expanding use of botulinum toxin
TRANSCRIPT
www.elsevier.com/locate/jns
Journal of the Neurological S
Review
Expanding use of botulinum toxin
Roongroj Bhidayasiri a,b,c, Daniel D. Truong c,*
aDepartment of Neurology, UCLA Medical Center, David Geffen School of Medicine at UCLA, Los Angeles, CA 90095, USAbMovement Disorders Group, Division of Neurology, Chulalongkorn University Hospital, Bangkok, Thailand
cThe Parkinson’s and Movement Disorder Institute, 9940 Talbert Ave, Fountain Valley, CA 92708, USA
Received 26 July 2004; received in revised form 14 April 2005; accepted 18 April 2005
Available online 28 June 2005
Abstract
Botulinum toxin type A (BTX-A) is best known to neurologists as a treatment for neuromuscular conditions such as dystonias and
spasticity and has recently been publicized for the management of facial wrinkles. The property that makes botulinum toxin type A useful for
these various conditions is the inhibition of acetylcholine release at the neuromuscular junction. Although botulinum toxin types A and B
(BTX-A and BTX-B) continue to find new uses in neuromuscular conditions involving the somatic nervous system, it has also been
recognized that the effects of these medications are not confined to cholinergic neurons at the neuromuscular junction. Acceptors for BTX-A
and BTX-B are also found on autonomic nerve terminals, where they inhibit acetylcholine release at glands and smooth muscle. This
observation led to trials of botulinum neurotoxins in various conditions involving autonomic innervation. The article reviews the emerging
use of botulinum neurotoxins in these and selected other conditions, including sialorrhea, primary focal hyperhidrosis, pathological pain and
primary headache disorders that may be of interest to neurologists and related specialists.
D 2005 Elsevier B.V. All rights reserved.
Keywords: Botulinum toxin; Sialorrhea; Drooling; Hyperhidrosis; Pathological pain; Headache
Contents
. . . . . . . 1
. . . . . . . 2
. . . . . . . 3
. . . . . . . 5
. . . . . . . 5
. . . . . . . 6
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2. Sialorrhea . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3. Primary focal hyperhidrosis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4. Conditions of pathological pain. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4.1. Headache disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4.2. Musculoskeletal pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . 6Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
1. Introduction
Botulinum toxin type A (BTX-A) is best known to
neurologists as a treatment for neuromuscular conditions
0022-510X/$ - see front matter D 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.jns.2005.04.017
* Corresponding author. Tel.: +1 714 378 5062; fax: +1 714 378 5061.
E-mail address: [email protected] (D.D. Truong).
such as dystonias and spasticity and has recently been
publicized for the management of facial wrinkles. The
property that makes botulinum toxin type A useful for these
various conditions is the inhibition of acetylcholine release
at the neuromuscular junction [1]. The efficacy of BTX-A
without systemic side effects has led to the rapid develop-
ment of its application in various conditions in addition to
ciences 235 (2005) 1 – 9

R. Bhidayasiri, D.D. Truong / Journal of the Neurological Sciences 235 (2005) 1–92
dystonia and spasticity, including hypersecretory disorders,
tics, tremor, stuttering, different pain syndromes, detrusor
sphincter dyssynergia or overactivity and gastrointestinal
smooth muscle/sphincter spasms [2–5]. Following local
injection into muscles, the toxin enters the nerve terminal
via endocytosis, interacts with intracellular proteins
(SNARE proteins) and inhibits the vesicular release of the
acetylcholine (Ach) neurotransmitter at the neuromuscular
junction [1,6]. Inhibition of Ach produces chemical dener-
vation and paralysis of the striated muscles. Paralysis
usually peaks 2 weeks after the injection. Because of the
Table 1
Current evidence of botulinum toxin in various disorders with the least
reasonable trial of evidence shown to be at least moderately effective by
BTX-A
(1) Focal dystonias
Blepharospasma
Cervical dystoniaa
Spasmodic dysphonia
Meige syndrome
Writer’s cramp
Foot dystonia
Oromandibular dystonia
Axial dystonia
Occupational cramps
(2) Tremor
Dystonia head tremor
Essential head tremor
Essential hand tremor
Palatal tremor
(3) Hemifacial spasma
(4) Focal spasticity in adults
Lower limb
Upper limb
(5) Focal spasticity in children
Upper limb
Lower limb
(6) Ophthalmic conditions
Strabismusa
Ptosis
(7) Autonomic disorders
Focal hyperhidrosis
Gustatory sweating
Hyperlacrimation
Sialorrhea
(8) Urological disorders
Detrusor sphincter dyssynergia
Hyperreflexive bladder
Vaginismus
(9) Gastrointestinal disorders
Anal fissure
Achalasia
Upper esophageal sphincter
Anismus
(10) Pain
Tension-type headache
Migraine
Low back pain
Chronic daily headache
Myofascial pain
(11) Wrinkles (Glabellar wrinklesa)
a Indicates conditions that have been approved by the United States Food
and Drug Administration; modified from Moore [105].
molecular turnover within the neuromuscular junction and
neuronal sprouting, neuronal activity begins to return at 3
months, with restoration of complete function at approx-
imately 6 months [7].
BTX-A is 1 of 7 botulinum neurotoxin serotypes known
alphabetically as types A to G [8]. Although these toxins
have different intracellular targets, their biological activity at
the neuromuscular junction is similar. Of these serotypes,
only A and B are currently available as commercial
preparations [9]. Types C and F have also been used in
humans, but only on an experimental basis [10,11]. The first
commercial preparation of botulinum neurotoxin to be used
clinically was based on the A serotype (Botox\), and this
product continues to be used in many countries throughout
the world. Another preparation based on the A serotype
(Dysport\) was later introduced in several countries and
may become available in the United States within several
years. In the year 2000, a product based on the B serotype
(Myobloc\/Neurobloc\) became commercially available.
Although all of these formulations inhibit acetylcholine
release, they do so at different doses [7,9,12]. Thus, all of
these products are used clinically at different unit doses that
may vary up to several orders of magnitude [9].
