unclassified ad number new limitation change from
TRANSCRIPT
UNCLASSIFIED
AD NUMBER
AD850510
NEW LIMITATION CHANGE
TOApproved for public release, distributionunlimited
FROMDistribution authorized to U.S. Gov't.agencies and their contractors;Administrative/Operational Use; MAR 1969.Other requests shall be referred toCommanding Officer, Fort Detrick, Attn:SMUFD-AE-T, Frederick, MD 21701.
AUTHORITY
SMUFD, D/A ltr, 17 Feb 1972
THIS PAGE IS UNCLASSIFIED
TRANSLATION NO.
DATL:
00
DDC AVAILABILITY NOTICE
This document is subject to special exportcontrols and each transmittal to foreign
governments or foreign nationals may bemade only with prior approval of CommandingOfficer, Fort Detrick, ATTN: SMUFD-AE-T,
Frederick, Md. 21701
DEPARTMENT OF THE ARMYFort Detrick
Frederick, Maryland
I I I I
Tran.Icltion 'No. T-701-1
Author: U.F. Gruber, Basel, Switzerland
Tit1: Intestinal factors in shock: enterotoxin (Intestinale Faktoren im
Schock: Dar.tcoxine).
Jour.-ml: Lanyenbeck's Archives for Clinical Surgery (Langenbecks Archiv fur
Klinische Chirugie). 319: 909-925 (1967).
March 1969
Briefly and in sum nary, th course of the hemodynanic changes in the
splanchnic region during severe shock can be represented as follows:
As a renilt of the decrease in tho cardizc minute-volune (in suriory limited
mostly to cardiogenic- or hypo-volemia), there is a relatively markeJ decrease
in the timic-flo volume with a significant increase in resistnce (1, 56, 123).
This is the rsult of the particularly strong adrenergic intervention and consi-
tivity of catecholamine in the splanchnic region in comparison with the other
vascular flow regions (9, 60, 70, 90, 101, 107).
Hypoxic chnnges (6L4, 113), therefore, appear relatively early in a region
* lo; in 02 but with a high 02 consunption (13, 137). As a result, the 02 absorption
can re;main decreased in soite of restored flow even after transfusion (33, 125).
Other regions, such as the liver, are able to convert Lmmediately to aerobic nieta-
boliem.
As a consequence of these changes, large amomnts of plasma are lost (87, 91,
93, 131) as a result of the increased permeability of the capillaries (97, 106).
Under certain conditirns, a temporary poolirg can be observed in the upper intes-
tinal regions (78, 80). In this regards, the erythrocytes become sequestered (55,
133) since the pro-capillary sphinctors lose their tonus earlier than do the post-
capillary ores (88). In this manner, the loss of volume, especially plasma volume,
intenrifies the hypovolemia in the sense of a postive feed-back mechanism (scheme).
Not all of these findings have been confirmed in humans. The partially
contradictory results can be explained on the anatomical differences in the species
tested, various means of narcosis, nature, severity, and duration of the chock
model employed as well as by factors involving methodology (1, 16, 37, L4, 56, 108,
122, 128, l12). However, basically these n:'hanisms should follow the same course
in laboratory animals and in humans.
0 -2 --
;s a result, it is understandable why several authors deuling with various
fonin of shock involving intestinal and liver bleeding and also chances of
sur-ival ach- cved favorable results after the administration of the following
vaco-=tivc zu:bztances:
ibensnyia. (15, 5L, 67, 80, 10h, 131)
Chlorproaszine (72, 80, 121)
iscproterenol (11, 79)
Fhe nylalnine-lysine-vasopressin (6, 7, 69, 68, 66, 95) not, however, in
the case of the employment of cltecholanines (11, 70, 75, 88, 98).
In this connection, good results have also been obtained by the use of low
molecular wiziht dextrans (10, 38, 42, 3, 84, 129, 130, 133), celior block or
denervrtion (17a, 10h, 105, 110) and hypothermy (87) for amelioration of the
intestinal perfusion and elimination of the state of shock.
The splonchnic region has a special significance in the event of shock when
viewed from a hcmodynamic view point. Tn this case, it is a caestion os to Whether
these circulatory factors are implicated in the secondary changes in the tissues
which affect the entire organism and could be responsible for the more rapid
onset of irreversibility before overall 02 deficit makes survival impossible.
in this regard, the following observations are presented:
1. In the upper intestine, there are significant pathological-anatomical
alteraticns.
IT. Resection of the intestines in rats and dogs during hemorrhagic (80, 975
112) znd cndotoxic ohock (48, 133) leads to a significant prolongation of the
survival time. The only investigation (lO) that led to a contrary conclusion had
so many methodological errors that it does not have to be taken into consideration
during this discussion.
-3-.
111. An, increase in the intestinal blood flow as a result of isolated
perfusion of the arteria mosenterica suporior (AMS) improves survval chances
of animal,- undcrgoin,, ehock (18, 86, 87, 93, 135),
Blattberr (29), however, made thc assu~rption that the protective effect is
not the result of perfusion as such since the animal's own blood is not effective.
The don~or blo,- J must ccrc frar. a healthy rabbit.
Tho resul.ts msentioned in 1, 11, and 111, however, car. o~nly be explained on a
hecdynzr.ic bz-sis and do not prvide definite Proof for the presence of spccific
intestL:.r~nl factcors.
Additionol aspectz. are provided by the follo-oing facts:
IV. Since the entire intestinal tract repres.ents a large reservoir of bacteria,
rcrocr,.n sm -ere considered veryj early as an asserntial element in shock patho-
genesic. As oar'li -- : 19UT, J.C. Aub (Ib) in an extrenely clear work explainecd that,
in aJ.dt-i;n To los-s of vulumie anid bacterial factcrs, no other toxic eonponents of
rny oth.;r kic ould Ix f to explain the -shock probLsr1.
in the invustigatic'ns ;:! Firw (50,51) and his c-ULIrkers (5il, 7L1 , 10h, 110,
ll5, ,131) ~.~~zdin '3 114), art attempt WC;E mado t,: OIttritlutu (10finite
&.ignifczc t.o endotoxin in the pathogenesis of ircesbcshock. Although
the comprehensive in1testigAtIons stirvi]'ted thorough rczcarc,-. 1nto the 51iock
prbeit has been assmned that very Li1ttle significance can be attributed to
endctcxin as being an important factor fcr th-e following rcasons (67, 81, 103,
1316):
(1) In germi-free animals, the s3bock- proceedr- in exactly the same manner as in
ordinary animals (J.47).
Fine had argued thc-t erndotoxins were prcent in the food. H{owever, the same
reactiona were obverved in germ-free vniro.le which had Ition fed a sai-ynthetic
fcod sterilized in a dry oven
(2) The cxpcritcnts of Fine have not been reproducible in other laboratories
and pre-treatment with antibiotics has turned out to be unsuccessful even in his
ow. hn63 (7, 2h, 65, 76, 86, 96).
(3) Fine himnelf has shown that incubated aurecmycin, which is practically
without effect on microorganisns, VIl neverthelesz protect against shock (7W).
Lin and Zwcifach (89) assumed that antibiotics have a protective effect on the
mucous memlranes of the intestines and that this effect is unrelated to their
bacteriortatic effect.
(L) Chlocr.phenicol, which is an effective antibiotic for gram-negative
microorganis s, has no protective effect (74, 89).
(5) Mice, that have been made 10 times more sensitive to endotoxin, cannot
be killed by the injection of blood of dogs irreversibly shocked with endotoxin
(132).
(6) A hypotensive peptide has been detected in the cecum of germ-free rats
(59). The amount of this substance decreases.markedly upon the introdction of
microorganisms (13). Certain bacteria, therefore, could exert a protective
function (12, hl).
V. in the case of mechanical ileus, in addition to the loss of volume,
bacteria or their products have also been implicated as responsible for the toxic
propcrties of the peritoneal exudates and the intestinal contents (9, 7, 30).
kc.nundsen (8) also observed in germ-free rats a protein originating from the
intestinal wall which increased toxicity. It was not hemoglobin or one of its
derivatives. The results allow a comparison with the conditions during irreversi-
ble shock and indicate a possible participation of the intestinal wall.
Because the intestines and liver are dependent on each other anatomically and
functionally, it seemed advisable to consider the latter also in our observations
VT. Blockage of the reticulo-endothelial system (RES) increases the sensi-
tivity to shock (145). Durirg shock, the ability of the RES to eliminate endo-
toxin from the blood is dccreased (115, lh). Also, its ability to eliminnte
bacteria (50) and colloid particles (23, IL 6 ) is diminished. This tmpairu:nt
of the, so-called granulopectic activity is considcred by mary authors to be a
Cignificant factor in shock ptthogencsis (3, 27, 53, l10). In that regards,
one must also consider substances which block the RES to be hepato-toxic.
