multi-factorial forensic age estimation
TRANSCRIPT

MULTI-FACTORIAL FORENSIC AGE ESTIMATION
Combining magnetic resonance imaging of the third molars, the left wrist and both clavicles
JANNICK DE TOBEL


march 2019 A dissertation submitted to Ghent University and Catholic University Leuven
in partial fulfilment of the requirements for the Joint Degree of Doctor in Health Sciences and Biomedical Sciences, respectively.
co-promoter Prof. Dr. Constantinus Politis
promoters
Prof. Dr. Koenraad Verstraete Prof. Dr. Patrick Thevissen
MULTI-FACTORIAL FORENSIC AGE ESTIMATION
Combining magnetic resonance imaging of the third molars, the left wrist and both clavicles
JANNICK DE TOBELUGent 20051808 KU Leuven 0652217

Table of contents
promoters
Prof. Dr. Koenraad Verstraete Universiteit Gent Prof. Dr. Patrick Thevissen Katholieke Universiteit Leuven
co-promoter
Prof. Dr. Constantinus Politis Katholieke Universiteit Leuven
superv isory committee
Prof. Dr. Marc De Leeuw (postuum) Universiteit Gent Em. Prof. Dr. Marc Espeel Universiteit Gent Prof. Dr. Reinhilde Jacobs Katholieke Universiteit Leuven Prof. Dr. Wim Van de Voorde Katholieke Universiteit Leuven
examinat ion committee
Prof. Dr. Maria Cadenas de Llano Pérula Katholieke Universiteit Leuven Prof. Dr. Jan Casselman Universiteit Gent, Universiteit Antwerpen Prof. Dr. Karel Deblaere Universiteit Gent Prof. Dr. Helen Liversidge Queen Mary University of London Prof. Dr. Luc Marks Universiteit Gent Prof. Dr. Luc Martens (chair public defence) Universiteit Gent Prof. Dr. Johan Vande Walle (chair internal defence) Universiteit Gent Dr. Martin Urschler Ludwig Boltzmann Institut für Klinisch-Forensische Bildgebung Graz
ISBN 9789082552522 graphic design by Janine Kopatz www.janinekopatz.com
© Jannick De Tobel, 2019
All rights reserved. No part of this thesis may be reproduced or transmitted in any form or by any means, without prior written permission of the authors, or when appropriate, from the publishers of the publications.

Preface ................................................................................................................................................................ 7List of abbreviations ......................................................................................................................................... 9
PART 1 InceptionChapter 1 General introduction: Forensic age estimation now and in the future ............................ 12Chapter 2 Study objectives and design ................................................................................................... 30
PART 2 Age estimation based on third molars MRIChapter 3 Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation....................................................................................... 38Chapter 4 Forensic age estimation based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging ................................................................... 54Chapter 5 Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging ......................................................................... 72Chapter 6 Magnetic resonance imaging of third molars in forensic age estimation: comparison of the Ghent and Graz protocols focusing on apical closure ..................... 100
PART 3 Age estimation based on wrist MRIChapter 7 Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fitsall staging technique and age estimation model apply? ............................. 118
PART 4 Age estimation based on clavicle MRIChapter 8 The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation .................................................................................................. 144Chapter 9 Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation ..................................................................................... 164
PART 5 Age estimation based on multi-factorial MRIChapter 10 The use of magnetic resonance imaging in forensic age estimation of living children and subadults systematically reviewed .................................................... 188Chapter 11 Multi-factorial age estimation: a Bayesian approach combining dental and skeletal magnetic resonance imaging .......................................................................... 232
PART 6 ConclusionChapter 12 General discussion: New state of the art and future prospects ....................................... 258
Table of contents
Table of contents

PART 7 EpilogueSummary ....................................................................................................................................................... 281Samenvatting ................................................................................................................................................ 285Conflict of interest statement ...................................................................................................................... 289Scientific acknowledgements ...................................................................................................................... 291Personal contribution .................................................................................................................................. 295Personal acknowledgements ....................................................................................................................... 297Persoonlijk dankwoord ............................................................................................................................... 303Curriculum vitae .......................................................................................................................................... 309
Table of contents

7
At the inception of this PhD project, in December 2011, the migration crisis of 2015 was still pending. In the course of previous years, author-ities increasingly called upon medical professionals to estimate age in unaccompanied minor refugees. Meanwhile, age estimation in sports also gained interest to ensure fair play. However, the increasing demand for age estimation raised concerns with respect to its ethical justification and accuracy. Different nongovernmental organisations and profession-al associations expressed their concerns and even stated that medical professionals should not be implicated in age estimation. Actually, pro-fessionals who were conducting age estimation shared those concerns, and in response launched new research to try to optimise age estimation practice. In this climate, which is elaborated in Part 1 of this thesis, the current PhD project germinated.
This PhD project was one of those responses to the concerns regard-ing age estimation, along with several other European research projects. Founded on years of experience in this field, Ghent University, Catholic University Leuven and the Netherlands Forensic Institute joined forces to develop a new approach. Using magnetic resonance imaging (MRI) to study the development of different anatomical sites in adolescents and young adults aimed at countering several concerns concurrently. Given that several research groups simultaneously started this type of research, an ethical, reliable and accurate approach to estimate age seemed im-minent. The major asset of the MRI approach lies in its ability to inte-grate information from different anatomical sites in the same individ-ual, which allows deriving one statistically sound multi-factorial age estimate, instead of several single age estimates. This was never reached using radiographs – which is still the gold standard imaging modality in age estimation – because reference studies that combined information were never conducted and are now considered unethical.
To date, several research groups have published their single site MRI approach and results for age estimation. We have studied three anatom-ical sites, which are consecutively elaborated upon in Parts 2 to 4 of this thesis. Remarkably, the several research groups independently came up with very similar imaging techniques, which might facilitate the next
PrefaceGhent, October 18th, 2018
8
step: creating reference studies of sufficiently large sample sizes. Whether or not MRI data can be pooled to reach this goal, was studied in Chapter 10.
But single site MRI does not suffice. To provide a nuanced age es-timation, the multi-factorial MRI approach seems to be the way to go, especially now that two groups – including ours, in Chapter 11 – have independently demonstrated that the multi-factorial MRI approach out-performs all single site approaches.
Although none of the research groups had a validated comprehensive MRI approach ready for age estimation by 2015, Sweden has used knee MRI in practice to estimate age in unaccompanied minors. Moreover, hand/wrist MRI has been used in football tournaments. With these ini-tial steps taken, and knowing that more European groups are expected to report their multi-factorial results, age estimation practice might be off to a new start, countering the disadvantages of the current practice.
Preface

9
List of abbreviations
μCT micro computed tomographyμMRI micro magnetic resonance imagingρerror correlation coefficient between the errors of two modelsAGFAD Arbeitsgemeinschaft für Forensische AltersdiagnostikAUC area under the curveCBCT cone-beam computed tomographyCI confidence intervalCISS constructive interference in the steady stateCT computed tomographyDCNN deep convolutional neural networkEASO European Asylum Support OfficeEC ethics committeeEND end stageEU-28 28 Member States of the European UnionFIFA Fédération Internationale de Football AssociationFPR false positive rate (minors who are wrongfully classified as adults)FS fat saturationFSE fast spin echoICC intra-class correlation coefficientIND immigration and naturalisation serviceIPR in-plane resolutionIQR interquartile rangeLO lateral obliqueM3 third molarMAE mean absolute errorMe medianMFA multi-factorial age estimationML maximum likelihoodMPR multi-planar reconstructionMRI magnetic resonance imaging
N number of participants or anatomical structuresNA not applicableNFI Netherlands forensic instituteNPV negative predictive valuePA postero-anteriorPI prediction intervalPICOS population/participants, intervention, control, outcome, study typePPV positive predictive valuer Spearman correlation coefficientR² Coefficient of determinationRMSE root mean squared errorROC receiver operator characteristicRRF regression random forestSAR specific absorption rateSD standard deviationSE (Ch. 7) T1-weighted spin echo MR-sequenceSE (Ch. 5 & 12) standard errorSens sensitivity (proportion of correctly classified adults)SNR signal-to-noise ratioSSA single site age estimationSWIFT sweep imaging with Fourier TransformationTE echo timeTFS threefold stratification signTR repetition timeTSE turbo spin echoUMR unaccompanied minor refugeeUMR unaccompanied minor refugeesUTE ultrashort echo timeVIBE T1-weighted gradient echo volumetric interpolated breath-hold examination MR-sequencey yearsZTE zero echo time


11
PART 1
Inception

12
CHAPTER 1
PARTS OF TH I S CHAPTER WERE PUBL I SHED AS :
De Tobel J, de Haas MB, van Wijk M, Verstraete KL, Thevissen PW. De toekomst van forensische leeftijdsschatting bij levende adolescenten en jongvolwassenen: magnetische resonantie beeldvorming en automatisering. In: Aps JKM, Boxum SC, De Bruyne MAA, Jacobs R, van der Meer WJ, Nienhuijs MEL, eds. Het Tandheelkundig Jaar 2018. Houten: Bohn Stafleu van Loghum, 2018; p. 1-19. [Dutch]
CONS IDERAT IONS DESCR I BED IN TH I S CHAPTER WERE PARTLY
P RESENTED AT THE FOLLOWING CONFERENCE :
De Tobel J, de Haas M, van Wijk M, Phlypo I, Verstraete K, Thevissen P. The future of age estimation: living up to the ethical demands? The importance of dental ethics and law, International Dental Ethics and Law Society (IDEALS); Amsterdam, The Netherlands; August 23, 2018.

13
Forensic age estimation now and in the future
GENERAL INTRODUCT ION
Current practice
Forensic age estimation in living adoles-cents and young adults is used in crim-inal, civil and asylum procedures. The result of the procedure is twofold. First, a point prediction of age is given with an indication of the uncertainty (e.g. 95% confidence interval). Second, the proba-bility is given that the examined person has reached a specific legally relevant age threshold, which in most countries lies between 14 and 22 years of age [52]. Moreover, in sports, age estimation is used to make sure athletes participate in the right age category [9].
Asylum procedures
Immigration into Europe rapidly in-creased during the last decade, reaching a peak in 2015, which was called the migra-tion crisis. In that year, almost 1.3 million asylum applications were registered in the 28 Member States of the European Union (EU-28) [17]. This was the highest num-ber since the turn of the millennium. Un-fortunately, human traffickers saw this as an opportunity to increase their activities. Upon request, they would also provide falsified identification documents. Ref-ugees might want to appear older, e.g. to avoid separation from adults with whom they have arrived, or to hide child brides. On the other hand, refugees might want to appear younger, e.g. to ensure protec-tion and judicial guiding.
With 39.000 asylum applicants in 2015, Belgium was rated eighth in the Europe-an Union ranking of countries with high refugee immigration rates [17]. The Neth-erlands were seventh, with 43.000 appli-cations, and Germany topped the list with nearly 441.800 applications. Overall 29% of these refugees were minors, i.e. aged less than 18. Almost 88.700 applications in the EU-28 were from unaccompanied minor refugees [17].
Asylum procedure with age estimation in Belgium
Table 1.1 shows absolute numbers for applicants in Belgium from 2008 to 2018 [21]. The asylum procedure for unaccom-panied minor refugees (UMR) differs from the one for adults. The Guardianship Service appoints a guardian to the UMR, who ensures appropriate housing, social and judicial protection, and psychologi-cal counselling [20]. When no identifying documents are at hand or when the police or the Foreigners Affairs Office doubt the UMR’s age, a medical age estimation can be requested [19]. The Belgian govern-ment can consult several hospitals to per-form age estimation, in order to guarantee a rapid clarification about the real age of the young refugee [59]. Unfortunately, no uniform national guidelines have been established regarding the age estimation procedure, leading to different approach-es in different hospitals [19]. In Leuven University Hospital, the triple test is per-

14
formed, which can render two scenarios [64, 65]:
1 The dentition is assessed on a pano-ramic radiograph, and the left hand/wrist is assessed on a postero-ante-rior (PA) radiograph. If the perma-nent teeth (except third molars) or the hand/wrist bones are still devel-oping, then these radiographs suf-fice.
2 If the permanent teeth (except third molars) and the hand-wrist bones are mature, then both clavicles are assessed on either a PA radiograph or a 10-15° lateral oblique (LO) ra-diograph (Figures 1.1 to 1.3).
Developmental stages are allocated to the anatomical structures and based on those developmental data, a point prediction of age is given, with a 95% confidence inter-val (CI) and the probability that the age of 18 has been reached. To date, this is the most scientifically valid approach, com-
plying with the recommendations of the international Study Group on Forensic Age Diagnostics (Arbeitsgemeinschaft für Forensische Altersdiagnostik, AGFAD) [51, 52].
However, in Belgium, every institute that performs age estimation can choose freely which anatomical structures, im-aging modalities, staging techniques and age estimation methods they want to use. This might cause conflicting results, which hinder the asylum procedure [22].
Asylum procedure with age estimation in the Netherlands
In the Netherlands, the asylum procedure for UMR differs from the one in Belgium. The guardian is appointed by NIDOS (child protection service for refugees) and ensures the well-being of the UMR. Throughout the entire procedure, judicial advice is provided. The asylum applica-tion is handled by the Immigration and Naturalisation Service (IND), who re-
De Tobel J. Multi-factorial forensic age estimation. Chapter 1: 12-28.
TABLE 1 . 1 — ABSOLUTE NUMBERS FOR ASYLUM APPLICANTS IN BELGIUM. Considering 2018, numbers were
only avai lable unt i l the end of September. Note that the number of adults and minors do not add up to
the number of age est imations, s ince the results of some age examinations were not avai lable yet .
YEAR SELF-DECLARED UNACCOMPA-
NIED MINOR REFUGEES
NUMBER OF AGE
ESTIMATIONS
ADULT MINOR
2008 1887 401 245 156
2009 2501 441 322 1 19
2010 2510 390 324 66
201 1 3258 1042 729 313
2012 281 1 953 689 264
2013 2090 666 503 163
2014 1780 537 370 167
2015 5047 1 187 814 373
2016 2927 1296 902 394
2017 31 1 1 675 479 196
2018 3075 694 479 189

15
General introduction: Forensic age estimation now and in the future
quests an age estimation if necessary. Contrary to Belgium, age estimation is performed centralised by the Netherlands Forensic Institute (NFI), according to a uniform protocol [38]. No panoramic dental radiograph is obtained, while the hand/wrist and clavicle radiographs are [2]. Moreover, no point prediction of age is given, but only the possibility to be an adult is discussed. Therefore, instead of allocating developmental stages, it is only assessed whether or not the bone is fully mature. Thus, several scenarios are pos-sible. First, a PA radiograph of the left hand/wrist is obtained.
1 If this radiograph demonstrates that the distal radius is not mature, no radiographs of the clavicles are ob-tained. A developing radius is con-sidered to imply a high probability for the clavicles not to be mature either. Thus, minority cannot be ex-cluded.
2 If the hand/wrist bones are mature, one PA radiograph of the sternal ends of the clavicles is obtained.
a If the radiograph demonstrates that the clavicles are not mature, no fur-ther radiographs are obtained, since minority cannot be excluded.
b If the radiograph does not clearly demonstrate that the clavicles are not mature, then LO radiographs of both clavicles are obtained. If the mature clavicles are confirmed on all three radiographs, this is consid-ered proof of adulthood.
Thus, an UMR is only considered as an adult if the left hand/wrist as well as both clavicles are considered mature.
Asylum procedure with age estimation in an international perspective
The disparities between Belgian institutes and between the Belgian and Dutch ap-proaches demonstrate the wide variety in age estimation procedures. Table 1.2 summarises the different parts of the age estimation procedure that are applied throughout Europe. The table is based on a report by the European Asylum Sup-port Office (EASO) [16], and was updated through personal communication with professionals [4, 6]. Additionally, the pro-cedures in Colombia [50], Indonesia [36], Japan [28], Thailand [46], and the USA [40, 44] were displayed.
This variety in procedures reflects the uncertainty inherent to age estimation, with no approach clearly outperforming another. This could be attributed to the lack of information on how to combine different age estimation results from dif-ferent sites. The variety in procedures also reflects how different authorities feel about ionising radiation, which is banned for age estimation in some coun-tries.
Sports
Youth sports competitions are organized in various age categories from as low as under-13 up to under-21 [15]. Unfortu-nately, sometimes it is suspected that the chronological age of the participating players does not correspond to the age stated on official documents [15]. In some

16
FIGURE 1 . 1 — RADIOGRAPHS AND CORRESPONDING MRI OF 17-YEAR-OLD MALES. F igures a and f- i are from
the same par t ic ipant , whi le Figures b-e and j- l are from another par t ic ipant .
De Tobel J. Multi-factorial forensic age estimation. Chapter 1: 12-28.

17
a Panoramic radiograph. Root development
in the lower third molars can easi ly be
assessed (arrows). Upper third molars are
harder to assess due to superposit ion
(arrowheads).
b Postero-anterior radiograph of the c lav-
ic les’ sternal ends (arrowheads). The
assessment is impossible due to superposi-
t ion.
c, d Lateral obl ique radiograph of the r ight
and left c lavic le’s sternal ends, respect ive-
ly. In between the arrowheads, the min-
eral ised secondary growth centre can be
discerned.
e Postero-anterior radiograph of the left
wrist . The physeal plates of the radius and
ulna are not fu l ly br idged (arrowheads).
f Sagittal MR-image of the palatal root of 18
(arrowhead).
g Sagittal MR-image of the palatal root of
28 (arrowhead). The roots of 38 are also
depicted (arrow), but in this s l ice, the
apices are not included, because they are
s ituated more buccal ly.
h Sagittal MR-image of the buccal roots of 18
(arrowhead) and the roots of 48 (arrow).
i Sagittal MR-image of the buccal roots of
28 (arrowhead) and the root apices of 38
(arrow).
j Anterior coronal MR-image of the c lavic les’
sternal ends. No growth centre is depicted.
k Poster ior coronal MR-image of the c lavi-
c les’ sternal ends. In it iated growth centre
mineral isat ion is depicted bi lateral ly be-
tween the arrows.
l Coronal MR-image of the left wrist . The
physeal plates of the radius and ulna are
not fu l ly br idged (arrowheads).
General introduction: Forensic age estimation now and in the future

18
FIGURE 1 .2 — RADIOGRAPHS AND CORRESPONDING MRI OF A 24-YEAR-OLD (A AND F-I ) AND 21-YEAR-OLD
(B-E AND J-L) MALE.
De Tobel J. Multi-factorial forensic age estimation. Chapter 1: 12-28.

19
a Panoramic radiograph. Root development
in the lower third molars can easi ly be
assessed (arrows). Upper third molars are
not assessable due to superposit ion (ar-
rowheads).
b Postero-anterior radiograph of the c lav-
ic les’ sternal ends (arrowheads). The
assessment is impossible due to superposi-
t ion.
c, d Lateral obl ique radiograph of the r ight
and left c lavic le’s sternal ends, respect ive-
ly. In between the arrowheads, the min-
eral ised secondary growth centre can be
discerned. The del ineation of the growth
centre and the degree of br idging in the
physeal plate are very unclear.
e Postero-anterior radiograph of the left
wrist . The physeal plates of the radius and
ulna are ful ly br idged (arrowheads).
f Sagittal MR-image of the palatal root of 18
(arrowhead).
g Sagittal MR-image of the palatal root of
28 (arrowhead).
h Sagittal MR-image of the buccal roots of 18
(arrowhead) and the roots of 48 (arrow).
I i Sagittal MR-image of the buccal roots of
28 (arrowhead) and the roots of 38 (ar-
row).
j Anterior coronal MR-image of the c lavic les’
sternal ends. In it iated bridging of the phy-
seal plate is depicted bi lateral ly between
the arrows.
k Poster ior coronal MR-image of the c lavi-
c les’ sternal ends. In it iated bridging of the
physeal plate is depicted bi lateral ly be-
tween the arrows.
l Coronal MR-image of the left wrist . The
physeal plates of the radius and ulna are
ful ly br idged (arrowheads).
FIGURE 1 .3 — RADIOGRAPHS AND CORRESPONDING MRI OF A 30-YEAR-OLD FEMALE.
a Postero-anterior radiograph of the c lav-
ic les’ sternal ends (arrowheads). The as-
sessment of the left c lavic le is impossible
due to superposit ion.
b, c Lateral obl ique radiograph of the r ight
and left c lavic le’s sternal ends, respect ive-
ly (arrowheads). Both c lavic les are ful ly
mature, i .e. their physeal plates are com-
pletely br idged.
d Coronal MR-image of the c lavic les’ sternal
ends (arrowheads). They are ful ly mature.
General introduction: Forensic age estimation now and in the future
20
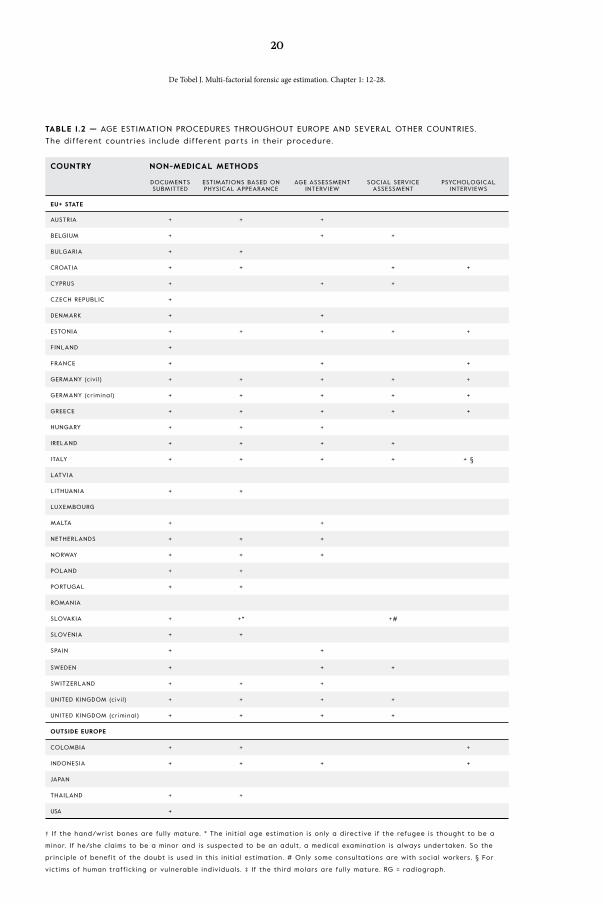
TABLE 1 .2 — AGE ESTIMATION PROCEDURES THROUGHOUT EUROPE AND SEVERAL OTHER COUNTRIES.
The different countr ies inc lude different par ts in their procedure.
† If the hand/wrist bones are ful ly mature. * The in it ia l age est imation is only a direct ive i f the refugee is thought to be a
minor. If he/she claims to be a minor and is suspected to be an adult , a medical examination is always under taken. So the
principle of benefit of the doubt is used in this in it ia l est imation. # Only some consultat ions are with social workers. § For
vict ims of human traff ick ing or vulnerable indiv iduals . ‡ If the third molars are ful ly mature. RG = radiograph.
COUNTRY NON-MEDICAL METHODS
DOCUMENTS SUBMITTED
ESTIMATIONS BASED ON PHYSICAL APPEARANCE
AGE ASSESSMENT INTERVIEW
SOCIAL SERVICE ASSESSMENT
PSYCHOLOGICAL INTERVIEWS
EU+ STATE
AUSTRIA + + +
BELGIUM + + +
BULGARIA + +
CROATIA + + + +
CYPRUS + + +
CZECH REPUBLIC +
DENMARK + +
ESTONIA + + + + +
FINLAND +
FRANCE + + +
GERMANY (c iv i l ) + + + + +
GERMANY (cr iminal) + + + + +
GREECE + + + + +
HUNGARY + + +
IRELAND + + + +
ITALY + + + + + §
LATVIA
LITHUANIA + +
LUXEMBOURG
MALTA + +
NETHERLANDS + + +
NORWAY + + +
POLAND + +
PORTUGAL + +
ROMANIA
SLOVAKIA + +* +#
SLOVENIA + +
SPAIN + +
SWEDEN + + +
SWITZERLAND + + +
UNITED KINGDOM (civ i l ) + + + +
UNITED KINGDOM (cr iminal) + + + +
OUTSIDE EUROPE
COLOMBIA + + +
INDONESIA + + + +
JAPAN
THAILAND + +
USA +
De Tobel J. Multi-factorial forensic age estimation. Chapter 1: 12-28.

21
MEDICAL METHODS
DENTAL OBSERVATION PHYSICAL DEVELOPMENT
SEXUAL MATURITY OBSERVATION
HAND/WRIST RADIOGRAPH
CLAVICLES RADIOGRAPH
DENTAL RADIOGRAPH OTHER
+ + + + + Clavic les CT†
+ + + + †
+ + +
+ + + + +
+ + +
+
+ + +
+ + + + +
+ + +
+ + +
+ + +
+ + + + + Clavic les CT†
+ + +
+ + + + Pelvic bone RG
+ + + + +
+ + + + +
+ +
+ +
+ Pelvic bone RG
+ +
+ + +
+ + + +
+ + + Four th r ib RG
+ + + + + Elbow RG
+ + + + †
+ +
+ + Knee MRI
+ + +
+ Clavic les MRI‡
+ + + + +
+
+ + + + + Proximal humerus RG
+ + + + +
+ +
General introduction: Forensic age estimation now and in the future

22
sports, relatively older players may have physical advantages over their younger peers (for example physical strength or endurance). Thus, they might be more likely to be identified as talented. By con-trast, in other sports, relatively younger athletes might be favoured (for example because of more elasticity) [71]. More-over, in some countries births are not meticulously registered, so the exact age of individuals is not known. These age discrepancies impede fair play and might compromise the health and safety of ath-letes (e.g. psychological stress or physi-cal injuries). As a consequence, reliable methods for age estimation are sought [15]. Although radiation exposure is not justifiable or ethically acceptable in these cases, radiographic methods remain the gold standard imaging modalities [15].
Staging techniques and age estimation methods
To register development of anatomical structures that act as age indicators, stages can be allocated based on medical imag-ing. The criteria that define the different stages comprise the staging technique. How those stages relate to age has been reported in reference studies which in-cluded samples of populations of known chronological age. That way, implement-
ing the stages to estimate age comprises an age estimation method. Age estima-tion methods differ in their statistical ap-proach from merely descriptive analysis to advanced statistical modelling. Thus, in case of doubt about the chronological age, it can be estimated by checking how the allocated developmental stages occur in the reference population. Different ref-erence studies are available for different anatomical structures, each with their own staging technique and age estimation method.
Ethically justifiable age estimation
Age estimation gives rise to several ethical concerns. In view of future prospects, two major ethical aspects should be highlight-ed. Firstly, age estimation should strive for the most accurate point prediction, keep-ing the uncertainty interval as narrow as possible. This means that age estimation methods need to comply with the scien-tific state-of-the-art [69]. Still, since den-tal and skeletal development are prone to inter-individual variability, the result will always be an estimation. To date, an age determination is not possible. If and to what extent ethnical background affects development depends on the age indica-tor (dental or skeletal) and remains a sub-
TABLE 1 .3 — EFFECTIVE RADIATION DOSE OF IMAGING FOR AGE ESTIMATION [26, 33, 34, 37, 51 ] .
EXAMINATION EFFECTIVE DOSE (MILLISIEVERT)
Panoramic radiograph 0.009 - 0.026
CBCT upper and lower jaws 0.045 - 0.860
CT maxi l lofacial 0.860 - 1 .500
Hand/wrist radiograph 0.0001
CBCT wrist 0.007 - 0.010
Clavic les radiograph (per radiograph) 0.003 – 0.2
CT clavic les 0.4 – 0.8
De Tobel J. Multi-factorial forensic age estimation. Chapter 1: 12-28.

23
ject of debate [25, 30, 35, 41, 53, 58, 66, 68, 78, 82]. Overall, between-race differences seem inferior to inter-individual differ-ences within the race [31, 65, 66, 68, 73].Furthermore, the use of posteroanterior radiographs of the clavicles’ sternal ends is considered obsolete. Additional lateral oblique radiographs are necessary to de-crease uncertainty about the developmen-tal stage [79, 80]. Some authors have stat-ed that clavicle CT is the only appropriate imaging modality to verify if the age of 18 or 21 has been reached [80]. In particu-lar, CT allows for a high resolution vis-ualisation of mineralised tissues, such as bones and teeth [39]. Therefore, it seems the most appropriate imaging modality for age estimation based on skeletal and dental development.
However, CT interferes with the sec-ond ethical concern: the use of ionising radiation without a medical indication [69], knowing that children and adoles-cents are more susceptible to the carcino-genic effects of ionising radiation [47]. Digital panoramic dental and hand/wrist radiographs only cause a minimal radi-ation exposure, but some authors find the use of CT ethically unacceptable in children (Table 1.3). Since modern tech-niques such as cone beam CT (CBCT) apply lower radiation doses than conven-tional CT [33, 34, 37], they might become ethically justifiable for forensic use in the near future. To date, only one reference study using CBCT for dental age esti-mation in adolescents and young adults has been published [3], while skeletal age estimation based on CBCT has not been studied in this context.
Moreover, in some countries, the use of ionising radiation is prohibited in civil
and asylum procedures [32]. Consequent-ly, several authors stressed the need for reference studies using imaging modal-ities free of ionising radiation [5, 26, 29, 51, 56, 75]. Similarly, in their updated practical guide for age estimation, EASO states that radiation-free medical meth-ods should be considered prior to radia-tion methods [16].
Future prospects
MRI as an alternative or complementary to radiographs
Rationale
The interest in MRI for age estimation originated from the two major disadvan-tages of the current gold standard:
— A radiograph depicts a two-dimen-sional (2D) projection of three-di-mensional (3D) structures, which might mask certain details, imped-ing the most accurate age estima-tion.
— Radiographs require the use of ion-ising radiation.
These disadvantages correspond with the ethical concerns that were discussed ear-lier. Furthermore, as a technique free of ionising radiation, MRI seems more suit-able than ultrasound because interpreting the images is easier and more straightfor-ward to explain to judicial professionals [8]. Moreover, ultrasound does not always allow to visualise the entire anatomical site and anatomical variants might hin-der the assessment [23]. Several research groups are studying the use of MRI for age estimation, in an attempt to develop
General introduction: Forensic age estimation now and in the future

24
a new standard. The studies were inde-pendently initiated around the year 2007, causing the different groups to publish on similar topics at the same time. This raises questions about the different approaches, but also strengthens conclusions, since researchers agree on the essentials of the MRI approach.
Technical aspects of MRI
Image acquisition using radiographs or CT is straightforward, with the emitted X-rays being absorbed or transmitted by the tissues [39]. The relative absorption rate corresponds with the signal intensity in the image, which makes radiographs and CT relatively easy to interpret.
By contrast, image acquisition us-ing MRI is more complex, with radio waves sent out by a powerful magnet in a sequence of very short pulses [39]. Each pulse causes the emission of a responding pulse of radio waves from the tissues. Se-quence parameters can be altered, which alters the signal intensities of different tis-sues to better visualise the tissue or con-dition of interest [39]. Thus, interpreting MRI can be challenging for physicians and dentists. Several key aspects of MRI are essential for a basic understanding. Firstly, mineralised tissues, such as teeth and bone cortex, generate almost no sig-nal when standard MR-sequences are applied. This explains why those tissues appear black in the images. In a dental fol-licle, the mineralised tissue is surrounded by fluid, which appears white and, there-fore, contrasts sharply with the enamel and dentin. Thus, early stages of dental development are very clear in the MR-im-ages (Figure 1.1). By contrast, late stages are harder to discern, because they involve
the disappearing of the dental follicle and the closing of the apex (Figure 1.2). The lack of contrast between dental tissue and bone cortex can hinder the assessment. In developing bones, physeal cartilage can clearly be discerned from bone cortex or it blends into the surrounding tissues. When the physeal plate starts to bridge, bone bridges appear as a blurring of the physeal cartilage or as black interruptions of the physeal plate (Figures 1.1 and 1.2).
Research groups studying MRI for age estimation
In this joint PhD project, Ghent University and Catholic University Leuven studied if forensic age estimation in adolescents and subadults could be improved by multi-fac-torial MRI, including all third molars, the left wrist and both clavicles. Since 2012, a reference database was prospectively built comprising MRI of those three anatomical sites in healthy volunteers from 14 to 26 years old. The aim was to include at least ten participants per sex per age category of one year. From 2007 to 2012, a similar database was collected, including the left wrist and both clavicles of participants from 16 to 26 years old [26, 27].
In Germany, two large scale projects started simultaneously with our Belgian group, around the year 2007. The first was a multicentre study to collect MRI ref-erence data on the development of third molars, the left wrist, both clavicles and the left knee. Their aim was to include 25 participants per sex per age category of one year from 12 to 24 years old [24, 42, 43, 54, 70, 77]. The second project was funded by the Fédération Internation-ale de Football Association (FIFA) and scanned football players with MRI to op-
De Tobel J. Multi-factorial forensic age estimation. Chapter 1: 12-28.

25
timise the applications in sports [55, 73, 76, 81]. MRI has already been applied in international football competitions. By comparing the wrist images of young elite players with those of players in regional competitions, Dvorak et al. (2007) dis-covered that 6 to 35% of the elite players might have been over-aged for their cate-gory [10]. When the FIFA announced that they would conduct a wrist MRI in ran-domly selected players at the U-17 World Cup in 2009, some teams who qualified for the competition replaced up to fifteen players from their original selection [10].
In Austria, a large scale project started simultaneously with the current PhD pro-ject, in the year 2011. MRI reference data was collected of the same three anatom-ical sites – third molars, left hand/wrist, and both clavicles – in male volunteers. The aim was to include at least 300 male participants [1, 60, 74].
Other researchers in France [7, 48, 49, 56], Italy [57, 72], Denmark [61], Nor-way, Sweden, Turkey [11-14], China [18], Japan [62, 63] and very recently the USA [45] have been working on MRI in age estimation too, or they still are. However, their studies did not prospectively include multi-factorial MRI, except for the Nor-wegian and Swedish studies. Unfortunate-ly, to date, no results have been reported from the latter two studies.
Multi-factorial age estimation
Inter-individual variability in growth rates of different anatomical structures caus-es uncertainty in age estimation. When considering only one anatomical site, this uncertainty bears the risk of an ethically unacceptable error, i.e. wrongfully classi-
fying a minor as an adult. Moreover, in a forensic context, the benefit of the doubt needs to be granted in all cases, by assum-ing the youngest possible age. Incorporat-ing information from different anatomical sites might nuance the point prediction of age and reduce uncertainty, which reduc-es the risk of a faulty classification. How-ever, when a statistical model is developed for age estimation, one needs to realise that growth rates from different anatom-ical structures in one individual are cor-related. To what extent they correlate was unknown at the start of this PhD project. Fortunately, a statistical framework that handles this correlation in an appropriate way had been developed already [67].
acknowledgements
The author wishes to thank Cezar Capi-taneanu, Michiel de Haas, Kathy Kasper, Akiko Kumagai, Talia Marroquin, Rizky Merdietio Boedi, Philippe Pede, Pisha Pittayapat, Graham Roberts and César Sanabria Medina for providing informa-tion on the age estimation procedures in their countries.
references
[1] Baumann P, Widek T, Merkens H, Boldt J, Petrovic A, Urschler M, Kirnbauer B, Jakse N, Scheurer E. Dental age estimation of living persons: Comparison of MRI with OPG. Forensic Sci Int. 2015;253(0):76-80.
[2] Bontrager KL. Textbook of radiographic positioning and related anatomy. 4th ed. St. Louis, Missouri, United States of America: Mosby, 1997.
[3] Cantekin K, Sekerci AE, Buyuk SK. Dental computed tomo-graphic imaging as age estimation: morphological analysis of the third molar of a group of Turkish population. Am J Forensic Med Pathol. 2013;34(4):357-62.
[4] Capitaneanu C. Personal communication with De Tobel J. Octo-ber 21, 2018.
General introduction: Forensic age estimation now and in the future

26
[5] Cunha E, Baccino E, Martrille L, Ramsthaler F, Prieto J, Schu-liar Y, Lynnerup N, Cattaneo C. The problem of aging human remains and living individuals: a review. Forensic Sci Int. 2009;193(1-3):1-13.
[6] de Haas MB. Personal communication with De Tobel J. October 23, 2018.
[7] Dedouit F, Auriol J, Rousseau H, Rouge D, Crubezy E, Telmon N. Age assessment by magnetic resonance imaging of the knee: a preliminary study. Forensic Sci Int. 2012;217(1-3):232 e1-7.
[8] Dedouit F, Saint-Martin P, Mokrane FZ, Savall F, Rousseau H, Crubezy E, Rouge D, Telmon N. Virtual anthropology: useful radiological tools for age assessment in clinical forensic medi-cine and thanatology. Radiol Med. 2015;120(9):874-86.
[9] Dvorak J, George J, Junge A, Hodler J. Age determination by magnetic resonance imaging of the wrist in adolescent male football players. Br J Sports Med. 2007;41(1):45-52.
[10] Dvorak J, George J, Junge A, Hodler J. Application of MRI of the wrist for age determination in international U-17 soccer com-petitions. Br J Sports Med. 2007;41(8):497-500.
[11] Ekizoglu O, Hocaoglu E, Can IO, Inci E, Aksoy S, Bilgili MG. Magnetic resonance imaging of distal tibia and calcaneus for forensic age estimation in living individuals. Int J Legal Med. 2015;129(4):825-31.
[12] Ekizoglu O, Hocaoglu E, Can IO, Inci E, Aksoy S, Sayin I. Sphe-no-occipital synchondrosis fusion degree as a method to esti-mate age: A preliminary, magnetic resonance imaging study. Aust J Forensic Sci. 2016;48(2):159-70.
[13] Ekizoglu O, Hocaoglu E, Inci E, Can IO, Aksoy S, Kazimoglu C. Forensic age estimation via 3-T magnetic resonance imaging of ossification of the proximal tibial and distal femoral epiphyses: Use of a T2-weighted fast spin-echo technique. Forensic Sci Int. 2016;260:102.e1-7.
[14] Ekizoglu O, Inci E, Ors S, Kacmaz IE, Basa CD, Can IO, Kranioti EF. Applicability of T1-weighted MRI in the assessment of fo-rensic age based on the epiphyseal closure of the humeral head. Int J Legal Med. 2018.
[15] Engebretsen L, Steffen K, Bahr R, Broderick C, Dvorak J, Janarv PM, Johnson A, Leglise M, Mamisch TC, McKay D, Micheli L, Schamasch P, Singh GD, Stafford DE, Steen H. The Inter-national Olympic Committee Consensus statement on age determination in high-level young athletes. Br J Sports Med. 2010;44(7):476-84.
[16] European Asylum Support Office (EASO). Practical Guide on Age Estimation, Second edition. EASO Practical Guides Series. Malta2018.
[17] European Commission. Asylum statistics. [updated 20 April 2016; cited 2016 15 August]; Available from: http://ec.europa.eu/eurostat/statistics-explained/index.php/Asylum_statistics#.
[18] Fan F, Zhang K, Peng Z, Cui JH, Hu N, Deng ZH. Forensic age estimation of living persons from the knee: Comparison of MRI with radiographs. Forensic Sci Int. 2016;268:145-50.
[19] Federale Overheidsdienst Justitie. Identifcatie van een niet-be-geleide minderjarige vreemdeling. Federale Overheidsdienst Justitie; [cited 2016 16 August]; Available from: http://justitie.belgium.be/nl/themas_en_dossiers/kinderen_en_jongeren/niet-begeleide_minderjarige_vreemdelingen/dienst_voogdij/identifcatie_van_een_niet-begeleide_minderjarige_vreemde-ling.
[20] Federale Overheidsdienst Justitie. Zorg voor een niet-bege-leide minderjarige vreemdeling. Federale Overheidsdienst Justitie; [cited 2016 16 August]; Available from: http://justitie.belgium.be/nl/themas_en_dossiers/kinderen_en_jongeren/niet-begeleide_minderjarige_vreemdelingen/dienst_voogdij/zorg_voor_een_niet-begeleide_minderjarige_vreemdeling.
[21] Federale Overheidsdienst Justitie. [Statistics of the Guardian-ship Service]. October 18, 2018.
[22] Fournier K. [Age estimation of unaccompanied minors ques-tioned: defining the issue, analysis and recommendations]. Platform for refugee children, 2017.
[23] Gonsior M, Ramsthaler F, Gehl A, Verhoff MA. Morphology as a cause for different classification of the ossification stage of the medial clavicular epiphysis by ultrasound, computed tomogra-phy, and macroscopy. Int J Legal Med. 2013;127(5):1013-21.
[24] Guo Y, Olze A, Ottow C, Schmidt S, Schulz R, Heindel W, Pfeiffer H, Vieth V, Schmeling A. Dental age estimation in living individuals using 3.0 T MRI of lower third molars. Int J Legal Med. 2015;129(6):1265-70.
[25] Haglund M, Mornstad H. A systematic review and meta-analy-sis of the fully formed wisdom tooth as a radiological marker of adulthood. Int J Legal Med. 2018.
[26] Hillewig E, De Tobel J, Cuche O, Vandemaele P, Piette M, Ver-straete K. Magnetic resonance imaging of the medial extrem-ity of the clavicle in forensic bone age determination: a new four-minute approach. Eur Radiol. 2011;21(4):757-67.
[27] Hillewig E, Degroote J, Van der Paelt T, Visscher A, Vandemaele P, Lutin B, D’Hooghe L, Vandriessche V, Piette M, Verstraete K. Magnetic resonance imaging of the sternal extremity of the clavicle in forensic age estimation: towards more sound age es-timates. Int J Legal Med. 2013;127(3):677-89.
[28] Kumagai A. Personal communication with De Tobel J. Novem-ber 1, 2018.
[29] Kumagai A, Willems G, Franco A, Thevissen P. Age estimation combining radiographic information of two dental and four skeletal predictors in children and subadults. Int J Legal Med. 2018;Epub ahead of print.
[30] Liversidge HM. Timing of human mandibular third molar for-mation. Ann Hum Biol. 2008;35(3):294-321.
[31] Liversidge HM, Smith BH, Maber M. Bias and accuracy of age estimation using developing teeth in 946 children. Am J Phys Anthropol. 2010;143(4):545-54.
[32] Lockemann U, Fuhrmann A, Püschel K, Schmeling A, Geserick G. Arbeitsgemeinschaft für Forensische Altersdiagnostik der Deutschen Gesellschaft für Rechtsmedizin. Rechtsmedizin. 2004;14(2):123-6.
De Tobel J. Multi-factorial forensic age estimation. Chapter 1: 12-28.

27
[33] Ludlow JB, Timothy R, Walker C, Hunter R, Benavides E, Sam-uelson DB, Scheske MJ. Effective dose of dental CBCT-a meta analysis of published data and additional data for nine CBCT units. Dentomaxillofac Radiol. 2015;44(1):20140197.
[34] Lurie AG. Doses, Benefits, Safety, and Risks in Oral and Maxil-lofacial Diagnostic Imaging. Health physics. 2019;116(2):163-9.
[35] Meijerman L, Maat GJR, Schulz R, Schmeling A. Variables af-fecting the probability of complete fusion of the medial clavicu-lar epiphysis. Int J Legal Med. 2007;121(6):463-8.
[36] Merdietio Boedi R. Personal communication with De Tobel J. November 30, 2018.
[37] Nardi C, Salerno S, Molteni R, Occhipinti M, Grazzini G, Norberti N, Cordopatri C, Colagrande S. Radiation dose in non-dental cone beam CT applications: a systematic review. Radiol Med. 2018;123(10):765-77.
[38] Netherlands Forensic Institute. [Protocol Age Assessment]. 2014.
[39] Novelline RA, Squire LF. Squire’s fundamentals of radiology: La Editorial, UPR, 2004.
[40] Office of Refugee Resettlement. Children Entering the United States Unaccompanied: Section 1. 2015 [updated January 30, 2015; cited 2018 October 10]; Available from: https://www.acf.hhs.gov/orr/resource/children-entering-the-united-states-un-accompanied-section-1.
[41] Olze A, van Niekerk P, Schulz R, Ribbecke S, Schmeling A. The influence of impaction on the rate of third molar mineralisation in male black Africans. Int J Legal Med. 2012;126(6):869-74.
[42] Ottow C, Krämer JA, Olze A, Schmidt S, Schulz R, Wittschieber D, Heindel W, Pfeiffer H, Ribbecke S, Vieth V, Schmeling A. Magnetresonanztomographiestudie zur Altersschätzung von unbegleiteten minderjährigen Flüchtlingen. Rechtsmedizin. 2014;25:12-20.
[43] Ottow C, Schulz R, Pfeiffer H, Heindel W, Schmeling A, Vieth V. Forensic age estimation by magnetic resonance imaging of the knee: the definite relevance in bony fusion of the distal femoral- and the proximal tibial epiphyses using closest-to-bone T1 TSE sequence. Eur Radiol. 2017;27(12):5041-8.
[44] Outten-Mills D, Schmidt A, Bobman H, Brown S. Age Deter-mination Practices for Unaccompanied Alien Children in ICE Custody. Department of Homeland Security - Office of Inspec-tor General. 2009.
[45] Pennock AT, Bomar JD, Manning JD. The Creation and Valida-tion of a Knee Bone Age Atlas Utilizing MRI. J Bone Joint Surg Am. 2018;100(4):e20.
[46] Pittayapat P. Personal communication with De Tobel J. October 25, 2018.
[47] Ramsthaler F, Proschek P, Betz W, Verhoff MA. How reliable are the risk estimates for X-ray examinations in forensic age estimations? A safety update. Int J Legal Med. 2009;123(3):199-204.
[48] Saint-Martin P, Rerolle C, Dedouit F, Bouilleau L, Rousseau H, Rouge D, Telmon N. Age estimation by magnetic resonance im-aging of the distal tibial epiphysis and the calcaneum. Int J Legal Med. 2013;127(5):1023-30.
[49] Saint-Martin P, Rerolle C, Dedouit F, Rousseau H, Rouge D, Telmon N. Evaluation of an automatic method for forensic age estimation by magnetic resonance imaging of the distal tibial epiphysis--a preliminary study focusing on the 18-year thresh-old. Int J Legal Med. 2014;128(4):675-83.
[50] Sanabria Medina C. Personal communication with De Tobel J. October 30, 2018.
[51] Schmeling A, Dettmeyer R, Rudolf E, Vieth V, Geserick G. Fo-rensic Age Estimation. Dtsch Arztebl Int. 2016;113(4):44-50.
[52] Schmeling A, Geserick G, Reisinger W, Olze A. Age estimation. Forensic Sci Int. 2007;165(2-3):178-81.
[53] Schmeling A, Reisinger W, Loreck D, Vendura K, Markus W, Geserick G. Effects of ethnicity on skeletal maturation: consequences for forensic age estimations. Int J Legal Med. 2000;113(5):253-8.
[54] Schmidt S, Ottow C, Pfeiffer H, Heindel W, Vieth V, Schmeling A, Schulz R. Magnetic resonance imaging-based evaluation of ossification of the medial clavicular epiphysis in forensic age assessment. Int J Legal Med. 2017;131(6):1665-73.
[55] Schmidt S, Vieth V, Timme M, Dvorak J, Schmeling A. Ex-amination of ossification of the distal radial epiphysis using magnetic resonance imaging. New insights for age estima-tion in young footballers in FIFA tournaments. Sci Justice. 2015;55(2):139-44.
[56] Serin J, Rerolle C, Pucheux J, Dedouit F, Telmon N, Savall F, Saint-Martin P. Contribution of magnetic resonance imaging of the wrist and hand to forensic age assessment. Int J Legal Med. 2016;130(4):1121-8.
[57] Serinelli S, Panebianco V, Martino M, Battisti S, Rodacki K, Marinelli E, Zaccagna F, Semelka RC, Tomei E. Accuracy of MRI skeletal age estimation for subjects 12-19. Potential use for subjects of unknown age. Int J Legal Med. 2015;129(3):609-17.
[58] Serinelli S, Panetta V, Pasqualetti P, Marchetti D. Accuracy of three age determination X-ray methods on the left hand-wrist: a systematic review and meta-analysis. Leg Med (Tokyo). 2011;13(3):120-33.
[59] Smeyers S. De toename van het aantal niet-begeleide minder-jarige vreemdelingen. In: Staatssecretaris voor Asiel en Migratie bmAV, toegevoegd aan de minister van Veiligheid en Binnen-landse Zaken, ed. Brussel: De Kamer van volksvertegenwoordi-gers, 13 November 2015.
[60] Štern D, Kainz P, Payer C, Urschler M. Multi-Factorial Age Estimation from Skeletal and Dental MRI Volumes. In: Inter-national Workshop on Machine Learning in Medical Imaging. Quebec City, Canada: Springer, 2017; p. 61-9.
[61] Tangmose S, Jensen KE, Villa C, Lynnerup N. Forensic age es-timation from the clavicle using 1.0T MRI-Preliminary results. Forensic Sci Int. 2014;234:7-12.
General introduction: Forensic age estimation now and in the future
28
[62] Terada Y, Kono S, Tamada D, Uchiumi T, Kose K, Miyagi R, Yamabe E, Yoshioka H. Skeletal age assessment in chil-dren using an open compact MRI system. Magn Reson Med. 2013;69(6):1697-702.
[63] Terada Y, Kono S, Uchiumi T, Kose K, Miyagi R, Yamabe E, Fujinaga Y, Yoshioka H. Improved reliability in skeletal age assessment using a pediatric hand MR scanner with a 0.3T per-manent magnet. Magn Reson Med Sci. 2014;13(3):215-9.
[64] Thevissen P, Willems G. [The Triple Test: The K.U.Leuven-pro-tocol for age estimation of unaccompanied minor refugees]. In: Aps JKM, Brand HS, Duyck J, van Es RJJ, Jacobs R, Vissink A, eds. Het Tandheelkundig Jaar 2013. Houten: Bohn Stafleu van Loghum, 2013; p. 175-90.
[65] Thevissen PW. Dental age estimation: striving for an optimal approach [Doctoral thesis]. Leuven: Leuven University Press, 2013.
[66] Thevissen PW, Alqerban A, Asaumi J, Kahveci F, Kaur J, Kim YK, Pittayapat P, Van VM, Zhang Y, Fieuws S, Willems G. Hu-man dental age estimation using third molar developmental stages: Accuracy of age predictions not using country specific information. Forensic Sci Int. 2010;201(1-3):106-11.
[67] Thevissen PW, Fieuws S, Willems G. Human dental age estima-tion using third molar developmental stages: does a Bayesian approach outperform regression models to discriminate be-tween juveniles and adults? Int J Legal Med. 2010;124(1):35-42.
[68] Thevissen PW, Fieuws S, Willems G. Human third molars devel-opment: Comparison of 9 country specific populations. Foren-sic Sci Int. 2010;201(1-3):102-5.
[69] Thevissen PW, Kvaal SI, Dierickx K, Willems G. Ethics in age estimation of unaccompanied minors. J Forensic Odontostom-atol. 2012;30 Suppl 1:84-102.
[70] Timme M, Ottow C, Schulz R, Pfeiffer H, Heindel W, Vieth V, Schmeling A, Schmidt S. Magnetic resonance imaging of the distal radial epiphysis: a new criterion of maturity for determin-ing whether the age of 18 has been completed? Int J Legal Med. 2017;131(2):579-84.
[71] Timme M, Steinacker JM, Schmeling A. Age estimation in com-petitive sports. Int J Legal Med. 2017;131(1):225-33.
[72] Tomei E, Semelka RC, Nissman D. Text-atlas of skeletal age de-termination: MRI of the hand and wrist in children: John Wiley & Sons, 2013.
[73] Tscholl PM, Junge A, Dvorak J, Zubler V. MRI of the wrist is not recommended for age determination in female football players of U-16/U-17 competitions. Scand J Med Sci Sports. 2016;26(3):324-8.
[74] Urschler M, Grassegger S, Štern D. What automated age estima-tion of hand and wrist MRI data tells us about skeletal matura-tion in male adolescents. Ann Hum Biol. 2015;42(4):358-67.
[75] Urschler M, Krauskopf A, Widek T, Sorantin E, Ehammer T, Borkenstein M, Yen K, Scheurer E. Applicability of Greu-lich-Pyle and Tanner-Whitehouse grading methods to MRI when assessing hand bone age in forensic age estimation: A pilot study. Forensic Sci Int. 2016;266:281-8.
[76] Vieth V, Schulz R, Brinkmeier P, Dvorak J, Schmeling A. Age estimation in U-20 football players using 3.0 tesla MRI of the clavicle. Forensic Sci Int. 2014;241c:118-22.
[77] Vieth V, Schulz R, Heindel W, Pfeiffer H, Buerke B, Schmeling A, Ottow C. Forensic age assessment by 3.0T MRI of the knee: proposal of a new MRI classification of ossification stages. Eur Radiol. 2018.
[78] Willems G, Lee SS, Uys A, Bernitz H, Cadenas de Llano-Peru-la M, Fieuws S, Thevissen P. Age estimation based on Willems method versus new country-specific method in South African black children. Int J Legal Med. 2017.
[79] Wittschieber D, Ottow C, Schulz R, Puschel K, Bajanowski T, Ramsthaler F, Pfeiffer H, Vieth V, Schmidt S, Schmeling A. Forensic age diagnostics using projection radiography of the clavicle: a prospective multi-center validation study. Int J Legal Med. 2016;130(1):213-9.
[80] Wittschieber D, Ottow C, Vieth V, Kuppers M, Schulz R, Hassu J, Bajanowski T, Puschel K, Ramsthaler F, Pfeiffer H, Schmidt S, Schmeling A. Projection radiography of the clavicle: still rec-ommendable for forensic age diagnostics in living individuals? Int J Legal Med. 2015;129(1):187-93.
[81] Wittschieber D, Vieth V, Timme M, Dvorak J, Schmeling A. Magnetic resonance imaging of the iliac crest: age estima-tion in under-20 soccer players. Forensic Sci Med Pathol. 2014;10(2):198-202.
[82] Zhang A, Sayre JW, Vachon L, Liu BJ, Huang HK. Racial differ-ences in growth patterns of children assessed on the basis of bone age. Radiology. 2009;250(1):228-35.
De Tobel J. Multi-factorial forensic age estimation. Chapter 1: 12-28.


30
CHAPTER 2

31
Study objectives and design
I NCEPT ION
Study objectives
The current PhD project was set up as a response to the shortcomings of the cur-rent gold standard approach to estimate age in living adolescents and subadults. The study was founded on the following general study hypothesis:
Forensic age estimation in living adoles-cents and subadults is the most accurate when it is based on the multi-factorial MRI evaluation of all third molars, the left wrist and both clavicles.
Consequently, the following specific study objectives were established:
1 To collect a reference dataset of MR images of third molars, left wrist and both clavicles. These images will be registered simultaneously in each participant.
2 To develop an MRI scanning proto-col for all third molars.
3 To compare the third molars’ MRI with the current gold standard im-aging, i.e. radiographs.
4 To stage the development of each age predictor based on the MRI. Existing 2D staging techniques will be modified or new methods will be developed. Reproducibility of the staging techniques will be tested.
5 To fit a statistical age estimation model on the reference data set, for each age predictor individually, as well as combining all registered age predictors. In all these models Bayes’ rule will be applied to coun-ter drawbacks of other regression methods.
6 To validate this model and to com-pare its performance with existing models.
Fortunately, this project was built on pre-vious research by our group, in which objectives 2 and 3 had already been met for the left wrist and both clavicles. Ob-jectives 4 and 5 were also partially met for both clavicles in this previous research.
Additional study objectives were estab-lished during the process:
1 To compare our MRI protocol for third molars with the Graz protocol.
2 To study how motion artefacts affect stage allocation to the clavicles’ ster-nal ends on MRI.
3 To review the use of MRI in age es-timation of living children and sub-adults.

32
Study design
This project was approved by the Ethics Committee of Ghent
University Hospital with project number EC/2011/0842.
To collect the MRI reference data set, the age predictors were studied in healthy Belgian and Dutch participants between 14 and 26 years old (at least ten per sex per age category of one year, n ≥ 260). They were all Caucasian and from mod-erate to high socio-economic class. They were recruited by means of posters, e-mail and oral announcements in public places where young people gather and in the waiting rooms of dentists and medical doctors.
In this study population, MRI was per-formed at Ghent University Hospital with a 3 Tesla scanner. Detailed imaging was required to discern the small age-related changes in dental and bone development. Therefore, existing scanning protocols as described in literature were tested and compared to new or modified protocols. The set-up for the scans is illustrated in Figures 2.1 to 2.3. Furthermore, clinically indicated panoramic radiographs of study participants were collected in dental offic-es. No additional radiographs were made for this study.
Multiple observers with expertise in forensic age estimation assessed the de-velopment of the different age predictors based on the collected MR-images. In-ter- and intra-observer agreement were studied. For third molars, results were compared to the assessments based on ra-diographs.
a The par t ic ipant bites a s i l icone paste to
indiv idual ise the bite plate.
b During the scan, the par t ic ipant c loses her/
his mouth around the bite plate, which is
attached to a frame. The surface coi ls
are f ixed around the cheeks.
c Set-up before the par t ic ipant is s l id into
the gantry.
FIGURE 2. 1 — SET-UP FOR THE MRI SCAN OF THE
THIRD MOLARS.
Consequently, the extracted data on de-velopment of the different age predictors was used to develop statistical models for age estimation. The validity of these mod-
De Tobel J. Multi-factorial forensic age estimation. Chapter 2: 30-34.

33
Study objectives and design
a Indiv idual ly shaped vacuum pi l low with the
loop coi l stabi l ised in a rubber device.
b Prone posit ioning with the sternoclavicular
jo ints central ly on the loop coi l .
c Set-up before the par t ic ipant is s l id into the
gantry.
a The left hand and wrist are posit ioned in the
coi l in such a way that the focus is on the
physeal plates of radius and ulna.
b The coi l is c losed and the hand and wrist are
supported using pi l lows.
c Set-up before the par t ic ipant is s l id into the
gantry.
FIGURE 2.3 — SET-UP FOR THE MRI SCAN OF BOTH
CLAVICLES.
FIGURE 2.2 — SET-UP FOR THE MRI SCAN OF THE
LEFT WRIST.
The stepwise pathway that was followed to reach the study objectives is depicted in Figure 2.4.
els was tested and compared to existing models reported in literature.

34
FIGURE 2.4 — THE STEPWISE PATHWAY OF DIFFERENT ASPECTS THAT WERE STUDIED IN THIS PHD PROJECT
TO REACH THE MAIN STUDY OBJECTIVE. These aspects correspond with the study repor ts that resulted
from this PhD project and their corresponding chapters in this thesis .
De Tobel J. Multi-factorial forensic age estimation. Chapter 2: 30-34.


37
PART 2
Age estimation based on third molars MRI

38
CHAPTER 3
TH I S CHAPTER ADDRESSED THE FOLLOWING STUDY OB JECT IVE :
Objective 2: To develop an MRI scanning protocol for all third molars.
TH I S CHAPTER WAS PUBL I SHED AS :
De Tobel J, Hillewig E, Bogaert S, Deblaere K, Verstraete K. Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation. Ann Hum Biol. 2017; 44:130-139. [A1; Journal Impact Factor 2017 1.531; Biology Q3; Public, Envi-ronmental & Occupational Health Q3; Peer reviewed]
RESULTS DESCR I BED IN TH I S CHAPTER WERE PARTLY
P RESENTED AT THE FOLLOWING CONFERENCES :
De Tobel J, Hillewig E, Bogaert S, Deblaere K, Politis C, Verstraete K, Thevissen P. Third molar magnetic resonance imaging (MRI) in forensic age estimation: protocol develop-ment and considerations for use. American Academy of Forensic Sciences (AAFS) 69th Annual Scientific Meeting; New Orleans, USA; February 16, 2017. p 867-868.
De Tobel J, Hillewig E, Bogaert S, Deblaere K, Verstraete K. MRI of the third molars: developing a protocol suitable for age estimation. 18th Meeting of the Study Group on Forensic Age Diagnostics, Arbeitsgemeinschaft für Forensische Altersdiagnostik (AG-FAD); Berlin, Germany; March 20, 2015.

39
Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation
OR IG INAL RESEARCH
Abstract
Background — Established dental age estimation methods in subadults study the development of third molar root apices on radiographs. In living individuals however, avoiding ionizing radiation is expedient. Studying dental development with mag-netic resonance imaging complies with this requirement, add-ing the advantage of imaging in three dimensions. Aim — To elaborate the development of an MRI protocol to visualize all third molars for forensic age estimation, with particular atten-tion to the development of the root apex. Subjects and meth-ods — Ex vivo scans of porcine jaws and in vivo scans of ten volunteers aged 17-25 years were performed to select adequate sequences. Studied parameters were T1 versus T2 weighting, ul-trashort echo time (UTE), fat suppression, in-plane resolution, slice thickness, 3D imaging, signal-to-noise ratio and acquisi-tion time. A bilateral four-channel flexible surface coil was used. Two observers evaluated the suitability of the images. Results — T2-weighted images were preferred to T1-weighted images. To clearly distinguish root apices in (almost) fully developed third molars an in-plane resolution of 0.33 × 0.33 mm² was deemed necessary. Taking acquisition time limits into account, only a T2 FSE sequence with slice thickness of 2 mm generated images with sufficient resolution and contrast. UTE, thinner slice T2 FSE and T2 3D FSE sequences could not generate the desired resolution within 6.5 minutes. Conclusion — Three Tesla MRI of the third molars is a feasible technique for forensic age esti-mation, in which a T2 FSE sequence can provide the desired in-plane resolution within a clinically acceptable acquisition time.
Key Words
• surface head coil
• apical development
• subadult
AFF IL IAT IONS
1 Department of Radiology and
Nuclear Medicine, Ghent Univer-
sity, Belgium
2 Ghent Institute for Functional
and Metabolic Imaging (GIFMI)
Funding for this research was entirely
provided by the department of
Radiology and Nuclear Medicine at
Ghent University.
The authors declare that there are
no conflicts of interest.
JANN ICK DE TOBEL 1 ELKE H I LLEW IG 1
STEPHAN I E BAGAERT 2
K AREL L . D EBLAERE 1 KOENRAAD L . VERSTRAETE 1

40
Studying the development of indi-viduals and populations is the core of human biology. It can be elabo-rated by studying human remains or by studying the living [22]. Both approaches imply multidisciplinar-
ity, with contributions of archaeologists, biologists, anthropologists, geneticists, endocrinologists, radiologists, forensic medical doctors and forensic odontol-ogists [19]. Studying the relationship between development and age is a sub-domain of human biology in which the same multidisciplinarity applies [18]. The developing skeleton and dentition can be used as biological maturity indicators to estimate chronological age [4]. This relationship has been studied using ra-diographs of developing bones and teeth in both deceased and living individuals. Information on skeletal and dental age is useful in population studies, evolutional studies, clinical follow up in paediatrics and orthodontics, asylum procedures, civil and criminal procedures, adoption cases and sports [6]. Although previous research has already revealed many as-pects of skeletal and dental development, authors keep stressing the importance of further investigation to enable scientists and authorities to optimize and standard-ize age estimation practices [3, 16].
The current paper focuses on the de-velopment of third molars and the way it can be studied in the living. In adoles-cents and young adults the development of third molars is a useful age indicator [5, 28]. The complete cycle of third mo-lar development is traversed between the eighth and 25th year of life [17]. It can be evaluated on panoramic radiographs and is divided into stages [9]. Although a panoramic radiograph has a relatively
low radiation dose (0.026 mSv [26]), in some countries it cannot be used because radiation is prohibited in asylum and civil procedures [20]. Also for age estimation in sports, radiation exposure is not justifi-able or ethically acceptable [7].
Magnetic resonance imaging (MRI) is an imaging technique free of ionizing radiation. In addition, it enables a 3D vis-ualization which might provide comple-mentary information for age estimation, compared to the 2D projection on radio-graph. This has already been demonstrat-ed for age estimation based on MRI of the clavicles [12] and hand/wrist MRI [32].
Performing basic MRI, the scanner sends out a pulse which generates a signal in the tissues. This signal is received in a coil, which is positioned as close to the an-atomical region of interest as possible, in order to generate sufficient signal intensi-ty on the image. A series of sequences is embedded in a scanning protocol. Imag-es are made up of pixels (e.g. 0.50 × 0.50 mm², this is called in-plane resolution) with a slice thickness (e.g. 2.00 mm), thus resulting in a voxel (e.g. 0.50 × 0.50 × 2.00 mm³). In MRI many sequence parameters are related. Changing one parameter, will cause changes in other parameters. For instance, increasing in-plane resolution – thus reducing pixel size – will require a longer acquisition time to achieve the same image quality (i.e. the same signal-to-noise ratio) when all other parameters are left unchanged [33].
Mineralized tissues such as teeth and cortical bone yield almost no signal with standard MR sequences, appearing black on the image [33]. In the dental follicle mineralized dental tissue is surrounded
Introduction
De Tobel J. Multi-factorial forensic age estimation. Chapter 3: 38-52.

41
by watery content creating sufficient con-trast, so early stages of tooth development are clearly displayed on MRI. Later stages are more challenging, as the most impor-tant characteristics are the remnant of the dental follicle and closing of the apex. In these stages the lack of contrast between dental tissue and bone might impede the assessment. Specific MR sequences to vis-ualize highly mineralized tissues such as teeth have been developed for clinical use. Feasible in vivo approaches include ultra-short echo time (UTE) [2, 21] and SWeep Imaging with Fourier Transformation (SWIFT) [14] sequences. However, clini-cal studies using these sequences did not focus on root apices or third molars.
To our knowledge results from two research groups have been published on MRI of third molars for age estimation. Using a surface coil, Ottow et al. (2014) and Guo et al. (2015) used a T2 turbo spin echo (TSE) sequence with measured voxel size = 0.50 × 0.65 × 2.00 mm³ and recon-structed voxel size = 0.19 × 0.19 × 2.00 mm³ [24]. They only studied left lower third molars (when this was not present, the right one was studied). However, The-vissen et al. (2013) found that the accura-cy of age estimation based on the lower left third molar improved significantly when the stage of the upper left third mo-lar was added to the regression model [11, 29]. Using an 8-channel multifunction-al coil, Baumann et al. applied a 3D TSE and a 3D constructive interference in the steady state (CISS) sequence [1]. In both sequences the resolution was 0.6 × 0.6 × 1.0 mm³. They evaluated all molars. Both groups concluded that dental MRI seems to be suitable for dental age estimation. No details were given about how the used sequences were developed.
The purpose of this study was to elaborate the development of a clinically feasible MRI protocol to visualize all four third molars for forensic age estimation, with particular attention to distinguishing the highest developmental stages.
Study population
Initially, a pig head was scanned ex vivo, since porcine teeth have simi-lar dimensions as human teeth. For
in vivo human scans, approval of the local ethics committee was obtained as well as written informed consent from every par-ticipant, and in case of minors from their parents. Ten volunteers (seven females of 17-25 years old, three males of 23-24 years old) were randomly recruited. They had had no surgical removal of any second or third molar. Agenesis of both lower third molars was seen in one participant, while another one showed agenesis of the lower right third molar.
Image acquisition
Scans were performed with 3T MRI (Magnetom Trio Tim, Siemens, Erlangen, Germany). A bilateral four-channel flexi-ble surface head coil (Model NMP-001D-ST-4, Nova Medical Inc., Wilmington, USA) for parallel imaging was used.
Based on the available literature on dental MRI [2, 8, 14, 31] and in house experience with imaging of the brain and clavicles, several approaches were tested to design an adequate scanning protocol. The initial MRI investigations were con-ducted from December 2011 until March 2012. In January 2015, this protocol was evaluated and compared with more recent literature [13, 15, 24]. Scanning parame-
Methods
Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation

42
ters of the most important tested sequenc-es are provided in Table 3.1.
Ex vivo testing
To scan the porcine jaws, the whole pig head was heated by steam to 20 °C. Fig-ure 3.1 shows how it was then wrapped in plastic film and positioned for the scan. T2-weighted images were acquired in sagittal and axial planes. A UTE sequence was also performed.
In vivo optimization
For in vivo scanning, an acquisition time of maximum 6 minutes 30 seconds was considered acceptable [23]. This limit was set because the desired protocol should be feasible in a clinical setting. To ensure
a stable head position an individual bite plate was made for each participant, using an addition silicone (Futar D®, Ketten-bach, Eschenburg, Germany). This plate was attached to a custom-made frame for brain imaging, which was placed over the head of the participant. During the scan the mouth was closed, with the incisors and canines captured in the set silicone, minimizing motion artefacts. Figure 3.2 demonstrates the set-up for imaging.
The first step was to determine wheth-er a T1- or a T2-weighted sequence should be used. Both were tried in two volunteers. Sagittal and axial images were acquired. The T2 sequence that was used here will from now on be referred to as the reference T2 sequence (TR 5084 ms, TE 74 ms, 3 averages, flip angle 120 de-
TABLE 3. 1 — TECHNICAL PROPERTIES OF THE TESTED MR SEQUENCES.
SUBJECTS SEQUENCE PLANE REPETITION
TIME (MS)
ECHO TIME (MS) AVERAGES
IN VIVO T1 FLASH Sagittal 255 2.96 3
HUMAN Reference T2 FSE Sagittal 5084 74 3
T2 FSE Axial 4290 74 3
T2 FSE Coronal 4080 74 3
T2 FSE non FS Sagittal 5084 74 3
T2 3D FSE Axial 3200 467 2
Thin S l ice T2 FSE Sagittal 7270 66 3
T2 FSE doubled
averages
Sagittal 5084 74 6
T2 FSE decreased
IPR
Sagittal 5084 74 3
T2 FSE increased
IPR
Sagittal 5680 67 3
T2 FSE increased
IPR and doubled
averages
Sagittal 5680 67 6
IN VITRO T2 FSE Sagittal 5084 74 3
PORCINE T2 FSE Axial 4290 74 3
3D UTE Axial 5.85 TE 1 0.07
TE 2 3.75
2
FS = FAT SATURATION; IPR = IN-PLANE RESOLUTION; SNR = SIGNAL-TO-NOISE RATIO; TE = ECHO TIME.
De Tobel J. Multi-factorial forensic age estimation. Chapter 3: 38-52.

43
Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation
FLIP ANGLE
(DEGREES)
FAT SUP-
PRESSION
VOXEL SIZE
(MM³)
FIELD OF VIEW
(MM)
RELATIVE SNR ACQUISITION
TIME (MIN:S)
70 None 0.49 × 0.49 × 2 .0 220 1 .00 5:43
120 FS 0.33 × 0.33 × 2.0 150 1.00 6:33
120 FS 0.33 × 0.33 × 2 .0 150 1 .00 6:49
120 FS 0.33 × 0.33 × 2 .0 150 1 .00 6:29
120 None 0.33 × 0.33 × 2 .0 150 1 .00 6:28
/ None 0.80 × 0.80 × 0.80 240 1 .00 5:41
120 FS 0.50 × 0.50 × 1 .7 150 1 .00 6:49
120 FS 0.33 × 0.33 × 2 .0 150 1 .4 1 14 :56
120 FS 0.50 × 0.50 × 2 .0 225 2.25 6:28
120 FS 0.20 × 0.20 × 2 .0 90 0.36 14: 19
120
FS 0.20 × 0.20 × 2 .0 90 0.51 25:41
120 FS 0.33 × 0.33 × 2 .0 150 1 .00 6:33
120 FS 0.33 × 0.33 × 2 .0 150 1 .00 6:49
14 None 1 .04 × 1 .04 × 1 .04 150 1 .00 5:51
a The whole head was kept intact . Surface
coi ls were taped around the jaws.
b Corresponding schematic representation of
the posit ion of the coi ls . The centre of fo-
cus l ies around the premolar teeth (arrow).
grees, fat saturation, voxel size 0.33 × 0.33 × 2.0 mm³, FOV 150 mm, acquisition time 6 minutes 33 seconds).
Next, several parameter changes of the reference sequence were tested in new volunteers. To limit the total scanning time for the participants, different se-quences were tested in different individu-als. However, in all of them the reference T2 sequence was performed. In addition to sagittal and axial images, coronal slices were acquired with the T2 sequence.
To counter the obvious disadvantage of a relatively large slice thickness of 2 mm, both a 3D T2 sequence and a thin slice T2 sequence were tested. The 3D T2 images were acquired in the axial plane and sagittal reconstructions were made (n = 4). The minimum voxel size that could
FIGURE 3. 1 — SET UP FOR THE EX VIVO MRI SCAN
OF PORCINE JAWS.

44
be reached within the set time constraints was 0.80 × 0.80 × 0.80 mm³. The thin slice T2 sequence generated sagittal images with 0.50 × 0.50 × 1.7 mm³ voxels (n = 3).
To check the influence of in-plane res-olution without decreasing slice thickness, pixel size of the reference T2 sequence was enlarged to 0.50 × 0.50 mm² (n = 1). Finally sagittal T2-weighted scans were performed beyond a clinically acceptable acquisition time, to see whether a large improvement of image quality could be obtained (n = 2). Averages were doubled to increase signal-to-noise ratio (SNR). Then in-plane resolution was increased to 0.20 × 0.20 mm² by reduction of the field of view (FOV) to check if this higher res-olution would result in more clearly dis-tinguishable apices and consequently an easier evaluation. Pixel size reduction im-plicates a loss in SNR, which can partially be compensated for by increasing averag-es. Therefore, a sequence was performed
with in-plane resolution 0.20 × 0.20 mm² with a smaller FOV and doubled averages.
Image analysis
Two observers interpreted the images. The first observer (JDT), a medical doctor studying dentistry, had one year of expe-rience in evaluating dental radiographs. The second observer (EH), a researcher at the radiology department with five years of experience in skeletal age estimation on radiographs and MRI, started with no experience in dental imaging.
Images were considered suitable for age estimation if the different develop-mental stages could be distinguished. Suitability of the images was evaluated by both observers in consensus. Images were evaluated on a Barco MFGD 3420 mon-itor with 3 megapixel resolution (Barco, Kortrijk, Belgium) using K-PACS V 1.6.0 DICOM viewing software.
FIGURE 3.2 — SET-UP FOR THE IN VIVO
MRI SCAN.
a The par t ic ipant bites into a s i l i -
cone paste to create an individu-
al bite plate.
b The bite plate is attached to the
frame.
c Cranio-anterior v iew of the set-
up for the scan. The par t ic ipant
c loses the mouth around the bite
plate during the scan. Surface
head coi ls are posit ioned next to
the cheeks.
d Lateral overview of the set-up for
the scan.
De Tobel J. Multi-factorial forensic age estimation. Chapter 3: 38-52.

45
Statistical analysis
For analysis, the data were transferred from Microsoft Excel 2010 to SPSS Sta-tistics 22.0 (IBM SPSS Statistics for Win-dows, Armonk, NY). Descriptive statis-tics were calculated. Statistical tests were performed two-sided and evaluated at the 0.05 significance level. Combined results for upper third molars were reported, be-cause in all variables results and P-values for the right third molar were similar to those for the left one. The same applied to lower third molars.
The proportion of suitable images for each in vivo tested MR sequence was calculated. These proportions were com-pared with the proportion of the reference T2 sequence by a McNemar’s test. Because only one ex vivo scan was performed, re-sults of the evaluation of this scan were not statistically analysed.
Image acquisition
Ex vivo testing
Compared to the T2 images, the UTE im-ages showed insufficient spatial resolution to allocate developmental stages to the teeth (Figure 3.3). Thus, the T2 sequence was selected to continue the optimization.
In vivo optimization
With acquisition times of 5 minutes 43 seconds and 6 minutes 33 seconds respec-tively, both the T1 and the T2 sequences met the time requirements. The soft tis-sues of the pulp and the dental follicle were more clearly depicted on T2-weight-ed images (Figure 3.4) than on T1-weight-ed images (Figure 3.5). This also implied better visibility of the hard dental tissues, because of better contrast (Table 3.2).
Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation
Results
TABLE 3.2 — PROPORTION OF SUITABLE IMAGES FOR EACH IN VIVO TESTED MR SEQUENCE. P-values were
generated by comparing each sequence to the reference T2 FSE sequence (bold) by a McNemar test .
Stat ist ical ly s ignif icant differences are shaded.
SEQUENCE UPPER THIRD MOLARS LOWER THIRD MOLARS
SUITABLE IMAGES P-VALUE SUITABLE IMAGES P-VALUE
T1 FLASH 83.3% (5/6) 1 .000 80.0% (4/5) 1 .000
Reference T2 FSE Sagittal 100.0% (18/18) 100.0% (16/16)
T2 FSE Axial 83.3% ( 15/18) 0.250 58.8% ( 10/17) 0.016
T2 FSE Coronal 68.8% ( 1 1/ 16) 0.063 80.0% (12/15) 0.250
T2 FSE non FS 100.0% (4/4) NA 50.0% (2/4) 0.500
T2 3D FSE 66.7% (8/12) 0. 125 45.5% (5/1 1 ) 0.031
Thin S l ice T2 FSE 80.0%) (8/10) 0.500 70.0% (7/10) 0.250
T2 FSE doubled averages 100.0% (4/4) NA 100.0% (4/4) NA
T2 FSE decreased IPR 100.0% (6/6) NA 83.3% (5/6) 1 .000
T2 FSE increased IPR 75.0% (3/4) 1 .000 100.0% (4/4) NA
T2 FSE increased IPR
and doubled averages
100.0% (4/4) NA 100.0% (4/4) NA
FS = FAT SATURATION; IPR = IN-PLANE RESOLUTION; NA = NOT APPLICABLE.

46
FIGURE 3.3 — SAGITTAL IMAGES OF
A LOWER THIRD PREMOLAR IN THE 6
MONTHS OLD MALE PIG.
a T2 weighted image. The open root
apex (arrow) can be dist inguished
from the surrounding remnant of
the dental fol l ic le.
b Corresponding UTE image. The
soft t issue of the dental fol l ic le
cannot be dist inguished from the
pulp t issue at the apex (arrow).
FIGURE 3.4 — SAGITTAL IMAGES OF A
LOWER THIRD MOLAR IN A 23-YEAR-OLD
MALE.
a, b Consecutive reference T2-weight-
ed images.
c, d Corresponding schematic repre-
sentation. The mesial root is fu l ly
developed, with a c losed apex
(arrows). The apex of the distal
root is st i l l open (arrowheads).
This sequence is cal led the refer-
ence sequence in this paper, as
other sequences were compared
to this one.
FIGURE 3.5 — CORRESPONDING T1
WEIGHTED IMAGES.
These images are equivalent to the
images shown in Figure 3.4 . Only the
ful ly developed mesial root apex can be
dist inguished (arrow). The apex of the
distal root cannot be evaluated with
suff ic ient cer tainty.
FIGURE 3.6 — CORRESPONDING T2
WEIGHTED NON-FAT SUPPRESSED IMAGES.
These images are equivalent to the
images shown in Figure 3.4 .
a The ful ly developed mesial root
can be dist inguished (arrow).
b The apex of the distal root can-
not be dist inguished from the
surrounding bone marrow.
De Tobel J. Multi-factorial forensic age estimation. Chapter 3: 38-52.

47
The watery content of the remnant of the dental follicle was clearly distinguisha-ble with fat suppression. Compared to the reference T2 sequence, eliminating fat saturation resulted in a more difficult evaluation of root apices in lower third molars (Figure 3.6, Table 3.2).
In the younger participants, third molars with large remnants of the dental follicle and wide (funnel shaped) open apices were seen. Because in these teeth more soft tissue was present around the apex, the resolution reached with 3D T2, thin slice T2 and T2 with 0.50 × 0.50 mm² in-plane resolution was sufficient to allo-cate a developmental stage. To distinguish an almost closed apex from a closed one in older participants, both the 3D T2 se-quence and the thin slice T2 sequence provided images of insufficient in-plane resolution (Figure 3.7, Figure 3.8). Also the adjusted T2 sequence with in-plane resolution 0.50 × 0.50 mm² was insuffi-cient for this purpose in one case (Figure 3.9, Table 3.2). By contrast, using the ref-erence T2 sequence with its in-plane res-olution of 0.33 × 0.33 mm², all root apices were depicted with sufficient detail for staging.
Doubling averages of the reference T2 sequence resulted in a relative SNR increase of 41% with an acquisition time of 14 min-utes 56 seconds, but did not generate a better representation of the apices (Figure 3.10). Neither did an in-plane resolution of 0.20 × 0.20 mm² (Figure 3.11), not even with doubled averages (Figure 3.12).
Image and statistical analysis
Comparing all in vivo tested sequences with the reference sagittal T2, the Mc-
Nemar test detected only two statisti-cally significant differences (Table 3.2). Lower third molars were not assessable on axial T2 images in 58.8% (95% confi-dence interval (CI) for the difference in proportions [15.9% ; 66.8%], P=0.016), compared to 100% assessable molars on sagittal T2 images. On 3D T2 images only 45.5% of lower third molars could be as-sessed (95% CI [14.5% ; 78.7%], P=0.031). Despite the lack of statistically significant differences in other comparisons, both observers considered the superiority of the reference T2 sequence clinically sig-nificant, especially for third molars in higher developmental stages.
Based on the presented results it was concluded that the reference T2-weighted MR images were best suitable to evaluate third molar root apices for age estimation. Fat
suppression proved to be valuable to dis-tinguish the developing tooth from the surrounding bone and bone marrow. This corresponds to findings of Manoliu et al. (2016) [21]. A resolution of 0.50 × 0.50 mm² was sufficient to evaluate open fun-nel shaped apices. However, to determine whether an individual has reached the age of 18, a closed root apex needs to be dis-tinguished from an almost closed one. In one case an in-plane resolution of 0.33 × 0.33 mm², as in the reference T2 sequence, was necessary for this purpose. The con-cerning tooth would be allocated a lower developmental stage based on the imag-es of lower resolution (0.50 × 0.50 mm²). This implies that the benefit of the doubt would be granted, since the estimated age would be younger than that based on the images of higher resolution (0.33 × 0.33 mm²). A further increase in resolution (0.20 × 0.20 mm²) did not outweigh the
Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation
Discussion

48
FIGURE 3.8 — CORRESPONDING THIN
SLICE ( 1 .7 MM) T2 FSE IMAGES.
These images are equivalent to the
images shown in Figure 3.4 . Only the
ful ly developed mesial root apex can be
dist inguished (arrow). The apex of the
distal root cannot be evaluated with
suff ic ient cer tainty with an in-plane
resolut ion of 0.50 × 0.50 mm².
FIGURE 3.9 — CORRESPONDING T2 FSE
IMAGES WITH IN-PLANE RESOLUTION
0.50 × 0.50 MM² AND REGULAR SLICE
THICKNESS OF 2 MM.
These images are equivalent to the
images shown in Figure 3.4 . Only the
ful ly developed mesial root apex can be
dist inguished (arrow). The apex of the
distal root cannot be evaluated with
suff ic ient cer tainty.
FIGURE 3. 10 — CORRESPONDING T2 FSE
IMAGES WITH DOUBLED AVERAGES.
These images are equivalent to the im-
ages shown in Figure 3.4 . Both the me-
sial (arrow) and the distal (arrowhead)
root can be evaluated. Compared to the
reference sequence, the gain in s ignal-
to-noise rat io is negl igible.
FIGURE 3.7 — CORRESPONDING T2 3D
FSE IMAGES.
These images are equivalent to the im-
ages shown in Figure 3.4 . Because of the
low in-plane resolut ion (0.80 × 0.80mm²),
staging of the root development is
uncer tain .
De Tobel J. Multi-factorial forensic age estimation. Chapter 3: 38-52.

49
disadvantage of a longer acquisition time. Neither did a gain in SNR by increasing averages and hence acquisition time.
To improve image quality the use of intra-oral coils has been suggested [14, 15, 30]. However, to study the develop-ing root apices of third molars a surface coil might be sufficient for three reasons. Firstly, Idiyatullin et al. (2014) calculated the Biot-Savart magnetostatic approxima-tion of the radiofrequency field and re-ported figures of simulations for one-wire loop coils [15]. These figures suggest that a comparable SNR could be reached at the root apices with a conventional extra-oral coil as with an intra-oral coil. Secondly, they reported that it was difficult to po-sition the intra-oral coil sufficiently pos-teriorly to visualize the distal teeth [15].
Moreover, an extra-oral coil is more com-fortable than an intra-oral one, which might reduce motion artefacts. Finally, developing root apices of third molars are often situated relatively far from the oc-clusal plane. In the maxilla they follow the upward curvature of the tuberosity. In the mandible they often lie more lateral than the crown. Thus, their distance to the in-tra-oral coil is increased compared to the other teeth, while the distance to an ex-tra-oral coil is decreased.
Recently two studies were published about a dedicated surface coil for den-tal 3T MRI [10, 25]. The use of this four-channel surface coil (NORAS MRI Products GmbH, Höchberg, Germany) was compared with a standard combined 12-channel head and two-channel neck
FIGURE 3. 1 1 — CORRESPONDING T2 FSE
IMAGES WITH IN-PLANE RESOLUTION
0.20 × 0.20 MM².
These images are equivalent to the im-
ages shown in Figure 3.4 . Both the me-
sial (arrow) and the distal (arrowhead)
root can be evaluated. Compared to the
reference sequence, the gain in resolu-
t ion does not improve the assessabi l i ty
of the roots.
FIGURE 3. 12 — CORRESPONDING T2 FSE
IMAGES WITH IN-PLANE RESOLUTION
0.20 × 0.20 MM² AND DOUBLED AVER-
AGES.
These images are equivalent to the
images shown in Figures 3.4 and 3. 1 1 .
Compared to the T2 FSE sequence with
in-plane resolut ion 0.20 × 0.20 mm²,
the s ignal- to-noise rat io is h igher, but
it does not improve the assessabi l i ty of
the roots. Compared to the reference
sequence, the gain in resolut ion does
not improve the assessabi l i ty of the
roots either.
Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation

50
coil (Siemens Healthcare, Erlangen, Ger-many). Using identical standard MRI pa-rameters the surface coil yielded a SNR gain of about 300% compared to the head/neck coil [25]. Adjustment of sequence parameters resulted in a further optimi-zation with the surface coil, such as an in-creased spatial resolution (voxel size 0.26 × 0.35 × 1.5 mm³) [10]. However, since the surface coil was positioned anteriorly on the face, a significant signal decrease was noted posterior to the mandibular angle [10]. This might imply that this kind of coil is not optimal to study root apices of third molars.
A limited acquisition time is essential to maximize comfort of participants [23] and reduce the chance of motion artefacts [30]. A clinically acceptable time limit of 6 minutes 30 seconds was suggested by Na-sel et al. [23]. The proposed T2 sequence lives up to this recommendation with its acquisition time of 6 minutes 33 seconds.
The major limitation to the reference T2 sequence is that it is not a 3D se-quence. The slice thickness of 2 mm con-trasts sharply with the in-plane resolution of 0.33 × 0.33 mm². The tested sequences with a smaller slice thickness could not combine the requested resolution with a clinically acceptable acquisition time. Nonetheless, if in the future a method for automatic age estimation from third mo-lar MRI would be developed, a sequence with an almost isotropic voxel size is nec-essary. At least the difference between the in-plane resolution and the slice thickness should be limited. Such a method has re-cently been developed for left hand MRI by Stern et al. [27].
Conclusion
The results in this paper suggest that MRI of the third molars could act as an alter-native technique for age estimation. This corresponds to findings of other research groups [1, 11, 24]. The proposed imaging protocol will be used in further research to study its advantages compared to the evaluation of third molars on panoramic radiographs. Baumann et al. stated that MRI seems to be equally suited for dental age estimation as panoramic radiographs [1]. Moreover it has to be studied whether MR images in all planes are necessary or if images in one plane would suffice. To confirm the value of third molar MRI for age estimation, country specific reference samples should be scanned with adequate protocols. Results of a German reference sample between 12 and 24 years old have been published [11]. To include all devel-opmental stages of third molars the refer-ence sample should include individuals from 8 to 24 years old [17].
In conclusion, a T2 FSE MR se-quence at 3T can generate images of the third molars suitable for age estimation. The proposed scanning protocol provides the desired spatial resolution to distinguish closed root
apices from almost closed ones, within a clinically acceptable acquisition time. Further research should determine if this protocol shows enough advantages to be used as an alternative to age estimation based on panoramic radiographs. Final-ly a reference study using this protocol is needed before considering the use of this method for age estimation in practice.
De Tobel J. Multi-factorial forensic age estimation. Chapter 3: 38-52.

51
acknowledgements
The authors wish to thank Prof. Dr. Piet-er Cornillie and Rudy De Tobel for their help in the initial phase of the study. We thank all the volunteers who participat-ed. We also want to express our gratitude to Em. Prof. Dr. Marc Kunnen, Louis Si-moen, Inès Phlypo and Geert Dermaut for their help with the creation and pro-cessing of the images in this paper. Finally we thank Dr. Helen Liversidge, Dr. Djau-dat Idiyatullin, Prof. Dr. Patrick Thevissen and Inès Phlypo for their critical appraisal of the manuscript.
references
[1] Baumann P, Widek T, Merkens H, Boldt J, Petrovic A, Ur-schler M, Kirnbauer B, Jakse N, Scheurer E. Dental age es-timation of living persons: Comparison of MRI with OPG. Forensic Sci Int. 2015;253(0):76-80.
[2] Bracher AK, Hofmann C, Bornstedt A, Boujraf S, Hell E, Ul-rici J, Spahr A, Haller B, Rasche V. Feasibility of ultra-short echo time (UTE) magnetic resonance imaging for identifi-cation of carious lesions. Magn Reson Med. 2011;66(2):538-45.
[3] Buckberry J. The (mis)use of adult age estimates in osteolo-gy. Ann Hum Biol. 2015;42(4):323-31.
[4] Cameron N. Can maturity indicators be used to esti-mate chronological age in children? Ann Hum Biol. 2015;42(4):302-7.
[5] Cole TJ. The evidential value of developmental age imaging for assessing age of majority. Ann Hum Biol. 2015;42(4):379-88.
[6] Cunha E, Baccino E, Martrille L, Ramsthaler F, Prieto J, Schuliar Y, Lynnerup N, Cattaneo C. The problem of aging human remains and living individuals: a review. Forensic Sci Int. 2009;193(1-3):1-13.
[7] Engebretsen L, Steffen K, Bahr R, Broderick C, Dvorak J, Janarv PM, Johnson A, Leglise M, Mamisch TC, McKay D, Micheli L, Schamasch P, Singh GD, Stafford DE, Steen H. The International Olympic Committee Consensus state-ment on age determination in high-level young athletes. Br J Sports Med. 2010;44(7):476-84.
[8] Ferretti F, Malventi M, Malasoma R. Dental magnetic reso-nance imaging: study of impacted mandibular third molars. Dentomaxillofac Radiol. 2009;38(6):387-92.
[9] Gleiser I, Hunt EE, Jr. The permanent mandibular first molar: its calcification, eruption and decay. Am J Phys An-thropol. 1955;13(2):253-83.
[10] Gradl J, Horeth M, Pfefferle T, Prager M, Hilgenfeld T, Ga-reis D, Baumer P, Heiland S, Bendszus M, Hahnel S. Appli-cation of a Dedicated Surface Coil in Dental MRI Provides Superior Image Quality in Comparison with a Standard Coil. Clin Neuroradiol. 2016.
[11] Guo Y, Olze A, Ottow C, Schmidt S, Schulz R, Heindel W, Pfeiffer H, Vieth V, Schmeling A. Dental age estimation in living individuals using 3.0 T MRI of lower third molars. Int J Legal Med. 2015;129(6):1265-70.
[12] Hillewig E, De Tobel J, Cuche O, Vandemaele P, Piette M, Verstraete K. Magnetic resonance imaging of the medial ex-tremity of the clavicle in forensic bone age determination: a new four-minute approach. Eur Radiol. 2011;21(4):757-67.
[13] Hovener JB, Zwick S, Leupold J, Eisenbeibeta AK, Scheife-le C, Schellenberger F, Hennig J, Elverfeldt DV, Ludwig U. Dental MRI: imaging of soft and solid components without ionizing radiation. J Magn Reson Imaging. 2012;36(4):841-6.
[14] Idiyatullin D, Corum C, Moeller S, Prasad HS, Garwood M, Nixdorf DR. Dental magnetic resonance imaging: making the invisible visible. J Endod. 2011;37(6):745-52.
[15] Idiyatullin D, Corum CA, Nixdorf DR, Garwood M. In-traoral approach for imaging teeth using the transverse B1 field components of an occlusally oriented loop coil. Magn Reson Med. 2014;72(1):160-5.
[16] Larsen ST, Arge S, Lynnerup N. The Danish approach to forensic age estimation in the living: how, how many and what’s new? A review of cases performed in 2012. Ann Hum Biol. 2015;42(4):342-7.
[17] Liversidge HM. Timing of human mandibular third molar formation. Ann Hum Biol. 2008;35(3):294-321.
[18] Liversidge HM, Buckberry J, Marquez-Grant N. Age estima-tion. Ann Hum Biol. 2015;42(4):299-301.
[19] Liversidge HM, Chaillet N, Mornstad H, Nystrom M, Rowl-ings K, Taylor J, Willems G. Timing of Demirjian’s tooth formation stages. Ann Hum Biol. 2006;33(4):454-70.
[20] Lockemann U, Fuhrmann A, Püschel K, Schmeling A, Ges-erick G. Arbeitsgemeinschaft für Forensische Altersdiagnos-tik der Deutschen Gesellschaft für Rechtsmedizin. Rechts-medizin. 2004;14(2):123-6.
[21] Manoliu A, Ho M, Nanz D, Dappa E, Boss A, Grodzki DM, Liu W, Chhabra A, Andreisek G, Kuhn FP. MR neurographic orthopantomogram: Ultrashort echo-time imaging of man-dibular bone and teeth complemented with high-resolution morphological and functional MR neurography. J Magn Re-son Imaging. 2016.
[22] Marquez-Grant N. An overview of age estimation in foren-sic anthropology: perspectives and practical considerations. Ann Hum Biol. 2015;42(4):308-22.
Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation

52
[23] Nasel C, Gahleitner A, Breitenseher M, Czerny C, Solar P, Imhof H. Dental MR tomography of the mandible. J Com-put Assist Tomogr. 1998;22(3):498-502.
[24] Ottow C, Krämer JA, Olze A, Schmidt S, Schulz R, Wittsch-ieber D, Heindel W, Pfeiffer H, Ribbecke S, Vieth V, Schmeling A. Magnetresonanztomographiestudie zur Al-tersschätzung von unbegleiteten minderjährigen Flüchtlin-gen. Rechtsmedizin. 2014;25:12-20.
[25] Prager M, Heiland S, Gareis D, Hilgenfeld T, Bendszus M, Gaudino C. Dental MRI using a dedicated RF-coil at 3 Tesla. J Craniomaxillofac Surg. 2015;43(10):2175-82.
[26] Ramsthaler F, Proschek P, Betz W, Verhoff MA. How reli-able are the risk estimates for X-ray examinations in fo-rensic age estimations? A safety update. Int J Legal Med. 2009;123(3):199-204.
[27] Stern D, Ebner T, Bischof H, Grassegger S, Ehammer T, Urschler M. Fully automatic bone age estimation from left hand MR images. Med Image Comput Comput Assist Interv. 2014;17(Pt 2):220-7.
[28] Thevissen PW, Fieuws S, Willems G. Human dental age estimation using third molar developmental stages: does a Bayesian approach outperform regression models to dis-criminate between juveniles and adults? Int J Legal Med. 2010;124(1):35-42.
[29] Thevissen PW, Fieuws S, Willems G. Third molar de-velopment: evaluation of nine tooth development reg-istration techniques for age estimations. J Forensic Sci. 2013;58(2):393-7.
[30] Tymofiyeva O, Boldt J, Rottner K, Schmid F, Richter EJ, Jakob PM. High-resolution 3D magnetic resonance imaging and quantification of carious lesions and dental pulp in vivo. Magma. 2009;22(6):365-74.
[31] Tymofiyeva O, Rottner K, Jakob PM, Richter EJ, Proff P. Three-dimensional localization of impacted teeth us-ing magnetic resonance imaging. Clin Oral Investig. 2010;14(2):169-76.
[32] Urschler M, Grassegger S, Stern D. What automated age estimtion of hand and wrist MRI data tells us about skel-etal maturation in male adolescents. Ann Hum Biol. 2015;42(4):358-67.
[33] Westbrook C. MRI at a Glance. 2nd ed. Hoboken, NJ: Wiley-Blackwell, 2010.
De Tobel J. Multi-factorial forensic age estimation. Chapter 3: 38-52.


54
CHAPTER 4
TH I S CHAPTER ADDRESSED THE FOLLOWING STUDY OB JECT IVE :
Objective 3: To compare the third molars’ MRI with the current gold standard imaging, i.e. radiographs.
PARTS OF TH I S CHAPTER WERE PUBL I SHED AS :
De Tobel J, Hillewig E, Verstraete K. Forensic age estimation based on magnetic reso-nance imaging of third molars: converting 2D staging into 3D staging. Ann Hum Biol. 2017; 44:121-129. [A1; Journal Impact Factor 2017 1.531; Biology Q3; Public, Environ-mental & Occupational Health Q3; Peer reviewed]
RESULTS DESCR I BED IN TH I S CHAPTER WERE PARTLY PRESENTED
AT THE FOLLOWING CONFERENCES :
De Tobel J, Hillewig E, Bogaert S, Deblaere K, Politis C, Verstraete K, Thevissen P. Third molar magnetic resonance imaging (MRI) in forensic age estimation: protocol develop-ment and considerations for use. American Academy of Forensic Sciences (AAFS) 69th Annual Scientific Meeting; New Orleans, USA; February 16, 2017. p 867-868.
De Tobel J, Hillewig E, Verstraete K. Age estimation based on MRI of the third mo-lars: transferring 2D staging into 3D staging. Symposium on Age Estimation, Society for the Study of Human Biology (SSHB) in association with the British Association for Biological Anthropology and Osteoarchaeology (BABAO); Oxford, United Kingdom; December 9-11, 2014.