Although botulinum toxin types A and B (BTX-A and
BTX-B) continue to find new uses in neuromuscular
conditions involving the somatic nervous system, it has
also been recognized that the effects of these medications
are not confined to cholinergic neurons at the neuro-
muscular junction [13,14]. Acceptors for BTX-A and
BTX-B are also found on autonomic nerve terminals, where
they inhibit acetylcholine release at glands and smooth
muscle [15]. This observation led to trials of botulinum
neurotoxins in various conditions involving autonomic
innervation [16–18]. The rest of this article considers the
emerging use of botulinum neurotoxins in these and selected
other conditions that may be of interest to neurologists and
related specialists (Table 1).
2. Sialorrhea
Excessive drooling, which occurs in many different
neurological conditions, may pose significant risks of
choking with aspirations and pneumonia and may affect
patients’ social activities and self-image. Up to 20% of
patients with bulbar amyotrophic lateral sclerosis (ALS) and
78% of patients with Parkinson’s disease (PD) manifest this
problem [19]. It is usually caused by swallowing dysfunc-
tion, although primary sialorrhea rarely occurs. The
mechanism of action by which botulinum toxins reduce
saliva production may relate to the inhibition of cholinergic
autonomic parasympathetic and postganglionic sympathetic
acetylcholine release, which innervates the salivary glands.
Over the past few years, BTX-A has been studied for the
treatment of sialorrhea associated with parkinsonism,
cerebral palsy, head and neck carcinoma, neurodegenerative

R. Bhidayasiri, D.D. Truong / Journal of the Neurological Sciences 235 (2005) 1–9 3
diseases, stroke and ALS [20–33]. Although most of the
published literature describes open pilot studies with
relatively small groups of patients, up to two-thirds of the
patients experienced a marked or moderate improvement of
drooling after treatment of both parotid glands or the parotid
and submandibular glands combined, as determined by
patient ratings of drooling severity, objective measurement
of salivary flow by sialometry and weight of dental rolls
(Table 2). More recently, larger scale clinical trials have
been conducted and confirmed with favorable results
[34,35]. Encouraging results of BTX-B in sialorrhea have
recently been reported in two studies involving 25 patients
with parkinsonism [36,37]. Indeed, BTX-B may prove to be
a particularly effective treatment for sialorrhea due to an
apparent predilection for autonomic neurons. Dysphagia and
dry mouth occur more frequently from BTX-B than BTX-A,
probably reflecting preferential blockade of autonomic
neurons [38–40].
Generally, results have been encouraging with the
reported duration of the beneficial response varying from
7 weeks to 7 months. Most of these studies did not report
any significant adverse events with botulinum toxin
injections in the treatment of sialorrhea, except for local
pain, infection, dry mouth, transient dysphagia and weak-
ness of mouth opening and closure [20–24,36,37]. How-
ever, BTX-A was associated with recurrent jaw dislocation
in one patient with ALS [41]. Another study reported
marked deterioration of dysphagia and local infection of the
gland when the toxin was injected transductally in ALS
patients [26]. Most other studies have used ultrasound
guidance to direct injections into the parotid and/or
submandibular glands.
The results of these studies suggest that botulinum
neurotoxin therapy may be useful for the treatment of
sialorrhea, with a low risk of side effects. The highest safe
Table 2
Summary of selected studies on botulinum toxin in sialorrhea (n >5)
Authors Design Technique Number (n), Diagnosis
Botox\
Ellies et al. [21] Open U/S 13, carcinoma, neurodege
Bothwell et al. [32] Open Blind 9, CP
Pal et al. [24] Open Blind 9, PD
Giess et al. [31] Open U/S 5, ALS
Porta et al. [25] Open U/S 10, ALS, PD, CP, SSPE,
Suskind and Tilton [23] Open U/S 22, CP
Jongerius et al. [34] Controlled U/S 45, CP
Dogu et al. [33] Open U/S, Blind 15, PD
Dysport\
Mancini et al. [20] Controlled U/S 20, PD, MSA
Lipp et al. [35] Controlled Blind 32, ALS, PD, CBD, MSA
Myobloc\
Racette et al. [36] Open Blind 9, Parkinsonism
Ondo et al. [37] Controlled Blind 16, PD
U/S: ultrasound; CP: cerebral palsy; PD: Parkinson’s disease; ALS: amyotrophic
atrophy; SSPE: subacute sclerosing panencephalitis.
individual dose is not known and may be very low in some
patients, particularly in patients suffering from ALS, who
may be unusually sensitive to botulinum toxin. The risk can
be minimized by cautiously increasing the dose and the
number of glands treated in subsequent cycle. The positive
results of the open-labeled studies are supported by those of
small, placebo-controlled trials; further larger scale con-
trolled studies would add significantly to the literature.
3. Primary focal hyperhidrosis
Hyperhidrosis refers to excessive sweating and may be
focal or generalized. Focal hyperhidrosis usually affects
palms or soles of the feet (60%), axillae (40%) and the face
(10%) [42]. Rarely, other areas are involved. The majority
of hyperhidrosis studies have been published in dermato-
logic journals, and it is possible that this indication is not
widely recognized in the neurology community. Further-
more, patients with hyperhidrosis may seek treatment from
their general practitioners or dermatologists instead of
neurologists. Focal hyperhidrosis is most often essential or
idiopathic. A positive family history is present in 30–50%
of cases suggesting a genetic component [43]. However, the
scant literature available on the etiology of primary focal
hyperhidrosis suggests that it may be caused by neurogenic
overactivity of the sweat glands in the affected area [44].
Ross syndrome is a rare form of focal hyperhidrosis of
unknown etiology, characterized by progressive anhidrosis
due to degeneration of sudomotor fibers, associated with
compensatory hyperhidrosis in areas in which sudomotor
fibers remain intact [45].
For patients with mild hyperhidrosis, topical antiper-
spirants containing aluminum chloride hexahydrate may be
effective [46]. Anticholinergic agents, such as glycopyrro-
Region Dose per side (U) Duration (months)
nerative, stroke Parotid, SM 50–65 (total) 3
Parotid 5 2
Parotid 7.5–15 2 (approximately)
Parotid 6–20 >3
encephalopathy Parotid, SM 15–40 4–7
Parotid, SM 20–40 N/A
SM 20–25 Up to 6
Parotid 15 2–6
Parotid, SM 450–500 (total) 1
Parotid 18.75–75 3
Parotid 1000 3.5
Parotid, SM 250–1000 >1
lateral sclerosis; CBD: corticobasal degeneration; MSA: multiple system

Fig. 2. Axillary hyperhidrosis before (A) and 2 weeks after (B) botulinum
toxin type A injection in the right axilla.
