incidence of adenovirus infections in pediatric … · • s.c. oncoematologia pediatrica e centro...
TRANSCRIPT
1
INCIDENCE OF ADENOVIRUS INFECTIONS IN PEDIATRIC AND ADULT ALLOGENEIC
HEMATOPOIETIC CELL TRANSPLANT RECIPIENTS IN EUROPE
Sebastian Voigt,1 Cécile Pochon,2 Kanchan Rao,3Antonio Pérez-Martínez,4 Marco Zecca,5 Enrikas Vainorius,6 Tom Brundage,6
Artak Khachatryan,7 Essy Mozaffari,6 Garrett Nichols6
1Charité-Universitätsmedizin Berlin, Department of Pediatric Oncology/Hematology/Stem Cell Transplantation, Berlin, Germany; 2University Hospital of Nancy, Allogeneic Hematopoietic Stem Cell Transplantation Unit, Department of Hematology, Vandoeuvre-lès-Nancy, France;
3Great Ormond Street Hospital for Children NHS Foundation Trust, London, United Kingdom; 4Hospital Universidad Autónoma de Madrid, Madrid, Spain;
5Fondazione IRCCS Policlinico San Matteo, Pediatric Hematology/Oncology, Pavia, Italy; 6Chimerix, Durham, NC, United States;
7Analytica-Laser, London, United Kingdom

Disclosures
SV, CP, KR, APM, and MZ are investigators in the AdVance study sponsored by Chimerix
EV, TB, EM, and GN are employees of the study sponsor, Chimerix
AK is an employee of Analytica-Laser, a research consultancy who conducted the study on behalf of the sponsor, Chimerix
2

Allo-HCT recipients are at increased risk of viral infection
Viral infections may lead to life-threatening conditions that further complicate the management of allogeneic-hematopoietic cell transplant (allo-HCT) recipients1,2
Pediatric allo-HCT patients are at particularly high risk for development of adenovirus (AdV) infections2
Current evidence regarding AdV epidemiology after allo-HCT is generally limited to single-center studies2,3
3
1Lin R and Liu Q, J Hematol Oncol. 2013;6:94. 2Lion T. Clin Microbiol Rev. 2014;27:441-62. 3Ison M. Clin Infect Dis. 2006;43:331-9.

The AdVance study AdVance is a retrospective, multicenter,
multinational study of the incidence, management, and clinical outcomes of AdV infection in allo-HCT recipients
• Data were from transplants between January 2013 and September 2015 at participating centers
• Quantitative and qualitative data were extracted for AdV infection, AdV viremia,and AdV viremia ≥1000 copies/mL within 6 months of transplanto Results were stratified by age
(pediatric [<18 years] vs adult)
4
10
12
9
10
17
1
50 centers in total

Objectives
As part of the AdVance study, the incidence of AdV infection was evaluated in pediatric and adult allo-HCT recipients
Other presentations of AdVance data at EBMT 2018:• The next presentation will share data on the outcomes of AdV infection
• Two posters are also presenting AdVance results today:
o B043 shares results of a practice patterns survey
o B073 presents the impact of AdV infection on hospitalization duration among pediatric allo-HCT recipients
5

