independent feedback on clinical audit performance: a multi-professional pilot study
TRANSCRIPT
Clinical Governance: An International JournalIndependent feedback on clinical audit performance: a multi-professional pilot studyPaul Bowie Pat Quinn Ailsa Power
Article information:To cite this document:Paul Bowie Pat Quinn Ailsa Power, (2009),"Independent feedback on clinical audit performance: a multi-professional pilot study", Clinical Governance: An International Journal, Vol. 14 Iss 3 pp. 198 - 214Permanent link to this document:http://dx.doi.org/10.1108/14777270910976148
Downloaded on: 27 April 2015, At: 04:28 (PT)References: this document contains references to 28 other documents.To copy this document: [email protected] fulltext of this document has been downloaded 763 times since 2009*
Users who downloaded this article also downloaded:Howard J. Klein, Aden E. Heuser, (2008),"The learning of socialization content: A framework forresearching orientating practices", Research in Personnel and Human Resources Management, Vol. 27 pp.279-336
Access to this document was granted through an Emerald subscription provided by 465347 []
For AuthorsIf you would like to write for this, or any other Emerald publication, then please use our Emerald forAuthors service information about how to choose which publication to write for and submission guidelinesare available for all. Please visit www.emeraldinsight.com/authors for more information.
About Emerald www.emeraldinsight.comEmerald is a global publisher linking research and practice to the benefit of society. The companymanages a portfolio of more than 290 journals and over 2,350 books and book series volumes, as well asproviding an extensive range of online products and additional customer resources and services.
Emerald is both COUNTER 4 and TRANSFER compliant. The organization is a partner of the Committeeon Publication Ethics (COPE) and also works with Portico and the LOCKSS initiative for digital archivepreservation.
*Related content and download information correct at time of download.
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)
Independent feedback on clinicalaudit performance:
a multi-professional pilot studyPaul Bowie, Pat Quinn and Ailsa Power
NHS Education for Scotland, Glasgow, UK
AbstractPurpose – The purpose of this paper is to investigate the acceptability and educational impact ofindependent feedback on the clinical audit performance of different groups of healthcare professionalsby trained colleagues.
Design/methodology/approach – This is a pilot study involving review of the criterion audit andsignificant event analysis (SEA) attempts of west of Scotland dentists, pharmacists, physiotherapists,practice managers and nurse practitioners by trained colleagues using validated instruments. Audit,SEA and feedback reports were content-analysed. Data on pre- and post-study attitudes, experiencesand knowledge levels were collected by questionnaire. T-tests for differences in mean group scoreswere calculated, along with 95 per cent confidence intervals for mean differences. A difference in meanscores of 1.0 or greater would be indicative of educational gain.
Findings – A total of 34 participants submitted 54 audit and SEA reports, with 20 submitting both(58.9 per cent). In total, 14/20 audits (75.0 per cent) and 26/34 SEAs (76.5 per cent) contained evidence ofappropriate learning needs and action(s) implemented for healthcare improvement. Feedback focusedon knowledge and skills in applying audit methods; demonstrating insight into deficiencies;highlighting appropriate learning needs; and implementing change. Audit knowledge and skill scoresincreased by a mean difference of $1.0 for most stages of audit and SEA method (p , 0:001). Strongagreement on the value of independent feedback on clinical audit was reported.
Research limitations/implications – The study highlights some of the difficulties in applyingaudit methods across professions and highlights the added value of feedback by trained colleagues,but is limited in size.
Practical implications – Integrating clinical audit and peer feedback with continuing professionaldevelopment obligations may facilitate greater engagement and more effective quality improvement,but will require a policy change and additional resource.
Originality/value – This small study provides further evidence of the acceptability and educationalimpact of independent feedback on clinical audit performance for healthcare professionals.
Keywords Clinical audit, Peer review, Feedback, Quality improvement
Paper type Research paper
IntroductionIn the past decade a greater emphasis has been placed on the need for all healthprofessionals in the UK to participate in continuing professional development (CPD)(Scottish Office Department of Health, 1998). Reflecting on clinical practice and
The current issue and full text archive of this journal is available at
www.emeraldinsight.com/1477-7274.htm
The authors extend their thanks to all health care professionals who participated in this studyand the members of the peer group networks who provided feedback. They also thank Dr JohnMcKay, NHS Education for Scotland, for commenting on earlier drafts of this paper and Dr LilianMurray, University of Glasgow, for statistical advice. This research was funded by NHSEducation for Scotland.
CGIJ14,3
198
Received 24 October 2008Revised 18 February 2009Accepted 13 March 2009
Clinical Governance: An InternationalJournalVol. 14 No. 3, 2009pp. 198-214q Emerald Group Publishing Limited1477-7274DOI 10.1108/14777270910976148
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)
identifying learning needs are important components of CPD (Royal College ofNursing, 2003; Scottish Executive et al., 2003; British Dental Association, 2007).Investigating significant events, undertaking clinical audit and seeking peer feedbackare all proposed as objective methods of highlighting potential learning needs(Chartered Society of Physiotherapy, 2003; McLaren et al., 2007). Participation in theseactivities may also make important organisational contributions to improvinghealthcare quality as part of the UK clinical governance (Scottish Office Department ofHealth, 1998) and patient safety agendas (National Patient Safety Agency, 2005).
However, the clinical audit evidence base suggests that there are a number ofobstacles that impede its success as an effective mechanism for change – despite itswidespread endorsement by policymakers (Department of Health, 2006) andprofessional hierarchies (Scottish Executive et al., 2003; Royal College of Nursing,2003; Chartered Society of Physiotherapy, 2003). For many health professionals audit isstill a marginal activity with low priority. Lack of engagement is a serious concern(Davies et al., 2006). Ever increasing workloads, poor leadership, inadequateunderstanding of audit methods, distrust and hostility, and limited resources andtime are often cited as factors inhibiting participation (Johnston et al., 2000; NationalInstitute for Clinical Excellence, 2002). It is assumed by policymakers that cliniciansintuitively understand audit methods and posses the necessary knowledge, skills andprofessional attributes to apply these to a satisfactory standard. The reality is thatmuch audit is poorly designed and frequently fails largely because all of thefundamental stages of the audit cycle are not always adequately completed (Bowieet al., 2007; McKay et al., 2006; Miles et al., 1996). Similar methodological failings havebeen identified for significant event analysis (SEA) – a qualitative method of audit –when undertaken by many health care teams (Bowie et al., 2008a). The consequencesare potentially serious in that crucial opportunities to improve the quality and safety ofhealthcare may be missed and finite time and resources can be wasted.
Given the reaffirmation by national decision-makers of the priority role of clinicalaudit in improving healthcare quality and safety (Healthcare Commission, 2007) andcontributing to professional appraisal and regulation (Department of Health, 2006),tackling these deficiencies and educational gaps should be of prime concern. One obviousapproach to raising audit performance is through targeted education and training atundergraduate and postgraduate level, but this is not often a priority in alreadycondensed course curricula and effective examples are limited (Campbell et al., 1993).
