· web viewlonger courses (>13 weeks) decrease the rate of perianal fistula relapse. when csa...
TRANSCRIPT
Immune mediated Diseases – WITS branch April 2018
DR Dave MillerJHB Specialist Veterinary Centre011 [email protected]
List of immune mediated disease – from memory of cases diagnosed recently
Mutisystemic:- SLE
Skin:- PF, DLE, L-P pododermatitis etc - Atopy- Food allergy- All hypersensitivities- SLE [Polysystemic]- Symmetrical Lupoid Onchitis [SLO]- Perianal fistulae’s /furunculosis
Blood:- IMHA- IMTP- pure red cell aplasia- aplastic anaemia, - amegakaryocytic thrombocytopenia and - steroid-responsive neutropaenia.- SLE [Polysystemic]- Blood Tx reactions
As a general rule, in dogs these disorders are most commonly primary, whereas in cats they are more likely to be secondary.
Joints:- IMPA/IMA – non erosive and erosive- Immune mediated synovitis - SLE [Polysystemic]
Muscle - Polymiositis
Masticatory Miositis [MM or MMM]
Neuro Muscular: - MG - myaesthenia gravis
All Lympho-Plamacytic disease:= Imbalance between immune system and symbiotic bacteria:- IBD / Crone’s- L-P RHINITIS
- L-P pododermatitis [Cushion pad disease]
CNS [Can be heritable]:- GME- NME- Eosinophilic meningitis- SRM- Optic Neuritis- Immune Cerebellitis/Little White Dog shaker syndrome
ENDOCRINE [Can be heritable]:- Diabetes- Hypoadrenocorticism/Addissons- Hypothyroidism
Heart:- Forms of pericarditis and pleuritis - SLE [Polysystemic]
Kidneys:- Glomurulonephritis
List of Therapies:- Sun avoidance- Dietary change- Metronidasole and B12- Doxycycline and Niacinamide/Nicotinamide- Glucocorticoids- Cyclosporin- Steroid sparing – Azathioprine, Cyclophosphamide, Lufeneron,
Mycophenolate- Gamma globulin infusions- Plasmaphoresis- Splenectomy- Cytosine Arabinoside- Procarbazine- Lomustine / CeeNu
Tests:- Coombs- ANA- LE- Anti platelet tests- MG antibodies- Type II fibre antibody tests [MM]- Histopathology- Joint tap

- CSF tap- B/s - ISA
Why?Immune responses are, of necessity, toxic! They have evolved to destroy things: bacteria, viruses, fungi, parasites, infected host cells, perhaps even tumour cells. Because of that, all animals have evolved sophisticated means for controlling immune responses—T-reg cells, cytokines, receptors and their ligands, apoptosis, the thymus itself, positive selection, negative selection, central tolerance, and peripheral tolerance all help to control immune responses and try to limit the opportunities for animals’ immune systems to turn against their hosts.
In spite of all the checks and balances and all of the selections that occur, immune systems sometimes overreact to innocuous agents and sometimes turn on self. The diseases that result are immune-mediated diseases or hypersensitivities.
Immune-mediated diseases fall into four major categories, types I–IV. Antibodies mediate the first three of these categories, and they are immediate-type hypersensitivities. T cells mediate type IV responses, including delayed-type hypersensitivities (DTHs). Ag = antigen; CTL = Tc cells.(Illustration: William Zaun)
TYPE II HYPERSENSITIVITIES AND AUTOIMMUNE DISEASES:Antibodies of type II hypersensitivities are anti-self antibodies, which makes most type II hypersensitivities autoimmune diseases. For example, immune-mediated haemolytic anaemia (IMHA) is a relatively common disorder of dogs, especially in
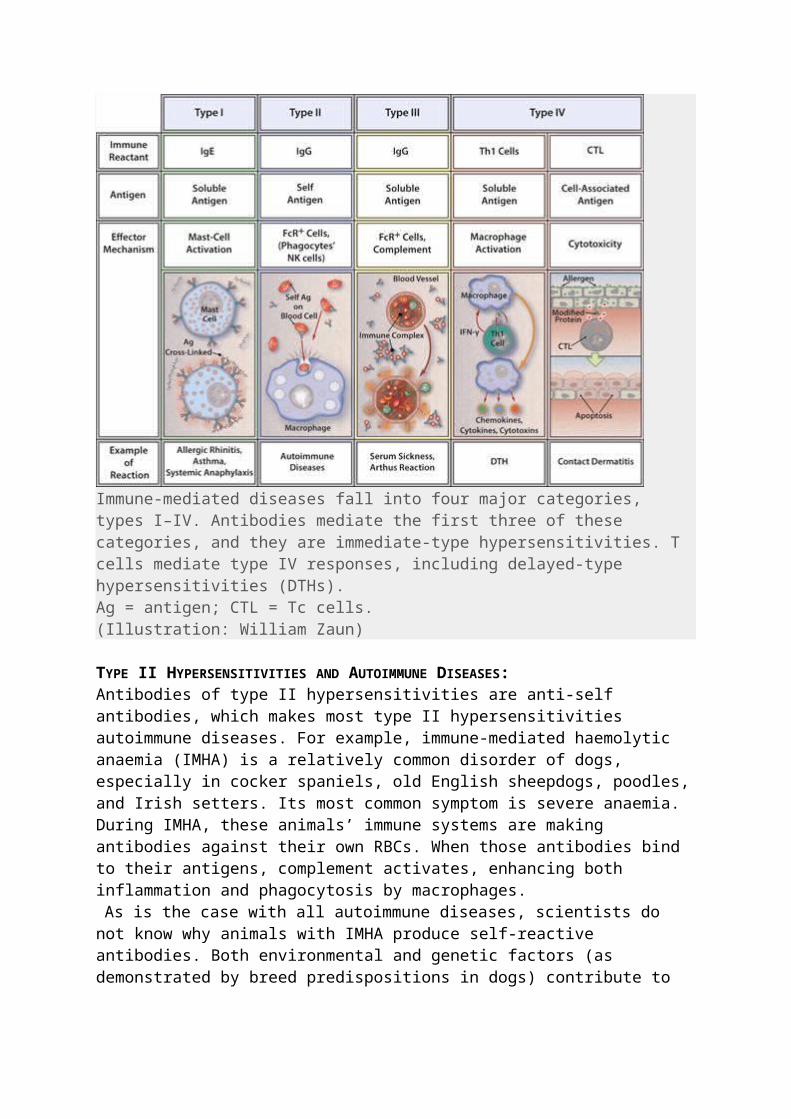
cocker spaniels, old English sheepdogs, poodles, and Irish setters. Its most common symptom is severe anaemia. During IMHA, these animals’ immune systems are making antibodies against their own RBCs. When those antibodies bind to their antigens, complement activates, enhancing both inflammation and phagocytosis by macrophages. As is the case with all autoimmune diseases, scientists do not know why animals
with IMHA produce self-reactive antibodies. Both environmental and genetic factors (as demonstrated by breed predispositions in dogs) contribute to these diseases. In most cases, the essential genetic factors remain unknown.
