exercise limitation in obstructive lung disease
TRANSCRIPT
DOI 10.1378/chest.114.4.965 1998;114;965-968Chest
Cristina Murariu, Herberto Ghezzo, Joseph Milic-Emili and Henry Gautier DiseaseExercise Limitation in Obstructive Lung
http://chestjournal.chestpubs.org/content/114/4/965
services can be found online on the World Wide Web at: The online version of this article, along with updated information and
ISSN:0012-3692)http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(
written permission of the copyright holder.this article or PDF may be reproduced or distributed without the priorDundee Road, Northbrook, IL 60062. All rights reserved. No part of Copyright1998by the American College of Chest Physicians, 3300Physicians. It has been published monthly since 1935.
is the official journal of the American College of ChestChest
1998 by the American College of Chest Physicians by guest on April 11, 2012chestjournal.chestpubs.orgDownloaded from

Exercise Limitation in Obstructive LungDisease*Cristina Murariu, MD; Herherto Ghezzo, PhD; Joseph Milic-Emili, MD; andHenry Gautier, MD
Objective: To study the relationship of resting pulmonary function to maximal exercise poweroutput (Wmax) in obstructive lung disease (OLD).Setting: University Hospital Pulmonary Function Laboratory.Subjects: Twenty-five patients with OLD (6 with asthma and 19 with COPD).Methods: Measurement of pulmonary lung function, resting arterial blood gases, and maximalsymptom-limited exercise on a cycle ergometer.Results and conclusions: In OLD, the only significant contributor to Wmax was the inspiratorycapacity (r2 = 0.66; p < 0.001). (CHEST 1998; 114:965-968)
Key words: arterial Po2; inspiratory capacity; maximal power output; routine lung function; spirometryAbbreviations: Dlco = single breath diffusing capacity; FRC = functional residual capacity; IC = inspiratory capac¬ity; IRV = inspiratory reserve volume; OLD = obstructive lung disease; Vt = tidal volume; Vrmax = maximal tidalvolume during exercise; Wmax = maximal exercise power output
HP he relationship between resting lung function¦*¦ variables (FEV1? FVC, etc) and maximal poweroutput (Wmax) during exercise has been studiedextensively in patients with obstructive lung disease(OLD). In general, it has been found that Wmax is
loosely related to FEVj.1 This is not surprising sincethere is an association of FEVt and maximal exerciseventilation, and maximal exercise ventilation plays a
dominant role in determining Wmax.2 Patients withOLD often exhibit expiratory flow limitation even atrest (ie, the expiratory flows are maximal under theprevailing condition).34 Tidal expiratory flow limita¬tion promotes an increase in functional residualcapacity (FRC) (dynamic hyperinflation) with con¬
comitant decrease in inspiratory capacity (IC) andinspiratory reserve volume (IRV).56 In normal sub¬jects, the tidal volume (Vt) during exercise usuallyincreases at the expense of both the IRV and theexpiratory reserve volume, and even during Wmax,there remains a substantial IRV.56 In contrast, inOLD patients who exhibit tidal expiratory flow lim¬itation, any increase in Vt during exercise necessarilyoccurs at the expense of the IRV, and the end-
*From the Service d'Explorations Fonctionnelles Respiratoires(Drs. Murariu and Gautier), Hopital St. Antoine, Paris, France,and Meakins-Christie Laboratories McGill University (Drs.Ghezzo and Milic-Emili), Montreal, Canada.Manuscript received September 25, 1997; revision accepted April23, 1998.Correspondence to: Cristina Murariu, MD, Lahoratoire de Physi-ologie Respiratoire, Faculte de Medecine St. Antoine, 27, rue
Chaligny, 75012, Paris, France
inspiratory volume eventually approaches the totallung capacity.56 Thus, in OLD, the maximal Vtduring exercise (Vrmax) should depend mostly on
the magnitude of resting IC. Since the exercisecapacity is related to Vrmax,5 there should also be a
close association of Wmax to IC. To our knowledge,the latter has not been investigated in OLD patients.To test this hypothesis, in the present investiga¬
tion, we have assessed the relationship of Wmax toIC in 25 OLD patients. In addition, we also mea¬
sured the relationship ofWmax to FEV1? FVC, FRC,and resting arterial Po2 and CO diffusing capacity(Dlco). Previously a loose association of Wmax to
FEV1? FVC, and Dlco was found in OLD patients.1
Materials and Methods
SubjectsWe studied 25 patients (16 male) with OLD, of whom 19 had
COPD and 6 had asthma. Their diagnosis was made according tothe recommendations of the American Thoracic Society.7 Theanthropometric characteristics are given in Table 1. At the timeof the study, all patients were in stable clinical and functionalstate, and had no contraindications for exercise testing. Patientswith evidence of cardiovascular disorders were excluded. Toavoid any potential influence of medication on testing, treatmentwith all respiratory drugs was withheld for at least 12 h prior toevaluation. All patients gave informed consent.
