abdominal rectopexy for complete rectal prolapse: preliminary results of a new technique
TRANSCRIPT

Int J Colorectal Dis (2005) 20:180–189DOI 10.1007/s00384-004-0650-0 O R I G I N A L A R T I C L E
Angelo Di GiorgioDaniele BiacchiSimone SibioFabio AccarpioGiovanni SinibaldiLea PetrellaFrancesca Romana CappielloPaolo Sammartino
Abdominal rectopexyfor complete rectal prolapse:preliminary results of a new technique
Accepted: 7 July 2004Published online: 20 November 2004� Springer-Verlag 2004
A. Di Giorgio · D. Biacchi · S. Sibio ·F. Accarpio · G. Sinibaldi · F. R. Cappiello ·P. Sammartino ())Department of Surgery “Pietro Valdoni”,University of Rome “La Sapienza”,Rome, Italye-mail: [email protected].: +39-6-49972210Fax: +39-6-49972210
L. PetrellaDepartment of Studi Geoeconomici,Linguistici, Statistici, Storiciper l’Analisi Regionale,University of Rome “La Sapienza”,Rome, Italy
Abstract Purpose: Although thetechnique for the surgical repair ofrectal prolapse has advanced over theyears, no ideal procedure has beenfound. We aim to test a new surgicalprocedure for abdominal rectopexythat uses the greater omentum tosupport the rectum below the recto-pexy, to reconstruct the anorectalangle and dispense with the need forsynthetic mesh, thus reducing the riskof infection. Methods: A series of tenpatients, all young and medically fit,underwent repair surgery for rectalprolapse with the new rectopexytechnique. Some patients had con-comitant sigmoidectomy. Preopera-tive and postoperative assessmentincluded a clinical examination, analmanometry and defecography. Re-sults: Follow-up lasted a mean of56.4 months. None of the patients hadrecurrent rectal prolapse or infection.Postoperative assessment at24 months disclosed significant im-provements in all the bowel andsphincter variables assessed. The 8patients who had severe incontinencepreoperatively had notably improvedand 4 were fully continent, 3 moder-ately incontinent, and only 1 patienthad persistently high levels of in-
continence. In only 1 patient whoinitially had severe incontinence,continence completely regressed andsevere constipation developed. Max-imal basal pressure values increasedsignificantly after surgery(p=0.0025), although they increasedslightly less evidently in patients inwhom marked incontinence persistedat postoperative follow-up. Maximalvoluntary contraction pressure alsoincreased significantly after surgery(p=0.0054), although the valueschanged less than those for basalpressure. During rest, squeeze andstraining, and in all the patients whoregained continence, even those whorecovered it only partly, surgerysubstantially reduced the anorectalangle. The reduction during rest wasstatistically significant (p=0.0062).Conclusions: The rectopexy tech-nique we tested in patients with rectalprolapse avoids the need for syntheticmesh, and provides good results interms of bowel and sphincter func-tion, without infection or recurrence.
Keywords Rectal prolapse · Newtechnique for rectopexy · Rectopexytechnique · Surgery for rectalprolapse · Prolapse
Introduction
Complete rectal prolapse is a socially disabling conditionthat still has a highly controversial multifactorial etiology[1]. Despite the numerous surgical procedures proposed
for treating rectal prolapse, choosing the ideal operationstill remains a perplexing problem for the surgeon. Thechoice depends mainly on the patient’s age, surgical risk,coexisting functional symptoms, including incontinenceor constipation, and the surgeon’s familiarity with a par-

181
ticular surgical approach [2]. Although consensus islacking on the most appropriate surgical technique fortreating rectal prolapse [3, 4], all agree that surgery hastwo principal aims: to bring the prolapsed rectum underlong-lasting control and to improve bowel and sphincterdysfunction (constipation and incontinence). The opera-tive technique we propose is an abdominal posteriorrectopexy with an omentoplasty that fixes the rectum tothe presacral fascia with the edges of the pelvic perito-neum, which improves the patient’s functional symptomsand avoids the use of a synthetic mesh. Our aims in re-viewing this series were to see whether this new ab-dominal repair procedure effectively provides long-last-ing control of rectal prolapse and to assess the surgicaloutcome in terms of bowel and sphincter function (con-stipation and incontinence).
Patients and methods
Between January 1996 and December 2002, a total of 36 consec-utive patients were admitted to our Department and treated forrectal prolapse. Of these 36 patients, 26, all elderly and infirm,underwent perineal rectosigmoidectomy according to the Altemeierprocedure [5] and the remaining 10 (9 women and 1 man; mean age44.7, range 21–68 years), younger patients who were medically fit,constituted the objective of this study and underwent abdominalrectopexy with the new technique.
All patients had a documented complete rectal prolapse duringstraining defined as a “circumferential full-thickness intussuscep-tion of the rectal wall with protrusion beyond the anal canal” ac-cording to the criteria stated at the Tripartite Consensus Conference
of Definitions for Anorectal Physiology and Rectal Cancer held inWashington DC on 1 May 1999 [6]. Patients with internal prolapseand mucosal prolapse were excluded from the present analysis.Two of the 10 patients selected had undergone hysterectomy foruterine prolapse and 3 hemorrhoidectomy; none of the patients hadhad a previous operation for rectal prolapse. Preoperative assess-ment included a clinical examination, colonoscopy, and analmanometry (AM), with the intention of evaluating the maximalbasal pressure (MBP), maximal voluntary contraction pressure(MVCP), and defecography.
Postoperative results were evaluated in the absence of anycomplaints by a simple physical examination 6 months after theoperative procedure. Thereafter, all diagnostic tests were repeatedyearly for the first 2 years and a questionnaire was also mailed to allpatients for the remaining follow-up time.
Incontinence was graded using a modified version of Kirwan’sincontinence score (grade 0: continent; grade I: incontinent forflatus; grade II: incontinent for liquid stools; grade III: incontinentfor liquid stools and daily soiling; and grade IV: total fecal in-continence) [7]. Constipation in our study was defined as less thantwo bowel movements a week, difficulty in bowel emptying re-quiring straining or dependent use of laxatives or enemas. Sphincterfunction was assessed by anal manometry according to a techniquepreviously described by Hiltunen [8].
All patients underwent defecography to study the anorectalangle (ARA) and the pelvic floor descent (PFD); the ARA wasmeasured as the angle between the luminal axis of the anal canaland the long axis of the rectum; pelvic floor descent was defined asthe perpendicular distance between the position of the anorectalangle and the pubococcygeal line according to previously publishedcriteria [9, 10]. Changes in both variables were assessed at rest,during maximum pelvic floor contraction (squeeze) and duringattempted defecation (straining).