In recognition of the difficulties in this area, NHS Education for Scotland (NES) – aspecial health authority with responsibility for the education and training of the NHSworkforce – introduced a voluntary feedback model for reviewing the clinical auditactivities of general medical practitioners (GPs). This has enabled GPs to submitexamples of two methods of clinical audit - criterion based audit and significant eventanalysis - for independent review by trained peers as part of regional arrangements forCPD. The model was introduced in the west of Scotland deanery in 2000 andestablished nationally in 2007. It has been previously described in detail (Bowie et al.,2005b), while evidence for its acceptability, feasibility and educational impact ingeneral practice and hospital medicine has grown steadily (McKay et al., 2007, 2006,Bowie et al., 2005a; McGregor et al., 2005).
The purpose of the model is to facilitate engagement in audit methods and providedevelopmental feedback on the quality of audit attempts. The underlying philosophy is
Clinical auditperformance
199
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)

based firmly on formative educational principles and the feedback follows best practiceby aiming to be objective, positive, fair, clear and specific. The aim of the feedback is toprovide thepractitioner with informationonhowsuccessfully aclinical audit activity wascarried out and guide individuals on improving their performance in this area(Chur-Hansen and Koopowitz, 2005). Engagement with the medical model has beenmoderate butencouraging witharound35per cent ofGPprincipals in thewestofScotlandhaving submitted at least one audit example for peer feedback (McKay et al., 2006).
This feedback model is currently limited to GPs but should in theory be transferablegiven the symmetry of CPD and clinical governance expectations for all healthcareprofessionals. Given the potential rewards for improving clinical audit practices on amulti-professional basis through a targeted educational intervention, the possibility ofextending this model of learning to other members of the healthcare workforce clearlymerits investigation. The main aim of this pilot study, therefore, was to investigate theacceptability and educational impact of independent feedback on the clinical auditperformance of different groups of healthcare professionals.
MethodsA summary of the study project design and timeline is outlined in Table I.
Participants and settingsEvery second general practice in the Greater Glasgow NHS Board area was randomlyselected from a descending alphabetical list of all 128 practices. Identified practiceswere sent a letter outlining the study purpose and inviting practices to nominate apractice manager or nurse to participate, with 30 practices expressing an initial interest(23.4 per cent).
Physiotherapists were voluntarily recruited from the NHS Greater Glasgow BackPain Team, which had agreed to pilot the use of SEA and independent feedback.Dentists and pharmacists were recruited from SEA peer review network groups newlyestablished in NHS Scotland in 2006.
Clinical audit training and allocated tasksParticipants all attended single half-day training sessions in February 2007 on clinicalaudit methods and were provided with relevant educational support materials forfuture reference. As well as a focus on understanding the technical side of auditmethods, the training emphasised the need for participants to demonstrate leadership,organisational, motivational and negotiation skills when engaging their healthcareteams. All participants agreed to attempt to complete either one or two clinical audittasks – a completed criterion-based audit cycle and/or a significant event analysis. Atime-scale of six months was set for completion of both tasks that were to be submittedin standard report formats to NES for review and feedback.
Educational review and feedbackIn this model both SEA and criterion audit have defined standardised methods (McKayet al., 2006; Bowie et al., 2007). Reviewers in all peer networks underwent appropriatetraining and calibration (a check on inter-rater reliability) to learn how to formativelyassess audit and/or SEA reports using the validated assessment instruments (Loughet al., 1995; McKay et al., 2007) and provide developmental feedback. Materials
CGIJ14,3
200
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)

submitted by participants were screened for confidentiality issues and then forwardedto two trained reviewers in the appropriate peer group for assessment. The feedbackwas returned to a NES coordinator who undertook a third review and combined allfeedback before returning this in the form of a detailed letter to the submittingpractitioner for their consideration. The absence of established peer review groups forphysiotherapy and practice nursing led to their efforts being evaluated by reviewersfrom the GP network.
Data collectionAll participants completed a pre and post study four-part evaluation questionnaire.The first two sections focused on respondents’ experiences of audit and SEA andestimations of their knowledge and skill levels. The third section consisted of a series
Project stage Timescale Description
One October-December 2006 Training of audit/SEA reviewers (dentists andpharmacists)
Two January 2007 Recruitment of study participants and locationsPractice managers and practice nurses – NHSGreater GlasgowCommunity physiotherapists – NHS GreaterGlasgowGeneral dental practitioners – West of ScotlandCommunity pharmacists – NHS Scotland
Three February 2007 Delivery of training in audit and SEA methodsParticipants attended a single half-day introductorytraining session covering both methodsParticipants agreed to undertake an audit and/orSEA task and submit a written report to NHSEducation for Scotland for feedback from trainedcolleagues within the next six monthsParticipants complete a pre-study evaluationquestionnaire of perceived knowledge, skills andexperiences related to audit and SEA
Four April-October 2007 Independent review and feedback completedParticipants completed audit and SEA reportssubmitted for review and feedbackWritten feedback provided to participants two tofour weeks after submission
Five April-November 2007 Post-study evaluation questionnaires completedParticipants completed and returned questionnaireswithin three weeks of receiving feedback letters
Six November 2007-February 2008 Analysis and reporting of study dataAudit and SEA reports content analysed by researchteamsWritten feedback letters content analysed byresearch teamsQuestionnaire data analysed by research teamPreliminary report of findings sent to participantsand professionals heads of department
Table I.Details of project stages
and timetable inchronological date order
Clinical auditperformance
201
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)
of attitudinal statements about the acceptability and educational impact of the receivedfeedback on their clinical audit efforts. The final section collected demographic dataand encouraged free text responses on participants’ experiences of taking part.Respondents indicated their level of agreement with all statements on a five-pointrating scale.
Data analysisAll audit and SEA reports and associated feedback letters were jointly analysed forcontent by both authors. Key themes were identified around the types of topics studiedand the main learning and change that reportedly took place. The feedback issueshighlighted by reviewers were subjected to identical analysis.
Questionnaire data were input into a Microsoft Excel spreadsheet and analysed. Preand post intervention differences in mean rating scale scores for the group werecalculated. T-tests for differences in mean group scores were calculated, along with 95per cent confidence intervals for mean differences. We determined that a difference inmean group scores of 1.0 or greater would be indicative of overall educational gain.
