lawyer's guide to forensic medicine
TRANSCRIPT


LAWYER’S GUIDE TOFORENSIC MEDICINE
Cavendish Publishing
Limited
CPLondon • Sydney


LAWYER’S GUIDE TOFORENSIC MEDICINE
Second Edition
Bernard Knight, CBE, MD, DSc (Hon), LLD (Hon), BCh, MRCP, FRCPath, Dip Med Jur
Barrister of Gray’s InnEmeritus Professor of Forensic Pathology, University of Wales College of Medicine
Cavendish Publishing
Limited
CPLondon • Sydney

Published in Great Britain 1998 by Cavendish Publishing Limited, The GlassHouse, Wharton Street, London WC1X 9PX, United Kingdom.Telephone: +44 (0) 171 278 8000 Facsimile: +44 (0) 171 278 8080E-mail: [email protected] our Home Page on http://www.cavendishpublishing.com
First published by William Heinemann Medical Books 1982
© Knight, Bernard 1998First edition 1982Second edition 1998
All rights reserved. No part of this publication may be reproduced, stored in aretrieval system, or transmitted, in any form or by any means, electronic,mechanical, photocopying, recording, scanning or otherwise, except under theterms of the Copyright Designs and Patents Act 1988 or under the terms of alicence issued by the Copyright Licensing Agency, 90 Tottenham Court Road,London W1P 9HE, UK, without the permission in writing of the publisher.
Knight, BernardLawyer’s Guide to Forensic Medicine – 2nd edn1. Medical jurisprudenceI. Title614.1
ISBN 1 85941 159 2
Printed and bound in Great Britain

PREFACE
The 16 years that have elapsed since the first edition of this book have seenmany changes which require significant updating of the text. Some entrieshave been deleted and others added, to reflect the changing priorities in theinterface between medicine and the law.
This book has apparently filled a previously vacant niche in lawyer’slibraries – on one occasion, I had the uncomfortable experience of standingin the witness box while both prosecuting and defence counsel, as well asthe judge, quoted passages to me from their own copies.
Due to restrictions of space, the text is sometimes telegraphic and doesnot purport to be of great literary quality but, hopefully, the content isuseful, comprehensible and free from unexplained medical jargon.
Within this small compass, it is impossible to provide references to alltopics, but a list of standard forensic medical texts is provided, which willdirect the reader to the relevant literature.
Bernard KnightLisvane, Cardiff
1998
v


CONTENTS
vii
Preface v
PART I: ANATOMICAL DRAWINGS 1Anatomical directions 2Structures of the thorax and upper abdomen (anterior view) 3Structures of the thorax and upper abdomen (posterior view) 4Posterior view of kidneys and spleen (showing relationship
to pleural cavity) 5Structures of the thorax and neck 6The aorta and its branches 7Surface outlines of heart and lungs 8Surface markings of the heart 9Relationships of female and male genital organs 10
PART II: ALPHABETICAL ENTRIES 11Abdominal injury 12Abortion 13Abortion legislation 15Abrasions 17Adipocere 18Age estimation 19AIDS 21Air embolism 21Air-gun injuries 22Air passage obstruction 23Alcohol (ethyl) 24Alcohol (methyl) 28Amnesia 29Amphetamines 29Anaesthetic deaths 30Aneurysms 33Aorta 35Arm-lock deaths 37Arteries 37Asbestos 38Asphyxia 38Aspirin poisoning 42Autopsy 43
Barbiturates 45Bestiality 45Bite marks 46Black eye 47Bladder 48

Lawyer’s Guide to Forensic Medicine
viii
Blisters 49Blood groups 50Blood pressure 50Blood splashes 51Brain death 52Bruises 54Burial 56Burns 57
‘Café coronary’ 61Cannabis 61Carbon monoxide poisoning 63Cardiac arrest 64Cardiomyopathies 65Cerebral haemorrhage 65Cerebral oedema 67Child abuse syndrome 67Child destruction 70Choking 71Circle of Willis 72Cocaine 72Cold injury (hypothermia) 72Concussion 74Consent to treatment 75Contre-coup injury 76Cooling of the body 78Coronary artery disease 80Coroner, deaths reportable to 83Cot death 84Cremation (legal requirements) 85Creutzfeldt-Jakob disease 86Cut throat 87
Death certification 89Death, signs of 90Decomposition of dead body 91Defence injuries 92Dental identification 92Diatom test in drowning 93Diffuse axonal injury (DIA) 95Disseminated intravascular coagulopathy (DIC) 96DNA 96Drowning and immersion 97Drugs and medicines 100

Contents
ix
Ecstasy 101Electrocution 101Embolism 103Entomology 104Epilepsy 104Expectation of life 104Exhumation 107Explosion injuries 109Extradural haemorrhage (or haematoma) 110
Fabricated injuries (self-inflicted injuries) 112Fat embolism 112Femur, fracture of 113Fingernail marks 114Firearm wounds 115Foetus (fetus) 118Foreign bodies 119Fractures 119Frontal sinus identification 120
Gangrene 122General Medical Council (GMC) 122Glass injuries 124Glue sniffing (solvent abuse) 125
Haemorrhage 126Hair 126Hanging 127Head injury 128Heart 130Hepatitis 132Heroin 132Histology 133Human Tissue Act 1961 133Hymen 135Hyoid bone 135Hyperpyrexia or hyperthermia 138Hypostasis (post-mortem lividity) 139
Identification 141Immersion 142Incised wounds 142Infanticide 143Intestine 144

Lawyer’s Guide to Forensic Medicine
x
Jaw, injuries to 147
Kicking 148Kidneys 149
Lacerations 150Larynx 150Ligature 152Live birth 153Liver 155Longevity 156LSD (lysergic acid diethylamide) 156
Malignant hyperthermia 158Masochistic (sexual) asphyxia 158Methadone 159Misuse of Drugs Act 1971 159Mobility and activity after injury 162Morphine 163Mummification 164Mutilation 164Myocardial infarction 165Myocarditis 166
Neck-hold deaths 168Necrosis 168
Obscure or negative autopsy 169
Patterned injuries 171Petechial haemorrhages 173Pneumoconioses 174Poisoning 177Positional or postural asphyxia 178Post-mortem entomology 181Pregnancy 182Procurator Fiscal 183Pulmonary embolism and deep vein thrombosis 185
Rape 188Reflex cardiac arrest 191Rib fractures 191Rigor mortis 192

Contents
xi
Scalds 194Scalp wounds 194Scars 195Semen 196Sexual intercourse 197Skeletal identification 198Skull fractures 199Smothering 202Sodomy 203Solvent abuse 204Spleen 204Spontaneous combustion 205Stab wounds 205Stature, estimation of 208Status lymphaticus 208Sterilisation 209Still-birth 210Stomach 211Strangulation 212Subarachnoid haemorrhage (or haematoma) 215Subdural haemorrhage (or haematoma) 218Sudden natural death 220Suffocation 223
Tattoos 224Thrombosis 224Throttling 225Thyroid gland 225Time since death 226Traffic accidents 230Transplantation of organs and tissues 234Trauma and disease 236Traumatic asphyxia 240
Vagal inhibition (reflex cardiac arrest) 242Vertebral artery injury 243Vital reaction 243
Whiplash injury 245
Appendix: Recommended Reading 247
Index 249


PART I: ANATOMICAL DRAWINGS
Lawyer’s Guide to Forensic Medicine
2
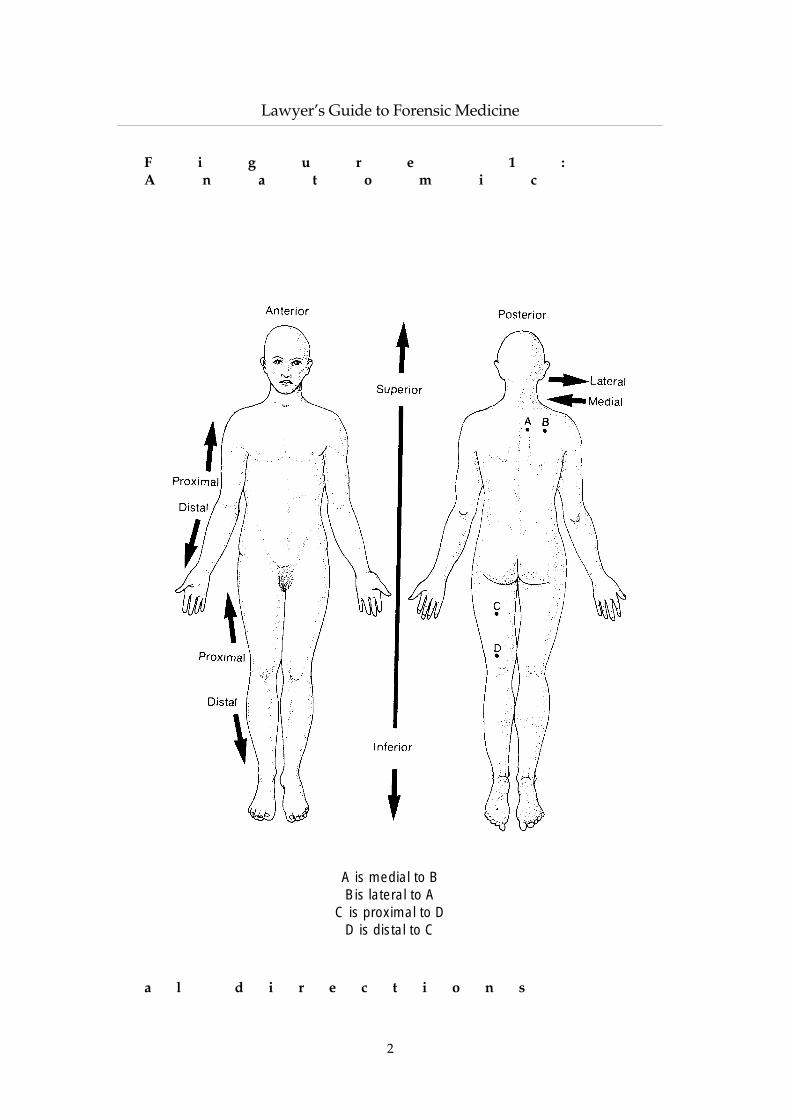
F i g u r e 1 :A n a t o m i c
a l d i r e c t i o n s
A is medial to BBis lateral to A
C is proximal to DD is distal to C

Part I: Anatomical Drawings
3
F i g u r e 2 : S t r u c t u r e s o f t h et h o r a x a n d u p p e ra b d o m e n
( a n t e r i o r v i e w )

Lawyer’s Guide to Forensic Medicine
4
F i g u r e 3 : S t r u c t u r e s o f t h et h o r a x a n d u p p e ra b d o m e n
( p o s t e r i o r v i e w )

Part I: Anatomical Drawings
5
F i g u r e 4 :P o s t e r i o rv i e w o f k i d n e y s a n d
s p l e e n ( s h o w i n gr e l a t i o n s h i p
t op l e u r a lc a v i t y )

Lawyer’s Guide to Forensic Medicine
6
F i g u r e 5 : S t r u c t u r e s o f t h et h o r a x a n d n e c k

Part I: Anatomical Drawings
7
F i g u r e 6 : Thea o r t a
a n d i t s b r a n c h e s

Lawyer’s Guide to Forensic Medicine
8
F i g u r e 7 : S u r f a c eo u t l i n e s o f t h eh e a r t a n d l u n g s

Part I: Anatomical Drawings
9
F i g u r e 8 : S u r f a c em a r k i n g s o f t h eh e a r t

Lawyer’s Guide to Forensic Medicine
10
F i g u r e 9 :R e l a t i o n s h i p so f f e m a l e
Relationship of female genital organs
Relationship of male genital organs

PART II: ALPHABETICAL ENTRIES

ABDOMINAL INJURY
A blow or kick upon the abdomen can cause severe, even fatal internal injury.There need not be any mark on the skin, especially if clothing is interposed.Though bruising or abrasions may be seen externally, rupture of internalorgans can occur with no visible skin mark.
Most common injuries
Rupture of the spleen (qv) which lies in the left upper part of the abdomen.Fatal haemorrhage may occur from impact on the upper left abdomen orlower ribs.
Rupture of the intestine (qv), especially in children as part of child abusesyndrome. The upper small intestine may be lacerated or even divided whereit crosses the projection of the spinal column, due to direct blows in the centreor upper part of the abdomen. This can be delayed if the injury first makes theintestinal wall non-viable, then it tears a day or two later.
The mesentery, the membranous root of the intestine may be lacerated in asimilar fashion, leading to severe haemorrhage.
Rupture of the liver (qv) often occurs in traffic accidents and falls from aheight due to heavy impact on the abdomen or lower chest. Also seen in kicksto the abdomen.
Rupture of the stomach or large bowel, but this happens less often than theabove.
In all these instances, severe illness or death may be due to:(a) haemorrhage into the peritoneal cavity (the free space around the organs),
especially from liver, spleen and mesentery; or(b) infective or chemical peritonitis, with shock when intestine or stomach is
perforated into the abdominal cavity.
Rarely, death may occur instantaneously from a blow in the central abdomen:this is due to cardiac arrest from so called ‘vagal inhibition’ (qv) and wherethere are no external or internal signs of violence, the diagnosis rests upon thecircumstances and exclusion of other causes.
Lawyer’s Guide to Forensic Medicine
12

Part II: Abortion
ABORTION
Synonymous with the older term ‘miscarriage’, meaning the expulsion of apregnancy from the womb before the 24th week of gestation. Later than this,the process is usually called a premature birth, though these are not legaldefinitions.
A considerable proportion – up to 40% – of fertilised ova fail to proceed tofull term, most of them aborting at such an early stage that pregnancy may noteven have been apparent.
The causes of natural abortion include any severe general illness in themother, but especially acute fevers, congestive heart disease, hypertensionwith kidney disease, etc. In spite of these risks, a large proportion ofpregnancies in ill women do not abort, though the strain of the pregnancymay cause further deterioration in the health of the woman.
A defect in the ovum or foetus is one of the most common causes ofaborting, this being a genetic safety device to reduce the incidence ofmalformed individuals. Abortion may be at a very early stage when the actualdefect is indiscernible.
Trauma and violence is rarely a factor, though it can be grounds forlitigation if alleged to have been precipitated by some accident or assault. Asthe incidence of natural abortion is said to be of the order of 10% of allrecognisable pregnancies, it can never be definitely stated that a particulartraumatic event was the inevitable cause, though a close association in timewill naturally strengthen the probability.
Induced abortion
This may be illegal or medically induced under permissive legislation (forBritain, the Abortion Act 1967).
Methods employed include the following:
Dilatation of the neck of the womb and curettage (scraping) of the products ofconception. Usually performed by medically trained persons, either legally or,rarely now in Britain, criminally.
Suction aspiration. The removal of the foetus and membranes by suctionthrough a tube inserted into the womb via the cervix. Now the most common,rapid and complication-free method, usually employed during termination ofearly pregnancy by legitimate means. A very rare complication is airembolism (qv), though in theory this should not occur.
Hysterotomy. The opening of the womb by surgical operation through theabdomen, similar to a Caesarean section. Usually used in the later stages ofpregnancy. Sterilisation is often performed at the same time.
13

Drugs. Usually ineffective and taken by the woman herself in an effort toabort. A wide and largely useless pharmacopoeia exists, such as herbalremedies, purgatives, quinine. Substances such as lead and ergot may havesome effect but are dangerous to the mother. Medical drugs like pituitrin andprostaglandin are effective, but only near full term as inducers of labour.
External physical stimuli. Riding, bicycling, hot baths, enemas and violence tothe abdomen are all without effect, but severe violence may cause injury,sometimes fatal, to the mother.
Uterine syringing. Formerly the most common means of effective illegalabortion, using a Higginson enema syringe to inject fluid into the uterusthrough the neck of the womb (cervix). The purpose is to peel off thepregnancy sac from the walls of the womb by fluid pressure: once loosened, itis expelled by the uterus. Effective, but potentially dangerous method.
Injection of irritant substances into the womb through the cervix. Performedlegally and illegally by use of such substances as Utus paste, which causesexpulsion of the displaced and irritated embryo sac.
Hazards of abortion
Infection. Formerly the most common complication, especially of criminalabortion. With antibiotics and greater involvement of medical and nursingoperators, the incidence is greatly reduced. Anaerobic infection by gas-gangrene-type bacteria is a particular danger.
Haemorrhage can occur from vaginal damage or perforation from inepttechnique, especially by the woman herself. Damage to the neck of the wombor the womb itself also a hazard. The placental bed of the pregnancy sac maybleed profusely, especially in later pregnancy.
Air embolism (qv) from Higginson syringing was one of the most common fatalsequelae of illegal abortion, though now almost unknown in Britain.
Rapid shock effects of abortion. Not common, but may be immediate fromcardiac arrest due to interference with the neck of the womb (see ‘Vagalinhibition’).
Poisoning (for example, toxic effects of substances such as permanganate ofpotash applied to the neck of the womb) or antiseptics containing phenolicsubstances douched into the vagina or syringed into the cervix.
Lawyer’s Guide to Forensic Medicine
14

Part II: Abortion Legislation
ABORTION LEGISLATION
Offences Against the Person Act 1861 did not contemplate any exclusion formedical reasons. Section 58 made it a felony for a woman (if she be pregnant)or any other person (whether she was pregnant or not) to procure or intend toprocure an abortion. Section 59 concerned the supply of poisons orinstruments for the purpose of abortion.
Pharmacy and Medicine Act 1941 made it unlawful to advertise goods in termscalculated to lead to their use in abortion.
Infant Life (Preservation) Act 1929 first mention that medical abortion might notbe unlawful – ‘no person shall be found guilty of an offence unless it is provedthat the act was not done in good faith for the purpose only of preserving thelife of the mother’.
15
Figure 10: Hazards of abortion

The later Abortion Act and Human Fertilisation and Embryology Act make itimpossible for a medical practitioner to be charged under the 1929 Act.
Abortion Act 1967 (as amended by the Human Fertilisation andEmbryology Act 1990)
It is not unlawful for a registered medical practitioner to terminate apregnancy provided that two registered medical practitioners form theopinion in good faith:(a) that the pregnancy has not exceeded the 24th week and that continuance
of the pregnancy would involve greater risk than if the pregnancy wereterminated, of injury to the physical or mental health of the pregnantwoman or any existing child of her family; or
(b) that the termination is necessary to prevent grave permanent injury to thephysical or mental health of the pregnant woman; or
(c) that the continuation of the pregnancy would involve risk to the life of thepregnant woman greater than if the pregnancy were terminated; or
(d) that there is a substantial risk that if the child were born, it would sufferfrom physical or mental abnormalities as to be seriously handicapped.
Notes
(a) Any two doctors may so certify and the actual operation may be carriedout by a third doctor. However, it is most common for a generalpractitioner and a consultant obstetrician to certify, and frequently thelatter is the operator.
(b) In assessing the risk to the woman or to her family, account must be takenof her actual or reasonably foreseeable environment.
(c) The termination of pregnancy may only be carried out either in a NationalHealth Service hospital or in premises approved for the purpose by theSecretary of State.
(d) In an emergency, the opinion of one doctor is sufficient only on thegrounds that abortion is immediately necessary to save the life or preventgrave permanent injury to the pregnant woman.
(e) Documentation must comply with the requirements of the AbortionRegulations (1968), the termination being notified to the appropriate ChiefMedical Officer. These must be completed either before or within 24 hoursof the completion of the operation. Records must be retained for at leastthree years.
(f) Conscientious objection to taking part in abortions is to be upheld amongstmedical and nursing staff, except when the operation is necessary to savethe life or avoid grave damage to the woman.
Lawyer’s Guide to Forensic Medicine
16

Part II: Abrasions
(g) The 1990 amendment placed an upper limit of 24 weeks’ gestation (inplace of the previous 28) only on the first ground for termination. There isno time limit on the three subsequent grounds.
ABRASIONS
These are the most superficial type of wounds, in which the injury does notpenetrate through the full thickness of the skin. A pure abrasion thereforedoes not bleed, as no blood vessels are present in the epidermis (the upperlayer of the skin), but in most cases the injury, unless merely a very superficialscrape, does involve the tips of the corrugated papillae of the underlyingdermis and therefore some bleeding usually occurs.
17
Figure 11: Characteristics of abrasions

Abrasions are also called ‘scratches’ or ‘grazes’, the former referring to asingle linear abrasion and the latter to multiple parallel abrasions due to atangential contact with a rough surface. A ‘gravel rash’ is a colloquial term fora graze caused by sliding impact with a road surface, often seen in trafficinjuries and to a lesser degree in simple falls to the ground. These multipleparallel marks are also known as ‘brush abrasions’.
In these and other abrasions, the direction of the injury can often bedetermined by close inspection of the ends of the scratches, where tags of skinwill be piled up at the end furthest from the initial point of contact. Where aweapon or object hits the skin, its direction will be towards the skin tags,whereas if a moving body skids along a rough surface, the direction will beaway from the end of the graze that shows skin tags.
Abrasions take the imprint of the object which caused them better thanbruises and a clear pattern may be imprinted on the skin (see ‘Patternedinjuries’).
After death, extensive abrasions become leathery and dark reddish brown,especially where friction has occurred as in grazes and ligature marks. In theliving, drying of the surface scab, where present, may also heighten theprominence of an abrasion after a few hours or a day.
Abrasions are sometimes caused on the assailant when a victim isattacked, due to defence actions by the victim. In such instances, forensicexamination of finger-nail scrapings may reveal fragments of skin which canbe DNA analysed, to assist in the identification of the assailant.
Abrasions frequently occur in association with bruises (qv) and lacerations(qv) to form mixed lesions.
ADIPOCERE
A long term post-mortem change in body fat, leading to partial preservationof the soft tissues. Fats are converted to adipocere, a crumbly grey material,which may persist for many years as an alternative to the usual putrefaction.The cheeks, breasts and buttocks are most obviously preserved, but patchyconversion of any part of the body fat may occur. Features may even berecognisable if facial fat is preserved. The process usually needs a wetenvironment, either in water or in damp burials, but this is not invariable. Theadipocere may retain bullet holes or other evidence of violence usually lostduring putrefaction. Adipocere formation usually takes several months tooccur, but may happen within a few weeks in the right conditions.
Chemically, adipocere is a complex mixture of waxes and soaps due to theaction of water on body fat. Fatty acids are a predominant constituent. Thewater necessary for conversion may be provided from the original bodywater, so a damp environment is not absolutely essential.
Lawyer’s Guide to Forensic Medicine
18

Part II: Age Estimation
AGE ESTIMATION
Required in both living and dead, either for identification or for determiningage of criminal responsibility, inheritance, in sexual offences, marriage,employment, immigration, military service, etc – also in foetuses and infantsto determine the stage of maturity (see ‘Foetus’).
Up to about age 25, development of the skeleton affords a reasonablyaccurate means of age determination. The bones mature by developing‘ossification centres’, which are foci of chalky calcium in the cartilage
19
Figure 12: Development of the femur

precursors. These progressively enlarge and eventually fuse together atrelatively constant ages, the last being between 20–25 years. These ossificationcentres, usually at ‘epiphyses’ or growing ends of the bones, can be detectedby X-ray in the living as well as by direct exposure in the dead. Textbooks offorensic medicine and of radiology give tables for the times of appearance andfusion, but caution must be employed in the degree of accuracy expected, asgirls tend to fuse up to one year earlier than boys and, in the tropics, theremay be two to three years advance in bony changes compared to Europe. Theadvice of an experienced radiologist, pathologist or anatomist is necessary asto the expected degree of accuracy in any given circumstance.
Other most useful tools are the teeth, especially in children. The first set ofteeth (‘milk’ or ‘deciduous’ teeth) begin to appear at about the sixth monthafter birth and the second set of permanent teeth begin to erupt at about sixyears. The last tooth is the ‘wisdom’ tooth or third permanent molar, whichmay not appear until 20–25 years. Where the issue is important, the opinion ofa forensic odontologist is essential.
Lawyer’s Guide to Forensic Medicine
20
Figure 13: Development of the teeth

Part II: Air Embolism
After 25 years, the determination of age becomes very imprecise,compared with children, where accuracy measured in weeks can be attainedby special dental techniques. Certain specialised tests of teeth may give an agein the mature adult to within five to seven years, but only on dead subjects.Once the skeleton is fully matured at about 25 years, accuracy only of thenearest decade can be expected in the living, based on general appearancesand the onset of degenerative changes. In the skeleton of the dead, specialtechniques such as pubic bone examination may give a much better result, butexpert anthropological advice is required. Considerable space is devoted tothis subject in standard textbooks of forensic pathology which should beconsulted for details, but it is vital to appreciate the inherent inaccuracies,especially in the mature living person, and to accept the biological variations(sexual, ethnic, nutritional and individual) in the development of children,especially where body height and weight are concerned.
AIDS
Acronym for Acquired Immune Deficiency Syndrome, where the body’simmunological defences are impaired by the action of HIV (human immunedeficiency virus). This loss of defence is against foreign material, includingbacteria, fungi, other micro-organisms and tumour cells, and particularlyreduces the T-lymphocytes, the major defensive mechanism.
This allows a range of opportunist infections to thrive, includingcandidiasis, cytomegalic virus, cryptosporosis, pneumocystis cariniipneumonia, tuberculosis, etc. In addition, a type of cancer, called Kaposi’ssarcoma may develop, due to the loss of the normal destruction of malignantcells by the immune system.
It should be noted that death is not from HIV itself, but of theconsequences of HIV infection, which is a spectrum of secondary infectionsconstituting AIDS. There may be a number of years between infection withHIV and the development of AIDS – a period now able to be prolonged bydrug treatment – and some persons with HIV infection seem not to go on todevelop AIDS.
AIR EMBOLISM
Introduction of air or other gas into circulatory system. Small amounts may betolerated but, beyond a threshold volume (which is very variable from case tocase), bubbles in heart, brain or coronary arteries may cause death.
21

Causes
Induced criminal abortion from the use of a Higginson enema syringe, now avery rare event. Here, instead of fluid, air is inadvertently pumped into thewomb and penetrates the open veins of the separated placental bed to gainaccess to the circulation. Can be a very rare complication of therapeuticabortion by suction (see ‘Abortion’).
Surgical operations on the neck or chest, above heart level, where air may besucked into opened veins. Thyroid operation is most common circumstance,though rare. Cut throat also an uncommon cause. The induction of artificialpneumothorax and pneumoperitoneum also carry risks of embolism.
During transfusion, where bottle empties and air enters vein – especially ifbeing introduced under pressure from gas cylinder. The introduction offlexible plastic containers has greatly reduced this danger.
A few homicidal instances, where air is deliberately introduced by syringe intoarm veins; usually so called ‘mercy killings’ by doctors, for example, theSander and Montemerano cases in the USA.
In divers, when rapid decompression allows gas bubbles to form.
Diagnosis
This is best made by radiology (bubbles seen in heart and large blood vessels).At autopsy, a special technique is needed. It is not necessary to open the chestand heart under water. After X-rays, the large veins and right side of the heartmust be carefully palpated and examined for contained bubbles. Once thevessels and chambers are opened, the bubbles rapidly vanish. The diagnosismust exclude gas formed by decomposition. There are many difficulties ininterpretation, for instance, false bubbles may be seen in brain surface vessels.Radiology is the only really reliable method of detection, either before or afterdeath. Volume of air needed is a matter of controversy: as little as 10 ml hasbeen fatal, while over 100 ml has been survived. Other authorities say that60–100 ml is a minimum fatal volume.
AIR-GUN INJURIES
Air-rifles and pistols can cause lethal injuries, either in the .177 or .22 inchcalibres. Most deaths occur from penetration of the skull and brain, especiallyin children and young persons, the pellet being able to traverse the entirewidth of the interior of the skull and impact against the further side. Thoughthe slug is small, a wide track of damage may be present in the brainsubstance, as with all projectile injuries.
Lawyer’s Guide to Forensic Medicine
22

Part II: Air Passage Obstruction
A common, usually non-fatal, injury is damage to the eye, frequentlycausing blindness in that eye.
As well as head injuries, the pellet can penetrate the chest and cause deathor severe injury from damage to the heart or great blood vessels.
Some control over air weapons was brought in as a result of several deathsin children. This was the Air-Guns and Shotguns, etc, Act 1962, nowincorporated in later Firearms Acts. This made it an offence for a child under14 years to have an air weapon or ammunition and for anyone under 17 yearsto have an uncovered gun in a public place.
The Firearms (Dangerous Weapons) Rules 1969 make the maximumallowable muzzle energy of an air-rifle 16 joules (12 ft/lb) and a pistol 8 joules(6 ft/lb).
AIR PASSAGE OBSTRUCTION (see also ‘Choking’)
Blockage of back of throat (pharynx), voice box (larynx), windpipe (trachea) orlung tubes (bronchi) by foreign objects or material. For external obstructiondue to constriction of neck, obstruction of nose and mouth, etc, see‘Suffocation’, ‘Strangulation’.
Main causes
Internal blockage of air passages is usually due to food material, toys,dentures, extracted teeth, blood, etc. There are two types of food obstruction:
Food just eaten, before it is swallowed into stomach. Common in senile andmentally defective people, including children. Also in the so called ‘cafécoronary’ (qv), confused with heart attacks whilst eating. In all these cases, thefood is fresh and undigested. It may impact in the entrance to the voice box (atthe glottis) or in the windpipe and cause death either by asphyxia, due toblockage of air, or (much more often) from sudden reflex cardiac arrest (qv).
Food regurgitated from stomach, the so called ‘aspiration of vomit’, or ‘inhalationof stomach contents’. Considerable caution is required in accepting such adiagnosis from post-mortem findings, unless corroborated by clinicalobservation. Many pathologists use this as a cause of death, though it may notbe possible to prove. Spurious aspiration of vomit is often really due to agonalor even post-mortem spillage of stomach contents into air passages.Regurgitation is common in death throes; also post-mortem handling of bodyby porters and undertakers has been shown to move stomach contents intolarynx. A quarter of all autopsies reveal some gastric contents in the air
23

passages, but this cannot be accepted as genuine unless someone saw theaspiration take place during life. Only true proof of aspiration at post-mortemis acid digestion in lungs, with a cellular reaction seen under the microscope:not visible unless aspiration occurred some time before death, probably inexcess of many minutes after entry of vomit into lungs.
The mere finding of food particles in the lungs under the microscope is notevidence of death from aspiration; it can be sucked down during the dyingprocess – and if artificial respiration has been given it has no significance atall.
Other causes
Other causes of air passage blockage include gags in the back of the mouth;though these may allow breathing via nose passages at first, mucus andswelling in the nasal passages may close the airway later and cause death.Seen in tied-up watchmen during robbery, etc.
Inhalation of teeth after extraction, false teeth, small toys and other objectsmay also block air passages. Blood from facial and mouth injuries, especiallyin unconscious victims of assault, may also block air tubes. There may or maynot be ‘asphyxial signs’ of blue face, petechial haemorrhages in eyes. These arefrequently absent in choking, due to the rapid death from cardiac arrest.
ALCOHOL (ETHYL)
A very complex toxicological and physiological subject: much uncertainty andcontroversy surrounds the relationship between the amount taken and thebehavioural effects, due to great variation in a number of factors, includingthe following.
Absorption
Alcohol is normally rapidly absorbed after drinking, both from the stomachlining and especially from the first part of the intestine (duodenum andjejunum). The rate of absorption differs according to various factors.
Presence of food in the stomach. A full stomach dilutes the swallowed alcoholand reduces its contact with the stomach wall, so absorption is slowed. A fattymeal retards absorption, partly by delaying the transfer of stomach contentsinto the intestine where alcohol absorption is maximal. Persons who have hada stomach operation, such as partial gastrectomy or a gastro-jejunostomy(usually for peptic ulcers) will absorb alcohol more quickly, as the swallowed
Lawyer’s Guide to Forensic Medicine
24

Part II: Alcohol (Ethyl)
drink will almost immediately enter the upper intestine where absorption ismore rapid.
The concentration of the alcohol. About 20% alcohol in the drink is optimal forquick absorption. Very strong liquor may irritate the stomach wall and slowabsorption by production of mucus on the lining. Very weak alcohol naturallyhas less active substance per volume for absorption and so raises the bloodlevel more slowly. Large volume drinks, such as beer, absorb more slowlythan small volume spirits because the bulk prevents the alcohol from reachingthe walls of the stomach or intestine, which is a prerequisite for absorption.
Carbon dioxide bubbles. In ‘aerated’ diluents for drinks (lemonade and tonic,etc), these are said to increase the rate of absorption. Sparkling wines, such aschampagne, may have the same enhancing effect on absorption, probably dueto the large surface area of the bubbles carrying alcohol molecules to thestomach wall.
Personal variation. Marked variation exists in the rate of absorption, includingthe build of a person, the length of the intestinal canal and the size of thestomach (both related to area of absorptive surface) and other unknownidiosyncratic factors, such as the proportion of alcohol which passesunabsorbed through the intestinal canal. Habitual drinkers appear to have theability to destroy alcohol more quickly.
All these factors make it impossible accurately to calculate the blood levelat a certain time after a certain amount of drink, but a generalisation would bethat after a single ‘dose’ of alcohol on an empty stomach, a maximum bloodlevel is reached within 30–60 minutes, though, if the dose is large, this timemay be prolonged up to a couple of hours. If taken as spirits the level willpeak rapidly, but diluted drink, such as beer or alcoholic drink on a fullstomach, will be partly eliminated during the period of absorption and thus amuch lower, longer peak will occur.
Elimination of the alcohol
Once absorbed, the alcohol will be progressively lost because of:(a) excretion in the breath, urine and sweat; this amounts to less than 10% of
the total;(b) destruction by chemical processes in the tissues, mainly the liver,
accounting for the major part of elimination.
These processes begin as soon as the first alcohol appears in the blood fromabsorption, so the maximum blood level is a dynamic equilibrium betweenthe rates of absorption and elimination. Naturally, further intake of drink afterthe first will escalate the absorption phase and will soon overtake themaximum rate of elimination, which is generally taken to be about 9–15 ml
25

per hour (about the amount in a small whisky) and a figure of about 15 mgper 100 ml of blood is an acceptable rule of thumb for the drop in bloodalcohol per hour once absorption has ceased, though more recent researchfavours a figure of 18 mg/100 ml/hour.
However, this figure is by no means sacrosanct and must vary greatly indifferent persons, especially habitual drinkers, who are able to eliminatealcohol much faster. Normal rates of between 11–25 mg/100 ml/hour havebeen found experimentally and it is said that the rate is especially irregularduring the first few hours after the cessation of drinking – the period in whichmost medico-legal interest lies.
Chronic alcoholics (not intermittent ‘binge’ drinkers) can eliminate muchfaster, even up to 40 mg/100 ml/hour.
Alcohol diffuses evenly throughout all the water in the body. It attains ahigher level in the urine, due to selective withdrawal of water by the kidneys.The excess is in the ratio of between 1.2:1 to 1.4:1, a mean of 1.3:1 being usuallyquoted.
Naturally, where urine alcohol is used as a quantitative measure, anystored urine in the bladder before drinking began must be emptied to avoid adilution effect: hence the requirement under the Road Traffic Act for a secondsample to be collected after a minimum of 20 minutes. Though a level of 107mg/100 ml is accepted as the minimum level for conviction under this Act,urine/blood ratios are not constant enough for the use of urine as a reliableindicator of the blood level.
Breath alcohol is a much better index, as there is an immediate equilibriumestablished between blood and ‘alveolar air’ – air in the smallest air sacs of thelungs; 2,100 ml of alveolar air contain the same amount of alcohol as 1.0 ml ofblood, though accuracy is reduced by the dilution with dead-space air fromthe large bronchial tubes which has not been equilibrated with blood and alsoby the change in temperature of the air as it is expired. However, manycountries accept the ratio as good enough for the establishment of minimumblood concentrations for road traffic testing.
Because alcohol diffuses into all the body water, but not into fat, womenattain a higher blood concentration (20–30% greater) than men, for a givendose of alcohol in persons of the same weight. This does not depend on overtobesity, but on the ‘pannunculus adiposus’, a layer of fat under the skin.
Because of all these variables, it is not possible accurately to back-calculateeither the amount of alcohol taken from a knowledge of the blood alcohol, northe likely blood level to be expected from the drinking of certain amounts ofliquor. Different persons will have different biochemical responses to alcoholand even the same person will have different responses at different times,especially in relation to their dietary habits. Therefore the over-optimistic tablesof conversion which were formerly relied upon cannot be justified, except asthe roughest of guides where large potential errors may have to be admitted.
Lawyer’s Guide to Forensic Medicine
26

Part II: Alcohol (Ethyl)
Even more than the unforeseeable biochemical results, the physiologicaland behavioural sequelae cannot be related with any accuracy to the amountof drink taken.
The physiological effects of alcohol
Alcohol is entirely depressant in effect and the apparent stimulatory action ofsmall-to-moderate amounts is due to depression of the inhibitory control ofthe highest centres in the brain, giving rise to the social lubricant ofloquaciousness and other apparently stimulant effects. ‘Sobriety disguisethman’ (wrote de Quincey), but once this removal of inhibition is past, a furtherrise of alcohol levels causes progressive descent through stupor to coma, andfinally death from paralysis of the lower brain functions of breathing control.
It is impossible to relate behaviour to levels of blood alcohol, except in thevery broadest terms, but judgment, co-ordination and reaction time may beimpaired by low levels in the region of 20–40 mg/100 ml. A number ofjurisdictions have minimum levels for motor vehicle driving much lower thanthe British 80 mg/100 ml, which at the time of writing is under considerationfor lowering to 50 mg.
On ordinary clinical testing, as opposed to sophisticated techniques, fewsigns can be detected below about 80–100 mg/100 ml, though many peoplemay show euphoria, garrulousness, loss of concentration, etc, after reaching50–70 mg/100 ml.
From 100–150 mg/100 ml, flushed face, poor sensory perception and slightincoordination may be expected and from this range up to 250 mg/100 ml, thewhole range of behavioural abnormalities and progressive signs will bepresent.
These include impaired mental ability, yawning and sighing, reddenedeyes, tremor and incoordination, impaired gait and staggering, dilated pupils,heavy breathing and possibly vomiting. However, great variation occurs indifferent people and in the same person at different times. General health andspecific illness can markedly affect the level of impairment.
During the Blennerhassett research before the introduction of evidentialbreath testing, it was found that most volunteers became nauseous and sickby 150 mg/100 ml.
Over 200 mg/100 ml, severe drunkenness is likely to be present, except inhabitual drinkers who may appear relatively normal up to very high bloodlevels, though objective signs are usually present.
Vomiting, incoherence, circulatory collapse with pallor and sweating leadup to the dangerous levels of 350–400 mg/100 ml, where coma may ensue anddeath can take place at any point from here onwards.
27

Occasionally, levels of 500–600 mg/100 ml may be seen in habituateddrinkers, though death is likely at these levels, in spite of many reportedexceptions, which can exceed 1000 mg/100 ml.
Natural disease may mimic or exaggerate the effects of alcohol. Thefollowing non-exhaustive list comprises the most common conditions:
Carbon monoxide poisoning, especially in motor vehicles.
Diabetes: either high or low blood sugar states. The latter, due to excessinsulin-like drugs or loss of a meal, may be the closest mimic of all todrunkenness.
A cerebral vascular defect, such as a ‘stroke’ or incipient vascular catastrophe.
Head injury, often related either to a traffic accident or some assault whereintoxication may be co-existent.
Epilepsy, including the pre- or post-fit state.
Kidney or liver failure and other toxic biochemical states.
Intoxication with drugs other than alcohol, especially narcotics, barbiturates,other hypnotics, antihistamines, etc.
Numerous neurological and psychiatric conditions.
ALCOHOL (METHYL)
A common industrial chemical, which has often given rise to illness and deathwhen drunk either accidentally or deliberately. It is broken down in the bodymuch more slowly than ethanol and can thus accumulate even from amoderate intake.
Some chronic abusers drink methylated spirit, often flavoured with cheapwine (red Biddy, etc) and appear to be less sensitive to its toxic effects.Methylated spirit is duty-exempt ethyl alcohol denatured by the addition ofabout 9% methyl alcohol, together with offensive-tasting substances such asnaphtha, pyridine and a violet dye.
Industrial and surgical spirit consist of ethyl alcohol and about 5% methyl,without the other disgustants.
Pure methyl alcohol has been used as a motor antifreeze and deaths haveoccurred from its drinking, between 60–200 ml being a fatal dose. Lowerblood levels than ethyl alcohol are dangerous or fatal, 80 mg/100 ml being adangerous level. It persists in the blood for several days, being excreted anddestroyed much more slowly than ethanol. The general effects are similar, butit has a specific effect on the optic nerves, causing failure of vision andsometimes permanent blindness. Muscle weakness, cramps, abdominal pains,
Lawyer’s Guide to Forensic Medicine
28

Part II: Amphetamines
depression of breathing and toxic damage to liver and kidneys arecharacteristic.
AMNESIA
Loss of memory, either transient or permanent. An extremely commondefence to criminal actions, obviously over-used in proportion to the amountof true amnesia seen in clinical practice.
Post-concussional (retrograde) amnesia. There is a delay in imprinting sensationsand experiences into the memory. This is a protective mechanism to prevent alater disturbing appreciation of traumatic events, for example, the memory ofbeing hit by a car. Thus after recovery from any concussion due to headinjury, there is a period of amnesia for events prior to the concussion, whichmay vary from a few seconds to a few hours. This is the most common type ofgenuine loss of memory. It may also be seen after electric shock.
Alcoholic amnesia is very common, occurring in between 60–80% of chronicalcoholics, as well as the acutely drunk.
Epilepsy (qv).
Many toxic, infective and drug-induced causes.
Hypoglycaemia. Low blood sugar, either as an inherent state or in uncontrolleddiabetics on insulin.
Failure of registration of sensation as in (a) above, but due to emotion, fear,repression of guilt, hysteria and numerous psychiatric conditions.
Amnesia is not likely to be due to organic causes if it is an isolated instance.
AMPHETAMINES (see also ‘Ecstasy’)
Drugs originally developed to dispel fatigue by stimulating brain activity:later used in obesity to reduce appetite. The side effects and misuse byaddiction led to amphetamine use being abandoned in legitimate medicineand it is no longer prescribed or legally manufactured in Britain. Now a wellknown illicit drug, often known as ‘speed’. Its clandestine manufacture isrelatively simple, as is its even more popular derivative ‘ecstasy’.
Though rarely fatal except in large doses, amphetamine can lead tomarked psychological disturbances. The acute phases of ingestion showrestlessness, insomnia, excitability, impaired judgment and distorted sense oftime. Psychotic states, similar to schizophrenia, may ensue with continued
29

usage and withdrawal may bring depression and suicidal tendencies.A cyclic misuse is common, in which the stimulant effect of amphetamine
is alternated with barbiturates, dependence forming to both substances. Aswell as amphetamine itself, usually in the form of its sulphate, a wide range ofchemicals with similar properties exists, including methylamphetamine,dextro-amphetamine, methyl phenidate, phenylephrine and many others, allof which may be misused.
All these drugs produce a rise in blood pressure, which may induce asudden cardiovascular catastrophe, such as a cerebral haemorrhage. Thoughrarely producing direct fatal poisoning, 30 mg has been reported as causingdeath, though the toleration of addiction may allow several hundredmilligrams per day to be ingested.
ANAESTHETIC DEATHS
Usually a misnomer, as most deaths are associated with an anaesthetic, ratherthan due to it.
Deaths during or soon after surgical procedures may be due to:(a) the disease or injury for which the operation was performed, especially if
the operation was a ‘heroic’ attempt at saving the life;(b) a poor preoperative condition of the patient: usually the operation will
again be an urgent procedure, otherwise it would have been delayed untilthe patient’s condition could be improved;
(c) other concomitant diseases, such as heart or lung complaints, other thanthe condition for which the operation is being performed. Again, thesituation would usually be urgent enough for this risk to be taken, after a‘risk-benefit’ assessment;
(d) some accident or other defect in the surgical technique, rather than ananaesthetic mishap. Such a defect need not be negligent, for example,where anatomical or other complications exist;
(e) a true anaesthetic death is due to the effects of the anaesthetic agent itself –relatively rare – or, more often, to a defect in its administration.
Disease or injury cause the largest proportion of deaths associated withsurgical operations. Surgical mishaps include gross haemorrhage fromslipped ligatures, uncontrolled oozing and damage to blood vessels fromclamps and sharp instruments. Accidental perforation of an organ, removal ofthe wrong organ or part of an organ and air embolism (qv) also contribute tothis group.
Deaths during surgical operations, or other diagnostic procedures
Lawyer’s Guide to Forensic Medicine
30

Part II: Anaesthetic Deaths
requiring an anaesthetic, are customarily referred to the coroner in Englandand Wales if they occur during the anaesthetic or within 24 hours of itsadministration. In Scotland, there is a statutory duty to report ‘anaesthetic’deaths to the Procurator Fiscal, by means of a completed standardquestionnaire.
Other jurisdictions have varying, but broadly similar requirements forcases in which surgical procedures and anaesthetics may have contributed todeath.
It should be noted that the ‘24 hour’ rule in England and Wales is notexclusory, in that any death, however long after a medical or surgicalintervention, where a doctor thinks that the procedure may have contributed,should be reported to the coroner, for example, a pulmonary embolism (qv)two weeks after operation.
True anaesthetic deaths and mishaps vary according to the methodemployed.
Local anaesthesia
This depends upon the deadening of nerves supplying the operation zone bythe injection of a cocaine-like substance or a synthetic homologue. Widelyused in dentistry and minor operations, but increasingly advocated for majorsurgery because of the speed of recovery and lack of complications seen ingeneral anaesthesia. To reduce the spread of the local anaesthetic beyond theoperative zone, a substance such as adrenaline is usually added to constrictthe blood vessels of the area – this may give rise to dangers in itself. Dangersof local anaesthesia include ‘hypersensitivity’ to the drugs, especially if theydiffuse away from the operative area. It is said that most allegedhypersensitivity is really overdosage, but there are undoubtedly cases inwhich an individual idiosyncrasy can give rise to a severe or fatal reaction.
Straight overdosage of the agent or vasoconstrictive additive is probablythe most common hazard: accidental injection into a blood vessel, instead ofinto the tissues or nerve sheath, may also give sudden death or dramaticadverse reactions, usually by poisoning the respiratory centres in the brain orthe heart. Where local anaesthetics are sprayed or injected onto highlyabsorptive surfaces such as the interior of the nose or throat, the suddenabsorption may again give rise to serious or fatal effects.
In essence, the dangers usually consist of sudden over-absorption of eitheran excessive dose or of too rapid absorption of a dose which would have beensafe if spread over a longer period. The overall rate of complications fromlocal anaesthesia is about 1:2000, rarely fatal in nature.
Spinal and epidural anaesthesia
31

A variety of local anaesthesia, where the drug is either injected into the fluidaround the lower spinal cord or into the nerve roots outside the dura, thesheath around the spinal cord (epidural anaesthesia). Either method achievessensory numbing of the lower part of the body; commonly used in childbirth.
The dangers of true spinal anaesthesia are that the agent may diffuseupwards and involve vital centres in the upper part of the cord: it thus cannotbe used for operations above the abdomen. It also paralyses the nervescontrolling blood vessel tension and may lead to dangers from low bloodpressure.
Other dangers exist from contamination of syringes and apparatus bysterilising and cleansing agents such as phenols and detergents, which cancause permanent paraplegia and tetraplegia (paralysis of two or four limbs) oreven death. A number of older litigation cases arising from this cause led tospinal anaesthesia falling into relative disrepute for some years.
To avoid these dangers, epidural anaesthesia was developed, especiallyfor childbirth. The dangers are less but still exist, being mainly that ofpermanent nerve paralysis, the risks of which are calculated to be about 1 inevery 10,000 anaesthetics.
General anaesthesia
The abolition of pain by producing total unconsciousness. Basically acontrolled narcosis which paralyses the upper centres of the brain byadministering substances which reduce the oxygen uptake, for example,barbiturates or nitrous oxide gases. Numerous substances are now used, forexample, halothane, cyclopropane, trichlorethylene, etc.
All anaesthetics have risks but, relative to the millions given each year, thedangers are small and are usually due to factors other than the inherenttoxicity of the actual anaesthetic agent itself. The greatest danger is ‘hypoxia’or ‘anoxia’, that is, a reduction or absence of oxygen supply to the patient dueto negligent administration or equipment failure. This may lead to death orpermanent brain damage, with a vegetable-like survivor.
Such mishaps are usually due to an error in administration or tomalfunction of the equipment, such as a wrongly connected or filled gascylinder, incorrect or blocked tube connections or defective supervision by theanaesthetist.
During anaesthesia, the autonomic nervous system is depressed less thanother parts. This leads to an increased sensitivity to vagal stimuli, which maylead to sudden heart stoppage (see ‘Vagal inhibition’). This is more likely tooccur if there is any degree of oxygen lack. Such stimuli might arise fromerrors in introducing tubes into the air passages, vomit entering the airpassages and other anaesthetic techniques. The detailed discussion of the
Lawyer’s Guide to Forensic Medicine
32

Part II: Aneurysms
many risks is a matter for expert anaesthetic opinion, but the followingparticular hazards must be mentioned.
Halothane anaesthesia, though a widely used and very effective technique, hasacquired a reputation for causing liver damage in a small proportion of cases,especially where several separate anaesthetics using halothane have beenadministered, even widely spaced in time. A number of surveys have beencarried out on its use, but with no constancy of agreement on the risks.
Malignant hyperpyrexia (qv) may also occur after certain anaesthetics andrelaxant agents, including halothane and suxamethonium.
Ether and chloroform, now of historical interest only in most parts of the world,had the dangers of inflammability for the former and liver damage for thelatter.
Cyclopropane is a powerful and useful gas, but again has the dangers of fireand explosion.
A number of anaesthetic agents are directly toxic to the heart muscle and mayprecipitate irregularities and fatal arrest, though these major complications arerare except when administered by inexperienced staff who fail to monitor andanticipate the various permutations of danger signs. A large British survey(Lunn and Mushin) indicated that the majority of deaths was due toinexperience of the anaesthetist and failure to adopt proper precautions whenindicated. It has been calculated that deaths associated with generalanaesthesia comprise about 0.2–0.6% of administrations, but that thoseattributable directly to the anaesthetic procedure rather than other factors areonly between 0.03 and 0.1%.
The autopsy on a death associated with anaesthesia is often unhelpful inproviding positive information, except where death has been due to factorsother than the anaesthetic, for example, surgical complications. Toxicologicalanalysis for residual anaesthetic agents is rarely useful and is difficult tointerpret. The pathologist can usually assist by excluding certain factors, butthe overall investigation of an anaesthetic death depends heavily upon clinicalrecords and a review of the procedure by an experienced anaesthetist.
ANEURYSMS
A swelling on a blood vessel, usually an artery. It arises at a point ofweakness, due to the internal blood pressure distending the vessel wall, muchas a motor inner-tube will swell at one point if overinflated. Beyond athreshold point, the swelling will burst, causing an aneurysmal rupture, oftena fatal event.
33

Lawyer’s Guide to Forensic Medicine
34
Figure 14: Types of arterial aneurysm

Part II: Aorta
Causes
Atheromatous degeneration. The most common variety, most frequently in theaorta (qv). Due to degeneration of the wall from atheroma, athero-sclerosis or‘hardening of the arteries’ – all synonyms for the common fibro-fattybreakdown of the wall. Aneurysms of the aorta may rupture and form a hugehaemorrhage in the back of the abdomen, with often rapidly fatal results. Aslow leak may be repaired surgically, by a synthetic bypass or grafttransplantation.
Dissecting aneurysm. Softening of the central zone of the aortic wall due to‘medio-necrosis’, a degenerative condition. A potential space may form, likethe filling in a sandwich. If blood under high pressure finds it way into thisspace (usually by tearing through a patch of atheroma in the lining) then acleavage plane will open and fill with blood. This may strip the aortic wallfrom pelvis to heart and kill the patient by bursting through into thepericardium (bag around the heart) causing a haemopericardium or cardiactamponade, which rapidly embarrasses the heart’s action by preventing fillingof the chambers.
Syphilitic aneurysm. A complication of tertiary syphilis, now very rare inBritain due to the treating of primary and secondary syphilis. Almost alwaysaffects the arch of the aorta and may produce a large bulge which mayrupture.
Traumatic aneurysm. Due to firearm, explosive or other wounds damaging anarterial wall, often in a limb. Sometimes a false connection is made with anadjacent vein, causing an arterio-venous aneurysm or anastomosis.
Mycotic aneurysm. Due to an infection, usually blood-borne, damaging thewall.
Berry, congenital or cerebral aneurysm (see also ‘Subarachnoid haemorrhage’).This is a small swelling on an artery at the base of the brain on the Circle ofWillis (qv). Rupture is a common cause of sudden headache, collapse anddeath in young and middle-aged adults. Though called ‘congenital’, theaneurysms are not present at birth, but develop as age and blood pressureincrease. They arise at points of weakness in the structure of the wall of brainarteries, usually at junctions. The relationship of exertion, trauma and alcoholin rupture of a berry aneurysm has profound medico-legal connotations.
AORTA
The main artery of the body, leading out of the heart to supply all tissues.Shaped like a round handled walking stick, it begins at the aortic valve at the
35

upper border of the heart, behind the upper part of the breast bone. It curvesbackwards and downwards to run along the front of the spine in the chest,penetrates the diaphragm to enter the back of the abdomen and divides intotwo large branches to the legs, at a level just below the umbilicus.
Medico-legal importance
Stab wounds of the chest may perforate the aorta, leading to rapid deathunless surgical repair is possible. On the right side of the upper part of thebreast bone (sternum), the aorta is very near the surface and here even a smallpenknife can cause a fatal wound. As the pressure in the aorta rises to 120 mm
Lawyer’s Guide to Forensic Medicine
36
Figure 15: Position of aorta

Part II: Arteries
mercury with each heart beat (and over 200 mm mercury in persons withhypertension), any defect in the wall will bleed torrentially and rapidly filleither the sac around the lung (pleural cavity) or the bag around the heart(pericardium), causing a cardiac tamponade. Stab wounds of the chest mayonly bleed internally and several pints may fill the chest cavity without anysignificant amount leaking externally.
Diseased swellings of the aorta, called ‘aneurysms’ (qv) are commoncauses of natural sudden death when they burst.
In traffic accidents, in occupants in motor cars, a severe deceleration injurymay lead to aortic tearing, which is often the cause of death. In such awhiplash, the spine is violently flexed and extended (bent in a forward andbackwards direction) and the aorta may be ripped as it follows this distortion.Another mechanism may be the abrupt traction of the heart on the root of theaorta during violent deceleration. Where the descending aorta joins the spine(at the level of the junction of the curved arch of the aorta with the straightsection) the tethering of the straight part to the spine may lead to transversehorizontal tears in the lining and other layers of the aortic wall. These may bemultiple and appear as rungs of a ladder when viewed from the inside. Thefull thickness of the aortic wall may be torn, in which case the blood underhigh pressure will leak out into the surrounding body cavities, usually thepleural space in the chest.
ARM-LOCK DEATHS
See ‘Neck-hold deaths’.
ARTERIES
Vessels supplying oxygenated blood to the tissues (with the exception of thepulmonary arteries which convey blood from the heart to the lungs and arethin-walled as the pressure is relatively low). Arteries are thick-walled toresist high pressure within, which varies between 70–120 mm mercury in thenormal person (see ‘Blood pressure’).
The arterial wall contains muscle and elastic fibres to accommodatepulsation at every heart beat. The vessels all originate from the aorta (qv) andbranch progressively down to the smallest branches or ‘arterioles’, which aremicroscopic in size, but still retain elastic fibres. From these the finaldistributing branches arise, the capillaries.
In the condition of ‘hypertension’ or high blood pressure, the arterial wallsthicken to resist the increased internal strain.
37