Pyrexia of Unknown Origin [PUO/FUO]:In one retrospective study of 50 dogs with fever for ≥1 weeks duration, 36/50 had a final diagnosis. 24/50 dogs were diagnosed with non-infectious inflammatory diseases; 9 dogs had an infectious disease; and 3 had a neoplastic disease. Another study of 22 dogs with PUO showed that 36% were diagnosed with inflammatory and immune-mediated diseases. Finally, the underlying cause was diagnosed in 51/66 dogs in one retrospective study. A diagnosis was achieved within 7 days of referral for 74% of them. Of these cases, 34.8% were diagnosed with immune-mediated disease, with the most frequent diagnoses being steroid-responsive meningitis and polyarthritis.Compared to dogs, primary immune-mediated diseases and neoplasia are less likely to cause FUO in cats. Infectious causes of fever are more common in cats. In one retrospective study of 106 cats with fever, 41/106 were diagnosed with an infectious disease. Other diagnoses included inflammatory conditions (19/106), neoplasia (13/106), immune-mediated disease (6/106).
Immune Mediated Haemolytic Anaemia (IMHA):- Formerly known as autoimmune haemolytic anaemia or AIHA)
Immune-mediated haemolytic anaemia (IMHA) is an often fatal disease with mortality rates reported as high as 50–70% within the first 6-12 months with significantly higher incidence in the first two weeks of treatment!
The destruction of the red blood cells is a result of a type II (antibody-mediated) hypersensitivity reaction in which cells are lysed after the binding of immunoglobulins and complement, or both. IgG or IgM antibodies are directed against the red blood cell membrane. Intravascular haemolysis is a result of IgM-mediated intravascular complement activation in contrast to IgG-mediated extravascular haemolysis by macrophages within the mononuclear phagocytic system, primarily in the liver and spleenSaid another way, IMHA is the condition where the body’s immune system attacks and removes its own red blood cells, thus leading to severe anaemia. Dogs are usually presented for weakness, lethargy, anorexia, pale mucous membranes, jaundice, or discoloured urine. There is a weak association between recent vaccination and IMHA. Assessment of historical tick attachment, drugs (sulfas), toxins (zinc, onions) and other concurrent systemic signs may make infectious or neoplastic causes more likely. Some studies suggest a seasonal increase of IMHA cases in the spring and summer in the northern hemisphere.
Physical Examination:Pallor, weakness, depression, or jaundice. Fever may be present and in IMHA usually does not indicate an infectious aetiology. Systolic heart murmur may be present due to decrease viscosity of the blood. Tacchycardia and tacchypnoea may be present due to low oxygen delivery. Animals with concurrent Immune mediated Thrombocytopaemia [ITP] may have petechia or ecchymoses and ocular exam may reveal uveitis or petechia.
Diagnosis:Anaemia, > 40% spherocytosis in most cases, ISA positive in small % of cases, Coombs positive in many cases [diagnosis made on combination of all tests]
Therapy:Once you have diagnosed IMHA, set your client up for the long haul. A treatment commitment of at least one week is important to see if you can make it thru the initial phase, since that is about how long it takes for the immunosuppressive therapy to start to be effective. Treatment will continue at least 4–6 months and possibly the rest of the animal's life. The following are tables that describe ways you can treat IMHA. Remember, there is more than one way to treat biological systems, and that each patient requires custom management. Excluding Babesiosis induced cases, I always start a second immune suppressive drug at the time of diagnosis. Partially due to the high costs of care and due to “the want to” decrease the glucocorticoids sooner due to their side-effects. Thromboembolic complications are now know to be an important cause of morbidity and mortality in dogs with IMHA. The use of low dose aspirin, which can be given safely with glucocorticoids, is now considered standard IMHA therapy.Uncomplicated IMHA:
Patient is eating and drinking Not tacchypnoeic at rest Ht ≥15% at presentation Reticulocytosis is ≥60,000 at presentation [regerative] No obvious agglutination of RBCs Not intravascular haemolysis with red serum
Drug:Prednisone 2 mg/kg PO divided BID until the PCV is normalAzathioprine 2 mg/kg oid for 3 weeks (IN ALL CASES except Babesiosis)GI protectant Omeprazole (1 mg/kg PO BID 1H pre food)Aspirin 0.5 to 1 mg/kg PO Q 24 or Clopidogrel 2–3 mg/kg PO Q 24Blood Tx as needed decided on clinical signs NOT PCV
Expected response: Stable or rising heamatocrit within 7 days
Drug tapering: Prednisone
Always recheck the PCV before changing drug doses and recheck 7-10 days later
Once the PCV is normal or if side effects or glucocorticoids too severe Decrease the current dose by approximately 25%/time

Do not decrease the dose more frequently than every 4-6-8 weeksDo not change dose without rechecking the PCVWhen taper from 1 mg/kg/day GO TO 1 mg/kg every 2nd day [EOD],
NOT ½ mg/kg/day Azathioprine
After 3–4 weeks – change to every other day [EOD] GI protectant
I taper and stop over 2-4 weeks when the prednisone dose is at 1 mg/kg/dayIf there is no response within 7-10 days = complicated cases Complicated IMHA:
Patient is not eating and drinking Tacchypnoeic at rest Hct is ≤15 % at presentation
Inadequate regeneration on FBC - Reticulocytosis is ≤60,000 at presentation Agglutination of RBCs = ISA positive Intravascular haemolysis present
OR - Fails to respond to meds after 7-10 daysMedications – same as above and add:
IV fluids – Ringers with 1-2 vials potassium added (avoid jugular catheterization if possible as it increases risk of thromboembolic disease)Blood transfusions as needed to keep patient alive while waiting for drug response
AND – IF HAVE IV lineHeparin – 300U/kg/day CRI or 70-100 U /kg 3x/day s/c [ideal dose not determined yet]Add a 3rd medication – most reach for Cyclosporine 10mg/kg/day
Drug tapering: IV fluids are discontinued when the patient is eating and drinking
Heparin is discontinued when IV catheters are removedIf inadequate response needs added meds/changed meds:
Other Therapies for IMHA:
Cyclosporine [Atopica/Neoral]- 10 mg/kg/day orally- Therapeutic serum concentrations are 200–400 ng/ml. - often first choice treatment for complicated IMHA cases ahead of
azathioprine.
Mycophenolate Mofetil [Cellcept]:10–20 mg/kg PO BID. Very little information in veterinary medicine for use in IMHA/ITP, but experiences are promising.
Human Gamma Globulin:0.5–1.0 gram/kg intravenously over 4–12 hours. May be repeated within 48 hours.

Leflunomide:2–4 mg/kg/day. Treatment that has shown some efficacy for the treatment of immune mediated diseases.
Cyclophosphamide:Due to haemorrhagic cystitis I do not use this drug in critically ill patients BUT is one of my medications of choice for immune mediated polyarthritis.
Splenectomy:Absolute "last resort". Some recent studies may show benefit. Try prove splenic haemophagocytois with FNA and make sure that these patients do not have infectious diseases (especially Babesia and Ehrliciosis) before doing this.
Blood Transfusion:There is no "magic" number for when to do a transfusion. I base it on clinical signs and the rate at which the PCV is dropping. Ideally, cross-matched blood will be administered, but at a minimum, donors should be screened for infectious diseases.If have time or if it is not 1st transfusion:
Major X-match Recipient serum to donor RBC
Minor X-match Donor serum to recipient RBC
Antibiotics:Antibiotics are not indicated for idiopathic IMHA, but Babesiosis is treated and doxycycline is used pending the results of infectious disease testing or on suspicion of E canis.