Pulmonary Function Tests
Before exercise, each patient underwent routine lung functionstudies. The FEVj and FVC, together with IC, were measured in
CHEST /114/4/ OCTOBER, 1998 965
1998 by the American College of Chest Physicians by guest on April 11, 2012chestjournal.chestpubs.orgDownloaded from
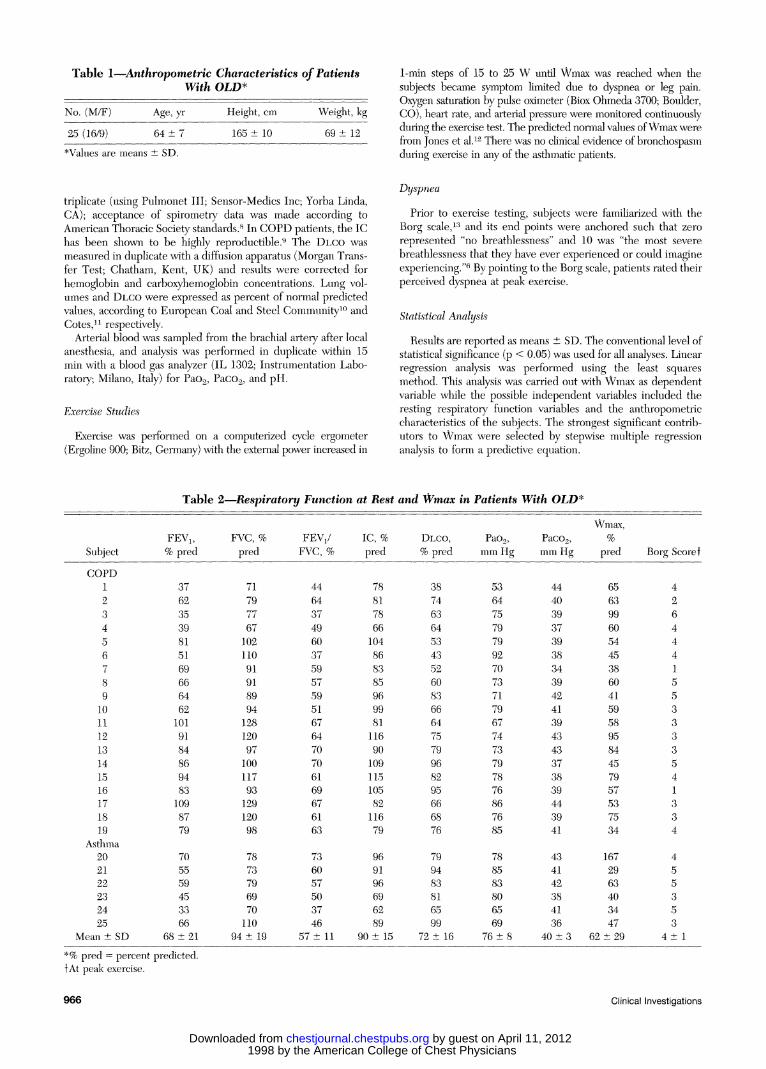
Table l-.Anthropometric Characteristics of PatientsWith OLD*
No. (M/F) Age, yr
25 (16/9) 64:
*Values are means ± SD.
