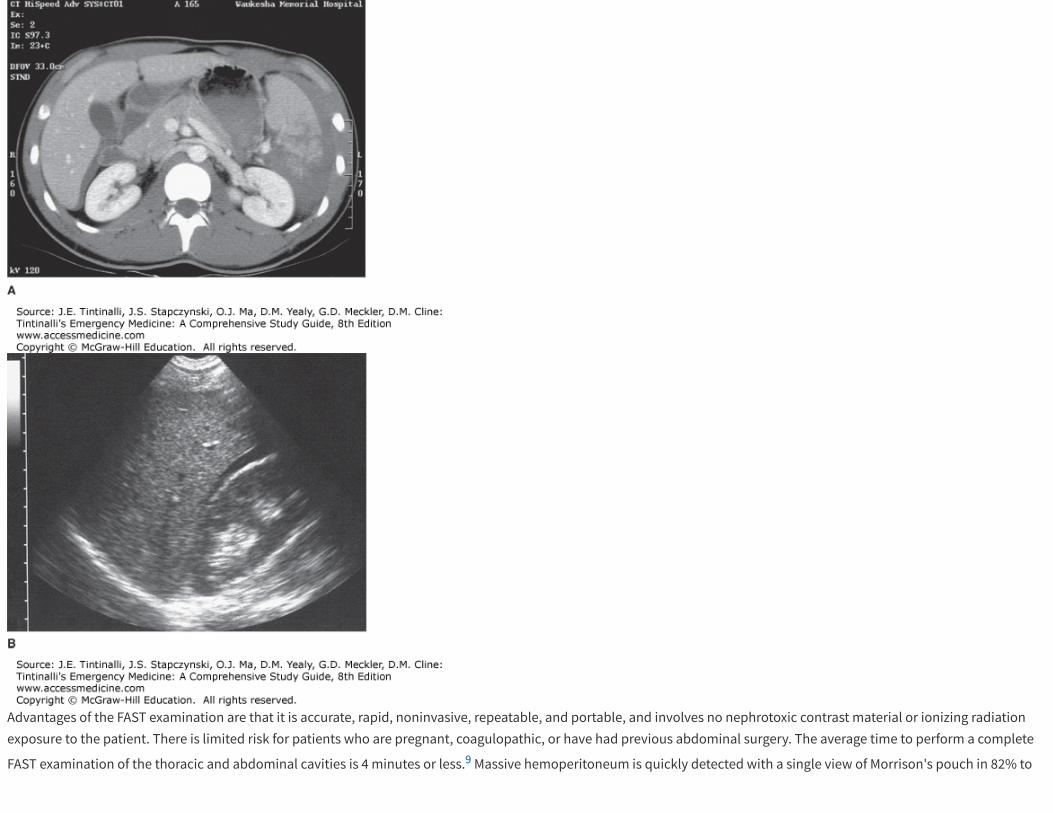
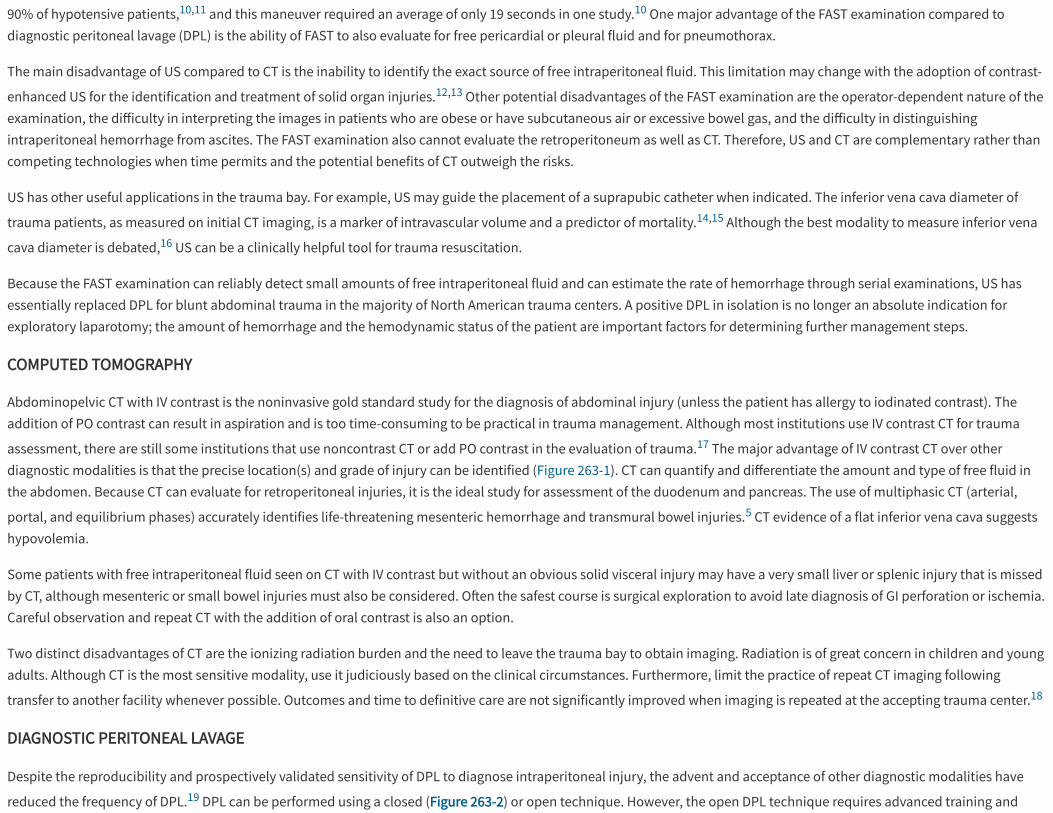
The focused assessment with sonography for trauma (FAST) examination is a widely accepted primary diagnostic study. The underlying premise of the FAST exam is that manyclinically significant injuries will be associated with free intraperitoneal fluid (Figure 263-1). The greatest benefit of FAST is the rapid identification of free intraperitoneal fluidin the hypotensive patient with blunt abdominal trauma.
FIGURE 263-1.
Hemoperitoneum. The abdominal IV contrast CT. A. A fractured spleen with surrounding hematoma is demonstrated, but a small stripe of fluid is also present above the rightkidney in Morrison's pouch. B. A right intercostal oblique US view from the same patient reveals a thin stripe of fluid in Morrison's pouch. [Reproduced with permission fromMa OJ, Mateer JR, eds: Ma and Mateer's Emergency Ultrasound, 3rd ed. © 2014, McGraw-Hill, Inc. New York.]
Advantages of the FAST examination are that it is accurate, rapid, noninvasive, repeatable, and portable, and involves no nephrotoxic contrast material or ionizing radiationexposure to the patient. There is limited risk for patients who are pregnant, coagulopathic, or have had previous abdominal surgery. The average time to perform a complete
FAST examination of the thoracic and abdominal cavities is 4 minutes or less.9 Massive hemoperitoneum is quickly detected with a single view of Morrison's pouch in 82% to
90% of hypotensive patients,10,11 and this maneuver required an average of only 19 seconds in one study.10 One major advantage of the FAST examination compared todiagnostic peritoneal lavage (DPL) is the ability of FAST to also evaluate for free pericardial or pleural fluid and for pneumothorax.