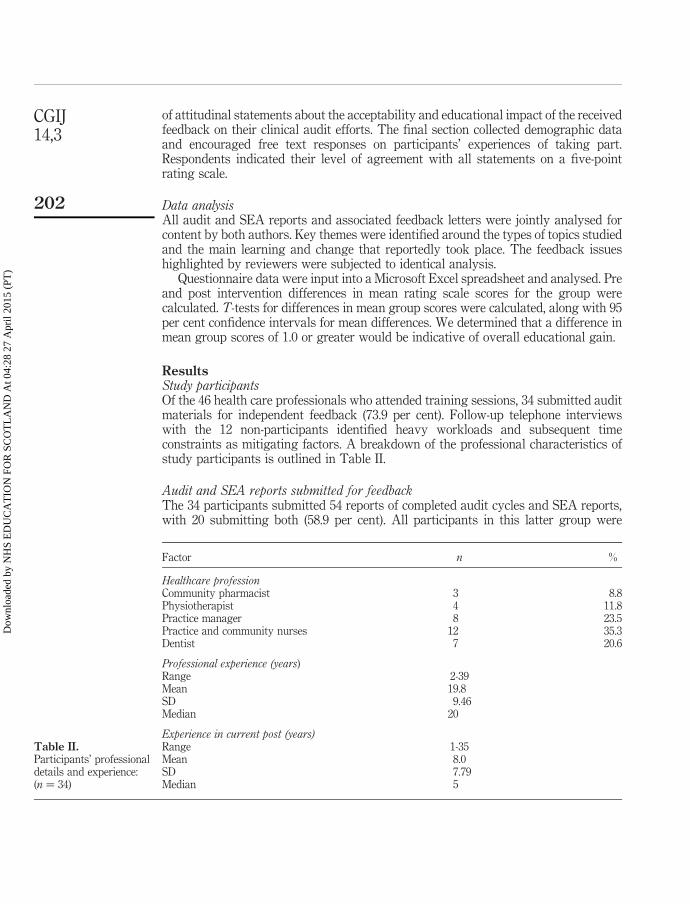
ResultsStudy participantsOf the 46 health care professionals who attended training sessions, 34 submitted auditmaterials for independent feedback (73.9 per cent). Follow-up telephone interviewswith the 12 non-participants identified heavy workloads and subsequent timeconstraints as mitigating factors. A breakdown of the professional characteristics ofstudy participants is outlined in Table II.
Audit and SEA reports submitted for feedbackThe 34 participants submitted 54 reports of completed audit cycles and SEA reports,with 20 submitting both (58.9 per cent). All participants in this latter group were
Factor n %
Healthcare professionCommunity pharmacist 3 8.8Physiotherapist 4 11.8Practice manager 8 23.5Practice and community nurses 12 35.3Dentist 7 20.6
Professional experience (years)Range 2-39Mean 19.8SD 9.46Median 20
Experience in current post (years)Range 1-35Mean 8.0SD 7.79Median 5
Table II.Participants’ professionaldetails and experience:(n ¼ 34)
CGIJ14,3
202
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)
practice managers, pharmacists or practice nurses. The remaining 14 physiotherapists,dentists and a community nurse submitted a single SEA report only.
Previous experience of criterion audit and SEAIn terms of audit experience, 17 of the 20 participants (85 per cent) who submitted acriterion audit project had previously been involved in audit as part of a health careteam. Of these, ten had gained experience in their current post of being the main personleading a project (50 per cent), while eight from the whole group (40 per cent) hadpreviously written-up a completed audit cycle report.
For the 34 participants who submitted SEA reports, 28 (82 per cent) had beeninvolved previously in discussing a significant event informally with colleagues; 24(70.5 per cent) had highlighted a significant event which was discussed with thehealthcare team in a formal meeting situation; and 18 (52.9 per cent) had been the leadperson charged with analysing a significant event in their current post. A total of 19had previous experience of writing-up a completed SEA report (55.8 per cent).
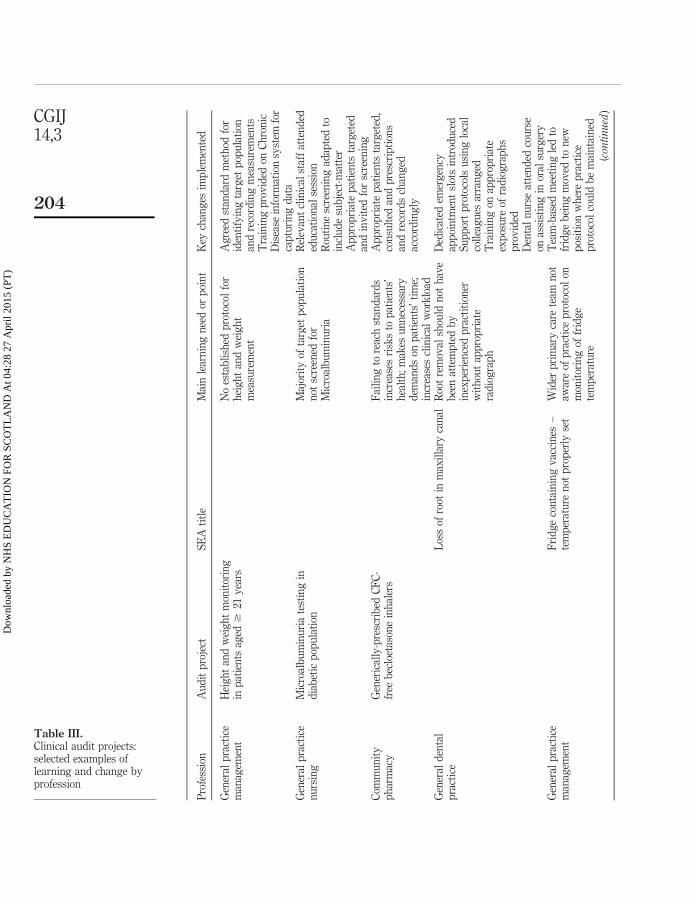
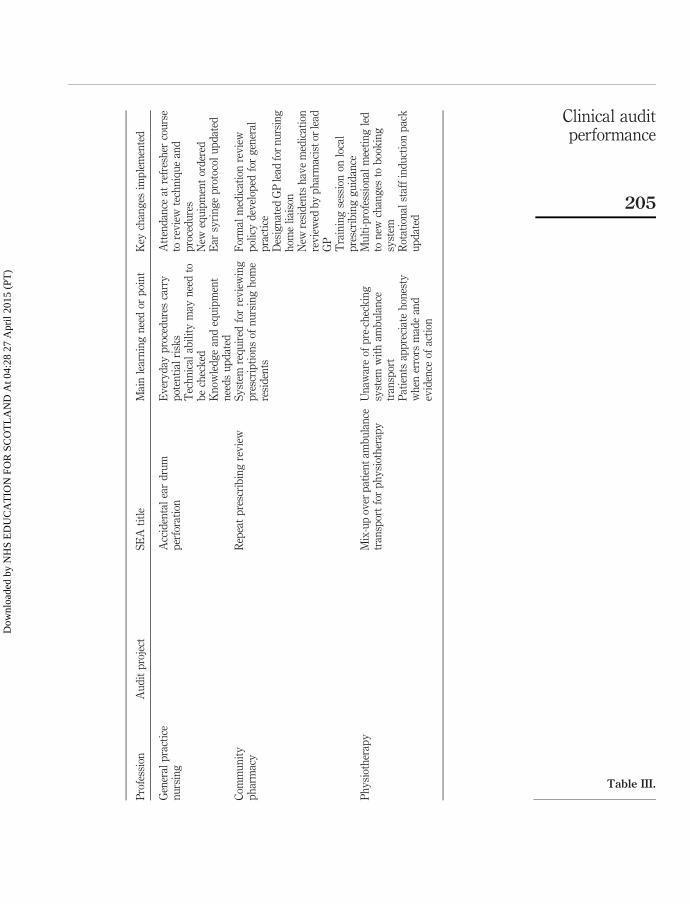
Learning and changeThe review process judged 14/20 audit reports (75.0 per cent) and 26/34 SEA reports(76.5 per cent) to contain sufficient evidence of learning and change that wasappropriate to the topics being investigated. The reviewers agreed that the actionsimplemented under the leadership of participants were relevant, potentiallysustainable and likely to lead to improvements in the quality and safety ofhealthcare. Typical examples of specific learning and change resulting from clinicalaudit efforts are highlighted in Table III.