55
Forensic age estimation based on magnetic resonance imaging of third molars:
converting 2D staging into 3D staging
OR IG INAL RESEARCH
Abstract
Aim — To prospectively study root stage assessment of third molars in age estimation using 3 Tesla magnetic resonance im-aging (MRI) and to compare this with panoramic radiographs, in order to provide considerations for converting 2D staging into 3D staging and to determine the decisive root. Subjects and methods — All third molars were evaluated in 52 healthy participants aged 14-26 years using MRI in three planes. Three staging methods were investigated by two observers. In sixteen of the participants, MRI findings were compared with findings on panoramic radiographs. Results — Decisive roots were pal-atal in upper third molars and distal in lower third molars. Fif-ty seven percent of upper third molars were not assessable on the radiograph, while 96.9% were on MRI. Upper third molars were more difficult to evaluate on radiographs than on MRI (P<0.001). Lower third molars were equally assessable on both imaging techniques (93.8% MRI, 98.4% radiograph), with no difference in level of difficulty (P=0.375). Inter- and intra-ob-server agreement for evaluation was higher in MRI than in radiographs. In both imaging techniques lower third molars showed greater inter- and intra-observer agreement compared to upper third molars. MR images in the sagittal plane proved to be essential for staging. Conclusion — In age estimation, 3T MRI of third molars could be valuable. Some considerations are however necessary to transfer known staging methods to this 3D technique.
Key Words
• third molar root
• panoramic radiograph
• surface head coil
• subadult
AFF IL IAT IONS
1 Department of Radiology and
Nuclear Medicine, Ghent Univer-
sity, Belgium
Funding for this research was entirely
provided by the department of
Radiology and Nuclear Medicine at
Ghent University.
The authors declare that there are
no conflicts of interest.
JANN ICK DE TOBEL 1 ELKE H I LLEW IG 1
KOENRAAD L . VERSTRAETE 1

56
Forensic age estimation in living adolescents and young adults is used in criminal, civil and asylum procedures. The estimation usually has to assess the probability that the examined person has reached a spe-
cific legally relevant age threshold, which in most countries lies between 14 and 22 years of age [22]. Age estimation is also used in sports to make sure athletes par-ticipate in the right age category [8].
The current recommendation for age estimation in living adolescents and young adults – as suggested by the inter-national Study Group on Forensic Age Diagnostics – is a combination of the fol-lowing medical examinations:
— a physical examination including anthropometric data, signs of sex-ual maturation and potential devel-opmental disorders,
— a radiograph of the left hand and wrist,
— a dental examination with clinical assessment of the dentition and an evaluation of a panoramic radio-graph [22, 23].
If the hand and wrist bones appear fully developed on the radiograph an addition-al radiograph or computed tomography (CT) of the medial clavicular epiphysis should be made to establish whether the person has attained 21 years of age [22, 23]. Since these methods use ionizing ra-diation one must comply with the ethical principles. In most countries the use of X-ray examinations without any medi-cal indication is only allowed in criminal procedures. Since it is prohibited in asy-
lum and civil procedures, age estimation is limited to a physical and dental exam-ination. This significantly decreases the accuracy. Therefore it would be valuable to develop protocols for age estimation based on non-ionizing imaging tech-niques [22]. Three dimensional imaging could also counter the problem of super-position. Several studies investigated the use of magnetic resonance imaging (MRI) for skeletal age estimation [7, 8, 12, 14, 21, 24, 28] and for dental age estimation [3, 20]. However, none of these studies dis-cussed the differences between staging on radiographs and on MRI.
The purpose of our research was to prospectively evaluate the use of 3 Tesla (3T) MRI of third molars in age estima-tion. Moreover it was investigated wheth-er the known staging methods – devel-oped for radiography – could be applied to evaluate MR images.
Study population
The approval of the local ethics com-mittee was obtained. Written in-formed consent was obtained from
every participant, and in case of minors from their parents. All participants were healthy Caucasian volunteers between 14 and 26 years old. The sample consisted of two individuals per chronological age per gender (N = 52), without surgical re-moval of any second or third molar. Only persons with at least three third molars present – both impacted and non-im-pacted – were included. Individual teeth were named according to the Internation-al Standards Organization Designation System. Participants were examined with 3T MRI (Magnetom Trio Tim, Siemens, Erlangen, Germany) between March 2012
Introduction
Methods
De Tobel J. Multi-factorial forensic age estimation. Chapter 4: 54-70.

57
and October 2014. When a recent (within six months prior to the scan) panoramic radiograph was available, the participant’s permission was requested to obtain this radiograph from his or her dentist (n = 16). These sixteen participants were also approximately evenly distributed among ages and genders.
Image acquisition
MRI was performed according to the pro-tocol described in De Tobel et al. (2017) [6]. Fast spin echo (FSE) T2 sequences in three planes were used, with a bilater-al four-channel flexible surface head coil (Model NMP-001D-ST-4, Nova Medical Inc., Wilmington, USA). A custom made bite bar individualized with an addition silicone (Futar D®, Kettenbach, Eschen-burg, Germany) minimized moving arte-facts.
When a recent digital panoramic ra-diograph was available (n = 13), this was obtained from the dentist in DICOM-for-mat. Analogue radiographs (n = 3) were digitalized with Perrenity DICOM Burner 4.10 before they were evaluated. The in-terval between the panoramic radiograph and the MRI varied from -17 to 189 days (mean 79, median 58, standard deviation 72.2).
Image analysis
All images were anonymized and assessed separately by two observers. The first ob-server (JDT) was a medical doctor stud-ying dentistry. He had been involved in research on age estimation for five years including three years in evaluating dental radiographs and MRI. The second observ-er (EH) was a researcher at the radiology
department who had been studying skel-etal age estimation on radiographs and MRI for seven years, but without expe-rience in dental imaging. Both observers were trained by an experienced researcher in the field of dental age estimation. For this training, images of (study and non-study) participants of all age ranges were selected. All assessments were conducted on a Barco MFGD 3420 monitor with 3 megapixel resolution (Barco, Kortrijk, Belgium) using K-PACS V 1.6.0 DICOM viewing software. Inter-observer agree-ment was calculated. To assess intra-ob-server agreement, the first observer eval-uated the images twice individually with a three weeks interval.
To avoid biased adjudication of stages, MR images were evaluated independently from radiographs. First, the suitability of each imaging technique for forensic age estimation was evaluated. If an observer judged the image quality to be insuffi-cient, he/she was asked to describe the reason from a number of choices. On MRI these choices were: artefacts due to motion of the participant, other artefacts (e.g. susceptibility due to metal), poor im-age quality (e.g. poor signal-to-noise ra-tio), poor positioning of the coil, apex in between slices, other. On panoramic ra-diographs choices were: superposition of other anatomical structures, artefacts due to motion of the participant, artefacts due to metal, poor image quality (e.g. irradia-tion dose too low), ageing of the non-dig-ital radiograph, other.
If the images were considered suita-ble, the molars were staged according to the methods described by Demirjian et al. (1973) (Table 4.1), Köhler et al. (1994) (Table 4.2) and Olze et al. (2010) (Table
Forensic age estimation based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging

58
4.3). The updated Demirjian method was used as described by Levesque and Demirjian (1980). These three methods represent different ways of staging de-velopment in teeth: based on anatomical characteristics, on estimated final dimen-sions and on surrounding tissues, respec-tively. An overview of Demirjian and Köhler stages on radiographs and on MRI are shown in Figures 4.1 to 4.7. To allo-cate a stage to a molar on MRI, the asses-sors used all the images of a sequence that depicted the molar by scrolling through them to decide which stage was appropri-ate. This was first done based on only the sagittal images. Afterwards, the observers used the combination of sagittal, axial and coronal images, registering the planes they considered essential to assign a tooth stage.
During the training, the observers en-countered some uncertainties in staging on MRI and radiography that were not described in literature. Moreover, consid-erations for converting the staging meth-ods from radiography to MRI were sug-gested (Table 4.4).
Although the Demirjian method sug-gested considering the distal root in mo-lars, applying MRI might allow deciding on a different decisive root, especially since upper molars were studied too. Therefore, since the first observer had more experience with dental imaging, he started by staging all roots separately on MRI, in order to determine the decisive root per third molar. Based on this deci-sion the second observer staged only the decisive root. For the second assessment
TABLE 4. 1 — DEVELOPMENTAL STAGES FOR MOLARS AS DEFINED BY LEVESQUE AND DEMIRJIAN ( 1980).
STAGE DESCRIPTION
STAGE A A beginning of calc if icat ion is seen at the superior level of the crypt in the form of an
inver ted cone or cones. There is no fus ion of these calc if ied points .
STAGE B Fusion of the calcif ied points forms one or several cusps which unite to give a regularly
out l ined occlusal surface.
STAGE C a) Enamel formation is complete at the occlusal surface. I ts extension and convergence
towards the cervical region is seen.
b) The beginning of a dentinal deposit is seen.
c) The out l ine of the pulp chamber has a curved shape at the occlusal border.
STAGE D a) The crown formation is completed down to the cemento-enamel junct ion.
b) The pulp chamber has a trapezoidal shape. The project ion of the pulp horns i f
present , gives an out l ine shaped l ike an umbrel la top.
c) Beginning of root formation is seen in the form of a spicule.
STAGE E a) In it ia l formation of the radicular bifurcation is seen in the form of either a calc if ied
point or a semi- lunar shape.
b) The root length reaches at least one-third of the crown height .
STAGE F a) The calc if ied region of the bifurcation has developed fur ther down from its semi-
lunar stage to give the roots a more def in ite and dist inct out l ine with funnel
shaped endings.
b) The root length equal to or greater than the crown height .
STAGE G The wal ls of the distal root canal are now paral le l and its apical end is st i l l par t ial ly
open.
STAGE H a) The apical end of the distal root canal is completely c losed.
b) The periodontal membrane has a uniform width around the root and the apex.
De Tobel J. Multi-factorial forensic age estimation. Chapter 4: 54-70.

59
TABLE 4.2 — DEVELOPMENTAL STAGES FOR THIRD MOLARS AS DEFINED BY KÖHLER ET AL. ( 1994).
STAGE DESCRIPTION
STAGE I Crown one-half mineral ized.
STAGE I I Crown three-quarters mineral ized.
STAGE I I I Crown completely mineral ized.
STAGE IV Init ia l root formation.
STAGE V Roots one-quar ter mineral ized.
STAGE VI Roots one-half mineral ized.
STAGE VI I Roots three-quar ters mineral ized.
STAGE VI I I Nearly fu l l root length. Divergent wal ls of the canal .
STAGE IX Ful l root length. Paral le l wal ls of the canal .
STAGE X Ful l root length. Convergent wal ls of the canal .
TABLE 4.3 — DEVELOPMENTAL STAGES FOR THIRD MOLARS AS DEFINED BY OLZE ET AL. (2010).
STAGE DESCRIPTION
STAGE 0 The periodontal l igament is v is ib le along the ful l length of al l roots.
STAGE I The periodontal l igament is invis ib le in one root from apex to more than
half root .
STAGE I I The periodontal l igament is invisible along almost the ful l length of one
root or along part of the root in two roots or both.
STAGE I I I The periodontal l igament is invis ib le along almost the ful l length of two
roots.
(to calculate intra-observer agreement) the first observer only evaluated the deci-sive root.
Finally, the observers were asked about the level of difficulty they experienced to stage the molars based on each imaging technique: impossible, high (very dif-ficult), moderate (rather difficult), low (rather easy) or very low (very easy). This parameter reflected the quality of the im-age for age estimation and not the intrin-sic difficulty of the staging method.
Statistical analysis
For analysis, the data were transferred from Microsoft Access 2010 to SPSS Sta-
tistics 22.0 (IBM SPSS Statistics for Win-dows, Armonk, NY). Descriptive statis-tics were calculated. Statistical tests were performed two-sided and evaluated at the 0.05 significance level. When com-parisons were made between MRI and radiography or within radiography, only the sixteen participants who had a radi-ograph were included in the tests. When comparisons were made within MRI, all 52 participants were included. Combined results for upper third molars were re-ported, because in all variables results and P-values for tooth 18 were similar to those for tooth 28. The same applies to lower third molars.
Forensic age estimation based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging

60
FIGURE 4. 1 — SAGITTAL MR IMAGES OF
THIRD MOLARS IN DEMIRJIAN STAGE D,
KÖHLER STAGE IV.
On each image the white arrow indi-
cates the spicule of the decis ive root .
a Upper third molar.
b Lower third molar. No panoram-
ic radiographs depict ing these
teeth were avai lable.
FIGURE 4.2 — IMAGES OF THIRD MOLARS
IN DEMIRJIAN STAGE E, KÖHLER STAGE V.
a, c The same upper third molar is de-
picted, respect ively on panoramic
radiograph and sagittal MRI .
b, d The same lower third molar is de-
picted, respect ively on panoramic
radiograph and sagittal MRI .
White arrows indicate the decis ive roots,
which are assessable on al l images.
Moreover a developing furcation is v is i-
ble (white arrowheads).
FIGURE 4.3 — IMAGES OF THIRD MOLARS
IN DEMIRJIAN STAGE F, KÖHLER STAGE VI .
a, c The same upper third molar is de-
picted, respect ively on panoramic
radiograph and sagittal MRI .
b, d The same lower third molar is de-
picted, respect ively on panoramic
radiograph and sagittal MRI .
White arrows indicate the decis ive roots,
which are assessable on al l images.
De Tobel J. Multi-factorial forensic age estimation. Chapter 4: 54-70.

61
FIGURE 4.4 — IMAGES OF THIRD MOLARS
IN DEMIRJIAN STAGE F, KÖHLER STAGE VI I .
a, c The same upper third molar is de-
picted, respect ively on panoramic
radiograph and sagittal MRI .
b, d The same lower third molar is de-
picted, respect ively on panoramic
radiograph and sagittal MRI .
White arrows indicate the decis ive roots,
which are assessable on al l images.
FIGURE 4.5 — IMAGES OF THIRD MOLARS
IN DEMIRJIAN STAGE F, KÖHLER STAGE VI I I
a, c The same upper third molar is de-
picted, respect ively on panoramic
radiograph and sagittal MRI .
b, d The same lower third molar is de-
picted, respect ively on panoramic
radiograph and sagittal MRI .
White arrows indicate the decis ive roots,
which are assessable on al l images.
Forensic age estimation based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging

62
FIGURE 4.6 — IMAGES OF THIRD MOLARS
IN DEMIRJIAN STAGE G, KÖHLER STAGE IX.
a, c The same upper third molar is de-
picted, respect ively on panoramic
radiograph and sagittal MRI .
b, d The same lower third molar is de-
picted, respect ively on panoramic
radiograph and sagittal MRI .
White arrows indicate the assessable
decis ive roots. Due to superposit ion,
evaluation of the apex was impossible in
f igure a (black arrow).
TABLE 4.4 — CONSIDERATIONS FOR CONVERTING THE STAGING METHODS FROM RADIOGRAPHY TO MRI .
METHOD STAGE DESCRIPTION
Demir j ian
Köhler
D
IV
Beginning of root formation is seen in the form of a spicule. This spicule was
interpreted as a straight structure in contrast to the curved appearance of
the root spicule in the higher stages.
Köhler V The root was considered one-quar ter complete when the spicule began show-
ing a curved shape, regardless of the presence of the radicular bifurcation.
Demir j ian E The presence of the root furcation was not considered the main criterion since
some third molars had only one root and the furcation might be formed later
when the molar is a taurodont [ 16] . Instead the criterion of root length reach-
ing one-third of the crown height was considered the most important.
Demir j ian E As soon as a hypo-intense point was seen on any image at a location where
the bifurcation would be expected, this stage was al located. However, no
c lar ity could be given about a threshold for the intensity of this point , s ince
in MRI s ignal intensity is not uniformly determined by the composit ion of the
t issue. (By contrast , in CT the Hounsf ie ld units do uniformly depend on t issue
composit ion.)
Demir j ian F The endings of the root were considered funnel shaped when this shape per-
sisted for some mil l imetres.
Demir j ian H The distinction between stage G and H should not be based on one pixel with
relatively lower signal intensity. When the walls at the apex of the root canal
show relatively thick dentin, then stage H is more appropriate then stage G.
Demir j ian H The apex may be diff icult to locate in lower third molars, s ince the extension
of the mandibular canal – which contains the neurovascular str ing entering
the root apex – may mimic the appearance of the root canal (F igure 4. 10).
However, this extension is located more caudal ly than the apex of the molar.
De Tobel J. Multi-factorial forensic age estimation. Chapter 4: 54-70.

63
FIGURE 4.7 — IMAGES OF THIRD MOLARS
IN DEMIRJIAN STAGE H, KÖHLER STAGE X.
a, c The same upper third molar is de-
picted, respect ively on panoramic
radiograph and sagittal MRI .
b, d The same lower third molar is de-
picted, respect ively on panoramic
radiograph and sagittal MRI .
White arrows indicate the assessable
decis ive roots. Due to superposit ion,
evaluation of the apex was impossible in
f igure a (black arrow).
Note that the mesial root of the low-
er third molar is in Demir j ian stage G,
Köhler stage IX , as can be seen on the
radiograph b and on the sagittal MR
image d (white arrowheads).
Based on the evaluation of the first observ-er, the proportion of assessable images of the different roots on MRI was compared using a McNemar’s test. This led to the choice of the decisive roots. The results of both observers were combined to evaluate the suitability of the images for the alloca-tion of developmental stages (McNemar’s test), to report the level of difficulty this allocation entailed (Wilcoxon matched-pairs signed-ranks test) and to determine which planes were essential for staging on MRI. Intra-class Correlation Coefficient (ICC) was calculated to quantify intra- and inter-observer variability.
Because of the small study sample, no subgroup analyses were done by tooth stage, age group or gender.
In most of the fully developed third molars the visibility of the periodon-tal ligament on MRI was insufficient to assess stages as described by Olze
et al. (2010). Therefore this method could not be applied. Thus staging for this study
was done using the methods of Demirjian et al. (1973) [15] and Köhler et al. (1994).
Choice of decisive roots
The choice of decisive roots was based on two items: assessability of the differ-ent roots within a tooth and their rela-tive developmental stage. In upper third molars, assessability of the roots differed significantly (Table 4.5). The palatal root was the most suitable for staging, since 98% (100/102) were assessable (Figure 4.8). This differed significantly from the proportion assessable mesiobuccal roots (82/95 = 86%, P = 0.003) and distobuccal roots (71/93 = 76%, P = 0.004).
When all roots were visible on MRI, the development of the palatal root was either at the same level as the buccal roots (72/82 = 88%) or at a lower stage (8/82 = 10%). By contrast, no significant differ-ence in assessability was seen between both roots in lower third molars. In most of the cases the distal root was equally de-
Results
Forensic age estimation based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging

64
veloped as the mesial root (78/96= 81%) or at a lower stage (13/96 = 14%). Thus the distal root was considered decisive.
Staging on panoramic radiograph versus MRI
Suitability of the imaging techniques
When the evaluation of a root was impos-sible on the radiograph, this was always due to superposition of other anatom-ical structures (Figures 4.6 and 4.7). On MRI this was due to insufficient image quality (e.g. poor signal-to-noise ratio), insufficient contrast between apex and surrounding cortex (Figure 4.9) or the tip of the apex falling in between slices. The number of assessable upper third molars on MRI (62/64 = 97%) differed signifi-cantly from the number on radiograph (37/64 = 58%) with P < 0.001. In the lower jaw however, there was no significant dif-ference (P = 0.375) .with 94% (60/64) as-sessable molars on MRI and 98% (63/64) on radiograph.
Difficulty of the assessment
When an upper third molar appeared as-sessable, staging was less difficult based on MRI than on the radiograph (Table 4.6). A Wilcoxon matched-pairs signed-ranks test to compare the level of diffi-
culty between assessments on both im-aging techniques showed a significant difference with P < 0.001. For lower third molars however, the level of difficulty did not significantly differ between MRI and radiography (P = 0.438). In all evaluated teeth the assessment was more difficult at the higher developmental stages – of both the Demirjian and Köhler staging method – compared with the lower ones.
Inter- and intra-observer variability
No inter-observer variability could be cal-culated for tooth 18 on panoramic radi-ograph, since one observer allocated the same stage to every 18 (thus, the variable was a constant). Regardless of the imaging technique, the staging of the lower third molars (ICC from 0.82 to 0.95) was asso-ciated with less variability than the stag-ing of the upper third molars (ICC from 0.40 to 0.90). The agreement between observers was higher in the evaluation of MRI (ICC from 0.85 to 0.95) than in the evaluation of panoramic radiographs (ICC from 0.40 to 0.86) (Table 4.7). This also applied to intra-observer agreement of the first observer (ICC from 0.94 to 0.98 for MRI and from 0.13 to 0.98 for ra-diographs).
TABLE 4.5 — ASSESSABILITY OF THE DIFFERENT ROOTS BASED ON MRI .
ELEMENTS ROOT ASSESSABLE IMAGES
Upper third molars Palatal
Mesiobuccal
Distobuccal
98% (100/102)
86% (82/95)
76% (71/93)
Lower third molars Distal
Mesial
97% (100/103)
97% (97/100)
De Tobel J. Multi-factorial forensic age estimation. Chapter 4: 54-70.

65
a The palatal root shows an apex in Demir j ian stage F, Köhler stage VI I (arrow).
b No apices can be evaluated on this image.
c The distobuccal root is assessable. I t is in Demir j ian stage F, Köhler stage VI I (arrow). On this
image the mesiobuccal root appears to show its apex (arrowhead), but the adequate image for
assessment is the more buccal one.
d The apex of the mesiobuccal root is in Demir j ian stage F, Köhler stage VI I I (arrow). The distobuccal
root should not be assessed on this image (arrowhead).
FIGURE 4.8 — CONSECUTIVE SAGITTAL MR IMAGES OF 18 FROM PALATAL TO BUCCAL, WITH A SLICE THICK-
NESS OF 2 MM.
Results
FIGURE 4.9 — CONSECUTIVE SAGITTAL
MR IMAGES OF 18 FROM BUCCAL TO PAL-
ATAL, WITH A SLICE THICKNESS OF 2 MM.
The contours of the root wal ls are not
c learly dist inguishable from surrounding
t issues (arrows).
FIGURE 4. 10 — CONSECUTIVE SAGITTAL
MR IMAGES OF 38 FROM BUCCAL TO
LINGUAL, WITH A SLICE THICKNESS OF
2 MM.
a The extension of the mandibular
canal mimics the appearance of
the root canal of the distal root
( in between arrowheads).
b The actual apex of the distal root
(arrow).
Forensic age estimation based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging

66
Essential planes for MRI
The sagittal MR images proved to be es-sential for staging in 99% (191/194) of the assessable upper third molars. Axi-al (25/194 = 13%) and coronal (30/194 = 16%) images were only essential in a small minority of upper third molars. In assessable lower third molars the ob-servers considered the sagittal images to be essential in 100% (190/190) of cases. Axial images were only important for 4% (7/190), while 6% (12/190) of the coronal images contributed to the allocation of a developmental stage to lower third mo-lars. Moreover, in six upper third molars (6/194 = 3.1%) combining the sagittal images with axial or coronal ones led to a different stage than the stage that was al-located based on the sagittal images alone. Twice (2/194 = 1.0%) a Demirjian stage H (Köhler stage X) was changed to stage G (stage IX). Three times (3/194 = 1.5%) it was the other way round. And once (1-194 = 0.5%) Demirjian stage F (Köhler stage VIII) was changed to stage G (stage IX). In three lower third molars changes were made. Twice (2/190= 1.0%) Demirji-an stage G (Köhler stage IX) was changed to stage H (stage X). Once (1/190 = 0.5%) Köhler stage VII was changed to stage VI (both Demirjian stage F).
The current recommendations re-garding imaging for forensic age estimation in living adolescents and young adults have two major draw-backs. Firstly, they imply radiation
exposure without clinical indication, which raises ethical questions [27]. In some countries the use of ionizing radia-tion is prohibited in asylum and civil pro-cedures, leading to a decrease in the pos-sibilities to estimate age accurately [22]. Secondly, on radiographs superposition can interfere with the correct assignment of developmental stages, e.g. when the hard palate is superimposed over roots of the upper teeth. This problem is overcome by 3D imaging techniques. In an attempt to counter these drawbacks the use of 3T dental MRI in this field of study was prospectively investigated in this paper. Since the known staging methods were developed for radiographic images, it was timely to explore if radiographic staging methods were appropriate for MRI.
Choice of decisive roots
Reference studies about age estimation on radiographs did not specify which root of the upper third molars was being evalu-ated [25]. Pilot studies on dental MRI also failed to clarify which root is most
Discussion
TABLE 4.6 — LEVEL OF DIFFICULTY ASSOCIATED WITH ALLOCATING A DEVELOPMENTAL STAGE TO A THIRD
MOLAR (N=64).
ELEMENTS IMAGING
TECHNIQUE
LEVEL OF DIFFICULTY
IMPOSSIBLE HIGH MODERATE LOW VERY LOW
Upper third
molars
MRI
Radiograph
3%
42%
(2)
(27)
14%
23%
(9)
( 15)
33%
23%
(21 )
( 15)
16%
8%
( 10)
(5)
34%
3%
(22)
(2)
Lower third
molars
MRI
Radiograph
6%
2%
(4)
( 1 )
13%
14%
(8)
(9)
30%
25%
(19)
( 16)
19%
31%
( 12)
(20)
33%
28%
(21 )
( 18)
De Tobel J. Multi-factorial forensic age estimation. Chapter 4: 54-70.

67
adequate [3, 20]. In our sample the pala-tal root proved to be best suited, while in lower third molars this was the distal root. However, this was concluded based on the assessment of one observer. Further research comparing relative root develop-ment in a same tooth, evaluated by sever-al observers, is necessary to confirm our findings. In literature contradictory opin-ions exist about the decisive root in lower third molars. Friedrich et al. (2003) report that the mesial root shows tendency to an increased growth speed, compared to the distal root, but the difference was not sta-tistically significant. They claim that the more advanced root should be considered decisive, which is in contrast to the ben-efit of the doubt. Authors that used the Demirjian method however, considered the distal root decisive [17].
Staging on panoramic radiograph versus staging on MRI
Suitability of the imaging techniques
Almost half of the upper third molars in our study were not assessable on pano-ramic radiograph, which corresponds to findings of Baumann et al. (2015). Most previous reports investigate lower third molars and omit upper third molars from the analyses [1, 10, 18]. However, Thevis-sen et al. (2013) found that the accuracy of age estimation based on the lower third molar improved significantly when the stage of the upper third molar was add-ed to the regression model. In our study, investigating upper third molars with MRI increased the proportion of assess-able ones to a similar level (97%) as the proportion assessable lower third molars (94%). Moreover, the projection on ra-diographs might hide information about
Forensic age estimation based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging
TABLE 4.7 — INTEROBSERVER VARIABILITY ( INTRACLASS CORRELATION COEFFICIENT) FOR STAGING THIRD
MOLARS ON MRI AND ON PANORAMIC RADIOGRAPH. NA = Not appl icable, because one of both observers
al located the same stage to every 18.
IMAGING TECHNIQUE ELEMENT INTEROBSERVER VARIABILITY
DEMIRJIAN KÖHLER NUMBER
OF CASES
ICC 95% CI ICC 95% CI
MRI 18 0.85 0.73 - 0.91 0.86 0.76 - 0.92 45
28 0.90 0.84 - 0.95 0.86 0.76 - 0.92 47
38 0.93 0.88 - 0.96 0.95 0.92 - 0.98 44
48 0.94 0.89 - 0.97 0.91 0.82 - 0.95 47
Panoramic radiograph 18 NA NA 0.40 -0.38 - 0.86 7
28 0.79 0.24 - 0.96 0.84 0. 13 - 0.97 8
38 0.82 0.56 - 0.94 0.83 0.53 - 0.94 15
48 0.85 062 - 0.94 0.86 0.66 - 0.95 16

68
the direction of the root. On MRI propor-tions of the tooth can be estimated more accurately than on radiographs, because tilting can be taken into account to esti-mate tooth dimensions. Herein lies the biggest difference between the staging on 2D radiographs – on which a projection is depicted – and staging on 3D MR im-ages – on which a section is depicted. In Figure 4.4b it is clear that the lower third molar is tilted mesially, but nothing can be concluded about buccolingual inclina-tion. Figure 4.4d shows the apices of the roots, but not the crown which is depict-ed on more lingual slices. Thus, in Figure 4.4b the length of the tooth might be un-derestimated.
Difficulty of the assessment
Staging upper third molars was signifi-cantly easier on MRI than on panoram-ic radiograph. This was not observed for lower third molars. In both imaging tech-niques observers found it more difficult to stage molars that were in the highest stages (Demirjian G and H, Köhler IX and X). In earlier stages a wide open apex and its surrounding follicle were always clear-ly depicted on an MR image, whereas an (almost) closed apex could fall in between MR slices or blend into the surrounding cortex.
Inter- and intra-observer variability
De Angelis et al. (2014) stressed that den-tal age estimation should be performed by experienced observers, as is the case for age estimation based on imaging of other anatomical structures [29]. How-ever our MRI results showed that staging of third molars could be done with great agreement between the experienced and
inexperienced observer, after adequate training.
The low number of assessable upper third molars on panoramic radiograph yielded wide 95% confidence intervals for inter- and intra-observer variability compared to MRI. In literature the cal-culations of this variability are often not reported in detail [5, 17].
Essential planes for MRI
Due to the anatomy of third molars, sagit-tal MR images are best suited for allocat-ing a developmental stage. Axial or coro-nal images can be helpful in case of doubt. This might occur when a molar is tilted or when the apex is not clearly visible on the sagittal images in higher stages (Demirji-an G and H, Köhler IX and X). In lower stages sagittal slices are sufficient.
Study limitations and future prospects
There are four limitations to our study that need consideration. The first one lies in the small study sample. Too few pano-ramic radiographs could be compared to a corresponding MRI to draw strong con-clusions about the value of MRI. Moreo-ver, the time interval between radiograph and MRI is a drawback. Ideally both im-aging techniques should be applied on the same day, but this was not feasible at our institution. Furthermore the influence of impaction and of extracted premolars was not investigated. In literature it is suggest-ed that extractions might accelerate third molar eruption [9] and if or how this re-lates to formation is unclear. The influ-ence of impaction is controversial [10, 19]. A larger reference sample is needed
De Tobel J. Multi-factorial forensic age estimation. Chapter 4: 54-70.

69
Conclusion
to counter these first three limitations, but also to compare the value of different staging methods and to develop a statisti-cal model for age estimation.
A final study limitation is the slice thickness (2 mm) of the used MR se-quences. De Tobel et al. (2017) [6] point-ed out the balance between slice thickness and spatial resolution. Although a 3D se-quence would prevent the apex from fall-ing in between MR slices, insufficient res-olution would also compromise adequate staging.
The results in this paper suggest that dental MRI may act as an alternative tech-nique for age estimation. Its advantages justify further investigation. It would also be useful to combine dental MRI with MRI of other anatomical structures used for age estimation, e.g. wrist MRI. The value of this approach to estimate the age of individuals with more precision has been stressed by several authors [2, 4, 11, 13, 23, 26]. The lack of ionizing radiation in MRI offers opportunities to study the development of anatomical structures longitudinally [7].
In conclusion, 3T MRI of third molars has advantages compared to panoramic radiographs, possi-bly making it useful in forensic age estimation practice. Some consid-erations are however necessary to
transfer known staging methods to this 3D technique, as described in this paper. Further research is necessary to validate and improve the use of MRI in forensic dental age estimation.
acknowledgements
The authors wish to thank all the partic-ipants and everybody who helped with the recruitment. We are very grateful to Dr. Helen Liversidge for discussing stage assessment and comparing 2D with 3D images. Moreover, she provided invalua-ble language advice. We wish to thank the dentists who allowed us access to their patient records software in order to re-trieve the panoramic radiographs. With special thanks to Rik Jamaels for enabling the gathering of these radiographs. We are pleased to acknowledge the organ-izational and administrative help given by Katrien Saegerman. Also the critical appraisal of the document by Inès Phly-po is appreciated. Finally we express our gratitude to Prof. Dr. Marc Kunnen for his help with processing of the images in this paper.
references
[1] Bassed RB, Briggs C, Drummer OH. Age Estimation and the Developing Third Molar Tooth: An Analysis of an Australi-an Population Using Computed Tomography. J Forensic Sci. 2011;56(5):1185-91.
[2] Bassed RB, Briggs C, Drummer OH. Age estimation using CT imaging of the third molar tooth, the medial clavicular epiphysis, and the spheno-occipital synchondrosis: A multi-factorial approach. Forensic SciInt. 2011.
[3] Baumann P, Widek T, Merkens H, Boldt J, Petrovic A, Ur-schler M, Kirnbauer B, Jakse N, Scheurer E. Dental age es-timation of living persons: Comparison of MRI with OPG. Forensic Sci Int. 2015;253(0):76-80.
[4] Cameriere R, De Luca S, Biagi R, Cingolani M, Farronato G, Ferrante L. Accuracy of three age estimation methods in children by measurements of developing teeth and car-pals and epiphyses of the ulna and radius. J Forensic Sci. 2012;57(5):1263-70.
[5] Cameriere R, Ferrante L, De Angelis D, Scarpino F, Galli F. The comparison between measurement of open apices of third molars and Demirjian stages to test chronological age of over 18 year olds in living subjects. Int J Legal Med. 2008;122(6):493-7.
[6] De Tobel J, Hillewig E, Bogaert S, Deblaere K, Verstraete K. Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation. Ann Hum Biol. 2017;44(2):130-9.
Forensic age estimation based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging

70
[7] Dedouit F, Auriol J, Rousseau H, Rouge D, Crubezy E, Telm-on N. Age assessment by magnetic resonance imaging of the knee: a preliminary study. Forensic Sci Int. 2012;217(1-3):232 e1-7.
[8] Dvorak J, George J, Junge A, Hodler J. Age determination by magnetic resonance imaging of the wrist in adolescent male football players. Br J Sports Med. 2007;41(1):45-52.
[9] Fanning EA. Third molar emergence in Bostonians. Am J Phys Anthropol. 1962;20(3):339-45.
[10] Friedrich RE, Ulbricht C, Ljuba ABvM. The influence of wisdom tooth impaction on root formation. Ann Anat. 2003;185(5):481-92.
[11] Garamendi PM, Landa MI, Ballesteros J, Solano MA. Relia-bility of the methods applied to assess age minority in living subjects around 18 years old. A survey on a Moroccan origin population. Forensic Sci Int. 2005;154(1):3-12.
[12] Hillewig E, De Tobel J, Cuche O, Vandemaele P, Piette M, Verstraete K. Magnetic resonance imaging of the medial ex-tremity of the clavicle in forensic bone age determination: a new four-minute approach. Eur Radiol. 2011;21(4):757-67.
[13] Hillewig E, Degroote J, Van der Paelt T, Visscher A, Vande-maele P, Lutin B, D'Hooghe L, Vandriessche V, Piette M, Ver-straete K. Magnetic resonance imaging of the sternal extrem-ity of the clavicle in forensic age estimation: towards more sound age estimates. Int J Legal Med. 2013;127(3):677-89.
[14] Kramer JA, Schmidt S, Jurgens KU, Lentschig M, Schmeling A, Vieth V. Forensic age estimation in living individuals us-ing 3.0T MRI of the distal femur. Int J Legal Med. 2014.
[15] Levesque GY, Demirjian A. The inter-examiner variation in rating dental formation from radiographs. J Dent Res. 1980;59(7):1123-6.
[16] Liversidge HM. Timing of human mandibular third molar formation. Ann Hum Biol. 2008;35(3):294-321.
[17] Liversidge HM, Marsden PH. Estimating age and the like-lihood of having attained 18 years of age using mandibular third molars. Br Dent J. 2010;209(8):E13.
[18] Mincer HH, Harris EF, Berryman HE. The A.B.F.O. study of third molar development and its use as an estimator of chronological age. J Forensic Sci. 1993;38(2):379-90.
[19] Olze A, van Niekerk P, Schulz R, Ribbecke S, Schmeling A. The influence of impaction on the rate of third molar mineralisation in male black Africans. Int J Legal Med. 2012;126(6):869-74.
[20] Ottow C, Krämer JA, Olze A, Schmidt S, Schulz R, Wittsch-ieber D, Heindel W, Pfeiffer H, Ribbecke S, Vieth V, Schmeling A. Magnetresonanztomographiestudie zur Al-tersschätzung von unbegleiteten minderjährigen Flüchtlin-gen. Rechtsmedizin. 2014;25:12-20.
[21] Saint-Martin P, Rerolle C, Dedouit F, Bouilleau L, Rousseau H, Rouge D, Telmon N. Age estimation by magnetic reso-nance imaging of the distal tibial epiphysis and the calcane-um. Int J Legal Med. 2013;127(5):1023-30.
[22] Schmeling A, Geserick G, Reisinger W, Olze A. Age estima-tion. Forensic Sci Int. 2007;165(2-3):178-81.
[23] Schmeling A, Grundmann C, Fuhrmann A, Kaatsch HJ, Knell B, Ramsthaler F, Reisinger W, Riepert T, Ritz-Timme S, Ros-ing FW, Rotzscher K, Geserick G. Criteria for age estimation in living individuals. Int J Legal Med. 2008;122(6):457-60.
[24] Terada Y, Kono S, Tamada D, Uchiumi T, Kose K, Miyagi R, Yamabe E, Yoshioka H. Skeletal age assessment in chil-dren using an open compact MRI system. Magn Reson Med. 2013;69(6):1697-702.
[25] Thevissen PW, Fieuws S, Willems G. Human dental age estimation using third molar developmental stages: does a Bayesian approach outperform regression models to dis-criminate between juveniles and adults? Int J Legal Med. 2010;124(1):35-42.
[26] Thevissen PW, Kaur J, Willems G. Human age estimation combining third molar and skeletal development. Int J Legal Med. 2012;126(2):285-92.
[27] Thevissen PW, Kvaal SI, Dierickx K, Willems G. Ethics in age estimation of unaccompanied minors. J Forensic Odontos-tomatol. 2012;30 Suppl 1:84-102.
[28] Vieth V, Schulz R, Brinkmeier P, Dvorak J, Schmeling A. Age estimation in U-20 football players using 3.0 tesla MRI of the clavicle. Forensic Sci Int. 2014;241c:118-22.
[29] Wittschieber D, Schulz R, Vieth V, Kuppers M, Bajanowski T, Ramsthaler F, Puschel K, Pfeiffer H, Schmidt S, Schmeling A. Influence of the examiner's qualification and sources of error during stage determination of the medial clavicular ep-iphysis by means of computed tomography. Int J Legal Med. 2014;128(1):183-91.
De Tobel J. Multi-factorial forensic age estimation. Chapter 4: 54-70.


72
CHAPTER 5
TH I S CHAPTER ADDRESSED THE FOLLOWING STUDY OB JECT IVES :
Objective 1: To collect a reference dataset of MR images of third molars, left wrist and both clavicles. These images will be registered simultaneously in each participant.
Objective 4: To stage the development of each age predictor based on the MRI. Existing 2D staging techniques will be modified or new methods will be developed. Reproduci-bility of the staging techniques will be tested.
Objective 5: To fit a statistical age estimation model on the reference data set, for each age predictor individually, as well as combining all registered age predictors. In all these models Bayes’ rule will be applied to counter drawbacks of other regression methods. Objective 6: To validate this model and to compare its performance with existing models.
TH I S CHAPTER WAS PUBL I SHED AS :
De Tobel J, Phlypo I, Fieuws S, Politis C, Verstraete K, Thevissen P. Forensic age estima-tion based on development of third molars: a staging technique for magnetic resonance imaging. J Forensic Odontostomatol. 2017; 35:117-140. [A2; Not included in Journal Citation Reports; Peer reviewed]
RESULTS DESCR I BED IN TH I S CHAPTER WERE PARTLY PRESENTED
AT THE FOLLOWING CONFERENCE :
De Tobel J, Phlypo I, Fieuws S, Politis C, Verstraete K, Thevissen P. Forensic age estima-tion based on development of third molars: a staging technique for magnetic resonance imaging. Triennial International Organization for Forensic Odonto-Stomatology (IO-FOS) Conference. Leuven, Belgium; September 15, 2017. p 21

73
Forensic age estimation based on development of third molars: a staging technique
for magnetic resonance imaging
OR IG INAL RESEARCH
Abstract
Background — The development of third molars can be evaluated with med-
ical imaging to estimate age in subadults. The appearance of third molars on
magnetic resonance imaging (MRI) differs greatly from that on radiographs.
Therefore a specific staging technique is necessary to classify third molar de-
velopment on MRI and to apply it for age estimation. Aim — To develop a
specific staging technique to register third molar development on MRI and
to evaluate its performance for age estimation in subadults. Materials and
methods — Using 3T MRI in three planes, all third molars were evaluated in
309 healthy Caucasian participants from 14 to 26 years old. According to the
appearance of the developing third molars on MRI, descriptive criteria and
schematic representations were established to define a specific staging tech-
nique. Two observers, with different levels of experience, staged all third mo-
lars independently with the developed technique. Intra- and inter-observer
agreement were calculated. The data were imported in a Bayesian model for
age estimation as described by Fieuws et al. (2016). This approach adequately
handles correlation between age indicators and missing age indicators. It was
used to calculate a point estimate and a prediction interval of the estimated
age. Observed age minus predicted age was calculated, reflecting the error
of the estimate. Results — One-hundred and sixty-six third molars were
agenetic. Five percent (51/1096) of upper third molars and 7% (70/1044) of
lower third molars were not assessable. Kappa for inter-observer agreement
ranged from 0.76 to 0.80. For intra-observer agreement kappa ranged from
0.80 to 0.89. However, two stage differences between observers or between
staging sessions occurred in up to 2.2% (20/899) of assessments, probably
due to a learning effect. Using the Bayesian model for age estimation, a mean
absolute error of 2.0 years in females and 1.7 years in males was obtained.
Root mean squared error equalled 2.38 years and 2.06 years respectively. The
performance to discern minors from adults was better for males than for
females, with specificities of 96% and 73% respectively. Conclusion — Age
estimations based on the proposed staging technique for third molars on
MRI showed comparable reproducibility and performance as the established
methods based on radiographs.
Key Words
• magnetic resonance imaging
• staging technique
• third molars
• age estimation
• subadult
AFF IL IAT IONS
1 Department of Radiology and
Nuclear Medicine, Ghent Univer-
sity, Belgium
2 Department of Oral Health
Sciences – Forensic Dentistry,
KU Leuven and Department of
Dentistry – University Hospitals
Leuven, Belgium
3 Department of Oral and Maxillo-
facial Surgery, Leuven University
Hospital, Belgium
4 Department of Head, Neck and
Maxillofacial Surgery, Ghent
University Hospital, Belgium
5 Department of Dentistry –
Special Care in Dentistry, PaeCo-
MeDiS, Ghent University, Ghent,
Belgium
6 Leuven Biostatistics and Sta-
tistical Bioinformatics Centre
(L-BioStat), Leuven, Belgium
Funding for this research was entirely
provided by the department of Radi-
ology and Nuclear Medicine at Ghent
University and the department of
Forensic Dentistry at KU Leuven.
The authors declare that there are
no conflicts of interest.
JANN ICK DE TOBEL 1 2 34 I N ÈS PHLYPO 5
STEFFEN F I EUWS 6 CONSTANT INUS POL I T I S 3
KOENRAAD L . VERSTRAETE 1 PATR ICK W. THEV I S SEN 2

74
Staging third molars’ development
The development of third molars can be evaluated with medical im-aging to estimate age in subadults
by allocating developmental stages. A staging technique should cover the en-tire maturation sequence of the structure that is evaluated [31, 49]. Thevissen et al. (2013) pointed out that the choice of staging technique should depend on the number of stages in the period of interest [49]. Moreover, stages should be defined unambiguously with clear threshold be-tween them [49]. In forensic context, the most important question to be answered is whether or not the individual is a minor or an adult. Therefore, in most countries, an adequate staging technique should en-compass stages defined by changes that occur around the 18th birthday. A balance should be sought between a comprehen-sive method with a sufficient number of stages and a performant method with suf-ficient reproducibility and accuracy [43]. Stage characteristics should be straight-forward and simple, in order to facilitate the learning process for observers and to exclude stage overlap caused by different interpretations.
Numerous staging techniques have been described, all of them based on ra-diological appearance of developing teeth [35, 49]. In all published papers on dental age estimation based on MRI of third mo-lars, the radiological staging techniques were extrapolated without any MR spe-cific validity testing [5, 12, 13, 20, 38]. All of them used the Demirjian staging technique, whereas De Tobel et al. (2017) used both the Demirjian and the Köhler technique [14, 28]. Demirjian stages are
defined by objective criteria, while Köhler stages are based on predictions of crown and root lengths. De Tobel et al. reported considerations to take into account when transferring Demirjian and Köhler stages to MRI. Still, major concerns remain re-garding the different appearance on MRI compared with radiographs, which can-not be overcome using the existing stag-ing techniques. Therefore, a specific stag-ing technique is necessary to classify third molar development on MRI and to apply it for age estimation.
Statistical approach to age estimation
It has been stated that a Bayesian approach renders the most appropriate age estima-tion using developmental stages [23, 47]. Although the prediction outcome does not strongly outperform the classical re-gression result, it circumvents some as-sumptions that are not true in age estima-tion: (1) a linear relationship between age and stages, (2) a normal distribution of the variation of age around the mean with a constant variance and (3) uncorrelated development of the different anatomical structures [23, 45]. The major drawback of a Bayesian approach is its computation-al burden when combining multiple de-pendent predictors. However, this can be circumvented. Fieuws et al. (2016) report-ed a practical approach using Bayes’ rule combining multiple age indicators based on Boldsen et al. (2002) [6, 16]. The ad-hoc procedure allows constructing an ap-proximate confidence interval without the need to model the multivariate correlation structure between the indicators [16].
Introduction
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.

75
Aims
The aims of the current study were (1) to develop an MRI specific staging tech-nique for the development of third molars and (2) to evaluate the age estimation per-formance of a Bayesian approach using this MRI specific staging.
Study population
The local ethics committee approved the study and written informed consent was obtained from every participant. In case the participant was a minor, the parents’ consent was also obtained. A study sample of 309 healthy Belgian and Dutch Caucasian volunteers (163 females,
146 males) were prospectively includ-ed. Table 5.1 shows the age distribution of the participants per sex. Additionally, four younger children were scanned (two
girls of age 7 and 11; two boys of age 9 and 13). Their images were used to illustrate certain stages, but they were not included for analyses. Part of the study population was included in previous papers [12, 13]. None of the participants were relatives up to the third degree. Neither had any of them had any removal of a third molar. Socio-economic background was docu-mented. Teeth were named according to the International Standards Organisation Designation System.
Image acquisition
Between March 2012 and May 2017, 3T MRI was conducted according to the pro-tocol described in De Tobel et al. (2017) with a Siemens scanner (Magnetom Trio Tim, Siemens, Erlangen, Germany) [12]. Fast spin echo (FSE) T2 images were available in three planes. Sagittal images were made along the long axis of the teeth per side. Axial images were made paral-lel to the occlusal plane, whereas coronal images were made perpendicular to the occlusal plane (Figure 5.1). A bilateral flexible four-channel surface head coil (Model NMP-001D-ST-4, Nova Medi-cal Inc., Wilmington, NC, USA) and an individualised bite bar were used. In ten cases (3.2%), the scan had to be done over because of motion artefacts (9 cas-es) or wrong coil positioning (1 case). In three cases the head positioning was too extended at the neck, causing motion ar-tefacts because the participant could not keep the lower teeth still in the bite plate. This was resolved in the second scan by making a new bite plate, allowing for a more neutral neck position.
Materials and M
ethods
Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging
TABLE5 5. 1 — NUMBER OF PARTICIPANTS PER AGE
PER SEX.
AGE (Y) FREQUENCY
FEMALE MALE TOTAL
14 1 1 1 1 22
15 1 1 10 21
16 10 10 20
17 1 1 10 21
18 13 10 23
19 15 14 29
20 20 10 30
21 14 1 1 25
22 12 12 24
23 12 10 22
24 1 1 1 1 22
25 13 12 25
26 10 15 25
TOTAL 163 146 309

76
Image analysis
MRI specific staging technique
The considerations recommended by De Tobel et al. (2017) [13], together with other concerns made by the authors of the current study, were included to devel-op an MRI specific staging technique for third molar development.
The allocation of stages based on MRI should be conducted scrolling through the whole stack of slices depicting the considered tooth. When a fluid contain-ing structure is seen in the jaw where the third molar is expected, stage 0 can be al-located. In fact, one can only be sure that a third molar is present when calcification appears (stage 1). After all, the crypt may be a cyst in which no tooth will develop (this situation is similar when evaluating radiographs). Therefore stage 0 should not be included in any analysis for age es-timation. Since the youngest participants in the study sample were 14 years of age, it could be decided that the third molar was agenetic when no possible crypt or calci-fied tooth part was seen at the third molar region [31, 48].
Since on regular MR-images no distinc-tion can be made between enamel, dentin and cementum, criteria based on these materials were omitted. For instance, the cemento-enamel junction cannot be iden-tified on MR-images. As a consequence, the MR crown height was defined as be-ing the distance between the tips of the cusps and the pulp horns (Figures 5.2 and 5.3). Corresponding to Demirjian’s rules, when the different cusps are not at the same level, the midpoint between them is considered the highest reference point. Similarly, the lowest reference point is the midpoint between the pulp horns. Lines to define MR crown height should be per-pendicular to the tooth axis. New crite-ria based on this MR crown height were formulated. The MR crown height clear-ly differs from the clinical crown height, which – in contrast to radiographs or CT – cannot be determined on MRI. When evaluating relative lengths, a pair of di-viders can be used to compare MR root lengths with MR crown height. In border-line cases, the measure tool of the viewing software can be used to compare absolute measures. MR root length is measured from the nearest pulp horn to the most apical point of the root, at the least devel-
a Coronal MRI showing al l four third molars enclosed within the boxes of sagittal s l ices.
b Coronal MRI showing al l four third molars enclosed within the box of axial s l ices.
c Sagittal MRI showing the r ight third molars enclosed within the box of coronal s l ices.
FIGURE 5. 1 — YELLOW BOXES DEPICT THE STACK OF SCANNED MRI SLICES.
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.

77
oped root wall (Figures 5.2 and 5.3). The least developed root should be considered in case different roots are in different de-velopmental stages.
Stages 3, 4 and 5 depend on MR root length compared with MR crown height. In case doubt prevails even after using the measure tool, the youngest stage should be allocated. Because the measure tool can only be used on one slice, it is impos-sible to measure tooth proportions when the tooth is depicted over multiple imag-es. Still, when a certain MR root length is nearly reached on one slice and the root is spread over multiple consecutive sagittal slices, the higher stage can be allocated (Figure 5.4). After all, one has to take into account that the MR-sequence has a slice thickness of 2 mm. In the final stages, the root dentin at the apex changes from thin and parallel (stage 6), over thicker and converging (stage 7), to thick and closed (stage 8).
All of these considerations resulted in the stages defined in Table 5.2 and Fig-ure 5.5. To have reached a certain stage, the appearance of the root has to comply with the given criteria. When two crite-
ria are given, the molar has reached the stage if the first criterion applies. When three criteria are given, the first two have to apply to allocate the concerning stage. Both schematic representations of mono-radicular third molars and multiradicular third molars are given. Examples of the appearance of the different stages on MRI are shown in Figures 5.6 to 5.8.
Observers and media
Images were anonymised and evaluated by two observers independently. Observ-ers were blinded to the age of the partici-pant. Five participants per age per gender between 14 and 26 years old were assessed in a first session. After four months, both observers evaluated all 309 participants in a second session. The first observer (J.D.T.) was a resident at maxillofacial surgery studying forensic dentistry. He had been involved in research on age estimation for 8 years, including 6 years of dental age estimation. The second ob-server (I.P.) was a dentist in the first year after graduation. She had been involved in dental age estimation research for 1 year.
Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging
FIGURE 5.2 — DEFINITION OF MR CROWN HEIGHT AND MR ROOT LENGTH
ON MRI . L ines are perpendicular to the tooth axis . Distances (arrows) are
evaluated along the tooth axis .
Line D is at the distal cusp t ip, whi le M is at the mesial cusp t ip. Line C
represents the midpoint between the distal and mesial cusp t ips. Line H
is at the pulp horns, which are both at the same level . Line A is at the
most apical point of the roots, which are al l at the same l ine.
The distance between l ines C and H is the MR crown height . The distance
between l ines H and A is the MR root length. In this case MR root length
is more than one and a half MR crown height , so the tooth is in stage 5.

78
TABLE 5.2 — DESCRIPTIVE CRITERIA FOR DEVELOPMENTAL STAGES OF THIRD MOLARS ON MRI .
STAGE DESCRIPTION
STAGE 0 The crypt of the third molar is suspected without any calc if icat ion. .
STAGE 1 A beginning of calc if icat ion is seen at the superior level of the crypt in the form of an
inver ted cone or cones. There is no fus ion of these calc if ied points
STAGE 2 a) Fusion of the calc if ied points forms one or several cusps which unite to give a
regular ly out l ined occlusal surface.
b) The outl ine of the pulp chamber has a f lat or curved shape at the occlusal border.
c) In it ia l formation of the radicular bifurcation is seen in the form of a hypo-intense
calc if ied point .
STAGE 3 a) The pulp chamber has a trapezoidal shape. The out l ine of the pulp horns is pointy
and shaped l ike an umbrel la top.
b) Fur ther downshaping of the crown and/or beginning of root formation is seen in
the form of a spicule. The spicule is shor ter than MR crown height .
c) The calc if ied region of the bifurcation has developed fur ther into a hypo-intense
semi- lunar shape.
STAGE 4 a) MR root length reaches at least one MR crown height .
b) The calc if ied region of the bifurcation st i l l has a semi- lunar shape or has devel-
oped fur ther down.
STAGE 5 a) MR root length reaches at least one and a half MR crown height .
b) The calc if ied region of the bifurcation has developed fur ther down from its
semi- lunar shape to give the roots a more def in ite and dist inct out l ine with funnel
shaped endings. The funnel shape pers ists for some mi l l imetres ( i .e. i t is not l imited
to a few pixels on the image)
STAGE 6 a) The wal ls of the distal root canal are paral le l and its apical end is st i l l par t ial ly
open.
b) The wal ls at the apex of the root canal show relat ively thin dentin .
c) Remnants of the dental fol l ic le are seen in the form of a hyper- intense area sur-
rounding the apex.
STAGE 7 a) The wal ls of the distal root canal are convergent and its apical end is st i l l par t ial ly
open.
b) The wal ls at the apex of the root canal show relat ively thin dentin .
c) Remnants of the dental fol l ic le are seen in the form of a hyper- intense area sur-
rounding the apex.
STAGE 8 a) The apical end of the distal root canal is completely c losed.
b) The wal ls at the apex of the root canal show relat ively thick dentin .
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.

79
a, b Lower r ight mandibular third molar depicted on two consecutive MRI s l ices. S l ice a is s ituated
more buccal ly than s l ice b. The pulp chamber has a trapezoidal shape, corresponding to stage 3.
To exclude stage 4, MR crown height and MR root length have to be evaluated as i l lustrated in
images c , d.
c Copy of image a, with marked landmarks and distances to consider in order to al locate a stage.
Lines are perpendicular to the tooth axis . Distances (arrows) are evaluated along the tooth axis .
L ine Dc is at the distal cusp t ip, whi le Mc is at the mesial cusp t ip. L ine C represents the midpoint
between the distal and mesial cusp t ips. L ine Dh is at the distal pulp horn whi le l ine Mh is at the
mesial pulp horn. L ine H represents the midpoint between the distal and mesial pulp horns. L ine
Da is at the most apical point of the distal root . L ine Ma is at the most apical point of the mesial
root .
The distance between l ines C and H is the MR crown height based on this s l ice. The distance be-
tween l ines Dh and Da is the distal MR root length, whi le the distance between l ines Mh and Ma is
the mesial MR root length.
d Copy of image b. Both cusp t ips are at the same level on this s l ice, represented by l ine C. MR
crown height is larger than on the previous image, whereas the distal MR root length is smal ler.
To al locate a stage, MR crown height on image d is the most appropriate, whi le the distal MR root
length on image c is the most appropriate. Because the third molar is t i l ted bucco-l ingual ly, the
observer has to scrol l through consecutive s l ices to decide on the most appropriate measures to
consider. In s l ice c the crown is transsected more buccal ly, so par t of the crown is not depicted.
By contrast , the distal root apex is s ituated more buccal ly than the crown, so it is best depicted
in s l ice d. Because the distal root is shor ter than MR crown height , this third molar is in stage 3.
FIGURE 5.3
Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging
Images were assessed using a Barco MFGD monitor (3280 x 2048 pixels, Bar-co, Kortrijk, Belgium).Studied variables
Using Microsoft Access forms, both observers assessed the images gathering data on four variables. First, a develop-mental stage was allocated or it was de-cided that the tooth could not be evaluat-ed. Reasons for the latter were included in Table 5.3 [13].
Second, it was documented which root was considered to decide on the stage. Third, assessability of the roots was
noted (Table 5.4). Fourth, observers indi-cated which planes they used to allocate a stage, allowing for combinations to be ticked off.
Statistical analysis
All data were transferred from Microsoft Access to SPSS Statistics 24.0 (IBM SPSS Statistics for Windows, Armonk, NY, USA) and SAS 9.4 (SAS Institute, Cary NC, USA). Descriptive statistics were cal-culated. Results of the second session by both observers were combined to report on the root used to stage, assessability of the roots and essential planes.

80
FIGURE 5.5 — SCHEMATIC REPRESENTATION OF DEVELOPMENTAL STAGES OF THIRD MOLARS ON MRI . Miner-
al ized t issues appear black on MRI . By contrast , the dental fol l ic le, pulpal t issues, the periodontal space
and sal iva appear white. The upper panels show stages for mult iradicular molars, whi le in the lower panels
stages for monoradicular molars are shown (this also corresponds with the appearance of the palatal root
in upper molars, albeit upside down).
FIGURE 5.4 — LOWER RIGHT MANDIBULAR THIRD MOLAR DEPICTED ON CONSECUTIVE MRI SLICES FROM BUC-
CALLY TO LINGUALLY. MR crown height is most appropriately measured on s l ice d. When MR root length
would only be based on s l ice c , stage 3 would be al located. In fact the tooth is in stage 4, s ince MR root
length on s l ice b is s l ight ly longer than MR crown height and the root is depicted over several s l ices (keep-
ing in mind that s l ice thickness is 2 mm).
A paired Wilcoxon test was used to com-pare development between upper and lower third molars on the same side and to compare left and right third molars in the same jaw. Inter- and intra-observ-er agreement regarding stage allocation were quantified using proportion agree-ment and weighted kappa statistics. Cross tabulation of the observations allowed checking for systematic differences. The difference in marginal score distribution (between two observers or between two measurement occasions) was verified with Bowker’s test of symmetry.
The data from the first observer were im-plemented into a continuation-ratio mod-el for ordinal data assuming conditional independence, to obtain a posterior den-sity curve of age per stage per sex. These curves represent the distribution of the probability to be a certain age for a giv-en pattern of stages. From those curves, a point estimate of age and an appropriate prediction interval can be derived [16]. To correct for conditional dependence, a validated ad-hoc procedure was applied to the curves and the corresponding pre-diction intervals [16]. Participants with all
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.
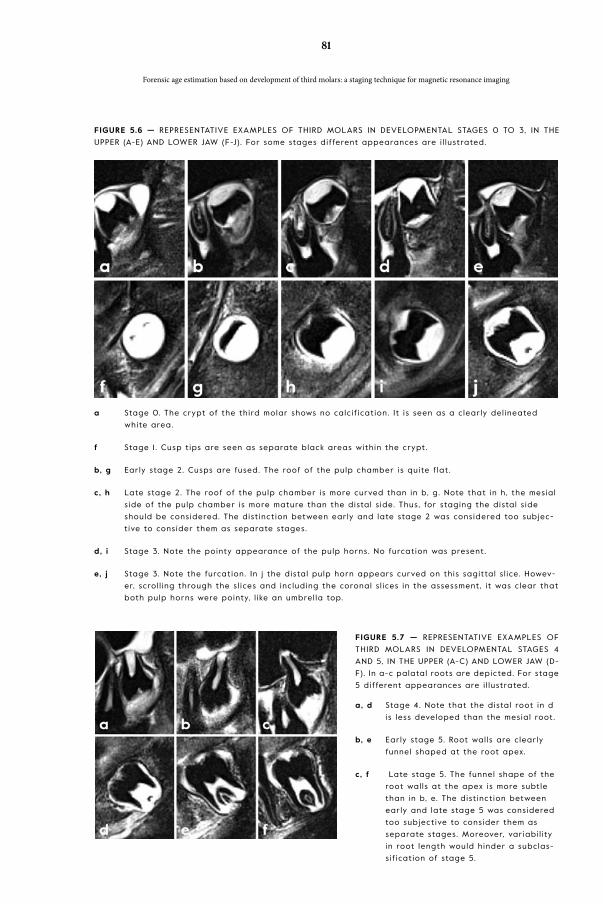
81
Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging
FIGURE 5.6 — REPRESENTATIVE EXAMPLES OF THIRD MOLARS IN DEVELOPMENTAL STAGES 0 TO 3, IN THE
UPPER (A-E) AND LOWER JAW (F-J). For some stages different appearances are i l lustrated.
a Stage 0. The crypt of the third molar shows no calc if icat ion. I t is seen as a c learly del ineated
white area.
f Stage 1 . Cusp t ips are seen as separate black areas within the crypt .
b, g Early stage 2. Cusps are fused. The roof of the pulp chamber is quite f lat .
c, h Late stage 2. The roof of the pulp chamber is more curved than in b, g. Note that in h , the mesial
s ide of the pulp chamber is more mature than the distal s ide. Thus, for staging the distal s ide
should be considered. The dist inct ion between early and late stage 2 was considered too subjec-
t ive to consider them as separate stages.
d, i Stage 3. Note the pointy appearance of the pulp horns. No furcation was present .
e, j Stage 3. Note the furcation. In j the distal pulp horn appears curved on this sagittal s l ice. Howev-
er, scrol l ing through the s l ices and including the coronal s l ices in the assessment , i t was c lear that
both pulp horns were pointy, l ike an umbrel la top.
FIGURE 5.7 — REPRESENTATIVE EXAMPLES OF
THIRD MOLARS IN DEVELOPMENTAL STAGES 4
AND 5, IN THE UPPER (A-C) AND LOWER JAW (D-
F). In a-c palatal roots are depicted. For stage
5 different appearances are i l lustrated.
a, d Stage 4. Note that the distal root in d
is less developed than the mesial root .
b, e Early stage 5. Root wal ls are c learly
funnel shaped at the root apex.
c, f Late stage 5. The funnel shape of the
root wal ls at the apex is more subtle
than in b, e. The dist inct ion between
early and late stage 5 was considered
too subject ive to consider them as
separate stages. Moreover, variabi l i ty
in root length would hinder a subclas-
s i f icat ion of stage 5.

82
a, e Stage 6. The width of the root canal differs depending on tooth anatomy. St i l l , paral le l root wal ls
are c lear. Note that the thin dentin at the apex in a might give the impress ion of a smal l funnel
shape. However, i t is stated in the cr iter ia for stage 5 that the funnel shape should be more ex-
tensive than is seen in this example. Therefore, stage 6 is appropriate.
b, f Stage 7. The apices have clearly star ted clos ing. In f remnants of the dental fol l ic le can be seen
as white areas surrounding root apices.
c, g Stage 8. The apical dentin is relat ively thin , but c learly continuous.
d, h Stage 8. Not only is the apical dentin continuous, but in these examples it is also relat ively thick .
FIGURE 5.8 — REPRESENTATIVE EXAMPLES OF THIRD MOLARS IN DEVELOPMENTAL STAGES 6 TO 8, IN THE
UPPER (A-D) AND LOWER JAW (E-H). In a-d palatal roots are depicted. For stage 8 different appearances
are i l lustrated.
TABLE 5.3 — REASONS FOR THE MRI BEING NOT ASSESSABLE, WITH THEIR FREQUENCIES.
REASON FOR BEING NOT ASSESSABLE UPPER THIRD MOLARS LOWER THIRD MOLARS
Insuff ic ient contrast between apex t ip
and surrounding bone
2.6% (28/1096) 2. 1% (22/1044)
Apex t ip fal ls in between s l ices 0.5% (6/1096) 1 .8% ( 19/1044)
Poor coi l posit ioning 0.0% (0/1096) 0.0% (0/1044)
Poor image qual ity
(e.g . poor s ignal- to-noise rat io)
0.3% (3/1096) 0.4% (4/1044)
Ar tefacts due to motion of the par t ic ipant 0.9% ( 10/1096) 1 .5% ( 16/1044)
Other ar tefacts (e.g. susceptibi l i ty due to
metal)
0.4% (4/1096) 0.6% (6/1044)
Other, please specify 0.0% (0/1096) 0.3% (3/1044)
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.

83
FIGURE 5.9 — INFLUENCE OF AGENETIC THIRD MOLARS ON THE POSTERIOR DENSITY IN MALES. The four third
molars are repor ted in the fol lowing sequence: 18 28 38 48. They are represented by the stage they are
in (“6” in this example) or by “.” i f they are agenetic . The posterior density becomes smal ler as a funct ion
of increasing information.
available third molars in stage 8 were not included in the analysis (N = 28). Hence, the prediction pertains to subjects with not all available third molars fully devel-oped. Motivation for this approach was that the point prediction (and thus the er-ror) for participants with fully developed third molars is heavily influenced by the age range of included participants.
The ad-hoc procedure was based on application of Bayes’ rule, using continu-ation-ratio models assuming conditional independence. The model takes third molar position into account, so that even when one or more third molars are age-netic, the other third molars contribute to the model. The influence of agenetic third molar(s) to the posterior density distribution was illustrated in Figure 5.9. Non-proportional odds were allowed in the continuation-ratio model. Linearity was assumed for the relation between age and the logits. Note that for the same rea-son, the more simplistic model assuming proportional odds would lead to a more stable solution. Due to the low number of scores equal to 2, these were combined with scores 3 into a single level. Evalua-
tion of the performance was based on 10-fold cross-validation and the approach was performed separately for males and females. The creation of the folds was stratified on age category (1 year interval).
Observed age minus predicted age was calculated, reflecting the error of the estimate. The maximum likelihood (ML) estimate was given as point prediction (this equals the modus of the posterior distribution of age), as well as the mean and 95% trimmed mean of the posterior distribution. The interval estimate (pre-diction interval) for age corresponded to the 95% age values of highest probabili-ty density. The difference between the posterior density assuming conditional independence and the correction by the ad-hoc procedure was illustrated in Fig-ure 5.10. The proportion of cases, whose chronological age fell inside the 95% confi-dence interval (CI), known as coverage, was calculated. Since the ML estimate is known not to minimize the root mean squared er-ror (RMSE), the mean of the posterior dis-tribution, as well as the mean of the posteri-or distribution in the prediction interval (= trimmed mean) were also reported.
Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging

84
TABLE 5.4 — RELATIVE ASSESSABILITY OF THE DIFFERENT ROOTS
ELEMENTS ASSESSABLITY FREQUENCY
UPPER THIRD MOLARS Only the staged root is assessable 4% (32/914)
Other roots are also assessable 81% (739/914)
Only the staged root is present 16% ( 143/914)
LOWER THIRD MOLARS Only the staged root is assessable 2% (16/844)
Other roots are also assessable 97% (817/844)
Only the staged root is present 3% (27/844)
Spearman correlation between chrono-logical age and staging was calculated, as well as Pearson correlation between chronological age and error of the esti-mated age. The first reflecting the degree of change in development explained by a change in age. The latter reflecting the degree of bias of the age estimate. Accura-
cy, sensitivity, specificity, positive predic-tive value (PPV) and negative predictive value (NPV) were used to evaluate the minor-adult distinction. Accuracy repre-sented the proportion of correctly clas-sified subjects. Sensitivity indicated the proportion of correctly classified adults, while specificity indicated the propor-
FIGURE 5. 10 — VISUALISATION OF THE AD-HOC PROCEDURE TO CONSTRUCT AN APPROXIMATE CONFIDENCE
INTERVAL WITHOUT THE NEED TO MODEL THE MULTIVARIATE CORRELATION STRUCTURE BETWEEN THE INDI-
CATORS.
The black continuous curve refers to the posterior density assuming condit ional independence. The grey
dashed curve presents the density obtained after appl icat ion of the ad-hoc procedure (Boldsen et al .
2002). At the top r ight are the stages for each third molar with their respective point predict ion of age
based on the maximum l ikel ihood est imate, the 95% predict ion interval and the poster ior probabi l i ty to be
a minor. At the top left are the combined results , f i rst without correct ion and second after correct ion ap-
ply ing the ad-hoc procedure. Note that without correct ion the predict ion interval is ar t i f ic ia l ly too narrow.
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.

85
TABLE 5.5 — PATTERNS OF AGENESIS OF ONE
OR MORE THIRD MOLARS WITH THEIR FREQUEN-
CIES.
AGENETIC ELEMENTS FREQUENCY
18 6
28 3
38 7
48 6
18, 28 7
38, 48 14
18, 38 2
18, 48 2
28, 38 1
18, 28, 38 1
18, 38, 48 3
28, 38, 48 2
18, 28, 38, 48 10
TOTAL 64
tion of correctly classified minors. PPV equalled the proportion of adults within estimated adults. NPV was the proportion of minors within estimated minors. The area under the receiver operator charac-teristic (ROC) curve (AUC) reflected the percentage of times that a randomly se-lected individual from the older age cat-egory would have a more advanced root compared to a randomly chosen individ-ual from the younger age category. Final-ly, the AUC probability to be older than 18 years was calculated.
Statistical tests were performed two-sided and evaluated at the 0.05 sig-nificance level.
Tooth development and assessability
In the study sample, agenesis of one or more third molars was frequently seen: teeth 18, 28, 38 and 48 were agenetic in 40, 30, 50 and 46 out of 309 cases respec-tively (Table 5.5).
Tables 5.4 and 5.6 summarise results on the relative assessability of the different roots and root used to stage per third mo-lar. The root used to stage was always the least developed assessable root. These re-sults included all assessable third molars from stage 4 on. No stage could be allo-cated in 5% (51/1096) of upper and 7% (70/1044) of lower third molars (Table 5.3). In a few cases monoradicular third molars were encountered (Table 5.4). Nineteen percent of the upper third mo-lars had non-assessable (mostly buccal) roots, compared to only 3% of lower third molars (mesial or distal were approxi-mately equally distributed).
Essential plane
Sagittal images were essential to allocate a stage in 95% (1040/1096) of assessa-ble upper third molars. Only in a few upper third molars did the coronal (5% = 55/1096) plane contribute to staging, while the axial images were never useful. In lower third molars frequencies were 92% (966/1044), 4% (41/1044) and 1% (9/1044) for sagittal, coronal and axial images respectively. Coronal and/or ax-ial images proved to be useful when the tooth was extremely tilted, when the apex seemed to fall in between sagittal slices or to differentiate stage 2 from stage 3.
Staging and age estimation
In fourteen participants all third molars were not allocated a stage, because they were either agenetic (n = 10) or non-as-
Results
Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging

86
TABLE 5.6 — FREQUENCY OF ROOT USED TO STAGE (LEAST DEVELOPED).
ELEMENTS ROOT USED TO STAGE FREQUENCY
Upper third molars Palatal 88% (741/838)
Mesiobuccal 9% (75/838)
Distobuccal 3% (22/838)
Lower third molars Mesial 1 1% (91/845)
Distal 89% (754/845)
sessable due to motion artefacts (n = 2) or susceptibility to metal (n = 2). A system-atic difference in development between upper and lower third molars was statisti-cally confirmed (P = 0.001 right, P < 0.001 left), with lower third molars overall being in the same or more advanced stages than upper ones. Left and right third molars in the same jaw did not differ significantly in development (P = 0.283 upper, P = 0.085 lower).
Reproducibility of staging
Table 5.7 shows inter- and intra-observer agreement for stage allocation. Table 5.8 shows the cross tabulation of frequencies of allocated stages by both observers at both staging sessions. A one stage differ-ence was frequently seen. Two stage dif-ferences were also encountered between staging sessions in 1.3% (5/379) and 1.4% (5/350) of assessments, and between ob-servers in 1.4% (5/364) and 2.2% (20/899) of assessments. Moreover, a systematic difference in allocated stages was noticed for both observers. In the second session more frequently a higher stage was allo-cated. Bowker’s test of symmetry indicat-ed no statistically significant asymmetry between both staging sessions for observ-er 1 (P = 0.21), while it was significant for observer 2 (P < 0.001). This also result-
ed in a significant asymmetry between both observers in the second session (P < 0.001), while in the first session asymme-try was not significant (P = 0.51).
Age estimation
Summary statistics regarding age distri-bution per stage of the lower left third mo-lar are shown in Table 5.11, in order to be able to compare the results with other re-search. Notice that the minimum age in stage 7 was over 18 years for females and males. An overview of chronological age and estimated age for the study sample is presented in Figure 5.11. Figure 5.12 pre-sents posterior distributions of the Bayes-ian approach. Table 5.9 shows examples of point predictions with prediction inter-vals and probabilities to be adult for dif-ferent patterns of allocated stages per sex.
Applying the Bayesian model for age estimation, using the mean of the pos-terior distribution as point prediction rendered better results than using the trimmed mean or ML estimate. The mean absolute error was 2.0 years in females (median (Me) = 1.7, interquartile range (IQR) 0.8–2.7) and 1.7 years in males (Me = 1.6, IQR 0.6–2.5) based on the mean of the posterior distribution. The mean error was 0.1 years in females (Me = 0.0, IQR
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.

87
TAB
LE
5.7
— R
EPRO
DU
CIB
ILIT
Y O
F S
TAG
ING
TH
IRD
MO
LA
R D
EV
ELO
PMEN
T. T
he p
roport
ion
agre
emen
t as
wel
l as
two v
ersi
ons
of
the
wei
ght
ed k
appa a
re r
eport
ed for
all
third m
ola
rs
com
bin
ed, a
s w
ell f
or
each
thi
rd m
ola
r se
para
tely. T
he k
appa w
ith
the
linea
r w
eight
s is
the
wei
ght
ed k
appa, t
ypic
ally
rep
ort
ed in
most
agre
emen
t st
udie
s. T
he k
appa w
ith
qua
dra
tic
wei
ght
s is
sim
ilar
to t
he in
tra-c
lass
corr
elation
(ICC
). N
ote
tha
t re
sults
base
d a
ggre
gate
d d
ata
fro
m t
he four
thi
rd m
ola
rs d
o n
ot
take
into
acc
oun
t th
e co
rrel
ation
bet
wee
n th
e fo
ur t
hird
mola
rs.
EL
EM
EN
TIN
TR
A-O
BSE
RV
ER
AG
RE
EM
EN
TIN
TE
R-O
BSE
RV
ER
AG
RE
EM
EN
T
Ag
ree
me
nt
(SE)
We
igh
ted
ka
pp
aA
gre
em
en
t (S
E)
We
igh
ted
ka
pp
a
Lin
ea
r (S
E)
Qu
ad
rati
c (
SE)
Lin
ea
r (S
E)
Qu
ad
rati
c
(SE)
Ob
serv
er
1Se
ssio
n 1
All t
hir
d m
ola
rs(N
= 3
79
)0
.76
0 (
0.0
22)
0.8
73
(0
.013
)0
.95
4 (
0.0
06
)(N
= 3
64)
0.8
08
(0
.02
1)0
.89
3 (
0.0
12)
0.9
59
(0
.00
6)
180
.72
2 (
0.0
46
)0
.85
7 (
0.0
25
)0
.95
3 (
0.0
09
)0
.86
8 (
0.0
36
)0
.93
2 (
0.0
19)
0.9
77
(0
.00
7)
28
0.7
60
(0
.04
3)
0.8
48
(0
.03
0)
0.9
33
(0
.017
)0
.78
1 (0
.04
2)
0.8
66
(0
.02
8)
0.9
44
(0
.015
)
38
0.7
69
(0
.04
4)
0.8
90
(0
.02
3)
0.9
66
(0
.00
8)
0.7
73
(0
.04
5)
0.8
68
(0
.02
9)
0.9
46
(0
.015
)
48
0.7
91
(0.0
43
)0
.88
9 (
0.0
25
)0
.95
9 (
0.0
12)
0.8
09
(0
.04
2)
0.9
03
(0
.02
2)
0.9
68
(0
.00
8)
Ob
serv
er
2Se
ssio
n 2
All t
hir
d m
ola
rs(N
= 3
50
)0
.76
0 (
0.0
22)
0.8
34
(0
.015
)0
.95
4 (
0.0
06
)(N
= 8
99
)0
.620
(0
.016
)0
.79
0 (
0.0
10)
0.9
22
(0
.00
5)
180
.713
(0
.04
9)
0.8
46
(0
.02
8)
0.9
45
(0
.012
)0
.64
8 (
0.0
32)
0.8
03
(0
.02
1)0
.92
6 (
0.0
10)
28
0.6
74 (
0.0
49
)0
.80
4 (
0.0
32)
0.9
19 (
0.0
17)
0.6
17 (
0.0
32)
0.7
84
(0
.02
1)0
.920
(0
.010
)
38
0.7
74 (
0.0
46
)0
.87
7 (
0.0
27
)0
.95
8 (
0.0
10)
0.5
88
(0
.03
4)
0.7
64
(0
.02
3)
0.9
07
(0
.012
)
48
0
.65
5 (
0.0
51)
0.8
09
(0
.03
0)
0.9
31
(0.0
13)
0.6
24
(0
.03
3)
0.8
04
(0
.019
)0
.93
3 (
0.0
08)
N =
NU
MB
ER
OF
ASSESSED
TH
IRD
MO
LA
RS;
SE =
STA
ND
AR
D E
RRO
R.
Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging

88
-1.7–1.8) and males (Me = 0.0, IQR -1.4–1.9). Root mean squared error equalled 2.38 (95% confidence interval (CI) 2.11–2.65) for females and 2.06 (95% CI 1.79–2.33) for males. Coverage of the 95% pre-diction interval was 94.7% (142/150) for females and 91.4% (107/117) for males.Moreover, the error of the age estimate clearly depended on age. The dependency was lowest using the mean of the poste-rior distribution as point prediction with
Spearman correlation (r) for mean error in females equal to 0.51 (95% CI 0.38–0.62, P < 0.001) and in males equal to 0.50 (95% CI 0.35–0.62, P < 0.001). For mean absolute error r = 0.10 in females (95% CI -0.06–0.25, P = 0.22) and r = 0.29 in males (95% CI 0.11–0.44, P = 0.0017).
Performance of the Bayesian proce-dure to discriminate between minors and adults is summarized in Table 5.10. In
FIGURE 5. 1 1 — GRAPHS COMPARING CHRONOLOGICAL AGE (DOTS) WITH THE POINT (TRIANGLE) AND INTER-
VAL (LINE) PREDICTION IN FEMALES (A) AND MALES (B). THE POINT PREDICTION IS THE ML ESTIMATE.
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.

89
Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging
TAB
LE
5.8
— C
RO
SS T
AB
UL
AT
ION
OF
FR
EQ
UEN
CIE
S O
F A
LLO
CA
TED
SC
OR
ES B
Y B
OT
H O
BSERV
ER
S I
N B
OT
H S
TAG
ING
SESSIO
NS.
INT
RA
-OB
SE
RV
ER
AG
RE
EM
EN
TIN
TE
R-O
BSE
RV
ER
AG
RE
EM
EN
T
Ob
serv
er
1 Sta
ge
se
ssio
n 1
Se
ssio
n 1
Sta
ge
ob
serv
er
2
F
RE
QU
EN
CY
23
45
67
8TO
TAL
FR
EQ
UE
NC
Y2
34
56
78
TO
TAL
Sta
ge
sess
ion
2
24
00
00
00
4Sta
ge
ob
serv
er
1
24
00
00
00
4
30
52
30
00
05
53
15
16
00
00
58
40
65
86
00
070
40
54
72
10
00
73
50
011
50
11
06
35
00
56
40
10
70
60
01
133
79
06
06
00
05
35
41
45
70
00
111
30
54
77
00
01
54
83
57
80
00
02
21
57
80
80
00
02
104
55
7
TO
TAL
45
87
370
51
61
62
379
TO
TAL
55
65
89
14
26
34
93
64
Ob
serv
er
2Sta
ge
se
ssio
n 1
Se
ssio
n 2
Sta
ge
ob
serv
er
2
F
RE
QU
EN
CY
23
45
67
8TO
TAL
FR
EQ
UE
NC
Y2
34
56
78
TO
TAL
Sta
ge
sess
ion
2
24
20
00
00
6Sta
ge
ob
serv
er
1
220
70
00
00
27
31
40
10
00
04
23
57
73
01
00
011
3
40
143
30
00
04
74
04
64
743
00
145
50
02
276
00
09
85
00
211
22
90
014
3
60
02
152
75
15
06
00
13
310
23
03
169
70
00
06
33
115
07
00
00
33
75
1412
2
80
00
02
22
33
57
80
00
012
61
107
180
TO
TAL
55
65
89
13
56
04
53
50
TO
TAL
25
88
97
220
179
166
124
89
9

90
forensic age estimation in the living, one should strive for an approach with high specificity and NPV (specificity being the major concern). Estimating age based on the ML estimate rendered the highest specificity in females and males. The high-est NPV was obtained using the mean of the posterior distribution as point pre-diction of age. The AUC was very similar for all three point predictions. The AUC probability to be older than 18 years was 0.869 (95% CI 0.811–0.926) for females and 0.948 (95% CI 0.908–0.988) for males.
Staging third molars’ development
Considerations for developing a staging technique
Staging development of third molars has been developed based on radiographs. However, with the increasing demand of imaging for age estimation that does not use ionizing radiation [15], MRI is being studied for dental age estimation by sev-eral research groups [5, 12, 13, 20, 38]. Since the appearance of teeth on MRI differs greatly from that on radiographs, a mere extrapolation of radiographical stages seems inappropriate. After all, cri-teria for staging based on crown height and root length cannot be applied when the cemento-enamel junction cannot be identified unambiguously. Dedicated MR sequences, in which it is possible to dif-ferentiate between the hard dental tissues, have been developed [7, 25, 34]. However, their use is not common practice yet, ren-dering them unavailable for forensic pur-poses. Therefore, a universally applicable MRI specific staging technique for third molar development was proposed in this paper.
Some authors stated that predictions of crown height and root length should be avoided because, especially in third mo-lars, dimensions are highly variable and unpredictable [48]. Predictions always imply subjectivity, while objective criteria for stages should be pursued. It has been reported that precision of the staging technique might be reduced – i.e. com-promise the feasibility to register all of the stages correctly – if thresholds between stages are based on predictions of lengths of tooth parts [11, 49]. Moreover, the fully developed crown height cannot be used to predict the future mature root length [1]. In the current study, it was considered inappropriate to include a stage in which MR root length would be at least twice MR crown height, because it was noticed that the roots of some third molars never reached this length, even when fully ma-tured. In literature, it was also stated that because of variability between second and third molars, predictions of third molar lengths should not be based on or com-pared with the dimensions of neighbour-ing teeth [48]. Therefore, only objective criteria were used in the proposed staging technique.
To differentiate between stage 5 and stage 6, one could check the tooth’s erup-tion. In stage 5 it is still in infra-occlusion, while in stage 6 it has reached the occlu-sal plane. However, third molars are often impacted or they over-erupt (when they don’t have an antagonising tooth), which makes these characteristics inapplicable. Therefore, eruption was not included in the criteria for MR specific staging.
Discussion
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.

91
FIGURE 5. 12 — POSTERIOR DENSITY FOR ALL POSSIBLE HOMOGENEOUS STAGE PATTERNS (SAME STAGE FOR
ALL THIRD MOLARS) IN MALES.
When al l th ird molars are in stages equal to or lower than three (3333), the distr ibut ion of age is r ight-
skewed. This smoothly evolves to a left-skewed age distr ibut ion when al l th ird molars are ful ly mature
(8888). Around the age of 18 years, most indiv iduals have third molars in stage 5. Per s ituation the proba-
bi l i ty to be adult is represented by the area under the posterior density curve to the r ight of the 18 years
threshold (grey ver t ical l ine).
TABLE 5.9 — EXAMPLES OF POINT PREDICTIONS WITH PREDICTION INTERVALS AND PROBABILITIES TO BE
ADULT FOR DIFFERENT PATTERNS OF ALLOCATED STAGES PER SEX. Point predict ions of age are based on
the mean of the posterior distr ibut ion. Note that the lower l imit of the predict ion interval in the low-
est stage ref lects the minimum age in the study sample. S imi lar ly, the upper l imit in the highest stages
equals the maximum age in the study sample.
ELEMENT POINT
PREDICTION
95% PREDICTION
INTERVAL
PROBABILITY
TO BE ADULT
18 28 38 48
Females
3 3 3 3 15.53 ( 14 .00–18.33) 0.0600
4 4 4 4 16.89 ( 14 .00–20.78) 0.2496
5 5 5 5 18.59 ( 14 .35–22.74) 0.5760
6 6 6 6 21 .88 ( 17.76–26.73) 0.9509
7 7 7 7 23.96 (20. 15–27.00) 0.9956
8 8 8 8 24.68 (21 . 17–27.00) 0.9989
Males
3 3 3 3 15.03 ( 14 .00–16.68) 0.0037
4 4 4 4 16.90 (14 .35–19.45) 0. 1765
5 5 5 5 17.75 ( 15.35–20.33) 0.3746
6 6 6 6 20. 17 ( 16.79–24.08) 0.8883
7 7 7 7 22.85 ( 19.25–27.00) 0.9926
8 8 8 8 23.76 (20.04–27.00) 0.9976
Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging

92
Tooth development and assessability
It can be considered a limitation of the cur-rent study that both participants with and without third molar impaction, agenesis or extraction of other teeth were included to generate the model for age estimation. However, in the general population sev-eral patterns of agenesis/extraction/im-paction are present and it is not feasible to take all different patterns into account for age estimation. It has been stated that agenesis and impaction might delay third molar development [17, 19, 21, 27, 28, 30, 36, 37], while extractions might accelerate it [22, 53]. It is our intention in future re-search to study this on MRI in the current study population.
In about 90% of upper third molars the palatal root was the least developed one, meaning it was either less developed or equally developed as the buccal roots. Also in about 90% of lower third molars the distal root was the least developed. These numbers are lower than reported based on a subset of the current study population (98% and 95% respectively) [13]. In some cases not all roots could be assessed on MRI. This was more frequent in the upper jaw, mainly due to the small dimensions of the buccal roots, as previ-ously reported by De Tobel at al. (2017) [13]. Few studies reported on the relative development of different roots within the same third molar [17]. In any case, the least developed root should be consid-ered, to grant the benefit of the doubt.
TABLE 5. 10 — PERFORMANCE TO DISCRIMINATE BETWEEN MINORS AND ADULTS.
PREDICTED AGE
BASED ON
ML ESTIMATE MEAN TRIMMED MEAN
RATE (95% CI)
Females Accuracy 77.3 (69.8–83.8) 79.3 (72.0–85.5) 78.0 (70.5–84.4)
Sensit iv ity 78.9 (70.0–86. 1 ) 84.4 (76.2–90.6) 82.6 (74. 1–89.2)
Specif ic ity 73.2 (57.0–85.8) 65.8 (49.4–79.9) 65.8 (49.4–79.9)
PPV 88.7 (80.6–94.2) 86.8 (78.8–92.6) 86.5 (78.4–92.4)
NPV 56.6 (42.3–70.2) 61 .4 (45.5–75.6) 58.7 (43.2–73.0)
AUC 0.865 (0.809–0.922) 0.873 (0.817–0.928) 0.874 (0.818–0.929)
Males Accuracy 90.6 (83.8–95.2) 90.6 (83.8–95.2) 89.7 (82.8–94.6)
Sensit iv ity 91 .0 (82.4–96.3) 92.3 (84.0–97. 1 ) 91 .0 (82.4–96.3)
Specif ic ity 89.7 (75.8–97. 1 ) 87.2 (72.6–95.7) 87.2 (72.6–95.7)
PPV 94.7 (86.9–98.5) 93.5 (85.5–97.9) 93.4 (85.3–97.8)
NPV 83.3 (68.6–93.0) 85.0 (70.2–94.3) 82.9 (67.9–92.8)
AUC 0.950 (0.912–0.988) 0.949 (0.909–0.988) 0.949 (0.909–0.988)
Accuracy = propor t ion of correct ly c lass if ied subjects ; Sensit iv ity = propor t ion of correct ly c lass if ied
adults ; Specif ic ity = propor t ion of correct ly c lass if ied minors ; PPV = propor t ion of adults within est imated
adults ; NPV = propor t ion of minors within est imated minors ; AUC = area under the ROC curve.
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.

93
Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging
TABLE 5. 1 1 — DESCRIPTIVE STATISTICS OF AGE DISTRIBUTION PER SEX PER STAGE FOR THIRD MOLAR 38.
38 STAGE FREQUENCY MEAN SE SD MEDIAN MIN MAX
Females 1 0 - - - - - -
2 1 14 .40 - - 14 .40 14.40 14.40
3 17 16.50 0.50 2.20 15.80 14. 10 21 .00
4 15 17.70 0.60 2.30 18.40 14.70 20.60
5 28 18.50 0.30 1 .80 18.80 15.40 21 .90
6 26 20.90 0.60 2.80 21 .20 15.50 25.60
7 16 23.30 0.60 2.50 23.90 18.60 26.80
8 37 23.40 0.30 2. 10 23.80 19.30 26.80
Males 1 0 - - - - - -
2 2 14 . 10 0.00 0.00 14. 10 14 . 10 14 .20
3 16 15.30 0.30 1 . 10 14 .90 14. 10 17.70
4 12 16.80 0.50 1 .90 16.20 14.40 20.90
5 5 18.20 0.80 1 .70 18.80 15.60 19.90
6 15 19.90 0.60 2.20 19.20 17. 10 24.30
7 10 21 . 10 0.70 2. 10 20.50 18.70 24.90
8 52 24.00 0.30 2.20 24.40 19.00 27.00
Baumann et al. (2015) mentioned that 5% (15/307) of molars could not be assessed, due to technical reasons (e.g. motion ar-tefacts), equally distributed among upper and lower jaw. However, this also includ-ed first and second molars. In the study by Guo et al. (2015) 2% (13/530) of lower third molars could not be assessed due to insufficient image quality. In the current study slightly higher numbers of non-as-sessable teeth were encountered with 5% (51/1096) of upper and 7% (70/1044) of lower third molars. Whether this should be attributed to the MRI scanner and/or MRI sequence used, could be subject of future studies. However, the used se-quence proved to be the most suitable af-ter a selection process in De Tobel et al. (2017) [12].
Essential plane
Regarding the plane in which slices are deemed suitable for stage allocation, De Tobel et al. (2017) reported that sagittal slices were essential in 99% of cases [13]. They contributed this to the anatomy of third molars. This corresponds with the current number of 94%. Coronal and ax-ial slices were less frequently useful in the current study (4% and 0% respectively) than in the previous study (11% and 8% respectively) [13].
Statistical approach to age estimation
Reproducibility of staging
It has been stated that reproducibility de-pends on the staging technique [26]. In-

94
ter- and intra-observer agreement in the current study were similar to or lower than those reported in previous studies on third molar development, as seen on 3D imaging modalities (Table 5.12) [3, 5, 10, 13, 20]. It appears that studies includ-ing a larger sample of staged molars had relatively lower reproducibility values. Possibly, more easy to stage cases ended up in the small subsamples, used for re-producibility calculations. Furthermore, one might expect that staging based on computed tomography (CT) would be more reproducible than based on MRI, since MRI is more prone to artefacts and is more influenced by surrounding tissue and motion. From Table 5.12 however, it is clear that staging on MRI shows sim-ilar reproducibility as on CT. Although the presented staging technique did not outperform the established techniques (developed on radiographs), one could question the suitability of the Demirjian technique, since it is based on criteria that cannot be visualised with MRI, and the Köhler technique, since it is based on pre-dictions of root lengths which are highly variable [48].
Although intra- and inter-observer agreement was high, a substantial propor-tion of disagreement remained (Tables 5.7 and 5.8). Two striking observations can be made: two stage differences occurred and systematically a higher stage was al-located during the second staging session. Both observations might be explained by a learning curve. In the first session, more often when observers doubted about the appropriate stage, the lower stage was allocated. Possibly they were more confi-dent during the second session, with the first observer being more confident than
TAB
LE
5.1
2 —
REPRO
DU
CIB
ILIT
Y O
F S
TAG
ING
TH
IRD
MO
LA
R D
EV
ELO
PMEN
T B
ASED
ON
3D
IM
AG
ING
MO
DA
LIT
IES.
RE
FE
RE
NC
EIM
AG
ING
MO
DA
LIT
Y
EL
EM
EN
TS
STA
GIN
G
TEC
HN
IQU
E
INT
RA
-OB
SE
RV
ER
AG
RE
EM
EN
TIN
TE
R-O
BSE
RV
ER
AG
RE
EM
EN
T
STA
TIS
TIC
N
STA
TIS
TIC
N
Ba
um
an
n (
20
15)[
5]
MR
IA
ll m
ola
rsD
em
irji
an
-
-C
oh
en’s
ka
pp
a0
.51
312
Gu
o (
20
15)[
20
]M
RI
Lo
we
r le
ft t
hir
d m
ola
rD
em
irji
an
Ka
pp
a0
.89
60
Ka
pp
a0
.83
60
De
To
be
l (2
017
)[13
]M
RI
All t
hir
d m
ola
rsD
em
irji
an
ICC
0.9
4-0
.97
48
-50
ICC
0.8
5-0
.94
44
-47
Kö
hle
rIC
C0
.96
-0.9
74
8-5
0IC
C0
.86
-0.9
54
4-4
7
Cu
rre
nt
MR
IA
ll t
hir
d m
ola
rsW
eig
hte
d k
ap
pa
Ag
ree
me
nt
0.8
0-0
.89
0.6
6-0
.79
35
0-3
79
35
0-3
79
We
igh
ted
ka
pp
a
Ag
ree
me
nt
0.7
6-0
.80
0.7
7-0
.87
89
9
89
9
Ba
sse
d (
20
11)[
3]
CT
Lo
we
r th
ird
mo
lars
De
mir
jia
nKa
pp
a
Ag
ree
me
nt
0.9
49
0.9
6
25
25
Ka
pp
a
Ag
ree
me
nt
0.8
42
0.8
8
25
25
Ca
nte
kin
(20
13)[
10]
CB
CT
Lo
we
r th
ird
mo
lars
De
mir
jia
nKa
pp
a0
.89
670
Ka
pp
a0
.69
270
(CB
)CT =
(co
ne
be
am
) co
mp
ute
d t
om
og
rap
hy;
ICC
= i
ntr
a-c
lass
co
rre
lati
on
co
eff
icie
nt;
MR
I = m
ag
ne
tic r
eso
na
nce
im
ag
ing
; N
= n
um
be
r o
f a
sse
sse
d m
ola
rs
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.