All ten patients were given preoperative per oral mechanicalbowel lavage with electrolyte solution. Antibiotic prophylaxis wasgiven during the induction of general anesthesia. All patients un-
Table 1 Preoperative and postoperative (24 months) evaluations
Patients Sex Age Kirwan’sscore
Constipation MeanMBP(cmH2O)
MeanMVCP(cmH2O)
ARA (degree) PFD (cm)
R Sq St R Sq St
Preoperative evaluation1 Female 21 4 No 11 42 123 115 140 6.6 4.8 10.22 Male 42 3 No 15 38 120 116 132 5.6 3.0 7.13 Female 43 2 No 23 49 107 101 120 5.4 3.0 8.44 Female 35 3 No 17 39 118 110 142 5.8 5.2 9.15 Female 37 3 No 13 40 121 117 145 6.5 3.8 9.76 Female 68 4 No 11 36 125 108 138 7.0 6.6 10.07 Female 55 0 Yes 40 52 100 94 110 3.5 2.3 5.48 Female 39 3 No 18 41 120 113 145 5.9 4.4 7.29 Female 61 4 No 19 38 128 116 150 6.5 5.6 8.610 Female 46 0 Yes 36 51 107 99 125 3.2 2.7 6.1
Postoperative evaluation (24 months)1 Female 21 1 No 35 48 108 91 120 4.0 2.4 6.02a Male 42 0 No 37 49 103 96 110 3.8 2.3 6.83 Female 43 0 No 38 47 110 90 125 3.8 2.3 6.74a Female 35 1 No 36 48 102 93 128 3.9 3.0 6.55 Female 37 0 No 39 49 104 94 118 6.4 3.8 9.06a Female 68 3 No 21 38 120 107 140 7.2 6.8 10.37a Female 55 0 No 41 65 102 94 115 3.8 2.7 7.08 Female 39 0 Yes 38 51 107 92 124 4.1 3.0 6.79 Female 61 1 No 35 50 102 94 130 4.4 3.8 7.110a Female 46 0 No 38 52 101 93 125 3.4 2.2 7.6
a Patient submitted for colic resection
182
derwent rectopexy using the new technique after a laparotomyapproach under general anesthesia.
Five of the 10 patients underwent rectopexy and sigmoid re-section (patients 2, 4, 6, 7, and 10); in 2 of these (7 and 10) sigmoidresection was indicated for severe constipation and in 3 (patients 2,4, and 6) by the intraoperative finding of a dolichosigmoid (Ta-ble 1).
Informed consent was obtained from all patients. None of thepatients were lost to follow-up and the mean follow-up of the entiregroup was 56.2 months (range 24–84 months).
Surgical technique
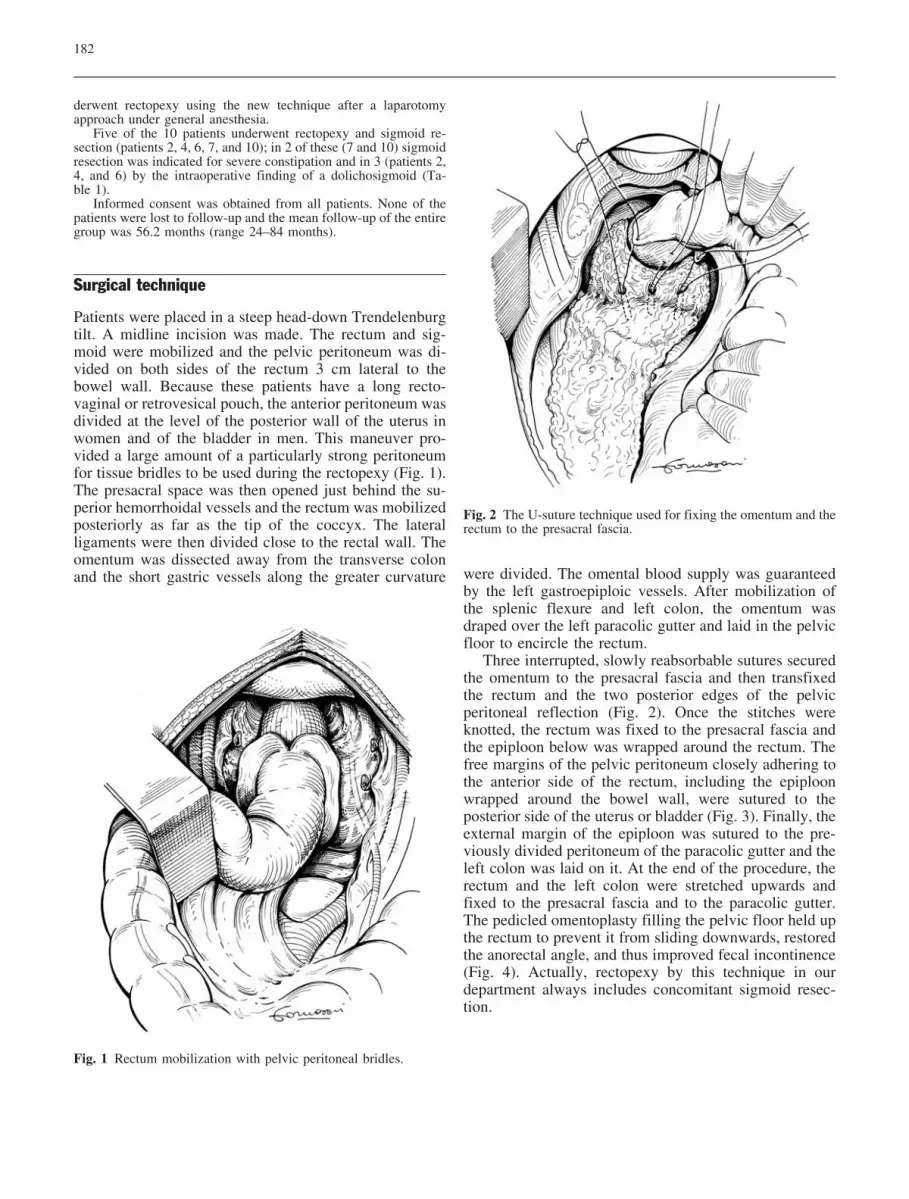
Patients were placed in a steep head-down Trendelenburgtilt. A midline incision was made. The rectum and sig-moid were mobilized and the pelvic peritoneum was di-vided on both sides of the rectum 3 cm lateral to thebowel wall. Because these patients have a long recto-vaginal or retrovesical pouch, the anterior peritoneum wasdivided at the level of the posterior wall of the uterus inwomen and of the bladder in men. This maneuver pro-vided a large amount of a particularly strong peritoneumfor tissue bridles to be used during the rectopexy (Fig. 1).The presacral space was then opened just behind the su-perior hemorrhoidal vessels and the rectum was mobilizedposteriorly as far as the tip of the coccyx. The lateralligaments were then divided close to the rectal wall. Theomentum was dissected away from the transverse colonand the short gastric vessels along the greater curvature were divided. The omental blood supply was guaranteed
by the left gastroepiploic vessels. After mobilization ofthe splenic flexure and left colon, the omentum wasdraped over the left paracolic gutter and laid in the pelvicfloor to encircle the rectum.
