angiotensin ii and atherosclerosis
TRANSCRIPT

Angiotensin II and AtherosclerosisDaiana Weiss, MD, Dan Sorescu, MD, and W. Robert Taylor, MD, PhD
Numerous clinical and laboratory data are now avail-able supporting the hypothesis that the renin–angioten-sin system is mechanistically relevant in the pathogene-sis of atherosclerosis. The traditional role of the renin–angiotensin system in the context of blood pressureregulation has been modified to incorporate the conceptthat angiotensin II (Ang II) is a potent proinflammatoryagent. In vascular cells, Ang II is a potent stimulus for thegeneration of reactive oxygen species. As a result, AngII upregulates the expression of many redox-sensitivecytokines, chemokines, and growth factors that have
been implicated in the pathogenesis of atherosclerosis.Extensive data now confirm that inhibition of the renin–angiotensin system inhibits atherosclerosis in animalmodels as well as in humans. These studies providemechanistic insights into the precise role of Ang II inatherosclerosis and suggest that pharmacologic inter-ventions involving the renin–angiotensin system may beof fundamental importance in the treatment and preven-tion of atherosclerosis. Q2001 by Excerpta Medica,Inc.
Am J Cardiol 2001;87(suppl):25C–32C
The renin–angiotensin system has emerged as oneof the essential links in the pathophysiology of
vascular disease. Historically, the most important ef-fect of angiotensin II (Ang II) was considered to be theneurohormonal regulation of arterial blood pressure.Plasma-derived Ang II exerts potent vasoconstrictoreffects on resistance arteries. In addition Ang II re-leases aldosterone from the adrenal glands, which inturn enhances renal tubular sodium reabsorbtion re-sulting in an increase in the effective circulatingplasma volume.1
Although these acute hemodynamic effects can becompensatory in acute hemorrhagic conditions, it hasbecome apparent that chronic exposure of cardiovas-cular tissues to Ang II produces paradoxically patho-logic effects. Indeed, it now appears that Ang II is acentral integrator of multiple processes critically im-plicated in vascular pathophysiology. Ang II has beenshown to regulate the growth and migration of smoothmuscle cells and fibroblasts, apoptosis of endothelialcells, and differentiation of monocytes into macro-phages. Moreover, Ang II can induce potent inflam-matory responses in vascular cells by stimulating therelease of growth factors (eg, platelet-derived growthfactor, transforming growth factor-b, insulin-likegrowth factor-I), cytokines (eg, interleukin-6, interleu-kin-1), and chemokines (eg, monocyte chemoattrac-tant protein-1 and interleukin-8) (Table 1). For review,see Schmidt-Ott et al.2 Ang II can also alter the extra-cellular matrix remodeling via activation of metallopro-teinases (matrix metalloproteinase-2, matrix metallopro-teinase-9)3 and induce a procoagulant state.4
The complexity and diversity of cellular responsesto Ang II is further complicated by the presence ofmultiple pathways for generating Ang II. The classicsource of Ang II is circulating plasma-derived Ang II.Angiotensinogen produced by the liver is cleaved by
renin (released from the kidney) to generate angioten-sin I. Next, angiotensin-converting enzyme (ACE)(identical to kininase II, which degrades bradykinin)present on endothelial cells in the pulmonary vascu-lature finalizes the conversion of angiotensin I toactive Ang II. However, it is now apparent that an-other, perhaps more important source of Ang II is thelocal, tissue-based production of Ang II by cardiacmuscle and the vascular wall.
Bernstein et al5 have recently demonstrated the po-tential importance of tissue-bound ACE using a uniquegenetic model. Tissue ACE is normally anchored to theplasma membrane by a specialized transmembrane do-main. Mice were generated with a deletion of the anchordomain such that there was a release of all tissue-boundAng II into plasma. Interestingly, these mice developedlow blood pressure and inability to concentrate urine—aphenotype identical to complete disruption of ACE gene.These findings suggested that the disruption of the an-chorage of the tissue ACE induces a functional stateidentical to the complete deficiency of ACE.5,6 It hasbeen demonstrated that ACE, Ang II, and Ang II recep-tors are present in human atherosclerotic lesions. Fur-thermore, these components of the renin–angiotensinsystem are produced by all cellular components of thevascular wall: macrophages, smooth muscle cells, endo-thelial cells, and fibroblasts.7 In addition, it has beenrecently found that in normal and diseased vascular tis-sues, Ang II can also be formed via chymase, a neutralendopeptidase produced abundantly by vascular cells. Itis important to note that although the kinetics of thisenzyme are similar to those of ACE, this enzyme is notaffected by ACE inhibitors.8 Thus, local production ofAng II within the arterial wall is important in the normalregulation of arterial tone and is potentially critical to thepathogenesis of atherosclerosis.
OXIDATIVE STRESS AS AMECHANISTIC LINK BETWEENANGIOTENSIN II ANDATHEROSCLEROSIS
Perhaps the most intriguing aspect of the AngII-mediated events in the arterial wall is the almost
From the Department of Medicine, Division of Cardiology, EmoryUniversity School of Medicine and The Atlanta Veterans Affairs Med-ical Center, Atlanta, Georgia, USA.
Address for reprints: W. Robert Taylor, MD, PhD, Emory Univer-sity, Division of Cardiology, 1639 Pierce Drive, Suite 319 WMB,Atlanta, Georgia 30322. E-mail: [email protected].
