metabolic syndrome is associated with markers of subclinical atherosclerosis in a french...
TRANSCRIPT

Atherosclerosis 186 (2006) 345–353
Metabolic syndrome is associated with markers of subclinicalatherosclerosis in a French population-based sample
N. Ahluwalia a,b,∗, L. Drouet c, J.-B. Ruidavets b, B. Perret d, J. Amar b,e,H. Boccalon f, H. Hanaire-Broutin g, J. Ferrieres b
a Department of Nutritional Sciences, Pennsylvania State University, USAb INSERM Unit 558, Toulouse, France
c Department of Haematology, Lariboisiere Hospital, Paris, Franced INSERM Unit 563 and Biochemistry Department, CHU, Toulouse, France
e Department of Internal Medicine and Arterial Hypertension, CHU Purpan, Toulouse, Francef Department of Vascular Medicine, CHU Rangueil, Toulouse, France
g Department of Diabetology, CHU Rangueil, Toulouse, France
Received 4 February 2005; received in revised form 28 June 2005; accepted 18 July 2005Available online 29 August 2005
A
au(s1mcvw©
K
1
sct
tm
DC
0d
bstract
Metabolic syndrome (MetS) is associated with increased risk of cardiovascular disease (CVD). The relation of MetS with early stages oftherosclerosis, more important from a prevention perspective, has not been evaluated extensively. We examined the association of MetS,sing WHO and NCEP definitions, with number of carotid and femoral plaques; carotid intima-media thickness (IMT); pulse wave velocityPWV) in a random population-based sample of 1153 French adults (35–65 year). Impact of inflammatory factors (C-reactive protein andoluble intercellular adhesion molecule-1) on these parameters was also evaluated. Prevalence of MetS was 14.5 (CI: 12.3–16.0) and 17.5 (CI:5.1–20.2)%, using NCEP and WHO definitions, respectively. MetS significantly predicted number of plaques, IMT, and PWV after adjust-ent for traditional risk factors (P < 0.05). Inflammatory factors predicted peripheral plaques only. The risk of subclinical atherosclerosis was
onsiderably increased with MetS (P < 0.05); odds ratios ranged 1.80–2.15 with NCEP definition, and 1.48–1.97 with WHO definition. Indi-iduals meeting both NCEP and WHO definitions had slightly greater risk of increased plaques, IMT, and PWV. MetS was strongly associatedith subclinical atherosclerosis and aortic stiffness, and can be used as a surrogate marker for high CVD risk, deserving aggressive treatment.2005 Elsevier Ireland Ltd. All rights reserved.
eywords: Metabolic syndrome; Insulin resistance syndrome; Carotid intima-media thickness; Pulse wave velocity; Atherosclerotic plaques; Inflammation
. Introduction
Metabolic syndrome (MetS), also called insulin resistanceyndrome, is characterized by the concurrence of cardiovas-ular disease (CVD) risk factors namely impaired glucoseolerance, obesity, dyslipidemia, and hypertension. Studies
Abbreviations: CVD, cardiovascular disease; CRP, C-reactive pro-ein; MetS, metabolic syndrome; sICAM-1, soluble inter-cellular adhesion
olecule-1∗ Corresponding author. Present address: INSERM U558, Hopital Paule Viguier, 330 Avenue de Grande Bretagne, TSA 70034, 31059 Toulouse,edex 9, France. Tel.: +33 5 61 52 18 70; fax: +33 5 62 26 42 40.
E-mail address: [email protected] (N. Ahluwalia).
on insulin resistance syndrome have utilized various defi-nitions, encompassing in some manner these components.Thus, to aid in research and clinical application of MetS, theWHO consultation for the classification of diabetes and itscomplications [1–3] and the National Cholesterol Educationprogram (NCEP) Adult Treatment Panel III [4] have recentlypublished definitions. Both WHO and NCEP definitions ofMetS revolve around the four components, but have slightlydifferent tests and/or cut-offs [1–5].
Various epidemiological studies have related MetS toincreased risk of developing type 2 diabetes and CVD [3,6–9].An increase in mortality due to CVD, as well as all causemortality was noted in Finnish men with MetS [3]. Recent
021-9150/$ – see front matter © 2005 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.atherosclerosis.2005.07.021

346 N. Ahluwalia et al. / Atherosclerosis 186 (2006) 345–353
analyses of the US NHANES II follow-up data by Maliket al. [10] also show increased CVD mortality in indi-viduals with the syndrome. However, the relationship ofMetS with early stages of CVD, which is even more impor-tant from a prevention perspective, has not been examinedextensively.
Several studies have shown that the individual compo-nents of MetS are associated with measures of subclin-ical atherosclerosis, such as carotid intima-media thick-ness (IMT), and discrete atherosclerosis (number ofcarotid–femoral plaques), as well as pulse wave velocity(PWV) [11–13]. Few studies have, however, examined therelationship of MetS as an entity with these measures ofsubclinical atherosclerosis [13–17] as well as with coronaryartery calcium score [18,19]. The literature examining therelationship of MetS and PWV, a non-invasive measure ofarterial stiffness, is also limited particularly in the US andEurope [15–17]. Further increase in carotid IMT and PWVhas been related to the number of MetS components in recentstudies [13,16].
It is important to examine the relationship of MetS withearly stages of atherosclerosis from a clinical and pub-lic health perspective, so as to direct appropriate treatmentefforts early for optimal patient care. Thus, we examined therelationship of MetS, defined using the NCEP and WHO cri-teria, with several measures of subclinical atherosclerosis andapoii
2
2
(TsacniCnjCta
sucs
were recorded by trained staff. A physical examination wasperformed in the morning and a fasting blood sample wasdrawn.
2.2. Clinical measurements
2.2.1. Blood pressure (BP) and resting heart rateBP measurements were performed with a standard sphyg-
momanometer using cuff size adapted to the subject’s armcircumference. After at least a 5-min rest, carotid–femoralPWV was measured in supine position. Immediately after,heart rate and BP were measured twice in supine position.The average of the two BP measurements was used for sta-tistical analysis.
2.2.2. Discrete plaquesPlaques were assessed qualitatively, using high-resolution
B-mode ultrasonography, in carotid and femoral artery beds[11,23]. Plaques were defined as a distinct area identifiedeither with a focal area of hyperechogenicity relative to adja-cent segments and/or a focal protrusion into the lumen ofthe vessel, composed of only calcified deposits or a combi-nation of calcified and non-calcified material. The presenceof atherosclerotic plaques was investigated in the right andin the left common carotid arteries, internal, and externalcarotid arteries (including carotid bulbs) and femoral arteries(
2
mtlTcmeaf
2
mlwurswta
2
b
rterial distensibility examined simultaneously, in a randomopulation based sample in Southwestern France. Becausef increasing evidence on the important role of inflammationn CVD [11,16] we also examined the effect of inflammationn modifying these associations.
