lapjag reny ruptur dg corpal
TRANSCRIPT

LAPORAN JAGA RESIDENBAGIAN ILMU KESEHATAN MATA
SELASA, 18 MARET 2014 PUKUL : 07.00 WIB S/D
RABU, 19 MARET 2014 PUKUL : 07.00 WIB
Residen Jaga :
Jaga II : dr. Tesha Ratnafury dr. Nurul Widiati
Jaga I : dr. Reny Violeta dr. Dian Ariani
Jaga Magang : dr. Faika
1
Konsulen Jaga : dr. Riani Erna, SpM

Data dasar Permasalahan Assesment PlanningF/Lk/48 thn/ Luar kota.KU: Mata kanan terkena pelantingan granit saat memotong lantai granit ± 4jam SMRSRPP: ± 4 jam SMRS, mata kanan terkena pelantingan granit (keramik lantai) saat sedang memotong lantai, dari arah depan, penderita tidak memakai kaca mata pelindung, keluar darah (+), nyeri (+), keluar cairan berwarna kehitaman (+), keluar cairan seperti putih telur - tidak tahu, penderita tidak melakukan tindakan apapun pada matanya, dan lansung ke RS Charitas. Di RS setempat, tidak dilakukan tindakan apapun, dan langsung dirujuk ke RSMH.
VOD: 0
Palpebra : Tampak ruptur palpebra full thickness memanjang dari arah jam 1, 3mm dari canthus medial, ke arah jam 7, 20 mm dari canthus medial, sepanjang 60 mm. Darah (+), tampak corpus alienum tertancap pada luka, panjang ± 20mm, tepi luka rata.
Sklera : Belum dapat dinilaiKonjungtiva : Belum dinilaiKornea : Tampak ruptur fullthickness dari arah jam 1-jam 7 dengan CA (+)
BMD :Iris :Pupil :Lensa :Segmen posterior :
• Trauma terbuka bola mata dengan komplikasi laserasi kornea full thickness OD
• laserasi palpebra full thickness OD
dd/ Destroyed eye OD
ICD X: H44.6 dan
ICD IX: 16.3 14.6, 08.74
Informed ConsentMRSPro eksplorasi trauma dan ekstraksi corpus alienum OD dengan AUPro Konsul anestesiPro konsul PDLPro Rontgen Torak dan Ro orbitaPro cek LabLevofloxacin ED 1 gtt / jamPro Ceftriaxone 1x1gr IVPro inj Tetagam IMBelum
dapat dinilai
STATUS GENERALIS
Keadaan umum : BaikKesadaran : kompos mentisTD : 140/80 mmHgNadi : 80x/menitRespiratory rate : 24x/menitTemperatur : afebris

FOTO PASIEN

RONTGEN ORBITA

STATUS OFTALMOLOGIKUSVOD : 0 VOS : 6/6
TIOD : tidak dilakukan TIOS : 18,5 mmHg
KBM simetris
GBM Belum dapat dinilai

OD OS
palpebra Palpebra :Tampak ruptur palpebra full thickness memanjang dari arah jam 1, 3mm dari canthus medial, ke arah jam 7, 20 mm dari canthus medial, sepanjang 60 mm. Darah (+), tampak corpus alienum tertancap pada luka panjang ±20mm, tepi luka rata.
tenang
konjungtiva Belum dapat dinilai tenang
kornea Tampak ruptur fullthickness dari arah jam 1-jam 7 dengan CA (+)
jernih
sklera Belum dapat dinilai tenang

BMD Belum dapat dinilai Sedang
Iris Belum dapat dinilai Gambaran baik
Pupil Belum dapat dinilai Bulat, sentral, RC (+), ø 3 mm
Lensa Belum dapat dinilai Jernih

SEGMEN POSTERIOR
Segmen Posterior : RFOD (-) RFOS(+)
FOD : Tidak dilakukan
FOS :
Papil : Bulat, batas tegas, warna merah normal,
c/d 0.3 a/v : 2/3
Makula : RF (+)N
Retina : kontur pembuluh darah baik, perdarahan (-), eksudat (-)

DIAGNOSA :
• Trauma terbuka bola mata dengan komplikasi laserasi kornea full thickness OD
• Laserasi palpebra full thickness OD
dd/ Destroyed eye OD

PENATALAKSANAAN :Informed ConsentMRSPro eksplorasi trauma dan ekstraksi corpus alienum OD dengan AUPro Konsul anestesiPro konsul PDLPro Ro Torak dan Ro orbitaPro cek LabLevofloxacin ED 1 gtt / jamPro Ceftriaxone 1x1gr IVPro inj Tetagam IM

INTRA OPERATIF




Identifikasi intraoperatif : Ditemukan corpus alienum berupa mata pisau gerinda pemotong granit, ukuran 20mm x 30 mm
Ditemukan laserasi palpebra superior dan inferior, memanjang dari arah jam 1 ke jam 7, sepanjang 60mm
Ditemukan massa choroid dan vitreus
Ditemukan laserasi sklera, 10 mm dr limbus superior, memanjang hingga 14 mm dari limbus inferior
Ditemukan laserasi kornea fullthickness OD
Ditemukan massa lensa dalam kondisi hancur
Diputuskan penatalaksanaan : Eviscerasi dengan DFG