Feedback issues highlightedA range of feedback issues was identified by clinical audit reviewers (Table IV). Thesewere mainly concerned with technical and human factors related to participants’knowledge, skills and behaviour in applying both improvement methods;demonstrating insight into why aspects of health care delivery may be deficient;highlighting appropriate learning needs; and also leading the healthcare team in theimplementation of agreed change and ensuring sustainability. However, reviewers alsoraised issues and made suggestions for participants to reflect upon which were basedon their own experiences and ideas as a way of potentially further enhancing thequality and safety of patient care being described in the audit and SEA reports.
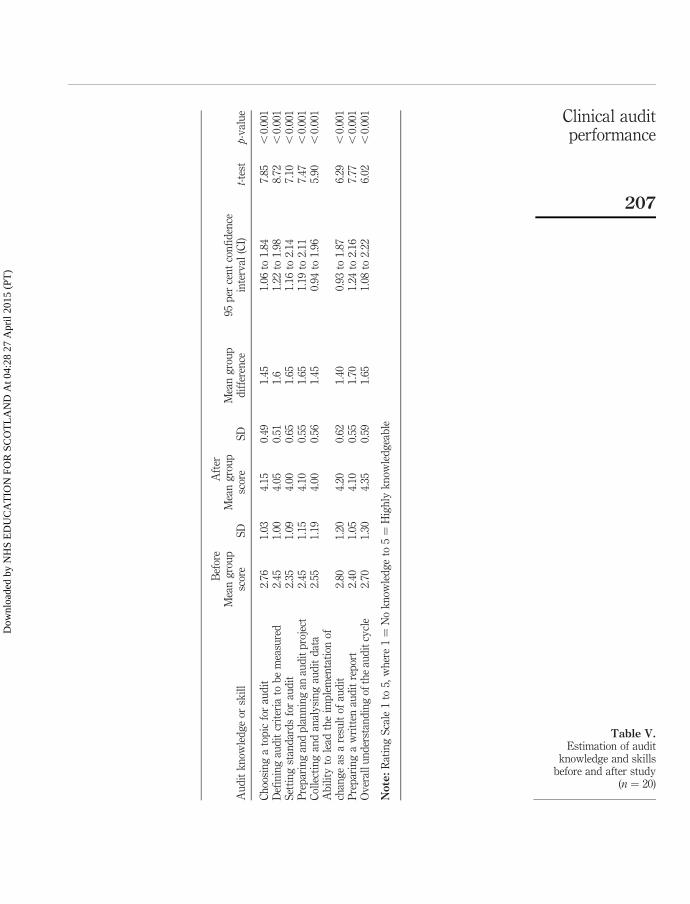
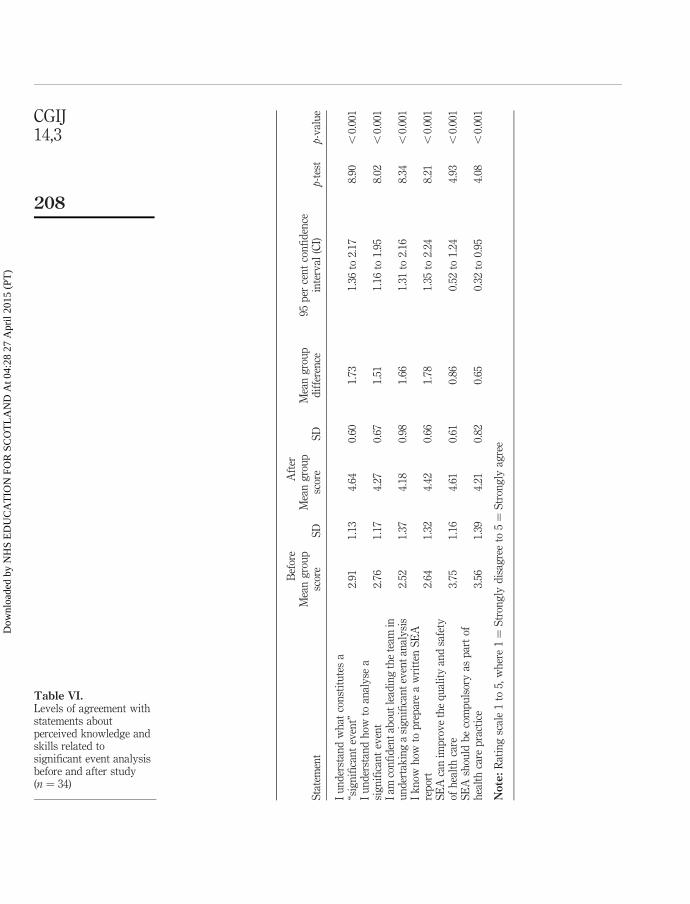
Pre- and post-study estimation of audit and SEA knowledge and skillsParticipants estimated that their levels of knowledge and skills of both audit and SEAto have increased after attempting both activities and receiving independent feedbackcompared with their estimated levels before they took part. Tables V and VI highlightstatistical post study differences in participants’ estimated knowledge and skill levelsfor most stages of the defined criterion audit and SEA methods.