Height, cm
165 ± 10
Weight, kg69 ± 12
1-min steps of 15 to 25 W until Wmax was reached when thesubjects became symptom limited due to dyspnea or leg pain.Oxygen saturation by pulse oximeter (Biox Ohmeda 3700; Boulder,CO), heart rate, and arterial pressure were monitored continuouslyduring the exercise test. The predicted normal values ofWmax were
from Jones et al.12 There was no clinical evidence of bronchospasmduring exercise in any of the asthmatic patients.
triplicate (using Pulmonet III; Sensor-Medics Inc; Yorba Linda,CA); acceptance of spirometry data was made according toAmerican Thoracic Society standards.8 In COPD patients, the IChas been shown to be highly reproductible.9 The Dlco was
measured in duplicate with a diffusion apparatus (Morgan Trans¬fer Test; Chatham, Kent, UK) and results were corrected forhemoglobin and carboxyhemoglobin concentrations. Lung vol¬umes and Dlco were expressed as percent of normal predictedvalues, according to European Coal and Steel Community10 andCotes,n respectively.
Arterial blood was sampled from the brachial artery after localanesthesia, and analysis was performed in duplicate within 15min with a blood gas analyzer (IL 1302; Instrumentation Labo¬ratory; Milano, Italy) for Pao2, PaCO£, and pH.
Exercise Studies
Exercise was performed on a computerized cycle ergometer(Ergoline 900; Bitz, Germany) with the external power increased in
DyspneaPrior to exercise testing, subjects were familiarized with the
Borg scale,13 and its end points were anchored such that zero
represented "no breathlessness" and 10 was "the most severe
breathlessness that they have ever experienced or could imagineexperiencing."6 By pointing to the Borg scale, patients rated theirperceived dyspnea at peak exercise.
Statistical AnalysisResults are reported as means ± SD. The conventional level of
statistical significance (p < 0.05) was used for all analyses. Linearregression analysis was performed using the least squaresmethod. This analysis was carried out with Wmax as dependentvariable while the possible independent variables included theresting respiratory function variables and the anthropometriccharacteristics of the subjects. The strongest significant contrib¬utors to Wmax were selected by stepwise multiple regressionanalysis to form a predictive equation.
Table 2.Respiratory Function at Rest and Wmax in Patients With OLD*
Wmax,
SubjectFEVi, FVC, % FEVr/ IC, % Dlco, Pao2, Paco2, %
%predpred FVC, % pred % pred mm Hg mm Hg pred Borg Scoref
COPD123456789
10111213141516171819
Asthma202122232425
Mean SD
3762353981516966646210191848694831098779
705559453366
68 ±21
7179776710211091918994128120971001179312912098
7873796970110
94 ± 19
44643749603759575951676470706169676163
736057503746
57 ± 11
788178661048683859699811169010911510582
11679
969196696289
90 ± 15
38746364534352608366647579968295666876
799483816599
72 ± 16
53647579799270737179677473797876867685
788583806569
76 ±8
44403937393834394241394343373839443941
434142384136
40 ±3
65639960544538604159589584457957537534
1672963403447
62 ±29
4264441553333541334
455353
4± 1
*% pred = percent predicted.fAt peak exercise.