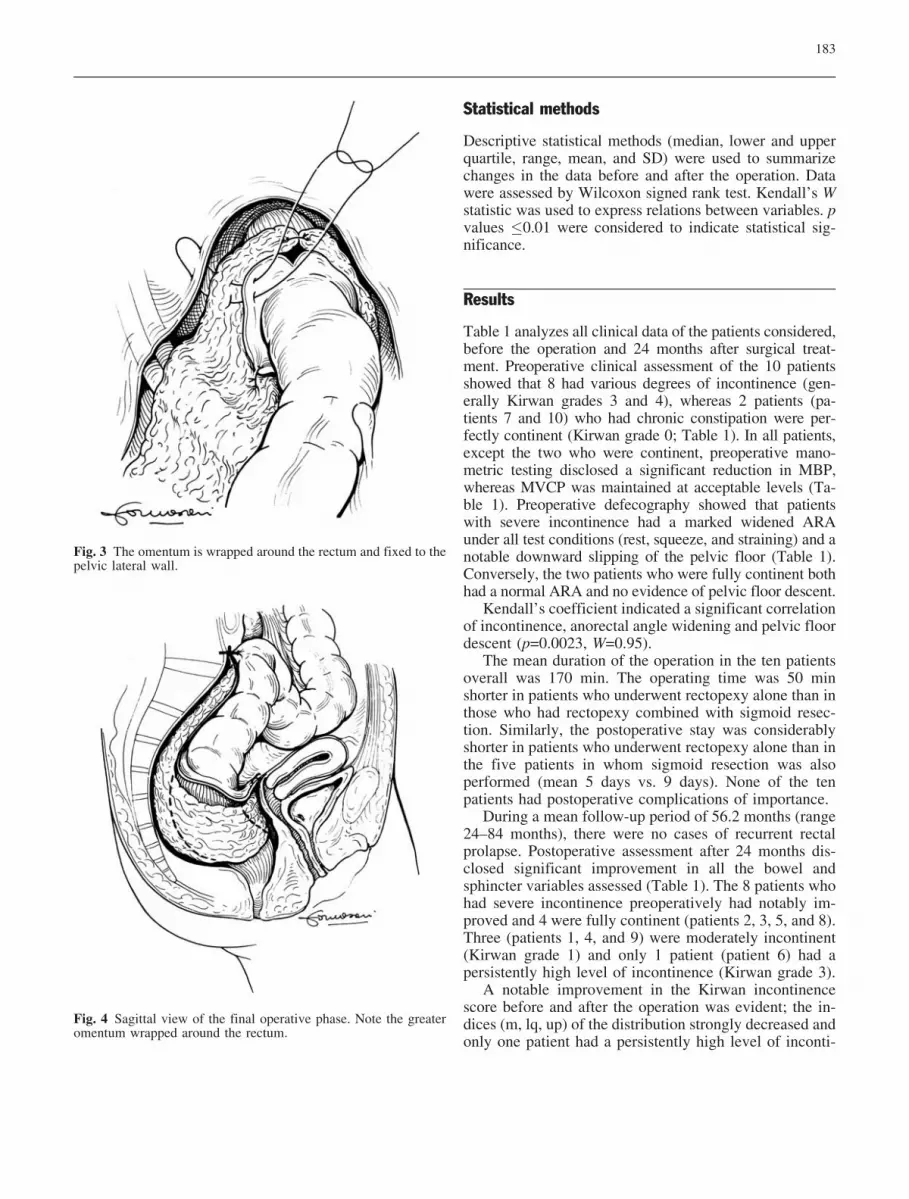
Three interrupted, slowly reabsorbable sutures securedthe omentum to the presacral fascia and then transfixedthe rectum and the two posterior edges of the pelvicperitoneal reflection (Fig. 2). Once the stitches wereknotted, the rectum was fixed to the presacral fascia andthe epiploon below was wrapped around the rectum. Thefree margins of the pelvic peritoneum closely adhering tothe anterior side of the rectum, including the epiploonwrapped around the bowel wall, were sutured to theposterior side of the uterus or bladder (Fig. 3). Finally, theexternal margin of the epiploon was sutured to the pre-viously divided peritoneum of the paracolic gutter and theleft colon was laid on it. At the end of the procedure, therectum and the left colon were stretched upwards andfixed to the presacral fascia and to the paracolic gutter.The pedicled omentoplasty filling the pelvic floor held upthe rectum to prevent it from sliding downwards, restoredthe anorectal angle, and thus improved fecal incontinence(Fig. 4). Actually, rectopexy by this technique in ourdepartment always includes concomitant sigmoid resec-tion.
Fig. 1 Rectum mobilization with pelvic peritoneal bridles.
Fig. 2 The U-suture technique used for fixing the omentum and therectum to the presacral fascia.
183
Statistical methods
Descriptive statistical methods (median, lower and upperquartile, range, mean, and SD) were used to summarizechanges in the data before and after the operation. Datawere assessed by Wilcoxon signed rank test. Kendall’s Wstatistic was used to express relations between variables. pvalues �0.01 were considered to indicate statistical sig-nificance.
Results
Table 1 analyzes all clinical data of the patients considered,before the operation and 24 months after surgical treat-ment. Preoperative clinical assessment of the 10 patientsshowed that 8 had various degrees of incontinence (gen-erally Kirwan grades 3 and 4), whereas 2 patients (pa-tients 7 and 10) who had chronic constipation were per-fectly continent (Kirwan grade 0; Table 1). In all patients,except the two who were continent, preoperative mano-metric testing disclosed a significant reduction in MBP,whereas MVCP was maintained at acceptable levels (Ta-ble 1). Preoperative defecography showed that patientswith severe incontinence had a marked widened ARAunder all test conditions (rest, squeeze, and straining) and anotable downward slipping of the pelvic floor (Table 1).Conversely, the two patients who were fully continent bothhad a normal ARA and no evidence of pelvic floor descent.
Kendall’s coefficient indicated a significant correlationof incontinence, anorectal angle widening and pelvic floordescent (p=0.0023, W=0.95).
