feasibility of a day-camp model of modified constraint-induced movement therapy with and without...
TRANSCRIPT

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [Karolinska Institute Library]On: 1 September 2009Access details: Access Details: [subscription number 909766720]Publisher Informa HealthcareInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Physical & Occupational Therapy In PediatricsPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t792304027
Feasibility of a Day-Camp Model of Modified Constraint-Induced MovementTherapy With and Without Botulinum Toxin A Injection for Children WithHemiplegiaAnn-Christin Eliasson ab; Karin Shaw b; Eva Pontén c; Roslyn Boyd de; Lena Krumlinde-Sundholm a
a Department of Woman and Child Health, Astrid Lindgren Children's Hospital, Karolinska Institute,Stockholm, Sweden b Habilitation Services for Children and Youth, Stockholm, Sweden c Department ofPediatric Orthopedic Surgery, Astrid Lindgren Children's Hospital, Karolinska Institute, Stockholm, Sweden d
Brain Research Institute, Melbourne, Australia e Queensland Cerebral Palsy and Rehabilitation ResearchCentre, School of Medicine, University of Queensland, Brisbane, Australia
Online Publication Date: 01 August 2009
To cite this Article Eliasson, Ann-Christin, Shaw, Karin, Pontén, Eva, Boyd, Roslyn and Krumlinde-Sundholm, Lena(2009)'Feasibility ofa Day-Camp Model of Modified Constraint-Induced Movement Therapy With and Without Botulinum Toxin A Injection for ChildrenWith Hemiplegia',Physical & Occupational Therapy In Pediatrics,29:3,311 — 333
To link to this Article: DOI: 10.1080/01942630903011123
URL: http://dx.doi.org/10.1080/01942630903011123
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

Feasibility of a Day-Camp Model ofModified Constraint-Induced Movement
Therapy With and Without Botulinum ToxinA Injection for Children With Hemiplegia
Ann-Christin EliassonKarin ShawEva Ponten
Roslyn BoydLena Krumlinde-Sundholm
Ann-Christin Eliasson, PhD, is a registered occupational therapist and a professorat the Department of Woman and Child Health, Astrid Lindgren Children’s Hospital,Karolinska Institute, at the Habilitation Services for Children and Youth, Stockholm,Sweden.
Karin Shaw, MSc, is a registered physical therapist working with the HabilitationServices for Children and Youth, Stockholm, Sweden.
Eva Ponten, PhD, MD, is a specialist in hand surgery and orthopedic surgery workingwith the Department of Pediatric Orthopedic Surgery, Astrid Lindgren Children’s Hospital,Karolinska Institute, Stockholm, Sweden.
Roslyn Boyd, PhD, is a registered physical therapist associated with the Brain ResearchInstitute, Melbourne, and an associate professor in the Queensland Cerebral Palsy andRehabilitation Research Centre, School of Medicine, at the University of Queensland,Brisbane, Australia.
Lena Krumlinde-Sundholm, PhD, is a registered occupational therapist at the Depart-ment of Woman and Child Health, Astrid Lindgren Children’s Hospital, Karolinska Insti-tute, Stockholm, Sweden.
The authors wish to express their gratitude to the participants at the day camp as wellas their camp colleagues, Beatrice Bonnier, Asa Karlsson, Karin Nyhlen, Annika Pahlen,Magnus Hansson, Sara Jonsson, and Barry Shaw, who made this project possible. Theywould also like to thank Frida Sandberg for collecting all the data and Brian Hoare forscoring all the videos. Finally they would like to acknowledge the Stockholm HabilitationService research unit, Stiftelsen Sunnerdahls Handikappfond, Norrback-Eugeniastiftelsen,the Swedish Research Council and Stockholm County Council, the Center for Health CareSciences, National Health and Medical Research Council (NHMRC) Career Developmentfellowship, and the Queensland Smart State award (Australia) for supporting this research.
Address correspondence to: Ann-Christin Eliasson, Neuropediatric Research UnitQ2:07, Astrid Lindgren Children’s Hospital, SE-171 76 Stockholm, Sweden (e-mail:[email protected]).
Physical & Occupational Therapy in Pediatrics, Vol. 29(3), 2009Available online at http://www.informaworld.com/POTP
C© 2009 by Informa Healthcare USA, Inc. All rights reserved.doi: 10.1080/01942630903011123 311
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009
312 PHYSICAL & OCCUPATIONAL THERAPY IN PEDIATRICS
ABSTRACT. The objective of the study was to investigate the feasi-bility of modified constraint-induced (CI) therapy provided in a 2-weekday-camp model with and without intramuscular botulinum toxin type A(BoNT-A) injections for children with congenital cerebral palsy. Sixteenchildren with congenital hemiplegia, Manual Ability Classification Sys-tem (MACS) level I and II, aged 8–17 years, participated in a CI therapyday camp; of whom five participants (aged 11–16 years) received in-tramuscular BoNT-A prior to CI therapy. Assessments were conducted4 months and 2 weeks before (baselines 1 and 2), immediately after,and 6 months after the day camp. For the children who received BoNT-A, no statistical analyses were conducted due to the small size of thesample. In this group, consistent improvement was only found accord-ing to the Melbourne Unilateral Limb Assessment. The children whoreceived only the CI therapy demonstrated improvements in the Jebsen–Taylor Hand Function Test (p = .04) at posttest, but improvementswere not sustained at 6-month follow-up. No significant improvementwas obtained for the Melbourne Assessment or the Assisting Hand As-sessment. Children in both groups improved on specially trained tasks:frisbee golf, stacking blocks, and in-hand manipulation. Feedback fromthe participants suggests that the day-camp model is a feasible inter-vention following intramuscular BoNT-A injections. The results suggestthat children with congenital hemiplegia with varying severity of im-pairment in hand function may benefit from CI therapy, but not everychild demonstrates improvements in hand function. The characteristicsof children who respond the best to CI therapy are not clear.
