resistant hypertension, ppt
TRANSCRIPT

Lady DavisInstitute
Resistant hypertension
Ernesto L. Schiffrin CM, MD, PhD, FRSC, FRCPC
Physician-in-Chief, Sir Mortimer B. Davis-Jewish General Hospital, Canada Research Chair in
Hypertension and Vascular Research, Lady Davis Institute for Medical Research,
Vice-Chair, Department of Medicine, McGill University, Montreal, PQ, Canada.
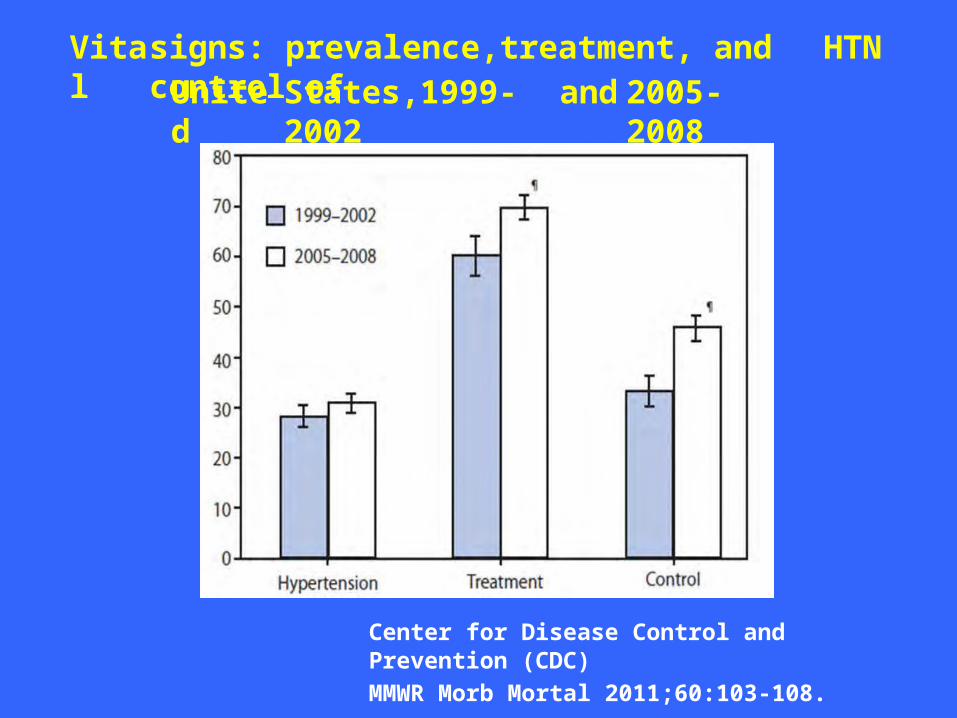
Vital
signs: prevalence,treatment, and control of
HTNUnited
States,1999-2002
and 2005-2008
Center for Disease Control and Prevention (CDC)MMWR Morb Mortal 2011;60:103-108.
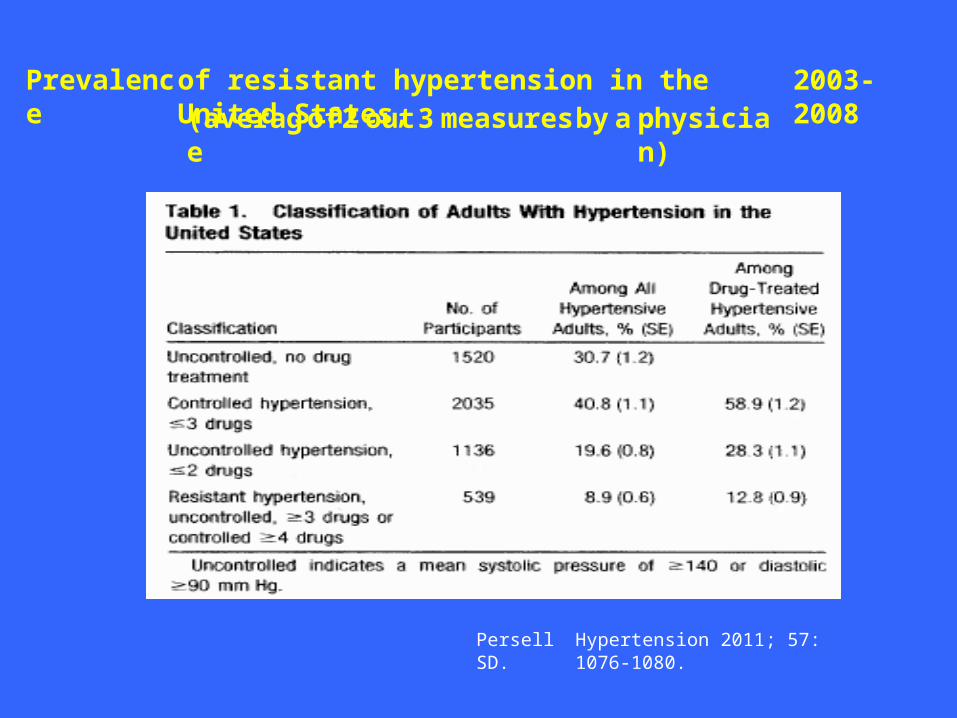
Prevalence
of resistant hypertension in the United States,
2003-2008(averag
eof2 out3 measuresby a physicia
n)
Persell SD.
Hypertension 2011; 57: 1076-1080.
Resistant vs refractory hypertensionResistant hypertension is hypertension that doesrespond to adequate doses of 3-4 or moreantihypertensive drugs.It represents 10-15% of the general hypertensive population.Refractory hypertension is defined as BP that
not
remains uncontrolled after 3 visits to a hypertensionclinic within a minimum 6-month follow-up period.Secondary causes of hypertension, obesity, diabetes, sleep disordered breathing and excess salt intake or use of AINS drugs are among some of the findings associated with resistant or refractory hypertension.
