punjab academy of forensic medicine & toxicology ... - pafmat
TRANSCRIPT
Punjab Academy of Forensic Medicine & Toxicology
JOURNAL OF
Volume:18,Number:01JanuarytoJunePublication:HalfYearly
ISSN:0972-5687
2018
APeerReviewedJournalon
ForensicMedicine,Toxicology,AnalyticalToxicology,ForensicScience,EnvironmentalPollution,
ForensicPathology,ClinicalForensicMedicine,Identi�ication,LegalMedicine,StateMedicine,
MedicalJurisprudence,MedicalEthics,ForensicNursing,ForensicOdontology,ForensicAnthropology,
ForensicPsychiatryandotherAlliedbranchesofMedicineandScience
dedicatedtoadministrationofJustice.
• Indexed with Index Copernicus (Poland), Scopus (Elsevier Products), IndMed (ICMR New Delhi), Safetylit, Worldcat Library & WHO Hinari
• Available online at Indian Journals.com and pafmat.com• UGC Approved (Sr. No. 97, Journal No.19445)
Place of Publication: Bathinda (Punjab) India
• JPAFMAT is also having PubMed/NLM catalogue number (NLM Unique ID: 101232466).

PUNJAB ACADEMY OF FORENSIC MEDICINE AND TOXICOLOGY
(Registration No. 139 / 1998-99, Chandigarh)
HO: Department of Forensic Medicine, Govt. Medical College Patiala (Punjab) 147001
PresidentDr. D. S. Bhullar
Vice PresidentDr. Rajiv Joshi
General SecretaryDr. Akashdeep Aggarwal
Editor-in-ChiefDr. Parmod Kumar Goyal
Finance SecretaryDr. Shilekh Mittal
Joint EditorDr. Amandeep Singh
Dr. Ashok Chanana
Dr. Ishwar Tayal
Dr. Dasari Harish
Dr. Preetinder S. Chahal
Dr. Puneet Khurana
Dr. Ajay Kumar
Dr. Amit Singla
Dr. Ashwani Kumar
Dr. Deep Rattan Mittal
Dr. O.P. Aggarwal
Dr. S.S. Oberoi
Dr. Balbir Kaur
Dr. Gurmanjit Singh
Dr. K.K. Aggarwal
Dr. R.K. Sharma
Dr. R.K. Gorea
Dr. Vijaypal Khanagwal
Executive Members
Advisors
GOVERNING COUNCIL (2017 - 2019)
Patron
Dr Jagdish Gargi
Advisors
Dr J. S. Dalal
Dr Harish Tuli
Dr Maj. Gen (Rtd.) Ajit Singh
President
Dr. R. K. Gorea
Vice President
Dr. D. S. Bhullar
Secretary
Dr. Sat Pal Garg
Treasurer
Dr. Nirmal Dass
Executive Members
Dr A S Thind,
Dr Jagjiv Sharma,
Dr Kuldeep Kumar,
Dr I. S. Bagga,
Dr Baljit Singh
FOUNDER GOVERNING COUNCIL OF PAFMAT
Special Invitee
Dr. Adish Goyal Dr. Mukul Chopra
J Punjab Acad Forensic Med Toxicol 2018;18 (1) ISSN : 0972-5687
Joint SecretaryDr. Didar Singh Walia
Web MasterDr. Dildar Singh
Assistant EditorDr. Satinder Pal Singh
From the Desk of Editor-in-Chief
I am pleased to present the first issue of the year 2018 of Journal of Punjab Academy of Forensic Medicine & Toxicology. I am
thankful to the authors and contributors for the scientific articles and research papers which are being published in this issue. I am
also thankful to the editorial team for supporting me in its publication and the members of the Academy for giving me the
opportunity to serve as Editor-in-Chief of the journal. My special thanks to Joint Editor Dr Amandeep Singh and Assistant Editor Dr
Satinder Pal Singh for their support and sincere efforts for timely publication and release of this issue.
The Journal publishes original research papers, review articles, case reports and review of books on Forensic Medicine and
Toxicology. The Journal highlights the achievements of the academy and its members. This journal is meant for achieving the aims
and goals of the academy to expand the academic activities, spread the knowledge and latest research in the field of Forensic
Medicine and Toxicology.
My request to all the members of academy to share interesting case reports/photographs of medico legal cases for publication
and benefit of readers. Even case photographs can be sent on whattsapp after hiding the identity.
Any suggestions and advice for further improving the standards and quality of the journal will be highly appreciated and may
be sent to me through email or my whattsapp no. 9876005211.
J Punjab Acad Forensic Med Toxicol 2018;18 (1) ISSN : 0972-5687
ISSN Numbers:
ISSN-L: 0972-5687, p-ISSN: 0972-5687, e-ISSN: 0974-
083X.
Indexed with:
IndexCopernicushttp://journals.indexcopernicus.com/karta.p
hp?id=4715
Scopus (SCI):
http://www.scimagojr.com/journalsearch.php?q=199001949
14&ip=sid&clean=0
Volume of Distribution:
300 copies.
Funding Bodies: Punjab Academy of Forensic Medicine &
Toxicology, Donations from Philanthropists and manuscript
handling charges
Address for submission of articles Online (Soft Copy):
Copyright:
No part of this publication may be reprinted or republished
without the prior permission of Editor-in-Chief of Journal of
Punjab Academy of Forensic Medicine & Toxicology.
Submission of all papers to the journal is understood to imply
that it is not being considered for publication elsewhere.
Submission of multi-authored paper implies that the consent
of each author has been taken. Researchers/Authors should
adhere to publication requirements that submitted work is
original, not plagiarized, ethical an has not been published
elsewhere.
Every effort has been made not to publish any inaccurate or
misleading information. However, the Editor-in-Chief, the
Joint Editor or any member of the editorial committee accept
no liability in consequences of such statements. For any further
information/query please contact with Editor-in-Chief.
Dr Parmod Kumar Goyal
1

2
*From the Desk of Editor-in-Chief 01
*Contents 2-3
* Editorial : Theory of Relative Justice 4-5
Imran Sabri, Sayed A. Quadri
*Original Research Papers
1. Correlation Study Between Fingerprint Patterns and Rh Blood Group 6-9
Smitha Rani, Balaraj BM
2. Chromatographic Separation of Ephedrine, Pseudoephedrine and Phenyl Propanolamine on 10-12
Silica Gel –G Layers Using Different Solvent Systems
Kavita Goyal, Neha Tomar, R. K. Sarin, S.K. Shukla
3. Lightning Deaths in Tigray Region, Northern Ethiopia 13-16
Rajeev Varma, Enyew Debash, Sesen Tsegaye, Dharmaraya Ingale
4. Informed Consent In A Medical Treatment – KAP Study 17-24
Nidhi Sachdeva, Vivek Srivastava, Ashok Najan
5. Profile of Medico Legal Cases at Netaji Subhash Chandra Bose Medical College 25-27 Jabalpur, Madhya Pradesh
Vivek Srivastava, Ashok Najan, Pradeep Kumar Markam, Shivoham Shukla
6. Gaps in Nursing Training on Biomedical Waste Management and Handling: 28-32
Situational analysis at a Tertiary Care Public Hospital
Ravinder Nath Bansal, Sonu Gupta
7. A Study of Completed Suicide Among Women in the Reproductive Age Group From 33-37
Coastal Karnataka
Haneil Larson D'Souza, Prashantha Bhagavath, Francis NP Monteiro, Tanuj Kanchan
Suresh Kumar Shetty, Jagadish Rao P.P, Pavanchand Shetty H
8. An Alternative Method for Extraction and Cleaning of Bones From Buried Cadavers 38-40
Monika Gupta, Parmod Goyal, Navita Aggarwal
9. For Ethical Doctors: Does selection process for Medical students require a change? 41-43
Mrinal Kanti Jha, Jagadish Biswas, Tilak Bose, Shyam Sekhar Choudhury
10. Multiple Linear Regression to Determine Stature Using Hand and Feet Dimensions Among 44-49
Central Indian Population.
Anudeep Singh
11. Determination of the Sequence of Strokes Made from the Same Color and Type of the Ink 50-53
Manisha Mann, Sudhir Kumar Shukla, Seema Rani Pathak
12. A Study On Waste Disposal Management In A Tertiary Care Hospital 54-57
Pratik V Tarvadi
13. Wound Dating By Gross And Histopathological Examination of Abrasions- 58-62
An Autopsy Based Study
Prashanthi Krishna Dharma Ramasamy Devaraj, Thanka J, Sampath Kumar, Selva Arasi
14. Reprotoxic Effects of Noon tea on Drosophila Melanogaster 63-65
Lovleen, Altaf Hussain, Bhupendra Koul
Punjab Academy of Forensic Medicine & Toxicology
JOURNAL OF
ISSN:0972-5687
Volume:18,Number:01JanuarytoJunePublication:HalfYearly
Contents

Punjab Academy of Forensic Medicine & Toxicology
JOURNAL OF
ISSN:0972-5687
Volume:18,Number:01JanuarytoJunePublication:HalfYearly
Contents
15. Epidemiological Profile, Pattern of Skull Fractures and Intracranial Haemorrages in 66-68
Fatal Road Traffic Accident Victims: An Autopsy Study
Munish Kumar, Sukhdeep Singh, Yatiraj Singi
*Case Reports
1. Accessory Lobes of Liver - A rare malformation noticed during autopsy 69-70
Vijay Arora, Arun Gautam
2. Pericardial Rupture without Cardiac Injury or Herniation 71-72
Vikram Palimar, Kaushal Kishore, Sajan Babu, Chandni Gupta
3. Elongated Styloid Process (Eagle Syndrome) - A rare finding at autopsy 73-74
Yogesh Kumar Vashist, Sakshi Sharma, Bhagwat Rajput, Anil Garg, Rahul Chawla, Gaurav Sharma
*Review Article
1. Role of Forensic Odontologists in Child Abuse Detection and reporting : A Review 75-77
Pooja Puri, SK Shukla, I. Haque
2. Nanotechnology And Its Applications In Forensic Sciences- A Boon To Legal Justice 78-83
Jaskaran Singh, Neeta Raj Sharma, Chelsea Marie Joseph, Dattatraya Khisse, Savreet Kaur,
Pratibha Rani, Divya Sahu
*Correspondence
1. Suggestion for MPT act, “abortion on demand”? 84
Lalit Kumar
2. Recommendations Sent to Government of Punjab for Bringing Necessary Amendments in the 85-87
Punjab Anatomy Act.
Priti Chaudhary, Parmod Kumar Goyal
*Instructions to Authors 88
*Life Membership Form 89
*Book Review 90
*Life Members PAFMAT 91-92
3

Editorial
INTRODUCTION :
A famous quote by William E. Gladstone is “Justice [1]Delayed is Justice Denied” . But what if the justice is not
done at all, or justice has been done in favour of accused which
obviously is injustice to the victim. Justice is defined according
to dictionary.com as “the quality of being just; righteousness, [2]equitableness, or moral rightness.” . Justice and injustice are
relative terms, as justice for one may be injustice to the other
party. Absolute justice as per Merriam Webster dictionary is [3]“free from imperfection” . It can be interpreted that absolute
justice is a perfect trait, and, since only God is perfect hence
only He can deliver it. As human beings could be imperfect in
their judgment, it can impact criminal justice administration
and absolute justice cannot be assured in true sense. In this
article we will look into a few imperfections prevalent in our
existing criminal justice administration system. “The Theory
of Relative Justice” implies that “we are living in a world of
Relative Justice” which need not be necessarily absolute
justice.
Utilitarianism, on the other hand, deals with the concerns of
majority and cannot be regarded as justice, however it could be
labeled as an ethical term. Ethics and law differ in that ethics
are social guidelines based on moral principles and values
while laws are rules and regulations that have specific penalties [6 ]and consequences when violated . The practice of
Utilitarianism has been debatable as legal understanding may
differ.
A 14 year old boy arrested in a country on complaint of school
staff who suspects him to make a clock bomb later turns out to
be a case of racial prejudice. This incidence was covered by [7]media which highlighted profound private information . Had
there been a similar incidence occurred with a student of
different background, the fate could have been otherwise.
Other similar incidences are reported albeit the names of the
accused/victim. In the above mentioned case the victim has
been accused as criminal. Now the question arises that who is
the criminal in actuality? or whom can we blame ? the media,
the school staff, the police or the society. In reality all of them
are fulfilling their duties. Then who is the real culprit? In this
instance it can be said that “Doctrine of Relative Justice” has
prevailed. In order to protect the rights of majority population,
we have compromised the rights of the minority.[8]A certain country bans a particular dress , while another
[9]makes it mandatory . In this situation, a particular dress is
legal in one country but illegal in other. Therefore a country
may take legal action against people wearing that dress while
another country legally enforces the wearing of that dress.
Absolute justice states that everyone should have the freedom
to wear the dress of their choice. The society however
sometimes defines its dress code according to the norms set by
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687
4
Theory of Relative Justice1. Imran Sabri, Assistant Professor, Division of Forensic Medicine*
2. Sayed A. Quadri, Assistant Professor, Division of Microbiology, Department of Biomedical Sciences*
*College of Medicine, King Faisal University, Al-Ahsa, Kingdom of Saudi Arabia
Corresponding Author
Dr. Imran Sabri,
Assistant Professor, College of Medicine, King Faisal
University, Al-Ahsa, Kingdom of Saudi Arabia
Contact : +966565554107
Email : [email protected], [email protected]
KEYWORDS : Justice, Relative Justice,Theory
Article History:Received: 17 January 2018Received in revised form: 29 May 2018Accepted on: 29 May 2018Available online: 1 July 2018
ABSTRACT :
Justice is defined according to dictionary.com as “the quality of being just; righteousness, equitableness, or moral
rightness”. Justice and injustice are relative terms, as justice for one may be injustice to the other. “The Theory of Relative Justice”
implies that “we are living in a world of Relative Justice”. In order to protect the rights of majority population, we have
compromised the rights of the minority. If it were to happen that the minority becomes the majority “The Theory of Relative
Justice” will still prevail. “The Doctrine of Relative Justice” is an applied approach in which the benefits of majority population are
of paramount consideration and perhaps application of Relative justice may not be a bad choice. “The Theory of Relative Justice”
can be considered independent of majority and minority status. Practicing relative justice may be considered a better approach than
practicing no Justice. Absolute Justice may seem to be a utopian dream to some; however it is desirable and achievable.

it and the rights of individual stand violated. Now in the afore
mentioned instance certain nations may actively discourage
the full covering of the body or face and in a similar way, rules
governing sports activities may restrict use of clothing's. These
issues could also be considered as violation of the rights of
individuals and hence doctrine of relative justice is also
applicable here.
DISCUSSION:
Justice for one may be injustice to other, in the cases mentioned
above. Justice, Law, Ethics, Social Norms etc are applied in
relative context in the society. How is it possible that we have
different laws for same crime or different criminal justice
administration system for different sections of the society?
This could only happen if criminal justice administration
system is biased on the bases of religion, caste, skin color,
seeking dominance, region etc.
“The Doctrine of Relative Justice” is an applied approach in
which the benefits of majority population are of paramount
consideration and perhaps application of Relative justice may
not be a bad choice, as at least we are giving justice to the
majority population while restricting the rights of the minority.
If it were to happen that the minority becomes the majority
“The Theory of Relative Justice” will still prevail.
CONCLUSION:
It could be concluded that “The Theory of Relative Justice” is
prevalent across the world. Absolute Justice seems to be
merely a textbook term and doesn't seem to be practiced. “The
Theory of Relative Justice” can be considered independent of
majority and minority status. Practicing relative justice may be
considered a better approach than practicing no Justice.
Absolute Justice may seem to be a utopian dream to some;
however it is desirable and achievable.
Ethical approval : None/Not Applicable
Funding : None/Self-Funded
Conflicts of interest : No conflicts of interest.
REFERENCES :
1. "William E. Gladstone Quotes." BrainyQuote.com.
X p l o r e I n c , 2 0 1 8 . 2 9 M a y 2 0 1 8 .
https://www.brainyquote.com/quotes /william_e_gladsto
ne_101551
2. Dictionary.com [Internet] Justice [Cited on April 1, 2018]
. Available from
http://www.dictionary.com/browse/justice
3. Merriam Webster Dictionary Internet] Absolute [Cited on
April 1, 2018] . Available from https://www.merriam-
webster.com/dictionary/absolute .
4. John Rawls. A Theory of Justice By John Rawls-Revision
Edition . Massachusetts . Harvard University Press 1999.
Available from
h t t p s : / / b o o k s . g o o g l e . c o m . s a / b o o k s ?
id=kvpby7HtAe0C&printsec=frontcover#v=onepage&q
&f=false
5. Henry R, West. [Internet] Utilitarialism [Cited on May 29,
2018]. Available from
https://www.utilitarianism.com/utilitarianism.html
6. What Is the Difference Between Ethics and Law?
[Internet]. Available from
h t t p s : / / w w w. r e f e r e n c e . c o m / g o v e r n m e n t -
p o l i t i c s / d i ff e r e n c e - b e t w e e n - e t h i c s - l a w -
1b772dd7ebc7cd74# [Cited on April 1, 2018].
7. Ashley Fantz, Steve Almasy and AnneClaire Stapleton,
CNN. Muslim teen Ahmed Mohamed creates clock,
shows teachers, gets arrested [Internet] September 16,
2015. [Cited on April 1, 2018] Available From
https://edition.cnn.com/2015/09/16/us/texas-student-
ahmed-muslim-clock-bomb/ .
8. Lizzei Dearden. China bans burqas and 'abnormal' beards
in Muslim province of Xinjiang [Internet] May 30, 2017
[ C i t e d o n A p r i l 1 , 2 0 1 8 ] Av a i l a b l e f r o m
http://www.independent.co.uk/news/world/asia/china-
burqa-abnormal-beards-ban-muslim-province-xinjiang-
veils-province-extremism-crackdown-freedom-
a7657826.html
9. The Economist. [Internet] Saudi Arabia's dress code for
women.[Cited on April 2, 2018] Available from
h t tp : / /www.economis t . com/b logs /economis t -
explains/2015/01/economist-explains-20.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687
5

Original Research Paper
Corresponding Author
Dr. Smitha Rani
Assistant Professor
Department of Forensic Medicine and Toxicology,
J.S.S Medical College, , JSS Academy of Higher
Education and Research, Sri Shivarathreeshwara Nagar,
Bannimantap, Mysore-570015, Karnataka, India.
Telephone no: 09886673946
Email: [email protected]
KEYWORDS : Rh Blood Group, Fingerprint Print Pattern, Identification.
Article History:Received: 23 March 2018Received in revised form: 29 April 2018Accepted on: 29 April 2018Available online: 01 July 2018
INTRODUCTION :
Identification means determination of the individuality of a
person based on certain physical characteristics unique to that [1]individual . It is the most important component in medico
legal practice. Identity of a person may be absolute (complete)
or partial (incomplete). Complete identification is the absolute
determination of the individuality of the person. Incomplete or
partial identification is the ascertainment of only a few facts
whereas the other facts are unknown.
The various comparative techniques for identification are
dental patterns and restorations, finger, palm and foot prints,
superimposition technique, neutron activation analysis, [2]anthropometry and trace evidence comparisons . Among the
various comparative data techniques listed above, Personal
identification through fingerprints has long been recognized
and is regarded as the greatest contribution to the police force.
Study of fingerprints as a method of identification is also
known as Dactylography or Dactyloscopy or Henry – Galton [3]system of identification . The finger print patterns are
distinctive and permanent in individuals. The pattern is
different even in identical twins.
Similar to fingerprints, blood as trace evidence is an extremely
important entity of medico legal practice. In Forensic Science
and Medicine, the ABO and Rh blood group system have been
a major focus, since the record of this blood group system is a
very prevalent one. A, B and O (H) antigens on erythrocytes are
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00001.8
6
ABSTRACT :
Introduction: Establishment of identity is an important component of medico legal practice. Among the various comparative data
techniques available for identification, fingerprints has long been regarded as the greatest contribution to the police force.
Objective:To establish a possible relationship between fingerprint pattern and Rh blood group.
Methods: The present cross-sectional study was carried out on 500 (250 male & 250 female) subjects of Indian origin above the age
of 18 years, who were selected randomly from the students & staff members from various educational institutions of JSS Academy
of Higher Education and Research, Mysuru.
Results: 93.8% subjects in the study were Rh positive, of which 31.8% belonged to blood group O, 29.8% belonged to blood group
B, 24.8% belonged to blood group A and 7.4% belonged to blood group AB. Among Rh negative individuals, blood group B and O
had same frequency amounting to 2.2%. 1.8% subjects belonged to Blood group A and none of the subjects in the study were AB
negative. Fingerprint pattern analysis showed that, loops were the most common pattern in the study followed by whorls and arches
respectively among both Rh positive and Rh negative individuals. A non significant association was observed between fingerprint
pattern and Rh blood group.
Conclusion: The association between Rh blood group and fingerprint pattern was not significant. Hence the result of this study
infers that Rh blood group is not an effective tool in predicting the primary fingerprint pattern of the individual when Rh blood group
is known.
Correlation Study Between Fingerprint Patterns and Rh Blood Group1. Smitha Rani, Assistant Professor*
2. Balaraj BM, Professor*
*Department of Forensic Medicine and Toxicology, JSS Academy of Higher Education and Research, Mysuru, Karnataka,
India.

present since birth and can be determined from soft tissues,
hair, nails, dental tissues and bone and in about 80 % of the
individuals. They can be demonstrated in all body fluids except
the cerebrospinal fluid.
Aside from the antigens of the ABO system, those of
the Rh system are of the great clinical importance. The “Rh
factor”, named after Rhesus monkey because it was first
studied using the blood of this animal, is a system composed
primarily of the C, D and E antigens, although it actually
contains many more. Unlike the ABO antigens, the Rh system
has not been detected in tissues other than the red cells. D is far
the most antigenic component, and the term “Rh-positive”
means that the individual has agglutinogen D. The “Rh-
negative” individual has no D antigen and forms the anti-D
agglutinin when injected with D-positive cells. The Rh typing
serum used in routine blood typing is anti-D serum. 85% of the
Caucasians are D-positive and 15% are D-negative; over 99%
of the Asians are D-positive. Unlike the antibodies of the ABO
system, anti-D antibodies do not develop without the exposure
of a D-negative individual to D-positive red cells by
transfusion or entrance of fetal blood into maternal [4]circulation .
Both Fingerprint pattern and blood group are
genetically determined. The inheritance of dermatoglyphic
features is said to be polygenic, where individual gene
contribute a small additive effect. Even the genetic basis for
inheritance of blood groups is well established. Fingerprint
pattern and blood group have been extensively but separately
studied. Hence the present study is aimed at studying the
correlation between these two important comparative data
techniques to serve the process of positive identification.
MATERIALS AND METHODS :
After approval by institutional ethics committee, 500 subjects
(250 male and 250 female) of Indian origin and above 18 years
of age were analyzed. Subjects with leprosy, electrical injury,
radiation exposure and those with recent blood transfusion
which cause permanent impairment of finger print pattern
were excluded from the study.
Convenience sampling technique was adopted. Informed
written consent was obtained prior to taking the prints and
determining the blood group. The study was undertaken in the
Department of Forensic Medicine & Toxicology, JSS Medical
College, JSS Academy of Higher Education and Research,
Mysuru,Karnataka, India.
Blood Group Determination :
Blood samples were collected by finger prick with a sterile
lancet, after cleaning the puncture site with 70% ethyl alcohol.
Rapid slide test was done as an assay procedure to determine
the blood group using SPANCLONE monoclonal antibodies
(Blood grouping antisera).
Fingerprint Recording :
The subjects were asked to wash and dry their hands to remove
dirt and grease. Inkless fingerprint pad, square in shape,
measuring 2 inch x 1.5 inch was used to obtain the fingerprints.
The subject was asked to keep his / her arm relaxed and not to
try to help in rolling the fingers as this may cause smearing.
Then the finger bulbs were rolled on the fingerprint pad – “the
thumbs were rolled towards the subject's body and the fingers
were rolled away from the body, i.e. thumb in fingers out
method” (Figure 1).
Figure 1: Ink being smeared on the fingertip by rolling the
finger on inkless fingerprint pad.
And then the rolled impressions of each finger were obtained in
the allotted space for that finger on the Proforma (Figure 2).
Single inkless finger print pad was used to record 800 rolled
impressions.
Figure 2: Inked fingertip being rolled on the proforma to
obtain fingerprint.
Statistical Analysis:
The data obtained was analyzed statistically using SPSS
(Statistical Programme for Social Sciences, version 16.0)
computer software package. Descriptive statistics,
contingency co-efficient test were applied and p-value <0.05
was considered as significant.
7
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00001.8
RESULTS :
Distribution of cases according to Rh blood group
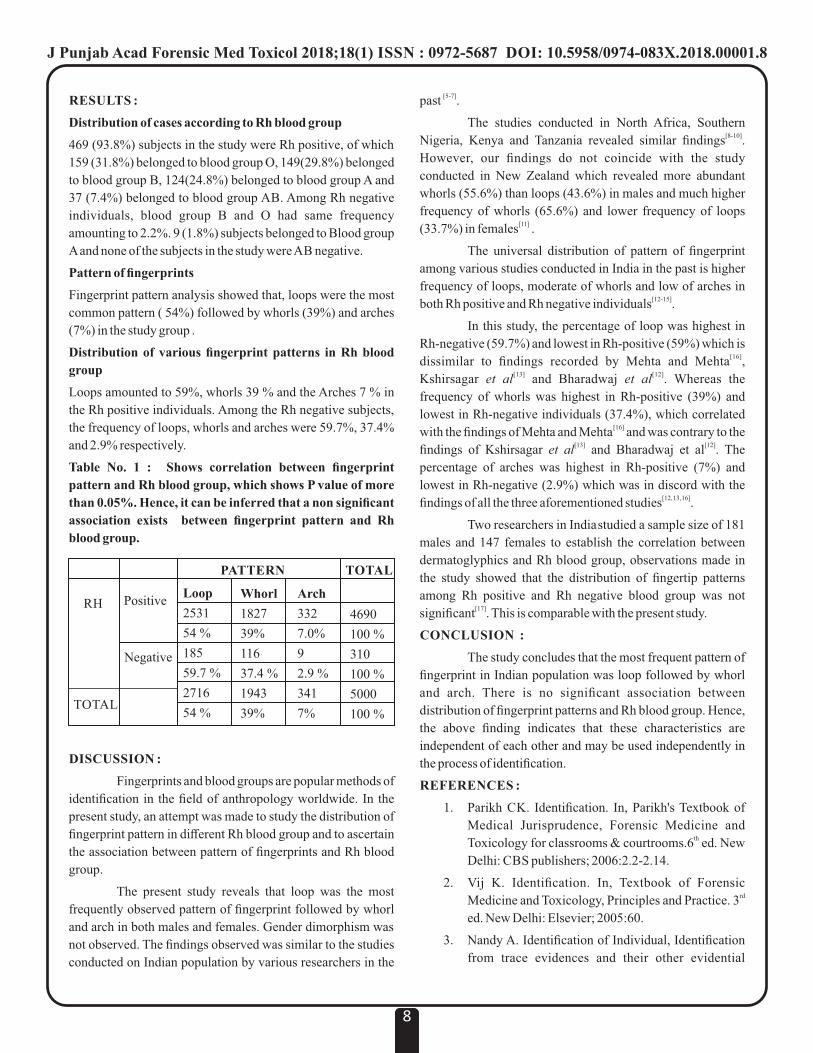
469 (93.8%) subjects in the study were Rh positive, of which
159 (31.8%) belonged to blood group O, 149(29.8%) belonged
to blood group B, 124(24.8%) belonged to blood group A and
37 (7.4%) belonged to blood group AB. Among Rh negative
individuals, blood group B and O had same frequency
amounting to 2.2%. 9 (1.8%) subjects belonged to Blood group
A and none of the subjects in the study were AB negative.
Pattern of fingerprints
Fingerprint pattern analysis showed that, loops were the most
common pattern ( 54%) followed by whorls (39%) and arches
(7%) in the study group .
Distribution of various fingerprint patterns in Rh blood
group
Loops amounted to 59%, whorls 39 % and the Arches 7 % in
the Rh positive individuals. Among the Rh negative subjects,
the frequency of loops, whorls and arches were 59.7%, 37.4%
and 2.9% respectively.
Table No. 1 : Shows correlation between fingerprint
pattern and Rh blood group, which shows P value of more
than 0.05%. Hence, it can be inferred that a non significant
association exists between fingerprint pattern and Rh
blood group.
DISCUSSION :
Fingerprints and blood groups are popular methods of
identification in the field of anthropology worldwide. In the
present study, an attempt was made to study the distribution of
fingerprint pattern in different Rh blood group and to ascertain
the association between pattern of fingerprints and Rh blood
group.
The present study reveals that loop was the most
frequently observed pattern of fingerprint followed by whorl
and arch in both males and females. Gender dimorphism was
not observed. The findings observed was similar to the studies
conducted on Indian population by various researchers in the
[5-7]past .
The studies conducted in North Africa, Southern [8-10]Nigeria, Kenya and Tanzania revealed similar findings .
However, our findings do not coincide with the study
conducted in New Zealand which revealed more abundant
whorls (55.6%) than loops (43.6%) in males and much higher
frequency of whorls (65.6%) and lower frequency of loops [11](33.7%) in females .
The universal distribution of pattern of fingerprint
among various studies conducted in India in the past is higher
frequency of loops, moderate of whorls and low of arches in [12-15]both Rh positive and Rh negative individuals .
In this study, the percentage of loop was highest in
Rh-negative (59.7%) and lowest in Rh-positive (59%) which is [16]dissimilar to findings recorded by Mehta and Mehta ,
[13] [12]Kshirsagar et al and Bharadwaj et al . Whereas the
frequency of whorls was highest in Rh-positive (39%) and
lowest in Rh-negative individuals (37.4%), which correlated [16]with the findings of Mehta and Mehta and was contrary to the
[13] [12]findings of Kshirsagar et al and Bharadwaj et al . The
percentage of arches was highest in Rh-positive (7%) and
lowest in Rh-negative (2.9%) which was in discord with the [12, 13, 16]findings of all the three aforementioned studies .
Two researchers in Indiastudied a sample size of 181
males and 147 females to establish the correlation between
dermatoglyphics and Rh blood group, observations made in
the study showed that the distribution of fingertip patterns
among Rh positive and Rh negative blood group was not [17]significant . This is comparable with the present study.
CONCLUSION :
The study concludes that the most frequent pattern of
fingerprint in Indian population was loop followed by whorl
and arch. There is no significant association between
distribution of fingerprint patterns and Rh blood group. Hence,
the above finding indicates that these characteristics are
independent of each other and may be used independently in
the process of identification.
REFERENCES :
1. Parikh CK. Identification. In, Parikh's Textbook of
Medical Jurisprudence, Forensic Medicine and thToxicology for classrooms & courtrooms.6 ed. New
Delhi: CBS publishers; 2006:2.2-2.14.
2. Vij K. Identification. In, Textbook of Forensic rdMedicine and Toxicology, Principles and Practice. 3
ed. New Delhi: Elsevier; 2005:60.
3. Nandy A. Identification of Individual, Identification
from trace evidences and their other evidential
8
PATTERN TOTAL
RH
TOTAL
Positive
Negative
Loop
2531
54 %
185
59.7 %
2716
54 %
Whorl
1827
39%
116
37.4 %
1943
39%
Arch
332
7.0%
9
2.9 %
341
7%
4690
100 %
310
100 %
5000
100 %
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00001.8
values. In, Principles of Forensic Medicine including rdToxicology.3 ed. Kolkata: New Central Book
Agency (P) Ltd; 2010: 89.nd4. Ganong WF. Review of Medical Physiology.22 ed.
Singapore: The McGraw-Hill Companies;2005:537-
39.
5. Gangadhar M R, Rajashekara R K. Finger
dermatoglyphics of Adikarnatakas: a scheduled caste
population of Mysore city, Karnataka. Man India
1993;83(1&2):183-93.
6. Nithin MD, Balaraj BM, Manjunatha B, Mestri SC.
Study of fingerprints classification and their gender
distribution among South Indian population. Journal
of Forensic and Legal Medicine 2009;16:460-463.
7. V Maled, V Khode, D Maled, A Jain, S Male, K
Ruikar. Pattern of Fingerprints in different ABO and
Rh blood groups. Journal of Indian Academy of
Forensic Medicine 2015;37 (2) : 124-26.
8. Fayrouz INE, Farida N, Irshad AH. Relation between
fingerprints and different blood groups. Journal of
Forensic and Legal Medicine 2012;19:18-21.
9. Igbigbi PS, Msamati BC. Palmer and digital
dermatoglyphic traits of Kenyan & Tanzanian
subjects. West Afr. J Med 2005;24(1):26-30.
10. Jaga B N, Igbigbi P S . Digital and palmar
dermatoglyphics of the Ijaw of Southern Nigeria. Afr.
J Med Sci. 2008;37(1):1-5.
11. Ching Cho. A finger dermatoglyphics of the New
Zealand Samoans. Korean J Bio Sci 1998;2:507-511.
12. Bharadwaj A, Saraswat PK, Agrawal SK, Banerji P,
Bharadwaj S. Pattern of fingerprints in different ABO
blood groups. Journal of Forensic Medicine &
Toxicology 2004;26(1):6-9.
13. Kshirsagar SV, Burgul SN, Kamkhedkar SG.
Maharastra A. Study of fingerprint patterns in ABO
blood group. J Anat Soc India 2003;52:82-115.
14. Mahajan AA. Dermatoglyphics and ABO Blood
Group. Thesis Submitted for MS Anatomy,
Aurangabad; 1986.
15. Shivhare PR, Sharma SK, Ray SK, Minj A, Saha K.
Dermatoglyphic Pattern in Relation to ABO, Rh
Blood Group and Gender among the Population of
Chhattisgarh. Int J Sci Stud 2017;4(11):61-65.
16. Mehta AA, Mehta AA. Palmar dermatoglyphis in
ABO, Rh blood groups. Int J Biol Med Res
2011;2:961-64.
17. K s h i r s a g a r S V, G u n d r e S D . S t u d y o f
dermatoglyphics in Rh blood group. Anatomica
Karnataka 2012;6(1):70-73.
Acknowledgement :
Authors thank all subjects who volunteered to participate in
the study .
Funding : Nil
Conflict of Interest : Nil
9
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00001.8

J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00002.X
Chromatographic Separation of Ephedrine, Pseudoephedrine and Phenyl Propanolamine on Silica Gel –G Layers Using Different Solvent Systems
1. Kavita Goyal, Assistant Director, Chemistry Forensic Science Laboratory, G.N.C.T, New Delhi
2. Neha Tomar, Research Associate, Amity Institute of Forensic Sciences, Amity University, Noida
3. Dr. R. K. Sarin, Director RFSL, Amravathi, Andhra Pradesh
4. S.K. Shukla, Professor and Head, Amity Institute of Forensic Sciences, Amity University, Noida
Original Research Paper
Corresponding AuthorDr. Neha Tomar, Research Associate, Amity Institute of Forensic Sciences, Amity University, Noida Contact No. : +91 81303-21327E-mail : [email protected]
KEYWORDS : Ephedrine, Pseudoephedrine, Phenyl, Propanolamine, Silica Gel-G Layers, Thin Layer Chromatography
Article History:Received: 16 April 2018Received in revised form: 15 June 2018Accepted on: 15 June 2018Available online: 1 July 2018
INTRODUCTION:
Over the years,the use of Ephedrine, Pseudoephedrine and
Phenylpropanolamine [Figure 1-3] in drugs have been
increasing. These drugs are easily available as over the counter
medicine acting as bronchodilators and have been found in
combination with paracetamol, antihistamines etc. for
treatment of various ailments in human and have direct impact
on Central Nervous System. On account of its numerous
effects, there is an increase in manufacture of synthetic drugs
where they are being prepared or modified for various illicit
uses. These drugs are widely produced in clandestine
laboratories and used by athletes. The illicit use of these drugs
lies in their being used as Precursor Chemicals for the
preparation of Amphetamines and Amphetamine Type
Stimulants (ATS). These are similar in structure to
[1]amphetamines and methamphetamines . Ephedrine increases
post-synaptic noradrenergic receptor activity by directly
activating post-synaptic α-receptors and β-receptors.The bulk
of its effect comes from the pre-synaptic neuron being unable
to distinguish between real adrenaline or noradrenaline from [2]ephedrine . The illicit use of these drugs is responsible for
large number of criminal cases being referred to forensic
science laboratories for analysis of samples. Such cases pose a
serious challenge forensic chemists to choose an appropriate
and easy protocol for rapid and accurate detection and
determination of these drug. Thin layer chromatography is a
versatile, fast, easy, robust and economical technique and thus
was chosen for separation and identification of these drugs.
10
ABSTRACT:
Ephedrine, Pseudoephedrine and Phenylpropanolamine are available in combination with antihistamines, Guaifenesin,
Dextromethorphan and paracetamol. These drugs have been widely used for illicit purpose and sometimes multiple doses of these
drugs are taken by athletes for quick relief as therapeutic medicine that crosses the maximum recommended dose and gives positive
test results in dope test analysis. Clandestine laboratories use these medicines as a precursor to manufacture numerous illicit drugs.
Such cases pose a challenge to forensic scientists due to their quick elimination from human body, lack of suitable detection
protocol, complicated and similar chemical structures. The present paper presents Chromatographic separation of Ephedrine,
Pseudoephedrine and Phenylpropanolamine using 27 solvent systems. The drugs were best separated and detected in n-butyl
acetate: Acetone: 1- Butanol: 5 M Ammonia: Methanol (hRf 80, 91, 54) and Ethyl Acetate: Butanone: Formic Acid: Water (hRf
37, 30, 45)
Figure 1: Ephedrine Figure 2: Pseudoephedrine Figure 3 : Phenylpropanolamine

MATERIALS AND METHODS :
Standard / Sample solutions: The standard drugs were
procured from Indian Pharmacopoeia and the samples were the
seized drugs referred by the investigating agencies to Forensic
Science Laboratory. 100 samples were separated and identified
using various solvent systems. The standard/ sample was
dissolved in 5ml distilled water, made slightly basic (pH 9) and
extracted in Chloroform: Ether (3:1), thrice, taking 10ml each
time, to ensure maximum recovery of the drug. The collected
organic solvent fraction layers were collected, air-dried and [3-4]used for spotting . All other chemicals used and were of
Analytical grade. Deionized water was used in all necessary [5]steps .
Preparation of Solvent System/ Mobile Phase: 27 different
solvent systems were prepared and studied as per details given
in Table. An attempt was made to observe the separation of
Ephedrine, Pseudoephedrine and phenylpropanolamine.
TLC Plates: TLC pre-coated plates silica made by Merck
silica gel G 60 F, layer thickness 0.25mm, was used for
spotting [Figure 4].
Figure 4 : TLC with ninhydrin and iodoplatinate
reagents
11
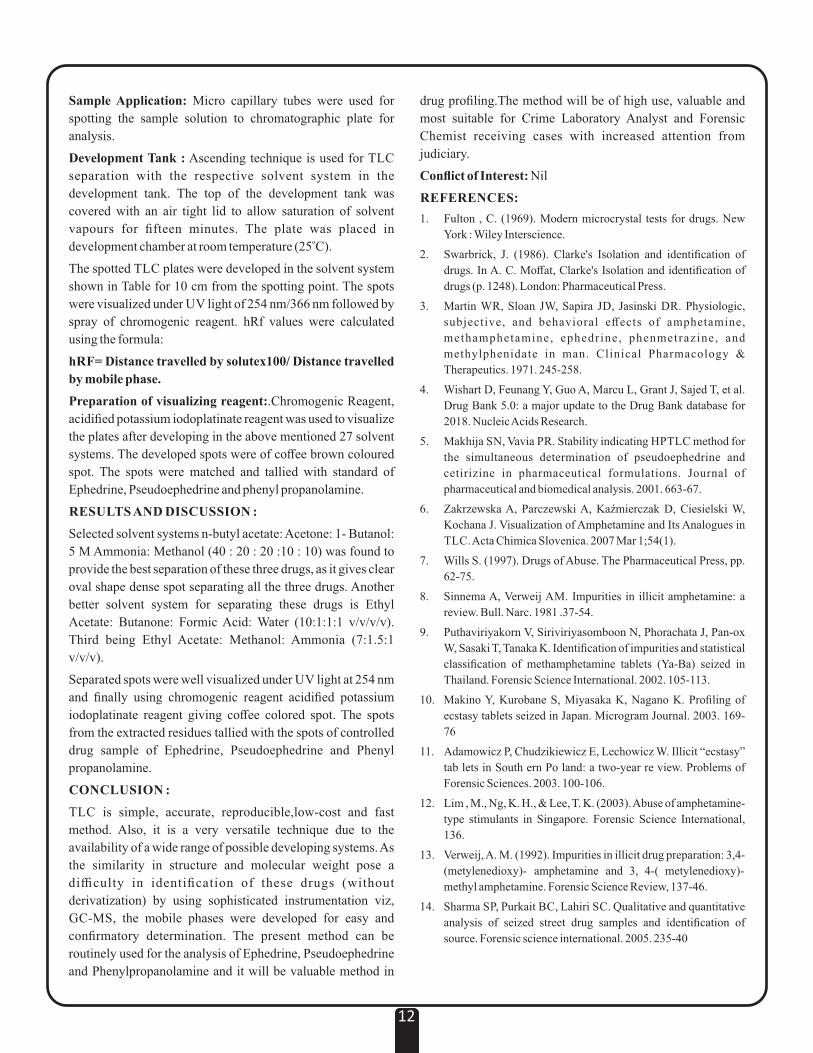
Table : hRF values of Ephedrine, Pseudoephedrine and Phenylpropanolamine in different solvent systems
S. No.
1.2.3.4.5.6.7.8.9.10.11.12.13.14.15.16.17.18.19.20.21.22.23.24.25.26.27.
Ethanol : Methanol: Ammonia(25 %) - 85:10:5 v/v/vChloroform: Ethyl Acetate : Toluene : Methanol : Acetic Acid- 39:39:77:39:6Toluene : Ethyl Acetate: Methanol: Formic acid- 10 : 3:1:2Ethyl Acetate : Butanone :Formic Acid: H O - 10:1:1:12
Chloroform: Methanol- 40 :1n- Hexane : Ethyl Acetate - 9:1Chloroform: Methanol- 7:1n-butyl acetate : acetone : 1- Butanol: 5 M Ammonia: Methanol- 40 : 20 : 20 :10 : 10Toluene : Ethyl Acetate: Methanol- 8:1:1Chloroform Cyclohexane : Acetic Acid- 4:4:2 :
Methanol: Ammonia - 100:1.5Chloroform: Methanol - 9:1Acetone MethanolMethanol : 1- Butanol - 60:40Chloroform: Acetone - 80:20Ethyl Acetate: Methanol: Ammonia --85:10:5Ethyl Acetate Ethyl Acetate : Ethanol- 90:10Chloroform Methanol: Propionic acid - 72:18:10 :
Cyclohexane : Toluene : Diethyl amine - 75 :15:10Chloroform Ammonia :2- propanol - 5:15:80 :
Ethyl Acetate : Methanol: Ammonia - 7:1.5:1Methylene chloride: Ammonia: 2- Propanol – 5:15:80n- hexane: Toluene: 1,4 dioxane–3:3:11,4 dioxane: Methanol: Chloroform: Ammonia – 6:2:2:1 Ethyl acetate: n- heptane – 1:1
Solvent Systems Phenypropanolamine
Ephedrine Pseudoephedrine
482001450502185404074604000000003031011903
5575005600
302001370203218005103205011065012739011708
4968002600
321802300302229105103504630902012336001358
4371002400
Sample Application: Micro capillary tubes were used for
spotting the sample solution to chromatographic plate for
analysis.
Development Tank : Ascending technique is used for TLC
separation with the respective solvent system in the
development tank. The top of the development tank was
covered with an air tight lid to allow saturation of solvent
vapours for fifteen minutes. The plate was placed in odevelopment chamber at room temperature (25 C).
The spotted TLC plates were developed in the solvent system
shown in Table for 10 cm from the spotting point. The spots
were visualized under UV light of 254 nm/366 nm followed by
spray of chromogenic reagent. hRf values were calculated
using the formula:
hRF= Distance travelled by solutex100/ Distance travelled
by mobile phase.
Preparation of visualizing reagent:.Chromogenic Reagent,
acidified potassium iodoplatinate reagent was used to visualize
the plates after developing in the above mentioned 27 solvent
systems. The developed spots were of coffee brown coloured
spot. The spots were matched and tallied with standard of
Ephedrine, Pseudoephedrine and phenyl propanolamine.
RESULTS AND DISCUSSION :
Selected solvent systems n-butyl acetate: Acetone: 1- Butanol:
5 M Ammonia: Methanol (40 : 20 : 20 :10 : 10) was found to
provide the best separation of these three drugs, as it gives clear
oval shape dense spot separating all the three drugs. Another
better solvent system for separating these drugs is Ethyl
Acetate: Butanone: Formic Acid: Water (10:1:1:1 v/v/v/v).
Third being Ethyl Acetate: Methanol: Ammonia (7:1.5:1
v/v/v).
Separated spots were well visualized under UV light at 254 nm
and finally using chromogenic reagent acidified potassium
iodoplatinate reagent giving coffee colored spot. The spots
from the extracted residues tallied with the spots of controlled
drug sample of Ephedrine, Pseudoephedrine and Phenyl
propanolamine.
CONCLUSION :
TLC is simple, accurate, reproducible,low-cost and fast
method. Also, it is a very versatile technique due to the
availability of a wide range of possible developing systems. As
the similarity in structure and molecular weight pose a
difficulty in identification of these drugs (without
derivatization) by using sophisticated instrumentation viz,
GC-MS, the mobile phases were developed for easy and
confirmatory determination. The present method can be
routinely used for the analysis of Ephedrine, Pseudoephedrine
and Phenylpropanolamine and it will be valuable method in
drug profiling.The method will be of high use, valuable and
most suitable for Crime Laboratory Analyst and Forensic
Chemist receiving cases with increased attention from
judiciary.
Conflict of Interest: Nil
REFERENCES:
1. Fulton , C. (1969). Modern microcrystal tests for drugs. New
York : Wiley Interscience.
2. Swarbrick, J. (1986). Clarke's Isolation and identification of
drugs. In A. C. Moffat, Clarke's Isolation and identification of
drugs (p. 1248). London: Pharmaceutical Press.
3. Martin WR, Sloan JW, Sapira JD, Jasinski DR. Physiologic,
subjective, and behavioral effects of amphetamine,
methamphetamine, ephedrine, phenmetrazine, and
methylphenidate in man. Clinical Pharmacology &
Therapeutics. 1971. 245-258.
4. Wishart D, Feunang Y, Guo A, Marcu L, Grant J, Sajed T, et al.
Drug Bank 5.0: a major update to the Drug Bank database for
2018. Nucleic Acids Research.
5. Makhija SN, Vavia PR. Stability indicating HPTLC method for
the simultaneous determination of pseudoephedrine and
cetirizine in pharmaceutical formulations. Journal of
pharmaceutical and biomedical analysis. 2001. 663-67.
6. Zakrzewska A, Parczewski A, Kaźmierczak D, Ciesielski W,
Kochana J. Visualization of Amphetamine and Its Analogues in
TLC. Acta Chimica Slovenica. 2007 Mar 1;54(1).
7. Wills S. (1997). Drugs of Abuse. The Pharmaceutical Press, pp.
62-75.
8. Sinnema A, Verweij AM. Impurities in illicit amphetamine: a
review. Bull. Narc. 1981 .37-54.
9. Puthaviriyakorn V, Siriviriyasomboon N, Phorachata J, Pan-ox
W, Sasaki T, Tanaka K. Identification of impurities and statistical
classification of methamphetamine tablets (Ya-Ba) seized in
Thailand. Forensic Science International. 2002. 105-113.
10. Makino Y, Kurobane S, Miyasaka K, Nagano K. Profiling of
ecstasy tablets seized in Japan. Microgram Journal. 2003. 169-
76
11. Adamowicz P, Chudzikiewicz E, Lechowicz W. Illicit “ecstasy”
tab lets in South ern Po land: a two-year re view. Problems of
Forensic Sciences. 2003. 100-106.
12. Lim , M., Ng, K. H., & Lee, T. K. (2003). Abuse of amphetamine-
type stimulants in Singapore. Forensic Science International,
136.
13. Verweij, A. M. (1992). Impurities in illicit drug preparation: 3,4-
(metylenedioxy)- amphetamine and 3, 4-( metylenedioxy)-
methyl amphetamine. Forensic Science Review, 137-46.
14. Sharma SP, Purkait BC, Lahiri SC. Qualitative and quantitative
analysis of seized street drug samples and identification of
source. Forensic science international. 2005. 235-40
12