The mean duration of the operation in the ten patientsoverall was 170 min. The operating time was 50 minshorter in patients who underwent rectopexy alone than inthose who had rectopexy combined with sigmoid resec-tion. Similarly, the postoperative stay was considerablyshorter in patients who underwent rectopexy alone than inthe five patients in whom sigmoid resection was alsoperformed (mean 5 days vs. 9 days). None of the tenpatients had postoperative complications of importance.
During a mean follow-up period of 56.2 months (range24–84 months), there were no cases of recurrent rectalprolapse. Postoperative assessment after 24 months dis-closed significant improvement in all the bowel andsphincter variables assessed (Table 1). The 8 patients whohad severe incontinence preoperatively had notably im-proved and 4 were fully continent (patients 2, 3, 5, and 8).Three (patients 1, 4, and 9) were moderately incontinent(Kirwan grade 1) and only 1 patient (patient 6) had apersistently high level of incontinence (Kirwan grade 3).
A notable improvement in the Kirwan incontinencescore before and after the operation was evident; the in-dices (m, lq, up) of the distribution strongly decreased andonly one patient had a persistently high level of inconti-
Fig. 4 Sagittal view of the final operative phase. Note the greateromentum wrapped around the rectum.
Fig. 3 The omentum is wrapped around the rectum and fixed to thepelvic lateral wall.
184
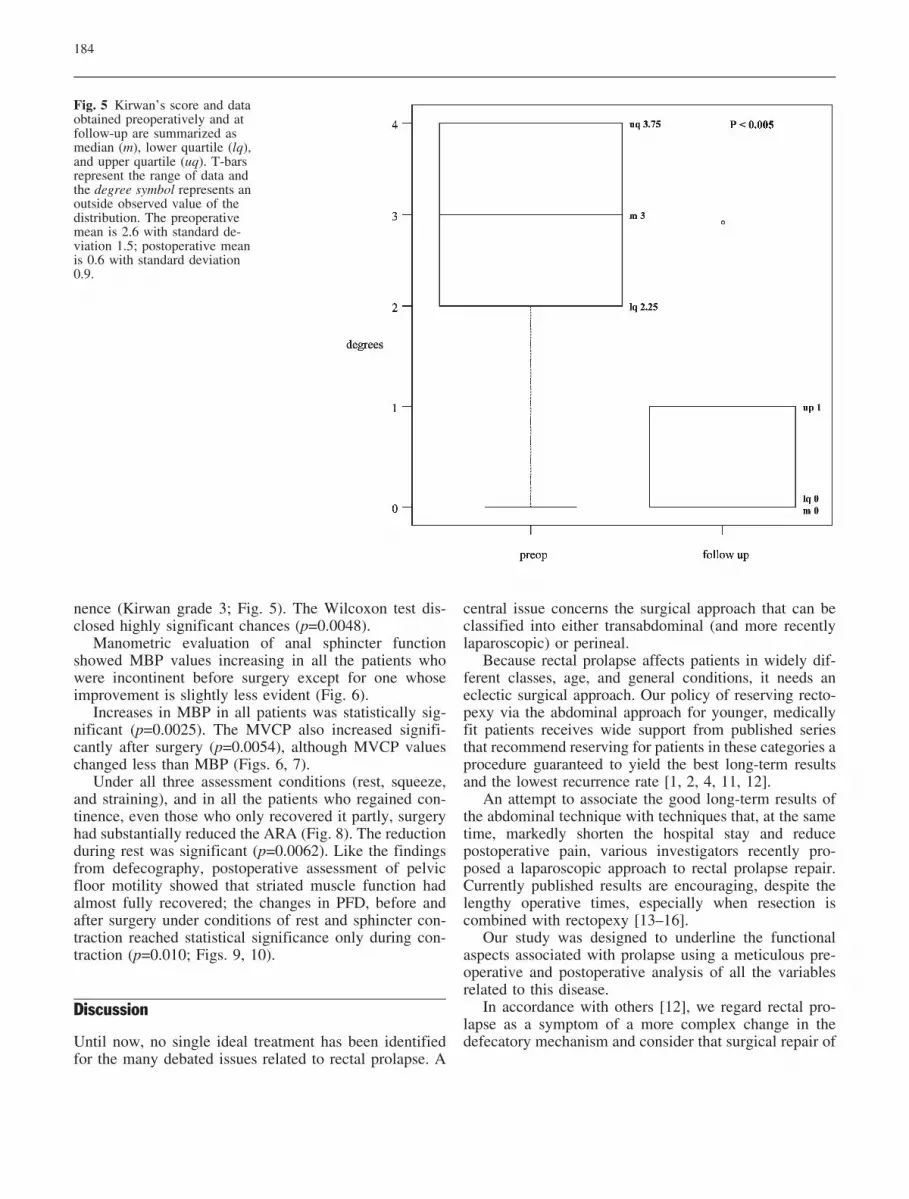
nence (Kirwan grade 3; Fig. 5). The Wilcoxon test dis-closed highly significant chances (p=0.0048).