Attitudes to independent feedbackLevels of agreement with a series of attitudinal statements about the value ofindependent feedback for clinical audit activities and participating in this type ofeducational model are outlined in Table VII. It is evident that the vast majority of
Clinical auditperformance
203
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)
Pro
fess
ion
Au
dit
pro
ject
SE
Ati
tle
Mai
nle
arn
ing
nee
dor
poi
nt
Key
chan
ges
imp
lem
ente
d
Gen
eral
pra
ctic
em
anag
emen
tH
eig
ht
and
wei
gh
tm
onit
orin
gin
pat
ien
tsag
ed$
21y
ears
No
esta
bli
shed
pro
toco
lfo
rh
eig
ht
and
wei
gh
tm
easu
rem
ent
Ag
reed
stan
dar
dm
eth
odfo
rid
enti
fyin
gta
rget
pop
ula
tion
and
reco
rdin
gm
easu
rem
ents
Tra
inin
gp
rov
ided
onC
hro
nic
Dis
ease
info
rmat
ion
syst
emfo
rca
ptu
rin
gd
ata
Gen
eral
pra
ctic
en
urs
ing
Mic
roal
bu
min
uri
ate
stin
gin
dia
bet
icp
opu
lati
onM
ajor
ity
ofta
rget
pop
ula
tion
not
scre
ened
for
Mic
roal
bu
min
uri
a
Rel
evan
tcl
inic
alst
aff
atte
nd
eded
uca
tion
alse
ssio
nR
outi
ne
scre
enin
gad
apte
dto
incl
ud
esu
bje
ct-m
atte
rA
pp
rop
riat
ep
atie
nts
targ
eted
and
inv
ited
for
scre
enin
gC
omm
un
ity
ph
arm
acy
Gen
eric
ally
-pre
scri
bed
CF
C-
free
bec
loet
ason
ein
hal
ers
Fai
lin
gto
reac
hst
and
ard
sin
crea
ses
risk
sto
pat
ien
ts’
hea
lth
;m
akes
un
nec
essa
ryd
eman
ds
onp
atie
nts
’ti
me;
incr
ease
scl
inic
alw
ork
load
Ap
pro
pri
ate
pat
ien
tsta
rget
ed,
con
sult
edan
dp
resc
rip
tion
san
dre
cord
sch
ang
edac
cord
ing
ly
Gen
eral
den
tal
pra
ctic
eL
oss
ofro
otin
max
illa
ryca
nal
Roo
tre
mov
alsh
ould
not
hav
eb
een
atte
mp
ted
by
inex
per
ien
ced
pra
ctit
ion
erw
ith
out
app
rop
riat
era
dio
gra
ph
Ded
icat
edem
erg
ency
app
oin
tmen
tsl
ots
intr
odu
ced
Su
pp
ort
pro
toco
lsu
sin
glo
cal
coll
eag
ues
arra
ng
edT
rain
ing
onap
pro
pri
ate
exp
osu
reof
rad
iog
rap
hs
pro
vid
edD
enta
ln
urs
eat
ten
ded
cou
rse
onas
sist
ing
inor
alsu
rger
yG
ener
alp
ract
ice
man
agem
ent
Fri
dg
eco
nta
inin
gv
acci
nes
–te
mp
erat
ure
not
pro
per
lyse
tW
ider
pri
mar
yca
rete
amn
otaw
are
ofp
ract
ice
pro
toco
lon
mon
itor
ing
offr
idg
ete
mp
erat
ure
Tea
m-b
ased
mee
tin
gle
dto
frid
ge
bei
ng
mov
edto
new
pos
itio
nw
her
ep
ract
ice
pro
toco
lco
uld
be
mai
nta
ined
(con
tinued
)
Table III.Clinical audit projects:selected examples oflearning and change byprofession
CGIJ14,3
204
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)
Pro
fess
ion
Au
dit
pro
ject
SE
Ati
tle
Mai
nle
arn
ing
nee
dor
poi
nt
Key
chan
ges
imp
lem
ente
d
Gen
eral
pra
ctic
en
urs
ing
Acc
iden
tal
ear
dru
mp
erfo
rati
onE
ver
yd
ayp
roce
du
res
carr
yp
oten
tial
risk
sT
ech
nic
alab
ilit
ym
ayn
eed
tob
ech
eck
edK
now
led
ge
and
equ
ipm
ent
nee
ds
up
dat
ed
Att
end
ance
atre
fres
her
cou
rse
tore
vie
wte
chn
iqu
ean
dp
roce
du
res
New
equ
ipm
ent
ord
ered
Ear
syri
ng
ep
roto
col
up
dat
ed
Com
mu
nit
yp
har
mac
yR
epea
tp
resc
rib
ing
rev
iew
Sy
stem
req
uir
edfo
rre
vie
win
gp
resc
rip
tion
sof
nu
rsin
gh
ome
resi
den
ts
For
mal
med
icat
ion
rev
iew
pol
icy
dev
elop
edfo
rg
ener
alp
ract
ice
Des
ign
ated
GP
lead
for
nu
rsin
gh
ome
liai
son
New
resi
den
tsh
ave
med
icat
ion
rev
iew
edb
yp
har
mac
ist
orle
adG
PT
rain
ing
sess
ion
onlo
cal
pre
scri
bin
gg
uid
ance
Ph
ysi
oth
erap
yM
ix-u
pov
erp
atie
nt
amb
ula
nce
tran
spor
tfo
rp
hy
siot
her
apy
Un
awar
eof
pre
-ch
eck
ing
syst
emw
ith
amb
ula
nce
tran
spor
tP
atie
nts
app
reci
ate
hon
esty
wh
ener
rors
mad
ean
dev
iden
ceof
acti
on
Mu
lti-
pro
fess
ion
alm
eeti
ng
led
ton
ewch
ang
esto
boo
kin
gsy
stem
Rot
atio
nal
staf
fin
du
ctio
np
ack
up
dat
ed
Table III.
Clinical auditperformance
205
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)

participants were strongly positive in their response levels in agreeing about theeducational value and potential need for external and independent feedback. There wasno difference in attitudes between participants who received in-depth feedback andthose receiving limited feedback on performance i.e. confirmation of good practice. Aselection of comments from participants on their opinions of the role of this type offeedback on clinical audit performance is outlined in Table VIII.
DiscussionThis pilot study aimed to establish whether an existing medical model of external andindependent feedback on audit and SEA attempts was potentially acceptable and ofeducational value to a multi-professional group of healthcare professionals. Thefindings demonstrate that the overwhelming majority of study participants were ableto successfully complete a clinical audit task(s) within a six-month period and did notobject to the principle of independent review of their performances. The feedback theyreceived was perceived to be professionally acceptable by the vast majority ofparticipants. Similarly, the findings show that most participants reported increasedlevels of knowledge and skills in the application of both audit and SEA techniquesafter receiving their feedback. The implication is that this type of independentfeedback had a positive educational impact on participants. It may also contribute tovalidating the reported learning, change and potential healthcare improvement thatwas facilitated by most participants’ clinical audit attempts. Overall the findingssuggest that this medical model may potentially be transferable to other professions asa generic educational support mechanism for improving clinical audit practice andpotentially adding value to the CPD process. Against this background, the pilot study
Audit projects SEA reports
Unclear or confused criteriaNo clear or defined standard(s) setStandards defined not related to criteriaNo justification for standard levels setTime-scale set to achieve standards not evident orunrealisticNo evidence or insufficient evidence ofpreparation and planning or teamworkData collected were not related to criteria/standardsFailure to compare data with criteria/standardsNumerical errors in data presentedData were poorly presented or difficult to interpretFailure to implement necessary changeFailure to describe change agreed andimplementedInadequate change implementedDescription of change poor or confusedFailure to outline what was learnedFailure to explain why results improvedFailure to explain why results got worseFailure to document how change will be sustained
Not a healthcare significant eventFailure to fully describe what happenedInadequate description of why event happenedWrong interpretation of why the event happenedFailure to describe why the event happenedInadequate description of learning needs, pointsor related issuesLack of insight demonstratedFailure to describe any learning issuesInsufficient details of change describedInadequate action takenInappropriate action takenChange discussed, but failed to take necessaryactionFailure to discuss or take action
Table IV.Summary examples offeedback issues providedby reviewers toparticipants
CGIJ14,3
206
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)
Bef
ore
Aft
er
Au
dit
kn
owle
dg
eor
skil
lM
ean
gro
up
scor
eS
DM
ean
gro
up
scor
eS
DM
ean
gro
up
dif
fere
nce
95p
erce
nt
con
fid
ence
inte
rval
(CI)
t-te
stp-
val
ue
Ch
oosi
ng
ato
pic
for
aud
it2.