Administration of citrated blood increasos the limited dotoxifying function
of the RES (109) and it was shown earlier thrat citratu in vito iinfluences the
activity of leucocytes (2).
In addition, vasoactive substances such as histamines, scrotonin, and
bradykinin, depending on dosage, restrict the function of the RES (27).
Furthermore, there is the Questicn whether the large quantity of denatured
proteins and cell aggregates in transfused blcod can restrict the blood supply
of the liver by increasing viscosity and in this manner restrict its function
(TLl).
Blattberg and Levy have assumed that in the course of severe shock, a RES
depressor substance (RES-DS) is produced in the gastrointestinal tract and enters
the system via the portal vein (22, 25). This material is formed during AMS
shock (arteria mesentericurn superior occlusion) in the rat and in the dog (2b,
25) as well as during hemorrhagic shock in the dog (21-23). The RES-DS can be
trans.mitted via various carriers (blood, plasma, plasma-dialysate) frcn rat to
rat and from rat to dog. On the basis of chromatographic separations and puri-
fications, it appears to a small molecule. Its mechanism of action does not
involve blockage of the RES (26).
Levy and Blattberg and co-workers (9, 28, 18, 20, 85) have found that in
the post-transfusion phase after hemorrhagic shock in the dog, the irmune system
becoces involved. This appears to ultimately correlated with damage to the
RES function.
Various authors have asstied that during severe shock, there is no formation
of enterotoxins but that the liver loses its ability to inactivate metabolites
which are normally present (15, hi, 80, 113).
Battbeg (23) and Lillebei (196) have demonstrated that perfusion of the
liver does not have any effect. On the other hand, chIorprcmazirn and diberzylin
i-Prorv chances of survival only as long as the liver is present (15, 80, 86, 121).
IMI. Bounous and co-workers (33) (sjr.-arized in 62) after extensive examina-
tions believe that the metabolism of the mucous mebrarns of the intestires and
the production of protective macin are affected before pathological-anatmical
alterations can be observed and before other regions shcw similar changes (35,
3h, 31, 36). These investigators were able to demonstrate that purification of
isolated coils of the intestine or prophylactic administration of trasylol inhi-
bited the typical symptoms of hemorrhagic necrosis frCa appearing during irreversible
shock in the dog and the rat (3A, 32). They assumed that trypsin and chymotrypsin
have a special significance but pointed out there is much less trypsin present in
the human intestine. The prophylactic ligature of the pvncreatic ducts also has
a protective effect on the intestines and prolongs survival time. Therefore, it
is possible that toxic products of the intestinal constituents pass through the
previously dcmaged mucous membranes (see E.E. Smith, Surg. Gynec. Obstet. 125: 15
(1967)).
TIII. Barii and Allgower (39, 4o) found a toxic substance in the intestinal
walls of burned animals =f:in animals with hemorrhagic shock. This factor is
active zgainst mice which are refractive to endotoxin. They assumed that it was
forzed during the hypoxic phase in the intestinal wall.
The results mentioned in V - VIII do not present absolute evidence for the
formation of toxic substances in the intestinal tract or for a decreased function
of detoxiCication of the liver. There are many gaps - severe controls, too small
anoants of experimental material, missing statistical evaluations, confirmation
F4-7-
in other animals by other authors, and lack of data for humans. 'Tcverthlcss,
they certainly deserve our full attention.
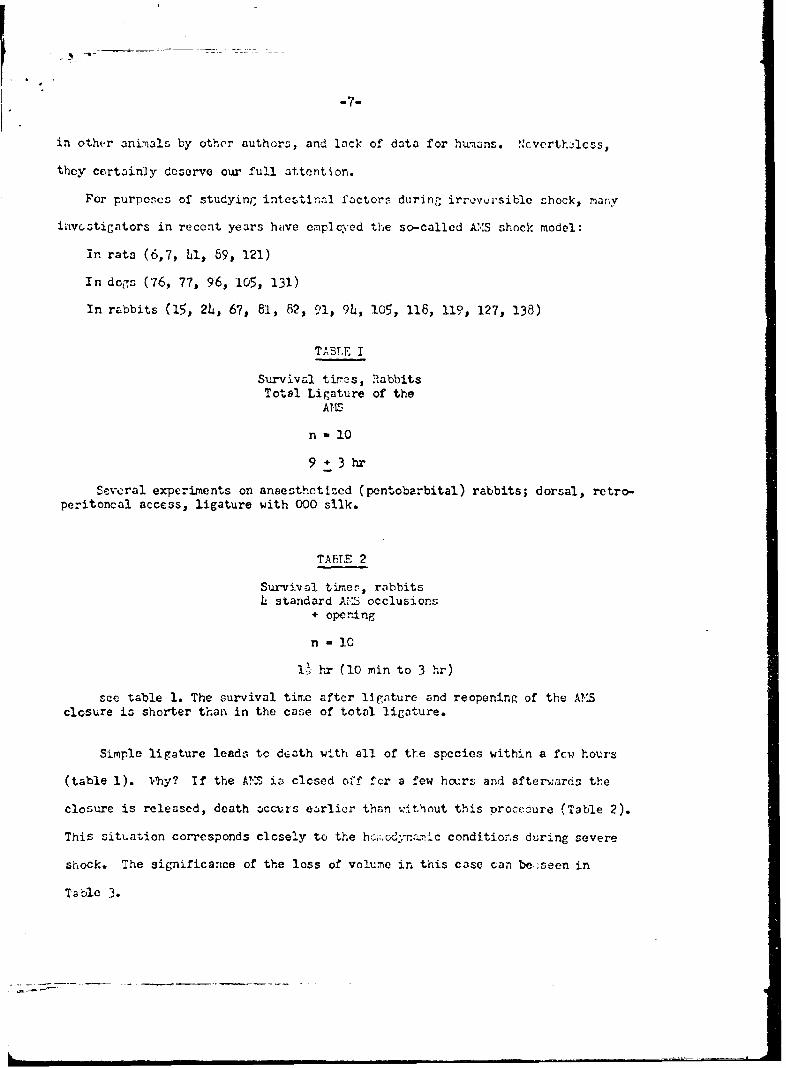
For purposes of studying intestinnl factors during irro\,'rsible shock, many
investigators in recent years have emplcyed the so-called AMS shock model:
In rats (6,7, hl, 89, 121)
In dogs (76, 77, 96, 105, 131)
In rabbits (15, 24, 67, 81, 82, 91, 9h, 105, 116, 119, 127, 138)
TABLE I
Survival ttirs, RabbitsTotal Ligature of the
AT£T,
n a 10
9+ 3 hr
Several experiments on anaesthetized (pentobarbital) rabbits; dorsal, retro-peritoncal access, ligature with 000 sIlk.
TABT 2
Survival times, rabbitsL, standard AV.S occlusions
+ openring
n -10
11 hr (10 min to 3 hr)
see table 1. The survival time after ligature and reopening of the AMSclosure is shorter than in the case of total ligature.
Simple ligature leads to death with all of the species within a few hours
(table 1). Vhy? If the AT- in closed off for a few hours and afterwards the
closure is released, death occurs earlier than .ithout this procedure (Table 2).
This situation corresponds closely to the hod'om~ ic conditions during severe
shock. The significance of the loss of volume in this case can be..seen in
Table 3.