Some arteries, notably the carotids in the neck, have intrinsic nerveendings to detect and measure pressure changes These have great forensicimportance, as external pressure, as in manual strangulation (qv), may causesudden death from heart stoppage.
Tearing or laceration of a large artery causes torrential haemorrhage anddeath if not rapidly staunched. The time of survival depends on the size of theartery, the size and nature of the defect and the age and condition of thevictim. Paradoxically, if an artery is completely transected, the bleeding maybe less than if partly torn, as the severed vessel can retract due to its muscleand elastic tissue, thus reducing or even stopping the rate of blood loss.
ASBESTOSIS
See ‘Pneumoconiosis’.
ASPHYXIA
An unsatisfactory term which has come to mean ‘deprivation of air’, thoughthe literal meaning is ‘absence of pulsation’, which in some ways is oftennearer the truth. More exact modern terms for lack of air (essentially oxygen)are ‘hypoxia’ for partial, and ‘anoxia’ for total deprivation.
In a medico-legal context, true asphyxia refers to mechanical deprivationof air by obstruction of the gas exchange system.
May be due to:(a) lack of oxygen in the surrounding gaseous environment, for example, a closed
room with a gas fire or a ship’s tank that has been sealed for a long period(see ‘Suffocation’);
(b) blockage of the external breathing orifices (see ‘Smothering’);(c) blockage of the internal air passages (see ‘Choking’);(d) pressure on the neck which may block the air passages (see ‘Strangulation’,
‘Throttling’); or(e) fixation of the chest preventing breathing movements (see ‘Traumatic
asphyxia’).
Other causes of asphyxia, not usually involved in forensic issues, are asfollows:
Disease of the lungs, such as extensive pneumonia, industrial lung diseases suchas pneumoconiosis or some infant conditions which prevent gas transferacross the lung membranes.
Lawyer’s Guide to Forensic Medicine
38

Part II: Asphyxia
Chronic heart failure, which fail to shift the oxygen-laden blood around thebody.
Severe anaemias and other blood disorders which cause a deficiency in theoxygen-carrying capacity of the blood.
Some forms of poisoning which either prevent oxygen-carrying by the blood (see‘Carbon monoxide’) or prevent uptake of oxygen by the body cells (forexample, cyanide).
39
Figure 17: Causes of mechanical asphyxia

However, mechanical obstructions provide most medico-legal problems,discussed under the various headings given above. There has been aconsiderable shift of opinion in recent years about the ‘signs of asphyxia’ andthe true role of asphyxia in these conditions. The ‘classic signs’ of asphyxia arenow suspect and in many cases a very critical interpretation must be made, asartefacts and non-specific appearances can easily cloud the issues.
The ‘classical’ signs of asphyxia, both in the living and dead, are outlinedbelow.
Congestion (reddening of skin and tissues) and cyanosis (purplish coloration).This can be due to both blockage of veins preventing blood returning to theheart, as in pressure around the neck, and to depletion of oxygen in the bloodwhich has been prevented from passing through the lungs. However, it issuch a non-specific finding (seen in congestive conditions such as heart failureand very commonly after deaths from many causes) that alone, it is ofnegligible significance. Above a strangulation mark on the neck, it has moresignificance if the rest of the body is pale, but this is due to obstruction ofreturning blood, rather than oxygen lack.
Fluidity of the blood and over-distension of the right side of the heart; these areutterly non-specific signs which may be related to many modes of death andeven to post-mortem changes – of no significance whatsoever.
Petechial haemorrhages (qv). These may occur in the face, eyes and membranouscoverings of heart and especially lungs (where they were formerly known asTardieu’s spots). Many ‘petechiae’ are post-mortem artefacts and manyapparent petechiae are not haemorrhages at all. Even when genuine, they canbe seen in greater or lesser numbers on the lungs in many autopsies and theirsignificance is now very much in doubt, unless numerous and whenassociated with other signs of mechanical asphyxia. Alone, they aremeaningless as an indicator of asphyxia.
Bleeding from nostrils or ears. This is a consequence of raised pressure in theveins of the head after constriction of the neck and is not related to asphyxiaitself.
It will be seen that most of the ‘classical signs’, which veteran US pathologistLester Adelson calls the ‘redundant quintet’, are signs of raised venouspressure from pressure on the neck. The most florid signs occur in ‘traumaticasphyxia’, where venous return is prevented by fixation of chest movements.Most other signs are due to strangulation and the signs are therefore due notto oxygen lack, but to raised pressure in obstructed veins.
Adelson, whose account of the forensic interpretation in his book Pathologyof Homicide (1974, Springfield, Illinois: Charles Thomas), is the best expositionof the subject, admirably summarises thus:
Lawyer’s Guide to Forensic Medicine
40

Part II: Asphyxia
The general signs of asphyxia, either singly or in combination, are merelyconsistent with, though not diagnostic of asphyxia. To establish that deathoccurred from mechanical asphyxia, reliable local indications of lethalobstructing trauma must be demonstrable. In other words, the pathologistmust find unequivocal evidence of the means by which the airway wasobstructed.
The time taken for ‘asphyxia’ to occur is a matter of controversy anduninformed theorising. At least half the cases of strangulation die quicklywith a pale face, due to rapid, even almost instantaneous death from carotidartery pressure (see ‘Strangulation’).
If death is due to ‘pure’ asphyxia, such as an irrespirable atmosphere or aplastic bag over the head, without the added factor of pressure on bloodvessels, then the time factor is a matter of conjecture, as no controls have beenmeasured in the human for obvious reasons.
41
Figure 16: Classical features in strangulation

To attain the signs of venous obstruction described above, probably aminimum of 15–30 seconds unremitting pressure is necessary. This willproduce congestion, blueness and small haemorrhages in the eyes. Pureblockage of the windpipe or larynx is hardly possible without pressure onblood vessels, so ‘pure’ asphyxia from neck pressure is not seen. As breath canbe held for several minutes, death could not occur from pure asphyxial neckpressure for at least a minute, but this is of little practical moment instrangulation, because of the co-existence of the other factors which canprecipitate death at any time from zero seconds to the full blown asphyxialpicture of congestion and bleeding.
In suffocation and choking, where external pressure is not a factor, thenpure asphyxia can occur, but again they produce a very variable time scale.Many sudden obstructions of the air passages cause instant death fromcardiac arrest (for example, café coronary (qv)), as can obstruction of the facewith plastic bags. At the other end of the spectrum, survival from completeobstruction has occurred after three, four or even more minutes, where reliefhas been forthcoming.
Thus it is impossible to be dogmatic about the length of time required toproduce an asphyxial death, a matter often led in criminal trials where thedetermination of an assailant may be an important issue in the prosecution ordefence. All that is safe to say in medical evidence is that where signs ofpressure on the neck or obstruction of the air passages are present, then:(a) if the face is pale and there are no small haemorrhages in the eyes or skin,
death must have been very rapid due to cardiac arrest;(b) if congestive/asphyxial signs are present, then obstruction or pressure
must have been maintained for at least a quarter of a minute. This estimateis arbitrary, but is a reasonable minimum time.
ASPIRIN POISONING
Acetyl-salicylic acid is one of the oldest and most widely used analgesics (painrelievers). Though generally very safe, it is toxic in large amounts and somepersons have an idiosyncratic sensitivity to normal doses (varying from a rashto sudden death).
Recent research has shown that aspirin has a mild tranquillising effect aswell as analgesic: it also has the effect of reducing blood-clotting ability, whichmay lead to dangerous bleeding from stomach ulcers or even from an intactstomach.
Forensically, aspirin was formerly a common suicidal agent in Britain butfatalities are now rarely seen. It is still used as a suicidal gesture method,especially in teenage girls. It also causes accidental poisoning in children.
Lawyer’s Guide to Forensic Medicine
42

Part II: Autopsy
The medicinal dose in adults is 1–2 tablets of 300 mg each, but far largerdoses are given for rheumatic and arthritic conditions. The lethal dose variesenormously and some persons who swallow a whole bottle of 100 tablets (30gm) may suffer no more than ringing in the ears. However, this dose mayoften be fatal, though nausea and vomiting may be self-protective byremoving the substance from the stomach.
Deaths in children have been reported after only a few tablets. The clinicalsymptoms of aspirin toxicity include nausea, tinnitus (ear ringing), sweating,confusion and shock. The breathing may first be stimulated, then depressed.Bleeding from the stomach or bowel may occur. Severe acidosis of the blood,which might mimic diabetic acidosis, can develop.
The blood level of toxic doses is also variable, but above 50–90 mg/100 mlthe danger of death exists, though patients on long term salicylate treatmentmay tolerate similar levels without ill effect. A particular danger of aspirinoverdosage is delayed death. A person may present at hospital with minimalsymptoms, such as tinnitus, and be discharged from casualty afterexamination, only to die at home during the next few hours or even a daylater. This has been cause for negligence allegations against doctors, and allcases of undoubted aspirin overdosage should be admitted for overnightobservation.
Autopsy appearances may reveal gastric irritation and perhaps signs ofbleeding in the stomach lining. Other organs and serous membranes may alsohave haemorrhagic manifestations, but nothing specific may be found inexamination, the diagnosis resting upon the history and analyses of bodyfluids.
AUTOPSY
Now the most common name for a full post-mortem examination by apathologist. The latter term is still very frequent in Britain, but elsewhere isnot synonymous with an autopsy, as it may mean merely an external scrutinyof a body.
‘Autopsy’ strictly means ‘seeing for oneself’. A better term is ‘necropsy’, anexamination of the dead, a word gaining acceptance, especially in America.
An autopsy is performed to achieve one or more of the followingobjectives:(a) to determine the cause of death;(b) to determine the nature and extent of disease;(c) to record and describe any injuries and to offer an interpretation as to their
mode of infliction;(d) to estimate the time since death;
43

(e) to assist in identifying the deceased where this is in doubt;(f) to estimate the expectation of life in certain cases where injuries have
prematurely terminated life;(g) in the new-born, to determine whether live birth occurred; and(h) to obtain samples and fluids for analysis and other ancillary investigations.
The law concerning permission for autopsy varies widely in differentjurisdictions, but basically there are two types: clinical or medico-legal.
The clinical autopsy is to investigate the extent of disease and theeffectiveness of treatment and often to utilise the results in medical audit orresearch. This type of autopsy almost invariably requires some form ofconsent, either ante mortem from the deceased or post-mortem from therelatives (see ‘Human Tissue Act 1961’).
The medico-legal or forensic autopsy is at the behest of law enforcementauthorities where the cause of death is unnatural, suspicious or unknown.Here, permission is not required in most jurisdictions, the autopsy beingordered by legal authority. In England and Wales, this authority is containedin the various Coroner’s Acts and Rules (qv).
Lawyer’s Guide to Forensic Medicine
44

Part II: Bestiality
BARBITURATES
A group of hypnotic drugs used to induce sleep or sometimes anaesthesia, orto sedate and quieten agitated or epileptic patients. Formerly prescribed invast quantities as ‘sleeping pills’, but active restraints by doctors and saferalternatives have made their legitimate prescribing rare in Britain, althoughthey are easily available on the illicit market.
There are four types of barbiturate (see below), related to their speed ofaction: all are derivatives of barbitone or barbituric acid.
Long acting, such as barbitone or phenobarbitone. Therapeutic dose ofphenobarbitone is about 50–100 mg, fatal dose upwards of 1–4 g, but withgreat variation. Blood levels in coma and death are of the order of 5–8 mg/100ml.
Intermediate acting, such as amylobarbitone, butobarbitone and allobarbitone.Therapeutic dose 50–200 mg, dangerous dose around 1–2 g. Blood levels infatal or comatose cases between 2–5 mg/100 ml.
Short acting, such as pentobarbitone and cyclobarbitone. Therapeutic dosesbetween 200–400 mg, dangerous dose about 1 g. Blood levels in coma about1 mg/100 ml.
Ultra short acting drugs given as intravenous injection for induction of generalanaesthesia or short anaesthetics for dental and minor operations. Examplesare thiopentone (Pentothal) and methohexobarbitone.
The short acting barbiturates, such as cyclobarbitone and quinalbarbitone,may cause death from heart failure (ventricular fibrillation) within 20 minutesin large doses. Other drugs cause extended coma which may result in deathfrom respiratory depression. In long coma, bronchopneumonia may be themode of death: blisters on the skin are sometimes seen (see ‘Blisters’).
BESTIALITY
Sexual connection with animals. In English law, it is an offence under theSexual Offences Act 1956 and can be committed by either man or woman, ifintercourse per vaginam occurs.
In Scotland, this is a common law crime and appears to be applicable onlyto men.
Medical aspects are similar to those relevant in rape, but modified byphysical disparity depending upon the size of the animals concerned. Forensicscience evidence is more important than medical aspects; it is concerned withthe detection of human and animal semen and blood, species differentiation of
45

animal blood, semen, hairs, faeces, etc. Both serological and microscopictesting used, especially DNA.
BITE MARKS
Present on the skin in some cases of assault, especially sexual and in childabuse.
In sexual assaults, there may be actual bites or less severe ‘love bites’, thelatter often taking the form of multiple suction marks (a shower of small pin-head haemorrhages sometimes in the shape of pursed lips). Actual bites maybe deep and sometimes sadistic. Common sites are the side of the neck andthe breasts. Nipples may be injured or even bitten off.
The teeth in any bites may cause bruising, abrasion or lacerationsdepending upon the force used. Bites may occasionally be inflicted on thethighs, abdomen, buttocks or vulva and where more severe than mere sexualenthusiasm, indicate a sadistic element. Increasingly, they are being seen insporting injuries, especially to ears in rugby matches. Occasionally, policeofficers are bitten during attempted arrests.
Bites are not infrequently seen in battered child syndrome, usuallyinflicted by the mother. They may be on any part of the body, but especiallyarm, leg, buttock or cheek. Usually not as severe as in sexual cases, but mayleave a clear imprint of the teeth.
In any bite mark, observation and measurement may match up with thedentition of the assailant or exclude alleged assailants. In child abusesyndrome, the excuse is sometimes made that the bite was due to a pet dog oranother child of the family. The pattern of the bite can be compared with thespacing and shape of the suspect’s teeth.
Photography of the bite is essential before it fades, as it is to have anexamination performed by a dentist skilled in forensic work (a forensicodontologist). Casts (rubber or PVC, etc) can be made of marks if stillpalpable. Also swabs of the area may reveal the DNA pattern of the assailantfrom the saliva.
Occasionally, bite marks may have a forensic aspect if left in objects at thescene of a crime, for example, in cheese, apples, chewing gum, etc, whichagain may help to identify the culprit.
Lawyer’s Guide to Forensic Medicine
46

Part II: Black Eye
BLACK EYE
Bruising in the loose tissues of the upper and/or lower eyelids, medicallytermed a ‘peri-orbital haematoma’.
Most often due to a direct blow in the eye, frequently from a fist. Unlikelyto occur from a fall onto a flat surface, as the arch of the eyebrow, cheek boneand nose protect the eye itself. However, if there are abrasions, bruises orlacerations on these surrounding areas, it is possible that a black eye can occurfrom impact, including a fall, with an object larger than a fist.
Fist blows causing a black eye frequently also damage the skin over theupper edge of the cheek bone, the nose (especially the bridge, which may befractured) and the eyebrow, which may be split.
As well as bruising in the lids, there may be marked swelling of thetissues, which can close the eye. This does not appear immediately, as can thebruising, but may take minutes or hours to develop. The bruising mayincrease over hours, but some is always apparent immediately after injury.
47
Figure 18: Production of black eye

Though a black eye usually heals completely, there can be internal damageto the eye, such as a detached retina or dislocated lens or haemorrhages intothe vitreous. These are more common in children, as part of child abusesyndrome (qv).
A kick in the eye region can obviously cause a black eye, but there isusually more surrounding damage than from a fist blow, such as laceration ofthe cheek and eyebrow and perhaps fractures of the facial skeleton.
A black eye can occur from causes other than a direct blow in the eye:(a) A bruise or laceration of the forehead or scalp above the eye may allow
blood to track downwards under the scalp. It flows by gravity over theeyebrow ridge and can then accumulate in the loose tissues of the eyelids.This process takes hours or a day or more to complete.
(b) A severe head injury, especially a fall onto the back of the head, may causea fracture of the front of the base of the skull (see ‘Contre-coup’). Blood canthen leak down into the interior of the eye sockets from damaged brainmembranes and appear in the white of the eye and the eyelids, causingblackening and often swelling of the lids. In such cases, the victim isusually unconscious.
A black eye, from whatever cause, will undergo the usual colour changes ofany bruise. When fresh, it is dark red to purple and may increase in intensityin the first day or so as more blood accumulates – the bruise ‘coming out’. Infatal cases, in common with bruises elsewhere, it may appear more markedone or more days after death.
In life, the speed of colour changes depends on the original intensity andindividual variations, but a green-brown colour may be expected in two tothree days, passing through paler green and yellow during the next week orso until fading occurs. The rate of these changes is very variable and ismarkedly slowed in old people (see ‘Bruises’).
BLADDER
The urinary bladder, in the lower abdomen, behind the pelvic bone, is aroughly spherical organ which can enlarge to many times its empty size byvirtue of its elastic, muscular wall. Normally protected behind the pubis, a fullbladder can rise to the level of the umbilicus and be vulnerable to rupturefrom blows or kicks on the abdomen.
Two tubes enter the back of the bladder, the ureters, bringing urine fromthe kidneys. One tube leaves the bladder, the urethra, conveying urine to theoutside. In the male this may become sheared or ruptured by severe pelvicinjury, either pelvic fractures or kicks in the genitals.
Lawyer’s Guide to Forensic Medicine
48

49
Part II: Blisters
BLISTERS
Dome-shaped swellings on the skin, formed in the thickness of the epidermis,the outer layer. They contain fluid, but may be collapsed and empty eitherduring life or after death. Blisters may be formed ante or post-mortem.
Main types of forensic interest
Burns. Blisters of any size may occur in medium-severity burns. Less severeburns do not blister, more severe destroy the skin. Burn blisters may occurbefore or after death and it is often difficult or impossible to differentiatebetween them if they occur peri-mortally (at the time of death). This hasimportant forensic importance, related to the possibility of a dead body beingdisposed of in a fire. Classical differentiation is said to be (a) a red margin toliving blister, and (b) fluid containing high concentration of protein if formedduring life. In practice, these points may be of little help if death occurredsoon after burning.
Electricity. A firm contact electrical mark is usually in the form of a blister, dueto the heating effect of the current passing through the high resistance of theskin at the entry point. There is usually no fluid in the blister, which collapses.Often a pale surrounding halo, due to blood vessels constricted by the shock.Microscopic examination of the edge of the blister may show alignment orpolarisation of the nuclei of the skin cells, celled ‘streaming’ due to thepassage of electricity, but this may also be seen in purely thermal burns.
Post-mortem decomposition causes blisters in the moist stage of putrefaction.Large areas of skin may rise and become filled with clear bloody fluid. Whenthese burst, there is ‘skin slippage’ of sheets of outer skin layers. The times atwhich this occurs is variable, but in average temperate conditions is from oneweek onwards after death.
‘Barbiturate’ blisters are a misnomer for those seen in any case of coma. Thecause is obscure, but is due partly to gravitational accumulation of fluid dueto immobility and partly due to oxygen lack in the skin. As well as drugsinducing long coma, like barbiturates, they may be seen in carbon monoxidepoisoning, natural cerebral haemorrhage, etc. Often seen on dependent partssuch as buttocks, thighs, calves, loins.
Many diseases give rise to blisters, usually from infections, for example,smallpox, chicken-pox, etc. Also in skin diseases, such as pemphigus. Thefluid from contagious diseases is often highly infectious.

Lawyer’s Guide to Forensic Medicine
50
BLOOD GROUPS
The forensic use of blood groups and other constituents of blood (especiallyDNA) fall into two sections: (a) the identification and comparison of bloodstains on clothing, weapons, etc; and (b) the investigation of disputedpaternity issues.
These topics (together with a few less common uses, such as theidentification of parts of fragmented bodies or the separation of new-borninfants whose identity is confused in maternity hospitals) constitute thescience of ‘forensic serology’, which has now grown to such complexity that itis a discipline in its own right, similar to forensic dentistry or forensictoxicology. The expertise and technology necessary for the properinvestigation of legal issues in which serology is involved must come fromspecialists in the field.
Such expertise is provided in Britain by the Home Office Forensic ScienceLaboratory Service; several academic departments of forensic medicine andsome private laboratories have expert serologists.
The advent of DNA technology in the late 1980s has made blood groupand many other blood constituent tests, such as enzymes, largely redundant.
BLOOD PRESSURE
The contractions of the heart produce a head of pressure in the arteries whichis necessary to maintain the flow of blood to the small arterioles and hence tothe tissues via the final capillary bed, the blood returning to the heart throughthe veins.
This pressure is produced by the left ventricle as it contracts during‘systole’, the relaxed phase being called ‘diastole’. The aortic valve betweenthe left ventricle and the aorta (the main blood vessel leaving the heart)ensures that blood does not fall back into the heart during diastole. However,the pressure in the aorta is greater during systole as the blood jet is thrownout, than in diastole when the pressure is static at the valve. There is thereforea range of blood pressure between ‘diastolic’ end ‘systolic’. This leads to apulsation synchronous with the heart beat, the pulse at the wrist or neck beingdue to the pressure difference arriving in rhythmic waves from the heart. Thenormal diastolic pressure is about 70 mm of mercury and the systolic about120 mm of mercury; these are often written as ‘mm Hg’ or, in differentmodern units, as ‘kilopascals’. The normal range varies, but is usuallybetween 110/70 and 140/80 mm/Hg. The two pressures are conventionallywritten as ‘systolic over diastolic’.

Part II: Blood Splashes
Anything significantly higher than the upper limit of these values isabnormal, being termed ‘high blood pressure’ or ‘hypertension’. Grosshypertension may reach 240/130 or even more.
The dangers of hypertension are numerous: physical rupture of an arterymay lead to ‘strokes’ (cerebral haemorrhage), nose bleeds or eye damage:formation and rupture of aneurysms, kidney failure, heart failure due toinability of the heart to maintain the extra work and an increased risk ofcoronary artery disease.
A low blood pressure is usually the result of some acute injury or illness,such as blood loss, shock, etc. If below 80/50 there is danger of death fromfailure of perfusion of the tissues, especially heart, kidney and brain.Chronically low blood pressure may be seen in debilitating diseases andadrenal failure (Addison’s disease). Acute low blood pressure needs urgenttreatment with drugs and/or transfusion of blood or fluids.
BLOOD SPLASHES
When free blood flies through the air, the shape of the resulting splash canindicate the direction and hence the original position of the weapon or victimand sometimes the minimum number of blows.
51
Figure 19: Direction of blood splashes

Lawyer’s Guide to Forensic Medicine
52
A blood drop in the air is spherical, but on impact releases a small globule,so that on hitting a surface tangentially, a splash resembling a printedexclamation mark will be formed, with the dot in the leading position. Themore glancing the impact, the longer will be the stem of the mark. Conversely,a splash hitting perpendicularly will be circular.
In most cases, such blood splashes will have been thrown off from aweapon which is carrying blood from a wound which has bled profusely,especially the scalp. Usually, the first blow will not carry much blood, as thereis often a momentary delay in the escape of blood from ruptured vessels,unless the vessel is a large one. In repeated violence with a weapon,subsequent blows will pick up blood, which will then be flung off on theupswing. This may travel a number of feet, to strike walls, ceiling or furniture,etc, and give a pattern which can indicate the direction. Though there is aconsiderable and variable scatter from each swing, the general direction canbe assessed and any marked variation attributed to a change of direction orpoint of origin. Over-interpretation must be avoided as, although generalpatterns are useful, each shower contains spots with a wide variety oftrajectories. Bleeding directly from a blood vessel rarely leaves such spots;only arterial blood gushes with any force and this tends to be a jet rather thana shower. Even a large artery will not gush more than a couple of feet from thebody. Veins and capillaries only ooze and the blood is never projected fromthe body, other than by gravitational fall.
BRAIN DEATH
With the advent of modern medical techniques, the brain may die, that is,irreversibly cease functioning, without the inevitable cessation of other vitalfunctions of heart and breathing, which can be artificially supported.
This state of brain death is taken in many jurisdictions to be synonymouswith the death of the individual. In Britain, no statutory definition of deathexists, the decision of the medical attendants being sufficient, whatevercriteria they use. There is an increasing tendency to certify the time of death asthat when brain death is unmistakably present. The matter is currently ofgreat importance, because of the ability to maintain brain-dead patients forlong periods on artificial ventilation and circulation; and also because of theneed to declare death before organs are taken for transplantation.
The brain may die in stages, the higher functions of sentient thought andconsciousness being more vulnerable than the basic functions of breathingand heart control. The higher functions are carried out by the cerebral cortexin the upper areas of the brain, whilst the more basic functions are situated inthe brain stem and upper spinal cord.

Part II: Brain Death
Brain death may be due to the following:
Severe head injury with direct trauma to the brain.
Swelling of the brain (cerebral oedema) following trauma (which includessurgical operation).
Intoxication by a wide range of drugs, such as barbiturates and otherdepressants.
Deprivation of the blood supply to the brain, either by disease or injury to themain arteries in the neck or by failure of the blood pressure for more than aminimum of three minutes, as in a treated cardiac arrest.
Deprivation of the oxygen content of the blood, even if the circulation ismaintained, may lead to brain ‘anoxia’ or ‘hypoxia’, a mishap sometimesoccurring during anaesthesia or by events such as mechanical obstruction tobreathing, as in crowd disasters such as at Hillsborough.
Brain swelling is a common sequel to head injuries, even if there is no fractureof the skull or laceration of the brain. It may lead to brain death because a risein intracranial pressure may exceed the supplying blood pressure and thusprevent blood from circulating through the brain.
If the brain stem survives and the cerebral cortex dies, there will bepermanent coma, but spontaneous breathing may persist and life maycontinue indefinitely (‘persistent vegetative state’ – PVS) as in cases such asKaren Quinlan and the Hillsborough victim Tony Bland which had suchprofound medico-legal consequences; in both these cases, court orders wereobtained to allow discontinuation of nourishment to allow death to take place.
Death may eventually supervene due to feeding difficulties, emaciationand infections such as bronchopneumonia. If the brain stem fails, thenbreathing will cease and conventional death will rapidly follow unlessartificial ventilation by machine is instituted. It is this situation which posessuch difficulties in the ethical and legal sphere, both from the definition ofdeath and the moral consequences of maintaining a vegetative patient todistress relatives and the monopolisation of scarce and expensive medicalresources.
A Code of Practice (The Removal of Cadaveric Organs for Transplantation,1979, London: DHSS) has consolidated and clarified the previous clinicalcriteria for diagnosing brain death. These are based on the recommendationsof the 1976 Conference of Royal Colleges and Faculties of the UnitedKingdom:(a) the patient is deeply comatose, this not being due to drugs, hypothermia
or metabolic disturbance;(b) the patient is being maintained on a ventilator because spontaneous
respiration had become inadequate or had ceased altogether (relaxant orother drugs having been excluded as a cause);
53

(c) there should be no doubt that the condition is irreversible and thediagnosed cause has been fully established. Diagnostic tests for braindeath include:• all brain stem reflexes are absent (fixed pupils, no corneal reflex, no
vestibulo-occular reflexes, no gag reflex, etc);• no respiratory movements occur when the patient is disconnected
from the ventilator, after ensuring that the arterial carbon dioxidetension rises above the threshold for stimulation of breathing;
(d) testing should be repeated. The interval between tests varies according tothe definitions of previous criteria, but may be as long as 24 hours.
(See also ‘Transplantation of organs and tissues’.)
BRUISES
Otherwise known as ‘contusions’, bruises are injuries characterised by leakageof blood from blood vessels under an intact skin. They are often associatedwith the two other types of wound, the abrasion and the laceration. Thecolour of a fresh bruise depends on the amount of blood extravasated fromthe vessels and the depth at which this occurs, as well as upon anypigmentation of the overlying skin. However, they are commonly reddishblue when fresh but varying from a deep purple-blue (almost black in someinstances) to a pinkish red.
A deep bruise does not reproduce the shape of the injuring object asfaithfully as the surface abrasion, due to the padding effect of the overlyingskin, but sometimes such a pattern may be discernible, such as the radiatorgrille of a vehicle.
Some bruises are in the uppermost layer of the skin immediately under theepidermis and are then called ‘intradermal’. These are often confused withabrasions, but there is no grazing of the outer dead layer of skin cells. Suchintradermal bruises may faithfully reproduce the pattern of the impactingobject, such as the tread of a shoe or the weave of a coarse cloth.
Small discoid bruises, about half an inch in diameter (sometimes called‘sixpenny’ bruises), are typical of finger-tip pressure, especially when multipleand sometimes side by side. These are commonly seen from gripping of thesoft upper arm by an assailant and also in child abuse syndrome.
Bruises may not always appear exactly at the site of impact of the injuringobject, due to tissue planes diverting the blood. Bruising may be delayed up tosome hours after injury (the bruise ‘coming out’), as the blood may have tofilter up from deeper layers or dense tissue planes.
Lawyer’s Guide to Forensic Medicine
54
Part II: Bruises
The intensity of the bruise is generally comparable to the amount of force,except in certain lax areas such as the eyelids – or where there is a propensityto easy bleeding, such as some haemorrhagic diseases or senile states. Oldpeople bruise so easily that the term ‘spontaneous bruising’ is sometimesused, though there must always be some minimal amount of trauma.Children also bruise easily, due to the softness of their tissues and thetransparency of their skin.
Bruising cannot occur where dense tissues surround the blood vesselssuch as the palm of the hand and sole of the foot. Visible bruising is lessapparent in the scalp (partly due to the presence of hair) unless associatedwith lacerations and abrasions, though deep bruising is commonly seen underthe fibrous sheet (aponeurosis) beneath the scalp.
Lax tissues such as the eyelids bruise very easily (see ‘Black eye’).Estimating the age of a bruise is fraught with inaccuracies, but a sequence
of colour changes can be recognised. The initial purplish red becomes brownin one to three days, then successively develops through greenish brown,greenish yellow, yellowish brown, tan and yellow before vanishing.Photographic studies have claimed that if a greenish hue is visible, the bruisemust be at least 18 hours since infliction, but there is great variation in thesequence and timing of colour changes. The colour changes vary from theedge to the centre of a substantial bruise, being more advanced at the margins,a large bruise showing several colours simultaneously.
All but the most florid of these colours may be obscured by racialpigmentation. The above colour changes proceed over a very variable timescale and no accurate calendar can be prepared for dating.
Children and young adults heal their bruises far more quickly than theaged, who may retain their bruises almost permanently.
Complete resolution of a large bruise may take up to three weeks. Ayellowish green bruise must have been inflicted at least several days earlier,but no justifiable opinion can be offered to date bruises in a succession ofnumbered days.
Microscopic examination may assist only slightly in dating bruises, asthere is great variation in the date at which the healing process develops,initiated by the appearance of white blood cells, usually many minutes oreven hours after infliction. Special stains to reveal iron pigment(haemosiderin) derived from red blood cells can be used – a positive findingof iron granules indicates that the bleeding took place at least 36 hours earlier,as long as the victim survived that long.
Where a number of bruises of the same order of size are present on thesame victim, then significant differences in colour indicate that they wereinflicted at times separated by at least a few days, even if no absolute datingcan be given. This lack of simultaneous production is important in child abusesyndrome, where continued violence may have been taking place.
55

A bruise may shift after infliction under the influence of gravity. A bruiseon the forehead may slide down and pass over the eyebrow ridge to appear inthe eyelids as a black eye, and bleeding from a fractured hip can sink to thelower thigh.
Bruises cannot be inflicted after death, but considerable violence maycause a mark in the tissues, such as crushed muscle and an abrasion, which isunlikely to be mistaken for a true bruise.
Bruises formed at or near the time of death cannot be firmly differentiatedinto ante mortem and post-mortem injuries. Though blood pressure falls tozero when the heart stops, thus removing most of the cause of leakage ofblood from vessels, there may be some passive movement of blood fromarteries into veins for about 20 minutes after death, due to arterial contraction,and this might allow some slight bruising to occur even after the heart ceasesto beat, though the injury will almost always have been suffered before theheart stops.
Bruises usually appear much more prominent as the post-mortem intervalincreases. Bruises seen soon after death may appear much darker and largersome hours later and even worse in a day or two. Other bruises too feeble tobe seen immediately after death may appear next day and this may causesome discrepancies between an initial prosecution autopsy and a subsequentexamination carried out for the defence at a later date.
The explanation is that the skin becomes paler in most areas as blood sinksto the back under gravity, causing greater contrast between the bruise and theskin; also a bruise may diffuse from deeper layers towards the surface as thehaemoglobin leaks from the red blood cells.
BURIAL
Now the least common method of disposal of the dead, compared withcremation.
After the issue of either a medical certificate of the cause of death by adoctor or a coroner’s certificate, the death is registered by the Registrar ofBirths and Deaths. He issues a certificate of disposal which allows the funeraldirector and cemetery authorities to bury the body.
After burial, the speed of decomposition varies greatly according to theenvironment of the grave, the season and the initial condition of the body.However, the rate of decay is greatly reduced compared to a body left on thesurface. Animal predators are reduced (rodents, fly maggots, etc). In aconventional coffined burial, the rate of decomposition is much slower than ashallow clandestine internment. Factors such as brick-lined grave or vault, dryconditions, non-acid soil, lack of flooding, all retard decay. In a wet grave,
Lawyer’s Guide to Forensic Medicine
56

Part II: Burns
57
especially in acid-peaty soil with a variable water table, the body may vanish(even bones) within 10–20 years. In dry, sandy conditions, good preservationmay be seen after centuries. Some wet graves may produce adipocereformation (qv) which may also preserve the body for many years. The valueof exhumation (qv) is very variable and unpredictable due to these inconstantfactors, and no accurate forecast can be made of the condition of the body –thus where the indications for exhumation exist, it is always a worthwhileprocedure.
BURNS
Injury due to a variety of physical agents, including dry and moist heatcorrosive substances, ultra-violet light, X-ray and other radiations andelectricity. Usual cause is heat, most often dry. This can lead to burns ofvarying severity, now classified in three grades after Hebas, each of whichincorporates a pair of the six grades of the older classification of Dupuytren.
Grade 1. Burns which heal leaving no skin scar because the full thickness of theepidermis is not killed. Reddening (erythema), swelling and blistering are thehallmarks.
Grade 2. Where full-thickness destruction of skin will lead to scar formationafter healing. When fresh, these burns may show shrivelled, coagulated skinsurrounded by areas of first degree burns.
Grade 3. Severe destruction of skin and underlying tissues such as muscle andeven bone. There may be charring of these tissues. Some classifications ofburns incorporate Grade 3 into Grade 2, using epidermal damage as the solecriterion.
The grades are not necessarily related to danger to life, which is more afunction of the area involved. Where more than half the body surface isinvolved, even in superficial first degree burns, recovery is unlikely, except inchildren, who may survive 60%. In old people, 20% or even 10% surface burnsmay be fatal. Conversely, charring of a limb may be compatible with recovery,if the initial severe shock stages are survived.
In calculating the approximate area involved, the ‘rule of nine’ is oftenused, designating each part of the limbs and trunk as multiples of 9% of thetotal surface (see Figure 20).
Medico-legal aspects of fatal burns
Were the burns sustained before or after death? The possibility of disposal of ahomicide by burning must always be considered.

Lawyer’s Guide to Forensic Medicine
58
Burns seen at autopsy may be ante mortem, post-mortem or both. Burnssustained during life show a ‘vital reaction’ (qv) in that the margins of theburns are reddened and may be blistered. However, where death hassupervened rapidly (that is, the burns are ‘peri-mortal’) this sign is absent. Atleast several minutes’ survival are required for unequivocal vital signs toappear. Where ante mortem blisters are present, it is said that the containedfluid is rich in protein, but that post-mortem blisters contain watery fluid orgas. However, in practice, this method of differentiation is seldom possible orhelpful. Microscopic examination for signs of early vital reaction in equivocalcases is less useful than standard textbooks suggest (see ‘Vital reaction’).
Other significant factors
Apart from the burns, other factors are significant:
Smoke. In most fires, smoke is produced and is inhaled by the living victim.Soot particles are then present in the throat, larynx and air passages, oftendeep in the lungs. Though passive deposition after death may occur via theopen mouth, the presence of soot below the larynx is indicative of breathinghaving been present during the fire. Similarly, soot particles may be present inthe gullet and stomach through swallowing. Rapid flash fires, especiallypetrol fires in vehicles and aircraft, may not always produce smoke nor carbonmonoxide (see below) and death may also be too rapid to allow absorption.Where flames and hot gases are inhaled, the air passages may be burnedinternally.
Carbon monoxide. Most fires, especially house fires with smouldering fabricsand woodwork, produce large quantities of carbon monoxide (qv). This canonly enter the body via breathing and not through the skin, so any raisedblood level (above the few per cent seen in smokers and city dwellers)indicates that life was present during the fire. Most victims of house fires havean appreciable level of carbon monoxide in the blood, for example, 20–50%saturation, and this is frequently the cause of death or at leastunconsciousness, before the fire reaches the victim. It is important to note thatthe presence of soot and carbon monoxide confirms life during the fire, butthat the converse is not necessarily true. The absence of these signs does notindicate that the person was dead, though the general rule is most helpful.
Heat injuries. A body recovered from a conflagration often shows certaininjuries which might arouse suspicion. Second or third degree burns cause‘heat contractures’, where the limbs are flexed into the so called ‘pugilisticattitude’, due to the shortening of the flexor muscles more than the extensors.In addition, shrinkage of the skin may cause extensive splits, especially overlarge joints such as elbow, knee and shoulder, often precipitated bymovements during recovery by firemen, but also spontaneously. These mayresemble wounds, but there is no bleeding and structures such as vessels and

Part II: Burns
59
Figure 20: ‘Rule of nine’ for estimating area of burns

fibres survive in the depths of the splits, which show no vital reaction. Theymay occur on the scalp, where they may look even more suspicious, especiallyif associated with a ‘heat haematoma’ inside the skull. This heat haematoma isa collection of blood, often considerable in amount, which develops betweenthe inside of the skull and the outermost brain membrane, the dura. It is seenwhere direct heat has impinged on the outside of the head, but the appearancecan be confused with a true extradural haematoma (qv), which is always dueto mechanical trauma to the head. The blood in a heat haematoma is frothyand chocolate coloured and is due to boiling out of blood from vessels in themembranes and skull, though the precise mechanism is unclear. It has givenrise to a number of instances of spurious allegations of homicide concealed byfire.
Causes of death in bodies recovered from fires
Natural causes. Strokes and heart attacks may have preceded the fire and oftencaused it, for example, when an old person collapses in the act of lighting afire or gas stove.
Pre-conflagration injuries. Homicidal, suicidal or accidental.
Injuries caused during the fire. Falling masonry and roof beams.
Carbon monoxide poisoning, asphyxia from oxygen lack, and other irrespirable gasessuch as carbon dioxide.
Poisoning from toxic fumes. Recent research has shown that burning plasticsfrom upholstery and fittings can produce very noxious gases such as cyanide,phosgene and nitrous compounds.
In death from burns, the immediate cause may be:(a) tissue destruction and/or severe primary shock, pain, etc;(b) delayed shock and loss of fluid from large areas of burns;(c) biochemical disturbances from electrolyte disorders in large areas of
burning;(d) kidney failure (delayed several days) due to tissue damage and ‘acute
tubular nephrosis’;(e) infection and toxaemia from septic burns;(f) pneumonias, especially after inhalation of flames or hot gas which may
also cause rapid death from pulmonary oedema (waterlogging of thelungs); and
(g) gastro-intestinal lesions, such as bleeding or perforation from acuteulceration of the stomach or rarely duodenum (the so called, butuncommon, Curling’s ulcer). These are manifestations of stress caused bythe burning, similar to adrenal haemorrhage.
Lawyer’s Guide to Forensic Medicine
60

Part II: Cannabis
61
‘CAFÉ CORONARY’
A colloquial medical term, coined after a series of deaths described in theUSA, where supposed coronary deaths were shown to be due to blockage ofthe throat by recently ingested food, before it has been swallowed into thestomach.
The original series mostly involved men in restaurants, who sat back intheir chairs dead whilst eating a meal. Autopsy revealed that the most likelydiagnosis of heart attack was incorrect, there being a mass of freshly eatenfood impacted in the larynx (the voice box). The deaths were not classicallyasphyxial, being rapid and usually silent, with no marked congestion of theface or other supposedly classical signs of asphyxia (see ‘Air passageobstruction’).
Deaths from impaction of a bolus of unswallowed food must bedistinguished from inhalation or aspiration of vomit, which is theregurgitation of stomach contents, already completely swallowed. Death fromthis latter event is much less common than death statistics allege, as it is afrequent agonal and even post-mortem event.
True ‘café coronaries’ are more common than previously thought andfrequently take place in old people’s homes and mental institutions, wheresenile or demented persons bolt their food rapidly, without chewing. It is alsoseen in mentally deficient children in institutions and in victims ofneurological disability, such as motor neurone disease and head injuries.
The rapid and often undramatic mode of death appears due to suddencardiac arrest, due to the sudden impaction of food in the sensitive larynx,rather than to frank obstruction of the air passages.
CANNABIS
Extract of the Indian hemp plant, Cannabis sativa, the active substances beingcannabinol and tetrahydro-cannabinol. The leaves and flowers contain theactive principles. The potency varies according to the method of cultivation.Various names for cannabis include marijuana, bhang, hashish, ganga, grass,etc. Absorption is by smoking or eating any part of the plant or the resinextracted from it, which is more potent than the untreated leaves or floweringtops.
There is no evidence that casual indulgence causes any physical harm andcannabis can never cause death from direct toxic action. There is someevidence that long-continued use may lead to physical harm (includingpossible genetic damage), though the effects of the drug remain a matter ofconsiderable controversy.

Lawyer’s Guide to Forensic Medicine
62
The effects of cannabis vary from nil in some persons, to marked mentalsensations, though the substance is not ‘hallucinogenic’ in the true meaning ofthe word.
Common effects include euphoria, distortion of time, enhancement ofcolours, sounds and rhythm, a dream-like state, liability of emotionsconfusion. It is not habit forming in most persons and there are no truewithdrawal symptoms. Long usage appears to reduce concentration andefficiency and may have a deleterious effect on any coincident mental illness.
There are effective methods for the analytical detection of the cannabinolsin human tissues and body fluids, which persist for some days after using thesubstance.
CARBON MONOXIDE POISONING
Once one of the most common fatal poisonings in urban and industrial areas,it is far less frequent now that the gas supply no longer contains monoxide,due to replacement by natural gas.
The most common sources of poisoning are now motor exhaust fumes,industrial leakages and defective domestic heating appliances.
Carbon monoxide kills in two ways. First, it has 300 times the affinity forcombining with the haemoglobin of the red blood cells than has oxygen. Thusit is a very successful competitor for oxygen, even in low concentrations, anddeprives the body tissues of oxygen by occupying oxygen-carrying capacity inthe red blood cells. Secondly, it has recently been shown to dissolve in theplasma (liquid part of the blood) and to have a direct toxic effect on thechemistry of the body cells supplied by that blood.
The level of monoxide is usually expressed as a percentage saturation ofthe haemoglobin. Though the normal level is nil, smokers and city dwellersmay have 3–5% saturation.
Symptoms, such as headache and nausea, may begin from 15% accordingto the individual response. Old persons are usually more susceptible andoften are anaemic, so that less haemoglobin is available for oxygen transport.From 40–50% there is incoordination, slurred speech, vomiting andprogressive impairment of consciousness and death is likely at any levelabove 50–60%. Death may occur at 30% in old and debilitated persons, andyoung children. No strict correlation between levels and expected effects canbe made, except in the broadest terms.
Due to the high affinity of carbon monoxide for haemoglobin, minuteconcentrations can build up to dangerous or fatal levels. One part in 1,000 ofair may cause 50–60% saturation within two to three hours. One part in 100may lead to coma within 15 minutes.

Part II: Carbon Monoxide Poisoning
63
A few breaths of undiluted monoxide, as in industrial or laboratoryexposure, may be sufficient to kill.
The middle ranges of saturation may cause symptoms identical withdrunkenness, with which this type of poisoning may be confused, especiallyin transport accidents.
Where a dead body is recovered from a fire, the presence of monoxide inthe blood is sure evidence that the victim was alive during the fire, but theopposite is not true, especially in violent flash or petrol fires. No monoxideneed be inhaled, even though the victim was alive at the onset of theconflagration. This is of medico-legal importance in allegations of disposal of adead body by fire (see ‘Burns’).
Approximate relationship of concentration of monoxide in blood tosymptoms and signs:(a) no effects below about 15%, apart from possible slight headache;(b) at 15–30%, severe headache, confusion, sickness, visual defects, weakness.
May be similar to drunkenness in some victims;(c) at 30–60%, stupor deepening to coma, vomiting, convulsions. Death in
some cases, especially in old people below this level;(d) above 60%, coma and death in the majority.
This relationship is very variable: two persons who die side by side in thesame room may have markedly differing monoxide concentrations whenmeasured at autopsy.
Sources of monoxide poisoning
Motor vehicle exhaust fumes, 4–7% monoxide. A 1.5 litre car engine will generatea fatal level of monoxide in a closed single garage in about five minutes tick-over time.
Faulty heating appliances (gas or solid fuel). Even if fuelled on monoxide-freenatural gas, a defect in the burners or choked flue will cause incompletecombustion in absence of sufficient oxygen, so that monoxide is produced inaddition to relatively less harmless dioxide. Examples are bathroom waterheaters and butane appliances in caravans and boats.
Solid fuel stoves may also generate monoxide if the air supply is restricted.
Blast furnace gas and coal gas (rarely encountered in UK due to use of naturalgas) contains 7–10% monoxide.

Lethal levels
Due to the stability of carboxyhaemoglobin in the red blood cells comparedwith oxyhaemoglobin, fatal levels can build up from very low atmosphericconcentrations. One part per 1,000 can cause a lethal concentration of 60% inthe blood within 3 hours’ exposure. One per cent can cause coma within a fewminutes.
After recovery from non-fatal exposure, there may be transient andpermanent brain damage, as monoxide causes degeneration in the deeperparts of the brain. Both neurological and psychiatric disturbances maydevelop and become permanent.
CARDIAC ARREST
Stoppage of the heart, usually sudden and unexpected, is the usual meaningof ‘cardiac arrest’. Ultimate cause of death in everyone except where braindeath is used as definition.
Numerous causes, but usually related either to intrinsic heart disease or toacute external causes, such as electric shock, over-stimulation of vagus nerve(for example, pressure on neck), anaesthesia, etc.
Sudden cardiac arrest is the only cause for virtually instantaneous death,as seen in a sudden collapse with no signs of life immediately afterwards.Even pulmonary embolism (qv) or cerebral haemorrhage (qv) does not causesuch an instantaneous death.
Cardiac arrest is potentially reversible by cardiac massage or electricalstimulation applied to the chest, unless there is severe intrinsic damage to theheart.
Treatment is most likely to succeed when arrest not due to heart diseases,for example, electric shock or vagal inhibition.
Cardiac arrest for more than three minutes may cause irreversible braindamage from deprivation of blood supply, so resuscitation should be avoidedif arrest took place more than five minutes earlier, or there may be the risk ofrestoring heart function to a vegetative patient – though cases are on recordwhere full brain function has been restored after six or even nine minutes ofcardiac arrest.
Cardiac arrest strictly means complete stoppage of the contractions of theheart muscle, but ‘ventricular fibrillation’ and other defects of rhythm may bepreliminary stages before arrest. In ventricular fibrillation, the heart muscletwitches instead of pumping in a co-ordinated fashion. This may be correctedby cardiac massage, drugs or electrical defibrillation applied to the chest wall.
Lawyer’s Guide to Forensic Medicine
64

Part II: Cerebral Haemorrhage
65
External cardiac massage often causes trauma to the chest (fractured ribsor breast bone, bruised muscles and haemorrhage on surface of the heart, etc)which can be mistaken for signs of injury unless the pathologist is aware ofthe possible artefact.
CARDIOMYOPATHIES
A group of heart diseases of unknown cause, usually found in young adultsand which may be a cause of sudden unexpected death in the age groupyounger than that associated with coronary disease.
Not common, but a forensic pathologist might see one or two per year in abusy coroner’s autopsy service.
Sometimes associated with exertion and a number of apparently healthysportsmen have died during a game and been found to have acardiomyopathy. It is sometimes familial and where a death occurs, siblingsand children may need to be screened for evidence of similar heartabnormality.
The two main types are:
Hypertrophic obstructive cardiomyopathy (HOCM) where there is a large heartwith a very thick left ventricle. This thickening is sometimes asymmetrical anda pad of muscle may partly obstruct the outflow tract for blood leaving the leftventricle. Histologically, the muscle fibres of the heart may be arranged inbizarre patterns.
Congestive cardiomyopathy (COCM) where the heart is large and globular, butthe chambers are dilated rather than thickened and the main feature iscongestive cardiac failure. These are less associated with sudden death thanHOCM and run a slower course.
Cardiomyopathy is sometimes confused with myocarditis (qv), which alsocauses sudden death in the younger age group.
CEREBRAL HAEMORRHAGE
Usually refers to natural disease causing bleeding into substance of brain, asopposed to traumatic bleeding (see ‘Extradural haemorrhage’, ‘Subduralhaemorrhage’ or natural ‘Subarachnoid haemorrhage’, all into membranes ofbrain). Any injury lacerating the brain will cause some intracerebral bleeding,but the usual meaning is bleeding due to spontaneous rupture of an arterywithin the brain substance.

Often called a ‘stroke’ if it leads to paralysis or other neurological defect,but this indefinite term can apply to other disorders of the cerebral circulationsuch as thrombosis. The clinical distinction between haemorrhage andthrombosis may be impossible without ancillary investigations such as CATscan or magnetic resonance imaging (MRI).
Causes of cerebral haemorrhage
Hypertension (high blood pressure). Most common cause, leading to tearing ofsmall artery, often the ‘artery of cerebral haemorrhage’ which is one of thelenticulo-striate branches of the middle cerebral artery. This lies near the mainnerve tracts which carry the ‘motor’ (outgoing) nerve fibres and damage islikely to cause a paralysis or weakness of the opposite limbs. If thehaemorrhage occurs in the speech area of the left cerebral hemisphere, it maycause speech defect. Large cerebral haemorrhage may cause coma and death,either rapid or delayed any length of time. The normal blood pressure is about120/70 mm of mercury, but in hypertension, the pressure may rise to over200/120 (see ‘Blood pressure’).
Atheroma (arteriosclerosis). Either independently or more often in combinationwith high blood pressure, atheroma of the cerebral arteries may weaken thevessel wall and lead to cerebral haemorrhage.
Congenital or developmental abnormalities of blood vessels in the brain may leadto bleeding. Most common is the ‘berry aneurysm’ (qv) of the Circle of Willis(qv), leading to the subarachnoid haemorrhage (qv). Sometimes, this mayburst through the brain substance, rather than into membranes. Another causemost common in children and young adults is an ‘angioma’, an abnormalcluster of blood vessels, sometimes of a tumorous nature. Rupture of this maylead to haemorrhage and severe disability or death. The medico-legalsignificance of this group is the controversial relationship of any trauma to therupture and the consequent degree of civil or criminal responsibility.
Another frequent medico-legal problem is the need to distinguish causefrom effect in autopsy findings. A large cerebral haemorrhage may be foundin a person with a head injury, presumed due to a fall. Did the naturalhaemorrhage cause the fall or did the haemorrhage occur because of thetrauma of the fall? Sometimes, this dilemma cannot be resolved from autopsyappearances alone. Though a large, solitary haemorrhage in the depths of thebrain is more likely to be natural than traumatic, there are numerousexceptions. Assistance may be gained from:(a) the history and circumstances, such as witnessed collapse before striking
the head, more likely to be the result of a natural ‘stroke’;(b) other evidence of significant intracranial damage and bleeding may tend
towards attributing all to injury;
Lawyer’s Guide to Forensic Medicine
66

Part II: Child Abuse Syndrome
67
(c) the presence or absence of evidence of high blood pressure (medicalhistory, large heart, etc.) and diseased brain arteries;
(d) investigations such as CAT scan and MRI.
CEREBRAL OEDEMA
Swelling of the brain, most often due to head injury. Fluid may pass from theblood vessels in the brain into the inter-cellular spaces in the substance of thebrain, when a diffuse impact force passes through the tissues.
A severe blow or fall may temporarily paralyse the functions of the highernerve cells (neurones) causing transient unconsciousness (see ‘Concussion’).
This may be followed by brain swelling, which can occur rapidly, certainlywithin an hour and probably more quickly. It seems more common amongstchildren and is a frequent cause of death in child traffic accidents, even whenthere appears to be no structural damage to the brain, such as bruising orlaceration, etc.
Progressive oedema is dangerous and may lead to raised intracranialpressure, as the brain is enclosed within the rigid box of the skull and cannotexpand, except to push down against the only exit, the foramen magnum,where the spinal cord emerges. In this area of the skull is the vital midbrain,which carries the control centres for breathing – so oedema may lead toparalysis of breathing, the patient then needing artificial ventilation.
Cerebral oedema may also cause widening of the sutures (seams) betweenthe skull bones in very small infants. It also causes ‘papilloedema’, blurring ofthe optic discs in the eyes, due to pressure – this is one of the diagnosticmethods for brain swelling, to seek papilloedema by looking in the eyes withan ophthalmoscope, though CAT and MRI scans now add to the diagnostictools.
The pressure can also cause retinal haemorrhages (qv) in the eye; this maybe wrongly ascribed to primary injury such as the shaking, so beloved ofpaediatricians, when in fact it may be secondary to cerebral oedema.
Cerebral oedema may often co-exist with diffuse axonal injury (qv), bothbeing due to mechanical disruption of the micro-structure of the brain.
CHILD ABUSE SYNDROME
Also known as ‘battered baby’, ‘battered child’, or ‘non-accidental injury inchildhood’ (NAI) syndrome.

Lawyer’s Guide to Forensic Medicine
68
First described in mid 19th century by Tardieu in Paris, then forgottenuntil revived by American paediatrician Caffey in 1946, then known as‘Caffey’s syndrome’.
Salient features
(a) Repetitive physical (and often sexual and psychological) injury to a childby parent, guardian or temporary custodian.
(b) Main injuries: bruising of skin, fractures of bones, damage to internalorgans, especially brain and abdomen.
(c) About 60% recurrence after first injury, 10% mortality if no adequateintervention.
(d) Battering parents were frequently themselves battered children, thisbehaviour pattern being accepted as the norm.
(e) Parents often young: ‘father’ frequently a consort, rather than biologicalparent.
(f) After severe abuse, disparity between clinical findings and the parentalexplanation, which is evasive and inconstant, often varying betweenmother and father.
(g) Usually an inexplicable delay between serious injury and the seeking ofmedical or other assistance, especially in fatal cases. A London seriesshowed an average of 20 hours’ delay in seeking a doctor.
(h) Bruises usually on face (around mouth, eyes and ears), arms (especiallygrip marks above and below elbows), legs, abdomen and chest. Frequentlycircular ‘sixpenny bruises’ from adult fingertips. Black eyes, bruised earsand lips common, also tears inside lining of lips.
(i) Internal eye damage common: suspected victims should have expertophthalmological examination. Retinal and vitreous haemorrhage,detached retina and dislocated lens frequent, from slaps and punches;retinal bleeding usually secondary to brain injury and swelling, thoughsome may be due to shaking.
(j) Fatalities most often due to fractured skull and/or internal brain damage,especially subdural haemorrhage (qv), followed in frequency byabdominal injuries.
(k) Typical fractures common, around elbows, wrist, knees, due to tractionand twisting of limbs. Also from squeezing of chest and blows or falls onthe head. Radiology essential to detect multiple fractures and fractures of differentages, indicating intermittent abuse. In small infants, typical pattern offractured ribs, which break in sequence down the back, parallel to thespine, from side to side squeezing. by adult hands around the chest. After

Part II: Child Abuse Syndrome
69
some weeks, these heal with ‘callus’ formation, presenting a typical ‘stringof beads’ appearance on X-ray.Front rib fractures rare in infants, almost unknown due to attempts atresuscitation.Similarly, bruises may be of different colours and thus duration.
(l) Many bizarre injuries, such as cigarette burns, scalds, radiant heat burns.Bites not uncommon, usually from mother. Such cases must have expertdental examination to compare with dentition of adult, as often allegedthat other children or even pets caused marks.
(m)Affects all age groups of children, but most common under three yearsand even more so under 18 months, especially fatal cases. High risk ofpermanent brain damage with mental impairment, even where death doesnot occur.
(n) In recent years, a vogue has arisen amongst paediatricians andpathologists to refer to ‘shaken baby syndrome’ in abused infants withhead injury, but doubt has been cast upon the frequency of shaking asopposed to impact.Because an impact upon the head, especially against a flat surface, needleave no mark on or under the scalp, nor a fractured skull, this absence ofovert external injury led many clinicians to think that shaking must havebeen the cause – though in many instances, this explanation was stillaccepted even when there was evidence of a scalp impact. Experimental research has shown that an impact provides energy of theorder of 50 times greater than shaking and is far more likely to be the trueexplanation; some doctors now hedge by calling it ‘shaken impactsyndrome’.
(o) Much controversy may arise about the force required (especially thedistance of a fall) to fracture the skull of an infant and/or cause braindamage.It must be appreciated that a skull fracture may easily be caused. Weber, in1985, found that dead infants dropped passively from only 80 cm (32 in)onto a hard floor all suffered skull fractures, and even when dropped ontoa variety of soft surfaces, a proportion still fractured.However, many persons, including infants, may suffer a skull fracturewith no resulting disability – it is damage to the skull contents which isdangerous.Any injury of sufficient force to cause a skull fracture has the potential tocause brain damage or haemorrhage into the brain membranes, but this byno means always occurs.Thus a fall or impact which causes a skull fracture need not be life-threatening if it does not also cause intracranial damage; conversely, fatalbrain damage can occur in the absence of a fractured skull.