Clinical features of 8295 patients with resistant
hypertension classified on the basis of ABPM• Prevalence of resistant hypertension in the
Spanish ABPMregistry• Resistance defined by BP in office ≥140/90 mmHg andantihypertensive drugs
≥ 3
•••
12.2% of 68,045After ABPM: 62.5% wereAfter ABPM :55.9%
true resistant ≥130/80 mmHg
≥135/85 mmHg
• Selected population
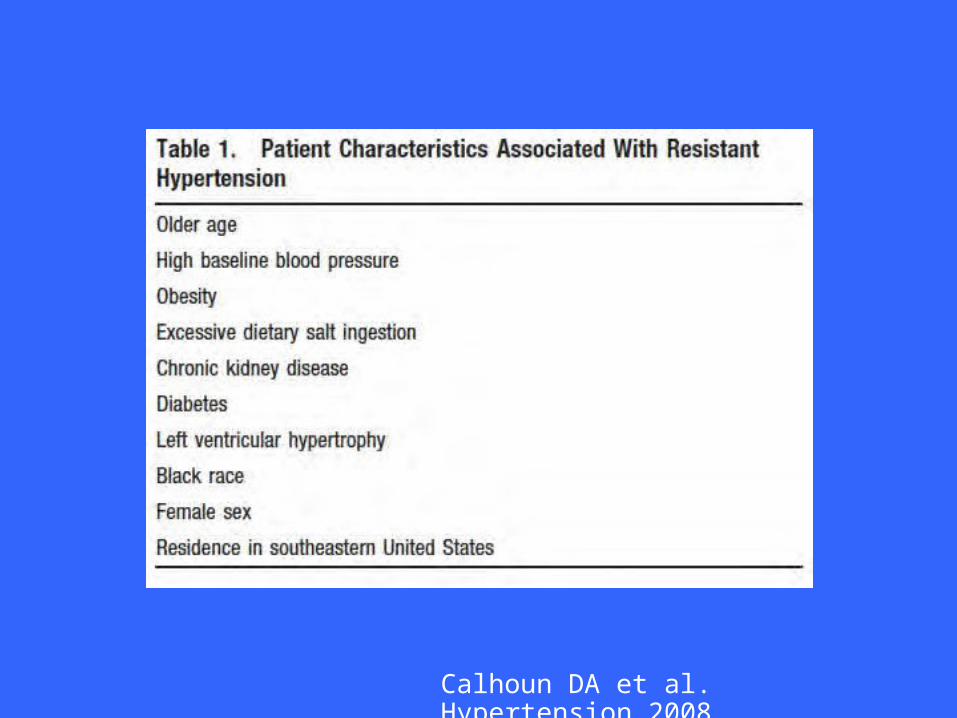
Calhoun DA et al. Hypertension 2008
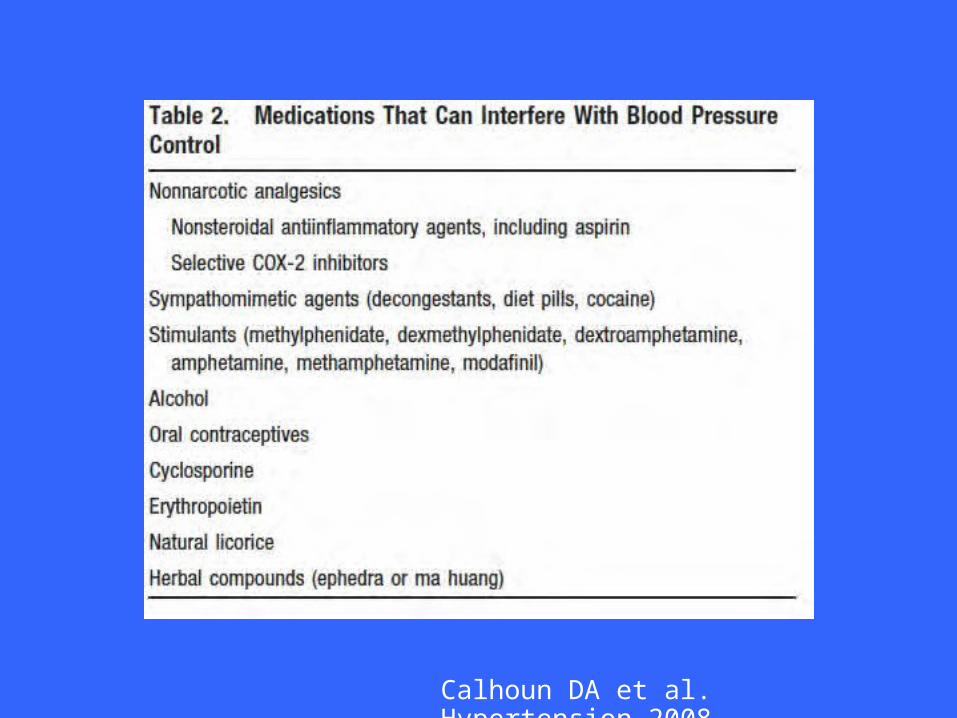
Calhoun DA et al. Hypertension 2008
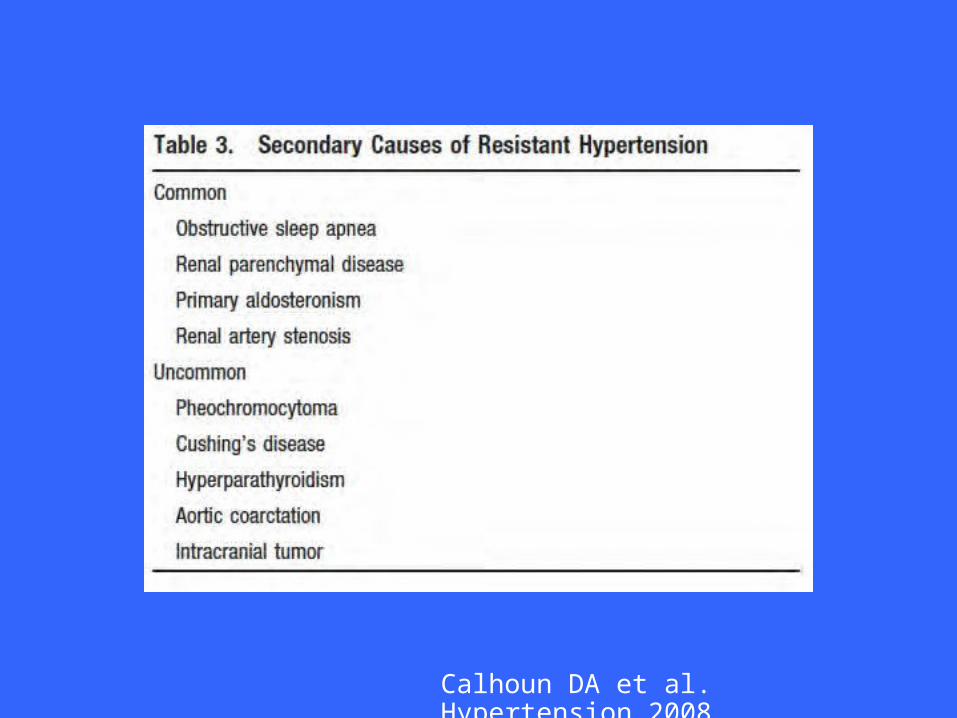
Calhoun DA et al. Hypertension 2008
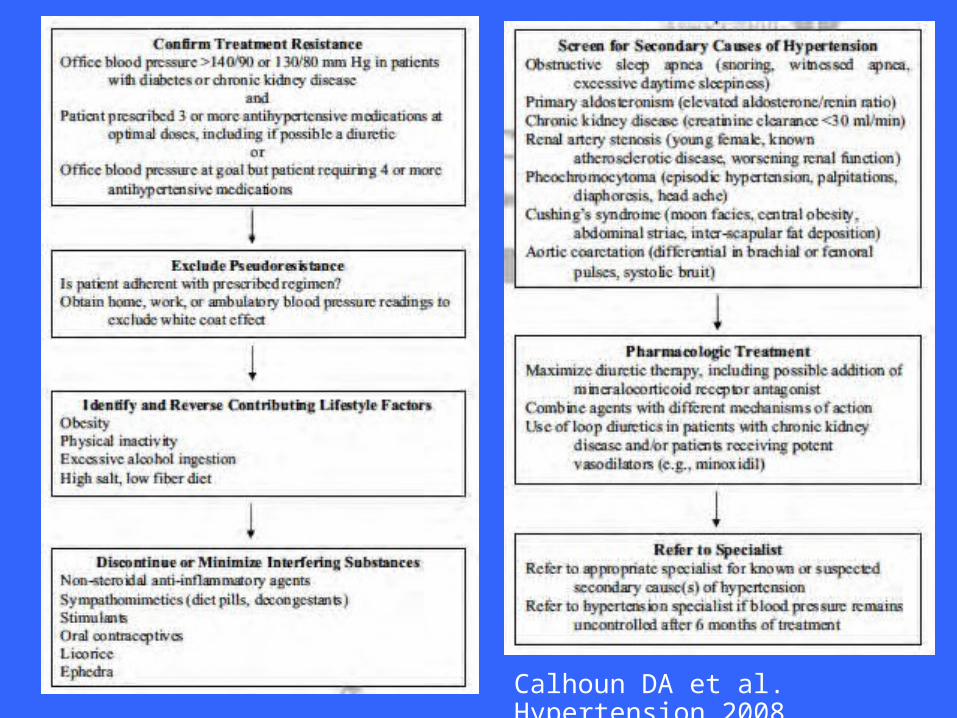
Calhoun DA et al. Hypertension 2008
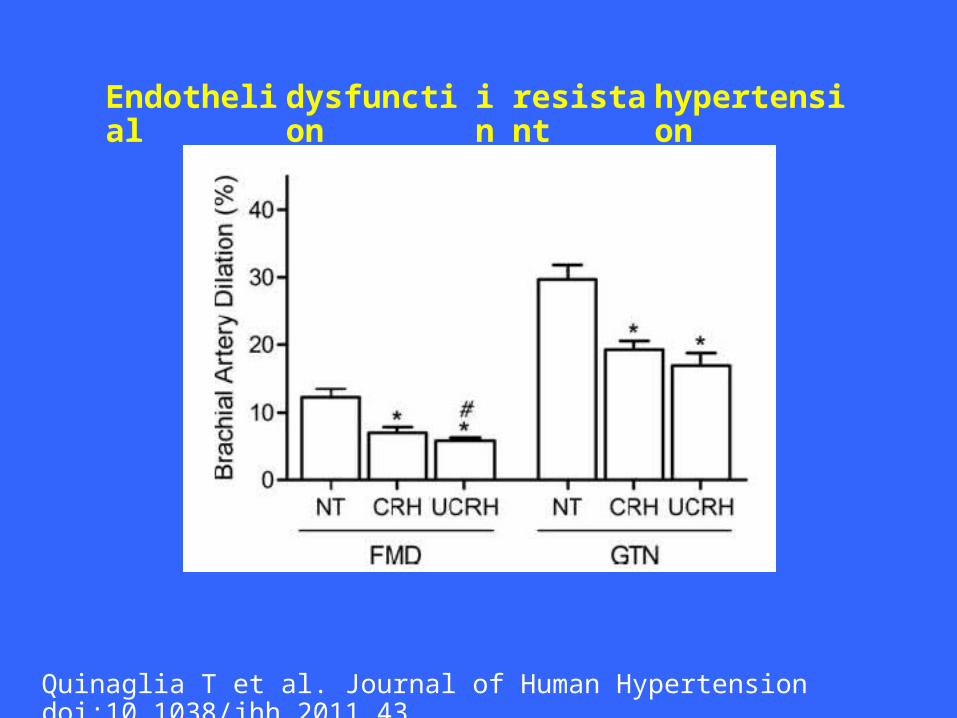
Endothelial
dysfunction
inresistant
hypertension
Quinaglia T et al. Journal of Human Hypertension doi:10.1038/jhh.2011.43