The main disadvantage of US compared to CT is the inability to identify the exact source of free intraperitoneal fluid. This limitation may change with the adoption of contrast-
enhanced US for the identification and treatment of solid organ injuries.12,13 Other potential disadvantages of the FAST examination are the operator-dependent nature of theexamination, the di�iculty in interpreting the images in patients who are obese or have subcutaneous air or excessive bowel gas, and the di�iculty in distinguishingintraperitoneal hemorrhage from ascites. The FAST examination also cannot evaluate the retroperitoneum as well as CT. Therefore, US and CT are complementary rather thancompeting technologies when time permits and the potential benefits of CT outweigh the risks.
US has other useful applications in the trauma bay. For example, US may guide the placement of a suprapubic catheter when indicated. The inferior vena cava diameter of
trauma patients, as measured on initial CT imaging, is a marker of intravascular volume and a predictor of mortality.14,15 Although the best modality to measure inferior vena
cava diameter is debated,16 US can be a clinically helpful tool for trauma resuscitation.
Because the FAST examination can reliably detect small amounts of free intraperitoneal fluid and can estimate the rate of hemorrhage through serial examinations, US hasessentially replaced DPL for blunt abdominal trauma in the majority of North American trauma centers. A positive DPL in isolation is no longer an absolute indication forexploratory laparotomy; the amount of hemorrhage and the hemodynamic status of the patient are important factors for determining further management steps.
