em_hep_28_en.pdf - world health organization (who)
TRANSCRIPT

W f ' 3 L D I i 9 P LTI" C'FGPD'IZP. i'1C.N Regional Office f o r t h e E a s t e ~ n h?editerranean
Ei:GLISH ONLY
REFORT ON THE SEfi?INkR O N SCHQOL HEALTH EDUCATION
KULVAIT, 1 4 2 0 MARCH 1966

T h e v iews e x p r e s s e d in t h i s R e p o r t do not n e c e s s a r i l y r e f l ec t t h e off ic ial policy of the World Heal th Crganizat ion.
T h i s document h a s been p r e p a r e d by the Tl?rEO Regional Office for t h e E a s t e r n P ied i te r ranean f o r G o v e r n ~ l e n t s of Wember S t a t e s in the Seg ion and for those who par t ic ipa ted in t he S e m i n a r . A l imi ted number of cop ie s i s ava i lab le on r e q u e s t f o r p e r s o n s officially o r professional ly conce rned with the f i e ld of school heal th education.

Participants and Observers who Attended the W H O Seminar on School Health Education held in Kuwait from 14 - 20 March 1966

WHO EMRO
TABLE OF CONTENTS
Page
............... 1. Background and Objectives ........ 2. Opening Session and Organization ............................... 3. Appraisal ......................... 4. Acknowledgement
CHAPTER I1 NAT'URE AND SCOPE OF SCHOOL HEALTH EDUCATION . CHA- I11 SCHOOL HEALTH SERVICES AND SCHOOL HEALTH
EDUCATION I N THE COUNTRIES OF THE EASTEW MEDITERRANEAN REGION
1. General Remarks on School Health Needs and Services i n the Eastern Mediterranean Region ..................................
2. Description of School Health Services and Schnol Health Education i n the countries of the astern Mediterranean Region ..... 33
CHAPTER TV SCHOOL HEALTH EDUCATION I N THE CON?TMT OF . EDUCATION AND HEALTH
. . . . . . . . . . Panel Discussion ........................ 49
CHAPTER V AN OVERVIEW OF BASIC NFBDS
1. Nutrition i n School Health Services and ........................ Health Education 2. Mental Health o f the School Child i n the
Present Transitional Stage of Rapidly Developing Nations. Dialogue followed by .............................. Discussion ......... 3. Some Notes on School Sanitation

EM/IBP/~~ page ii
WHO EMRO
TABLE: OF CONTENTS (cont Id)
CHAPTER VII
ANNMB
ANNEX C
A N N M D
ANNEXE
4. Health Contents i n the Textbooks of the F'rirnary and Secondary Schools i n Some of the Countries of the Eastern Mediterranean Region ..................................
5. Research i n School Health Education and ...................... the ~ e a c h e r ' s Role
EXAMPLES OF SOME SPECIFIC PROGRAMMES I N THE REGION
1. A Note on Teacher Training and Curriculum Development .............................
2. ~ e a c h e r s ' Preparation i n Health Education An Experiment i n the United Arab Republic
3. Health Education i n Secondary Schools - The Pattern i n Pakistan .................
4. School Health Education - Joint Cooperation Between Ministry o f Public Health and Ministry of Education i n Ethiopia .......
5. Audio-Visual Aids i n School. Health Eduoation ...............................
COMMI- WORK AND RECOMMENDATIONS
1. Committee !'ark .......................... ......................... 2. Recommendations
LIST OF PARTICIPANTS, OBSERVERS AND NATIONAL PREPARATORY coI"lMIm
LIST OF COMMI- MEMBERS
AGENDA
PROGRAMME O F THE SEMINAR
LIST OF DOCUMENTS AND BACKGROUND MATERIAL
Page

WHO EMRO
1. Background and Objectives
School health educatior; can only become meaningful i f it is trans- formed in to the pat tern of behaviour of the chi ld during h i s school days and afterwards, 8ccepting health as a value and as an asset . !The u l t i - mate aim of school health education, therefore, is not only the acquisi- t i on of some knowledge of nature of disease, morphology of the causative .-- agent and personal hygiene but a l so the acceptance of heal th behaviour as pas* of everyday l i f e . I n the endeavour t o reach t h i s aim, the following three elements are essent ia l p a r t s of every sound health education pro- gramme :
a. well established school health services f o r the students and school personnel;
b. healthful school environment, physical, soc ia l and mental;
c . organized 5eal th instruction.
'L'he increasing a t tent ion given t o educaLiv11 LugeLher w i t 1 1 regulations ', concerning compehsory-education has resuzted . in-a -rapid grouFth.of school . attendance i n t h i s Region. According t o the UN estimates i n the academic
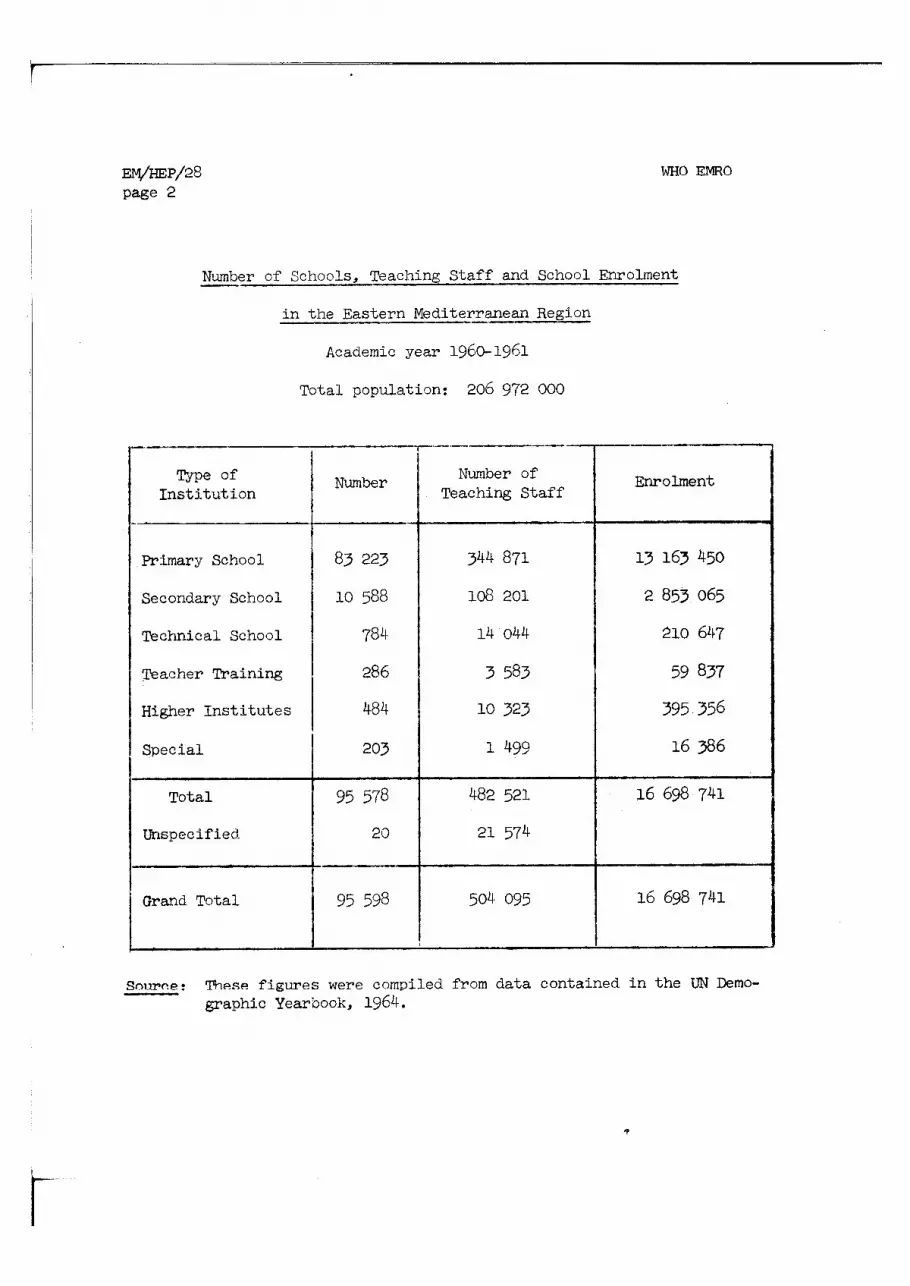
year 1960.1961, there were almost 17 million people i n this Region attend- ing primary or higher schools taught by over half a million teachers i n more than 95 000,training institutions: One cannot over-emphasize the .- - *.- . . value of-health Bducation fo r such a large group of stuclent population,
I many of whom are i n t h e i r formative years of l i f e . The following tab le explains the above point:
WHO EMRO
Number of Schools, Teaching Staff and School Enrolment - i n the Eastern Mediterranean - Region
Academic year 1960- 1961
Total population: 206 972 000
Source: These figures were compiled from data contained i n the UN Demo- - graphic Yearbook, 1964.
Enrolment
1 13 163 450
2 853 065
210 647
59 837
395 356
16 386
-- Type of
Ins t i tu t ion
Primary School
Secondary School
Technical School
Teacher Training
Number
83 223
10 588
784
286
7-. --
Nwnber of Teaching Staff
344 871
108 201
14 044
3 583
Total
Unspecified
Grand Total
10 323
1 499
482 521
21 574
504 095
95 578
20
95 598
Higher Ins t i tu tes 1 484
16 698 741
16 698 741
Special 203

WHO EMRO
This attention 'to eclucatlon i n tfle Reggion 1s a very enCOWaglng phenomenon. The importance f o r s t r e s s ing hea l th and hea l th education a s par t of t h i s t r a i n i n g is c lear .
The need f o r ac t ive cooperation between education and hea l th autho- r i t i e s i n matters deal ing with school hea l th and school hea l th education has long been accepted by t h e World Health Organization Regional Office f o r t h e Eastern Flediterranem. The Six th Session of t he Regional Committee (1956) i n i ts Technical Discussion on hea l th education emphasized t h e need f o r ac t ive coaperation, and f o r placing r e spons ib i l i t y f o r hea l th education i n schools j o i n t l y w i t h both education and hea l th au thor i t i e s .
I n these discussions "special emphasis w a s placed on t h e value and need f o r promoting c lose r cooperation between teachers, parents, school hea l th personnel and community resources1".
The Seminar on Health Education of t he Public i n t h e Eastern Mediter- ranean Region, which was held i n Teheran from 28 October t o 9 November 1958, a l s o pinpointed t h i s col laborat ion.
The following suggestions emerged from the discussions on the subject of school hea l th education:
"1. During t h e i r basic t ra in ing , s tudent teachers should rece ive s inp le and > r a c t i c a l i n s t ruc t ion on the basic f a c t s regarding t h e promotion and protec t ion of t h e i r own and t h e schoolchi ld ' s heal th, cn; x i h e cause and prevention of l o c a l public hea l th problems.
2. The cooperation of the education a u t h o r i t i e s should be sought so t h a t hea l th education can be continued and expanded i n t h e secondary schools2".
Document ~1fl/RC6/~ech. ~ i s c ./lg, page 8 - 11.
Seminar on Health Education of t h e Pulslic i n t h e Eastern Mediterranean Region, 1958. Final Report: Alexandria (m ), 1959.

Following the above Technical Discussion and the 1955 Seminar, the Regional Office i n i ts contacts with the Governments has continuously stressed the need fo r such joifit e f fo r t . This present Seminar vas con- ceived and developed t o give further impetus t o cooperative measures already well advanced i n many of the countries of the Region.
Objectives of the Iresent Seminar .--. --- Basel: on these considerations, the following objectives were selected
fo r the present Seminar:
a. reviewing the s ta tus of health education a c t i v i t i e s a s par t of the school health serviues carried u u t i r ~ primary and secondary schools o? the cc7mtries of t h i s Region;
b. diacuooing the health education needs of school chil&-en, taking in to account the f a c i l i t i e s and the provisions;
c. sharing experience on the means of developing bet ter health education ac t i v i t i e s and t ra in ing i n schools;
d. studying the curriculum development i n schools and the significant ro le of health education, qual i ta t ively and quantitatively, i n t h i s curriculum;
e. studying the health education aspect i n the curricula of teacher t ra in ing ins t i tu t ions .
On the international level valuable cooperation ex i s t s between WHO and other UN agencies. For example, there have been a number of joint meetings with UNESCO i n various regions and a l so a t WHO Heaclquarters i n Geneva. WHO Technical Report Series No. 193, dealing with teachers preparation i n health education, is the outcome of one of these joint ef for ts . The recent joint project however was the preparation of a document "planning fo r Health Education i n ~choo l s " by Professor C.E. Turner, WO/UNESCO Consultant. The r e su l t s of t h i s ac t ive cooperation between these two agencies have been published In form of a book, d is t r ibuted t o a l l part icipants. Coop-.ratiori with UNICEF i n the f i e l d of school health education has a lso been very encouraging. The document prepared on the

WHO EMRO
Teachers' Preparation i n Health ducati ion' provides an example. Further- more, UNICEF offered three fellowships f o r part icipation i n t h i s Seminar. Cooperation a lso ex i s t s between WHO and FAO, especial ly i n the f i e l d of nutr i t ion education. The same holds t rue f o r other UN specialized agencies and various other international agencies.
This, obviously, is not an exhaustive account of the amount of co- operation between WHO and other UN agencies and other international bodies interested i n the f i e l d of school health education. Such an account would i t s e l f be a voluminous document.
The following resolution w a s made during the Technical Discussions of the Fifteenth Session of the Regional Committee w h i c h was held i n Addis Ababa i n September 1965~:
he Regional C o r n m i t t c c ,
"Having studied with in te res t the document on School Health i n the Eastern Mediterranean Region, presented by the Regional Director;
"Considering t ha t school health services a re among the major needs of t h i s Region;
" ~ o t i n g the development of various a c t i v i t i e s i n school health services and school health education i n a number of countries of t h i s Region fo r promotion of these services,
i. "MPRESSES i ts sa t is fact ion with the s tudies made by the World Health Organization i n a few countries of the Region;
2. "ENDORSES the recommendations made i n the document under review;
Kamel, W.H. and Sonbaty, M.M., Teachers ' Preparation i n Health Educa- t i o n - A n Experiment i n the United Arab Republic, 1966, (EM/SEM. SCH. HLTH. EDUC . /7 )

WHO EMRO
3. "RECOMMENDS that the governments give high p r io r i ty t o school health services including :
a. health services f o r cl?il&en, an6 other students i n various stages of t he i r education;
b. health services f ~ r school personnel;
c. health of the school environment;
d. school health education;
e . teachers ' preparatior, i n healt'n education;
f . mental health of scl-loo1 children;
g. inclusion of public health in to the curricula of the schools.
4. "RECOMMENDS medical colleges and schools t o give special a t tent ion t o school health and health education;
I1 5. REQUESTS the Regional Director t o make further surveys on school health services and health education and t o provide assistance t o the governments, a s required, i n school health services and school health education in order t o develop and promote the health of the school children".
It is very pleasant t o note the trend i n organizing or planning act ive cooperation between ministr ies of health and of education, and with other ministr ies such as youth, guidance etc. . i n the f i e l d of school health educa- tion.
During the l a s t two years i n a t l e a s t t en countries of the Region seminars have been organized between the two ministr ies of health and education, bringing together the medical and educational author i t ies t o discuss and share experiences on promotion of school health services and school health education. In these seminars emphasis has been given t o school health education, a s part of school health services on the one hand and of the t o t a l community and national health on the other, thus making school health education not a separate en t i t y but part of a wider sphere. Attention has occasionally been given t o making the school a community

centre, bringing in parents and other citizens to the school for dis- cussions on improvement of the health of the community. Also attention to provision of recreation facilities and health education in physical education programmes is increasing.
Obviously,the more attention given to the school as a dynamic centre of change and improvement in the community for the present and future, the more effective will be the schcol health ed- cation activities and that has been a major aim of this Serninar.
2. Opening Session and Organization
The Seminar on School Health Education sponsored by the World Health Organization with the cooperation of the Government of Kuwait was held in the Nursing College, Ministry of Public Health, Kuwait, from 14 - 20 March 1966.
Forty-one participants from sixteen countries of the Eastern Mediter- ranean Region and nine observers representing UN and some international agencies interested in school health education attended the Meetings. The participants included, senior administrators, planners, policy makers, health educators and teachers from Ministries of Health and of Education of the countries of the Region.
Inaugural Statement by H.E. Tke Ministcr of Public Health, Kuwd;it
In his inaugural speech H.E. El Sayed Abdul Aziz El Feleig, Minister of Publio Hcalth, Kuwait, welcomed the participants on behalf of His Highness The Amir and the Government and statel! that s he cultural and historical background shared by countries of the Eastern Mediterranean Region will make it easy for us to increase our cooperation in this rcspcct in order to raise the health standard of our people. The Government and people of Kuwait heartily welcome such cooperation which would yield substancial benefits to all and cause peace and friendship to prevail in our world in compliance with the charter of the United Nations and constitution of the World Health Organization which provides that the health of all people is fundamental to the attainment of peace and security and is "dependent upon the fullest co- operation of individuals and states".

WHO mo
Excerpt of the Address bjr Dr. A.H. Taba, WHO Director, EMR
I n h i s address D r . A.H. Taba, Director of the Eastern Mediterranean Regional Office of WHO thanked H i s Highness the A r n i r and the Government of Kuwait for t h e i r hospi ta l i ty and the Governments of the Region fo r accepting the invi ta t ion of libTHO fo r part icipation i n the Seminar. Dr. Taba s ta ted t ha t "The increasing a t tent ion t o education on the one hand and t c health on the other as the dynarnic forces of change i n the communities brings t o the a t tent ion the need fo r focussing on school health education i n a l l countries.
"There are, according t o conservative estimates over 17 million students studying in primary and secondary schoolo in th is Region taught
by over half a million teachers. This i n i t s e l f is a big enterprise and a growing endea.vour, considering the f ac t t ha t not every child of the school-age io attending echo01 at prcsent and that plans are under w a y i n the majority of countries f o r spreading education t o a l l school-age children.
"The Sta te of Kuwait is a shining example of achievement i n t h i s respect, f o r according t o the l a t e s t data, 97 000 students a re attending primary and secondary schools. That is, over 20 per cent of the en t i re population.
"It becomes imperative a t t h i s stage of rapid development, therefore, t ha t a t tent ion be given t o the education of younger generation i n the f i e l d of health not only fo r the present healthful l iv ing but f o r accepting health a s a value and a s an asse t f o r future l i f e .
"The World Health Organization, since i ts inception and by its con- s t i t u t i on has placed much emphasis on the health of the younger age-groups and, through its projects and! consultations with the Government and by symposia and expert committee meetings and semipars has directed a t tent ion t o the importance of education of t h i s group i n the f i e l d of health.
('It is fo r the f i r s t time, however, t ha t t h i s Region is bringing to- gether the eminent experts, planners, administrators and educators from Ministries of Health and of Education t o discuss and share experience on matters regarding school health education.

WHO EMRO
"It is the general feeling "Liat sch~vl health education wlth lts important role is not limite2 to the health instructions given in the class-rooms, and the a i m of this Seminar is to discuss school health education not only as far as instruction is concerned but also in regard to the total health and educational experience that the child feels in his school days".
Audience with His Highness The Arnir
His Highness Sheikh Sabah A1 Salem A1 Sabah, The Arnir of Kuwait, received the participants and other representatives of UN and other international agencies and the WHO Secretariat, in audience. He wel- comed all and emphasized the need for increased attention to health education of school children and general public.
Or.sanization of the Seminar
In the first plenary session the following were elected as Seminar Officers by the participants:
Mr. Berges Hamoud Berges, (~uwait) Chairman
Dr. Mohamed Mahmood El-Sonbaty, (UAR) Vice- Chairman
Dr. Ibrahim Alamuddin, (~ordan) Vice- Chairman
Dr. Z.G. Panos, (cyprus) Viue- Chairman
Dr. K. Shayer. (11-zq) Rapporteur
The Seminar was composed of plenary sessions and four committees.
Visits were also arranged to a number of schools, kindergmtens, school clinics, the Al-Sabah Hospital, the Kuwait Oil Company, the Water Distillation Plant and the Museum.
3. Appraisal
In the last session of the Seminar a questionnaire was distributed to participants inviting their comments and suggestions for the improvement of similar seminars and to find out in what ways - in their opinion - such seminars may have tangible results. The prnticipants and observers

E M / H E P / ~ ~ page 10
WHO EPmO
were asked not t o s ign t h e i r names on the questionnaire sheets . Out of f i f t y questionnaires d i s t r ibu ted th i r ty- four responses were received.
The f i v e questions were a l l "open-end" questioils allowing f o r a var ie ty of responses. Later the responses were categorized under d i f f e ren t sect ions.
The o r ig ina l questions were a s follows:
1. What fea tures o f t he Seminar were especia l ly he lpful t o you?
2. What fea tures were not helpful?
3 . What suggestions have you f o r improving s imi lar seminars?
4. How do you propose t o make r e s u l t s of the seminar known i n your country?
5. What follow-up measures w i l l you attempt?
Following are the answers received 6ivided i n t o a number of in ter - dependent sect ions. It is very encouraging t o note t h a t the majority of the par t ic ipants found the seminar s t imulat ing and have made recommendations f o r t h e implementation of the recommendations.
1. What fea tures of the Seminar were especia l ly he lpful t o you?
Responses
A l l f ac to r s were found useful 8
A. Organization and approaches t h a t were found useful:
Committee work Free discussion with pa r t i c ipan t s V i s i t s Sharing experience Panel discussions Technical papers Ef f i c i en t organization of the Seminar

WHO Ern0 ~ M / H E p j / 2 8 ' page 11
Responses
Presence of both health and education disciplines 1 Literature distributed 1 High caliber of staff 1 Plenary sessions 1
B. Contents which were foulid helpful:
Planning for school community relationships 4 Preparation of teachers 4 Statements by participants 4 Audio-vlsual alds in school health education 2 Strengthening curricula of primary and secondary schools 2
2. The features t'mt were not helpful:
No answer 16 Nothing 13 Group discussions 2 Participarts raising their own problems 1 Too many subjects discussed 1 Time limitations 1
3 . Suggestions for improving similar seminars: \- -
A. How the present seminar n o i ~ l c ! have been imaroved?
By extension of time 13 By ~ise of Arabic language 9 By better planning I"or field visits 2 By arranging sight seeing tours 1 By more emphasis on role of woman 1 By inviting finance and planning people to see the importance of school health education 1
By inviting non-governmental agencies interested in school health education 1
EM/HEP/~~ page 12
WHO EMRO
Responses
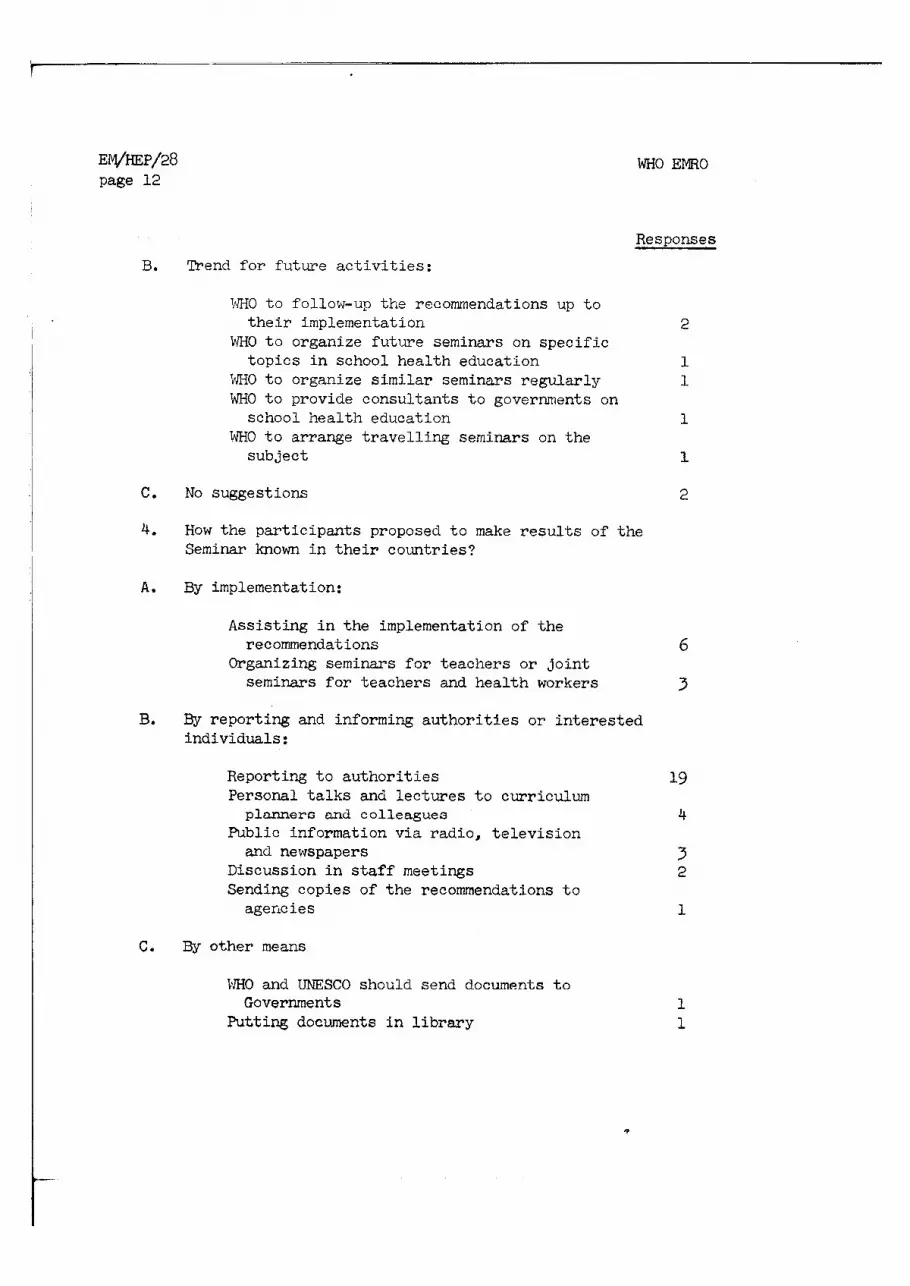
B. Trend for future activities:
IdHO to follotu-up the recommendations up to their implementation 2
WHO to organize future seminars on specific topics in school health education 1
WHO to organize similar seminars regularly 1 WHO to provide consultants to governments on school health education 1
WHO to arra,nge travelling seminars on the subject 1
C. No suggestions 2
4. HOW the participants proposed to make results of the Seminar known in their countries?
A. By implementation:
Assisting in the implementation of the recommendations
Organizing seminars for teachers or joint seminars for teachers and health workers
B. By reporting and informing authorities or interested individuals:
Reporting to authorities Personal talks and lectures to curriculum planners and colleagues
Public information via radio, television and newspapers
Discussion in staff meetings Sending copies of the recommendations to agerrc ies
C. By other means
lJHO and UNESCO should send documents to Governments
Putting documents in library

WHO EMRO
D. Noanswer
5. What fellow up measures will participants attempt?
A. By direct action:
Personal consideration in planning Initiation of research, studies and evaluation
Forming a coordination committee for the implementation of the recommendations
Contacting authorities to see if the recommendations were implemented
Proposing a scheme for school health education to be included in development plans
WHO/EMRO should publish a quarterly bulletin on health education as a follow-up measure
C. No answer
nesponses
2
B. By proposals and contacts:
4. Acknowledgement
The particlpalis and representatives at the closing oeosion expressed their deep gratitude to His Highness The Arnir of Kuwait, the Government and especially the Ministry of Public Health for all the courtesy and hospitality extendcd to them throughout the Seminar. They also thanked the National Preparatory Committee for making a11 arrangements. Thanks were also expressed to the Eastern Mediterranean Regional Office of the World Health Organization for planning and conducting a Seminar on such an important topic.

CHAPTER I1
This is a time of change i n public health and i n education. Old goals and methods are being reevaluated and new ones explored. Many health ~roblems plaauing nations over the years are now within reach of prevention or control. New health problems a re r i s i ng as conditions which engender them develop. Urbanization, human mobility, modern agri- cu l tu ra l practices, and indust r ia l iza t ion a r e among soc ia l and technical developments af fect ing health. A s peoples ' expectations f o r a be t t e r l i f e expand, and as an increasing number of children at tend school, edu- cational leaders are reappraising t h e i r goals, curricula, and methods. The great explosion of knowledge is likewise making its impact on educa- tion. I n the midst o f these dynamic changes, school heal th education is a l so changing.
What is school heal th education?
School heal th education, a s the term w i l l be used here, is that education f o r health which takes place within schools o r under the general guidance of school-related personnel. In one sense, it is a process by which agents of education, such as teachers and health workers, exer t t h e i r influence so a s t o a f fec t the heal th behaviour of pupils. I n another sense, it may be thought of as the changes which occur i n heal th behaviour, individually or col lec t ively - t k a t is, i n what people under- stand, how they feel , and what they do i n respect t o health. Though the
Based on the paper presented and the discussions of the Seminar

WHO EMFlO
primary focus i n school health education is on pupil health, school heal th education programmes must deal ac t ively with health needs of home, school and comunity. Pupils do not l i v e i n a vacuum; t h e i r health is affected by conditions around them and the school, through its educational ef for ts , can play an important par t i n improving these conditions. School health education, then, can be thought of a s dealing with the f u l l range of heal th needs t ha t i n any way impinge upon the well-being of pupils, and of the homes, schools and communities i n which they l i v e and work.
School health education includes individual heal th counseling, informal health teaching (and learning), and systematic health instruction. Some of the most important health education takes place on a one-to-one baais between pupils and teachers o r health workers who are i n d i rec t contact with a child. The chi ld who is malnourished o r who has an eye infection needs individual assistance as may also his parents. The young person who attends a clinic because of ill heal th needs t o understand what may be wrong with him and what he himself may do t o become well. Health is frequently a personal matter requiring personal at tention. Individualized health education is an essent ia l par t of every school health education programme.
Opportunities f o r informal health teaching and learning occur through- out the school day. In r u r a l areas where children may help with basic sani ta t ion needs, such a s providing water, disposing of wastes, and handling of food, the pupils with guidance can often work out safe and sani tary pro- cedures, even with the simplest of equipment, and learn important heal th principles i n the process. I n many communities, modern school buildings have been constructed, providing f a c i l i t i e s which pupils must learn t o use i n a safe and sanitary manner. I f pupils can have a par t i n adjusting l ight ing and seating, or i n inaugurating cleanliness and sa fe ty measures, a t the same time learning why ce r ta in measures a re preferable t o others, much worthwhile health education can take place. Within community l i f e , opportunities likewise ex i s t f o r informal heal th education. I n some countries, f o r example, young people serve as volunteers i n c l i n i c s and hospitals and i n other community health ef for ts , thus, learning through firsthand experience about health needs as well a s resources and programmes available t o deal with needs, Daily events, when adequately exploited by educators and health workers, can become teachable moments t ha t not only add realism and i n t e r e s t t o health education but may bring r e su l t s i n desirable health action.