J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00003.1
Lightning Deaths in Tigray Region, Northern Ethiopia
Rajeev Varma Manukonda, Assistant Professor, Department of Forensic Medicine and Toxicology, Govt Medical College,
Ambikapur, Chhattisgarh.
Enyew Debash*, S esen Tsegaye*
DharmarayaIngale, Professor and Head, Department of Forensic Medicine and Toxicology, Karuna Medical College,
Palakkad, Kerala.
*Resident, Department of Forensic Medicine and Toxicology, Ayder Comprehensive Specialized Hospital, College of Health
Sciences, Mekelle University, Mekelle, Ethiopia.
Original Research Paper
Corresponding Author
Dr. Rajeev Varma Manukonda
Assistant Professor,
Govt Medical College, Ambikapur, Chhattisgarh. 497001
E-mail: [email protected]
KEYWORDS : Thunderbolt lightning, Lightning deaths, Safety precautions, Litchenburg figures, Blast effect,
Mechanism of lightning.
Article History:Received: 17 March 2018Received in revised form: 25 March 2018Accepted on: 25 March 2018Available online: 1 July 2018
INTRODUCTION :
“Lightning kills 25 amid extensive drought in East Africa:
Sudan Tribune, 27th July 2011.” This news in one of the online
news channels initiated the thought of studying deaths related
to lightning in Tigray region of northern Ethiopia. The global
incidence of lightning is studied in some parts of the world but
no such studies have been done on the Tigray region of
northern part of Ethiopia. The African continent as such
receives the highest lightning strikes with Congo basin toping
the list.
The Optical Transient Detector (OTD) is a space-based
instrument used to detect and locate lightning discharges to
Earth. Statistical analysis to the data collected by OTD
revealed that Earth receives nearly 1.4 billion flashes annually
which are roughly 39-49 flashes per second. Analysis of the
data collected by OTD also revealed an interesting fact that the
ratio of flashes to land and water is nearly 10:1 which means
that the land experiences 10 times more flashes than water
bodies. Ethiopia being a land locked country, is particularly
vulnerable to lightning. The Congo basin, which includes
Democratic Republic of Congo and Rwanda, is considered to _2 _1have peak mean annual flash density of 80 fl km yr highest in
the African continent. Ethiopia has a mean annual flash density _2 _1 [1]of 33.1 fl km yr is not further down the list .
13
ABSTRACT :
Introduction: An individual found dead in an isolated place with torn clothing, disrupted footwear, evidence of burn marks on the
body, lacerations and fractured bones will really present a confusing picture to the investigation authorities and the autopsy surgeon
as to the involvement of foul play. Similar picture can be present in a person struck with thunderbolt lightning. Though the manner
of death is suggestive of homicide. It is in reality due to lightning stroke which is accidental in 100% of cases. The present study is
undertaken to understand the various presentation of victims of lightning and to achieve the other mentioned formulated study
objectives.
Objectives: To study the prevalence of deaths due to lightning during the study period, demographic profile of victims, the various
injuries sustained and mechanisms involved in lightning stroke and the various safety precautions to be undertaken during an event
of thunderstorm.
Methods: A Cross-sectional study design for the study of deaths due to lightning. Data collected in a data collection sheet
developed considering the various study variables.The data collected is analyzed with SPSS statistical software 16.
Results :Majority of the victims are farmers (87%) in the age group of 31-50 years (78.2%) with a male predominance ratio of 7:1.
Conclusion: The importance of lightning deaths should be understood and research in this much neglected field should be
intensified. A clear understanding of mechanism of lightning and varied presentations of these injuries is essential to arrive at a
conclusion in a rather confused autopsy picture.People should be educated about the hazards of lightning and the safety precautions
discussed should penetrate the deepest core of the society.
Some of the news relating to lightning strokes which shook the
African continent and grabbed media attention are listed [2]below :
l Kenyans Alarmed as Lightning kills 20 people within one thweek : Julalo, 05 July 2011.
l Lightning Kills 19 in Gombe, Yobe, Bauchi - Man Loses thTwo Wives, Two Children : Vanguard, 29 June 2011.
thl Lightning Kills 3 Children The New Times, 28 June 2011.
l Lightning kills 7 school children in Darfur : Gulf News, th17 August 2010.
MATERIALS AND METHODS : After approval from
institutional ethical review board, present retrospective study
was conducted on 23 cases of lightning fatalities over a period
of two years from September 2015 to August 2017 at
Department of Forensic Medicine and Toxicology of Ayder
Comprehensive Specialized Hospital. Detailed history was
collected from investigating officers and family members. The
circumstances relating to the death were carefully analyzed.
The cases which are concluded to have died due to lightning,
are included in the study. Cases in which conclusion is not
arrived are excluded from the study. A data sheet was prepared
with various study variables for data collection. Collected data
was analyzed with SPSS 16 software. Data was cross checked
to keep missing data to zero percent.
RESULTS : A total of 356 autopsies were performed during
the study period, out of which 23 deaths were due to
thunderbolt lightning. Among these cases male are 20 (87%)
and females are 3 (13%). Majority of the victims (47.8%)
belong to 31-40 years age group followed by 41-50 years. 31-
50 years accounted for majority of the victims (78.2%).
Majority of the victims were farmers (87%) (Table 1).
Table 1 : Age Wise Distribution of Cases
Month Wise Distribution of Cases :
Seventy four percent of the deaths occurred during the
Ethiopian summer months (June, July and August) followed
by 22% of deaths during the autumn season (March, April and
May). Sixty one percent of the deaths occurred in the middle of
the week during Wednesday.
Time Wise Distribution of Cases :
Majority of the death (52%) occurred between 12 pm to 6 pm
followed by 35% of deaths occurring between 6am-12 pm and
6 pm -12 am.
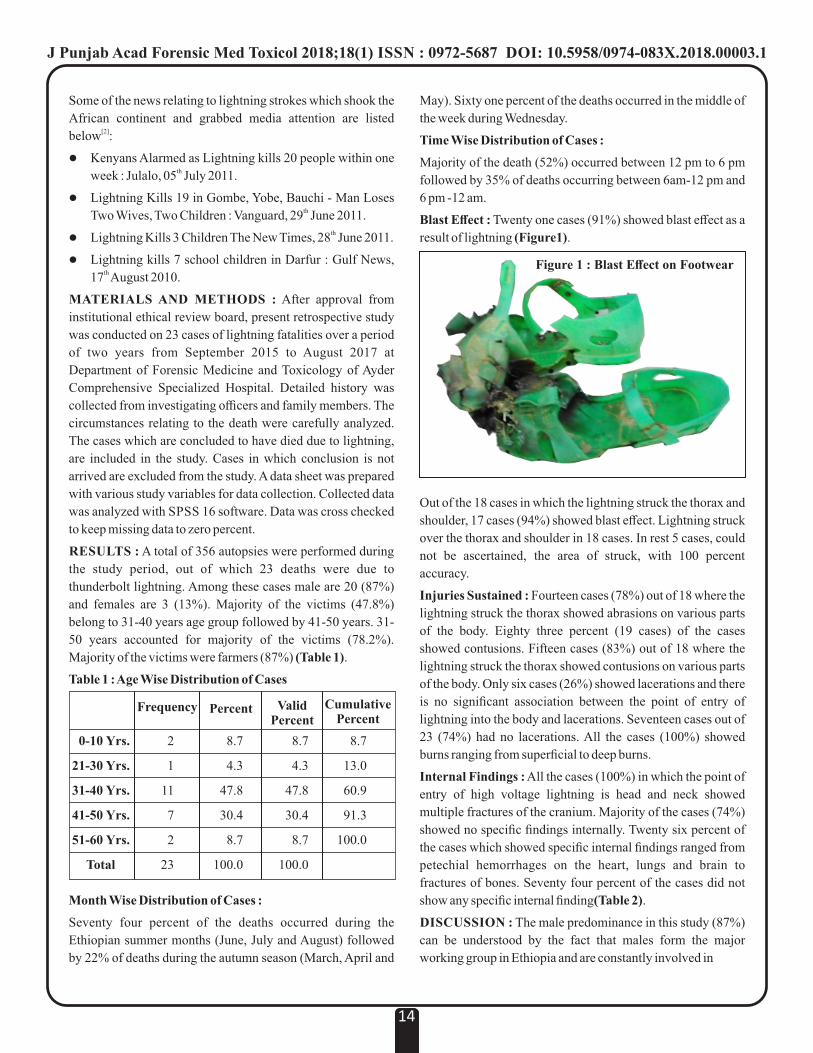
Blast Effect : Twenty one cases (91%) showed blast effect as a
result of lightning (Figure1).
Out of the 18 cases in which the lightning struck the thorax and
shoulder, 17 cases (94%) showed blast effect. Lightning struck
over the thorax and shoulder in 18 cases. In rest 5 cases, could
not be ascertained, the area of struck, with 100 percent
accuracy.
Injuries Sustained : Fourteen cases (78%) out of 18 where the
lightning struck the thorax showed abrasions on various parts
of the body. Eighty three percent (19 cases) of the cases
showed contusions. Fifteen cases (83%) out of 18 where the
lightning struck the thorax showed contusions on various parts
of the body. Only six cases (26%) showed lacerations and there
is no significant association between the point of entry of
lightning into the body and lacerations. Seventeen cases out of
23 (74%) had no lacerations. All the cases (100%) showed
burns ranging from superficial to deep burns.
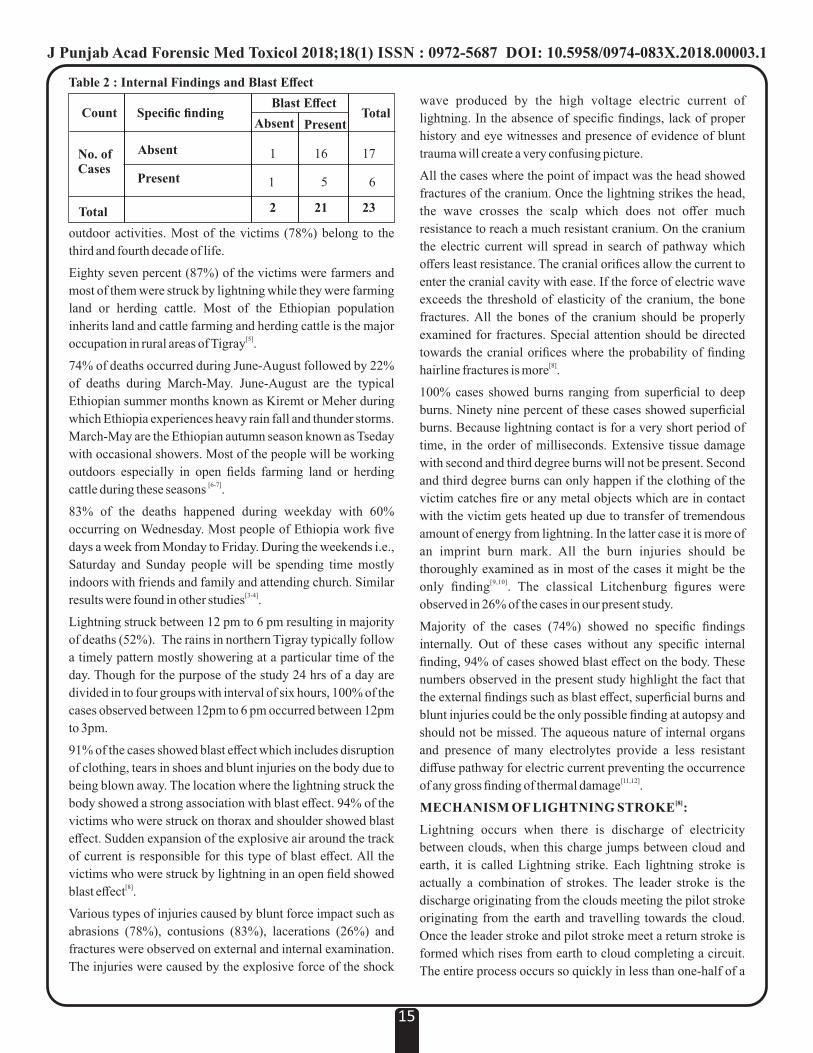
Internal Findings : All the cases (100%) in which the point of
entry of high voltage lightning is head and neck showed
multiple fractures of the cranium. Majority of the cases (74%)
showed no specific findings internally. Twenty six percent of
the cases which showed specific internal findings ranged from
petechial hemorrhages on the heart, lungs and brain to
fractures of bones. Seventy four percent of the cases did not
show any specific internal finding(Table 2).
DISCUSSION : The male predominance in this study (87%)
can be understood by the fact that males form the major
working group in Ethiopia and are constantly involved in
14
0-10 Yrs.
21-30 Yrs.
31-40 Yrs.
41-50 Yrs.
51-60 Yrs.
Total
Frequency Percent ValidPercent
CumulativePercent
2
1
11
7
2
23
8.7
4.3
47.8
30.4
8.7
100.0
8.7
4.3
47.8
30.4
8.7
100.0
8.7
13.0
60.9
91.3
100.0
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00003.1
Figure 1 : Blast Effect on Footwear
Total
Count Total
1
1
2
16
5
21
17
6
23
Specific finding
Absent
Present
Blast Effect
Absent Present
No. ofCases
outdoor activities. Most of the victims (78%) belong to the
third and fourth decade of life.
Eighty seven percent (87%) of the victims were farmers and
most of them were struck by lightning while they were farming
land or herding cattle. Most of the Ethiopian population
inherits land and cattle farming and herding cattle is the major [5]occupation in rural areas of Tigray .
74% of deaths occurred during June-August followed by 22%
of deaths during March-May. June-August are the typical
Ethiopian summer months known as Kiremt or Meher during
which Ethiopia experiences heavy rain fall and thunder storms.
March-May are the Ethiopian autumn season known as Tseday
with occasional showers. Most of the people will be working
outdoors especially in open fields farming land or herding [6-7]cattle during these seasons .
83% of the deaths happened during weekday with 60%
occurring on Wednesday. Most people of Ethiopia work five
days a week from Monday to Friday. During the weekends i.e.,
Saturday and Sunday people will be spending time mostly
indoors with friends and family and attending church. Similar [3-4]results were found in other studies .
Lightning struck between 12 pm to 6 pm resulting in majority
of deaths (52%). The rains in northern Tigray typically follow
a timely pattern mostly showering at a particular time of the
day. Though for the purpose of the study 24 hrs of a day are
divided in to four groups with interval of six hours, 100% of the
cases observed between 12pm to 6 pm occurred between 12pm
to 3pm.
91% of the cases showed blast effect which includes disruption
of clothing, tears in shoes and blunt injuries on the body due to
being blown away. The location where the lightning struck the
body showed a strong association with blast effect. 94% of the
victims who were struck on thorax and shoulder showed blast
effect. Sudden expansion of the explosive air around the track
of current is responsible for this type of blast effect. All the
victims who were struck by lightning in an open field showed [8]blast effect .
Various types of injuries caused by blunt force impact such as
abrasions (78%), contusions (83%), lacerations (26%) and
fractures were observed on external and internal examination.
The injuries were caused by the explosive force of the shock
wave produced by the high voltage electric current of
lightning. In the absence of specific findings, lack of proper
history and eye witnesses and presence of evidence of blunt
trauma will create a very confusing picture.
All the cases where the point of impact was the head showed
fractures of the cranium. Once the lightning strikes the head,
the wave crosses the scalp which does not offer much
resistance to reach a much resistant cranium. On the cranium
the electric current will spread in search of pathway which
offers least resistance. The cranial orifices allow the current to
enter the cranial cavity with ease. If the force of electric wave
exceeds the threshold of elasticity of the cranium, the bone
fractures. All the bones of the cranium should be properly
examined for fractures. Special attention should be directed
towards the cranial orifices where the probability of finding [8]hairline fractures is more .
100% cases showed burns ranging from superficial to deep
burns. Ninety nine percent of these cases showed superficial
burns. Because lightning contact is for a very short period of
time, in the order of milliseconds. Extensive tissue damage
with second and third degree burns will not be present. Second
and third degree burns can only happen if the clothing of the
victim catches fire or any metal objects which are in contact
with the victim gets heated up due to transfer of tremendous
amount of energy from lightning. In the latter case it is more of
an imprint burn mark. All the burn injuries should be
thoroughly examined as in most of the cases it might be the [9,10]only finding . The classical Litchenburg figures were
observed in 26% of the cases in our present study.
Majority of the cases (74%) showed no specific findings
internally. Out of these cases without any specific internal
finding, 94% of cases showed blast effect on the body. These
numbers observed in the present study highlight the fact that
the external findings such as blast effect, superficial burns and
blunt injuries could be the only possible finding at autopsy and
should not be missed. The aqueous nature of internal organs
and presence of many electrolytes provide a less resistant
diffuse pathway for electric current preventing the occurrence [11,12]of any gross finding of thermal damage .
[8] MECHANISM OF LIGHTNING STROKE :
Lightning occurs when there is discharge of electricity
between clouds, when this charge jumps between cloud and
earth, it is called Lightning strike. Each lightning stroke is
actually a combination of strokes. The leader stroke is the
discharge originating from the clouds meeting the pilot stroke
originating from the earth and travelling towards the cloud.
Once the leader stroke and pilot stroke meet a return stroke is
formed which rises from earth to cloud completing a circuit.
The entire process occurs so quickly in less than one-half of a
15
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00003.1
Table 2 : Internal Findings and Blast Effect

second the entire flash is perceived as one single stroke. [13-14]SAFETY PRECAUTIONS :
1. If you are anticipating thunderstorm and the hair on
your body stands or skin tingles, it indicates strong
electric field. Seek shelter immediately.
2. The varied landscapes of Tigray region offer vast
open fields and high mountains. These open fields
with high projecting objects should be avoided.
3. If you are caught in open fields crouch down like a
baseball catcher so that the smallest possible target is
presented and do not lay flat on the ground. The only
thing touching the ground should be the balls of your
feet.
4. Cover both ears with hands tightly. This will
minimize hearing loss from loud thunder clap.
5. The agricultural lands in most part of Tigray are
nurtured by wells found adjacent to the land which
are used to store water for farming. It is advisable to
get out of water and move away from water bodies.
6. Seek shelter in a closed building. Stay away from
metal conductors, doors, windows and plumbing.
7. In an open field do not seek shelter under isolated
trees or buildings. Majority of lightning strikes occur
on isolated tall trees.
8. If you are caught in a vehicle, roll the window glass
and avoid contact with metal conductors
9. Avoid using mobile phones, radio, computer and
transistors.
10. Follow 30-30 rule. When the time gap between
visualization and hearing a thunder is less than or
equal to 30 sec, immediately seek shelter.
CONCLUSION :
The observations made in the present study are only the tip of
an iceberg. Lightning deaths are much more prevalent and their
incidence is increasing every year. More research has to be
undertaken to properly address and understand the problem
and prepare for major disasters due to lightning. The family
members, health care professionals and police personnel
should be educated regarding the precautions to be undertaken
while dealing with a case of lightning deaths. The safety
precautions discussed above should be taught to the people of
remote areas who are most vulnerable.
LIMITAIONS OF STUDY :
During our study period of two years, 23 deaths occurred due
to lightning were autopsied. This number cannot be used for
calculating true prevalence rate of deaths due to lightning in
Tigray region for various reasons such as, not all deaths due to
lightning are being reported to police and not all reported cases
are being autopsied. The reason for this is most of the Tigray
region has remote rural areas which don't have access to proper
and timely transport, the financial burden the family has to bare
while transporting the body for examination and back to
cremation ground back in the remote rural areas and lack of
knowledge that such type of deaths need to be reported to
police for postmortem examination.
Funding: Nil
Conflicts of Interest: None
REFERENCES :
1. Christian HJ, Blakeslee RJ, Boccippio DJ, Boeck WL,
Buechler DE, Driscoll KT, et al. Global frequency and
distribution of lightning as observed from space by the
Optical Transient Detector. J Geophys Res. 2003;108.
2. Mary AK, Gomes C. Lightning Accidents In Uganda. In:
2012 International Conference on Lightning Protection
(ICLP), Vienna, Austria. 2012. p. 1–6.
3. Guntheti BK, Singh UP. Profile and Analysis of Lightning
Victims Brought to MGH , Khammam ; Telangana State. J
Indian Acad Forensic Med. 2015;37(3):258–62.
4. Korah MK, Guria J, Mahto T, Bhengra A. Profile and
Analysis of Lightning Victims Brought To RIMS ,. IOSR J
Dent Med Sci. 2016;15(11):26–9.
5. Gebre-selassie A, Bekele T. A Review of Ethiopian
Agriculture : Roles , Policy and Small-scale Farming
Systems. 1999.
6. Korecha D, Barnston AG. Predictability of June –
September Rainfall in Ethiopia. Mon Weather Rev.
2006;135:628–50.
7. Seleshi Y, Zanke U. Recent changes in rainfall and rainy
days in ethiopia. Int J Climatol. 2004;24:973–83.
8. Anne A, Lewis ME. Understanding the principles of
lightning injuries. J Emerg Nurs. 1997;(December
1997):535–41.
9. Ritenour AE, Morton MJ, Mcmanus JG, Barillo DJ,
Cancio LC. Lightning injury : A review. Burns.
2008;34:585–94.
10. Cooray V, Cooray C, Andrews CJ. Lightning caused
injuries in humans. J Electrostat. 2007;65:386–94.
11. Saukko P, Knight B. Knights Forensic Pathology. 3rd ed.
London: Hodder Arnold; 2004. p333.
12. Vij K. Text book of forensic medicine and toxicology.
Principles and practice. 5th ed. India: Elsevier; 2011. p179 .
13. Zimmermann C, Cooper MA, Holle RL. L ightning Safety
Guidelines. Ann Emerg Med. 2002;(June):0–5.
14. Col L, Nagesh I V, Col L, Bhatia P, Mohan CS, Lamba
BNS. A bolt from the blue : Lightning injuries. Med J
armed forces india. 2015;71:134–37
16
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00003.1
Informed Consent in Medical Treatment – KAP Study1. Nidhi Sachdeva, Assistant Professor*
2. Vivek Srivastava, Associate Professor*
3. Ashok Najan, Assistant Professor*
*Netaji Subhash Chander Bose Medical College, Jabalpur.
Original Research Paper
Corresponding Author
Dr. Nidhi Sachdeva,
Assistant Professor,
Department of Forensic Medicine
Netaji Subhash Chander Bose Medical College, Jabalpur.
Contact : +91 95890-04138
Email : [email protected]
KEYWORDS : Informed Consent, Awareness, Medico-legal.
Article History:Received: 15 March 2018Received in revised form: 25April 2018Accepted on: 25 April 2018Available online: 1 July 2018
INTRODUCTION :
The element of consent is one of the critical issues in the area of
medical treatment today. It is well known that the patient must
give valid consent to medical treatment; and it is his
prerogative to refuse treatment even if the said treatment will
save his or her life. No doubt this raises many ethical debates
and falls at the heart of medical law today. The earliest
expression of this fundamental principle, based on autonomy, [1] is found in the Nuremberg Code of 1947 .The code makes it
mandatory to obtain voluntary and informed consent of human
subjects. Similarly, the Declaration of Helsinki adopted by the
World Medical Association in 1964 emphasizes the
importance of obtaining freely given informed consent for
medical research by adequately informing the subjects of the
aims, methods, anticipated benefits, potential hazards, and [2] discomforts that the study may entail . The circle of legal
development in the area (i.e., consent) appears to be almost
complete when the apex court in India recently ruled that, it is
not just the 'consent' or 'informed consent' (as it is known
worldwide) but it shall also be 'prior informed consent'
generally barring some specific cases of emergency. This
places a medical professional in a tremendous dilemma.
Hence, it is time to revisit the area of 'consent and medical
treatment' to understand the sensitive and underpinning
elements. Informed consent is an integral part of patient-
centered medical care. It occurs in almost every patient
encounter. Documenting your discussion with the patient is
important. In general, it is always useful to note that "patient
understands plan" at the end of a patient note.
Consent can be either expressed or implied. Expressed
consent may be written or verbal. Implied consent is indicated
by the demeanor and behavior of the patient and is adequate for
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00004.3
17
ABSTRACT:
Introduction: The circle of legal development in the area (i.e., consent) appears to be almost complete when the apex court in India
recently ruled that, it is not just the 'consent' or 'informed consent' (as it is known worldwide) but it shall also be 'prior informed
consent' generally barring some specific cases of emergency. Doctors are increasingly being criticized for imposing treatment
without adequate consent.
Objective: The: present study was conducted to know the level of awareness, knowledge and actual practice pattern of the informed
consent among all age groups of practicing doctors (Both clinical and Non-clinical branches).
Material and Method: The questionnaire was designed which comprised of around 19 questions, to test the knowledge of how,
when and in what form the consent has to be taken, attitude of the physician, when they are taking the consent and to know the actual
practice pattern which is being practiced.
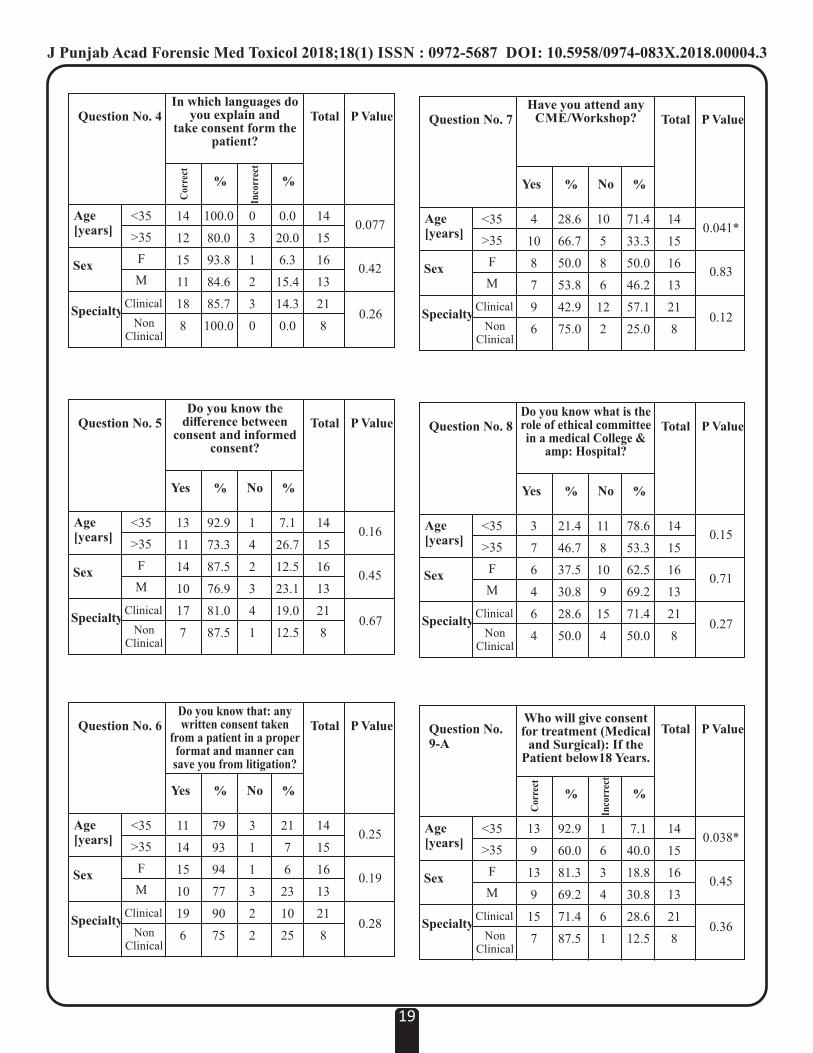
Result: In the present study it was found that doctors of age more than 35 years, only 73.3 % knew about the difference between
consent and informed consent. In Doctors of less than 35 years of age, 92.9 % knew the difference.In the present study it was found
none of the senior doctors have faced any litigation as compared to the junior doctors. This shows that the risk of practioners facing
litigation is increasing day by day.
Conclusion: There is a continuous need of up gradation of Medico legal knowledge in the form of CMEs, workshops, Medico-legal
lectures in other platforms like specialized conferences etc.

knowledge about informed consent while giving treatment to
their patients. The questionnaire used has been included.
Chi Square test applied, P value is significant if p<0.05 and
highly significant if p<0.01.
RESULTS : Questions and Answers are tabulated below :
Question No. 1
How do you obtain consent
before any treatment procedure?
verbal or written
Cor
rect
Inco
rrec
t
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
11
15
15
11
19
7
78.6
100.0
93.8
84.6
90.5
87.5
3
0
1
2
2
1
21.4
0.0
6.3
15.4
9.5
12.5
14
15
16
13
21
8
0.058
0.42
0.81
routine general examinations but special examinations such as
vaginal, rectal etc, require express consent to be taken. For
more complicated diagnostic and therapeutic procedures like
endoscopy or for surgical procedures, written consent is
essential.
Doctors are increasingly being criticized for imposing
treatment without adequate consent. Capacity remains the
cornerstone of the Medico-legal doctrine of informed consent.
Although capacity to consent is ultimately a legal construct,
doctors of all specialties must assess their patient's capacity to
consent on a variety of issues. Although guidelines are
available, there is no gold standard for the assessment of
capacity. Doctors in general are expected to know the standard
for capacity, but may at times apply them incorrectly.
As far as possible, consent must be obtained after explaining
the nature and consequences of the treatment procedure being
contemplated in the presence of disinterested third party such
as nurse or receptionist. This is termed as informed consent.
Failure to take informed consent can expose a doctor to legal
action if anything goes wrong during a particular procedure.
Informed consent help patients make informed decisions about [11,12]their proposed treatments . The concept of informed
[13,14]consents is rooted in moral, cultural, and legal principles .
Informed consents are often perceived as necessary for legal [15]protection against malpractice claims . Present Study has
been conducted to know about level of theoretical knowledge
of doctors with the actual implementation in their routine
practice and to compare actual and correct use of informed
consent among medical and surgical fields.
MATERIALS AND METHODS :
The present KAP study is a cross sectional & hospital based
study performed on 29 randomly selected Medical
practitioners (faculty members both young and old, males and
females, clinical and non-clinical, of the different specialties),
via a questionnaire after taking prior permission from dean and
medical superintendent. Doctors were very supportive,
encouraging and enthusiastic while answering the
Questionnaire. Coding was done to interpret answers
statistically. 1- for yes, 2- for No. After preparing master
chart, results were interpreted using SPSS IBM 20 software.
Identity of the doctors were not disclosed. Post analysis a
seminar was conducted about informed consent.
The questionnaire comprised of 19 questions, to test the
knowledge of how, when and in what form the consent has to
be taken, attitude of the physician, when they are taking the
consent and to know the actual practice pattern which is being
practiced. 11 questions (1-11) were included to test the
Knowledge, 3 questions (12-14) to test the attitude and 5
questions (15-19) to know about how they practice their
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00004.3
18
Question No. 2Whether consent is taken
in proper printed format or on plain paper
orPatient own hand writing
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
6
13
10
9
14
5
42.9
86.7
62.5
69.2
66.7
62.5
8
2
6
4
7
3
57.1
13.3
37.3
30.8
33.3
37.5
14
15
16
13
21
8
0.013*
0.71
0.82
Cor
rect
Inco
rrec
t
Question No. 3Before taking consent,
what information isgiven to the patient?
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
14
10
15
9
18
6
100.0
66.7
93.8
69.2
85.7
75.0
0
5
1
4
3
2
0.0
33.3
6.3
30.8
14.3
25.0
14
15
16
13
21
8
0.017*
0.082
0.49
Cor
rect
Inco
rrec
t
Question No. 7Have you attend any
CME/Workshop?
Yes No
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
4
10
8
7
9
6
28.6
66.7
50.0
53.8
42.9
75.0
10
5
8
6
12
2
71.4
33.3
50.0
46.2
57.1
25.0
14
15
16
13
21
8
0.041*
0.83
0.12
Question No. 8Do you know what is therole of ethical committeein a medical College &
amp: Hospital?
Yes No
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
3
7
6
4
6
4
21.4
46.7
37.5
30.8
28.6
50.0
11
8
10
9
15
4
78.6
53.3
62.5
69.2
71.4
50.0
14
15
16
13
21
8
0.15
0.71
0.27
Question No.9-A
Who will give consent for treatment (Medical
and Surgical): If the Patient below18 Years.
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
13
9
13
9
15
7
92.9
60.0
81.3
69.2
71.4
87.5
1
6
3
4
6
1
7.1
40.0
18.8
30.8
28.6
12.5
14
15
16
13
21
8
0.038*
0.45
0.36
Cor
rect
Inco
rrec
t
Question No. 6Do you know that: any written consent taken
from a patient in a properformat and manner cansave you from litigation?
Yes No
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
11
14
15
10
19
6
79
93
94
77
90
75
3
1
1
3
2
2
21
7
6
23
10
25
14
15
16
13
21
8
0.25
0.19
0.28
Question No. 5Do you know the
difference between consent and informed
consent?
Yes No
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
13
11
14
10
17
7
92.9
73.3
87.5
76.9
81.0
87.5
1
4
2
3
4
1
7.1
26.7
12.5
23.1
19.0
12.5
14
15
16
13
21
8
0.16
0.45
0.67
Question No. 4In which languages do
you explain andtake consent form the
patient?
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
14
12
15
11
18
8
100.0
80.0
93.8
84.6
85.7
100.0
0
3
1
2
3
0
0.0
20.0
6.3
15.4
14.3
0.0
14
15
16
13
21
8
0.077
0.42
0.26
Cor
rect
Inco
rrec
t
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00004.3
19
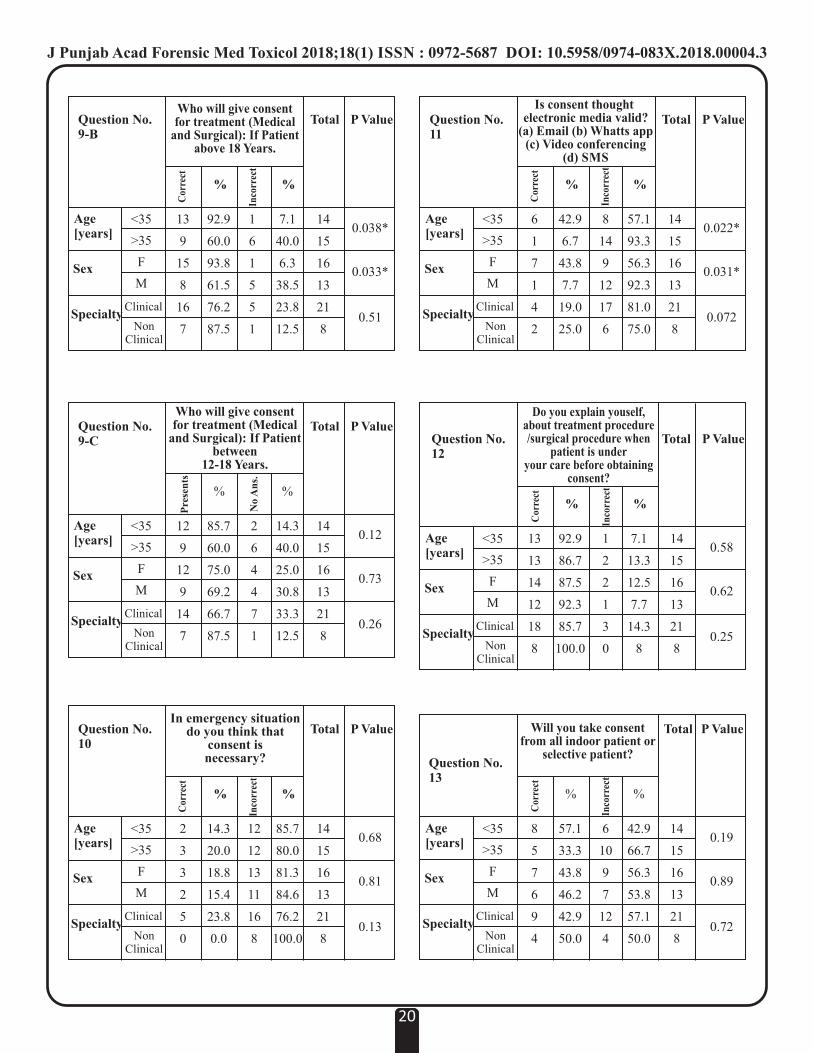
Question No.12
Do you explain youself,about treatment procedure/surgical procedure when
patient is underyour care before obtaining
consent?
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
13
13
14
12
18
8
92.9
86.7
87.5
92.3
85.7
100.0
1
2
2
1
3
0
7.1
13.3
12.5
7.7
14.3
8
14
15
16
13
21
8
0.58
0.62
0.25
Cor
rect
Inco
rrec
t
Question No.11
Is consent thought electronic media valid?
(a) Email (b) Whatts app (c) Video conferencing
(d) SMS
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
6
1
7
1
4
2
42.9
6.7
43.8
7.7
19.0
25.0
8
14
9
12
17
6
57.1
93.3
56.3
92.3
81.0
75.0
14
15
16
13
21
8
0.022*
0.031*
0.072
Cor
rect
Inco
rrec
t
Question No.9-B
Who will give consent for treatment (Medical
and Surgical): If Patient above 18 Years.
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
13
9
15
8
16
7
92.9
60.0
93.8
61.5
76.2
87.5
1
6
1
5
5
1
7.1
40.0
6.3
38.5
23.8
12.5
14
15
16
13
21
8
0.038*
0.033*
0.51
Cor
rect
Inco
rrec
t
Question No.9-C
Who will give consent for treatment (Medical
and Surgical): If Patientbetween
12-18 Years.
Pre
sen
ts
No
An
s.
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
12
9
12
9
14
7
85.7
60.0
75.0
69.2
66.7
87.5
2
6
4
4
7
1
14.3
40.0
25.0
30.8
33.3
12.5
14
15
16
13
21
8
0.12
0.73
0.26
Question No.10
In emergency situationdo you think that
consent is necessary?
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
2
3
3
2
5
0
14.3
20.0
18.8
15.4
23.8
0.0
12
12
13
11
16
8
85.7
80.0
81.3
84.6
76.2
100.0
14
15
16
13
21
8
0.68
0.81
0.13
Cor
rect
Inco
rrec
t
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00004.3
20
Will you take consent from all indoor patient or
selective patient?
Age [years]
Sex
SpecialtyClinical
Non Clinical
<35
>35
F
M
8
5
7
6
9
4
Cor
rect
Question No.13
Total P Value
% %
57.1
33.3
43.8
46.2
42.9
50.0
6
10
9
7
12
4
42.9
66.7
56.3
53.8
57.1
50.0
14
15
16
13
21
8
0.19
0.89
0.72
Inco
rrec
t

Question No.15
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
6
12
10
7
11
6
42.9
80.0
62.5
53.8
52.4
75.0
8
3
6
6
10
2
57
20
38
46
48
25
14
15
16
13
21
8
0.039*
0.63
0.26
How do you take consentin
(a) Proper Format (b) Plane Paper
(c) Approved Printed Format
Cor
rect
Inco
rrec
t
Do you take informed consent(a) Before any surgical procedure?
(b) In case of poor prognosis(c) For staying in a hospital with
available facilities(d) All indoor patients.
(e) All of the above.
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
12
7
11
7
9
7
85.7
46.7
68.8
53.8
42.9
87.5
2
8
5
6
12
1
14.3
53.3
31.3
46.2
57.1
12.5
14
15
16
13
21
8
0.027*
0.41
0.031*
Cor
rect
Inco
rrec
t
Question No.14
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00004.3
21
Cor
rect
Inco
rrec
t
Question No.16
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
10
13
13
10
18
5
71.4
86.7
81.3
76.9
85.7
62.5
4
2
3
3
3
3
28.6
13.3
18.8
23.1
14.3
37.5
14
15
16
13
21
8
0.31
0.72
0.17
Do you think format for all treatment is same
or different Question No.19-B
Yes No
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
8
10
10
8
17
3
57.1
66.7
62.5
61.5
81.5
37.5
6
5
6
5
4
5
42.9
33.3
37.3
38.5
19.0
62.5
14
15
16
13
21
8
0.59
0.96
0.023*
While examining the Accused of rape, informed
consent should betaken or not?
Question No.18
Yes No
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
1
0
1
0
1
0
7.1
0.0
6.3
0.0
4.8
0.0
13
15
15
13
20
8
92.9
100.0
93.8
100.0
95.2
100.0
14
15
16
13
21
8
0.29
0.54
0.53
Have you faced any litigation Because of nottaking proper informed
consent?
Question No.19-A
Yes No
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
11
13
14
10
18
6
78.6
86.7
87.5
76.9
85.7
75.0
3
2
2
3
3
2
21.4
13.3
12.5
23.1
14.3
25.0
14
15
16
13
21
8
0.56
0.45
0.49
While examining the victim of rape, informed
consent should betaken or not?
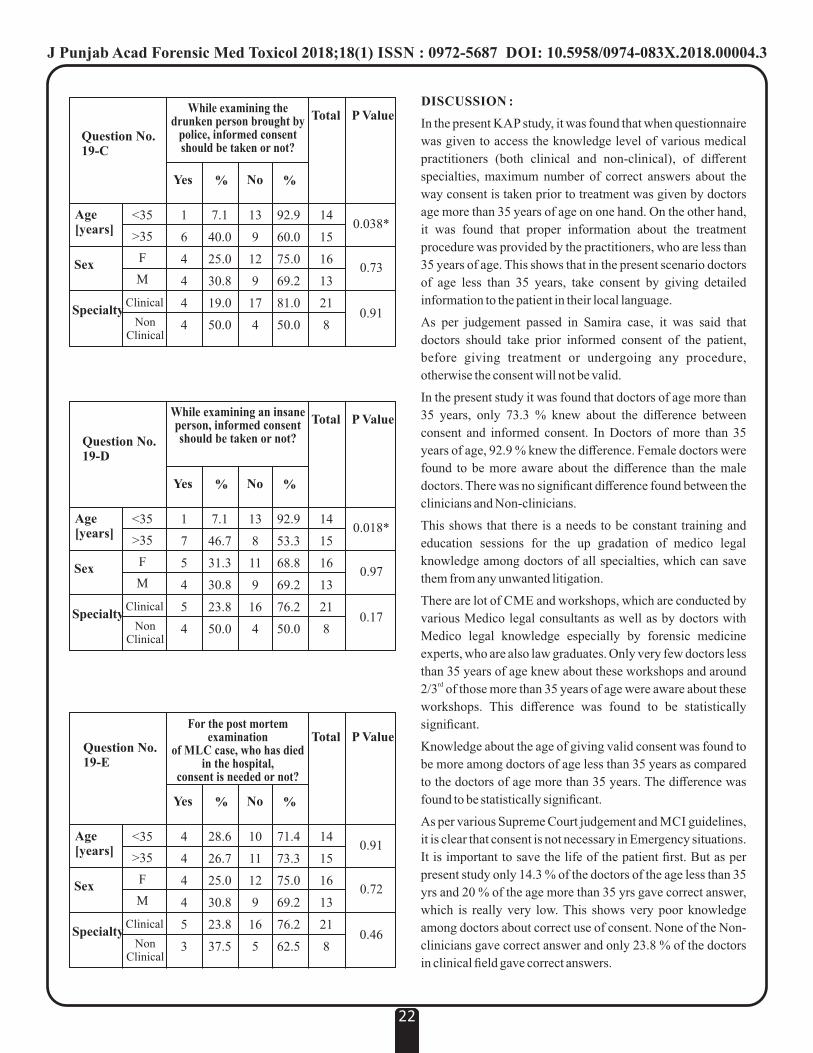
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00004.3
22
Question No.19-E
Yes No
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
4
4
4
4
5
3
28.6
26.7
25.0
30.8
23.8
37.5
10
11
12
9
16
5
71.4
73.3
75.0
69.2
76.2
62.5
14
15
16
13
21
8
0.91
0.72
0.46
For the post mortem examination
of MLC case, who has died in the hospital,
consent is needed or not?
Question No.19-C
Yes No
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
1
6
4
4
4
4
7.1
40.0
25.0
30.8
19.0
50.0
13
9
12
9
17
4
92.9
60.0
75.0
69.2
81.0
50.0
14
15
16
13
21
8
0.038*
0.73
0.91
While examining the drunken person brought by
police, informed consent should be taken or not?
Question No.19-D
Yes No
Total P Value
Age [years]
Sex
SpecialtyClinical
Non Clinical
% %
<35
>35
F
M
1
7
5
4
5
4
7.1
46.7
31.3
30.8
23.8
50.0
13
8
11
9
16
4
92.9
53.3
68.8
69.2
76.2
50.0
14
15
16
13
21
8
0.018*
0.97
0.17
While examining an insaneperson, informed consent should be taken or not?
DISCUSSION :
In the present KAP study, it was found that when questionnaire
was given to access the knowledge level of various medical
practitioners (both clinical and non-clinical), of different
specialties, maximum number of correct answers about the
way consent is taken prior to treatment was given by doctors
age more than 35 years of age on one hand. On the other hand,
it was found that proper information about the treatment
procedure was provided by the practitioners, who are less than
35 years of age. This shows that in the present scenario doctors
of age less than 35 years, take consent by giving detailed
information to the patient in their local language.
As per judgement passed in Samira case, it was said that
doctors should take prior informed consent of the patient,
before giving treatment or undergoing any procedure,
otherwise the consent will not be valid.
In the present study it was found that doctors of age more than
35 years, only 73.3 % knew about the difference between
consent and informed consent. In Doctors of more than 35
years of age, 92.9 % knew the difference. Female doctors were
found to be more aware about the difference than the male
doctors. There was no significant difference found between the
clinicians and Non-clinicians.
This shows that there is a needs to be constant training and
education sessions for the up gradation of medico legal
knowledge among doctors of all specialties, which can save
them from any unwanted litigation.
There are lot of CME and workshops, which are conducted by
various Medico legal consultants as well as by doctors with
Medico legal knowledge especially by forensic medicine
experts, who are also law graduates. Only very few doctors less
than 35 years of age knew about these workshops and around rd2/3 of those more than 35 years of age were aware about these
workshops. This difference was found to be statistically
significant.
Knowledge about the age of giving valid consent was found to
be more among doctors of age less than 35 years as compared
to the doctors of age more than 35 years. The difference was
found to be statistically significant.
As per various Supreme Court judgement and MCI guidelines,
it is clear that consent is not necessary in Emergency situations.
It is important to save the life of the patient first. But as per
present study only 14.3 % of the doctors of the age less than 35
yrs and 20 % of the age more than 35 yrs gave correct answer,
which is really very low. This shows very poor knowledge
among doctors about correct use of consent. None of the Non-
clinicians gave correct answer and only 23.8 % of the doctors
in clinical field gave correct answers.