. Materials and methods
.1. Description of study design and subjects
A population-based sample of 1153 middle-aged adults35–65 year) was randomly selected from the electoral rolls inoulouse area to participate in the III French MONICA cross-ectional survey on cardiovascular risk factors, between 1995nd 1997 [20,21]. The goal of MONICA project was toompare the frequency, prognosis, and management of coro-ary heart disease and CVD risk factors. Subjects providednformed consent following protocols approved by the Ethicsommittee (Comite Consultatif de Protection des Person-es dans la Recherche Biomedicale, Lille, France). All sub-ects were Caucasian and none had clinical evidence ofVD. Data on 896 subjects who had complete informa-
ion on all variables of interest were used for the presentnalysis.
Subjects provided information on demographic variables,ocio-economic status, medical history including medicationse, smoking, and alcohol consumption, as well as physi-al activity using a questionnaire with the aid of medicaltaff [22]. Height, weight, and waist and hip circumference
including femoral bifurcations).
.2.3. Common carotid IMTHigh-resolution B-mode ultrasonography was used to
easu2re the common carotid IMT. The IMT was defined ashe distance between the media/adventitia interface and theumen/intima interface, avoiding the sites of plaque [11,23].he IMT was measured on the right and on the left commonarotid arteries, on the far wall exclusively. Twelve measure-ents were made in total: three points at two locations on
ach artery, proximal, and middle. The mean value of IMTt the 12 sites was used as the overall common carotid IMTor statistical analyses.
.2.4. PWVAortic stiffness was assessed by carotid–femoral PWV
easurement with a semi-automatic device (Complior, Gargees Gonesse, France) [12]. The two pressure waveformsere digitised. The time delay (t) between the two pressurepstrokes was automatically calculated. This procedure wasepeated on 10 cardiac cycles and the mean value was used fortatistical analysis. The distance covered by the pulse waveas measured on the surface of the body and represented
he distance between the two recording sites (D). PWV wasutomatically calculated as PWV = D/t.
.3. Biological analyses
Serum total cholesterol and triglycerides were measuredy enzymatic methods (Roche Diagnostics, Mannheim,

N. Ahluwalia et al. / Atherosclerosis 186 (2006) 345–353 347
Germany). HDL cholesterol was measured in the supernatantafter sodium phosphotungstate/magnesium chloride pre-cipitation (Roche Diagnostics, Mannheim, Germany). LDLcholesterol was determined by the Friedewald equation.Plasma insulin was measured by a radioimmunoassay(BioRad, France). Fasting plasma glucose was measuredwith a hexokinase-glucose-6-phosphate dehydrogenasemethod. Inflammation was assessed based on C-reactiveprotein (CRP) and soluble inter-cellular adhesion molecule-1 (sICAM-1) levels [11]. CRP was measured by animmunonephelemetric method (Dade Behring MarburgGmbH, Marburg, Germany); the assay had a sensitivity of0.2 mg/L. Serum sICAM-1 levels were determined using animmunoenzymatic method (Beckman-Coulter, Marseille,France).
2.4. MetS: operational definitions
We used the working definitions of MetS suggestedby the NCEP Expert panel [4] and the WHO consulta-tion for the classification of diabetes and its complications[1]. Using the NCEP guidelines [4], MetS was defined asthe presence of at least three of the following five crite-ria: fasting glucose (≥6.1 mmol/L [110 mg/dL]); abdomi-nal obesity characterized by increased waist circumference(M: >102 cm; F: >88 cm); serum triglycerides (≥1.7 mmol/L[<s
t[InrhqccosH(
2
cacWsmbwa
as well as inflammatory factors namely CRP and sICAM-1. Logistic regression analysis with backward selection wasused to estimate the age- and sex-adjusted odds ratio asso-ciated with MetS for number of plaques, IMT, and PWV.There is no general agreement regarding the threshold beyondwhich IMT can be considered as abnormal; cut-offs between0.75 and 1 mm have been associated with higher risk [24].In the current analyses, we used a cut-off of 0.71 mm forIMT that corresponded to the 90th percentile in our cohort,as it was close to the threshold used in previous studies;and it allowed a sufficient number of subjects in each classof IMT (≥ or <90th percentile). We reiterated the analysesusing 80th and 75th percentiles as cut-offs and found similarresults to those using the cut-off of 90th percentile. Thus, wechose to present here the findings using 90th percentile ascut-off for both IMT and PWV. For atherosclerotic plaques,we examined the distribution of the number of plaques inthe study cohort and used various cut-offs (≥1, ≥2, and ≥3plaques) to perform logistic regression. Because the numberof subjects with >4 plaques was small, we pooled these sub-jects into ≥3 atherosclerotic plaques category. Irrespectiveof the cut-off used for atherosclerotic plaques our findingson its association with variables of interest (MetS) wereunchanged. Thus, the results using cut-off ≥2 plaques are pre-sented to avoid excessive number of false positive subjectsin the group with atherosclerotic plaques and have highers
aqtnd
3
fd(fMAnottiPighmI
150 mg/dL]); low HDL cholesterol (M: <1.04 mmol/L; F:1.29 mmol/L [M: <40 mg/dL; F: <50 mg/dL]); or hyperten-ion (≥130/85 mmHg).
The definition of MetS according to the WHO consulta-ion [1] was recently modified for epidemiological studies3] as proposed by the European Group for the Study ofnsulin Resistance [2]. We used this modified WHO defi-ition of MetS [3] involving evidence of impaired glucoseegulation (fasting glucose ≥6.1 mmol/L [110 mg/dL]) oryperinsulinemia (based on fasting insulin levels in the upperuartile of the non-diabetic population, i.e. >14 IU/L) inonjunction with at least two of the following components:entral obesity characterized by waist to hip ratio (>0.90)r BMI (>30 kg/m2); dyslipidemia characterized by elevatederum triglycerides (≥1.7 mmol/L [150 mg/dL]) and/or lowDL cholesterol (<0.9 mmol/L [35 mg/dL]); or hypertension
≥140/90 mmHg).