966 Clinical Investigations
1998 by the American College of Chest Physicians by guest on April 11, 2012chestjournal.chestpubs.orgDownloaded from
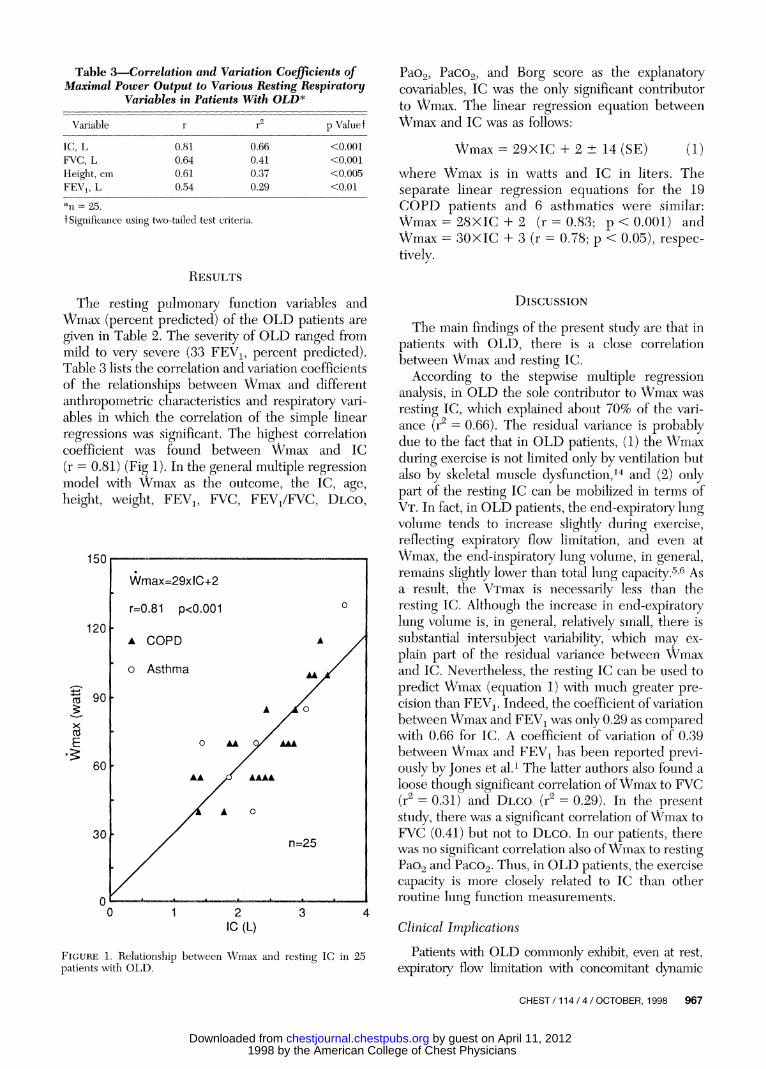
Table 3.Correlation and Variation Coefficients ofMaximal Power Output to Various Resting Respiratory
Variables in Patients With OLD*
Variable p Value!
IC, LFVC, L
Height, cmFEV1? L
0.810.640.610.54
0.660.410.370.29
<0.001<0.001<0.005<0.01
*n = 25.f Significance using two-tailed test criteria.
Results
The resting pulmonary function variables andWmax (percent predicted) of the OLD patients are
given in Table 2. The severity of OLD ranged frommild to very severe (33 FEVX, percent predicted).Table 3 lists the correlation and variation coefficientsof the relationships between Wmax and differentanthropometric characteristics and respiratory vari¬ables in which the correlation of the simple linearregressions was significant. The highest correlationcoefficient was found between Wmax and IC(r = 0.81) (Fig 1). In the general multiple regressionmodel with Wmax as the outcome, the IC, age,height, weight, FEVj, FVC, FEV/FVC, Dlco,
150
Pao2, Paco2, and Borg score as the explanatorycovariables, IC was the only significant contributorto Wmax. The linear regression equation betweenWmax and IC was as follows:
Wmax = 29XIC + 2 ± 14 (SE) (1)where Wmax is in watts and IC in liters. Theseparate linear regression equations for the 19COPD patients and 6 asthmatics were similar:Wmax = 28XIC + 2 (r = 0.83; p < 0.001) andWmax = 30XIC + 3 (r = 0.78; p < 0.05), respec¬tively.
DISCUSSION
The main findings of the present study are that in
patients with OLD, there is a close correlationbetween Wmax and resting IC.
