botulinum toxin assessment, intervention and after-care for lower limb spasticity in children with...
TRANSCRIPT

Botulinum toxin assessment, intervention and after-care for upperlimb hypertonicity in adults: international consensus statement
G. Sheeana, N. A. Lanninb, L. Turner-Stokesc, B. Rawickid and B. J. Snowe
aNeurosciences, University of California, San Diego, CA, USA; bRehabilitation Studies Unit, Sydney Medical School, The University of
Sydney, Ryde, NSW, Australia; cKing�s College London School of Medicine, Harrow, Middlesex, UK; dVictorian Paediatric Rehabilitation
Service, Monash Medical Centre, Clayton, Vic., Australia; and eDepartment of Neurology, Auckland City Hospital, Auckland, New Zealand
Keywords:
brain injury, consensus
statement, spasticity,
stroke, systematic review,
upper extremity
Received 9 July 2009
Accepted 14 May 2010
Upper limb spasticity affecting elbow, wrist, and finger flexors can be safely and
effectively reduced with injections of botulinum toxin type-A (BoNT-A). It has been
best studied in adults in the context of post-stroke spasticity. The clinical benefits
include reduction in pain and deformity, improvement in washing and dressing the
upper limb, and a reduction in caregiver burden (Class I evidence, recommendation
level A). Some patients show improvement in function performed by active movement
of the affected upper limb (Class III evidence, recommendation C), but predicting and
measuring this is difficult, and further research is needed. An individually based ap-
proach to treatment and outcome measurement is preferred (Class IV, recommen-
dation U). More research is needed to resolve many unknown issues of assessment and
treatment, using research methods appropriate to the question.
Introduction
As with other body areas, spasticity in the upper limb
(UL) can produce pain and deformity, and can interfere
with function. The relatively small size of the UL
muscles makes them attractive targets for botulinum
toxin type-A (BoNT-A) injection. The general
approach to management is similar to other body areas
in terms of assessment, goal setting, and outcome
measurement. The authors therefore have attempted to
limit overlap, only repeating that which is valuable in
the context of UL spasticity and that which will allow
this consensus to serve as a stand-alone document.
Objective
The purposes of this international consensus statement
are to provide guidance about �best practice� to clini-
cians in the assessment and treatment of upper limb
hypertonicity in adults and to identify areas for future
research based on gaps in the literature. Literature was
searched and appraised using a conventional evidence
hierarchy. The highest levels of evidence available were
used to develop recommendations, with randomized
controlled trials (RCTs) and systematic reviews
preferentially sought. Only when RCT or systematic
review evidence was not available, was lower level
evidence and practice-based evidence included to
answer clinical questions raised at the International
BoNT Consensus Workshop. Expert opinion where
included have been clearly labelled and should be
interpreted with judicious caution. Recommendations
for research were made based on the gaps indentified in
the literature. All recommendations were graded based
on the American Academy of Neurology evidence
classification [1]. The authors were both researchers and
clinicians with experience in BoNT and were a multi-
disciplinary team including rehabilitation physicians, an
occupational therapist, and neurologists.
Which patients should be treated?
The mainstay of treatment for spasticity is the preven-
tion and relief of provocative factors (infection, noci-
ceptive stimuli, tight clothing, etc.) and a regimen of
care that includes positioning, stretching and (where
relevant) the facilitation of active movement to main-
tain muscle length and prevent soft tissue contracture.
BoNT-A treatment should be viewed as an adjunct to a
neurorehabilitation programme rather than the other
way around. An algorithm for treatment with BoNT-A
is presented in Fig. 1.
Decisions about whether and how a patient�s UL
spasticity should be treated are individually determined.
These decisions may be influenced by the chronicity,
Correspondence: Dr G. Sheean, Clinical Professor of Neurosciences,
UCSD, Director of Neuromuscular Division, 402 Dickinson St, Suite
190, San Diego, CA 92103-8465, USA (tel.: +1 619 543 5300;
fax: +1 619 543 5793; e-mail: [email protected]).
74� 2010 The Author(s)
Journal compilation � 2010 EFNS
European Journal of Neurology 2010, 17 (Suppl. 2): 74–93 doi:10.1111/j.1468-1331.2010.03129.x

severity, and distribution of the spasticity as well as
weakness, the presence and severity of co-morbidities,
the availability of support and the goals of treatment.
Spasticity is not always harmful, but it can be painful
and distressing. Unlike the lower limb, spasticity in the
UL is rarely functionally useful.
The effects of spasticity are most commonly
described at the level of impairment [2] (hypertonicity,
associated reactions, limb deformity, etc.). However, it
is also important to consider the impact on function.
Functional activities may be divided into the following
two categories:
• Active function, where a functional task is performed
byactivemovement of the individual�s affected limb, or
• Passive function, where a task is carried out on the
affected limb by the individual using the unaffected
limb, or by a carer [3,4].
Evidence for effectiveness
Botulinum toxin has been clearly shown to reduce
clinical indicators of UL spasticity (Class I evidence);
however, functional improvement, and not just reduc-
tion in spasticity itself should be the goal of therapy
(Class IV). Following treatment, there can be improve-
ments in symptoms (pain), and �passive function� (carer
management of dressing the UL, hygiene of the hand,
elbow and axilla) and cosmetic limb position (Class I)
[5]. Individually tailored BoNT-A treatment has also
been shown to improve caregiver burden for tasks such
as hygiene, cutting fingernails and dressing (Class I) [6].
Given the two studies with consistent results, we
recommend BoNT-A treatment for the reduction in
pain and improvement in passive function in patients
with UL spasticity, using individualized injection pat-
terns and treatment goals established for each patient
(Level A rating) [5,6]. There are three studies specifically
addressing shoulder pain associated with post-stroke
spasticity that included injection into the subscapularis
muscle. Two studies showed clear reduction in pain
(Yelnik et al., Lim et al.: Class 1) [7,8], whilst the third
study did not (de Boer) [9]. Given this contradiction and
methodological variations, we recommend considering
injections into shoulder girdle muscles to reduce
shoulder pain (Level U).
No randomized controlled study has shown clear
benefit in active function of the spastic UL [4,10].
Inconsistency of improvements in active function has,
however, been noted in open-label studies, with some
studies reporting benefit [11–14] whilst others have not
[15–17]. Paediatric studies in which participants
received BoNT-A injections and occupational therapy
Patient presents with problem
due to focal spastic motor overactivity
Patient* satisfaction achieved?
Cost-effective? Decide parameters for re-injection
If quantitative difference, review treatment plan
If qualitative difference, re-evaluate role ofBoNT in treatment
Review patient’s expectations*
Disability goals achieved?
Search for confounding factors and treat accordingly
Still a problem?No further Rx
Continue therapy
Consider alternativetreatments
Consider alternativetreatments
Yes
Yes
Yes
Yes
Yes
Yes
No
Still a problem?
Consider BoNT and discuss costs,
risks, benefits
NoYes
Technical goals achieved (impairments)?
Review• Treatment plan• Confounding variables
* and caregiver
Review
Inject and continue with adjunctive Rx
Perform baseline evaluation
Acceptable?
Formulate management plan
1. Define clinical problem – impairment, disability, handicap2. Choose outcome measures and timing of review3. Treatment plan a. Injection plan b. Adjunctive treatment
No
No
No
Re-evaluate causal relationship between
impairments and disability
No
No
Physical therapy:OT, PT
Hyperkinetic (involuntary movements)
Spasms (flexor, extensor, adductor)
Associated reactions
Mass movements
Action-induced spastic dystonia†Evaluated by tone and active or passive range of movement. The hyperkinetic spastic
forms occur when the spastic muscle contractions produce involuntary movements while
in the hypokinetic forms the muscle contractions impair movement, active or passive.
2. Define disability in terms of
a. Function
i. Active
ii. Passive
b. Symptoms
i. Pain
ii. Cosmetic
iii. Unwanted involuntary movements
3. Confounding variables
a. Musculoskeletal
i. Soft tissue stiffness
ii. Joint calcification
b. Aggravating factors
i. Noxious stimulation
ii. Medications
Notes:
1. Technical goal is to reduce impairments = spastic motor over activity, which is of 2 types:
Hypokinetic (impairment of movement)†
Spasticity
Static spastic dystonia
Spastic co-contraction
Figure 1 Algorithm: managing spasticity.
BoNT-A consensus statement: AUL 75
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

