renal failure and abdominal hypertension after liver transplantation: determination of critical...
TRANSCRIPT

Renal Failure and Abdominal Hypertension After Liver Transplantation: Determination of Critical
Intra-Abdominal Pressure Gianni Biancojore, * Lucia Bindi, Anna Maria Romanelli, ' Massimo Bid, * Antonella Boldrini, * Giovanni Consani, *Augusta Dmella, * Lucio Urbani,'
Frdnco Filipponi,' and Franco Mosca'
There is growing interest in measuring intra-abdominal pressure (LAP) in postsurgical and critically ill patients because increased pressure can impair various organs and functions. The aim of this study was to evaluate the effect of different LAP levels on the postoperative renal function of subjects undergoing orthotopic liver transplantation. LAP was measured every 8 hours with the urinary bladder pressure method for at least 72 hours after surgery. At the end of the study, the patients were classified on the basis of their LAP values: I 18 mm Hg (group A), 19 to 24 mm Hg (group B), 1 25 mm Hg (group C). The three groups were compared in terms of the incidence of acute renal failure (defined as blood creatinine > 1.5 mg/dL or an increase in the same of > 1.1 mg/dL within 72 hours of surgery), hourly diuresis, blood creatinine, the filtration gradient, hemodynamic variations, and outcome. The incidence of renal failure was higher among the subjects in group C (P < .05 versus group A and < .01 versus group B), who also had higher creatinine levels (P < All), a greater need for diuretics (P < . O l ) and a worse outcome (P < .05). Receiver Operator Characteristic curve analysis showed that an abdominal pressure of 25 mm Hg had the best sensitivity/specificity ratio for renal failure. An intra-ab- dominal pressure of 1 25 mm Hg is an important risk factor for renal failure in subjects undergoing liver trans- plant. (Liver TranspZ2002;8:1175-1181.)
hypertension, or the massive intravenous infusion of fluids and blood components.7.9
Acute renal failure (ARF) is a frequent complication in liver transplant patients. Before surgery, renal func- tion may be jeopardized by a frequently latent hepato- renal syndrome that reduces the recovery of kidney function, frequent recourse to diuretics or nephrotoxic antibiotics, or difficulties in achieving hydroelectrolytic homeostasis.lO,l After the transplantation, renal dys- function may be caused by the use of immunosuppres- sive agents, transplanted organ dysfunction, the use of nephrotoxic antibiotics or major hemodynamic distur- bances.11,12 In any case, postoperative ARF greatly influences the outcome of OLT patients in terms of survival and the length of hospitalization. l2
Despite the interest in abdominal hypertension,3 no generalized consensus has yet been reached concerning what should be considered a high level of IAP, and the published studies have used very different values vary- ing from 10 mm Hg to 25 mm Hg.3,9,13-17
Given the absence of specific data, the aim of this study was to evaluate the effect of different IAP levels on
0 the renal function of cirrhotic patients undergoing
ver the last few years, there has been growing OLT. In particular, we wanted to establish the critical interest in measuring intra-abdominal pressure level of abdominal pressure above which renal dysfunc-
(MP) in postsurgical and critically ill patients.lJ2 The abdomen (and particularly the gut) plays a primary role in the genesis of multiorgan dysfunction (MODS) and, from this point of view, IAP is a valid prognostic indi- cator of the general condition of critically ill patients because intra-abdominal hypertension (IAH) can impair the function of various organs, particularly the kidneys, heart, and lung^.^-^
Patients undergoing orthotopic liver transplantation (OLT) are frequently at risk of IAH before surgery (because of tense ascites9) and during the postoperative phase, when high abdominal pressure may be attribut- able to different causes: the accumulation of blood and clots in the abdominal cavity, the placement of perihe- patic or retrohepatic packs to control nonsurgical bleed- ing, intestinal edema or congestion caused by portal
tion becomes significantly more frequent in the imme- diate postoperative period.
From the *Division o f Anesthesia & Intensive Care, Post-Surgical and Transplant Intensive Care Unit, Aziendu Ospedaliera Pisana, Ospedale di Cisanello; the flnstitute o f Clinical Physiology, Department o f Epidemiology and Biostatistics, National Research Council, S. Cataldo; and the $Department o f Generaland Transplantation Surgey, University School of Medicine, Ospedale di Cisanello, Pisa, Itab.
Address reprint requests to Gianni Biancofore, MD, U TI. Trapi- anti, Ospedale Cisanello, Via Paradisa 2, 56100 Pisa, Itah. Telephone 0039-050-996885/996815; FAX. 0039-050-996984; E-mail: g. bianco$ore@med. unipi.it
Liver Diseases Copyright 0 2002 by the American Association for the Study o f
1527-6465/02/0812-0012$35.00/0 doi:lO. 1053/jltss.2O02.36246
Liver Transplantation, VoL 8, No 12 (December), 2002: pp 1175-1 181 1175

1176 Biancofiore et a1
Materials and Methods
The study involved a population of subjects consecutively undergoing O L T at our center. The exclusion criteria were a preoperative diagnosis of renal dysfunction (defined as a blood creatinine level of more than 1.5 mg/dL) and the onset of hemodynamic, infective, respiratory or graft function problems (defined on the basis of standard criteria'83'9) dur- ing the study period, which, in the opinions of the attending physicians, were sufficiently serious to be considered possible causes of renal failure.