Baseline characteristics for pediatric patients
6
Sex Male 1099 (63%)
Age Median years 7
Underlying condition
Malignant 1111 (64%)
Non-malignantimmunodeficient 427 (25%)
Non-malignant immunocompetent 200 (11%)
Graft type
Bone marrow 934 (54%)
Peripheral blood stem cell 549 (31%)
Cord blood 255 (15%)
Donor type1
Matched-related 490 (28%)
Matched-unrelated 701 (40%)
Mismatched 179 (10%)
Haploidentical 270 (15%)
ConditioningMyeloablative 1481 (85%)
Non-myeloablative 257 (15%)
T-cell depletion
Ex-vivo 283 (16%)
Serotherapy (ATG) 753 (43%)
Serotherapy (Campath) 252 (15%)
None 450 (26%)
Patients were from centers in Italy (431 patients), UK (388), Spain (324), France (214), Germany (214), Netherlands (91), and Czech Republic (76)
n recipients (%), unless otherwise stated. 1Non-exclusive categories
Allo-HCT recipients n=1738
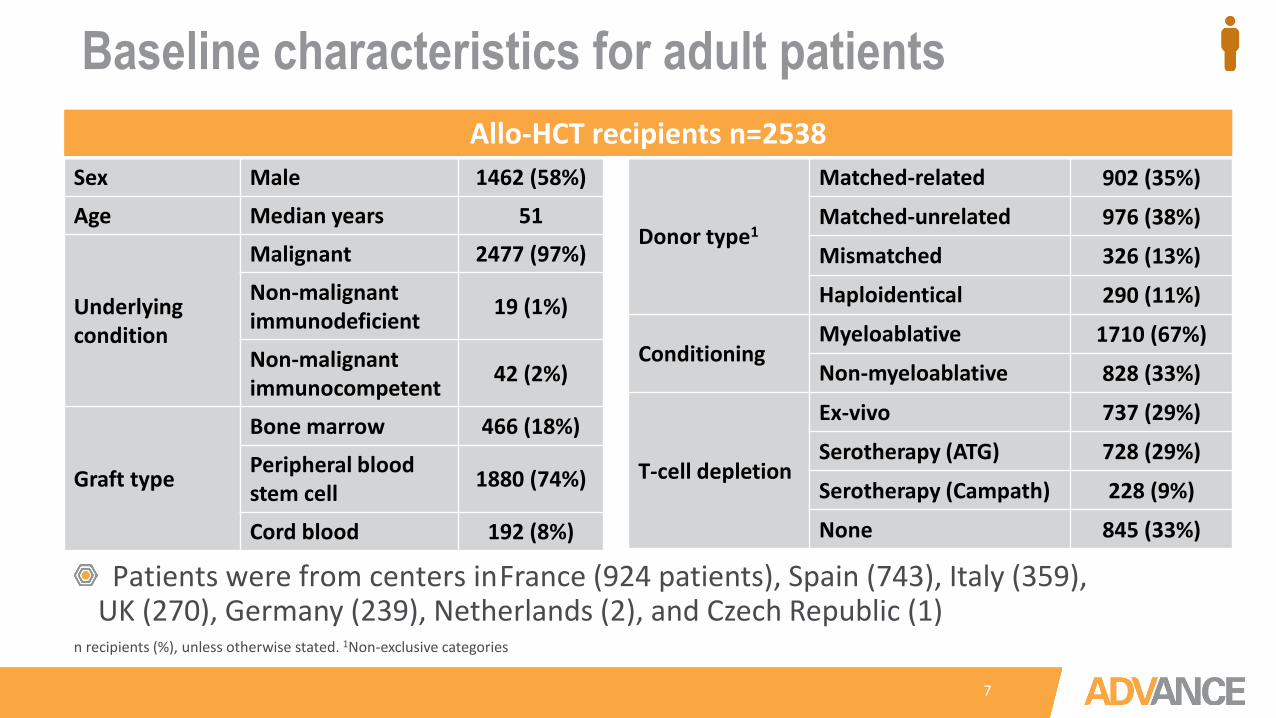
Baseline characteristics for adult patients
7
n recipients (%), unless otherwise stated. 1Non-exclusive categories
Sex Male 1462 (58%)
Age Median years 51
Underlying condition
Malignant 2477 (97%)
Non-malignantimmunodeficient 19 (1%)
Non-malignant immunocompetent 42 (2%)
Graft type
Bone marrow 466 (18%)
Peripheral blood stem cell 1880 (74%)
Cord blood 192 (8%)
Donor type1
Matched-related 902 (35%)
Matched-unrelated 976 (38%)
Mismatched 326 (13%)
Haploidentical 290 (11%)
ConditioningMyeloablative 1710 (67%)
Non-myeloablative 828 (33%)
T-cell depletion
Ex-vivo 737 (29%)
Serotherapy (ATG) 728 (29%)
Serotherapy (Campath) 228 (9%)
None 845 (33%)
Patients were from centers in France (924 patients), Spain (743), Italy (359), UK (270), Germany (239), Netherlands (2), and Czech Republic (1)
Allo-HCT recipients n=2538