demonstrated greater improvements in self-care and
upper-extremity movement function than those chil-
dren who received BoNT-A or occupational therapy
only [18,19]. Although not demonstrated in adults,
these paediatric findings suggest that, when combined
with functional, activity-based interventions, BoNT-A
may provide an opportunity to improve the functional
use of a spastic UL. However, there is often a time lag
between maximum reduction in spasticity and func-
tional gain [20], possibly reflecting time taken to learn
how to use the new reduction in hypertonicity. We
therefore conclude that improvement in active function
of the UL may occur in some patients (recommendation
C, Class III) but not necessarily simultaneously with
reduction in spasticity.
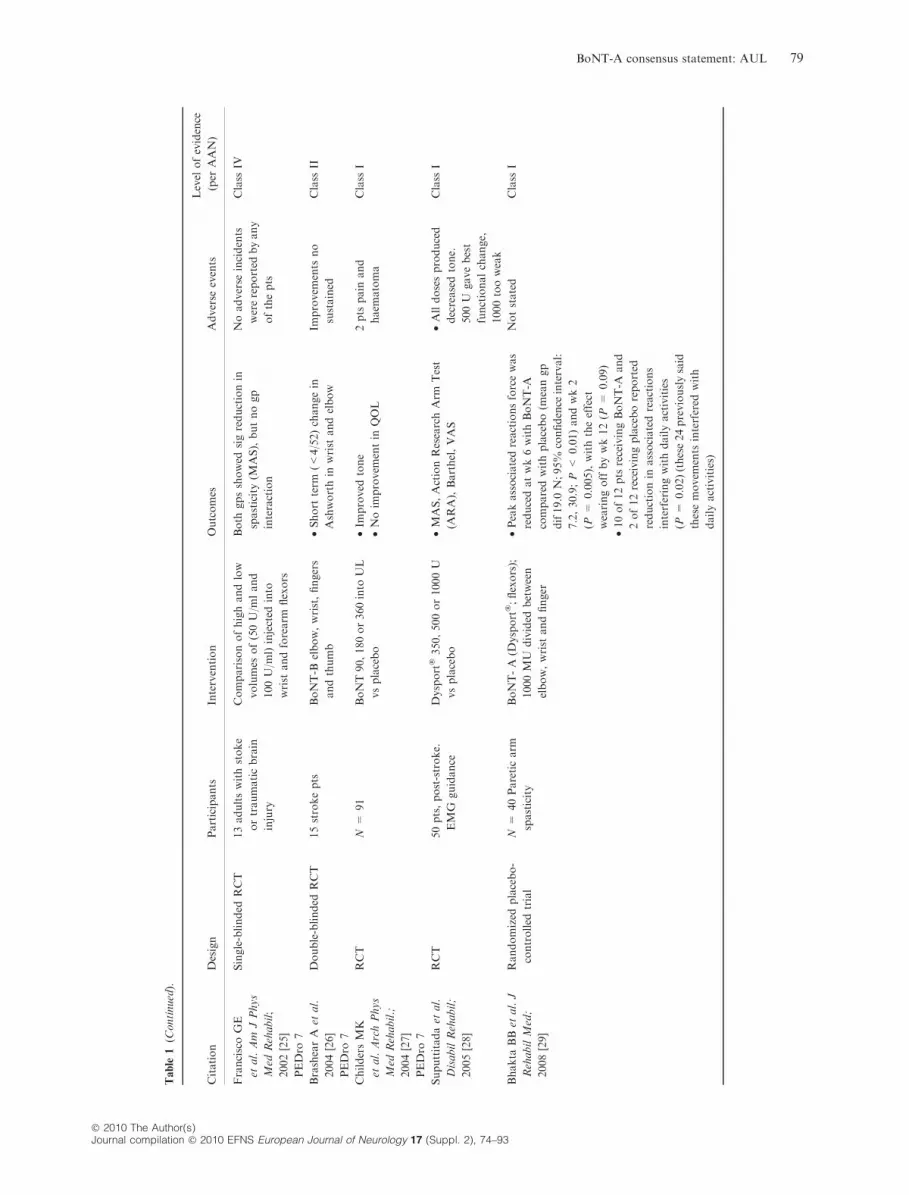
Evidence for the use of BoNT-A in the UL for adults
is summarized in Table 1. Papers were included if they
were Class I (AAN), that is, double-blinded random-
ized, controlled trials with adequate methods, with an
additional requirement of adequate statistical power.
Recommendation 1
In summary, the following is recommended:*
• The effects of spasticity should be described at the level of both
impairment and impact on function (active; passive)
• Treatment decisions should be based on individual evaluation,
including chronicity, severity, and distribution of the spasticity and
weakness; the presence and severity of co-morbidities, such as
contracture; the availability of support; and the goals of treatment
• BoNT-A treatment is appropriate for the reduction in pain and
improvement in passive function in patients with UL spasticity,
using individualized injection patterns and treatment goals estab-
lished for each patient
*Expert opinion
What is the best way to assess?
Treatment should be individually tailored to the spastic
muscles that are judged to be causing the disability.
Patients who are most likely to benefit from treatment
with BoNT-A are those in whom focal or multi-focal
UL spasticity is making a substantial contribution to a
clinical problem. Patients in whom the dominant
problem is fixed contracture or those with generalized
spasticity are unlikely to benefit from management with
BoNT-A.
Assessment must therefore measure the clinical phe-
nomena (including muscle contracture, pain and joint
range of movement) as well as the passive and active
functional impairments experienced by the patient.
The key steps in patient assessment are as follows:
(i) To confirm the patient meets patient selection cri-
teria (outlined in Table 2).
(ii) To identify and agree on the goals of treatment by:
s Identifying functional impairments (both pas-
sive and active) and differential contributions
of components the UL deformity, and
s Understanding the extent to which spasticity
and muscle overactivity, weakness and con-
tracture contribute to the UL functional
impairments.
(iii) To determine the current levels of therapy received
and potential arrangements for follow-up therapy.
(iv) To define and agree on how overall outcome will be
determined.
Goals for intervention
Goals for treatment typically include managing symp-
toms, preventing or slowing down the progression of
impairments, and improving passive or active function.
Occasionally, goals relate to process, for example to
optimize the effects of other interventions such as
therapy or systemic medication. Common treatment
goals are outlined in Table 3.
Having identified the main goal areas, clearly defined
treatment goals should be collaboratively determined
with the patient and their carers. Agreed goals should
be SMART (i.e. specific, measurable, achievable, real-
istic and timed). The expected outcome, thus carefully
defined, should be agreed by all parties to be worth-
while, and the time-point for evaluation should be set in
advance [33].
Baseline assessment
Baseline assessment should include evaluation of the
spasticity itself. The Ashworth (or Modified Ashworth)
and Tardieu scales provide a clinical indicator of
spasticity, assessing resistance to passive movement.
• The Ashworth scale provides a baseline indicator of
severity and may indicate clinically important chan-
ges, though validity, reliability and sensitivity have
limitations [34].
• The Tardieu scale, which has a velocity component to
its measurement of tone, has demonstrated higher
validity, reliability and clinical utility for the clinical
measurement of spasticity [34].
It is important to distinguish hypertonia by spasticity
from that due to soft tissue changes because of the
additional treatment options available for spasticity.
So, despite potentially taking longer, use of the Tardieu
scale is recommended over the Ashworth wherever
possible, as research findings suggest that the Tardieu
Scale is able to differentiate spasticity from soft tissue
hypertonia, whereas the Ashworth Scale cannot [35]. It
76 G. Sheean et al.
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

Table
1Evidence
fortheuse
ofBoNT-A
inupper
limbhypertonicityin
adults
Citation
Design
Participants
Intervention
Outcomes
Adverse
events
Level
ofevidence
(per
AAN)
Sim
psonDM
etal.Neurology,
1996
PEDro
8[21]
Randomized,double-
blinded,placebo-
controlled,
multicenterclinical
trial
N=
39chronic
UL
spasticityafter
stroke
ULIM
injectionsofatotal
dose
ofeither
75,150,or
300U
ofBoNT-A
or
placebo(biceps,flexorcarpi
radialis,
andflexorcarpi
ulnarismuscles)
•300U
BoNT-A
resulted
insigmean
decrease
inwrist
flexortoneof1.2
(P=
0.028),1.1
(P=
0.044),and
1.2
(P=
0.026)points
andelbow
flexortoneof1.2
(P=
0.024),1.2
(P=
0.028),and1.1
(P=
0.199)
atwks2,4,and6post-injection.
•In
theplacebogp,tonereductionat
thewristwas0.3,0.2,and0.0
andat
theelbow
was0.3,0.3,and0.6
at
wks2,4,and6post-injection.
•BoNT-A
gpsreported
sig
improvem
entonthephysicianand
patientGlobalAssessm
entof
Response
totx
atwks4and6post-
injection
Nostatisticallysigdif.No
seriousAEs
Class
I
BakheitAM
etal.
Stroke;
2000[22]
PEDro
8
Prospective,
randomized,double-
blinded,placebo-
controlled,dose-
rangingstudy
N=
83ULspasticity
after
stroke
BoNT-A
/Dysport
�500,1000,
1500U
•AlldosesofBoNT-A
showed
sig
reductionfrom
baselineofmuscle
tonecomparedwithplacebo.
•Effectonfunctionaldisabilitywas
notstatisticallysigandwasbestat
dose
1000U.
•Txwaseffectiveatdosesof500,
1000,and1500U.
•Optimaldose
fortx
ofpts
with
residualvoluntary
movem
ents
in
theULappears
tobe1000U
Nostatisticallysigdif
Class
I
Bhakta
BBet
al.J
Neurol
Neurosurg
Psychiatry;2000
[6]
Randomized,double-
blinded,single-
centretrial
N=
40
•1000MU
ofBoNT-A
(Dysport
�)vsplacebo
dilutedin
10ml0.9%
saline.
•Flexibilitywasallowed
betweenpts
inthedose
of
trialdruggiven
to
individualmuscles.
•Dose
selectionfor
individualmusclesbasedon
clinicaljudgem
entbyone
investigator
•Betweengpdifsnotreported.
•Statisticallysignificantlygreater
improvem
ents
reported
inBoNT-A
gpvsplacebofor:
•disabilityatwk6(w
orn
off
by
wk12)
•carerburden
atwk6(continued
atwk12)
•forearm
flexorspasticityatwks
6(continued
atwk12)
•elbow
flexorspasticityatwk2
only
•Noim
provem
ents
inarm
pain,and
gripstrength
wasreducedwith
BoNT-A
•BoNT-A
gp:2pts
developed
self-lim
itingarm
pain
within
1wkof
injectionand1ptreported
worseningofmuscle
spasm
•NoseriousBoNT-A
-related
AEsreported.
•In
theplacebogp,1pt
reported
herpes
labialis
7dayspost-injection,1pt
reported
2transient
ischaem
icattacks12days
post-injection,and1pthad
exacerbationofcardiac
failure
4wksafter
tx
Class
II
BoNT-A consensus statement: AUL 77
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

Table
1(C
ontinued).
Citation
Design
Participants
Intervention
Outcomes
Adverse
events
Level
ofevidence
(per
AAN)
SmithSJet
al.
ClinRehabil;
2000[23]
PEDro
7
Double-blinded
placebo-controlled
randomized
dose-
rangingstudy
21(19post-stroke,
twopost-head
injury)
Pts
randomized:0(sterile
saline),500,1000or
1500MU
ofIM
BoNT-A
(Dysport
�).
Rangeofmusclesinjected
andthusdose
depended
on
distributionofspasticity
•Combiningdata
from
all
dosesofBoNT
therewasa
sigreductionin
spasticityat
thewrist
andfingers
associatedwithagreater
rangeofpassivemovem
ent
atthewrist
andless
finger
curlatrest
•Nochangein
ULdisability
•Sig
increase
inpts
�global
assessm
entofbenefit
•BoNT-A
generally
welltolerated
•Noincreased
weakness
•1ptdeveloped
hip
pain
(feltunrelated
toinjection)
•1pthad
�flu-like
symptoms�for
2dayspost-
injection
•1ptcomplained
ofa
tendency
for
affectedlimbwith
sensory
neglect
to
occasionallyget
caughtin
thespokes
ofthewheelchair
after
the1000Mu
dose
Class
I
BakheitAM
etal.
EurJNeurol;
2001[24]
PEDro
8
Double-blinded,
multicentreRCT
N=
59
OnecycleofDysport
�
(1000U)injected
into
five
musclesin
thearm
and
forearm
(fixed
regim
en)vs
placebo
•Sig
improvem
ents
in
spasticity,rangeof
movem
entandglobal
benefitatendofstudy
Nosigdifin
pain,Barthel
index
ornumber
ofgoals
attained
20pts
inplacebogp
and16in
BoNT
gp
reported
AEs
Nonemajorand
most
notrelatedto
thestudy
Nosigdifin
AE
reportingbetween
gps
Class
I
BrashearA
etal.
NEnglJMed;
2002[5]
PEDro
7
Double-blinded,
multicentreRCT
126pts
withpost-
strokespasticity
OnecycleBoNT-A
(BOTOX
�)into
wrist
and
fingersvsplacebo.
Primary
outcome:
self-
report
ofdisabilityat6wks
•62%
BOTOX
�vs17%
placeboim
proved
byat
least
onepointonthe
disabilityscale
(P<
0.001).BoNT-A
reducedspasticityin
the
wrist
andfingers,andits
associateddisability
•Note
thatbetween-gps
comparisonsoncontinuous
outcomes
notreported
Nostatisticallysigdif
betweengps
Class
II
78 G. Sheean et al.
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93
Table
1(C
ontinued).
Citation
Design
Participants
Intervention
Outcomes
Adverse
events
Level
ofevidence
(per
AAN)
FranciscoGE
etal.Am
JPhys
Med
Rehabil;
2002[25]
PEDro
7
Single-blinded
RCT
13adultswithstoke
ortraumaticbrain
injury
Comparisonofhighandlow
volumes
of(50U/m
land
100U/m
l)injected
into
wrist
andforearm
flexors
Both
gpsshowed
sigreductionin
spasticity(M
AS),butnogp
interaction
Noadverse
incidents
werereported
byany
ofthepts
Class
IV
BrashearA
etal.
2004[26]
PEDro
7
Double-blinded
RCT
15strokepts
BoNT-B
elbow,wrist,fingers
andthumb
•Short
term
(<4/52)changein
Ashworthin
wrist
andelbow
Improvem
ents
no
sustained
Class
II
ChildersMK
etal.ArchPhys
Med
Rehabil.;
2004[27]
PEDro
7
RCT
N=
91
BoNT90,180or360into
UL
vsplacebo
•Im
proved
tone
•Noim
provem
entin
QOL
2pts
pain
and
haem
atoma
Class
I
Suputtitadaet
al.
DisabilRehabil;
2005[28]
RCT
50pts,post-stroke.
EMG
guidance
Dysport
�350,500or1000U
vsplacebo
•MAS,ActionResearchArm
Test
(ARA),Barthel,VAS
•Alldosesproduced
decreasedtone.
500U
gavebest
functionalchange,
1000tooweak
Class
I
Bhakta
BBet
al.J
RehabilMed;
2008[29]
Randomized
placebo-
controlled
trial
N=
40Pareticarm
spasticity
BoNT-A
(Dysport
�;flexors);
1000MU
divided
between
elbow,wrist
andfinger
•Peakassociatedreactionsforcewas
reducedatwk6withBoNT-A
comparedwithplacebo(m
eangp
dif19.0
N;95%
confidence
interval:
7.2,30.9;P
<0.01)andwk2
(P=
0.005),withtheeffect
wearingoffbywk12(P
=0.09)
•10of12pts
receivingBoNT-A
and
2of12receivingplaceboreported
reductionin
associatedreactions
interferingwithdailyactivities
(P=
0.02)(these24previouslysaid
thesemovem
ents
interfered
with
dailyactivities)
Notstated
Class
I
BoNT-A consensus statement: AUL 79
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