KEYWORDS. Botulinum toxin A, constraint-induced movement ther-apy, group therapy, hand function, hemiplegia, upper extremity
Constraint-induced (CI) movement therapy has gained attention as anintervention for children with congenital hemiplegia. Despite its promise,the evidence concerning the effects is tentative at best (Charles & Gordon,2005; Hoare, Wasiak, Imms, & Carey, 2007). It is difficult to compare theresults between studies, as there are considerable variations in the methodsand modes of delivery of interventions as well as the outcome measuresused (Charles & Gordon, 2005). One challenge has been the developmentof a child-oriented approach, and different methods have been described(Bonnier, Eliasson, & Krumlinde-Sundholm, 2006; Eliasson, Krumlinde-Sundholm, Shaw, & Wang, 2005; Gordon, Charles, & Wolf, 2005). Another
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009
Eliasson et al. 313
intervention for children with congenital hemiplegia is intramuscular in-jections of botulinum toxin type A (BoNT-A), which aims to diminishmuscle overactivity (Corry, Cosgrove, Walsh, McClean, & Graham, 1997)and improve the quality of movement when combined with various mod-els of upper-limb training (Fehlings, Rang, Glazier, & Steele, 2000). Asystematic review concluded that there is uncertainty in the results (Park& Rha, 2006). Some studies indicated positive results of BoNT-A withusual training and care (Fehlings et al., 2000; Lowe, Novak, & Cusick,2006), but no additional benefits over upper-limb training alone have beenreported for others (Speth, Leffers, Janssen-Potten, & Vles, 2005; Wallen,O’Flaherty, & Waugh, 2007). No studies have examined intensive trainingafter BoNT-A injection; at most training was provided three times a weekfor 12 weeks (Speth et al., 2005). The protocols commonly included dif-ferent aspects of occupational therapy in addition to specifically targetinghand training. The effectiveness of CI therapy of high intensity followingintramuscular injections of BoNT-A has not been examined.
A modified CI training paradigm, developed and used in our earlier stud-ies and in clinical practice in the Stockholm region, has been enjoyed bythe participants, and many have shown significant and sustained improve-ments in hand function (Bonnier et al., 2006; Eliasson et al., 2005). Thekey ingredient in the “Stockholm paradigm” was restraining the dominanthand by a stiff glove to elicit intensive use and training of the impairedhand. Furthermore, the content and structure of the training was developedto make it enjoyable and motivating and was adapted to the ability levelsof individual children within the group, giving numerous opportunitiesfor repetitive practice (Bonnier et al., 2006; Eliasson et al., 2005; Gordonet al., 2005). The training focused on hand use, practiced by performingcomplete tasks and motivating activities. Participants were encouraged todiscover various strategies for solving tasks requiring different types ofhand use (Skold, Josephsson, & Eliasson, 2004). The training was basedon knowledge generated from the motor learning and motor control lit-erature and also from knowledge of characteristics of the impaired hand(Eliasson, 2006; Haugen & Mathiowetz, 1989; Smith & Wrisberg, 2001).This training paradigm is somewhat different from the CI therapy describedby Taub and colleagues, in which specific components or part practice ofmovements are practiced by using shaping techniques (Gordon et al., 2005;Taub et al., 1994).
An issue of concern for intervention studies is the selection of assess-ments for optimal understanding and interpretation of the results. Inter-ventions need to be evaluated from a broad perspective, and more impor-tantly there is a need to measure the elements targeted in the intervention
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009
314 PHYSICAL & OCCUPATIONAL THERAPY IN PEDIATRICS
(Majnemer & Mazer, 2004). Few assessments of hand function, however,are validated for individuals with hemiplegic cerebral palsy with adequatereliability and demonstrated responsiveness to change. The wide variationof assessments that have been used in research might be because of thelack of suitable assessments or consensus on what is important to measure(Charles & Gordon, 2005).
Results from studies indicate that speed, force control, coordination,and dexterity are components of hand use that may improve following CItherapy (Charles & Gordon, 2005; Hoare et al., 2007; Taub et al., 2007).Typically there is a relationship between skillful hand use and speed ofperformance, demonstrated for example by age-related norms from upper-limb scales like the Bruininks–Oseretsky Test of Motor Proficiency (Bru-ininks & Bruininks, 2006). Even though children with cerebral palsy donot follow typical development, the relation between skilled performanceand speed of performance seems relevant so that a timed test would beuseful.
Another important issue is whether there is a transfer effect from uni-lateral training (in CI therapy) to bimanual performance, which would bethe hoped-for outcome for participants with hemiplegia. For BoNT-A in-tervention the aims are to weaken relatively overactive muscles (agonists)so that the relatively weaker antagonists can act more normally on thejoints. Botulinum toxin also reduces the spasticity in the injected muscles.Accordingly, muscle tone, quality of movements, grip strength, and speedare important to measure (Park & Rha, 2006; Reeuwijk, van Schie, Becher,& Kwakkel, 2006).
Our previous day-camp model of CI therapy for adolescents with con-genital hemiplegia was successful in that the participants gained improvedhand function; however, the sample was small (n = 9) (Bonnier et al.,2006). The purpose of this study was first to investigate if a day-campmodel of CI therapy is a feasible intervention in children and adolescentswith congenital hemiplegia after intramuscular BoNT-A injections andsecond whether the results of our previous study (Bonnier et al., 2006)could be replicated.
METHOD
Design
This study used a prospective design with two baselines with 4 monthsbetween assessments, posttreatment assessment, and a 6-month follow-up.
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009

Eliasson et al. 315
Recruitment of Participants
Written invitations to attend a day camp with CI therapy were distributedto potential participants in the Stockholm City County through their ther-apists. The target participants were persons with congenital hemiplegia,aged 8–18 years and attending mainstream schools, with reduced handfunction but able to grasp and lift a 500-g bottle with the impaired hand,to ensure a minimal level of grasping ability and strength. Families ofchildren suitable and interested in intramuscular injections of BoNT-A asa complementary treatment to CI therapy were referred to an experiencedhand surgeon for decisions about suitability. The final decision of groupassignment was based on the family’s wishes and the professional judg-ments of the most suitable treatment (Rosenbaum, 2004). The groups werethose of (a) participants who were suitable and willing to combine intra-muscular BoNT-A injections with CI therapy (CI therapy and BoNT-Agroup) and (b) participants only interested in the day camp (CI therapygroup). Informed consent was obtained from all participating families, andthe study was conducted after approval from the research ethics committeeat the Karolinska University Hospital in accordance with ethical standardsof human experimentation and with the Helsinki Declaration of 1975 asrevised in 1983.