Consent through Electronic media viz Teleconferencing,
SMS, what's app etc. is not valid as per present Supreme Court
judgement till date. No valid literature regarding the same is
available.
The treating physician should explain to their patient
themselves, about the treatment procedure as patient is under
his duty of care. If patient is not able to understand anything,
patient has the right to get his doubts clear from the treating
physician. The treating physician should tell about all the
possible complication that can occur due to the procedure or
due to the disease per se, otherwise if any untoward
complication arise, then the treating physician is held
negligent for the same. In the present study, only 92.9 % of the
doctors of age less than 35 years explain the procedure and
related complications to the patient themselves and only 86.7
% of the doctors of age more than 35 years does the same. It
should be 100 % and nothing less is acceptable.
Very few percentage of the female practitioners explain the
procedure themselves to their patient as compared to the males.
When the clinicians were compared with the non- clinicians
the ratio was (85.7 % vs. 100 %).
Taking informed consent in a proper format and in the proper
manner is more important for the treating physician. While
non-clinical doctors generally take consent before doing any
survey for Research purposes. This shows lack of awareness,
knowledge or the underutilization of the knowledge, which the
doctors gain in their under graduation level by studying the
subjects regarding medical law.
In our country, where the number of litigation cases are
increasing day by day, doctors are growing towards practicing
defensive medicine compared to preventive medicine. Doctors
are always tense at the back of their mind. It is very important
for them to save their neck and practice with proper
precautions to avoid unnecessary mental and financial
harassment. Therefore proper informed consent, in the
language the patient understands should always be taken,
before starting treatment procedure of all the indoor patients.
Ideally informed consent should be taken before any treatment
procedure. If the prognosis is poor and the hospital has limited
facilities, this should be properly explained to the patient and
proper informed consent in the proper format should be taken.
In the present study, it was found that only 46 % of the doctors
above 35 years of age and 85.7 % of the doctors less than 35
years practice this. This difference was found to be statistically
significant (p value = 0.027)
Very few doctors in the clinical field actually practice this, on
the contrary 87.5 % of the clinicians are aware about the same.
So it is clear that knowledge and the actual practice of the
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00004.3
23
clinicians are different. This is unethical and therefore more
and more doctors are landing themselves in the litigation.
Format to take consent for different treatment procedure,
should be different. It should cover all aspects of the treatment
and complications related to a particular procedure. Then only
it can be held valid. 71.4 % of the doctors of age less than 35
years of age and 86.7 % of the doctors more than 35 years of
age are aware of this concept.
In the present study only 1 clinician less than 35 years of age,
had to face litigation for not taking proper informed consent.
None of the doctor more than 35 years of age faced any such
litigation.
Every medical practitioner in their undergraduate curriculum
are taught about the concept of informed consent, which is
covered under Medical Law and Ethics, with various relevant
to them, in actual practice. But in the present study, on the
whole only 70 – 80 % doctors are aware about how to proceed
in situations like examination of rape victim, examination of
rape accused, examination of drunken people, examination of
insane person and death of Medico Legal case in a hospital.
As per section 164 A of CrPc, doctor does not need to take
consent while examining a person accused of rape, but the
consent is mandatory while examining a victim of rape.
An Insane person cannot give a legal consent. The valid
consent can only be given by the immediate guardian of the
insane person.
Under section 53 of CrPc, consent is not needed before
examining a drunken person brought by the police.
Consent is not necessary from the next of kin of deceased
person involved in a MLC case. Consent is mandatory before
pathological autopsy and not before Medico legal autopsy.
CONCLUSION :
The present study was conducted to know the level of
awareness, knowledge and actual practice pattern of the
informed consent among all age groups of practicing doctors
(both clinical and Non-clinical branches)
It was found that none of the senior doctors have faced any
litigation as compared to the junior doctors. This shows that the
risk of practioners facing litigation is increasing day by day.
The following points are concluded from the present study.
1. There is lack of application of the theoretical
knowledge and correlation in various situations
among practioners.
2. The consent are not being taken in a proper format,
because of the lack of knowledge and sheer
carelessness of the practitioners. So in this changing
era, one need to be extra careful about all these legal

things, because these things can result in both mental
as well as financial harassment.
3. As the medical profession has come under the
umbrella of Consumer Protection act, more and more
dissatisfied patients file complaints to retrieve their
money. The patients are more educated and aware of
their rights than before, so the practioners needs to be
more careful and legally sound. The doctor- patient
relationship has undergone a sea change, and the
patients are more of a customer/client to the doctor.
Now a days the ethical committee plays a very important role
in an institutional setup. There is a continuous need of up
gradation of Medico legal knowledge in the form of CMEs,
workshops. Medico-legal lectures in other platforms like
specialized conferences etc.
REFERENCES :
1. Shaha KK, Patra AP, Das S. The importance of informed
consent in medicine. Sch J App Med Sci. 2013; 1(5):455-
63.
2. Samira Kohli versus Dr Prabha Manchanda (2008) 2
SCC1:2008 ACJ 747: AIR 2008 SCI 385: JT 2008(1)
SC399 (2008)1 Scale 442
3. Shukla V, Tripathi R. Chikitsa Sthana. Ch. 13, Verse
no.176- 177, Part-II.2007. Charaka Samhita; p. 314.
4. Valiathan MS. Bioethics and Ayurveda. Indian J Med
Ethics. 2008; 5:29–30.
5. Nandimath OV. Consent and medical treatment: The legal
paradigm in India. Indian J Urol. 2009; 25:343–7.
6. Kumar NK. Bioethics activities in India. East Mediterr
Health J. 2006;12:56–65.
7. Kumar N, Ravindran GD, Bhan A, Srivastava JS, Nair
VM. The India experience. J Acad Ethics. 2009;
6:295–303.
KNOWLEDGE
Q.1 How do you obtain before any treatment procedure?
(a) Verbal Consent (b) Written Consent
Q.2 Whether consent is taken in proper printed format or on
plain paper?
(a) Printed Format (b) Plain Paper
(c) Patient own hand written Consent
Q.3 Before taking consent, what information is given to the
patient?
(a) All relevant information about ailment and treatment
option.
(b) Significant risk Involved in procedure.
(c) All available alternative treatment option.
(d) All of the above.
Q.4 In which languages do you explain and take consent form
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00004.3
24
the patient?
Q.5 Do you know the difference between consent and
informed consent.
(a) Yes (b) No
Q.6 Do you know that: any written consent taken from a
patient in a proper format and manner can save you from
litigation.
(a) Yes (b) No
Q.7 Have you attend any CME / Workshop?
Q.8 Do you know what is the role of ethical communities in a
medical College & Hospital?
Q.9 Who will give consent for treatment (Medical and
Surgical): If the Patient age is:
(a) Below 18 Years. (b) Above 18 Years.
(c) Between 12-18 Years.
Q.10 In emergency situation do you think that consent is
necessary?
(a) Yes (b) No
Q.11 Is consent thought electronic media valid?
(a) Email (b) What's app
(c) Video conferencing (d) SMS
ATTITUDE
Q.12 Do you explain yourself to the patient about treatment
procedure / surgical procedure when patient is under your
duty of case before obtaining consent?
(a) Yes (b) No
Q.13 Will you take consent from all indoor patient or selective
patient?
Q.14 Do you take informed consent-
(a) Before any surgical procedure.
(b) In case of poor prognosis.
(c) For starting in a hospital with available facilities
(d) All indoor patients.
(e) All of the above.
PRACTICE
Q.15 How do you take consent in
(a) Proper Format (b) Plain Paper
(c) Approved Printed Format
Q.16 Do you think format for all treatment is same or different?
Q.17 Have you come across any circumstance: When you have
taken consent:
(a) During the procedure. (b) After the procedure.
Q.18 Have you faced any litigation Because of not taking proper
informed consent?
Q.19 In the under mentioned medical legal conditions informed
consent should be taken or not:
(a) Examination of victim of Rape.
(b) Examination of accused of Rape.
(c) Examination of a drunken person brought by police.
(d) Examination of an insane.
(e) Death in a hospital of an MLC case followed by –
Body to be sent for post mortem examination.

J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00005.5
Original Research Paper
Corresponding Author
Dr. Ashok Najan
Assistant professor,
Department of Forensic Medicine, NSCB Medical
College Jabalpur
Contact : 97522-12017
Email: [email protected]
KEYWORDS : Medico Legal Case, Casualty, Profile
Article History:Received: 1 March 2018Received in revised form: 2 March 2018Accepted on: 2 March 2018Available online: 1 July 2018
INTRODUCTION :
A medico-legal case is “a case of injury or illness where the
attending doctor, after eliciting history and examining the
patient, thinks that some investigation by law enforcement
agencies is essential to establish and fix responsibility for the [1]case in accordance with the law of the land” . Emergency
department plays a vital role in functioning of any hospital.
Ours is a tertiary care hospital providing medical care to vast
population in Mahakaushal region of Madhya Pradesh. A large
number of cases of these are medico legal cases which mandate
c o m p u l s o r y d o c u m e n t a t i o n a f t e r e m e r g e n c y
treatment.Medico legal cases constitute substantial proportion
of workload in tertiary care hospitals. Study of profile of
medico legal cases is helpful to know the burden of medico
legal cases on different specialty departments of the hospital, to
identify load of preventable medical emergencies and also to
know the crime in particular area.
MATERIAL AND METHODS :
After getting approval from IEC, present retrospective study
was conducted on 912 medico-legal cases attended on OPD
basis and admitted in the month of September 2017 in the
emergency department of NSCB Medical College and
Hospital Jabalpur. Documentation of age, gender, manner,
number of departments referred or from which opinion is
sought, type of cases was confirmed from the hospital and also
police records. The data was collected and analyzed. The
objectives of the study was to know cause, manner and
profiling of medico legal cases.
OBSERVATIONS:
Out of 912 cases, 301 (33%) were in the age group of 21-30
years followed by 31-40 years (21.49%) (Table 1).
In respect to gender distribution, 694 (76.09%) were male as
compared to 215 (23.15%) female and male to female ratio was
3.22:1 in this study (Table 2).
Manner of blunt injuries other than road traffic accidents, in
maximum cases i.e.153 (57.73%) is homicidal, followed by
accidental i.e 110 cases (42.96%) which include fall from .
height, cow goring, dog bite, human bite cases. (Table 3)
Manner of sharp injuries in maximum cases is homicidal 18
(69.23%) cases (Table 4)
Maximum cases reported were of road traffic accidents 323
25
1. Vivek Srivastava, Associate Professor, Department of Forensic Medicine, NSCB Medical College Jabalpur
2. Ashok Najan, Assistant professor, Department of Forensic Medicine, NSCB Medical College Jabalpur
3. Pradeep Kumar Markam, Casualty Medical Officer, Emergency Department, NSCB Medical College Jabalpur
4. Shivoham Shukla, Casualty Medical Officer, Emergency Department, NSCB Medical College Jabalpur
ABSTRACT :
Introduction: Medico legal cases constitute substantial proportion of workload in tertiary care hospitals. Methods and material:
The study was conducted retrospectively during the month of September 2017 to know cause, manner and to make profiling of
medico legal cases. Results: Maximum cases i.e.301 (33.00%) were reported in the age group of 21-30 years. Male to female ratio
was 3.22:1. Manner of blunt injuries other than road traffic accidents, is homicidal i.e. 153 (57.73%) cases. Manner of sharp injuries
in maximum cases is homicidal 18 (69.23%) cases. Maximum medico legal cases were referred to Surgery department i.e. 492
(53.94%). Discussion: Sharp injuries were found in 27 (02.96%) cases in which predominant manner of death was homicidal i.e.18
cases (69.23%). Most common medico legal cases were RTA followed by fall from height, snake bite. This finding is consistent
with findings of other studies. Conclusion: Most common injury involved in these cases is blunt injury. In cases of sharp injuries
commonly manner of production is homicidal in nature. Surgery, orthopedics departments most commonly involved in medico
legal cases. Opinion of single department is most commonly sought by CMO’s.
Profile of Medico Legal Cases at Netaji Subhash Chandra Bose Medical College Jabalpur, Madhya Pradesh

J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00005.5
26
Table 3 : Manner of Blunt Injuries (other than Road Traffic Accidents)
Homicidal
Accidental
Suicidal
153 (57.73%)
110 (42.96%)
02 (00.75%)
Table 1 : Age Wise Distribution of Medical Legal Cases
Age (yrs)
Number
0-10 11-20 21-30 31-40 41-50 51-60 61-70 71-80 81-90
51(05.59%)
149(16.13%)
301(33.00%)
196(21.49%)
109(11.95%)
60(06.05%)
37(04.05%)
07(0.76%)
02(0.21%)
Table 2 : Gender Wise Distribution of Cases
Sex
Number
Males Females
110 (42.96%) 02 (23.57%)
Table 4 : Manner of Sharp Injuries
Homicidal
Accidental
Suicidal
18 (69.23%)
7 (26.92%)
1 (03.84%)
Type of Case
Road Traffic Accident
Fall From Height
Snake Bite
Poisoning
Brought Dead
Burns
Dog Bite
Alcohol Poisoning
Scorpion Bite
Cow Goring
Hanging
Human Bite
Unconscious
Drowning
Electric Shock
Fire Cracker
Fox Bite
Hot Oil Burns
Injection Cellulitis
Table 5 : Type of Medical Legal Cases
No. of Cases
323 (35.41%)
100 (10.96%)
72 (07.89%)
56 (06.14%)
32 (03.50%)
26 (02.85%)
21 (02.30%)
21 (02.30%)
07 (00.76%)
06 (00.65%)
05 (00.54%)
03 (00.33%)
3 (00.33%)
2 (00.22%)
2 (00.22%)
01 (00.10%)
01 (00.10%)
01 (00.10%)
01 (00.10%)
Departments Referred
Surgery
Orthopedics
Medicine
ENT
Ophthalmology
Pediatrics
CMO
Obstetrics & Gynecology
Dentistry
Table 6 : Opinion Sought per MLC from other Specialty Department
No. of Cases
492(53.94%)
257(28.17%)
189(20.72%)
68(07.45%)
19(02.10%)
08(00.87%)
07 (00.76%)
02 (00.20%)
01 (00.10%)
(35.41%) followed by fall from height 100 (10.96%) snake
bite72 (07.89%) poisoning 56 (06.14%) (Table 5).
Maximum medico legal cases were referred to Surgery
department i.e.492 (53.94%) followed by orthopedics
257(28.17%) cases, Medicine 189 (20.72%) cases, ENT
department 68 (07.45%) cases (Table 6).

In 736 (80.70%) cases CMO sought opinion from one
department and in 146 (16.00%) cases they sought opinion
from more than one department. (Table 7)
DISCUSSION:
In our study most common age group involved in Medico-legal
cases was 21-30 years as this age group is socially and
occupationally involved in outdoor activities. This outdoor
activity and active life style make this age group more
vulnerable to such hazards. This finding is similar to findings [2]of the studies done by Garg V and Verma S K , Salgado MS
[3] [4]and Colombage SM , Sahdev P and Lacqua MJ , and Singh B [5]and Dogra .
Male to female ratio was 3.22:1 which is not consistent with [2]finding of the study done by Garg V and Verma S. K .
Most common medico legal cases were RTA followed by fall
from height, snake bite.This finding is consistent with findings [2,6,7]of other studies . This could be due to the fact that Jabalpur
is a divisional headquarters and daily a large population is
moving towards and away from Jabalpur with heavy traffic.
Most of the surrounding districts of Jabalpur are agriculturally
highly active which expose the population to insecticidal
poisons and snake bites. Besides cases of burns, dog bite, and
alcohol poisonings are also common.
In our study blunt injuries were observed n 595 (65.24%) case
Similar finding differs from study done by Arif M, Rasool SH, [7]Ali SMH who observed that almost two third of the victims
suffered from blunt injuries (64.77%). Blunt injuries other than
road traffic accident were observed in 272 (29.82%) cases.
Manner of blunt injuries other than road traffic accidents, in
maximum cases i.e. 110 (42.96%) is accidental (Table 3),
which include fall from height, cow goring, dog bite, human
bite etc.
Sharp injuries were found in 27 (02.96%) cases in which
predominant manner of death was homicidal i.e.18 cases
(69.23%)(Table 4). Our findings differ from those of study [7] done by Arif M, Rasool SH, Ali SMH who observed sharp
weapon injuries in 8.8% cases.
Single department opinions were most commonly sought but
more than one department opinions were also sought.
Maximum opinions were sought from Surgery followed by
Orthopedics and Medicine department which is consistent [2]with workload of these departments in other studies .
Cases of sexual assault are dealt with at other civil hospitals in
Jabalpur and not at our medical college.
CONCLUSION:
Most commonly males in young age group are involved in
medico legal cases. Most common injury involved in these
cases is blunt injury. Excluding road traffic accidents most
commonly blunt injuries are homicidal in nature. In cases of
sharp injuries manner of production is commonly homicidal in
nature.
Cases of road traffic accidents are most common cause of
medico legal cases.
Most commonly medico legal cases were handled by Surgery
and Orthopedics departments Opinion of single department is
most commonly sought by CMO's.
Conflict of interest: None
Source of funding: Self
REFERENCES :
1. Dogra TD, Rudra A. Lyon's Medical Jurisprudence &
Toxicology. 11th Ed. Delhi Law House. 2005:367.
2. Garg V, Verma S.K. Profile of Medico-legal Cases at
Adesh Institute of Medical Sciences and Research,
Bathinda, Punjab J Indian Acad Forensic Med, 2010.
32(2); 150-52.
3. Salgado MSL, Colombage SM. Analysis of fatalities
in road accidents. Forensic Sci Int. 1998; 36: 91-96.
4. Sahdev P, Lacqua MJ, Singh B, Dogra TD. Road
Traffic fatalities in Delhi: causes, injury patterns and
incidence of preventable deaths. Accidental Ann
Prev. 1994; 26: 377-84.
5. Friedman Z, Kungel C, Hiss J, Marganit B, Stein M,
Shapira S. The Abbreviated injury scale – a valuable
tool for forensic documentation of trauma. Am J
Forensic Med Pathol. 1996;17(3):233-8
6. Malhotra S., Gupta R.S. A study of the workload of
the casualty department of a large city hospital.
Health and Population - Perspectives & Issues.
1992.15(l&2); 68-76.
7. Mahajan A, Dhillon S, Sekhon H. Profile of Medico
Legal Cases in Shimla (June 2008- December 2008).
Medico-Legal Update, 2011. 11 (2); 64- 66.
8. Arif M, Rasool SH, Ali SMH. Profile of medicolegal
cases; accident & emergency department of services
h o s p i t a l , L a h o r e . P r o f e s s i o n a l M e d J .
2017;24(3):366-369.
27
Number of Departments
One
More than one
Table 7 : Opinion Sought Departments
No. of Cases
736 (80.70%)
146 (16.00%)

Original Research Paper
Corresponding Author
Dr Sonu Gupta
Lecturer,
Dashmesh Institute and Research Dental Sciences, Faridkot.
Contact : +91 92176-66699
Email : [email protected]
KEYWORDS : Hospital, Healthcare, Medical College, Public Sector, Bio-Medical Waste training
Article History:Received: 29 April 2018Received in revised form: 19 June 2018Accepted on: 19 June 2018Available online: 1 July 2018
INTRODUCTION:
Growing health care industry has been seeing parallel growth
of generated bio-medical waste which requires scientific
approach for its management. Many studies have been done on
Bio-Medical Waste (BMW) management in the past assessing
and describing knowledge, attitude and practices at various
Health Care Organisations (HCO). Hospitals have been
working hard to maintain standards for biomedical waste [1]management as notified by Government of India . Studies
have reported that potential infectious waste to be segregated [2]as BMW is approximately 340 gm to 2 kg per bed . Typically
inpatient general wards at medical colleges with 30 beds are
likely to generate 9-15 kg of bio-medical waste, which when
divided into 3 shifts shall translate into 3-5 kg of BMW to be
segregated in each shift. This again gets divided among doctors
and nurses on duty at a particular time. Successful
implementation of Bio-Medical Waste (Management and [ 3 - 4 ]Handling) Rules (B M W M H) requires s incere
implementation efforts in terms of training, administrative
focus and uniformity across organizations. While BMWMH
defines the colour coding and end point requirements from the
HCO's; it becomes imperative for the organizations to define
their systems, processes, responsibility assignments and
monitoring systems. BMWMH have left it for the
organization to educate and endow adequate training to their
employees and staff generating and handling Bio-Medical
Waste (BMW). BMWMH training is a part of nursing study [5]curriculum , additionally nursing students are required to
attend their clinical postings on regular basis. Post
employment in-service training must include two components;
one to inform about BMWMH rules with respective
organization policies and second to provide conceptual clarity.
While earlier studies were focused on knowledge, attitude and
practices at various organizations, current study focuses to
identify reasons for possible lapses in BMWMH.
OBJECTIVES:
This study was conducted to assess the differences in
conceptual clarity on BMWMH among diploma and graduate
nurse and identify areas requiring management focus.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00006.7
Gaps in Nursing Training on Biomedical Waste Management and Handling:
Situational analysis at a Tertiary Care Public Hospital1. Ravinder Nath Bansal, Deputy Medical Superintendent, GGS Medical College Hospital, Faridkot.
2. Sonu Gupta, Lecturer, Dashmesh Institute of Research and Dental Sciences, Faridkot.
28
ABSTRACT:
Introduction: Growing health care industry has been seeing parallel growth of generated Bio-Medical Waste (BMW) which
requires scientific approach for its management. Hospitals have been working hard to maintain levels of standards for Bio-Medical
Waste (Management and Handling) Rules (BMWMH) as notified by Government of India. BMWMH have left it for the
organization to define their systems, processes, responsibility assignments and monitoring systems and to educate and endow
adequate training to their employees and staff generating and handling BMW. While earlier studies were focused on knowledge,
attitude and practices at various organizations, current study focuses to identify reasons for possible lapses in BMWMH.
Objective: The objectives of this study were to assess the differences in conceptual clarity on BMWMH among diploma and
graduate nurse and identify areas requiring management focus. Method: Study was conducted at a tertiary care public sector
Medical College. Validated questionnaire was used where by questionnaire was specifically framed to assess the clarity on basic
concepts behind the BMWMH.
Result: Graduate nurses were found to have higher conceptual clarity compare to diploma holder nurses. Training levels were
found to be below national averages in tertiary care hospitals. Study goes on to identify, suggest methods and actionables for tertiary
care institutions to improve compliance to BMWMH rules which can also be replicated for other healthcare organizations.
BMWHM rules and 74% nurses assessed their confidence
levels to be more than 50% (Table 3).
On comparing the self assessed confidence levels significant
(p=0.00) differences were found between Diploma and
Graduate nurses with graduate nurses responding as being
more confident. Following this respondents filled the
questionnaire and the last question asked the respondents to
specify if, they felt that they required further training on
BMWMH (Table 4).
Paired t-test was run to identify if, there were significant
differences in confidence levels before the start of test and felt
training needs after the test. It was found that there was
significant differences with p=0.000.
MATERIALS AND METHODS:
For the purpose of study GGS Medical College, Faridkot,
Punjab (a tertiary care public sector) was selected by choice
being easily accessible to the researchers. This institute was
established more than 35 years ago and currently has an
average OPD of more than 1800 patients per day with more
than 36000 admissions per year supported by 700 plus beds
and being manned by 1000 plus personnel including more than
280 nurses. Government Medical College was chosen
expecting higher awareness levels being teaching institution.
Following NULL hypothesis was formed H 1: that is there is 0
no significant difference in knowledge and awareness levels
between diploma holder and graduate nurses.
STUDY INSTRUMENT:
Based on the previous studies, available guidelines and
applicable rules, a structured questionnaire was formed.
Questionnaire was got validated out and pilot study was
conducted. Consent was obtained from the college.
Questionnaire consisted of two parts namely: respondent's
demographic profile and awareness on BMWMH rules.
Questionnaire was specifically framed to assess the clarity on
basic concepts behind the BMWMH.
SAMPLE SIZE AND SAMPLING:
All the nurses at the college were contacted and a cross
sectional study was performed. Pre-defined questionnaire was
distributed to all the nurses. They were met in small groups,
consent was obtained and study objectives were explained
while ensuring confidentiality of responses.
STATISTICAL ANALYSIS:
After the survey responses were fed in Microsoft Excel
software. Further assessment was done applying mean,
median, t-test using statistical package (SPSS, Ver.20).
RESULT :
Feedback was received from 240 nurses with females being
91% (n=291). Graduate nurses were 69% and the rest were
diploma (GNM) holders. It was found that almost all the
participants were in regular job and had been in the profession
for more than 1 year. No formal training was received by 16%
of them even though they had completed nursing studies
including diploma and graduation course and had been in job
for more than 1 year. Only 45% of the nurses had received
training session within last one year (Table 1).
Nurses trained by nursing incharges were 30% and by
administrators 37% (Table 2).
Before starting filling specific questions, respondents were
asked for self assessment (the first question of the
questionnaire) of their confidence on knowledge about the
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00006.7
29
Trainer
Administrator
BMW Coordinator
Faculty/Doctor/HOD
Infection Control Nurse
No Response
Nurse of that Area
Grand Total
Table 2 : Training Session Delivery Trends
N
90
18
18
30
42
42
240
%age
37.5
7.5
7.5
12.5
17.5
17.5
Table 3 : Pre Test Confidence Levels
Confidence
100%
75% to 100%
50% to 75%
< 50%
No Response
Grand Total
GNM
33
81
48
3
165
B.Sc
3
60
9
3
75
N
36
141
57
3
3
240
%
15.00
58.75
23.75
1.25
1.25
Table 1: Time When Last Trained/Orientation Session Delivered
Training in BMW
Never
< 1 year
> 1 year ago
No response
Total
n
39
108
75
18
240
%age
16.25
45.00
31.25
7.50
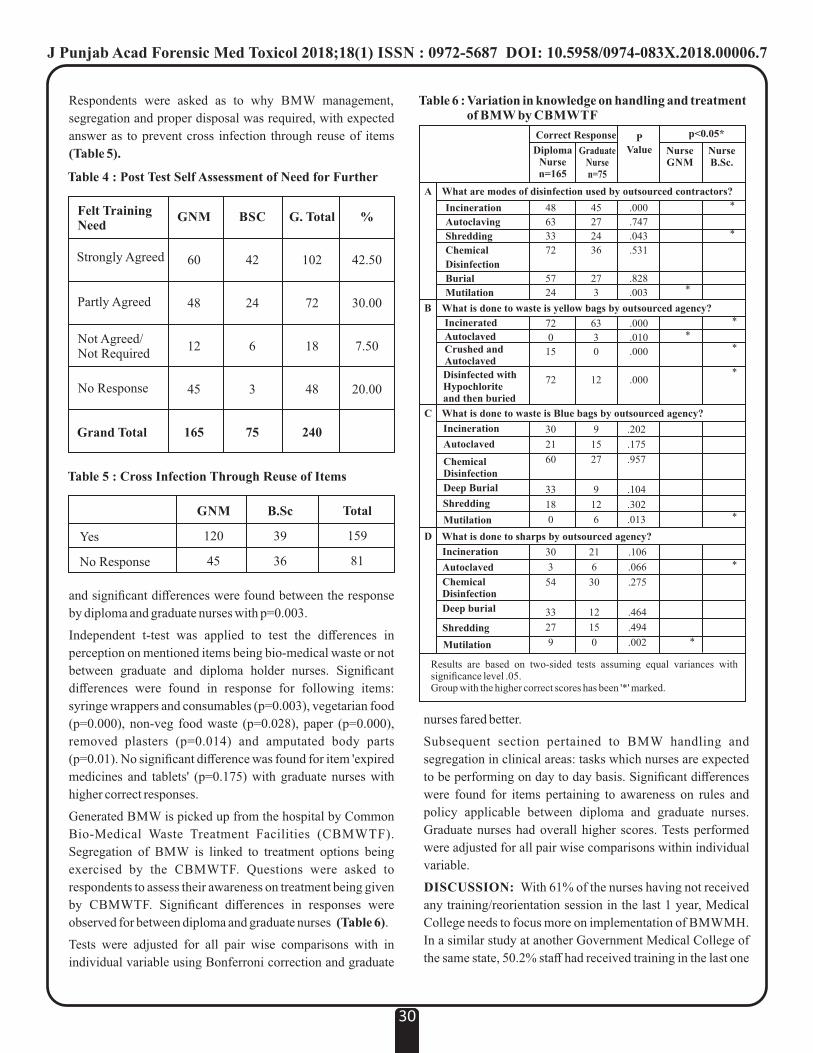
nurses fared better.
Subsequent section pertained to BMW handling and
segregation in clinical areas: tasks which nurses are expected
to be performing on day to day basis. Significant differences
were found for items pertaining to awareness on rules and
policy applicable between diploma and graduate nurses.
Graduate nurses had overall higher scores. Tests performed
were adjusted for all pair wise comparisons within individual
variable.
DISCUSSION: With 61% of the nurses having not received
any training/reorientation session in the last 1 year, Medical
College needs to focus more on implementation of BMWMH.
In a similar study at another Government Medical College of
the same state, 50.2% staff had received training in the last one
Table 6 : Variation in knowledge on handling and treatment of BMW by CBMWTF
Incineration
Autoclaving
Shredding
Chemical
Disinfection
Burial
Mutilation
What is done to waste is yellow bags by outsourced agency?
Incinerated
AutoclavedCrushed and Autoclaved
Disinfected with Hypochlorite and then buried
What is done to waste is Blue bags by outsourced agency?
Incineration
Autoclaved
Chemical Disinfection
Deep Burial
Shredding
Mutilation
What is done to sharps by outsourced agency?
Incineration
Autoclaved
Chemical Disinfection
Deep burial
Shredding
Results are based on two-sided tests assuming equal variances with significance level .05. Group with the higher correct scores has been '*' marked.
Correct Response
DiplomaNursen=165
GraduateNursen=75
PValue
p<0.05*
NurseGNM
NurseB.Sc.
What are modes of disinfection used by outsourced contractors?
Mutilation
A
B
C
D
48
63
33
72
57
24
45
27
24
36
27
3
.000
.747
.043
.531
.828
.003 *
*
*
72
0
15
72
63
3
0
12
.000
.010
.000
.000
*
*
*
*
30
21
60
33
18
0
9
15
27
9
12
6
.202
.175
.957
.104
.302
.013 *
*
*
30
3
54
33
27
9
21
6
30
12
15
0
.106
.066
.275
.464
.494
.002
Respondents were asked as to why BMW management,
segregation and proper disposal was required, with expected
answer as to prevent cross infection through reuse of items
(Table 5).
and significant differences were found between the response
by diploma and graduate nurses with p=0.003.
Independent t-test was applied to test the differences in
perception on mentioned items being bio-medical waste or not
between graduate and diploma holder nurses. Significant
differences were found in response for following items:
syringe wrappers and consumables (p=0.003), vegetarian food
(p=0.000), non-veg food waste (p=0.028), paper (p=0.000),
removed plasters (p=0.014) and amputated body parts
(p=0.01). No significant difference was found for item 'expired
medicines and tablets' (p=0.175) with graduate nurses with
higher correct responses.
Generated BMW is picked up from the hospital by Common
Bio-Medical Waste Treatment Facilities (CBMWTF).
Segregation of BMW is linked to treatment options being
exercised by the CBMWTF. Questions were asked to
respondents to assess their awareness on treatment being given
by CBMWTF. Significant differences in responses were
observed for between diploma and graduate nurses (Table 6).
Tests were adjusted for all pair wise comparisons with in
individual variable using Bonferroni correction and graduate
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00006.7
30
Table 5 : Cross Infection Through Reuse of Items
Yes
No Response
GNM
120
45
B.Sc
39
36
Total
159
81
Table 4 : Post Test Self Assessment of Need for Further
Felt Training Need
Strongly Agreed
Partly Agreed
Not Agreed/Not Required
No Response
Grand Total
GNM
60
48
12
45
165
BSC
42
24
6
3
75
G. Total
102
72
18
48
240
%
42.50
30.00
7.50
20.00

[6]year while the national average among tertiary care hospitals [1]has been reported at 66.7% . As shown in Table 2 structured
training programs were found to be lacking with some of the
nurses being trained by nurse trainers, some by faculty and rest
trained by administrators. There seemed to be no uniformity in
training/trainers pattern. It is possible that different
instructors/trainers have different teaching content: leading to
difference in opinions/perceptions among nurses. Training
programs had no fixed timing and schedule. On discussion
with the hospital head it was found that there was no defined
BMW coordinator, train the trainer program and thus no
uniformity in trainings. Felt training need were found to be
significantly more than the pretest confidence levels.
Questionnaire was designed specifically to assess the
conceptual clarity. Post test nurses realized that there is lot
more for them to know and be aware of. This possible gap is
likely to be due to deficient training programs which possibly
cover only portion of BMWMH and training being provided
on need to know basis only instead of comprehensive training.
Lack of clarity on overall picture limits the staff's decision
making ability which can result in lapses.Significant difference
was found in confidence levels of diploma and graduate nurses
with graduate nurses having higher confidence levels. This
difference can be attributed either to higher education status,
better curriculum of graduate course or better faculty of higher
education institutes. Pre test nurses assessed their awareness
levels at higher levels which could be based on their
assumption on knowledge of limited tasks which they have
been performing on day to day basis and post test they felt that
more information and training was required. Such difference
was found to be statistically highly significant (p=0.000) using
paired T-test. Gaps identified require to be bridged by
comprehensive training programs. Studies have shown
significant increase in awareness in the hospital setup after [7]training .
With respect to tasks being performed by CBMWTF graduate
nurses fared better and there were significant difference in the
knowledge levels. With little training programs at the current
work place (which shall be same for diploma and graduate
nurses), such difference can be attributed to their nursing
education curriculum. Items with significant differences
highlight and specify the portion of training program which
need to be covered better. Nursing curriculum has been found [5]to include teaching on BMWMH . Gaps in the training and
education programs as identified in the studies includes
training on management by CMBTF, colour coding for
segregation for uncommon items, logic behind color coding.
While it has been discussed above that there were significant
differences in diploma and graduate nurses. Yet it needs to be
noted that even if one of staff members has a different thought
then errors in the form of non-compliances are bound to
happen. The question that arises is how can there be variation
in practice within the same organization? This variation needs
to be dealt with by the HCO's to bring down their errors which
can result into non-compliances. Further structured induction
program is one solution should be mandatory in HCO's to
bring down variation rates within the organization.
CONCLUSION: Organizations need to define their standard
operating procedures for BMWMH. While the required
outcomes in terms of color coding have been defined under
BMWMH for ensuring uniformity in terms of colour coding of
bags and collection bins, what needs to be addressed is the
uniformity in implementation and forming Standard Operating
Procedures (SOP's). Organizations need to define their
training teams, train their trainers and empowering trainers
with sufficient material for information and educating staff
members on regular basis and through induction program.
Difference in SOP's and implementation plans among various
organizations may lead to confusion to employees switching
their jobs and students moving to another institution,
especially when subsequently joined organizations do not
conduct induction sessions. Medical college may be taking the
implementation of BMWMH heedlessly by being inadequate
in forming SOP's, structured training, implementation and
review programs. Scenario is likely to be same in other similar
institutions. Organizations not having structured training
teams and programs are likely to have non-compliances which
can be measured either by organizational audit or by assessing
the staff awareness levels. Training program should not be
limited to awareness on ward level functions but must be
comprehensive covering all aspects to improve nurse's
decision making skills. Success lies in imparting training while
medicos and paramedics are still students. Conceptual clarity
can help staff and students understand with reasoning thus
providing better knowledge, ability to correlate the rules and
act with organization policies and enabling them to take
informed decision in all situations.
Acknowledgement: We express our gratitude and thanks
towards all who have directly or indirectly helped us to
complete this study and to the participating respondents.
Limitations of the Study: 1. Individual bias of the
respondents. 2. Study being conducted at a single institution.
Conflict of interest: There is no conflict of interest.
REFERENCES:
1. INCLEN Program Evaluation Network (IPEN)
study group. Bio-medical waste management:
situational analysis & predictors of performances in
25 districts across 20 Indian States. Indian J Med Res
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00006.7
31

2 0 1 4 ; 1 3 9 ( 1 ) : 1 4 1 - 5 3 . A v a i l a b l e a t :
h t tp : / /www.ncbi .n lm.nih .gov/pmc/ar t ic les
/PMC3994730/#!po=83.3333.
2. Pandey A, Ahuja S, Madan M, Asthana AK. Bio-
Medical Waste Management in a Tertiary Care
Hospital: An Overview. Journal of Clinical and
Diagnostic Research 2016;10(11):DC01-3.
DOI:10.7860/JCDR/2016/22595.8822
3. Government of India. Ministry of Environment and
Forests Gazette Notification No.460, dated 27th July
1998, New Delhi , pp.10-20. Available at :
http://envfor.nic.in/legis /hsm/ biomed.html.
4. Government of India ministry of Environment,
Forest and Climate change, Notification dated 28th
March, 2016, New Delhi, pp.1-37. Published in the
Gazette of India, Extraordinary, Part II, Section 3,
Sub-section (i).
5. Chauhan AS, Chauhan SR, Pati S, Pati S. Teaching of
Biomedical Waste in India: A Mapping Exercise. Ntl
J Community Med 2016;7(5):386-90.
6. Verma V, Sharma ML, Oberoi S, Singh A.
Biomedical waste management at tertiary level
hospital–Rajindra Hospital [Government Medical
College], Patiala-A situational analysis. Int J Med
R e s R e v 2 0 1 6 ; 4 ( 1 1 ) : 2 0 5 4 - 8 .
doi:10.17511/ijmrr.2016.i11.26.
7. Sarotra P et al. Health care professional training in
biomedical waste management at a tertiary care
hospital in India. J Biomed Res 2016;30(2):168-70
8. World Health Organization (WHO). Wastes from
healthcare activities. Fact sheet No. 253, Geneva.
2009.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00006.7
32
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00007.9
Original Research Paper
Corresponding Author
Dr. Prashantha Bhagavath,
Forensic Advisor,
International Committee of the Red Cross, New Delhi
Contact : +91 94486-24014
Email : [email protected]
KEYWORDS : Suicide, Women, Reproductive age group, South India
Article History:Received: 2 April 2016Received in revised form: 30 April 2016Accepted on: 16 May 2016Available online: 1 July 2018
INTRODUCTION :
Suicide not only affects the single individual who takes his life,
but also his/her immediate circle community at large. It may be
anticipated that everyone during the “intolerable moments” in
his or her life will succumb to the idea to put an end to it all. In
fact suicidal thoughts, threats and attempted suicide are a [1]common human phenomena . Given the size of the
population, almost 30% of all cases of fatal deliberate self-
harm worldwide are seen in China and India. The number of
incidents of fatal deliberate self-harm in India is comparable to
those put together in the four European countries with the
highest number of fatal deliberate self-harm incidents (Russia,
[2]Germany, France and Ukraine) . More than one hundred
thousand people (1,25,017) in India lost their lives by
committing suicide during the year 2008 with an overall [3]suicide rate of being 10.8 per 100,000 population . Karnataka
state in South India had a suicide rate of 21.2/100000 which is [3]nearly double the national average for the year 2008 . These
statistics reveal that suicide is a major problem faced not just
by the developed world but even the developing countries.The
causes and methods of suicides vary greatly between males [4]and females . Though in absolute numbers more men commit
suicide than women, there are various complexities associated
with female suicides. Self-inflicted injuries accounts for 6-7%
A Study of Completed Suicide Among Women in the Reproductive Age Group From
Coastal Karnataka1. Haneil Larson D'Souza, Associate Professor*
2. Prashantha Bhagavath, Forensic Advisor, International Committee of the Red Cross, New Delhi
3. Francis NP Monteiro, Professor, Department of Forensic Medicine, A J Institute of Medical Sciences and Research Centre,
Mangalore
4. Tanuj Kanchan, Associate Professor, Department of Forensic Medicine, All India Institute of Medical Sciences, Jodhpur
5. Suresh Kumar Shetty, Professor and Head*
6. Jagadish Rao P.P, Associate Professor*
7. Pavanchand Shetty H, Associate Professor*
*Department of Forensic Medicine, Kasturba Medical College Mangalore, Manipal Academy of Higher Education
(M.A.H.E), Manipal
ABSTRACT :
Introduction: Though in absolute numbers more men commit suicide than women, there are various complexities associated with
female suicides. The studies on suicides among women based on whether or not they are in the reproductive age group may lead to
greater understanding of specific factors attributable to this particular sub-population of women.
Materials and Methods: Women in the reproductive age group who died as a result of fatal deliberate self-harm were autopsied at
the Department of Forensic Medicine, Kasturba Medical College, Manipal during January 2010 and September 2011.
Results: 44 women suicides were included. Thirty-one of the victims (70%) were aged above 19 years (adults) and 13 (30%) were
adolescents. In 11 cases (25%) the motive was either not mentioned or could not be ascertained. Out of the remaining 33 victims,
the most common reason for committing suicide was health related issues (n=16). Among the suicide methods, poisoning was the
most common, seen in 28 of the victims (64%). In 41 cases (93%) the place of occurrence of the incident was indoors. Thirty of the
victims (68%) were hospitalised after the suicide attempt.
Conclusion:It is recommended that psychiatric assessment should be considered for women with chronic and vague symptoms of
ill health not responding to treatment, as a possible manifestation of the underlying psychiatric disease, which then turns into the
primary motive for suicide for women in the reproductive age group.
33
of all the deaths worldwide in females in the age group between [5-6]fifteen and forty-four years . It has been observed that
economic and social influences and factors have led most
Indian males to commit suicide. The situation is different
among women. Emotional and personal causes have been the
main contributors to incidents of fatal deliberate self-harm in [3]Indian women . Women specific factors include societal
influences; marital status and stressors associated with it,
failed relationships, socio-economic inequality are just a few [7] of the factors that influence suicidal behaviour in women .The
proportion of female victims by 2008 in India was
comparatively more under the heads 'Dowry Dispute' (98.1%),
'Illegitimate Pregnancy' (91.6%), 'Physical Abuse (Rape,
Incest etc.)' (72.8%), 'Barrenness/Impotence (Not having
children)' (65.5%), 'Divorce' (62.2%),'Cancellation/Non-
settlement of marriage' (53.5%) and 'Suspected/Illicit
Relations' (50.8%). The present research was undertaken to
study the factors affecting completed suicides among the
women in the reproductive age group from a coastal region of
South India.
MATERIALS AND METHODS :
The material for the study comprised of cases involving
women in the reproductive age group (from onset of
menarche till menopause) who died as a result of fatal
deliberate self-harm and whose autopsies were performed at
the mortuary of the Department of Forensic Medicine,
Kasturba Medical College, Manipal during January 2010 and
September 2011. The confirmation of the reproductive age
group was based on correlation of age and histological features
of the uterus in the reproductive age group. Women outside the
reproductive age group, and cases wherein the manner of death
was in doubt were excluded from the study. Data regarding age
of the victim, date of suicidal attempt, method adopted to
commit suicide, place of occurrence, whether hospitalized or
not, the date of death and survival period were collected from
the information furnished by the Karnataka State Police and
the hospital records of Kasturba Hospital, Manipal.
RESULTS :
During the study period, a total of 44 women who were in the
reproductive age group as confirmed from histological
examination of the uterus were included in the study. Thirty-
one of the victims (70%) were adults over the age group of 19
years and 13 of the victims (30%) were adolescents (Table
No.1).
The youngest victim was 11 years old and the oldest victim was
48 years. The motive behind the suicides are shown in Table
No. 2.
In 11 cases (25%) the motive was either not mentioned or could
not be ascertained. Out of the remaining 33 victims, the most
common reason for committing suicide was health related
issues as reported in 16 victims (36%). In two victims the
health related issue was specific to uterine pain. In one case, it
was stated that the victim could not cope with the health
problems of her husband. The next most common motive for
committing suicide was relationship related issues among
eight victims (18%). For relationship related issues, three
victims cited reasons of loneliness due to the loss of/ being
away from a loved one. Three victims were involved in failed
romantic relationships; while one victim cited family discord
and the other marital discord as the motives behind the suicide.
Six victims (14%) committed suicide due to either
frustration/depression. The underlying reason for the
frustration/depression was not mentioned/ could not be
ascertained. For two victims (5%), the suicide was a result of
academic failure and one victim (2%) committed suicide as a
result of being unemployed and unable to find work.
Among the methods of fatal deliberate self-harm adopted by
the victims, poisoning was the most common, seen in 28 of the
victims (64%) as shown in Table 3.
The next most common method adopted was hanging in10
victims (23%). Four of the victims (9%) died due to self-
immolation. One victim (2%) resorted to being run over by a
train while in another (2%) the method was fall from height.
In 41 cases (93%) the place of occurrence of the incident was
34
Table No. 2 : Motive for Suicide
Motive Number (n=44)
Motive unascertainable
Heath related issues
Relationship related issues
Depression/Frustration
Academic
Unemployment
11 (25%)
16 (36%)
8 (18%)
6 (14%)
2 (5%)
1 (2%)
Table No. 1: Age Distribution of the Study Group
11-19 years 20-48 years Total (n=44)
13 (30%) 31 (70%) 44 (100%)
Table No. 3 : Methods Adopted by the Victim
Poison consumption
Hanging
Self-immolation
Run over by a train
Fall from height
Method adopted Number (Total n = 44)
28 (64%)
10 (23%)
4 (9%)
1 (2%)
1 (2%)
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00007.9

indoors while in three cases (7%) it was outdoors. Thirty of the
victims (68%) were hospitalized while the other 14 (42%)
were not. Of the hospitalized patients, 25 of the admitted cases
(83%) were after consumption of poison, hanging accounted
for three (10%) and the self-immolation for two cases (7%).
Information regarding time interval between suicide attempt
and death i.e. the survival period could only be ascertained for
admitted cases. Among the cases admitted after poison
consumption the minimum period of survival was a couple of
hours and the maximum period of survival was 17 days. In the
three hospitalized hanging cases, one victim survived for a
couple of hours and another survived for five days. Among the
two cases admitted for burn injuries following self-
immolation, the period of survival was five days and eight
days, respectively.
DISCUSSION :
The main gender difference seen in suicidal behavior
worldwide, is that the rate of completed suicides in women are [9]lower than men, the exception being China .The same is true
in India as well. However the reported sex ratio of 4:5.8 in [10,11]India is low when compared internationally . The reasons
[10,12]for this seem to be diverse . The higher suicide rate in the
male gender has been stated, as being due to the more rigorous
subjection of men variations and stressors of daily living and [13,14]life when compared to females . Suicide is best studied and
researched as a multi-factorial event, with biological,
relationship, psychological, social and cultural factors, to [10,15,16]name just a few .
According to an earlier analysis of the National Crime Records
Bureau, fatal deliberate self-harm is among the top ten causes
of death in India. Fatal deliberate self-harm is also among the
top three causes of death in India between the ages of sixteen [17]and thirty-five . It can therefore be deduced from the present
study that people in the early stages of their lives are more
predisposed to getting affected by the turmoil of life. They
then unfortunately opt for self-harm over trivial issues.
It is known that the mortality risk for fatal deliberate self-harm
associated with a psychiatric illness such as depression is many [18]times the risk faced by the general population . The WHO
suicide statistics suggest that mental disorders (depression and
substance abuse) are associated with more than ninety percent
of all cases of suicide. Also psychological autopsy approach to
death investigation has revealed that psychiatric disorders are
present in about ninety percent of people who are victims of
fatal deliberate self-harm. These people also contribute
between forty-seven to seventy-four percent of the population [19]at risk of suicide . So also a study in Wolverhampton
ascertained a positive psychiatric history in 64.5% cases of [20]suicide . Our findings are in contrast to the findings observed
by the above-mentioned workers wherein the health related
issues dominated followed by relationship related issues,
frustration/depression, academic failure and unemployment.
This lower incidence of depression, a well-documented and
researched risk factor for destructive self-harm worldwide has
been previously documented in poisoning self-destructive [21 ]mortalities in the region . In India, studies using
psychological autopsies have reported that suicide is related to
interpersonal conflicts, marital discord, alcoholism, financial [22]problems and unemployment . A study undertaken in
Singapore also ascertained that illness (51%) was the [23]predominant factor associated with suicide . However the
study included both physical and mental illness as a single
entity.With regards to the suicide with unemployment as the
motive, suicide rates are high in people without gainful
employment.The reasons for this relationship are however [12]complex . As previously mentioned, high rates of suicide are
associated with mental illness. Mental illness can thus be seen [24]as a common factor of both unemployment and suicide .
Among the methods of fatal deliberate self-harm adopted by
the victims, poisoning was the most common, followed by
hanging, self-immolation etc. This is in agreement with the
study done by Banerjee et al which stated that poisoning with
insecticides was the most common mode of suicide among [25]Indian women . This also in accordance of the fact that as a
generalization, men may be said to have a tendency to choose
more violent means of self-destruction (such as shooting).
Women on the other hand may be seen to prefer less violent [26]methods to end their lives (such as poisoning) . It has been
observed that in the less developed and agricultural hinterland
of many developing countries, intake of pesticides is the
method of choice for self-destruction. This may be due to the
perceived advantages of easy availability, enhanced toxicity [27]and poor storage . As many as thirty percent of global self-
[27]destruction deaths might involve intake of pesticides . In
concurrence of our findings, females of Geneva, Brazil and
Israel adopted common methods like poisoning and fall from [28-30]height for committing suicide . It has been observed in the
Southern Part of India and in countries like Pakistan, Japan,
Austria and England that the commonest method used by [31-35]females for committing suicide was by hanging . Chao et al,
in their study on changing trends of suicide by poisons in
Singapore, points out that until the early sixties, corrosive
acids and alkali, inorganic chemicals, heavy metals and plant [36]alkaloids were the mainstay of poisons principally used . The
seventies and eighties witnessed a swing towards
pharmaceutical products. The early nineties saw a peak of
alcohol, insecticides such as malathion, paraquat and [36]household items such as detergents, and antiseptics .
According to the study conducted by Bhatia et al and Agarwal
35
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00007.9
et.al, the common methods used in suicide include drowning, [37-38]hanging, poisoning and burning . Methods of self-
destruction and self-harm can be said to echo the availability of
these methods. Pattern of self-destruction in the vicinity
depends upon a multitude of factors and their interplay. These
include obtainability and access of the method, the socio-
economic status and also not to forget the prevailing socio-
religious influences. Knowing the pattern of suicide in an area
not only helps in early management of such cases but also [39]allows taking early preventive measures . Forty one out of
forty four females preferred to commit suicide inside the four
walls of the house. This high incidence at home can be
attributed to the preference of the victims for a familiar home
environment. This is in agreement with a study reported from [33]Southern India .
It is necessary for the death investigators to be knowledgeable
of the many scenarios, stressor and risk factors, methods,
methodology as well as deterrents that may be encountered in
investigating such incidents. We recommend psychiatric
assessment for women with chronic and vague symptoms of ill
health not responding to treatment, as a possible manifestation
of underlying psychiatric disease. Left untreated or
misdiagnosed, many women may be committing suicide for
manageable psychiatric conditions.
REFERENCES :
1. Retterstol N. Suicide: A European Perspective.
Cambridge: University Press; 1990.p.1-20.
2. Bertolote JM, Fleischmann A. A global perspective in
the epidemiology of suicide. Suicidologi 2002; 7(2): 6-
8.
3. National crime records bureau. Accidental deaths and
suicides in India: ADSI. 2008. Available from:
http://ncrb.nic.in/accdeaths.htm[accessed on 2011
Sept30].
4. Kanchan T, Menon A, Menezes RG. Methods of choice
in completed suicides: gender differences and review
of literature. J Forensic Sci. 2009;54:938-42.
5. World Health Organisation. Facts and Figures about
suicides. Geneva: WHO; 1999.
6. Monk M. Epidemiology of suicide. Epidemiol Rev
1987; 9:51-69. 11.
7. Roy A. Suicide. Baltimore: Williams & Wilkins;
1986.p.17-40.
8. Young people's health: a challenge for society. Report
of a Study Group on Young People and Health for All
by the Year 2000, Technical Report Series. Geneva:
World Health Organization; 1986.p.11-12.
9. Philips MR, Liu H, Zhang Y. Suicide and social change
in China. Cult Med Psychiatry 1999; 23(1):25-50.
10. World Health Organisation. World report on violence
and health. Geneva: WHO; 2002.
11. Girdhar S, Leenaars AA, Dogra TD, Leenaars L,
Kumar G. Suicide notes in India: what do they tell us?
Arch Suicide Res 2004; 8:179-85.
12. Hawton K, Van Heeringen K. The international
handbook of suicide and attempted suicide. Chichester:
Wiley; 2000.
13. Stack S. Suicide: a 15 year review of the sociological
literature. Part II: modernization and social integration
perspectives. Suicide Life Threat Behav 2000; 24:
362–74.
14. Girard C. Age, gender and suicide: a cross national
analysis. Am Sociol Rev 1993; 58: 553–74.
15. Shneidman E. Definition of suicide. New York: John
Wiley & Sons; 1985.p.6-26.
16. Leenaars A. Psychotherapy with suicidal people.
Chichester: Wiley; 2004.
17. Vyas JN, Ahuja N. Text book of Postgraduate
Psychiatry. New Delhi: Jaypee Brothers Medical
Publishers; 1999.p.527-550.
18. Harris EC, Barraclough B. Excess mortality of mental
disorder. Br J Psychiatry 1998; 173: 11–53.
19. Cavanagh JTO, Carson AJ, Sharpe M, Lawrie SM.
Psychological autopsy studies of suicide: a systematic
review. Psychol Med 2003; 33: 395–405.
20. Scott KW Suicide of Wolverhampton (1976-1990).
Med Sci Law 1994; 34 (2), 99-105.
21. Kanchan T, Menezes RG. Suicidal poisoning
mortalities in Southern India: gender differences. J
Forensic Legal Med 2008; 15 :7–14.
22. Gururaj G, Isaac MK, Subbakrishna DK, Ranjani R.
Risk factors for completed suicides: a case–control
study from Bangalore, India. Inj Control Saf Promot
2004; 11:183–91.
23. Peng KL, Choo AS. Suicide in Singapore, 1986. Aust
NZ J Psychiatry 1992; 26 (4): 599-608.
24. B l a k e l y TA , C o l l i n g s S C D , A t k i n s o n J .
Unemployment and suicide: evidence for a causal
association? J Epidemiol Community Health 2003; 57:
594–600.
25. Banerjee G, Nandi DN, Nandi S, Sarkar S, Boral GC,
Ghash A. The vulnerability of Indian women to suicide:
a field study. Indian J Psychiatry 1990; 32:305–8.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00007.9
36
26. Denning DG, Conwell Y, King D, Cox C. Method
choice, intent, and gender in completed suicide.
Suicide Life Threat Behav 2000; 30: 282–88.
27. Gunnell D, Eddleston M, Phillips MR, Konradsen F.
The global distribution of fatal pesticide self-
poisoning: systematic review. BMC Public Health
2007; 7: 357.
28. La Harpe R. Suicide in the Geneva canton (1971-1990).
An analysis of the forensic medicine autopsy sample.
Arch Kriminol 1995; 195(3-4): 65-74.
29. Leon ML, Barros MB. Suicide mortality: gender and
socio-economic differences. Rev Sande Publica 2003;
37 (3), 357-63.
30. Nachman R, Yanai O, Goldin L, Swartz M, Barak Y,
Hiss J. Suicide in Israel: 1985-1997. J Psychiatry Neuro
Sci 2002; 27 (6): 423-8.
31. Saeed A, Bashir MZ, Khan D, Iqbal J, Raja KS,
Rehmon A. Epidemiology of suicide in Faisalabad. J
Ayub Med Coll Abbottabad 2002; 14 (4):34-7.
32. Yamamoto Y, Yamada M, Fukunaga T, Tatsuno V.
Statistical studies on suicides in Shiga Prefecture
during the 15-year period, 1974 to 1988. Nippon
Hoigaku Zasshi 1990; 44 (2), 190-8.
33. Namboodiri VMD.Conscise Text book of Psychiatry. nd2 ed. New Delhi: Reed Elsevier India Private Ltd;
2005.p. 292-30.
34. Etzersdorfer E, Fischer P, Sonneck G. Epidemiology of
suicide in Austria 1980 to 1990. Wien Klin Wochenschr
1992; 104(19): 594-9.
35. Cooper PN, Milroy CM. Violent suicide in South
Yorkshire, England. J. Forensic Sci 1994; 39 (3):657-
67.
36. Chao TC, Danny ST, Bloodworth BC. Common
poisons in Singapore- Past & present. Med Sci
Law1992; 32 (2): 139-147.
37. Aggawal NK, Bhatia MS, Aggarwal BBL. Pattern of
suicide in North East Delhi. Indian J Soc Psychiatry
1994; 10: 20-22.
38. Bhatia MS, Aggarwal NK, Aggarwal BBL. Pattern of
suicide ideators, attempted suicide & completed
suicide in a tertiary care teaching hospital. Indian Pract
1998; 51: 776-780.
39. Kumar A, Krishan Vij. Trends of poisoning in
Chandigarh - A six year autopsy study. Journal of
Forensic Medicine & Toxicology 2001; 18(1); 8-11.
37
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00007.9