Table
1(C
ontinued).
Citation
Design
Participants
Intervention
Outcomes
Adverse
events
Level
ofevidence
(per
AAN)
Mayer
NH
etal.
ArchPhysMed
Rahabil;2008
[30]
Parallel-gp,RCT
with
blinded
outcome
assessm
ent.
(injectiontechnique
randomized)
N=
31adults
acquired
brain
injury
(21traumatic
brain
injury,8
stroke,
and2
hypoxic
encephalopathy)
Motorpointinjections
occurred
atonesite
inthe
biceps(60U,2.4
ml)and1
site
inthebrachioradialis
(30U,1.2
ml).
Distributedinjectionsat
foursitesin
thebicepsand
twositesin
the
brachioradialis(15U,
0.6
mlper
site).Totaldose
(90U)andvol(3.6
ml)were
constantforboth
gps;only
injectionsitesand
localizationtechniques
varied
betweengps
•Post-interventiontestingat3wks:
nosigdifsbetweengps(P
range,
0.31–0.82across
3outcome
measures)
•Within
each
gp,sigtx
effectswere
observed
onalloutcomemeasures
(allP<
0.01)
•Fortheuninjected
brachialis
muscle,electromyographic
reductionwasgreaterforthe
distributedgp
NoseriousAEs
Class
III
McC
rory
P,et
al.
JRehabilMed;
2009[31a]
Multicentre,
randomized,double-
blinded,placebo-
controlled
study
N=
96meanage
59.5
years)
‡6monthspost-
stroke(m
ean
5.9
years)
hem
iplegic
stroke
andsevere/moderate
spasticityfollowing
stroke
BoNT-A
injection(D
ysport
�)
orplacebo.(range750–
1000U)into
principal
spastic
musclesofdistalUL
atwk0;re-txatwk12
Sig
reduction(M
ASmeasure)in
muscle
spasticityforBoNT-A
-vs
placebo,atalltime-points.
Significantlygreaterattainmentof
person-centred
goals.Nosigdifin
QOL
BoNT-A
:67%
AEs(5.5%
tx
related)
Placebo:62%
AEs(9.5%
tx
related)
TheseAEs
generallymild.
Nodeaths;no
hospitalizations
fortx-related
events.
Noinstances
respiratory
failure
or
swallowing
problemsto
suggestdistance
muscular
weakness
Class
I
BoNT-A
,Botulinum
toxin
type-A;AE,adverse
events;RCT,randomized
controlled
trial;pts,patients;tx,treatm
ent;yr,year;U,units;IM
,intramuscular;sig,significant;dif,difference;gp/s,group/s;
wk/s,week/s;mnth/s,month/s;UL,upper
limb;MAS,Modified
Ashworthscale;QOL,quality
oflife;MU:Mouse
Units.
80 G. Sheean et al.
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

should be acknowledged, however, that research to date
has primarily been undertaken in larger muscle groups
such as the elbow flexors and that there is limited
research investigating the validity or reliability of either
measure in the smaller muscle groups that are com-
monly injected. Surface or needle electromyography can
also help to show whether active muscle contraction is
contributing to hypertonia.
Once the specific goals for treatment have been iden-
tified, the outcomemeasures that will be used to evaluate
the effects of intervention are chosen and recorded at
baseline. An outcome measure should be clearly defined,
easily measured, and ideally can be objectively or inde-
pendently confirmed. Thesemay be either a standardized
measure or, more commonly in clinical practice, an
individualized measure. For example, one of the most
sensitive individualized methods for evaluating outcome
Table 2 Preliminary checklist for patient selection [32]
• Problem attributed to focal or multi-focal UL spasticity, rather
than fixed contracture
• Provocative factors for spasticity have been excluded or treated
• Condition likely to respond to BoNT-A injection
• No contraindications to BoNT-A injection
• Goals of treatment have been determined, with patient input
• Arrangements in place for implementation of appropriate physical
treatment strategies and monitoring
• Appropriate outcome measures identified
• Informed consent for treatment from patient, or family assents on
their behalf
Adapted from: Royal College of Physicians, British Society of
Rehabilitation Medicine, Chartered Society of Physiotherapy, Asso-
ciation of Chartered Physiotherapists Interested in Neurology. Spas-
ticity in adults: management using botulinum toxin. National
guidelines. London: RCP, 2009.
Copyright � 2009 Royal College of Physicians. Adapted by permission.
Table 3 Common treatment goals and some objective measurements that may be used to record them
ICF level Goal area
Some examples of goals for
treatment
Measurements to record goal
achievement
Impairment
symptom
management
Relief of symptoms • Pain relief
• Muscle spasm frequency
• Involuntary movements e.g.
associated reactions
• Numerical or Visual analogue pain scores
• Spasm frequency counts
• The Associated Reaction Rating Scale [38]
Avoiding progression of
impairment
• Prevention of contractures and
deformity – ease of splint
application and prolonged use
• Optimizing posture and seating to
improve tissue viability
• Torque-controlled Goniometry [39]
• Goniometry (without controlling torque
forces)
• Anatomical distances (e.g. finger-palm
distance)
• Digital photos of position
Activity Passive function
Decrease carer burden
• Ease of moving, handling and
positioning
• Routine day-to-day care (e.g.
axillary hygiene, dressing)
Individual measures
• Carer ratings of ease of care (e.g. score out
of 10)
Standardized measures
• The Leeds Adult Spasticity Impact scale
(LASIS)
• The Arm Activity Scale (ArMa) (Passive
subscale)
Active function Improved ability in the following
tasks:
• Dexterity and reaching
• Self-care e.g. washing, dressing
• Eating/drinking
• Sexual activity
• Mobility e.g. balance, quality or
gait pattern or endurance of
wheelchair propulsion
Individual measures
• Self-rated ease of accomplishing activity
Video recordings
Standardized measures
• Motor function scales, e.g. The Action
Research Arm Test (ARAT), UL Motor
Assessment Scale (UL-MAS);
• Self-report UL use scales e.g. Motor
Activity Log (MAL) or Arm Activity Scale
(ArMa) (Activity subscale)
Participation Aesthetic and postural
appearance
Improve body image
Improve fit of clothes
• Self-rated body image
• Digital photos
Process goals
Enhance impact of
conventional
rehabilitation
intervention
Optimize effectiveness of
therapies
Reduce use of systemic
medication to treat
spasticity
Inform potential surgical
treatment
BoNT-A consensus statement: AUL 81
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