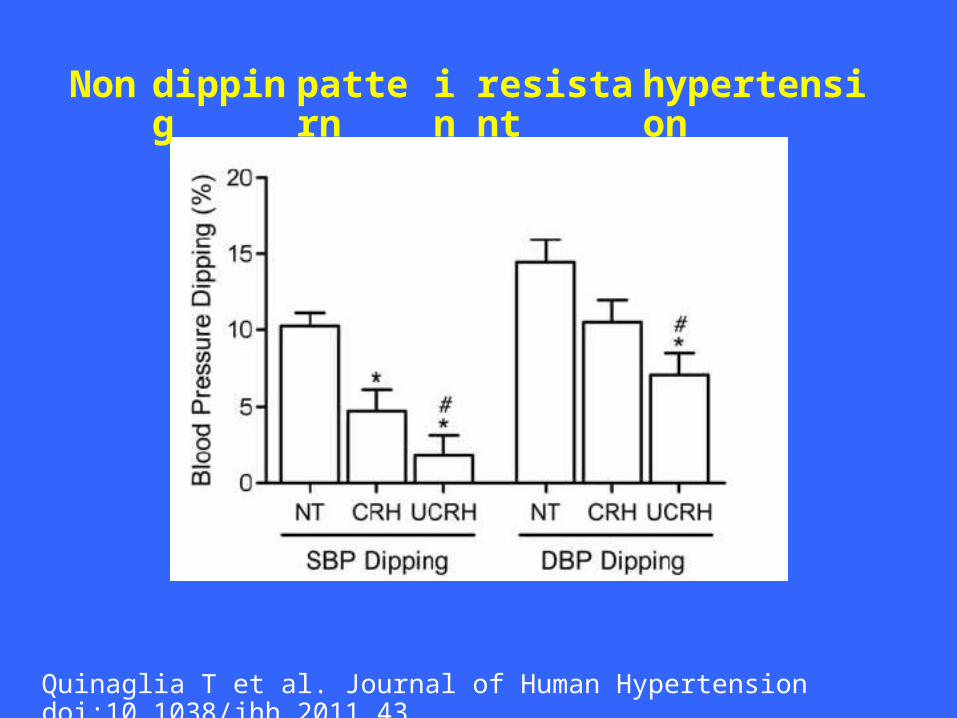
Non dipping
pattern
inresistant
hypertension
Quinaglia T et al. Journal of Human Hypertension doi:10.1038/jhh.2011.43
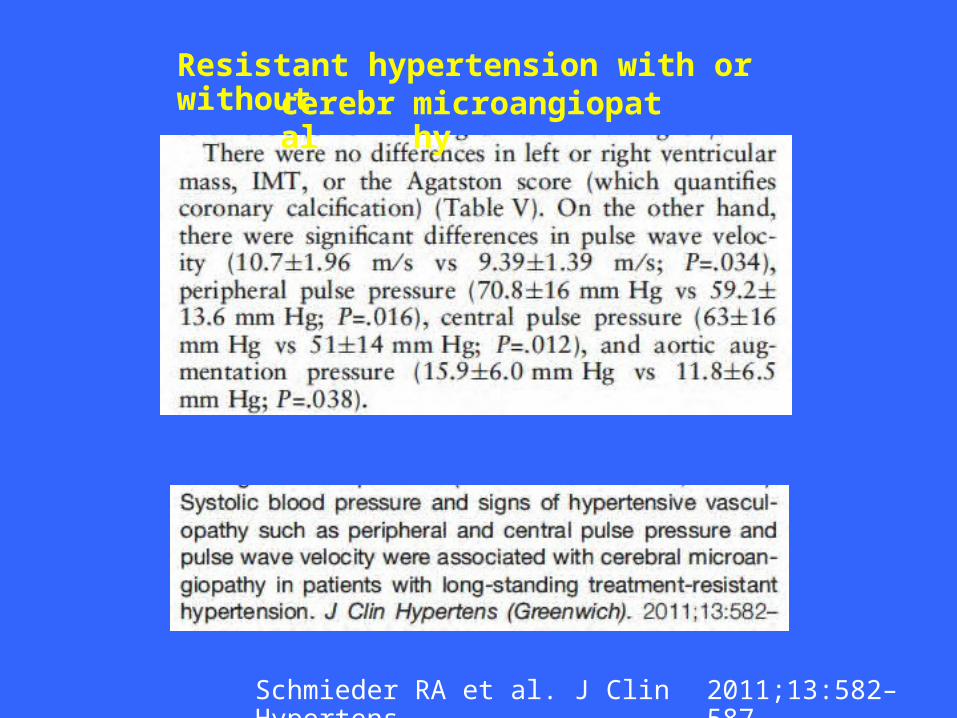
Resistant hypertension with or withoutcerebr
almicroangiopathy
Schmieder RA et al. J Clin Hypertens.
2011;13:582–587.
How to approach resistant hypertension
The general treatment approach:
1.adding or titrating diuretic therapy,2.changing the diuretic class to one appropriate for the patient’s kidney function,3.using medications with complementary mechanisms of action, and4.adding a mineralocorticoid antagonist to the antihypertensivedrug regimen.
How to approach resistant hypertension
1.
RAS blocker + diuretic + CCB + MR antagonist with or withouta beta-blockerThiazide diuretics: chlorthalidone @ 25 mg⁄ d, preferred formost patients.CKD: loop diuretic, most commonly furosemide at 20 mg to40 mg twice daily.
