interictal and postictal language testing accurately lateralizes language dominant temporal lobe...
TRANSCRIPT

Epilepsia, 49(1):22–32, 2008doi: 10.1111/j.1528-1167.2007.01209.x
FULL-LENGTH ORIGINAL RESEARCH
Interictal and postictal language testing accuratelylateralizes language dominant temporal lobe complex
partial seizures∗Maya J. Ramirez, ∗†Bruce K. Schefft, ∗Steven R. Howe, ‡Hwa-Shain Yeh,
and †Michael D. Privitera
Departments of ∗Psychology and †Neurology, University of Cincinnati, and ‡Department of Neurosurgery,University of Cincinnati Medical Center, Cincinnati, Ohio, U.S.A.
SUMMARYPurpose: Noninvasive tests that accurately localizeseizure onset provide great value in the presurgi-cal evaluation of patients with intractable epilepsy.This study examined the diagnostic utility of threeexpressive language disturbances in lateralizinglanguage-dominant (DOM) temporal lobe complexpartial seizures: (1) the postictal language delay(PILD; time taken to correctly read a test phraseout loud immediately following seizures); (2) theproduction of postictal phonemic paraphasic errors(PostPE); and (3) interictal phonemic paraphasicerrors (InterPE).Methods: All 60 subjects underwent inpatientvideo/EEG monitoring and had surgically con-firmed temporal lobe epilepsy (TLE). We deter-mined the presence and number of PostPE and,PILD times (in s) for 212 seizures, and InterPE onthe Boston Naming Test (BNT). Each technique’sdiagnostic usefulness was evaluated via logistic re-gression and ROC curve analysis. Sensitivity, speci-
ficity, positive predictive value and negative predic-tive values were computed.Results: PILD, PostPE and InterPE production wereequally effective and accurate in lateralizing DOMseizure onset. Patients with DOM TLE had a longerPILD and committed more PostPE and InterPEthan those with nondominant (NDOM) TLE. Re-spective sensitivity and specificity values were asfollows: PILD (84%, 86%), PostPE (94%, 64%), andInterPE (97%, 86%). No single predictor was sig-nificantly better but a combination model yieldedenough incremental utility to collectively outper-form each separate predictor model.Conclusions: Interictal language testing is as ac-curate as postictal language testing in predictingDOM lateralization of TLE. Clinicians should alsoattend to the quality of errors produced during in-terictal and postictal language testing.KEY WORDS: Paraphasic error, postictal languagedelay, Epilepsy, Confrontation naming, Confronta-tion naming, Postictal language testing.
Noninvasive methods that can localize or lateralize theepileptogenic focus are preferred in the evaluation ofepilepsy surgery candidates. Prior studies have shown thatpostictal and interictal language disturbances can accu-
Accepted May 9, 2007; Online Early publication July 21, 2007.This work was part of the first author’s Master’s Thesis, chaired by the
second author in the Department of Psychology, University of Cincinnati,Cincinnati, Ohio.
Address correspondence and reprint requests to Bruce K. Schefft, De-partment of Psychology, Dyer Hall, ML 376, University of Cincinnati,Cincinnati, OH, 45221-0376. E-mail: [email protected]
Blackwell Publishing, Inc.C© 2008 International League Against Epilepsy
rately differentiate language dominant (DOM) from lan-guage nondominant (NDOM) temporal lobe complex par-tial seizures (Mayeux et al., 1980; Koerner and Laxer,1988; Gabr et al., 1989; Privitera et al., 1991; Schefft et al.,2003; Busch et al., 2005; Fargo et al., 2005). Since the ini-tial findings of Koerner and Laxer (1988) and Gabr et al.(1989), a handful of subsequent studies have further es-tablished the diagnostic value of postictal language dis-turbance in temporal lobe epilepsy (TLE) (Privitera et al.,1991; Devinsky et al., 1994; Fakhoury et al., 1994; Adamet al., 2000; Leutmezer, 2002; Loddenkemper and Kota-gal, 2005). Specifically, Privitera et al. (1991) reported thathaving a postictal language delay (PILD; the amount oftime that elapses from the end of an ictal discharge until a
22

23
Interictal and Postictal Language Testing
patient first correctly reads a test phrase aloud) greater thanor equal to 60 s provided greater diagnostic accuracy ofDOM TLE than MRI, interictal EEG, ictal EEG and over-all neuropsychological assessment. Moreover, 33% of allNDOM TLE patients in their sample could read the testphrase during the seizure itself, whereas none of the DOMTLE patients was able to so. Studies conducted by Fickeret al. (2001) and Goldberg-Stern et al. (2004) further spec-ified this. They found that NDOM temporal lobe seizuresand DOM frontal lobe seizures only produced a prolongedPILD when seizure activity also spread to the DOM tempo-ral lobe. Thus, prolonged PILD (≥60 s) occurrence may bespecific to the DOM temporal lobe and not just indicativeof DOM hemispheric involvement.
Phonemic paraphasic errors are unique expressive lan-guage disturbances in which there is an incorrect phonemeor morpheme substitution (i.e., when an individual isshown a target picture of a “muzzle” and he or sheinstead calls it a “muzzler” (Kaplan et al., 1983)). Pos-tictal paraphasic errors were first reported as a lateraliz-ing sign by Jackson (1898) in the nineteenth century, butthe introduction of video/EEG seizure recording has al-lowed more consistent detection (McKeever et al., 1983;Koerner and Laxer, 1988; Gabr et al., 1989). The diagnos-tic utility of postictal paraphasias is limited by the find-ing that most patients with dominant temporal lobe com-plex partial seizures do not speak spontaneously in the ic-tal and early postictal states. Moreover, the repetitive pre-sentation of the test phrase in the postictal period markedlyincreases the elicitation of postictal paraphasic errors (Priv-itera et al., 1991). Longer PILD elicits more frequent pre-sentation of the sign, which provides greater opportunityto commit postictal paraphasias. However, Privitera andcolleagues (1991) observed that for their sample, phone-mic paraphasic errors were the only dysphasic languageerrors produced during the postictal period, and that theyoccurred exclusively in patients with DOM temporal lobeseizure onset.
Schefft et al. (2003) investigated the diagnostic utilityof interictal paraphasic errors (InterPE) on two measuresof confrontation naming ability, the Boston Naming Test(BNT) (Kaplan et al., 1983) and the Visual Naming Test(VNT) (Benton and Hamsher, 1983), which are sensitiveto patient production of InterPE. Schefft and colleaguesfound that one InterPE was 6.8 times more likely in in-dividuals with a left (DOM) seizure focus compared withindividuals with a right (NDOM) focus. They also found arobust effect of global intelligence on BNT performance.The overall predictive ability of BNT performance and In-terPE production to accurately lateralize seizure focus im-proved among patients with Full Scale IQs ≥ 90. Using theBNT, Fargo et al. (2005) analyzed the overall frequencyand type of paraphasic naming errors produced by indi-viduals with confirmed DOM and NDOM TLE as well asthose without epilepsy (individuals with psychogenic non-
epileptic seizures). Other types of paraphasic errors (e.g.,verbal-semantic paraphasic errors, circumlocutions, etc.)that were examined did not yield the degree of diagnos-tic differentiation between DOM and NDOM TLE patientsas did the presence of at least one phonemic paraphasic er-ror. Overall, Fargo et al. (2005) found that DOM TLE pa-tients produced significantly more InterPE’s than both theNDOM and control groups.
Although Schefft et al. (2003) and Fargo et al. (2005)suggested that the quality of expressive language errorsthat occur between seizures are diagnostically useful, nei-ther study addressed the potential diagnostic value ofpostictal language disturbances (i.e., during the PILD).Privitera et al. (1991) demonstrated the presence and im-portance of the PILD as it relates to seizure origin inthe DOM temporal lobe; however, they performed limitedanalysis of the method’s diagnostic utility (i.e., no ROCcurve analyses, etc). Additionally, no follow-up analyseswere performed examining the usefulness of the PILD ascompared with other language measures. Moreover, Fickeret al. (2001) and Goldberg-Stern et al.’s (2004) findingsthat prolonged PILD can also occur in individuals withsecondary seizure propagation cast doubt on the estab-lished diagnostic utility (i.e. specificity) of the PILD. Pro-longed PILD due to secondary seizure generalization isclearly diagnostically different from prolonged PILD dueto DOM temporal lobe seizure onset. Lastly, interictal lan-guage measures provide a distinct advantage over postic-tal measures as testing can occur at any time, whereas thePILD can only be measured once a seizure has been de-tected. In light of the limitations of previous studies, thepresent study used a larger, surgically confirmed sample toconduct a comprehensive analysis of the diagnostic utilityof PILD and both InterPE and PostPE for DOM seizurelateralization.