Participants
Sixteen participants with congenital hemiplegia of functional levels I andII of Manual Ability Classification System (MACS; Eliasson et al., 2006),aged 8–17 years, were entered (Table 1). Based on parental preferencechildren were entered into the following groups:
(a) CI therapy and BoNT-A group: Five participants were suitable forbeing injected and willing to be injected with intramuscular BoNT-A(Botox©R , Allergan, Inc., Irvine, CA) 2 weeks prior to CI therapy.
(b) CI therapy group: Eleven participants were included in the group re-ceiving CI therapy alone. Participant demographics are reported forboth groups in Table 1.
Measures
The Jebsen–Taylor Hand Function Test (JTHFT) was used to measuredexterity using the six timed (in seconds) subtests with the writing test
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009

316 PHYSICAL & OCCUPATIONAL THERAPY IN PEDIATRICS
TABLE 1. Characteristics of Children With Hemiplegia, Ordered From theMildest to the Severest Hand Function Based on the Jebsen–Taylor HandFunction Test
Subject Gender Age Side First Baseline (s) Strength (N) Sensibilitya MACS
CI therapy group1 F 16 L 49 155 Good 12 M 12 R 108 38 Good 23 M 12 R 111 44 Decreased 24 M 17 R 146 111 Poor 25 M 10 R 162 24 Decreased 26 M 11 R 165 58 Good 27b M 8 L 182 72 Good 28c F 10 R 235 22 Good 29 M 13 L 341 44 Good 2
10 F 8 L 604 12 Poor 211 M 12 R 693 15 Poor 2
BoNT-A and CI therapy group12 F 13 R 179 35 Poor 213b F 16 R 189 77 Good 214c M 14 L 201 101 Good 215 M 11 R 226 54 Good 216c F 15 L 715 36 Poor 2
aSee the Method section for explanation.bDid not participate in 6-month follow-up.cHave had surgery more than 2 years ago.
excluded (Taylor, Sand, & Jebsen, 1973). If a subtest was not completedwithin 2 min a score of 120 s was assigned on that subtest (Gordon, Charles,& Wolf, 2006). Maximal time was consequently limited to 720 s for eachindividual. The test–retest data of the JTHFT is fairly strong (Taylor et al.,1973).
The Melbourne Unilateral Upper Limb Assessment (Melbourne Assess-ment) is a standardized test for children, aged 5–15 years, with neurologicalimpairment (Randall, Carlin, Chondros, & Reddihough, 2001). It measuresquality of movement related to reach, grasp, release, and manipulation in16 tasks. The test is video recorded, and the raw score sum is converted toa percentage scale (1–100). The test is validated for children with cerebralpalsy with strong intra- and inter-rater reliability as well as with test–retestvalidity (Randall et al., 2001)
The Assisting Hand Assessment (AHA) is a standardized test for chil-dren with unilateral upper-limb impairments, which measures the ef-fectiveness with which a child makes use of his/her impaired hand in
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009
Eliasson et al. 317
bimanual activities (Krumlinde-Sundholm & Eliasson, 2003). The AHAis designed and validated for children with unilateral impairment, betweenthe ages of 18 months and 12 years. Its intra- and inter-rater reliability isstrong (Holmefur, Krumlinde-Sundholm, & Eliasson, 2007; Krumlinde-Sundholm, Holmefur, Kottorp, & Eliasson, 2007). For participants over 12years of age, an adolescent version of the test was used. The AHA is scoredfrom video with 22 items rated on a 4-point scale, resulting in a 22–88 rawscore range; the higher the score, the higher the child’s performance.
Grip strength was measured using the electronic measuring device Grip-pit and recorded in N (Nordenskiold & Grimby, 1993). The instrument isvalidated for use with children, and there are norms for Swedish children(Hager-Ross & Rosblad, 2002).
The two-point discrimination test (2PD) was used to measure sensibil-ity (Krumlinde-Sundholm & Eliasson, 2002). Sensibility was consideredgood when 2PD was possible at 3 mm, reduced if 7 mm of spacing wasdiscriminated, and poor when it was not possible to discriminate 7 mmspacing.
The in-hand manipulation task (Exner, 2001) involves moving a penlinearly (from the point to the top of the pen) along the pads of the fingers(pen shift task). The task was practiced for approximately 5 min each dayduring the day camp. Through the use of video analysis, the shift task wasscored from 0 to 8 (0 = no transfer of the pen, 8 = translation in bothdirections) (Bonnier et al., 2006).
Frisbee golf is a game in which the goal is to traverse a 350-foot longcourse, ending with the frisbee in a basket in the fewest number of throws(Bonnier et al., 2006). Each consecutive throw is made from where thefrisbee comes to rest after the last throw. On the first and last days ofthe camp the total number of throws needed to complete the course wasrecorded. The participants practiced frisbee golf on five occasions duringthe day camp.
The ability to stack blocks in towers was assessed on the first and lastdays of the camp and measured as the total height in cm. The task waspracticed for 10 min a day. Any form of construction was allowed whilepracticing, but the measured height was only legitimate for towers built insingle file with wooden blocks (with sides of 3 cm).
Procedure
The assessments were conducted by an occupational therapist not in-volved in the day camp. Another independent occupational therapist,
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009
318 PHYSICAL & OCCUPATIONAL THERAPY IN PEDIATRICS
not aware of the order of assessments and treatment groups, scored theparticipants’ performance on the video-based assessments. The assess-ment for the first baseline occurred 4 months before the day camp. Thesecond, preintervention baseline assessment was performed 2 weeks be-fore the day camp commenced. The third, postintervention assessment wasperformed the week after the day camp ended, and the fourth assessmentwas performed 6 months later, i.e., at follow-up. Measures of the in-handmanipulation task, frisbee golf, and stacking blocks were only performedat the second baseline and directly after the day camp.