.5. Statistical analysis
Statistical analysis was performed using the SAS statisti-al software (SAS Institute Inc., Cary, NC, USA). Univariatenalyses were conducted using t-test. Associations betweenategorical variables were examined by chi-square analysis.e used linear regression analysis to examine the relation-
hip of MetS (defined using WHO and NCEP guidelines) witheasures of subclinical atherosclerosis and arterial distensi-
ility. Other independent variables included in the modelsere traditional factors, such as age, sex, smoking, physical
ctivity level, family history of CVD, and LDL-cholesterol
pecificity.To compute percentiles for each of these markers of
therosclerosis, data were first ordered. Then the rank of theuantile was calculated as follows: C = (N + 1)/n, where N ishe total number of records, n the quantile order, and C is theumber of subjects in each class; n = 10 was used to estimateeciles.
P < 0.05 was considered statistically significant.
. Results
The study cohort consisted of 53% males and 47%emales. The prevalence of MetS by NCEP and WHOefinitions was similar: 14.5 (CI: 12.3–16.0) and 17.5CI: 15.1–20.2)%, respectively. MetS was less prevalent inemales as compared to males, with both NCEP (F: 12.1%;
: 16.6%) and WHO definitions (F: 10.2%; M: 24.0%).s expected, an increase in the prevalence of MetS wasoted with increasing age (Table 1; P < 0.05). The presencef MetS, irrespective of the definition used, was charac-erized by significantly higher plasma insulin, glucose, andriglyceride levels as well as increased abdominal adipos-ty, blood pressure, pulse pressure, and heart rate (Table 1;< 0.05). HDL cholesterol levels were significantly lower
n the group with MetS (Table 1; P < 0.05). Consequently, areater proportion of individuals with the syndrome were onypocholesterolemic, antidiabetic, or antihypertensive treat-ent as compared to those without MetS (Table 1; P < 0.05).
nterestingly, markers of subclinical inflammation (CRP and

348 N. Ahluwalia et al. / Atherosclerosis 186 (2006) 345–353
Table 1Clinical and laboratory parameters in the study cohort by presence of metabolic syndrome (n = 896)
MetS by NCEP definition MetS by WHO definition
Yes (n = 130) No (n = 766) P Yes (n = 157) No (n = 739) P
Age (%) <0.0001 <0.000135–44 year 15.4 37.3 17.2 37.845–54 year 36.9 34.1 35.7 34.255–64 year 47.7 28.6 47.1 28.0
Sex (men, %) 60.8 51.7 0.0553 72.6 48.9 <0.0001
Smoking (%) 0.03 0.03Yes 14.6 23.1 15.2 23.2No 85.4 76.9 84.8 76.8
Moderate to high physical activity (%)* 35.4 49.1 0.0038 42.0 48.2 0.1619Familial history of premature cardiovascular disease† 18.5 13.3 0.1187 17.2 13.4 0.2134Plasma insulin (mU/L) 18.7 ± 9.1‡ 10.6 ± 10.2 <0.0001 19.4 ± 8.7 10.2 ± 10.1 <0.0001Plasma glucose (mmol/L) 6.34 ± 1.08 5.57 ± 1.09 <0.0001 6.42 ± 1.15 5.52 ± 1.05 <0.0001BMI (kg/m2) 30.7 ± 4.2 24.4 ± 3.3 <0.0001 29.8 ± 4.2 24.4 ± 3.3 <0.0001Waist to hip ratio 0.95 ± 0.07 0.87 ± 0.08 <0.0001 0.96 ± 0.06 0.87 ± 0.08 <0.0001Waist circumference (cm) 102.3 ± 9.8 84.1 ± 11.0 <0.0001 100.5 ± 9.3 83.9 ± 11.2 <0.0001Systolic blood pressure (mmHg) 145.3 ± 16.9 128.2 ± 16.0 <0.0001 144.4 ± 17.6 127.8 ± 15.7 <0.0001Diastolic blood pressure (mmHg) 86.8 ± 10.1 78.7 ± 9.6 <0.0001 86.8 ± 10.0 78.4 ± 9.5 <0.0001Mean pressure (mmHg) 106.3 ± 10.8 95.2 ± 10.8 <0.0001 105.9 ± 11.1 94.9 ± 10.6 <0.0001Pulse pressure (mmHg) 58.5 ± 14.6 49.5 ± 11.5 <0.0001 57.6 ± 14.7 49.4 ± 11.4 <0.0001Heart rate (beat/mn) 69.6 ± 9.3 66.8 ± 8.8 0.0008 68.8 ± 9.0 66.9 ± 8.8 0.0166Total cholesterol (mmol/L) 5.98 ± 0.96 5.82 ± 1.00 0.0805 5.93 ± 0.99 5.82 ± 1.00 0.2076HDL cholesterol (mmol/L) 1.12 ± 0.35 1.50 ± 0.43 <0.0001 1.17 ± 0.33 1.51 ± 0.44 <0.0001LDL cholesterol (mmol/L) 4.05 ± 0.90 3.84 ± 0.95 0.0269 3.99 ± 0.92 3.85 ± 0.95 0.1039Triglycerides (mmol/L) 1.97 ± 1.11 1.03 ± 0.46 <0.0001 1.82 ± 1.06 1.03 ± 0.47 <0.0001CRP (ng/mL) 2.99 ± 3.90 1.46 ± 3.42 <0.0001 2.69 ± 3.72 1.47 ± 3.46 <0.0001sICAM-1 (ng/mL) 292.1 ± 100.1 263.4 ± 90.5 0.0011 283.1 ± 87.6 264.3 ± 93.2 0.0206Diabetes§ (%) 20.8 3.4 0.0011 20.4 2.8 <0.0001Hypertension# (%) 76.2 26.5 <0.0001 80.9 23.7 <0.0001Hypercholesterolemia** (%) 56.9 41.5 0.0011 56.1 41.1 0.0006Antidiabetic treatment (%) 8.5 2.1 <0.0001 10.2 1.5 <0.0001Antihypertensive treatment (%) 35.4 9.9 <0.0001 35.0 9.1 <0.0001Hypocholesterolemic treatment (%) 24.6 11.4 <0.0001 22.3 11.4 0.0002
Values are % unless otherwise indicated.* Two levels of leisure time physical activity were defined: no regular physical activity or light physical activity (i.e. less than once a week); and moderate
physical activity (i.e. 20 minutes at least, once or twice a week) or high physical activity (i.e. 20 min at least, three times a week or more).** Plasma cholesterol ≥6.15 mmol/L or medical treatment.† Family history of premature stroke, angina, myocardial infarction or peripheral arterial disease.‡ Mean ± S.D.# Systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg or medical treatment for hypertension.§ Hyperglycemia or medical treatment.
sICAM-1) were significantly higher in the group with MetSas compared to those without MetS (Table 1; P < 0.05).