25C©2001 by Excerpta Medica, Inc. 0002-9149/01/$ – see front matterAll rights reserved. PII S0002-9149(01)01539-9

complete overlap with proposed mechanisms ofatherogenesis. Many of the phenomena implicated inatherosclerosis can be reproduced by Ang II. Athero-sclerosis is an inflammatory disease of vascular wallinitiated and amplified by vascular oxidative stress.9
Ang II is also a very potent stimulus for both inflam-mation and oxidative stress.2 The important potentialsources of oxidative stress in vascular tissue are:(1) oxidized low-density lipoprotein (LDL); (2)phagocytic and nonphagocytic nicotinamide adeninedinucleotide phosphate (NADPH) oxidases, whichproduce superoxide anion (O2z
2), which is convertedby superoxide dismutases to hydrogen peroxide; (3)xanthine oxidase; (4) lipooxygenases; and (5) cyto-chrome P450-monooxygenases.
Oxidized LDL, Ang II, and atherosclerosis: One of theearliest events in atherogenesis is endothelial dysfunc-tion. Abnormal endothelial cells exhibit upregulationof the intercellular adhesion molecules E-selectin,vascular cell adhesion molecule-1, and intercellularadhesion molecule-1, which causes increased adhe-siveness to circulating monocytes. Adherent mono-cytes migrate into the subendothelium and differenti-ate into macrophages.10 Interestingly, Ang II can in-crease expression of the same adhesion molecules(E-selectin, vascular cell adhesion molecule-1, andintercellular adhesion molecule-1) and can enhancethe recruitment of local macrophages into the athero-sclerotic plaque.11
Elevated LDL and Ang II also induce monocytechemotaxis through upregulation of monocyte che-moattractant protein-1, CC chemokine receptor 2 (the
macrophage receptor for monocyte chemoattractantprotein-1).11–13 LDL, in turn, attracts macrophagesand is modified oxidatively in the subendothelialspace by macrophage-derived lipooxygenase, myelo-peroxidase, or NADPH oxidase, and converted intooxidized LDL (Figure 1).14 Once produced locally,oxidized LDL has dramatic effects on local vascularhomeostasis and endothelial cell cytotoxicity15 in ad-dition to stimulating migration and mitogenesis ofmacrophages and smooth muscle cells.14
Ang II and oxidized LDL influence, in a dualfashion, each other’s production and effects on thetarget cell. Hypercholesterolemia increases Ang IItype 1 receptor expression on vascular smooth musclecells, which potentially enhances the responses ofvascular smooth muscle cells to Ang II. This effect isblocked by hydroxymethyl glutaryl coenzyme A(HMG-CoA) reductase inhibitors in human coronaryartery disease.16,17 Reciprocally, Ang II upregulatesthe receptor for oxidized LDL (LOX-1) on both en-dothelial cells and macrophages and increases thecellular uptake of oxidized LDL contributing to mac-rophage activation and endothelial dysfunction.18,19
Human and animal studies have suggested that Ang IIis required in vivo for the oxidation of LDL. Forexample the Ang II receptor antagonist losartan andthe ACE inhibitor fosinopril inhibit LDL oxidation inthe murine apolipoprotein E knockout model of hy-percholesterolemia.20,21 A direct consequence of theactivation of macrophages by Ang II or oxidizedLDL is that these activated cells also secrete proin-flammatory cytokines (eg, tumor necrosis factor-a,
TABLE 1 Growth Factors, Adhesion Molecules, and Cytokines Stimulated by Angiotensin II that Have also Been Implicated in thePathogenesis of Atherosclerosis
Cytokines, Chemokines,and Growth Factors Cellular Source Function Reference
Osteopontin SMC, macrophages Migration of SMC 53VCAM-1 EC, SMC Monocyte adherence 11ICAM-1 EC Leukocyte adhesion to the vascular endothelium 54E-selectin EC Adherence, migration of monocytes and T
lymphocytes55
TNF-a EC, SMC, macrophages SMC proliferation; endothelial cell recruitmentof monocytes via adhesion molecules
37
MCP-1 EC, SMC, macrophages, Activated T-cell chemoattractant; inducesmonocyte migration
1236
IL-1 EC, SMC SMC proliferation; production of growthfactors, cytokines
37
IL-6 SMC, macrophages Induction of b-cell differentiation; T-cellactivation; induction of acute phase proteins;stimulation of matrix-degrading enzymes
56
IL-8 EC, SMC, macrophages,monocytes
Activated T-cell chemoattractant; angiogenicfactor; stimulates SMC migration andproliferation
37
IGF-1 SMC SMC hypertrophy 57PDGF EC, SMC macrophages SMC proliferation; chemoattractant for SMC
and monocytes58
TGF-b SMC, fibroblasts SMC hypertrophy, fibroblast differentiation intomyofibroblasts, promotes collagen synthesisand fibrosis
59
bFGF SMC SMC proliferation after injury 60
bFGF 5 basic fibroblast growth factor; EC 5 endothelial cell; ICAM 5 intercellular adhesion molecule; IGF-1 5 insulin-like growth factor-1; IL-1 5 interleukin-1;IL-6 5 interleukin-6; IL-8 5 interleukin-8; MCP-1 5 monocyte chemoattractant protein-1; PDGF 5 platelet-derived growth factor; SMC 5 smooth muscle cells; TGF-b 5
transforming growth factors-b; TNF-a 5 tumor necrosis factor-a; VCAM-1 5 vascular cellular adhesion molecule-1.