All of the patients underwent the same anesthetic proce- dure: after intravenous induction with fentanyl (0.2 mg), thiopental sodium (4 mg/kg), and succinylcholine (1 mg/kg) and orotracheal intubation, narcosis was maintained with sevofluorane at inhalatory concentrations between 1% and 2.5% in a 50% oxygen/air respiratory mixture administered with low flows of fresh gas (2 L/min). The anesthetic protocol was completed by an intravenous infusion of fentanyl (0.1 mg/h) and atracurium besylate (0.01 mg/kg/min).
The native liver was removed after the suprahepatic and subhepatic clamping of the subdiaphragmatic vena cava after the establishment of an extracorporeal venovenous bypass. All of the liver transplantations were performed by the same sur- geon (F.F.)
At the end of the procedure, all of the patients were trans- ferred to the intensive care unit (ICU) where they were weaned from ventilatory support as soon as possible in accor- dance with a technique described elsewhere.20
The immunosuppressive protocol included oral cyclo- sporin A (10 mg/d begun on the same day as the operation and then adjusted to maintain a trough blood concentration of 200 to 250 ng/dL) and methylprednisolone (10 mg/kg intraoperatively, subsequently reduced by 50% every day until reaching a prednisolone dose of 20 mg/d). Immunosup- pression was completed by means of the intravenous admin- istration of basiliximab 20 mg on the first and fourth postop- erative day.
Intraoperative and postoperative hemodynamic monitor- ing included the invasive measurement of arterial blood pres- sure, central venous pressure (CVP), pulmonary capillary wedge pressure (PCWP) and cardiac performance (CCO/ SV02 Thermodilution Catheter; Edwards Life Sciences LLC, Irvine, CA).
IAP was measured every eight hours with the urinary blad- der pressure technique for at least the first 72 hours after transplantation; the measurements were continued beyond this period in some cases because of the persistence of high IAP levels.
As previously proposed for postsurgical patients with abdominal hypertension, renal function was measured by means of 24-hour hourly urinary output and blood creatinine levels, measured on the second and fourth postoperative day. 5-l6 ARF was defined as blood creatinine values of > 1.5 mg/dL or an increase of > 1.1 mg/dL within 72 hours of surgeryl5; IAH and ARF were considered potentially related when the time interval between their onsets was less than 48
hours.15 The filtration gradient (FG), which is considered to be a key factor in evaluating renal function in patients with high IAP levels, was calculated every day. The FG corresponds to the mechanical force across the glomerulus'5 and can be easily calculated because it is equal to the difference between glomerular filtration pressure and proximal tubule pressure; in subjects with IAH, the first is equal to the difference between mean arterial pressure (MAP) and IAP, and the sec- ond is equivalent to IAP itself.l5 Consequently:
FG = MAP - (2 X IAP)
At the end of the study, the patients were divided into groups on the basis of their mean daily IAP levels: 5 18 mm Hg (group A), 19 to 24 mm Hg (group B) and 2 25 mm Hg (group C). None of the patients was switched from one group to another because no significant changes in mean IAP were observed during the course of the study.
Intra-Abdominal Pressure Measurements
IAP can be measured directly by connecting a manometer to a catheter positioned in the abdominal cavity, or indirectly by measuring the pressure of intra-abdominal hollow organs such as the rectum, stomach or urinary bladder; urinary blad- der pressure currently is considered to be the clinical reference standard3 because the bladder is a structure with highly com- pliant walls; its pressure reflects intra-peritoneal pressure.