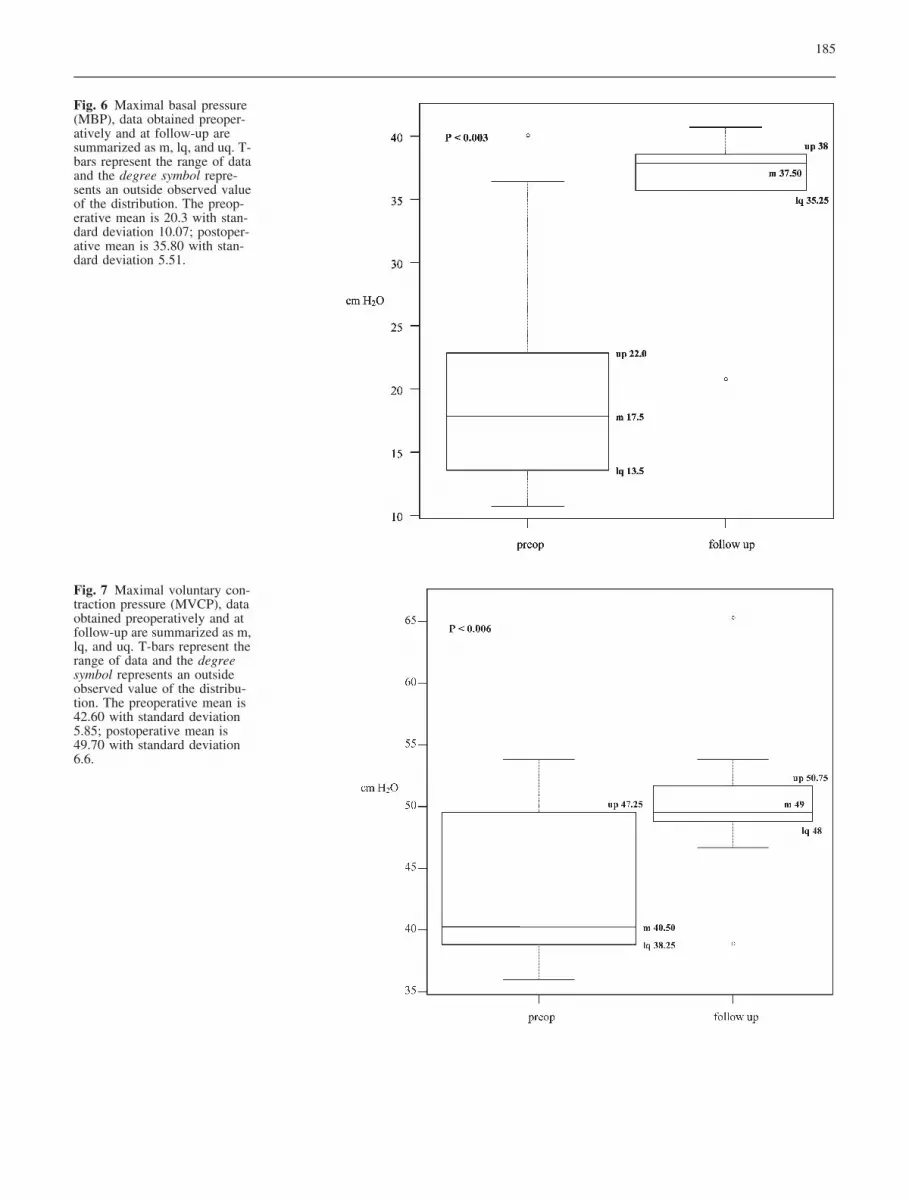
Manometric evaluation of anal sphincter functionshowed MBP values increasing in all the patients whowere incontinent before surgery except for one whoseimprovement is slightly less evident (Fig. 6).
Increases in MBP in all patients was statistically sig-nificant (p=0.0025). The MVCP also increased signifi-cantly after surgery (p=0.0054), although MVCP valueschanged less than MBP (Figs. 6, 7).
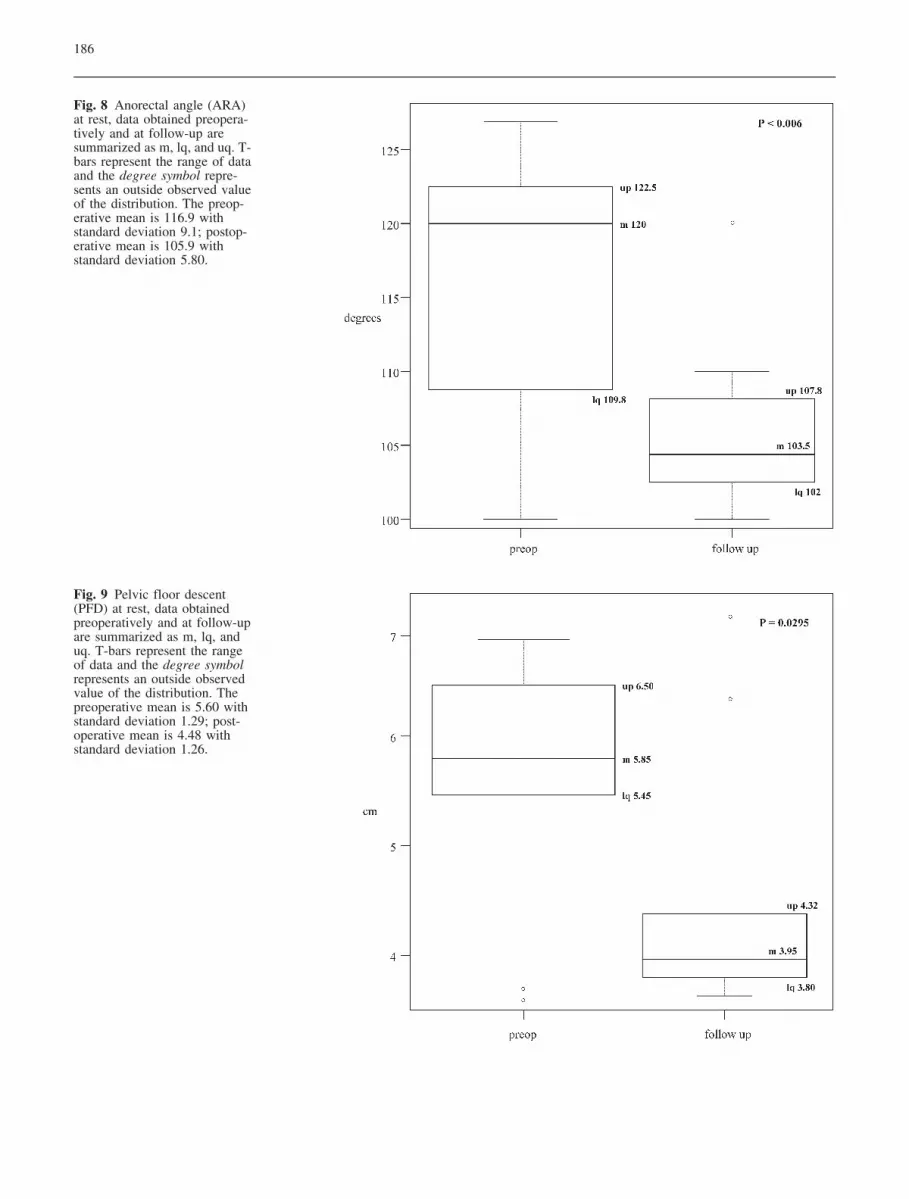
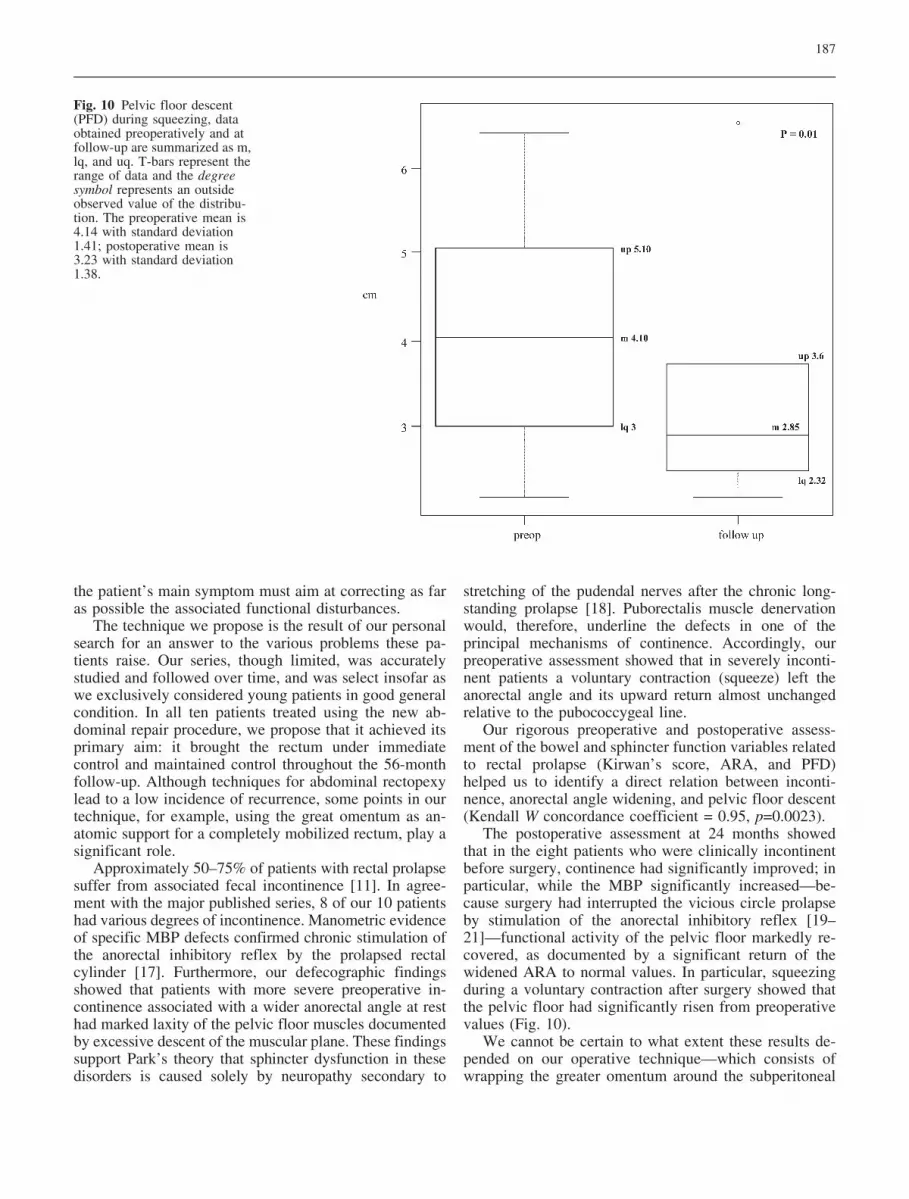
Under all three assessment conditions (rest, squeeze,and straining), and in all the patients who regained con-tinence, even those who only recovered it partly, surgeryhad substantially reduced the ARA (Fig. 8). The reductionduring rest was significant (p=0.0062). Like the findingsfrom defecography, postoperative assessment of pelvicfloor motility showed that striated muscle function hadalmost fully recovered; the changes in PFD, before andafter surgery under conditions of rest and sphincter con-traction reached statistical significance only during con-traction (p=0.010; Figs. 9, 10).
Discussion
Until now, no single ideal treatment has been identifiedfor the many debated issues related to rectal prolapse. A
central issue concerns the surgical approach that can beclassified into either transabdominal (and more recentlylaparoscopic) or perineal.
Because rectal prolapse affects patients in widely dif-ferent classes, age, and general conditions, it needs aneclectic surgical approach. Our policy of reserving recto-pexy via the abdominal approach for younger, medicallyfit patients receives wide support from published seriesthat recommend reserving for patients in these categories aprocedure guaranteed to yield the best long-term resultsand the lowest recurrence rate [1, 2, 4, 11, 12].
An attempt to associate the good long-term results ofthe abdominal technique with techniques that, at the sametime, markedly shorten the hospital stay and reducepostoperative pain, various investigators recently pro-posed a laparoscopic approach to rectal prolapse repair.Currently published results are encouraging, despite thelengthy operative times, especially when resection iscombined with rectopexy [13–16].
Our study was designed to underline the functionalaspects associated with prolapse using a meticulous pre-operative and postoperative analysis of all the variablesrelated to this disease.
In accordance with others [12], we regard rectal pro-lapse as a symptom of a more complex change in thedefecatory mechanism and consider that surgical repair of