A s important as individual health counseling and informal health teaching are, they need t o be accompanied by systematic health instruction. Such ins t ruct ion may take place through separate health classes or be in- corporated i n other par ts of the curriculum such a s i n science and home economics. The manner i n which t h i s is done varies widely from school system t o school system.
0b.lectives of school health education
ObJectives of school health education are determined i n large measures by heal th needs and developments on the one hand and by broad purposes of education on the other.
As health conditions change, goals f o r health eciucation i n schools may likewise change. Though t h i s Region has made rapid s t r i de s i n the control of such diseases as.malaria, tuberculosis, and trachoma, I am to ld that much yet remains t o be done, nevertheless, t o eliminate these and other de- b i l i t a t i ng diseases. I n t h i s Region, a s i n other par ts of the world, mal- nutri t ion, poor personal hygiene practices, chronic i l lness , and insanitary environment demand constant at tention.
I n the past, education on health dea l t mainly with personal heal th habits and the nature and cause of i l l ne s s and disease. In many instances, l i t t l e posit ive action fo r improvement was possible with exis t ing knowledge. However, modern methods of prevention and control make feas ible such atitii- t i ona l objectives as fostering use of preventive and treatment f a c i l i t i e s . Many heal th problems today c m be solved only through the widest understand- ing and cooperation of the people concernea. I n recognltlon of t h i s fact the World Health Organization, i n what has now become a c lass ic statement has said:
he aim of health education is t o help people t o achieve health by t h e i r own actions and effor ts . Health eaucation begins therefore with the i n t e r e s t of people i n improving t h e i r conditions of living, and aims a t developing a sense of responsibi l i ty f o r t h e i r own health betterment as individuals and as members of families, communities, or government^."^
World H e a l t h Organization Expert Committee on Health Education of the
Public, First Report: Geneva, 1954 (world Health Organization Technical Report Series No. 89)

WHO EMRO
Universally, educators are res ta t ing broad purpose of education i n the l i gh t of changing t ines . Schools of the past, t r ad i t ion bound, existed primarily t o transmit and perpetuate knowledge from one generation t o another. In contrast, goals commonly expressed by educators today include increasing national unity, strengthening citizenship, ra is ing the l i t e racy ra te , and educating people t o become responsible and productive members of society.
The time has arrived when leaders i n school health education must re- define objectives t o be rnore nearly In harmony with the changing goals of health and education. No longer can schools be s a t i s f i ed with the mere transmission of health fac t s . Important as f a c t s are, f a c t s alone a re inadequate t o evoke improvements i n health behaviour which are so necessary for a strong and productive citizenship. Objectives i n school health educa- t ion must be directed toward helping children t o a t t a i n heal th goals on a ra t iona l basis and through t h e i r own actfons and e f fo r t s ,
A discussion of school health education objectives would not be complete without mention of social , po l i t i ca l , economic and re l ig ious factors t ha t influence the nature and scope o f health education ef fo r t s .
I n most cultures the home exerts the greatest influence on the child. By the time the chi ld reaches school, many of h i s health habits have become well established. Throughout school years, the values he attaches t o health are often determined by those values held within the family unit, values often deeply rooted i n t r ad i t ion . A question not eas i ly answered is t o what extent the school should dis turb child-parent relat ionships through promoting health objectives t ha t run counter t o those i n the home, especially when home objectives are contrary t o sound health practices. School objectives must often be modified or adapted t o be consonant w i t h values held by the hume and other socla l lns t l tu t fons outside the School, Y e t , should not the schools seek t o influence these values i n appropriate ways?
I n determining and f u l f i l l i n g health education objectives, schools may f ind common cause with other agencies and organizations, Governmental agencies, a s fo r health, soc ia l welfare, and agriculture, influence health objectives through the policies they s e t and the funds they provide. Voluntary health associations and f ra te rna l and c ivic groups have health education goals and programmes which often can be synchronizcd with those

WHO m o
of schools. Professional organizations i n the f i e l d s of health and education can prov1.de valuable leadership. The teachings of the great re l ig ions are cogent with health implications and re l ig ious leaders are potential colleagues fo r health betterment. Through community development e f fo r t s and other concerted programmes, these many individuals and groups may unite fo r the comrncln purpose of improving the health and well-being of both children and adults.
Content of school health education
While objectives help point the way fo r heal th education, the content provides the substance. Sound school health education, a s already stated, deals with health needs and in te res t s of children and of the homes, schools, and community of which they are a part . It takes in to account psychologi- cal, sociological, cultural , po l i t i c a l and economic factors, and the avail- a b i l i t y of resources. It is based on s c i en t i f i c a l l y sound health fac ts . What we teach, then, m u s t be determined by a variety of fac tors i f it is t o become t ransla ted in to desirable health action.
I n some areas, standard health teaching sy l l ab i developed a t national, provincial, or loca l levels prescribe what sha l l be taught i n each grade. Too frequently, the untrained or unimaginative teacher follows these guides with l i t t l e consideration f o r loca l health conditions. The chi ld of a coastal community and the chi ld l iv ing i n a r i d lands have the same basic nutr i t ion needs but foods available t o each may be quite d i f ferent . Sanita- t i on problems are universal but assume di f ferent forms under varying environmental conditfons. lJl-lile one community may have l i t t l e or no water, another may have enough water but so highly polluted t ha t special measures must be taken t o make it safe f o r hum'm consumption. Certain diseases may be more prevalent i n one area than i n another. Health teaching guides can be helpful i n suggesting content of health education. Their value is increased however, i f they a r e used f lexibly and i n accord with regional or loca l conditions.
I n r e a l i s t i c health teaching, the needs of the children themselves should have primary at tention. These needs a re re la ted largely t o biologic- a l processes, such as eating, elimination, exercise and sleeping; t o preventing or controlling conditions which may cause or aggravate physical defects, i l lnesses , disease, and injuries; and t o sound emotional and soc ia l development. Though such needs pers i s t throughout l i fe , they vary i n t h e i r manifestations a t d i f fe ren t maturity levels, thus suggesting possible changes

EM/HEP/~~
page 20
WHO EMRO
i n teaching emph~sis ns children progress through school. By analyzing developmental character is t ics of ~ n i l c ' , ~ e n a t d i f ferent age levels and under d i f fer ing cul tura l conditions, and by considering childrens' readiness t o learn and breadth of in teres t , a ra t ional basis can be reached fo r the selection of health education content. Though some generalizations can be
I
I made on t h i s basis, each teacher should be encouraged t o determine i n h i s own s i tua t ion th? specif ic chi ld health problems requiring a t tent ion a t a given time. I must s t r e s s emphatically a t t h i s point, however, t ha t teachers and other school yersonnel responsible f o r t ra in ing the young need the help of medical author i t ies i n locating and defining these problems.
Mention has been made more than once of home, school and community health needs which a l so mag become the foc l f o r productl.ve health education i n schools. Here again, health autl lori t ies can help point out those needs demanding special a t tent ion i n a speci f ic local i ty .
Methods of school health education
Methods of health education are determined not only by the nature of a problem but a lso by ways i n which learning takes place. Learning is an active process occurring tbxough the l ea rner ' s own e f fo r t s a s he in te rac t s with h i s environment. Learning has both an emotional and a ra t iona l basis. It is more than mere absorption of knowledge.
In many ochool o g ~ t c m ~ , hcalth cducstion methods have not kept pace
with other methods of education. Yet health education, a more recent innovation i n mr?Tr ;nb?f-lC. could take the lead through experimenting with methods appliosble t o a w i d e range of interes-Ls.
Too frequently health has bee11 taught by ro t e learnin@; and heal th f a c t s have been studied w i t h l i t t l e o r no plan f o r t h e i r t r a n s l a t i o n in to action. Children need t o work act ively on problems meaningful t o them i n order t o convert theory in to practice. The problem-solving method is one effect ive way.
I n c r a t i n g s i tuat ions which fos te r learning, it is well t o recognize tha t se l f - se t goals have strong motivational value and problem-solving methods, when properly used, provide a r a t i cna l approach t o decision making and action. Learning of more las t ing value is l ike ly t o occur when pupils themselves, individuall~r or i n groups, se lec t problems from r e a l l i f e si tua- t ions and take steps t o solve the problems. Such an approach is more than

WHO m a 0 ~M/'h3~/20 page 21
an in te l l ec tua l exercise. Facts gathered i n the process are be t t e r understood, retained, and applied when they are oriented. toward action. Individual or group commitment may r e su l t i n l a s t ing behaviour change.
Though problem solving is only one of a number of methods which can be used advantageously i n school health education, it has been stressed here because of i ts pertinence i n contributing t o desirable health goals. Other methods often used i n health eductition include various forms of discussions, drarnatizatfons, f i e l d experiences, experimentation, and the use of audio-visual materials. "Learning through doingn had become an axiom i n education. Part icipation of pupils i n health act ion programmes and through volunteep services gravid-es a ~ r a c t i c a l way of ~ u t t i n g t h i s principle in to practice.
Evaluating school health education practices - Foremost i n evaluating school health education should be an attempt
t o determine whether a programme is accomplishing what . i t has s e t out t o do. Since school health education today aims t o bring about health improvements i n the pupils themselves, and i n conditions surrounding the pupils, then such questions as the follov~ing need t o be pursued: Is the health of an individual chi ld or a group of children be t t e r a s a r e s u l t of a speci f ic health education effor t? Are the children taking more responsibi l i ty f o r t h e i r own health commensurate with t h e i r stages of development? What are t h e i r a t t i tudes toward a speci f ic health study? Are they passively following instructions or a re they enthusias t ica l ly and in te l l igen t ly working t o bring about a health improvement? What changes a r e evident i n the home and community as well a s i n the school? Unfortunately, i n working f o r a limited time with a group of children, a teacher cannot always hope t o f i n d c lea r evidence of progress or of achievements a t t r lbutable t o his own e f fo r t s . Pupil heal th progress is often slow; r e su l t s of teaching a re cumulative and may extend over many years. Yet through observation, interviews, study of health records, surveys and other evaluative procedures, improvements may be discernible. Moreover, schools can obtain information which w i l l be invaluable i n planning future health education programmes.
School health education practices may a l so be evaluated by examining the programme i t s e l f t o determine whether its objectives, content, methods and materials follow generally accepted standards in health and in education

E M / H E P / ~ ~ page 22
WHO EMRO
and are appropriate t o a speci f ic s i tuat ion. Many of the points developed i n t h i s paper suggest directions fo r such evaluation so w i l l not be repeated here.
Evaluation is an essent ia l part of every well-planned school health education programme. To be meanirqful it must be bu i l t in to the programme from the s t a r t and become a continuous process. Only when pupils, teachers, parents, health workers and community leaders share i n evaluation, and use the information gained, can l as t ing health progress be expected.
I n concluding t h i s statement on the nature and scope of school health education, recognition is given t o the influence of those whose responsi- b i l i t y it is. A t the heart of every sound programme are teachers who are professionally qualified, emotionally adjusted, and genuinely interested i n children and t h e i r health. The degree t o which teachers succeed i n the d i f f i c u l t and ever changing task of health education is dependent not only upon t h e i r training, but a lso upon the support and guidance they receive from medical leaders, health authori t ies, school administrators, and the public.

SCHOOL HEALTH SERVICES A h 9 SCHOOL KEALTH EDUCATION I N THE COUNTRIES OF THE EASTERN MEDITECRRANEAN REGION
GENERAL FEMMNS ON SCHOOL HEALTH NEEDS AND SERVICES IN THE E A S ~ N MEDITERRANEAN REGION^
I INTRODUCTION . .
Thn-ing the last twenty years, many cor~ntries of this Region have recognized the importance of the health of school-age children. Increas- ing emphasis is being given t o the school health services as more and more children a re entering primary schools every year.
I n the preamble of the consti tut ion of the World Health Organization, it was already declared t ha t "healthy development of the chi ld is of basic importance; the a b i l i t y t o l i ve harmoniously i n a changing t o t a l environ- ment is essen t ia l t o such development". Accordingly, the Organization has, i n the broadest possible sense, assigned an important place t o the protec- t i o n and promotion of child health within i ts global programme. This holds t rue both fo r the child s t i l l l iv ing i n the ra ther secluded environment of the family and fol- t k s zY1.,301 chi ld being exposed t o the greater r i s k and hazards of the outside environment.
I n 1950, the WHO Expert Committee on School Health Services discussed the needs f o r special health services f o r the school-age children and fo r a health programme fo r t h i s segment of the population, Which is undergoing
1
Based on' the paper presentkd and the discussions of the Seminar

WHO EMRO
physical, mental, emotional and soc ia l changes. The Expert Committee, i n its report, referred speci f ica l ly t c the responsibi l i t ies of the country "for revising its health policies f o r school-age children". Compulsory educa- tion, enforcing parents by law t o subject t h e i r children t o the school author i t ies f o r a considerable period of time, embodies the f u l l responsi- b i l i t y of the law-maker for t h e i r health and well-being. Consequently, school health services cannot be regarded as voluntary or "optional"
I services of the community, but a s obligatory services t o be provided by , the law-enforcing authority, i .e . the government. I
I I I1 SCHOOL HEALTH SERVICES
Organization and Administration
Wide variat ions ex i s t i n the organization and administratinn nf school health services i n the Region. In Aden, Iraq, Jordan, Kuwait, Pakistan, Somalia, the United Arab Republic and Yemen, the school health services are administered through the Ministry of Public Health. In Ethiopia, Iran, Qatar, Saucli Arabia and the Syrian Arab Republic, these services are ad- ministered by the Ministry of Educatfon. I n some countries, a specia l school health department i s responsible f o r t h i s service whilst i n other countries, one of the administrative un i t s i n the ministry concerned deals with school health amongst other things.
The s taf f ing of the school health department varies i n the d i f fe ren t countries, but it is usuallyheaded by a medical d i rector . A t the provin- c i a l and local level the administration of the school health a c t i v i t i e s is the responsibil i ty of e i the r the ass i s t an t d i rector or the d i s t r i c t health off icer the municipal health o f f i ce r s o r medical off icers of the school health centres or units .
Private schools are covered i n some countries by the established school heal th services, but they mostly have t h e i r own system of heal th care which is usually under the supervision of the school health department. In fac t , many small private schools have pract ica l ly no health services a t a l l ; and some, on the contrary, have excellent health services.
2. Functions
A t the central level, the functions are f u l l y o r partly carried out i n the di f ferent countries and mostly include: establishment of pol ic ies

WHO EMRO
on protection and promotion of the health of school children; issuance and enforcement of regulations governing the school health programme; planning organization and supervision of the di f ferent school health services; revision of curricula with regard t o the teaching of heal th subjects; t ra in ing of health personnel; budgetting and assessment of school health services ancl supervision and advice t o loca l levels . A t the local level, the functions of the school health teams ( i n school health polyclinics, centres, units, e t c . ) usually include periodical medical examinations, screening of schocl children, detection of diseases and defects, treatment of s ick children and school personnel, immunization and control of communicable diseases, supervision of school sanitat ion, counselling of students, parents and teachers i n chi ld growth and develop- ment, part icipation in and extension of heal th e.ducation fo r teachers, students and parents and record- keeping.
I n the vil lages and r u r a l areas, the r u r a l health centres or un i t s are responsible f o r the health supervision of school children.
3 . Activit ies
It is most encouraging t o note the wide range of a c t i v i t i e s carr ied out by the exist ing school health services:
Periodical Examinations a r e usually carried out on a l l school children upon f i r s t admission t o primary schools and thereaf ter upon admission t o preparatory and secondary schools. Sometimes, a fourth msdical examination is made In the thsr? year secondary school, before completion of studies, Sometimes parents are asked t o attend the examination of t h e i r cllildren In primary schools. Teachers are not often invited or obliged t o attend the child ' s examination. However, the parents ' and teachers ' presence is desirable and w i l l enable the physician (if in teres ted and glven sufficient time) t o carry out properly h i s function a s a health counsellor t o the parents, child and teacher.
Findings a t medical examinations have c lea r ly demonstrated t ha t a f a i r l y high percentage of children had some health defects other than dental, which required special a t tent ion and treatment.
Vaccination and Immunization Programmes of a l l school children have produced valuable results. In addition to mallp pox mooination,

systematic imm-w~izatfon is reported t o be undertaken i n the majority of the countries against other &iseases su.ch as: diphtheria, tetanus, tuberculosis, poliomyelitis, TAB and cholera. The vaccination calendar f o r re-vaccinaticn and fo r b ~ o s t e ~ doses varies according t o the country.
Accident Prevention Accidents are ii10s-t l i k e ly t o occur during school -- -- years and a re ail important cause u f death and disabil-ity. Necessary care and measures fo r accident prevention are talien i n most countries through health education, school health societ ies, precautions within the school buildings and supervision of the school environment and through the provision of schools with f i r s t - a i d equipment and medicaments.
Dental Health Services are being provided by the school health services or c l i n i c s i n the majority of the countries, but mostly i n urban areas. School health uni ts are often equipped by mobile dental uni ts designed fur LL-eaLmer l t i n schools. 7% of the stuaents examined tiTough a p i l o t project, i n one country, were faund i n need of dental treatment.
Mental Health Services and Child Guidance are s t i l l lacking i n the maJority - of countries i n the Region. A few special schools fo r retarded children have been established &d are under the supervision of the Ministry of Education. Mentally retarded children have t h e i r own t ra in ing centres under the supervision of the Ministry of Social Affairs. Child guidance c l in ics , although limited i n number, have accommodated some needs.
Care fo r Handicapped School Children has been given special a t tent ion i n some ccwt r i e s , where special schools have been establishec5 fo r the blind, the deaf-mute and paralytic children, as woll as speoial C ~ ~ E E C G for the children with visual disorders or hearing impairment. Health services have a l so been provided t o special schools fo r the deaf and fo r the physically handicapped.
Early detection of visual and auditory defects i n children is very important. Surveys t o be carried out i n schools might reveal i n a large number of children with l a t e r a l hearing defects which could in te r fe re with learning, It is important t o discover the chi ld who is mentally handicap- ped i n order t o ensure t h a t special a t tent ion be given t o the promotion of h i s health and t o the special problem of h i s education.

Nutrition and School Feeding Many countries in this Region are conscious of the nutrition prcblems of school children anc! are carrying out sup- plementary feeding programmes, although some of these countries are faced with budgetary difficulties, owing to their limited local resources,
School Sanitation Many countries in the Region are giving considerable attention to the construction of a new and adequately equipped school buildings in their long-term development plans. However, the sanitary conditions in most of the existing schools (often occupying old rented buildings) are not adequate. Most of these schools have been renovated to secure the indispensable sanitary facilities but the sanitary conditions are still hardly satisfactory. Rural communities with limited resources are particularly handicapped in their efforts to remedy the situation. Wherever bad construction, poor ventilation and lighting, lack of washing and inadequate drinking faciliti~s exist as w e l l as any other unsanitary latrines or similar deficiencies, children absorb wrong ideas and learn harmful habits, difficult to unlearn later and contradictory to what they are being taught by the teachers and the school health personnel in this respect.
Prevalent Diseases of School Children
From the information made available from countries and from other sources, findings at school medlcal examinations revealed that, in addition to dental, visual and hearing defects, there are many diseases, which are prevalent among the school children in this Region. Among these diseases, the following have been reported: enteric infections; parasitic diseases, such as billtarziasis, ankylostomiasis, ascariasis, other helminthic in- fections, amoebiasis; virus infections, particularly chicken-pox, polio- myelitis, mumps, measles; other bacterial diseases such as diphtheria, pertussis and tetanus; communicable eye diseases, mainly trachoma, con- junctivitis~ skin infections, scabies and favus; tuberculosis and malaria. Many efforts are being made in most countries to get these diseases under control.
5. Sports andRecreation
Physical training and sports have widely developed in schools of this Region and have been encouraged by governments. Camping, tours and excursions receive inel-easirig at ter l t ion by -the authorltles concerned. Attendance in camp is sometimes undertaken to educate children in a health- ful mode of living.

EM/HEP/2tj I
page 28 WHO EMRO
6. School Health Centres
~ There are various types of schocl hea l th cent res o r u n i t s a t d i f f e ren t
i l eve l s of a c t i v i t i e s an? s t a f f ing , v:i?icli 2rovid.e preventive and curatf ve I s e rv ices f o r school ch i ldren i n the count r ies cf t he Region. Usually, a 1 -clinic i n the cap i t a l , adequately equipped and s ta f fed , serves about I I
20 000 - 30 000 school chi ldren. I n the c i t i e s , a school hea l th u n i t serves 10 000 chi ldren. In v i l l ages where school hea l th serv ices a r e a p a r t of t h e r u r a l hea l th service, a rural hea l th u n i t is responsible f o r
I about 5 000 general population and a l s o supervises the hea l th of school children. In some countries, attempts have been made t o provide one
I school medical officer for 4 000 - 8 000 childrenj one dental surgeon for
I 8 000 - 10 000; one school hea l th nurse o r hea l th v is i tor /dresser f o r I
I 1 500 - 3 000. 7. Auxiliary Health Workers
I n some areas of t h e world and i n many count r ies of t h i s Region, it is impossible, f o r many years t o come, t o employ an adequate nwnber of physi- c ians and qua l i f i ed nurses within the school hea l th programme. A t present, much of the work i n some a reas is done by aux i l i a r i e s , such a s h e a l t h a s s i s t an t s , dressers , compounders and nurse a ids . However, t he re is s t i l l a shortage of hea l th a u x i l i a r i e s working i n many hea l th f i e l d s including school heal th.
8. Record Keeping andEvalua t ion
The importance of hea l th records i s measured mainly by t h e ex tent t o which they m e useful t o t h e s t a f f i n helping the c h i l d t o obtain maximum health, within t h e l i m i t s of h i s p o t e n t i a l i t i e s .
The.schoo1 hea l th record cards used i n school hea l th serv ices i n t h i s Region a r e more o r l e s s s imi lar . Usually r e s u l t s of individual medical examinations, which a re recordeci and coded by t h e healtl i worker, a r e checked by the physician, s t a t i s t i c a l l y analysed and interpreted, and subsequently r eg i s t e red and tabulated. However, there i s no indica t ion that t h e information col lec ted is always being properly u t i l i zed .

WHO EMRO
9. Role of Non-Govcrmzntal and International Agencies i n A ----
School Health Services
Non-governmental agencies pla;: i n general, a minimal r o l e i n school health services i n this Region, owing t o the f a c t t ha t the majority of schools belong t o the Government. I n a few countries, however, they a s s i s t the Government i n f u l f i l l i n g its obligations.
111 SCHOOL EALTH EDUCATION
This subject has been deal t with by many speakers and i n other technical papers and needs no c m p h s i s hcrc. It has bccn fclt dceirablc that emphasis be given t o the ro le of the school health team, par t icular ly the teacher, i n school health education.
The school health service is taking an increasing part i n health educa- t i o n i n schools and, consequently, i ts work is a l so becoming more closely interwoven with education.
I V RECOMMENDATIONS
The Regional Committee a t i ts Fifteenth Session held i n October 1965, endorsed the following recommendations:
1. School health services should be established and developed simul- taneously with the educational system of a country, par t icular ly i n countries with compulsory edu~at ion.
2. The responsibi l i ty fo r the establishment, development and super- vision of.schoo1 health services should r e s t with the Government and its executive authori t ies, preferably the ministr ies of health and education.
3 . School health services should be designed and operated so as t o meet the health an6 educational needs of a l l school children, taking in to account the considerable physical, mental and soc ia l changes occurring during t h i s important segment of the l i fet ime of the whole population.
4. School health services should preferably be integrated i n to the general health services of the country, forming an important part of the health services provided t o the population.

WHO EMRO
5. School h e a l t h scrvices si-iould be d i r ec t ed and operate2, i f possible, by s p e c i a l l y trainee? an2 qua l i f i ed personnel, who should be employed fu l l - t ime a t t he c e n t r a l =an?. p r m i n c i a l l evc l s .
6. School hea l th department sliould employ educators, s an i t a ry 1 engineers, s o c i a l workers, s t a t i s k i c i a n s and psychologis-t;~, where
appropriate i n addi t ion t o doctors and names. I n t he absence of q u a l i f i e d personnel, use shoulu be ma& sf s p e c i a l l y t r a i n e d a u x i l i a r y personnel a s an inter im measurc.
7. Plans f o r new school buildings, renovation of o ld ones, operat ion and s ~ ~ p e r v i s i o n of existing school premises, should talre i n t o considerat ion recognized basic s an i t a ry requirements. These should be codi f ied i n ~ nat iona l minimum and optimum standards.
I
8, The school hea l th programme should comprise:
a. Regular comprehensive medical examinations of ch i ldren upon admission tc school, a t r e g u l a ~ i n t e r v a l s of at l e a s t t h ree years, -and upon leaving school.
b. I n addi t ion t o compulsory vaccinat ion aga ins t smallpox compulsory immunization aga ins t d iphther ia , te tanus, tuberculos is and pol iomyeli t is .
c. A den-tal hea l th programme including r egu la r screening by qua l i f i ed d e z t i s t s , org&?izcd den ta l care ar.L den ta l h e a l t h education.
d. A hea l th education programme f o r ch i ldren and teachers, including teaching of important hea l th subjec ts , wi th in t h e cu r r i cu l a of primary and secondary schools a s wel l a s of teacher t r a i n i n g col leges.
e . Nutr i t ion eS.ucatien and s~~pplernentary feeding programmes.
f . C a r e of handicapped chi ldren, p a r t i c u l a r l y those with v i sua l and audi tory de fec t s a s wel l a s s p e c i a l c l a s se s o r courses f o r t he blind, deaf-mute and pa ra ly t i c chi ldren.

WHO EMRO
g. A comprehensive gymnastics and physical culture programme with its proper place in the curriculunl, including sports, excursions, summer camps under consultation and supervision of the school physician.
h. A mental health and child guidance programme, including regular clinics, with the participation of parents and sometimes teachers.
i. A p=.o@;ranme on safety and accident prevention in childhood.
9. School health reoords should bc established and kept, containing major physical and health data of the individual childi, findings of medical examinations, vaccinations and immunization, therapeutic measures, absent- eeism and other pertinent information.
10. School health services should be regularly evaluated in regard to organization, staffing, efficiencies and deficiencies to safeguard adequate functioning.
11. School health services should be especially considered as an integral part of national development plans, in view of their importance for the healtn of the nation.
The Regional Committee for the Eastern Mediterranean also adopted a resolution in which it recomrneded that Governments give high priority to all facets of schocl liealth services1.
1 Text of the resolution may be found in page 5 of this report

WHO EMRO
2. DESCRIPTION OF SCHOOL J3EALTH SE9VICES AND SCHOOL HEALTH EDUCATION IN THE C O U I ~ I E S OF THE EASTERN MEDITERRANEAN REGION^
ADEN
School health services were established i n Aden i n 1964 under a fu l l - time medical off icer fo r the purpose of curative and preventive services i n schools. This function includes extension of health education t o teachers, stuzents and t he i r parents.
There dl-e 47 scliuols in A d e n w i t h an e s t i r n t t l u d emulment ul: 20 000 students.
Courses on health and nut r i t ion are given t o students in primary schools.
There are plans fo r more a c t i v i t i e s concerning health education with the involvement of teachers. It is, however, noted t h a t since the establishment of school health services, teachers have taken more in te res t i n the health of t he i r students and discuss such subjects f ree ly with the school physician and the nurses.
CYPRUS
There are 853 schools, primary anti secondary i n Cyprus with a t o t a l number of 123 293 stud.en_ts and 4 085 teachers. The duty of the health services of t h i s group i s entrusted chiefly with the medical and para- medical. personnel, par t icular ly those working i n r u r a l areas. A limited amount of health education i n the form of t a l k s on healtn topics is carried out by the health personnel i n the schools.
1 Based on: a. informatirn received from the Governments of the Region
fo r the Technical Discussions i n the Fifteenth Session of the Regional Committee, AdGis Ababa, 1965
b. statements given by part icipants throughout the Seminar on School Health Education, Kuwait, 1966

WHO EMRO
Plans are underway fo r establishing a closer cooperation between the Health and Education Ministries fo r the promotion of school health services and health education. Parentbeacher Association plays an important ro le i n tine health and welfare of t h e students.
The curricula f o r primary and secondary schools contain elements of health e i the r as a speci f ic topic or integrated with other topics. The curricula are presently review and it is f e l t t h a t more a t tent ion t o community health is needed a s the p ~ e s e n t curricula emphasize anatomy and physiology.
A study on school health education was made i n Cyprus and it was suggested t ha t therewas an urgent need fo r the revision of health education in schools. According t o t h i s study, children of the primary schools need health education:
1. To develop habits and a t t i tudes of healthful l iv ing by guidance on :
a. safe ty and sanitat ion;
b. interpersonal relat ions;
c . routlne ac t lv l t l e s , such as school lunch, routine physical examination, etc.
2 . Tu reali~e Ll~e value uT scl~uul llealLh services:
a. detection, prevention and treatment of communicable diseases;
b. correction of defects.
3. To learn about:
a. development of t h e i r body and its various functions;
b. emotional and soc ia l adjustment;
c. personal hygiene;

WHO EMRO EM/HEP/~~ page 35
d. safety;
e. community health.
In addition, children o f secondary school need guidance on special topics re la t ing t o t h e i r age md needs especially i n reference t o com- plexi t ies associai:ecl with ac'!?lescence. Their erflotional and soc ia l needs require careful supervision and counselling.
r en t a l health o f the sclhool child needs increased a t tent ion and teachers need t o he retrained an< guided i n giving due a t tent ion t o t h i s Important ILem.
ETHIOPIA
I n recent years there has Seen a great awareness i n the inclusion of health educaticn i n science, home economics and physlcal education. This has created the need fo r including the school health programme i n the curriculum of teacher-training ins t i tu t ions . To up-grade the school health programme, the Ministry of Public Health on the request of the Ministry of Education conducts in-service t ra in ing fo r teachers and school administrators. The Faculty of Education of the Haile Selassie I University requires t ha t a l l students of education have three hours of health education per week fo r a f u l l semester.
A permanent joint meeting be-tween the Ministries of Public Health and of Edi~r.a,t.ion has beer1 azi-SlisheL \:it:? the responsibility of;
1. Formulating plans and policies f o r a r e a l i s t i c cooperative school health programme.
2. Establishing minimum standards fo r a well-coordinated service.
3 . Coordinating the ac t i v i t i e s of various agencies involved i n school health programmes a t a l l levels .
4. Pulling together the resources (personnel, f inancial , e tc . ) available t o the betterment o f school health programmes,
5. Avoiding duplication of function between the Ministries and other agencies involved i n tihe school health programme.

: EM/HEP/~~ I pace 36 I
I IRAN
WHO Ern0
The responsibil i ty f o r the health o f the school children and personnel r e s t s with the Directorate of School Health Services under the Ministry of Education. This Department has 102 school health centres of which 13 are i n Teheran and 89 i n other provinces. In r u r a l areas and where the a r e c t o r a t e s has no centres, such services are carr ied out by the Ministry of Health. There are over 2 million students i n Iran out of which over 1.5 million attend primary schools.
Good cooperation ex i s t s between the Ministries of Health and of Educa- tion as well as with voluntary agencies on matters concerning school health and education. Of the voluntary agencies, the National Society f o r the Protection of Children is especial ly act ive i n t h i s f i e ld .
Attention has been given t o health education and guidance of the students on a l l levels whenever possible. !Be teaching of health has been duly emphasized i n a l l teachers ' t ra in ing programmes.
Health clubs have been organized i n a number of schools and i n these clubs students are assuming active roles.
I n the curricula f o r primary and secondary schools the following top ics received emphasis: personal hygiene, community health, prevention of communicable diseases, f i r s t a id and nutr i t ion.
!The Division of Public Health Education of the Ministry of Public Health is a l so ass is t ing the Directorate of School Health Services i n various forms such as i n giving refresher courses t o teachers.
The School Health Services were oreanized i n the Ministry of Education i n 1946 but i n 1954 were transferred t o the Ministry of Health with a wider scope and s t a f f .
The duties of t h i s department are as follows:
1. Preventive services.
2. Curative services.
3. Educational services.

WHO EMRO
Several pilo", p~o ;ec t s were launcketi including introduction of health education i n pi-eventive and curative services. Special teams were sent t o schools f o r th? purpose of health education of children and the r e su l t s have been encourc?gir_g. I.t pi7~scl?,t t:?era are 4 507 schools i n Iraq with the t o t a l of 1 058 @82 students. Heal"; services are carried out i n 20 school dispensaries throughout the co:~ntry anCk wherever such dispensaries do not exist , the services are cnrried ov-t b] the respective departments of health.
The School Etealth Services sad the Health Education Directorate co- operate i n screening of the students ailfi education i n needed areas. Audio- visual materials are special ly designed by the l a t t e r Division t o meet speci f ic needs of school children i n various areas.
Effor ts have been made t o ir,vol.ve teachers i n school health services and much Is expected from teachers who have Jolned the refresher t ra ln lng courses. These courses are held C w 3 . i ~ summer sessions by close co- operation between Ministries of Health and of Education.
JORDAN
There is no autonomous rnachiner:; f o r school health services i n Jordan. However, school health forms part af the public health services. Recently, funds were made available f o r -the assignment of t en physicians on full-time b a o i ~ t o work on school hcalth ~ c r v i o c ~ throql-~out thc country. ~ h i k woilld lead t o a more systematic school healti; services i n the educational ins t i tu - t ions.
The school children i n Jordan comprise 20% of the en t i re population, 2$ of which are studying abroad. Since the e f fec t of the environment upon health is recognized, the Government has b u i l t 464 schnqls w i t h proper sanitary conditions and i s planning t~ build many more. By 1970 over 85s of the school children w i l l be accommodated i n the Government buildings.
The Curriculum Department of the Ministry of Education has given due a t tent ion t o inclusion of health a s a topic i n various textbooks. Also the Ministry of Education has revised the health content of teacher t ra in ing programmes. But s t i l l more ac t i v i t i e s need t o be done i n t h i s f i e l d .
. .- - .

WHO EMRO
KUWAIT
The aim of hea l th education f n the schools of Kuwait is primari ly t o help the pupil t o be healthy 2n6 stsj. heal ti?^. This important t a s k is d e a l t with d i f f e ren t ly i n differei l t s tages.
I n Kuwait there a re three d i f f e ren t s tages i n the educational system:
1. F~imary school - 4 years (6 t o 10 age-groups)
2. Intermediate school - 4 years (10 t o 14 age-groups)
3 . Secondary school - 4 years (14 t o 18 age-groups)
F'rimary school
There l-ave been separate courses on hea l th i n primary schools, but, recent ly the Ministry of Education has abandoned the idea and hea l th is incorporated with other topics. The topics emphasized i n the primary school are: cleanliness, personal and environmental; nu t r i t i on ; hea l th habi t s and pract ices; meaning of hea l th and diseases and prevention of some contagious diseases.
Intermediate school
There is a separate period per week devoted t o hea l th topics including cleanliness, care of t h e body organs, da i ly hea l th prac t ices and habits , s implif ied human anatomy and physiology; a?? introduction t o f i r s t aid, human nut r i t ion , prevention of a number of comrn~micable diseases; and vaccination and immunization.
I n addition, g i r l s receive an addi t ional course i n ch i ld care during the third year of t h i s s tage.
The completion of the intermedia-ke school marks the end of the com- pulsory education i n Kuwait.
Secondary school
No special coursc cxists i n health for the secondary school students. However, i n the study of various sciences including biology, chemistry and physics, important elements of health, including paras i tes , fungi, poisons and thc cffeotsof the environment and heredity nn health are inc1i:r l~d.

