uij - urotoday international journal
TRANSCRIPT
©2012 Digital Science Press, Inc. / UIJ / Vol 5 / Iss 1 / February http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
www.urotodayinternationaljournal.comVolume 5 - February 2012
Table of Contents: February, 2012
Review
• LowerUrinaryTractManagementinPatientswithNeurologicalDisease
MarcusJDrake,FranciscoMJCruz
Lower Urinary Tract Dysfunction
• DutasteridewithAs-NeededTamsulosininMenatRiskofBenignProstaticHypertrophyProgression
PaulFSiami,KnoxBeasley
Overactive Bladder
• PrevalenceandRiskFactorsAssociatedwithOveractiveBladder
Christopher Chee Kong Ho, Teo Chee Yang, Phang Lay Fang, Nur Aziyana Noor Azizi, Farah Lyna Darwin,NurAfifahMohdGhazi,GuanHeeTan,EngHongGoh,PraveenSingam,BadrulhishamBahadzor,ZulkifliMdZainuddin
Penile Cancer
• ClinicalEpidemiologicStudyofPenileCancerintheStateofPernambuco,Brazil
RógersonTenóriodeAndrade,MarinadeAndradeLimaArcoverde,FábiodeOliveiraVilar,MisaelWanderleySantosJr,NicodemosTelesPontesFilho,SalvadorVilarCorreiaLima
Ureteric Calculi
• PercutaneousNephrolithotomyintheSupinePositionwithUltrasound-GuidedRenalAccess
HammoudaSherif,OsamaAbdelwahab,AbdelazizOmar,IbrahimEraky
Case Reports
• ARareCauseofAcuteUrinaryRetentioninaYoungFemale:LeiomyomaBladderBikashBawri,RajeevTPuthenveetil,SaumarJBaruah,SasankaKBarua,PuskalKBagchi
• InflammatoryPseudotumoroftheUrachusRajKumarSharma,VirKumarJain,SMukherjee,SNMondal,DKarmakar
• Lymphoepithelioma-like Carcinoma of the Bladder: Is the Prognosis Different from ConventionalBladderCarcinoma?Eng Hong Goh, Akhavan Adel, Praveen Singam, Christopher Chee Kong Ho, Guan Hee Tan, BadrulhishamBahadzor,ZulkifliMdZainuddin,IsaMohamedRose
UroToday International Journal®UIJ

©2012 Digital Science Press, Inc. / UIJ / Vol 5 / Iss 1 / February http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
• Mondor’sDiseaseofthePenis:AForgottenEntityKapilSingla,AshishKSharma,SistlaBViswaroop,GaneshGopalakrishnan,SangamVKandasami
• RetroperitonealTextilomaMimickinganAdrenalTumorRahulDevraj,VedamurthyPogulaReddy,SuryaPrakashVaddi,AjitVikram,SreedharD
• TeratoidWilmsTumorinaChild:ACaseReportJameelHishamBardesi,AhmedJalalAl-Sayyad
• TreatmentofPost,High-Intensity-FocusedUltrasoundUrethralStricturewithNovelLong-termStent
OmriNativ,SarelHalachmi,BoazMoskovitz,OferNativ
• UreteralDiverticuluminAdults:DiagnosticProblemsandTherapeuticImplications
SatâaSallami,SamiBenRhouma,AliHorchani
UroToday International Journal®UIJ
Marcus J Drake,1 Francisco MJ Cruz2
1University of Bristol, Bristol Urological Institute, Southmead Hospital, Bristol, United Kingdom2Department of Urology, Hospital São João, Faculty of Medicine of Porto and IBMC, Alameda Hernani Monteiro, Porto, PortugalSubmitted April 26, 2011 - Accepted for Publication January 17, 2012
www.urotodayinternationaljournal.comVolume 5 - February 2012
Lower Urinary Tract Management in Patients with Neurological Disease
ABSTRACT
Lower urinary tract dysfunction is common in patients with neurological disease. Storage and/or voiding function
can be affected, leading to bothersome symptoms. However, preventing upper urinary tract deterioration is a
greater clinical priority, requiring identification of patients at risk, early intervention where indicated, and ongoing
surveillance. An initial assessment requires a comprehensive evaluation, including wider issues such as aspirations
for independent living, cognitive function, manual dexterity, and mobility. Measures to improve urine storage
include antimuscarinic drugs, botulinum injections, or surgical procedures. For voiding dysfunction, intermittent
catheterization is by far the most effective and most widely applicable approach, with additional benefits for
urinary storage. The assessment of urinary tract function and treatment selection requires a multidisciplinary
approach in the context of full rehabilitation or support.
KEYWORDS: Neurourology; Detrusor overactivity; Urodynamics; Antimuscarinics; Botulinum toxin A
CORRESPONDENCE: Marcus J Drake, MA, DM, FRCS (Urology), University of Bristol, Bristol Urological Institute, Southmead Hospital, Bristol, BS10 5NB, United Kingdom ([email protected]).
CITATION: UroToday Int J. 2012 Feb;5(1):art 95. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.13
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/ 10.3834/uij.1944-5784.2012.02.13
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
INTRODUCTION
The initial clinical evaluation of the urinary tract in a patient with neurological disease is crucial as presentations and prognoses vary, and the outcome is dependent on an accurate assessment. The key aims are: 1) to detect risk factors for the future (especially renal failure), 2) to optimize life expectancy, and 3) to evaluate symptoms, thereby guiding management to optimize quality of life.
There are useful guidelines published by international
organizations, such as the International Consultation on Incontinence and the European Association of Urology [1,2]. National consensus statements have also been developed (for example [3,4]).
Fundamentally, neurological patients should be assessed by a suitably trained health care professional who has specialized knowledge of lower urinary tract dysfunction, and the appropriate follow-up surveillance is needed at intervals. Lower urinary tract (LUT) issues have to be managed in the context of the wider health issues of the individual. These include directly

UroToday International Journal®
review
Lower Urinary Tract Management in Patients with Neurological Disease
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.13
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
relevant aspects, such as bowel and sexual function, and the impact of LUT dysfunction on psychological, domestic, social, and employment rehabilitation. Accordingly, multidisciplinary expertise is needed in medical teams managing patients with neurological disease, where the urological element is one of several important aspects.
CLINICAL EVALUATION
Medical History
The neurological diseases a urologist sees most commonly are spinal cord injury (SCI), multiple sclerosis (MS), and spina bifida (myelomeningocele). The range of possible neurological diseases is substantial, with many unfamiliar to the urologist. In general, they can be considered as follows:
1. Level(s) of nervous system affected: brain, upper motor neuron spinal, lower motor neuron spinal, peripheral, and combination of the above
2. Sensory and/or motor deficit3. Complete or incomplete neurological impairment4. Cognition5. Possible progression of neurology
After the neurological disease has been understood, the general history covers: 1) social factors and the patient’s motivation, 2) relevant surgery, 3) drug history, 4) bowel function, 5) gynecological/obstetric history and hopes for future fertility, and 6) sexual function.
Additionally, urinary tract history covers: 1) possible alarm signs, such as pain, urinary tract infection, hematuria, and fever that warrants further specific diagnosis, 2) LUT symptoms related to storage and voiding phases, including urinary incontinence and bladder sensation, 3) current bladder management methods, including intermittent catheterization, and 4) urinary infections (remembering the symptoms are unreliable where sensation below the neurological lesion is impaired [5]).
Symptom assessment tools are important to catalogue problems and their severity [6]. A bladder diary gives information about frequency, daytime and nighttime voiding frequency, voiding volume, incontinence, and urgency episodes [7]. This is useful for making treatment decisions and assessing response.
Examination
The examination aims to: 1) locate neurological lesions, 2) establish if other organ systems are affected; e.g., bowels,
3) establish lower urinary tract function (storage, voiding), 4) detect unexpected problems; e.g., lower motor neuron deficits may point towards secondary changes needing early intervention (e.g., syringomyelia in spinal cord injuries), and 5) influence further management options (coordination and cognitive tests are rarely untaken but may be appropriate as they influence the choice of management options).
A general urological examination looks for distended bladder/hydronephrosis, prostate size, pelvic organ prolapse (POP), continence/fecal impaction, and sacral/dependent sores. A focused neurological examination looks at key features, such as: 1) lower limb reflexes and bulbocavernosus reflexes, sensory dermatomes (fine touch and pin prick) of the lower limbs, and perianally effects, to see which spinal cord segments are affected, 2) anal tone and voluntary pelvic-floor squeeze, and 3) the evaluation of other facets; for example, coordination or blood pressure (lying and standing) should be considered.
INVESTIGATION
Urinalysis
Asymptomatic bacteriuria may subsequently turn into a urinary tract infection, which may become severe due to a lack of awareness of early symptoms in people with impaired sensory function.
Serum Tests of Renal Function
Allowance has to be made for muscle mass, considering disease is often lower in able-bodied individuals, and it will influence the normal range for serum creatinine values.
Imaging Tests
Specific tests depend on the findings of a clinical evaluation. In most cases, the following are appropriate: 1) ultrasound, to look for upper urinary tract (UUT) changes, 2) hydronephrosis, post-void residual, calcification, and other lesions, and 3) flow rate testing.
Flow rate patterns include normal, interrupted, prostatic, or stricture. The interrupted pattern is commonly seen in neurological patients and signifies poorly sustained detrusor contractions, straining, or dyssynergia. Artifacts have to be excluded.
Other tests are required, according to specific clinical requirements:
UIJ
UroToday International Journal®
review
Lower Urinary Tract Management in Patients with Neurological Disease
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.13
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
1. IVU / CTU: many neurological patients are at risk of forming urinary tract stones, and
2. spine/brain imaging: if there is doubt as to neurological lesion location or progression; however, this is most appropriately discussed with the relevant neurologist.
URODYNAmICS
Urodynamics is an invasive test with risks attached, so careful consideration is needed before proceeding with formal filling cystometry and pressure/flow studies. The EAU guidelines make a grade A recommendation that urodynamic investigation is necessary to document the (dys)function of the LUT.
Key urodynamic questions can be addressed by videourodynamics (VUDS):
1. Are the patient’s kidneys at risk because of LUT dysfunction? 2. What is the cause of a patient’s LUT symptoms?
Certain neurological patients may be considered at risk of LUT deterioration (especially SCI and spina bifida). They will generally need pressure flow studies. Those neurourological patients who, in the opinion of the managing clinician, are at a lower risk of renal dysfunction, and who have LUT symptoms, should only have invasive pressure flow studies if conservative treatment has failed, the patient is bothered by the symptoms, and they are fit for management interventions.
Invasive urodynamic tests should be in accordance with the International Continence Society good urodynamic practices [8]. Key issues are: use a slow filling rate (at least at the start of filling), and minimize the risk of artifactual reduction in compliance. The use of video screening is important because of the range of apparent filling and voiding abnormalities. In most cases, the bladder should be emptied at the start of filling, though the investigator may vary this according to the circumstances.
1. Filling cystometry2. To detect detrusor overactivity3. To ascertain the cause of incontinence4. To check leak point pressures5. To look for vesicoureteric reflux6. To check compliance7. To find cystometric capacity8. To evaluate pelvic-floor support9. Voiding studies10. To exclude bladder outlet obstruction or identify its site, if
present11. To gauge detrusor contractility12. To look at problems of coordination of outlet and bladder
contraction (detrusor-sphincter dyssynergia [DSD])13. Post-void residual
Detrusor leak point pressure (DLPP) is assessed in patients with reduced filling compliance (for example, patients with myelomeningocele, or where there is a neurological lesion of the sacral spinal cord). The DLPP is the detrusor pressure associated with leakage. When the compliance curve exceeds the outlet resistance, high values cause anxiety for future upper urinary tract function [9]. (Abdominal leak point pressure is a different concept, unrelated to the risk of renal impairment, giving an indication of incontinence severity in patients with normal bladder compliance).
Electromyography (EMG) can register the activity of the external urethral sphincter, the periurethral striated musculature, the anal sphincter, or the striated pelvic-floor muscles. It signifies the patient’s ability to control the pelvic floor and objectively identifies DSD, though the pressure trace alone can be used to deduce the presence of DSD in the absence of EMG recording
Ambulatory urodynamics uses natural filling by the kidneys. It can be used where conventional VUDS fails to reproduce a patient’s symptoms. For example, wheelchair users with stress incontinence symptoms may not be able to exert themselves sufficiently to elicit stress incontinence in the confines of a standard urodynamic test. Ambulatory testing should allow them the freedom to undertake the activity that reliably elicits symptoms.
The ice water test is fast-filling cystometry with cooled saline. The ice water test has reportedly distinguished between an upper motor neuron lesion (UMNL) and lower motor neuron lesion (LMNL) [10]. It is not widely used outside a research setting.
Safety for the Patient During UDS
Specific issues require caution when undertaking a VUDS test in neuropathic patients.
1. UTI: Urine should be screened before filling cystometry. If bacteriuria is present, the test should be deferred until resolved, or prophylaxis should be administered.
2. Autonomic dysreflexia [11]: A life-threatening complication of SCI above T6, in which extreme hypertension arises acutely in response to a noxious stimulus below the injury
UIJ
UroToday International Journal®
review
Lower Urinary Tract Management in Patients with Neurological Disease
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.13
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
level. Severe headache can be followed by intracerebral hemorrhage and death. If the patient complains of headache, the bladder should be emptied. Other stimuli should be excluded (i.e., any additional noxious stimulus below the neurological level), antihypertensives should be administered (e.g., sublingual nifedipine), and monitoring instituted.
3. Latex allergies: Neuropathic patients are at risk of a latex allergy [12] and may manifest an anaphylactic response [13]. Latex-free settings for VUDS are important, as a remarkably small level of exposure can trigger an anaphylactic response.
4. Erroneous conclusions: If VUDS is not carried out satisfactorily, inappropriate management decisions may result.
TREATmENT
Treatments are often a compromise between 2 main objectives: firstly, the protection of the upper urinary tract from deleterious effects of high intravesical pressures, and secondly, the improvement of storage and voiding symptoms. Restoration of nervous system function is not currently possible, but it is a hope for many patients.
Risk of Renal Failure in Neurological Disease
Upper urinary tract deterioration, which may be clinically “silent” until advanced, is a crucial factor in neurourological management. Four main risk factors have been identified for upper urinary tract damage in MS [14]: 1) the duration of MS, 2) the presence of an indwelling catheter, 3) high-amplitude neurogenic detrusor contractions, 4) permanent high detrusor pressure, and 5) DSD.
Accordingly, these factors warrant consideration of more active surveillance of the upper urinary tract. However, the factors are debatable in context. There is a paucity of irrefutable evidence relating to the risk factors of renal deterioration in modern practice, and for the range of neurological diseases. For example, in SCI, an indwelling catheter protects against subsequent deterioration [15].
BEHAVIORAL TREATmENT
Triggered Reflex Voiding
Triggered reflex voiding comprises maneuvers performed by the patient to trigger reflex detrusor contractions, such as suprapubic percussion. The integrity of the sacral reflex
pathways is a requirement. Patients who may benefit are those with suprasacral spinal cord lesions who are able to collect urine in a socially acceptable way. The presence of severe DSD must be excluded.
Bladder Expression (Credé and Valsalva Maneuvers)
Bladder expression has been recommended to patients with an underactive detrusor combined with an underactive sphincteric mechanism. It is no longer supported by most clinicians due to the risk of infection, vesicoureteral reflux, hernias, and rectogenital prolapses.
Toileting Assistance
Toileting assistance aims to correct habitual patterns of liquid intake and urination, to improve bladder control under urgency, and to teach patients how to reduce incontinence episodes. Techniques include timed voiding, prompted voiding, habit retraining, bladder retraining, and a patterned response to urgency.
CATHETERS
Overall, the evidence base for catheter use in neurourology is limited [16]. Excellent intermittent catheterization (IC) outcomes in neurogenic patients with various LUT dysfunctions put it in the management forefront.
Intermittent Catheterization
Intermittent catheterization (IC) can protect renal function and facilitate the achievement of urinary continence, either alone or in combination with other treatments. The frequency of catheterizing should be tailored according to fluid intake, bladder capacity, and detrusor pressure. Frequent urinary tract infections (UTIs) can occur, but prophylactic antibiotics are not recommended, and active treatment should be confined to symptomatic UTI. One fifth of the patients on long-term IC will experience urethral complications; e.g., bleeding and stricture. Sterile IC is associated with lower bacteriuria/infection risk as opposed to clean IC. Fully sterile approaches, using entirely sterile materials, including gloves and forceps, are most frequently advocated for intensive care units. Auto-lubricated catheters, which require immersion for a few seconds in drinking water to activate the lubricating film, are catheters of 12 to 14 Fr and are suitable for most adult male and female patients.
Indwelling Urethral and Suprapubic Catheters
UIJ