761.
034.
150.
491.
451.
06to
1.84
7.85
,0.
001
Defi
nin
gau
dit
crit
eria
tob
em
easu
red
2.45
1.00
4.05
0.51
1.6
1.22
to1.
988.
72,
0.00
1S
etti
ng
stan
dar
ds
for
aud
it2.
351.
094.
000.
651.
651.
16to
2.14
7.10
,0.
001
Pre
par
ing
and
pla
nn
ing
anau
dit
pro
ject
2.45
1.15
4.10
0.55
1.65
1.19
to2.
117.
47,
0.00
1C
olle
ctin
gan
dan
aly
sin
gau
dit
dat
a2.
551.
194.
000.
561.
450.
94to
1.96
5.90
,0.
001
Ab
ilit
yto
lead
the
imp
lem
enta
tion
ofch
ang
eas
are
sult
ofau
dit
2.80
1.20
4.20
0.62
1.40
0.93
to1.
876.
29,
0.00
1P
rep
arin
ga
wri
tten
aud
itre
por
t2.
401.
054.
100.
551.
701.
24to
2.16
7.77
,0.
001
Ov
eral
lun
der
stan
din
gof
the
aud
itcy
cle
2.70
1.30
4.35
0.59
1.65
1.08
to2.
226.
02,
0.00
1
Note:
Rat
ing
Sca
le1
to5,
wh
ere
1¼
No
kn
owle
dg
eto
5¼
Hig
hly
kn
owle
dg
eab
le
Table V.Estimation of audit
knowledge and skillsbefore and after study
(n ¼ 20)
Clinical auditperformance
207
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)
Bef
ore
Aft
er
Sta
tem
ent
Mea
ng
rou
psc
ore
SD
Mea
ng
rou
psc
ore
SD
Mea
ng
rou
pd
iffe
ren
ce95
per
cen
tco
nfi
den
cein
terv
al(C
I)p-
test
p-v
alu
e
Iu
nd
erst
and
wh
atco
nst
itu
tes
a“s
ign
ifica
nt
even
t”2.
911.
134.
640.
601.
731.
36to
2.17
8.90
,0.
001
Iu
nd
erst
and
how
toan
aly
sea
sig
nifi
can
tev
ent
2.76
1.17
4.27
0.67
1.51
1.16
to1.
958.
02,
0.00
1I
amco
nfi
den
tab
out
lead
ing
the
team
inu
nd
erta
kin
ga
sig
nifi
can
tev
ent
anal
ysi
s2.
521.
374.
180.
981.
661.
31to
2.16
8.34
,0.
001
Ik
now
how
top
rep
are
aw
ritt
enS
EA
rep
ort
2.64
1.32
4.42
0.66
1.78
1.35
to2.
248.
21,
0.00
1S
EA
can
imp
rov
eth
eq
ual
ity
and
safe
tyof
hea
lth
care
3.75
1.16
4.61
0.61
0.86
0.52
to1.
244.
93,
0.00
1S
EA
shou
ldb
eco
mp
uls
ory
asp
art
ofh
ealt
hca
rep
ract
ice
3.56
1.39
4.21
0.82
0.65
0.32
to0.
954.
08,
0.00
1
Note:
Rat
ing
scal
e1
to5,
wh
ere
1¼
Str
ong
lyd
isag
ree
to5¼
Str
ong
lyag
ree
Table VI.Levels of agreement withstatements aboutperceived knowledge andskills related tosignificant event analysisbefore and after study(n ¼ 34)
CGIJ14,3
208
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)

Health care professional Comment
Community physiotherapist (B) “SEA is an excellent form of CPD activity. A formalreport of this with external feedback is appropriateevidence for my portfolio . . . Physiotherapy staffshould be exposed to this . . . ”
General practice nurse (A) “I totally agree that audits and SEA should be anintegral part of our professional practice. However,management have to be supportive in allocation oftime and resources . . . ”
Practice manager (B) “I found the whole process very rewarding and I amglad I took part. External peer review is very usefulas it is completely unbiased with no personal feelingtowards the person doing the work”
General practice nurse (C) “One of the main aspects I have learned from thisprogramme – TIME – staff need protected time”
Community physiotherapist (D) “A relatively new experience that was bothchallenging and rewarding. Peer review was focusedand relevant. I will continue to submit reports of anySEAs in future”
Practice manager (E) “I enjoyed completing the audit as I had noexperience. The information was very useful and Ihave used the skills gained to complete audits for theQuality Practice Award that we are workingtowards. Overall I found it very beneficial for mydevelopment”
Table VIII.Selected comments from
participants on theirstudy experiences and
attitudes towards clinicalaudit methods and the
feedback model
Statement Mean score SD
I fully understand the concept of educational reviewand feedback 4.12 0.65It is a good idea to get external, independent feedbackon improving aspects of my work 4.64 0.57I was apprehensive about having my SEA reportcritically reviewed 3.59 1.22I don’t believe external peer review of audit is feasiblein the workplace 1.89 0.93External peer review of audit should be more widelyused in health care 4.19 0.83I found the feedback I received to be educationallyusefulAudit (n ¼ 20) 4.52 0.51SEA 4.44 0.51I would submit examples for review and feedback inthe futureAudit (n ¼ 20) 3.96 0.95SEA 4.26 0.86
Note: Rating scale 1 to 5, where 1 ¼ Strongly disagree to 5 ¼ Strongly agree
Table VII.Post-study levels of
agreement withattitudinal statements
about independent reviewby trained colleagues
(n ¼ 34)
Clinical auditperformance
209
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)

was largely successful in meeting its aim. However it is unclear if this approach isfeasible on a long-term basis without sustainable investment from relevant educationaldecision-makers.
A minority of potential study participants was unable to participate – even withinthe timeframe outlined – citing familiar well-documented barriers which confirms thatengagement in audit activity may never be a feasible proposition for some individualsin the current climate. Additionally, a lack of expertise in audit method is oftenreported as an obstacle by many healthcare professionals, with limited exposure toeducation and training a major contributory factor (Johnston et al., 2000). The findingssuggest that lack of expertise and experience was also a factor for many participantsprior to the study. Although many may also believe that they understand audit theory,we know that they can fail to grasp the range of leadership, technical and otherprofessional attributes necessary to undertake successful, completed audit projects(Johnston et al., 2000; Bowie et al., 2007). From a medical perspective, independent anddevelopmental feedback from trained colleagues has been beneficial in highlightingrelevant learning needs and providing informed guidance (McKay et al., in press a).Evidence from this study indicates that this may also be true with other health careprofessionals.