Lawyer’s Guide to Forensic Medicine
70
There is no known quantum of force which will inevitably cause braindamage (which includes subdural haemorrhage). It is conventionallyclaimed that a fall from adult waist height is the minimum to cause suchdamage, but there are cases on record of lower falls causing subduralhaemorrhage, such as Japanese reports where infants have sustained asubdural haemorrhage when falling over only from a sitting position.This whole area is one of considerable controversy, especially in the veryextensive medical literature and entrenched positions are held by expertson both sides (see also ‘Subdural haemorrhage’, ‘Skull fractures’,‘Abdominal injury’).
CHILD DESTRUCTION
The deliberate killing of a child capable of being born alive before it has aseparate existence. Prior to 1929, this was neither the offence of abortion underthe Offences Against the Person Act 1861, nor infanticide, nor murder, as therewas no separate existence.
The Infant Life (Preservation) Act 1929 closed the loophole by making it anoffence for any person, with intent to destroy the life of a child capable ofbeing born alive, to carry out a wilful act causing the child to die before it hadan existence independent of its mother. A statutory defence to this charge,now largely overtaken by the Abortion Act 1967, was that the act was done ingood faith for the purpose only of preserving the life of the mother.
This Act required (s 1(2)) evidence that the woman had at any materialtime been pregnant for a period of 28 weeks or more, as prima facie evidencethat she was pregnant of a child capable of being born alive. Thus a statutorythreshold of 28 weeks’ gestation was established for foetal viability, a legalconcept that does not necessarily coincide with medical fact, as foetuses lessthan 28 weeks may survive with modern obstetrical procedures. Conversely, afoetus of more than 28 weeks may not be viable for other medical reasons.Later legislation under the Abortion Act reduced the 28 weeks to 24, tocoincide more realistically with modern advances in obstetrics.
The concept of actual live birth does not enter into the definition of childdestruction, being important in infanticide. Similarly, ‘separate existence’ doesnot have to be proved, only the viability (by maturity) which in theory shouldallow a separate existence.
The Infant Life (Preservation) Act was the first statute to mention thepossibility that destruction of the foetus might not always be unlawful,though in a much more restricted way than the later Abortion Act.
The 1990 amendment to the Abortion Act 1967 (the Human Fertilisationand Embryology Act) means that a registered medical practitioner cannotnow be guilty of an offence under the 1929 Act.

Part II: Choking
CHOKING
Usually refers to internal obstruction of air passages by foreign material.Sometimes used loosely to cover other forms of mechanical obstruction, suchas strangulation (qv) (see also ‘Air passage obstruction’).
Internal obstruction is usually due to the following:
Gagging or obstruction of mouth, for example, watchman tied up during robberywith cloth stuffed in mouth. Initially may be able to breathe through noseuntil swelling and mucus block this alternative airway.
Food just swallowed – see ‘Café coronary’.
Food regurgitated from stomach, but caution needed as this is frequently anagonal or even post-mortem phenomenon (see ‘Air passage obstruction’).
Inhaled foreign objects, such as toys, bottle teats and household objects inchildren: dentures, extracted teeth, etc, in adults.
71
Figure 21: Choking

Acute infections, such as diphtheria and Haemophilus influenzae epiglottitis inchildren; also rupture of pharyngeal abscess.
Choking may give rise to extreme congestive signs in face and neck (see‘Asphyxia’) with purple-red coloration and swelling of face, with sometimesblood spots in eyes (petechiae), the latter only if there is forcible coughing anddistress. However, many victims die quietly and suddenly from cardiac arrestand show no congestion. These gave rise to misnamed ‘café coronary’syndrome.
Treatment must be rapid and consist of removing the obstruction byinstrumentation or the Heimlich manoeuvre or making an emergencytracheostomy, that is, an opening in the windpipe below the larynx, which isthe usual site of obstruction. Cardiac massage and artificial respiration may berequired.
CIRCLE OF WILLIS
A ring or rather pentagon of arteries at the base of the brain, named afterThomas Willis, a 17th century physician. The circle forms a bypass system forthe vital blood supply of the brain, supplied by the two vertebral arteries andthe two internal carotid arteries, so that if one artery is blocked, blood can bediverted through the ring. Aneurysms (qv) may occur at junctions on thiscircle and cause subarachnoid haemorrhage (qv).
COCAINE
A common drug of abuse, taken by injection or sniffing. the effects come onwithin minutes of injection, but more slowly after sniffing.
‘Crack’ is free-base cocaine, made by heating with baking soda to releasethe free base from the cocaine salt. Its effects come on and pass off morequickly.
The dangers of cocaine include a rise in blood pressure, sweating,hyperactivity and a risk of sudden heart failure or a brain haemorrhage.
COLD INJURY (HYPOTHERMIA)
Most common in old people, but also seen in children. Less common inyounger adults, except in extreme environmental conditions. If bodytemperature (normally 37°C) drops to 28°C or less, recovery is unlikely. Nowa relatively common condition even in European winters, related to low
Lawyer’s Guide to Forensic Medicine
72

Part II: Cold Injury (Hypothermia)
73
environmental temperature. Senility and poor living conditions causes mostcases in old people. Poverty, senile dementia, withdrawal into recluse state,poor housing, nutrition, thyroid deficiency (myxoedema) and lack of domesticheating may lead to hypothermia, even in moderately cold weather.
Also seen in unconscious or stuporose persons, from injury, alcohol, drugsor natural disease, if exposed for extended period to cold. Unclothed victimsof assault in the open may die of hypothermia rather than their injuries.Exposure on mountains, in cold water, open moorland, etc, may causehypothermia, especially if exhaustion present.
Figure 22: Circle of Willis

General signs
Pink or dusky pink colour of skin, especially over large joints like knees, hipsand elbows due to pooling of blood in skin, and persistence of oxygenatedhaemoglobin due to small uptake of oxygen by cold, inactive tissues.
Sometimes skin blistering. In actual ‘frostbite’, extremities like fingers,toes, nose, cheeks, may become bright red and eventually the tissues die, withlater disintegration and separation of the tissues. Internally, signs slight orabsent in many cases, but general bright red colour of blood, may be acutehaemorrhages in lining of stomach, occasionally haemorrhage into adrenalglands, and haemorrhage or necrosis of pancreas. Diagnosis rests largely oncircumstances, temperature during life and absence of other demonstrablecause of death in fatal cases.
CONCUSSION
Unconsciousness following head injury, more accurately ‘a transitory periodof unconsciousness resulting from a blow on the head, unrelated to any injuryto the brain which is apparent to the unaided eye’. Pure concussion, as justdefined, lasts for not more than 5–10 minutes. If unconsciousness is longer,then physical brain damage must be presumed.
Post-concussional state of considerable forensic importance. May beautomatism, similar to post-epileptic state, in which behaviour is purposefuland possibly criminal, but of which the victim is unaware. False explanationsof the circumstances of the injury may be uttered in this state, but which fadeand cannot be recollected by the victim when he later returns to normal.
Long term post-concussional symptoms may give rise to civil actions forloss of faculty, etc. These include intractable headaches, loss of memory,irritability, dizziness and vertigo, visual, olfactory and auditory sensorydefects, decreased perception and speed of thinking. Where fits supervene,physical damage to the brain should be suspected (see ‘Traumatic epilepsy’).It is very unusual for a significant degree of brain damage to occur in absenceof some concussion, though length of unconsciousness is not related toseverity of damage.
Concussion is an important clinical feature – usually any patient coming tohospital with a history of concussion, however transient, is investigated andadmitted for observation, to exclude serious intracranial damage, such asextradural haemorrhage (qv).
Concussion is usually associated with some degree of retrograde amnesia(qv), that is, loss of memory for events immediately preceding the injury. Thisis due to the normal delay in registering events in the memory, a protectivedevice to avoid recollection of actual injury.
Lawyer’s Guide to Forensic Medicine
74

Part II: Consent to Treatment
75
CONSENT TO TREATMENT
All medical care must take place with informed consent of varying degree.The most common type of consent is implied, where the actions anddemeanour of the patient implicitly provide consent. Thus the presentation ofa person at a doctor’s surgery, out-patients or clinic implies that the patient iswilling to undergo examination and treatment, up to a certain degree ofcomplexity.
This degree covers the usual diagnostic methods of interview, inspection,palpation, percussion and auscultation (with stethoscope). Even here, theusual courtesies of speech on the part of the doctor may reinforce the consent,such as a request to undress or to allow a pulse or blood pressure to be taken.
Beyond these simple matters, consent must be express, a specific requestbeing made by the doctor and acquiescence obtained. This extends to intimateexaminations, such as rectal or vaginal examinations, to any procedureintroducing an instrument or needle into an orifice or beneath the skin, etc.The patient may require some explanation as to why this is necessary, thisthen becoming informed consent.
For complex or potentially hazardous procedures, such as surgicaloperations, anaesthetics, sophisticated X-ray techniques and many others,written, informed, express consent is highly advisable.
Written consent is no better than oral consent in law, but is much moreeasily proved if later disputes occur. It is usual to have both oral and writtenconsent for any substantial procedure witnessed by an impartial witness. Arelative of the patient is less satisfactory, as in any retrospective dispute, theymay well not be unbiased.
The concept of informed consent relies upon the right of every patient tobe fully cognisant of what is wrong with him and what is to be done about it.However, though in theory every proposed item of treatment should bepreceded by a full explanation, this must be modified by a clinical judgmentabout the effects of such information upon the patient. The two attitudes maywell conflict. A full recital of possible risks of an operation may cause thepatient to reject what might be a life or health-saving procedure.
Consent is normally obtained from mentally capable adults, that is, over16 years of age, though this age limit may be lowered if the doctor judges thatthe younger person can understand and make rational judgments, otherwiseconsent is given on behalf of minors by the parent, guardian or person in locoparentis.
In urgent situations, no consent is needed to save life or ameliorate seriouseffects of injury or disease. However, the procedure should be limited to themost urgent matters.

Lawyer’s Guide to Forensic Medicine
76
In the case of severely mentally incapacitated persons, the consent ofrelatives is obtained if they live at home, but in an institution, the consent isgiven by the officers of the hospital, even if relatives are available.
Where a patient is unconscious, then consent may be obtained fromrelatives, but in urgent situations generally, the prime consideration is what isbest for the patient, consent being waived on the principle that a doctor actingin good faith has an ethical duty to carry out all necessary treatment in theexpectation that his actions will be upheld in any subsequent litigation.
A similar concept now applies in the case of children of parents holdingstrict religious views about certain forms of treatment, for example, bloodtransfusion in Jehovah’s Witnesses, though recourse is made to the courts incertain cases.
CONTRE-COUP INJURY
Refers almost entirely to brain damage, though rarely applied to lungbruising.
When a moving head strikes the ground or other fixed surface, the braindamage is frequently sustained diametrically opposite the point of impact,hence the term ‘contre-coup’. Conversely, when a weapon strikes a stationary,unsupported head, the brain damage is under the point of impact, the socalled ‘coup’ injury.
Contre-coup injury may be accompanied by a coup injury, but often thereis little or no damage at the site of impact. Contre-coup damage is seen whenthe head strikes either at the side or the back of the head, the injury then beingon the opposite side or the front of the brain respectively. The damage neednot be exactly 180 degrees from the impact site, often being more diffuse, butstill in the general area most distant from the impact.
Occasionally, contre-coup brain damage may be seen on the opposite sideof one cerebral hemisphere, rather than on the opposite side of the wholebrain.
It is almost unknown for a fall onto the front of the head to cause contre-coup damage at the back of the brain.
The mechanism is obscure and controversial, but shearing stresses,rotational forces and shock waves have all been incriminated.
Medico-legally, contre-coup is most useful in corroborating anunwitnessed claim that a head injury was due to a fall, rather than a blowupon the head, that is, to help differentiate an accident or other fall from adirect assault upon the head. Experimental work in Japan has shown that onimpact, there is a momentary vacuum or suction effect within the cranium atthe site of contre-coup.

Part II: Contre-Coup Injury
77
The absence of contre-coup does not rule out a fall, but its presence isalmost certain proof of a moving head suddenly being arrested in its motion.There may be a fracture of the skull at the point of impact, but not necessarilyso. There is often a laceration or bruise at the site, but many falls onto a flatsurface may leave no mark.
There may be contre-coup fractures – where a fall occurs onto the back ofthe head, the frontal lobes of the brain may be severely damaged, evenpulped. Beneath these frontal lobes, the very thin bone that overlies the roof ofthe eye sockets may be fractured by the same contre-coup forces. This mayallow blood from local bleeding to enter the eye sockets (orbits) and appear atthe eyelids as deep bruising.
This may be confused with black eyes from direct violence and furthercomplicate the interpretation of an assault (see ‘Black eye’).
Where a supported head is struck on the opposite side by a weapon, as ina head already lying on the ground or firm surface so that it cannot moveaway, then contre-coup damage may also be seen.
In the chest, sometimes a heavy fall may produce a type of contre-coupbruising in the lung tissue.
Figure 23: Coup and contre-coup injuries

COOLING OF THE BODY (See also ‘Time since death’)
A very variable process, used as a basis for estimating time since death.There are considerable inaccuracies in this estimation, even when theoptimum data are available, which is often not the case.
The normal mouth temperature of the body at death is 37°C (98.4°F). Thearmpit temperature is about 2°C less and the commonly used rectaltemperature about 1°C higher. The ‘normal’ temperature may vary by 1°Cfrom one time of the day to another.
The rationale of the test is that, after death, cessation of metabolicprocesses causes failure of temperature maintenance, so a measurement of thefalling temperature will allow a calculation of the time elapsed.
Variable factors
Many variable factors involved, all contributing errors.
Temperature at death may not be 37°C: raised in infections, after vigorousexertion just before death and some brain haemorrhages. Lowered inhypothermia (qv) from environmental causes, but not in haemorrhage asoften erroneously stated, nor raised in ‘asphyxia’, as formerly claimed. Thelatter error probably arose because many strangulations were associated withviolent struggling, which raised the body temperature from muscularexertion.
Rate of cooling is very variable, with no constant linear relationship betweentemperature and time. There is usually a ‘plateau’ of normal rectaltemperature immediately after death due to lag in cessation of metabolism.This may be half an hour to two hours, or even more, in duration. Then aprogressive fall for about the first day until temperature is near environmental– but does not reach environmental unless freezing conditions prevail (orenvironment is warmer than body, as in tropics, where bodies may never cool,but actually warm up) Thus the only useful part of a temperature graph isduring first day, but the angle and regularity of this graph is very variable.
It has long been assumed that during the first few hours, the bodytemperature drops by about 1°C (1.5°F) per hour, a highly unsafe assumption.Some doctors add an arbitrary 3 hours to this ‘rule of thumb’ to allow for theplateau, but this is unsatisfactory. The answer cannot be relied upon, and aftertaking into account other factors to be considered below, can only be used asmid point of a wide range of times, such as ‘probably between six and 12 hours’.
Clothing naturally modifies the rate of cooling, the spectrum being fromcomplete nudity to heavy swaddling.
Lawyer’s Guide to Forensic Medicine
78

Part II: Cooling of the Body
79
Posture is another factor related to the exposed surface area. A body in acurled up foetal position will cool more slowly than one spread-eagled.
Body shape affects cooling. The mass/surface area ratio is different in a slimperson compared with a corpulent one, apart from the fat insulation factor. Achild has a greater area/mass ratio and will cool more quickly.
A fat person will retain heat better due to the subcutaneous layer of fatacting as a heat insulator.
Oedema (waterlogging) from heart failure or kidney disease will retain heatlongest, due to the high specific heat of water. This has been found to be amore potent factor than fat.
Environmental conditions are all-important. Cold, heat, wind, draughts, rainand humidity all alter the rate of heat loss, but they may not be constantthroughout the period since death, that is, temperature changes due toweather, rain, wind, etc, or variation indoors from dying fires to exhaustedgas or electricity meters. Thus no calculations can compensate for variation ofthe cooling rate, especially if the variations are unknown.
Artificial factors may cause gross distortion of the expected cooling rate, forexample, hot water bottles, electric blankets, radiant heat from fires.
It is therefore obvious that no meaningful calculations can be made for allpossible permutations of these factors. A century of research has failed toimprove methods much – for instance, taking two temperatures several hoursapart to attempt to gauge the slope of the cooling graph has made no materialadvance. Accuracy is impossible and errors of 100% are possible.
It is fatuous and misleading for an expert witness to offer a ‘time sincedeath’ expressed as a single point of time, especially if it is ‘accurate’ to a fewminutes. The best that can be done is offer a ‘bracket’ which straddles areasonably wide period and, even then, errors are not infrequent. To attemptunreasonable accuracy is to invite ridicule.
A great deal of research has gone into the heat physics and mathematics ofbody cooling and numerous formulae exist.
One of the best known is that of Henssge, which is available as a computerprogram and a nomogram. This is reproduced under ‘Time since death’, but itmust be noted that the smallest range of error, giving 95% confidence, is 5.2hours.
Other methods of estimating ‘time since death’, such as potassium in theeye fluid, the residual electrical stimulatability of muscles and a variety ofbiochemical parameters, are equally uncertain, as most depend ultimately onchanges in temperature.
The use of hypostasis (qv), rigor (qv), stomach contents (qv), etc, are evenless helpful.

CORONARY ARTERY DISEASE
One of the most common causes of death (especially in men) and the mostcommon cause of sudden death in Western-style society. Due to blockage ornarrowing of the coronary arteries by atherosclerosis (atheroma) which supplyblood to the muscle mass of the heart.
There are two main coronary arteries, both arising from the aorta (qv) justabove the aortic valve. The left artery divides into the anterior descendingbranch and into the circumflex branch; these supply the front and left side ofthe heart. The right coronary artery has no major branch, but supplies theright side of the heart.
Lawyer’s Guide to Forensic Medicine
80
Figure 24: Coronary artery disease

Part II: Coronary Artery Disease
The blockage is a degenerative condition of the arterial wall and lining,which either blocks (occludes) or narrows (stenoses) the channel (lumen). Theblockage is due either to thickening of the wall by fibro-fatty masses(atheroma) or to thrombosis on the damaged wall, which blocks the lumenpartially or completely. In either event, the heart muscle beyond the point ofblockage becomes deprived of blood. If this deprivation leads to death of thatzone of muscle (necrosis), this constitutes a myocardial infarct (qv). If thepatient survives the infarct, the dead muscle is replaced by a non-functioningfibrous scar.
Where no actual infarct occurs (as in the majority of fatal cases) the longstanding starvation of blood may lead to a diffuse replacement by fibroustissue, or the muscle may survive intact but in an impaired state of vitality.Such a heart is chronically unstable and may suffer a number of sequelae, theseverity partly depending upon the area of the heart involved:(a) weakening of pumping action may lead to chronic cardiac failure, with
clinical signs of failure;(b) electrical instability of muscle may lead to sudden failure and death;(c) irregularities of rhythm, of any type. May lead to sudden death from
ventricular fibrillation (twitching of the muscle instead of regularpumping) or to lesser degrees of rhythm defects.
It is important to appreciate that most fatal cases of coronary artery disease donot have a demonstrable new defect, such as recent thrombosis or infarct.Cases dying in hospital under recent medical care are a ‘selected population’due to the onset of symptoms and have a higher proportion of recent newlesions. Sudden, unexpected deaths may reveal nothing new at autopsy apartfrom their long standing coronary disease. Newer techniques, such as enzymeestimations, may reveal new disease in a proportion of these, but it is oftenimpossible to demonstrate that any fresh event has taken place immediatelybefore a sudden fatal collapse.
Any person with more than 70–80% narrowing of a major branch of acoronary artery is a candidate for sudden death.
Complications
A number of complications of coronary artery disease exist:
Infarction and fibrosis (as described above).
Rupture of the heart through a softened infarct. Common in older people withweak, senile muscle, especially old women. Occurs on the second or third dayafter onset – leads to filling of the bag around the heart (pericardium) withblood. This is known as a ‘cardiac tamponade’ or ‘haemopericardium’ and israpidly fatal.
81

Lawyer’s Guide to Forensic Medicine
82
Mural thrombosis. Blood clot may settle on the inner surface of the infarctinside the cavity of the heart: fragments may break off and be washed away inthe bloodstream, causing embolism (qv) of other organs such as brain orkidneys.
The muscles holding the valve flaps may rupture if infarcted and the septum(partition between the chambers) may rupture, though these are rare.
When healed, a large infarct may produce an extensive sheet of fibrous tissue,which may then bulge under the blood pressure within the heart cavities andform a ‘cardiac aneurysm’.
Any person with substantial coronary artery disease is may die at any time,especially if the conducting system of fibres which convey the rhythmiccontractions is involved. Such persons are far more vulnerable to suddenshocks, either physical or emotional, and can be precipitated into fatal cardiacarrest or other cardiac abnormalities by assaults, emotional trauma or suddenphysical exertion. Thus there is a strong relationship between sudden deathsin these people to a variety of external stimuli, many of which have bothcriminal and civil relevance in a legal sense (see ‘Trauma and disease’).
CORONER, DEATHS REPORTABLE TO
According to the Coroner’s Rules 1953–80 (Consolidated), deaths should bereported to the coroner:(a) when no doctor has treated the deceased in his or her last illness;(b) when the doctor attending the patient did not see him or her within 14
days before the death or after death;(c) when the death occurred during an operation or before recovery from
anaesthetic;(d) when the death was sudden and unexplained or attended by suspicious
circumstances;(e) when the death might be due to an industrial injury or disease or to
accident, violence, neglect or abortion or to any kind of poisoning.
Though not specifically mentioned, other deaths are invariably reported to thecoroner, including deaths in legal custody, deaths of persons receiving anindustrial disability pension or war pension and any cases in whichnegligence (medical or otherwise) has been alleged to have contributed to thedeath.

Part II: Coroner, Deaths Reportable to
Though not a statutory provision, it is conventional for the coroner torequire deaths to be reported to him where such death has occurred during asurgical operation or under anaesthetic or within 24 hours of recovery fromthese. Similarly, it is usual for the coroner to request notification of deathsoccurring within 24 hours of emergency admission to hospital.
There are local variations in the requirements of individual coroners aboutthe types of death of which they require notification.
In addition, there is a statutory duty upon Registrars of Births and Deathsunder reg 51 of the Registration of Births, Deaths and Marriages Regulations1968 to refer certain deaths to the coroner:(i) Where a registrar is informed of the death of any person before the
expiration of 12 months from the date of the death he shall report thedeath to the coroner on a form provided by the Registrar General if thedeath is one:(a) in respect of which the deceased was not attended during his last
illness by a medical practitioner; or(b) in respect of which the registrar has been unable to obtain a duly
completed certificate of cause of death; or(c) with respect to which it appears to the registrar, from the particulars
contained in such a certificate or otherwise, that the deceased wasseen by the certifying medical practitioner neither after death norwithin 14 days before death; or
(d) the cause of which appears to be unknown; or (e) which the registrar has reason to believe to have been unnatural or to
have been caused by violence or neglect, or by abortion, or to havebeen attended by suspicious circumstances; or
(f) which appears to the registrar to have occurred during an operationor before recovery from the effect of an anaesthetic; or
(g) which appears to the registrar from the contents of any medicalcertificate to have been due to industrial disease or industrialpoisoning.
(ii) Where the registrar has reason to believe, with respect to any death ofwhich he is informed or in respect of which a certificate of cause of deathhas been delivered to him, that the circumstances of the death were suchthat it is the duty of some person or authority other than himself to reportthe death to the coroner, he shall satisfy himself that it has been reported.
(iii)The registrar shall not register any death which he has himself reported tothe coroner, or which to his knowledge it is the duty of any other personor authority to report to the coroner, or which to his knowledge has beenreported to the coroner, until he has received a coroner’s certificate or anotification that the coroner does not intend to hold an inquest.
83

Lawyer’s Guide to Forensic Medicine
84
COT DEATH
Colloquial term for Sudden Infant Death Syndrome or SIDS.Called ‘crib death’ in North America. Most common single cause of infant
mortality after first week of life. At three months of age, more common thanall other causes of death combined. Incidence was about one death in every500 births, but since about 1991, the number in most Western countries hasdropped significantly. In UK, the rate is now less than half its formerincidence, said to be due to recommendations to sleep infants face up, reducesmoking in the vicinity and to avoid overheating.
SIDS has been known since antiquity (Old Testament) but cause is stilluncertain, being a common end result of a number of coincident factors.
There is no single cause, it is a multifactorial event where severalpredisposing factors come together to cause death.
Culmination is respiratory failure, due to sleep apnoea (cessation ofbreathing during sleep).
Features
(a) Definite age range, most common at about three to four months, majoritybetween two and eight months, though can occur between two weeks andtwo years.
(b) Slightly more common in male babies, marked increase in risk formembers of twin pair. More common in premature and under-birthweightinfants.
(c) Marked social class incidence (more in ‘working class’) but no social groupimmune.
(d) Marked seasonal incidence, from October to April in northern hemisphere.(e) Typical circumstances: child well or has slight illness (a cold, snuffles or
diarrhoea) on previous night. Put to bed then found dead in morning, ordies in early part of day; 80% found dead in sleeping place before noon.
Autopsy findings are nil or relatively trivial, insufficient to arrive at definitecause of death.
Numerous theories over the years, but probably a combination of factors,including sleep, a slight infection and a maldevelopment or immaturity of thebreathing regulatory mechanism. Respiratory infection may often be ‘trigger’that sets off a chain of events leading to oxygen deprivation in blood,enhancing sleep apnoea.

Part II: Cremation (Legal Requirements)
85
Practical considerations
Cot death is not suffocation from inhalation of vomit (qv) or negligence onpart of mother. Such allegations by doctors or coroners reinforce universalguilt of mother, which may lead to anxiety, neurosis or even suicide.Counselling necessary to alleviate family discord from recrimination.
Controversy exists as to the incidence of maternal suffocation amongst theoverall numbers of cot deaths. Some paediatric evidence, such as coverttelevision cameras, to indicate that some mothers attempt to smother theirinfants, even in hospital – called the Munchausen by proxy syndrome.
However, pathologically, there are no positive autopsy signs in eitherSIDS or suffocation, so no means to differentiate them. Recently, somepathologists allege that finding haemorrhages in the lungs at autopsy (and oldiron pigment in the lungs as evidence of previous episodes) is indicative ofsuffocation; this claim is hard to accept, as it is virtually impossible to obtaintest and control samples, as the basis on which the two groups are separatedhas no other criteria, so the claim is self-fulfilling.
Where two or more SIDS occur in the same family, such a suspicion isstrengthened, but impossible to prove in individual cases. Since the dramaticfall in ‘true’ SIDS since 1991, it is claimed that the proportion of suspiciousdeaths is thus greater, but the burden of proof of suffocation is usuallyunattainable, though some illogical bias on the part of some doctors can leadto injustice.
CREMATION (LEGAL REQUIREMENTS)
A clumsy, anachronistic legislation exists, originating in statutes dating backto 1903. Now, cremation is the method of disposal in 75% of deaths, but anoutdated system persists, in spite of recommendations of the Brodrick report,entitled Report of the Committee on Death Certification and Coroners, Cmnd 4510,1971, London: HMSO.
Series of documents required for cremation:
Form A: application by family or executors, to be countersigned by person ofrepute, for example, magistrate or clergyman.
Form B: first medical certificate given by doctor who issues death certificate.Can be any doctor who attended in deceased’s last illness, even provisionallyregistered house officer. He must declare any relationship with and anypecuniary benefit from the will of the deceased. Must view the body, afterdeath.

Lawyer’s Guide to Forensic Medicine
86
Form C: confirmatory medical certificate given by a doctor who has been fullyregistered for at least five years. He must also examine the body and discussthe death with the first doctor. He must also declare any interest and not be ageneral practice partner of the first doctor. Ideally, he should not be in thesame hospital team either (DHSS advice) but this is often disregarded. If anautopsy has been performed, the pathologist usually gives Form C.
Exemption from Form C granted if an autopsy has been carried out by apathologist qualified for at least five years and the doctor signing Form Bknows the result of the autopsy before certifying the cause of death.
Form D: rarely used, but is a request from the medical referee of thecrematorium for an autopsy, if he is not satisfied with the two medicalcertificates. Such cases usually proceed via the coroner’s system.
Form E: issued by the coroner, replacing previous forms.
Form F: approving certificate by medical referee of crematorium.
Form G: completion certificate from the crematorium superintendent to certifythat cremation has been carried out.
The Brodrick report recommended that this cumbersome system be replacedby a more comprehensive death certificate which will allow any form ofdisposal. Note that doctors can only give their two certificates if the case hasnot been reported to the coroner.
CREUTZFELDT-JAKOB DISEASE (CJD)
Several forensic implications exist over this neurological disease. It is infective,but is not due to a bacterium or virus. The cause is a prion, an abnormalprotein which has the potential to replicate itself in brain tissue.
It is related to scrapie, an ancient disease of sheep and to kuru, a similardisease transmitted by cannibalism of brain tissue in New Guinea. BSE (Bovinespongiform encephalopathy) of cattle is virtually identical to CJD.
Though CJD has occurred rarely and sporadically in humans for manyyears, a ‘new variant CJD’ has appeared in the last decade, about 25 casesbeing reported in Britain to date. It is untreatable and invariably fatal. Thepresumed incubation period for classical CJD is thought to be many years,though as the source of infection is unknown, this is difficult to establish. Thenew variant CJD occurs mostly in younger people and seems to have a rapidincubation period.
Medico-legal implications surround the safety of food and also oftherapeutic substances. The development of CJD by recipients of growthhormone extracted from pooled human cadaver pituitary glands led to amajor negligence action against the Department of Health in 1997.

Part II: Cut Throat
There is also a potential problem, as with HIV and hepatitis, of thepossibility of infection by – and to – health care workers and mortuary staffand pathologists. Special precautions have to be taken in performingautopsies on CJD victims, especially as prions do not seem susceptible to theusual methods of disinfection and sterilisation.
CUT THROAT
Slashing wound(s) on front of neck, most often suicidal, occasionallyhomicidal. Accidental infliction almost unknown, except from falling throughglass window.
Suicidal
Almost always ‘tentative cuts’, sometimes numerous where hesitant trialincisions are made. This feature is the best distinction from homicidal cutthroat. Suicide may be abandoned at this stage in favour of another method,but where successful, a major slash is usually made parallel to the tentativecuts. Many attempts fail, due to throwing back the head, so that thevulnerable great blood vessels slide back behind the shelter of thesternomastoid muscles.
A suicidal slash is usually obliquely across the throat, from high up on theleft side (in right handed victims) under the angle of the jaw. The woundtends to be deeper where it begins and tails off to a shallower cut at itstermination on the lower part of the opposite side of the throat.
Often, other signs of attempted self-destruction, either contemporary orprevious, especially cuts on the inside of the wrist (again, frequently multipletentative cuts). Wrist cutting is usually not fatal, due to over-extension of thewrist joint allowing the radial artery to slide into a protected position.
Homicidal
No multiple shallow tentative cuts, though there may be several majorslashes. These may be in different directions and may involve the face andchest as well. As the head is not thrown back, as in suicides, the skin is not onthe stretch, so ragged wounds may be caused through the lax skin. Theseverity and depth may be extreme, even involving the spinal column.However, undoubted suicides can occasionally cause extreme injury tothemselves. Defence injuries (qv) may be seen in murder, but are naturallyabsent in suicide.
87

Lawyer’s Guide to Forensic Medicine
88
Common features
Whatever the motivation, both types have some common features:(a) even where the windpipe is slashed open below the larynx, the power of
speech may be retained;(b) considerable physical activity is possible for some time after severe cut
throat injuries, unless a carotid artery has been severed leading to rapidexsanguination;
(c) the cause of death is blood loss, especially if a carotid artery is cut.Bleeding from jugular veins may be gross, but is a ‘welling up’ rather thanthe active arterial spurting of carotid damage, which may spurt blood adistance of several feet.
Death may also be due to blood blocking the air passages, either through awound in the larynx or windpipe or through the mouth.
Air embolism (qv) is another rare, but recognised complication if a largeneck vein is opened. Damage to the larynx or windpipe may rarely cause anasphyxial type death by the cut tissues blocking the air flow.

Part II: Death Certification
DEATH CERTIFICATION
A registered medical practitioner has a statutory duty under the Births andDeaths Registration Acts to give a certificate of the medical cause of death inall cases where he has attended the deceased during life. This attendance isnot further defined, but working regulations of Registrars of Births andDeaths indicate that a certificate is not acceptable without notification to thecoroner or Procurator Fiscal if more than 14 days has elapsed between the lastattendance and the death. However, some years ago, the Registrar Generalrequired that a certificate should be issued in all cases where the doctor hadbeen in attendance, whatever the time period, even though he also reports thecase to the coroner. This cuts across the long established practice and thematter is not yet clearly resolved.
Whether or not a certificate is issued, the doctor should report the death tothe coroner if:(a) he has not attended the patient for a potentially lethal condition in the last
two weeks;(b) he is not sure of the cause of death;(c) he is not completely satisfied that the death was due to natural causes.
The present law does not oblige the doctor to see the body after death, thoughit is most unwise not to do so.
The cause of death is recorded according to international conventions, thesequence being that adopted by the World Health Organisation, modelled onthe original devised by the British Registrar General.
Part 1 records the disease or condition leading directly to death, which issubdivided into three antecedent causes (a), (b) and (c). Thus (a) must be dueto (b), which must be due to (c). The basic pathological condition is that on thelowermost line and is the one which will be used for statistical purposes.
For example, 1(a) Ruptured myocardial infarction due to (b) coronarythrombosis due to (c) coronary athero-sclerosis.
Often, only one or two lines are used. Modes of death or symptomatology,etc, should not be included in the cause of death, for example, ‘Heart failure’or ‘Coma’, unless qualified on a subsequent line below.
Part 2 records ‘any other significant conditions which contributed to deathbut which were not related to the conditions in Part 1’. This section isfrequently misused as a depository for secondary pathological conditions,which usually are not strictly part of the death process.
The standard of death certification is very poor and is worsening Severalsurveys have revealed that the recorded cause of death, without the benefit ofan autopsy, is incorrect in about 50% of cases, of which half are substantialerrors.
89

Lawyer’s Guide to Forensic Medicine
90
DEATH, SIGNS OF
No legal definition of death in most countries, other than the conventionalmedical criteria which vary according to the circumstances, especially inrelation to organ donation for transplantation surgery.
Death may be somatic or cellular. The first refers to the permanentcessation of organised life which characterises the individual, that is,breakdown of integrated bodily systems such as breathing, circulation andnervous control. This is the conventional definition of death, but with theavailability of modern life support techniques, all three major functions neednot now fail together. It is usually the nervous control by the brain which hasfailed, but respiration and sometimes heart function can be maintainedartificially. At this point, it becomes a matter of definitions, semantics andreligious and ethical debate as to the presence of life (see ‘Brain death’).
Cellular death is more straightforward, in that once breathing andcirculation have ceased, the body tissues die progressively on a tissue andcellular level. Various tissues survive for different lengths of time: brain cellsdie in a few minutes, whereas connective tissue cells may last for many hours.
Organs such as cornea, skin or kidneys may be viable for transplantationfor hours or even days if preserved under appropriate conditions.
To return to somatic death, the conventional signs (in the absence ofartificial support systems) are:(a) loss of consciousness;(b) flaccidity of the muscles (though they may react to mechanical and electric
stimulation for some hours, until rigor mortis sets in);(c) cessation of the circulation (no pulse at wrist or neck, no heart beat at
chest, no heart sounds through stethoscope);(d) no respiratory movements or sounds of air entry into lungs;(e) loss of corneal reflex (sensitivity of front of eye);(f) loss of tension in eyeball (the pupil of the eye may react to drugs for some
hours, but not to light);(g) special tests such as electroencephalogram (EEG) and electrocardiogram
(ECG) reveal a flat tracing of inactivity; and(h) observing the retina (back of the inside of the eye) with an
ophthalmoscope reveals fragmentation of blood column in the vessels.
All these tests may give equivocal results in deep coma, such as barbituratepoisoning.

Part II: Decomposition of Dead Body
91
DECOMPOSITION OF DEAD BODY
Important medico-legally as one of the ways in which time since death can beestimated, though like all methods, there are very wide margins of error.Decomposition (virtually synonymous with putrefaction except wheremummification (qv) occurs) is the only incontrovertible sign of cellular death,that is, death of the tissues as opposed to death of the organised functions.
The chronology of decomposition varies greatly with:(a) temperature of the environment (climate, season, interior heating, humidity,
clothing, etc);(b) nature of the environment (water, burial, animal predators, etc);(c) condition of body (obesity, dehydration, oedema, infections); and(d) refrigerated storage, either artificial or natural freezing.
General sequence of decomposition in ‘average’ temperateenvironment
Green discoloration of abdominal wall, usually over right lower segmentwhere caecum (large intestine) is nearest the surface. The third or fourth day isabout average for this, but in heated rooms or tropics may appear in 12–24hours. Retarded indefinitely in very cold conditions.
Diffuse reddish green discoloration of skin, especially in dependent parts,with ‘marbled’ appearance of superficial veins five to 10 days, though markedvariation.
Swelling of face, abdomen and genitals in male, with moist breakdown ofskin, blebs filled with thin bloody fluid and slippage of outer layers of skin,especially in dependent areas of trunk. Tongue and eyes may protrude, hairloosens from scalp, skin of feet and hands may peel in sock and glove fashionin two to three weeks.
Body becomes visually unidentifiable from facial appearance from thistime. Bloated appearance, body cavities may break down. Further stagesdepend upon presence or absence of animal and insect predators, such asmaggots, rats and dogs, according to situation of body. Time scale very hardto estimate, being so dependent on season, temperature and predators; likelyto be several weeks, but a body can be reduced to a skeleton in three to fiveweeks in optimum conditions of temperature and predation.
Skeletalisation (qv) progresses, usually complete in two years in temperatecountries, but extreme variations possible. Bones with fibrous tissue, cartilageand ligaments still attached, are probably less than five years since death. Drybones can be anything from two years to many millennia.
As always, environment is more important than time.

DEFENCE INJURIES
Injuries sustained in an attempt to ward off an assailant. Almost always onhands and arms, occasionally on thighs.
Incised wounds seen on fingers, hands and forearms where victim tries toprotect himself against attack from a sharp weapon. In knife attacks, the blademay be grasped, causing cuts on the inside aspect of the fingers, often at thecreases of the finger joints and on the palm and base of the thumb, especiallyin the web between thumb and index finger.
They may also occur on the outside (knuckles) from attempts to deflect theblade. Less frequently, they are present on the back of the wrist and forearm.The injuries may vary from small pricks to deep slashes which may severtendons or blood vessels.
In assault by blunt weapon, the typical defence injuries consist of bruiseson the backs of the hands, wrists and forearms, from efforts to ward off heavyblows. Rarely, there may be actual lacerations, depending on the type ofweapon used. Such bruises may sometimes be present right up the outer sideof the arms to the shoulder, where an arm is thrown across the face and headin an attempt at protection.
In attacks on the genitals, such as kicking, the thighs may be crossed in anattempt at protection and suffer blunt injuries.
DENTAL IDENTIFICATION
A highly specialised field which, in all but the simplest cases, requires theservices of a forensic odontologist (dentist with experience of medico-legaldentistry).
Major uses
(a) The identification of the recently dead (and, occasionally, the living).(b) Identification of skeletal material by means of the jaws.(c) The examination of bite marks, both on the body and on inanimate objects.(d) The estimation of age in the living (rarely required in Western countries).
Identification may be needed in individual cases or in mass disasters such asaircraft crashes, where dental identification may be the only means ofdistinguishing mutilated or burnt victims. The two main approaches inidentification from teeth are set out below.
Lawyer’s Guide to Forensic Medicine
92

Part II: Diatom Test in Drowning
93
Determination of broad groupings
Determination of broad groupings, such as human origin, age, sex and race. Agecan be determined with considerable accuracy in children and young personsfrom sequence of eruption of milk and permanent teeth. Other techniquesused in later age groups, such as attrition (wearing down) and rarefaction(porosity) of roots (modified Gustafson technique).
Recently, a new ageing technique has been developed which depends onthe progressive racemisation (conversion of stereo-isomers) of aspartic acid,an amino acid in the teeth.
Sex differences are slight in teeth, but jaw shapes differ. Race may bedetermined in some instances, such as ‘shovel shaped’ front teeth ofmongoloid races.
Determination of personal identity
Matching of dentition of unknown person with dental records of potentialmatches. Extractions, dentures, fillings, bridgework and many other referencepoints can be identified by an expert dentist, either by direct inspection or X-ray. For this matching technique to be successful, dental records must beavailable. DNA in the pulp of a tooth may also be used for identification, if amatching sample of that person’s DNA can be obtained.
Photographic and video superimposition of a skull upon facialphotographs of the putative subject are now often used. Also, a face may bebuilt up on an unknown skull, either by anatomical modelling by an expertmedical artist or by computer replacement techniques.
Forensic odontology is now a specialised discipline and, for reliableinterpretation, an experienced odontologist, rather than just any dentist, mustbe consulted.
DIATOM TEST IN DROWNING
Diatoms are microscopic water algae with a rigid case composed of silica.There are many thousands of forms of diatoms, which are different in freshwater from salt.
When a body (dead or alive) falls into water, fluid passes down the airpassages to the lungs. If life is still present, the heart will be beating and cantransport diatoms which penetrate the lung lining to distant parts of the body,but in a corpse this cannot occur.
Therefore, at autopsy, if specimens of bone marrow, blood, liver orkidneys are taken and digested with strong acid or detergents or enzymes, toremove soft tissue, the absorbed diatoms can be seen microscopically in thedrowned cases only.

Lawyer’s Guide to Forensic Medicine
94
Figure 25: Principles of the diatom test in drowning

Part II: Diffuse Axonal Injury (DAI)
95
As well as a test for drowning, as opposed to mere immersion, an expertbotanical opinion can distinguish sea diatoms from fresh water algae andeven identify the likely geographical source in some cases.
Certain factors are needed for successful interpretation, though someauthorities discount the reliability of the technique:(a) there must be diatoms in the water (absent seasonally and in pollution);(b) there must be strict safeguards at autopsy so as not to contaminate test
tissues by surface water on instruments;(c) the ubiquity of diatoms in environment (even air) must be appreciated,
though the number recovered in drowned cases greatly exceeds controlnumbers of diatoms.Some experts point to the huge load of diatoms in shellfish, which when
eaten, may reach the bloodstream by penetrating the gut wall and thus give aspurious positive result in target organs.
There is considerable controversy as to the practical value of this test fordrowning. A negative result certainly never excludes drowning and a positiveresult is indicative only, never probative.
DIFFUSE AXONAL INJURY (DAI)
An important concept in head injuries. In recent years, microscopic techniqueshave demonstrated that there is specific injury to nerve cells following severeimpact upon the head. Neurones, the essential cells of the nervous system,have a body and many radiating branches, the largest of which is the axon,which may be several feet long in some cells which control movement. Wherea severe mechanical insult to the brain occurs, many of these axons aredamaged and may leak their contents, forming a microscopic globularstructure called an axonal bulb or retraction globe. The process is called diffuseaxonal injury or DAI, which persists for a month or more in survivors.
This may be suspected by gross examination of the brain, when smallhaemorrhages may be seen in certain parts of the brain, but this must beconfirmed by microscopy.
DAI often accompanies cerebral oedema (brain swelling). It is useful, as itmay confirm that a substantial impact has occurred to the head, even in theabsence of any obvious bruising or laceration of the brain substance.
One problem is that no microscopic changes are visible in conventionalstaining techniques for a number of hours, usually more than 12 hours afterinjury, so the victim must survive this long for the microscopic diagnosis to bemade at autopsy. Recent research has shortened this period, by using ahistochemical method to search for beta-amyloid precursor protein, which mayreveal DAI within a few hours, perhaps even less than five after injury.

DISSEMINATED INTRAVASCULAR COAGULOPATHY (DIC)
A dangerous blood condition secondary to many causes, some of forensicimportance.
The blood develops a tendency to initiate its clotting propensitiesthroughout the body, converting fibrinogen to fibrin, which together withplatelets, small cells assisting in the coagulation process, may block smallvessels and lead to haemorrhage, infarction and organ failures.
Causes include:
Trauma, causing tissue damage and release of thromobogenic material.
Infections of many types.
Amniotic fluid embolism at childbirth (see ‘Embolism’).
Hypothermia and hyperthermia.
The dangers are blockage of the microvasculature with fibrin, andhaemorrhage due to the failure of the clotting system. It is a highly complexcondition, and where an expert is required to evaluate DIC, a haematologistspecialising in coagulation disorders would be most appropriate.
DNA
The introduction of DNA technology into forensic science has been the mostimportant advance since earlier this century, when blood groups were firstused in identification procedures.
The subject is vast, complex and expanding on a monthly basis;furthermore, in the UK it lies within the discipline of forensic science, ratherthan forensic medicine or pathology, so no useful explanation can beattempted in a small book such as this.
In summary, DNA is deoxyribonucleic acid, the carrier of all geneticinformation within the cell. It lies within the nucleus and also a different typeis in the mitochondria, the organelles embedded in the cell cytoplasm, theDNA of which is transmitted down the maternal line – and which may bemore useful in DNA work on ancient material such as bones.
DNA consists of two strands of sugar and phosphate molecules which aretwisted into a double helix, the strands being bound together by permutationsof four bases, adenine, guanine, thymine and cytosine, which form the rungs of aladder, there being ten such rungs to each twist of the helix. A single DNAmolecule may have millions of such links; genetic information is carried onsegments of a molecule, called a gene, separated by lengths of DNA whichappear to have no function.
Lawyer’s Guide to Forensic Medicine
96

Part II: Drowning and Immersion
97
In spite of repeated legal challenges, mainly in the USA, no two persons,other than identical twins, have been found to have identical DNA profiles,the possible number of permutations far exceeding the population of theworld.
From the forensic aspect, the uses are legion, but all depend upon thecomparison of a DNA sample from a person or from trace evidence, withDNA from a control, in order to prove or exclude identity. As with bloodgroups, merely obtaining a DNA profile in isolation is useless, unless there issomething to match it against. Exceptions are the ability to determine the sexof a sample and to determine whether or not it is human.
In paternity testing, DNA now allows positive determination ofparenthood, rather than the statistical likelihood or exclusion offered by bloodtyping in former years.
Sampling for DNA tests
The greatly increased sensitivity of laboratory techniques, such as thepolymerase chain reaction (PCR), now allow minute traces to be tested, butlarger samples are still preferable where possible. In blood, only the whitecells (leucocytes) carry DNA, as the red cells have no nucleus. At least 1 mland preferably 5 ml should be taken into an EDTA tube.
As with all tissue, live material is better than that from post-mortem, asdecomposition can interfere with testing.
Semen and seminal stains, vaginal fluid and swabs, should be air driedand kept at low temperature, if not taken immediately to the laboratory.
From autopsies, spleen, liver, muscle and bone marrow all provide plentyof nuclear material. Hair roots, with nucleated cells attached, were previouslyrequired for DNA testing, but now hair shafts themselves are sufficient.
Unless taken straight to the laboratory, deep freezing is the best method ofpreserving material for DNA analysis.
DROWNING AND IMMERSION
Not synonymous with the cause of death of all dead bodies recovered fromwater; many corpses from water did not die there and many did not drown.(a) May be a criminal death, disposed of by throwing body into water –
decomposition, passive transportation from the locus of death anddelayed recovery may hamper or defeat identification and recognition oftrue cause of death.
(b) Death from natural causes may have occurred before falling into water, forexample, heart attack in a boat or on bank.

Lawyer’s Guide to Forensic Medicine
98
(c) Death may have occurred during fall before entering water, from accidentor suicide, for example, by striking bridge parapet or other obstruction.
(d) Death may have occurred in water, but not from drowning (naturaldisease).
(e) Death may have resulted from injuries after entering water – impact withbottom or edge of swimming pool, river or lake: hitting bridge abutment,injuries from propeller of boat, etc.
(f) Death from sudden cardiac arrest (shock) from suddenly entering coldwater. More likely in drunken state or emotional tension. May be due tosudden cooling of skin especially if flushed from alcohol, or from a jet ofcold water impinging on the sensitive lining of nose or throat – the socalled ‘vagal inhibition’ (qv).
(g) True drowning may be demonstrable.
Drowning
Not merely asphyxia as formerly thought; a much more complex mechanism,different in salt water from fresh.
In fresh water drowning, there is massive absorption of water throughlungs, due to osmotic pressure effects. Blood volume may increase by 50%within one minute. This causes sudden strain on heart pumping function: also
Figure 26: Mechanism of fresh water drowning
Part II: Drowning and Immersion
dilution of plasma causes red cells to rupture, releasing potassium, which isheart muscle poison. These factors combine to cause death from heart failurebefore lack of oxygen takes effect.
Note that the great increase in blood volume may give a falsely reducedvalue for post-mortem analyses, such as alcohol or drugs, which may be 50%less than the true concentration immediately before death.
In salt water drowning, osmotic pressure differences prevent absorption ofwater and in fact withdraws water from the blood into the lungs, causingsevere pulmonary oedema, the source of the froth frequently seen at thenostrils in any type of drowning. However, heart failure is less rapid than infresh water drowning and survival is longer.
Signs of drowning
Variable, may be minimal or absent, especially if delay since death. So called‘dry lung drowning’ not infrequent and presents none of the so called classicalsigns.
Dry lung drowning means either that death was rapid due to cardiac arrest andis not drowning at all; or that all the water in the lungs has been absorbed intothe bloodstream, leaving no post-mortem waterlogging.
Autopsy diagnosis is then difficult, often by exclusion of other causes inconjunction with knowledge of circumstances.
Note that signs of immersion are not necessarily the signs of drowning –wrinkled skin, gooseflesh (cutis anserina), mud staining, sodden clothing.
Positive signs of drowning (often absent) are fine froth exuding from nostrilsand mouth or present in air passages. A delay of a few hours or more afterrecovery may allow froth to dissipate.
Over-distended lungs filling the chest cavity due to plugging of small airpassages by mucoid froth; sometimes large quantity of swallowed water inthe stomach, though this can occur post-mortem. Similarly, foreign materialsuch as weed or sand in the air passages may be a post or ante mortem sign.
Chemical tests, such as Gettler’s chloride test on the blood, have been discardedand are useless, even in freshly recovered bodies.
Diatom test (qv).
Time since immersion. Great variation, as in all timing of death. Depends ontemperature and contamination of water and on stagnant or fast flowingwater. On average, cooling is twice as fast in water as in air at the sametemperature. Whitening and wrinkling of skin of palms and feet occurs withinone or two hours, but a few minutes in a hot bath.
99

Lawyer’s Guide to Forensic Medicine
100
Later putrefactive changes slower than in air, but within two weeks, skinslippage and loosening of hair, with detachment of skin of hands and feetslightly later, though environment may cause variation in time of severalhundred per cent.
Adipocere (qv) may form, being most common in immersed bodies due tothe need for water to convert fat to soapy and waxy compounds. Minimumtime usually several weeks to a few months.
Injuries. May be ante mortem or inflicted after death from trauma in water.Marine or fresh water predators include crabs, fish, rats, etc. Injuries may befrom rough river bottom, rocks, piers, bridges, etc, or from propellers of high-speed outboard motors, which leave characteristic injuries of regularly spacedslashes.
Due to the washing action of water, no haemorrhage remains aroundexternal injuries and it is very difficult to distinguish the two groups. Internalinjuries should present no problems.
Former claims about time of surfacing of body, posture of male and femalecorpses, etc, are now discounted as useless speculation, as so many variablesexist.
DRUGS AND MEDICINES
See ‘Misuse of Drugs Act 1971’

Part II: Electrocution
101
ECSTASY (see also ‘Amphetamine’)
A so-called ‘recreational drug’ of abuse, a derivative of amphetamine,chemically being 3:4-methylene dioxymethamphetamine (MDMA), also called‘XTC’.
Although there have been a number of well publicised deaths, consideringthe widespread usage of the substance amongst young people, its toxicity isrelatively low.
A moderate dose of 75–100 mg produces effects within 20–60 minutes.Its actions are similar to that of amphetamine (‘speed’) with sometimes
spasm of jaw muscles and grinding of teeth, and the hyperactivity of theusers, especially at prolonged ‘raves’, can lead to dehydration, hightemperature, loss of sodium and exhaustion and muscle damage.
The deaths are likely to be due to some personal hypersensitivity, ratherthan the usual slower complications.
ELECTROCUTION
For electrocution, fatal or otherwise, to occur there must be a passage ofelectricity through the body from an entry to an exit point. Without thispassage there are no ill-effects, as in birds perched on overhead cables. Theentry is usually a live conductor and the exit either an earthed object oranother conductor at zero potential, such as the neutral line of the supply.
The biological damage depends on the amount, that is, both the time andthe amperage of current flowing through the body, but the pressure, that is,the voltage, is related to this as per Ohm’s Law (current = voltage/resistance).Fifty milliamperes flowing across the heart for a few seconds is very likely tobe fatal. To achieve this current flow, the voltage is usually in excess of 100 v,though death has been recorded at 50 v and even 24 v, though the time of flowwas long. Most electrocutions occur from domestic supply voltage of 240 v.
The resistance of the thick dry skin of the palm of the hand is of the orderof one million ohms, but when damp, from sweat or wetness, it is reduced to afew hundred ohms, thus greatly increasing the current flow.
Most electrocutions (about 80–100 fatalities a year in the UK) occur frompassage of a current from a hand, either to earth via the feet or via the oppositehand. Death is usually due to fibrillation and arrest of the heart muscle. Lessoften, death is asphyxial from paralysis of the breathing muscles of chest anddiaphragm. Much less often, current enters the head, as in workers onoverhead wires and electrified railways. Here, direct brain damage may occur,including paralysis of the breathing centres in the brain stem.