26C THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 87 (8A) APRIL 19, 2001
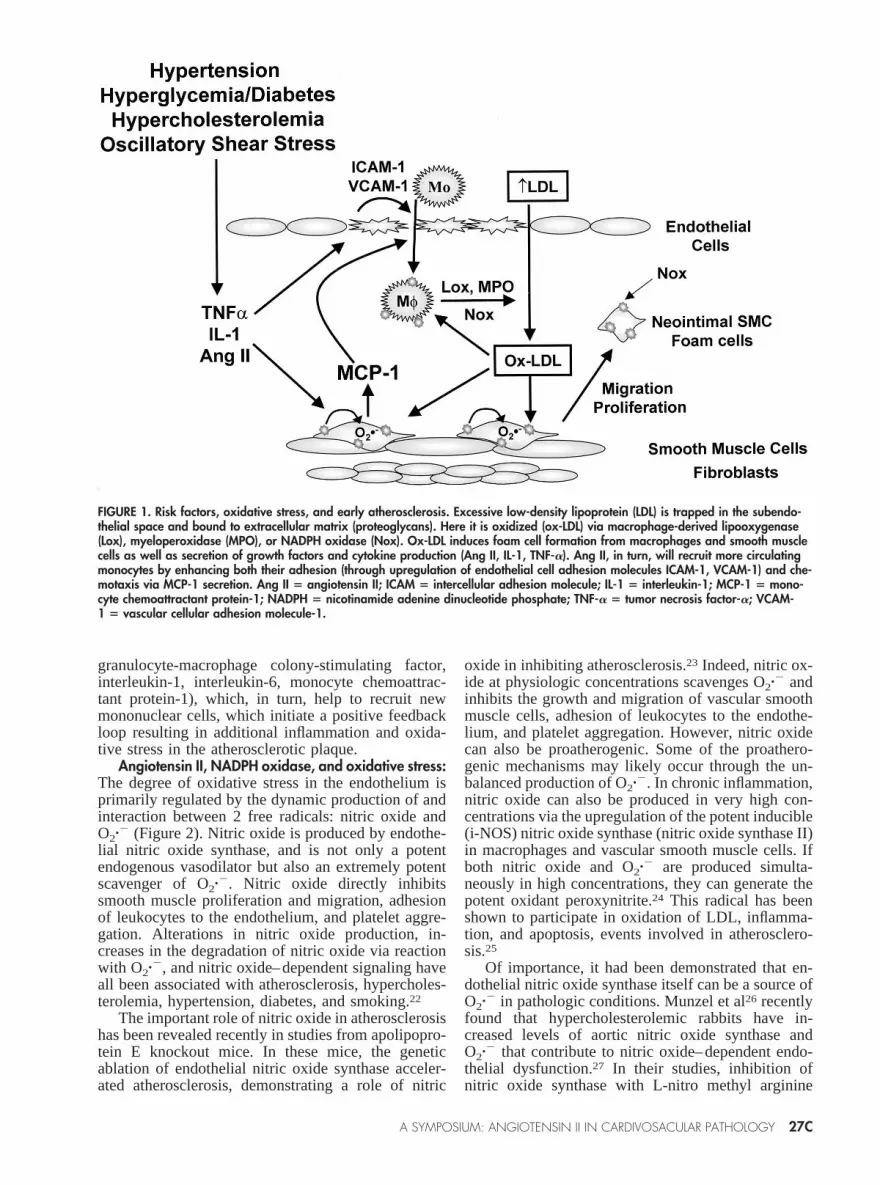
granulocyte-macrophage colony-stimulating factor,interleukin-1, interleukin-6, monocyte chemoattrac-tant protein-1), which, in turn, help to recruit newmononuclear cells, which initiate a positive feedbackloop resulting in additional inflammation and oxida-tive stress in the atherosclerotic plaque.
Angiotensin II, NADPH oxidase, and oxidative stress:The degree of oxidative stress in the endothelium isprimarily regulated by the dynamic production of andinteraction between 2 free radicals: nitric oxide andO2z
2 (Figure 2).Nitric oxide is produced by endothe-lial nitric oxide synthase, and is not only a potentendogenous vasodilator but also an extremely potentscavenger of O2z
2. Nitric oxide directly inhibitssmooth muscle proliferation and migration, adhesionof leukocytes to the endothelium, and platelet aggre-gation. Alterations in nitric oxide production, in-creases in the degradation of nitric oxide via reactionwith O2z
2, and nitric oxide–dependent signaling haveall been associated with atherosclerosis, hypercholes-terolemia, hypertension, diabetes, and smoking.22
The important role of nitric oxide in atherosclerosishas been revealed recently in studies from apolipopro-tein E knockout mice. In these mice, the geneticablation of endothelial nitric oxide synthase acceler-ated atherosclerosis, demonstrating a role of nitric
oxide in inhibiting atherosclerosis.23 Indeed, nitric ox-ide at physiologic concentrations scavenges O2z
2 andinhibits the growth and migration of vascular smoothmuscle cells, adhesion of leukocytes to the endothe-lium, and platelet aggregation. However, nitric oxidecan also be proatherogenic. Some of the proathero-genic mechanisms may likely occur through the un-balanced production of O2z
2. In chronic inflammation,nitric oxide can also be produced in very high con-centrations via the upregulation of the potent inducible(i-NOS) nitric oxide synthase (nitric oxide synthase II)in macrophages and vascular smooth muscle cells. Ifboth nitric oxide and O2z
2 are produced simulta-neously in high concentrations, they can generate thepotent oxidant peroxynitrite.24 This radical has beenshown to participate in oxidation of LDL, inflamma-tion, and apoptosis, events involved in atherosclero-sis.25
Of importance, it had been demonstrated that en-dothelial nitric oxide synthase itself can be a source ofO2z
2 in pathologic conditions. Munzel et al26 recentlyfound that hypercholesterolemic rabbits have in-creased levels of aortic nitric oxide synthase andO2z
2 that contribute to nitric oxide–dependent endo-thelial dysfunction.27 In their studies, inhibition ofnitric oxide synthase with L-nitro methyl arginine
FIGURE 1. Risk factors, oxidative stress, and early atherosclerosis. Excessive low-density lipoprotein (LDL) is trapped in the subendo-thelial space and bound to extracellular matrix (proteoglycans). Here it is oxidized (ox-LDL) via macrophage-derived lipooxygenase(Lox), myeloperoxidase (MPO), or NADPH oxidase (Nox). Ox-LDL induces foam cell formation from macrophages and smooth musclecells as well as secretion of growth factors and cytokine production (Ang II, IL-1, TNF-a). Ang II, in turn, will recruit more circulatingmonocytes by enhancing both their adhesion (through upregulation of endothelial cell adhesion molecules ICAM-1, VCAM-1) and che-motaxis via MCP-1 secretion. Ang II 5 angiotensin II; ICAM 5 intercellular adhesion molecule; IL-1 5 interleukin-1; MCP-1 5 mono-cyte chemoattractant protein-1; NADPH 5 nicotinamide adenine dinucleotide phosphate; TNF-a 5 tumor necrosis factor-a; VCAM-1 5 vascular cellular adhesion molecule-1.