-8-
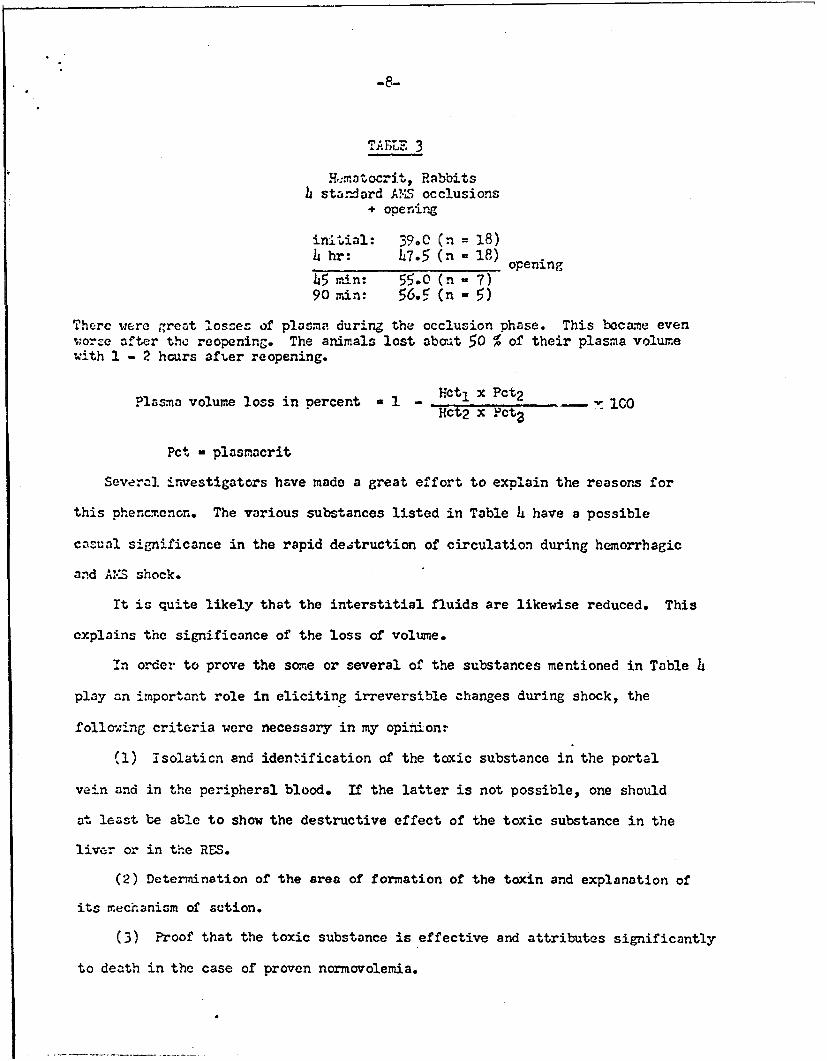
TABLE 3
H.matocrit, Rabbitsh standard A?.LS occlusions
+ opening
initVial: 39°0 (n = 18)h hr: 07.5 (n 18) opening
L5 min: 55.0 (n = 7)90 min: 56.5 (n - 5)
There were great losces of plasma during the occlusion phase. This bcame evenvorse after the reopening. The animals lost abat 50 % of their plasma volumewith 1 - 2 hours afier reopening.
?lasma volume loss in percent a 1 - Hct I x Pct2Hct2 x Fcta
Pct - plasmacrit
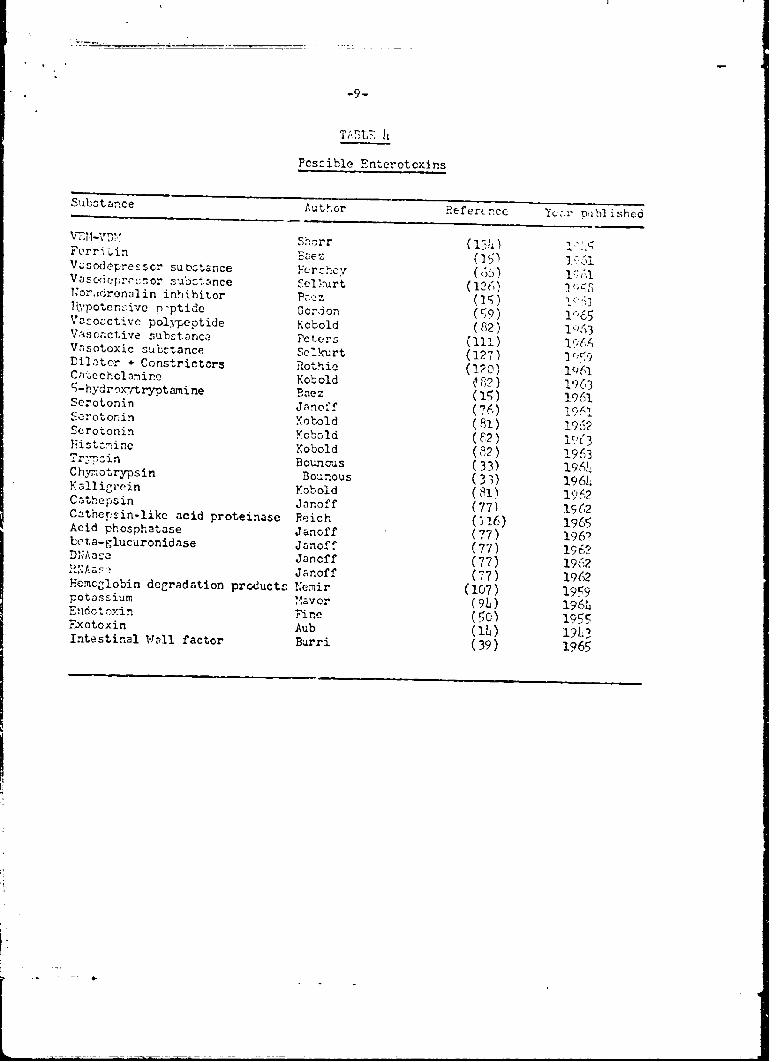
Several, investigators have made a great effort to explain the reasons for
this phencmenon. The various substances listed in Table 4 have a possible
ctiual significance in the rapid deAruction of circulation during hemorrhagic
and AS shock.
It is quite likely that the interstitial fluids are likewise reduced. This
explains the significance of the loss of volume.
In order to prove the some or several of the substances mentioned in Table
play an important role in eliciting irreversible changes during shock, the
follring criteria were necessary in my opinion.
(1) isolaticn and identification of the toxic substance in the portal
vein and in the peripheral blood. If the latter is not possible, one should
at least be able to show the destructive effect of the toxic substance in the
liver or in the RES.
(2) Determination of the area of formation of the toxin and explanation of
its mechanism of action.
(3) Proof that the toxic substance is effective and attributes significantly
to death in the case of proven normovolemia.
-9-
T;-LF, IL
Pcszj' ble Enterotoxins
Substa nce Reftrcncr Y mib shehd
Forrirr -P 3e -V .;sodcresrsor sub:;tarnce FcQrzc (6k) 1Vascieprcior b eeSl:<-Urt(16NO'r-idrenalin inhihitor (~71yPoten,-.",r n-ptide CGorjOn (19) 16v~OczciCtvc polypeotide Kobold (82) I P,")3Vsctjesubzt;nue Peters (111) I(.1Vis.'Otoxic -,A zt once Sc' kurt (127) lr;9fliLntor + Constrictors Rothie (ipo) 1461Ca' c cholimire Kobold kiF) ) 19635-hydr-' xytryptami ne B-acz (15) 1961Scrotonin Jnnofi' (976)
ScZrotonin Kobold(2)13Histc-nine Yobold(2)96
T:-znBouncus (33) 9( 'Chyrmotrypsin Bounous (3) 196hKalligrein Yobold (81) 1962Cothepsin Jinoff (77) 1 (2Czithersin-likc acid proteinase Reich (1!6) 16Acid phosphatase Janoff (7)1965Lcta-glucuronidase janoof (77) 196?D'Nia Jancff (77) 196?~ZNasJanoff (7)1902Eenclobin degradation product-o Inir (107) 1959Potassium Vavor (90 ~ 1961,E-idotoxin Fire 5~0) 1955Exotoxjn Ab(14) 191.?Intestinal Wall factor Burni (39) 1965
-13-
T () r:ansfcraci'-ity of the toxic principle to another an-.al, for example,
by inj..-ction, tranz:.usion, c;.- y crossed (syste...ic) circulation.
In these ca::es, the shocked aninal does not have to die since a healthy
o.'nI can :etuslv combat the toxin succezsfully. It app-ars, therefore,
poazihie that the subst.ances in question have been exanined several times in
arinl,; ;-roinrc.-,versible shock. They can also be tested after liver
d:-> nrodu by 13 blockage for exanple. In this regards, one must consider
at cq i,. likely the vasonotor control has to be also influenced if a vasonctive
scbsta.: should lad to the collapse of the circulatory system.
Thus far, no investigator has been able to fulfill all of these criteria.13 I. Of the substances mentioned in Table h, it is most likely that the
vazoactivu ones are the one Vhich are the toxins. The effect is probably due
to a rIxturc of vasoconntrictive as well as vasodilatative substances. At present,
there is not evidence available (for serotonin, ace (118)).
ad 2. The fact that such substances are prsent in the blood of the portal
vein is uncontestable. On the other hand, there is still the question as to
v:hether they are derived from the intestinal wall or intestinal contents. Also
thero ir still the question as to which of kinds of cells they originate from
(-ec tables 5 and 6).
ad 3. An extremely small n=.ber of irnestigators have considered the sig-
nificance of the voltme factor. From the plasma volume and hematocrit determina-
tions-carried out by various authors (41, 44, 93, 121, 131), it is assumed that
in the intestiral tract, the whole plasma volume can disappear into the wall or
into the lumen. Only strict volumetric controls can be used as proof for m.echan-
isms other than the loss of plasma. It is possible to conceive that ultimately
toxins that happen to be present intensify the loss of plasma.