Fig. 5 Kirwan’s score and dataobtained preoperatively and atfollow-up are summarized asmedian (m), lower quartile (lq),and upper quartile (uq). T-barsrepresent the range of data andthe degree symbol represents anoutside observed value of thedistribution. The preoperativemean is 2.6 with standard de-viation 1.5; postoperative meanis 0.6 with standard deviation0.9.
185
Fig. 6 Maximal basal pressure(MBP), data obtained preoper-atively and at follow-up aresummarized as m, lq, and uq. T-bars represent the range of dataand the degree symbol repre-sents an outside observed valueof the distribution. The preop-erative mean is 20.3 with stan-dard deviation 10.07; postoper-ative mean is 35.80 with stan-dard deviation 5.51.
Fig. 7 Maximal voluntary con-traction pressure (MVCP), dataobtained preoperatively and atfollow-up are summarized as m,lq, and uq. T-bars represent therange of data and the degreesymbol represents an outsideobserved value of the distribu-tion. The preoperative mean is42.60 with standard deviation5.85; postoperative mean is49.70 with standard deviation6.6.
186
Fig. 8 Anorectal angle (ARA)at rest, data obtained preopera-tively and at follow-up aresummarized as m, lq, and uq. T-bars represent the range of dataand the degree symbol repre-sents an outside observed valueof the distribution. The preop-erative mean is 116.9 withstandard deviation 9.1; postop-erative mean is 105.9 withstandard deviation 5.80.
Fig. 9 Pelvic floor descent(PFD) at rest, data obtainedpreoperatively and at follow-upare summarized as m, lq, anduq. T-bars represent the rangeof data and the degree symbolrepresents an outside observedvalue of the distribution. Thepreoperative mean is 5.60 withstandard deviation 1.29; post-operative mean is 4.48 withstandard deviation 1.26.
187
the patient’s main symptom must aim at correcting as faras possible the associated functional disturbances.
The technique we propose is the result of our personalsearch for an answer to the various problems these pa-tients raise. Our series, though limited, was accuratelystudied and followed over time, and was select insofar aswe exclusively considered young patients in good generalcondition. In all ten patients treated using the new ab-dominal repair procedure, we propose that it achieved itsprimary aim: it brought the rectum under immediatecontrol and maintained control throughout the 56-monthfollow-up. Although techniques for abdominal rectopexylead to a low incidence of recurrence, some points in ourtechnique, for example, using the great omentum as an-atomic support for a completely mobilized rectum, play asignificant role.