The MetS group differed significantly from correspondinggroup without MetS on all variables related to subclini-
cal atherosclerosis and arterial distensibility, irrespectiveof the definition of MetS used (Table 2). Specifically,individuals with MetS had significantly greater carotidIMT and carotid–femoral PWV and were approximately
Table 2Markers of subclinical atherosclerosis and arterial stiffness by metabolic syndrome (n = 896)
MetS by NCEP definition MetS by WHO definition
Yes (n = 130) No (n = 766) P Yes (n = 157) No (n = 739) P
% with ≥2 carotid–femoral plaques* 30 (22.3–38.7) 14.6 (11.2–17.3) <0.001 30.6 (23.5–38.4) 13.9 (11.5–16.4) <0.001% with ≥2 carotid plaques* 25.4 (18.2–33.8) 11.2 (9.1–13.7) <0.001 23.6 (17.2–31.0) 11.1 (8.3–13.6) <0.001Carotid intima-media thickness (mm)† 0.64 ± 0.11 0.58 ± 0.09 <0.001 0.63± 0.11 0.58 ± 0.09 <0.001Pulse wave velocity (m/s)† 9.88 ± 1.83 8.82 ± 1.63 <0.001 9.85 ± 1.92 8.78 ± 1.60 <0.001
* % and 95% CI in parenthesis.† Mean ± S.D.

N. Ahluwalia et al. / Atherosclerosis 186 (2006) 345–353 349
Table 3Predictors of subclinical atherosclerosis and arterial stiffness (n = 896)
Carotid–femoral plaques(0–8)
Carotid plaques (0–6) Intima-media thickness(mm)
Pulse wave velocity(m/s)
β S.E. P β S.E. P β S.E. P β S.E. P
Using NCEP definition for metabolic syndromeAge (years) 0.069 0.005 <0.0001 0.035 0.003 <0.0001 0.005 0.0003 <0.0001 0.067 0.006 <0.0001Sex (women vs. men) −0.743 0.087 <0.0001 −0.333 0.057 <0.0001 −0.025 0.006 <0.0001 −0.564 0.108 <0.0001
Smoking (#cigarettes/day) Trend 0.002 Trend 0.072 Trend 0.002 Trend 0.365≥11 vs. 0 0.380 0.138 0.006 0.149 0.091 0.101 0.037 0.009 <0.0001 0.217 0.172 0.2091–10 vs. 0 0.269 0.145 0.063 0.093 0.095 0.328 0.004 0.010 0.713 −0.123 0.180 0.496
CRP (mg/L) 0.027 0.012 0.024 0.012 0.008 0.143 0.0007 0.0008 0.383 0.023 0.015 0.121sICAM-1 (mg/L) 2.132 0.489 <0.0001 0.924 0.321 0.004 −0.007 0.032 0.826 0.248 0.609 0.684Moderate to high physical
activity (%)0.101 0.085 0.236 0.073 0.056 0.194 0.004 0.006 0.426 −0.144 0.106 0.176
Familial history of prematurecardiovascular disease†
0.102 0.121 0.399 0.043 0.080 0.585 0.002 0.008 0.834 −0.046 0.151 0.761
LDL cholesterol (mmol/L) 0.078 0.046 0.087 0.022 0.030 0.472 0.004 0.003 0.193 0.072 0.057 0.204MetS by NCEP definition
(yes/no)0.421 0.124 0.001 0.227 0.082 0.006 0.032 0.008 0.0001 0.684 0.155 <0.0001
Using WHO definition for metabolic syndromeAge (years) 0.065 0.005 <0.0001 0.034 0.003 <0.0001 0.005 0.0003 <0.0001 0.068 0.007 <0.0001Sex (women vs. men) −0.690 0.086 <0.0001 −0.309 0.055 <0.0001 −0.023 0.006 <0.0001 −0.526 0.111 <0.0001
Smoking (#cigarettes/day) Trend 0.002 Trend 0.097 Trend 0.0004 Trend 0.376≥11 vs. 0 0.406 0.136 0.003 0.141 0.087 0.104 0.036 0.009 <0.0001 0.229 0.175 0.1911–10 vs. 0 0.212 0.141 0.132 0.053 0.090 0.551 0.0003 0.010 0.978 −0.159 0.181 0.381
CRP (mg/L) 0.035 0.012 0.005 0.020 0.008 0.013 0.001 0.0008 0.126 0.032 0.016 0.043sICAM-1 (mg/L) 1.971 0.484 <0.0001 0.803 0.308 0.009 −0.011 0.033 0.744 0.449 0.622 0.471Moderate to high physical
activity (%)*0.130 0.083 0.119 0.010 0.053 0.061 0.004 0.006 0.538 −0.130 0.107 0.227
Familial history of prematurecardiovascular disease†
0.092 0.120 0.443 0.038 0.077 0.620 0.0005 0.008 0.956 −0.042 0.155 0.786
LDL cholesterol (mmol/L) 0.078 0.045 0.088 0.017 0.029 0.558 0.003 0.003 0.359 0.060 0.058 0.303MetS by WHO definition (yes/no) 0.249 0.119 0.037 0.054 0.076 0.479 0.021 0.008 0.009 0.620 0.154 <0.0001
* Two levels of leisure time physical activity were defined: no regular physical activity or light physical activity (i.e. less than once a week) and moderatephysical activity (i.e. 20 min at least, once or twice a week) or high physical activity (i.e. 20 min at least, three times a week or more).† Family history of premature stroke, angina, myocardial infarction or peripheral arterial disease diagnosed before 60 years among fathers and before 65
years among mothers.
two times more likely to have ≥2 atherosclerotic plaquescompared to subjects without the syndrome (Table 2; P< 0.05).
As expected, age and sex were significant predictors of alldependent variables examined in the linear regression mod-els (Table 3). Smoking predicted the total number of plaques(carotid and femoral) and IMT but generally did not predictnumber of carotid plaques or PWV. Interestingly, inflamma-tion factors namely CRP and sICAM-1 predicted the num-ber of plaques (carotid–femoral plaques) but not IMT orPWV (Table 3). In addition, sICAM-1 also predicted carotidplaques (Table 3; P < 0.05). After adjustment for the tradi-tional risk factors and inflammation, MetS (using NCEP defi-nition) predicted number of carotid–femoral plaques, numberof carotid plaques, carotid IMT, and PWV. Similar resultswere noted with MetS using the WHO definition with theexception of lack of association with carotid plaques (Table 3;P < 0.05). The odds ratios (adjusted for age and sex) for mark-ers of early stages of atherosclerosis and arterial distensibilitywere approximately 2 (Fig. 1; P < 0.05), and ranged from 1.80
Fig. 1. Age and sex adjusted odds ratio for subclinical atherosclerosis andarterial stiffness.