-11-
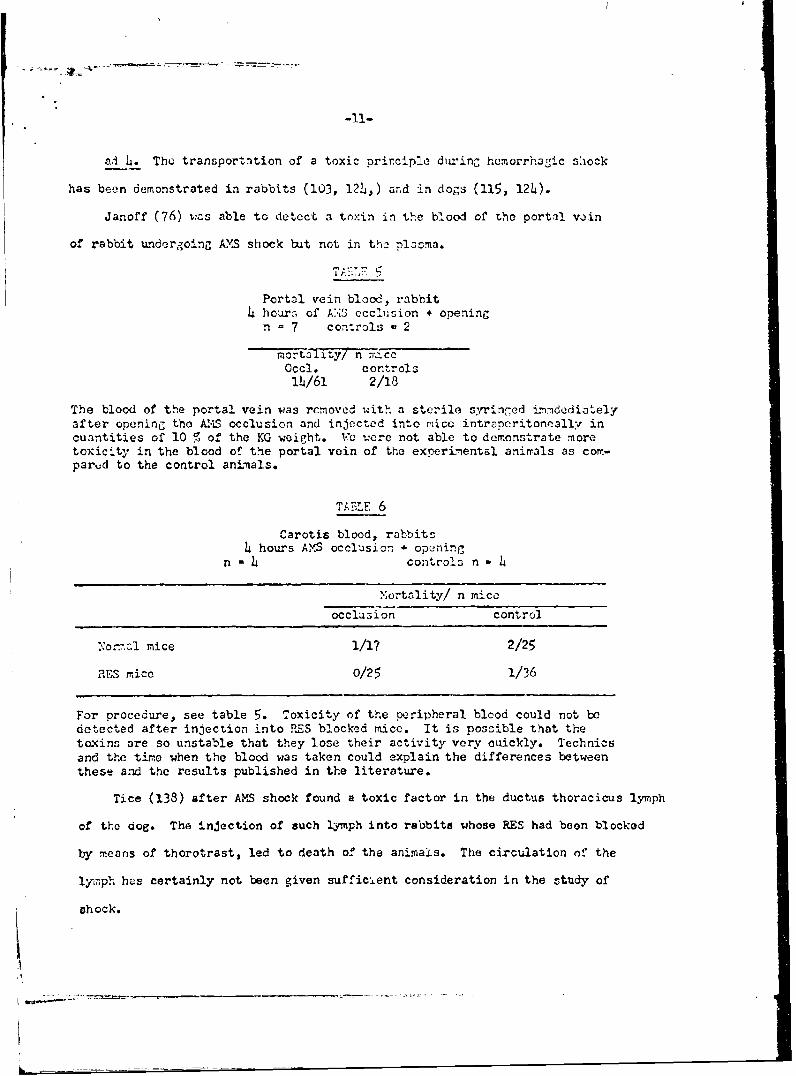
ad L. The transportation of a toxic principle du-ing hemorrhagic shock
has been demonstrated in rabbits (103, 124,) and in dogs (115, 124).
Janoff (76) vas able to detect a toxin in the blood of the portil vAin
of rabbit undergoing AYS shock but not in tha plasma.
Portal vein blood, rabbit4 hours of A:.S occlusion + opening
n - 7 controls -2
nortolity/ n r.ccOccl. controls
14/61 2/18
The blood of the portal vein was removed with a sterile syringed imdcdiatelyafter opening the A.S occlusion and injected into mice intrncritoneally incuantities of 10 Z of the KG weight. Vu were not able to demonstrate moretoxicity in the blood of the portal vein of the experimental animals as com-parud to the control animals.
TABLE 6
Carotis blood, rabbitshours AMS occlusion + opeaning
n -1 controla n - h
Nortality/ n mice
occlusion control
yornal mice 1/1? 2/25RES mice 0/25 1/36
For procedure, see table 5. Toxicity of the peripheral blood could not bedetected after injection into RES blocked mice. It is possible that thetoxins are so unstable that they lose their activity very ouickly. Technicsand the tire when the blood was taken could explain the differences betweenthese and the results published in the literature.
Tice (138) after AMS shock found a toxic factor in the ductus thoracicus lymph
of tho dog. The injection of such lymph into rabbits whose RES had boon blocked
by means of thorotrast, led to death of the animals. The circulation of the
lymph has certainly not been given sufficient consideration in the study of
shock.
L
-12-
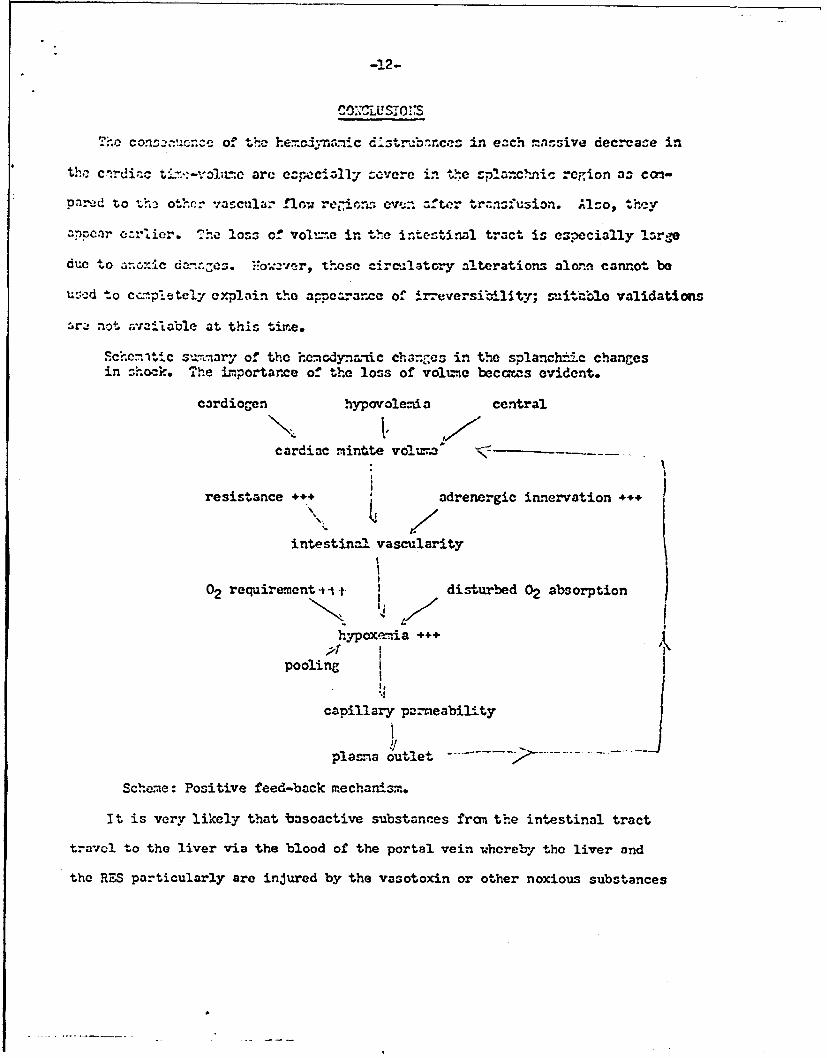
,O.,cLusiO:,S
The con n:-unc-2 of te he. n-.ic d-str -b'.ncez in each ..a.Sive decrease in
the clrdiac t%--vol1L-c arc eczpcialYy covere in the -planchpic r-egion oa co-
pnod to t othr vascular flow rei,-onr ovn after trznsfusion. Alco, they
PPOae oz-lier. "he loss of vol,-,e in the intestinal tract is espcially large
due to anoxic dann~. es. Fow:vr, these circilatory alterations alonn cannot be
usecd to cc.-pietcly explain t:ho appcaarmc of irreversilelity; suitablo validations
ar not available at this tirr.e.
Scecniltic s,-.rnry of the hcm.dynanic charnzcs in the splanch:ic changesin shock. The importarce of the loss of vol=,o beccmas evident.
cardiocn hypovolerda centralK 1/cardiac mintte vol, " a
resistance +++ adrenergic innervation ..+
intestinal vascularity
02 requirement t i t I disturbed 02 absorption
hypoxemia +++
pooling I
capillary p-rneability
plasna outlet .