UroToday International Journal®
review
Lower Urinary Tract Management in Patients with Neurological Disease
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.13
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
Short-term urethral catheterization is needed in the initial phase of spinal shock. It is not appropriate in the longer term. A dilated (“patulous”) urethra can result in women, and urethritis, trauma, and stricture can form in men. If patients cannot perform IC, a suprapubic catheter (SPC) is preferable. Due to bladder cancer risks [17], regular cystoscopy is necessary after 5 to 10 years.
PHARmACOLOGICAL TREATmENT
Drugs for Detrusor Smooth Muscle Relaxation
Antimuscarinic agents
Antimuscarinic drugs aim to decrease reflex incontinence by delaying nonvoluntary detrusor contraction in patients who void spontaneously or empty the bladder by triggered voiding. They also aim to decrease high intravesical pressure in patients with DSD. In conjunction with IC, 70% of patients with less severe neurogenic LUT dysfunction may achieve continence. The evidence base for this patient group is small. Muscarinic receptor antagonists cause a variety of side effects, including dry mouth and constipation. They are contraindicated in closed angle glaucoma. Oxybutynin, tolterodine, propiverine, and trospium are the most extensively studied in the treatment of neurogenic LUT dysfunction. They significantly reduce micturition frequency and the number of urinary incontinence episodes, and they increase maximal cystometric capacity. Often, these patients will require doses higher than those recommended by the manufacturers [18,19]. The addition of a second antimuscarinic agent may also be tried in patients for whom urinary incontinence or detrusor pressure is not adequately controlled with 1 single agent [19].
Intravesical instillation is an interesting option. Sometimes purified oxybutynin preparations are available, usually as vials containing 5 mg. In most countries, there are no such formulations. Thus, 5 mg of oxybutynin tablets are crushed and dissolved in 30 ml of distilled water or saline and instilled 2 or 3 times per day. They are left until the next voiding, as maximum effect may take 2 to 4 hours.
Acetylcholine release inhibitors
Botulinum toxin (BoNT/A) impedes the release of neurotransmitters from nerve endings. It is increasingly used in neurogenic LUT dysfunction [20,21]. In the bladder, the blockade of acetylcholine release reduces detrusor contractility, and it may affect afferent nerve function. In the sphincter, it
will decrease urethral closing pressure.
BTX-A in Neurogenic Detrusor Overactivity
Schürch and colleagues [22] reported a bladder injection of BoNT/A for neurogenic detrusor overactivity (NDO) of a spinal origin resistant to anticholinergic drugs, in a patient who emptied the bladder by IC. Each patient received 300 units of onabotulinum A (Botox) diluted in saline (10 UI/ml) and injected in 30 different locations above the trigone. A significant increase in bladder capacity and a significant decrease in maximum detrusor voiding pressure were still present 36 weeks later. A multicentric European study with Botox in 200 neurogenic LUTD patients using IC or an indwelling catheter achieved continence in 73%, most benefitting at 9 months [23]. A recent and large randomized clinical trial with spinal cord injury and multiple sclerosis patients showed that 200 and 300 units of onabotulinum A were equally effective to improve or cure urinary incontinence and decrease detrusor pressure, but adverse events, mainly urinary retention and urinary tract infections, were more frequent with the 300 unit dose [24].
Patients should understand that, following BoNT/A, urinary retention is likely, and patients should be willing to accept a transient period of IC. A minimum interval of 3 months between BoNT/A injections might be considered to reduce the risk of antibody formation. Mild muscular weaknesses in the upper extremities of patients with complete cervical cord lesions rarely arise.
Drugs That Decrease Bladder Outlet Resistance
Alpha-1 adrenergic antagonists
Evidence to support the use of alpha-1 adrenergic blockers in neurogenic LUT dysfunction is sparse. Alpha-blockers may also contribute to decreased excessive sweating, secondary to autonomic dysreflexia [25].
Urethral sphincter injections of BTX-A
BoNT/A injected in the urethral sphincter aims to decrease bladder outlet resistance and facilitate bladder emptying, as an alternative to urethral sphincterotomy. It can be undertaken in conjunction with bladder injections [26]. Decreased urethral closure pressure, bladder pressure during voiding, and post-void residual urine are seen, and episodes of autonomic dysreflexia are reduced [27].
Central nervous system polysynaptic inhibitors
UIJ

UroToday International Journal®
review
Lower Urinary Tract Management in Patients with Neurological Disease
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.13
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
Baclofen is a GABAB receptor agonist that decreases the release of sensory neurotransmitters in the spinal cord. In theory, this may depress the activation of the bladder reflexes. However, oral baclofen has demonstrated poor efficacy in the treatment of neurogenic DO (perhaps due to poor CNS penetration). Improvement of NDO is seen with intrathecal administration of baclofen.
Substances That Decrease Sensory Input
Capsaicin extracted from hot chili peppers and resiniferatoxin (RTX) extracted from euphorbia resinifera, a cactus-like plant abundant in Northern Africa, are the most well studied compounds of the vanilloid family. These compounds have been in use clinically, and were found to have benefits. They are not commercially available, but they remain a source of potential development for future therapeutic interventions. The name “vanilloid” derives from the presence of a homovanillyl ring. Compounds with similar properties may not possess this ring. Vanilloid substances bind to a receptor belonging to the transient receptor family, a vanilloid 1 subtype (TRPV1, or VR1 or in the old terminology) that occurs in the membrane of type C, unmyelinated sensory fibers. This causes a brief excitation followed by a prolonged desensitization during which the neuron is unresponsive to natural stimuli.
SURGICAL TREATmENT
Many patients with chronic debilitating LUTS, refractory to conservative measures, will eventually require surgical procedures. Such procedures require careful evaluation of the patient. Careful urodynamic evaluation is important to establish the range of upper urinary tract dysfunctions present, so that appropriate plans can be made according to clinical need. For example, for a patient who hopes to achieve continence, the urodynamic evaluation of the bladder and the outlet enables the clinician to identify potential needs in relation to achieving sufficient stable reservoir capacity and a catheterizable continent outlet.
Operations That Decrease Outlet Resistance
DSD can be difficult to manage, and the currently available options have important limitations [28].
Sphincterotomy
Transurethral sphincterotomy (TUS) aims to reduce intravesical pressure mediated by bladder contractions against a contracted
sphincter, and it may reduce episodes of autonomic dysreflexia. TUS applies to male patients, as a penile condom catheter will be needed subsequently to collect urine. Prosthesis infection and penile erosions are too high to use an implant to aid condom use. TUS is expected to be a permanent solution but there is a significant rate of failure [29], and severe bleeding or stricture formation can occur.
Permanent urethral stents
The application of permanent urethral stents in the area of the urethral sphincter may constitute an alternative to TUS [30]. However, stent placement may trigger autonomic dysreflexia, and migration, encrustation, infections, or fistula are problems and outcomes that are uncertain.
Operations That Decrease Detrusor Contractility
Bladder augmentation with intestine
Bladder augmentation should be undertaken only when less invasive measures fail to create a low-pressure continent reservoir of sufficient volume. Bladder augmentation with a detubularized intestinal segment is well established. In short, 20 to 30 cm of ileum is isolated and detubularized, and then sutured over a transverse cystostomy [31]. Outcomes can be reasonable but may not be sustained [32], while complications might include urine reabsorption, urolithiasis, obstruction due to mucus accumulation, frequent UTIs, bladder rupture, and some risks of cancer development in the region of the intestinal patch. Most patients will require IC.
Bladder auto augmentation
Bladder auto augmentation (detrusor myectomy) [33] involves extraperitoneally stripping the detrusor layer from the dome and anterior surface of the bladder wall to create a large epithelial diverticulum. The technique is now infrequently used.
Neuromodulation and denervation procedures
Neuromodulation of the posterior sacral roots has been investigated in idiopathic DO. Some centers have reported results in NDO, but it is not widespread. Sacral neuromodulation was recently shown to have the potential to prevent NDO in patients with spinal cord injury if initiated at the phase of spinal shock [34]. This intriguing observation was carried out in a small number of patients and requires confirmation.
Subtrigonal denervation using phenol injections provided
UIJ

UroToday International Journal®
review
Lower Urinary Tract Management in Patients with Neurological Disease
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.13
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
inconsistent results and major complications, so it is no longer in use.
Operations That Increase Sphincteric Resistance
Artificial urinary sphincters have been frequently used in patients with congenital neuropathies. Success rates vary between 70 to 95%, with a revision rate of 16 to 60%. It is effective in most male patients [35]. In female patients, there can be significant problems [36].
Operations That Modulate Detrusor Contractility
Sacral anterior root stimulation to modulate detrusor contractions
Brindley and Craggs developed sacral anterior root stimulation, which is indicated in patients with suprasacral spinal cord lesions exhibiting severe DSD and autonomic dysreflexia. It comprises a posterior S2-S4 complete rhizotomy and the implantation of electrode stimulators on the intact sacral anterior roots. Anterior root stimulation activates simultaneous detrusor contractions when voiding is desired. It also activates urethral closure, but the latter fatigues quickly. Positive outcomes have been reported [37]. It can also be used to facilitate bowel emptying, and some males use it for erections. muscle augmentation
The restoration of bladder function by the use of an electrically stimulated muscle flap can be achieved by wrapping the latissimus dorsi muscle around the atonic bladder, retaining its innervation and blood supply [38]. The technique has not entered widespread practice.
Urinary diversion
An ileal conduit may be appropriate to prevent the deterioration of the upper urinary tract in highly selected patients. A continent reservoir may be offered to patients who have normal renal function and enough manual dexterity to catheterize the reservoir. Patients who maintain the bladder in situ have a risk of developing severe pyocystitis (pus accumulation in the dysfunctional bladder). In some women, this can be managed by vaginocystostomy.
Bladder reinnervation
Xiao and colleagues, following a series of animal experiments, reinnervated the bladder of volunteers with NDO and DSD
by transferring motor nerves in the L5 ventral root onto the S2/3 ventral root. Micturition was later initiated by stimulating the L5 dermatome. However, the useful results reported [39] have yet to be reproduced by other centers, raising significant uncertainty about the procedure.
CONCLUSION
Neurourology is a challenging subspecialty requiring considerable resources. Careful specialized evaluations are needed to identify the risk factors for renal deterioration. Symptom management requires a fastidious approach to diagnosis and a realistic insight into the patient’s preserved functions in order to identify realistic options to restore bladder storage function and emptying. Patients should have access to the full range of therapeutic options, and the more complex cases should be managed in appropriate specialist centers. REFERENCES
1. Abrams P, Andersson KE, Birder L, et al. Fourth International Consultation on Incontinence Recommendations of the International Scientific Committee: Evaluation and treatment of urinary incontinence, pelvic organ prolapse, and fecal incontinence. Neurourol Urodyn. 2010;29(1):213-240. Pubmed ; CrossRef
2. Stöhrer M, Blok B, Castro-Diaz D, et al. EAU guidelines on neurogenic lower urinary tract dysfunction. Eur Urol. 2009;56(1):81-88. Pubmed ; CrossRef
3. Fowler CJ, Panicker JN, Drake M, et al. A UK consensus on the management of the bladder in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2009;80(5):470-477. Pubmed
4. Ruffion A, de Sèze M, Denys P, et al. [Groupe d’Etudes de Neuro-Urologie de Langue Francaise (GENULF) guidelines for the management of spinal cord injury and spina bifida patients]. Prog Urol. 2007;17(3):631-633. Pubmed ; CrossRef
5. Linsenmeyer TA, Oakley A. Accuracy of individuals with spinal cord injury at predicting urinary tract infections based on their symptoms. J Spinal Cord Med. 2003;26(4):352-357. Pubmed
6. Abrams P, Avery K, Gardener N, Donovan J. et al. The International Consultation on Incontinence Modular Questionnaire. J Urol. 2006;175(3 pt 1):1063-1066. Pubmed ; CrossRef
UIJ
UroToday International Journal®
review
Lower Urinary Tract Management in Patients with Neurological Disease
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.13
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
7. Bright E, Drake MJ, Abrams P. Urinary diaries: evidence for the development and validation of diary content, format, and duration. Neurourol Urodyn. 2011; 30(3):348-352. Pubmed ; CrossRef
8. Schäfer W, Abrams P, Liao L, et al. Good urodynamic practices: uroflowmetry, filling cystometry, and pressure-flow studies. Neurourol Urodyn. 2002;21(3):261-274. Pubmed ; CrossRef
9. Ghoniem GM, Bloom DA, McGuire EJ, Stewart KL. Bladder compliance in meningomyelocele children. J Urol. 1989; 141(6):1404-1406. Pubmed
10. Geirsson G, Lindström S, Fall M. Pressure, volume and infusion speed criteria for the ice-water test. Br J Urol. 1994;73(5):498-503. Pubmed ; CrossRef
11. Khastgir J, Drake MJ, Abrams P. Recognition and effective management of autonomic dysreflexia in spinal cord injuries. Expert Opin Pharmacother. 2007;8(7):945-956. Pubmed ; CrossRef
12. Ozkaya E, Coskun Y, Turkmenoglu Y, Samanci N. Prevalance of latex sensitization and associated risk factors in Turkish children with spina bifida. Pediatr Surg Int. 2010;26(5):535-538. Pubmed ; CrossRef
13. Lieberman P. Anaphylactic reactions during surgical and medical procedures. J Allergy Clin Immunol. 2002;110(2 suppl):S64-S69. Pubmed ; CrossRef
14. de Sèze M, Ruffion A, Denys P, et al. The neurogenic bladder in multiple sclerosis: review of the literature and proposal of management guidelines. Mult Scler. 2007;13(7):915-928. Pubmed ; CrossRef
15. Drake MJ, Cortina-Borja M, Savic G, Charlifue SW, Gardner BP. Prospective evaluation of urological effects of aging in chronic spinal cord injury by method of bladder management. Neurourol Urodyn. 2005;24(2):111-116. Pubmed ; CrossRef
16. Jamison J, Maguire S, McCann J. Catheter policies for management of long term voiding problems in adults with neurogenic bladder disorders. Cochrane Database Syst Rev. 2004;(2):CD004375. Pubmed
17. Pannek J. Transitional cell carcinoma in patients with spinal cord injury: a high risk malignancy? Urology. 2002;59(2):240-244. Pubmed ; CrossRef
18. O’Leary M, Erickson JR, Smith CP, et al. Effect of controlled-release oxybutynin on neurogenic bladder function in spinal cord injury. J Spinal Cord Med. 2003;26(2):159-162. Pubmed
19. Amend B, Hennenlotter J, Schäfer T, Horstmann M, Stenzl A, Sievert KD. Effective treatment of neurogenic detrusor dysfunction by combined high-dosed antimuscarinics without increased side-effects. Eur Urol. 2008;53(5):1021-1028. Pubmed ; CrossRef
20. Giannantoni A, Mearini E, Del Zingaro M, Santaniello F, Porena M. Botulinum A toxin in the treatment of neurogenic detrusor overactivity: a consolidated field of application. BJU Int. 2008;102(suppl 1):2-6. Pubmed ; CrossRef
21. Apostolidis A, Dasgupta P, Denys P, et al. Recommendations on the Use of Botulinum Toxin in the Treatment of Lower Urinary Tract Disorders and Pelvic Floor Dysfunctions: A European Consensus Report. Eur Urol. 2009;55(1):100-119. Pubmed ; CrossRef
22. Schürch B. [Bladder dysfunction after spinal and peripheral nerve lesions]. Ther Umsch. 2000;57(11):690-697. Pubmed ; CrossRef
23. Reitz A, Stöhrer M, Kramer G, et al. European experience of 200 cases treated with botulinum-A toxin injections into the detrusor muscle for urinary incontinence due to neurogenic detrusor overactivity. Eur Urol. 2004;45(4):510-515. Pubmed ; CrossRef
24. Cruz F, Herschorn S, Heesakkers J, et al. Efficacy and safety of onabotulinumtoxina in patients with urinary incontinence due to neurogenic detrusor overactivity. Eur Urol Suppl. 2011;10(2):190. CrossRef
25. Chancellor MB, Erhard MJ, Hirsch IH, Stass WE Jr. Prospective evaluation of terazosin for the treatment of autonomic dysreflexia. J Urol. 1994;151(1):111-113. Pubmed
26. Safari S, Jamali S, Habibollahi P, et al. Intravesical injections of botulinum toxin type A for management of neuropathic bladder: a comparison of two methods. Urology. 2010;76(1):225-230. Pubmed ; CrossRef
UIJ
UroToday International Journal®
review
Lower Urinary Tract Management in Patients with Neurological Disease
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.13
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
27. Karsenty G, Baazeem A, Elzayat E, Corcos J. Injection of botulinum toxin type A in the urethral sphincter to treat lower urinary tract dysfunction: a review of indications, techniques and results. Can J Urol. 2006;13(2):3027-3033. Pubmed
28. Ahmed HU, Shergill IS, Arya M, Shah PJ. Management of detrusor-external sphincter dyssynergia. Nat Clin Pract Urol. 2006;3(7):368-380. Pubmed ; CrossRef
29. Pan D, Troy A, Rogerson J, et al. Long-term outcomes of external sphincterotomy in a spinal injured population. J Urol. 2009;181(2):705-709. Pubmed ; CrossRef
30. Abdul-Rahman A, Ismail S, Hamid R, Shah J. A 20-year follow-up of the mesh wallstent in the treatment of detrusor external sphincter dyssynergia in patients with spinal cord injury. BJU Int. 2010;106(10):1510-1513. Pubmed ; CrossRef
31. Bramble FJ. The clam cystoplasty. Br J Urol. 1990;66(4):337-341. Pubmed ; CrossRef
32. Hasan ST, Marshall C, Robson WA, Neal DE. Clinical outcome and quality of life following enterocystoplasty for idiopathic detrusor instability and neurogenic bladder dysfunction. Br J Urol. 1995;76(5):551-557. Pubmed ; CrossRef
33. Cartwright PC, Snow BW. Bladder autoaugmentation: partial detrusor excision to augment the bladder without use of bowel. J Urol. 1989;142(4):1050-1053. Pubmed
34. Sievert KD, Amend B, Gakis G, et al. Early sacral neuromodulation prevents urinary incontinence after complete spinal cord injury. Ann Neurol. 2010;67(1):74-84. Pubmed ; CrossRef
35. Chartier-Kastler E, Genevois S, Gamé X, et al. Treatment of neurogenic male urinary incontinence related to intrinsic sphincter insufficiency with an artificial urinary sphincter: a French retrospective multicentre study. BJU Int. 2011;107(3):426-432. Pubmed ; CrossRef
36. Chartier-Kastler E, Van Kerrebroeck P, Olianas R, et al. Artificial urinary sphincter (AMS 800) implantation for women with intrinsic sphincter deficiency: a technique for insiders? BJU Int. 2011;107(10):1618-1626. Pubmed ; CrossRef
37. Vignes JR, Bauchet L, Ohanna F. Dorsal rhizotomy combined with anterior sacral root stimulation for neurogenic bladder. Acta Neurochir Suppl. 2007;97(pt 1):323-331. Pubmed ; CrossRef
38. Ninkovic M, Stenzl A, Schwabegger A, et al. Free neurovascular transfer of latisstmus dorsi muscle for the treatment of bladder acontractility: II. Clinical results. J Urol. 2003;169(4):1379-1383. Pubmed ; CrossRef
39. Xiao CG. Reinnervation for neurogenic bladder: historic review and introduction of a somatic-autonomic reflex pathway procedure for patients with spinal cord injury or spina bifida. Eur Urol. 2006;49(1):22-28. Pubmed
UIJ
Paul F Siami, Knox BeasleyResearch Institute of Deaconess Clinic, Evansville, IN, USASubmitted October 24, 2011 - Accepted for Publication December 15, 2011
www.urotodayinternationaljournal.comVolume 5 - February 2012
Dutasteride with As-Needed Tamsulosin in Men at Risk of Benign Prostatic Hypertrophy Progression
ABSTRACT
Purpose: The primary aim of this study was to investigate whether initial therapy with dutasteride followed by
dutasteride with as-needed tamsulosin can prevent symptom progression in patients at a high risk of clinical
progression of benign prostatic hyperplasia (BPH).
Patients and Methods: This study was an open-label, single-site pilot study of 63 patients. Patients were men > 50
years of age, with a clinical diagnosis of BPH based on medical history, symptom scores, and medical exams. Each
patient was prescribed 0.5 mg once daily of dutasteride for 1 year, at which time 0.4 mg once daily of tamsulosin
was added. After 3 months of combination therapy, subjects were counseled to taper or discontinue tamsulosin
and to restart only on an as-needed basis. Patients returned to the clinic at 6, 9, and 12 months when they were
evaluated and drug compliance was measured.
Results: Adding tamsulosin to dutasteride resulted in a 41% improvement in IPSS and a 62% improvement in Qmax
after 3 and 6 months, respectively, which were maintained regardless of subsequent tamsulosin use.
Conclusion: The partial or total withdrawal of tamsulosin after 1 year of 5-ARI, followed by combination therapy
for 3 months, resulted in little or no deterioration of LUTS in men with BPH in the final 12 months of the study.
Dutasteride after 1 year (n = 63) Dutasteride + tamsulosin As-needed tamsulosin
Baseline 3 months 6 months 9 months 12 months
IPSS 19.80 11.76 11.30 12.07 11.31
Qmax 9.75 n/a 15.84 n/a 20.43
KEYWORDS: Dutasteride; Tamsulosin; Benign prostatic hyperplasia
CORRESPONDENCE: Paul F Siami, MD, 3521 Lincoln Ave, Evansville, IN 47714 USA ([email protected]).
CITATION: UroToday Int J. 2012 Feb;5(1):art 93. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/ 10.3834/uij.1944-5784.2012.02.11
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)