95
Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging
the other. However, since some degree of uncertainty remained, more divergent re-sults were obtained, compared to the first session. The learning effect was present in both observers, although observer 1 was more experienced than observer 2. An explanation might be that although ob-server 1 had seen more teeth on MRI than observer 2 and he had staged some series of third molars on MRI and panoramic radiograph for previous research, he had never staged a series this large. As was stated by other researchers, more experi-enced observers generate more consistent results [24, 29, 33, 40, 52]. An alternative explanation for two stage differences was when the considered third molar was de-picted over several slices. In those cases one observer might have been more con-servative and allocate the lower stage be-cause in most slices that seemed appropri-ate. By contrast, the other observer might have reasoned that the root was in a high-er stage, incorporating the slice thickness. When age estimation is done in practice, it is wise to assess the images with at least two observers and allocate stages in con-sensus.
Finally, also calibration of the ob-servers influences reproducibility. Both observers were from the same research group and were trained in a similar way. It would be useful to see which results would be obtained by an independent observer, e.g. someone from another re-search group. Anyway, future research is necessary to verify the reproducibility of the proposed staging technique.
The only way to eliminate inter- and intra-observer variability is to conduct automated age estimation. Urschler et al. (2015) reported promising re-
sults on automated age estimation based on hand and wrist MRI.[51]. Whether or not this approach can be extrapolated to other anatomical structures, such as third molars, is subject of further research [44].
Age estimation
Baumann et al. (2015) demonstrated that compared with staging on MRI, slightly lower stages were allocated to the same third molar on panoramic radiographs [5]. Guo et al. (2015) found that the mini-mum age for a fully mature 38 on MRI was 19.57 years for females and 17.77 years for males [20]. Consequently, it seems that a mature third molar 38 on MRI could act as a sign of adulthood in females. In the current sample minimum ages were not used to discern minors from adults. In-stead probabilities were calculated using the Bayesian model. When homogeneous stage pattern 8 is seen, it is highly prob-able that an individual is over 18 years old (99.89% in females, 99.76% in males). However, around the age of 18, most in-dividuals will have third molars in stage 5 (Figure 5.12).
With a mean absolute error of 2.0 years in females and 1.7 years in males, age estimation based on MRI of third molars is less accurate than a similar ap-proach based on radiographs which had an overall mean absolute error of 1.13 years (Me = 0.89, IQR 0.44–1.62) [47]. Third molar stages of 2513 individuals were included in their Bayesian model. It can be expected that age estimation per-formance based on MRI would increase when the reference sample would be larger. However, third molars are not rou-tinely scanned with MRI, so retrospective data collection is impossible. Since several

96
research groups are gathering third molar MRI data prospectively, joining forces could generate a more robust age estima-tion model.
The performance to discern minors from adults was better for males than for females, with specificities of 96% and 73% respectively. The AUC equalled 0.873 for females and 0.949 for males. Based on lower left third molar staging on radio-graphs, Liversidge and Marsden (2010) reported a specificity of 96% (females and males combined) [32]. However, they re-ported separate statistics for the different stages, since they did not apply statistical modelling to estimate age. In their study AUC was 0.904 (95% CI 0.889–0.919) [32]. Based on staging all third molars on radiographs, Thevissen et al. (2010) reported that specificity ranged between 33% and 87%, without obvious better re-sults for either sex, using country-specific data in a Bayesian model [46]. An AUC of 0.853 was reported in another paper by the same research group [47].
Because of the inherent inter-indi-vidual variability of development, several anatomical structures should be incor-porated into the ad-hoc procedure. It has been demonstrated that combining the information of several developing struc-tures increases accuracy of age estimation [2, 4, 8, 9, 18, 39, 50]. However, when combinations are used for age estimation, appropriate statistical methods should be used. Simple regression will generate un-realistically narrow prediction intervals. Instead, a Bayesian approach has been demonstrated to be the most suitable statistical method [16, 41, 42]. In view of adding information of other anatomical structures to the ad-hoc procedure used
in the current study, the upper age limit of the study population (26 years of age) was higher than in other studies about third molar development (25 years of age [32], 24 years of age [20], 23 years of age [5], 22 years of age [47]).
A mere extrapolation of staging techniques for third molar devel-opment based on radiographs to MRI was considered inappropriate. Therefore, an MRI specific staging technique was proposed. Repro-
ducibility was similar to other staging techniques. Although embedding this technique into a Bayesian model for age estimation did not outperform estab-lished age estimation methods based on radiographs, it opens the perspective of combining developmental MRI informa-tion for age estimation. Other anatomical structures can be added to the used third molars model.
acknowledgements
We would like to thank all the partici-pants and everybody who helped with the recruitment. In particular, we are grate-ful to Rudy De Tobel, Griet Parmentier, Leen De Paepe and Gaetan Van de Vyvere for recruiting the last participants in the younger age categories. Special thanks to the department of Orthodontics at Ghent University Hospital, for allowing us to recruit among their patients. We also ac-knowledge the help by Maarten Peleman from the radiology department at Ghent University Hospital.
Conclusion
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.

97
references
[1] Altalie S, Thevissen P, Willems G. Classifying stages of third molar development: crown length as a predictor for the ma-ture root length. Int J Legal Med. 2014;129(1):165-9.
[2] Baccino E, Ubelaker DH, Hayek LA, Zerilli A. Evaluation of seven methods of estimating age at death from mature human skeletal remains. J Forensic Sci. 1999;44(5):931-6.
[3] Bassed RB, Briggs C, Drummer OH. Age Estimation and the Developing Third Molar Tooth: An Analysis of an Australi-an Population Using Computed Tomography. J Forensic Sci. 2011;56(5):1185-91.
[4] Bassed RB, Briggs C, Drummer OH. Age estimation using CT imaging of the third molar tooth, the medial clavicular epiphysis, and the spheno-occipital synchondrosis: a multi-factorial approach. Forensic Sci Int. 2011;212(1-3):273.e1-5.
[5] Baumann P, Widek T, Merkens H, Boldt J, Petrovic A, Ur-schler M, Kirnbauer B, Jakse N, Scheurer E. Dental age es-timation of living persons: Comparison of MRI with OPG. Forensic Sci Int. 2015;253(0):76-80.
[6] Boldsen JL, Milner GR, Konigsberg LW, Wood JW. Transi-tion analysis: a new method for estimating age from skel-etons. In: Hoppa RD, Vaupel JW, eds. Paleodemography: Age Distributions from Skeletal Samples. 1st ed. Cambridge: Cambridge University Press, 2002; p. 73-106.
[7] Bracher AK, Hofmann C, Bornstedt A, Boujraf S, Hell E, Ul-rici J, Spahr A, Haller B, Rasche V. Feasibility of ultra-short echo time (UTE) magnetic resonance imaging for identifi-cation of carious lesions. Magn Reson Med. 2011;66(2):538-45.
[8] Cameriere R, De Luca S, Biagi R, Cingolani M, Farronato G, Ferrante L. Accuracy of three age estimation methods in children by measurements of developing teeth and car-pals and epiphyses of the ulna and radius. J Forensic Sci. 2012;57(5):1263-70.
[9] Cameriere R, Ferrante L. Age estimation in children by measurement of carpals and epiphyses of radius and ulna and open apices in teeth: A pilot study. Forensic Sci Int. 2008;174(1):60-3.
[10] Cantekin K, Sekerci AE, Buyuk SK. Dental computed tomo-graphic imaging as age estimation: morphological analysis of the third molar of a group of Turkish population. Am J Forensic Med Pathol. 2013;34(4):357-62.
[11] Corradi F, Pinchi V, Barsanti I, Manca R, Garatti S. Optimal age classification of young individuals based on dental ev-idence in civil and criminal proceedings. Int J Legal Med. 2013;127(6):1157-64.
[12] De Tobel J, Hillewig E, Bogaert S, Deblaere K, Verstraete K. Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation. Ann Hum Biol. 2017;44(2):130-9.
[13] De Tobel J, Hillewig E, Verstraete K. Forensic age estima-tion based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging. Ann Hum Biol. 2017;44(2):121-9.
[14] Demirjian A, Goldstein H, Tanner JM. A new system of den-tal age assessment. Hum Biol. 1973;45(2):211-27.
[15] European Asylum Support Office (EASO). Practical Guide on Age Estimation, Second edition. EASO Practical Guides Series. Malta2018.
[16] Fieuws S, Willems G, Larsen-Tangmose S, Lynnerup N, Boldsen J, Thevissen P. Obtaining appropriate interval esti-mates for age when multiple indicators are used: evaluation of an ad-hoc procedure. Int J Legal Med. 2016;130(2):489-99.
[17] Friedrich RE, Ulbricht C, Ljuba ABvM. The influence of wisdom tooth impaction on root formation. Ann Anat. 2003;185(5):481-92.
[18] Garamendi PM, Landa MI, Ballesteros J, Solano MA. Relia-bility of the methods applied to assess age minority in living subjects around 18 years old. A survey on a Moroccan origin population. Forensic Sci Int. 2005;154(1):3-12.
[19] Gelbrich B, Hirsch A, Dannhauer KH, Gelbrich G. Agenesis of second premolars and delayed dental maturation. J Oro-fac Orthop. 2015;76(4):338-50.
[20] Guo Y, Olze A, Ottow C, Schmidt S, Schulz R, Heindel W, Pfeiffer H, Vieth V, Schmeling A. Dental age estimation in living individuals using 3.0 T MRI of lower third molars. Int J Legal Med. 2015;129(6):1265-70.
[21] Guo YC, Yan CX, Lin XW, Zhang WT, Zhou H, Pan F, Wei L, Tang Z, Liang F, Chen T. The influence of impaction to the third molar mineralization in northwestern Chinese popu-lation. Int J Legal Med. 2014;128(4):659-65.
[22] Halicioglu K, Toptas O, Akkas I, Celikoglu M. Permanent first molar extraction in adolescents and young adults and its effect on the development of third molar. Clin Oral Investig. 2014;18(5):1489-94.
[23] Hillewig E, Degroote J, Van der Paelt T, Visscher A, Van-demaele P, Lutin B, D’Hooghe L, Vandriessche V, Piette M, Verstraete K. Magnetic resonance imaging of the sternal extremity of the clavicle in forensic age estimation: towards more sound age estimates. Int J Legal Med. 2013;127(3):677-89.
[24] Hogge JP, Messmer JM, Doan QN. Radiographic identifica-tion of unknown human remains and interpreter experience level. J Forensic Sci. 1994;39(2):373-7.
[25] Idiyatullin D, Corum C, Moeller S, Prasad HS, Garwood M, Nixdorf DR. Dental magnetic resonance imaging: making the invisible visible. J Endod. 2011;37(6):745-52.
[26] Kimmerle EH, Prince DA, Berg GE. Inter-observer variation in methodologies involving the pubic symphysis, sternal ribs, and teeth. J Forensic Sci. 2008;53(3):594-600.
Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging

98
[27] Knell B, Schmeling A. Einfluss der Retention auf die Weisheitszahnmineralisation. Rechtsmedizin. 2010;20(6):469-74.
[28] Köhler S, Schmelzle R, Loitz C, Puschel K. [Development of wisdom teeth as a criterion of age determination]. Ann Anat. 1994;176(4):339-45.
[29] Koot MG, Sauer NJ, Fenton TW. Radiographic human iden-tification using bones of the hand: a validation study. J Fo-rensic Sci. 2005;50(2):263-8.
[30] Lebbe A, Cadenas de Llano-Perula M, Thevissen P, Verdon-ck A, Fieuws S, Willems G. Dental development in patients with agenesis. Int J Legal Med. 2017;131(2):537-46.
[31] Liversidge HM. Timing of human mandibular third molar formation. Ann Hum Biol. 2008;35(3):294-321.
[32] Liversidge HM, Marsden PH. Estimating age and the like-lihood of having attained 18 years of age using mandibular third molars. Br Dent J. 2010;209(8):E13.
[33] Lynnerup N, Belard E, Buch-Olsen K, Sejrsen B, Damgaard-Pedersen K. Intra- and interobserver error of the Greulich-Pyle method as used on a Danish forensic sample. Forensic Sci Int. 2008;179(2-3):242 e1-6.
[34] Manoliu A, Ho M, Nanz D, Dappa E, Boss A, Grodzki DM, Liu W, Chhabra A, Andreisek G, Kuhn FP. MR neurographic orthopantomogram: Ultrashort echo‐time imaging of man-dibular bone and teeth complemented with high‐resolution morphological and functional MR neurography. J Magn Re-son Imaging. 2016;44(2):393-400.
[35] Olze A, Bilang D, Schmidt S, Wernecke KD, Geserick G, Schmeling A. Validation of common classification systems for assessing the mineralization of third molars. Int J Legal Med. 2005;119(1):22-6.
[36] Olze A, Otto A, Tsokos M. Einfluss der Retention auf die Mineralisationsgeschwindigkeit dritter Molaren. Rechts-medizin. 2012;22(2):110-4.
[37] Olze A, van Niekerk P, Schulz R, Ribbecke S, Schmeling A. The influence of impaction on the rate of third molar mineralisation in male black Africans. Int J Legal Med. 2012;126(6):869-74.
[38] Ottow C, Krämer JA, Olze A, Schmidt S, Schulz R, Wittsch-ieber D, Heindel W, Pfeiffer H, Ribbecke S, Vieth V, Schmeling A. Magnetresonanztomographiestudie zur Al-tersschätzung von unbegleiteten minderjährigen Flüchtlin-gen. Rechtsmedizin. 2014;25:12-20.
[39] Pinchi V, De Luca F, Focardi M, Pradella F, Vitale G, Ric-ciardi F, Norelli GA. Combining dental and skeletal evidence in age classification: Pilot study in a sample of Italian sub-adults. Leg Med (Tokyo). 2016;20:75-9.
[40] Pinchi V, Norelli GA, Caputi F, Fassina G, Pradella F, Vin-centi C. Dental identification by comparison of antemor-tem and postmortem dental radiographs: influence of operator qualifications and cognitive bias. Forensic Sci Int. 2012;222(1-3):252-5.
[41] Prince DA, Kimmerle EH, Konigsberg LW. A Bayesian approach to estimate skeletal age-at-death utilizing dental wear. J Forensic Sci. 2008;53(3):588-93.
[42] Prince DA, Konigsberg LW. New formulae for estimating age-at-death in the Balkans utilizing Lamendin’s dental tech-nique and Bayesian analysis. J Forensic Sci. 2008;53(3):578-87.
[43] Serin J, Rerolle C, Pucheux J, Dedouit F, Telmon N, Savall F, Saint-Martin P. Contribution of magnetic resonance im-aging of the wrist and hand to forensic age assessment. Int J Legal Med. 2016;130(4):1121-8.
[44] Štern D, Kainz P, Payer C, Urschler M. Multi-Factorial Age Estimation from Skeletal and Dental MRI Volumes. In: International Workshop on Machine Learning in Medical Imaging. Quebec City, Canada: Springer, 2017; p. 61-9.
[45] Thevissen PW. Dental age estimation: striving for an opti-mal approach [Doctoral thesis]. Leuven: Leuven University Press, 2013.
[46] Thevissen PW, Alqerban A, Asaumi J, Kahveci F, Kaur J, Kim YK, Pittayapat P, Van VM, Zhang Y, Fieuws S, Wil-lems G. Human dental age estimation using third molar developmental stages: Accuracy of age predictions not using country specific information. Forensic Sci Int. 2010;201(1-3):106-11.
[47] Thevissen PW, Fieuws S, Willems G. Human dental age estimation using third molar developmental stages: does a Bayesian approach outperform regression models to dis-criminate between juveniles and adults? Int J Legal Med. 2010;124(1):35-42.
[48] Thevissen PW, Fieuws S, Willems G. Third molar develop-ment: measurements versus scores as age predictor. Arch Oral Biol. 2011;56(10):1035-40.
[49] Thevissen PW, Fieuws S, Willems G. Third molar de-velopment: evaluation of nine tooth development reg-istration techniques for age estimations. J Forensic Sci. 2013;58(2):393-7.
[50] Thevissen PW, Kaur J, Willems G. Human age estimation combining third molar and skeletal development. Int J Legal Med. 2012;126(2):285-92.
[51] Urschler M, Grassegger S, Stern D. What automated age estimation of hand and wrist MRI data tells us about skeletal maturation in male adolescents. Ann Hum Biol. 2015;42(4):358-67.
[52] Wittschieber D, Schulz R, Vieth V, Kuppers M, Bajanowski T, Ramsthaler F, Puschel K, Pfeiffer H, Schmidt S, Schmeling A. Influence of the examiner’s qualification and sources of error during stage determination of the medial clavicular ep-iphysis by means of computed tomography. Int J Legal Med. 2014;128(1):183-91.
[53] Yavuz I, Baydas B, Ikbal A, Dagsuyu IM, Ceylan I. Effects of early loss of permanent first molars on the develop-ment of third molars. Am J Orthod Dentofacial Orthop. 2006;130(5):634-8.
De Tobel J. Multi-factorial forensic age estimation. Chapter 5: 72-98.


100
CHAPTER 6
TH I S CHAPTER ADDRESSED THE FOLLOWING STUDY OB JECT IVE :
Objective 7: To compare our MRI protocol for third molars with the Graz protocol.
TH I S CHAPTER WAS PUBL I SHED AS :
De Tobel J, Parmentier G, Phlypo I, Descamps B, Neyt S, Van De Velde W, Politis C, Verstraete K, Thevissen P. Magnetic resonance imaging of third molars in forensic age estimation: comparison of the Ghent and Graz protocols focusing on apical closure. Int J Legal Med. 2018; Epub ahead of print [A1; Journal Impact Factor 2017 2.316; Medicine, Legal Q1; Peer reviewed]
RESULTS DESCR I BED IN TH I S CHAPTER WERE PARTLY PRESENTED
AT THE FOLLOWING CONFERENCE :
De Tobel J, Parmentier G, Phlypo I, Descamps B, Neyt S, Van De Velde W, Verstraete K, Thevissen P. Magnetic resonance imaging of third molars in forensic age estimation: comparison of the Ghent and Graz protocols focusing on apical closure. 21st Meeting of the Study Group on Forensic Age Diagnostics, Arbeitsgemeinschaft für Forensische Altersdiagnostik (AGFAD); Berlin, Germany; March 16, 2018.
De Tobel J, Parmentier G, Phlypo I, Descamps B, Neyt S, Van De Velde W, Thevissen P, Verstraete K. Magnetic Resonance Imaging (MRI) of Third Molars in Forensic Age Estimation: Validation of the Gent and Graz Protocols. American Academy of Forensic Sciences (AAFS) 70th Annual Scientific Meeting; Seattle, USA; February 23, 2018. p 640.

101
Magnetic resonance imaging of third molars in forensic age estimation: comparison of the Ghent and Graz protocols
focusing on apical closure
OR IG INAL RESEARCH
Abstract
Aim — To compare the Ghent and Graz magnetic resonance imaging (MRI) protocols for third molars, focusing on the as-sessment of apical closure. To study the influence of (1) voxel size and (2) head fixation using a bite bar. To compare both pro-tocols with a ground truth of apical development. Materials and methods — In eleven healthy volunteers 3T MRI was conduct-ed, including four Ghent sequences and two Graz sequences, with and without bite bar. After removal, 39 third molars were scanned with 7T µMRI and µCT to establish the ground truth of apical development. Three observers in consensus evaluat-ed assessability and allocated developmental stages. Results — The Ghent T2 FSE sequence (0.33 x 0.33 x 2 mm³) was more assessable than the Graz T1 3D FSE sequence (0.59 x 0.59 x 1 mm³). Comparing assessability in both sequences with bite bar rendered P = 0.02, whereas comparing those without bite bar rendered P < 0.001. Within the same sequence, the bite bar in-creased assessability, with P = 0.03 for the Ghent T2 FSE and P = 0.07 for the Graz T1 3D FSE. Considering µCT as ground truth for staging, allocated stages on MRI were most frequently equal or higher. Among in vivo protocols, the allocated stages did not differ significantly. Conclusion — Imaging modality-specific and MRI sequence-specific reference data are needed in age es-timation. A higher in-plane resolution and a bite bar increase assessability of apical closure, whereas they do not affect stage allocation of assessable apices.
Key Words
• age determination by teeth
• molar, third
• adolescent
• adult
• magnetic resonance imaging
AFF IL IAT IONS
1 Department of Radiology and
Nuclear Medicine, Ghent Univer-
sity, Belgium
2 Department of Head, Neck and
Maxillofacial Surgery, Ghent
University Hospital, Belgium
3 Department of Oral and Maxillo-
facial Surgery, Leuven University
Hospitals, Belgium
4 Department of Imaging and Pa-
thology – Forensic Odontology,
KU Leuven, Belgium
5 Department of Dentistry – Spe-
cial Care in Dentistry, PaeCoMe-
DiS, Ghent University, Belgium
6 Department of Dentistry – Com-
munity Dentistry and Oral Public
Health, PaeCoMeDiS, Ghent
University, Belgium
7 IbiTech-Medisip-Infinity lab,
Ghent University, Belgium
8 MOLECUBES NV, Ghent, Belgium
9 Department of Oral and Maxillo-
facial Surgery, General Hospital
Saint-Lucas, Ghent, Belgium
JANN ICK DE TOBEL 1 2 34 GR I ET I . L . PARMENT I ER 1 2 3
I N ÈS PHLYPO 56 BENED ICTE DESCAMPS 7
SARA NEY T 4
WIM L . VAN DE VELDE 9 CONSTANT INUS POL I T I S 3
KOENRAAD L . VERSTRAETE 1 PATR ICK W. THEV I S SEN 2
This study has received funding by the American Society of Forensic Odontology
(ASFO) in form of its Research Grant 2017.
Sara Neyt declares a relationship with the following company: MOLECUBES NV
(Gent, Belgium). The µCT scans for this study were performed free of charge by
this company. The other authors of this manuscript declare no relationships with
any companies, whose products or services may be related to the subject matter
of the article.

102
Forensic dental age estimation is ap-plied in criminal, civil, and asylum procedures, as well as in sport com-petitions [23, 25]. The estimation at best includes a predicted age, an un-certainty measure, and the proba-
bility of having reached a specific relevant age threshold [14, 24, 28]. In living ado-lescents and young adults, the gold stand-ard in dental age estimation includes the clinical examination of the dentition and the evaluation of a panoramic radiograph. However, to increase accuracy, dental age estimation should be combined with oth-er suitable age estimation methods (e.g. skeletal age estimation based on hand/wrist and clavicles) [5, 8, 21, 26].
X-ray examinations for age estimation imply ionizing radiation exposure with-out medical indication, leading to deon-tological and ethical controversy [29]. Therefore, using ionizing radiation is pro-
hibited for asylum and civil procedures in some European countries [19]. Moreover, superposition on plain radiographs can lead to misinterpretation of the develop-mental status of the anatomical structures of interest [12].
To counter these drawbacks, magnetic resonance imaging (MRI) is of particu-lar interest in forensic age estimation. Although not routinely used in clinical dental practice, dedicated MRI has been demonstrated to adequately depict per-iodontal space, apical foramen, cortical and trabecular bone [6, 7]. To our knowl-edge dental age estimation by third mo-lars MRI has only been studied by three research groups [1-4, 11, 26]. Guo et al. (2015) described an MRI protocol for a 3T Philips scanner, while Baumann et al. (2015) and De Tobel et al. (2017) used a 3T Siemens scanner. MRI sequences of the latter two research groups will further
IntroductionTABLE 6. 1 — OVERVIEW OF THE APPLIED MRI AND CT PROTOCOLS, WITH THEIR PARAMETERS.
IMAGING
MODALITY
PROTOCOL SEQUENCE PLANE TR (MSEC) TE (MSEC) AVERAGES
In v ivo MRI Ghent T2 FSE Sagittal 5084 74 3
Thin S l ice T2
FSE
Sagittal 7270 66 3
T2 FSE Axial 4290 74 3
T2 FSE Coronal 4080 74 3
Graz T1 3D FSE Sagittal 175 10 1
3D CISS Axial 5.25 2.28 2
In vitro µMRI T2 FSE Coronal 3661 37. 1 10
ZTE (Sagittal ) 2 NA 4
IMAGING
MODALITY
TRAJEC-
TORY
CONTINUOUS
ROTATIONS
PROJEC-
TIONS /
ROTATION
TUBE CUR-
RENT (µA)
In v itro µCT Circular 4 720 460
TA = acquis it ion t ime; FOV = f ie ld of v iew; FS = fat suppress ion; NA = not appl icable; TE = echo t ime; TR =
repetit ion t ime
De Tobel J. Multi-factorial forensic age estimation. Chapter 6: 100-114.

103
on be referred to as the Graz and Ghent protocol, respectively.
The current study tested both Siemens protocols. They differ in type of coil, type of fixation, and voxel size. The Ghent pro-tocol uses a flexible coil, so fixation in a bite bar is applied to minimize motion. The Graz protocol uses a more rigid coil, so support by pillows is deemed sufficient. Furthermore, De Tobel et al. (2017) sug-gested that an in-plane resolution of 0.33 x 0.33 mm² is necessary to discern the stages of apical closure [2]. However, their study sample was small with only 10 par-ticipants and their suggestion was based on only one case. By contrast, Baumann et al. (2015) used an in-plane resolution of 0.59 x 0.59 mm² in 19 female and 8 male volunteers [1].
The current study aimed to compare the Ghent and Graz magnetic resonance
imaging (MRI) protocols for third molars, focusing on the assessment of apical clo-sure. Firstly, it was aimed to evaluate how staging apical closure for age estimation is affected by (1) voxel size and (2) head fixation using a bite bar. Secondly, it was aimed to compare both protocols with a ground truth of apical development.
Study population
This project was approved by the Ghent University Hospital Eth-ics Committee. Written informed consent was obtained from all vol-unteers, and in case of minors, from their parents. In a prospective cross-sectional design, a conveni-ence sample of eleven volunteers (5
females, 6 males, 17-30 years of age) was recruited at the department of Oral and Maxillofacial Surgery at Ghent Hospital and in a private practice, both in Gh-
Materials and M
ethods
TABLE 6. 1 (CONTINUED)
NUMBER OF
SLABS
FLIP
ANGLE
(DEGREES)
FS VOXEL SIZE (MM³) FOV (MM²) NUMBER OF
SECTIONS
TA
(MIN:SEC)
1 120 Yes 0.33 x 0.33 x 2.0 150 x 150 32 inter leaved 6:33
1 120 Yes 0.47 x 0.47 x 1 .7 150 x 150 32 inter leaved 6:49
1 120 Yes 0.33 x 0.33 x 2.0 150 x 150 27 inter leaved 6:49
1 120 Yes 0.33 x 0.33 x 2.0 150 x 150 17 inter leaved 6:29
2 150 Yes 0.59 x 0.59 x 1 .0 150 x 150 56 inter leaved 9:58
2 30 No 0.59 x 0.59 x 1 .0 150 x 150 56 sequential 8 :39
1 90 Yes 0, 167 x 0, 167 x 0,3 17.2 x 17.2 20 inter leaved 7: 19
1 2 NA 0, 167 x 0, 167 x 0, 167 25 x 25 150 6:31
TUBE
VOLTAGE
(KVP)
VOXEL SIZE (MM³) FOV (MM²) TA (MIN)
50 0.05 x 0.05 x 0.05 70 x 40 4
Magnetic resonance imaging of third molars in forensic age estimation: comparison of the Ghent and Graz protocols focusing on apical closure

104
FIGURE 6. 1 — SET-UP FOR THE IN VIVO
MRI SCAN.
a Cranio-anterior view. The
par t ic ipant c loses the mouth
around the bite plate during
the scan. Surface head coi ls
are posit ioned next to the
cheeks.
b Posit ioning without bite bar.
Relat ive f ixat ion of the head
and the coi ls was ensured by
pi l lows.
(Written informed consent was ob-
tained from the par t ic ipant for pub-
l icat ion of these images.)
FIGURE 6.2 — SET-UP FOR THE IN
VITRO µCT (MOLECUBES NV, GHENT,
BELGIUM).
a Close-up of the posit ioned
specimens for µCT.
b Caudal overview of the posi-
t ioning of the specimens for
µCT.
FIGURE 6.3 — SET-UP FOR THE IN VI-
TRO 7T µMRI.
a Close-up of the posit ioned
specimen for the ZTE se-
quence.
b Caudal v iew of the posit ioning
of the specimen and the coi l
for the ZTE sequence
c Close-up of the posit ioned
specimen in formal in 3% solu-
t ion for the T2 FSE sequence.
d Caudal v iew of the posit ioning
of the specimen and the coi l
for the T2 FSE sequence.
e Caudal overview of the µMRI
set-up.
a
c
b
d d
De Tobel J. Multi-factorial forensic age estimation. Chapter 6: 100-114.

105
ent, Belgium. Inclusion criteria were not based on age or sex, because of inter-indi-vidual variability regarding development and agenesis [16]. Instead, patients sched-uled for surgical removal of third molars were asked to participate when at least one lower third molar was in a stage of apical closure on panoramic radiograph. The surgeons were instructed to preserve all pieces of the removed third molars in labelled containers with formalin 3%. Ex-clusion criteria were dental developmen-tal disorders and consanguinity among participants up to the third degree.
Image acquisition
A clinically indicated panoramic radi-ograph was obtained from the hospital or private practice. MRI was performed at Ghent University Hospital with a 3T scanner (Magnetom Trio Tim, Siemens, Erlangen, Germany), with the interval be-tween the radiograph and the MRI rang-ing from 28 to 479 days (mean 87, median 41). Table 6.1 shows an overview of imag-ing modalities, protocols and sequences. In the Ghent protocol [2], two groups of sequences were considered for evaluation: (1) sagittal, axial and coronal T2 fast spin echo (FSE), and (2) sagittal thin slice T2 FSE. The latter sequence was particularly included to study the influence of voxel size, because its in-plane resolution and slice thickness were intermediate between the first sequences and the Graz sequenc-es (Table 6.1). The Graz sequences were developed at the Ludwig Boltzmann Insti-tute for Clinical Forensic Imaging, Graz, Austria [1]. Researchers from this group were contacted to obtain the correct pa-rameters to apply their T1 3D FSE and 3D constructive interference in steady state (CISS) sequences.
A bilateral four-channel flexible surface head coil (model NMP-001D-ST-4, Nova Medical Inc., Wilmington, USA) for par-allel imaging was used. To ensure a stable head position and minimize motion arte-facts, an individual bite bar was made for each participant, as described by De To-bel et al. (2017) [2]. Both the Ghent and Graz protocols were conducted with and without the bite bar (Figure 6.1). Without bite bar, relative fixation was ensured by Velcro straps and pillows. To eliminate the effect of fatigue, the scanning process was randomized: the protocols – either with or without bite bar – were applied in a miscellaneous order. However, scans without bite bar were not conducted in the first two participants because insuffi-cient time was scheduled. From then on, half an hour extra was scheduled for the other participants.
In four cases, specific absorption rate (SAR) limits were exceeded when the Graz T1 3D FSE scan was started. There-fore, the number of slabs was reduced to one and TR was changed from 175 to 174, 193, 258, or 285, changing the acquisition times from 9:58 min to 9:54, 10:57, 14:40 and 16:07 min, respectively.
The interval between the MRI and surgical removal ranged from 2 to 11 days (mean 7, median 7). After surgical re-moval, all third molars were scanned with µCT (X-Cube, MOLECUBES NV, Gh-ent, Belgium) (Figure 6.2) and 7T µMRI (Pharmascan, Bruker BioSpin, Ettlingen, Germany) at the Infinity lab (IbiTech-Me-disip, Ghent University, Belgium) (Figure 6.3). These high resolution in vitro imag-ing modalities were chosen to establish a ground truth of apical development. Mi-cro-CT was selected because of its ability
Magnetic resonance imaging of third molars in forensic age estimation: comparison of the Ghent and Graz protocols focusing on apical closure
106
to reach extremely small voxel sizes and lower noise than MRI. Regarding µMRI, a zero echo time (ZTE) sequence was select-ed for its capability to discern the different dental hard tissues [15, 32]. Additionally, a T2 FSE sequence was applied because it depicts the tooth similar to the in vivo T2 sequences. Before positioning in the scan-ner, every tooth was visually examined for orientation. In case of fragmented teeth, all fragments were positioned as to resem-ble the original anatomical situation for the ZTE sequence. To enhance contrast in the T2 FSE sequence, teeth were scanned inside a syringe filled with formalin 3%. Hence, an anatomical reconstruction of fragments was impossible for the latter scan. All imaging was conducted between February and April 2017.
Image analysis and visual inspection
The clinical panoramic radiographs were not considered for analysis, because in some cases the interval between the ra-diograph and in vivo MRI was too large. The images of all molars were anonymized and randomized before evaluation. Every surgically removed tooth was evaluated before micro-imaging to assess possible iatrogenic damage and to decide on a visual developmental stage. These stages were allocated according to De Tobel et al. (2017) [4], since their staging technique into eight stages accounts for the specific appearance of dental tissues on MRI. This staging technique was also applied to all images: in vivo and in vitro, MRI and CT. Details about the staging technique were included in chapter 5. For reference imag-es – which have been suggested to increase inter-observer agreement [17] – the origi-nal paper [4] should be consulted.
Three observers – JDT, GP and IP – eval-uated the teeth and the images in consen-sus. They had over 5 years of experience in evaluating dental radiographs. Two of them – JDT and IP – had 6 and 1 year of experience, respectively, as researchers on dental age estimation using MRI.
If no consensus was reached, the im-ages were analyzed by a fourth observer (PWT) to resolve disputes. He had more than 10 years of experience studying den-tal development for age estimation and over 30 years of experience in evaluating dental radiographs. Non-assessable imag-es were documented and specified with one of the following causes:
— insufficient contrast between apex tip and surrounding bone;
— apex tip falls in between slices;— poor coil positioning;— poor image quality (e.g. poor signal
to noise ratio);— artefacts due to motion of the par-
ticipant;— other artefacts (e.g. susceptibility
due to metal);— other.
Images were evaluated and staged on a Barco MDCC-6130 monitor (3280 x 2048 pixels, Barco, Kortrijk, Belgium) using Synedra View Personal and Amide view-ing freeware, for MRI and CT, respec-tively. If possible (i.e. for Graz sequences, µMRI and µCT), multiplanar reconstruc-tion (MPR) was considered.
Statistical analysis
Data were collected using Microsoft Excel 2010 and were transferred to SPSS Statis-tics 24 (IBM SPSS Statistics for Windows,
De Tobel J. Multi-factorial forensic age estimation. Chapter 6: 100-114.

107
Results
Armonk, NY). Descriptive statistics were calculated, and assessability and staging were compared with McNemar and Wil-coxon matched-pairs signed-ranks tests, respectively. Additionally, intra-class cor-relation coefficients (ICCs) were calculat-ed to quantify the agreement in staging between MRI protocols. All tests were considered two-sided at 0.05 significance level.
In the eleven participants a total of 39 third molars were available for µCT and µMRI. Four third molars were either agenetic or removed at
an earlier time. One third molar was se-verely damaged during surgery. Eight lower third molars were removed in frag-ments, but remained suitable for assess-ment.
In all Graz 3D CISS images, the con-trast between the pulpal tissue and the hard tissue of the root was insufficient to allocate a stage. Therefore this sequence was omitted from analysis. In all other sequences, sagittal slices were decisive to allocate a stage when MPR was evaluated. Likewise, when Ghent T2 FSE was used, the axial and coronal images did not con-tribute to stage allocation. Figures 6.4 and 6.5 show corresponding slices of an upper and lower third molar, respectively, as seen on all imaging modalities. The fig-ures demonstrate that voxel size and head fixation by a bite bar influence staging both in lower stages (stages 5-6) of apical development as well as in higher stages (stages 7-8).
Visual inspection was considered most efficient to observe fractures and chipping of the roots. In two molars, a fragment of the apex had chipped off dur-
ing surgery, but this did not affect staging: in one tooth the decisive roots for staging were undamaged, and in the other tooth the roots were in stage 6 on in vivo as well as in vitro scans. Visual inspection did not offer an added value in staging the third molars, since it did not allow for assessment of the internal anatomy and configuration of the root canals. The com-bination of the small voxel size and the inherent high-contrast of µCT rendered the optimal depiction of the specimens. Hence, imaging with µCT was considered as the ground truth to compare the assess-ability and staging of third molars’ apical closure.
Assessability
In practice, two settings are applied in research on a large scale: Ghent T2 FSE with bite bar and Graz T1 3D FSE without bite bar [1-4, 26, 30]. Comparing the per-centages of assessable scans in these situa-tions – respectively 97% (31/32) and 59% (19/32) – rendered P < 0.001. Comparing both sequences with bite bar rendered P = 0.02, with 100% (35/35) being assessable in Ghent T2 FSE and 80% (28/35) in Graz T1 3D FSE.
Overall, the bite bar significantly in-creased the number of assessable scans compared to scans without bite bar (Fig-ure 6.6). With bite bar, Ghent T2 FSE – the sequence with the highest in-plane resolution – rendered more assessable cases than the other sequences.
Difficulties for in vivo staging were either due to motion artefacts or subopti-mal contrast between the hard dental tis-sues and the surrounding bone. Still, the contrast between the different dental hard
Magnetic resonance imaging of third molars in forensic age estimation: comparison of the Ghent and Graz protocols focusing on apical closure

108
FIGURE 6.4 — CORRESPONDING IMAGES OF AN UPPER THIRD MOLAR WITH ON TOP AN INDICATION OF THE
IMAGING MODALITY AND ITS TYPE.
For in v ivo scans, the top panels show images obtained using the bite bar, whereas the bottom panels
show corresponding images obtained without bite bar. The circ le indicates the root apex. Al located stages
were: stage 5 (a,c ,g) ; stage 6 (b,d,h , i , j ) ; stage 7 (e). Graz 3D CISS images were excluded, s ince overal l , they
were of insuff ic ient qual ity to al locate a stage. 3D = three-dimensional , µCT = micro computed tomography,
µMRI = micro magnetic resonance imaging, CISS = construct ive interference in steady state, FSE = fast spin
echo, T1 = T1-weighted, T2 = T2-weighted, ZTE = zero echo t ime.
FIGURE 6.5 — CORRESPONDING IMAGES OF A LOWER THIRD MOLAR WITH ON TOP AN INDICATION OF THE
IMAGING MODALITY AND ITS TYPE.
For in v ivo scans, the top panels show images obtained using the bite bar, whereas the bottom panels
show corresponding images obtained without bite bar. The circ le indicates the root apex. Al located stag-
es were: stage 6 (g) ; stage 7 (a,c ,f ) ; stage 8 (b,d). Image h was decided not to be assessable because of
motion ar tefacts. Graz 3D CISS images (e) were excluded, s ince overal l , they were of insuff ic ient qual ity
to al locate a stage. 3D = three-dimensional , µCT = micro computed tomography, µMRI = micro magnetic
resonance imaging, CISS = construct ive interference in steady state, FSE = fast spin echo, T1 = T1-weighted,
T2 = T2-weighted, ZTE = zero echo t ime.
De Tobel J. Multi-factorial forensic age estimation. Chapter 6: 100-114.

109
TABLE 6.2 — FREQUENCIES OF RELATIVE STAGING BASED ON MRI COMPARED WITH µCT. P-values and ICCs
indicate the difference and the agreement , respect ively, between staging based on the considered MRI
versus based on µCT.
SEQUENCE N CT = MR CT < MR CT > MR P ICC 95% CI
µMR T2 FSE 39 21 14 4 0.018 0.81 [0.65 ; 0.90]
µMR ZTE 37 20 9 8 0.817 0.73 [0.53 ; 0.85]
Ghent T2 FSE 38 20 14 4 0.016 0.74 [0.54 ; 0.86]
Ghent thin s l ice
T2 FSE
32 14 14 4 0.016 0.73 [0.49 ; 0.86]
Graz T1 3D FSE 28 13 13 2 0.005 0.75 [0.53 ; 0.88]
CI = conf idence interval ; ICC = intra-class correlat ion coeff ic ient
TABLE 6.3 — FREQUENCIES OF RELATIVE STAGING BASED ON MRI WITH BITE BAR COMPARED WITH MRI WITH-
OUT BITE BAR. P-values and ICCs indicate the difference and the agreement , respect ively, between staging
based on the considered MRI with versus without bite bar.
SEQUENCE N BITE BAR =
NO BITE BAR
BITE BAR <
NO BITE BAR
BITE BAR >
NO BITE BAR
P ICC 95% CI
Ghent T2 FSE 26 17 4 5 0.739 0.82 [0.64 ; 0.92]
Ghent thin s l ice
T2 FSE
23 1 1 4 8 0.065 0.45 [0.09 ; 0.72]
Graz T1 3D FSE 19 12 4 3 1 .000 0.65 [0.27 ; 0.85]
CI = conf idence interval ; ICC = intra-class correlat ion coeff ic ient
TABLE 6.4 — FREQUENCIES OF RELATIVE STAGING BASED ON GHENT T2 FSE COMPARED WITH GRAZ T1 3D
FSE, both with bite bar. P-value and ICC indicate the difference and the agreement , respect ively, between
staging based on Ghent T2 FSE compared with Graz T1 3D FSE, both with bite bar.
N GHENT = GRAZ GHENT < GRAZ GHENT > GRAZ P ICC 95% CI
28 15 8 5 0.317 -0.03 [-0.27 ; 0.27 ]
CI = conf idence interval ; ICC = intra-class correlat ion coeff ic ient
Magnetic resonance imaging of third molars in forensic age estimation: comparison of the Ghent and Graz protocols focusing on apical closure

110
tissues in µMRI ZTE provided no added value for staging.
Staging
Three types of comparisons were dis-played in Tables 6.2 to 6.4. Firstly, con-sidering µCT as ground truth for staging, the allocated stages on MRI were most frequently equal (about half of the third molars) or higher (Table 6.2). Even stag-ing based on µMRI did not always cor-respond with staging on µCT. Based on µCT, the following ground truth results of staging were obtained: stages 5 to 8 were allocated eight (21%), nine (23%), fifteen (38%) and seven (18%) times, respective-ly. Overall, a difference of up to two stages occurred between all MRI and µCT. Al-though stages allocated on Ghent T2 FSE showed more absolute correspondence
with µCT than stages allocated on the other in vivo sequences, ICCs were sim-ilar among in vivo sequences.
Secondly, whether or not the bite bar was used did not render statistically sig-nificant differences in stages allocated to assessable third molars (Table 6.3). However, agreement between findings with and without bite bar was lower for sequences with relatively lower in-plane resolution.
Thirdly, the difference between stag-ing on Ghent T2 FSE and Graz T1 3D FSE – both using the bite bar – was not statistically significant either (Table 6.4). Nonetheless, agreement between these two sequences proved to be non-existent, as reflected by an ICC approaching zero.
FIGURE 6.6 — PERCENTAGE OF ASSESSABLE THIRD MOLARS PER MRI SEQUENCE TYPE, E ITHER WITH OR WITH-
OUT USING THE BITE BAR. 3D = three-dimensional , FSE = fast spin echo, T1 = T1-weighted, T2 = T2-weighted.
De Tobel J. Multi-factorial forensic age estimation. Chapter 6: 100-114.

111
Discussion
Apical closure involves the smallest morphological changes in dental development with the largest impact on forensic age estimation, since these changes occur around the age
threshold of 18 years [18, 28]. In younger ages, the changes involve larger structures, with the differences between MRI proto-cols presumably being less pronounced. The current study focused on staging api-cal closure. Correlating the stages to the chronological age of the participants was beyond the scope of this study, since this correlation has been reported in literature [4, 26].
In the current study, the low noise in µCT images allowed studying apex mor-phology in great detail. Therefore, this imaging modality was considered the ground truth for comparison. Remark-ably, the differences between staging on any MRI versus µCT were clinically and statistically significant, except for µMR ZTE. This confirms the need for imag-ing modality-specific reference data for age estimation. Other authors agreed with this statement: regarding developing teeth, both Guo et al. (2015) and Bau-mann et al. (2015) highlighted differenc-es in age distribution per developmental stage when MRI was compared with radi-ographs [1, 11]. Moreover, this statement was confirmed for the developing hand/wrist and clavicle, including MRI, CT, and radiographs [9, 13, 27, 31].
In a multi-factorial age estimation ap-proach, Stern et al. (2017) only included results from the Graz T1 3D FSE [26], which confirms our finding to omit the CISS from analysis. Consequently, in research on dental age estimation, two Siemens MRI sequences are applied on
a large scale: Ghent T2 FSE with bite bar and Graz T1 3D FSE without bite bar [1, 3]. They mainly differ in acquisition ap-proach and voxel size.
Image acquisition
The longer acquisition time of 9:58 min of the Graz T1 3D FSE compared to the Ghent T2 FSE with 6:33 min, could be considered a drawback. Nasel et al. (1998) proposed 6:30 min as a clinically accept-able acquisition time [20]. Moreover, a 3D sequence is more prone to motion ar-tefacts than a 2D sequence [10, 22]. Not only was this confirmed by comparing the proportion of assessable cases when the bite bar was not used – which was lower in Graz T1 3D FSE (59%) than in Ghent T2 FSE (81%) – but also by the higher ICC for Ghent T2 FSE.
However, the arms of the Noras CPC coil that was used in Graz are more rig-id than those of the Nova Medical sur-face head coil used in the current study. This implies that motion might be more impeded by the Noras coil. Therefore, comparisons between Ghent sequences with bite bar and Graz sequences without bite bar should be considered cautious-ly. More certain conclusions about the relative image quality of both protocols can only be made when the original se-quences would be used with both coils in the same individual at the same scanning session, which proved not to be feasible in the current study. By contrast to the used Nova Medical four-channel surface head coil, the Noras CPC coil used in the origi-nal Graz protocol contains eight channels, presumably rendering higher signal-to-noise ratio when resolution and acquisi-tion time are kept constant.
Magnetic resonance imaging of third molars in forensic age estimation: comparison of the Ghent and Graz protocols focusing on apical closure

112
Image analysis
A first consideration regarding image analysis is the voxel size. The slice thick-ness of 2.0 mm in Ghent T2 FSE was a drawback, since it impeded MPR. How-ever, the availability of MPR in the Graz 3D FSE sequence could not make up for its lower in-plane resolution of 0.59 x 0.59 mm² compared to the in-plane resolu-tion of 0.33 x 0.33 mm² of the Ghent T2 FSE. Consequently, more cases could be assessed based on the Ghent T2 FSE than based on the Graz T1 3D FSE. According-ly, in literature the latter resolution has been deemed necessary to distinguish an almost closed apex from a closed one [2]. Moreover, the current study confirmed that a different resolution can result in a different stage allocation. With an ICC close to zero, Ghent T2 FSE and Graz T1 3D FSE proved to render divergent stag-ing results. Compared to the stage on µCT, more frequently a higher stage was allocated based on the Graz T1 3D FSE than on the Ghent T2 FSE. This could be explained by the different in-plane reso-lutions. A small opening at the root apex in stage 7 based on Ghent T2 FSE (0.33 x 0.33 mm²) might be indiscernible on Graz T1 3D FSE (0.59 x 0.59 mm²) and inter-preted as being closed (stage 8).
However, a lower in-plane resolution can also result in the allocation of a lower stage, as was reported in a previous study [2] and was confirmed by the current re-sults. Thus, staging and its corresponding age distribution cannot be extrapolated from one sequence to another. Therefore, when either of these sequences would be used in age estimation practice, se-quence-specific reference data of age dis-tribution are needed (in addition to the
need for imaging modality-specific refer-ence data).
To study how the differences between the Ghent and Graz protocols affect age estimation, future research could (1) test the performance of the Bayesian age esti-mation model based on the Ghent proto-col [4] in the Graz study sample, and (2) test the performance of automatic age es-timation based on the Graz protocol [26] in the Ghent study sample. If the results of both comparisons are similar to the orig-inal cross-validation results, it could be presumed that both protocols are inter-changeable. However, the current study contradicts this hypothesis.
A second consideration regarding im-age analysis is the image plane. De Tobel et al. [4] reported that sagittal MR images were essential for staging upper and lower third molars in 95% and 92% of cases, re-spectively. Axial images contributed in 0% and 1% respectively, and coronal images in 5% and 4% respectively. The current study showed similar findings. In case of the Ghent T2 FSE, only sagittal images contributed to stage allocation. In other sequences, when MPR was available, the sagittal images were preferred as well.
Although the sagittal images might suffice for stage allocation by human observers, a major disadvantage of 2D sequences is that they are unsuitable for automated evaluation if a large discrep-ancy exists between in-plane resolution and slice thickness. More isotropic voxels allow the software to consider the 3D vol-ume of the developing structure, which might increase the accuracy of age esti-mation. In that prospect, the Graz T1 3D FSE is being studied [26, 30].
De Tobel J. Multi-factorial forensic age estimation. Chapter 6: 100-114.

113
Conclusion
The third consideration regarding image analysis relates to the ground truth. We chose µCT to compare all MRIs with. Al-ternatively, future research could study the ex vivo third molars histologically. However, to our knowledge, a histologi-cal threshold has not been proposed yet to distinguish a closing apex from a fully mature apex with an opening for the neu-rovascular structures.
Study limitations
The current study faced three limitations. Firstly, the protocol used by Guo et al. (2015) could not be evaluated because only Siemens scanners were available at our institution. Secondly, only a small study population was included and only in 9/11 participants all MRI sequences were conducted. Still, sufficient data were available to draw conclusions about the applicability of the studied MRI sequenc-es. Finally, with the available coil at our institution, it was only possible to mim-ic the Graz approach, not to reproduce it. Nonetheless, comparison with their original images confirmed that a similar quality was reached for the T1 3D FSE in the current study. The quality of the CISS images however, was inferior to the actual CISS that is being conducted in Graz.
In conclusion, third molars often appeared to be in a higher devel-opmental stage on MRI compared with µCT. Therefore, imaging mo-dality-specific reference data are
needed in age estimation practice. More-over, MRI sequence-specific reference data are needed. To increase the propor-tion of assessable third molar apices using MRI, a higher in-plane resolution is more important than a smaller slice thickness.
A further increase of that proportion can be obtained by using a bite bar. By con-trast, the voxel size and the bite bar do not affect stage allocation if the apices are as-sessable. Images of the Ghent protocol al-low to interpret the highest proportion of third molars available for age estimation.
acknowledgements
We are very grateful to all participants and everybody who helped with recruitment. We wish to express our most sincere grat-itude and appreciation to Martin Urschler for making the exact parameters of the Graz protocol available for our research and for his critical appraisal of the manu-script. We also want to thank Dominique Neyts for her critical review of the man-uscript. Lastly, we gratefully acknowledge the contribution of Geert Dermout and Louis Simoen in the production of the figures.
references
[1] Baumann P, Widek T, Merkens H, Boldt J, Petrovic A, Ur-schler M, Kirnbauer B, Jakse N, Scheurer E. Dental age es-timation of living persons: Comparison of MRI with OPG. Forensic Sci Int. 2015;253(0):76-80.
[2] De Tobel J, Hillewig E, Bogaert S, Deblaere K, Verstraete K. Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation. Ann Hum Biol. 2017;44(2):130-9.
[3] De Tobel J, Hillewig E, Verstraete K. Forensic age estima-tion based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging. Ann Hum Biol. 2017;44(2):121-9.
[4] De Tobel J, Phlypo I, Fieuws S, Politis C, Verstraete K, The-vissen P. Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging. J Forensic Odontostomatol. 2017;35(2):125-45.
[5] Fieuws S, Willems G, Larsen-Tangmose S, Lynnerup N, Boldsen J, Thevissen P. Obtaining appropriate interval esti-mates for age when multiple indicators are used: evaluation of an ad-hoc procedure. Int J Legal Med. 2016;130(2):489-99.
Magnetic resonance imaging of third molars in forensic age estimation: comparison of the Ghent and Graz protocols focusing on apical closure

114
[6] Flugge T, Hovener JB, Ludwig U, Eisenbeiss AK, Spittau B, Hennig J, Schmelzeisen R, Nelson K. Magnetic resonance imaging of intraoral hard and soft tissues using an intraoral coil and FLASH sequences. Eur Radiol. 2016;26(12):4616-23.
[7] Gaudino C, Cosgarea R, Heiland S, Csernus R, Beomonte ZB, Pham M, Kim TS, Bendszus M, Rohde S. MR-Imaging of teeth and periodontal apparatus: an experimental study comparing high-resolution MRI with MDCT and CBCT. Eur Radiol. 2011;21(12):2575-83.
[8] Gelbrich B, Frerking C, Weiss S, Schwerdt S, Stellzig-Eisen-hauer A, Tausche E, Gelbrich G. Combining wrist age and third molars in forensic age estimation: how to calculate the joint age estimate and its error rate in age diagnostics. Ann Hum Biol. 2015;42(4):389-96.
[9] George J, Nagendran J, Azmi K. Comparison study of growth plate fusion using MRI versus plain radiographs as used in age determination for exclusion of overaged football players. Br J Sports Med. 2012;46(4):273-8.
[10] Gourtsoyiannis NC. Clinical MRI of the abdomen: why, how, when. Berlin: Springer Science & Business Media, 2011.
[11] Guo Y, Olze A, Ottow C, Schmidt S, Schulz R, Heindel W, Pfeiffer H, Vieth V, Schmeling A. Dental age estimation in living individuals using 3.0 T MRI of lower third molars. Int J Legal Med. 2015;129(6):1265-70.
[12] Gustafson G, Koch G. Age estimation up to 16 years of age based on dental development. Odontol Revy. 1974;25(3):297-306.
[13] Hillewig E, De Tobel J, Cuche O, Vandemaele P, Piette M, Verstraete K. Magnetic resonance imaging of the medial ex-tremity of the clavicle in forensic bone age determination: a new four-minute approach. Eur Radiol. 2011;21(4):757-67.
[14] Hillewig E, Degroote J, Van der Paelt T, Visscher A, Vande-maele P, Lutin B, D'Hooghe L, Vandriessche V, Piette M, Ver-straete K. Magnetic resonance imaging of the sternal extrem-ity of the clavicle in forensic age estimation: towards more sound age estimates. Int J Legal Med. 2013;127(3):677-89.
[15] Hovener JB, Zwick S, Leupold J, Eisenbeibeta AK, Scheife-le C, Schellenberger F, Hennig J, Elverfeldt DV, Ludwig U. Dental MRI: imaging of soft and solid components without ionizing radiation. J Magn Reson Imaging. 2012;36(4):841-6.
[16] Levesque GY, Demirijian A, Tanguay R. Sexual dimorphism in the development, emergence, and agenesis of the mandib-ular third molar. J Dent Res. 1981;60(10):1735-41.
[17] Levesque GY, Demirjian A. The inter-examiner variation in rating dental formation from radiographs. J Dent Res. 1980;59(7):1123-6.
[18] Liversidge HM. Timing of human mandibular third molar formation. Ann Hum Biol. 2008;35(3):294-321.
[19] Lockemann U, Fuhrmann A, Püschel K, Schmeling A, Ges-erick G. Arbeitsgemeinschaft für Forensische Altersdiagnos-tik der Deutschen Gesellschaft für Rechtsmedizin. Rechts-medizin. 2004;14(2):123-6.
[20] Nasel C, Gahleitner A, Breitenseher M, Czerny C, Solar P, Imhof H. Dental MR tomography of the mandible. J Com-put Assist Tomogr. 1998;22(3):498-502.
[21] Pinchi V, De Luca F, Focardi M, Pradella F, Vitale G, Ric-ciardi F, Norelli GA. Combining dental and skeletal evidence in age classification: Pilot study in a sample of Italian sub-adults. Leg Med (Tokyo). 2016;20:75-9.
[22] Saloner D. The AAPM/RSNA physics tutorial for resi-dents. An introduction to MR angiography. Radiographics. 1995;15(2):453-65.
[23] Schmeling A, Dettmeyer R, Rudolf E, Vieth V, Geserick G. Fo-rensic Age Estimation. Dtsch Arztebl Int. 2016;113(4):44-50.
[24] Schmeling A, Geserick G, Reisinger W, Olze A. Age estima-tion. Forensic Sci Int. 2007;165(2-3):178-81.
[25] Schmeling A, Grundmann C, Fuhrmann A, Kaatsch HJ, Knell B, Ramsthaler F, Reisinger W, Riepert T, Ritz-Timme S, Ros-ing FW, Rotzscher K, Geserick G. Criteria for age estimation in living individuals. Int J Legal Med. 2008;122(6):457-60.
[26] Štern D, Kainz P, Payer C, Urschler M. Multi-Factorial Age Estimation from Skeletal and Dental MRI Volumes. In: International Workshop on Machine Learning in Medical Imaging. Quebec City, Canada: Springer, 2017; p. 61-9.
[27] Tangmose S, Jensen KE, Lynnerup N. Comparative study on developmental stages of the clavicle by postmortem MRI and CT imaging. J Forensic Radiol Imaging. 2013;1(3):102-6.
[28] Thevissen PW, Fieuws S, Willems G. Human dental age estimation using third molar developmental stages: does a Bayesian approach outperform regression models to dis-criminate between juveniles and adults? Int J Legal Med. 2010;124(1):35-42.
[29] Thevissen PW, Kvaal SI, Dierickx K, Willems G. Ethics in age estimation of unaccompanied minors. J Forensic Odontos-tomatol. 2012;30 Suppl 1:84-102.
[30] Unterpirker W, Ebner T, Stern D, Urschler M. Automatic third molar localization from 3D MRI using random regres-sion forests. . In: Proceedings of the 19th Conference on Medical Image Understanding and Analysis (MIUA). Lin-coln, United Kingdom2015; p. 195-200.
[31] Urschler M, Krauskopf A, Widek T, Sorantin E, Ehammer T, Borkenstein M, Yen K, Scheurer E. Applicability of Greu-lich-Pyle and Tanner-Whitehouse grading methods to MRI when assessing hand bone age in forensic age estimation: A pilot study. Forensic Sci Int. 2016;266:281-8.
[32] Weiger M, Pruessmann KP, Bracher AK, Kohler S, Lehmann V, Wolfram U, Hennel F, Rasche V. High-resolution ZTE im-aging of human teeth. NMR Biomed. 2012;25(10):1144-51.
De Tobel J. Multi-factorial forensic age estimation. Chapter 6: 100-114.


117
PART 3
Age estimation based on wrist MRI

118
CHAPTER 7
TH I S CHAPTER ADDRESSED THE FOLLOWING STUDY OB JECT IVES :
Objective 1: To collect a reference dataset of MR images of third molars, left wrist and both clavicles. These images will be registered simultaneously in each participant.
Objective 4: To stage the development of each age predictor based on the MRI. Existing 2D staging techniques will be modified or new methods will be developed. Reproduci-bility of the staging techniques will be tested.
Objective 5: To fit a statistical age estimation model on the reference data set, for each age predictor individually, as well as combining all registered age predictors. In all these models Bayes’ rule will be applied to counter drawbacks of other regression methods.
Objective 6: To validate this model and to compare its performance with existing models.
TH I S CHAPTER WAS PUBL I SHED AS :
De Tobel J, Hillewig E, de Haas MB, Van Eeckhout B, Fieuws S, Thevissen PW, Verstraete KL. Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all stag-ing technique and age estimation model apply? Eur Radiol. 2019. Epub ahead of print. [A1; Journal Impact Factor 2017 4.027; Radiology, Nuclear Medicine & Medical Imaging Q1; Peer reviewed]
RESULTS DESCR I BED IN TH I S CHAPTER WERE PARTLY PRESENTED
AT THE FOLLOWING CONFERENCE :
De Tobel J, de Haas M, Thevissen P, Verstraete K. Forensic age estimation based on T1 SE and VIBE wrist MRI sequences: opposite or complementary? 20th Meeting of the Study Group on Forensic Age Diagnostics, Arbeitsgemeinschaft für Forensische Altersdiag-nostik (AGFAD); Berlin, Germany; March 17, 2017.

119
Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age
estimation model apply?
OR IG INAL RESEARCH
Abstract
Aim — Providing recommendations for wrist MRI in age esti-mation by determining (1) which anatomical structures to in-clude in the statistical model, (2) which MRI sequence to con-duct, and (3) which staging technique to apply. Materials and methods — Radius and ulna were prospectively studied on 3T MRI in 363 healthy Caucasian participants (185 females, 178 males) between 14 and 26 years old, using T1 spin echo (SE) and T1 gradient echo VIBE. Bone development was assessed applying a 5-stage staging technique with several amelioration attempts to optimise staging. A Bayesian model rendered point predictions of age and diagnostic indices to discern minors from adults. Results — All approaches rendered similar results, with none of them outperforming the others. A single bone assess-ment of radius or ulna sufficed. SE and VIBE sequences were both suitable, but needed sequence-specific age estimation. A one-fits-all 5-stage staging technique –with substages in stage 3 – was suitable and did not benefit from profound substaging. Age estimation based on SE radius resulted in a mean absolute error of 1.79 years, a specificity (correctly identified minors) of 93%, and a discrimination slope of 0.640.Conclusion — Radius and ulna perform similarly to estimate age, and so do SE and VIBE. A one-fits-all staging technique can be applied.
Key Words
• age determination by skeleton
• wrist
• adolescent
• adult
• resonance imaging
AFF IL IAT IONS
1 Department of Radiology and
Nuclear Medicine, Ghent Univer-
sity, Belgium
2 Department of Imaging and Pa-
thology – Forensic Odontology,
KU Leuven, Belgium
3 Department of Head, Neck and
Maxillofacial Surgery, Ghent
University Hospital, Belgium
4 Department of Forensic Anthro-
pology, Netherlands Forensic
Institute, Den Haag, the Nether-
lands
5 KU Leuven – University of
Leuven & Universiteit Hasselt,
Department Public Health and
Primary Care, I-BioStat, Leuven,
Belgium
Funding for this research was entirely
provided by the department of Radi-
ology and Nuclear Medicine at Ghent
University, and the department of Im-
aging and pathology - Forensic Odon-
tology at KU Leuven.
The authors declare that there are no
conflicts of interest.
JANN ICK DE TOBEL 1 2 3 ELKE H I LLEW IG 1
MICH I EL B . D E HAAS 4 BRAM VAN EECKHOUT 1
STEFFEN F I EUWS 5 PATR ICK W. THEV I S SEN 2
KOENRAAD L . VERSTRAETE 1

120
Established methods for forensic age estimation in the living use radi-ographs and computed tomography (CT) to study the development of anatomical structures. However, the use of ionizing radiation limits their
forensic applicability in several countries [29]. Consequently, magnetic resonance imaging (MRI) has been studied for age estimation using different approaches [10, 20, 26, 34, 42]. Therefore, evidence-based recommendations are necessary to im-plement MRI in age estimation practice. Three aspects can be considered for this implementation: anatomical structures to include, MRI sequence types, and staging technique. The current study aims to pro-vide recommendations for each of these aspects.
Anatomical structures
Age estimation focusing on the age threshold of 18 years should include ana-lysing wrist development [6, 28, 38]. Using MRI, 11 developing hand/wrist features were used by Urschler et al. (2015) [45]. By contrast, Serin et al. (2016) demon-strated that age estimation results based on combined developmental information of distal radius, distal ulna and proximal first metacarpal bone did not outperform those based on the distal radius alone [32]. Consequently, other authors only analysed the distal radius [12-14, 17, 31, 32, 42, 44]. Because of these varying ap-proaches in literature and since the distal ulna and radius are the last regions to ma-ture in the hand/wrist, the current study aims to analyse both of them, to verify which structure should be included for an optimal age estimation.
MRI sequence types
Two MRI sequence types have been re-ported to study hand/wrist development: T1-weighted spin echo images (SE) with-out fat suppression [13, 14, 17, 21, 31, 32, 42, 44, 46] and T1-weighted gradient echo VIBE images (VIBE) with fat suppression [21, 34, 45, 46]. Since the relative value of both sequence types remains unclear, they were both analysed in the current study.
Staging techniques for wrist development
Different staging techniques for wrist de-velopment have been applied to MRI. The most elaborate staging technique for long bone development was established for clavicle CT and includes five stages with several substages and profound substag-ing (Table 7.1) [24, 30, 31, 48]. However, those substages might not be consecutive, questioning their relevance for age esti-mation [15, 42, 50]. Additionally, on MRI, a threefold stratification sign (TFS) could be of interest to subdivide stages 3c and 4, but its relevance to age estimation needs to be explored [31, 42]. Hence, the current study aims to provide a comprehensive staging technique, keeping the balance between a sufficient number of stages and sufficient reproducibility [40].
Study population
Healthy Caucasian volunteers were prospectively included between Jan-uary 2008 and May 2017. Part of this sample has been used in previous studies [7, 8, 10, 19, 20]. The current study population included for anal-ysis comprised 363 individuals (185 females, 178 males) between 14 and
Introduction
Materials and M
ethods
De Tobel J. Multi-factorial forensic age estimation. Chapter 7: 118-140.

121
26 years old (Table 7.2). Ethical approval and informed consent were obtained.
Image acquisition
Three Tesla MRI of the left wrist was con-ducted using a Siemens scanner (Mag-netom Trio Tim, Siemens) with two MRI sequences:
— SE (TR 534 ms, TE 16 ms, flip angle 150°, no fat suppression, voxel size 0.20 × 0.20 × 2.0 mm³, 2:43 min);
— VIBE (TR 12.7 ms, TE 4.82 ms, flip angle 10°, fat suppression, voxel size 0.40 × 0.40 × 0.40 mm³, 5:57 min).
Participants were positioned supine, with their left wrist in a dedicated 8-channel coil (Invivo).
Image analysis
MRI datasets were anonymised and blinded for the age of the participants. Three observers assessed different parts
TABLE 7. 1 — DESCRIPTIVE CRITERIA FOR DEVELOPMENTAL STAGES OF LONG BONES ON CT OR MRI . MOST
ELABORATE STAGING REPORTED IN LITERATURE SO FAR.
1 Ossif icat ion centre is invis ib le (= not yet oss if ied).
2 Ossif icat ion centre is v is ib le (= oss if ied), non-union of the epiphysis and metaphysis .
2a The lengthwise epiphyseal measurement is one third or less compared to the widthwise
measurement of the metaphyseal ending.
2b The lengthwise epiphyseal measurement is over one third unt i l two thirds compared to
the widthwise measurement of the metaphyseal ending.
2c The lengthwise epiphyseal measurement is over two thirds compared to the widthwise
measurement of the metaphyseal ending.
3 Physeal plate is par t ial ly oss if ied (= bone trabeculae cross the physeal plate from ossif i-
cat ion centre to metaphysis).
3a The epiphyseal-metaphyseal fus ion completes one third or less of the former gap be-
tween epiphysis and metaphysis .
3aa Lengthwise measurement of the epiphysis is one third or lower compared with the width-
wise measurement of the metaphyseal ending.
3ab Lengthwise measurement of the epiphysis is between one third and two thirds compared
with the widthwise measurement of the metaphyseal ending.
3ac Lengthwise measurement of the epiphysis is over two thirds compared with the widthwise
measurement of the metaphyseal ending.
3b The epiphyseal-metaphyseal fus ion completes over one third unt i l two thirds of the for-
mer gap between epiphysis and metaphysis .
3c The epiphyseal-metaphyseal fus ion completes over two thirds of the former gap between
epiphysis and metaphysis .
4 Complete union of the epiphysis and metaphysis (= physeal plate is completely oss if ied).
Physeal scar is st i l l v is ib le.
4a Threefold strat if icat ion s ign is v is ib le.
4b No threefold strat if icat ion s ign.
5 Complete union of the epiphysis and metaphysis . Physeal scar is indiscernible.
Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply?
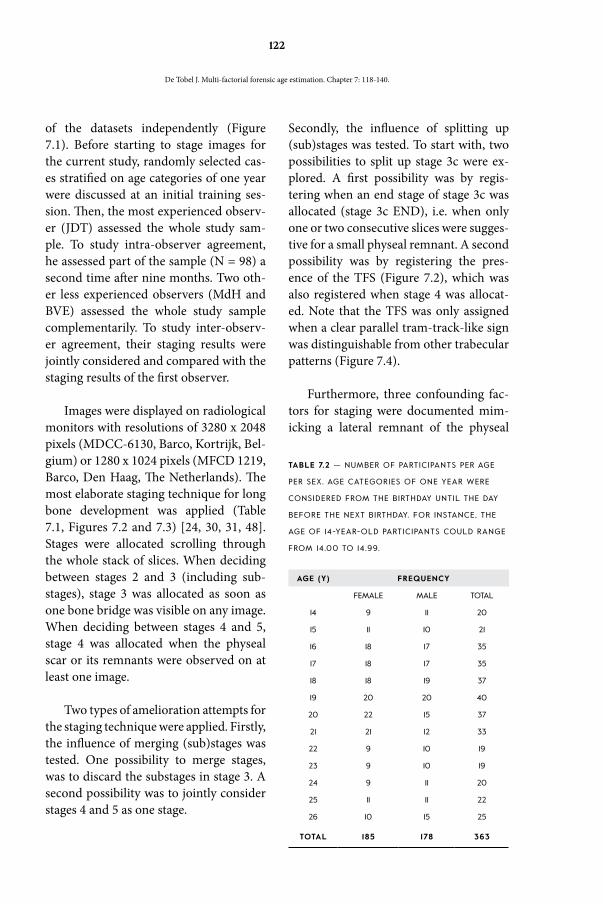
122
of the datasets independently (Figure 7.1). Before starting to stage images for the current study, randomly selected cas-es stratified on age categories of one year were discussed at an initial training ses-sion. Then, the most experienced observ-er (JDT) assessed the whole study sam-ple. To study intra-observer agreement, he assessed part of the sample (N = 98) a second time after nine months. Two oth-er less experienced observers (MdH and BVE) assessed the whole study sample complementarily. To study inter-observ-er agreement, their staging results were jointly considered and compared with the staging results of the first observer.
Images were displayed on radiological monitors with resolutions of 3280 x 2048 pixels (MDCC-6130, Barco, Kortrijk, Bel-gium) or 1280 x 1024 pixels (MFCD 1219, Barco, Den Haag, The Netherlands). The most elaborate staging technique for long bone development was applied (Table 7.1, Figures 7.2 and 7.3) [24, 30, 31, 48]. Stages were allocated scrolling through the whole stack of slices. When deciding between stages 2 and 3 (including sub-stages), stage 3 was allocated as soon as one bone bridge was visible on any image. When deciding between stages 4 and 5, stage 4 was allocated when the physeal scar or its remnants were observed on at least one image.
Two types of amelioration attempts for the staging technique were applied. Firstly, the influence of merging (sub)stages was tested. One possibility to merge stages, was to discard the substages in stage 3. A second possibility was to jointly consider stages 4 and 5 as one stage.
Secondly, the influence of splitting up (sub)stages was tested. To start with, two possibilities to split up stage 3c were ex-plored. A first possibility was by regis-tering when an end stage of stage 3c was allocated (stage 3c END), i.e. when only one or two consecutive slices were sugges-tive for a small physeal remnant. A second possibility was by registering the pres-ence of the TFS (Figure 7.2), which was also registered when stage 4 was allocat-ed. Note that the TFS was only assigned when a clear parallel tram-track-like sign was distinguishable from other trabecular patterns (Figure 7.4).
Furthermore, three confounding fac-tors for staging were documented mim-icking a lateral remnant of the physeal
TABLE 7.2 — NUMBER OF PARTICIPANTS PER AGE
PER SEX. AGE CATEGORIES OF ONE YEAR WERE
CONSIDERED FROM THE BIRTHDAY UNTIL THE DAY
BEFORE THE NEXT BIRTHDAY. FOR INSTANCE, THE
AGE OF 14-YEAR-OLD PARTICIPANTS COULD RANGE
FROM 14.00 TO 14 .99.
AGE (Y) FREQUENCY
FEMALE MALE TOTAL
14 9 11 20
15 11 10 21
16 18 17 35
17 18 17 35
18 18 19 37
19 20 20 40
20 22 15 37
21 21 12 33
22 9 10 19
23 9 10 19
24 9 11 20
25 11 11 22
26 10 15 25
TOTAL 185 178 363
De Tobel J. Multi-factorial forensic age estimation. Chapter 7: 118-140.

123
plate: blood vessels, persisting lateral fis-sures or surrounding soft tissue (Figure 7.5). Finally, if images were not assessable, the reason was registered.
Statistical analysis
SPSS Statistics 25.0 (IBM SPSS Statistics for Windows, Armonk, New York, USA) and SAS 9.4 (SAS Institute, Cary NC, USA) were used for statistical analyses. Descrip-tive statistics were calculated, and statisti-cal tests were performed two-sided with
the significance level equal to 0.05. Unless otherwise stated, reported results were based on the first observer’s assessments. Females and males were considered to-gether, since similar results were obtained when sex-specific results were calculated.
Weighted kappa statistics and tests for symmetry (extension of the McNe-mar test) were used to evaluate the inter- observer reliability of staging and the agreement between staging obtained with SE and VIBE.
TABLE 7.3 — FREQUENCIES OF CONFOUNDING FACTORS MIMICKING A LATERAL REMNANT OF THE PHYSEAL
PLATE. N = 726 ASSESSMENTS.
LATERAL FISSURE BLOOD VESSEL SOFT TISSUE
Radius SE 30 4. 13% 44 6.06% 52 7. 16%
VIBE 30 4. 13% 235 32.37% 129 17.77%
Ulna SE 6 0.83% 24 3.31% 12 1 .65%
VIBE 5 0.69% 67 9.23% 34 4.68%
FIGURE 7. 1 — SCHEMATIC OVERVIEW OF THE MRI ASSESSMENTS BY THREE OBSERVERS. Observer 1 assessed
par t of the sample twice to study intra-observer agreement . Observers 2 and 3 assessed the whole study
sample complementari ly. Therefore, they were joint ly considered to study inter-observer agreement .
Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply?
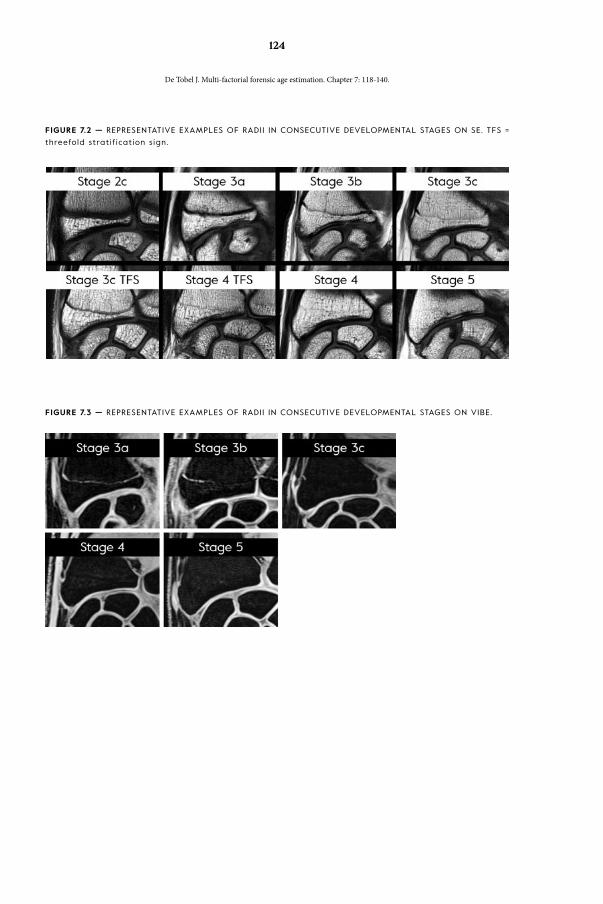
124
FIGURE 7.2 — REPRESENTATIVE EXAMPLES OF RADI I IN CONSECUTIVE DEVELOPMENTAL STAGES ON SE. TFS =
threefold strat if icat ion s ign.
FIGURE 7.3 — REPRESENTATIVE EXAMPLES OF RADI I IN CONSECUTIVE DEVELOPMENTAL STAGES ON VIBE.
De Tobel J. Multi-factorial forensic age estimation. Chapter 7: 118-140.

125
FIGURE 7.4
a SE radius in stage 4. The phy-
seal scar is c learly v is ib le
(black/white arrowheads).
b Corresponding VIBE. A pos-
s ible physeal scar is hardly
discernible (black/white ar-
rowheads). A s imi lar trabec-
ular pattern is v is ib le more
proximal ly (white arrowheads).
Therefore, stage 5 was al lo-
cated.
FIGURE 7.5 — CONFOUNDING FACTORS FOR STAGING THAT MIMIC A REMNANT OF THE PHYSEAL PLATE.
Corresponding SE radius (a, b, c) and VIBE radius (d, e, f ) .
a, d A lateral f issure (white arrowheads) is l ined by cor tex and shows no s igns of possible bridging. An
axial ly transsected blood vessel (white arrows) can be encountered anywhere in the bone.
b, e A longitudinal ly transsected blood vessel (white arrows) shows less c learly on SE than on VIBE. Note
that this vessel runs more distal ly than the physeal scar.
c, f A longitudinal ly transsected blood vessel (white arrow) is only vis ib le on VIBE and runs more distal ly
than the lateral remnants of the physeal plate (black/white arrows).
Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply?

126
A linear model with three factors (sex, stage, sequence) was used to compare the mean age of participants with their radius or ulna in particular (sub)stages, and to verify if the difference in mean age depend-ed on sequence. Stages obtained with both sequences were considered as independent samples for this analysis, although the same subject appeared twice. In the model, the variance of age was allowed to differ be-tween the stages. Independent t-tests were used to compare age between two stages. A one-way ANOVA was used to compare age between more than two stages.
Age estimation was based on applica-tion of Bayes’ rule, with a continuation ra-tio model for the distribution of the stage
[4, 16]. Ten-fold cross-validation was used to handle overfitting. Two aspects of age estimation were studied to quan-tify and compare performance: (1) point prediction for age and (2) the ability to discern minors from adults.
Regarding the first aspect, the modus is the ‘most likely’ age estimate. Howev-er, it is known not to minimise the error [39]. Therefore, the mean was used as point prediction, more specifically the 5% trimmed mean, i.e. the mean in the 95% prediction interval. The mean absolute error (MAE) was evaluated, as measure of accuracy. The Wilcoxon signed rank test was used to compare the MAE.
TABLE 7.4 — DESCRIPTIVE STATISTICS PER SE RADIUS STAGE WITH VIBE INFO IN STAGE 4.
SE RADIUS
STAGE
2C 3A 3B 3C 4/5 4/5 4/5 4/5
VIBE RADIUS
STAGE
NC NC NC NC NC 3c 4 5
Females N 18 5 55 109 12 9 87
MEAN 15.24 16.38 18. 10 22.09 21 .33 19.91 22.38
MEDIAN 15.27 16.26 17.88 21 .70 20.60 19.88 22.37
SD 0.88 1 . 13 1 .88 2.59 2.57 1 .30 2.57
MINIMUM 14. 10 14 .90 14.30 17. 10 17. 10 18. 10 17.90
MAXIMUM 17.80 18.00 22.40 26.90 25.70 21 .70 26.90
P25 14.64 15.44 16.75 19.99 19.55 18.7 1 20.20
P75 15.57 17.39 19.33 24.26 23.74 21 .24 24.79
Males N 7 45 3 25 99 3 9 86
MEAN 15.01 16.35 17.40 18.97 22.76 20.71 21 .44 23.03
MEDIAN 14.65 16.25 17. 18 18.95 22.68 20.59 20.78 23. 1 1
SD 1 .02 1 .24 0.39 1 .58 2.70 0.81 2 .63 2.63
MINIMUM 14.20 14. 10 17.20 15.40 17. 10 20.00 19. 10 18. 10
MAXIMUM 17.00 19.00 17.90 23. 10 27.00 21 .60 26.60 27.00
P25 14.25 15.53 17. 17 18.02 20.62 19.97 19.45 20.88
P75 15.34 17. 18 NA 19.60 25.35 NA 23.23 25.49
NC = not considered; P25 = f irst quar t i le ; P75 = third quar t i le ; SD = standard deviat ion.
De Tobel J. Multi-factorial forensic age estimation. Chapter 7: 118-140.
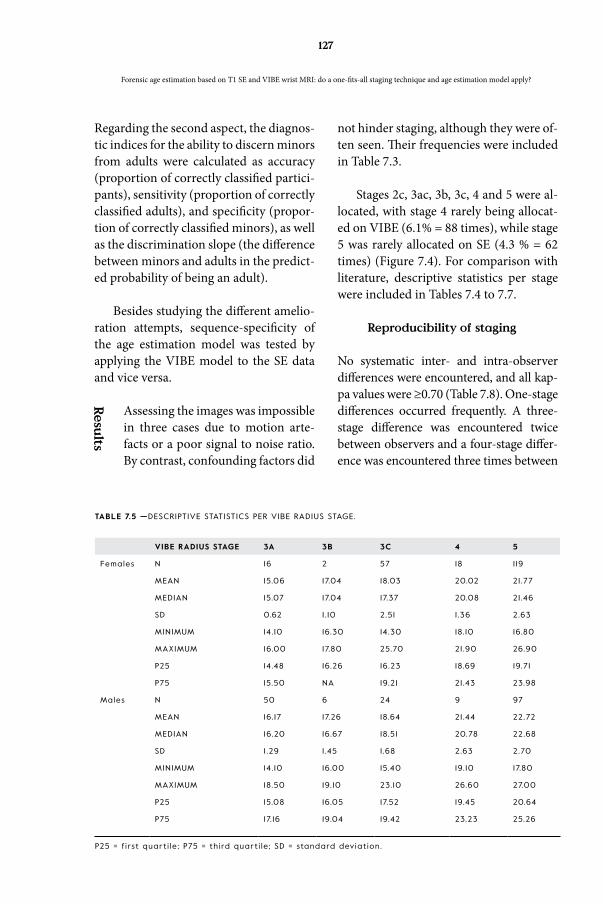
127
Regarding the second aspect, the diagnos-tic indices for the ability to discern minors from adults were calculated as accuracy (proportion of correctly classified partici-pants), sensitivity (proportion of correctly classified adults), and specificity (propor-tion of correctly classified minors), as well as the discrimination slope (the difference between minors and adults in the predict-ed probability of being an adult).
Besides studying the different amelio-ration attempts, sequence-specificity of the age estimation model was tested by applying the VIBE model to the SE data and vice versa.
Assessing the images was impossible in three cases due to motion arte-facts or a poor signal to noise ratio. By contrast, confounding factors did
not hinder staging, although they were of-ten seen. Their frequencies were included in Table 7.3.
Stages 2c, 3ac, 3b, 3c, 4 and 5 were al-located, with stage 4 rarely being allocat-ed on VIBE (6.1% = 88 times), while stage 5 was rarely allocated on SE (4.3 % = 62 times) (Figure 7.4). For comparison with literature, descriptive statistics per stage were included in Tables 7.4 to 7.7.
Reproducibility of staging
No systematic inter- and intra-observer differences were encountered, and all kap-pa values were ≥0.70 (Table 7.8). One-stage differences occurred frequently. A three-stage difference was encountered twice between observers and a four-stage differ-ence was encountered three times between
ResultsTABLE 7.5 —DESCRIPTIVE STATISTICS PER VIBE RADIUS STAGE.
VIBE RADIUS STAGE 3A 3B 3C 4 5
Females N 16 2 57 18 1 19
MEAN 15.06 17.04 18.03 20.02 21 .77
MEDIAN 15.07 17.04 17.37 20.08 21 .46
SD 0.62 1 . 10 2.51 1 .36 2.63
MINIMUM 14. 10 16.30 14.30 18. 10 16.80
MAXIMUM 16.00 17.80 25.70 21 .90 26.90
P25 14.48 16.26 16.23 18.69 19.71
P75 15.50 NA 19.21 21 .43 23.98
Males N 50 6 24 9 97
MEAN 16. 17 17.26 18.64 21 .44 22.72
MEDIAN 16.20 16.67 18.51 20.78 22.68
SD 1 .29 1 .45 1 .68 2.63 2.70
MINIMUM 14. 10 16.00 15.40 19. 10 17.80
MAXIMUM 18.50 19. 10 23. 10 26.60 27.00
P25 15.08 16.05 17.52 19.45 20.64
P75 17. 16 19.04 19.42 23.23 25.26
P25 = f irst quar t i le ; P75 = third quar t i le ; SD = standard deviat ion.
Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply?

128
TABLE 7.6 — RELATIVE FREQUENCIES (%) OF RADI I IN THE DIFFERENT STAGES, PER AGE CATEGORY OF ONE
YEAR. ONLY OBSERVER 1 ’S RESULTS ARE DISPLAYED.
SE
QU
EN
CE
SE VIBE
Sex Age
(y)
N 2c 3ac 3b 3c 4 5 N 2c 3ac 3b 3c 4 5
FEM
AL
ES
14 10 80 10 10 1 1 73 27
15 1 1 64 36 12 50 50
16 18 1 1 17 72 18 1 1 6 78 6
17 18 6 6 78 1 1 20 5 70 25
18 18 39 61 23 22 26 52
19 20 30 70 25 16 12 72
20 22 23 77 27 19 1 1 70
21 21 19 81 21 10 29 62
22 9 1 1 89 12 100
23 9 100 1 1 9 91
24 9 100 1 1 9 91
25 12 100 1 1 18 82
26 10 100 10 100
MA
LES
14 1 1 36 64 1 1 100
15 10 20 70 10 10 90 10
16 17 94 6 19 74 16 1 1
17 18 6 50 17 22 6 19 58 5 32 5
18 19 26 37 37 19 26 26 47
19 20 5 35 55 5 22 9 32 14 45
20 15 27 73 16 6 13 81
21 12 0 100 12 8 17 75
22 10 0 100 10 100
23 10 10 90 10 10 90
24 1 1 0 100 1 1 100
25 1 1 0 100 12 8 92
26 15 0 100 15 7 93
De Tobel J. Multi-factorial forensic age estimation. Chapter 7: 118-140.

129
TABLE 7.7 — RELATIVE FREQUENCIES (%) OF ULNAE IN THE DIFFERENT STAGES, PER AGE CATEGORY OF ONE
YEAR. ONLY OBSERVER 1 ’S RESULTS ARE DISPLAYED.
SE
QU
EN
CE
SE VIBE
Sex Age
(y)
N 2c 3ac 3b 3c 4 5 N 2c 3ac 3b 3c 4 5
FEM
AL
ES
14 10 90 10 10 80 10 10
15 1 1 64 18 18 12 42 25 25 8
16 18 22 22 28 28 18 1 1 1 1 6 1 17
17 18 1 1 50 39 21 5 5 43 5 43
18 18 6 94 23 9 30 61
19 20 15 85 25 8 16 76
20 22 5 91 5 27 22 78
21 21 5 90 5 21 24 76
22 10 100 12 100
23 9 89 1 1 1 1 100
24 9 89 1 1 1 1 9 91
25 12 83 17 1 1 100
26 10 90 10 10 100
MA
LES
14 1 1 55 45 1 1 9 91
15 10 20 80 10 10 90
16 17 6 88 6 19 74 16 1 1
17 18 6 56 22 17 19 63 5 26 5
18 19 37 5 16 42 19 32 32 37
19 20 5 15 75 5 22 9 5 23 23 41
20 15 87 13 16 13 6 81
21 12 17 75 8 12 17 17 67
22 10 80 20 10 100
23 10 80 20 10 100
24 1 1 82 18 1 1 100
25 1 1 82 18 12 100
26 15 93 7 15 7 93
Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply?

130
observers. Within observers, the largest difference was a two-stage difference.
Anatomical structures
Table 7.9 summarises age estimation performance of the different tested ap-proaches. Regarding the accuracy of point prediction, no statistically significant dif-ferences could be demonstrated between radius and ulna separately. Although combined information of radius and ulna statistically significantly outperformed separate information per structure, this was clinically insignificant, since the MAE differences ranged from -0.09 to 0.16.
Regarding the ability to discern mi-nors from adults, the highest specific-ity (93%) was obtained for the radius. By contrast, the highest discrimination slopes were obtained with combined in-formation of radius and ulna.
MRI sequence types
The observers judged staging on VIBE to be easier than on SE because of the high contrast with adjacent bone (Figure 7.3), and the lack of a chemical shift artefact, which caused blurring on the SE images (Figure 7.2). Conversely, the physeal scar was hard to discern on VIBE (Figure 7.4).
Consequently, staging differed sys-tematically between SE and VIBE, with lower stages being allocated on SE than VIBE (P < 0.0001 in the symmetry tests for radius as well as for ulna). Weighted kappas and their 95% confidence inter-val (CI) equalled 0.550 (0.504;0.595) and 0.595 (0.551;0.638) for radius and ulna, respectively, confirming the differences between both sequence types. One-stage
TAB
LE
7.8 —
REPRO
DU
CIB
ILIT
Y O
F S
TAG
ING
RA
DIU
S A
ND
UL
NA
DEV
ELO
PMEN
T P
ER
MR
I SEQ
UEN
CE.
AN
ATO
MIC
AL
ST
RU
CT
UR
E
SE
QU
EN
CE
INT
ER
-OB
SE
RV
ER
1-2
INT
ER
-OB
SE
RV
ER
1-3
INT
RA
-OB
SE
RV
ER
P-v
alu
eW
eig
hte
d ka
pp
a
(95
%C
I)
Nu
mb
er
of c
ase
s
P-v
alu
eW
eig
hte
d ka
pp
a
(95
%C
I)
Nu
mb
er
of c
ase
s
P-v
alu
eW
eig
hte
d ka
pp
a
(95
%C
I)
Nu
mb
er
of c
ase
s
Radius
SE
0.3
71
0.7
96
(0.74
4;0
.84
8)
26
61.0
00
0.7
70
(0.6
79
;0.8
61)
95
1.00
00
.85
6 (0
.78
1;0.9
31)
98
VIB
E0
.26
80
.69
9 (0
.62
8;0
.770
)2
65
0.3
170
.69
6 (0
.59
3;0
.79
8)
94
1.00
00
.84
3 (0
.76
4;0
.92
3)
98
Ulna
SE
0.4
47
0.7
94
(0.74
7;0.8
42)
26
41.0
00
0.8
36
(0.7
64
;0.9
09
)9
50
.99
90
.82
2 (0
.742
;0.9
01)
98
VIB
E0
.94
90
.78
5 (0
.720
;0.8
49
)2
64
0.4
120
.774
(0.6
94
;0.8
54)
94
0.9
98
0.8
36
(0.7
61;0
.910
)9
8
CI =
Co
nfid
en
ce
inte
rva
l; P-v
alu
e =
P-v
alu
e fo
r test o
f sym
me
try (e
xten
sion
of th
e M
cN
em
ar te
st).
De Tobel J. Multi-factorial forensic age estimation. Chapter 7: 118-140.

131
differences occurred frequently, whereas two-stage differences were encountered only twice for radius and twice for ulna. Hence, applying the sequence-specific model rendered better point prediction ac-curacy and diagnostic indices (Table 7.9).
Regarding the accuracy of point pre-diction, MAE did not differ significantly between SE or VIBE within one anatom-ical structure. Neither did the diagnostic indices for discerning minors from adults differ systematically between sequence types (Table 7.9).
Staging techniques for wrist development
Two aspects of the amelioration attempts need clarification. First, note that the TFS was only visible in SE, since it is part of the physeal scar. Neither in stage 3c nor in stage 4 did the TFS improve age esti-mation performance. Second, it was no-ticed that radii in SE stage 4 showed a dispersion in VIBE stages from 3c to 5. Thus, one amelioration attempt was to add VIBE information to SE information in SE stage 4. To illustrate the Bayesian ap-proach, Figure 7.6 displays posterior den-sity curves of age for SE radius with added VIBE information in males.
Regarding point prediction, none of the amelioration attempts remarkably out-performed the original staging technique (Table 7.9). Although statistically signif-icant differences were obtained between suggested substages for mean age (Table 7.10) as well as for MAE (Table 7.9), the differences in MAE were too small to be of clinical significance (range -0.02 to 0.24 years). Note that merging stages rendered the least accurate point predictions.
Similarly, regarding the ability to discern minors from adults, none of the amelio-ration attempts remarkably outperformed the original staging technique. Merging SE radius stages 4 and 5 considerably de-creased specificity (Table 7.9), suggesting that these stages should be considered separately. By contrast, merging SE radi-us stage 3 rendered the highest specificity, but caused a major decrease in sensitiv-ity (Table 7.9), suggesting that substages in stage 3 should also be considered sep-arately. This avoids an artificially high number of wrongly identified adults that would only marginally increase the num-ber of correctly identified minors.
For comparison with literature, prob-abilities of being an adult per stage per sex were included in Tables 11 to 13. Remark-ably, looking at these probabilities for the different amelioration attempts, stage 3c END still seems valuable for the radius, although this is not reflected by the diag-nostic indices in Table 7.9. For instance, the probability of being an adult was 0.937 for males with SE radius stage 3c END. When the 3c END radii were excluded from stage 3c, that probability dropped from 0.737 to 0.664.
Reproducibility of staging
Inter-observer agreements with Co-hen’s kappa ranging from 0.23 [5] to 0.97 [42] have been reported in
literature on wrist MRI for age estima-tion, with kappa >0.80 in most studies [5, 13, 27, 31, 32, 42, 44]. The inter-observer agreements in the current study ranged from 0.71 to 0.81, which might be due to the difference in experience [49] and re-flects the difficulty of the interpretation.
Discussion
Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply?

132
TABLE 7.9 — AGE ESTIMATION PERFORMANCE BASED ON RADIUS AND ULNA DEVELOPMENT, PER MRI SE-
QUENCE AND ATTEMPTS TO AMELIORATE THE STAGING TECHNIQUE.
ANATOMICAL
STRUCTURE
SEQUENCE AMELIORATION
ATTEMPT
ACCURACY OF POINT PREDICTION
CONSIDERING
ALL CASES
CONSIDERING THE SUBSET OF CASES WITHIN
THE RELEVANT STAGES
MAE (Y) N MAE
REFERENCE #
MAE
AMELIO-
RATION
P-VALUE MAE
DIFFERENCE ‡
Radius
+ Ulna
SE None 1 .72 NA
VIBE None 1 .78 NA
Radius SE None 1 .79 NA NA
VIBE None 1 .90 NA NA
SE Merge stage 3 1 .95 150 1 . 17 1 .56 < 0.001
VIBE Merge stage 3 2.03 143 1 .34 1 .66 < 0.001
SE Merge stages 4
and 5
1 .93 172 2.25 2.26 0. 183 †
VIBE Merge stages 4
and 5
2.02 187 2.36 2.35 0.687 †
SE Stage 3c END 1 .78 80 1 .40 1 .35 0.707
VIBE Stage 3c END 1 .87 74 1 .66 1 .53 0.042
SE Stage 3c TFS 1 .80 80 1 .40 1 .42 0.584
SE Stage 4 TFS 1 .80 205 2.27 2.29 < 0.001
SE Add VIBE info to
SE stage 4
1 .77 205 2.27 2.23 0. 162
Ulna SE None 1 .88 NA
VIBE None 1 .82 NA
SE Merge stage 3 1 .98 109 0.96 1 .29 < 0.001
VIBE Merge stage 3 2.03 124 1 .03 1 .40 < 0.001
SE Merge stages 4
and 5
1 .93 228 2.33 2.38 0.082
VIBE Merge stages 4
and 5
2.05 232 2.35 2.35 0. 127
SE Stage 3c END NA §
VIBE Stage 3c END 1 .83 48 0.97 1 .00 0.705
SE Stage 3c TFS NA §
SE Stage 4 TFS 1 .84 224 2.36 2.29 0. 103
SE Add VIBE info to
SE stage 4
1 .78 224 2.36 2. 18 0.031
Radius SE VIBE model * 1 .98 355 1 .8 1 1 .97 0.006
VIBE SE model ° 1 .43 165 1 .39 1 .43 0. 166
END = end stage; CI = conf idence interval ; N = total number of par t ic ipants in relevant stages; NA = not
appl icable; MAE = mean absolute error ; TFS = threefold strat if icat ion s ign; y = years.
# Reference for comparison is the original equivalent (radius or ulna; SE or VIBE). ‡ P-value from Wilcoxon
s igned rank test comparing MAE. † Based on the second observer ’s assessment . § Too few cases in one
category.
De Tobel J. Multi-factorial forensic age estimation. Chapter 7: 118-140.

133
TABLE 7.9 (CONTINUED)
DISCERNING MINORS FROM ADULTS
CONSIDERING ALL CASES
ACCURACY (95%CI)
SENSITIVITY (95%CI) SPECIFICITY (95%CI) DISCRIMINATION SLOPE
91 .2 (87.8 ;93.9) 94.0 (90.4;96.6) 84.7 (76.6;90.8) 0.725
92.3 (89.0;94.8) 95.6 (92.3 ;97.8) 84.7 (76.6;90.8) 0.721
89.8 (86.2 ;92.7) 88.5 (83.9;92.2) 92.8 (86.3 ;96.8) 0.640
89.8 (86.2 ;92.7) 90.9 (86.6;94. 1 ) 87.4 (79.7;92.9) 0.584
86.2 (82.2 ;89.6) 81 .0 (75.6;85.6) 98.2 (93.6;99.8) 0.51 1
87.9 (84. 1 ;9 1 . 1 ) 84.9 (79.9;89. 1 ) 94.6 (88.6;98.0) 0.492
86. 1 (82.2 ;89.5) 94.4 (90.8;96.9) 67.6 (58.0;76. 1 ) 0.571
85.2 (81 . 1 ;88.7) 85. 1 (80. 1 ;89.3) 85.5 (77.5 ;91 .5) 0.494
92.0 (88.7;94.6) 92.5 (88.5 ;95.4) 91 .0 (84. 1 ;95.6) 0.683
89.3 (85.6;92.2) 93.3 (89.4 ;96.0) 80.2 (71 .5 ;87. 1 ) 0.615
89.0 (85.3 ;92.0) 88.5 (83.9;92.2) 90. 1 (83.0;94.9) 0.647
89.8 (86.2 ;92.7) 88.5 (83.9;92.2) 92.8 (86.3 ;96.8) 0.640
89.8 (86.2 ;92.7) 88.5 (83.9;92.2) 92.8 (86.3 ;96.8) 0.640
91 .7 (88.4 ;94.4) 94.0 (90.4;96.6) 86.5 (78.7;92.2) 0.652
92.3 (89.0;94.8) 95.6 (92.3 ;97.8) 84.7 (76.6;90.8) 0.676
89.5 (85.9;92.5) 90.9 (86.6;94. 1 ) 86.5 (78.7;92.2) 0.574
85.4 (81 .3 ;88.9) 82.9 (77.7;87.4) 91 .0 (84. 1 ;95.6) 0.465
88.0 (84.2 ;91 .2) 90.7 (86.4 ;94.0) 82.0 (73.6;88.6) 0.584
88.5 (84.8 ;91 .7) 92.7 (88.8 ;95.6) 79. 1 (70.3;86.3) 0.526
92.3 (89.0;94.8) 95.6 (92.3 ;97.8) 84.7 (76.6;90.8) 0.672
91 .7 (88.4 ;94.4) 94.0 (90.4;96.6) 86.5 (78.7;92.2) 0.652
92.6 (89.4 ;95.0) 93.7 (89.9;96.3) 90. 1 (83.0;94.9) 0.682
89.6 (85.9;92.6) 88.4 (83.8 ;92. 1 ) 92.3 (85.4 ;96.6) 0.536
81 .2 (74.4 ;86.9) 61 .7 (48.2 ;73.9) 92.4 (85.5 ;96.7) 0.414
* Restr icted to SE stages 3ac, 3b, 3c, and 4 (too few subjects in stage 5). Applying the SE-sequence-specif ic
model in these cases resulted in RMSE = 2.26 and MAE = 1 .8 1 . ° Restr icted to VIBE stages 3ac, 3b, 3c, and 4
(too few subjects in stage 5). Applying the VIBE-sequence-specif ic model in these cases resulted in RMSE
= 1 .90 and MAE = 1 .29.
Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply?