Pediatric allo-HCT recipientsn=1738
Any AdV infection1
n=558 (32%)
AdV viremia1
n=395 (23%)
AdV viremia ≥1000 copies/mL1
n=241 (14%)≥1000
1 in 3 pediatric HCT recipients had an AdV infection
8
1Within 6 months of transplant
93% (519/558) of AdV infections were identified as part of routine screening practices
• See poster B043 for more details on practice patterns
Less than half of patients with AdV infection had viremia ≥1000 copies/mL

2 in 5 had a concurrent dsDNA viral infection
Of 241 pediatric allo-HCT recipients with AdV viremia ≥1000 copies/mL:• 66% had ≥1 concurrent infection (bacterial/fungal/viral)1
• 27% had CMV coinfection1
9
dsDNA viral coinfection1
n=241CMV 65 (27%)EBV 42 (17%)BKV 22 (9%)CMV, EBV, and/or BKV 103 (43%)
≥1000
n recipients (%). CMV, Cytomegalovirus; EBV, Epstein–Barr virus; BKV, BK virus. 1At the time of first AdV infection identification. Non-exclusive categories

Adult allo-HCT recipientsn=2538
Any AdV infection1
n=141 (6%)
AdV viremia1
n=77 (3%)
AdV viremia ≥1000 copies/mL1
n=39 (2%)
6% of adult HCT recipients had an AdV infection
10
1Within 6 months of transplant
≥1000
72% (101/141) of AdV infections were identified as part of routine screening practices
• See poster B043 for more details on practice patterns

2 in 3 had a concurrent dsDNA infection
Of 39 adult allo-HCT recipients with AdV viremia ≥1000 copies/mL:• 79% had ≥1 concurrent infection (bacterial/fungal/viral)1
• Half (51%) had CMV coinfection1
11
dsDNA viral coinfection1
n=39CMV 20 (51%)EBV 9 (23%)BKV 9 (23%)CMV, EBV, and/or BKV 26 (67%)
n recipients (%). CMV, Cytomegalovirus; EBV, Epstein–Barr virus; BKV, BK virus. 1At the time of first AdV infection identification. Non-exclusive categories
≥1000