is that of Goal Attainment Scaling (GAS) [36]. GAS has
been used to demonstrate clinically important changes in
the context of UL spasticity management [31b,37]. GAS
will be discussed again in the section on evaluation of
treatment outcomes.
Some assessments that may be used to define goals, as
well as baseline performance levels are shown in Table 3.
Recommendation 2
In summary, the following is recommended:*
• Goals for treatment typically include managing symptoms,
preventing or slowing down the progression of impairments, and
improving passive or active function
• Treatment goals should be collaboratively determined with the
patient and their carers
• Establish baseline spasticity using reliable and valid scale
• Distinguish hypertonia caused by spasticity from that because of
soft tissue changes
• Outcome measures should be chosen and recorded at baseline
*Expert opinion
What is the optimal botulinum toxinintervention regimen?
There is no clear evidence from the literature to guide
optimal timing of interventions (e.g. early versus late),
frequency of interventions, dilutions, injection sites, or
doses. Accurate localization of injected muscles is likely
to result in improved benefit and requires a good
knowledge of surface anatomy. Muscle localization can
also be confirmed using such technology as neuromus-
cular electrical stimulation, ultrasound, or EMG. EMG
is useful to confirm the presence of muscle overactivity
and that the injection needle is within muscle tissue.
However, accurate identification of a specific muscle is
difficult with EMG because of the patient�s loss of
selective activation of individual muscles and because
many other muscles in the same compartment may be
overactive. Electrical stimulation is more accurate for
localization, particularly of small muscles controlling
the fingers and thumb, and for difficult to reach mus-
cles, such as subscapularis, pronator quadratus, and
individual finger flexor fascicles.
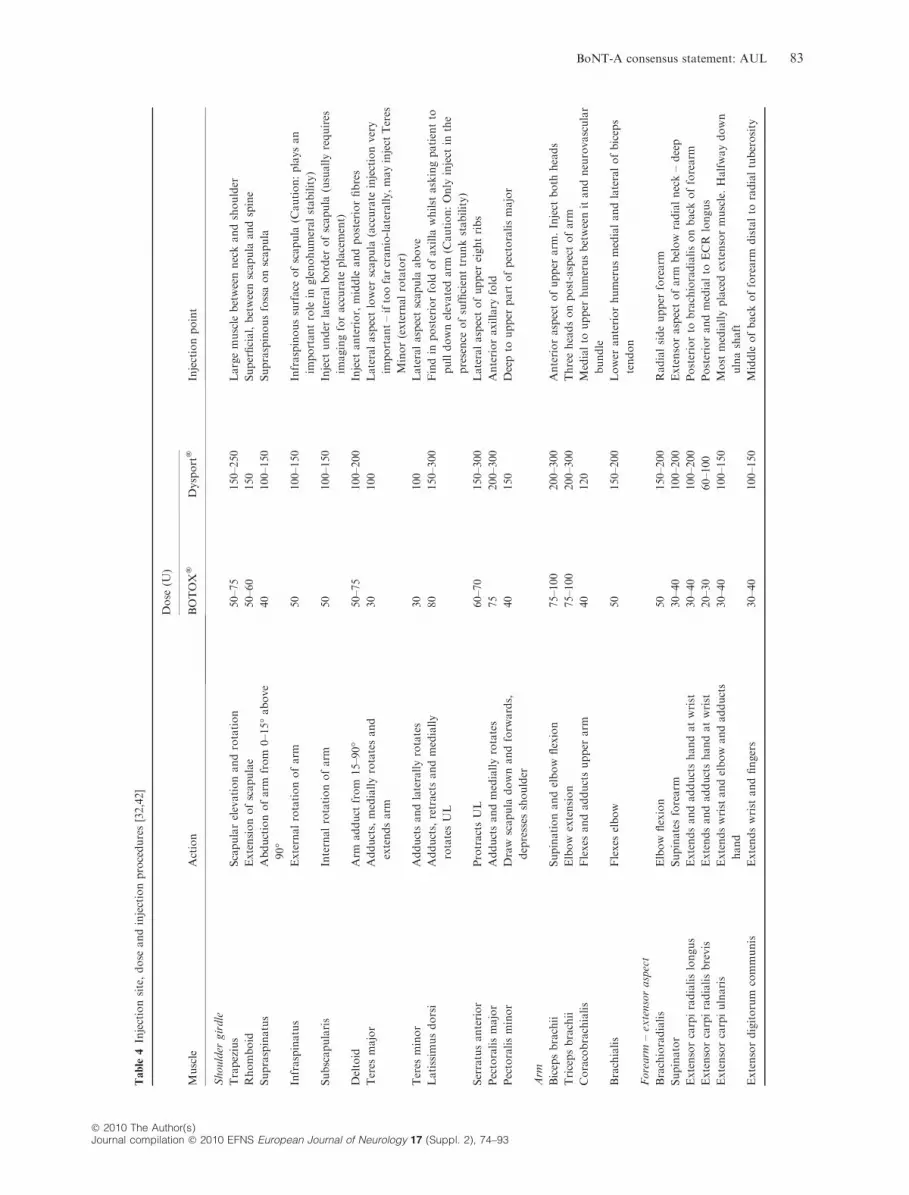
Table 4 summarizes suggestions for dosing in differ-
ent muscles based on recommendations of experienced
injectors derived from the UK guidelines. In general,
total dosing per session in the UL would not usually
exceed 400 units of BOTOX� (Allergan, Irvine, CA,
USA) or 750 units of Dysport� (Ipsen, Paris, France).
Some injectors prefer to use multiple injection tech-
niques and lower concentrations (more dilute) for larger
muscles. High-volume injections or end-plate targeting
produce better results in the biceps brachii [40], and
although intuitively sensible for other muscles, this is at
present a matter for clinical judgement.
Initiating regimen
Botulinum toxin type-A should be consideredwhen there
is an absence of absolute contraindications, and after
relative contraindications have been weighed carefully.
There is no arbitrary minimum duration of symp-
toms before treatment should be initiated, although it is
appropriate to commence when the spasticity is a sig-
nificant impediment to beginning occupational therapy
or physiotherapy, or when the problem has reached a
plateau or is worsening despite such therapies. A trial of
oral antispasticity agents is unnecessary for focal UL
spasticity [41].
The therapy or neurorehabilitation programme
should be continued following the injection. This may
require the addition of techniques that were not possi-
ble prior to BoNT-A injection, such as stretching or
fitting orthotics to improve passive function, or motor
training for active functional goals (see later).
Reinjection
Reinjection of the originally injected muscles may be
performed, after a minimum of 3 months, if it is clear
that the spastic motor overactivity being treated is
returning, despite continuing therapy, guided by the
baseline and outcome measures already identified.
Recommendation 3
In summary, the following is recommended:*
• Patients most likely to benefit from BoNT-A have focal or multi-
focal UL spasticity
• BoNT-A treatment should:
s be viewed as adjunct to a neurorehabilitation programme;
programme should be continued after injection
s only be considered in the absence of absolute contraindications
s commence when the spasticity is a significant impediment to
therapy or when problem is worsening or plateaus.
• Muscle localization may be based on surface anatomy, EMG
neuromuscular electrical stimulation, ultrasound or other appro-
priate imaging (e.g. CT)
*Expert opinion
What are the optimal adjunctiveinterventions?
Therapeutic intervention and BoNT-A
Spasticity management involves a multi-disciplinary
approach that includes:
82 G. Sheean et al.
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93
Table
4Injectionsite,dose
andinjectionprocedures[32,42]
Muscle
Action
Dose
(U)
Injectionpoint
BOTOX
�Dysport
�
Shoulder
girdle
Trapezius
Scapularelevationandrotation
50–75
150–250
Largemuscle
betweenneckandshoulder
Rhomboid
Extensionofscapulae
50–60
150
Superficial,betweenscapula
andspine
Supraspinatus
Abductionofarm
from
0–15
�above
90
�40
100–150
Supraspinousfossaonscapula
Infraspinatus
Externalrotationofarm
50
100–150
Infraspinoussurface
ofscapula
(Caution:playsan
importantrole
inglenohumeralstability)
Subscapularis
Internalrotationofarm
50
100–150
Inject
under
lateralborder
ofscapula
(usuallyrequires
imagingforaccurate
placement)
Deltoid
Arm
adduct
from
15–90
�50–75
100–200
Inject
anterior,middle
andposteriorfibres
Teres
major
Adducts,mediallyrotatesand
extendsarm
30
100
Lateralaspectlower
scapula
(accurate
injectionvery
important–iftoofarcranio-laterally,mayinject
Teres
Minor(externalrotator)
Teres
minor
Adductsandlaterallyrotates
30
100
Lateralaspectscapula
above
Latissim
usdorsi
Adducts,retractsandmedially
rotatesUL
80
150–300
Findin
posteriorfold
ofaxilla
whilst
askingpatientto
pulldownelevatedarm
(Caution:Only
inject
inthe
presence
ofsufficienttrunkstability)
Serratusanterior
ProtractsUL
60–70
150–300
Lateralaspectofupper
eightribs
Pectoralismajor
Adductsandmediallyrotates
75
200–300
Anterioraxillary
fold
Pectoralisminor
Draw
scapula
downandforw
ards,
depresses
shoulder
40
150
Deepto
upper
part
ofpectoralismajor
Arm
Bicepsbrachii
Supinationandelbow
flexion
75–100
200–300
Anterioraspectofupper
arm
.Inject
both
heads
Tricepsbrachii
Elbow
extension
75–100
200–300
Threeheadsonpost-aspectofarm
Coracobrachialis
Flexes
andadductsupper
arm
40
120
Medialto
upper
humerusbetweenitandneurovascular
bundle
Brachialis
Flexes
elbow
50
150–200
Lower
anteriorhumerusmedialandlateralofbiceps
tendon
Forearm
–extensoraspect
Brachioradialis
Elbow
flexion
50
150–200
Radialsideupper
forearm
Supinator
Supinatesforearm
30–40
100–200
Extensoraspectofarm
below
radialneck–deep
Extensorcarpiradialislongus
Extendsandadductshandatwrist
30–40
100–200
Posteriorto
brachioradialisonback
offorearm
Extensorcarpiradialisbrevis
Extendsandadductshandatwrist
20–30
60–100
Posteriorandmedialto
ECR
longus
Extensorcarpiulnaris
Extendswrist
andelbow
andadducts
hand
30–40
100–150
Most
mediallyplacedextensormuscle.Halfwaydown
ulnashaft
Extensordigitorum
communis
Extendswrist
andfingers
30–40
100–150
Middle
ofback
offorearm
distalto
radialtuberosity
BoNT-A consensus statement: AUL 83
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

Table
4(C
ontinued).
Muscle
Action
Dose
(U)
Injectionpoint
BOTOX
�Dysport
�
Extensordigitiminim
iExtends5th
finger
30–40
50–100
Medialto
extdigitorum
Extensorpollicislongus
Extendsalljoints
ofthumb
20–30
50–100
Midwaydownback
offorearm
Extensorpollicisbrevis
ExtendsCMC
andMCPjoints
of
thumb
20–25
50–75
Distalthirdofforearm
.Palpate
bymovingCMC
and
MCPjoints
Adductorpollicis
longus
Adductsthumbandhand
20–40
50–100
Proxim
alto
extpollicisbrevisonback
offorearm
.
Palpate
action
Extensorindicis
Extendsforefinger
20–30
50–100
Foundmedialofmost
lateraltendonofExtdigit
communis
Forearm
–Flexoraspect
SuperficialflexormusclesPronatorteres
Pronatesforearm
andflexes
elbow
30–40
100–200
Medialborder
ofanteriorcubitalfossa–medialto
brachialartery
Flexorcarpiradialis
Flexes
wrist
andelbow
30–40
100–200
Upper
forearm
just
below
bicipitalaponeurosisand
medialto
pronatorteres
Flexorcarpiulnaris
Flexes
andadductshandatwrist
30–40
100–150
Upper
forearm
medialaspectofflexorsurface
below
bicipitalaponeurosis.Medialto
FCR.Observeaction
ofwrist
flexion.
Flexordigitorum
superficialis
PIP
jointflexorandMCPjointflexor
25–30
100–200
Middle
offorearm
halfwaydownto
either
sideof
palm
aristendon
Flexordigitorum
profundus
Flexes
allfinger
joints
30–40
100–200
Upper
thirdofforearm
.Deepmuscle
abovelateral
border
ofulna
Flexorpollicislongus
Flexes
alljoints
ofthumb
20–30
100–150
Mid
forearm
over
anterioraspectofradius
Flexorpollicisbrevis
Pronatorquadratus
Pronatesforearm
20–30
100–150
Approach
muscle
from
extensoraspectofforearm
just
proxim
alto
wrist
andadvance
throughinterosseous
mem
brane
Lumbricals
10
Adaptedfrom:RoyalCollegeofPhysicians,British
SocietyofRehabilitationMedicine,
Chartered
SocietyofPhysiotherapy,AssociationofChartered
Physiotherapists
Interested
inNeurology.
Spasticityin
adults:managem
entusingbotulinum
toxin.Nationalguidelines.London:RCP,2009.Copyright
�2009RoyalCollegeofPhysicians.Adaptedbypermission.Adaptedfrom
BrinMuscle
andNerve.
1997;6:S208–S220.ReproducedwithpermissionofJohnWiley
&Sons,Inc.
84 G. Sheean et al.
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