350 N. Ahluwalia et al. / Atherosclerosis 186 (2006) 345–353
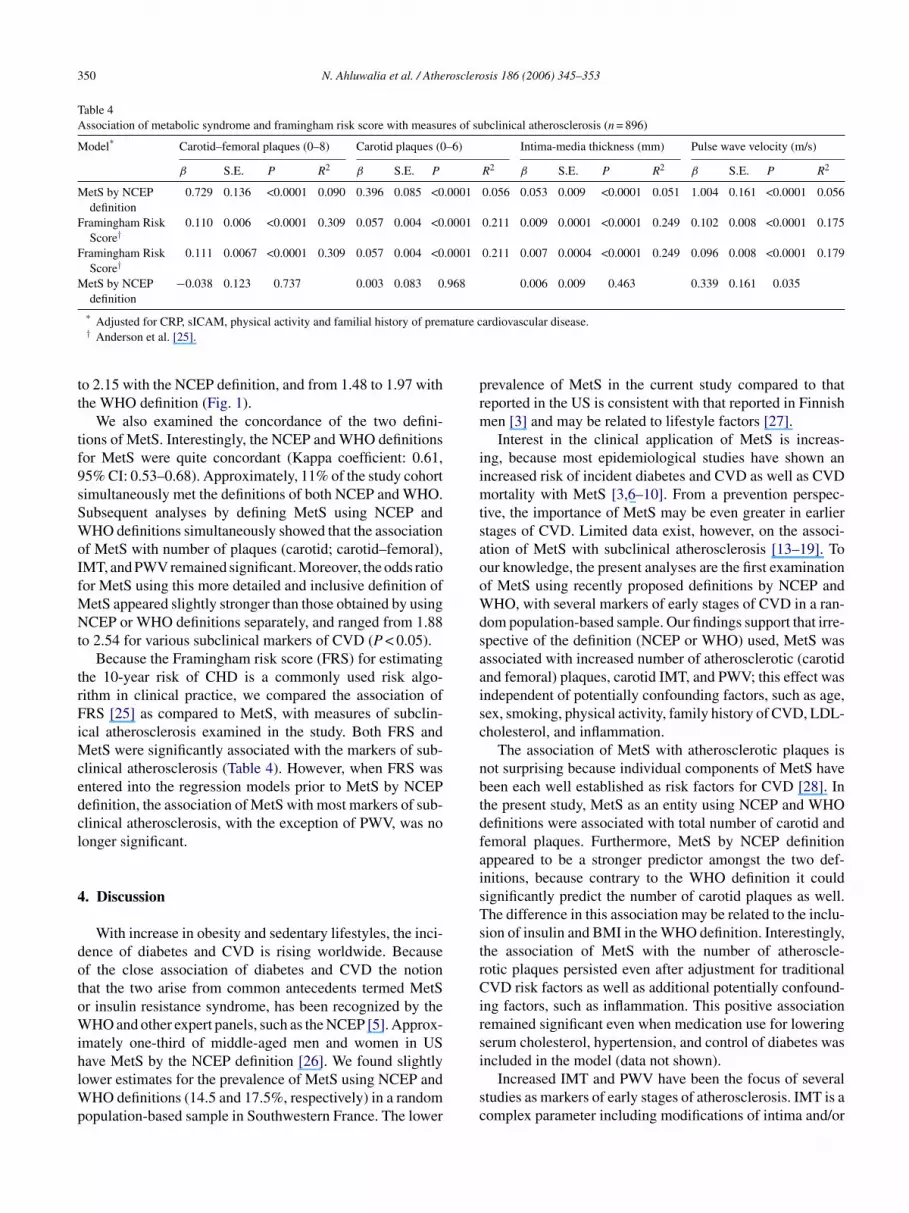
Table 4Association of metabolic syndrome and framingham risk score with measures of subclinical atherosclerosis (n = 896)
Model* Carotid–femoral plaques (0–8) Carotid plaques (0–6) Intima-media thickness (mm) Pulse wave velocity (m/s)
β S.E. P R2 β S.E. P R2 β S.E. P R2 β S.E. P R2
MetS by NCEPdefinition
0.729 0.136 <0.0001 0.090 0.396 0.085 <0.0001 0.056 0.053 0.009 <0.0001 0.051 1.004 0.161 <0.0001 0.056
Framingham RiskScore†
0.110 0.006 <0.0001 0.309 0.057 0.004 <0.0001 0.211 0.009 0.0001 <0.0001 0.249 0.102 0.008 <0.0001 0.175
Framingham RiskScore†
0.111 0.0067 <0.0001 0.309 0.057 0.004 <0.0001 0.211 0.007 0.0004 <0.0001 0.249 0.096 0.008 <0.0001 0.179
MetS by NCEPdefinition
−0.038 0.123 0.737 0.003 0.083 0.968 0.006 0.009 0.463 0.339 0.161 0.035
* Adjusted for CRP, sICAM, physical activity and familial history of premature cardiovascular disease.† Anderson et al. [25].
to 2.15 with the NCEP definition, and from 1.48 to 1.97 withthe WHO definition (Fig. 1).
We also examined the concordance of the two defini-tions of MetS. Interestingly, the NCEP and WHO definitionsfor MetS were quite concordant (Kappa coefficient: 0.61,95% CI: 0.53–0.68). Approximately, 11% of the study cohortsimultaneously met the definitions of both NCEP and WHO.Subsequent analyses by defining MetS using NCEP andWHO definitions simultaneously showed that the associationof MetS with number of plaques (carotid; carotid–femoral),IMT, and PWV remained significant. Moreover, the odds ratiofor MetS using this more detailed and inclusive definition ofMetS appeared slightly stronger than those obtained by usingNCEP or WHO definitions separately, and ranged from 1.88to 2.54 for various subclinical markers of CVD (P < 0.05).