A SYMPOSIUM: ANGIOTENSIN II IN CARDIVOSACULAR PATHOLOGY 27C

blocked the increased production of O2z2. Thus,
they were able to conclude that in their modelsystem, endothelial nitric oxide synthase was theprimary source of excessive O2z
2 production. Further-more, pretreatment with an Ang II receptor blockeralso inhibited the nitric oxide synthase-derivedO2z
2 thereby implicating Ang II in hypercholesterol-emia-induced O2z
2 release. Endothelial nitric oxidesynthase generates nitric oxide by transferring elec-trons from NADPH to L-arginine through the vitamintetrahydrobiopterin. If tetrahydrobiopterin is in rela-tive deficiency compared with the amount of nitricoxide synthase, this will halt the electron flow andresult in less nitric oxide production and redirection ofelectron flow toward oxygen to produce O2z
2. Thisphenomenon of conversion of nitric oxide productioninto O2z
2 through uncoupling of endothelial nitricoxide synthase has been suggested to be relevant tohuman atherosclerosis. For example, the same groupdemonstrated that administration of BH4 correctedimpaired nitric oxide–dependent endothelial relax-ation in chronic smokers. Furthermore, the same im-provement of vasorelaxation was achieved when vita-min C was used to scavenge O2z
2, suggesting that theadministration of tetrahydrobiopterin resulted in bothincreased production of nitric oxide and a concomitantreduction in O2z
2 production, resulting in improvedendothelial-dependent vasodilatation.28
Although several other sources of vascular O2z2
have been identified, the most important are thephagocytic and nonphagocytic oxidases. The phago-cytic NADPH oxidase (nox2, or NADPH oxidase 2)was identified as a potent source of O2z
2 .20 yearsago. It is an enzyme in macrophages that consists of 2plasma membrane proteins (gp91phox and p22phox)that are activated by the cytoplasmic complex rac/p47/p67 assembled upon stimulation with phorbol esther,tumor necrosis factor-a. Upon activation, 2 electronsare transferred from NADPH to molecular oxygen andform O2z
2. The O2z2 is released by phagocytes in
bursts and either is used in lysosomes for microbialkilling or can be released into the extracellular spacewere it is dismutated by superoxide dismutase to hy-drogen peroxide.
The nonphagocytic oxidases are NADPH-depen-dent oxidases that are present in all vascular cells(endothelial cells, smooth muscle cells, and fibro-blasts).29 One characteristic of the nonphagocytic oxi-dases is that they release O2z
2 in minibursts (1,000-fold lower in magnitude than the phagocytic type) andperhaps in very compartmentalized fashion. The ulti-mate role for O2z
2 generated by NADPH oxidasesappears to be intracellular signaling in response toagonists as opposed to extracellular secretion.30
Griendling et al31 made the seminal observationthat Ang II potently induces activation of NADPHoxidase activity in vascular smooth muscle cells (Fig-ure 3). Subsequently, it has been demonstrated that ap22phox-based NADPH oxidase is required for bothin vitro and in vivo Ang II-induced vascular hypertro-phy.32,33 Furthermore, this response appears to bespecific for Ang II because norepinephrine, which also
induces hypertension does not increase NADPH oxi-dase activity. Subsequently, the same group and othershave identified that the specific redox-sensitive path-ways involve the p38MAPK34 and the survival kinaseAkt35 substantiating the concept that there are specificintracellular redox-sensitive signaling cascades con-trolled by endogenous reactive oxygen species. Fromthese studies has emerged the concept that many bio-logic effects of Ang II are mediated at the cellularlevel through O2z
2 generated by the nonphagocyticNADPH oxidase.
Ang II increases the inflammation of the vascularwall by recruiting macrophages via the upregulationof monocyte chemoattractant protein-1 productionfrom vascular cells (Figure 1).12 Of importance,monocyte chemoattractant protein-1 induction in vas-cular smooth muscle cells by Ang II is dependent onthe activation of NADPH oxidase.36 Monocyte che-moattractant protein-1 is essential in atherogenesisbecause it is one of the most potent chemoattractantsfor monocytes that propagate atherosclerosis in thevascular wall. Another example is the induction ofinterleukin-6 upon stimulation with Ang II via thejanus kinase/signal transducers and activators of tran-scription (JAK/STAT) pathway, which is also entirelydependent on stimulation of endogenous vascularNADPH oxidase.37 Interleukin-6 is a potent proin-flammatory cytokine, which is responsible for induc-tion of acute phase reactant proteins from liver duringacute or chronic inflammatory states. It has a potentmitogenic effect on vascular smooth muscle cells.38 Itis also an activator of macrophages39 and has beenlinked recently to human coronary artery disease andacute coronary syndromes. Both Ang II and interleu-kin-6 co-localize in the human atherosclerotic plaquesin the macrophages present in the shoulder region ofthe plaque, a region that has been suggested to beprone to plaque rupture in acute coronary syndromes.Thus, Ang II–mediated production of O2z
2 has beenproposed to be a pivotal mechanism in the develop-ment of atherosclerosis.