WHO EfJlRO
Teacher training-irnktitutes -.
There a re two teacher t ra in ing i n s t i t u t e s i n Kuwait. One fo r boys and one f o r g i r l s . The dura-Lion of study is four years a f t e r the intermediate stage.
I n the f i r s t and t h i rd gears health is incorporated i n the general sciences bubject. This includesstudg of zoology, physiology, anatomy and physics. Often, reference is made t o health and the diseases caused by parasites, by chemical and physicalagents such as sunstroke, etc.
111 Lhe t h i rd and fourth years , however, a w e e k l y per iod is devoted t o health as a topic. In t h i s two years' course the following are taught:
1. H e a l t h services i n Kuwait
2. Nutrition
3. Routine medical examination
4. Studjr of common diseases i n Kuwait
5. Immunity
6. F i r s t a id and safe ty
It is f e l t that l n planning health education much is accomplished outside the class-room. Thus, leadership of the students is encouraged by organizing health clubs i n which students assume act ive ro l e i n the discussion of the health topics and i n the implementation of ce r ta in programmes.
LEBANON
The Health Education Section of the Ministry is ass i s t ing the primary schools by arranging discussions on health, using the mobile f i lm un i t s i n schools and dis t r ibut ing health materials i n schools on important health topics.
However, it is found t ha t more is needed t o be done i n t h i s regard. It is found t ha t i n the preparation of the teacher more a t tent ion is needed
WHO BIvlKV
i n the inclusion of the hea l th topLcs. This requi res more ac t ive col- laborat ion between the two Ministr ies of Health and of Education. A cooperation is needed t o develop the cwricula based on the need, under- standing and age requiremenLs of t h e children. This i s only possible a f t e r the preparation of a plan between the two Ministr ies and the f inanc ia l provision f o r such a ;ror!r.
Attempts have been made i n t h i s regard by incorporating hea l th i n a number of courses.
A Committee f o r the revis ion of a l l school cu r r i cu la is envisaged. Based on experience the following items shoi~ld be gjven priority:
1. Training of teachers on heal th matters
2. In tegra t ion of hea l th topics i n primary and secondary schools
3. Inclusion of hea l th education and public hea l th a s a top ic of t r a in ing f o r a l l who a re involved i n teaching.
4. Cooperation between schools and a l l hea l th workers.
5. Assisting school au thor i t i e s i n the provision of hea l th education material
6. Study of the needs of school children.
7. Need f o r r e g u l a t i ~ n s on school hea l th f o r a l l public and pr iva te schools.
PAKISTAN
Health education i n schools is c a r ~ l e c i out Jo in t ly by t h e school hea l th services and heal th education u n i t s under the supervision of the provincial hea l th departments.
I n West Pakistan, i n some areas medical examinations of s tudents have been s t a r t e d with the cooperation of the Department of Education. Ws w i l l give a beginning f o r fur ther ing heal th education i n schools by col lec t - ing informtion on health problems and conditions of Lfiu students.

WHO EMRO EM/IXP/28 page 41
I n East Pakistan, i n urban areas the school medical o f f i ce r s have been entrusted with the duty of organizing health education a c t i v i t i e s i n schools with the collaboration of teachers.
I n general, health education as a topic of instruction is incorporated i n sciences and especially i n physical education. In 1959-60 the Commission on National Education l a i d special emphasis on the teaching of health and physical education by s ta t ing that : "physical education has become a much more inclusive f i e l d than cal l i s thenics and drills; it includes provision fo r promoting the health of the school child, f o r guarding him against i l l ne s s and weakness, and fo r the correction of defects .......... It must concern
1 I1 itself with matters of hygiene and public health ........ . A s a resul t , the programme of phjrsical education i n the secondary schoobs,
fo r example, general science includes t u p i u s ourlcerri ir lg personal cleanliness,
sanitation, ventilation, water and sewage disposal. For g i r l s , i n home economics the following courses are integrated: nu t r i t ion and balanced die t , f l i e s and pests, sanitat ion, personal hygiene, f i r s t a id etc..
In teacher t ra in ing ins t i tu t ions more e f fo r t s are needed i n the di rect ion of health teaching, However, some a c t i v i t i e s have already been carried out. Ebr example, i n East Palcistan provision has been made i n almost a l l teacher t ra in ing ins t i tu t ions fo r a physician extending a var ie ty of health services t o children fncluiding health education and a l l such institutions havc pre- scribed courses i n health.
SAUDI ARABIA
The School Health Services function under the Ministry of Education and is responsible f o r the health services of a l l school children.
Much a t tent ion is being given t o health education of the students during the school inspections and by radio and publications.
Ban0 &ha, S., Health Education i n Secondary Schools - The Pattern i n PAistan, 1966 (EM/SEM. SCH.HLTH.EDUC./~O)

EM/HEP/~~ page 42
WHO EMRO
Also meetings arc organized with the tcachers i n each school when the health problems of the school children a m discussed, and cooperation of teachers i n coping with the problcms sought. In t h i s connection, coopera- t i o n ex i s t s between the Dlinistry of Education and the Ministry of Health i n the provision of needed material, equipment and. s t a f f services.
Health instruction is given t o students on topics such as nutri t ion, f i r s t a id and sanitat ion. This Is especial ly emphasized i n secondary schools where attentiori is a lso given t o endemic diseases and methods of controll ing tliem.
I n the teacher t r a i n i n g i n s t i t u t i o n s the following courses are given; anatomy and physiology; microbiology; i n t e s t i na l diseases and t h e i r methods of prevention; nutri t ion; school health; health education. Zachers are al&0 rc~ponoiblc for hcslth obecrvations of thcir studcnts and arc t o inform
the head master on any deviations occurring among the children.
SOMALIA
The health of the school child is the responsibi l i ty of the Health Department. Regulations require t ha t a l l school children be vaccinated against smallpox.
I n the Northern Province, it is required t ha t a l l students be examined annually and r e su l t s of the examination recorded.
Some teaching of health is included i n the curriculum of primary and intermediate schools.
In g i r l s ' schools the subject of nutr i t ion i s given added importance. A plan is under way fo r revision of the curriculum i n which adequate a t tent ion has been given t o the health aspects of the curriculum.
SUDAN
There are 570 0 0 students attending schools i n the Sudan. The Ministry of Health is planning t o es tabl ish a Central Division of Social Health and a School Health Clinic i n each provincial headquarters. The present 37 dispensaries each a t present serving about 20 000 students w i l l l a t e r serve the schools i n which they are located.

WHO EMRO
Health topics, including nutri t ion, are taught a t a l l levels of a l l schools. In the secondary school, health has been taught as par t of science. This method is now being changed and a se r ies of health books are being prepared and it is planned t o assign specif ic periods t o teaching of health.
Science teachers are responsible fo r teaching health i n secondary schools and physical education teachers t o teach safe ty and f i r s t aid. A health club has been organized i n the teacher t ra in ing college with functions of health education by group work method.
In the elementary schools the fo l l vwi lu topics are included I n the syllabus of the fourth year as p a r t of subject on "Life and Health": elemen- t a ry physiology; anatomy of important organs; some common diseases and t he i r methods of prevcntion including malaria; dysen+eryj s leeping s i ckr~ess ; influ- enza; smallpox; bi lharzia and i n t e s t i na l worms; f i r s t a id f o r wounds; burns and fractures.
I n the hygiene book f o r g i r l s i n the f i r s t year of the intermediate, a t tent fon is given t o food and nutri t ion, exercise, le isure and sleep, water sanitat ion, f i r s t aid, dental care, care of the body organs such a s eyes and ears and i n the t h i rd year the syllabus includes chi ld development, pregnancy, anti-natal and post-natal care, disease of childhood and personal hygiene.
SYRIA
General education i n Syria is divided i n three stages plus the stage for teacher training, male and female.
Primary stage
I n t h i s stage, health is incorporated with other subjects and is mostly based on observations of various teachers. The topics i n t h i s stage include personal cleanliness, prevention of more prevalent communicable diseases and some elements of nutri t ion.
In the f i f t h grade, the curriculum requires t ha t under "Elements of Science and Health ducat ion" some more a t t e n t i ~ n be given t o speci f ic topics i n health such a s environmental sanitat ion, e tc .
Preparatory stage
WHO EMRO
I n t h i s stage health is given n3re prominence. Attention is given t o show the relat ionship between health and l i f e . In the f i r s t year, water pollution,diseases of the respiratory t r a c t , housing, lighting, f i r s t a id and home nursing are taught. In the second year a t tent ion is given t o nutr i t ion and food sanitat ion. In the t h i rd year some other communicable diseases such a s tuberculosis, typhoid, smallpox, etc, are discussed.
Secondary stage
I n the secondary schools the elements of health are incorporated i n the course of biology. I n physiology the di f ferent organs of the body and the diseases affecting them are discussed. When studying parasi tes, insects, fungi, worms, e tc . the re la t ion between man and these organisins are stressed. Also included are studies i n bi lharziasis , malaria, body resistance against infection e tc . .
School health education i n teacher t ra in ing ins t i tu t ions
I n the male and female teacher t ra in ing ins t i tu t ions , health is a separate subject of study ent i t led: "School Health and Health Education" w h e r e the f o l l u w i r ~ L u p i u s are discussed: school sanltat lon; school day; curriculum development i n the f i e l d of health; nutri t ion; communicable diseases; periodic medical examinations; child health; mental heal th of the ~chool child; first aid and nursing.
TUNISIA
Close t o 800 000 or nearly 18% of the t o t a l population of Tunisia attend primary and secondary schools, a tremendous increase since 1956. The health services for t h i s group is carried out by the Department of School Health Services which has become very active since 1962. The national development plan envisages the establishment of six school health centres with dentistry, general medicine and specialized services i n cardio- logy, mental health, ear, nose and t'moat and ophthalmology. A project is also foreseen fo r a mobile health unit t o regularly v i s i t the schools i n the ru r a l areas.

Cooperation ex i s t s between the Ministry of Health, Ministry of Education and the newlj established Ministry of Social Affairs i n the f i e l d of school health education. The Latter Ministry is responsible f o r health education through its 13 regional health education centres.
I n primary schools, health instruction is incorporated with other items or as a separate topic.
I n the first two years, it is a par t of moral and soc ia l education where students are given notions of health and care of the body, nu t r i t ion and other essen t ia l elements.
I n the subsequent four years, the topic of health received more at tention. In the t h i rd and fourth years, community health is emphasized by introducing topics such a s water sanitat ion, diseases such a s trachoma, insects and parasites, heat and safety.
I n the f i f t h and s i x th years topics dealing with skin diseases, f i r s t aid, dental health, nu t r i t ion and digestion, blood circulat ion, parasites, eyes and t h e i r hygiene, respiratory t r a c t and diseases such as tuberculosis are mentioned .
In addition, i n g i r l s ' schools more a t t en t ion is being given t o maternal and chi ld health and problems associated with pregnancy and chi ld b i r th .
I n the secondary schools, specia l textbooks ex i s t f o r the teaching of health where ce r ta in diseases a re dea l t with i n de ta l l .
UNI'IIED ARAB REPUBLIC
School Health Services i n the United Arab Republic s t a r t ed i n 1835 with the Education Council and remained with the Ministry of Education till 1957. Since then t h i s Department has been t ransferred t o the Ministry of' Health. To-day t h i s Department has a s t a f f of 438,school physicians and a number of spec ia l i s t s including in ternis ts , general and orthopedic surgeons; nempjychiatr ists; radiologists; edr, nose and throat spec3.alists; dermatologists; den t i s t s and a group of health v is i tors ; nurses; pharmacists; socia l workers; e tc . who take care of over 3 million students i n more than 8 000 straining institutions.
WHO m o
Health services and health education a re linked t o encourage teachers t o take an active part i n the health a f f a i r s by organizing short t ra in ing courses and refresher programmes fo r them and by encouraging the school health personnel fo r taking active p a r t i n health education. Parents are also included i n the health education scheme by coordination of a c t i v i t i e s with the section responsible fo r public health education and by encouraging them t o attend c l i n i c s with t he i r children and by arranging special educa-
1 t iona l a c t i v i t i e s f o r them . The system of education i n the United Arab Republic normally includes
s i x years of primary compulsory education, three years of intermediate and three years of secondary s tudies followed by university education. The teacher t ra in ing i n s t i t u t e s t a r t s a f t e r the intermediate school and con- tinues fo r f ive years.
Health k i a s a special syllabus i n the 4th, 5th and 6th grades of primary schools, a l l grades of intermediate schools and i n various forms i n d i f ferent branches i n secondary schools and teacher t ra in ing i n s t i t u t e s . A t the secondary schools no special syllabus ex i s t s on health fo r g i r l s . However, a course on "first a id and preliminary nursing" was i n i t i a t ed i n 1965.
Some elements of health are correlated with other subjects such as microbiology i n the course of biology and simple anatomy and physiology and first aid In the physical education i n secondary schools.
Extra-curricular and co-curricular a c t i v i t i e s a l so help t o a great extent In health education of the Students such a s i n morning Inspections or i n special school socie t ies such as dramatic a r t , home economics, teams of physical education, summer camps, etc. .
I n the teacher t r a in ing ins t i tu te , school health and health education receive prominent consideration. I n t h i s course the purpose is t o prepare teachers not only t o teach health topics but t o be able t o help the chi ld t o grow healthy. Thus, the curriculum not only covers items on communic- able diseases, f i r s t a id and safe ty but on such topics as growth and development, counselling and guidance and mental health.
Kamel, W.H. and Sonbaty, M.M., Teachers' Preparation i n Health Educa- t i on - An experiment i n the United Arab Republic, 1966, (~S~.~CH.HLTH.EDUC.[~)

YEMEN
A law has been passed by the Council of Ministers t o es tabl ish a Department of School Health i n the Ministry of Health and t o es tabl ish school health uni ts i n c i t i e s of ~ a n a ' a , Taiz and. Hodeida. Later such uni ts w i l l a l so be established i n the eight provinces.
The curricula f o r eleinentary and secondary schools contain courses on health and are usually incorporated with other topics even though specia l t e x t s ex i s t f o r health; for example, i n the fourth grade of elementary school i n the course on agriculture, elements of nutr i t ion. In the fifth year nutrition, water, digestion and absorbation and i n t e s t i na l parasi tes are discussed. In the s i x th year water, vent i la t ion f i r s t aid, respiratory t r a c t and diseases of respiratory system are taught.
In the preparatory schools, bi lharziasis , ascariasis , malaria, tuberculosis, typhoid, trachoma, etc. are taught a s part of science courses.
I n genera1,health and science are taught a s one uni t i n secondary school and not a s a separate subject.

CHAPTER IV
SCHOOL HEALTH MlUCATION I N THE C O m T OF EDUCATION AND HEALTH
Panel Discussion
Panel Members: Dr . J. Singh, UNESCO (Kuwait) Dr. G. Jallad, WHO, EMR (Alexandria) Dr. A. Hurbli, WESCO (Beirut) Dr. J. Burton, h'HO, Headquarters (Geneva) - Moderator
Dr. Wtrton: Do we need t o j u s t i f y health education? Indeed It is c l ea r that health services can help an overburdened disease services t o deal with t h e i r task. Tnere are many diseases t ha t can be prevented by immunization, by sani ta t ion and by other service measures. But, looking a t the changing picture of the diseases we see that there are many conditions which cannot be Qealt w i t h by a service alone.
If you ask f o r instance the subject of nutri t ion, how much can a service do about it? It can give a mcnl, but, can it change what a mother does i n the family? What can a service do about mental health? It can deal with casualties, but, can it change the way i n which a mother o r a fa ther brings up a child? O r the venereal diseases! Yes, one can t r e a t the pat ient i f he comes t o the c l in ic . But, can one do a great deal through a service i n order t o prevent venereal diseases?
Many people would say, of course, t ha t heal th services include heal th education automatically. But unfortunately, i n practice they do not unless health education is put forward as a de f in i t e item.
In the new pattern of disease, we are qui te often dealing with a way of l i f e rather than a bacterium and the way of l i f e is real ly influenced by education. The way of l i f e depends on be l i e f s and customs and expectations t h a t people have about t h e i r future. These things are fac to rs which can be influenced by education.

WHO Ern0
Modern education has ra ised people ' s expectations. They demand more. People w i l l not only expect more, but, they w i l l have a vocabulary t o express t he i r wishes. This is another important aspect of health education, It a s provide the public with the means of communication with health workers.
One of the greatest d i f f i cu l t i e s i n relat ionships is the d i f f i cu l t y of comunication v h k h neither the doctors are taught how t o communicate with the public, nor the public has the vocabulary t o communicate with the health people.
Having said that , one comes t o the or iginal point that i f jus t i f i ca t ion for health education is clear, why are problems of developing health education i n practice so d i f f i c u l t and so great?
I would l i ke t o ask Dr. Singh if he would wish t o express some views on planning of health education and with national planning generally.
Dr . Sinffb: Thank you very much. Since I am largely concerned with planning, I would l i ke t o say t ha t we do not make these plans ourselves. We ask others t o make the i r plans, t o put forward t h e i r demands, their requireme-n%@.-..@ only study them and we t r y t o r e l a t e those demands t o the f inancia l resources of the country. Therefore, when an item of any programme does not get enough recognition, it is not r ea l l y the f au l t of the planners, it is usually the f au l t of those who have not been able t o put forward a very convincing case fo r t h e i r demands.
The planners' ro le is t ha t of coordination and integration; and i f they have not given health education the f inancia l a t tent ion it deserves, the short-coming may be elsewhere.
Now, it seems tha t although the importance of health education is agree6 upon by a l l , it is not c lear how t h i s is t o be achieved.
To begin with, modern health education attempts suffer f'rom practices of the past where emphasis was placed only on study of those subjects. The emphasis was mostly on information and largely concerned with a course in the curriculum. The subject dealing with l i f e , the problem d i rec t ly re la ted t o l i f e si tuation, have not received proper attention.
It is not only health education which has suffered from this . The general education suffers as well. For, i n the majority of the countries,

WHO mo
general education is highly academic and not related to the requirements of l i fe , t o needs either of students or of the societies.
There is a need for realization by those who prescribe curricula t o devote greater attention to re la te education t o the needs and requirements of the students, of the community and of the country.
Health education should receive the highest pr ior i ty because whatever exists i n the world exis ts for human beings and the happiness and welfare of human beings is largely governed by the i r physical and mental efficiency.
In some countries, there are no adequate finances f o r school health education. In some others, not enough recognition as t o the need. Still, i n some others, there are not adequtely trained personnel and teachers t o do it. planner^ must take a l l these in to aonsideratfon and plan t o meet a l l of these needs.
p. EW-ton: Now, according t o Dr. Singh, i f health education does not get adequate support from planners it is because a good enough case has not been made. I would l ike to ask Dr. Jallad i f he fee ls that f'rom the health point of view a good case might be made. We obviously have two kinds of needs depending on the viewpoints. Needs as seen by 8 health worker and the need as seen by the economist.
Dr Jallad- Thank you Dr. Burton. School health is receiving increasing -* attention i n the countries of the Eastern Mediterranean Region. These services are conducted by the Ministry of Health i n some countries and by the Mnistry of Education i n others and occasionally both Ministries are working cooperatively i n this field. In order t o provide adequate health services including health education i n schools, the best way is that both Ministries plan and work jointly i n that activity.
In the f i e ld of school health i n general, the role of teacher as a member of the health team needs strengthening. There is no doubt that the role of the teacher i n school health ac t iv i t ies is a general one and not only limited t o giving instruction on health. After the parents, the teacher is the one who has the-longest contact with the child and can I n f f W m h i s behaviour .

WHO EMRO
!lb arouse teaahers ' interest in the school health ac t iv i t ies and t o ass i s t the school health team without jeopardizing teacher's academic role, adJustments should be made in the time-table of the respective teachers. lhis has been suggested previously and wherever practised has been found successfbl.
Obviously, i n many cases one sees a lack of qualified s ta f f and t h i s will be the situation for many years t o come. But, occasionally a vacuum i s seen between the direct services and education when close cooperation and understanding does not exis t between the team entrusted with health services on the one hand and teachers and school administrators on the other.
QYJS, the preparation and training of different personnel working i n the school health team is a great need.
Also, it should be noted that i n the majority of schools record is kept on the health s ta tus of each child but there is no indication that the information collected is always properly utilized. The records w i l l no doubt help i n planning and evaluating of such services i f they are properly utilized.
Dr. Iiurbli: I think it was right ly mentioned that the teacher is the main key t o the whole situation and his training for assuming this function is highly essential. Here it should be mentioned that even with the best curriculum health education takes place only and only i f it follows the nonnal pattern of learning, i.e., it is not only concerned with information but with right a t t i tude about health and f inal ly with the correct health behaviour .
Wherever there is a system of education i n which emphasis is put on memorization, the child wil l not rea l ly learn for h is att i tudes and behaviour are not taken into consideration,
Right a t t i tude is very important i n health matters. If you want a child t o have a certain health practice, he must, of course, have the r ight a t t i tude for it. He practises for a while and then it becomes a habit, a pattern of behaviour.
Furthermore, the situation and f a c i l i t i e s must permit putting a desire, an attitude lnto practice. We always teach our children t o wash the i r hands But, are soaps available alwars? So comethe need for UNICEF and its

WHO EMRO
supporting service i n health education. We t r ea t the child for trachoma but he has already contaminated other members of his family by using the common towel.
Health education is a cooperative effor t between the school and the community.
Health education, as I said before, needs some supporting services and one of the most important supporting service is research, research into the h t t e r n s of behaviour and underlying reasons for such behaviour. We should study the child and the community and find out the barriers i n achieving the goal of health education.
The teacher should not only understand the child but also the community from which the child comes.
I&, Burton: I think by now, a number of important points have been brought up by the panel members. I wonder i f anyone i n the audience would l ike t o contribute t o this discussion.
Mr. Koleilat (UNICEF) : Mr. Chairman, following Dr. Hurbli ' s statement about the supporting services for health education, I wish t o add that UNICEF has provided soaps and towels t o many schools and communities. Also milk is provided t o schools when nutri t ion is taught. In order t o augment ac t iv i t ies i n nutrition eaucation, some communities are provided with fishlings so tht they could develop their own f i s h ponds.
Dr. MOarefi (WHO, EMIU): I enJoyed very much the presentation by %he four panel members. One point, however, needs some elaboration and that is the problem of child against home. Schools are agents of change and i n t h i s Region changes are so rapid that result in rapid changes of sooial values for which parents are not prepared. Thus, occasionally a si tuation is developed where children revolt against home. New against old! It is true the Pamnt/)lleacher Associations can be of help in this matter, but, in many cases, the attempts have not been successful,
May be it would be necessary that school health education becomes a part of colMmrnity health education and may be other attempts should be made. I would appseciate i f this matter is further discussed,

WHO EMRO
Ato o Beshah (Ethiopia): I agree tha t a l l attempts should be made t o f a c l l i E acceptance of health behaviour by the child. But we have t o be careful not t o discourage teaching of health i f f a c i l i t i e s do not exis t at home.
Dr. Sin&: A very important issue has been raised as t o the relationship between home and school. When you teach something a t school and the child finds different si tuation a t home, there is a psychological conflict within himself and there might be some unpleasmtness between the parent and the child. How are we going t o overcome that situation? That is the question!
In this connection, I would l ike t o say that t h i s phenomenon is not a new one. There has always been a conflict between the younger and older generatians apart from w h a t the child learns a t school. Sometimes it is also impractical t o provide t o the community whatever it is provided a t scho01,for the community is a large area and i s largely consisted or people with se t patterns of behaviour. This we have t o face and do our best hoping that the child himself when he grows up would be able t o somehow influence the behaviour of h is parents.
I do not deny that there is a need for doing something for the corn- munity through the general health education services. But, I do not f ee l t h a t the school health education should be diluted a t a l l . Sometimes it is said that the role of teachers and the i r active work with the comrmnity must be enYLancecl. Well It is a very good thing t o say but l e t us also see the part of the teacher. '1Pne teacher a f te r a l l is a human being with certain responsibilities and ordinarily a heavy load of work a t school. If we add t o hls responslbilities, 1L might affect his educational task and will affect h is own physical and mental efficiency. We must realize his limitations. I f an ambitious programme is made, we may not succeed. There- fore, the side or the teacher must also be realized when making reeonmend- ations .
Dr. Harfouche (AW) : Elr. Chairman, a f e w remarks that I would l ike t o make are real ly inspired by the very valuzble comments that I heard i n the l a t t e r part of the Session.
1. In order t o help this Region i n developing its hutnan resources we have t o learn many thinzs, Before we proceed with doing these things we have t o define the -- why. Tnere i s a great value i n health. Yet, uk fortunately, t h i s idea -- heal-lh a s a value - has not adequately matured.

WHO EMRO
The preamble of the constitution of the World Health Organization has defined health as a value and certainly there is a great deal t o be done i n the implementation of t h i s idea.
I f we take health as a value and realize t h i s value as a basis for a great philosophy, then the planners w i l l see it and the teachers w i l l see it and we can see our way through! -
2. Unfortunately, the contents of what we teach is not always based on our knowledge of the fact, of the att i tudes of the people, of the i r practices, and of the i r physical and emotional needs. Unless we investi- gate these factors very thoroughly, there is l i t t l e we can do t o make health a value.
3- We have made, i n many cases,a dead process out of teaching health because of isolatlng it. Although much has been done for higher specializ- ation, for better information, for a greater wealth of knowledge.
However, for health education t o become a dynamic process, it has t o be integrated with a l l health services i n a l l programmes. I fully agree with w h a t has been said tha t health education is only a park of general education a t a l l levels, a l l f ie lds and i n a l l phases.
It was mentioned that use should be made of health records. But, before that we should teach ourselves how t o collect data and we hope that t h i s is one of the important things we t r y t o emphasize i n our teaching -- how t o collect data and how t o mz&e recorded material more useful for better planning.
Dr. Buyton: Thank you very much. A nwnber of important points were brought up i n t h i s panel discussion by the participants. They may be summarized as follows:
1. A workable plan with justlfications must be made for school health education.
2. Ministries of Health and of Education must cooperate closely i n school health education
3. In school health education stress must be made on learning and not only on teaching.
4. The child and his home and the child's emotional stresses must be taken into account while planning and conducting school health education activities.
5. Teachers must modify the curriculum and content to suit the cultural arad local needs.
6. Teachers' loads must be considered in order not to saorifice quality for quantity.
With this r e s d , I wish to thank all who participated in the diecuoaiona.

WHO Em0
C H A m V
AN OVERVIEW OF BASIC NEEDS
The re la t ion between nu t r i t ion and well-being is widely recognized. It i~ known that the human body cannot function efficiently and adequately i n the absence of proper nutri t ion. A well-nourished child has a good chance of becoming a useful productive adult. Adequate nu t r i t ion is essen t ia l f o r mental development, par t icular ly during school l i f e ; i f t h i s is achieved, there is a good chance t h a t the adult w i l l be userul and productive too. Failure t o maintain good nutri t ion, on the other hand, can r e su l t i n i l l ne s s or death a t an ear ly age and hence the loss of a considerable cap i ta l investment which the family cannot afford.
The question now raised is: how far are the above conclusions re- cognized by parents? I n some countries it is sa id t h a t when the cow d ies the whole family mourns, but when the chi ld d ies only the mother f e e l s t he loss. Deatti is looked on i n many countries a s inevitable but when an economic asse t such as a cow dies then there is genuine sorrow based on economic ra ther t'm emotiorai considerations. So far as the human infant is concerned, there often are no economic considerations associated with its death; i l lness , death, hunger and poverty a re accepted as par t of l i f e and there is often l i t t l e o r no concept of a l i f e i n which these conditions do not exist .
1 Based on the paper presented and the discussions of the Seminar

WHO m o
School health education may play a predominant role in changing attitudes, but it is also necessary to help the child being educated to achieve adequate health and physical and mental development, A child may accept the importance of an adequate diet through formal education at school, but, if it is to see for itself and experience good feeding practices, the lessons will be learned more easily and the practical benefits accepted and understood. School feeding should thus have a high priority in practical nutritiori education programmes.
Most administrations in developing countries are only prepared to invest in services which have all obvious immediate value and which have a reasonable cost. Feeding children is believed to be prohibitive and hence impracticable. It is unfortunate that, in most instances, school feeding projects do involve the go~arsnents in enormous expenditure, 81- though this high cost is not always necessary. Where school feeding has been implemented it has tended to be based on the European or North American pattern, involving a school dining-room service with well-equipped kitchens and trained staff preparing and serving a well-balanced diet. There are at the other end of the scale, adequate opportunities for providing a simple snack at minimal cost with minimal facilities yet which meets home diet deficiencies .
1 An experiment was devised initially to see if a snack could be provided for children who of necessity had to walk several kilometres to school every day and v:hose ho~e diet was deficient in protein. The food to be supplied had to conf'orm to the following criteria:
1. The food had to be capable of being manufactured in the country f??m locally available foodstuffs;
2. A single ration of the foodstuffs had to supply at least 25 grams of protein per child per day;
3. The food had to be capable of preparation on an open fire with the simplest equipment;

WHO mo
4. Its cost was t o be no more than three US cents per day;
5. It had t o prove palatable over a prolonged period of time.
The effects on the health and physique of the children of the various foodstuffs tested were recorded over the 2Wday duration of the t r i a l . The t r i a l fndicated foods, whose palatabili ty w a s not accepted; it showed how easily it Is t o organize a school snack; and it showed the benefit of feeding i n terms of increased height and weight and in improvement of haemoglobin levels no matter what food was given. One of the surprising developments of the t r i a l was that although no child had ever thought of bringing food t o eat a t school before the t r l a l , a s soon as the trial started then pupils brought from the i r own homes food which supplemented the snack provided by the school, so that a substantial meal was i n fac t Wing conswnea by the children.
The snack provides a talking point for discussion; the periodic weight and height checks stimulate interest i n personal physique and subsidiary health education, such as hand-washing before the meal can be readily introduced.
There seems t o be l i t t l e reason why a school snack should not be provided by most countries i n t h i s Region, provided the programme is carefully planned.
The periodic recording of height and weight has been mentioned i n oonneotion w i t h an experiment. Suah recordings are, however, an essential pmt of any school feeding programme, for not only does physique become of personal interest but the effect of the feeding programme on the child physique can be observed by the child itself, its parents, teachers and administrators alike. Once it bemesknown that supplementation of the home d ie t has beneficial effects, further interest i n food i n the home is likely t o be aroused. As a long-term measure the child tha t has benefited *om school feeding w i l l wish h is own children t o be fed similarly and also t o receive a d ie t that w i l l assure the i r well-being and optimal physical development. Personal physique graphs on which the child ' s development is recorded have proved t o be of great value i n stimulating interest and evaluating the school feeding programme and many schools now have a record of the child's physique from the time of joining school.