Because the Framingham risk score (FRS) for estimatingthe 10-year risk of CHD is a commonly used risk algo-rithm in clinical practice, we compared the association ofFRS [25] as compared to MetS, with measures of subclin-ical atherosclerosis examined in the study. Both FRS andMetS were significantly associated with the markers of sub-clinical atherosclerosis (Table 4). However, when FRS wasentered into the regression models prior to MetS by NCEPdefinition, the association of MetS with most markers of sub-clinical atherosclerosis, with the exception of PWV, was nolonger significant.
4
dotoWihlWp
prevalence of MetS in the current study compared to thatreported in the US is consistent with that reported in Finnishmen [3] and may be related to lifestyle factors [27].
Interest in the clinical application of MetS is increas-ing, because most epidemiological studies have shown anincreased risk of incident diabetes and CVD as well as CVDmortality with MetS [3,6–10]. From a prevention perspec-tive, the importance of MetS may be even greater in earlierstages of CVD. Limited data exist, however, on the associ-ation of MetS with subclinical atherosclerosis [13–19]. Toour knowledge, the present analyses are the first examinationof MetS using recently proposed definitions by NCEP andWHO, with several markers of early stages of CVD in a ran-dom population-based sample. Our findings support that irre-spective of the definition (NCEP or WHO) used, MetS wasassociated with increased number of atherosclerotic (carotidand femoral) plaques, carotid IMT, and PWV; this effect wasindependent of potentially confounding factors, such as age,sex, smoking, physical activity, family history of CVD, LDL-cholesterol, and inflammation.
The association of MetS with atherosclerotic plaques isnot surprising because individual components of MetS havebeen each well established as risk factors for CVD [28]. Inthe present study, MetS as an entity using NCEP and WHOdefinitions were associated with total number of carotid andfemoral plaques. Furthermore, MetS by NCEP definitionaisTstrCirsi
sc
. Discussion
With increase in obesity and sedentary lifestyles, the inci-ence of diabetes and CVD is rising worldwide. Becausef the close association of diabetes and CVD the notionhat the two arise from common antecedents termed MetSr insulin resistance syndrome, has been recognized by theHO and other expert panels, such as the NCEP [5]. Approx-
mately one-third of middle-aged men and women in USave MetS by the NCEP definition [26]. We found slightlyower estimates for the prevalence of MetS using NCEP and
HO definitions (14.5 and 17.5%, respectively) in a randomopulation-based sample in Southwestern France. The lower
ppeared to be a stronger predictor amongst the two def-nitions, because contrary to the WHO definition it couldignificantly predict the number of carotid plaques as well.he difference in this association may be related to the inclu-ion of insulin and BMI in the WHO definition. Interestingly,he association of MetS with the number of atheroscle-otic plaques persisted even after adjustment for traditionalVD risk factors as well as additional potentially confound-
ng factors, such as inflammation. This positive associationemained significant even when medication use for loweringerum cholesterol, hypertension, and control of diabetes wasncluded in the model (data not shown).
Increased IMT and PWV have been the focus of severaltudies as markers of early stages of atherosclerosis. IMT is aomplex parameter including modifications of intima and/or
N. Ahluwalia et al. / Atherosclerosis 186 (2006) 345–353 351
media of the arterial wall; and PWV is a marker of arterial dis-tention, increased PWV reflects increased arterial stiffness.Several studies have shown an association between increasedIMT and CVD [11,29,30] as well as between increased PWVand CVD [12,31–33]. There is limited information in theliterature, however, on the relationship of MetS with sub-clinical CVD markers, such as IMT and PWV. Our findingof increased IMT in persons with MetS in this population-based sample in France is consistent with the findings ofGolden et al. and McNeill et al. with 45–64 year olds in theUS [13,14]. These authors also showed that the componentsof MetS had a synergistic rather than additive effect on IMT[13]. In addition, our finding of increased IMT and PWV insubjects with MetS in the current study is consistent with thefindings of Nakanishi et al. [15] and Tomiyama et al. [16]with middle-aged Japanese men and of Li et al. [17] in aracially mixed sample of adults in USA. Importantly, in thecurrent study even after adjustment for traditional risk factorsfor CVD as well as inflammation and treatment for diabetes,hypertension and hypercholesterolemia, the association ofMetS with increased IMT and PWV persisted, highlight-ing the significance of identifying individuals with MetS fortargeting treatment efforts against all components of the syn-drome. Similarly, when individuals with diabetes (n = 54)were excluded from analysis, the findings of a significantassociation of MetS (irrespective of the definition used) witha
ipsImrbCbrIcceetibMsMdttw
im
with early stages of atherosclerosis have not only been few butalso generally did not include inflammation in their design.Thus, to our knowledge the current study is the first to simul-taneously examine the impact of MetS and inflammationfactors on several markers of subclinical CVD examined in-conjunction. In keeping with the building evidence on the roleof inflammation in CVD, inflammatory factors were signif-icant predictors of total number of atherosclerotic plaquesbut not IMT or PWV in the current study. This findingis consistent with results from a longitudinal study whereinflammation was shown to be associated with generation ofatherosclerotic lesions [37]. In response to pro-inflammatorycytokines, various adhesion molecules including ICAM-1,are expressed on the surface of endothelial cells and mediatethe adhesion and migration of circulating leukocytes, thusplaying a critical role in the formation of foam cells and fattystreaks in the early development of atherosclerosis [38]. Thiscould partly explain our finding of CRP and sICAM-1 emerg-ing as significant predictors of the number of plaques but notIMT or PWV. Contrary to these findings, others have reportedan association of inflammation with carotid IMT [39] andPWV [16].