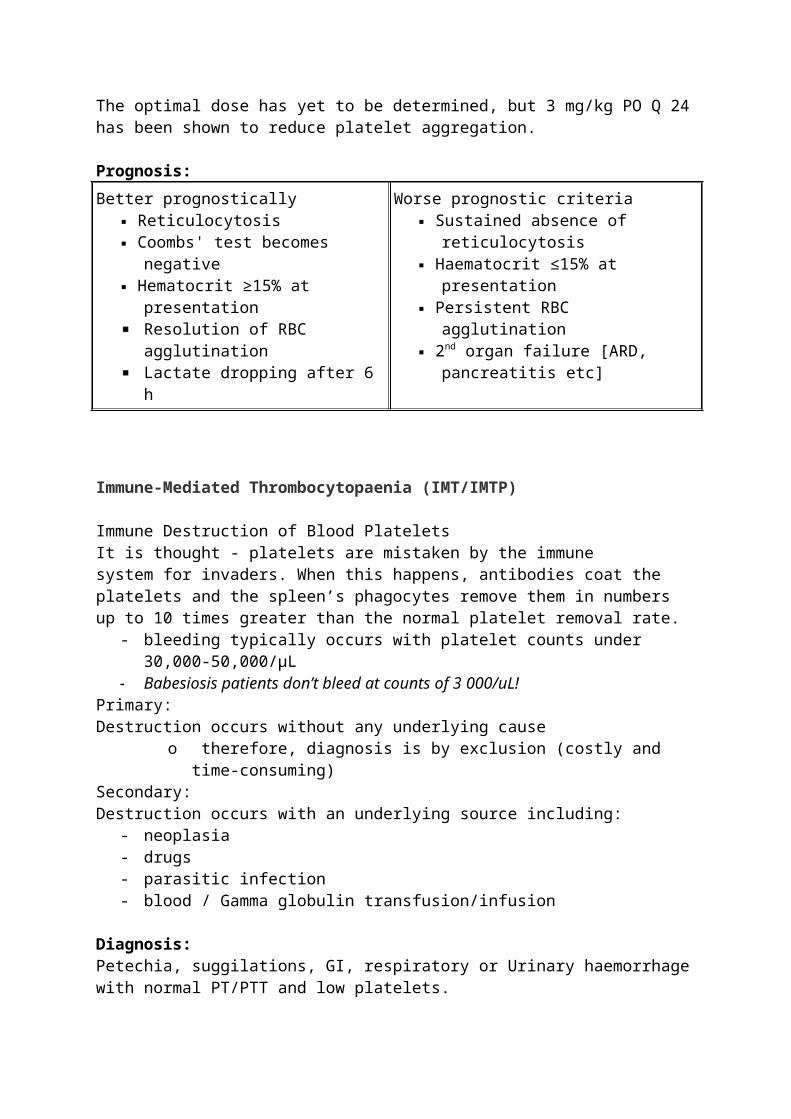
Heparin:Recommendation - 300–900 U/kg/day as a CRI with the goal of increasing their APTT 1.5 times their baseline. OR 100 units/kg tid S/C if can’t do a CRIPlavix/Clopidogrel:- should have the same effect as aspirin, but there is less data in veterinary medicine justifying its use over aspirin. The optimal dose has yet to be determined, but 3 mg/kg PO Q 24 has been shown to reduce platelet aggregation.
Prognosis:Better prognostically
Reticulocytosis Coombs' test becomes negative Hematocrit ≥15% at presentation
Resolution of RBC agglutinationLactate dropping after 6 h
Worse prognostic criteria Sustained absence of reticulocytosis Haematocrit ≤15% at presentation Persistent RBC agglutination 2nd organ failure [ARD, pancreatitis
etc]
Immune-Mediated Thrombocytopaenia (IMT/IMTP)

Immune Destruction of Blood PlateletsIt is thought - platelets are mistaken by the immune system for invaders. When this happens, antibodies coat the platelets and the spleen’s phagocytes remove them in numbers up to 10 times greater than the normal platelet removal rate.
- bleeding typically occurs with platelet counts under 30,000-50,000/µL- Babesiosis patients don’t bleed at counts of 3 000/uL!
Primary: Destruction occurs without any underlying cause
o therefore, diagnosis is by exclusion (costly and time-consuming)Secondary: Destruction occurs with an underlying source including:
- neoplasia- drugs- parasitic infection- blood / Gamma globulin transfusion/infusion
Diagnosis:Petechia, suggilations, GI, respiratory or Urinary haemorrhage with normal PT/PTT and low platelets.
Therapy:As for IMHA discussed above with the exceptions of:
- can often be controlled with single agent prednisolone- Vincristine IV can be used as emergency therapy to rapidly increase platelet
numbers - Gamma-globulin infusions, a therapy for IMHA and IMTP can also be a trigger
for IMTP- Splenectomy – Standard therapy for chronic ITP in humans but has shown
NO benefit in veterinary studies.- Plasma or blood transfusions do not help with platelet numbers
Immune-Mediated Polyarthritis:
Immune-mediated polyarthritis (IMPA) is a relatively common disease/syndrome in the dog. The immune-mediated polyarthropathies are divided into two major categories: erosive (or deforming) and nonerosive (or nondeforming).
Pathophysiology:Immune-mediated non-erosive polyarthritis is believed to be driven by a Type III hypersensitivity reaction, where immune complexes comprised of antigen bound to antibody accumulate in the joint space. Implicated antigens are typically found in the systemic circulation, but can originate from within the joint space itself. Idiopathic or viruses such as distemper virus, other microbial agents, neoplasia, drug haptens or even dietary elements. In addition, antibodies directed against self-antigens, such as heat shock proteins, immunoglobulins (rheumatoid factors) and nuclear elements (antinuclear antibodies) can also form complexes that accumulate in the joint space. The presence of immune complexes in the joint space activates complement along the synovial membrane and within the synovial fluid. Complement fixation results in

tissue damage and release of cytokines, some of which attract neutrophils. Initially, mononuclear cell infiltration occurs that is followed by neutrophils. Inflammation leads to weakening of intra-articular and peri-articular structures. Eventual joint instability may develop and result in osteoarthritis. These neutrophils also release cytokines and lysosomal enzymes that cause further tissue damage. Immune-mediated, nonerosive polyarthritis (IMPA) is characterized by inflammation of the synovium secondary to deposition of immune complexes in the joint. At least in the early stages, radiographic evidence of joint destruction is absent. Affected dogs often have combinations of joint pain, swelling, lameness, and fever. Typically, more than one joint is involved and signs may be intermittent or chronically recurrent.
Classification[s]:Immune-mediated nonerosive polyarthritis is loosely divided into four types:
- idiopathic, - reactive, - systemic lupus erythematosus (SLE), and - breed-associated IMNPA.
Idiopathic polyarthritis is by far the most common form of nonerosive immune-mediated polyarthritis in the dog. With idiopathic disease, no trigger is identified. Reactive polyarthritis is often associated with systemic diseases (e.g. gastrointestinal disorders, pancreatitis, bacterial cystitis or pneumonia, meningitis, possibly bartonellosis) or administration of certain drugs (e.g. sulfonamides). Breed-associated IMPA has been described in the Bernese Mountain dog, akita, weimaraner, German shorthaired pointer, beagle, and spaniels.