Approximately 50–75% of patients with rectal prolapsesuffer from associated fecal incontinence [11]. In agree-ment with the major published series, 8 of our 10 patientshad various degrees of incontinence. Manometric evidenceof specific MBP defects confirmed chronic stimulation ofthe anorectal inhibitory reflex by the prolapsed rectalcylinder [17]. Furthermore, our defecographic findingsshowed that patients with more severe preoperative in-continence associated with a wider anorectal angle at resthad marked laxity of the pelvic floor muscles documentedby excessive descent of the muscular plane. These findingssupport Park’s theory that sphincter dysfunction in thesedisorders is caused solely by neuropathy secondary to
stretching of the pudendal nerves after the chronic long-standing prolapse [18]. Puborectalis muscle denervationwould, therefore, underline the defects in one of theprincipal mechanisms of continence. Accordingly, ourpreoperative assessment showed that in severely inconti-nent patients a voluntary contraction (squeeze) left theanorectal angle and its upward return almost unchangedrelative to the pubococcygeal line.
Our rigorous preoperative and postoperative assess-ment of the bowel and sphincter function variables relatedto rectal prolapse (Kirwan’s score, ARA, and PFD)helped us to identify a direct relation between inconti-nence, anorectal angle widening, and pelvic floor descent(Kendall W concordance coefficient = 0.95, p=0.0023).
The postoperative assessment at 24 months showedthat in the eight patients who were clinically incontinentbefore surgery, continence had significantly improved; inparticular, while the MBP significantly increased—be-cause surgery had interrupted the vicious circle prolapseby stimulation of the anorectal inhibitory reflex [19–21]—functional activity of the pelvic floor markedly re-covered, as documented by a significant return of thewidened ARA to normal values. In particular, squeezingduring a voluntary contraction after surgery showed thatthe pelvic floor had significantly risen from preoperativevalues (Fig. 10).
We cannot be certain to what extent these results de-pended on our operative technique—which consists ofwrapping the greater omentum around the subperitoneal
Fig. 10 Pelvic floor descent(PFD) during squeezing, dataobtained preoperatively and atfollow-up are summarized as m,lq, and uq. T-bars represent therange of data and the degreesymbol represents an outsideobserved value of the distribu-tion. The preoperative mean is4.14 with standard deviation1.41; postoperative mean is3.23 with standard deviation1.38.

188
References
1. Eu KW, Seow-Choen F (1999) Func-tional problems in adult rectal prolapseand controversies in surgical treatment.Br J Surg 84:904–911
2. Kim Do S, Tsang CBS, Wong WD,Lowry AC, Golberg SM, Madoff RD(1999) Complete rectal prolapse; evo-lution of management and results. DisColon Rectum 42:460–469
3. Jacobs LK, Lin YJ, Orkin BA (1997)The best operation for rectal prolapse.Surg Clin North Am 77:49–70
4. Azimuddin K, Khubchandani IK, RosenL, Stasik JJ, Riether RD, Reed JF(2001) Rectal prolapse: a search for the“best” operation. Am Surg 67:622–627
rectal segment below the rectopexy, thus restoring anacute angle between the rectum and the anus—or on thefact that interrupting the prolapse phenomenon allows thepelvic floor muscles to recover their normal function.Probably both phenomena contributed to this result, andundoubtedly a technique that brings the bowel back asnear as possible to its original anatomical condition isrecommended.
Restoring a correct angle between the anus and therectum through a specific surgery technique has beenrecently highlighted by other authors, as well as a methodenabling the recovering of continence [22].
The only patient in whom severe incontinence per-sisted over time was the oldest patient in our series andthe one who had the most long-standing prolapse. Asothers have already noted, old age makes continencedifficult to restore after abdominal rectopexy [23].
Lastly, a controversial matter that many underline ispostoperative constipation after rectopexy and the role ofsigmoid resection in the treatment of prolapse. Eventhough constipation may complicate rectopexy for full-thickness rectal prolapse [24], it also coexists, albeit in alower percentage than incontinence (30–60%), as a func-tional disturbance in patients with prolapse [11]. In pa-tients with complete rectal prolapse, constipation is aproblem that depends not only on slower intestinal transitbut also reflects a complex phenomenon linked to an overtoutlet syndrome caused by paradoxical contraction of thepelvic floor muscles during defecation [25]. Evidencenevertheless shows that in these cases attempts at defe-cation lead to the same mechanism—stretching of thepudendal nerve and pelvic floor dysfunction—that canultimately cause prolapse followed by incontinence [26,27]. Another possible cause of constipation after rectopexyis transection of the lateral rectal ligaments [28], althoughthe latest research fails to confirm this hypothesis [29].Consensus opinion agrees that patients who have consti-pation when rectal prolapse is diagnosed must undergorectopexy with concomitant sigmoid resection [30–32].Some also think that this approach serves not simply toprevent postoperative constipation, but also, by shorteningthe left colon, could avoid repeated intussusceptions, a keyfactor in the clinical outcome of prolapse [33–35].
In five patients in this series, rectopexy includedconcomitant sigmoid resection for chronic preoperative
constipation and intraoperative findings of a dolichosig-moid. Postoperative constipation developed in only onepatient after rectopexy alone had resolved the prolapsealong with severe coexisting incontinence. In this patientas well, a concomitant sigmoid resection would mostprobably have prevented the postoperative constipationfrom developing. Our current clinical practice now en-visages sigmoid resection as an integral part of the rec-topexy technique. It is precisely the indispensable asso-ciation of a sigmoid resection with rectopexy for rectalprolapse that raises a further indication for our use of thegreat omentum. As previously stated, in our techniqueepiploonplasty serves two specific functions. The first isto support the rectum below the rectopexy, thus providingmechanical support and making it easier to reconstruct theanorectal angle. Its second function is to substitute thesynthetic mesh commonly used to create scarring scle-roses at the level of rectopexy with the presacral plane,thereby definitively fixing the rectum in its position.Using the omentum has the advantage that during recto-pexy, with concomitant sigmoid resection, it avoids re-course to synthetic materials along with inherent risks ofinfection [36]. No infection developed in our series.
Conclusions
The abdominal rectopexy technique we used in this serieshas two distinctive features: it reconstructs the bowel asclosely as possible to its original anatomical condition anddoes so using exclusively autologous tissues. It thereforedispenses with the need for synthetic materials, an im-portant advantage when rectopexy has to be combinedwith sigmoid resection. The meticulous protocol we usedfor studying bowel and sphincter function provided evi-dence that our surgical technique not only brings rectalprolapse under control over time but more importantly, byrestoring the anorectal angle and restoring sphincterfunction, it corrects prolapse and substantially improvespreoperative incontinence, a common complaint in patientswith rectal prolapse. Despite the small number of cases inthis series, because we selected patients who were youngand medically fit, the thorough diagnostic work and reg-ular follow-up of patients over time support these results.