It was hypothesized that, as compared with individu-als with NDOM TLE, individuals with DOM TLE would:(a) have a significantly longer PILD, (b) commit morePostPEs, and (c) commit more InterPEs on a confronta-tion naming task. This study also reevaluated the effect ofglobal intelligence on the predictive accuracy of these threemethods.
METHOD
ParticipantsWe conducted a retrospective study of 60 participants
(32 DOM TLE, 28 NDOM TLE) who were evaluated onthe Epilepsy Monitoring Unit (EMU) at University Hos-pital in Cincinnati, OH. This research was fully approvedby the University of Cincinnati Institutional Review Boardand all participants provided informed written consentprior to participation at the time of their admission.
The EMU is a medical inpatient facility where all pa-tients undergo prolonged 24-hour video/EEG monitoring
Epilepsia, 49(1):22–32, 2008doi: 10.1111/j.1528-1167.2007.01209.x

24
M. J. Ramirez et al.
to differentiate epileptic from nonepileptic seizures, andto localize the epileptogenic region for presurgical eval-uation in patients with focal epilepsy. Individuals on theEMU also participate in comprehensive neuropsychologi-cal assessment to measure interictal neurocognitive func-tioning. This study included sequential patients who metall of the following criteria: (a) surgically confirmed di-agnosis of either language dominant (DOM) or languagenondominant (NDOM) temporal lobe epilepsy (TLE);patients were considered accurately localized if surgicaloutcome included at least a 90% reduction in seizure fre-quency (Engel Class I and II seizure outcome) at ap-proximately 1 year of follow-up, (b) confirmed languagedominance by intracarotid amobarbital test or intraop-erative electrocorticography testing; (c) Wechsler AdultIntelligence Scale-III or WAIS-R Full Scale IQ of 70and above; (d) normal MRI or structural brain lesionslimited to mesial temporal areas such as mesial temporalsclerosis, low grade tumor or vascular malformation (e) age17or older; (f) received the 60-item version of the BostonNaming Test (BNT); (g) minimum of eight years of ed-ucation; (h) English as the native language; (i) no priorbrain surgery; and (j) absence of a comorbid neurologi-cal or serious psychiatric disorder as screened via medicalrecords and psychological self-report measures includingthe Minnesota Multiphasic Personality Inventory, secondedition, and the Beck Depression Inventory, second edition(e.g., Multiple Sclerosis, Schizophrenia). Serious psychi-atric disorder was defined as schizophrenia, autism, or se-vere bipolar disorder.
Participants in this study were part of a larger sampleof over 1,000 patients who were evaluated on the EMUbetween January 1994 and January 2005. Of these pa-tients, approximately 40% (400) were diagnosed as hav-ing epileptic seizures and 186 met the inclusion criteria fora non-surgically confirmed TLE diagnosis (i.e., via video-EEG monitoring). Of these 186 TLE patients, 101 under-went temporal lobectomy and 80 (36 left, 44 right) metthe seizure outcome criteria of at least a 90% reduction inseizure frequency. Three patients were excluded becauseof missing data. Postictal language testing could not becompleted for 10 patients because of the following rea-sons: secondary generalized seizures (n = 4), no responseto presentation of the sign during postictal language test-ing (n = 1), no seizures recorded during monitoring (n =2), did not undergo postictal language testing (n = 2), ordata was not available (n = 1). In addition patients withindependent seizure onset from both temporal lobes wereexcluded (n = 1). All patients included in the study hadexaminations on the EMU that yielded all three languagedisturbance indices. In addition, individuals for whom lan-guage dominance could not be determined (n = 5) were ex-cluded as were those with mixed language dominance (n =6) according to intracarotid amobarbital test (IAT) results.Standard IAT procedures at this epilepsy center include in-
jection of both hemispheres of the brain. One patient wasincluded who was right hemisphere language dominant, ac-cording to IAT. This patient’s data were consistent withthose patients who were left hemisphere language domi-nant. Language dominance for 11 patients was confirmedvia intraoperative language mapping, whereas the rest un-derwent IAT. Language results for all IATs were conclu-sive. Application of these inclusion criteria resulted in asample of 60 (32 DOM TLE, 28 NDOM TLE).
ProceduresSince 1988, all video/EEG monitoring reports at this
center include descriptions of ictal and postictal behav-ior and document the duration of the PILD. All availablevideo/EEG-monitoring reports were reviewed for PILD (inseconds) and presence of PostPE production. These lan-guage disturbances were assessed by the attending physi-cians (all fellowship trained epileptologists) who reviewedthe video-monitoring footage to determine the PILD andpresence of PostPE. Since most patients had multipleseizures during prolonged video/EEG monitoring, an av-erage of all recorded PILD times was calculated for eachpatient and used in the analyses. Average paraphasic er-ror production was not used as a number of people did notcommit any language errors during testing and the rangewas limited from 0-6.
MeasuresThe following is a description of EMU procedures for
assessing postictal language disturbance. The EEG techni-cian entered the patient’s room upon identifying a seizurebased on EEG and patient behavior changes. During theseizure (defined by ictal discharge), the EEG technicianpresented the patient with a test phrase from the BostonDiagnostic Aphasia Examination (Goodglass and Kaplan,1972) to read aloud (“They heard him speak on the radiolast night.”). Throughout the ictal and postictal period, theEEG technician continued to instruct the patient to read thesign until the patient correctly read it aloud. The time fromthe end of the EEG ictal discharge until the patient readthe sign correctly was the PILD for that seizure. Both thePILD (in seconds) as well as the presence of PostPEs wereevaluated with these procedures. In computing the numberof PostPEs per patient the current study used the total num-ber of errors committed after all recorded seizures for eachpatient.
The Boston Naming Test (BNT) (Kaplan et al., 1983)is a well-known confrontation naming measure. Duringthis test the patient is presented with a stimulus card andasked to name aloud the stimuli, line drawings of com-mon objects, pictured on the card (Kaplan et al., 1983).The BNT was administered using standard clinical proce-dures. Medical charts were reviewed to obtain BNT scores,the presence and number of interPEs and language dom-inance information. Presence of paraphasic errors on theBNT was rated according to previously established criteria
Epilepsia, 49(1):22–32, 2008doi: 10.1111/j.1528-1167.2007.01209.x

25
Interictal and Postictal Language Testing
(Goodglass and Kaplan, 1983; Ardila and Rosselli, 1993;Goodglass et al., 1997; Fargo et al., 2005). The currentstudy only used the categorical distinction of phonemicparaphasic errors as empirical investigation has demon-strated very limited diagnostic utility for any other types ofparaphasic errors in lateralizing TLE (i.e., verbal-semantic,circumlocution, etc.) (Fargo et al., 2005; Schefft et al.,2003). Phonemic paraphasic errors occur when there is anincorrect phoneme or morpheme substitution, such as say-ing the word “hap” when the target word is “hat.” Theseerror ratings were reviewed by the staff clinical neuropsy-chologist (B.K.S.) to ensure accuracy.
AnalysisCorrelations, independent-sample t-tests and χ2 tests
were conducted to assess between-group differencesand relationships among the various demographic andneuropsychological variables. Logistic regression was usedto model the probability of belonging to the DOM group(when compared with the NDOM group). Logistic regres-sion models the logit, which is the natural logarithmictransformation of the odds that an observation is in onegroup as opposed to the other (i.e., the odds of DOM TLEgroup membership). The utility of each predictor is mea-sured by the regression coefficient β, and exp(β) is theodds ratio, an estimate of the change in the odds of groupmembership for the target group as the predictor variableincreases by one unit. Separate logistic regression analyseswere performed for PILD and for the number and presenceof InterPEs and PostPEs to evaluate the utility of each as apredictor of DOM seizure focus.