• Proactive identification and relief of provocative
factors
• Positioning and handling in a range of positions to
vary the stretch on different muscles and body parts
throughout the 24-h day
• An active programme of occupational therapy or
physiotherapy with the following aims
s Maintaining muscle and soft tissue length across
joints
s Facilitating care giving (improvements in passive
function)
s Motor training to increase active participation in
tasks (improvements in active function)
Botulinum toxin type-A can make an important con-
tribution to a comprehensive rehabilitation programme
by decreasing spasticity making it easier to stretch and
maintain the length of soft tissues.
Evidence for effectiveness of adjunctive interventions
The evidence for effectiveness of �adjunctive therapeu-
tic intervention� is hard to extract from the literature
for a number of reasons. Therapy intervention con-
stitutes �normal treatment� for spasticity, and so is of-
ten coupled with BoNT-A both in trials and in clinical
practice. However, the interventions are rarely de-
scribed in detail, rather referred to simply as �treatment
in line with routine practice�. They are so well accepted
that to deprive the patient of this routine treatment has
ethical implications. As yet there are only two ran-
domized trials published in adult populations in which
the effect of adjunctive therapy plus BoNT-A injec-
tions into UL musculature has been compared to
BoNT-A injections alone [43,44]. Therefore, the inde-
pendent effects of BoNT-A treatment alone versus
those of therapy alone versus those generated by the
combination of the two are largely unknown [45]. In
any event, this discussion misses the point that in
clinical practice the BoNT-A injection is really the
adjunctive treatment.
Table 5 lists the adjunctive UL therapies that have
been used in the published literature to date, with evi-
dence of effectiveness of the therapies included.
Frequency and duration of adjunctive therapy
There is no standard regimen of adjunctive therapy that
is widely applied after BoNT-A injection into the UL
[44] and this is not surprising given the diversity of
presentation of clinical problems. At the current time,
therapists must rely on professional judgment to
determine potential changes and areas of improvement
in spasticity patients following BoNT-A injections.
In the absence of formal research evidence, other
guidelines [32] recommend a therapy review to assess
and plan adjunctive therapy at approximately 7–
14 days after injection when the clinical effect of spas-
ticity reduction is evident.
In studies that have provided UL therapies in con-
junction with BoNT-A injections into the UL of adults
with neurological conditions, the frequencies of therapy
provided post-injection are listed in Table 6.
Recommendation 4
In summary, the following is recommended:*
• Mainstay of spasticity management is a multi-disciplinary approach
• BoNT-A can make an important contribution to a comprehensive
rehabilitation programme
*Expert opinion
Management algorithm
The algorithm (Figure 1) introduces a new classification
of the positive phenomena of the upper motor neurone
(UMN) syndrome, borrowing from movement disor-
ders by dividing them into hyperkinetic (producing
unwanted involuntary movement) and hypokinetic
(restricting active and passive movement). Whilst this
classification has no technical implications (dosing,
sites, dilution, etc.) it does emphasize that the UMN
syndrome is essentially a movement disorder, that there
are many more types of spastic motor overactivity than
basic spasticity, and helps provide a visualizable foun-
dation for the phenomena.
Evaluation of treatment outcomes
The evaluation of treatment outcomes should involve
goal attainment, measures of symptoms or impairments,
and measures of active/passive function depending on
the goals for treatment. It may also be appropriate to
assess whether there has been an improvement at the
level of participation, including well-being or quality of
life, and to consider cost-effectiveness.
No single outcome measure will wholly evaluate
treatment benefits as individual goals differ.
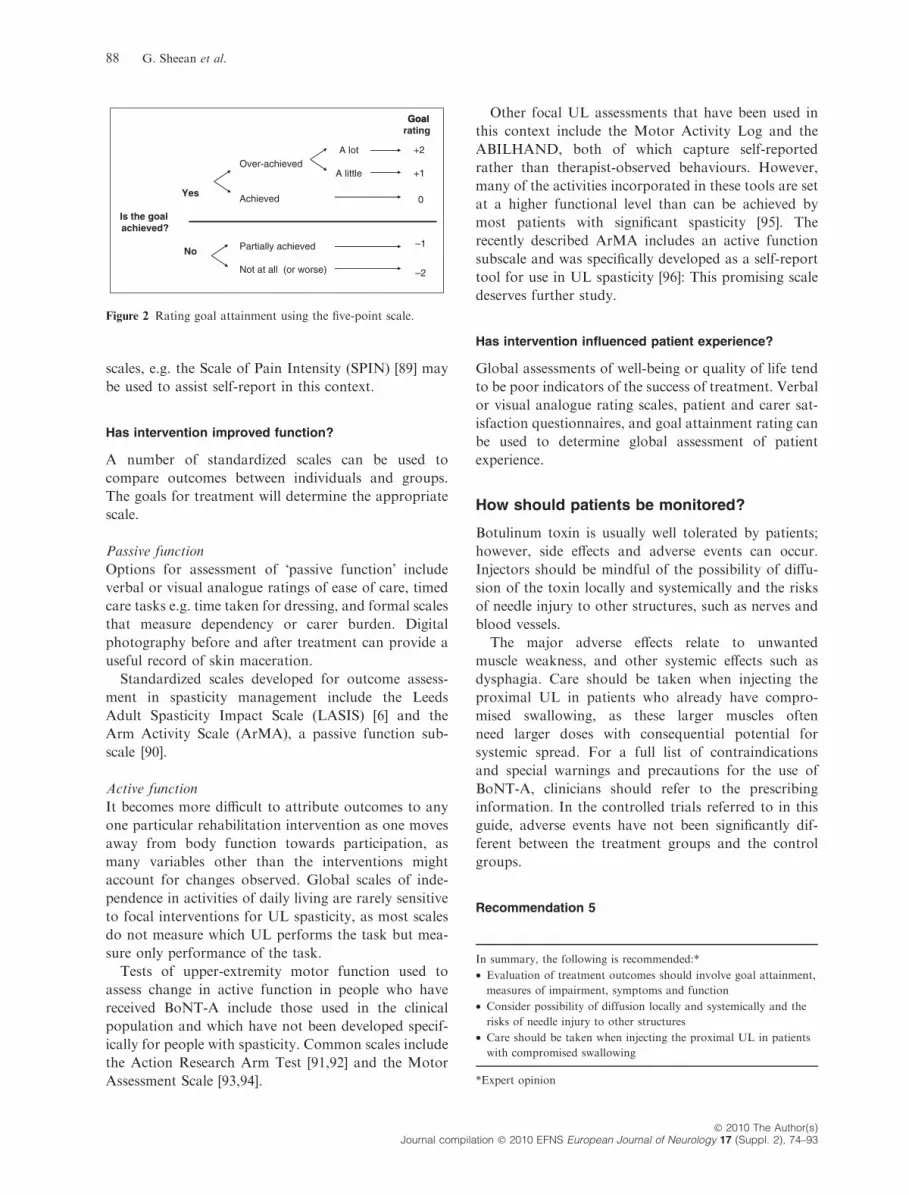
Have the treatment goals been achieved?
One of the simplest and most sensitive methods for
evaluating outcome from treatment is to record the
achievement of the specific goals using GAS as
described by Kiresuk and Sherman 1968 [36].
Achievement of individual goals is recorded on a
5-point scale from )2 to +2 (see Fig. 2 for decision
BoNT-A consensus statement: AUL 85
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93
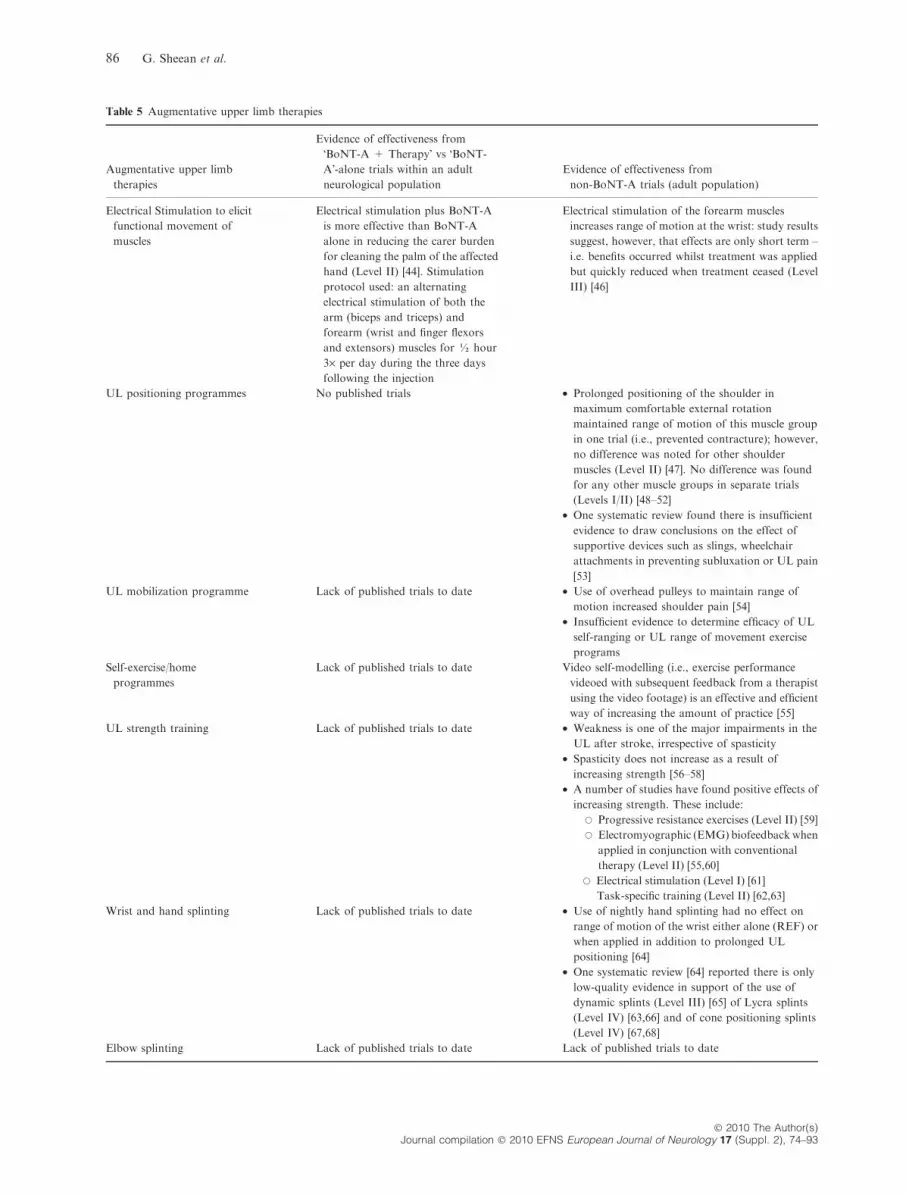
Table 5 Augmentative upper limb therapies
Augmentative upper limb
therapies
Evidence of effectiveness from
�BoNT-A + Therapy� vs �BoNT-
A�-alone trials within an adult
neurological population
Evidence of effectiveness from
non-BoNT-A trials (adult population)
Electrical Stimulation to elicit
functional movement of
muscles
Electrical stimulation plus BoNT-A
is more effective than BoNT-A
alone in reducing the carer burden
for cleaning the palm of the affected
hand (Level II) [44]. Stimulation
protocol used: an alternating
electrical stimulation of both the
arm (biceps and triceps) and
forearm (wrist and finger flexors
and extensors) muscles for ½ hour
3· per day during the three days
following the injection
Electrical stimulation of the forearm muscles
increases range of motion at the wrist: study results
suggest, however, that effects are only short term –
i.e. benefits occurred whilst treatment was applied
but quickly reduced when treatment ceased (Level
III) [46]
UL positioning programmes No published trials • Prolonged positioning of the shoulder in
maximum comfortable external rotation
maintained range of motion of this muscle group
in one trial (i.e., prevented contracture); however,
no difference was noted for other shoulder
muscles (Level II) [47]. No difference was found
for any other muscle groups in separate trials
(Levels I/II) [48–52]
• One systematic review found there is insufficient
evidence to draw conclusions on the effect of
supportive devices such as slings, wheelchair
attachments in preventing subluxation or UL pain
[53]
UL mobilization programme Lack of published trials to date • Use of overhead pulleys to maintain range of
motion increased shoulder pain [54]
• Insufficient evidence to determine efficacy of UL
self-ranging or UL range of movement exercise
programs
Self-exercise/home
programmes
Lack of published trials to date Video self-modelling (i.e., exercise performance
videoed with subsequent feedback from a therapist
using the video footage) is an effective and efficient
way of increasing the amount of practice [55]
UL strength training Lack of published trials to date • Weakness is one of the major impairments in the
UL after stroke, irrespective of spasticity
• Spasticity does not increase as a result of
increasing strength [56–58]
• A number of studies have found positive effects of
increasing strength. These include:
s Progressive resistance exercises (Level II) [59]
s Electromyographic (EMG) biofeedbackwhen
applied in conjunction with conventional
therapy (Level II) [55,60]
s Electrical stimulation (Level I) [61]
Task-specific training (Level II) [62,63]
Wrist and hand splinting Lack of published trials to date • Use of nightly hand splinting had no effect on
range of motion of the wrist either alone (REF) or
when applied in addition to prolonged UL
positioning [64]
• One systematic review [64] reported there is only
low-quality evidence in support of the use of
dynamic splints (Level III) [65] of Lycra splints
(Level IV) [63,66] and of cone positioning splints
(Level IV) [67,68]
Elbow splinting Lack of published trials to date Lack of published trials to date
86 G. Sheean et al.
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