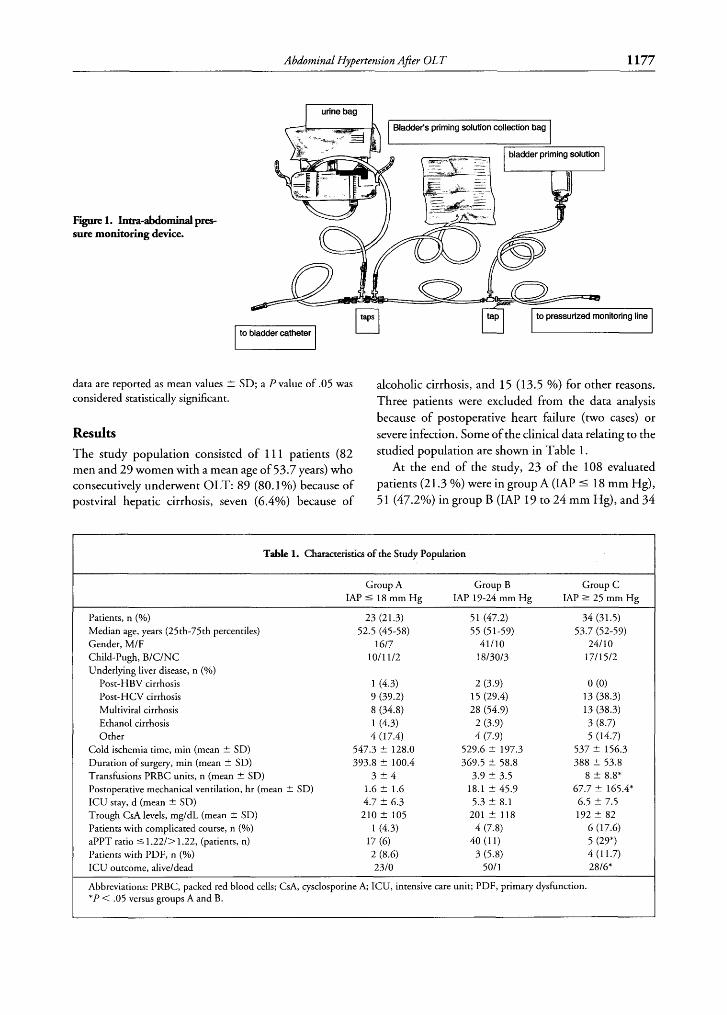
W e used a method similar to that originally proposed by Kron in 1984,21 which involves connecting a manometer to the bladder by means of a disposable needle inserted in the sample collection port of the vescical catheter. Figure 1 shows the device specially developed by the nursing staff at our ICU, which, after being sterilized with ethylene oxide, is applied to the vescical catheter and thus allows IAP to be measured safely, easily, and repeatably.
After filling the bladder with 100 mL of saline, its pressure is measured by rotating a tap to connect it to a pressurized monitoring line. After the measurement has been made, the fluid used to fill the bladder is drained into a separate bag (using a second tap) to prevent it from becoming mixed with the patient's urine and, thus, altering the results of subsequent laboratory tests. Furthermore, the health workers performing the procedure are protected from the risks of accidental needle puncture and urine contamination, and the system guarantees that the urine drain is always externally closed and, thus, prevents the risk of urinary infections caused by repeated IAP measurements.
Statistical Analysis
The data were analyzed with STATA software (release 7.0, Stata Corp, College Station, T X ) and the Chi-squared test according to Pearson, the Chi-squared test according to Yates, and the t-test for unpaired data. The IAP cutoff point for ARF, i.e., the IAP value having the best ratio between sensi- tivity (the ability to identify true positives) and specificity (the ability to identify true negatives) was selected by means of ROC (Receiver Operator Characteristic) curve analysis. The
Abdominal Hypertension Afier OL T 1177
Figure 1. Insra-aMominalpres- sure monitoring device.
data are reported as mean values +- SD; a P value of .05 was alcoholic cirrhosis, and 15 (1 3.5 %) for other reasons. considered statistically significant. Three patients were excluded from the data analysis
because of postoperative heart failure (two cases) or Results severe infection. Some of the clinical data relating to the
The study population consisted of 1 1 1 patients (82 studied Population are shown in men and 29 women with a mean age of 53.7 years) who At the end of the study, 23 of the 108 evaluated consecutively underwent OLT: 89 (80.1%) because of patients (21.3 %> were in groupA (MP 5 18 mm Hg), postviral hepatic cirrhosis, seven (6.4%) because of 51 (47.2%) in group B (MP 19 to 24 mm Hg), and 34
Table 1. Characteristics of the Study Population
Group A Group B Group C IAP 5 18 mm Hg IAP 19-24 mm Hg IAP 2 25 mm Hg
Patients, n (%) 23 (21.3) 51 (47.2) 34 (31.5) Median age, years (25th-75th percentiles) 52.5 (45-58) 55 (51-59) 53.7 (52-59) Gender, MIF 1617 41/10 241 10 Child-Pugh, BICINC 1011 112 1813013 1711512 Underlying liver disease, n (Yo)
Post-HBV cirrhosis 1 (4.3) 2 (3.9) 0 (0) Post-HCV cirrhosis 9 (39.2) 15 (29.4) 13 (38.3) Multiviral cirrhosis 8 (34.8) 28 (54.9) 13 (38.3) Ethanol cirrhosis 1 (4.3) 2 (3.9) 3 (8.7) Other 4 (17.4) 4 (7.9) 5 (14.7)
Cold ischemia time, min (mean ? SD) 547.3 ? 128.0 529.6 5 197.3 537 2 156.3 Duration of surgery, min (mean ? SD) 393.8 ? 100.4 369.5 t 58.8 388 5 53.8 Transfusions PRBC units, n (mean 2 SD) 3 ? 4 3.9 2 3.5 8 5 8.8* Postoperative mechanical ventilation, hr (mean -t SD) 1.6 ? 1.6 18.1 2 45.9 67.7 & 165.4* ICU stay, d (mean ? SD) 4.7 ? 6.3 5.3 2 8.1 6.5 5 7.5 Trough CsA levels, mgldL (mean 5 SD) 210 5 105 201 -t 118 192 2 82 Patients with complicated course, n (Yo) 1 (4.3) 4 (7.8) 6 (17.6) aPPT ratio 5 1.22/> 1.22, (patients, n) 17 (6) 40 (1 1) 5 (29*) Patients with PDF, n (Yo) 2 (8.6) 3 (5.8) 4 (11.7) ICU outcome, aliveldead 2310 501 1 28/6*
Abbreviations: PRBC, packed red blood cells; CsA, cysclosporine A; ICI.7, intensive care unit; PDF, primary dysfunction. *P < .05 versus groups A and B.