COMPUTED TOMOGRAPHY
Abdominopelvic CT with IV contrast is the noninvasive gold standard study for the diagnosis of abdominal injury (unless the patient has allergy to iodinated contrast). Theaddition of PO contrast can result in aspiration and is too time-consuming to be practical in trauma management. Although most institutions use IV contrast CT for trauma
assessment, there are still some institutions that use noncontrast CT or add PO contrast in the evaluation of trauma.17 The major advantage of IV contrast CT over otherdiagnostic modalities is that the precise location(s) and grade of injury can be identified (Figure 263-1). CT can quantify and di�erentiate the amount and type of free fluid inthe abdomen. Because CT can evaluate for retroperitoneal injuries, it is the ideal study for assessment of the duodenum and pancreas. The use of multiphasic CT (arterial,
portal, and equilibrium phases) accurately identifies life-threatening mesenteric hemorrhage and transmural bowel injuries.5 CT evidence of a flat inferior vena cava suggestshypovolemia.
Some patients with free intraperitoneal fluid seen on CT with IV contrast but without an obvious solid visceral injury may have a very small liver or splenic injury that is missedby CT, although mesenteric or small bowel injuries must also be considered. O�en the safest course is surgical exploration to avoid late diagnosis of GI perforation or ischemia.Careful observation and repeat CT with the addition of oral contrast is also an option.
Two distinct disadvantages of CT are the ionizing radiation burden and the need to leave the trauma bay to obtain imaging. Radiation is of great concern in children and youngadults. Although CT is the most sensitive modality, use it judiciously based on the clinical circumstances. Furthermore, limit the practice of repeat CT imaging following
transfer to another facility whenever possible. Outcomes and time to definitive care are not significantly improved when imaging is repeated at the accepting trauma center.18
DIAGNOSTIC PERITONEAL LAVAGE
Despite the reproducibility and prospectively validated sensitivity of DPL to diagnose intraperitoneal injury, the advent and acceptance of other diagnostic modalities have
reduced the frequency of DPL.19 DPL can be performed using a closed (Figure 263-2) or open technique. However, the open DPL technique requires advanced training and
Abbreviation: RBC = red blood cell.
expertise. Some advocate the use of DPL in the hemodynamically unsTable patient with concern for intra-abdominal injury when the FAST exam is negative.19 Table 263-2 lists
criteria for laparotomy based on DPL results.20
TABLE 263-2
Criteria for Positive Diagnostic Peritoneal Lavage
>10 mL free flowing blood immediately on aspiration
>15,000 RBC/mm3 in abdominal wounds or >25,000 RBC/mm3 in lower chest wounds
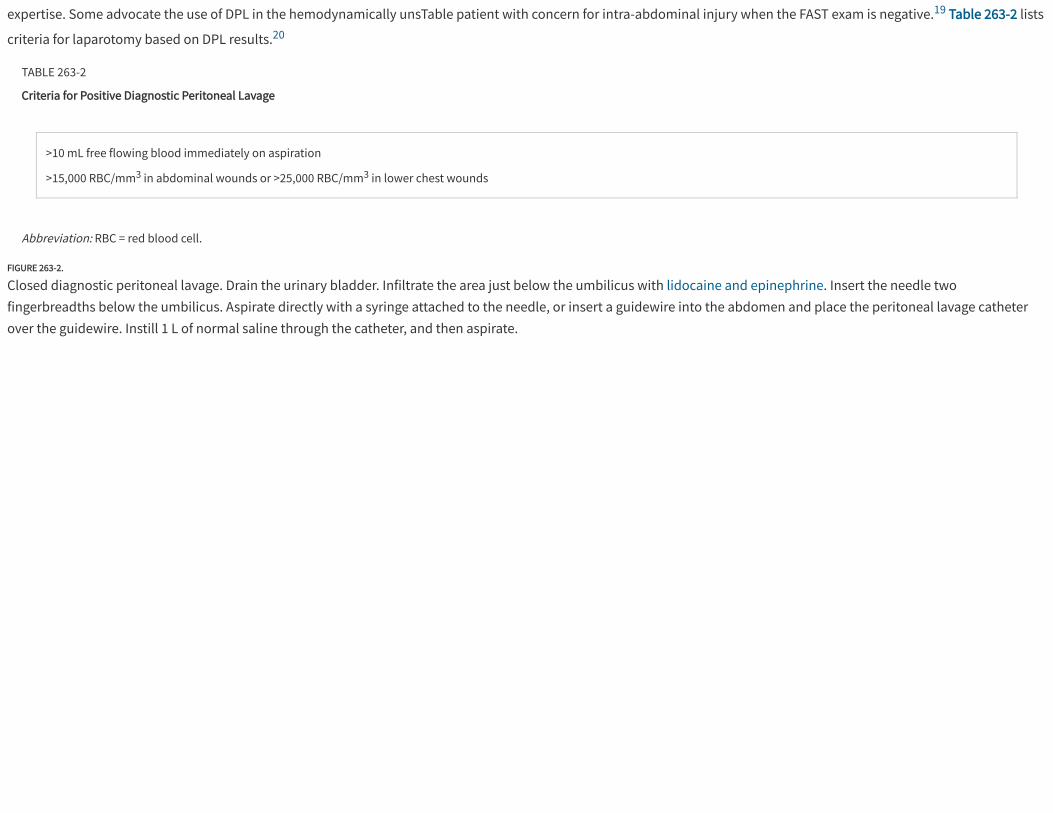
FIGURE 263-2.