Several studies have recently documented a directlink between NADPH oxidase and human atheroscle-rosis. First, immunohistochemical studies have dem-onstrated the presence of a p22phox-based oxidase inhuman coronary arteries in all cell types that is up-regulated in advanced atherosclerotic plaques.40 Sec-ond, a p22pox polymorphic variant that potentiallyinhibits the function of NADPH oxidase is associatedwith decreased oxidative stress and less extensivecoronary artery disease.41,42 Third, an increase infunctional NADPH oxidase activity has been shown tocorrelate with coronary artery disease independent ofother traditional risk factors in patients.43
Angiotensin II accelerates atherosclerosis in apoli-poprotein E mice: Epidemiologically, Ang II has beenlinked to left ventricular hypertrophy, congestive heartfailure, renal failure, and atherosclerosis.44,45 Unex-pectedly, several major trials for human heart failure(Cooperative North Scandinavian Enalapril SurvivalStudy [CONSENSUS], Study of Left VentricularDysfunction [SOLVD], and Survival and Ventricular
28C THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 87 (8A) APRIL 19, 2001

FIGURE 2. Potential sources of oxidative stress induced by angiotensin II (Ang II) in atherosclerosis. In the normal, physiologic statethe superoxide (O2z2) produced by the nonphagocytic nicotinamide adenine dinucleotide phosphate (NADPH) oxidases serve to con-trol the vascular wall tone through dynamic interactions with nitric oxide. O2z2 is converted to hydrogen peroxide by extracellularsuperoxide dismutase (SOD). Although O2z2 is a vasoconstrictor, nitric oxide and hydrogen peroxide are potent vasodilators. Physio-logic pathways are depicted with a continuous line, pathologic pathways with a discontinuous line. In pathologic conditions, localproduction of Ang II, tumor necrosis factor (TNF)-a or oscillatory shear stress induces upregulation of NADPH oxidases or xanthineoxidase, which, in turn, will increase the production of O2z2. This will inactivate nitric oxide and generate peroxynitrite (ONOO•).Hypercholesterolemia upregulates local production of Ang II. Ang II results in a shift of the activity of endothelial nitric oxide synthase(e-NOS) from nitric oxide production toward O2z2 production, which further contributes to increased oxidative stress.VSMC 5 vascu-lar smooth muscle cells.
FIGURE 3. Nicotinamide adenine dinucleotide phosphate (NADPH) oxidase is a major source for intracellular hydrogen peroxide gen-eration in response to angiotensin II (Ang II). Vascular smooth muscle cells (VSMCs) were untreated (A), stimulated with Ang II alonefor 4 hours (B), or treated with Ang II in presence of diphenyleneiodonium (an inhibitor of NADPH oxidases) and incubated with theperoxide-sensitive fluorophore DCF-DA (C). VSMCs transfected with antisense p22phox (which downregulates the NADPH oxidase)were treated with Ang II for 4 hours before incubation with dichlorofluorescein diacetate (DCF-DA) (D). Images were obtained by la-ser confocal microscopy. (Reproduced with permission from Hypertension.33)
A SYMPOSIUM: ANGIOTENSIN II IN CARDIVOSACULAR PATHOLOGY 29C

Enlargement [SAVE]) found that enalapril, a standardACE inhibitor, reduced the incidence of acute coro-nary events in patients with heart failure by 25%.46
The potential etiologic link between Ang II and hu-man atherosclerosis has been further strengthened re-cently by the reports from the Heart Outcomes Pre-vention Evaluation (HOPE) trial, which demonstratedthat ACE inhibition reduced the rates of death, myo-cardial infarction, and stroke in patients with athero-sclerosis.47
These trials are in agreement with the mechanisticstudies performed in animal models of atherosclerosisin which administration of drugs, which interfere withthe renin–angiotensin system, can delay or amelioratethe development of atherosclerosis. For example, cap-topril has been shown to inhibit atherosclerosis in boththe Watanabe rabbit model48 and the apolipoprotein Eknockout mouse model of atherosclerosis.49 Similarly,losartan has been shown to reduce atherosclerosis incholesterol-fed monkeys.50 In addition, Warnholtz etal51 found that treatment with the Ang II type 1receptor antagonist BAY 10-6734 normalized O2z
2
and endothelial function and reduced early atheroscle-rotic lesion formation in the Watanabe rabbit model.Furthermore, it has been recently shown that enalaprilpartially blocked the accelerated atherosclerosis pro-duced by combining the apolipoprotein E and endo-thelial nitric oxide synthase knockout mice. Takentogether, these data begin to provide a substantialfoundation to support the hypothesis that Ang II–mediated production of O2z
2 is a critical pathogenicmechanism of atherosclerosis.23
In a more direct approach to demonstrate a role forAng II in atherosclerosis progression, our group hasrecently assessed the effect of chronic Ang II infusionon atherosclerosis progression in the apolipoprotein Eknockout mice.52 Apolipoprotein E–deficient micelack apolipoprotein E, the cofactor that is required forthe clearance of the LDL cholesterol particles and alsoimportant in high-density lipoprotein reverse choles-terol transport from tissue to plasma. Therefore, theplasma cholesterol level of apolipoprotein E mice is
very high (2,000–3,000 mg/dL when they are fed anatherogenic diet), and they develop spontaneously ad-vanced atherosclerosis but only after 6 months of life.To test whether Ang II accelerates atherosclerosis, theapolipoprotein E knockout mice were fed either anormal chow diet or atherogenic diet with or withoutAng II treatment for 8 weeks. Ang II raised systolicblood pressure from approximately 90 to 150 mm Hgthroughout the study. At the end of the study theaortas were harvested, fixed, and quantified for theatherosclerotic lesion content. Theen-facequantifica-tion of the descending aorta showed a dramatic accel-eration of atherosclerosis (from'4% in control miceto '70% of total aortic area) in Ang II-treated mice.Furthermore, at 12 weeks most of the animals on AngII and high fat were deceased secondary to cardiovas-cular morbidity (bowel ischemia, myocardial infarc-tion, and strokes). The cellular composition of thelesions showed a prominent macrophage infiltration ofatherosclerotic plaques with a very friable lipid coresuggesting that Ang II-accelerated atherosclerosisthrough a direct effect on vascular inflammation. Be-cause Ang II also produced hypertension, in a separateseries of experiments we infused norepinephrine inapolipoprotein E mice as to produce an increase in theblood pressures as was seen with Ang II infusion.Although increasing blood pressure with norepineph-rine clearly accelerated atherosclerosis, the magnitudeof the increase was minimal when compared with theresponse seen with Ang II (Figure 4). Therefore, weconcluded that the increase in atherosclerosis seenwith Ang II infusion was due primarily to the humoraleffects of Ang II as opposed to the secondary mechan-ical effects of elevated blood pressure.