J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00008.0
An Alternative Method for Extraction and Cleaning of Bones From Buried Cadavers 1. Monika Gupta, Professor, Anatomy*
2. Parmod Goyal, Professor & Head, Forensic Medicine*
3. Navita Aggarwal, Professor & Head, Anatomy*
*Adesh Institute of Medical Sciences & Research (AIMSR), Bathinda (Punjab)
Original Research Paper
Corresponding Author
Dr. Parmod Goyal,
Professor & Head, Forensic Medicine
Adesh Institute of Medical Sciences & Research, Bathinda
(Punjab)
Contact No. : 98760-05211
E-mail : [email protected]
KEYWORDS : Extraction, Cleaning, Bones, Burial, Buried bodies
Article History:Received: 7 March 2018Received in revised form : 8 June 2018Accepted on: 8 June 2018Available online: 1 July 2018
INTRODUCTION :
The human bones are an integral tool in the study of anatomy.
Bones are necessary not only for teaching anatomy but also
provide three dimensional instructions in osteology as well as
understanding the sites of soft tissue insertion and the course of
neurovascular structures in a region. Knowledge of bones also
required for planning of various surgeries and assessing the [1-2]efficacy of orthopaedic devices .
In the absence of original human bones, artificial bones made
of plaster of paris or glass fibre or plastic replica are used in
many health care institutions, which do not provide the actual
picture especially of bone ridges/elevations/tubercles etc but at [1-2]the same time too much costly . The source of original
human bones is human bodies only. With the efforts of many
Non Governmental Organisations (NGO’s) and inclusion of
voluntary body donation clause in the Anatomy acts,
successful Body donations programmes are running in many
medical institutions of the country. As a result many medical [3]institutions are receiving even excess of cadavers . But it has
been seen that even in such medical instituitions, sufficient
number of dry bones are not available for studying, for First
Year MBBS students, orthopedics faculty, post graduate
students , ENT surgeons and oral and maxillofacial surgeons.
If a first year mbbs student has dry bones in his hostel room, it
help in better understanding of anatomical structures
especially of limbs and head and neck.
The insufficient number of dry bones is due to absence of any
guidelines for extraction of bones from cadavers. Bones
require soft tissue removal, bleaching and colouring before
being used for teaching purpose. Various methods mentioned
in literature for bone cleaning are boiling, maceration, use of [4-11]enzymes, insect and burial excavation etc . We have used the
burial excavation method. In our institute authors had [2]conducted a previous study and found use of hydrogen
peroxide as a useful tool for cleaning of bones. But over a
period of time, authors felt that although cleaning of bones
with hydrogen peroxide is a good method but many times
especially in long bones and skull, small tag of soft tissue
remain intact and over times some part of bones become
brittle.So we experimented with an alternative method of bone
cleaning. Although present method is lengthy, more time
consuming and required comparatively more hard work but the
ultimate recovered bones were more clean, completely devoid
of soft tissues, more appealing to the eyes and nice to touch.
38
ABSTRACT :
Introduction : Bones are required for studying the human anatomy, osteology etc. Artificial available bones are costly and do not
bear expressions.Various methods of extraction and cleaning are in use. In the present study method adopted at our institute is
shared.
Methodology : Dissected bodies were buried in the burial ground attached to anatomy department. Remains were extracted after
one year. cleaned with water and brush followed by immersion in H O . followed by rinsing in water, drying in shade followed by 2 2
varnishing and colouring.
Results: Obtained bones were free from flesh and smell. Varnishing and colouring gave more better picture.
Conclusion: Method is lengthy and tedious and required lot of hard work but resultant bones were in good condition.
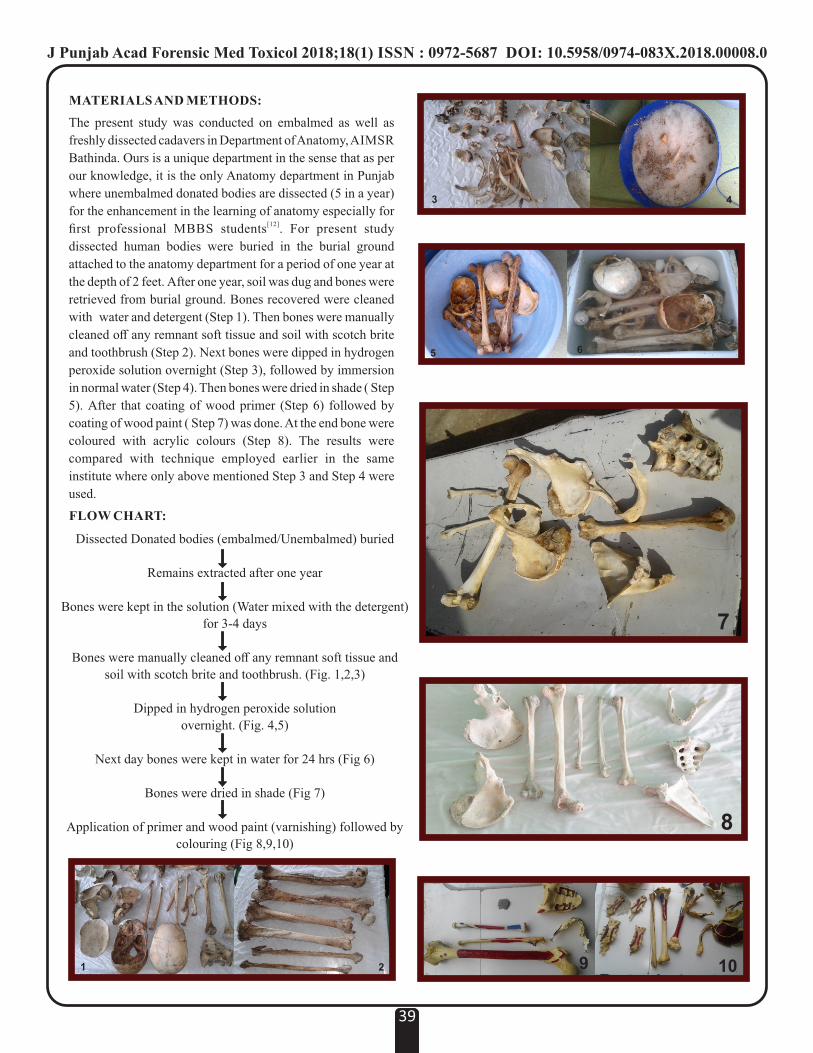
MATERIALS AND METHODS:
The present study was conducted on embalmed as well as
freshly dissected cadavers in Department of Anatomy, AIMSR
Bathinda. Ours is a unique department in the sense that as per
our knowledge, it is the only Anatomy department in Punjab
where unembalmed donated bodies are dissected (5 in a year)
for the enhancement in the learning of anatomy especially for [12]first professional MBBS students . For present study
dissected human bodies were buried in the burial ground
attached to the anatomy department for a period of one year at
the depth of 2 feet. After one year, soil was dug and bones were
retrieved from burial ground. Bones recovered were cleaned
with water and detergent (Step 1). Then bones were manually
cleaned off any remnant soft tissue and soil with scotch brite
and toothbrush (Step 2). Next bones were dipped in hydrogen
peroxide solution overnight (Step 3), followed by immersion
in normal water (Step 4). Then bones were dried in shade ( Step
5). After that coating of wood primer (Step 6) followed by
coating of wood paint ( Step 7) was done. At the end bone were
coloured with acrylic colours (Step 8). The results were
compared with technique employed earlier in the same
institute where only above mentioned Step 3 and Step 4 were
used.
FLOW CHART:
39
1 2
3 4
5 6
7
8
9 10
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00008.0
Dissected Donated bodies (embalmed/Unembalmed) buried
Remains extracted after one year
Bones were kept in the solution (Water mixed with the detergent)
for 3-4 days
Bones were manually cleaned off any remnant soft tissue and
soil with scotch brite and toothbrush. (Fig. 1,2,3)
Dipped in hydrogen peroxide solution
overnight. (Fig. 4,5)
Next day bones were kept in water for 24 hrs (Fig 6)
Bones were dried in shade (Fig 7)
Application of primer and wood paint (varnishing) followed by
colouring (Fig 8,9,10)
RESULT :
The bones obtained after this procedure were clean, intact and
their quality was better compared with the bones extracted
with previous technique. Application of wood primer resulted
in consumption of less amount of wood paint so the cost
involved in cleaning got reduced.
LIMITATIONS :
Since the wood primer was of white colour, Resultant bones
seem to be of white colour. Next time we shall try to procure
transparent wood primer.
CONCLUSION :
Although the procedure may appear to be labour requiring but
it is comfortable, cost effective, ecofriendly and suitable
method for obtaining the human bone specimens from the
cadavers. Bones obtained looked good, strong and suitable for
teaching purpose.
ACKNOWLEDGEMENT :
l The Families and the deceased for donating the bodies for
noble contributions toward the mankind.
l Dera Saccha Sauda Sirsa organization and Taraksheel
Society, Punjab for motivating peoples regarding
voluntary body donations.
l Management and Staff of Adesh University for their
continuous support, guidance and encouragement.
REFERENCES:
1. Modi B S, Puri N, Patnaik VVG. Evaluation of
Techniques for Cleaning Embalmed Cadaver Bones. Int J
Anat Res 2014; 2(4):810-13.
2. Aggarwal N, Gupta M, Goyal P K, Kaur J. An Alternative
Approach to Bone Cleaning Methods for Anatomical
Purposes. Int J Anat Res 2016; 4(2):2216-21.
3. Goyal P K, Monika G. Study of the profile of cadavers
donated to the Anatomy Department of a Private Medical
College of Punjab for Medical Research vis a vis Body
Donation Programme. A First Hand Experience of Five
Years, Journal of Research in Medical Education &
Ethics. 2011;1(3):176-9.
4. Cleaning methods - SEABIRD OSTEOLOGY.
Available from: http://www.shearwater.nl/index.php?
file= kop131. php. (last accessed on 20 April 2018).
5. Mair S, Swift B. Detergent An Alternative Approach to
Traditional Bone Cleaning Methods for Forensic Practice.
Am J Forensic Med Pathol. 2004; 25(4):276- 84.
6. Simonsen KP, Rasmussen AR, Mathisen P, Petersen H,
Borup F. A Fast Preparation of Skeletal Materials Using
Enzyme Maceration. J Forensic Sci 2011; 56(2):480-4.
7. Motz VA ,Garner , Schultz B. Defleshing of Embalmed
Human Cadaveric Bone in situ. Available from http:/
/www.lifescitrc.org/resource.cfm? submissionID =2230
(last accessed on 20 April 2018).
8. Sullivan LM, Romney CP. Cleaning and Preserving
Animal Skulls. The University of Arizona-A Cooperative
E x t e n s i o n . A v a i l a b l e f r o m h t t p : / /
extension.arizona.edu/sites/extension.arizona.edu/
files/pubs/az1144.pdf (last accessed on 20 April 2018).
9. Fenton TW, Birkby WH, Cornelison J. A fast and safe
non-bleaching method for skeletal preparation. J Forensic
Sci.2003;48:274-6.
10. Mishra S Rj, Singh R, Shukla R, Passey J, Singh S,
Sushobhana. Burial, Excavation and Chemical Cleaning -
An Economical Approach for Extraction of Human Bones
from Embalmed Dissected Cadavers in India.
International Journal of Anatomy, Radiology and Surgery
2016;5(3): 14-18
11. Okada DM, De Sousa AM, Huertas RA, Suzuki FA.
Surgical simulator for temporal bone dissection training.
Braz J Otorhino laryngol. 2010;76:575–78. ( Plastic
replica)
12. Goyal PK, Gupta M, Kaur J.Autopsy as a tool for learning
gross anatomy during 1st year MBBS. Int J Appl Basic
Med Res. 2016;6(3): 230–32.
40
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00008.0

J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00009.2
For Ethical Doctors: Does selection process for Medical students require a change?1. Mrinal Kanti Jha, Associate Professor*
2. Jagadish Biswas, Assistant Professor Department of Forensic Medicine and Toxicology, North Bengal Medical College,
Sushruta Nagar, Darjeeling. West Bengal.
3. Tilak Bose, Administrative Officer, IIM Rohtak
4. Shyam Sekhar Choudhury, Demonstrator*
*Department of Forensic Medicine and Toxicology, KPC Medical College. Jadavpur, Kolkata 700032
Original Research Paper
Corresponding Author
Dr. Jagadish Biswas,
Assistant Professor
Department of Forensic Medicine and Toxicology, North
Bengal Medical College, Sushruta Nagar, Darjeeling.
KEYWORDS : Ethical Doctor, Restructure of selection process for Medical students, Reducing unethical practice by doctors.
Article History:Received: 26 May 2018Received in revised form: 18 June 2018Accepted on: 18 June 2018Available online: 1 July 2018
INTRODUCTION:
There has been a rise in unethical practices by doctors. These
have been brought to light by the print and electronic media,
and have given rise to an atmosphere of scepticism in society.
Doctors are probably no longer considered noble professionals
or healers who would always do the patient good. Rather, they
are service providers, and the patients the service users. This
change may have come about partly because of the corrupt and
unethical practices of a few doctors, resulting in a loss of trust [1]in the doctor–patient relationship .
Some of disturbing recent news include: June 10, 2017-Doctor
injured in nursing home attack after patient's death, Aug
13,2015-2 junior doctors beaten up at SSKM Hospital, Jan
11,2016-A PG trainee at R G Kar admitted in ICU after he was
assaulted by a mob, Jun 22,2016- Junior doctor assaulted at
SSKM Hospital, Mar 24, 2017- Doctors attacked at RG Kar
Medical College, Feb 15, 2017-Mob vandalism at CMRI [2]Hospital . The attacks on doctors are more due to lack of
doctor-patient relationship or understanding of medical ethics
than anything else.
It is expected that the principles of ethics would either come
from within or that budding doctors would imbibe morality
from parents at home.Among the earliest influences on child
behaviour are the attitudes and behaviours of the parents.
Therefore, parental behaviours have a strong influence on
children. Studies have shown that parental and environmental
influences have a significant role in promoting pro-social [3]behaviours among children . Parental role has a significant
influence on moral values of children.
Ethics is moral conduct of right and wrong in a civil society,
which comes from within. It is a branch of Philosophy.
Medical Ethics guides doctors in dealing with their patients,
for the best possible outcome. Unlike Law which is enforced
on an individual after commission of crime, ethics prevents
individual from committing wrong. As per Definition:
Medical ethics deals with moral principles which should
guide the members of medical profession, in dealing with [4]each other, with patients and with the state . India can boast
41
ABSTRACT:
Introduction: There is an increase in unethical practice by doctors, which is widely, publicized both by electronic and print media.
This is due to lack of understanding of Medical ethics or moral values involved in doctor-patient relationship. One of the methods to
reduce unethical practice can be selection of medical students based on core ethical knowledge as was done in ancient India.
Objective: To evaluate core ethical knowledge among medical students, before ethics is taught to them in class by teachers and find
out means to recruit medical students who are sound in ethics for future ethical doctors.
Material and Method: An anonymised, questionnaire-based, cross-sectional survey of students.
Result: 51.80% of students in the study had core ethical knowledge.
Conclusion: If all selected students have core ethical values and knowledge, unethical practice by doctors will automatically
diminish. Ancient India had stringent selection process for pupils who were admitted as medical students,they were honest,
humble, temperate, generous. This is practiced in medical schools across US and Europe. This is high time we should change the
process of selection to prevent unethical practices and revert to selection of students as was done in ancient India.
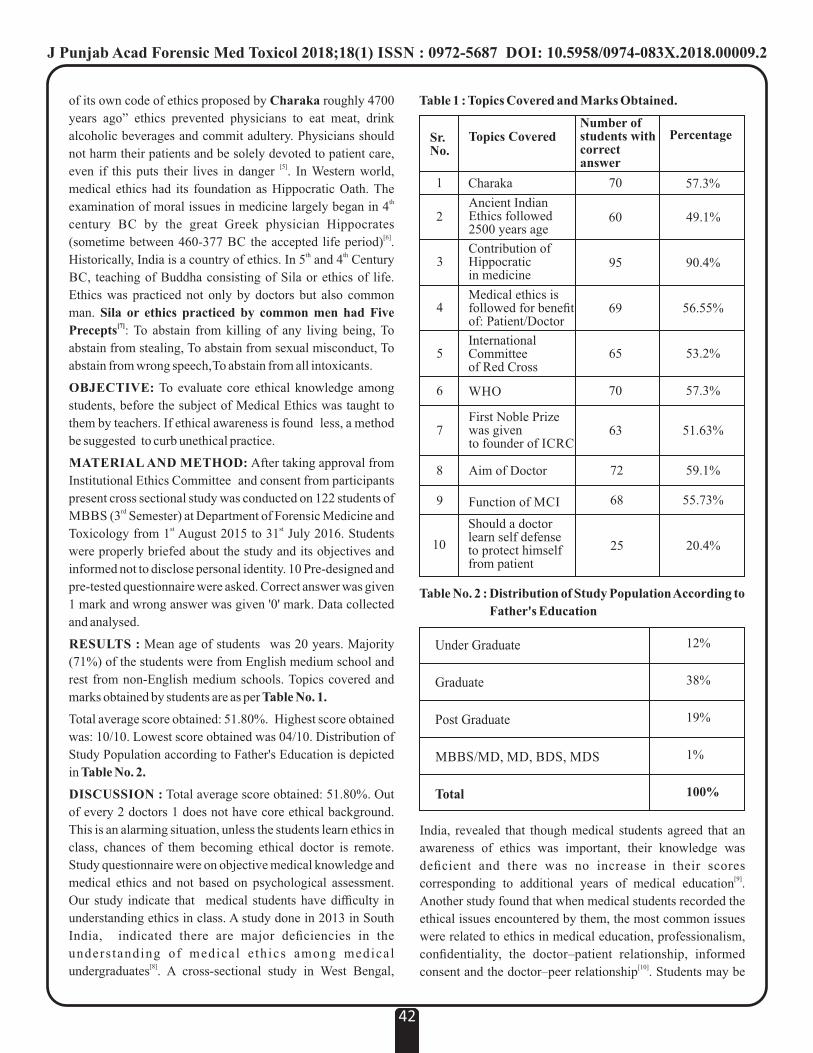
Table 1 : Topics Covered and Marks Obtained.
Charaka
Ancient Indian Ethics followed 2500 years age
Contribution of Hippocratic in medicine
Medical ethics is followed for benefit of: Patient/Doctor
International Committee of Red Cross
WHO
First Noble Prize was given to founder of ICRC
Aim of Doctor
Function of MCI
Should a doctor learn self defense to protect himself from patient
1
2
3
4
5
6
7
8
9
10
Topics Covered
70
60
95
69
65
70
63
72
68
25
Number of students with correct answer
57.3%
49.1%
90.4%
56.55%
53.2%
57.3%
51.63%
59.1%
55.73%
20.4%
PercentageSr.No.
of its own code of ethics proposed by Charaka roughly 4700
years ago” ethics prevented physicians to eat meat, drink
alcoholic beverages and commit adultery. Physicians should
not harm their patients and be solely devoted to patient care, [5]even if this puts their lives in danger . In Western world,
medical ethics had its foundation as Hippocratic Oath. The thexamination of moral issues in medicine largely began in 4
century BC by the great Greek physician Hippocrates [6](sometime between 460-377 BC the accepted life period) .
th thHistorically, India is a country of ethics. In 5 and 4 Century
BC, teaching of Buddha consisting of Sila or ethics of life.
Ethics was practiced not only by doctors but also common
man. Sila or ethics practiced by common men had Five [7]Precepts : To abstain from killing of any living being, To
abstain from stealing, To abstain from sexual misconduct, To
abstain from wrong speech, To abstain from all intoxicants.
OBJECTIVE: To evaluate core ethical knowledge among
students, before the subject of Medical Ethics was taught to
them by teachers. If ethical awareness is found less, a method
be suggested to curb unethical practice.
MATERIAL AND METHOD: After taking approval from
Institutional Ethics Committee and consent from participants
present cross sectional study was conducted on 122 students of rdMBBS (3 Semester) at Department of Forensic Medicine and
st stToxicology from 1 August 2015 to 31 July 2016. Students
were properly briefed about the study and its objectives and
informed not to disclose personal identity. 10 Pre-designed and
pre-tested questionnaire were asked. Correct answer was given
1 mark and wrong answer was given '0' mark. Data collected
and analysed.
RESULTS : Mean age of students was 20 years. Majority
(71%) of the students were from English medium school and
rest from non-English medium schools. Topics covered and
marks obtained by students are as per Table No. 1.
Total average score obtained: 51.80%. Highest score obtained
was: 10/10. Lowest score obtained was 04/10. Distribution of
Study Population according to Father's Education is depicted
in Table No. 2.
DISCUSSION : Total average score obtained: 51.80%. Out
of every 2 doctors 1 does not have core ethical background.
This is an alarming situation, unless the students learn ethics in
class, chances of them becoming ethical doctor is remote.
Study questionnaire were on objective medical knowledge and
medical ethics and not based on psychological assessment.
Our study indicate that medical students have difficulty in
understanding ethics in class. A study done in 2013 in South
India, indicated there are major deficiencies in the
unders tanding of medical e thics among medical [8]undergraduates . A cross-sectional study in West Bengal,
42
Under Graduate
Graduate
Post Graduate
MBBS/MD, MD, BDS, MDS
Total
12%
38%
19%
1%
100%
Table No. 2 : Distribution of Study Population According to
Father's Education
India, revealed that though medical students agreed that an
awareness of ethics was important, their knowledge was
deficient and there was no increase in their scores [9]corresponding to additional years of medical education .
Another study found that when medical students recorded the
ethical issues encountered by them, the most common issues
were related to ethics in medical education, professionalism,
confidentiality, the doctor–patient relationship, informed [10]consent and the doctor–peer relationship . Students may be
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00009.2
either unaware of the code of conduct or the principles of
ethics, or unable to translate the knowledge into actual
practice.Education of father was taken into account, since vast
part of, ethics and morality is taught at home. Education of
father may serve as a pointer to condition at home. In USA and
Europe students have to pass MCAT a multiple-choice
examination where Physical science, biology, critical thinking, [11]and verbal skills are all tested in a 5-hour computerized test .
This is followed by interview which finds ethical knowledge,
self less service provided by the students in addition if the
student is honest, humble, temperate, generous, and hard-
working. In ancient India Sushruta Samhita describes in detail
the internal character and external built of a pupil who are to be
admitted as a medical student. This admission process was
very stringent. A medical student was expected to be honest, [12]humble, temperate, generous, and hard-working . He was not
supposed to be enamored with women or engage in gambling
or hunting. His memory and academic performance were also [13]given importance .
CONCLUSION:
This study is an eye opener. Almost 50% of students of Medical
College so not have core ethical knowledge. Other studies also
points out that it is difficult to obtain knowledge on ethics from
Medical College. Time has come to change the process of
selection of Medical Students to have ethical doctors in our
Country. It can be done in the way as was done in past by
ancient Indian Doctors, which is followed by many Countries
of west except our country.
Stringent selection criteria can be adopted coupled with
interview, projects and work done for the service of ill and
unwell person in addition to multiple-choice examination
where Physics, Biology, Chemistry, Critical Thinking and
Verbal Skills can tested in a computerized test. If the selection
of Medical Students can be stream lined, only can we expect
ethical doctor population.
REFERENCES:
1. Chattopadhyay S. Corruption in healthcare and medicine:
why should physicians and bioethicists care and what
should they do? Indian J Med Ethics. 2013 Jul-
Sep;10(3):153-9.
2. The Times of India, Kolkata, Saturday, June 10, 2017,
page 39, column 1
3. Knafo A, Plomin R. Prosocial behavior from early to
middle childhood: genetic and environmental influences
on s tabi l i ty and change. Dev Psychol . 2006
Sep;42(5):771-86.
4. VV Pillay .Textbook of Forensic Medicine and thToxicology, 18 edition, Hyderabad Paras Medical
Publisher. 2017 page 30
5. English V et el. Medical ethics today. The BMA hand ndbook of ethics and law. 2 edition, page 25
6. Nandy A. Principals of Forensic Medicine including rdToxicology, 3 edition reprint, New Central Book
Agency(P) Ltd, Kolkata 700009, 2010 page 24rd7. Lay U K. Manual of Vipassana Meditation. 3 edition
reprint, Vipassana Research Institute, Dhamma Giri.
Igatpuri422403, 2010 Page 40.
8. Arun Babu T, Venkatesh C, Sharmila V. Are tomorrow's
doctors aware of the code of medical ethics? Indian J Med
Ethics. 2013 Jul-Sep;10(3):192-4.
9. Chatterjee B, Sarkar J. Awareness of medical ethics
among undergraduates in a West Bengal Medical College.
Indian J Med Ethics. 2012 Apr-Jun;9(2):93-100.
10. Fard NN, Asghari F, Mirzazadeh A. Ethical issues
confronted by medical students during clinical rotations.
Med Educ. 2010 Jul;44(7):723-30.
11. h t t p : / / s t u d y. c o m / r e q u i r m e n t s t o b e c o m e a
doctor.html.downloaded on 10 Oct. 17
12. Nuraliev YN. Doctor's ethics in ancient east written
classics and in the works of middle age medical scientists.
In: Abdi WH, Asimov MS, Bag AK, Khairullayev MM,
Mikulinsky SR, Mukherjee SK, et al., editors. Interaction
between Indian and Central Asian Science and
Technology in Medieval Times. Medicine, Technology,
Arts and Crafts, Architecture and Music. Vol. II. New
Delhi: Indian National Science Academy; 1990. pp. 11–8.
13. Lochan K. Varanasi: Chaukhambha Sanskrit Bhawan;
2003. Medical education. Medicines of Early India: With
Appendix on a Rare Ancient Text. Ch. 4; pp. 90–103.
43
PROFORMA
Sex: Age: Religion :
Name of School/ Location :
Medical of Instruction in School : English/ Hindi/ Bengali
Education and Occupation of Father :
Q 1. India has its own Code of Medical Ethics, composed by
Charaka: Yes/ No
Q2. In Ancient India, Ethics was strictly followed , who
contributed : Buddha/Patanjali/ Both
Q3. What is Contribution of Hippocratic in Medicine : Ethics/
Oath
Q4. Medical Ethics is followed for benefit of : Patent/Doctor
Q5. International Red Cross says-treat enemy soldiers also:
Yes/No
Q6. Where is HQ of WHO : Geneva / New York
Q7. First Noble Prize was given to founder of : WHO/
International Red Cross
Q8. Aim of a Doctor : Cure / Prevention / Teach
Q9. Function of MCI : Recognize Medical College/ Set Medical
syllabus/ Both
Q10. Should a doctor learn Karate (self defense) to protect himself
form patients: Yes/ No
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00009.2

Multiple Linear Regression to Determine Stature Using Hand and Feet Dimensions Among Central Indian Population.
1. Anudeep Singh, Senior Lecturer, Department of Anatomy, Faculty of Medicine, Saujana Putra Campus, MAHSA
University, Jenjarum, Selangor, Malaysia. 42610
Original Research Paper
Corresponding Author
Dr. Anudeep Singh
Senior Lecturer,
Department of Anatomy, Faculty of Medicine, Saujana
Putra Campus, MAHSA University, Jenjarum, Selangor,
Malaysia. 42610
Contact No. : +60163546930
E-mail : [email protected]
KEYWORDS : Hand and foot measurements, Stature estimation, Forensic anthropometry, Forensic anthropology, Central India.
Article History:Received: 2 April 2018Received in revised form: 18 June 2018Accepted on: 18 June 2018Available online: 1 July 2018
INTRODUCTION :
Anthropometric data collected from different races, age and
sex groups is greatly useful for designing products for
ergonomics, biomedical engineering, surgery and especially in [1-3]forensic medicine . Anthropologists have always been
interested in computing stature using measurements of
different parts of the body, as stature is one of the most [4-8]important factors in profiling the individuals . These data are
extremely useful in countries where techniques like DNA or
dental markers, which can be used for identification, are
expensive or not easily available.
The human remains, as the result of wars, airplane crashes,
traffic accidents, criminal mutilation and dismemberment and
other mass disasters, are present in different forms. The
primary challenge for any medico-legal investigator in
identifying unknown human remains is the development of a
biological profile via the estimation of race, sex, age and [9-10]stature . Using population specific standards is the most
[11]accurate and generally accepted method .
The estimation of stature from various skeletal parameters has [12- 18]been performed in different studies . Studies have also been
done where stature as well as gender is estimated from [19-29]dimensions of hands and feet .
There is currently a dearth of gender based studies done among
the population from central India. Thus, the purpose of the
present study was to analyse the relationship between the
measurements of the hand and foot dimensions and the stature
and to devise linear and multiple regression equations for each
gender. There are differences among populations due to
variations of race and ethnicity thus region based study of
subjects is necessary to have population specific forensic [30-33]standards .
MATERIALS AND METHODS :
After taking approval from research review committee of the
university and informed consent from participants the study
was conducted in Bhopal, India which is a region in central part
of India. All the measurements were taken in centimeters in a
reasonably well lit room by author himself to avoid inter-
observer error in methodology. 140 healthy subjects (70
female and 70 male) between the age group of 20 to 25 years
were chosen randomly. Sliding calliper was used for hand/feet
measurements and Stadiometer was used to measure vertical
height for stature estimation. The subjects were made to stand
on the level platform barefoot and erect against the stadiometer
bar with head in the Frankfurt plane for stature. Length and
width of hand and foot were measured separately of the left and
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00010.9
44
ABSTRACT :
Introduction : The identification of body parts is essential of biological profiling. Present study aims to use hand and feet
measurements to estimate stature based on sex.
Material and Methods : The study included 140 adults with 70 male and 70 female from central India. The age group was between
18 to 25 years. Length and breadth of both hands and feet were taken into account.. A descriptive analysis was done and regression
equations were derived to estimate the stature for each gender.
Results : The correlation coefficient was significantly positive between measurements and stature in both sexes. The stature
prediction accuracy ranged from ±3.49 - ±4.25 in males and ±0.86 – ±1.37 in females.
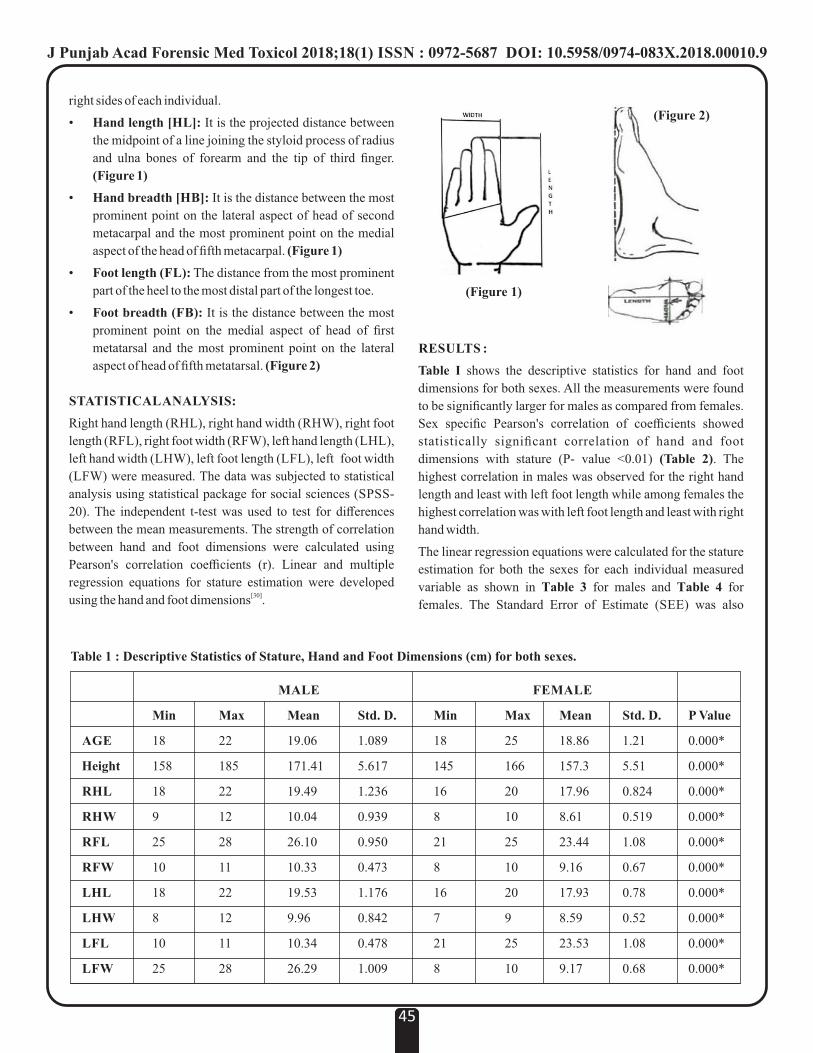
right sides of each individual.
• Hand length [HL]: It is the projected distance between
the midpoint of a line joining the styloid process of radius
and ulna bones of forearm and the tip of third finger.
(Figure 1)
• Hand breadth [HB]: It is the distance between the most
prominent point on the lateral aspect of head of second
metacarpal and the most prominent point on the medial
aspect of the head of fifth metacarpal. (Figure 1)
• Foot length (FL): The distance from the most prominent
part of the heel to the most distal part of the longest toe.
• Foot breadth (FB): It is the distance between the most
prominent point on the medial aspect of head of first
metatarsal and the most prominent point on the lateral
aspect of head of fifth metatarsal. (Figure 2)
STATISTICAL ANALYSIS:
Right hand length (RHL), right hand width (RHW), right foot
length (RFL), right foot width (RFW), left hand length (LHL),
left hand width (LHW), left foot length (LFL), left foot width
(LFW) were measured. The data was subjected to statistical
analysis using statistical package for social sciences (SPSS-
20). The independent t-test was used to test for differences
between the mean measurements. The strength of correlation
between hand and foot dimensions were calculated using
Pearson's correlation coefficients (r). Linear and multiple
regression equations for stature estimation were developed [30]using the hand and foot dimensions .
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00010.9
45
(Figure 2)
(Figure 1)
MALE FEMALE
Min Max Mean Std. D. Min Max Mean Std. D. P Value
AGE 18 22 19.06 1.089 18 25 18.86 1.21 0.000*
Height 158 185 171.41 5.617 145 166 157.3 5.51 0.000*
RHL 18 22 19.49 1.236 16 20 17.96 0.824 0.000*
RHW 9 12 10.04 0.939 8 10 8.61 0.519 0.000*
RFL 25 28 26.10 0.950 21 25 23.44 1.08 0.000*
RFW 10 11 10.33 0.473 8 10 9.16 0.67 0.000*
LHL 18 22 19.53 1.176 16 20 17.93 0.78 0.000*
LHW 8 12 9.96 0.842 7 9 8.59 0.52 0.000*
LFL 10 11 10.34 0.478 21 25 23.53 1.08 0.000*
LFW 25 28 26.29 1.009 8 10 9.17 0.68 0.000*
Table 1 : Descriptive Statistics of Stature, Hand and Foot Dimensions (cm) for both sexes.
RESULTS :
Table I shows the descriptive statistics for hand and foot
dimensions for both sexes. All the measurements were found
to be significantly larger for males as compared from females.
Sex specific Pearson's correlation of coefficients showed
statistically significant correlation of hand and foot
dimensions with stature (P- value <0.01) (Table 2). The
highest correlation in males was observed for the right hand
length and least with left foot length while among females the
highest correlation was with left foot length and least with right
hand width.
The linear regression equations were calculated for the stature
estimation for both the sexes for each individual measured
variable as shown in Table 3 for males and Table 4 for
females. The Standard Error of Estimate (SEE) was also

J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00010.9
46
Table 3 : Linear Regression Equations for the Estimation of Stature (in cm) from Hand and Foot Dimensions in Males.
Males
Linear Regression Equation SEE R� P Value
S =102.52 + 3.53 × RHL 3.55 0.60 <0.001
S =145.55 + 2.57 × RHW 5.10 0.17 <0.001
S =124.03 + 1.81 × RFL 5.38 0.08 <0.001
S =94.18 + 7.47 × RFW 4.39 0.38 <0.001
S =100.89 + 3.61 × LHL 3.70 0.56 <0.001
S =143.45 + 2.80 × LHW 5.13 0.16 <0.001
S =133.74 + 1.43 × LFL 5.46 0.05 <0.001
S =95.96 + 7.29 × LFW 4.43 0.37 <0.001
Table 4 Linear Regression Equations for the Estimation of Stature (in cm) From Hand and Foot Dimensions in Females.
Females
Linear Regression Equation SEE R� P Value
S = 49.30 + 6.01 × RHL 2.42 0.809 <0.001
S = 84.48 + 8.45 × RHW 3.35 0.629 <0.001
S = 43.73 + 4.84 × RFL 1.66 0.909 <0.001
S = 88.86 + 7.47 × RFW 2.26 0.831 <0.001
S = 43.99 + 6.32 × LHL 2.39 0.810 <0.001
S = 84.62 + 8.46 × LHW 3.28 0.644 <0.001
S = 41.77 + 4.91 × LFL 1.38 0.936 <0.001
S = 89.42 + 7.40 × LFW 2.25 0.833 <0.001
Variables Value of ‘r’
Male Female
RHL 0.778** 0.900**
RHW 0.431** 0.796**
RFL 0.307** 0.954**
RFW 0.630** 0.913**
LHL 0.756** 0.902**
LHW 0.421** 0.806**
LFL 0.257*** 0.968**
LFW 0.621** 0.914**
Table 2 : Pearson’s Correlation Between Stature and Hand and Foot Dimensions.
calculated. It predicts the deviation of the estimated stature
from the actual stature (lower values indicate more reliable
stature estimates). The SEE was between ±3.55 (right hand
length) and ±5.46 (left foot length) for the males and was
between ±2.42 (right hand length) and ±3.35 (right hand
width) for the females. The regression coefficients were found
to be statistically significant for all of the derived equations.
Multiple regression equations (Table 5 and 6) were derived to
assess whether using multiple variables would increase the
accuracy of predicting stature. This showed a reduce SEE,
±3.37 for males and ±0.86 for females. The regression
formulae were developed for all hand and foot, in case
individual hand or foot of either side are found to be
dismembered.
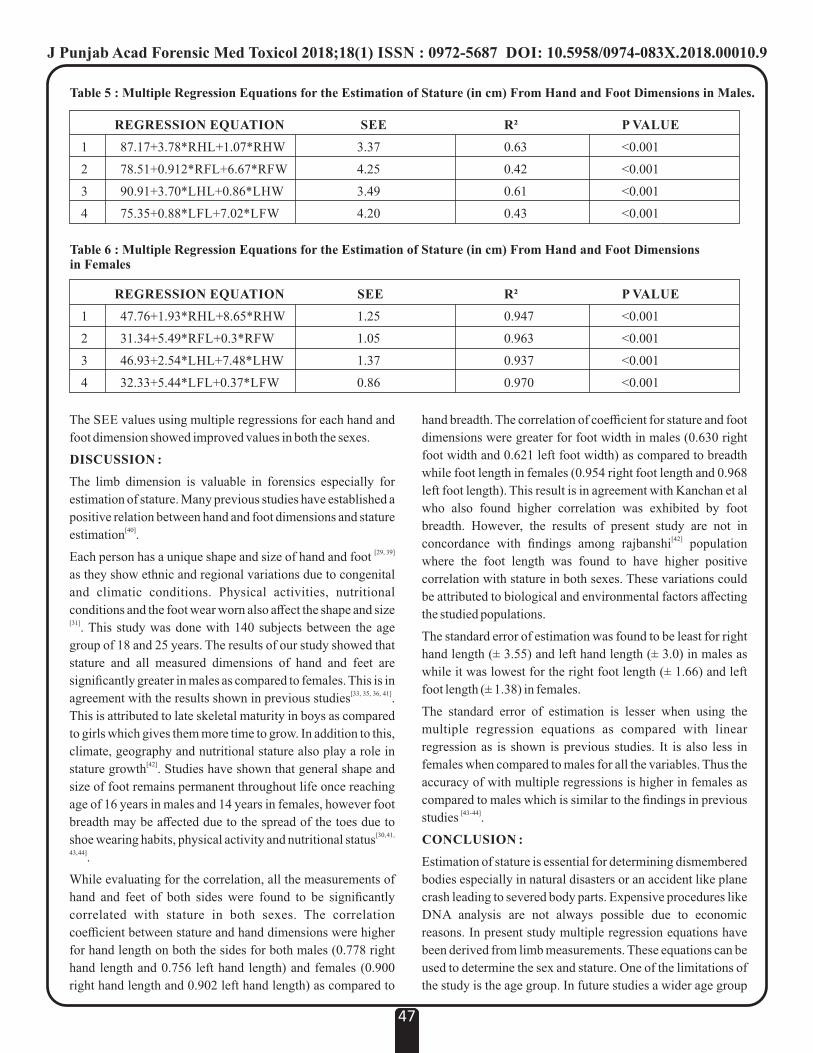
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00010.9
47
The SEE values using multiple regressions for each hand and
foot dimension showed improved values in both the sexes.
DISCUSSION :
The limb dimension is valuable in forensics especially for
estimation of stature. Many previous studies have established a
positive relation between hand and foot dimensions and stature [40]estimation .
[29, 39]Each person has a unique shape and size of hand and foot
as they show ethnic and regional variations due to congenital
and climatic conditions. Physical activities, nutritional
conditions and the foot wear worn also affect the shape and size [31]. This study was done with 140 subjects between the age
group of 18 and 25 years. The results of our study showed that
stature and all measured dimensions of hand and feet are
significantly greater in males as compared to females. This is in [33, 35, 36, 41]agreement with the results shown in previous studies .
This is attributed to late skeletal maturity in boys as compared
to girls which gives them more time to grow. In addition to this,
climate, geography and nutritional stature also play a role in [42]stature growth . Studies have shown that general shape and
size of foot remains permanent throughout life once reaching
age of 16 years in males and 14 years in females, however foot
breadth may be affected due to the spread of the toes due to [30, 41, shoe wearing habits, physical activity and nutritional status
43, 44].
While evaluating for the correlation, all the measurements of
hand and feet of both sides were found to be significantly
correlated with stature in both sexes. The correlation
coefficient between stature and hand dimensions were higher
for hand length on both the sides for both males (0.778 right
hand length and 0.756 left hand length) and females (0.900
right hand length and 0.902 left hand length) as compared to
hand breadth. The correlation of coefficient for stature and foot
dimensions were greater for foot width in males (0.630 right
foot width and 0.621 left foot width) as compared to breadth
while foot length in females (0.954 right foot length and 0.968
left foot length). This result is in agreement with Kanchan et al
who also found higher correlation was exhibited by foot
breadth. However, the results of present study are not in [42]concordance with findings among rajbanshi population
where the foot length was found to have higher positive
correlation with stature in both sexes. These variations could
be attributed to biological and environmental factors affecting
the studied populations.
The standard error of estimation was found to be least for right
hand length (± 3.55) and left hand length (± 3.0) in males as
while it was lowest for the right foot length (± 1.66) and left
foot length (± 1.38) in females.
The standard error of estimation is lesser when using the
multiple regression equations as compared with linear
regression as is shown is previous studies. It is also less in
females when compared to males for all the variables. Thus the
accuracy of with multiple regressions is higher in females as
compared to males which is similar to the findings in previous [43- 44]studies .
CONCLUSION :
Estimation of stature is essential for determining dismembered
bodies especially in natural disasters or an accident like plane
crash leading to severed body parts. Expensive procedures like
DNA analysis are not always possible due to economic
reasons. In present study multiple regression equations have
been derived from limb measurements. These equations can be
used to determine the sex and stature. One of the limitations of
the study is the age group. In future studies a wider age group
Table 5 : Multiple Regression Equations for the Estimation of Stature (in cm) From Hand and Foot Dimensions in Males.
REGRESSION EQUATION SEE R� P VALUE
1 87.17+3.78*RHL+1.07*RHW 3.37 0.63 <0.001
2 78.51+0.912*RFL+6.67*RFW 4.25 0.42 <0.001
3 90.91+3.70*LHL+0.86*LHW 3.49 0.61 <0.001
4 75.35+0.88*LFL+7.02*LFW 4.20 0.43 <0.001
Table 6 : Multiple Regression Equations for the Estimation of Stature (in cm) From Hand and Foot Dimensions in Females
REGRESSION EQUATION SEE R� P VALUE
1 47.76+1.93*RHL+8.65*RHW 1.25 0.947 <0.001
2 31.34+5.49*RFL+0.3*RFW 1.05 0.963 <0.001
3 46.93+2.54*LHL+7.48*LHW 1.37 0.937 <0.001
4 32.33+5.44*LFL+0.37*LFW 0.86 0.970 <0.001
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00010.9
48
can be studied.
REFERENCES :
1. Chaichankul C, Tanavalee A, Itiravivong P.
Anthropometric measurements of knee joints in Thai
population: correlation to the sizing of current knee
prosthesis. The Knee 2011;18:5-10.
2. Yue B, Varadarajan KM, Ai S, Tang T, Rubash HE, Li
G. Differences of Knee Anthropometry Between
Chinese and White Men and Women. The Journal of
a r t h r o p l a s t y 2 0 1 1 ; 2 6 ( 1 ) : 1 2 4 - 3 0 .
doi:10.1016/j.arth.2009.11.020.
3. Tseng, Chun-Yang & Wang, I-Jan & Chu, Chih-
Hsing. Parametric Modeling of 3D Human Faces
using Anthropometric Data. IEEE International
Conference on Industrial Engineering and
E n g i n e e r i n g M a n a g e m e n t 2 0 1 5 . 1 0 . 11 0 9
/IEEM.2014.7058686.
4. Athawale, M. C. Estimation of height from lengths of
fo rea rm bones - A s tudy o f one hundred
Maharashtrian male adults of ages between twenty-
five and thirty years. Am j Phys Anthropol
1963;21:105-12.
5. Charnalia V. Anthropological study of the foot and its
relationship to stature in different castes and tribes of
Pondicherry state. Journal of Anatomical Society of
India 1961; 10:26-30.
6. Jit I, Singh S. Estimation of stature from clavicles.
The Indian Journal of Medica l Research
1956;44(1):137-55.
7. Joshi N, Patel M, Dongre A. Regression equation of
height from ulnar length. The Indian Journal of
Medical Research 1964;52:1088-91.
8. Shroff A, Vare A. Determination of height from
length of superior extremity and its segments. Journal
of Anatomical Society of India. 1979;28:53-57.
9. Ahmed A A. Estimation of stature using lower limb
measurements in Sudanese Arabs. J Forensic Leg
Med. 2013;20(5):483-88.
10. Ahemad N, Purkait R. Estimation of stature from
hand impression: a nonconventional approach. J
Forensic Sci. 2011);56(3):706-09.
11. Ishak, N, Hemy N, Franklin D. Estimation of stature
from hand and handprint dimensions in a Western
Australian population. Forensic Sci Int 2012;216(1-
3):199.e1-7.
12. Kalia S, Shetty SK, Patil K, Mahima VG. Stature
e s t ima t ion us ing odon tomet ry and sku l l
anthropometry. Indian J Dent Res.2008;19(2): 150-4.
13. Krishan K. Estimation of stature from cephalo-facial
anthropometry in north Indian population. Forensic
Sci Int. 2008;181(1-3):52.e51-56.
14. Agnihotri A K, Kachhwaha S, Googoolye K, Allock
A. Estimation of stature from cephalo-facial
dimensions by regression analysis in Indo-Mauritian
population. J Forensic Leg Med 2011;18(4):167-72.
15. Menezes R, Nagesh K, Monteiro F, Kumar G,
Kanchan T, Uysal S et al. Estimation of stature from
the length of the sternum in South Indian females. J
Forensic Leg Med 2011;18(6): 242-45.
16. Giroux C L, Wescott D J. Stature estimation based on
dimensions of the bony pelvis and proximal femur. J
Forensic Sci 2008;53(1): 65-68.
17. Pelin C, Duyar I, Kayahan EM, Zagyapan R,
Agildere AM, Erar A. Body height estimation based
on dimensions of sacral and coccygeal vertebrae. J
Forensic Sci 2005;50(2): 294-97.
18. Nagesh K R, Pradeep G K. Estimation of stature from
vertebral column length in South Indians. Leg Med
Tokyo 2006;8(5):269-272.
19. De Mendonca M C. Estimation of height from the
length of long bones in a Portuguese adult population.
Am J Phys Anthropol 2000;112(1):39-48.
20. Pelin I C, Duyar I. Estimating stature from tibia
length: a comparison of methods. J Forensic Sci
2003;48(4):708-12.
21. Chibba K, Bidmos M A. Using tibia fragments from
South Africans of European descent to estimate
maximum tibia length and stature. Forensic Sci Int
2007;169(2-3): 145-51.
22. Anudeep S, Mahindra N, Anil K. An Anthropometric
Study of the Humerus in Adults. RRJMHS
2014;July-September;3(3):77-82.
23. Bidmos M A. Estimation of stature using fragmentary
femora in indigenous South Africans. Int J Legal Med
2008;122(4):293-99.
24. Bidmos M. A. Metatarsals in the estimation of stature
i n S o u t h A f r i c a n s . J F o r e n s i c L e g M e d
2008;15(8):505-09.
25. Mahakkanukrauh P, Khanpetch P, Prasitwattanseree
S, Vichairat K, Troycase D. Stature estimation from
long bone lengths in a Thai population. Forensic Sci
Int 2011;210(1-3): 279.e271-77.
26. Bidmos M, Asala S. Calcaneal measurement in