UroToday International Journal®
original study
Dutasteride with As-Needed Tamsulosin in Men at Risk of Benign Prostatic Hypertrophy Progression
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
INTRODuCTION
There is little doubt about the existence of benign prostatic hyperplasia (BPH) in men in the United States. Prevalence is at 40% in men 60 years of age and 90% for men 80 years or older [1]. Symptomatic BPH left untreated can progress to a worsening of symptoms, obstruction, acute urinary retention, infection, and the need for surgery [2]. Lower urinary tract symptoms (LUTS) typically arise from the prostate or bladder. Symptoms are classified into obstructive or irritative, and they can be rated on a scale, such as the International Prostate Symptom Score (IPSS). Currently, there are 2 drug classes with different mechanisms of action, which are the mainstay of the medical management of BPH. One class is the alpha-antagonist (α-blocker) and the second are the 5-alpha-reductase inhibitors (5-ARI). Efficacy with either agent as monotherapy has been demonstrated in other trials [3,4]. The use of these 2 classes in combination therapy to control LUTS due to BPH has been established in a number of studies [1,5].
Barkin et al. have demonstrated that BPH symptom relief can be maintained after withdrawal of the alpha-blocker tamsulosin from sustained combination therapy of dutasteride and tamsulosin. However, it has not been shown whether patients with BPH, who are at high risk for symptom progression and who achieve optimal improvement of symptoms on combination therapy followed by withdrawal of the alpha-blocker, will maintain the degree of improvement relative to the continuous coadministration of the 2 agents.
The objective of this study is to look at men with BPH who are at a high risk for symptom progression and who achieve optimal improvement of symptoms on combination therapy followed by withdrawal of the alpha-blocker. Will returning the alpha-blocker on an as-needed basis for symptom control maintain the degree of improvement relative to the continuous coadministration of the 2 agents?
This study in men with moderate to severe symptomatic BPH investigated the efficacy and safety of treatment with dutasteride (0.5 mg) once daily for 1 year and tamsulosin (0.4 mg), administered once daily for 3 months. Subjects were then counseled to begin flexible dosing of tamsulosin, if possible, taking it only on an as-needed basis, depending on the severity of symptoms and the clinical outcome.
METHODS
Study Design
This single-site, open-label study included 63 men > 50 years of age, with clinical diagnoses of BPH. Baseline assessments prior to beginning the study included eligibility criteria, medical history, physical exams (including digital rectal examination [DRE]), concomitant medication, hematology, serum chemistry, serum PSA, prostate volume by transrectal ultrasound (TRUS), maximum urine flow (Qmax), post-void residue (PVR), urinalysis, adverse events, BPH symptoms (IPSS), AUR (surgery/resource utilization), BPH impact index (BII), and evidence of urinary tract infection (UTI). Those subjects meeting all inclusion and exclusion criteria began combination therapy with 0.5 mg once daily of dutasteride and 0.4 mg once daily of tamsulosin for the first 3 months. Subjects then returned to the clinic every 3 months, for the next 9 months, for symptom assessment, dutasteride continuance counseling, and placement on flexible tamsulosin dosing on an as-needed basis according to symptom decline or improvement.
At the 3-month study visit, concomitant medications, adverse events, and vital signs were recorded. Subjects were questioned for evidence of UTI, AUR, hematuria, and hematospermia, and asked to complete the BII, PPSM, and IPSS. Any unused study medication was collected and counted, and a new 3-month supply was dispensed. Subjects were counseled to:
1. continue dutasteride on a daily basis, 2. discontinue, taper, or restart their tamsulosin as symptoms
might dictate, and 3. return to the clinic in 3 months.
At the 6-month study visit, the same assessments from the previous visit were again made, with the addition of PVR and urine flowmetry. A new supply of study medications was dispensed, subjects were counseled to discontinue, taper, or restart their tamsulosin as symptoms might dictate, and return to the clinic in 3 months. Subjects were counseled to:
1. continue dutasteride on a daily basis, 2. discontinue, taper, or restart their tamsulosin as symptoms
might dictate, and 3. return to clinic in 3 months.
At a 9-month study visit, concomitant medications, adverse events, and vital signs were recorded. Subjects were questioned for evidence of UTI, AUR, hematuria, and hematospermia, and asked to complete the BII, PPSM, and IPSS. Any unused study
UIJ

UroToday International Journal®
original study
Dutasteride with As-Needed Tamsulosin in Men at Risk of Benign Prostatic Hypertrophy Progression
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
medication was collected and counted, and a new 3-month supply was dispensed. Subjects were counseled to:
1. continue dutasteride on a daily basis, 2. discontinue, taper, or restart their tamsulosin as symptoms
might dictate, and3. return to the clinic in 3 months.
Subjects returned to the clinic at 12 months. Unused study medications were collected and counted. Subjects were evaluated as before, which included hematology, chemistry, total serum PSA, PVR, and flowmetry. Subjects were thanked and discharged from study participation.
LUTS were assessed at screening, baseline, and every 3 months using the self-administered IPSS questionnaire, including the BPH-related health status evaluation (question 8). PSA, hematology, and serum chemistries were performed at baseline, 6-month, and 12-month visits. Quality of life (QoL) was assessed using the PPSM and BII every 3 months. Qmax and PVR measurements were made at the initial screening, baseline, 6-month visit, and 12-month visit. TRUS was performed at the initial screening. Evidence for UTI, hematuria, and hematospermia was assessed every 3 months.
Study Population
Men > 50 years of age with a clinical diagnosis of BPH by medical history and physical exam, including digital rectal examination, were enrolled in the study. Other entry criteria were IPSS > 12, prostate volume > 30 cc (TRUS), total serum PSA > 1.5 ng/ml, Qmax > 5 and < 15 ml/second, minimum voided volume > 125 ml (based on 2 voids), and the ability to give informed consent and comply with the protocol for 1 year. Exclusion criteria were total serum PSA > 10 ng/ml, history or evidence of prostate cancer, previous prostate surgery, cystoscopic examination or catheterization within 7 days prior to screening, AUR within 3 months prior to screening, post-void residual volume > 250 ml, a history of breast cancer, any history or current use of drugs that would enhance or diminish the action of the study drugs or the occurrence of side effects (including anabolic steroids), the use of phytotherapy for BPH, renal insufficiency, malignancy other than basal-cell carcinoma, hypersensitivity to any study component, or participation in another study concurrently.
Study Endpoints
The primary endpoints were to determine the proportion of subjects who were able to discontinue tamsulosin without deterioration of symptoms and the average amount of
tamsulosin saved by those able to reduce or discontinue its usage. Effectiveness was assessed using IPSS and Qmax, while quality of life was measured by BII and PPSM. Safety was measured by UTI and AUR incidence and resource utilization. Pharmacoeconomic impact was calculated via direct tablet count.
Statistical Considerations
This was an open-label, single-arm observational study. All subjects were included in the intent-to-treat population. The population was analyzed in 4 dynamic cohorts based on tamsulosin usage after 3 months of combination therapy.
1. No change in dose as initiated at baseline.2. Increased or restarted tamsulosin after tapering or
discontinuing. 3. Reduced tamsulosin dosage.4. Discontinued tamsulosin completely.
The percent change in tamsulosin usage was based on the actual amount used based on pill count. For IPSS, Qmax, and QoL assessments, the values and change from month 0 were compared at month 3, month 6, month 9, and month 12.
RESuLTS
Subject Demographics and Disposition
Sixty-three subjects were enrolled in the study and entered into the combination therapy phase. Fifty-four subjects completed the study, 6 subjects discontinued due to adverse events, 2 subjects withdrew consent, and 1 subject was lost to follow-up (Tables 1 and 2). The mean age was 66 and the majority of
Table 1. Baseline characteristics.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11t1
Baseline parameters Value*
Age (years) 66.63
IPSS 19.8
PSA (nag/mL) 4.73
Prostate volume 57.65 cc
Qmax 9.75 ml/sec
PVR volume 82.33 ml*Unless otherwise noted, values are means.
UIJ
UroToday International Journal®
original study
Dutasteride with As-Needed Tamsulosin in Men at Risk of Benign Prostatic Hypertrophy Progression
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
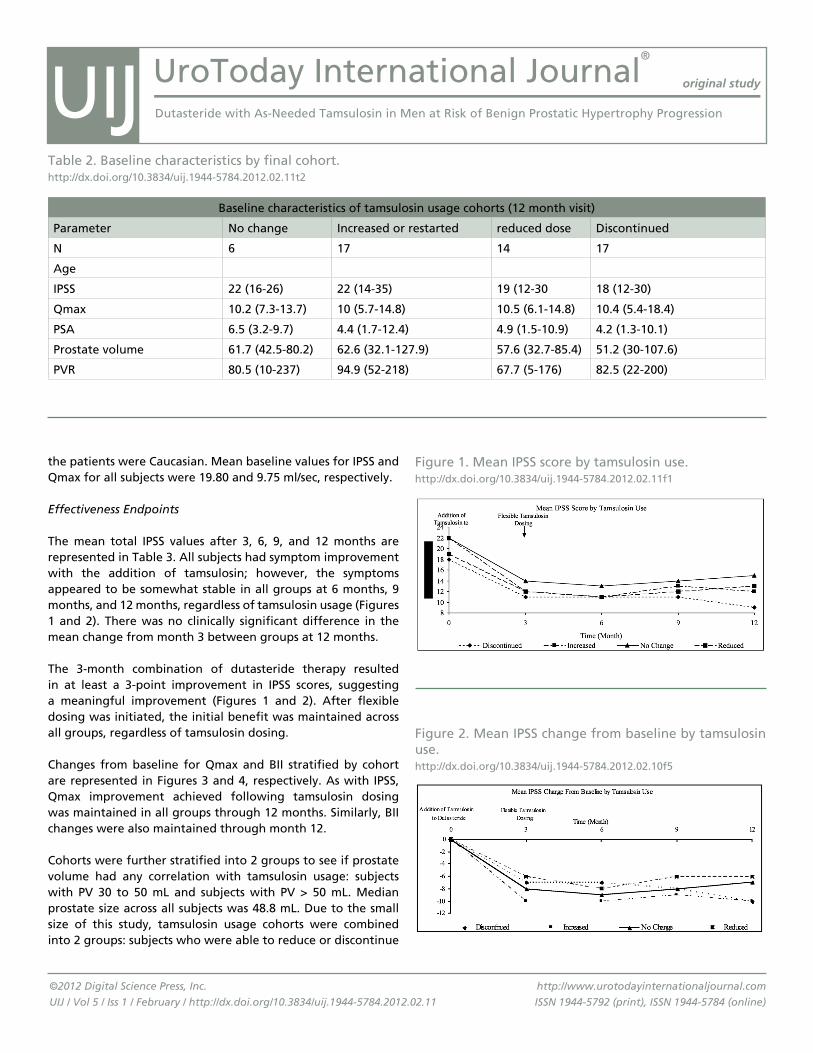
Baseline characteristics of tamsulosin usage cohorts (12 month visit)
Parameter No change Increased or restarted reduced dose Discontinued
N 6 17 14 17
Age
IPSS 22 (16-26) 22 (14-35) 19 (12-30 18 (12-30)
Qmax 10.2 (7.3-13.7) 10 (5.7-14.8) 10.5 (6.1-14.8) 10.4 (5.4-18.4)
PSA 6.5 (3.2-9.7) 4.4 (1.7-12.4) 4.9 (1.5-10.9) 4.2 (1.3-10.1)
Prostate volume 61.7 (42.5-80.2) 62.6 (32.1-127.9) 57.6 (32.7-85.4) 51.2 (30-107.6)
PVR 80.5 (10-237) 94.9 (52-218) 67.7 (5-176) 82.5 (22-200)
Table 2. Baseline characteristics by final cohort.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11t2
the patients were Caucasian. Mean baseline values for IPSS and Qmax for all subjects were 19.80 and 9.75 ml/sec, respectively.
Effectiveness Endpoints
The mean total IPSS values after 3, 6, 9, and 12 months are represented in Table 3. All subjects had symptom improvement with the addition of tamsulosin; however, the symptoms appeared to be somewhat stable in all groups at 6 months, 9 months, and 12 months, regardless of tamsulosin usage (Figures 1 and 2). There was no clinically significant difference in the mean change from month 3 between groups at 12 months.
The 3-month combination of dutasteride therapy resulted in at least a 3-point improvement in IPSS scores, suggesting a meaningful improvement (Figures 1 and 2). After flexible dosing was initiated, the initial benefit was maintained across all groups, regardless of tamsulosin dosing.
Changes from baseline for Qmax and BII stratified by cohort are represented in Figures 3 and 4, respectively. As with IPSS, Qmax improvement achieved following tamsulosin dosing was maintained in all groups through 12 months. Similarly, BII changes were also maintained through month 12.
Cohorts were further stratified into 2 groups to see if prostate volume had any correlation with tamsulosin usage: subjects with PV 30 to 50 mL and subjects with PV > 50 mL. Median prostate size across all subjects was 48.8 mL. Due to the small size of this study, tamsulosin usage cohorts were combined into 2 groups: subjects who were able to reduce or discontinue
Figure 1. Mean IPSS score by tamsulosin use.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11f1
Figure 2. Mean IPSS change from baseline by tamsulosin use.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.10f5
UIJ

UroToday International Journal®
original study
Dutasteride with As-Needed Tamsulosin in Men at Risk of Benign Prostatic Hypertrophy Progression
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
tamsulosin usage, and subjects who either had no change or increased tamsulosin usage, respectively (Table 5).
The Patient Perception of Study Medication (PPSM) questionnaire was evaluated case by case. While these patients reported outcomes that were inconsistent across all measures in all cohorts, it appears to the investigator that trends were consistent with the objective measures also employed in this study.
Safety Profile and Tolerability
Tolerability has been well established in previous studies, in both monotherapy and combination regimens. Adverse events emergent in this study are reported in Table 4. Of 149 total adverse events reported, only 27 were designated as possibly or probably study-drug related: 8 had altered ejaculation, 4 had vertigo, 3 had fatigue, 2 had nasal congestion, 2 had gynecomastia, 2 had erectile dysfunction, 2 had decreased libido, 1 had urgency incontinence, 1 had headache, 1 had rash, and 1 had postural hypotension. Two subjects were discontinued from study participation while the remainder completed the study. No subjects experienced AUR that required utilization of resources, such as catheterization or surgery.
Six subjects experienced 11 serious adverse events but none were study related. There was 1 death, but the remaining subjects completed the study.
DISCuSSION
Men with BPH often present with a wide constellation of LUTS that respond well to pharmacotherapy. Long-range studies have demonstrated that both dutasteride and tamsulosin can
Table 3. Changes in mean values for IPSS and Qmax, for all subjects.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11t3
Baseline 3 months
6 months
9 months
12 months
IPSS 19.8 11.76 11.3 12.07 11.31
Qmax 9.75 n/a 15.84 n/a 20.43
Figure 3. Qmax changes from baseline by tamsulosin use.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11f3
Figure 4. BII changes from baseline by tamsulosin use.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11f4
Number of patients with at least 1 adverse event, by body system
Body system Total Drug related
Body as a whole 7 3
Cardiovascular system 18 1
Digestive system 9 1
Endocrine system 6 2
Hemic and lymphatic system 0 0
Metabolic and nutritional disorders 2 0
Musculoskeletal system 18 0
Nervous system 19 4
Respiratory system 31 1
Skin and appendages 15 2
Urogenital system 24 13
Table 4. Adverse events by body system.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11t4
UIJ