1178 Biancofiore et al
A 65
B
40 i
gr.A gr.6 LJ gr.C E:: 15 10 gr.A gr.6 gr.C
C 50
20
15
l- §
gr.A gr.6 gr.C
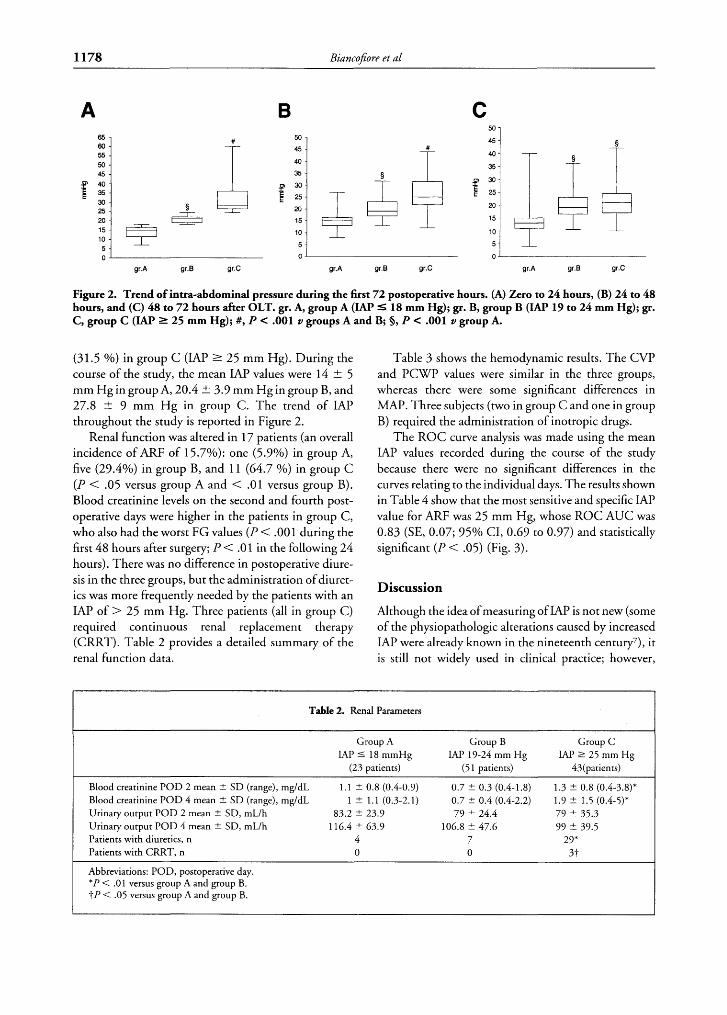
Figure 2. Trend of intra-abdominal pressure during the first 7 2 postoperative hours. (A) Zero to 24 hours, (B) 24 to 48 hours, and (C) 48 to 7 2 hours after OLT. gr. A, group A (IAP S 18 mm Hg); gr. B, group B (LAP 19 to 24 mm Hg); gr. C, group C (W' 1 25 mm Hg); #, P C .001 v groups A and B; 0, P C .001 v group A.
(3 1.5 Yo) in group C (IAP 2 25 mm Hg). During the course of the study, the mean LAP values were 14 2 5 mm Hg in group A, 20.4 t 3.9 mm Hg in group B, and 27.8 t 9 mm Hg in group C. The trend of IAP throughout the study is reported in Figure 2.
Renal function was altered in 17 patients (an overall incidence of ARF of 15.7%): one (5.9%) in group A, five (29.4%) in group B, and 1 1 (64.7 %) in group C (P < .05 versus group A and < .01 versus group B). Blood creatinine levels on the second and fourth post- operative days were higher in the patients in group C, who also had the worst FG values (I) < .001 during the first 48 hours after surgery; P < .01 in the following 24 hours). There was no difference in postoperative diure- sis in the three groups, but the administration of diuret- ics was more frequently needed by the patients with an IAP of > 25 mm Hg. Three patients (all in group C) required continuous renal replacement therapy (CRRT). Table 2 provides a detailed summary of the renal function data.
Table 3 shows the hemodynamic results. The CVP and P C W values were similar in the three groups, whereas there were some significant differences in MAP. Three subjects (two in group C and one in group B) required the administration of inotropic drugs.