INSTRUKSI POST OP:
Ciprofloxacin 2 x 500mg
Asam mefenamat 3x500mg
Kloramfenikol EO 3x1

FOLLOW UP RABU, 19 MAR 2014:
VOD : - VOS : 6/6
TIOD : - TIOS : 15.6 mmHg
KBM simetris
GBM

OD OS
Palpebra Blepharorrhaphy (+)Tampak Jahitan di palpebra superior (5 jahitan) dan di
palpebra inferior (4 jahitan) jahitan baik, darah (-), pus (-)
Tenang
Konjungtiva - Tenang
Kornea - Jernih

BMD - Sedang
Iris - Gambaran baik
Pupil - Bulat, sentral, RC (+), ø 3 mm
Lensa - Jernih

SEGMEN POSTERIOR
Segmen Posterior : RFOD (-) RFOS(+)
FOD : -
FOS :
Papil : Bulat, batas tegas, warna merah normal, c/d 0,3, a/v : 2/3
Makula : RF (+)N
Retina : kontur pembuluh darah baik

FOTO PASIEN Foll.UP post op hari ke-1

DIAGNOSA :
Post Eviscerasi OD a/i trauma terbuka bola mata dengan komplikasi laserasi kornea full thickness OD + laserasi sklera OD + prolaps isi bola mata OD
Penatalaksanaan :
Ciprofloxacin 2x500mg
Asam mefenamat 3 x 500 mg
Kloramfenikol EO 3x1 OD
Acc Rawat jalan, KU 3 hari ke Poli mata.

Thank You...



BETTS CLASIFICATION
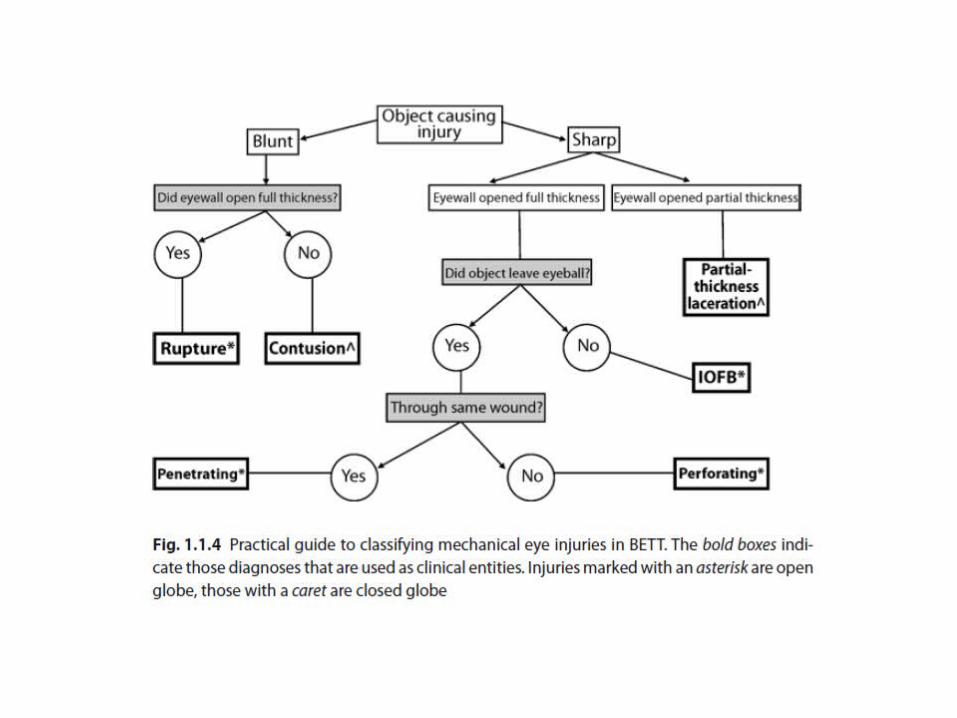


- Closed globe injury: No full- thickness wound of eyewall- Open globe injury: Full- thickness wound of the eyewall- Lamellar laceration: Partial- thickness wound of the eyewall- Rupture: Full- thickness wound of the eyewall, caused by a blunt object- Laceration: Full- thickness wound of the eyewall, caused by a sharp object
BETTS (Birmingham Eye Trauma Terminology System) DEFINITION :

Menurut Birmingham Eye Trauma Terminology (BETT), trauma mata dibagi menjadi:5
Tertutup
Kontusio: tidak ada luka pada bola mata
Laserasi lamellar: hanya mengenai setengah dari ketebalan dinding bola mata.
Terbuka
Laserasi: mengenai seluruh ketebalan dinding bola mata yang disebabkan benda tajam
Penetrasi: satu agen menyebabkan satu luka masuk
Benda asing dalam mata: sama dengan penetrasi tetapi dikelompokan sendiri karena memerlukan penanganan berbeda.
Perforasi: terdapat luka masuk dan luka keluar
Ruptur: mengenai seluruh ketebalan dinding bola mata yang disebabkan benda tumpul