134
TABLE 7. 10 —AGE DIFFERENCE BETWEEN SUBSTAGES BASED ON DIFFERENT AMELIORATION ATTEMPTS.
AN
ATO
MIC
AL
ST
RU
CT
UR
E
SE
QU
EN
CE
AM
EL
IOR
AT
ION
AT
TE
MP
T
CO
NSID
ER
ED
SU
BSE
T O
F C
ASE
S
FO
R C
OM
PAR
ISO
N
OF
ME
AN
AG
E
LO
WE
R S
UB
STA
GE
MID
DL
E S
UB
STA
GE
HIG
HE
R S
UB
STA
GE
P-V
AL
UE
AG
E
DIF
FE
RE
NC
E ‡
N MEAN
AGE
(SD)
N MEAN
AGE
(SD)
N MEAN
AGE
(SD)
RA
DIU
S
SE Merge stage 3 Stages 3a, 3b and 3c
62 16. 1 ( 1 .25)
8 16.8 ( 1 .03)
80 18.4 ( 1 .83)
< 0.001
VIBE Merge stage 3 Stages 3a, 3b and 3c
62 15.8 ( 1 .24)
7 16.9 ( 1 . 13)
74 18.3 (2 .27)
< 0.001
SE Merge stages 4 and 5
Stages 4 and 5
165 22.4 (2 .63)
7 23.0 (2 .72)
0.528 †
VIBE Merge stages 4 and 5
Stages 4 and 5
27 23. 1 (2 .66)
160 22. 1 (2 .75)
0. 1 12 †
SE Stage 3c END Stage 3c without or with END
63 17.9 ( 1 .59)
17 20.0 ( 1 .76)
< 0.001
VIBE Stage 3c END Stage 3c without or with END
53 17.9 (2 .22)
21 19. 1 (2 .25)
0.057
SE Stage 3c TFS Stage 3c without or with TFS
50 18.4 ( 1 .89)
30 18.3 ( 1 .75)
0.674
SE Stage 4 TFS Stage 4 with or without TFS
94 22.4 (2 .83)
1 1 1 22.5 (2 .46)
0.875
SE Add VIBE info to SE stage 4
VIBE stages 3c, 4 and 5
14 21 .3 (2 .38)
18 20.7 (2 . 16)
173 22.7 (2 .61 )
0.002
UL
NA
SE Merge stage 3 Stages 3a, 3b and 3c
67 16.2 ( 1 .30)
12 16.7 ( 1 .03)
30 18.3 ( 1 .66)
< 0.001
VIBE Merge stage 3 Stages 3a, 3b and 3c
66 16.0 ( 1 .35)
12 16.5 ( 1 .30)
48 17.8 ( 1 .58)
< 0.001
SE Merge stages 4 and 5
Stages 4 and 5 224 21 .7 (2 .83)
20 23.4 (2 . 13)
0.010
VIBE Merge stages 4 and 5
Stages 4 and 5 27 20.2 ( 1 .77)
210 22.2 (2 .77)
< 0.001 *
SE Stage 3c END Stage 3c without or with END
29 18. 1 ( 1 .56)
1 2 1 .6 (NA)
NA §
VIBE Stage 3c END Stage 3c without or with END
40 17.7 ( 1 .60)
8 18.2 ( 1 .52)
0.385
SE Stage 3c TFS Stage 3c without or with TFS
28 18.2 ( 1 .72)
2 18.5 (0.20)
NA §
SE Stage 4 TFS Stage 4 with or without TFS
43 21 .3 (2 .57)
18 1 21 .9 (2 .88)
0.21 1
SE Add VIBE info to SE stage 4
VIBE stages 3c, 4 and 5
15 18.8 ( 1 .73)
24 20.2 ( 1 .79)
185 22.2 (2 .79)
< 0.001
END = end stage; N = number of participants in subgroup; NA = not applicable; SD = standard deviation; TFS = threefold stratification
sign. ‡ P-value from independent t-test comparing age between two stages, or from one-way ANOVA comparing age between three
stages. † Based on the second observer’s assessment. § Too few cases in one category. * Based on the other observer P = 0.299.

135
TABLE 7. 1 1 — PROBABILITIES OF
BEING AN ADULT PER STAGE PER
SEX FOR SE RADIUS WITH ADDED
VIBE INFORMATION FOR STAGE 4.
TABLE 7. 12 — PROBABILITIES
OF BEING AN ADULT PER
STAGE PER SEX FOR SE
RADIUS + ULNA.
TABLE 7. 13 — PROBABILITIES
OF BEING AN ADULT PER STAGE
PER SEX FOR VIBE
RADIUS + ULNA.
SE R
ad
ius sta
ge
VIB
E R
ad
ius sta
ge
P ≥ 18 y
SE R
ad
ius sta
ge
SE U
lna
stag
e
P ≥ 18 y
VIB
E R
ad
ius sta
ge
VIB
E U
lna
stag
e
P ≥ 18 y
Female Male Female Male Female Male
2c 0.021 2c 2c 0.001 3a ≤ 3a < 0.001 0.043
3a 0.008 0. 100 2c 3a 0.010 3a 3b < 0.001 0.084
3b 0. 103 0.364 2c 3b 0.079 3a 3c 0.002 0.332
3c 0.431 0.740 2c 3c 0.431 3a 4 0.043 0.551
4/5 3c 0.91 1 0.928 2c 4 0.624 3a 5 0.071 0.677
4/5 4 0.772 0.963 2c 5 0.665 3b ≤ 3a 0.008 0.086
4/5 5 0.969 0.986 3a 2c 0.008 3b 3b 0.023 0. 137
3a 3a 0.001 0.040 3b 3c 0.070 0.419
3a 3b 0.001 0. 145 3b 4 0.501 0.633
3a 3c 0.022 0.487 3b 5 0.658 0.748
3a 4 0.098 0.644 3c ≤ 3a 0.019 0.295
3a 5 0. 172 0.676 3c 3b 0.050 0.362
3b 2c 0.044 3c 3c 0. 122 0.692
3b 3a 0.007 0. 130 3c 4 0.629 0.856
3b 3b 0.005 0.277 3c 5 0.768 0.921
3b 3c 0. 105 0.669 4 ≤ 3a 0.048 0.554
3b 4 0.361 0.809 4 3b 0. 1 13 0.605
3b 5 0.549 0.835 4 3c 0.218 0.879
3c 2c 0.212 4 4 0.808 0.967
3c 3a 0.038 0.340 4 5 0.908 0.988
3c 3b 0.022 0.496 5 ≤ 3a 0.088 0.625
3c 3c 0.287 0.850 5 3b 0. 193 0.669
3c 4 0.665 0.933 5 3c 0.313 0.913
3c 5 0.824 0.947 5 4 0.908 0.980
4/5 2c 0.583 5 5 0.966 0.994
4/5 3a 0. 181 0.638
4/5 3b 0.099 0.746
4/5 3c 0.675 0.974
4/5 4 0.960 0.995
4/5 5 0.990 0.997
Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply?

136
Anatomical structures
Combined assessment of radius and ulna did not outperform separate assessments, neither regarding accuracy of the point prediction, nor regarding the ability to discern minors from adults. This corre-sponds with findings of Serin et al. (2016) [32]. Conversely, Urschler et al. (2015) included hand and wrist bones on VIBE [45], suggesting that hand bones could add age information to the wrist model. However, no comparing studies have been conducted so far between hand/wrist and wrist alone.
MRI sequence types
Both wrist SE and VIBE have been re-ported in literature on age estimation. The subjective finding that the physeal plate appears more clear-cut on VIBE corre-
sponds with the findings of Urschler et al. (2016) [46] and Hojreh et al. (2018) [21], and is caused by fat suppression. Conversely, SE clearly depicts the physeal scar. Together with the blurry appearance of the physeal plate, the latter can be ex-plained by the chemical shift artefact [25], which causes an enlarged appearance of the physeal cartilage. Fat suppression in VIBE avoids chemical shift artefacts. These differences result in different age estimation models. Therefore, MRI se-quence-specific reference data should be used. This has also been demonstrated for age estimation based on third molars’ MRI [9].
Combining information of different sequences is common in a clinical con-text, but has only once been suggested in forensic age estimation by Vieth et al. [47]. Their combined staging technique
FIGURE 7.6 — POSTERIOR DENSITY OF AGE PER RADIUS STAGE IN MALES. SE is considered and when stage
4 is al located, addit ional VIBE staging al lows for a differentiat ion within that group. Al l distr ibut ions of
age are r ight-skewed. Around the age of 18 years, most indiv iduals have a radius in stage 3b or 3c. Per
curve, the point predict ion of age corresponds with the tr immed mean, and the probabi l i ty to be adult is
represented by the area under the curve to the r ight of the 18 years threshold (grey ver t ical l ine).
De Tobel J. Multi-factorial forensic age estimation. Chapter 7: 118-140.

137
allowed discerning minors from adults based on the distal femoral epiphysis. By contrast, the current study did not render better results by adding VIBE informa-tion to SE.
Moreover, the high field MRI might not even be necessary to study hand/wrist development. Several authors have suc-cessfully applied open 0.2-0.3T scanners to study the hand/wrist for age estimation [1, 33, 35-37, 43]. However, only one of those studies included participants older than 18 [33]. An open scanner is more appropriate for children, who might be scared of lying in the small bore of a large scanner. By contrast, 3T MRI seemed appropriate in the current study, since it focussed on subadults and young adults, and was part of a larger project that also included MRI of third molars [10] and clavicles.
Staging techniques for wrist development
The current study confirmed the appli-cability of the 5-stage staging technique to assess radius and ulna development, including substages to stage 3. Merging stages decreased age estimation perfor-mance, while splitting up stages did not ameliorate age estimation performance.
Splitting up clavicular stage 3a into 3aa, 3ab and 3ac has been suggested on clavicle CT [48]. However, in the current study only stage 3ac was seen. Further-more, two possibilities to split up stage 3c were encountered. A first possibility was by registering END, which might valuable to correctly identify minors. In judicial context this is the major concern. How-ever, only the probabilities to be adult
suggested any value of this substage. A larger study sample will be needed to ver-ify the value of stage 3c END. A second possibility to split up stage 3c was by reg-istering the TFS on SE [31]. The TFS can be explained by the laminar structure of the maturing metaphysis-physis-epiphy-sis complex [23]. It has been hypothesised that this sign occurs gradually before the physeal scar condenses into a single line. Accordingly, it has been suggested to split up stage 4, with or without a TFS [42]. However, current results suggest that the TFS is of no value for age estimation. Even our 25- and 26-year-olds demon-strated no trend regarding the presence (or disappearance) of the TFS, which contrasts with Timme et al. (2017), who only included subjects until age 24. An-other possibility to split up stage 4 on SE radius was to add VIBE information. This allowed a further differentiation of age within that group, but did not outperform the original approach. Unfortunately, no other studies have combined SE and VIBE information of the wrist to estimate age.
Recommendations and future prospects
The current findings and the available lit-erature demonstrated that no anatomical structure should be preferred over anoth-er and that both SE and VIBE are equal-ly suitable. A one-fits-all 5-stage staging technique with substages 3a, 3b and 3c can be applied based on the corresponding se-quence-specific reference data.
Moreover, compared to literature, the methods in the current study seem to perform equally well regarding the distinction between minors and adults,
Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply?

138
but perform worse regarding the point prediction of age. Few MRI studies have applied a model to estimate age and have reported MAE and diagnostic indices. For hand/wrist, a MAE of 0.85 in males has been reported, applying an automated age estimation method [45]. For third molars, a MAE of 1.7 years in males and 2.0 years in females have been reported, with cor-responding specificities of 96% and 73%, respectively [10]. Combined MRI of third molars, both clavicles and the left hand/wrist rendered a MAE of 1.14 and 89% correctly classified minors [34].
The search for the optimal distinction between minors and adults is character-istic for forensic age estimation, which should always strive for the highest pos-sible proportion of correctly classified mi-nors and report appropriate confidence intervals around the point prediction of age [4, 16]. Traditionally, age estimation put too much focus on the point predic-tion, which increases the risk of over- or underestimation of the age. After all, age estimation will always be prone to in-ter-individual variation, impeding a true age determination. Fortunately, more recent literature and ongoing research focus more on the uncertainty intervals and probabilities to have reached the 18-year-threshold [3, 39]. It should be stressed that they are part of the age es-timation results and should always be re-ported [22].
This ensures an appropriate use of medical imaging for forensic age esti-mation. Conversely, many authors have stated that age estimation based on for instance the Greulich and Pyle atlas [18] or the Demirjian method [11] should not be applied in age estimation, since they
were developed to detect developmen-tal disorders. However, when reference studies have validated certain methods of age estimation, their use is scientifically justified. If their use is ethically justified remains debatable [2, 41], but when fo-rensic age estimation is compared with other forensic clinical activities, it seems similar: the medical expertise is used to answer a question asked by an authority, with respect for the individual’s integrity but in a societal context.
Study limitations
Finally, two limitations of the current study need to be taken into account. First, the suitability of stages 1 to 2b and substages of 3a could not be stud-ied, with age 14 as our lower cut-off. By contrast, the sample of participants up to age 26 did allow studying stages 4 and 5, which is more important considering the 18-year-threshold. Second, the relative-ly small study sample hindered to draw strong conclusions, especially regarding the amelioration attempts of the staging technique. Profound substaging some-times resulted in too few cases to allow any analysis.
To estimate age in adolescents and subadults based on wrist MRI, it suffices to apply a one-fits-all 5-stage staging technique – optimised with substages in stage 3 – to either ra-dius or ulna on T1 SE or VIBE. The
age estimate and the probability to have reached a threshold age need to be based on sequence-specific reference data.
Conclusion
De Tobel J. Multi-factorial forensic age estimation. Chapter 7: 118-140.

139
acknowledgements
The authors wish to express their grat-itude to all participants and everyone who helped with recruitment. Thank you Maarten Peleman and Dries Ovaere to install the viewing software on the de-partment’s computers. Finally, we wish to acknowledge Inès Phlypo for her indis-pensable critical appraisal of the manu-script.
references
[1] Abdelbary MH, Abdelkawi MM, Nasr MA. Age determina-tion by MR imaging of the wrist in Egyptian male football players. How far is it reliable? Egyptian Journal of Radiology and Nuclear Medicine. 2018;49(1):146-51.
[2] Aynsley-Green A, Cole T, Crawley H, Lessof N, Boag L, Wal-lace R. Medical, statistical, ethical and human rights consid-erations in the assessment of age in children and young peo-ple subject to immigration control. British medical bulletin. 2012;102(1):17-42.
[3] Bleka O, Wisloff T, Dahlberg PS, Rolseth V, Egeland T. Ad-vancing estimation of chronological age by utilizing avail-able evidence based on two radiographical methods. Int J Legal Med. 2018.
[4] Boldsen JL, Milner GR, Konigsberg LW, Wood JW. Transi-tion analysis: a new method for estimating age from skel-etons. In: Hoppa RD, Vaupel JW, eds. Paleodemography: Age Distributions from Skeletal Samples. 1st ed. Cambridge: Cambridge University Press, 2002; p. 73-106.
[5] Bolívar J, Sandoval Ó, Osorio J, Dib G, Gallo J. Relationship of chronological age and sexual maturity with skeletal ma-turity by magnetic resonance imaging of the distal radial epiphysis in adolescent football players. Apunts Medicina de l'Esport. 2015;50(188):129-37.
[6] Cunha E, Baccino E, Martrille L, Ramsthaler F, Prieto J, Schuliar Y, Lynnerup N, Cattaneo C. The problem of aging human remains and living individuals: a review. Forensic Sci Int. 2009;193(1-3):1-13.
[7] De Tobel J, Hillewig E, Bogaert S, Deblaere K, Verstraete K. Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation. Ann Hum Biol. 2017;44(2):130-9.
[8] De Tobel J, Hillewig E, Verstraete K. Forensic age estima-tion based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging. Ann Hum Biol. 2017;44(2):121-9.
[9] De Tobel J, Parmentier GIL, Phlypo I, Descamps B, Neyt S, Van De Velde WL, Verstraete KL, Thevissen PW. Magnetic resonance imaging of third molars in forensic age estima-tion: comparison of the Ghent and Graz protocols focusing on apical closure. Int J Legal Med. 2018;Epub ahead of print.
[10] De Tobel J, Phlypo I, Fieuws S, Politis C, Verstraete KL, The-vissen PW. Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging. J Forensic Odontostomatol. 2017;35(2):117-40.
[11] Demirjian A, Goldstein H, Tanner JM. A new system of den-tal age assessment. Hum Biol. 1973;45(2):211-27.
[12] Dvorak J. Detecting over-age players using wrist MRI: sci-ence partnering with sport to ensure fair play. Br J Sports Med. 2009;43(12):884-5.
[13] Dvorak J, George J, Junge A, Hodler J. Age determination by magnetic resonance imaging of the wrist in adolescent male football players. Br J Sports Med. 2007;41(1):45-52.
[14] Dvorak J, George J, Junge A, Hodler J. Application of MRI of the wrist for age determination in international U-17 soccer competitions. Br J Sports Med. 2007;41(8):497-500.
[15] Ekizoglu O, Hocaoglu E, Inci E, Can IO, Aksoy S, Sayin I. Estimation of forensic age using substages of ossification of the medial clavicle in living individuals. Int J Legal Med. 2015;129(6):1259-64.
[16] Fieuws S, Willems G, Larsen-Tangmose S, Lynnerup N, Boldsen J, Thevissen P. Obtaining appropriate interval esti-mates for age when multiple indicators are used: evaluation of an ad-hoc procedure. Int J Legal Med. 2016;130(2):489-99.
[17] George J, Nagendran J, Azmi K. Comparison study of growth plate fusion using MRI versus plain radiographs as used in age determination for exclusion of overaged football players. Br J Sports Med. 2012;46(4):273-8.
[18] Greulich W, Pyle SI. Radiographic atlas of skeletal develop-ment of the hand and wrist. 2nd ed. Stanford, CA: Stanford University Press, 1959.
[19] Hillewig E, De Tobel J, Cuche O, Vandemaele P, Piette M, Verstraete K. Magnetic resonance imaging of the medial ex-tremity of the clavicle in forensic bone age determination: a new four-minute approach. Eur Radiol. 2011;21(4):757-67.
[20] Hillewig E, Degroote J, Van der Paelt T, Visscher A, Vande-maele P, Lutin B, D'Hooghe L, Vandriessche V, Piette M, Ver-straete K. Magnetic resonance imaging of the sternal extrem-ity of the clavicle in forensic age estimation: towards more sound age estimates. Int J Legal Med. 2013;127(3):677-89.
[21] Hojreh A, Gamper J, Schmook MT, Weber M, Prayer D, Herold CJ, Noebauer-Huhmann IM. Hand MRI and the Greulich-Pyle atlas in skeletal age estimation in adolescents. Skeletal Radiol. 2018.
[22] International Organization for Forensic Odonto-Stomatol-ogy (IOFOS). Recommendations for Quality Assurance: Dental Age Estimation. Leuven 2018.
[23] Jaramillo D, Connolly SA, Mulkern RV, Shapiro F. De-veloping epiphysis: MR imaging characteristics and histologic correlation in the newborn lamb. Radiology. 1998;207(3):637-45.
[24] Kellinghaus M, Schulz R, Vieth V, Schmidt S, Pfeiffer H, Schmeling A. Enhanced possibilities to make statements on the ossification status of the medial clavicular epiphysis us-ing an amplified staging scheme in evaluating thin-slice CT scans. Int J Legal Med. 2010;124(4):321-5.
Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply?

140
[25] McGibbon CA, Bencardino J, Palmer WE. Subchondral bone and cartilage thickness from MRI: effects of chemi-cal-shift artifact. MAGMA. 2003;16(1):1-9.
[26] Ottow C, Schulz R, Pfeiffer H, Heindel W, Schmeling A, Vieth V. Forensic age estimation by magnetic resonance imaging of the knee: the definite relevance in bony fu-sion of the distal femoral- and the proximal tibial epiphy-ses using closest-to-bone T1 TSE sequence. Eur Radiol. 2017;27(12):5041-8.
[27] Sarkodie BD, Botwe BO, Pambo P, Brakohiapa EK, Mayeden RN. MRI age verification of U-17 footballers: The Ghana study. J Forensic Radiol Imaging. 2018;12:21-4.
[28] Schmeling A, Dettmeyer R, Rudolf E, Vieth V, Geserick G. Fo-rensic Age Estimation. Dtsch Arztebl Int. 2016;113(4):44-50.
[29] Schmeling A, Geserick G, Reisinger W, Olze A. Age estima-tion. Forensic Sci Int. 2007;165(2-3):178-81.
[30] Schmeling A, Schulz R, Reisinger W, Muhler M, Wernecke KD, Geserick G. Studies on the time frame for ossification of the medial clavicular epiphyseal cartilage in conventional radiography. Int J Legal Med. 2004;118(1):5-8.
[31] Schmidt S, Vieth V, Timme M, Dvorak J, Schmeling A. Ex-amination of ossification of the distal radial epiphysis using magnetic resonance imaging. New insights for age estima-tion in young footballers in FIFA tournaments. Sci Justice. 2015;55(2):139-44.
[32] Serin J, Rerolle C, Pucheux J, Dedouit F, Telmon N, Savall F, Saint-Martin P. Contribution of magnetic resonance im-aging of the wrist and hand to forensic age assessment. Int J Legal Med. 2016;130(4):1121-8.
[33] Serinelli S, Panebianco V, Martino M, Battisti S, Rodacki K, Marinelli E, Zaccagna F, Semelka RC, Tomei E. Accu-racy of MRI skeletal age estimation for subjects 12-19. Po-tential use for subjects of unknown age. Int J Legal Med. 2015;129(3):609-17.
[34] Štern D, Kainz P, Payer C, Urschler M. Multi-Factorial Age Estimation from Skeletal and Dental MRI Volumes. In: International Workshop on Machine Learning in Medical Imaging. Quebec City, Canada: Springer, 2017; p. 61-9.
[35] Terada Y, Kono S, Tamada D, Uchiumi T, Kose K, Miyagi R, Yamabe E, Yoshioka H. Skeletal age assessment in chil-dren using an open compact MRI system. Magn Reson Med. 2013;69(6):1697-702.
[36] Terada Y, Kono S, Uchiumi T, Kose K, Miyagi R, Yamabe E, Fujinaga Y, Yoshioka H. Improved reliability in skeletal age assessment using a pediatric hand MR scanner with a 0.3T permanent magnet. Magn Reson Med Sci. 2014;13(3):215-9.
[37] Terada Y, Tamada D, Kose K, Nozaki T, Kaneko Y, Miyagi R, Yoshioka H. Acceleration of skeletal age MR examina-tion using compressed sensing. J Magn Reson Imaging. 2016;44(1):204-11.
[38] Thevissen PW. Dental age estimation: striving for an optimal ap-proach [Doctoral thesis]. Leuven: Leuven University Press, 2013.
[39] Thevissen PW, Fieuws S, Willems G. Human dental age estimation using third molar developmental stages: does a Bayesian approach outperform regression models to dis-criminate between juveniles and adults? Int J Legal Med. 2010;124(1):35-42.
[40] Thevissen PW, Fieuws S, Willems G. Third molar de-velopment: evaluation of nine tooth development reg-istration techniques for age estimations. J Forensic Sci. 2013;58(2):393-7.
[41] Thevissen PW, Kvaal SI, Dierickx K, Willems G. Ethics in age estimation of unaccompanied minors. J Forensic Odontos-tomatol. 2012;30 Suppl 1:84-102.
[42] Timme M, Ottow C, Schulz R, Pfeiffer H, Heindel W, Vieth V, Schmeling A, Schmidt S. Magnetic resonance imaging of the distal radial epiphysis: a new criterion of maturity for determining whether the age of 18 has been completed? Int J Legal Med. 2017;131(2):579-84.
[43] Tomei E, Sartori A, Nissman D, Al Ansari N, Battisti S, Rubi-ni A, Stagnitti A, Martino M, Marini M, Barbato E, Semelka RC. Value of MRI of the hand and the wrist in evaluation of bone age: Preliminary results. J Magn Reson Imaging. 2014;39(5):1198-205.
[44] Tscholl PM, Junge A, Dvorak J, Zubler V. MRI of the wrist is not recommended for age determination in female football players of U-16/U-17 competitions. Scand J Med Sci Sports. 2016;26(3):324-8.
[45] Urschler M, Grassegger S, Štern D. What automated age estimation of hand and wrist MRI data tells us about skeletal maturation in male adolescents. Ann Hum Biol. 2015;42(4):358-67.
[46] Urschler M, Krauskopf A, Widek T, Sorantin E, Ehammer T, Borkenstein M, Yen K, Scheurer E. Applicability of Greu-lich-Pyle and Tanner-Whitehouse grading methods to MRI when assessing hand bone age in forensic age estimation: A pilot study. Forensic Sci Int. 2016;266:281-8.
[47] Vieth V, Schulz R, Heindel W, Pfeiffer H, Buerke B, Schmeling A, Ottow C. Forensic age assessment by 3.0T MRI of the knee: proposal of a new MRI classification of ossification stages. Eur Radiol. 2018.
[48] Wittschieber D, Schmidt S, Vieth V, Schulz R, Püschel K, Pfeiffer H, Schmeling A. Subclassification of clavicular sub-stage 3a is useful for diagnosing the age of 17 years. Rechts-medizin. 2014;24(6):485-8.
[49] Wittschieber D, Schulz R, Vieth V, Kuppers M, Bajanowski T, Ramsthaler F, Puschel K, Pfeiffer H, Schmidt S, Schmeling A. Influence of the examiner's qualification and sources of error during stage determination of the medial clavicular ep-iphysis by means of computed tomography. Int J Legal Med. 2014;128(1):183-91.
[50] Wittschieber D, Schulz R, Vieth V, Kuppers M, Bajanowski T, Ramsthaler F, Puschel K, Pfeiffer H, Schmidt S, Schmeling A. The value of sub-stages and thin slices for the assessment of the medial clavicular epiphysis: a prospective multi-center CT study. Forensic Sci Med Pathol. 2014;10(2):163-9.
De Tobel J. Multi-factorial forensic age estimation. Chapter 7: 118-140.



143
PART 4
Age estimation based on clavicle MRI

144
CHAPTER 8
TH I S CHAPTER ADDRESSED THE FOLLOWING STUDY OB JECT IVE :
Objective 8: To study how motion artefacts affect stage allocation to the clavicles’ sternal ends on MRI.
TH I S CHAPTER WAS SUBM ITTED FOR PUBL ICAT ION AS :
De Tobel J, van Wijk M, Alberink I, Hillewig E, Phlypo I, van Rijn RR, Thevissen PW, Verstraete KL, de Haas MB. The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation. Int J Legal Med. Submitted on October 24, 2018 [A1; Journal Impact Factor 2017 2.316; Medicine, Legal Q1; Peer reviewed].
This paper has been peer reviewed and a revised version is being prepared for submission.
RESULTS DESCR I BED IN TH I S CHAPTER WERE PARTLY PRESENTED
AT THE FOLLOWING CONFERENCE :
De Tobel J, van Wijk M, Hillewig E, Phlypo I, Alberink I, van Rijn R, Thevissen P, Ver-straete K, de Haas M. The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation. 6th International Society of Forensic Radiology and Imaging (ISFRI) Congress; Odense, Denmark; May 12, 2017. p 64.

145
The influence of motion artefacts on magnetic resonance imaging of the clavicles
for age estimation
OR IG INAL RESEARCH
Abstract
Aim — To determine how motion affects stage allocation to the clavicle’s sternal end on MRI. Materials and methods — Eight-een volunteers (9 females, 9 males) between 14 and 30 years old were prospectively scanned with 3T MRI. One resting state scan was followed by five intentional motion scans. Additionally, a control group of 72 resting state scans were selected from previ-ous research. Firstly, six observers allocated developmental stag-es to the clavicles independently. Secondly, they re-assessed the images, allocating developmental statuses (immature, mature). Finally, the resting state scans of the 18 volunteers were assessed in consensus to decide on the ‘correct’ stage/status. Results were compared between groups (control, prospective resting state, prospective motion), and between staging techniques (stages/statuses). Results — Inter-observer agreement was low (Krip-pendorff α 0.23-0.67). The proportion of correctly allocated stages (64%) was lower than correctly allocated statuses (83%). Overall, intentional motion resulted in fewer assessable images and less images of sufficient evidential value. The proportion of correctly allocated stages did not differ between resting state (64%) and motion scans (65%), while correctly allocated sta-tuses were more prevalent in resting state scans (83% versus 77%). Remarkably, motion scans did not render a systematically higher or lower stage/status, compared to the consensus. Con-clusion — Intentional motion frustrates clavicle MRI for age estimation. Still, in case of obvious disturbances, the forensic expert will consider the MRI unsuitable as evidence. Thus, the development of the clavicle as such and the staging technique seem to play a more important role in a faulty age estimation.
Key Words
• age determination by skeleton
• clavicle
• magnetic resonance imaging
• motion artefact
AFF IL IAT IONS
1 Department of Diagnostic
Sciences – Radiology, Ghent
University, Belgium
2 Department of Imaging and Pa-
thology – Forensic Odontology,
KU Leuven, Belgium
3 Department of Head, Neck and
Maxillofacial Surgery, Ghent
University Hospital, Belgium
4 Department of Oral and Maxillo-
facial Surgery, Leuven University
Hospitals, Belgium
5 Department of Forensic Anthro-
pology, Netherlands Forensic
Institute, The Hague, The Neth-
erlands
6 Department of Oral Health
Sciences – Special Needs in Den-
tistry, Ghent University, Belgium
7 Department of Radiology, Uni-
versity of Amsterdam, Academic
Medical Center, Amsterdam, The
Netherlands
This study received funding from the
Dutch Immigration and Naturalisation
Service (IND).
The authors declare that there are
no conflicts of interest.
JANN ICK DE TOBEL* 1 2 34 MAYONNE VAN W I J K* 5
I VO ALBER INK 5 ELKE H I LLEW IG 1
I N ÈS PHLYPO 6
R ICK R . VAN R I JN 7 PATR ICK W. THEV I S SEN 2
KOENRAAD L . VERSTRAETE 1 MICH I EL B . D E HAAS 5
* De Tobel J and van Wijk M equally contributed to this paper.

146
Magnetic resonance imaging (MRI) has been studied by several research groups to visualise developing struc-tures for forensic age estimation in living adolescents and subadults. Developing structures for which
MRI protocols have been reported in fo-rensic literature include long bones and teeth [3, 4, 6, 16, 19, 24, 26, 44]. Most pro-tocols will include a method of fixation or stabilisation of the region of interest, since MRI acquisition requires several minutes and is prone to motion artefacts. For ex-ample, the wrist can be fixed with a flexi-ble cloth belt [34] or stabilised in the coil using pillows [38] or a vacuum bed [40]. The head can be fixed by an individual-ised bite plate [4]. This minimises motion artefacts that might impede an adequate assessment of the developmental stage of the considered anatomical structure.
However, when clavicles are stud-ied for age estimation, absolute fixation is impossible and breathing artefacts are unavoidable. Hillewig et al. (2011) report-ed the use of a specially shaped vacuum pillow and rubber device to position the coil during the scan of the sternal ends of the clavicles. Moreover, they scanned in prone position to decrease breathing arte-facts [16]. Authors of more recent publi-cations agreed that scanning in prone po-sition resulted in less breathing artefacts [33, 42].
Since absolute fixation is impossible when the clavicles are scanned, more ex-tensive movements than breathing move-ments are possible. If participants would be aware of the capability of motion to disturb the age diagnostics, they might conduct intentional movements. One can assume that mainly older subjects would
try to frustrate the examination to try to appear younger. Intentional motion has been noted in practice during X-ray ex-aminations of clavicles or hand/wrist by the authors (Figure 8.1). Therefore, the aim of the current study was to deter-mine the influence of motion on stage allocation to the sternal end of both clav-icles based on MRI. It was hypothesised that intentional motion artefacts would impede stage allocation, whereas mere breathing artefacts would not.
Study population and staging technique
The study was approved by the eth-ics committee of Ghent University Hospital. From every participant, written informed consent was ob-tained. In case of minors, the parents’ informed consent was also obtained.
Healthy Belgian and Dutch Cauca-sian volunteers between 14 and 30 years old were prospectively included to par-ticipate in motion scans (Table 8.1). The participants were part of a sample of a larger ongoing study at Ghent University. They were selected based on the expect-ed developmental stage of their clavicles, aiming for a balanced sample that would cover all stages of development. The stag-ing technique by Schmeling (2004), mod-ified by Kellinghaus (2010) was used to assess the images [20, 27]. Because of the low number of participants with clavicles in stage 2, no substaging was included for that stage. Moreover, since Hillewig et al. (2013) demonstrated that the physeal scar could not be distinguished on clavicle MRI [17], stages based on the presence or absence of the physeal scar were not in-cluded (Table 8.2).
Introduction
Materials and M
ethods
De Tobel J. Multi-factorial forensic age estimation. Chapter 8: 144-162.

147
In a total of 18 participants, one motionless resting state scan and five motion scans were conducted. Moreover, for every mo-tion scan that would be assessed, a resting state matched control scan was included (Figure 8.2). Matching was done based on the developmental stages of the clavicles, allocated in consensus. Since five motion scans were conducted per participant and every motion participant already had one resting state scan, an additional 72 rest-ing state scans were needed. Therefore, 55 participants were retrospectively selected from the study sample of Hillewig et al. (2013), complemented with 17 partici-
pants from the sample of the larger ongo-ing study at Ghent University. Regarding the scans from Hillewig et al. (2013), only cases were selected in which at least three out of four observers had agreed on the stage. Regarding the scans from the larger ongoing study, cases were selected based on preliminary staging results.
Image acquisition and motion protocol
Three Tesla MRI (Magnetom Trio Tim, Siemens, Erlangen, Germany) was per-formed using a loop-shaped surface coil
The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation
a Standard PA rest ing state. The r ight c lavic le is assessable and appears fu l ly mature. The left c lav-
ic le cannot be assessed, due to superposit ioning.
b Left anterior obl ique 10° rest ing state, intended to better visual ise the left c lavic le. The left c lavi-
c le is assessable and appears fu l ly mature.
c Standard PA whi le moving both shoulders caudal ly. The r ight c lavic le is assessable, whi le the left
one is not , due to superposit ion.
d Left anterior obl ique 10° whi le moving the left shoulder from 10° to 45° . None of both c lavic les
can be assessed. Because of the overly turned left shoulder, a (remnant of the) growth plate
and epiphysis would be projected over the metaphysis .
FIGURE 8. 1 — CORRESPONDING RADIOGRAPHS OF BOTH CLAVICLES. Al l radiographs were produced poste-
ro-anterior ly (PA), but they were mirrored here to correspond with the standard view of imaging.

148
according to the T1 gradient-echo VIBE protocol by Hillewig et al. (2011) (TR/TE 10/2.9; voxel size 0.7 × 0.7 × 0.9 mm³; ma-trix 536 × 576 pixels; FOV 400 mm; flip angle 20°; water excitation filter; acquisi-tion time 4 minutes 2 seconds). Partici-pants were positioned prone. Prospective scans were conducted between June and November 2015. Retrospectively selected control scans had been conducted be-tween April 2009 and May 2015.For the motion study, six scans in two sessions of three consecutive scans were conducted in every participant. For all of them, the first scan was a resting state scan without intentional motion. The ap-plied scanning sequence filled k-space in a linear way. The position of the sternal ends of the clavicles was in the centre of the images, corresponding with k-space being filled at half the acquisition time.
Thus, the influence of motion on image quality was less at the beginning and at the end of the acquisition time, while it peaked at half the acquisition time. Therefore, the participant was instructed to move voluntarily at 2 minutes 1 second during the motion scans.
Participants moved in five distinctive ways (Figure 8.2), four of which were standardised movements designed by the authors:
— cough twice,— move both shoulders twice anteriorly,— move both shoulders twice posteriorly,— move both shoulders twice cranially.
One movement (further on referred to as ‘freestyle’) was invented by the partic-ipant in advance, after a short explanation about the purpose of the movements and without prior knowledge about the stand-ardised movements. It was explained that by moving, a participant would intend to disturb the image in order to impede as-sessment. On the other hand, the move-ment should be quite discrete, since it should remain unnoticed by the scanning personnel.
In order to eliminate the influence of fatigue on the latter scans, the order of the motion scans was randomised, so that a specific order would only occur once.
Image analysis
All images were anonymised and every scan was allocated a random code, in or-der to randomly distribute motion scans and resting state scans. Six observers (JDT, MvW, MdH, EH, RvR, KV) assessed the images. Their level of experience and
TABLE 8. 1 — AGE AND SEX DISTRIBUTION OF THE
MOTION STUDY POPULATION
AGE (Y) FREQUENCY
FEMALE MALE
14 0 2
15 1 1
16 0 1
17 0 1
20 1 0
21 3 0
23 1 0
24 1 0
25 1 1
26 0 2
27 0 1
30 1 0
TOTAL 9 9
De Tobel J. Multi-factorial forensic age estimation. Chapter 8: 144-162.

149
The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation
TABLE 8.2 — APPLIED STATUSES AND STAGES. Staging cr iter ia for the sternal end of the c lavic le were
based on Schmel ing et al . (2004) and Kel l inghaus et al . (2010), modif ied for MRI . Stages 1 to 3 were com-
bined into one status, “ Immature”, whereas stage 4 corresponded with status “Mature”.
STATUS STAGE STAGE CRITERIA
IMMATURE 1 Ossif ication centre is invisible (= not yet ossif ied).
2 Ossif ication centre is vis ible (= ossif ied), non-union of the epiphysis and metaphysis.
3 Growth plate is partial ly ossif ied (= bone trabeculae cross the growth plate from
ossif ication centre to metaphysis).
3a The epiphyseal-metaphyseal fusion completes one third or less of the former gap
between epiphysis and metaphysis.
3b The epiphyseal-metaphyseal fusion completes over one third unti l two thirds of the
former gap between epiphysis and metaphysis.
3c The epiphyseal-metaphyseal fusion completes over two thirds of the former gap
between epiphysis and metaphysis.
MATURE 4 Complete union of the epiphysis and metaphysis (= growth plate is completely
oss if ied).
FIGURE 8.2 — SCHEMATIC OVERVIEW OF THE STUDY POPULATION. All 180 scans were assessed by six observers.

150
the monitors used for the assessments are shown in Table 8.3. Training occurred by assessing two training cases with known motion artefacts in consensus. These cas-es were not included for analysis.
Firstly, each observer individually as-sessed both clavicles simultaneously. Four variables were considered. For every one of them, the observer took the whole se-quence of slices into account.
1 It was recorded if motion could be noticed on one or more images of the sequence.
2 A stage of epiphyseal development of the clavicles (Table 8.2) was allo-cated. No exact measurements were done whilst assessing the MR-imag-es. Instead, the degree of fusion was estimated by the observers. During staging, the benefit of the doubt was always granted. This means that in cases of reasonable doubt, the younger stage was allocated. If the evaluation proved to be impossible, a reason was reported (anatomical impediment, insufficient technical quality, motion artefacts, other). This staging technique corresponds with the current practice in Bel-gium, albeit currently still applied to radiographs [36, 37].
3 Then, the observer judged if the im-ages could be used as forensic evi-dence in a court of law. After all, an observer might be sufficiently confi-dent to allocate a stage within a re-search setting, but consider the im-ages of insufficient quality to declare the allocated stage in a court setting.
4 Finally, observers described the ease of the assessment, i.e. to allocate a stage or to decide that the images were not assessable and to judge the evidential value (easy, not easy/not difficult, difficult).
To eliminate the learning effect of assess-ing the images, the first 20 cases were ran-domly repeated in the second half of the dataset. These cases were disregarded in the analyses.
Secondly, the six observers re-assessed all scans independently from the previous assessment, collecting data on the above described four variables, but with an al-ternative to the staging technique. This time, only two statuses were considered: immature or mature (Table 8.2). This sta-tus technique corresponds with the cur-rent practice in the Netherlands, albeit currently still applied to radiographs [22].
Finally, five out of the six original observers (JDT, MvW, MdH, EH, KV) assessed the resting state scan of the 18 prospectively included participants in consensus, joined by an additional ob-server (PT).
Statistical analysis
For analysis, the data were transferred from Microsoft Access 2010 to Micro-soft Excel 2010, SPSS Statistics 22.0 (IBM SPSS Statistics for Windows, Armonk, NY, USA) and Matlab R217a (Mathworks Inc., Natick, MA, USA). Descriptive sta-tistics were calculated and statistical tests were performed two-sided and evaluated at the 0.05 significance level.
De Tobel J. Multi-factorial forensic age estimation. Chapter 8: 144-162.

151
Influences other than motion
In order to be able to study the influence of motion artefacts, other influences had to be taken into account first. To study the influences other than motion, the pro-portions of the four study variables were compared between resting state scans of the control group and those of the pro-spective group.
Reproducibility of the process was studied using the Krippendorff α coeffi-cient, a statistical measure of the agree-ment achieved when coding a set of units. The coefficient is well fit for nominal data
with a considerable amount of missing data, which was the case here. In these tests, stages were considered as nominal instead of ordinal data, because of the relatively large number of participants in stages 1 and 4, while those stages might be confused. The SPSS software of Hayes and Krippendorff was used, including the ability to bootstrap the results [14]. Rules of thumb describe that one may rely on data with α ≥ 0.80, consider data with 0.80 > α ≥ 0.67 fit to draw tentative conclusions, and to discard data with α < 0.67. Bootstrap intervals were used to construct 95% confidence intervals (CI) for Krippendorff α.
The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation
TABLE 8.3 — OBSERVERS’ BACKGROUND AND MONITOR PROPERTIES.
OBSERVER BACKGROUND MONITOR
PROFESSION LEVEL OF EXPERIENCE BRAND TYPE RESOLUTION
(P IXELS)
EH Researcher at
Radiology
9 years of interpret ing
MR-images as researcher
on age est imation
Barco MDCC-6130 3280 x 2048
JDT Resident Oral
and Maxi l lofacial
Surgery
7 years of interpret ing
MR-images as researcher
on age est imation
Barco MDCC-6130 3280 x 2048
KV Professor Radiol-
ogy and Medical
Imaging
more than 25 years of
experience as musculo-
skeletal radiologist ; in-
volved in age est imation
for more than 25 years
Toshiba 173HT02-T01 1920 x 1080
MdH Physical Anthro-
pologist
7 years of interpret ing
X-ray images as re-
searcher on age est i-
mation
Barco MDCC-6130 2048 x 1640
MvW Forensic Anthro-
pologist
5 years of interpret ing
X-ray images as re-
searcher on age est i-
mation
Barco MDCC-6130 2048 x 1640
PT Professor Foren-
s ic Odontology
12 years of interpret-
ing X-ray images as
researcher on age est i-
mation
Barco MDCC-6130 3280 x 2048
RvR Professor Foren-
s ic and Paediat-
r ic Radiology
14 years of experience
as c l in ical paediatr ic
radiologist
Barco MDCC-6130 2048 x 1640

152
To detect possible population bias, the inter-observer agreement of the image assessment was compared between the 18 prospectively included participants’ rest-ing state scans and the 72 controls. Since this was done for each observer separate-ly, matched pairs were considered in a Wilcoxon rank-sum test.
To study the influence of the imag-ing technique, the stages allocated by the different observers were compared with the consensus stages. When the allocated stage corresponded with the consensus stage, this was called a ‘correctly allocated
stage’. When all observations would ran-domly differ from the consensus, this would reflect the difficulty in interpret-ing the MRI. This also allowed studying observer bias and checking for the need to weigh the assessments of different ob-servers or even the need to exclude an ob-server (if his/her allocated stages would differ systematically from the consensus and the other observers). Status allocation was studied in the same way. Thus, the in-fluence of staging technique was reflected by differences between allocating stages versus statuses.
TABLE 8.4 — RESULTS OF STAGE AND STATUS ALLOCATION, PER POPULATION GROUP AND TYPE OF SCAN.
POPULATION TYPE OF SCAN VARIABLE STAGE ALLOCATION
AVERAGE RANGE
Control Rest ing Motion ar tefacts 51% (219/432) 17% ( 12/72) -
state Assessable 83% (358/432) 67% (48/72) -
Inter-observer agreement 0.53 [0.46 -
Suff ic ient evidence in cour t 72% (310/432) 54% (39/72) -
Easy assessment 31% ( 136/432) 4% (3/72) -
Prospective Rest ing Motion ar tefacts 74% (80/108) 44% (8/18) -
state Assessable 71% (77/108) 50% (9/18) -
Inter-observer agreement 0.23 [0. 12 -
Correct ly al located 64% (49/77) 44% (4/9) -
Suff ic ient evidence in cour t 55% (59/108) 28% (5/18) -
Easy assessment 17% ( 18/108) 0% (0/18) -
Prospective Motion Motion ar tefacts 89% (483/540) 77% (69/90) -
Assessable 43% (233/540) 23% (21/90) -
Inter-observer agreement 0.58 [0.50 -
Correct ly al located 65% (151/233) 48% (21/44) -
Suff ic ient evidence in cour t 28% (151/540) 10% (9/90) -
Easy assessment 36% (193/540) 10% (9/90) -
P-value (Control ) = P-value of Wi lcoxon rank-sum test comparing results between the rest ing scans in the
control and prospective populat ions. P-value (Motion) = P-value of Wi lcoxon s igned-rank test comparing
results between rest ing state and motion scans in the prospective populat ion.
De Tobel J. Multi-factorial forensic age estimation. Chapter 8: 144-162.

153
Influence of motion
To study the influence of motion, the pro-portions of the four study variables were compared between prospective resting state scans and motion scans. A final step was to compare the proportion of correct-ly allocated stages and statuses based on:
— resting state scans,— motion scans,— scans in which the observer indicat-
ed that the images could be used as evidence in a court of law.
A Wilcoxon matched-pairs signed-rank test was used for these analyses.
All reported results were based on the evaluation of the right clavicle. Results for the left clavicle were similar. Table 8.4 summarises the results of the
studied variables in the different groups.
Influences other than motion
Population bias
The upper and middle parts of Table 8.4 display the results of resting state scans in
The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation
Results
TABLE 8.4 (CONTINUED)
STATUS ALLOCATION
P-VALUE AVERAGE RANGE P-VALUE
85% (61/72) 0.002 52% (223/432) 32% (23/72) - 90% (65/72) < 0.001
92% 66/72) 0.007 84% (363/432) 65% (47/72) - 92% (66/72) 0. 132
0.60] 0.39 [0. 16 - 0.61 ]
89% (64/72) 0.013 69% (299/432) 50% (36/72) - 85% (61/72) 0.048
69% (50/72) 0.003 48% (208/432) 17% ( 12/72) - 100% (72/72) 0.331
100% (18/18) 81% (87/108) 44% (8/18) - 100% (18/18)
94% (17/18) 75% (81/108) 61% ( 1 1/ 18) - 94% (17/18)
0.34] 0.67 [0.49 - 0.84]
77% ( 10/13) 83% (67/81) 69% (9/13) - 92% (1 1/ 12)
83% (15/18) 56% (61/108) 28% (5/18) - 94% (17/18)
33% (6/18) 40% (43/108) 1 1% (2/18) - 100% (18/18)
99% (89/90) 0.001 84% (452/540) 59% (53/90) - 100% (90/90) 0.433
62% (56/90) < 0.001 51% (275/540) 37% (33/90) - 72% (65/90) < 0.001
0.65] 0.39 [0. 12 - 0.61 ]
80% (40/50) 0.550 77% (21 1/275) 53% (26/49) - 90% (38/42) 0.070
46% (41/90) < 0.001 37% (202/540) 24% (22/90) - 57% (51/90) 0.005
62% (65/90) 0.010 52% (282/540) 30% (27/90) - 100% (90/90) 0.021
Range = Range of frequencies encountered by different observers. For inter-observer agreement . the
95% bootstrap interval is displayed instead.
154
the control and prospective populations, respectively. A population bias was noted, with scans in the prospective population showing more motion artefacts, and con-sequently being more difficult to assess. This needs to be taken into account when interpreting all other results.
Imaging technique, observer bias and staging technique
Inter-observer agreement was low, with α ranging from 0.23 to 0.67. The middle part of Table 8.4 summarises resting state scan results of stage/status allocation in the prospective population. The propor-tion of correctly allocated stages was low (64%). Results per observer indicated that this was not due to one or more observers performing worse than others. By con-trast, the proportion of correctly allocated statuses was higher (83%). However, al-locating statuses instead of stages did not result in more assessable images or more images of sufficient evidential value. Over-all, the process of status allocation was con-sidered easier than stage allocation.
Influence of motion
To illustrate the motion artefacts, Figure 8.3 shows one corresponding slice of the six conducted scans from the same par-ticipant. Figure 8.4 illustrates the resulting variation in allocated stages and statuses.
The lower part of Table 8.4 summaris-es motion scan results. Motion artefacts were more frequent than in resting state scans, indicating that intentional motion did affect the images. Hence, motion re-sulted in fewer assessable images and less images of sufficient evidential value. The
proportion of correctly allocated stages did not differ significantly between rest-ing state scans (64%) and motion scans (65%). By contrast, correctly allocated statuses were more prevalent in resting state scans (83% versus 77%). Surpris-ingly, when the observer was confident to take the images to court as evidence, the proportions of correctly allocated stages (58%; 121/210) was lower than in imag-es of low evidential value (68%; 69/101). Conversely, correctly allocated statuses in these cases were 80% (209/261) and 73% (69/94) respectively.
Overall, the process of assessing mo-tion scans was considered easier than assessing resting state scans. After all, in case of clear image distortion by motion, it was easy to decide to discard the images. By contrast, when the artefacts were more subtle, it was harder to discern intentional motion from physiological motion arte-facts.
Furthermore, Tables 8.5 and 8.6 sum-marise all observers’ allocated stages/sta-tuses based on motion scans, compared to consensus stage/status. Motion scans did not render a systematically higher or lower stage/status, compared to the con-sensus stages/statuses. Neither did the ability to assess correlate with stage/sta-tus. Intentional motion lead to wrongfully allocating a younger stage (stage 1 to 3) to a fully mature clavicle in 35% (24/68) of assessable cases. For status allocation, this was in 56% (41/73) of assessable cases. Conversely, wrongfully deciding on a ful-ly mature clavicle was less frequent with 19% (32/165) for stages and 11% (23/202) for statuses.
De Tobel J. Multi-factorial forensic age estimation. Chapter 8: 144-162.

155
The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation
TABLE 8.5 — CROSS TABULATION OF ALLOCATED STAGES BASED ON MOTION SCANS BY ALL OBSERVERS,
PER CONSENSUS STAGE.
INDIVIDUAL STAGE ALLOCATION (ALL MOTION SCANS AND ALL OBSERVERS COMBINED)
CONSENSUS
STAGE
1 2 3 4 NOT ASSESSABLE
1 23% (27/120) 1% ( 1/ 120) 4% (5/120) 6% (7/120) 67% (80/120)
2 - - - - - - - - - -
3 6% (16/270) 1% (4/270) 30% (80/270) 9% (25/270) 54% (145/270)
4 7% (1 1/ 150) 1% ( 1/ 150) 8% ( 12/150) 29% (44/150) 55% (82/150)
TABLE 8.6 — CROSS TABULATION OF ALLOCATED STATUSES BASED ON MOTION SCANS BY ALL OBSERVERS,
PER CONSENSUS STATUS.
INDIVIDUAL STATUS ALLOCATION
(ALL MOTION SCANS AND ALL OBSERVERS COMBINED)
CONSENSUS STATUS IMMATURE MATURE NOT ASSESSABLE
Immature 46% (179/390) 6% (23/390) 48% (188/390)
Mature 27% (41/150) 21% (32/150) 51% (77/150)
In this case, scans were conducted in the fol lowing order: a, d, f ; c , b, e. Note that because of the break
in between the third and four th sequence, the posit ion of the par t ic ipant changed.
FIGURE 8.3 — ONE CORRESPONDING SLICE OF THE SIX CONDUCTED SCANS FROM THE SAME PARTICIPANT.
Al located stages and statuses are displayed in Figure 8.4 .
a Rest ing state scan.
b Cough twice.
c Move both shoulders
twice anterior ly.
d Move both shoulders
twice posterior ly.
e Move both shoulders
twice cranial ly.
f Freestyle motion. In
this case the par t ic-
ipant chose to move
the shoulders poste-
r ior ly, corresponding
with the movement
in d.

156
a Although consensus stage 1 was al located to the rest ing state scan, indiv idual observers al located
stages 1 , 3 or 4 .
b This dispers ion was also seen based on the motion scans. Note that one observers judged al l motion
scans to be unsuitable for stage al location, whi le others al located a stage to al l of them.
c Al locating a status, al l observers agreed on an immature c lavic le.
d This agreement was also seen based on the motion scans. Note that the observer who had judged
all motion scans to be unsuitable to allocate a stage, did find those scans suitable for status allocation.
FIGURE 8.4 — ALLOCATED STAGES (A, B) AND STATUSES (C, D) TO THE RIGHT CLAVICLE OF THE SAME PAR-
TICIPANT AS SHOWN IN FIGURE 8.3, BASED ON THE DIFFERENT SCANS, PER OBSERVER.
Discussion
Motion
The current study demonstrated that at a certain degree of motion, assessment becomes impossible and
the images rendered unsuitable as evi-dence. Deciding this is relatively easy and does not depend on staging technique. When this is obvious during the scan-ning session, a rescan can be done. This corresponds with the way radiographs are
obtained in current age estimation. If a ra-diograph proves to be unsuitable, a new radiograph is made [22].
Motion artefacts are known to dis-turb MR-images of the clavicles for age estimation in the living [17, 29, 33]. It has been reported that the magnitude of the disturbing effect is directly proportion-al to the magnetic field strength [41], so artefacts become more important, as line
De Tobel J. Multi-factorial forensic age estimation. Chapter 8: 144-162.

157
by line, higher field scanners are replacing lower field scanners all around the world. Table 8.7 displays the frequencies of un-tenable MRIs that have been reported in age estimation literature. However, these studies only included participants who volunteered to be scanned. One can as-sume that they tried their best to lie still during the image acquisition. Conversely, in age estimation practice, the examinee might try to frustrate the image by volun-tary motion. This might result either in unusable images or in a faulty assessment of the clavicle’s development. Neverthe-less, the observer needs to decide whether or not the images are of sufficient quality to be of judicial evidence.
However, motion artefacts might be caused by breathing or by the pulsations of the blood vessels near the clavicles, even in resting state scans. Those cannot be distinguished from artefacts caused by small intentional movements. There-fore, the current study aimed to quantify the effect of intentional motion on stage allocation. Results demonstrated that mo-tion artefacts bear the risk of wrongfully assessing the clavicle’s development, re-gardless of the developmental stage. No trend could be demonstrated regarding the direction of this wrong assessment, i.e. no systematic over- or under-staging. Remarkably, development was not signif-icantly more correctly assessed in resting state scans than in motion scans.
Therefore, age estimation based on clavicle MRI might benefit from further reducing motion artefacts. One way to do this, is to decrease acquisition time. Us-ing an open compact 0.3T MRI to apply a 3D coherent gradient-echo sequence, Terada et al. (2016) demonstrated that
compressed sensing with an acceleration factor of 3 rendered the optimal protocol to study hand/wrist development for age estimation [35]. This resulted in an ac-quisition time of 55 seconds instead of 2 minutes 44 seconds. Similarly, Neumay-er et al. (2018) used a 3D FLASH VIBE sequence on 3T MRI to study hand/wrist [23]. They undersampled their data to study acceleration factors between 4 and 20. They suggested that an acceleration factor up to 7.49 was feasible for age es-timation by a radiologist. This corre-sponded with an acquisition time of 15 sec instead of 3 min 46 sec. Automatic age estimation [39] was possible within the range of reported minimum standard errors, based on images with an accelera-tion factor up to 19.58. Both publications suggest that a major reduction in acqui-sition time would be possible to study hand/wrist for age estimation. However, it remains unclear if this could also apply to MRI of other anatomical regions – such as clavicles – to estimate age.
In pulmonary MRI, motion artefacts can be avoided by using either a coached breathing procedure or an active breathing control device in combination with seg-mented k-space acquisition [1]. That way, data acquisition only occurs while breath-ing is suspended. However, this might not be feasible for age estimation practice, since it respectively requires good compliance of the participant and an external device, which adds to the cost of the procedure.
Staging technique
The influence of motion artefacts on stage and status allocation proved to be sim-ilar. Rather than depending on motion artefacts, correctly assessing the clavicle’s
The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation

158
TABLE 8.7 — FREQUENCIES OF MOTION ARTEFACTS AND REPRODUCIBILITY OF ASSESSING CLAVICULAR
DEVELOPMENT BASED ON 3D IMAGING MODALITIES. Note that different stat ist ics have been repor ted to
quantify reproducibi l i ty of staging, and that the number of stages varies between studies.
IMAGING
MODALITY
SUBJECTS REFERENCE UNTENABLE IMAGES
DUE TO MOTION
ARTEFACTS
NUMBER OF
APPLIED
STAGES
MRI Liv ing Hi l lewig et al . 201 1 [ 16] 1 .0% 4
Hi l lewig et al . 2013 [ 17 ] 2 .8% 4
Tangmose et al . 2014 [33] - 4
- 2 (statuses)
Vieth et al . 2014 [42] 5.9% 9
MRI Deceased Tangmose et al . 2013 [32] 4
Tangmose et al . 2014 [33] 4
Schmidt et al . 2016 [28] 9
CT Living Schulze et al . 2006 [30] - 4
Bassed et al . 201 1 [2] - 5
Mi lenkovic et al . 2014 [21 ] - 5
Wittschieber et al . 2014 [43] - 5
- 9
Ekizoglu et al . 2015a [8] - 5
5
Ek izoglu et al . 2015b [7 ] - 6
El Morsi et al . 2015 [9] - 5
Frankl in et al . 2015 [ 1 1 ] - 5
Houper t et al . 2016 [ 18] - 9
Gurses et al . 2016 [ 12] - 9
Gurses et al . 2017 [ 13] - 9
9
Ramadan et al . 2017 [25] - 9
CT Deceased Tangmose et al . 2013 [32] 4
ICC = intra-class correlat ion coeff ic ient ; N = number of par t ic ipants.
development seemed to depend on the staging technique. After all, status allo-cation was more frequently correct than stage allocation. This is in line with status allocation being more frequently consid-ered as an easy process, as opposed to stage allocation. Thus, the interpretation of the clavicle MRI is more difficult when
one needs to allocate a stage than when one only needs to decide if the clavicle is mature. By contrast, Hillewig et al. (2013) demonstrated that stage 1 can be mistak-en for a stage 4 and vice versa [17], a prob-lem which was confirmed in the current study (Figure 8.4) and is not countered by status allocation.
De Tobel J. Multi-factorial forensic age estimation. Chapter 8: 144-162.

159
TABLE 8.7 (CONTINUED)
INTRA-OBSERVER AGREEMENT INTER-OBSERVER AGREEMENT
STATISTIC N STATISTIC N
- - ICC 0.743 - 0.787 121
Cohen’s kappa 0.75 20 Fleiss’ kappa 0.74 - 0.76 220
kappa (prone) 0.675 32 kappa 0.077 - 0. 125 49 - 53
kappa (prone) 0.788 32 kappa 0.040 - 0.446 55
- - - -
Cohen’s kappa 0.685 94 - -
Cohen’s kappa 0.662 47 kappa 0.410 - 0.447 45 - 47
weighted kappa 0.992 80 weighted kappa 0.986 80
- - Cohen’s kappa 0.63 - 0.80 100
kappa 0.866 20 kappa 0.734 20
Cohen’s kappa 0.817 - 0.832 308 Cohen’s kappa 0.678 - 0.708 308
- - Cohen’s kappa 0.494 - 0.674 710
- - Cohen’s kappa 0.470 - 0.605 710
Cohen’s kappa 0.768 503 Cohen’s kappa 0.826 503
weighted kappa 0.928 503 weighted kappa 0.946 503
Cohen’s kappa 0.916 193 Cohen’s kappa 0.868 193
kappa 0.854 kappa 0.753
Cohen’s kappa 0.915 - 0.945 50 Cohen’s kappa 0.889 50
Cohen’s kappa 0.82 319 Cohen’s kappa 0.96 319
kappa 0.857 - 0.887 725 kappa 0.871 725
kappa 0.900 - 0.909 254 kappa 0.890 254
weighted kappa 0.960 - 0.964 254 weighted kappa 0.957 254
Cohen’s kappa 0.901 100 Cohen’s kappa 0.884 601
Cohen’s kappa 0.61 1 94 - -
Reproducibility and imaging technique
The difficult interpretation of the clavicle MRI is reflected by the low reproducibil-ity of the process. Surprisingly, status al-location did not render higher inter- and intra-observer agreements than stage
allocation. By contrast, Tangmose et al. (2014) reported higher values for repro-ducibility statistics when allocating sta-tuses (Table 8.7). Note that the low values of Krippendorff α cannot directly be com-pared with literature, since other statistics were reported. Still, the reproducibility statistics for clavicle assessments dis-
The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation

160
played in Table 8.7 are lower than those for other long bones, with kappa > 0.80 in most studies [5]. Since the clavicles’ de-piction on CT is more clear-cut, relatively higher reproducibility statistics have been reported than with MRI [15]. However, great disparity exists among reported re-producibility statistics. This might indi-cate that the clavicle as a bone is hard to assess, rather than the MRI as an imaging technique being hard to assess.
Strengths, weaknesses and future prospects
With 18 participants, the population in which intentional motion was studied was small. Moreover, a population bias was noted, which might obfuscate the conclu-sions. This might have been caused by the selection of control scans from Hillewig et al. (2013). Since cases were only se-lected when three out of four observers had agreed on the stage, those scans were more likely less affected by artefacts. Still, intentional motion showed the potential to disturb the images without them being considered of insufficient quality to hold as judicial evidence. Consequently, the risk of a wrong assessment of the clavicle’s development was evident. Since inten-tional motion cannot be derived from the image, the only way to detect intentional motion – and to prevent a wrong assess-ment – is to monitor the examinee during the scan. This could simply be done by someone keeping an eye on the examinee at all times during the scan, or by video-taping the examination.
With six observers, this study included a wide variety of observers’ backgrounds, their experience with MRI, and their ex-perience with age estimation. Some ob-
servers were more cautious and decided to discard the images as evidence more often than other observers. This reflects the wide variety of practitioners who are performing age estimation currently [10]. As long as there is no internationally de-fined and accepted approach to estimate age, the inter-observer variety of assess-ments will add dispersion to the already large inter-individual variety of develop-ment. Therefore, in practice, assessments of the clavicle should always be based on a consensus between at least two observ-ers. This is not limited to clavicle MRI, but applies to all imaging techniques and all anatomical structures. Fortunately, a promising step towards a more uniform age estimation process has been made by Stern et al. (2017), introducing fully auto-mated multi-factorial age estimation [31]. In a next step, the value of this approach needs to be explored in validation studies. Moreover, motion artefacts will undoubt-edly have occurred in their sample and it remains unclear how machine learning handled them.
Intentional motion frustrates clavi-cle MRI for age estimation. Still, in case of obvious disturbances, the fo-rensic expert will consider the MRI unsuitable as evidence. Thus, the development of the clavicle as such
and the staging technique seem to play a more important role in a faulty age esti-mation. Although status allocation might be a safer approach then stage allocation, validation studies are needed to verify this statement.
Conclusion
De Tobel J. Multi-factorial forensic age estimation. Chapter 8: 144-162.

161
acknowledgements
We wish to thank all participants and everybody who helped with recruitment. Special thanks to Patrick Davis for his critical appraisal of the manuscript.
references
[1] Arnold JF, Morchel P, Glaser E, Pracht ED, Jakob PM. Lung MRI using an MR-compatible active breathing control (MR-ABC). Magn Reson Med. 2007;58(6):1092-8.
[2] Bassed RB, Drummer OH, Briggs C, Valenzuela A. Age es-timation and the medial clavicular epiphysis: analysis of the age of majority in an Australian population using computed tomography. Forensic Sci Med Pathol. 2011;7(2):148-54.
[3] Baumann P, Widek T, Merkens H, Boldt J, Petrovic A, Ur-schler M, Kirnbauer B, Jakse N, Scheurer E. Dental age es-timation of living persons: Comparison of MRI with OPG. Forensic Sci Int. 2015;253(0):76-80.
[4] De Tobel J, Hillewig E, Bogaert S, Deblaere K, Verstraete K. Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation. Ann Hum Biol. 2017;44(2):130-9.
[5] De Tobel J, Hillewig E, de Haas MB, Van Eeckhout B, Fieuws S, Thevissen P, Verstraete K. Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging tech-nique and age estimation model apply? In progress. 2018.
[6] Dvorak J, George J, Junge A, Hodler J. Age determination by magnetic resonance imaging of the wrist in adolescent male football players. Br J Sports Med. 2007;41(1):45-52.
[7] Ekizoglu O, Hocaoglu E, Inci E, Can IO, Aksoy S, Sayin I. Estimation of forensic age using substages of ossification of the medial clavicle in living individuals. Int J Legal Med. 2015;129(6):1259-64.
[8] Ekizoglu O, Hocaoglu E, Inci E, Sayin I, Solmaz D, Bilgi-li MG, Can IO. Forensic age estimation by the Schmeling method: computed tomography analysis of the medial clav-icular epiphysis. Int J Legal Med. 2015;129(1):203-10.
[9] El Morsi DA, Abo El-Atta HM, ElMaadawy M, Tawfik AM, Batouty NM. Age Estimation from Ossification of the Me-dial Clavicular Epiphysis by Computed Tomography. Int J Morphol. 2015;33(4).
[10] European Asylum Support Office (EASO). Practical Guide on Age Estimation, Second edition. EASO Practical Guides Series. Malta2018.
[11] Franklin D, Flavel A. CT evaluation of timing for ossification of the medial clavicular epiphysis in a contemporary West-ern Australian population. Int J Legal Med. 2015;129(3):583-94.
[12] Gurses MS, Inanir NT, Gokalp G, Fedakar R, Tobcu E, Ocakoglu G. Evaluation of age estimation in forensic med-icine by examination of medial clavicular ossification from thin-slice computed tomography images. Int J Legal Med. 2016;130(5):1343-52.
[13] Gurses MS, Inanir NT, Soylu E, Gokalp G, Kir E, Fedakar R. Evaluation of the ossification of the medial clavicle ac-cording to the Kellinghaus substage system in identifying the 18-year-old age limit in the estimation of forensic age-is it necessary? Int J Legal Med. 2017;131(2):585-92.
[14] Hayes AF, Krippendorfff K. Answering the call for a stand-ard reliability measure for coding data. Communication methods and measures. 2007;1(1):77-89.
[15] Hermetet C, Saint-Martin P, Gambier A, Ribier L, Sautenet B, Rerolle C. Forensic age estimation using computed to-mography of the medial clavicular epiphysis: a systematic review. Int J Legal Med. 2018;132(5):1415-25.
[16] Hillewig E, De Tobel J, Cuche O, Vandemaele P, Piette M, Verstraete K. Magnetic resonance imaging of the medial ex-tremity of the clavicle in forensic bone age determination: a new four-minute approach. Eur Radiol. 2011;21(4):757-67.
[17] Hillewig E, Degroote J, Van der Paelt T, Visscher A, Van-demaele P, Lutin B, D’Hooghe L, Vandriessche V, Piette M, Verstraete K. Magnetic resonance imaging of the sternal extremity of the clavicle in forensic age estimation: towards more sound age estimates. Int J Legal Med. 2013;127(3):677-89.
[18] Houpert T, Rérolle C, Savall F, Telmon N, Saint-Martin P. Is a CT-scan of the medial clavicle epiphysis a good exam to attest to the 18-year threshold in forensic age estimation? Forensic Sci Int. 2016;260:103.e1-.e3.
[19] Jopp E, Schröder I, Maas R, Adam G, Püschel K. Proximal tibial epiphysis in magnetic resonance imaging. Rechts-medizin. 2010;20(6):464-8.
[20] Kellinghaus M, Schulz R, Vieth V, Schmidt S, Pfeiffer H, Schmeling A. Enhanced possibilities to make statements on the ossification status of the medial clavicular epiphysis us-ing an amplified staging scheme in evaluating thin-slice CT scans. Int J Legal Med. 2010;124(4):321-5.
[21] Milenkovic P, Djuric M, Milovanovic P, Djukic K, Zivkovic V, Nikolic S. The role of CT analyses of the sternal end of the clavicle and the first costal cartilage in age estimation. Int J Legal Med. 2014;128(5):825-39.
[22] Netherlands Forensic Institute. [Protocol Age Assessment]. 2014.
[23] Neumayer B, Schloegl M, Payer C, Widek T, Tschauner S, Ehammer T, Stollberger R, Urschler M. Reducing acquisi-tion time for MRI-based forensic age estimation. Sci Rep. 2018;8(1):2063.
[24] Ottow C, Krämer JA, Olze A, Schmidt S, Schulz R, Wittsch-ieber D, Heindel W, Pfeiffer H, Ribbecke S, Vieth V, Schmeling A. Magnetresonanztomographiestudie zur Al-tersschätzung von unbegleiteten minderjährigen Flüchtlin-gen. Rechtsmedizin. 2014;25:12-20.
The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation

162
[25] Ramadan SU, Gurses MS, Inanir NT, Hacifazlioglu C, Feda-kar R, Hizli S. Evaluation of the medial clavicular epiphysis according to the Schmeling and Kellinghaus method in liv-ing individuals: A retrospective CT study. Leg Med (Tokyo). 2017;25:16-22.
[26] Saint-Martin P, Rerolle C, Dedouit F, Bouilleau L, Rousseau H, Rouge D, Telmon N. Age estimation by magnetic reso-nance imaging of the distal tibial epiphysis and the calcane-um. Int J Legal Med. 2013;127(5):1023-30.
[27] Schmeling A, Schulz R, Reisinger W, Muhler M, Wernecke KD, Geserick G. Studies on the time frame for ossification of the medial clavicular epiphyseal cartilage in conventional radiography. Int J Legal Med. 2004;118(1):5-8.
[28] Schmidt S, Henke CA, Wittschieber D, Vieth V, Bajanowski T, Ramsthaler F, Puschel K, Pfeiffer H, Schmeling A, Schulz R. Optimising magnetic resonance imaging-based evalua-tion of the ossification of the medial clavicular epiphysis: a multi-centre study. Int J Legal Med. 2016;130(6):1615-21.
[29] Schmidt S, Ottow C, Pfeiffer H, Heindel W, Vieth V, Schmeling A, Schulz R. Magnetic resonance imag-ing-based evaluation of ossification of the medial clavic-ular epiphysis in forensic age assessment. Int J Legal Med. 2017;131(6):1665-73.
[30] Schulze D, Rother U, Fuhrmann A, Richel S, Faulmann G, Heiland M. Correlation of age and ossification of the medial clavicular epiphysis using computed tomography. Forensic Sci Int. 2006;158(2-3):184-9.
[31] Štern D, Kainz P, Payer C, Urschler M. Multi-Factorial Age Estimation from Skeletal and Dental MRI Volumes. In: International Workshop on Machine Learning in Medical Imaging. Quebec City, Canada: Springer, 2017; p. 61-9.
[32] Tangmose S, Jensen KE, Lynnerup N. Comparative study on developmental stages of the clavicle by postmortem MRI and CT imaging. J Forensic Radiol Imaging. 2013;1(3):102-6.
[33] Tangmose S, Jensen KE, Villa C, Lynnerup N. Forensic age estimation from the clavicle using 1.0T MRI-Preliminary results. Forensic Sci Int. 2014;234:7-12.
[34] Terada Y, Kono S, Tamada D, Uchiumi T, Kose K, Miyagi R, Yamabe E, Yoshioka H. Skeletal age assessment in chil-dren using an open compact MRI system. Magn Reson Med. 2013;69(6):1697-702.
[35] Terada Y, Tamada D, Kose K, Nozaki T, Kaneko Y, Miyagi R, Yoshioka H. Acceleration of skeletal age MR examina-tion using compressed sensing. J Magn Reson Imaging. 2016;44(1):204-11.
[36] Thevissen P, Willems G. [The Triple Test: The K.U.Leu-ven-protocol for age estimation of unaccompanied minor refugees]. In: Aps JKM, Brand HS, Duyck J, van Es RJJ, Jacobs R, Vissink A, eds. Het Tandheelkundig Jaar 2013. Houten: Bohn Stafleu van Loghum, 2013; p. 175-90.
[37] Thevissen PW. Dental age estimation: striving for an opti-mal approach [Doctoral thesis]. Leuven: Leuven University Press, 2013.
[38] Tomei E, Sartori A, Nissman D, Al Ansari N, Battisti S, Rubi-ni A, Stagnitti A, Martino M, Marini M, Barbato E, Semelka RC. Value of MRI of the hand and the wrist in evaluation of bone age: Preliminary results. J Magn Reson Imaging. 2014;39(5):1198-205.
[39] Urschler M, Grassegger S, Stern D. What automated age estimation of hand and wrist MRI data tells us about skeletal maturation in male adolescents. Ann Hum Biol. 2015;42(4):358-67.
[40] Urschler M, Krauskopf A, Widek T, Sorantin E, Ehammer T, Borkenstein M, Yen K, Scheurer E. Applicability of Greu-lich-Pyle and Tanner-Whitehouse grading methods to MRI when assessing hand bone age in forensic age estimation: A pilot study. Forensic Sci Int. 2016;266:281-8.
[41] van Gelderen P, de Zwart JA, Starewicz P, Hinks RS, Duyn JH. Real-time shimming to compensate for respiration-in-duced B0 fluctuations. Magn Reson Med. 2007;57(2):362-8.
[42] Vieth V, Schulz R, Brinkmeier P, Dvorak J, Schmeling A. Age estimation in U-20 football players using 3.0 tesla MRI of the clavicle. Forensic Sci Int. 2014;241c:118-22.
[43] Wittschieber D, Schulz R, Vieth V, Kuppers M, Bajanowski T, Ramsthaler F, Puschel K, Pfeiffer H, Schmidt S, Schmeling A. Influence of the examiner’s qualification and sources of error during stage determination of the medial clavicular ep-iphysis by means of computed tomography. Int J Legal Med. 2014;128(1):183-91.
[44] Wittschieber D, Vieth V, Timme M, Dvorak J, Schmeling A. Magnetic resonance imaging of the iliac crest: age estima-tion in under-20 soccer players. Forensic Sci Med Pathol. 2014;10(2):198-202.
De Tobel J. Multi-factorial forensic age estimation. Chapter 8: 144-162.


164
CHAPTER 9
TH I S CHAPTER ADDRESSED THE FOLLOWING STUDY OB JECT IVES :
Objective 1: To collect a reference dataset of MR images of third molars, left wrist and both clavicles. These images will be registered simultaneously in each participant.
Objective 4: To stage the development of each age predictor based on the MRI. Existing 2D staging techniques will be modified or new methods will be developed. Reproduci-bility of the staging techniques will be tested.
Objective 5: To fit a statistical age estimation model on the reference data set, for each age predictor individually, as well as combining all registered age predictors. In all these models Bayes’ rule will be applied to counter drawbacks of other regression methods.
Objective 6: To validate this model and to compare its performance with existing models.
TH I S CHAPTER WAS SUBM ITTED FOR PUBL ICAT ION AS :
De Tobel J, Hillewig E, van Wijk M, Fieuws S, Thevissen PW, Verstraete KL. Staging cla-vicular development on magnetic resonance imaging: pitfalls and suggestions for age es-timation. J Magn Reson Imaging. Submitted on November 28, 2018 [A1; Journal Impact Factor 2017 3.612; Radiology, Nuclear Medicine & Medical Imaging Q1; Peer reviewed].
This paper has been peer reviewed and a revised version is being prepared for submission.
RESULTS DESCR I BED IN TH I S CHAPTER W ILL BE PRESENTED
AT THE FOLLOWING CONFERENCE :
De Tobel J, Hillewig E, van Wijk M, Fieuws S, Thevissen PW, Verstraete KL. Staging Clavicular Development on Magnetic Resonance Imaging: Pitfalls and Suggestions For Age Estimation. American Academy of Forensic Sciences (AAFS) 71st Annual Scientific Meeting; Baltimore, USA; February 22, 2019.

165
Staging clavicular development on magnetic resonance imaging: pitfalls and
suggestions for age estimation
OR IG INAL RESEARCH
Abstract
Background — Magnetic resonance imaging (MRI) of the clavicle’s sternal end has been studied for age estimation. Several pitfalls have been noted, but how they affect age estimation performance remains unclear. Aim — To elaborate on these pitfalls and to make suggestions for a proper use of clavicle MRI for forensic age estimation. It was hypothesised that age estimation would benefit from (1) discarding stages 1 and 4/5; (2) including profound substages 3aa, 3ab, and 3ac; (3) combining left and right clavicles; and (4) excluding morpholog-ical variants. Study type — Prospective cross-sectional. Population — Healthy Caucasian volunteers between 11 and 26 years old (277 females, 247 males). Field strength/sequence — 3 Tesla, T1-weight-ed gradient echo volumetric interpolated breath-hold examination (VIBE) MR-sequence. Assessment — Two observers applied the most elaborate staging technique for long bone development and docu-mented morphological variants. Statistical tests — Weighted kappa quantified reproducibility of staging. Bayes’ rule was applied for age estimation with a continuation ratio model for the distribution of the stages. According to the hypotheses, different models were tested. Mean absolute error (MAE) differences between models were com-pared, as were MAEs between cases with and without morphological variants. Results — Weighted kappa equalled 0.82 for intra-observer and 0.64 for inter-observer agreement. Stages 1 and 4/5 were allocated interchangeably in 4.4% (19/436). Age increased steadily in profound substages of stage 3, but improvement in age estimation was not sig-nificant. The model that included both clavicles and discarded stages 1 and 4/5 yielded an MAE of 1.97 years, a root mean squared error of 2.60 years, and 69% correctly classified minors. Morphological vari-ants rendered significantly higher MAEs (right 3.84 years, P = 0.015; left 2.93 years, P = 0.022). Data Conclusion — Striving for the safest approach, hypotheses (3) and (4) were confirmed, while hypotheses (1) and (2) remain to be investigated in larger studies.
Key Words
• age determination by skeleton
• clavicle
• adolescent
• adult
• magnetic resonance imaging
AFF IL IAT IONS
1 Department of Diagnostic
Sciences – Radiology, Ghent
University, Belgium
2 Department of Imaging and Pa-
thology – Forensic Odontology,
KU Leuven, Belgium
3 Department of Oral and Maxillo-
facial Surgery, Leuven University
Hospitals,, Belgium
4 Department of Forensic Anthro-
pology, Netherlands Forensic
Institute, The Hague, the Nether-
lands
5 KU Leuven – Leuven University &
Hasselt University, Department
Public Health and Primary Care,
I-BioStat, Leuven, Belgium
Funding for this study was entirely
provided by the Department of
Diagnostic Sciences – Radiology at
Ghent University, and the Department
of Imaging and Pathology – Forensic
Odontology at KU Leuven.
The authors declare that there are
no conflicts of interest.
JANN ICK DE TOBEL 1 2 3 ELKE H I LLEW IG 1
MAYONNE VAN W I J K 4 STEFFEN F I EUWS 5
PATR ICK W. THEV I S SEN 2 KOENRAAD L . VERSTRAETE 1

166
Although magnetic resonance im-aging (MRI) has been studied by several research groups for foren-sic age estimation, it has not found its way to common practice yet. Its major assets are the lack of ionizing
radiation and a 3D depiction of the re-gion of interest. However, MRI also shows drawbacks such as long acquisition times and susceptibility to artefacts. A particu-larly challenging region of interest is the sternal end of the clavicle, which is stud-ied when the age threshold of 18 years is of importance [20]. Few studies have ap-plied MRI of this region in the living [9, 14, 15, 24, 26, 29], which might be due to the prevalence of motion artefacts, im-peding an assessment of development.
Regarding early and late clavicular de-velopment, two pitfalls have been point-ed out in literature. Firstly, Hillewig et al. (2011) highlighted that the physeal scar was hard to discern on MRI, regardless of the applied sequence [14]. This was con-firmed in a larger study sample [15], whilst the physeal scar had not disappeared in any of Schmidt et al’s (2017) participants [24]. The latter was probably due to the younger upper age limit in Schmidt et al. (2017) (24.9 years compared to 26.9 in [15]). Secondly, in ten out of 220 partici-pants in Hillewig et al. (2013), the sternal end was judged to be fully mature, while the participants were relatively young and showed a partially open distal physis on radius MRI. The authors concluded that the fully mature stage was wrongfully al-located, and that in fact, the earliest stage should have been allocated, in which the epiphysis has not started mineralisation yet. They corrected their data according-ly, but still one case remained of a girl (18.1 years old) with a fully mature radius
and possibly a clavicle that was wrongly judged to be mature [15]. By contrast, this problem was not encountered by Schmidt et al. (2017). They stated that discerning early from late clavicular development should be based solely on the sternal end’s morphology, not on the hand/wrist status [24].
Regarding physeal bridging, substag-es proved to be useful in determining whether or not the age thresholds of 18 and 21 years old had been reached [24, 29]. However, none of these studies re-ported the corresponding probabilities to have reached those age thresholds associ-ated with the different substages. A final pitfall is the variability in morphology of the clavicle’s sternal end. A deviation from a straight, or slightly concave or convex shape can be considered a variant. Since these variants might develop in an aber-rant way, they are mostly excluded for age estimation.
The current study aims to elaborate on these pitfalls and to make suggestions for a proper use of clavicle MRI in this field. It was hypothesised that age estimation per-formance would increase by (1) discard-ing stages 1 and 4/5; (2) including sub-stages 3aa, 3ab, and 3ac; (3) combining left and right clavicles; and (4) excluding morphological variants.
Study population
Healthy Belgian and Dutch Cauca-sian volunteers between 11 and 26 years old were prospectively includ-ed between March 2012 and May 2017, rendering 298 participants (158 females, 140 males, Table 9.1). Part of this population was included
Introduction
Materials and M
ethods
De Tobel J. Multi-factorial forensic age estimation. Chapter 9: 164-184.

167
in earlier studies [5-8, 14, 15]. Recreation-al athletes were excluded if they practiced a sport in which the shoulder was unilat-erally more loaded (e.g. javelin-throwing, shot-put).
Additionally, the study population of Hillewig et al. (2013) was included. Although they only included 220 par-ticipants in their paper, more scans were available from participants between 11 and 30 years old, rendering a total of 226 participants (119 females, 107 males). Therefore, the current study population comprised 524 participants (277 females, 247 males). Every one of them granted informed consent, and in case of minors also the parents. The study was approved by the Ghent University hospital ethics committee.
Image acquisition
According to the Hillewig et al. (2011) protocol 3T MRI of the sternal ends of both clavicles was conducted in prone position with a Siemens Magnetom Trio Tim scanner (Siemens, Erlangen, Ger-many) and a surface loop coil [14]. Since Hillewig et al. (2013) demonstrated that the physeal scar was hard to discern, even on a dedicated T1 fast spin echo sequence, only their T1 gradient echo volumetric interpolated breath-hold examination (VIBE) sequence was applied (TR 10.00 ms, TE 2.92 ms, flip angle 20°, water ex-citation, voxel size 0.7 × 0.7 × 0.9 mm³, acquisition time 4:02 min) [15].
Image analysis
After anonymising the images, two ob-servers assessed them independently and blinded for the age of the participants.
The first observer (JDT) had 8 years of ex-perience with MRI for age estimation. He assessed the total study population a first time, and additionally assessed a random selection of 110 participants a second time, after a two week interval. The sec-ond observer (MvW) had 1 year of expe-rience with MRI for age estimation. She only assessed the new prospective group once.
Using radiological monitors with res-olutions of 3280 × 2048 pixels (MDCC-6130, Barco, Kortrijk, Belgium) or 1280 × 1024 pixels (MFCD 1219, Barco, Den Haag, The Netherlands) both observ-ers considered the whole stack of slices to allocate developmental stages to both clavicles. They applied the most elaborate staging technique that is currently availa-ble for long bone development (Table 9.2, Figures 9.1 and 9.2), which was designed based on CT studies. This technique was composed of five main stages (1 to 5) [21], some of which were further split up into substages (a to c) [17], and even profound substaging for one substage (aa to ac) [30]. When deciding between stages 2 and 3 (including substages), stage 3 was allo-cated as soon as a bone bridge was visible on any image. However, stage 3 was only allocated (instead of stage 2) if the bone bridge(s) were of similar signal intensity as the epiphysis. If the epiphysis was still completely surrounded by a line of higher signal intensity, stage 2 was allocated (ben-efit of the doubt). No actual measurements of dimensions were made. Instead, dimen-sions were estimated by scrolling through the sequence. When two separate ossifying epiphyseal islands were present, their com-bined dimensions were considered.
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

168
FIGURE 9. 1 — REPRESENTATIVE EXAMPLES OF CLAVICLES IN CONSECUTIVE DEVELOPMENTAL STAGES. De-
scr ipt ive cr iter ia for the stages are included in Table 9.2 . In the pathway each clavic le fol lows, each row
is compulsory, but columns might be sk ipped. For example, the fol lowing sequence of stages is possible :
1 – 2a – 2b – 3ab – 3b – 3c – 4.
Note the irregular border of stage 1 , as compared to the smooth border in stages 4 and 5. In profound
substages of stage 3a, white arrows indicate the few bone bridges. In stage 4, white arrowheads indicate
the physeal scar.
De Tobel J. Multi-factorial forensic age estimation. Chapter 9: 164-184.

169
TAB
LE
9.1
— N
UM
BER
OF
PA
RT
ICIP
AN
TS P
ER
AG
E P
ER
SEX
, A
ND
IN
BO
TH
GRO
UPS O
F T
HE S
TU
DY
PO
PU
LA
TIO
N.
Pa
rtic
ipa
nts
wit
h n
o a
sse
ssa
ble
cla
vic
le w
ere
dis
pla
yed
sep
ara
tely
.
AT L
EA
ST O
NE
ASSE
SSA
BL
E C
LA
VIC
LE
NO
ASSE
SSA
BL
E C
LA
VIC
LE
NEW
PRO
SPEC
TIV
E G
RO
UP
HIL
LEW
IG E
T A
L.
(20
13)
TO
TAL
TO
TAL
Ag
e (
y)Fe
ma
leM
ale
Su
bto
tal
Fe
ma
leM
ale
Su
bto
tal
Fe
ma
leM
ale
Tota
lFe
ma
leM
ale
Tota
l
11-1
31
01
00
01
01
11
2
149
716
10
110
717
24
6
1511
819
10
112
820
02
2
1610
1020
109
1920
193
90
00
1711
102
110
1020
21
20
41
00
0
1813
102
310
919
23
194
20
00
1915
132
810
919
25
22
47
01
1
20
1810
28
87
152
617
43
10
1
21
1210
22
105
152
215
37
00
0
22
1110
21
99
1820
193
92
02
23
1110
21
1210
22
23
20
43
00
0
24
1111
22
1110
21
22
21
43
00
0
25
1112
23
811
1919
23
42
20
2
26
1012
22
109
1920
21
41
01
1
27
00
01
23
12
30
00
28
00
02
35
23
50
00
29
00
00
11
01
10
00
30
00
02
13
21
30
00
TO
TAL
154
133
28
711
510
52
20
26
92
38
50
78
917
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

170
a Stage 2b was al located, although stage 3ab seems apparent . Zooming in al lowed detect ing a
continuous hyperintense l ine representing the physeal plate. Although the hypointense cor t ices of
the epiphysis and the metaphysis approached each other, they did not form an uninterrupted bone
bridge yet (black/white arrow).
b Stage 3ac was al located, although the bone bridges are hypointense compared to the epiphysis
(white arrows). St i l l , the bridges c learly interrupted the physeal plate and were of s imi lar intensity
as the metaphysis’ cor tex.
c Stage 4 with a more intense appearance of the bone marrow than was shown in Figure 9. 1 . White
arrowheads indicate the physeal scar.
d Stage 2c with trabecular bone mimick ing the physeal scar (white arrowheads).
FIGURE 9.2 — CLARIFICATION EXAMPLES OF STAGING.
Furthermore, morphological variance was documented and it was indicated if it impeded stage allocation. Finally, when images were deemed of insufficient quali-ty for assessment, these were documented and the reason(s) stated.
Statistical analysis
All analyses were conducted with SPSS Statistics 25.0 (IBM SPSS Statistics for Windows, Armonk, New York, USA) and SAS 9.4 (SAS Institute, Cary NC, USA). Statistical tests were performed two-sided with the significance level equal to 0.05.Reproducibility of staging was assessed by weighted kappa statistics and tests for symmetry (extension of the McNemar test). Additionally, cross tables were gen-erated to provide detailed information on staging results.
Results of observer 1 were used for age estimation, based on the application of
Bayes’ rule with a continuation ratio mod-el for the distribution of the stages [2, 13]. To handle overfitting, ten-fold cross-val-idation was used. Moreover, participants with a morphological variant were ex-cluded to develop the age estimation model. According to the four hypotheses, models were created, with an additional model to test the effect of merging stages 4 and 5. Thus, five approaches were tested: (1) using the original staging; (2) merg-ing substages 3aa, 3ab, and 3ac into one stage 3a; (3) merging stages 4 and 5; (4) discarding stages 1 and 4/5; and (5) com-bining left and right clavicles.
Unless otherwise stated, combined results of both sexes were reported re-garding age estimation performance of the models, since sex-specific results were similar. Two groups of age estimation outcome measures were studied: point prediction of age and the ability to dis-cern minors from adults. Regarding point
De Tobel J. Multi-factorial forensic age estimation. Chapter 9: 164-184.
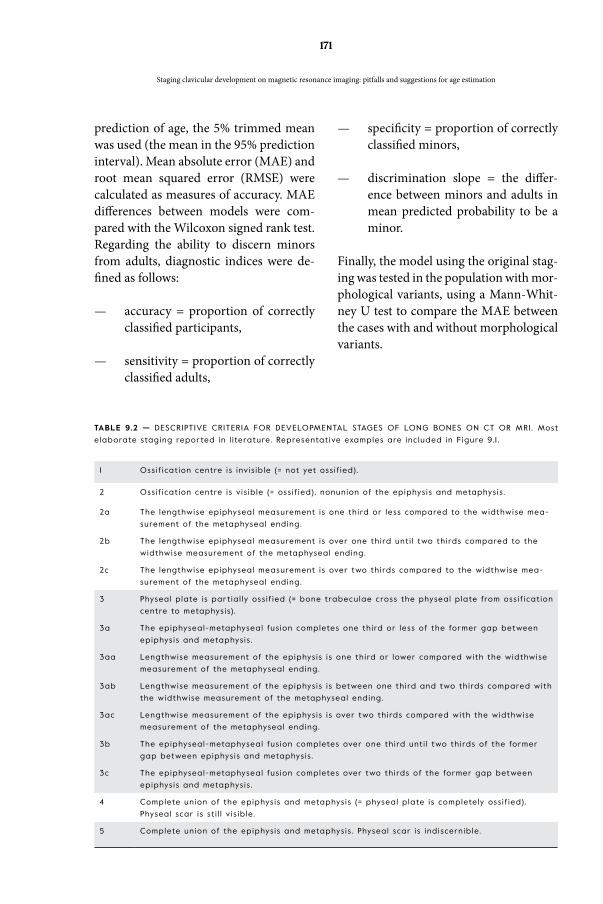
171
TABLE 9.2 — DESCRIPTIVE CRITERIA FOR DEVELOPMENTAL STAGES OF LONG BONES ON CT OR MRI . Most
elaborate staging repor ted in l i terature. Representative examples are included in Figure 9. 1 .
1 Oss if icat ion centre is invis ib le (= not yet oss if ied).
2 Ossif icat ion centre is v is ib le (= oss if ied), nonunion of the epiphysis and metaphysis .
2a The lengthwise epiphyseal measurement is one third or less compared to the widthwise mea-
surement of the metaphyseal ending.
2b The lengthwise epiphyseal measurement is over one third unt i l two thirds compared to the
widthwise measurement of the metaphyseal ending.
2c The lengthwise epiphyseal measurement is over two thirds compared to the widthwise mea-
surement of the metaphyseal ending.
3 Physeal plate is par t ial ly oss if ied (= bone trabeculae cross the physeal plate from ossif icat ion
centre to metaphysis).
3a The epiphyseal-metaphyseal fus ion completes one third or less of the former gap between
epiphysis and metaphysis .
3aa Lengthwise measurement of the epiphysis is one third or lower compared with the widthwise
measurement of the metaphyseal ending.
3ab Lengthwise measurement of the epiphysis is between one third and two thirds compared with
the widthwise measurement of the metaphyseal ending.
3ac Lengthwise measurement of the epiphysis is over two thirds compared with the widthwise
measurement of the metaphyseal ending.
3b The epiphyseal-metaphyseal fus ion completes over one third unt i l two thirds of the former
gap between epiphysis and metaphysis .
3c The epiphyseal-metaphyseal fus ion completes over two thirds of the former gap between
epiphysis and metaphysis .
4 Complete union of the epiphysis and metaphysis (= physeal plate is completely oss if ied).
Physeal scar is st i l l v is ib le.
5 Complete union of the epiphysis and metaphysis . Physeal scar is indiscernible.
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation
prediction of age, the 5% trimmed mean was used (the mean in the 95% prediction interval). Mean absolute error (MAE) and root mean squared error (RMSE) were calculated as measures of accuracy. MAE differences between models were com-pared with the Wilcoxon signed rank test. Regarding the ability to discern minors from adults, diagnostic indices were de-fined as follows:
— accuracy = proportion of correctly classified participants,
— sensitivity = proportion of correctly classified adults,
— specificity = proportion of correctly classified minors,
— discrimination slope = the differ-ence between minors and adults in mean predicted probability to be a minor.
Finally, the model using the original stag-ing was tested in the population with mor-phological variants, using a Mann-Whit-ney U test to compare the MAE between the cases with and without morphological variants.

172
In the prospective group, 20 partic-ipants needed a rescan because the first scan was of insufficient quality. In three female participants, the rescan
was conducted in supine position with fix-ation of the coil, because in prone position, the distance between the coil and the clavi-cles was too large due to body morphology.
Descriptive results
Early and late development
The age distributions within stage 1 on the one hand and stages 4/5 on the other demonstrated two facts (Figure 9.3, Table 9.3). Firstly, the age distribution within stage 4 did not differ from that within stage 5. Secondly, the outliers of the age distributions in stage 1, as well as in stages 4 and 5, suggested that these stages were allocated interchangeably. This was con-firmed by the cross tabulation in Table 9.4, and illustrated in Figure 9.4. Con-
sidering all clavicles that had received a stage by both observers, stages 1 and 4/5 were allocated interchangeably in 4.4% (19/436). Note that trabecular bone might mimic the physeal scar in stages 2 and 3, which implies that it is an unreliable char-acteristic to discern stage 1 from stage 4 (Figure 9.2d). Furthermore, stages 1 and 3c were allocated interchangeably in 1.8% (8/436; Figure 9.4d).
Substages of epiphyseal growth and physeal bridging
The age did not seem to increase from stage 2a to 2b (Figure 9.3, Table 9.3). Moreover, frequencies within substages of stage 2 decreased from low to high sub-stages. By contrast, substages of stage 3 were encountered in a sufficient number of participants, including profound sub-stages of stage 3a. Figure 9.3 shows an in-creasing age from low to high (profound) substages.
FIGURE 9.3 — AGE DISTRIBUTIONS PER
STAGE PER SEX. Note the older age
out l iers in stage 1 , and the younger
age out l iers in stages 4 and 5. The
horizontal reference l ine indicates
the age of 18.
Results
De Tobel J. Multi-factorial forensic age estimation. Chapter 9: 164-184.