BoNT-A Injection
The five children receiving BoNT-A were injected after the secondbaseline assessment, 2 weeks prior to the day camp. This ensured that thepeak effect of the BoNT-A injection had been reached before entering thecamp. The 4-month baseline period thus served as a pretreatment controlperiod.
Dosage of BoNT-A was calculated on the basis of body weight, andselection of injected muscles was determined by observation of the par-ticipant’s individual motor patterns in functional tasks (Table 2). Targetmuscles for injections (diluted to 100 U Botox/ml normal saline) werelocated using an EMG amplifier and muscle stimulator. A total dose of2–4 U/kg body weight was given. The muscles were injected through thesame insulated 27-gauge needle (Allergan) that was used for the elec-trical stimulation to locate the target muscle. Topical dermal anesthetic(EMLA©R ) combined with nitrous oxide inhalation or midazolam was usedto minimize pain due to the injections.
Day Camp
The duration of the day camp was 7 hr per day, over 9 days, for a 2-week summer period (total 63 hr). The camp was held in a favorable openrecreational area and was conducted by occupational therapists, physicaltherapists, and volunteers. The training program primarily consisted ofdaily recreational activities of interest to the participants. Each participantwas given a restraining glove to be worn on the unimpaired dominant hand.The glove prevented finger flexion and fine manipulation but enabled grosshand movements and stabilizing for bimanual gross grasp. The day-campmodel was a replication of our earlier day camp (Bonnier et al., 2006; Elias-son, Bonnier, & Krumlinde-Sundholm, 2003). Activities were specifically
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009

Eliasson et al. 319
TABLE 2. Muscles Injected With BoNT-A and Change in Grip Strength
Grip Strength (N)
Subject Indication Injection Baseline 2 Posttreatment
12 Diminished thumb abductionduring initiation of grip.Impaired supination.
AddP, FPB, PQ 50 67
13 Volar flexion of wrist during grip.Impaired supination.
FCU, FCR, PT, PQ 97 78
14 Volar flexion of wrist and flexionof thumb during initiation ofgrip. Adduction and internalrotation of shoulder.
FCU, FPB,subscapularis
91 102
15 Volar flexion of wrist andadduction of thumb duringinitiation of grip. Difficulty inextending fingers andrelease. Impaired supination.Diminished reaching capacity.
FCU, FCR, FDP, AddP,PQ, biceps
45 36
16 Flexed thumb and fingers flexedin MCP, extended in PIP andDIP during initiation of grip.Upper arm adducted tothorax.
FPB, opponens,interosseus muscles,AddP, TM, pectoralis
28 30
Note: AddP = adductor pollicis, FPB = flexor pollicis brevis, PT = pronator teres, PQ = pronator quadratus,FCU = flexor carpi ulnaris, FCR = flexor carpi radialis, FDP = flexor digitorum profundus, TM = teres major,MCP = metacarpophalangeal joint, PIP = proximal interphalangeal joint, DIP = distal interphalangeal joint.
selected to include both gross motor function of the upper extremity andhand manipulation tasks. Examples of gross motor activities are playingfrisbee golf, basketball, boule, and water games. Specific fine-motor boardgames and dice and card games were incorporated into daily activities.Furthermore, participants engaged in activities of daily living such as thepreparation of meals, eating, and washing of dishes. The program includedchallenging activities that require use of both hands such as rock climbingand canoeing. During these tasks the glove was not used.
Overall, the attendance in the modified training program was good;the participants were engaged in the training and completed the expectedtasks. Following completion of the day camp, all participants were askedfive open questions about their perceptions of the day camp in a paperquestionnaire: The questions were as follows: What was the best? Whatwas the most important? What was the hardest? Which activity was the
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009
320 PHYSICAL & OCCUPATIONAL THERAPY IN PEDIATRICS
most boring? Which activity was the most fun? Participants recorded theirresponses anonymously.
Data Analysis
The data were not normally distributed; therefore, nonparametric statis-tics were used. The median and 25–75 percentiles were computed for eachstandardized measure. For the CI therapy group (n = 11) the overall effectwas calculated by the Friedman ANOVA, and the Wilcoxon matched-pairtest was used to measure the difference between scores at different as-sessment times. To assess whether the treatment effect was related to theseverity of the impairment in hand use as measured by the JTHFT, anapproach suggested by Kirkwood and Sterne (2003) was used. The corre-lation between the effect of treatment (pretreatment score on the JTHFTminus posttreatment score on the JTHFT) and the average of pre- andposttreatment measures (the sum of pretreatment and posttreatment scoreson the JTHFT divided by two) were calculated. The level of statisticalsignificance was set at p < .05. For the CI therapy and BoNT-A group,individual results and medians are reported due to the small number ofparticipants (n = 5). No comparisons between groups were made.
RESULTS
The median and 25–75 percentiles for each standardized measure ateach of the four assessments are reported by group in Table 3. Data weremissing for two participants, one from each group, at 6-month follow-up(Table 1).
Children Who Received CI Therapy and BoNT-A
Standardized Measures
As only five participants received BoNT-A prior to CI therapy, no groupcomparisons could be made, and individual results are reported. Two ofthe five participants improved on the JTHFT (lower time score) directly af-ter the day camp. The scores were sustained results at 6-month follow-up(Figure 1a). All five participants had improved in the quality of move-ment on the Melbourne Assessment immediately posttraining; however,the effect was not sustained at 6-month follow-up (Figure 2a and Table 3).
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009

TAB
LE3.
Res
ults
ofS
tand
ardi
zed
Mea
sure
sfo
rC
hild
ren
Rec
eivi
ngC
IThe
rapy
and
Chi
ldre
nR
ecei
ving
Bot
hC
IThe
rapy
and
BoN
T-A
.Med
ian
and
25–7
5P
erce
ntile
sA
reR
epor
ted
CIT
hera
py,n
=11
CIT
hera
pyan
dB
oNT-
A,n
=5
Fol
low
-Up,
Fol
low
-Up,
Test
Bas
elin
e1
Bas
elin
e2
Pos
tinte
rven
tion
n=
10B
asel
ine
1B
asel
ine
2P
ostin
terv
entio
nn
=4
Jebs
en(s
)16
5(1
11–3
41)
160
(113
–287
)10
9(7
8–26
0)a,
b14
2(8
4–32
2)ac
220
1(1
89–2
26)
145
(123
–209
)12
2(1
12–1
36)
122
(100
–129
)M
elbo
urne
(%)
77(6
3–84
)77
(65–
86)
78(6
4–86
80(6
5–87
)77
(55–
81)
76(5
7–82
)81
(65–
85)
72(5
8–85
)A
HA
(raw
scor
e)60
(52–
62)
60(5
4–62
)60
(57–
63)
58(5
4–60
)58
(50–
62)
59(5
3–62
)57
(52–
62)
57.5
(52.