Every point on a receiver-operator characteristic (ROC)curve represents a combination of a sensitivity and speci-ficity value. Receiver-operator characteristic (ROC) curveswere constructed for each model; the area under each curve(AUC, or c) was calculated as an index of the ability ofeach predictor to lateralize TLE. The software programMedCalc was used to assess the AUCs. To compare AUCsthe standard error of the difference between the two AUCsmust be calculated. MedCalc does this while employingHanley and McNeil’s parametric method in which the AUCis equivalent to the Wilcoxon statistic and the standard er-ror is computed using exponential approximation (Hanelyand McNeil, 1983). Multiple logistic regression was alsoused to investigate whether combinations of these predic-tors might significantly improve diagnostic accuracy. Sen-sitivity, specificity, positive predictive value (PPV), andnegative predictive value (NPV), and ROC curve anal-ysis were used to assess the diagnostic utility of eachmodel. Because of the moderating effect of global intel-ligence (Full Scale Intelligence Quotient (FSIQ) ≥ 90) onBNT performance (Schefft et al., 2003), additional analy-ses were performed on all predictors using FSIQ ≥90 as acut point. FSIQ ≥90 was used as these analyses were con-ducted to evaluate the utility of the predictors when intel-
lectual functioning is largely intact. FSIQ ≥90 is the stan-dard clinical demarcation between intact and below aver-age intellectual functioning.
RESULTSPreliminary analyses
Independent-sample t-tests and χ2 tests of independence(Table 1) revealed no significant differences between theDOM and NDOM TLE groups in terms of age, education,(global) intelligence, sex, handedness or race. The NDOMgroup had a higher FSIQ mean and was slightly older thanthe DOM group, although the differences were not signifi-cant (α = .05). As expected, t-tests of neuropsychologicalvariables revealed significant group differences for meanPILD, mean number of PostPE’s, and mean number of In-terPEs (Table 1). Follow-up outcome for all participantswas assessed between 1 and 10 years after surgery. Two-hundred and twelve seizures were assessed overall with 98in the DOM and 114 in the NDOM TLE group. In addition,PILD ranged from 0–1560 s (∼26 min).
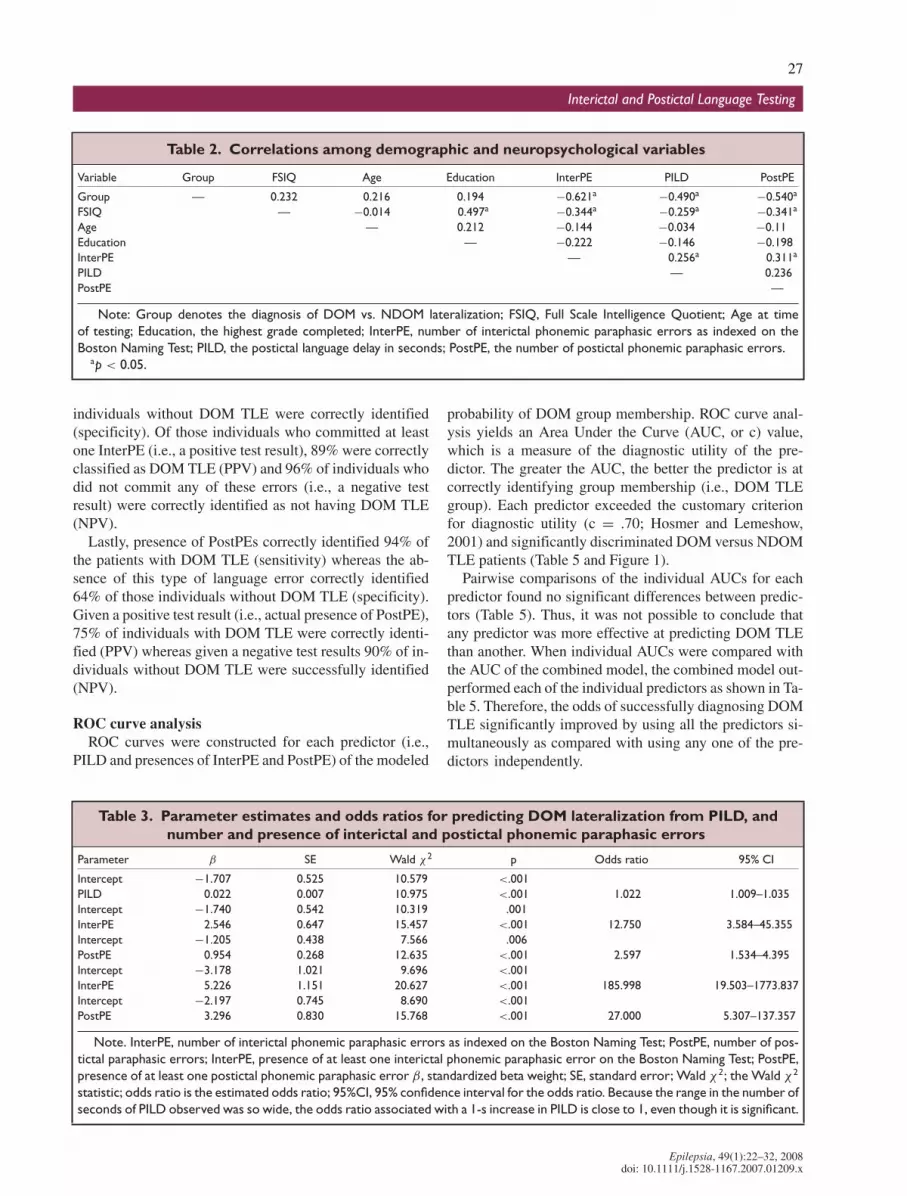
A correlation matrix of demographic and neuropsycho-logical variables is presented in Table 2. The followingsignificant relationships were found: (a) FSIQ and yearsof education were positively correlated; (b) FSIQ andInterPE production were negatively correlated; (c) nega-tive correlations were found among the three language in-dices; (d) there was a positive correlation between PILDand phonemic error production; (e) all three language mea-sures were positively related to DOM seizure onset.
Logistic regression modelsLogistic regression was used to evaluate the predictive
utility of the PILD to lateralize epileptogenic seizure focusto the DOM hemisphere. Separate regressions were alsorun to evaluate the utility of the number as well as thepresence of InterPEs and PostPEs for the same task. Ta-ble 3 presents the individual parameter estimates for eachmodel as well as the estimated odds ratios for each predic-tor. Overall, each predictor was able to accurately lateralizeDOM seizures to the DOM temporal lobe.
For PILD, the odds of belonging to the DOM TLE groupwere greater for higher PILD values. Therefore, the longerthe PILD time the more likely that the patient was cate-gorized as a member of the DOM TLE group. However,the relatively small odds ratio associated with the PILD isdeceptive since PILD was measured in seconds. Thus, theodds ratio indexed the change in the odds associated witheach 1-s increase in PILD. The PILD had the widest rangeof all the predictors spanning 0 to >1000 s. The averagePILD for the DOM and NDOM TLE group were 288.76sand 37.82s, respectively. Because of the measurement ofthe PILD in seconds the odds ratio is small. Had the PILDbeen measured in minutes, it would have increased the sizeof the odds ratio. Therefore, the phenomenon is of clinicalsignificance despite the small odds ratio.
Epilepsia, 49(1):22–32, 2008doi: 10.1111/j.1528-1167.2007.01209.x

26
M. J. Ramirez et al.
Table 1. Comparisons of DOM (N = 32) and NDOM (N = 28) groups
M SD d t df p
FSIQ DOM 90.78 13.21 −0.47 1.82 58 0.074NDOM 97.11 13.69
Age DOM 32.72 10.99 −0.44 1.69 58 0.096NDOM 37.57 11.22
Education DOM 12.56 2.09 −0.39 1.51 58 0.138NDOM 13.43 2.36
% df χ2 p Odds ratio
Sex DOM 56% female 1 0.58 0.448 0.674NDOM 46% female
Race DOM 91% white 1 0.81 0.367 0.358NDOM 96% white
Handedness DOM 88% right 1 0.34 0.562 0.657NDOM 82% right
M SD d t df p
InterPE DOM 1.59 0.98 1.56 6.17 55.91 <0.001NDOM 0.25 0.7
PILD DOM 288.76 304.64 1.11 4.56 33.76 <0.001NDOM 37.82 60.31
PostPE DOM 2.47 1.65 1.26 5.02 54.24 <0.001NDOM 0.68 1.09
Note: The t-tests reported for these variables involve Satterthwaite’s adjustment for heterogeneity of variance. FSIQ is theaverage full scale intelligence quotient according to the Wechsler Adults Intelligence Scale—Revised (WAIS-R) and WAIS-III.Education is years of education completed. Comparisons for sex were between female and male; for race were between white andnonwhite patients; and for handedness were between left and right hand dominant.