Closed diagnostic peritoneal lavage. Drain the urinary bladder. Infiltrate the area just below the umbilicus with lidocaine and epinephrine. Insert the needle twofingerbreadths below the umbilicus. Aspirate directly with a syringe attached to the needle, or insert a guidewire into the abdomen and place the peritoneal lavage catheterover the guidewire. Instill 1 L of normal saline through the catheter, and then aspirate.
DIAGNOSIS IN PENETRATING TRAUMA
The same diagnostic tools are available for evaluation of intraperitoneal injury in the patient with penetrating trauma (CT, US, and DPL). Mandatory exploration for patients
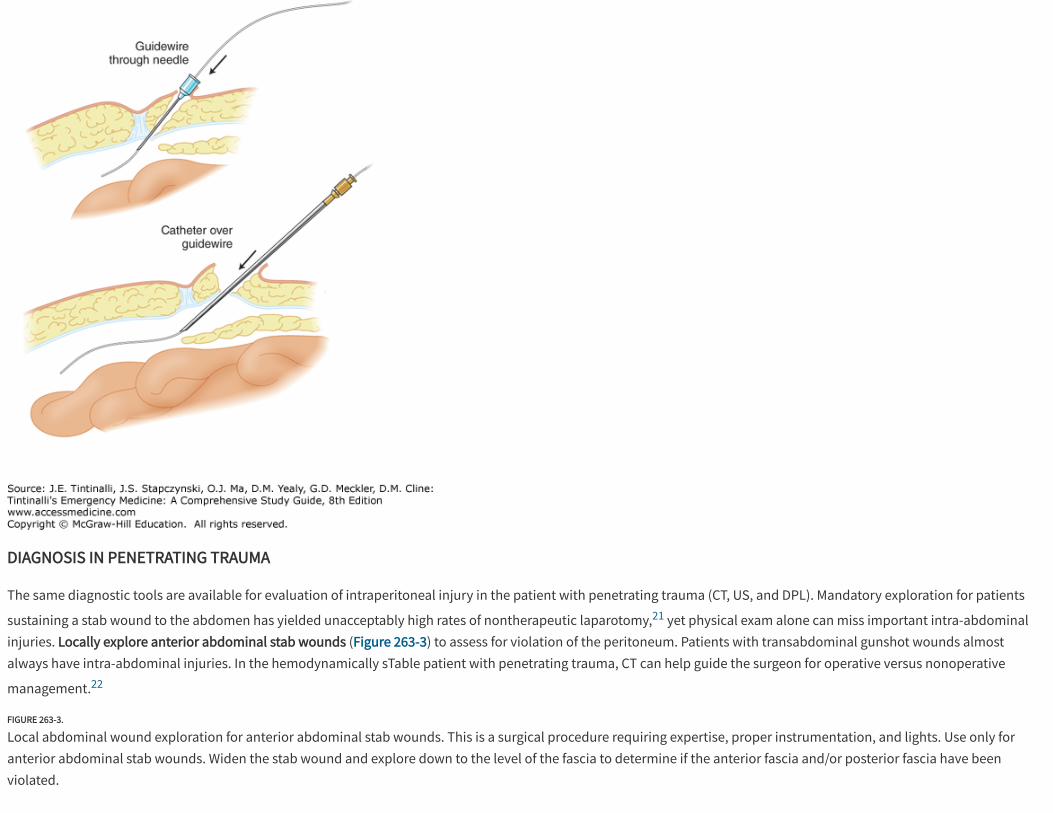
sustaining a stab wound to the abdomen has yielded unacceptably high rates of nontherapeutic laparotomy,21 yet physical exam alone can miss important intra-abdominalinjuries. Locally explore anterior abdominal stab wounds (Figure 263-3) to assess for violation of the peritoneum. Patients with transabdominal gunshot wounds almostalways have intra-abdominal injuries. In the hemodynamically sTable patient with penetrating trauma, CT can help guide the surgeon for operative versus nonoperative