Scheme: Positive feed-back mechanism.
It is very likely that basoactive substances fran the intestinal tract
travc to the liver via the blood of the portal vein whereby the liver and
the RES particularly are injured by the vasotoxin or other noxious substances
-13-
during detoxification and phagocytosis. This would explain the offect on the
whole organism that is observed.k
The bacterial factor, cspecially endotoxin, if at all.will play a si ni-
cantly smaller role in hyoovalemic shock than has been azsu-iod in the past.
This doas not mean, however, that b cterial factors are not cssontial in
soptic shockl It should also be mentioned that many authors have emplorcd
endotoxin in the laboratory to simulate shock. This shoiad not be interpreted
as meaning that endotoxin plays a major role in the initiation of irreversible
shock.
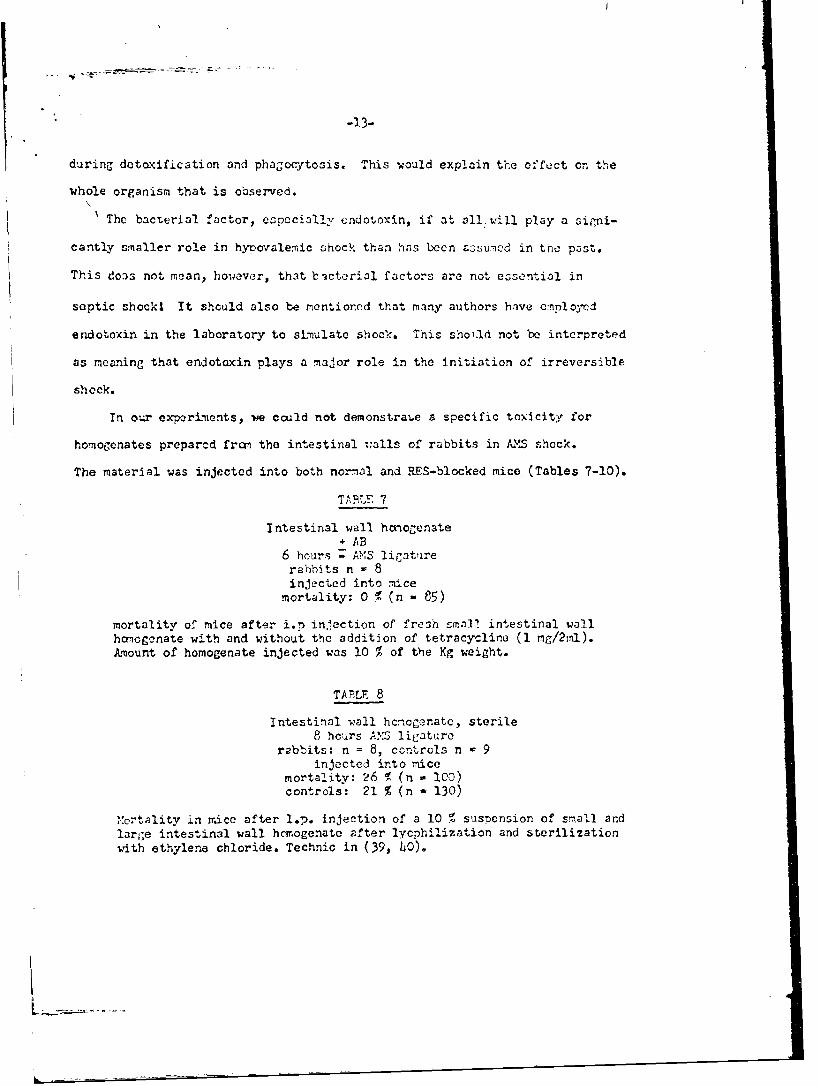
In our experiments, we could not demonstrabe a specific toxicity for
homogenates prepared fron the intestinal Walls of rabbits in Ak.5 shock.
The material was injected into both normal and RES-blocked mice (Tables 7-10).
TAB 1 7
Intestinal wall honogenate+ AB
6 hours - AvS ligaturerabbits n = 8injected into mice
mortality: 0 1 (n - 85)
mortality of mice after i.p injection of fresh smna] intestinal wallhoiogcnate with and without the addition of tetracycline (I mg/2rnl).Amount of homogenate injected was 10 O of the Kg weight.
TABLE 8
Intestinal wall hcnogenatc, sterile8 hcurs A.S ligature
rabbits: n = 8, ccntrols n - 9injected into mice
mortality: 26 1 (n - IC0)controls: 21 % (n - 130)
,ortality in r.ice after l.p. injection of a 10 % suspension of small andlarvae intestinal wall hcmogenate after lycphilization and sterilizationwith ethylene chloride. Technic in (39, LO).
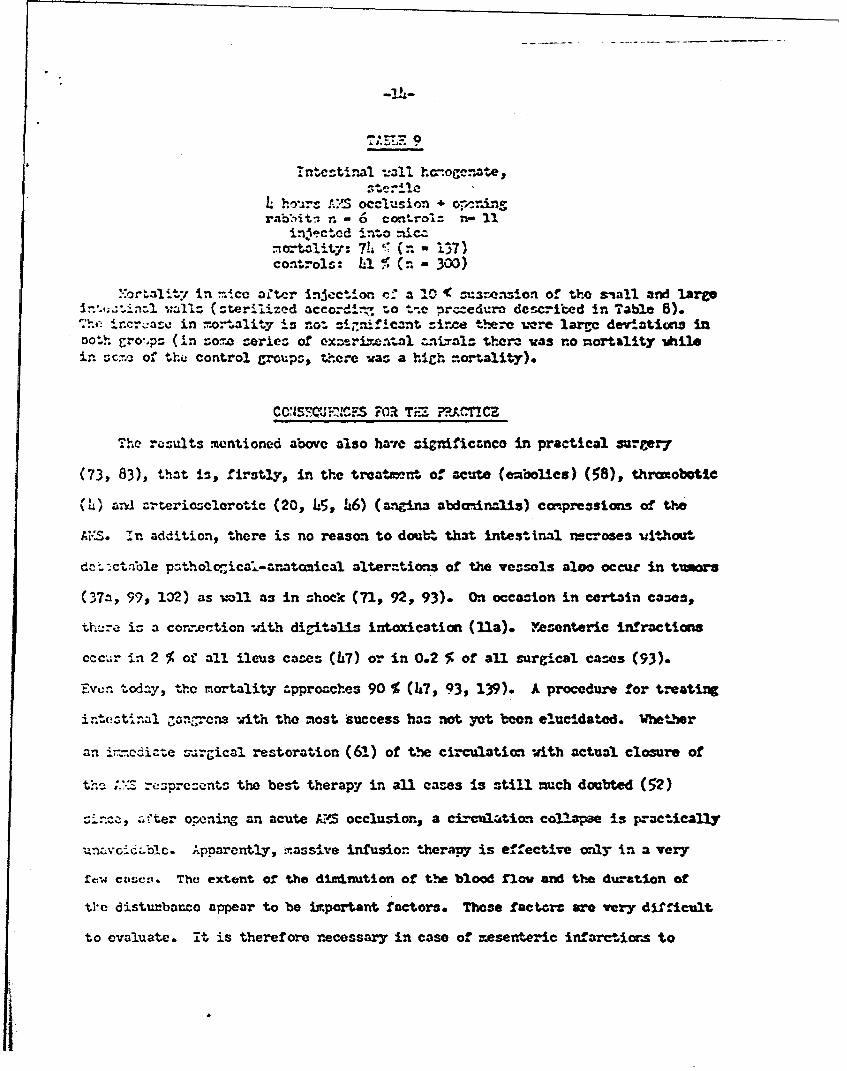
Intcstinal -.all ha-~oge.-te,
L hoirs AS occlusion + o-r -rinrnbiitn r. - 6 con'ro!= n- 11
injected into nicz.not al4t): 74 (r. - 137)controls: .% (n - 300)
-or* .in-e a.*.e at,.r inJction r-,; a "0 1( =-=enion of the "all and lare'-n l (sterilized accord :- to tn~e prccedure dcscried in Table 8).
Tht incr:azc in mo-'ality is not =i.niflcant since thre L-.e larrc deviations inboth E.o,.ps (in so-r.z eries of exneari=tal znials thera vas no mortality -hilein sre of th control groups, there was a high -ortallty).