tree) and composite T scores are derived for the chosen
goal set using the standard formula [31b, 37].
Has intervention improved impairment?
Use of the Tardieu and Ashworth scales to evaluate
hypertonicity has already been discussed. Documenta-
tion of improvement in range of movement may be
recorded through goniometry or anatomical distances
(e.g. fingers to palm), although these are prone to
observer error. In practice, the achievement of impair-
ment-related goals, such as ability to apply a splint or
orthosis, may be more relevant.
In the context of research, standardized torque forces
should ideally be used when documenting change in
passive range [88], but it is accepted that this may not be
practical in the clinical situation.
Has intervention improved symptoms?
Visual analogue scales and verbal rating scales can be
used to record symptoms such as pain or perceived
muscle stiffness before and after treatment. The pa-
tient is typically asked to classify the severity of their
target symptom with a numerical score out of 10,
or on a verbal scale e.g. �none – mild – moderate –
severe�.Some patients with cognitive or communication dif-
ficulties may have difficulty in responding to a standard
verbal or visual analogue scale. Pictorial graphic rating
Table 5 (Continued).
Augmentative upper limb
therapies
Evidence of effectiveness from
�BoNT-A + Therapy� vs �BoNT-
A�-alone trials within an adult
neurological population
Evidence of effectiveness from
non-BoNT-A trials (adult population)
Casting for contracture
management
Lack of published trials to date • A systematic review of casting (i.e., casting at the
wrist or elbow which may have been one cast or a
series of casts) in people with traumatic brain
injury or stroke found casting improves range of
motion immediately following cast removal [69]
• An RCT of elbow casting found a mean
improvement in muscle extensibility of 11� (95%
confidence interval )21� to 0�) favouring the cast
group one day after removal, but that any effect
from cast-wear had almost completely
disappeared by the follow-up 4 weeks after (mean
difference 2�, 95% CI )13� to 17�). UL function
results showed no between-group differences [70]
Surgical release of elbow
flexor tendons
Lack of published trials to date Lack of published trials to date
Facilitation training for arm
extension and reach and
grasp
Lack of published trials to date Studies on UL activity have found the following:
• Task-specific training in conjunction with strength
training was superior to neuro-developmental
therapy [63]. Task-specific training was also
superior to repetition alone in improving UL
activity [71]
• Repetitive protraction of the arm was superior to
placebo in the severely disabled [72]. There is
conflicting evidence for bilateral retraining [73–
76]. No improvement in activity has been reported
by higher level trials [73–76].
• Neither NDT [77] nor sensorimotor integration
[78] was more effective than the orthopaedic
approach in improving UL activity
• Joint position feedback in conjunction with
conventional therapy improved the quality of
reaching [79]
• Robot-assisted shoulder–elbow movement
improved reaching [80–82]
• Constraint-induced movement therapy improved
UL activity [83]
Training of carer in moving
and handling of limb
Lack of published trials to date Lack of published trials to date
BoNT-A consensus statement: AUL 87
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93
scales, e.g. the Scale of Pain Intensity (SPIN) [89] may
be used to assist self-report in this context.
Has intervention improved function?
A number of standardized scales can be used to
compare outcomes between individuals and groups.
The goals for treatment will determine the appropriate
scale.
Passive function
Options for assessment of �passive function� include
verbal or visual analogue ratings of ease of care, timed
care tasks e.g. time taken for dressing, and formal scales
that measure dependency or carer burden. Digital
photography before and after treatment can provide a
useful record of skin maceration.
Standardized scales developed for outcome assess-
ment in spasticity management include the Leeds
Adult Spasticity Impact Scale (LASIS) [6] and the
Arm Activity Scale (ArMA), a passive function sub-
scale [90].
Active function
It becomes more difficult to attribute outcomes to any
one particular rehabilitation intervention as one moves
away from body function towards participation, as
many variables other than the interventions might
account for changes observed. Global scales of inde-
pendence in activities of daily living are rarely sensitive
to focal interventions for UL spasticity, as most scales
do not measure which UL performs the task but mea-
sure only performance of the task.
Tests of upper-extremity motor function used to
assess change in active function in people who have
received BoNT-A include those used in the clinical
population and which have not been developed specif-
ically for people with spasticity. Common scales include
the Action Research Arm Test [91,92] and the Motor
Assessment Scale [93,94].
Other focal UL assessments that have been used in
this context include the Motor Activity Log and the
ABILHAND, both of which capture self-reported
rather than therapist-observed behaviours. However,
many of the activities incorporated in these tools are set
at a higher functional level than can be achieved by
most patients with significant spasticity [95]. The
recently described ArMA includes an active function
subscale and was specifically developed as a self-report
tool for use in UL spasticity [96]: This promising scale
deserves further study.
Has intervention influenced patient experience?
Global assessments of well-being or quality of life tend
to be poor indicators of the success of treatment. Verbal
or visual analogue rating scales, patient and carer sat-
isfaction questionnaires, and goal attainment rating can
be used to determine global assessment of patient
experience.
How should patients be monitored?
Botulinum toxin is usually well tolerated by patients;
however, side effects and adverse events can occur.
Injectors should be mindful of the possibility of diffu-
sion of the toxin locally and systemically and the risks
of needle injury to other structures, such as nerves and
blood vessels.
The major adverse effects relate to unwanted
muscle weakness, and other systemic effects such as
dysphagia. Care should be taken when injecting the
proximal UL in patients who already have compro-
mised swallowing, as these larger muscles often
need larger doses with consequential potential for
systemic spread. For a full list of contraindications
and special warnings and precautions for the use of
BoNT-A, clinicians should refer to the prescribing
information. In the controlled trials referred to in this
guide, adverse events have not been significantly dif-
ferent between the treatment groups and the control
groups.
Recommendation 5
In summary, the following is recommended:*
• Evaluation of treatment outcomes should involve goal attainment,
measures of impairment, symptoms and function
• Consider possibility of diffusion locally and systemically and the
risks of needle injury to other structures
• Care should be taken when injecting the proximal UL in patients
with compromised swallowing
*Expert opinion
Yes
No
Over-achieved
Achieved
Is the goal achieved?
A lot
A little
+2
+1
0
Partially achieved
Not at all (or worse)
–1
–2
GoalratingGoal
Figure 2 Rating goal attainment using the five-point scale.
88 G. Sheean et al.
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

Future directions
At present, there are deficiencies in knowledge at all
levels of management of adult UL spasticity with
BoNT-A, except the very few associated with Class I
evidence already described, and also regarding the
safety of the drug.
The knowledge gaps require that most of the paper
is based on low levels of evidence, chiefly expert
opinion.
Future goals for research and clinical practice may
include:
• Study techniques to accentuate the paralytic effect of
the toxin.
s Study injection technique – dilution, injection site,
localization method.
s Develop electrical stimulation post-injection.
• Studies to predict improvement in active move-
ment, designed from a perspective that BoNT-A is
used as an adjunct to standard, ideally proven,
therapies.
• Develop and study measures of active upper limb
function sensitive to reduction in spasticity – includ-
ing further evaluation of the ArMa.
• Study the role of early injection BoNT-A as pre-
ventive for development of contracture or unmasking
potential for active movement.
• Develop internationally agreed datasets to facilitate
large prospective cohort studies conducted in the
context of real-life clinical practice to identify which
patients respond best to which approaches.
Acknowledgements
The Cerebral Palsy Institute sincerely thank the Prin-
cipal Authors involved in the development and leader-
ship of these International Consensus Statements,
including: Professor H. Kerr Graham; Professor John
Olver; Associate Professor Victor S.C. Fung; Associate
Professor Barry Rawicki; Dr Barbara J. Singer and
Dr Iona Novak. The authors gratefully acknowledge
Dr Stephen de Graaff for the review of this paper.
Table 6 Frequency of therapy post-injection
Study Therapy frequency Level of evidence*
Hesse S et al. Clin Rehabil.
1998;12(5):381–8 [44]
ES for ½ hr per session, three sessions per day for 3 days following BoNT-A
injections
II
Giovannelli M et al. Clin Rehabil.
2007; 21: 331–337 [43]
Daily physiotherapy for 15 consecutive days after injection. Patients received
therapy to maintain muscle length through passive or active exercise, and
stretching regimen on injected area (40 min each session): soft movements of
joints with short pauses at final position and reciprocal movements
II
Carda S et al. Clin Rehabil
2005;19:621–626 [84]
Adhesive taping worn 24-h/day for 6 days and checked daily III
Thermoplastic palmar splint positioned for maximal stretching in conjunction with
daily stretching exercises and electrical stimulation of injected muscles for 5 days.
Total daily time required for this treatment was about 90 min. In addition,
60 min was required for splint modelling during 1st day
Levy CE et al. Am J Phys Med
Rehabil 2007;86:696–706 [45]
Exercise therapy commenced within 1 week of BONT-A treatment. Its intensity
was 1 h, 3· per week, duration 4 wks
III
Subjects who met eligibility criteria for CIMT at the conclusion of exercise therapy
(4-wks post-injection) were then entered into a 2-wk course of CIMT. CIMT
consisted of 6 h of intensive upper-limb training 5 days/wk for 2 wks
Rodriquez AA et al. Am J Phys Med
Rehabil 2000; 79: 44–47 [85]
Stretch using a short-hand �weight-bearing� orthosis for 1 min 5 times/day and on
hands and knees (3-point) 5–10 min/day. All subjects used a wrist-hand
antispasticity ball orthosis for night use. After stretching, subjects participated in
self-directed training of voluntary finger and wrist extension as appropriate to
their level of active extension (implied daily; frequency and total amount of
therapy not reported)
IV
Sun SF et al. Physical Therapy 86
(10):1387–1397 [86]
4-wk modified CIMT programme: 2 h of training each day three times weekly and
�told to wear the restraint as long as possible and for at least 5 h of his waking
hours per day during the study period�
V
Denham SP. American Journal of
Occupational Therapy 2008;61:473–
479 [87]
Occupational therapy began the day following injection, and was scheduled 3·week for 6 weeks, then 2· week for 6 weeks. Following one-on-one therapy, the
participant was started on a functional home programme for 6 weeks including
overnight splint wear, daily passive stretching and AROM exercises followed by a
minimum of three functional activities
V
*Level of evidence refers specifically to the level of evidence supporting the therapy intervention, not the BoNT-A comparison. Thus, the therapy
protocol provided in conjunction with BoNT-A in a BoNT-A RCT would be classified as being level III (case series) if there was not a control
group who received BoNT-A without therapy.
BoNT-A consensus statement: AUL 89
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