UroToday International Journal®
original study
Dutasteride with As-Needed Tamsulosin in Men at Risk of Benign Prostatic Hypertrophy Progression
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
initiate rapid improvement and maintain that level of relief for an extended period. We also know that combination therapy provides enhanced symptom relief when compared to monotherapy. Unfortunately, the number of study-drug related adverse events increase with combination therapy, as demonstrated in the combination of Avodart and tamsulosin (CombAT) trial.
Remarkably, all subjects maintained similar improvement from baseline at 1 year, regardless of whether the subject:
1. made no change in tamsulosin usage as initiated at baseline,
2. restarted tamsulosin after tapering or discontinuing tamsulosin,
3. reduced tamsulosin usage, or4. discontinued tamsulosin completely.
These data suggest that:
1. in patients whose symptoms are not adequately controlled on a 5-ARI alone, the addition of tamsulosin shows an additional benefit in symptom improvement, and
2. after maximal improvement has been seen in combination therapy, individualization of the tamsulosin dose based upon the patient’s clinical status dosing might be possible (coadministration with dutasteride and tamsulosin or monotherapy with dutasteride).
Furthermore, analysis of tamsulosin usage by prostate volume revealed that patients with smaller prostates (30 to 50 mL) were more likely to reduce or discontinue tamsulosin usage, whereas patients with larger prostates (> 50 mL) had similar outcomes across all cohorts.
We also observed that those subjects who started with the
PV = 30-50 mL PV > 50 mL
Reduced/discontinued tamsulosin
18 13
No change/increased tamsulosin
10 13
Table 5. Number of patients in each cohort, further divided by prostate volume.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11t5
highest IPSS scores at baseline, and who had derived the greatest benefit from adding tamsulosin, tended to stay on combination therapy or added tamsulosin after discontinuing at 3 months. This may have resulted from reluctance to discontinue symptom relief or the perception of symptoms returning after discontinuing combination therapy. Those subjects who were on dutasteride monotherapy at 1 year seemed to trend toward further improvement, but the sample size was insufficient to produce confirmatory results. No subjects experienced AUR or required utilization of resources for safety issues, underscoring the safety of all of the self-selected regimens.
CONCLuSION
This study, while small in size, suggests that symptom relief in subjects with BPH may be maintained or improved with dutasteride monotherapy following symptom optimization with dutasteride and tamsulosin combination therapy for 3 months. The limitations to this trial are it’s size and observational design. Prostate volume may be a key clinical parameter to the use of intermittent combination of tamsulosin and dutasteride. A larger prospective, statistically adequate, double blind placebo-controlled study will be needed to corroborate our results.
REfERENCES
1. Roehrborn CG, Siami P, Barkin J, et al. The effects of dutasteride, tamsulosin and combination therapy on lower urinary tract symptoms in men with benign prostatic hyperplasia and prostatic enlargement: 2-year results from the CombAT study. J Urol. 2008;179(2):616-612. PubMed ; CrossRef
2. Emberton M, Cornel EB, Bassi PF, et al. Benign prostatic hyperplasia as a progressive disease: a guide to the risk factors and options for medical management. Int J Clin Pract. 2008;62(7):1076-1086. PubMed ; CrossRef
3. Kirby RS, Roehrborn P, Boyle P, Bartach G, et al. Efficacy and tolerability of doxazocin and finasteride, alone or in combination, in treatment of symptomatic benign prostatic hyperplasia: The Prospective European Doxazocin and Combination Therapy (PREDICT) trial. Urology. 2003;61(1):119-126. PubMed ; CrossRef
4. Lepor H, Williford WO, Barry MJ, et al. The effects of Terazosin, finasteride, or both in benign prostatic hyperplasia. Veterans Affairs Cooperative Studies Benign Prostatic Hyperplasia Study Group. N Eng J Med. 1996;335(8):533-539. PubMed ; CrossRef
UIJ
UroToday International Journal®
original study
Dutasteride with As-Needed Tamsulosin in Men at Risk of Benign Prostatic Hypertrophy Progression
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.11
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
5. McConnel JD, Roehrborn CG, Bautista OM, et al. The long term effect of doxazosin, finasteride, and combination therapy on clinical progression of BPH. N Engl J Med. 2003;349(25):2387-2398. PubMed ; CrossRef
6. Barkin J, Guimarães M, Jacobi G, et al. Alpha-blocker therapy can be withdrawn in the majority of men following initial combination therapy with the dual 5alpha-reductase inhibitor dutasteride. Eur Urol. 2003;44(4):461-466. PubMed ; CrossRef
UIJ

Christopher CK Ho, Teo Chee Yang, Phang Lay Fang, Nur Aziyana Noor Azizi, Farah Lyna Darwin, Nur Afifah Mohd Ghazi, Guan Hee Tan, Eng Hong Goh, Praveen Singam, Badrulhisham Bahadzor, Zulkifli Md ZainuddinUrology Unit, Department of Surgery, Faculty of Medicine, Universiti Kebangsaan Malaysia Medical Centre, Jalan Yaacob Latiff, Bandar Tun Razak, 56000 Cheras, Kuala Lumpur, Malaysia Submitted November 7, 2011 - Accepted for Publication November 23, 2011
www.urotodayinternationaljournal.comVolume 5 - February 2012
Prevalence and Risk Factors Associated with Overactive Bladder
ABSTRACT
Introduction: The pathophysiology and management of overactive bladder (OAB) has been the subject of intensive
research, but the prevalence of OAB in the community has not been well documented. This study aims to determine
the prevalence of OAB among men and women attending the Universiti Kebangsaan Malaysia Medical Centre
(UKMMC). This study also shows the impact of OAB on daily life activities and associated risk factors.
Methods: Four hundred respondents, aged between 18 to 70 years and visiting UKMMC, were interviewed and
scored using the validated OAB screener. Information on sociodemographic data, the effects of OAB on daily living
activities, and possible risk factors were included in the questionnaire.
Results: The prevalence of overactive bladder in the study population was 42%. The most common symptom
complaint was nocturia (94%). Gender (p = 0.004) and family history (p = 0.016) were related to a higher prevalence
of overactive bladder. Males were significantly affected with the odd ratio of 1.792 compared to females. Race,
age, monthly income, occupation, family, and smoking history were not associated with OAB. The most commonly
affected activity of daily living in OAB patients is sleep disturbance (43.5%).
Conclusion: The study has shown that the prevalence of OAB is relatively high in the Malaysian community,
especially among males, and those with a positive family history. This has warranted closer attention to the issue.
Preemptive measures should be taken by health care givers, the government, and the community to raise OAB
awareness among society.
KEYWORDS: Prevalence; Overactive bladder; Daily living activities; Risk factors
CORRESPONDENCE: Christopher CK Ho, Department of Surgery, Faculty of Medicine, Universiti Kebangsaan Malaysia Medical Centre, Jalan Yaacob Latiff, Bandar Tun Razak, 56000 Cheras, Kuala Lumpur, Malaysia ([email protected]).
CITATION: UroToday Int J. 2012 Feb;5(1):art 88. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/ 10.3834/uij.1944-5784.2012.02.06
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
INTRODuCTION
The International Continence Society (ICS) defines overactive
bladder (OAB) as “urgency, with or without urge urinary incontinence (UI), usually associated with frequency and nocturia” [1]. However, many studies have used different