Our interesting finding that both MetS and inflammationwere independently associated with subclinical measures ofatherosclerosis suggests that multiple mechanisms underlieinflammation including the commonly acknowledged asso-crlscuofni
oscowibmdOMwrtftndv
therosclerotic plaques, carotid IMT, and PWV persisted.Our approach of examining multiple markers of subclin-
cal atherosclerosis simultaneously namely atheroscleroticlaques, carotid IMT, and PWV in the study cohort makes thetudy design stronger. We took this approach because carotidMT, atherosclerotic plaques, and PWV are complementaryeasures, which explore various dimensions of atheroscle-
osis (anatomic, functional changes). Moreover, evidence isuilding that increased PWV is a surrogate risk factor forVD not only in hypertensive and renal patients [34,35],ut also in non-hypertensive subjects [33], as well as in aepresentative French population based sample [12]. CarotidMT explores a very specific localized vascular region namelyarotid artery while the presence of plaques in femoral andarotid arteries could represent broader diffusion and a morextended state of atherosclerosis. In recent analyses, McNeillt al. [14] extrapolated the findings of Chambless et al. [36],o the observed 40-�m excess in IMT associated with MetSn their study to suggest that the 5-year risk of CHD woulde increased by 17 and 9% among women and men withetS, respectively. Considering these reports [14,36], we
peculate that the increase in carotid IMT associated withetS observed in the current study, in the order of 50–60 �m
epending on the definition (NCEP or WHO) used, suggestshat the increase in 5-year risk of CHD would be similar tohat observed by McNeill et al. (at least 17 and 9% amongomen and men, respectively, in presence of MetS) [14].An additional strength of this study is the inclusion of
nflammatory factors, CRP, and sICAM-1, in the regressionodels. Previous studies examining the relationship of MetS
iation of obesity and inflammation; excess adipose tissueeleases inflammatory cytokines that may elicit higher CRPevels [5]. This observation is consistent with recent reportshowing the capability of high sensitivity CRP to predictoronary events after adjusting for traditional risk factorssed in the Framingham risk estimate, as well as similarbservations in older adults with adjustment for risk factorsor CVD [40–42]. Taken together, these results support theotion that pro-inflammatory state is implicated directly innsulin resistance and atherogenesis [5].
In clinical practice, the Framingham risk algorithm [25] isften used to estimate the 10-year risk of CHD. In the presenttudy, although both FRS and MetS were significantly asso-iated with all of the markers of subclinical atherosclerosis,nly the association of MetS with PWV remained significanthen FRS was entered into the models before MetS. This is
n contrast to the finding of a significant association of MetSy NCEP definition with coronary artery calcium, anotherarker of subclinical atherosclerosis, which was indepen-
ent of subjects’ 10-year CHD risk based on the FRS [19,43].ur findings are, however, consistent with those reported bycNeill et al. [9] and Stern et al. [44] showing that individualsithout diabetes or CVD, but with MetS, were at increased
isk for long-term cardiovascular outcomes, although statis-ical models suggested that most of that risk was accountedor by the FRS. We concur with McNeill et al. [9] that iden-ification of individuals with MetS is important as it may,evertheless, provide opportunities to intervene earlier in theevelopment of shared disease pathways that predispose indi-iduals to both CVD and diabetes.

352 N. Ahluwalia et al. / Atherosclerosis 186 (2006) 345–353
We recognize that the two approaches for CVD risk assess-ment are complementary and are correlated. It is well recog-nized that FRS determines the evolution of CVD over anextended time period (10 years) while MetS may be morepredictive of onset of diabetes; this could not be analyzed inthe present study because of its cross-sectional nature. Futurelongitudinal studies should evaluate the contribution of MetSversus FRS in predicting diabetes and CHD.
In conclusion, our findings show that MetS is stronglyassociated with subclinical atherosclerosis and arterial mark-ers of CVD (with both WHO and NCEP definitions). Further-more, both definitions of MetS provided similar associationswith early stages of atherosclerosis. The risk of subclini-cal CVD was slightly higher when both definitions wereused simultaneously to identify individuals with MetS. Inaddition, inflammation factors were significant predictors ofatherosclerotic plaques. The clinical applications of thesefindings are important: efforts should be placed at diagnos-ing MetS as an entity so as to identify individuals at highrisk for subclinical atherosclerosis; interventions should betargeted to simultaneously treat all components of MetS. Insummary, clinically MetS may be considered as a surrogatemarker for high risk of subclinical CVD and should be treatedaggressively as an entity.
A
sIHdl
R
[7] Resnick HE, Jones K, Ruotolo G, et al. Insulin resistance,the metabolic syndrome, and risk of incident cardiovascular dis-ease in non-diabetic American Indians. Diab Care 2003;26:861–7.
[8] Nakanishi N, Takatorige T, Fukuda H, et al. Components of themetabolic syndrome as predictors of cardiovascular disease andtype 2 diabetes in middle-aged Japanese men. Diab Res Clin Pract2004;64:59–70.
[9] McNeill AM, Rosamond WD, Girman CJ, et al. The metabolicsyndrome and 11-year risk of incident cardiovascular diseasein the atherosclerosis risk in communities study. Diab Care2005;28:385–90.
[10] Malik S, Wong ND, Franklin SS, et al. Impact of the metabolicsyndrome on mortality from coronary heart disease, cardiovascu-lar disease, and all causes in United States adults. Circulation2004;110:1245–50.
[11] Bongard V, Elias A, Bal dit Sollier C, et al. Soluble intercel-lular adhesion molecule-1 is associated with carotid and femoralatherosclerosis but not with intima-media thickness in a population-based sample. Atherosclerosis 2002;164:297–304.
[12] Amar J, Ruidavets JB, Chamontin B, Drouet L, Ferrieres J. Arterialstiffness and cardiovascular risk factors in a population-based study.J Hypertens 2001;19:381–7.
[13] Golden SH, Folsom AR, Coresh J, et al. Risk factor groupingsrelated to insulin resistance and their synergistic effects on subclin-ical atherosclerosis. Diabetes 2002;51:3069–76.
[14] McNeill AM, Rosamond WD, Girman CJ, et al. Prevalence ofcoronary heart disease and carotid arterial thickening in patientswith the metabolic syndrome (The ARIC Study). Am J Cardiol2004;94:1249–54.
[15] Nakanishi N, Suzuki K, Tatara K. Clustered features of the metabolic
[
[
[
[
[
[
[
[
[
[
[
cknowledgements
We are grateful to the subjects for their participation in thetudy. This study was supported by grants from the Nationalnstitute for Health and Medical Research, France, Nationalealth Surveillance System, France, la Federation Francaisee Cardiologie, la Fondation pour la Recherche Medicale anda Fondation de France.
eferences
[1] Alberti KG, Zimmet PZ. Definition, diagnosis and classification ofdiabetes mellitus and its complications. Part I. Diagnosis and classifi-cation of diabetes mellitus provisional report of a WHO consultation.Diab Med 1998;15:539–53.
[2] Balkau B, Charles MA. Comment on the provisional report from theWHO consultation. Diab Med 1999;16:442–3.
[3] Lakka H-M, Laaksonen DE, Lakka TA, et al. The metabolic syn-drome and total and cardiovascular disease mortality in middle-agedmen. JAMA 2002;288:2709–16.
[4] Executive Summary of the Third Report of the National CholesterolEducation Program (NCEP). Expert Panel on Detection, Evaluation,and Treatment of High Blood Cholesterol in Adults (adult TreatmentPanel III). JAMA 2001;285:2485–97.