Erosive – Vey rare <1% of Immune arthritides: In canine rheumatoid arthritis, a disease characterized by erosive joint damage, antibody directed against Type II collagen has been found along the joint surface as well as rheumatoid factors within the joint fluid. In addition, chronic persistent synovitis exists that is characterized by perivascular accumulation of mononuclear cells, indicating a possible Type IV hypersensitivity component to this destructive disease. T lymphocytes, macrophages and fibroblasts release matrix-degrading enzymes such as metalloproteinases, which cause cartilage degeneration and further inflammation.Rheumatoid factor is an autoantibody with specificity for the constant region (Fc) portion of an immunoglobulin molecule. Many infectious and inflammatory diseases can be associated with the presence of rheumatoid factor in the serum, including infectious arthritis and osteoarthritis. Testing for rheumatoid factor is indicated if bilateral symmetrical, erosive changes are present in joint radiographs, especially if distal joints are affected. A positive test would support a diagnosis of rheumatoid arthritis in a dog in which erosion of articular cartilage is present but extra-articular manifestations of immune disease are absent, especially if joint cultures are negative.
Physical Examination Findings: - intermittent signs including stiffness, difficulty in rising, lameness, swollen,
warm and painful joints, lethargy and depression, anorexia, lymphadenopathy, polydipsia, and fever, sore back or lifting of tail. Shifting leg lameness is another common sign
Of 101 dogs presented for unexplained pyrexia, 22% had immune-mediated polyarthritis. When only one joint is affected, it is usually the elbow. Spinal pain was found in 18/62 dogs with immune-mediated polyarthritis, most pronounced in the tail. Many dogs with immune-mediated arthritis hold the tail down and react painfully when the tail is manipulated or extended.
Diagnosis:Diagnosis is made with a negative joint culture in a dog with non degenerative neutrophils dominating the cytology. C-reactive protein and Interleukin-6 in peripheral blood are significantly elevated in the disease state and decrease with a positive response to therapy and may be useful in diagnosing and monitoring response to therapy.
Therapy:Target the underlying cause if applicable, and concurrently address pain and inflammation. The overall goal of therapy is to achieve long-term remission with the lowest possible dose of medication, and to prevent recurrence of joint inflammation.
NSAIDs are occasionally sufficient in mild cases like post vaccinal or post drug induced self limiting cases [authors opinion] but most dogs with IMNPA require corticosteroids or other immunosuppressive drugs. If steroids are indicated for further treatment, NSAIDS should be discontinued for at least 48 hours before glucocorticoids are administered. Misoprostol can be added to help avoid or treat gastric ulceration induced by NSAIDs.
Corticosteroid Therapy: Corticosteroids alone may put the disease in remission in some dogs. Prednisone may be initially started at 1-2 mg/kg PO q 12 hrs for 10-14 -21 days.
1. Drug-induced polyarthritis, for example, requires discontinuation of the inciting drug and possibly a short tapering course of glucocorticoids.
2. Polyarthritis/polymyositis use a combination of cyclophosphamide and a tapering dose of prednisone with varying success.
3. RMA have been successfully treated with prednisone alone or a combination of prednisone and azathioprine.
4. Juvenile onset polyarthritis in Akita dogs has also been treated with multidrug protocols including a combination of prednisone and azathioprine, but with a less reliable positive outcome.
5. Type II to Type IV idiopathic polyarthritis, joint inflammation will usually resolve when the underlying disease process is successfully identified and treated or removed. Occasionally, however, additional treatment with analgesics and possibly glucocorticoids will be required.
6. Type II (reactive) polyarthritis triggered by infection, immunosuppressive doses of steroids will be contraindicated. Tick borne diseases, however, may benefit from concurrent treatment with doxycycline and a tapering dose of glucocorticoids.
7. Sulfasalazine has been used to treat cases of Type III (enteropathic) arthritis and rheumatoid arthritis associated with gastrointestinal disease, and

provides a combination of antibacterial, anti-inflammatory and immunosuppressive properties.
8. Type I (uncomplicated) idiopathic polyarthritis, a tapering dose of glucocorticoids is indicated if symptoms persist after more conservative treatment protocols have failed. Immunosuppressive doses of prednisone, prednisolone or methylprednisone (2–3 mg/kg/day once daily or divided) can be started initially. This dose is administered until there is no cytologic evidence of joint inflammation or the clinical signs of arthritis are no longer present. The dose can then be tapered every 4-6 weeks by 25–30% until 1 mg/kg EOD is acheived. Tapering glucocorticoids too quickly can lead to relapses that may be less responsive to treatment than the original manifestation of the disease. The addition of supplementary immunosuppressive agents should be considered if clinical or cytological remission is not attained or if relapse occurs during treatment with steroids alone. If side effects with glucocorticoids or other immunosuppressive agents are intolerable, monotherapy with leflunomide can also be considered.
Cytotoxic Therapy: In cases refractory to prednisone [Most cases in my experience] or for dogs with intolerable side effects to prednisone, additional drugs may be considered.1) Azathioprine
- 2 mg/kg PO q 24 hrs for 3-4 weeks, then 2 mg/kg PO EOD.2) Cyclophosphamide - 1.5-2.5 mg/kg or 50 mg/m2
for 4 days/week. - dosed in early morning with a soup on breakfast and locked out for min. 6 hours- Often also dose Furosemide at 1-2 mg/kg with the soup- discontinued 1-3 months after remission or if myelosuppression or haemorrhagic cystitis occurs.
Immunomodulating Drugs: In a study of 14 affected dogs, leflunomide given at 2.5-3.5 mg/kg OiD for 1-6 weeks resulted in complete remission in 8 dogs, partial response in 5 dogs, and minimal response in 1 dog. Mild thrombocytopenia, leukopaenia, and elevated cholesterol occurred but were not clinically significant.
A study of 20 dogs that compared single agent cyclosporine therapy (5 mg/kg PO q 12 hrs) to prednisone therapy found success rates were similar.Mycophenolate, used together with prednisolone, at a slowly increasing dose to watch for level of GI toxicity also has been shown to have clinical success in resistant cases
Prognosis:Swelling and pain should respond within 7 days BUT repeat arthrocentesis is needed to show resolution of neutrophils before the first tapering of medication to ensure that the patient is in true remission.In terms of prognosis, IMPA may be a one-time event; it may continue indefinitely unless treated long term; or it may recur as therapy is tapered or terminated. In one report of 39 cases, a complete cure was documented in 56% of the dogs. Continuous medication was required in 18% (7/39); relapses were treated successfully in 13% (5/39); and 15% (6/39) of the dogs died or were euthanized as a result of the disease.

Measuring acute phase protein levels, C-reactive protein, is significantly elevated prior to treatment in dogs with IMPA, and also when the disease is active during relapse. The prognosis for long-term remission appears to be better in those dogs with various forms of idiopathic polyarthritis in which C-reactive protein concentrations normalize rapidly after starting glucocorticoids.
Extra Pain Control:In early stages of disease some dogs are too painful to move:
- Gabbapentin, Amantadine and Acetaminophen and maybe Tramahexal 4x/day are added to achieve pain control until glucocorticoids decrease inflammation.