Lawyer’s Guide to Forensic Medicine
102
Figure 27: Clinical effects of electrocution

Part II: Embolism
Fatality likely if a good earth; as in wet ground, damp concrete, metalpipes, etc. Exit on feet may be marked by electrical burns corresponding withmetal boot studs.
Signs
Electrical burn (more accurately ‘mark’) on skin, usually of hands. Difficult tosee in clenched fist of rigor mortis. May be tiny and insignificant. Firm contactmark is a collapsed blister. An intermittent or ‘jump’ spark burn shows acentral yellow core of melted skin, with a pale surrounding zone. No otherspecific changes: said to be ‘streaming’ of nuclei of skin cells due to electricalpolarisation, but this may be seen in thermal burns as well.
Other signs such as ‘fragmentation of heart muscle’ are spurious. Rigor mortis is known to supervene much more quickly after
electrocution. Cardiac arrest from electricity is the condition par excellencewhich may respond to prolonged cardiac massage and artificial respiration.
EMBOLISM
The movement of an abnormal substance through the blood vessels, withsubsequent impaction at the first junction where the larger vessel divides intobranches. Embolism may occur in either arteries or veins, but its harmfuleffects are almost always in arteries, especially the pulmonary artery.
The abnormal substance may be any of the following, which are furtherdescribed under the first three headings:
Thrombo-embolism, where blood clot is washed along the vessels. This is by farthe most common type, most important medico-legally (see ‘Pulmonaryembolism’).
Air embolism, where air or other gas gains entry through a defect in a vein (see‘Air embolism’).
Fat embolism, usually following a bone fracture, where the marrow fat leaksinto ruptured blood vessels. It may also be seen as a post-mortem artefact insevere burns. Almost all fractures – and many soft tissue injuries involvingfatty areas such as the buttocks – result in minor fat embolism, but almost allis filtered out by the lung capillary bed. Only if so much is released that itpenetrates the lungs, can it reach the arterial circulation and cause problems oreven death by impacting in small vessels in the brain, heart and kidneys (see‘Fat embolism’).
103

Amniotic fluid embolism, from the contents of the pregnancy sac; the fluidaround the foetus may be forced into the circulation during or followingchildbirth, especially when complications such as ruptured uterus occur.
The fluid contains skin squames of keratin from the baby, which may beidentified at post-mortem by microscopic examination of the lungs. Death ispresumed to occur from some ‘allergic’ response to the protein in the fluid,causing profound shock and collapse. A frequent complication isdisseminated intravascular coagulopathy (DIC) (qv).
Bone marrow embolism in fractures. The blood-forming tissue in the marrowcavities of bones often becomes dislodged into the circulation when fracturesoccur. This may be helpful in distinguishing ante mortem from post-mortemfractures, when investigating, for instance, air crashes. For embolism of distantorgans to occur, the circulation must naturally have been in operation at thetime of fracture, that is, the victim was still alive.
Foreign body embolism: rare, but shotgun pellets have embolised into vitalblood vessels such as a coronary artery.
ENTOMOLOGY
The study of insect infestation on bodies (see ‘post-mortem entomology’).
EPILEPSY
A common neurological disease with frequent medico-legal aspects. There aretwo main types of epilepsy:(a) grand mal, where fits involving physical movement occur;(b) petit mal, where the episodes consist of transient unconsciousness without
fits.
There is also psychomotor epilepsy, characterised by a disorder of behaviourwhich may manifest itself as antisocial or criminal acts. Epilepsy may bethought of as a sporadic disturbance of brain activity leading either to loss offunction (unconsciousness) or active movement (fits). Everyone is a potentialepileptic, but the normal threshold is too high for stimuli to be effective,except in extreme conditions such as electric shock, high fevers and somepoisons. The threshold is much lower in children, for example, the commonconvulsions of high temperature.
A certain proportion of people retain a low threshold and are actual orpotential epileptics, this potential usually being diagnosable by electro-encephalography (EEG). There is a definite familial tendency to epilepsy. In
Lawyer’s Guide to Forensic Medicine
104

Part II: Expectation of Life
both grand mal and petit mal, a premonitory ‘aura’ is common, which maytake many forms, including sensory abnormalities of sight, hearing or smell.After the fit, a post-epileptic state is common, again pleomorphic, butcommonly deep sleep, disordered behaviour or ‘post-epileptic automatism’,where a certain pattern of actions is irresistible. During this state, antisocial,dangerous or criminal acts may be carried out.
Petit mal consists of sudden loss of senses and consciousness – the ‘fallingsickness’. There may be danger to the patient or to those in his care. In thegrand mal attack, a preliminary ‘tonic’ state occurs where the muscles aretensed, followed by a ‘clonic’ state where rhythmical muscle contractionsconstitute the classical fit. The tongue may be bitten, respiration is preventedand physical injuries may occur.
Where fits are continuous or repeated with little interval, the condition of‘status epilepticus’ exists. This may cause death from exhaustion or injury, butepileptics can suddenly die for no discernible reason, even when not in statusor even in a fit. There is modern evidence that many epileptics have damageto their heart muscle from repeated attacks of oxygen lack during previousfits. Death may also occur from asphyxia when an unsupervised epileptic hasa fit with his face in a pillow – or drowns in a bath. Epileptics usually haveamnesia for a variable period before, during and after a fit, which again mayhave profound legal connotations in regard to criminal responsibility.
Applications for motor vehicle driving licences must reveal any propensityto fits and usually an epileptic will not be allowed to drive. However, this is amatter for determination in each case, dependent upon medical opinion as tothe complete suppression of fits by appropriate drugs, such as Epanutin(phenytoin) and similar and more modern medicaments. The use of theelectro-encephalograph (EEG) is not always reliable, as a much largerproportion of the population have an epileptiform EEG than those whoactually show any signs of fits.
Most epilepsy is ‘idiopathic’, that is, there is no morphological abnormalityvisible on examination of the brain. A small proportion is ‘traumatic epilepsy’,which may arise from old brain injury, such as a previous fracture of the skull,which causes pressure on the brain or some abnormality which can berecognised at autopsy. This variety has particular legal aspects due to thecompensation issues relating to the original causative injury.
EXPECTATION OF LIFE
The years of life expected to remain to a man or woman at any given age havebeen statistically assessed in actuarial tables. This is a blanket calculation forthe whole population, not taking into account the state of health of anyindividual.
105

The expected longevity of a particular person may assume considerablelegal importance where life has been prematurely terminated by an unnaturalevent, predominantly transport or occupational accidents. Where a civil actionin negligence succeeds, the potentially large damages may be significantlyreduced if it is shown that the expectation of life of the deceased would havebeen shortened by some natural disease, even if the accident had not occurred.
Medical opinion is usually sought to affirm or deny such a reduction ofexpectation of life. This is based on a study of the medical records during lifeand the post-mortem findings after death.
The main diseases likely to reduce expectation of life are cardiovascular,and coronary artery disease is easily the most frequent problem. It must besaid that medical opinion on this matter is fraught with uncertainty andspeculation, especially where heart disease is concerned. Where a cancer isinvolved, opinions may be firmer, though even there, the natural history ofthe disease and the alternative modes of treatment make prognosis far fromaccurate.
In degenerative arterial disease, though some clinicians will give opinionswith considerable confidence, the truth is that huge variations in prognosisexist, with no means of anticipating what would have been the actualoutcome. There are some statistical surveys of the prognosis of various gradesof coronary artery disease (qv) but the individual multiple variations of thestate of the vessels and of the heart muscle make it impossible to apply thesewith confidence to any given person.
A person found at autopsy to have, say, 80% narrowing of the main leftcoronary artery, but no signs of current or past damage in the heart muscle,may have dropped dead next day – or may have lived for 20 years.
Where the heart muscle shows fibrosis from previous infarction, theprognosis is much worse, but again he may have lived for ten years, whereasthe first man may have died next week. There is no way to be accurate aboutthis matter and medical experts have to ‘pick a figure from the air’, basedloosely on the grade of disease found at autopsy or recorded in the medicalhistory.
All that can usefully be offered is to suggest, on the balance ofprobabilities, that a person with potentially lethal disease would probably notsurvive until the actuarial date for average life span – and to hazard areasonable guess as to the proportionate reduction of that period, which canonly be speculative.
Lawyer’s Guide to Forensic Medicine
106

Part II: Exhumation
EXHUMATION
The raising of a body after burial is most often carried out for administrativereasons, such as the removal of a burial site or the re-burial of the person insome other grave. In the medico-legal context, exhumation is performed toallow a post-mortem examination of the corpse, either for the first time or as are-examination. The length of time for which exhumation is worthwhile variesaccording to the nature of the examination required and the likelyenvironmental conditions of the burial. In peaty, waterlogged ground, a bodymay vanish, including the bones, within 10–20 years; whereas in dry, welldrained soil, soft tissues may survive for many years in a recognisable state.Previous embalming also retards decomposition.
Where poisons are being sought, the physical state of the body is lessimportant and drugs such as barbiturates may be found after at least 8–10years: heavy metallic poisons such as arsenic, antimony and lead may berecovered after many more years, again depending upon the local conditions.
Where anatomical and morphological evidence is being sought, theprospects of success are less, but if the conditions of preservation are good,then exhumation may be worthwhile up to 5–10 years after burial, dependingupon the nature of the disease or injuries suspected.
If examination of the bones is required, as for identification purposes, thenthis period may be extended almost indefinitely.
Where poisons are being sought, it is vital to obtain control material fromthe coffin, its internal lining and from the adjacent soil above, below and at thesides of the casket.
The law concerning exhumation varies from country to country, but wherecrime or some important civil claim rests upon the outcome, it is usual forpermission to be sought from a judicial or executive authority.
In England and Wales, exhumations are only lawful if authorised by acoroner, the Home Secretary or a faculty of the Ordinary (that is, a bishop).
The coroner for the district in which the deceased died theoretically hasthe power to order exhumation in cases in which he did not hold an inquestwhen the death took place, so that he can subsequently hold such an inquest Ifhe had held an inquest, then his jurisdiction has ceased. In practice, it seemsnow that the procedure in all cases is to make application to the HomeSecretary for an exhumation. Good cause has to be shown why such aprocedure is necessary.
The procedure adopted at an exhumation mainly concerns identificationof the body and the avoidance of public offence. It is now rare for the actualexamination to be carried out in some inadequate shed at the edge of acemetery. The churchwarden, sexton, superintendent of the burial ground or asurveyor must definitely identify the grave plot with reference to plans and
107
records. Where the coffin is recovered (usually behind screens at an early hourof the day) a funeral director should identify the name plate and coffin as thatwhich he buried. The coffin lid is loosened at the graveside to allow the escapeof noxious fumes and then the coffin removed to a properly equippedmortuary for examination by a pathologist well experienced in forensicautopsies. Again, the grave clothes and coffin furniture should be identifiedby the undertaker, where possible.
When the examination is complete, the body is usually reburied in thesame grave, either in the same coffin or another if the original was in a badcondition.
The value of the examination is naturally very variable (as stated) but,where the issues are serious, the information gained may often be more usefulthan might be expected, certainly within the first few years after burial.
EXPLOSION INJURIES
The rise in terrorist activity in many parts of the world has caused theincidence of explosion trauma to increase markedly.
Formerly seen only in the military or industrial accident situation, thedetonation of explosive devices causes a wide spectrum of injuries. In general,the destructive power of ‘home made’ devices, even when quite sophisticatedin terms of the arming and firing components, is far less than military bombs,mines and shells, due to the less powerful explosive compounds used andalso to a less massive confining container around the charge. This difference isreflected in the nature of the injuries, as pure blast damage is uncommon interrorist devices except at very close range and is most often seen when apremature detonation kills or injures the terrorist himself (so called ‘owngoal’).
Types of injury
Penetration, laceration and abrasions by bomb fragments. The casing of the device,adjacent loose objects, and sometimes metal missiles deliberatelyincorporated, fly away from the focus of the detonation and impinge uponany body in their path. At relatively close range, this produces a typicalpicture of multiple, stippled wounds of varying size and depth, the skinsometimes being ‘peppered’ as in shotgun blasts, though the marks areusually of very uneven size. Death may occur from larger fragmentspenetrating vital structure and this may occur up to many yards away fromthe explosion.
Lawyer’s Guide to Forensic Medicine
108

Part II: Explosion Injuries
Gross injuries and disruption of the body. Complete dismemberment andevisceration is not a common feature of terrorist bombs except at minimumrange, usually when the victim is holding or carrying the device or standingdirectly over it. Even in the latter situation, the damage tends to be polarisedto the nearest part of the body and can give good evidence for reconstructingthe position of the victim, for example, destroyed legs suggest a bomb on theground with the victim standing next to it or frontal abdominal and thighinjuries suggest the device was held on the lap. In all types of close rangeexplosion, the skin is often darkened and discoloured from the effects of thechemicals and products of explosion, as well as from burns and dirt blastedinto the skin by the explosion.
Injuries and fatalities may often occur not from the direct effects of thedevice, but from secondary damage such as falling masonry or roof beamswhen a building collapses or burns from fires started by the bomb. Crushing,internal injuries, traumatic asphyxia (qv) and direct fractures and traumapresent the same features as similar injuries in other circumstances.
Burns from the direct effect of the explosion may occur if the victim is nearthe device, but other effects from direct trauma are more likely to be fatal ifthe range is small enough to allow heat effects.
Blast injuries in the true sense are not common in the terrorist situation, asmentioned earlier, unless military devices have been obtained. However, theymay be seen in confined spaces and industrial fatalities. Blasting in miningand quarrying or massive explosions in munitions or chemical factories mayproduce severe blast effects. This effect is due to a wave of high pressure airtravelling away from the focus of explosion at about the speed of sound. Thehigh pressure front is followed by a zone of negative pressure. A pressure ofover 100 lb/sq in is necessary to produce significant damage to a person andthis can be generated by the adjacent detonation of a 70lb charge. However,the effects diminish by the inverse square law with distance, so that thischarge would produce only 15 lb/sq in at 30 ft distance. The shock waveinjures by direct transmission through the body surface. Organs with arelatively uniform composition, such as liver and muscle, suffer little damage,but where an organ has a variable composition, especially with junctionsbetween air and solid components (such as lung), then severe damage mayoccur. Disruption and haemorrhage are common due to the shock waveacting with differing intensity on different tissues. The ear is also oftendamaged in blast injuries.
Where injury is severe, identification becomes a problem and even theestimation of how many victims were involved may present difficulties. Acareful post-mortem examination is essential in order to reconstruct the eventsas fully as possible.
109

Lawyer’s Guide to Forensic Medicine
110
EXTRADURAL HAEMORRHAGE (OR HAEMATOMA)
Accumulation of blood and blood clot between the inner aspect of the skulland the outermost layer of the brain membranes (the dura mater). Sometimescalled ‘epidural’ haemorrhage.
Invariably the result of a head injury, usually with a fracture of the skull,but between 9% and 19% of cases occur without skull fracture, mostly inyoung people with a more elastic skull. The middle meningeal artery isusually the source of bleeding, as it runs in a groove or tunnel up the inside ofthe skull above the ear. The middle meningeal is involved in 54% and theposterior meningeal in 21%.
Rupture of one of these vessels, usually due to a fracture line crossing thevessel, allows blood to escape into the potential space between skull and dura.
The blood and clot slowly accumulates over hours or up to a day, duringwhich there may be no or slight symptoms after recovery from the probabletransient concussion (qv). This ‘latent’ or ‘lucid interval’ is typical ofextradural haemorrhage. Eventually, the haemorrhage reaches a size sufficientto press on the brain. This leads to unconsciousness, often neurological signsof weakness of the opposite side, and other symptoms and signs detectable bya neurological examination. These may progress to a fatal result if surgicalintervention to open the skull and evacuate the blood clot is not undertaken. Itwas formerly held that this was the type of head injury that responded best tosurgery, but more recent opinion suggests that the mortality rate remains higheven after operation.
The progressive enlargement of the extradural haemorrhage (EDH) willindent the underlying brain and sometimes push that hemisphere of the brainacross the midline. The brain stem becomes compressed into the base of theskull by the swelling of the rest of the cranial contents above it.
Death is due to raised intracranial pressure leading to failure of the vitalcentres in the brain stem which control breathing and heart function. Failureof a doctor to diagnose or anticipate the risk of an extradural haemorrhage hasled to many allegations of negligence, both in general practitioners and in Aand E doctors. Many patients have attended and been discharged home, onlyto be re-admitted to die in a coma the following day.

Part II: Extradural Haemorrhage (or Haematoma)
111
Figure 28: Extradural haemorrhage

Lawyer’s Guide to Forensic Medicine
112
FABRICATED INJURIES (SELF-INFLICTED INJURIES)
Superficial self-inflicted injuries with often a characteristic pattern, but notsuicidal in intent.
Motives
(a) To cover some criminal activity, for example, robbery or fraud, by allegingrobbery with violence against themselves.
(b) To feign injury for insurance, compensation or malingering reasons or toelicit sympathy for some personal reason.
(c) To support a false allegation of assault against another person.(d) Psychiatric origin, for example, woman fabricating sexually orientated
attack. Also gross mutilation, often genital, by paranoid schizophrenic,often with religious basis.
Apart from the last type, injuries are usually trivial and present no threat tolife.
Features
(a) Usually multiple, parallel scratches of uniform, slight depth.(b) They avoid vital and sensitive areas such as eyes, nose, mouth.(c) Often confined to, or more marked on left side in right handed persons.(d) Usual sites are face, forehead, sides of neck, front of chest, backs of hands
(especially left) and back of shoulders.(e) Are absent in inaccessible sites such as the lower back.
Often do not correspond with fabricated damage to overlying clothing. Grossinjuries due to severe self-mutilation in psychiatric patients usually involveamputation of genital organs, cut throat and sometimes self-blinding.
FAT EMBOLISM
Blockage of small arteries by globules of fat (see also ‘Embolism’). Commoncondition after fractures, but rarely of fatal degree.
After fractures or extensive injury to fatty tissues such as buttocks, fatescapes into the bloodstream through torn veins. May also occur in surgicaloperations on bones, joints or breast. Origin is the fat stores in bone marrow oradipose tissue under skin.

Part II: Femur, Fracture of
113
Globules are carried to lungs, where most are held up by the tinycapillaries, but if the volume of fat exceeds a certain (variable) threshold, itescapes from the further end of the lung circulation and enters the left side ofthe heart and hence the arterial system.
Globules can then block small branches of vital arteries, especially in thebrain and coronary vessels and cause small haemorrhages at the impactionsite. Most frequent action is to damage the nerve centres in the brain stem,leading to coma and death from heart and lung failure. Often a latent intervalof a day or two between fractures and onset of coma – causes difficulty indifferentiation of head injury (especially extradural haemorrhage) fromcerebral fat embolism.
Fat may be recognised in body fluids, such as sputum or urine, but thisoccurs quite often when no fatal cerebral embolism occurs.
Small haemorrhage in skin often a sign of fat emboli. post-mortem findingof fat globules in lungs is of no particular significance, as it is so common.After death from burning, spurious post-mortem fat embolism may be found,due to melting and boiling of fat after death.
Some academic controversy exists as to true source of fat – whetherdirectly from fat stores in bones and tissues, or by chemico-physical alterationof normal emulsified fat in blood into larger globules.
FEMUR, FRACTURE OF
The most common domestic accident, very frequent in old people, especiallywomen, due to increasing rarefaction of bone and subsequent brittleness.Death rate is relatively high, though greatly improved in recent years due tosurgical repair by hip replacement and other metal prostheses. The bones ofold people become more fragile due to ‘osteoporosis’ of skeleton as whole,where the calcium content is reduced. The neck of the femur, just below thehip joint, bears most stress and easily fractures due to any fall or serious twist.
Dangers of fractured femur
Rapid death from pain, shock and blood loss. The latter might be considerable intosurrounding tissues and muscles and in old people, often anaemic, the loss ismore serious. In healthy, younger persons fractured femur due to seriousaccidents, such as traffic injuries, may be fatal from gross shock andhaemorrhage. The fracture is then usually of the shaft, rather than the neck.
Bronchopneumonia may supervene within days or weeks. Sometimes called‘hypostatic’, because immobility in bed, shallow breathing due to pain and

Lawyer’s Guide to Forensic Medicine
114
accumulation of lung fluids and secretions due to flat posture, encourage thegrowth of infective bacteria.
Pulmonary embolism (qv) is common, due to tissue damage, immobility in bedand pressure on calves of legs.
The so called ‘spontaneous fracture’ of the femur is a misnomer, and reallymeans a fracture with minimal trauma, even turning over in bed, due to thepresence of some disease process such as a tumour or severe brittleness (see‘Fractures’).
FINGER-NAIL MARKS
Superficial abrasions or shallow lacerations on skin. Seen most often instrangulation and in child abuse syndrome.
In strangulation, they are most commonly inflicted by the victim, whostruggles to tear the hands of the assailant or a ligature from the neck.Scratches are often vertical, running up and down the front and sides of theneck beneath the chin, but may be along the line of a ligature. Even in self-hanging, nailmarks may be seen alongside the rope, from reflex scrabbling.
Other nail marks may be from the assailant, but usually shorter, crescenticmarks due to static pressure, often associated with disc-shaped bruises fromfinger-tip pressure.
In still-born infants and suspected infanticides, spurious signs ofstrangulation may be due to finger-nails imprinted or dragged along infant’sneck in frantic effort at self-delivery by lone, often inexperienced youngmother.
Finger-nail scratches may be linear, due to dragging along skin surface, orsemi-lunar, due to static digging in. In the latter, care is needed ininterpretation of direction of hand when inflicted, as it has been shown thatthe concavity of the mark may in fact be caused by convexity of nail, due toelastic rebound of skin under tension.
Skin and blood may be trapped under the finger-nails of a scratchinghand; scrapings or trimmings of such nails may allow the forensic laboratoryto confirm the presence of skin and blood, to confirm its human origin, todetermine its sex and to determine the individual, by DNA technology, all ofwhich can differentiate the victim from the assailant.

Part II: Firearm Wounds
FIREARM WOUNDS
Two main types, according to weapon: (a) from smooth bore shotguns; and(b) from rifled weapons – revolver, automatic pistol, rifle, machine gun, etc.
Smooth bore weapon wounds
The shotgun emits numerous small projectiles in a narrow extended cone,thus the size of wound increases with distance from muzzle. There are twomain types of shotgun – 12-bore (larger) and 410 (smaller). Cartridges containshot, propellant powder or granules, and plastic, felt or cardboard discs, cupsand wads, all of which may contribute to the wound.
Entrance wound. Features of entry wound vary, according to distance ofdischarge:(a) contact: circular, but often split due to entry of gases, especially over bony
areas such as skull. May be a muzzle mark on skin, but not common.Burning of margins, hairs. Bruising around hole, with soot and powdersoiling. Great internal disruption, especially when fired into head. Pinkcoloration of tissues from carbon monoxide in gases. Wads and discs inwound as well as shot. Single large hole, no spread of shot;
(b) near-contact: circular, unless very near when split to admit gases. Burntmargins, soot and powder tattooing, though less with modern propellants.Wads and cups in wound;
(c) mid-range: up to two metres. Some burning and powder tattooing at lowerend of range, depending on weapon and ammunition. Large single hole,maybe irregular margins. A few stray satellite pellet holes may begin at afew feet range;
(d) distant discharge: over two metres. Progressive enlargement of pelletpattern with diminution of central hole until latter vanishes at about sevento 10 yards. Diameter of pellet spread in inches roughly equals range inyards, but this varies greatly with weapon and ammunition. No burningor powder tattooing. Wads, plastic cups and discs travel two to four yards,but occasionally up to six yards. Distant ‘peppering’ rarely fatal unlessassociated heart disease or shot through eye, etc.
Shotgun wounds rarely exit through trunk but may traverse limb or neck,especially when fired into mouth in suicides.
115

Lawyer’s Guide to Forensic Medicine
116
Figure 29: 12-bore shotgun injuries

Part II: Firearm Wounds
Rifled weapon wounds
Much higher muzzle velocity than shotgun (up to 3,000 ft/second). Also thesingle projectile is heavier, so energy (2 mv2) much greater than with shotgunpellet. Thus, both entrance and exit wounds frequently occur, though modernmilitary weapons may have very high velocity and small bullet, designed tofragment in the body and thus deliver all their kinetic energy without lossfrom exiting.
Entrance wound. Features of entry wound vary, according to distance ofdischarge:(a) if contact, may be ragged or stellate tear due to entry of gas. Bruising and
mark from muzzle (not due to recoil as often stated in textbooks, as recoiltakes the muzzle away – it is due to gas pressure forcing tissues againstmuzzle);
(b) near discharge: soot immediately around hole, though modern propellantrelatively ‘clean’. May be unburnt propellant flakes on skin. At shortrange, same features, though round hole, with inverted edges. May besoiled if lead or lubricated bullet. Abrasion ring or friction from passage ofbullet through outer skin layer. General appearance like lead pencil thrustthrough skin, with inverted margins;
(c) distant shot cannot be gauged as to range, once distance too far. Hole smalldue to steady gyro trajectory of bullet: at extreme range (may be over amile with a rifle) the bullet may begin to oscillate or even tumble andcause a bigger wound;
(d) size of hole need not correspond to calibre of bullet, due to elastic recoil ofskin – hole usually smaller unless very close discharge or a tumblingbullet.
Exit wounds
Usually larger, more irregular (stellate or cruciate) with everted margins.However, some exit wounds hard to differentiate from entry. If solid objectstruck within body, then tumbling or fragmentation of bullet or bonystructures may cause larger, ragged or even multiple exit wounds. If skin atexit site supported, for example, by trouser or brassière band or pressureagainst wooden door, then the exit wound may not be everted and may looklike entry.
Direction of shot
This is better estimated with rifled weapon by projecting a line from entry andexit wounds, though deviation may occur from striking internal structures,especially bone. Interpretation of direction must take into account the postureof the body at time of impact – this may not be known and may beunexpected.
117

Direction is more difficult in shotgun wound due to diffuse nature ofpellet spread – X-ray may assist. Skin wound is helpful – circular pellet spreadin frontal discharge, becomes progressively more elliptical as shot comes fromside.
In rifle wound, direction affects circular or elliptical shape to lesser extent:undercutting of wound edges in oblique impact. Smoke blackening in neardischarge may assist in assessing direction, especially with shotgun: ellipticalin oblique discharge.
FOETUS (FETUS)
Foetal state exists between conception until birth (or in law, until separateexistence). ‘Embryo’ is usually taken to mean the very early stages of gestationbefore the detailed human shape is attained.
Though in law, a foetus attains ‘viability’ at the age of 24 weeks’ gestation,modern obstetrical care allows some younger infants to survive. At 36 weeksthe foetus attains ‘maturity’, though birth is usually several weeks later thanthis, around the 40th week.
Length of gestation – see ‘Pregnancy’
Foetal development
At full term of about 40 weeks, the foetus shows:(a) a weight of 2,550–3,500 g;(b) a crown–heel length of 48–52 cm, crown–rump length 28–32 cm, head
circumference of 33–38 cm;(c) the finger and toe-nails have grown beyond the tips of the digits (not
reliable);(d) the head hair is more than 2 cm in length;(e) the male’s testes are present in the scrotum and the female’s labia close the
vaginal opening; and(f) ossification centres are present in the lower end of the femur (thigh) –
about 6 mm diameter – and upper end of the tibia (shin) in 80% of infants,as well as in the cuboid of the heel.
At 36 weeks, the length is about 45 cm and the weight around 2,200 g. At 28weeks, the length is about 35 cm and the weight 900–1,100 g.
Lawyer’s Guide to Forensic Medicine
118

Part II: Fractures
119
The Haase Rule for length of gestation is that, up to the 20th week, thelength in centimetres is equal to the square of the age in lunar months.
Beyond the 20th week, the length in centimetres, divided by five, is the agein months.
FOREIGN BODIES
Intrusive deposition of foreign matter into tissues or body cavities. Usuallyrefers to solid, inorganic (often metallic) objects, rather than to bacteria orliving organisms.
Foreign bodies can be introduced into the body as follows:(a) From trauma, such as firearm or explosive injury, traffic or transport
accidents or any penetrating injury carrying foreign material into wound.Industrial accidents another common cause, as well as DIY accidents athome with power tools, hammers and chisels, etc.Foreign bodies may enter through skin wound, into eye, mouth or airpassages, etc. Food bones may penetrate stomach or intestine.
(b) During surgical operations: foreign bodies such as surgical instruments,swabs, needles, etc, retained after surgical procedure completed.
(c) Children and mental patients, more so than normal adults, may introduceforeign bodies into throat, stomach, larynx, windpipe, anus, vagina, etc. Insome forms of sexual aberration, foreign bodies may be introduced intobladder via the urinary passages or into the rectum via the anus.
Surgical exploration or visual detection via gastroscope or bronchoscope maybe needed.
X-rays almost always used to detect and localise internal foreign bodies,especially if object is radio-opaque. Glass fragments, common in motoraccidents, are almost always visible on X-ray.
Foreign bodies have particular relevance in medical malpractice actions,either because of retention after operation or because of failure of doctors tosearch adequately for foreign body on attendance at an Accident andEmergency department.
FRACTURES
Physical discontinuity of a bone due to mechanical stress. Amount of stressrequired to exceed fracture threshold related to condition of bone, forexample, osteoporosis or rarefaction of bone in senility and in some kidney orendocrine diseases which have abnormal calcium metabolism.

Lawyer’s Guide to Forensic Medicine
120
Certain diseases with abnormal fragility of bones, such as some varieties ofosteogenesis imperfecta, are often invoked in defence against child abuse.
Where a localised focus of disease exists in a bone, such as a secondarytumour from a distant cancer, then the so called ‘pathological fracture’ mayoccur. This is often termed ‘spontaneous’, but still requires some trauma,albeit minimal.
If fracture associated with breach of skin, called ‘compound’, with risk ofinfection.
Fracture at a joint termed ‘fracture dislocation’, common in spine. Inchildren, bones are more pliable and less brittle, so fractures are oftenincomplete, called ‘greenstick’, with angulation but no complete loss ofcontinuity.
Dangers of fractures
Immediate pain, shock and haemorrhage. Bleeding can be severe, either externallyin a compound fracture or internally around bone. This bleeding itself maycontribute substantially to death, especially in anaemic old people. Pre-existing heart disease may be exacerbated to cause sudden or rapid death.
Infection of tissues, especially in compound fracture.
Kidney failure due to crushing of muscles or low blood pressure from shockand haemorrhage.
Bronchopneumonia, especially in the aged, due to enforced immobility allowingstagnation and infection of lung secretions.
Fat embolism (qv) within a day or two.
Pulmonary embolism (qv) usually within a week or two, due to deep veinthrombosis in legs, following tissue trauma and immobility.
Failure or long delay in healing and subsequent deformity.
Complication of treatment, for example, anaesthesia, tight plasters, need forextensive surgical repair, etc.
FRONTAL SINUS IDENTIFICATION
The frontal sinuses are convoluted air spaces within the bone of the skull, inthe centre of the forehead, extending outwards above the eyes. Their patternas seen on X-ray is unique to every individual, as characteristic as fingerprints:this applies especially to the scalloped upper border of the sinuses, as well asto their general size and shape.

Part II: Frontal Sinus Identification
Used in identification, even of badly decomposed or burned body,especially in mass disasters such as air crashes. The sinuses are protected fromeven severe charring by fire. Must have a pre-existing X-ray available forcomparison, obtained from hospital or other records. Complete reliability inmatching if this is compared with post-mortem X-rays of skull.
Chronic infection, such as sinusitis, may blur or even distort theradiographic individuality, but this is a relatively uncommon source ofdifficulty in matching sinuses.
121

Lawyer’s Guide to Forensic Medicine
122
GANGRENE
Death of tissues, usually an extremity such as fingers, toes, arm or leg, usuallydue to failure of adequate circulation. Tissues surrounding wounds can alsobecome gangrenous, as well as internal organs such as appendix. Gangrene oflimbs may be dry desiccation or moist putrefaction: the tissues usuallydiscolour and go through spectrum of red, purple, black or green.
A particularly virulent form of gangrene is known as ‘fasciitis’, due torapid spread of an infection through the tissues of a limb or trunk.
Causes
Loss of blood supply, such as arterial degeneration in diabetes or arterio-sclerosis. Also when artery is blocked by embolism (qv) and in frostbite,where blood supply ceases.
Infection, which may be primary or follow an injury to the affected part.May also supervene in tissues dying from lack of blood supply. Great dangerof death from septicaemia or local toxaemia.
Gas gangrene
This is a particular type of infective gangrene due to anaerobic bacteria (whichshun oxygen), usually B perfringens (formerly known as Clostridium welchii).Putrid smell and puffy tissues due to gas formation. Used to be almostinvariably fatal without amputation, but antibiotics now effective in earlierstages.
GENERAL MEDICAL COUNCIL (GMC)
Originally established by the Medical Act (1858) to allow the public todistinguish between qualified doctors and quacks.
Primary duties are to:(a) maintain the Medical Register;(b) supervise medical education;(c) exercise disciplinary function over medical profession;(d) establish standards of medical ethics and professional conduct; and(e) investigate defects in physical and mental health of doctors relating their
fitness to practice.

Part II: General Medical Council (GMC)
123
The GMC is directly responsible to the Privy Council and consists of memberselected by registered medical practitioners every five years, membersnominated by university medical schools and Royal Colleges, and laymembers nominated by the Privy Council.
Medical Register
British doctors may be fully or provisionally registered. The latter are newgraduates who must spend at least 12 months in approved house officerappointments and show proof of satisfactory progress before being admittedto full registration.
Overseas doctors may be granted either full or limited registrationdepending upon complex arrangements relating to their previous medicaleducation and fluency in English. Most will have to sit the PLAB (Professionaland Linguistics Assessment Board) examinations to gain admission to theRegister.
The Register now also give indications as to the speciality of fully trainedregistrants. UK registration must be granted to EEA nationals qualifying intheir own country.
Disciplinary functions of the GMC
Complaints about the professional behaviour of doctors reach the GMC:(a) from all convictions of doctors in criminal courts via the police;(b) from official bodies such as NHS trusts and health authorities;(c) on sworn statements from members of the public; and(d) from divorce cases, now only if the aggrieved party alleges a breach of
professional behaviour.
All complaints are examined by a member of the GMC, the PreliminaryScreener. Trivial, obviously unfounded or fatuous complaints are eliminated,the remainder go to the Preliminary Proceedings Committee for consideration(similar to committal proceedings). The doctor may be invited at this stage toanswer the complaint. If a prima facie case is considered to exist, the case goesto the Professional Conduct Committee, where a full hearing is held withwitnesses on oath and legal representation on both sides.
The Committee decides whether there has been ‘serious professionalmisconduct’ and may:(a) dismiss the complaint;(b) admonish the doctor;

Lawyer’s Guide to Forensic Medicine
124
(c) postpone judgment – in effect, a probationary period of any length, duringwhich the doctor must obtain proof of good behaviour in order to avoid anadverse judgment;
(d) suspend the doctor’s registration for a period not exceeding one year; or(e) direct the Registrar to erase the doctor’s name from the Register. In this
case, an appeal may be made to the Judicial Committee of the PrivyCouncil. If the appeal is not upheld, the doctor may apply at 10 monthintervals for restoration of his name to the Register.
A doctor erased or suspended from the Register loses all privileges as aregistered medical practitioner.
A Health Committee investigates doctors whose fitness to practice may beimpaired by any physical or mental disability.
A more recent development is the establishment of professionalperformance machinery as, formerly, complaints about a poorly performingdoctor, who was not committing professional misconduct, could not be dealtwith. Now such doctors are investigated, monitored and may be required toundergo re-training. If they fail to improve or refuse to co-operate, they maybe removed from the Register.
GLASS INJURIES
In general, similar to incised wounds by knives and razors, but may be evenmore cleanly cut due to the exquisitely sharp edge. The wound lacks anymarginal bruising, which may be seen on some knife injuries where theweapon is not very sharp. There may be slicing of the skin in an undercutfashion, so that an oblique cut is made into the thickness of the skin by thevery sharp edge – this may cut through hair roots in hairy parts, revealing astippled appearance.
Where the glass fragment is irregular, the wound may also be misshapen,even bizarre. A sharp spicule may cause a stab wound. Fragments of glassmay detach and can be seen on X-ray, as almost all glass is radio-opaque,contrary to popular belief.
The damage caused by shattered windscreen glass is highly characteristicdue to the nature of the uniform fragments of pre-toughened glass used inmotor vehicles. The face is the usual site of injury and may be covered bymultiple small V- or Y-shaped abrasions and shallow lacerations.
Other glass injuries are often seen in bar brawls where a shattereddrinking glass is used as a weapon. Severe facial injuries are common, due toprojections and spicules of glass smashing or penetrating the skin.

Part II: Glue Sniffing (Solvent Abuse)
It may be difficult or impossible to tell from the wounds whether a glasswas used intact and smashed on the victim’s face, or whether the glass waspre-smashed to be used as a weapon. Substantial glasses may not break onimpact and then the features are naturally that of blunt injury only.
Glass-type cuts can be caused by broken pottery, such as a coffee mug, ifthe glaze is exposed as a sharp cutting edge by an oblique fracture of thepottery.
Glass injuries, sometimes fatal, can also occur from persons falling orbeing pushed through a window or glass door.
GLUE SNIFFING (SOLVENT ABUSE)
A common form of drug abuse, mostly amongst children and teenagers,though no age is exempt. Many organic compounds, especially halogenatedhydrocarbons, may be used, such as the solvents used in proprietary glues.These have potent effects on the brain when inhaled, similar to chloroform ortrichloethylene, though in fact the most common solvent of glues such as‘Evo-stik’ is toluene, which is not a halogenated compound. Many othersubstances, such as typewriter correcting fluid (for example, Tippex), gasoline,paint strippers, fire extinguisher fluid, cellulose solvent, etc, are misused in asimilar fashion. Another form of inhalation abuse is from aerosol cans ofvarious substances, including that used to treat sprained muscles. Lighter fueland hydrocarbon gases, such as butane and propane, may also be inhaled.
A particular danger of inhaled pressurised gases is the possibility ofsudden death from a vagal inhibition (qv) type reaction when the refrigeratingeffect of released gas impinges on the back of the throat. This has been seen anumber of times with the use of small cylinders of butane intended forcigarette lighters.
Solvents are easily available and cheap, often shoplifted; users inhale thefumes from glue extruded from the tubes and pass into a presumably pleasantstate of disorientation and even coma.
The substance is often squeezed into a plastic bag, which is placed over theface or head. This in itself is dangerous, even without the presence of solvent,as it can cause asphyxia very rapidly. Though most solvent sniffing has nopermanent ill effects, there is a danger of sudden death from an effect on theheart, which can fibrillate or arrest. The mechanism is thought to be asensitisation by the solvent of the heart muscle to catecholamines, adrenaline-like compounds generated by the body. These can send the heart into a stateof abnormal rhythm.
Vomiting and choking are also possible and in a small proportion of longterm users, the toxic solvents can cause irreversible liver disease.
125

Lawyer’s Guide to Forensic Medicine
126
HAEMORRHAGE
Loss of blood from body surface or into body cavities or tissues. Danger to lifeis related to (a) volume lost, (b) speed of loss, and (c) fitness and age of person.
Total volume of blood in body is about six litres (10 pints). Rapid loss oftwo pints is dangerous to life, but much more can be lost over a longer period(days) if volume is made up from other body fluids.
Persons with anaemia (thin blood) or any other systemic disease are atgreater risk from the effects of haemorrhage.
Internal haemorrhages
Bleeding into alimentary canal may appear in vomit (haematemesis), oftenbrown due to alteration by stomach acid, or may appear in stools (melaena),usually black unless massive or bleeding low down in canal, when it mayremain red. Many causes, including peptic ulcers (of stomach or duodenum),cancer of stomach or intestines, or internal injuries.
Bleeding into air passages and lungs is usually bright red due tooxygenation and is frothy from mixture with air (haemoptysis). Causesinclude tuberculosis, cancer and chest injuries.
Bleeding into heart bag (pericardium) rapidly fatal due to embarrassmentof heart’s filling capacity – ‘cardiac tamponade’. Usual causes are a rupturedaortic aneurysm (qv) or a ruptured myocardial infarct (qv).
Bleeding into abdominal cavity (haemoperitoneum) usually occurs fromtrauma such as ruptured liver or spleen or bruised intestines.
Bleeding into chest cavities (pleura) from wounds of lung or leakage fromlarge blood vessels, such as aorta. Common in chest stab wounds. Uterine andvaginal bleeding from abortions, menstruation and disease.
Small pin-head haemorrhages in eyes and skin, called petechiae (qv).When larger, called ecchymoses.
Haemorrhage inside skull (see ‘Extradural haemorrhage’, ‘Subarachnoidhaemorrhage’ and ‘Subdural haemorrhage’).
A relatively small volume of blood spilt upon a flat surface may give afalse impression of a large amount lost.
HAIR
Modified skin composed of keratin, the same protein as the epidermis (outerlayer of skin). Extruded from small follicle or ‘silo’ embedded in skin. Growsat about half a millimetre per day on head and face.

Part II: Hanging
127
Hairs can be identified as to species and sometimes to race. Since theadvent of DNA techniques, the sex and personal identity can be obtainedfrom the root cells and even the shaft.
Characteristics of hair displayed by thickness, external skull pattern, cross-sectioned shape, relative size of cortex and medulla (inner and outer layers),colour, etc.
Apart from DNA, no way of matching individual hairs to any one person,but marked dissimilarity in colour, shape and texture may exclude matching.Pubic and armpit hair different in texture from head hair.
Other characteristics of hair include the presence of artificial colour orbleach; whether the hair has been cut or has a natural end; whether it has beenplucked out with the root or shed naturally in the cycle of ‘moulting’.
Some racial characteristics may also be present in hair, the negroid typebeing elliptical in cross-section, the mongoloid being circular, with caucasianintermediate. The whole subject is complex and requires the assistance of aforensic biologist.
HANGING
Death due to suspension by the neck: usually not truly ‘asphyxial’ in nature(see ‘Asphyxia’).
Almost always accidental or self-inflicted. Homicidal hanging virtuallyimpossible, unless victim shows signs of restraint (bruises, etc) or isincapacitated by drink, drugs, fear, etc. Accidental hangings seen in childrenentangled in cot harness and in young male adults as a result of masochisticpractices (qv).
Mechanisms
Death is often rapid, virtually instantaneous, due to jerk on carotid arteries,producing reflex cardiac arrest (qv). This is the most common singlemechanism, even in the short drop employed by suicides. The face is usuallypale, with no congestion or petechial haemorrhages in eyelids or lips. Thelatter is seen in a proportion of cases, especially where the hanging is‘incomplete’, that is, where the body is not fully suspended clear of the floor,but slumped with partial support.
Few post-mortem signs internally. Hyoid bone (qv) usually not fractured.In the slower deaths, constriction of neck veins and airway obstruction,
due to raising of tongue against the palate at the back of the throat.Obstruction of jugular veins causes dark congestion and purple cyanosis of

Lawyer’s Guide to Forensic Medicine
128
face and neck above ligature. Pin-point petechial haemorrhages may appear inface, eyelids, whites of eyes, etc (see ‘Asphyxia’). Less common than suddendeath hangings.
There may be terminal convulsions which can kick over stool or chair, etc.May be reflex scrabbling at rope, leaving fingermarks.
The rope or cord commonly becomes imprinted onto the skin of the neck,causing a groove. The pattern of the weave frequently remains. After death,the hanging mark usually becomes parchment-like or leathery due to drying.
Soft fabrics can be used for hanging, even folded towels, scarves, etc. Theymay leave a narrow groove like a rope, due to pressure from tension bands inthe fabric.
Even shoe laces, string and belts may be used, especially in deaths incustody, where ingenuity leads to improvisation of available material.
Except sometimes when a slip knot is used, the partly circumferentialmark will show a defect at the point of suspension, where the vertical tensionon the knot carries the ligature away from the skin. This is usually at the backof the neck or under one ear, but may rarely be in front of the chin.
There need be no high suspension point, hanging being quite possiblefrom doorknobs and bedposts, the slumped weight of the body beingsufficient.
The post-mortem hypostasis (qv) should be in the legs and hands. In hanging with a long rope (as in judicial hanging), the vertebrae of the
neck may become fractured or dislocated, with damage to the spinal cord andspinal shock. Complete disruption of the spine may occur with stretching ofthe neck, or even decapitation.
HEAD INJURY
Many varieties, with varying classifications. External damage is notnecessarily related to intracranial damage, which is the serious consequence.
Types of head injury
Scalp damage. Lacerations bleed copiously due to profuse blood supply, butrarely fatal unless extensive scalping as in some traffic accidents. Blunt injuriesto scalp may cause wounds which closely resemble knife, axe or cleaverwounds, because of splitting over firm support of skull. Differentiation fromincised wounds:

Part II: Head Injury
(a) edges show rim of bruising;(b) hairs often bridge the gash;(c) strands of fibrous tissue may survive in depths of wound.
Where the scalp injury (laceration or bruise) is on the front of the head, ifvictim survives more than a few hours, may get a black eye due to bloodtracking down under the scalp and accumulating in the eye socket (see ‘Blackeye’). Scalp injuries may continue to bleed profusely after death, especiallyfrom dependent wounds.
Skull fractures (qv) may or may not be associated with either scalp damage orunderlying brain damage; 25% of head injuries with fatal brain damage do nothave a skull fracture.
Many skull fractures, including those in infants, may cause no disability atall and may remain undiagnosed in life. It is the damage to the cranialcontents which is dangerous.
Intracranial damage is the major danger to life in head injuries, the scalp andskull lesions usually being only a concomitant indicator of substantial trauma.Brain damage may be superficial and/or deep and meningeal haemorrhage(see ‘Extradural haemorrhage’, ‘Subdural haemorrhage’ and ‘Subarachnoidhaemorrhage’) very common.
The brain itself may suffer:(a) contusions (that is, bruised either on the surface of the cortex or deep
inside);(b) lacerations on the surface;(c) deep haemorrhages (which must be carefully differentiated from natural
haemorrhages, which may have caused an accidental injury, rather than bethe result of an injury);
(d) occult damage to brain substance, causing cerebral oedema (qv) and diffuseaxonal injury (DAI) (qv). Common in closed head injuries and in children.Examination of brain needs special techniques to demonstrate microscopicdamage of DAI, but this cannot be seen unless victim survives for at least anumber of hours;
(e) where a moving object strikes a stationary head, usually a ‘coup’ braininjury occurs under the point of impact. Where a moving head strikes afixed surface (as in falls or projection from a vehicle), then if the back orside of the head is the site of impact, ‘contre-coup’ damage (qv) occurs tothe diametrically opposite part of the brain.
129

HEART
The heart is about the size of a fist, varying in weight between 280–380 g innormal adults. Marked variation in size, related to body weight and build.The estimates given in many anatomical textbooks are smaller than usuallyseen in contemporary British subjects at autopsy. New tables are at variancewith older estimates.
A large, athletic young man may have a heart of 420 g but this is the upperlimit of normal unless the subject is of very large build. Above this, there isusually disease present, most often high blood pressure, which enlarges theheart due to the extra work required to pump against hypertension.
A small heart is seen in old age, unless disease keeps it large. A senileheart may be only 200 g or even less.
The heart lies inside a thin bag, the pericardium, which normally has onlya moistening of fluid for lubrication. Increase of this fluid is an ‘effusion’ andinflammation of the bag is ‘pericarditis’.
The main bulk of the heart mass is formed from the left ventricle whichoverlaps the right ventricle and forms the apex or bottom point, which is oftenvulnerable to knife wounds.
The heart lies obliquely in the chest, the apex being five to seven cm to theleft of the midline in the fifth intercostal space (gap between fifth and sixthribs). It thus lies inside and slightly below the left male nipple, though there isappreciable variation (see Part I, Figures 7 and 8).
The surface of the heart lies about three to four cm below the surface of theskin in the apex region, though this naturally varies with the amount of fatand muscle on the person.
Much of the heart is protected by the breast bone, but part of the leftventricle and a narrow band of the right ventricle are accessible each side, andvulnerable to knife stabs. The aorta (qv) is also vulnerable in the secondintercostal space, where it lies superficially.
Wounds of the heart from knives usually puncture a ventricle allowingblood to escape into the pericardium, where death occurs from blood lossand/or ‘cardiac tamponade’, that is, prevention of the heart’s action bystopping filling due to the constricting action of the tensed pericardial bag.Paradoxically, wounds of the right ventricle may be more lethal than those ofthe higher pressure left ventricle, due to the lack of the self-sealing property ofthe thick-walled left chamber.
Lawyer’s Guide to Forensic Medicine
130
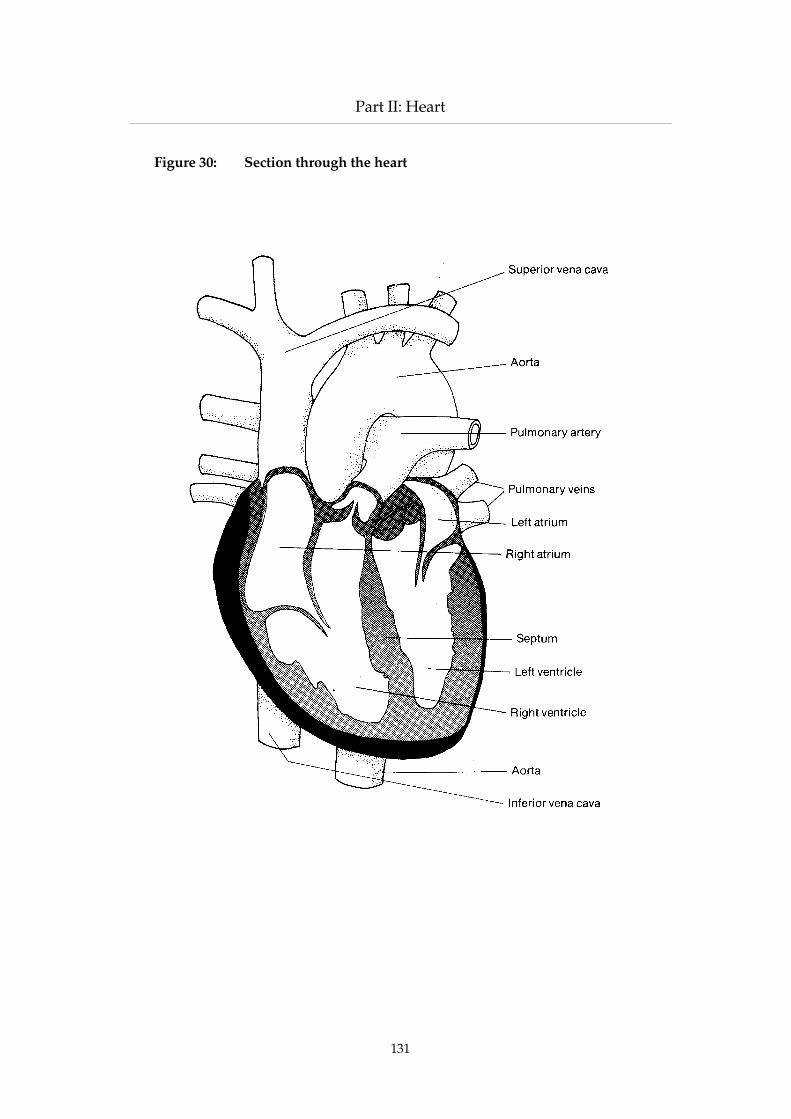
Part II: Heart
131
Figure 30: Section through the heart

HEPATITIS
Inflammation of the liver, usually due to viruses, though other micro-organisms can affect the liver, mainly through the bile ducts (cholangitis).
Viral hepatitis is of three main types:
Hepatitis A, contracted through eating infected food. It is usually benign,though deaths can occur and the liver damage may be progressive.
Hepatitis B and C, contracted through virus entering the body direct, viainjections, blood transfusions, and sexual intercourse.
Shared unsterile syringes used by drug abusers, hetero and homosexualcarriers, contaminated blood products and possibly infected health careworkers such as surgeons and dentists may be the agent of infection.
HEROIN
Heroin is both a potent medicinal substance and a common drug of misuse,being a chemical derivative of morphine. It can be manufactured legally orillicitly by a relatively simple laboratory procedure. It is di-acetyl-morphine(diamorphine) and has about five times the effect of morphine, dose for dose.A potent pain killer, it is the most dangerous drug of addiction and itsmanufacture has been banned by a number of countries, as other analgesicscan be used in its place.
It is active in the same way as morphine, and can be taken by swallowing,sniffing or injection. The symptoms of overdosage are similar to, but moreprofound than morphine. Overdosage in addicts is often due to a new sourceof the drug being obtained which has not been ‘cut’ as much as the previoussupply, that is, not diluted so much with a variety of substances such asglucose or lactose.
Although many deaths are due to overdosage of heroin, rapid death mayalso occur from hypersensitivity on lower dosage – this may occur with firsttime users or habituated takers.
Stupor, coma and especially depression of breathing are the hallmarks ofheroin and morphine poisoning. Waterlogging of the lungs (pulmonaryoedema) is a specific feature of heroin intoxication or hypersensitivity.Infections from the use of shared, dirty and unsterile injection equipment arecommon, as in morphine addicts, and death from septicaemia is a well knowncomplication of addiction, as is infection by HIV and hepatitis.
Lawyer’s Guide to Forensic Medicine
132

Part II: Human Tissue Act 1961
HISTOLOGY
The study of tissues under the microscope; when abnormalities are sought, itis histopathology.
Clinical histopathologists study tissue from operations for disease,especially cancer; tissues are (or should be) taken routinely from post-mortems to seek occult disease not visible at the gross dissection.
Tissue is placed in 10% formalin (formaldehyde in water or saline) andprocessed in the laboratory, this taking a few days, though there is a rapidfrozen method. The tissue is embedded in paraffin wax blocks and thinsections cut and stained on glass slides, usually by the haematoxylin and eosinmethod (H and E), though there are hundreds of special stains.
Modern advances include histochemistry, where certain substances,especially enzymes, are rendered visible, and immunocytochemistry, whereantigens and antibodies are labelled to become visible.
Histology may occasionally provide vital medico-legal evidence and slidesmay need to be re-examined by experts for the defence where the issuesindicate.
HUMAN TISSUE ACT 1961
The statute governing the donation of organs and tissues, the obtaining ofpermission for post-mortem examination and, less importantly, thesubstitution of cremation for burial of bodies used for anatomical dissection.
The major provision of the Act is to regularise the obtaining of humantissues and organs for transplantation, therapeutic use, medical research andteaching, though there are some deficiencies in the drafting of the Act whichhave given rise to ambiguities in interpretation. Tissues may be taken from adeceased person by the person lawfully in possession of the body, for theabove purposes, if:(a) the deceased during life expressed a request in writing (or orally in the
presence of two witnesses) that he desired any or specified tissues to beused for such purposes; or
(b) after having made reasonable inquiries, the person in possession of thebody has no reason to believe that neither the deceased nor the survivingspouse or any surviving relative had any objection.
The person lawfully in possession of the body is almost invariably anadministrator of a hospital or institution, or a deputy.
The removal of tissue must be carried out by a fully registered medicalpractitioner who must satisfy himself that life is extinct (for definition of
133

death, see ‘Death, signs of’). No such removal may be performed without theconsent of the coroner (or Procurator Fiscal in Scotland) in deaths which maybe the subject of an inquest. Authority for removal of tissues cannot be givenby a person entrusted with the body only for the purposes of interment orcremation.
A defect in the wording of this Act is that ‘reasonable inquiries’ are subjectto wide interpretation end ‘any surviving relative’ can also give rise todifficulties. In actual practice, instead of the person in possession of the body‘making reasonable inquiries as may be practicable to exclude objections’, apositive act of permission for post-mortem examination is sought from thenearest available relative in the shape of a signed and witnessed form ofconsent. For transplantation, written permission is not usually obtained, but anote confirming the relatives’ lack of objection is recorded in the clinical notes.
Though in law the pre-mortal consent of the deceased is sufficientauthority for donation of organs, it is unlikely for this to be done in the face ofadamant post-mortem objection from near relatives. However, with theincreasing use of the kidney donor card, now being extended to other organs,it is usual for the spouse or other near relative to be the witness signatory, solater objection in these cases would be very uncommon.
Following medical scandals relating to commercial exploitation of donors,which ended in disciplining of some doctors by the General Medical Council,the Human Organ Transplants Act 1989 limited the scope of donation byliving donors by restricting transplantation between persons who were notgenetically related and created a regulatory authority to police such activities.
Post-mortem examinations
Similar provisions extend under the Human Tissue Act 1961 to theperformance of post-mortem examinations (but only so called ‘clinicalautopsies’ not under the direction of the coroner or Procurator Fiscal, whereno permission is required). As before, authority for post-mortem examinationmay be granted if the person lawfully in possession of the body is satisfiedthat the deceased left written or witnessed oral permission (a rare event) or issatisfied after such reasonable inquiries as may be practicable that thedeceased had not objected and that the surviving spouse or any other relativedo not object.
The lack of objection is invariably confirmed by positive written witnessedpermission. The standard Health Service form of consent has now twoclauses: (a) in relation to the post-mortem examination itself, and (b)permission to remove ‘limited amounts of tissue for therapeutic purposes,teaching and research’. This latter clause may be deleted by a relative if sodesired.
Lawyer’s Guide to Forensic Medicine
134

Part II: Hyoid Bone
The Human Tissue Act 1961 does not extend to Northern Ireland, whichhas a similar Act dated 1962.
HYMEN
Membrane at the lower end of the vagina. Various forms when intact, whichmust be distinguished from damage due to first intercourse. An intact hymenmay be completely imperforate, a condition which requires surgical treatment,as the products of menstruation are unable to escape. The aperture may bevery small, insufficient to allow normal intercourse, though this is notnecessarily a bar to pregnancy, which can occur from semen being depositedupon the vulva or even between the thighs.
The usual form of intact hymen is a wavy-edged fold of mucousmembrane with smooth margins. This may or may not allow penilepenetration. After intercourse, the membrane is usually damaged, tearing inone or more places. This rapidly heals up within a few days, leaving a smoothedge, but can usually be distinguished from an intact hymen by the presenceof indentations which extend back to the level of the vaginal wall.
After repeated intercourse or childbirth, the hymen virtually disappears, afew remnants being called ‘carunculae myrtiformes’.
Soon after rupture of the hymen, whether by penile penetration, or bymasturbation, the edges of the torn hymen will show slight bleeding, swellingand perhaps bruising.
Hymenal damage is not synonymous with rape or forcible intercourse,such damage often being present after any full penetration. Other injuriesabove or below the hymen must be sought to corroborate a charge of rape.The hymen is sometimes examined for damage by inserting a glass globe on astem into the vagina and partly withdrawing it so that the hymenal marginsare spread over the globe. An inflatable balloon, containing a light for trans-illumination, has also been developed for this purpose, but a carefulconventional gynaecological examination will give satisfactory evidence whencarried out by an experienced practitioner.
HYOID BONE
A small horseshoe-shaped bone in the upper part of the larynx or voice box, ofconsiderable forensic significance because of its use as an indicator of violenceapplied to the neck. (See also ‘Larynx’.)
135