CONCLUSIONIn summary there is accumulating evidence from
both clinical studies and laboratory investigations thatthe renin–angiotensin II system represents a critical,causal link in the pathogenesis of human atheroscle-rosis. The current studies provide mechanistic insightsinto the precise role of Ang II in atherosclerosis,
FIGURE 4. Angiotensin II (Ang II) dramatically accelerates atherosclerosis in Apolipoprotein E (apoE)knockout mice. Shown are the en-face preparations of aortas from apoE null mice fed with athero-genic diet alone, atherogenic diet and Ang II, or norepinephrine (NE) for 8 weeks. (Adapted fromCirculation.52)
30C THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 87 (8A) APRIL 19, 2001

which suggest that pharmacologic interventions in-volving the renin–angiotensin system may be of fun-damental importance in the treatment and preventionof atherosclerosis.
1. Guyton AC. Abnormal renal function and autoregulation in essential hyper-tension.Hypertension1991;18:III49–III53.2. Schmidt-Ott KM, Kagiyama S, Phillips MI. The multiple actions of angioten-sin II in atherosclerosis.Regul Pept2000;93:65–77.3. Rajagopalan S, Meng XP, Ramasamy S, Harrison DG, Galis ZS. Reactiveoxygen species produced by macrophage-derived foam cells regulate the activityof vascular matrix metalloproteinases in vitro: implications for atheroscleroticplaque stability.J Clin Invest1996;98:2572–2579.4. Vaughan DE. The renin-angiotensin system and fibrinolysis.Am J Cardiol1997;79:12–16.5. Esther CR, Marino EM, Howard TE, Machaud A, Corvol P, Capecchi MR,Bernstein KE. The critical role of tissue angiotensin-converting enzyme asrevealed by gene targeting in mice.J Clin Invest1997;99:2375–2385.6. Esther CR Jr, Howard TE, Marino EM, Goddard JM, Capecchi MR, BernsteinKE. Mice lacking angiotensin-converting enzyme have low blood pressure, renalpathology, and reduced male fertility.Lab Invest1996;74:953–965.7. Pratt RE. Angiotensin II and the control of cardiovascular structure.J Am SocNephrol1999;10(suppl 11):S120–S128.8. Arakawa K, Urata H. Hypothesis regarding the pathophysiological role ofalternative pathways of angiotensin II formation in atherosclerosis.Hypertension2000;36:638–641.9. Alexander RW. Theodore Cooper Memorial Lecture: hypertension and thepathogenesis of atherosclerosis. Oxidative stress and the mediation of arterialinflammatory response: a new perspective.Hypertension1995;25:155–161.10. Nakashima Y, Raines EW, Plump AS, Breslow JL, Ross R. Upregulation ofVCAM-1 and ICAM-1 at atherosclerosis-prone sites on the endothelium in theApoE-deficient mouse.Arterioscler Thromb Vasc Biol1998;18:842–851.11. Tummala PE, Chen XL, Sundell CL, Laursen JB, Hammes CP, AlexanderRW, Harrison DG, Medford RM. Angiotensin II induces vascular cell adhesionmolecule-1 expression in rat vasculature: a potential link between the renin-angiotensin system and atherosclerosis.Circulation 1999;100:1223–1229.12. Capers QT, Alexander RW, Lou P, De Leon H, Wilcox JN, Ishizaka N,Howard AB, Taylor WR. Monocyte chemoattractant protein-1 expression inaortic tissues of hypertensive rats.Hypertension1997;30:1397–1402.13. Han KH, Tangirala RK, Green SR, Quehenberger O. Chemokine receptorCCR2 expression and monocyte chemoattractant protein-1-mediated chemotaxisin human monocytes: a regulatory role for plasma LDL.Arterioscler ThrombVasc Biol1998;18:1983–1991.14. Chisolm GM, Steinberg D. The oxidative modification hypothesis of athero-genesis: an overview.Free Radic Biol Med2000;28:1815–1826.15. Li D, Yang B, Philips MI, Mehta JL. Proapoptotic effects of ANG II in humancoronary artery endothelial cells: role of AT1 receptor and PKC activation.Am JPhysiol1999;276:H786–H792.16. Nickenig G, Jung O, Strehlow K, Zolk O, Linz W, Scholkens BA, Bohm M.Hypercholesterolemia is associated with enhanced angiotensin AT1-receptorexpression.Am J Physiol1997;272:H2701–H2707.17. Nickenig G, Baumer AT, Temur Y, Kebben D, Jockenhovel F, Bohm M.Statin-sensitive dysregulated AT1 receptor function and density in hypercholes-terolemic men.Circulation 1999;100:2131–2134.18. Morawietz H, Rueckschloss U, Niemann B, Duerrschmidt N, Galle J, HakimK, Zerkowski HR, Sawamura T, Holtz J. Angiotensin II induces LOX-1, thehuman endothelial receptor for oxidized low-density lipoprotein.Circulation1999;100:899–902.19. Li DY, Zhang YC, Philips MI, Sawamura T, Mehta JL. Upregulation ofendothelial receptor for oxidized low-density lipoprotein (LOX-1) in culturedhuman coronary artery endothelial cells by angiotensin II type 1 receptor acti-vation.Circ Res1999;84:1043–1049.20. Hayek T, Attias J, Coleman R, Brodsky S, Smith J, Breslow JL, Keidar S. Theangiotensin-converting enzyme inhibitor, fosinopril, and the angiotensin II re-ceptor antagonist, losartan, inhibit LDL oxidation and attenuate atherosclerosisindependent of lowering blood pressure in apolipoprotein E deficient mice.Cardiovasc Res1999;44:579–587.21. Hayek T, Aviram M, Heinrich R, Sakhnini E, Keidar S. Losartan inhibitscellular uptake of oxidized LDL by monocyte-macrophages from hypercholes-terolemic patients.Biochem Biophys Res Commun2000;273:417–420.22. Harrison DG. Cellular and molecular mechanisms of endothelial cell dys-function.J Clin Invest1997;100:2153–2157.23. Knowles JW, Reddick RL, Jennette JC, Shesely EG, Smithies O, Maeda N.Enhanced atherosclerosis and kidney dysfunction in eNOS(-/-)Apoe(-/-) mice areameliorated by enalapril treatment.J Clin Invest2000;105:451–458.24. O’Donnell VB, Freeman BA. Interactions between nitric oxide and lipidoxidation pathways: implications for vascular disease.Circ Res2001;88:12–21.25. White CR, Brock TA, Chang LY, Crapo J, Briscoe P, Ku D, Bradley WA,Gianturco SH, Gore J, Freeman BA, et al. Superoxide and peroxynitrite inatherosclerosis.Proc Natl Acad Sci U S A 1994;91:1044–1048.26. Munzel T, Li H, Mollnau H, Hink U, Matheis E, Hartmann M, Oelze M,
Skatchkov M, Warnholtz A, Duncker L, Meinertz T, Forstermann U. Effects oflong-term nitroglycerin treatment on endothelial nitric oxide synthase (NOS III)gene expression, NOS III-mediated superoxide production, and vascular NObioavailability.Circ Res2000;86:E7–E12.27. Oelze M, Mollnau H, Hoffmann N, Warnholtz A, Bodenschatz M, SmolenskiA, Walter U, Skatchkov M, Meinertz T, Munzel T. Vasodilator-stimulatedphosphoprotein serine 239 phosphorylation as a sensitive monitor of defectivenitric Oxide/cGMP signaling and endothelial dysfunction.Circ Res 2000;87:999–1005.28. Heitzer T, Brockhoff C, Mayer B, Warnholtz A, Mollnau H, Henne S,Meinertz T, Munzel T. Tetrahydrobiopterin improves endothelium-dependentvasodilation in chronic smokers: evidence for a dysfunctional nitric oxide syn-thase.Circ Res2000;86:E36–E41.29. Griendling KK, Sorescu D, Ushio-Fukai M. NAD(P)H oxidase: role incardiovascular biology and disease.Circ Res2000;86:494–501.30. Griendling KK, Sorescu D, Lassegue B, Ushio-Fukai M. Modulation ofprotein kinase activity and gene expression by reactive oxygen species and theirrole in vascular physiology and pathophysiology.Arterioscler Thromb Vasc Biol2000;20:2175–2183.31. Griendling KK, Minieri CA, Ollerenshaw JD, Alexander RW. Angiotensin IIstimulates NADH and NADPH oxidase activity in cultured vascular smoothmuscle cells.Circ Res1994;74:1141–1148.32. Ushio-Fukai M, Zafari AM, Fukui T, Ishizaka N, Griendling KK. p22phox isa critical component of the superoxide-generating NADH/NADPH oxidase sys-tem and regulates angiotensin II-induced hypertrophy in vascular smooth musclecells.J Biol Chem1996;271:23317–23321.33. Zafari AM, Ushio-Fukai M, Akers M, Yin Q, Shah A, Harrison DG, TaylorWR, Griendling KK. Role of NADH/NADPH oxidase-derived H2O2 in angio-tensin II-induced vascular hypertrophy.Hypertension1998;32:488–495.34. Ushio-Fukai M, Alexander RW, Akers M, Griendling KK. p38 Mitogen-activated protein kinase is a critical component of the redox-sensitive signalingpathways activated by angiotensin II: role in vascular smooth muscle cell hyper-trophy.J Biol Chem1998;273:15022–15029.35. Ushio-Fukai M, Alexander RW, Akers M, Yin Q, Fujio Y, Walsh K,Griendling KK. Reactive oxygen species mediate the activation of Akt/proteinkinase B by angiotensin II in vascular smooth muscle cells.J Biol Chem1999;274:22699–22704.36. Chen XL, Tummala PE, Olbrych MT, Alexander RW, Medford RM. Angio-tensin II induces monocyte chemoattractant protein-1 gene expression in ratvascular smooth muscle cells.Circ Res1998;83:952–959.37. Kranzhofer R, Schmidt J, Pfeiffer CA, Hagl S, Libby P, Kubler W. Angio-tensin induces inflammatory activation of human vascular smooth muscle cells.Arterioscler Thromb Vasc Biol1999;19:1623–1629.38. Ikeda U, Ikeda M, Oohara T, Oguchi A, Kamitani T, Tsuruya Y, Kano S.Interleukin 6 stimulates growth of vascular smooth muscle cells in a PDGF-dependent manner.Am J Physiol1991;260:H1713–H1717.39. Cochran FR, Finch-Arietta MB. Interleukin-6 can prime THP-1 macrophagesfor enhanced production of tumor necrosis factor-alpha in response to LPS.Immunopharmacology1992;23:97–103.40. Azumi H, Inoue N, Takeshita S, Rikitake Y, Kawashima S, Hayashi Y, ItohH, Yokoyama M. Expression