According to the stepwise multiple regressionanalysis, in OLD the sole contributor to Wmax was
resting IC, which explained about 70% of the vari¬ance (r2 = 0.66). The residual variance is probablydue to the fact that in OLD patients, (1) the Wmaxduring exercise is not limited only by ventilation butalso by skeletal muscle dysfunction,14 and (2) onlypart of the resting IC can be mobilized in terms ofVt. In fact, in OLD patients, the end-expiratory lungvolume tends to increase slightly during exercise,reflecting expiratory flow limitation, and even atWmax, the end-inspiratory lung volume, in general,remains slightly lower than total lung capacity.56 Asa result, the Vrmax is necessarily less than theresting IC. Although the increase in end-expiratorylung volume is, in general, relatively small, there issubstantial intersubject variability, which may ex¬
plain part of the residual variance between Wmaxand IC. Nevertheless, the resting IC can be used to
predict Wmax (equation 1) with much greater pre¬cision than FEVj. Indeed, the coefficient of variationbetween Wmax and FEVX was only 0.29 as comparedwith 0.66 for IC. A coefficient of variation of 0.39between Wmax and FEVX has been reported previ¬ously by Jones et al.1 The latter authors also found a
loose though significant correlation ofWmax to FVC(r2 = 0.31) and Dlco (r2 = 0.29). In the presentstudy, there was a significant correlation ofWmax toFVC (0.41) but not to Dlco. In our patients, therewas no significant correlation also ofWmax to resting
Figure 1. Relationship between Wmax and resting IC in 25patients with OLD.
Pao2 and Paco2. Thus, in OLD patients, the exercisecapacity is more closely related to IC than otherroutine lung function measurements.
Clinical ImplicationsPatients with OLD commonly exhibit, even at rest,
expiratory flow limitation with concomitant dynamicCHEST/114/4/OCTOBER, 1998 967
1998 by the American College of Chest Physicians by guest on April 11, 2012chestjournal.chestpubs.orgDownloaded from

pulmonary hyperinflation, which promotes increasedinspiratory work, impairment of inspiratory musclefunction, and adverse effects of hemodynamics 4-5 Theincreased FRC due to dynamic hyperinflation is axiom-
atically associated with a decreased IC. Because ofexpiratory flow limitation, the maximal Vt (and henceventilation) during exercise is closely related to restingIC.5-6 Therefore, there should be also a close associa¬tion between resting IC and working capacity, as foundin the present study. This implies diat in OLD patients,the IC, which is easy to measure, is an excellent indexof dynamic hyperinflation, and hence of the status andprogress of their disease. Furthermore, measurementof IC has been shown to provide useful information on
the effects of bronchodilatators15 and surgical treat¬ment16 on hyperinflation in OLD patients. However,the IC is not as commonly used in die clinical assess¬
ment ofOLD as FEVx, FVC, and FRC. The FEVX andFVC, however, are poorly related to both exercise
performance and dyspnea,4 while measurement ofFRC is complicated and costly.
Dyspnea, impaired exercise tolerance, and re¬
duced quality of life are common complaints ofOLDpatients. Since reduced exercise capacity shows onlya weak link to lung function impairment measured interms of FEV1? FVC, and Dlco,1 it has been arguedthat in OLD patients, factors other than lung func¬tion impairment (eg, peripheral muscle weaknessand deconditioning) are important contributors toreduced exercise tolerance.1718 Based on IC, how¬ever, the present results indicate that lung functionimpairment is the major contributor to reducedexercise tolerance in OLD.
In conclusion, our study shows that in OLD, thereis a close association between the maximal exercise
capacity and the resting IC. Therefore, measurementof IC may provide a simple tool for monitoring thefunctional status and progress of OLD patients.