WHO Em0
There is a tendency to consider the school period in isolation, whereas, fkom the point of view of development, school age is only p&rt of a period of physiological development, the most critical part of which is probably during the pre-school years, a time when the child is largely unprotected by health and social services. It would therefore seem logical that any school feeding programme should make provision for extension of service to pre-school children as soon as this becomes practicable. Thus, the school health service should be a means of teaching beyond its immediate chronological boundaries to other fields where preparation for school takes place.
In some countries this has been achieved through ment/lreacher Associations, which have developed, with assistance from the school, a meal service in the villages which may be entirely provided by the villasera themselves1. Such programmes have not only the advantage of providing much needed diet supplements, but also have other useful side effects, such as introducing nutritionally desirable foods into the diet encouraging local food production, educating mothers in better methods of food preparation and stimulating and promoting food hygiene habits. Such programnes having important side effects mean, of course, that the school' should exert some supervision over them.
Part of our existing difficulties in promoting a better knowledge of nutritfon is attributable tn the miscnnceptions of nutrition as a scientif- ic subject. m e popular concept is that it is a subJect which studies diets, nutrients, obesity and metabolic disease, often in a theoretical manner, This concept is a product of Western Universities which naturally concern themselves with problems pertaining to their sophisticated mode of life. The concept in Europe and North America is started during school, when the student is introduced to the theory of the physiology and pathology of nutrition but is denied any practical introduction on the application of scientific knowledge of nutrition, which in reality involves subjects as varied as social customs, food and food habits, health economics, trade and legislation.
1 WHO Progress Summary Report on Bayambang (~hilippines) Applied Nutrition Project, July 1965
WHO EMRO
There is a tendency for the curricula and syllabuses of the Western World t o be adopted i n educational systems of the developing countries, thus perpetuating a system which does not re la te t o prevailing problems. It is important t o ensure that the science of nutri t ion i n its widest terms be integrated into curricula and teaching i n schools i n the develop- ing countries. A t the end of a school career the student should have been exposed t o a l l the various facets of nutri t ion and become fu l ly aware of its implication i n l i f e . Fortunately, this concept is being increasingly recognized and an important meet- organized by FAO/UNESCO/ WHO was convened, which dealt with the teachers ' role i n nutri t ion educa- tionl.
One of the d i f f icu l t ies i n implementing a nutri t ion programme is the multi-faceted approach which is so necessary. Several disciplines are involved and when the curricula for nutri t ion eaucatlon comes up for con- sideration, health, agricultural and education interest may In some instances be a t variance. There is thus a special need for careful col- laborative planning and discussion by educationalists, health authorit ies and agriculturalists i f the teaching of nutri t ion i n schools is t o be effective and practical. This has been already done with success and in one country i n t h i s Region rural science curricula and senior science curricula have been revised and made most practicable as a resul t of conJo%nt action by FAO, UNESCO and WHO representatives. There is l i t t l e doubt about the potential value or such revised curricula; tho main problem now is t o promote interest i n a l l countries so that the school graduate of the f'uture has not only a better understanding of the theory of nutri t ion but alsu its practical implementations.
1 Joint F A O / W S C O ~ ~ O Meeti% on the Teachers ' Role i n Nutrition Education, Report, P a r i s , 1965 ( U N E S C O / E D / ~ ~ ~ )

WHO EMRO
IMENTAL HEALTH O F THE SCHOOL CHILD I N THE PRESENT TFtANSITIONAL STAGE OF RAPIDLY DFVELOPING NATIONS
Dialogue followed - by Discussion
UT. ~ebo 'z -zama.n i r ran): Mental health has t o do not only w ~ t h the care of the diseased mind but a l so w i t h the prevention of mental disorder and the development of normal personality, and adjustment t o society.
Do school children actual ly have special mental health problems? The answer is positive, f a r the sudden t rans i t ion from home t o school causes overwhelming changes. I n the school the child is placed i n a si tuation, completely urdmown hitherto, demanding adjustment t o a large group of homogeneous strangers, and adaptation t o a new type of authority. H i s emotion3 are an a l ternat ing blond of i n t c n ~ i v c mtioipat ion, fear, rejection, wonder, and gaiety in' a way not known before. He is expected t o produce a de f in i t e r e s u l t within a de f in i t e time period.
Now l e t us ask whethzr there a re any speci f ic mental health problems common t o the school children of rapidly developing nations? This question we dl1 attempt to answer by dealing with some special fea tures of developing countries, and clearing up ce r ta in defini t ions. We w i l l deal with the following:
1. Who is the school child?
. - - -
2. Children who need special help
3. Who should deal with t~-vubled children? - - " - - - *

4. The teacher and the mental health of the pupil
5. Poverty and mental health
6. Home against school
WHO EMRO
7. Family s ize
8. Complications 'of polygamy
9. Inadequar: y of schools.
1. Who is the school child?
Defining who the school chi ld is, does not pose an easy task. Should we consider kindergartens and nursery schools a s an in tegra l par t of the elementary school programme or not? What is the permissive attendance age and what is the upper l i m i t of the school age? Is the school chi ld he who is subject t o the compulsory school attendace laws. Are these laws universal?
I f one does not consider the kindergarten and nursery school as an in tegral part of the elementary schnnl programme, then current practice is almost universal i n placing age 6 or 5 as the lower limit of the elementary school. I n developing countries, however, we must make fur ther d i s t inc t ion between potential and actual school children. W r not all , but only a f ract ion of the children of school age, in rapidly developing nations, a re attending school. According t o a study made by UNESCO on school attendance i n academic year 1958-1959, almost over 50 per cent of a l l potent ia l primary school children i n two great regions of the World, Asia and Africa, were, for various reasons, not able t o benefi t from the most basic educational f ac i l i t - ies. Thus, when we t a l k about the school chi ld i n developing countries, unwittingly, we overlook the other half of those unfortunate potent ia l school children who are not ac tual ly attending the school1.
1 For the main types and causes of discrimination and inequali ty of opportunity i n education see:
a ) Arnrnoun, C.D., Study of Discrimination i n Education, New York, United Nations, 1957
b) Juvigny, Pa, Towards E q u a l i t y in Education, Paris, UNESCO, 1962

WHO EMRO
2. Children - who need spec'ial help
From the preventive aspect of mental heal th a l l children need help. But there are childre3 who need special help. Different western surveys, appear t o agree i n finding tha t approximately 3 per cent of the school population is suffering from serious psychiatric conditions requiring intensive treatment, and t h a t another 10 t o 12 per cent, having milder troubles, need some other form of special help1. A s a matter of emergency, these findings could be, temporarily, applied t o western culture, as well as t o the s i tua t ion i n developing countries.
3. Who should deal with troubled children?
Psychiatrists, school psychologists, school soc ia l workers, guidar~ce councelors a re frequently named among those who should deal with the school children. But, since f a c i l i t i e s and personnel f o r dealing with emotional disturbances of children a re far below the need, teachers f o r y e a s t o come w i l l remain the principal resource fo r dealing with emotionally troubled children.
This point should be taken in to consideration i n professional prepara- ticnof teachers since they w i l l of necessity be dealing with problems of emotionally dioturbed childrcn.
4. The teacher and the mental heal th of the pupil
Tfie teachert-> o w men-Lal health is an in tegra l par t of the pupils ' healthy personality deve-lopment. In no other profession is good mental health more essential than i n teaching. The work demands a high degree of s t a b i l i t y - a capacity t o withstand pressures, and most important-of all, the s k i l l of working aggressions off in to channels d i f fe ren t *om the work si tuation. The energies of children, and the turmoil of the class- room inevitably create tensions within the teacher. These tensions must f ind healthy release i n work and recreations. Teachers who a re unable t o discover mechanisms of release a r e apt t o become i r r i t ab l e , emotionally disturbed, anc! malad justed2.
1 The Encyclopedia of Mental Health, 1963, V. 5, 1806
2 Blair, G.M. and others, Educational P~ych~logy , 2nd ed., New York, MacMillan, 1962

I EM/HEp/28
1 page 66 WHO EMRO
How many teachers are maladjusted? Perhaps the most comprehensive studies of the condition of the mental health and adjustment of teachers are those of I?enton1 and ~ i c k s ~ . Both Fenton and Hicks estimated t ha t about 20 per cent of the teachers i n t h e i r sample were i n need of psycho- logical and psychiatric assistance.
The need fo r be t t e r screening of teachers a s well a s ava i l ab i l i ty of f a c i l i t i e s fo r diagnosis and treatment cf mental troubles become obvious from the above survey. The s i tua t ion has been worsened by the conditions influenced by rapid change and continued need fo r re-adjustment. Many teacllers In t h l s part of the world are sudderlly faced w i L h Lhe task of educating great number of people especial ly i n an area where the d ras t i c need necessi tates emphasis on quantity.
This was especially t rue i n l a t e 1940's and ear ly 1950's where countrieswere abruptly faced with the task of educating masses a s par t of t h e i r developmental programmes. UNESCO has given evidence fo r t h i s f ac t i n reports from Afghanistan, Burma, Libya and Viet-Nam among 0 t h e r s 3 ' ~ , 5 ' ~ .
In many countries facing the problem of i l l i t e r acy , the governments are forced t o reduce the course of teacher t ra in ing t o a few months.
1 Fenton, N., Mental Hygiene i n School Practice, Palo Alto, Stanford University Press, 1943
2 Hicks, F.R., "The Mental Health of ~eachers" , Contribution t o Educa- tion, No. 123, Tennessee, George Peabody College, 1943 -
3 UNESCO Mission t o Afghanistan. Report. Paris, 1952. p.53
4. UNESCO Mission t o Burma. . Repor+,. Paris, 1952. p.20
5 UNESCO Mission t o Libya. Report. Paris, 1952. p.20
6. UNESCO Secondary Education i n Asia. Report. Paris, 1962. p.139

WHO EMRO
5. Poverty and mental health
Perhaps it would not be too much t o say that a s t r ik ing c r i t e r ion fo r many of the developing nations is poverty. Poverty has been r ighly cal led the grandmother of a l l evi ls . Those who a re born i n to the world of poverty a re not only deprived of most of the material comforts of l i f e , but many a re a l so stunted i n t he i r emotional, in te l l ec tua l and soc ia l development, and thus ef fect ively prevented from real iz ing t h e i r human potent ia l i t ies . It has been indicated t ha t there a re two di f ferent meanings f o r poverty:
a. A r e la t ive term indicating the absence of the comforts of l i f e and an adequate supply of the necessi t ies.
b. M o r a t : pr-ecisely defined as that p o i n t at which d e p r i v a t i o n makes impossible the maintenance of physical efficiency1.
The kind of poverty which seems t o be more the f a t e of developing countries is of the second type.
According t o the United Nations S t a t i s t i c a l Office, half of the people of the world l ive i n countries t ha t have per capi ta incomes of l e s s than $100, some of them much less . In br ief , two-third of the world's population live i n countries where yearly incomes average less than $ 150 Der person only . . . .2. We are talking about the mental health these people's children!
, .
Different studies have shown the close connection which ex i s t s between poverty and personal rnalad justment3. Not Etll children who come f r u m under- privileged families are problem children by any means, but s t a t i s t i c a l l y speakfng, low socio-economic s ta tus breeds conditions unfavorable t o sound adjustment. The American President 's Task R r c e on Manpower Conservation found that :
1 Sloan, H.S. and Zurcher, A.J., Dictionary of Economics, 4th rev. ed., New York, Barners a& Noble; --1961
2 W e , G., Poverty i n Plenty, New York, Kennedy and sons, 1964, p. 29
--.
3 Sheldon and Eleanor Glueck, Unraveling Juvenile Delinquency, New York, !.&e Commonwealth M d , 1950

EM/HEP/~~ page 68
WHO Ern0
". . . . One th i rd of the nations ' youth woulcl, on examination, be unqualified on the basis of standards established fo r mi l i tary service, Moreover, proverty is the principal reason why these young men f a i l t o meet those physical anci mental standards ...
These findings a re dramatic evidence t ha t the problem of poverty is s t i l l very much with us, and t ha t i ts soc ia l and economic costs are heavj ...
Physical and mental d-isease, delinquency and crime, high infant mortality, loss of productive capacity - a l l of these are part of the environment of poverty1 ." Even i n higly developed countries, schools located i n lower-class
neighbowhood a re often in fe r io r i n quality. The so cal led "Slum Schools" have special problems and characterist ics2.
Thus, they who need more receive l ess . Therefore, the elimination of poverty becomes a major mental health problem i n i t s e l f .
As t o the f a c i l i t i e s ,
" ~ e n t a l health care f o r school children and chi ld guidance are stlll lacking i n the majority of the countries of the astern Mediterranean) ~ e ~ i o n 3 . "
And i n oLher slrnilar parks of the world the case Is not too different . But, as Bernard remarks, the problem of the mental health of the poor is not only the inadequacy of f a c i l i t i e s , it is ra ther t o f ind more efficacious
- ---
1 Poverty i n Plenty, ibid., p. 25-26
Broom, Leonard and Phil ip Selznick, Sociology, 3rd ed., New York, Harper and Raw, 1963, p.472
Eecker, S.B., "Social-class variat ions i n the teacher-pupil relat ion- ship1', Journal of Educational Sac iology, 1952, 25, 451- 465
3 Document E ~ C l5/%ch. ~ i sa . /2 , p. 6

WHO EMRO
kinds of mental health services t o reach a l l segments of the needy popul- ations, and t o eliminate the poverty - the main spring of most evi ls - i t s e l f .
6. Home against school
Of a l l the groups of which a person is a member, the most important f o r h i s destiny is the family. It is i n the family tliat the ch i l d a r r ives a t a conception of s e l f . Research by sociologists, psychiatr ists , psychologists and c 7 d t m a l anthropologists a l l show the paramount importance of the rarnily in shaping personality. The counselling expericncc has also shown tha t success i n dealing with the behaviour problems of children of ten involves the f ea s ib i l i t y of t r ea t ing d i f f i c u l t i e s i n t h e i r relat ionships t o their parents and. in the relation~hipo of thc pments to each other.
And, on the other hand, growing up i n a broken, insecure, or poverty- s t r icken home a f fec t s the values, a t t i tudes , and motivation of children i n re la t ion t o school and work. Especially where the ever-increasing use of communication media such as radio, te levis ion and films a r e demonstrating other and more a t t rac t ive s ides t o everyday l i f e . Children are strongly conditioned i n the family se t t ing by unconscious, a s well a s exp l i c i t in- s t ruct ion through word and example, on the par t of parents and other members of the family. The educat.i onal attainments of gasents exert a strong Pre- disposing influence upon the relat ionship between them and t h e i r children. When the parents a re more educated,' children seem t o f e e l more sa t i s f i ed .
1 Msr.ont.~ntrnent with parents among teen-agers is almost universal . But, i n the developing cocrit-.ies, the case is more serious. Lack of understand- ing i n the family is the major complaint of most of the youth of developing
2 nations . For example, Persian l i t e r a tu r e which i n the old days was highly respectful towards parents and t h e i r a t t i tudes and r ights, is not always so at present. The cri t icism and evidence of the f r i c t i o n between old and new
1 Gessell, Youth, the years from ten t o sixteen, New York, Harper and mothers, 1956, p. 303-304
2 Sahebo'z-Zamani, ProBlems of 'youth i n a developing country - Iran

FEIO EMRO
values is not infrequent. A wave of i e t t e r s denoting t h i s phenomenon is received by press ant?. radlo daily. This is not inerelj- an Iranian pheno- menon. Observers of develcping nations report s imilar s i tuat ions else- where. Nuri Eren, writing on the sucia l problem of ''Turkey today", notes as follows:
"1n a comparison of the daily l i f e of an average family i n Ankara, Adnara, Istanbul or Isrnir, with t ha t of the twenties, only the food woulc! be found mchanged .... The teen-agers f ree ly express t h e i r views .... Only the subject of marriage is not argued. Both the parents and the younger generation are conscious of the clash i n t h e i r outlook; the elders st i l l regarding it on arrangement between families, the younger fo lk acceptirq it as a matter nf individual c h n i n e . This difference i n outlook they prefer not t o discuss1."
I n other words, many youth and t h e i r families i n developing countries l i ve together without understanding each other, but with tormenting scruples and doubts resul t ing from confl ict ing values and sudden cu l tu ra l change.
The comprehension of passing t rad i t iona l values and the emergence of the new ones is almost universal. But most dramatic is the r i s i ng conf l ic t resul t ing from the encounter of the native cu l tu ra l values of developing areas and those of the west. Their co-existence i n t r ans i t iona l stage poses much social , a s well a s individual, complications.
Rejection of the old values is very much common amon@; the younger generation of the developing nations. Even the Manus, whose primitive culture Margaret Mead reported is "growing up i n New ~uinea" , and who made according t o Mead, the cu l tu ra l giant s tep from the Stone Age t o the Space Age, a re not f ree from t h i s rejection2,
Among the factors contributing t o juvenile delinquency i n Africa, the students of "The International African instituten, speak with emphasis of
1 N u r i Eren, Turkey today and tomorrow, London, Pal l Mall Press, 1963, p. 161-162
2 Mead, Me, New l i ve s f o r old, New York, New Am. Library, 1961, p. 42

WHO m o
poverty, the disintegration of the family system and of the conflict of cultural values1 .
In this situation of conflicting values the home is more the guardian of tradition, and the school the agent of westernization; and this brings about a home-against- school situation, which exerts an irritable influence on the mind of school chileen. It is not very uncommon that some parents even become jealous when they find a child in a household discussion, for example, expressing a point of view different from the parents and obstinate- ly holding to this contradiction by citing the teacher as a final authority. In some cases a father may find that his son admires some man teacher more than the father; or a mother may find that a girl reverse some woman teacher. Due to all of this, special measures must be sought through adult education courses and the parent/teacher association, to bridge this widening gap.
In most of the developing countries, unfortunately, the parent-teacher relationship is either totally lacking or it is practiced on a very limited scale.
The home may supplement or complement school experience or it may act to neutralize or negate their effects. Baldwin and Osborne made a detailed study of home-school relations in six schools. They found as the school authorities learned to know the parents betLer t h e y acquirad more confidence in their judgment, similarly, as the parents learned to how the school better, they more fully understood the problems faced by the school2.
1 UNESCO Social Implications of Industrialization and Urbanization in Africa, South of the Sahara. Paris, 1956. p.82
2 - Baldwin, Sara E., "~ome-'~chool Relationships; Philosophy and
Practice", - Progressive Education Association, 1935
Encyclopedia of Educational Research, 3rd ed. by C.W. Harris, New York, MacMillan, p:' 802 - 806

WHO EMRO
7. Family Size - Studies have sllorqn tile impact of family s ize on education, personality
development and tha hsnlth of i Ls mem1>cYs, Basil Bernstein, i n an investig- ation, found thnt s ~ ~ c c ? s s i n learning, ai~d more fundamentally the growth of intelligence, may be closely re la ted t o the type of language learned from ea r l i e s t years. ZqFs 1-3s been explained by the theory of John Nisbet t ha t the well-knotn ifi-,-ey?e ;.elation of intel l igence and family s ize is par t ly due t o the lesser development of language through the more limited contacts of children ~ ~ 5 t h thei? parents i n l ~ g o families1. Some fur ther evidence has been provided by Zean Floud and her collaborators, and by Elizabeth F'razer, a l l indicating t ha t the children of small-sized families do bet ter
2 i n school, while children from large families were found t o be handicapped . On the matter of health i n re la t ion t o family size, again Hare and
Shaw i n a study of 499 urban families have shown tha t the:
" ~ a t e s of various indices of i l l -hea l th fo r mothers and t o a lesser extent fo r fathers, increased progressively with the number of t he i r ~ h i l d r e n 3 , ~ '
One of the outstanding characterist ic features of the family i n the developing countries is its relatively large size. The UNESCO aUtnOrS O f
"Culture and Human ~ e r t i l i t y " , writing on " ~ s i a n Pattern of Family Life", s t a t e as follows:
Nishet, J., "Family Environnent and Inkelligcnce", Eugenics Review,
1953, 45
Floud, J.E., Halseg, A.H. and Martin, F.M., Social Class and Educational Opportunity, Heinemann, 1956, Chapter 6
Bazer, E., Jp, , Epviroment and the S c h s , London, University Press, 1959
Ottoway, A. K. C, , Education and Society, London, Routledge and Kegan Paul, 1962, p. 130 - 132-
3 The Br i t i sh Journal of Psychiatry, 1965. 3, 464 - 466

"Under conditions where about half of all infants born alive die before reaching maturity, the anxiety for sons, even for the .assured survival of a single son, results in large families ...1."
However it may be, the fact is that family size in developing countries, with all its consequences, is notably larger than in the western countries.
8. Complications of polygamy
Polygamy is a custom almost exclusively found among developing nations. Needless to say, if a community is called polygamous, it is not necessarily assumed that polygamy is the rule, but merely that it is permitted under certain circumstances! Polygamy is declining. However, it is still practised. A by-product of polygamy is the increase of half related persons, i.e. children of the various wives of a husband, being involved in a half- relationship. !%is step-relationship has been, through the ages, the kernel of hostility and conflict within the family.
Although there are no statistics at hand nevertheless the conditions seem to require more consideration in the developing countries.
9. Inadequacy of schools
It is not an exaggeration to say that the future of human civilization depends, to a great degree, upon how well schools fulfil their objectives and how well children learn the skills which will enable them to face the crises of tomorrow 3- modern concepts of educational theories the emphasis is more on reaching into the culture to satisfy purposes rather than on assembling elements of the culture and imposing $hem on the pupil. Thus, the aim of the school is, more or less, to prepare children and youth for life. It may be said, that the aim of the school is living, a purposeful living. Are the schools of developing nations fulfilling this aim?
Unfortunately, however, most education in most schools is:
".. . unilineal and that all the pupils, regardless of differing aptitudes and abilities, are pressed into one pattern.21'
. --. .*.-
1 Lorimer, F., Culture ahd Human Fertility, Paris, UNESCO, 1954, p. 160-161
2 UNESCO Secondary Education in Asia. Report. Paris, 1962. p. 61-62

WHO EMRO
and
he kind of education imparted in many schools is still bookish 1 and determined by the needs of examinations rather than by the country's
i economic development. l"
I I Thus, the schools of developing countries, if they tend to be con-
servative, radically a?lbitious educational bodies, fail to cope with the I requirements of the rapidly transitional stage of these changing cultures I and are apt to produce a herd of sophisticated, unsatisfied, dependent, help-
less, suspicious, suffering and rebellious angry youth. So in many cases inadequate curricula of developing countries can, and indeed do, easily turn the integrative factor of education in mental health into a disintegrative one.
Fortunately, however, many authorities in the Governments have recognized this trend and are carefully studying the clash between the old and new values, between the needs and possibilities, between quality and quantity.
In summary, this is an age of rapid transition like of which has seldom humanity seen and this change has brought about consequences some of which have mixed impacts.
A number of nations and health and education authorities have given due attention to this trend by guiding youth for creative use of their leisure time and for better education of both the young and the old to accept new values. Other nations will undoubtedly follow the trend. The fact that to a great extent the social malady has been diagnosed, even if no treatment has as yet been administered, is a very promising and hopeful sign indeed!

WHO EMS0
Dr. Koutsakos ( ~ y p r u s ) : A s an attempt i n solving problems of mental - health of the gchool chi ld i n the present stage of rapid transi t ion, I t r y t o b r i e f l y discuss what w2 are doing i n Cyprus. Educational author- i t i e s , school healtn services and teachers i n Cyprus, have heen fo r the past f i ve or s i x yems focu.dsing a t tent ion on the mental health problems of the school child,
A school psychological service was established i n 1960 having two psychologists. In 1964 a counselling service was established serving a l l the secondary schools. One may ask, however, whether or not mental heal th consti tutes a big problem i n Cyprus. The impression t ha t mental health is growing t o becomz a problem i n Cyprus has been substantiated by a number of studies and surveys carried out by the Pancyprian Society fo r Mental Health, the School Psychological Service and i n the Teachers Training College. The School ~sychoiogical Services have prepared on experimental bas is the mental health record of individual students. They have a lso worked on the adjust- ment and standardization of the intel l igence t es t s . The same service has a l so dealt therapeutical ly with a number of cases of maladjustments, emotion- a l s t r e s s and other psychological anomalies among school children. Further- more, special classes f o r retarded children and t ra in ing programmes f o ~ nurses and t ra ine rs of retarded children have been organized.
Other points which need mentioning a re the personal re la t ionship of the students and recognition of individual differences. This is based on the concepts of m e n t ~ l h 2 ~ l t h . For t h i s reason a c lass with a smaller number of students is preferred. The r a t i o i n the c lasses i n Cyprus is at present 31 pupils per teacher i n the primary and 25 i n the secondary schools, A t the same time recognition and acceptance of individual differences have been duly studied i n the teacher t ra in ing ins t i tu t ions ,
The education of parents i n matters of mental health is another of the basic conditions. Much has been done i n Cyprus i n t h i s regard and many methods including meetings, instructions, newspapers, radio and te levis ion lmve been used f o r t h i s purpose. This programme is conducted by the f u l l cooperation of heal th and education author i t ies a s well a s the s c i en t i f i c associations such a s the Pancyprian Society f o r Paedagogical Research and the parent/teacher associations. Mental health ins t ruct ion is one of the main subjects in the teaoher training colleges with the ultimate a i m of promoting knowledge and practice i n mental health. Also, short courses and seminars f o r teachers a re organized on t h i s topic.

WHO EMRO
Sex education has received some a t tent ion i n the school curricula. A cer ta in amount of instruction on sex education is already i n the curriculum o f t h e secondary schools. Yet, it is f e l t t ha t teachers approach t o t h i s complex subject should be sought, taking in to consideration its mental health aspects,
This is a brief account of what is being done a t present i n Cyprus. It is only a beginning and the following s teps are a l so needed t o betaken:
1. More intensive ins t ruct ion of teachers, special ly teachers of the seoondary echools on the subject of mental health and in regard t o the a t t i tude toward students.
2 More systematic action in parcnt/tcacher associations for . improving teacher-pupil and parent-child relationships.
3. Better adjustment of the school curricula t o the needs and in te res t s of the students.
4. More recreational oppor-t;unities i n the schools.
5. More a t tent ion t o the secondary school students special ly those coming from ru r a l areas.
6. Extension of services of school psychological services.
7. Closer ident i f ica t ion of mental health problems by research and surveys.
Dr. Singh (UNESCG): A point I raised yesterday about the function of teachers may have been misunderstood. When I sa id is t ha t teachers should not be overburdened, I was not referr ing t o the school functions.
What the teacher does i n the school and what he is expected to do in the school is part of h i s duty. Education is concerned largely with offering or assuring the maximum condition which would contribute t o the optimum development of childrens' personality.

WHO EMRO
The duty of the teacher is not simply to teach the subject but t o provide educational atmosphere. It is to provide a l l conditions which w i l l aid i n the development of the child -- physical development, mental development and emotional development. 'kerefore, the attention to the to t a l development of the child is a responsibility of the teacher.
Mr. Madi (Lebanon): There are a number of factors which need attention:
1. Mental health problems of the school-age children not attending school need due consideration.
2. The education of parents as t o the health problems of children should not be neglected.
Most often when mental health problems are occurring among children the parents usually take a defensive at t i tude and are not able t o accept the fac t that the child may be mentally ill just i n the same way that he can be physically ill or may have personality or maladjustment prbblems.
3. There is a need for some psychological services available t o teachers.
Miss Doss (FAO): Both i n the discussions of yesterday and today it was stated that involvement of teachers i n the home and the community activ- i t i e s was inescapable. But, It should rluL be expected that a teacher do a l l of these on his or her spare time. Thus, f a c i l i t i e s should be provided so that the teacher can devote part of his time t o a programme of work i n the community and homes. alis of course should be related t o his teaching.
Dr. Harfouche (AUB): It should be reminded that when a child begins school he is ' s i x years old and a number of problems i n mental health as well a s in physical health have already taken root. Therefore, we have t o refer t o the personality problems i n man's first and most important teacher, h i s mother. I f we real ly want t o have a f u l l grasp of the problems i n the school health services we have t o coordinate these activ- i t i e s with maternal and child health services and with the ac t iv i t ies of those who are i n contact with the mother, i n the pre-natal, post-natal and period of pre-school years.
WHO m o
SOtvZ TU'OTES O;$ SCIIOL'L SANITATION
The school is an expznsive anc; im2ortant community facility. To ensure every opportunity for the youngey generation to improve on its elders some commuii?ities are willing to spend one third or more of their public funds on building and running their schools. Such an activity should obviously be well-planned from all points of view.
Most of the environmental factors with whioh sanitmistns are usually
concerned may afPect the school child, wlio during the years of greatest physical growth spends half of his waking hours in school. Boarding school students spend most of their time in the school environment, The learning process itself is aided by good environmental conditions which permit the child to concentrate efficiently on his school work. In addition, various environmental factors which can be controlled affect the likelihood of disease transmission and of accidents.
Thought should be given to school sanitation at all stages: before a site is selected, when the building is being designed and built and its accessories are being chosen and installed, in providing for the operation and maiptenance of the buildim, and in the class curricula devoted to hygiene'. The importance of these considerations should be emphasized when budgets for school construction and maintenance are discussed.
1
See example on "~e~uirements of Schools in the ~udan", p. 86 - 90 of this Report

EM/HEP/~~ page 80
WHO Ern0
I1 LOCATION OF SCHOOLS
The school child should not be tired by too long a walk or ride when he reaches school, and the young child should, if possible, be able to reach school without having to cross heavily travelled streets. Central locations are thus advantageous. But even more important than ready accessibility in choosing a location for a school are adequate space and light and freedom from excessive noise and polluted air. In sub-urban communities it may be possible to satisfy all these requirements without difficulty or heavy expense. In rural areas long distances from house to school, especially at secondary level, may be inevitable. In city centres, where land is scarce and expensive, space for athletics may be minimal, and poor light and air may be unavoidable.
For these reasons, the choice of school location should be carefully made and specific steps taken to offset specific unfavourable environmental factors in the chosen site. For instance, boarding arrangements or buses will usually be needed for secondary school children in rural areas. On the other hand, a city school with poor natural lighting and noisy environ- ment may need to depend largely on artificial light and conditioned air. Similarly, where children are obliged to cross busy thoroughfares to reach school, pedestrian over- or under-passes may be built.
Speclslc standards for school grounds are not easy to fix or maintaln but may be useful as a guide. In some American cities approximately the following have been adopted:
1, Space: 1/2 hectare per 100 children plus 2 hectares in elementary schools or plus 4 hectares in secondary schools,
2. Accessibility: 1 km walk (elementary) or 3 km walk (secondary), or 1/2-hour bus ride (elementary) or 1-hour bus ride (secondary).
3. Schoold grounds: free of insects, rodents, noise, bad air.
4, Water, electricity, sewerage, fire and police service available.
I11 DESIGN OF SCHOOL BUILDING
The school building should be laid out in such a way as to give class- rooms the most advantageous orientation, depending on local climatic conditions.
Administrative services should be centralized. Noisy ac t iv i t i e s , such as machine shops and music rehearsal rooms, should be separated as mush as possible from study class-rooms. In large schools the auditorium is potential ly useful f o r various community a c t i v i t i e s and should be designed and located within the building with t h i s i n mind. In case of need f o r emergency egress, upper storeys ( i f any) should have two or more stairways t o the ground level. Stairways should be wide, not steep and well- l i t . Outside doors should be wide and hung so a s t o swing toward the outside of the building.
The class-room should be a pleasant and comfortable room. Its physical qua l i t i e s have an e f fec t on the school-child's a b i l i t y t o concentrate on h i s lessons. Satisfactory temperature, ventilation, l ight ing and acoustics can t o a large extent be assured i n the design of the room. What is then lack- i ng can be provided t o any desired degree of excellence i n decorating and equipping the room.
A great deal of research has been done with the aim of determining optimum standards based on physiological and psychological considerations, Studies have a l so been made t o determine whether natura l vent i la t ion and l ight ing have any basically superior qua l i t i e s a s compared w i t h a r t i f i c i a l ones. Those who design school buildings should be acquainted with the up- to-date r e su l t s of t h i s work. A t the same time they should recognize t ha t conclusions reached fo r schools i n other climatic and economic cunditions cannot be blindly adopted i n t h e i r own countries. Similar s tudies are necessary i n t h i s part of the world.
Max imum use should be made of nautra l heating, vent i la t ion and l ight ing i n the design of schools i n most Eastern Medditerranean communities. Tempera- tures are moderate, sunlight is strong, stormy w e a t h e r is infrequent, and budgets a r e limited. This means t ha t rooms should be large, high-ceilinged, and have ample window-space. Room-heating i n winter, where needed, may be accomplished or supplemented by d i rec t sunlight. Otherwise, d i r ec t sunlight i n class-rooms should be avoided, A i r movement i n hot weather can be accomplished by putting windows on two s ides of the room and by various kinds of vents. I h s t o r sand may be a problem. Indigenous building methods o f fe r many suggestions on how t o insula te rooms and heat, cool and vent i la te them. 'Ihese should be taken i n to consideration i n designing school buildings as they may mab m o r e c o m f o r t a b l e s c h o o l - r o o m s and at the s a m e t i m e save m o n e y .
-, 1

EM/HEp/28 WHO EMRO page 82
Natural l ighting is usually easy t o assure i n the countries of t h i s Region. Since the sky brightness is greater than i n Europe and North America, window areas can be correspondingly less . Windows should extend t o theoei l ingand the fur thes t desk should not be more than twice as far from the window as the height of the window above the desk tops. Windows are usually required t o be between 1 5 d 20 percent of the f loor area (e.g. , a room of 6 x 10 m. would need windows of 9 t o 12 m? area).
1 Dormitories i n boarding schools must be designed so tha t sleeping children w i l l be adequately separated (e.g., beds by 1 meter, heads by 2 m. ).
IV EQUIPMENT AND DECORATION i
While they a re normally inclu6eci i n the design of a school, equipment and i n t e r i o r decorating can be modified even a f t e r construction is finished and so are deal t with separately i n t h i s paper.
Equipment includes water supply, sewage disposal ins ta l la t ions , space heating, cooling and venti lat ing f ac i l i t i e s , restaurant and kitchen f a c i l i t i e s , e l e c t r i c l ight ing (and sometimes power supply) and f i r e pro- t ec t ion devices. In te r io r decorating of hygienic in te res t includes ceil ings, walls and f loors of class-rooms, halls, stairways, wash-rooms, kitchens and gymnasiums, a s well a s choice and colour of furni ture and chalk- boarda.
The most important single item is cer ta in ly a clean water supply for drinking, hadwaahing, and possibly also fo r t o i l e t s , showers and kitchen use. If running water is available, 20 t o 80 l i t r e s per student per day may be needed.
If the school is not connected t o the community sewerage system, a sep t ic tank and t i l e disposal f i e l d w i l l need t o be b u i l t on the grounds. I n the absence of runnipg water, p i t l a t r i ne s w i l l be bu i l t . Handwashing f a c i l i t i e s near the l a t r i ne s are needed.
One drinking fountain, one wash basin and three WC's ought t o be provided fo r each 100 children i n the school. (For boys, three urinals and one WC per hundred may be allowed). Spring-loaded or "waste-not" -type taps may be provided t o conserve water. If chlldren take past i n a t h l e t i c s during school hours, showers should be provided a t the r a t e of a t l e a s t three per hundred children.