UroToday International Journal®
original study
Prevalence and Risk Factors Associated with Overactive Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
definitions of OAB in their results, which have made comparisons across studies difficult, and the prevalence rates have differed widely [2-6].
Using the ICS definition, a study among Asian men in 11 countries found that the estimated prevalence of OAB among men was 29.9% [7], whereas another study done on women showed the prevalence of OAB was 54.1% [8]. Also, from these 2 studies, it was found that OAB was more common among professional workers (43%), high-income groups (26%, income of > RM 2660), and urban dwellers (64%). With increased age, there was an increased incidence of OAB; i.e., the prevalence was 53% in men aged > 70 years [7,8]. Other than that, there is a significant relationship between OAB and a positive family history [7,8].
A study was conducted on the role of nicotine in the micturition reflex in rats. It was found that nicotine had significant stimulation on the nicotinic acetylcholine receptors on bladder activity [9]. Another population-based study done in Finland showed that a history of smoking may increase the risk of lower urinary tract symptoms, with the odds ratios of 1.39 and 1.34 for current and former smokers, respectively, compared to men who never smoked [10]. However, additional research on the association of smoking and OAB needs to be done to establish this possible linkage more clearly.
OAB has a significant impact on the quality of life of men who are affected by disturbing urinary symptoms [11,12]. Wagner et al. (2002) also reported a significant association between OAB and urinary tract infection, fall injuries, and more frequent visits to their physicians [13]. In the NOBLE study, Stewart et al. (2003) found that OAB has a significant impact on quality of life, quality of sleep, and mental health, in both men and women [5]. Studies have found that most people with OAB used non-medical coping strategies and would like to speak with a health care provider about their disturbing symptoms [14,15].
The pathophysiology and management of OAB has been the subject of intensive research, but the prevalence of OAB in the community has not been well documented [16,17]. Published reports on the effects of OAB on quality of life are also limited [10], suggesting that OAB is generally under-diagnosed and under-treated [18]. Globally, except for a European report [19], there has been no comprehensive epidemiological survey on OAB. We, therefore, aim to conduct a population-based study in a multiethnic population in Malaysia and determine the prevalence of OAB in men and women. We also study how OAB affects the activity of daily living in this group and if there are any associated sociodemographic and health-related attributes.
OAB can be treated, which involves behavioral therapy, physiotherapy, and pharmacotherapy. Most clinicians would start treatment by physiotherapy through bladder training, which is a reasonable first-line therapy. However, pharmacotherapy allows the patient to improve more rapidly. Anticholinergic drugs are the main pharmacotherapy agents, such as oxybutynin and tolterodine. A study was conducted to determine the effectiveness of anticholinergic drugs in the treatment of OAB. Results have shown that anticholinergics produce significant improvements in OAB symptoms; however, the effectiveness of these drugs is still unclear [20].
The general objective of this research was to study the epidemiology of overactive bladder among men and women attending UKMMC. Our specific objective was to determine the prevalence of OAB in the population in UKMMC, the sociodemographic and health-related attributes in this population, the impact on activities of daily living in OAB patients, and, last but not least, to identify the risk factors associated with OAB.
MATERIALS AND METHODS
The Research and Ethical Committee, Faculty of Medicine, University Kebangsaan, Malaysia (FF-291-2010), approved this research.
This is a cross-sectional, face-to-face, community-based survey. It was conducted in all the clinics, the main lobby, the visitor’s lobby, and all the departments in UKMMC, except the urology clinic. Private rooms were sought in the designated locations to ensure respondent confidentiality. The fieldwork took 4 months. The respondents were men and women, aged between 18 to 70 years, coming to UKMMC. They were patients from all clinics, the relatives of the patients, and the staff of UKMMC (except the urology clinic). Two hundred men and 200 women were randomly selected for this study (convenience sampling). Patients, relatives, and staff in UKMMC who refused to participate; those unable to respond to the questionnaire accordingly; those who have other obvious pathological problems, such as urinary tract infection, stones, BPH, etc.; or patients who are being treated in the urology clinic were excluded from this study.
The diagnostic criteria of OAB was based on the International Continence Society (ICS) definition of OAB: “OAB is urgency, with or without urge urinary incontinence (UI), usually associated with frequency and nocturia after the exclusion of any obvious pathology such as infection or stones.”
UIJ
UroToday International Journal®
original study
Prevalence and Risk Factors Associated with Overactive Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
We used the questionnaires from the OAB screener —OAB-V8 study—and collected data on the symptoms of urgency, frequency, nocturia, and urge urinary incontinence, and how each of these symptoms bothered them. Having the score of 8 or greater indicated that the respondent had overactive bladder. For sociodemography, health status, and daily living activity disturbance, a questionnaire was designed to document the participants’ sociodemographic data; e.g., age, gender, race, etc.).
The questionnaire was self-administered by the respondents who were assisted by medical students, when necessary. During the face-to-face interview, written consent was obtained from the respondents.
The prevalence of OAB symptoms (urgency, frequency, nocturia, and urge incontinence) was described in percentages. The association between these symptoms and the sociodemographic data and health status were analyzed using the chi-square test. All data were entered and analyzed using the Statistical Package for the Social Sciences (SPSS), version 19, and OpenEpi (www.openepi.com/OE2).
RESuLTS
Study Population Demographics
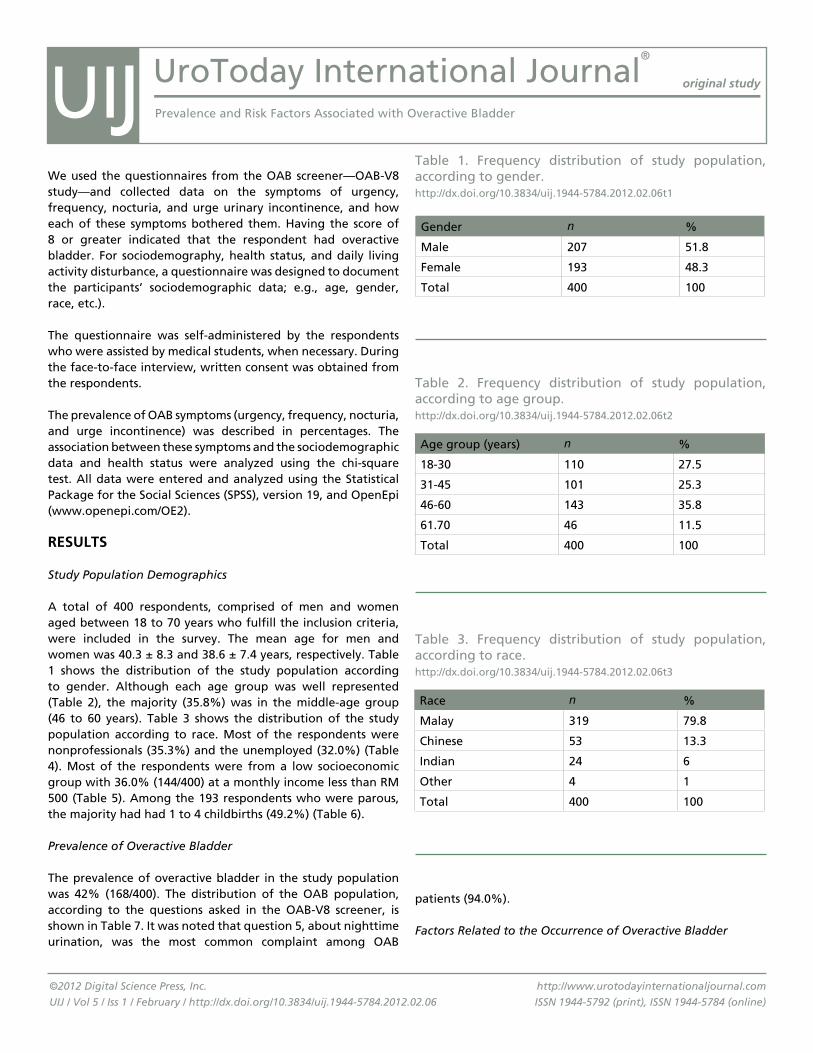
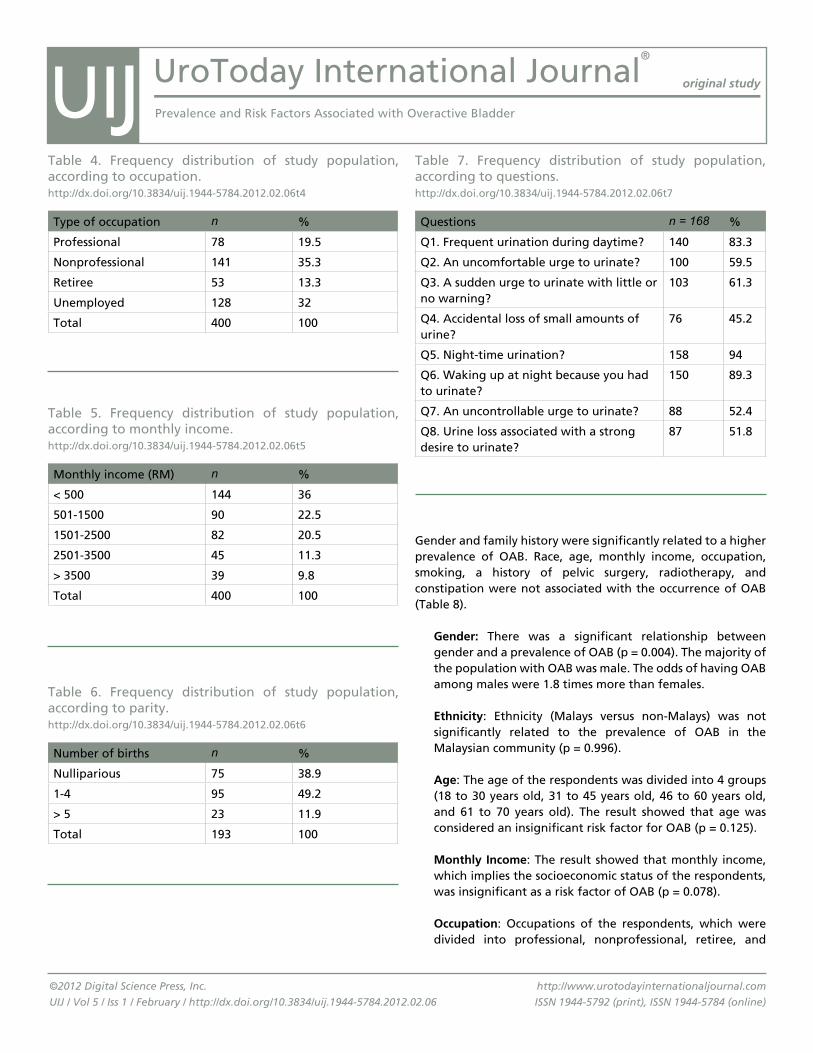
A total of 400 respondents, comprised of men and women aged between 18 to 70 years who fulfill the inclusion criteria, were included in the survey. The mean age for men and women was 40.3 ± 8.3 and 38.6 ± 7.4 years, respectively. Table 1 shows the distribution of the study population according to gender. Although each age group was well represented (Table 2), the majority (35.8%) was in the middle-age group (46 to 60 years). Table 3 shows the distribution of the study population according to race. Most of the respondents were nonprofessionals (35.3%) and the unemployed (32.0%) (Table 4). Most of the respondents were from a low socioeconomic group with 36.0% (144/400) at a monthly income less than RM 500 (Table 5). Among the 193 respondents who were parous, the majority had had 1 to 4 childbirths (49.2%) (Table 6).
Prevalence of Overactive Bladder
The prevalence of overactive bladder in the study population was 42% (168/400). The distribution of the OAB population, according to the questions asked in the OAB-V8 screener, is shown in Table 7. It was noted that question 5, about nighttime urination, was the most common complaint among OAB
patients (94.0%).
Factors Related to the Occurrence of Overactive Bladder
Gender n %
Male 207 51.8
Female 193 48.3
Total 400 100
Age group (years) n %
18-30 110 27.5
31-45 101 25.3
46-60 143 35.8
61.70 46 11.5
Total 400 100
Race n %
Malay 319 79.8
Chinese 53 13.3
Indian 24 6
Other 4 1
Total 400 100
Table 1. Frequency distribution of study population, according to gender.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06t1
Table 2. Frequency distribution of study population, according to age group.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06t2
Table 3. Frequency distribution of study population, according to race.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06t3
UIJ
UroToday International Journal®
original study
Prevalence and Risk Factors Associated with Overactive Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
Gender and family history were significantly related to a higher prevalence of OAB. Race, age, monthly income, occupation, smoking, a history of pelvic surgery, radiotherapy, and constipation were not associated with the occurrence of OAB (Table 8).
Gender: There was a significant relationship between gender and a prevalence of OAB (p = 0.004). The majority of the population with OAB was male. The odds of having OAB among males were 1.8 times more than females.
Ethnicity: Ethnicity (Malays versus non-Malays) was not significantly related to the prevalence of OAB in the Malaysian community (p = 0.996).
Age: The age of the respondents was divided into 4 groups (18 to 30 years old, 31 to 45 years old, 46 to 60 years old, and 61 to 70 years old). The result showed that age was considered an insignificant risk factor for OAB (p = 0.125).
Monthly Income: The result showed that monthly income, which implies the socioeconomic status of the respondents, was insignificant as a risk factor of OAB (p = 0.078).
Occupation: Occupations of the respondents, which were divided into professional, nonprofessional, retiree, and
Type of occupation n %
Professional 78 19.5
Nonprofessional 141 35.3
Retiree 53 13.3
Unemployed 128 32
Total 400 100
Table 4. Frequency distribution of study population, according to occupation.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06t4
Monthly income (RM) n %
< 500 144 36
501-1500 90 22.5
1501-2500 82 20.5
2501-3500 45 11.3
> 3500 39 9.8
Total 400 100
Table 5. Frequency distribution of study population, according to monthly income.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06t5
Number of births n %
Nulliparious 75 38.9
1-4 95 49.2
> 5 23 11.9
Total 193 100
Table 6. Frequency distribution of study population, according to parity.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06t6
Questions n = 168 %
Q1. Frequent urination during daytime? 140 83.3
Q2. An uncomfortable urge to urinate? 100 59.5
Q3. A sudden urge to urinate with little or no warning?
103 61.3
Q4. Accidental loss of small amounts of urine?
76 45.2
Q5. Night-time urination? 158 94
Q6. Waking up at night because you had to urinate?
150 89.3
Q7. An uncontrollable urge to urinate? 88 52.4
Q8. Urine loss associated with a strong desire to urinate?
87 51.8
Table 7. Frequency distribution of study population, according to questions.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06t7
UIJ
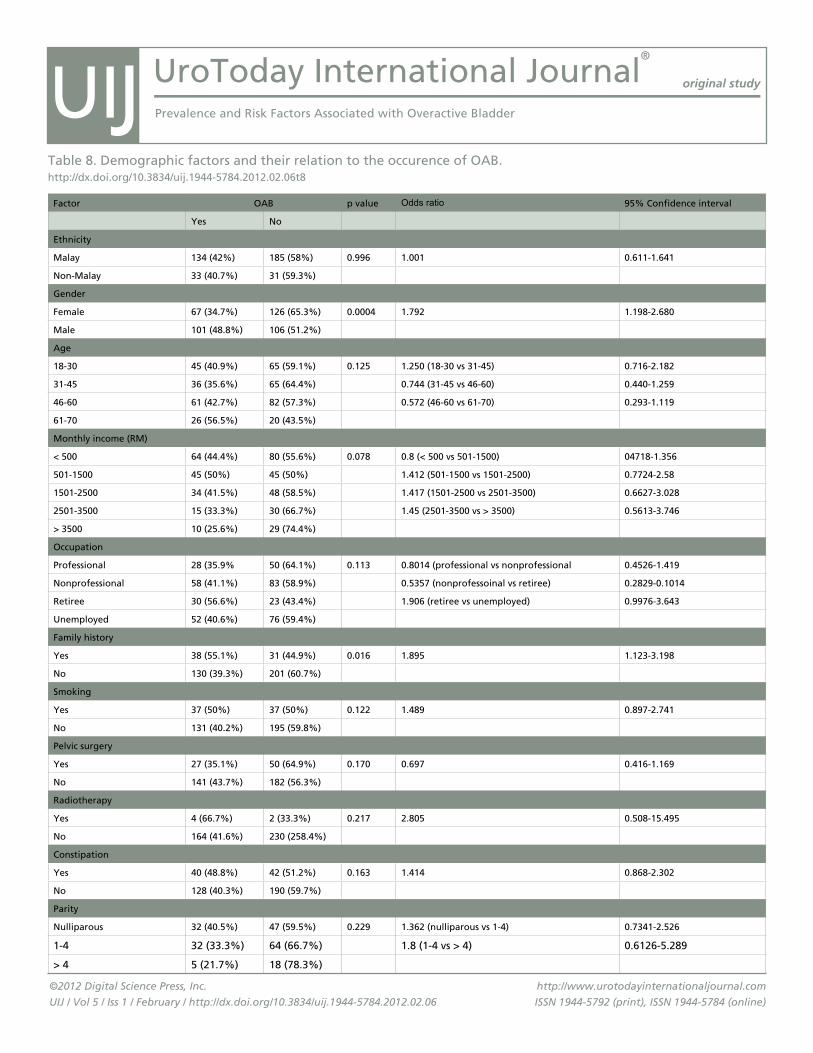
UroToday International Journal®
original study
Prevalence and Risk Factors Associated with Overactive Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
Factor OAB p value Odds ratio 95% Confidence interval
Yes No
Ethnicity
Malay 134 (42%) 185 (58%) 0.996 1.001 0.611-1.641
Non-Malay 33 (40.7%) 31 (59.3%)
Gender
Female 67 (34.7%) 126 (65.3%) 0.0004 1.792 1.198-2.680
Male 101 (48.8%) 106 (51.2%)
Age
18-30 45 (40.9%) 65 (59.1%) 0.125 1.250 (18-30 vs 31-45) 0.716-2.182
31-45 36 (35.6%) 65 (64.4%) 0.744 (31-45 vs 46-60) 0.440-1.259
46-60 61 (42.7%) 82 (57.3%) 0.572 (46-60 vs 61-70) 0.293-1.119
61-70 26 (56.5%) 20 (43.5%)
Monthly income (RM)
< 500 64 (44.4%) 80 (55.6%) 0.078 0.8 (< 500 vs 501-1500) 04718-1.356
501-1500 45 (50%) 45 (50%) 1.412 (501-1500 vs 1501-2500) 0.7724-2.58
1501-2500 34 (41.5%) 48 (58.5%) 1.417 (1501-2500 vs 2501-3500) 0.6627-3.028
2501-3500 15 (33.3%) 30 (66.7%) 1.45 (2501-3500 vs > 3500) 0.5613-3.746
> 3500 10 (25.6%) 29 (74.4%)
Occupation
Professional 28 (35.9% 50 (64.1%) 0.113 0.8014 (professional vs nonprofessional 0.4526-1.419
Nonprofessional 58 (41.1%) 83 (58.9%) 0.5357 (nonprofessoinal vs retiree) 0.2829-0.1014
Retiree 30 (56.6%) 23 (43.4%) 1.906 (retiree vs unemployed) 0.9976-3.643
Unemployed 52 (40.6%) 76 (59.4%)
Family history
Yes 38 (55.1%) 31 (44.9%) 0.016 1.895 1.123-3.198
No 130 (39.3%) 201 (60.7%)
Smoking
Yes 37 (50%) 37 (50%) 0.122 1.489 0.897-2.741
No 131 (40.2%) 195 (59.8%)
Pelvic surgery
Yes 27 (35.1%) 50 (64.9%) 0.170 0.697 0.416-1.169
No 141 (43.7%) 182 (56.3%)
Radiotherapy
Yes 4 (66.7%) 2 (33.3%) 0.217 2.805 0.508-15.495
No 164 (41.6%) 230 (258.4%)
Constipation
Yes 40 (48.8%) 42 (51.2%) 0.163 1.414 0.868-2.302
No 128 (40.3%) 190 (59.7%)
Parity
Nulliparous 32 (40.5%) 47 (59.5%) 0.229 1.362 (nulliparous vs 1-4) 0.7341-2.526
1-4 32 (33.3%) 64 (66.7%) 1.8 (1-4 vs > 4) 0.6126-5.289
> 4 5 (21.7%) 18 (78.3%)
Table 8. Demographic factors and their relation to the occurence of OAB.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06t8
UIJ
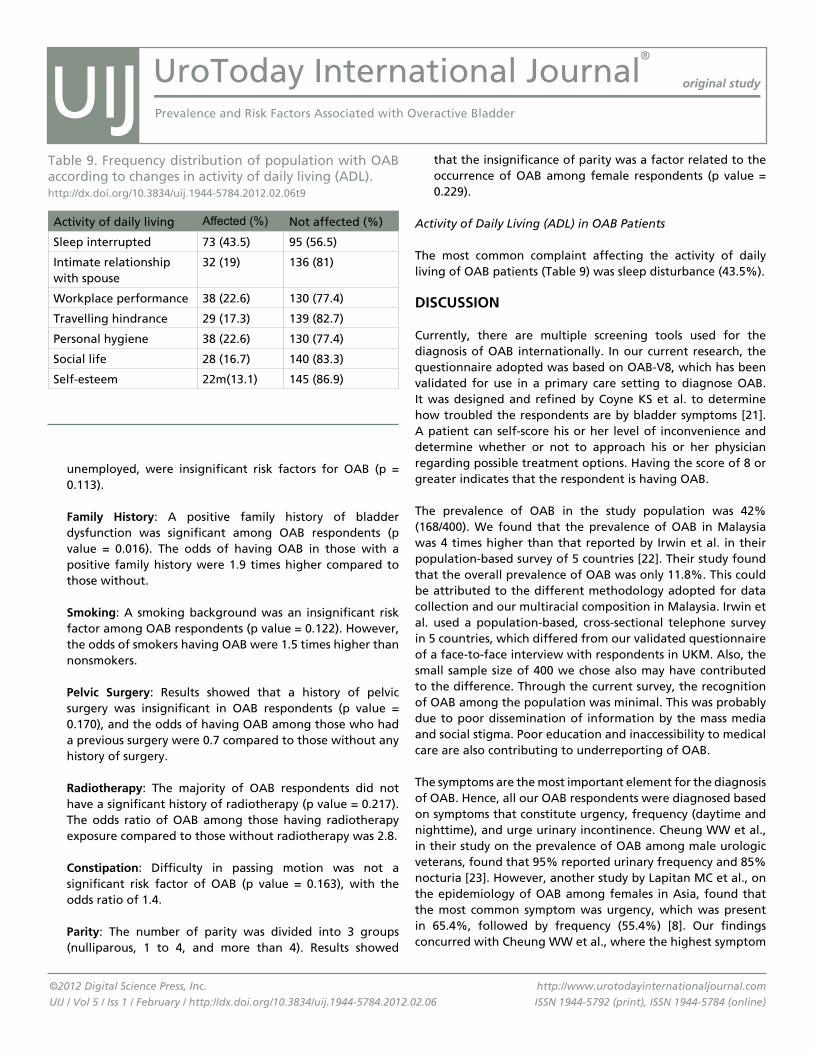
UroToday International Journal®
original study
Prevalence and Risk Factors Associated with Overactive Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
unemployed, were insignificant risk factors for OAB (p = 0.113).
Family History: A positive family history of bladder dysfunction was significant among OAB respondents (p value = 0.016). The odds of having OAB in those with a positive family history were 1.9 times higher compared to those without.
Smoking: A smoking background was an insignificant risk factor among OAB respondents (p value = 0.122). However, the odds of smokers having OAB were 1.5 times higher than nonsmokers.
Pelvic Surgery: Results showed that a history of pelvic surgery was insignificant in OAB respondents (p value = 0.170), and the odds of having OAB among those who had a previous surgery were 0.7 compared to those without any history of surgery.
Radiotherapy: The majority of OAB respondents did not have a significant history of radiotherapy (p value = 0.217). The odds ratio of OAB among those having radiotherapy exposure compared to those without radiotherapy was 2.8.
Constipation: Difficulty in passing motion was not a significant risk factor of OAB (p value = 0.163), with the odds ratio of 1.4.
Parity: The number of parity was divided into 3 groups (nulliparous, 1 to 4, and more than 4). Results showed
that the insignificance of parity was a factor related to the occurrence of OAB among female respondents (p value = 0.229).
Activity of Daily Living (ADL) in OAB Patients
The most common complaint affecting the activity of daily living of OAB patients (Table 9) was sleep disturbance (43.5%).
DISCuSSION
Currently, there are multiple screening tools used for the diagnosis of OAB internationally. In our current research, the questionnaire adopted was based on OAB-V8, which has been validated for use in a primary care setting to diagnose OAB. It was designed and refined by Coyne KS et al. to determine how troubled the respondents are by bladder symptoms [21]. A patient can self-score his or her level of inconvenience and determine whether or not to approach his or her physician regarding possible treatment options. Having the score of 8 or greater indicates that the respondent is having OAB.
The prevalence of OAB in the study population was 42% (168/400). We found that the prevalence of OAB in Malaysia was 4 times higher than that reported by Irwin et al. in their population-based survey of 5 countries [22]. Their study found that the overall prevalence of OAB was only 11.8%. This could be attributed to the different methodology adopted for data collection and our multiracial composition in Malaysia. Irwin et al. used a population-based, cross-sectional telephone survey in 5 countries, which differed from our validated questionnaire of a face-to-face interview with respondents in UKM. Also, the small sample size of 400 we chose also may have contributed to the difference. Through the current survey, the recognition of OAB among the population was minimal. This was probably due to poor dissemination of information by the mass media and social stigma. Poor education and inaccessibility to medical care are also contributing to underreporting of OAB.
The symptoms are the most important element for the diagnosis of OAB. Hence, all our OAB respondents were diagnosed based on symptoms that constitute urgency, frequency (daytime and nighttime), and urge urinary incontinence. Cheung WW et al., in their study on the prevalence of OAB among male urologic veterans, found that 95% reported urinary frequency and 85% nocturia [23]. However, another study by Lapitan MC et al., on the epidemiology of OAB among females in Asia, found that the most common symptom was urgency, which was present in 65.4%, followed by frequency (55.4%) [8]. Our findings concurred with Cheung WW et al., where the highest symptom
Activity of daily living Affected (%) Not affected (%)
Sleep interrupted 73 (43.5) 95 (56.5)
Intimate relationship with spouse
32 (19) 136 (81)
Workplace performance 38 (22.6) 130 (77.4)
Travelling hindrance 29 (17.3) 139 (82.7)
Personal hygiene 38 (22.6) 130 (77.4)
Social life 28 (16.7) 140 (83.3)
Self-esteem 22m(13.1) 145 (86.9)
Table 9. Frequency distribution of population with OAB according to changes in activity of daily living (ADL).http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06t9
UIJ