Vasodilators, centrally acting antihypertensive agents, and alpha-adrenergic blockers added if failure to control BP.
2.
3.
4.
How to approach resistant HTN
•Adherence needs to be assessed by asking thepatient about medication use, perceptionsabout medication efficacy, and presence ofadverse effects, if any.Patients must be seen every 4 to 8 weeks, with more frequent visits for patients with uncontrolled BP.
•
Resistant HTN treatment
•Use of a MR antagonist in addition to adiuretic, particularly chlorthalidone, inaddition to a full dose of a RAS blocker and aCCB is usually associated with control rates ofresistant hypertension >80%.
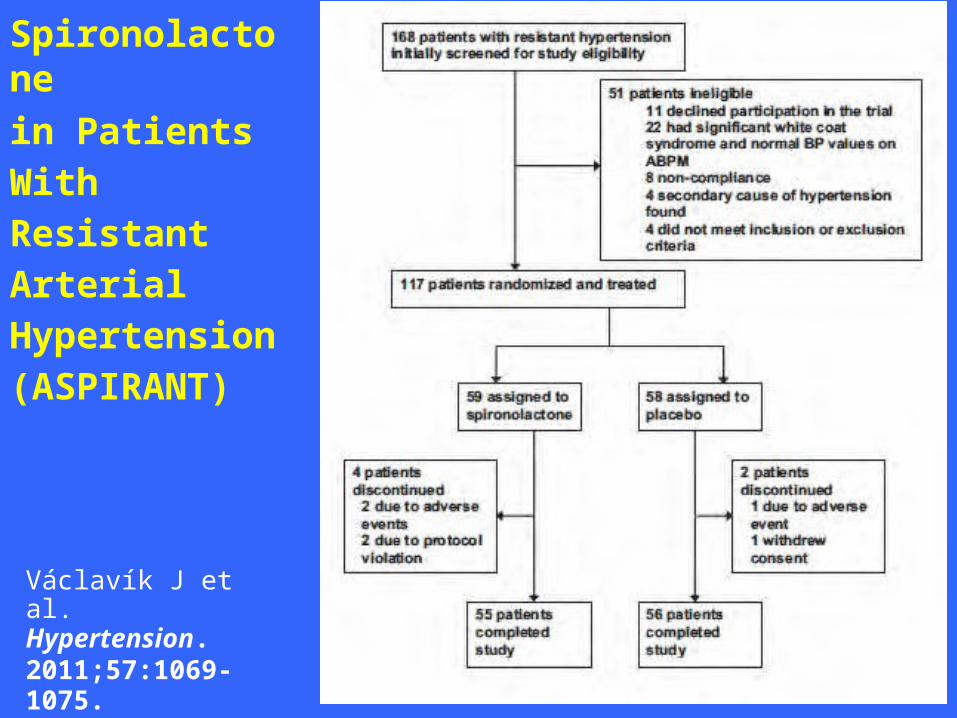
Spironolactonein Patients WithResistantArterialHypertension(ASPIRANT)
Václavík J et al.Hypertension.2011;57:1069-1075.