Klasifikasi Trauma Mata Terbuka (Open Globe Injury):6
Tipe
Ruptur
Penetrasi
Benda asing
Perforasi
Campuran
Grade (visual acuity)
> 20/40
20/50 sampai 20/100
19/100 sampai 5/200
4/200 sampai hanya persepsi cahaya
Tidak ada persepsi cahaya
Pupil
Positif, relative afferent pupillary defect pada mata yang terkena
Negatif, relative afferent pupillary defect pada mata yang terkena
Zona (lihat gambar)
Kornea dan Limbus
Limbus sampai 5 mm posterior sclera
Posterior sampai 5 mm dari limbus.













Lid Margin RepairTh ere are a number of diff erent techniques available for repairing lid margins, but the principles are the same. It is important to accurately align the three surfaces of the lid (skin, gray line, and conjunctiva) for an adequate time for healing to occur.If a tarsal plate suture is used then additional skin sutures can be removed early (1 week), but if gray line and skin sutures are used without a cardinal tarsal suture, then they must be left in for 2 to 3 weeks to allow proper healing, especially if the wound is under tension such as when a proportion of the lid length has been removed in tumor removal or entropion repair. A cardinal tarsal suture should be placed horizontally parallel to the lid margin about 1 mm from its surface and should be within the lid substance entirely. In other words, the suture should not protrude through either skin at the front of the lid or conjunctiva at theback. A well-placed tarsal suture will provide the necessary strength and tension for the lid margin to heal with no notching, and will allow early removal of supplementary skin and lid margin sutures.


Grading system for traumatic hyphemas:
Grade 1 hyphema—layered blood occupying less than one third of the anterior chamber
Grade 2 hyphema—blood filling one third to one half of the anterior chamber
Grade 3 hyphema—layered blood filling one half to less than total
Grade 4 hyphema—total clotted hyphemas, of ten referred to as blackball or eightball hyphema




Cefadroxil adalah antibiotika semisintetik golongan sefalosforin untuk pemakaian oral. Cefadroxil bersifat bakterisid dengan jalan menghambat sintesa dinding sel bakteri. Cefadroxil aktif terhadap Streptococcus beta-hemolytic, Staphylococcus aureus (termasuk penghasil enzim penisilinase), Streptococcus pneumoniae, Escherichia coli, Proteus mirabilis, Klebsiella sp, Moraxella catarrhalis

Like most adrenocortical steroids, methylprednisolone is typically used for its anti-inflammatory effects. However, glucocorticoids have a wide range of effects, including changes to metabolism and immune responses. The list of medical conditions for which methylprednisolone is prescribed is rather long, and is similar to other corticosteroids such as prednisolone. Common uses include arthritis therapy and short-term treatment of bronchial inflammation or acute bronchitis due to various respiratory diseases. It is used both in the treatment of acute periods and long-term management of autoimmune diseases, most notably Systemic lupus erythematosus.

Hifema merupakan keadaan dimana terdapat darah di dalam bilik mata depan, yaitu daerah di antara kornea dan iris, yang dapat terjadi akibat trauma tumpul yang merobek pembuluh darah iris atau badan siliar dan bercampur dengan humor aqueus (cairan mata) yang jernih

Komplikasi Ruptur Korneo sklera
Endophthalmitis , yang terjadi pada 2-7% pasien dengan trauma okular
Katarak
Kerusakan Iris
Glaukoma , yang dapat terjadi akut atau lambat, kemungkinan berhubungan dengan resesi sudut
Hyphema
Perdarahan vitreous
Detasemen retina
Epitel downgrowth
Uveitis
Edema makula Cystoid
SO

Untuk mencegah atropi papil saraf optik dilakukan pembedahan bila:
- tekanan bola mata maksimal > 50 mmHg selama 5 hari
- tekanan bola mata maksimal > 35 mmHg selama 7 hari
Untuk mencegah imbibisi kornea dilakukan pembedahan bila:
tekanan bola mata rata-rata > 25mmHg selama 6 hari
bila terdapat tanda-tanda dini imbibisi korneaUntuk mencegah sinekia posterior perifer
Dilakukan pembedahan bila:- hifema total bertahan selama 5 hari- Hifema difus bertahan selama 9 hari

Levofloxacin is a later-generation antibacterial agent of the fluoroquinolone class that exhibits a broad spectrum of in vitro activity. It has been demonstrated to be effective in the treatment of a wide range of community- and hospital-associated infections.
The main indications for treatment are bacterial blepharitis and conjunctivitis, bacterial keratitis – especially when associated with contact lenses – and endophthalmitis, where it is provided as an additional therapeutic agent

Levofloxacin acts by inhibiting two bacterial enzymes that control the topological state of DNA: DNA gyrase, encoded by the genes gyrA and gyrB, and topoisomerase IV, encoded by the genes parC and parE (grlA and grlB in S. aureus)