UroToday International Journal®
original study
Prevalence and Risk Factors Associated with Overactive Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
complaint among OAB patients was nocturia [23].
A study by Stewart WF et al., conducted in a US population, showed that the overall prevalence of OAB was similar between men (16.0%) and women (16.9%) [5]. A study conducted in Venezuela showed females were more affected than males (25.6% in women versus 13.7% in men, p < 0.005) [24]. A study conducted in the US (New York) shows that OAB was present in 60.5% of men and 48.3% of women (p = 0.058) [23]. Our finding was somehow consistent with the latter where there was a significant relationship between gender and the prevalence of OAB, with the majority of the OAB population being male. The odds of having OAB among males were 1.8 times more than females.
The previous study has shown that increased age is a strong risk factor associated with OAB, and it has been proposed that this is due to decreasing bladder capacity, estrogen deficiency, degenerative neuronal control, and connective tissue changes as age progresses [8,25]. This finding is supported by the National Overactive Bladder Evaluation (NOBLE) study, which showed that the prevalence of OAB symptomatology increases with age in both men and women [8]. However, we found that the age of the respondents was considered an insignificant risk factor for OAB. Surprisingly, there was evidence of a decreasing trend in OAB patients as age increases, suggesting that somehow, with increasing age, one may have protective factors toward OAB. Unfortunately, up to date, there is no specific research being done on this pattern, and the reason is unknown. One of the limitations from our research was that the number of respondents from each age group was not evenly distributed and bias of the result may exist.
So far, there was no research done to investigate the influence of ethnicity towards OAB. In Malaysia, there was no specific research done to compare the 3 main races, namely the Malay, Chinese, and Indian population. It was found that the difference between the prevalence of OAB among the ethnic groups (Malay versus non-Malay) was insignificant (p = 0.996, OR = 1.001). The relationship between overactive bladder with occupation and monthly income were also insignificant. The result was similar with the outcome of the study conducted on Asian women [8]. However, the odds ratio for monthly income showed an increasing trend. This pattern was consistent with a study done on Asian men, which reported a higher incidence of OAB in the high-income group [7]. This might be related to their awareness towards OAB symptoms, as well as the need to seek treatment among this group.
Previous studies have related many risk factors to OAB, such
as relevant smoking history and childbirth history, among others [7,8]. A genetic locus (D13S171) was found in patients with detrusor overactivity (DO) or OAB phenotypes in a study revealing its genetic linkage in Australia and the United Kingdom [26]. A positive family history of OAB symptoms was evident and proved significant in this study (p = 0.016, OR = 1.895), therefore suggesting a possible genetic predisposition. However, more studies should be done to validate this theory.
In a study on the roles of central and peripheral nicotinic receptors in the micturition reflex in rats, nicotinic acetylcholine receptor activation of the C-fiber afferent nerves in the bladder induces detrusor overactivity. Other than that, the receptors in the spinal cord and brain have an excitatory and inhibitory effect on the bladder, as well, indicating that there is influence on the bladder lining from nicotine exposure [9]. Yet, smoking history was insignificant in our study (p = 0.122, OR = 1.489). It may be due to the sample distribution of the male-to-female ratio being about 0.5. The smoking prevalence rate was higher among Malaysian males compared to women (49.2% compared to 3.5%, respectively) in a study where 4 countries (Singapore, the Philippines, Vietnam, and Malaysia) were explored pertaining to gender and tobacco issues. Therefore, our results may be biased in that only the male respondents have a significant influence on smoking history [27].
Studies have shown that prior pelvic and reconstructive surgeries may denervate the bladder [28,29]. Patients who underwent a hysterectomy may experience OAB symptoms postoperatively due to the disruption of autonomic nerve fibers running along the pelvic plexus. However, this pathophysiology is not well understood, and most studies only involved women post hysterectomy or post pelvic organ prolapse (POP) surgery. Therefore, this opens a new opportunity to study pelvic surgeries as a predictive factor of OAB in both genders. Nevertheless, prior pelvic surgery was found insignificant in our study (p = 0.170, OR = 0.697).
There was no evidence of radiotherapy being a significant risk factor in causing OAB symptoms (p = 0.217, OR = 2.805). Though researchers have investigated the possibility of pelvic radiotherapy effects on the bladder causing urinary incontinence [35], there is not yet a definitive pathophysiology to this condition. Therefore, more objective research should be done, specifically to evaluate this risk factor.
There was no clear evidence to relate constipation as a risk factor to OAB (p = 0.163, OR = 1.414). However, other studies have revealed its significant occurrence with OAB, which further exacerbate the symptoms [30-32]. This is due to a shared
UIJ

UroToday International Journal®
original study
Prevalence and Risk Factors Associated with Overactive Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
pathophysiology, a side effect of the antimuscarinic drugs in treating OAB, or due to dietary reasons in order to control the OAB symptoms. Along with poor fluid intake, constipation has been a common complaint among OAB patients.
Research has been conducted, revealing multiparity (parity of > 4) as a risk factor in causing OAB symptoms, and that multiparous women were 1.5 times more at risk than the nulliparous, or those with only 1 pregnancy [8]. Even so, in this current study, there was no evidence of parity being significant in OAB (p = 0.229), though it was found that there is a trend increase with a parity increase (OR nulliparous versus a parity of 1 to 4 = 1.362, and OR parity of 1 to 4 versus multiparous women = 1.8). It is said that childbearing and childbirth may damage the peripheral nerves in the pelvis, resulting in a hyperactive bladder [33,34]. However, subjects were randomly approached in this study, with 198 female respondents. Of those, 69 were positive for OAB. Among those who were positive, only 5 were multiparous (7.25%). Thus, the majority of female subjects were either considered nulliparous, 32/69 (46.38%), or with parity < 5, also 32/69 (46.38%). This has a significant impact on the aforementioned factor and, therefore, may not be applicable in its validity.
The impact of OAB in daily life has been emphasized in several studies. Wagner et al. reported a significant association between OAB and urinary tract infection, fall injuries, and frequent visits to physicians [13]. In the NOBEL study, Stewart WF et al. found that OAB has a significant impact on the quality of life, quality of sleep, and mental health in both men and women [5]. In this study, the impact on sleep, intimate relationships with spouses, workplace performance, travel, personal hygiene, social life, and self-esteem in OAB patients was brought to attention. Most patients complained that sleep disturbance had the most troublesome impact (43.5%). This was consistent with the aforementioned nocturia symptoms as the most bothersome among OAB patients. The impact on ADL was followed by a change in workplace performance and personal hygiene, which equaled 22.6% for both. In regards to the impact of the remaining factors: intimate relationships with spouse were 19%, travelling hindrance was 17.3%, social life was 16.7%, and, lastly, self-esteem was 13.1%.
Other factors that have not been analyzed in this study are the volumetric fluid intake, as well as dietary issues. An increased fluid intake will result in increased urine production. This will cause frequency, as well as nocturia. Besides that, certain drinks, such as alcohol and caffeine, have diuretic effects that will result in OAB symptoms, such as frequency and nocturia. Indeed, it has been shown that the reduction of fluid input by
25% produces a significant improvement in urgency, frequency, and nocturia [36].
CONCLuSION
The study has shown that the prevalence of OAB is relatively high in the Malaysian community, especially among males and those with a positive family history. This has warranted closer attention to the issue. Preemptive measures should be taken by the health care givers, the government, and the community to raise awareness of OAB among society. Among the effective measures proposed are the incorporation of OAB knowledge in curricular education, better coverage by the mass media, improvement in health care policy, and better education of the public by health care workers. Meanwhile, more studies should be done to further prove risk factors associated with the occurrence of OAB in Malaysia.
REFERENCES
1. Abrams P, Cardozo L, Fall M, Griffiths D, Rosier P, Ulmsten U, et al. The standardization of terminology of lower urinary tract function: report from the Standardization Sub-committee of the International Continence Society. Neurourol Urodyn. 2002;21(2):167-178. PubMed ; CrossRef
2. Corcos J, Schick E. Prevalence of overactive bladder and incontinence in Canada. Canadian J Urol. 2004;11(3):2278-2284. PubMed
3. Homma Y, Yamaguchi O, Hayashi K, Neurogenic Bladder Society Committee. An epidemiological survey of overactive bladder symptoms in Japan. Br J Urol. 2005;96(9):1314-1318. PubMed ; CrossRef
4. Milsom I, Abrams P, Cardozo L, Roberts RG, Thüroff J, Wein AJ. How widespread are the symptoms of an overactive bladder and how are they managed? A population-based prevalence study. Br J Urol. 2001;87(9):760-766. PubMed
5. Stewart WF, Van Rooyen JB, Cundiff GW, Abrams P, Herzog AR, Corey R, et al. Prevalence and burden of overactive bladder in the United States. World J Urol. 2003;20(6):327-336. PubMed
6. Temml C, Heidler S, Ponholzer A, Madersbacher S. Prevalence of the overactive bladder syndrome by applying the International Continence Society definition. Eur Urol. 2005;48(4):622-627. PubMed ; CrossRef
UIJ
UroToday International Journal®
original study
Prevalence and Risk Factors Associated with Overactive Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
7. Moorthy P, Lapitan MC, Quek PL, Lim PH. Prevalence of Overactive Bladder in Asian Men: An Epidemiological Survey. BJU Int. 2004;93(4):528-531. PubMed ; CrossRef
8. Lapitan MC, Chye PL, Asia-Pacific Continence Advisory Board. The Epidemiology of Overactive Bladder among Females in Asia: A Questionnaire Survey. Int Urogynecol J Pelvic Floor Dysfunct. 2001;12(4):226-231. PubMed ; CrossRef
9. Masuda H, Hayashi Y, Chancellor MB, Kihara K, de Groat WC, de Miguel F, et al. Roles of peripheral and central nicotine receptors in micturition reflex in rats. J Urol. 2006;176(1):374-379. PubMed ; CrossRef
10. Milsom I, Stewart W, Thüroff JW. The prevalence of overactive bladder. Am J Manag Care. 2000;6(suppl 11):S565-573. PubMed
11. Liberman JN, Hunt TL, Stewart WF, Wein A, Zhou Z, Herzog AR, et al. Health related quality of life among adults with symptoms of overactive bladder: results from a US community-based survey. Urology. 2001;57(6):1044-1050. PubMed ; CrossRef
12. Coyne KS, Payne C, Bhattacharyya SK, Revicki DA, Thompson C, Corey R, et al. The impact of urinary urgency and frequency on health related quality of life in overactive bladder: results from a national community survey. Value Health. 2004;7(4):455-463. PubMed ; CrossRef
13. Wagner TH, Hu TW, Bentkover J, LeBlanc K, Stewart W, Corey R, et al. Health related consequences of overactive bladder. Am J Manag Care. 2002;8(suppl 19):S598-607. PubMed
14. Ricci JA, Baggish JS, Hunt TL, Stewart WF, Wein A, Herzog AR, et al. Coping strategies and health care seeking behavior in US National sample of adults with symptoms suggestive of overactive bladder. Clin Ther. 2001;23(8):1245-1259. PubMed ; CrossRef
15. Irwin DE, Milsom I, Kopp Z, Abrams P, EPIC Study Group. Symptom bother and health care seeking behavior among individuals with overactive bladder. Eur Urol. 2008;53(5):1029-1037. PubMed ; CrossRef
16. Payne CK. Epidemiology, pathophysiology, and evaluation of urinary incontinence and overactive bladder. Urology. 1998;51(suppl 2A):3-10. PubMed ; CrossRef
17. Chu FM, Dmochowski R. Pathophysiology of Overactive Bladder. Am J Med. 2006;119(3, suppl 1):3-8. PubMed ; CrossRef
18. Wein AJ. Overactive bladder: Defining the disease. Am J Manag Care. 2000;6(suppl 11):S559-564. PubMed
19. Hempel C, Wienhold D, Benken N, Eggersmann C, Thüroff JW. Definition of overactive bladder and epidemiology of urinary incontinence. Urology. 1997;50(suppl 6A):4-14. PubMed ; CrossRef
20. Herbison P, Hay-Smith J, Ellis G, Moore K. Effectiveness of anticholinergic drugs compared with placebo in the treatment of OAB: systematic review. BMJ. 2003;326(7394):841-844. PubMed ; CrossRef
21. Coyne KS, Zyczynski T, Margolis MK, Elinoff V, Roberts RG. Validation of an overactive bladder awareness tool for use in a primary care setting. Adv Ther. 2005;22(4):381-394. PubMed ; CrossRef
22. Irwin D, Milsom I, Hunskaar S, Reilly K, Kopp Z, Herschorn S, et al. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50(6):1306-1314. PubMed ; CrossRef
23. Cheung WW, Khan NH, Choi KK, Bluth MH, Vincent MT. Prevalence, evaluation and management of overactive bladder in primary care. BMC Fam Pract. 2009;10:8. PubMed ; CrossRef
24. Dávila HA, López V, Nieves L, Colantuono A, Guaiquirián L, Sánchez P, et al. [Demographic distribution and prevalence of overactive bladder in Venezuela]. Actas Urol Esp. 2010;34(2):176-180. PubMed
25. Moorthy P, Lapitan MC, Quek PL, Lim PH. Prevalence of overactive bladder in Asian men: an epidemiological survey. BJU Int. 2004;93(4):528-531. PubMed ; CrossRef
26. Morris AR, Mullan G, Roscioli T, Buckley MF, Moore KH. A Genetic Linkage Study of Detrusor Overactivity. Neurourol Urodyn. 2003;22(5):460-461.
27. Morrow M, Barraclough S. Tobacco Control and Gender in South-east Asia. Part II: Singapore and Vietnam. Health Promot Int. 2003;18(4):373-380. PubMed ; CrossRef
UIJ
UroToday International Journal®
original study
Prevalence and Risk Factors Associated with Overactive Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.06
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
28. Zullo MA, Manci N, Angioli R, Muzil L, Panici PB. Vesical Dysfunctions After Radical Hysterectomy for Cervical Cancer: A Critical Review. Crit Rev Oncol Hematol. 2003;48(3):287-293. PubMed ; CrossRef
29. de Boer TA, Kluivers KB, Withagen MI, Milani AL, Vierhout ME. Predictive Factors for Overactive Bladder Symptoms After Pelvic Organ Prolapse Surgery. Int Urogynecol J. 2010;21(9):1143-1149. PubMed ; CrossRef
30. Coyne KS, Cash B, Kopp Z, Gelhorn H, Milsom I, Berriman S, et al. The Prevalence of Chronic Constipation and Faecal Incontinence Among Men and Women With Symptoms of Overactive Bladder. BJU Int. 2011;107(2):254-261. PubMed ; CrossRef
31. Abrams P, Freeman R, Anderström C, Mattiasson A. Tolterodine, A New Antimuscarinic Agent: As Effective but Better Tolerated Than Oxybutynin in Patients with an Overactive Bladder. Br J Urol. 1998;81(6):801-810. PubMed ; CrossRef
32. Wyman JF, Burgio KL, Newman DK. Practical Aspects of Lifestyle Modifications and Behavioural Interventions in the Treatment of Overactive Bladder and Urgency Incontinence. Int J Clin Pract. 2009;63(8):1177-1191. PubMed ; CrossRef
33. Allen RE, Hosker GL, Smith ARB, Warrell DW. Pelvic Floor Damage and Childbirth: A Neurophysiological Study. Br J Obstet Gynaecol. 1990;97(9):770-779. CrossRef
34. Snooks SJ, Swash M, Setchell M, Henry MM. Injury to Innervation of Pelvic Floor Sphincter Musculature in Childbirth. Lancet. 1984;324(8402):546-550. CrossRef
35. Rackley R, DeBlieux PMC, Firoozi F, et al. Urinary incontinence. http://emedicine.medscape.com/article/452289-overview#aw2aab6b2b4. Updated June, 2011. Accessed June 24, 2011.
36. Hashim H, Abrams P. How should patients with an overactive bladder manipulate their fluid intake? BJU Int. 2008;102(1):62-66. PubMed ; CrossRef
UIJ

Rógerson Tenório de Andrade,1 Marina de Andrade Lima Arcoverde,2 Fábio Oliveira Vilar,1 Misael Wanderley Santos Jr,1 Nicodemos Teles Pontes Filho,3 Salvador Vilar Correia Lima1
1Department of Urology, Federal University of Pernambuco, Recife, Brazil2Federal University of Pernambuco, Recife, Brazil3Post-graduation Program of Pathology, Federal University of Pernambuco, Recife, BrazilSubmitted September 27, 2011 - Accepted for Publication December 9, 2011
www.urotodayinternationaljournal.comVolume 5 - February 2012
Clinical Epidemiologic Study of Penile Cancer in the State of Pernambuco, Brazil
ABSTRACT
Introduction: Penile cancer is a malignant disease that has an uneven geographical distribution. Brazil is one of the
countries with the highest incidence of penile cancer, although epidemiological studies are rare. Poor hygiene, the
presence of phimosis, HPV infection, and low socioeconomic status seem to be some important risk factors. The
objective of this study is to know the clinical and epidemiological data on new cases of penile cancer in the state of
Pernambuco, located in the northeast region of Brazil, and contribute to the national study of the Brazilian Society
of Urology.
Methods: We selected from a plethora of new penile cancer cases diagnosed from August 2008 to June 2009, at
the department of urology of 5 referral hospitals of the National Health System. Interviews were conducted with a
clinical, epidemiological questionnaire adapted from the questionnaire used by the SBU in the first epidemiological
study of penile cancer. All patients gave written, informed consent for inclusion in the sample. This study was
approved by the ethics committees of the institutions involved.
Results: In 11 months of the study, 32 new cases of penile cancer were enrolled and analyzed in 5 referral hospitals
in Pernambuco. The average age of lesion diagnosis was 59.2 years (SD ± 14.3 years), with 50% of cases diagnosed
in patients over 60 years. Regarding schooling, 92% were illiterate or had only a primary level of schooling, and
none advanced beyond the second grade. Assessing the antecedents and habits, it was found that 8 patients (32%)
had at least 1 case of a lifelong STD, 14 patients (56%) reported a history of phimosis, and only 4 (16%) underwent
circumcision, 3 of which during adulthood. Smoking was an addiction reported by 56.2% of patients. The average
time between the appearance of the lesion and the diagnosis of penile cancer was higher than 10 months.
Conclusion: Penile cancer in referral hospitals of Pernambuco usually involves men older than 60 years, with low
education, a history of smoking, uncircumcised genitalia, and with delayed access to specialized medical care. It is
necessary to create campaigns for the prevention and guidance of this most affected population.
KEYWORDS: Circumcision; Epidemiology; Penile cancer; Phimosis; Risk factors
CORRESPONDENCE: Marina de Andrade Lima Arcoverde, Federal University of Pernambuco, Recife, Brazil ([email protected]).
CITATION: UroToday Int J. 2012 Feb;5(1):art 91. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.09
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/ 10.3834/uij.1944-5784.2012.02.09
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)