5–61
.5)
Grip
stre
ngth
(N)
44(2
4–72
)38
(21–
82)
40(2
4–84
)42
(25–
76)
54(4
0–78
)50
(45–
91)
67(3
6–78
)52
(44–
89.5
)
ap
<.0
5.bT
heW
ilcox
onm
atch
ed-p
air
test
was
calc
ulat
edbe
twee
nba
selin
e2
and
post
inte
rven
tion.
c Cal
cula
ted
betw
een
base
line
1an
dfo
llow
-up.
321
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009

322 PHYSICAL & OCCUPATIONAL THERAPY IN PEDIATRICS
FIGURE 1. Dexterity measured in seconds by the JTHFT in the involved handobtained on four occasions: two baseline assessments before intervention,postintervention and at 6-month follow-up. Individual data for (a) individualchildren who received both CI therapy and BoNT-A (n = 5) and (b) the CItherapy group alone (n = 11; n = 10 at 6-month follow-up). The thick dottedline represents the median results.
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009

Eliasson et al. 323
FIGURE 2. Quality of movements as measured by the Melbourne UnilateralUpper Limb Assessment on four occasions: two baseline assessments beforeintervention, after intervention and at 6-month follow-up. Individual data for (a)individual children who received both CI therapy and BoNT-A (n = 5, with oneparticipant missing at 6-month follow-up) and (b) the CI therapy group alone(n = 11; n = 10 at 6-month follow-up). The thick dotted line represents themedian results.
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009
324 PHYSICAL & OCCUPATIONAL THERAPY IN PEDIATRICS
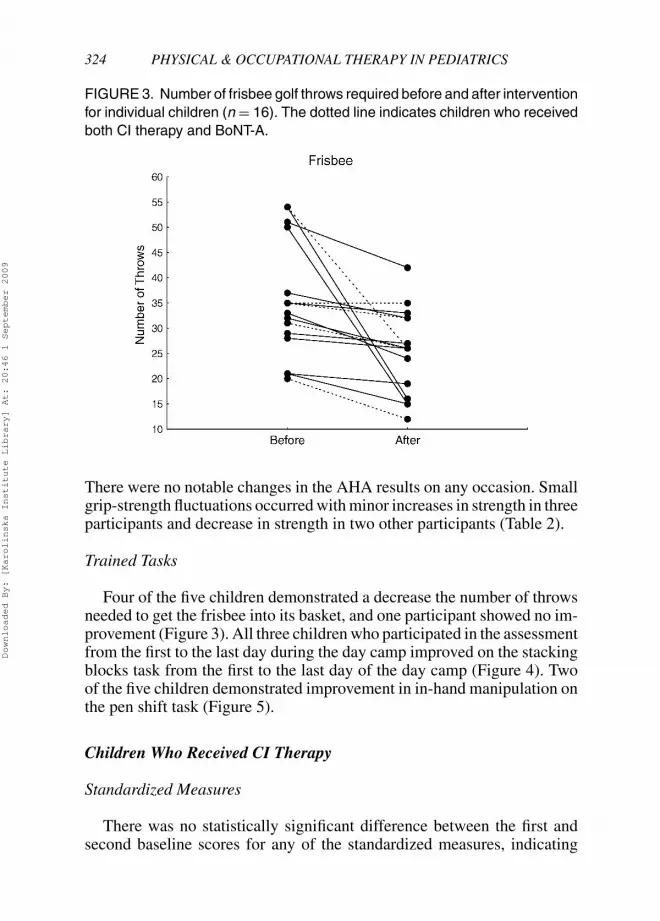
FIGURE 3. Number of frisbee golf throws required before and after interventionfor individual children (n = 16). The dotted line indicates children who receivedboth CI therapy and BoNT-A.
There were no notable changes in the AHA results on any occasion. Smallgrip-strength fluctuations occurred with minor increases in strength in threeparticipants and decrease in strength in two other participants (Table 2).
Trained Tasks
Four of the five children demonstrated a decrease the number of throwsneeded to get the frisbee into its basket, and one participant showed no im-provement (Figure 3). All three children who participated in the assessmentfrom the first to the last day during the day camp improved on the stackingblocks task from the first to the last day of the day camp (Figure 4). Twoof the five children demonstrated improvement in in-hand manipulation onthe pen shift task (Figure 5).
Children Who Received CI Therapy
Standardized Measures
There was no statistically significant difference between the first andsecond baseline scores for any of the standardized measures, indicating
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009

Eliasson et al. 325
FIGURE 4. Height in cm of stacked blocks obtained before and after inter-vention for individual children (n = 14). The dotted lines indicate children whoreceived both CI therapy and BoNT-A.
FIGURE 5. Score for in-hand manipulation, i.e, vertical pen transition alongthe fingers before and after the intervention (n = 16). The dotted lines indicatechildren who received both CI therapy and BoNT-A.
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009
326 PHYSICAL & OCCUPATIONAL THERAPY IN PEDIATRICS
the stability of performance in the control period (no training). The chil-dren demonstrated a significant improvement in speed and dexterity onthe JTHFT (overall effect chi-square = 8.93, p = .03) with a decreasein the median time from 160 to 109 s between the pre- and postcampassessments (p = .04). Wilcoxon matched-pair analysis indicated that theimprovements were not sustained at 6-month follow-up (p = .95) (Figure1b and Table 3).
The children did not demonstrate an improvement in quality of move-ment on the Melbourne Assessment (overall effect chi-square = 0.23, p =.9; Figure 2a and Table 3). There were no changes in bimanual perfor-mance on the AHA (overall effect chi-square = 4.48, p = .21) or the taskmeasuring grip strength (p = .2; Table 3).