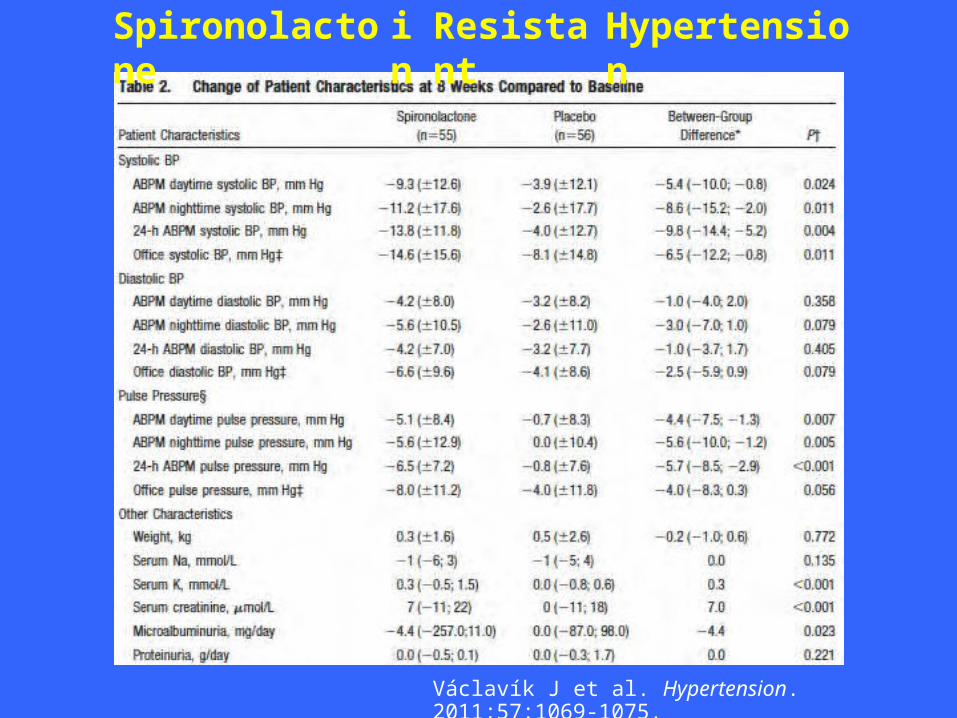
Spironolactone
inResistant
Hypertension
Václavík J et al. Hypertension. 2011;57:1069-1075.
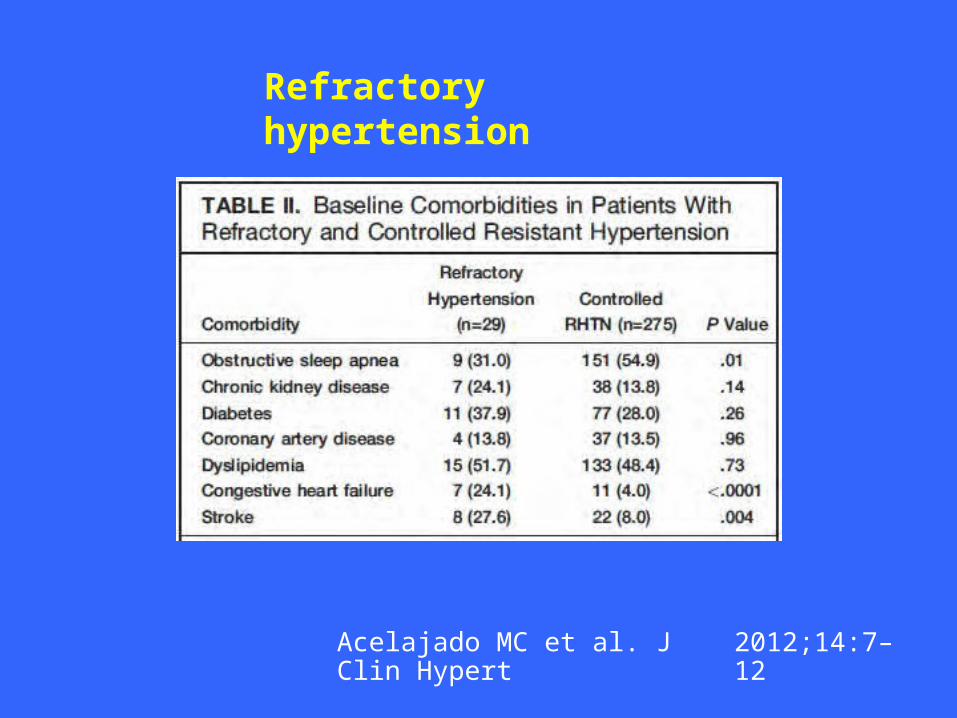
Refractory hypertension
Acelajado MC et al. J Clin Hypert
2012;14:7–12
Refractory
hypertension
Acelajado MC et al. J Clin Hypert
2012;14:7–12
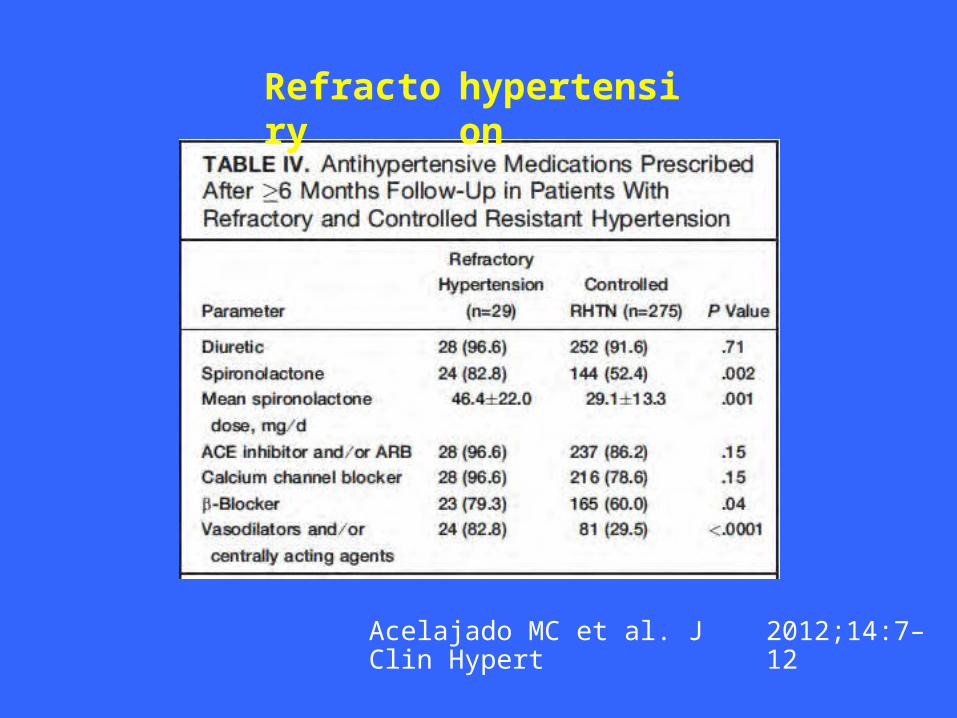
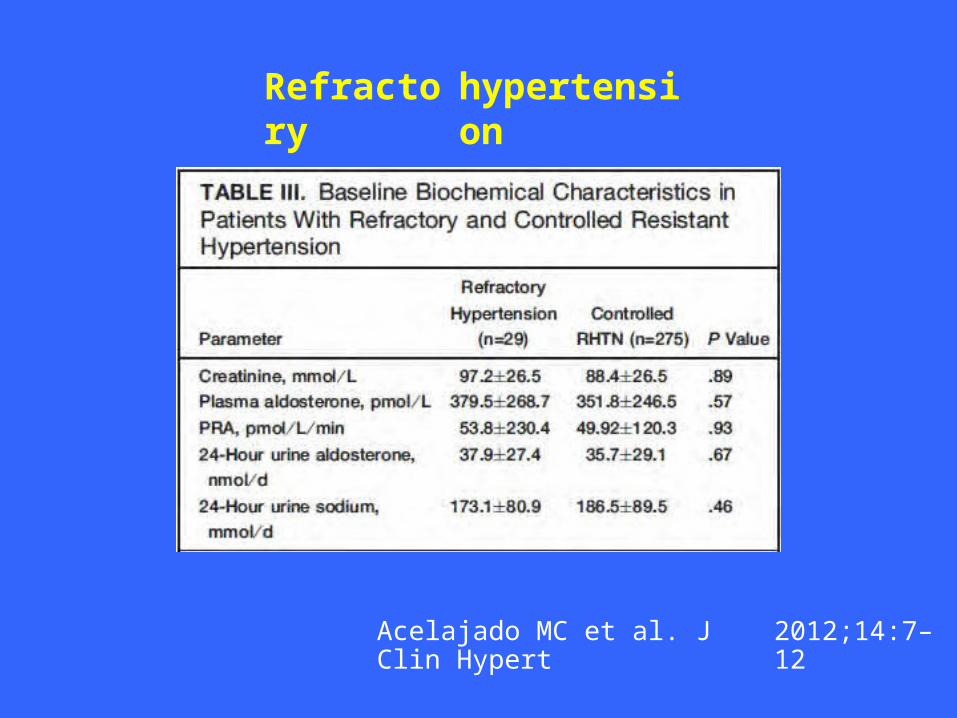
Refractory
hypertension
Acelajado MC et al. J Clin Hypert
2012;14:7–12