InterPE, number of phonemic paraphasic errors produced on the Boston Naming Test; PostPE, number of phonemic paraphasicerrors produced during the postical period; PILD, the postictal language delay time in seconds.
Similarly, as the number of InterPEs on the BNT in-creased, the odds of belonging to the DOM TLE groupincreased. In other words, the more phonemic paraphasicerrors that were produced on the BNT, the more likely thatthe patient was to be predicted a member of the DOM TLEgroup. Similar results were observed across independentanalyses of all three remaining predictors; number of Post-PEs and presence of PostPE and InterPEs. Odds of DOMTLE group membership were positively associated with agreater number of PostPE produced. Additionally, the pres-ence of at least one InterPE or one PostPE was also posi-tively related to DOM TLE group membership.1
Multiple logistic regressionFor the multiple logistic regression model, the variables
presence of InterPE and PostPE, and PILD were added atthe same time. The combined model including the averagePILD and presence of InterPE and PostPEs was significant
1Both sets of analyses examining number and presence of phone-mic paraphasic errors were significant; however, the interpretation ofthe number of paraphasic errors will not easily carry over to a clini-cal setting. Moreover, absence and presence of language errors are morediagnostically relevant indicators that fit well into the medical paradigm.Therefore, due to improved diagnostic relevance and ease of use the fol-lowing analyses evaluating diagnostic utility focused on the presence andnot the number of phonemic paraphasic errors produced.
(χ2all = 9.997, p = .019; Table 4). According to this model,
larger values of all three lateralizing techniques predictedDOM TLE group membership. Therefore, if a patient hasa longer PILD and commits even one InterPE and PostPE,the greater the likelihood that he or she will be a memberof the DOM TLE group.
Diagnostic utility
Sensitivity, Specificity, PPV, NPVThe sensitivity, specificity, positive predictive value
(PPV) and negative predictive value (NPV) were evaluatedfor each predictor, using Privitera et al.’s (1991) criterioncutoff PILD ≥ 60 and the presence of InterPE and Post-PEs (Table 6). The base rate of DOM TLE in this samplewas 53%. By using a PILD criterion cutoff of ≥ 60 s, 84%of patients in this sample were identified correctly as hav-ing DOM TLE (sensitivity), and 86% of patients withoutDOM TLE were correctly identified (specificity). Given apositive test result, 87% of those individuals were correctlyidentified (PPV) with DOM TLE and 83% were correctlyidentified as not having DOM TLE (NPV).
Using the presence of InterPEs as an indicator ofDOM seizure onset, 97% of individuals with DOM TLEwere correctly identified (sensitivity), whereas 86% of
Epilepsia, 49(1):22–32, 2008doi: 10.1111/j.1528-1167.2007.01209.x
27
Interictal and Postictal Language Testing
Table 2. Correlations among demographic and neuropsychological variables
Variable Group FSIQ Age Education InterPE PILD PostPE
Group — 0.232 0.216 0.194 −0.621a −0.490a −0.540a
FSIQ — −0.014 0.497a −0.344a −0.259a −0.341a
Age — 0.212 −0.144 −0.034 −0.11Education — −0.222 −0.146 −0.198InterPE — 0.256a 0.311a
PILD — 0.236PostPE —
Note: Group denotes the diagnosis of DOM vs. NDOM lateralization; FSIQ, Full Scale Intelligence Quotient; Age at timeof testing; Education, the highest grade completed; InterPE, number of interictal phonemic paraphasic errors as indexed on theBoston Naming Test; PILD, the postictal language delay in seconds; PostPE, the number of postictal phonemic paraphasic errors.
ap < 0.05.
individuals without DOM TLE were correctly identified(specificity). Of those individuals who committed at leastone InterPE (i.e., a positive test result), 89% were correctlyclassified as DOM TLE (PPV) and 96% of individuals whodid not commit any of these errors (i.e., a negative testresult) were correctly identified as not having DOM TLE(NPV).
Lastly, presence of PostPEs correctly identified 94% ofthe patients with DOM TLE (sensitivity) whereas the ab-sence of this type of language error correctly identified64% of those individuals without DOM TLE (specificity).Given a positive test result (i.e., actual presence of PostPE),75% of individuals with DOM TLE were correctly identi-fied (PPV) whereas given a negative test results 90% of in-dividuals without DOM TLE were successfully identified(NPV).
ROC curve analysisROC curves were constructed for each predictor (i.e.,
PILD and presences of InterPE and PostPE) of the modeled
Table 3. Parameter estimates and odds ratios for predicting DOM lateralization from PILD, andnumber and presence of interictal and postictal phonemic paraphasic errors
Parameter β SE Wald χ2 p Odds ratio 95% CI
Intercept −1.707 0.525 10.579 <.001PILD 0.022 0.007 10.975 <.001 1.022 1.009–1.035Intercept −1.740 0.542 10.319 .001InterPE 2.546 0.647 15.457 <.001 12.750 3.584–45.355Intercept −1.205 0.438 7.566 .006PostPE 0.954 0.268 12.635 <.001 2.597 1.534–4.395Intercept −3.178 1.021 9.696 <.001InterPE 5.226 1.151 20.627 <.001 185.998 19.503–1773.837Intercept −2.197 0.745 8.690 <.001PostPE 3.296 0.830 15.768 <.001 27.000 5.307–137.357
Note. InterPE, number of interictal phonemic paraphasic errors as indexed on the Boston Naming Test; PostPE, number of pos-tictal paraphasic errors; InterPE, presence of at least one interictal phonemic paraphasic error on the Boston Naming Test; PostPE,presence of at least one postictal phonemic paraphasic error β , standardized beta weight; SE, standard error; Wald χ2; the Wald χ 2
statistic; odds ratio is the estimated odds ratio; 95%CI, 95% confidence interval for the odds ratio. Because the range in the number ofseconds of PILD observed was so wide, the odds ratio associated with a 1-s increase in PILD is close to 1, even though it is significant.
probability of DOM group membership. ROC curve anal-ysis yields an Area Under the Curve (AUC, or c) value,which is a measure of the diagnostic utility of the pre-dictor. The greater the AUC, the better the predictor is atcorrectly identifying group membership (i.e., DOM TLEgroup). Each predictor exceeded the customary criterionfor diagnostic utility (c = .70; Hosmer and Lemeshow,2001) and significantly discriminated DOM versus NDOMTLE patients (Table 5 and Figure 1).
Pairwise comparisons of the individual AUCs for eachpredictor found no significant differences between predic-tors (Table 5). Thus, it was not possible to conclude thatany predictor was more effective at predicting DOM TLEthan another. When individual AUCs were compared withthe AUC of the combined model, the combined model out-performed each of the individual predictors as shown in Ta-ble 5. Therefore, the odds of successfully diagnosing DOMTLE significantly improved by using all the predictors si-multaneously as compared with using any one of the pre-dictors independently.
Epilepsia, 49(1):22–32, 2008doi: 10.1111/j.1528-1167.2007.01209.x

28
M. J. Ramirez et al.
Table 4. Parameter estimates and estimated odds ratio for all-predictor model predicting DOMlateralization
Parameter β SE Wald χ2 p Odds ratio 95% CI
Intercept −7.509 2.460 9.317 0.002PILD 0.022 0.010 5.203 0.023 1.023 1.003–1.042InterPE 6.047 2.031 8.862 0.003 422.691 7.890–22645.130PostPE 3.137 1.467 4.575 0.032 23.038 1.300–408.217
Note. This is the model that includes all predictors.InterPE, presence of interictal phonemic paraphasic errors as indexed on the Boston Naming Test; PostPE and the presence
of postictal phonemic paraphasic errors; PILD, postictal language delay in seconds. Because the range in the number of secondsof PILD observed was so wide, the odds ratio associated with a one second increase in PILD is close to 1, even though it is significant.