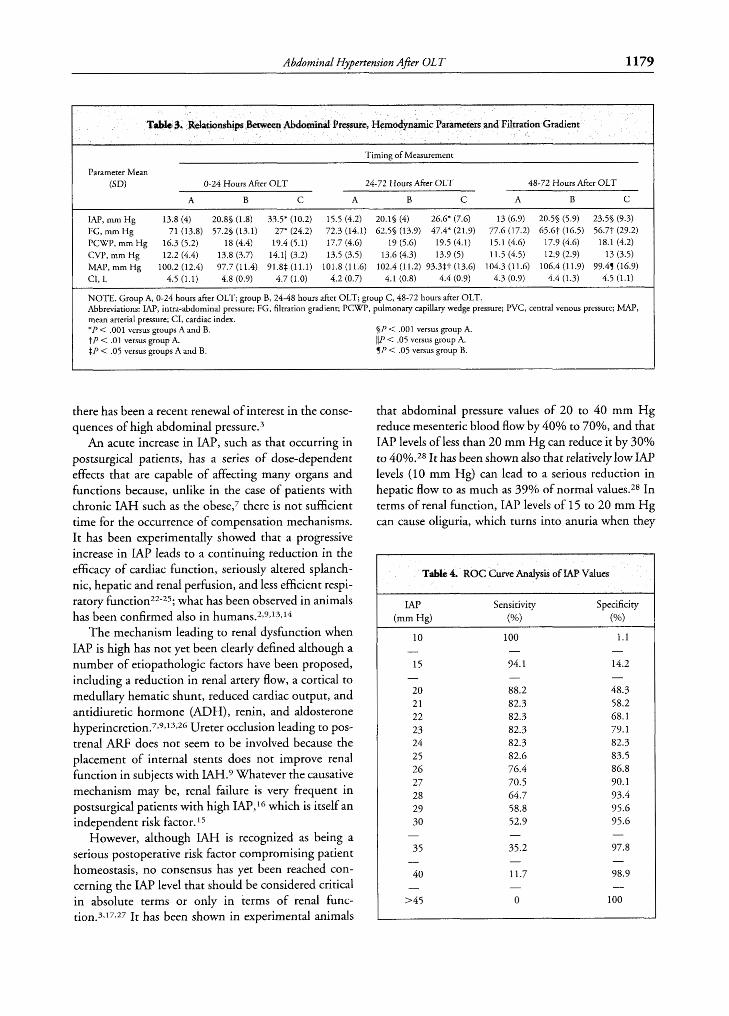
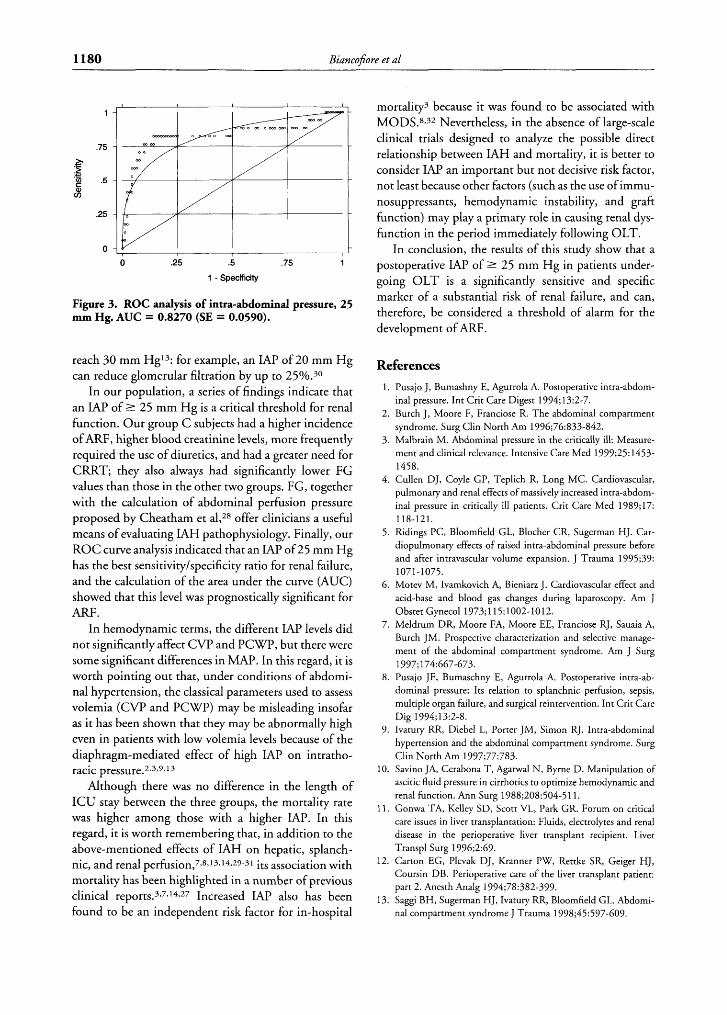
The ROC curve analysis was made using the mean LAP values recorded during the course of the study because there were no significant differences in the curves relating to the individual days. The results shown in Table 4 show that the most sensitive and specific IAP value for ARF was 25 mm Hg, whose ROC AUC was 0.83 (SE, 0.07; 95% CI, 0.69 to 0.97) and statistically significant (P < .OS) (Fig. 3).