management.22
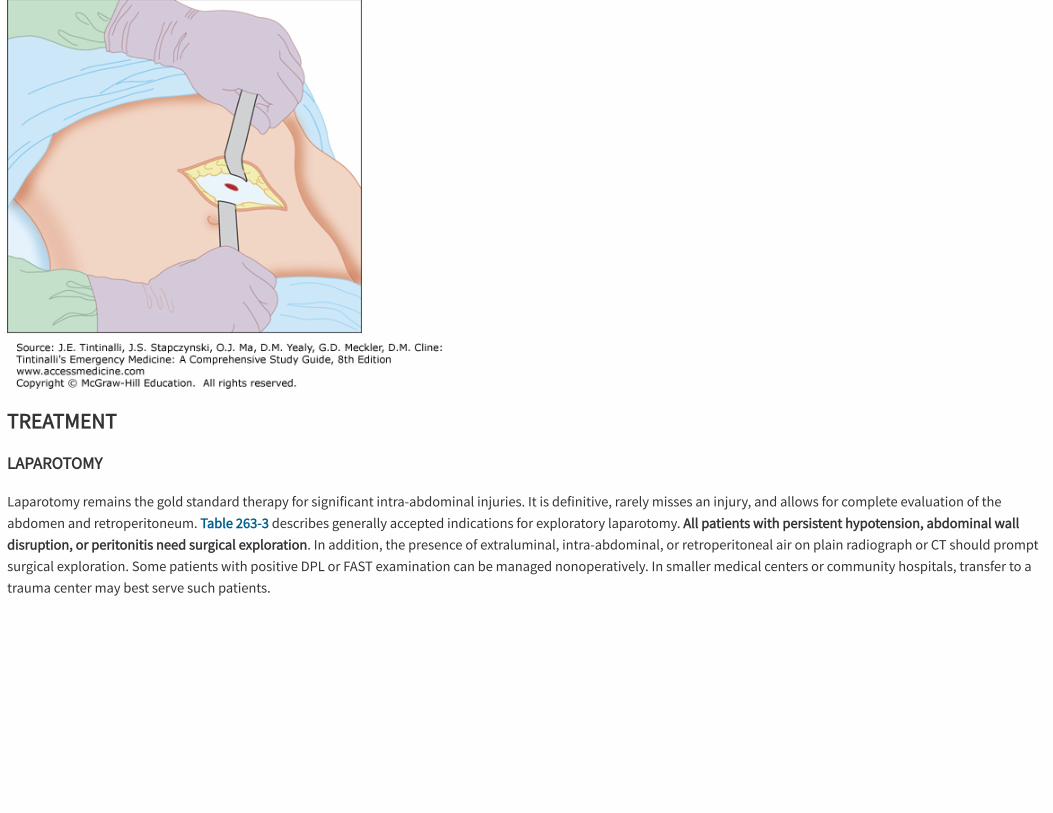
FIGURE 263-3.
Local abdominal wound exploration for anterior abdominal stab wounds. This is a surgical procedure requiring expertise, proper instrumentation, and lights. Use only foranterior abdominal stab wounds. Widen the stab wound and explore down to the level of the fascia to determine if the anterior fascia and/or posterior fascia have beenviolated.
TREATMENT
LAPAROTOMY
Laparotomy remains the gold standard therapy for significant intra-abdominal injuries. It is definitive, rarely misses an injury, and allows for complete evaluation of theabdomen and retroperitoneum. Table 263-3 describes generally accepted indications for exploratory laparotomy. All patients with persistent hypotension, abdominal walldisruption, or peritonitis need surgical exploration. In addition, the presence of extraluminal, intra-abdominal, or retroperitoneal air on plain radiograph or CT should promptsurgical exploration. Some patients with positive DPL or FAST examination can be managed nonoperatively. In smaller medical centers or community hospitals, transfer to atrauma center may best serve such patients.