WHO EMRO
Space heating, cooling and venti lat ing equipment (including a i r conditioning equipment) is not of great importance i n most communities of t h i s Region a t present. I n some very hot regions schools, l i k e a l l other ac t iv i t i e s , close during the ho t tes t hours of the day. A i r conditioning might be considered i n such places i n the in te res t s of greater work efficiency (as it has been i n o i l company off ices) . Conventional air conditioning dehumidifies the a i r , and is needed i n hunid climates, I n dry climates various kinds of "desert coolers" can be used which derive t h e i r cooling e f fec t from the evaporation of water and which are f a r cheaper t o buy and t o operate. I n some circumstances a fan placed i n the ceiling t e exhaust a i r from the room and discharge it through a roof vent is helpful. 'Ib be effective, such a fan should be capable of withdrawing a quanti ty of air equal t o the room's volume every minute.
Depending upon the Inherent f l r e hazard of Wle sc2lvol building some f i r e f ight ing equipment may be provided, on the premises. I f the school is located i n an upper storey of an exist ing building with a s ingle stair- way, an outside metal f i r e stairway may need t o be provided.
Most schools have some -food service f a c i l i t i e s , ranging from snack- counters t o complete restaurant f a c i l i t i e s . Provisions must be made i n even the simplest of these f o r clean and e f f i c i en t storage, preparation and serv- ing of food. Walls and f loors should be of t i l e or other hard, washable surface, Cupboards ahould c l o ~ e t igh t ly and be screened against insects and rodents. A r e f r ige ra to r should be available i f milk is served. Tables and counters where food is prepared and served should be smooth and impervious 30 .they can be kcpt cl-can. Si-ovtss should be vented. A sink with hot water is needed f o r dish-v~ashing,a second sink fo r r ins ing ( i f possible), and a rack f o r a i r drying of dishes. I n large ins t i tu t ions automatic dish-washing equipment may be justified, Preparation, serving and washing-up should be carried out i n separate par ts of the room, or i n d i f fe ren t rooms. Cleaning materials and insecticides should be stored separate from foods. A c lose t should be provided where food handlers can keep t h e i r uniforms and hang t h e i r s t r e e t clothes, a s well a s a t o i l e t and wash basin. Garbage should be kept i n a closed receptable i n the kitchen. I f there is no municipal refuse collection, the school needs a refuse p i t with a t i g h t cover and an inciner- a to r f o r paper. The dining area should a l so have smooth, washable f loor (and tables and chairs, i f provided). Simple, chip-resistant crockery o r p las t i c dishes should be used. Where complete meals are served compartmented p las t i c or metal trays, on which the meals are served di rect ly , a re convenient and f a c i l i t a t e dish-washing procedures. .

WHO EMRO
School-room and corridor f loors are subject t o tremendous wear. They must be hard, smooth and res i s tan t t o cleaning materials. Asphalt t i l e is a t t rac t ive , but deter iora tes ra ther rapidly. Concrete tends t o get dusty. Rubber, p las t i c and linoleum surfaces are good; terrazzo is excellent, but slippery; a non-skid surface is required i f t h i s material is used.
Cheap, cleanable but sound-proof materials should be used fo r school- rooms walls. The surface should not be glossy (except i n wash-rooms and kitchens) but should have a r e f l e c t i v i t y of 60 - 70%. This is achieved by using l i gh t pas te l colours. In hot climates "cool" colours (blue and grecn) are favoured. Chalk-board today is often green ra ther than black. To f a c i l i t a t e seeing it, the lower par t of the walls and a s t r i p around the chalk-boards is painted a darker colour. Ceilings should be f inished in w h i t e plaster.
I n most circumstances i n t h i s Region, natural illumination from the windows w i l l suffice f o r day-time classes. Elect r ic l i gh t s w i l l be provided fo r evening classes and sometimes t o supplement daylight on dark days. According t o present illumination standards enough l i gh t should be provided t o give an illumination of 10 t o 30 foot-candles on the darkest desk topl . Incadescent bulbs should be enclosed i n frosted glass globes t o diffuse the l ight . I f lamps are going t o be extensively used fluor- escent 1-s may be chosen; they are more expensive in initial cost but operate more e f f i c ien t ly (and coolly) and hence more cheaply.
As s ta ted a t the outset, the considerations i n th i s seotion apply equally t o new school buildings and t o old ones. It is not necessary t o wait u n t i l a new building is provided t o improve school children's environment.
V REPAIR AND MAINTENANCE
Like every building, a school needs periodic repai rs and constant maintenance. Adequate budgetary provision must be made t o cover da i ly cleaning, annual plastering and painting, seasonal overhauling of heating,
1 I n a typical case of a class-room 10 x 7 m large with lamps 2 m above desk tops, f ive 200-watt lamps spaced i n an "x" w i l l give about 10 foot-candles illumination.

WHO EMRO
plumbing and other systems, replacement o f e l ec t r i c lamps, etc. Special a t tent ion should be paid t o safety factors, such a s t es t ing and recharging f i r e extinguishers,
VI TEACHING GOOD SANiTATION
School children are a favourite target f o r advice on public heal th and sanitation. Posters depicting unhygienic and hygienic ways of con- ducting various household ac t i v i t i e s adorn the class-room walls i n many communities. I n many schools instruction is given on personal hygiene and public health.
Such instruction, however, cannot have f u l l impact i f the physical means t o put it i n practice a re absent. How can you persuade a chi ld t o form good study habits at home when h i s school bench is crowded and badly l i t ? What does a lecture on safe water and excreta disposal mean t o a child i n a school with neither of them? What use is it t o teach food sanitat ion and permit the school canteen t o operate i n a f i l t h y manner? Why t a l k about hand-washing i f wash basin and soap are not available i n the school?
On the other hand, i f the author i t ies provide the basic sanitary needs fo r a school, i t should not be d i f f i c u l t f o r teachers t o stimulate the school children's in te res t and sense of pride am responslbll l ty In using the f a c i l i t i e s properly and i n helping maintain them. It can a lso be fore- seen t ha t children f'rom such a school w i l l take ideas home and gradually introduce some GL 'cilei11 ~ n t o the home environment, no matterv liuw cunser- vative a re local ways.
VII RESPONSIBILITY O F HEALTH ADMINISTRATTON3
In most countries the intervention of health author i t ies i n school sanitat ion is limited t o health education ac t iv i t i es . Physical planning of schools, design and equipping of school buildings, and surveillance of the sanitary condition of schools are the sole responsibil i ty of education authori t ies.
It is evident that health ministrigs &d local health admid-stratioris should be interested in the matter whenever the health and comfort of school children are threatened. There is in f ac t scope fo r considerable act iv i ty , mainly i n the f i e l d of sani tary engineering. As suggested i n this paper,

EM/HEP/28 page 86
WHO EMRO
such in te res t should begin with the selection of school s i t e s and the study of ce r ta in aspects of school building designs. Out of experience gained, codes would be developed or revised.
I BOY'S ELEMENTARY SCHOOLS
Maximum of 50 pupils per c lass and 4 classes per school-age of pupils 7 - 12 (average).
i Number : 4 class-rooms f o r a f u l l school of f o ~ ~ r classes.
ii Floor space: 8 ft2 (0.76 m2) f o r pupils under 8 years of age.
8 1/2 f t 2 (0.82 m2) f o r pupils over 8 and under 11 years of age.
10 f t 2 (0.97 rn2) f o r pupils over 11 years of age with a space of 6 f t (1.8 m) between the black- board and the f ront row of the pupils.
iii Dimensions : In order t o conform t o ( i i ) above and a t the same time sa t i s fy educational requirements.
One class-room 8.5 m by 5.5 m. Two class-rooms 9 m by 5 m. One class-room 11.5 m by 5.5 m.
i v Cubic space per pupil : A minimum of:
3 100 f t f o r pupils under 8 years. of age.
136 f'b3 f o r pupils over 8 yeass of age.
v Height of inside walls : A minimum of 12 f t (3.7 m)
1 Information received *om the Government of the Sudan, July 1965

WHO m o
v i Seating space: Each pupil should be allowed 20 inches1(50 cm).
v i i Black-board : Should be e i ther b u i l t i n to or fixed t o the end wall.
v i i i Window space : Should be not l e s s than 1/8 of the f loor area and should not include the door. Window shut ters should be divided in to two sections.
ix Ventilators : Should be provided. They should be of the cheapest type with mosquito wiring.
x Lighting : Should come from both sides, i f possible, i. e. from north and south, but a t any r a t e from the side t o the l e f t of the pupils,. i.e. from the north. There should be no window i n the black-board wall.
x i Floors : Should be made of hard, permanent material such a s w i l l permit of adequate cleaning.
x i i Shelves and cupboards : Shelving should be provided on class-room
walls; a lso bui l t - in cupboards, where the construction allows.
b. Offioes
Each school. should have two offices, one fo r head master and another a s a common room for the rssistant masters,
c. Verandahs and sunshades
Verandahs should be provided on the southern side of the-main block of class-rooms and sunshades on the southern side of the two subsidiary class- rooms. Sunshades should a lso be provided on the cas t w a l l of the eastern class-room of the main block while t h e i r provision is furCher desirable on the western rooms.
As i n standard design.

WHO EMRO
e. Latrines
The following accommodation of e i the r bucket or p i t l a t r i ne compartments should be provided:
1 f o r s t a f f 5 for the f i r s t 100 pupils 3 f o r each succeeding 100 pupils
A l l l a t r ines should be constructed t o standard type as l a i d down i n the Tlrocal Public Health Regulations.
f . Water supply
ShoulU come f r o m pure sourceb. Where zeers (pottery storage jara) are used, arrangements should be made fo r the water t o be drawn off by t ap and f o r the supply t o be capable of being cooled and s t e r i l i z ed where necessary. Zeer houses should be contructed t o standard type.
g. Washing f a c i l i t i e s
Should be provided i n a l l schools.
h. Sisc of playground
2 2 A minimum of 20 f t (1.9 m ) per pupil should be allowed, exclusive of
the area occupied by buildings and absorption beds.
I1 GIRL'S ElXPIENTARY SCHOOLS
Maximum of 30 - 40 pupils per class. Age of pupils 7 - 12 years.
i Number : 4 class-rooms fo r a f u l l school of four classes. and a domestic science room.
A needlework room, which is included i n the standard design, is considered t o be desirable but not essential .

WHO EMRO
ii Floor space : A s i n the case of boys' schools.
iii Dimensions : In order t o conform t o ( i i ) above and a t the same time s a t i s fy educational requirements.
4 class-rooms 7.5 x 5.5 m
N.B. The number of g i r l s i n the 3rd and 4th year classes - very ra re ly reaches even the 30 mark.
i v Cubic space per pupil : A s i n the case of boys ' schools.
v Height of inside walls : A s i n the case of boys' schools.
v i Seating space : AS i n the case of boys' schools.
v i i Black-board : A s i n the case of boys ' schools.
v i i i Window space: A s i n the case of boys' schools.
ix Ventilators : A s i n the case of boys' schools.
x Floors : A s i n the case of boyst schools.
xi Lighting : A s i n the case of boys' schools.
x i i Shelves and cupboards : A s i n the case of boys' schools.
Not required.
c. Verandahs and sunshades
As i n the case of boyst schools.
d. Store-rooms
One is required.
WHO EMRO
e. Latrines
I I
I A s i n the case of boys' schools, except t h a t no addit ional l a t r i ne I is required fo r the s t a f f where l iv ing quarters a re provided fo r the
1 school mistresses on the premises.
f . Water supply
A s i n the case of boys' schools.
g. Washing f a c i l i t i e s
A s i n the case of boys' schools.
h, Size of playground
A s i n the case of boys' schools.
I11 INTERMEDIATE SCHOOLS (and others above t ha t l eve l )
a. The minimum f loor space provided per pupil should be 12 ft2 (1.1 m2).
b. The recommendations s e t f o r t h above regarding elementary schools i n respect of verandahs, sunshades, venti lators, lighting, la t r ines , etc., should likewise apply to schools of a higher grade.
c. G i r l s ' school .*-. -- -.
The Committee considered it t o be most desirable t ha t quarters f o r mistresses on the premises should be provided i n a l l schools.
Boarding schools
i Dormitories : There should be a space of 6 ft (1.8 m) between heads and 3 ft (0.9 m ) between beds t o apply t o pupils of a l l ages. .
ii Washing f a c i l i t i e s : Adequate arrangements must be made, but where
t ap water is available showers should be provided a t a minimum r a t e of 5 per 100 pupils.

WHO mo
4. HEALTH COMENTS IN THE TEXTBOOKS OF THE PRIMARY AM) SECONDARY SCHOOLS IN SOME OF THE COUNTRIES OF THE
EASTERN MEDI'IERRANEAN REGION1
Although the most important role in health educatfon is undoubtedly played by the teacher, yet the school textbook is an indispensable and valuable aid in health teaching. Attention should therefore be paid to the quality of health textbooks.
The textbnok for health should not aim simply at the acquisition of basic ideas and the memorization of some facts, It should aim at foster- ing health habits, changing health behaviour, and helping future citizens to solve their own problems. The information given should correspond to the latest knowledge and be of a high educational and scientific standard.
I CRITERIA FOR HEALTH TEXTBOOKS
The following criteria are proposed for the preparation (or evaluation) of health textbooks.
Health material
1.1 The health material should be accurate.
1.2 It should be adapted to interests and needs of pupils. Needs of each age should be studied before advising the curriculun~ of health for each grade of education and ultimately the textbook.
1 Based on the paper presented and the discussions of the Seminar

1.3 m e health material should be presented and organized so that it will be in the frame of experience of the child and related to local conditions and problems.
-
1.4 The health material should be adapted to the mental capacity of the children for whom it is intended. Particular care should be given to vocabulary and modes of expression used for primary schools, so that difficulties in comprehension are not added to those arising from the knowledge to be assimilated.
1.5 The method of presentation of health material in the textbooks must take in to consideration the ~ c i e n t i f i c methods of education as regards how children acquire knowledge and modify their behaviour. Therefore, it is recommended that eclbcational specialists, public health speoialists and teachers i n charge of classes for corresponding levels of education collaborate in the drafting.
2. Education aids
2.1 Illustrations aid in comprehension and assimilation, especially in textbooks for beginners. Although illustrations tend to increase the cost price, especially when coloured (which is more interesting for young pupils), yet some illustrations are particularly needed to make the text- book more educatio~ally valuable and accepted.
2.2 The health education textbook should preferably give a summary after each lesson or chapter for the points to be stressed in the subject studied; also a series of questions or a list of activities or practical work. All these give an opportunity for discussion and encourage change of ideas.between teachez? and pupils which are greatly needed for change of attitudes and behaviour.
2.3 It is desirable that textbooks point to reference books, pamphlets, guides for teachers or other aids available for f'urther help to teacher and pupils.
3. The textbook itself ----
1 The appearance of the health textbook is important as it has an effect on the mentzl heelth of the pupil, especially at the primary school. Tl?e child's textbook may be the first health book in the home and so its appearance should be appealing, in spite of the extra cost needed.

IrRK) EMRO
3.2 Very careful attention should be paid t o readability of the textbooks. The type-size and c lar i ty are important, especially for text- books of the f i r s t school years. Bigger type-size and wider interspacing are needed for younger pupils, which w i l l gradually decrease t o ordinary printing as they get older. The quality and colour of paper is important for clarity. The binding or cover should also be considered.
I1 STUDY OF HEALTH TEXTBOOKS
Over f i f t y health and science textbooks of ten countries of t h i s Region were studied by the writer.
In a l l these countries the subject of hygiene is studied i n the primary stage of education mostly correlated t o science. In others it is studied under the subjcct of general science.
In the intermediate stage some countries specify curricula for health teaching either separately or correlated with science, while i n others health material studied is considered under other subjects as general science and biology. In one country no health topica that deserve mentioning are studied i n t h i s stage.
I n the secondary stage of education no textbook is provided for health teaching, yet an overall study of the general curriculum reveals various health topics mentioned in the science curriculum and biology.
No information on occupational health was included i n most of the textbooks used i n technical schools.
1, Health material
1.1 The health material conforms t o the scient i f ic facts and ideas i n almost a l l textbooks provided, A few items i n some textbooks are not quite i n accordance with recent knowledge of public health.
A few of the important health facts and behaviour i n some items are not mentioned or mentioned without the necessary stress, while there are a few facts mentioned which are not needed for the special age of children.
1.2 The method of presentation of the health materlal Itself is, as such, suitable,

WHO Em0
Some chapters in many of the textbooks are perfectly presented to satisfy both scientific health ideas, as well as the recent development of educational methods. Some of the textbooks present the knowledge and behaviour expected as a story or in disucssions which are interesting and attractive for young children. Sometimes, however, the material presented could be put in a more practical way.
1.3 Although the material presented in most textbooks, is suitable to the age comprehension of pupils to whom it is intended, occasiowlly it is found to be somewhat complicated or difficult to understand.
2. Material presented
The material presented in the tevtbooks could be considered relevant to the needs of the children f o r whom it is prepared. With rare exoept- ions it is related to the problems of the local environment. Yet how far it fulfils the needs and aids in solving the local problems could not be ascertained without studying all curricula and textbooks of every stage of education in continuity,
Tlze print-size and interspacing used in most books are suitable and conform to the age o f the nhjldren. Most textbooks intended for young children and some for older children have big type-size and wide inter- spacing which made them clearer and more attractive. In one textbook, however, the ink has blotted to the back pages makjng it difficult to read.
There are -y explanatory figures in almost all textbooks making them more valuable and impressive. Some figures need correction, as they are not easily understood.
Questions are given at the end of each chapter in some textbooks; this is very useful, Only three textbooks for teachers' schools are pro- vided; curricula textbooks of teacherst schools need special study.
4. A n overall evaluation -- The contents in health books, with very few exceptions, are accurate.
The methods of presentation and educational aids in most textbooks are suitable. Yet revision is greatly needed every few years to meet the latest scientific developments i n both health material and eduoational methods.

IEXXARCH IN SCHOOL HEALTH EDUCATION AND THE TEACHWS' ROLE?
School health education present a very challenging and rewarding f ie ld for research i n the countries of the Eastern Mediterranean Region where :
1. over 17 million of the population attend schoolj
2. there is an almost geometrical progression of enrolment i n primary schools i n a number of countries of the Region; and
3. the stage of transit ion is very rapid, bringing with it changes i n problems, needs and values.
Education is the pocess; health, the content; and school the dimension. The combination of these three essentials, coupled with the fact tha t the ultimate goal is the impact upon the behaviour maintenance o r change; not only of a single child but of all children, the soclety and the comnunity; makes the challenge multiphasic indeed! Meeting t h i s challenge, which for want of a more descriptive word may be called *sucial engineeri- i n the f i e ld of health", is not ~umething that can be done solely by a weekly lecture on health.
It is therefore, timely that some of the premises upon which a great number of school health education ac t iv i t ies are based should be carefully scrutinized.
1 Based on the paper presented and the discussions of the Seminar

WHO m o
There are a number of premises needing scrutiny depending on the country and the situation. Two m e cited below as examples:
1. Health is taught in schools so that a child is:
a. prepared for healthy living at present3
b. prepared to make correct decisions on health matters when he becomes an adult.
This premise pre-supposes:
i the child's freedom of choice in selection of healthful habits, in spite of his possibly uneducated parents;
ii 'availability of facilities in the community f& ,
implementation of desirable practice;
iii a retention factor of several years from the time .
the child is taught to the time that he has established his own home.
. - -. - - - - .- These pre-supp6ditions may or may not be true, or may only '&&ally
be true. Thus, should not the school be more linked with the heel, and should not school health education be part of community health education?
- ,
- - 2. The attention to health education in many of the'prbary schools
of the Regi0n.i~ occasional, if not incidental. Usually, no special course or text exists for this subject whereas there &e special courses and texts in secondary schools2. This practice has been transplanted
.I.
Salman, M.H., Link between School and Home in Health Education, 1966 (EM/SEM.SCH.HLTH.ED'C@./~~).
Sweilim, S., Health contents in the Textbooks of the Primary and Secondary Schools in some of the Countries of the Eastern Mediter- ranean Region, 1966, (WSEM. SCH. HLTH,EDUC./13)

WHO EMRO
from western cultures. Considering the drastic drop-out of students between primary and secondary schools (school enrolment for six y e u s of primary school education i n the Region i n 1960-1961 was 13 163 450 and for s ix years of secondary school education in the same period 2 853 305 ):
1. Should there be more emphasis on health i n primary schools i n the form of special courses?
2. Are children of 6 - 12 years of age capable of understanding technical health topics?
3. If so, how should they be taught? and
4. Are the teachers prepared f o r the task?
The above are two of many fundamental questions inviting thoughtful consideration. They are stated as a basis for discussion and' solutions suggested m e by no means conclusive. There are many other si tuations with or without the same degree of importance each of which needing a special design and special s k i l l for research.
It should not be construed, however, that i n the f i e ld of school heal%h educatiorl every research design by nature is a complex one needing a team of health specialists, behavioural science workers and stat is t ic ians. Much can also be done by a single teacher with sharp eyes, keen desire and searching mind.
If health records are kept f o r each child with the assistance of school health personnel and if these records are cumulative and the teacher records his observations on each child, a very sound basis for group and individual teaching is prepared; for "what a mother might think of is af l i t t l e importance because it happened several times before without disaster t o her par t icular child, ... the teacher thinks of i n relat ion
1 . . Introduction to the Seminar on School Health Education, 1966,
(~SEM.SCH.HLTH.EDUC./~).

WHO EMFlO
to all children in her care, . .. (and therefore) sees as a deviation from the expected behaviour or learning activity of a group of children of approximately the same age1*,
No matter what other techniques are used, the value of observation and recording should never be ignored. Observation is a foundation upon which much of the research is based. I%ny epidemics probably have been prevented through careful observation and reporting, "An interested and observant teacher can be of tremendous aid to parents and school health specialists in helping them understand needs of a child. As a trained observer who spends a great deal of time with the children, the teacher can be alert to the subtlechange of appearance or behaviour which may herald the onset of disease. Certain specific procedures when carried out by the teacher in the schools add immeasur- ably to the originality of the health programme in the school. The fundamental method is a continuous observation and not just an inspection at a particular moment2".
On simple marginal punch cards, teachers can punch various observ- ations and at any time sort out f'requencies of each deviation f'rom the established pattern as a basis for teaching.
Fortunately, even though in almost all countries of the Region curricula and syllabi are approved centrally, as evidenced by reports of tlw Governments teachers have some degree of freedom in introducing topics of local and general importance. Therefore, the leadership in teaching pertinent health' problems rests with the teacher whether he does it by hlmsell or invites the specialist Tor the purpose.
Research in a field such as school health education with all its ramifications is a needed one. Many of the premises need questioning. Technological developments change needs and values and this change may necessitate examining previous approaches and old premises.
1 Wheatley, G.M., What Teacher Sees, Metropolitan Wfe Insurance Co., p.2.
2 World Health Organization Expert Committee on School Health Services. Report on the First Session: Geneva, 1951 (world Health Organization Technical Report Series No. 30)

WHO -0
This should be the path of scient i f ic thought. ELusctions change and with the change of f'unctions forms should follow without the bias of our prejudice or personal preference, f o r "science is but a method; an observation accurately made and f'ree of compromise t o bias of desire, and undderred by consequence, is sciencelft.
d
1 Zinser, H., Atlantic Monthlx, July 1929

WHO m o EM/HEP/28 page 101
EXAMPLES 03 SObE SPECIFIC PROGRAMMES IN THE REGION
. .
UNESCO wishes t o express i ts appreciation of the e f for t s of the Government of Kuwait and the World Health Organization t o promote school health ac t i v i t i e s b-y organizing t h i s Seminar on School Health Education. It welcomes the opportunity t o acquaint the part icipants i n the Seminar with some of i ts ac t i v i t i e s i n teacher t ra ining and curriculum deve lop ment. Such ac t i v i t i e s consti tute one of the channels fo r putting in to practice the recommendations on health education t o be adopted during t h i s Seminar. UNESCO proposes t o transmit these recommendations t o a l l its off icers concerned, in one wzy or another, with health education i n the schools.
The two main types of teacher t ra ining ac t i v i t i e s aided by UNESCO are directed towards:
a. the t ra ining of secondary teachers i n ins t i tu t ions financed- with assistance from the United Nations Special Fund and
b. the t ra ining of primary school teachers with assistance of the United Nations children's Fund (UNICEF).
In the two f i e ld s under consideration, namely, teacher t ra ining and curriculum development, UNESCO provides technical guidance and the services of experts.
1 Abstract nf t.he paper p~epared f o r the seminar by the UNESCO Secretariat

EM/HEP/~~ page 102
WHO EMRO
Special importance is attached t o the in-service t ra in ing of primary and secondary school teachers. A lasge nwnber of practising teachers, many of whom have received inadequate training, can be reached t-qh intensive refresher courses, These courses have proved a most e f f i c ien t and effect ive means of transmitting information on health and hygiene and so of ra is ing the standard of health education i n schools.
In addition t o its e f fo r t s i n national set t ings, UNESCO has ass i s t ed i n the establishment of a "~eg iona l Training Centre of Senior Educational Personnel in the Arab States'' i n Beirut and a "Regional School Building Centre f o r ~ f k i c a " i n Khartoum. Both of these Centres have a c t i v i t i e s which are indirect ly re la ted t o the subject of health education. In part icular the l a t t e r centre is concerned i n t e r alia with the environmental health of the school, and the former with the general problems of curriculum planning, including health education, and the provision of a l l types of school services, including school health services.
A br ief r6sutn6 of UNESCO a c t i v i t i e s i n Member Sta tes invited t o par t ic ipate i n this Seminar is given below:
ADEN
A project f o r improving r u r a l primary education and teacher t ra in ing aided by UNICEF and UNESCO has been I n operatlon slnce 1964. The project
consists of in-service t ra in ing fo r untrained primary teachers and the pre- service t ra in ing of teachers, including the t ra in ing of women teachers. UNESCO wi l l probadly LC y20Vidlng an expert In vrornerlls Leac1ie1- training.
Instructors from the Ministries both of Education and Hea1tl-i-are pro- . ,- -
vided with in-service training. Die training of women teachers includes teaching of hygiene, chi ld care, cooking and sewing, i n addit ion t o the usual academic subjects.
CYPRUS
No relevant ac t iv i t i e s .
A three-year teacher-training project a ss i s t ed by UNICEF and UNESCO began operations in 19@+. Existing teacher t ra in ing i n s t i t u t e s have been

WHO EMRO
strengthened, a new i m x i t u t e established and summer courses arranged f o r teachers i n service. UNESCO has provided the services of an adviser on primary teacher t ra in ing,
There is a lso a p i m fo r ass i s t ing the t ra in in& of secondary school teachers i n the Faculty of Education of the m i l e Selassie I University by the UN Special FQ-J m d U ' S C O , Tri? cou.se of study is of the usual type with some empliasis on i n s i ruc t i o l i n tl72 teaching of English, and the sciences (chemistry, biology and physics). The planned annual out- put a t the end o-i' t x f i f t h year of the p-oject is 120 teachers, men and women, f o r employment i n the higher grades of the secondary schools and 122 teachers f o r employment i n the junior grades of the secondary schools.
IRAN
The Army of Knowledge was created by H i s Imperial Majesty The Shah t o bring elementary education t o the vil lages. Young men who have completed secondary education take a four-month course of mi l i tary and teacher t ra in ing i n l i e u of mi l i tary service, and spend the following fourteen months i n the vil lages. Their work consists of regulas school teaching and community education, including l i t e r acy and adult education.
Since qualif ied supervisors and teacher educators f o r these new teachers a re badly needed, a course fo r 200 men selectecl from among the former sergeant teachers who had successfully completed t h e i r v i l lage work was begun i n January 1965, organized by the National Teacher Training College. UlESCd U ~ Y ~ G I U L ~ jo int ly ~ ~ a i ; l - , i i & the Government of Iran i n organizing t h i s t ra in ing course. Training of the supervisors lasts one academic year. In 1965 the courses were ass is ted by four UNESCO experts recrui ted under the Expanded Programme of Technical Assitance. F'ield practice takes place i n about twenty vi l lages under the supervision of the UNESCO experts. After the f i r s t year of t ra in ing the f i f t y most
. successfLiL students are allowed t o continue f o r three addit ional years of study at the NatLonal Training College leading t o a B.A. i n Ehcat ion.
The work of the UNESCO experts is expected t o continue through 1966.
In connection with the establishment of compulsory primary education and sh i f t ing emphasis t o a more pract ica l primary school curriculum with inorcased trdnine; i n health educatinn and s r i ~ n n e , TJN-rCRP and UNESCO are
E M / H E P / ~ ~ page 104
WHO EMRO
cooperating i n a two-year project u n t i l the end of 1967. The plan includes provision for in-service t ra in ing of teachers and the extension of pre-service teacher training. Both the urban and rural programmes of
I I
primary teachers' education emphasize pract ica l t ra in ing i n science,
I health and hygiene. Tne services of an expert i n teacher t r a in ing have been provided since 19a, and an addit ional expert i n the f i e l d of women's teacher t ra in ing is t o be provided i n 1966.
JORDAN
A project t o improve the levels of nu t r i t ion and home economics i n r u r a l areas by strengthening t ra in ing i n women's teacher t ra in ing centres has been undertaken with the assistance of UNICEF, The Government estab- l ished a rural teacher t ra in ing college fo r women, providing a two-year course with speclal emphasls on nu t r i t ion and child care and appropriate teaching methods. UNESCO has been consulted on the setting-up of the project, but has not ac t ively part icipated i n its operation.
Between 1960 and 1965 UNESCO provided Jordan with two experts: one i n r u r a l teacher t ra in ing and one i n educational psychology. A t present two UNESCO experts, one i n curriculum development and one i n textbook production, are working together on the revision of the curricula of the primary and secondary schools. There is no doubt t ha t health education w i l l come up in thc comes of the diocuosions regarding the revision of general science curricula f o r primary schools.
I KUWAIT
UNESCO assistance i n the f i e l d of education has consisted mainly of the provision n f short-term consultant services, A recent four-month mission of an expert i n the f i l e d of teacher t ra in ing w a s undertaken i n connection with plans fo r establishing t ra in ing fo r teachers in-service. The assistance of an adviser on the planning of education has been provid- ed since 1964. UNESCO w i l l a lso p~ovide the services of two consultants: one i n eciucational guidance and the other i n ext ra curricular a c t i v i t i e s .
A jo in t WCEF/UNESCO in-service t ra in ing project was i n operation f'rom 1962 t o 1964, Its main or ienta t ion was toward accelerated t ra in ing t o meet the country's need fo r qualif ied teachers i n primary and complement- ary schools. Two UNESCO teacher t ra in ing experts cooperated i n the work

WHO Em0
undertaken for the project, but have now finished the i r period of service. It is now foreseen that a further phase of the project w i l l be implemented i n 1966. Special emphasis w i l l be given t o the improvement of nutri t ion and home economics i n the teacher training curricalm, particularly oriented towards the practical needs of rural schools. One of the UNESCO experts i n teacher training w i l l return t o ass i s t i n the project,
A t present discussions are taking place for assistance of the UN Special Fund and UNESCO i n the development of a higher college for teacher training i n Tripoli. The college, which began operating la te i n 1965 i n temporary quarters, w i l l t r a i n teachers for Libyan intermediate and second- e y schools as well as instnlctors for primary teacher training institutions. There w i l l be an annual intake of about 120 trainees per year for a four- year course. The training,course is of the standard type with emphasis on the usual scient i f ic and a r t s disciplines. There is, however, an option for students t o study domestic science i n which undoubtedly a large part will be given to nutri t ional studies.
A joint UNICEF/UNESCO project i n 1963 - 1964 concentrated on improv- ing the training of rural primary schoolteachers i n Adult Education Centres. One of the aims of the project was the improvement of the teaching of general science anu hygiene i n the rura l primary schools. There was also tYle traln- ing of women teachers i n home economics and child care. The success of the project resulted i n its expat ion and continuation unt i l June 1966. The expanded project incluaes greater emphasis on primary school Sclence and hygiene, A t present a new project t o pay special attention t o the training of g i r l s i n home economics, hygiene and nutrition, is being studied for operation i n 1966 - 1968.
PAKISTAN
Since the publication of the Educakion Commission Report i n 1959, particular importance has been attached to teacher training and curriculum revision i n Fakistan, New curricula and syllabuses were introduced for primary and secondary schools i n 1961. The primary school curriculum has been reorientated t o make it less academic and more practical.
UNESCO's help, i n cooperation with UNICEF, is mainly concentrated on secondary education. A survey of secondary education was carried out i n

WHO EMRO
1963 by a UNESCO consultant, with the f inancia l assistance of UNICEF, t o study part ioularly the s i tua t ion i n the f i e l d of science teaching. After considering the report of the consultant, the Government requested the a i d of W S C O and UlbTCEF i n the improvement of secondary science teaching i n both East and West Pakistan.
I I The jo int UNESCO/UNICEF project on secondary science teaching s t a r t ed
i n 1965, and aims a t preparing stzdents be t t e r f o r the needs of a modern economy by introducing in to secondary schools d ivers i f ied e lect ive courses such a s woodwork, metalwork, applied e lec t r i c i ty , agriculture, commerce and home economics.
The t ra in ing of secondary school teachers i s t o be strengthened by the provision of teacher equipment t ra in ing k i t s and of equipment t o schools i n East and West Pakistan. The equlpment is being providlecl Dy UNICEF. The Government is appointing a science teaching supervisory team of f i ve super- visors i n each province t o v i s i t schools renefving tlae new equipment. UNESCO is providing, under the Expanded Programme of Technical Assistance, two experts t o work with the teams i n East and West Pakistan.
QPm
No programmes concerning teacher t ra in ing or curriculum development art: in opcratiun. Huwever , an educational planning expert ha& oubmittcd a report ( i n November 1965) containing some recommendations with relevance t o health education. The recommendations mainly concern the organization of the School I I e a l t h Depbrtment i n thc t t inistry of Education and of the school meals service, but he a lso suggests t ha t lessons i n the elementary school i n the Arabic language be used t o impart a s much useful. information m possiblc i n general sciences, hygiene and i n social sriences,
SAUDI ARABIA
A plan t o es tabl ish a four-year teacher t r a in ing college with ass i s t - ance from the UN Special F'und is now under study. The college is t o t r a i n teachers fo r secondmy schools and ins t ructors f o r primary teacher t r a in ing ins t i tu t ions , with p r io r i ty t o be given t o t ra in ing teachers of science, mathematics and modern languages, It is haped t ha t the first intake of students w i l l be enrolled before the end of the year 1966. When the college operates a t f u l l capacity it w i l l have some 480 student enrolment and w i l l graduate some 120 secondary school teachers per year.