Discussion
Although the idea of measuring of LAP is not new (some of the physiopathologic alterations caused by increased IAP were already known in the nineteenth century'), it is still not widely used in clinical practice; however,
Table 2. Renal Parameters
. Group A
TAP 5 18 mmHg (23 patients)
Blood creatinine POD 2 mean rt SD (range), mg/dL 1.1 rt 0.8 (0.4-0.9) Blood creatinine POD 4 mean % SD (range), mg/dL 1 -+ 1.1 (0.3-2.1) Urinary output POD 2 mean rt SD, mL/h 83.2 * 23.9 Urinary output POD 4 mean rt SD, mL/h 116.4 rt 63.9 Patients with diuretics, n 4 Patients with CRRT, n 0
Group B TAP 19-24 mm Hg
(5 1 patients)
0.7 2 0.3 (0.4-1.8) 0.7 ? 0.4 (0.4-2.2) 79 rt 24.4
106.8 ? 47.6 7 0
Group C IAP 2 25 mm Hg
43(patients)
1.3 rt 0.8 (0.4-3.8)* 1.9 ? 1.5 (0.4-5)' 79 5 35.3 99 5 39.5
29* 31-
Abbreviations: POD, postoperative day. *P < .01 versus group A and group B. ?P < .05 versus group A and group B.
Abdominal Hypertension After OL T 1179
Timing of Measurement
Parameter Mean ( W 0-24 Hours M e r O L T 24-72 Hours After OLT 48-72 Hours After OLT
A B C A B C A B C
IAP, mm Hg 13.8 (4) 20.85 (1.8) 33.5' (10.2) 15.5 (4.2) 20.15 (4) 26.6' (7.6) 13 (6.9) 20.55 (5.9) 23.55 (9.3) FG, mm Hg 71 (13.8) 57.2% (13.1) 27* (24.2) 72.3 (14.1) 62.55 (13.9) 47.4* (21.9) 77.6 (17.2) 65.6t (16.5) 56.77 (29.2) PCWP, m m H g 16.3 (5.2) 18 (4.4) 19.4 (5.1) 17.7 (4.6) 19 (5.6) 19.5 (4.1) 15.1 (4.6) 17.9 (4.6) 18.1 (4.2) CVP, m m H g 12.2 (4.4) 13.8 (3.7) 14.111 (3.2) 13.5 (3.5) 13.6 (4.3) 13.9 (5) 11.5 (4.5) 12.9 (2.9) 13 (3.5) MAP, mm Hg 100.2 (12.4) 97.7 (11.4) 91.8$. (11.1) 101.8 (11.6) 102.4 (11.2) 93.337 (13.6) 104.3 (11.6) 106.4 (11.9) 99.45 (16.9) CI, L 4.5 (1.1) 4.8 (0.9) 4.7 (1.0) 4.2 (0.7) 4.1 (0.8) 4.4 (0.9) 4.3 (0.9) 4.4 (1.3) 4.5 (1.1)
NOTE. Group A, 0-24 hours after OLT; group B, 24-48 hours after OLT; group C, 48-72 hours after OLT. Abbreviations: IAP, intra-abdominal pressure; FG, filtration gradient; PCWP, pulmonary capillary wedge pressure; PVC, central venous pressure; MAP, mean arterial pressure; CI, cardiac index. *P < .001 versus groups A and B. §P < .001 versus group A. tP < .01 versus group A. 111' < .05 versus group A. $P < .05 versus groups A and B. 5P < .05 versus group B.