Abbreviations: DPL = diagnostic peritoneal lavage; FAST = focused assessment with sonography for trauma.
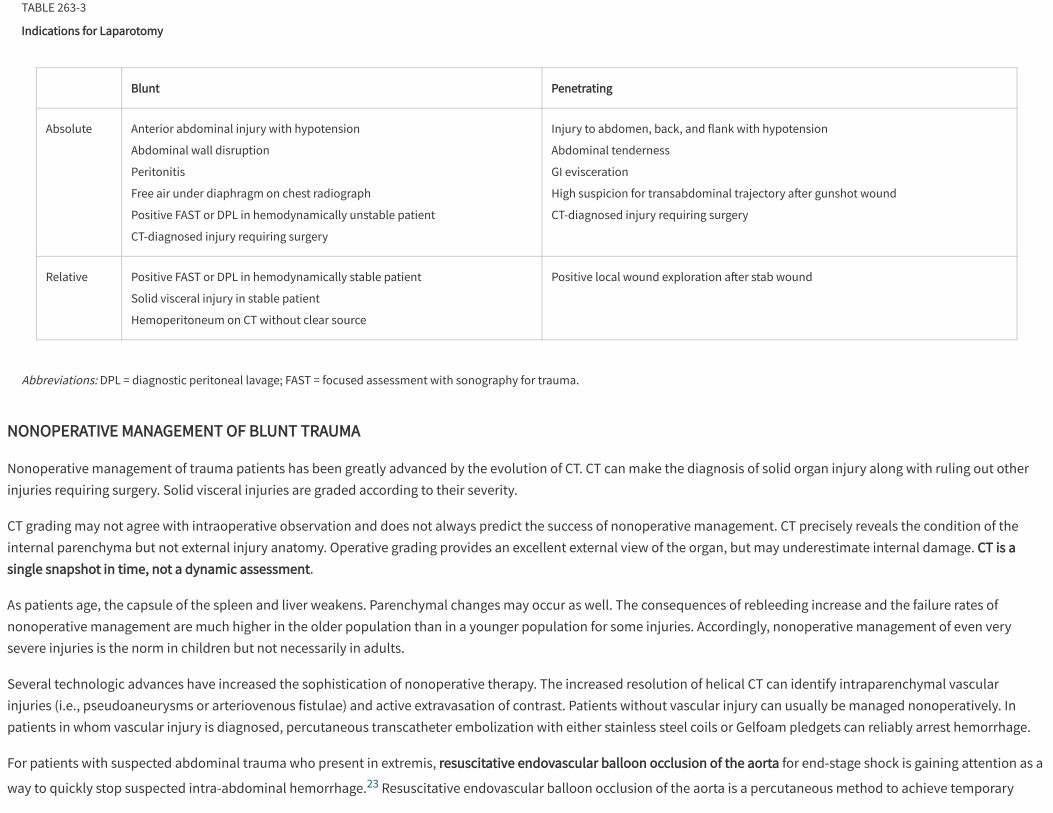
TABLE 263-3
Indications for Laparotomy
Blunt Penetrating
Absolute Anterior abdominal injury with hypotension
Abdominal wall disruption
Peritonitis
Free air under diaphragm on chest radiograph
Positive FAST or DPL in hemodynamically unstable patient
CT-diagnosed injury requiring surgery
Injury to abdomen, back, and flank with hypotension
Abdominal tenderness
GI evisceration
High suspicion for transabdominal trajectory a�er gunshot wound
CT-diagnosed injury requiring surgery
Relative Positive FAST or DPL in hemodynamically stable patient
Solid visceral injury in stable patient
Hemoperitoneum on CT without clear source
Positive local wound exploration a�er stab wound
NONOPERATIVE MANAGEMENT OF BLUNT TRAUMA
Nonoperative management of trauma patients has been greatly advanced by the evolution of CT. CT can make the diagnosis of solid organ injury along with ruling out otherinjuries requiring surgery. Solid visceral injuries are graded according to their severity.
CT grading may not agree with intraoperative observation and does not always predict the success of nonoperative management. CT precisely reveals the condition of theinternal parenchyma but not external injury anatomy. Operative grading provides an excellent external view of the organ, but may underestimate internal damage. CT is asingle snapshot in time, not a dynamic assessment.