Masticatory Myositis:
Masticatory Muscle myositis (MMM or MM) is inflammation of the muscles of mastication, namely the temporalis, masseter, and pterygoid muscles and they have unique myosin fibres, designated as 2M fibres. The development of autoimmunity against 2M fibres is the proposed pathogenesis of this disease. The major antigen targeted by autoantibodies has been identified as masticatory myosin binding protein-C (mMyBP-C). Canine MM is characterized by initial swelling and inflammatory cell (sometimes eosinophilic) infiltration of the muscles, followed by degeneration, fibrosis, and atrophy. Clinical Signs:Acute stage - muscles may swell or enlarge and be painful. The dog may be reluctant to open its mouth and appetite may be decreased. This acute stage may go unnoticed, especially in long-haired dogs. If untreated, damaged myofibers are replaced with fibrotic connective tissue.Chronic stage - is characterized by severe atrophy of masticatory muscles and secondary enophthalmos. Some dogs with severe fibrosis develop trismus DiagnosisPhysical Examination Findings: In a clinical study of 18 affected dogs, all 18 were reluctant or unable to open their mouths at the time of presentation. Muscle swelling was found in 10 dogs and pain was noted with palpation of the muscles in 6 dogs. Ten dogs had muscle atrophy and 8 dogs had ocular signs, including exophthalmos (n=6), unilateral blindness (n=1), and conjunctivitis (n=2)Immunological Assays: The masticatory muscle type 2M autoantibody test can demonstrate circulating auto-antibodies in some (but not all) cases. The 2M antibody test is an ELISA-based test that is very sensitive and specific. A negative antibody titer may occur in end-stage canine MM and in cases that have been given immunosuppressive dosages of corticosteroids for >7-10 days. Muscle Biopsy: Specimens taken from the temporalis or masseter muscle often confirm the diagnosis
Immunosuppressive therapy is the mainstay of treatment, if the disease is diagnosed before it has become end stage.1) Corticosteroids are typically administered first. Even if muscle atrophy is present, steroids are often given in an attempt to prevent further fibrosis, to alleviate pain, and to combat any residual inflammation. a) Prednisone is initiated at 1-2 mg/kg PO q 12 hrs until clinical signs abate. The
dosage is then decreased to the lowest alternate-day dosage that keeps the dog free of signs. Alternate-day therapy may be required for as long as for 4-6 months. b) A sample protocol is to give 2 mg/kg/day PO x 3 weeks, then 1 mg/kg/day PO x 6-8 weeks, then 1 mg/kg/day PO x every 2nd day 6-8 weeks, then 0.5 mg/kg PO EOD for at least 3-4 months. If the patient continues to do well (i.e. based on resolution of muscle swelling and pain; normal or improved jaw motion; but not necessarily improvement in muscle atrophy), then the dosage can be decreased to 0.5 mg/kg PO q 3rd day for another 1-2 months. c) Dexamethasone is a viable alternative to prednisone, especially in those dogs with intolerable polydipsia/polyuria.2) Azathioprine may be given at 1-2 mg/kg PO q 24 hrs x 3 weeks or longer, and eventually tapered to QOD for 4-6 months or longer. .a) Cyclosporine (Atopica®) may be given at 5 mg/kg PO q 12 hrs. b) Mycophenolate mofetil (CellCept) may be considered at the dosage used for pemphigus foliaceus (10-13 mg/kg PO q 8 hrs for 4 months), although gastrointestinal side effects are common. Prognosis is often good for dogs diagnosed during the acute stage of the disease, particularly if marked fibrosis and myofiber destruction are absent. Even chronic cases with marked fibrosis may respond partially, although the likelihood of reversing severe muscle atrophy is poor.
Steroid-responsive meningitis-arteritis (SRMA)Steroid-responsive meningitis-arteritis (SRMA) is currently the most widely accepted term describing a disease syndrome that causes meningitis in medium- and large-breed dogs less than two years of age. The syndrome was first recognized in young laboratory Beagles, and was referred to as 'Beagle pain syndrome'. Other breeds that are predisposed to SRMA include the Boxer, Bernese Mountain Dog, Akita and German Short Haired Pointer and in RSA we seem to see a lot of Weimeraners. Typically, affected animals present with an acute onset of neck pain, fever and lethargy.
Cerebrospinal fluid analysis reveals inflammation and an increase in protein. More specifically, a high level of immunoglobulin A is found both systemically and intrathecally. Paired measurements of IgA in the serum and CSF have proven useful for diagnosing SRMA. The combination of immune-mediated polyarthritis and apparent SMRA is more common than suspected. Up to one in three dogs with IMPA also has spinal pain, which may often be due to SMRA. Spinal pain was most commonly demonstrated in the cervical region when the head was flexed or extended. It is recommended that a CSF tap be performed on all dogs suspected IMPA that have concurrent joint and spinal pain.
Therapy:If the CSF tap is > 70-80% neutrophils therapy is single agent glucocorticoidsBut with mixed cell pleocytosis the addition of Cytozar to the regime shows benefit.
Granulomatous Meningoencephalomyelitis (GME):GME is an aseptic, inflammatory disease of the central nervous system (CNS) of dogs that affects primarily white matter and perivascular areas. The cause is unknown but is thought to be delayed-type hypersensitivity involving major
histocompatibility class 2, with a predominance of CD3 antigen-positive T lymphocytes. A recent study showed that macrophages/microglia that infiltrate brain lesions producing IL-17 are more important in GME than T cells.
This causes a perivascular accumulation of mononuclear cells (i.e. lymphocytes, plasma cells, reticuloendothelial cells). GME lesions can affect one or more parts of the CNS, such as the brainstem, cerebello-vestibular area, cerebrum, optic nerves, and/or spinal cord. Clinical signs vary based on the areas affected but is usually multi-focal. 1) Disseminated or multifocal form affects multiple areas of the brain and may mimic encephalitis. This form is usually very progressive and pleocytosis (increased white blood cells) is often found on cerebrospinal fluid (CSF) analysis. 2) Focal form mimics an expanding mass and is very difficult to distinguish from neoplasia on neurological examination or brain scans.3) Ocular form usually causes vision loss and is the least commonly found form. GME is a differential diagnosis for acute onset blindness and optic neuritis.
All can have an acute onset or a more slowly progressive onset but the course is progressive. Seizures, mental dullness (doff) and central vestibular signs are common manifestations. Cerebellar signs, quadriparesis, paraparesis, and/or cranial nerve deficits can also occur.
Diagnosis:A definitive diagnosis of GME is made only by biopsy and histopathology of samples obtained at necropsy. However, a presumptive diagnosis can be made on signalment, history, clinical signs, advanced imaging, and CSF analysis. Elimination of encephalitides (e.g. canine distemper virus, Neospora caninum, Toxoplasma gondii, systemic mycoses, and CNS lymphosarcoma) is sometimes necessary.
MRI findings typically include multiple hyperintensities on T2-weighted or FLAIR sequences, with a predilection for CNS white matter. MRI findings are not pathognomonic for GME and must be differentiated from other forms of meningoencephalitis and neoplasia.
CSF Analysis: Elevation of total protein and a predominantly mononuclear pleocytosis (with or without neutrophils) are typical findings.
Disease description:GME occurs most often in young to middle-aged dogs. Small dogs are affected more often than large breed dogs. Certain breeds appear to be predisposed, including the miniature poodle, Yorkshire Terrier, Maltese, dachshund, West Highland white terrier, and Chihuahua. However, any breed of dog may be affected.