there has been a recent renewal of interest in the conse- quences of high abdominal pressure.3
An acute increase in IAP, such as that occurring in postsurgical patients, has a series of dose-dependent effects that are capable of affecting many organs and functions because, unlike in the case of patients with chronic IAH such as the obese,7 there is not sufficient time for the occurrence of compensation mechanisms. It has been experimentally showed that a progressive increase in IAP leads to a continuing reduction in the efficacy of cardiac function, seriously altered splanch- nic, hepatic and renal perfusion, and less efficient respi- ratory f ~ n c t i o n ~ ~ - ~ 5 ; what has been observed in animals has been confirmed also in human~.~,9>'3,'*
The mechanism leading to renal dysfunction when IAP is high has not yet been clearly defined although a number of etiopathologic factors have been proposed, including a reduction in renal artery flow, a cortical to medullary hematic shunt, reduced cardiac output, and antidiuretic hormone (ADH), renin, and aldosterone hyperincretion.7~9,'3,~G Ureter occlusion leading to pos- trenal ARF does not seem to be involved because the placement of internal scents does not improve renal function in subjects with IAH.9 Whatever the causative mechanism may be, renal failure is very frequent in postsurgical patients with high IAP,16 which is itself an independent risk factor. 5
However, although IAH is recognized as being a serious postoperative risk factor compromising patient homeostasis, no consensus has yet been reached con- cerning the IAP level that should be considered critical in absolute terms or only in terms of renal func- tion.3,17>27 It has been shown in experimental animals
that abdominal pressure values of 20 to 40 mm Hg reduce mesenteric blood flow by 40% to 70%, and that IAP levels of less than 20 mm Hg can reduce it by 30% to 40%.28 It has been shown also that relatively low MP levels (10 mm Hg) can lead to a serious reduction in hepatic flow to as much as 39% of normal values.28 In terms of renal function, IAP levels of 15 to 20 mm Hg can cause oliguria, which turns into anuria when they
Table 4. ROC Curve Analysis of LAP Values
IAP Sensitivity Specificity (mm Hg) ( W ( W
10 100 1.1 - - -
15 94.1 14.2
20 88.2 48.3 21 82.3 58.2 22 82.3 68.1 23 82.3 79.1 24 82.3 82.3 25 82.6 83.5 26 76.4 86.8 27 70.5 90.1 28 64.7 93.4 29 58.8 95.6 30 52.9 95*6
35 35.2 97.8
40 11.7 98.9
- - -
- - -
- - -
- - -
>45 0 100
1180 Biancofore et al
l
.75
'5 4 3
.- c .- g .5
c%
.25
0 I
0 .25 .5 .75 l
l - Specificity
Figure 3. ROC analysis of intra-abdominal pressure, 25 mm Hg. AUC = 0.8270 (SE = 0.0590).
reach 30 mm Hg'3: for example, an MP of 20 mm Hg can reduce glomerular filtration by up to 25%.30
In our population, a series of findings indicate that an IAP of 2 25 mm Hg is a critical threshold for renal function. Our group C subjects had a higher incidence of ARF, higher blood creatinine levels, more frequently required the use of diuretics, and had a greater need for CRRT; they also always had significantly lower FG values than those in the other two groups. FG, together with the calculation of abdominal perfusion pressure proposed by Cheatham et a1,28 offer clinicians a useful means of evaluating IAH pathophysiology. Finally, our ROC curve analysis indicated that an IAP of 25 mm Hg has the best sensitivity/specificity ratio for renal failure, and the calculation of the area under the curve (AUC) showed that this level was prognostically significant for ARF.
In hemodynamic terms, the different LAP levels did not significantly affect CW and PCWP, but there were some significant differences in MAP. In this regard, it is worth pointing out that, under conditions of abdomi- nal hypertension, the classical parameters used to assess volemia (CV? and PCWP) may be misleading insofar as it has been shown that they may be abnormally high even in patients with low volemia levels because of the diaphragm-mediated effect of high IAP on intratho- racic press~re.~,3,9,~3
Although there was no difference in the length of ICU stay between the three groups, the mortality rate was higher among those with a higher LAP. In this regard, it is worth remembering that, in addition to the above-mentioned effects of IAH on hepatic, splanch- nic, and renal perfu~ion,7,8,13,'~.~9-31 its association with mortality has been highlighted in a number of previous clinical reports.3,7,14,27 Increased IAP also has been found to be an independent risk factor for in-hospital
mortality3 because it was found to be associated with MODS.8,32 Nevertheless, in the absence of large-scale clinical trials designed to analyze the possible direct relationship between IAH and mortality, it is better to consider IAP an important but not decisive risk factor, not least because other factors (such as the use of immu- nosuppressants, hemodynamic instability, and graft function) may play a primary role in causing renal dys- function in the period immediately following OLT.
In conclusion, the results of this study show that a postoperative LAP of 2 25 mm Hg in patients under- going OLT is a significantly sensitive and specific marker of a substantial risk of renal failure, and can, therefore, be considered a threshold of alarm for the development of ARF.
References 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
Pusajo J, Bumashny E, Agurrola A. Postoperative intra-abdom- inal pressure. Int Crit Care Digest 1994;13:2-7. Burch J, Moore F, Franciose R. The abdominal compartment syndrome. Surg Clin North Am 1996;76:833-842. Malbrain M. Abdominal pressure in the critically ill: Measure- ment and clinical relevance. Intensive Care Med 1999;25:1453- 1458. Cullen DJ, Coyle GP, Teplich R, Long MC. Cardiovascular, pulmonary and renal effects of massively increased intra-abdom- inal pressure in critically ill patients. Crit Care Med 1989;17:
Ridings PC, Bloomfield GL, Blocher CR, Sugerman HJ. Car- diopulmonary effects of raised intra-abdominal pressure before and after intravascular volume expansion. J Trauma 1995;39:
Motev M, Ivamkovich A, Bieniarz J. Cardiovascular effect and acid-base and blood gas changes during laparoscopy. Am J Obstet Gynecol 1973;115:1002-1012. Meldrum DR, Moore FA, Moore EE, Franciose RJ, Sauaia A, Burch JM. Prospective characterization and selective manage- ment of the abdominal compartment syndrome. Am J Surg
Pusajo JF, Bumaschny E, Agurrola A. Postoperative intra-ab- dominal pressure: Its relation to splanchnic perfusion, sepsis, multiple organ failure, and surgical reintervention. Int Crit Care Dig 1994; 13:2-8. Ivatury RR, Diebel L, Porter JM, Simon RJ. Intra-abdominal hypertension and the abdominal compartment syndrome. Surg Clin North Am 1997;77:783. Savino JA, Cerabona T, Agarwal N, Byrne D. Manipulation of ascitic fluid pressure in cirrhotics to optimize hemodynamic and renal function. Ann Surg 1988;208:504-511. Gonwa TA, Kelley SD, Scott VL, Park GR. Forum on critical care issues in liver transplantation: Fluids, electrolytes and renal disease in the perioperative liver transplant recipient. Liver Transpl Surg 1996;2:69. Carton EG, Plevak DJ, Kranner PW, Rettke SR, Geiger HJ, Coursin DB. Perioperative care of the liver transplant patient: part 2. Anesth Analg 1994;78:382-399. Saggi BH, Sugerman HJ, Ivatury RR, Bloomfield GL. Abdomi- nal compartment syndrome J Trauma 1998;45:597-609.