The correlation between severity of impairment in hand use (using themean of pretest and posttest of the JTHFT) and improvement on the JTHFT(difference between pre- and postintervention; see the Method section)was r = 0.04. The correlation indicates that the participant’s severity ofimpairment in hand use was not related to change in hand use followingintervention.
Trained Tasks
Children who received CI therapy demonstrated significant improve-ments in the specifically practiced tasks. In frisbee golf, the number ofthrows needed to get the frisbee into the basket decreased from the firstday of camp to the last day of camp from a median of 33 throws to 26throws (p = .003; Figure 3). Stacking blocks as high as possible also im-proved from a median of 27 cm to 43 cm (p = .005) from the first to thelast day of the day camp (Figure 4). In-hand manipulation increased froma median of 2 points to 3 points postintervention (p = .02; Figure 5).
Participants’ Experience of the Day Camp
Overall, the participants enjoyed the camp. They reported that the bestthing about the day camp was meeting new friends with the same problemsas themselves; the feeling of not being alone with this type of disability wascommonly mentioned. Several participants reported conflicting feelings,saying that the training was both the most important and the most difficultissue. Typically, they had not expected that wearing the glove would be asdifficult as it turned out to be. Several participants reported that it was “fun”or very encouraging to recognize the improvement, for example, whenplaying frisbee golf. One child reported that not noticing any improvement
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009
Eliasson et al. 327
during the camp was tough for her. The activities reported to be the mostfun were rock climbing, building and climbing on crates, and water games.When asking about the most boring activities several participants answeredthat they could not come up with anything, whereas others mentioned thatthe structured hand training including the in-hand manipulation task wasboring. Once a day, there was a group discussion in which the participantscould discuss the training and how they felt about it. This conversationwas mentioned as important, with some participants emphasizing that itwas both important and very hard to talk about themselves. Although thetraining was mentioned as important, it was the whole concept includingthe environment for the day camp—friends and activities—which madethis event important for the participants.
DISCUSSION
All participants could successfully participate in the modified CI ther-apy day-camp program. There was no difference in the carrying through,engagement, or participation between the training activities for the par-ticipants with or without BoNT-A. The main results from the CI therapyalone group support the results from the previous day camp organized ina similar way (Bonnier et al., 2006; Eliasson et al., 2003), demonstratingimproved speed of performance and improvements in specifically trainedtasks. In the participants who also received injections of BoNT-A, a consis-tent change was only found oi the Melbourne Assessment. Children whoreceived only the CI therapy, however, did not demonstrate changes in theMelbourne Assessment.
To our knowledge, this is the first report of the combination of intramus-cular BoNT-A injections followed by intensive training. The results variedamong the five children. The only outcome in which a trend was seen thatcould be related to effects from BoNT-A was in the Melbourne Assess-ment. All five participants demonstrated improved quality of movementsdirectly after the day camp, but the effect was not sustained at the 6-monthfollow-up, a result probably related to the transitory effects of BoNT-A.Decreased grip strength after BoNT-A has been reported (Fehlings et al.,2000) but did not occur in this study. Children demonstrated almost nochange in grip strength, and no evidence of fatigue was reported. The find-ing that the children who received BoNT-A injections could complete thetraining sessions is encouraging.
The improvements in speed and dexterity measured by the JTHFT sup-port the outcomes previously reported (Bonnier et al., 2006; Charles,
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009

328 PHYSICAL & OCCUPATIONAL THERAPY IN PEDIATRICS
Wolf, Schneider, & Gordon, 2006; Gordon et al., 2006). In our study,however, none of the children in the CI therapy group sustained the im-provements at the 6-month follow-up. Among the 14 participants avail-able for follow-up, 9 had improved JTHFT scores compared to beforethe day camp (baseline 2). As illustrated in Figure 1, the performanceof participants both with and without BoNT-A varied considerably. Thishighlights the question that which children with congenital hemiplegia aremost likely to benefit from CI therapy? Unfortunately, the combination ofBoNT-A and CI therapy does not, so far, provide any new insights into thisquestion.
The findings suggest that children with a wide spectrum of hand usemay benefit from CI therapy. The participants in this study had moresevere limitations on hand function than the participants in the first daycamp (Bonnier et al., 2006; Eliasson et al., 2003). The median time toperform the JTHFT before the day camp was 160 s compared with 72 sin the previous study (Bonnier et al., 2006; Eliasson et al., 2003). Time toperform the JTHFT improved 32% among children in this study, comparedwith a 31% improvement in our previous study (Eliasson et al., 2003). Ourperspective is also supported by Gordon and coauthors, who reported aJTHFT baseline above 240 s and significant and sustained improvements(Charles et al., 2006; Gordon et al., 2006).
There was no transfer of the improvement from one-handed training tobimanual performance as measured by the AHA. The AHA has previouslydemonstrated responsiveness to change following a longer treatment periodof CI therapy in younger children (Eliasson et al., 2005). It is possible thata 2-week unimanually oriented treatment duration is too brief to changethe habitual use of the hands in bimanual activities or that changes inbimanual function are harder to achieve in this sample of older individuals.The AHA has been used in a study with an intensive, 2-week bimanualtreatment approach (hand–arm bimanual intensive therapy or HABIT) inwhich improvements in bimanual functioning were demonstrated (Gordonet al., 2007). Further studies are needed to evaluate which treatments leadto improved bimanual performance, probably the most important aspect ofhand function in people with unilateral disabilities.
In contrast to the varying results of the standardized assessments, most ofthe children demonstrated improvement in the specifically practiced tasks(mostly novel tasks) of in-hand manipulation, throwing the frisbee, andstacking blocks. Individuals receiving BoNT-A improved within the samerange as children who received only CI therapy. This finding emphasizes thepremise “You learn what you practice” as suggested in the outcome of ourearlier day camp (Bonnier et al., 2006). It also suggests that improvements
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009

Eliasson et al. 329
in hand use were quite specific, and transfer effects to a more generallyimproved hand function as measured by the different standardized tests arenot obvious.