Therapy:Prednisone may be tried 1-2 mg/kg PO q 12-24 hrs for one month then tapered to 1 mg/kg EOD or the lowest dose possible that control the signs. Response is variable and clinical signs often recur as the dose is tapered so the author always uses polytherapy with added Cytosine arabinoside. Survival times 8 to 100 days are reported

Cytosine arabinoside is given 50 mg/m2 SC q 12 hrs x 2 days, and repeated q 3 wks. To increase treatment efficacy, cytosine is usually administered in combination with prednisone. In one study, survival times ranged from 78-603 days when cytosine arabinoside was administered q 3 wks in conjunction with prednisolone.Procarbazine can be tried at 25-50 mg/m2/day PO. The lower dose is associated with fewer side effects. This antineoplastic drug can be used as a monotherapy or in conjunction with prednisone. Since it is available in 50 mg capsules, it may have to be re-compounded to get an appropriate dose.Cyclosporine can be given at 6 mg/kg PO q 12 hrs. Administer it either 1 hour before or 2 hours after feeding to guarantee consistent and best absorption. Although passage through the blood-brain barrier is poor, since GME is a perivascular disease and the blood-brain barrier is disrupted during inflammation, it is believed that a therapeutic concentration can be reached in the CNS. In one study, dogs that received a combination of corticosteroids and cyclosporine had a median survival time of 620 days (range 8-870 days) compared with those that received only corticosteroids (median survival time of 28 days, range of 3-63 days.Leflunomide may be tried 1.5-4 mg/kg PO q 24 hrs. Dosage is adjusted as necessary to result in plasma trough level of 20 ug/mL. In one study it was started 2-3 months after glucocorticoids had begun. It was possible to reduce the glucocorticoid doses maintaining leflunomide, for as long as 12 months.Lomustine may be given at 50-70 mg/m2 PO q 3-4 wks. In one study, oral administration of lomustine combined with prednisolone had similar efficacy to just prednisolone alone.Azathioprine has been tried at 2 mg/kg PO q 24 hrs. It can be added to prednisone when side effects of prednisone become severe or if prednisone alone has failed.Radiation therapy may be beneficial for the focal form of GME based on longer survival times (median >404 days) compared to cases treated only with corticosteroids.
Sterile Nodular Panniculitis (SNP, NP):- a suspected immune-mediated disease of dogs and cats.
Nodular Panniculitis (NP) is an inflammatory disease of subcutaneous fat. Affected animals develop deep, firm to cystic, subcutaneous nodules that may fistulate into the overlying dermis and lead to ulcerations and draining tracts.Prednisolone can be used at anti-inflammatory or immunosuppressive doses. - 1-2 mg/kg PO q 12 hrs until lesions regress or resolve. - Attempt to taper and then discontinue therapy after remission is achieved- usually within 3-8 weeks.. Cyclosporine (Atopica/Neoral)
- 7 mg/kg PO q 24 hrs, then tapered once the signs resolve.- Cyclosporine may be required to achieve remission, and to decrease severity
and frequency of recurrences.Vitamin E - an adjunctive systemic therapy for panniculitis.
- 400 IU PO q 12 hrs or 13.5 IU/kg/day PO.
- given 2 hours before a meal for maximum effectivenessDoxycycline with Niacinamide/Nicotinamide:
Dogs < 10 kg, 5-10 mg/kg doxycycline dosed oid and niacinamide 250 mg dosed Tid Dogs > 10 kg, 5-10 mg/kg doxycycline dosed oid and niacinamide 500 mg dosed.

Doxycycline and niacinamide appear to be more helpful as a sole therapy in DLE, Symmetrical Lupoid Onchitis [SLO], Nodular steatitis/pansteatitis, forms of Lympho-plamacytic disease and mild cases of pemphigus foliaceus.It can take several weeks for tetracycline and niacinamide to have a clinical effect. Once remission occurs with tetracycline and niacinamide, the frequency of administration can be decreased to once or twice a day.
Feline Steatitis:Therapy is directed at correcting the diet, and identifying and treating any underlying disease. Feed a well-balanced diet. Eliminate fish products from the diet of patients with steatitis.Supplementation with vitamin E (α-tocopherol acetate) at 10-25 IU PO q 12 hrs can be beneficial. S-adenosylmethionine (SAMe) at 18 mg/kg/day PO also has antioxidant properties that may be beneficial in the treatment of steatitis.For SNP cases with multiple lesions, systemic immunomodulating agents are indicated. Most of these cases respond well to systemic glucocorticoids. Other patients may respond to cyclosporine at 5 mg/kg/day PO, if immunosuppression is needed. Active infection and other causes of subcutaneous nodules/fistulas must be ruled out before starting corticosteroids or cyclosporine.
Perianal Fistulae’s/Furunculosis:
Currently, an immune-mediated pathogenesis is suspected. The disease responds to various immunosuppressive drugs, such as prednisone, azathioprine, cyclosporine, and tacrolimus. In German shepherd dogs, there may be a link between colitis and perianal fistulas similar to the development of perianal fistulas in people with Crohn's Disease. Additionally, high levels of expression of selected cytokine mRNA in perianal fistula lesions and the disease’s responsiveness to cyclosporine supports a T cell-mediated inflammatory response.
Specific Therapy:Although surgical treatment of perianal fistulae was previously done, medical therapy with immune-modulating drugs is now the treatment of choice. Medical management is divided into two phases: 1) Induction phase, which is undertaken until clinical signs resolve. Higher drug doses are used in the induction phase.2) Maintenance phase, which aims to keep clinical signs in remission. As with other
immune-mediated skin disorders, lifelong therapy is often needed and secondary bacterial infections must be controlled.
Topical Therapy with Tacrolimus:Tacrolimus (Protopic) mechanism of action is similar to that of cyclosporine. It is 10-100 times more potent than cyclosporine and is applied topically as a thin film to affected areas q 12-24 hrs.Tacrolimus - 0.1% can be used alone if clinical signs are mild and the dog accepts topical therapy. In one study, 50% (5/10) of dogs had complete resolution after 16 weeks of tacrolimus treatment.Tacrolimus can also be used alone as a maintenance therapy to minimize recurrence of perianal fistulas in dogs that are in remission after

cyclosporine therapy. Administer tacrolimus for 4 weeks beyond clinical resolution and then apply it less often in a tapering fashion (i.e. every other day, twice weekly) and then less often indefinitely as maintenance or preventive therapy.
Systemic Medical Therapy:Systemic therapy can be used alone or in combination with topical therapy. Cyclosporine is the preferred systemic drug and has been evaluated in multiple studies.Cyclosporine (Atopica, Neoral)
- most effective dose has not been established. In general, higher doses of CsA result in faster clinical improvement.