References1 Jones NG, Jones G, Edwards RHT. Exercise tolerance in
chronic airway obstruction. Am Rev Respir Dis 1971; 103:477-491
2 Clark THJ, Freedman S, Campbell EJM, et al. The ventila¬tory capacity of patients with chronic airway obstruction. ClinSci 1969; 36:307-316
3 Koulouris NG, Valta P, Lavoie A, et al. A simple method todetect expiratory flow limitation during spontaneous breath¬ing. Eur Respir J 1995; 8:306-313
4 Eltayara L, Becklake MR, Volta CA, et al. Relationshipbetween chronic dyspnea and expiratory flow-limitation in
patients with chronic obstructive pulmonary disease. Am JRespir Crit Care Med 1996; 154:1726-1734
5 Koulouris NG, Dimopoulou I, Valta P, et al. Detection ofexpiratory flow limitation during exercise in COPD patients.J Appl Physiol 1997; 82:723-731
6 O'Donnell DE, Webb KA. Exertional breathlessness in pa¬tients with chronic airflow limitation: the role of lung hyper¬inflation. Am Rev Respir Dis 1993; 148:1351-1357
7 American Thoracic Society. Standards for the diagnosis andcare of patients with chronic obstructive pulmonary disease(COPD) and asthma. Am Rev Respir Dis 1987; 136:225-244
8 American Thoracic Society. Standardization of spirometry.Am J Respir Crit Care Med 1995; 152:1107-1136
9 Yan S, Kaminski D, Sliwinski P. Reliability of inspiratorycapacity for estimating end-expiratory lung volume changesduring exercise in patients with chronic obstructive pulmo¬nary disease. Am J Respir Crit Care Med 1997; 156:55-59
10 Quanjer PH. Standardized lung function testing. Clin RespirPhysiol 1983; 19:1-95
11 Cotes JE. Lung function: assessment and application inmedicine. 4th ed. Oxford: Blackwell, 1979; 329-387
12 Jones NL, Makrides L, Hitchcock C, et al. Normal standardsfor an incremental progressive cycle ergometer test. Am Rev
Respir Dis 1985; 131:700-70813 Borg GAV. Psychophysiological basis of perceived exertion.
Med Sci Sports Exerc 1982; 14:377-38114 Maltais F. Oxidative capacity of the skeletal muscle and lactic
acid kinetics during exercise in normal subjects and in
patients with COPD. Am J Respir Crit Care Med 1996;153:288-293
15 Boczkowski J, Murciano D, Pichot M-H, et al. Expiratory/ flowlimitation in stable asthmatic patients during resting breath¬ing. Am J Respir Crit Care Med 1997; 156:752-757
16 Murciano D, Pichot M-H, Boczkowski J, et al. Expiratory/ flowlimitation in COPD patients after single lung transplantation.Am J Respir Crit Care Med 1997; 155:1036-1041
17 Hamilton N, Killian KJ, Summers E, et al. Muscle strength,symptom intensity, and exercise capacity in patients withcardiorespiratory disorders. Am J Respir Crit Care Med 1995;152:2021-2031'
18 Gosselink R, Troosters T, Decramer M. Peripheral muscleweakness contributes to exercise limitation in COPD. Am JRespir Crit Care Med 1996; 153:976-980
968 Clinical Investigations
1998 by the American College of Chest Physicians by guest on April 11, 2012chestjournal.chestpubs.orgDownloaded from
DOI 10.1378/chest.114.4.965 1998;114; 965-968Chest
Cristina Murariu, Herberto Ghezzo, Joseph Milic-Emili and Henry GautierExercise Limitation in Obstructive Lung Disease
April 11, 2012This information is current as of
http://chestjournal.chestpubs.org/content/114/4/965Updated Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/114/4/965#related-urlsThis article has been cited by 9 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtmlfound online at: Information about reproducing this article in parts (figures, tables) or in its entirety can bePermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
"Services" link to the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the
Citation Alerts
PowerPoint slide format. See any online figure for directions. articles can be downloaded for teaching purposes inCHESTFigures that appear in Images in PowerPoint format
1998 by the American College of Chest Physicians by guest on April 11, 2012chestjournal.chestpubs.orgDownloaded from