Pediatric Adult
Median time to first AdV viremia ≥1000 copies/mL: 26 days (IQR: 13, 56)
Median time to first AdV viremia ≥1000 copies/mL: 61 days (IQR: 33, 91)
AdV viremia ≥1000 copies/mL develops more quickly in pediatric patients
12
IQR, interquartile range (1st, 4th)
≥1000
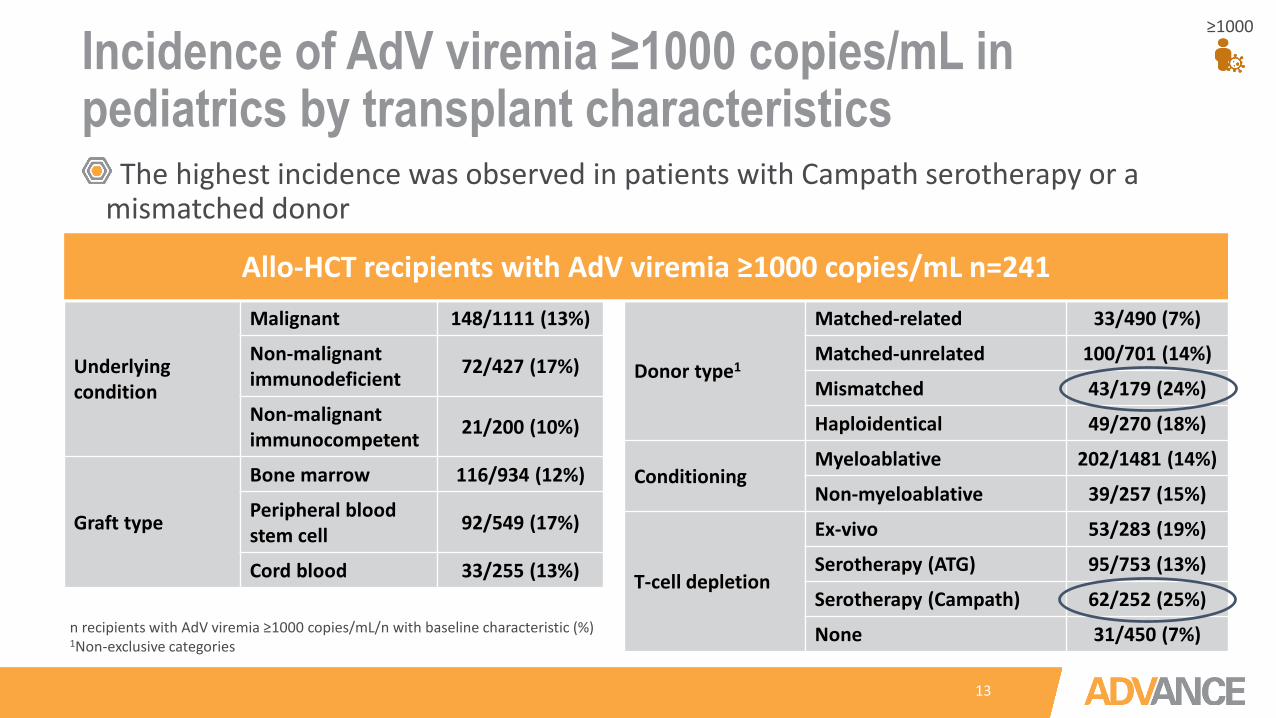
Incidence of AdV viremia ≥1000 copies/mL in pediatrics by transplant characteristics
13
The highest incidence was observed in patients with Campath serotherapy or a mismatched donor
Pediatric allo-HCT recipients with AdV viremia (≥1000 copies/mL); n=241
Underlying condition
Malignant 148/1111 (13%)
Non-malignantimmunodeficient 72/427 (17%)
Non-malignant immunocompetent 21/200 (10%)
Graft type
Bone marrow 116/934 (12%)
Peripheral blood stem cell 92/549 (17%)
Cord blood 33/255 (13%)
Pediatric allo-HCT recipients with AdV viremia (≥1000 copies/mL); n=241
Donor type1
Matched-related 33/490 (7%)
Matched-unrelated 100/701 (14%)
Mismatched 43/179 (24%)
Haploidentical 49/270 (18%)
ConditioningMyeloablative 202/1481 (14%)
Non-myeloablative 39/257 (15%)
T-cell depletion
Ex-vivo 53/283 (19%)
Serotherapy (ATG) 95/753 (13%)
Serotherapy (Campath) 62/252 (25%)
None 31/450 (7%)n recipients with AdV viremia ≥1000 copies/mL/n with baseline characteristic (%) 1Non-exclusive categories
≥1000
Allo-HCT recipients with AdV viremia ≥1000 copies/mL n=241
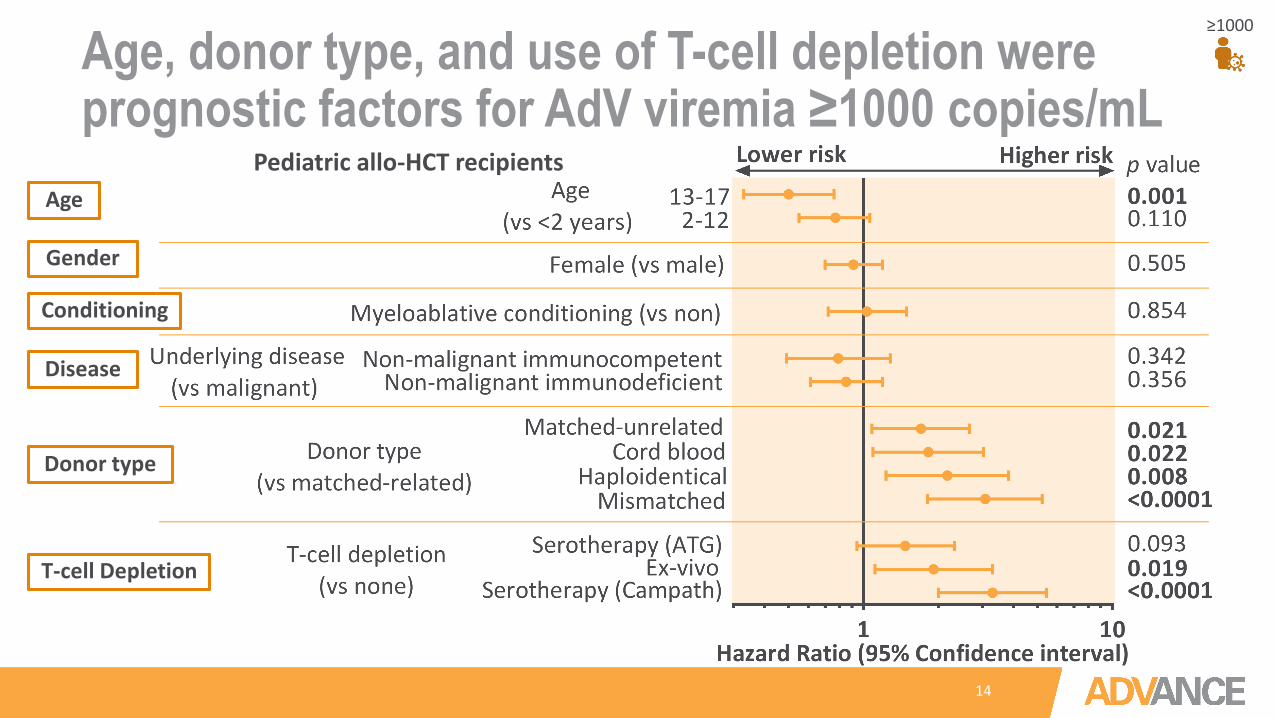
Age, donor type, and use of T-cell depletion were prognostic factors for AdV viremia ≥1000 copies/mL
14
≥1000
Pediatric allo-HCT recipientsAge
Disease
Donor type
T-cell Depletion
Conditioning
Gender

