trauma-informed practice - calswec
TRANSCRIPT
Version3.3|2017
CommonCore3.0
Trauma-informedPractice
TraineeGuide

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide 2
TableofContentsIntroductiontoCommonCore.........................................................................................3
CurriculumIntroduction...................................................................................................4
Agenda.............................................................................................................................5
LearningObjectives..........................................................................................................6
HelpingTraumatizedChildren:AGuideforCaregivers....................................................7
ReMoved:DiscussionQuestions.....................................................................................24
HowtoFlourishinSocialWork......................................................................................25
AdverseChildhoodExperiences:ResearchBrief|July2014.........................................25
BirthParentswithTraumaHistoriesandtheChildWelfareSystem..............................38
Scenario:BirthParentswithTraumaHistory................................................................41
EssentialElementsofTrauma-InformedChildWelfarePractice....................................42
CompassionFatigueSelf-Test:AnAssessment..............................................................47
Bibliography...................................................................................................................49
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide 3
IntroductiontoCommonCore
California’sCommonCoreCurriculaforChildWelfareWorkersistheresultoftheinvaluableworkandguidanceofagreatmanypeoplethroughoutthechildwelfaresysteminCaliforniaandacrossthecountry.Itwouldbeimpossibletolistalloftheindividualswhocontributed,butsomegroupsofpeoplewillbeacknowledgedhere.TheContentDevelopmentOversightGroup(CDOG)asubcommitteeoftheStatewideTrainingandEducationCommittee(STEC)providedoverallguidanceforthedevelopmentofthecurricula.ConvenedbytheCaliforniaSocialWorkEducationCenter(CalSWEC)andtheCaliforniaDepartmentofSocialServices(CDSS),CDOGmembershipincludesrepresentativesfromtheRegionalTrainingAcademies(RTAs),theUniversityConsortiumforChildrenandfamiliesinLosAngeles(UCCF),andLosAngelesCountyDepartmentofChildrenandFamilyServices.InadditiontoCDOG,aCommonCore3.0subcommitteecomprisedofrepresentativesfromtheRTAs,theResourceCenterforFamilyFocusedPractice,andcountiesprovidedoversightandapprovalforthecurriculumdevelopmentprocess.Alongtheway,manyotherpeopleprovidedtheirinsightandhardwork,attendingpilotsofthetrainings,reviewingsectionsofcurricula,orprovidingotherassistance.California’schildwelfaresystemgreatlybenefitsfromthiscollaborativeendeavor,whichhelpsourworkforcemeettheneedsofthestate’schildrenandfamilies.IncompliancewiththeIndianChildWelfareAct(1978)andtheCaliforniaPracticeModel,socialworkersmustidentifyAmericanIndian/AlaskaNativechildreninthesystem.ForanoverviewofImplementingtheIndianChildWelfareActview:https://www.youtube.com/watch?v=BIQG65KFKGsThecurriculumisdevelopedwithpublicfundsandisintendedforpublicuse.Forinformationonuseandcitationofthecurriculum,pleasereferto:http://calswec.berkeley.edu/CalSWEC/Citation_Guidelines.doc
FORMOREINFORMATIONonCalifornia’sCoreCurricula,aswellasthelatestversionofthiscurriculum,pleasevisittheCaliforniaSocialWorkEducationCenter(CalSWEC)website:http://calswec.berkeley.edu
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide 4
CurriculumIntroduction
Thiscurriculumisdesignedtoprovideanoverviewoftrauma-informedpracticesinchildwelfare.Traineeswillhaveanopportunitytolearnmoreaboutthebasicterms,definitions,andconceptsrelatedtotrauma-informedpractice.Childrenandadultswhoareimpactedbytraumamayhavelife-longconsequencesifthereisnotanappropriateintervention.Traineeswilllearnskillstoidentifyandaddresstraumaresponsesinthechildren,youth,andadultsinvolvedinthechildwelfaresystem.Additionally,traineeswillbeprovidedwithresourcesandtoolstohelpmanagesecondarytraumaticstressandcompassionfatigue,withafocusonself-care.
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide 5
Agenda
Welcome,ReviewoftheAgendaandLearningObjectives 9:00–9:30am
TraumaBasics 9:30–10:30am
BREAK 10:30–10:45am
TraumaBasics(cont’d) 10:45–12:00pm
LUNCH 12:00–1:00PM
AdverseChildhoodExperiences 1:00–1:50pm
HistoricalTraumaandCulture 1:50–2:20pm
BREAK 2:20–2:35pm
ChildWelfare’sResponsetoTrauma 2:35–2:50pm
Self-Care 2:50–3:15pm
Post-Test 3:15–3:45pm
Wrap-up 3:45–4:00pm
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide 6
LearningObjectives
Knowledge
K1.Thetraineewillbeabletodescribetherelationshipbetweenaperson’sculture,experiencesofindividual,familialand/orhistorictrauma,andhisorherbehaviorsorresponses.
K2.Thetraineewillbeabletoidentifybehaviorsofchildrenandparentsinresponsetotraumaortraumatriggersandwaystosupportpositiveadjustment.
K3.Thetraineewillbeabletodescribehowchildtraumaticstressisexacerbatedbyongoingstressorsinachild’senvironmentandwithinthechildwelfaresystem.
K4.Thetraineewillbeabletoidentifythreethingssocialworkerscandotomitigatetheimpactofandhealtraumaforchildrenandfamilies.
K5.Thetraineewillbeabletodescribetheeffectofpersonaltraumahistoryandsecondarytraumaticstressonsocialworkersandtheirresponsestofamiliesandchildren.
Skills
S1.Usingacaseexample,thetraineewillbeabletorecognize,identify,andassesssymptomsoftraumaticstresswithinadevelopmentalandculturalcontext.
S2.Usingacaseexample,thetraineewillbeabletodemonstratethreethingssocialworkerscandotomitigatetheimpactofandhealtraumaforchildrenandfamilies
Values
V1.Thetraineewillvaluereferringchildrenwithatraumahistoryforathoroughtraumaassessmentandspecifictrauma-relatedmentalhealthservices.
V2.Thetraineewillvalueworkingtopreventormitigatetheimpactoftraumaticstressbyusingtrauma-informedresponses.
V3.Thetraineewillvaluethedifferentrolesforsocialworkersandmentalhealthprovidersinprovidingtrauma-informedservices.
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide 7
HelpingTraumatizedChildren:AGuideforCaregiversByDr.BrucePerry
! !
All Rights Reserved © 2014 Bruce D. Perry and The ChildTrauma Academy
Helping Traumatized Children A Brief Overview for Caregivers Bruce D. Perry, M.D., Ph.D. CAREGIVER SERIES www.ChildTrauma.org
This booklet is one in a series developed by the ChildTrauma Academy to assist parents, caregivers, teachers and various professionals working with maltreated and traumatized children.
Fall$16#
08!Fall$

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide 8
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide 9
!
All Rights Reserved © 2014 Bruce D. Perry and The ChildTrauma Academy
!!
3!
The acute post-traumatic period is characterized by an attempt by the
child to reorganize, reevaluate and restore their pre-traumatic world. Many of the emotional, behavioral and cognitive signs and symptoms of the acute post-traumatic period are due to these efforts. Unfortunately, children often do not have the same capacity to understanding or explaining most traumatic experiences. Young children may make many false assumptions about the event – “the tornado came because God was mad.”
As with most situations, children seek answers and comfort from adults around them, yet we often feel helpless in this role. Indeed, most traumatic experiences challenge the most mature and experienced adult. While adults do not have all the answers, they can help children better understand the traumatic event and the ways we respond following trauma.
This booklet addresses some of the key issues related to the child's complex set of reactions that often follow traumatic events. While focused on caregivers, this information may be helpful to caseworkers, teachers, other family and other adults working and living with traumatized children.
This simple guide is intended to inform and provide general principles -- it is not intended to be comprehensive or to exclude other observations or approaches to helping traumatized children. The more we understand these children and the impact of traumatic experiences, the more compassionate and wise we can be as we try to help these children.

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide10
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide11
!
All Rights Reserved © 2014 Bruce D. Perry and The ChildTrauma Academy
!!
5!
animals. “Is Mickey Mouse scared?” Or as they put their stuffed animals under the bed, they may explain “They have to go hide because the bad guy is coming with a gun.” The child will experience and process the very same material differently at different times following the trauma. In the long run, the opportunity to process and re-process many times will facilitate healthy coping. This re-processing may take place throughout the development of a given child. Even years after the original trauma, a child may ‘revisit’ the loss and struggle to understand it from their current developmental perspective. An intensity of emotional feelings will often be seen on various anniversary dates following the trauma (e.g., one week, one month and one year). Children may develop unusual fears of specific days – “Bad things happen on Fridays.” One of the most important elements in this process is that children of different ages have different styles of adapting and different abilities to understand abstract concepts often associated with trauma such as death, hate or the randomness of a tornado’s path or a drunk driver hitting their car.