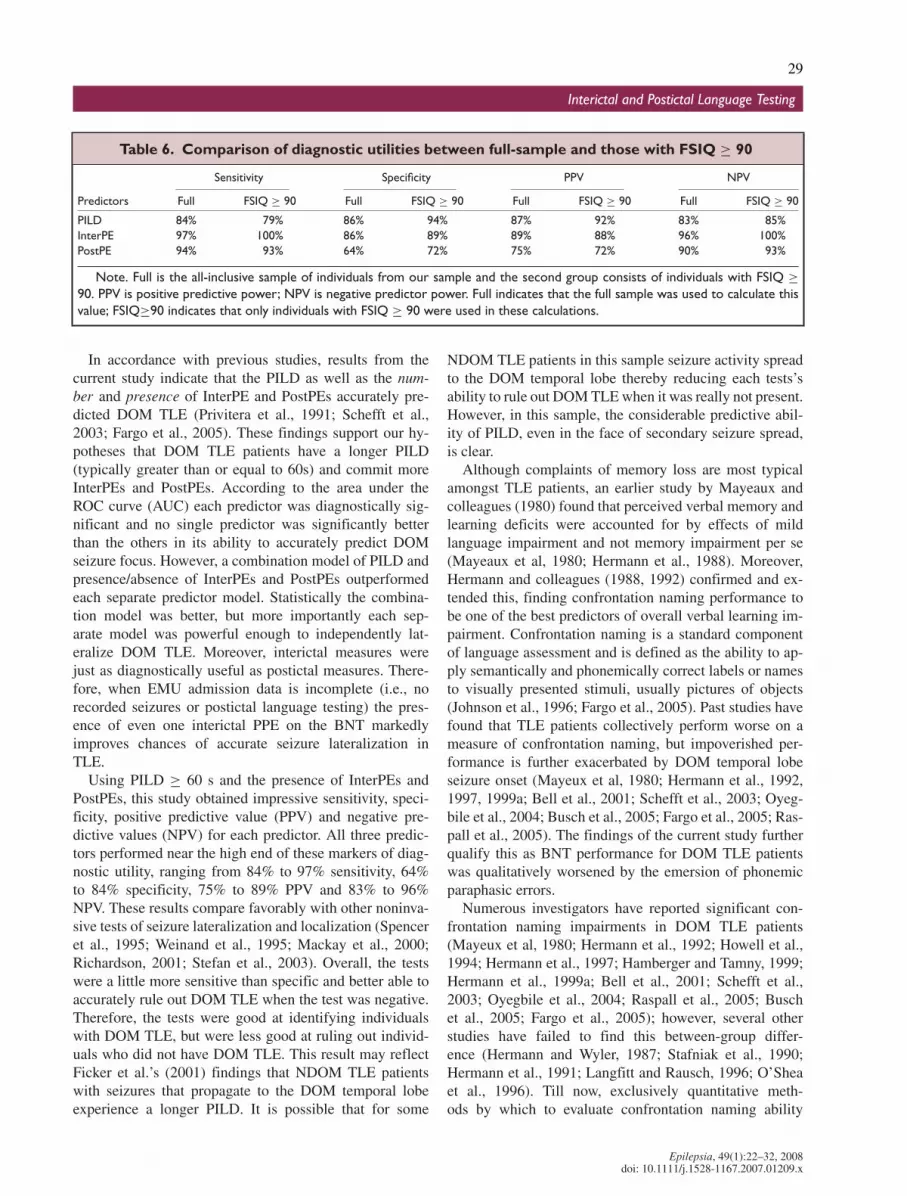
Secondary analyses with FSIQ ≥ 90 cut pointUsing a FSIQ ≥ 90, 32 (14 DOM, 18 NDOM) of the
original 60 patients were included in these analyses. Whena FSIQ ≥ 90 was used as a cut point the AUC of allthe models improved. Both the combined model and thepresence of InterPE model achieved quasi-separation (i.e.,100% of DOM patients were categorized correctly, and89% of the NDOM patients were correctly categorized),rendering it impossible to perform a logistic regression.Without the model produced by logistic regression to backtransform the data into predicted probabilities, pairwiseAUC analyses could not be conducted.
For individuals with FSIQ ≥ 90 (when compared withthe full sample), PILD sensitivity was marginally reduced,as was PPV for presence of InterPEs and sensitivity andPPV for presence of PostPEs. However, the majority ofdiagnostic utility indices across all three predictors im-proved: for PILD, values of specificity, PPV and NPV in-creased; for InterPEs, sensitivity, specificity and NPV im-
Table 5. Area under the curve (AUC) andpairwise comparisons
Predictor AUC P (area = 0.5)
PILD 0.902 <.0001InterPE 0.913 <.0001PostPE 0.790 <.0001All Three 0.991 <.0001Pairwise comparisons
between predictorsComparison Diff. between areas pPILD/InterPE 0.011 0.845InterPE/PostPE 0.123 0.070PILD/PostPE 0.112 0.078Pairwise comparisons between
predictors and allpredictor model
All 3/PILD 0.088 0.009All 3/InterPE 0.078 0.033All 3/PostPE 0.200 0.000
Note: The comparison column includes the predictors usedin the pairwise comparison of AUCs.
proved; and for PostPE production, specificity and NPVimproved (see Table 6 for comparisons). In addition, theAUCs (c) of all three predictors were enhanced. Therefore,taken together, these results indicate a better overall diag-nostic accuracy for all independent and combined predic-tors using FISQ ≥ 90.
DISCUSSION
Few studies in the epilepsy literature have evaluated thequality of language errors committed on tests of confronta-tion naming ability. The present study considered the di-agnostic utility of the number and presence of InterPEsproduced on the BNT in lateralizing seizure focus to theDOM hemisphere (Schefft et al., 2003). It also reassessedthe diagnostic usefulness of PILD as well as the numberand presence of PostPEs. Past research suggests that theselanguage disturbances accurately lateralize seizure focus tothe DOM hemisphere; however, their diagnostic utilitieshad not been comprehensively evaluated (Privitera et al.,1991; Ficker et al., 2001).
Figure 1.Graph comparing ROC curves for PILD, and presenceof interictal and postictal phonemic paraphasic errors.Epilepsia C© ILAE
Epilepsia, 49(1):22–32, 2008doi: 10.1111/j.1528-1167.2007.01209.x
29
Interictal and Postictal Language Testing
Table 6. Comparison of diagnostic utilities between full-sample and those with FSIQ ≥ 90
Sensitivity Specificity PPV NPV
Predictors Full FSIQ ≥ 90 Full FSIQ ≥ 90 Full FSIQ ≥ 90 Full FSIQ ≥ 90
PILD 84% 79% 86% 94% 87% 92% 83% 85%InterPE 97% 100% 86% 89% 89% 88% 96% 100%PostPE 94% 93% 64% 72% 75% 72% 90% 93%
Note. Full is the all-inclusive sample of individuals from our sample and the second group consists of individuals with FSIQ ≥90. PPV is positive predictive power; NPV is negative predictor power. Full indicates that the full sample was used to calculate thisvalue; FSIQ≥90 indicates that only individuals with FSIQ ≥ 90 were used in these calculations.
In accordance with previous studies, results from thecurrent study indicate that the PILD as well as the num-ber and presence of InterPE and PostPEs accurately pre-dicted DOM TLE (Privitera et al., 1991; Schefft et al.,2003; Fargo et al., 2005). These findings support our hy-potheses that DOM TLE patients have a longer PILD(typically greater than or equal to 60s) and commit moreInterPEs and PostPEs. According to the area under theROC curve (AUC) each predictor was diagnostically sig-nificant and no single predictor was significantly betterthan the others in its ability to accurately predict DOMseizure focus. However, a combination model of PILD andpresence/absence of InterPEs and PostPEs outperformedeach separate predictor model. Statistically the combina-tion model was better, but more importantly each sep-arate model was powerful enough to independently lat-eralize DOM TLE. Moreover, interictal measures werejust as diagnostically useful as postictal measures. There-fore, when EMU admission data is incomplete (i.e., norecorded seizures or postictal language testing) the pres-ence of even one interictal PPE on the BNT markedlyimproves chances of accurate seizure lateralization inTLE.