R. Bhidayasiri, D.D. Truong / Journal of the Neurological Sciences 235 (2005) 1–94
nium bromide or propantheline bromide or beta blockers
can be effective, although their side effects limit the use.
Iontophoresis, or the introduction of an ionized substance
through the skin using direct current, may be effective for
some cases of plantar and palmar hyperhidrosis, but is
less useful in the axillary regions. In addition, it is a time-
consuming procedure in which the hands are soaked in
tap water with an electric current for up to 30 min.
Transthoracic endoscopic sympathectomy can be consid-
ered in severe cases of palmar hyperhidrosis [44] but
wound infection, hemorrhage, pneumothorax, Horner’s
syndrome, brachial plexus injuries, post-sympathetic neu-
ralgia, gustatory sweating and phrenic nerve damage are
among the possible complications. Intradermal injection of
BTX-A has recently been shown to be effective in
patients with gustatory sweating (Frey’s syndrome),
axillary sweating, palmoplantar sweating, or compensatory
sweating [47–49].
The development of botulinum toxin as a treatment of
hyperhidrosis came from the initial observation of hypo- or
anhidrosis in patients with botulism. Although the mech-
anism of action of botulinum toxin in focal hyperhidrosis is
unknown, it is probably different from that in dystonic
disorders. Swartling et al. [50] demonstrated that the sweat
glands were structurally normal before the botulinum toxin
therapy but that the lumen diminished after subsequent
injections, suggesting the mechanism of denervation. In
addition to several small controlled studies, the benefits of
BTX-A on patient quality of life and objective sweating in
primary axillary and palmar hyperhidrosis have been
documented in large-scale, randomized, controlled trials
[47,48,51–64]. These studies mainly involved patients with
moderate to severe hyperhidrosis. Results showed that up
to 94% of patients in the BTX-A group were responders, in
contrast to 36% of patients in the placebo group [51].
Ninety-eight percent of patients with axillary hyperhidrosis
in one multicenter study said that they would recommend
this therapy to others [62]. The duration of action of
botulinum toxin varied between 4 and 12 months with a
mean duration of 7 months after a single treatment session
(Figs. 1 and 2). Frontal hyperhidrosis also responded well
Fig. 1. Palmar hyperhidrosis before (A) and 2 weeks after (B
to the treatment with BTX-A with a reduction in sweating
of 75% for a period of at least 5 months [65]. Long-term
effects were reported, especially in gustatory sweating, and
satisfaction with treatment remained consistently high with
no diminution of effect with repeated treatments [66].
Twenty-eight percent of patients did not require more than
one injection, indicating a long-lasting benefit of more than
16 months in a substantial proportion of patients. The
adverse event that was different between the BTX-A and
placebo groups was infection, which surprisingly had a
higher incidence in the placebo group [51]. Other side
effects, which were minimal, included painful injections
and small local hematomas. Although several studies have
reported beneficial effects of BTX-B in the treatment of
hyperhidrosis, systemic side effects such as visual accom-
modation difficulties and dry mouth, as well as pain at the
injection site, limit its widespread use [40,67–69]. Table 3
provides detailed information from the literature on the
sites of injection, the doses used and the duration of action
after injections of BTX-A for both axillary and palmar
hyperhidrosis.
Overall, the efficacy and safety of BTX-A is established
in the treatment of primary, focal hyperhidrosis based on the
published controlled and open trials, as well as the
regulatory approval of at least one of the type A products
) botulinum toxin type A injection in the right hand.
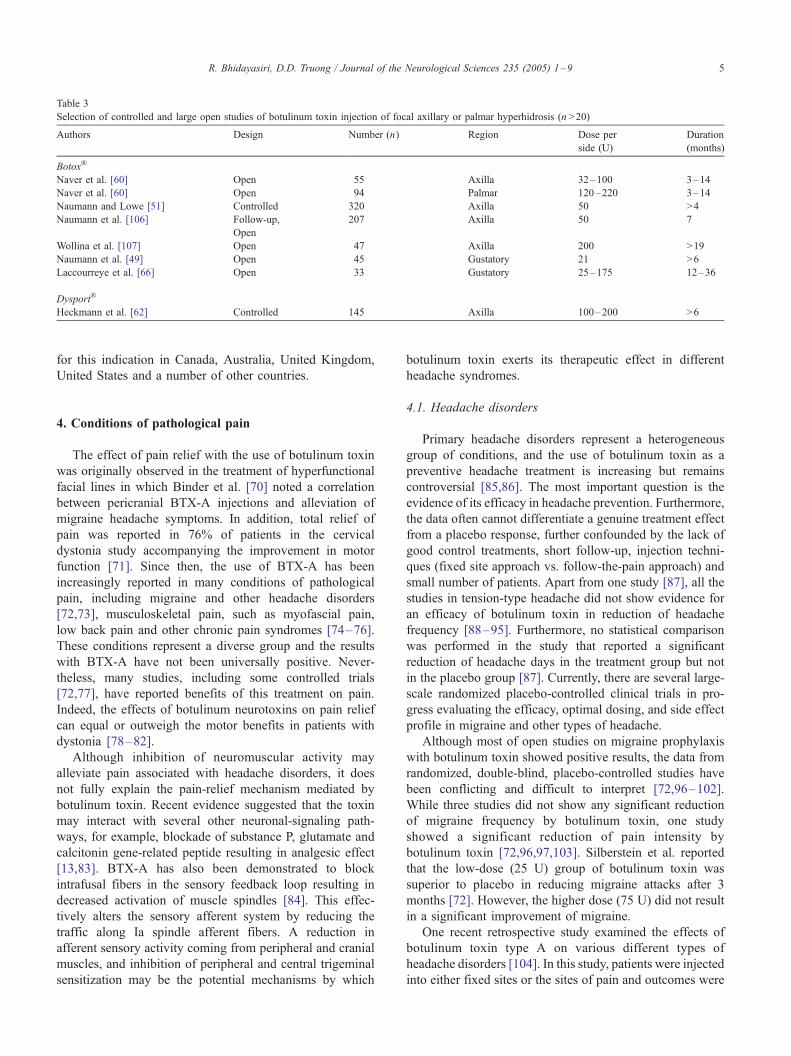
Table 3
Selection of controlled and large open studies of botulinum toxin injection of focal axillary or palmar hyperhidrosis (n >20)
Authors Design Number (n) Region Dose per
side (U)
Duration
(months)
Botox\
Naver et al. [60] Open 55 Axilla 32–100 3–14
Naver et al. [60] Open 94 Palmar 120–220 3–14
Naumann and Lowe [51] Controlled 320 Axilla 50 >4
Naumann et al. [106] Follow-up,
Open
207 Axilla 50 7
Wollina et al. [107] Open 47 Axilla 200 >19
Naumann et al. [49] Open 45 Gustatory 21 >6
Laccourreye et al. [66] Open 33 Gustatory 25–175 12–36
Dysport\
Heckmann et al. [62] Controlled 145 Axilla 100–200 >6
R. Bhidayasiri, D.D. Truong / Journal of the Neurological Sciences 235 (2005) 1–9 5
for this indication in Canada, Australia, United Kingdom,
United States and a number of other countries.