3. Should I talk to others about the traumatic event? Yes. Inform adults and children in the child's world what has happened. Let teachers, counselors, parents of the child's friends and, if appropriate, the child's peers know some of the pain that this child is living with. Sometimes this can allow the people in the child's life to give them the small amount of tolerance, understanding or nurturing that will smooth the way. People can often be intolerant or insensitive when dealing with the traumatized child "Isn't it about time they got over this?” When you see that this is occurring don't be shy about taking this person aside and educating them about the long-lasting effects of traumatic events and the long process of recovery.
4. How long to these reactions last? An acute post-traumatic change in feeling, thinking and behaving is normal – persistence or extreme symptoms are not. Many clinicians working with traumatized have noted that the persistence of symptoms beyond three months is associated with increased risk for problems. If symptoms of re-experiencing, avoidance, fearfulness, sleep problems, nightmares, sadness or poor school or social functioning persist beyond three months, they need to be addressed. If they persist for six months or if the symptoms interfere with any aspect of
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide12
!
All Rights Reserved © 2014 Bruce D. Perry and The ChildTrauma Academy
!!
6!
functioning, you should have the child see a professional. If the child is in therapy, communicate this with the therapist. Find out if school performance has been affected. Watch for changes in patterns of play and loss of interest in activities. Be observant. Be patient. Be tolerant. Be sympathetic. These children have been terrified and hurt. In many cases, some form of post-traumatic symptom can last for many years. Indeed, more than thirty percent of children living through traumatic stress develop some form of post-traumatic stress disorder (PTSD) . This is a chronic disorder requiring the attention of mental health professionals.
5. Do children understand events accurately? Young children often make false assumptions about the causes of major events. Unfortunately these assumptions may include some sense that they were at fault for the event -- including the death of a loved one. Adults often assume that causality is clear -- dying in a car accident, being shot in a drive-by shooting, dying in a fire. The child may very easily distort an event and make the wrong conclusions about causality. Mom died in the car accident because she was coming to get me at school. The other driver was mad at her. My brother is dead because he was helping me with my homework. The person that shot my brother was shooting at me and hit my brother because he was in my room. The tornado was God's way of punishing my family. In many of these distorted explanations, children assume some degree of responsibility for the traumatic event. This can lead to very destructive and inappropriate feelings of guilt. Be clear. Explore the child's evolving sense of causality. Correct and clarify as you see false reasoning develop. Over time, the ability of the child to cope is related to the ability of the child to understand. While some elements of trauma seem beyond understanding, this can be explained to a child -- some things we don't know. Don't let the child develop a sense that there is a secret about the event -- this can be very destructive. Let the child know that adults can not and will not understand some things either.
6. Do all children have problems after traumatic events? The majority of children experiencing trauma will have some change in their behavior and emotional functioning. In addition to the symptoms listed above,
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide13
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide14
!
All Rights Reserved © 2014 Bruce D. Perry and The ChildTrauma Academy
!!
8!
2. Provide a consistent, predictable pattern for the day. Make sure the
child has a structure to the day and knows the pattern. Try to have consistent times for meals, school, homework, quiet time, playtime, dinner and chores. When the day includes new or different activities, tell the child beforehand and explain why this day's pattern is different. Don't underestimate how important it is for children to know that their caretakers are 'in control.' It is frightening for traumatized children (who are sensitive to control) to sense that the people caring for them are, themselves, disorganized, confused and anxious. There is no expectation of perfection; caretakers themselves have often been affected by the trauma and may be overwhelmed, irritable or anxious. If you find yourself being this way, simply help the child understand why, and that these reactions are normal and will pass.
3. Be nurturing, comforting and affectionate, but be sure that this is in
an appropriate ‘context.’ For children traumatized by physical or sexual abuse, intimacy is often associated with confusion, pain, fear and abandonment. Providing a hug, a kiss and other physical comfort to a young child can be very reassuring. A good working principle for this is to be physically affectionate when the child seeks it. When the child walks over and touches you, return in kind. The child will want to be held or rocked – feel free. On the other hand, try not to interrupt the child's play or other free activities by grabbing them and holding them. Further, be aware that many children from chronically distressed settings may have what we call attachment problems. They will have unusual and often inappropriate styles of interacting.
Do not tell or command them to 'give me a kiss' or 'give me a hug.' Abused children often take commands very seriously. It reinforces a very malignant association linking intimacy/physical comfort with power (which is inherent in a caregiving adult's command to 'hug me').
4. Discuss your expectations for behavior and your style of ‘discipline’ with the child. Make sure that there are clear 'rules' and consequences for breaking the rules. Make sure that both you and the child understand beforehand the specific consequences for compliant and non-compliant behaviors. Be consistent when applying consequences. Use flexibility in
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide15
!
All Rights Reserved © 2014 Bruce D. Perry and The ChildTrauma Academy
!!
9!
consequences to illustrate reason and understanding. Utilize positive reinforcement and rewards. Avoid physical discipline.
5. Talk with the child. Give them age appropriate information. The more the child knows about who, what, where, why and how the adult world works, the easier it is to 'make sense' of it. Unpredictability and the unknown are two things which will make a traumatized child more anxious, fearful, and therefore, more symptomatic. They may be more hyperactive, impulsive, anxious, and aggressive and have more sleep and mood problems. Without factual information, children (and adults) 'speculate' and fill in the empty spaces to make a complete story or explanation. In most cases, the child's fears and fantasies are much more frightening and disturbing than the truth. Tell the child the truth, even when it is emotionally difficult. If you don't know the answer yourself, tell the child. Honesty and openness will help the child develop trust.
6. Watch closely for signs of re-enactment (e.g., in play, drawing,
behaviors), avoidance (e.g., being withdrawn, daydreaming, avoiding other children) and physiological hyper-reactivity (e.g., anxiety, sleep problems, behavioral impulsivity). All traumatized children exhibit some combination of these symptoms in the acute post-traumatic period. Many exhibit these symptoms for years after the traumatic event. When you see these symptoms, it is likely that the child has had some reminder of the event, either through thoughts or experiences. Try to comfort and be tolerant of the child's emotional and behavioral problems. These symptoms will wax and wane - sometimes for no apparent reason. The best thing you can do is to keep some record of the behaviors and emotions you observe (keep a diary) and try to observe patterns in the behavior.
7. Protect the child. Do not hesitate to cut short or stop activities that are
upsetting or re-traumatizing for the child. If you observe increased symptoms in a child that occur in a certain situation or following exposure to certain movies, activities and so forth, avoid these activities. Try to restructure or limit activities that cause escalation of symptoms in the traumatized child.

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide16

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide17
!
All Rights Reserved © 2014 Bruce D. Perry and The ChildTrauma Academy
!!
11!
The human brain has multiple ways to "recall" experience. Indeed, the brain is designed to store and recall information of all sorts – motor, vestibular, emotional, social and cognitive. When you walk, play the piano, feel your heart race in an empty parking lot at night, feel calmed by the touch of a loved one or create a "first impression" after meeting someone for first time, you are using memory. All incoming sensory information creates neuronal patterns of activity that are compared against previously experienced and stored patterns. New patterns can create new memories. Yet the majority of these stored memory templates are based upon experiences that took place in early childhood – the time in life when these patterns of neuronal activity were first experienced and stored. And the majority of our 'memories' are non-cognitive and pre-verbal. It is the experiences of early childhood that create the foundational organization of neural systems that will be used for a lifetime. This is why, contrary to popular perception, infants and young children are more vulnerable to traumatic stress – including sexual abuse. If the original experiences of the infant with primary caregiving adults involve fear, unpredictability, pain and abnormal genital sensations, neural organization in many key areas will be altered. For example, abnormal associations may be created between genital touch and fear, thereby laying the foundation for future problems in psychosexual development. Depending upon the specific nature of the abuse, the duration, the frequency and the time during development, a host of problems can result. In many ways, the long-term adverse effects of sexual abuse in infancy are the result of memories – physiological state memories, motor-vestibular memories and emotional memories, which in later years can be triggered by a host of cues that are pervasive. Incestuous abuse in infancy is most destructive in this regard. It will result in the association of fear, pain and unpredictability into the very core of future human functioning – the primary relational templates. If these original 'templates' for all future relationships are corrupted by sexual exploitation and abuse, the child will have a lifetime of difficulties with intimacy, trust, touch and bonding – indeed the core elements of healthy development and functioning throughout the lifecycle will be altered. Furthermore, if the child is maltreated or abused during early childhood, they may not have any cognitive "memory" and be completely unaware that the source of their fears, difficulties with intimacy and relationships has its roots in this betrayal in infancy. This can lead to problems with self-esteem and, will make any therapeutic efforts more difficult.

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide18
!
All Rights Reserved © 2014 Bruce D. Perry and The ChildTrauma Academy
!!
12!