J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00010.9
49
estimation of stature of South African blacks. Am J
Phys Anthropol 2005;126(3):335-42.
27. Bidmos, M. Adult stature reconstruction from the
calcaneus of South Africans of European descent. J
Clin Forensic Med 2006;13(5):247-52.
28. Krishan, K. Estimation of stature from footprint and
foot outline dimensions in Gujjars of North India.
Forensic Sci Int 2008;175(2-3):93-101.
29. Zeybek G, Ergur I, Demiroglu Z. Stature and gender
estimation using foot measurements. Forensic Sci Int
2008;181(1-3):54.e51-55.
30. Akhlaghi M, Sheikhazadi A, Khosravi N, Pournia Y,
Saberianary SH. The value of the anthropometric
parameters of the tibia in the forensic identification of
the Iranian population over the age of 20. J Forensic
Leg Med 2011;18(6): 257-63.
31. Case, D. T. and Ross A. H. Sex determination from
hand and foot bone lengths. J Forensic Sci
2007;52(2):264-270.
32. Robinson, M. S. and Bidmos M. A. An assessment of
the accuracy of discriminant function equations for
sex determination of the femur and tibia from a South
African population. Forensic Sci Int 2011;206(1-
3):212.e211-15.
33. Krishan, K. Kanchan T, Sharma A. Sex determination
from hand and foot dimensions in a North Indian
population. J Forensic Sci 2011;56(2):453-59.
34. Kanchan, T. and Rastogi P. Sex determination from
hand dimensions of North and South Indians. J
Forensic Sci 2009;54(3):546-50.
35. Kanchan, T, Menzes G, Moudgil R, Kaur R. Kotian
M S, Garg K. Stature estimation from foot length
using universal regression formula in a North Indian
population. J Forensic Sci 2010;55(1):163-66.
36. Philip TA. Formulae for estimating stature from foot
size by regression method. Journal of Indian Academy
Forensic Medicine. 1990;12(2):57-62.
37. Geetha G N, Swathi, Sunita, Arvind A. Estimation of
Stature From Hand and Foot Measurements in a Rare
Tribe of Kerala State in India.J Clin Diagn
Res2015;9(10): Hc01-04.
38. Krishan, K. Determination of stature from foot and its
segments in a north Indian population. Am J Forensic
Med Pathol 2008;29(4):297-03.
39. Lohman, T. G, Roche A. Martorell R. Anthropometric
standardization reference manual. Champaign, IL,
(1988); Human Kinetics Books.
40. Krishan K, Kanchan T, Passi N. Estimation of stature
from the foot and its segments in a sub-adult female
population of North India. Journal of Foot and Ankle
Research. 2011;4:24. doi:10.1186/1757-1146-4-24.
41. Ashizawa K, Kumakura C, Kusumoto A, Narasaki S.
Relative foot size and shape to general body size in
Javanese, Filipinas and Japanese with special
reference to habitual footwear types. Ann Hum Biol
1997;24(2): 117-29.
42. Sen, J. and Ghosh S. Estimation of stature from foot
length and foot breadth among the Rajbanshi: an
indigenous population of North Bengal. Forensic Sci
Int 2008;181(1-3): 55.e51-56.
43. Kanchan T, Menezes RG, Moudgil R, Kaur R, Kotian
MS, Garg RK. Stature estimation from foot
dimensions. Forensic Sci Int 2008;179(2-3):
241.e241-45.
44. Krishan K, Sharma A. Estimation of stature from
dimensions of hands and feet in a North Indian
population. J Forensic Leg Med 2007;14(6):327-32.

50
Original Research Paper
Corresponding Author
Dr Seema Rani Pathak,
Professor and Head,
Department of Chemistry, Biochemistry and Forensic
Sciences, Amity School of Applied Science (ASAS), Amity
University, Gurugram, Haryana- 122413, India.
Contact : +919871803613
Email : [email protected]
KEYWORDS : Homogenous Strokes, Three-Dimensional Analysis, Ball Point Pens, Gel Pens.
Article History:Received: 13 April 2018Received in revised form: 25 April 2018Accepted on: 25 April 2018Available online: 1 July 2018
INTRODUCTION :
Forensic Document examination is one of the oldest branch of
Forensic sciences and till now being used for investigation of
the documents. One of the most challenging part in Forensic
Questioned Document is the determination of sequence of
strokes or in other words sequence of two intersecting lines [1]placed on a writing surface . Sequence of strokes means, the
sequence in which words or alphabets are placed or written on
writing surface. The need for investigation of sequence of
strokes arises when it is alleged that a statement is written after
a signature was done on the document, the two handwritings
touch at the same point or this examination can be performed to
learn which of the two writings that touch was last written. The
examination of sequence determination is very important job
to fix the accountability of the document.There are many cases
in which the signatory claims that the document he signed may
be disputed as the paragraph or sentence written just above his
signature was not present when he signed it. The most common
examples are blank paper signatures, addition in security
documents like cheques, etc. The dispute could be settled if we
could determine the sequence of writings when they are
intersecting (whether the paragraph was written first or the
signature). The importance of sequence of strokes Forensic
Questioned Documents was first mentioned by Albert S
Osborn in his book “Questioned Documents”. He stated that
“in various situations it is not possible to tell the correct
chronological order of two crossed lines and under these
situations a strong evidence should be made. This evidence
should be supported by observations from instruments. These
observations should be clear enough that a layman is able to
conclude the correct sequence of crossed lines”. Albert S
Osborn also said that the time interval between two writing is
also an influential factor. Examining the sequence of stroke is
not easy because there are several factors which affect the
analysis process like, writing instrument, types of ink, the
number of intersections, the color intensity of the lines [2]intersecting each other, the color of the ink and much more .
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00011.0
Determination of the Sequence of Strokes Made from the Same Color and Type of the Ink
1. Manisha Mann, Research Scholar*
2. Sudhir Kumar Shukla, Professor and Head, Amity Institute of Forensic Sciences (AIFS), Amity University, Noida.
3. Seema Rani Pathak, Professor and Head*
* Department of Chemistry, Biochemistry and Forensic Sciences, Amity School of Applied Science (ASAS), Amity
University, Gurugram, Haryana- 122413, India.
ABSTRACT :
Investigation of the sequence of strokes is an integral part in Forensic Questioned Document Examination. With the modernization,
forgers are also using modern methods for forging the documents and hence making the examination process more tedious. The
present study focuses on investigating the sequence of two intersected lines made from same type and color of the ink using
Confocal microscope and Docucenter Nirvis. Oil-based and liquid based inks in the color black was used for making the sample.
All the intersections made were homogenous in nature.The samples were first analysed under Docucenter Nirvis and then finally
examined under Confocal microscope for more accuracy. It was found that the Confocal microscope covered all the area in which
the Docucenter Nirvis lacked in the analysis and gave more confident result. The three dimensional feature of Confocal microscope
aided the study and the authors was able to find the correct sequence of the lines placed on the writing surface.
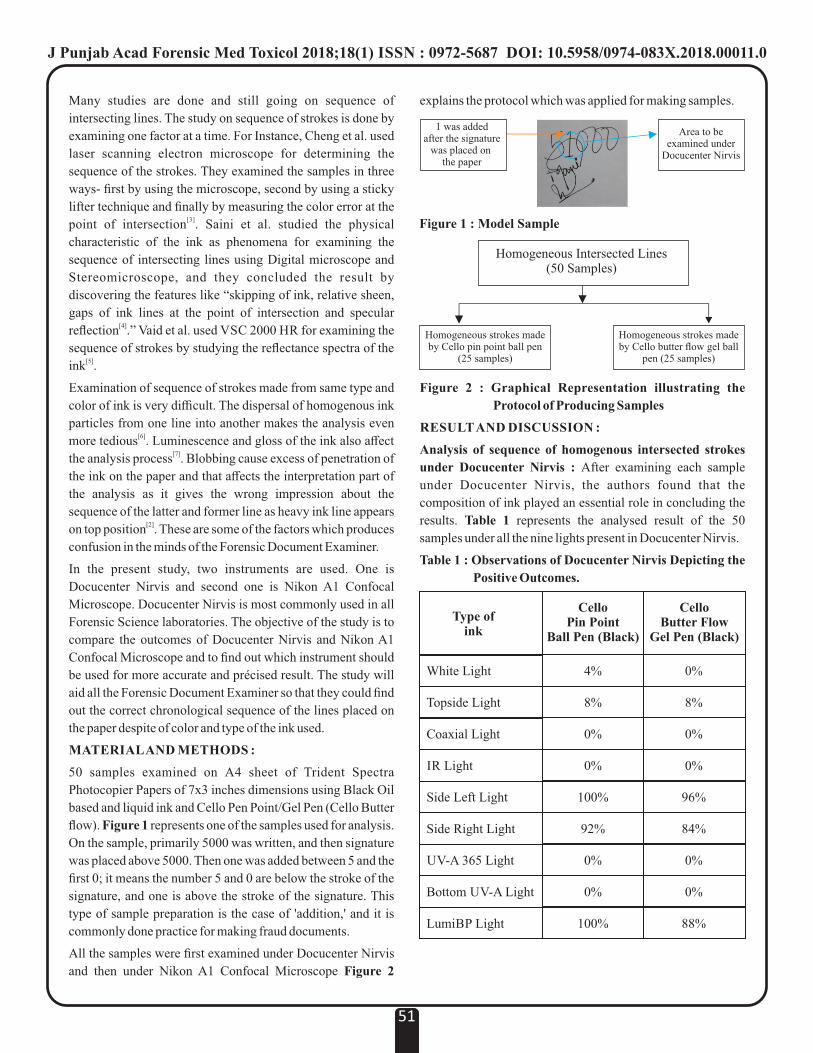
Many studies are done and still going on sequence of
intersecting lines. The study on sequence of strokes is done by
examining one factor at a time. For Instance, Cheng et al. used
laser scanning electron microscope for determining the
sequence of the strokes. They examined the samples in three
ways- first by using the microscope, second by using a sticky
lifter technique and finally by measuring the color error at the [3]point of intersection . Saini et al. studied the physical
characteristic of the ink as phenomena for examining the
sequence of intersecting lines using Digital microscope and
Stereomicroscope, and they concluded the result by
discovering the features like “skipping of ink, relative sheen,
gaps of ink lines at the point of intersection and specular [4]reflection .” Vaid et al. used VSC 2000 HR for examining the
sequence of strokes by studying the reflectance spectra of the [5]ink .
Examination of sequence of strokes made from same type and
color of ink is very difficult. The dispersal of homogenous ink
particles from one line into another makes the analysis even [6]more tedious . Luminescence and gloss of the ink also affect
[7]the analysis process . Blobbing cause excess of penetration of
the ink on the paper and that affects the interpretation part of
the analysis as it gives the wrong impression about the
sequence of the latter and former line as heavy ink line appears [2]on top position . These are some of the factors which produces
confusion in the minds of the Forensic Document Examiner.
In the present study, two instruments are used. One is
Docucenter Nirvis and second one is Nikon A1 Confocal
Microscope. Docucenter Nirvis is most commonly used in all
Forensic Science laboratories. The objective of the study is to
compare the outcomes of Docucenter Nirvis and Nikon A1
Confocal Microscope and to find out which instrument should
be used for more accurate and précised result. The study will
aid all the Forensic Document Examiner so that they could find
out the correct chronological sequence of the lines placed on
the paper despite of color and type of the ink used.
MATERIAL AND METHODS :
50 samples examined on A4 sheet of Trident Spectra
Photocopier Papers of 7x3 inches dimensions using Black Oil
based and liquid ink and Cello Pen Point/Gel Pen (Cello Butter
flow). Figure 1 represents one of the samples used for analysis.
On the sample, primarily 5000 was written, and then signature
was placed above 5000. Then one was added between 5 and the
first 0; it means the number 5 and 0 are below the stroke of the
signature, and one is above the stroke of the signature. This
type of sample preparation is the case of 'addition,' and it is
commonly done practice for making fraud documents.
All the samples were first examined under Docucenter Nirvis
and then under Nikon A1 Confocal Microscope Figure 2
explains the protocol which was applied for making samples.
Figure 2 : Graphical Representation illustrating the
Protocol of Producing Samples
RESULT AND DISCUSSION :
Analysis of sequence of homogenous intersected strokes
under Docucenter Nirvis : After examining each sample
under Docucenter Nirvis, the authors found that the
composition of ink played an essential role in concluding the
results. Table 1 represents the analysed result of the 50
samples under all the nine lights present in Docucenter Nirvis.
Table 1 : Observations of Docucenter Nirvis Depicting the
Positive Outcomes.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00011.0
51
Homogeneous Intersected Lines(50 Samples)
Figure 1 : Model Sample
Type ofink
CelloPin Point
Ball Pen (Black)
CelloButter Flow
Gel Pen (Black)
White Light
Topside Light
Coaxial Light
IR Light
Side Left Light
Side Right Light
UV-A 365 Light
Bottom UV-A Light
LumiBP Light
4%
8%
0%
0%
100%
92%
0%
0%
100%
0%
8%
0%
0%
96%
84%
0%
0%
88%
1 was added after the signature
was placed on the paper
Area to be examined under
Docucenter Nirvis
Homogeneous strokes made by Cello pin point ball pen
(25 samples)
Homogeneous strokes made by Cello butter flow gel ball
pen (25 samples)
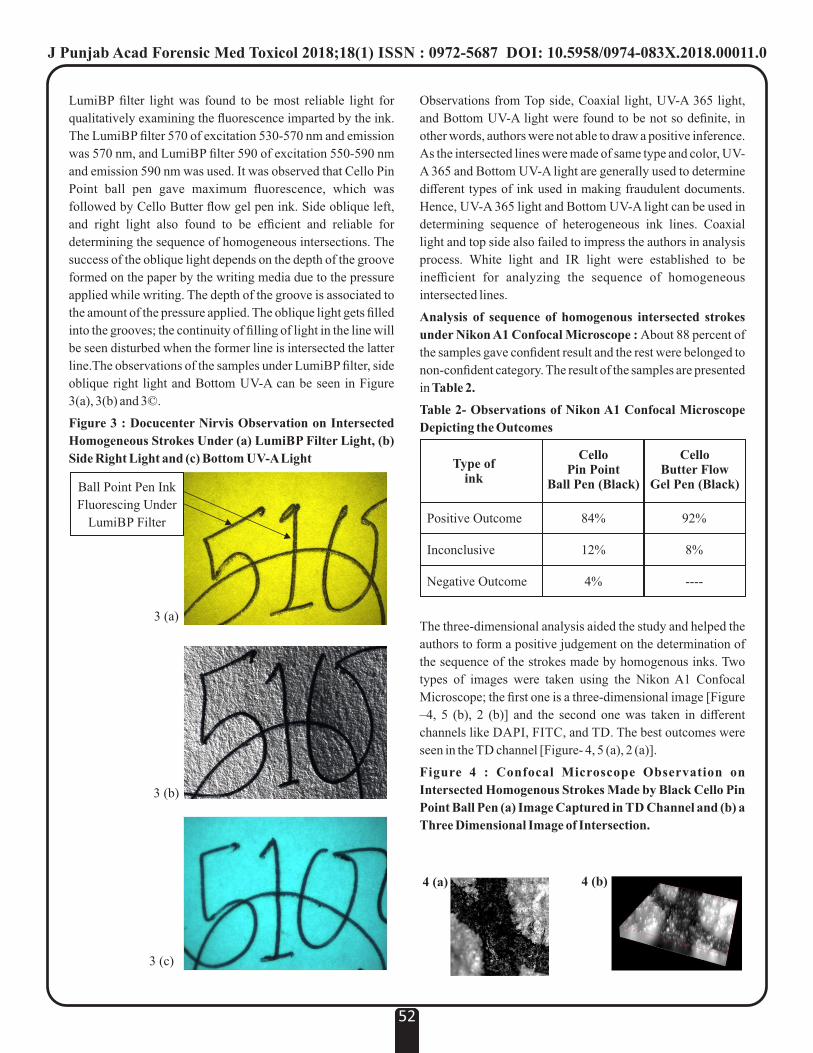
LumiBP filter light was found to be most reliable light for
qualitatively examining the fluorescence imparted by the ink.
The LumiBP filter 570 of excitation 530-570 nm and emission
was 570 nm, and LumiBP filter 590 of excitation 550-590 nm
and emission 590 nm was used. It was observed that Cello Pin
Point ball pen gave maximum fluorescence, which was
followed by Cello Butter flow gel pen ink. Side oblique left,
and right light also found to be efficient and reliable for
determining the sequence of homogeneous intersections. The
success of the oblique light depends on the depth of the groove
formed on the paper by the writing media due to the pressure
applied while writing. The depth of the groove is associated to
the amount of the pressure applied. The oblique light gets filled
into the grooves; the continuity of filling of light in the line will
be seen disturbed when the former line is intersected the latter
line.The observations of the samples under LumiBP filter, side
oblique right light and Bottom UV-A can be seen in Figure
3(a), 3(b) and 3©.
Figure 3 : Docucenter Nirvis Observation on Intersected
Homogeneous Strokes Under (a) LumiBP Filter Light, (b)
Side Right Light and (c) Bottom UV-A Light
Observations from Top side, Coaxial light, UV-A 365 light,
and Bottom UV-A light were found to be not so definite, in
other words, authors were not able to draw a positive inference.
As the intersected lines were made of same type and color, UV-
A 365 and Bottom UV-A light are generally used to determine
different types of ink used in making fraudulent documents.
Hence, UV-A 365 light and Bottom UV-A light can be used in
determining sequence of heterogeneous ink lines. Coaxial
light and top side also failed to impress the authors in analysis
process. White light and IR light were established to be
inefficient for analyzing the sequence of homogeneous
intersected lines.
Analysis of sequence of homogenous intersected strokes
under Nikon A1 Confocal Microscope : About 88 percent of
the samples gave confident result and the rest were belonged to
non-confident category. The result of the samples are presented
in Table 2.
Table 2- Observations of Nikon A1 Confocal Microscope
Depicting the Outcomes
The three-dimensional analysis aided the study and helped the
authors to form a positive judgement on the determination of
the sequence of the strokes made by homogenous inks. Two
types of images were taken using the Nikon A1 Confocal
Microscope; the first one is a three-dimensional image [Figure
–4, 5 (b), 2 (b)] and the second one was taken in different
channels like DAPI, FITC, and TD. The best outcomes were
seen in the TD channel [Figure- 4, 5 (a), 2 (a)].
Figure 4 : Confocal Microscope Observation on
Intersected Homogenous Strokes Made by Black Cello Pin
Point Ball Pen (a) Image Captured in TD Channel and (b) a
Three Dimensional Image of Intersection.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00011.0
52
Ball Point Pen Ink
Fluorescing Under
LumiBP Filter
3 (a)
3 (b)
3 (c)
Type ofink
CelloPin Point
Ball Pen (Black)
CelloButter Flow
Gel Pen (Black)
Positive Outcome
Inconclusive
Negative Outcome
84%
12%
4%
92%
8%
----
4 (b)4 (a)

Three dimensional feature of the Nikon A1 Confocal
Microscope aided the authors to draw a definite conclusion
irrespective of color and type of ink used. The three-
dimensional image was handy, as the depth of the grooves
made by the writing media on the paper was observable and the
sequence of writing media strokes made on the paper could be
recognized.Pen pressure created by the writer also helped in
the analysis process. Higher the pen pressure, higher the ability
to find the sequences of overlapping pen strokes.
Figure 5 : Confocal Microscope Observation on
Intersected homogenous strokes made by black Cello
Butterflow gel pen (a) image captured in TD channel and
(b) a three dimensional image of intersection.
CONCLUSION :
Overall, the Nikon A1 Confocal microscope is a versatile
instrument for the analysis of the sequence of strokes. The
properties of the confocal microscope helped in the process of
the examination, especially the three-dimensional images
were extremely helpful for inspecting the sequence of the
strokes made by the homogeneous ink. The three-dimensional
analysis was valuable in determining the exact sequence of the
intersected strokes irrespective of the color and type of ink
used.After evaluating all the interpretations, it can be
established that the Docucenter Nirvis can be used for
determining the correct sequence of homogeneous intersected
lines, but up to a certain extent only. Out of all nine lights used
for analysis, LumiBP filter, Sidelight left, and right gave
positive results.LumiBP light is the best choice for analyzing
the intersected lines made from the ballpoint pen.The confocal
microscope is highly recommended for examining the
sequence of the strokes made by the black color ink. Its use is
not limited to low pen pressure. Further research is going on
sequence of strokes made by other types of inks like Pilot pen
ink and Fountain ink.
REFERENCES :
1. Brito L R, Martins A R, Braz A, Chaves A B, Braga J,
Pimentel M F. Critical review and trends in forensic
investigations of crossing ink lines. TrAC Trends in
Analytical Chemistry 2017;94:54-69.
2. Osborn A S.(1910) Sequence of writing as shown by
crossed strokes. In Questioned Document (pp. 375-
393). The Lawyer's Co-operative publishing Co.
3. Cheng K, Chao C, Jeng B, Lee S. A New Method of
Identifying Writing Sequence with the Laser
Scanning Confocal Microscope. Journal of Forensic
Sciences J. Forensic Sci. 1998;43(2)348-52.
4. Saini K, Kaur R, Sood N. Determining the sequence
of intersecting gel pen and laser printed strokes — A
comparative study. Science & Justice2009;49:286-
291.
5. Vaid B A, Rana R S, Dhawan C. Determination of
sequence of strokes through reflection spectra.
Problems of Forensic Sciences,2017;LXXXVII:
193-203.
6. C l a y b o u r n M , A n s e l l M . U s i n g R a m a n
Spectroscopy to solve crime: inks, questioned
documents and fraud. Science & Justice. 2000;
40(4):261-271.
7. Wilkinson T J, Perry D L, Martin M C, Mc Kinney W
R, Cantu A A. Use of Synchrotron Reflectance
Infrared Spectromicroscopy as a Rapid, Direct, Non-
destructive Method for the Study of Inks on Paper.
Applied Spectroscopy, 2002; 56(6):800-803.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00011.0
53
5 (a) 5 (b)

Original Research Paper
Corresponding Author
Dr Pratik V Tarvadi,
Professor & Head,
Department of Forensic Medicine and Toxicology, Pacific
Institute of Medical Sciences, Ambua Road, Umarda, Udaipur
Contact : +91 98453-06634
Email : [email protected]
KEYWORDS : Biomedical Waste, Knowledge, Management
Article History:Received: 10 May 2018Received in revised form: 10 May 2018Accepted on: 22 May 2018Available online: 1 July 2018
INTRODUCTION :
Biomedical waste or infectious waste or medical waste is
defined as solid waste generated during the diagnosis, testing,
treatment, research or production of biological products for
humans or animals. Biomedical waste includes syringes, live
vaccines, laboratory samples, body parts, bodily fluids and [1]waste, sharp needles, cultures and lancets . While biomedical
waste management means a technique, of dealing with
biomedical waste, from the point of generation to the disposal
of waste. As per the reports from developing countries
approximately 1-2 kgs per bed per day, whereas in developed
countries approximately 1-5 kgs of waste / bed / day is [2]generated. In India it is estimated to be 2.0 kgs /bed/day .
Biomedical Wastes in health care facilities are generated
commonly from wards, delivery rooms, operating theaters,
emergency, outpatient services, laboratories, pharmaceutical
and chemical stores. Hospital staff (doctors, nurses, health care
assistants, maintenance personnel, support personnel for waste
handling, transportation and laundry) working at these places,
patients and their visitors, and waste management facility
employees and scavengers are at high risk of exposure to
nosocomial infection resulting from biomedical wastes. The
management of the wastes plays a vital role in its management.
The management involves the following steps: generation,
segregation, collection, on-site transportation, on-site storage,
offsite transportation (optional), treatment and disposal of the
waste, with Segregation being the most important step in the [1-6]process of biomedical waste management .
Improper handling of biomedical waste increases the airborne
pathogenic micro-organisms, which would affect the hospital
environment and the community. Improper disposal of
Biomedical waste also carries a vital importance. If it is
disposed in open dumps, it increases the risk of injury from
sharps and the spread of infectious diseases to waste handlers
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00012.2
A Study On Waste Disposal Management In A Tertiary Care Hospital1. Pratik V Tarvadi, Professor & Head, Department of Forensic Medicine and Toxicology, Pacific Institute of Medical
Sciences, Ambua Road, Umarda, Udaipur
54
ABSTRACT:
Introduction: Hospital wastes pose a significant impact on health and environment. The quantity of the Hospital (Bio-Medical)
Waste generated varies depending on the hospital polices and practices and also the type of care that is provided. According to a
WHO report, globally, around 85% of the hospital wastes are actually non hazardous, 10% are infective (hence, hazardous), and
the remaining 5% are non-infectious but hazardous (chemical, pharmaceutical and radioactive).
Objectives: To collect information on the collection, treatment, handling, hauling, and disposal of medical wastes and determine
the type of hazardous medical wastes produced in hospital.
Material and Methods: Our study was done at a tertiary care hospital. Information regarding the biomedical waste was obtained
through observation and interview with the help of a validated questionnaire prepared for the respective medical and paramedical
staff of relevant departments.
Results: Our study revealed that the staff had knowledge of the biomedical waste handling but lacked the practical handling of the
waste. The predominant waste noticed in the hospital was human anatomical waste, solid waste, liquid waste and chemical waste.
We observed that the collection of waste from each department was twice a day (morning and evening) and was transported to the
government approved waste disposal locations.
Conclusion: Every hospital should have regular trainings regarding knowledge and practical application pertaining to handling of
Biomedical waste, which will inturn help in protecting themselves, patients and move towards a healthy society.
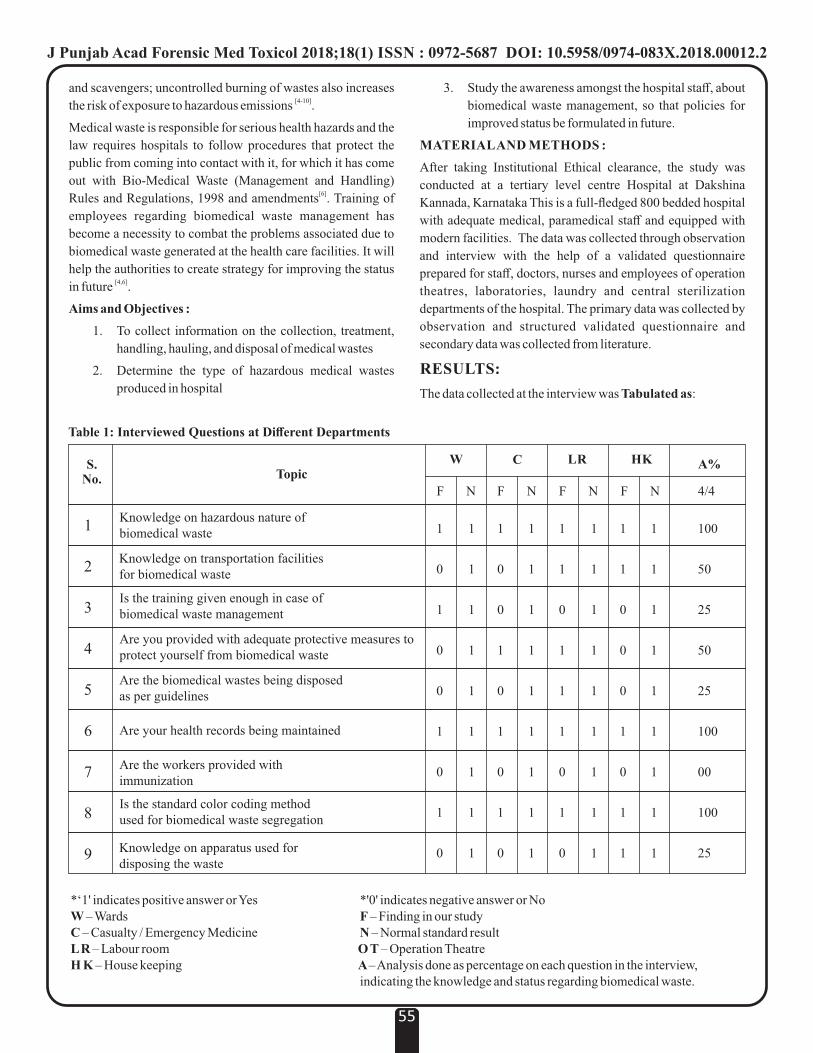
and scavengers; uncontrolled burning of wastes also increases [4-10]the risk of exposure to hazardous emissions .
Medical waste is responsible for serious health hazards and the
law requires hospitals to follow procedures that protect the
public from coming into contact with it, for which it has come
out with Bio-Medical Waste (Management and Handling) [6]Rules and Regulations, 1998 and amendments . Training of
employees regarding biomedical waste management has
become a necessity to combat the problems associated due to
biomedical waste generated at the health care facilities. It will
help the authorities to create strategy for improving the status [4,6]in future .
Aims and Objectives :
1. To collect information on the collection, treatment,
handling, hauling, and disposal of medical wastes
2. Determine the type of hazardous medical wastes
produced in hospital
3. Study the awareness amongst the hospital staff, about
biomedical waste management, so that policies for
improved status be formulated in future.
MATERIAL AND METHODS :
After taking Institutional Ethical clearance, the study was
conducted at a tertiary level centre Hospital at Dakshina
Kannada, Karnataka This is a full-fledged 800 bedded hospital
with adequate medical, paramedical staff and equipped with
modern facilities. The data was collected through observation
and interview with the help of a validated questionnaire
prepared for staff, doctors, nurses and employees of operation
theatres, laboratories, laundry and central sterilization
departments of the hospital. The primary data was collected by
observation and structured validated questionnaire and
secondary data was collected from literature.
RESULTS:
The data collected at the interview was Tabulated as:
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00012.2
55
S.No. Topic
W C LR HK A%
F N F F FN N N
Knowledge on hazardous nature of biomedical waste
Knowledge on transportation facilities for biomedical waste
Is the training given enough in case of biomedical waste management
Are you provided with adequate protective measures to protect yourself from biomedical waste
Are the biomedical wastes being disposed as per guidelines
Are your health records being maintained
Are the workers provided with immunization
Is the standard color coding method used for biomedical waste segregation
Knowledge on apparatus used for disposing the waste
1
2
3
4
5
6
7
8
9
1
0
1
0
0
1
0
1
0
1
1
1
1
1
1
1
1
1
1
0
0
1
0
1
0
1
0
1
1
1
1
1
1
1
1
1
1
1
0
1
1
1
0
1
0
1
1
1
1
1
1
1
1
1
1
1
0
0
0
1
0
1
1
1
1
1
1
1
1
1
1
1
4/4
100
50
25
50
25
100
00
100
25
Table 1: Interviewed Questions at Different Departments
*‘1' indicates positive answer or Yes *'0' indicates negative answer or NoW – Wards F – Finding in our studyC – Casualty / Emergency Medicine N – Normal standard resultL R – Labour room O T – Operation Theatre H K – House keeping A – Analysis done as percentage on each question in the interview, indicating the knowledge and status regarding biomedical waste.

Table No. 1 indicates the awareness of biomedical waste and
about its management among the hospital staff. It is very clear
from the table that though they have the knowledge about
biomedical waste but due to inadequate training given to them,
they do not have the practical application and knowledge of
waste management. From our findings, it was interpreted that
the institution is playing its part in waste management, but the
application is not there at the action level.
Table No. 2 enumerates the wastes produced in each
department.
In our study, we observed that the frequency of collection of
waste from each department was twice a day, Morning
between 8.00 am to 9.00 am and evening 4.00 pm to 5.00 pm,
and transported to storage place. From the storage place to
disposal center, the waste is collected on alternate days. The
general waste is shifted to Vamchur, while the hazardous waste
is shifted to Mulky, for its further treatment and disposal.
(Table 3)
S.No. Topic W C LR OT
1
2
3
4
5
6
7
8
9
1
0
1
0
1
1
1
1
1
Human anatomical waste
Animal waste
Microbiological Waste
Waste sharp
Discarded medicine & cytotoxic drugs
Solid waste
Liquid waste
Incineration ash
Chemical waste
1
0
1
1
0
1
1
1
1
1
0
1
1
1
1
1
0
1
1
0
0
0
0
1
1
1
1
Table 2 : Types of Biomedical Waste
DISCUSSION :[6]As per Biomedical Waste Management Rules, 1998 , “every
hospital generating biomedical waste needs to set up requisite
Biomedical waste treatment facilities on site or ensure
requisite treatment of waste at common treatment facility”.
Management of these waste is very important in all hospitals
and also important is the hospital staff having adequate
information regarding hospital waste and its management and
also be adequately trained for hospital waste management to
avoid nosocomial infections arising due to biomedical waste in
the hospital. In our study we observed that the hospital staff
though had the knowledge of the hazardous effects of the
biomedical waste but lacked the knowledge regarding its
transportation and were not adequately trained in biomedical
waste management.
In our study we observed that, adequate protective clothing
were though provided, but were not used, which can result in
infection to self while managing or transporting biomedical
wastes. As per Biomedical waste Management and handling [6]rules 1998 , Health care waste management workers should
be given proper protective clothing, provide immunization and
training to them. The hospital is doing its part, but inadequacy
from the workers in following the guidelines was noted.
In our study we observed that, sparing animal waste, all the
types of wastes are produced in our hospital, specifically the
departments we did our study on. These include general and
hazardous, which implies that it is very vital for the hospital
staff to be adequately trained and prepared in handling and
disposal of these wastes.
In our study we observed that the hospital was following the
Rules book in terms of maintaining color coded containers for
proper segregation of waste material, but apart from the data
about colour coding it was observed that the hospital staff did
not have adequate information regarding the disposal of
wastes.[10-11]As per handling of biomedical waste management , it is
mentioned that the color coded bags in the wards should be
emptied at-least once a day, preferably twice a day and the
wastes should be sent to the disposal at-least on alternate days.
It was observed in our study that the transportation of the waste
was done twice a day and at the time which did not interfere
with other activities like peak working hours and meal times.
Also the wastes were transported from the hospital storage
place to the disposal place for further treatment every alternate
day.
CONCLUSION AND RECOMMENDATIONS:
Biomedical waste management deals with biomedical waste,
from the point of generation to the disposal of waste. Our study
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00012.2
56
S.No.
Topic W C LR OT
1
2
3
Frequency of CollectionTime of Collection – Morning
Time of Collection – Evening
Table 3: Transportation Timings
Twice
8-9am
4-5pm
Twice
8-9am
4-5pm
Twice
8-9am
4-5pm
Twice
8-9am
4-5pm

J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00012.2
57
dealt with the departments where the most infectious
biomedical waste is generated. Among all the wastes, only
animal wastes are not generated at our hospital.
In our study we observed that the studied departments
followed proper color coding segregation and collection
procedure. The frequency of waste collection was twice in a
day and the transport of waste from the department to the area
of disposal was on alternate days. Disposal of these wastes was
being done in accordance to the guidelines. As the hospital is
providing proper training to the staff, they are well aware about
the nosocomial infection due to improper biomedical waste
management. As no research or any statistical study is present
regarding any nosocomial infection resulting from Biomedical
wastage, we are of the opinion that a study is required to be
done to keep the hospital updated about the relation between
nosocomial infection and biomedical waste management.
Our team also had observed that the hospital is providing the
necessary basic protective measures but due to lack of training
the hospital staff is not well aware about the safety measures
they need to comply to. Hence it is of paramount importance
that all the hospital staff should be provided adequate training
regarding biomedical waste management. Also it is important
that hospital management should depute few paramedical
staff, properly trained in courses that provide training for
biomedical waste management who can work as supervisors in
biomedical waste management, to give a healthy hospital
atmosphere and prevent nosocomial infection to the hospital
staff, in particular workers of biomedical waste management
team.
The hospital authority should also look into re-design a
separate lift or stair case to transport the wastes other than
patient circulation area, so as to prevent the exposure of
biomedical waste to the already weakly immunized patients
present in the wards.
We observed in our study, that with certain limitations and
shortcomings also, the hospital is trying their level best to
effectively handle the Biomedical waste management and to
protect themselves and the patients from the hazardous nature
of the biomedical waste.
LIMITATION OF STUDY :
Ÿ The study is limited to only one hospital
Ÿ Short study period
FUNDING: None
ACKNOWLEDGEMENTS:
Ÿ My teacher and guide, Dr. Mahabalesh Shetty, M.D.,
Professor and Head, Department of Forensic Medicine, K S
Hegde Medical Academy, Mangalore for his constant
encouragement, constructive criticism, continuous
motivation and personal attention throughout this study.
Ÿ D r. Sampath Kumar , Dr. Sher ley , Nurs ing
Superintendent and all the participants, who spent their
valuable time for their kind help and assistance in
answering my questionnaire for the data collection.
REFERENCES :
1. Mathur P, Patan S, Shobhawat S. Need of Biomedical Waste
Management System in Hospitals - An Emerging issue - A
Review. Curr World Environ 2012;7(1):117-124
2. Grover P.D. Management of Hospital Wastes – An overview.
Proceedings of National workshop on Management of Hospital
Waste;1998:16-18.
3. S. Saini, S.S. Nagarajan, R.K. Sarma, Knowledge, Attitude and
Practices of Bio-Medical Waste Management Amongst Staff of a
Tertiary Level Hospital in India, Journal of the Academy of
Hospital. 2005; 17(2): 01-12
4. World Health Organization. Preparation of National Health-
Care Waste Management Plans in Sub-Saharan Countries.
Guidance Manual (Cited 20 February 2018). Available from:
http://www.who.int/water_sanitation_health/medicalwaste/en/
guidancemanual.pdf
5. World Bank. Health Care Waste Management in India. (Cited 25
February 2018). Available from:
http://siteresources.worldbank.org/INTRANETENVIRONM
ENT/1705736-1127758054592 / 20677728 / HCWMText.pdf
6. Ministry of Environment and Forests. Government of India.
( C i t e d 2 5 F e b r u a r y 2 0 1 8 ) . Av a i l a b l e f r o m :
http://envfor.nic.in/legis/hsm/biomed.html
7. World Health Organization. Management of solid health-care
waste at primary health-care centres. A Decision-Making guide.
(Cited 25 February 2018). Available from:
http://www.searo.who.int/entity/emergencies/documents/List_
of_Guidelines_for_Health_Emergency_solid-health-
care_waste.pdf?ua=1
8. World Health Organization. Health Care Waste Management.
Guidance for the development and implementation of a National
Action Plan (Cited 25 February 2018) Available from:
http://www.who.int/water_sanitation_health/medicalwaste/en/
napguidance.pdf
9. Mathur V, Dwivedi S, Hassan M, Misra R. Knowledge, attitude,
and practices about biomedical waste management among
healthcare personnel: A cross-sectional study. Indian J
Community Med. 2011;36(2):143–5
10. International Committee of the Red Cross. Medical Waste
Management. (Cited 1 March 2018). Available from:
https:/www,icrc.org/eng/assets/files/publications/icrc-002-
4032.pdf
11. World Health Organization. Safe Management of Bio-medical
Sharps Waste in India. A Report on Alternative Treatment and
Non-Burn Disposal Practices. (Cited 1 March 2018). Available
from:
h t t p s : / / w w w . h e a l t h c a r e - w a s t e . o r g /
fileadmin/user_upload/resources/Safe-management-bio-
medical-sharps-waste-India-2005.pdf
Original Research Paper
Corresponding Author
Dr Thanka J,
Professor,
Department of Pathology, Sri Ramachandra Medical
College & Research Institute, Porur, Chennai – 600116
Contact : 94440-47907
Email : [email protected]
KEYWORDS : Gross Changes, Histopathology, Dating of Abrasions.
Article History:Received: 21 April 2018Received in revised form: 4 June 2018Accepted on: 4 June 2018Available online: 1 July 2018
INTRODUCTION :
A wound or injury is defined as damage to any part of the body [1]due to application of mechanical force . Forensic experts are
frequently asked to comment on the age of injuries and the
interpretat ion may have significant medico-legal [2]consequences . Three basic lesions are recognized:
[3]Abrasions, Contusions and Lacerations . Age of wounds can
be determined by (i) Gross changes (ii) Histopathology [4](iii)Enzyme histo-chemistry and Immuno-histochemistry . In
Indian setting, generally, we adopt the “naked eye
examination” method to date an injury. It is difficult to
determine exactly the age of an injury on the basis of its [5]appearance by the naked eye . Hence this study of wound
dating of abrasions from macroscopic and microscopic level
was taken up in our set up, to look into the accuracy by
comparing with the age determined by colour changes and
microscopic examination with that of the known time of
infliction of injury.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00013.4
58
Wound Dating By Gross And Histopathological Examination of Abrasions
- An Autopsy Based Study 1. Prashanthi Krishna Dharma Ramasamy Devaraj, Assistant Professor, Department of Forensic Medicine, Sri
Muthukumaran Medical College & Research Institute, Chikkarayapuram, Chennai – 600069
2. Thanka J, Professor, Department of Pathology, Sri Ramachandra Medical College & Research Institute, Porur, Chennai –
600116
3. Sampath Kumar, Professor and Head, Department of Forensic Medicine,Sri Ramachandra Medical College & Research
Institute, Porur, Chennai – 600116
4. Selva Arasi, Third Year Post Graduate Student, Department of Forensic Medicine,Sri Ramachandra Medical College &
Research Institute, Porur, Chennai – 600116
ABSTRACT :
Introduction: Abrasions are the commonly encountered blunt force injuries. Exact ageing of wound is inevitable in routine
forensic investigations. Each phase in wound healing such as inflammation, proliferation, and maturation helps us understand the
chain of events in wound healing. This study was done to determine the age of abrasions since the time of infliction till death by
histopathology and gross examination.
Materials and Methods: Postmortem study of wound dating by gross and histopathological examination of abrasions was
carried out in the Department of Forensic Medicine, in Sri Ramachandra Medical College. Cases subjected to medico legal
autopsy having well demarcated abrasions were taken up for the study. A total of 37 abrasions were studied by microscopy in
correlation with the gross changes at various time interval. Abrasions ranging from 0 hour to a maximum of 21 days were studied.
Cases with known time of infliction of injury were included in the study and cases in a state of decomposition were excluded from
the study.
Results: Microscopic changes corresponds to the gross changes in abrasions whereas, with various co-morbid conditions wounds
showed disparity by delaying healing process.
Conclusion: This study reveals us when subjective evaluation of gross findings are combined with the histopathological
examination, the reliability and precision of dating wounds increases in comparison with gross findings alone, especially before
giving opinions.
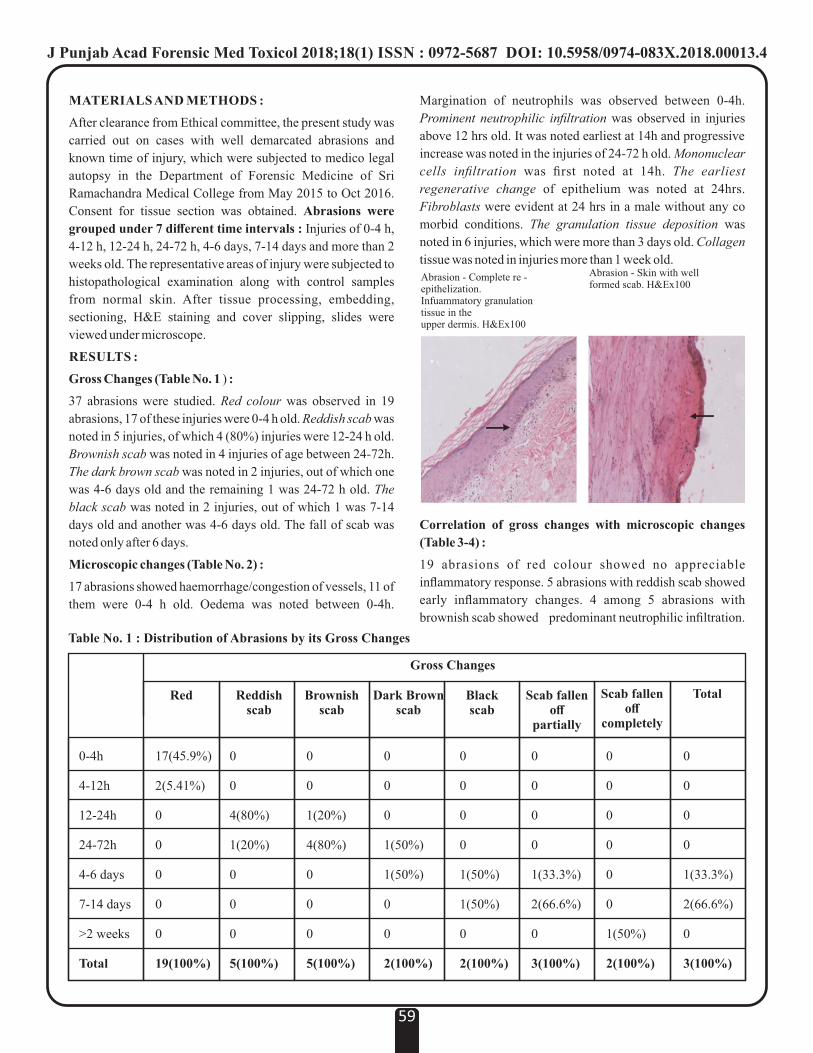
MATERIALS AND METHODS :
After clearance from Ethical committee, the present study was
carried out on cases with well demarcated abrasions and
known time of injury, which were subjected to medico legal
autopsy in the Department of Forensic Medicine of Sri
Ramachandra Medical College from May 2015 to Oct 2016.
Consent for tissue section was obtained. Abrasions were
grouped under 7 different time intervals : Injuries of 0-4 h,
4-12 h, 12-24 h, 24-72 h, 4-6 days, 7-14 days and more than 2
weeks old. The representative areas of injury were subjected to
histopathological examination along with control samples
from normal skin. After tissue processing, embedding,
sectioning, H&E staining and cover slipping, slides were
viewed under microscope.
RESULTS :
Gross Changes (Table No. 1 ) :
37 abrasions were studied. Red colour was observed in 19
abrasions, 17 of these injuries were 0-4 h old. Reddish scab was
noted in 5 injuries, of which 4 (80%) injuries were 12-24 h old.
Brownish scab was noted in 4 injuries of age between 24-72h.
The dark brown scab was noted in 2 injuries, out of which one
was 4-6 days old and the remaining 1 was 24-72 h old. The
black scab was noted in 2 injuries, out of which 1 was 7-14
days old and another was 4-6 days old. The fall of scab was
noted only after 6 days.
Microscopic changes (Table No. 2) :
17 abrasions showed haemorrhage/congestion of vessels, 11 of
them were 0-4 h old. Oedema was noted between 0-4h.
Margination of neutrophils was observed between 0-4h.
Prominent neutrophilic infiltration was observed in injuries
above 12 hrs old. It was noted earliest at 14h and progressive
increase was noted in the injuries of 24-72 h old. Mononuclear
cells infiltration was first noted at 14h. The earliest
regenerative change of epithelium was noted at 24hrs.
Fibroblasts were evident at 24 hrs in a male without any co
morbid conditions. The granulation tissue deposition was
noted in 6 injuries, which were more than 3 days old. Collagen
tissue was noted in injuries more than 1 week old.
Correlation of gross changes with microscopic changes
(Table 3-4) :
19 abrasions of red colour showed no appreciable
inflammatory response. 5 abrasions with reddish scab showed
early inflammatory changes. 4 among 5 abrasions with
brownish scab showed predominant neutrophilic infiltration.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00013.4
59
Table No. 1 : Distribution of Abrasions by its Gross Changes
Gross Changes
Red Reddishscab
Brownishscab
Dark Brownscab
Blackscab
Scab fallenoff
partially
Scab fallenoff
completely
Total
0-4h
4-12h
12-24h
24-72h
4-6 days
7-14 days
>2 weeks
Total
17(45.9%)
2(5.41%)
0
0
0
0
0
19(100%)
0
0
4(80%)
1(20%)
0
0
0
5(100%)
0
0
1(20%)
4(80%)
0
0
0
5(100%)
0
0
0
1(50%)
1(50%)
0
0
2(100%)
0
0
0
0
1(33.3%)
2(66.6%)
0
3(100%)
0
0
0
0
0
0
1(50%)
2(100%)
0
0
0
0
1(33.3%)
2(66.6%)
0
3(100%)
0
0
0
0
1(50%)
1(50%)
0
2(100%)
Abrasion - Complete re - epithelization.Infuammatory granulation tissue in the upper dermis. H&Ex100
Abrasion - Skin with well formed scab. H&Ex100
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00013.4
60
Table No. 4 : Distribution of Abrasions by its Gross Changes
Microscopic changes Earliest appearance Routine appearance
Congestion/ hemorrhage 0 min 0-4 h
Oedema formation 0 min 0-4 h
Margination of polymorphs 1 hr 50 mts 0-4 h
Early infiltration of neutrophils - 4-12 h
Predominant neutrophilic infiltration 14 hrs 12-24 h
Mononuclear cell infiltration 14hrs 24-72 h
Fibroblast formation 24hrs 30 mts 71-78 h
Granulation tissue deposition 24hrs 30 mts 4-6 days
Collagen tissue deposition 10 days13hrs 24mts 7-14 days
Regression phase - >2 weeks
Table No. 2 : Distribution of Abrasions by its Microscopic Changes
Microscopic Scoring
0-4h
4-12h
12-24h
24-72h
4-6 days
7-14 days
>2 weeks
11
0
4
2
0
0
0
Age ofInjury
0 1 2 3 4 5 6 7 8 9
2
0
0
0
0
0
0
2
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
2
5
2
2
4
0
0
1
1
1
3
0
0
0
0
1
3
2
0
0
0
0
1
3
2
0
0
0
0
0
0
1
1
0
0
0
0
0
0
0
Score :
0- Haemorrhage and/or Congestion of vessels
1- Oedema formation
2- Margination of polymorph cells
3- Early infiltration of neutrophil cells
4- Predominant neutrophil infiltration with poorly
differentiated mononuclear cells.
5- Predominant mononuclear cell infiltration
6- Fibroblast formation
7- Granulation tissue with rich leucocyte infiltration and much
fibroblasts
8- Collagen tissue deposition
9- Cellular reaction subsides, fibroblast are more active with
increased collagen formation (regression phase)
Table No. 3 : Correlation of Gross Changes with microscopic Changes in Abrasions
Microscopic Scoring
Red
Reddish Scab
Brownish Scab
Dark Brown
Black Scab
Scab Fallen Off Partially
Scab Fallen Off Completely
11
3
1
1
0
0
0
GrossChanges
0 1 2 3 4 5 6 7 8 9
2
0
0
0
0
0
0
1
0
0
0
0
0
0
0
0
0
0
0
0
0
0
2
4
2
1
2
1
0
1
1
0
1
2
0
0
0
1
1
1
2
0
0
0
1
1
1
1
0
0
0
0
0
0
1
1
0
0
0
0
0
0
0