UroToday International Journal®
original study
Clinical Epidemiologic Study of Penile Cancer in the State of Pernambuco, Brazil
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.09
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
INTRODuCTION
Penile cancer is a malignant disease that has a curiously uneven geographical distribution [1]. In Europe, the incidence is rare, and varies between 0.1 and 0.9 per 100 000 males. In the US, it varies between 0.7 and 0.9 per 100 000 males. However, the incidence of penile cancer is significantly higher when dealing with developing countries in regions such as Africa, Asia, and South America, where it can reach 20 per 100 000 males [2]. In these countries, penile cancer remains a major public health issue since it represents 10 to 20% of all malignancies in men [2].
Penile cancer represents approximately 2 percent of all cancers in males in Brazil, with most cases reported in the north and the northeast regions [3]. In these areas, penile carcinoma outnumbers, in some states, even the cases of prostate and bladder cancer [4]. Although the etiology of cancer is unknown, poor hygiene, the presence of phimosis, HPV infection, and low socioeconomic status are known risk factors [5]. Age is one of the main risk factors while ethnicity is not [6,7].
Phimosis is present in 75 to 90% of penile cancer cases [8]. The incidence of penile cancer is extremely low, reaching less than 1 percent of all diagnosed cancers, in countries where circumcision is a common practice [6]. The prophylactic effect of circumcision in penile carcinoma appears to be related to less retention of the smegma that has, arguably, a carcinogenic and inflammatory effect in animals [9].
Another factor that may predispose the development of penile carcinoma is HPV infection. In some reports, the association between penile cancer and HPV reaches over 30% of the patients, revealing the oncogenic effect of the virus, also in men [7,10]. Other skin lesions, such as Queirat erythroplasia, Bowen’s disease, and balanitis xerotic, can also develop into squamous cell carcinoma (SCC) in the penile region [11], the first 2 already considered by some authors as carcinoma in situ since they are composed of dysplastic characteristic cells [12].
Some studies reveal that SCC is the most common type of penile cancer, accounting for more than 95% of the cases [11, 23]. Penile cancer primarily spreads through the lymphatic system. Inguinal lymph nodes are usually the first site of metastasis [11]. The treatment is mainly surgical, which may be a simple resection, partial, or complete amputation and emasculation [6].
Recife, the capital of Pernambuco, has a penile cancer incidence of 6.8/100 000 [13], which is higher than American and European
rates, but quite similar to both north and northeast regions of Brazil where this type of cancer is mostly located [3]. Therefore, the primary objective of this study is to analyze the clinical and epidemiological profile of penile cancer in Pernambuco, contributing to the Brazilian epidemiological tracing initiated by the Brazilian Society of Urology, and also to prove the under-reported cases of penile cancer in the state in Pernambuco in that previous study. The outcome data, such as disease-specific survival rate, type of surgery performed, and functional outcomes, does not meet the interest of this work.
METHODS
This work was carried out in Pernambuco State, located in the northeast region of Brazil, through a multicenter study conducted in 5 referral hospitals, for the treatment of urological cancer in the state; all 5 were part of the National Health System.
We studied every new case of penile carcinoma diagnosed and admitted in the urology services of these institutions, from August 2008 to June 2009, representing a total of 32 patients. We excluded from the study all patients diagnosed with disease at a stage of premalignancy, those with inconclusive histopathological examinations, as well as those who refused to participate. The hospitals’ protocols on penile cancer were followed properly.
Through an interview with the selected patients, we filled out a clinical, epidemiological questionnaire, adapted from the questionnaire used by the Brazilian Society of Urology in the first epidemiological study of penile cancer [3].
The variables in the questionnaire were age, education level, a history of STD or preneoplastic disease, a partner with a history of HPV infection or cervical cancer, smoking, a history of phimosis and/or performing circumcision, the time between the appearance of the lesion and the diagnosis, site of the lesion, and histology.
Age was a categorical factor in this research, divided by decades of life. Schooling was divided into illiterate, primary education (elementary and middle school), secondary education (high school), and tertiary education (college and university). For patients who underwent circumcision, it was classified according to when the surgery took place (childhood, adolescence, or adulthood). The lesion was classified according to the involvement of the region, such as glans; foreskin; shaft; base; glans and foreskin; glans, foreskin, and shaft; or the entire penis. According to the histological differentiation, the lesions
UIJ
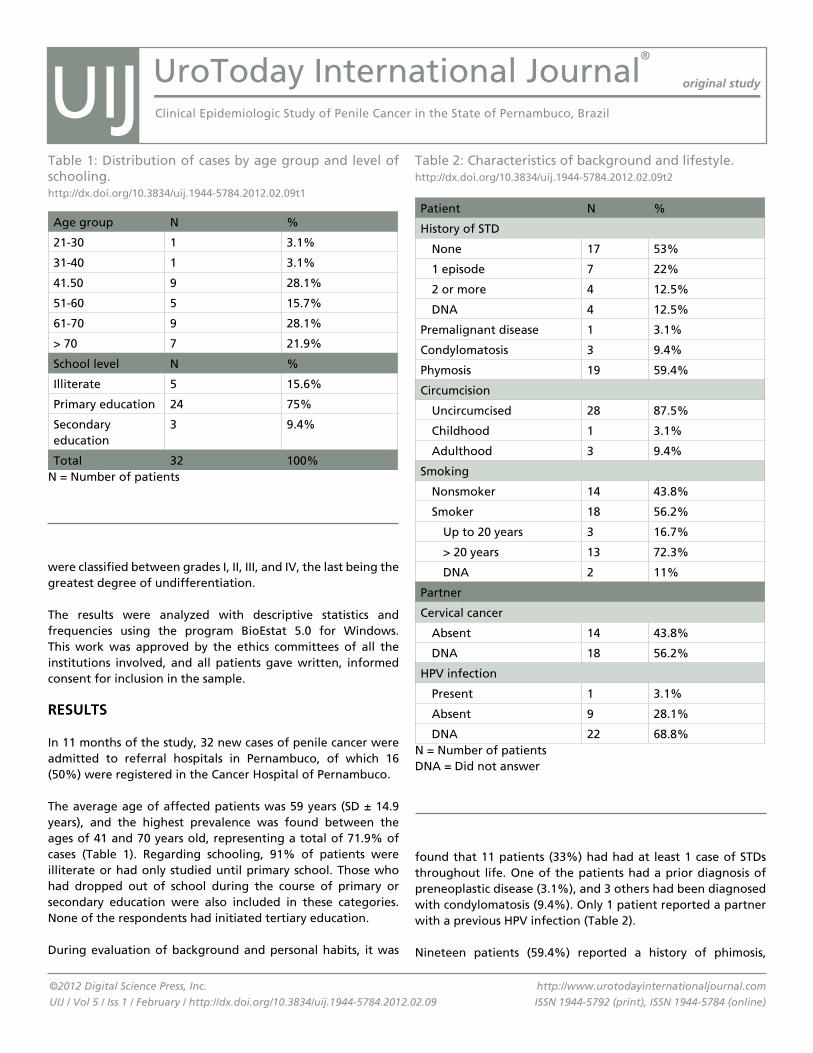
UroToday International Journal®
original study
Clinical Epidemiologic Study of Penile Cancer in the State of Pernambuco, Brazil
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.09
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
were classified between grades I, II, III, and IV, the last being the greatest degree of undifferentiation.
The results were analyzed with descriptive statistics and frequencies using the program BioEstat 5.0 for Windows. This work was approved by the ethics committees of all the institutions involved, and all patients gave written, informed consent for inclusion in the sample.
RESuLTS
In 11 months of the study, 32 new cases of penile cancer were admitted to referral hospitals in Pernambuco, of which 16 (50%) were registered in the Cancer Hospital of Pernambuco.
The average age of affected patients was 59 years (SD ± 14.9 years), and the highest prevalence was found between the ages of 41 and 70 years old, representing a total of 71.9% of cases (Table 1). Regarding schooling, 91% of patients were illiterate or had only studied until primary school. Those who had dropped out of school during the course of primary or secondary education were also included in these categories. None of the respondents had initiated tertiary education.
During evaluation of background and personal habits, it was
found that 11 patients (33%) had had at least 1 case of STDs throughout life. One of the patients had a prior diagnosis of preneoplastic disease (3.1%), and 3 others had been diagnosed with condylomatosis (9.4%). Only 1 patient reported a partner with a previous HPV infection (Table 2).
Nineteen patients (59.4%) reported a history of phimosis,
Table 1: Distribution of cases by age group and level of schooling.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.09t1
Age group N %
21-30 1 3.1%
31-40 1 3.1%
41.50 9 28.1%
51-60 5 15.7%
61-70 9 28.1%
> 70 7 21.9%
School level N %
Illiterate 5 15.6%
Primary education 24 75%
Secondary education
3 9.4%
Total 32 100%N = Number of patients
Table 2: Characteristics of background and lifestyle.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.09t2
Patient N %
History of STD
None 17 53%
1 episode 7 22%
2 or more 4 12.5%
DNA 4 12.5%
Premalignant disease 1 3.1%
Condylomatosis 3 9.4%
Phymosis 19 59.4%
Circumcision
Uncircumcised 28 87.5%
Childhood 1 3.1%
Adulthood 3 9.4%
Smoking
Nonsmoker 14 43.8%
Smoker 18 56.2%
Up to 20 years 3 16.7%
> 20 years 13 72.3%
DNA 2 11%
Partner
Cervical cancer
Absent 14 43.8%
DNA 18 56.2%
HPV infection
Present 1 3.1%
Absent 9 28.1%
DNA 22 68.8%N = Number of patientsDNA = Did not answer
UIJ

UroToday International Journal®
original study
Clinical Epidemiologic Study of Penile Cancer in the State of Pernambuco, Brazil
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.09
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
poor genital hygiene, and both are important factors in the development of the disease [13]. The level of schooling in this study was used as a socioeconomic status meter and revealed that over 90% of patients had not exceeded the level of primary education. Since the northeast still has an illiteracy rate of 18.7% [14], and one of the lowest incomes per capita in Brazil, it is expected that this region contributes to a large portion of total penile cancer in the country, which, according to the Brazilian Society of Urology, corresponds to 40% [3]. There is evidence that lack of hygiene in the genital region makes the individual more vulnerable to HPV infection, this being one of the links between poor hygiene and penile cancer. On the other hand, it is notable that the socioeconomic-cultural status interferes in the time between the onset of the lesion and the diagnosis, since people with low purchasing power have greater difficulties accessing specialists, and they usually rely on alternatives or popular therapies without proven effect.
Although the mechanism of action of HPV and other STDs in the formation of oncogenic cells is not fully elucidated, some studies show a strong association between them [15]. HPV seems to act by altering the cell cycle by the expression of viral proteins that interact with cellular proteins. These cellular proteins disrupt the strict cell-cycle control by tumor suppressing genes, which turns the infection into a strong precursor of tumors [7]. In our study, 34% of patients (n = 11) reported previous cases of unspecified STDs, while another 12.5% did not answer the question. Additionally, 9.4% of interviewed patients (n = 3) reported the presence of condylomatous lesions in the penis. In a study published in 2008, HPV-positive DNA was detected in 72% cases of penile carcinoma patients with squamous cell, while in another study, the association between penile cancer and HPV infection was 30.5% [16]. It is important to remember that the data collected in our research was not confirmed by laboratory tests, but still indicates the importance of sexually transmitted diseases as a risk factor for penile cancer. Furthermore, due to the low social-intellectual level of the patients, the use of a written questionnaire made it difficult to learn precise information about previous HPV infection, although, at the time, no patients had active HPV lesions.
Another identified risk factor was the presence of phimosis, found in 59.4% of our cases. Studies report that phimosis, as well as chronic inflammation of the glans, increases the odds of developing penile cancer by 10 [17]. In turn, the practice of circumcision is a good way to prevent the neoplasm since it is performed soon after birth, decreasing the risk of developing the pathology by 3 [18]; however, when performed later in adulthood, it does not offer the same protection [5]. In our study, 4 patients had undergone circumcision as adults,
of which only 4 (12.5%) were circumcised. Smoking was an addiction reported by 56.2% of patients, with an average of 29.3 years of addiction for patients who smoke.
Regarding diagnosis, the average time between the appearance of the lesion and the diagnosis of penile cancer was 10.8 months (SD ± 2.08 months), and the sizes of the lesions ranged from 0.7 to 10 cm, with an average 4.08 cm lesion. The most affected areas were the glans and/or the prepuce, representing a total 71.8% of cases.
The predominant histologic type was well differentiated SCC (lesions I) found in 26 patients (81.25%), followed by the pattern of moderately differentiated cell carcinoma (lesions II) in 2 patients (9.4%). Only 1 case had a diagnosis of mucoepidermoid carcinoma. Another patient had a histopathological diagnosis of papillary hyperplasia, as well differentiated SCC, when the previous biopsy was diagnosed. A single patient had grade IV injury, with the presence of undifferentiated cells.
In surgical treatment, there were 21 partial penectomies (65.6%), 10 total penectomies (31.3%), and 1 circumcision (3.1%).
DISCuSSION
Brazil is one of the countries with the highest incidence of penile cancer in the world, and even then, epidemiological studies are rare. Recently, the Brazilian Society of Urology (SBU) conducted a national study on penile cancer, aiming to outline an epidemiological profile of the disease in the country [3] and adopt preventive, diagnostic, and prophylactic measures. In that study, Pernambuco contributed with only 1 case, for a total of 110 reported cases in 6 months across the country. Our research demonstrates that the occurrence of penile cancer in the state of Pernambuco is much higher, making it clear that they were underreported since there is notification of 32 new cases in 11 months.
Penile cancer occurs more frequently in men after the sixth decade of life [6]. In the current sample, 50% of patients were over 60 years. Of the total cases analyzed, only 1 (3.1%) was aged 35 years, this incidence being significantly lower than the 10% reported by Nardi [3]. On the other hand, a high prevalence of penile cancer was noticed among the age group between 41 to 60 years, representing 43.8% of the total. This emphasizes the importance of close monitoring of nonelderly patients with suspicious penile lesions.
The low socioeconomic cultural status is closely related to
UIJ

UroToday International Journal®
original study
Clinical Epidemiologic Study of Penile Cancer in the State of Pernambuco, Brazil
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.09
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
and even then, the tumor took place, which agrees with the literature. Although there is no data showing the relationship between personal hygiene, phimosis, and penile cancer, some scholars believe that good hygiene is the key to preventing both the development of phimosis and the tumor once they are strictly related [2,19,20].
It was observed that 56.2% (n = 18) of patients in this study were smokers, and 72.3% (n = 13) had smoked for more than 20 years. According to a study by Daling et al., male smokers are more likely to develop invasive penile carcinoma [21]. Another study argues that the incidence of penile cancer is 2.4 times greater for those who are or were smokers, with the largest number found in the group of men that smoked more than 20 cigarettes per day [22]. There are suspicions that the same way that nicotine accumulates in the secretion of the cervix in women smokers could accumulate in the secretions of the penis, developing its carcinogenic effect in the region [23]. It is noted, therefore, that smoking, along with the presence of phimosis, is presented as an extremely important risk factor for penile cancer.
The average time between the appearance of the lesion and the diagnosis exceeded 10 months, which is an alarming number. It reveals the patient’s difficulty in accessing a specialist. This number may also result from the ignorance of the population and its fear of surgical treatment. This delay in diagnosis radically affects the treatment of the disease, and usually leaves mutilating surgery as the only viable treatment. In 65.5% of the patients, partial penectomy was performed. Total penectomy was performed in 31.3% of the patients, and only 1 patient (3.1%) was treated with circumcision. Therefore, early diagnosis is of great importance for a better resolution of the disease. It may also avoid radical surgery and its physical, psychological, and sexual impact.
CONCLuSION
This study found an epidemiological pattern of penile cancer in the state of Pernambuco was similar to that observed in the rest of the country, with a higher prevalence of penile cancer among men after the sixth decade of life, with a low education level, with an uncircumcised penis, a history of smoking, and those who do not seek medical care immediately. These findings show the immediate necessity to create a national campaign for prevention and guidance of matters regarding penile cancer, particularly for the low-income male population, which is the most affected class.
REfERENCES
1. Barbosa Júnior AA, Athanázio PR, Oliveira B. [Cancer of the penis: study of its geographic pathology in the State of Bahia, Brazil]. Rev Saúde Pública. 1984;18(6):429-435. PubMed ; CrossRef
2. Pizzocaro G, Algaba F, Horenblas S, Solsona E, Tana S, Van Der Poel H, et al. EAU Penile Cancer Guidelines 2009. Eur Urol. 2010;57(6):1002-1012. PubMed ; CrossRef
3. Favorito LA, Nardi AC, Ronalsa M, Zequi SC, Sampaio FJ, Glina S. [Epidemiologic study on penile cancer in Brazil]. Int Braz J Urol. 2008;34(5):587-591. PubMed ; CrossRef
4. Instituto Nacional do Câncer. Câncer de Pênis. http://www2.inca.gov.br/wps/wcm/connect/tiposdecancer/site/home/penis. Accessed December 15, 2010.
5. Dagher R, Selzer ML, Lapides J. Carcinoma of the penis and the anti-circumcision crusade. J Urol. 1973;110(1):79-80. PubMed
6. De Paula AAP, Almeida Netto JC, Cruz AD, Freitas R Jr. Carcinoma epidermóide do pênis: considerações epidemiológicas, histopatológicas, influência viral e tratamento cirúrgico. Rev Bras de Cancerol. 2005;51(3):243-252.
7. Reis AA, De Paula LB, Paula AA, Saddi VA, Cruz AD. [Clinico-epidemiological aspects associated with penile cancer]. Ciên Saúde Colet. 2010;15(suppl 1):1105-1111. PubMed ; CrossRef
8. Srougi M, Simon SD. Câncer do pênis. Em Câncer Urológico. 1995;447-468.
9. Micali G, Innocenzi D, Nasca MR, Musumeci ML, Ferraú F, Greco M. Squamous cell carcinoma of the penis. J Am Acad Dermatol. 1996;35(3 pt 1):432-451. PubMed ; CrossRef
10. Carvalho NS, Kannenberg AP, Munaretto C, Yoshioka D, Absy MCV, Ferreira MA, et al. Associação entre HPV e câncer peniano: revisão da literatura. J Bras Doenças Sex Transm. 2007;19(2):92-95.
11. Leite KRM. Patologia Cirúrgica do Câncer do Pênis. Int Braz J Urol. 2007;32(1):8-19.
UIJ
UroToday International Journal®
original study
Clinical Epidemiologic Study of Penile Cancer in the State of Pernambuco, Brazil
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.09
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
12. Begliomini H. [Penile multifocal superficial carcinoma. Emphasis to toluidine blue test]. Rev Col Bras Cir. 2001;28(3):235-237. CrossRef
13. Fonseca AG, Pinto JASA, Marques MC, Drosdoski FS, Fonseca Neto LOR. Estudo epidemiológico do câncer de pênis no Estado do Pará, Brasil. Rev Pan-Amaz Saude. 2010;1(2):85-90.
14. Brazilian Institute for Geography and Statistics -IBGE. National Research for Sample of Home (PNAD) 2009. http://www.ibge.gov.br/home/presidencia/noticias/noticia_ visualiza.php?id_noticia=1708. Accessed January 18, 2011.
15. Scheiner MA, Campos MM, Ornellas AA, Chin EW, Ornellas MH, Andrada-Serpa MJ. Human papillomavirus and penile cancers in Rio de Janeiro, Brazil: HPV typing and clinical features. Int Braz J Urol. 2008;34(4):467-476. PubMed ; CrossRef
16. Bezerra AL, Lopes A, Santiago GH, Ribeiro KC, Latorre MR, Villa LL. Human papillomavirus as a prognostic factor in carcinoma of the penis. Cancer. 2001;91(12):2315-2321. PubMed ; CrossRef
17. Dillner J, von Krogh G, Horenblas S, Meijer CJ. Etiology of squamous cell carcinoma of the penis. Scand J Urol Nephrol Suppl. 2000;(205):189-193. PubMed
18. Schoen EJ, Oehrli M, Colby C, Machin G. The Highly Protective Effect of Newborn Circumcision Against Invasive Penile Cancer. Pediatrics. 2000;105(3):e36. PubMed
19. Frisch M, Friis S, Kjaer SK, Melbye M. Falling incidence of penis cancer in an uncircumcised population. BMJ. 1995;311(7018):1471. PubMed ; CrossRef
20. Maiche AG. Epidemiological aspects of cancer of the penis in Finland. Eur J Cancer Prev. 1992;1(2):153-158. PubMed ; CrossRef
21. Daling JR, Madeleine MM, Johnson LG, Schwartz SM, Shera KA, Wurscher MA, et al. Penile cancer: Importance of circumcision, human papillomavirus and smoking in in situ and invasive disease. Int J Cancer. 2005;116(4):606-616. PubMed ; CrossRef
22. Tseng HF, Morgenstern H, Mack T, Peters R. Risk Factors for Penile Cancer: Results of a Population-based Case-Control study in Los Angeles County (United States). Cancer Causes Control. 2001;12(3):267-77. PubMed ; CrossRef
23. Runowicz CD, Lymberis S, Tobias D. Cervical Neoplasia and Cigarette Smoking: Are They Linked? Medscape Womens Health. 1997;2(3):2. PubMed
UIJ