CCSTCJ'FN. -- T7-n RAC.TrE
Th results mentioned above also have zignificanco in practical surgery
(73, 83), that is, firstly, in the treatzr-e of acute (embolies) (58), thruobotie
(4) anI zrterimclerotic (20, 5, 6) (angina abdoinlis) Compressions of the
AI:S. In addition, there is no reason to doubt that intestinal necroses uithout
ctat.ue patholZicad-anatomical alterations of the vessels aloo occur in tumors
(37a, 99, 12) as =1ll as in shocx (71, 92, 93). On occasion in certain cases,
there is a connection "ith digitalis intoxication (fla). esonteric infractions
cccur in 2 % of all ileus cases (07) or in 0.2 % of all surgical cases (93).
Even todny, the mortality approaches 90 % (47, 93, 139). A procedure for treating
intestina1 ganlrcna with the most success has not yet been elucidated. Whether
an i-.-cdiae surgical restoration (61) of the circulation with actual closure of
th. ;.:.z rezprecents the best therapy in all cases is still much doubted (52)
:i*no., c.-ter opening an acute AM occlusion, a cf-ciiltion. collapse is practically
un:xvodzblc. Apparently, massive infusion 4herapy is effectiv only in a very
rcw ca ,. The extent of the dinnution of the blood fIo and the duation of
tie disturbanco appear to be mportant factors. These factort are very difficult
to evaluate. it is therefore necessary in case of meserveric infarctiors to
consiCier tx'oatm'cr~t ty iso1ntod rerifusion of the .. r:-,.-A'n (91t~), the pcrfoz-,imcc
of a splarmcnic blcckode (52, l10) ani~/or t-ne uz c of chiorpro:., sir, di1.onzylin,
and hypertonic solutions of lom:-mcocul32_-: , (c:ru,tce tnbln 1(t). Tt
in mre that in all cizes, !Lr,-c vi>r (2-3 U.,tc ;' Orn) of' t and
cdextranr s-hould I-- aonni.tcred. Az izir t'.c uoo cl' vniocitive subAt-irces are
concervcdp such zs octcpressir., xjith rQ.-rds to hurans, there is not erncuih
in~form-ation L.v.tilable (66). In a c.:ie of a sim'pe int-st rnol. necrosic, only a
surcical intervention (resection plus eventual vnscular operation) has any
chance ofl succeos.
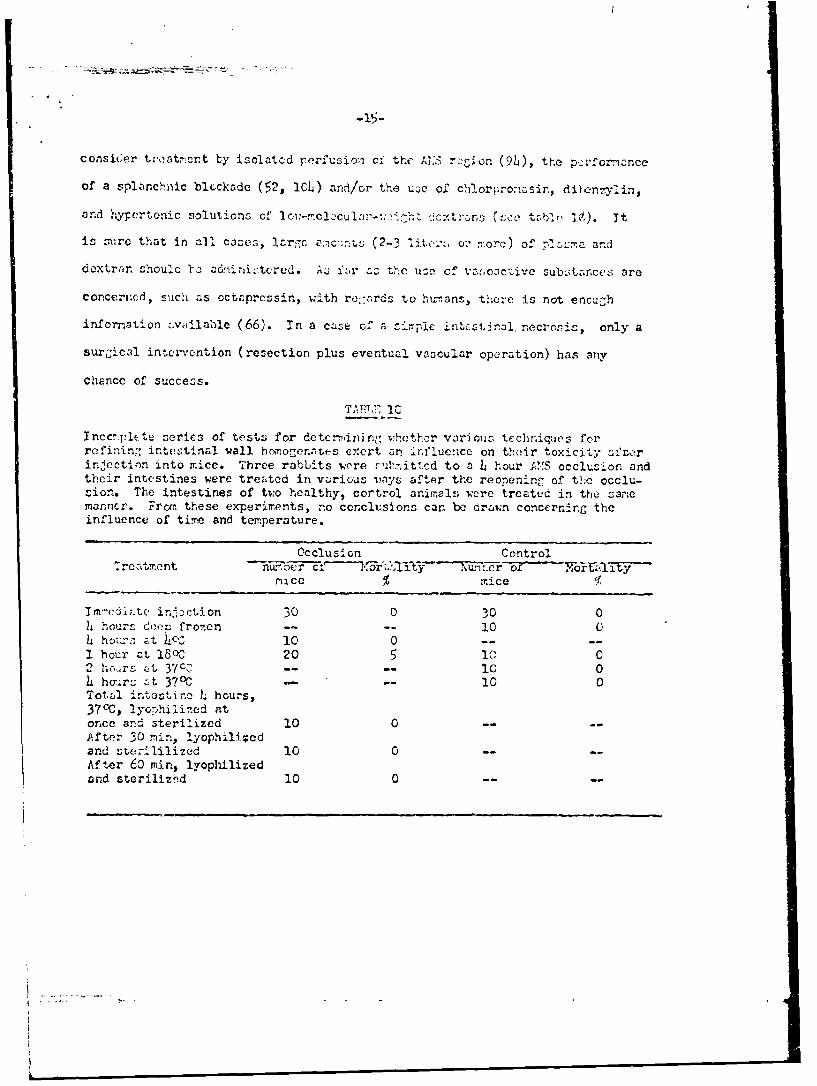
Incc-:pp(hte series of test:; for detcrminin,- vhethcr various techn~iquies forrefinin- intestinal wall hcmiiogernnt.es exert zi in~fluen~ce on th(Ar toxicity 3,utor
injection into mice. Three rabbits wore ri-nrittcd to a L hour A"iS occlksion andtheir intestines were treated in vzarious Monys ai't~r the reopening of the occlu--ion. The intestines of tvo, healthy, oortrol animals vere trcated in the !;arlermarncr. From, these experinrents, no cconclusions car. be drziwn concernin~g theinfluence of time- and temperature.
Occluslon ControlTreat,'rnent Ru
mice % ice
Im-cdlhite in'Pctilon 30 0 30 0It "hours doer; frozen - 10 0hi hozur. -t L-03 10 0 --
1 hour ct 1800 20 502or A 37c,7- - 10 0Ithour-, ,t 37'C - 10 0Totajl intustino L hours,3700, 2yophilized atonce and sterilized 10 0 --
.After 30 ninr, lyophili-*edand sterililized 10 0 --
Af ter 60 min, lyophilizedan~d steriliznd 10 0 --
.:O C.lcnchriic rezicn has ani e:ze siz-aificance In c-evere shock as
tfc' C1ct 0±:n.z d*&z .-_o43-C?.cFF z'P':' carly Ard nro very pro-
acr.id ,z djr of i-.rcvcrs4i*1e d'i.z~z iz cspecially ;-reat (circ. rtois
~ :re cz-. b. decetcd in otzher vvtu~z retoz rLM leadz to l.-.rc losses
3:- _-z.. r c-n.1t of anoxic alerztioaz in t .tCzItr.:s tract.. Tt i ! v A; r
C~j ha~t va:ocwc-z arictve Zs -. Il zz vzzcd!il:-o-. rubztzr c',- travel fr= the
i~a~ cortont., or frcn thc ed wTl in'to t~c porta~l vef~n and dzr.oze
t'.x livc.r. 7rcy y b:e 1zo rcvporftle for the ir-ctof the furncticn of
L~ r:~ ~1 K.~Oh~l g yrter.. This &,=3 not apzczr 'Co cte recult of Ondo-
,:_a: the nunwrou su"C.tances hat have been~ considered o-- pocriblein?.e.4 ral t"-Pr, no Iv c- :lte r itified as a cauvativ ec.
Ce.r -!:,nifiecncc ir. hr-n ahock iz still not clear.
jco trxc~y~n'c alterations in the splancbr.±c region, as they teceir in
iri.wvv-ible chcckp zrr capable of Imir. reproduced in thc artecria rwentericz
curerior (A:-=) shock ne-5l. The inforztion obtvined from'. Vhis model haz
practical c1incai significance in the treatment of -wesenteric blcd flowa dis-
Qtr=incc., e:=ccially in accenteric irfzrctions, in which ca=e it is considered
a-~; t least to orteriez irst h.ve inferior blood flcw before
c1'.n-dcal .r. ',tc:-_ appear. These aspects ame probably more frequent than generally
:-i.nte'stinal gangrene without any detectable organic necroses in the A.S
reg;ion ca.n lso occur in hunrans. It is cuestionble wImhther an i-mediate vascular
r~r~ialrestoration of the intestinal blood flcj in cases of actual occl-usion is
tn best terapy except vhen there is a clear necrosiz. Isolated perfuzion of
the .03 rcgion, ad.inistration of chlorprca=sir., dibenzylin,, octopressin, and
lc--.ccur-%oight doxtrans, coliacal blockade, have to be considered, the
-17 -
most important treatment, hcver, is Luficic:;t rcplaceIcnt of pi. 3n • Several
liters of plasma may be necessary.