The Cerebral Palsy Institute also gratefully
acknowledges the unrestricted educational grant
received from Allergan to support the project. It should
be noted that no authors were provided with any funds
to participate in the project. Funds were solely used for
independent project management and professional
editing from an independent medical writer. A project
charter was developed by the Cerebral Palsy Institute
and independent project officer based on a literature
review of International Consensus Statements. As part
of this charter, Allergan had no access to the manu-
scripts at any point throughout the project duration
and had no right of scientific veto. Authors were
recruited to the project using the following criteria: had
published research on BoNT or the associated adjunc-
tive therapies; were from varying professions repre-
senting the team typically involved with a patient for
this indication of BoNT; were preferentially from
varying countries and continents; had experience of
using different preparations of BoNT so as to minimize
potential sources of bias; had experience working with
children and adults; and were willing to volunteer to
work in a multi-disciplinary author team. Potential
authors were excluded if they were or had ever been
employees of any of the BoNT pharmaceutical
companies.
Conflicts of interest
Barry Snow has acted as a paid consultant to Allergan
by attending an advisory board on the use of botulinum
toxin for headache. Lynne Turner Stokes has received
honoraria and consultancy fees from Ipsen Ltd relating
to research and clinical use of Botulinum Toxin, some
of which are referred to in this work.
References
1. American Academy of Neurology. AAN classification ofevidence for therapeutic intervention. 2004. http://www.neurology.org. (accessed 23/01/2009)
2. World Health Organization. International Classification ofFunctioning, Disability and Health (ICF). Geneva: WorldHealth Organization, 2001.
3. Esquenazi A, Mayer N. Botulinum toxin for the man-agement of muscle overactivity and spasticity after stroke.Curr Atheroscler Rep 2001; 3: 295–298.
4. Sheean GL. Botulinum treatment of spasticity: why is it sodifficult to show a functional benefit? Curr Opin Neurol2001; 14: 771–776.
5. Brashear A, Gordon MF, Elovic E, et al. Intramuscularinjection of botulinum toxin for the treatment of wrist andfinger spasticity after a stroke. N Engl J Med 2002; 347:395–400.
6. Bhakta BB, Cozens JA, Chamberlain MA, Bamford JM.Impact of botulinum toxin type A on disability and carerburden due to arm spasticity after stroke: a randomised
double blind placebo controlled trial. J Neurol NeurosurgPsychiatry 2000; 69: 217–221.
7. Yelnik AP, Colle FM, Bonan IV, Vicaut E. Treatment ofshoulder pain in spastic hemiplegia by reducing spasticityof the subscapular muscle: a randomised, double blind,placebo controlled study of botulinum toxin A. J NeurolNeurosurg Psychiatry 2007; 78: 845–848.
8. Lim J-Y, Koh J-H, Paik N-J. Intramuscular botulinumtoxin-A reduces hemiplegic shoulder pain: a randomized,double-blind, comparative study versus intraarticular tri-amcinolone acetonide. Stroke 2008; 39: 126–131.
9. de Boer KS, Arwert HJ, de Groot JH, Meskers CGM,Rambaran Mishre AD, Arendzen JH. Shoulder pain andexternal rotation in spastic hemiplegia do not improve byinjection of botulinum toxin A into the subscapularmuscle. J Neurol Neurosurg Psychiatry 2008; 79: 581–583.
10. Elia AE, Filippini G, Calandrella D, Albanese A. Botu-linum neurotoxins for post-stroke spasticity in adults: asystematic review. Mov Disord 2009; 24: 801–812.
11. Woldag H, Hummelsheim H. Is the reduction of spasticityby botulinum toxin a beneficial for the recovery of motorfunction of arm and hand in stroke patients? Eur Neurol2003; 50: 165–171.
12. Slawek J, Bogucki A, Reclawowicz D. Botulinum toxintype A for upper limb spasticity following stroke: anopen-label study with individualised, flexible injectionregimens. Neurol Sci 2005; 26: 32–39.
13. Rousseaux M, Kozlowski O, Froger J. Efficacy of botu-linum toxin A in upper limb function of hemiplegic pa-tients. J Neurol 2002; 249: 76–84.
14. Caty GD, Detrembleur C, Bleyenheuft C, et al. Effect ofupper limb botulinum toxin injections on impairment,activity, participation, and quality of life among strokepatients. Stroke 2009; 40: 2589–2591.
15. Lagalla G, Danni M, Reiter F, Ceravolo MG, ProvincialiL. Post-stroke spasticity management with repeated bot-ulinum toxin injections in the upper limb. Am J Phys MedRehabil 2000; 79: 377–384.
16. Wang HC, Hsieh LF, Chi WC, Lou SM. Effect of intra-muscular botulinum toxin injection on upper limb spas-ticity in stroke patients. Am J Phys Med Rehabil 2002; 81:272–278.
17. Miscio G, Del Conte C, Pianca D, et al. Botulinum toxinin post-stroke patients: stiffness modifications and clinicalimplications. J Neurol 2004; 251: 189–196.
18. Russo RN, Crotty M, Miller MD, Murchland S, Flett P,Haan E. Upper-limb botulinum toxin A injection andoccupational therapy in children with hemiplegic cerebralpalsy identified from a population register: a single-blind,randomized, controlled trial. Pediatrics 2007; 119: 1149–1158.
19. Chin TY, Duncan JA, Johnstone BR, Graham HK.Management of the upper limb in cerebral palsy. J PediatrOrthop 2005; 14: 389–404.
20. Francis HP, Wade DT, Turner-Stokes L, Kingswell RS,Dott CS, Coxon EA. Does reducing spasticity translateinto functional benefit? An exploratory meta-analysis.J Neurol Neurosurg Psychiatry 2004; 75: 1547–1551.
21. Simpson DM, Alexander DN, O�Brien CF, et al. Botu-linum toxin type A in the treatment of upper extremityspasticity: a randomised, double-blind, placebo-controlledtrial. Neurology 1996; 46: 1306–1310.
22. Bakheit AM, Thilmann AF, Ward AB, et al. A random-ized, double-blind, placebo-controlled, dose-ranging study
90 G. Sheean et al.
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

to compare the efficacy and safety of three doses ofbotulinum toxin type A (Dysport�) with placebo inupper limb spasticity after stroke. Stroke 2000; 31: 2402–2406.
23. Smith SJ, Ellis E, White S, Moore AP. A double-blindplacebo-controlled study of botulinum toxin in upper limbspasticity after stroke or head injury. Clin Rehabil 2000;14: 5–13.
24. Bakheit AM, Pittock S, Moore AP, et al. A randomized,double-blind, placebo-controlled study of the efficacy andsafety of botulinum toxin type A in upper limb spasticityin patients with stroke. Eur J Neurol 2001; 8: 559–565.
25. Francisco GE, Boake C, Vaughn A. Botulinum toxin inupper limb spasticity after acquired brain injury: arandomised trial comparing dilution techniques.Am J Phys Med Rehabil 2002; 81: 355–363.
26. Brashear A, McAfee AL, Kuhn ER, Fyffe J. Botulinumtoxin type B in upper-limb poststroke spasticity: a double-blind, placebo-controlled trial. Arch Phys Med Rehabil2004; 85: 705–709.
27. Childers MK, Brashear A, Jozefczyk P, et al. Dose-dependent response to intramuscular botulinum toxintype A for upper-limb spasticity in patients after a stroke.Arch Phys Med Rehabil 2004; 85: 1063–1069.
28. Suputtitada A, Suwanela NC. The lowest effective dose ofbotulinum A toxin in adult patients with upper limbspasticity. Disabil Rehabil 2005; 27: 176–184.
29. Bhakta BB, O�Connor RJ, Cozens JA. Associated reac-tions after stroke: a randomized controlled trial of theeffect of botulinum toxin type A. J Rehabil Med 2008; 40:36–41.
30. Mayer NH, Whyte J, Wannstedt G, Ellis CA. Compara-tive impact of 2 botulinum toxin injection techniques forelbow flexor hypertonia. Arch Phys Med Rehabil 2008; 89:982–987.
31a.McCrory P, Turner-Stokes L, Baguley I, et al. Botulinumtoxin A for the treatment of upper limb spasticity followingstroke: amulti-centre randomized placebo-controlled studyof the effects on quality of life and other person-centredoutcomes. J Rehabil Med 2009; 41: 536–544.
31b.Turner-Stokes L, Baguley I, De Graff S, McCrory P,Katrak P, Davies L, Hughes A. Goal attainment scalingin the evaluation of treatment of upper limb spasticitywith botulinum toxin: a secondary analysis from adouble blind placebo controlled randomised clinical trial.J Rehabil Med 2010; 42: 81–89.
32. Royal College of Physicians, British Society of Rehabili-tation Medicine, Chartered Society of Physiotherapy,Association of Chartered Physiotherapists Interested inNeurology. Spasticity in Adults: Management Using Bot-ulinum Toxin. National guidelines. London: RCP, 2009.
33. Wade DT. Evidence relating to goal planning in rehabil-itation. Clin Rehabil 1998; 12: 273–275.
34. Mehrholz J, Wagner K, Meissner D, et al. Reliability ofthe Modified Tardieu Scale and the Modified AshworthScale in adult patients with severe brain injury: a com-parison study. Clin Rehabil 2005; 19: 751–759.
35. Patrick E, Ada L. The Tardieu Scale differentiates con-tracture from spasticity whereas the Ashworth Scale isconfounded by it. Clin Rehabil 2006; 20: 173–182.
36. Kiresuk TJ, Sherman RE. Goal attainment scaling: ageneral method for evaluating comprehensive communitymental health programs. Community Ment Health J 1968;4: 443–453.
37. Ashford S, Turner-Stokes L. Goal attainment for spas-ticity management using botulinum toxin. Physiother ResInt 2006; 11: 24–34.
38. Macfarlane A, Turner-Stokes L, De Souza L. The Asso-ciated Reaction Rating Scale: development and pre-liminary evaluation of a clinical tool to measureassociated reactions in the hemiplegic upper limb.Clin Rehabil 2002; 16: 726–735.
39. Harvey L, King M, Herbert R. Reliability of a tool formeasuring the length of long finger flexor muscles.J Hand Ther 1995; 7: 251–254.
40. Gracies JM, Lugassy M, Weisz DJ, et al. Botulinum toxindilution and endplate targeting in spasticity: a double-blind controlled study. Arch Phys Med Rehabil 2009; 90:9–16.
41. Sheean G. Botulinum toxin should be first-line treatmentfor poststroke spasticity. J Neurol Neurosurg Psychiatry2009; 80: 359.
42. Brin MF. Dosing, administration, and a treatment algo-rithm for use of botulinum toxin A for adult-onset spas-ticity. Spasticity Study Group. Muscle Nerve 1997; 6:
S208–S220.43. Giovannelli M, Borriello G, Castri P, Prosperini L,
Pozzilli C. Early physiotherapy after injection of botu-linum toxin (Bt) increases the beneficial effects on spas-ticity in patients with multiple sclerosis. Clin Rehabil 2007;21: 331–337.
44. Hesse S, Reiter F, Konrad M, Jahnke MT. Botulinumtoxin type A and short-term electrical stimulation in thetreatment of upper limb flexor spasticity after stroke: arandomized, double-blind, placebo-controlled trial. ClinRehabil 1998; 12: 381–388.
45. Levy CE, Giuffrida C, Richards L, Wu S, Davis S,Nadeau SE. Botulinum toxin A, evidence-based exercisetherapy, and constraint-induced movement therapy forupper-limb hemiparesis attributable to stroke: apreliminary study. Am J Phys Med Rehabil 2007; 86: 696–706.
46. Pandyan AD, Granat MH, Stott DJ. Effects of electricalstimulation on flexion contractures in the hemiplegicwrist. Clin Rehabil 1997; 11: 123–130.
47. Ada L, Goddard E, McCully J, Stavrinos T, Bampton J.30 minutes of positioning reduces the development ofexternal rotation but not flexion contracture in theshoulder after stroke: a randomized controlled trial. ArchPhys Med Rehabil 2005; 86: 230–234.
48. Dean CM, Mackey FH, Katrak P. Examination ofshoulder positioning after stroke: a randomised controlledpilot trial. Aust J Physiother 2000; 46: 35–40.
49. Horsley SA, Herbert RD, Ada L. Four weeks of dailystretch has little or no effect on wrist contracture afterstroke: a randomised controlled trial. Aust J Physiother2007; 53: 239–245.
50. Turton AJ, Britton E. A pilot randomized controlled trialof a daily muscle stretch regime to prevent contractures inthe arm after stroke. Clin Rehabil 2005; 19: 600–612.
51. de Jong LD, Nieuwboer A, Aufdemkampe G. Contrac-ture preventive positioning of the hemiplegic arm in sub-acute stroke patients: a pilot randomized controlled trial.Clin Rehabil 2006; 20: 656–667.
52. Gustafsson L, McKenna K. A program of static-posi-tional stretches does not reduce hemiplegic shoulder painor maintain shoulder range of motion - a randomizedcontrolled trial. Clin Rehabil 2006; 20: 277–286.
BoNT-A consensus statement: AUL 91
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