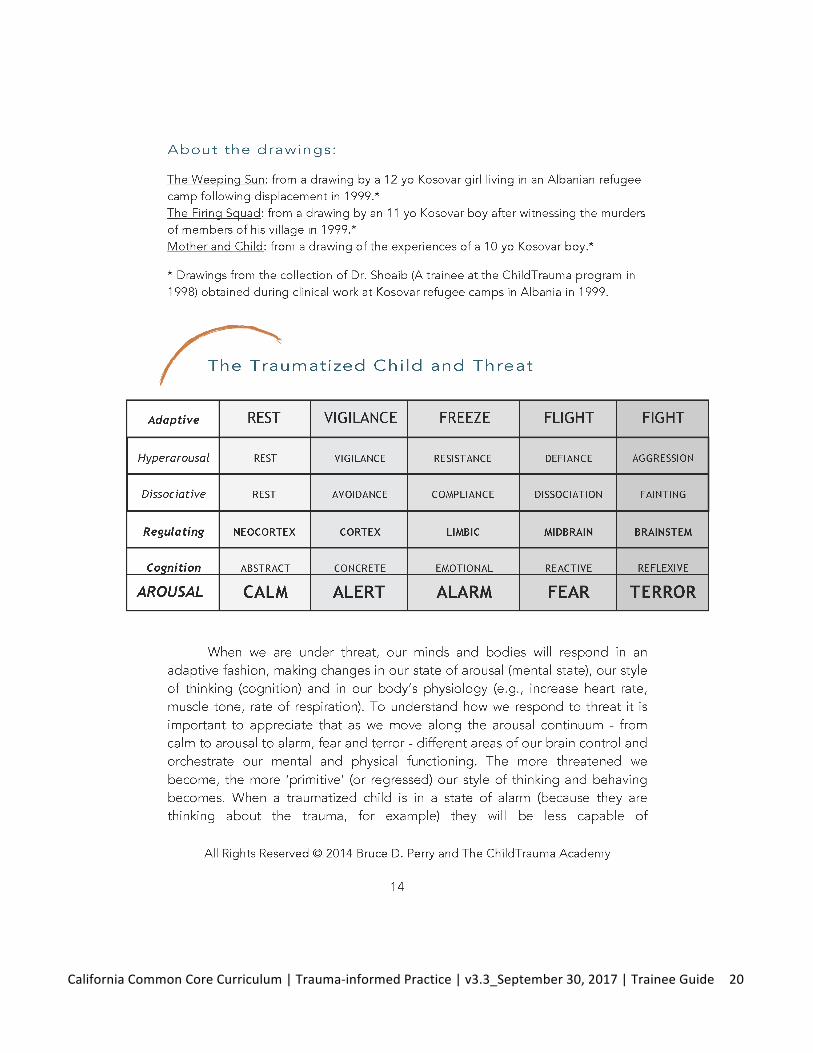
2. Can trauma during infancy arrest cognitive, emotional or behavioral development? The abuse of an infant is often accompanied by extreme disruptions of normal caregiving behaviors and by extreme and prolonged stress responses. Altered caregiving and a prolonged stress response will alter the development of the infant. The major mediators of emotional, cognitive and social environment and, therefore, learning during infancy are the primary caregivers. Development in all domains can be disrupted if these primary relationships are compromised. As mentioned above, it is almost inevitable that emotional, behavioral and cognitive development will be arrested by early traumatic experience. 3. Are there physiological changes in the brain resulting from a traumatic event? As mentioned above, the brain is designed to change in response to experience. Indeed, all experience changes the brain. With traumatic experiences, the changes are in those parts of the brain involved in the stress and fear responses. Many studies with adults and, now with children, have demonstrated a host of neurophysiological changes that are related to traumatic stress. While many more well-controlled studies are needed, it is likely that certain brainstem catecholamine systems (e.g., locus coeruleus noradrengergic), limbic areas (e.g., amygdala), neuroendocrine (e.g., hypothalamic-pituitary-adrenal axis) and cortical systems involved in regulating stress and arousal may all be altered in traumatized children. 4. Do infants display problems similar to older children who are traumatized or abused? The long-term problems that result from maltreatment will vary as a function of several keys factors: what is the nature of the abuse, the duration, frequency, intensity, time during development and the presence of attenuating factors such as other caring, attentive caregivers in the child's life. In general, however, with all traumatic experiences, the earlier in life, the less "specific" and more pervasive the resulting problems appear to be. For example, when traumatized as an adult, there is a specific increase in sympathetic nervous system reactivity when exposed to cues associated with the traumatic event. With young children, following traumatic stress, there appears to be a generalized increase in autonomic nervous system reactivity in addition to the cue-specific reactivity. Due to the sequential and functionally interdependent nature of development, traumatic disruption of the organization and functioning of neural system can result in a cascade of related disrupted
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide19
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide20
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide21
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide22

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide23