118-121.
1071-1075.
1997;174:667-673.

Abdominal Hypertension After OL T 1181
14. Cullen DJ, Coyle JP, Teplick R. Cardiovascular, pulmonary, renal effects of massively increased intra-abdominal pressure in critically ill patients. Crit Care Med 1989;17:118-121.
15. Sugrue M, Jones F, Deane SA, Bishop G, Bauman A, Hillman K. Intra-abdominal hypertension is an independent cause of post- operative renal impairment. Arch Surg 1999;134:1082-1085.
16. Sugrue M, Buist MD, Hourihan F, Deane S, Baumann A, Hill- man K. Prospective study of intra-abdominal hypertension and renal function after laparotomy. Br J Surg 1995;82:235-238.
17. McNelis J, Marini CP, Jurkiewicz A, Fields S, Caplin D, Stein D, et al. Predictive factors associated with the development of abdominal compartment syndrome in the surgical intensive care unit. Arch Surg 2002;137: 133-136.
18. American College of Chest Physisicians/Socety of Critical Care Medicine Consensus Conference. Crit Care Med 1992;20:864- 874.
19. McDonald M, Perkins JD, Ralph D, Carirhers RL. Postopera- tive care: Immediate. In: Maddrey WC, Sorrel MF editors. Transplantation of the Liver, 2"d edition. Nonvalk, W. Apple- ton & Lange, 1996: 171 -206.
20. Biancofiore G, Romanelli AM, Bindi L, Consani G, Boldrini A, Battistini M, et al. Very early tracheal extubation without prede- terminated criteria in a liver transplant recipient population. Liver Transpl2001;7:777-782.
21. Kron IL, Hartman PK, Nolan SP. The measurement of intra- abdominal pressure as a criterion for abdominal re-exploration. Ann Surg 1984;199:28-30.
22. Mutoh T, Lamm WJ, Embree LJ. Abdominal distension alters regional pleural pressures and chest wall mechanics in pig in vivo. J Appl Physiol 199 1 ;70:26 1 1-26 18.
23. Mutoh T, Lamm WJ, Embree LJ. Volume infusion produces
abdominal distension, lung compression and chest wall stiffen- ing in pigs. J Appl Physiol 1992;72:575-582.
24. Diebel LN, Wilson RF, Dulchavsky SA, Saxe J. Effect of increased intra-abdominal pressure on hepatic arterial, portal venous and hepatic microcirculatory blood flow. J Trauma 1992; 33:279-283.
25. Nakatami T, Sakamoto Y, Kaneko I, Ando H, Kobayashy K. Effects of intra-abdominal hypertension on hepatic energy metabolism in a rabbit model. J. Trauma 1998;44:446-543.
26. Bradley SE, Bradley GP. The effect of increased intra-abdominal pressure on renal function in man. J Clin Invest 1947;26:1010- 1022.
27. Sugrue M. Intra-abdominal pressure. Clin Intensive Care 1995;
28. Cheatham ML, White MW, Sagraves SG, Johnson JL, Block EFJ. Abdominal perfusion pressure: A superior parameter in the assessment of intra-abdominal hypertension. J Trauma 2000;49:
29. Diebel L, Dulchavsky S, Wilson R. Effect of increased intra- abdominal pressure on mesenteric artery and intestinal mucosal blood flow. J Trauma 1992;33:45-49.
30. Diebel LN, Wilson W, Dulchavsky SA, Saxe J. Effect of increased intra-abdominal pressure on hepatic arterial, portal venous and hepatic microcirculatory blood flow. J Trauma 1992;
3 1. Bradley SE, Bradley GP. The effect of increased intra-abdominal pressure on renal function in man. J Clin Invest 1947;26: 10 10- 1022.
6~76-79.
62 1-627.
33~279-283.
32. Eddy V, Nunn C, Morris JA. Abdominal compartment syn- drome. Surg Clin North Am 1997;74:801-8 1 1.