In fact, though the hyoid has gained most attention as an indicator ofstrangulation, it is the superior horns of the thyroid cartilage, which lie below thehyoid, which are much more vulnerable and are better indicators of neckpressure.
The hyoid bone is about three to four cm in size, both from side to side andfront to back. It consists of a firm bar of bone in front (the body), from whichtwo horns curve backwards to form the greater horns or cornuae. There isusually another pair of small spurs arising from the base of the greater horns,but these have no medico-legal significance.
When the neck is squeezed from side to side, as in manual strangulation(and much less often in ligature or hanging compression), the hyoid mayfracture, usually on one side, but very occasionally on both sides. The fractureitself is clinically inconsequential, being unassociated with any dangeroussequelae, but it is an index of substantial trauma to the neck – though certaincriteria must be strictly applied to ensure that an apparent hyoid fracture isgenuine.
The following points are relevant: (a) fractures only occur when the hyoid is calcified, that is, where the
structure is bony rather than cartilaginous or gristly. Such calcification,sufficient to allow fracturing, is almost never seen in young people below
Lawyer’s Guide to Forensic Medicine
136
Figure 31: The hyoid bone

Part II: Hyoid Bone
the age of about 20. Calcification is progressive with age and mostfractured hyoids are seen in middle-aged and elderly victims;
(b) a large proportion of hyoids have natural joints between the body and thehorns, which are mobile and can give the impression of a fracture,especially to a pathologist insufficiently experienced in medico-legal work.The joints may be on one or both sides and a unilateral joint may bemistaken for a fracture. X-ray assists in recognising a joint, but also theposition of the joint is different from the usual site of fracture. Joints areusually at the junction of body with horn, whereas a true fracture is almostalways towards the tip of the greater horn, often within a cm of the tip.However, recent work has shown that the tips are often naturally mobiledue to extra joints or separate calcification of the extremity;
(c) a fracture must be shown to have occurred during life to have anysignificance. Though not as common as sometimes stated in forensicmedicine textbooks, the accidental fracture of a hyoid may occur duringremoval of the neck structures at autopsy. Ideally, a fracture causedduring life should reveal a small haemorrhage surrounding the fracturesite, due to blood being extravasated while the circulation is stillfunctioning. A post-mortem fracture will theoretically reveal no suchbleeding. Unfortunately, in a small number of cases, this sign is unreliable,as even a post-mortem fracture can allow slight passive bleeding to stainthe adjacent tissues and be visible in microscopic sections. Conversely,definite ante mortem fractures proven on other grounds, such asassociated laryngeal damage, may have no discernible haemorrhage.However, the presence of bleeding at the fracture site is usually a valuablecorroborative indicator of injury during life;
(d) it is common for X-rays to be taken of the larynx in strangulation cases andthe X-ray film to be produced in evidence. The demonstration of a fractureby this means does not form incontestable proof of strangulation – itmerely confirms that the hyoid is fractured, but cannot assist indifferentiating ante mortem from post-mortem infliction. Other criteria oflaryngeal damage, such as haemorrhage into the overlying ‘strap’ musclesof the neck, other laryngeal fractures and possibly haemorrhage into thelining membrane of the larynx, are more helpful in establishing trauma.An X-ray may be valuable in demonstrating a joint rather than a fractureand in detecting separate ossification of the tips of the horns. Such a jointhas been missed both on dissection and on X-ray by pathologists, andwhere X-rays are available, a defence opinion should be sought as to thegenuine nature of an alleged fracture;
(e) more often, the superior horns of the thyroid cartilage, which are belowand parallel to the hyoid horns, are fractured in pressure on the neck –though it must be emphasised that many deaths from such strangulation
137

reveal neither fractures of the hyoid nor thryoid, especially in youngvictims;
(f) significant, though not great, pressure has to be applied to the neck tofracture a horn, and there is great variation in the fragility of the bone. Inmany old people, the calcified, almost chalky bone is extremely brittle andwill break easily;
(g) it is possible to fracture the hyoid by a blow or a fall onto the neck, ratherthan by manual pressure, but this is exceedingly rare. It is also possible tocrack other cartilages in the larynx, such as the larger thyroid plate or thecricoid cartilage; this may be caused by strangling or by a direct blow tothe neck and rarely to a fall on some projection.The significance of hyoid fractures is always dependent upon otherfindings in strangulation, such as finger-tip bruises in the skin, bruising ofthe muscles in the neck and other signs in the larynx such as mucosalhaemorrhages. The solitary finding of a fractured hyoid with nocorroborative injuries can never be accepted as proof of strangulation;
(h) ligature strangulation causes hyoid fracture far less often than manualstrangulation, though it can occur. Hanging seldom fractures the hyoidbone.
HYPERPYREXIA OR HYPERTHERMIA
Condition of raised body temperature, sometimes fatal. Normal mouthtemperature is 37°C (98.4°F); rectal temperature about 1°C higher.
Causes
Heat exhaustion, due to salt depletion and dehydration from environmentalcauses, such as climate or boiler rooms, etc.
Heat hyperpyrexia, due to a failure of body temperature-regulatingmechanisms, again from environmental conditions.
Severe infections, the true ‘fever’ caused by micro-organisms, viruses and theirtoxins disturbing the heat regulatory centres.
Certain brain lesions, especially pontine haemorrhage, affecting the heatregulatory centres in the pons of the brain stem.
Malignant hyperthermia (qv), a condition usually following anaesthesia withhalothane or suxamenthonium drugs, though it can arise with simple nitrousoxide anaesthesia. The temperature may rise to 42°C in this condition.
Lawyer’s Guide to Forensic Medicine
138

Part II: Hypostasis (Post-Mortem Lividity)
139
HYPOSTASIS (POST-MORTEM LIVIDITY)
Gravitational settling of the blood after death. Hypostasis is more descriptive,‘lividity’ being an older and inaccurate term.
When the circulation ceases at death, the veins and the partly contractedsmall arteries relax and allow blood to flood passively into the smaller vessels.Gravity causes most of it to sink to the most dependent parts, though there isusually an earlier stage of blotchiness, even on upper skin surface, due to localvariation in degree of vessel dilatation. This early stage may commence withinan hour after death or may be delayed or absent. The main hypostasis mayalso begin within an hour or two and is well marked within four to five hoursin the average case. However, the timing is quite unreliable as an index of the timesince death. Hypostasis may be minimal or even undetectable in some cases,especially anaemic old persons and some infants. Hypostasis persists untilovertaken by decomposition, usually several days later. In deeply pigmentedbodies, especially racial coloration, hypostasis may be difficult or impossibleto detect.
The usual pattern is of hypostasis on the back of the body, neck and backof arms and legs in persons lying face-up after death. There are white patchesover the shoulder blades and buttocks where pressure against the supportingsurface has excluded the blood. When the body has lain in some otherposition, the hypostasis will be situated appropriately, unless the body hasbeen moved since death.
It was formerly believed that hypostasis became fixed some hours afterdeath and therefore could not move again if the body was disturbed. This ismost unreliable, as hypostasis may move, either totally or partially, at anytime after death. Tests such as trying to blanch rigor by finger pressure, toderive information about time since death, are used by some continentalpathologists, but are quite unreliable.
The colour of the hypostasis is of more forensic use than its totallyunpredictable timing. A cherry red hue is diagnostic of carbon monoxidepoisoning. A darker red is suggestive of cyanide and brownish colours maybe due to methaemoglobin or sulphaemoglobin, usually due to industrialexposure. In death from hypothermia (qv) the skin may be bright pink orbrownish pink, due to unreduced oxy-haemoglobin in the tissues. This mayeven be seen as a post-mortem phenomenon in bodies from cold water andalso after refrigeration.
Many corpses have a dark blue or purple hypostasis due to a congestivedeath with de-oxygenated blood in the tissues. Caution must be observed innot associating this with an asphyxial process, unless other criteria are present(see ‘Asphyxia’). Skin haemorrhages within areas of dependent hypostasis arecommon as a post-mortem phenomenon some hours or even days after death,

especially over the shoulders and back – they have no significance and mustnot be confused with true petechiae.
Hypostasis occurs in the organs as well as the skin and producesdiscoloration in the heart and intestines, etc, which have been misinterpretedas disease or injury by inexperienced pathologists.
The blotchy stage of hypostasis may be mistaken for bruises, but oncutting into the areas, the blood will be seen to be within the vessels if theappearance is due to hypostasis. If the tissues are stained with blood, then abruise is present: microscopical examination may be required to confirm theextravasation of blood in doubtful cases.
Lawyer’s Guide to Forensic Medicine
140

Part II: Identification
IDENTIFICATION
The establishment of the individuality of a living or dead person. Forensicmedical evidence is required when from unconsciousness, debility, mentalabnormality or, rarely, deliberate refusal, identity cannot be provided directlyby a living person; or when, in the case of the dead, lack of witnesses or thestate of the body present direct identification.
The problem resolves itself into the following questions:(a) What is the sex?(b) What is the age?(c) What are the height and weight?(d) What is the race?(e) What is the personal identity?
In the case of fragmented, scanty or bony remains, an additional questionmight be: are the remains human? This requires expert anatomical andperhaps laboratory serological investigation to differentiate between humanand animal origin.
In the living
The sex, approximate age, stature and race may be self-evident in most cases,though an accurate estimate of age (especially in young persons) may berequired (see ‘Age estimation’). Personal identity is usually the prime questionin the living and the following are the usual paths of investigation:(a) facial recognition, directly or by photography, by means of witnesses. A
number of remarkable errors have been reported in respect ofphotographic recognition;
(b) finger, palm and sole prints are unique if undamaged, but there must bematching prints on record for comparison;
(c) lip prints, vein patterns on the back of the hand and the configuration ofthe ear have been claimed as unique criteria, but they are hardly likely tobe on record ante mortem as a means of comparison;
(d) teeth and dentures may provide definite matching (from structure,number, extractions, fillings and other dental work) if dental records areavailable (see ‘Dental identification’);
(e) height and weight may exclude identity, but can never confirm it. Errors inprevious estimation and changes in weight can complicate the issue;
(f) congenital defects (moles, birthmarks, limb deformities, etc), scars ofinjuries or surgical operations, tattoos, asymmetries, etc, may be specificenough to assist in identity;
141

(g) blood typing, these days almost exclusively through DNA;(h) occupational stigmata (for example, coal miner’s blue scars) may assist,
but are far less numerous and specific than in former years.
In the dead
The same criteria as above can be used in the intact body but, wheredecomposition or skeletalisation has occurred, or where only fragments areavailable, additional help may be obtained from:(a) radiography of certain bones and teeth, for example, frontal sinuses which
are unique to every person. However, previous X-rays must be availablefor matching;
(b) direct measurement of bones for estimation of height, sex and race (see‘Skeletal identification’);
(c) photo or video superimposition and computerised or anatomical facialreconstruction.
Identification of the dead may be required (a) in single instances, toinvestigate a crime or the cause of death and to restore the body to relativesfor disposal, or (b) in mass disasters such as air crashes, where large numbersof bodies, often fragmented and perhaps burnt, need to be identified forinvestigative, compensatory and ethical reasons. This process requires ahighly organised operation, with skilled experts such as pathologists anddentists on the scene.
IMMERSION
See ‘Drowning and immersion’.
INCISED WOUNDS
Wounds made by sharp cutting weapon (knife, razor, cleaver, etc) or brokenglass, pottery glaze, etc.
Subdivided into cuts or slashes, where the length is greater than the depth,and stabs, where the depth is greater than the width.
The word ‘cut’ is unsatisfactory and ambiguous in medico-legalterminology, as it can mean either a laceration or an incised wound.
An incised wound shows clean-cut edges with no crushing or bruising. Onthe scalp, it can be confused with a laceration unless closely examined (see‘Scalp’).
Lawyer’s Guide to Forensic Medicine
142

Part II: Infanticide
Incised wounds can bleed copiously, especially on the head; they canbleed more than blunt lacerations, as blood vessels are not crushed, but slit.Deep stab wounds have danger of profuse internal haemorrhage frompenetrated large vessels, but any slash may lead to fatal bleeding if majorartery involved.
As with stab wounds, the severity of the wound depends mostly on theweapon. Sharp points and edges will produce long, deep cuts with littlephysical effort. Factors such as strength and sex of assailant, toughness of skinand age of victim of little importance compared with efficiency of cuttingedge.
Incised wound usually gapes, with eversion of centre of wound, the totallength of which may shorten due to elasticity of skin and contraction ofunderlying muscles. Appearances depend on anatomical area wounded.Gaping is not a reliable index of infliction during life, when wounds are foundon corpse.
Post-mortem bleeding is often profuse (especially on head), especially ifwound is dependent after death, allowing blood to escape by gravity. Ifwound made some time before death (many minutes or hours), then vitalreaction (qv) may be seen in edges. This is the only definite proof of antemortem infliction, unless bleeding is torrential and arterial, spurting in nature,indicating active heart beat. Potentially fatal complications of incised woundsare haemorrhage, infection and air embolism.
A long knife wound where the skin is loose (for example, the abdomen)may cause a zig-zag incision, due to the skin being pushed in front of theblade in an irregular fashion.
INFANTICIDE
Until 1922, the unlawful killing of any infant was murder. In that year, the notinfrequent occurrence of mental stress in the mother leading to such killingwas legally recognised by the Infanticide Act, which was repealed and re-enacted with certain amendments in 1938.
This created an alternative charge to murder with lesser penalties, if awoman by any wilful act of commission or omission causes the death of herchild being under the age of 12 months, it being shown that the balance of hermind was disturbed by reason of her not having fully recovered from theeffect of giving birth or from lactation consequent upon the birth.
Several medical points are of importance:(a) only the mother can plead this lesser charge;(b) although the Act allows a 12 month period, most killings occur within the
first few hours or even minutes after birth;
143

(c) only the clearest evidence of deliberate killing by an act of commission oromission is proceeded upon;
(d) the law presumes a still-birth and the onus is upon the prosecution toprove a separate existence (not just a live birth);
(e) indictments are relatively few, because (1) identifying the mother of aconcealed, often decomposed, infant is difficult; (2) pathological proof oflive birth is difficult and evidence of separate existence even more difficult;and (3) proof of a wilful act causing death is difficult, especially if byomission;
(f) in many cases, insufficient medical evidence leads to an alternative chargeof concealment of birth.
See also ‘Live birth’.
INTESTINE
Lower part of alimentary canal or gastro-intestinal tract. Reaches from exit ofstomach (pylorus) to anus. Entirely within the abdomen. Divided into:(a) the duodenum, about 25 cm long, into which the bile and pancreatic ducts
open;(b) the small intestine about 5 m long, the first part of which is the jejunum
and the lower part the ileum;(c) the large intestine or colon, subdivided into caecum (which carries the
appendix), the ascending, transverse, descending and finally sigmoidcolon;
(d) the rectum passing down through the pelvis to the anus.
Medico-legal significance
Intestine sometimes ruptured by blows on the front of the abdomen, as inchild abuse or kicking in the adult. External marks on the skin need not bepresent even with gross internal injury. In infants, the duodenum may besevered by a blow compressing it across the unyielding bone of the spinalcolumn, which lies at the back of the abdominal cavity.
Intestine is tethered by a membrane called the mesentery. This may beruptured or perforated by blows on the abdomen. Where the intestine ispenetrated by injury, death may be due to shock and haemorrhage or to aperitonitis caused by leakage of contents into the peritoneal cavity.
Lining of the intestine may be damaged by many poisons: for example,arsenic, antimony and other heavy metals may cause diffuse damage, withdiarrhoea.
Lawyer’s Guide to Forensic Medicine
144

Part II: Intestine
145
Figure 32: Alimentary canal and intestines

Natural perforation of intestine is a relatively common occurrence,frequently fatal:(a) perforated duodenal ulcer (a chronic peptic ulcer) floods the peritoneal
cavity with digestive juices and food, causing acute chemical peritonitis orinfective peritonitis if prolonged;
(b) perforated diverticulitis (small pouches on the large intestine) may cause afaecal peritonitis and rapid death, usually in old people. Cancer of thelarge intestine may also perforate.
Lawyer’s Guide to Forensic Medicine
146

Part II: Jaw, Injuries to
147
JAW, INJURIES TO
The lower jaw, or mandible, is a horseshoe-shaped bone which turns up at thefree ends into flat plates (‘rami’) which run in a back to front plane. At the topsof these plates are the ‘condyles’, two rollers which fit into grooves on theunder-surface of the base of the skull, forming simple hinge joints.
The upper jaw is the maxilla, the lower part of the face, continuous with therest of the skull. It may suffer extensive fractures in facial injuries, especiallykicking.
Blows on the point of the jaw may cause a violent impact to be transmittedupwards via these joints, which may lead to concussion or even braindamage, though it is unusual for the floor of the skull to be fractured in thisway.
A violent blow to the jaw may cause it to be fractured, the site varyingaccording to the point of impact. A blow on the point of the jaw may crack thejaw in the front midline, through the ‘symphysis’ or front seam. A blow on theside may split the jaw either through the tooth-bearing region or through anascending ramus either at the rear angle of the jaw or higher towards the joint.It is possible for a blow on the side to fracture the opposite side, either solelyor in addition to a fracture on the same side. Dislocation of the joints mayoccur from a side blow.
A fractured jaw can be a relatively serious injury, needing expert andurgent treatment, sometimes with wiring together of the fragments. The liningof the mouth or gums may be ripped, when the fracture is said to be‘compound’, with the broken bone exposed. Detachment of teeth and severebleeding may pose a risk to life from blockage of the mouth and air passages,but most simple fractures are unlikely to be lethal.
A relatively common combination of injuries, sometimes fatal, is a blow onthe jaw which causes the victim to fall backwards (especially if drunk) from astanding position onto the back of the head, with the likely sequel of laceratedscalp, and possibly fractured skull and brain damage. In this type of injury,there would probably be ‘contre-coup’ brain damage (qv).

KICKING
Kicking is a common method of inflicting serious, sometimes fatal injury. Theshod foot, especially the heavy boot currently in fashion amongst aggressiveyouths, forms a potentially lethal weapon which runs no risk of contraveninglegislation restricting the carrying of more obvious weapons.
Injuries may be caused by the foot delivering a direct swinging blow.Here, the force delivered is greater than that from a fist, due to the largermusculature of the leg and the added weight of foot and footwear. Anothermechanism is stamping downwards, usually on a victim already on the floor.The heel may be used and there may be a backward component to the action,causing shearing stresses in the tissues.
Another very injurious method is to stamp with the heel or sole, thentwist, which can cause tearing of the skin and tissues. Occasionally, a femaleshoe with a sharp, narrow heel may be involved, when actual stab woundscan be inflicted.
Where a kick glances tangentially across the skin surface, severe shearingstresses may be inflicted, with tearing of the surface. Direct kicks can causesevere internal damage. Where clothing is interposed, there may be noexternal damage, but rupture of the liver, intestine, spleen or lung can occurfrom extreme violence. Kicks in the male genitals may cause death from painor may raise a very large blood-filled swelling in the scrotum. The urethra(urine passage) may be ruptured.
Kicks in the neck are especially dangerous: the windpipe or larynx may beruptured and death occur from blockage of the airway or reflex cardiac arrest(qv). The muscles of the neck may be ruptured and extensive bruising mayoccur, especially under the angle of the jaw, which may be fractured,sometimes in several places.
One recently recognised danger of kicking in the neck region is that ofsubarachnoid haemorrhage (qv) due to rupture of a vertebral artery or othervessel in the base of the skull. Kicks high in the neck, below the ear, areespecially prone to cause this injury.
Kicks on the head may lacerate the scalp and fracture the skull and causeany type of internal head injury.
The differentiation of kicks from punches may be difficult or impossible,but certain pointers exist. Kicks are rarely seen in the centre of the chin orforehead. The degree of surface damage is often greater in kicking and scuffmarks and even patterned abrasions from the sole or heel may be visible.Bony injury beneath surface bruising is more common in kicking, due to thegreater force employed. Kicks are often delivered into concavities of the body,such as under the jaw, the loin, the armpit area of the exposed side and thegroin. The prominence of the cheek and eyebrow may be kicked, especially
Lawyer‘s Guide to Forensic Medicine
148

Part II: Kidneys
with a glancing blow, and the face may be ground under a stamping heel,causing fracture of the nose. In general, the best method of differentiatingkicks from punches lies in the greater degree of damage inflicted and also thepresence of patterned marks from toe-caps, sole or heel.
KIDNEYS
Paired organs in the back of the abdominal cavity, which filter waste productsand excess fluid from the blood.
Kidney (renal) failure
This may be due to many causes, some of medico-legal importance:(a) intrinsic kidney disease, such as nephritis;(b) failure of blood supply, including low blood pressure in shock after injury
or surgical operations;(c) crush syndrome, due partly to (b) and also to blockage by muscle
haemoglobin from damaged limbs;(d) acute tubular necrosis – a manifestation of shock, partly synonymous with
(b) where low blood pressure and sometimes toxic substances causedamage to the kidney tubules;
(e) poisoning by a wide variety of substances, including infections.
Temporary kidney failure
This can be treated by dialysis, which eliminates the waste products until thekidney recovers – this is most successful in causes such as shock andpoisoning. Where the kidneys are irreversibly damaged, either dialysis mustcontinue for life or a kidney transplant must be performed.
Dialysis may be either via the bloodstream (haemodialysis), where thebloodstream is diverted through an external filter system, or by peritonealdialysis, where large volumes of fluid are washed through the abdominalcavity, removing the waste products through the thin membranes of theperitoneum which cover the intestines.
149

LACERATIONS
The third class of wounds, being more serious than bruises or abrasions (qv).A laceration is defined as a wound which penetrates the full thickness of theskin and, of necessity, severs blood vessels and leads to bleeding. Beneath theskin is the subcutaneous layer of loose fibrous tissue containing many arteries,veins and nerves. The laceration may extend more deeply and involve muscleand ‘fascia’, the thin sheets of fibrous tissue which separate the various musclecompartments.
Lacerations may be ragged, where due to blunt or tearing impact, or clean-cut, where caused by a cutting instrument (see ‘Incised wounds’). However,where a blunt injury occurs over a firm base, especially the head, a clean splitmay be inflicted (see ‘Head injury’, ‘Scalp wounds’).
The edges of a blunt laceration tend to be inverted and bruised, though thelatter may be confined to a narrow rim. The danger to life depends upon thesite and extent of the injury. If large blood vessels underlie the wound, such asthe neck, armpit or groin, then fatal haemorrhage may occur. If the skin loss isprofound, such as with a ‘flaying’ laceration of a limb due to the rotatingimpact of a vehicle wheel, then gross shock, haemorrhage and infection mayprove fatal. Bleeding may be more profuse from an irregular laceration thanfrom a clean knife slash, as in the latter, complete transection of blood vesselsmay allow elastic retraction and reduced bleeding, whereas tearing andpartial rupture in a blunt injury may keep the vessel open.
LARYNX
The voice box or ‘Adam’s apple’, more prominent in males. Consists of acomplex cartilaginous box at the upper end of the windpipe, with its entranceprotected by a flap (epiglottis) which prevents food from entering from theadjacent pharynx (back of the throat).
Immediately above the main part of the larynx (thyroid cartilage) is ahorseshoe-shaped bone, the hyoid (qv).
The upper end of the thyroid cartilage also has two slim horns (cornuae orsuperior horns) which lie parallel to the horns of the hyoid bone and are joinedto them by a membrane. This is of importance in fracture of the horns duringstrangulation (see ‘Hyoid bone’, ‘Strangulation’).
At the lower end of the larynx is a single ring of cartilage, shaped like asignet ring, which is the cricoid; this may be fractured in the front from severepressure or a blow. The main plates of the thyroid cartilage may also becracked from severe strangling pressure or a direct blow, either from a kick orvehicle accident, or a Karate-type chop.
Lawyer‘s Guide to Forensic Medicine
150

Part II: Larynx
The interior of the larynx may become blocked and cause death fromsudden cardiac arrest or asphyxia. The entrance or glottis may be blocked byfood just swallowed (see ‘Choking’) or swelling of the membranous margins.This is called ‘glottal oedema’ and may occur from allergy, such as stings orspecific food; from infection such as Haemophilus influenzae in children; orfrom inhalation of irritant fumes.
151
Figure 33: Larynx and hyoid bone

Blockage from dentures, small toys or any foreign inhaled object may alsocause sudden unexpected death (see ‘Choking’).
The urgent treatment of a blocked larynx is tracheotomy, the making of ahole in the windpipe just below the larynx, unless an endo-tracheal tube canbe inserted through the mouth.
LIGATURE
Surgically, a tight constricting thread applied to a blood vessel to staunchbleeding.
Forensically, a strangling band applied around the neck; all manner ofmaterials may be used, from thin wires to flat bands of fabric. The ligatureusually leaves a characteristic mark, red during life, but becomes brown,leathery and parchment-like from drying after death.
The pattern of the ligature, such as spiral rope or woven cord, may beclearly imprinted. The same features are seen in hanging (qv) but the positionon the neck is different. In homicidal strangling, the mark will run more orless horizontally and a cross-over point is often visible. In suicidal strangling,there may be several loops of ligature and a knot or other means ofmaintaining the pressure. The latter features by no means preclude self-application before unconsciousness and death supervene.
A ligature fractures the laryngeal structures less often than manualstrangulation, but hyoid and thyroid cartilage damage sometimes occur.Congestive changes and petechiae are often seen, more frequently than inmanual strangulation, as there is less likelihood of sudden cardiac arrest frompressure on the carotid sinuses, which finger pressure may provoke.
As in manual strangulation, there may well be bruising of the neck, lessoften from the assailant, but vertical scratches are frequent from the victimscrabbling at the ligature in an attempt to remove it.
Bruising may occur in the tissues under the ligature, but generally there isless trauma than in manual strangulation. Where the ligature has been appliedover clothing, the skin mark may be minimal or absent, but the weave of thefabric may be imprinted on the skin, as in manual strangulation, where handpressure is applied over a collar.
A wide band of fabric can be used as a ligature, but on bare skin, this oftenleaves a narrow mark due to tension lines in the stretched fabric. Also, wherea wide band has been used, it is possible to kill by constriction without leavingany mark on the neck, especially in children.
In post-mortems on infants or, sometimes, on fat people, skin creases onthe neck have been mistaken for ligature marks. These are pale areascontrasting with the more reddened area of hypostasis.
Lawyer‘s Guide to Forensic Medicine
152

Part II: Live Birth
The signs that a ligature was applied during life include the obviouscongestion and petechial haemorrhages above the mark, with often sometissue swelling; and, sometimes, a line of small dotted haemorrhages along theline of the ligature.
LIVE BIRTH
Not synonymous with ‘separate existence’, though the latter must include livebirth. As defined by the Births and Deaths Registration Act, a still-birth is onewhere the child has issued forth from its mother after the 24th week ofpregnancy and which did not at any time after being completely expelledfrom its mother, breathe or show any other signs of life; thus, a live birth isdefined by implication from this description.
These legal definitions do not coincide completely with medicalinterpretation – for instance, to a doctor, a baby might be obviously alivewhen half-born, but if those signs of life fade before the feet are expelled fromthe maternal passages, then legally, there was no separate existence. Thistheoretical discrepancy led to the Infant Life (Preservation) Act (1929) to coverchild destruction.
Again, with modern obstetrical expertise, foetuses under 24 weeks can belive-born (even at 18 weeks, though they are unlikely to survive) and maysurvive from about 22 weeks.
Separate existence requires the extrusion of the whole infant from thebody of the mother, but this does not include the umbilical cord or placenta(afterbirth).
Proof of live birth
For a charge of murder or infanticide to lie, evidence of separate existencemust be offered. This, as stated above, is not medically synonymous with livebirth, but unless live birth can be proved, then legally, a separate existencecannot have occurred.
Witnessed observation at the time of delivery is the best and only absoluteproof of live birth, but in most forensic situations this is lacking due to thecircumstances. The debate then revolves around the retrospective examinationof a dead infant.
Establishment of breathing is usually the only helpful criterion. When achild is being born, a point is reached where its head is first exposed to the airand it is then able to breathe. At or about the same time, the placenta becomesfunctionally detached from the lining of the womb and can no longer delivermaternal oxygen. This provides a stimulus for the initiation of air breathing.
153

Such breathing may begin whilst most of the baby’s body is still within thematernal birth canal, so a separate existence has not yet been legallyestablished. Where a pathologist examines a dead new-born child, it can bevery difficult or impossible to give a firm opinion on whether breathing didbegin. Lungs which have not breathed are solid, dark red, collapsed andairless, whilst those where breathing has become established for a fewminutes become spongy, pink, crepitant (crinkly to the touch) and light intexture.
However, there is a whole spectrum between these two obvious states andwhere there are any signs of post-mortem decomposition (as so often happensin concealed births or delayed examinations), no reliable opinion can beoffered.
For many years, the so called ‘hydrostatic test’ was employed todistinguish lungs that had breathed, but this has now been completelydiscredited by most experienced medico-legists, though some still erroneouslycling to its fallacious results. The rationale was to drop the lungs and/orpieces of lung into water, to see if they would float. Sinking meant nobreathing, floating meant that breathing had occurred. However, even withlater enforced modifications, such as the complete exclusion of lungs with anytrace of decomposition (which produces gas from putrefactive processes) andvarious mystical manoeuvres such as compressing and treading lungfragments in cloths, the test is quite fallacious. The best description of thehydrostatic test was given by Professor Polson, who said, many years ago, ‘thetest was suspect even in 1900 and requires no detailed discussion, because it isnow known to have no value’.
In spite of this and other authoritative opinions, such as Shapiro andGordon, reliance is still placed in the test in some quarters, without scientificfoundation. The best that can be said for it is that floating lungs have noevidential value; if they sink, then they were likely to have come from a still-birth. Of course, any attempts at resuscitation completely negate anyassessment of the condition of the lungs.
Other pathologists rely upon the microscopic appearance of the lungs, butthis also is fraught with uncertainty in the frequently marginal cases whererespiration may only have lasted for a short period. The argument that theheight of the cells lining the air passages is an index of breathing (highcolumnar cells – no breathing; low flattened cells – breathing) has been shownto be related to maturity of the infant, not a function of respiration.
The most reliable test is the naked-eye examination by an experiencedpathologist of the fresh lungs at autopsy. Where definite pinkness, sponginessand crepitation are apparent, then respiration probably occurred. Anythingless than these definite signs is unacceptable and the benefit of the doubt mustbe given.
Lawyer‘s Guide to Forensic Medicine
154

Part II: Liver
The umbilical cord progressively shrivels after birth and drops off somedays later. This is a late sign and is not helpful in the majority of cases where astill-birth has to be distinguished from death very shortly after delivery. In thefirst day the cord becomes shrivelled, but this may also happen in a still-birth.In a live baby, a reddened zone of separation is seen at the umbilicus in 36–48hours and the cord is usually cast off before the end of the first week.
Food in the stomach is naturally a sign of live birth.If the baby has been washed and tended (with removal of the cheesy
vernix from the skin), it is likely to have been a live birth, but not necessarilyso.
Air in the stomach is not a reliable sign, as both post-mortem changes andartificial respiration can produce this appearance, apart from the activeswallowing of air.
Maceration. Where a new-born baby is macerated, that is, decomposed in acertain way which indicates death in utero, then still-birth is established.Similarly, very gross congenital deformities, sufficient to make the child amonster, may usually (but not invariably) be taken to be incompatible with aseparate existence.
The whole problem is fraught with uncertainties and the invariable rulefor the pathologist must be to assume still-birth unless there isincontrovertible evidence of live birth. As this is usually based on evidence ofbreathing, the pathologist is unable to say that this is also definite evidence ofa separate existence, as breathing can and does occur whilst the baby is stillnot fully extruded from the mother.
Evidence of feeding, and separation of the cord, must be demonstrative ofa separate existence.
LIVER
The largest organ of the body, situated in the upper abdomen, almost entirelyprotected under the edge of the rib cage. The usual weight is about 1,500 g: indisease states, such as alcoholic fatty degeneration, this may increase to twicenormal size, but after prolonged disease, such as cirrhosis, it may shrinkbelow the normal weight.
The liver performs most of the chemical processes connected withmetabolism and the processing of digested food, but has many otherfunctions, such as producing bile – a substance which both provides analkalising medium for digestion in the intestines and removes the wasteproduced by the breakdown of old blood cells.
Many diseases afflict the liver. One of the most common is a virusinfection called ‘infective hepatitis’ or ‘yellow jaundice’, of which there are
155

three main types, Hepatitis A, B and C. The first – and least dangerous – isusually spread via the gastro-intestinal tract, the other two by virus gainingdirect access to the body, as in injections, including drug abuse, transfusions,or by sexual intercourse.
Jaundice, which is an accumulation of bile products in the blood, can becaused by any process which either prevents the outflow of bile (‘obstructivejaundice’), for example, gallstones or cancer of the pancreas or liver, or fromliver failure, in which damage to the liver cells fails to clear the bile pigment(‘bilirubin’) from the blood.
Alcohol is the most common liver poison. Taken over a considerableperiod (at least a couple of years) even moderate excess of alcohol may lead tofatty degeneration and enlargement of the liver – partly due to a direct toxiceffect and partly due to poor nutrition, especially proteins and vitamins,which is common in heavy drinkers.
If the fatty degeneration persists for a long time, then the liver cells maydie and the organ may contract and become nodular and fibrotic, thecondition known as cirrhosis.
The liver is vulnerable to heavy impact upon the abdomen and lowerchest, such as may be suffered in traffic accidents or kicking. The organ mayrupture or tear, allowing blood to escape into the abdominal cavity. It hasremarkable powers of repair and regeneration.
LONGEVITY
See ‘Expectation of life’.
LSD (LYSERGIC ACID DIETHYLAMIDE)
The initials are derived from the German Lyserge Saure Diethylamid.One of the group of psychoactive drugs, often termed ‘psychedelic’ or
‘hallucinogenic’, though this description is not strictly accurate. Other drugswith a broadly similar action include mescaline and extracts from certainfungi, such as psilocybin from the Liberty Cap, a European magic mushroom.
Minute amounts of these drugs can cause gross distortions of perception,with visual and auditory fantasies. Though not physically dangerous in atoxicological sense, mechanical injury and even death may occur from rashacts undertaken whilst this abnormal state persists, such as falling fromheights under the impression that the subject can fly, or attempting to stopmoving trucks with one hand. Occasionally, the sensual distortions are so
Lawyer‘s Guide to Forensic Medicine
156

Part II: LSD (Lysergic Acid Diethylamide)
gross as to lead to acute psychic disturbances. True dependence andwithdrawal symptoms do not occur with these drugs.
157

MALIGNANT HYPERTHERMIA
A condition of high body temperature almost exclusively associated withanaesthesia, where the use of some anaesthetic agents and muscle relaxantstrigger a metabolic change in the muscles, with great heat production,sometimes reaching 43°C, the normal being 37°C.
Succinylcholine relaxant and halogenated anaesthetics, especiallyhalothan, are the most frequent initiators of hyperthermia.
It occurs about once in every 10,000 anaesthetics, estimates ranging fromone in 5,000 to one in 70,000.
It is familial and other relatives should be tested in case they are exposedto the same danger.
MASOCHISTIC (SEXUAL) ASPHYXIA
A common form of sexual deviation, almost totally confined to men, usuallyadolescent to middle-aged. Very few female instances quoted in worldliterature.
Fatal cases encountered because of failure of equipment, but this isobviously only the tip of the iceberg of successful deviants. Sexual pleasure,presumably orgasmal, is obtained by achieving transient deprivation of bloodto the brain, usually by pressure on the neck or blockage of the breathingpassages.
A running noose tightened by extending the legs or by a counterweight ismost frequent, though enveloping the head in plastic or pressing the faceagainst some occluding fabric is sometimes encountered. The syndrome isusually signposted by other evidence of deviation, especially transvestism,bondage, masks, pornography, mirrors, etc. Some are bizarre in the extremeand may involve solvent inhalation, the use of anaesthetic gases, etc.
The vast majority of deaths are accidental and represent a failed episode ina long established habit. A proportion seem to have some intrinsic ‘deathwish’ element, as the mechanics of the procedure would appear to admit of noprospect of survival. However, there still may be no definite intent to commitsuicide and most cases are undoubtedly non-suicidal, as can be seen byattempts to pad the neck to avoid a mark from the noose and other evidenceof a repetitive trait.
Lack of awareness of this relatively common accident leads someuninformed coroners to label them as ‘suicides’, which may have undesirablelegal and social consequences for the family. Not infrequently, a young boy,even down to the age of 12, may be found hanged. There is usually a sexualelement in these deaths, albeit occult or obscure, even though they may be
Lawyer‘s Guide to Forensic Medicine
158

Part II: Misuse of Drugs Act 1971
wrongly attributed to ‘experimenting with ropes after seeing televisionWesterns’!
METHADONE
An opiate pharmaceutical which is a powerful analgesic, but also intended forthe replacement treatment of heroin and morphine addicts. It has become adrug of abuse in itself, deaths in Scotland in 1995 exceeding those from heroin.
It is usually prescribed as a syrup, widely available on the illicit drugmarket. Overdose is common, whether as a prescribed replacement for heroinor used as the sole drug of abuse.
MISUSE OF DRUGS ACT 1971
In 1973, this Act came into force to sweep away the previous legislation of theDangerous Drugs Acts and the Drugs (Prevention of Misuse) Act 1964.
A drug is defined by the World Health Organisation as ‘any substance,other than those required for the maintenance of normal health, that whentaken into the living organism may modify one or more of its functions’.
The WHO definition of drug dependence is ‘a state, psychic andsometimes also physical, resulting from the interaction between a livingorganism and a drug, characterised by behavioural and other responses thatalways include a compulsion to take the drug on a continuous or periodicbasis in order to experience the psychic effects and sometimes to avoiddiscomfort of its absence. Tolerance may or may not be present.’
The current Act was designed to control the misuse of drugs of manykinds, but especially narcotics and other drugs of dependence. It categorisesdrugs of dependence into various degrees of harmfulness and grades thepenalties for misuse. It also brings UK law into line with internationalagreements on drugs.
It controls unlawful possession and trafficking, prescribing and supply,trading and production of such drugs, and affords means of constantsurveillance of drug dependence in the UK. It also has provisions fornotification of addicts and the fostering of education and research in relationto drug dependence. The Act applies to Northern Ireland as well as toEngland, Wales and Scotland. It contains 23 sections and 5 Schedules.
159

Some major provisions
Section 1 established a statutory body called the ‘Advisory Council on theMisuse of Drugs’, which advises the government on all aspects of the drugproblem, with particular emphasis on the social aspects. This Council has atleast 20 members, drawn from the medical, dental, veterinary, pharmaceuticaland chemical industries.
Section 2 deals with the categorisation of drugs of dependence, classingthem into three groups, Class A, Class B and Class C, graded for penaltypurposes:
Class A lists the most dangerous drugs of dependence such as morphine,heroin, cocaine, pethidine, LSD, methadone, cannabinol and injectableamphetamines.
Class B contains addictive drugs of intermediate potency including oralamphetamines, cannabis plant material and resin, codeine, dihydrocodeine,methylamphetamine, and a number of other synthetic substances includingcertain barbiturates.
Class C drugs are rarely involved in dependence but are included for the sakeof completeness. These include substances such as certain benzodiazapines,chlorophentermine, meprobamate, pipradrol, etc.
The classification into the three groups above is mainly for the purposes ofcategorising the maximum penalties which may be applied for offences, onthe basis of the drug’s potential harmfulness when misused.
A totally different classification is used for the purposes of the controls tobe applied to their use for legitimate purposes. This is the classification whichmainly concerns the pharmacist and is set out not in the actual Act, but in theRegulations.
This second classification is broken down into four schedules:
Sched 1: Prohibited drugs, except with Home Office authority, for example,cannabis, LSD, raw opium, ecstasy.
Sched 2: Full controlled drug requirements in relation to prescribing, safecustody, keeping of registers, for example, diamorphine, pethidine, cocaine.
Sched 3: Barbiturates, meprobamate, pentazocine, etc.
Sched 4: Benzodiazapines, etc.
Sched 5: Preparations containing small amounts of controlled drugs.
Further legislation under the Act is the reconfirmation in 1973 of theNotification of and Supply to Addicts Regulations. A person is regarded asbeing addicted to a drug if (and only if) he has, as a result of repeatedadministration, become so dependent on a drug that he has an overpowering
Lawyer‘s Guide to Forensic Medicine
160

Part II: Misuse of Drugs Act 1971
desire for the administration of it to be continued. Under the regulations, anydoctor who attends a person whom he considers is addicted to any drug inthe following list, must within seven days furnish certain particulars to theChief Medical Officer of the Home Office.
No doctor may administer or authorise the supply of cocaine ordiamorphine or their salts to an addicted person except for the purposeorganic disease or injury, unless he is licensed to do so by the Secretary ofState.
Sections 3, 4 and 5 concern the import or export of controlled drugs, theproduction, supply or an offer to supply such drugs and the possession ofdrugs of dependence. Apart from exempted persons, such as doctors, dentists,veterinary surgeons, etc, it is an offence to possess or to attempt to possess acontrolled drug unless to prevent an offence or to hand the drug to somesuitable person.
Section 6 makes it an illegal act under any circumstances to cultivate thecannabis plant.
Section 7 contains the exemptions granted by the Home Secretary tocertain drugs or to persons from the foregoing sections. This is naturallyintended to allow those persons properly entitled to handle such drugs toobtain the legal possession of such substances. A number of other sectionscontrol the use of premises for the preparation and smoking of opium,cannabis, etc, and a number of other matters mainly of concern to the police.
Sections 10 and 11 control the packaging, labelling, transport and disposalof control drugs and the documentation of possession and transactions. Thissection particularly concerns doctors and pharmacists. It also includes thenotification of addicts to the proper authority by doctors, as brought into forceby the previous legislation. This notification of addicts was reconfirmed in theNotification of and Supply to Addicts Regulations 1973.
Section 13 concerns prohibitions for failure to notify addicts andauthorising prescribing to addicts. Though neither of these matters is anoffence under the Act, they would lead to an investigation and to possibleprohibition of prescribing in the case of an individual practitioner who floutsthe regulations.
Section 15 provides that if the Home Secretary considers that a doctor isprescribing in an irresponsible manner in respect of drugs of dependence, hecan refer the matter to a professional panel for quick action and depending ontheir advice, the doctor may be prohibited from further prescribing of suchdrugs. Other sections provide for safeguards relating to withdrawal of theright to prescribing and describe tribunals and advisory bodies withnominated members from such bodies as the GMC, the Royal Colleges andthe BMA.
161

Section 17 states that the Home Secretary may require any doctor orpharmacist to provide information about prescriptions if it appears that thereis a social problem arising in a certain area.
MOBILITY AND ACTIVITY AFTER INJURY
Except in gross destructive injury of the brain, heart or large blood vessels, it isunsafe to be dogmatic about the ability or inability of an injured person tomove and to perform certain acts. Especially in brain injuries, the ability towalk, speak and perform co-ordinated movements may be retained evenwhere there has been gross cerebral damage, especially if confined to thefrontal areas. Similarly, it is possible for suicides repeatedly to shoot or stabthemselves in the head, neck or chest, even where some or all of the woundswould, individually, appear to be rapidly fatal.
Though most gross injuries are indeed associated with sudden andimmediate loss of consciousness and function, this is by no means a uniformresponse. In head injuries, unless the damage involves vital areas of the brain,it is unsafe to deduce the ability, or lack of it, from purely post-mortemfindings.
Neither can an autopsy prove or exclude the presence of a period ofconcussion after a head injury, though a strong probability might beexpressed if evidence of a forceful impact is obtained.
More confident assumption of instant incapability may be made if:(a) heart function must have ceased abruptly, such as in cardiac arrest
(provable by witnesses, not autopsy), large penetrating injuries of the heartor gross rupture of the aorta, where sudden catastrophic loss of bloodpressure must have led to immediate deprivation of blood supply to thebrain;
(b) where extensive brain damage has affected the brain stem and upperspinal cord, involving the control centres for heart and breathing.
In cases of severe chest injury, such a ‘flail chest’ from multiple rib fractures orsevere external or internal bleeding, a clinical opinion may be more valuablethat that of an autopsy pathologist, though even experienced clinical advicemust be viewed with the acceptance of very wide physiological variation.
Lawyer‘s Guide to Forensic Medicine
162

Part II: Morphine
MORPHINE
The unripe seed capsules of the poppy Papaver somniferum provide crudeopium, which contains a mixture of natural narcotic alkaloids. These includemorphine, codeine, thebaine, papaverine, etc. From morphine, severalderivatives can be made including heroin (qv), which has about five times thenarcotic power of morphine.
Morphine can be taken by mouth, smoked or be injected. The fatal dose isimpossible to estimate, due to personal variation and the great tolerancewhich addicts develop: in the latter, many times a therapeutic dose has to betaken in order to attain any narcotic effects.
The therapeutic dose is of the order of eight to 20 mg. In a non-habituatedadult, a likely fatal dose might be about 180 mg . Much lower doses havekilled and anything over 60–100 mg is potentially dangerous, 250 mg usuallycausing death.
Addicts can tolerate far higher levels, equal to fatal amounts in non-habituated persons.
Liver and lung disease form dangerous conditions for morphine takers, asthe liver is responsible for detoxifying the drug and the depressant effect onbreathing makes it unwise to administer morphine to those with chestdiseases.
The effects of morphine appear within half an hour of swallowing andwithin minutes of injection (usually into an arm or leg vein, as with heroin).Fatal overdoses usually kill within six to 12 hours, though deaths haveoccurred within the hour. Preliminary euphoria is followed by drowsiness,weakness, headache, giddiness, deepening into stupor and then coma if thedose is large enough. The pupils of the eye are contracted, until just beforedeath, when they often become large. Death occurs from depression ofrespiration, with eventual cessation of breathing.
Post-mortem signs are limited to non-specific appearances of a congestivedeath, but there may be marks of injection on the limbs, especially at the bendof the elbow, the forearm or thigh. These may be scarred and infected, due tothe unhygienic methods of ‘mainlining’ with unsterile syringes and medicinedroppers, as with heroin.
Addicts who share needles with each other run a substantial risk ofcontracting viral hepatitis, a frequently fatal infective jaundice, as well as HIV.
Toxicological analysis may recover morphine from the blood, urine or skinaround an injection site and also from the bile on the gall bladder. However,even fatal poisoning cases may give disappointing results on autopsy analysis,especially on blood levels, which may be extremely low or even negative inundoubted morphine deaths.
163

MUMMIFICATION
A relatively uncommon type of post-mortem change in temperate climates, inwhich the body undergoes drying and partial preservation instead ofputrefying. It requires a dry environment, warmth and a current of airassisting the process. Most commonly seen in the bodies of new-born infants,sometimes in infanticide or concealment of birth, who are hidden in a dryplace, such as an attic, cupboard or chimney. The lack of bacteria in the babyrecently delivered from a sterile womb discourages putrefaction and the bodymay become dry, hard and shrivelled.
Adults dying in hay lofts or attics may undergo the same change, the skinbecoming brown, hard and tightly stretched, though the features may remainrecognisable for long periods.
The leathery tissues may persist for many years, eventually beingdestroyed by moths, beetles, mice and other predators. The body may escapedetection because of the absence of the smell of putrefaction. The gauntfeatures may become covered with moulds or fungus.
Mummification is much more common in dry desert climates where theprocess of artificial mummification was first suggested by the frequency ofnatural conversion (Egypt and South America).
MUTILATION
The deliberate disfigurement or dismemberment of the living or dead body.May be from sadistic or sado-sexual motives, where horrific injuries can beinflicted: or may be self-inflicted (see ‘Fabricated injuries’).
Additionally, mutilation of murdered bodies may be to facilitateconcealment or transport and to hinder identification.
Types of mutilation
Sadistic mutilation is almost invariably inflicted upon a woman by a man andtypical patterns exist, the damage usually having a sexual orientation. Knifewounds are by far the most common – slashes and stabs involving breast,genitals, abdomen, buttocks and thighs are typical. Stabs into the breast maybe multiple and sometimes are patterned, for example, radial or circular.Injuries may be confined to the nipple, including complete amputation orbites far more severe than those seen in amorous excitement. Sometimes, thewhole breast may be removed, usually as part of fatal injuries or post-mortemmutilation.
Lawyer‘s Guide to Forensic Medicine
164

Part II: Myocardial Infarction
The abdomen and pubic region are also targets for sado-sexual attack – thepubic eminence or the vulva may be slashed. The abdomen may be openedand in extreme cases of the ‘Jack the Ripper’ type, intestines and other organs,including the womb, may be removed and may be displayed in ritual fashion.
Penetration of the abdomen, either directly through the front wall or pervaginam by a variety of instruments and weapons, is also a well known‘Ripper’ perversion, sometimes associated with bizarre bondage andpatterned wounds. Slashes and stabs on the buttocks and injuries to the analregion also have sado-sexual connotations. Less clearly defined sexualmotives may lead to decapitation, again sometimes associated with ritual acts(the Byrne case).
Post-mortem mutilation may be a variant of the above injuries, but atotally different motive exists as an attempt to dispose of a dead body, usuallythe victim of homicide. The object is to divide the body both to make thedisposal of smaller fragments easier, and also to make identificationimpossible. Clandestine cremation may be attempted or even passing thebody through a waste disposer (Lofrumento, USA). More often, disposal byburial or in water is employed.
The possibility of surgical experience is often discussed, but in practicesuch expertise is rarely present (for example, Fred West), though several casesin recent years have involved butchers. The instruments used need not beparticularly specialised nor sharp, as the Byrne (Birmingham) decapitation,which was performed with a blunt table knife. The forensic science aspectsresolve around the recovery of blood and tissue traces from the scene,including drains and pipes and the possibility of DNA matching.
Forensic medical aspects include the anatomical proof of human remainsand the determination of sex, age and other identity (qv).
MYOCARDIAL INFARCTION
Death of part of the heart muscle due to blockage of a coronary artery. One of the forms of ‘heart attack’, but all such attacks certainly need not be
infarcts. Death may ensue at any time after the onset of the infarct, fromimmediate sudden death to survival for many years, but an infarct alwaysleaves the residual danger of a subsequent infarct or death from one of theother sequelae of coronary artery disease (qv).
The most common cause of a myocardial infarct is a coronary thrombosis,though this again is not invariable. The features classically consist of pain inthe chest passing down one or both arms or to the back, sweating, sickness,pallor, breathlessness and collapse, but there is a wide spectrum of symptomsand indeed, many infarcts are ‘silent’ or are mistaken for ‘indigestion’, beingdemonstrable only as a retrospective finding at post-mortem examination.
165

At the moment of blockage of a coronary artery, usually by a thrombus,the dramatic signs of infarction do not commence. There is a latent periodwhich may be hours or even a day or so until a threshold point is reachedwhen the symptoms begin. This makes the diagnosis of an infarct difficult atpost-mortem, if death has occurred soon after the blockage, and makes theinterpretation of some accidents equally difficult. For instance, a man maycollapse at the wheel of his car or the pilot of an aircraft may becomeincapacitated at the controls. Though long standing coronary artery diseasecan be seen at post-mortem, there may be no fresh abnormality to explain theaccident and insufficient time may have elapsed for an infarct to be visible tothe naked eye (up to 24 hours) or even to standard microscopical examination(8–12 hours). There are newer methods available using enzymes andfluorescence microscopy which can reveal infarction within 3–6 hours, butspecialist techniques are needed. This has profound medico-legal importancein accident investigation and even in criminal cases, where death following anassault can be shown to be due to, or contributed to, by a heart attack.
Where a myocardial infarct is not fatal (the majority of cases), healing ofthe muscle occurs and a fibrous scar develops, taking about three months toattain its permanent appearance.
Any person with such scarring is always vulnerable to heart disorders andthe risk of sudden death from instability of the heart muscle function(arrhthymias, ventricular fibrillation and cardiac arrest).
It is now statistically proven that sudden severe exertion can precipitatesudden death in persons with coronary artery disease, but these are rarelyacute myocardial infarcts.
MYOCARDITIS
An inflammation of the heart muscle, often fatal. Many general infections mayinclude the heart, such as diphtheria, but the term is usually reserved forinflammatory conditions of obscure cause, sometimes viral.
A type which has been blamed for many sudden unexpected deaths inyoung adults is called isolated myocarditis or sometimes Fiedler’s or Saphir’smyocarditis.
For a firm diagnosis, post-mortem microscopic evidence of aninflammatory cell reaction and areas of heart muscle necrosis (qv) must beobtained.
Criteria have sometimes been relaxed and a few scattered inflammatorycells seen in the heart muscle are insufficient for a firm diagnosis. A survey offatal transport accidents in the RAF and in Australia, where natural diseasecould have played no part, showed that an appreciable number of victims had
Lawyer‘s Guide to Forensic Medicine
166

Part II: Myocarditis
minimal signs in the heart that might in other circumstances have been calledmyocarditis.
167

NECK-HOLD DEATHS
Deaths usually in police custody, though some occur during otheraltercations.
Like positional or postural asphyxia (qv), this was first reported in theUSA, when a standard police restraint method, using an arm around theoffender’s neck, led to a series of deaths. The police arm-lock was of twotypes, one where the forearm was used as a bar across the front of thesubject’s throat and another, soon proscribed, used the crook of the elbowcentred on the throat. The latter is more dangerous, as the forearm and upperarm form the limbs of a ‘V’ which can impinge on the carotid sinuses andcause cardiac arrest (see ‘Vagal inhibition’). The forearm bar was thought to besafe, but it can also cause death, either by blocking the airway by pressing thelarynx upwards and backwards, or by cardiac arrest from general pressure onthe neck, especially in adrenaline-mediated circumstances of a violentstruggle.
In Britain, arm-locks are now excluded from police procedures, because ofa series of fatalities.
NECROSIS
Death of living tissue, usually from deprivation of blood supply (calledinfarction), physical damage (mechanical injury, heat, cold, electricity,chemicals, radiation, etc) or infection.
Medico-legally, more important types include necrosis of heart muscle (see‘Myocardial infarction’), or periphery of limbs from embolism (qv) of mainarteries or cold injury, and necrosis of brain, often called softening, whichleads to strokes.
Lawyer‘s Guide to Forensic Medicine
168