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide24
ReMoved:DiscussionQuestions
RRReeeMMMooovvveeeddd::: DDDiiissscccuuussssssiiiooonnn QQQuuueeessstttiiiooonnnsss
What strikes you about this video? How did the abuse history of this child impact her later behavior / interactions with others? What triggers fight / flight / freeze responses for this child? How did the adults who were trying to help, unknowingly mimic the behaviors of adults who had been hurtful in her life? What could they have done to be “deliberately different”? What actions by adults were healing for this child?
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide25
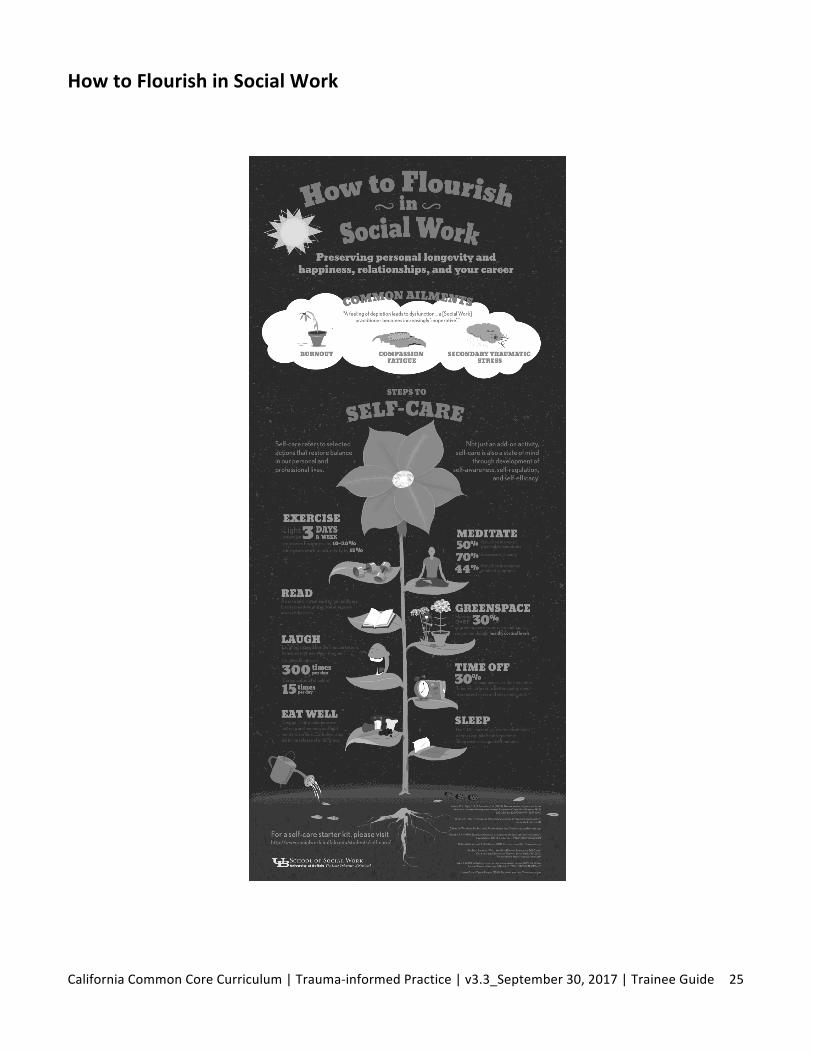
HowtoFlourishinSocialWork
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide26
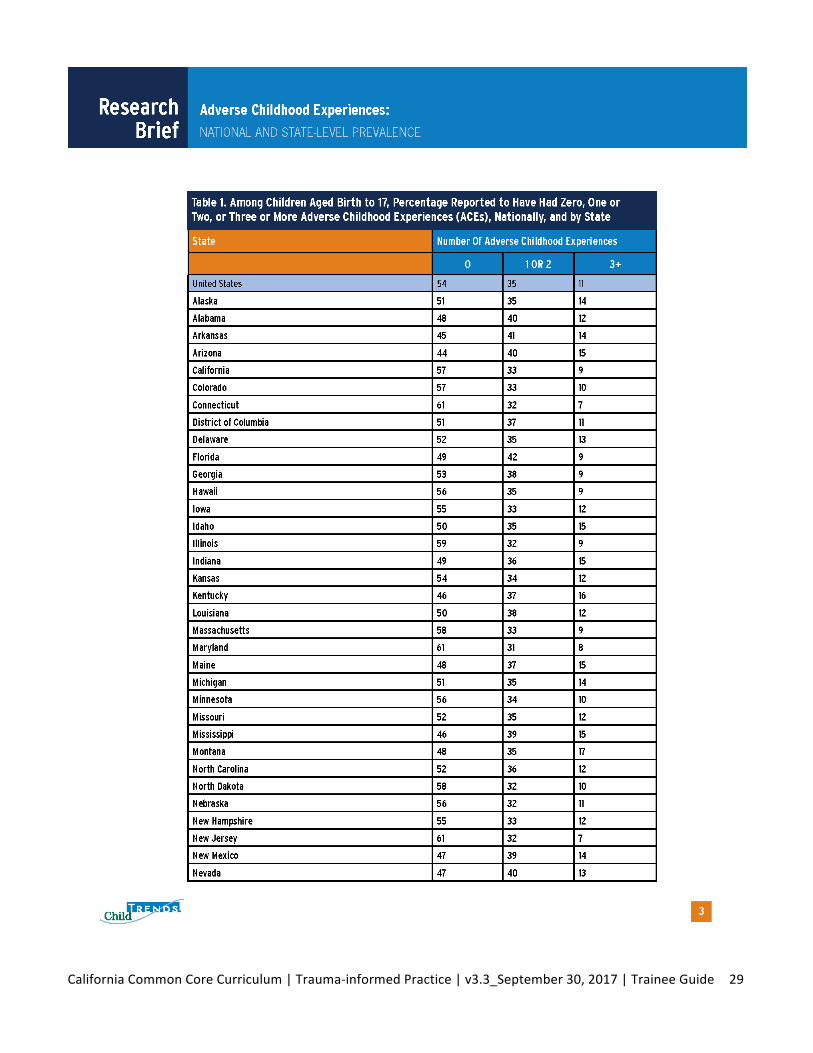
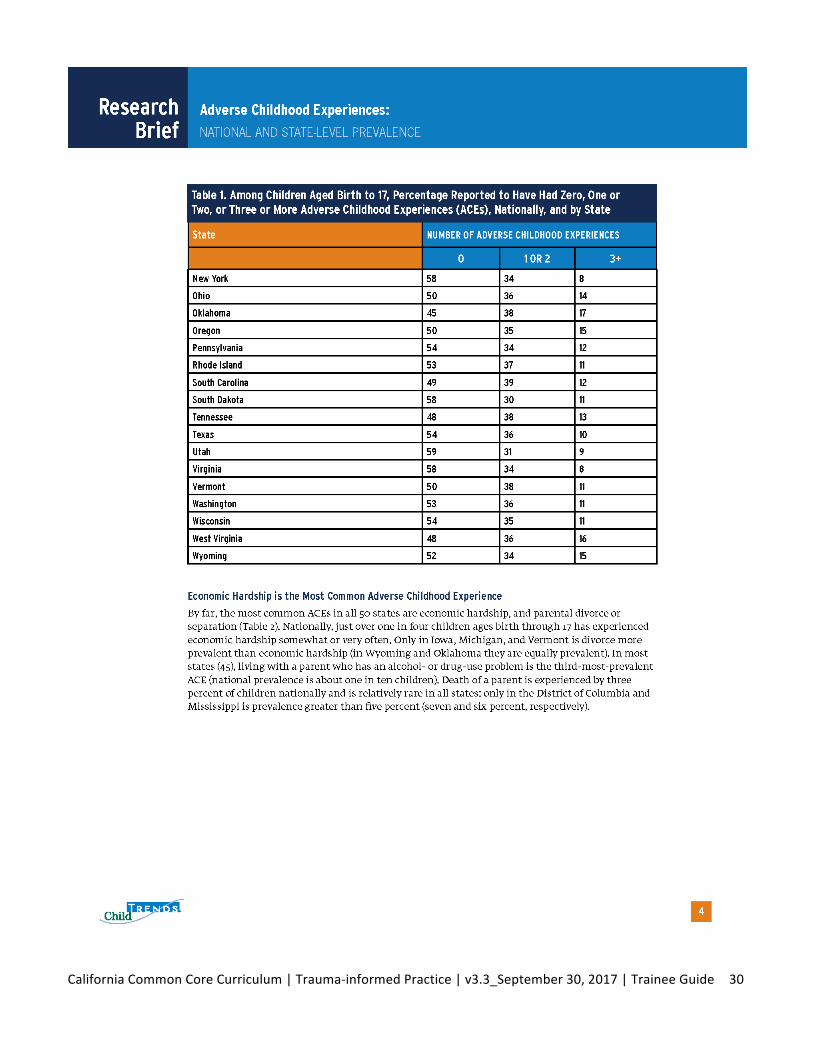
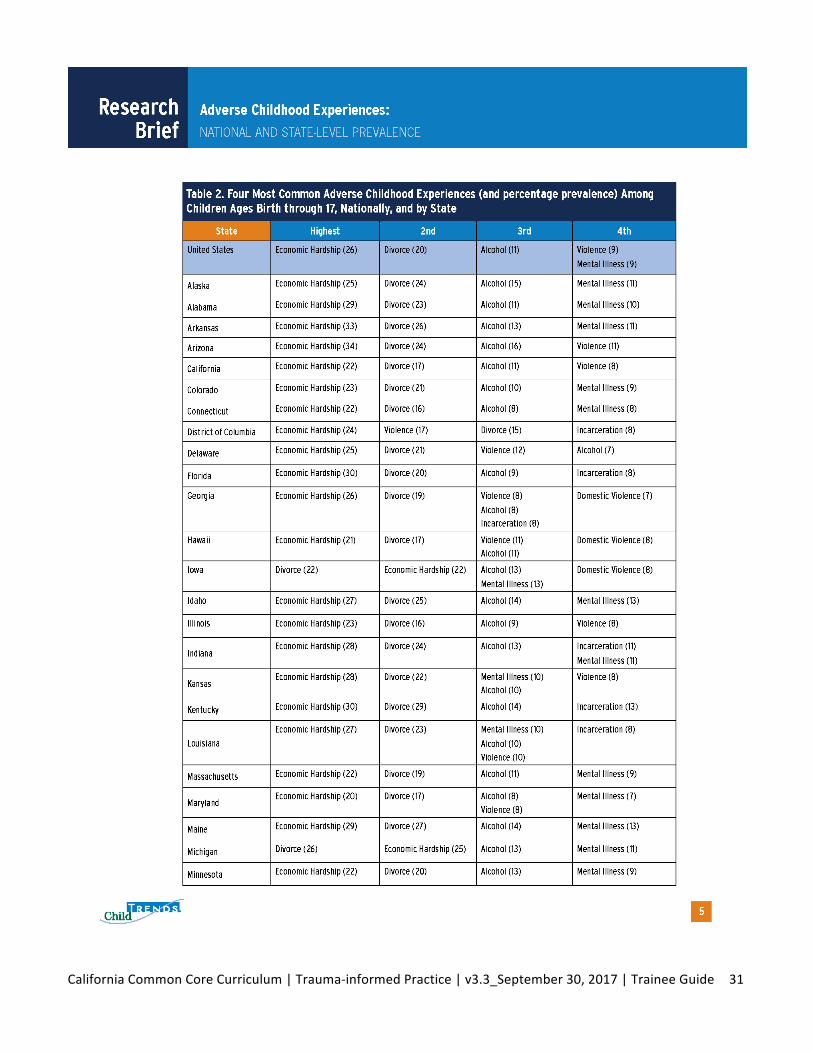
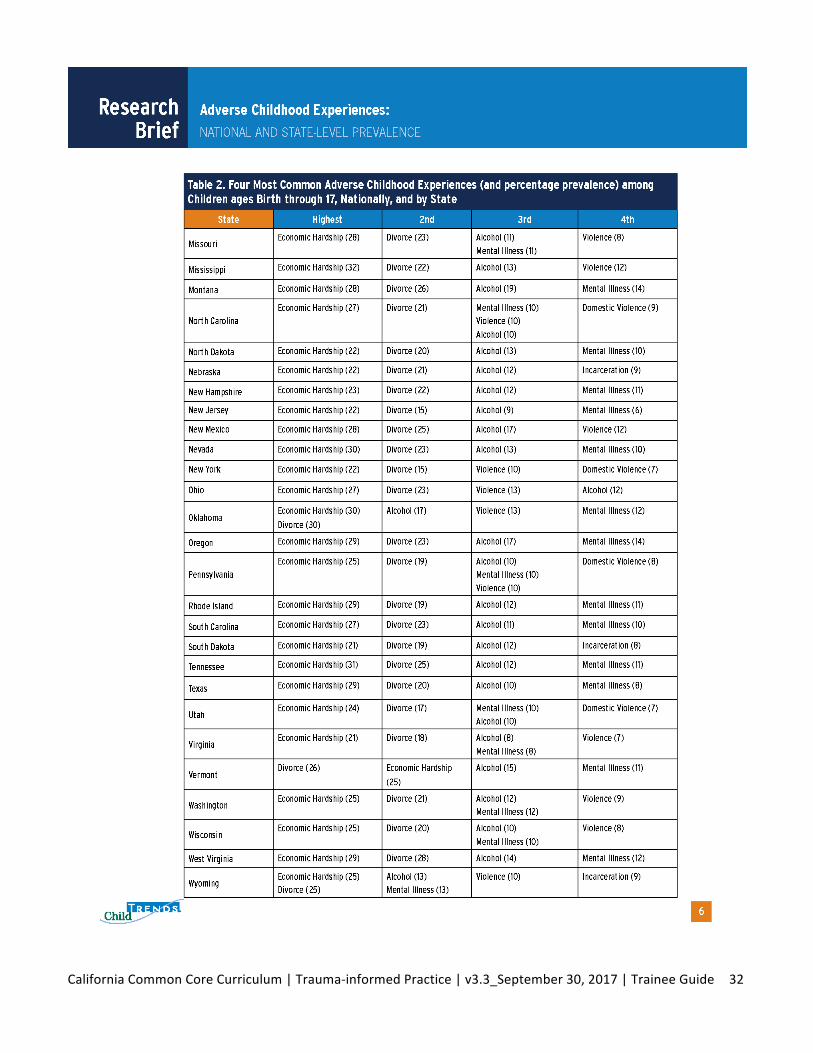
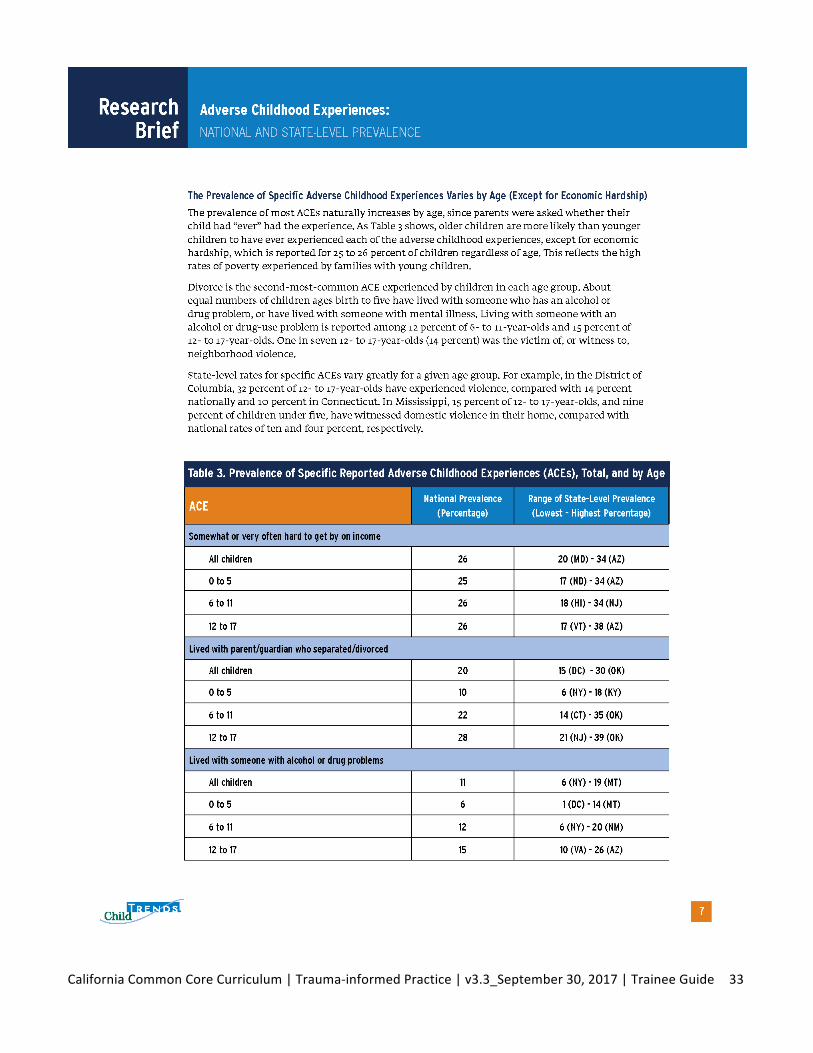
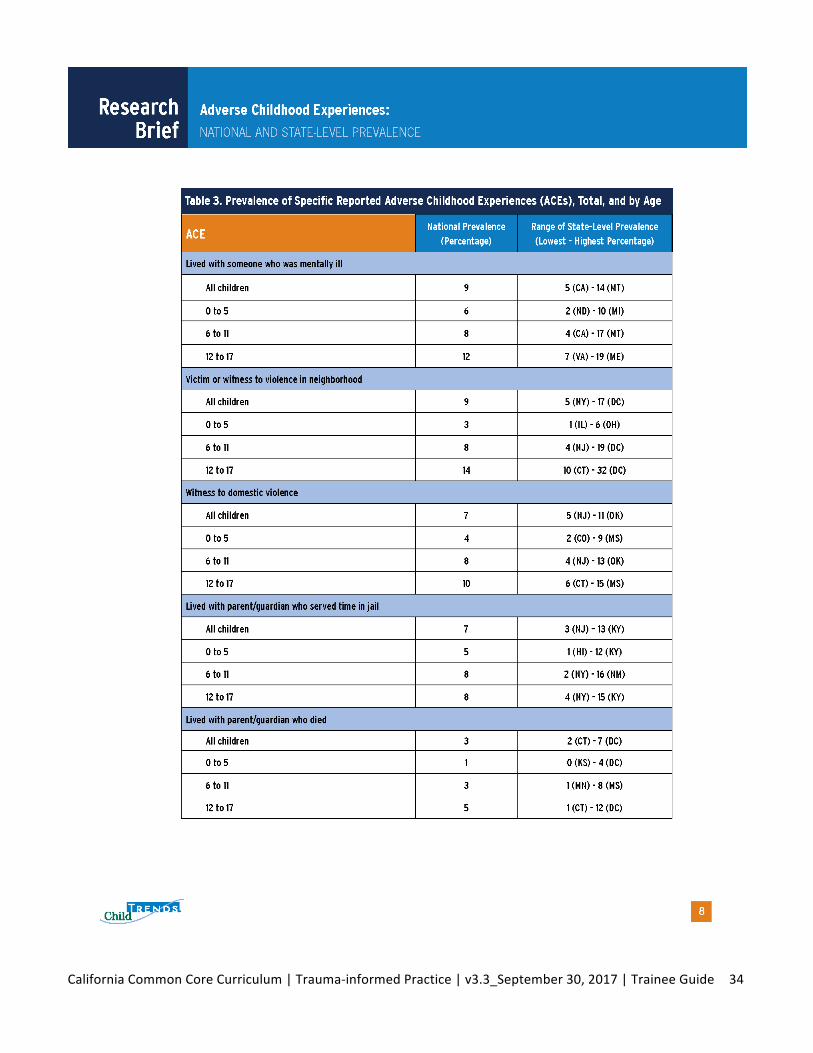
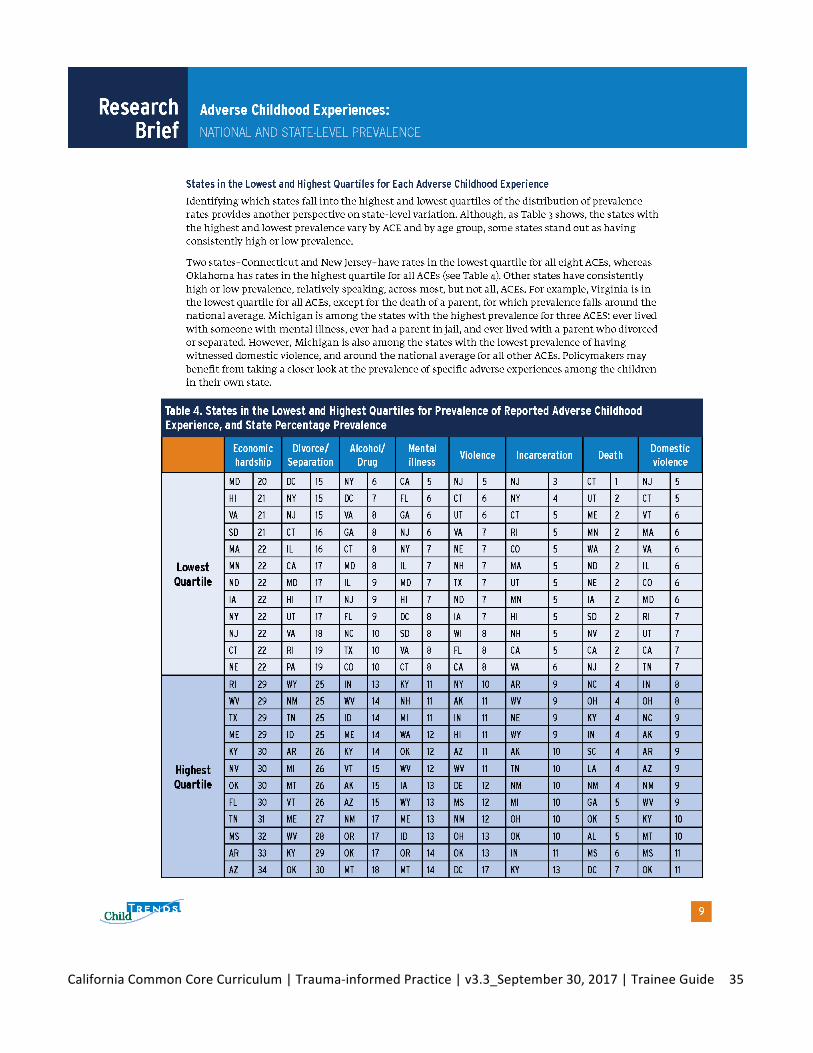
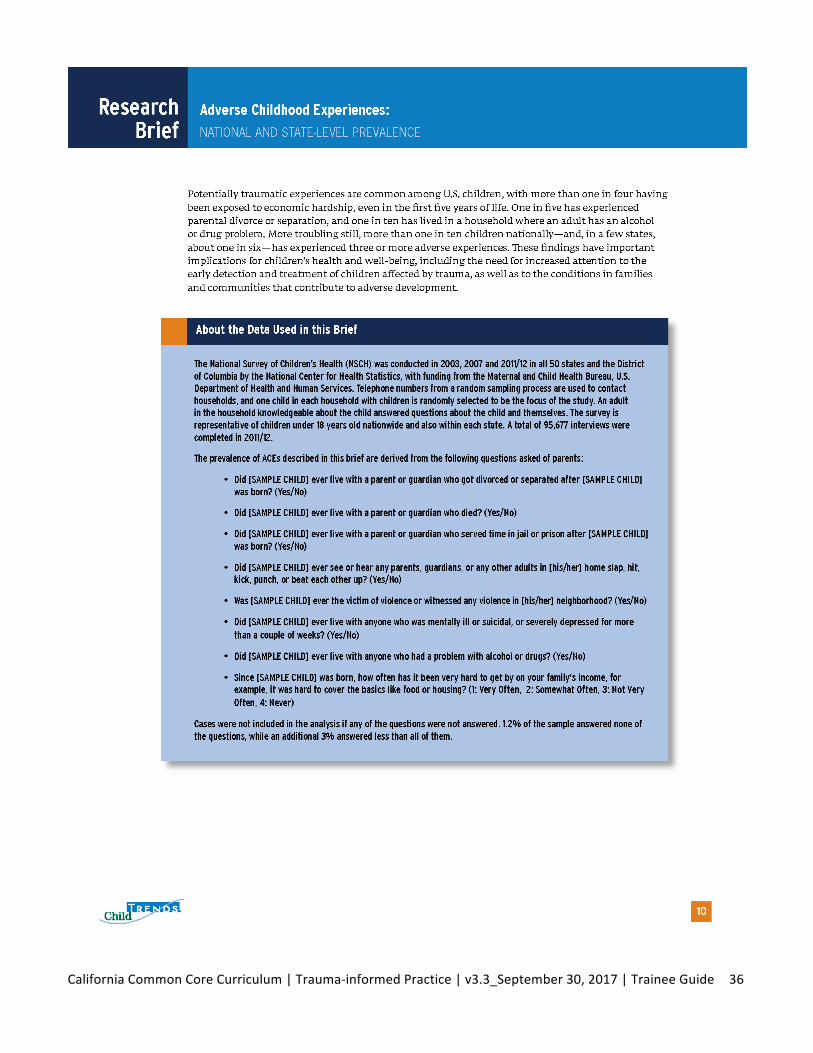
AdverseChildhoodExperiences:ResearchBrief|July2014

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide27
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide28
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide29
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide30
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide31
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide32
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide33
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide34
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide35
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide36
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide37
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide38
BirthParentswithTraumaHistoriesandtheChildWelfareSystem:AGuideforChildWelfareStaff
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide39
Birth Parents with Trauma Histories and the Child Welfare System: A Guide for Child Welfare Staff – March 20112
workers and parents meet the child welfare system’s goals of safety, permanency, and well-being of children and families.
How Can Trauma Affect Parents?
A history of traumatic experiences may:
n Compromise parents’ ability to make appropriate judgments about their own and their child’s safety and to appraise danger; in some cases, parents may be overprotective and, in others, they may not recognize situations that could be dangerous for the child.
n Make it challenging for parents to form and maintain secure and trusting relationships, leading to: • Disruptions in relationships with infants, children, and adolescents, and/or negative
feelings about parenting; parents may personalize their children’s negative behavior, resulting in ineffective or inappropriate discipline.