53. Ada L, Foongchomcheay A, Canning C. Supportivedevices for preventing and treating subluxation of theshoulder after stroke. Cochrane Database Syst Rev 2002;Issue 4. Art. No.: Cd003863. Doi:10.1002/14651858.Cd003863.
54. Kumar R, Metter EJ, Mehta AJ, Chew T. Shoulder painin hemiplegia. The role of exercise. Am J Phys MedRehabil 1990; 69: 205–208.
55. McCLellan R, Ada L. A six week, resource-efficientmobility program after discharge from rehabilitationimproves standing in people affected by stroke: placebo-controlled randomised controlled trial. Aust J Physiother2004; 50: 163–167.
56. Inglis J, Donald MW, Monga TN, Sproule M, Young MJ.Electromyographic biofeedback and physical therapy ofthe hemiplegic upper limb. Arch Phys Med Rehabil 1984;65: 755–759.
57. Teixeira-Salmela LF, Olney SJ, Nadeau S, Brouwer B.Muscle strengthening and physical conditioning to reduceimpairment and disability in chronic stroke survivors.Arch Phys Med Rehabil 1999; 80: 1211–1218.
58. Heckmann J, Mokrusch T, Krockel A, Warnke S, Von S,Neundorfer B. EMG-triggered electrical muscle stimula-tion in the treatment of central hemiparesis after a stroke.Eur J Phys Med Rehabil 1997; 7: 138–141.
59. Morris SL, Dodd KJ, Morris ME. Outcomes ofprogressive resistance strength training following stroke: asystematic review. Clin Rehabil 2004; 18: 27–39.
60. Basmajian JV, Kukulka CG, Narayan MG, Takebe K.Biofeedback treatment of foot-drop after stroke com-pared with standard rehabilitation technique: effects onvoluntary control and strength. Arch Phys Med Rehabil1975; 56: 231–236.
61. Glanz M, Klawansky S, Stason W, Berkey C, ChalmersTC. Functional electrostimulation in poststroke rehabili-tation: a metaanalysis of the randomized controlled trials.Arch Phys Med Rehabil 1996; 77: 549–553.
62. Duncan P, Studenski S, Richards L, et al. Randomizedclinical trial of therapeutic exercise in subacute stroke.Stroke 2003; 34: 2173–2180.
63. Winstein CJ, Rose DK, Tan SM, Lewthwaite R, ChuiHC, Azen SP. A randomized controlled comparison ofupper-extremity rehabilitation strategies in acute stroke: apilot study of immediate and long-term outcomes. ArchPhys Med Rehabil 2004; 85: 620–628.
64. Lannin NA, Horsley SA, Herbert R, McCluskey A,Cusick A. Splinting the hand in the functional positionafter brain impairment: a randomized, controlled trial.Arch Phys Med Rehabil 2003; 84: 297–302.
65. McPherson JJ, Becker H, Franszczak N. Dynamic splintto reduce the passive component of hypertonicity. ArchPhys Med Rehabil 1985; 66: 249–252.
66. Gracies JM, Marosszeky JE, Renton R, Sananam J,Gandevia SC, Burke D. Short-term effects of dynamiclycra splints on upper limb in hemiplegic patients. ArchPhys Med Rehabil 2000; 81: 1547–1555.
67. Dayoff N. Rethinking stroke: soft or hard devices toposition hands. Am J Nurs 1975; 75: 1142–1144.
68. Jamison SL, Dayhoff NE. A hard hand-positioning deviceto decrease wrist and finger hypertonicity: a sensorimotorapproach for the patient with nonprogressive braindamage. J Nurs Res 1980; 29: 285–289.
69. Lannin NA, Novak I, Cusick A. A systematic review ofupper extremity casting for children and adults with cen-
tral nervous system motor disorders. Clin Rehabil 2007;21: 963–973.
70. Moseley AM, Hassett LM, Leung J, Clare JS, HerbertRD, Harvey LA. Serial casting versus positioning for thetreatment of elbow contractures in adults with traumaticbrain injury: a randomized controlled trial. Clin Rehabil2008; 22: 406–417.
71. Nelson DL, Konosky K, Fleharty K, et al. The effects ofan occupationally embedded exercise on bilaterallyassisted supination in persons with hemiplegia. Am JOccup Ther 1996; 50: 639–646.
72. Feys HM, De Weerdt WJ, Selz BE, et al. Effect of atherapeutic intervention for the hemiplegic upper limb inthe acute phase after stroke: a single blind, randomized,controlled multicenter trial. Stroke 1998; 29: 785–792.
73. Lewis GN, ByblowWD. Neurophysiological and behavio-ural adaptations to a bilateral training intervention inindividuals following stroke. Clin Rehabil 2004; 18: 48–59.
74. Luft AR, McCombe-Waller S, Whitall J, et al. Repetitivebilateral arm training and motor cortex activation inchronic stroke: a randomized controlled trial. J Am MedAssoc 2004; 292: 1853–1861.
75. McCombe Waller S, Whitall J. Fine motor control inadults with and without chronic hemiparesis: baselinecomparison to nondisabled adults and effects of bilateralarm training. Arch Phys Med Rehabil 2004; 85: 1076–1083.
76. Mudie MH, Matyas TA. Responses of the densely hemi-plegic upper extremity to bilateral training. NeurorehabilNeural Repair 2001; 15: 129–140.
77. Gelber D, Josefcyz P, Herrman D, Good D, Verhulst S.Comparison of two therapy approaches in the rehabili-tation of the pure motor hemiparetic stroke patient.J Neurol Rehabil 1995; 9: 191–196.
78. Jongbloed L, Stacey S, Brighton C. Stroke rehabilitation:sensorimotor integrative treatment versus functionaltreatment. Am J Occup Ther 1989; 43: 391–397.
79. Maulucci RA, Eckhouse RH. Retraining reaching inchronic stroke with real-time auditory feedback.Neurorehabilitation 2001; 16: 171–182.
80. Lum PS, Burgar CG, Shor PC, Majmundar M, Van derLoos M. Robot-assisted movement training comparedwith conventional therapy techniques for the rehabilita-tion of upper-limb motor function after stroke. Arch PhysMed Rehabil 2002; 83: 952–959.
81. Volpe BT, Krebs HI, Hogan N, Edelstein OL, Diels C,Aisen M. A novel approach to stroke rehabilitation:robot-aided sensorimotor stimulation. Neurology 2000;54: 1938–1944.
82. Fasoli SE, Krebs HI, Stein J, Frontera WR, Hughes R,Hogan N. Robotic therapy for chronic motor impair-ments after stroke: follow-up results. Arch Phys MedRehabil 2004; 85: 1106–1111.
83. Van Peppen RPS, Kwakkel G, Wood-Dauphinee S,Hendriks HJM, Van Der Wees PJ, Dekker J. The impactof physical therapy on functional outcomes after stroke:what�s the evidence? Clin Rehabil 2004; 18: 833–862.
84. Carda S, Molteni F. Taping versus electrical stimulationafter botulinum toxin type A injection for wrist and fingerspasticity. A case-control study. Clin Rehabil 2005; 19:
621–626.85. Rodriquez AA, McGinn M, Chappell R. Botulinum toxin
injection of spastic finger flexors in hemiplegic patients.Am J Phys Med Rehabil 2000; 79: 44–47.
92 G. Sheean et al.
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93

86. Sun SF, Hsu CW, Hwang CW, Hsu PT, Wang JL, YangCL. Application of combined botulinum toxin type A andmodified constraint-induced movement therapy for anindividual with chronic upper-extremity spasticity afterstroke. Phys Ther 2006; 86: 1387–1397.
87. Denham SP. Augmenting occupational therapy treatmentof upper-extremity spasticity with botulinum toxin A: acase report of progress at discharge and 2 years later. AmJ Occup Ther 2008; 61: 473–479.
88. Harvey L. Management of People with Spinal CordInjuries: a Guide for Physiotherapists. London: Elsevier,2008.
89. Jackson D, Horn S, Kersten P, Turner-Stokes L. Devel-opment of a pictorial scale of pain intensity for patientswith communication impairments: initial validation in ageneral population. Clin Med 2006; 6: 580–585.
90. Ashford S, Slade M, Turner-Stokes L. Preliminaryevaluation of internal consistency and reliability of thearm activity measure (ArmA). Proceedings of the Societyfor Rehabilitation Research. Clin Rehabil 2008; 22: 856–863.
91. Carroll D. A quantitative test of upper extremity function.J Chronic Dis 1965; 18: 479–491.
92. Lyle RC. A performance test for assessment of upper limbfunction in physical rehabilitation treatment and research.Int J Rehabil Res 1981; 4: 483–492.
93. Carr JH, Shepherd RB, Nordholm L, Lynne D. Investi-gation of a new motor assessment scale for strokepatients. Phys Ther 1985; 65: 175–180.
94. Lannin NA. Reliability, validity and factor structure ofthe upper limb subscale of the Motor Assessment Scale(UL-MAS) in adults following stroke. Disabil Rehabil2004; 26: 109–116.
95. Ashford S, Slade M, Malaprade F, Turner-Stokes L.Evaluation of functional outcome measures for the hem-iparetic upper limb – a systematic review. J Rehabil Med2008; 40: 787–795.
96. Ashford S, Slade M, Turner-Stokes L. Development ofthe Arm Activity Measure for assessment of activity in thehemiparetic arm. 5th World Congress for NeuroReha-bilitation, Brazilia, Brazil. Sept. 2008. Neurorehabil NeuralRepair 2008; 22: 514–640.
BoNT-A consensus statement: AUL 93
� 2010 The Author(s)Journal compilation � 2010 EFNS European Journal of Neurology 17 (Suppl. 2), 74–93