4. Conditions of pathological pain
The effect of pain relief with the use of botulinum toxin
was originally observed in the treatment of hyperfunctional
facial lines in which Binder et al. [70] noted a correlation
between pericranial BTX-A injections and alleviation of
migraine headache symptoms. In addition, total relief of
pain was reported in 76% of patients in the cervical
dystonia study accompanying the improvement in motor
function [71]. Since then, the use of BTX-A has been
increasingly reported in many conditions of pathological
pain, including migraine and other headache disorders
[72,73], musculoskeletal pain, such as myofascial pain,
low back pain and other chronic pain syndromes [74–76].
These conditions represent a diverse group and the results
with BTX-A have not been universally positive. Never-
theless, many studies, including some controlled trials
[72,77], have reported benefits of this treatment on pain.
Indeed, the effects of botulinum neurotoxins on pain relief
can equal or outweigh the motor benefits in patients with
dystonia [78–82].
Although inhibition of neuromuscular activity may
alleviate pain associated with headache disorders, it does
not fully explain the pain-relief mechanism mediated by
botulinum toxin. Recent evidence suggested that the toxin
may interact with several other neuronal-signaling path-
ways, for example, blockade of substance P, glutamate and
calcitonin gene-related peptide resulting in analgesic effect
[13,83]. BTX-A has also been demonstrated to block
intrafusal fibers in the sensory feedback loop resulting in
decreased activation of muscle spindles [84]. This effec-
tively alters the sensory afferent system by reducing the
traffic along Ia spindle afferent fibers. A reduction in
afferent sensory activity coming from peripheral and cranial
muscles, and inhibition of peripheral and central trigeminal
sensitization may be the potential mechanisms by which
botulinum toxin exerts its therapeutic effect in different
headache syndromes.
4.1. Headache disorders
Primary headache disorders represent a heterogeneous
group of conditions, and the use of botulinum toxin as a
preventive headache treatment is increasing but remains
controversial [85,86]. The most important question is the
evidence of its efficacy in headache prevention. Furthermore,
the data often cannot differentiate a genuine treatment effect
from a placebo response, further confounded by the lack of
good control treatments, short follow-up, injection techni-
ques (fixed site approach vs. follow-the-pain approach) and
small number of patients. Apart from one study [87], all the
studies in tension-type headache did not show evidence for
an efficacy of botulinum toxin in reduction of headache
frequency [88–95]. Furthermore, no statistical comparison
was performed in the study that reported a significant
reduction of headache days in the treatment group but not
in the placebo group [87]. Currently, there are several large-
scale randomized placebo-controlled clinical trials in pro-
gress evaluating the efficacy, optimal dosing, and side effect
profile in migraine and other types of headache.
Although most of open studies on migraine prophylaxis
with botulinum toxin showed positive results, the data from
randomized, double-blind, placebo-controlled studies have
been conflicting and difficult to interpret [72,96–102].
While three studies did not show any significant reduction
of migraine frequency by botulinum toxin, one study
showed a significant reduction of pain intensity by
botulinum toxin [72,96,97,103]. Silberstein et al. reported
that the low-dose (25 U) group of botulinum toxin was
superior to placebo in reducing migraine attacks after 3
months [72]. However, the higher dose (75 U) did not result
in a significant improvement of migraine.
One recent retrospective study examined the effects of
botulinum toxin type A on various different types of
headache disorders [104]. In this study, patients were injected
into either fixed sites or the sites of pain and outcomes were

R. Bhidayasiri, D.D. Truong / Journal of the Neurological Sciences 235 (2005) 1–96
measured as the number of headache days per month,
headache intensity (0–3 scale), or both. Of the 271 patients
in this study series, 29 had episodic migraine, 17 had episodic
tension-type headache, 71 had mixed headache and 154 had
chronic daily headache. BTX-A treatment significantly re-
duced the number of headache days per month from appro-
ximately 19 to 8. BTX-A injections also decreased headache
intensity from amean of 2.4 points to 1.8 points. Both of these
differences were statistically significant. Of 263 patients
surveyed, 225 (85.6%) reported improvement in headache
frequency and intensity. The effectiveness of injections was
not related to the reason for treatment or injection technique,
or a variety of other variables. These results suggested that the
outcome of botulinum neurotoxin therapy was quite good for
the treatment of a variety of different headache disorders and
injection procedures. However, the reason that some patients
failed to respond and some studies failed to detect benefits of
botulinum toxin injections remains unknown [91]. Given the
large placebo effect noted in many headache studies,
psychological variables may play a role.
4.2. Musculoskeletal pain
An example of one study that examined the effects of
BTX-A on pain is a report of 31 consecutive patients with
chronic low back pain who were randomly assigned to active
treatment or placebo control [77]. Pain was measured on a
visual analog scale and disability was assessed using the
Oswestry Low Back Pain Questionnaire (OLBPQ). Results
showed that 73% of patients treated with BTX-A reported
more than 50% improvement in pain, in contrast to 25% in
the placebo group at 3 weeks post-injection. Improvements
on the OLBPQ were observed in 67% of patients treated with
BTX-A in contrast to 19% of those treated with placebo.