• Challenges in relationships with caseworkers, foster parents, and service providers and difficulties supporting their child’s therapy.
n Impair parents’ capacity to regulate their emotions.
n Lead to poor self-esteem and the development of maladaptive coping strategies, such as substance abuse or abusive intimate relationships that parents maintain because of a real or perceived lack of alternatives.
n Result in trauma reminders—or “triggers”—when parents have extreme reactions to situations that seem benign to others. These responses are especially common when parents feel they have no control over the situation, such as facing the demands of the child welfare system. Moreover, a child’s behaviors or trauma reactions may remind parents of their own past trauma experiences or feelings of helplessness, sometimes triggering impulsive or aggressive behav-iors toward the child. Parents also may seem disengaged or numb (in efforts to avoid trauma reminders), making engaging with parents and addressing the family’s underlying issues difficult for caseworkers and other service providers.
n Impair a parent’s decision-making ability, making future planning more challenging.
n Make the parent more vulnerable to other life stressors, including poverty, lack of education, and lack of social support that can worsen trauma reactions.
Although parents may experience the child welfare system as re-traumatizing because it removes their power and control over their children, there is potential for it to support their trauma recovery and strengthen their resilience. Caseworkers, as representatives of the child welfare system, can themselves serve as triggers to parents with trauma histories or can, through careful use of non-threatening voice and demeanor, be bridges to hope and healing. Viewing birth parents through a “trauma lens” helps child welfare staff—and parents themselves—see how their traumatic experiences have influenced their perceptions, feelings, and behaviors.2
How can caseworkers use a trauma-informed approach when working with birth parents?3
Caseworkers cannot reverse the traumatic experiences of parents, but they can:
2 Although the focus of this fact sheet is birth parents, we acknowledge that other adults—including non-parent partners, grandparents, and step-parents—may also have histories of traumatic experiences and could benefit from trauma-informed child welfare practice as well.
3 For information about trauma-informed child welfare practice go to www.NCTSN.org/products/child-welfare-trauma-training-toolkit-2008.
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide40
n Understand that parents’ anger, fear, or avoidance may be a reaction to their own past traumatic experiences, not to the caseworker him/herself.
n Assess a parent’s history to understand how past traumatic experiences may inform current functioning and parenting.