Using PILD ≥ 60 s and the presence of InterPEs andPostPEs, this study obtained impressive sensitivity, speci-ficity, positive predictive value (PPV) and negative pre-dictive values (NPV) for each predictor. All three predic-tors performed near the high end of these markers of diag-nostic utility, ranging from 84% to 97% sensitivity, 64%to 84% specificity, 75% to 89% PPV and 83% to 96%NPV. These results compare favorably with other noninva-sive tests of seizure lateralization and localization (Spenceret al., 1995; Weinand et al., 1995; Mackay et al., 2000;Richardson, 2001; Stefan et al., 2003). Overall, the testswere a little more sensitive than specific and better able toaccurately rule out DOM TLE when the test was negative.Therefore, the tests were good at identifying individualswith DOM TLE, but were less good at ruling out individ-uals who did not have DOM TLE. This result may reflectFicker et al.’s (2001) findings that NDOM TLE patientswith seizures that propagate to the DOM temporal lobeexperience a longer PILD. It is possible that for some
NDOM TLE patients in this sample seizure activity spreadto the DOM temporal lobe thereby reducing each tests’sability to rule out DOM TLE when it was really not present.However, in this sample, the considerable predictive abil-ity of PILD, even in the face of secondary seizure spread,is clear.
Although complaints of memory loss are most typicalamongst TLE patients, an earlier study by Mayeaux andcolleagues (1980) found that perceived verbal memory andlearning deficits were accounted for by effects of mildlanguage impairment and not memory impairment per se(Mayeaux et al, 1980; Hermann et al., 1988). Moreover,Hermann and colleagues (1988, 1992) confirmed and ex-tended this, finding confrontation naming performance tobe one of the best predictors of overall verbal learning im-pairment. Confrontation naming is a standard componentof language assessment and is defined as the ability to ap-ply semantically and phonemically correct labels or namesto visually presented stimuli, usually pictures of objects(Johnson et al., 1996; Fargo et al., 2005). Past studies havefound that TLE patients collectively perform worse on ameasure of confrontation naming, but impoverished per-formance is further exacerbated by DOM temporal lobeseizure onset (Mayeux et al, 1980; Hermann et al., 1992,1997, 1999a; Bell et al., 2001; Schefft et al., 2003; Oyeg-bile et al., 2004; Busch et al., 2005; Fargo et al., 2005; Ras-pall et al., 2005). The findings of the current study furtherqualify this as BNT performance for DOM TLE patientswas qualitatively worsened by the emersion of phonemicparaphasic errors.
Numerous investigators have reported significant con-frontation naming impairments in DOM TLE patients(Mayeux et al, 1980; Hermann et al., 1992; Howell et al.,1994; Hermann et al., 1997; Hamberger and Tamny, 1999;Hermann et al., 1999a; Bell et al., 2001; Schefft et al.,2003; Oyegbile et al., 2004; Raspall et al., 2005; Buschet al., 2005; Fargo et al., 2005); however, several otherstudies have failed to find this between-group differ-ence (Hermann and Wyler, 1987; Stafniak et al., 1990;Hermann et al., 1991; Langfitt and Rausch, 1996; O’Sheaet al., 1996). Till now, exclusively quantitative meth-ods by which to evaluate confrontation naming ability
Epilepsia, 49(1):22–32, 2008doi: 10.1111/j.1528-1167.2007.01209.x

30
M. J. Ramirez et al.
have produced mixed results. However, the current studyprovides evidence that the quality of performance be-tween DOM and NDOM TLE patients is, indeed, different(Schefft et al., 2003; Fargo et al., 2005).
Previous studies have also indicated that FSIQ moder-ates BNT performance (Mayeux et al., 1980; Schefft et al.,2003; Busch et al., 2005); however its potential effect onPILD and postictal and interictal PPE production was un-clear. The current study replicated Schefft et al.’s (2003)findings and in fact, more robust effects were observedand extended to other indices of DOM TLE (i.e., postictalPPE production and PILD). Although FSIQ ≥ 90 appearedto marginally improve diagnostic utility, this perceived in-crease may not be as useful in practice. A considerableeffect was obtained without the FSIQ moderator, furtherdemonstrating the robustness of each indices predictiveutility. The strength of these findings may be attributed tothe use of a surgically confirmed sample. Surgical con-firmation in this sample intimated accurate diagnosis ofDOM TLE. Without using a surgically confirmed sample,previous studies only found a moderate effect, whereas theuse of a surgically confirmed sample in the current studyyielded a greater magnitude of effect.
Schefft et al. (2003) posited two explanations to accountfor the moderating effect of intelligence on BNT perfor-mance that may extend to the postictal language indices.The first is that the BNT is more challenging for TLE pa-tients with FSIQ < 90 making them more likely to per-form more poorly on it. Similarly, this difficulty level mayalso predispose individuals with FSIQ < 90 to commitmore paraphasic errors. Second, Schefft and colleaguessuggested that a lower FSIQ may indicate greater dif-fuse cognitive involvement diminishing overall neurocog-nitive performance. Thus, individuals with FSIQ < 90may perform more poorly across numerous tasks and cog-nitive domains. Hypothesis one explains poor BNT per-formance and paraphasic error production for individualswith FSIQ < 90. However, it does not adequately explainthe moderating effect of FSIQ on postictal language. Thespecific tasks and patient behaviors required in pos-tictal language assessment are simpler than those re-quired for sufficient BNT performance. Therefore, inherentdifficulties attributed to the task do not effectively ex-plain PostPE production and longer PILD. Hence, hypoth-esis two may provide a better explanation for the currentfindings.
Naming deficits are considered the most substantial lan-guage morbidity associated with DOM TLE (Seidenberget al., 2005). A number of studies have highlighted thefunctional importance of the DOM temporal lobe in ade-quate naming performance (Mayeux et al., 1980; Hermannet al., 1997; Hermann et al., 1999a, 1999b; Schefft et al.,2003; Fargo et al., 2005; Seidenberg et al., 2005). Imagingstudies have implicated activation of DOM temporal lobestructures including the fusiform gyrus, inferior temporal
gyrus and hippocampus in naming ability (Henry et al.,1998; Zelkowicz et al., 1998; Martin et al., 1999; Sawrieet al., 2000; Maess et al., 2002; Abrahams et al., 2003; Sei-denberg, et al., 2005). Henry and colleagues (1998) foundthat adequate naming performance was associated with in-creased cerebral blood flow in the left fusiform gyrus ofthe left temporal lobe, while this was not observed in left(DOM) temporal lobe epilepsy patients. Moreover, Seiden-berg et al. (2005) found left (DOM) temporal lobe vol-ume to be more highly predictive of naming performancethan right (NDOM) temporal lobe volume. The findingthat DOM TLE patients produced more InterPE’s on theBNT than individuals with a relatively intact DOM tem-poral lobe provides further evidence for the importance ofDOM temporal lobe integrity in phonemic paraphasic errorproduction and overall naming performance.
Further support for the relationship between DOMtemporal lobe function and phonemic paraphasic errorproduction is found in previous studies suggesting left(DOM) temporal lobe specialization in processing phono-logical information (Levelt et al., 1991; Fedio et al.,1997; N’Kaoua et al., 2001; Lambon Ralph et al., 2002).In a study investigating the effects of unilateral sodiumamytal injections to both the left and right hemisphere,Fedio et al. (1997) found that normal semantic func-tions of the left hemisphere were augmented by theright hemisphere, while phonological processing was me-diated exclusively by the left hemisphere. Additionally,N’Kaoua et al. (2001) found left hemispheric specializa-tion of phonological processing involving the left tem-poral lobe, with semantic aspects of word generation in-volving both temporal lobes. The ability of interictal andpostictal phonological language errors (phonemic para-phasic errors) to successfully lateralize seizure focus tothe DOM temporal lobe provides further evidence forthis apparent DOM temporal lobe specialization. Fur-thermore, this may explain the predominance of seman-tically based language errors produced by both DOMand NDOM TLE patients on the BNT as both tempo-ral lobes are implicated in semantic aspects of word pro-cessing while only the left is associated with phonologicalaspects.