- Longer courses (>13 weeks) decrease the rate of perianal fistula relapse.When CsA is used as a single agent, the dose is 4-8 mg/kg PO q 24 hrs and it is continued until no lesions are present. However, reported CsA dosages have ranged from 1.5-7.5 mg/kg PO q 24 hrs to 4-10 mg/kg PO q 12 hrs.NB - Give CsA on an empty stomach, either 1 hour before a meal or 3-4 hours after a meal.Cyclosporine results in improvement of perianal fistulas within 1-2 weeks. In one study, most cases (85%, 17/20 dogs) resolved within 16 weeks.Perianal fistulas recur in 33-50% of cases that have had therapy discontinued so maintenance therapy is currently recommended and options include either using intermittent CsA or topical tacrolimus.Prednisone An immunosuppressive dose is used to induce remission, then the dosage is reduced. Prednisone has lower efficacy than CsA and is not the first-choice for systemic therapy. In a study, one-third of the dogs responded completely, one-third partially improved, and one-third had no response.Alternatively, prednisone at 3-4 mg/kg PO q 24 hrs or divided q 12 hrs has been used in conjunction with azathioprine or metronidazole (10-15 mg/kg PO q 12 hrs), or with a novel protein diet.
In the authors opinion, relapse of perianal fistulas is decreased considerably in dogs maintain on a novel or hydrolysed diet.
Symmetrical Lupoid Onchitis [SLO]:
When only the claw and no surrounding tissue is involved then immune-mediated diseases such as SLO (common), lupus erythematosus and pemphigus vulgaris (both rare) should be considered. If paronychia and/or footpad involvement is present, then pemphigus foliaceus is of primary concern.
SLO - Initially there is an acute loss of the claws from one or two toes, followed by loss of more claws within days to weeks - typically all feet are affected, but not always. Pain, lameness or finding claws in the house are the first clinical signs. Secondary bacterial infections are relatively common. Following claw loss, abnormal claws regrow, that are short, soft, brittle, crumbling and may be misshapen. - German Shepherd dog, Giant/Standard/Miniature Schnauzer, Rottweiler, Greyhound, Bearded Collie and Norwegian Gordon and English Setter and RSA Rhodesian Ridgeback?. Treat secondary infection with systemic antimicrobials.

Under general anesthesia, remove loose or deformed claws Tetracycline and niacinamide (see previous cases for doses
once significant regrowth noted (4–6 months) decrease the frequency of administration of both drugs to once daily. If good response is maintained for 4–6 months on once-per-day therapy, treatment is stopped. Recurrence may occur - start therapy as previously.
Pentoxifylline is beneficial in 50–60% of cases; 15–25 mg/kg BID; 3-month trial; for patients experiencing normal regrowth, after 6–9 months of therapy, consider stopping medication.
Glucocorticoids are effective but rarely necessary. Prednisone/prednisolone starting at 1–2 mg/kg/day; often used at the initiation of therapy (e.g., first 3 or 4 weeks), along with other drugs such as fatty acids or pentoxifylline or doxycycline/niacinamide - all of which have a slower onset of benefit to help reduce pain. It has been suggested that this more aggressive therapy, early in the disease may improve the overall prognosis.
Cyclosporine therapy, starting at 5 mg/kg/day has been noted to benefit the problem.
Refractory cases or patients who are intolerant of the above therapies can be managed with 20 nail, P3 amputations. Individuals generally do well without claws.
Keeping the nails trimmed to prevent contact with the ground may be of significant benefit.
Blood Transfusion Reactions Blood transfusion reactions are adverse events that occur during or following a transfusion of any blood product. Transfusion reactions can be classified as non-immunologic or immunologic, and categorized as acute or delayed.Immunologic reactions include allergic reactions, haemolysis, serum sickness, febrile non-haemolytic transfusion reaction, and transfusion-related acute lung injury. Acute transfusion reactions occur from within seconds of the start of the transfusion to as late as 48 hours after the transfusion.
Allergic reactions are type I hypersensitivity reactions. They are mediated by IgE and lead to mast cell degranulation, with the production and release of various inflammatory mediators (e.g. histamine, prostaglandins, leukotrienes). Allergic reactions can result in anaphylaxis.Haemolytic transfusion reactions can be acute or delayed, and are classified as type II hypersensitivity reactions. Acute haemolytic transfusion reactions occur in the presence of preexisting antibodies against erythrocytes, while delayed haemolytic reactions occur from production of antibodies against erythrocytes. Subsequent exposure to the same antigens on erythrocytes will cause an acute haemolytic transfusion reaction.Serum sickness is caused by a type III hypersensitivity reaction. Serum antibodies form immune complexes with unbound antigens. Normally these complexes are eliminated by binding to platelets or erythrocytes, or through the mononuclear phagocyte system. However, these clearance mechanisms can be overwhelmed by the high antigenic load from a transfusion and immune complexes then become deposited on blood vessel walls, leading to vasculitis.

Febrile non-hemolytic transfusion reaction occurs from an immune response to leukocyte antigens in a blood product, as opposed to erythrocyte antigens. These reactions rarely occur but have been reported following transfusion of red blood cell products that have been stored for long periods of time.2
Preventive Measures:Cross matching and/or blood typing are recommended in order to minimize the risk of incompatibility between donor and recipient. Cross matching examines the effect of recipient serum antibodies on donor erythrocytes (major crossmatch) and the effect that donor serum has on recipient cells (minor crossmatch).Blood typing can identify which canine blood group is present in blood donors, products, and recipients. Dogs have at least eight different blood groups. Dog erythrocyte antigen (DEA) 1.1 and 1.2 are two of the most important blood groups since these blood types are commonly implicated in transfusion reactions. Naturally occurring antibodies against DEA 1.1 and 1.2 are uncommon, so acute transfusion reactions are rare with a first blood transfusion. However, antibody induction occurs following a transfusion and can lead to reactions with subsequent transfusions. Naturally occurring antibodies against DEA 7 may be present in 15% of canines and lead to a delayed haemolytic transfusion reaction. Ideally, blood donors should be DEA 1.1 and 1.2 negative or a universal donor. Universal donors are negative for multiple DEA antigens and are only positive for DEA 4.
Diabetes Mellitus:Diabetes mellitus is considered a multifactorial disease. In most dogs, it is thought that an immune-mediated process leads to destruction of insulin-secreting pancreatic βeta cells, which leads to absolute insulin deficiency. Various βeta cell antibodies have been identified in people with Type I DM; however, no large studies of anti-βeta-cell antibodies have been reported in dogs.
Hypothyroidism:In thyroiditis, the thyroid is infiltrated with lymphocytes, plasma cells, and macrophages. As the condition progresses, thyroid parenchyma is destroyed and replaced by fibrous connective tissue. Thyroiditis is an immune-mediated disease in which cellular destruction occurs due to binding of thyroid autoantibodies to the follicular cells, with subsequent antibody-dependent, cell-mediated toxicity. Months to years may be required to produce clinical signs of hypothyroidism, and some patients with thyroiditis do not develop hypothyroidism. Circulating thyroid autoantibodies may be present but they may decline once a large portion of the thyroid is destroyed. Thyroiditis is a heritable trait.
Pemphigus Foliaceus [PF]:
The pemphigus variants occur when autoantibodies target the desmosomes between keratinocytes. Pemphigus foliaceus is often a chronic skin condition with a waxing and waning course. Clients should be aware of the very high possibility of disease recurrence after remissionPrednisone is initially started at 2 mg/kg/day orally in dogs, and prednisolone is initially started at 2 to 4 mg/kg/day orally in cats

Many use high-dose pulse oral and intravenous glucocorticoid administration to treat pemphigus foliaceus in dogs, these high dosages (oral prednisone at 10 mg/kg/day or intravenous methylprednisolone succinate at 11 mg/kg/day) are typically given for three days followed by a much lower dose of oral prednisone (0.5 to 2 mg/kg/day). High-dose glucocorticoid administration is used primarily in severe pemphigus foliaceus cases in which quick remission of signs is required.