n Remember that traumatized parents are not “bad” and that approaching them in a punitive way, blaming them, or judging them likely will worsen the situation rather than motivate a parent.
n Build on parents’ desires to be effective in keeping their children safe and reducing their children’s challenging behaviors.
n Help parents understand the impact of past trauma on current functioning and parenting, while still holding them accountable for the abuse and/or neglect that led to involvement in the system. For many parents, understanding that there is a connection between their past experiences and their present reactions and behavior can empower and motivate them.
n Pay attention to ways trauma can play out during case conferences, home visits, visits to children in foster care, court hearings, and so forth. Help parents anticipate their possible reactions and develop different ways to respond to stressors and trauma triggers
n Refer parents to trauma-informed services whenever possible. Parents will be more likely to attend services that address their needs. Generic interventions that do not take into account parents’ underlying trauma issues—such as parenting classes, anger management classes, counseling, or substance abuse groups—may not be effective.
n Become knowledgeable about evidence-supported trauma interventions to include in service planning. Linkages with programs that deliver trauma-informed services can support caseworkers in developing a plan that meets their clients’ needs.4
n Advocate for the development and use of trauma-informed services in the community.
How can child welfare professionals protect themselves from secondary traumatic stress?
When child welfare staff work with traumatized families and directly see or hear of traumatic events, they can experience extreme distress and sometimes secondary or vicarious traumatic stress.5 Supervisors, caseworkers, and administrators can—and should—find ways to take care of themselves and their staff and to address their own trauma reactions. Simply taking a walk at lunch or recognizing when they are getting overwhelmed or frustrated can make a difference.
Staff supervision can also be used to process the experience of working with traumatized clients.
This fact sheet is one in a series of factsheets discussing parent trauma in the child welfare system. To view others, go to http://www.nctsnet.org/resources/topics/child-welfare-system
4 For information on adult trauma treatments and interventions, go to: National Center for PTSD at http://www.ptsd.va.gov; Sidran Institute at http://www.sidran.org; California Evidence-based Clearinghouse for Child Welfare at http://www.cebc4cw.org; and the National Registry of Evidence-based Programs and Practices at http://www.nrepp.samhsa.gov. For help locating local adult trauma services,contact area rape crisis centers, domestic violence shelters, or Red Cross chapters.