Part II: Obscure or Negative Autopsy
OBSCURE OR NEGATIVE AUTOPSY
Though the autopsy is vastly superior to clinical examination in determiningthe cause of death, between 5–10% of autopsies provide no satisfactoryanswer, even when the most extensive investigations are made. These aremost frequent in children and young adults. The ‘cot death’ (qv) or SuddenInfant Death Syndrome accounts for some, where by definition, nomorphological findings are apparent.
In young adults, sudden unexpected death remains unexplained in a smallbut significant proportion, sometimes associated with extreme exertion on thesports field. When all ancillary investigations, such as microscopicexamination of tissues, microbiology, toxicology and virology, prove negativethen the cause must remain ‘unascertainable’. Occasionally seen in olderpersons, these examinations may be termed an ‘obscure’ or ‘negative’ autopsy.The mechanism of death is due to some occult malfunction which leaves nomorphological or chemical signs.
The death is presumed to be due to natural causes, usually a suddencardiac arrest or other form of heart failure, though this cannot be objectivelydemonstrated.
The reason that more cases appear to occur in young persons may largelybe explained by the fact that they do not have the overlay of arterialdegenerative disease that is so common after middle age. Where a man of 60drops dead, for instance, the true cause of death may in reality be just asoccult as that of the 20 year old football player on the next mortuary table. Butbecause the older man is likely to have some degree of coronary arterydisease, or thickened left ventricle due to high blood pressure, there is anatural and understandable tendency for the pathologist to ascribe the deathto that, even though the extent of the disease may be only marginallysufficient.
Another cause of apparently negative autopsy findings is an insufficientlythorough post-mortem examination. In reviewing such cases, a very detailedexamination of the coronary system may reveal a blocked vessel that waspreviously overlooked. Microscopic (histological) examination may revealdisease unapparent to the naked eye (a myocarditis – inflammation of theheart muscle – for instance). Less often, bacteriological or virologicalinvestigations may reveal a pathogenic infection. More often, analysis of bodyfluids and organs may show some toxic substance, including a high level ofalcohol, which might not have been suggested by the circumstances.
Where a thorough examination still provides no satisfactory explanation,the pathologist must resist the temptation to offer a speculative cause of deathbased on minimal findings, which he would not accept in other circumstances.To the younger pathologist especially, such a temptation is increased by thefear of censure for failing to provide an answer. All pathologists are naturally
169

influenced to some degree by the need to satisfy the coroner or other lawofficer, as well as the family, by providing some explanation. However, it iswell known and accepted that a small proportion of autopsies remain obscure,and truth should not yield to expediency.
Lawyer‘s Guide to Forensic Medicine
170
Part II: Patterned Injuries
PATTERNED INJURIES
Abrasions give the most detail of the nature of an inflicting object. Bruisesshow a more blurred pattern, but sometimes are useful, especially some timeafter infliction when surrounding swelling subsides. Intra-dermal bruising, inthe uppermost layer of the skin, may provide a good reproduction of theimpacting object and is often mistaken for an abrasion. After death, theintensity of abrasion damage is usually enhanced due to drying of the baredskin surface and bruises usually become more visible, albeit progressivelyblurring over time. Lacerations rarely give an accurate imprint of an inflictingobject, unless the outline is particularly distinctive, such as a large wrench, etc.(See, also, ‘Abrasions’, ‘Bruises’, ‘Lacerations’).
Types of patterned injury
A geometric pattern, often in vehicle accidents, may occur when the grid of aradiator, headlamp rim, mascot or tyre tread is imprinted on the skin. Hardfabric, such as the cord weave of a driving glove, may mark the skin, as inheavy slaps on a cheek. Woven or plaited cords or thongs, as in ligatures orwhips, may leave a clear pattern.
Pressure through woven fabric, such as strangulation through a polo-necked jumper, may leave a clear imprint, as may a neck chain.
Recognisable patterns can form from blows from distinctive weapons, such as ahammer-head, spanner, etc. The exact size need not be matched by the skinmark, as both the elasticity of the skin and tissue swelling may distort themark. Also, the impact may be glancing and a sliding mark of larger size maybe inflicted.
The clearest patterns arise from a perpendicular impact without anytangential movement. Where deep injury exists under the skin, as in adepressed fracture of the skull, the size of the internal injury may be largerthan the causative weapon, due to spreading of the force of impact and theintervention of the overlying soft tissues.
A bar or rod commonly leaves a distinctive pattern of two parallel lines ofbruising, with undamaged tissue between. This is due to the direct pressureexpelling blood from the central zone, but the skin edges being forcedinwards, causing shearing damage and bleeding from small vessels in thesemarginal zones.
A ‘target’ bruise is due to the impact of a spherical object, such as a hard sphere(for example, a squash ball) or even a round hammer-head, and may cause a‘target’ bruise, with a central pale area surrounded by a zone of haemorrhage.
171

Finger-tip bruises are disc-shaped and about 1–2 cm in diameter, often ingroups, sometimes suggesting or indicating a row of finger-tips. Commonlyseen in child abuse, where they are situated above and below large joints suchas elbow or knee, or the chest or abdomen, on the neck or on the sides of thetrunk from gripping by adult fingers. Also seen in adults on the upper andlower arms, from gripping during an altercation. Common on the neck inmanual strangulation.
Finger-nail marks may be linear (scratches) due to moving friction of the nailsalong the skin. These may be multiple and parallel; scrapings of the nails ofthe assailant (or victim where scratches are defensive) may reveal blood andskin remnants which can be identified by DNA.
Static finger-nail marks are usually crescentic. If deep and bleeding, theyusually mean a rapid impact rather than steady pressure. Note that thecurvature of the crescent may be in the opposite direction to that of theinflicting nail, due to elastic recoil of the skin when the nails are removed.
A contact wound from a firearm (qv) sometimes shows an abrasion or bruisefrom the rim of the muzzle, sometimes with a characteristic impression of theforesight or other shaped part of the muzzle. This is often erroneously called a‘recoil imprint’, but is not due to the recoil of the weapon, which alwaysmoves the gun away from the skin. It is due to gas entering the wound andballooning the skin against the muzzle.
‘Brush’ abrasions or grazes are linear scratches due to tangential impact,commonly seen from skidding across a road surface (‘gravel rash’), but mayoccur from a glancing blow, especially a kick.
Lawyer‘s Guide to Forensic Medicine
172
Figure 34: Mechanism of bruising from a rod or bar

Part II: Petechial Haemorrhages
PETECHIAL HAEMORRHAGES
Tiny pin-head sized haemorrhages, found in the skin, eyelids, eyes andinternal membranes such as the pleura (covering of the lungs) andpericardium (membrane around the heart).
Petechial haemorrhages, especially on the lungs or heart, were formerlythought to be diagnostic of asphyxia (qv), but this is quite incorrect. Theycertainly can appear in asphyxia, but are often absent: conversely, they arecommonly present in non-asphyxial conditions, and can even appear post-mortem.
True petechiae are caused by a sharp rise in pressure in the veins, so manytypes of congestive death, from heart disease and other natural causes as wellas trauma, may cause damming back of the blood in the veins as the heart failsterminally. Such congestive changes in the organs may be accompanied bypetechiae, but rarely in the skin.
In the forensic context, where the veins are mechanically blocked, as inpressure on the neck from strangulation, then the rise in venous bloodpressure may cause marked congestion and produce petechiae above the levelof obstruction. However, if death ensues rapidly, from cardiac arrest (see‘Strangulation’), then insufficient time elapses for the congestion andpetechiae to develop. This time is very variable, but is probably longer than 30seconds.
Petechiae from pressure on the neck are seen in the loose skin of the uppereyelids, in the skin of the cheeks, forehead, chin and neck, in the inside of theeyelids and on the whites of the eyes.
In the chest, they may occur under the pleural membranes (subpleuralpetechiae or ‘Tardieu spots’). These were once thought to be proof ofasphyxia, but are commonly seen in all types of death, especially in thefissures and near the root of the lung, where a few petechiae may usually befound. However, if numerous and taken in conjunction with facialhaemorrhages and evidence of pressure on the neck or obstruction ofbreathing, they are useful confirmatory findings if interpreted cautiously.
Petechiae may also be seen on the surface of the heart and on the thymusgland in infants – this gland lying above the heart. It has been shown by trialphotographic studies (Gordon and Shapiro) that petechiae can actuallydevelop on the surface of the heart in the course of a post-mortem; also,petechiae commonly appear in areas of dependent hypostasis after death (see‘Hypostasis’) so there is no doubt that they can be a post-mortemphenomenon. However, petechiae in the eyes or facial skin are usuallyevidence of a congestive process, though this is by no means synonymouswith asphyxia (qv). It should be noted that petechiae in the eyes can occurafter violent sneezing or in whooping cough, again due to a sudden rise invenous blood pressure.
173

The most gross congestion and petechiae are seen in the so called‘traumatic asphyxia’ (qv), due to damming back of blood from fixation of thechest.
The whole topic of ‘asphyxial petechiae’ is undergoing very critical reviewin forensic medical circles and the old classical interpretations should beaccepted with great caution, as it is now clear that the appearances are highlynon-specific.
PNEUMOCONIOSES
Industrial lung diseases due to inhalation of dust; now all scheduled diseasesunder the Industrial Injuries Act, such as coal workers’ anthraco-silicosis,asbestosis, slate workers’ and quarry workers’ silicosis, baggasosis, byssinosis,etc.
It must be appreciated that the mere inhalation and retention of dust in thelungs does not constitute a disease. There must be some response (‘hostreaction’) by the body, which leads to pathological changes which cause animpairment of function of the lungs, or to some other abnormality, forexample, tumour formation in asbestos exposure. An analogy may be drawnwith the hands of a mechanic, which, though dirty, are no less efficient. Thisdistinction is sometimes not appreciated by those engaged in compensationprocedures.
Coal workers’ pneumoconiosis
Medically, ‘anthraco-silicosis’. Coal is carbon, mixed with various amounts ofother rocks. It is the silica which is dangerous, not the carbon. The coal dustreaches the furthest parts of the lung (small bronchi or air passages and the aircells or ‘alveoli’) and may remain there inert, causing nothing more than ‘dustretention’, which is not a disease state. Commonly, the body reacts to the silicain the dust and forms small nodules of fibrous tissue. This is simplepneumoconiosis and is graded in life according to the X-ray appearances, inaccordance with the 1971 International Labour Office Classification ofRadiographs of Pneumoconiosis.
Category 1: few small, rounded opacities.
Category 2: numerous small, rounded opacities, normal lung markingstill visible.
Category 3: numerous small, rounded opacities, obscuring the normallung markings.
Lawyer‘s Guide to Forensic Medicine
174

Part II: Pneumoconioses
The size of the X-ray opacities or shadows are measured in an ascending scaleas ‘p’, ‘q’ and ‘r’.
A more serious condition is complicated pneumoconiosis or progressivemassive fibrosis (PMF), where infection, either septic or tuberculous, appearsas a progression from simple pneumoconiosis. The opacities are more than 1cm in size and may reach 10 or 15 times that size in advanced cases. It is thecomplicated disease, or PMF, that forms a danger to life and causes severedisability. The role of simple pneumoconiosis in causing symptoms isdisputed and it never leads to death.
Large opacities on X-ray (PMF) are classified as Categories ‘A’, ‘B’ and ‘C’,according to the size of the shadow.
According to many authorities, simple pneumoconiosis is symptomless.Any symptoms experienced by men without complicated disease is attributedto coincidental lung disease, the most common being chronic bronchitis andemphysema, which is now itself accepted as occupational, contrary to formermedical opinion.
Category ‘A’ PMF is also held officially to be without symptoms, disablingdisease being due to Category ‘B’ and ‘C’ masses.
Miners with either rheumatoid arthritis or an occult tendency to rheumaticdisease may get a special type of lung opacity, called the Caplan lesion. It isnot necessarily related to the degree of lung function disability. ExtensivePMF leads to obstruction of the lung circulation and to loss of lung function,as well as to congestive heart failure. It is the only cause of death in coalworkers’ pneumoconiosis, leading to ‘cor pulmonale’, heart failure due torestricted circulation through the lungs, though concomitant chronicbronchitis and emphysema have their own mortality, again partly fromcongestive cardiac failure and partly from impaired oxygen exchange in thelungs.
Coal miners do not get any increased risk of lung cancer; in fact the rate isslightly lower than in the general population. Though PMF is often associatedwith tuberculosis, there is no increased risk of contracting the disease as aresult of occupation, only a variation in the nature of the infection as a resultof dust in the lungs. This is not true of silicosis, seen in gold miners andquarry workers, which predisposes to tuberculous infection.
Silicosis
A pneumoconiosis contracted in many industries including quarrying, goldmining, slate work, stone dressing, ceramics, etc. Like coal workers’ disease, itmay be simple or complicated, but there is a greater degree of fibrosis.Tuberculosis is a frequent complication, silica appearing to facilitate infection,unlike the situation with anthraco-silicosis.
175

Asbestosis
Asbestos is ubiquitous in the urban environment and almost everyone has asmall number of asbestos fibres in their lungs. Like other pneumoconioses,damage occurs only when there is a host reaction to the substance. Thenumber of mineral fibres in a lung can be assessed after post-mortem byashing a sample of lung and counting the resistant fibres.
Three types of dangerous sequelae to substantial asbestos exposure exist:Asbestosis is a pneumoconiosis due to fibrosis of the lungs and is
comparable to the previous conditions, though the fibrosis is more diffuse andusually involves the pleura, the coverings of the lungs.
An increased risk of lung cancer, indistinguishable from the cancers whicharise spontaneously or as a result of smoking. Such cancers occur in a third toa half of cases of asbestosis, smokers with asbestosis being much more at risk,of the order of a 20 fold increase. It should be noted that increased lung canceronly occurs in the victims of actual asbestosis, not in persons merely exposedto asbestos dust.
Mesothelioma: there is a well substantiated connection between asbestosexposure (not necessarily asbestosis) and the type of tumour called‘mesothelioma’ which usually affects the pleura and, less often, the lining ofthe abdominal cavity. The condition is accepted (where related to anindustrial history of asbestos exposure) as a compensatable scheduled diseaseunder the Industrial Injuries Acts. The disease is invariably fatal, but may takeup to 15–20 years after exposure to become manifest. A substantial exposureto asbestosis is usually necessary for mesothelioma to develop. It must beappreciated, however that in about 15% of cases of this tumour, no exposureto asbestosis can ever be proved, the condition arising spontaneously.
The various types of asbestos have widely different and dangerous effectsThere are six varieties, but only three (white, blue and brown) are usedextensively in industry. Blue asbestos (crocidolite) has a particular danger ofmesothelioma production and is now banned from import into the UK. Whiteasbestos (chrysolite) now forms 90% of world production and is relativelyharmless. The dangers of the different types are thought to be to the physicalshape of their fibres, rather than to chemical effects. The tiny, sharp fibres arethought to damage cells physically, especially their DNA, which explains theirtumour-provoking properties.
‘Asbestos bodies’ are microscopic fibres found in the lung, coated withyellow iron-containing protein. They are not evidence of asbestosis, but ofasbestos exposure: a considerable proportion of all urban dwellers have suchexposure, but it is quantitatively greater in certain workers, such as laggers,shipbuilders and breakers, and in the asbestos supply and packing industries.
Lawyer‘s Guide to Forensic Medicine
176

Part II: Poisoning
Farmer’s lung
A pneumonia-like illness with an allergic basis, due to various moulds(especially Micropolyspora faeni) from damp hay. It may be an acute illness ormay be a long standing condition. Rarely fatal, it may lead to permanent lungdamage and severe disability. Now a scheduled industrial disease, but rarelyseen in Britain now, due to changes in farm practice with hay drying andsilage making.
POISONING
General features
Toxicology is a separate science in its own right, as are forensic serology anddentistry. The vast and ever-increasing number of toxic substances in themodern environment makes it impossible to offer any comprehensive surveyof poisoning, but some features of immediate medico-legal importance can beidentified.
First, the whole subject tends to fall naturally into two parts:(a) the technology of analysing biological fluids and organs for toxic
substances;(b) the interpretation of the results provided by the analyst.
Laboratory analysis
The first topic has no place in this book, except to emphasise that toxicology isa task for full time experts, where the occasional dilettante is quite out ofplace. Even though a person may be an expert general chemist, unless he orshe is constantly involved in the technology of poisons detection, their worthas an expert witness is very much reduced.
In the UK, the Home Office forensic science laboratories have the greatestexpertise in criminal cases or for the coroner in accidental or suicidalpoisoning. Some university departments of forensic medicine have goodtoxicological facilities and the area toxicological laboratories of the NationalHealth Service also carry out drug analysis. Where a defence solicitor requireshis own analysis, either private forensic or commercial laboratories, the publicanalyst service or some specialist laboratories in industry or the universitysphere can provide the necessary expertise.
The matter of samples is vital, as the site, type and amount of biologicalspecimen required may crucially affect the value of the analysis. Thelaboratory should be consulted when an analysis is required, to give guidanceon the nature, storage and transport of the samples.
177

For example, blood samples for alcohol analysis must be placed into a tubecontaining an adequate amount of fluoride, to inhibit micro-organisms whichmay distort the alcohol content before analysis is carried out.
In post-mortem toxicology, sampling is also vital and gross errors can ariseunwittingly if material is taken inappropriately. It has been shown in recentyears, especially by Professor Derrick Pounder of Dundee, that there is a veryuneven distribution of many substances in the dead body.
It is unsafe to take blood samples for many substances, especially alcoholand most drugs, from the heart, large blood vessels in the chest, neck andabdomen. This is because substances in the stomach, gut and even airpassages, after regurgitation, may diffuse from those sites after death intoadjacent blood vessels and the heart, giving a spuriously high result, often ofhigh concentration.
Blood samples should be taken from peripheral veins, such as the femoral,which are remote from sources of contamination.
It should be repeated here (see ‘Drowning’) that fresh water drowning isaccompanied by a marked rapid increase in blood volume and thereforedrugs and alcohol may be diluted by as much as 50% in a post-mortem bloodsample, compared to the true concentration immediately before death.
A variety of biological fluids and tissues may be used for analysis,including blood, urine, vitreous fluid from the eye (which resists post-mortemchange longer than blood), stomach contents, intestinal contents, and hair (forheavy metals, etc).
Interpretation
The interpretation of results is often more difficult than the provision of aquantitative analysis result.
Owing to biological and other variations, the end result may bear little orno relationship to the amount of poison taken, and the amount needed tocause death or disability may vary enormously from person to person or evenin the same person at different times. As with alcohol, the following factorshave to be taken into account:
Absorption. The speed and completeness of absorption of the poison into thebody (whether by mouth, inhalation or skin), will often determine whether atoxic level is attained in the blood and tissues. If the poison is eliminated asfast as it is absorbed, then no ill effects may occur.
Elimination may be by excretion of the intact toxic substance or detoxificationof it by the body’s chemical processes. Excretion of the original drug may bevia the urine, faeces, breath or skin or a combination of all methods. Theproducts of detoxification may also be excreted in a similar way.
Lawyer‘s Guide to Forensic Medicine
178

Part II: Poisoning
The concentration (‘level’) in the blood represents a dynamic balance between theabove processes of absorption and elimination. If the entry of the poison isfaster than elimination, then a build-up will occur, which will be reflected by arising blood level.
Once the intake of the toxic substance ceases, then elimination will cause afalling blood level, unless death supervenes, when all active detoxificationand excretion cease. However, lethal damage may already have been done,which then complicates the interpretation of the analysis results. For instance,a person may take such an overdose of sleeping tablets that grave depressionof the brain centres occurs. Prolonged coma may then result in death, yet onceall the drug has been absorbed from the alimentary tract, the processes ofelimination carry on until death. Thus a very low blood level may exist at thetime of death (which is the level detected in a post-mortem blood sample) andin the absence of circumstantial evidence, the actual cause of death may behard to substantiate. Where the victim was habitually taking therapeuticdoses of the drug, then the levels measured after death may be within thetherapeutic range, which makes it difficult to prove an overdose fromlaboratory results alone. Many drugs, such as tranquillisers and anti-depressants, pose the same problem for the pathologist and toxicologist.
Some poisons are cumulative, because their excretion is extremely slow. Inthese cases, even minute amounts of the substance absorbed may build up todangerous or lethal levels. Substances such as arsenic and colchicine (autumncrocus) are in this category.
Post-mortem decay may cause some poisons to be present in misleadinglylow concentration after death. Conversely, alcohol may rise after death, due tothe action of yeasts and other micro-organisms on body constituents,especially if the environmental temperature is high. However, some poisons,such as metallic compounds or barbiturates, may be detected in the bodymany years after death.
Some toxic substances are rapidly converted into other chemicals in thebody and may not be recoverable in the original form, such as the very rapidconversion of heroin to morphine. An expert knowledge of toxicologicalchemistry is needed for the degradation substance to be anticipated andsought in the samples.
All these factors make the interpretation of results very difficult, and it iscommon in fatal cases for the amount of drug or poison recovered to be lessthan the usually accepted fatal minimum.
Again, the published ranges for dangerous and lethal levels of the variouspoisons vary markedly. Owing to biological variation, the susceptibility ofdifferent people can vary greatly to a given amount of a toxic substance.Tolerance can develop from long usage, but also idiosyncrasy or sensitivitymay lead to death or severe illness in amounts which should normally beinnocuous.
179

The physical effects of poisons vary greatly according to the substanceabsorbed. Poisoning may occur in suicidal, accidental or homicidalcircumstances and industrial exposure may give rise to civil litigation, all ofwhich may require expert investigation and toxicological analysis. Wheredeath has occurred, though the technical aspects of sample analysis and theproduction of a quantitative result, together with advice on the normal,therapeutic, toxic and usually fatal concentrations, are the province of thechemist, the interpretation of those results should be the function of thepathologist, clinical toxicologist or other expert medical witness.
He has to interpret the result in the light of the full findings, which mayinclude co-existing natural disease, injuries or other modifying factors whichrequire the bare quantitative analysis results to be viewed in a different light.The decision as to whether a certain blood or tissue level of poison causeddeath or disability should not be left to the analyst, though as stated above,the medical witness may often seek his advice as to conventional ranges forthe particular substance under examination.
POSITIONAL OR POSTURAL ASPHYXIA
A recently recognised cause of death, most often occurring in police custody,but sometimes in accidental situations.
First named in the USA, it arose when prisoners where ‘hog-tied’, havingtheir hands pinioned behind their back and their ankles tied. They wereplaced face down in vehicles and found to be dead within minutes.
Further cases were then recognised in other countries, where prisoners,especially large or obese, were left face-down with their wrists handcuffedbehind their back, sometimes in police vehicles or in police stations.
Death is due to restriction of the ability to breathe, as the weight of thebody is upon the front of the chest and the arms are not available to assistlifting the trunk from the floor. As a consequence, inhalation is restricted andoxygen lack may develop. Existing heart disease or inebriation worsens thesituation, but is not essential.
Postural asphyxia may also occur when a person gets stuck in an invertedor jack-knifed position, such as attempting to climb through a fanlightwindow; other deaths have occurred during masochistic practices (qv) wherebondage or bizarre positions, sometimes inverted, lead to restriction ofbreathing.
Lawyer‘s Guide to Forensic Medicine
180

Part II: Post-Mortem Entomology
POST-MORTEM ENTOMOLOGY
The study of the infestation of the dead body by insects and other fauna is avery specialised subject, its expertise confined to only one or two zoologists inthe UK.
There are many pitfalls in interpretation and even expert forensicbiologists and pathologists cannot claim much specialist knowledge inestimating the time since death on the basis of the infestation.
Factors such as the ambient temperature, the season and, above all, theactual species and variety of sarcosaprophagous insect involved, alwaysrequire the best opinion possible.
The stage of maturation of certain fly maggots, usually Diptera, may beused as an aid to estimating the time since death of infested bodies. Both liveand alcohol-acetic-acid preserved maggots should be submitted for thisexamination.
Main infesting insects are the blue-bottle (Calliphora), green-bottle (Lucilia)and the house-fly (Musca). Beetles, moths and larger beetles may also bepresent at later stages.
Most common insect to infest the cadaver is the common blue-bottle. Eggsmay be laid shortly after death (or even before if the victim is debilitated orcomatose), but only in daylight and above 12°C temperature. The eyes,nostrils and mouth are the most common sites, or any wounds upon the skin.The blue-bottle favours fresh tissue rather than putrefied bodies. Smallmaggots may appear within 8–14 hours of egg laying, these being called thefirst ‘instar’. The speed of hatching depends upon environmental temperature.An instar is a stage in the life history between two successive castings of theouter skin of the maggot. The first instar persists for another 8–14 hours, thenthe skin is cast to form the second instar of larger maggots, which live for 2–3days. The third instar lives for six days, after which the insect pupates in aquiescent phase for about 12 days. The first empty pupa may be seen afterabout 22 days. The blue-bottle larva possesses an enzyme which liquefiestissues, so that numerous holes appear in the skin and the maggots can spreaddeeply into the tissue. This hastens putrefaction. Blue-bottles are active in theenvironment from early spring until late autumn. The green-bottle is similarin almost all respects to the blue-bottle as far as the life history is concerned.
The common house-fly (Musca domestica) is less common on bodies, thehouse-fly favouring putrid matter and manure. However, bodies are attackedon some occasions, the eggs hatching in about 12 hours. The first instar lastsfor 36 hours, the second for 1–2 days and the third for 3–4 days.
The rationale of using maggot infestation as an index of the time of deathgives a minimum time dependent upon the stage of maturation. However,various generations of maggots may be present at the same time, due tosuccessive egg layings.
181

Other insects may assist over the longer period and even the absence ofcertain fauna, either on the body or in the underlying ground, may be ofsignificance in timing death.
It is emphasised that the assistance of an expert entomologist is necessary.
PREGNANCY
Signs of pregnancy
(a) Cessation of menstruation.(b) Breast changes – swelling, darkening and prominence of tubercles of
nipple.(c) Morning sickness – variable.(d) Softening and congestive coloration of neck of womb.(e) Palpation signs (‘ballotment’) of enlarging womb.(f) Enlargement of womb – rises out of the pelvis by eighth week, reaches
umbilicus by 24th week, at full term is under the ribs.(g) X-ray confirmation – never performed except for urgent medical reasons
because of potential malformation dangers of radiation to foetus in earlypregnancy.
(h) ‘Quickening’ of foetal movements and contractions of womb.(i) Laboratory tests. Many available, depending on change in hormones
during pregnancy. Reliably positive from about 12–15 days afterconception.
(j) Foetal heart sounds heard through stethoscope.(k) Ultrasound and other imaging techniques.
Duration of pregnancy
Can be a matter of considerable importance in divorce, inheritance, etc.The average length is calculated from the date of the last missed period to
the birth and is 280 days (40 weeks, or 10 lunar months). Variations can occurdue both to length of pregnancy itself and to the length of the menstrualperiod, but 10 days either way is the usual maximum divergence, exceptwhere early birth occurs from some obstetrical cause. In most women, birthwill take place at the time of what would have been the 10th menstrualperiod, but as conception usually takes place some 10 days after the onset ofthe period, the actual length of gestation is nearer 270 days. Sperm cannotsurvive for long in the female genital tract, but fertilisation may occur up to aday or so after intercourse.
Lawyer‘s Guide to Forensic Medicine
182

Part II: Procurator Fiscal
All births before 38 weeks are premature and all over 40 weeks aredelayed.
Consideration of short pregnancies must take into account a comparabledegree of immaturity in the infant. A 24 week foetus can survive with modernmedical care.
The maximum length of gestation is uncertain, though 354 days has beenverified medically and several leading cases have accepted a long period:Gaskill (1921) – 331 days; Hadlum (1948) – 349 days; Wood (1949) – 346 days,though Preston-Jones (1951) was rejected at 360 days.
PROCURATOR FISCAL
In Scotland, there is no coroner system, the investigation of certain categoriesof death being the duty of the Procurators Fiscal, to whom such deaths arereported by police, doctors, the public and Registrars of Births and Deaths.Though a Procurator Fiscal can investigate any death which he thinks requiresit, the following is the advisory list published by the Crown Office:(a) any death uncertified by a doctor;(b) any death caused by an accident arising out of the use of a vehicle,
including an aircraft, ship or train;(c) any death arising out of industrial employment, by accident, industrial
disease or industrial poisoning;(d) any death due to poisoning;(e) any death where the circumstances would seem to indicate suicide;(f) any death where there are indications that it occurred as a result of
medical mishap;(g) any death resulting from an accident;(h) any death following abortion or attempted abortion;(i) any death apparently caused by fault or neglect on the part of another
person;(j) any death occurring in legal custody;(k) any death of a new-born child whose body is found;(l) any death (occurring not in a house) where deceased’s residence is
unknown;(m)death by drowning;(n) death of a child from suffocation (including overlaying);(o) any death which may be the sudden infant death syndrome;(p) where the death occurred from food poisoning or infectious disease;
183

(q) any death as a result of burning, scalding, fire or explosion;(r) deaths of foster children;(s) any other death due to violent, suspicious or unexplained cause;(t) any death where a complaint from the next of kin is received by a Health
Board or NHS Trust and the complaint is about the medical treatment witha suggestion that it might have contributed to the death of the patient.
There are special provisions concerning deaths associated with medical care,including:(a) deaths which occur unexpectedly having regard to the clinical condition of
the deceased;(b) deaths which are clinically unexplained;(c) deaths seemingly attribitable to a therapeutic or diagnostic hazard;(d) deaths which are apparently associated with a lack of medical care;(e) deaths which occur during the actual administration of an anaesthetic,
local or general;(f) deaths which may be due to an anaesthetic.
When apprised of a death, the Procurator Fiscal makes further enquiries viathe police, his only form of investigative agency. There is no exact parallel tothe English ‘coroner’s officer’ but investigations are carried out on theProcurator Fiscal’s behalf by uniformed or plain clothes officers, seconded forduty as ‘sudden death officers’. The CID may be involved where necessary.The police make investigations in all cases except those concerning anaestheticdeaths, for which there is a special procedure.
Certain categories of death, such as criminality, suicide, medical mishap,those of police officers in accidents, fires and explosions, and cases involving acontinuing public hazard, etc, must be reported by the Procurator to theCrown Office.
Details of the Procurator Fiscal’s procedures are contained in Crown Officeregulations.
PULMONARY EMBOLISM AND DEEP VEIN THROMBOSIS
Blood clot (more accurately ‘thrombus’) may form in veins, almost alwaysthose in the deep veins of the calf of the leg – much less often in other sites,such as the pelvis (even where there is pelvic vein thrombosis, there is usuallyalso deep vein thrombosis (DVT)).
This DVT is very common, but usually causes no ill-effects apart fromswelling and pain in the leg, which may be absent in many cases. If a partbecomes detached, it is conveyed through the veins to the right side of the
Lawyer‘s Guide to Forensic Medicine
184

Part II: Pulmonary Embolism and Deep Vein Thrombosis
heart and thence to the lungs via the pulmonary arteries. Branching of thepulmonary arteries provides the first obstruction to the thrombus, whichlodges at the first intersection too small to allow its passage. If large, the clotwill block the major branches and cause rapid death from obstruction of thecirculation (pulmonary embolism). If smaller, the fragments will pass furtherinto the lung, causing non-fatal symptoms or even having no apparent effect.They may cause local areas of lung damage due to deprivation of the bloodsupply, called pulmonary infarcts.
This pulmonary embolism (PE) is a common condition and a frequentcause of sudden death after a variety of causes, such as surgical operations,fractures of the leg, injuries of many types and prolonged immobility in bed.
185
Figure 35: Pulmonary embolism

Certain drugs have a variable risk of encouraging DVT, such asoestrogens, including oral contraceptive pills, though the risk is usually verysmall and is only revealed in large statistical analyses.
Pulmonary embolism is often unsuspected by doctors and is the cause ofdeath most frequently undiagnosed before an autopsy is performed. Fewerthan half the deaths from pulmonary embolism have been anticipated byclinicians, when confirmed by post-mortem examination. DVT may presentno signs and therefore the subsequent pulmonary embolism may be quiteunexpected. If DVT is recognised and especially if small pulmonary infarctshave occurred, then the administration of anti-coagulant drugs such asheparin may prevent further DVT and potential pulmonary embolism. Failureto do so has resulted in many medical negligence actions.
Pulmonary embolism may occur at any time after trauma or operation, etc,but is most common at about two weeks following injury. However, anyperiod from a day or two to several months is possible, though with aprogressively longer interval, it becomes harder to attribute the embolismdirectly to the injury, as about one-fifth of all fatal pulmonary emboli occur inthe absence of the usual precipitating factors.
It is therefore a matter of probabilities as to the causal relationship of anoperation, injury or bed rest to a fatal embolism and this has profoundmedico-legal connotations. For example, where criminal proceedings arisefrom a death due to pulmonary embolism following a traffic accident or anassault, it has to be shown that the fatal outcome was due to the effects of theinjury causing DVT and hence pulmonary embolism. As many emboli come‘out of the blue’, this causal relationship is difficult to establish ‘beyondreasonable doubt’.
If the pulmonary embolism occurs, say, two weeks after the injury, thenthe connection is strongly suspected, though never absolutely provable. If it isdelayed until two months, then it is very much more difficult to prove the linkbetween injury and death.
The age of the thrombus, both that in the lungs and that remaining in thedeep veins, is of vital importance as, if it can be shown to pre-date the injury,then the causal relationship is destroyed. Unfortunately, dating such thrombiis very difficult and uncertain, even on microscopic examination: expertadvice is needed. Opinions as to date may vary between experts and in anycase cannot be measured with any accuracy, except during the few daysfollowing commencement. At a later stage, a time scale must be measured atbest in weeks.
Lawyer‘s Guide to Forensic Medicine
186

Part II: Pulmonary Embolism and Deep Vein Thrombosis
Predisposing factors for deep vein thrombosis
Increased clotting tendency of the blood, occurring as a natural defensivemechanism after injury (including surgical operation).
Stagnation (‘stasis’) of blood in the veins due to bed rest during immobilitycaused by injuries, fractures, coma, etc. This stasis is due to minimal muscleaction, which fails to massage the blood back from the legs.
Pressure on the calves of the legs during immobility in bed: this causesobliteration of the veins and direct passive trauma to their walls.
Local tissue damage to muscles and veins, as in injuries and fractures of the legs.
Certain drugs, such as oral contraceptives, etc.
These factors are present in patients who have had surgery or tissue trauma orwho are confined to bed for other reasons, yet DVT and hence pulmonaryembolism can frequently occur in apparently healthy and mobile persons,10–20% having none of the predisposing factors just mentioned.
187

RAPE
In most jurisdictions, the essential feature of rape is penile penetration. If thiscannot be proved, then only a lesser sexual offence can be maintained.
Medical evidence of penetration
Recovery of semen from the depths of the vagina. Deposition of semen uponthe vulva or thighs can occur from intra-crural ejaculation (between thethighs). Pregnancy is well known to occur from such external ejaculation andtherefore subsequent pregnancy is not strict proof of vaginal intercourse (see‘Semen’).
Injury to the female genitalia is strong evidence of forcible intercourse,though penetration by fingers or some instrument may produce the samesigns. Also over-enthusiastic voluntary intercourse may cause some damage,though rarely as severe as in rape.
Injuries associated with rape may include the following:
Reddening, swelling and bruising of the vulva. These may also be signs ofenergetic voluntary intercourse, especially in difficult circumstances ofclandestine love making, but severe degrees are inevitably the result of rape,especially in children.
Rupture of the hymen. This membrane may be naturally prominent or almostabsent. The orifice may be wide enough to allow intercourse without ruptureor may be completely imperforate. In the usual circumstances it is torn duringfirst deep intercourse. If recent, within a day or two, there will be slightbleeding and reddened inflammatory reactions at the site of the tear. Thehymenal tear soon heals and subsequent intercourse usually leaves no furthersigns. Childbirth normally obliterates the remnants of the hymen. Rupture orpermanent dilatation of the hymen may occur from the use of tampons formenstruation or from manual masturbation (see ‘Hymen’).
Injuries to the vaginal wall. These may occur externally at the back, edge of theorifice of the vagina, adjacent to the anus. A tear may occur from violentpenetration or from disparity of size of the vaginal opening and the penis.This may be seen in adult intercourse with a young girl or child, but can occurat later ages. It is almost never a sign of voluntary intercourse, except inmarked disproportion of organ size. The tear may extend backwards into theanus and may cause a severe injury, especially in a child. Other injuries mayoccur to the internal walls of the vagina. These may vary from bruising andabrasions to lacerations. Fatal tears may occur in violent rape and in rapeupon children. The vagina may be split in a child by a large adult penis andthe peritoneal cavity entered, with death or severe illness from haemorrhage
Lawyer‘s Guide to Forensic Medicine
188

Part II: Rape
and peritonitis. The posterior fornix (the upper cul-de-sac beyond the neck ofthe womb) may be torn by a penis of much greater length than the immaturevagina. Lesser degrees of damage may occur to any part of the female organs,from friction from either penis, fingers or mouth. The usual signs of suchinjury include bruising, swelling, redness and abrasions.
Venereal infections may be discovered on medical or forensic laboratoryexamination. Occasionally, such infections may be matched bacteriologicallywith a similar infection in the suspect, though this is not absolute proof ofpenetration. The infection is usually gonorrhoea. HIV infection may occur, butdiagnosis may be delayed as even on blood testing, sero-conversion may takeseveral months.
189
Figure 36: Female external genitals

Other signs found on medical examination are not those indicative ofpenetration, but may assist in corroborating sexual activity.
Injuries on the thighs, buttocks and abdomen. Finger-nail scratches on the innerside of the upper thighs are especially significant, from efforts to force openthe legs. Finger-tip bruises in the same area and on the buttocks and small ofthe back also suggest forcible clutching of the woman or girl.
Scratches and bruises on the buttocks, shoulder blades, backs of thighs andcalves may also suggest forcible contact with the ground. Where relevant,soiling by dirt, earth, leaves, etc, may be found on the skin or clothing in theseareas.
Blood or semen stains on the thighs, pubic hair, abdomen or buttocks may berecoverable and afford valuable forensic science evidence.
Hairs foreign to the girl may be recovered from her pubic hair or clothing.
Marks on the breast are relatively common, including finger bruises, nailscratches and bites. Mouth marks may accompany bites, being typically ovalgroups of small haemorrhages called ‘suction petechiae’. Other bites may befound on the neck, abdomen and pubic area, but naturally may occur involuntary sexual intercourse.
Lawyer‘s Guide to Forensic Medicine
190
Figure 37: Relationship of female genital organs

Part II: Rib Fractures
Anal and oral intercourse may be without consent: the appropriate swabs andother samples may reveal semen, though this is unlikely in the mouth exceptin rape associated with murder. The injuries to the anus are described under‘Sodomy’.
REFLEX CARDIAC ARREST
See ‘Vagal inhibition’.
RIB FRACTURES
There are 12 pairs of ribs, all attached by joints to the vertebrae of the thoracicspine at the back; all but the lower two pairs are joined directly or indirectly tothe breast bone (sternum) in front. The ribs are joined together by thincontinuous sheets of muscle, the ‘intercostals’.
In breathing, the ribs hinge forwards and upwards on inspiration, thusexpanding the volume of the chest cavity and drawing in air.
Fractures of ribs are relatively common and, if not too extensive, are notdangerous to life. They commonly occur during cardiac massage and artificialrespiration. Hazards are:(a) flail chest, where numerous rib fractures, usually on both sides at the front,
prevent the bellows function described above and impair the breathingability;
(b) penetrating fractures, where broken rib ends stab or tear the underlyinglung and cause a pneumothorax (air in the pleural cavities between ribsand lung) preventing respiration.
Pressure or impact on the front of the chest, such as impact with a steeringwheel or fascia in car crashes – or stamping in an assault, can cause anteriorfractures, often running in a line down the outer side of the front of the chest.This is often called the anterior axillary line, if in line with the front of thearmpit, or mid-clavicular line if in line with the centre of the collar bone. Furtherback, they may be in the posterior axillary line, which is midway around theside of the chest.
Posterior fractures are not common in adults except from a violent impactsuch as a vehicle strike on a pedestrian or a fall from a height.
In infants, posterior fractures are commonly seen in child abuse, sometimesin a vertical line parallel to and near to the spine, where the back of the ribangles in to its attachment. This is typical of side to side pressure, as when thesmall infant is gripped under each armpit by adult hands and squeezed.
191

The child often survives and a line of ‘callus’, that is, lumps of calcium dueto the healing process, may be seen visually at post-mortem or on X-rayskeletal survey, as a ‘string of beads’, often on both sides.
Controversy surrounds anterior rib fractures in infants, as they are veryrare, due to the pliability of soft bone and gristle – the defence claim, that theymay be due to resuscitation, as in adults, is difficult to substantiate.
RIGOR MORTIS
Stiffening of the muscles after death. Due to complex chemical changesassociated with permanent oxygen lack and accumulation of lactic acid. Thisleads to conversion of the contractile proteins of the muscle into a stiff gel,which persists in this state until the onset of putrefaction causes softening.
Although rigor mortis develops uniformly throughout the body, it usuallybecomes first apparent in the smaller muscles, due to the lesser mass involved.Thus, it appears first in the muscles of the face and jaw, the limbs stiffeninglater, though in no fixed order.
As a measure of time since death, rigor is very unreliable.Like all chemical processes it is temperature-dependent. In warm
conditions, rigor mortis appears quickly and passes off more quickly, due tothe early onset of decomposition. In the cold, it may be delayed markedly andin freezing conditions, may not appear at all (though actual freezing of thebody fluids in extreme frost may cause stiffening). When a cold body isbrought into a warmer environment, then true rigor may quickly appear.
In average temperature conditions, rigor may be detected within 2–6 hoursand be generally present within the first 8–12 hours, though very widevariations can occur.
Fully developed rigor may last in ‘average’ conditions for a further 24hours and then begin to fade during the next day. The old rule of thumb that‘rigor takes 12 hours to come on, lasts for 12 hours and takes 12 hours to passoff’ can be relied upon only for its unreliability!
Rigor frequently is present up to the third or fourth day and may still bedetectable after a week in some cases, especially in cold conditions. It isimpossible for rigor and signs of decomposition to co-exist.
Virtually every textbook will quote a different range and all can bejustified due to the lack of constancy of this labile phenomenon. An analysisby Mallach of opinions in textbooks and medical papers over a long periodshowed variations of between 30 minutes and seven hours for the onset ofrigor; of 2–20 hours for full rigidity; and 24–96 hours for persistence of fullrigor.
Lawyer‘s Guide to Forensic Medicine
192

Part II: Rigor Mortis
The time to fade from full rigor varied from 24–192 hours, so it can be seenthat the evidential value is slight.
One fairly reliable fact about rigor is that it comes on much more rapidlyafter death from electrocution – and also tends to appear quickly after severeexertion just before death.
In children and frail, old people, it is frequently faint and transitory,depending to a considerable extent on the amount of muscle mass present.
As an index of time since death, it has very limited value and any opiniongiving an exact time or a range of units of less than 3–5 hours during the firstday is an untenable over-interpretation.
A more justifiable rule of thumb is that if a body is flaccid and warm, it hasprobably been dead less than six hours; if flaccid and cold, it has been deadmore than about 2–3 days. If cold and stiff, it is likely to have died betweenhalf a day and two days earlier.
Cadaveric spasm
This is a very rare form of rigor mortis which is said to come oninstantaneously at death, though some authorities deny its existence.
It is ill-understood, but invariably associated with sudden, violent death incircumstances of intense exercise or emotion. Battle casualties may show suchspasm but, in civilian practice, it is very occasionally seen in deaths such asdrowning, where in the death agony, the victim seizes a branch or weeds inan attempt to save himself. These may then be found clutched tightly in thehand before ordinary rigor could develop. Very rarely, a suicide may grip apistol in such cadaveric spasm, though the forensic implications are morerelevant to crime fiction than to legal practice.
193

SCALDS
Burns due to moist heat from hot liquids or vapours; usually superficial withno deep tissue destruction as in many dry burns. Danger due to area involved,rather than depth.
Effects from pain, primary shock and loss of function: later effects fromdisturbances of fluid balance through weeping skin areas, infection of skin, orintercurrent infections such as pneumonia. More serious in old people.
The ‘Rule of nine’ calculates area involved by assuming each limb to be 9%of total body area, front and back of chest each 9%, front and back of abdomeneach 9%, remaining 9% formed by head, neck, perineum, etc (see ‘Burns’).
Adults have poor outlook for survival if more than 40% burned, much lessin old people. Children may survive more than half total area being burned.
Scalding is usually accidental, but may be deliberate in child abuse. Bothtime and temperature contribute to scalding: water at only about 50°C maycause scalds if applied for long enough, as in a hot bath.
The temperature decreases rapidly away from the point of initial contactand scalding is thus less severe towards the periphery, when the liquid issplashed. This does not apply to immersion. Splashes may be visible by theshape of the scalds. Redness and blisters are the common signs of scalding.Clothing protects almost completely against splashes, the scalds beingconfined to exposed areas.
SCALP WOUNDS
Profuse bleeding occurs from wounds on the very vascular scalp, thoughrarely dangerous to life. Simultaneous injury to contents of skull is the majordanger. Scalp wounds may bleed considerably after death, especially if headleft in dependent posture (see also ‘Head injury’).
Forensic importance in the possibility of identification of causative weapon.Fine detail of wounds obscured by interposition of hair, but general patternmay be imprinted, for example, hammer-head, large spanner or metal bar.
Confusion may arise between blunt instrument and cutting weapon, asformer may cause sharply incised wound because of crushing effect overunderlying hard skull. Differentiated by slightly bruised edges, fibrousstrands crossing wound depths and intact hairs in blunt injury, compared totrue cutting weapon.
Swelling of the scalp more prominent than wounds elsewhere, due to thevascularity and the unyielding skull beneath, which prevents downwardspressure of a haemorrhage under the skin. The scalp may accumulate amassive collection of blood (haematoma) up to 3 cm thick.
Lawyer‘s Guide to Forensic Medicine
194

Part II: Scars
SCARS
Healed injuries of the skin, either from trauma or surgical operations.Composed of fibrous tissue covered with new epithelium (skin cells). Thelatter does not carry the usual skin appendages such as hair or sweat glands.
Scars of surgical incisions or of simple cuts consist of a thin segment offibrous tissue binding the opposing edges of the defect. More extensive scars,such as those of burns, may be irregular in shape and depth, often wrinkledand bound down at intervals to underlying structures.
Scars pass through a sequence of changes after the initial injury:(a) the wound is first filled with blood clot and serum which loosely binds the
edges together. Within hours, healing begins and new skin is visible in aday or two;
(b) depending on the width of the wound, the blood clot becomes ‘organised’,that is, new blood vessels and young fibrous tissue covered with new skingrow across the surface under the most superficial layer of the scab ofdried blood, which eventually falls off to reveal the new skin;
(c) the young fibrous scar is at first red in colour, then bluish, and graduallybecomes pale over many months until it reaches a final silvery pink stage.This is dependent upon the size of the defect, but it usually is completewithin 6–12 months.
195
Figure 38: Sharp and blunt scalp wounds

Many factors affect the speed of scar formation, such as age and health of thepatient, the presence of infection in the wound and the size and position of thewound. Vitamin deficiencies and other ill-understood personal variationsmake exact dating of a scar impossible within wide limits. Once the white-silver stage is reached, no change occurs for rest of life.
Scars cannot be removed, but a wide scar can be reduced to a narrowlinear scar by careful restorative surgery.
The presence or absence of a skin scar is sometimes of vital forensicimportance in identification of a person, alive or dead (for example, theTichborne and Crippen cases). Old scars may be very difficult to differentiatefrom skin creases. In the living, brisk rubbing will cause the adjacent skin toredden, but not the scar. In the dead, microscopic examination and stainingtechniques will reveal an absence of elastic fibres, sweat and sebaceous glandsat the site of the scar.
SEMEN
The male procreative fluid consists of the essential cellular elements, thespermatozoa and the fluid medium in which they are dispersed. The formerare formed in the two testes from precursor parent cells in the seminiferoustubules. This process takes about 60 days to maturation. Mature sperms arestored in the epididymis, adjacent to the testis in the scrotum. Here they are ina minimum of fluid and are not mobile, being in a state of suspendedanimation.
When orgasm occurs, the epididymis voids part of its contents along eachvas deferens, the tubes which lead up from the scrotum to the neck of thebladder. Here the primary fluid is diluted with a much larger volume ofsecretion from the two seminal vesicles and the prostate gland, whichcontribute the larger part of the bulk of the ejaculate. These glands addfructose and other chemical substances, which immediately activate thespermatozoa and make them motile, so that they can compete to seek andfertilise the female ovum in the uterus.
The constituents of the semen form the basis for forensic tests for seminalstains. A very high content of the enzyme acid phosphatase is detectable onscreening tests. The most satisfactory legal proof that a stain is seminal is themicroscopic identification of sperm, either heads or intact sperms with tails.However, with the increase in vasectomised men, lack of sperm may lead togreater dependence on chemical and serological tests for semen. Antibodies tosemen can be used to detect semen by immunological techniques which arequite specific, and the advent of DNA technology allows definiteidentification of the semen against blood or other tissue samples from anindividual, replacing the older blood group and other tests.
Lawyer‘s Guide to Forensic Medicine
196

Part II: Sexual Intercourse
The examination of garments for seminal stains by the use of ultra-violetlight is a useful screening test, but is by no means specific as pus, urine, bloodand other biological fluids may also give positive fluorescence.
SEXUAL INTERCOURSE
The signs indicating that sexual intercourse has taken place may be recent orlate (see also ‘Rape’).
Recent intercourse
Semen in the vagina may be absent if no ejaculation, or a condom used.Vasectomy removes spermatozoa from the semen, but the chemical tests
remain positive.Evidence of recent tearing of the hymen. Bleeding, slight swelling, redness
and a tear which usually extends to the wall of the vagina (see ‘Hymen’).However, intercourse can occur without hymenal damage when that structureis lax or has a large aperture.
Tear of the perineum (bridge of skin between the back edge of the vaginalorifice and the anus) can only be caused (apart from childbirth) by over-dilatation of the introitus (vaginal opening) by either a penis or the forcibleinsert of fingers or some object, usually in a child or young girl. All theseagents are evidence of over-stretching of the vaginal orifice, but notnecessarily by a male organ. It is impossible for the perineum to be torn bynormal activities such as jumping or falling, etc. An injury to the crutch mightcause generalised damage to the area, but the isolated tear of the perineumcan only arise from overstretching of the vaginal opening.
Previous intercourse
Widely dilated vagina and vulval orifice are likely to be due to habitualintercourse and/or childbirth, but are not inevitably due to this. Conversely,the usual appearance of a closed vaginal opening has no significance eitherway.
Even a single act of intercourse can tear the hymen into a condition whichis not then altered significantly by further intercourse, though the hymentends to become less prominent as time goes by and may be almost eliminatedby childbirth. Within a day or so after first intercourse, the bleeding, swellingand raw edges of the hymenal tears become healed (see ‘Hymen’).
197

Evidence of current or previous pregnancy is strong evidence ofintercourse, though many pregnancies have arisen from extra-vaginal sexualrelations (see also ‘Rape’).
SKELETAL IDENTIFICATION
The forensic examination of bones is a common task for pathologists and aseries of questions needs to be answered in a logical sequence.
Are the remains bones?
Sometimes artefacts such as stones, wood, etc, may be assumed by laypersons, including police, to be bones. A plaster facsimile used by medicalstudents was another false alarm seen by the author.
Are the bones human?
Where substantial remains or fragments are recovered, anatomical recognitionis sufficient, the necessary knowledge of anatomy depending on the amountof material. Where small pieces are involved, expert anatomical or evenveterinary opinion is needed. If visual recognition fails, then the forensiclaboratory can determine the species by serological tests, in which extracts ofthe bone are matched against immune sera from various animals. For this tosucceed, the remains can rarely be older than five or 10 years since death.However, recent advances in DNA technology have allowed sex and personalidentity to be determined even on very old bones.
If human, what sex are they?
Apart from DNA, this is entirely an anatomical exercise and depends on thenature and amount of the recovered remains. If a skull or pelvis is available,sexing is about 95% certain. Long bones such as thigh also have good sexualcharacteristics, as do the lower spine and the shoulder blade and breast bone.Before puberty, the sexual differences are slight or absent.
What age was the person at death?
Age determination (qv) decreases in accuracy with increasing maturity. Theage of the foetus can be determined within weeks, and that of a child to withinmonths. Using expert dental techniques (see ‘Identification’), the age of aninfant may be determined in ideal circumstances with an accuracy of days orweeks.
Up to the age of about 20, ageing is relatively accurate. The eruption of theteeth (milk and permanent), the appearance of ossification centres(‘epiphyses’) at the ends of bones, the fusion of these epiphyses with the main
Lawyer‘s Guide to Forensic Medicine
198

Part II: Skull Fractures
bone and other maturing processes offer much information. In middle age, theevidence is much less, but changes in the pubic symphysis of the pelvis, wearpattern of the teeth, etc, can assist. Radiological evidence of the remodelling ofthe internal structure of some bones, such as the neck of the femur, is useful inspecialist hands.
The closing of the seams (sutures) in the skull has fallen into disuse inrecent times, but some authorities say that the fusion on the inside of thecranium is relatively accurate, to within a decade up to 60 years.
In old age, very little accuracy is possible, apart from general senileappearances of toothless jaws, more fragile bones, etc.
What height was the deceased?
See ‘Stature, estimation of’.
What is the race?
Less exact data is available, but shovel-shaped front teeth in mongoloids,longer thigh bones in negroid, different facial bone pattern in negroids andmongoloids may assist.
Any individual identifying features?
Healing fractures with calcified ‘callus’ may match a known injury. The datingof such healing is impossible within wide limits. Old deformities fromcongenital defects or polio, etc, may be detectable. Surgical intervention to thebones from old infections or fractures may be seen (prostheses such as metalpins, replaced joints, etc).
Radiologically, bones may be matched with pre-existing X-rays in someinstances, especially if some unusual feature exists. The skull is usuallyunique, as are frontal sinuses (qv) and can give absolute identity match if pre-mortal X-rays are available. In all skeletal identification problems, the servicesof an expert are needed, including forensic pathologist, anthropologist,dentist, anatomist, radiologist and laboratory scientist.
SKULL FRACTURES
A fracture of the skull is usually no danger to life in itself (except whenfragments of a depressed fracture may press upon or penetrate the brain). Inmost cases, the fracture is merely an indicator of substantial trauma to thehead and the same force which fractured the skull may also cause internalbrain damage, which is the essential and dangerous lesion.
199

About 25% of fatal head injuries have no fracture of the skull, yet the braindamage caused death.
Types of fracture
Fissured or linear
A relatively simple fracture line running in a straight or curved direction. Ifthis line crosses a major meningeal artery rupture of the vessel may give riseto an extradural haematoma (qv).
Depressed
Here one or more fragments may be tilted downwards to press upon orpenetrate the membranes or brain. In certain circumstances, especially in thetemporal area, such a depression may eventually give rise to epilepsy (qv).
Pond fracture
A circular fracture, often depressed centrally, due to a focal impact. It mayhave concentric circles and radial lines, suggesting spider-web shape. A blowfrom a round-headed hammer, etc, may cause such a fracture.
Comminuted fracture.
Multiple fracture lines causing complete separation of bone fragments,sometimes with gross destruction of contour of head and pulping ofunderlying brain. Seen in railway and traffic accidents or where repeatedviolent blows from a blunt instrument are applied to the head.
Horizontal fracture
A heavy blow or blows on the side of the head may cause a horizontal fractureto run around the circumference of the head, with secondary fracture linesremote from the point of impact; seen particularly in infants subjected toimpact on the head.
Contre-coup
A fall onto the back of the head may cause contre-coup (qv) fractures of thethin bone over the eye sockets at the opposite end of the skull, alwaysassociated with brain damage on the undersurface and tips of the frontal andtemporal lobes.
Lawyer‘s Guide to Forensic Medicine
200

Part II: Skull Fractures
Ring fracture
A fall onto the feet from a height may cause a ‘ring fracture’ of the back of theskull around the foramen magnum, where the force transmitted up the spinalcolumn implodes the top of the spine into the skull.
Hinge fracture
Hinge fracture of base of skull is common in severe head injury, often fromimpact on either side of the head. A fracture line often crosses a line ofweakness on the floor of the skull, usually across the middle fossae through
201
Figure 39: Types of skull fracture

the pituitary fossa. This is the so called ‘hinge’ or ‘motor cyclist’s fracture’ butcan be seen in any heavy impact on the skull. This fracture may cross half theskull or may traverse it completely, thus hinging the base of the skull into twomovable halves.
The force necessary to fracture a skull is hard to evaluate, but is less thangenerally thought. In the case of infants, much discussion and controversyexists as to the height from which a child must be dropped to cause a skullfracture, though a more vital question is the force needed for brain damage orintracranial membrane bleeding.
Weber in Germany (1985) showed that passive falls in dead infants fromonly 80 cm (32 in) onto a firm floor caused fractures in all cases and evendropping from a similar distance onto various padded surfaces alsosometimes caused fractures.
The question sometimes arises, in adults, as to whether a thin skull allowsfractures to occur with less force. The answer must be in the affirmative,though it does not appear to be a major factor.
Skull fractures do not necessarily occur at the point of impact – they can beremote from this, but usually on the same side of the head. Lines of structuralweakness determine the actual site and extent of the fractures.
An impact on the side or top of the head commonly causes an obliquelydownward fracture of the side of the skull (the temporo-parietal area), whichmay turn inwards across the base of the skull if the force is great. An impacton top of the head may cause fractures of both sides, especially in infants.
SMOTHERING
Another indefinite term in the ‘asphyxia’ category, usually employed toindicate death from mechanical obstruction of the external air passages (noseand mouth).
Death can ensue rapidly with no classical signs of asphyxia (qv), which arenow outdated, leaving no physical signs to be demonstrable at autopsy.
Suffocation, where proven, may occur from soft material, such as a pillowbeing forcibly held over the face – or where an incapacitated person, such asthose drunk, drugged or suffering from an epileptic fit, lies face down on asoft surface. The weight of the head plus sealing of the mouth and nostrilswith saliva, vomit, etc, prevents ingress of air.
Most of these deaths leave no objective post-mortem signs, such as facialcongestion, cyanosis or petechiae, which are usually due to constriction of theneck causing damming of the blood return through the neck veins.
Lawyer‘s Guide to Forensic Medicine
202

Part II: Sodomy
Another well known cause is a plastic bag over the head, a not uncommonmethod of suicide. Here congestive petechial signs are virtually alwaysabsent, so if the bag is removed by someone before the body is found, then nocause of death is apparent.
Suffocation was formerly wrongly indicted as a frequent cause of ‘cotdeath’ (qv) (sudden death in infancy – SIDS), where it was for centuries called‘overlaying’, meaning the suffocation of an infant in bed with an adult.Though it is likely that some presumed SIDS are maternal suffocations, thiscan never be proved pathologically (unless there is physical damage to themouth and lips), yet some doctors illogically allege that they can determinethis as a cause of death, usually by misreading the frequent appearance (70%)of petechiae on the intra-thoracic organs of true SIDS, as evidence of‘asphyxia’. Recently it is being claimed by some pathologists that the presenceof patchy haemorrhage in the lungs is an indicator of suffocation rather thantrue SIDS, but this supposition is untenable.
Where considerable pressure has been applied to the face and nose of avictim, either by a hand or enveloping fabric, there may be bruising of the lips,especially inside, where they are forced onto the teeth. Patchy whitening ofthe lower face, due to irregular but normal post-mortem hypostasis (qv),especially in children, must not be mistaken for evidence of suffocatingpressure, as it has been in the past by inexperienced or biased doctors.
SODOMY
Strictly, the active element in male homosexuality: the passive recipient ofanal intercourse is the ‘pederast’, though etymologically this should refer toyoung boys. The whole activity is also termed ‘buggery’. These terms havecome to be used less exactly.
The passive recipient may show signs of either acute penetration orchronic participation in anal intercourse. Where recent, possibly forciblepenetration has occurred (especially in young boys), the anal margins may bereddened, inflamed or bruised. There may be a split in the margin of the anus,with bleeding or signs of infection or healing if examination is delayed. Theorifice may remain dilated and the sphincter muscle may be incontinent.There may still be signs of lubricant, if the act was voluntary. Forensicexamination of swabs from the anus and rectum may reveal semen, lubricantand possibly venereal infection.
Care must be taken in interpreting the degree of dilatation of the anus indead bodies where sodomy is suspected: after death, the anus may relaxmarkedly, especially in children, and give the spurious appearance ofdilatation. Such an appearance should only be accepted if other signs ofpenetration also exist.
203

Where the recipient is an habitual pederast, the anus may be permanentlydilated and lie at the bottom of a funnel-shaped depression, though thisappearance has been exaggerated in former textbooks and is often merely ananatomical variation seen in control cases. The skin of the surrounding areamay be thickened and glazed, with a loss of the usual abrupt margin betweenskin and pink mucous membrane at the edge of the anus, though there areother innocent causes for this, such as chronic infections. The sphincter maybe permanently incontinent. Lubricant, semen and evidence of venerealinfection may be found.
The active partner or assailant may show little or no signs of penetration,as in rape cases, unless violence has occurred. The glans penis may bereddened, abraded or bruised, especially at the edges of the corona (margin ofthe glans). Rarely, the frenulum (band of fibrous tissue under the glans) maybe damaged. Lubricants, such as jelly, Vaseline or even hair cream may berecovered by forensic examination and faecal soiling or even blood may beseen.
SOLVENT ABUSE
(See ‘Glue sniffing’)
SPLEEN
Organ the size of a small fist, hidden under the lower rib margin in the leftupper part of the abdomen. Not vital to life, concerned with elimination ofunwanted red cells and bacteria in the bloodstream and with immunityproduction. Main forensic importance is rupture due to blunt injury to theabdomen, common in assaults (especially kicking) and traffic accidents.
It is a soft, pulpy organ within a thin fibrous capsule. Injury can split thecapsule and lead to severe haemorrhage into the abdominal (peritoneal)cavity. Prompt surgical removal needed to avoid fatal internal blood loss.There may be a delayed rupture due to blood accumulating beneath the intactcapsule, which then tears some hours after injury, allowing a latent periodwith little or no clinical signs.
A spleen enlarged by disease (such as malaria) is much more vulnerable toinjury.
Lawyer‘s Guide to Forensic Medicine
204

Part II: Stab Wounds
SPONTANEOUS COMBUSTION
A persistent myth, centuries old, which claims that a living human body canspontaneously burst into flames and be consumed.
There are numerous cases on record, familiar to most forensic pathologists,where a body has been found with part or even most of the corpse consumedby fire, with little or no fire damage to the immediately adjacentsurroundings.
However, virtually all these cases occur near a hearth where there is anupdraught; there is always some source of ignition, such as fire or cigarette;and the victim is often an alcoholic. Even so, some cases are remarkable, inthat only a pair of feet in unburnt slippers may remain; or there is a holeburned through the carpet and floorboards with no surroundingconflagration.
Experiments have shown that human fat, wrapped around fabric as awick, can burn away completely in a current of air; it is however, hard tounderstand how much of a skeleton can vanish, given that even formal high-temperature cremation may not destroy large bones.
STAB WOUNDS
The most frequent method of homicide in the UK. Stab wounds are incisedwounds in which the depth is greater than the width. Most stabs are causedby a knife or similar weapon such as a chisel, screwdriver or ice pick, butslivers of glass, metal rods, circular prods and even wooden stakes can inflictstab wounds, either homicidally, suicidally or accidentally.
The depth of penetration, as opposed to a slashed wound, increases therisk of damaging some vital internal structure, usually in the chest orabdomen, the most common danger being internal haemorrhage. In the chest,the heart, lungs and great blood vessels form the most lethal target.
Features
Skin wound. Appearance may be deceptive, as the elasticity of the skin maycause the ends of the wound to come together, with some gaping of the centre,so that the length is less than the width of the blade after withdrawal.
Also, with a tapering blade, its width at the estimated point of maximumpenetration must be correlated with the wound length. Conversely, the skinwound may be longer than the blade width, due to ‘rocking’ of the knife in thewound. The angle of withdrawal may be different to that of penetration, also
205

causing the wound to enlarge. If the blade is twisted before withdrawal, a ‘V-shaped’ wound may result.
Also, re-introduction after partial penetration, perhaps at a different angle,may further complicate the interpretation. Where one end of the wound issharply cut and the other blunt, it may be inferred that a one-edged weaponwas used, but there are fallacies in this interpretation. Even a blunt edge maycause the skin to split, leaving a sharp end. When the blade is forcibly driven
Lawyer‘s Guide to Forensic Medicine
206
Figure 40: Characteristics of knife wounds

Part II: Stab Wounds
up to the hilt, an abrasion or bruise may be imprinted on the skin around thewound, though this is not seen very often.
Depth. A knife may inflict a wound deeper than the total length of the blade,due to deformation and indentations of the surface with a forcible stab,especially in the pliable abdomen. Even the rib cage may momentarily indent,allowing the tip to reach a point deeper than that measured at autopsy.
Direction. Caution must be used in interpreting the angle of approach of theknife, from a study of the orientation of the track in the body. The posture ofthe victim at the time of infliction cannot be assumed to be upright andforward facing in every case. A wound apparently inflicted downwards intothe chest, for example, may have been made horizontally into the chest of acrouching victim. Neither can the orientation of each wound in a multiplestabbing be related to a static victim, as turning and twisting of both victimand assailant can lead to great variation in the relative positions of each.
Degree of force. Invariably an issue in homicide, being related to determinationand intent, but one very difficult to quantify, other than in terms like ‘slight,moderate or forceful’. Very subjective descriptions often applied with littlerelation to actual situation. Pathologists should never employ pejorative termssuch as ‘frenzied’, as this imputes a state of mind impossible to determinefrom post-mortem appearances and which lies in the realm of psychiatry.
Experiments have shown that:(a) the most important factor in penetration is the sharpness of the extreme tip
of the blade. With a very sharp tip, a knife can be introduced up to the hiltby the pressure of only one finger;
(b) speed of approach. A rapid stab will penetrate the skin with minimal force(like a dart) whereas the same knife pressed slowly against the surface willrequire far more effort for penetration;
(c) the skin acts as an ‘elastic reservoir’ – it is the most resistant tissue apartfrom bone or cartilage and once punctured, the knife will slide into thechest or abdomen without further force being required, as if penetratingthe membrane of a drum. Thus a deep wound is not necessarily a ‘savageblow’ in the chest or abdomen;
(d) in the frequent defence of ‘falling on the knife’, such a mechanism is easilypossible and does not require a sharp-tipped knife to be supported on thehip or elsewhere. The momentum of a falling body will allow transfixionto occur before the inertia of the knife and supporting hand allow them tobe pushed backwards;
(e) the edges of the knife above the tip are of little importance in facilitatingentry. Once the tip is through, the rest easily follows;
(f) factors such as senile skin and different areas of the body have littlerelevance in ease of penetration, compared to the two major factors of tipsharpness and speed of entry.
207

STATURE, ESTIMATION OF
In the living, direct measurement is available. In the intact corpse, a similarmethod gives an approximation to the live height, but due to relaxation of themuscles and changes in the spinal discs, etc, there may be a discrepancy of atleast 2.5 cm (1 in) with the living stature. The dead body usually lengthenswithin this range.
Where a decomposed or mutilated or skeletalised body is the subject formeasurement, the stature must be estimated indirectly. This is best done by anaccurate measurement of limb bones, especially the thigh bone (femur),though the shin (tibia) or upper arm (humerus) may be used. Where acomplete skeleton or decomposed body is available, this method may besupplemented by direct measurement, but considerable inaccuracies areinvolved due to loss of spinal discs and cartilage or disconnection of the axialskeleton and limbs in the putrefied body.
Using long bones, reference can be made to established anatomical tablessuch as those of Pearson or Trotter and Glesor, or Dupertuis and Hadden.These given a margin of error to be expected using the method, which may beup to 5 cm (2 in).
Potential errors exist because of:(a) inaccuracies in measuring the isolated bone, including whether joint cartilage
persists. Specific parameters must be adhered to and special equipmentsuch as an osteological board used for measurement;
(b) racial and sex errors cannot always be compensated for – the tables wereconstructed for certain ethnic groups and may not be strictly applicable todifferent material;
(c) improving nutrition, in modern communities, causes the older tables to beno longer applicable to contemporary body dimensions.
All these factors may combine to introduce appreciable errors whenattempting to extrapolate total stature from a single bone. As a very roughapproximation, the length of the femur (thigh bone) can be taken as 27% of thetotal body length and the tibia (shin bone) about 22%.
STATUS LYMPHATICUS
Sometimes known also as ‘status thymo-lymphaticus’, this hypothetical entityis now virtually of historical interest only and is regarded as untenable as anexplanation of sudden death.
In vogue in the first part of this century, the alleged condition consisted ofa persistence of the thymus gland in adults (a gland in the upper part of the
Lawyer‘s Guide to Forensic Medicine
208
Part II: Sterilisation
chest normally shrinking at puberty), together with over-profuse lymphglands and lymphoid tissue in the body and under-development of the largeblood vessels, especially the aorta.
Persons (usually younger adults) with this condition were thought to beespecially prone to sudden death from relatively trivial causes, which left nosigns to be demonstrable at autopsy. The syndrome was often confused orlinked with ‘vagal inhibition’ (qv). After some energetic debate andcontroversy in the medical press between the wars, the existence of statuslymphaticus fell into disuse.
Most forensic pathologists would agree that no such condition can besubstantiated on morphological grounds, though sometimes an autopsyreveals a persistent thymus and prominent lymphoid tissue in a victim of anobscure sudden death. However, it seems very doubtful whether anystatistical support could be found to substantiate the hypothesis. Thesyndrome has been invoked mostly to explain deaths under anaesthetic andduring relatively minor operations, for which there might be betterexplanations.
STERILISATION
The inhibition of procreative ability by surgical operation. May be irreversibleor reversible, the latter sometimes spontaneously.
In the male, usually achieved by ‘vasectomy’, which involves tying andcutting each vas deferens, the ducts which convey sperm from the testes to theneck of the bladder. This process does not significantly reduce the volume ofejaculate, which is formed mainly by the prostate gland and the seminalvesicles.
Vasectomy is a simple surgical procedure performed under localanaesthetic without the necessity of admission to hospital. A temporarycomplication may be the formation of a haematoma (collection of blood) at theoperation site.
Occasionally, the vas deferens may spontaneously rejoin and allowfertility to be restored. Following vasectomy, other contraceptive methodsmust be continued for up to three months or until semen samples are shownto be permanently free from viable spermatozoa. About 1% of vasectomiesrevert and occasionally a negative sperm test at three months may becomepositive again later, for reasons not yet adequately explained.
In the female, a similar sterilisation technique may be performed on thefallopian or uterine tubes which convey the ova from the ovaries to the womb,these being tied and transected on each side. This may be done by openoperation or via ‘laparoscopy’, an instrument being introduced through a
209

small incision. Sterilisation may also be performed during operations for othergynaecological conditions, including termination of pregnancy and byhysterectomy.
Naturally, sterilisation is an inevitable by-product of many gynaecologicaloperations, especially hysterectomy (removal of the womb or removal of bothovaries or uterine tubes). However, the removal of one ovary and the oppositetube need not lead to sterility, as ova can cross the abdominal cavity to reachthe other tube.
Like the vas deferens, occasionally, tied uterine tubes may spontaneouslyre-open and both circumstances have given rise to litigation for negligenttechnique where an unwanted pregnancy has resulted. This is more frequentwhen the tubes are blocked by metal clips, rather than being cut throughsurgically.
STILL-BIRTH
Any child which has issued forth from its mother after the 24th week ofpregnancy and which did not, at any time after being completely expelledfrom its mother, breathe or show any other signs of life (Births and DeathsRegistration Acts). The original legislation, such as the 1953 Act, laid down 28weeks’ gestation, but in other legal contexts, due to improved obstetrical care,this has been reduced to 24 weeks – though even less mature foetuses of 22 oreven 20 weeks may be born alive and some survive.
Unless witnessed by a doctor, midwife or other responsible person, theretrospective diagnosis of a still-birth is difficult, unless maceration (signs ofdeath in utero) or gross malformation is present (see ‘Live birth’).
A still-birth must be registered before disposal: the special still-birthcertificate can be completed by a doctor or midwife, if they were eitherpresent at the birth or examined the body afterwards (an unsatisfactory meansof determination). If both were present, the doctor has precedence over themidwife in signing the certificate.
In the absence of such a certificate, a statutory declaration by an informantmay be accepted, though this is rare.
The causes of still-birth are varied and often obscure. Even autopsy cannotreveal a cause in a significant proportion – and cannot be decisive even aboutthe fact of still-birth within the narrow definition given above (see ‘Livebirth’).
The most common cause certified for still-births is ‘placental and cordconditions’, with disease and malformation of the foetus and diseases andabnormalities of pregnancy as other major reasons.
Lawyer‘s Guide to Forensic Medicine
210

Part II: Stomach
STOMACH
Primary receptacle for food, in which acid digestion takes place. Whencomplete, the exit from the stomach (pylorus) opens to allow contents to passinto duodenum, where bile neutralises the acid and alkaline digestion beginsin intestine.
The timing of death from stomach contents is highly unsatisfactory. Verymisleading opinions have been offered by pathologists, as the rate of digestionis almost useless in determining the time since the last meal. Fluid passes veryrapidly through the stomach, so food plus a large volume of liquid will leavethe stomach quickly.(a) There is great individual variation and even the same person has varying
rates at different occasions.(b) The type of food varies the rate, for example, high carbohydrate hastens
and fatty substances slow the speed of stomach emptying.(c) Physical and emotional stresses can retard or completely stop digestion.
Thus, even if the time of the last meal is known, the autopsy appearances ofthe stomach contents, both quantitatively and qualitatively are not a reliableguide to the time since death, especially if that was preceded by a period ofinjury, fear or other stress. Only in a sudden, unexpected death can anyapproximate conclusions be drawn, but even these vary within wide limits.Where disability, coma, etc, exist, food may remain undigested for days untileventual death.
In normal physiological circumstances, an ‘average’ meal may remain inthe stomach for two to four hours, before gradually seeping through thepylorus. But the whole concept of timing death by this means is fraught witherror. More useful is the nature of food found at autopsy, if still recognisable;this may be related to the content of a known meal and thus death can bepresumed to have taken place after that particular meal and before the nextscheduled meal.
Certain drugs may be recognisable in stomach contents, especially thosewith a strong smell, like cyanide, phenols or alcohol. Others may be coloured,like the blue of amytal capsules or the red of Seconal. Actual tablets, powderor capsules may be visible.
The condition of the stomach lining may be significant, for example,erosion from corrosive substances like acids, alkalis, or less irritative poisonslike aspirin or some alkaline barbiturates. Shallow acute ulcers, often withbleeding, may be seen in hypothermia (qv) or stress conditions such as headinjuries. Chronic alcoholism may cause gastritis, with thickening, corrugationand mucous coating of the lining. A perforation of a gastric ulcer is an acutesurgical emergency, as the release of acid contents into the abdominal cavitymay cause sudden collapse and rapid death from chemical peritonitis.
211

STRANGULATION (See also ‘Asphyxia’)
Pressure on the neck, either manual or by ligature. Manual strangulationsometimes called throttling (qv).
The old view that it caused death or disablement merely by ‘cutting off theair’ is now recognised to be untenable. Great medico-legal significance in themechanisms, which are complex and variable.
Features
When the neck is compressed, the following factors may operate:
Obstruction of the large veins (jugulars) which return blood from the head to theheart. The pressure inside the veins is low and only slight pressure is requiredto impede or obstruct the flow. This leads to ‘backing up’ of blood in the faceand head, seen as congestion and blueness (cyanosis) due to accumulation ofdeoxygenated blood in the skin.
Prolonged unremitting pressure for at least 15–30 seconds leads to ruptureof over-distended small veins in skin, lips and eyes, leading to petechialhaemorrhages (qv) and frank bleeding from nostrils and ears.
This is due to rise of pressure in the veins, because arteries (which are notobstructed at this level of squeezing) are pumping blood into the head, andthis blood cannot escape down the neck. Also oxygen lack in the vein wallsmay contribute, though this is a minor and rather doubtful factor.
The haemorrhages in the whites of the eyes (petechiae) are thus mainly asign of venous obstruction, not central oxygen-lack due to ‘cutting off the air’at the windpipe.
When the neck is constricted, these changes develop progressively as timegoes on, but the actual length of time necessary for their production variesconsiderably and is not capable of being exactly determined. It probably takesin excess of a quarter of a minute for eye petechiae to appear and often muchlonger. Dogmatic opinions are common, but ill-founded on fact. Thecompleteness and constancy of the pressure on the neck, together withindividual variations, prevent accurate estimation of this minimum time,which is often of legal importance in relation to intent and determination.
Pressure on the great arteries in the neck (the carotid arteries which supply bloodto the head and the brain). The pressure of blood inside these is far higherthan in the veins and consequently total obstruction requires far more effort. Ifboth right and left carotid arteries are obstructed, almost immediateunconsciousness will occur due to deprivation of oxygenated blood to thebrain.
Lawyer‘s Guide to Forensic Medicine
212

Part II: Strangulation
Continuous pressure for more than 3–5 minutes (an unlikely scenario)could cause irreversible brain damage, but probably death from reflex cardiacarrest (see below) would occur long before this point.
Carotid sinus pressure. Where the carotid arteries divide in the upper part of theneck into internal and external carotids, there exists on each side a sensitivepressure receptor called the carotid sinus, together with adjacent nerves in the
213
Figure 41: Strangulation

sheath of the artery. These monitor blood pressure, and operate a bio-feedback system to regulate blood pressure, but a sudden squeeze or impactupon these can lead to drastic slowing or even stoppage of the heart – the socalled ‘vagal inhibition’ (qv).
This is a common cause of death in pressure on the neck, especially inmanual strangulation, and can occur instantly when the neck is gripped.Reflex nerve impulses go from the carotid sinuses and sheath via the glosso-pharyngeal nerves to the brain stem, where they stimulate the tenth cranialnerve nucleus. This initiates impulses down the vagus nerves to the heart andcan slow or stop it altogether. A more acceptable name than vagal inhibitionfor this common mechanism is ‘reflex cardiac arrest’. In its pure form, itaccounts for at least half the deaths from manual strangulation and mayaccount for the remainder, even if it is delayed until sufficient time has passedfor the congestive-petechial signs to appear.
Obstruction of the air passages was classically held at one time to be the onlycause of death. In fact sufficient compression to stop the air flow of the stiff,rigid cartilage of the larynx or windpipe (trachea) is very difficult. A moreusual mechanism is for the larynx to be lifted up so that the tongue blocks theback of the throat. In any event, pure deprivation of air can be survived formany minutes, during which death from one of the other mechanisms aboveis more likely to occur. Fractures of the hyoid bone or laryngeal cartilages areindicators only of pressure on the neck and not of the mechanism of death (see‘Hyoid bone’).
There is thus an opportunity for a number of causes to operate duringstrangulation.
If the face is pale at death, then by definition, the carotid/cardiac reflexmechanism must have occurred, as death was too rapid for any of thecongestive changes to have taken place.
If the face is congested and petechial haemorrhages (qv) are present, thensudden immediate cardiac arrest could not have occurred in the early periodof strangulation, probably about 15–30 seconds minimum duration.
No maximum time can be inferred, as a shift of the strangling fingers ortightening of the grip may cause carotid pressure to supervene at any pointalong the ‘congestive-asphyxial’ path and the pathological appearancescannot indicate any time period.
From pure (and exceptionally rare) obstruction of the air passages, deathwould not be expected to occur for at least several minutes and numerouscases of failed near-strangulation have indicated that a prolonged period ofthrottling can be survived. Many of the survivors had gross congestivechanges in the face, indicating that their survival was due to a lack of thecarotid reflex mechanism.
Lawyer‘s Guide to Forensic Medicine
214

Part II: Subarachnoid Haemorrhage (or Haematoma)
This mechanism is more likely to occur in manual strangulation, due to thefocal impact of finger-tips into the groove in front of the sternomastoidmuscles where the arteries lie, but it can often occur in ligature strangulation.It is very common in hanging, due to the sudden jerking impact of a fallaffecting the carotid structures.
It must be emphasised again that evidence of physical damage to the neckstructures, especially the larynx, is evidence only of violence to the neck andnot to an asphyxial mechanism.
Sometimes, actual evidence of carotid trauma can be found by carefuldissection of the arteries, revealing tears of the inner lining of the wall.
The most significant forensic point, especially from the aspect of thedefence in a criminal trial, is that signs of pressure on the neck with a pale facemeans rapid death, whilst congestion and haemorrhages mean a delayeddeath, though a time factor is impossible to state with any accuracy, but isprobably in excess of 15–30 seconds.
SUBARACHNOID HAEMORRHAGE (OR HAEMATOMA)
Bleeding beneath the arachnoid, the inner layer of the two membranescovering the brain. Common condition, with frequent medico-legalconnotations, occurring as follows:
General head injuries
As part of any head injury in which the brain surface is damaged; often occurswith associated subdural bleeding.
Ruptured cerebral (berry) aneurysm
As a natural disease due to rupture of a cerebral artery, usually at the base ofthe brain. Most often, the rupture is due to leakage or bursting of a (berry)aneurysm of the Circle of Willis (qv), but in about 15% of cases, no aneurysmcan be demonstrated at either operation or autopsy.
A less common cause is bleeding from a congenital anomaly of the bloodvessels on the surface of the brain, such as an angioma (a benign tumour ofblood vessels) or other vascular malformation.
Subarachnoid haemorrhage from a ruptured cerebral aneurysm is acommon cause of sudden collapse and is frequently fatal, especially inyounger and middle-aged adults. As women have less coronary artery diseasein this age group, it is a relatively frequent cause of sudden death in women ofchild-bearing age, the other causes being pulmonary embolism or acomplication of pregnancy.
215

Cerebral aneurysms (qv) are often called ‘berry’ or ‘congenital’ aneurysms,though the actual aneurysm is not congenital. Rather there is a weakness ofthe wall of an artery where a junction occurs in the Circle of Willis, due tocongenital, perhaps embryological, factors. This weakness is subject toincreasing internal stress as the blood pressure rises in middle age, so that aswelling develops, usually at a junction of two vessels. This balloons and mayeventually burst, causing blood under arterial pressure to escape into thesubarachnoid space. Extra exertion, such as sport or sexual intercourse, mayraise the blood pressure sufficiently to cause the rupture, but it can occurspontaneously during rest. Emotion and physical exertion seem to be factorsin raising blood pressure and increasing blood flow.
It is usually claimed that alcohol enhances the onset and severity of asubarachnoid bleed, but there is little physiological proof of this. The claimthat it dilates cerebral blood vessels seems irrelevant in relation to the largernon-muscular vessels at the base of the brain and the walls of the aneurysmitself.
As mentioned below, where subarachnoid bleeding is associated withtrauma, the latter is usually sustained in a scenario where alcohol is much inevidence, such as a bar brawl or public house fight. This does not mean thatthe pharmacological action of alcohol is relevant, only that fighting and drinkusually go together.
It has also not been proven that direct injury to the head can precipitate arupture, due to the deeply situated and well protected site of the Circle ofWillis. However, rupture during or soon after a fight, assault or even threat ofviolence may well be related to the emotional and physical stress involved,with a consequent adrenaline response and a rise in pulse rate and bloodpressure.
The symptoms of a ruptured cerebral aneurysm and consequentsubarachnoid haemorrhage may vary from severe headache to sudden, rapiddeath. A victim may fall to the ground and die on the spot from a massivebleed. However, many patients have premonitory smaller bleeds and mayrecover spontaneously. Others may be operated upon, the surgeon often beingable to clip the bleeding vessel and effect a complete cure.
Traumatic subarachnoid haemorrhage
A very important topic in relation to fatal assaults.This type of subarachnoid haemorrhage commonly occurs from trauma
specifically applied to the upper part of the side of the neck, though impact onthe back or side of the head can also cause the same internal damage. This cancause a rupture of one of the arteries forming part of the vertebro-basilar systemat the base of the brain.
Lawyer‘s Guide to Forensic Medicine
216

Part II: Subarachnoid Haemorrhage (or Haematoma)
The two vertebral arteries come up tunnels in the sides of the vertebrae ofthe spinal column in the neck and then penetrate the dural membrane thatlines the skull and spinal canal, to enter the base of the skull through the largehole (foramen magnum) where the spinal cord emerges.
The left and right vertebral arteries then join together on the base of thebrain to form the single basilar artery, which supplies blood to the rear of thebrain, which includes the vital centres for breathing, etc.
A blow on the side of the neck (usually below the ear) or less often on theside of the head, can suddenly rotate and incline the head in such a way as tostress the arteries of the vertebro-basilar system and cause a rupture, givingrise to a subarachnoid haemorrhage, which can be rapidly fatal.
Such a blow need not be of great magnitude, though it has to besubstantial.
It can be delivered by a blunt weapon or by a kick; it is unusual for a fistblow to cause this tear, though it is not impossible. A fall onto a flat surfacecannot cause the injury, but if the fall is onto some projection, then it canoccur.
The mechanism of traumatic subarachnoid haemorrhage is ill-understood.It was formerly thought always to be due to tearing of a vertebral arteryoutside the skull, in the tunnel in the uppermost (first) cervical vertebra andthat the blood then tracked through the dural membrane into thesubarachnoid space. The rapidity and volume of blood inside the craniummade this hypothesis unlikely, and it is now widely accepted that there is atear of the vertebral or basilar artery or one of their branches within thecranium – even if there also happens to be a concomitant small bleed outsidethe skull in the upper part of the extracranial vertebral artery.
The difference is academic from a legal aspect – the injury is due to traumato the neck or head, whatever the mechanics of the bleed.
In practical terms, it may be difficult or impossible for the pathologist toidentify the bleeding point, which may be obscured by blood clot andimpossible to preserve intact during removal of the tissues at autopsy.
Various techniques are used, including post-mortem radiography afterinjecting the vessels with radio-opaque fluid; better is the slow decalcificationof the neck and lower skull bones, which takes weeks, then careful dissectionof the vessels. Even then, it may not be possible to identify the actual bleedingpoint.
Death may occur very rapidly – typically, after a fracas in the street or bar,a man is struck on the neck and collapses to the floor, being dead whenemergency services attend. The reason for such rapid death is obscure, butseems to be due to sudden release of blood around the vital centres in thebrain stem, which the vertebro-basilar system supplies.
217

SUBDURAL HAEMORRHAGE (OR HAEMATOMA)
Bleeding between the inner and outer membranes of the brain, that is, belowthe dura and above the arachnoid. Always caused by injury to the head, eventhough this might be so trivial as to pass unnoticed, especially in old people.
The source of the bleeding is from the veins which cross the subduralspace from the surface of the brain to reach the venous sinuses – large bloodchannels in the dura.
Subdural haemorrhage (SDH) is most common in infancy and old age, butcan occur at any time of life where there is a head injury. Unlike extraduralhaemorrhage (qv), subdural haemorrhage commonly occurs without fractureof the skull.
In infants, it is a common finding in alleged child abuse and was the majorcomponent of the original description by Caffey in 1946. Many clinicians andsome pathologists always attribute SDH to violent shaking, but it is now clearthat impact of the head from a blow or fall is much more common, even if thescalp and skull show no injury from contact with a flat surface or object.Subdural haemorrhage is the most common cause of death in child abuse (qv).
The pressure on the brain may cause neurological signs and symptomsand eventually death from raised intracranial pressure affecting the vitalcentres in the brain stem. However, many SDHs are relatively small and thereal danger is from actual direct brain damage and brain swelling, often withdiffuse axonal injury (qv), the SDH being a concomitant indicator of trauma tothe head.
In old people, subdural haemorrhage is not uncommon, due to the senileshrinkage of the brain which increases the width of the subdural space andmakes the fragile vessels more vulnerable due to stretching and shearingstresses. Often found at autopsy as an incidental finding in old persons. Maythen be a ‘chronic’ subdural haemorrhage, the haemorrhage (also called a‘haematoma’) persisting for months or years. May be symptomless or givingrise to false diagnosis of ‘stroke’ or senile dementia. May have been caused bya trivial head injury which is not recorded in the clinical history.
An old subdural haemorrhage, at whatever age of victim, is brown incolour due to altered blood pigment and after weeks or months, may have athick fibrous capsule. In infants especially, the age of an SDH may be of vitallegal importance (as in the Louise Woodward case in Boston, Mass), because ofaccess and alibi issues for the time of injury.
A fresh SDH is dark red, and this will not change to naked-eye inspectionfor at least a few days when a brownish tinge appears, though no rigid timescale can be applied.
Lawyer‘s Guide to Forensic Medicine
218

Part II: Subdural Haemorrhage (or Haematoma)
On microscopic examination, no change can be seen for at least 36 hours,when by special stains for the iron-containing pigment haemosiderin,granules of iron may be seen not earlier than this time.
Progressively from then, signs of absorption and healing appear, but againno definite time sequence can be established within wide limits.
An acute subdural haemorrhage is common in all types of head injury,whatever the age of the victim – seen especially in blunt trauma and trafficaccidents. Death from pressure on the brain may be averted by surgicalintervention – holes are drilled in the skull to evacuate the blood clot, butthere is often associated brain damage which itself may be fatal.
After a head injury, there is often a latent interval (after a short period ofconcussion (qv)) before blood accumulates either in the extradural position orsubdurally. The length of this ‘lucid interval’ is very variable, from a fewminutes to many hours or even days in the subdural haemorrhage of oldervictims.
A ‘thin-film’ subdural haemorrhage has little clinical significance, beingvery common in all sorts of trivial head injury. Only when substantial enoughto cause generalised or localised pressure on the surface of the brain (due tobeing confined within the rigid skull), does it present a danger to life.However, even minor degrees of subdural haemorrhage are often associated
219
Figure 42: Position of subdural haemorrhage

with other types of intracranial damage, such as brain bruising, lacerations,oedema (brain swelling) or deep haemorrhages and injury to the brain.
An SDH may re-bleed at a later date, either spontaneously or after asecond episode of trauma, sometimes minimal in severity. This is of greatimportance in child abuse, where the second bleed may occur during thecustody of a different carer, as in the Woodward case.
SUDDEN NATURAL DEATH
Most sudden or rapid unexpected deaths from natural causes are due to acatastrophe in the cardiovascular system, even if topographically situated insome major organ such as the brain. Where death is virtually instantaneous (a‘drop-down’ death) the cause can only be in the heart, due to a sudden cardiacarrest. Even massive strokes, pulmonary embolism, etc, do not kill as quicklyas sudden failure of the heart. Sudden unexpected death is most often due tocardiac causes and the most common single reason is coronary artery disease(qv) in men in Western-type society.
Sudden natural death in women of child-bearing age (15–50) is likely to bedue to:(a) a complication of pregnancy, such as abortion, ectopic pregnancy;(b) pulmonary embolism from deep leg vein thrombosis;(c) subarachnoid haemorrhage from a ruptured berry aneurysm;(d) heart disease of various types.
Coronary artery disease in women was formerly one or two decades later thanin men, due to the protective effects of female hormones, but in recent yearshas developed earlier, probably due to an increase in smoking.
Common causes of sudden natural death
Cardiovascular(a) Coronary artery disease (qv). Coronary thrombosis and myocardial
infarction are pathological subconditions of the general disease. Oftencalled ‘ischaemic heart disease’, ischaemia being a reduced blood supply,but this term is not quite synonymous with coronary artery disease, ashypertensive heart disease and some types of valve lesion are alsoischaemic.
(b) Valve disease, especially aortic stenosis. This is a common disease,especially in elderly men. The aortic valve becomes narrowed andstiffened by chalky deposits, restricting the pumping outflow andreducing the pressure in the coronary arteries.
Lawyer‘s Guide to Forensic Medicine
220

Part II: Sudden Natural Death
221
Figure 43: Common causes of sudden natural death

(c) Hypertensive heart disease – strain on the heart due to working against ahigh peripheral pressure (see ‘Blood pressure’).
(d) Congenital heart disease, depending on the type and severity, may berelatively rare cause of sudden death, usually in young people. Surgicalcorrection has greatly reduced this category.
(e) Cardiomyopathy and myocarditis (qv) – relevant in younger adults.(f) Aneurysm of aorta (qv) – common cause in older people, when rupture
occurs.
Nervous system(a) Subarachnoid haemorrhage (qv) from a ruptured berry aneurysm or brain
artery: important cause in young to middle-aged.(b) Cerebral haemorrhage (qv).(c) Cerebral thrombosis – rarely cause of sudden death, but leads to a ‘stroke’.(d) Epilepsy (qv) – can cause sudden death, even if no actual fit or status
epilepticus at the time.
Abdominal causes (a) Massive gastro-intestinal bleeding from peptic ulcer, oesophageal varices
in cirrhosis of liver or, rarely, cancers.(b) Perforation of the gut, either a peptic ulcer of stomach or duodenum, or
cancer or diverticulosis of large intestine.(c) Complication of pregnancy, such as massive haemorrhage from abortion
or ectopic pregnancy.
Chest causes(a) Haemorrhage (haemoptysis) from lungs or air passages, due to
tuberculosis or cancer.(b) Bronchial asthma – sudden death can occur even if no acute attack or
status asthmaticus present: formerly, many deaths were due to toxiceffects on heart of broncho-dilator sprays.
An appreciable number of sudden deaths in young to middle-aged adultsreveal no cause at post-mortem (see ‘Obscure autopsy’). These must beascribed to sudden failure of the heart muscle from occult causes and have tobe recorded as ‘unascertainable’.
Lawyer‘s Guide to Forensic Medicine
222

Part II: Suffocation
SUFFOCATION
A variety of the asphyxial group of conditions, though the nomenclature isunsatisfactory. Usually taken to mean deprivation of air supply to the lungs,either from absence of respirable gas in the atmosphere (such as entering a.room exhausted of oxygen by a gas fire or a pit or silo filled with carbondioxide) – or mechanical obstruction of the mouth, nose or air passages,though the latter is often called ‘smothering’ (qv).
Though included in the rather vague category of ‘asphyxia’, death fromsuffocation may be so rapid as to exclude oxygen lack, for example, a childmay die quickly if a plastic bag is pulled over its head or a worker may dropdead on entering a chamber devoid of oxygen. Here cardiac arrest isprecipitated by some ill-understood vagal reflex, rather than pure oxygendeprivation.
223

TATTOOS
Performed by pricking pigments under the skin with a manual or electricneedle. The permanency depends on the skill of the operator and on thenature of the pigment. The red colour tends to diffuse in time; more so thanthe black, which is particulate carbon rather than a dye.
A tattoo is permanent unless the skin and underlying subcutaneous tissueare removed, either surgically or by scarring by some injurious means, such asdeep burning or corrosive substances.
Tattooing can transmit several diseases, especially virus hepatitis andsyphilis.
Forensically, the main interest of tattoos is in identification of both livingand dead. They survive most injuries except deep burns. Superficial burnsmay obscure tattoos, but when the burned epidermis is removed at surgicalcleansing or autopsy, the tattoo survives in the deep layers of the skin.
Even moderate degrees of post-mortem decomposition, as in drowning,do not destroy tattoos, which can be seen when the peeled layers areremoved. Only when actual putrefaction of all tissues begins do they becomeindiscernible.
Tattooing of persons under 16 is illegal in Britain, under the provisions ofthe Tattooing of Minors Act 1969.
THROMBOSIS
Coagulation of blood within the vessels during life. Often called ‘clotting’, butthis strictly means the coagulation of blood after it is shed from the body,outwith the blood vessels.
Thrombosis is a complex mechanism involving many factors in both theblood itself and the vessel wall. Thrombus consists of fibrin (an insolubleprotein formed by precipitation of a soluble precursor, fibrinogen) mixed withred blood cells and also ‘platelets’, tiny cell fragments which circulate in theblood. These help to initiate the clotting process by providing substanceswhich convert fibrinogen to fibrin; they also mechanically plug any smalldefects in the vessel wall to stop leakage.
The thrombus, the actual clot in the vessels, is laid down in successivestrata, made up of layers of fibrin, red and white blood cells and platelets. Thestrata represent chronological layers of deposition; in large thrombi, such as inan aortic aneurysm, they are called the ‘lines of Zahn’.
Thrombi may occur in arteries or in veins. Precipitating factors may bestagnation of blood, as in deep vein thrombosis; local damage to the vessel
Lawyer‘s Guide to Forensic Medicine
224

Part II: Thyroid Gland
wall, as in an injury; an increased propensity of the blood to coagulate aftertissue damage anywhere in the body; or to degenerative changes in the vesselwall, especially atheroma (see ‘Coronary artery disease’).
Estimation of the duration of a thrombus since formation is complex andinexact. It depends upon naked eye and microscopic evaluation, dependentupon the expertise of the pathologist. Differentiation of ante mortemthrombus from post-mortem clot is less difficult, but where ante mortemthrombus forms very soon before death, then microscopy is needed, and if thecoagulation is peri-mortal then a reliable answer may not be possible.
Thrombosis in veins leads to danger of pulmonary embolism (qv) and, inarteries, leads to death of the tissues supplied by the thrombosed vessel, dueto deprivation of blood supply. Examples include myocardial infarction andgangrene of the foot, also ‘strokes’ due to thrombosis of brain arteries.
THROTTLING
An imprecise term, usually indicating manual pressure on the neck, ratherthan due to a ligature (garrotting). ‘Manual strangulation’ is a preferable term(see ‘Strangulation’).
THYROID GLAND
A gland in the neck, just below the larynx. It consists of two fleshy lobes, oneon either side of the windpipe, connected by a narrow isthmus.
It is an important endocrine gland, its main function being the productionof thyroxine, an iodine-containing compound which is vital in controlling therate of metabolism. Enlargement of the gland is common due to a variety ofcauses including overactivity and iodine deficiency.
Overactivity of the gland leads to hyperthyroidism, also known asexophthalmic goitre or Graves’ disease. Here there is over-excitability, raisedheart rate, flushing, prominence of the eyes and danger of heart failure.Removal of part of the gland is one treatment, though anti-thyroid drugs havegreatly reduced the need for surgical operation. The latter has importantmedico-legal aspects, in that the recurrent laryngeal nerve, which controlsspeech, may be damaged during operation and may lead to an action forsurgical negligence.
Reduced function of the thyroid is more common. If it occurs in infancy,the child is a cretin, being dull, sluggish and mentally retarded. If acquiredduring adult life (most common in older women), it leads to hypothyroidismor ‘myxoedema’, so called from the thickened appearance of the skin,
225

especially the face. Loss of eyebrow hair, mental sluggishness, sensitivity tocold, coarsening of the features, thickening of the skin of the hands andthinning of head hair are typical. The blood vessels are said to be more fragileand haemorrhages may occur more readily.
Persons so affected are much more likely to suffer hypothermia (qv). Thereare also mental changes (‘myxoedema madness’) which may have medico-legal consequences. Treatment is by the administration of thyroxine or thyroidextract.
Behind or embedded within the thyroid gland are the tiny parathyroidglands, usually four in number, which have a vital role in controlling calciummetabolism. Negligence actions have occurred because these have beeninadvertently removed or damaged during thyroid operations.
TIME SINCE DEATH
This is one of the most important, yet most inaccurate and controversial topicsin forensic medicine. For many years, numerous pathologists have conductedresearch and published methods of improved techniques in estimating thetime since death, but the procedure is still fraught with uncertainties.
Most methods ultimately depend upon the rate of cooling of the body, aschemical changes are mediated by temperature, including rigor mortis,enzyme changes and other chemical estimations. The various aspects arediscussed under the following entries – see ‘Cooling of body’, ‘Decompositionof dead body’, ‘Hypostasis’, ‘Post-mortem entomology’, ‘Rigor mortis’ – butas a general observation, it can be said that most methods tend tounderestimate the time, rather than overestimate it.
No estimate given in units of less than one hour is realistic, even quiteclose to the time since death; indeed, one of the most widely used methods(Henssge) gives a minimum bracket of ± 2.8 hours.
As the probable interval lengthens, so does the potential error increase.Estimations based on temperature are only valid during the first day afterdeath in temperate climates.
The environment is all-important in attempting to estimate the time.Unfortunately, in the criminal circumstances where the information is mostvital, accurate corroboration is often lacking to allow the doctor to check hismethods. Also the temperature, air currents, winds, humidity, etc, of a sceneof death may vary widely before the body is discovered, introducingunknown errors.
It is unrealistic for a doctor to offer a single time as his estimate of the timeof death: a ‘bracket’ should be given, stating the most likely minimum andmaximum extent of the period during which death probably took place.
Lawyer‘s Guide to Forensic Medicine
226

Part II: Time Since Death
Other methods of estimating the time of death include potassium analysisof the vitreous fluid from the eye – an inexact method, but potentially usefulwhen the body has been dead for more than a day or so.
Residual electrical activity in the muscle is recommended by someauthorities, but requires special equipment and expertise.
The use of stomach contents (qv) for timing death has severe limitations.See overleaf for Henssge nomogram method.
227

Henssge’s nomogram method for estimating the time since death from asingle rectal temperature, where the environmental temperature is below23°C. The nomogram expresses the death time (t) by:
The nomogram is related to the chosen standard, that is, naked bodyextended lying in still air. Cooling conditions differing from the chosenCooling conditions differing from the chosen standard may beproportionally adjusted by corrective factors of the real body weight, giving thecorrected body weight by which the death time is to be read off. Factors above 1.0 maycorrect thermal isolation conditions and factors below 1.0 may correct conditionsaccelerating the heat loss of a body.
How to read off the time of death:
(a) connect the points of the scales by a straight line according to the rectal andambient temperature. It crosses the diagonal of the nomogram at a special point;
(b) draw a second straight line going through the centre of the circle, below left of thenomogram, and the intersection of the first line and the diagonal.
The second line crosses the semicircles which represent the body weights.
At the intersection of the semicircle of the body weight, the time of death can beread off.
The second line touches a segment of the outermost semicircle. Here can be seenthe permissible variation of 95%.
Trectum - Tambient
37.2 - Tambient= 1.25 exp (B t) - 0.25 exp (5B t); B = -1.2815(kg-0.625) + 0.0284
Figure 44: Henssge’s nomogram
Lawyer‘s Guide to Forensic Medicine
228

Part II: Time Since Death
229
Example: temperature of the rectum 26.4°C; ambient temperature 12°C; body weight90kg.
Result: time of death 16 ± 2.8 hours. Statement: the death occurred within 13.2 and 18.8(13 and 19) hours before the time of measurement (with a reliability of 95%).
Note: if the values of the ambient temperature and/or the body weight (see correctivefactors) are called into question, repeat the procedure with other values that might bepossible. The range of death time can be seen in this way.
Requirements for use:
(a) no strong radiation (for example, sun, heater, cooling system);
(b) no strong fever or general hypothermia;
(c) no uncertain* severe changes of the cooling conditions during the point betweenthe time of death and examination (for example, the place of death must be thesame as where the body was found);
(d) no high thermal conductivity of the surface beneath the body.**
* Known changes can be taken into account: a change of the ambient temperaturecan often be evaluated (for example, contact the weather station); use the meanambient temperature of the period in question. Changes by the operations of theinvestigators (for example, taking any cover off) since finding the body arenegligible: take the conditions before into account.
** Measure the temperature of the surface beneath the body too. If there is asignificant difference between the temperature of the air and the surfacetemperature , use the mean.
Dry clothing/covering
naked1–2 thin layers
naked1–2 thin layers2–3 thin layers1–2 thick layers3–4 thin layers
more thin/thicklayers
thick bedspread + clothing combined
In air
movingmoving
stillstill
moving orstill
without influence
Correctivefactor0.350.50.70.70.750.91.01.11.21.21.31.4...1.8...2.4
Wet throughclothing/coveringWet body surface
nakednakednaked
1–2 thin layers
2 or more thick
2 thick layersmore than 2 thick
layers
In air
movingmoving
moving
stillstill
In waterflowing
still
Empiric corrective factors of the body weight:
Note: for the selection of the corrective factor in any case, only the clothing or coveringof the lower trunk is relevant. Personal experience is needed; nevertheless, this isquickly achieved by consistent use of the method.

TRAFFIC ACCIDENTS
The type of injury varies widely according to the location of the victim, that is,pedestrian, cyclist, motor-cyclist, car driver, front-seat passenger or rearpassenger and with the use or absence of safety equipment.
Pedestrians
Worldwide, pedestrians are the most frequent victims of road accidents,comprising over half of the estimated million deaths and 15 million injuries. InBritain, about 28% of deaths are pedestrians (1980–90), but only 19% in theUSA. For each death there are about eight significantly injured pedestrians.About 84% are struck by the front of a vehicle; nearside impact is morecommon than offside in the UK.
Injuries can be divided into primary and secondary injuries.
Primary injuries
Impact due to initial blow from vehicle, frequently on legs by bumper bar, orhip region from frontal grille or bonnet edge. Larger vehicles, such as trucksor buses, may make primary impact higher on body, which affects laterevents.
Where a car strikes the legs, because this is below the centre of gravity ofthe body, the upper part is often rotated towards the oncoming vehicle andthe victim is lifted up onto the bonnet. Severe injuries may then occur fromstriking the windscreen, which may shatter, or striking the windscreen pillaror upper rim. Severe head injuries may occur from this impact.
By now, the car is almost invariably decelerating, but the body havingacquired forward momentum by being lifted up, continues to move forward,sliding off the front or side of the bonnet to receive secondary injuries fromhitting the ground.
Secondary injuries
Further injuries may occur from being run over either by the same car beforebraking is complete or by an adjacent vehicle. If the victim is not lifted ontothe car, he may be projected forwards (and later run over) or thrown obliquelyto the side. In any event, secondary injuries, frequently more lethal than theprimary impact, may occur. The most common is a head injury from strikingthe ground or nearby structures. Other secondary injuries include fracturedpelvis and ribs and limb fractures.
Lawyer‘s Guide to Forensic Medicine
230

Part II: Traffic Accidents
Localised injuries may occur from door handles, mirrors, headlamp rims,mascots, etc, though deliberate improvements in car design have reduced thenumber of such projecting hazards.
A considerable proportion of pedestrian victims are found to have asignificant level of alcohol in their blood.
What was the speed of the vehicle?
An estimate of the speed of a vehicle is sometimes requested, based on theinjuries suffered by the pedestrian. This cannot be done, in spite of someclaims by medical experts. Death can occur at speeds as low as 15 mph, yetother pedestrians have survived high speed impacts. The injuries depend onthe part of the body struck and other variables. Scooping-up onto the bonnetcan also occur at speeds as low as 15 mph.
An estimate of speed is only sometimes possible by the evaluation of non-medical evidence, such as skid-marks and vehicular damage.
Motor cyclists
These suffer injuries to each extremity of the body, head injuries beingsustained in 80% of fatalities. The usual sequel of events is forward projectionfrom the machine on impact. The rider strikes the ground or other obstaclehead first and, at high speed, the crash helmet affords little chance of survival.At lower speeds it makes an appreciable difference, largely by presenting asmooth surface to the ground so that deceleration can be relatively gradual.Thus any projection on the helmet, such as a peak, defeats the object.
A typical injury has been called the ‘motor-cyclist’s fracture’, being a sideto side crack across the base of the skull due to violent impact on the side ofthe head. A ring fracture of the base is also common, as is a broken neck.
Leg injuries occur when the lower limbs are trapped under the fallingmachine. As in all traffic accidents, the danger of subsequent injuries fromother vehicles (especially on high speed roads such as motorways) is notsufficiently appreciated. Another injury occurs when a motor-cyclist drivesunder the back of a truck, known as ‘tailgating’ – severe head or neck injuries,or even decapitation, may occur.
Pedal cyclists
Because of the lower speeds, the gross head injuries seen in motor cyclists arenot so common, but are still frequent, though crash helmets are increasinglybeing worn. The primary impact from a car or truck may cause lower rib orpelvic fractures, but most damage occurs from secondary injuries due to beingprojected or falling from the unstable machine.
231

Vehicle occupants
The injuries differ according to the position of the victim in the car, the frontseat passenger being the most vulnerable. However, statistically, the driver ismost often injured, due to the fact that he is so frequently the only occupant.
Rear-seat passengers have less chance of death or severe injuries, thoughafter the use of seat belts by front-seat occupants became mandatory, and thefitting of air bags more common, the proportion of death and serious injury tothose in the back increased. This led to the compulsory use of rear seat belts.
Children in the front seat, either alone or on the lap of an adult, have adisproportionately high injury rate, and in many European countries, it isillegal for them to occupy this position.
Injuries to the front seat passenger
In one series of fatal accidents, 55% of front-seat passengers suffered fracturedskulls, as against 42% of drivers. Spinal neck injuries occurred in 35% ofpassengers and 30% of drivers. Passengers suffered brain damage in 64%,drivers in 53%.
As most car accidents consist of a frontal impact, there is usually violentdeceleration. If an unyielding object is struck, the deceleration equals thecontact speed of the car and if two vehicles collide, the ‘G forces’ equal thesum of their speeds.
This gross deceleration lifts the unbelted passenger from the seat andprojects him forwards. The first contact is usually the knees, lower legs orthighs against the parcel shelf or fascia, depending on the car design. Thismay cause abrasions, lacerations or fractures to the legs.
Then the upper part of the body folds forwards, but still rises as a wholeand may be smashed against and/or through the windscreen. The body maybe completely ejected through the glass and land in the road, to suffersecondary injuries and perhaps running over. Alternatively, the head maystrike the rim of the windscreen or side pillar or ‘A-frame’, causing severelacerations and head injury. The shattered toughened glass leavescharacteristic abrasions on the face, resembling multiple V-shaped or Y-shaped abrasions and lacerations.
The deceleration commonly causes a ‘whiplash’ injury (qv). The head isthrown violently down on the neck in a frontal impact ‘hyperflexion’ and afraction of a second later, when the vehicle stops, the head swings back overthe seat, causing a ‘hyperextension’ stress, which is more dangerous thanhyperflexion. This cracking whiplash effect can dislocate or fracture the spine,either in the neck region (cervical) or back region (thoracic or dorsal). The
Lawyer‘s Guide to Forensic Medicine
232

Part II: Traffic Accidents
vertebrae can be crushed or displaced, with the danger of distorting the spinalcanal, spinal cord injury and paralysis (tetraplegia or quadriplegia) (qv).
Safety equipment
The use of a restraint harness, head rest or air bag reduces the dangers.A diagonal shoulder-plus-lap strap seat belt reduces mortality by about
25%. The head rest reduces the hyperextension risk of whiplash, but none ofthese compromise devices purports to reduce all injuries.
The protective functions of a seat belt are:(a) to prevent or reduce the contact with the windscreen and fascia;(b) to retain the person in the vehicle if the side door bursts open, as
commonly happens, with the risk of ejection and secondary injuries andrunning over by other vehicles, especially on motorways;
(c) the significant stretching of the belt fabric increases the deceleration timeand reduces the G forces on the body; and
(d) the considerable total area of the seat belt in contact with the body spreadsthe deceleration forces over a greater area of the body, compared todissipation of the same force over a small zone, which would cause severeor fatal injury, especially on the head.
Both driver and front seat passenger may be injured if the engine andtransmission, even the front suspension, are intruded backwards into thepassenger compartment – and if the roof or sides are imploded towards them.In these instances, the seat belt is obviously of no protective value.
Head rests prevent backward hyperextension, which contribute to neckinjuries, but like seat belts, cannot prevent forward hyperflexion.
Air bags momentarily prevent forward movement of the upper part of thebody and keep the occupant off the windscreen and fascia; this also preventshyperflexion neck injuries to some extent.
There are injuries reported from air bags, including friction burns to theface and, rarely, fatalities.
Injuries to drivers
These are less common than those to passengers alongside them, dueprobably to (a) the slight warning due to greater concentration on roadconditions, with subsequent bracing before impact; and (b) the protectionafforded by the steering wheel.
Though the steering wheel can inflict its own injuries on the driver, it isstill more of an asset than a liability, acting as a brace and preventing so much
233

forward projection. However, the wheel can crush ribs, breast bone, chest andabdominal contents. Especially when broken, the wheel spokes can causegross injuries to the heart and lungs. Modern wheels are made to telescope orconcertina on their shaft and are thus less lethal, but injuries to the organs ofthe chest and upper abdomen, such as a torn liver, are more common indrivers than in passengers.
The drivers may sustain fractures of arms from bracing on the steeringwheel, and of legs or pelvis from pressing on the foot pedals at the moment ofimpact.
Rear-seat passengers
Fatalities less common than in the front seat occupants, but there are stillpotentially lethal risks. The passengers may be projected forwards onto thefront seat occupants or even thrown through the windscreen. Injuries frominterior fittings, such as door handles, window winders, mirrors and lightsmay occur, especially as, if the car overturns, the occupants may be whirledaround the periphery of the compartment. Ejection may also occur, sometimesthrough the rear window.
Side-impact injuries
Naturally the occupants on the side of impact will suffer most, but the vehiclemay be overturned and all may be injured. Trapping due to distortion of thepassenger compartment may occur. The use of side impact reinforcementsystems in modern cars reduces, but cannot eliminate, injuries from this cause.
Fire is relatively uncommon in car crashes, in spite of the argumentsformerly made by anti-seat belt protesters. A Canadian survey showed thatonly 24 out of 1,297 motor car accident victims died of burns – of these, onlythree were in passenger seats.
TRANSPLANTATION OF ORGANS AND TISSUES
Transplants may be:(a) a homograft, when tissue from the same person is moved to another site, for
example, skin grafts or a digit moved to replace damaged ormaldeveloped fingers. No legal problems apart from usual informedconsent and no problems with tissue rejection.
Lawyer‘s Guide to Forensic Medicine
234

Part II: Transplantation of Organs and Tissues
Auto blood transfusion is another example, when blood taken from aJehovah’s Witness patient before operation is returned to them whenrequired;
(b) a heterograft, where part of another person (or even animal) is transplanted.The oldest and most frequent is blood transfusion, but now also includescorneae of eyes, kidneys, hearts, liver, lung, pancreas and bone marrow.
Tissues or organs may be from (a) live donors, usually a relative, or (b) from adead donor (cadaveric transplantation).
Live donation requires fully informed consent from a mentally competentadult; though no special legal requirements exist, it is ethically desirable thattime be allowed for a full explanation to be given to the donor of the potentialrisks so that he may, if he so wishes, obtain further medical and, possibly,spiritual advice. The issue revolves mainly around the donation of one of apaired organ (usually kidney) where the possibility of future failure of theremaining organ might endanger health or life. Naturally, it is illegal toremove a vital non-paired organ, even with consent, as, in even the mostemotive circumstances of a parent wishing to donate to a mortally sick child,such a procedure would be homicide.
Since scandals surrounding the commercial exploitation of donorsemerged, the Human Organ Transplant Act 1989 established strict rules overthe procedure and set up a Regulatory Authority to police them.
Where the donated tissue is easily regenerated (for example, blooddonation) no legal problems arise. It is highly unusual for an adult to givepermission for donation from a child, but in the case of blood or bone marrow,which again is quickly regenerated, such donation does occur, especiallywhen a close relationship such as a twin or sibling is involved.
Nb: the guiding principle in live donation is that the benefit to therecipient should exceed the possible harm to the donor by a considerablemargin.
Cadaveric transplantation is, naturally, the only source of unpaired organs,such as the heart, and is the largest source (in Europe) of paired organs suchas the kidney. In Britain, the legal aspects of cadaveric donation are regulatedby the Human Tissue Act 1961 (qv) and most other jurisdictions have similarlegislation. It is in this context that definitions of death and brain death (qv)are of importance.
Further legal problems have arisen over the possible transmission ofinfective diseases such as HIV, hepatitis and CJD (Creutzfeldt-Jakob Disease)(qv).
HIV-contaminated blood products given to haemophiliacs and growthhormone from human pituitaries contaminated with CJD gave rise toextensive litigation in recent years; corneal grafts have also inadvertently beentaken from infected donors.
235