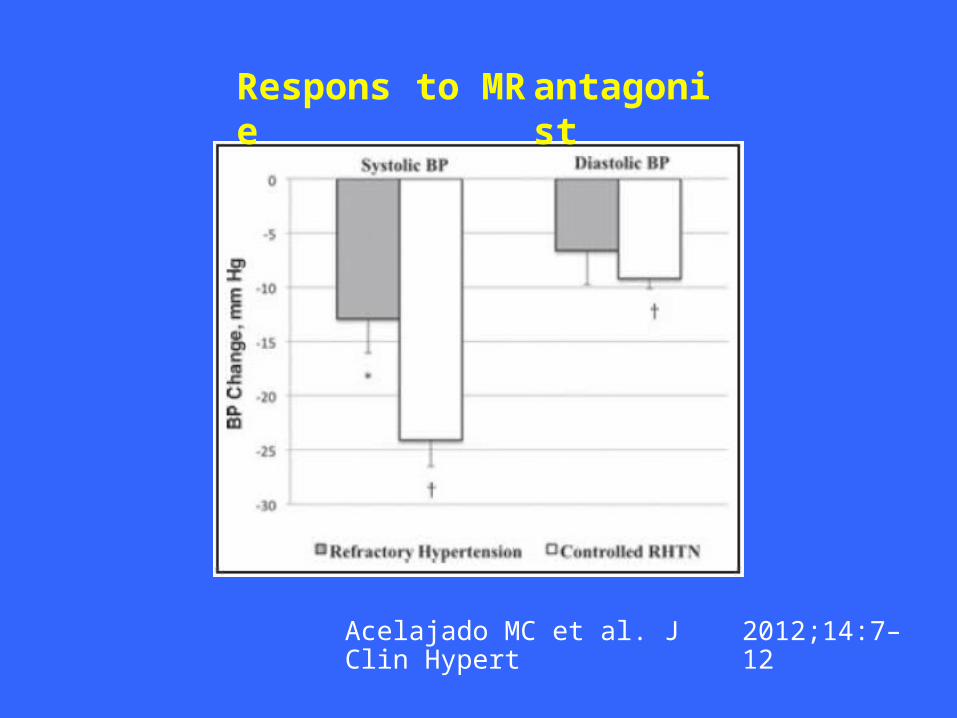
Response
to MR antagonist
Acelajado MC et al. J Clin Hypert
2012;14:7–12
Refractory hypertension: mechanisms
•No evidence of greater fluid retention inrefractory HTN vs controlled resistant HTNsince aldosterone or PRA levels notsuppressedGreater role of increased cardiac output and
• ⁄or vascular resistance: enhanced sympatheticdrive and ⁄ or increased peripheral resistancesecondary to local or circulating pressoragents?