1 among 2 abrasions with dark brown scab showed
granulation tissue, macrophages and congestion . 2 abrasions
with black scab showed granulation tissue. One among 3
abrasions with scab fallen off partially showed collagen tissue
deposition . Scab was fallen off completely in one abrasion
which showed granulation tissue.
By comparing gross changes with microscopic changes, all the
injuries of 4-6 days duration showed grossly dark brown
except one which was black, whereas all their histological
pictures showed granulation tissue formation, which
confirmed the age of injury to be more than 4 days old. Scab
was fallen off completely in more than 2weeks old abrasions
and showed dense collagen tissue with decreased cellular
reaction.
DISCUSSION :
Maximum Number of cases observed were males and most of
the injuries were due to RTA. Maximum number of cases were
observed in the age group between 21-30 years. 17 out of 19
abrasions showing red colour were below 4 hrs of age. This
was in agreement with the study conducted by Sharma A et al : [6]he noted redness from 10 min up to 7 hours . It was observed
in another study that majority of cases on the first day were [4]dark red . Reddish scab was usually noted between 12-24 hrs.
Similar observation was made by Sharma A et al in their [6,8]study . An author also quotes that reddish scab forms by 8-24
[7] rdh .Brownish scab was noted on the 3 day. Dark brown scab
was noted after 63 hrs. Black scab was observed after 5 days. [6]Sharma A et al found hard brown scab 27 h onwards and an
author also quotes that by 4th and 5th day the scab looks dark [7]brown . However this was in disagreement with another
study, where they observed dark red scab instead of dark th [4]brownish scab on 5 day . The fall of scab was noted only after
6 days. Scab was fallen off completely in an abrasion of more
than 2weeks old. In a similar study by Sharma A et al found [6]that, the black scab started separating 7 days onwards and
thalso the author quotes that by 6 day it is blackish and it starts
falling off from the margins. A big scab takes a few more days [7]to fall off . However, this was in disagreement with the study,
where they observed dark brown scab instead of black scab on th [4]the 9 day .
Microscopy revealed loss of epithelial layer in all abrasions.
Loss of rete ridges was a prominent feature in all the pressure
abrasions. Haemorrhage/congestion of vessels and early
inflammatory changes were noted in abrasions of age less than
14 hours. Predominant neutrophilic infiltration was noted after
14hrs. Mononuclear cell infiltration was first noted at 14h. In a
similar study by Sharma A et al early mononuclear infiltration [6]was observed at 13h .The earliest regenerative change of
epithelium was noted at 24hrs.Granulation tissue was
predominantly noted after 5days.Collagen tissue formation
was noted in a wound more than 10 days old.
By comparing gross with microscopic changes, injuries of 4-6
days old with dark brown & black scabs showed granulation
tissue formation, which confirmed their age to be more than 4
days old.
Scab were fallen off completely and dense collagen tissue with
decreased cellular reaction were seen in abrasions of more than
2 weeks old. Deposition of granulation tissue was observed
routinely by 4-6days.
This observation is in agreement with the author - granulation [8]tissue formation is seen by 5-8 days and another author also
[1]quotes the similar finding . There may be significant delay of
fall of scab in septicaemia.
CONCLUSION :
The pattern of healing of abrasions by both gross and
microscopic appearance was uniform. For Indian population
with dark skin, gross changes by naked eye examination for
dating the injuries gives a rough estimate, thus subjecting the
samples for histo-pathological examination would be more
accurate, whereas gross changes are well appreciated in the fair
skinned people to some extent. Future studies should include
more number of cases comprising a) different age groups b)
each type of injury c) associated co-morbities d) different sites
to get a more detailed survey. In examination by
histopathology, the presence of artefacts in the form of sand,
mud particles, grease, paint & glass pieces etc. are to be kept in
mind.
Acknowledgement: Nil
Conflict of Interest : None
Limitations of Study : Samples studied were from
refrigerated bodies.
REFERENCES :
1. Knight B. The Pathology of wounds. In: Saukko P
(ed.)Knight's Forensic Pathology .3 rd ed London: Arnold
publishers; 2004. p. 136,166-69.
2. Pilling M.L, Vanezis P, Johnston A. Visual assessment of
the timing of bruising by forensic experts. J Forensic Leg
Med. 2010;17(3): 143-49.
3. Vij K. Mechanical Injuries. In: Vij K (ed.) Textbook of
Forensic Medicine and Toxicology. New Delhi: Reed
Elsevir India Private Limited; 2014. p. 203.
4. Aggrawal A. Mechanical Injuries. In: Aggrawal A (ed.)
Textbook of Forensic Medicine and Toxicology. New
Delhi: Avichal Publishing Company; 2014. p. 232.
5. Kumar L, Chaitanya B.V, Agarwal S.S, Bhastia B.K. Age
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00013.4
61

J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00013.4
62
Related Changes in Mechanical and thermal Injuries-A
Pos t Mor tem Study. J Indian Acad Forens ic
Med.2011;33(2): 149-51.
6. Sharma A, Dikshit P.C, Aggrawal A, Mandal A.K. A Post
mortem study of histopathological findings to determine
the age of abrasion and laceration. Journal of Forensic
Medicine and Toxicology. 2010;27(1): 43-46.
7. Nandy A. Mechanical injuries. In: Nandy A
(ed.)Principles of Forensic Medicine and Toxicology.
New Delhi: New central book agency; 2000. p. 342,352.
8. Payne JJ, Busttil A, Smack W, (eds). Pathophysiology of
wound healing. In: Forensic Medicine, Clinical and
Pathological Aspects. London, England: Greenwich
Medical Media Ltd; 1977:83–87.
9. Reddy K.S.N. Medico-legal Aspects Of Wounds .
In:Murthy 0.P (ed.) The Essentials of Forensic Medicine
and Toxicology. Hyderabad: Om Sai Graphics; 2013.
10. Janssen W, Forster S. Forensic histopathology. Berlin:
Springer-Verlag:2011.
11. Vinay J, Harish S, Mangala GSR, Hugar BS. A Study on
P o s t m o r t e m Wo u n d D a t i n g b y G r o s s a n d
Histopathological Examination of Abrasions. The
American Journal of Forensic Medicine and Pathology.
2017;38(2):167–73.
12. Vinay J. Postmortem study of wound dating by gross and
histopathological examination of blunt injuries. Thesis,
2011;2014: 1-101.

Original Research Paper
Corresponding Author Dr. Lovleen
Assistant Professor
Department of Zoology, School of Bioengineering and
Biosciences, Lovely Professional University, Phagwara,
India
Contact : +91 94178-52950
Email : [email protected]
KEYWORDS : Noon Tea, Reprotoxic Effects, Drosophila melanogaster
Article History:Received: 22 May 2018Received in revised form: 22 June 2018Accepted on: 22 June 2018Available online: 1 July 2018
INTRODUCTION :
Noon tea (Kashmiri tea or Gulabi chai) is a special traditional
beverage, of Kashmir area, in India. Noon chai is composed of
Camella Sinensis, salt and a pinch of baking soda. Limited use
of noon tea possess many health benefits as it is powerful
antioxidant, inhibits formation of blood clots in intact blood
vessels, chances of heart attack and stroke wards off. The
Kashmiri tea (noon chai) is refreshing in the heat and resists the
cold in winters. The L-theanine, an amino acid component of
the tea helps to reduce the anxiety and stress, gaseous
distension, and intestinal spasms. Use of baking soda in noon
chai increases the alkalinity of the blood, which is useful in
muscle functionality. Major benefits of noon chai is, it
increases mental alertness, reduces headache and increase the [1]fluid levels in the body . Presence of oxalate in tea reduces the
[2]kidney stone formation by 8% in females and 14% in males .
But excessive use of noon chai is associated with induction of
gastric cancer in human beings and excess amount of sodium
bicarbonate can cause edema, alkalosis, heart failure,
hypertension, hypervolemic hypernatremia and also cause
urinary alkalinisation. It has been reported that 40% of gastric
cancer occur due to noon chai in Kashmir. It has been identified
that people suffering from anemia should avoid use of
Kashmiri tea as it contains polyphenolics which prevents
absorption of iron. It had been reported that regularly
consumption of noon chai enhance the level of ethylamine,
methyamine and pyrolidine in body, which are ultimately are
responsible for gastric cancer. Furthermore, noon tea cause
inflammation and generates free radicals of nitrogen and [1]oxygen which are carcinogenic .
MATERIALS AND METHODS :
As very limited data is available on reprotoxic consequences of
noon tea, therefore considering specific cognition, present
research work, had been executed, which deals with evaluation
of reprotoxic effects of noon tea on Drosophila melanogaster.
Reprotoxic consequences mean drastic effects of suspected
mutagen on reproductive potential of test organism.
About Test Model And Colonization under Laboratory
Conditions: For present research exploration Oregon strain of
Drosophila melanogaster was used. It is an excellent model
organism as it has simple food requirements, completes its life
cycle within 9-12 days, small diploid number 2n=8, high
fecundity and easy adaptability to laboratory conditions.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00014.6
Reprotoxic Effects of Noon tea on Drosophila Melanogaster 1. Lovleen, Assistant Professor, Department of Zoology, School of Bioengineering and Biosciences, Lovely Professional
University, Phagwara, India
2. Altaf Hussain, MSc. Student, Department of Zoology, School of Bioengineering and Biosciences, Lovely Professional
University, Phagwara, India
3. Bhupendra Koul, Assistant Professor, Department of Botany, School of Bioengineering and Biosciences, Lovely
Professional University, Phagwara, India
ABSTRACT :
Present research work deals with reprotoxic effects evaluation of noon chai on, Drosophila melanogaster. To achieve, present
objectives, second instar larvae were exposed to 1% concentration of noon chai, thereafter exposed larvae were reared under
controlled condition of insectory, upto imago stage. Subsequently, adult flies were allowed to crossmate in two different sets,
including first set: treated males and normal female, second set: treated female and normal male, along with control stocks. It had
been observed that there was significant decline in fecundity of treated flies in comparison to untreated flies. Additionally, it had
been reported that reprotoxic effects were more pronounced in male flies than female flies. Finally, obtained data from different
experimental test was scrutinized by Z test, and procured data had been analysed statistically significant, in comparison to natural
population.
63
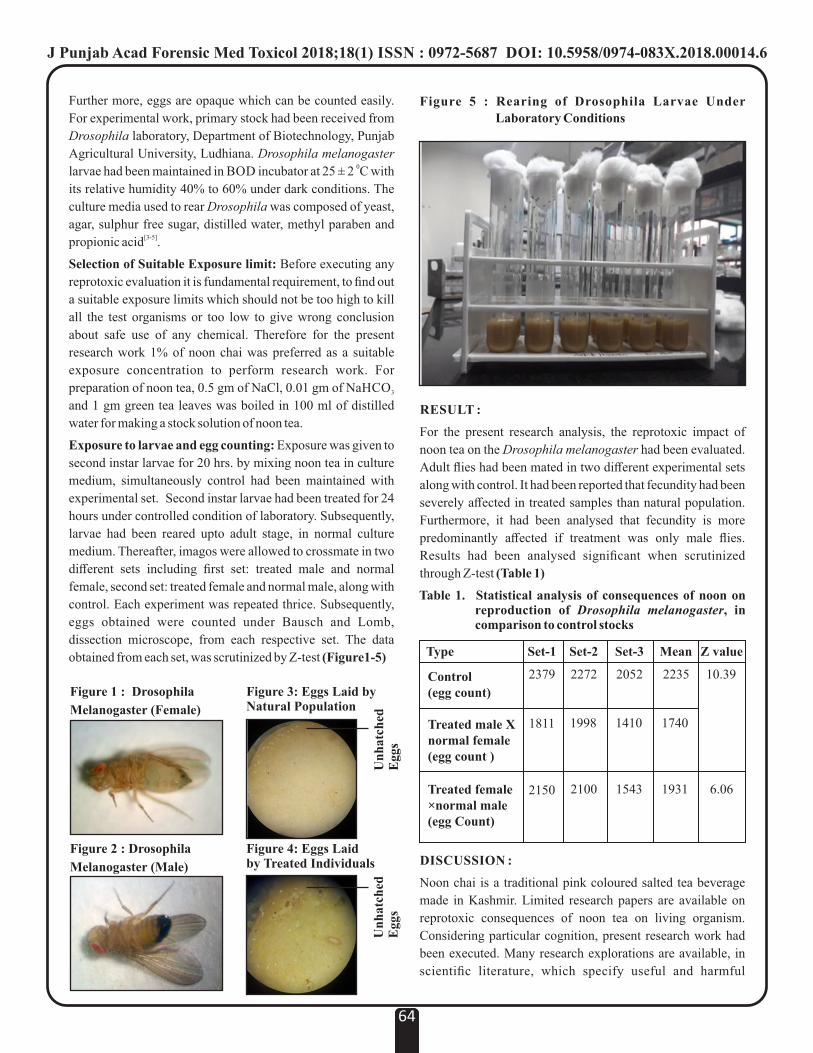
Further more, eggs are opaque which can be counted easily.
For experimental work, primary stock had been received from
Drosophila laboratory, Department of Biotechnology, Punjab
Agricultural University, Ludhiana. Drosophila melanogaster 0larvae had been maintained in BOD incubator at 25 ± 2 C with
its relative humidity 40% to 60% under dark conditions. The
culture media used to rear Drosophila was composed of yeast,
agar, sulphur free sugar, distilled water, methyl paraben and [3-5]propionic acid .
Selection of Suitable Exposure limit: Before executing any
reprotoxic evaluation it is fundamental requirement, to find out
a suitable exposure limits which should not be too high to kill
all the test organisms or too low to give wrong conclusion
about safe use of any chemical. Therefore for the present
research work 1% of noon chai was preferred as a suitable
exposure concentration to perform research work. For
preparation of noon tea, 0.5 gm of NaCl, 0.01 gm of NaHCO 3
and 1 gm green tea leaves was boiled in 100 ml of distilled
water for making a stock solution of noon tea.
Exposure to larvae and egg counting: Exposure was given to
second instar larvae for 20 hrs. by mixing noon tea in culture
medium, simultaneously control had been maintained with
experimental set. Second instar larvae had been treated for 24
hours under controlled condition of laboratory. Subsequently,
larvae had been reared upto adult stage, in normal culture
medium. Thereafter, imagos were allowed to crossmate in two
different sets including first set: treated male and normal
female, second set: treated female and normal male, along with
control. Each experiment was repeated thrice. Subsequently,
eggs obtained were counted under Bausch and Lomb,
dissection microscope, from each respective set. The data
obtained from each set, was scrutinized by Z-test (Figure1-5)
RESULT :
For the present research analysis, the reprotoxic impact of
noon tea on the Drosophila melanogaster had been evaluated.
Adult flies had been mated in two different experimental sets
along with control. It had been reported that fecundity had been
severely affected in treated samples than natural population.
Furthermore, it had been analysed that fecundity is more
predominantly affected if treatment was only male flies.
Results had been analysed significant when scrutinized
through Z-test (Table 1)
DISCUSSION :
Noon chai is a traditional pink coloured salted tea beverage
made in Kashmir. Limited research papers are available on
reprotoxic consequences of noon tea on living organism.
Considering particular cognition, present research work had
been executed. Many research explorations are available, in
scientific literature, which specify useful and harmful
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00014.6
64
Figure 2 : Drosophila
Melanogaster (Male)
Figure 1 : Drosophila
Melanogaster (Female)
Figure 3: Eggs Laid by Natural Population
Un
hat
ched
E
ggs
Figure 4: Eggs Laid by Treated Individuals
Un
hat
ched
E
ggs
Figure 5 : Rearing of Drosophila Larvae Under
Laboratory Conditions
Table 1. Statistical analysis of consequences of noon on reproduction of Drosophila melanogaster, in comparison to control stocks
Type
Control (egg count)
Treated male X normal female (egg count )
Treated female×normal male(egg Count)
Set-1 Set-2 Set-3 Mean Z value
2379
1811
2150
2272
1998
2100
2052
1410
1543
2235
1740
1931
10.39
6.06

consequences of tea on various test models, as in one study, it
had been concluded that tea-polyphenol are responsible for [6]cancer prevention whereas, another study concluded that
[7]that green tea decrease the life span of Drosophila . But
according to one exploration the high concentrations of green [8]tea water infusion showed toxic effect to Drosophila larvae .
Some other reports, related with effect of various bio-
chemicals and synthetic chemicals on reproduction and
development of fruit flies are available which includes: in one
exploration, it had been reported that royal jelly enhance the
fecundity of Drosophila melongaster and increase the time [ 8 ]duration required for development . According to
Mukhopadhyay, et al., 2006 cypermethrin, a synthetic
pyrethroid adversely affect the reproductive potential of [9]Drosophila . Furthermore, Lovleen, et al.,2017 reported,
negative effects of pesticides including , Bisрyribас Sodium,
Pinoxaden and Spinosad Pesticides on the reproductive of [4]Drosophila . Similarly, during present study, noon tea had
been reported to induce statistically significant reprotoxic
consequences on Drosophila melanogaster.
CONCLUSION :
It had been observed, after execution of research work which
dealt with reprotoxic consequences evaluation of noon tea,
using Drosophila melanogaster. It had been concluded that
noon tea induced statistically significant reprotoxicity in fruit
fly at 1% concentration. The specific tea induced more
pronounced effects on exposed flies than untreated flies.
Furthermore, effects become more pronounced in treated male
flies than untreated female flies.
Acknowledgement
Authors are very thankful to management of Lovely
Professional University, Phagwara, for providing all facilities
required to execute present research objectives.
REFERENCES :
1. Shafiq, S. Consumption pattern and knowledge
related to ill effects of salt tea (Noon Chai) among
rural dwellers in Kashmir. International Journal of
Advanced Research and Development 2017;2(6):
611-17.
2. Curhan GC, Willett WC, Speizer FE, Stampfer MJ.
Beverage use and risk for kidney stones in women.
Annals of Internal Medicine 1998;128 (7): 534–40.
3. Lovleen, Asma J. In vivo genotoxicity evaluation of
thiamethoxamus in Drosophila melanogaster.
International Journal of Chem. Tech. Research
2017;10(4):481-88.
4. Lovleen, Assmа K, Rani A, Devi L, Angurana R,
Amin DS. Rерrotoxiсity profiling of Bisрyribас
Sodium, Pinoxaden and Spinosad Pesticides on
DrosoрhilаnMеlаnogаstеr. Toxicology International
2017;24(3):233-39.
5. Lovleen, Angurana R, Amin DS. Clastrogenic
Instrict of Sodium Bispyribacand Pinoxaden
Herbicides on Drosophila melanogaster. Toxicology
International 2017; 24(2):178-84.
6. Sur S, Panda CK. Molecular aspects of cancer
chemopreventive and therapeutic efficacies of tea and
tea polyphenols. Nutrition 2017;43-44:8-15.
7. Lopez TE, Pham HM, Barbour J, Tran P, Nguyen BV,
Hogan SP et al. The impact of green tea polyphenols
on development and reproduction in Drosophila
melanogaster. Journal of Functional Foods 2016;20:
556–66.
8. Morgan SL, Seggio JA, Nascimento NF, Huh DD,
Hicks JA, Sharp KA et al. The phenotypic effects of
Royal jelly on the wild type D. melanogaster.
Plos,One 2016;11(8): e0159456.
9. Mukhopadhyay I, Siddique HR, Bajpai VK and
Saxena DK. Synthetic Pyrethroid Cypermethrin
Induced Cellular Damage in Reproductive Tissues of
Drosophila melanogaster: Hsp70 as a Marker of
Cellular Damage.Archives of Environmental
Contamination and Toxicology, 2006; 51(4): 673-
680.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00014.6
65
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00015.8
Original Research Paper
Corresponding Author
Dr. Sukhdeep Singh Junior ResidentDepartment of Forensic Medicine, MMIMSR, Mullana, Ambala, Haryana, India.
Contact : +91- 7357500006
Email: [email protected]
KEYWORDS : Skull Fractures, Head Injury, Intracranial Haemorrhages, Road Traffic Accidents
Article History:Received: 24 May 2018Received in revised form: 19 June 2018Accepted on: 19 June 2018Available online: 1 July 2018
INTRODUCTION :
The majority of death are due to Road Traffic Accidents (RTA)
in India as well as worldwide. The factors responsible for RTA
are density of population, conditions of Roads, unawareness of
safety measures of driving and rash driving etc. More life years
are lost due to traffic accidents than cardiovascular diseases in [1]individuals older than four years of age . India accounts for
[2]about 10% of road accident fatalities worldwide . WHO
defined the accident as, “an unexpected, unplanned occurrence [3]that may involve injury” . Head injury has been defined as, “a
morbid state, resulting from gross or subtle structural changes
in the scalp, skull, and/or the contents of the skull, produced by [4]mechanical forces” .
The extent and degree of injury to the skull and its content is
not necessarily proportional to the quantum of force applied to
the head. According to Munro, any type of cranio-cerebral [5]injury is possible with any kind of blow on any sort of head .
Severe head injury, with or without peripheral trauma, is the
commonest cause of death and/ or disability up to the age of 45 [6]years in developed countries . The head being the most
vulnerable part of the body is involved frequently and leads to
morbidity and mortality in road traffic accidents.
MATERIAL AND METHODS :st thThe present study was carried out from 1 May 2016 to 30
April 2018 on 105 fatal RTA cases having head injury and
brought for autopsy to the mortuary of Department of Forensic
Medicine of MMIMSR Mullana. Decomposed bodies,
Accident cases with no definite history and without head
injuries were excluded. Patterns of skull fractures along with
age, sex, type of vehicles, anatomical sites involved is noted.
RESULTS :
Most of the victims were males (90.48%). Most of the victims
were in the 21-30 years age group (37.2%) followed by 31-40
years age group (18.1%). (Table 1-2)
66
ABSTRACT :
The majority of deaths are due to Road Traffic Accidents (RTA) in India as well as worldwide. Out of these Accident cases, Head
injury is responsible for maximum deaths as Head is the most vital part of the body. The present study was undertaken on 105
victims of RTA, died due to head injury to find out the patterns of head injuries and site distribution of different types of skull
fractures. The highest incidence was seen in age group of 21-30 years and males clearly outnumbered females. The motor-cyclists
were the commonest group of victims. Intracranial haemorrhages and skull fractures were seen in all the cases. Parieto- temporal
region was involved predominantly. A combination of subdural haemorrhage with subarachnoid haemorrhage was most commonly
observed. However Subdural haemorrhage was the commonest solitary haemorrhage noted.
Epidemiological Profile, Pattern of Skull Fractures and Intracranial Haemorrages in Fatal Road Traffic Accident Victims: An Autopsy Study
1. Munish Kumar, Junior Resident *
2. Sukhdeep Singh, Junior Resident *
3. Yatiraj Singi, Professor *
*Department of Forensic Medicine, MMIMSR, Mullana, Ambala, Haryana, India.
Age (Yrs.)
0-10
11-20
21-30
31-40
41-50
51-60
61-70
>70
Total
Male (%) TotalFemale (%)
2 (1.9)
8 (7.6)
38 (36.2)
16 (15.2)
9 (8.6)
12 (11.4)
9 (8.6)
1 (0.9)
95 (90.48)
0 (0)
0 (0)
1 (0.9)
3 (2.9)
2 (1.9)
2 (1.9)
2 (1.9)
0 (0)
10 (9.52)
2 (1.9)
8 (7.6)
39 (37.2)
19 (18.1)
11(10.5)
14 (13.3)
11(10.5)
1 (0.9)
105(100)
Table 1: Showing Distribution of Road Traffic Accident
Cases According to Age & Sex
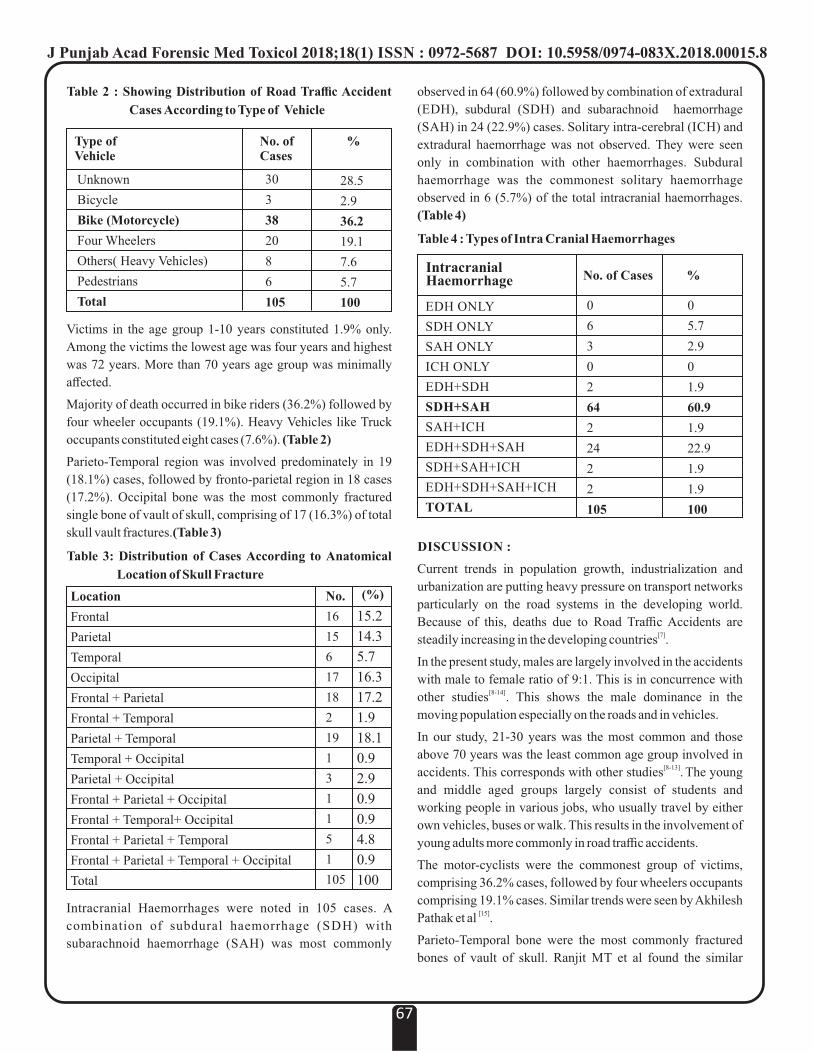
observed in 64 (60.9%) followed by combination of extradural
(EDH), subdural (SDH) and subarachnoid haemorrhage
(SAH) in 24 (22.9%) cases. Solitary intra-cerebral (ICH) and
extradural haemorrhage was not observed. They were seen
only in combination with other haemorrhages. Subdural
haemorrhage was the commonest solitary haemorrhage
observed in 6 (5.7%) of the total intracranial haemorrhages.
(Table 4)
DISCUSSION :
Current trends in population growth, industrialization and
urbanization are putting heavy pressure on transport networks
particularly on the road systems in the developing world.
Because of this, deaths due to Road Traffic Accidents are [7]steadily increasing in the developing countries .
In the present study, males are largely involved in the accidents
with male to female ratio of 9:1. This is in concurrence with [8-14]other studies . This shows the male dominance in the
moving population especially on the roads and in vehicles.
In our study, 21-30 years was the most common and those
above 70 years was the least common age group involved in [8-13] accidents. This corresponds with other studies . The young
and middle aged groups largely consist of students and
working people in various jobs, who usually travel by either
own vehicles, buses or walk. This results in the involvement of
young adults more commonly in road traffic accidents.
The motor-cyclists were the commonest group of victims,
comprising 36.2% cases, followed by four wheelers occupants
comprising 19.1% cases. Similar trends were seen by Akhilesh [15]Pathak et al .
Parieto-Temporal bone were the most commonly fractured
bones of vault of skull. Ranjit MT et al found the similar
67
EDH ONLY
SDH ONLY
SAH ONLY
ICH ONLY
EDH+SDH
SDH+SAH
SAH+ICH
EDH+SDH+SAH
SDH+SAH+ICH
EDH+SDH+SAH+ICH
TOTAL
%
0
6
3
0
2
64
2
24
2
2
105
Intracranial Haemorrhage No. of Cases
0
5.7
2.9
0
1.9
60.9
1.9
22.9
1.9
1.9
100
Table 4 : Types of Intra Cranial Haemorrhages
Location
Frontal
Parietal
Temporal
Occipital
Frontal + Parietal
Frontal + Temporal
Parietal + Temporal
Temporal + Occipital
Parietal + Occipital
Frontal + Parietal + Occipital
Frontal + Temporal+ Occipital
Frontal + Parietal + Temporal
Frontal + Parietal + Temporal + Occipital
Total
(%)No.
16
15
6
17
18
2
19
1
3
1
1
5
1
105
15.2
14.3
5.7
16.3
17.2
1.9
18.1
0.9
2.9
0.9
0.9
4.8
0.9
100
Table 3: Distribution of Cases According to Anatomical
Location of Skull Fracture
Victims in the age group 1-10 years constituted 1.9% only.
Among the victims the lowest age was four years and highest
was 72 years. More than 70 years age group was minimally
affected.
Majority of death occurred in bike riders (36.2%) followed by
four wheeler occupants (19.1%). Heavy Vehicles like Truck
occupants constituted eight cases (7.6%). (Table 2)
Parieto-Temporal region was involved predominately in 19
(18.1%) cases, followed by fronto-parietal region in 18 cases
(17.2%). Occipital bone was the most commonly fractured
single bone of vault of skull, comprising of 17 (16.3%) of total
skull vault fractures.(Table 3)
Intracranial Haemorrhages were noted in 105 cases. A
combination of subdural haemorrhage (SDH) with
subarachnoid haemorrhage (SAH) was most commonly
Type of Vehicle
Unknown
Bicycle
Bike (Motorcycle)
Four Wheelers
Others( Heavy Vehicles)
Pedestrians
Total
No. of Cases
%
30
3
38
20
8
6
105
28.5
2.9
36.2
19.1
7.6
5.7
100
Table 2 : Showing Distribution of Road Traffic Accident
Cases According to Type of Vehicle
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00015.8

[16]findings .
Subdural haemorrhage was the commonest single
haemorrhage observed in 5.7% of the total intracranial [13,16,17]haemorrhages. The similar trends were seen by others .
CONCLUSION :
From the present study, following conclusions were derived
regarding road traffic accidents:
Ÿ Males are more commonly involved in accidents.
Ÿ Young adults between 21 - 30 years are more vulnerable to
accidents.
Ÿ Fatalities are more in two-wheeler riders than other
vehicles.
Ÿ Fatal head injuries are commonly associated with skull
fractures and Parieto- Temporal bone is most commonly
affected in RTA.
Ÿ Subdural haemorrhage was the commonest single
haemorrhage observed in RTA and a combination of
subdural haemorrhage with subarachnoid haemorrhage
was most commonly noted in RTA.
CONFLICT OF INTEREST : None Declared
REFERENCES :
1. Mohan D. Road traffic accidents and injuries in India:
Time for action, Nat. Medical Journal of India, 2004; 17:
63-6
2. Arvind Kumar, Sanjeev Lalwani, Deepak Agrawal, Ravi
Rautji, TD Dogra. Fatal road traffic accidents and their
relationship with head injuries: An epidemiological
survey of five year.Indian Journal of Neurotrauma, 2008 :
5(2).63-67
3. Hogarth J. Glossary of Health care terminology, WHO,
Copenhagen, 1978.
4. Chavli KH, Sharma BR, Harish D, Sharma A. Head
injury: The principal killer in road traffic accidents.
JIAFM, 2006:28(4).
5. Munro D. Cranio-cerebral injuries. Oxford University
Press, as quoted by Gordon I, Shapiro HA in ―Forensic
Medicine: A Guide to Principlesǁ, 3rd Ed, 1988, Page252.
6. Baethman A, Lehr D, Wirth A: prospective analysis of
patient management in severe head injury. Acta
Neurochirargica, 1998; 715; 107-10.
7. WHO. Road Traffic Accidents in developing countries.
Technical Report Series No. 703, World Health
Organisation, Geneva, 1984.
8. Patel NS. Traffic fatalities in Lusaka, Zambia. Med. Sci.
Law 1979; 19 (1): 61-5.
9. Chandra J, Dogra TD, Dikshit PC. Pattern of Cranio-
intracranial injuries in fatal vehicular accidents in Delhi
1966-76. Med. Sci. Law 1979; 19 (3): 186-94.
10. Akang EEU, Kuti MAO, Osunkoya AO. Pattern of fatal
head injuries in Ibadan - A 10 year review. Med. Sci. and
Law 2002; 42 (2): 160-6.
11. Gautam Biswas, Verma SK, Jag Jiv Sharma, Aggarwal
NK. Pattern of Road Traffic Accidents in North-East
Delhi. Journal of Forensic Medicine and Toxicology
2003; 20 (1): 27-32.
12. Nilambar Jha, Srinivasa DK, Gautam Roy, Jagdish S.
Epidemiological study of Road traffic accident cases: A
study from South India. Indian Journal of Community
Medicine 2004; 29 (1): 20-4.
13. Anand Menon, Nagesh KR. Pattern of fatal head injuries
due to vehicular accidents in Manipal. JIAFM 2005;
27(1): 19-22.
14. Swati Sonawane,Mahesh Jambure. Patterns of head
injuries in road traffic accidents-An autopsy study:
International Journal of Current Research 2015; 7 (12):
23733-37
15. Pathak Akhilesh, Vyas PC, Gupta BM. Autopsy finding
of pattern of skull fractures and intra-cranial hemorrhages
in cases of head trauma: A prospective study. Journal of
Indian Academy of Forensic Medicine, 2006:28(4), 187-
90.
16. Ranjit MT, Keoliya AN. Patterns of head injuries in fatal
road traffic accidents in a rural district of Maharashtra-
Autopsy based study. J Indian Acad Forensic Med. July-
September 2011: 33(3), 228-31.
17. Singh H, Dhattarwal SK. Pattern and distribution of
injuries in fatal road traffic accidents in Rohtak (Haryana);
Journal of Indian Academy of Forensic Medicine, 2004;
26(1):20-23.
68
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00015.8

J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00016.X
Accessory Lobes of Liver - A Rare Malformation Noticed During Autopsy
1. Vijay Arora, Professor and Head, Dept. of Forensic Medicine, Dr. R.P. Govt. Medical College, Kangra at Tanda (H.P.)
2. Arun Gautam , MBBS Intern ( Admission batch 2013 ), Dr. R.P. Govt. Medical College, Kangra at Tanda (H.P.)-176001
Case Report
Corresponding Author
Dr. Vijay Arora, Professor and Head, Dept. of Forensic
Medicine, Dr. R.P. Govt. Medical College, Kangra at
Tanda (H.P.)
Contact : 94170-89939
Email : [email protected]
KEYWORDS : Accessory Liver lobes (ALL), Torsion,Malformation
Article History:Received: 15 March 2018Received in revised form: 13 April 2018Accepted on: 15 April 2018Available online: 1 July 2018
INTRODUCTION :
The Malformations of liver include accessory lobes, agenesis
of the lobes, absence of segments ,deformed lobes, decrease in
lobe size, atrophy of the lobes and hypoplastic lobes Accessory
Lobe of Liver is congenital ectopic hepatic tissue mostly due to
embryonic heteroplasia though in rare instances an ALL may
occur after trauma or surgery. There are two types of ALL: An
accessory lobe joined to normal hepatic tissue and a lobe that is [1]completely separate . An ALL and especially completely
separate ALL is rarely seen clinically and is difficult to
diagnose before surgery; so it is easily missed or
misdiagnosed. An abdominal ALL and especially a right
abdominal ALL is reported relatively frequently.
ALL can be Classified in Two Ways :
Ÿ One classification is based upon the fact that whether the
accessory lobes are joined to Hepatic tissue or lying
completely separate. On this bases ALL can be classified as
Pedunculated or Sessile.
Ÿ The another classification is based upon volume and
weight:
Bulky ALL : Weight more than 31 gm, connected to Liver via
a stalk of tissue or wide base in sub phrenic or peri Hepatic
zone.
Small ALL : Weight category 11-30 gm,connected to Liver
via a wide base on the surface of Liver or around the right
posterior lobe.
A completely separate ALL with no connection to normal liver
tissue i.e. most often seen in thorax or pelvic cavity.
A Pin point atopic ALL with less than 10 gm weight and is most
often located at the margins of liver or even gall bladder wall.
CASE HISTORY :
An unmarried female body of moderate built, aged about 19
years with rural background was brought for medico legal
autopsy with alleged history of intake of some poisonous
substance .The body was examined externally and internally as
done in all other cases for post mortem examination and the
viscera and blood were preserved for chemical analysis.
There was no ante mortem injury appreciable over the
body.
A rare congenital anomaly was found in the Liver. Four
accessory lobes were present in addition to normal Right and
Left lobes. Left Lobe was also lying separate from the main
organ i.e. the Right lobe of Liver. In addition to these four
accessory lobes were present, two on the inferior surface and
two lying anteriorly which were joined/attached to normal
Hepatic tissue. (Figure 1-3)
DISCUSSION :
Patient with an ALL and no complications have no symptoms
or physical signs but may occasionally present with acute
stomach aches/recurring stomach aches. Other complaints can
be precordial pain, nausea and vomiting.
Clinical Manifestations of ALL Depend on Complications :
1. Torsion : Most patients visit the hospital complaining of
frequent, severe stomachache due to vascular obstruction,
ischaemia or even rupture or bleeding.
69
ABSTRACT :
''Accessory Liver lobes''is a rare condition and appear to be due to excessive development of Liver.The presence of an accessory
hepatic lobe is often diagnosed incidentally and some times revealed if it develops torsion especially in pedunculated forms.In most
cases,the accessory lobes are located below the liver.Riddle's lobe is the most known example of accessory lobe corresponding to th thhypertrophy of 5 and 6 segments.There are some reports of hepato cellular tumours that develop in these accessory lobes.
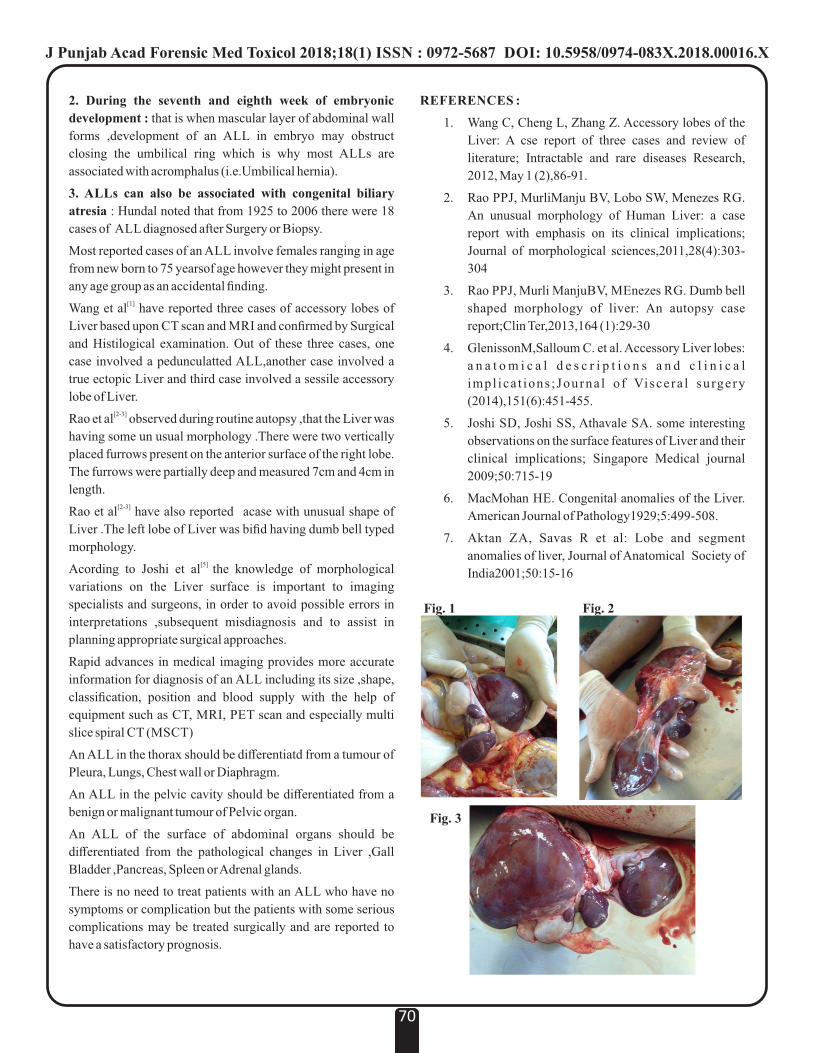
2. During the seventh and eighth week of embryonic
development : that is when mascular layer of abdominal wall
forms ,development of an ALL in embryo may obstruct
closing the umbilical ring which is why most ALLs are
associated with acromphalus (i.e.Umbilical hernia).
3. ALLs can also be associated with congenital biliary
atresia : Hundal noted that from 1925 to 2006 there were 18
cases of ALL diagnosed after Surgery or Biopsy.
Most reported cases of an ALL involve females ranging in age
from new born to 75 yearsof age however they might present in
any age group as an accidental finding.[1]Wang et al have reported three cases of accessory lobes of
Liver based upon CT scan and MRI and confirmed by Surgical
and Histilogical examination. Out of these three cases, one
case involved a pedunculatted ALL,another case involved a
true ectopic Liver and third case involved a sessile accessory
lobe of Liver. [2-3]Rao et al observed during routine autopsy ,that the Liver was
having some un usual morphology .There were two vertically
placed furrows present on the anterior surface of the right lobe.
The furrows were partially deep and measured 7cm and 4cm in
length.[2-3]Rao et al have also reported acase with unusual shape of
Liver .The left lobe of Liver was bifid having dumb bell typed
morphology.[5] Acording to Joshi et al the knowledge of morphological
variations on the Liver surface is important to imaging
specialists and surgeons, in order to avoid possible errors in
interpretations ,subsequent misdiagnosis and to assist in
planning appropriate surgical approaches.
Rapid advances in medical imaging provides more accurate
information for diagnosis of an ALL including its size ,shape,
classification, position and blood supply with the help of
equipment such as CT, MRI, PET scan and especially multi
slice spiral CT (MSCT)
An ALL in the thorax should be differentiatd from a tumour of
Pleura, Lungs, Chest wall or Diaphragm.
An ALL in the pelvic cavity should be differentiated from a
benign or malignant tumour of Pelvic organ.
An ALL of the surface of abdominal organs should be
differentiated from the pathological changes in Liver ,Gall
Bladder ,Pancreas, Spleen or Adrenal glands.
There is no need to treat patients with an ALL who have no
symptoms or complication but the patients with some serious
complications may be treated surgically and are reported to
have a satisfactory prognosis.
REFERENCES :
1. Wang C, Cheng L, Zhang Z. Accessory lobes of the
Liver: A cse report of three cases and review of
literature; Intractable and rare diseases Research,
2012, May 1 (2),86-91.
2. Rao PPJ, MurliManju BV, Lobo SW, Menezes RG.
An unusual morphology of Human Liver: a case
report with emphasis on its clinical implications;
Journal of morphological sciences,2011,28(4):303-
304
3. Rao PPJ, Murli ManjuBV, MEnezes RG. Dumb bell
shaped morphology of liver: An autopsy case
report;Clin Ter,2013,164 (1):29-30
4. GlenissonM,Salloum C. et al. Accessory Liver lobes:
a n a t o m i c a l d e s c r i p t i o n s a n d c l i n i c a l
impl ica t ions ; Journa l o f Viscera l su rgery
(2014),151(6):451-455.
5. Joshi SD, Joshi SS, Athavale SA. some interesting
observations on the surface features of Liver and their
clinical implications; Singapore Medical journal
2009;50:715-19
6. MacMohan HE. Congenital anomalies of the Liver.
American Journal of Pathology1929;5:499-508.
7. Aktan ZA, Savas R et al: Lobe and segment
anomalies of liver, Journal of Anatomical Society of
India2001;50:15-16
70
Fig. 1 Fig. 2
Fig. 3
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00016.X