Studies comparing the diagnostic usefulness of audi-tory and visual naming provide further evidence of lefttemporal lobe specialization in naming (Bell et al., 2003;Hamberger and Seidel, 2003). In fact, results from thesestudies indicate that there are modality-specific regions ofthe temporal lobe differentially responsible for executingvisual versus auditory naming tasks with anterior mesialand lateral regions more involved in auditory naming (Bellet al., 2003; Hamberger and Siedel, 2003). Moreover, Ham-berger and Seidel (2003) found significant qualitative dif-ferences (i.e., response time tip-of-the tongue phenomena)in naming performance for left compared with right TLEpatients. The results of the current study are consistent
Epilepsia, 49(1):22–32, 2008doi: 10.1111/j.1528-1167.2007.01209.x

31
Interictal and Postictal Language Testing
with this general idea that qualitative differences in namingperformance exist between DOM (left) and NDOM (right)TLE patients, regardless of test modality.
The considerable diagnostic accuracy of PILD, Inter-PEs and PostPEs has significant clinical implications; how-ever, there are methodological limitations which shouldbe noted. First and foremost, this study used a retrospec-tive data set. Although this type of data collection savedtime and resources, using retrospective data minimized theinvestigator’s control over the quality and availability ofthe information obtained. However, since 1988a standardprotocol for testing postictal language has been in placein the EMU and over 10,000 seizures have been assessedusing this simple, repeatable protocol. Specifically, somepatients were excluded from the study for the followingreasons: administration error on the BNT, lack of pos-tictal language testing and early departure from inpatientvideo/EEG monitoring. In some instances language domi-nance records (IAT) could not be located while in other in-stances records may have already been destroyed in accor-dance with hospital policy. The removal of patients fromthis study because of these methodological problems mayhave reduced the representativeness of this surgically con-firmed epilepsy sample. As a result of the decreased sam-ple size, people with structural lesions were not excluded.However, inclusion of these individuals may actually makethis sample more representative of DOM TLE patients whoactually undergo surgical intervention.
A final caveat relates to the quality of responses ob-served during postictal language testing. In reviewing pa-tient records, during postictal language testing some pa-tients never responded to presentation of the sign. In someinstances where this was the only seizure recorded dur-ing their admission, these patients were excluded fromthe study. Despite its problematic nature, this phenomenonis a potentially interesting one. Future studies of postic-tal language should include this “nonresponse” responsetype as it may yield even greater clarity and understand-ing of the nature of postictal language in DOM TLEpatients.
In addition to more thorough qualitative assessment ofPILD response types, future investigation should morecomprehensively investigate the moderating effect of FSIQon PILD and production of InterPEs and PostPEs. Sincelogistic models could not be computed for two of the lan-guage indices, pairwise comparisons of AUCs could notbe conducted. Although, the results of this study suggestedbetter diagnostic accuracy with a FSIQ ≥ 90, further in-vestigation into the significance and underlying cause ofthis observed moderating effect, particularly for the postic-tal measures, could make an important contribution to ourcurrent understanding of the brain-behavior relationship.
Although these language indices reflect only a smallpiece of the diagnostic puzzle, each one works to fur-ther enhance it. Since each method of lateralization was
equally as effective at correctly distinguishing DOM TLEfrom NDOM TLE, the use of any one of these measurescan add to the localization process. For individuals whosePILDs are not testable (i.e., only GTCs are captured, etc.)the use of interictal language measures provides an effec-tive and easily obtained clinical alternative to augment di-agnosis. Moreover, in general as diagnostic information iscompounded it makes the localization process better andfacilitates faster more accurate diagnoses, which permitsearlier more effective treatments including surgical inter-vention. By facilitating better treatments at earlier stagesof the disease, it is the hope that the monetary, cognitive,social, psychological, and quality of life costs associatedwith long-term unconfirmed diagnoses (e.g., multiple mon-itorings, lost income due to un- or under-employment, de-pression, social isolation, etc.) can be tempered thereby im-proving quality of patient care.
ACKNOWLEDGMENTSWe thank the Epilepsy Foundation of America who funded this
project through a predoctoral research fellowship.
REFERENCES
Abrahams S, Goldstein LH, Simmons A, Brammer MJ, Williams SCR,Giampietro VP, Andrew CM, Leigh PN. (2003) Functional magneticresonance imaging of verbal fluency and confrontation naming usingcompressed image acquisition to permit overt responses. Hum BrainMapp 20;29–40.
Adam C, Adam C, Rouleau I, Saint-Hilaire JM. (2000) Postictal aphasiaand paresis: a clinical and intracerebral EEG study. Can J Neurol Sci27:49–54.
Ardila A, Rosselli M. (1993) Language deviations in aphasia: a frequencyanalysis. Brain Lang 44:165–180.
Bell BD, Herman BP, Woodard AR, Jones JE, Rutecki PA, Sheth R, DowCC, Seidenberg M. (2001) Object naming and semantic knowledge intemporal lobe epilepsy. Neuropsychology 15:434–443.
Bell BD, Seidenberg M, Hermann BP, Douveille K. (2003) Visual and au-ditory naming in patients with left or bilateral temporal lobe epilepsy.Epilepsy Res 55:29–37.
Benton AL, Hamsher K deS. (1983) Multilingual aphasia examination,Revised ed. Department of Neurology, University of Iowa Hospitals,Iowa City.
Busch RM, Frazier TW, Haggerty KA, Kubu CS. (2005) Utility of theBoston naming test in predicting ultimate side of surgery in patientswith medically intractable temporal lobe epilepsy. Epilepsia 46:1773–1779.
Devinksy O, Kelley K, Yacubian EM, Sato S, Kufta CV, Theodore WH,Porter RJ. (1994) Postictal behavior: a clinical and subdural electroen-cephalographic study. Arch Neurol 51:254–259.
Fakhoury T, Abou-Khalil B, Peguero E. (1994) Differentiating clinicalfeatures of right and left temporal lobe seizures. Epilepsia 35:1038–1044.
Fargo JD, Schefft BK, Dulay MF, Privitera MD, Yeh HS. (2005) Con-frontation naming in individuals with temporal lobe epilepsy: aquantitative analysis of paraphasic error subtypes. Neuropsychology19:603–611.
Fedio O, August A, Patronas N, Sato S, Kufta C. (1997) Semantic,phonological and perceptual changes following left and right intrac-arotid injection (Wada) with a low amytal dosage. Brain Cogn 33:98–117.
Ficker D, Shukla R, Privitera MD. (2001) Postictal language dysfunctionin complex partial seizures: effect of contralateral ictal spread. Neu-rology 56:1590–1592.
Epilepsia, 49(1):22–32, 2008doi: 10.1111/j.1528-1167.2007.01209.x
32
M. J. Ramirez et al.
Gabr M, Leuders H, Dinner D, Dinner D, Morris H, Wylie E. (1989)Speech manifestations in lateralization of temporal lobe seizures. AnnNeurol 25:82–87.
Goldberg-Stern H, Gadoth N, Cahill W, Privitera M. (2004) Languagedysfunction after frontal lobe seizures. Neurology 62:1637–1638.
Goodglass H, Kaplan E. (1972) The assessment of aphasia and re-lated disorders, 2nd Edition; Boston Diagnostic Aphasia ExaminationBooklet; 16 test stimulus cards; Boston Naming Test; Boston NamingTest scoring booklet.
Goodglass H, Kaplan E. (1983) The assessment of aphasia and relateddisorders. Lea & Febiger, Philadelphia.
Goodglass H, Wingfield A, Hyde MR, Gleason JB, Bowles NL,Gallagher RE. (1997) The importance of word-initial phonology: er-ror patterns in prolonged naming efforts by aphasic patients. J Int Neu-ropsychol Soc 3:128–138.