Acelajado MC et al. J Clin Hypert 2012;14:7–12
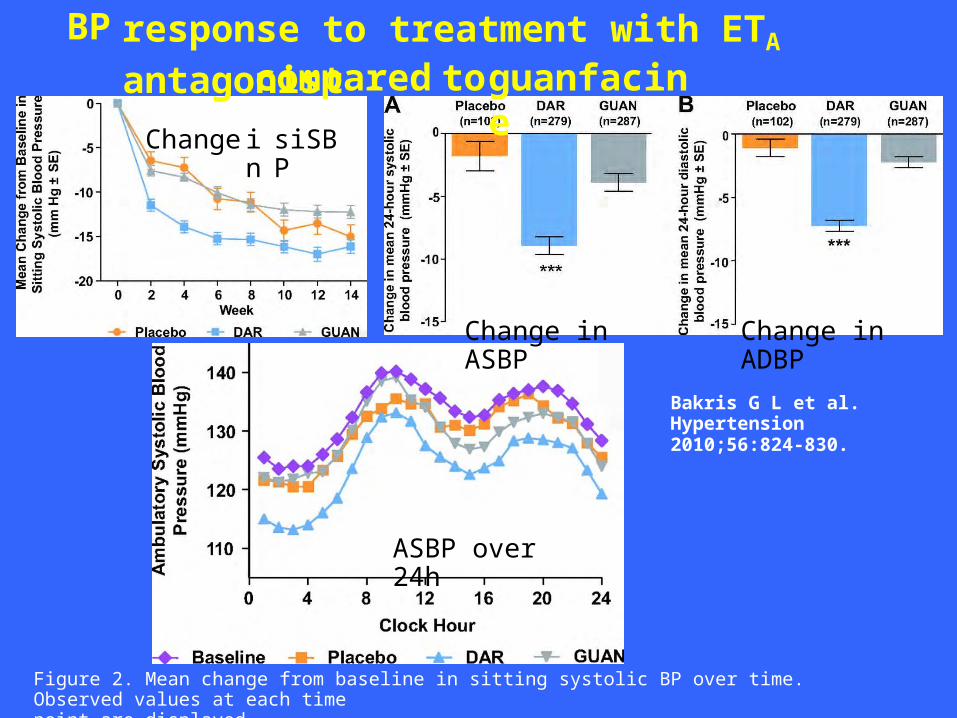
BP response to treatment with ETA antagonistcompared toguanfacin
eChangeinsiSBP
Change in ASBP
Change in ADBP
Bakris G L et al.Hypertension 2010;56:824-830.
ASBP over 24h
Figure 2. Mean change from baseline in sitting systolic BP over time. Observed values at each timepoint are displayed.
New approaches to refractory HTN
• Catheter-Based Radiofrequency RenalSympathetic Denervation• Baroreceptor stimulation
Catheter-Based Radiofrequency Ablation
ofRena
lSympathetic
Nerves
The SYMPLICITY-HTN results showed that
six months
after theablation, average office BP in the renal-
denervation group wasreduced by 32/12 mm Hg (average baseline 178/96 mm Hg), whereas it did not differ from baseline in the control group. Between-group differences in BP at six months were 33/11 mm Hg (p<0.0001).
Renal sympathetic denervation in patients with treatment-
resistant hypertension (The Symplicity HTN-2 Trial): a
randomised controlled trial
Simplicity HTN- 2 investigators ( Murray D Esler) Lancet
376;1903-1909
2010:
Objective: Activation of the sympathetic renal system is
involved in the pathogenesis of hypertensionRCT in patients wint BP>150 mmHg taking
3 drugs:denervation + Rx or Rx
aloneMeasured systolic BP at 6 monthsProcedures: Catheter SYMPLICITY in renal arteries
renal
4-6 low-intensity stimulations on the renal artery
BP 178/97 mmHg in patients 57-year old (male=60%) taking mean of 5.2 drugs (35% more than 5 )
a

SymplicityHTN-2 Tri
al
The Lancet 2010;376: 1903-1909
Symplicity HTN-1 Investigators
Catheter-Based Renal Sympathetic Denervation for Resistant Hypertension:Durability of Blood Pressure Reduction Out to 24 Months153 patients with catheter-based renal sympathetic denervation at 19 centersHypertension. 2011;57:911-917.
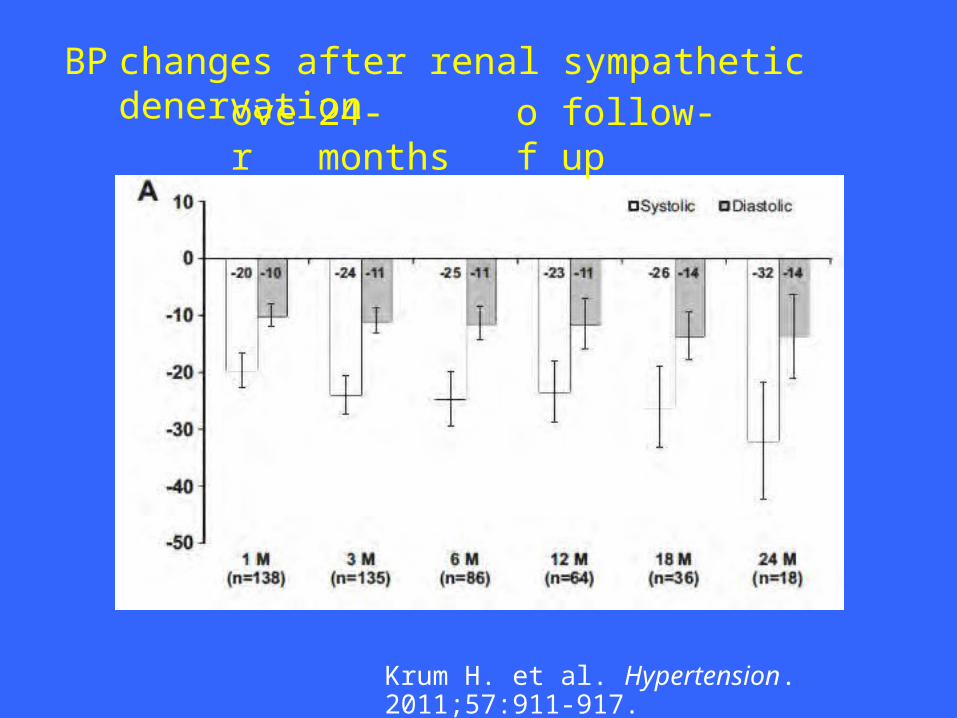
BP changes after renal sympathetic denervationove
r24-months
of
follow-up
Krum H. et al. Hypertension. 2011;57:911-917.