The general feedback provided to study participants not unsurprisingly replicatedthat previously reported for medical practitioners submitting both criterion audit(Bowie et al., 2007) and SEA reports (Bowie et al., 2005a) for peer review. However,while acknowledging the small study size there was a clear decrease in the volume andextent of learning and change issues raised by reviewers compared to those studiesinvolving medical practitioners. A mitigating factor may be that study participantshad a clear advantage as they were exposed to targeted education and training in bothaudit techniques prior to the study, while most doctors would have submitted withoutsuch formal and focused training.
The majority of study participants were highly experienced in terms of theiraverage length of service both as career professionals and in their current posts. Yet, interms of engagement with and exposure to the different stages of audit methods therewas wide variation in experience. Many lacked leadership experience of audit andSEA, and writing-up related reports. This perhaps reflects the lack of claritysurrounding the specific audit expectations for individual clinicians. For example, it isunclear whether “undertaking clinical audit” means taking on a project leadership roleand assuming responsibility for report authorship. Or is adopting a less active (orpassive) contributory role sufficient evidence of engagement in clinical audit? Theambiguities contained in various policy documents (Scottish Executive, 1998;Department of Health, 2006) and the lack of systems to verify engagement andperformance arguably hinder progress and thus contribute to the continued mixedfortunes of audit as an effective quality improvement method.
CPD is now a mandatory expectation of regulatory bodies for the majority ofprofessional disciplines in the UK. From this perspective, we would suggest that thevery act of submitting an audit or SEA report by a healthcare professional as part ofthe model confers either a level of confidence in their ability or potential insight intotheir educational need in these areas. But more importantly, the direct alignment of theclinical audit process with this type of CPD approach offers a multitude of potentialbenefits to the healthcare system. For the participant, it informs professional
CGIJ14,3
210
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)

performance and provides external recognition of workplace experiential learning. Forthe patient, it enhances the quality and safety of those aspects of healthcare that areunder scrutiny. For the NHS organisation, it has a potential clinical governancefunction in facilitating engagement in audit through the CPD route and in qualityassuring performance. Finally for the policymaker and professional regulator, it addsvalue and contributes to the robustness of CPD systems through the provision ofexternal, independent and objective evidence of performance (Department of Health,2006).
If clinical audit is to be taken seriously and clinicians are to be fully engaged, thenpolicymakers will need to co-ordinate and revitalise the efforts of a range ofstakeholders including health care regulators, medical colleges, professionalassociations, patients’ representatives, health authorities and higher educationinstitutions. The chief medical officer in England has called for a “reinvigoration” ofclinical audit (Department of Health, 2006) to ensure that it “takes its rightful place” ininfluencing NHS policy in the same way research and education already contributes.Medical appraisal, particularly in general practice in NHS Scotland (Scottish Executiveet al., 2003), has focused on providing evidence of competence in clinical audit methodsas a core professional activity, which is a start in demonstrating across the boardengagement. Other clinical professions should view this approach as one way ofimproving audit engagement and assuring knowledge of a defined approach.
It is clear overall that quality improvement education and training at undergraduateand postgraduate levels, and as part of continuing professional development, shouldhave a much greater and integrated focus in all healthcare professions. A morestrategic approach to aligning audit with clinical education is necessary and we need torethink how this can be realistically achieved. A long-term educational strategy will bepivotal to equipping clinicians with the necessary skills and professional attributes toallow them to engage in the process knowledgably and with confidence. However, thiswill take political will and serious time, commitment and resources, but it has thepotential to pay dividends. For example, the summative assessment of GPs’ auditprojects as part of vocational training provided evidence of clinicians’ ability to planand execute a completed cycle of effective audit in a pressurised workplaceenvironment and in time-limited circumstances (Campbell et al., 1993).
Study limitations and strengthsThe study numbers are small so the findings must be viewed in this context.Participants were volunteers and are not representative of their professions. Thefindings are likely to be biased because of the self-selected study population, whopotentially perceived value in participation. The motivations of those who did notparticipate were not investigated. It will be necessary to explore experiences andimpact of the model with larger groups of health care professionals once peer networksare better established. The use of a questionnaire to assess pre- and post-interventionratings of knowledge, skills and attitudes is limited because responses are self-reportedand cannot be verified. Similarly, we assumed that participants took the lead role indirecting and reporting the audit projects in conjunction with their healthcare teams,but how this was conducted in practice may have varied. Improvements in the qualityand safety of care reported by participants were not independently verified.
Clinical auditperformance
211
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)

GP reviewers evaluated the audit materials of some other professional groups,which may have been further enhanced if done by true peers. The reviewers’judgments and the feedback provided were done so using the methods outlined, butother approaches may have led to alternative conclusions. However, a key strength ofthe model is that it has been designed by practitioners for practitioners to developrather than criticise individual audit performance. Indeed, peer reviewers perceive theirrole to be a privileged and highly important professional duty.
Practical implicationsIf this model is to become more widely accepted, its practical use in the context ofsupporting professional appraisal and the clinical governance agendas of NHSorganisations must be further explored. The evidence for the feedback model in termsof its validity, acceptability and educational impact is growing (McKay et al., in press a,b) and there have been calls for it to be aligned with the GP appraisal system inScotland as one means of adding value to this process (Murie et al., in press). However,a justified limitation is whether it is “feasible” on a larger scale and on amulti-professional basis in terms of the cost implications and organisationalcommitment required.
From a health service perspective, we would suggest that setting up regionalmulti-professional peer networks and providing a minimum of training is not an overlyonerous or expensive task, given the potential rewards for CPD and the quality ofhealth care. Clinical governance leadership may be a key factor in developing this typeof initiative and providing sustainable support locally. Existing resources – such asclinical governance support staff – could arguably be targeted more effectively as theymay have a valuable role to play in managing and contributing to such an educationalmodel alongside peer networks. There is evidence that their clinical audit assessmentsas part of the feedback model are comparable with established peer reviewers (Bowieet al., 2008b), which may not be surprising because of their specialist experience inadvising healthcare professionals in these matters. A further strategy would be toutilise the experience of trained professional peers from established networks to“champion” the educational value of participation locally within both the service andtheir own professional associations, which may have a major influence from a CPDperspective.
ConclusionClinical audit attempts by healthcare professionals are often unchecked and ineffectivewhich may lead to non-engagement and missed opportunities to improve the qualityand safety of patient care. This small study adds further evidence of the potential valueof independent feedback by trained reviewers in quality assuring the audit process,validating good practice and providing guidance for improvement, where necessary.Given the overall evidence base for clinical audit, NHS organisations and policymakersshould consider exploring how engagement in this activity can be linked more directlywith CPD obligations as one way of ensuring participation and verifying the quality ofperformance.