Appraisal of Measures
Our proposal that BoNT-A might change other aspects of hand functionthan CI therapy alone was supported, because it was just the BoNT-Agroup that demonstrated changes in quality of movements as measuredwith the Melbourne Assessment. This assessment has been used in BoNT-Astudies (Boyd, 2004; Speth et al., 2005; Wallen et al., 2007) but not forevaluation of CI therapy, which suggests that other investigators share ourassumption that this instrument may be sensitive to changes related toeffects of BoNT-A. Testing speed with a timed test such as the JTHFT isrecommended as a general measure of (unilateral) hand capacity, whichis addressed in CI therapy. Baseline measures however varied, suggestingthat stability is a potential issue for children with congenital hemiplegia.The most functionally important aspect of hand function in people withunilateral impairments is probably the ability to perform daily activities,which mostly involve bimanual performance. In this study children did notdemonstrate change in the AHA; nevertheless we recommend includingbimanual function as an outcome.
Limitations
To investigate the feasibility of the CI therapy in combination withBoNT-A, we invited families with children potentially suitable for the in-tramuscular BoNT-A treatment and interested in CI therapy. The numberof potential participants interested in receiving injections of BoNT-A waslower than expected. The parents were given the opportunity to decidethe treatment methods after being informed by experts about suitable op-tions for their children. Most families and children were interested in justattending the CI therapy program. This resulted in the major limitationof this study: uneven numbers of participants in the two groups and thelow numbers in the BoNT-A group, which made statistical comparisonsimpossible.
The two-baseline prospective design aimed to examine stability overtime when no change was expected and to serve as a pretreatment controlperiod. The fluctuation in baseline indicates that a single subject designwith repeated baseline measurements is preferable. The data from the
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009

330 PHYSICAL & OCCUPATIONAL THERAPY IN PEDIATRICS
first and second baseline for the JTHFT were not stable and unexpected,because the test has been the primary outcome measure in several studies(Bonnier et al., 2006; Charles, Lavinder, & Gordon, 2001; Charles et al.,2006; Gordon et al., 2006). We did not expect changed performance on theJTHFT in a 4-month period for this age group. From clinical experience weknow that assessments measuring speed may be difficult to use in peoplewith varying muscle tone. Clearly, the JTHFT needs further investigationof both stability and sensitivity for change in persons with cerebral palsy.
Implication for Practice
The results suggest that children and adolescents with congenital hemi-plegia with varying impairment of the hand may benefit from CI therapy,but not every child demonstrates improvements in hand function. The prin-cipal features of the best responders to CI therapy are not clear. However, itseems important to ensure that the training is intensive, with the duration ofthe program long enough and the content carefully selected so as to engagethe participants. It is an enormous challenge for the participants in termsof effort and time; so the families and participants have to be preparedand well motivated for the program. Day camps may provide social andpersonal benefits for participants such as meeting new friends and learninga lot about themselves and their disability.
Declaration of interest: The authors report no conflicts of interest. Theauthors alone are responsible for the content and writing of the paper.
REFERENCES
Bonnier, B., Eliasson, A. C., & Krumlinde-Sundholm, L. (2006). Effects of constraint-induced movement therapy in adolescents with hemiplegic cerebral palsy: A daycamp model. Scandinavian Journal of Occupational Therapy, 13, 13–22.
Boyd, R. N. (2004). Central and peripheral effects of botulinum toxin A in childrenwith cerebral palsy. Australia: La Trobe University.
Bruininks, R., & Bruininks, B. (2006). Bruininks–Oseretsky Test of Motor Proficiency:Second edition. Minneapolis, MN: Pearson Education.
Charles, J., & Gordon, A. M. (2005). A critical review of constraint-induced movementtherapy and forced use in children with hemiplegia. Neural Plasticity, 12, 245–261.
Charles, J., Lavinder, G., & Gordon, A. M. (2001). Effects of constraint-inducedtherapy on hand function in children with hemiplegic cerebral palsy. PediatricPhysical Therapy, 13, 68–76.
Charles, J. R., Wolf, S. L., Schneider, J. A., & Gordon, A. M. (2006). Efficacy of achild-friendly form of constraint-induced movement therapy in hemiplegic cerebral
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009
Eliasson et al. 331
palsy: A randomized control trial. Developmental Medicine and Child Neurology,48, 635–642.
Corry, I. S., Cosgrove, A. P., Walsh, E. G., McClean, D., & Graham, H. K. (1997).Botulinum toxin A in the hemiplegic upper limb: A double-blind trial. Develop-mental Medicine and Child Neurology, 39, 185–193.
Eliasson, A. C. (2006). Sensorimotor integration of normal and impaired developmentof precision movement of the hand. In A. Henderson & C. Pehoski (Eds.), Handfunction in the child: Foundations for remediation (2nd ed., pp. 45–62). Mosby.
Eliasson, A. C., Bonnier, B., & Krumlinde-Sundholm, L. (2003). Clinical experienceof constraint induced movement therapy in adolescents with hemiplegic cerebralpalsy — a day camp model. Developmental Medicine and Child Neurology, 45,357–359.
Eliasson, A. C., Krumlinde-Sundholm, L., Shaw, K., & Wang, C. (2005). Effects ofconstraint-induced movement therapy in young children with hemiplegic cerebralpalsy: An adapted model. Developmental Medicine and Child Neurology, 47, 266–275.
Eliasson, A. C., Krumlinde-Sundholm, L., Rosblad, B., Beckung, E., Arner, M.,Ohrvall, A. M., & Rosenbaum, P. (2006). The Manual Ability Classification Sys-tem (MACS) for children with cerebral palsy: Scale development and evidence ofvalidity and reliability. Developmental Medicine and Child Neurology, 48, 549–554.
Exner, C. E. (2001). Development of hand skills. In J. Case-smith (Ed.), Occupationaltherapy for children (4th ed., pp. 289–328). St. Louis, MO.: Mosby.
Fehlings, D., Rang, M., Glazier, J., & Steele, C. (2000). An evaluation of botulinum-Atoxin injections to improve upper extremity function in children with hemiplegiccerebral palsy. Journal of Pediatrics, 137, 331–337.