of NADH/NADPH oxidase p22phox in humancoronary arteries.Circulation 1999;100:1494–1498.41. Cahilly C, Ballantyne CM, Lim DS, Gotto A, Marian AJ. A variant ofp22(phox), involved in generation of reactive oxygen species in the vessel wall,is associated with progression of coronary atherosclerosis.Circ Res2000;86:391–395.42. Inoue N, Kawashima S, Kanazawa K, Yamada S, Akita H, Yokoyama M.Polymorphism of the NADH/NADPH oxidase p22 phox gene in patients withcoronary artery disease.Circulation 1998;97:135–137.43. Guzik TJ, West NE, Black E, McDonald D, Ratnatunga C, Pillai R, ChannonKM. Vascular superoxide production by NAD(P)H oxidase: association withendothelial dysfunction and clinical risk factors.Circ Res2000;86:E85–E90.44. Brunner HR, Laragh JH, Baer L, Newton MA, Goodwin FT, Krakoff LR,Bard RH, Buhler FR. Essential hypertension: renin and aldosterone, heart attackand stroke.N Engl J Med1972;286:441–449.45. Gibbons GH. The pathophysiology of hypertension: the importance of an-giotensin II in cardiovascular remodeling.Am J Hypertens1998;11:177S–181S.46. Yusuf S, Pepine CJ, Garces C, Pouleur H, Salem D, Kostis J, Benedict C,Rousseau M, Bourassa M, Pitt B. Effect of enalapril on myocardial infarction andunstable angina in patients with low ejection fractions.Lancet1992;340:1173–1178.47. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of anangiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events inhigh-risk patients: the Heart Outcomes Prevention Evaluation Study Investigators[Published errata appear inN Engl J Med2000 March 9;342:748 and 2000 May4;342:1376].N Engl J Med2000;342:145–153.48. Chobanian AV, Haudenschild CC, Nickerson C, Drago R. Antiatherogeniceffect of captopril in the Watanabe heritable hyperlipidemic rabbit.Hypertension1990;15:327–331.49. Hayek T, Attias J, Smith J, Breslow JL, Keidar S. Antiatherosclerotic andantioxidative effects of captopril in apolipoprotein E-deficient mice.J CardiovascPharmacol1998;31:540–544.50. Strawn WB, Chappell MC, Dean RH, Kivlighn S, Ferrario CM. Inhibition ofearly atherogenesis by losartan in monkeys with diet-induced hypercholesterol-emia.Circulation 2000;101:1586–1593.
A SYMPOSIUM: ANGIOTENSIN II IN CARDIVOSACULAR PATHOLOGY 31C

51. Warnholtz A, Nickenig G, Schulz E, Macharzina R, Brasen JH, Skatchkov M,Heitzer T, Stasch JP, Griendling KK, Harrison DG, Bohm M, Meinertz T, MunzelT. Increased NADH-oxidase-mediated superoxide production in the early stagesof atherosclerosis: evidence for involvement of the renin-angiotensin system.Circulation 1999;99:2027–2033.52. Weiss D, Kools JJ, Taylor, WR. Angiotensin II–induced hypertension accel-erates the development of atherosclerosis in apoE-deficient mice.Circulation2001;103:448–454.53. deBlois D, Lombardi DM, Su EJ, Clowes AW, Schwartz SM, Giachelli CM.Angiotensin II induction of osteopontin expression and DNA replication in ratarteries.Hypertension1996;28:1055–1063.54. Pastore L, Tessitore A, Martinotti S, Toniato E, Alesse E, Bravi MC, Ferri C,Desideri G, Gulino A, Santucci A. Angiotensin II stimulates intercellular adhe-sion molecule-1 (ICAM-1) expression by human vascular endothelial cells andincreases soluble ICAM-1 release in vivo.Circulation 1999;100:1646–1652.55. Grafe M, Auch-Schwelk W, Zakrzewicz A, Regitz-Zagrosek V, Bartsch P,Graf K, Loebe M, Gaehtgens P, Fleck E. Angiotensin II-induced leukocyte
adhesion on human coronary endothelial cells is mediated by E-selectin.Circ Res1997;81:804–811.56. Han Y, Runge MS, Brasier AR. Angiotensin II induces interleukin-6 tran-scription in vascular smooth muscle cells through pleiotropic activation of nu-clear factor-kappa B transcription factors.Circ Res1999;84:695–703.57. Delafontaine P, Lou H. Angiotensin II regulates insulin-like growth factor Igene expression in vascular smooth muscle cells.J Biol Chem1993;268:16866–16870.58. Naftilan AJ, Pratt RE, Dzau VJ. Induction of platelet-derived growth factorA-chain and c-myc gene expressions by angiotensin II in cultured rat vascularsmooth muscle cells.J Clin Invest1989;83:1419–1424.59. Gibbons GH, Pratt RE, Dzau VJ. Vascular smooth muscle cell hypertrophyvs. hyperplasia: autocrine transforming growth factor-beta 1 expression deter-mines growth response to angiotensin II.J Clin Invest1992;90:456–461.60. Itoh H, Mukoyama M, Pratt RE, Gibbons GH, Dzau VJ. Multiple autocrinegrowth factors modulate vascular smooth muscle cell growth response to angio-tensin II.J Clin Invest1993;91:2268–2274.
32C THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 87 (8A) APRIL 19, 2001