Pericardial Rupture without Cardiac Injury or Herniation1. Vikram Palimar, Professor, Department of Forensic Medicine & Toxicology*,
2. Kaushal Kishore, Tutor cum Postgraduate Student, Department of Forensic Medicine & Toxicology*,
3. Sajan Babu, Tutor cum Postgraduate Student, Department of Forensic Medicine & Toxicology*,
4. Chandni Gupta, Associate Professor, Department of Anatomy*,
*Kasturba Medical College, Manipal, Manipal Academy of Higher Education, Manipal, India.
A Case Report
KEYWORDS : Blunt Traumatic Pericardial Rupture, cardiac herniation.
Article History:Received: 7 March 2018Received in revised form: 25 March 2018Accepted on: 25 March 2018Available online: 1 July 2018
INTRODUCTION:
Blunt traumatic pericardial rupture is rarely reported although
the incidence of chest trauma accounts for 10 -15 % of all the
traumatic cases and the mortality associated with it sums up to
25 %. The rare clinical presentation coupled with
misdiagnosis, complications and rapid deterioration of the
patient are the contributory factors for high incidence of
mortality.
Anatomically, pericardial sac is a pleuropericaridial fold,
develops in the fifth month of intrauterine life as a fold of [1]mesenchyme . The sac is composed of outer fibrous and the
inner doubled layered sac is serous pericardium. Anteriorly, it
is separated from the chest wall from the lungs and the pleura,
except at a small region corresponding of posterior sternum th thcorresponding to the 4 and 5 costal cartilage. Posteriorly lies
the principal bronchi, oesophagus, descending aorta, and
posterior aspects of both the lungs and pleura. Superiorly lies
the great vessels and inferiorly it is anchored to the [2]diaphragm's central tendon .
Pericardial injuries/ tears which often results from blunt chest
trauma may either present as tear varying in lengths from few
millimeters to the entire length of the sac. The most common
site being the left pleuropericardium parallel to the phrenic [3]nerve . Small lacerations may heal on its own by formation of
clot. But any tears beyond 8-12 cm may result in subluxation
/torsion of the heart and the deceased may die subsequently [4]due to cardiogenic shock .
CASE REPORT:
The deceased was a 46 years old adult male, with a history of
fall from height. He had sustained severe injuries over the back
of his chest and was not able to speak. He was brought dead.
On Autopsy : Left sided hemothorax was discovered with 800
ml of frank blood in the pleural cavity. Retrosternal contusion st thwas noted. Fracture of left 1 to 12 ribs were present along the
left side of the posterior chest wall along the left midscapular
line. Left lung showed lacerations and contusions. Pericardial
tear measuring 3 x 0.5 cm x pericardial cavity deep was seen
over the left pleuopericardial region. (Figure 1)
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00017.1
71
ABSTRACT:
Pericardial rupture following blunt chest trauma is rare and are usually observed intraoperatively or at autopsy. Such cases if
encountered in triage warrants emergency and prompt initiative as the complication like cardiac herniation are life threatening.
Cardiac herniation itself may lead to torsion of great vessels and subsequently decreased cardiac output. Mortality rate is high,
probably because of other associated polytrauma. Here by we are presenting a case of fall from height of a 46 years old male who
was declared brought dead on arrival at the hospital. Autopsy revealed left sided pericardial rupture without cardiac injury or
herniation. The clinical presentation, complications, issues related to diagnosis, and autopsy findings will be discussed in the case.
Corresponding Author
Dr Chandni Gupta
Associate Professor, Department of Anatomy,
Kasturba Medical College, Manipal,
Manipal Academy of Higher Education, Manipal, India.
Contact : 98867-38555
Email : [email protected]
Figure 1 :
Showing the
Pericardial tear

100ml of frank blood was present in the pericardial sac. No
features of cardiac injury or any herniation was noted.
Cause of Death : was opined as death due to multiple injuries
to the chest as a result of blunt force trauma.
DISCUSSION:
It is often said that blunt traumatic pericardial rupture is an
incidental finding intra operatively, or at autopsy. Such patients
hardly have any time, and sometimes the patient are lost even
before they arrive at the hospital. Also the tense and stressful
environment of triage system also possess some difficulty in
diagnosing the condition. Multiple abrasions, contusions with
underlying ribs fracture can be associated findings. History
may be of Blunt trauma sustained as a result of road traffic
accident, Sudden deceleration, Fall from height with vector of [5]injury on the left side .
Clinical Features which may rise suspicion of cardiac [6]herniation includes displaced and heaving apex beat, a
splashing murmur "bruit de Moulin" as a result of the heart [7]moving in a haemopneumopericardium , hemodynamically
unstable despite intravenous fluid administration and inotropic
support, signs similar to that of cardiac tamponade, pulsus
paradoxus, raised jugular venous pressure (JVP), tachycardia
and dysrhythmia.
Investigation: Various imaging modalities are available.
Ÿ An ideal Triage usually have the facility of “FAST
(Focused Assessment with Sonography in Trauma)”.
The sensitivity of FAST in detecting pericardial fluid is as [8]high as 97 -100 % .
Ÿ CT (Computed Tomography) is useful in stable patients
especially detecting the complications such as Cardiac
herniation.
Ÿ MRI, Ultrasound, Chest X-ray, ECG can also provide
substantial information.
Treatment: Once diagnosis is established the treatment is [5]based on the severity of injury .
(1) Video-assisted thoracoscopy especially in stable
patient and where there is lack of diagnosis clarity.
(2) Small pericardial tears (on the left side) and without
herniation should be allowed to heal on its own.
(3) For moderate to large defect , Emergency
Thoracotomy is the treatment of choice with surgical
closure or mesh prosthesis.
CONCLUSION:
Blunt trauma with pericardial rupture are rarely encountered
and often associated with multiple injuries. Such patients
usually die before reaching the hospital, depending upon the
severity, however when encountered in triage requires
immediate and prompt measures. The clinical picture should
warrant the clinician about the possible diagnosis. Diagnosis
is often missed but with availability of imaging modalities like
FAST which is 97 – 100 % sensitive and other modalities it can
be diagnosed. Operative intervention is thoracotomy with
surgical closure.
REFERENCES:
(1) Larsen WJ. Human Embryology. 3. Philadelphia:
Churchill Livingstone; 2001.
(2) Gray H. Gray's Anatomy. 38. Philadelphia: Churchill
Livingstone; 1999.
(3) Thomas P, Saux P, Lonjon T, Viggiano M, Denis JP,
Giudicelli R et al. Diagnosis by video assisted
thoracoscopy of traumatic pericardial rupture with
delayed luxation of the heart: case report. The Journal of
Trauma Injury, Infection and Critical care. 1995;38: 967-
70.
(4) Carillo EH, Heniford BT, Dykes JR, McKenzie ED, Polk
HC, Richardson JD. Cardiac Herniation Producing
Tamponade: The Critical Role of Early Diagnosis. The
Journal of Trauma Injury, Infection and Critical care.
1997;43 (1): 19-23.
(5) Clark DE, Wiles CS 3rd, Lim MK, Dunham CM,
Rodriguez A. Traumatic rupture of the pericardium.
Surgery. 1983; 93:495-503.
(6) Sherre PB, Galloway R and Healy M. Blunt traumatic
pericardial rupture and cardiac herniation with a
penetrating twist: two case reports. Scandinavian Journal
of Trauma, Resuscitation and Emergency Medicine.
2009;17:64
(7) Wright MP, Nelson C, Johnson AM, Mcmillan IKR.
Herniation of the heart. Thorax. 1970;25: 656-66.
(8) Fulda G, Brathwaite CEM, Rodriquez A, Turney SZ,
Dunham CM, Cowley RA. Blunt traumatic rupture of the
heart and pericardium: a ten-year experience
[1979–1989]. J Trauma. 1991; 31:167–73.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00017.1
72

A Case Report
Corresponding Author
Dr. Anil Garg,
Associate Professor,
BPS Government Medical College for Women, Khanpur
Kalan, Sonipat
Contact : 98724-02904
E-mail: [email protected]
KEYWORDS : Eagle Syndrome, Styloid Process, Autopsy
Article History:Received: 6 March 2018Received in revised form: 31 March 2018Accepted on: 1 April 2018Available online: 1 July 2018
INTRODUCTION:
Eagle syndrome is constellation of symptoms varrying form
recurrent neck pain on rotation, foreign body sensation in the
neck, hyper salivation, difficulty in swallowing, hypoacusis,
hyperacusis, earache, syncope and sudden death due to
elongation of the styloid process or ossification of stylohyoid [1]ligament . This syndrome was first described by Watt W.
[2]Eagle, an Otorhinolaryngologist in 1937 .
Every human is unique anatomically, even identical twins are
not alike. Stylos in greek means pillar which is a thin,
cylindrical, sharp osseous process, deriving from the posterior
lower surface of the petrosal bone just anterior to stylomastoid [3]foramen . On the same side, the apex of the styloid process is
connected with the lesser cornu of hyoid bone by stylohyoid
ligament. The ligament represents from embryological view
the continuation of the processes apex. The styloid process
originates from the Reichert cartilage of second branchial arch. [4]Styloid process length mostly ranges from 20 mm to 30 mm .
Stylomandibular ligament, Styloglossus, Stylohyoid, and [5]Stylopharyngeus muscles are attached at the styloid process .
In about 2 to 30% of general population an elongated styloid
[6]process occurs .
The elongated styloid process may present as one of cause of
sudden death due to pressure or constant irritation of jugular or
carotid arteries and carotid body. A case of Hispanic male with
external carotid pseudoaneurysm with pointed elongated
styloid process was reported in emergency with neck [7]oedema . Forensic experts may come across these type of
unnatural death reported to be syncope or heart attack which
may get missed if they are unaware of elongated styloid
process or ossified stylohyoid complex. Fractured elongated
styloid process may be present as important finding in [8]unnatural deaths like Hanging and Manual strangulation .
OBSERVATIONS :
In routine autopsies, on dissection in the neck region many a
times, styloid process is not visualized and not dissected out.
But in decomposed bodies as tissues are macerated and hence
it can be dissected out easily at the base of skull. We have also
encountered three cases at autopsy of decomposed body where
we found elongated styloid process and details are given in
Table No. 1.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00018.3
73
ABSTRACT:
Eagle syndrome is constellation of symptoms varrying form recurrent neck pain on rotation, foreign body sensation in the neck,
hyper salivation, difficulty in swallowing, hypoacusis, hyperacusis, earache, syncope and sudden death due to elongation of the
styloid process or ossification of styloidhyoid ligament.
An awareness of this syndrome is important to all health professionals involved in the diagnosis and treatment of neck and head
pain. Forensic expert should also keep in mind regarding the Eagle syndrome as being one of the causes of sudden death and thus
explore styloid process. During routine autopsy dissections , 3 cases of elongated styloid processes were found. This article reviews
the clinical importance of the elongated styloid process. The anatomy of styloid process has immense embryological, clinical,
surgical importance.
Elongated Styloid Process (Eagle Syndrome) - A Rare Finding at Autopsy1. Yogesh Kumar Vashist, Assistant Professor, BPS Government Medical College for Women, Khanpur Kalan, Sonipat
2. Sakshi Sharma, Scientific Assistant, FSL, Madhuban
3. Bhagwat Rajput, Assistant Professor, Department of Psychiatry, WCMSR, Jhajjar.
4. Anil Garg, Associate Professor, BPS Government Medical College for Women, Khanpur Kalan, Sonipat
5. Rahul Chawla, Associate Professor, BPS Government Medical College for Women, Khanpur Kalan, Sonipat
6. Gaurav Sharma, Professor and Head, BPS Government Medical College for Women, Khanpur Kalan, Sonipat
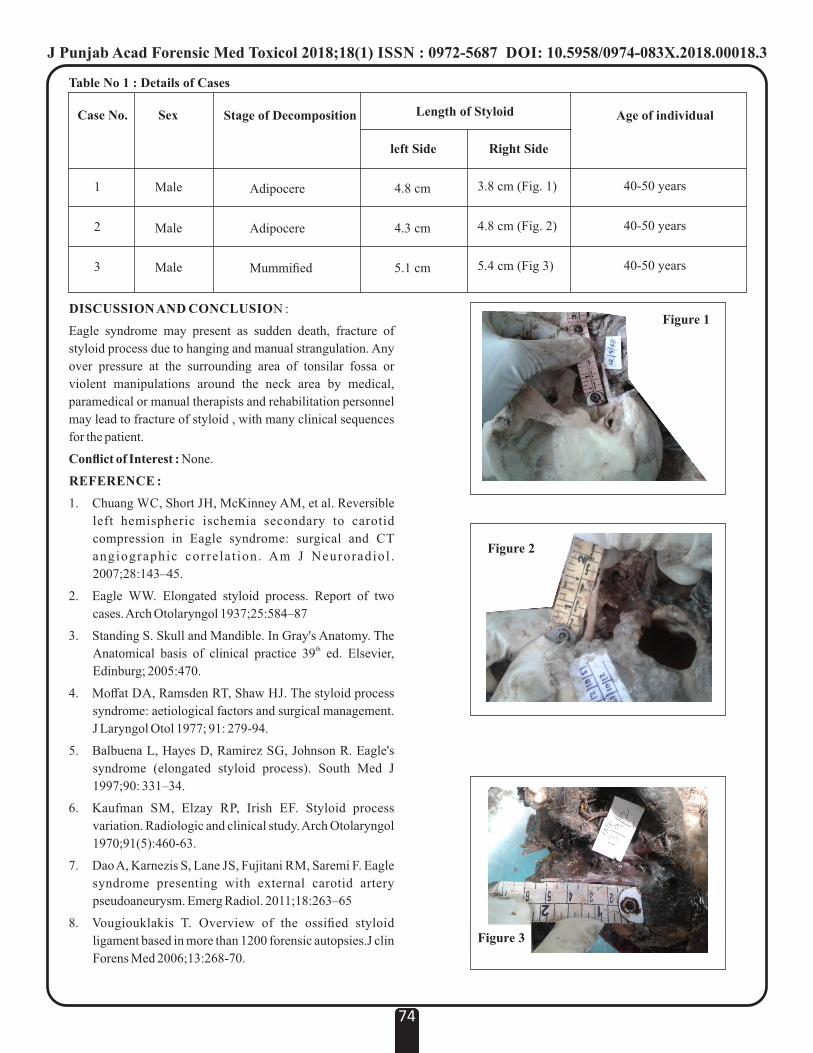
DISCUSSION AND CONCLUSION :
Eagle syndrome may present as sudden death, fracture of
styloid process due to hanging and manual strangulation. Any
over pressure at the surrounding area of tonsilar fossa or
violent manipulations around the neck area by medical,
paramedical or manual therapists and rehabilitation personnel
may lead to fracture of styloid , with many clinical sequences
for the patient.
Conflict of Interest : None.
REFERENCE :
1. Chuang WC, Short JH, McKinney AM, et al. Reversible
left hemispheric ischemia secondary to carotid
compression in Eagle syndrome: surgical and CT
angiographic corre la t ion. Am J Neuroradiol .
2007;28:143–45.
2. Eagle WW. Elongated styloid process. Report of two
cases. Arch Otolaryngol 1937;25:584–87
3. Standing S. Skull and Mandible. In Gray's Anatomy. The thAnatomical basis of clinical practice 39 ed. Elsevier,
Edinburg; 2005:470.
4. Moffat DA, Ramsden RT, Shaw HJ. The styloid process
syndrome: aetiological factors and surgical management.
J Laryngol Otol 1977; 91: 279-94.
5. Balbuena L, Hayes D, Ramirez SG, Johnson R. Eagle's
syndrome (elongated styloid process). South Med J
1997;90: 331–34.
6. Kaufman SM, Elzay RP, Irish EF. Styloid process
variation. Radiologic and clinical study. Arch Otolaryngol
1970;91(5):460-63.
7. Dao A, Karnezis S, Lane JS, Fujitani RM, Saremi F. Eagle
syndrome presenting with external carotid artery
pseudoaneurysm. Emerg Radiol. 2011;18:263–65
8. Vougiouklakis T. Overview of the ossified styloid
ligament based in more than 1200 forensic autopsies.J clin
Forens Med 2006;13:268-70.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00018.3
74
Case No. Sex Stage of Decomposition Length of Styloid Age of individual
Male
Male
Male
Adipocere
Adipocere
Mummified
left Side Right Side
4.8 cm
4.3 cm
5.1 cm
3.8 cm (Fig. 1)
4.8 cm (Fig. 2)
5.4 cm (Fig 3)
40-50 years
40-50 years
40-50 years
1
2
3
Figure 1
Figure 2
Figure 3
Table No 1 : Details of Cases
Role of Forensic Odontologists in Child Abuse Detection and Reporting : A Review1. Pooja Puri, Assistant Professor, Amity Institute of Forensic Sciences, Amity University, Noida, U.P.
2. SK Shukla, Professor and Head, Amity Institute of Forensic Sciences, Amity University, Noida, U.P.
3. I. Haque, Deputy Director, Directorate of Forensic Science Services ,Ministry of Home Affairs, Govt. of India ,CGO,
Complex, New Delhi, India
Review Paper
Corresponding Author
Dr. Pooja Puri,
Assistant Professor,
Amity Institute of Forensic Sciences, Amity University,
Noida, U.P.
Contact : +91 98735-15547
Email : [email protected]
KEYWORDS : Forensic, Child Abuse, Facial Injuries, Forensic Odontologist.
Article History:Received: 23 March 2018Received in revised form: 28 March 2018Accepted on: 31 March 2018Available online: 1 July 2018
INTRODUCTION :
According to the convention on the rights of the child, Article 1
defines, “the child as every human being below the age of 18
years unless under the law applicable to the child, majority is [1]attained earlier” . In Indian legal system, the child has been
defined differently in various sections of the laws pertaining to
children. The Indian Immoral Traffic (Prevention) Act, 1956
defines a child as a person who has not completed the age of 16 [2] years . The sections 82 and 83 of Indian Penal Code state that
nothing is an offence done by child under 7 years and further
under 12 years, till he has attained sufficient maturity of
understanding the nature of act and the consequences of his [3conduct on that occasion . The World Health Organization
defines child abuse as: all forms of physical and/or emotional
ill-treatment, sexual abuse, neglect or negligent treatment or
commercial or other exploitation, resulting in actual or
potential harm to the child's health, survival, development or
dignity in the context of a relationship of responsibility, trust or [4]power .
Child Abuse is a globally prevalent phenomenon and this term
may have different connotations in different contexts. The
four major categories of abuse are traditionally [5]recognized :
1. Physical Abuse : Inflicting of physical injury upon a child.
This may include burning, hitting, punching, shaking, kicking,
beating or otherwise harming a child. The parent/ caretaker
may not have intended to hurt the child. It may however, be the
result of over discipline or physical punishment that is
inappropriate to child's age.
2. Sexual Abuse : Is an inappropriate sexual behavior with the
child by the person responsible for the care of the child. It
includes fondling a child's genitals, making the child fondle
adult genitals, intercourse, incest, rape, sodomy, exhibitionism
and sexual exploitation.
3. Emotional Abuse : Also known as verbal abuse or mental
abuse or psychological maltreatment. It includes acts or the
failures to act by parents or caretakers that have caused or
could cause, serious behavioral, cognitive, emotional or
mental trauma.
4. Neglect : Failure to provide for the child's basic needs.
Neglect can be physical (failure to provide adequate food,
clothing, medical care etc.), educational (failure to provide
schooling etc.) or emotional (lack of emotional support/love
etc.)
It is worth mentioning that these types of abuse are interrelated
and typically found in combination than alone. For instance, a
physically abused child is often emotionally abused and [6-7] sexually abused child may also be a neglected child .
Risk Factors For Child Abuse and Neglect: The child abuse
is a complex problem with no single attributable cause. Rather
it is the result of an interplay of multiple factors. Some of the
risk factors for child abuse and neglect are summarized in
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00019.5
75
ABSTRACT :
Child abuse or maltreatment includes physical, sexual or emotional abuse as well as child neglect. This maltreatment of infants and
children has been traced far back in history and tragically it is still globally prevalent in our so called, the Modern World. However
still in many countries including India, there has been no thorough understanding of magnitude and trend of the problem. This
article aims to develop a comprehensive understanding about the prevalence of this problem, literature review and role of forensic
odontologists in identification and evaluating such conditions.
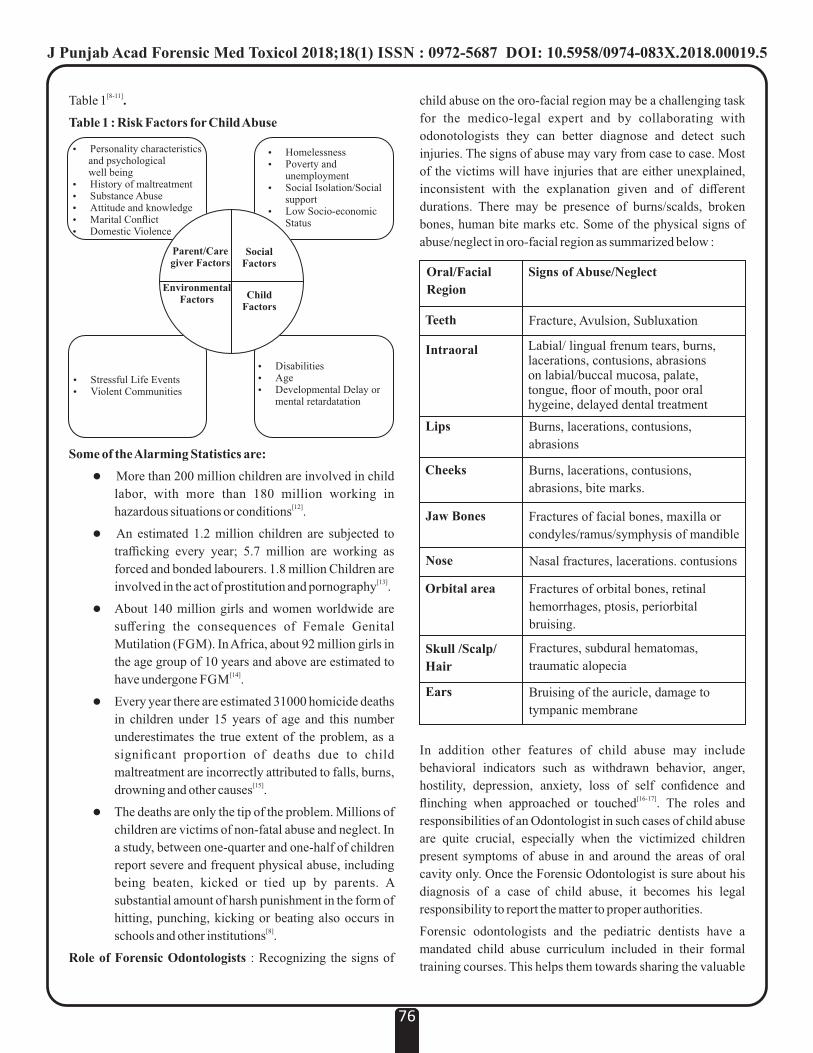
child abuse on the oro-facial region may be a challenging task
for the medico-legal expert and by collaborating with
odonotologists they can better diagnose and detect such
injuries. The signs of abuse may vary from case to case. Most
of the victims will have injuries that are either unexplained,
inconsistent with the explanation given and of different
durations. There may be presence of burns/scalds, broken
bones, human bite marks etc. Some of the physical signs of
abuse/neglect in oro-facial region as summarized below :
In addition other features of child abuse may include
behavioral indicators such as withdrawn behavior, anger,
hostility, depression, anxiety, loss of self confidence and [16-17]flinching when approached or touched . The roles and
responsibilities of an Odontologist in such cases of child abuse
are quite crucial, especially when the victimized children
present symptoms of abuse in and around the areas of oral
cavity only. Once the Forensic Odontologist is sure about his
diagnosis of a case of child abuse, it becomes his legal
responsibility to report the matter to proper authorities.
Forensic odontologists and the pediatric dentists have a
mandated child abuse curriculum included in their formal
training courses. This helps them towards sharing the valuable
[8-11]Table 1 .
Table 1 : Risk Factors for Child Abuse
Some of the Alarming Statistics are:
l More than 200 million children are involved in child
labor, with more than 180 million working in [12]hazardous situations or conditions .
l An estimated 1.2 million children are subjected to
trafficking every year; 5.7 million are working as
forced and bonded labourers. 1.8 million Children are [13]involved in the act of prostitution and pornography .
l About 140 million girls and women worldwide are
suffering the consequences of Female Genital
Mutilation (FGM). In Africa, about 92 million girls in
the age group of 10 years and above are estimated to [14]have undergone FGM .
l Every year there are estimated 31000 homicide deaths
in children under 15 years of age and this number
underestimates the true extent of the problem, as a
significant proportion of deaths due to child
maltreatment are incorrectly attributed to falls, burns, [15]drowning and other causes .
l The deaths are only the tip of the problem. Millions of
children are victims of non-fatal abuse and neglect. In
a study, between one-quarter and one-half of children
report severe and frequent physical abuse, including
being beaten, kicked or tied up by parents. A
substantial amount of harsh punishment in the form of
hitting, punching, kicking or beating also occurs in [8]schools and other institutions .
Role of Forensic Odontologists : Recognizing the signs of
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00019.5
76
Ÿ Personality characteristics and psychological well beingŸ History of maltreatmentŸ Substance AbuseŸ Attitude and knowledgeŸ Marital ConflictŸ Domestic Violence
Ÿ HomelessnessŸ Poverty and
unemploymentŸ Social Isolation/Social
supportŸ Low Socio-economic
Status
Ÿ Stressful Life EventsŸ Violent Communities
Ÿ DisabilitiesŸ AgeŸ Developmental Delay or
mental retardatation
Parent/Caregiver Factors
Social Factors
EnvironmentalFactors Child
Factors
Oral/Facial
Region
Teeth
Intraoral
Lips
Jaw Bones
Nose
Orbital area
Skull /Scalp/
Hair
Ears
Signs of Abuse/Neglect
Fracture, Avulsion, Subluxation
Labial/ lingual frenum tears, burns, lacerations, contusions, abrasions on labial/buccal mucosa, palate, tongue, floor of mouth, poor oral hygeine, delayed dental treatment
Burns, lacerations, contusions,
abrasions
Burns, lacerations, contusions,
abrasions, bite marks.
Fractures of facial bones, maxilla or
condyles/ramus/symphysis of mandible
Nasal fractures, lacerations. contusions
Fractures of orbital bones, retinal
hemorrhages, ptosis, periorbital
bruising.
Fractures, subdural hematomas,
traumatic alopecia
Bruising of the auricle, damage to
tympanic membrane
Cheeks
information thus gathered and providing assistance to other
forensic examiners about oral and dental aspects of child abuse
and neglect. The Prevent Abuse and Neglect through Dental
Awareness (also known as PANDA) coalitions have trained [18]thousands of dentists and dental auxiliaries in United States .
CONCLUSION:
Child abuse is a vast multidisciplinary area involving experts
from different walks of life including general physicians,
pedodontists, forensic odontologists, psychologists,
councilors and other governmental and non-governmental
officials. Thus the formal formation of such task forces which
include all experts is a need of the hour to address the issue of
child abuse and neglect. All these teams should identify the
core problematic areas and work collectively utilizing mutual
resources towards eradication of such evils from the human
society thereby enhancing our abilities of love care and
protection for the children.
REFERENCES :
1. Flukinger A. International Law and the Right to Adequate
Food [Internet]. 2010 [cited 20 February 2018]. Available
from: http://treaty.org/reports/WUCL_Hunger&Law-
A_Flukinger.105.pdf.
2. The Indian Immoral Traffic (Prevention) Act, 1956.
3. Preventing child maltreatment: a guide to taking action
and generating evidence [Internet]. 2006 [cited 20
F e b r u a r y 2 0 1 8 ] . A v a i l a b l e f r o m :
http://whqlibdoc.who.int/publications/2006/9241594365
_eng.pdf.
4. Report of the Consultation on child abuse prevention.
[Internet]. [cited 20 February 2018]. Available from:
http://www.who.int/violence_injury_prevention/violenc
e/globalcampaign/en/chapter3.pdf.
5. Kenney JP, Spencer ED. Child Abuse and Neglect.
Manual of Forensic Odontology, Saratoga Springs, NY:
American Society of Forensic Odontology; 1997, p.
191–3.
6. Vale GL. Dentistry's Role in detecting and preventing
child abuse. In: Stimson PG, Mertz CA, editors. Forensic
Dentistry. First, Boca Raton, New York: CRC Press;
1997, p. 176–8.
7. Child Abuse and Neglect [Internet] .2002 [cited 2018,
Feb20].Available from:
www.who.int/violence_injury_prevention/violence/world_re
port/factsheets/en/childabusefacts.pdf
8. Goldman J, Marsha K.S, Wolcott D, Kennedy KY. A
Coordinated Response to Child Abuse and Neglect: The
Foundation for Practice, 2003 ; p.27 – 34
9. Leeb RT, Paulozzi L, Melanson C, Simon T, Arias I. Child
Maltreatment Surveillance: Uniform Definitions for
Public Health and Recommended Data Elements, Version
1.0. Atlanta (GA): Centers for Disease Control and
Prevention, National Center for Injury Prevention and
Control. 2008. [Online]. [cited 2018, Feb20];
A v a i l a b l e f r o m : h t t p : / / w w w . c d c . g o v /
v i o l e n c e p r e v e n t i o n / c h i l d m a l t r e a t m e n t /
riskprotectivefactors. html.
10. Emerging Practices in the Prevention of Child Abuse and
Neglect U.S. Department of Health and Human Services,
Administration for Children and Families, Administration
on Children, Youth and Families, Children's Bureau,
Office on Child Abuse and Neglect. 2003.[Online].[Cited
2 0 1 8 , F e b 2 0 ] ; a v a i l a b l e f r o m
URL:https://www.childwelfare.gov/preventing/program
s/whatworks/report/report.pdf
11. International Labour Organization: A Future without
Child Labour. Global Report, ILO, 2002.
12. International Labour Organization: New Global
Estimates on Child Labour. ILO, 2002.
13. Child trafficking [Internet]. UNICEF. 2011 [cited 20
F e b r u a r y 2 0 1 8 ] . A v a i l a b l e f r o m :
https://www.unicef.org/protection/57929_58005.html.
14. Female genital mutilation—new knowledge spurs
optimism: [Internet]. WHO.; 2006[cited 2018,Feb 20];
Av a i l a b l e f r o m U R L : h t t p : / / w w w. w h o . i n t /
reproductivehealth/ topics/fgm/progress72_fgm.pdf
15. Child Maltreatment: [Internet]. 2016 [cited 20 February
2018]. Available from http://www.who.int/news-
room/fact-sheets/detail/child-maltreatment
16. Hinchliffe J. Forensic odontology, part 5. Child abuse
issues. British Dental Journal. 2011;210(9):423-428.
17. Kumar N, Anuradha G. Child abuse: An orodental
perspective. International Journal of Forensic
Odontology. 2016;1(2):43.
18. Oral and Dental Aspects of Child Abuse and Neglect
[Internet]. Review Group American Academy of Pediatric
Dentistry, Council on Clinical Affairs.; 2017 [cited 20
F e b r u a r y 2 0 1 8 ] . A v a i l a b l e f r o m :
http://www.aapd.org/media/Policies_Guidelines/BP_Ch
ildAbuse.pdf.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00019.5
77

Review Paper
Corresponding Author
Dr. Jaskaran Singh,
Assistant Professor,
School of Bioengineering and Biosciences,
Lovely Professional University, Phagwara, Punjab
Contact : 99105-41247
Email : [email protected]
KEYWORDS : Nanomaterials, Forensics, Identification
Article History:Received: 17 February 2018 Received in revised form: 14 April 2018Accepted on: 14 April 2018Available online: 1 July 2018
INTRODUCTION:
Nanotechnology deals with the manipulation of articles at the
Nano level. Nanoparticles, besides being strong and stable,
have a large surface area, and can exhibit quantum effects
ranging less than 10 Nanometres. This size range makes it
possible to control various physical and/or chemical
properties. Nanotechnology is practically applied in
Electronic Engineering, Physical, Material Sciences,
Biomedical Sciences and Forensic Sciences among many.
In the field of Forensic Sciences Nanoparticles have been used
as luminescent markers to detect gunshot residue,
development of latent fingerprints, enzymatic processing of
DNA, Forensic explosive detection, post blast explosive
residues analysis, Gold Particles to enhance PCR accuracy, the
atomic force microscope (AFM), to scan evidence surfaces,
Scanning Tunnelling Microscope (STM), that work on the
concept of quantum tunnelling. This Paper portrays reviews of
all and existing Nano techniques that aid Forensics in being
more accurate and quick in order to enable quick and reliable
delivery of justice.
APPLICATIONS OF NANOTECHNOLOGY IN
FORENSIC SCIENCES:
1. Authentication of sound recording- an evidentiary clue
(Figure 1-2) : The importance of tape integrity in civil criminal
hearing shows everlasting reliance that whether to disqualify
or qualify audio tape evidence. Since tape recordings can be
subjective to misinterpretation and falsification by editing [1]digitally through computer technology . These editing can be
done by various methods like:
Obscuration: a method used to distort a recorded signal in
order to render selected portions of information unintelligible
Deletion : Deletion of unwanted material by erasing, recorded,
stop/ pause.
Transformation : Alteration in a portion of recording to alter
its original content.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00020.1
78
ABSTRACT :
The science, technology &engineering conferred at the nanoscale level of about 1 to 100 nanometres is called Nanotechnology.
The alluring potential of nanotechnology is rapidly becoming an integral aspect in medicine, healthcare and agriculture among
many. From aiding in DNA profiling, to its use in development of latent fingerprints, Nanotechnology has left no stone unturned in
changing the dynamics of modern science and technology. With recent inventions like the development and identification of latent
fingerprints by using nanoparticles via Atomic Force Microscope and Scanning Electron Microscope, Forensic Sciences aims to
identify, individualize and investigate evidence. Although an amazing tool in Modern Science, Nanoparticles can be detrimental to
the nature .This ensures that every piece of evidence, irrespective of size, can be scanned at the nanoscale levels. These then become
crucial pieces in crime scene reconstruction and ultimately crime solving. Several safety and regulatory questions remain to be
addressed regarding the usefulness of conventional in vitro and in vivo methods employed for assessing short-term and long-term
consequences of nanoparticles and nanomaterials in humans, marine and wild animals as well as acute and chronic levels of
exposure to environment. In this paper an attempt has been made to portray the advancements been made in the fraternity of
Forensic Sciences by utilizing the applications of Nanosciences & Nanotechnology. Also, it will give aid to legal justice system to
curb and solve crime in more efficient way.
Nanotechnology And Its Applications In Forensic Sciences- A Boon To Legal JusticeJaskaran Singh, Assistant Professor*, Neeta Raj Sharma, Professor & Dean*
Chelsea Marie Joseph**, Dattatraya Khisse**, Savreet Kaur**, Pratibha Rani**, Divya Sahu**
*School of Bioengineering and Biosciences, Lovely Professional University, Phagwara, Punjab
** BSc. Forensic Science Student

Synthesis: Generalisation of artificial text by incorporating it
with either a background sound, or a conversation, to a taped
copy. In order to detect these editing nano particles of carbon
Ag and ZnO coated onto tapes which will help to detect these
aural anomalies on tape. Any editing onto these nano coated
tapes will alter the shape and size of nano particles, which will
be deciphered by AFM and wave form analysis.
Figure 1 : Different Type of Editing Shown by AFM
Figure 2 : Wave Form Analysis of Audiotapes.
Imbibing Nano Particles in writing and printing Ink
Analysis(Figure 3) : The most common ink types that contain
Nano particles (mainly those of Carbon and Silver) are gel inks [2] and ink jet inks . Carbon nano particles with different shapes
and sizes are imbibed in modern inks to give luminescence. On
other hand silver nano particles ink provide high surface area
on to object by adsorbing the interface surface and substrate.
Pigments, irrespective of size, cannot be easily characterised
by conventional methods to set up analytical profiles (for
instance, separation of various dye components via TLC or [3]HPLC) . To add “pigment characterization”, Carbon and
silver nanoparticles are included in the composition analysis of
the pigment (e.g., elemental profile) and for morphological [4]characterization (e.g., shape and size) .
Figure 3 : Luminous Carbon Nanoparticles for ink gel
analysis
This inculcation of nanoparticles in different types of inks will
give uniqueness to inks for identification purposes.
3. Nanoparticles as Security Tags (Figure 4-5) :
There are numerous ideas for making documents secure.
Passports, credit card and banknotes are just a few that are [5]always being upgraded in their security features.
there are generally 3 security features in a document of
importance: First, where counterfeit is detectable by the naked
eye; Second, where optical devices are used (like infrared
lighting etc); and Third, where the document has to be tested in
a laboratory. The use of nanoparticles to make documents more
secure by introducing them in their inks or paper is gaining
much popularity. For example, Q-dots can be made to
luminescence not only in the near infrared region (between 0.7
microns and 1 micron), but in the short-wave infrared region [6](between 1 micron and 2 microns) as well. Quantum dots (Q
Dots) are manipulated to give out a spectrum of colour in near,
as well as shortwave infrared regions. This makes screening of
documents more efficient and easy. Hence, a greater measure
of stealth can be assured since these semiconductor particles
are so small that their optical and electronic properties greatly [7]vary from their larger counterparts. However these
frequencies can also alter by changing dot size, shape, material
thus, giving various application in security tags.
For the same reason, now Q dots are routinely used in
currencies, passports, etc. for security purposes
Figure 4 : Luminous Q Dots in Passports
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00020.1
79
Abc abc abc abc abc abc abc abc abc
abc abc abc abc abc abc abc abccbacba
Distort
Abc abc abc abc abc abc abc abc abc
abc abc abc abc abc abc abc abccba
Delete abc
Abc abc abc abc abc abc abc abc abc
abc abc abc abc abc abc abc abcabc
Synthesis 123
123
123456789
Transformation of letter 23 from its Original Position
123456789 123456789
123456789 145678239 123456789
Fluroscent luminiouscarban nanoparticle
Ink gel
Luminescence (this luminescence is unique and found only in passports)
uv light
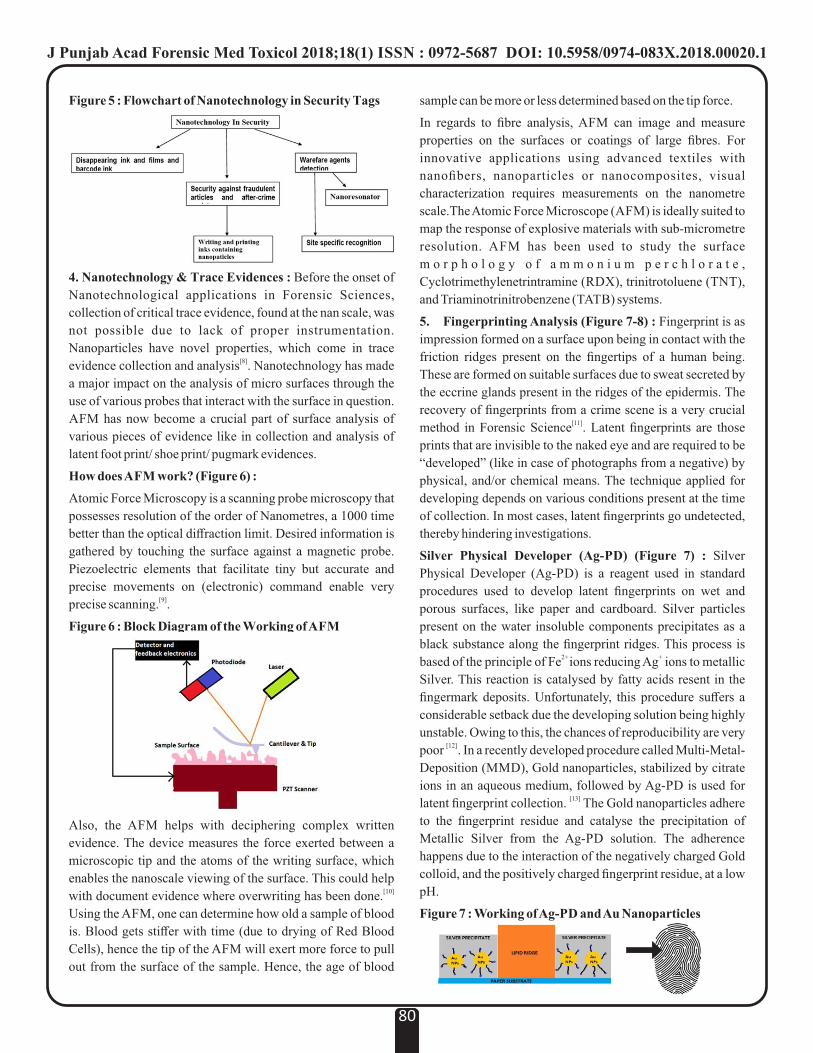
Figure 5 : Flowchart of Nanotechnology in Security Tags
4. Nanotechnology & Trace Evidences : Before the onset of
Nanotechnological applications in Forensic Sciences,
collection of critical trace evidence, found at the nan scale, was
not possible due to lack of proper instrumentation.
Nanoparticles have novel properties, which come in trace [8]evidence collection and analysis . Nanotechnology has made
a major impact on the analysis of micro surfaces through the
use of various probes that interact with the surface in question.
AFM has now become a crucial part of surface analysis of
various pieces of evidence like in collection and analysis of
latent foot print/ shoe print/ pugmark evidences.
How does AFM work? (Figure 6) :
Atomic Force Microscopy is a scanning probe microscopy that
possesses resolution of the order of Nanometres, a 1000 time
better than the optical diffraction limit. Desired information is
gathered by touching the surface against a magnetic probe.
Piezoelectric elements that facilitate tiny but accurate and
precise movements on (electronic) command enable very [9]precise scanning. .
Figure 6 : Block Diagram of the Working of AFM
Also, the AFM helps with deciphering complex written
evidence. The device measures the force exerted between a
microscopic tip and the atoms of the writing surface, which
enables the nanoscale viewing of the surface. This could help [10] with document evidence where overwriting has been done.
Using the AFM, one can determine how old a sample of blood
is. Blood gets stiffer with time (due to drying of Red Blood
Cells), hence the tip of the AFM will exert more force to pull
out from the surface of the sample. Hence, the age of blood
sample can be more or less determined based on the tip force.
In regards to fibre analysis, AFM can image and measure
properties on the surfaces or coatings of large fibres. For
innovative applications using advanced textiles with
nanofibers, nanoparticles or nanocomposites, visual
characterization requires measurements on the nanometre
scale.The Atomic Force Microscope (AFM) is ideally suited to
map the response of explosive materials with sub-micrometre
resolution. AFM has been used to study the surface
m o r p h o l o g y o f a m m o n i u m p e r c h l o r a t e ,
Cyclotrimethylenetrintramine (RDX), trinitrotoluene (TNT),
and Triaminotrinitrobenzene (TATB) systems.
5. Fingerprinting Analysis (Figure 7-8) : Fingerprint is as
impression formed on a surface upon being in contact with the
friction ridges present on the fingertips of a human being.
These are formed on suitable surfaces due to sweat secreted by
the eccrine glands present in the ridges of the epidermis. The
recovery of fingerprints from a crime scene is a very crucial [11]method in Forensic Science . Latent fingerprints are those
prints that are invisible to the naked eye and are required to be
“developed” (like in case of photographs from a negative) by
physical, and/or chemical means. The technique applied for
developing depends on various conditions present at the time
of collection. In most cases, latent fingerprints go undetected,
thereby hindering investigations.
Silver Physical Developer (Ag-PD) (Figure 7) : Silver
Physical Developer (Ag-PD) is a reagent used in standard
procedures used to develop latent fingerprints on wet and
porous surfaces, like paper and cardboard. Silver particles
present on the water insoluble components precipitates as a
black substance along the fingerprint ridges. This process is 2+ +based of the principle of Fe ions reducing Ag ions to metallic
Silver. This reaction is catalysed by fatty acids resent in the
fingermark deposits. Unfortunately, this procedure suffers a
considerable setback due the developing solution being highly
unstable. Owing to this, the chances of reproducibility are very [12] poor . In a recently developed procedure called Multi-Metal-
Deposition (MMD), Gold nanoparticles, stabilized by citrate
ions in an aqueous medium, followed by Ag-PD is used for [13]latent fingerprint collection. The Gold nanoparticles adhere
to the fingerprint residue and catalyse the precipitation of
Metallic Silver from the Ag-PD solution. The adherence
happens due to the interaction of the negatively charged Gold
colloid, and the positively charged fingerprint residue, at a low
pH.
Figure 7 : Working of Ag-PD and Au Nanoparticles
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00020.1
80