173TA
BL
E 9
.3 —
DESC
RIP
TIV
E S
TAT
IST
ICS O
F T
HE A
GE D
IST
RIB
UT
ION
S P
ER
STA
GE P
ER
SID
E.
Mo
rph
olo
gic
al
va
ria
nts
we
re e
xclu
de
d.
STA
GE
12
A2
B2
C3A
A3A
B3A
C3
B3
C4
5
RIG
HT
FEM
AL
ES
N13
187
12
14
52
819
49
37
20
Me
an
15.7
918
.13
17.5
520
.41
18.0
319
.25
20
.64
20
.32
23.1
22
4.6
72
3.4
9
Me
dia
n15
.35
17.8
616
.76
20
.41
17.8
819
.23
19.7
020
.53
23.0
32
4.8
02
5.1
4
Min
imu
m14
.06
15.3
915
.40
20
.41
14.2
715
.27
16.0
016
.89
16.0
215
.37
11.9
3
Ma
xim
um
21.0
72
3.4
72
1.6
520
.41
22
.64
24
.25
26
.19
23.2
82
8.6
33
0.5
23
0.0
5
P2
514
.72
16.3
415
.53
20
.41
16.5
917
.90
18.9
018
.74
21.
75
23.8
52
3.4
1
P75
16.0
018
.96
19.5
120
.41
19.1
920
.36
22
.23
21.
53
24
.68
26
.28
25.5
3
MA
LES
N2
29
30
33
21
316
32
39
15
Me
an
17.7
518
.13
18.6
8-
19.0
019
.72
20
.37
21.3
72
3.4
02
4.4
92
3.5
8
Me
dia
n16
.30
17.4
518
.23
-19
.02
19.3
619
.52
21.
23
23.9
72
4.9
32
5.1
3
Min
imu
m14
.08
15.7
917
.03
-15
.11
16.5
718
.95
18.8
217
.05
14.1
115
.41
Ma
xim
um
26
.09
22
.82
20
.77
-2
6.8
32
3.0
82
2.6
52
4.3
12
9.6
13
0.0
52
8.7
1
P2
515
.01
16.2
217
.03
-17
.23
18.5
718
.95
20
.10
21.
79
23.2
72
2.4
3
P75
19.4
219
.12
20
.77
-20
.65
20
.82
22
.65
22
.23
25.3
92
6.4
92
6.0
2
LE
FT
FEM
AL
ES
N7
23
132
65
12
32
64
94
816
Me
an
16.2
117
.34
17.7
318
.38
17.7
718
.98
19.8
42
1.8
32
3.0
12
4.2
32
4.0
5
Me
dia
n15
.54
17.3
716
.76
18.3
816
.95
18.7
319
.50
21.0
92
2.8
62
4.7
52
5.0
7
Min
imu
m14
.06
14.6
415
.40
16.8
614
.27
15.2
717
.04
16.9
819
.71
14.3
911
.93
Ma
xim
um
23.0
62
3.4
72
1.9
319
.91
22
.64
23.6
42
3.9
02
6.2
02
8.6
33
0.5
22
6.8
3
P2
514
.35
15.3
916
.00
16.8
615
.45
17.8
718
.46
20
.04
21.3
52
3.2
12
3.8
9
P75
16.2
618
.10
19.5
119
.91
20
.37
20
.05
20
.53
24
.25
24
.34
25.8
32
6.3
4
MA
LES
N13
24
40
162
77
20
38
31
19
Me
an
16.1
617
.90
17.7
4-
19.6
719
.69
20
.70
20
.96
23.7
62
4.3
72
4.5
7
Me
dia
n15
.64
17.3
017
.63
-19
.41
19.4
62
1.2
92
1.13
24
.20
25.1
72
4.9
3
Min
imu
m14
.08
14.4
416
.57
-15
.41
16.2
616
.94
18.3
717
.05
14.1
116
.09
Ma
xim
um
22
.51
24
.44
19.1
2-
24
.47
24
.31
23.4
52
4.4
83
0.0
52
7.72
28.7
7
P2
514
.65
16.3
316
.80
-17
.47
18.6
718
.95
19.7
92
1.8
72
3.1
32
3.7
8
P75
16.7
019
.34
18.6
8-
21.8
220
.77
22
.65
21.8
52
5.6
92
6.3
42
6.4
9
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

174
FIGURE 9.4 — CASES OF EARLY AND LATE DEVELOPMENT THAT WERE CONFUSED BY THE OBSERVERS.
a Stages 1 and 5 were al located. The gir l ’s age was 1 1 .9 years old.
b Stages 1 and 4 were al located. The man’s age was 22.5 years old. White arrowheads indicate what
was interpreted by one observer as a physeal scar.
c Stages 1 and 5 were al located. The man’s age was 25.2 years old.
d Stages 1 and 3c were al located. The man’s age was 26.9 years old. A white arrow indicates what
was interpreted as a remnant of the physeal scar by one observer. Conversely, the other observer
interpreted this as an MRI ar tefact that blurred the cor t ical l in ing.
a F ish mouth morphological variant that did not impede staging. Stage 2a was al located.
b F ish mouth morphological variant that did not impede staging. Stage 3ab was al located.
c F ish mouth morphological variant that did not impede staging. Stage 3b was al located.
d Tr ident morphological variant that impeded staging.
e F ish mouth morphological variant that impeded staging. Note the unclear aspect at the centre of
the sternal end.
f Wrench/bowl morphological variant that impeded staging. Note the hypointense cor tex cranial ly
and caudal ly compared to the centre.
g Hypoplast ic sternal end that impeded staging.
h Hypoplast ic caudal end with irregular border that impeded staging.
FIGURE 9.5 — MORPHOLOGICAL VARIANTS OF THE CLAVICLE’S STERNAL END.
De Tobel J. Multi-factorial forensic age estimation. Chapter 9: 164-184.

175
TABLE 9.4 — CROSS TABULATION OF FREQUENCIES OF ALLOCATED STAGES PER OBSERVER. Left and r ight
were considered joint ly, and clavic les were only inc luded if they had received a stage by both observers.
CURRENT STUDY OBSERVER 2 STAGE TOTAL
1 2a 2b 2c 3aa 3ab 3ac 3b 3c 4 5
OBSERVER 1
STAGE
1 22 0 0 0 1 0 0 0 0 2 1 26
2a 10 21 2 0 4 4 1 0 2 0 0 44
2b 0 2 0 0 1 12 0 0 0 0 0 15
2c 0 0 0 0 0 1 2 0 0 0 0 3
3aa 3 1 2 0 7 18 1 0 3 1 1 37
3ab 0 1 3 0 2 32 15 8 1 0 0 62
3ac 0 0 0 0 1 5 26 3 1 0 0 36
3b 0 0 0 0 0 1 1 13 19 2 0 36
3c 2 0 0 0 0 0 0 4 67 3 0 76
4 10 0 0 0 0 0 0 0 23 35 4 72
5 6 0 0 0 0 0 0 0 5 17 1 29
TOTAL 53 25 7 0 16 73 46 28 121 60 7 436
Light ly shaded cel ls indicate agreement between observers. Dark ly shaded cel ls indicate interchanged
early and late development .
TABLE 9.5 — FREQUENCIES OF FACTORS THAT IMPEDE STAGING (UPPER PANEL) AND FREQUENCIES OF ASSESS-
ABLE MORPHOLOGICAL VARIANTS (LOWER PANEL), PER OBSERVER.
OBSERVER 1 (N = 1048) OBSERVER 2 (N = 596)
Not assessable RIGHT LEFT TOTAL RIGHT LEFT TOTAL
Poor coi l posit ioning ( in coronal plane, e.g. too
high, too far r ight)4 0 4 0 0 0
Poor image qual ity (e.g. poor s ignal- to-noise
rat io)6 3 9 12 12 24
Artefacts due to motion of the par t ic ipant 14 12 26 57 57 1 14
Uncer tain f issure caudal ly 1 0 1 0 0 0
Insuff ic ient contrast between clavic le and sur-
rounding t issues1 0 1 2 1 3
Morphological variant
Fish mouth 5 7 12 2 2 4
Hypoplast ic sternal end 0 1 1 1 0 1
Tr ident 0 1 1 0 0 0
Wrench/bowl 4 2 6 5 6 1 1
Undefined 0 0 0 1 3 4
TOTAL 35 26 61 80 81 161
Assessable morphological variant
Fish mouth 13 21 34 6 5 1 1
Tr iangular indentation 1 2 3 0 0 0
Trident 1 1 2 0 0 0
Wrench/bowl 3 3 6 6 9 15
Undefined 0 0 0 1 0 1
TOTAL 18 27 45 13 14 27
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

176
Statistical analyses
Reproducibility
The two observers demonstrated a differ-ent attitude towards assessing the images. Overall, the first observer was bolder than the second one, with 5.8% (61/1048) and 27% (161/596) of all clavicles judged to be unsuitable for assessment, respectively
(Table 9.5). Motion artefacts, poor image quality and morphological variants often impeded the assessments. Nonetheless, staging morphological variants was more often possible than impossible (Figure 9.5, Table 9.5). Furthermore, clavicles were more frequently unsuitable for as-sessment in the youngest age categories (Table 9.1).
TABLE 9.6 —AGE ESTIMATION PERFORMANCE OF DIFFERENT APPROACHES.
SIDE MODIFIED
STAGING
ACCURACY OF
POINT PREDIC-
TION
DISCERNING MINORS FROM ADULTS
MAE
(Y)
RMSE
(Y)
ACCURACY
(95%CI)
SENSITIVITY
(95%CI)
SPECIFICITY
(95%CI)
DISCRIMI-
NATION
SLOPE
RIGHT None † 2.06 2.81 80.9 (77.0;84.5) 86. 1
(82.0;89.6)
64.2
(54.3 ;73.2)
0.363
Merge
stage 3a
† 2.04 2.83 82.0 (78.2 ;85.5) 93.0
(89.8 ;95.5)
46.2
(36.5 ;56.2)
0.316
Merge
stages 4
and 5
† 2.05 2.81 80.9 (77.0;84.5) 86. 1
(82.0;89.6)
64.2
(54.3 ;73.2)
0.363
Discard 1
and 4/5
‡ 2.05 2.67 77.4 (72.3 ;82.0) 82. 1
(76.5 ;86.7)
62.0
(49.7;73.2)
0.327
LEFT None † 1 .98 2.72 82.5 (78.7;85.9) 84.9
(80.7;88.4)
74.5
(65. 1 ;82.5)
0.433
Merge
stage 3a
† 1 .98 2.72 85.7 (82.2 ;88.8) 93.6
(90.5;95.9)
59.4
(49.5 ;68.9)
0.418
Merge
stages 4
and 5
† 1 .98 2.71
82.5 (78.7;85.9)84.9
(80.7;88.4)
74.5
(65. 1 ;82.5)0.433
Discard 1
and 4/5
‡ 1 .98 2.60 83.9 (79.5 ;87.7) 90.4
(86.0;93.7)
63.8
(52.2 ;74.2)
0.406
RIGHT
+ LEFT
None † 1 .93 2.70 83.9 (80.2;87. 1 ) 87.2
(83.2 ;90.4)
72.9
(63.4 ;81 .0)
0.445
Discard 1
and 4/5
§ 1 .97 2.60 82. 1 (77.6;85.9) 86. 1
(8 1 .3 ;90.0)
69.4
(58.5 ;79.0)
0.395
CI = conf idence interval ; MAE = mean absolute error ; N = total number of par t ic ipants in relevant stages;
RMSE = root mean squared error : y = years.
† The whole study populat ion was included for analyses. ‡ Par t ic ipants whose clavic le was in stage 1 or
4/5 were excluded. § Par t ic ipants whose both c lavic les were in stage 1 or 4/5 were excluded.
De Tobel J. Multi-factorial forensic age estimation. Chapter 9: 164-184.

177
Considering the clavicles that received a stage from both observers, large discrep-ancies were encountered between them (Table 9.4). Still, one-stage differences were the most frequent. Weighted kap-pa equalled 0.82 (95% confidence inter-val (CI) [0.77 – 0.87]) for intra-observer agreement, whereas it was 0.64 (95% CI [0.58 – 0.70]) for inter-observer agree-ment. Statistically significant asymmetry in stage allocation was noted (P = 0.0005), with observer 1 systematically allocat-ing lower stages. Similar reproducibility statistics were obtained when discarding stages 1 and 4/5 (weighted kappa 0.77 for intra-, and 0.67 for inter-observer).
Models for age estimation
Morphological variants were seen uni-laterally in 27 participants and bilaterally in 18, leaving 479 participants to develop the age estimation models. Applying these models, age estimation performance of five approaches was compared.
A first approach used the original staging technique. Due to the relatively low fre-quencies in certain substages of stage 2, these substages were not included in the models. Instead, stage 2 was included as one stage.
The second and third approaches merged stages. Regarding the point pre-diction of age, merging stages 3aa, 3ab and 3ac into stage 3a did not decrease the accuracy of point predictions (Tables 9.6 and 9.7). Neither did merging stages 4 and 5, since although the difference in MAE was statistically significant, a difference of 0.02 years was clinically irrelevant (Table 9.7). Regarding the ability to discern mi-nors from adults, merging stage 3a con-siderably decreased specificity (Table 9.6), which needs to be avoided in forensic age estimation. By contrast, merging stages 4 and 5 did not affect specificity.
The fourth approach discarded stages 1 and 4/5. One was mistaken for another
TABLE 9.7 — EfFECT OF MODIFIED STAGING ON AGE ESTIMATION ACCURACY. ONLY CASES WITHIN THE STUD-
IED STAGES WERE INCLUDED FOR ANALYSES.
SIDE MODIFIED
STAGING
ACCURACY OF POINT PREDICTION
N MAE
reference (y) #
MAE
modif icat ion (y)
P-value MAE
difference *
RIGHT Merge stage
3a
151 1 .85 1 .8 1 0.596
Merge stages 4
and 5
1 1 1 2 .37 2.33 0.303
LEFT Merge stage
3a
130 1 .7 1 1 .7 1 0.313
Merge stages 4
and 5
1 14 2.24 2.22 0.034
MAE = mean absolute error ; N = total number of par t ic ipants in relevant stages; y = years. # Reference
for comparison is the original equivalent without modif icat ion. * P-value from Wilcoxon s igned rank test
comparing MAE.
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation
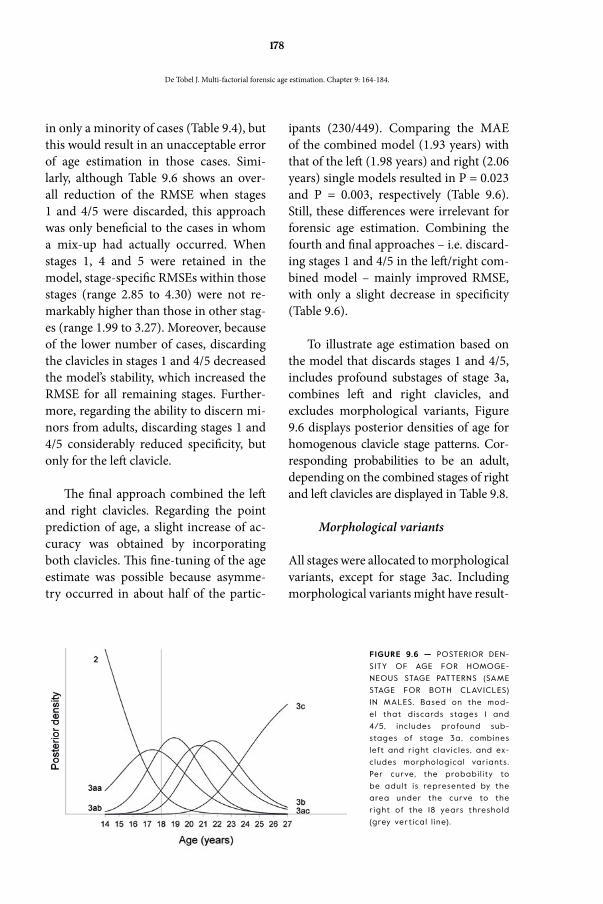
178
in only a minority of cases (Table 9.4), but this would result in an unacceptable error of age estimation in those cases. Simi-larly, although Table 9.6 shows an over-all reduction of the RMSE when stages 1 and 4/5 were discarded, this approach was only beneficial to the cases in whom a mix-up had actually occurred. When stages 1, 4 and 5 were retained in the model, stage-specific RMSEs within those stages (range 2.85 to 4.30) were not re-markably higher than those in other stag-es (range 1.99 to 3.27). Moreover, because of the lower number of cases, discarding the clavicles in stages 1 and 4/5 decreased the model’s stability, which increased the RMSE for all remaining stages. Further-more, regarding the ability to discern mi-nors from adults, discarding stages 1 and 4/5 considerably reduced specificity, but only for the left clavicle.
The final approach combined the left and right clavicles. Regarding the point prediction of age, a slight increase of ac-curacy was obtained by incorporating both clavicles. This fine-tuning of the age estimate was possible because asymme-try occurred in about half of the partic-
ipants (230/449). Comparing the MAE of the combined model (1.93 years) with that of the left (1.98 years) and right (2.06 years) single models resulted in P = 0.023 and P = 0.003, respectively (Table 9.6). Still, these differences were irrelevant for forensic age estimation. Combining the fourth and final approaches – i.e. discard-ing stages 1 and 4/5 in the left/right com-bined model – mainly improved RMSE, with only a slight decrease in specificity (Table 9.6).
To illustrate age estimation based on the model that discards stages 1 and 4/5, includes profound substages of stage 3a, combines left and right clavicles, and excludes morphological variants, Figure 9.6 displays posterior densities of age for homogenous clavicle stage patterns. Cor-responding probabilities to be an adult, depending on the combined stages of right and left clavicles are displayed in Table 9.8.
Morphological variants
All stages were allocated to morphological variants, except for stage 3ac. Including morphological variants might have result-
FIGURE 9.6 — POSTERIOR DEN-
SITY OF AGE FOR HOMOGE-
NEOUS STAGE PATTERNS (SAME
STAGE FOR BOTH CLAVICLES)
IN MALES. Based on the mod-
el that discards stages 1 and
4/5, inc ludes profound sub-
stages of stage 3a, combines
left and r ight c lavic les, and ex-
cludes morphological variants.
Per curve, the probabi l i ty to
be adult is represented by the
area under the curve to the
r ight of the 18 years threshold
(grey ver t ical l ine).
De Tobel J. Multi-factorial forensic age estimation. Chapter 9: 164-184.

179
Discussion
ed in unacceptable errors in age estima-tion. Indeed, applying the original model to the cases with morphological variants resulted in significantly higher MAEs (right 3.84 years, P = 0.015; left 2.93 years, P = 0.022). Note, however, that this com-parison was based on all stages aggregated and might thus be biased by a difference in distribution of the stages between cases with and without morphological variants.
Suggestions for age estimation practice
Taking all the reported considera-tions into account, several sugges-
tions can be made for an appropriate age estimation based on MRI of the clavicles’ sternal ends. Firstly, the authors suggest discarding stages 1 and 4/5, because con-fusing them would result in an unaccept-able error. Secondly, both clavicles should be incorporated, to avoid a decrease of specificity and because morphological variance might occur unilaterally. Third-ly, morphological variants should be dis-carded for age estimation. Additionally, including profound substaging of stage 3a might allow to fine-tune the age estima-tion and increase the proportion of cor-rectly classified minors. Note that regard-ing substages of stage 2, no suggestions for further refinement could be made because of the low frequencies in those substages.
Early and late development
The current findings confirmed the possi-ble mix-up of stage 1 and stages 4 and 5, which caused a modest increase in RMSE. Since RMSE highly weights large errors, it seems logical that discarding the con-fused stages of early and late development
rendered a better performance. When merely considering MAE, one could over-look this effect. Although only a minority of cases benefitted from discarding stages 1 and 4/5, it seems safer not to estimate age based on early and late clavicle de-velopment than to risk such a large er-ror. The mix-up has been noted before by Hillewig et al. (2013), because of the rela-tively young minimum age in their final stage [15]. To solve this, they suggested combining the clavicle information with wrist information. If the physeal plate of the distal radius is not observed to be fully bridged, this would suggest that a clavicle stage 1 would be appropriate, and not a
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation
TABLE 9.8 — PROBABILITIES OF BEING AN ADULT
FOR DIFFERENT PATTERNS OF RIGHT AND LEFT
CLAVICLE STAGES PER SEX.
CLAVICLE STAGE P ≥ 18 Y
RIGHT LEFT FEMALE MALE
- 3ac 0.785 0.797
- 3c 0.977 0.979
3ab 3ab 0.540 0.562
3ab 3ac 0.757 0.765
3ab 3b 0.917 0.921
3ab 3c 0.959 0.962
3ac 3ab 0.713 0.725
3ac 3ac 0.866 0.871
3ac 3b 0.963 0.965
3ac 3c 0.984 0.985
3b - 0.800 0.814
3b 3ab 0.736 0.745
3b 3ac 0.870 0.875
3b 3b 0.959 0.961
3b 3c 0.980 0.982
3c - 0.972 0.975
3c 3ab 0.929 0.932
3c 3ac 0.971 0.973
3c 3b 0.994 0.995
3c 3c 0.998 0.998

180
stage 4 or 5. However, when bridging in the radius is complete, it remains unclear whether the clavicle is in early or late de-velopment. Thus, more research is needed to verify how information from other age indicators could correct potentially con-fused clavicle stages. Furthermore, the mix-up of early and late development also occurred in a study focusing on motion artefacts in clavicle MRI [9]. Although the authors reported a case in which the mix-up was annulled by applying a different staging technique, that technique – which only distinguishes immature form mature – still bears the risk of mixing up a ful-ly immature clavicle with a fully mature one. Therefore, discarding stages 1 and 4/5 seems the safest approach in age es-timation.
Discarding stages 1 and 4/5 also elim-inates the issue of whether stages 4 and 5 should be merged or not. The value of the physeal scar for age estimation has always been doubted, in studies on the clavicle [15, 26], as well as in studies on other long bones [3, 4, 12]. Correspondingly, the current findings suggested no loss in age estimation performance by merging stages 4 and 5. However, the disappear-ance of the physeal scar might be impor-tant in individuals who are older than the current sample. Moreover, stages 3c and 4 were still encountered in the oldest age categories of the current study, even when participants had exceeded the age of 26. This implies that in some individuals, cla-vicular development continues into the late twenties and it cannot be excluded that stages 3c and 4 still occur after age 30. This also means that ages within those stages were underestimated in the current study, as well as in all other available stud-ies on clavicle MRI for age estimation [15,
22-26, 29]. Therefore, it could be useful to include a relatively older study sample in future studies to check if the age distribu-tions within stages 4 and 5 do drift apart, and to find the real age distribution with-in stages 3c and 4.
Substages of epiphyseal growth and physeal bridging
The appearance of physeal ossification varies, which might explain discrepan-cies between observers. This variety also explains that a stage 2a for one observer might be interpreted as a stage 3aa by another observer. The same applies to stages 2b/3ab and 2c/3ac. Moreover, the chronology of stages is not straight for-ward. For instance, the existence of stage 3aa indicates that stages 2b and 2c were never reached by this clavicle. Stage 3ab indicates that stage 2c was never reached. Furthermore, the prevalence of substages of stage 2 decreased in higher substages, which might indicate that bridging of the physeal plate often does not wait until the plate has reached its full width.
In literature, stage 2 was rarely seen by Hillewig et al. (2013) [15], whereas it was more prevalent in other MRI studies on clavicular development [24, 26, 29]. Similar to the current findings, Schmidt et al. (2017) reported a decreasing prev-alence with increasing substages of stage 2 [24]. Remarkably, the lack of increase in ages within the substages only applied to males in their study. Moreover, similar to the current findings, Vieth et al. (2014) re-ported younger ages within stage 3a than in stage 2c. Thus, since stage 2 is probably only briefly present, it seems unnecessary to split it up into substages. Moreover, disregarding substages in stage 2 better
De Tobel J. Multi-factorial forensic age estimation. Chapter 9: 164-184.

181
restores the chronology of stages. Unfor-tunately, the low frequencies in the cur-rent sample did not allow researchers in this project to study how the application of, versus merging of, substages of stage 2 would affect age estimation performance.
Furthermore, four aspects can be dis-cussed considering profound substages of stage 3a. Firstly, the increase in ages with-in those substages advocates their use. Secondly, the lack of an evidently worse age estimation performance by merging the profound substages of stage 3a might be explained by a larger model instabili-ty when the substages are incorporated. The instability increases by the increase in categories and fewer cases per cate-gory. Thirdly, merging stage 3a caused a drastic decrease of specificity (> 15%), which should be avoided in forensic age estimation. Fourthly, regarding stage 3ab, current age distributions corresponded well with those reported by Wittschieber et al. (2014) on CT [30]. They suggest-ed that stage 3ac might be useful to de-termine if the 17-year-old threshold had been reached, since they only encoun-tered stage 3ac in individuals over 17. By contrast, stage 3ac was encountered at younger minimum ages in the cur-rent study, with a minimum of 16.0 years in females and 16.9 years in males. This can be explained by the small number of clavicles in stage 3a in the CT study (20 in females, 34 in males) compared to the current study (174 in females, 107 in males). Moreover, both studies should not be compared directly, since they applied different imaging modalities [14, 25, 28].
Combining both sides
As a consequence of including profound substages of stage 3a, asymmetry was more prevalent in the current study pop-ulation (51%; 230/449) than in literature. MRI studies reported a prevalence ranging from 9% (19/220) [15] to 16.4% (37/225) [29], while in CT studies the range was 6% (18/300) [27] to 18% (108/604) [1]. However, none of those studies applied profound substages of stage 3a. Moreo-ver, it was noted that the left clavicle was more often clearly depicted than the right in the current population. This might be due to positioning errors arising as a re-sult of the participants tending to slightly move away from the scanning personnel or a small shift to the right whilst try-ing to press down the coil’s connection cable. Remarkably, age estimation sole-ly based on the left clavicle performed similar to the combination of both sides, with a clinically irrelevant difference be-tween them. Still, since both are scanned simultaneously and morphological var-iants may occur unilaterally, the authors suggest to include both in the MRI scan. This complies with earlier suggestions [1, 15, 19, 20]. Moreover, when stages 1 and 4/5 are discarded, combining both clavi-cles increases the specificity (+7.4% right; +5.6% left).
While the current model allowed incorporating either clavicle separately or both clavicles simultaneously, in lit-erature, age estimation is mostly based on only one clavicle. When different de-velopmental stages were observed in left and right clavicles, some authors used the more advanced side for final evalua-tion [10, 11, 17, 18, 30, 31]. This is called the minimum-age-concept, in which the
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

182
point prediction of age is based on the highest minimal age [19, 20]. In other words, when left and right clavicles are in different stages, the minimum age within the highest of both stages is considered to decide if the 18-year-threshold has been reached. By contrast, when the point prediction is based on the within-stage age distribution, the less advanced side should be decisive [16]. Both approach-es comply with the benefit of the doubt, which should always be granted in a fo-rensic context.
Factors that impede staging
MRI of the clavicles has proven to be prone to factors that impede staging for age esti-mation. Schmidt et al. (2017) reported an overall exclusion rate of 14.8% (99/669) [24]. Two factors in particular have been described. Firstly, anatomic morpholog-ical variants are frequently seen in clav-icles. In most studies these variants are excluded, because it is assumed that stag-ing might be compromised, resulting in age estimation errors [10, 11, 17, 18, 29-31]. However, it had never been studied if clavicles with an aberrant morphology of the sternal end develop in a different fash-ion from regularly shaped clavicles. The current findings confirmed that exclud-ing morphological variants is indeed ap-propriate. Only 2.1% of clavicles (20/973) could not be incorporated in the model, because of their aberrant morphology. By contrast, Vieth et al. (2014) reported to have excluded 21.3% (61/286) of clavicles for this reason [29]. Secondly, motion ar-tefacts might impede staging [9]. In our total population this occurred in 2.7% (26/979). In literature 2.8% (50/1760) [15] and 7.4% (18/243) [29] have been report-ed. The prone position helps to reduce
these artefacts [14, 26]. Fortunately, it has been demonstrated that observers recog-nise obvious motion artefacts and conse-quently exclude them for age estimation purposes [9]. Therefore, motion artefacts do not lead to more faulty staging of the clavicle’s development [9].
Study limitations and future prospects
Although the current findings allow us to propose suggestions for a proper use of clavicle MRI for forensic age estimation, these need to be validated in independent samples before they can be considered generally applicable. After all, the studied approach was constrained by three lim-itations, with the relatively small study population as a first limitation. This was reflected in low numbers of clavicles in certain stages. However, those low num-bers might also be caused by the devel-opment of the clavicle as such, with bone bridges already appearing in early epiphy-seal development.
A second limitation was inherent to studying how merging stages affects age estimation performance. Firstly, merging stages can imply throwing away informa-tion (hence, a decrease in performance is expected), but can also lead to a more sta-ble model (hence, yielding an increase in cross-validated performance). The latter especially holds in smaller samples and il-lustrates the difficulty of deriving recom-mendations from the comparison of the models’ performances. Secondly, the ab-sence of a significant performance wors-ening after merging stages, is no evidence that stages can safely be merged. There-fore, proposed suggestions were not only based on age estimation performance, but
De Tobel J. Multi-factorial forensic age estimation. Chapter 9: 164-184.

183
also on the chronology of development and age distributions within stages.
A third limitation was the relatively low reproducibility of staging. De Tobel et al. (submitted) summarized reproduc-ibility statistics of staging clavicular de-velopment on MRI, and concluded that it is generally lower than for other long bones [9]. Thus, the current results did not seem to be aberrant. Until validated automated methods become available, the low reproducibility of staging clavicular development on MRI will remain a major concern in the field of age estimation.
In conclusion, age estimation in adolescents and subadults based on clavicle MRI is prone to pitfalls. The safest approach incorporates both clavicles in the model and excludes morphological variants.
Additionally, only including stages of epi-physeal growth (stage 2) or physeal bridg-ing (stage 3) in the age estimation model, might help to avoid unacceptably large errors. The role of substages of stage 2 and profound substages of stage 3a remains unclear.
acknowledgements
Our sincerest gratitude goes to all partic-ipants and everyone who helped recruit-ing them. Thank you Inès Phlypo, for your keen eye for details while reviewing the manuscript. Furthermore, we want to thank Patrick Davis for his critical ap-praisal of the manuscript.
references
[1] Bassed RB, Briggs C, Drummer OH. The incidence of asym-metrical left/right skeletal and dental development in an Australian population and the effect of this on forensic age estimations. Int J Legal Med. 2012;126(2):251-7.
[2] Boldsen JL, Milner GR, Konigsberg LW, Wood JW. Transi-tion analysis: a new method for estimating age from skel-etons. In: Hoppa RD, Vaupel JW, eds. Paleodemography: Age Distributions from Skeletal Samples. 1st ed. Cambridge: Cambridge University Press, 2002; p. 73-106.
[3] Davies C, Hackman L, Black S. The epiphyseal scar: chang-ing perceptions in relation to skeletal age estimation. Ann Hum Biol. 2015;42(4):348-57.
[4] Davies C, Hackman L, Black S. The persistence of epiphy-seal scars in the distal radius in adult individuals. Int J Legal Med. 2016;130(1):199-206.
[5] De Tobel J, Hillewig E, Bogaert S, Deblaere K, Verstraete K. Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation. Ann Hum Biol. 2017;44(2):130-9.
[6] De Tobel J, Hillewig E, Verstraete K. Forensic age estima-tion based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging. Ann Hum Biol. 2017;44(2):121-9.
[7] De Tobel J, Parmentier GIL, Phlypo I, Descamps B, Neyt S, Van De Velde WL, Verstraete KL, Thevissen PW. Magnetic resonance imaging of third molars in forensic age estima-tion: comparison of the Ghent and Graz protocols focusing on apical closure. Int J Legal Med. 2018;Epub ahead of print.
[8] De Tobel J, Phlypo I, Fieuws S, Politis C, Verstraete KL, The-vissen PW. Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging. J Forensic Odontostomatol. 2017;35(2):117-40.
[9] De Tobel J, van Wijk M, Alberink I, Hillewig E, Phlypo I, van Rijn RR, Thevissen P, Verstraete K, de Haas MB. The influ-ence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation. Int J Legal Med. 2018;Sub-mitted on October 24.
[10] Ekizoglu O, Hocaoglu E, Inci E, Can IO, Aksoy S, Sayin I. Estimation of forensic age using substages of ossification of the medial clavicle in living individuals. Int J Legal Med. 2015;129(6):1259-64.
[11] Ekizoglu O, Hocaoglu E, Inci E, Sayin I, Solmaz D, Bilgi-li MG, Can IO. Forensic age estimation by the Schmeling method: computed tomography analysis of the medial clav-icular epiphysis. Int J Legal Med. 2015;129(1):203-10.
[12] Faisant M, Rerolle C, Faber C, Dedouit F, Telmon N, Saint-Martin P. Is the persistence of an epiphyseal scar of the knee a reliable marker of biological age? Int J Legal Med. 2015;129(3):603-8.
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation
Conclusion

184
[13] Fieuws S, Willems G, Larsen-Tangmose S, Lynnerup N, Boldsen J, Thevissen P. Obtaining appropriate interval esti-mates for age when multiple indicators are used: evaluation of an ad-hoc procedure. Int J Legal Med. 2016;130(2):489-99.
[14] Hillewig E, De Tobel J, Cuche O, Vandemaele P, Piette M, Verstraete K. Magnetic resonance imaging of the medial ex-tremity of the clavicle in forensic bone age determination: a new four-minute approach. Eur Radiol. 2011;21(4):757-67.
[15] Hillewig E, Degroote J, Van der Paelt T, Visscher A, Van-demaele P, Lutin B, D’Hooghe L, Vandriessche V, Piette M, Verstraete K. Magnetic resonance imaging of the sternal ex-tremity of the clavicle in forensic age estimation: towards more sound age estimates. Int J Legal Med. 2013;127(3):677-89.
[16] Houpert T, Rérolle C, Savall F, Telmon N, Saint-Martin P. Is a CT-scan of the medial clavicle epiphysis a good exam to attest to the 18-year threshold in forensic age estimation? Forensic Sci Int. 2016;260:103.e1-.e3.
[17] Kellinghaus M, Schulz R, Vieth V, Schmidt S, Pfeiffer H, Schmeling A. Enhanced possibilities to make statements on the ossification status of the medial clavicular epiphysis us-ing an amplified staging scheme in evaluating thin-slice CT scans. Int J Legal Med. 2010;124(4):321-5.
[18] Kellinghaus M, Schulz R, Vieth V, Schmidt S, Schmeling A. Forensic age estimation in living subjects based on the ossifi-cation status of the medial clavicular epiphysis as revealed by thin-slice multidetector computed tomography. Int J Legal Med. 2009.
[19] Rudolf E, Kramer J, Schmidt S, Vieth V, Winkler I, Schmeling A. Intraindividual incongruences of medially os-sifying clavicles in borderline adults as seen from thin-slice CT studies of 2595 male persons. Int J Legal Med. 2017.
[20] Schmeling A, Dettmeyer R, Rudolf E, Vieth V, Geserick G. Forensic Age Estimation. Dtsch Arztebl Int. 2016;113(4):44-50.
[21] Schmeling A, Schulz R, Reisinger W, Muhler M, Wernecke KD, Geserick G. Studies on the time frame for ossification of the medial clavicular epiphyseal cartilage in conventional radiography. Int J Legal Med. 2004;118(1):5-8.
[22] Schmidt S, Henke CA, Wittschieber D, Vieth V, Bajanowski T, Ramsthaler F, Puschel K, Pfeiffer H, Schmeling A, Schulz R. Optimising magnetic resonance imaging-based evalua-tion of the ossification of the medial clavicular epiphysis: a multi-centre study. Int J Legal Med. 2016;130(6):1615-21.
[23] Schmidt S, Muhler M, Schmeling A, Reisinger W, Schulz R. Magnetic resonance imaging of the clavicular ossification. Int J Legal Med. 2007;121(4):321-4.
[24] Schmidt S, Ottow C, Pfeiffer H, Heindel W, Vieth V, Schmeling A, Schulz R. Magnetic resonance imag-ing-based evaluation of ossification of the medial clavic-ular epiphysis in forensic age assessment. Int J Legal Med. 2017;131(6):1665-73.
[25] Tangmose S, Jensen KE, Lynnerup N. Comparative study on developmental stages of the clavicle by postmortem MRI and CT imaging. J Forensic Radiol Imaging. 2013;1(3):102-6.
[26] Tangmose S, Jensen KE, Villa C, Lynnerup N. Forensic age estimation from the clavicle using 1.0T MRI-Preliminary results. Forensic Sci Int. 2014;234:7-12.
[27] Ufuk F, Agladioglu K, Karabulut N. CT evaluation of medial clavicular epiphysis as a method of bone age determina-tion in adolescents and young adults. Diagn Interv Radiol. 2016;22(3):241.
[28] Vieth V, Kellinghaus M, Schulz R, Pfeiffer H, Schmeling A. Beurteilung des Ossifikationsstadiums der medialen Klavi-kulaepiphysenfuge. Rechtsmedizin. 2010;20(6):483-8.
[29] Vieth V, Schulz R, Brinkmeier P, Dvorak J, Schmeling A. Age estimation in U-20 football players using 3.0 tesla MRI of the clavicle. Forensic Sci Int. 2014;241c:118-22.
[30] Wittschieber D, Schmidt S, Vieth V, Schulz R, Püschel K, Pfeiffer H, Schmeling A. Subclassification of clavicular sub-stage 3a is useful for diagnosing the age of 17 years. Rechts-medizin. 2014;24(6):485-8.
[31] Wittschieber D, Schulz R, Vieth V, Kuppers M, Bajanowski T, Ramsthaler F, Puschel K, Pfeiffer H, Schmidt S, Schmeling A. The value of sub-stages and thin slices for the assessment of the medial clavicular epiphysis: a prospective multi-center CT study. Forensic Sci Med Pathol. 2014;10(2):163-9.
De Tobel J. Multi-factorial forensic age estimation. Chapter 9: 164-184.



187
PART 5
Age estimation based on multi-factorial MRI

188
CHAPTER 10
TH I S CHAPTER ADDRESSED THE FOLLOWING STUDY OB JECT IVE :
Objective 9: To review the use of MRI in age estimation of living children and subadults.
TH I S CHAPTER WAS SUBM ITTED FOR PUBL ICAT ION AS :
De Tobel J, Bauwens J, Parmentier G, Franco A, Pauwels N, Verstraete K, Thevissen P. The use of magnetic resonance imaging in forensic age estimation of living children and subadults systematically reviewed. Ped Radiol. Submitted on March 4, 2019 [A1; Journal Impact Factor 2017 1.826; Pediatrics Q2; Radiology, Nuclear Medicine & Medical Im-aging Q3; Peer reviewed].
RESULTS DESCR I BED IN TH I S CHAPTER WERE PARTLY PRESENTED
AT THE FOLLOWING CONFERENCES :
De Tobel J, Bauwens J, Parmentier G, Franco A, Pauwels N, Verstraete K, Thevissen P. The use of magnetic resonance imaging in forensic age estimation of living children and subadults systematically reviewed. 22nd Meeting of the Study Group on Forensic Age Diagnostics, Arbeitsgemeinschaft für Forensische Altersdiagnostik (AGFAD); Berlin, Germany; March 15, 2019.
De Tobel J, Parmentier G, Pauwels N, Verstraete K, Thevissen P. The Use of Magnetic Resonance Imaging (MRI) in Forensic Age Estimation of Living Children, Adolescents, and Subadults: Protocol for a Systematic Review and Preliminary Results. American Academy of Forensic Sciences (AAFS) 70th Annual Scientific Meeting; Seattle, USA; February 23, 2018. p 641.

189
The use of magnetic resonance imaging in forensic age estimation of living children and
subadults systematically reviewed
REV I EW
Abstract
The use of MRI in age estimation of living children and sub-adults has been explored extensively during the past decade. The current systematic review aims to provide a comprehensive overview that can guide age estimation practice and future re-search. Therefore, MEDLINE, Embase and Web of Science were searched. Additionally, cited and citing articles and study regis-ters were searched. Two review authors independently selected articles, recorded study characteristics, conducted data extrac-tion, and assessed risk of bias. Study populations including living subjects up to 30 years were considered. Authors were contacted for further details and data if these were unclear, missing or in a format unsuitable for analysis. After full-text screening, 55 stud-ies were included in qualitative analysis and 33 in quantitative analysis. Most studies included European (Caucasian) popula-tions. Studies were highly biased by their study populations and MR-sequences varied widely, as did staging techniques. There-fore, pooling of the age distribution data was not appropriate. Age estimation performance was in line with the gold standard, which uses radiographs, with mean absolute errors ranging from 0.85 to 2.0 years. The proportion of correctly classified minors ranged from 65% to 91%. The current review results can help medical professionals to decide on the preferred approach for specific cases. Moreover, they can help judicial professionals to interpret the evidential value of age estimation results.
Key Words
• magnetic resonance imaging
• age estimation
• child
• adolescent
• young adult
AFF IL IAT IONS
1 Department of Diagnostic
Sciences – Radiology, Ghent
University, Belgium
2 Department of Forensic Od-
ontology, Catholic University
Leuven, Belgium
3 Department of Oral Diseases
and Maxillofacial Surgery, Maas-
tricht UMC+, The Netherlands
4 Ghent Knowledge Centre for
Health, Ghent University, Belgium
Funding for this research was entirely
provided by the department of
Radiology and Nuclear Medicine at
Ghent University.
The authors declare that there are
no conflicts of interest.
JANN ICK DE TOBEL 1 2 3 J E ROEN BAUWENS 1
GR I ET I . L . PARMENT I ER 1 ADEM IR FRANCO 2
NELE S . PAUWELS 4 KOENRAAD L . VERSTRAETE 1
PATR ICK W. THEV I S SEN 2

190
Description of the issue
When birth records or other official identification documents reporting the age of an individual are unavail-able in criminal, civil and asylum
procedures, forensic age estimation can be deemed necessary by the authorities. The estimation usually has to contain a predicted age together with a measure of the uncertainty, and the probability that the examined person has reached a specif-ic legally relevant age threshold. In most countries the age threshold lies between 14 and 22 years of age, representing chil-dren and subadults [78]. Furthermore, in sports, age estimation is used to ensure fair play by checking if athletes participate in the correct age category [25].
Description of the intervention
Established methods for age estimation mainly use radiographs to evaluate teeth, carpal bones and long bones, which are still developing in children and subadults. The 2D radiographic registrations have two major drawbacks. Firstly, they imply an exposure to radiation without a clini-cal indication, resulting in deontological and ethical issues [103]. In some coun-tries, the use of ionizing radiation is even prohibited in asylum and civil procedures [61]. Secondly, on plain radiographs, su-perposition can yield mistakes or impede allocating a developmental status to the anatomical structures of interest [40].
To counter these drawbacks, several research groups have been studying the use of magnetic resonance imaging (MRI) to register the developmental status of the considered anatomical site. Since the details necessary to study development
might not be clear in routine clinical MRI, several dedicated MRI protocols have been developed.
Why is it important to do this review?
The different MRI approaches were re-ported in pilot studies and cross-sectional reference studies. Compared to reference studies of age estimation based on radio-graphs of developing teeth or bones, the MRI studies all included a relatively small study population. Therefore, pooling of the MRI data might increase age esti-mation performance. However, a review of these MRI studies is indispensable to study if pooling is appropriate. To the best of our knowledge, no systematic review has been published on the subject yet.
Objectives
To review the use of MRI for forensic age estimation in living children and sub-adults. To provide a comprehensive over-view that can guide age estimation prac-tice and future research.
Research questions
General
1 How does the development of dif-ferent anatomical structures, as registered on MRI, relate to chron-ological age in living children and subadults?
2 What is the performance of age es-timation based on development of different anatomical structures as registered on MRI?
Introduction
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

191
Specific
3 Which anatomical structures pro-vide the best MRI information to discern minors from adults?
4 How is age estimation on MRI af-fected by population characteristics and MRI technique?
Protocol design
The review protocol was drafted according to the Cochrane Guide-lines for review protocols (http://training.cochrane.org/) [98], and registered in Prospero, interna-tional prospective register of sys-tematic reviews (http://www.crd.york.ac.uk/PROSPERO), with reg-
istration number CRD42017061043). This project was approved by the Ghent University Hospital Ethics Committee (EC 2017/0024, with Belgian registration number B670201730806), as part of an ongoing larger project (EC 2011/0842, B670201112782). The reporting of the systematic review complies with the PRISMA statement [58, 64].
Selection of studies
Criteria for considering studies for this review (PICOS)
S Types of studies How does the development of dif-
ferent anatomical structures, as registered on MRI, relate to chron-ological age in living children and subadults?
Cross-sectional observational stud-
ies were included. When a pilot
study was published, followed by a more recent study including a larg-er study population, only the final publication was included for the review. When the final publication was not published yet, results of the pilot publication were considered. Furthermore, cohort observational studies were included, but only re-sults of one moment in time were extracted to avoid bias. Case reports and case series were also included, since they might provide informa-tion on minimum and/or maxi-mum age per developmental stage. Review articles were excluded. Fur-thermore, no restrictions were made based on the country of publication, language or publication date.
P Types of participants Study populations including living
children, subadults and adults up to 30 years old were considered. After the age of 30, age estimation is no longer based on development, but rather on degenerative changes [13, 87]. Moreover, studies which only included deceased individuals were excluded, since MRI is influenced by body temperature [72] and mo-tion artefacts [21].
I Types of interventions MRI of any field strength was in-
cluded studying hard tissue de-velopment related to age. Authors should refer to the staging tech-nique used to assess development. When measurements were made, the way of obtaining them should be described clearly. It was considered inappropriate to compare the age distributions within developmen-
Materials and M
ethods
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

192
tal stages based on MRI with those based on radiographs, since it has been demonstrated that imaging technique specific reference data are required [19, 33, 44, 91, 114, 115].
C Types of controls The control for age estimation per-
formance was the chronological age.
O Types of outcome measures The included papers should provide
any of these outcome measures:
— Descriptive statistics on age distri-bution within the different devel-opmental stages of the considered anatomical structures.
— Probabilities of attaining certain threshold ages, diagnostic indices.
— Statistics on the performance of the age estimation model.
Search methods
According to the described eligibility criteria, literature was searched in MED-LINE (via the PubMed interface), Embase (via the embase.com interface), and Web of Science. The search strings are reported in the Appendix. Furthermore, reference lists of included studies were searched for additional suitable papers, and papers citing the included studies were searched using Web of Science and Google Schol-ar. Finally, grey literature was searched by consulting the following study registers: the United States' ClinicalTrials.gov, EU Clinical Trials Register, the United King-doms' ISRCTN registry, German Clinical Trials Register (DRKS). All searches were conducted on September 2, 2018.
Reviewing process and selection of studies
Two authors conducted every step of the reviewing process independently. The first author (JDT) was a reviewer throughout the whole process. Other authors (JB, GP, AF) acted as second reviewers. After a first selection of articles based on title and abstract, the authors considered and com-pared their selection to achieve a consen-sus. Of the retained abstracts, the full text paper was checked independently for eli-gibility. Discrepancies between reviewers were identified at this stage and were re-solved by discussion to reach consensus. A record was kept of reasons for exclud-ing studies at each step (either title and abstract, or full text). Reasons for exclu-sion were checked in the following order:
1 Pilot of other reference.
2 Wrong study design (S): review.
3 Wrong population (P): deceased in-dividuals, insufficient data to differ-entiate within the group of 1 to 30 years of age.
4 Wrong intervention (I): MRI study-ing soft tissue.
5 Wrong outcome measures (O): no data on age distribution or age esti-mation performance.
References were managed and duplica-tions removed with Endnote software. Covidence software (Covidence system-atic review software, Veritas Health Inno-vation, Melbourne, Australia. Available at www.covidence.org) was used for study selection. The process and the results of
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

193
the literature search and study selection were presented in the PRISMA flowchart (Figure 10.1).
Data extraction and management
Study characteristics and outcome data were extracted by two reviewers inde-pendently. The study characteristics table summarised data on study population, MRI approach, staging technique, sta-tistical analysis, and observers. The data extraction table summarised data on missing data, correlation between stages and age, age distributions within stages, reproducibility of staging, regression for-mulas, and age estimation performance.
When multiple records were identi-fied of the same study, they were collated, so that the unit of interest in the review was the study, rather than each record.
Quality assessment of studies
Risk of bias assessment of included studies
Risk of bias was assessed by two review-ers independently using a dedicated tool based on the EPOC overview [11] and QUADAS-2 [119]. Questions were phrased in such a way that the preferred approach corresponded with answering “yes”. In case the answer was “no”, the rea-sons for high risk of bias were elaborated.
Dealing with missing data
When information was missing in a paper, only graphs were reported or clarification was needed, the authors were contacted by e-mail or telephone. When the au-
thors did not provide additional data, but graphs were reported in their paper, data were extracted from the graphs using cali-bration and the measuring tool in Adobe Photoshop CS2. For missing values due to images not being assessable, the reasons were registered. Moreover, it was evaluat-ed whether missing values depended on age, imaging sequence or research group.
Assessment of heterogeneity
Methodological heterogeneity was checked by comparing biological origin of participants and types of MR sequence. Statistical heterogeneity was taken into account by comparing the different types of statistical models that were used.
Moreover, it was evaluated whether the type of sequence generated hetero-geneity. If necessary, a subgroup analysis was performed per type of sequence.
Selection of studies and data
The database search rendered 391 single records (Figure 10.1). Search-
ing study registers generated one relevant ongoing study: the Swedish Age Assess-ment Study (SAAS). However, no addi-tional data for this review were provided. Furthermore, six additional records were identified by networking at conferences on forensic science and imaging.
One hundred full-text articles were screened for eligibility, rendering 55 pa-pers suitable for qualitative analysis. Next, searching cited and citing references ren-dered 16 additional articles that were as-sessed for eligibility.
Results
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

194
FIGURE 10. 1 — FLOWCHART SHOWING THE PROCESS OF LITERATURE SEARCH AND STUDY SELECTION.
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

195
Early studies tended to include only de-scriptions of the bones’ developmental changes on MRI [42]. They lacked details on age distribution within certain devel-opmental stages. Other early studies did not report sex-specific data [8, 9, 12, 57]. Although these studies were included for qualitative synthesis, they were unsuitable for data extraction.
Moreover, 23 studies did not report the statistics on age distribution that were needed for quantitative synthesis [8, 9, 12, 36, 42, 51, 52, 57, 63, 69, 75, 77, 90, 93, 95-97, 109, 114, 118]. When the study design indicated that such data should be availa-ble, the authors were contacted. Out of 32 authors that were contacted, only 13 re-sponded, with ten of them providing the requested data or statistics [3, 5, 16-18, 20, 49, 111, 113, 114]. This led to 33 studies suitable to create the overview graphs in Figure 10.3.
Characteristics and quality of included studies
Study characteristics
Results on age distribution were affected by the study characteristics displayed in Tables 10.1-10.3. In those tables, studies are grouped according to anatomical site from head to toe: skull, teeth, chest, upper limb, hip, and lower limb. Note that only one study has been published which inte-grates information from several anatomi-cal sites into one age estimate (multi-fac-torial age estimation = MFA) [89].
The first type of characteristics con-cerned the study populations (Table 10.1). Most studies included European (Cauca-sian) populations. In addition, there were
limited studies including African, Asian and Latin American populations. Healthy volunteers or athletes were recruited pro-spectively or patient records were searched retrospectively, excluding pathology. Only one study included patients with possible growth disorders, but their focus was on the agreements between X-ray based bone age and MRI based bone age, rather than on chronological age [114]. Furthermore, the age range of the study populations var-ied widely, with some studies only includ-ing minors, while others included partici-pants from birth to age 30.
Secondly, the MRI approaches were recorded (Table 10.2). The included scan-ning protocols used scanners with field strengths from 0.2T to 3T. The low field open scanners did not render the highly detailed images necessary for staging and substaging of both the epiphyseal and physeal development, but they allowed assessing individual bone development of the hand/wrist [95, 109]. Conversely, to study developing teeth and clavicles, 3T appears to be necessary [5, 17, 18, 20, 39, 82, 93, 116]. Most protocols used surface coils or dedicated extremity coils. A head/neck coil was used at an alternative site by two groups: to study the hand/wrist [46, 90, 113, 114], and to study the clavicles [90]. Positioning was often not reported in retrospective studies. By contrast, it proved to be major issue in the study of clavicles, since the prone position reduced motion artefacts [44, 93]. In an attempt to avoid motion artefacts in other structures, specific fixation was applied by a bite bar [15], and stabilisation was applied by vac-uum pillows [44, 114].
T1 sequences were most frequently used to study bone development, where-
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

196
as for teeth, T2 sequences were most fre-quent. The voxel size of those sequenc-es varied widely. Retrospective studies mostly lacked specifics on this, but some reported slice thicknesses ranging from 2 to 4 mm. In-plane resolution was never lower than 1.0 × 1.0 mm² and high res-olutions were reached in all anatomical sites, with a minimum of 0.188 × 0.188 mm² [3]. Unfortunately, the study with the highest resolution [3] did not report the acquisition time. Since 6 minutes 30 seconds could be considered the maxi-mum acceptable acquisition time [65], only the teeth and the iliac crest exceeded this threshold.
Thirdly, staging techniques and the statistical processing were compared (Ta-ble 10.3). Regarding dental development, the staging techniques were based on ra-diographs [23, 53]. . However, since the cemento-enamel junction is indiscernible using the reported MRI sequences, these staging techniques were said to be inap-propriate for MRI [18]. Consequently, an MRI-specific technique was reported [18, 20]. Regarding bone development, staging techniques were developed based on radiographs and CT. In contrast to the
dental staging techniques, the criteria for staging bone development did not include tissues which are indiscernible on MRI. Therefore, the staging techniques could integrally be applied to MRI. Moreover, they could be grouped when their stages overlapped. The most elaborate staging technique (Table 10.4) was developed by a German research group and combined stages [81], substages [50] and profound substaging [121]. When applicable, oth-er staging techniques were transposed to this staging technique to compare studies (Figure 10.3). In addition to this general staging technique, two staging techniques should be considered MR-sequence-spe-cific: Dedouit [22, 30] and Vieth [117]. Similarly, four MR-specific signs of bone development have been reported: the threefold stratification sign in wrist MRI [16, 84, 107], and the metaphyseal stripe [57], the oreo-sign and the crack-sign [69] in knee MRI.
In an attempt to combine information from different bones, Auf der Mauer et al. (2018) calculated the sum of the stag-es in three knee bones [3]. Similarly, the Tomei [110] and Tanner-Whitehouse [94] hand/wrist atlas techniques calculate a
FIGURE 10.2 —CLARIFICATION OF WHAT THE BOX-PLOTS IN FIGURE 10.3 INDICATE. When the f irst choice sta-
t ist ics were not avai lable, the second choice stat ist ics were used to create the graph instead. When the
second choice stat ist ics were not avai lable, the third choice stat ist ics were used. This needs to be taken
into account when interpret ing the graphs.
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

197
ANATOMICAL STRUCTURE
REFERENCE YEAR STUDY DESIGN
EXCLUDED REFERENCE BECAUSE OF CORRESPONDENCE
GEOGRAPHICAL POPULATION
NUMBER OF FEMALES
AGE RANGE (YEARS)
NUMBER OF MALES
AGE RANGE (YEARS)
Spheno-occipital synchondrosis
Ekizoglu 2016a RCS NA Turkish 623 7 - 21 455 7 - 21
Molars Baumann 2015 PCS NA Living in Austria 18 13.50 - 23.1 8 13.7 - 21.3
Lower left third molar Guo 2015 PCS NA German 248 12.32 - 24.98 269 12.14 - 24.98
Third molars De Tobel 2017b PCS NA Belgian 26 14.46 - 26.81 26 14.25 - 26.8
Third molars De Tobel 2017c PCS NA Belgian and Dutch 146 14.0 - 26.8 163 14.1 - 27.0
Clavicle Hillewig 2013 PCS Hillewig 2011 Belgian 110 16.0 - 26.9 110 16.1 - 26.9
Clavicle Tangmose 2014 PCS NA Mainly European Caucasian, four from Middle East, Asia or Africa
16 NA 39 NA
Clavicle Vieth 2014 PCS NA German 0 NA 152 18.1 23.0
Clavicle Schmidt 2017 PCS NA German 310 12.1 - 25.0 260 12.1 - 24.9
Clavicle De Tobel Submitted PCS Hillewig 2011, 2013 Belgian and Dutch 264 14.06 - 30.52 199 14.08 - 30.05
Manubrium Martínez Vera 2017 RCS NA Austrian 0 NA 130 13.01 24.98
Proximal humerus Ekizoglu 2018 RCS NA Turkish hospital 188 12.2 - 30.7 240 12.1 - 30.6
Left distal radius Dvorak 2007 PCS NA Swiss, Malay, Algerian and Argentinan
0 NA 496 14 - 19
Left distal radius George 2012 PCS NA Malaysian Malay 0 NA 150 15 - 19.0
Left distal radius Bolivar 2015 PCS NA Colombian 0 NA 60 12 - 18
Left distal radius Rashid 2015 PCS NA Iraqi 0 NA 179 13 - 18
Left distal radius Tscholl 2016 PCS NA African (Tanzania), Asian (Malaysia), European (Germany), Latin American (Brazil)
487; T 140; M 129; G 117; B 101
13.25 - 19.29 0 NA
Left distal radius Abdelbary 2018 PCS NA Egyptian 0 NA 61 13 18
Left distal radius Sarkodie 2018 PCS NA Ghanaian 0 NA 286 13 16
Left distal radius Schmidt 2015 PCS NA German 0 NA 152 18.1 22.9
Left hand/wrist Serin 2016 RCS NA French hospital 156 9 - 25 107 9 - 25.0
Left distal radius Timme 2017 PCS NA NA 333 12.10 - 24.9 335 12.1 - 24.9
Left wrist De Tobel 2019 PCS NA Belgian and Dutch 185 14.10 - 26.9 178 14.10 - 27.0
Left hand/wrist Tomei 2014 PCS NA Italian 78 11 - 17 101 11 - 17
Left hand/wrist Serinelli 2015 PCS NA Italian 74 12.0 - 18.83 77 12 - 19.08
Left hand/wrist Terada 2013 PCS NA Japanese 43 4.1 - 16.4 50 4.1 - 16.4
Left hand/wrist Terada 2014 PCS NA Japanese 23 3.4 - 15.7 65 3.4 - 15.7
Left hand/wrist Terada 2016 PCS NA Japanese 24 4.4 - 15.3 35 4.4 - 15.3
Left hand/wrist Urschler 2016 PCS NA Austrian 4 7.57 - 14.06 14 7.92 - 16.82
Left hand/wrist Hojreh 2018 PCS Hojreh 2017 European; Iranian, Argentinian, Malian, Philippine excluded for current results
29 12 - 19.8 17 12.8 - 18.5
Left hand/wrist Urschler 2015 PCS Stern 2014 Austrian 0 NA 102 13 - 20
Iliac crest Wittschieber 2014 PCS NA German 0 NA 152 18.0 - 22.9
Proximal femur Vo 2015 PCS NA NA 17 8 - 16 26 10 - 18
Sacrum Bollow 1997 PCS NA German hospital 43 8 - 17 71 8 - 17
Sacrum Bray 2016 RCS NA British hospital 36 10.17 - 18.92 19 10.17 - 18.92
Patellofemoral joint Kim 2014 RCS NA NA 51 5 - 22 46 5 - 22
Distal femur Saint-Martin 2015 RCS NA French hospital 0 NA 214 14 - 20
Knee Dedouit 2012 RCS NA French hospital 152 10.1 - 30.9 138 10.3 - 30.3
Knee Ekizoglu 2016b RCS NA Turkish hospital 198 10 - 30 305 10 - 30
Knee Harcke 1992 PCS NA NA 27 0 - 20 33 0 - 20
Knee Laor 2002 RCS NA American hospital 100 0 - 40 97 0 - 40
Proximal tibia Jopp 2010 PCS NA German 0 NA 41 15.73 - 19.82
Distal femur Krämer 2014a RCS NA German hospital 124 10.1 - 30.8 166 10.1 - 30.8
Proximal tibia Krämer 2014b RCS NA German hospital 124 10.1 - 30.8 166 10.1 - 30.8
Knee Fan 2016 RCS NA West China Han 139 11.0 - 29.48 183 11.00 - 29.9
Knee Ottow 2017 PCS NA German 333 12.11 - 25.0 325 12.05 - 24.98
Knee Auf der Mauer 2018 PCH NA German 0 NA 36 15.25 - 20.66
Knee Vieth 2018 PCS NA German 350 12.11 - 24.98 344 12.05 - 24.98
Knee Pennock 2018 RCS NA American hospital 421 2 - 19 438 2 - 19
Knee Craig 2004 RCS NA American hospital 5 3.8 - 15.6 9 3.8 - 15.6
Knee Kercher 2009 RCS NA NA 21 10 - 15 10 10 - 15
Ankle Saint-Martin 2013 RCS NA French hospital 100 8 - 25 80 8 - 25
Distal tibia Saint-Martin 2014 RCS NA French hospital 60 8 - 25 60 8 - 25
Ankle Ekizoglu 2015 RCS NA Turkish hospital 70 8 - 25 97 8 - 25
MFA Stern 2017 PCS NA Austrian 0 NA 103 13.01 - 24.89
MFS = multi-factorial; MFA = multi-factorial age estimation; NA = not applicable or not reported; PCH = prospective cohort; PCS = prospective cross-sectional; RCS = retrospective cross-sectional
MFS = mult i-factorial ; MFA = mult i-factorial age est imation; NA = not appl icable or not repor ted; PCH =
prospective cohor t ; PCS = prospective cross-sect ional ; RCS = retrospective cross-sect ional
TABLE 10. 1 — POPULATION CHARACTERISTICS OF ELIGIBLE STUDIES. Studies are grouped per anatomical
s ite and ordered per staging technique.
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

198
ANATOMICAL
STRUCTUREREFERENCE YEAR MRI SCANNER COIL POSITIONING MR SEQUENCE VOXEL SIZE (mm³) ACQUISITION TIME
Spheno-occipital
synchondrosisEkizoglu 2016a 1.5T Siemens NA NA
in text T1 SE; figure
captions say T2ST 2-4 mm NA
Molars Baumann 2015 3T Siemens 8-channel multifunctional coil Supine T1 3D TSE; 3D CISS 0.6 × 0.6 × 1.0 9:47 and 8:57
Lower left third molar Guo 2015 3T Philips16-channel surface head/neck
coilSupine T2 TSE
M 0.50 × 0.65 × 2.0,
R 0.19 × 0.19 × 2.05:36
Third molars De Tobel 2017b 3T Siemens4-channel flexible surface head
coilSupine T2 FSE 0.33 × 0.33 × 2.0 S 6:33; A 6:49; C 6:29
Third molars De Tobel 2017c 3T Siemens4-channel flexible surface head
coilSupine T2 FSE 0.33 × 0.33 × 2.0 S 6:33; A 6:49; C 6:29
Clavicle Hillewig 2013 3T SiemensLoop-shaped surface coil with 11
cm bore
Prone on vacuum
pillowT1 GE VIBE 0.7 × 0.7 × 0.9 4:02
Clavicle Tangmose 2014 1T Siemens Surface coil Supine; prone T2 3D GE 0.7 × 0.7 × 1.5 6:04
Clavicle Vieth 2014 3T Philips 2 elliptical loop shaped surface Prone 3D FFE 0.7 × 0.7 × 1.4 5:41
Clavicle Schmidt 2017 3T Philips Surface coil Prone T1 3D FFE FSM 0.69 × 0.70 × 1.4,
R 0.29 × 0.29 × 0.75:41
Clavicle De Tobel Submitted 3T SiemensLoop-shaped surface coil with 11
cm boreProne T1 VIBE 0.7 × 0.7 × 0.9 4:02
Manubrium Martínez Vera 2017 3T Siemens Neck coil Supine T1 3D VIBE WE 0.9 × 0.9 × 0.9 NA
Proximal humerus Ekizoglu 2018 1.5T Siemens Extremity coil NA T1 TSE 0.5 × 0.5 × 3.5 1:44
Left distal radius Dvorak 2007 1T or 1.5T Wrist coilWrist above the head
or at the sideT1 SE ≤ 0.5 × ≤ 0.5 × 3 NA
Left distal radius George 2012 1.5T Siemens Wrist coilProne both hands
outstretchedT1 FSE 0.39 × 0.39 × 3 NA
Left distal radius Bolivar 2015 1.5T Siemens Wrist coilWrist above the head
or at the sideT1 SE ≤ 0.5 × ≤ 0.5 × 3 NA
Left distal radius Rashid 2015 1.5T Siemens Surface coilWrist above the head
or at the sideT1 FSE 0.5 × 0.5 × 3 5:48
Left distal radius Tscholl 2016 1T or 1.5T Wrist coilWrist above the head
or at the sideT1 SE ≤ 0.5 × ≤ 0.5 × 3 NA
Left distal radius Abdelbary 2018 0.31T open 8-channel hand/wrist coilSupine hand next to
bodyT1 SE ST 3 mm < 7:00
Left distal radius Sarkodie 2018 1.5T GE or Toshiba Wrist coilWrist above the head
or at the sideT1 SE ≤ 0.5 × ≤ 0.5 × 3 NA
Left distal radius Schmidt 2015 3T Philips 2 elliptical loop shaped surface NA T1 TSE 0.4 × 0.5 × 1.5 6:00
Left hand/wrist Serin 2016Philips, Siemens, GE,
ToshibaExtremity coils NA T1 SE ST 2-5 mm NA
Left distal radius Timme 2017 3T Philips16-channel surface head/neck
coilNA T1 TSE
M 0.4 × 0.5 × 2.5,
R 0.2 × 0.2 × 2.53:33
Left wrist De Tobel 2019 3T Siemens Wrist coilSupine hand next to
bodyT1 SE; T1 VIBE
0.20 × 0.20 × 2.0;
0.40 × 0.40 × 0.402:43; 5:57
Left hand/wrist Tomei 2014 0.2T G-Scan open Hand/wrist coil NA T1 3D SE 0.73 × 1.09 × 1.3 1:39 (twice if necessary)
Left hand/wrist Serinelli 2015 0.2T G-Scan open Small coil NA T1 3D SE 0.73 × 1.09 × 1.3 NA
Left hand/wrist Terada 2013 0.3T Neomax open 1-channel dedicated coil Seated 3D GE 0.39 × 0.78 × 1.56 2:44
Left hand/wrist Terada 2014 0.3T Shin-Etsu open 1-channel dedicated coil Seated 3D GE 0.39 × 0.78 × 1.56 2:44
Left hand/wrist Terada 2016 0.3T Shin-Etsu open 1-channel dedicated coil Seated 3D GE 0.39 × 0.78 × 1.57 2:44
Left hand/wrist Urschler 2016 1.5T Siemens Head coil
Prone with
outstrectched arm on
vacuum bed
T1 3D VIBE; T1 SE; T2
3D GE
0.43 × 0.43 × 0.9;
0.86 × 0.86 × 2.0;
0.86 × 0.86 × 0.9
3:08 ; 1:00 ; 2:21
Left hand/wrist Hojreh 2018 1.5T Siemens Head/neck coilProne with
outstrectched armT1 3D VIBE WE 0.4 × 0.4 × 1.5 2:26
Left hand/wrist Urschler 2015 3T Siemens Head/neck coilProne with
outstrectched armT1 3D FLASH VIBE 0.45 × 0.45 × 0.9 < 4:00
ANATOMICAL
STRUCTUREREFERENCE YEAR MRI SCANNER COIL POSITIONING MR SEQUENCE VOXEL SIZE (mm³) ACQUISITION TIME
Iliac crest Wittschieber 2014 3T Philips 8-channel SENSE cardiac coil NA T1 3D GE 0.49 × 0.49 × 2.2 17:47
Proximal femur Vo 2015 1.5T GESurface coil anterior + spine coil posteriorly
Supine T1 3D spoiled GE ST 1 mm NA
Sacrum Bollow 1997 1.5T Philips Body coilSupine with elevated legs
T1 SE, T2* opposed-phase FFE, dynamic T1 opposed-phase FFE
dynamic 11:12
Sacrum Bray 2016 1.5T Siemens NA NA
T1 TSE, STIR, T1 Turbo Inversion Recovery Magnitude, postcontrast T1, DWI
1.0 × 1.0 × 3-5; 2.5 × 2.5 × 8
NA
Patellofemoral joint Kim 2014 1.5T GE Knee coil NAintermediate, T1, T2, and PD; FSE
ST 3-4 mm NA
Distal femur Saint-Martin 2015 1.5T Philips NA NA T1 TSE NA NA
Knee Dedouit 2012 1.5T Philips Extremity coil NA FSE PD ST 3.5-4 mm 4:00
Knee Ekizoglu 2016b 3T Siemens Knee coil NA T2 TSE ST 3.5 mm 2:20
Knee Harcke 1992 0.5T HP VistaKnee coil (> 6 years old) or head coil (< 6 years old)
NAT1 SE, field-echo, T2 SE
NA NA
Knee Laor 2002 1.5T GEExtremity coil, torso phased-array coil, or quadrature head coil
NA
intermediate, T1, or T2; SE, FSE, some with inversion recovery; 3D spoiled gradient-recalled-echo; some with gadolinium contrast
ST 3-5 mm NA
Proximal tibia Jopp 2010 1.5T or 3T Philips Knee coil NA1.5 T T1 TSE and PD SPIR; 3T T1 TSE and STIR long TE SENSE
ST 1.5T C 3.0 mm, S 3.5 mm; 3T C 3.0 mm, S 4.0 mm
Distal femur Krämer 2014a 3T Siemens 15-channel knee coil NA T1 TSE 0.4 × 0.4 × 3.0 1:57
Proximal tibia Krämer 2014b 3T Siemens 15-channel knee coil NA T1 TSE 0.4 × 0.4 × 3.0 1:57
Knee Fan 2016 1.5T Philips or Siemens Knee coil NA T1 TSE NA NA
Knee Ottow 2017 3T Philips Surface coil NA T1 TSEM 0.6 × 0.77 × 3, R 0.31 × 0.31 × 3
3:51
Knee Auf der Mauer 2018 3T Philips 8-channel knee coil NA T1 SENSE 0.1875 × 0.1875 × 2 NA
Knee Vieth 2018 3T Philips Surface coil NA T1 TSE; T2 TSE SPIRM 0.6 × 0.77 × 3, R 0.31 × 0.31 × 3; M 0.6 × 0.76 × 3, R 0.31 × 0.31 × 3
3:51; 3:08
Knee Pennock 2018 1.5T Extremity coil NA T1 NA NA
Knee Craig 2004 1T or 1.5T GE NA NA3D fat-suppressed spoiled GRASS
ST 1.0-2.0 mm NA
Knee Kercher 2009 1.5T or 3T NA NA T1 NA NA
Ankle Saint-Martin 2013 1.5T Philips Extremity coil NA T1 SE ST 2-4 mm 4:00
Distal tibia Saint-Martin 2014 1.5T Philips Extremity coil NA T1 SE ST 2-4 mm 4:00
Ankle Ekizoglu 2015 1.5T Siemens Extremity coil NA T1 SE 0.5 × 0.5 × 3.5 mm 4:00
MFA Stern 2017 3T SiemensT 8-channel multifunctional coil and CW head/neck coil
TC Supine and W prone with outstrectched arm
T PD TSE; CW T1 3D GE
T 0.59 × 0.59 × 1.0; C 0.9 × 0.9 × 0.9; W 0.45 × 0.45 × 0.9
NA
TABLE 10.2 — MRI CHARACTERISTICS OF ELIGIBLE STUDIES. STUDIES ARE GROUPED PER ANATOMICAL SITE
AND ORDERED PER STAGING TECHNIQUE.
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

199
ANATOMICAL
STRUCTUREREFERENCE YEAR MRI SCANNER COIL POSITIONING MR SEQUENCE VOXEL SIZE (mm³) ACQUISITION TIME
Spheno-occipital
synchondrosisEkizoglu 2016a 1.5T Siemens NA NA
in text T1 SE; figure
captions say T2ST 2-4 mm NA
Molars Baumann 2015 3T Siemens 8-channel multifunctional coil Supine T1 3D TSE; 3D CISS 0.6 × 0.6 × 1.0 9:47 and 8:57
Lower left third molar Guo 2015 3T Philips16-channel surface head/neck
coilSupine T2 TSE
M 0.50 × 0.65 × 2.0,
R 0.19 × 0.19 × 2.05:36
Third molars De Tobel 2017b 3T Siemens4-channel flexible surface head
coilSupine T2 FSE 0.33 × 0.33 × 2.0 S 6:33; A 6:49; C 6:29
Third molars De Tobel 2017c 3T Siemens4-channel flexible surface head
coilSupine T2 FSE 0.33 × 0.33 × 2.0 S 6:33; A 6:49; C 6:29
Clavicle Hillewig 2013 3T SiemensLoop-shaped surface coil with 11
cm bore
Prone on vacuum
pillowT1 GE VIBE 0.7 × 0.7 × 0.9 4:02
Clavicle Tangmose 2014 1T Siemens Surface coil Supine; prone T2 3D GE 0.7 × 0.7 × 1.5 6:04
Clavicle Vieth 2014 3T Philips 2 elliptical loop shaped surface Prone 3D FFE 0.7 × 0.7 × 1.4 5:41
Clavicle Schmidt 2017 3T Philips Surface coil Prone T1 3D FFE FSM 0.69 × 0.70 × 1.4,
R 0.29 × 0.29 × 0.75:41
Clavicle De Tobel Submitted 3T SiemensLoop-shaped surface coil with 11
cm boreProne T1 VIBE 0.7 × 0.7 × 0.9 4:02
Manubrium Martínez Vera 2017 3T Siemens Neck coil Supine T1 3D VIBE WE 0.9 × 0.9 × 0.9 NA
Proximal humerus Ekizoglu 2018 1.5T Siemens Extremity coil NA T1 TSE 0.5 × 0.5 × 3.5 1:44
Left distal radius Dvorak 2007 1T or 1.5T Wrist coilWrist above the head
or at the sideT1 SE ≤ 0.5 × ≤ 0.5 × 3 NA
Left distal radius George 2012 1.5T Siemens Wrist coilProne both hands
outstretchedT1 FSE 0.39 × 0.39 × 3 NA
Left distal radius Bolivar 2015 1.5T Siemens Wrist coilWrist above the head
or at the sideT1 SE ≤ 0.5 × ≤ 0.5 × 3 NA
Left distal radius Rashid 2015 1.5T Siemens Surface coilWrist above the head
or at the sideT1 FSE 0.5 × 0.5 × 3 5:48
Left distal radius Tscholl 2016 1T or 1.5T Wrist coilWrist above the head
or at the sideT1 SE ≤ 0.5 × ≤ 0.5 × 3 NA
Left distal radius Abdelbary 2018 0.31T open 8-channel hand/wrist coilSupine hand next to
bodyT1 SE ST 3 mm < 7:00
Left distal radius Sarkodie 2018 1.5T GE or Toshiba Wrist coilWrist above the head
or at the sideT1 SE ≤ 0.5 × ≤ 0.5 × 3 NA
Left distal radius Schmidt 2015 3T Philips 2 elliptical loop shaped surface NA T1 TSE 0.4 × 0.5 × 1.5 6:00
Left hand/wrist Serin 2016Philips, Siemens, GE,
ToshibaExtremity coils NA T1 SE ST 2-5 mm NA
Left distal radius Timme 2017 3T Philips16-channel surface head/neck
coilNA T1 TSE
M 0.4 × 0.5 × 2.5,
R 0.2 × 0.2 × 2.53:33
Left wrist De Tobel 2019 3T Siemens Wrist coilSupine hand next to
bodyT1 SE; T1 VIBE
0.20 × 0.20 × 2.0;
0.40 × 0.40 × 0.402:43; 5:57
Left hand/wrist Tomei 2014 0.2T G-Scan open Hand/wrist coil NA T1 3D SE 0.73 × 1.09 × 1.3 1:39 (twice if necessary)
Left hand/wrist Serinelli 2015 0.2T G-Scan open Small coil NA T1 3D SE 0.73 × 1.09 × 1.3 NA
Left hand/wrist Terada 2013 0.3T Neomax open 1-channel dedicated coil Seated 3D GE 0.39 × 0.78 × 1.56 2:44
Left hand/wrist Terada 2014 0.3T Shin-Etsu open 1-channel dedicated coil Seated 3D GE 0.39 × 0.78 × 1.56 2:44
Left hand/wrist Terada 2016 0.3T Shin-Etsu open 1-channel dedicated coil Seated 3D GE 0.39 × 0.78 × 1.57 2:44
Left hand/wrist Urschler 2016 1.5T Siemens Head coil
Prone with
outstrectched arm on
vacuum bed
T1 3D VIBE; T1 SE; T2
3D GE
0.43 × 0.43 × 0.9;
0.86 × 0.86 × 2.0;
0.86 × 0.86 × 0.9
3:08 ; 1:00 ; 2:21
Left hand/wrist Hojreh 2018 1.5T Siemens Head/neck coilProne with
outstrectched armT1 3D VIBE WE 0.4 × 0.4 × 1.5 2:26
Left hand/wrist Urschler 2015 3T Siemens Head/neck coilProne with
outstrectched armT1 3D FLASH VIBE 0.45 × 0.45 × 0.9 < 4:00
ANATOMICAL
STRUCTUREREFERENCE YEAR MRI SCANNER COIL POSITIONING MR SEQUENCE VOXEL SIZE (mm³) ACQUISITION TIME
Iliac crest Wittschieber 2014 3T Philips 8-channel SENSE cardiac coil NA T1 3D GE 0.49 × 0.49 × 2.2 17:47
Proximal femur Vo 2015 1.5T GESurface coil anterior + spine coil posteriorly
Supine T1 3D spoiled GE ST 1 mm NA
Sacrum Bollow 1997 1.5T Philips Body coilSupine with elevated legs
T1 SE, T2* opposed-phase FFE, dynamic T1 opposed-phase FFE
dynamic 11:12
Sacrum Bray 2016 1.5T Siemens NA NA
T1 TSE, STIR, T1 Turbo Inversion Recovery Magnitude, postcontrast T1, DWI
1.0 × 1.0 × 3-5; 2.5 × 2.5 × 8
NA
Patellofemoral joint Kim 2014 1.5T GE Knee coil NAintermediate, T1, T2, and PD; FSE
ST 3-4 mm NA
Distal femur Saint-Martin 2015 1.5T Philips NA NA T1 TSE NA NA
Knee Dedouit 2012 1.5T Philips Extremity coil NA FSE PD ST 3.5-4 mm 4:00
Knee Ekizoglu 2016b 3T Siemens Knee coil NA T2 TSE ST 3.5 mm 2:20
Knee Harcke 1992 0.5T HP VistaKnee coil (> 6 years old) or head coil (< 6 years old)
NAT1 SE, field-echo, T2 SE
NA NA
Knee Laor 2002 1.5T GEExtremity coil, torso phased-array coil, or quadrature head coil
NA
intermediate, T1, or T2; SE, FSE, some with inversion recovery; 3D spoiled gradient-recalled-echo; some with gadolinium contrast
ST 3-5 mm NA
Proximal tibia Jopp 2010 1.5T or 3T Philips Knee coil NA1.5 T T1 TSE and PD SPIR; 3T T1 TSE and STIR long TE SENSE
ST 1.5T C 3.0 mm, S 3.5 mm; 3T C 3.0 mm, S 4.0 mm
Distal femur Krämer 2014a 3T Siemens 15-channel knee coil NA T1 TSE 0.4 × 0.4 × 3.0 1:57
Proximal tibia Krämer 2014b 3T Siemens 15-channel knee coil NA T1 TSE 0.4 × 0.4 × 3.0 1:57
Knee Fan 2016 1.5T Philips or Siemens Knee coil NA T1 TSE NA NA
Knee Ottow 2017 3T Philips Surface coil NA T1 TSEM 0.6 × 0.77 × 3, R 0.31 × 0.31 × 3
3:51
Knee Auf der Mauer 2018 3T Philips 8-channel knee coil NA T1 SENSE 0.1875 × 0.1875 × 2 NA
Knee Vieth 2018 3T Philips Surface coil NA T1 TSE; T2 TSE SPIRM 0.6 × 0.77 × 3, R 0.31 × 0.31 × 3; M 0.6 × 0.76 × 3, R 0.31 × 0.31 × 3
3:51; 3:08
Knee Pennock 2018 1.5T Extremity coil NA T1 NA NA
Knee Craig 2004 1T or 1.5T GE NA NA3D fat-suppressed spoiled GRASS
ST 1.0-2.0 mm NA
Knee Kercher 2009 1.5T or 3T NA NA T1 NA NA
Ankle Saint-Martin 2013 1.5T Philips Extremity coil NA T1 SE ST 2-4 mm 4:00
Distal tibia Saint-Martin 2014 1.5T Philips Extremity coil NA T1 SE ST 2-4 mm 4:00
Ankle Ekizoglu 2015 1.5T Siemens Extremity coil NA T1 SE 0.5 × 0.5 × 3.5 mm 4:00
MFA Stern 2017 3T SiemensT 8-channel multifunctional coil and CW head/neck coil
TC Supine and W prone with outstrectched arm
T PD TSE; CW T1 3D GE
T 0.59 × 0.59 × 1.0; C 0.9 × 0.9 × 0.9; W 0.45 × 0.45 × 0.9
NA
TABLE 10.2 (CONTINUED)
A = axial ; C (voxel s ize) = c lavic le ; C (acquis it ion t ime) = coronal ; GE (scanner) = General E lectr ic ; M =
measured; MFA = mult i-factorial age est imation; NA = not apl l icable or not repor ted: R = reconstructed; S
= sagittal ; ST = s l ice thickness ; T = teeth; W = wrist . Sequences: DWI = diffus ion-weighted imaging, FLASH
= fast low angle shot , FFE = fast f ie ld echo; FS = fat saturation; FSE = fast spin echo; GE = gradient echo;
PD = proton-density-weighted; SE = spin echo; SENSE = sensit iv ity encoding; SPIR = spectral-presatura-
t ion-with- invers ion-recovery; STIR = shor t- tau-invers ion-recovery; T 1 = T1-weighted; T2 = T2-weighted; TSE
= turbo spin echo; VIBE = volume-interpolated breath-hold examination; WE = water excitat ion.
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

200
TABLE 10.3 — CHARACTERISTICS OF ANALYSES IN ELIGIBLE STUDIES. Studies are grouped per anatomical
s ite and ordered per staging technique.
AN
ATO
MIC
AL S
TRU
CTU
RE
REF
EREN
CE
YEA
RST
AG
ING
TEC
HN
IQU
EN
UM
BER
OF
STA
GES
STATI
STIC
AL A
NA
LYSI
SN
UM
BER
OF
OBSE
RVER
SPR
OFE
SSIO
NA
L B
AC
KGRO
UN
D
Sphe
no-o
ccip
ital
sync
hond
rosi
sEk
izoglu
2016
aBa
ssed
5Si
mple
line
ar
regre
ssio
n2
Radio
logis
t and
fore
nsic
path
olo
gis
t
Mola
rs (m
iner
aliz
ation)
Baum
ann
2015
Dem
irjia
n8
Des
crip
tive
2Den
tist
s
Mola
rs (e
ruption)
Baum
ann
2015
Olz
e4
Low
er le
ft t
hird
mola
rG
uo20
15Dem
irjia
n8
Des
crip
tive
1Den
tist
s
Third m
ola
rsDe
Tobel
2017
bDem
irjia
n8
Des
crip
tive
2M
edic
al d
oct
or/
den
stis
try
stud
ent
and
rese
arc
her
at
radio
logy
Third m
ola
rsDe
Tobel
2017
bKö
hler
10
Third m
ola
rsDe
Tobel
2017
cDe
Tobel
8Ba
yesi
an
2Re
siden
t O
MFS
and
den
tist
Cla
vicl
eH
illew
ig20
13Kr
eitn
er (c
fr. S
chm
elin
g 1,
2, 3
, 4/5
)4
Baye
sian
4Ra
dio
logis
ts a
nd P
hD-s
tuden
t
Cla
vicl
eTa
ngm
ose
2014
Krei
tner
(cfr. S
chm
elin
g 1,
2, 3
, 4/5
)4
Des
crip
tive
3M
D, r
adio
logis
t, fore
nsic
ant
hropolo
gis
t
Cla
vicl
eV
ieth
2014
Schm
elin
g a
nd K
ellin
gha
us9
Des
crip
tive
2N
A
Cla
vicl
eSc
hmid
t20
17Sc
hmel
ing a
nd K
ellin
gha
us9
Des
crip
tive
2N
A
Cla
vicl
eDe
Tobel
Subm
itte
d
Kelli
ngha
us a
nd W
itts
chie
ber
, dis
card
ing s
tages
1 and
4/5
, dis
card
ing s
ubst
ages
of
stage
2 (2
,
3aa, 3
ab, 3
ac,
3b, 3
c)
6Ba
yesi
an
2Re
siden
t O
MFS
and
fore
nsic
ant
hropolo
gis
t
Manu
brium
Mart
ínez
Ver
a20
17N
o s
tagin
g, m
easu
rem
ents
and
sha
pe
variations
; sem
i-aut
om
atic
segm
enta
tion
NA
Prin
cipal c
om
pone
nt
ana
lysi
s and
mul
tiple
line
ar
regre
ssio
n
NA
NA
Prox
imal h
umer
usEk
izoglu
2018
Schm
elin
g a
nd K
ellin
gha
us9
Des
crip
tive
2Ra
dio
logis
ts
Left
dis
tal r
adiu
sDvo
rak
200
7Dvo
rak
6Des
crip
tive
3Ra
dio
logis
ts a
nd n
euro
logis
t
Left
dis
tal r
adiu
sG
eorg
e20
12Dvo
rak
6Des
crip
tive
3Ra
dio
logis
ts
Left
dis
tal r
adiu
sBo
livar
2015
Dvo
rak
6Des
crip
tive
3Ra
dio
logis
ts a
nd s
port
s m
edic
ine
phy
sici
an
Left
dis
tal r
adiu
sRa
shid
2015
Dvo
rak
6Des
crip
tive
2Ra
dio
logis
ts
Left
dis
tal r
adiu
sTs
choll
2016
Dvo
rak
6Des
crip
tive
2N
A
Left
dis
tal r
adiu
sA
bdel
bary
2018
Dvo
rak
6Si
mple
line
ar
regre
ssio
n,
AN
OVA
3Ra
dio
logis
ts
Left
dis
tal r
adiu
sSa
rkodie
2018
Dvo
rak
6Des
crip
tive
3Ra
dio
logis
ts
Left
dis
tal r
adiu
sSc
hmid
t20
15Sc
hmel
ing a
nd K
ellin
gha
us, i
nclu
din
g T
FS11
Des
crip
tive
2Fo
rens
ic p
hysi
cian
Left
hand
/wrist
Serin
2016
Jopp (c
fr. S
chm
elin
g 2
, 3, 4
/5)
3Ba
yesi
an,
tra
nsitio
n2
Resi
den
t and
sen
ior
fore
nsic
path
olo
gis
t
Left
dis
tal r
adiu
sTi
mm
e20
17Sc
hmel
ing a
nd K
ellin
gha
us, i
nclu
din
g T
FS11
Des
crip
tive
2N
A
Left
wrist
De
Tobel
2019
Schm
elin
g a
nd K
ellin
gha
us; S
E st
age
4/5
subst
ages
base
d o
n V
IBE
stage
(3c,
4, 5
)7
Baye
sian
2Re
siden
t O
MFS
and
fore
nsic
ant
hropolo
gis
t
Left
hand
/wrist
Tom
ei20
14To
mei
Sum
of
score
s (rang
e 9-8
5)Si
mple
line
ar
regre
ssio
n2
Radio
logis
ts
Left
hand
/wrist
Serine
lli20
15To
mei
Sum
of
score
s (rang
e 9-8
5)Des
crip
tive
2N
A
Left
hand
/wrist
Tera
da
2013
Tann
er-W
hite
hous
e-2-
Japan
RUS
Sum
of
score
sSi
mple
line
ar
regre
ssio
n2
Ort
hoped
ic s
pec
ialis
ts
Left
hand
/wrist
Tera
da
2014
Tann
er-W
hite
hous
e-2-
Japan
RUS
Sum
of
score
sSi
mple
line
ar
regre
ssio
n3
Ort
hoped
ic s
pec
ialis
ts a
nd r
adio
logis
t
Left
hand
/wrist
Tera
da
2016
Tann
er-W
hite
hous
e-2-
Japan
RUS
Sum
of
score
sSi
mple
line
ar
regre
ssio
n2
Ort
hoped
ic s
pec
ialis
t and
radio
logis
t
Left
hand
/wrist
Urs
chle
r20
16G
reul
ich-
Pyle
; Tann
er-W
hite
hous
e-2
Age
cate
gories
; sum
of
score
sDes
crip
tive
2Ra
dio
logis
ts
Left
hand
/wrist
Hojreh
2018
Gre
ulic
h-Py
leA
ge
cate
gories
Des
crip
tive
2Ra
dio
logis
ts
Left
hand
/wrist
Urs
chle
r20
15C
ont
inuo
usA
ge
cate
gories
RRF
NA
NA
AN
ATO
MIC
AL S
TRU
CTU
RE
REF
EREN
CE
YEA
RST
AG
ING
TEC
HN
IQU
EN
UM
BER
OF
STA
GES
STATI
STIC
AL A
NA
LYSI
SN
UM
BER
OF
OBSE
RVER
SPR
OFE
SSIO
NA
L B
AC
KGRO
UN
D
Iliac
cres
tW
itts
chie
ber
2014
Web
b (c
fr. S
chm
elin
g 1,
2, 3
, 4)
8Des
crip
tive
1N
A
Prox
imal f
emur
Vo
2015
Adju
sted
Dvo
rak;
ang
le o
f N
ötz
li6; c
ont
inuo
us a
ngle
sA
NO
VA3
Radio
logis
ts
Sacr
um S
ABo
llow
1997
Bollo
w (c
fr. S
chm
elin
g 2
, 3, 4
/5);
ADC
cont
inuo
us3
Des
crip
tive
3Ra
dio
logis
ts
Sacr
um L
ABo
llow
1997
Bollo
w3
Sacr
um S
ABra
y20
16Bo
llow
(cfr. S
chm
elin
g 2
, 3, 4
/5);
ADC
cont
inuo
us3
AN
OVA
2Ra
dio
logis
ts
Pate
llofe
mora
l join
tKi
m20
14O
pen
/clo
sing
or
close
d; m
easu
rem
ents
2Re
gre
ssio
n2
Radio
logis
ts
Dis
tal f
emur
Sain
t-M
art
in20
15Fu
sed o
r no
t2
Des
crip
tive
2Fo
rens
ic p
ath
olo
gis
ts
Knee
Ded
oui
t20
12Ded
oui
t5
Trans
itio
n2
Radio
logis
t and
fore
nsic
path
olo
gis
t
Knee
Ekiz
oglu
2016
bDed
oui
t5
Des
crip
tive
2Ra
dio
logis
ts
Knee
Harc
ke19
92
Harc
ke (c
fr. K
ellin
gha
us 2
a/2
b, 2
c, 3
, 4/5
)4
None
NA
NA
Knee
Laor
200
2
Laor
(met
aphy
seal s
trip
e; c
fr. S
chm
elin
g 2
with
stripe,
3 w
ith
stripe,
4/5
with
stripe,
4/5
no
stripe)
4Des
crip
tive
2 co
nsen
sus
Radio
logis
ts
Prox
imal t
ibia
Jopp
2010
Jopp (c
fr. S
chm
elin
g 2
, 3, 4
/5)
3Des
crip
tive
2Ra
dio
logis
ts
Dis
tal f
emur
Kräm
er20
14a
Schm
elin
g a
nd K
ellin
gha
us9
Des
crip
tive
2N
A
Prox
imal t
ibia
Kräm
er20
14b
Schm
elin
g a
nd K
ellin
gha
us9
Des
crip
tive
2Ra
dio
logis
ts
Knee
Fan
2016
Kram
er (c
fr. K
ellin
gha
us 2
, 3a, 3
b, 3
c, 4
, 5)
6Si
mple
line
ar
regre
ssio
n2
NA
Knee
Ott
ow20
17Sc
hmel
ing a
nd K
ellin
gha
us9
Des
crip
tive
2N
A
Knee
Auf
der
Maue
r20
18Jo
pp (c
fr. S
chm
elin
g 2
, 3, 4
/5) and
SKJ
3Des
crip
tive
3Fo
rens
ic p
ath
olo
gis
t
Knee
Vie
th20
18V
ieth
6Des
crip
tive
2N
A
Knee
Penn
ock
2018
Penn
ock
Age
cate
gories
Des
crip
tive
2N
A
Knee
Cra
ig20
04
Cont
inuo
usA
reas
at
super
ior-
infe
rior
MIP
,
volu
mes
Sim
ple
line
ar
regre
ssio
nN
ARa
dio
logis
ts
Knee
Kerc
her
200
9Ph
ysea
l volu
me
cont
inuo
usN
ASi
mple
line
ar
regre
ssio
nN
AN
A
Ank
leSa
int-
Mart
in20
13Jo
pp (c
fr. S
chm
elin
g 2
, 3, 4
/5)
3Ba
yesi
an,
tra
nsitio
n2
Fore
nsic
path
olo
gis
ts, t
rain
ed b
y se
nior
radio
logis
t
Dis
tal t
ibia
Sain
t-M
art
in20
14N
o s
tagin
g, s
igna
l int
ensi
ty 3
D o
r 2D
gra
ph
Min
or
or
adul
tDes
crip
tive
NA
NA
Ank
leEk
izoglu
2015
Jopp (c
fr. S
chm
elin
g 2
, 3, 4
/5)
3Des
crip
tive
2Ra
dio
logis
ts
MFA
Ster
n20
17C
ont
inuo
usA
ges
as
out
put
RRF
and
DC
NN
NA
NA
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