WHO EMRO
UNESCO is providing Saudi Arabia w i t h an expert i n primary teacher training curricula which are being revised and upgraded.
SOMALIA
A project concernirr the expansion of primary education and the improvement of teacher t ra ining has been i n operation since 1964 with the assistance of UNICEF, W S C O and FAO. Emphasis i s placed on the provision of fully t rained teachers by means of evening and vacation courses fo r un- trained teachers and the expansion of exist ing t ra ining centres, Rural science has been introduced into the curriculum of the teacher t ra ining programme i n order t o develop the teaching of pract ical aspects of nutri- t i on and health education. The plan also pays part icular a t tent ion t o the education of g i r l s and women i n such subjects a s nutrition, hygiene, child care, home management, etc.
The services of a number of experts working closely with t h i s project have been provided by UNESCO: four i n teacher training; one i n r u r a l science.
SUDAN
A combined UNESCO/UMCEF project i n the f i e l d of primary teacher training has been ln operation since 1964. The ubject was to t r a in about
1 000 underqualified teachers of junior elementary schools and vi l lage schools each summer vacation (April t o ~ u n e ) a t various teacher t ra ining institutions. A praposal Lo revise the project was made in 1365 so as to include home economics courses fo r elementary and intermediate teachers in g i r l s ' schools. This proposal is yet t o be examined by the UNICEF Board. A Joint FAO/UNICEF project in the field of nutrition education includes the in-service t ra ining of domestic science teachers.
A t ra ining i n s t i t u t e fop secondary school teachers has been i n operation since 1962, ass is ted by the UN Special Fund and UNESCO. The course of study l a s t s four years and gtves emphasis t o science. About 120 students are t o be gradwt;ed annually fo r service i n secondary'schools, In addition short t ra ining courses fo r teachers in-service are provided for.
SYRIA
No relevant ac t iv i t i es ,

E M / H E P / ~ ~ page 108
WHO EMRO
TUNISIA
A secondary school teacher training institute i n Tunis has been enlarged with the assistance of the UN Special Fund and UNESCO. The in s t i t u t e t r a in s students i n three sections; general studies (including language studies and science); industr ia l studies; and commercial studies. (The commercial studies section receives no Special Fund assist- ance). A "second-cycle" course fo r t ra ining teachers of the upper second- ary school classes is being gradually introduced with the main purpose of providing applied science teachers t o upper secondary technical courses.
A UNICEF project in which UNESCO has participated has been in opera- t ion since 1963 t o improve the pract ical content of the primary school curriculum. The plan includes the t ra ining of primary school teachers in a certain number of practiostl subjects, including child care and home economics at the Normal School fo r Women of Montfleury. Men's primary teacher t ra ining curricula have, under t h i s project, been adapted i n three regions - urban, ru r a l and coastal - t o the needs of the respective en- vironments. Class-room teaching aids have a lso been developed fo r the teaching of science.
There has also been a nutr i t ion programme fo r mothers and children ass is ted by UNICEF, WHO and FA0 i n which UNESCO has cooperated principally in providing the services of an expert i n audio-visual teaching aids. The project was l a t e r transformed into a p i lo t project fo r the coordination and development of health, socia l and educational programmes i n urban areas. Another project fo r r u r a l areas i n under consideration.
UNITED ARAB REPIBLIC
A UNICEF-aided project i n the f i e l d of health education was under- taken in 1965. UNESCO has acted i n an advisory ro le i n connection with the project, but is taking no active part. The plan is t o provide in- service t ra ining courses t o instructors of teacher t ra ining i n s t i t u t e s and inspectors concerning health education. The syllabus covers such topics
. as environmental health, physical and mental health of students, nutri t ion, the organization of school health services. The project is t o last four years, f r o m 1965 t o 1969. I n the second phase of the programme, in- service training courses w i l l be organized for primary school teachers.
WHO Ern0
YEMEN
A joint UNICEF~UNESCO project covering pre-service and in-service t ra ining of elementary school teachers was expended i n l a t e 1965 t o cover pre-service teacher t ra ining and the t ra ining of g i r l s i n home economics.
The in-service t ra ining of teachers i n evening and holiday classes w i l l be continued through 1966. In addition, a f i r s t group of teacher t ra iners a re enrolled i n three teacher t ra ining i n s t i t u t e s f o r the school year 1965/66. The beginning classes w i l l be composed of about t h r i t y students i n caoh i n s t i t u t e i n addition t o f i f t e en students enrolled i n a primary teacher t ra ining c lass fo r g i r l s , making a t o t a l of about 100 students i n all. The i n s t i t u t e s wi l l offer a three-year course. UNESCO provides under the Expanded Programme of Technical Assistance, two teacher t ra ining experts, one of whom has science teaching background. The science teaching programme i n the teacher t ra ining i n s t i t u t e s covers some health education. The syllabus of the in-service t ra ining programme includes a u n i t cal led lfgeneral science and health education and t h e i r teaching methods".
A f i r s t attempt t o introduce home economics t ra ining in to the curri- culuin w i l l be made a t the three exist ing schools fo r g i r l s i n Sana'a, Taiz and Hodeida. The programme w i l l include home-cookery, dress-making, sewing, home-management, hygiene and chi ld care and w i l l be taught i n elght classes, a t the f i f t h and s ix th grades of elementary schools and i n the f i r s t and second grades of preparatory schools, for t w ~ lessons per week. bout 960 g i r l s i i r - G L L ~ . three schools w i l l receive this instruction. III
addition, in each of the three schools, home economics classes w i l l be taught t o groups of about t h i r t y women during four afternoons per week. The programme w i l l be similar t o t ha t taught t o the school g l r l s , anit will s t r e s s personal and environmental hygiene, nu t r i t ion and chi ld care.
The en t i re project is conducted under the responsibil i ty of the Government with the technical advice of TJNESCO and the material assistance of UNICEF. FA0 provides advice and guidance i n the technical aspects of the home economics programme.
Finally, reference should a lso be made t o the educational programme of UNBWA. UNESCO cooperates with UNRWA i n the administration and planning of

E M / H E P / ~ ~ page 110
WHO EMRO
t h i s programme and assumes responsibil i ty fo r i ts technical guidance. The services of nineteen UNESCO s t a f f members are made available fo r the purposes of t h i s work. These s t a f f members include the Director of the educational programme, and the principal s t a f f of the UNRWA/UNESCO Ins t i t u t e of Education, located i n Beirut. The Ins t i tu te has an active in-service t ra ining programme.
Up t o 1964 the loments Teacher Training Centre i n Rarnallah ( ~ o r d a n ) provided a three-year post-preparatory course. Since the 1964/65 school year the course was changed t o a two-year post-secondary course with an annual intake of 100 students. This Centre is p a r t of the combined women's Teacher Training/Vocational Training Centre i n Ramallah. On the vocational t ra ining side a variety of courses such as dress-making, needlework, hair- dressing, secretar ia l , infant-care, re-nursiw and home economics have been offered. Eighty-eight g i r l s graduated i n 1964, the f i r s t year of operation of the Centre. The Centre w i l l t r a i n 200 students i n the teacher t ra ining branch and 350 i n the vocational training courses during the current academic year.

WHO EMRO E M / H E P / ~ ~ page 111
'E~C3.Lt iS ' PiiEPARATION IN HEALTH EDUCATION AN EXFERIPEBJT IN m-i UNITED ARAB REPUBLIC^
The primary school teacher i s considered the best person t o contribute s ignif icant ly t o the health of school children. He is most f i t t e d t o create "health consciousness" in his puplls. H i s heal th knowledge, be- haviour, in te res t and enthusiasm, i. e. leadership, a re indispensable f o r the healthful up-bringing of h i s pupils. Therefore, proper preparation of p r i m a r y school tcachero f o r health ducali ion meets increasing in te res t i n %he United Arab Republic,
Many attempts have been made t o up-grade the teaching of health i n primary schools. The syllabus of health ins t ruct ion i n teachers t ra in ing ins t i tu t ions was repeatedly revised t o f u l f i l the requirements of pros- pective teachers i n the f i e l d of school health and-health education.
A new textbook was recently published according t o the revised syllabus. Yet it is observed that, the teachers of health i n teachers training insti- tu t ions and health inspectors need fur ther char i f ica t ion and specia l t ra in- ing i n order t o be more e f f i c ien t and pract ica l i n the preparation of more in teres ted and understanding primary school teaohers.
- .
Teachers already a t work i n primary schools a l so need more i n t e r e s t and suf f i c ien t understanding as regards t he i r active role i n hcalth protec- t i o n and promotion of t h e i r pupils, especial ly as regards heal th education.
1 Based on the paper presented and the discussions of the Seminar

EM/HEP/~~ page 112
WHO EMRO
Many in-service t ra in ing courses, seminars and conferences were held fo r teachers of primary schools both a t the national and regional levels; a lso a few attempts were made t o t r a i n i n the f i e l d of health education teachers of teacher t ra in ing ins t i tu t ions . Some of the courses f o r primary school teachers were held specia l ly on school health and health education; i n other courses, health was considered an item of the general t ra in ing planned fo r class-room teachers and few in this t ra in ing had a planned follow-up. Yet no organized general plan t o include a l l teachers of primary schools i n the Republic (whether student teachers or teachers already a t work) was previously implemented.
I n t h i s a r t i c l e an organized project t o upgrade heal th education i n primary schools i n the United Arab Republic is presented, This project was planned and conducted by both Ministries of Education and Public Health with the technical advice of WHO and the material assistance of UNICEF.
The proJect was planned with the following objectives:
1. Long-term objectives
To improve the qual i ty and quantity of health education made available f o r school children, and t o prepare them f o r assuming t h e i r ac t ive ro l e i n the promotion of health i n the c o m i t y , and eventually t o r a i s e the standard o r healtn o r the community.
2. Immediate objectives
To provide teachers with suff ic ient i n t e r e s t and c lear understanding of t h e i r functions i n the improvement of heal th of primary school children by:
a. improved health education as regar& health material, methods and means of how children change behaviour and acquire health habits ;
b. be t t e r understanding of simple heal th measures as regards school health a c t i v i t i e s and environmental problems and t h e i r role, as re la ted t o them;
c. be t t e r cooperation between school personnel, health personnel and parents f o r the benefit of t h e i r children.

WHO m o
The plan is t o give proper and adequate training i n health, school health and health education, for one and a half months "Phase A", t o teachers and responsible personnel for preparation and guidance of primary school teachers.
These trained leaders w i l l be responsible, i n cooperation with regional health personnel, for organizing simple training courses locally for head masters, head mistresses and teachers of a l l primary schools i n the i r governorates, "Phase 3". It is planned that i n five years all teachers working i n primary schools w i l l have had in-service training i n health education, while a t the same time more adequate preparation of new teachers by the trained teac'hers w i l l be going on.
The leaders i n "Phase A" were selected t o be:
1. From the teaching s taff of teachers training i n s t i t ~ t ~ s :
a. inspectors and senior teachers of science and hygiene (80);
b. teachers of school health and health education (311);
c. teachers of physical education (175).
A s health education and physical education have some common ultimate objectives, so interest and understanding of these teachers w i l l strengthen health education act ivi t ies .
d. teachers of psychology and education (186).
These teachers were selected on tne assumption that they would help the project by the application of methods and means of education they teach t o health education; in addition, for correlation i n the psychology syllabus . 2. From the primary schools ' administrat3m:
1 a. General inspectors of primary schools (328), as the i r confidence and interest are strongly needed both for encouragement and
1 These inspectors are responsible for supervision and guidance of a l l educational a c t i v i t i e ~ i n primary school8 in their domaln ;LncluBlng health education.

EM/HEp/28 page 114
WHO EMRO
guidance of health education ac t iv i t i e s , and contribution i n planning and execution of regional t ra in ing courses f o r primary school teachers;
b. inspeotors of s ience and hygiene of f i f t h and s i x th grades of E primary schools .
The f i r s t "phase A" course w a s held i n the summer of 1965 fo r six weeks i n the H i g h I n s t i t u t e of Pdblic Health, Alexandria. A Joint Advisory Board w a s formed of representatives of the Ministries of Education and Public Health and the Nutrition Ins t i tu te . This Board was responsible f o r the overall planning of the project. An Executive Committee of f i ve members was formed from members of the Advisory Board t o execute and follow up the training progrcwnmc and also t o give due consjderation t o evaluation of the project.
~ i ~ h t ~ - t w o ' teachers and inspectors (according t o the afore-mentioned selection) from the di f ferent governorates of the Republic attended the course. Training was i n the form of lec tures fo r a l l part icipants. In the seminars, workshops and f i e l d v i s i t s , they were divided in to four groups; each group was guided by two consultants, often one from the teaching staff and the other f r o m +,he health s t a f f . A discussion guide was prepared and dis t r ibuted daily.
HealLh educa t iu l i a ids in forms of films, elides, pamphlets and posters were selected and presented during or just a f t e r the lectures. A l l lec- tu res (except four) were typed and dis t r ibuted i n time.
Recommendations were made by each group fo r each topic discussed, ?&en recommendations of the four groups were collected and reviewed by a committee of members from the Executive Committee and the groups.
1 The f i r s t four grades have class-room teachers.
2 127 w e r e selected but, owing t o delayed f inal approval of the project, some of the selected personnel were attached t o other t ra in ing courses; a lso the Conference of the Arab Teachers of Science was being held a t the same time.

WHO m o
A committee of members of the teaching staff, Executive Committee and participants was formed to rearrange the final recommendations at the end of the course. These recommendations were very helpful in exposing needs, local problems, difficulties and facilities for solution, as seen by ex- perienced workers, in the different environmental conditions; they were discussed with the consultants.
The topics studied broadly were1:
1. Lectures
1.1 Environmental health
1.2 Physical and emotional. health including:
a. growth and development;
b. personal and community health.
1 . Nutrition
1.4 Health services, school health services and related public health services
1.5 Health education
These were presented and aiscussed in 84 hours of lectures and an 82-hour seminar.
2. Workshops (2G hours) in the following:
a. Mrst aid
b. The comprehensive physical examinations
c. Health education audio-visual aids
3. Field trips (24 hours) - related health, educationand social services, were visited,
1 See "course Content for In-service Training in Health ducat ion", p. 118 - 120 of this Report.

EM/HEP/~~ page 116
WHO EMRO
Follow-up is planned t o be made by the Executive Committee, or its representatives, i n the f ield, so as t o observe the application of t h i s in-service training i n day-to-day ac t i v i t i e s of trained teachers and inspectors (leaders ),
To evaluate t h i s t ra ining course and improve the teaching i n subsequent courses, a follow-up t ra ining course of one week's duration is planned t o be held a f t e r one year of f i e l d ac t i v i t y f o r a l l part icipants of this course. This w i l l be an opportunity f o r presentation and discussion of ac t iv i t i es , d i f f i cu l t i e s met and exchange of experiences. It w i l l give some idea a s t o the effectiveness of the teaching and its appl icabi l i ty i n the f ie ld . Participants can receive further training and experience i n areas requiring more cia-ification.
EVALUATION
The following were considered i n the evaluation of the first course:
1. Attendance: Participants a t f i r s t thoughtthat the period of the course was too long; but a f t e r a few days, almost a l l of them were quite interested and enthusiastic. Almost a l l were active i n discussions, and t h e teaching clarified many of their -blwu@its ant3 experlences. A l l part icipants attended regularly except for ra re obligatory causes.
2, Appraisal was m a d c of the extent uf Lhe participants ' comprehension of the courses by the consultants i n the seminars.
3. Twenty-six nf the p a r t i a i p m t s presented papers about health problems i n t h e i r environment and sometimes t h e i r opinions fo r solution.
These were arranged by a consultant of the Ekecutive Committee and submitted fo r discussion by a l l a f t e r the lectures o r i n the sub-groups.
4. Twelve topics were chosen from the di f ferent subjects studied, and provided for research so that -each participant could write an a r t i c l e on the subject of his interest. and experience. The l ib ra ry of the High Ins t i tu te of Public Health was used fo r reference, i n additiofi t o book& upp plied f r o m the Ministry of Public Health. These papers were corrected by the spec ia l i s t s and most were excellent.

WHO m o
5. Three questionnaires were prepared and f i l l e d in: . -
? . . . - .
5.1 The f i r s t was considered a Bas= 'qr;restionnaire, t o have an
- - - - idea about the i ~ t e r e s t and a c t i v i t i e s of part icipants i n school health and health education before the course.
5.2 The second w a s put t o know the opinion of part icipants about the course i t s e l f .
5.3 The t h i rd was a questionnaire t o know the opinion of the lectubers and consultants about the t ra in ing course.
Many of the questionnaire r e su l t s pointed t o the need of more' consider- a t ion t o the pract ica l side, especial ly i n f i r s t a id 'and f i e l d applications. This w i l l be considered i n future courses.
Each of the following four years w i l l have two similar courses for leaders, Trainees of the f i r s t course, a f t e r t h e i r week's follow-up course, w i l l , i n cooperation and with the assistance of loca l health personnel, plan and develop loca l t ra in ing courses f o r a l l primary schoolteachers.
Kamel, W.H., Directions i n Training of Teachers of Primary Schools, 1965 Documentation and Fese-rck Centre f o r Education, Cairo, UAR ( i n Arabic).
Karnel, W.H., School health Education i n the United Arab Republic, 1961 Thesis f o r D.P.H. Degree, High I n s t i t u t e of Public Health, Alexandria, UAR.
UNICEF Project of Up-grading Health Education Teaching i n the Primary Schools of the United Arab Republic. Plan of Operation. Cairo, 1964.

EM/HEp/28 page 118
Course Content for In-Service Training in Health Education
WHO EMRO
Lecture Seminar Workshop hours - hours - hours -
I EMTIRONPENTAL HEALTH 12 12 - 1. School building and premises, including hand-washing and toilet facilities, class- room arrangement, lighting and ventilation, heating, kitchen sanitation, school canteen and dining hall, etc.
2. Water supply, resources and use
3. Refuse and,sewage disposal
4, . Harmful insects and rodents, means of control and eradication
5. Safety and safety measures
I1 PmSICAL AND EMOTIONAL IIlWX'H OF THE s m N T
A; Growth and development
1. Growth and development of the child and its health education implications:
Physical Mental Social Emotional
2. Problems of handicapped children and their health, education implications (including hearing, vision, physical defects mental deficiencies speech defect and emotional deviations)

WHO EMRO E M / H E Y / ~ ~ page 119
Lecture Seminar Workshop hours - hours
7 hours -
3 . Rehabilitation
4. Recreation and i ts value i n socia l growth and development
B. Personal health and community health
1. Personal cleanliness, and its implication i n male an& female students, including persorial health and grooming
2. Communicable diseases - principles and general control measures with a t tent ion to important communicable diseases in the country.
3. Dental health
4. Mental health
5. other topics of importance
6. Nutrition: Food and i ts re la t ion t o public health Food contamination and poisoning Health conditions i n places fo r pre- paration, storage and consumption of food The school feeding regulations fo r persons engaged i n food Nutrition educationand ro l e of schools
I11 HEALTH SERVICES
1. Organization and functions of the Ministry of Public Health:
School Health Service Department Health Education Section Voluntary health services i n the United Arab Republic, such a s Red Crescent, etc.
2. Health Services i n the School periodic comprehensive medical examination;

EM/HEP/~~
page 120 WHO EMRO
Lecture Seminar . Workshop hours - hours hours -
Role of the teacher i n comprehensive medical examinations
3. Health of the teacher and schooi personnel
4. First a id
N HEALTH EDUCATION
1. Philosophy and purpose
2. School health education as par t of education community health
3. Health problems i n school and community
4. Habits, culture and customs
5. School day, health procedures
6. Role of teachers i n observation and screening
7. Cooperation between home, school and community
8. Correlation of health w i t h other topics
9. Health i n various grade levels; c r i t e r i a f o r determining topics
10. Pract ica l application i n prevention of infectious diseases
11. Health education and audio-visual aids

WHO EMRO EM/HE;P/~~ page 121
HEALTH EDUCATION I N SECONDARY SCHOOLS - THE PATIBRN I N PAKISTAN^
I ADMINISTRATIVE SET-UP OF HEALTH EDUCATION
Health education i n schools i n Pakistan is carried out by the Ministry of Health and Ministry of Education in close association with the t.wo provincial departments of health and education.
mere are three health education bureaux in the cnuntry, i-e., Direct- orate of Family Planning and Health Education and two provincial health education bureaux, working i n close cooperation with a l l the s i s t e r ministries and off ic ial and non-official agencies, which are connected with the health and social welfare of the people. They maintain contacts with the Departments of Education, Social Work, Labour Welfare, Basic Democracies and the Bureau of National Reconstruction.
Qne health educator is posted i n each of the six Regions of West Pakistan and four Regions of East Pakistan under the control of two provin- c i a l health education bureaux i n the Health Department. Regional health educators camy out health education ac t iv i t ies i n the schools, rural health centres, MCH centres, school health clinics, family planning clinics, etc. Through t h i s se t up a large number of schools i n the villages are also covered (8@ of the population i n Pakistan l ives i n the villages). Activ- ities of these regional health educators are coordinated by the health education officers i n the provincial health departments and the health education wing of the provincial education department.
Based on the paper presented and the discussions of the Seminar

EM/HEP/~~ page 122
WHO EMRO
Direct health education services i n schools by the health education ----- off icers aye as follows: ----- -"--
1. Assisting teachers, i n making health ins t ruct ion meaningful and pract ica l through the u t i l i z a t i on of group discussions, f i e l d t r i p s , and through the r e l a t i 02 of information material t o personal family and com- munity healt'n pi1og,-eiaes, and othe? health education techniques.
2. Assisting i n correlat ing health ins t ruct ion with other par ts of the school health wogrcme and other school subjects.
3. Encouraging active part icipation ul: s c h v v l representatives i n com- munity health programmes, health councils, e t ~ .
4. ~ot ' ivat ir ig Leaoller-s tu assume the important r o l e they can play i n health programmes.
I 5. Bringing up-to-date material t o the a t t en t ion of heachers and drawing
i . t h e i r a t tent ion t o new sc i en t i f i c information.
6. Assisting teachers i n the in terpre ta t ion of both school and community health programmes; t o assist them i n improving t h e i r observational and screening techniques, use and upkeep of cumulative heal th records.
7. Working tirough parent groups i n helping parents gain an understand- ing of good health practices and t o motivate them t o provide f a c i l i t i e s , serviees and deb, ,,,, .A,.,, b ~ L L . , fo r the gocd health of t h e i r children.
I1 'I3-E ROLE O F IBATJT3 EDUCATION A S PART O F THE CURRICULUM
I n secondary schools, health education is included i n the courses on physical education, general science and socia l studies. Home economics, an e lect ive subject of the g i r l s i n the secondary schools, includes topics on health and hygiene. Health education is included a s an in tegra l part of physical education in the exist ing curricula of a l l schools. Health education and pf7;~sical education are given three periods a week. Periods are a l l o t t ed i n such e way tha t every child has an opportunity t o learn the techniques of games, a th le t ics , educational gymanstics, apparatus and a g i l i t y work. P;.ovision is made fo r health education i n the exis t ing curricula, but, i n actual practice, many schools st i l l do not a l l o t enough time fo r teaching health t o the school children. One of the objectives

WHO EMRO
of school health education is t o f a c i l i t a t e the formation of correct health habits, and a more functional approach is needed i n t h i s respect. It could be achieved by providing and guiding school children through vari'ous health education opportunities i n the school environment.
Health education, a s included i n general science, soc ia l s tudies and home economics, has been considered insuff ic ient t o meet the heal th educa- t i o n needs of the pupils. In most schools the subject is taught by teachers who do not have suff ic ient t ra in ing i n health education. Health education is taught as part of the other subjects. There is a shortage of sui table books on health education fo r use i n schools, except f o r e lec t ive physiology and hygiene.
I n developing an effect ive school health education programme i n Pakistan, the r igh t kind of attitude and coopcrat ivc s p i r i t have not always been forthcoming from heads of schools and medical off icers of school heal th services. However, gradually the school author i t ies a re rea l iz ing the value of a school health education programme and the school medical o f f i ce r s are gaining more in te res t i n t h e i r work, with both s ides becoming more cooperat- ive.
Inadequate f a c i l i t i e s , including limited space, poor school building insuff ic ient arrangements f o r l i g h t and ventilation, improper seating nrrangnments, inadequate provision fo r safe d r i n k i w water and sani tary excreta disposal system, ex i s t i n many of our schools and adversely e f fec t the formation of be t t e r heal th babits of school children and students. Lack of adequate educa-l;imal material on di f ferent health topics is a l so a great handicap i n teaching health education i n the schools.
I n 1959-60, the Commission on National Education l a i d special emphasis on the teaching of health and physical education.
Some of the most important items i n the physical and health education syllabus recommended fo r secondary schools may be enumerated as follovrs:
1. Cleanliness
2. Sanitat ion
3. Ventilation

EM/HE~,'~S page 124
WHO EMRO
4. Pur i t ies and impurities of water
5. Drainage and refuse disposal
6. Disinfectants
7. Exercises
8. Group ac t i v i t i e s
9. Games
10. Education gymnastics
11. Personal hygiene.
A s regards the integration of health education with subjects of secondary schools, such as genera! science, socia l studies and 'home econom- ics, some significant topics are mentioned below:
1. Role of air, water heat and l igh t i n human l i f e
2. Necessity fo r food and balanced d i e t
3. Houseflies and mosquitoes
4. Circul a f . 0 ~ 1 ~ and digestive system
5. Personal hygiene
6. Hospltal and child welfare ancl health and recreation centres
7. Public sani ta t ion
8. Clothing
9. Helping the sick t o get well.
Thus, we f ind t ha t a t l e a s t some provision on health education has been made in the existing curriculum of the primary and secondary schools. Our teachers consti tute the most important aspect of our national building

WHO Ern0
programmes. With a l f t t l e in te res t an& devotion t o these important programmes, they could perform a fundamental du ty by helping the students t o understand t h e i r basic health problems. They czn inculcate good health habits among the students by creating a sound concept of healthful l iv ing and changing t h e i r faul ty a t t l tudes . They could thus prove themselves useful i n the health promotional programme of chilcken and pupils.
The Curriculum Committee j s strongly of the view tha t the amount of knowledge which an educated c i t i z en needs t o meet the demands of a sc ient i f - i c society can only be given t o the pupils i f teachers of good qual i ty are provided and effect ive teaching aids, charts, graphs, maps, films, radio, tape-recording, models; booklets, posters, exhibits, television, etc., and other information media, are placed a t t he i r disposal. I f the means of ins t ruct ion are not impr~ved i n these two directions, the curriculum and the syllabuses w i l l remain a deaa l eLLer * i n the CaGC of most schonls, and
educational reform w i l l hardly serve i ts purpose.
The syllabuses of a l l teachers t ra in ing ins t i tu t ions include health education as a compulsory subject. The curricLllwn is mainly concerned with the teaching methods of health education, but it is a l so importan-t; t o study the actual s t a t u s of health education i n the schools.
In East Pakistan provisions have been made i n almost a l l teachers tr3lllUlg Instilutions for a dootor-cum-hygiene teacher who extends heal th services t o the trainees. I n some t ra in ing ins t i tu t ions fkee medicines and a f u l l time compounder are a lso provided during the t ra in ing period. The Lrnpurtance ol a neiilbki, class-roam environment is al'fiays impressed upon the trainees. In this respect the subjects l i ke education i n psychology, chi ld development, physical education and health education encourage the teachers t o provide good health education services in the schools.
Besides these t ra in ing programmes, or ienta t ion courses on school heal th services a re a l so held fo r school medical officers, school teachers, sani tary inspectors and health ass i s t an t s i n cooperation with the Directo- r a t e of Health ServiCes and the Education Extension Centre,
According t o the Commission on National Education a l l teachers t ra in- ing colleges i n the country will have t o adopt t h e i r methodology t o modern techniques and lay greater emphasis on the use of modern t ra in ing f a c i l i t - ies and u t i l i z a t i on of available loca l material. Such an approach w i l l have not only educational but a lso economic value f o r the country.