Both of these effects were statistically significant. No side
effects were reported by patients in this study.
In the treatment of musculoskeletal pain, BTX-A is
typically used as part of a multimodal therapeutic program
[74]. It has been suggested that botulinum neurotoxin
therapy may improve pain by reducing muscle tone and
overactivity, perhaps enabling greater benefit from physical
therapy designed to restore normal muscle length and
biomechanical balance [74]. Given this conception of the
role of botulinum neurotoxins in musculoskeletal pain,
studies that include a multimodal regimen may be more
likely to find positive results with botulinum toxin therapy.
Thus, one of the challenges of future research is to design
studies that would test this and other hypotheses in order to
determine the appropriate patients and conditions under
which botulinum toxin helps alleviate pain.
5. Conclusion
The disorders discussed here for which botulinum
neurotoxin therapies are emerging represent only a portion
of the novel applications of these treatments that have been
reported in the literature. BTX-A has been found to improve
sialorrhea, hyperhidrosis and pain with few side effects.
Although BTX-B has been less studied due to its more
recent introduction into clinical use, it also appears
promising for many of these disorders. Ultimately, these
compounds are useful because they inhibit acetylcholine
release following local injections, a property that may be
capitalized upon in the treatment of many different focal
disorders in which reduced cholinergic tone is desired. This
basic property sets the stage for additional novel uses in the
future.
Acknowledgments
Roongroj Bhidayasiri, MD, MRCP(UK) is supported by
Lilian Schorr Postdoctoral Fellowship of Parkinson’s Dis-
ease Foundation (PDF) and Parkinson’s Disease Research,
Education and Clinical Center (PADRECC) of West Los
Angeles Veterans Affairs Medical Center.
Daniel D. Truong, MD, is supported by the Parkinson’s
and Movement Disorder Foundation and the Long Beach
Memorial Foundation.
References
[1] Simpson LL. The origin, structure, and pharmacological activity of
botulinum toxin. Pharmacol Rev 1981;33(3):155–88.
[2] Cordivari C, Misra VP, Catania S, Lees AJ. New therapeutic
indications for botulinum toxins. Mov Disord 2004;19(Suppl
8):S157.
[3] Rohrich RJ, Janis JE, Fagien S, Stuzin JM. Botulinum toxin: expan-
ding role in medicine. Plast Reconstr Surg 2003;112(5 Suppl):1S–3S.
[4] Jankovic J, Brin MF. Botulinum toxin: historical perspective and
potential new indications. Muscle Nerve Suppl 1997;6:S129–45.
[5] Klein AW. The therapeutic potential of botulinum toxin. Dermatol
Surg 2004;30(3):452–5.
[6] Rossetto O, Seveso M, Caccin P, Schiavo G, Montecucco C. Tetanus
and botulinum neurotoxins: turning bad guys into good by research.
Toxicon 2001;39(1):27–41.
[7] Brin MF. Botulinum toxin: chemistry, pharmacology, toxicity, and
immunology. Muscle Nerve Suppl 1997;6:S146–68.
[8] Eleopra R, Tugnoli V, Quatrale R, Rossetto O, Montecucco C.
Different types of botulinum toxin in humans. Mov Disord
2004;19(Suppl 8):S53–9.
[9] Sampaio C, Costa J, Ferreira JJ. Clinical comparability of marketed
formulations of botulinum toxin. Mov Disord 2004;19(Suppl 8):
S129–36.
[10] Eleopra R, Tugnoli V, Rossetto O, Montecucco C, De Grandis D.
Botulinum neurotoxin serotype C: a novel effective botulinum toxin
therapy in human. Neurosci Lett 1997;224(2):91–4.
[11] Greene PE, Fahn S. Response to botulinum toxin F in sero-
negative botulinum toxin A-resistant patients. Mov Disord 1996;
11(2):181–4.
[12] Odergren T, Hjaltason H, Kaakkola S, Solders G, Hanko J, Fehling
C, et al. A double blind, randomised, parallel group study to
investigate the dose equivalence of Dysport and Botox in the
treatment of cervical dystonia. J Neurol Neurosurg Psychiatry
1998;64(1):6–12.

R. Bhidayasiri, D.D. Truong / Journal of the Neurological Sciences 235 (2005) 1–9 7
[13] Dressler D, Adib Saberi F. Botulinum toxin: mechanisms of action.
Eur Neurol 2005;53(1):3–9.
[14] Silberstein SD. Review of botulinum toxin type A and its clinical
applications in migraine headache. Expert Opin Pharmacother
2001;2(10):1649–54.
[15] Black JD, Dolly JO. Selective location of acceptors for botulinum
neurotoxin A in the central and peripheral nervous systems. Neuro-
science 1987;23(2):767–79.
[16] Naumann M, Jost W. Botulinum toxin treatment of secretory
disorders. Mov Disord 2004;19(Suppl 8):S137–41.
[17] Jost WH, Naumann M. Botulinum toxin in neuro-urological
disorders. Mov Disord 2004;19(Suppl 8):S142–5.
[18] Brisinda G, Bentivoglio AR, Maria G, Albanese A. Treatment with
botulinum neurotoxin of gastrointestinal smooth muscles and
sphincters spasms. Mov Disord 2004;19(Suppl 8):S146–56.
[19] Glickman S, Deaney CN. Treatment of relative sialorrhoea with
botulinum toxin type A: description and rationale for an injection
procedure with case report. Eur J Neurol 2001;8(6):567–71.
[20] Mancini F, Zangaglia R, Cristina S, Sommaruga MG, Martignoni E,
Nappi G, et al. Double-blind, placebo-controlled study to evaluate
the efficacy and safety of botulinum toxin type A in the treatment of
drooling in parkinsonism. Mov Disord 2003;18(6):685–8.
[21] Ellies M, Laskawi R, Rohrbach-Volland S, Arglebe C. Up-to-date
report of botulinum toxin therapy in patients with drooling caused by
different etiologies. J Oral Maxillofac Surg 2003;61(4):454–7.