201
TABLE 10.3 (CONTINUED)
AN
ATO
MIC
AL S
TRU
CTU
RE
REF
EREN
CE
YEA
RST
AG
ING
TEC
HN
IQU
EN
UM
BER
OF
STA
GES
STATI
STIC
AL A
NA
LYSI
SN
UM
BER
OF
OBSE
RVER
SPR
OFE
SSIO
NA
L B
AC
KGRO
UN
D
Sphe
no-o
ccip
ital
sync
hond
rosi
sEk
izoglu
2016
aBa
ssed
5Si
mple
line
ar
regre
ssio
n2
Radio
logis
t and
fore
nsic
path
olo
gis
t
Mola
rs (m
iner
aliz
ation)
Baum
ann
2015
Dem
irjia
n8
Des
crip
tive
2Den
tist
s
Mola
rs (e
ruption)
Baum
ann
2015
Olz
e4
Low
er le
ft t
hird
mola
rG
uo20
15Dem
irjia
n8
Des
crip
tive
1Den
tist
s
Third m
ola
rsDe
Tobel
2017
bDem
irjia
n8
Des
crip
tive
2M
edic
al d
oct
or/
den
stis
try
stud
ent
and
rese
arc
her
at
radio
logy
Third m
ola
rsDe
Tobel
2017
bKö
hler
10
Third m
ola
rsDe
Tobel
2017
cDe
Tobel
8Ba
yesi
an
2Re
siden
t O
MFS
and
den
tist
Cla
vicl
eH
illew
ig20
13Kr
eitn
er (c
fr. S
chm
elin
g 1,
2, 3
, 4/5
)4
Baye
sian
4Ra
dio
logis
ts a
nd P
hD-s
tuden
t
Cla
vicl
eTa
ngm
ose
2014
Krei
tner
(cfr. S
chm
elin
g 1,
2, 3
, 4/5
)4
Des
crip
tive
3M
D, r
adio
logis
t, fore
nsic
ant
hropolo
gis
t
Cla
vicl
eV
ieth
2014
Schm
elin
g a
nd K
ellin
gha
us9
Des
crip
tive
2N
A
Cla
vicl
eSc
hmid
t20
17Sc
hmel
ing a
nd K
ellin
gha
us9
Des
crip
tive
2N
A
Cla
vicl
eDe
Tobel
Subm
itte
d
Kelli
ngha
us a
nd W
itts
chie
ber
, dis
card
ing s
tages
1 and
4/5
, dis
card
ing s
ubst
ages
of
stage
2 (2
,
3aa, 3
ab, 3
ac,
3b, 3
c)
6Ba
yesi
an
2Re
siden
t O
MFS
and
fore
nsic
ant
hropolo
gis
t
Manu
brium
Mart
ínez
Ver
a20
17N
o s
tagin
g, m
easu
rem
ents
and
sha
pe
variations
; sem
i-aut
om
atic
segm
enta
tion
NA
Prin
cipal c
om
pone
nt
ana
lysi
s and
mul
tiple
line
ar
regre
ssio
n
NA
NA
Prox
imal h
umer
usEk
izoglu
2018
Schm
elin
g a
nd K
ellin
gha
us9
Des
crip
tive
2Ra
dio
logis
ts
Left
dis
tal r
adiu
sDvo
rak
200
7Dvo
rak
6Des
crip
tive
3Ra
dio
logis
ts a
nd n
euro
logis
t
Left
dis
tal r
adiu
sG
eorg
e20
12Dvo
rak
6Des
crip
tive
3Ra
dio
logis
ts
Left
dis
tal r
adiu
sBo
livar
2015
Dvo
rak
6Des
crip
tive
3Ra
dio
logis
ts a
nd s
port
s m
edic
ine
phy
sici
an
Left
dis
tal r
adiu
sRa
shid
2015
Dvo
rak
6Des
crip
tive
2Ra
dio
logis
ts
Left
dis
tal r
adiu
sTs
choll
2016
Dvo
rak
6Des
crip
tive
2N
A
Left
dis
tal r
adiu
sA
bdel
bary
2018
Dvo
rak
6Si
mple
line
ar
regre
ssio
n,
AN
OVA
3Ra
dio
logis
ts
Left
dis
tal r
adiu
sSa
rkodie
2018
Dvo
rak
6Des
crip
tive
3Ra
dio
logis
ts
Left
dis
tal r
adiu
sSc
hmid
t20
15Sc
hmel
ing a
nd K
ellin
gha
us, i
nclu
din
g T
FS11
Des
crip
tive
2Fo
rens
ic p
hysi
cian
Left
hand
/wrist
Serin
2016
Jopp (c
fr. S
chm
elin
g 2
, 3, 4
/5)
3Ba
yesi
an,
tra
nsitio
n2
Resi
den
t and
sen
ior
fore
nsic
path
olo
gis
t
Left
dis
tal r
adiu
sTi
mm
e20
17Sc
hmel
ing a
nd K
ellin
gha
us, i
nclu
din
g T
FS11
Des
crip
tive
2N
A
Left
wrist
De
Tobel
2019
Schm
elin
g a
nd K
ellin
gha
us; S
E st
age
4/5
subst
ages
base
d o
n V
IBE
stage
(3c,
4, 5
)7
Baye
sian
2Re
siden
t O
MFS
and
fore
nsic
ant
hropolo
gis
t
Left
hand
/wrist
Tom
ei20
14To
mei
Sum
of
score
s (rang
e 9-8
5)Si
mple
line
ar
regre
ssio
n2
Radio
logis
ts
Left
hand
/wrist
Serine
lli20
15To
mei
Sum
of
score
s (rang
e 9-8
5)Des
crip
tive
2N
A
Left
hand
/wrist
Tera
da
2013
Tann
er-W
hite
hous
e-2-
Japan
RUS
Sum
of
score
sSi
mple
line
ar
regre
ssio
n2
Ort
hoped
ic s
pec
ialis
ts
Left
hand
/wrist
Tera
da
2014
Tann
er-W
hite
hous
e-2-
Japan
RUS
Sum
of
score
sSi
mple
line
ar
regre
ssio
n3
Ort
hoped
ic s
pec
ialis
ts a
nd r
adio
logis
t
Left
hand
/wrist
Tera
da
2016
Tann
er-W
hite
hous
e-2-
Japan
RUS
Sum
of
score
sSi
mple
line
ar
regre
ssio
n2
Ort
hoped
ic s
pec
ialis
t and
radio
logis
t
Left
hand
/wrist
Urs
chle
r20
16G
reul
ich-
Pyle
; Tann
er-W
hite
hous
e-2
Age
cate
gories
; sum
of
score
sDes
crip
tive
2Ra
dio
logis
ts
Left
hand
/wrist
Hojreh
2018
Gre
ulic
h-Py
leA
ge
cate
gories
Des
crip
tive
2Ra
dio
logis
ts
Left
hand
/wrist
Urs
chle
r20
15C
ont
inuo
usA
ge
cate
gories
RRF
NA
NA
AN
ATO
MIC
AL S
TRU
CTU
RE
REF
EREN
CE
YEA
RST
AG
ING
TEC
HN
IQU
EN
UM
BER
OF
STA
GES
STATI
STIC
AL A
NA
LYSI
SN
UM
BER
OF
OBSE
RVER
SPR
OFE
SSIO
NA
L B
AC
KGRO
UN
D
Iliac
cres
tW
itts
chie
ber
2014
Web
b (c
fr. S
chm
elin
g 1,
2, 3
, 4)
8Des
crip
tive
1N
A
Prox
imal f
emur
Vo
2015
Adju
sted
Dvo
rak;
ang
le o
f N
ötz
li6; c
ont
inuo
us a
ngle
sA
NO
VA3
Radio
logis
ts
Sacr
um S
ABo
llow
1997
Bollo
w (c
fr. S
chm
elin
g 2
, 3, 4
/5);
ADC
cont
inuo
us3
Des
crip
tive
3Ra
dio
logis
ts
Sacr
um L
ABo
llow
1997
Bollo
w3
Sacr
um S
ABra
y20
16Bo
llow
(cfr. S
chm
elin
g 2
, 3, 4
/5);
ADC
cont
inuo
us3
AN
OVA
2Ra
dio
logis
ts
Pate
llofe
mora
l join
tKi
m20
14O
pen
/clo
sing
or
close
d; m
easu
rem
ents
2Re
gre
ssio
n2
Radio
logis
ts
Dis
tal f
emur
Sain
t-M
art
in20
15Fu
sed o
r no
t2
Des
crip
tive
2Fo
rens
ic p
ath
olo
gis
ts
Knee
Ded
oui
t20
12Ded
oui
t5
Trans
itio
n2
Radio
logis
t and
fore
nsic
path
olo
gis
t
Knee
Ekiz
oglu
2016
bDed
oui
t5
Des
crip
tive
2Ra
dio
logis
ts
Knee
Harc
ke19
92
Harc
ke (c
fr. K
ellin
gha
us 2
a/2
b, 2
c, 3
, 4/5
)4
None
NA
NA
Knee
Laor
200
2
Laor
(met
aphy
seal s
trip
e; c
fr. S
chm
elin
g 2
with
stripe,
3 w
ith
stripe,
4/5
with
stripe,
4/5
no
stripe)
4Des
crip
tive
2 co
nsen
sus
Radio
logis
ts
Prox
imal t
ibia
Jopp
2010
Jopp (c
fr. S
chm
elin
g 2
, 3, 4
/5)
3Des
crip
tive
2Ra
dio
logis
ts
Dis
tal f
emur
Kräm
er20
14a
Schm
elin
g a
nd K
ellin
gha
us9
Des
crip
tive
2N
A
Prox
imal t
ibia
Kräm
er20
14b
Schm
elin
g a
nd K
ellin
gha
us9
Des
crip
tive
2Ra
dio
logis
ts
Knee
Fan
2016
Kram
er (c
fr. K
ellin
gha
us 2
, 3a, 3
b, 3
c, 4
, 5)
6Si
mple
line
ar
regre
ssio
n2
NA
Knee
Ott
ow20
17Sc
hmel
ing a
nd K
ellin
gha
us9
Des
crip
tive
2N
A
Knee
Auf
der
Maue
r20
18Jo
pp (c
fr. S
chm
elin
g 2
, 3, 4
/5) and
SKJ
3Des
crip
tive
3Fo
rens
ic p
ath
olo
gis
t
Knee
Vie
th20
18V
ieth
6Des
crip
tive
2N
A
Knee
Penn
ock
2018
Penn
ock
Age
cate
gories
Des
crip
tive
2N
A
Knee
Cra
ig20
04
Cont
inuo
usA
reas
at
super
ior-
infe
rior
MIP
,
volu
mes
Sim
ple
line
ar
regre
ssio
nN
ARa
dio
logis
ts
Knee
Kerc
her
200
9Ph
ysea
l volu
me
cont
inuo
usN
ASi
mple
line
ar
regre
ssio
nN
AN
A
Ank
leSa
int-
Mart
in20
13Jo
pp (c
fr. S
chm
elin
g 2
, 3, 4
/5)
3Ba
yesi
an,
tra
nsitio
n2
Fore
nsic
path
olo
gis
ts, t
rain
ed b
y se
nior
radio
logis
t
Dis
tal t
ibia
Sain
t-M
art
in20
14N
o s
tagin
g, s
igna
l int
ensi
ty 3
D o
r 2D
gra
ph
Min
or
or
adul
tDes
crip
tive
NA
NA
Ank
leEk
izoglu
2015
Jopp (c
fr. S
chm
elin
g 2
, 3, 4
/5)
3Des
crip
tive
2Ra
dio
logis
ts
MFA
Ster
n20
17C
ont
inuo
usA
ges
as
out
put
RRF
and
DC
NN
NA
NA
AD
C =
ap
pa
ren
t d
iffu
sio
n c
oe
ffic
ien
t; A
NO
VA
= a
na
lysi
s o
f va
ria
nce
; D
CN
N =
de
ep
co
nvo
luti
on
al
ne
ura
l n
etw
ork
; L
A =
la
tera
l a
po
ph
yse
s;
MFA
= m
ult
i-fa
cto
ria
l a
ge
est
ima
tio
n;
MIP
= m
axi
mu
m i
nte
nsi
ty p
roje
cti
on
, N
A =
no
t a
pp
lica
ble
or
no
t re
po
rte
d;
RR
F =
ra
nd
om
re
gre
ssio
n
fore
st;
SA
= s
eg
me
nta
l a
po
ph
yse
s; S
KJ
= c
um
mu
lati
ve
sco
re o
f th
e k
ne
e j
oin
t; T
FS =
th
ree
fold
str
ati
fica
tio
n s
ign
.
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

202
b Proximal humerus – Most elaborate staging technique
FEMALES MALES
a Spheno-occipital synchodrosis – Bassed staging technique
FEMALES MALES
FIGURE 10.3 —AGE DISTRIBUTIONS PER DEVELOPMENTAL STAGE OF DIFFERENT ANATOMICAL STRUCTURES
PER SEX. Staging techniques for development were grouped if they were s imi lar. Main stages were joint ly
indicated on top of the graph. Note that stages were re-named according to the most elaborate staging
technique (Table 10.4), i f appropriate. Below the main stages, the number of par t ic ipants per boxplot is
indicated. Age is displayed on the ordinate, uniformly cal ibrated for al l graphs. References are abbrevi-
ated on the abscissa including the f irst letter of the f irst author’s last name and the year of publ icat ion.
Numbers added to a reference with a hyphen indicate different observers, e.g . B2015-2 C = stage C al lo-
cated by observer 2 in Baumann et al . (2015). Per graph, results from the same study are indicated by the
same colour of the box-plots.
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.
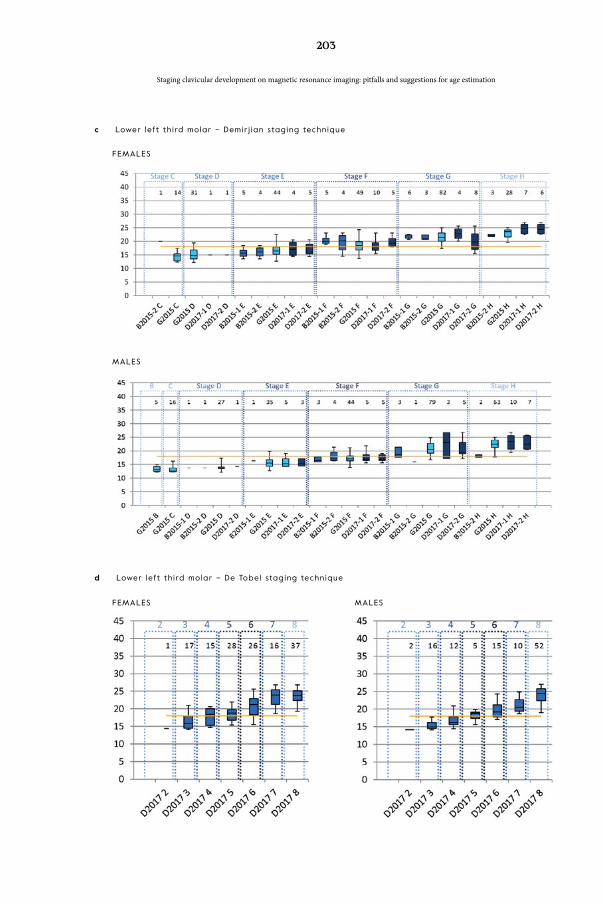
203
d Lower left third molar – De Tobel staging technique
FEMALES MALES
c Lower left third molar – Demir j ian staging technique
FEMALES
MALES
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

204
e Sternal end of the c lavic les – Most elaborate staging technique. When both c lavic les were recorded
separately, the suff ix -L indicates the left c lavic le, whi le the suff ix -R indicates the r ight c lavic le.
FEMALES
MALES
f Left hand/wrist spin echo (S2015) and VIBE (U2015 and H2018) sequence – At las and automated
technique. Note that S2015 appl ied the MRI-specif ic at las, H2018 appl ied the Greul ich-Pyle at las,
and U2015 appl ied an automated method.
FEMALES
MALES
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

205
g Left distal radius spin echo sequence – Dvorak staging technique. SA = Latin American; AF = Afr ican;
EU = European; AS = Asian.
FEMALES
MALES
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

206
h Left distal radius spin echo sequence – Most elaborate staging technique. For D2019, the stages
between brackets correspond with added VIBE information.
FEMALES
MALES
i Left distal radius VIBE sequence – Most elaborate staging technique
FEMALES MALES
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

207
k Distal femur – Dedouit staging technique
FEMALES MALES
j Distal femur – Most elaborate staging technique
FEMALES
MALES
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

208
m Proximal t ibia – Dedouit staging technique
FEMALES MALES
l Proximal t ibia – Most elaborate staging technique
FEMALES
MALES
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

209
n Distal femur – Vieth staging technique
FEMALES MALES
o Proximal t ibia – Vieth staging technique
FEMALES MALES
p Proximal f ibula – Most elaborate staging technique
FEMALES MALES
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

210
q Knee – Knee joint score
(sum of Jopp stages of each knee bone)
MALES
r Il iac crest – Most elaborate staging technique
MALES
s Distal t ibia – Most elaborate staging technique
FEMALES MALES
t Calcaneum – Most elaborate staging technique
FEMALES MALES
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

211
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation
sum of individual bone scores. Converse-ly, the Greulich-Pyle hand/wrist [38] and Pennock knee [69] atlas techniques use standard images per age category instead of scores. Finally, (semi-)automatic tech-niques extract continuous data from the MRI to relate them to age [8, 12, 51, 63, 90, 113].
When the latter techniques were ap-plied, regression was mostly performed to relate the continuous data of devel-opment to age. This was also reported to relate ordinal staging data to age, albeit in a minority of included papers. Most papers only reported descriptive statistics on age per stage in tables. Those statistics
were summarised in Figure 10.3 and will be elucidated further on. Furthermore, a few papers applied Bayes’ rule to nuance the age estimation, which has been stat-ed to be more appropriate than linear re-gression [16, 17, 20, 73, 85]. Finally, ad-vanced machine learning was applied to estimate age in two papers, but no details on the statistical approach were reported [90, 113]. The latter studies, together with four others, applied cross-validation [16, 17, 20, 63, 90, 113], while one study tested their results on a validation sample [69].
A final characteristic in relation to image analysis lies in the observers’ back-ground and experience. Table 10.3 clearly
TABLE 10.4 — DESCRIPTIVE CRITERIA FOR DEVELOPMENTAL STAGES OF LONG BONES ON MRI .
1 Ossif icat ion centre is invis ib le (= not yet oss if ied).
2 Ossif icat ion centre is v is ib le (= oss if ied), nonunion of the epiphysis and metaphysis .
2a The lengthwise epiphyseal measurement is one third or less compared to the widthwise mea-
surement of the metaphyseal ending.
2b The lengthwise epiphyseal measurement is over one third unt i l two thirds compared to the
widthwise measurement of the metaphyseal ending.
2c The lengthwise epiphyseal measurement is over two thirds compared to the widthwise measure-
ment of the metaphyseal ending.
3 Physeal plate is par t ial ly oss if ied (= bone trabeculae cross the physeal plate from ossif icat ion
centre to metaphysis).
3a The epiphyseal-metaphyseal fus ion completes one third or less of the former gap between
epiphysis and metaphysis .
3aa Lengthwise measurement of the epiphysis is one third or lower compared with the widthwise
measurement of the metaphyseal ending.
3ab Lengthwise measurement of the epiphysis is between one third and two thirds compared with
the widthwise measurement of the metaphyseal ending.
3ac Lengthwise measurement of the epiphysis is over two thirds compared with the widthwise mea-
surement of the metaphyseal ending.
3b The epiphyseal-metaphyseal fus ion completes over one third unt i l two thirds of the former gap
between epiphysis and metaphysis .
3c The epiphyseal-metaphyseal fus ion completes over two thirds of the former gap between epiph-
ysis and metaphysis .
4 Complete union of the epiphysis and metaphysis (= physeal plate is completely oss if ied). Physeal
scar is st i l l v is ib le.
5 Complete union of the epiphysis and metaphysis . Physeal scar is indiscernible.

212
demonstrates the multidisciplinary na-ture of age estimation. Some studies re-ported how many years of experience the observers had, either in their discipline (range 2 to 20 years) [9, 31], or with age estimation (range 1 to 9 years) [16, 17].
Risk of bias assessment
Table 10.5 demonstrates that bias was a major concern in almost all included studies. Selection bias was caused by in-cluding elite football players, who might be advanced in their development [76], or by including patients in whom develop-mental disorders could not be ruled out [8, 52, 57, 114]. Furthermore, the small study samples resulted in an uneven dis-tribution among age categories [1, 3, 5, 9, 12, 22, 25, 28, 30, 31, 33, 42, 46, 49, 52, 55, 56, 73, 74, 76, 84, 92, 109, 111, 113, 114, 118], or frequencies per age were not re-ported [57]. Retrospective studies did not report the biological origin of the pop-ulation, while some prospective studies included different ethnic groups [25, 93, 111], or only a few individuals of another ethnic group [46]. Moreover, only a few studies reported socio-economic status of their study participants.
Performance bias was caused by par-ticipants being scanned for a clinical indi-cation, which was not in agreement with the review question. The second source of performance bias considered the inter-pretation of the images and was caused by applying a staging technique which might not be suitable for MRI [5, 18, 39, 46, 95-97, 114], or by focusing on development, rather than age estimation [8, 9, 12, 42, 51, 52, 57].
Attrition bias was caused by lacking infor-mation about why data were missing [25], or by more missing values in certain age categories [17, 25, 93]. Especially in clavi-cle studies, motion artefacts and anatom-ical shape variants caused missing data, ranging from 1% [44] to 36% [17]. Molars were not assessable on MRI in 0-15% [5], the left wrist in 1% [16] to 14% [97], and a knee scan was repeated up to three times in case of motion artefacts [67].
Detection bias was a minor issue, since it can be assumed that observers were blinded for the age of participants, even when it was not reported. Blinding for sex seems less important, since in practice the sex is also known.
Reporting bias was caused as a result of neglecting to specify which observer’s results were reported. Although several studies received funding from govern-mental agencies or sports associations, they were not considered to cause con-flicts of interest.
Other sources of bias were manifold:
— not sex-specific [8, 9, 12, 51, 57];
— a small age range of the study popu-lation (i.e. 5 years or less) [36, 49, 77, 84, 116, 122];
— a lower age limit close to 18 (i.e. less than 2 years lower than 18) [84, 116, 122];
— an upper age limit close to 18 (i.e. less than 2 years higher than 18) [1, 7-9, 25, 36, 46, 69, 71, 86, 111, 118];
— an upper age limit younger than 18 [76, 95-97, 109, 114];
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

213
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation
— age expressed in years without frac-tions, so that subjects who exceeded 6 months of a year would be counted as reaching the upcoming age [1];
— only birth years were recorded, no birth dates [30];
— unclear statistical approach [114].
Because of the highly biased nature of most studies, it was decided not to con-duct meta-analysis on the age distribu-tions per stage. Moreover, it remains un-clear if data from an anatomical site can safely be pooled, when the MRI sequences are not identical. To date, only one study compared scanning protocols in the same individuals, but their sample was too small to draw strong conclusions [19].
Quantitative synthesis
Age distributions in relation to development
Statistics were extracted from boxplots for the following references: [7, 25, 73, 85]. Moreover, the following authors provid-ed additional data: Markus Auf der Mau-er [3, 49], Jannick De Tobel [16-18, 20], Astrid Junge [111], and Martin Urschler [113, 114].
To provide a clear overview, statistics on age distributions per stage were dis-played in box-plots. Figure 10.2 explains how differences in reported data were han-dled to create the graphs in Figure 10.3. Note that some boxplots (in early stages) entirely fall below the 18-year-threshold, while others (in late stages) lie entirely above the threshold. Cut-off stages for these absolute statements regarding child-
hood and adulthood are summarised in Table 10.6.
To quantify how well the age distri-butions increased with increasing stag-es, several studies reported correlation coefficients. The Pearson correlation coefficient was reported for the manu-brium (0.66-0.73) [63], and hand/wrist (0.90-0.92) [96, 109]. The Spearman cor-relation coefficient was reported for the spheno-occipital synchondrosis (0.73-0.86) [29], clavicle (-0.043-0.77) [45, 93], proximal humerus (0.63-0.65) [31], distal radius (0.07-0.77) [36, 76], hand/wrist (0.94-0.96) [85], proximal femur (0.79-0.83) [118], distal femur (0.76-0.85) [3, 30], proximal tibia (0.76-0.85) [3, 30], proximal fibula (0.77) [3], and knee (0.80-0.98) [3, 69]. Remarkably, the correlation coefficients were mostly higher in males than in females.
Furthermore, two studies applied transition analysis and reported mean ages of transition from one stage to anoth-er [22, 73]. They only applied main stages, without substaging.
Reproducibility of staging
Although different statistics were used to quantify reproducibility, the majority of studies reported reproducibility statistics > 0.80 (Table 10.7). However, for all ana-tomical sites except the ankle, at least one study reported considerably lower values [5, 7, 17, 22, 93, 114, 118]. No relation between those lower values and MR-se-quence or staging technique seemed ap-parent.
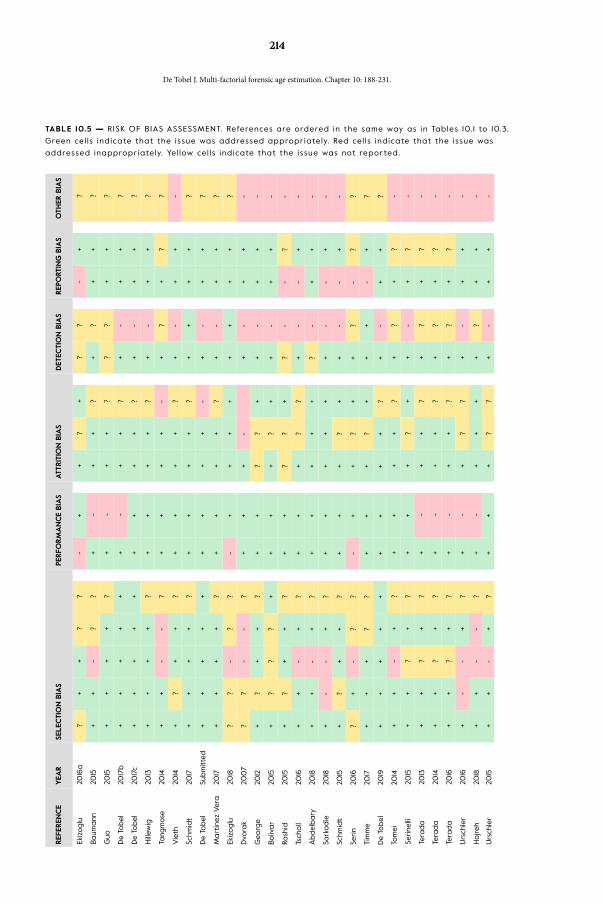
214
TABLE 10.5 — RISK OF BIAS ASSESSMENT. References are ordered in the same way as in Tables 10. 1 to 10.3.
Green cel ls indicate that the issue was addressed appropriately. Red cel ls indicate that the issue was
addressed inappropriately. Yel low cel ls indicate that the issue was not repor ted.
REF
EREN
CE
YEA
RSE
LEC
TIO
N B
IAS
PERFO
RM
AN
CE
BIA
SATT
RIT
ION
BIA
SD
ETEC
TIO
N B
IAS
REP
ORT
ING
BIA
SO
THER
BIA
S
Ekiz
oglu
2016
a?
++
??
-+
+?
+?
?-
+?
Baum
ann
2015
++
-?
?+
-+
+?
+?
++
?
Guo
2015
++
++
?+
-+
+?
??
++
?
De
Tobel
2017
b+
++
++
+-
++
?+
-+
+?
De
Tobel
2017
c+
++
++
++
++
?+
-+
+?
Hill
ewig
2013
++
++
?+
++
+?
+-
++
?
Tang
mose
2014
++
--
?+
++
+-
+?
+?
?
Vie
th20
14+
?+
+?
++
++
?+
-+
+-
Schm
idt
2017
++
++
?+
++
+?
++
++
?
De
Tobel
Subm
itte
d+
++
++
++
++
-+
-+
+?
Mart
ínez
Ver
a20
17+
++
+?
++
++
?+
-+
+?
Ekiz
oglu
2018
??
-?
?-
++
++
++
++
?
Dvo
rak
200
7?
?-
-?
++
+-
+-
++
-
Geo
rge
2012
+?
++
?+
+?
?+
+-
++
-
Boliv
ar
2015
+?
??
++
++
?+
+-
++
-
Rash
id20
15+
?+
+?
++
??
+?
--
?-
Tsch
oll
2016
++
-+
?+
++
??
+-
-+
-
Abdel
bary
2018
++
-+
?+
++
++
?-
++
-
Sark
odie
2018
+-
-+
?+
++
++
+-
-+
-
Schm
idt
2015
+?
++
?+
++
?+
+-
-+
-
Serin
2016
?+
-?
?-
++
?+
+?
-?
?
Tim
me
2017
++
+?
?+
++
?+
++
-+
?
De
Tobel
2019
++
++
++
++
+?
+-
++
?
Tom
ei20
14+
+-
+?
++
++
?+
?+
?-
Serine
lli20
15+
+?
+?
++
+?
++
-+
?-
Tera
da
2013
++
?+
?+
-+
+?
+?
+?
-
Tera
da
2014
++
?+
?+
-+
+?
+?
+?
-
Tera
da
2016
++
?+
?+
-+
+?
+?
+?
-
Urs
chle
r20
16+
--
+?
+-
+?
?+
-+
+-
Hojreh
2018
++
--
?+
-+
++
+?
++
-
Urs
chle
r20
15+
+-
+?
++
+?
?+
-+
+-
REF
EREN
CE
YEA
RSE
LEC
TIO
N B
IAS
PERFO
RM
AN
CE
BIA
SATT
RIT
ION
BIA
SD
ETEC
TIO
N B
IAS
REP
ORT
ING
BIA
SO
THER
BIA
S
Witts
chie
ber
2014
+?
++
?+
++
+?
+-
++
-
Vo
2015
++
-?
?+
++
??
+?
++
-
Bollo
w19
97?
-?
??
--
++
??
?+
+-
Bra
y20
16?
+-
??
--
++
??
?+
+-
Kim
2014
+-
-?
?-
-?
??
++
++
?
Sain
t-M
art
in20
15?
++
??
-+
??
?+
-+
??
Ded
oui
t20
12+
+-
??
-+
+?
++
+-
??
Ekiz
oglu
2016
b?
+-
??
-+
??
??
?-
?-
Harc
ke19
92
?+
-?
?-
-?
??
??
??
?
Laor
200
2+
-?
??
-+
?+
++
+?
-
Jopp
2010
++
-+
++
++
?+
+-
-+
-
Kräm
er20
14a
?+
-?
?-
++
??
++
+?
?
Kräm
er20
14b
?+
-?
?-
++
??
++
+?
?
Fan
2016
?+
-+
?-
++
?+
??
-?
?
Ott
ow20
17?
++
+?
++
++
++
++
+?
Auf
der
Maue
r20
18+
+-
++
++
++
++
--
+?
Vie
th20
18?
++
+?
++
++
++
++
+?
Penn
ock
2018
++
+?
?-
++
??
+-
-+
-
Cra
ig20
04
?+
-?
?-
-?
?+
??
+?
-
Kerc
her
200
9?
+?
??
--
+?
??
??
?-
Sain
t-M
art
in20
13?
+-
??
-+
+?
++
+-
+?
Sain
t-M
art
in20
14?
+-
??
-+
+?
++
++
+?
Ekiz
oglu
2015
?+
-?
?-
++
?+
??
+?
?
Ster
n20
17+
++
+?
++
+?
++
-+
+?
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

215
TABLE 10.5 (CONTINUED)
Was there no other possible bias?
Was there no conflict of interest from
funding?
Were the observers blinded for the sex of
the participants?
Were reasons for not assessable images
specified?
Did the study population show a uniform
biological origin?
Do the included patients match the
review question?
Was the interpretation of the index test
in agreement with the review question?
Were missing values equally distributed
among ages?
Did the study population show a uniform
socio-economic status (SES)?
Was there no selective outcome
reporting?
Were the observers blinded for the age
of the participants?
Were incomplete outcome data ade-
quately addressed?
Was the study population evenly distrib-
uted in age?
Did the study avoid inappropriate
exclusions?
Was the index test and its conduct in
agreement with the review question?
REF
EREN
CE
YEA
RSE
LEC
TIO
N B
IAS
PERFO
RM
AN
CE
BIA
SATT
RIT
ION
BIA
SD
ETEC
TIO
N B
IAS
REP
ORT
ING
BIA
SO
THER
BIA
S
Ekiz
oglu
2016
a?
++
??
-+
+?
+?
?-
+?
Baum
ann
2015
++
-?
?+
-+
+?
+?
++
?
Guo
2015
++
++
?+
-+
+?
??
++
?
De
Tobel
2017
b+
++
++
+-
++
?+
-+
+?
De
Tobel
2017
c+
++
++
++
++
?+
-+
+?
Hill
ewig
2013
++
++
?+
++
+?
+-
++
?
Tang
mose
2014
++
--
?+
++
+-
+?
+?
?
Vie
th20
14+
?+
+?
++
++
?+
-+
+-
Schm
idt
2017
++
++
?+
++
+?
++
++
?
De
Tobel
Subm
itte
d+
++
++
++
++
-+
-+
+?
Mart
ínez
Ver
a20
17+
++
+?
++
++
?+
-+
+?
Ekiz
oglu
2018
??
-?
?-
++
++
++
++
?
Dvo
rak
200
7?
?-
-?
++
+-
+-
++
-
Geo
rge
2012
+?
++
?+
+?
?+
+-
++
-
Boliv
ar
2015
+?
??
++
++
?+
+-
++
-
Rash
id20
15+
?+
+?
++
??
+?
--
?-
Tsch
oll
2016
++
-+
?+
++
??
+-
-+
-
Abdel
bary
2018
++
-+
?+
++
++
?-
++
-
Sark
odie
2018
+-
-+
?+
++
++
+-
-+
-
Schm
idt
2015
+?
++
?+
++
?+
+-
-+
-
Serin
2016
?+
-?
?-
++
?+
+?
-?
?
Tim
me
2017
++
+?
?+
++
?+
++
-+
?
De
Tobel
2019
++
++
++
++
+?
+-
++
?
Tom
ei20
14+
+-
+?
++
++
?+
?+
?-
Serine
lli20
15+
+?
+?
++
+?
++
-+
?-
Tera
da
2013
++
?+
?+
-+
+?
+?
+?
-
Tera
da
2014
++
?+
?+
-+
+?
+?
+?
-
Tera
da
2016
++
?+
?+
-+
+?
+?
+?
-
Urs
chle
r20
16+
--
+?
+-
+?
?+
-+
+-
Hojreh
2018
++
--
?+
-+
++
+?
++
-
Urs
chle
r20
15+
+-
+?
++
+?
?+
-+
+-
REF
EREN
CE
YEA
RSE
LEC
TIO
N B
IAS
PERFO
RM
AN
CE
BIA
SATT
RIT
ION
BIA
SD
ETEC
TIO
N B
IAS
REP
ORT
ING
BIA
SO
THER
BIA
S
Witts
chie
ber
2014
+?
++
?+
++
+?
+-
++
-
Vo
2015
++
-?
?+
++
??
+?
++
-
Bollo
w19
97?
-?
??
--
++
??
?+
+-
Bra
y20
16?
+-
??
--
++
??
?+
+-
Kim
2014
+-
-?
?-
-?
??
++
++
?
Sain
t-M
art
in20
15?
++
??
-+
??
?+
-+
??
Ded
oui
t20
12+
+-
??
-+
+?
++
+-
??
Ekiz
oglu
2016
b?
+-
??
-+
??
??
?-
?-
Harc
ke19
92
?+
-?
?-
-?
??
??
??
?
Laor
200
2+
-?
??
-+
?+
++
+?
-
Jopp
2010
++
-+
++
++
?+
+-
-+
-
Kräm
er20
14a
?+
-?
?-
++
??
++
+?
?
Kräm
er20
14b
?+
-?
?-
++
??
++
+?
?
Fan
2016
?+
-+
?-
++
?+
??
-?
?
Ott
ow20
17?
++
+?
++
++
++
++
+?
Auf
der
Maue
r20
18+
+-
++
++
++
++
--
+?
Vie
th20
18?
++
+?
++
++
++
++
+?
Penn
ock
2018
++
+?
?-
++
??
+-
-+
-
Cra
ig20
04
?+
-?
?-
-?
?+
??
+?
-
Kerc
her
200
9?
+?
??
--
+?
??
??
?-
Sain
t-M
art
in20
13?
+-
??
-+
+?
++
+-
+?
Sain
t-M
art
in20
14?
+-
??
-+
+?
++
++
+?
Ekiz
oglu
2015
?+
-?
?-
++
?+
??
+?
?
Ster
n20
17+
++
+?
++
+?
++
-+
+?
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

216
TABLE 10.6 — ABSOLUTE STATEMENTS REGARDING THE AGE THRESHOLD OF 18 YEARS.
MINOR ADULT
ANATOMICAL
STRUCTURE
STAGE ANATOMICAL
STRUCTURE
STAGE
FEM
AL
ES
Spheno-occipital syn-
chondrosis
Bassed stage 1 Lower left third molar Demir j ian
stage H
Lower left third molar * up to De Tobel stage 2 Lower left third molar * from De Tobel
stage 7 on
Proximal humerus up to Kel l inghaus stage
3a
Left hand/wrist SE * Tomei at las
skeletal age 18
Left hand/wrist SE * Tomei at las up to skele-
tal age 17
Left distal radius SE * Schmel ing
stage 5
Left hand/wrist VIBE Greul ich-Pyle at las up to
skeletal age 16
Distal femur * Dedouit stage 5
Left distal radius SE Dvorak stage 1 Distal femur * Vieth stage 6
Left distal radius SE * up to Kel l inghaus stage
3a
Left distal radius VIBE up to Kel l inghaus stage
3b
Distal femur up to Kel l inghaus stage
2c
Distal femur * up to Dedouit stage 2
Distal femur * up to Vieth stage 2
Proximal t ibia up to Kel l inghaus stage
2c
Proximal t ibia up to Dedouit stage 2
Proximal t ibia up to Vieth stage 4
Proximal f ibula up to Kel l inghaus stage
3c
Distal t ibia up to Schmel ing stage 2
Calcaneum up to Schmel ing stage 3
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

217
TABLE 10.6 (CONTINUED)
MINOR ADULT
ANATOMICAL
STRUCTURE
STAGE ANATOMICAL
STRUCTURE
STAGE
MA
LES
Spheno-occipital
synchondrosis
Bassed stage 1 Lower left third molar * from De Tobel
stage 7 on
Lower left third molar up to Demir j ian stage D Proximal humerus * Schmel ing
stage 4
Lower left third molar * up to De Tobel stage 2 Left hand/wrist VIBE Urschler auto-
mated skeletal
age 19
Proximal humerus * up to Kel l inghaus stage
3a
Left distal radius SE Schmel ing
stage 5
Left hand/wrist SE Tomei at las up to skele-
tal age 17
Distal femur * Dedouit stage 5
Left hand/wrist VIBE Greul ich-Pyle at las up to
skeletal age 17
Distal femur * Vieth stage 6
Left hand/wrist VIBE Urschler up to automat-
ed skeletal age 15
Proximal t ibia * Dedouit stage 5
Left distal radius Dvorak stage 1 Proximal t ibia * Vieth stage 6
Distal femur * up to Dedouit stage 2
Distal femur * Vieth stage 1
Proximal t ibia * Dedouit stage 1
Proximal t ibia * up to Vieth stage 3
Proximal f ibula up to Schmel ing stage 2
Knee SKJ up to 5
Distal t ibia up to Schmel ing stage 2
Calcaneum up to Schmel ing stage 2
SE = T1 spin echo sequence; SKJ = cumulat ive score of the knee joint ; VIBE = T1 gradient echo volumetr ic
interpolated breath-hold examination. * Anatomical structure and staging technique which al low abso-
lute statements about minority as wel l as adulthood.
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

218
TABLE 10.7 — REPRODUCIBILITY STATISTICS IN THE INCLUDED STUDIES. References are ordered in the same
way as in Tables 10. 1 to 10.3.
AN
ATO
MIC
AL
STRU
CTU
RE
REF
EREN
CE
YEA
RIN
TER-
OBSE
RVER
VA
RIA
BIL
ITY
INTR
A-O
BSE
RVER
VA
RIA
BIL
ITY
MEA
SURE
VALU
EN
PA
RTIC
IPA
NTS
N S
TRU
CTU
RES
N O
BSE
RVER
SM
EASU
RE
YEA
RN
PA
RTIC
IPA
NTS
N S
TRU
CTU
RES
N O
BSE
RVER
S
Sphe
no-o
ccip
ital
sync
hond
rosi
sEk
izoglu
2016
aC
ohe
n's
kappa
0,9
07
1078
1078
2C
ohe
n's
kappa
0,9
54
1078
1078
1
Wei
ght
ed k
appa
0,9
81W
eight
ed k
appa
0,9
90
Mola
rs (m
iner
aliz
ation)
Baum
ann
2015
Cohe
n's
kappa
0,5
118
262
mola
rs2
NA
Mola
rs (e
ruption)
Baum
ann
2015
Cohe
n's
kappa
0,5
718
274
mola
rs2
NA
Low
er le
ft t
hird
mola
rG
uo20
15Ka
ppa
0,8
360
60
2Ka
ppa c
oef
ficie
nt0
,89
60
60
1
Third m
ola
rsDe
Tobel
2017
ICC
0.8
5-0
.94
5218
3 m
ola
rs2
ICC
0.9
4-0
.98
52N
ot
spec
ified
1
Third m
ola
rsDe
Tobel
2017
ICC
0.8
6-0
.95
5218
3 m
ola
rs2
ICC
0.9
4-0
.98
52N
ot
spec
ified
1
Third m
ola
rsDe
Tobel
2017
Wei
ght
ed k
appa
0,7
90
309
899
2W
eight
ed k
appa
0,8
7313
037
92
18De
Tobel
2017
0,8
03
309
899
218
0,8
5713
037
92
28De
Tobel
2017
0,7
84
309
899
228
0,8
4813
037
92
38De
Tobel
2017
0,7
64
309
899
238
0,8
90
130
379
2
48De
Tobel
2017
0,8
04
309
899
248
0,8
8913
037
92
Cla
vicl
eH
illew
ig20
13Fl
eiss
' kappa
0.7
6 le
ft, 0
.74
right
220
440
4C
ohe
n's
kappa
0,7
520
Not
spec
ified
1
Cla
vicl
eTa
ngm
ose
2014
Kappa (s
tages
1-3
colla
pse
d)
-0.0
04-
0.4
14; p
rone
posi
tion
0.0
40-0
.446
49-5
398-
106;
pro
ne
posi
tion
26-3
2
3Ka
ppa
0.6
69;
pro
ne
posi
tion
0.7
88
53; p
rone
posi
tion
3210
6; p
rone
posi
tion
64
1
Cla
vicl
eV
ieth
2014
NA
NA
Cla
vicl
eSc
hmid
t20
17W
eight
ed k
appa
0,9
8780
160
2W
eight
ed k
appa
0,9
91
8016
01
Cla
vicl
eDe
Tobel
subm
itte
dW
eight
ed k
appa
0,6
40N
A40
02
Wei
ght
ed k
appa
0,7
66
NA
186
1
Manu
brium
Mart
ínez
Ver
a20
17N
AN
A
Prox
imal h
umer
usEk
izoglu
2018
Cohe
n's
kappa
0,8
2842
842
82
Cohe
n's
kappa
0,8
98
NA
NA
NA
Left
dis
tal r
adiu
sDvo
rak
200
7C
orr
elation
coef
ficie
nt0
.91-0
.92
496
496
3N
A
Left
dis
tal r
adiu
sG
eorg
e20
12Sp
earm
an
0,9
150
150
3N
A
Left
dis
tal r
adiu
sBo
livar
2015
Kappa
0,2
360
60
3Ka
ppa
0,7
96
61
Left
dis
tal r
adiu
sRa
shid
2015
NA
NA
Left
dis
tal r
adiu
sTs
choll
2016
Kappa
0,9
2848
748
72
NA
Left
dis
tal r
adiu
sA
bdel
bary
2018
Wei
ght
ed k
appa
0,8
2861
61
2N
A
Left
dis
tal r
adiu
sSa
rkodie
2018
Kappa
0,9
528
628
63
NA
Left
dis
tal r
adiu
sSc
hmid
t20
15Ka
ppa
0,8
830
302
Kappa
0,9
430
301
Left
dis
tal r
adiu
sSe
rin
2016
Cohe
n's
kappa
0,8
126
326
32
Cohe
n's
kappa
0,9
326
326
31
Left
dis
tal u
lna
Serin
2016
0,8
826
326
32
0,9
426
326
31
Left
pro
xim
al fi
rst
met
aca
rpus
Serin
2016
0,8
426
326
32
0,9
526
326
31
Left
dis
tal r
adiu
sTi
mm
e20
17C
ohe
n's
kappa
0,9
7410
010
02
Cohe
n's
kappa
0,9
8810
010
02
Left
dis
tal r
adiu
s SE
De
Tobel
2019
Wei
ght
ed k
appa
0,7
92
361
361
2W
eight
ed k
appa
0,8
5698
98
1
Left
dis
tal r
adiu
s V
IBE
Wei
ght
ed k
appa
0,7
1235
935
92
Wei
ght
ed k
appa
0,8
4398
98
1
Left
hand
/wrist
Tom
ei20
14Pe
ars
on
0.9
5 F,
0.9
7 M
78 F
, 10
1 M17
9 x
9 b
one
s2
NA
Left
hand
/wrist
Serine
lli20
15Pe
ars
on
0.9
7 F,
0.9
8 M
151
151 x
9 b
one
s2
Bla
nd-A
ltm
an
plo
tsN
A15
115
1 x 9
bone
s1
Left
hand
/wrist
Tera
da
2013
Pears
on
0.9
22-0
.926
8383
x 13
bone
s2
Pears
on
0,9
5883
83 x
13 b
one
s1
Left
hand
/wrist
Tera
da
2014
Pears
on
0.8
80-0
.935
8888
x 13
bone
s3
Pears
on
0,9
1888
88 x
13 b
one
s1
Left
hand
/wrist
Tera
da
2016
Pears
on
0.9
56-0
.964
5959
x 13
bone
s2
Pears
on
0,9
5959
59 x
13 b
one
s1
Left
hand
/wrist
Urs
chle
r20
16W
eight
ed k
appa
GP
0.74;
TW
2 0
.51
18G
P 18
; TW
2 18
x
13 b
one
s2
NA
Left
hand
/wrist
Hojreh
2018
ICC
0.9
5 F;
0.9
7 M
33; 1
722
; 15
2N
A
Left
hand
/wrist
Urs
chle
r20
15N
AN
A
AN
ATO
MIC
AL
STRU
CTU
RE
REF
EREN
CE
YEA
RIN
TER-
OBSE
RVER
VA
RIA
BIL
ITY
INTR
A-O
BSE
RVER
VA
RIA
BIL
ITY
MEA
SURE
VALU
EN
PA
RTIC
IPA
NTS
N S
TRU
CTU
RES
N O
BSE
RVER
SM
EASU
RE
YEA
RN
PA
RTIC
IPA
NTS
N S
TRU
CTU
RES
N O
BSE
RVER
S
Iliac
cres
tW
itts
chie
ber
2014
NA
NA
Prox
imal f
emur
Vo
2015
ICC
0,6
94
4386
3IC
C0
,788
4386
1
Sacr
umBo
llow
1997
NA
NA
Sacr
umBo
llow
1997
Pate
llofe
mora
l join
tKi
m20
14N
AN
A
Dis
tal f
emur
Sain
t-M
art
in20
15C
ohe
n's
kappa
0,8
621
421
42
Cohe
n's
kappa
0,8
621
421
41
Dis
tal f
emur
Ded
oui
t20
12C
ohe
n's
kappa
0,8
629
029
02
Cohe
n's
kappa
0,9
629
029
01
Prox
imal t
ibia
Ded
oui
t20
12C
ohe
n's
kappa
0,6
329
029
02
Cohe
n's
kappa
0,9
629
029
01
Dis
tal f
emur
Ekiz
oglu
2016
bC
ohe
n's
kappa
0,8
3650
350
32
Cohe
n's
kappa
0,9
1950
350
31
Wei
ght
ed k
appa
0,9
54
Wei
ght
ed k
appa
0,9
78
Prox
imal t
ibia
Ekiz
oglu
2016
bC
ohe
n's
kappa
0,8
8550
350
32
Cohe
n's
kappa
0,9
61
503
503
1
Wei
ght
ed k
appa
0,9
79W
eight
ed k
appa
0,9
93
Knee
Harc
ke19
92
NA
NA
Knee
Laor
200
2N
AN
A
Prox
imal t
ibia
Jopp
2010
NA
NA
Dis
tal f
emur
Kräm
er20
14a
Kappa
0,8
530
302
Kappa
0,9
430
301
Prox
imal t
ibia
Kräm
er20
14b
Kappa
0,8
530
302
Kappa
0,8
830
301
Dis
tal f
emur
Fan
2016
ICC
0,9
4632
232
22
ICC
0,9
67
322
322
1
Prox
imal t
ibia
Fan
2016
ICC
0,9
7832
232
22
ICC
1,00
032
232
21
Prox
imal fi
bul
aFa
n20
16IC
C0
,931
322
322
2IC
C0
,965
322
322
1
Dis
tal f
emur
Ott
ow20
17Ka
ppa
0,9
41115
1152
Kappa
0,9
61
115115
1
Prox
imal t
ibia
Ott
ow20
17Ka
ppa
0,9
51115
1152
Kappa
0,9
71115
1151
Knee
Auf
der
Maue
r20
18Fl
eis'
kappa
0,8
4036
104
3N
A
Dis
tal f
emur
Auf
der
Maue
r20
18Fl
eis'
kappa
0,7
99
3610
43
NA
Prox
imal t
ibia
Auf
der
Maue
r20
18Fl
eis'
kappa
0,8
8636
104
3N
A
Prox
imal fi
bul
aA
uf d
er M
aue
r20
18Fl
eis'
kappa
0,8
3336
104
3N
A
Dis
tal f
emur
Vie
th20
18C
ohe
n's
kappa
0,9
1310
010
02
Cohe
n's
kappa
0,9
1410
010
01
Prox
imal t
ibia
Vie
th20
18C
ohe
n's
kappa
0,8
4710
010
02
Cohe
n's
kappa
0,8
9310
010
01
Knee
Penn
ock
2018
ICC
0,9
5732
332
32
ICC
0,9
92
323
323
NA
Knee
Cra
ig20
04
NA
NA
Knee
Kerc
her
200
9N
AN
A
Dis
tal t
ibia
Sain
t-M
art
in20
13C
ohe
n's
kappa
0,8
418
018
02
Cohe
n's
kappa
0,9
718
018
01
Calc
ane
umSa
int-
Mart
in20
13C
ohe
n's
kappa
0,9
018
018
02
Cohe
n's
kappa
0,9
718
018
01
Dis
tal t
ibia
Sain
t-M
art
in20
14N
AN
A
Dis
tal t
ibia
Ekiz
oglu
2015
Cohe
n's
kappa
0,8
3416
716
72
Cohe
n's
kappa
0,8
8316
716
72
Calc
ane
umEk
izoglu
2015
Cohe
n's
kappa
0,8
02
167
167
2C
ohe
n's
kappa
0,8
1116
716
72
MFA
Ster
n20
17N
AN
A
F = females ; GP = Greul ich-Pyle at las technique; ICC = intra-class correlat ion coeff ic ient ; M = males ;
NA = not appl icable or not repor ted; SE = spin echo MR-sequence; TW2 = Tanner-Whitehouse-2 at las technique;
VIBE = volumetr ic interpolated breath-hold examination MR-sequence
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

219
TABLE 10.7 (CONTINUED)
AN
ATO
MIC
AL
STRU
CTU
RE
REF
EREN
CE
YEA
RIN
TER-
OBSE
RVER
VA
RIA
BIL
ITY
INTR
A-O
BSE
RVER
VA
RIA
BIL
ITY
MEA
SURE
VALU
EN
PA
RTIC
IPA
NTS
N S
TRU
CTU
RES
N O
BSE
RVER
SM
EASU
RE
YEA
RN
PA
RTIC
IPA
NTS
N S
TRU
CTU
RES
N O
BSE
RVER
S
Sphe
no-o
ccip
ital
sync
hond
rosi
sEk
izoglu
2016
aC
ohe
n's
kappa
0,9
07
1078
1078
2C
ohe
n's
kappa
0,9
54
1078
1078
1
Wei
ght
ed k
appa
0,9
81W
eight
ed k
appa
0,9
90
Mola
rs (m
iner
aliz
ation)
Baum
ann
2015
Cohe
n's
kappa
0,5
118
262
mola
rs2
NA
Mola
rs (e
ruption)
Baum
ann
2015
Cohe
n's
kappa
0,5
718
274
mola
rs2
NA
Low
er le
ft t
hird
mola
rG
uo20
15Ka
ppa
0,8
360
60
2Ka
ppa c
oef
ficie
nt0
,89
60
60
1
Third m
ola
rsDe
Tobel
2017
ICC
0.8
5-0
.94
5218
3 m
ola
rs2
ICC
0.9
4-0
.98
52N
ot
spec
ified
1
Third m
ola
rsDe
Tobel
2017
ICC
0.8
6-0
.95
5218
3 m
ola
rs2
ICC
0.9
4-0
.98
52N
ot
spec
ified
1
Third m
ola
rsDe
Tobel
2017
Wei
ght
ed k
appa
0,7
90
309
899
2W
eight
ed k
appa
0,8
7313
037
92
18De
Tobel
2017
0,8
03
309
899
218
0,8
5713
037
92
28De
Tobel
2017
0,7
84
309
899
228
0,8
4813
037
92
38De
Tobel
2017
0,7
64
309
899
238
0,8
90
130
379
2
48De
Tobel
2017
0,8
04
309
899
248
0,8
8913
037
92
Cla
vicl
eH
illew
ig20
13Fl
eiss
' kappa
0.7
6 le
ft, 0
.74
right
220
440
4C
ohe
n's
kappa
0,7
520
Not
spec
ified
1
Cla
vicl
eTa
ngm
ose
2014
Kappa (s
tages
1-3
colla
pse
d)
-0.0
04-
0.4
14; p
rone
posi
tion
0.0
40-0
.446
49-5
398-
106;
pro
ne
posi
tion
26-3
2
3Ka
ppa
0.6
69;
pro
ne
posi
tion
0.7
88
53; p
rone
posi
tion
3210
6; p
rone
posi
tion
64
1
Cla
vicl
eV
ieth
2014
NA
NA
Cla
vicl
eSc
hmid
t20
17W
eight
ed k
appa
0,9
8780
160
2W
eight
ed k
appa
0,9
91
8016
01
Cla
vicl
eDe
Tobel
subm
itte
dW
eight
ed k
appa
0,6
40N
A40
02
Wei
ght
ed k
appa
0,7
66
NA
186
1
Manu
brium
Mart
ínez
Ver
a20
17N
AN
A
Prox
imal h
umer
usEk
izoglu
2018
Cohe
n's
kappa
0,8
2842
842
82
Cohe
n's
kappa
0,8
98
NA
NA
NA
Left
dis
tal r
adiu
sDvo
rak
200
7C
orr
elation
coef
ficie
nt0
.91-0
.92
496
496
3N
A
Left
dis
tal r
adiu
sG
eorg
e20
12Sp
earm
an
0,9
150
150
3N
A
Left
dis
tal r
adiu
sBo
livar
2015
Kappa
0,2
360
60
3Ka
ppa
0,7
96
61
Left
dis
tal r
adiu
sRa
shid
2015
NA
NA
Left
dis
tal r
adiu
sTs
choll
2016
Kappa
0,9
2848
748
72
NA
Left
dis
tal r
adiu
sA
bdel
bary
2018
Wei
ght
ed k
appa
0,8
2861
61
2N
A
Left
dis
tal r
adiu
sSa
rkodie
2018
Kappa
0,9
528
628
63
NA
Left
dis
tal r
adiu
sSc
hmid
t20
15Ka
ppa
0,8
830
302
Kappa
0,9
430
301
Left
dis
tal r
adiu
sSe
rin
2016
Cohe
n's
kappa
0,8
126
326
32
Cohe
n's
kappa
0,9
326
326
31
Left
dis
tal u
lna
Serin
2016
0,8
826
326
32
0,9
426
326
31
Left
pro
xim
al fi
rst
met
aca
rpus
Serin
2016
0,8
426
326
32
0,9
526
326
31
Left
dis
tal r
adiu
sTi
mm
e20
17C
ohe
n's
kappa
0,9
7410
010
02
Cohe
n's
kappa
0,9
8810
010
02
Left
dis
tal r
adiu
s SE
De
Tobel
2019
Wei
ght
ed k
appa
0,7
92
361
361
2W
eight
ed k
appa
0,8
5698
98
1
Left
dis
tal r
adiu
s V
IBE
Wei
ght
ed k
appa
0,7
1235
935
92
Wei
ght
ed k
appa
0,8
4398
98
1
Left
hand
/wrist
Tom
ei20
14Pe
ars
on
0.9
5 F,
0.9
7 M
78 F
, 10
1 M17
9 x
9 b
one
s2
NA
Left
hand
/wrist
Serine
lli20
15Pe
ars
on
0.9
7 F,
0.9
8 M
151
151 x
9 b
one
s2
Bla
nd-A
ltm
an
plo
tsN
A15
115
1 x 9
bone
s1
Left
hand
/wrist
Tera
da
2013
Pears
on
0.9
22-0
.926
8383
x 13
bone
s2
Pears
on
0,9
5883
83 x
13 b
one
s1
Left
hand
/wrist
Tera
da
2014
Pears
on
0.8
80-0
.935
8888
x 13
bone
s3
Pears
on
0,9
1888
88 x
13 b
one
s1
Left
hand
/wrist
Tera
da
2016
Pears
on
0.9
56-0
.964
5959
x 13
bone
s2
Pears
on
0,9
5959
59 x
13 b
one
s1
Left
hand
/wrist
Urs
chle
r20
16W
eight
ed k
appa
GP
0.74;
TW
2 0
.51
18G
P 18
; TW
2 18
x
13 b
one
s2
NA
Left
hand
/wrist
Hojreh
2018
ICC
0.9
5 F;
0.9
7 M
33; 1
722
; 15
2N
A
Left
hand
/wrist
Urs
chle
r20
15N
AN
A
AN
ATO
MIC
AL
STRU
CTU
RE
REF
EREN
CE
YEA
RIN
TER-
OBSE
RVER
VA
RIA
BIL
ITY
INTR
A-O
BSE
RVER
VA
RIA
BIL
ITY
MEA
SURE
VALU
EN
PA
RTIC
IPA
NTS
N S
TRU
CTU
RES
N O
BSE
RVER
SM
EASU
RE
YEA
RN
PA
RTIC
IPA
NTS
N S
TRU
CTU
RES
N O
BSE
RVER
S
Iliac
cres
tW
itts
chie
ber
2014
NA
NA
Prox
imal f
emur
Vo
2015
ICC
0,6
94
4386
3IC
C0
,788
4386
1
Sacr
umBo
llow
1997
NA
NA
Sacr
umBo
llow
1997
Pate
llofe
mora
l join
tKi
m20
14N
AN
A
Dis
tal f
emur
Sain
t-M
art
in20
15C
ohe
n's
kappa
0,8
621
421
42
Cohe
n's
kappa
0,8
621
421
41
Dis
tal f
emur
Ded
oui
t20
12C
ohe
n's
kappa
0,8
629
029
02
Cohe
n's
kappa
0,9
629
029
01
Prox
imal t
ibia
Ded
oui
t20
12C
ohe
n's
kappa
0,6
329
029
02
Cohe
n's
kappa
0,9
629
029
01
Dis
tal f
emur
Ekiz
oglu
2016
bC
ohe
n's
kappa
0,8
3650
350
32
Cohe
n's
kappa
0,9
1950
350
31
Wei
ght
ed k
appa
0,9
54
Wei
ght
ed k
appa
0,9
78
Prox
imal t
ibia
Ekiz
oglu
2016
bC
ohe
n's
kappa
0,8
8550
350
32
Cohe
n's
kappa
0,9
61
503
503
1
Wei
ght
ed k
appa
0,9
79W
eight
ed k
appa
0,9
93
Knee
Harc
ke19
92
NA
NA
Knee
Laor
200
2N
AN
A
Prox
imal t
ibia
Jopp
2010
NA
NA
Dis
tal f
emur
Kräm
er20
14a
Kappa
0,8
530
302
Kappa
0,9
430
301
Prox
imal t
ibia
Kräm
er20
14b
Kappa
0,8
530
302
Kappa
0,8
830
301
Dis
tal f
emur
Fan
2016
ICC
0,9
4632
232
22
ICC
0,9
67
322
322
1
Prox
imal t
ibia
Fan
2016
ICC
0,9
7832
232
22
ICC
1,00
032
232
21
Prox
imal fi
bul
aFa
n20
16IC
C0
,931
322
322
2IC
C0
,965
322
322
1
Dis
tal f
emur
Ott
ow20
17Ka
ppa
0,9
41115
1152
Kappa
0,9
61
115115
1
Prox
imal t
ibia
Ott
ow20
17Ka
ppa
0,9
51115
1152
Kappa
0,9
71115
1151
Knee
Auf
der
Maue
r20
18Fl
eis'
kappa
0,8
4036
104
3N
A
Dis
tal f
emur
Auf
der
Maue
r20
18Fl
eis'
kappa
0,7
99
3610
43
NA
Prox
imal t
ibia
Auf
der
Maue
r20
18Fl
eis'
kappa
0,8
8636
104
3N
A
Prox
imal fi
bul
aA
uf d
er M
aue
r20
18Fl
eis'
kappa
0,8
3336
104
3N
A
Dis
tal f
emur
Vie
th20
18C
ohe
n's
kappa
0,9
1310
010
02
Cohe
n's
kappa
0,9
1410
010
01
Prox
imal t
ibia
Vie
th20
18C
ohe
n's
kappa
0,8
4710
010
02
Cohe
n's
kappa
0,8
9310
010
01
Knee
Penn
ock
2018
ICC
0,9
5732
332
32
ICC
0,9
92
323
323
NA
Knee
Cra
ig20
04
NA
NA
Knee
Kerc
her
200
9N
AN
A
Dis
tal t
ibia
Sain
t-M
art
in20
13C
ohe
n's
kappa
0,8
418
018
02
Cohe
n's
kappa
0,9
718
018
01
Calc
ane
umSa
int-
Mart
in20
13C
ohe
n's
kappa
0,9
018
018
02
Cohe
n's
kappa
0,9
718
018
01
Dis
tal t
ibia
Sain
t-M
art
in20
14N
AN
A
Dis
tal t
ibia
Ekiz
oglu
2015
Cohe
n's
kappa
0,8
3416
716
72
Cohe
n's
kappa
0,8
8316
716
72
Calc
ane
umEk
izoglu
2015
Cohe
n's
kappa
0,8
02
167
167
2C
ohe
n's
kappa
0,8
1116
716
72
MFA
Ster
n20
17N
AN
A
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

220
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.
TABLE 10.8 — ABILITY TO DISCERN MINORS FROM ADULTS. Regarding predict ive probabi l i t ies , stages or
combinations of stages are displayed between brackets. Regarding third molars, stages apply to 18, 28,
38, and 48, respect ively. Regarding clavic les, stages apply to the left and r ight c lavic le, respect ively.
Regarding diagnost ic indices, sex-specif ic results were not repor ted in al l studies. Instead, some studies
repor ted non-sex-specif ic results
MFA
= m
ult
i-fa
cto
ria
l a
ge
est
ima
tio
n;
NA
= n
ot
ap
plica
ble
or
no
t re
po
rte
d.
AN
ATO
MIC
AL
ST
RU
CT
UR
ER
EF
ER
EN
CE
YE
AR
PR
ED
ICT
IVE
PR
OB
AB
ILIT
IES
P(A
GE
< 1
8 Y
EA
RS)
SE
NSIT
IVIT
YSP
EC
IFIC
ITY
F
EM
AL
ES
MA
LES
FEM
AL
ES
MA
LES
FEM
AL
ES
MA
LES
Th
ird
mo
lars
De
To
be
l20
17(6
66
6)
0.0
49
1;
(77
77
) 0
.00
44
;
(88
88)
0.0
011
(66
66
) 0
.111
7;
(77
77
) 0
.00
74;
(88
88)
0.0
02
4
82
.69
1.06
5.8
87.
2
Cla
vic
les
Hille
wig
20
13(3
,3)
0.2
58
;
(3,4
) 0
.06
7;
(4,3
) 0
.070
;
(4,4
) 0
.00
8
(3,3
) 0
.15
9;
(3,4
) 0
.02
6;
(4,3
) 0
.02
9;
(4,4
) 0
.00
2
NA
NA
Cla
vic
les
De
To
be
lsu
bm
itte
d(3
b,
3c)
0.0
05
9;
(3c,
3b
) 0
.019
8;
(3c,
3c)
0.0
02
3
(3b
, 3
c)
0.0
05
3;
(3c,
3b
) 0
.018
2;
(3c,
3c)
0.0
019
86
.16
9.4
Ma
nu
bri
um
Ma
rtín
ez
Ve
ra
NA
NA
91.
18
2.4
Le
ft d
ista
l ra
diu
sSe
rin
20
16N
AN
A10
0.0
92
.58
9.9
92
.5
Le
ft w
rist
SE
De
To
be
l20
19(4
/5
) 0
.05
47
(4/5
) 0
.017
18
8.5
92
.8
Le
ft w
rist
VIB
ED
e T
ob
el
20
19(4
) 0
.25
70
;
(5)
0.0
84
0
(4)
0.0
54
7;
(5)
0.0
24
8
90
.98
7.4
Dis
tal
tib
iaSa
int-
Ma
rtin
20
13(4
) 0
.32
8(4
) 0
.02
6N
AN
A
Ca
lca
ne
um
Sa
int-
Ma
rtin
20
13(4
) 0
.35
3(4
) 0
.06
4N
AN
A
Dis
tal
tib
ia a
nd
ca
lca
ne
um
Sa
int-
Ma
rtin
20
13N
AN
A9
7.7
91.
778.6
90
.6
Dis
tal
tib
iaSa
int-
Ma
rtin
20
14N
AN
A9
4.3
97.
47
1.2
65.5
MFA
Ste
rn20
17N
AN
A9
3.2
88.6

221
Discussion
Age estimation performance
Regression formulas were reported in [1, 12, 29, 63, 95]. Corresponding coefficients of determination ranged from 0.40 [12] to 0.85 [95]. When statistical models were applied to estimate age, two aspects were considered to quantify age estimation performance: (1) the point prediction of age with its uncertainty, and (2) the ability to discern minors from adults.
The first aspect is reflected by the mean absolute error (MAE) and root mean squared error (RMSE). Only a few studies reported MAE. For females, MAE reached 2.0 years studying third molars [20]. For males, it reached 1.7 years study-ing third molars [20], 0.85 years studying the left hand/wrist [113], and 1.14 years combining third molars, both clavicles and the left hand/wrist [90]. Not sex-spe-cific, MAE reached 1.97 years studying both clavicles [17], and 1.79 years study-ing the left wrist [16]. Moreover, the effect of large differences between chronological and estimated age was quantified by the RMSE in three studies: for females RMSE was 2.38 years and for males 2.06 years, studying third molars [20], while it was 2.60 years studying both clavicles [17], and 2.24 years studying the left wrist [16]. The latter values were not sex-specific.
The second aspect is reflected by pre-dictive probabilities to be younger/older than 18 and by diagnostic indices (Table 10.8). For diagnostic indices in the cur-rent review, reported statistics were re-calculated so specificity would reflect the proportion of correctly classified minors, whereas sensitivity would reflect the pro-portion of correctly classified adults.
Characteristics and quality of included studies
The current systematic review pro-vides an overview of how hard tis-
sue development registered with MRI relates to age. Included studies showed high risk of bias, mainly due to their study population. Since a wide age range was studied, from birth to age 30, large ref-erence populations are indispensable. It has been suggested that at least 10 partici-pants per age category of one year per sex should be included per anatomical struc-ture [79]. Moreover, the age range of the study population affects lower and upper limits of age distributions within devel-opmental stage, as well as the mean age. This phenomenon is called ‘age mimicry’ and has been a major issue in age estima-tion for decades [6]. Ideally, a reference study should include participants with an age range starting several years before the studied anatomical structure starts its de-velopment, and ending several years after the structure has reached full maturity. For instance, an ideal reference study on third molars’ development might include participants between 6 and 28 years old [59]. Unfortunately, these ideally designed studies are scarce even using radiographs, which can easily be done retrospectively. Therefore, it seems self-evident that using MRI, those ideally designed studies will be rarer still. Only for the clavicles’ sternal end did two studies encompass the entire development with lower and upper age margins beyond developmental chang-es [17, 82]. For other structures, pooling the data of different studies might address this issue, but before this is done, it needs to be studied if it is safe to pool data ob-tained with different MR-sequences. Af-ter all, it has been demonstrated that age
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation

222
distributions within stages might differ between sequences for third molars [19] and for the left wrist [16]. Moreover, dif-ferent sequences may lead to different staging techniques, impeding the pooling of data [22, 30]. On the other hand, dif-ferent sequences might provide comple-mentary information, to allow for a more nuanced age estimation [16, 117].
Compared to age estimation studies using radiographs, MRI study popula-tions were relatively small, which could be attributed to the MRI technique. Since developmental stages are based on details, such as bone bridging and apical closure of teeth, routine clinical MRI is mostly not suitable for age estimation. Only larg-er anatomical structures, such as knee and ankle bones, show sufficient details on clinical MRI. This also explains why only those structures have been studied for age estimation in retrospective studies [9, 12, 22, 28-31, 33, 51, 52, 55-57, 69, 73-75]. Smaller structures require a dedicated scanning protocol, with a dedicated coil and sufficiently high in-plane resolution (Table 10.2), and thus, require a prospec-tive study design.
Ethnic differences between popu-lations have been studied using radi-ographs. Conclusions vary, with some authors claiming that inter-individual variability within ethnic group is larger than inter-ethnic variability [41, 59, 99, 101, 120], and others claiming that so-cio-economic status is more important than ethnicity [80]. By contrast, differ-ences between ethnic groups have been demonstrated too [66, 123]. Presuma-bly, trends in those studies also apply to MRI, but ethnic differences have only been studied for hand/wrist MRI [1, 7, 25,
111]. Moreover, these studies were only conducted in football players, who might be more advanced in their development than a general population of the same age [26, 62, 76, 108]. After all, their advanced development might be part of their tal-ent, i.e. their advanced development might contribute to better performance in sports. Thus, they might be scouted at an earlier age and be more likely to move on to elite sports. The study by Sarkodie et al. (2018) [77] was excluded for quantita-tive analysis, because it only included elite football players. At the other end of the spectrum, skeletal development in gym-nasts might be delayed, allowing more elasticity at a relatively older age [62, 108]. Maybe different standards should be ap-plied to athletes, to take into account their possible advanced or delayed skeletal age.
Quantitative synthesis
Bone development has been studied with MRI at most joints of the appendicular skeleton. The only site of the axial skele-ton that has been studied was the sphe-no-occipital synchondrosis. Combined, these anatomical sites cover development from childhood to adulthood. By con-trast, dental development has only been studied with MRI in molars, while in children up to age 14, the development of other permanent teeth is essential to esti-mate age [2, 60].
The graphs (Figure 10.3) revealed some remarkable concerns about how stages relate to age. Firstly, only few an-atomical sites and staging techniques provided a steady increase of age with in-creasing stage, with all participants in the first stage well below the 18-year-thresh-old and those in the final stage well above
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

223
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation
it in both sexes. They were Dedouit stag-ing of the distal femur (Figure 10.3k) and Vieth staging of the distal femur (Figure 10.3n). De Tobel staging of the lower left third molars came close, but the mini-mum ages of the final stage were still close to 18 (Figure 10.3d).
Secondly, the high maximum ages in stage 1 of clavicular development, and the low minimum ages in stages 4 and 5 sug-gest that those stages might be confused (Figure 10.3e) [17, 45]. This hinders a logical increase of age with an increase in stages.
Thirdly, although in wrist MRI, Dvorak stage 1 coincides with Schmeling stage 2, Dvorak stage 1 has never been re-ported above the age of 18 (Figure 10.3g), while Schmeling stage 2 has been report-ed in one male of 18.6 years old (Figure 10.3h) [85]. At the other end of the spec-trum, in third molar MRI, De Tobel stage 8 coincides with Demirjian stage H. The first has not been reported below the age of 18 (Figure 10.3d), while the latter has in males (Figure 10.3c) [5, 39].
Fourthly, the influence of the study populations’ age ranges is obvious. For in-stance, Figure 10.3e demonstrates that the boxplots of the male participants in Vi-eth et al. (2014) are situated at the upper ends of other studies’ box plots for lower stages, while they are at the lower end of other studies’ box plots for higher stages. This can be explained by the narrow age range (5 years) of participants in Vieth et al. (2014). The same applies to Schmidt et al. (2015) in Figure 10.3h. Fifthly, the iliac crest does not seem useful for age estima-tion, since ages within stages all overlap. However, this study suffered from high
population bias, with the same narrow age range of participants as Vieth et al. (2014) and Schmidt et al. (2015).
Finally, the introduction of substages was clearly an attempt to provide more accurate age estimation around the age of 18. They provide a more gradual increase of age with increasing stage than the main stages.
However, there is more to certain stag-ing techniques than the graphs revealed. Some MRI-specific characteristics of skeletal structures have been studied, but their relevance to age estimation remains unclear. The threefold stratification sign was stated to be useful by Timme et al. (2017) [107] while De Tobel et al. (2019) [16] could not confirm its use. Other signs such as the metaphyseal stripe [57], the oreo-sign and the crack-sign [69] still need to be explored in future studies.
Furthermore, considering how stages relate to age, correlation coefficients and coefficients of determination need to be interpreted cautiously, since they depend on the age distribution of the study pop-ulation. Relatively high coefficients have been reported for single site age estima-tion (SSA) based on MRI. Still, they are expected to increase by MFA, as has been demonstrated for MFA based on radi-ographs and CT [4, 10, 24, 83, 87, 102]. Although only one study on MFA based on MRI has been published [90], all re-searchers in this field prefer MFA over SSA [78]. Stern et al. (2017) combined all four third molars, both clavicles and the left hand/wrist [90]. This combination complies with international recommen-dations, but is only partly supported by the current results of the review. Table

224
10.6 suggests that in females, combining third molars, the left hand/wrist and the knee might render a more robust model for age estimation. For males, combining third molars, the proximal humerus and the knee might be ideal. However, in prac-tice, a uniform approach for both sexes is desirable. Moreover, a sound statistical approach should be applied to combine the information, taking into account the possible conditional dependence of the included anatomical sites. Otherwise, ar-tificially narrow uncertainty intervals of the point prediction and artificially high probabilities will cause the judicial evi-dence to appear stronger than it really is [6, 34, 54].
Another major concern regarding age estimation based on MRI is the low repro-ducibility of staging that has been point-ed out by some authors (Table 10.7). An obligatory quality control of centres that perform age estimation still lacks, caus-ing large discrepancies between results from different centres [35]. This already affects the current gold standard of age estimation, using radiographs, and its ef-fect might be even larger using MRI, con-sidering the complexity of interpreting different MR sequences. Therefore, stag-ing development should be based upon a consensus between experts. These experts should be experienced in age estimation as well as being experienced in interpret-ing the imaging modality at hand.
To solve this problem, automated approaches have been developed to as-sess radiographs for age estimation [104, 106]. Since validation studies support the use of these approaches, they are applied in current age estimation practice [105]. Such an automated approach has been de-
veloped and optimised for MRI, but still needs to be validated [27, 89-91, 112, 113]. Moreover, should the same automated ap-proaches be used internationally, discrep-ancies between age estimation performed in different institutes would, presumably, be eliminated [32, 48]. Furthermore, stag-ing development should be a consensus between experts. These experts should be experienced in age estimation as well as being experienced in interpreting the im-aging modality at hand.
Few MRI studies have developed models for age estimation and reported statistical measures of age estimation per-formance. Remarkably, the same applies to X-ray studies. Studying radiographs of third molars, Thevissen et al. (2010) re-ported a MAE of 1.13 years [100]. Know-ing that their study population included 2513 participants, one might presume that such a MAE value would also be reached by larger MRI studies. Note that this val-ue is almost equal to the one reached by the MFA MRI study by Stern et al. (2017) [90]. Therefore, the limiting effect of the small study populations in MRI studies might be overcome by the possibility to study multiple anatomical sites with MRI. As a final remark, note that studies apply-ing Bayes’ rule to estimate uncertainty of the point prediction are not hampered by ‘age mimicry’ and counter false assump-tions that are made when linear regression is applied [34]. Therefore, interpreting confidence intervals from those studies should be preferred over those obtained from age distribution tables or regression.
Strengths and weaknesses
This systematic review provides a compre-hensive overview of literature that is cur-
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

225
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation
rently available on age estimation based on MRI. It puts the studies in perspective, allowing medical professionals to de-cide on which approach seems the most valuable in their casework, and allowing judicial advisors to interpret the eviden-tial value of the age estimation results. According to the PRISMA guidelines, all steps of the review were independently conducted by two reviewers, to avoid er-rors in the reported data.
However, this review also faced two limitations. Firstly, the search string did not include a part on “development”. In-stead only “age estimation” and its vari-ants were used. Therefore, there remains the possibility that studies on develop-ment were missed, which may, in turn, have highlighted other MRI-specific signs that might be of interest to age estima-tion. On the other hand, the encountered studies on development – without a focus on age estimation – were excluded from quantitative analysis, since their data was not sufficiently extensively reported. Sec-ondly, pooling of the data was considered inappropriate, because of discrepancies between the MRI approaches and the staging techniques. New studies are nec-essary to compare the age distributions within stages using different MRI ap-proaches in the same population.
Future prospects
Since the intervention of interest was MRI, results of the initial search included many studies on brain development and degeneration. However, in literature on age estimation in children, adolescents and subadults, the developing brain is generally not considered. After all, struc-tural changes in the brain are mostly stud-
ied in older patients, when degeneration occurs related to age (or disease). Howev-er, changes in the developing brain might be useful for age estimation in younger individuals. Another strength of MRI is the possibility to study dynamic changes in the body, such as diffusion in the brain or blood flow in the heart [14, 37, 43, 47, 68, 70].
Therefore, since inter-individual vari-ation remains a challenge in age estima-tion, adding soft tissue information might allow for a more nuanced age estimation than that solely based on hard tissue in-formation. Moreover, studying functional and anatomical age-related changes in a research context is justifiable because of the lack of ionizing radiation. MRI even enables longitudinal evaluation of the changes over the years in an ethically jus-tifiable way. However, to date, the bridge between hard and soft tissue development remains unexplored.
SSA using MRI has been studied extensively, providing several ref-erence studies, which all included a relatively small study sample. Al-though a review might solve this
issue by pooling the data, this was cur-rently not appropriate, because of a wide variety in study characteristics. As a next step in the field, MFA studies are immi-nent, since MRI avoids the use of ionizing radiation and, consequently, allows the study of multiple anatomical sites. The current review results can guide those MFA studies. Moreover, (published and imminent) MFA studies can help medical professionals to decide on the preferred approach for specific cases, and they can help judicial professionals to interpret the evidential value of age estimation results.
Conclusion

226
acknowledgements
We wish to thank Tom Verschoore (Bi-metra, Ghent University Hospital), for his advice regarding the review protocol.
Furthermore, we want the acknowledge Karoline Elisivdatter Nyhagen for pro-viding us the reference list of her bach-elor’s thesis at the University of Central Lancashire entitled “Age Estimation in the Living Using Magnetic Resonance Imaging – A Review of Current Methods Identifying the 18-Years-Old Threshold”, which rendered two additional references to screen. We also thank Michiel de Haas (Netherlands Forensic Institute) and Mar-tin Urschler (Ludwig Boltzmann Institute for Clinical Forensic Imaging) for provid-ing us additional papers.
Our sincerest gratitude goes out to the authors who provided additional data for this review: Markus Auf der Mauer [3, 49], Astrid Junge [111], Martin Urschler [113, 114]. Furthermore, special thanks to Peter Roozenbeek for his advice and help to create the perfect graphs.
Finally, we kindly acknowledge Patrick Davis and Inès Phlypo for their critical review of the manuscript.
references
[1] Abdelbary MH, Abdelkawi MM, Nasr MA. Age determina-tion by MR imaging of the wrist in Egyptian male football players. How far is it reliable? Egyptian Journal of Radiology and Nuclear Medicine. 2018;49(1):146-51.
[2] AlQahtani SJ, Hector MP, Liversidge HM. Brief communi-cation: The London atlas of human tooth development and eruption. Am J Phys Anthropol. 2010;142(3):481-90.
[3] Auf der Mauer M, Saring D, Stanczus B, Herrmann J, Groth M, Jopp-van Well E. A 2-year follow-up MRI study for the evaluation of an age estimation method based on knee bone development. Int J Legal Med. 2018.
[4] Bassed RB, Briggs C, Drummer OH. Age estimation using CT imaging of the third molar tooth, the medial clavicular epiphysis, and the spheno-occipital synchondrosis: a multi-factorial approach. Forensic Sci Int. 2011;212(1-3):273.e1-5.
[5] Baumann P, Widek T, Merkens H, Boldt J, Petrovic A, Ur-schler M, Kirnbauer B, Jakse N, Scheurer E. Dental age es-timation of living persons: Comparison of MRI with OPG. Forensic Sci Int. 2015;253(0):76-80.
[6] Boldsen JL, Milner GR, Konigsberg LW, Wood JW. Transi-tion analysis: a new method for estimating age from skel-etons. In: Hoppa RD, Vaupel JW, eds. Paleodemography: Age Distributions from Skeletal Samples. 1st ed. Cambridge: Cambridge University Press, 2002; p. 73-106.
[7] Bolívar J, Sandoval Ó, Osorio J, Dib G, Gallo J. Relationship of chronological age and sexual maturity with skeletal ma-turity by magnetic resonance imaging of the distal radial epiphysis in adolescent football players. Apunts Medicina de l'Esport. 2015;50(188):129-37.
[8] Bollow M, Braun J, Kannenberg J, Biedermann T, Schau-er-Petrowskaja C, Paris S, Mutze S, Hamm B. Normal morphology of sacroiliac joints in children: magnetic resonance studies related to age and sex. Skeletal Radiol. 1997;26(12):697-704.
[9] Bray TJ, Vendhan K, Roberts J, Atkinson D, Punwani S, Sen D, Ioannou Y, Hall-Craggs MA. Association of the apparent diffusion coefficient with maturity in adolescent sacroiliac joints. J Magn Reson Imaging. 2016;44(3):556-64.
[10] Cameriere R, Ferrante L. Age estimation in children by measurement of carpals and epiphyses of radius and ulna and open apices in teeth: A pilot study. Forensic Sci Int. 2008;174(1):60-3.
[11] Cochrane Effective Practice and Organisation of Care (EPOC). EPOC Resources for review authors. 2017 [March 15, 2017]; Available from: epoc.cochrane.org/epoc-resourc-es-review-authors.
[12] Craig JG, Cody DD, Van Holsbeeck M. The distal femoral and proximal tibial growth plates: MR imaging, three-di-mensional modeling and estimation of area and volume. Skeletal Radiol. 2004;33(6):337-44.
[13] Cunha E, Baccino E, Martrille L, Ramsthaler F, Prieto J, Schuliar Y, Lynnerup N, Cattaneo C. The problem of aging human remains and living individuals: a review. Forensic Sci Int. 2009;193(1-3):1-13.
[14] Das SK, Wang JL, Bing L, Bhetuwal A, Yang HF. Regional Values of Diffusional Kurtosis Estimates in the Healthy Brain during Normal Aging. Clin Neuroradiol. 2017;27(3):283-98.
[15] De Tobel J, Hillewig E, Bogaert S, Deblaere K, Verstraete K. Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation. Ann Hum Biol. 2017;44(2):130-9.
[16] De Tobel J, Hillewig E, de Haas MB, Van Eeckhout B, Fieuws S, Thevissen P, Verstraete K. Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply? Eur Radiol. 2019;Epub ahead of print:1-12.
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

227
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation
[17] De Tobel J, Hillewig E, van Wijk M, Fieuws S, Thevissen P, Verstraete K. Staging clavicular development on magnetic resonance imaging: pitfalls and recommendations for age estimation. J Magn Reson Imaging. 2019;Submitted on No-vember 28, 2018.
[18] De Tobel J, Hillewig E, Verstraete K. Forensic age estima-tion based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging. Ann Hum Biol. 2017;44(2):121-9.
[19] De Tobel J, Parmentier GIL, Phlypo I, Descamps B, Neyt S, Van De Velde WL, Verstraete KL, Thevissen PW. Magnetic resonance imaging of third molars in forensic age estima-tion: comparison of the Ghent and Graz protocols focusing on apical closure. Int J Legal Med. 2018;Epub ahead of print.
[20] De Tobel J, Phlypo I, Fieuws S, Politis C, Verstraete KL, The-vissen PW. Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging. J Forensic Odontostomatol. 2017;35(2):117-40.
[21] De Tobel J, van Wijk M, Alberink I, Hillewig E, Phlypo I, van Rijn RR, Thevissen P, Verstraete K, de Haas MB. The influ-ence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation. Int J Legal Med. 2019;Sub-mitted on October 24, 2018.
[22] Dedouit F, Auriol J, Rousseau H, Rouge D, Crubezy E, Telm-on N. Age assessment by magnetic resonance imaging of the knee: a preliminary study. Forensic Sci Int. 2012;217(1-3):232 e1-7.
[23] Demirjian A, Goldstein H, Tanner JM. A new system of den-tal age assessment. Hum Biol. 1973;45(2):211-27.
[24] Demirturk Kocasarac H, Sinanoglu A, Noujeim M, Helva-cioglu Yigit D, Baydemir C. Radiologic assessment of third molar tooth and spheno-occipital synchondrosis for age estimation: a multiple regression analysis study. Int J Legal Med. 2016;130(3):799-808.
[25] Dvorak J, George J, Junge A, Hodler J. Age determination by magnetic resonance imaging of the wrist in adolescent male football players. Br J Sports Med. 2007;41(1):45-52.
[26] Dvorak J, George J, Junge A, Hodler J. Application of MRI of the wrist for age determination in international U-17 soccer competitions. Br J Sports Med. 2007;41(8):497-500.
[27] Ebner T, Štern D, Donner R, Bischof H, Urschler M. To-wards automatic bone age estimation from MRI: localization of 3D anatomical landmarks. Med Image Comput Comput Assist Interv. 2014;17(Pt 2):421-8.
[28] Ekizoglu O, Hocaoglu E, Can IO, Inci E, Aksoy S, Bilgili MG. Magnetic resonance imaging of distal tibia and calcaneus for forensic age estimation in living individuals. Int J Legal Med. 2015;129(4):825-31.
[29] Ekizoglu O, Hocaoglu E, Can IO, Inci E, Aksoy S, Sayin I. Spheno-occipital synchondrosis fusion degree as a method to estimate age: A preliminary, magnetic resonance imaging study. Aust J Forensic Sci. 2016;48(2):159-70.
[30] Ekizoglu O, Hocaoglu E, Inci E, Can IO, Aksoy S, Kazimoglu C. Forensic age estimation via 3-T magnetic resonance im-aging of ossification of the proximal tibial and distal femoral epiphyses: Use of a T2-weighted fast spin-echo technique. Forensic Sci Int. 2016;260:102.e1-7.
[31] Ekizoglu O, Inci E, Ors S, Kacmaz IE, Basa CD, Can IO, Kranioti EF. Applicability of T1-weighted MRI in the assess-ment of forensic age based on the epiphyseal closure of the humeral head. Int J Legal Med. 2018.
[32] European Asylum Support Office (EASO). Practical Guide on Age Estimation, Second edition. EASO Practical Guides Series. Malta2018.
[33] Fan F, Zhang K, Peng Z, Cui JH, Hu N, Deng ZH. Forensic age estimation of living persons from the knee: Comparison of MRI with radiographs. Forensic Sci Int. 2016;268:145-50.
[34] Fieuws S, Willems G, Larsen-Tangmose S, Lynnerup N, Boldsen J, Thevissen P. Obtaining appropriate interval esti-mates for age when multiple indicators are used: evaluation of an ad-hoc procedure. Int J Legal Med. 2016;130(2):489-99.
[35] Fournier K. [Age estimation of unaccompanied minors questioned: defining the issue, analysis and recommenda-tions]. Platform for refugee children, 2017.
[36] George J, Nagendran J, Azmi K. Comparison study of growth plate fusion using MRI versus plain radiographs as used in age determination for exclusion of overaged football players. Br J Sports Med. 2012;46(4):273-8.
[37] Grady CL, Garrett DD. Understanding variability in the BOLD signal and why it matters for aging. Brain Imaging Behav. 2014;8(2):274-83.
[38] Greulich W, Pyle SI. Radiographic atlas of skeletal develop-ment of the hand and wrist. 2nd ed. Stanford, CA: Stanford University Press, 1959.
[39] Guo Y, Olze A, Ottow C, Schmidt S, Schulz R, Heindel W, Pfeiffer H, Vieth V, Schmeling A. Dental age estimation in living individuals using 3.0 T MRI of lower third molars. Int J Legal Med. 2015;129(6):1265-70.
[40] Gustafson G, Koch G. Age estimation up to 16 years of age based on dental development. Odontol Revy. 1974;25(3):297-306.
[41] Haglund M, Mornstad H. A systematic review and me-ta-analysis of the fully formed wisdom tooth as a radiologi-cal marker of adulthood. Int J Legal Med. 2018.
[42] Harcke HT, Synder M, Caro PA, Bowen JR. Growth plate of the normal knee: evaluation with MR imaging. Radiology. 1992;183(1):119-23.
[43] Helpern JA, Adisetiyo V, Falangola MF, Hu C, Di Marti-no A, Williams K, Castellanos FX, Jensen JH. Preliminary evidence of altered gray and white matter microstructural development in the frontal lobe of adolescents with atten-tion-deficit hyperactivity disorder: A diffusional kurtosis imaging study. J Magn Reson Imaging. 2011;33(1):17-23.

228
[44] Hillewig E, De Tobel J, Cuche O, Vandemaele P, Piette M, Verstraete K. Magnetic resonance imaging of the medial ex-tremity of the clavicle in forensic bone age determination: a new four-minute approach. Eur Radiol. 2011;21(4):757-67.
[45] Hillewig E, Degroote J, Van der Paelt T, Visscher A, Van-demaele P, Lutin B, D'Hooghe L, Vandriessche V, Piette M, Verstraete K. Magnetic resonance imaging of the sternal ex-tremity of the clavicle in forensic age estimation: towards more sound age estimates. Int J Legal Med. 2013;127(3):677-89.
[46] Hojreh A, Gamper J, Schmook MT, Weber M, Prayer D, Herold CJ, Noebauer-Huhmann IM. Hand MRI and the Greulich-Pyle atlas in skeletal age estimation in adolescents. Skeletal Radiol. 2018.
[47] Hsu JL, Van Hecke W, Bai CH, Lee CH, Tsai YF, Chiu HC, Jaw FS, Hsu CY, Leu JG, Chen WH, Leemans A. Microstruc-tural white matter changes in normal aging: A diffusion ten-sor imaging study with higher-order polynomial regression models. NeuroImage. 2010;49(1):32-43.
[48] International Organization for Forensic Odonto-Stomatol-ogy (IOFOS). Recommendations for Quality Assurance: Dental Age Estimation. Leuven 2018.
[49] Jopp E, Schröder I, Maas R, Adam G, Püschel K. Proximal tibial epiphysis in magnetic resonance imaging. Rechts-medizin. 2010;20(6):464-8.
[50] Kellinghaus M, Schulz R, Vieth V, Schmidt S, Pfeiffer H, Schmeling A. Enhanced possibilities to make statements on the ossification status of the medial clavicular epiphysis us-ing an amplified staging scheme in evaluating thin-slice CT scans. Int J Legal Med. 2010;124(4):321-5.
[51] Kercher J, Xerogeanes J, Tannenbaum A, Al-Hakim R, Black JC, Zhao J. Anterior cruciate ligament reconstruction in the skeletally immature: an anatomical study utilizing 3-dimen-sional magnetic resonance imaging reconstructions. J Pedi-atr Orthop. 2009;29(2):124-9.
[52] Kim HK, Shiraj S, Anton C, Horn PS. The patellofem-oral joint: do age and gender affect skeletal maturation of the osseous morphology in children? Pediatr Radiol. 2014;44(2):141-8.
[53] Köhler S, Schmelzle R, Loitz C, Puschel K. [Development of wisdom teeth as a criterion of age determination]. Ann Anat. 1994;176(4):339-45.
[54] Konigsberg LW. Multivariate cumulative probit for age es-timation using ordinal categorical data. Ann Hum Biol. 2015;42(4):368-78.
[55] Kramer JA, Schmidt S, Jurgens KU, Lentschig M, Schmeling A, Vieth V. Forensic age estimation in living individu-als using 3.0 T MRI of the distal femur. Int J Legal Med. 2014;128(3):509-14.
[56] Kramer JA, Schmidt S, Jurgens KU, Lentschig M, Schmeling A, Vieth V. The use of magnetic resonance imaging to ex-amine ossification of the proximal tibial epiphysis for foren-sic age estimation in living individuals. Forensic Sci Med Pathol. 2014;10(3):306-13.
[57] Laor T, Chun GF, Dardzinski BJ, Bean JA, Witte DP. Poste-rior distal femoral and proximal tibial metaphyseal stripes at MR imaging in children and young adults. Radiology. 2002;224(3):669-74.
[58] Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interven-tions: explanation and elaboration. Bmj. 2009;339:b2700.
[59] Liversidge HM. Timing of human mandibular third molar formation. Ann Hum Biol. 2008;35(3):294-321.
[60] Liversidge HM, Smith BH, Maber M. Bias and accuracy of age estimation using developing teeth in 946 children. Am J Phys Anthropol. 2010;143(4):545-54.
[61] Lockemann U, Fuhrmann A, Püschel K, Schmeling A, Ges-erick G. Arbeitsgemeinschaft für Forensische Altersdiagnos-tik der Deutschen Gesellschaft für Rechtsmedizin. Rechts-medizin. 2004;14(2):123-6.
[62] Malina RM. Skeletal age and age verification in youth sport. Sports medicine (Auckland, NZ). 2011;41(11):925-47.
[63] Martinez Vera NP, Holler J, Widek T, Neumayer B, Eham-mer T, Urschler M. Forensic age estimation by morphomet-ric analysis of the manubrium from 3D MR images. Forensic Sci Int. 2017;277:21-9.
[64] Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred re-porting items for systematic reviews and meta-analyses: the PRISMA statement. Bmj. 2009;339:b2535.
[65] Nasel C, Gahleitner A, Breitenseher M, Czerny C, Solar P, Imhof H. Dental MR tomography of the mandible. J Com-put Assist Tomogr. 1998;22(3):498-502.
[66] Olze A, van NP, Schmidt S, Wernecke KD, Rosing FW, Ges-erick G, Schmeling A. Studies on the progress of third-mo-lar mineralisation in a Black African population. Homo. 2006;57(3):209-17.
[67] Ottow C, Schulz R, Pfeiffer H, Heindel W, Schmeling A, Vieth V. Forensic age estimation by magnetic resonance imaging of the knee: the definite relevance in bony fu-sion of the distal femoral- and the proximal tibial epiphy-ses using closest-to-bone T1 TSE sequence. Eur Radiol. 2017;27(12):5041-8.
[68] Paydar A, Fieremans E, Nwankwo JI, Lazar M, Sheth HD, Adisetiyo V, Helpern JA, Jensen JH, Milla SS. Diffusional kurtosis imaging of the developing brain. AJNR Am J Neu-roradiol. 2014;35(4):808-14.
[69] Pennock AT, Bomar JD, Manning JD. The Creation and Val-idation of a Knee Bone Age Atlas Utilizing MRI. J Bone Joint Surg Am. 2018;100(4):e20.
[70] Pfefferbaum A, Sullivan EV, Hedehus M, Lim KO, Adal-steinsson E, Moseley M. Age-related decline in brain white matter anisotropy measured with spatially corrected echo-planar diffusion tensor imaging. Magn Reson Med. 2000;44(2):259-68.
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

229
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation
[71] Rashid NR, Aliasghar A, Shaker QM. Magnetic resonance imaging of the left wrist: assessment of the bone age in a sample of healthy Iraqi adolescent males. J Fac Med Bagh-dad. 2015;57(1):22-6.
[72] Ruder TD, Hatch GM, Siegenthaler L, Ampanozi G, Mathier S, Thali MJ, Weber OM. The influence of body tempera-ture on image contrast in post mortem MRI. Eur J Radiol. 2012;81(6):1366-70.
[73] Saint-Martin P, Rerolle C, Dedouit F, Bouilleau L, Rousseau H, Rouge D, Telmon N. Age estimation by magnetic reso-nance imaging of the distal tibial epiphysis and the calcane-um. Int J Legal Med. 2013;127(5):1023-30.
[74] Saint-Martin P, Rerolle C, Dedouit F, Rousseau H, Rouge D, Telmon N. Evaluation of an automatic method for forensic age estimation by magnetic resonance imaging of the distal tibial epiphysis--a preliminary study focusing on the 18-year threshold. Int J Legal Med. 2014;128(4):675-83.
[75] Sarkodie B, Ofori E, Pambo P. MRI to determine the chron-ological age of Ghanaian footballers. S Afr J Sports Med. 2013;25(3):3.
[76] Sarkodie BD, Botwe BO, Pambo P, Brakohiapa EK, Mayeden RN. MRI age verification of U-17 footballers: The Ghana study. J Forensic Radiol Imaging. 2018;12:21-4.
[77] Schmeling A, Dettmeyer R, Rudolf E, Vieth V, Geserick G. Forensic Age Estimation. Dtsch Arztebl Int. 2016;113(4):44-50.
[78] Schmeling A, Geserick G, Reisinger W, Olze A. Age estima-tion. Forensic Sci Int. 2007;165(2-3):178-81.
[79] Schmeling A, Reisinger W, Loreck D, Vendura K, Markus W, Geserick G. Effects of ethnicity on skeletal maturation: consequences for forensic age estimations. Int J Legal Med. 2000;113(5):253-8.
[80] Schmeling A, Schulz R, Reisinger W, Muhler M, Wernecke KD, Geserick G. Studies on the time frame for ossification of the medial clavicular epiphyseal cartilage in conventional radiography. Int J Legal Med. 2004;118(1):5-8.
[81] Schmidt S, Ottow C, Pfeiffer H, Heindel W, Vieth V, Schmeling A, Schulz R. Magnetic resonance imag-ing-based evaluation of ossification of the medial clavic-ular epiphysis in forensic age assessment. Int J Legal Med. 2017;131(6):1665-73.
[82] Schmidt S, Schramm D, Ribbecke S, Schulz R, Wittschieber D, Olze A, Vieth V, Ramsthaler HF, Pfischel K, Pfeiffer H, Geserick G, Schmeling A. [Forensic age estimation in juve-niles and young adults: Reducing the range of scatter in age diagnosis by combining different methods]. Arch Kriminol. 2016;237(1-2):25-37.
[83] Schmidt S, Vieth V, Timme M, Dvorak J, Schmeling A. Ex-amination of ossification of the distal radial epiphysis using magnetic resonance imaging. New insights for age estima-tion in young footballers in FIFA tournaments. Sci Justice. 2015;55(2):139-44.
[84] Serin J, Rerolle C, Pucheux J, Dedouit F, Telmon N, Savall F, Saint-Martin P. Contribution of magnetic resonance im-aging of the wrist and hand to forensic age assessment. Int J Legal Med. 2016;130(4):1121-8.
[85] Serinelli S, Panebianco V, Martino M, Battisti S, Rodacki K, Marinelli E, Zaccagna F, Semelka RC, Tomei E. Accu-racy of MRI skeletal age estimation for subjects 12-19. Po-tential use for subjects of unknown age. Int J Legal Med. 2015;129(3):609-17.
[86] Shi L, Jiang F, Ouyang F, Zhang J, Wang Z, Shen X. DNA methylation markers in combination with skeletal and den-tal ages to improve age estimation in children. Forensic Sci Int Genet. 2017;33:1-9.
[87] Solheim T. A new method for dental age estimation in adults. Forensic Sci Int. 1993;59(2):137-47.
[88] Štern D, Ebner T, Bischof H, Grassegger S, Ehammer T, Urschler M. Fully automatic bone age estimation from left hand MR images. Med Image Comput Comput Assist Interv. 2014;17(Pt 2):220-7.
[89] Štern D, Kainz P, Payer C, Urschler M. Multi-Factorial Age Estimation from Skeletal and Dental MRI Volumes. In: International Workshop on Machine Learning in Medical Imaging. Quebec City, Canada: Springer, 2017; p. 61-9.
[90] Štern D, Payer C, Lepetit V, Urschler M. Automated age es-timation from hand MRI volumes using deep learning. In: International Conference on Medical Image Computing and Computer-Assisted Intervention. 2016:194-202.
[91] Tangmose S, Jensen KE, Lynnerup N. Comparative study on developmental stages of the clavicle by postmortem MRI and CT imaging. J Forensic Radiol Imaging. 2013;1(3):102-6.
[92] Tangmose S, Jensen KE, Villa C, Lynnerup N. Forensic age estimation from the clavicle using 1.0T MRI--preliminary results. Forensic Sci Int. 2014;234:7-12.
[93] Tangmose S, Jensen KE, Villa C, Lynnerup N. Forensic age estimation from the clavicle using 1.0T MRI-Preliminary results. Forensic Sci Int. 2014;234:7-12.
[94] Tanner JM, Whitehouse RH, Cameron N, Marshall WA, Healy MJR, Goldstein H. Assessment of skeletal maturity and prediction of adult height (TW2 method). 2nd ed. Lon-don: Academic Press Limited, 1983.
[95] Terada Y, Kono S, Tamada D, Uchiumi T, Kose K, Miyagi R, Yamabe E, Yoshioka H. Skeletal age assessment in chil-dren using an open compact MRI system. Magn Reson Med. 2013;69(6):1697-702.
[96] Terada Y, Kono S, Uchiumi T, Kose K, Miyagi R, Yamabe E, Fujinaga Y, Yoshioka H. Improved reliability in skeletal age assessment using a pediatric hand MR scanner with a 0.3T permanent magnet. Magn Reson Med Sci. 2014;13(3):215-9.
[97] Terada Y, Tamada D, Kose K, Nozaki T, Kaneko Y, Miyagi R, Yoshioka H. Acceleration of skeletal age MR examina-tion using compressed sensing. J Magn Reson Imaging. 2016;44(1):204-11.