5 Secondary or vicarious traumatic stress (also called compassion fatigue) describes trauma reactions in helping professionals following extensive exposure to clients’ retelling of their trauma experiences, for more information on self-care, go to: http://www.nctsnet.org/nctsn_assets/pdfs/CWT3_SHO_STS.pdf
Established by Congress in 2000, the National Child Traumatic Stress Network (NCTSN) is a unique collaboration of academic and community-based service centers whose mission is to raise the standard of care and increase access to services for traumatized children and their families across the United States. Combining knowledge of child development, expertise in the full range of child traumatic experiences, and attention to cultural perspectives, the NCTSN serves as a national resource for developing and
disseminating evidence-based interventions, trauma-informed services, and public and professional education.
The views, policies, and opinions expressed are those of the authors and do not necessarily reflect those of SAMHSA or HHS.
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide41
Scenario:BirthParentswithTraumaHistory
Carolisaparentwithwhomyouareworking.Visitswithher2-year-olddaughter,Angelique,arescheduledtotakeplaceatthechildwelfareagencyofficeonTuesdaysandThursdaysforonehour.Forthelastfourvisits,Carolhaseitherno-showedorhastestedpositiveformethamphetaminepriortothevisitationtime.Carolhasn’tseenAngeliqueinmorethantwoweeks.YouaremeetingwithCaroltotalkaboutthevisitationplanandtrytocollaborateaboutwhatcanbeputinplacetomakethevisitsagoodexperienceforherandherdaughter.Inthepast,whenyouhavemetwithCarol,shehasoftengottenupsetandraisedhervoicewithyou.Shehasstatedonseveraloccasionsthatthecaregiverhatesherandthatthesystemisriggedtokeepherkidawayfromher.

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide42
EssentialElementsofTrauma-InformedChildWelfarePractice
1Child Welfare Trauma Training Toolkit: The Essential Elements | March 2008 The National Child Traumatic Stress Network
www.NCTSN.org
The Essential Elements of Trauma-Informed Child Welfare Practice
1. Maximize the child’s sense of safety.
Why it’s essential After traumatic events are over, a child may continue to experience insecurity, both physically and emotionally. A sense of safety is critical for physical and emotional growth and functioning, appetite, digestion, and sleep. Both physical and psychological safety are important, at home and within service settings. If children or their caregivers are living in an unsafe setting, this needs to be addressed immediately. Workers need to provide a psychologically safe setting for children and families while inquiring about emotionally painful and difficult experiences and symptoms. Workers must explain clearly the limits of confidentiality and how certain information must be shared with other appropriate authorities.
2. Assist children in reducing overwhelming emotion.
Why it’s essential Trauma can result in such intense fear, anger, shame, and helplessness that the child feels overwhelmed by his or her emotions. This overwhelming emotion may delay the development of age-appropriate self-regulation. Emotions experienced prior to language development may be very real for the child but difficult to express or communicate verbally. Trauma may be “stored” in the body in the form of physical tension or health complaints.
3. Help children make new meaning of their trauma history and current experiences.
Why it’s essential Child trauma can result in serious misunderstandings about safety, personal responsibility, and self-concept. It can disorganize and distort the connections between thoughts, feelings, and behaviors, and disrupt the encoding and processing of memory. Traumatic experiences may be difficult for children to communicate, thereby undermining their confidence and the social support they might receive from others. School age and older children need to do more than just recall or repetitively replay trauma details; they need help developing a coherent understanding of their traumatic experience. The child needs to feel safe enough to face emotional experiences, begin to make sense out of what happened to him/her, and express this to others.
Module 1, Activity 1C; Module 7, Activity 7A

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide43
2Child Welfare Trauma Training Toolkit: The Essential Elements | March 2008 The National Child Traumatic Stress Network
www.NCTSN.org
4. Address the impact of trauma and subsequent changes in the child’s behavior, development, and relationships.
Why it’s essential Traumatic events can affect many aspects of the child’s life beyond the initial trauma response and may create new or secondary problems. These effects may be adaptive in the short-term but can, in the long-term, become counterproductive and interfere with a child’s recovery. These effects can include difficulties in school and relationships or health-related problems (e.g., weight gain) and substance abuse. Other consequences of trauma—or secondary adversities—can also include changes in the family system precipitated by a traumatic event. It may be important to address these issues along with, or before, trauma-focused treatment. Problems in these areas may be so extreme, pronounced, or troublesome that they mask other underlying traumatic stress symptoms.
5. Coordinate services with other agencies.
Why it’s essential Traumatized children and their families are often involved with multiple service systems, including law enforcement, child welfare, the courts, schools, primary care, and mental health. Service providers working with traumatized children should endeavor to develop common protocols and frameworks for documenting trauma history, exchanging information, coordinating assessments, and planning and delivering care. In contrast to a fragmented approach, cross-system coordination views the child as a whole person. When different systems have many different and potentially competing priorities, there is risk that children and their families will receive mixed or confusing messages—or simply fall through the cracks.
6. Utilize comprehensive assessment of the child’s trauma experiences and their impact on the child’s development and behavior to guide services.
Why it’s essential Millions of children experience some sort of trauma every year. Short-term effects might include behavioral difficulties or emotional and health problems. Long-term effects might include depression, anxiety disorders, PTSD, delinquency, substance abuse and relationship problems. Trauma-specific standardized clinical measures identify the types and severity of symptoms the child is experiencing. A thorough assessment identifies potential risk behaviors (i.e., danger to self, danger to others) and aims to determine interventions that will ultimately reduce risk. Assessment also tells us why a child may be reacting in a particular way and the behavior’s connection to his/her experiences of trauma. Proper assessment provides input for the development of treatment goals with measurable objectives designed to reduce the negative effects of trauma.

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide44
3Child Welfare Trauma Training Toolkit: The Essential Elements | March 2008 The National Child Traumatic Stress Network
www.NCTSN.org
7. Support and promote positive and stable relationships in the life of the child.
Why it’s essential Children form and maintain relationships to important figures in their lives through bonding and attachment. Being separated from an attachment figure, particularly under traumatic and uncertain circumstances, can be very stressful for a child. Within the child welfare system, the risk of separation from parents, siblings, and other important figures in a child’s life is common (i.e., removal from home, multiple foster home placements, changes in school and/or community).
Establishing permanency for children in the child welfare system is critical if children are to form and maintain positive attachments. Child welfare workers can play a huge role in encouraging and promoting the positive relationships in a child’s life and minimizing the extent to which these relationships are disrupted by constant changes in placement. If a parent or caregiver is not available following a traumatic event, it is important for child welfare workers to understand that it may be necessary to engage other familiar and positive figures, such as teachers, neighbors, siblings, and/or relatives, to help provide comfort and consistency for the child. Depending on the age of a child, friends may also play an important role in supporting a child who has been exposed to trauma. Promoting these positive relationships is a well-respected child welfare best practice and is also critical to a child’s sense of safety and well-being, particularly during a stressful time.
8. Provide support and guidance to the child’s family and caregivers.
Why it’s essential Children experience their world in the context of family relationships. Parents, kin, and other caregivers are the full-time and long-term supports for their children, and they will typically be involved in the child’s life longer than will the child welfare or mental health professional. In many cases, the family system is experiencing traumatic stress along with the child. Promoting resilience and improving coping skills among family members helps them deal with traumatic events and also prepares them for future challenges. Finally, family members are critical participants in service planning and delivery within systems of care.
Resource families have some of the most challenging and emotionally draining roles in the entire child welfare system. They must be prepared to welcome a new child into their home at any hour of the day or night, manage a wide array of emotions and behaviors, and cope with agency regulations, policies, and paperwork. They are also expected to provide mentoring support and aid to birth families while at the same time attaching to the children and youth in their care. They must prepare simultaneously for the child’s reunification with his/her

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide45
4Child Welfare Trauma Training Toolkit: The Essential Elements | March 2008 The National Child Traumatic Stress Network
www.NCTSN.org
family or for the possibility of making a lifelong commitment to the child through adoption or legal custodianship.
Relatives caring for children and youth face many of the same challenges that other resource parents face and several that are unique. Unlike foster families who are not related to the young people they care for, relatives may not have been seeking this role at this time in their lives. However, they have stepped up to the challenge in order to be there in a time of need or crisis in their family. Thus, they are often dealing with their own conflicting emotions and experiences of trauma and crisis. Meeting the needs of the children they love, responding to the requirements of the agency and courts, and sorting out their own feelings about the children’s parents and the situation that brought them to their home, can be overwhelming at times.