As patients age, the capsule of the spleen and liver weakens. Parenchymal changes may occur as well. The consequences of rebleeding increase and the failure rates ofnonoperative management are much higher in the older population than in a younger population for some injuries. Accordingly, nonoperative management of even verysevere injuries is the norm in children but not necessarily in adults.
Several technologic advances have increased the sophistication of nonoperative therapy. The increased resolution of helical CT can identify intraparenchymal vascularinjuries (i.e., pseudoaneurysms or arteriovenous fistulae) and active extravasation of contrast. Patients without vascular injury can usually be managed nonoperatively. Inpatients in whom vascular injury is diagnosed, percutaneous transcatheter embolization with either stainless steel coils or Gelfoam pledgets can reliably arrest hemorrhage.
For patients with suspected abdominal trauma who present in extremis, resuscitative endovascular balloon occlusion of the aorta for end-stage shock is gaining attention as a
way to quickly stop suspected intra-abdominal hemorrhage.23 Resuscitative endovascular balloon occlusion of the aorta is a percutaneous method to achieve temporary
1.
2.
3.
4.
5.
6.
occlusion of the aorta, to maintain or increase perfusion to the heart and lungs in the setting of shock from blunt and penetrating injury, and to avoid the morbidity of athoracotomy for control of the proximal aorta. The femoral artery is accessed, typically percutaneously with US guidance. Using the Seldinger technique, a sheath isintroduced, and a latex balloon is placed inside the sheath, with sheath length and balloon size based on the level of the aorta to be occluded. For resuscitative endovascularballoon occlusion of the aorta, the aorta is divided into the following three zones: I, descending thoracic aorta between the origin of the le� subclavian and celiac arteries; II,between the celiac and lowest renal artery; and III, the lowest renal artery and the aortic bifurcation. The balloon is inflated to get inflow control of the aorta. For example, formassive bleeding from a pelvic fracture, the balloon can be inflated below the renal arteries providing control of bleeding until definitive surgical care or embolization is
done.24 Sixty minutes of resuscitative endovascular balloon occlusion of the aorta is tolerated and recoverable. Further studies are under way before widespread clinicalapplication.
DISPOSITION AND FOLLOW-UP
Patients with significant intra-abdominal injury need admission to the surgical or trauma service for definitive surgical intervention or observation. Given the high rate ofconcomitant injuries, even patients who su�er minor abdominal injury may need hospitalization to manage other injuries. In patients in whom ED discharge is considered,discuss appropriate follow-up and careful instructions for return to the ED. Patients who develop fever, vomiting, increased pain, or symptoms suggestive of blood loss (e.g.,dizziness, weakness, fatigue) should return promptly for reevaluation.
REFERENCES
Demetriades D, Murray J, Charalambides K et al.: Trauma fatalities: time and location of hospital deaths. J Am Coll Surgeons 198: 20, 2003. [PubMed: 14698307]
Intravia JM, DeBeradino TM: Evaluation of blunt abdominal trauma. Clin Sports Med 32: 211, 2013. [PubMed: 23522502]
Scalea TM, Goldstein AS, Phillips TF et al.: An analysis of 161 falls from a height: the "jumper syndrome." J Trauma 26: 06, 1986. [PubMed: 3735467]
Rozycki GS, Root HD: The diagnosis of intraabdominal visceral injury. J Trauma 68: 1019, 2010. [PubMed: 20453755]
Wu CH, Wang LJ, Wong YC et al.: Contrast-enhanced multiphasic computed tomography for identifying life-threatening mesenteric hemorrhage and transmural bowelinjuries. J Trauma 71: 543, 2011. [PubMed: 21336192]
Malinoski DJ, Patel MS, Yakar DO et al.: A diagnostic delay of 5 hours increases the risk of death a�er blunt hollow viscous injury. J Trauma 69: 84, 2011. [PubMed: 20622582]