EM/HEP/28 page 126
WHO Ern0
I11 THE ROLE O F HEALTH EDUCATION A S PART O F THE SCHOOL HEALTH SERVICES
Health education i n schools is carried out by the school heal th services unit and health education units, under the control of provincial health departments. Each regional health education uni t i n West Pakistan consists of one health educator, one projectionist , one artist, one driver for the van which is equipped with projection camera and tape-recorder.
School health services uni t i n West Pakistan comprises of one medical officer; one compounder; one laboratory ass is tant ; one radiologist. Some un i t s are not mobile and, instead of a radiologist , a nurse or heal th v i s i to r is posted with the school rned iaa l of f icer .
Recently, i n some areas of West Pakistan a medical check-up of a l l students has been s t a r t e d . This is an im~or t an t s t ep i n spreading heal th
I education a c t i v i t i e s i n the r u r a l areas through the cooperation of teachers
! and physicians.
The school health programme needs t o be interpreted i n the home. Many disturbances i n students' physical and mental health are intimately connected with family problems. Contacts between parents, teachers and school physicians can prove very useful i n such cases. The health v is i tor , nurse, compounder and other health workers should take an act ive par t i n the health education of parents and students.
School health c l in ics , i f properly organized, can play an important part i n bringiag about a favourable change i n the a t t i tudes of students with regard t o t h e i r health. School physicians should cooperate w i t h the teaching s t a f f i n planning the health education programme of the school.
In East Pakistan, the health uepartment, besides providing health services t o the students through i ts school health programme, shares a good deal of responsibi l i ty i n the f i e l d of school health education both i n the r u r a l and urban areas with the department of education, school authori ty and community at large. In urban areas, the school medical off icers have been entrusted with the responsibil i ty of organizing health education ac t i v i t i e s i n the schools i n cooperation with the teachers and the a l l i e d agencies i n the community. So far as the ru r a l areas a re concerned these ac t i v i t i e s a re organized by the loca l public health person- nel, .Such a s medical officers of the rural health ccntres and the Thana Dispensaries, sanitary inspectors and health ass is tants . The health

WHO EMRO
education centres headed by t ra ined health education officers, extend a l l possible cooperation i n the organization and development of health education ac t i v i t i e s i n the schools.
IV OTHER HEALTH EDUCATION A C T I V I T I E S
The School Health Committee
The health of the school children cannot be considered i n i so la t ion fkom community health problems. Hsaith problems of the community have a de f in i t e influence upon the health of the school-going children. Under the school health education programme there is provision to create an awareness among the community people about the local health problem and t o e n l i s t t h e i r act ive par t ic ipat ion fo r solving the same i n cooperation w i t h the ochool and othcr l o o s l community agencies, There is prnvisinn f o r forming a school health committee, by taking members from community leaders, various community agencies, community soc ia l workers, community health workers, etc., a s well a s from the school children and teachers.
Recreational f a c i l i t i e s
For the development of' sound mental health of the school children, recreational a c t i v i t i e s a re essential . I n the absence of recreational f a c i l i t i e s , the school children may become involved i n various anti-social ac t iv i t i e s . This fac tor is pa r t i cu lw ly responsible f o r the increasing incidence of juvenile delinquency i n the schools of urban areas. Consider- i ng the need of recreation fo r school chilcken, the Directorate of Public Instruction has made it a condition precedent t o have a playground attached t o a school before giving recognition t o a new school. %sides recrea- t i ona l ac t iv i t i e s , the school children should be involved i n various physical a c t i v i t i e s , e.g. gardening, cleaning school premises, etc. This w i l l inculcate the s p i r i t of dignity of labour and w i l l d iver t t h e i r m i n d s from e v i l thoughts.
Health needs of g i r l students
The school health education programme should focus on the specia l health needs of the g i r l students. After school education, many g i r l students get married and start family l i f e . Through the school heal th education programme they should be given the basic family education relat-
ing t o health, e.g., various aspects re la t ing t o maternal and chi ld health,

EM/IIEP/~~ page 128
WHO m o
1 food sani ta t ion and preservations, home economics and personal hygiene 1 r e l a t ing t o the special female problems, e tc , !Re exist ing home economics i syllabus, however, includes some of the above-mentioned aspects of health
I education.
Social a c t i v i t i e s
I To f a c i l i t a t e the soc ia l development of the school children, it is necessary t ha t various soc ia l a c t i v i t i e s be organized. Many schools have regular programmes of soc ia l and cu l tu ra l ac t iv i t i e s , such as v i s i t s t o in teres t ing places, and meetings and gatherings. These ac t i v i t i e s , of course,' should be organized on a wide scale covering a s many schools as posslbf e.
V RECOlvIMENDATIONS FOR IMPROVING THE EXISTING SCHOOL HEALTH EDUCATION PROGRAMME
1. I n order t o provide effect ive health education t o school children, the 'school curriculum may include health education as an independent compulsory examination subject both a t the primary and secondary levels. The subject should be taught by a teacher t ra ined i n health education. A health educa- t i o n t ra in ing programme fo r the teachers should be organized regularly, so t h a t a t l e a s t one teacher from every school may receive intensive training. A separate period should be a l l o t t ed i n the school time tab le f o r teaching health education.
2. Health education i n the teacher t ra in ing ins t i tu t ions should be improved by providing a teacher w i t h specialized t ra in ing in health educa- t i o n t o every teacher t ra in ing ins t i tu t ion.
3. More coordinated e f fo r t among various re la ted agencies and personnel should be i n i t i a t ed fo r the ef fect ive working of the school health educa- t ion programme . 4. Effective periodic evaluation procedure should be evolved t o assess the strength and weakness of the school health education programme, and accordingly changes i n the programme should be made from time t o time.
5. Regular health education conferences and in-service t ra in ing program- mes should be launched i n both the urban and r u r a l areas with the coopera- t i o n of the school management committees, teachers, block-development members, loca l in f luen t ia l s and the public health personnel.
WHO m o
6. mere should be provision for a t l e a s t one school health c l i n i c f o r every 2 000 students.
7. There should be adequate provision fo r necessary equipment f o r school health education, including material l i ke t ex t books, journals, heal th films and other reading material on health.
8. There should a lso be a regular survey of the health s t a t u s of the school children t o determine the in tens i ty of the problems and t o design and develop health education programmes accordingly.
9. Schools and communities m e the two fundamental areas where heal th education takes place; therefore, they should be given top p r i o r i t y i n a national health education programme.
10. Each and every health and soc ia l workers whether voluntary or govern- mental, should act ively associate himself i n motiva-bing community, school community and school population f o r adopting a wholesome a t t i t ude towards heal th education.
11. There should be coordination and cooperation i n a l l the soc ia l groups working fo r the improvement of schools and communities.
12. A l l Lht: rrleilia uf rrlass uur1unur~iuaLiur1 s l ~ v u l i l be u t i l i z e d fur mi effect- ive health education programme fo r secondary schools.
WHO EMRO
4. SCHOOL HEALTH EDUCATION - J O I N T COOPERATION BETWEXN MINISTRY OF PUBLIC HEALTH AHD MINISTRY OF EDUCATION IN ETHIOPIA^
The early establishment of schools pr ior t o the development of health centres i n i t i a l l y resulted i n the Ministry of Education taking a l l the responsibi l i t ies of administering public health services fo r school children. It has been only i n the last decade, especially following the establishment of health centres i n the rural areas t ha t the Ministry of Public Health began t o share the responsibi l i t ies of a school heal th programme. . .
In implementing a functional programme of school health, the Ministry of Public Health follows the general policy of complete c o o p ~ a t i o n with the school author i t ies i n a l l school health ac t iv i t i es ,
The Ministry of Education and the Ministry of Public Health a re cognizant of the fac t t ha t cooperation between the two w i l l expedite matters and avoid duplication and wastage of time and e f for t . The two Ministries have now established a smoother relat lonship than ever before.
Among the ac t i v i t i e s participated i n by both Ministries are:
National Level
The two Ministries kave eqaged i n the production of school health materials such as pamphlets and booklets.
Based on the paper presented and the discussions of the Seminar

The Ministry of Public Health a s s i s t s the Ministry of Education i n the t ra in ing programme and ce r t i f i ca t ion of school dressers. It a l s o par t ic i - pates i n the summer workshops of school dressers.
The Ministry of Public Health reviews and ed i t s the health educational materials produced by the Ministry of Education.
The two Ministries cooperate i n the development of the school curricu- l u m t o include health subjects t o be correlated i n other subjects a s much as possible.
The Ministry of Public Health believes t ha t i f health is t o be included i n the elementary school curriculum, it is imperative t ha t teachers get some courses i n health education while i n t ra in ing and during t h e i r in- service training. It has ass is ted the Ministry of Education i n conducting summer workshops a l l over the Empire.
Provincial Level
A t the provincial level, the provincial medical o f f i ce r and the school author i t ies work together t o safeguard the health of the school population.
The provincial medical off icer v i s i t s schools when necessary and the provincial s t a f f a s s i s t s school dressers i n vaccinating the school children,
Sanitarians make regular sani ta t ion inspection of the schools, give advice, and help t o improve the sani tary conditions.
Arrangements a re a lso made with the school master f o r the medical s t a f f t o teach health courses i n the schools.
Local LRvel
The jo int e f f o r t s of the two Ministries are c lea r ly seen a t the local level ,
Great care is being taken by the health centre s t a f f t o coordinate t h e i r school health with the exist ing programme being carried out by the school dresser i n order t o avoid duplication and wastage of t i m e and effort.

WHO EMRO
The sixty-one health centres throwhout the Empire ?+re s i tuated i n towns or v i l lages where school or schools already existed and are giving health services t o the school children a s one of the regular health a c t i v i t i e s of the health centre. The s t a f f members of a health centre consist of the health officer , two community nurses and two sanitarians. The health workers usually spend a t l e a s t one afternoon per week f o r school health.
The health workers make arrangements ~ L t h the school master so t ha t cer ta in hours may be al located from dif ferent classes t o enable the health worker t o give health teachings a s one part o f t h e i r regular class. Thesc health teachings are a part of the health centre ' s health education programme and most of them are lec tures on such subjects a s personal hygiene, communicable diseases psirticularly f o r t h e i r transmission and prevention, importance of sanitation and vaccination, etc. In some schools, the health workers have organized special clubs fo r g i r l s of the high grades t o teach them the Materml and Child Health subjects. However, this needs continual e f fo r t s and the subjects should be selected careful ly t o meet the needs of those par t icular areas and grades of students.
Because of the limited ava i lab i l i ty of s t a f f and time i n the heal th centres, a t present, physical examinations are carr ied out only among the first and l a s t years of students i n order t o f ind out t h e i r defects f o r correction and t o give them proper advice before they leave the school.
Trachoma is very common among school children i n the country. There- fore, the health workers have been paying special a t tent ion t o control of trachoma i n the schools. !This programme needs much help and cooperation fYom school teachers, par t icular ly during the treatment stage.
The health workers, par t icular ly the sanitarians, make regular sani ta t ion inspections of the school and give advice and help on the improvement of safe ty water-supply anct l a t r i ne f a c i l i t i e s . Special a t tent ion has also been paid i n the development of the hand washing and bathing or shower f a c i l i t i e s i n the school.
The health workers a l so supervise the preparation and d i s t r ibu t ion of UNICEF milk supply.

EM/HEP/~~ page 134
WHO EMRO
Future Plans
I n the long run both the Ministry of Education and Ministry of Public Health contemplate on modifying t h e i r e f fo r t s i n v i t a l i z ing the school health programme. This would be done by establishing a committee whose responsibi l i t ies would be:
1. To formulate plans and policies t o serve guidelines of r e a l i s t i c cooperative school health programme.
2. To es tabl ish minimwn standards f o r well coordinated service.
3. To coordinate the a c t i v i t i e s of the various agencies involved i n school health programme a t all levels.
4. To pu l l together the resources (personnel, finance, e tc . ) available t o the betterment of school health programme,
5. To avoid duplication and misunderstanding between the two Ministries and other agencies involved i n school health programme.

WHO EMRO
5.
In h i s day-to-day work with pupils, a teacher must help the pupils t o know, t o want, t o love, and t o do. In order t o help pupils form good health habits and develop a sense of responsibil i ty fo r the public's health, he must have a t h i s disposal suitable a ids and materials. More- over, he must be able t o use these a ids with intel l igence and discretion and with due regard t o t h e i r respective functions and t o the par t icular aim in mind.
I AUDIO-VISUAL AIDS NEEDED BY THE TEACHER
A matter of primary concern t o the class-room teacher is t o have at h i s disposal such audio-visual a ids as are sui table t o the purpose of the health education programme of his grade. The problem of acquiring these aids i s a f a i r l y easy one i n countries which possess ins t i tu t ions of t h e i r own fo r producing the aids required. But i n countries where no such ins t i tu t ions ex i s t the problem of acqulrlng the required aids becomee d i f f i c u l t and assumes a challenging aspect t o a l l conscientious educators.
I f a country does not produce the required aids, or produocs t h e m on a very badequate scale, can it effectively and successfully adopt such &ds a s are produced and effect ively used i n a di f ferent country?
A number of foreign made flannelgraphs were studied with the purpose of exploring the prospects of u t i l i z i ng them i n the implementation of the
Based on the paper presented and the discussions of the Seminar

WHO EMRO
education programme of the Syrian Arab Republic. They were found t o be very cleverly and conscientiously designed fo r stimulating class-room discussions which would bring t o l i g h t the students' motives of behaviour and leave a favourable e f fec t on t h e i r future behaviour. It soon became evident, however, t ha t those flannelgraphs which were used i n a country of diyferent cu l tu ra l and economic se t t ing could not so effect ively be used i n the new environment and t ha t a great deal of the general design pattern of those flannelgraphs would have t o be changed or modified t o s u i t the character is t ic local conditions. But i f such adaptation is sometimes possible, a s i n flannelgraphs, it is very often out o f the question i n the case of most foreign produced motion pict.ures where usual- l y no degree of technical s k i l l would be enough t o adapt them successfully t o the needs of the loca l environment.
I n h i s bock ducatio ion sani ta i re t t , Dr. Jules Gilbert warns against one country borrowing the health education programme of another. If t h i s is t rue with respect t o programmes, it is cer ta in ly t rue a l so with respect t o the a ids and means t ha t are speci f ica l ly made fo r a par t icular programme. Each country w i l l then have t o r e l y on i t s e l f i n making whatever a ids and means are needed fo r the implementation of its own programmes. This does not mean, however, t ha t a country should not t r y t o p rof i t from the exper- iences a cqa red by another country i n the f i e l d of planning, production, pre-testing and evaluation of audio-visual materials, nei ther does t h i s exclude the poss ibi l i ty of one country prof i t ing from the educational materials made by another when both have similar soc ia l and cu l tu ra l character is t ics , On the contrary, when such is the case, the exchange of educational materiais should be encouraged1. If such s imi la r i ty does not exist , the use of only those materials which could be adapted t o the import- ing country's character is t ics should be encouraged,
When preparing audio-visual aids, the responsible educational ins t i - tu t ion must f i r s t take in to account:
a. The a b i l i t y of these a ids t o help the teacher i n developing h i s pupils ' physical, mental and soc ia l health within the scope of t h e i r par t icular age-group, needs and character is t ics .
1 UNESCO Inter-American Health Education Seminar. Report. Paris, 1957.

WHO EMRO
b. Their a b i l i t y t o help the teacher i n correcting such bad habits a s a pupil may have acquired a t home.
c. Their a b i l i t y t o introduce such new experiences t o his pupils a s would conduct them on the road of a healthy adult l i f e .
These aids w i l l , however, f a i l t o stimulate the children t o the desired course of act ion unless t h e i r preparation is based on a factual understanding of the children's needs and habits.
A second step, therefore, i n preparing class-room aids should be t o carry out such studies and surveys a s w ~ u l d help t o provide the required information about the children's pre-school zcquired habi ts and beliefs .
In the l i g h t of these guiding principles and i n collaboration with a number of educators and school teachers, a representative survey study of fourth, f i f t h and s i x th elementary grade pupils i n Damascus schools w a s carried out i n 1959. The purpose of this survey study was t o appraise the children's health knowledge and habits with a view t o drawing up an experimental health education programme f o r Syrian elementary grades and f o r determining what audio-visual aids should be used i n the implementation of t h i s programme.
Pupils were asked t o answer a wide range of questions re la t ing t o such matters as cleanliness, hygiene, communicable diseases, safe ty pre- cautious, r es t , play 2nd dai ly meals. It would be out of place here t o dwell on the s t a t i s t i c a l r e su l t s of t ha t survey, but it should be mention- ed t h a t -the information obtained from the pupils ' answers have opened up new horizons i n planning out many of the audio-visual aids needed i n the implementation of the basic health education programme on Lhe levels of the family, the school and the general public.
This survey has also been of great use i n preparing a number of t e le - vision programmes directec! t o the family and t o various age-groups of children up t o the age of thir teen. !The information obtained from the answers of the children supplied the substance of those programmes which took the f ~ r m of dramatical representations portraying the habits, manners and problems of a t ~ p i c a l Damascus family ana suggesting solutions t o t h e i r problems.

WHO EMRO
I n one programme i n connection with communicable diseases, the number of responses received by m a i l from children of age-group 10 - 12 of Damascus, to ta l l ed t o 422.
Considering the f ac t t ha t not a l l the children who wished t o respond were, f o r a number of reasons, able t o do so, and t ha t i n case of children who did actual ly respond, parents and s ib l ings had ass is ted i n finding answers t o questions posed. One w i l l r ea l i ze the great i n t e r e s t shown by te levis ion audience i n following health programmes.
I1 COOPERATION EETWEEN HEALTH A I D EDUCATIONAL AUTHORITIES
From the foregoing it becomes apparent how important it is t o es tabl ish active cooperation between health a d educational author i t ies f o r the purposc of planning a sahool health education programme, preparing its materials, pre-testing the qual i ty of these resources and evaluating the effectiveness of the programme during a ce r ta in period of time a f t e r the beginning of i ts application, and f o r introducing whatever modifications may be considered imperative t o make it answer the changing conditions i n the l i gh t of the achieved resul ts .
111 AUDIO-VISUAL RESOURCES I N SCHOOL HEALTH EDUCATION
School health education has numerous audio-visual resources a t its disposal. Each of these is used i n a manner character is t ic of the object- ive aimed a t and the environment it is supposed t o serve. These re- sources have develogec! so great ly t ha t it is no longer admissible t o confine education t o the old method which depended largely on theoret ica l lessons. Every teaching s i tua t ion now has its own methods and media and, however good a method or a medium may be, it can only be effect ively used by a competent and well-trained teacher who can make h i s pupils take an active part i n finding solutions t o t h e i r health problems. He must not forget, however, that these instruments a re designed t o a i d him and not t o take h i s place i n the class-room. A teacher who is s a t i s f i ed with displaying health posters, films and f i lm-s t r ips can hardly claim t o have performed his duties i n health education. Such a ids a re meant t o help h i m i n h i s teaching and i n stimulating group discussions aimed a t solving his pupils ' problems. Talking things over gives children an opportunity t o share experiences, develop the capacity of feel ing fo r and with others, f ind wholesome solutions t o the common problems t ha t inevltably accompany each stage of t h e i r growth, and integrate new concepts in to t h e i r own background of experience.

WHO Em0
Some of the best audio-visual aids for stimulating such discussions a t school are the following:
1. Booklets and Leaflets
Booklets and l e a f l e t s used i n teaching health are usually intended t o serve as reinforcing material for the spoken word and should, therefore, be written i n short, simple terms and i l lus t ra ted with pictures or sketches for a t t ract ing the interest of the children.
2. Practical Demonstration
The method of practical demonstration is certainly the easiest, cheapest and most effective i n school health education. The animal feed- ing experiment is an excellent example tha t can be used a t any learning level1. Chlldren m i g h t , ruz. enanlpla, be requested to demonstrate the effect of a well balanced d i e t on health by watching the growth of a number of chickens fed by them over a period of t i m e .
This kind of practical experiment is recommended i n demonstrating such health topics such as house f l i e s or the method t o be followed i n bathing a baby.
3. Motion Pictures
Motion pictures have a great appeal t o children. A film can show sk i l l , action, baclkg20urlSi information and facts. It can also a s s i s t i n building attitilcles, s t , imulatc? emotions and demostrate solutions t o problems.
In order t o perform its function as an excellent visual aid t o school health education, a film must be clear and t o the point. The teacher must prepare the questions which he w i l l put t o his pupils on the subject of the film with the aim of stimulating group discussions. I n t h i s way the subject of the film w i l l be more vividly incorporated into the children's experience.
1 Teacher's Activity Book for a Programme i n Nutrition and Health, Minneapolis, The Department of hrblic Relations, 1954

EM/HEp/28 page 140
WHO EMRO
It is possible f o r the health educator t o f i l n very successful and cheap motion pictures dealing with local health education problems. The author has filmed a great number of s i l e n t motion pictures on such problems as cleanliness, f l ies. , and qusck medicine. While each of those films was being shown, personal comments were given on the par t icular occasion and discussions which followed were even more stimulating than he had dared t o hope.
4. Film-Strips - The f i l m s t r i p is a very pract ica l a i d t o the teacher and can be made
to deal w i t h anjz topic o f human relat ionships and many aspects of heal th education. This a id has a l so the advantage o f not requiring so many technicians and specialized personnel as are required i n producing motion pictures. The f i lm-str ig projector has the advantage of being cheap and simple t o handle, Another advantage of the f i lm-str ip is its great f lexi - b i l i t y . Any one picture can be retained on the screen or returned t o l a t e r i n the lesson.
F i lm-s t r ips have t h e i r own commentaries and questions suggested f o r discussion. They are usually of great help t o the teacher, but a well- experienced teacher w i l l have no d i f f i cu l t y i n framing questions of h i s own t o s u i t the demands of the loca l environment and occasion.
Slides 5. - Films and fiL,i-stL;p; a;-2 sometimes not available with respect t o one
o r other of the topics which touch upon school health education. In such cases the film-slide can be used very effect ively by the teacher. He can make his own collection, e i the r i n colour or i n black and white, on any number of subjects needed fo r stimulating the In te res t of his class, These f i lm-sl ides which are snapped by the teacher himself w i l l moreover have the advantage of b r ing ing in to the class-room such informative and stimulating pictures as are r e a l l y ca l led f o r by the occasion. Being designed by the teacher himself and not by a foreign 2nd remote hand, t h e i r appeal t o the students w i l l i n a l l l ikelihood be very considerable. Many students w i l l a l so l i ke t o make t h e i r own collect ions of s l i de s and, with the loca l scenes and characters they represent, the group discussions which follow would be most effective i n i l l u s t r a t i ng some of the most important points i n health education.

WHO m o E M / H E P / ~ ~ ..
page 141
6. The Flannelgraph
The flannelgraph is cer ta in ly the most f l ex ib le a i d i n school health education. The flannelgraph forms a picture with moving par t s which can be constructed very eas i ly at school. A i l we need i s a sheet of .f lanne1 t o cover the black-board. The i l l u s t r a t i ons used may be symbols or out- l i n e pictures mounted on t h i n l i n t , sand paper or b lot t ing paper. Talent- ed students may be asked t o help i n preparing the pictures or symbols which w i l l form the mobile par ts of the i l lus t ra t ion . Flazmelgraphs can be purely symbolic t o i l l u s t r a t e any hsal th o r anatomy subject such a s the structure of the eye, or can be made i n the form of a s tory on such sub- jects as malaria o r h o m e safety. But the most in teres t ing of these is the multiple-choice flannelgraph, a s it allows most par t ic ipat ion from the group. It can be designed on any number of topics such as nutri t ion, personal hygiene, chain of infection, chi ld development and so on.
A flannelgraph can be constructed within a few hours. When the multiple-choice flannelgraph is used with the f u l l par t ic ipat ion of the group, discussion is a laost inevitable, since there is .bound t o be dis- agreement i n the group about the re la t ive positions of the pictures o r symbols and when every member of the group has t o make his choice, this w i l l help t o involve the en t i re group i n the learning si tuation.
7. Posters
Posters a r e used t o reinforce ce r ta in fundamental points explained i n lessons, or t o draw at tent ion t o some project o r aspect of school work. A poster gives a purely visual message and its success w i l l depend on Its a b i l i t y t o a t t r a c t a t tent ion t c i t s e l f by its design, o r ig ina l i ty and challenge.
Posters can also be used t o explain the various phases of a heal th problem with the aim of educating the viewer t o adopt a new course of act ion o r mode of behaviow.
Posters can be displayed singly or i n a series, depending upon the message it is desired t o convey. When fi lm-str ips are not available, a se r ies of simple expressive posters can be made t o perform some of the important functions of the f i lm-s t r ip .
EM/HEP/~~ page 142
WHO EMRO
The children can be encouraged t o design t h e i r own posters on a suggested health topic and t h i s would fur ther stimulate t h e i r in te res t and thus add t o the effectiveness of t h i s visual aid.
Photographs
Ordinary photographs can a lso serve a s a stimulating a id i n school health education. These can be taken by the teacher himself or he may ask h i s students t o take pictures on ce r ta in subjects of in te res t t o i l l u s t r a t e the exact point he wishes t o drive home. The pictures can then be enlarged and displayed t o serve as health posters.
9. The Black-Board
The black-board is no longer r e s t r i c t ed t o writing and i l lus t ra t ion , but a lso used as a base fo r flannelgraphs, screens, posters and pictures. One variety is a movable board, on one s ide of which a black cinemato- graphic screen is fixed t o be used i n broad daylight and on the other, a piece of f lannel , Such a board is more f lexible than the ordinary black- board and can become a very useful teaching aid.
10. Models
School health education can a l so make use of the three-dimensional model. It forms a r e a l a id i n stimulating the children's in te res t a s it gives them an opportunity t o f e e l a s well as see new material. Models would fur ther help the learning process i n the children i f they a re encouraged t o make t he i r own models, which might be small repl icas of large objects or enlargements from the or ig inal made t o show some important deta i ls .
11. The Tape-recorder
The uses o f the tape-recorder a re considerable In school health education. It encourages par t ic ipat ion both during the recording session and playback and furnishes the group with recorded discussions fo r l a t e r analysis.
Recordings should not be too long. One minute is recommended a s the time limit in amatcur rccording. If a rccording must for eomc reason be longer, it should be interrupted with discussions.

WHO EMRO
12. Role-playiq
Boya and g i r l s a t any grade l eve l a re very fond of role-playing, which i n f a c t serves t o offer reassurance t o the children t h a t t h e i r experiences and feel ings are shared by others. I f children are encouraged t o ac t out t h e i r problems, t h i s may help them t o discover be t t e r ways of handling them. Children a l so l i ke t o a c t the par ts of t h e i r parents, teachers and a l l those who occupy an important place i n t h e i r l ives . Besides sa t is fy- ing the children's emotional need t o f e e l "grown-up", role-playing can a l so conduct them t o gain a be t t e r understanding of the grown-up point of view. This i n i ts turn w i l l make the children want t o improve t h e i r behaviour so as t o get alone; well with others,
13. School Exhibitions
It would be a very- good idea t o inv i te the pupils ' families t o a school health exhibition displaying the school I s achievements i n the f i e l d of health education and t o s t r e s s the importance of continued cooperation between parents and teachers i n this f ie ld .
A l l students should be encouraged t o take par t i n the organization of the exhibits along with t h e i r teachers, each g o u p of students t o be responsible f o r a cer ta in l i n e of a c t i v i t i e s according t o t h e i r capacit ies and ta lents .
A school exhibition a l so provides an occasion f o r discussions between parents and teacher; on whatever heal th problems may confront them i n common. Ehch discussions may be very helpful i n planning cooperation and solving some of the most d i f f i c u l t problems conf'ronting schools and homes i n matters re la t ing t o health education.
I T CONCLUSIONS
There is no end t o the resources and materials on which a well- qualif ied teacher can draw i n the course of his work a t school, regardless of whether it is located i n vi l lage or town. He can make good use of the many occasions t ha t present themselves t o h i m i f he takes in to account h i s students ' in teres ts , needs, experiences and intel l igence, He w i l l never f a l l t o f ind some way fo r stimulating the act ive par t ic ipat ion of his students with a vlew t o solving t h e i r health problerns and making heal th education more functional and meaningful.

EM/HEp/28 page 144
WHO EMRO
Almost a l l children a r e natural ly creative. They love t o make things, t o draw pictures, t o write s t o r i e s and t o f ind out by doing. This intense cur ios i ty on the part of children makes it easy fo r the teacher t o provide a r i c h and varied programme of individual and group projects on health problems, and t o promote those a c t i v i t i e s t ha t would make each pupil come through h i s school experience with the best possible physical, mental and soc ia l well-being.

WHO EMRO
CHAPEX VII
CCmliTI'EE \:OX AND FECOlVIMENDATIONS
The Committee members were selected on the basis of their background and experience. It was tried to include in csoh Committee participants from both Ministries. Also effort was made to include both administrators as well as teachers and planners. Each Committee selected its own convenor and recorder. Repre~entativcs of UN and other international agencies were requested to participate in the Committees they wished. List of Committee members appear in Annex B,
The Committees dealt with the following subjects:
A. Planning for school - community health education
B. Strengthening health education in the curricula of elementary and secondary schools.
C, Methods and materials in school health education
D. Preparation of teachers and school health workers for their health education responsibilities
Fbllowing are the guidelines discussed in the Committees:
A. PLANNING FOR SCEOOL - COMMUNITY HEALTH EDUCATION 1. How may school health education gain recognition in long-term
national planning?
2. How can pertinent information on needs and requirements of pupils, community and colmtry be collected and studied as a basis for health edudation planning?

EM/HEP/~~ page 146
WHO EMRO
3. What factors are involved i n planning a "two-front approachn t o heal th education - That is, on the "school fYont" and on the "corn- munity front", so t ha t the two f ronts are well coordinated?
4. On what basis can planning contribute t o team-work?
B. STRENGTHENIXG HEALTH EDUCATION IN THE CURRICULA OF ELEMENTARY AND SECOI\DARY SCI1130LS
1. What factors a re involved i n determining curricula for:
a. chilcben a t d i f ferent age levels?
b. r u r a l a s d i s t r i c t from -mbm schools?
c, vocational anc! agr icul tura l schools?
e. l i t e r acy programmes?
2 . How may " l i f e si tuation" receive adequate a t t en t ion i n health education?
For example:
a. How could far t ic ipat ion i n community development a c t i v i t i e s become a par t of the regular school curriculum?
b. How could pract ica l health a c t i v i t i e s , such as those carried on by pupil health soc ie t i es and committees, become a part of regular class-room health instruction?
3. What help do school author i t ies and teachers need i n carrying out t h e i r health education responsibi l i t ies?
How can t h i s help be provided?
C. METHODS AND MATERIALS IN SCHOOL HEALTH EDUCATION
1. Are we interested i n "learning" or "teaching"? How may once's point of view af fec t once's methods?

WHO EMRO
2. How c= teaching (and learning) methods be improved so t ha t be t t e r a t t i tudes and practices are developed?
3. How can r e a l objects which a re readi ly available be used more extensively as teaching material i n health education?
4. In what wags can part icipation of pupils i n health - re la ted events i n the home, school, o r community become a worthwhile method of health teaching?
5. What needs t o be done i n the evaluation of materials s o t h a t those selected or prepared fo r health education are suitable for local use? What are the c r i t e r i a f o r t h e i r usefulness?
6. HOW can one determine wlletller the methods or materials being used i n school health education are effect ive i n bringirg about intended resu l t s?
D. PREPARATION OF TEACHERS AND SCHOOL HEALTH WORIWS FOR THEIR HEALTH EDUCATION ~SPONSIBILITIES
Teacher Education
1, How can pre-service health [email protected] of teachers be imgroved?
2. How can teachers in-service become be t t e r prepared as through:
a, on-the- job training?
b, refYesher courses?
c. other (special courses, workshops, e tc . )?
School Health Workers
1. The recommenda-t;ions have been made i n Wc15/R6 t h a t "medical colleges and schools give specia l a t t en t ion t o health education". How can t h i s be done?
2. How can school health workers in-service become be t t e r prepared i n heal th education, a s through:

WHO EMRO
a. on-the- job t raining?
b. refresher courses?
c. other (for example, special courses, workshops, etc. )?
The Cornmitteeslater presented t h e i r recommendations a t the plenary session. A detailed discussion was carried on and f ina l recommendations were approved as the recommendations emanated not from the Committees alone but f'rom the Seminar as a whole.
These reuommendations have already been distr ibuted t o both Ministries of Health and of Education of the countries of the Region f o r t h e i r con- siderat ion i n planning and implementation of a c t i v i t i e s i n school heal th education,

WHO mo EM/'I-IEP/~~ Page 149
2. RECOMMENDATIONS
I PLANNDG FOR SCHOOL - COMbKJNITY HEALTH EDUCATION
Planning i n the f i e ld of health education i n schools involves several special in teres ts . Planning i n i t s e l f can be an important educational experience fo r the planners. The importance of a good plan for submission t o the national planning commission j u s t i f i e s time and care i n its prepar- ation. The main planning procedures consist of survey, assessment, for- mulation of pulicy, plan of action, execution and evaluation.
The Committee recommends:
1. That legis la t ion making health education an integral and in- s t ruct ive programme be included i n tne s ta tu tes of a l l ministr ies concerned.
2. That an i n t e r ministerial committee (with appropriate sub-commit- t ees ) be set-up t o plan, coordinate and evaluate the country's health educ- a t ion services and determine a general policy;'- 'AS regards health education i n schools the f i r s t responsibil i ty of the committee should be t o prepare a plan t o be included i n the plans of the bfinistry of Education and/or Health fo r presentatinn t o ;the national planning commission. These plans should make provision for:
a, sw%eys 225 studies t o form the basis f o r assessing the nature and extent of the problem a s well a s the curriculum planning and evaluation; .
b. the se t t ing u i of an organization t o carry out health education i n schools;
c. the t r a i n i w of personnel; basic, post-graduate and in-service;
d. development of curricula;
e. materials and teaching aids;
f , , qtipends and scholarships fo r professional, and administrative personnel.
WHO EMRO
3. That budgetary provisions during t h i s period cover:
a. in-service t ra ining of exist ing teachers;
b. preparation of the curriculum for prinlary schools;
c. development of books, materials and teaching aids;
d. scholarships and stipends of service, administrative and consultant personnel.
4, That consideration be given during the first planning period to the f inancial and administrative provisions which are required t o introduce specia l is t teachers i n health education i n intermediate and secondary sohools . a STRFNGTHENING HEALTH EDUCATION IN THE CURRICULA OF EIEMENTARY
AND SECONDARY SCHOOLS
A. Health Education Curricula
1. The aim of health education curricula is t o inculcate i n students from the very beginning health at t i tudes, habit patterns and practices together with an in te l l igen t understanding of the "whyt' and the importance of these topics.
2. Time- table.
a. Health education should form a part of the primary school's curriculum i n such a manner as t o commensurate with other school subjects.
The subject should be incorporated in to a l l other school subjects. Every opportunity should be seized t o dwell on a pertinent aspect of the subject. However, t h i s intermittent treatment should not be haphazard, but, rather, within a carefully studied framework and a general plan.
b. It is advisable t o a l l o t a separate period fo r health education i n the time-table of intermediate and secondary schools t o ascertain t ha t students have acquired an accepted standard of health education.

WHO mo
3 The syllabus or curriculum of health education i n schools should comprise the following broad principles of health and ecology:
a. Personal and env i ron~enta l cleanliness - cleanliness of foodstuffs, drinking and bathing water, clothes and utensils , f r esh a i r , a i r pollution, etc..
b. Health habits, prectices and a t t i tudes - reading habits, posture, barefootednees, personal hygiene, table manners, proper use of bathrooms, disposal of waste, e tc .
c. Nutrition - gradation from such topics as the importance of a varied and balanced d i e t a s well a s eat ing habi ts t o a systematic study of nutri t ion. m e causes and prevention of malnutrition anci vitamin cleficiencles.
d. Human anatomy and physiology with reference t o common physio- logical disorders and care of d i f ferent systems.
e. The meaning of health and disease, dangers of infection, preventive measures, microbes and parasites.
f . Sanitat ion of the environment.
g. Endemic and common infectious and paras i t ic diseases, t h e i r symptoms, dangers of infection, preventive measures, innocul- a t ion ;;id .V-*CJ iration.
h. Elements of mental health - some principles of applied psychology. Sex education as an aspect n f physical and mental health education. G i r l s should be given, i n addition, a t the onset of puberty, a short course i n feminine hyglene, mother c ra f t , prenatal, infant and child care. This l a t t e r topic should be done i n close cooper- a t ion with the Ministry of Public Health.
i. First aid, safety and home nursing.
j. Public k a l t h f a c i l i t i e s exis t ing i n the local i ty , as well a s nationally, should get due consideration.