In all but homografts, great care and technical expertise must be employedto obtain the best possible compatibility between donor and recipient tissues.This invokes highly complex tissue typing to avoid rejection of the donatedorgan. Apart from the best possible matching of tissue types, energeticimmunosuppressive measures with drugs are carried on after transplantation.An exception is corneal grafting, the longest established technique for solidtissue transplantation, where such problems are minimal. In this instance,there is also little complication relating to moment of death, as corneal graftscan be taken from the cadaver up to a day or so after death.
In the cases of other organs, such as kidney, speed is of the essence and inEurope a centralised data bank (Eurotransplant) of waiting potentialrecipients is maintained on computer, ready to be matched immediately withnew donor material. In Britain, this service is based in Bristol.
Some religious sects, notably Jehovah’s Witnesses, have strong objectionsto any form of transplantation, including blood transfusion. Whilst adultmembers are entitled to withhold consent for such procedures, controversysurrounds their refusal to allow life-saving measures to be applied to theirchildren. Formerly, it was usual for the child to be rapidly taken into care, by acourt being convened at the bedside, but this has fallen into disuse and nowthe opinion of two doctors acting in good faith seems sufficient against thesuccess of any possible civil action for assault. The same would apply to theurgent treatment of an adult religious objector, if he was unconscious and inextremis: doctors who employed life-saving measures, such as bloodtransfusion, would be supported by their medical protection organisations inthe defence of any subsequent suit for assault, but every case differs and theethical, and even political, climate on this matter is ever-changing.
TRAUMA AND DISEASE
The role of trauma in the causation of disease is a potent source of medico-legal argument and in many cases the problem is insoluble. However, it mustbe emphasised that the probability of an injury giving rise to disease variesgreatly according to the type of disease under discussion and there can be nogeneralisation possible in this respect.
If injury be held to include certain toxic or irritative states, as well as directtrauma, then the field of positive causation is greatly widened. For example, itwill then include such things as chemical carcinogenesis, which is theinducement of tumours, such as the well established connection betweenasbestos and mesothelioma or the malignant diseases caused by radiation.
Returning to the possible effects on human tissues of direct injury, theprobability of such an effect has been greatly exaggerated in the past, withunwarranted conclusions being drawn in many places, usually because of the
Lawyer‘s Guide to Forensic Medicine
236

Part II: Trauma and Disease
prospect of financial compensation. Though there are certain diseases where aconnection, on the balance of probabilities, is thought to exist, such aconnection is usually incapable of absolute proof, as all these diseases are wellknown to occur quite spontaneously. For example, although the association ofasbestos exposure and mesothelioma tumour is well recognised (and includedin the schedule of industrial diseases), it must be remembered that 15% of allmesotheliomata occur without any apparent asbestos exposure.
Coronary artery disease
Though claims are commonly made that death or disability from coronaryartery disease (‘heart attacks’) are due to injury or over-exertion, this claimmust be carefully analysed.
There is no evidence whatsoever that injury or exertion can cause theunderlying disease, that is, trauma and effort play no part in the aetiology ofcoronary atheroma. However, in a person who already has coronary arterydisease, it cannot be denied that over-exertion may precipitate an acuteepisode in the natural history of the disease, usually myocardial infarction ordeath from ventricular fibrillation or cardiac arrest (qv).
Recent research has confirmed the association between exertion andsudden cardiac death. Mittleman in the USA investigated 1,228 patients withacute myocardial infarction and showed there was a sixfold increase inincidence during or within one hour of heavy physical exertion. In Germany,Willich researched 1,194 patients and showed a doubling of risk. Both surveysshowed that the risk was greater in those who were normally sedentary.
Trauma very rarely causes a coronary episode, unless there is substantialdirect injury to the front of the chest. Sudden over-exertion, such as the liftingof a heavy weight or a sudden stress beyond the usual physical capabilities ofthe person, may precipitate some form of exacerbation of the cardiaccondition, as stated above. However, it must be emphasised that suddencardiac deaths are so common in the absence of trauma or effort, that no realprospect of absolute proof can be hoped for in maintaining that the untowardresult was directly related to the injury or effort.
Other types of heart disease
Diseases such as hypertension, aortic valve disease and aortic aneurysms, etc,have similar relationships to injury and effort, there being no evidence that thelatter can give rise to the basic disease, but it must be admitted that a suddenstrain might precipitate complications of the disease. This is especially so if theeffort or stress of the injury causes a sudden rise in blood pressure, which maycause rupture of an atheromatous plaque in a diseased coronary artery or of
237

an aneurysm or precipitation of death from valvular disease or hypertensiveheart disease. The fact that such diseases frequently cause death or suddendisability, in the absence of such special circumstances, reduces the cause andeffect relationship considerably.
Tumours
The relationship between malignant disease and injury is a frequent source ofcontroversy. In general, there is very little evidence indeed to allow such acausal connection to be made, except where chemical or long standingirritative states exist. For instance, a cancer of the bladder may well followexposure to aniline in an industrial worker and this is well recognised. Againa person with asbestosis of the lungs has a high probability of contracting lungcancer and those exposed to asbestos may much less frequently develop amesothelioma though, as mentioned earlier, some 15% of mesotheliomata areunrelated to asbestos.
Physical trauma is much less likely to lead to tumours, except in a directmanner, where a jagged tooth may cause years of irritation, bleeding andinfection upon the tongue and lead to a cancer. However, it is inconceivablethat a single act of injury could give rise to a tumour, though this is oftenalleged. Most allegations have arisen because the detection of a tumourappears to date from shortly after the traumatic incident. However, in almostall cases, the attention drawn to the injured part is instrumental in bringing tolight the existence of the tumour which must have pre-existed in almost allcases. A blow on a part of the body may draw attention to a previouslyunnoticed lump, or the temporary signs of the injury may render the firstsigns of the tumour apparent.
Certain criteria, known as ‘Ewing’s postulates’, must be satisfied beforeany connection can be maintained (though, even then, there is no scientificway of proving anything other than a possibility):(a) the tumour must arise exactly at the site injured;(b) definite and substantial trauma must be proved;(c) the tumour must be confirmed pathologically;(d) the tissue at the site must have been healthy before the trauma;(e) a reasonable interval – neither too long or too short – must elapse between
the time of the trauma and the appearance of the tumour; and(f) though not one of the Ewing’s original postulates, there should be some
good scientific reason for ascribing the tumour formation to the injury –and this is rarely possible.
Lawyer‘s Guide to Forensic Medicine
238

Part II: Trauma and Disease
The interval necessary is also a difficult matter. Though few would acceptanything less than months, the upper limit may be very long. For instance,mesothelioma from asbestos may take 15–20 years to appear.
Brain tumours have presented many problems in relation to head injury,but there is no good evidence that a causal relationship exists. This statementmust be modified according to the type of tumour, as growths of themembranes (meningiomata) may have a slightly better chance of establishinga cause-and-effect relationship than growths of brain itself, such as a ‘glioma’.Courville, who is one of the best authorities on the subject, has come to theinvariable conclusion that in no case, evaluated from a clinical or pathologicalviewpoint, has a glioma proved to be of traumatic origin. As head injuries areso common in the general population, it is inevitable that tumour formationand a history of trauma must frequently coincide. It should be rememberedthat over 10% of a non-tumour-suffering population can recall a significanthead injury.
Infections
Here, the possibility of trauma being related is far greater, depending uponthe circumstances. Due either to an injury penetrating and carrying infectioninto the wound, or because tissue damage renders the body more susceptibleto ever-present contamination, then the possibility exists in greater or lesserdegree according to the circumstances. Again, expert evidence is required toevaluate the site, timing and other pathological factors, which might relate theinjury to the infection.
Damage to a limb, for instance, may give rise to osteomyelitis (infection ofthe bone) or a chest injury may rekindle a healing or dormant tuberculouscondition. Each case must be considered upon its particular circumstances,but the chances of connecting infection to injury are far greater than withtumours.
Epilepsy
The onset of fits after a focal head injury (almost always a localised skullfracture and/or brain damage) is well established, but direct evidence of alocal area of injury in a site that neurologically can be related to the fits mustbe produced, as well as assurance that no fits were suffered before the headinjury. It is difficult or impossible to differentiate the usual types of‘idiopathic’ (that is, of unknown cause) epilepsy from post-traumatic epilepsyunless there are localising signs which correspond to the area of injury. Sometypes of fits may be so localised, such as temporal lobe epilepsy, where theremay be olfactory or gustatory manifestations. In addition, the use of electro-
239

encephalography (EEG) may localise the focus of origin of the fits. Adepressed fracture, even when healed, may cause local pressure or irritationto the surface of the brain, which may be correlated with the focus of the fits tosubstantiate the claim of traumatic epilepsy. The age of onset may besignificant, as it is less likely for a person of mature years to begin idiopathicepilepsy, when there is a definite injury present consistent with theproduction of fits. The whole matter needs the most expert neurologicaladvice for resolution.
The possibility that a pre-existing disease actually caused or contributed to theaccident, which in turn led to the trauma, must be considered. This isespecially the case in fatal instances, where dependants claim that some stressor injury caused death and the subject himself is not available as a witness orfor clinical examination.
The problem arises even more often in relation to insurance andcompensation claims concerning transport accidents, where the relative role ofpre-existing disease, such as coronary occlusion or hypertension, is difficult toassess in retrospect as a potential cause of the fatal accident.
TRAUMATIC ASPHYXIA
An inappropriately named condition, where the most florid signs of‘asphyxia’ are seen. It is almost always accidental, due to pressureimmobilising the chest wall and preventing breathing movements. Veryoccasionally it can be homicidal, as in ‘Burking’, named after Burke and Hare,where the killers sat upon the chests of drunken victims to obtain cadavers foranatomical dissection.
Accidents, such as burial in earth, mud, sand, silo contents, grain bunkers,etc, may cause fixation of the chest, even though the mouth and nose areabove the surface. It is the most common cause of multiple deaths in crowdaccidents where collapse of barriers and crushing of the victims (such asHillsborough, Ibrox Park, Heisl Stadium and Bolton football disasters) leads topacking together of bodies so that the chest movements are restricted.
Another cause is the pinning of drivers beneath vehicles, especiallyagricultural tractors, which now must have a safety roll-bar or cab to guardagainst this particular accident.
The common factor is fixation of the chest by external pressure, eventhough the air passages are unobstructed at the nose and mouth. As the ribscannot move and the diaphragm cannot descend, no air can be drawn into thelungs. The frustrated violent attempts to breathe and the impairment of bloodreturn to the chest, which is normally assisted by movements of the thorax,
Lawyer‘s Guide to Forensic Medicine
240

Part II: Traumatic Asphyxia
causes gross congestion in the face and neck above the level of the collar bone.This area becomes red or purple in colour and numerous petechialhaemorrhages (qv) appear in the eyelids, whites of the eyes and skin of theface. Sometimes bloodshot whites of the eyes bulge through the lids, givingthe most classical example of asphyxia – more correctly called ‘congestivesigns’ due to impaired return of blood through the large veins to the heart.
241

VAGAL INHIBITION (REFLEX CARDIAC ARREST)
This term fell into considerable disrepute as a consequence ofoveremployment in past years as a rather loose excuse to explain many deathswhere no positive findings could be obtained by autopsy. However, usingdiscretion and reasonable criteria, the concept has genuine validity. Part of itsfall from grace resulted from confusion with ‘status lymphaticus’ (qv), an evenmore nebulous entity used to explain obscure sudden deaths.
In essence, vagal inhibition is a convenient and exact term describingsudden heart stoppage due to excessive nervous stimulation of the heart viathe vagus nerve, which is the paired (10th) cranial nerve which leaves the baseof the brain and courses down the neck, through the chest to terminate in theabdomen. It supplies many organs and structures with ‘parasympathetic’nerve fibres, which is part of the ‘autonomic nervous system’. This is notunder voluntary control and performs a myriad of functions concerned withthe workings of blood vessels, glands, heart, etc. The other component of thesystem is the ‘sympathetic’ nervous system, which is in balanced oppositionto the parasympathetic system.
The medico-legal significance is profound, in that any sudden unexpectedstimulus to many parts of the body can cause a burst of nerve impulses topass down the parasympathetic via the vagus, so slowing or stopping theheart. In contrast to sympathetic nerve activity (the ‘flight or fight’ responsewhich releases adrenaline and directly speeds up the heart), vagus impulsesslow the heart and in excess, can stop it altogether.
The type of stimulus which can trigger this vagal reflex includes suddencooling of the skin, as in falls into cold water; the abrupt entry of cold waterinto the back of the throat or air passages; touching or dilation of the neck ofthe womb as in abortions; and forensically most important, sudden pressureon the neck (qv). The latter causes nervous discharges to originate in thecarotid sinuses, which causes sudden death in a large proportion ofstrangulations, rather than an asphyxial death.
The likelihood of vagal inhibition is heightened when the victim is pre-sensitised by emotional tension. For instance, very apprehensive patients havedied instantly on having teeth extracted or small operations performed underlocal anaesthetic. The woman undergoing an abortion may die the momentthe cervix of the womb is touched or dilated. Other cases are on record wherestudent ‘rags’ have caused death when the skin was touched with ice in amock execution. Professor Keith Simpson records a case where a woman diedinstantly on rapidly gulping a glass of cold water and every pathologist hascases where similar events have occurred, leaving no traces at post-mortemexamination. Even a horrific or nauseating sight has caused sudden death andthe potential categories of such events are without limit.
Lawyer‘s Guide to Forensic Medicine
242

Part II: Vital Reaction
However, for such an explanation to be acceptable, the following criteriashould be applied:(a) no demonstrable abnormalities sufficient to cause death at autopsy (see
‘Obscure autopsy’);(b) the circumstances of the death allow of some situation such as described
above to have been present: unfortunately, in many cases, the death is notwitnessed; and
(c) no other more convincing explanation is forthcoming.
Where negative autopsy findings are combined with a completely unhelpfulhistory, it is more satisfactory to admit that the cause of death was‘unascertainable’ than to invoke vagal inhibition. It has been the lack of thiscaution that has allowed an otherwise reasonable explanation to fall intodisrepute and even ridicule.
VERTEBRAL ARTERY INJURY
See ‘Subarachnoid haemorrhage’.
VITAL REACTION
A term indicating the response of living body tissues to injury.By definition it can only occur during life and is therefore an index of ante
mortem injury. This is of considerable importance in forensic medicine in (a)attempting to establish that an injury was inflicted before death; and (b)possibly estimating the time of infliction before death.
The rather absolute acceptance of ante-mortem versus post-morteminfliction has become more indistinct in recent years, as it has becomeapparent that death is a process, not an event and that injuries inflicted at oraround the time of death (‘peri-mortal’) may not be so easily differentiated. Ithas been found, for instance, that white blood cells (leucocytes), which may beattracted to injured tissue, can remain mobile for many hours after thecessation of the heart and breathing, the conventional markers of life or death.
It is also apparent that the cellular response to injuries, with migration ofwhite blood cells and other tissue cells, is much more irregular than formerlythought; some undoubtedly ante mortem injuries may be without such acellular response for a long time after wound infliction.
The vital reaction may be sought by the naked eye, microscopichistological examination, or histochemical or other chemical means.
243

Naked eye evidence includes the signs of inflammation, viz, reddening andswelling. The edges of a wound or burn will usually show these signs ifsufficient time has elapsed before death supervenes. A minimum time is hardto quantify, but is usually of the order of several minutes in the case of burns,and longer in wounds.
Histological examination. Using conventional histological methods, bypreparing stained sections of tissue for examination under the microscope, themost important signs of vital reaction are oedema (swelling) and hyperaemia(dilatation of blood vessels), which are rather indeterminate signs. The bestcriterion is the appearance of migrant white blood cells (leucocytes) into theinjured part. The first cells to appear are the polymorphonuclear leucocytesand may be seen from a number of minutes to a few hours after injury.Unfortunately, their appearance is most irregular and if death occurs within ashort time (up to many hours) then none may be visible.
Chemical and histochemical tests. More recent research has shown that enzymesand other substances such as histamine and serotonin (all mediators in theinflammatory reaction, which is a precursor to healing) may appear within afew minutes after injury, in the zone adjacent to the main damage. The area ofactual tissue destruction may lose its pre-existing enzyme content.
This is an area of ongoing research, some of which is only just appearingin routine practice in the more advanced forensic centres. However, many ofthese sophisticated new enzyme techniques have not been adopted intogeneral use, due to their unreproducibility by those who did not develop themethods.
Lawyer‘s Guide to Forensic Medicine
244

Part II: Whiplash Injury
WHIPLASH INJURY
Spinal damage caused by violent bending and then straightening of thevertebral column. The most common cause is a traffic accident involvingmotor car occupants. Sudden deceleration from a frontal impact, oracceleration from impact in the rear, causes the head to swing back and forth,resulting in severe stresses to bones and joints of spine caused by the inertia ofthe heavy head. This may result in fracture and/or dislocation of the spinaljoints of the neck and upper chest.
There may be local damage to bones and joints of the spinal vertebra, withsubsequent fractures, dislocations, pain and tenderness, but the major dangeris injury to the spinal cord at the level of the injury, which may result in nervedamage, paralysis or even death.
The legs may be paralysed (paraplegia) or all four limbs (tetraplegia orquadriplegia). If the injury is high in the neck (above 3rd–5th vertebrae) thenerves which control breathing may be damaged and death ensue fromrespiratory paralysis.
Lesser degrees of injury may damage the nerve roots that pass out fromthe spinal canal, with impairment of motor function (movement) of parts ofthe upper limb or of sensory function leading to numbness, tingling, etc.
In addition to damage to the spine and spinal cord, a severe whiplash ofthe chest region may damage the aorta, which is attached to the front of thespine where the aortic arch becomes the descending aorta. The aorta may becompletely transected at this point or may show one or more transverse tearsin its lining due to whiplash stress: death from fatal internal bleeding mayresult (see ‘Aorta’).
245


APPENDIX
Adelson, L, The Pathology of Homicide, 1974, Springfield, Illinois: CharlesThomas.
Denny, R, None for the Road – Understanding Drink-Driving, 1997, Crayford:Shaw.
Di Maio, V and Di Maio, K, Forensic Pathology, 1989, New York: Elsevier.
Evand, KT and Knight, B, Forensic Radiology, 1981, Oxford: BlackwellScientific.
Knight, B (ed), Estimation of the Time Since Death, 1995, London: EdwardArnold.
Knight, B, Forensic Pathology, 2nd edn, 1996, London: Edward Arnold.
Knight, B, Legal Aspects of Medical Practice, 5th edn, 1992, London: Churchill-Livingston.
Knight, B, Simpson’s Forensic Medicine, 11th edn, 1997, London: EdwardArnold.
Mason, JK, Forensic Medicine for Lawyers, 3rd edn, London: Butterworths.
Mason, JK (ed), Pathology of Trauma, 2nd edn, 1993, London: Edward Arnold.
Mason, JK and McCall Smith, E, Law and Medical Ethics, 1983, London:Butterworths.
McLay, WDS (ed), Clinical Forensic Medicine, 2nd edn, 1996, London:Greenwich Medical Media.
Polson, C, Gee, D and Knight, B, Essentials of Forensic Medicine, 5th edn, 1985,Oxford: Pergamon Press.
Walls, H and Brownlie, A, Drink, Drugs and Driving, 2nd edn, 1985, London:Sweet & Maxwell.
Whittaker, D and Macdonald, F, A Colour Atlas Of Forensic Dentistry, 1989,London: Wolfe Medical.
247
RECOMMENDED READING


INDEX
Abdomen...........................................................3, 4injuries to .....................................................12
Abortion ........................................................13–17hazards of ........................................14, 15, 22induced ............................................13–14, 22legislation on.........................................15–17
Abortion Act 1967............................13, 16–17, 70
Abortion Regulations 1968...............................16
Abrasions ..............................................17–18, 108finger-nail marks ..............................114, 172
Accidentshanging ......................................................127see also Traffic accidents
Acetyl-salicylic acid (aspirin) poisoning ...............................................42–43
Acquired Immune Deficiency Syndrome (AIDS) .......................................21
Adipocere..............................................18, 57, 100
Advisory Council on the Misuse of Drugs........................................160
Age, estimation of...............................19–21, 141, 198–99
Air embolism...................................14, 21–22, 30, 88, 103
causes............................................................22diagnosis ......................................................22
Air passageobstruction of...........................23–24, 42, 61,
151–52choking ....................................23–24, 38,
71–72smothering ...............................38, 202–3strangulation.........................38, 212–15,
225suffocation.............................38, 202–03,
223
Air-gun injuries............................................22–23
Air-Guns and Shotguns, etc, Act 1962........................................................23
Alcoholethyl ........................................................24–28
absorption of..................................24–25elimination of.................................25–27physiological effects of..........27–28, 29,
156methyl ....................................................28–29
Allobarbitone......................................................45
Amnesia ................................................29, 74, 105
Amniotic fluid embolism ...............................104
Amphetamines.............................................29–30ecstasy ..................................................29, 101
Amylobarbitone.................................................45
Anaemia, asphyxia caused by .........................39
Anaesthesiadeath associated with ..........................30–33epidural ........................................................32general....................................................32–33hyperthermia and.....................................158local...............................................................31spinal ............................................................32
Anal intercourse (sodomy) ..............191, 203–04
Anatomyabdomen ....................................................3, 4anatomical directions...................................2anatomical drawings .............................2–10aorta and branches .......................................7genital organs..............................................10heart ............................................................8, 9kidney.............................................................5lungs ...............................................................8neck.................................................................6spleen..............................................................5thorax..........................................................3, 6
Aneurysms ......................................22, 33–35, 37, 66, 72, 82,
215–16causes............................................................35
Angioma..............................................................66
Anthraco-silicosis ......................................174–75
Aorta ..................................................7, 35–37, 245aneurysms .....................................35, 37, 222atheromatous
degeneration of....................................35stenosis .......................................................220
Arm-lock (neck-hold deaths).........................168
Arteries ..........................................................37–38asphyxia and.......................................212–13atheromatous
degeneration of .................35, 66, 80–81blockage,
see Embolismcoronary artery disease ..............80–82, 106,
220complications ..................81–82, 165–66trauma and.........................................237
subarachnoid haemorrhage.........................66, 72, 148,
215–17vertebro-basilar system.....................216–17
249

Arterio-venous aneurysm ................................35
Arterioles.............................................................37
Arteriosclerosis (atheroma) ...........35, 66, 80–81
Arthritis, rheumatoid......................................175
Asbestosis..................................................174, 176
Asphyxia .......................................................38–42causes of.................................................38–39choking............................................23–24, 38,
71–72hanging ................................................127–28masochistic practices .................127, 158–59petechial haemorrhages ...................40, 126,
173–74positional/postural..................................180signs of ...................................................40–42smothering ......................................38, 202–3strangulation................................38, 212–15,
225suffocation....................................38, 202–03,
223traumatic.......................................38, 40, 174,
240–41
Aspirin poisoning........................................42–43
Atheromatous degeneration of blood vessels .............................35, 66, 80–81
Automatism, post-epileptic ...........................105
Autopsy.........................................................43–44aspirin poisoning........................................43diagnosis of air embolism.........................22diatom test in drowning .....................93–95establishing live or still birth..........154, 210Human Tissue Act 1961 and ..................134objectives................................................43–44obscure or negative....................169–70, 222poison sampling .................................178–80
Baggasosis .........................................................174
Barbitone .............................................................45
Barbiturates.............................................30, 45, 49
Berry aneurysm ..............................34, 35, 66, 72, 215–16
Bestiality........................................................45–46
Beta-amyloid precursor protein detection.......................................................95
Birthlive.........................................................153–55still-birth ....................................114, 153, 210
Births and Deaths Registration Acts .....................................................153, 210
Bite marks ...................................................46, 190
Black eye..................................................47–48, 55
Bladder ................................................................48
Blast injuries ...............................................108–09
Bleeding,see Haemorrhage (bleeding)
Blisters .....................................................45, 49, 58
Bloodalcohol levels in ....................................25–26blood groups ...............................................50blood pressure ...............................37, 50–51,
66, 222disseminated intravascular
coagulopathy (DIC)....................96, 104fluidity of, asphyxia sign...........................40hypostasis (post-mortem
lividity) .........................................139–40splashes ..................................................51–52transfusion of, air embolism
caused by..............................................22
Blood vessels.........................................................7air embolism...................................14, 21–22,
30, 88, 103aneurysms ................................33–35, 37, 66,
72, 215–16, 222
angioma........................................................66aorta...........................................7, 35–37, 220,
222, 245arteries....................................................37–38
asphyxia and................................212–13atheromatous
degeneration...............35, 66, 80–81coronary artery disease.......80–82, 106,
165–66, 220, 237
subarachnoid haemorrhage .................66, 72, 148,
215–17vertebro-basilar system..............216–17
blockage, see Embolism
veinsdeep vein thrombosis................184–87,
224–25obstruction of.........................40, 42, 212petechial haemorrhages............40, 126,
173–74
Blue-bottles .......................................................181
Bone marrow embolism .................................104
Lawyer’s Guide to Forensic Medicine
250

Index
Bones (skeleton)decomposition processes
and.........................................................91estimation of age and ............19–20, 198–99fractures ...............................................119–20
femur.............................................113–14hyoid bone ..........................127, 135–38,
150, 151jaw .......................................................147ribs .................................................191–92skull.....................................129, 199–202
identification from .............................198–99osteoporosis...............................................113
Bovine Spongiform Encephalopathy (BSE) ...............................86
Bowel, rupture of ...............................................12
Brainbrain death ......................................52–54, 90cerebral aneurysm...................34, 35, 66, 72,
215–16cerebral haemorrhage..........................65–67causes of.................................................66–67cerebral oedema .................................67, 129cerebral vascular defects ...........................28extradural haemorrhage/
haematoma ..........................60, 110, 111head injuries and ......................................129
contre-coup injury ..........48, 76–77, 129necrosis.......................................................169tumours......................................................239
Breathalcohol levels ...............................................26proof of live birth ...............................153–54
Brodrick Report............................................85, 86
Bronchi, air passage obstruction .....................23
Bruising .........................................................54–56black eye ..........................................47–48, 55finger-tip bruising ....................................172mixed lesions...............................................18
Brush abrasions....................................17, 18, 172
Buggery (anal intercourse)...............191, 203–04
Burial..............................................................56–57exhumation after ..........................57, 107–08
Burns......................................................57–60, 109blisters ..........................................................49cause of death in bodies
recovered from fires .....................60, 63electrical .....................................................103medico-legal aspects............................57–58other significant factors.......................58, 60
rule of nine ....................................57, 59, 194scalds ..........................................................194severity of ..............................................57, 59spontaneous combustion ........................205
Butobarbitone.....................................................45
Byssinosis ..........................................................174
Cadaveric spasm..............................................193
‘Café coronary’.................................23, 42, 61, 71
Cancer, see Tumours
Cannabis........................................................61–62
Capillaries ...........................................................37
Caplan lesion ....................................................175
Carbon dioxide, absorption of ethyl alcohol and ........................................25
Carbon monoxide poisoning..............28, 39, 58, 62–63
lethal levels............................................62, 64sources of .....................................................63
Cardiac, see Heart
Cardiomyopathies.....................................65, 222
Carotid arteries ....................................38, 212–13
Carotid sinus ..............................................213–14
Carunculae myrtiformes ................................135
Cellular death .....................................................90
Cerebrum, see Brain
Certificates, death............................56, 85–86, 89
Chest, compression of (traumatic asphyxia)...................38, 40, 174,
240–41
Chest (thorax) ...................................................3, 6injuries
air-gun injuries ....................................22rib fractures..................................191–92
see also Heart; Lungs
Child destruction ...............................................70
Childrenabuse of ..................................................67–70
features of................................46, 48, 55, 68–70, 114, 191–92, 218
air-gun injuries......................................22, 23bruising ........................................................55cot death ................................84–85, 169, 203
251

Lawyer’s Guide to Forensic Medicine
252
estimation of age ..................20, 21, 141, 198infanticide............................................143–44rape of.........................................................188
Chloroform .........................................................33
Choking, air passage obstruction ......23–24, 38, 71–72
Circle of Willis..............................................72, 73berry aneurysm .............................34, 35, 66,
72, 215–16
Cirrhosis ....................................................155, 156
Clinical autopsy .................................................44
Clots, see Thrombosis
Coal workers’ pneumoconiosis (anthraco-silicosis) .............................174–75
Cocaine ..........................................................31, 72
Code of practice on removal of organs for transplantation ..................53–54
Cold injury (hypothermia).........................72–74signs......................................................74, 139
Colon..................................................................144
Comminuted skull fractures..........................200
Concussion..........................................................74post-concussional amnesia .................29, 74
Congenital aneurysm.................................35, 66, 215–16
Congestion, asphyxia sign ...............................40
Congestive cardiomyopathy (COCM)........................................................65
Consentto transplantation ..............................133–34,
234–36to treatment ...........................................75–76
Contre-coup injuries ............................48, 76–77, 129, 200
Contusion, see Bruising
Coronary artery disease ....................80–82, 106, 220
complications..........................81–82, 165–66thrombosis..................................165–66, 220,
225
Coronerdeaths reportable to .......................82–84, 89exhumation and........................................107
Coroner’s Acts....................................................44
Coroner’s Rules............................................44, 82
Cot death..............................................84–85, 169, 203
features...................................................84–85practical considerations.............................85
‘Crack’ cocaine ...................................................72
Cremation .....................................................85–86
Creutzfeldt-Jakob Disease (CJD) ......86–87, 235
Crib death .....................................................84–85
Cricoid cartilage.......................................150, 151
Curling’s ulcer....................................................60
Cuts, see Incised wounds; Lacerations
Cyanosis, asphyxia sign ...................................40
Cyclists, traffic accidents ................................231
Cyclobarbitone ...................................................45
Cyclopropane .....................................................33
Dangerous Drugs Acts ...................................159
Deathadipocere formation after ...........18, 57, 100age estimation after..............................19–21appearance of injuries after .........18, 48, 56,
58, 152associated with anaesthesia................30–33brain death ......................................52–54, 90burial after .............................................56–57
exhumation after...................57, 107–08certificates..................................56, 85–86, 89cooling of body after......................78–80, 99cot death........................................84–85, 169,
203cremation after......................................85–86decomposition,
see Decomposition of body
drowning ..............................................93–95, 97–100, 178
hanging ................................................127–28hypostasis (post-mortem
lividity) .........................................139–40identification after ....................................142
DNA technology .................................97exhumation and ..........................107–08from bones (skeleton).................198–99from frontal sinuses............120–21, 142tattoos..................................................224teeth.........................................92–93, 142
mummification after..........................91, 164

Index
mutilation after ...................................164–65neck-hold deaths ......................................168post-mortem entomology.........104, 181–82Procurator Fiscal and.........................183–84reportable to Coroner ....................82–84, 89rigor mortis..........................................192–93signs of .........................................................90stature estimation after............................208sudden natural death ........................220–22timing of....................................78–79, 91, 99,
139–40, 181–82, 192–93, 211,
226–29see also Autopsy
Decomposition of body ....................................91adipocere formation ....................18, 57, 100after burial .............................................56–57blisters ..........................................................49general sequence of....................................91insects and .................................................181maceration .................................................155
Deep vein thrombosis.................184–87, 224–25
Defence actions, injuries caused by ...............................................18, 92
Dental, see Teeth
Deoxyribonucleic acid (DNA) technology .................50, 96–97, 127
Depressed skull fractures...............................200
Dextro-amphetamine........................................30
Diabetes .........................................................28, 29
Diamorphine (heroin).............................132, 163
Diatom test in drowning ............................93–95
Diffuse axonal injury ..........................67, 95, 129
Dilatation and curettage ...................................13
Dislocation, fracture dislocation ...................120
Dissecting aneurysms .................................34, 35
Disseminated intravascular coagulopathy (DIC) ...........................96, 104
Divers, air embolism in.....................................22
Diverticulitis .....................................................146
DNA (deoxyribonucleic acid) technology...............................50, 96–97, 127
Drivers, traffic accidents...........................233–34
Drowning............................................97–100, 178diatom test in ........................................93–95signs of .................................................99–100
Drugs ...................................................................28abortion induced by...................................14amphetamines ......................................29–30anaesthetic .............................................31–33barbiturates .....................................30, 45, 49cannabis .................................................61–62cocaine....................................................31, 72ecstasy ..................................................29, 101glue sniffing...............................................125heroin..........................................................132LSD .......................................................156–57methadone.................................................159Misuse of Drugs Act 1971.................159–62morphine ...........................................132, 163
Drugs (Prevention of Misuse) Act 1964......................................................159
Dry lung drowning ...........................................99
Duodenal ulcer.................................................146
Duodenum........................................................144
Ecchymoses.......................................................126
Ecstasy .........................................................29, 101
Electricityblisters ..........................................................49electrocution........................................101–03
signs of ................................................103
Embolism ....................................................103–04air embolism...................................14, 21–22,
30, 103amniotic fluid embolism .........................104bone marrow embolism ..........................104fat embolism................................103, 112–13foreign body embolism ...........................104pulmonary embolism...............31, 103, 114,
184–87thrombo-embolism ..................................103
Entomology, post-mortem...............104, 181–82
Entrance woundsrifle ..............................................................117shotgun.......................................................115
Epidural anaesthesia .........................................32
Epidural (extradural) haemorrhage .....................................110, 111
Epilepsy...........................................28, 29, 104–05traumatic.............................................74, 105,
239–40
Ether.....................................................................33
253

Ethyl alcohol.................................................24–28absorption of .........................................24–25elimination of ........................................25–27physiological effects of..........27–28, 29, 156
Euthanasia, by air embolism ...........................22
Ewing’s postulates...........................................238
Exhumation ..........................................57, 107–08
Exit woundsrifle ..............................................................117shotgun.......................................................115
Exophthalmic goitre........................................225
Expectation of life ........................................105–6
Explosion injuries ........................................108–9
Extradural haematoma.....................60, 110, 111
Extradural haemorrhage ........................110, 111
Eyeinjuries
air-gun injuries ....................................22black eye...................................47–48, 55
retinal haemorrhage...................................67
Fabricated injuries ...........................................112
Farmer’s lung ...................................................177
Fasciitis ..............................................................122
Fatadipocere .......................................18, 57, 100alcohol absorption/
elimination and ...................................26fat embolism................................103, 112–13
Female genital organs.........................10, 188–91
Female sterilisation....................................209–10
Femur, fractures.........................................113–14
Fever (hyperpyrexia/hyperthermia).............................33, 138, 158
Fibrosiscoronary artery disease .....................81, 106pneumoconioses.................................174–77
Fiedler’s myocarditis.......................................166
Finger-nail marks ....................................114, 172
Finger-tip bruising...........................................172
Firearm wounds ................................115–18, 172rifled weapon wounds ......................117–18smooth bore weapons .....................115, 116
Firearms Acts......................................................23
Firearms (Dangerous Weapons) Rules 1969 ....................................................23
Fissured skull fractures...................................200
Flail chest...........................................................191
Flaying lacerations...........................................150
Flies ....................................................................181
Foetus...........................................................118–19child destruction.........................................70development of...................................118–19estimation of age.........................................19see also Abortion
Foodabsorption of ethyl
alcohol and.....................................24–25air passage obstruction and................23–24Creutzfeldt-Jakob Disease
(CJD) and........................................86–87
Foreign bodies..................................................119air passage obstruction
caused by..................................23, 24, 71foreign body embolism ...........................104
Forensic autopsy ................................................44
Fractures......................................................119–20femur ....................................................113–14hyoid bone..................................127, 135–38,
150, 151jaw...............................................................147ribs ........................................................191–92skull ............................................129, 199–202
Fresh water drowning ........................98–99, 178
Front seat passenger, traffic accidents ..............................................232–33
Frontal sinuses, identification from .....................120–21, 142
Fusiform aneurysm ...........................................34
Gags, air passage obstruction....................24, 71
Gangrene...........................................................122
Gas gangrene....................................................122
General anaesthesia.....................................32–33
General Medical Council (GMC)............122–24disciplinary functions........................123–24medical register ........................................123
Genital organs, see Female genital organs; Male genital organs
Glass injuries ..............................................124–25
Gliomas..............................................................239
Glottal oedema.................................................151
Lawyer’s Guide to Forensic Medicine
254

Index
Glue sniffing .....................................................125
Goitre .................................................................225
Grand mal epilepsy.................................104, 105
Gravel rash............................................17, 18, 172
Graves’ disease.................................................225
Grazes (abrasions) .......................................17–18
Green-bottles ....................................................181
Greenstick fractures ........................................120
Haematemesis ..................................................126
Haematomaextradural ....................................60, 110, 111heat haematoma .........................................60peri-orbital (black eye) ..................47–48, 55subdural...............................................218–20
Haemopericardium...........................................81
Haemoperitoneum ..........................................126
Haemoptysis.....................................................126
Haemorrhage (bleeding) ................................126abdominal injuries .....................................12abortion ........................................................14abrasions ......................................................17air passage obstruction
caused by..............................................24amphetamines.............................................30aneurysms and ..............................33, 35, 66,
215–16aortic .......................................................35, 37arterial ..........................................................38asphyxia signs.......................................40, 42cerebral haemorrhage..........................66–67death associated with
anaesthesia ...........................................30extradural haemorrhage .................110, 111internal .......................................................126petechial haemorrhages ...................40, 126,
173–74retinal haemorrhage...................................67subarachnoid haemorrhage ......66, 72, 148,
215–17subdural haemorrhage......................218–20sudden natural death and.......................222
Haemosiderin, detection of......................55, 219
Hair ..............................................................126–27
Halothane anaesthesia ......................................33
Hanging.......................................................127–28
Head injuries ........................................28, 128–29air-gun injuries............................................22amnesia following................................29, 74
concussion .............................................29, 74contre-coup injury.........................48, 76–77,
129, 200coup injury ....................................76, 77, 129diffuse axonal injury....................67, 95, 129epilepsy following..............................74, 105kicking........................................................148scalp injuries ..............................128–29, 142,
194–95skull fractures ...........................129, 199–202
Heart ....................................................8, 9, 130–31anaesthetics and....................................32, 33asphyxia caused by heart
failure ....................................................39‘café coronary’.......................................23, 61cardiac aneurysm .......................................82cardiac arrest..................................23, 64–65,
103, 127cardiac tamponade.....................81, 126, 130cardiomyopathies...............................65, 222cor pulmonale ...........................................175coronary artery disease ..............80–82, 106,
220complications ..................81–82, 165–66trauma and.........................................237
dissecting aneurysm and ..........................35massage..................................................64–65myocardial infarct........................81, 165–66myocarditis ...........................65, 166–67, 222necrosis...............................................168, 169rupture of...............................................81–82sudden natural death and ................220–22trauma and disease of .......................237–38vagal inhibition......................12, 14, 32, 125,
127, 242–43ventricular fibrillation ...............................64
Heat haematoma................................................60
Height, estimation of.......................................208
Henssge’s nomogram ..............................79, 226, 228–29
Hepatitis..............................................132, 155–56
Heroin................................................................132
Heterograft transplantation ...........................235
Higginson syringing ...................................12, 22
Hinge skull fractures.................................201–02
Histology...........................................................133
Histopathology ................................................133
Home Office Forensic Science Laboratory Service .............................50, 177
255

Homicideair embolism................................................22homicidal cut throat.............................87–88mutilation after .........................................164
Homograft transplantation......................234–35
Horizontal skull fractures ..............................200
House-flies ........................................................181
Human Fertilisation and Embryology Act 1990 ....................16, 17, 70
Human immune deficiency virus (HIV) ..........................................21, 235
Human Organ Transplantation Act 1989..............................................134, 235
Human Tissue Act 1961 ....................44, 133–35, 235
Hydrostatic test ................................................154
Hymen...............................................135, 188, 197
Hyoid bone........................................127, 135–38, 150, 151
Hyperpyrexia/hyperthermia..........33, 138, 158
Hypertension (high blood pressure) .........................................37, 51, 66,
222
Hyperthyroidism.............................................225
Hypertrophic obstructive cardiomyopathy (HOCM) ........................65
Hypostasis (post-mortem lividity) .........139–40
Hypotension (low blood pressure).................51
Hypothermia ................................................72–74signs......................................................74, 139
Hypothyroidism ........................................225–26
Hysterotomy.......................................................13
Identification ..............................................141–42dead .................................................92–93, 97,
107–08, 120–21, 142, 198–99,
224DNA technology ..........................96–97, 127exhumation and..................................107–08from bones (skeleton) ........................198–99from frontal sinuses...................120–21, 142from tattoos ...............................................224from teeth .....................................92–93, 141,
142living..............................................96–97, 127,
141–42
Idiopathic epilepsy ..........................................105
Incised wounds..........................................142–43glass injuries........................................124–25see also Stab wounds
Industrial Injuries Acts ...................................176
Infant Life (Preservation) Act 1929..........................................15, 70, 153
Infanticide...........................................143–44, 153
Infanticide Act 1922.........................................143
Infanticide Act 1938...................................143–44
Infectionabortion and ................................................14AIDS and......................................................21aneurysm caused by ..................................35burns and.....................................................60choking caused by......................................72gangrene ....................................................122hyperpyrexia/hyperthermia..................138trauma and ................................................239venereal infections ...................................189
Injuriesabdominal....................................................12abortion induced by...................................14abrasions........................................17–18, 108air-gun injuries......................................22–23aneurysm caused by ..................................35aorta........................................................36–37appearance after death.................18, 48, 56,
58, 152bite marks ............................................46, 190bruising................................18, 47–48, 54–56burns.......................................................58, 60child abuse......................................46, 48, 55,
67–70, 114, 191–92, 218
cold injury (hypothermia) ..........72–74, 139cut throat................................................87–88defence injuries.....................................18, 92disease and ..........................................236–40explosion injuries ...............................108–09eye.....................................................22, 47–48fabricated ...................................................112firearm wounds..........................115–18, 172fractures ...............................................119–20
femur.............................................113–14hyoid bone ..........................127, 135–38,
150, 151jaw .......................................................147ribs .................................................191–92skull.....................................129, 199–202
glass injuries........................................124–25
Lawyer’s Guide to Forensic Medicine
256

Index
head injuries..................................28, 128–29air-gun injuries ....................................22amnesia following ........................29, 74concussion......................................29, 74contre-coup injury .................48, 76–77,
129, 200coup injury.............................76, 77, 129diffuse axonal injury ............67, 95, 129epilepsy following .....................74, 105,
239–40kicking.................................................148scalp injuries .......................128–29, 142,
194–95skull.....................................129, 199–202
incised wounds..................................124–25, 142–43
jaw...............................................................147kicking..................................................148–49lacerations.......................................18, 87–88,
108, 114, 150mobility and activity after ......................162mutilation ............................................164–65patterned injuries .........................18, 171–72rape .......................................................188–89scar tissue.............................................195–96stab wounds............................36–37, 205–07traffic accidents..............................17, 18, 37,
124, 171, 172, 230–34
traumatic asphyxia......................38, 40, 174, 240–41
traumatic epilepsy.............................74, 105, 239–40
traumatic subarachnoid haemorrhage................................216–17
vital reaction.......................................58, 143, 243–44
whiplash injuries........................37, 232, 245
Insects, post-mortem entomology .................................104, 181–82
Intercostal muscles ..........................................191
Intestine.......................................................144–46natural perforation of ..............................146rupture of.............................................12, 144
Intradermal bruising .........................................54
Iron pigment (haemosiderin), detection of ..................................................55
Irritants, abortion induced by..........................14
Ischaemic heart disease ..................................220
Isolated myocarditis........................................166
Jaundice (hepatitis)............................132, 155–56
Jaw, injuries ......................................................147
Jehovah’s Witnesses ................................235, 236
Joints, fracture dislocation..............................120
Kicking injuries ..........................................148–49
Kidney ...........................................................5, 149failure ...................................................28, 149burns and.....................................................60
Knife wounds, see Stab wounds
Kuru .....................................................................86
Lacerations................................................108, 150cut throat................................................87–88
features..................................................88homicidal........................................87–88suicidal..................................................87
finger-nail marks ..............................114, 172mixed lesions...............................................18
Large intestine..................................................144
Larynx..........................................................150–52air passage obstruction .........23, 61, 151–52hyoid bone..................................127, 135–38,
150, 151
Legislation, on abortion..............................15–17
Life expectancy ..........................................105–06
Ligature .......................................................152–53
Lighter fuel........................................................125
Linear abrasions...........................................17, 18
Linear skull fractures ......................................200
Liver .............................................................155–56damage to ....................................33, 155, 156
rupture..........................................12, 156failure............................................................28hepatitis .......................................132, 155–56
Lividity (hypostasis) .................................139–40
Local anaesthesia ...............................................31
Longevity (expectation of life) ................105–06
LSD (lysergic acid diethylamide) ...........156–57
Lungs .....................................................................8air passage obstruction..............................23asphyxia caused by lung
disease...................................................39contre-coup injury................................76, 77drowning ...............................................98, 99
257

pneumoconioses.................................174–77proof of live birth ...............................153–54pulmonary embolism...............31, 103, 114,
184–87
Lymphatic system, status lymphaticus.........................................208–09
Lysergic acid diethylamide (LSD) ..........156–57
Maceration ........................................................155
Male genital organs ...........................................10kicking injuries..........................................148semen from..........................................196–97
Male sterilisation..............................................209
Malignant hyperpyrexia/hyperthermia ..............................33, 138, 158
Mandible (jaw), injuries..................................147
Marijuana......................................................61–62
Masochistic practices, asphyxia.......................................127, 158–59
Maxilla (jaw), injuries......................................147
Medical treatment, consent to ...................75–76
Medico-legal autopsy........................................44
Medio-necrosis ...................................................35
Melaena .............................................................126
Memory loss .......................................................29
Mesentery..........................................................144rupture of.............................................12, 144
Mesothelioma...........................................176, 238
Methadone........................................................159
Methohexobarbitone .........................................45
Methyl alcohol..............................................28–29
Methyl phenidate...............................................30
Methylamphetamine.........................................30
3:4-Methylene dioxymethamphetamine (MDMA; ecstasy) .................................29–30
Miscarriage, see Abortion
Misuse of Drugs Act 1971 ........................159–62
Mixed lesions......................................................18
Mobility and activity after injury..................162
Morphine...........................................................163heroin .................................................132, 163
Motor cyclists, traffic accidents .....................231
Mummification ..........................................91, 164
Mural thrombosis ..............................................82
Murder, see Homicide
Musclesintercostal muscles ...................................191rigor mortis..........................................192–93
Mutilation ...................................................164–65
Mycotic aneurysm .............................................35
Myocardial infarct ...............................81, 165–66
Myocarditis..........................................65, 166–67, 222
Myxoedema................................................225–26
Nails, finger-nail marks..........................114, 172
Neck .......................................................................6kicking injuries..........................................148neck-hold deaths ......................................168whiplash injuries........................37, 232, 245see also Throat
Necrosis.....................................................168, 169
Negative autopsy ..............................169–70, 222
Nerves, strangulation and .................38, 213–14
Nine, rule of..........................................57, 59, 194
Notification of and Supply to Addicts Regulations 1973 .................160–61
Obscure autopsy................................169–70, 222
Odontology, forensic...................................92–93
Oedemacerebral oedema .................................67, 129glottal oedema ..........................................151
Offences Against the Person Act 1861..................................................15, 70
Oral intercourse ...............................................191
Osteogenesis imperfecta.................................120
Osteoporosis .....................................................113
Papilloedema......................................................67
Parathyroid glands..........................................226
Pathological fractures .....................................120
Patterned injuries.................................18, 171–72
Pedal cyclists, traffic accidents ......................231
Pedestrians, traffic accidents ...................230–31
Penetrating rib fractures.................................191
Lawyer’s Guide to Forensic Medicine
258

Index
Penetration injuries .........................................108
Pentobarbitone ...................................................45
Pentothal .............................................................45
Peri-orbital haematoma (black eye)........................................47–48, 55
Pericarditis ........................................................130
Pericardium ................................................81, 130
Persistent vegetative state (PVS).....................53
Petechial haemorrhages ..........................40, 126, 173–74
Petit mal epilepsy ....................................104, 105
Pharmacy and Medicine Act 1941 ..................15
Pharynx, air passage obstruction....................23
Phenobarbitone ..................................................45
Phenylephrine ....................................................30
Pneumoconioses ........................................174–77
Pneumonia, burns and......................................60
Poisoning ..............................................28, 177–80abortion and ................................................14amphetamines.............................................30asphyxia caused by ....................................39aspirin.....................................................42–43carbon monoxide...........................28, 39, 58,
62–63exhumation and........................................107laboratory analysis.............................177–78interpretation ......................................178–80rupture of intestine lining and...............144toxic fumes...................................................60
Pond skull fractures ........................................200
Positional asphyxia..........................................180
Post-mortem examination, see Autopsy
Post-concussional amnesia ........................29, 74
Postural asphyxia ............................................180
Pregnancy ...................................................182–83duration of...........................................182–83signs of .......................................................182see also Abortion; Birth
Prions ...................................................................86
Procurator Fiscal ........................................183–84
Progressive massive fibrosis (PMF)............................................175
Psilocybin..........................................................156
Psychomotor epilepsy.....................................104
Pulmonary, see Lungs
Putrefaction, see Decomposition of body
Pyrexia (hyperpyrexia/hyperthermia).............................33, 138, 158
Quinalbarbitone .................................................45
Radiologyin child abuse ........................................68–69diagnosis of air embolism.........................22identification of bones and .....................199
Rape .............................................................188–91
Rear seat passenger, traffic accidents ............................................232, 234
Rectum...............................................................144anal intercourse (sodomy)........191, 203–04
Reflex cardiac arrest (vagal inhibition)...................12, 14, 32, 125,
127, 242–43
Registrar of Births and Deaths ............56, 83, 89
Registration of Births, Deaths and Marriages Regulations 1968 .....................83
Retinal haemorrhage.........................................67
Rheumatoid arthritis.......................................175
Rib fractures................................................191–92
Rifle wounds ..............................................117–18
Rigor mortis................................................192–93
Ring skull fractures .........................................201
Rule of nine...........................................57, 59, 194
Saccular aneurysm.............................................34
Safety equipment, traffic accidents and.................................233
Salt water drowning..........................................99
Saphir’s myocarditis........................................166
Scalds .................................................................194
Scalp injuries .....................................128–29, 142, 194–95
Scar tissue....................................................195–96
Scotland, Procurator Fiscal in..................183–84
Scrapie..................................................................86
Scratches (abrasions)...................................17–18
259

Lawyer’s Guide to Forensic Medicine
260
Self-inflicted (fabricated) injuries..................112
Semen ..........................................................196–97
Serology, forensic...............................................50
Sex, establishment from bones ......................198
Sexual deviationmasochistic practices .................127, 158–59mutilation ............................................164–65sodomy
(anal intercourse) ................191, 203–04
Sexual intercourse .....................................197–98previous ...............................................197–98rape .......................................................188–91recent ..........................................................197
Sexual offencesbestiality.................................................45–46rape .......................................................188–91sexual assaults.............................................46
Sexual Offences Act 1956..................................45
Shaken baby syndrome ....................................69
Shockabortion and ................................................14burns and.....................................................60
Shotgun wounds......................................115, 116
Side-impact injuries, traffic accidents.........................................234
Silicoses .......................................................174–75
‘Sixpenny’ bruising............................................54
Skeleton, see Bones (skeleton)
Skull, fractures .................................129, 199–202
Sleeping pills (barbiturates).................30, 45, 49
Small intestine ..................................................144
Smoke inhalation ...............................................58
Smothering ...........................................38, 202–03
Sodomy (anal intercourse)...............191, 203–04
Solvent abuse....................................................125
Somatic death .....................................................90
‘Speed’ ...........................................................29–30
Spinal anaesthesia..............................................32
Spine, whiplash injuries ...................37, 232, 245
Spleen.............................................................5, 204rupture of.............................................12, 204
Spontaneous bruising .......................................55
Spontaneous combustion ...............................205
Stab wounds ...............................................205–07aorta........................................................36–37
Stature, estimation of ......................................208
Status epilepticus .............................................105
Status lymphaticus ....................................208–09
Sterilisation .................................................209–10
Still-birth............................................................210birth.............................................................153finger-nail marks ......................................114
Stomach .............................................................211food regurgitation from ..........23–24, 61, 71rupture of.....................................................12ulcer, burns and..........................................60
Strangulation.......................................38, 212–15, 225
carotid artery nerves and..........................38finger-nail marks ..............................114, 172hyoid bone trauma and............135–38, 150,
151ligature .................................................152–53
Strokes ...........................................................28, 66
Subarachnoid haemorrhage .............66, 72, 148, 215–17
Subdural haemorrhage/haematoma..........................................218–20
Succinylocholine ..............................................158
Suction aspiration abortion..............................13
Sudden cardiac arrest .................................23, 64
Sudden Infant Death Syndrome (SIDS; cot death) ..........................84–85, 169,
203features...................................................84–85practical considerations.............................85
Sudden natural death ...............................220–22
Suffocation...........................................38, 202–03, 223
Suicidecut throat......................................................87hanging ......................................................127
Surgeryabortion..................................................13–14air embolism caused by.............................22consent to...............................................75–76death associated with
anaesthesia .....................................30–33
Syphilitic aneurysm...........................................35

Index
Tattooing of Minors Act 1969 ........................224
Tattoos ...............................................................224
Teethair passage obstruction
caused by..............................................24estimation of age and ..........................20–21identification from ......................92–93, 141,
142
Temperaturecold injury (hypothermia) ..........72–74, 139cooling of body after death...........78–80, 99
Thiopentone........................................................45
Thorax, see Chest (thorax)
Throatair passage obstruction..............................23cut............................................................87–88
features..................................................88homicidal........................................87–88suicidal..................................................87
Thrombo-embolism.........................................103
Thrombosis .................................................224–25coronary artery ..........................165–66, 220,
225deep vein thrombosis .......................184–87,
224–25mural ............................................................82
Throttling (strangulation) .................38, 212–15, 225
Thymus gland ..............................................208–9
Thyroid cartilage .............................136, 150, 151
Thyroid gland ............................................225–26
Toxic effects,see Poisoning
Trachea, air passage obstruction.....................23
Traffic accidents .........................................230–34aortic tearing ...............................................37glass injuries..............................................124motor cyclists ............................................231patterned injuries ........................17, 18, 171,
172pedal cyclists .............................................231pedestrians ..........................................230–31safety equipment and ..............................233vehicle occupants ...............................232–34
drivers...........................................233–34front seat passenger....................232–33rear seat passenger ...................232, 234side-impact injuries ..........................234
Transplantation....................................90, 234–36cadaveric donation...................................235code of practice on removal
of organs for...................................53–54consent to............................................133–34,
234–36heterograft transplantation.....................235homograft transplantation................234–35Human Tissue Act 1961 and ....133–34, 235live donation .............................................235
Trauma, see Injuries
Treatment, consent to..................................75–76
Tuberculosis......................................................175
Tumoursasbestosis and ...........................................176pathological fractures ..............................120trauma and ..........................................238–39
Umbilical cord, establishing live or still birth ................................................155
Ureters .................................................................48
Urethra.................................................................48
Urinealcohol levels ...............................................26bladder .........................................................48
Uterine syringing, abortion induced by.............................................14, 22
Vagal inhibition ............................12, 14, 32, 125, 127, 242–43
Vaginahymen ........................................135, 188, 197injuries to .............................................188–89
Vasectomy.........................................................209
Veinsdeep vein thrombosis .......................184–87,
224–25obstruction of,
asphyxia and..........................40, 42, 212petechial haemorrhages ...................40, 126,
173–74
Venereal infections ..........................................189
Ventricular fibrillation ......................................64
Vertebral artery, subarachnoid haemorrhage ................................66, 72, 148,
215–17
Vertebro-basilar system............................216–17
261

Lawyer’s Guide to Forensic Medicine
262
Vital reaction .............................................58, 143, 243–44
Voice box, see Larynx
Vomitaspiration of ..............................23–24, 61, 71haematemesis............................................126
Whiplash injuries...............................37, 232, 245
Windpipe, air passage obstruction...................................................23
World Health Organisation (WHO)........................................................159
X-rays, see Radiology