[22] Ellies M, Rohrbach-Volland S, Arglebe C, Wilken B, Laskawi R,
Hanefeld F. Successful management of drooling with botulinum
toxin A in neurologically disabled children. Neuropediatrics
2002;33(6):327–30.
[23] Suskind DL, Tilton A. Clinical study of botulinum-A toxin in the
treatment of sialorrhea in children with cerebral palsy. Laryngoscope
2002;112(1):73–81.
[24] Pal PK, Calne DB, Calne S, Tsui JK. Botulinum toxin A as treatment
for drooling saliva in PD. Neurology 2000;54(1):244–7.
[25] Porta M, Gamba M, Bertacchi G, Vaj P. Treatment of sialorrhoea
with ultrasound guided botulinum toxin type A injection in patients
with neurological disorders. J Neurol Neurosurg Psychiatry
2001;70(4):538–40.
[26] Winterholler MG, Erbguth FJ, Wolf S, Kat S. Botulinum toxin for the
treatment of sialorrhoea in ALS: serious side effects of a transductal
approach. J Neurol Neurosurg Psychiatry 2001;70(3):417–8.
[27] Bhatia KP, Munchau A, Brown P. Botulinum toxin is a useful
treatment in excessive drooling in saliva. J Neurol Neurosurg
Psychiatry 1999;67(5):697.
[28] O’Sullivan JD, Bhatia KP, Lees AJ. Botulinum toxin A as treatment
for drooling saliva in PD. Neurology 2000;55(4):606–7.
[29] Friedman A, Potulska A. Quantitative assessment of parkinsonian
sialorrhea and results of treatment with botulinum toxin. Parkinson-
ism Relat Disord 2001;7(4):329–32.
[30] Jongerius PH, Rotteveel JJ, van den Hoogen F, Joosten F, van Hulst
K, Gabreels FJ. Botulinum toxin A: a new option for treatment of
drooling in children with cerebral palsy. Presentation of a case series.
Eur J Pediatr 2001;160(8):509–12.
[31] Giess R, Naumann M, Werner E, Riemann R, Beck M, Puls I, et al.
Injections of botulinum toxin A into the salivary glands improve
sialorrhoea in amyotrophic lateral sclerosis. J Neurol Neurosurg
Psychiatry 2000;69(1):121–3.
[32] Bothwell JE, Clarke K, Dooley JM, Gordon KE, Anderson R, Wood
EP, et al. Botulinum toxin A as a treatment for excessive drooling in
children. Pediatr Neurol 2002;27(1):18–22.
[33] Dogu O, Apaydin D, Sevim S, Talas DU, Aral M. Ultrasound-guided
versus Fblind_ intraparotid injections of botulinum toxin-A for the
treatment of sialorrhoea in patients with Parkinson’s disease. Clin
Neurol Neurosurg 2004;106(2):93–6.
[34] Jongerius PH, van den Hoogen FJ, van Limbeek J, Gabreels FJ,
van Hulst K, Rotteveel JJ. Effect of botulinum toxin in the
treatment of drooling: a controlled clinical trial. Pediatrics 2004;
114(3):620–7.
[35] Lipp A, Trottenberg T, Schink T, Kupsch A, Arnold G. A
randomized trial of botulinum toxin A for treatment of drooling.
Neurology 2003;61(9):1279–81.
[36] Racette BA, Good L, Sagitto S, Perlmutter JS. Botulinum toxin B
reduces sialorrhea in parkinsonism. Mov Disord 2003;18(9):
1059–61.
[37] Ondo WG, Hunter C, Moore W. A double-blind placebo-controlled
trial of botulinum toxin B for sialorrhea in Parkinson’s disease.
Neurology 2004;62(1):37–40.
[38] Brashear A, Lew MF, Dykstra DD, Comella CL, Factor SA,
Rodnitzky RL, et al. Safety and efficacy of NeuroBloc (botulinum
toxin type B) in type A-responsive cervical dystonia. Neurology
1999;53(7):1439–46.
[39] Brin MF, Lew MF, Adler CH, Comella CL, Factor SA, Jankovic J, et
al. Safety and efficacy of NeuroBloc (botulinum toxin type B) in type
A-resistant cervical dystonia. Neurology 1999;53(7):1431–8.
[40] Dressler D, Benecke R. Autonomic side effects of botulinum toxin
type B treatment of cervical dystonia and hyperhidrosis. Eur Neurol
2003;49(1):34–8.
[41] Tan EK, Lo YL, Seah A, Auchus AP. Recurrent jaw dislocation after
botulinum toxin treatment for sialorrhoea in amyotrophic lateral
sclerosis. J Neurol Sci 2001;190(1–2):95–7.
[42] Cheshire WP, Freeman R. Disorders of sweating. Semin Neurol
2003;23(4):399–406.
[43] Mosek A, Korczyn A. Hyperhidrosis of the palms and soles. In:
Korczyn A, editor. Handbook of autonomic nervous system
dysfunction. New York’ Marcel Dekker; 1995.
[44] Lin TS, Fang HY. Transthoracic endoscopic sympathectomy in the
treatment of palmar hyperhidrosis–with emphasis on perioperative
management (1,360 case analyses). Surg Neurol 1999;52(5):453–7.
[45] Bergmann I, Dauphin M, Naumann M, Flachenecker P, Mullges W,
Koltzenburg M, et al. Selective degeneration of sudomotor fibers in
Ross syndrome and successful treatment of compensatory hyper-
hidrosis with botulinum toxin. Muscle Nerve 1998;21(12):1790–3.
[46] Atkins JL, Butler PE. Hyperhidrosis: a review of current manage-
ment. Plast Reconstr Surg 2002;110(1):222–8.
[47] Heckmann M, Breit S, Ceballos-Baumann A, Schaller M, Plewig G.
Side-controlled intradermal injection of botulinum toxin A in
recalcitrant axillary hyperhidrosis. J Am Acad Dermatol 1999;
41(6):987–90.
[48] Schnider P, Binder M, Kittler H, Birner P, Starkel D, Wolff K, et al.
A randomized, double-blind, placebo-controlled trial of botulinum
A toxin for severe axillary hyperhidrosis. Br J Dermatol 1999;
140(4):677–80.