1. Abel, F.L. and O.F. >:urphy: ier. J. ?'nyzlo1. 202, 978 (1962).
2. Allgo-,:cr, X. : !!ely. Cir. Acta 1L, 4n3 (19'"17).
3. _ _Toxic f; ctcrc in shock (w.th sreciz.l rcfrencc to birns). 7n cck,. D.: Shock (Schock), Perlin, Gottin,]cn, Heidelberg, Spriner, 1962.
4. Holy. Chir. Acta 30, L3 (1963).
5. and U.F. Gruber- Schweiz. Mcd. Wschr. 95, 1087 (1965).
6. Altura, P.M., S.C. Hershey, and V.D.P. Mazzia: Amer. J. Surr. 111, 186 (1966).
7. , R. Hsu, V.D.B. Mazzia, and S.C. Hershey: Proc. Soc. Exp. Biol. (N.Y.)
_Yf9_73'9 (1965).
8. Anindzen, E.: J. Surg. Res. L, 531 (196).
9. and T. Midtvedt: J. SurE. Rcs. 4, 306 (1V6).
10. Anderson, M.C., R.E. Geurkink, and D.?'. Sims: J. I-mer. Mcd. Ass. 192, 56L (1965).
11. Apel, A.J., J.P. Lintermans, G.L. Kul-ns, and W.G. Guntheroth: SurE. Gynac.Obstet. 123, 755 (1966).
12. , rnstrong J.R., J.D. Henoghan, and G.ti. Bornside: Pull. Soc. Tnt. Chir. 25,108 (1966.
13. Attinger, T.O. , I-. Sugnwara, A. Navarro, A. Riccetto, and R. Martin. Circulit.
Res. 19, 230 (1966).
1L. Aub, J.C.: New Engl. J. Med. 231, 71 (19LL).
15. Baez, S., S.G. Hershey, and E.A. Rovenstine: Amer. J. Physiol. 200, 125 (1961).
16. Ballinger, W.F. IT and H. Vollenw:eider: Surgery 48, 758 (1960).
17. Barnett, W.O., G. Truett, R. Williams, and J. Crowell: Ann. Surg. 157, 77 (1963).
17&. Berger, R.L., W.E. Novogradac, and J.J. 1rn e: Ann. Sur,. 162, 181 (1965).
18. Blattberg, B., P.O. Banning, R.E. Mehler, and M.N. Levy; Proc. Soc. Fxp. Biol.
(N.Y.) 107, 620 (1961).
19. and M.N. Levy: Proc. Soc. Exptl. Biol. (N.Y.) !Cli, 155 (1960).
-18-
20. Blattberg, P. and M.N. Levy: Amer. J. Physiol. 200, 98 (1961).
21. , Amer. J. Physiol. 203, h09 (1962).
22. , Amer. J. Physiol. 203, 867 (1962).
23. ------ _. , Amer. J. Physiol. 203, 111 (1962).
2L. - , Amer. J. Physiol. 202, 899 (1963).
25. - __ , Amer. J. Physiol. 209, 71 (1965).
26. __, Amer. J. Physiol. 210, 912 (1966).
27. • Amer. J. Physiol. 210, 569 (1966).
28. , C. Maldonado, and M.N. Levy: Amer. J. Physiol. 199, 623 (1960).
29. - Circulat. Res. 8, 920 (1960).
30. Bornside, G.H., C.E. Floyd, and I. Cohn: J. Surg. Res. 4, 233 (19 6 ).
31. Bounous, G.: Canad. J. Surg. 8, 332 (1965).
32. , R.A. Brown, D.S. Moulder, and L.O. Rampson, Arch. Surg. 91# 371 (1965).
33. , L.G. Hampson, and F.N Ourdt Arch. Surg. 87, 340 (1963).
3L. __ , Ann. Surg. 160, 650 (1964).
35. , P.G. Scholefield, L.B. Hampson, and F.N. Curdt J. Trauna 4, 42h (196b).
36. , A.H. McArdle, D.M. Hodges, L.G. Hampeon, and L.G. Fraser: Ann. Surg.I 3 (1966).
37. Bradley, S.E., P.A. Marks, P.C. Reynell, and J. Metters Trans. Assoc. Amer.Physicians 66, 295 (1953).
370. Brawley, R.K., W.C. Roberts, and A.G. Morrow: Arch. Surg. 92, 374 (1966).
38. Bridger, J.F. and W. Gillison: Lancet 1965 1, h92.
39. Burri, C. and M. Allgover: Scheiz. Med. vschr. 95, 808 (1965).
hO. * Z. Gee. Exp. Med. 139, 189 (1965).
hl. Carter, D. and A. Einheber: Surg. Oynec. Obstet. 122, 66 (1966).
L2. D'Angelo, C.J., L.M. Ameriso, and J.B. Tredways Circulation 27, 662 (1963).
3. Daniel, W.J., S.D. Mohamed, and N.A. Mathesont Lancet 1966 Is 567.
Uj. Delaney, J.P.t Surg. Form 17, 333 (1966).
LS. Dickinson, S.J. Amer. J. Oastroent. L5, 276 (1966).
-19-
h6. Editorial: Lancet 1964 II, 1222.
VY. Emmermann, H. Chirurg. 37, 349 (1966).
48. Evans, W.E. and J.C. Darint Surgery 60, 1026 (1966).
L9. Fell, C.? Amer. J. Physiol. 210, 863 (1966).
50. Fine, J.: Amn. Surg. 1U2, 361 (1955).
51. , Amer. T. Gastroent. 29, 596 (1958).
52. . . "
53. ", t.A. Ravin, S.H. Rutenberg, and F.B. Schweinburg: New
r J. Mod. 260, 214 (1959).
5L. Frank, E.D., H.A. Frank, S.W. Jacob, and J. Fine: Amer. J. Physiol. 202,7 (1962).
55. Friedman, J.J., Amer. J. Physiol. 200, 6Uh (1961).
56. _ , Circulat. Rea. 9, 561 (1961).
57. Fry, W.J. and R.O. Kraft: Surg. Gynec. Obstet. 117, h17 (1963).
58. Glotzer, D.J. and P. Glotzer; Arch. Surg. 93, 421 (1966).
59. Gordon, H.A.: Nature (London) 205, 571 (1965).
60. Gregg, D.E, In Bock, K.D., Shock (Schock), Berlin, Gottingen, Heidelberg,Springer, 1962.
61. Gumrich, H.: Langenbecke Arch. Klin. Chir. 308, 229 (1964).
62. Gurd, F.N., Amer. J. Surg. 110, 333 (1965).
63. Guyton, A.C. and J.W. Crowell, Fed. Proc. 20, 51 (1961).
6L. Hamrick, L.W. Jr. and J.D. Mayers, Circulat. Res. 3, 65 (1955).
65. Hardy, E.G., G.C. Morris, E.M. Yow, B.W. Haynes, and M.E. DeBakey: Ann.Surg. 139, 282 (1954).
66. Hershey, S.G. and B.M. Altura: Schweis. Med. Wschr. 96, 1L67,1516 (1966).
67. , S. Baez, and L.A. Rovenstine: Amer. J. Physiol. 200, 1239 (1961).
68. V.D.B. Mazzia, B.M. Altura, and L. Oyure: Anesthesiology 26, 179
69. ,9 ., L. Oyure, and K. Sirger: Proc. Soo. Exp. Biol. (N.Y.) 115,
s
-20-
70. Hinshaw, D.B., M. Peterson, W.M. Huse, 0.1. Stafford, and E.J. Joergensen:A1ner. J. Surg. 102, 22h (1961).
71. opkins, R.W., G. Sabgs, J. Penn, and F.A. Simeonet J. Amer. Med. Ass. 191,
731 (1965).
72. Tnrlis, F.G., L.G. Hampson, and F.N. Curd: Ann. Surg. h9, h3 (1959).
73. Jackson, D.B.: Occlusion of the superior mesenteric artery. Springfield, Ill.C.C. Tbomas, 1963.
7h. Jacob, S., H. Weiel, E. Gordon, H. Korman, F. Schweinburg, H. Frank, andJ. Fine: Amer. J. Physiol. 179, 523 (195h).