230
[98] The Cochrane Public Health Group. Guide for developing a Cochrane protocol. 2011.
[99] Thevissen PW, Alqerban A, Asaumi J, Kahveci F, Kaur J, Kim YK, Pittayapat P, Van VM, Zhang Y, Fieuws S, Wil-lems G. Human dental age estimation using third molar developmental stages: Accuracy of age predictions not using country specific information. Forensic Sci Int. 2010;201(1-3):106-11.
[100] Thevissen PW, Fieuws S, Willems G. Human dental age estimation using third molar developmental stages: does a Bayesian approach outperform regression models to dis-criminate between juveniles and adults? Int J Legal Med. 2010;124(1):35-42.
[101] Thevissen PW, Fieuws S, Willems G. Human third molars development: Comparison of 9 country specific populations. Forensic Sci Int. 2010;201(1-3):102-5.
[102] Thevissen PW, Kaur J, Willems G. Human age estimation combining third molar and skeletal development. Int J Legal Med. 2012;126(2):285-92.
[103] Thevissen PW, Kvaal SI, Dierickx K, Willems G. Ethics in age estimation of unaccompanied minors. J Forensic Odontos-tomatol. 2012;30 Suppl 1:84-102.
[104] Thodberg HH, Kreiborg S, Juul A, Pedersen KD. The Bon-eXpert method for automated determination of skeletal ma-turity. IEEE Trans Med Imaging. 2009;28(1):52-66.
[105] Thodberg HH, Savendahl L. Validation and reference values of automated bone age determination for four ethnicities. Acad Radiol. 2010;17(11):1425-32.
[106] Thodberg HH, van Rijn RR, Jenni OG, Martin DD. Auto-mated determination of bone age from hand X-rays at the end of puberty and its applicability for age estimation. Int J Legal Med. 2017;131(3).
[107] Timme M, Ottow C, Schulz R, Pfeiffer H, Heindel W, Vieth V, Schmeling A, Schmidt S. Magnetic resonance imaging of the distal radial epiphysis: a new criterion of maturity for determining whether the age of 18 has been completed? Int J Legal Med. 2017;131(2):579-84.
[108] Timme M, Steinacker JM, Schmeling A. Age estimation in competitive sports. Int J Legal Med. 2017;131(1):225-33.
[109] Tomei E, Sartori A, Nissman D, Al Ansari N, Battisti S, Rubi-ni A, Stagnitti A, Martino M, Marini M, Barbato E, Semelka RC. Value of MRI of the hand and the wrist in evaluation of bone age: Preliminary results. J Magn Reson Imaging. 2014;39(5):1198-205.
[110] Tomei E, Semelka RC, Nissman D. Text-atlas of skeletal age determination: MRI of the hand and wrist in children: John Wiley & Sons, 2013.
[111] Tscholl PM, Junge A, Dvorak J, Zubler V. MRI of the wrist is not recommended for age determination in female football players of U-16/U-17 competitions. Scand J Med Sci Sports. 2016;26(3):324-8.
[112] Unterpirker W, Ebner T, Štern D, Urschler M. Automatic third molar localization from 3D MRI using random regres-sion forests. . In: Proceedings of the 19th Conference on Medical Image Understanding and Analysis (MIUA). Lin-coln, United Kingdom2015; p. 195-200.
[113] Urschler M, Grassegger S, Štern D. What automated age estimation of hand and wrist MRI data tells us about skeletal maturation in male adolescents. Ann Hum Biol. 2015;42(4):358-67.
[114] Urschler M, Krauskopf A, Widek T, Sorantin E, Ehammer T, Borkenstein M, Yen K, Scheurer E. Applicability of Greu-lich-Pyle and Tanner-Whitehouse grading methods to MRI when assessing hand bone age in forensic age estimation: A pilot study. Forensic Sci Int. 2016;266:281-8.
[115] Vieth V, Kellinghaus M, Schulz R, Pfeiffer H, Schmeling A. Ossification stage of the medial clavicular epiphysis: Comparison of projectional radiography, computed tomog-raphy and magnetic resonance imaging. Rechtsmedizin. 2010;20(6):483-8.
[116] Vieth V, Schulz R, Brinkmeier P, Dvorak J, Schmeling A. Age estimation in U-20 football players using 3.0 tesla MRI of the clavicle. Forensic Sci Int. 2014;241c:118-22.
[117] Vieth V, Schulz R, Heindel W, Pfeiffer H, Buerke B, Schmeling A, Ottow C. Forensic age assessment by 3.0T MRI of the knee: proposal of a new MRI classification of ossification stages. Eur Radiol. 2018;28(8):3255-62.
[118] Vo A, Beaule PE, Sampaio ML, Rotaru C, Rakhra KS. The femoral head-neck contour varies as a function of physeal development. Bone Joint Res. 2015;4(2):17-22.
[119] Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, Leeflang MM, Sterne JA, Bossuyt PM. QUA-DAS-2: a revised tool for the quality assessment of diagnos-tic accuracy studies. Ann Intern Med. 2011;155(8):529-36.
[120] Willems G, Lee SS, Uys A, Bernitz H, Cadenas de Llano-Pe-rula M, Fieuws S, Thevissen P. Age estimation based on Wil-lems method versus new country-specific method in South African black children. Int J Legal Med. 2017.
[121] Wittschieber D, Schmidt S, Vieth V, Schulz R, Püschel K, Pfeiffer H, Schmeling A. Subclassification of clavicular sub-stage 3a is useful for diagnosing the age of 17 years. Rechts-medizin. 2014;24(6):485-8.
[122] Wittschieber D, Vieth V, Timme M, Dvorak J, Schmeling A. Magnetic resonance imaging of the iliac crest: age estima-tion in under-20 soccer players. Forensic Sci Med Pathol. 2014;10(2):198-202.
[123] Zhang A, Sayre JW, Vachon L, Liu BJ, Huang HK. Racial dif-ferences in growth patterns of children assessed on the basis of bone age. Radiology. 2009;250(1):228-35.
De Tobel J. Multi-factorial forensic age estimation. Chapter 10: 188-231.

231
Staging clavicular development on magnetic resonance imaging: pitfalls and suggestions for age estimation
APPENDIX
IN MEDLINE, THE FOLLOWING SEARCH STRING WAS USED:
1 “age determination by teeth”[MeSH Terms]
OR “age determination by skeleton”[MeSH
Terms] OR “determine age”[TIAB] OR “age
determination”[TIAB] OR “determined age”[-
TIAB] OR “determining age”[TIAB] OR “est i-
mate age”[TIAB] OR “age est imation”[TIAB]
OR “est imated age”[TIAB] OR “est imating
age”[TIAB] OR “assess age”[TIAB] OR “age
assessment”[TIAB] OR “assessed age”[TIAB]
OR “assess ing age”[TIAB] OR “measure
age”[TIAB] OR “age measurement”[TIAB] OR
“measured age”[TIAB] OR “measuring age”
[T IAB]
2 “magnetic resonance imaging”[MeSH Terms]
OR “MRI” [T IAB] OR “NMR imaging”[TIAB] OR
“magnetic resonance imaging”[TIAB] OR
“MR imaging”[TIAB] OR “nuclear magnetic
resonance imaging”[TIAB] OR “ imaging,
magnetizat ion transfer” [T IAB] OR “magneti-
zat ion transfer imaging”[TIAB]
3 1-2 AND
IN EMBASE, THE FOLLOWING SEARCH STRING WAS USED:
1 ‘dental age est imation’/exp OR ‘bone age
determination’/exp OR ‘determine age’ : t i ,ab
OR ‘age determination’ : t i ,ab OR ‘determined
age’ : t i ,ab OR ‘determining age’ : t i ,ab ‘est i-
mate age’ : t i ,ab OR ‘age est imation’ : t i ,ab
OR ‘est imated age’ : t i ,ab OR ‘est imating
age’ : t i ,ab OR ‘assess age’ : t i ,ab OR ‘age as-
sessment’ : t i ,ab OR ‘assessed age’ : t i ,ab OR
‘assess ing age’ : t i ,ab OR ‘measure age’ : t i ,ab
OR ‘age measurement’ : t i ,ab OR ‘measured
age’ : t i ,ab OR ‘measuring age’ : t i ,ab
2 ‘nuclear magnetic resonance imaging’/exp
OR ‘mri ’ : t i ,ab OR ‘nmr imaging’ : t i ,ab OR
‘magnetic resonance imaging’ : t i ,ab OR ‘mr
imaging’ : t i ,ab OR ‘nuclear magnetic reso-
nance imaging’ : t i ,ab OR ‘ imaging, magne-
t izat ion transfer ’ : t i ,ab OR ‘magnetizat ion
transfer imaging’ : t i ,ab
3 1-2 AND
IN WEB OF SCIENCE, THE FOLLOWING SEARCH STRING
WAS USED:
1 TS=(“determine age” OR “age determina-
t ion” OR “determined age” OR “determining
age” OR “est imate age” OR “age est imation”
OR “est imated age” OR “est imating age” OR
“assess age” OR “age assessment” OR “as-
sessed age” OR “assess ing age” OR “mea-
sure age” OR “age measurement” OR “mea-
sured age” OR “measuring age”)
2 TS=(“magnetic resonance imaging” OR “MRI”
OR “MR imaging” OR “nuclear magnetic res-
onance imaging” OR “NMR imaging” OR “ im-
aging, magnetizat ion transfer” OR “magne-
t izat ion transfer imaging”)
3 1-2 AND
IN STUDY REGISTERS, THE FOLLOWING SEARCH STRING
WAS USED:
“age est imation” OR “age determination” OR “age
assessment”
232
CHAPTER 11
TH I S CHAPTER ADDRESSED THE FOLLOWING STUDY OB JECT IVES :
Objective 1: To collect a reference dataset of MR images of third molars, left wrist and both clavicles. These images will be registered simultaneously in each participant.
Objective 4: To stage the development of each age predictor based on the MRI. Existing 2D staging techniques will be modified or new methods will be developed. Reproduci-bility of the staging techniques will be tested.
Objective 5: To fit a statistical age estimation model on the reference data set, for each age predictor individually, as well as combining all registered age predictors. In all these models Bayes’ rule will be applied to counter drawbacks of other regression methods.
Objective 6: To validate this model and to compare its performance with existing models.
TH I S CHAPTER WAS SUBM ITTED FOR PUBL ICAT ION AS :
De Tobel J, Fieuws S, Hillewig E, Phlypo I, van Wijk M, de Haas MB, Politis C, Verstraete KL, Thevissen PW. Multi-factorial age estimation: a Bayesian approach combining den-tal and skeletal magnetic resonance imaging. Eur Radiol. Submitted on January 26, 2019 [A1; Journal Impact Factor 2017 4.027; Radiology, Nuclear Medicine & Medical Imaging Q1; Peer reviewed].
RESULTS DESCR I BED IN TH I S CHAPTER WERE PRESENTED
AT THE FOLLOWING CONFERENCES :
De Tobel J, Hillewig E, Phlypo I, de Haas M, van Wijk M, Fieuws S, Verstraete K, The-vissen P. Multi-factorial age estimation: a Bayesian approach combining dental and skel-etal magnetic resonance imaging. 22nd Meeting of the Study Group on Forensic Age Diagnostics, Arbeitsgemeinschaft für Forensische Altersdiagnostik (AGFAD); Berlin, Germany; March 15, 2019.
De Tobel J, Hillewig E, Phlypo I, de Haas M, van Wijk M, Fieuws S, Verstraete KL, The-vissen PW. Magnetic Resonance Imaging (MRI) of Third Molars, Clavicles, and Wrists for Age Estimation: A Combined Bayesian Approach. American Academy of Forensic Sciences (AAFS) 71st Annual Scientific Meeting; Baltimore, USA; February 21, 2019.

233
Multi-factorial age estimation: a Bayesian approach combining dental and
skeletal magnetic resonance imaging
OR IG INAL RESEARCH
Abstract
Aim — To study age estimation performance of combined MRI data of all four third molars, the left wrist and both clavicles in a reference population of females and males. To study the value of adding anthropomorphic and sexual maturation data. Methods — Three Tesla MRI of the three anatomical sites was prospectively conducted from March 2012 to May 2017 in 14- to 26-year-old healthy Caucasian volunteers (160 females, 138 males). Development was assessed by allocating stages, anthro-pomorphic measurements were taken, and self-reported sexual maturation data were collected. All data was incorporated in a continuation-ratio model to estimate age, applying Bayes’ rule to calculate point and interval predictions. Two performance aspects were studied: (1) accuracy and uncertainty of the point prediction, and (2) diagnostic ability to discern minors from adults (≥ 18 years). Results — Combining information from different anatomical sites decreased the mean absolute error (MAE) compared to incorporating only one site (P < 0.0001). By contrast, adding anthropomorphic and sexual maturation data to the model did not further improve MAE (P = 0.11). In females, combining all three anatomical sites rendered a MAE equal to 1.41 years, a mean width of the 95% prediction intervals of 5.91 years, 93% correctly classified adults and 91% correctly classified minors. In males, the corresponding results were 1.36 years, 5.49 years, 94%, and 90%, respectively. Conclu-sion — All aspects of age estimation improve when multi-fac-torial MRI data of the three anatomical sites are incorporated. Anthropomorphic and sexual maturation data do not seem to add relevant information.
Key Words
• age determination by skeleton
• age determination by teeth
• adolescent
• adult
• magnetic resonance imaging
AFF IL IAT IONS
1 Department of Diagnostic
Sciences – Radiology, Ghent
University, Belgium
2 Department of Imaging and Pa-
thology – Forensic Odontology,
KU Leuven, Belgium
3 Department of Oral and Maxillo-
facial Surgery, Leuven University
Hospitals, Belgium
4 KU Leuven – Leuven University &
Hasselt University, Department
of Public Health and Primary
Care, I-BioStat, Leuven, Belgium
5 Department of Oral Health
Sciences – Special Needs in Den-
tistry, Ghent University, Belgium
6 Department of Forensic Anthro-
pology, Netherlands Forensic
Institute, The Hague, The Neth-
erlands
Funding for this study was entirely
provided by the Department of
Diagnostic Sciences – Radiology at
Ghent University and the Department
of Imaging and Pathology – Forensic
Odontology at KU Leuven.
The authors declare that there are
no conflicts of interest.
JANN ICK DE TOBEL 1 2 3 STEFFEN F I EUWS 4
ELKE H I LLEW IG 1 I N ÈS PHLYPO 5
MAYONNE VAN W I J K6
M ICH I EL B . D E HAAS 6 CONSTANT INUS POL I T I S 3
KOENRAAD L . VERSTRAETE 1 PATR ICK W. THEV I S SEN 2

234
Multi-factorial forensic age estima-tion is recommended by experts [28] and applied by most author-ities [15, 26]. In adolescents and young adults, combining the devel-opmental information of different
anatomical sites improves age estimation performance [28]. In the living, medi-cal imaging can be used to obtain this developmental information. Currently, radiographs and computed tomography (CT) are the commonly applied imaging modalities. Numerous studies on single anatomical sites are available (further on referred to as “single site age estimation” = SSA), with large reference studies most-ly based on retrospective data. Attempts to combine the information from single site studies have been made [4], but con-troversies about the appropriate statisti-cal approach remain [5, 19]. By contrast, studying multiple anatomical sites in the same reference population (further on referred to as “multi-factorial age esti-mation” = MFA) allows for more relevant conclusions about combined age estima-tion and the relative contribution of each site. However, studying development of multiple anatomical sites in a living ref-erence population would not be ethical if this requires exposure to ionising ra-diation without clinical indication. Con-sequently, MFA studies have been con-ducted on deceased populations [3], on clinically indicated imaging [6, 14, 19, 22-24, 27, 30, 33] or on magnetic resonance imaging (MRI) [31].
MFA studies on deceased populations can be conducted retrospectively as well as prospectively. Mostly, post-mortem full body CT is of high quality because there are no limitations regarding radia-tion exposure [18]. However, gathering a
sufficiently large reference population of adolescents and young adults might take a long time, since autopsies in this age co-hort are rare.
MFA studies applying MRI require a prospective study design. After all, clini-cal images of the knee and wrist might be of sufficient quality to visualise bridging physeal plates, but clinical maxillofacial and thorax scans will not depict the de-tails of developing teeth and clavicles, respectively [7, 20]. Moreover, different sites of interest for age estimation are un-likely to be scanned at the same time in a clinical context. Consequently, several research groups are collecting MRI data for MFA. The first results were published by Stern et al. (2018) [31]. Their approach was based on a fully automatic assessment of the MRI data and information was combined by deep convolutional neural networks. They demonstrated that MFA combining MRI data of all four third molars (further on numbered according to the World Dental Federation 18, 28, 38, 48), the left hand and both clavicles outperformed SSA as well as combining only two sites. Unfortunately, their study population only included males. They re-ported the diagnostic ability of the meth-od to discern minors from adults, as well as mean absolute errors of the point pre-diction. However, no prediction intervals (PI; i.e. uncertainty intervals of the point prediction) were reported nor was the coverage verified (i.e. the proportion of true ages falling within the 95% PI).
Moreover, few studies have combined developmental information from medical imaging with anthropometric and sexual maturation data. Overall, the studies in-dicated that anthropometric and sexual
Introduction
De Tobel J. Multi-factorial forensic age estimation. Chapter 11: 232-254.

235
maturation data contribute little to age estimation [2, 17].
Therefore, the current study aimed to combine the information of human ob-servers, who staged the development of all four third molars, the left wrist and both clavicles for MFA in a reference popula-tion of females and males, with specific attention to PIs and coverage. A second aim was to study the value of adding an-thropometric and sexual maturation data to MFA.
Study population
The Ghent University Hospital eth-ics committee approved the study. Subsequently, 298 healthy volun-teers were prospectively recruited from March 2012 to May 2017 (160 females, 138 males, Table 11.1). This convenience sample comprised Caucasians of Belgian and Dutch
ancestry of middle to high socio-econom-ic status. Exclusion criteria were surgical removal of any third molar, developmen-tal disorders, chronic diseases or chronic medication intake that might affect devel-opment, and contra-indications for MRI. Parts of the study population have been included in earlier publications on SSA [7-13]. All participants gave informed consent, and in minors, the parents also consented. The study design complied with recommendations for reference studies on age estimation [28].
Anthropometric, socio- economic and sexual maturation data
All data were collected by the first author (JDT), who is a medical doctor and a den-
tist. He also conducted the MRI (see be-low). In a questionnaire, participants were asked about anthropometry, socio-eco-nomic status, medical and dental history. To provide self-reported data on sexual maturation, the questionnaire also in-cluded drawings and explanations of the Tanner stages of pubic hair for both sexes [1]. Breast development was also includ-ed for females, while males assessed their testicular volumes using an orchidometer (intervals of 5 mL). Participants received the questionnaires beforehand, and all as-pects were discussed with the researcher at the day of data collection. After said discussion, a clinical dental examination was conducted to check for anomalies.
Image acquisition
Subsequently, 3T MRI (Magnetom Trio Tim, Siemens, Erlangen, Germany) was carried out according to published pro-
Materials and M
ethods
TABLE 1 1 . 1 — NUMBER OF PARTICIPANTS PER AGE
PER SEX.
AGE (Y) FREQUENCY
FEMALE MALE TOTAL
14 1 1 1 1 22
15 1 1 10 21
16 10 10 20
17 1 1 9 20
18 13 10 23
19 15 12 27
20 20 9 29
21 14 10 24
22 12 10 22
23 1 1 10 21
24 1 1 1 1 22
25 1 1 12 23
26 10 14 24
TOTAL 160 138 298
Multi-factorial age estimation: a Bayesian approach combining dental and skeletal magnetic resonance imaging

236
tocols for third molars [7], the left wrist [8] and both clavicles [20]. Third molars and both clavicles were only scanned with one sequence, i.e. a T2 TSE and a T1 VIBE sequence, respectively. However, the wrist was scanned with a T1 spin echo as well as a T1 VIBE sequence. Reported wrist results were based on the latter sequence.
Image analysis
The images were pseudonymised and de-velopment was studied by allocating stag-es to all third molars [12], the distal radius and ulna [8] and both clavicles [9]. Re-garding all three anatomical sites, differ-ent MRI-specific staging considerations were pointed out in the references studies, resulting in the staging techniques depict-ed in Figure 11.1. Criteria for these stag-es are included in Tables 11.2 and 11.3. Note that stages of early (stage 1) and late (stages 4 and 5) development of the clav-icles were discarded, since they might be confused [9, 21]. For each anatomical site, the whole stack of slices was considered. Different observers with different levels of
experience assessed the images, resulting in inter- and intra-observer agreements that have been reported in earlier studies [8, 9, 12]. The staging results of the most experienced observer (JDT) were used for statistical analyses in the current study.
Statistical analysis
Development at each anatomical site and each anthropometric or sexual matura-tion measure were considered as age indi-cators. Bayes’ rule was used to obtain the posterior distribution of age given these indicators, using an ad hoc procedure [5, 16] to obtain an appropriate PI which cor-rects for violation of the conditional inde-pendence assumption (see below). As in the original approach, a continuation-ra-tio model was used for all ordinal age indicators, such as the allocated develop-mental stages and the ordinal sexual mat-uration data. The approach was expanded for the current study to incorporate con-tinuous data too, using a linear regression model for body weight and length. Ten-fold cross-validation handled overfitting.
FIGURE 1 1 . 1 — STAGING TECHNIQUES TO ASSESS DEVELOPMENT AT THREE ANATOMICAL SITES.
De Tobel J. Multi-factorial forensic age estimation. Chapter 11: 232-254.

237
For each model, two aspects of age esti-mation performance were studied: (1) point prediction of age, with PIs to quan-tify uncertainty, and (2) the ability to dis-cern minors (<18 years old) from adults (≥ 18 years old). Regarding the point pre-diction, the 5% trimmed mean was used, i.e. the mean in the 95% PI. Uncertainty was quantified by 95% PI, while accura-cy and precision were studied by calcu-lating mean absolute error (MAE; error = chronological age – estimated age) and root mean squared error (RMSE). Comparing the RMSE with the RMSE obtained when using the mean observed age as prediction for every participant, a coefficient of determination (R²) was cal-culated to reflect the percentage of total variance in age explained by the model. Regarding the ability to discern minors from adults, diagnostic indices were de-fined as follows:
— accuracy = proportion of correctly classified participants,
— sensitivity = proportion of correctly classified adults,
— specificity = proportion of correctly classified minors,
— discrimination slope = the differ-ence between minors and adults in mean predicted probability to be a minor.
Differences in age estimation perfor-mance between the models were evaluated by Wilcoxon signed rank tests, comparing MAEs. Furthermore, the conditional in-dependence assumption was tested. In age estimation, two age indicators are condi-tionally independent if for a given age, the
developmental stage of one age indicator provides no information about the devel-opmental stage of the other age indicator. This was tested in two ways. Firstly, the coverage of the 95% PI was studied for the applied models, i.e. for the PIs assuming conditional independence as well as for the PIs corrected for possible violation of the conditional independence. Note that when the conditional independence as-sumption does not hold, the PIs assuming independence will be too narrow, causing the percentage of true chronological ages falling within the 95% PI being too low. Secondly, the Pearson correlation coeffi-cients (ρerror) were calculated between the errors of the different models. If the con-ditional independence assumption truly holds, this correlation should be close to zero.
MFA was studied by combining dif-ferent sets of age indicators in the model. The following age indicators comprised those different sets: all four third molars (T), the distal radius and ulna at the wrist (W), both clavicles’ sternal ends (C), an-thropomorphic and sexual maturation data (A). Those sets were incorporated into the model separately or using the fol-lowing combinations: T+W, T+C, W+C, T+W+C, T+W+C+A. SSA based on T was selected as a starting point for com-parisons, since third molars go through developmental changes throughout the entire age range of the study population. Conversely, developmental changes of W and C are more pronounced in younger and older age categories, respectively.
The number of included anatomi-cal structures per model varied because of missing data. For all structures, some missing data arose as a result of images
Multi-factorial age estimation: a Bayesian approach combining dental and skeletal magnetic resonance imaging

238
TABLE 1 1 .2 — DESCRIPTIVE CRITERIA FOR DEVELOPMENTAL STAGES OF THIRD MOLARS ON MRI . Reproduced
from the Open Access ar t ic le De Tobel et al . (2017) [ 12] .
STAGE DESCRIPTION
STAGE 0 The crypt of the third molar is suspected without any calc if icat ion.
STAGE 1 A beginning of calc if icat ion is seen at the superior level of the crypt in the form of an in-
ver ted cone or cones. There is no fus ion of these calc if ied points .
STAGE 2 a) Fusion of the calc if ied points forms one or several cusps which unite to give a regu-
lar ly out l ined occlusal surface.
b) The out l ine of the pulp chamber has a f lat or curved shape at the occlusal border.
c) In it ia l formation of the radicular bifurcation is seen in the form of a hypo-intense
calc if ied point .
STAGE 3 a) The pulp chamber has a trapezoidal shape. The out l ine of the pulp horns is pointy and
shaped l ike an umbrel la top.
b) Increasing concavity of the crown and/or beginning of root formation is seen in the
form of a spicule. The spicule is shor ter than MR crown height .
c) The calc if ied region of the bifurcation has developed fur ther into a hypo-intense
semi- lunar shape.
STAGE 4 a) MR root length reaches at least one MR crown height .
b) The calc if ied region of the bifurcation st i l l has a semi- lunar shape or has developed
fur ther down.
STAGE 5 a) MR root length reaches at least one and a half MR crown height .
b) The calc if ied region of the bifurcation has developed fur ther down from its semi- lunar
shape to give the roots a more def in ite and dist inct out l ine with funnel shaped end-
ings. The funnel shape pers ists for some mi l l imetres ( i .e. i t is not l imited to a few pixels
on the image).
STAGE 6 a) The wal ls of the distal root canal are paral le l and its apical end is st i l l par t ial ly open.
b) The wal ls at the apex of the root canal show relat ively thin dentin .
c) Remnants of the dental fol l ic le are seen in the form of a hyper- intense area surround-
ing the apex.
STAGE 7 a) The wal ls of the distal root canal are convergent and its apical end is st i l l par t ial ly
open.
b) The wal ls at the apex of the root canal show relat ively thin dentin .
c) Remnants of the dental fol l ic le are seen in the form of a hyper- intense area surround-
ing the apex.
STAGE 8 a) The apical end of the distal root canal is completely c losed.
b) The wal ls at the apex of the root canal show relat ively thick dentin .
De Tobel J. Multi-factorial forensic age estimation. Chapter 11: 232-254.

239
TABLE 1 1 .3 — DESCRIPTIVE CRITERIA FOR DEVELOPMENTAL STAGES OF LONG BONES ON MRI [8, 9] .
1 Ossif icat ion centre is invis ib le (= not yet oss if ied).
2 Ossif icat ion centre is v is ib le (= oss if ied), nonunion of the epiphysis and metaphysis .
3 Physeal plate is par t ial ly oss if ied (= bone trabeculae cross the physeal plate from ossif icat ion
centre to metaphysis).
3a The epiphyseal-metaphyseal fus ion completes one third or less of the former gap between
epiphysis and metaphysis .
3aa Lengthwise measurement of the epiphysis is one third or lower compared with the widthwise
measurement of the metaphyseal ending.
3ab Lengthwise measurement of the epiphysis is between one third and two thirds compared with
the widthwise measurement of the metaphyseal ending.
3ac Lengthwise measurement of the epiphysis is over two thirds compared with the widthwise
measurement of the metaphyseal ending.
3b The epiphyseal-metaphyseal fus ion completes over one third unt i l two thirds of the former
gap between epiphysis and metaphysis .
3c The epiphyseal-metaphyseal fus ion completes over two thirds of the former gap between
epiphysis and metaphysis .
4 Complete union of the epiphysis and metaphysis (= physeal plate is completely oss if ied). Re-
gardless of the physeal scar being discernible.
not being assessable. Furthermore, third molar data was missing in cases of agen-esis, and clavicle data if they were in the discarded stages 1, 4 or 5. Anthropomor-phic and sexual maturation data were not missing for any participant. Thus, if for in-stance the performance of T+C was stud-ied and a specific participant did not have T information, the prediction was solely based on C. If there was no information at all within a specific approach for a spe-cific participant, the following distinction was made between two quantifications: (1) the participant was excluded from the assessment (rendering performance re-sults based only on cases with no missing information), and (2) the prediction for this participant equaled the best available guess, which was chosen to be the mean of the prior distribution of age, i.e. a uni-form distribution from 14 to 26 years old (rendering performance results based on the entire study population). It was as-
sumed that the observed proportion of missing data for the age indicators was representative for the rate of missing data in a practical setting.
Statistical analyses were conducted with SAS 9.4 (SAS Institute, Cary NC, USA), and tests were performed two-sid-ed with the significance level equal to 0.05. Sex-specific results were reported when appropriate.
To illustrate the Bayesian approach to MFA using MRI, four cases were displayed in Figures 11.2 to 11.5.
Missing data
Table 11.4 summarizes the number of anatomical structures that were included in the models. Missing clavicle data was more frequent in the younger and older participants, because the earliest and lat-
Results
Multi-factorial age estimation: a Bayesian approach combining dental and skeletal magnetic resonance imaging

240
est stages were discarded. In all other age indicators, missing data showed no predi-lection for certain age categories.
As a result of the relatively small study sample, the frequency in certain stages was too low to allow for a stable model. Therefore, the following stages were in-corporated jointly into the models: radius and ulna stages 2/3a, 3b/3c, 4/5; clavicle stages 3aa/3ab/3ac.
Which age indicators should be included?
In general, incorporating more age indi-cators in the model resulted in higher R². However, adding anthropomorphic and sexual maturation data to the information from the anatomical sites only yielded a negligible increase in R² (0.002 to 0.014) (Table 11.5).
Secondly, the accuracy of the point prediction was considered. When cases without information were excluded, none of the anatomical sites outperformed the other for SSA (Table 11.6, upper panel).
Obviously, when clavicle information lacked, dental or wrist information was indispensable (Table 11.6, lower panel). Combining the three anatomical sites rendered the most accurate age estima-tion with MAE = 1.38 years (standard deviation (SD) 1.15), and MAE = 1.39 years (SD 1.17) when imputing mean age for cases without information (Ta-ble 11.6). Moreover, compared with SSA or combining only two anatomical sites, the MAE improvement was not only significant, but also forensically rele-vant ranging from 0.16 to 0.47 years (i.e. 58 to 171 days). Still, not all individuals benefit from MFA, compared to SSA, as demonstrated in Figure 11.6. Note that developmental changes occur at the three anatomical sites around the age of 18. Therefore, it seems logical that the overall performance of the model benefits from this combination. Finally, adding anthro-pomorphic and sexual maturation data to the model did not significantly reduce the mean error (P = 0.1138; P = 0.0941 when imputing mean age for cases without in-formation).
Thirdly, the uncertainty of the point prediction and the ability to discern mi-nors from adults were considered. Com-bining information narrowed down the 95% PIs and increased the value of diag-nostic indices (Table 11.5). Again, adding anthropomorphic and sexual maturation data only rendered marginal improve-ments. Moreover, results for males were better than for females.
Finally, Table 11.7 provides an over-view of probabilities to be an adult, for combinations that might be encountered in practice when the 18-year-threshold is questioned.
TABLE 1 1 .4 — NUMBER OF ANATOMICAL
STRUCTURES INCLUDED IN THE MODELS FOR
AGE ESTIMATION, PER SEX.
ANATOMICAL
STRUCTURE
FREQUENCY
FEMALE MALE TOTAL
Third molar 18 135 1 18 253
Third molar 28 145 120 265
Third molar 38 137 106 243
Third molar 48 137 106 243
Distal radius 157 136 293
Distal u lna 157 136 293
Right c lavic le 106 78 184
Left c lavic le 1 15 82 197
De Tobel J. Multi-factorial forensic age estimation. Chapter 11: 232-254.

241
Conditional independence
The coverage of the 95% PIs was appro-priate, ranging from 94.0 to 95.8% (Table 11.8), when they were corrected for the plausible violation of the conditional in-dependence assumption. However, when conditional independence was assumed, they were much too narrow, ranging from 77.2 to 91.2%. Moreover, the violation of the conditional independence assump-tion was confirmed by the correlation between the prediction errors when dif-ferent anatomical sites were incorporated into the models, with ρerror ranging from 0.12 (third molars and clavicles in fe-males) to 0.49 (third molars and wrist in males). Furthermore, the conditional in-dependence assumption was rejected for all anthropometric and sexual maturation data, either among them or between them and each of the anatomical sites, with ρerror ranging from 0.17 (clavicles and pubic hair in females) to 0.76 (testicular volume and pubic hair in males).
The current findings demonstrated that MFA outperforms SSA based on MRI to estimate age in adoles-cents and young adults of both sex-es. With an MAE of 1.41 years in fe-
males and 1.36 in males, combining MRI information of all four third molars, the left wrist and both clavicles yielded more accurate age estimations than using less information. Moreover, narrower 95% PIs were obtained, with a width of 5.91 years in females and 5.49 years in males. Furthermore, MFA combining all three anatomical sites reached the highest abil-ity to discern minors from adults, with a specificity of 91% in females and 90% in males, and a sensitivity of 93% in females and 94% in males. Adding anthropomor-
phic and sexual maturation data only marginally improved age estimation per-formance.
The current findings were consistent with those reported by Stern et al. (2018), who performed MFA based on MRI of the same combination of anatomical sites in 322 male Austrian volunteers from 13.0 to 25.0 years old [31]. They quantified the relative contribution of each anatom-ical site to age estimation. Third molars showed the most constant contribution throughout the studied age range. The hand/wrist’s contribution decreased with increasing age, whereas the clavicles’ con-tribution increased. Similar to our find-ings, they demonstrated that the combi-nation of all three structures is especially valuable around the age of 18. In their sample, the MAE even reached 1.01 years, and a specificity of 90% corresponded with a sensitivity of 93%. Since they ap-plied a fully automated approach to assess the images and estimate age, they coun-tered intra- and inter-observer variability, which remains a major disadvantage of human observers who stage development on imaging [13, 34]. However, they did not report PIs and it is unclear how con-ditional dependence is handled within their deep convolutional neural networks approach.
Those PIs are essential to forensic age estimation practice, since they allow the requesting authority to interpret the un-certainty. However, an appropriate statis-tical approach is required to calculate the PIs [5]. In a first possible approach, the correlation between the age indicators is modelled explicitly in a multivariate model for the conditional distribution in Bayes’ rule [32]. Unfortunately, this ap-
Discussion
Multi-factorial age estimation: a Bayesian approach combining dental and skeletal magnetic resonance imaging

242
FIGURE 1 1 .2 — EXAMPLE OF MULTI-FACTORIAL MRI
DATA USED FOR AGE ESTIMATION BASED ON THE
BAYESIAN APPROACH. This female par t ic ipant was
16.05 years old.
a - d Third molars 18, 28, 38, and 48, respect ively.
Al l th ird molars are in stage 6, except tooth
38 (c) which is in stage 5.
e The r ight c lavic le is in stage 1 ; the left c lav-
ic le in stage 2.
f The distal radius is in stage 3a.
g The distal u lna is in stage 3a.
h Poster ior density curves for s ingle s ite age
est imation and for mult i-factorial age est i-
mation.
De Tobel J. Multi-factorial forensic age estimation. Chapter 11: 232-254.

243
FIGURE 1 1 .3 — EXAMPLE OF MULTI-FACTORIAL MRI
DATA USED FOR AGE ESTIMATION BASED ON THE
BAYESIAN APPROACH. This male par t ic ipant was
19.41 years old.
a - d Third molars 18, 28, 38, and 48, respect ively.
Al l th ird molars are in stage 6, except tooth
38 (c) which is in stage 7.
e Both c lavic les are in stage 3aa.
f, g The distal radius and ulna are in stage 3c.
h Poster ior density curves for s ingle s ite age
est imation and for mult i-factorial age est i-
mation.
Multi-factorial age estimation: a Bayesian approach combining dental and skeletal magnetic resonance imaging

244
FIGURE 1 1 .4 — EXAMPLE OF MULTI-FACTORIAL MRI
DATA USED FOR AGE ESTIMATION BASED ON THE
BAYESIAN APPROACH. This male par t ic ipant was
19.56 years old.
a, b Third molar 18, with its buccal roots (a) and
its palatal root (b). This third molar is in
stage 4.
c, d Third molar 28, with its buccal roots (c) and
its palatal root (d). This third molar is in
stage 4. The lower third molars were age-
netic .
e The r ight c lavic le is unsuitable for staging,
due to poor image qual ity. The left c lavic le
is in stage 3ab.
f The distal radius is in stage 4.
g The distal u lna is in stage 4.
h Poster ior density curves for s ingle s ite age
est imation and for mult i-factorial age est i-
mation.
De Tobel J. Multi-factorial forensic age estimation. Chapter 11: 232-254.

245
FIGURE 1 1 .5 — EXAMPLE OF MULTI-FACTORIAL MRI
DATA USED FOR AGE ESTIMATION BASED ON THE
BAYESIAN APPROACH. This male par t ic ipant was
18.57 years old.
a - f Al l th ird molars are in stage 4.
a, b Palatal roots of third molars 18 and 28, re-
spect ively.
c, d Crown and apices of third molar 38, respec-
t ively.
e, f Crown and apices of third molar 48, respec-
t ively.
g Both c lavic les are in stage 3ab.
h The distal radius is in stage 3c.
i The distal u lna is in stage 3c. In this s l ice, i t
appears to be in a lower stage, but scrol l-
ing through the sequence demonstrates
that most of the physeal plate is br idged.
j Poster ior density curves for s ingle s ite age
est imation and for mult i-factorial age est i-
mation. Note that the procedure grants this
par t ic ipant the benefit of the doubt , i f the
18-year-threshold would be quest ioned.
Multi-factorial age estimation: a Bayesian approach combining dental and skeletal magnetic resonance imaging

246
TABLE 1 1 .5 — AGE ESTIMATION PERFORMANCE OF DIFFERENT MODELS WHICH INCLUDE DIFFERENT AGE IN-
DICATORS.
CASES WITHOUT
INFORMATION
ACCURACY
OF POINT
PREDICTION
UNCERTAIN-
TY OF POINT
PREDICTION
SEX N R² RMSE (Y) MAE (Y) WIDTH OF
95% PI
Mean SD
EXCLUDED
Females 154 T 0.317 2.378 1 .920 7.82 1 .88
158 W 0.255 2.621 2 .078 8. 15 2.96
121 C 0.230 2.304 1 .782 8.37 1 .86
160 A 0. 1 18 3. 103 2.464 10.42 2.63
159 T + W 0.418 2.027 1 .566 6.47 2.00
157 T + C 0.397 2. 1 10 1 .677 6.90 1 .8 1
158 W + C 0.342 2.296 1 .825 7.23 2.50
160 T + W + C 0.464 1 .887 1 .4 1 1 5.91 1 .88
160 T + W + C + A 0.478 1 .836 1 .353 5.76 1 .77
Males 131 T 0.467 2. 1 17 1 .706 6.79 2.33
136 W 0.457 2. 169 1 .775 6.74 2.43
94 C 0. 172 2.830 2. 124 8.40 1 .95
138 A 0. 155 3.361 2.672 10. 17 2.99
138 T + W 0.526 1 .861 1 .500 5.96 2.22
137 T + C 0.513 1 .905 1 .5 18 6.36 2.33
138 W + C 0.473 2.069 1 .628 6.20 2. 16
138 T + W + C 0.564 1 .732 1 .357 5.49 1 .96
138 T + W + C + A 0.566 1 .724 1 .342 5.45 1 .94
MEAN AGE IMPUTED Females 154 T 0.301 2.442 1 .963 7.99 2.03
158 W 0.251 2.637 2.089 8.20 2.98
121 C 0. 1 19 3.088 2.420 9.34 2.36
160 A 0. 1 18 3. 103 2.464 10.42 2.63
159 T + W 0.410 2.061 1 .589 6.51 2 .05
157 T + C 0.388 2. 137 1 .695 7.00 1 .94
158 W + C 0.336 2.318 1 .839 7.30 2.55
160 T + W + C 0.464 1 .887 1 .4 1 1 5.91 1 .88
160 T + W + C + A 0.478 1 .836 1 .353 5.76 1 .77
Males 131 T 0.449 2. 161 1 .736 7.07 2.58
136 W 0.452 2. 177 1 .785 6.82 2.51
94 C 0.084 3.613 2.904 9.66 2.45
138 A 0. 155 3.361 2.672 10. 17 2.99
138 T + W 0.526 1 .861 1 .500 5.96 2.22
137 T + C 0.502 1 .955 1 .547 6.40 2.38
138 W + C 0.473 2.069 1 .628 6.20 2. 16
138 T + W + C 0.564 1 .732 1 .357 5.49 1 .96
138 T + W + C + A 0.566 1 .724 1 .342 5.45 1 .94
De Tobel J. Multi-factorial forensic age estimation. Chapter 11: 232-254.

247
DISCERNING MINORS FROM ADULTS
ACCURACY SENSITIVITY SPECIFICITY DISCRIMINATION
SLOPE
77.3 78.8 73.2 0.477
89.9 93.9 79. 1 0.656
86.0 92.0 70.6 0.507
77.5 81 .2 67.4 0.362
86.2 85.3 88.4 0.641
84.7 84.2 86.0 0.582
92.4 93.9 88.4 0.682
92.5 93.2 90.7 0.706
90.6 91 .5 88.4 0.718
91 .6 92.4 89.7 0.715
94. 1 93.8 94.9 0.815
78.7 85.7 58.3 0.346
75.4 79.6 65.0 0.369
93.5 94.9 90.0 0.807
92.0 92.8 90.0 0.724
92.8 93.9 90.0 0.793
92.8 93.9 90.0 0.807
93.5 94.9 90.0 0.81 1
77.3 78.8 73.2 0.477
89.9 93.9 79. 1 0.656
86.0 92.0 70.6 0.507
77.5 81 .2 67.4 0.362
86.2 85.3 88.4 0.641
84.7 84.2 86.0 0.582
92.4 93.9 88.4 0.682
92.5 93.2 90.7 0.706
90.6 91 .5 88.4 0.718
91 .6 92.4 89.7 0.715
94. 1 93.8 94.9 0.815
78.7 85.7 58.3 0.346
75.4 79.6 65.0 0.369
93.5 94.9 90.0 0.807
92.0 92.8 90.0 0.724
92.8 93.9 90.0 0.793
92.8 93.9 90.0 0.807
93.5 94.9 90.0 0.81 1
In cases without information, the
mean of the prior distr ibut ion of
age was imputed as point predict ion
(20.5 years), and the width of the
95% predict ion interval equaled that
of the prior distr ibut ion of age
(0.95 × 13 = 12 .35 years).
A = anthropomorphic and sexual
maturation data; C = both c lavi-
cles ; MAE = mean absolute error ;
N = number of par t ic ipants ; P I =
predict ion interval ; R² = coeff i-
c ient of determination; RMSE =
root mean squared error ; SD =
standard deviat ion; T = third mo-
lars ; W = wrist = distal radius and
ulna; y = years. Sensit iv ity = per-
centage correct ly identif ied adults ;
Specif ic ity = percentage correct ly
identif ied minors ; Discr imina-
t ion s lope = difference between mi-
nors and adults in mean predict-
ed probabi l i ty to be a minor. A =
anthropomorphic and sexual matu-
ration data; C = both c lavic les ; MAE
= mean absolute error ; N = number
of par t ic ipants ; P I = predict ion in-
terval ; R² = coeff ic ient of determina-
t ion; RMSE = root mean squared er-
ror ; SD = standard deviat ion; T =
third molars ; W = wrist = distal ra-
dius and ulna; y = years. Sensit iv ity
= percentage correct ly identif ied
adults ; Specif ic ity = percentage cor-
rect ly identif ied minors ; Discr imina-
t ion s lope = difference between mi-
nors and adults in mean predict-
ed probabi l i ty to be a minor.
Multi-factorial age estimation: a Bayesian approach combining dental and skeletal magnetic resonance imaging

248TA
BL
E 1
1.6
— M
EA
N A
BSO
LU
TE E
RRO
R O
F A
GE E
ST
IMA
TIO
N C
OM
PAR
ED
IN
DIF
FER
EN
T M
OD
EL
S W
HIC
H I
NC
LU
DE D
IFF
ER
EN
T A
GE I
ND
ICA
TO
RS.
Fe
ma
les
an
d m
ale
s a
re c
on
-
sid
ere
d j
oin
tly.
Sh
ad
ed
ce
lls
of
P-v
alu
es
ind
ica
te s
tati
stic
ally s
ign
ific
an
t re
sult
s.
CA
SE
S W
ITH
OU
T
INF
OR
MA
TIO
N
AC
CU
RA
CY
OF
PO
INT P
RE
DIC
TIO
N
AG
E I
ND
ICA
TO
R(S
)M
AE (
Y)
SD
(Y
)A
GE I
ND
ICA
TO
R(S
)M
AE (
Y)
SD
(Y
)N
P-V
ALU
E M
AE D
IFF
ER
EN
CE *
EXC
LU
DED
T1.8
31.3
2C
1.9
31.6
820
60
.915
2
T1.8
31.3
5W
1.9
41.4
62
82
0.4
79
7
W2
.01
1.4
8C
1.9
41.6
72
130
.73
20
T1.8
21.3
4T +
W1.
52
1.20
28
5<
0.0
00
1
T1.8
21.3
4T +
C1.
59
1.2
32
85
< 0
.00
01
T1.8
21.3
4T +
W +
C1.3
71.
152
85
< 0
.00
01
T +
W1.
54
1.2
1T +
W +
C1.3
81.
152
97
0.0
04
1
T +
C1.6
01.
23
T +
W +
C1.3
81.
142
94
< 0
.00
01
W +
C1.
73
1.3
5T +
W +
C1.3
81.
152
96
< 0
.00
01
T +
W +
C +
A1.3
41.
17T +
W +
C1.3
81.
152
97
0.1
138
MEA
N A
GE
IMPU
TED
T1.8
61.3
9C
2.6
42
.05
29
8<
0.0
00
1
T1.8
61.3
9W
1.9
51.4
62
98
0.5
187
W1.9
51.4
6C
2.6
42
.05
29
8<
0.0
00
1
T1.8
61.3
9T +
W1.
55
1.2
22
98
< 0
.00
01
T1.8
61.3
9T +
C1.6
31.
26
29
8<
0.0
00
1
T1.8
61.3
9T +
W +
C1.3
91.
172
98
< 0
.00
01
T +
W1.
55
1.2
2T +
W +
C1.3
91.
172
98
0.0
04
1
T +
C1.6
31.
26
T +
W +
C1.3
91.
172
98
< 0
.00
01
W +
C1.
741.3
6T +
W +
C1.3
91.
172
96
< 0
.00
01
T +
W +
C +
A1.3
51.
17T +
W +
C1.3
91.
172
98
0.0
94
1
A =
an
thro
po
mo
rph
ic a
nd
se
xua
l m
atu
rati
on
da
ta;
C =
bo
th c
lavic
les;
N =
nu
mb
er
of
pa
rtic
ipa
nts
in
clu
de
d f
or
co
mp
ari
son
; M
AE =
me
an
ab
solu
te e
rro
r; S
D =
sta
nd
ard
devia
tio
n;
T =
th
ird
mo
lars
; W
= w
rist
= d
ista
l ra
diu
s a
nd
uln
a;
y =
ye
ars
. *
P-v
alu
e f
rom
Wilco
xon
sig
ne
d r
an
k te
st c
om
pa
rin
g M
AEs.
De Tobel J. Multi-factorial forensic age estimation. Chapter 11: 232-254.

249
FIGURE 1 1 .6 — CROSS-VALIDATED EF-
FECT OF COMBINING ANATOMICAL
SITES ON MEAN ABSOLUTE ERROR
(MAE). On average, MAE is reduced
when more information is incorporat-
ed into the model , but this does not
hold for al l par t ic ipants.
a Adding wrist information to
third molars information main-
ly renders large correct ions
of the error in younger par-
t ic ipants, whereas the effect
of adding wrist information
fades away in the older par-
t ic ipants.
b Adding clavic les information
to third molars information
mainly renders large correc-
t ions of the error in par t ic i-
pants in their early twenties,
whereas the effect of adding
clavic les information fades
away in the younger par t ic i-
pants.
c Adding wrist and clavic les
information to third molars
information renders large cor-
rect ions of the error in par t ic-
ipants up to age 23.
C = both c lavic les ; T = third molars ; W
= distal radius and ulna.
Multi-factorial age estimation: a Bayesian approach combining dental and skeletal magnetic resonance imaging

250
TABLE 1 1 .7 — PROBABILITIES OF BEING AN ADULT PER SEX, PER COMBINATION OF STAGE PATTERNS AT THE
DIFFERENT ANATOMICAL SITES. For third molars, homogenous stage patterns were displayed per jaw (upper
or lower). For c lavic les, only homogenous stage patterns were displayed. Moreover, only late stages of de-
velopment were displayed.
DEVELOPMENTAL STAGE PER ANTOMICAL STRUCTURE P ≥ 18 Y
18 28 38 48 DISTAL
RADIUS
DISTAL ULNA RIGHT
CLAVICLE
LEFT CLAVICLE FEMALE MALE
7 7 7 7 3b/3c 3b/3c 3b 3b 0.9858 0.9764
7 7 7 7 3b/3c 3b/3c 3c 3c 0.9984 0.9951
7 7 7 7 3b/3c 3b/3c - - 0.9561 0.9305
7 7 7 7 3b/3c 4/5 3b 3b 0.9977 0.9944
7 7 7 7 3b/3c 4/5 3c 3c 0.9999 0.9993
7 7 7 7 3b/3c 4/5 - - 0.9947 0.9791
7 7 7 7 4/5 3b/3c 3b 3b 0.9945 0.9934
7 7 7 7 4/5 3b/3c 3c 3c 0.9996 0.9992
7 7 7 7 4/5 3b/3c - - 0.9845 0.9759
7 7 7 7 4/5 4/5 3b 3b 0.9994 0.9990
7 7 7 7 4/5 4/5 3c 3c 1 .0000 0.9999
7 7 7 7 4/5 4/5 - - 0.9991 0.9957
7 7 8 8 3b/3c 3b/3c 3b 3b 0.9908 0.9922
7 7 8 8 3b/3c 3b/3c 3c 3c 0.9991 0.9989
7 7 8 8 3b/3c 3b/3c - - 0.9724 0.9722
7 7 8 8 3b/3c 4/5 3b 3b 0.9987 0.9987
7 7 8 8 3b/3c 4/5 3c 3c 1 .0000 0.9999
7 7 8 8 3b/3c 4/5 - - 0.9975 0.9946
7 7 8 8 4/5 3b/3c 3b 3b 0.9967 0.9984
7 7 8 8 4/5 3b/3c 3c 3c 0.9998 0.9999
7 7 8 8 4/5 3b/3c - - 0.9915 0.9934
7 7 8 8 4/5 4/5 3b 3b 0.9997 0.9999
7 7 8 8 4/5 4/5 3c 3c 1 .0000 1 .0000
7 7 8 8 4/5 4/5 - - 0.9997 0.9997
8 8 7 7 3b/3c 3b/3c 3b 3b 0.9904 0.9782
8 8 7 7 3b/3c 3b/3c 3c 3c 0.9991 0.9956
8 8 7 7 3b/3c 3b/3c - - 0.9710 0.9349
8 8 7 7 3b/3c 4/5 3b 3b 0.9987 0.9950
8 8 7 7 3b/3c 4/5 3c 3c 1 .0000 0.9994
8 8 7 7 3b/3c 4/5 - - 0.9973 0.9810
8 8 7 7 4/5 3b/3c 3b 3b 0.9965 0.9941
8 8 7 7 4/5 3b/3c 3c 3c 0.9998 0.9993
8 8 7 7 4/5 3b/3c - - 0.9909 0.9780
8 8 7 7 4/5 4/5 3b 3b 0.9997 0.9991
De Tobel J. Multi-factorial forensic age estimation. Chapter 11: 232-254.

251
TABLE 1 1 .8 — PERCENTAGE OF TRUE AGE FALLING
WITHIN THE 95% CONFIDENCE INTERVALS, I .E . COV-
ERAGE OF THE INTERVALS.
AGE INDICA-
TOR(S)
95% COVERAGE
NOT ASSUMING
CONDITIONAL
INDEPENDENCE
ASSUMING
CONDITIONAL
INDEPEN-
DENCE
T 95.8% 77.2%
W 94.6% 90.8%
C 94.9% 87.4%
A 95.0% 88.9%
T + W 95.6% 81 . 1%
T + C 94.2% 82.0%
W + C 94.6% 91 .2%
T + W + C 94.6% 85.9%
T + W + C + A 94.0% 81 .9%
A = anthropomorphic and sexual maturation data;
C = both c lavic les ; T = third molars ; W = wrist =
distal radius and ulna.
TABLE 1 1 .7 (CONTINUED)
DEVELOPMENTAL STAGE PER ANTOMICAL STRUCTURE P ≥ 18 Y
18 28 38 48 DISTAL
RADIUS
DISTAL ULNA RIGHT
CLAVICLE
LEFT CLAVICLE FEMALE MALE
8 8 7 7 4/5 4/5 3c 3c 1 .0000 1 .0000
8 8 7 7 4/5 4/5 - - 0.9997 0.9962
8 8 8 8 3b/3c 3b/3c 3b 3b 0.9940 0.9930
8 8 8 8 3b/3c 3b/3c 3c 3c 0.9995 0.9991
8 8 8 8 3b/3c 3b/3c - - 0.9827 0.9745
8 8 8 8 3b/3c 4/5 3b 3b 0.9993 0.9989
8 8 8 8 3b/3c 4/5 3c 3c 1 .0000 0.9999
8 8 8 8 3b/3c 4/5 - - 0.9989 0.9953
8 8 8 8 4/5 3b/3c 3b 3b 0.9980 0.9986
8 8 8 8 4/5 3b/3c 3c 3c 0.9999 0.9999
8 8 8 8 4/5 3b/3c - - 0.9954 0.9942
8 8 8 8 4/5 4/5 3b 3b 0.9998 0.9999
8 8 8 8 4/5 4/5 3c 3c 1 .0000 1 .0000
8 8 8 8 4/5 4/5 - - 0.9999 0.9998
18 = upper r ight third molar ; 28 = upper left third molar ; 38 = lower left third molar ; 48 = lower r ight
third molar.
Multi-factorial age estimation: a Bayesian approach combining dental and skeletal magnetic resonance imaging
252
proach becomes computationally com-plex when the number of age indicators increases and when they are of different types. This computational complexity is circumvented in a second approach by factorising the multivariate conditional distribution for the age indicators into univariate distributions, i.e. fitting a sep-arate model for each age indicator. How-ever, the resulting posterior distribution will be too narrow when the conditional independence assumption is violated and an adaption of the posterior distribution is required to obtain appropriate PIs [16]. Correspondingly, several authors rejected the conditional independence assump-tion, and stated that conditional depend-ence should be accounted for [5, 16, 29], which is supported by the current find-ings. Nevertheless, some authors did as-sume conditional independence between the different anatomical sites [4, 19, 25], i.e. correlations between them are solely attributable to age. For instance, Bleka et al. (2018) reported a mean width of the 95% PI equal to 4.6 years for females and 4.5 years for males, when third molars and hand/wrist information was combined based on radiographs. Unfortunately, they did not verify the coverage.
The major limitation of the current study was its relatively small sample size. This led to the combination of certain (sub)stages to avoid insufficient numbers within stages, which on its turn would hinder analyses. The prospective nature of MFA studies using MRI explains their relatively small sample sizes. Therefore, future studies should investigate if the results of the few MFA studies that have been conducted (or are still ongoing) can safely be combined to increase the sam-ple size. Such studies should bear in mind
the need for an appropriate statistical ap-proach to handle conditional dependence and differences in study populations.
In conclusion, MFA based on MRI of all third molars, the left wrist and both clavicles outperforms SSA or any combination of two age indi-cators. By contrast, adding anthro-pomorphic and sexual maturation
data does not improve age estimation performance.
acknowledgements
The authors wish to thank all participants and people who helped with their recruit-ment. Furthermore, we want to thank Pat-rick Davis for his critical appraisal of the manuscript.
references
[1] Adams J, Shaw N. A practical guide to bone densitometry in children. Camerton, Bath, UK: National Osteoporosis Soci-ety, 2004.
[2] Auf der Mauer M, Saring D, Stanczus B, Herrmann J, Groth M, Jopp-van Well E. A 2-year follow-up MRI study for the evaluation of an age estimation method based on knee bone development. Int J Legal Med. 2018.
[3] Bassed RB, Briggs C, Drummer OH. Age estimation using CT imaging of the third molar tooth, the medial clavicular epiphysis, and the spheno-occipital synchondrosis: a multi-factorial approach. Forensic Sci Int. 2011;212(1-3):273.e1-5.
[4] Bleka O, Wisloff T, Dahlberg PS, Rolseth V, Egeland T. Ad-vancing estimation of chronological age by utilizing avail-able evidence based on two radiographical methods. Int J Legal Med. 2018.
[5] Boldsen JL, Milner GR, Konigsberg LW, Wood JW. Transi-tion analysis: a new method for estimating age from skel-etons. In: Hoppa RD, Vaupel JW, eds. Paleodemography: Age Distributions from Skeletal Samples. 1st ed. Cambridge: Cambridge University Press, 2002; p. 73-106.
[6] Cameriere R, De Luca S, Biagi R, Cingolani M, Farronato G, Ferrante L. Accuracy of three age estimation methods in children by measurements of developing teeth and car-pals and epiphyses of the ulna and radius. J Forensic Sci. 2012;57(5):1263-70.
Conclusion
De Tobel J. Multi-factorial forensic age estimation. Chapter 11: 232-254.

253
[7] De Tobel J, Hillewig E, Bogaert S, Deblaere K, Verstraete K. Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation. Ann Hum Biol. 2017;44(2):130-9.
[8] De Tobel J, Hillewig E, de Haas MB, Van Eeckhout B, Fieuws S, Thevissen P, Verstraete K. Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply? Eur Radiol. 2019;Epub ahead of print:1-12.
[9] De Tobel J, Hillewig E, van Wijk M, Fieuws S, Thevissen P, Verstraete K. Staging clavicular development on magnetic resonance imaging: pitfalls and recommendations for age estimation. J Magn Reson Imaging. 2019;Submitted on No-vember 28, 2018.
[10] De Tobel J, Hillewig E, Verstraete K. Forensic age estima-tion based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging. Ann Hum Biol. 2017;44(2):121-9.
[11] De Tobel J, Parmentier GIL, Phlypo I, Descamps B, Neyt S, Van De Velde WL, Verstraete KL, Thevissen PW. Magnetic resonance imaging of third molars in forensic age estima-tion: comparison of the Ghent and Graz protocols focusing on apical closure. Int J Legal Med. 2018;Epub ahead of print.
[12] De Tobel J, Phlypo I, Fieuws S, Politis C, Verstraete KL, The-vissen PW. Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging. J Forensic Odontostomatol. 2017;35(2):117-40.
[13] De Tobel J, van Wijk M, Alberink I, Hillewig E, Phlypo I, van Rijn RR, Thevissen P, Verstraete K, de Haas MB. The influ-ence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation. Int J Legal Med. 2019;Sub-mitted on October 24, 2018.
[14] Demirturk Kocasarac H, Sinanoglu A, Noujeim M, Helva-cioglu Yigit D, Baydemir C. Radiologic assessment of third molar tooth and spheno-occipital synchondrosis for age estimation: a multiple regression analysis study. Int J Legal Med. 2016;130(3):799-808.
[15] European Asylum Support Office (EASO). Practical Guide on Age Estimation, Second edition. EASO Practical Guides Series. Malta2018.
[16] Fieuws S, Willems G, Larsen-Tangmose S, Lynnerup N, Boldsen J, Thevissen P. Obtaining appropriate interval esti-mates for age when multiple indicators are used: evaluation of an ad-hoc procedure. Int J Legal Med. 2016;130(2):489-99.
[17] Garamendi PM, Landa MI, Ballesteros J, Solano MA. Relia-bility of the methods applied to assess age minority in living subjects around 18 years old. A survey on a Moroccan origin population. Forensic Sci Int. 2005;154(1):3-12.
[18] Gascho D, Thali MJ, Niemann T. Post-mortem computed tomography: Technical principles and recommended pa-rameter settings for high-resolution imaging. Med Sci Law. 2018;58(1):70-82.
[19] Gelbrich B, Frerking C, Weiss S, Schwerdt S, Stellzig-Eisen-hauer A, Tausche E, Gelbrich G. Combining wrist age and third molars in forensic age estimation: how to calculate the joint age estimate and its error rate in age diagnostics. Ann Hum Biol. 2015;42(4):389-96.
[20] Hillewig E, De Tobel J, Cuche O, Vandemaele P, Piette M, Verstraete K. Magnetic resonance imaging of the medial ex-tremity of the clavicle in forensic bone age determination: a new four-minute approach. Eur Radiol. 2011;21(4):757-67.
[21] Hillewig E, Degroote J, Van der Paelt T, Visscher A, Vande-maele P, Lutin B, D'Hooghe L, Vandriessche V, Piette M, Ver-straete K. Magnetic resonance imaging of the sternal extrem-ity of the clavicle in forensic age estimation: towards more sound age estimates. Int J Legal Med. 2013;127(3):677-89.
[22] Kullman L. Accuracy of two dental and one skeletal age es-timation method in Swedish adolescents. Forensic Sci Int. 1995;75(2-3):225-36.
[23] Kumagai A, Willems G, Franco A, Thevissen P. Age estima-tion combining radiographic information of two dental and four skeletal predictors in children and subadults. Int J Legal Med. 2018;Epub ahead of print.
[24] Machado MA, Daruge Junior E, Fernandes MM, Lima IFP, Cericato GO, Franco A, Paranhos LR. Effectiveness of three age estimation methods based on dental and skeletal de-velopment in a sample of young Brazilians. Arch Oral Biol. 2018;85:166-71.
[25] Mostad P, Tamsen F. Error rates for unvalidated medical age assessment procedures. Int J Legal Med. 2018.
[26] Office of Refugee Resettlement. Children Entering the Unit-ed States Unaccompanied: Section 1. 2015 [updated January 30, 2015; cited 2018 October 10]; Available from: https://www.acf.hhs.gov/orr/resource/children-entering-the-unit-ed-states-unaccompanied-section-1.
[27] Pinchi V, De Luca F, Focardi M, Pradella F, Vitale G, Ric-ciardi F, Norelli GA. Combining dental and skeletal evidence in age classification: Pilot study in a sample of Italian sub-adults. Leg Med (Tokyo). 2016;20:75-9.
[28] Schmeling A, Grundmann C, Fuhrmann A, Kaatsch HJ, Knell B, Ramsthaler F, Reisinger W, Riepert T, Ritz-Timme S, Ros-ing FW, Rotzscher K, Geserick G. Criteria for age estimation in living individuals. Int J Legal Med. 2008;122(6):457-60.
[29] Seselj M. Relationship between dental development and skeletal growth in modern humans and its implications for interpreting ontogeny in fossil hominins. Am J Phys An-thropol. 2013;150(1):38-47.
[30] Shi L, Jiang F, Ouyang F, Zhang J, Wang Z, Shen X. DNA methylation markers in combination with skeletal and den-tal ages to improve age estimation in children. Forensic Sci Int Genet. 2017;33:1-9.
[31] Štern D, Payer C, Giuliani N, Urschler M. Automatic Age Estimation and Majority Age Classification from Multi-Fac-torial MRI Data. IEEE J Biomed Health Inform. 2018;Epub ahead of print.
Multi-factorial age estimation: a Bayesian approach combining dental and skeletal magnetic resonance imaging

254
[32] Thevissen PW, Fieuws S, Willems G. Human dental age estimation using third molar developmental stages: does a Bayesian approach outperform regression models to dis-criminate between juveniles and adults? Int J Legal Med. 2010;124(1):35-42.
[33] Thevissen PW, Kaur J, Willems G. Human age estimation combining third molar and skeletal development. Int J Legal Med. 2012;126(2):285-92.
[34] Wittschieber D, Schulz R, Vieth V, Kuppers M, Bajanowski T, Ramsthaler F, Puschel K, Pfeiffer H, Schmidt S, Schmeling A. Influence of the examiner's qualification and sources of error during stage determination of the medial clavicular ep-iphysis by means of computed tomography. Int J Legal Med. 2014;128(1):183-91.
De Tobel J. Multi-factorial forensic age estimation. Chapter 11: 232-254.



257
PART 6
Conclusion

258
CHAPTER 12

259
New state of the art and future prospects
GENERAL D I SCUSS ION
New state of the art
At the end of this PhD project, MRI in age estimation has evolved from a scarcely ex-plored method to an extensively studied approach. Since migration was a major concern of European authorities during the past decade, research on age estima-tion gained an unprecedented interest. At the same time, several non-governmental and professional groups intensified their criticism against age estimation, powered by major disadvantages of the current approaches. Among them, the use of ion-ising radiation without a medical indica-tion is most frequently highlighted. Fur-thermore, multi-factorial age estimation has been suggested repeatedly to increase accuracy of age estimation. Unfortunate-ly, reports on this topic remain scarce, since studying different anatomical sites in healthy volunteers using ionising ra-diation would not be ethically justifiable. Moreover, the lack of a nationally and internationally accepted standardised approach to age estimation contributes to the diversity in the procedure’s results, and, consequently, to a lack of confidence in the whole concept of age estimation. Thus, striving to optimise age estimation, several research groups have completed the pathway outlined in Figure 2.4 simul-taneously (Figure 12.1).
MRI protocol
Remarkably, the different groups inde-pendently came up with similar MR im-ages to implement for age estimation. Chapter 3 demonstrated how we distilled the third molar MRI protocol, trying to find the balance between image quality and feasibility in a forensic context [20]. The selected sagittal T2 FSE sequence still proves to be state of the art, with its high resolution as main strength. Its weakness lies in its slice thickness, which hindered the assessment in some cas-es [24]. Although a 3D sequence would overcome this weakness, in Chapter 6 we demonstrated that the advantage of the multi-planar reconstruction (MPR) only outweighs the longer acquisition time in a few cases [23]. In an ongoing study, this statement was confirmed by staging MRI of third molars in 327 males. There-fore, it seems unnecessary to apply a 3D sequence in all cases. Instead, it could be added if a third molar’s assessment proves to be impossible, based on the 2D se-quence. Moreover, an additional axial or coronal 2D sequence might suffice to al-low stage allocation.
The protocols that were applied to scan the wrist and the clavicles were de-veloped by Hillewig et al. Regarding wrist MRI, several research groups have applied and compared T1 SE and VIBE sequences [21, 48, 110]. Mostly, they concluded the VIBE to be more easily assessable. Only in

260
our study was age estimation performance compared between both sequences, indi-cating that they performed equally well [21]. Regarding clavicle MRI, the VIBE sequence had been distilled before this PhD project started [46]. Other groups applied sequences that rendered similar images [85, 99, 114].
Staging technique
In Chapter 4, it became clear that the es-tablished staging technique for third mo-lars on radiographs could not simply be applied to MRI. Several considerations were formulated, but it was decided to cre-ate an MRI-specific staging technique to allow incorporating the 3D information. This technique was elaborated in Chapter 5. Only two other MRI studies on dental age estimation have been published [8,
39]. Both of them did apply a radiograph-ic staging technique. Comparative studies are necessary to elucidate whether one staging technique outperforms the other.
By contrast, the way of assessing the images of the long bones was very similar between the research groups. Based on ra-diographs and later on CT, the most elab-orate staging technique was composed of five main stages (1 to 5), some of which were further split up into substages (a to c), and even profound substaging for one substage (aa to ac) [54, 82, 116]. Moreo-ver, MRI-specific signs were identified, and their use for age estimation studied [58, 87]. In Chapter 7, we applied the most elaborate staging technique to the distal radius and ulna. Moreover, we tested sev-eral amelioration attempts for staging, but they did not improve age estimation [21].
TABLE 12. 1 — EUROPEAN COUNTRIES IN WHICH RESEARCH ON THE USE OF MRI IN AGE ESTIMATION HAS BEEN
CONDUCTED OR IS STILL ONGOING.
De Tobel J. Multi-factorial forensic age estimation. Chapter 12: 258-276.

261
The elaborate staging technique was rec-ommended, including substages of stage 3, but no profound substages. Although the wrist – and particularly the distal ra-dius – is the most frequently studied ana-tomical site with MRI for age estimation [18], no other studies compared how the staging technique of wrist bones affected age estimation performance.
Similarly, the elaborate staging tech-nique was applied to the sternal end of both clavicles in Chapter 9. A previous study had highlighted the risk of mix-ing-up stages of early (stage 1) and late (stages 4 and 5) development of the clavi-cle [47], which was confirmed in our larg-er study [22]. Thus, to avoid unacceptable errors, the clavicles should be discarded if they are in one of those stages. Our study indicated that staging the clavicle on MRI is prone to several pitfalls, which had been indicated for CT already [117]. Al-though the latter CT study provided tips and tricks to correctly stage clavicles, they did not all seem to be transferable to MRI [22, 47, 99].
Instead of using human observers, an Austrian research group developed a fully automated age estimation method based on MRI [28, 93-97, 107, 109]. The deep convolutional neural network (DCNN) combines all third molars, the left hand/wrist and both clavicles. In a pilot study including 103 male participants from 13.0 to 25.0 years old, they first trained the net-work to derive age from the MRIs, solely based on the chronological age [94]. Next they trained the network to derive age based on the chronological age with add-ed stage information of all the sites. Those stages had been allocated in advance by two human observers. As expected, age
estimation improved when the networks were trained with both the age and the stage information. Conversely, in their final paper including 322 male partici-pants, no improvement was reached by adding stage information [95].
Which age indicators should be included?
In Chapter 5, all four third molars were incorporated into the age estimation model, since studies on panoramic radi-ographs had indicated that this rendered the best age estimation performance [77]. By contrast, Chapter 7 demonstrated that the performance did not improve when radius and ulna were combined in the model [21]. Neither did one of the bones outperform the other. Similarly, radius and ulna performed equally well in males in a previous study [89]. In females, how-ever, the radius outperformed the ulna. Moreover, combining radius and ulna did not render better results than solely incorporating radius. Still, the Austrian automated method incorporates 13 hand/wrist regions (including distal radius and ulna), but they have not reported how leaving out some of them would affect their age estimates [95, 97].
Furthermore, in Chapter 9, we demonstrated that the safest approach to estimate age based on clavicle MRI was to incorporate both clavicles and exclude shape variants. This was in line with other studies on MRI [47, 83, 85, 113, 114] and CT [7, 29, 34, 41, 42, 49, 55, 76, 79, 81, 88, 116-119, 121]. However, only one study incorporated the information from both clavicles [47]. Instead, the other studies only included the less developed [7, 29, 30, 49] or more developed [31, 32, 34,
General discussion: New state of the art and future prospects

262
41, 42, 54, 55, 73, 76, 79, 83, 85, 106, 114, 116, 119, 121] side. Moreover, no other research group studied how staging shape variants would affect age estimation.
As a final step, in Chapter 11, we com-bined the information of all third molars, the radius and ulna, and both clavicles in an MRI-based MFA approach. The statis-tical analyses pointed out that all three an-atomical sites need to be incorporated in the model to render optimal results [19]. Adding anthropomorphic and sexual ma-turity data to the model did not further improve age estimation, which corre-sponded with other studies [4, 35, 64].
In the considered age range of 14 to 26, dental age is solely defined by the third molars, while skeletal age can be studied in several bones, of which the clavicle is the last to complete development [105]. The relative contribution to age estima-tion of dental age compared to skeletal age seems ambiguous. Regarding the point prediction of age and its uncertainty, add-ing the third molars’ information to any skeletal age indicator improves the results, achieving lower RMSEs, lower MAEs, and narrower PI’s (Table 11.5). Regarding the ability to discern minors from adults, bet-ter diagnostic indices and discrimination slopes were reached by skeletal age indi-cators – whether or not combined – than when third molars’ information was add-ed. Overall, the best age estimation results were reached by combining third molars, wrist, and clavicles. Our findings were not consistent with those reported by Stern et al. (2018), whose male reference popula-tion ranged from 13 to 25 years of age [95]. They found that the relative contribution to age estimation of dental age compared to skeletal age was consistently worse.
They found a lower MAE and narrower PI for skeletal age indicators – whether or not combined – than for third molars. Di-agnostic indices were also better for skel-etal age indicators than for third molars. Overall, the best age estimation results were reached by combining third molars, hand/wrist, and clavicles, albeit only mar-ginally better than combining hand/wrist and clavicles.
By contrast, the review of SSA studies based on MRI in Chapter 10 suggested that an alternative combination of ana-tomical sites might be more valuable. In females, combining third molars, the left hand/wrist and the knee might have the strongest potential, while in males, com-bining third molars, the proximal hu-merus and the knee might be ideal [18]. However, this combination of anatomical sites has never been studied, not even us-ing other imaging modalities. In general, studies that combined multiple anatomi-cal sites to estimate age are scarce. Table 12.1 provides an overview of the applied imaging modalities and age indicators that have been studied to date.
Finally, one needs to realise that the added value of a certain anatomical site to the age estimation results depends on the demands of the requesting authority. It can be expected that adding more an-atomical sites would improve the results, but if this improvement is only marginal, then the lower number of sites suffices. This is a forensic consideration, rather than a statistical one, although it consid-ers the age estimation performance.
De Tobel J. Multi-factorial forensic age estimation. Chapter 12: 258-276.

263
Age estimation performance
The largest dispersion between the re-search groups is found in the way the data are handled to estimate age. Some groups limited their findings to descrip-tive statistics (Table 11.3), which limits the conclusions that can be drawn regard-ing age estimation performance. We are the only group that has applied a Bayes-ian approach to MFA based on MRI [19]. This allows to report a point prediction of age, the uncertainty of the point estimate, and a probability to be an adult [33]. The Austrian automated method applies a re-gression DCNN architecture. It has been reported how the point prediction of age is derived, as well as how minors are dis-cerned from adults [95]. However, it re-mains unclear how the network would calculate prediction intervals.
Comparing age estimation performance between studies is tricky, since study pop-ulations, staging techniques and statisti-cal approaches differ. Therefore, a direct comparison of performance statistics between studies is irrelevant. This needs to be taken into account when interpret-ing Tables 12.2 to 12.4. They summarise the most important findings from MFA studies based on different age indicators and different imaging modalities. Note that most studies are very recent. Regard-ing the point prediction of age, all stud-ies agreed that combining age indicators improved the outcome. Results are gen-erally better when only children and ad-olescents are included, compared to when also adults were included. However, in a forensic context, studies that included both adolescents and adults are indis-pensable, since the 18-year-threshold is
TABLE 12. 1 — AGE INDICATORS IN MULTI-FACTORIAL AGE ESTIMATION STUDIES.
IMAGING MODALITY OR
OTHER TECHNIQUE
AGE INDICATORS REFERENCES
Radiograph Seven lower permanent teeth + hand/wrist [ 1 1 - 13, 63, 74]
Seven lower permanent teeth + al l th ird molars
+ hand/wrist + cranial width + mandibular width
[57 ]
Lower third molars + hand/wrist [9, 35, 56]
Al l th ird molars + hand/wrist [36]
Left third molars + cervical ver tebrae + mandibular
measurements
[ 102]
Radiograph + DNA Seven lower permanent teeth + hand/wrist + DNA
methylat ion
[90]
Radiograph + CT Lower third molar + spheno-occipital synchondrosis
+ both c lavic les
[6]
Lower left third molar + hand/wrist + both c lavic les [86]
Radiograph + CBCT Lower third molar + spheno-occipital synchondrosis [25]
Radiograph + MRI Lower left third molar + distal femur [67 ]
MRI Al l th ird molars + hand/wrist + c lavic les [94, 95]
Al l third molars + wrist + c lavic les [ 19]
General discussion: New state of the art and future prospects

264
mostly questioned. Regarding the ability to discern minors from adults, the opti-mal balance between specificity and sen-sitivity is also reached by combining age indicators.
Limitations and future prospects of MFA based on MRI
Study population and statistical analyses
The major limitation of the currently available MFA studies is their relatively small study population. By contrast, nu-merous X-ray SSA reference studies based on third molar development included more than 1000 participants of a uniform geographical origin [3, 5, 10, 17, 26, 27, 50, 51, 62, 65, 68-71, 75, 77, 78, 103], with some even including more than 2000 [38, 44, 53, 60, 61, 66, 101], or more than 3000 [40, 59, 120]. They were systematically re-viewed in [43, 100]. Such large numbers were not reached for skeletal age studies. Still, some X-ray SSA reference studies based on hand/wrist development includ-ed more than 500 participants of a uni-form geographical origin [37, 80, 84, 98, 111, 115], with some including more than 700 [16, 52], or more than 1000 [2]. They were systematically reviewed in [1]. Fur-thermore, some CT SSA reference studies based on clavicle development included more than 500 participants of a uniform geographical origin [30, 55, 76, 88, 122], with one including more than 700 [41]. They were systematically reviewed in [45].
How large a number of females and males is required to develop an age esti-mation model is highly debatable. After all, a power analysis would rely on pre-defined levels of uncertainty. Obvious-
ly, the narrower the prediction intervals and the higher the diagnostic indices, the better. However, it seems useless to set a predefined cut-off for them. With such a cut-off, presumably a sample size of thousands would be necessary, since the proposed MFA approach in this thesis is sex-specific, and combines eight anatom-ical structures, which can be in at least six developmental stages. Therefore, it seems more logical to study which age indicators add information to the model and to re-port the age estimation performance that can be reached by them.
The proposed MFA approach in this thesis should only be applied in adoles-cents and young adults, since we only in-cluded participants from 14 to 26 years of age. The results of the approach depend on the prior distribution, which was cho-sen to be a uniform distribution from 14 to 26 years old. This implies that every individual starts the age estimation pro-cedure with an equal chance to be of any age between 14.00 and 26.99. However, in cases whose considered anatomical sites are in the lowest and highest stages, results of the proposed approach should be inter-preted with caution. Still, SSA results for the lowest and highest stages were report-ed, since they are necessary for MFA. For instance, a male with all four third molars in stage 8, radius and ulna in stage 4, and both clavicles in stage 3c, will have a dif-ferent age estimation than when one third molar is in stage 7. Moreover, individuals whose chronological age is at the lower or upper end of the spectrum are less likely to start the procedure, since there will be no doubt about being a minor or an adult. Thus, because of the study design, the pro-posed approach is highly suitable for age estimation around the age of 18.
De Tobel J. Multi-factorial forensic age estimation. Chapter 12: 258-276.

265
A strength of the proposed MFA ap-proach is its advanced statistical founda-tion. The combination of age indicators is handled appropriately, and proves that this combination is useful. Still, further research could focus on the influence of the prior distribution. Sironi et al. (2016) stated that this prior distribution should reflect the initial belief that an exam-iner may have about the chronological age of the examinee, based on personal knowledge or past experience [91]. For instance, the proportion of individuals who are classified as adults after they went through the age estimation procedure has been constant for years at 70% (Table 1.1). Therefore, one could redistribute the pri-or distribution of age to reflect this out-come. Incidentally, the uniform prior dis-tribution applied in this PhD thesis exactly corresponds with this proportion of 70% (4/9), since we studied four age categories of minors (14 to 17) and nine age catego-ries of adults (18 to 26). Moreover, it has been demonstrated that results are more robust against changes in the prior distri-bution when multiple age indicators are simultaneously taken into account [92].
As a next step, the proposed approach should be validated in other populations. The available MRI data from other re-search groups could act as validation samples. If the model’s performance in those populations would be similar to the cross-validated performance that was reported in Chapter 11, then the other groups’ data could be incorporated into the model to further increase its perfor-mance. After all, this would indicate that between-population differences and be-tween-MRI-sequence differences would be inferior to within-population differ-ences, i.e. biological variability. Because
of the cumbersome process of collecting new MRI data suitable for age estimation, combining the MRI data that has been collected during the past decade could mean a breakthrough for age estimation practice.
Unfortunately, most MRI studies only included Caucasian participants, since MRI scanners are widespread in Europe and other rich countries. So did the cur-rent PhD project, which established the basics of MRI for age estimation: the scanning protocols and the staging tech-niques. Thus, a Caucasian population sufficed. Whether age estimation perfor-mance of the established models is simi-lar when they are applied to other ethnic groups, should be the focus of future re-search. After all, individuals requiring age estimation mostly do not originate from rich countries. Unfortunately, popula-tion-specific MRI data from other ethni-cal groups will be even harder to obtain than population-specific X-ray data.
Image acquisition
Limitations of MFA based on MRI
The limited access to MR-scanners does not only hinder the design of reference studies. It might also hinder the practical implementation of the imaging modality for age estimation. Currently, waiting lists for MRI are relatively long. Therefore, the age estimation scans will need to be planned in between or after clinical scans. One possible solution would be to central-ise the scanning procedure. In European countries like Denmark and Switzerland, a forensic institute is established, which features an MR-scanner. In those cas-es, the scanner is immediately available,
General discussion: New state of the art and future prospects

266R
EF
ER
EN
CE
WA
Y O
F C
OM
BIN
ING
INF
OR
MA
TIO
N
IMA
GIN
G
MO
DA
LIT
Y
AN
ATO
MIC
AL
SIT
ES
MA
E (
Y)
PO
PU
LA
TIO
N,
FE
MA
LE
SM
AL
ES
NO
N-S
EX
-SP
EC
IFIC
AG
E R
AN
GE
(Y
)
Ca
me
rie
re
et
al. 2
00
8
[13
]
Mu
ltip
le l
ine
ar
reg
ress
ion
Ra
dio
gra
ph
(1)
Seve
n l
ow
er
pe
rma
ne
nt
tee
th [
14]
150
liv
ing
(2)
Ha
nd
/wri
st [
15]
0.0
8 (
SE 1
.19
) §
5 -
15
(3)
Co
mb
ine
d (
1) +
(2)
0.4
65
(IQ
R 0
.52
9)
§
(3)
0.5
53
(SE 0
.73
) §
Ste
rn e
t a
l.
20
17 [
94]
De
ep
co
nvo
luti
on
al
ne
u-
ral
ne
two
rk p
retr
ain
ed
on
sta
ge
s
MR
I(1
) A
ll t
hir
d m
ola
rs
103
liv
ing
(2)
Ha
nd
/wri
st
13.0
1 -
24
.89
(3)
Cla
vic
les
(4
) C
om
bin
ed
(1)
+ (
2)
+ (
3)
1.
14 (
SD
0.9
6)
Ku
ma
ga
i e
t
al. 2
018
[5
7]
Ba
yes’
ru
le w
ith
a m
ult
iva
ri-
ate
co
nti
nu
ati
on
ra
tio
mo
de
l
Ra
dio
gra
ph
(1)
Seve
n l
ow
er
pe
rma
ne
nt
tee
th a
nd
1.00
1.07
25
6 l
ivin
ga
ll t
hir
d m
ola
rs
4 -
20
(2)
Co
mb
ine
d (
1) +
Ce
rvic
al
ve
rte
bra
C3
0.9
61.0
2
(3)
Co
mb
ine
d (
1) +
Ha
nd
/wri
st0
.94
0.9
8
(4)
Co
mb
ine
d (
2)
+ H
an
d/w
rist
+ c
ran
ial
0.9
10
.95
wid
th +
ma
nd
ibu
lar
wid
th
Ma
ch
ad
o
et
al. 2
018
[63
]
Mu
ltip
le l
ine
ar
reg
ress
ion
Ra
dio
gra
ph
(1)
Seve
n l
ow
er
pe
rma
ne
nt
tee
th [
14]
0.7
30
.83
23
4 l
ivin
g(2
) H
an
d/w
rist
[15
]1.9
61.6
4
5 -
14
(3)
Co
mb
ine
d (
1) +
(2)
[13
]0
.87
0.7
4
Sh
i e
t a
l.
20
17 [
90
]
Mu
ltip
le l
ine
ar
reg
ress
ion
Ra
dio
gra
ph
s(1
) Seve
n l
ow
er
pe
rma
ne
nt
tee
th0
.54
0.6
3
124
liv
ing
(2)
Ha
nd
/wri
st0
.74
0.6
9
6 -
15
(3)
Co
mb
ine
d (
1) +
(2)
0.4
40
.51
(4)
Co
mb
ine
d (
3)
+ D
NA
me
thyla
tio
n0
.33
0.4
7
Ste
rn e
t a
l.
20
18 [
95
]
De
ep
co
nvo
luti
on
al
ne
ura
l
ne
two
rk w
ith
ou
t p
retr
ain
ing
on
sta
ge
s
MR
I(1
) A
ll t
hir
d m
ola
rs
1.4
2 (
SD
1.1
4)
32
2 l
ivin
g(2
) H
an
d/w
rist
1.
25
(SD
0.9
6)
13.0
- 2
5.0
(3)
Cla
vic
les
1.
22
(SD
0.9
5)
(4
) C
om
bin
ed
(1)
+ (
2)
1.
11 (
SD
0.9
5)
(5
) C
om
bin
ed
(1)
+ (
3)
1.
10 (
SD
0.8
7)
(6
) C
om
bin
ed
(2)
+ (
3)
1.0
4 (
SD
0.9
5)
(7
) C
om
bin
ed
(1)
+ (
2)
+ (
3)
1.0
1 (S
D 0
.74)
TABLE 12.2 — MEAN ABSOLUTE ERROR OF POINT PREDICTIONS BY MULTI-FACTORIAL AGE ESTIMATION.
De Tobel J. Multi-factorial forensic age estimation. Chapter 12: 258-276.

267
Cu
rre
nt
stu
dy [
19]
Ba
yes’
ru
le w
ith
a m
ult
iva
ri-
ate
co
nti
nu
ati
on
ra
tio
mo
de
l
MR
I(1
) A
ll t
hir
d m
ola
rs [
24]
2.0
(me
dia
n
1.7,
IQ
R
1.9
)
1.7
(m
ed
ian
1.6
, IQ
R 1
.9)
29
8 l
ivin
g(2
) H
an
d/w
rist
[2
1] 1
.82
1.7
7 1
.79
14 -
26
(3)
Cla
vic
les
[22
] 1
.95
1.9
9 1
.97
(4)
Co
mb
ine
d (
1) +
(2)
1.5
71.
50
1.5
4 (
SD
1.2
1)
(5)
Co
mb
ine
d (
1) +
(3
)1.6
81.
52
1.6
0 (
SD
1.2
3)
(6)
Co
mb
ine
d (
2)
+ (
3)
1.8
31.6
31.
73
(SD
1.3
5)
(7)
Co
mb
ine
d (
1) +
(2)
+ (
3)
1.4
11.3
61.3
8 (
SD
1.1
5)
IQR
= i
nte
rqu
art
ile
ra
ng
e;
MA
E =
me
an
ab
solu
te e
rro
r; S
D =
sta
nd
ard
devia
tio
n;
SE =
sta
nd
ard
err
or;
y =
ye
ars
.
§ M
ed
ian
ab
solu
te e
rro
r w
as
rep
ort
ed
in
ste
ad
of
me
an
ab
solu
te e
rro
r.
General discussion: New state of the art and future prospects

268
TABLE 12.3 — ROOT MEAN SQUARED ERROR OF POINT PREDICTIONS BY MULTI-FACTORIAL AGE ESTIMATION.
RE
FE
RE
NC
EW
AY
OF
CO
MB
ININ
G
INF
OR
MA
TIO
N
IMA
GIN
G
MO
DA
LIT
Y
AN
ATO
MIC
AL
SIT
ES
RM
SE
(Y
)
PO
PU
LA
TIO
N,
FE
MA
LE
SM
AL
ES
NO
N-S
EX
-SP
EC
IFIC
AG
E R
AN
GE
(Y
)
Th
evis
sen
et
al. 2
012
[10
2]
Mu
ltip
le l
ine
ar
reg
ress
ion
Ra
dio
gra
ph
(1)
Le
ft t
hir
d m
ola
rs3.9
92
.99
3.6
0
95
6 l
ivin
g(2
) C
erv
ica
l ve
rte
bra
e C
2,
C3,
C4
3.3
33.0
03.2
0
3 -
33
(3)
Ce
rvic
al
ve
rte
bra
C3
3.4
33.1
03.2
9
(4)
Co
mb
ine
d (
1) +
(2)
+ (
3)
1.75
1.2
21.
57
Ku
ma
ga
i
et
al.
20
18 [
57
]
Ba
yes’
ru
le w
ith
a m
ult
i-
va
ria
te c
on
tin
ua
tio
n r
ati
o
mo
de
l
Ra
dio
gra
ph
(1)
Seve
n l
ow
er
pe
rma
ne
nt
tee
th a
nd
1.2
51.3
5
25
6 l
ivin
ga
ll t
hir
d m
ola
rs
4 -
20
(2)
Co
mb
ine
d (
1) +
Ce
rvic
al
ve
rte
bra
C3
1.20
1.2
8
(3
) C
om
bin
ed
(1)
+ H
an
d/w
rist
1.19
1.2
2
(4
) C
om
bin
ed
(2)
+ H
an
d/w
rist
+ c
ran
ial
1.14
1.19
w
idth
+ m
an
dib
ula
r w
idth
Ma
ch
ad
o e
t
al. 2
018
[6
3]
Mu
ltip
le l
ine
ar
reg
ress
ion
Ra
dio
gra
ph
(1)
Seve
n l
ow
er
pe
rma
ne
nt
tee
th [
14]
0.9
21.0
6
23
4 l
ivin
g(2
) H
an
d/w
rist
[15
]2
.32
1.9
4
5 -
14
(3)
Co
mb
ine
d (
1) +
(2)
[13
]1.
100
.92
Sh
i e
t a
l.
20
17 [
90
]
Mu
ltip
le l
ine
ar
reg
ress
ion
Ra
dio
gra
ph
s(1
) Seve
n l
ow
er
pe
rma
ne
nt
tee
th0
.68
0.7
8
124
liv
ing
(2)
Ha
nd
/wri
st0
.94
0.9
5
6 -
15
(3)
Co
mb
ine
d (
1) +
(2)
0.5
20
.64
(4
) C
om
bin
ed
(3
) + D
NA
me
thyla
tio
n0
.40
0.5
8
Cu
rre
nt
stu
dy [
19]
Ba
yes’
ru
le w
ith
a m
ult
i-
va
ria
te c
on
tin
ua
tio
n r
ati
o
mo
de
l
MR
I(1
) A
ll t
hir
d m
ola
rs [
24]
2.3
82
.06
29
8 l
ivin
g(2
) H
an
d/w
rist
[2
1]2
.26
2.2
22
.24
14 -
26
(3)
Cla
vic
les
[22
]2
.55
2.6
82
.60
(4)
Co
mb
ine
d (
1) +
(2)
2.0
31.8
6
(5)
Co
mb
ine
d (
1) +
(3
)2
.11
1.9
1
(6)
Co
mb
ine
d (
2)
+ (
3)
2.3
02
.07
(7
) C
om
bin
ed
(1)
+ (
2)
+ (
3)
1.8
91.
73
RM
SE =
ro
ot
me
an
sq
ua
red
err
or;
y =
ye
ars
.
De Tobel J. Multi-factorial forensic age estimation. Chapter 12: 258-276.

269
TABLE 12.4 — SPECIFICITY OF DISCERNING MINORS FROM ADULTS BY MULTI-FACTORIAL AGE ESTIMATION.
RE
FE
RE
NC
EW
AY
OF
CO
MB
ININ
G
INF
OR
MA
TIO
N
IMA
GIN
G M
OD
AL
ITY
AN
ATO
MIC
AL
SIT
ES
SP
EC
IFIC
ITY
(%
)
PO
PU
LA
TIO
N,
FE
MA
LE
SM
AL
ES
NO
N-S
EX-S
PEC
IFIC
AG
E R
AN
GE
(Y
)
Ga
ram
en
di
et
al. 2
00
5 [
35
]
Fre
qu
en
tist
sta
-
tist
ics
Ra
dio
gra
ph
80
liv
ing
13 -
25
(1)
Lo
we
r ri
gh
t th
ird
mo
lar
§9
5 (
Se
ns
24)
(2)
Lo
we
r le
ft t
hir
d m
ola
r§
95
(Se
ns
28)
(3)
Ha
nd
/wri
st78
(Se
ns
68)
(4)
Tan
ne
r p
ub
ic h
air
§8
7 (
Se
ns
10)
(5)
Co
mb
ine
d (
1) +
(2)
+ (
3)
§9
7 (
Se
ns
21)
Ca
me
rie
re e
t a
l.
20
15 [
12]
Mu
ltip
le l
ine
ar
re-
gre
ssio
n
Ra
dio
gra
ph
29
1 livin
g
5 -
15
(1)
Seve
n l
ow
er
pe
rma
ne
nt
tee
th*
92
(Se
ns
83
)8
9 (
Se
ns
80
)
(2)
Ha
nd
/wri
st*
83
(Se
ns
96
)8
5 (
Se
ns
88)
(3)
Co
mb
ine
d (
1) +
(2)
*9
2 (
Se
ns
91)
93
(Se
ns
93
)
Ste
rn e
t a
l. 2
017
[94]
De
ep
co
nvo
luti
on
al
ne
ura
l n
etw
ork
pre
tra
ine
d o
n
sta
ge
s
MR
I
103
liv
ing
13.0
1 -
24
.89
(1)
All t
hir
d m
ola
rs
(2)
Ha
nd
/wri
st8
1.8
(Se
ns
96
.6)
(3)
Cla
vic
les
(4)
Co
mb
ine
d (
1) +
(2)
+ (
3)
88.6
(Se
ns
93.2
)
Mo
sta
d a
nd
Tam
sen
20
18
[67
]
Ba
yes’
ru
le w
ith
a m
ult
iva
ria
te
co
nti
nu
ati
on
ra
tio
mo
de
l
Ra
dio
gra
ph
an
d
MR
I #
126
94
an
d 3
26
liv
ing
(1)
Lo
we
r le
ft t
hir
d m
ola
r [4
3]
Sens
51
(FPR
3.1)
(2)
Dis
tal
fem
ur
[72
]
(3)
Co
mb
ine
d (
1) +
(2)
6
7 (
Se
ns
93
)
Cu
rre
nt
stu
dy
[19
]
Ba
yes’
ru
le w
ith
a m
ult
iva
ria
te
co
nti
nu
ati
on
ra
tio
mo
de
l
MR
I
29
8 l
ivin
g
14 -
26
(1)
All t
hir
d m
ola
rs [
24]
65.8
(Se
ns
84
.4)
87.
2 (
Se
ns
92
.3)
(2)
Ha
nd
/wri
st [
21]
92.8
(Se
ns
88.5
)
(3)
Cla
vic
les
[22
]6
9.1
(Se
ns
85.5
)70
.0 (
Se
ns
86
.8)
69.4
(Se
ns
86.1)
(4)
Co
mb
ine
d (
1) +
(2)
88.4
(Se
ns
85.3
)9
0.0
(Se
ns
94
.9)
(5)
Co
mb
ine
d (
1) +
(3
)8
6.0
(Se
ns
84
.2)
90
.0 (
Se
ns
92
.8)
(6)
Co
mb
ine
d (
2)
+ (
3)
88.4
(Se
ns
93.9
)9
0.0
(Se
ns
93.9
)
(7
) C
om
bin
ed
(1)
+ (
2)
+ (
3)
9
0.7
(Se
ns
93.2
)9
0.0
(Se
ns
93.9
)
FPR
= f
als
e p
osi
tive
ra
te =
min
ors
wh
o a
re w
ron
gfu
lly c
lass
ifie
d a
s a
du
lts;
Se
ns
= s
en
siti
vit
y =
co
rre
ctl
y c
lass
ifie
d a
du
lts;
Sp
ecif
icit
y =
co
rre
ctl
y c
lass
ifie
d m
i-
no
rs;
y =
ye
ars
. § T
he
cu
t-o
ff w
as
ba
sed
on
sta
ge
s, n
ot
on
ag
e e
stim
ate
. *
Th
e c
ut-
off
wa
s a
t 14
ye
ars
of
ag
e,
inst
ea
d o
f 18
. #
Da
ta e
xtra
cte
d f
rom
lit
era
ture
.
General discussion: New state of the art and future prospects

270
since its use only serves forensic purpos-es. A forensic MR-scanner might not even be necessary in every country. For age es-timation, it would suffice to have forensic MR-scanners in the countries at Europe’s outer borders.
Imaging the three anatomical sites according to our protocols takes 30 to 45 minutes, taking into account the time to change clothes, the acquisition times, and changing the coils and the position of the examinee to scan each structure separate-ly. To reduce the time, two possible solu-tions are being studied. Firstly, more pow-erful coils are currently available than the ones we started to use in 2012. Since the third molars and the clavicles might be scanned with one powerful head and neck coil, time would be saved, since changing the coil and the participant’s position would no longer be needed. Secondly, ac-celeration of the MR-sequences has been proposed. Using compressed sensing with an open 0.3T MR-scanner, Terada et al. (2016) demonstrated that suitable hand/wrist images were still obtained with a 55 seconds acquisition time. Using a 3T MR-scanner, Neumayer et al. (2018) re-ported suitable hand/wrist images with a 15 seconds acquisition time. These results look promising, but need to be validat-ed before they can be generally applied. Moreover, studies are needed to explore the possibilities of accelerating the se-quences for third molars and clavicles. An accelerated sequence for third molars is required to reach the combination of a high in-plane resolution with a 3D image acquisition, while this combination was already achieved in the current PhD pro-ject for wrist and clavicle sequences.
Additionally, the process needs to be ex-plained clearly, since the examinee needs to be slid in the bore, lie perfectly still, and the scanner is very loud. The explanation could be supported by a demonstration using a mock scanner. The combined ex-planation and demonstration takes about 20 minutes. Thus, in total, about one hour is needed to complete the MR-image ac-quisition for age estimation. Compared to radiographs, the process is more demand-ing for all who are involved. Consequently, the costs for the requesting authority are higher, i.e. about twice as high, according to Belgian pricing. Still, although scien-tists can propose and validate alternative approaches to improve age estimation, politicians need to weigh the benefits in relation to the disadvantages and consider the practical implementation.
Furthermore, the explanation might not suffice to comfort an examinee if he/she suffers from claustrophobia. In some cases, starting the examination with the wrist scan can help, since the head is not in the bore during that scan. After that, the clavicle scan should be conducted and the third molars should be scanned last. Finally, the use of a high magnetic field is contra-indicated if the examinee has suf-fered war trauma, which might have left metal parts in the body [99], or in case of ferromagnetic implants.
Limitations of MFA based on other imaging modalities
Acquiring radiographs and CT-scans is less overwhelming for the examinee than an MR-scan. Moreover, numerous refer-ence and validation studies for age estima-tion based on dental radiographs, hand/wrist radiographs and clavicle CT have
De Tobel J. Multi-factorial forensic age estimation. Chapter 12: 258-276.