[49] Naumann M, Zellner M, Toyka KV, Reiners K. Treatment of
gustatory sweating with botulinum toxin. Ann Neurol 1997;42(6):
973–5.
[50] Swartling C, Naver H, Pihl-Lundin I, Hagforsen E, Vahlquist A.
Sweat gland morphology and periglandular innervation in essential
palmar hyperhidrosis before and after treatment with intradermal
botulinum toxin. J Am Acad Dermatol 2004;51(5):739–45.
[51] Naumann M, Lowe NJ. Botulinum toxin type A in treatment of
bilateral primary axillary hyperhidrosis: randomised, parallel group,
double blind, placebo controlled trial. BMJ 2001;323(7313):596–9.
[52] Naumann MK, Hamm H, Lowe NJ. Effect of botulinum toxin type A
on quality of life measures in patients with excessive axillary
sweating: a randomized controlled trial. Br J Dermatol 2002;
147(6):1218–26.
[53] Schnider P, Binder M, Auff E, Kittler H, Berger T, Wolff K. Double-
blind trial of botulinum A toxin for the treatment of focal hyper-
hidrosis of the palms. Br J Dermatol 1997;136(4):548–52.
[54] Naumann M, Hofmann U, Bergmann I, Hamm H, Toyka KV, Reiners
K. Focal hyperhidrosis: effective treatment with intracutaneous
botulinum toxin. Arch Dermatol 1998;134(3):301–4.

R. Bhidayasiri, D.D. Truong / Journal of the Neurological Sciences 235 (2005) 1–98
[55] Naumann M, Bergmann I, Hofmann U, Hamm H, Reiners K.
Botulinum toxin for focal hyperhidrosis: technical considerations and
improvements in application. Br J Dermatol 1998;139(6):1123–4.
[56] Odderson IR. Axillary hyperhidrosis: treatment with botulinum toxin
A. Arch Phys Med Rehabil 1998;79(3):350–2.
[57] Shelley WB, Talanin NY, Shelley ED. Botulinum toxin therapy for
palmar hyperhidrosis. J Am Acad Dermatol 1998;38(2 Pt 1):227–9.
[58] Naumann M, Jost WH, Toyka KV. Botulinum toxin in the treatment
of neurological disorders of the autonomic nervous system. Arch
Neurol 1999;56(8):914–6.
[59] Glogau RG. Botulinum A neurotoxin for axillary hyperhidrosis. No
sweat Botox. Dermatol Surg 1998;24(8):817–9.
[60] Naver H, Swartling C, Aquilonius SM. Treatment of focal hyper-
hidrosis with botulinum toxin type A. Brief overview of method-
ology and 2 years’ experience. Eur J Neurol 1999;6:S117–20.
[61] Naver H, Swartling C, Aquilonius SM. Palmar and axillary hyper-
hidrosis treated with botulinum toxin: one-year clinical follow-up.
Eur J Neurol 2000;7(1):55–62.
[62] Heckmann M, Ceballos-Baumann AO, Plewig G. Botulinum toxin A
for axillary hyperhidrosis (excessive sweating). N Engl J Med
2001;344(7):488–93.
[63] Solomon BA, Hayman R. Botulinum toxin type A therapy for palmar
and digital hyperhidrosis. J Am Acad Dermatol 2000;42(6):1026–9.
[64] Karamfilov T, Konrad H, Karte K, Wollina U. Lower relapse rate of
botulinum toxin A therapy for axillary hyperhidrosis by dose
increase. Arch Dermatol 2000;136(4):487–90.
[65] Kinkelin I, Hund M, Naumann M, Hamm H. Effective treatment of
frontal hyperhidrosis with botulinum toxin A. Br J Dermatol
2000;143(4):824–7.
[66] Laccourreye O, Akl E, Gutierrez-Fonseca R, Garcia D, Brasnu D,
Bonan B. Recurrent gustatory sweating (Frey syndrome) after
intracutaneous injection of botulinum toxin type A: incidence,
management, and outcome. Arch Otolaryngol Head Neck Surg
1999;125(3):283–6.
[67] Baumann LS, Halem ML. Systemic adverse effects after botulinum
toxin type B (myobloc) injections for the treatment of palmar
hyperhidrosis. Arch Dermatol 2003;139(2):226–7.
[68] Baumann LS, Halem ML. Botulinum toxin-B and the management of
hyperhidrosis. Clin Dermatol 2004;22(1):60–5.
[69] Dressler D, Adib Saberi F, Benecke R. Botulinum toxin type B for
treatment of axillar hyperhidrosis. J Neurol 2002;249(12):1729–32.
[70] Binder WJ, Brin MF, Blitzer A, Schoenrock LD, Pogoda JM.
Botulinum toxin type A (BOTOX) for treatment of migraine
headaches: an open-label study. Otolaryngol Head Neck Surg
2000;123(6):669–76.
[71] Jankovic J, Schwartz K. Botulinum toxin injections for cervical
dystonia. Neurology 1990;40(2):277–80.
[72] Silberstein S, Mathew N, Saper J, Jenkins S. Botulinum toxin type A
as a migraine preventive treatment. For the BOTOX Migraine
Clinical Research Group. Headache 2000;40(6):445–50.
[73] Freund BJ, Schwartz M. Relief of tension-type headache symptoms
in subjects with temporomandibular disorders treated with botulinum
toxin-A. Headache 2002;42(10):1033–7.
[74] Lang AM. Botulinum toxin type A therapy in chronic pain disorders.
Arch Phys Med Rehabil 2003;84(3 Suppl 1):S69–73 [quiz S4–S5].
[75] Reilich P, Fheodoroff K, Kern U, Mense S, Seddigh S, Wissel J, et al.
Consensus statement: botulinum toxin in myofascial pain. J Neurol
2004;251(Suppl 1):I36–8.
[76] Sycha T, Kranz G, Auff E, Schnider P. Botulinum toxin in the
treatment of rare head and neck pain syndromes: a systematic review
of the literature. J Neurol 2004;251(Suppl 1):I19–30.
[77] Foster L, Clapp L, Erickson M, Jabbari B. Botulinum toxin A and
chronic low back pain: a randomized, double-blind study. Neurology
2001;56(10):1290–3.