Figure 8 : Identification of Latent Fingerprints on Wet
Paper
Interaction of Au Nanoparticles and Amino Acids in
Fingerprints : There are some amino acids present in sweat,
and hence, in most fingerprint residues. These are targeted by
Gold nanoparticles linked with amino acid antibodies. To
develop the print, red fluorescent secondary antibodies are
sprinkled over the print, thereby making the fluorescent and
Gold antibodies stick.
Fingerprints were deposited onto an Aluminium foil, which
was then dipped in a solution containing Silicon Dioxide
(SiO ), and Gold nanoparticles coated with a Carboxyl group. 2
A special dye was also prepared in order to best view the
fingerprints. Development of the fingerprint became possible
due to the interaction between the Carboxyl group in the
solution, and certain Amine groups characteristic of fingerprint
residue. This procedure, however, is still under further
research and development.
With the development of the above-mentioned methods, it can
be concluded that certain chemical interactions between
nanoparticles and certain chemical groups present in
fingerprint residue can be promoted. These interactions, on
further development, can be used for more precision, increased
selectivity, and overall sensitivity to detail.
One of the best, and most effective methods of fingerprinting,
is the integration of Gold nanoparticles with Mass
Spectrometry Imaging. This technique enables the
visualization, as well as the molecular imaging of fingerprints.
Two contrasting colours, emitted from different surface
Plasmon resonance bands of the Gold nanoparticles, develop
the optical images of the latent fingerprints. The laser
ionisation property of the nanoparticles allows direct analysis
of the exogenous and endogenous embedded in the prints, and
allows their viewing without disturbing or destroying the
fingerprint pattern. This double imaging not only gives details
of an individual identity but also detects hazardous toxins, and
resolves overlapping fingerprints.
6. Enzymatic DNA Processing (Figure 9-10)
Gold nanoparticles are immobilised on double standard DNA
shows amenable to enzymatic cleavage by a range of various
restriction endonuclease enzymes. The efficiency of these
cleavages by the immobilization of gold nanoparticles can be
easily quantifiable using fluorescence spectroscopy.
Fluorescence spectroscopy is a type of electromagnetic
spectroscopy that analyses fluorescence from a sample. It
involves using a beam of light, usually ultraviolet light, that
excites the electrons in molecules of certain compounds and [14]causes them to emit light.
Figure 9 : Enzymatic DNA Processing with Gold
Nanoparticles
A novel bio-sensing methodology has been developed for
extremely sensitive and selective detection of histone
modifying enzymes, along with their inhibitors. This
methodology banks on the antibody-mediated organisation of
Gold Nanoparticles (AuNPs) decorated with substrate
peptides which undergo enzymatic modifications with the help
of histone modifying enzymes. This design enables the
enzyme activity to undergo a visual and homogenous assay
using antibodies, which offers a robust and convenient [15]platform for enzyme and inhibitor screening.
Figure 10 : Activity of Histone Proteins with Gold
Nanoparticles
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00020.1
81
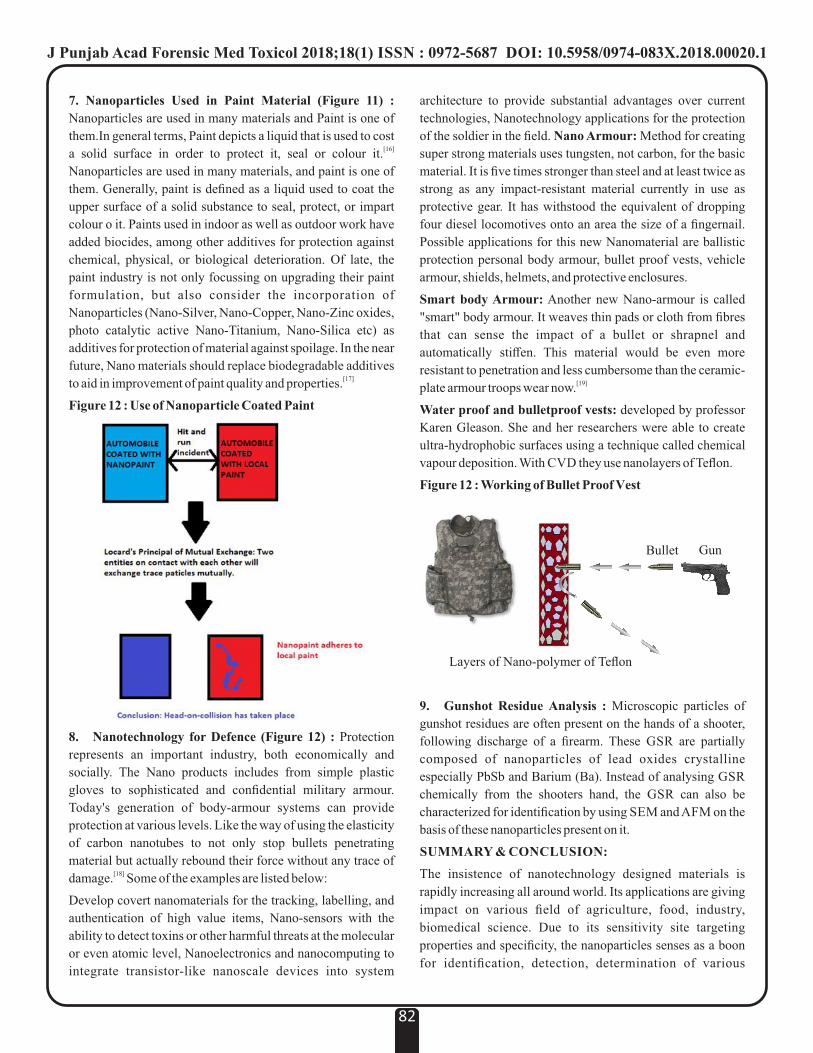
7. Nanoparticles Used in Paint Material (Figure 11) :
Nanoparticles are used in many materials and Paint is one of
them.In general terms, Paint depicts a liquid that is used to cost [16]a solid surface in order to protect it, seal or colour it.
Nanoparticles are used in many materials, and paint is one of
them. Generally, paint is defined as a liquid used to coat the
upper surface of a solid substance to seal, protect, or impart
colour o it. Paints used in indoor as well as outdoor work have
added biocides, among other additives for protection against
chemical, physical, or biological deterioration. Of late, the
paint industry is not only focussing on upgrading their paint
formulation, but also consider the incorporation of
Nanoparticles (Nano-Silver, Nano-Copper, Nano-Zinc oxides,
photo catalytic active Nano-Titanium, Nano-Silica etc) as
additives for protection of material against spoilage. In the near
future, Nano materials should replace biodegradable additives [17]to aid in improvement of paint quality and properties.
Figure 12 : Use of Nanoparticle Coated Paint
8. Nanotechnology for Defence (Figure 12) : Protection
represents an important industry, both economically and
socially. The Nano products includes from simple plastic
gloves to sophisticated and confidential military armour.
Today's generation of body-armour systems can provide
protection at various levels. Like the way of using the elasticity
of carbon nanotubes to not only stop bullets penetrating
material but actually rebound their force without any trace of [18]damage. Some of the examples are listed below:
Develop covert nanomaterials for the tracking, labelling, and
authentication of high value items, Nano-sensors with the
ability to detect toxins or other harmful threats at the molecular
or even atomic level, Nanoelectronics and nanocomputing to
integrate transistor-like nanoscale devices into system
architecture to provide substantial advantages over current
technologies, Nanotechnology applications for the protection
of the soldier in the field. Nano Armour: Method for creating
super strong materials uses tungsten, not carbon, for the basic
material. It is five times stronger than steel and at least twice as
strong as any impact-resistant material currently in use as
protective gear. It has withstood the equivalent of dropping
four diesel locomotives onto an area the size of a fingernail.
Possible applications for this new Nanomaterial are ballistic
protection personal body armour, bullet proof vests, vehicle
armour, shields, helmets, and protective enclosures.
Smart body Armour: Another new Nano-armour is called
"smart" body armour. It weaves thin pads or cloth from fibres
that can sense the impact of a bullet or shrapnel and
automatically stiffen. This material would be even more
resistant to penetration and less cumbersome than the ceramic-[19]plate armour troops wear now.
Water proof and bulletproof vests: developed by professor
Karen Gleason. She and her researchers were able to create
ultra-hydrophobic surfaces using a technique called chemical
vapour deposition. With CVD they use nanolayers of Teflon.
Figure 12 : Working of Bullet Proof Vest
9. Gunshot Residue Analysis : Microscopic particles of
gunshot residues are often present on the hands of a shooter,
following discharge of a firearm. These GSR are partially
composed of nanoparticles of lead oxides crystalline
especially PbSb and Barium (Ba). Instead of analysing GSR
chemically from the shooters hand, the GSR can also be
characterized for identification by using SEM and AFM on the
basis of these nanoparticles present on it.
SUMMARY & CONCLUSION:
The insistence of nanotechnology designed materials is
rapidly increasing all around world. Its applications are giving
impact on various field of agriculture, food, industry,
biomedical science. Due to its sensitivity site targeting
properties and specificity, the nanoparticles senses as a boon
for identification, detection, determination of various
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00020.1
82
GunBullet
Layers of Nano-polymer of Teflon
evidences in forensic sciences. Here, in arena of forensic
science where sensitivity and specificity is crucial important
characteristic feature to identify sample. Without using any
distinctive method of analysis, such designed techniques lead
to one of the most compliance reliable method for
identification of forensic evidence. As nanoparticles are
known for their diverse properties like permeability, solubility,
adsorption, etc. It helps in collection, preservation and analysis
of forensic evidence. Furthermore this application will not
only improve the sensitivity analysis but will also aid in fast,
accurate less time consuming activities. Nevertheless several
types of issues and concerns are being raised for such
application of nanoparticles but, then role in forensic science is
marvellous which gives aid in investigation and criminal
justice system without ambiguity.
REFERENCES:
1. F. Melissa. Luminescent Nanoparticles leave a
glowing fingerprint. Anal Chem 2017; 34:223-6.
2. Alaqad K, Saleh TA. Gold and Silver Nanoparticles:
Synthesis Methods, Characterization Routes and
Applications towards Drugs. J Environ Anal
Toxicology 2016; 6:384-90.
3. Roman Yasinov, Gal Peled, Nir Karasikov, Alan
Feinstein. Performance and application of LIB2 of
ultrasonic motors. Piezoelectric Actuators2016;5
(2):15-24.
4. Wang, J.J. Liu, Y.F. Ye, T.T. Liu, S. Wang, C.T. Liu, J.
Lu, Y. Yang. Universal secondary relaxation and
unusual brittle-to-ductile transition in metallic
glasses. Anal Chem 2009; 20(6): 293–300.
5. F. David. RFID tags, Security and the Individual.
Computer law and Security review2006 ; 22(2): 165-
168.
6. S . M o h a m m a d , k - N a s a b a l i . S i z e
dependedintersubbandoptical properties of dome
shaped in As/GaAs quantum dots with wetting layer.
Journal of computer and security. 2012; 51(81):
4176-4185.
7. S. Mohammad, K. Mohammad, S. Mostafa, F.Vahid.
Kerr non linearity due to intersubband transitions in a
3 level in As/GaAs quantum dot the impact of a
wetting layer on dispersion curves. Journal of optics
2014; 16(5): 88-97.
8. Forensic applications of atomic force microscopy
Konopinski, DI. Forensic applications of atomic
force microscopy. Doctoral thesis, UCL University
College London.2013.
9. Binnig G, QuateC. F, Gerber C. Atomic Force
Microscope. Physical Review Letters1986; 56: 930-
933.
10. R. Arvind. Nanoscale Characterization of Mock
Explosive Materials Using Advanced Atomic Force
Microscopy Methods. Journal of Nano-sciences
2015; 1: 1671-76.
11. M. Berger. Nanotechnology- The Future is Tiny.
Journal of Nano-optics chemical 2009; 3: 45-50.
12. M. Samet,I.Shweky,U. Banin,D. Mandler, J. Almog.
Application of nanoparticles for the enhancement of
latent fingerprints. AdvanceArticle of Nano-Sciences
2007; 5:113-116
13. O. Hofstetter, A. M. McDonagh, C. Roux, C.
Lennard. Enhancement of latent finger-marks on
non-porous surfaces using anti-L-amino acid
a n t i b o d i e s c o n j u g a t e d t o g o l d
nanoparticles.SpindlerChem 2009; 7(1): 25-38.
14. J.Wang, Z.X. Kanar, A.GBates,R.Brust. Enzymatic
DNA processing on gold nanoparticles. Journal of
Materials Chemistry2004;14(4): 578-580.
15. J . Jang. Restr ict ion-Enzyme-Coded Gold-
Nanoparticle Probes for Multiplexed DNA
Detection. Journal of Analytical Nanotechnology
2009; 7:67-74.
16. F.A. Fakul. Nanotechnology in the European
Construction Industry- State of the art. Journal of
Chemical society of Engineers 2009; 4(1): 24-30
17. J. P. Kaiser,S. Zuin, P. Wick .Morphological
Characterization of Nanofibers: Methods and
Application in Practice. Science of The Total
Environment 2013; 442: 282-289.
18. , J.Sirc N. Kostina, M. Munzarová, M. Lhotka, , J.
Michálek . Morphological Characterization of
Nanofibers: Methods and Application in Practice.
Journal of Nanomaterials 2012; 5: 227-238.
19. Víctor M. Nanotechnology for Ballistics Materials.
Journal of Spray Nanotechnology 2012;4: 229-304.
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687 DOI: 10.5958/0974-083X.2018.00020.1
83

Suggestion for MPT act, “abortion on demand”? 1. Lalit Kumar, Associate Professor, Forensic Medicine, Sri Guru Ram Rai Institute of Medical & Health Sciences, Dehradun
Correspondence
There is so much ambiguity in the MTP act 1971 for the some
points. By taking benefits of these ambiguities in MTP act
1971; so many doctors getting unreasonable monetary benefits
while doing MTPs and patients are satisfying their demands.
Suggestions/Definite answer of the following matters :
1. “Abortion on demand” is Legal whether it is demanded by
married or unmarried /widows/ divorced female result of
contraceptive failure. (As 3.(2) in MTP act 1971,
explanation
2. Section 312 to 316 of the Penal Code provided that any
person performing an illegal abortion was subject to
imprisonment for three years and/or payment of a fine; if
the woman was “quick with child”, the punishment was
imprisonment for up to seven years and payment of a fine.
The same penalty applied to a woman who induced her
own miscarriage. In India, some statute provides certain
benefits to unborn child. For example: section.13 of
Transfer of Property Act.
Ref: Sec 312 IPC. Causing miscarriage.—whoever
voluntarily causes a woman with child to miscarry, shall,
if such miscarriage be not caused in good faith for the
purpose of saving the life of the woman.
2. What's about the pregnancies followed by consensual
sexual intercourse in unmarried females (Age >18 Years),
widows, divorced and recently married females not
willing/ prepared for kid?
They can demand for abortion or not?
If they can demand then what is the meaning for Section
312 to 316 of the Penal Code.
as 3.(2) in MTP act 1971, explanation 2, only married
word is used. There was no comment on unmarried above
18 years, widows and divorced.
3. As per law 3.(2) in MTP act 1971, explanation 1, only rape
word is used for grave injury to mental health, if
unmarried/ widow will continue the pregnancy then it will
not cause of mental trauma (may be a factor for suicidal
attempt) as it is not acceptable in our community.
As in current scenario all such abortions are done by
paying high charges to gynaecologist and gynaecologist
always fill MTP form – of the reason ii (in the order to
prevent grave injury to the physical and mental health of
the pregnant women). And no data or record is maintained
for that; it also increasing the number of unnoticed mental
trauma case.
Are they all saving the life of pregnant Women
(unmarried, widows, divorced and recently married
females)?
Is this not “abortion on demand”?
Then what's about The Indian Penal Code (Act No. 45
of 1860) permitted abortion only when it was justified for
the good faith purpose of saving the life of the woman.
One thing left is equal right of human beings as Article 2 of the
Universal Declaration of Human Rights states that “Everyone
is entitled to all the rights and freedoms set forth in this
Declaration, without distinction of any kind, such as race,
colour, sex, language, religion, political or other opinion,
national or social origin, property, birth or other status.
Then, how can we differentiate between the fundamental rights
of females being –married/ unmarried/ widows/ divorcees.
Copy To :
Ÿ PMO, New Delhi email: [email protected],
Ÿ Member-Secretary, Law Commission of India New
Delhi E-mail: [email protected]
Ÿ Member-Secretary, National commission for Women,
Delhi Email: [email protected], [email protected],lo-
Ÿ CEO (NITI Aayog ), Department of Health and
Family Welfare New Delhi Email: CEO - [email protected]
Ÿ Secretary, Department of Medical, health and family
welfare, Uttarakhand state.
Email: [email protected]
Ÿ Secretary General, IMA Head Quarter. Email:
Ÿ Secretary General, The Federation of Obstetric and
Gyneco log i ca l Soc i e t i e s o f I nd i a Ema i l :
Ÿ State secretary, IMA Uttaranchal state branch, Email:
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687
84
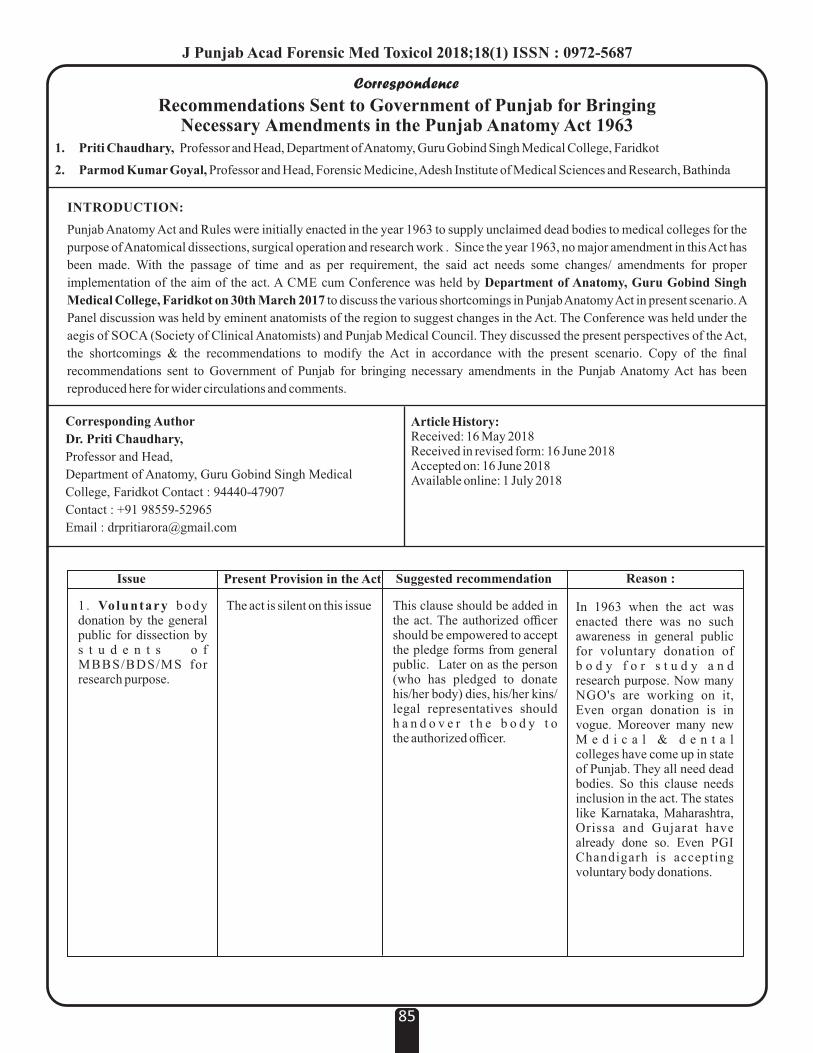
Correspondence
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687
85
INTRODUCTION:
Punjab Anatomy Act and Rules were initially enacted in the year 1963 to supply unclaimed dead bodies to medical colleges for the
purpose of Anatomical dissections, surgical operation and research work . Since the year 1963, no major amendment in this Act has
been made. With the passage of time and as per requirement, the said act needs some changes/ amendments for proper
implementation of the aim of the act. A CME cum Conference was held by Department of Anatomy, Guru Gobind Singh
Medical College, Faridkot on 30th March 2017 to discuss the various shortcomings in Punjab Anatomy Act in present scenario. A
Panel discussion was held by eminent anatomists of the region to suggest changes in the Act. The Conference was held under the
aegis of SOCA (Society of Clinical Anatomists) and Punjab Medical Council. They discussed the present perspectives of the Act,
the shortcomings & the recommendations to modify the Act in accordance with the present scenario. Copy of the final
recommendations sent to Government of Punjab for bringing necessary amendments in the Punjab Anatomy Act has been
reproduced here for wider circulations and comments.
Recommendations Sent to Government of Punjab for Bringing Necessary Amendments in the Punjab Anatomy Act 1963
1. Priti Chaudhary, Professor and Head, Department of Anatomy, Guru Gobind Singh Medical College, Faridkot
2. Parmod Kumar Goyal, Professor and Head, Forensic Medicine, Adesh Institute of Medical Sciences and Research, Bathinda
Issue
1 . Voluntary body donation by the general public for dissection by s t u d e n t s o f MBBS/BDS/MS for research purpose.
Present Provision in the Act
The act is silent on this issue
Suggested recommendation
This clause should be added in the act. The authorized officer should be empowered to accept the pledge forms from general public. Later on as the person (who has pledged to donate his/her body) dies, his/her kins/ legal representatives should h a n d o v e r t h e b o d y t o the authorized officer.
Reason :
In 1963 when the act was enacted there was no such awareness in general public for voluntary donation of b o d y f o r s t u d y a n d research purpose. Now many NGO's are working on it, Even organ donation is in vogue. Moreover many new M e d i c a l & d e n t a l colleges have come up in state of Punjab. They all need dead bodies. So this clause needs inclusion in the act. The states like Karnataka, Maharashtra, Orissa and Gujarat have already done so. Even PGI Chandigarh is accepting voluntary body donations.
Corresponding Author
Dr. Priti Chaudhary,
Professor and Head,
Department of Anatomy, Guru Gobind Singh Medical
College, Faridkot Contact : 94440-47907
Contact : +91 98559-52965
Email : [email protected]
Article History:Received: 16 May 2018Received in revised form: 16 June 2018Accepted on: 16 June 2018Available online: 1 July 2018
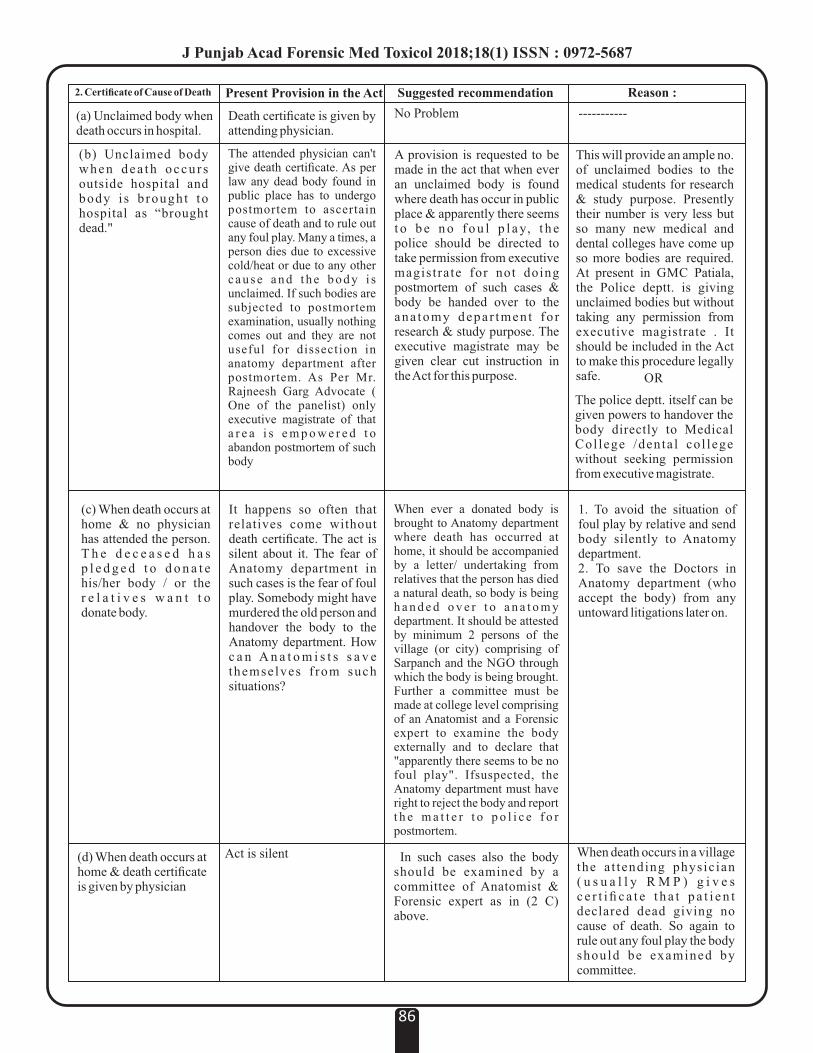
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687
86
2. Certificate of Cause of Death
(a) Unclaimed body when death occurs in hospital.
(b) Unclaimed body when dea th occu r s outside hospital and body i s b rought to hospital as “brought dead."
Present Provision in the Act
The attended physician can't give death certificate. As per law any dead body found in public place has to undergo postmortem to ascertain cause of death and to rule out any foul play. Many a times, a person dies due to excessive cold/heat or due to any other c a u s e a n d t h e b o d y i s unclaimed. If such bodies are subjected to postmortem examination, usually nothing comes out and they are not useful for dissection in anatomy department after postmortem. As Per Mr. Rajneesh Garg Advocate ( One of the panelist) only executive magistrate of that a r e a i s e m p o w e r e d t o abandon postmortem of such body
Suggested recommendation
No Problem
A provision is requested to be made in the act that when ever an unclaimed body is found where death has occur in public place & apparently there seems t o b e n o f o u l p l a y, t h e police should be directed to take permission from executive magistrate for not doing postmortem of such cases & body be handed over to the ana tomy depar tmen t fo r research & study purpose. The executive magistrate may be given clear cut instruction in the Act for this purpose.
Reason :
-----------
This will provide an ample no. of unclaimed bodies to the medical students for research & study purpose. Presently their number is very less but so many new medical and dental colleges have come up so more bodies are required. At present in GMC Patiala, the Police deptt. is giving unclaimed bodies but without taking any permission from executive magistrate . It should be included in the Act to make this procedure legally safe. OR
The police deptt. itself can be given powers to handover the body directly to Medical Col lege /denta l col lege without seeking permission from executive magistrate.
Death certificate is given by attending physician.
(c) When death occurs at home & no physician has attended the person. T h e d e c e a s e d h a s p l e d g e d t o d o n a t e his/her body / or the r e l a t i v e s w a n t t o donate body.
It happens so often that relatives come without death certificate. The act is silent about it. The fear of Anatomy department in such cases is the fear of foul play. Somebody might have murdered the old person and handover the body to the Anatomy department. How c a n A n a t o m i s t s s a v e themselves f rom such situations?
When ever a donated body is brought to Anatomy department where death has occurred at home, it should be accompanied by a letter/ undertaking from relatives that the person has died a natural death, so body is being h a n d e d o v e r t o a n a t o m y department. It should be attested by minimum 2 persons of the village (or city) comprising of Sarpanch and the NGO through which the body is being brought. Further a committee must be made at college level comprising of an Anatomist and a Forensic expert to examine the body externally and to declare that "apparently there seems to be no foul play". Ifsuspected, the Anatomy department must have right to reject the body and report t h e m a t t e r t o p o l i c e f o r postmortem.
1. To avoid the situation of foul play by relative and send body silently to Anatomy department.2. To save the Doctors in Anatomy department (who accept the body) from any untoward litigations later on.
(d) When death occurs at home & death certificate is given by physician
Act is silent In such cases also the body should be examined by a committee of Anatomist & Forensic expert as in (2 C) above.
When death occurs in a village the a t tending physic ian ( u s u a l l y R M P ) g i v e s c e r t i fi c a t e t h a t p a t i e n t declared dead giving no cause of death. So again to rule out any foul play the body should be examined by committee.
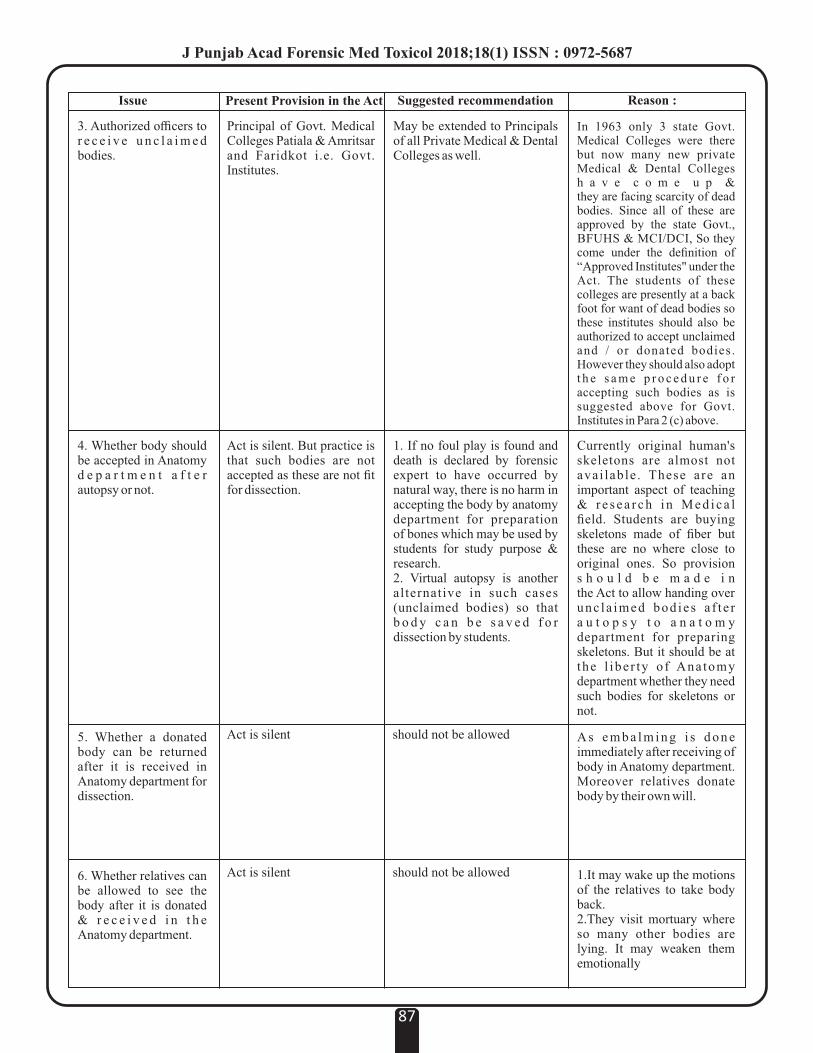
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687
87
Issue Present Provision in the Act Suggested recommendation Reason :
3. Authorized officers to r e c e i v e u n c l a i m e d bodies.
Principal of Govt. Medical Colleges Patiala & Amritsar and Faridkot i.e. Govt. Institutes.
May be extended to Principals of all Private Medical & Dental Colleges as well.
In 1963 only 3 state Govt. Medical Colleges were there but now many new private Medical & Dental Colleges h a v e c o m e u p & they are facing scarcity of dead bodies. Since all of these are approved by the state Govt., BFUHS & MCI/DCI, So they come under the definition of “Approved Institutes" under the Act. The students of these colleges are presently at a back foot for want of dead bodies so these institutes should also be authorized to accept unclaimed and / or donated bodies. However they should also adopt t h e s a m e p r o c e d u r e f o r accepting such bodies as is suggested above for Govt. Institutes in Para 2 (c) above.
4. Whether body should be accepted in Anatomy d e p a r t m e n t a f t e r autopsy or not.
Act is silent. But practice is that such bodies are not accepted as these are not fit for dissection.
1. If no foul play is found and death is declared by forensic expert to have occurred by natural way, there is no harm in accepting the body by anatomy department for preparation of bones which may be used by students for study purpose & research.2. Virtual autopsy is another alternative in such cases (unclaimed bodies) so that b o d y c a n b e s a v e d f o r dissection by students.
Currently original human's skeletons are almost not avai lable . These are an important aspect of teaching & r e s e a r c h i n M e d i c a l field. Students are buying skeletons made of fiber but these are no where close to original ones. So provision s h o u l d b e m a d e i n the Act to allow handing over unc la imed bod ies a f t e r a u t o p s y t o a n a t o m y department for preparing skeletons. But it should be at the l ibe r ty o f Ana tomy department whether they need such bodies for skeletons or not.
5. Whether a donated body can be returned after it is received in Anatomy department for dissection.
Act is silent should not be allowed A s e m b a l m i n g i s d o n e immediately after receiving of body in Anatomy department. Moreover relatives donate body by their own will.
6. Whether relatives can be allowed to see the body after it is donated & r e c e i v e d i n t h e Anatomy department.
Act is silent should not be allowed 1.It may wake up the motions of the relatives to take body back.2.They visit mortuary where so many other bodies are lying. It may weaken them emotionally

INSTRUCTIONS TO AUTHORS
Preparing a Manuscript For Submission to Journal of Punjab Academy of Forensic Medicine and Toxicology
Unpublished, Ethical, Un-Plagiarised original manuscript written in English should be sent to: Dr. Parmod Kumar Goyal,
Editor-in-Chief, Journal of Punjab Academy of Forensic Medicine and Toxicology by email at:
The Publication Particulars
The JPAFMAT is the official publication of the Punjab Academy of Forensic Medicine & Toxicology, published since
2001.
The Contents of the Journal
The journal accepts a range of articles of interest, under several feature sections as follows:
Original Papers: Includes conventional observational and experimental research.
Commentary: Intended for Reviews, Case Reports, Preliminary Report and Scientific Correspondences.
Letter to the Editor
Designed to be an avenue for dialogue between the authors of the papers published in the journal and the readers
restricted to the options expressing reviews, criticisms etc. It could also publish letters on behalf of the current
affairs in the field of Forensic Medicine in the country.
Editorial
Intended as a platform, for the Editor-in-Chief and for others with a keen interest in forensic medicine that wished
to comment on the current affairs.
Special Features
In the History of Indian Forensic Medicine, Book Review, Abstracts, Announcement etc, which appear frequently,
but not necessarily in every issue.
News and Notes
Intended for providing information of members and activities of the Academy and other such other organizations
affiliated to the Academy may appear frequently and not in every issue.
General Principles
The text of observational and experimental articles is usually (but not necessarily) divided into the following sections: Introduction,
Methods, Results, and Discussion. This so-called “IMRAD” structure is not an arbitrary publication format but rather a direct
reflection of the process of scientific discovery. Long articles may need subheadings within some sections (especially Results and
Discussion) to clarify their content. Other types of articles, such as case reports, reviews, and editorials, probably need to be
formatted differently. Electronic formats have created opportunities for adding details or whole sections, layering information,
cross linking or extracting portions of articles, and the like only in the electronic version. Double spacing all portions of the
manuscript— including the title page, abstract, text, acknowledgments, references, individual tables, and legends—and generous
margins make it possible for editors and reviewers to edit the text line by line and add comments and queries directly on the paper
copy. If manuscripts are submitted electronically, the files should be double-spaced to facilitate printing for reviewing and editing.
Authors should number all of the pages of the manuscript consecutively, beginning with the title page, to facilitate the editorial
process.
International Uniform Requirements
Please visit http://www.icmje.org/ for detailed instructions for manuscript submission.
Note : Manuscript handling charges Rs. 1000/- to be paid after acceptance.
88
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687
Format of Application for Membership
To
The General Secretary
Punjab Academy of Forensic Medicine & Toxicology (PAFMAT)
Dear Sir,
I wish to become a Life Member / Annual Member of PAFMAT. I am furnishing the required particulars below with a
request to enrol me in the academy. The fee of Rs. 1000 / Rs. ---- for Life Membership / Annul Membership is enclosed as a Demand
Draft with No________________ of _______________________________________Bank, in the name of PAFMAT along with
my two passport size photographs.
I have gone / will go through the rules and regulations of the academy and I agree to abide by the same.
PARTICULARS
1. Full Name ( in block letters )
2. Father's / Husband's name
3. Date of Birth
4. Qualification ( with name of university & date of passing )
5. Official Designation & Place of Posting
6. Permanent Address
7. Address for Correspondence ( subsequent change of address to be intimated)
8. Phone No. & Email
Place Yours Sincerely
Date
(Signature)
FOR USE OF PAFMAT
Membership Accepted with Life / Annual membership No. / PAFMAT / /
Dated
Treasurer Secretary President
Note : Payment can be made by NEFT in the account of academy (A/c No. 2082101026802, IFSC
CNRB0002082, CANARA BANK, Gopal Nagar, Amritsar) after telephonic talk with
President/Secretary/Treasurer. Scanned copy of the filled form can be sent by email to Secretary.
89
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687
90
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687
LM/PAFMAT/1/1998 Dr. R.K. Gorea
LM/PAFMAT/2/1998 Late Dr. Sat Pal Garg
LM/PAFMAT/3/1998 Dr. D.S. Bhullar
LM/PAFMAT/4/1998 Late Dr. A.S. Thind
LM/PAFMAT/5/2001 Dr. Hakumat Rai
LM/PAFMAT/6/2001 Dr. K.K. Aggarwal
LM/PAFMAT/7/2001 Dr. Jaswinder Singh
LM/PAFMAT/8/2001 Dr. Karamjit Singh
LM/PAFMAT/9/2001 Dr. Harjinder Singh
LM/PAFMAT/10/2001 Dr. Virender Pal Singh
LM/PAFMAT/11/2001 Dr. Ashok Chanana
LM/PAFMAT/12/2002 Dr. J.S. Dalal
LM/PAFMAT/13/2002 Dr. Jagdish Gargi
LM/PAFMAT/14/2002 Dr. R.S. Parsad
LM/PAFMAT/15/2002 Dr., Ajit Singh
LM/PAFMAT/16/2002 Dr. Harish Tuli
LM/PAFMAT/17/2002 Dr. S.K. Bal
LM/PAFMAT/18/2002 Dr. S.S. Sandhu
LM/PAFMAT/19/2002 Dr. Akashdeep Aggarwal
LM/PAFMAT/20/2002 Dr. Kuldeep Singh
LM/PAFMAT/21/2002 Dr. Vishal Garg
LM/PAFMAT/22/2002 Dr. S.S. Oberoi
LM/PAFMAT/23/2002 Late Dr. Ram Lubhaya
LM/PAFMAT/24/2003 Dr. Amandeep Singh
LM/PAFMAT/25/2003 Dr. Harkirat Singh
LM/PAFMAT/26/2003 Dr. I.S. Bagga
LM/PAFMAT/27/2004 Dr. Harpreet Singh
LM/PAFMAT/28/2004 Dr. Parminder Singh
LM/PAFMAT/29/2004 Dr. Anil Garg
LM/PAFMAT/30/2004 Dr. O.P. Aggarwal
LM/PAFMAT/31/2006 Dr. Gaurav Sharma
LM/PAFMAT/32/2006 Late Dr. Madhur Tayal
LM/PAFMAT/33/2006 Dr. Gurmanjit Rai Mann
LM/PAFMAT/34/2006 Dr. Didar Singh
LM/PAFMAT/35/2006 Dr. Kuldeep Singh
LM/PAFMAT/36/2006 Dr. Pankaj Gupta
LM/PAFMAT/37/2007 Dr. Karam Singh
LM/PAFMAT/38/2007 Dr. Baljit Singh
LM/PAFMAT/39/2007 Dr. Puneet Khurana
LM/PAFMAT/40/2007 Dr. Puneet Arora
LM/PAFMAT/41/2007 Dr. Prabhsharan Singh
LM/PAFMAT/42/2007 Dr. Dildar Singh
LM/PAFMAT/43/2007 Dr. Mian Abdur Rashid
LM/PAFMAT/44/2007 Dr. Shilekh Mittal
LM/PAFMAT/45/2007 Dr. B.R. Sharma
LM/PAFMAT /46/2007 Dr. D.Harish
LM/PAFMAT /47/2007 Dr. Krishna D. Chavali
LM/PAFMAT /48/2007 Dr. Ashwani Kumar
LM/PAFMAT /49/2007 Dr. Vikram Bains
LM/PAFMAT /50/2007 Dr. Kirpal Singh
LM/PAFMAT /51/2007 Dr. Gurbachan Singh
LM/PAFMAT /52/2007 Dr. Sangeet Dhillon
LM/PAFMAT /53/2008 Dr. Sukhbir Singh Chauhan
LM/PAFMAT /54/2008 Dr. Parminder Singh Bhatti
LM/PAFMAT /55/2008 Dr. Rakesh Kumar
LM/PAFMAT /56/2008 Dr. Jagbir Singh
LM/PAFMAT /57/2008 Dr. Karnveer Singh
LM/PAFMAT /58/2008 Dr. Rajiv K. Chowdhary
LM/PAFMAT /59/2008 Dr. Parmod Kumar Goyal
LM/PAFMAT /60/2008 Dr. Ajay Kumar
LM/PAFMAT/61/2009 Dr RK Sharma
LM/PAFMAT/62/2009 Dr Brij M. Gupta
LM/PAFMAT/63/2010 Dr Sunil Gambhi
LM/PAFMAT/64/2010 Dr Vijal Pal Khangwal
LM/PAFMAT/65/2010 Dr Rajiv Joshi
LM/PAFMAT/66/2010 Dr Manpreet Kaul
LM/PAFMAT/67/2010 Dr Sheikh AnayatUllah
LM/PAFMAT/68/2010 Dr Satinder Pal Singh
LM/PAFMAT/69/2011 Dr Preetinder Singh Chahal
LM/PAFMAT/70/2011 Dr Kulbhushan Garg
LM/PAFMAT/71/2011 Dr Imran Sabri
LM/PAFMAT/72/2011 Dr Bindu Aggarwal
LM/PAFMAT/73/2011 Dr Adish Goyal
LM/PAFMAT/74/2011 Dr Charak Sangwan
LM/PAFMAT/75/2011 Dr Pardeep Singh
LM/PAFMAT/76/2011 Dr Ishwer Tayal
LM/PAFMAT/77/2011 Dr Ripan Chanana
LM/PAFMAT/78/2012 Dr Gurvinder Singh Kakkar
LM/PAFMAT/79/2012 Dr Ravdeep Singh
LM/PAFMAT/80/2012 Dr Rohit Kumar Singal
LM/PAFMAT/81/2012 Dr Prabhdeep Singh
LM/PAFMAT/82/2012 Dr Jasbir Singh
LM/PAFMAT/83/2012 Dr Jatinder Pal Singh
LM/PAFMAT/84/2012 Dr Alok Kandpal
Life Members (PAFMAT)
91
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687
Life Members (PAFMAT)
LM/PAFMAT/85/2013 Dr Iram Khan
LM/PAFMAT/86/2013 Dr Charanpreet K. Pawar
LM/PAFMAT/87/2013 Dr Mukul Chopra
LM/PAFMAT/88/2013 Dr Mohit Gupta
LM/PAFMAT/89/2013 Dr Rahul Chawla
LM/PAFMAT/90/2013 Dr Maneel Grover
LM/PAFMAT/91/2014 Dr Y.S. Bansal
LM/PAFMAT/92/2014 Dr C.S. Gautam
LM/PAFMAT/93/2014 Dr S.P. Mandal
LM/PAFMAT/94/2014 Dr Murli . G
LM/PAFMAT/95/2014 Dr Anil Kumar Mittal
LM/PAFMAT/96/2014 Dr G.A. Sunil Kumar Sharma
LM/PAFMAT/97/2014 Dr Abhishek Yadav
LM/PAFMAT/98/2014 Dr Jagdev Kullar
LM/PAFMAT/99/2014 Dr Gurpreet Kaur Randhawa
LM/PAFMAT/100/2014 Dr Gursirat Singh Khokhar
LM/PAFMAT/101/2014 Dr Saginder Samara
LM/PAFMAT/102/2014 Dr Saginder Samaraj
LM/PAFMAT/103/2014 Dr Neha Sharma
LM/PAFMAT/104/2014 Dr Sunil Mahajan
LM/PAFMAT/105/2014 Dr Harshdeep Kashyap
LM/PAFMAT/106/2014 Dr Kiran Kumar
LM/PAFMAT/107/2014 Dr Swati Tyagi
LM/PAFMAT/108/2014 Dr Mini
LM/PAFMAT/109/2014 Dr Mandeep Kaur
LM/PAFMAT/110/2014 Dr Gurinder Singh
LM/PAFMAT/111/2014 Dr Minal
LM/PAFMAT/112/2014 Dr Kanchan Jyoti Heera
LM/PAFMAT/113/2014 Dr Manpinder Kaur Bhullar
LM/PAFMAT/114/2014 Dr Arashdeep Singh
LM/PAFMAT/115/2014 Dr Chamandeep Singh Bains
LM/PAFMAT/116/2014 Dr Maninder Singh
LM/PAFMAT/117/2014 Dr Akhilesh Agarwal
LM/PAFMAT/118/2014 Dr Guneet
LM/PAFMAT/119/2014 Dr Hitesh Bhatia
LM/PAFMAT/120/2015 Dr. Deep Rattan Mittal
LM/PAFMAT/121/2015 Dr. Arun Kumar Maria
LM/PAFMAT/122/2015 Dr. S Valliappan
LM/PAFMAT/123/2015 Dr. Preet Inder Singh
LM/PAFMAT/124/2015 Dr. Harvinder Singh Chhabra
LM/PAFMAT/125/2015 Dr. Bhoj Kumar Sahu
LM/PAFMAT/126/2016 Dr. Amarnath Mishra
LM/PAFMAT/127/2016 Dr. Shekhar Chumber
LM/PAFMAT/128/2016 Dr. Navroz Goyal
LM/PAFMAT/129/2016 Dr. Gurjeet Singh
LM/PAFMAT/130/2016 Dr. Deepika Kanwar
LM/PAFMAT/131/2016 Dr. Mohd. Amjad Bhatt
LM/PAFMAT/132/2016 Dr. Nikhil Mehta
LM/PAFMAT/133/2016 Dr. Charan Kamal
LM/PAFMAT/134/2016 Dr. Amit Singla
LM/PAFMAT/135/2017 Dr. Sukhdeep Singh
LM/PAFMAT/136/2017 Dr. Munish Kumar
LM/PAFMAT/137/2017 Dr. Arindam Chatterjee
LM/PAFMAT/138/2017 Dr. Ranjodh Jeet Singh
LM/PAFMAT/139/2017 Dr. Kanika Kohli
LM/PAFMAT/140/2017 Dr. Vinka Maini
LM/PAFMAT/141/2017 Dr. Ravi Tejpal
LM/PAFMAT/142/2017 Dr. Preet Mohinder Singh
LM/PAFMAT/143/2017 Dr. Satbir Singh
LM/PAFMAT/144/2017 Dr. Kamaljit Singh
LM/PAFMAT/145/2018 Dr. Mrinal Kanti Jha
LM/PAFMAT/146/2018 Dr. Vijay Arora
LM/PAFMAT/147/2018 Dr. Vivek Srivastava
LM/PAFMAT/148/2018 Dr. Pankaj Chhikara
LM/PAFMAT/149/2018 Dr. Lalit Kumar
LM/PAFMAT/150/2018 Dr. Prem Chandra Srivastava
LM/PAFMAT/151/2018 Dr. Niraj Kumar
LM/PAFMAT/152/2018 Dr. Om Parkash Saini
LM/PAFMAT/153/2018 Dr. Rajesh Kumar Verma
LM/PAFMAT/154/2018 Dr. Shailender Kumar
LM/PAFMAT/155/2018 Dr. B.L. Chaudhary
LM/PAFMAT/156/2018 Dr. Parmod Kumar Saini
LM/PAFMAT/157/2018 Dr. Rajendra Singh Kulhari
LM/PAFMAT/158/2018 Dr. Nidhi Sachdeva Agarwal
LM/PAFMAT/159/2018 Dr. Rajeev Varma
LM/PAFMAT/160/2018 Dr. Pragnesh Bharatkumar
Parmar
LM/PAFMAT/161/2018 Dr. Yatiraj Singi
LM/PAFMAT/162/2018 Dr. Navpreet Kaur
LM/PAFMAT/163/2018 Dr. Kunal Khanna
LM/PAFMAT/164/2018 Dr. Smitha Rani Shetty
LM/PAFMAT/165/2018 Dr. Vivekanshu Verma
LM/PAFMAT/166/2018 Dr. B.V. Naga Mohan Rao
92
J Punjab Acad Forensic Med Toxicol 2018;18(1) ISSN : 0972-5687

Glimpse of Mid Term CME on Medical Negligence & Assault on doctors
DEPARTMENT OF FORENSIC MEDICINEPUNJAB INSTITUTE OF MEDICAL SCIENCES, JALANDHAR
Organized by:Organized by:Organized by:
On Saturday, 12th May, 2018
J Punjab Acad Forensic Med Toxicol 2018;18 (1) ISSN : 0972-5687
Editorial Board
NationalAdvisoryBoardDr T.D. DograDr J.S. DalalDr R.K. GoreaDr O P AggarwalDr K K AggarwalDr Balbir KaurDr K. VijDr Dalbir SinghDr Sanjoy DassDr E.J. RodrigeusDr Gurudatta PawarDr D.S. BadkurDr Jagadeesh. N.
EditorialCommittee:Dr S. S. OberoiDr Sangeet DhillonDr Ishwar TayalDr Kuldeep SinghDr Harjinder SinghDr Harpreet SinghDr Parul KherDr Antara DebBarmanDr Gurpreet S. Sandhu
Dr OP MurtiDr V. V. PillayDr Shiv KochharDr R.K. SharmaDr N K AggarwalDr Amitabh ShrivastvaDr Shankar M. BakkannavarDr Mukesh YadavDr C.B. JaniDr. Vijal Pal KhanagwalDr. Samita SinhaDr. Manjot KaurDr. Karan MaheshwariMrs. Ritika Gupta, FSL Bathinda
SubscriptionInformationMembers of PAFMAT will receive the journal free of cost.
SubscriptionratesforNon-MembersandInstitutionsforYear2018Personal: Rs. 1,000/- Institutions: Rs. 3,500/-
Abroad : Postal Charges Extra
l Subscription request be sent on email to [email protected]
l Payments be made in Bank Account of Journal of Punjab Academy of Forensic Medicine (A/c No. 65075504236, State Bank of India, Branch Rajindra Hospital Patiala, IFS Code SBIN0050263
A copy will be sent free to the
member / subscriber provided the
claim is made within 2 months of the
publication of the issue and Rs.
100/- deposited in the Journal
account as postal Charges.
ClaimsforMissingIssue
Printed&Publishedby:Dr Parmod Kumar Goyal
Professor & Head,Department of Forensic Medicine & ToxicologyAdesh Institute of Medical Sciences & Research,
Bathinda (Pb.) India M. 9876005211, 0164-5055073E-mail: [email protected]
Printedat:Subhash Mittal Printing Press
Hospital Bazar, BathindaM. 99880-11022
e-mail: [email protected]
Editor-in-ChiefDr Parmod Kumar Goyal
Joint EditorDr Amandeep Singh
Assistant EditorDr Satinder Pal Singh
Web MasterDr Dildar Singh
J Punjab Acad Forensic Med Toxicol 2018;18 (1) ISSN : 0972-5687
Dr. Vivek SrivastavaDr. Sanjoy DasDr. Pardeep SinghDr. Monika GuptaDr. Navita AggarwalDr. Tanvir Kaur SidhuDr. Sandeep KaurDr. Priti ChaudharyDr. Vijay SuriDr. Saranpal SinghDr. Lovleen MarwahaDr. Tanuj KanchanDr. Raghuvendra K. Vidua
ManuscriptReviewCommittee