75. Jacobson, E.D.t Gastroenterology 50, 236 (1966).
76. Janoff, A., A.L. Nagler, S. Baez, and B.W. Zweifach: J. Exp. Med. 11l, 20h(1961).
77. , G. Weissmann, B.W. Zweifach, and L. Thomast J. Exp. Med. 116, h577M.
78. Johnson, P.C.: Amer. J. Physiol. 199, 589 (1960).
79. Johnson, D.G. and W.M. Parkinst Fed. Proc. 23, abstract 1885 (196).
80. Yelan, M. and B.W. Zweifach: Surg. Gynect. Obstet. 99, 707 (1954).
81. Kobold, E.E. and A.P. Thalt Surg. Forum 13, 35h (1962).
82. . Surg. Gynect. Obstet. 117, 315 (1963).
83. Lzufman, H., P.F. Nora, and A.L. Mittelpunkti Arch. Surg. 88, 102 (1964).
8L. Lepley, D. Jr., C.J. Mani, and E.H. Ellison: J. Surg. Res. 2, 403 (1962).
85. Trevy, .'.N., B. Blattborg, and J.L. Barlow: J. Lab. C21n. Med. 56, 165 (1960).
86. Lillehei, R.C.t Surgery L2, 103 (1957).
87. , B. oott, and F.A. Miller: Ann. Surg. 150, 543 (1959).
88. , J.K. Longerbeam, J.H. Bloch, and W.B. Hanax: Ann. Sur&. 160, 68 (1964).
89. Lin, M.K. and B.W. Zeifach: Proc. Soc. Exp. Biol. (N.Y.) 108, 27 (1961).
90. Longerbeam, J.K.,. R.C. Lillehei, and W.R. Scott: Surg. Forum 13, ? (1962).
91. - J. Amer. Med. Assoc. 181, 878 (1962).
92. Marston, A.: Lancet 1962 IT, 365.
93. 1 Ann. Roy. Coll. Surg. Engl. 35, 151 (1964).
-21-
91. Mayer, G.E., A.0. Lyall, K.M.R. Chrystal, and D.M. Proctor: Brit. J. Surg.50, 536 (1963).
95. Ma7cia, V.D.B., J.M. McKenna, L. Gyure, and S.G. Hersheye Fed. #roc. 23,539 (1960).
96. McCluskey. R.T., B.W. Zweifach W. Antopol, B. Benacerref, and A.L. Nagler:Amer. J. Pathol. 37, 2L5 (196W5.
97. McRae, J.M. Jr., ':!.R. Webb, S.S. Lee, J.D. Hardy, and J.C. Griffin: Surg.
Forum 9, 37 (1958).
98. Messmer, B., U. Middendorp, and E. Maranta: Helv. Chir. Acta 33, 521 (196?)
9. Mills, L.C. and J.H. Moyer: Schock and hypotension, Pathogenesis and treat-ment, New Yorks Grune and Stratton, 1965.
101. Muller, W. and L.L. Smith: Surg. Gynect. 117, 753 (1963).
102. Musa, B.U.*; Ann. Intern. Med. 63, 783 (1965).
103. Nagler, A.L. and B.W. Zweifach: J. Exp. Med. 114i 195 (1961).
10. Nahor, A., J. Milliken, and J. Fine: Ann. Surg. 163, 29 (1966).
105. R. Minton, and J. Fine: J. Amer. Med. Associ. 192, 600 (1965).
106. Nelson, R.M. and H.E. Noyes: Surg. Forum 3, L74 (1952).
107. Nemir, P. Jr., S.J. Much&, P.R. Hawthorne, and D.L. Dvabkin: Ann. Surg. 150,469 (1959).
108. Noer, R.J. Amer. J. Anat. 73, 293 (1943).
109. Oilodart, R. and A.R. Mansberger: Amer. J. Surg. 110, 302 (1965).
110. Palmerio, C., B. Zetterstrom, J. Shammah, E. Euchbaum, E. Frank, and J. FinesNew Engl. J. Med. 269, ?09 (1963).
111. Peters, R.M. and R.A. Carter: Ann. Surg. 164, 197 (1966).
ll1a. Polansky, B.J., R.L. Berger, and J.J. Brynez Circulation 30, 1 (196?).
112. Powers, L.H. and P.R. Schloerb: Surg. Forum 9, h0 (1963).
113. Price, H.L., S. Deutsch, B.E. Marshall, G.W. Stephen, M.O. Berg, and G.R.Neufeld, Circulat. Res. 18, L69 (1966).
I1h. Ravin; H.A. and J. Fines Progr. Surg. (Basel) 3, 102 (1963).
115. , F.B. Schweinberg, and J. Fine: Proc. Soc. Exp. Biol. (N.Y.) 99, ? (1958).
-22-
116. Reich, T., B.M. Pierolf, and B.M. Reynoldst J. Surg. Rea. 5, 116 (1965).
117. flrrnell, P.C., P.A. Marks, C. Chidsey, and S.E. Bradleyr Clin. Sci. 7,
i8. Rogonberg, J.C.u Clin. Res. 9, 396 (1963).
119. , R. Davis, W.H. Moran, and B. Zimmermann: Fed. Proc. 18, 503 (19??).
120. Rothe, C.F. and E.E. Selkurt: Amer. J. Physiol. 200, 1177 (1961).
121. Rovenstine, E.A., S.C. Hershey, S. Lanza, A. Baez, and S. Baez: Anesthesiology20, 290 (1959).
122. Sapirstein, L.A., N.M. Rickley, and E. Ogden: Science 122, 1138 (1955).
123. , E.H. Sapirstein, and A. Bredmmeyert Circulat. Res. 8, 135 (1960).
12L. Schwein)umrt, F.B., P.8. Shapiro, E.D. Frank, and J. Fine: Proc. Soc. Exp.Biol. (N.Y.) 95, 646 (1957).
125. Selkurt, E.E., P.J. Brecher, and G.A. Brecher: Circulat. Res. 4, 633 (1956).
126. Amer. J. Physiol.193, 599 (1958).
127. Amer. J. Physiol. 197, 281 (1959).
128. and C.F. Rothe: Proc. Soc. Exp. Biol. (N.Y.) 111, 57 (1962).
129. Sergeant, J.C.B.: Lancet 1965 Ip 139.
130. Lancet 1965 I, 65h.
131. Shapiro, P.B., B. Pronsther, E.P. Frank, and J. Fines Proc. Soc. Exp. Biol.(N.Y.) 97, 372 (1958).
132. Sherman, R.T. and H.E. Noyes J. Surg. Res. 3, L09 (1963).
133. Sherman, P.H D Krumhaar, T. Tanaka, L.R. Bennell, and J.V. Maloney Jr.:
Ann. Surg. 164, 23 (1966).
13L. Short, E., B.W. Zweifach, and R.F. Furchgott: Science 102, 189 (19L,5).
135. S.ith, J.J. and R.A. Grace: Amer. J. Physiol. 191, 135 (1957).
136. Nith, L.L., C.D. Reeves, and D.B. Hinshaw: Hemodynamic alterations and regionalblood flow in hemorrhagic shock. In L.C. Mills and J.H. Moyer: Shock andFjypotension, p. 373. New York: Grune and Stratton, 1965.
137. and U.P. Veragut, Progr. Surg. (Badel) 4, 55 (1964).
138. Tice, D.A. and A.E. Dumont: Surg. Forum 15, 86 (1964).

-23-
139. Van Zyl, J.J.W. and F.D. DuToitz Brits J. Surg. 53, 522 (1966).
i 10. Vick, J.A., L.E. Wittmers, M.M. Jordan, and L.B. Hinshawt Proc. Soc.Fxp. Biol. (N.Y.) 109, 200 (1962).
ILI. Wells, R.E. : Rheology of blood in low flow states. In L..C. Ylls and J.P.Moyer: Shock and Hypotension, p. 80. New York: Grune and Stratton, 1965.
1L2. 1*crner, A.Y., D.M. MacCanon, and S.H. Horvaths Amer. J. Physiol. 130, 62h
(1952).
1013. Wiseman, R.F. and H.A. Gordon: Nature (London) 205, 572 (1965).
14L. .zaitzer, T., N. Better, W. Rachlin, N. Atkins, E.F. Frank, and J. Fine:J. Exp. Med. 112, 1157 (1960).
1,45. Zweifach, B.W. : Ann. N.Y. Acad. Sci. 88, 203 (1960).
1I_6. and B. Benacerraft Circulat. Res. 6, 83 (1958).
IT7. , H.A. Gordon, M. Wagner, and J.A. Rsyniers: J. Exp. Med. 107, L37
1; ~r