9. Manage professional and personal stress.
Why it’s essential Child welfare is a high-risk profession, and child welfare workers are confronted every day—both directly and indirectly—with danger and trauma. Threats may come in from violent or angry family members. On top of this, hearing about the victimization and abuse of children can be very disturbing for the empathic child welfare worker and can result in feelings of helplessness, anger, and hopelessness. Those who are parents themselves or who have their own histories of childhood trauma might be at particular risk for the negative effects of secondary traumatic stress. Some professionals struggle with maintaining appropriate boundaries and with a sense of overwhelming personal responsibility. These challenges can be intensified in resource-strapped agencies, where there is little professional or personal support available. It is critical to address professional or personal stress because, if left unaddressed, it can result in burnout and undermine work performance, to the detriment of the children and families served. Signs of burnout might include avoidance of certain clients, missed appointments, tardiness, and lack of motivation.
Awareness and a plan that provides positive coping strategies are critical to preventing the potential risk of secondary traumatic stress to staff and to program success. Child welfare workers must have a thorough understanding of the impact of trauma on the child victims and families served. They also need to have an understanding of the impact this trauma may have on them. Staff can be stressed by hearing detailed reports of trauma from children on a daily basis and from having to deal with the powerful emotional responses and the impact of abuse and violence on the child. Dealing with a community system with limited resources that is not always responsive to the needs of these children can also be stressful to staff. The trauma suffered by these children can result in serious and chronic emotional and behavioral problems. Feeling frustrated when trying to deal with a complicated, often

CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide46
5Child Welfare Trauma Training Toolkit: The Essential Elements | March 2008 The National Child Traumatic Stress Network
www.NCTSN.org
insensitive system and experiencing the sense of “helplessness” when trying to heal these children make staff vulnerable to developing their own emotional and physical problems. Just as with the children themselves, staff members who work with victims are at risk of experiencing alterations in their thinking about their world, in their feelings, in their relationships, and in their lives.
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide47
CompassionFatigueSelf-Test:AnAssessment
COMPASSION FATIGUE SELF-TEST: AN ASSESSMENT
Answer the questions below to the best of your knowledge. There is no right or wrong answer.
Assign one of these numbers to each one of the questions below:
Responses: 1 = Very True 2 = Somewhat True 3 = Rarely True
You will find summation directions at the end of the test.
1. _____ When people get upset, I try to smooth things out.
2. _____ I am able to listen to other's problems without trying to "fix" them and/or take away their pain.
3. _____ My self-worth is determined by how others perceive me.
4. _____ When I am exposed to conflict, I feel it is my fault.
5. _____ I feel guilty when others are disappointed by my actions.
6. _____ When I make a mistake, I tend to be extremely critical of myself. I have difficulty forgiving myself.
7. _____ I usually know how I want other people to treat me.
8. _____ I tell people how I prefer to be treated.
9. _____ My achievements define my self-worth.
10. ____ I feel anxious in most situations involving confrontation.
11.____ In relationships, it is easier for me to "give" than to "receive".
12. ____ I can be so focused on someone I am helping that I lose sight of my own perceptions, interests and desires.
13. ____ It is hard for me to express sadness.
14. ____ To make mistakes means that I am weak.
15. ____ It is best to not "rock the boat" or "make waves."
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide48
16. ____ It is important to put people at ease.
17. ____ It is best not to need others.
18. ____ If I cannot solve a problem, I feel like a failure.
19. ____ I often feel "used up" at the end of the day.
20. ____ I take work home frequently.
21. ____ I can ask for help but only if the situation is serious.
22. ____ I am willing to sacrifice my needs in order to please others.
23. ____ When faced with uncertainty, I feel that things will get totally out of control.
24. ____ I am uncomfortable when others do not see me as being strong and self-sufficient.
25. ____ In intimate relationships, I am drawn to people who are needy or need me.
26. ____ I have difficulty expressing my differing opinion in the face of an opposing viewpoint.
27. ____ When I say "no," I feel guilty.
28. ____ When others distance from me, I feel anxious.
29. ____ When listening to someone's problems, I am more aware of their feelings than I am of my own feelings.
30. ____ I find it difficult to stand up for myself and express my feelings when someone treats me in an insensitive manner.
31. ____ I feel anxious when I am not busy.
32. ____ I believe that expressing resentments is wrong.
33. ____ I am more comfortable giving than receiving.
34. ____ I become anxious when I think I've disappointed someone.
35. ____ Work dominates much of my life.
36. ____ I seem to be working harder and accomplishing less.
37.____ I feel most worthwhile and alive in crisis situations.
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide49
38. ____ I have difficulty saying "no" and setting limits.
39. ____ My interests and values reflect what others expect of me rather than my own interests and values.
40. ____ People rely on me for support.
It is important for you to periodically review your self-care, along with your needs and action plans to meet those needs. If you find that you responded with a 1 (Very True) to more than 15 of these items, it's definitely time to take a close and careful look at self-care issues.
Copyright 1996: Dennis Portnoy, from OVEREXTENDED AND UNDERNOURISHED: A SELF-CARE GUIDE FOR PEOPLE IN HELPING ROLES. All rights reserved. Individuals may print this material for personal use only. Written permission is required for any other reproduction. For more information, go to www.myselfcare.org.
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide50
BibliographyArticleReferences:AmericanAcademyofPediatricsandDaveThomasFoundation.Parentingaftertrauma:understandingyour
child’sneeds,AGuideforFosterandAdoptiveParents,2013.RetrievedJanuary28,2015,fromhttp://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/healthy-foster-care-america/Documents/FamilyHandout.pdf
AmericanPsychologicalAssociation.Parentsandfamiliesarealsoaffected,andtheirresponsesaffecthow
childrenreacttotrauma:http://www.apa.org/pi/families/resources/children-trauma-tips.aspxCaliforniaDepartmentofSocialServices.(2016).Requirementsandguidelinesforcreatingandprovidingachild
andfamilyteam.All-countyletterno.16-84(Oct.7).CaliforniaDepartmentofHealthCareServices.(2016).ProvisionofICCandIHBSasmedicallynecessarythrough
EPSDTmentalhealthandsubstanceusedisorderservicesinformationnoticeno.16-004(Feb.5).ChadwickTrauma-InformedSystemsProject.(2013).Creatingtrauma-informedchildwelfaresystems:Aguidefor
administrators(2nded.).SanDiego,CA:ChadwickCenterforChildrenandFamilies.ChadwickTrauma-InformedSystemsProject.(2013).GuidelinesforApplyingaTraumaLenstoaChildWelfare
PracticeModel(1sted.).SanDiego,CA:ChadwickCenterforChildrenandFamilies.ChildWelfareCommittee,NationalChildTraumaticStressNetwork.(2008).Childwelfaretraumatrainingtoolkit:
Comprehensiveguide(2nded.).LosAngeles,CA,andDurham,NC:NationalCenterforChildTraumaticStress.
ChildWelfareCommittee,NationalChildTraumaticStressNetwork.(2013).Childwelfaretraumatrainingtoolkit:
Comprehensiveguide(3rded.).LosAngeles,CA,andDurham,NC:NationalCenterforChildTraumaticStress.
Hudnall,Stamm.2009-2012.ProfessionalQualityofLife:CompassionSatisfactionandFatigueVersion5
(ProQOL).www.proqol.orgNationalChildTraumaticStressNetwork.ResourcesforParentsandCaregivers.RetrievedJanuary28,2015,from
www.nctsnet.org/resources/audiences/parents-caregiversPerry,B.D.Helpingtraumatizedchildren:Abriefoverviewforcaregivers.CTAParentandCaregiverEducation
SeriesVolume1:Issue5,ChildTraumaAcademyPress,1999.RetrievedFebruary1,2015,fromhttp://childtrauma.org/cta-library/trauma-ptsd/
Pryce,Josephine,Sheckelford,Kimberly,Pryce,David.SecondaryTraumaticStressandtheChildWelfare
Professional.(2007).Osofsky,J.D.,Putnam,F.W.,&Lederman,C.(2008).Howtomaintainemotionalhealthwhenworkingwith
trauma.JuvenileandFamilyCourtJournal,59(4),91-102.
CaliforniaCommonCoreCurriculum|Trauma-informedPractice|v3.3_September30,2017|TraineeGuide51
SubstanceAbuseandMentalHealthServicesAdministration.SAMHSA’sConceptofTraumaandGuidanceforaTrauma-InformedApproach.HHSPublicationNo.(SMA)Rockville,MD:SubstanceAbuseandMentalHealthServicesAdministration,2014.
TheThreePillarsofTrauma-InformedCare,HowardBath.Reclaimingchildrenandyouth(Fall2008)Volume17,No.3:www.reclaiming.com
WebReferences:CentersforDiseaseControlandPrevention,AdverseChildhoodExperiences:http://www.cdc.gov/ace/about.htmTheChildTraumaAcademy:www.childtrauma.orgTheNationalChildTraumaticStressNetwork(NCTSN).BirthParentsWithTraumaHistoriesintheChildWelfare
System:AGuideforParents.http://www.nctsnet.org/sites/default/files/assets/pdfs/birth_parents_trauma_history_birth_parents.pdf