Gordon, A. M., Charles, J., & Wolf, S. L. (2005). Methods of constraint-inducedmovement therapy for children with hemiplegic cerebral palsy: Development ofa child-friendly intervention for improving upper-extremity function. Archives ofPhysical Medicine and Rehabilitation, 86, 837–844.
Gordon, A. M., Charles, J., & Wolf, S. L. (2006). Efficacy of constraint-inducedmovement therapy on involved upper-extremity use in children with hemiplegiccerebral palsy is not age-dependent. Pediatrics, 117, e363–e373.
Gordon, A. M., Schneider, J. A., Chinnan, A., & Charles, J. R. (2007). Efficacy of ahand-arm bimanual intensive therapy (HABIT) in children with hemiplegic cerebralpalsy: A randomized control trial. Developmental Medicine and Child Neurology,49(11), 830–838.
Hager-Ross, C., & Rosblad, B. (2002). Norms for grip strength in children aged 4–16years. Acta Paediatrica, 91, 617–625.
Haugen, J. B., & Mathiowetz, V. (1989). Contemporary task-oriented approach.In C. Trombly (Ed.), Occupational therapy for physical dysfunction (pp. 510–527). Philadelphia: Lippincott, Williams, and Wilkins.
Hoare, B. J., Wasiak, J., Imms, C., & Carey, L. (2007). Constraint-induced movementtherapy in the treatment of the upper limb in children with hemiplegic cerebralpalsy. The Cochrane Database of Systematic Reviews, (2): Art No. CD004149.
Holmefur, M., Krumlinde-Sundholm, L., & Eliasson, A. C. (2007). Interrater andintrarater reliability of the Assisting Hand Assessment. The American Journal ofOccupational Therapy, 61, 79–84.
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009

332 PHYSICAL & OCCUPATIONAL THERAPY IN PEDIATRICS
Kirkwood, B. R., & Sterne, J. A. C. (2003). Essential medical statistics. Oxford, UK:Blackwell Science.
Krumlinde-Sundholm, L., & Eliasson, A. C. (2002). Comparing tests of tactile sensi-bility: Aspects relevant to testing children with spastic hemiplegia. DevelopmentalMedicine and Child Neurology, 44, 604–612.
Krumlinde-Sundholm, L., & Eliasson, A. C. (2003). Development of the AssistingHand Assessment: A Rasch-built measure intended for children with unilateralupper limb impairments. Scandinavian Journal of Occupational Therapy, 10, 16–26.
Krumlinde-Sundholm, L., Holmefur, M., Kottorp, A., & Eliasson, A. C. (2007). TheAssisting Hand Assessment: Current evidence of validity, reliability, and respon-siveness to change. Developmental Medicine and Child Neurology, 49, 259–264.
Lowe, K., Novak, I., & Cusick, A. (2006). Low-dose/high-concentration localizedbotulinum toxin A improves upper limb movement and function in children withhemiplegic cerebral palsy. Developmental Medicine and Child Neurology, 48, 170–175.
Majnemer, A., & Mazer, B. (2004). New directions in the outcome evaluation ofchildren with cerebral palsy. Seminars in Pediatric Neurology, 11, 11–17.
Nordenskiold, U., & Grimby, G. (1993). Grip force in patients with rheumatoid arthritisand fibromyalgia and in healthy subjects: A study with the grippit instrument.Scandinavian Journal of Rheumatology, 22, 14–19.
Park, E. S., & Rha, D. W. (2006). Botulinum toxin type A injection for managementof upper limb spasticity in children with cerebral palsy: A literature review. YonseiMedical Journal, 47, 589–603.
Randall, M., Carlin, J. B., Chondros, P., & Reddihough, D. (2001). Reliability of theMelbourne assessment of unilateral upper limb function. Developmental Medicineand Child Neurology, 43, 761–767.
Reeuwijk, A., van Schie, P. E. M., Becher, J. G., & Kwakkel, G. (2006). Effects ofbotulinum toxin type A on upper limb function in children with cerebral palsy: Asystematic review. Clinical Rehabilitation, 20, 375–387.
Rosenbaum, P. (2004). Families and service providers forging effective connectionsand why it matters. In D. Scrutton, D. Damiano, & M. Mayston (Eds.), Clinicsin developmental medicine 161: Management of motor disorders of children withcerebral palsy (pp. 22–31). London: Mac Keith.
Skold, A., Josephsson, S., & Eliasson, A. C. (2004). Performing bimanual activities:The experiences of young persons with hemiplegic cerebral palsy. The AmericanJournal of Occupational Therapy, 58, 416–425.
Smith, R. A., & Wrisberg, C. A. (2001). Motor learning and performance: A problem-based learning approach (2nd ed.). Champaign, IL: Human Kinetics.
Speth, L. A. W. M., Leffers, P., Janssen-Potten, Y. J. M., & Vles, J. S. H. (2005).Botulinum toxin A and upper limb functional skills in hemiparetic cerebral palsy:A randomized trial in children receiving intensive therapy. Developmental Medicineand Child Neurology, 47, 468–473.
Taub, E., Crago, J. E., Burgio, L. D., Groomes, T. E., Cook, E. W., III, DeLuca,S. C., et al. (1994). An operant approach to rehabilitation medicine: Overcominglearned nonuse by shaping. Journal of the Experimental Analysis of Behaviour, 61,281–293.
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009

Eliasson et al. 333
Taub, E., Griffin, A., Nick, J., Gammons, K., Uswatte, G., & Law, C. R. (2007). Pe-diatric CI therapy for stroke-induced hemiparesis in young children. DevelomentalNeurorehabilitation, 10, 3–18.
Taylor, N., Sand, P. L., & Jebsen, R. H. (1973). Evaluation of hand function in children.Archives of Physical Medical and Rehabilitation, 54, 129–135.
Wallen, M., O’Flaherty, S. J., & Waugh, M. C. (2007). Functional outcomes of intra-muscular botulinum toxin type A and occupational therapy in the upper limbs ofchildren with cerebral palsy: A randomized controlled trial. Archives of PhysicalMedicine and Rehabilitation, 88, 1–10.
Downloaded By: [Karolinska Institute Library] At: 20:46 1 September 2009