CGIJ14,3
212
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)
References
Bowie, P., Pope, L. and Lough, M. (2008a), “A review of the current evidence base for significantevent analysis”, Journal of Evaluation in Clinical Practice, Vol. 14 No. 4, pp. 520-36.
Bowie, P., McCoy, S., McKay, J. and Lough, M. (2005a), “Learning issues raised by the peerreview of significant event analyses in general practice”, Quality in Primary Care, Vol. 13No. 2, pp. 75-84.
Bowie, P., McKay, J., Dalgetty, E. and Lough, J.R.M. (2005b), “A qualitative study of why generalpractitioners may participate in significant event analysis and educational peerassessment”, Quality & Safety in Health Care, Vol. 14 No. 3, pp. 185-9.
Bowie, P., McKay, J., Murray, L. and Lough, M. (2008b), “Judging the quality of clinical audit bygeneral practitioners: a pilot study comparing the educational assessments of medicalpeers and NHS audit specialists”, Journal of Evaluation in Clinical Practice, Vol. 14 No. 6,pp. 1038-43.
Bowie, P., Cooke, S., Lo, P., McKay, J. and Lough, M. (2007), “The assessment of criterion auditcycles by external peer review – when is an audit not an audit?”, Journal of Evaluation inClinical Practice, Vol. 13 No. 2, pp. 352-7.
British Dental Association (2007), “Continuing professional development”, available at: www.bda.org/education/education.cfm?ContentID¼307 (accessed 12 December 2007).
Campbell, L.M., Howie, J.G.R. and Murray, T.S. (1993), “Summative assessment: a pilot project inthe west of Scotland”, British Journal of General Practice, Vol. 43 No. 375, pp. 430-4.
Chartered Society of Physiotherapy (2003), Continuing Professional Development (CPD) Briefingand Policy Statement, CSP, London.
Chur-Hansen, A. and Koopowitz, L.F. (2005), “Formative feedback in teaching undergraduatepsychiatry”, Academic Psychiatry, Vol. 29 No. 1, pp. 66-8.
Davies, H., Powell, A. and Rushmer, R. (2006), Healthcare Professionals’ Views on ClinicianEngagement in Quality Improvement: A Literature Review, The Health Foundation,London.
Department of Health (2006), Good Doctors, Safer Patients: Proposals to Strengthen the System toAssure and Improve the Performance of Doctors and to Protect the Safety of Patients.A Report by the Chief Medical Officer, Department of Health, London.
Healthcare Commission (2007), “Developing the annual health check 2008/09 – have your say”,available at: www.healthcarecommission.org.uk/publicationslibrary.cfm?fde_id¼491(accessed 5 February 2009).
Johnston, G., Crombie, I.K., Alder, E.M., Davies, H.T.O. and Millard, A. (2000), “Reviewing audit:barriers and facilitating factors for effective clinical audit”, Quality in Health Care, Vol. 9No. 1, pp. 23-36.
Lough, J.R.M., McKay, J. and Murray, T.S. (1995), “Audit and summative assessment:a criterion-referenced marking schedule”, British Journal of General Practice, Vol. 45No. 400, pp. 607-9.
McGregor, J., Bowie, P. and McKay, J. (2005), “A pilot study of the feasibility of trainee hospitaldoctors undertaking significant event analysis”, British Journal of Hospital Medicine,Vol. 66 No. 9, pp. 477-80.
McKay, J., Bowie, P. and Lough, J.R.M. (2006), “Variation in the ability of general medicalpractitioners to apply two methods of clinical audit: a 5-year study of assessment by peerreview”, Journal of Evaluation in Clinical Practice, Vol. 12 No. 6, pp. 622-9.
Clinical auditperformance
213
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)

McKay, J., Pope, L., Bowie, P. and Lough, M. (in press a), “External feedback in general practice:a focus group study of trained peer reviewers of significant event analyses”, Journal ofEvaluation in Clinical Practice.
McKay, J., Shepherd, A., Bowie, P. and Lough, M. (in press b), “The acceptability and educationalimpact of a peer feedback model for significant event analysis in general practice”, MedicalEducation.
McKay, J., Murphy, D., Bowie, P., Schmuck, M.-L., Lough, M. and Eva, K.W. (2007),“Development and testing of an assessment instrument for the formative peer review ofsignificant event analyses”, Quality and Safety in Health Care, Vol. 16 No. 2, pp. 150-3.
McLaren, S., Woods, L., Boudioni, M., Lemma, F., Rees, S. and Broadbent, J. (2007), “Developingthe general practice manager role: managers’ experiences of engagement in continuingprofessional development”, Quality in Primary Care, Vol. 15 No. 2, pp. 85-91.
Miles, A., Bentley, P., Polychronis, A., Price, N. and Grey, J. (1996), “Clinical audit in the NationalHealth Service: fact or fiction?”, Journal of Evaluation in Clinical Practice, Vol. 2 No. 1,pp. 29-35.
Murie, J., McCrae, J. and Bowie, P. (in press), “The peer review pilot project: a potential system tosupport GP appraisal in NHS Scotland”, Education for Primary Care.
National Institute for Clinical Excellence (2002), Principles for Best Practice in Clinical Audit,Radcliffe Medical Press, Oxford.
National Patient Safety Agency (2005), Seven Steps to Patient Safety for Primary Care, NPSA,London.
Royal College of Nursing (2003), Nursing Education: A Statement of Principles, RCN, London.
Scottish Executive, NHS Education for Scotland, RCGP (Scotland) and BMA (Scotland) (2003),GP Appraisal: A Brief Guide, Scottish Executive, Edinburgh.
Scottish Office Department of Health (1998), Clinical Governance, MEL 75, Scottish Office,Edinburgh.
Further reading
Royal Pharmaceutical Society of Great Britain (2007), “Continuing professional development”,available at: www.rpsgb.org.uk/registrationandsupport/continuingprofessionaldevelopment/ (accessed 12 December 2007).
Corresponding authorPaul Bowie can be contacted at: [email protected]
CGIJ14,3
214
To purchase reprints of this article please e-mail: [email protected] visit our web site for further details: www.emeraldinsight.com/reprints
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)

This article has been cited by:
1. Carol Fawkes, Elena Ward, Dawn Carnes. 2014. Clinical audit in osteopathic practice: A Masterclass.International Journal of Osteopathic Medicine 17, 110-118. [CrossRef]
2. Kay Donnellon, Grace Hurford, Diane L. Cox. 2013. It's good to talk: auditing clinicians' interactions withpatients in a primary care setting. Clinical Governance: An International Journal 18:3, 220-227. [Abstract][Full Text] [PDF]
Dow
nloa
ded
by N
HS
ED
UC
AT
ION
FO
R S
CO
TL
AN
D A
t 04:
28 2
7 A
pril
2015
(PT
)