[78] Tsui JK, Eisen A, Stoessl AJ, Calne S, Calne DB. Double-blind study
of botulinum toxin in spasmodic torticollis. Lancet 1986;2(8501):
245–7.
[79] Greene P, Kang U, Fahn S, Brin M, Moskowitz C, Flaster E.
Double-blind, placebo-controlled trial of botulinum toxin injections
for the treatment of spasmodic torticollis. Neurology 1990;40(8):
1213–8.
[80] Lorentz IT, Subramaniam SS, Yiannikas C. Treatment of idiopathic
spasmodic torticollis with botulinum toxin A: a double-blind study
on twenty-three patients. Mov Disord 1991;6(2):145–50.
[81] Naumann M, Yakovleff A, Durif F. A randomized, double-masked,
crossover comparison of the efficacy and safety of botulinum toxin
type A produced from the original bulk toxin source and current bulk
toxin source for the treatment of cervical dystonia. J Neurol
2002;249(1):57–63.
[82] Brin MF, Fahn S, Moskowitz C, Friedman A, Shale HM, Greene
PE, et al. Localized injections of botulinum toxin for the treatment
of focal dystonia and hemifacial spasm. Mov Disord 1987;
2(4):237–54.
[83] Mense S. Neurobiological basis for the use of botulinum toxin in
pain therapy. J Neurol 2004;251(Suppl 1):I1–7.
[84] Rosales RL, Arimura K, Takenaga S, Osame M. Extrafusal and
intrafusal muscle effects in experimental botulinum toxin-A injec-
tion. Muscle Nerve 1996;19(4):488–96.
[85] Blumenfeld A. Botulinum toxin type A for the treatment of
headache: pro. Headache 2004;44(8):825–30.
[86] Welch KM. Botulinum toxin type A for the treatment of headache:
con. Headache 2004;44(8):831–3.
[87] Smuts JA, Baker MK, Smuts HM, Stassen J, Rossouw E,
Barnard P. Prophylactive treatment of chronic tension-type head-
ache using botulinum toxin type A. Eur J Neurol 1999;6(Suppl 4):
S99–102.
[88] Gobel H, Lindner V, Krack P, Heinze A, Gaartz N, Deuschl G.
Treatment of chronic tension-type headache with botulinum toxin.
Cephalalgia 1999;19:455.
[89] Rollnik JD, Tanneberger O, Schubert M, Schneider U, Dengler R.
Treatment of tension-type headache with botulinum toxin type A:
a double-blind, placebo-controlled study. Headache 2000;40(4):
300–5.
[90] Burch CM, Kokoska MS, Glaser DA, Hollenbeak CS. Treatment
of frontal tension headaches with botulinum toxin. Cephalalgia
2001;21:489–91.
[91] Schmitt WJ, Slowey E, Fravi N, Weber S, Burgunder JM. Effect of
botulinum toxin A injections in the treatment of chronic tension-type
headache: a double-blind, placebo-controlled trial. Headache
2001;41(7):658–64.
[92] Schulte-Mattler WJ, Krack P. The therapeutic effect of botulinum
toxin on tension-type headache: a multicenter, randomized, double-
blind, placebo-controlled study. Cephalalgia 2003;23:634.
[93] Schulte-Mattler WJ, Krack P. Treatment of chronic tension-type
headache with botulinum toxin A: a randomized, double-blind,
placebo-controlled multicenter study. Pain 2004;109(1–2):110–4.
[94] Ondo WG, Vuong KD, Derman HS. Botulinum toxin A for chronic
daily headache: a randomized, placebo-controlled, parallel design
study. Cephalalgia 2004;24(1):60–5.
[95] Padberg M, de Bruijn SF, de Haan RJ, Tavy DL. Treatment of
chronic tension-type headache with botulinum toxin: a double-blind,
placebo-controlled clinical trial. Cephalalgia 2004;24(8):675–80.
[96] Brin MF, Swope DM, O’Brian C, Abbasi S, Pogoda JN. Botox for
migraine: double-blind, placebo-controlled, region-specific evalua-
tion. Cephalalgia 2000;20:421–2.
[97] Schwaag S, Vollmer-Haase J, Rahmann A, Frese A, Husstedt I-W,
Evers S. Botulinum toxin A in the prophylactic treatment of
migraine-a randomised, double-blind, placebo-controlled study.
Cephalalgia 2003;23:702.
[98] Mauskop A. The use of botulinum toxin in the treatment of
headaches. Curr Pain Headache Rep 2002;6(4):320–3.
[99] Barrientos N, Chana P. Botulinum toxin type A in the prophylactic
treatment of migraine headache: a preliminary study. J Headaches
Pain 2003;4:146–51.

R. Bhidayasiri, D.D. Truong / Journal of the Neurological Sciences 235 (2005) 1–9 9
[100] Behmand RA, Tucker T, Guyuron B. Single-site botulinum toxin
type a injection for elimination of migraine trigger points. Headache
2003;43(10):1085–9.
[101] Tamura BM, Chang B. Botulinum toxin: application into acupunc-
ture points for migraine. Dermatol Surg 2003;29(7):749–54.
[102] Eross EJ, Dodick DW. Duration of migraine illness is a predictor for
response to botulinum toxin type A. Cephalalgia 2003;23:739.
[103] Evers S, Vollmer-Haase J, Schwaag S, Rahmann A, Husstedt IW,
Frese A. Botulinum toxin A in the prophylactic treatment of
migraine–a randomized, double-blind, placebo-controlled study.
Cephalalgia 2004;24(10):838–43.
[104] Blumenfeld A. Botulinum toxin type A as an effective prophylactic
treatment in primary headache disorders. Headache 2003;43(8):
853–60.
[105] Moore AP. Movement, visceral and autonomic disorders: use of
botulinum toxin. Hosp Med 2003;64:452–9.
[106] Naumann M, Lowe NJ, Kumar CR, Hamm H. Botulinum toxin type
a is a safe and effective treatment for axillary hyperhidrosis over 16
months: a prospective study. Arch Dermatol 2003;139(6):731–6.
[107] Wollina U, Karamfilov T, Konrad H. High-dose botulinum toxin type
A therapy for axillary hyperhidrosis markedly prolongs the relapse-
free interval. J Am Acad Dermatol 2002;46(4):536–40.