CATS often need different glucocorticoids : Dexamethasone – 2mg/cat/day till controlled then 1 mg/cat/day for a week or so then1mg/cat on M W Fri and ? taper? Taper furtherCyclosporine – 5-7-10 mg/kg/day
- cyclosporine monotherapy at 5 to 10 mg/kg/day was ineffective in managing pemphigus foliaceus signs in four out of five dogs but anecdotal reports of using cyclosporine at 10 mg/kg/day or greater to manage pemphigus foliaceus in dogs, especially those with milder presentations are reported.
- Cyclosporine is more effective for pemphigus foliaceus when used in combination with other therapies. In three dogs with pemphigus foliaceus already receiving azathioprine and glucocorticoids, oral cyclosporine at 7.5 to 10 mg/kg/day was used. All dogs were then able to have glucocorticoids discontinued within 3 months of adding the cyclosporine
Chlormabucil – ½ tab /cat every 2nd day with blood after 2-3 weeks and then 1-2 monthly
- 0.1 to 0.2 mg/kg orally every 24 to 48 hoursTriamcinolone 0.2 to 0.4 mg/kg/day and taper once controlledDOGS:Azathioprine is commonly started at 2 to 2.5 mg/kg/day orally in dogs
- azathioprine can take weeks to have an effectNiacinamide with tetracycline or doxycycline
- Tetracycline is an antibiotic that also modulates the immune system by suppressing neutrophil chemotaxis and lymphocyte activation. Tetracycline is used in combination with niacinamide for a variety of immune-mediated dermatologic conditions.
- For dogs < 10 kg, 250 mg each of tetracycline and niacinamide are given orally every eight hours. For dogs > 10 kg, the dose is 500 mg of each every eight hours. Tetracycline and niacinamide are typically not used in cats because it is difficult to administer these larger-sized oral medications to most cats. Doxycycline has the advantage of needing less frequent dosing than tetracycline. It has been substituted for tetracycline and used at a dose of 5 to 10 mg/kg orally in dogs every 12 to 24 hours. However, there is no documentation of the benefit of doxycycline when it is substituted for tetracycline to treat canine pemphigus foliaceus.
- Tetracycline and niacinamide appear to be more helpful as a sole therapy in mild cases of pemphigus foliaceus, especially those cases with lesions localized to the face. It can also be used in combination with glucocorticoids or azathioprine. It can take several weeks for tetracycline and niacinamide to have a clinical effect. Once remission occurs with tetracycline and niacinamide, the frequency of administration can be decreased to once or twice a day.

Systemic Lupus Erythematosus:
Systemic lupus erythematosus (SLE) is a multisystemic autoimmune disease characterized by the production of a variety of autoantibodies that form immune complexes.Full Blood Count: Anaemia, thrombocytopenia, leukopaenia, or leukocytosis can occur. Anaemia can be regenerative or non-regenerative. Haemolytic anemia is rare. Anaemia may or may not be Coombs’ positive.Urinalysis: 55 % of dogs and 40% of cats have renal abnormalities. Glomerulonephritis is the most typical disorder, and proteinuria is one of the earliest abnormalities noted. A urine protein:creatinine ratio should be evaluated in order to quantify urine protein levels.Synovial Fluid Analysis: Arthrocentesis may reveal cloudy synovial fluid. Decreased viscosity with poor mucin clot formation is common. Synovial fluid analysis reveals elevated cell counts, particularly non-degenerate neutrophils and monocytes. Antinuclear Antibody (ANA) Test: ANA tests detect antibodies directed against nuclear antigens. It is usually reported as a serum titer. Positive titers can occur in patients without SLE that have chronic infectious, inflammatory, or neoplastic disease. Therefore, a positive ANA test is not pathognomonic for SLE. False negatives can also occur ANA testing is not useful in patients without clinical abnormalities suggestive of SLE. ANA testing may be considered in patients with at least 2 major signs consistent with SLE. SLE cannot be diagnosed or excluded solely on the basis of ANA testing.Lupus Erythematosus (LE) Test: LE testing identifies phagocytized nuclear material within neutrophils and macrophages. A positive result is highly suggestive of SLE but sensitivity is low. The LE test is also difficult to perform. For these reasons, the LE test has been largely replaced by the ANA test.1-3
Dermatohistopathology: Skin biopsy can be performed to support the diagnosis but biopsy alone cannot definitively diagnose SLE. Abnormalities include thickening of the basement membrane zone; subepidermal vacuolation; hydropic or lichenoid interface dermatitis; and leukocytoclastic vasculitis.1
Diagnostic Criteria for SLE:Because no single test can definitively diagnose SLE in dogs and cats, it has been proposed the diagnosis be established if a patient manifests ≥3 of the following criteria simultaneously or over any period of time:1) Positive ANA test 2) Cutaneous lesions (e.g. depigmentation, erythema, erosions, ulcerations, crusts, scaling) with biopsy findings consistent with SLE3) Oral ulcerations4) Nonerosive, nonseptic arthritis involving two or more peripheral joints5) Renal disorders, such as glomerulonephritis or persistent proteinuria in the absence of a urinary tract infection6) Hemolytic anemia or thrombocytopenia, in the absence of offending drug therapy7) Leukopenia8) Polymyositis or myocarditis9) Serositis (i.e. inflammation of any serous membrane)10) Neurologic disorders, in the absence of a known cause11) Antiphospholipid antibodies
Corticosteroids are the primary therapy for SLE. Prednisolone at 1-2.2 mg/kg PO q 12-24 hrs is a reasonable starting dose. Induction doses are administered until remission of disease (i.e. resolution of clinical signs or laboratory changes). Doses are gradually tapered by reducing the amount given by 50% q 3-4 weeks to achieve the lowest dose that is effective at controlling clinical signs. Tapering is continued until a relapse occurs. It may be possible to stop medications in some patients but others require long-term maintenance therapy.Cats may respond better to triamcinolone or dexamethasone compared to prednisolone. Triamcinolone at 0.3-1 mg/kg PO q 12-24 hrs or dexamethasone at 0.1-0.2 mg/kg PO q 12-24 hrs are possible induction doses.Azathioprine is not recommended because it is toxic to cats. Chlorambucil may be tried at 15 mg/m2 PO q 24 hrs for 4 days and repeated q 3 weeks in conjunction with corticosteroids, if additional immunosuppression is needed. Alternatively, chlorambucil can be given at 2 mg total dose PO q 48-72 hrs. If used with prednisolone, taper the chlorambucil first.2 Alternative immunosuppressant medications for induction include cyclosporine at 5 mg/kg PO q 12-24 hrs, mycophenolate mofetil at 10 mg/kg PO q 12-24 hrs, or cyclophosphamide at 50 mg/m2 PO q 48 hrs or daily on 4 days/week. Use of the latter two drugs is off label in cats.
Canine atopic dermatitisA genetically predisposed inflammatory and pruritic allergic skin disease with characteristic clinical features associated with IgE antibodies most commonly directed against environmental allergens.
Inflammatory Bowel Disease [IBD]Atypical immune reaction to symbiotic bacteriaVsBacterial change affecting immune response