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
Lahiri R, Bhattacharya S: Pancreatic trauma. Ann R Coll Surg Engl 95: 241, 2013. [PubMed: 23676806]
Muroni, M, Provenza G, Conte S et al.: Diaphragmatic rupture with right colon and small intestine herniation a�er blunt trauma: a case report. J Med Case Rep 4: 289, 2010.[PubMed: 20735836]
Ma OJ, Mateer JR, Ogata M et al.: Prospective analysis of a rapid trauma ultrasound examination performed by emergency physicians. J Trauma 38: 879, 1995. [PubMed: 7602628]
Rozycki GS, Ochsner MG, Feliciano DV et al.: Early detection of hemoperitoneum by ultrasound examination of the right upper quadrant: a multicenter study. J Trauma45: 878, 1998. [PubMed: 9820696]
Wherrett LJ, Boulanger BR, McLellan BA et al.: Hypotension a�er blunt abdominal trauma: the role of emergent abdominal sonography in surgical triage. J Trauma 41:815, 1996. [PubMed: 8913209]
Khawaja OA, Shaikh KA, Al-Mallah MH: Meta-analysis of adverse cardiovascular events associated with echocardiographic contrast agents. Am J Cardiol 106: 742, 2010. [PubMed: 20723656]
Valentino M, Ansaloni L, Catena F et al.: Contrast-enhanced ultrasonography in blunt abdominal trauma: considerations a�er 5 years of experience. Radiol Med 114:1080, 2009. [PubMed: 19774445]
Liao YY, Lin HJ, Lu YH, Foo NP, Guo HR, Chen KT: Does CT evidence of a flat inferior vena cava indicate hypovolemia in blunt trauma patients with solid organ injuries? JTrauma 70: 1358, 2011. [PubMed: 21378583]
Johnson JJ, Garwe T, Albrecht RM et al.: Initial inferior vena cava diameter on computed tomography scan independently predicts mortality in severely injured patients.J Trauma 74: 741, 2013. [PubMed: 23425730]
Sefidbakht S: Letter to the editor in response to "Does CT evident of a flat inferior vena cava indicate hypovolemia in blunt trauma patients with solid organ injuries? JTrauma 70:1358-1261." J Trauma 71: 1092, 2011. [PubMed: 21986757]
Broder JS, Hamedani AG, Liu SW et al.: Emergency department contrast practices for abdominal/pelvic computed tomography: a national survey and comparison withthe American College of Radiology Appropriateness Criteria. J Emerg Med 44: 423, 2013.
18.
19.
20.
21.
22.
23.
24.
[PubMed: 23164558]
Emick DM, Carey TS, Charles AG, Shapiro ML: Repeat imaging in trauma transfers: a retrospective analysis of computed tomography scans repeated upon arrival to a level1 trauma center. J Trauma Acute Care Surg 72: 1255, 2012. [PubMed: 22673252]
Cha JY, Kashuk JL, Sarin EL et al.: Diagnostic peritoneal lavage remains a valuable adjunct to modern imaging techniques. J Trauma 67: 330, 2009. [PubMed: 19667886]
Hashemzadeh S, Mameghani K, Fouladi RF, Ansari E: Diagnostic peritoneal lavage in hemodynamically stable patients with lower chest or anterior abdominal stabwounds. Ulus Travma Acil Cerrahi Derq 18: 37, 2012. [PubMed: 22290048]
Renz BM, Feliciano DV: Unnecessary laparotomies for trauma: a prospective study of morbidity. J Trauma 38: 350, 1995. [PubMed: 7897713]
Como JJ, Bokhari F, Chiu WC et al.: Practice management guidelines for selective nonoperative management of penetrating abdominal trauma. J Trauma 68: 721, 2010. [PubMed: 20220426]
Scott DJ, Eliason JL, Rasmussen TE et al.: A novel fluoroscopy-free, resuscitative endovascular aortic balloon occlusion system in a model of hemorrhagic shock. JTrauma Acute Care Surg 75: 122, 2013. [PubMed: 23940855]
Martinelli T, Thony F, Declety P et al.: Intra-aortic balloon occlusion to salvage patients with life-threatening hemorrhagic shocks from pelvic fractures. J Trauma 68: 942,2010. [PubMed: 20173661]
USEFUL WEB RESOURCES
American Association for the Surgery of Trauma—http://www.aast.org
Eastern Association for the Surgery of Trauma (EAST)—http://www.east.org/portal
Western Trauma Association Algorithms—http://westerntrauma.org/algorithms/algorithms.html
McGraw Hill
Copyright © McGraw-Hill EducationAll rights reserved.Your IP address is 162.211.72.10 Terms of Use • Privacy Policy • Notice • Accessibility
Access Provided by: St. Joseph’s Healthcare SystemSilverchair