189
5. Altemeier WA, Culbertson WR, Scho-wengerdt C (1971) Nineteen years ex-perience with the one-stage perinealrepair of rectal prolapse. Ann Surg173:993
6. Lowry AC, Clifford LS, Simmang L,Boulos P, Chip Farmer K, Finan PJ,Hyman N, Killingback M, LubowskiDZ, Moore R, Penfold C, Savoca P,Stitz R, Tjandra JJ (2001) Consensusstatement of definitions for anorectalphysiology and rectal cancer. Dis ColonRectum 44:915–919
7. Sullivan ES, Corman ML, Devroede G,Rudd WWH, Schuster MM (1982) Analincontinence. Dis Colon Rectum 25:90–107
8. Hiltunen KM, Matikainen M, AuvinenO, Hietanen P (1986) Clinical andmanometric evaluation of anal sphincterfunction in patients with rectal prolapse.Am J Surg 151:489–492
9. Yoshioka K, Hyland G, Keighley MRB(1989) Anorectal function after ab-dominal rectopexy: parameters of pre-dictive value in identifying return ofcontinence. Br J Surg 76:64–68
10. Seok Choi J, Wexner SD, Soon Nam Y,Mavrantonis C, Salum MR, YagamuchiT, Weiss EG, Nogueras JJ, Fang YUC(2000) Intraobserver and interobservermeasurements of the anorectal angleand perineal descent in defecography.Dis Colon Rectum 43:1121–1126
11. Madoff RD, Mellgren A (1999) Onehundred years of rectal prolapse sur-gery. Dis Colon Rectum 42:441–450
12. Karulf RE, Madoff RA, Goldberg SM(2001) Rectal prolapse. Curr Probl Surg38:757–832
13. Stevenson AR, Stitz RW, Lumley JW(1998) Laparoscopic assisted resection-rectopexy for rectal prolapse: early andmedium follow-up. Dis Colon Rectum41:46–54
14. Bruch HP, Herold A, Schwander O(1999) Laparoscopic surgery for rectalprolapse and outlet obstruction. DisColon Rectum 42:1189–1194
15. Xynos E, Chrysos E, Tsiaoussis J,Epanomeritakis E, Vassilakis JS (1999)Resection rectopexy for rectal prolapse.The laparoscopic approach. Surg En-dosc 13:862–864
16. Kessler H, Jerby BL, Milsom JW(1999) Successful treatment of rectalprolapse by laparoscopic suture recto-pexy. Surg Endosc 13:858–861
17. Farouk R, Duthie GS, Macgregor AB,Bartolo DCC (1994) Recto-anal inhibi-tion and incontinence in patients withrectal prolapse. Br J Surg 81:743–746
18. Parks AG, Swash M, Urich H (1977)Sphincter denervation in anorectal in-continence and rectal prolapse. Gut18:656–665
19. Duthie GS, Bartolo DCC (1992) Ab-dominal rectopexy for rectal prolapse: acomparison of techniques. Br J Surg79:107–113
20. Farouk R, Duthie GS, Bartolo DCC,Macgregor AB (1992) Restoration ofcontinence following rectopexy forrectal prolapse and recovery of the in-ternal anal sphincter electromyogram.Br J Surg 79:439–440
21. Hiltunen KM, Matikainen M (1991)Improvement of continence after ab-dominal rectopexy for rectal prolapse.Int J Colorectal Dis 7:8–10
22. Lechaux JP, Atienza P, Goasguen N,Lechaux D, Bars I (2001) Prostheticrectopexy to the pelvic floor and sig-moidectomy for rectal prolapse. Am JSurg 182:465–469
23. Petri T, Aitola MD, Hiltunen KM,Martti J, Matikainen MD (1999) Func-tional results of operative treatment ofrectal prolapse over an 11 year period.Emphasis on transabdominal approach.Dis Colon Rectum 42:655–660
24. Gordon PH, Hoexter B (1978) Com-plications of the Ripstein procedure. DisColon Rectum 21:277–280
25. Agachan F, Pfeifer J, Wexner SD(1996) Defecography and proctography:results of 744 patients. Dis Colon Rec-tum 39:899–905
26. Sagar PM, Pemberton JH (1996) Ano-rectal and pelvic floor function: rele-vance to continence, incontinence andconstipation. Gastroenterol Clin NorthAm 25:163–182
27. Harewood GC, Coulie B, Camilleri H,Rath-Harwey D, Pemberton JH (1999)Descending perineum syndrome: studyof clinical and laboratory features andoutcome of pelvic floor retraining. AmJ Gastroenterol 94:126–130
28. Speakman CT, Madden MV, NichollsRJ, Kamm MA (1991) Lateral ligamentdivision during rectopexy causes con-stipation but prevents recurrence: re-sults of a prospective randomized study.Br J Surg 78:1431–1433
29. Mollen RMHG, Kuijpers JHC, VanHoek F (2000) Effects of rectal mobi-lization and lateral ligament division oncolonic and anorectal function. DisColon Rectum 43:1283–1287
30. Madoff RD, Williams JG, Wong WD,Rothemberger DA, Goldberg SM(1992) Long-term functional results ofcolon resection and rectopexy for overtrectal prolapse. Am J Gastroenterol87:101–104
31. Watts JD, Rothemberger DA, Buls JG,Goldberg SM, Mnivatvongs S (1985)The management of procidentia. 30years experience. Dis Colon Rectum28:96–102
32. Husa A, Sainio P, Von Smitten K(1988) Abdominal rectopexy and sig-moid resection (Frykman—Goldbergprocedure) for rectal prolapse. ActaChir Scand 154:221–224
33. Frykman HM, Goldberg SM (1969) Thesurgical treatment of procidentia. SurgGynecol Obstet 129:1225–1229
34. Luukkonen P, Mikkonen U, Jarvinen H(1992) Abdominal rectopexy with sig-moidectomy vs rectopexy alone forrectal prolapse. A prospective random-ized study. Int J Colorectal Dis 7:219–222
35. Huber FT, Stein H, Siewert JR (1995)Functional results after treatment ofrectal prolapse with rectopexy and sig-moid resection. World J Surg 19:138–143
36. Novell JR, Osborne MJ, Winslet MC,Lewis AAM (1994) Prospective ran-domized trial on ivalon sponge versussutured rectopexy for full-thicknessrectal prolapse. Br J Surg 81:904–906