Ely/HEp/28 WHO E r n page 152
The curriculum should be re-evaluated, revised and developed a t f ive years ' interval .
4. The above-mentioned outl ine of health education curriculum serves both ru r a l a s well a s urban schools, but emphasis s h i f t s t o charac- t e r i s t i c a l aspects ans special problems i n each area.
5. Health education i n vocational and agr icul tura l schools should have a firm broad basis of general health principles. The curriculum should be e l a s t i c and modified t o s u i t the d i f fe ren t specializations. In otlner words, the curriculum should ca te r f o r the health needs of the specialized student (and future worker) i n h i s trade in addition t o his needs as a member of the community a t large,
6. I n out-of-school youth ac t iv i t i e s , health education i n the form of pertinent topics should be discussed and practiced when appropriate.
7. Adults i n l i t e racy programmes should be exposed t o health education i n two ways:
a. Through incorporation of health topics i n the reading matter.
b. I n a more tangible and practical way tmough demonstration and practice of health ac t iv i t i e s , i n accordance with development plans i n the area.
B. Nature of Curricula and Co-Curricular Act iv i t ies
1. The schoolst sy l l ab i and curr icula shuuld deal w i t h community problems and programmes both theoret ica l ly and pract ica l ly with specia l emphasis on the pupils.!. ac t ive part icipation i n pract ica l e f fo r t s f o r the solution of these problems i n cooperation with community authori t ies.
2. Over and above the health education curriculum mentioned previously which encompases a l l pupils, those who a re so minded may be encouraged t o do co-curricular work of heal th nature.
This should be designed ae .an extension of the curriculum for those pupils who are strongly i n c l b d t o and a t t rac ted by t h i s type of work.

WHO EMRO
C. Methods and Neans of Helping Schools t o Attain Health Education Goals
School author i t ies and teachers should be helped t o f u l f i l t h e i r duties regarding health education i n the following ways:
1, They should be t ra i rnd properly i n health education and health practices. The t ra ining should bring them up t o a high level of competence i n health subject matter and technjques.
2. They should be prepared t o plan co-curricular health a c t i v i t i e s 'in schools. Their fngenuity and creative a b i l i t i e s should be encouraged i n order t o f a c i l i t a t e t h e i r work a s health leaders and examples.
3. Textbooks should be well written and amply i l l u s t r a t ed and they should be an enlightening factor.
4. Supervision of health education should be active and energetic and it should take in to consideration up-to-date methods and data.
Supervisors should be technical people belonging t o both the Ministry of Education and the Ministry of Public Health. These should form a consultant body t o the school author i t ies i n health matters and should work i n close cooperation with each other.
5. Family and parent education whether through parent/teacher associations, instruction and mass media, home v i s i t ing or any other means should be encouraged and developed,
6. Teachers shouldbe put i n b e t t e r socio- economic s ta tus since so much is required from them i n terms of work and responsibility. This cer ta inly w i l l help teachers towards emotional s t a b i l i t y which w i l l r e f l e c t \.re11 on t h e i r students.
7. Eslcouragement of local author i t ies t o take more active in te res t i n the health ac t i v i t i e s of the school.
8. Greater and closer cooperation between the Ministry of Education and the Ministry of Public Health a t a l l levels is essential .
It is part icularly recommended t ha t the doctor and nurse of the school shodd work very closely with the school author i t ies and consider themselves

WHO EMRO
as p a r t of the school system. A n interdepartmental cornrnittee should be s e t up t o coordinate work between the two Ministries and help i n the attainment of f u l l cooperation. Furthermore, the standard of public health should be equally ra ised t o f a c i l i t a t e health education i n schools.
9. School being par t of the comnunity, should not be only an exact repl ica of this community, or representing a section of it, but, should be a projection of what the community aspires t o be i n future. This concept also comprises the design of the school, its sanitary conditions, maintenance, amenities, etc., i n such a way a s t o make school environments an inspira t ion t o a more healthy community and a higher standard of living.
I11 METHODS AND MATERIALS I N SCHOOL HEALTH EDUCATION
"Teaching" and "learning" processes a r e complementary. Methods and materials i n education including health education are valuable t o the extent t ha t they fos te r learning. I n employing various methods and materials, much depends upon the teachers' a b i l i t y t o help the pupils learn actively and effectively. Consideration must be given t o basic principles of learning and the goals desired i n a par t icular teaching - learning si tuation. I n order t ha t methods and materials i n health education may contribute t o improved health behaviour, the following points should be taken in to consideration:
1. Both methods and materials should be selected and used i n ways t ha t s a t i s fy the needs and requirements of children as well as the charac- t e r i e t i co of the en\-ir.o;me:~t i n w h i c h they l ive. I n teaching heal th behaviour changes, teachers should not confine themselves t o t r ad i t iona l and c lass ica l methods of education.
2. Methods and materials should be selected so as t o contribute t o desired goals. They should be used f lexibly. The lecture method and discussion techniques may help the pupils t o gain information, while discussion techniques and problem solving methods should be continued t o stimulate c r i t i c a l thinking and actual behaviour change.
3. Conditions i n homes, school, or community may provide f e r t i l e s i tuat ions fo r pupil learning. The teacher should be a le r t ed t o poss i - b i l i t i e s fo r involving pupils i n such events as building a new well i n a village, helping with f l y control campaigns, investigating causes of school absences, or ass i s t ing with safe ty measures. By such methods,

WHO EMRO
pupils may gain vslc~5le -md~r.-i~xndi.~gz an3 clevelop a greater sense of responsibil i ty f o r cop-ing with +,i:z problems, Moreover, such endeavours may have a benef ic id offsc t on tlnz whole l i f e of the community.
4. Simple ri?aCla., i f ueed wall by a t ~ a i n e d teacher may become valuable teaching aicls. Xeal objccts , scch as foods, gardens and water supplies can serv3 as pr.zctiea1 te;, ? k i ~ & as-;erial.
5. Children should be e n c o ~ ~ e g s d md helged t o develop t h e i r own audio-visual materiel:; such a s flannelg?a.pks, posters, s l ides and photo- graphs *
6. Resources within sehbols md community should be explored and used t o the utmost. Eaalth o~*@aniza'tions both o f f i c i a l and voluntary may provide valuable asslstancc w i t t i rrral,erials. ~ommunicati.ons should be s a t i s f ac to r i l y established between schools and sources of teaching a ids so that the a ids which are developed or d is t r ibuted by such groups are sui table fo r school use. Tnis means t ha t schools should have act ive par t i n determining what type of health education aids they need.
7. Audio-visual materials produced fo r school or community use should be pretested and re tes ted u n t i l t h e i r effectiveness and usefulness a re assured. I n the preparation of materials, it is t o be real ized that:
a. the content should be technically sound and i n harmony with desired goals;
b. the material should be appropriate f o r the age leve l of the pupils and t he i r cu l tu ra l and socia l environment;
c , materials silould be a t t r ac t ive and understandable.
8. Evaluation of the effectiveness of health education methods and materials must be a continuous process. Evaluation may be done not only by periodic s t a t i s t i c a l smveys but a l so by assessment of r e su l t s on a continuous basis. A t a l l times the teacher should keep constantly i n mind t h a t educational methods and materials are aids t o learning and not the learning process i t s e l f .
9. Investigatior. and rezearch should be developed and encouraged t o serve a s basis f o r cffectjve planning and improvement of teaching materials and methods.

WHO EMRO
PREPARATION OF TEACHERS AND SCHOOL HEALTH W C m S FOR THEIR HEALTH EDUCATION RESPONSIBILITLES
A. Teacher Education
1. Pre-service health education of teachers
In order t o provide effect ive health education t o school children, teachers should receive proper t ra in ing on the subject i n the course of preparation f o r the teaching profession. It is, therefore, recommended t ha t the subject be given due importance i n the curriculum of the teacher t ra in ing ins t i tu t ions and be properly integrated with a l l i e d subjects; health education a s a subject, should a l so be fur ther strengthened and highlighted.
I n order t ha t teaching of the s ~ b j e c t a t the teacher t ra in ing l eve l becomes r ea l l y ef fect ive it should be taught by persons properly qualif ied t o teach t h i s par t icular subject.
2. Preparation of teacners in-service
To i n i t i a t e improvement i n the teaching of health education a t the teacher t ra in ing level, su i table curricula should be planned with due consideration given t o local conditions and environmental factors. A thorough programme would include:
- Instr7uction i n personal and conrnunity health as a pa r t of general education; an3
- i r ls t ruct ion regarding child health neeas, school health problems and programmes, methods and materials of heal th education, these should be considered an in tegral pa r t of the teachers ' professional education.
a. On-the- job t ra in ing
On-the-job t ra in ing of teachers is of much help towards fur ther improvement of t he i r teaching proficiency. In order t h a t t h e i r eff iciency as teachers of health eduoation my constantly and uninter- ruptedly be improved, frequent lec tures and discussion on the subject should be arranged and other in-service media used, such a s s t a f f

WHO EMRO
meetings, personal interviews and case conferences. Provision should be made fo r evaluating the teaching proficiency with regard t o both content and method, a t regular intervals .
b. Refresher courses - Provision should be made fo r organizing periodic refresher
courses on health education i n order t ha t teachers could remain abreast with the l a t e s t developments i n this f i e ld . It is fur ther recommended t ha t scholarships, stipends or allovrances be given t o the part icipants of these courses and t ha t t h e i r recommendations be properly recognized by the competent authori t ies. It is f e l t that such t ra in ing w i l l a t t r a c t the teachers already in-service f o r fur ther improvement i n t he i r professional work.
B. School Health Workers
1. Medical and a l l i e d ins t i tu t ions
The Seminar Committee, following the recommendations of the Eastern Mediterranean Regional Committee Meeting - 15th Session - and having discussed the subject i n a l l its aspects and on the basis of the needs of the countries of t h i s Region, urges " a l l medical colleges and schools of the Region t o give special al~ter-rtiul~ %o health educationff1. The subject should be integrated with the exist ing curricula of these ins t i tu t ions . Some ins t i tu t ions of the Region have already taken action t o t h i s effect .
Ins t i tu t ions preparing nurses and other heal th workers should include school health i n t h e i r curricula, and should likewise provide instruction i n health education inoluding school health education needs, programmes and methods.
2. In-Service Training of Health Workers -------.-
a. _On-the- job t ra in ing
School health and eciucation author i t ies should arrange f o r adequate and up-to-date individual and group t ra in ing of health

WHO EMRO
workers suZted t o their part icular needs. Such t ra in ing may be provided through personal guidance, s t a f f meetings, case conferences and provision of up-to-date reference materials including books, pamphlets, journals and others.
b. Ref'resher courses
Refresher t ra in ing courses should be arranged by the public health author i t ies i n conjunction with the department of education, i n order t ha t the work standard of the health workers can keep pace with the most up-to-date developments i n the f i e l d of health services, health education and education i n general.

A N N E X E S

WHO EMRO EM,~HEP/~~ Annex A page i
LIST OF PARTICIPANTS, 013S.ERV%RS AID N.4TIONAL F'REPARAMRY COMMI?TEE
PARTICIPANTS
ADEN lfr. Ibrahim Robleh Rogional Director, Education Ministry of Education liEiormalksar_ --
Dr. Ahmed Abdulla Basahai Medical Officer Ministry of Health Khormaksm
Dr. Z.G. Panos (Vice-chairman) Director, Medical Services Ministry of Health Nicosia
Dr. Ioannis Koutsakos Lectwer. i n Psychology and Philosophy Paemogica l Academy Ministry of Education Nicosia
Ato Mamo Beshah Chief, Health Education Section Ministry of Public Health Addis Ababa
-p/?8 Annex A page ii
WHO EMRO
ETHIOPIA (cont 'd)
I R A N
bks. Tebereh Wolde Gabriel Home Economist C1miculum Division Ministry of Education and Fine Arts Addis Ababa -
Dr. A. Teymour Kalali Director-General School Health Services Ministry of Education Teheran
Dr. Kazen Shayan (Rapporteur ) Director, Health Education Division Ministry of Public Health Teheran
Dr. M. H. Sahebo ' z-Zamani Director, Mental Health Division Mild3 Lry o f Publlc Health Teheran
Dr. Ghaib M. Mukhlis Director, Students Health Services Ministry of Public IIealth Baghdad
I@, Y.M. Farid Area Education Officer Baghdad, Rusaf a

WHO EMRO
HASHEMIrn KINGDOM OF JORDAN
Elp'HE~/28 Annex A page iii
D r . Ibrahim Alamuddin (Vice-Chairman) Director, Medical Services Amman -
Miss Lutfiyeh Ragheb Abu Laila Head, Eealth Education Division Ministry of Education
M r , Berges Hamoud Berges (chairman) Assistant Under-Secretary fo r Health Affairs Ministry 'of Public Health Kuwalt --
Dr. Ahmad Salama Director, Curative Services Ministry of Public Health Kuwait
Dr. Yahya Shaker Head, Paediatrlc Section Sabah Hospital , , Kuwait --
Dr. A w n i A 1 Nimar Hea~, School Health ?4inistr]-. of Public Health Kuwait
Dr. J3assan F. Abu Ghazaleh Acting Head, Health Education Ministry of Public Health Kuwait

E;M/HE;P/~~ Annex A Page i v
KUWAIT (cont ' d)
PAKISTAN
WHO Elm0
M r . Yousef Allam Acting Head, Health Affairs Ministry of Education Kuwait
Mr. Zuhair A l - K a r m i Senior Inspector of Science Ministry of Education K u w a i t
DP, Badih Fidaoui Head, Department of Social Hygiene Ministry of Public Health Beirut - M r . A.A. Madi Head, Division of Scholarship and
Cultural Missions Ministry of Education Beirut
Dr. Abdul Azim Quresht Assistant Director Public Health Directorate Peshawar
Dr. (ks.) Sadiqa Bano Agha Deputy Assistant Direct or- General Health,
!4CH and School Health Services Ministry of Health, Labour and Social Welfare (Health ~ i v i s i o n ) Islamabad

WHO EMRO
PAKISTAN (cont ' d ) M r . Syed Shafiqul Hossain Specialist Education Extension Centre Dacca -
Me. Fakhrul Islam Choudhry Assistant Educational Adviser Ministry of Education Islamabad
SAUDI ARABIA
SOMALIA
EM/HEp/28 Annex A Page v
TSr. Mohamed Ismail Hayati Director, School Health Education Ministry of Education Ri yad -
Dr. J. Ashi Director, Health Office Mecca - Mr. Nur Elmi Osman Head, Education and Training Ministry of Health and Labour Mogadishu
Kr. Sayecl Abdurahman Sayed Ali ~irector, Department of Education Ministry of Education Mogadishu

EM/HEP/~~ Annex A page v i
SUDAN
SYRIAN ARAB REPUBLIC
TUNISIA
WHO EMRO
Dr. Hamdi Sal ih Gabbani Province Medical Officer of Health Northern Province Atbara
Mr. Khalid Mohamed A l i Science Inspector Ministry of Education Khartoum
Dr. Adel-Sarnman Director, Division of Health Education Ministry of Health and Public Assistance Damascus
Dr. Jamil Mahfouz Director, School Health Services Ministry of Education IZamascus
Dr. Mohamed Taieb Hachicha Mecllcal Inspector Ministry of Public Health Tunis - Mr. Chamseddine Bendamire Chief, Social Services Ministry of National Education Tunis
WHO EMRO EM/HEP/~~ Annex A page vii
UNITED ARAB REPUBLIC
YEMEN
Dr. Mohammed Mahmood El-Sonbaty (vice-chairman) Director-General, School Health Administration
Ministry of Public Health Cairo -
Dr. Wasfia Hussein Kame1 Assistant Director, School Health Administration
Ministry of Public Health Cairo -
Dr. Moukhtar El Sayed El Sherif Deputy Chief, Health Education Section Ministry of Public Health Cairo - M r . Ahmed Moustafa Abdullah Science Inspector Egyptian Education Mission to Kuwait Ministry of Education Kuwait
Dr. Ahrned. Rached Abd El Mawla Government Hospital Taiz -
corny OBSERVER
UNITED ARAB REPUBLIC
Dr. Yehia Talaat Science Inspector Egyptian Education Mission to Kuwaft Ministry of Education Kuwait

EM/HEP/~~ Annex A page viii
WHO EMRO
REPRESENTATNES O F UNITED NATIOIJS B O D E S --
UNITED NATIONS Mr. S. Kar DEVELOPMENT BOARD Correspondent of the (WP) United Nations Development Programme
UNITED NATIONS EDUCATIONAL SCIENTIFlcC AND CULTURAL rnGANIzATTON (UNESCO )
UNITED NATIONS CHILMIEN'S FUND ( ~ C E F )
FOOD AND AGRICULTURE ORGAMZATlDN OF THE UNITED NATIONS (FA0
Dr. J. Singh UNESCO Adviser in Education Planning and Administration
c/o Planning Board Kuwait KUWAIT
Dr. A. Hurbli Deputy Director, Primary and Teacher Education
Department of Education UNRWA Headquarters Beirut LEBANON
M r . R.A. Koleiiat UNICEF Area Representative UNESCO Building Beirut LEBANON
Miss Mona Doss Regional Nutrition and Home Economics Officer
F A 0 Rcgional Off ice for the Near East
Cairo - UICETED ARAB REPUBLIC

WHO m o EM/HEP/~~ Annex A PWe
REPRESENTATIVES OF UNITED NATIONS BODIES (cont 'd)
UNITED NATIOPJS Mr. Shawqui A l i Hasna fU3LIEF AND WORKS Health Educator AGENCY FOR Department o f Health PUSTINE UlEiWA Headquarters REFWGEES (UNRWA) Beirut
LEBANON
OlXEFWPG FROM OTHE3I ORGANIZATIONS
UNI'lED STATES Miss Gloria Russo AGENCY BDR Health Education Adviser 1-TIONAL US A I D Mission DEVELOPMENT (US AID) Lahore
WEST PAKISTAN
LEAGUE OF l3ED CR033 IX-. Ctlaib M. MuklAis SOCIETIES Director, Students Health Services
and Member of the Iraqi Red .
Crescent Society rfinistry of Public Health Baghdad mc,
ARABIAN AMERICAN OIL COMPANY (ARA,"/K:O )
!@. Thomas Gray Supervisor, Health Education Unit ARAMCO Dhahran* SAUDI ARABIA

~M/m~/28 Annex A Page x
WHO SPECIAL CONSULTANT TO THE SEMINAR
Professor Ruth E. Grout Professor, Health Education School of Public Health
and College of Education University of Minnesota Minneapolis, Minnesota USA
WHO SECRETARIAT
Dr. A.H. Taba
Dr. J. Burton
Dr. A. Moarefi
Dr. G. Ja l lad
Miss P. Cartoudis
Chairman r
WHO EMRO
WHO Regional Director
Medical Officer Health Education Section
Regional Adviser on Health Education
Regional Adviser on Maternal and Child Health
Conference Officer
NATIONAL PREPARAMRY C O M I ' a m
Dr. Mohamed Hassan Salman, Director, Preventive Services
Members: (Ministry of Public Ik. Awni A 1 Nimar Health) Dr . Hassan F. Abu Ghazaleh
Mr. Farouq Qpddoumi
(Ministry of Educa- Mr. Yousef A l l a m t i on ) Mr. Hassan Abu Rahma

EM/HEP/~~ Annex B page i
LIST OF COMMITTEE MEMBERS
PLANKING FOR SCHOOL - COIJlMUNITY HEALTH EDUCATION
Convenor - Dr. Moukhtar El Sayed El Sherif (UAR)
Recorder - Miss Lutfiyeh Ragheb Abu Laila (~ordan)
mmbers of the Committee
Dr. A. Teymour Kalali (Dan)
Mr. Berges Hamoud Berges (~uwait )
Dr. Ahmad Salama (Kuwait)
Mr. Fakhrul Islam Choudhry (Pakistan)
Dr. A M u l Azi rn Q u r e s h l (Pakistan)
Dr. Mohamed Hayati (~audi Arabia)
Mr. Sayed Abdurahman Bayed Ali (,Somalia)
Dr. Ahmed Rached Abd El Mawla (Yemen)
Dr. J. Singll (UNESCO)
M r . R.A. Koleilat (UNICEF)
Pk. S.A. Hasna (UNRWA)
Dr. J. Burton

EM/HBP/~~ Annex B page ii
WHO EMRO
STRENGTHENIIqG IEALTH EDUCATION I N THE CURRICULA OF ELEMENTARY AND SECONDARY SCHOOLS
Convenor - Dr. Mohamed Mahmood El-Sonbaty (urn) Recorder - Mr. Zuhair Al-Karmi (Kuwait)
Members :of the Committee
Mr. Ibral~im Robleh. d den) . . .
Dr. Ioannis Koutsakos ( ~ y p r u s )
Nrs. Tebereh FJolde Gabriel (~thiopia)
Dr. Kazem Shayan (1ran)
Dr. Awni A1 Nimar (Kuwait)
Dr. Yahya Shaker (~uwait)
Dr. Badi h Ftda.niii (~ebanon)
Dr. ( ~ s . ) Sadiqa Bano A g h a (~akistan)
Miss Mona Doss (FAO)
Dr. J.K. Harfouche (AUB)
WHO Staff
Professor R.E. Grout

WHO Ern0 EM/HEp/28 Annex B page iii
-0DS AED M4'ER3S;~S I h SCHOOL - HEALTH EDUCATION
Members of the Cocni5toe - .--. Dr. Ahrnld Abdulla Bzsahai d den)
Dr. mssan I?. Abu Ghazaleh (Kuwait) 3 8
Dr. J. Ashi (Saudi Arabia)
M r . Khalid Mohamed A l i (Sudan)
Dr . Jamil PahTouz ( ~ y r i a )
Dr. Adel Samman ( ~ y r i a )
Mr. Chamseddine Bendamire (Tunisia)
Dr. Mohaned Taieb Hachicha (~unisia)
WHO Staff
Dr. G. Jallz?d
COMMITTEE "D"
PREPARATION OF ------.- TEP.CL3S !WD SCHOOL HEALTH WORKERS l?3R THEIR HEALTH EDUCATION FBS~ONSTbXLI,. 3s - ----,- -
Convenor - Dr. Ibrahim Alarnuddin (~o rdan )
Recorder - Mr. Syed Shafiqul Hossain (Pakistan)

EM/HEP/~~ Annex B page i v
WHO EMRO
COMMIW "D" (cont 'd)
PREPARATION O F TEACHERS AND SCHOOL HEALTH WORKERS FOR THEIR HEALTH EDUCATION FLESPONSIBILlTIES_
Members of the Committee
Dr. Z.G. Panos ( ~ y p r u s )
Ato Mammo Beshah ( ~ t h i o p i a )
Dr. M. H. Sahebo ' z- Zamani ( I ran)
Mr. Y.M. Farid (1raq)
Mr. Yousef Al lam ( ~ u w a i t )
IW. P J u r Elmi Osman (Somalia)
Dr. Hamdi S a l i h Gabbani ( ~ u d a n )
Dr. Wasfia Hussein Kame1 (UAR)
Dr. A. Hurbli (UNESCO)
Miss G. Russo (US ALD)
Mr. T. Gray (ARAMCO)
WHO S taf f
Dr. A. Moarefi
WHO EMRO EM/~t%p/28 Annex C page i
A G E N D A
1. Opening of the Szminar
2. Election of Officers
3. Adoption of the Agenda
4. Nature and Scope of School Health Education
5 . Health Education Needs of School Children and Cr i te r ia f o r Determining these Needs
6. School Health Services and School Health Education
7. Health Education Activit ies i n the Eastern Mediterranean Region:
a. Primary Schools
b. Secondary Schools
c . Teacher Training Ins t i tu t ions
8. Health Education in Currioulum Development
9. Health Education i n the Curriculum of Teacher Training Ins t i tu t ions
10. Nutrition Education i n Schools
11. Environmental Health of the School
12. Mental Eealth of the School Child
13. Methods and Materials i n School Health Education
14. Means of Developing Se t t e r Health Education Activit ies i n Schools - Cooperation of Various Agencies i n School Health Education
15. New Trends i n School Health Education

EM/HEP/28 Annex C page ii
6 Evaluation of Health Education Ac t iv i t i e s
17. Other Business
18. Approval of the Provisional Report of the Seminar
19. Closing Session
WHO EMRO

WHO Elm0 EM/HEP/~~ Annex D page i
1. MONDAY, 14 MARCH 1966
NURSING COLLEGE - Registration of Participants
- OPENING SESSION - Address by H.E. E l Sayed Abdul Aziz E l Feleig, Minister of Public Health, . , Kuwait
- Address by D r . A.H. Taba, WHO Director, ENR
- RECESS
- Audience with H i s Highness The A r n i r
- FIRST PIENARY SESSION - Election of Officers: A Chairman, 3 Vice-Chairmen, a Rapporteur
- Adoption df the Agenda
- INTRODUCTION by Dr. A: Moarefi WHO Adviser on Health Education
- PIATUFB AND SCOPE OF SCHOOL HEAL'IB EDUCATION by Professor R.E. Grout, WHO Special Consultant
- Reception by H;E; The ,Minister of Publi c Health

EM/HEP/~~ Annex D page ii
2. TUESDAY, 15 MARCH 1966
8.00 a.m. - 8.30 a.m. 8.30 a.m. - 10.30 a.m.
- Steering Committee - SECOND PLENARY SESSION - SCHOOL HEALTH EDUCATION PROBLElvkS
AND PROGRAMMES IN THE REGION
- STATEMENTS BY PARTICIPANTS - RECESS - CONTINUATION OF STATEMENTS BY
PARTICIPANTS AND REPRESENTATIVES
- SCHOOL HEALTH EDUCATION IN THE CONTEXT OF HEALTH AND EDUCATION
by Dr. J. Burton, WHO Headquarters by Dr. G. Jallad, WHO, EMRO by'Dr. J. Singh, UNESCO Expert by Dr. A, Hurbli, UNESCO Expert
- Visit to Al-Sabah Hospital - Reception by Dr. A.H. Taba, WHO
Director, EMR
- Steering Committee - THIRD PLENARY SESSION - MENTAL HEALTH OF rmE SCHOOL CHILD
- rnCESS
- INTRODUCTION TO COMMI- WORK
EM/HEP/~~ Annex D page iii
WHO EMRO
WEDNESDAY, 16 WW3-I 1966 (cont 'd)
11.00 a.m. - 2.00 P.m. - CON MI^ WORK Committee "A" - Planning for School - Cornunity Health' Education
Committee "B' - Strengthening Health Education in the Curricula of Elementary and Secondary Scnools
Conunittee "c" - Methods and Materials in School Health Education
Committee "D" - Prepasation of Teachers and School Health Workers for their Health Education Repponsibilities
4. THURSDAY, 17 MARCH 1966
8.30 a.m. - 12.00
2.30 p.m. - 3.00 p.m.
3.00 p.m. - 5.00 p.m.
5.00 p.m. - 6.00 p.m. 5. FRIDAY, 18 MARCH 196
- Visit to Kindergartens - Visit to Schools - Steering Committee . .
- COMMIT= hKBK (cont'd)
- Films and Exhibits . . . .
- Visit to "Kuwait Oil Companyt' - Visit to "Water Distillation
Plant" '

w='p/28 A I m a c D Page iv
8.00 a.m. - 8.30 a.m. - - - - Steering Committee - SVURTH PIENARY SESSION - Report of Committee "A" -. General
Discussion I
9.30 a.m. - 10.30 a.m. - Report of Committee "Bn - General Discussion
I I
10.30 a.m. - 11.00 a.m. - RECESS
7. s m y , 20 MARCH 19%
8.00 a.m. - 8.30 a.m.
8.30 a.m. - 10.30 a.m.
- Report of Committee "C" - General Discussion
- Report of Committee "Dn - General Discussion
- EVALUATSO~~ AND -H IN SCHOOL HEAZTH EDUCATION-
- Visit to the Museum - Reception at the Medical Association
at suleibikhat
- Steering Committee - FIm PIENARY SESSION - SCHOOL HEALTH EDUCATION IN
PERSPECTIVE
- RECESS
- Approval of the Provlsional Report - Closing Session

WHO EMRO WfEP/Q8 Annex E page i
LIST O F BASIC DOCWBI?I'S
Hi- OF THE sF2TtNA.R WSEM.SCH. HLTH.EDUT:./~
=ST OF PARTICIPANTS AND OBSERVERS EM/SEM.SCH.HL~TH.~XIC./'~
I ~ O D U C T I O N TO THE SEMINAR EM/sEM. SCH. HLTH.EDUC. / I (
by WHO Secretariat
by Professor Ruth E. Grout WHO Special Consultant .
by Dr. G. Jallad Regional Adviser on Mater.ml and Child Health
m c m PRFPARAT~ON FOR HEALTH ATIO ION - Wm. SCH. HLTH.EMK:.A AN EXPERImNT IN TH% UNITED ARAB REPUBLIC
by Dr. blasfia Hussein Kame1 Assistant Director, School Health Department, Cairo
and
Dr. Mohamed Mahmood El-Sonbaty Director-General, School Health Department, Cairo

-p/2a Annex E page ii
NVHiITION IN SCHOOL HEALTH SERVICES
WHO m o
by Dr. J.R.K. Robson Regional Adviser on Nutrition
HEALTH EDUCATION IN CURRICULUM DEVELOPMENT EM/=. SCH. HLTH.EDuc ./9 PLANNXPEf
by UNESCO Secretariat
HEALTH EDIEATION I N SECONDARY SCHOOLS
by Dr. Sadiqa Bano A g h a Health Division, Islamabad
SOME NOTES ON SCHOOL SANITATION EM/SEM. SCH. HL17H.EDUC. /11
by Mr. P.A. Stevens Regional Adviser on Environmental Health
MENTAL HEALTH O F THE SCHOOL CHILD I N THE EM/sEM. SCH. HLTH.EDUC ./12 PRESENT TRANSITIONAL STAGE OF RAPIDLY DFVELDPING NATIONS
by Dr. M.H. Sahebo '2-Zamani Director, Mental Health Division, 'Ileheran
HEALTH CONTENTS IN THE TEXTBOOKS OF THE EM/SEM. SCH. HLTH. EDUC ./13 P R W Y AND SECONDARY SCHOOLS I N SOME O F THE COlJNTRl3S OF THE E A S m MEDI-N REGION
by Dr. S. Sweilim Technical Adviser, Cairo

EM/W/28 Annex E page iii
AUDIO-VISUAL AIDS IN SCHOOL HEALTH EDUCATION EM/SEM. SCH. HLTH.EMK:. /14
by Dr. A. Sainman Director, Health Education Division, Damascus
LINK BE?WEEN SCHOOL AND HOME IN HEALTH EM/sEM. SCH.HLTH.EDVC ./is EDUCATION
by &. M.H. Salman Director, Preventive H e a l t h Services, Kuwait
SCHOOL HEALTH EDUCATION: JOINT E;~/sE;M. SCH. HLTH.EDUC .I16 COOPERATION BE- MIMmY OF PUBLIC HEALTH AND MINISTRY OF EDUCATION
by Ato -0 Beshah Chief, Health Education Sect ion, Addis Ababa
NEED RIR RESEfiRCH IN SCHOOL HEALTH EM/SEM. SCH. HLTH.EDUC./~~ EDUCATION WITH PARTICULAR HASI IS ON THE ROLE OF TEACHERS
by Dr. A. Moarefi Regional Adviser on Health Education
NOTTI ON THE ACTlJWl'IES OF UNFSCO IN THE E-M. SCH. HLTH. EDWC . /18 FIELDS OF TEACHER 'IRA- AND CURRICUUJM DEVELOPMENT
by W S C O Secretariat

EM/HEp/28 Annex E page i v
WHO . m o
LIST OF BACKGROUND MATERIAL
World Health Organization Expert Committee on School Health Services. M r s t Report: Geneva, 1951. (world Health Organization Technical Report Series No. 30).
World Health Organization Expert Committee on Health Education of the Public. First Report: Geneva, 199. (World Health Organization Technical Report Series No. 89).
worm ~ e a l t l z mganiiat lon Expert coml t t ee on Training of Health Personnel i n Health Education of the Public. Report: Geneva, 1958. (world Health Organization Technical Report Series No. 156).
WHO/UNESCO Expert Committee on Teacher Preparation fo r Health Education. Report : Gezleva, 1960. (World Health Organization Technical Report Series No. 193).
PAHO/WHO Inter-Regibnal Conference on the Postgradusbe Preparation af Iba l th lforlrera f o r Ilealth Education. Report: Geneva, 1964. (World Health Organization Technical Report Series No. 278).
World Hcalth Or~anizat ion Expcrt Committee on Health Problems of Adolescer-ze . Report : Geneva, 1965. (world Health Organization Technical Report Series No. 308).
Jof n t F.V~/UT\.ESCO/~C~O Meeting on the Teachers ' Role i n Nutrition Education, Paris, 7 - 12 September 1964.
UNESCO Sou?ce Eook, Planning fo r Health Education i n Schools, A study undertaken by Frofessor C.E. Turner,
Joint ~ F ~ / ~ E S C O European Symposium on the Preparation of Teachers fo r Health Educz%io;z, Paris, 7 - 16 December 1961
European Seminar on Child Health and the School, Noordwijk-aan-Zee, 21 - 31 August 1963.