271
been published [1, 43, 45, 100], making SSA based on these imaging modalities a well-studied approach. Furthermore, modern CT techniques require less irra-diation (Table 1.3) than conventional CT, which might increase their possibility of getting accepted for forensic diagnostics in the living. However, before these new techniques can be brought into forensic practice, they would require new refer-ence studies. Such reference studies could become available soon, because they can be conducted retrospectively. The high-er accessibility of CT compared to MRI, and the large amount of clinical scans with 1 mm slice thickness, guarantee a large amount of CT data suitable for SSA studies. By contrast, designing MFA stud-ies retrospectively is not feasible. Conse-quently, no suitable MFA reference stud-ies are available using radiographs and/or CT in living adolescents and young adults. Moreover, setting up such a prospective MFA study using radiographs and/or CT would currently not be approved anymore by any ethical committee. Thus, to date, only two suitable MFA studies have been published: Stern et al. (2018) [95] and De Tobel et al. (2019) [19], both of them based on MRI. Future research might fo-cus on how this MFA MRI information could be extrapolated to combine SSA radiographs/CT information in a statisti-cally appropriate way.
Image analysis
The proposed MFA approach based on MRI has another disadvantage: it still re-quires a human observer who stages de-velopment based on the images. Ideally, this observer is (1) an expert in age esti-mation, and (2) experienced in interpret-ing images of the applied modality. Too
often age estimation is based on staging by an observer who lacks experience in one of both aspects. Furthermore, inter-ob-server variability varies between anatomi-cal structures – with knee and wrist bones reaching relatively high agreement – but remains a downside to the procedure.
Therefore, automated image analysis and age estimation might mean the oth-er breakthrough for age estimation. Au-tomated methods have successfully been developed for hand/wrist radiographs [104, 108, 112]. Similarly, the Austrian au-tomated method for MRI was first devel-oped and optimised for hand/wrist [28, 93, 109]. When the hand/wrist method was established [96], it was extended with the four third molars and both clavicles [94, 95]. The method reached a promising age estimation performance, but is only available for males. It would be interesting to feed MRI’s from other research groups to the DCNN, to expand the reference population. However, the DCNN will need to be adapted to handle the differ-ent MRIs. For instance, compared to the Austrian images, our third molars were not scanned with a 3D sequence, and our wrist scans did not include the hand.
Conclusion
In conclusion, several research groups have demonstrated that MRI is a feasible and valuable imaging modality for age es-timation in living adolescents and young adults, countering the disadvantages of the currently applied modalities. When specific considerations and pitfalls are taken into account, and an appropriate statistical approach is used, MFA based on MRI has the potential to become the first internationally accepted standardised
General discussion: New state of the art and future prospects
272
method to estimate age. In a next step to strive for its practical implementation, the different research groups will need to join forces to validate age estimation models and eliminate observer-induced errors.
references
[1] Alshamrani K, Messina F, Offiah AC. Is the Greulich and Pyle atlas applicable to all ethnicities? A systematic review and meta-analysis. Eur Radiol. 2019.
[2] Andersen E. Comparison of Tanner-Whitehouse and Greu-lich-Pyle methods in a large scale Danish Survey. Am J Phys Anthropol. 1971;35(3):373-6.
[3] Arany S, Iino M, Yoshioka N. Radiographic survey of third molar development in relation to chronological age among Japanese juveniles. J Forensic Sci. 2004;49(3):534-8.
[4] Auf der Mauer M, Saring D, Stanczus B, Herrmann J, Groth M, Jopp-van Well E. A 2-year follow-up MRI study for the evaluation of an age estimation method based on knee bone development. Int J Legal Med. 2018.
[5] Bagherpour A, Anbiaee N, Partovi P, Golestani S, Afzali-nasab S. Dental age assessment of young Iranian adults using third molars: A multivariate regression study. J Forensic Leg Med. 2012;19(7):407-12.
[6] Bassed RB, Briggs C, Drummer OH. Age estimation using CT imaging of the third molar tooth, the medial clavicular epiphysis, and the spheno-occipital synchondrosis: a multi-factorial approach. Forensic Sci Int. 2011;212(1-3):273.e1-5.
[7] Bassed RB, Drummer OH, Briggs C, Valenzuela A. Age es-timation and the medial clavicular epiphysis: analysis of the age of majority in an Australian population using computed tomography. Forensic Sci Med Pathol. 2011;7(2):148-54.
[8] Baumann P, Widek T, Merkens H, Boldt J, Petrovic A, Ur-schler M, Kirnbauer B, Jakse N, Scheurer E. Dental age es-timation of living persons: Comparison of MRI with OPG. Forensic Sci Int. 2015;253(0):76-80.
[9] Bleka O, Wisloff T, Dahlberg PS, Rolseth V, Egeland T. Ad-vancing estimation of chronological age by utilizing avail-able evidence based on two radiographical methods. Int J Legal Med. 2018.
[10] Boonpitaksathit T, Hunt N, Roberts GJ, Petrie A, Lucas VS. Dental age assessment of adolescents and emerging adults in United Kingdom Caucasians using censored data for stage H of third molar roots. Eur J Orthod. 2011;33(5):503-8.
[11] Cameriere R, De Luca S, Biagi R, Cingolani M, Farronato G, Ferrante L. Accuracy of three age estimation methods in children by measurements of developing teeth and car-pals and epiphyses of the ulna and radius. J Forensic Sci. 2012;57(5):1263-70.
[12] Cameriere R, De Luca S, Cingolani M, Ferrante L. Meas-urements of developing teeth, and carpals and epiphyses of the ulna and radius for assessing new cut-offs at the age thresholds of 10, 11, 12, 13 and 14 years. J Forensic Leg Med. 2015;34:50-4.
[13] Cameriere R, Ferrante L. Age estimation in children by measurement of carpals and epiphyses of radius and ulna and open apices in teeth: A pilot study. Forensic Sci Int. 2008;174(1):60-3.
[14] Cameriere R, Ferrante L, Cingolani M. Age estimation in children by measurement of open apices in teeth. Int J Legal Med. 2006;120(1):49-52.
[15] Cameriere R, Ferrante L, Mirtella D, Cingolani M. Carpals and epiphyses of radius and ulna as age indicators. Int J Legal Med. 2006;120(3):143-6.
[16] Cantekin K, Celikoglu M, Miloglu O, Dane A, Erdem A. Bone age assessment: the applicability of the Greu-lich-Pyle method in eastern Turkish children. J Forensic Sci. 2012;57(3):679-82.
[17] Cantekin K, Yilmaz Y, Demirci T, Celikoglu M. Morpholog-ic analysis of third-molar mineralization for eastern Turkish children and youth. J Forensic Sci. 2012;57(2):531-4.
[18] De Tobel J, Bauwens J, Parmentier GIL, Franco A, Pauwels NS, Verstraete K, Thevissen P. The use of magnetic reso-nance imaging in forensic age estimation of living children and subadults systematically reviewed. In progress. 2019.
[19] De Tobel J, Fieuws S, Hillewig E, Phlypo I, van Wijk M, de Haas MB, Politis C, Verstraete K, Thevissen P. Multi-facto-rial age estimation: a Bayesian approach combining den-tal and skeletal magnetic resonance imaging Eur Radiol. 2019;Submitted on January 26, 2019.
[20] De Tobel J, Hillewig E, Bogaert S, Deblaere K, Verstraete K. Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estimation. Ann Hum Biol. 2017;44(2):130-9.
[21] De Tobel J, Hillewig E, de Haas MB, Van Eeckhout B, Fieuws S, Thevissen P, Verstraete K. Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estimation model apply? Eur Radiol. 2019;Epub ahead of print:1-12.
[22] De Tobel J, Hillewig E, van Wijk M, Fieuws S, Thevissen P, Verstraete K. Staging clavicular development on magnetic resonance imaging: pitfalls and recommendations for age estimation. J Magn Reson Imaging. 2019;Submitted on No-vember 28, 2018.
[23] De Tobel J, Parmentier GIL, Phlypo I, Descamps B, Neyt S, Van De Velde WL, Verstraete KL, Thevissen PW. Magnetic resonance imaging of third molars in forensic age estima-tion: comparison of the Ghent and Graz protocols focusing on apical closure. Int J Legal Med. 2018;Epub ahead of print.
[24] De Tobel J, Phlypo I, Fieuws S, Politis C, Verstraete KL, The-vissen PW. Forensic age estimation based on development of third molars: a staging technique for magnetic resonance imaging. J Forensic Odontostomatol. 2017;35(2):117-40
De Tobel J. Multi-factorial forensic age estimation. Chapter 12: 258-276.

273
[25] Demirturk Kocasarac H, Sinanoglu A, Noujeim M, Helva-cioglu Yigit D, Baydemir C. Radiologic assessment of third molar tooth and spheno-occipital synchondrosis for age estimation: a multiple regression analysis study. Int J Legal Med. 2016;130(3):799-808.
[26] Duangto P, Iamaroon A, Prasitwattanaseree S, Mahakka-nukrauh P, Janhom A. New models for age estimation and assessment of their accuracy using developing mandibular third molar teeth in a Thai population. Int J Legal Med. 2016.
[27] Duangto P, Janhom A, Prasitwattanaseree S, Mahakka-nukrauh P, Iamaroon A. New prediction models for dental age estimation in Thai children and adolescents. Forensic Sci Int. 2016;266:583.e1-.e5.
[28] Ebner T, Štern D, Donner R, Bischof H, Urschler M. To-wards automatic bone age estimation from MRI: localization of 3D anatomical landmarks. Med Image Comput Comput Assist Interv. 2014;17(Pt 2):421-8.
[29] Ekizoglu O, Hocaoglu E, Inci E, Can IO, Aksoy S, Sayin I. Estimation of forensic age using substages of ossification of the medial clavicle in living individuals. Int J Legal Med. 2015;129(6):1259-64.
[30] Ekizoglu O, Hocaoglu E, Inci E, Sayin I, Solmaz D, Bilgi-li MG, Can IO. Forensic age estimation by the Schmeling method: computed tomography analysis of the medial clav-icular epiphysis. Int J Legal Med. 2015;129(1):203-10.
[31] El Gerby KM, Azza SM, Mie SG. Using thin-slice multi-detector computed tomography in forensic age estimation based on the ossification status of the medial clavicular epiphysis among Egyptian subjects. The Medical Journal of Cairo University. 2013;81(2):221-7.
[32] El Morsi DA, Abo El-Atta HM, ElMaadawy M, Tawfik AM, Batouty NM. Age Estimation from Ossification of the Me-dial Clavicular Epiphysis by Computed Tomography. Int J Morphol. 2015;33(4).
[33] Fieuws S, Willems G, Larsen-Tangmose S, Lynnerup N, Bold-sen J, Thevissen P. Obtaining appropriate interval estimates for age when multiple indicators are used: evaluation of an ad-hoc procedure. Int J Legal Med. 2016;130(2):489-99.
[34] Franklin D, Flavel A. CT evaluation of timing for ossification of the medial clavicular epiphysis in a contemporary Western Australian population. Int J Legal Med. 2015;129(3):583-94.
[35] Garamendi PM, Landa MI, Ballesteros J, Solano MA. Relia-bility of the methods applied to assess age minority in living subjects around 18 years old. A survey on a Moroccan origin population. Forensic Sci Int. 2005;154(1):3-12.
[36] Gelbrich B, Frerking C, Weiss S, Schwerdt S, Stellzig-Eisen-hauer A, Tausche E, Gelbrich G. Combining wrist age and third molars in forensic age estimation: how to calculate the joint age estimate and its error rate in age diagnostics. Ann Hum Biol. 2015;42(4):389-96.
[37] Gungor OE, Celikoglu M, Kale B, Gungor AY, Sari Z. The reliability of the Greulich and Pyle atlas when applied to a Southern Turkish population. Eur J Dent. 2015;9(2):251-4.
[38] Gunst K, Mesotten K, Carbonez A, Willems G. Third mo-lar root development in relation to chronological age: a large sample sized retrospective study. Forensic Sci Int. 2003;136(1-3):52-7.
[39] Guo Y, Olze A, Ottow C, Schmidt S, Schulz R, Heindel W, Pfeiffer H, Vieth V, Schmeling A. Dental age estimation in living individuals using 3.0 T MRI of lower third molars. Int J Legal Med. 2015;129(6):1265-70.
[40] Guo YC, Yan CX, Lin XW, Zhang WT, Zhou H, Pan F, Wei L, Tang Z, Liang F, Chen T. The influence of impaction to the third molar mineralization in northwestern Chinese popu-lation. Int J Legal Med. 2014;128(4):659-65.
[41] Gurses MS, Inanir NT, Gokalp G, Fedakar R, Tobcu E, Ocakoglu G. Evaluation of age estimation in forensic med-icine by examination of medial clavicular ossification from thin-slice computed tomography images. Int J Legal Med. 2016;130(5):1343-52.
[42] Gurses MS, Inanir NT, Soylu E, Gokalp G, Kir E, Fedakar R. Evaluation of the ossification of the medial clavicle ac-cording to the Kellinghaus substage system in identifying the 18-year-old age limit in the estimation of forensic age-is it necessary? Int J Legal Med. 2017;131(2):585-92.
[43] Haglund M, Mornstad H. A systematic review and me-ta-analysis of the fully formed wisdom tooth as a radiologi-cal marker of adulthood. Int J Legal Med. 2018.
[44] Harris EF. Mineralization of the mandibular third molar: a study of American blacks and whites. Am J Phys Anthropol. 2007;132(1):98-109.
[45] Hermetet C, Saint-Martin P, Gambier A, Ribier L, Sautenet B, Rerolle C. Forensic age estimation using computed to-mography of the medial clavicular epiphysis: a systematic review. Int J Legal Med. 2018;132(5):1415-25.
[46] Hillewig E, De Tobel J, Cuche O, Vandemaele P, Piette M, Verstraete K. Magnetic resonance imaging of the medial ex-tremity of the clavicle in forensic bone age determination: a new four-minute approach. Eur Radiol. 2011;21(4):757-67.
[47] Hillewig E, Degroote J, Van der Paelt T, Visscher A, Vande-maele P, Lutin B, D'Hooghe L, Vandriessche V, Piette M, Ver-straete K. Magnetic resonance imaging of the sternal extrem-ity of the clavicle in forensic age estimation: towards more sound age estimates. Int J Legal Med. 2013;127(3):677-89.
[48] Hojreh A, Gamper J, Schmook MT, Weber M, Prayer D, Herold CJ, Noebauer-Huhmann IM. Hand MRI and the Greulich-Pyle atlas in skeletal age estimation in adolescents. Skeletal Radiol. 2018.
[49] Houpert T, Rérolle C, Savall F, Telmon N, Saint-Martin P. Is a CT-scan of the medial clavicle epiphysis a good exam to attest to the 18-year threshold in forensic age estimation? Forensic Sci Int. 2016;260:103.e1-.e3.
[50] Jafari A, Mohebbi S, Khami M, Shahabi MS, Naseh M, El-hami F, Shamshiri A. Radiographic evaluation of third mo-lar development in 5- to 25 year olds in tehran, iran. J Dent (Tehran). 2012;9(2):107-15.
General discussion: New state of the art and future prospects

274
[51] Johan NA, Khamis MF, Abdul Jamal NS, Ahmad B, Ma-hanani ES. The variability of lower third molar development in Northeast Malaysian population with application to age estimation. J Forensic Odontostomatol. 2012;30(1):45-54.
[52] Johnston FE. Skeletal age and its prediction in Philadephia children. Hum Biol. 1963;35:192-202.
[53] Jung YH, Cho BH. Radiographic evaluation of third mo-lar development in 6- to 24-year-olds. Imaging Sci Dent. 2014;44(3):185-91.
[54] Kellinghaus M, Schulz R, Vieth V, Schmidt S, Pfeiffer H, Schmeling A. Enhanced possibilities to make statements on the ossification status of the medial clavicular epiphysis us-ing an amplified staging scheme in evaluating thin-slice CT scans. Int J Legal Med. 2010;124(4):321-5.
[55] Kellinghaus M, Schulz R, Vieth V, Schmidt S, Schmeling A. Forensic age estimation in living subjects based on the ossifi-cation status of the medial clavicular epiphysis as revealed by thin-slice multidetector computed tomography. Int J Legal Med. 2009.
[56] Kullman L. Accuracy of two dental and one skeletal age es-timation method in Swedish adolescents. Forensic Sci Int. 1995;75(2-3):225-36.
[57] Kumagai A, Willems G, Franco A, Thevissen P. Age estima-tion combining radiographic information of two dental and four skeletal predictors in children and subadults. Int J Legal Med. 2018;Epub ahead of print.
[58] Laor T, Chun GF, Dardzinski BJ, Bean JA, Witte DP. Poste-rior distal femoral and proximal tibial metaphyseal stripes at MR imaging in children and young adults. Radiology. 2002;224(3):669-74.
[59] Lee SH, Lee JY, Park HK, Kim YK. Development of third molars in Korean juveniles and adolescents. Forensic Sci Int. 2009;188(1-3):107-11.
[60] Levesque GY, Demirijian A, Tanguay R. Sexual dimorphism in the development, emergence, and agenesis of the mandib-ular third molar. J Dent Res. 1981;60(10):1735-41.
[61] Li G, Ren J, Zhao S, Liu Y, Li N, Wu W, Yuan S, Wang H. Dental age estimation from the developmental stage of the third molars in western Chinese population. Forensic sci-ence international. 2012;219(1-3):158-64.
[62] Lucas VS, Andiappan M, McDonald F, Roberts G. Dental Age Estimation: A Test of the Reliability of Correctly Identi-fying a Subject Over 18 Years of Age Using the Gold Stand-ard of Chronological Age as the Comparator. J Forensic Sci. 2016;61(5):1238-43.
[63] Machado MA, Daruge Junior E, Fernandes MM, Lima IFP, Cericato GO, Franco A, Paranhos LR. Effectiveness of three age estimation methods based on dental and skeletal de-velopment in a sample of young Brazilians. Arch Oral Biol. 2018;85:166-71.
[64] Martinez Vera NP, Holler J, Widek T, Neumayer B, Eham-mer T, Urschler M. Forensic age estimation by morphomet-ric analysis of the manubrium from 3D MR images. Forensic Sci Int. 2017;277:21-9.
[65] Mesotten K, Gunst K, Carbonez A, Willems G. Dental age estimation and third molars: a preliminary study. Forensic Sci Int. 2002;129(2):110-5.
[66] Mesotten K, Gunst K, Carbonez A, Willems G. Chrono-logical age determination based on the root development of a single third molar: a retrospective study based on 2513 OPGs. J Forensic Odontostomatol. 2003;21(2):31-5.
[67] Mostad P, Tamsen F. Error rates for unvalidated medical age assessment procedures. Int J Legal Med. 2018.
[68] Nystrom ME, Ranta HM, Peltola JS, Kataja JM. Timing of de-velopmental stages in permanent mandibular teeth of Finns from birth to age 25. Acta Odontol Scand. 2007;65(1):36-43.
[69] Olze A, Taniguchi M, Schmeling A, Zhu BL, Yamada Y, Mae-da H, Geserick G. Comparative study on the chronology of third molar mineralization in a Japanese and a German pop-ulation. Leg Med (Tokyo). 2003;5 Suppl 1:S256-S60.
[70] Olze A, Taniguchi M, Schmeling A, Zhu BL, Yamada Y, Mae-da H, Geserick G. Studies on the chronology of third molar mineralization in a Japanese population. Leg Med (Tokyo). 2004;6(2):73-9.
[71] Orhan K, Ozer L, Orhan AI, Dogan S, Paksoy CS. Radio-graphic evaluation of third molar development in relation to chronological age among Turkish children and youth. Forensic Sci Int. 2007;165(1):46-51.
[72] Ottow C, Schulz R, Pfeiffer H, Heindel W, Schmeling A, Vieth V. Forensic age estimation by magnetic resonance imaging of the knee: the definite relevance in bony fu-sion of the distal femoral- and the proximal tibial epiphy-ses using closest-to-bone T1 TSE sequence. Eur Radiol. 2017;27(12):5041-8.
[73] Pattamapaspong N, Madla C, Mekjaidee K, Namwongprom S. Age estimation of a Thai population based on maturation of the medial clavicular epiphysis using computed tomogra-phy. Forensic Sci Int. 2015;246:123.e1-5.
[74] Pinchi V, De Luca F, Focardi M, Pradella F, Vitale G, Ric-ciardi F, Norelli GA. Combining dental and skeletal evidence in age classification: Pilot study in a sample of Italian sub-adults. Leg Med (Tokyo). 2016;20:75-9.
[75] Prieto JL, Barberia E, Ortega R, Magana C. Evaluation of chronological age based on third molar development in the Spanish population. Int J Legal Med. 2005;119(6):349-54.
[76] Ramadan SU, Gurses MS, Inanir NT, Hacifazlioglu C, Feda-kar R, Hizli S. Evaluation of the medial clavicular epiphysis according to the Schmeling and Kellinghaus method in liv-ing individuals: A retrospective CT study. Leg Med (Tokyo). 2017;25:16-22.
[77] Rozkovcova E, Dostalova T, Markova M, Broukal Z. The third molar as an age marker in adolescents: new approach to age evaluation. J Forensic Sci. 2012;57(5):1323-8.
[78] Rozkovcova E, Markova M, Mrklas L. Third molar as an age indicator in young individuals. Prague Med Rep. 2005;106(4):367-98.
De Tobel J. Multi-factorial forensic age estimation. Chapter 12: 258-276.

275
[79] Rudolf E, Kramer J, Schmidt S, Vieth V, Winkler I, Schmeling A. Intraindividual incongruences of medially os-sifying clavicles in borderline adults as seen from thin-slice CT studies of 2595 male persons. Int J Legal Med. 2017.
[80] Santoro V, Roca R, De Donno A, Fiandaca C, Pinto G, Tafuri S, Introna F. Applicability of Greulich and Pyle and Demiri-jan aging methods to a sample of Italian population. Foren-sic Sci Int. 2012;221(1-3):153.e1-5.
[81] Scharte P, Vieth V, Schulz R, Ramsthaler F, Püschel K, Ba-janowski T, Pfeiffer H, Schmeling A, Schmidt S, Wittsch-ieber D. Comparison of imaging planes during CT-based evaluation of clavicular ossification: a multi-center study. Int J Legal Med. 2017:1-7.
[82] Schmeling A, Schulz R, Reisinger W, Muhler M, Wernecke KD, Geserick G. Studies on the time frame for ossification of the medial clavicular epiphyseal cartilage in conventional radiography. Int J Legal Med. 2004;118(1):5-8.
[83] Schmidt S, Henke CA, Wittschieber D, Vieth V, Bajanowski T, Ramsthaler F, Puschel K, Pfeiffer H, Schmeling A, Schulz R. Optimising magnetic resonance imaging-based evalua-tion of the ossification of the medial clavicular epiphysis: a multi-centre study. Int J Legal Med. 2016;130(6):1615-21.
[84] Schmidt S, Koch B, Schulz R, Reisinger W, Schmeling A. Comparative analysis of the applicability of the skeletal age determination methods of Greulich-Pyle and Thiemann-Nitz for forensic age estimation in living subjects. Int J Legal Med. 2007;121(4):293-6.
[85] Schmidt S, Ottow C, Pfeiffer H, Heindel W, Vieth V, Schmeling A, Schulz R. Magnetic resonance imag-ing-based evaluation of ossification of the medial clavic-ular epiphysis in forensic age assessment. Int J Legal Med. 2017;131(6):1665-73.
[86] Schmidt S, Schramm D, Ribbecke S, Schulz R, Wittschieber D, Olze A, Vieth V, Ramsthaler HF, Pfischel K, Pfeiffer H, Geserick G, Schmeling A. [Forensic age estimation in juve-niles and young adults: Reducing the range of scatter in age diagnosis by combining different methods]. Arch Kriminol. 2016;237(1-2):25-37.
[87] Schmidt S, Vieth V, Timme M, Dvorak J, Schmeling A. Ex-amination of ossification of the distal radial epiphysis using magnetic resonance imaging. New insights for age estima-tion in young footballers in FIFA tournaments. Sci Justice. 2015;55(2):139-44.
[88] Schulz R, Mühler M, Mutze S, Schmidt S, Reisinger W, Schmeling A. Studies on the time frame for ossification of the medial epiphysis of the clavicle as revealed by CT scans. Int J Legal Med. 2005;119(3):142-5.
[89] Serin J, Rerolle C, Pucheux J, Dedouit F, Telmon N, Savall F, Saint-Martin P. Contribution of magnetic resonance im-aging of the wrist and hand to forensic age assessment. Int J Legal Med. 2016;130(4):1121-8.
[90] Shi L, Jiang F, Ouyang F, Zhang J, Wang Z, Shen X. DNA methylation markers in combination with skeletal and den-tal ages to improve age estimation in children. Forensic Sci Int Genet. 2017;33:1-9.
[91] Sironi E, Gallidabino M, Weyermann C, Taroni F. Probabil-istic graphical models to deal with age estimation of living persons. Int J Legal Med. 2016;130(2):475-88.
[92] Sironi E, Pinchi V, Pradella F, Focardi M, Bozza S, Taroni F. Bayesian networks of age estimation and classification based on dental evidence: A study on the third molar mineraliza-tion. J Forensic Leg Med. 2018;55:23-32.
[93] Štern D, Ebner T, Bischof H, Grassegger S, Ehammer T, Urschler M. Fully automatic bone age estimation from left hand MR images. Med Image Comput Comput Assist Interv. 2014;17(Pt 2):220-7.
[94] Štern D, Kainz P, Payer C, Urschler M. Multi-Factorial Age Estimation from Skeletal and Dental MRI Volumes. In: International Workshop on Machine Learning in Medical Imaging. Quebec City, Canada: Springer, 2017; p. 61-9.
[95] Štern D, Payer C, Giuliani N, Urschler M. Automatic Age Estimation and Majority Age Classification from Multi-Fac-torial MRI Data. IEEE J Biomed Health Inform. 2018;Epub ahead of print.
[96] Štern D, Payer C, Lepetit V, Urschler M. Automated age es-timation from hand MRI volumes using deep learning. In: International Conference on Medical Image Computing and Computer-Assisted Intervention. 2016:194-202.
[97] Štern D, Payer C, Urschler M. Automated Age Estimation from MRI Volumes of the Hand. Med Image Anal. Revision submitted.
[98] Suri S, Prasad C, Tompson B, Lou W. Longitudinal com-parison of skeletal age determined by the Greulich and Pyle method and chronologic age in normally growing children, and clinical interpretations for orthodontics. Am J Orthod Dentofacial Orthop. 2013;143(1):50-60.
[99] Tangmose S, Jensen KE, Villa C, Lynnerup N. Forensic age estimation from the clavicle using 1.0T MRI-Preliminary results. Forensic Sci Int. 2014;234:7-12.
[100] Thevissen PW. Dental age estimation: striving for an opti-mal approach [Doctoral thesis]. Leuven: Leuven University Press, 2013.
[101] Thevissen PW, Fieuws S, Willems G. Human dental age estimation using third molar developmental stages: does a Bayesian approach outperform regression models to dis-criminate between juveniles and adults? Int J Legal Med. 2010;124(1):35-42.
[102] Thevissen PW, Kaur J, Willems G. Human age estimation combining third molar and skeletal development. Int J Legal Med. 2012;126(2):285-92.
[103] Thevissen PW, Pittayapat P, Fieuws S, Willems G. Estimat-ing age of majority on third molars developmental stages in young adults from Thailand using a modified scoring tech-nique. J Forensic Sci. 2009;54(2):428-32.
[104] Thodberg HH, Kreiborg S, Juul A, Pedersen KD. The Bon-eXpert method for automated determination of skeletal ma-turity. IEEE Trans Med Imaging. 2009;28(1):52-66.
General discussion: New state of the art and future prospects

276
[105] Todd TW. Atlas of skeletal maturation, 1937.
[106] Ufuk F, Agladioglu K, Karabulut N. CT evaluation of medial clavicular epiphysis as a method of bone age determina-tion in adolescents and young adults. Diagn Interv Radiol. 2016;22(3):241.
[107] Unterpirker W, Ebner T, Štern D, Urschler M. Automatic third molar localization from 3D MRI using random regres-sion forests. . In: Proceedings of the 19th Conference on Medical Image Understanding and Analysis (MIUA). Lin-coln, United Kingdom2015; p. 195-200.
[108] Urschler M, Ebner T, Štern D. Integrating geometric config-uration and appearance information into a unified frame-work for anatomical landmark localization. Med Image Anal. 2018;43:23-36.
[109] Urschler M, Grassegger S, Štern D. What automated age estimation of hand and wrist MRI data tells us about skeletal maturation in male adolescents. Ann Hum Biol. 2015;42(4):358-67.
[110] Urschler M, Krauskopf A, Widek T, Sorantin E, Ehammer T, Borkenstein M, Yen K, Scheurer E. Applicability of Greu-lich-Pyle and Tanner-Whitehouse grading methods to MRI when assessing hand bone age in forensic age estimation: A pilot study. Forensic Sci Int. 2016;266:281-8.
[111] van Rijn RR, Lequin MH, Robben SG, Hop WC, van Kuijk C. Is the Greulich and Pyle atlas still valid for Dutch Cauca-sian children today? Pediatr Radiol. 2001;31(10):748-52.
[112] van Rijn RR, Lequin MH, Thodberg HH. Automatic deter-mination of Greulich and Pyle bone age in healthy Dutch children. Pediatr Radiol. 2009;39(6):591-7.
[113] Vieth V, Kellinghaus M, Schulz R, Pfeiffer H, Schmeling A. Beurteilung des Ossifikationsstadiums der medialen Klavi-kulaepiphysenfuge. Rechtsmedizin. 2010;20(6):483-8.
[114] Vieth V, Schulz R, Brinkmeier P, Dvorak J, Schmeling A. Age estimation in U-20 football players using 3.0 tesla MRI of the clavicle. Forensic Sci Int. 2014;241c:118-22.
[115] Wenzel A, Droschl H, Melsen B. Skeletal maturity in Austri-an children assessed by the GP and the TW-2 methods. Ann Hum Biol. 1984;11(2):173-7.
[116] Wittschieber D, Schmidt S, Vieth V, Schulz R, Püschel K, Pfeiffer H, Schmeling A. Subclassification of clavicular sub-stage 3a is useful for diagnosing the age of 17 years. Rechts-medizin. 2014;24(6):485-8.
[117] Wittschieber D, Schulz R, Pfeiffer H, Schmeling A, Schmidt S. Systematic procedure for identifying the five main os-sification stages of the medial clavicular epiphysis using computed tomography: a practical proposal for forensic age diagnostics. Int J Legal Med. 2017;131(1):217-24.
[118] Wittschieber D, Schulz R, Vieth V, Kuppers M, Bajanowski T, Ramsthaler F, Puschel K, Pfeiffer H, Schmidt S, Schmeling A. Influence of the examiner's qualification and sources of error during stage determination of the medial clavicular ep-iphysis by means of computed tomography. Int J Legal Med. 2014;128(1):183-91.
[119] Wittschieber D, Schulz R, Vieth V, Kuppers M, Bajanowski T, Ramsthaler F, Puschel K, Pfeiffer H, Schmidt S, Schmeling A. The value of sub-stages and thin slices for the assessment of the medial clavicular epiphysis: a prospective multi-center CT study. Forensic Sci Med Pathol. 2014;10(2):163-9.
[120] Zeng DL, Wu ZL, Cui MY. Chronological age estimation of third molar mineralization of Han in southern China. Int J Legal Med. 2010;124(2):119-23.
[121] Zhang K, Chen XG, Zhao H, Dong XA, Deng ZH. Forensic Age Estimation Using Thin-Slice Multidetector CT of the Clavicular Epiphyses Among Adolescent Western Chinese. J Forensic Sci. 2015;60(3):675-8.
[122] Zhao H, Dong XA, Zheng T, Qing SH, Deng ZH, Zhu GY. [Skeletal age estimation of sternal end of clavicle in Sichuan Han nationality youth using thin-section computed tomog-raphy]. Fa Yi Xue Za Zhi. 2011;27(6):417-20.
De Tobel J. Multi-factorial forensic age estimation. Chapter 12: 258-276.



279
PART 7
Epilogue


281
During the past decade, a substantial in-crease in immigration has proved very challenging for European countries. The migration crisis reached its peak in 2015 and currently transmigration is giving rise to further issues. To protect unac-companied minor refugees, authorities offer different services to minors than to adults. However, refugees might lack valid identification documents, raising doubt about their chronological age. In such cases, the authorities rely on scientists to estimate the age. Those scientists are med-ical doctors and dentists who use medical imaging to study the development of the considered individual. They determine the skeletal and dental age, which act as indicators to estimate the chronological age. Moreover, age estimation is used in sports to ensure that athletes participate in the right age category.
Current age estimation methods rely on radiographs and/or computed to-mography (CT) to visualise developing structures. However, these methods show major drawbacks. Firstly, they necessitate exposure to ionising radiation, without a medical diagnostic or therapeutic indica-tion. Thus, in certain countries, their use is considered not to be ethically justifiable in civil and asylum procedures. Neither is their use ethically justifiable to verify age in sports. Secondly, superposition of anatomical structures can hamper the in-terpretation of radiographs, because the image is a projection. Conversely, super-
Summary
position is eliminated when CT is used, since that imaging modality renders slices through the targeted structures. Thirdly, developmental information of different anatomical structures should be com-bined to increase the accuracy. However, large scale studies using ionising radia-tion to study development in healthy vol-unteers would not be ethically justifiable. Thus, to date, no uniform approach to combine the information of different ana-tomical structures has been proposed. Fi-nally, no internationally accepted stand-ardised approach is available to estimate age. This causes discrepancies between age estimation results from different insti-tutions, whether in different countries, or even from within the same country.
As a response to the drawbacks of the current approach, the use of magnetic res-onance imaging (MRI) is investigated as an alternative to radiographs and CT. This imaging modality renders slices through the examined anatomical structures, without using ionising radiation. Conse-quently, it allows studying different ana-tomical structures of the same individual simultaneously in an ethically justifiable way. The current PhD project includes the joint efforts made in Belgium and the Netherlands to strive for an optimisation of age estimation. The project builds upon the foundations laid at Ghent University and the Catholic University of Leuven, reinforced by the Netherlands Forensic Institute. The study population included

282
335 healthy Belgian and Dutch Caucasian volunteers from 14 to 26 years old (with some exceptions from 7 to 30 years old). They underwent 3 Tesla MRI of all third molars, the left wrist and both clavicles, since it is recommended to combine those three sites for age estimation in adoles-cents and young adults.
In a first step, suitable MRI protocols were developed to visualise the three ana-tomical sites. In the current PhD project, a high resolution sagittal T2 sequence was selected to visualise the third molars. The protocols for the left wrist and both clavi-cles had been developed during the earlier project at Ghent University. A coronal T1 spin echo and a T1 VIBE sequence were selected for the left wrist. Similarly, a T1 VIBE sequence proved to be the most suitable to study clavicles.
In a second step, we investigated if the current techniques to assess development on radiographs and CT could be trans-posed to MRI. Regarding third molars, an MRI-specific staging technique was deemed necessary. Wrist and clavicle as-sessment could be done with a CT staging technique, provided certain considera-tions were taken into account. Regarding the wrist, a one-fits-all staging technique could be applied to both MR-sequences. A technique with five main stages and substages of stage 3 rendered the best results. Regarding the clavicles, the same technique with five main stages and sub-stages of stage 3 was applied. However, it remains unclear if profound substag-es of stage 3a might allow fine-tuning of age estimation in a close range around the 18-year-threshold. Furthermore, we demonstrated that stages of early and late development can be confused. Therefore,
it seems safer to exclude clavicles in those stages from age estimation to avoid unac-ceptably large errors. On the other hand, discarding those stages implies a loss of information. Further research with larg-er study populations will be necessary to elucidate how clavicles in early and late stages of development could safely contribute to age estimation. Finally, our study demonstrated that both clavicles should be incorporated in the statistical model for age estimation.
The third step studied age estimation performance of the statistical models based on the assessment of MRI. The fol-lowing different aspects of age estimation were studied: (1) the accuracy of the point prediction of age, reflected by the mean absolute error (MAE); (2) the uncertainty of the point prediction , reflected by the 95% prediction intervals (PI); (3) the abil-ity to discern minors (< 18 years old) from adults (≥ 18 years old); and (4) the proba-bility of having reached the age of 18.
First of all, age estimation perfor-mance was compared between different staging techniques per anatomical site. This allowed selecting the optimal staging technique, which was subsequently incor-porated in multi-factorial age estimation models, i.e. models which combined the information of different age indicators. Combining the three anatomical sites yielded the best performance. Particularly around the age of 18, all three sites con-tributed significantly to the age estima-tion. Adding anthropomorphic and sexu-al maturity data was demonstrated to be of negligible value. Based on the current study population, the performance of the multi-factorial model was as follows:
Summary

283
— In females, the MAE equalled 1.41 years; the mean width of 95% PI equalled 5.91 years; the proportion of correctly classified adults was 93%; and the proportion of correct-ly classified minors was 91%.
— In males, the MAE equalled 1.36 years; the mean width of 95% PI equalled 5.49 years; the proportion of correctly classified adults was 94%; and the proportion of correct-ly classified minors was 90%.
With regard to the practical implemen-tation of MRI for age estimation, three additional studies were conducted. First-ly, we compared our third molars MRI protocol with the one that was devel-oped at the Ludwig Boltzmann Institut für Klinisch-Forensische Bildgebung in Graz, Austria. A higher resolution and stabilising of the head by means of a bite bar yielded more tooth apices that were suitable for assessment. Moreover, al-though the study sample was small, it was demonstrated that MR-sequence-specific reference data should be applied for age estimation. This corresponds with the need for MR-sequence-specific reference data of wrist MRI.
Secondly, it was studied how motion affects clavicle MRI for age estimation. In-tentional motion frustrated the procedure, rendering untenable images, but did not induce a systematic over- or under-estima-tion of age. Taking into account the afore-mentioned considerations for the staging of clavicles using MRI, the motion study confirmed that the clavicles’ development as such is hard to assess. The influence of motion and imaging modality are only sec-ondary effects to this inherent difficulty.
Finally, the literature on MRI for age es-timation was systematically reviewed. Different research groups have now col-lected multi-factorial MRI data in 300 or more healthy volunteers. For this data collection, the research groups designed prospective studies, which have all taken approximately the same time as the PhD project in this thesis. Therefore, the most efficient step to strive for MRI’s practical implementation in age estimation would be to combine the data of those groups. However, it remains unclear whether the data can safely be combined to create more robust age estimation models, since MR-protocols and staging techniques dif-fer between groups. With the current PhD project, a statistically appropriate method was presented, ready to be enriched with data from other groups.
Summary


285
Het voorbije decennium werd Europa geconfronteerd met een aanzienlijke toe-name aan immigranten. De migratiecrisis bereikte een hoogtepunt in 2015 en kent momenteel een heropflakkering door transmigratie. Om niet-begeleide min-derjarige vluchtelingen te beschermen, voorzien de autoriteiten maatregelen die verschillen van de maatregelen voor vol-wassenen. De vluchtelingen beschikken echter niet altijd over geldige identifica-tiebewijzen, waardoor er twijfel kan ont-staan over hun chronologische leeftijd. Autoriteiten doen dan beroep op weten-schappers om de leeftijd te schatten. Deze wetenschappers zijn meestal artsen en tandartsen die de ontwikkeling van het individu bestuderen op medische beeld-vorming. Zo worden de dentale en ske-lettale leeftijd bepaald en gebruikt om de chronologische leeftijd te schatten. Der-gelijke leeftijdsschatting wordt eveneens toegepast in competitiesport, om te ver-zekeren dat jongeren in de juiste leeftijds-categorie wedijveren.
De huidige methoden voor forensi-sche leeftijdsschatting maken gebruik van radiografieën en/of computertomo-grafie (CT) om de ontwikkeling in beeld te brengen. De methoden worden echter gekenmerkt door aanzienlijke nadelen. Ten eerste vereisen ze blootstelling aan ioniserende stralen, buiten een medisch diagnostische of therapeutische indica-tie om. In verschillende landen wordt dit dan ook als ethisch onverantwoord be-
Samenvatting
schouwd voor burgerlijke en asielproce-dures. Bovendien is stralingsblootstelling niet ethisch verantwoord om de leeftijd te verifiëren in sportcompetities. Ten twee-de kan de interpretatie van radiografieën onmogelijk zijn door superpositie, omdat het beeld een projectie is van verschillen-de structuren. Dit is niet het geval voor CT, omdat deze beeldvormingsmodaliteit sneden weergeeft doorheen de bestudeer-de structuren. Ten derde is het aangera-den om informatie te combineren van verschillende zich ontwikkelende anato-mische structuren om de nauwkeurigheid te verhogen. Het is echter ethisch onver-antwoord om bij een gezonde populatie op grote schaal verschillende anatomische regio’s gelijktijdig te bestuderen met ioni-serende stralen. Daardoor is er vooralsnog geen eenduidigheid over hoe de informa-tie van verschillende anatomische regio’s optimaal gecombineerd kan worden. Ten slotte is er geen internationaal erkende en gestandaardiseerde aanpak voor leeftijds-schatting. Dit zorgt voor discrepanties in de resultaten van de leeftijdsschatting tus-sen verschillende instituten, hetzij in ver-schillende landen, hetzij binnen eenzelfde land.
Om een antwoord te bieden op de be-schreven nadelen van de huidige aanpak, wordt magnetische resonantie beeldvor-ming (MRI) door verschillende Europe-se onderzoeksgroepen bestudeerd als al-ternatief voor radiografieën en CT. Deze beeldvormingsmodaliteit geeft sneden

286
weer doorheen de bestudeerde structu-ren, maar maakt geen gebruik van ioni-serende stralen. Dit laat dus ook toe om zonder ethische bezwaren verschillende anatomische regio’s gezamenlijk te bestu-deren bij eenzelfde individu. Het huidige PhD project bundelt de inspanningen die in België en Nederland gedaan zijn in een streven naar een geoptimaliseer-de leeftijdsschatting. Het project bouwt verder op twee eerdere projecten aan de Universiteit Gent (UGent) en de Katho-lieke Universiteit Leuven (KU Leuven) en werd versterkt door de inbreng van het Nederlands Forensisch Instituut (NFI). De onderzoekspopulatie bestond uit 335 ge-zonde Belgische en Nederlandse Kaukasi-sche vrijwilligers van 14 tot en met 26 jaar oud (met enkele uitzonderingen van 7 tot 30 jaar oud). Drie Tesla MR-scans werden genomen van alle derde molaren, de linker pols en beide sleutelbeenderen, aangezien het aangeraden wordt om deze drie regio’s te combineren voor leeftijdsschatting bij adolescenten en jongvolwassenen.
Een eerste stap bestond uit het ont-wikkelen van geschikte MR-scanproto-collen voor de drie anatomische regio’s. In het huidige PhD project werd een hoge resolutie T2-sequentie in het sagittale vlak als meest geschikt bevonden voor de visu-alisatie van de derde molaren. De proto-collen voor de linker pols en beide sleutel-beenderen werden in het eerdere project aan de UGent opgesteld. Voor de linker pols werden een coronale T1 spin echo en een T1 VIBE sequentie geselecteerd. Voor de sleutelbeenderen bleek eveneens de coronale T1 VIBE sequentie het meest geschikt.
In een tweede stap werd nagegaan of de huidige technieken om de ontwikke-
ling op de radiografieën en CT-beelden te beoordelen konden overgebracht worden naar MRI. Voor de derde molaren bleek een MRI-specifieke stageringstechniek nodig te zijn. Voor de pols- en de sleutel-beenderen bleek het mogelijk om de sta-geringstechniek van CT over te brengen, mits enkele overwegingen in acht werden genomen. Zo kon voor de pols eenzelfde stageringstechniek toegepast worden op de beide MR-sequenties en gaf een tech-niek met vijf hoofdstadia en substadia in stadium 3 de beste resultaten. Voor de sleutelbeenderen werd dezelfde techniek met vijf hoofdstadia en substadia in stadi-um 3 toegepast. Het bleef echter onduide-lijk of doorgedreven substadia in stadium 3a een verdere nuancering toelaten van leeftijdsschattingen rond de leeftijd van 18 jaar. Daarnaast werd vastgesteld dat vroege en late ontwikkelingsstadia om-gewisseld kunnen worden. Het lijkt dus veiliger om sleutelbeenderen die zich in die stadia bevinden uit te sluiten voor leeftijdsschatting, om zo onaanvaardbare fouten te vermijden. Anderzijds betekent het uitsluiten van deze sleutelbeenderen veel verlies aan informatie. Verder onder-zoek met grotere onderzoekspopulaties is nodig om uit te wijzen hoe het best kan omgegaan worden met sleutelbeenderen in vroege en late ontwikkelingsstadia. De studie toonde wel aan dat beide sleutel-beenderen best samen opgenomen wor-den in het statistisch model voor leeftijds-schatting.
In een derde stap werden de pres-taties van de statistische modellen voor leeftijdsschatting op basis van MRI on-derzocht. Verschillende aspecten van leeftijdsschatting werden hierbij belicht: (1) de nauwkeurigheid van de puntpre-dictie van de leeftijd in de vorm van de
Samenvatting

287
gemiddelde absolute fout (mean absolute error, MAE); (2) de onzekerheid van de puntpredictie in de vorm van 95% pre-dictie-intervallen (95% PI); (3) de moge-lijkheid om minderjarigen (< 18 jaar) te onderscheiden van meerderjarigen (≥ 18 jaar); en (4) de probabiliteit om de grens-leeftijd van 18 jaar bereikt te hebben.
Eerst werden de prestaties voor leef-tijdsschatting vergeleken voor de ver-schillende stageringstechnieken per ana-tomische regio. Op die manier werd de optimale stageringstechniek uitgeselec-teerd, die in een volgende stap geïncor-poreerd werd in multifactoriële leeftijds-schattingsmodellen, i.e. modellen die de informatie van verschillende leeftijdsindi-catoren combineren. De combinatie van de drie anatomische regio’s bleek het best te presteren. Voornamelijk rond de grens-leeftijd van 18 jaar levert elk van de drie regio’s een essentiële bijdrage aan de leef-tijdsschatting. De waarde van antropo-morfe en secundaire geslachtskenmerken was daarentegen verwaarloosbaar. Op basis van de huidige onderzoekspopulatie waren de prestaties van het multifactorië-le model als volgt:
— Voor vrouwen was de MAE gelijk aan 1,41 jaar, de gemiddelde breedte van het 95% PI 5,91 jaar, de propor-tie correct geïdentificeerde volwas-senen 93% en de proportie correct geïdentificeerde minderjarigen 91%.
— Voor mannen was de MAE gelijk aan 1,36 jaar, de gemiddelde breedte van het 95% PI 5,49 jaar, de propor-tie correct geïdentificeerde volwas-senen 94% en de proportie correct geïdentificeerde minderjarigen 90%.
Met het oog op de praktische implemen-tatie van MRI bij leeftijdsschatting wer-den nog drie studies uitgevoerd. Ten eer-ste werd het MRI protocol voor de derde molaren vergeleken met een protocol dat aan het Ludwig Boltzmann Institut für Klinisch-Forensische Bildgebung in Graz (Oostenrijk) werd ontwikkeld. Een hoge-re resolutie en stabilisatie van het hoofd door middel van een bijtblok leverde meer beoordeelbare tandapices op. Bo-vendien werd in de beperkte studiepopu-latie aangetoond dat MR-sequentie-speci-fieke referentiegegevens moeten toegepast worden. Dit komt overeen met de nood aan MR-sequentie-specifieke referentie-gegevens voor de pols.
Ten tweede werd de invloed van be-weging op de beoordeling van de sleu-telbeenderen onderzocht. Opzettelijke beweging verstoorde de beelden, waar-door ze frequenter als onbeoordeelbaar werden beschouwd. De beweging leidde echter niet tot een systematische over- of onderschatting van het ontwikkelingssta-dium. Samen met de vele overwegingen die bij de stageringstechniek voor de sleu-telbeenderen in acht genomen moeten worden, wees deze studie uit dat de ont-wikkeling van de sleutelbeenderen op zich moeilijk te beoordelen is. De invloed van beweging en van de beeldvormingsmoda-liteit zijn daar dan ook secundair aan.
Ten slotte werd een systematische be-oordeling gedaan van de literatuur over MRI voor leeftijdsschatting. Verschillen-de onderzoeksgroepen beschikken nu over multifactoriële MRI gegevens van 300 of meer gezonde vrijwilligers. Deze groepen zetten daarvoor prospectieve studies op die alle ongeveer even lang ge-lopen hebben als de studie in deze thesis.
Samenvatting

288
Daarom lijkt de meest efficiënte stap in het streven naar praktische implementatie van MRI voor leeftijdsschatting het com-bineren van de gegevens van de verschil-lende groepen. Door de verschillen in MR-protocollen en stageringstechnieken is het echter onduidelijk of deze gegevens
Samenvatting
veilig kunnen gecombineerd worden om meer robuuste modellen te ontwikkelen. Met het huidige PhD project staat er een statistisch adequate methode klaar die kan verrijkt worden met gegevens van an-dere groepen.

289
Sara Neyt declares a relationship with the following company: MOLECUBES NV (Gent, Belgium). The µCT scans for the study in Chapter 6 were performed free of charge by this company.
The other contributors to this thesis declare no relationships with any companies, whose products or services may be related to the subject mat-ter of the papers.
This study has received funding by the American Society of Forensic Odontology (ASFO) in form of its Research Grant 2017.
Conflict of interest statement

291
Scientific acknowledgements
Ivo Alberink Conducted the statistical analyses in chapter 8 andproof-read the corresponding paper.
Jeroen Bauwens Acted as a second reviewer for part of the systematic review in chapter 10 and conducted his own system-atic review on age estimation as a side project of the current PhD project.
Stephanie Bogaert Optimised dental MR sequences for chapter and proof-read the corresponding paper. Guided me through the PhD project with her expertise in scanning.
Maria Cadenas de Llano PérulaThe quality of this PhD thesis was improved based on her comments as a member of the examination committee.
Jan CasselmanThe quality of this PhD thesis was improved based on his comments as a member of the examination committee.
Patrick Davis Proof-read the papers of chapters 8, 9, 10, and 11.
Karel DeblaereDeveloped and optimised the dental MR sequences for chapter 3, and proof-read the corresponding paper. Moreover, the quality of this PhD thesis was improved based on his comments as a member of the examina-tion committee.
Michiel de HaasAssessed part of the sample in chapters 7 and 8. Wrote the Dutch part of the book chapter which was the foundation of chapter 1 in this thesis. Guided me through the PhD project with his expertise in age es-timation. Moreover, he proof-read most of the papers.
Benedicte DescampsAdvised us on the study design of chapter 6 and con-ducted the µMR scans for that chapter. Moreover, she proof-read the corresponding paper.
Ademir FrancoActed as a second reviewer for part of the systematic review in chapter 10.
Steffen FieuwsConducted the statistical analyses in chapters 5, 7, 9, and 11. Developed the statistical model for age estima-tion and extended it for continuous data in chapter 11.
Elke HillewigSet the foundations for the current project with her research on wrist and clavicle MRI for age estimation and was involved in the study design of the current project. She scanned a sample of more than 240 vol-unteers for her own project. MRI data of her sample were jointly used with the more recently collected data in chapters 7, 8, and 9. She also scanned part of the sample of chapter 8. Furthermore, she assessed part of the recent data for the papers in chapters 3, 4, and 8. Moreover, she proof-read most of the other pa-pers and guided me through the whole PhD process.
Every chapter in this thesis resulted from a team effort. I want to thank the following colleagues for their indispensable contributions to this project:

292
Scientific acknowledgements
Helen LiversidgeAdvised us for chapter 4, with her expertise in den-tal age estimation. She proof-read the corresponding papers of chapters 3 and 4. Moreover, the quality of this PhD thesis was improved based on her com-ments as a member of the examination committee.
Luc MarksThe quality of this PhD thesis was improved based on his comments as a member of the examination committee.
Griet Parmentier Recruited the participants for chapter 6 and assessed the images for that chapter. Acted as a second re-viewer for part of the systematic review in chapter 10.
Sara NeytAdvised us on the study design of chapter 6 and con-ducted the µCT scans for that chapter. Moreover, she proof-read the corresponding paper.
Constantinus Politis Advised us with his expertise in third molar devel-opment and watched over the management of the PhD project. Moreover, he proof-read chapter 1 and the papers of chapters 5 and 6.
Nele PauwelsAdvised us with her expertise in conducting system-atic reviews and proof-read the paper of chapter 10.
Inès PhlypoWas involved in every aspect of the project, from the design, to the recruitment, the assessments and the analyses. She assessed the dental MRIs of chapters 5 and 6, and scanned part of the sample in chapter 8. Furthermore, she proof-read every paper and every chapter in this thesis.
Patrick ThevissenSet the foundations for the current project with his research on dental age estimation. Guided me through every aspect of the project with his ex-pertise in age estimation and forensic odontology. Moreover, he closely followed-up on the progress of the project and the papers. He proof-read every paper and chapter in this thesis. Furthermore, he provided funding for the statistical processing.
Pieter VandemaeleDeveloped and optimised the MR sequences for chapters 7, 8, and 9. Advised us with his expertise in scanning.
Wim Van De VeldeFacilitated the recruitment of participants for chap-ter 6 and proof-read the corresponding paper.
Bram Van EeckhoutAssessed part of the sample in chapter 7 and proof-read the corresponding paper.
Rick van RijnAdvised us for the study design of chapter 8 and assessed the images for that chapter. Moreover, he proof-read the corresponding paper.
Mayonne van WijkAssessed part of the sample in chapters 8 and 9 and conducted statistical analyses for chapter 8. Wrote the Dutch part of the book chapter which was the foundation of chapter 1 in this thesis. Guided me through the PhD project with her expertise in age estimation. Moreover, she proof-read most of the papers.

293
Scientific acknowledgements
Koenraad VerstraeteSet the foundations for the current project, men-toring Elke Hillewig’s project and continuing with mine. Guided me through every aspect of the pro-ject with his expertise in MRI. Moreover, he watched over the progress of the project and the papers. He proof-read every paper and chapter in this thesis. Furthermore, he provided funding for the entire project, except for the statistical processing.
Martin UrschlerHe provided the details on their MRI protocol, which made the study in chapter 6 possible. He proof-read the corresponding paper. Moreover, he kept me post-ed about the progress in their research, which broad-ened my insight and facilitated a more profound dis-cussion of several papers. Finally, the quality of this PhD thesis was improved based on his comments as a member of the examination committee.

295
Personal contribution
My personal contribution to this thesis started with the study design and application for ethical approval. Subsequent amendments followed in the first years of the project, some of which were related to side projects such as those in chapters 6 and 8.
I initiated the development of the third molars MRI protocol. I recruited the participants, informed them, did the planning, and conducted the clinical examinations and MRI scans. I visited dental practices and spe-cialist departments to collect panoramic radiographs. I managed the data and guaranteed the pseudonymisation.
I designed the tables to collect the data and Access forms to reduce the risk of errors during the assessment of the images. I assessed all the im-ages for the different studies, and recruited and trained other observers. I conducted the statistical analyses in chapters 3, 4, and 6.
I reviewed the literature on age estimation and stayed up to date, allowing me to write well-founded introductions and discussions for every paper. I acted as the first reviewer for the systematic review in chapter 10 and selected suitable second reviewers.
I presented preliminary and final results at national and international conferences and built a multi-disciplinary network of researchers, practi-tioners and policy makers who are involved in age estimation. I wrote all the manuscripts in this thesis, submitted them to peer-reviewed journals, adjusted them according to the reviewers’ remarks and replied to those remarks if appropriate.
I contacted local authorities and organised discussions with the policy makers to gain insight into the practical implementation of age estimation. We also discussed the possibilities our new MRI approach might offer.


297
Personal acknowledgements
Koenraad VerstraeteFor feeding me ideas, for guiding me with respect for my freedom, for warning me for Murphy and Kafka, for providing me academic as well as fatherly wisdom.
Patrick ThevissenFor launching me into the small world of forensic odontology experts, for respecting research integrity above all, for teaching me to question other’s persua-sions, for making me a fair peer-reviewer, for keep-ing an eye on the ball at all times.
Constantinus PolitisFor sticking up for our profession, for enabling my aberrant pathway, for valuing my academic and fo-rensic work.
Elke HillewigFor scouting me when I was still a rookie, for appre-ciating my ideas from the start, for confiding me all of your data and MRI skills, for transforming from my supervisor into a friend whom I confide in.
Steffen FieuwsFor exponentially increasing my insight into ad-vanced statistics, for warning me about hasty con-clusions, for overwhelming me with results and then helping me to see the wood for the trees.
Michiel de HaasFor knowing everything there is to know about age estimation, for staying in the game despite the pro-fessional instability, for all your trips to Ghent, for all my trips to Hillegom, for appreciating Sociaal Incapabele Michiel.
Mayonne van WijkFor all your trips to Ghent, for my trip to Den Haag, for being the best clavicle stager ever, for being the muse of that Italian guy in Berlin every year again.
Rick van RijnFor teaching me and Elke about the peer-reviewing process, for staging all of those clavicles again and again, for almost slapping me when I call you pro-fessor van Rijn.
Pieter VandemaeleFor being my go-to when the scanner was acting up, for appreciating my autistic respect for keeping the scanner site tidy and well-organised.
Stephanie BogaertFor knowing the scanner inside out, for your love for basic structural MRI over functional tralala.
This PhD project allowed me to broaden my horizons and to meet the most interesting people around the world. I want to thank everyone I encountered during this journey. Starting off as colleagues with whom I philosophised about research and age estimation, most of them became friends with whom I also enjoyed the pleasures in life. Their support and respect made me to the person I am today, and I respect them all deeply. Furthermore, I want to acknowledge everyone I knew before I started this project, and who stuck with me, even though I was absorbed by the project at times. You all contributed to my scientific and personal growth.
Thank you,

298
Patricia ClementFor sharing the PhD life at MR, for bumping into each other whenever some training for researchers was organised, for being an excellent patient.
All the scanning colleagues at GIFMIFor your understanding when the time table was stretched.
Karel DeblaereFor believing in the dental MRI story, for being down-to-earth Karel even when I was still a student.
Benedicte Descamps and Sara NeytFor your dedication to find the best gold standard, for your accessibility when I was fighting another deadline.
All the medical imagers at MRI UZ GentFor saving me when a coil went missing or when I was on the wrong track while scanning.
Katrien Saegerman, Kathy Van Synghel, Evi De Mits, Céline Dedapper, Adriano Bono, Bieke De RooFor all of your organizing skills and administrative help, for finding a way either through the UZ or the UGent.
Lynn De Poorter, Marleen Vereecken, Katleen Verkammen, Brenda Aerts, Bieke TembuyserFor helping me through the extensive bureaucracy, for supporting the fight to organise my defences timely, which was the final episode of my PhD soap.
Janine KopatzFor your creative mind, for your own style, for being stubborn about some details, for giving in when I was stubborn.
Martin UrschlerFor being transparent about each other’s work, for creating ways to collaborate, for your T-shirts in Graz.
Helen LiversidgeFor your interest and help at the initiation of the project, for your down to earth approach to age es-timation.
Andreas SchmelingFor providing me insight into the most recent liter-ature as a peer-reviewer, for breaking through the embargo of IJLM.
All the people I met at AAFS, ASFO, IOFOS, ISFRI and AGFAD meetingsFor appreciating our work and striving for the opti-mal approach together.
All the master students of Forensic OdontologyFor appreciating my work and advice for your work, for being in the same boat, drowning in tasks.
Cezar Capitaneanu and Ademir FrancoFor sharing your experiences, for your contagious dedication to forensic odontology, for sharing your desk with Inès.
Patrick DavisFor your keen interest in my work, for the indis-pensable linguistic tips that go beyond non-native speakers, for the telephone calls philosophising about forensics and life.
Caroline Van Schoubroeck en Yvo VermylenFor your flexibility to plan the lectures, for your en-thusiasm and down to earth approach to turn me into an ethical court expert witness, for the lunches at Wok Dynasty.
Personal acknowledgements

299
Everyone at Forensic Medicine UZ LeuvenFor taking me in when I was still a student, for sup-porting my work from the start, for making me feel like a peer early on, for all the Forensic Parties.
All the people we met at the Cabinets of Asylum and Migration and of JusticeFor your transparency, for discovering that your frustrations exactly matched with ours, for your urge for improvement.
All my fellow students at Dentistry UGent For sharing your notes, for participating and recruit-ing, for valuing my academic work, for gossiping in the preclinic, for coming to get me for difficult ex-tractions, for taking over some of my endos, for en-tertaining me during boring lectures.
All the professors at Dentistry UGentFor your flexibility in planning, for recognising my potential, for supporting Inès.
Johan ApsFor sticking up for me in Dentistry, for valuing my work, for bumping into each other at the other side of the world, for keeping in touch.
Louis SimoenFor philosophising about MRI, the TMJ and re-search, for supporting the Red Devils together.
Gaetan Van de VyvereFor the parties at the OR, for het Geluidshuis, for the tractors, for being my idol as a surgeon and as a fam-ily man. You and Leen supported me from the start, and appreciated the aberrant pathway I was taking. Thank you Jules and Camille, for being in my life as long as you can remember, for being my enthusiastic youngest participants.
Marc CapiauTo save me in the final phase of the thesis, to know exactly how it feels when something is chronically 'almost finished', to be glad that we are in your team.
Herman Van den EyndeFor your no-nonsense approach during my time in Aalst, for setting the base for my surgical training, for recognising my academic qualities immediately and helping me to find a balance between my clinical and academic growth.
All the nurses and secretaries at OMFS OLV AalstFor distracting my patients while I was operating, for training, teaching, entertaining, gossiping and bullying me.
All the surgeons, nurses and secretaries at OMFS UZ LeuvenFor taking me in part-time, for valuing my academic work, for trying to create order in the chaos.
All the surgeons at Head and Neck Surgery UZ GentHubert Vermeersch, Philippe Deron, Katrien Bonte, Wouter Huvenne, Peter Tomassen. For your flexibil-ity, for your appreciation of OMFS, for valuing my ac-ademic work, for warning me about the final phase of my PhD, for the extracurricular activities.
Robin WillaertFor being my idol as a young surgeon, for valuing my aberrant pathway, for including me in your own research, for all the evenings we were about to leave and then still talked for over an hour.
All the nurses and secretaries at Head and Neck Surgery UZ GentFor valuing my work, for trying to convince me to come back to Gent, for the team buildings.
Personal acknowledgements

300
Lies PottelFor valuing my work, for taking on a new MRI pro-ject which allows the fusion with OMFS, for contin-uously taking the hurdles of that project, for embod-ying the project while I am not there.
Jan CasselmanFor your love for MRI, for increasing my under-standing of MRI, for taking me in for a new MRI project.
Johan AbeloosFor valuing my work, for believing in the power of MRI, for supporting our new MRI project, for trying to convince the Head and Neck surgeons.
All the surgeons at OMFS AZ Sint-Jan BruggeFor joining in on the new MRI project, for believing in the power of MRI.
All the medical imagers at MRI AZ Sint-Jan BruggeFor valuing my input while scanning, for increasing my understanding of MRI, for all the cookies and coffee.
Britt EngelenFor saving me when I erroneously thought I had the whole weekend to work on my thesis, for being my idol as a resident.
All the surgeons and students at OMFS Maastricht UMCBirgit van Lieshout, Veronique Timmer, David Kop-er, Auke van Mierlo, Maria Desmedt, Lauretta Vaas-sen, Cornelia Wilkert, Peter Kessler, Rick Claessen, Carine Leung en Niels Sluypers. For putting up with me being absorbed by this last phase of my PhD, for your flexibility in planning, for all of my first times in the OR, for teaching me that I am too kind, for dancing with me during the File Fuif, for drinks on Friday, for learning Flemish.
All the dental assistants and nurses at OMFS Maastricht UMC For striving for efficiency, for sharing the changing room, for making fun of the way I talk.
All the Flemish residents at OMFS and Head and Neck Surgery, and all the ASTsFor your flexibility in planning when I wanted to at-tend a conference or had a deadline coming up, for sharing your experiences and knowledge, for being in the same boat, for all the drinks and after parties.
Brecht De Cuyper and his familyFor the similar pathway we took for over 25 years, for entertaining me during lectures, for taking me with you traveling, for the dance classes, for Dance your PhD, for the squash matches, with or without shorts.
Rik Jamaels and his familyFor believing in me, for being there when I need to ventilate, for valuing my opinion and advice, for finding me when I can be of any help, for being my idols as a family, for trusting me in the milking pit, for complying with Admiral Freebee’s “Einstein brain”:
But you can't milk a cow with your hands in your pants.
The families De Tobel and VerhasseltFor supporting me on this non self-evident track, both academic as well as private, for participating in this project.
Personal acknowledgements

301
Jorge De TobelFor dragging me away from academia and work, for sharing the passion for horses, for being an en-cyclopaedia when it comes to breeding advice in Haflinger or Belgian draft horses, for helping around wherever you can. You know he means well when Admiral Freebee sings about you in “Einstein brain”:
Maybe God wanted to make something ugly but in great shape.
All my friends at the Friesian, Haflinger and Belgian draft horse studbooksFor sharing and stressing the beauty of the horses, for appreciating the way I handle horses, for appre-ciating my running skills, for valuing my work, for safeguarding my spot at the Friesian stallion show.
All my friends from my time in high school and in MedicineFor once in a while checking if I am still alive and kicking.
José Phlypo, Brigitte Vanrobaeys, Jelle Phlypo, Vicky Cafmeyer and their familiesFor taking me in, knowing all of my bad edges, for being my second home, for teaching me how to drink, for all the parties, for taking me swimming, for selecting the best pigs for Robin.
Rudy De TobelFor putting Jorge and me first, for passing me your horse sense, for granting me chances, for saving me when I locked myself out again, for saving me when I forgot my cable and the plane was about to leave, for saving me all of those other times.
Inès PhlypoFor the privilege of having you by my side. No words can encompass what you have contributed to this thesis or to the person I am today. The Strypes came close in their “I need to be your only”:
She’s the bag, she’s the leaf, she’s the sugarThe full cup baby, like no other
Personal acknowledgements


303
Persoonlijk dankwoord
Koenraad VerstraeteOm ideeën uit uw mouw te schudden, om me te be-geleiden met respect voor mijn vrijheid, om me te waarschuwen voor Murphy en Kafka, om me zowel academische als vaderlijke wijsheden mee te geven.
Patrick ThevissenOm me te lanceren in de kleine wereld van foren-sisch tandheelkundige experten, om onderzoeksin-tegriteit hoog in het vaandel te dragen, om me te leren anderen hun overtuigingen in vraag te stellen, om van mij een eerlijke peer-reviewer te maken, om over heel de lijn kort op de bal te spelen.
Constantinus PolitisOm het op te nemen voor onze professie, om mijn afwijkend traject mogelijk te maken, om mijn aca-demisch en forensisch werk te waarderen.
Elke HillewigOm me te ontdekken toen ik nog een groentje was, om van bij het begin mijn ideeën op prijs te stellen, om me al uw data en MR-vaardigheden toe te ver-trouwen, om te evolueren van mijn begeleider naar een vriendin bij wie ik alles kwijt kan.
Steffen FieuwsOm mijn inzicht in hogere statistiek exponentieel te doen toenemen, om me te waarschuwen voor over-haaste conclusies, om me te bedelven onder resul-taten en me dan te helpen om door de bomen het bos te zien.
Michiel de HaasOm alles te weten wat er te weten valt over leeftijds-schatting, om door te gaan ondanks de professione-le instabiliteit, voor al uw reizen naar Gent, voor al mijn reizen naar Hillegom, om Sociaal Incapabele Michiel op prijs te stellen.
Mayonne van WijkVoor al uw reizen naar Gent, voor mijn reis naar Den Haag, om de beste clavicular scoorder ooit te zijn, om elk jaar opnieuw de muze te zijn voor die Italiaan in Berlijn.
Rick van RijnOm Elke en mij te leren hoe we goede peer-revie-wers kunnen zijn, om al die clavicula’s keer op keer te scoren, om me bijna te slaan als ik u aanspreek met “professor van Rijn”.
Dankzij dit doctoraat heb ik mijn horizonten verruimd en wereldwijd de meest interessante personen ont-moet. Ik wil dan ook iedereen bedanken die ik op deze reis ben tegengekomen. Het begon meestal bij filosofe-ren over onderzoek en leeftijdsschatting, waarna de meesten vrienden werden met wie ik ook de deugden des levens mocht delen. Hun steun en respect maakte me tot de persoon die ik vandaag ben en ik respecteer hen allen eindeloos. Daarnaast wil ik ook iedereen bedanken die ik al kende voordat ik startte met dit doctoraat en die me bleven steunen, ook al werd ik dikwijls helemaal geabsorbeerd door dit project. Jullie hebben allen bijgedragen aan mijn wetenschappelijke en persoonlijke groei.
Dank u,
304
Pieter VandemaeleOm mijn redding te zijn als de scanner fars deed, om mijn autistisch respect te waarderen voor de netheid van de scannerruimte en de plaats van alle materialen.
Stephanie BogaertOm de scanner van binnen en van buiten te kennen, voor uw liefde voor gewoon structurele MRI boven functionele tralala.
Patricia ClementOm het doctoraatsleven op MR te delen, om elkaar tegen het lijf te lopen telkens er een opleiding voor onderzoekers georganiseerd werd, om een zalige pa-tiënt te zijn.
Al de scannende collegae op het GIFMIVoor jullie begrip als ik de agenda moest rekken.
Karel DeblaereOm te geloven in het dentale MRI verhaal, om ge-woon Karel te zijn, zelfs toen ik nog student was.
Benedicte Descamps en Sara NeytVoor jullie toewijding om de beste gouden stan-daard te vinden, voor jullie beschikbaarheid wan-neer ik weeral tegen een deadline aanliep.
All the medical imagers at MRI UZ GentOm me te redden wanneer er een coil vermist was of wanneer ik vanalles mis deed tijdens het scannen.
Katrien Saegerman, Kathy Van Synghel, Evi De Mits, Céline Dedapper, Adriano Bono, Bieke De RooVoor jullie organisatorische vaardigheden en admi-nistratieve hulp, om een weg te vinden, hetzij via het UZ, hetzij via de UGent.
Lynn De Poorter, Marleen Vereecken, Katleen Verkammen, Brenda Aerts, Bieke TembuyserOm me door de eindeloze bureaucratie te helpen, om me bij te staan in het gevecht om mijn verdedi-gingen georganiseerd te krijgen, wat de laatste episo-de besloeg van mijn doctoraatssoap.
Janine KopatzVoor uw creatieve geest, voor uw eigen stijl, om kop-pig vast te houden aan sommige details, om toe te geven wanneer ik koppig was.
Martin UrschlerOm transparent te zijn over elkaars werk, om mo-gelijkheden tot samenwerking te creëren, voor uw T-shirts in Graz.
Helen LiversidgeVoor uw interesse en hulp bij het begin van dit pro-ject, voor uw relativerende kijk op leeftijdsschatting.
Andreas SchmelingOm me als peer-reviewer een kijk te geven op de meest recente literatuur, om door het embargo met IJLM te breken.
Iedereen die ik ontmoet heb tijdens AAFS, ASFO, IOFOS, ISFRI en AGFAD bijeenkomstenOm ons werk te waarderen en samen te streven naar de optimale aanpak.
Alle masterstudenten Forensische TandheelkundeOm mijn werk te waarderen, om mijn advies bij jul-lie werk op prijs te stellen, om in hetzelfde schuitje te zitten verdrinkend in alle taakjes.
Cezar Capitaneanu en Ademir FrancoOm jullie ervaringen te delen, voor jullie besmette-lijke toewijding aan forensische tandheelkunde, om jullie bureau te delen met Inès.
Persoonlijk dankwoord
305
Patrick DavisVoor uw grote belangstelling voor mijn werk, voor de onmisbare taalkundige tips die voorbijgaan aan iemand die Engels niet als moedertaal heeft, voor de telefoontjes waarin we filosofeerden over forensi-sche en het leven.
Caroline Van Schoubroeck en Yvo VermylenVoor uw flexibiliteit om de lessen in te plannen, voor uw enthousiasme en nuchtere aanpak om van mij een ethische gerechtsdeskundige te maken, voor het middageten in Wok Dynasty.
Iedereen op Forensische Geneeskunde UZ LeuvenOm me op te nemen in de groep toen ik nog student was, om van bij het begin mijn werk te steunen, om me al vroeg het gevoel te geven dat ik gelijkwaardig was, voor alle Forensische Feesten.
Alle mensen die we ontmoet hebben op de Kabinetten Asiel en Migratie en JustitieVoor uw transparantie, om te ontdekken dat al uw frustraties exact overeen komen met die van ons, voor uw drang naar verbetering.
Al mijn medestudenten op Tandheelkunde UGent Om jullie nota’s te delen, om deel te nemen aan mijn onderzoek en er mensen voor te rekruteren, om mijn academisch werk te waarderen, voor het geroddel in de prekliniek, om mij te komen halen bij moei - lijke extracties, om sommige van mijn endo’s over te nemen, om mij te entertainen tijdens saaie lessen.
Alle professoren en lesgevers op Tandheelkunde UGentVoor uw flexibiliteit in de planning, om mijn poten-tieel te erkennen, om Inès te steunen.
Johan ApsOm voor mij op te komen in Tandheelkunde, om mijn werk op prijs te stellen, om elkaar tegen te ko-men aan de andere kant van de wereld, om contact te houden.
Louis SimoenOm te filosoferen over MRI, het kaakgewricht en onderzoek, om samen te supporteren voor de Rode Duivels.
Gaetan Van de VyvereVoor de feestjes in het OK, voor het Geluidshuis, voor de tracteurs, om mijn idool te zijn als chirurg en als familieman. Jij en Leen hebben me van bij de start gesteund en respecteerden het afwijkend traject dat ik aan het volgen was. Dank u Jules en Camille om al zo lang in mijn leven te zijn als jullie herin-neringen hebben en om mijn enthousiaste jongste deelnemers te zijn.
Marc CapiauOm me te redden in de finale fase van de thesis, om als geen ander te weten hoe het voelt wanneer iets chronisch 'bijna af ' is, om blij te zijn dat wij in uw team zitten.
Herman Van den EyndeVoor uw nuchtere aanpak tijdens mijn periode in Aalst, om de basis te leggen van mijn chirurgische opleiding, om mijn academische kwaliteiten direct te erkennen en om me te helpen het evenwicht te zoeken tussen mijn klinische en academische groei.
Alle verpleegsters en secretaressen op MKA OLV AalstOm op mijn patiënten in te spreken als ik aan het opereren was, om me op te leren, me te entertainen, te roddelen en mij te pesten.
Persoonlijk dankwoord

306
Alle chirurgen, verpleegsters en secretaressen op MKA UZ LeuvenOm mij part-time te laten werken, om mijn aca-demisch werk te waarderen, om te trachten orde te creëren in de chaos.
Alle chirurgen op Hoofd-Halschirurgie UZ GentHubert Vermeersch, Philippe Deron, Katrien Bonte, Wouter Huvenne, Peter Tomassen. Voor uw flexibi-liteit, voor uw waardering voor MKA, om mijn aca-demisch werk op prijs te stellen, om me te waarschu-wen voor de laatste fase van mijn doctoraat, voor de extra-curriculaire activiteiten.
Robin WillaertOm mijn idool te zijn als jonge chirurg, om mijn af-wijkend traject te waarderen, om mij te betrekken bij uw eigen onderzoek, voor alle avonden dat we gingen voortgaan en dan toch nog meer dan een uur zaten te babbelen.
Alle verpleegsters en secretariaatsmede- werkers op Hoofd-Halschirurgie UZ GentOm mijn werk te appreciëren, om mij te proberen overtuigen naar Gent terug te komen, voor de team buildings.
Lies PottelOm mijn werk te waarderen, om een nieuw MRI project op te zetten dat de fusie met MKA betekent, om continu te horden te nemen die dat project mee-brengen, om het project in goede banen te leiden nu ik daar niet meer ben.
Jan CasselmanVoor uw liefde voor MRI, om mijn inzicht in MRI te vergroten, om mij een nieuw MRI project toe te vertrouwen.
Johan AbeloosOm mijn werk te waarderen, om te geloven in het potentieel van MRI, om ons nieuw MRI project te steunen, om de Hoofd-Halschirurgen te proberen overtuigen.
Alle chirurgen op MKA AZ Sint-Jan BruggeOm mee in te stappen op het nieuwe MRI project, om te geloven in het potentieel van MRI.
Alle technologen medische beeldvorming op MR AZ Sint-Jan BruggeOm mijn input te waarderen tijdens het scannen, om mijn inzicht in MRI te vergroten, voor alle koek-jes en koffie.
Britt EngelenOm mij te redden wanneer ik verkeerdelijk dacht dat ik nog het hele weekend aan mijn thesis kon werken, om mijn idool te zijn als assistent.
Alle chirurgen en studenten op MKA Maastricht UMCBirgit van Lieshout, Veronique Timmer, David Koper, Auke van Mierlo, Maria Desmedt, Lauretta Vaassen, Cornelia Wilkert, Peter Kessler, Rick Claessen, Carine Leung en Niels Sluypers. Om het met mij uit te hou-den terwijl ik geabsorbeerd word door mijn docto-raat, voor uw flexibiliteit in de planning, voor al mijn eerste keren in het OK, om mij te leren dat ik te aardig ben, om samen met mij te dansen op de File Fuif, voor de borrels op vrijdag, om Vlaams te leren.
Alle tandartsassistentes en verpleegsters op MKA Maastricht UMCOm te streven naar efficiëntie, om de kleedkamer te delen, om mij uit te lachen met mijn tongval.
Persoonlijk dankwoord

307
Alle Vlaamse assistenten op MKA en Hoofd-Halschirurgie en alle AST’sVoor jullie flexibiliteit in planning wanneer ik naar een congres wilde of een aankomende deadline had, om jullie ervaringen en kennis te delen, om in het-zelfde schuitje te zitten, voor alle keren dat we iets gingen drinken en alle after parties.
Brecht De Cuyper en zijn familieVoor het gelijkaardig traject dat we meer dan 25 jaar lang bewandelden, om mij te entertainen tijdens de lessen, voor de danslessen, voor Dance your PhD, voor de squash matchen, met of zonder short.
Rik Jamaels en zijn familieOm in mij te geloven, om er te zijn als ik eens moet ventileren, om mijn mening en advies te vragen, om mij op te zoeken als ik met iets kan helpen, om mijn idolen te zijn als familie, om mij in de melkput te vertrouwen, om te voldoen aan het “Einstein brain” van Admiral Freebee:
But you can't milk a cow with your hands in your pants.
De families De Tobel en VerhasseltOm mij te steunen op dit niet-vanzelfsprekend tra-ject, zowel academisch als privé, om deel te nemen aan mijn onderzoek.
Jorge De TobelOm me weg te slepen van mijn werk, om de paar-denpassie te delen, om een encyclopedie te zijn als het komt op fokadvies voor Haflingers of Belgische trekpaarden, om te helpen waar en wanneer je kan. Je weet dat het goed bedoeld is als Admiral Freebee over u zingt in “Einstein brain”:
Maybe God wanted to make something ugly but in great shape
Al mijn vrienden bij de stamboeken van het Friese paard, de Haflinger en het Belgisch trekpaard Om de schoonheid van de paarden te delen en te be-nadrukken, voor de waardering voor de manier waar - op ik met de paarden omga en voor mijn loopkun-sten, om mijn werk op prijs te stellen, om voor mij een plaats te voorzien op de Friese hengstenkeuring.
Al mijn vrienden van toen ik in het middelbaar en in Geneeskunde zat Om af en toe eens te horen of ik nog leef.
José Phlypo, Brigitte Vanrobaeys, Jelle Phlypo, Vicky Cafmeyer en hun familiesOm mij in huis te halen, terwijl jullie al mijn scherpe kantjes kennen, om mijn tweede thuis te zijn, om mij te leren drinken, voor alle feestjes, om mij mee te nemen naar het zwembad, om de beste varkentjes te kiezen voor Robin.
Rudy De TobelOm Jorge en mij boven alles te stellen, om mij uw boerenverstand en paardenpassie door te geven, om mij kansen te geven, om mij te redden wanneer ik mijzelf weer eens had buitengesloten, om mij te redden wanneer ik mijn kabel vergeten was en de vlieger bijna ging vertrekken, om mij al die andere keren te redden.
Inès PhlypoVoor het voorrecht om u aan mijn zijde te hebben. Geen woorden kunnen bevatten wat jij hebt bij-gedragen aan deze thesis of aan de persoon die ik vandaag ben. The Strypes komen wel al dichtbij in hun “I need to be your only”:
She’s the bag, she’s the leaf, she’s the sugarThe full cup baby, like no other
Persoonlijk dankwoord


309
Curriculum Vitae
personal data
name Jannick De Tobeldate of birth October 27, 1987place of birth Jette, Belgiumnationality Belgian
professional addresses Maastricht University Medical Centre Oral diseases and Maxillofacial Surgery P. Debyelaan 25 NL – 6229 HX Maastricht
Ghent University Hospital Medical Imaging, MR -1K12 C. Heymanslaan 10 B – 9000 Gent
Leuven University Hospital Imaging and Pathology - Forensic Odontology Kapucijnenvoer 7 B – 3000 Leuven
home address Heisbroekstraat 13 B – 9290 Uitbergen
e-mail [email protected] phone +32 (0)485 16 10 79

310
professional career
Education
2018 Master of Forensic Odontology, Catholic University Leuven, Belgium2016 – present PhD student Biomedical Sciences, Catholic University Leuven, Belgium2016 – present PhD student Health Sciences, Ghent University, Belgium2015 – present Master in Specialist Medicine, Ghent University, Belgium2013 – 2015 Master of Dentistry, Ghent University, Belgium2011 – 2013 Bachelor of Dentistry, Ghent University, Belgium2008 – 2012 Master of Medicine, Major Hospital Doctor, Ghent University, Belgium2005 – 2008 Bachelor of Medicine, Ghent University, Belgium 2003 – 2005 Secondary school, Science-Mathematics (8h mathematics), Heilig-Hartinsituut
Halle, Belgium1999 – 2003 Secondary school, Latin-Greek, Heilig-Hartinsituut Halle, Belgium
Courses and specific competences
2018 Trauma basics course: Mandibular Fractures, Stryker and Academic Medical Center Amsterdam, the Netherlands
2018 Erasmus Course Head and Neck MRI, Bruges, Belgium2017 Systematic review course, CEBAM – Cochrane Belgium, University Hospital
Leuven, Belgium2015 Advanced surgical course: The Zygoma Concept, Nobel Biocare, Belgium2014 Profess basic International Conference on Harmonisation Good Clinical Practice
qualification training course, Ghent University, Belgium2011 Rechtsmedizin, Justus-Liebig-Universität Gießen, Germany2009 Principles of electrocardiography, Ghent University, Belgium2006 – 2009 Student-assistant Neurological examination, Ghent University, Belgium
Medical specialist in training
2019 Oral Diseases and Maxillofacial Surgery, Maastricht University Medical Center, the Netherlands
2018 Oral and Maxillofacial Surgery and Radiology, AZ Sint-Jan, Brugge, Belgium2017 – 2018 Head, Neck and Maxillofacial Surgery, University Hospital Gent, Belgium2016 – 2017 Oral and Maxillofacial Surgery, University Hospital Leuven, Belgium2015 – 2016 Oral and Maxillofacial Surgery, OLV Ziekenhuis Aalst, Belgium
Curriculum Vitae

311
publications
De Tobel J, Bauwens J, Parmentier G, Franco A, Pauwels N, Verstraete K, Thevissen P. The use of magnetic resonance imaging in forensic age estima-tion of living children and subadults systematically reviewed. Ped Radiol. Submitted on March 4, 2019.
De Tobel J, Fieuws S, Hillewig E, Phlypo I, van Wijk M, de Haas M, Politis C, Verstraete KL, Thevissen PW. Multi-factorial age estimation: a Bayesian ap-proach combining dental and skeletal magnetic res-onance imaging. Eur Radiol. Submitted on January 27, 2019.
De Tobel J, Hillewig E, van Wijk M, Fieuws S, The-vissen PW, Verstraete KL. Staging clavicular devel-opment on magnetic resonance imaging: pitfalls and suggestions for age estimation. J Magn Reson Imag-ing. Submitted on November 28, 2018.
De Tobel J, van Wijk M, Alberink I, Hillewig E, Phlypo I, van Rijn RR, Thevissen PW, Verstraete KL, de Haas MB. The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estimation. Int J Legal Med. Submitted on October 24, 2018.
De Tobel J, Hillewig E, de Haas MB, Van Eeckhout B, Fieuws S, Thevissen PW, Verstraete KL. Forensic age estimation based on T1 SE and VIBE wrist MRI: do a one-fits-all staging technique and age estima-tion model apply? Eur Radiol. 2019. Epub ahead of print.
De Tobel J, Parmentier G, Phlypo I, Descamps B, Neyt S, Van De Velde W, Politis C, Verstraete K, Thevissen P. Magnetic resonance imaging of third molars in forensic age estimation: comparison of the Ghent and Graz protocols focusing on apical closure. Int J Legal Med. 2018; E-pub ahead of print doi: 10.1007/s00414-018-1905-6.
Phlypo I, De Tobel J, Marks L, De Visschere L, Koole S. Integrating community service learning in under-graduate dental education: A controlled trial in a resi-dential facility for people with intellectual disabilities. Spec Care Dentist. 2018; 38:201-207
De Tobel J, Phlypo I, Fieuws S, Politis C, Verstraete K, Thevissen P. Forensic age estimation based on de-velopment of third molars: a staging technique for magnetic resonance imaging. J Forensic Odontos-tomatol. 2017; 35:117-140.
De Tobel J, Radesh P, Vandermeulen D, Thevissen P. An automated technique to stage lower third molar development on panoramic radiographs for age es-timation: a pilot study. J Forensic Odontostomatol. 2017; 35:42-54.
De Tobel J, Hillewig E, Verstraete K. Forensic age estimation based on magnetic resonance imaging of third molars: converting 2D staging into 3D staging. Ann Hum Biol. 2017; 44:121-129.
De Tobel J, Hillewig E, Bogaert S, Deblaere K, Ver-straete K. Magnetic resonance imaging of third molars: developing a protocol suitable for forensic age estima-tion. Ann Hum Biol. 2017; 44:130-139.
Hillewig E, De Tobel J, Cuche O, Vandemaele P, Pie-tte M, Verstraete K. Magnetic resonance imaging of the medial extremity of the clavicle in forensic bone age determination: a new four-minute approach. Eur Radiol. 2011; 21:757-767.
Curriculum Vitae

312
book chapter
De Tobel J, de Haas MB, van Wijk M, Verstraete KL, Thevissen PW. The future of forensic age estimation in living adolescents and young adults: magnetic resonance imaging and automation. In: Aps JKM, Boxum SC, De Bruyne MAA, Jacobs R, van der Meer WJ, Nienhuijs MEL, eds. Het tandheelkundig Jaar 2018. Houten: Bohn Stafleu van Loghum, 2018; p. 1-19. [Dutch]
international oral presentations
De Tobel J, Hillewig E, Phlypo I, de Haas M, van Wijk M, Fieuws S, Verstraete K, Thevissen P. Mul-ti-factorial age estimation: a Bayesian approach combining dental and skeletal magnetic resonance imaging. 22nd Meeting of the Study Group on Fo-rensic Age Diagnostics, Arbeitsgemeinschaft für Fo-rensische Altersdiagnostik (AGFAD); Berlin, Ger-many; March 15, 2019.
De Tobel J, Bauwens J, Parmentier G, Franco A, Pau-wels N, Verstraete K, Thevissen P. The use of mag-netic resonance imaging in forensic age estimation of living children and subadults systematically re-viewed. 22nd Meeting of the Study Group on Foren-sic Age Diagnostics, Arbeitsgemeinschaft für Foren-sische Altersdiagnostik (AGFAD); Berlin, Germany; March 15, 2019.
De Tobel J, Hillewig E, van Wijk M, Fieuws S, The-vissen PW, Verstraete KL. Staging Clavicular Devel-opment on Magnetic Resonance Imaging: Pitfalls and Suggestions For Age Estimation. American Academy of Forensic Sciences (AAFS) 71st Annu-al Scientific Meeting; Baltimore, USA; February 22, 2019.
De Tobel J, Hillewig E, Phlypo I, de Haas M, van Wijk M, Fieuws S, Verstraete KL, Thevissen PW. Magnetic Resonance Imaging (MRI) of Third Mo-lars, Clavicles, and Wrists for Age Estimation: A Combined Bayesian Approach. American Academy of Forensic Sciences (AAFS) 71st Annual Scientific Meeting; Baltimore, USA; February 21, 2019.
De Tobel J, de Haas M, van Wijk M, Phlypo I, Ver-straete K, Thevissen P. The future of age estimation: living up to the ethical demands? The importance of dental ethics and law, International Dental Ethics and Law Society (IDEALS); Amsterdam, The Neth-erlands; August 23, 2018.
De Tobel J, Parmentier G, Phlypo I, Descamps B, Neyt S, Van De Velde W, Verstraete K, Thevissen P. Magnetic resonance imaging of third molars in fo-rensic age estimation: comparison of the Ghent and Graz protocols focusing on apical closure 21st Meet-ing of the Study Group on Forensic Age Diagnostics, Arbeitsgemeinschaft für Forensische Altersdiagnos-tik (AGFAD); Berlin, Germany; March 16, 2018.
De Tobel J, Parmentier G, Pauwels N, Verstraete K, Thevissen P. The Use of Magnetic Resonance Im-aging (MRI) in Forensic Age Estimation of Living Children, Adolescents, and Subadults: Protocol for a Systematic Review and Preliminary Results. Ameri-can Academy of Forensic Sciences (AAFS) 70th An-nual Scientific Meeting; Seattle, USA; February 23, 2018. p 641.
De Tobel J, Parmentier G, Phlypo I, Descamps B, Neyt S, Van De Velde W, Thevissen P, Verstraete K. Magnetic Resonance Imaging (MRI) of Third Mo-lars in Forensic Age Estimation: Validation of the Gent and Graz Protocols. American Academy of Forensic Sciences (AAFS) 70th Annual Scientific Meeting; Seattle, USA; February 23, 2018. p 640.
Curriculum Vitae

313
De Tobel J, The use of MRI in forensic age estima-tion. Triennial International Organization for Fo-rensic Odonto-Stomatology (IOFOS) Conference. Leuven, Belgium; September 16, 2017. Workshop
De Tobel J, Phlypo I, Fieuws S, Politis C, Verstraete K, Thevissen P. Forensic age estimation based on de-velopment of third molars: a staging technique for magnetic resonance imaging. Triennial Internation-al Organization for Forensic Odonto-Stomatology (IOFOS) Conference. Leuven, Belgium; September 15, 2017. p 21
De Tobel J, Radesh P, Vandermeulen D, Thevissen P. Performance of an automated lower third molar staging technique on panoramic radiographs. Tri-ennial International Organization for Forensic Od-onto-Stomatology (IOFOS) Conference. Leuven, Belgium; September 15, 2017. p 26
De Tobel J, van Wijk M, Hillewig E, Phlypo I, Alber-ink I, van Rijn R, Thevissen P, Verstraete K, de Haas M. The influence of motion artefacts on magnetic resonance imaging of the clavicles for age estima-tion. 6th International Society of Forensic Radiology and Imaging (ISFRI) Congress; Odense, Denmark; May 12, 2017. p 64.
De Tobel J, de Haas M, Thevissen P, Verstraete K. Forensic age estimation based on T1 SE and VIBE wrist MRI sequences: opposite or complementary? 20th Meeting of the Study Group on Forensic Age Diagnostics, Arbeitsgemeinschaft für Forensis-che Altersdiagnostik (AGFAD); Berlin, Germany; March 17, 2017.
De Tobel J, Hillewig E, Bogaert S, Deblaere K, Politis C, Verstraete K, Thevissen P. Third molar magnetic resonance imaging (MRI) in forensic age estimation: protocol development and considerations for use. American Academy of Forensic Sciences (AAFS) 69th Annual Scientific Meeting; New Orleans, USA; February 16, 2017. p 867-868.
Phlypo I, De Tobel J, Marks L, De Visschere. Pilot study on the effects of oral health education for car-egivers in a residential setting for people with intel-lectual disabilities: a randomized controlled trial. 23rd International Association for Disability and Oral Health (iADH) Congress in conjunction with Special Care Dentistry Association (SCDA) 28th Annual Meeting; Chicago, USA; April 16, 2016.
De Tobel J, Hillewig E, Bogaert S, Deblaere K, Ver-straete K. MRI of the third molars: developing a protocol suitable for age estimation. 18th Meeting of the Study Group on Forensic Age Diagnostics, Ar-beitsgemeinschaft für Forensische Altersdiagnostik (AGFAD); Berlin, Germany; March 20, 2015.
De Tobel J, Hillewig E, Verstraete K. Age estimation based on MRI of the third molars: transferring 2D staging into 3D staging. Symposium on Age Esti-mation, Society for the Study of Human Biology (SSHB) in association with the British Association for Biological Anthropology and Osteoarchaeology (BABAO); Oxford, United Kingdom; December 10, 2014.
Hillewig E, De Tobel J, Cuche O, Piette M, Ver-straete K. Is 3T MRI of the sternal extremity of the clavicle a good method for assessing bone age? Eu-ropean Congress of Radiology, European Society of Radiology (ESR); Vienna, Austria; March 4, 2010.
Curriculum Vitae

314
research funding
2017 American Society of Forensic Odontology (ASFO) Research Grant, USA2018 Broaden your Horizon, Travel Grant, Catholic University Leuven, Belgium2018 Faculty Mobility Fund, Travel Grant, Ghent University, Belgium2018 Grant for a short study visit abroad, Fund for Scientific Research (FWO),
Flanders, Belgium2018 Interest-free loan, Foundation Fernand-Lazard, Belgium2019 Grant for participation in a conference abroad, Fund for Scientific Research
(FWO), Flanders, Belgium2019 Faculty Mobility Fund, Travel Grant, Ghent University, Belgium
reviewer
Clinical Oral Investigations Associate editor Prof. Dr. Reinhilde JacobsEuropean Radiology Editor in chief Prof. Dr. Yves MenuInternational Journal of Legal Medicine Editor Prof. Dr. Andreas SchemingJournal of Forensic Odontostomatology Editor in chief Prof. Dr. Vilma PinchiScientific Reports, Nature Group Editorial board member Dr. Marin Pilloud
assistant editor
Journal of Forensic Odontostomatology, Special issue 35(2) for the Triennial International Organization for Forensic Odonto-Stomatology (IOFOS) Conference. Editor in chief Prof. Dr. Patrick Thevissen.
membership
American Academy of Forensic Sciences (AAFS) Trainee AffiliateAmerican Society of Forensic Odontology (ASFO) MemberEuropean Association for Cranio-Maxillo-Facial Surgery (EACMFS) Trainee MemberInternational Society of Forensic Radiology and Imaging (ISFRI) PhD/Resident Member
advisory committees
2017 International Organization for Forensic Odonto-Stomatology (IOFOS) Quality Assurance Recommendations, Age estimation Working Group
2018 American Dental Association Standards Committee on Dental Informatics, Joint Working Group on Forensic Odontology Informatics, Standard No. 1077: Human Age Assessment by Dental Analysis
Curriculum Vitae


ISBN 9789082552522