Randomized controlled clinical trials
SimplicityHTN 3
DEPART ReSET MIRT DENER- HTN
PRAGUE-15 INSPIRE
Recruiting Y Y Y Y Y Y N
Intervention
RDN RDN RDN PVI+RDN RDN RDN RDN
No. patients
530 120 70 150 120 150 230
Catheter Simplicity
Simplicity
Simplicity
THERMOCOOL Simplicity
Simplicity
TBD
Completion 2013
2014
2012
2012
2014 2013
2016
Country USA Belgium Denmark Russia France Czech Rep.
Europe
Renal function
mGFR/cys C
eGFR/mGFR
Imaging renal arteries
Arteriogr (6) AngioCT (12,24, 36)

Center
requirements for application
of
RDN inrefracto
ryHTN
Modified from Joint UK Societies Consensus on RDN for treatment-resistant HTN
Experience Management of resistant hypertensionHigh volume interventional cardiology/radiologyProtocol Written protocol for work-up, procedure & f/u Written informed consent and ethics approval Plans for management of complications
Infrastructure
High quality CT/MRI Hemodynamics labMultidiscip
linary team
HTN specialists experienced in managing resistant HTN Interventional cardiologists/radiologists experienced in RDN and nephrologists and vascular surgeons
Transparency Participation in registration program
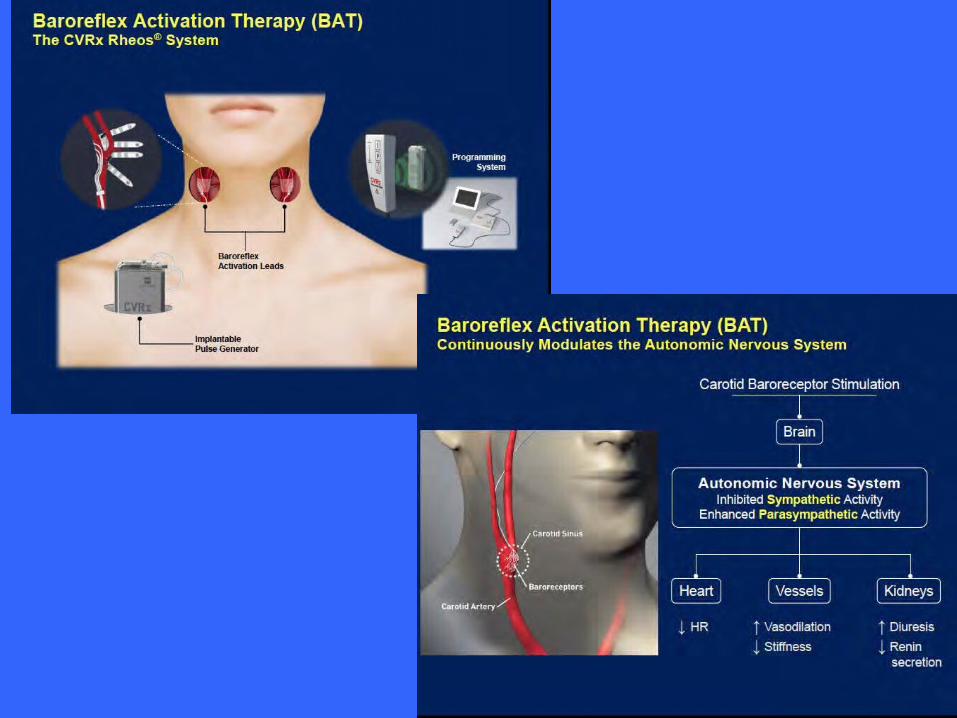
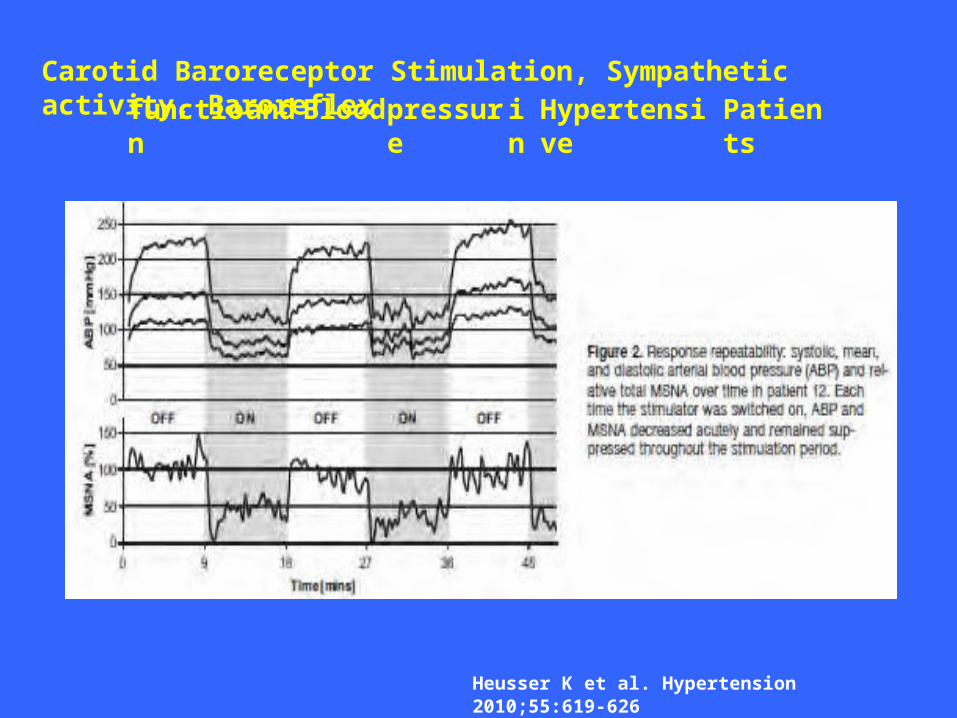
Carotid Baroreceptor Stimulation, Sympathetic activity, Baroreflexfunctio
nand Bloodpressur
einHypertensive
Patients
Heusser K et al. Hypertension 2010;55:619-626
Conclusion
Diagnosis, including ABPM
•••••
Exclude secondary causes3 drugs (RAS inhibitor, CCB,
diuretic)
+ MR blocker
Adherence to treatment, salt intakeF/u and only then consider invasive treatments
Gracias