Incidence of AdV viremia ≥1000 copies/mL in adults by transplant characteristics
15
The highest incidence was observed in those with Campath serotherapy
Adult allo-HCT recipients with AdV viremia (≥1000 copies/mL); n=39
Underlying condition
Malignant 38/2477 (2%)
Non-malignantimmunodeficient 1/19 (5%)
Non-malignant immunocompetent 0/42 (0%)
Graft type
Bone marrow 6/466 (1%)
Peripheral blood stem cell 29/1880 (2%)
Cord blood 4/192 (2%)
Adult allo-HCT recipients with AdV viremia (≥1000 copies/mL); n=39
Donor type1
Matched-related 8/902 (1%)
Matched-unrelated 19/976 (2%)
Mismatched 10/326 (3%)
Haploidentical 0/290 (0%)
ConditioningMyeloablative 21/1710 (1%)
Non-myeloablative 18/828 (2%)
T-cell depletion
Ex-vivo 9/737 (1%)
Serotherapy (ATG) 8/728 (1%)
Serotherapy (Campath) 16/228 (7%)
None 6/845 (1%)n recipients with AdV viremia ≥1000 copies/mL/n with baseline characteristic (%) 1Non-exclusive categories
≥1000
Allo-HCT recipients with AdV viremia ≥1000 copies/mL n=39