[5] Grundy SM, Brewer HB, Cleeman JI, Smith SC, Lenfant C.Definition of metabolic syndrome: report of the National Heart,Lung and Blood Institute/American Heart Association Conferenceon Scientific Issues Related to Definition. Circulation 2004;109:433–8.
[6] Hanson RI, Imperatore G, Bennett PH, Knowler WC. Components ofthe “metabolic syndrome” and incidence of type 2 diabetes. Diabetes2002;51:3120–7.
syndrome and the risk for increased aortic pulse wave velocity inmiddle-aged Japanese men. Angiology 2003;54:551–9.
16] Tomiyama H, Koji Y, Yambe M, et al. Elevated C-reactive proteinaugments increased arterial stiffness in subjects with the metabolicsyndrome. Hypertension 2005;45:997–1003.
17] Li S, Chen W, Srinivasan SR, Berenson GS. Influence of metabolicsyndrome on arterial stiffness and its age-related change in youngadults: the Bogalusa Heart Study. Atherosclerosis 2005;180:349–54.
18] Michos ED, Nasir K, Braunstein JB, et al. Framingham risk equa-tion underestimates subclinical atherosclerosis risk in asymptomaticwomen. Atherosclerosis 2005 May 19 [Epub ahead of print].
19] Kullo IJ, Cassidy AE, Peyser PA, et al. Association betweenmetabolic syndrome and subclinical coronary atherosclerosis inasymptomatic adults. Am J Cardiol 2004;94:1554–8.
20] Ferrieres J, Ruidavets JB. Association between resting heart rateand hypertension treatment in a general population. Am J Hypertens1999;12:628–31.
21] Ferrieres J, Ruidavets JB, Fauvel J, et al. Angiotensin I-convertingenzyme gene polymorphism in a low-risk European population forcoronary artery disease. Atherosclerosis 1999;142:211–6.
22] Ruidavets JB, Ducimetiere P, Arveiler D, et al. Types of alcoholicbeverages and blood lipids in a French population. J Epidemiol Com-munity Health 2002;56:24–8.
23] Ferrieres J, Elias A, Ruidavets JB, et al. Carotid intima-media thick-ness and coronary heart disease risk factors in a low-risk population.J Hypertens 1999;17:743–8.
24] Touboul JP, Crouse III JR. Intima-media thickness and atheroscle-rosis: predicting the risk? New York: Parthenon Publishing Group;1997.
25] Anderson KM, Odell PM, Wilson PW, Kannel WB. Cardiovasculardisease risk profiles. Am Heart J 1991;121:293–8.
26] Ford ES, Giles WH, Dietz WH. Prevalence of the metabolicsyndrome among US adults: findings from the third NationalHealth and Nutrition Examination Survey. JAMA 2002;287:356–9.

N. Ahluwalia et al. / Atherosclerosis 186 (2006) 345–353 353
[27] Ferrieres J. The French paradox: lessons for other countries. Heart2004;90:107–11.
[28] Meigs JB. The metabolic syndrome. BMJ 2003;327:61–2.[29] Salonen JT, Salonen R. Ultrasonographically assessed carotid mor-
phology and the risk of coronary heart disease. Arterioscler Thromb1991;11:1245–9.
[30] O’Leary DH, Polak JF, Kronmal RA, et al., Cardiovascular HealthStudy Collaborative Research Group. Carotid-artery intima andmedia thickness as a risk factor for myocardial infarction and strokein older adults. N Engl J Med 1999;7:14–22.
[31] Zureik M, Bureau JM, Temmar M, et al. Echogenic carotid plaquesare associated with aortic arterial stiffness in subjects with subclinicalcarotid atherosclerosis. Hypertension 2003;41:519–27.
[32] Safar ME, Levy BI, Struijker-Boudier H. Current perspectives onarterial stiffness and pulse pressure in hypertension and cardiovas-cular diseases. Circulation 2003;107:2864–9.
[33] Dernellis J, Panaretou M. Aortic stiffness is an independent pre-dictor of progression to hypertension in non-hypertensive subjects.Hypertension 2005;45:426–31.
[34] Laurent S, Katsahian S, Fassot C, et al. Aortic stiffness is an inde-pendent predictor of fatal stroke in essential hypertension. Stroke2003;34:1203–6.
[35] Pannier B, Guerin AP, Marchais SJ, Safar ME, London GM. Stiffnessof capacitive and conduit arteries: prognostic significance for end-stage renal disease patients. Hypertension 2005;45:592–6.
[36] Chambless LE, Heiss G, Golsom AR, et al. Association of coro-nary heart disease incidence with carotid arterial wall thicknessand major risk factors: the Atherosclerosis Risk in Commmunities(ARIC) study. Am J Epidemiol 1997;146:483–94.
[37] Hashimoto H, Kitagawa K, Hougaku H, et al. C-reactive proteinis an independent predictor of the rate of increase in early carotidatherosclerosis. Circulation 2001;104:63–7.
[38] Albelda SM, Smith CW, Ward PA. Adhesion molecules and inflam-matory injury. FASEB J 1994;8:504–12.
[39] Sitzer M, Markus HS, Mendall MA, et al. C-reactive protein andcarotid intimal medial thickness in a community population. J Car-diovasc Risk 2002;9:97–103.
[40] Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparisonof C-reactive protein and low-density lipoprotein cholesterol lev-els in the prediction of first cardiovascular events. N Engl J Med2002;347:1557–65.
[41] Chaves PH, Kuller LH, O’Leary DH, Manolio TA, Newman AB.Cardiovascular Health Study. Subclinical cardiovascular disease inolder adults: insights from the Cardiovascular Health Study. Am JGeriatr Cardiol 2004;13:137–51.
[42] Smith Jr SC, Anderson JL, Cannon III RO, et al. CDC/AHA Work-shop on Markers of Inflammation and Cardiovascular Disease: Appli-cation to Clinical and Public Health Practice. Report from the clinicalpractice discussion group. Circulation 2004;110:e550–3.
[43] Girman CJ, Rhodes T, Mercuri M, et al. The metabolic syn-drome and risk of major coronary events in the Scandinavian Sim-vastatin Survival Study (4S) and the Air Force/Texas CoronaryAtherosclerosis Prevention Study (AFCAPS/TexCAPS). Am J Car-diol 2004;93:136–41.
[44] Stern MP, Williams K, Gonzalez-Villalpando C, Hunt KJ, HaffnerSM. Does the metabolic syndrome improve identification of individ-uals at risk of type 2 diabetes and/or cardiovascular disease? DiabCare 2004;27:2676–81.