Hamberger MJ, Tamny TR. (1999) Auditory naming and temporal lobeepilepsy. Epilepsy Res 35:229–243.
Hamberger MJ, Seidel WT. (2003) Auditory and visual naming tests: nor-mative and patient data for accuracy, response time, and tip-of-the-tongue. J Int Neuropsychol Soc 9:479–489.
Hanley JA, McNeil BJ. (1983) A method of comparing the areas underreceiver operating characteristic curves derived from the same cases.Radiology 148:839–843.
Henry TR, Buchtel HA, Koeppe RA, Pennell PB, Kluin KJ, Minoshima S.(1998) Absence of normal activation of the left anterior fusiform gyrusduring naming in left temporal lobe epilepsy. Neurology 50:787–790.
Hermann BP, Wyler AR. (1987) Effects of anterior temporal lobectomyon language function: a controlled study. Ann Neurol 23:585–588.
Hermann BP, Wyler AR, Steenman H, Richey ET. (1988) The interrela-tionship between language function and verbal learning/memory per-formance in patients with complex partial seizures. Cortex 24:245–253.
Hermann BP, Wyler AR. (1991) Language function following anteriortemporal lobectomy. J Neurosurg 74:560–566.
Hermann BP, Seidenberg M, Haltiner A, Wyler AR. (1992) Adequacyof language function and verbal memory performance in unilateraltemporal lobe epilepsy. Cortex 28:423–433.
Hermann BP, Seidenberg M, Schoenfeld J, Davies K. (1997) Neuropsy-chological characteristics of the syndrome of mesial temporal lobeepilepsy. Arch Neurol 54:369–376.
Hermann BP, Perrine K, Chelune GJ, Barr W, Loring DW, Strauss E,Trenerry MR, Westerveld M. (1999a) Visual confrontation namingfollowing left anterior temporal lobectomy: a comparison of surgicalapproaches. Neuropsychology 13:3–9.
Hermann BP, Davies K, Foley K, Bell B. (1999b) Visual confrontationnaming outcome after standard left anterior temporal lobectomy withsparing versus resection of the superior temporal gyrus: a randomizedprospective clinical trial. Epilepsia 40:1070–1076.
Hosmer DW, Lemeshow S. (2001) Applied logistic regression, 2nd ed.John Wiley & Sons, Hoboken.
Howell RA, Saling MM, Bradley DC, Berkovic SF. (1994) Interictal lan-guage fluency in temporal lobe epilepsy. Cortex 30:469–478.
Jackson, JH. (1898) Relations of different divisions of the central nervoussystem to one another and to parts of the body. Lancet 1:79–87.
Johnson CJ, Paivo A, Clark JM. (1996) Cognitive components of picturenaming. Psychol Bull 120:113–139.
Kaplan E, Goodglass H, Weintraub S. (1983) Boston naming test, Reviseded. Lea & Febiger, Philadelphia.
Koerner M, Laxer KD. (1988) Ictal speech, postical language dysfunction,and seizure lateralization. Neurology 38:634–636.
Lambon Ralph MA, Moriarty L, Sage K. (2002) Anomia is simply a re-flection of semantic and phonological impairments: evidence from acase-series study. Aphasiology 16:56–82.
Langfitt J, Rausch R. (1996) Word-finding deficits persist after anterotem-poral lobectomy. Arch Neurol 53:72–76.
Levelt WJM, Schriefes H, Vorberg D, Meyer AS, Pechmann T, HavingaJ. (1991) The time course of lexical access in speech production: astudy of picture naming. Psychol Rev 98:122–142.
Leutmezer F, Baumgartner C. (2002) Postictal signs of lateralizing andlocalizing significance. Epileptic Disord 4:43–48.
Loddenkemper T, Kotagal P. (2005) Lateralizing signs during seizures infocal epilepsy. Epilepsy Behav 7:1–17.
Mackay CE, Webb JA, Eldridge PR, Chadwick DW, Whitehouse GH,Roberts N. (2000) Quanitative magnetic resonance imaging in con-secutive patients evaluated for surgical treatment of temporal lobeepilepsy. Magn Reson Imaging 18:1187–1199.
Maess B, Friederici AD, Damian M, Meyers AS, Levelt WJM. (2002)Semantic category interference in overt picture naming: sharpen-ing current density localization in PCA. J Cogn Neurosci 14:455–462.
Martin RC, Sawrie S, Hugg J, Gilliam R, Faught E, Kuzniecky R. (1999b)Cognitive correlates of HMRSI-detected hippocampal abnormalitiesin temporal lobe epilepsy. Neurology 53:2052–2058.
Mayeux R, Brandt J, Rosen J, Benson DR. (1980) Interictal memory andlanguage impairment in temporal lobe epilepsy. Neurology 30:120–125.
McKeever M, Holmes GL, Russman BS. (1983) Speech abnormalities inseizures: a comparison of absence and partial complex seizures. BrainLang 19:25–32.
N’Kaoua B, Lespinet V, Barasse A, Rougier A, Claverie B. (2001) Ex-ploration of hemispheric specialization and lexico-semantic processin unilateral temporal lobe epilepsy with verbal fluency tasks. Neu-ropsychologia 39:635–642.
O’Shea MF, Saling MM, Bladin PF, Berkovic SF. (1996) Does namingcontribute to memory self-report in temporal lobe epilepsy? J ClinExp Neuropsychol 18:98–109.
Oyegbile TO, Dow C, Jones J, Bell B, Rutecki P, Sheth R, SeidenbergM, Hermann BP. (2004) The nature and course of neuropsychologi-cal morbidity in chronic temporal lobe epilepsy. Neurology 62:1736–1742.
Privitera MD, Morris GL, Gilliam F. (1991) Postictal language assessmentand lateralization of complex partial seizures. Ann Neurol 30:391–396.
Raspall T, Donate M, Boget T, Carreno M, Donaire A, Agudo R,Bargallo N, Rumia J, Setoain X, Pintor, L, Salamero M. (2005) Neu-ropsychological tests with lateralizing value in patients with temporallobe epilepsy: reconsidering material-specific theory. Seizure 14:569–576.
Richardson MP. (2001) Functional imaging in epilepsy. Seizure 10:139–156.
Sawrie SM, Martin RC, Gilliam FG, Faught RE, Maton B, HuggJW, Bush N, Sinclair K, Kuzniesky RI. (2000) Visual confronta-tion naming and hippocampal function: a neural network study us-ing quantitative H magnetic resonance spectroscopy. Brain 123:770–780.
Schefft BK, Testa SM, Dulay MF, Privitera MD, Yeh HS. (2003) Pre-operative assessment of confrontation naming ability and interictalparaphasia production in unilateral temporal lobe epilepsy. EpilepsyBehav 4:161–168.
Seidenberg M, Geary E, Hermann. (2005) Investigating temporal lobecontribution to confrontation naming using MRI quantitative volumet-rics. J Int Neuropsychol Soc 11:358–366.
Spencer SS, Theodore WH, Berkovic SF. (1995) Clinical applica-tions: MRI, SPECT and PET. Magn Reson Imaging 13:1119–1124.
Stafniak P, Saykin AJ, Sperling M, Kester MS, Robinson LJ, O’ConnorMJ, Gur R. (1990) Acute naming deficits following dominant tempo-ral lobectomy: prediction by age at first risk for seizures. Neurology40:1509–1512.
Stefan H, Hummel C, Scheler G, Genow A, Druschky K, Tilz C,Kaltenhauser M, Hopfengartner R, Buchfelder M, Romstock J. (2003)Magnetic brain source imaging of focal epileptic activity: a synopsisof 455 cases. Brain 125:2396–2405.
Weinand ME, El-Saadany WF, Labiner DM, Talwar D, Ahern G. (1995)Subdural strip electrode monitoring and surgical decision making inrefractory epilepsy: validity and prognostic value of noninvasive lo-calizing data. J Epilepsy 8:131–138.
Zelkowicz BJ, Herbster AN, Nebes RD, Mintum MA, Becker JT. (1998)An examination of regional cerebral blood flow during object namingtasks. J Int Neuropsychol Soc 4:160–166.
Epilepsia, 49(1):22–32, 2008doi: 10.1111/j.1528-1167.2007.01209.x