Age, donor type, and use of T-cell depletion were prognostic factors for AdV viremia ≥1000 copies/mL
16
≥1000
Stepwise reduction in risk with increasing age
Adult and pediatric allo-HCT recipients
Age
Conclusions
17
Pediatric allo-HCT recipients are screened routinely, with 1 in 3 (32%) having an identified AdV infection in the 6 months following their transplant23% of recipients developed AdV
viremiaJust less than half of those with an
AdV infection (14%) had AdV viremia ≥1000 copies/mL
• dsDNA viral coinfection was common
Adult allo-HCT recipients are less routinely screened6% of recipients had an identified AdV
infection in the 6 months following their transplant3% developed AdV viremia2% had AdV viremia ≥1000 copies/mL • dsDNA viral coinfection was common
Pediatric Adult

Conclusions
18
AdultPediatric and adult
Patient age was an independent predictor of AdV viremia ≥1000 copies/mL in the 6-months following allo-HCT
• T-cell depletion and donor type are also independent risk factors
These results suggest a need for re-examination of screening approaches, particularly for younger and at-risk adults

19
SPAIN (12)• Hospital Universitario y Politécnico La Fe (2)• Hospital Universitario 12 de Octubre• Hospital Universitario La Paz• Hospital Universitario de Salamanca• Hospital Universitario Vall d'Hebrón• Hospital de la Santa Creu i Sant Pau (2)• Hospital Universitario Reina Sofía• Hospital Regional Universitario de Málaga• Hospital Infantil Universitario Niño Jesús• Hospital General Universitario Morales
Meseguer
UK (10)• Royal Manchester Children's
Hospital• Bristol Royal Children’s
Hospital• Sheffield Children's Hospital• St. James's University
Hospital and The General Infirmary, Leeds
• Great North Children's Hospital, Newcastle
• Great Ormond Street Hospital, London
• University College London Hospitals,
• University Hospital of Wales Cardiff
• The Royal Marsden Hospital, London
• Birmingham Children’s Hospital
The NETHERLANDS (1)• UMC Utrecht
GERMANY (7)• Charité Campus Virchow Klinikum• J. W. Goethe Universität• Medizinische Hochschule Hannover• Universitätsklinikum Jena• Universitätsklinikum Köln• Universitätsklinik Tübingen• Klinikum der Universität München (LMU)
CZECH REPUBLIC (1)• Hospital Motol, Praha
ITALY (9)• Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico Centro Trapianti Midollo Osseo, Milano• Hospital Casa Sollievo Sofferenza, San Giovanni Rotondo• Azienda Ospedale ‘Riuniti e Morelli’ Bianchi-Melacrino Centro Unico Regionale Trapianti Cellule
Staminali e Terapia Cellulare, Reggio Calabria • Pediatric Hematology/Oncology Department Policlinico San Matteo, Pavia
• Ospedale Civile Centro Trapianti Midollo Osseo Dip. Ematologia Medicina Trasfusionale e Biotecnologie, Pescara
• Pediatric Hematology/Oncology Department San Gerardo Hospital, Monza• S.C. Oncoematologia Pediatrica e Centro Trapianti Regina Margherita, Torino• Oncoematologia e TMO, Ospedale 'La Maddalena' Palermo• Ospedale Bambin Gesù-Dip. Oncoematologia Pediatrica e Medicina Transfusionale, Roma
FRANCE (10)• Robert Debré
Hospital, Paris• CHU Angers• Institut of
Hematology, Lyon• CHU Nancy• CHU Montpellier
• CHU Bordeaux• CHU Lyon• CHU Nantes• Saint Louis Hospital,
Paris• CHU Nice
The AdVance centers