Hammouda Sherif,1 Osama Abdelwahab,1 Abdelaziz Omar,1 Ibrahim Eraky2
1Urology Department, Faculty of Medicine, Benha University, Egypt2Urology and Nephrology Center, Mansura University, EgyptSubmitted November 4, 2011 - Accepted for Publication December 6, 2011
www.urotodayinternationaljournal.comVolume 5 - February 2012
Percutaneous Nephrolithotomy in the Supine Position with Ultrasound-Guided Renal Access
ABSTRACT
Aim: To evaluate PCNL in the supine position under ultrasound-guided puncture regarding its technical aspects,
success rate, and complications.
Patients and Methods: The study included 47 patients. All patients with renal and or upper ureteral stones were
included in this study, while patients with uncorrectable coagulopathy congenital anomalies in the kidney were
excluded. PCNL in the supine position was done under ultrasound-guided puncture while dilatation was done
under fluoroscopy.
Results: Twenty cases (42.5%) had pelvic stones, 18 cases (38.3%) had calyceal stones, 5 cases (10.6%) had multiple
stones, 1 case (2.1%) had upper ureteic stones, and 3 cases (6.4%) had stagehorn stones. Twenty-five cases (53.2%)
were right sided and 22 cases (46.8%) were left sided. Stone size was 2.9 ±1.029. Forty-two cases had radiopaque
stones (89.4%), while 5 cases had radiolucent stones (10.6%). Upper calyceal puncture was done in 2 cases, middle
calyceal puncture in 6 cases, lower calyceal puncture in 32 cases (68.1%), and multiple punctures in 9 cases. Stone
disintigration using pneumatic lithoclast was done in 31 cases (66%), and in toto stone extraction was done in 16
cases (34%). The mean operative time was 70 minutes (60 to 120 minutes). The intraoperative complications were
dilatation difficulties in 5 cases (10.6%) and bleeding requiring transfusion in 2 cases (4.2%). The stone-free rate
was achieved in 44 cases (93.6%) and residual stones more than 4 mm were detected in 3 cases (6.4%). The mean
hospital stay was 3.2 days (2 to 5 days). There was fever in 4 cases (8.5%) and urinary leakage in 3 cases (6.4%).
Conclusion: PCNL in the supine position under ultrasound-guided puncture is feasible, safe, and successful, with
minimal complications.
KEYWORDS: Supine position; PCNL; Stones
CORRESPONDENCE: Hammouda Sherif, MD, Benha University, Benha Elgdeeda, Benha,11513, Egypt ([email protected]).
CITATION: UroToday Int J. 2012 Feb;5(1):art 89. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.07
ABBREvIATIONS AND ACRONYMS
CT: Computed tomographyDJ: Double JESWL: Electrohydrolic lithotripsyIvU: Intravenous urographyPCS: Pelvicaliceal systemPCNL: Percutaneous nephrolithotomyURS: UreteroscopyUS: Ultrasonography
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/ 10.3834/uij.1944-5784.2012.02.07
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)

UroToday International Journal®
original study
Percutaneous Nephrolithotomy in the Supine Position with Ultrasound-Guided Renal Access
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.07
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
INTRODUCTION
Despite newer advances in stone surgery, including extracorporeal shockwave lithotripsy (ESWL) and flexible ureteroscopy (URS) with laser lithotripsy, the percutaneous approach is still the optimal method for minimally invasive, upper tract stone surgery [1]. Percutaneous nephrolithotomy (PCNL) in the prone position is accepted globally for its familiarity, excellent understanding of the anatomy in this position, and a reduced risk of visceral complications. However, there are various concerns regarding PCNL in the prone position, especially in the morbidly obese. Patients with compromised cardiopulmonary status and stature deformity are also not suitable for treatment in the prone position [2]. Moreover, in the conventional setting of the prone position, the hands of the urologists are in the field of the fluoroscopy, thus increasing the radiological hazards to medical personnel [3].Valdivia and associates [4] first described the supine position for percutaneous stone surgery. They suggested that the colon floats away from the kidney when the patient is in a supine position, which makes the colon less likely to be injured by a puncture made in the posterior axillary line. Hopper and colleagues [5] found that in a series of 90 prone and 500 supine abdominal CT scans, the bowel was posterior to the kidneys in 10 and 1.9% of cases, respectively. They suggested that the bowel might be more often encountered in the posterior of the kidney in the prone position compared to the supine position. Therefore, performing PCNL in the prone position may increase the risk of colon injury.
PCNL in the supine position has several advantages. First, it does not disturb blood circulation and respiration the way the prone position does. Second, the risk of iatrogenic colon injury is lower in the supine position. Third, this position is convenient for the anesthetist to observe the patient and switch to general anesthesia with endotracheal intubation, if necessary. Fourth, the angle between the horizontal plane and working tract is small, so it is easier to wash out stone fragments through the working sheath. In addition, urologists are made comfortable by sitting while performing the operation [6].
Ultrasonography (US) has made a significant impact in the field of urinary interventions. US guidance makes procedures safer, limiting the number of needle punctures and decreasing radiation exposure. In most cases, it is complementary to fluoroscopy, providing image guidance for different urinary procedures [7]. In addition to avoidance of contrast material administration, identification of all the tissue between the skin and kidney and the energy expenditure of the surgeon and other staff of the operating room decreases as it is not
necessary to wear a lead shield [8].
In this study, we evaluated PCNL in the supine position under an ultrasound-guided puncture in regards to its technical aspects, success rate, and complications. PATIENTS AND METhODS
This study included 47 patients (30 males and 17 females) admitted to the urology department of Benha University Hospital between January 2010 and December 2010. All patients with renal and or upper ureteral stones were included in this study, while patients with uncorrectable coagulopathy, congenital anomalies in the kidney, such as a horseshoe kidney, and ectopic pelvic kidney were excluded. Informed written consent was taken from all participants after the study protocol was approved by the Research Ethical Committee, Faculty of Medicine, Benha University.
All patients where investigated preoperatively via routine laboratory tests, pelviabdominal US, KUB, IVP, and spiral CT, when indicated.
PCNL in the supine position was done under high spinal anesthesia, with the patient placed in the supine position with the side harboring the stone close to the operating table (Figure 1).
Figure 1. Position of the patient.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.07f1
UIJ

UroToday International Journal®
original study
Percutaneous Nephrolithotomy in the Supine Position with Ultrasound-Guided Renal Access
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.07
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
The ipsilateral flank was elevated with a water bag, and the ipsilateral arm was laid on the thorax. Intravenous access was established in the contralateral arm after a standard cystourethroscopy and a 6 Fr, open-tip, ureteral catheter was inserted into the ipsilateral ureteral orifice.
A kidney puncture was done under real-time US (Toshiba), after distending the pelvicalyceal system with saline from the ureteric catheter for better US imaging and puncture. The puncture site and path were chosen in the mid axillary line, and then an 18-gauge puncture needle was advanced into the appropriate calyx using a needle-guiding system fixed to the US probe.
A US-guided puncture through the cup of the desired calyx was established. A 0.38, floppy-tip guide wire was advanced into the chosen calyx. Tract dilatation was performed after opacification of the PCS, with a contrast medium in a retrograde fashion, under fluoroscopic guidance using Alken dilators up to 27 Fr, except in 5 cases where hypermobile kidney balloon dilatation was used. A 30 Fr Amplatz sheath was used, and then a standard 26 Fr, rigid nephroscope was used for stone retrieval (Figure 2). A 26 Fr nephrostomy tube was fixed at the end of the procedure.
Patient demographics, body mass index (BMI), stone characteristics, operative time, intra- and postoperative complications, stone clearance, and the total number of sessions of the PCNL required were collected, tabulated, and analyzed using the Statistical Package of Social Science (SPSS), version 11, software. Suitable statistical techniques were computed (frequencies, mean, standard deviation, and range). RESULTS
Patient demographics and stone features were summarized in Tables 1 and 2. Intraoperative data of the study group were demonstrated in Table 3. Multiple punctures were done in 7 cases: lower and middle calices in 5 cases, lower and upper calices in 2 cases.
Intraoperative complications, including dilatation difficulties, were found in 5 cases (10.6%), and bleeding requiring transfusion was found in 2 cases (4.2%). Visceral injury did not occur in any of the studied cases.
The stone-free rate was achieved in 44 cases (93.6%). Residual stones more than 4 mm were detected in 3 cases (6.4%). Stone free was considered if there were no residual stones or stones less than 4 mm. Subsequent auxiliary procedures were used as DJ insertion and ESWL in 2 cases (4.2%), while in the third
Figure 2. PCNL in the supine position.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.07f2`
case of residual stones with prolonged leakage there was a 6 mm stone that passed spontaneously after 5 days without intervention. the mean hospital stay was 3.2 days (range 2 to 5 days).
Postoperative complications in the form of fever occured in 4 cases (8.5%) and urinary leakage in 3 cases (6.4%). There were insignificant differences (p = 0.018) between pre- and postoperative hemoglobin (11.3 ± 0.95, 10.8 ±1.3, respectively), as well as pre- and postoperative hematocrite value (32.7 ± 1.9, 31.2 ± 3.25, respectively; p = 0.003). DISCUSSION
The prone position has been the most commonly used position for PCNL, because this was the way the technique was invented; however, the main reason for perseverance with this position must be the apprehension of colonic and vascular injury [9]. Various modifications in patient positioning for PCNL emerged as urologists understood more of the surface anatomy of the kidney and related viscera. When patients were placed in the supine position for percutaneous nephrolithotomy, the ipsilateral flank was elevated with a 1L or 3L water bag, depending on a patient’s body mass [9]. Falahatkar and colleagues [8] performed complete supine PCNL without a rolled towel under the flank and no change in leg position. We
UIJ
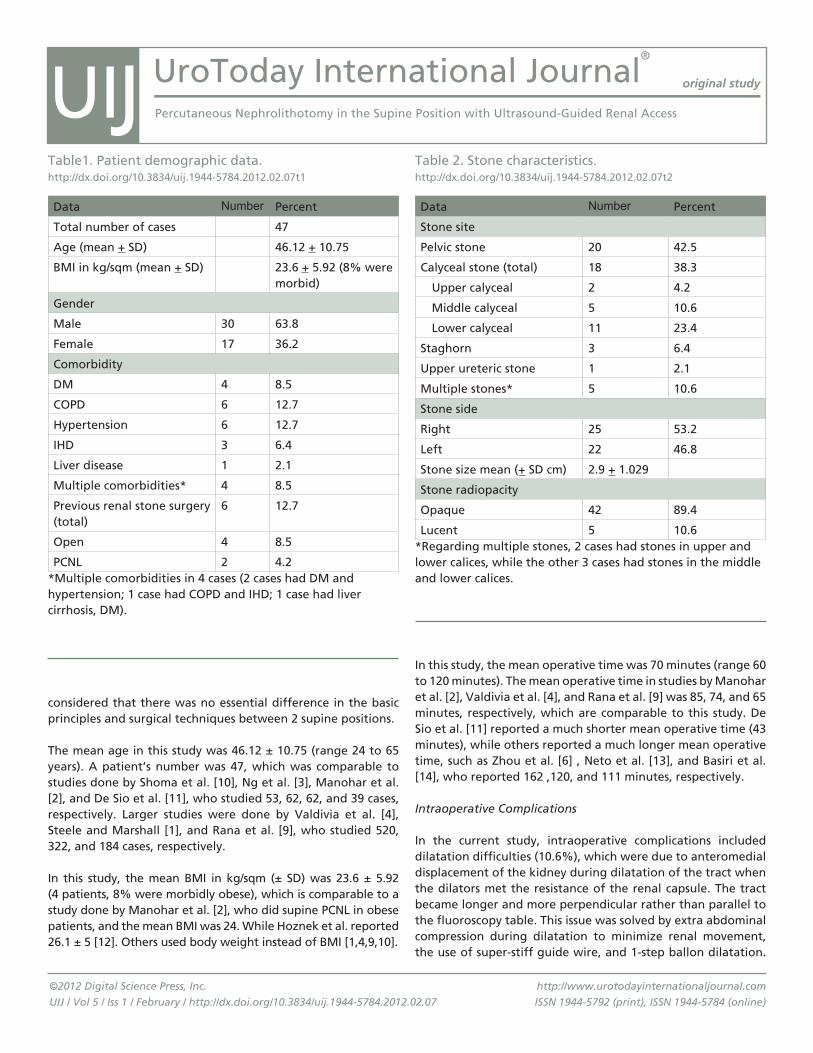
UroToday International Journal®
original study
Percutaneous Nephrolithotomy in the Supine Position with Ultrasound-Guided Renal Access
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.07
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
In this study, the mean operative time was 70 minutes (range 60 to 120 minutes). The mean operative time in studies by Manohar et al. [2], Valdivia et al. [4], and Rana et al. [9] was 85, 74, and 65 minutes, respectively, which are comparable to this study. De Sio et al. [11] reported a much shorter mean operative time (43 minutes), while others reported a much longer mean operative time, such as Zhou et al. [6] , Neto et al. [13], and Basiri et al. [14], who reported 162 ,120, and 111 minutes, respectively.
Intraoperative Complications
In the current study, intraoperative complications included dilatation difficulties (10.6%), which were due to anteromedial displacement of the kidney during dilatation of the tract when the dilators met the resistance of the renal capsule. The tract became longer and more perpendicular rather than parallel to the fluoroscopy table. This issue was solved by extra abdominal compression during dilatation to minimize renal movement, the use of super-stiff guide wire, and 1-step ballon dilatation.
considered that there was no essential difference in the basic principles and surgical techniques between 2 supine positions.
The mean age in this study was 46.12 ± 10.75 (range 24 to 65 years). A patient’s number was 47, which was comparable to studies done by Shoma et al. [10], Ng et al. [3], Manohar et al. [2], and De Sio et al. [11], who studied 53, 62, 62, and 39 cases, respectively. Larger studies were done by Valdivia et al. [4], Steele and Marshall [1], and Rana et al. [9], who studied 520, 322, and 184 cases, respectively.
In this study, the mean BMI in kg/sqm (± SD) was 23.6 ± 5.92 (4 patients, 8% were morbidly obese), which is comparable to a study done by Manohar et al. [2], who did supine PCNL in obese patients, and the mean BMI was 24. While Hoznek et al. reported 26.1 ± 5 [12]. Others used body weight instead of BMI [1,4,9,10].
Data Number Percent
Total number of cases 47
Age (mean + SD) 46.12 + 10.75
BMI in kg/sqm (mean + SD) 23.6 + 5.92 (8% were morbid)
Gender
Male 30 63.8
Female 17 36.2
Comorbidity
DM 4 8.5
COPD 6 12.7
Hypertension 6 12.7
IHD 3 6.4
Liver disease 1 2.1
Multiple comorbidities* 4 8.5
Previous renal stone surgery (total)
6 12.7
Open 4 8.5
PCNL 2 4.2*Multiple comorbidities in 4 cases (2 cases had DM and hypertension; 1 case had COPD and IHD; 1 case had liver cirrhosis, DM).
Table1. Patient demographic data.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.07t1
Data Number Percent
Stone site
Pelvic stone 20 42.5
Calyceal stone (total) 18 38.3
Upper calyceal 2 4.2
Middle calyceal 5 10.6
Lower calyceal 11 23.4
Staghorn 3 6.4
Upper ureteric stone 1 2.1
Multiple stones* 5 10.6
Stone side
Right 25 53.2
Left 22 46.8
Stone size mean (+ SD cm) 2.9 + 1.029
Stone radiopacity
Opaque 42 89.4
Lucent 5 10.6*Regarding multiple stones, 2 cases had stones in upper and lower calices, while the other 3 cases had stones in the middle and lower calices.
Table 2. Stone characteristics.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.07t2
UIJ
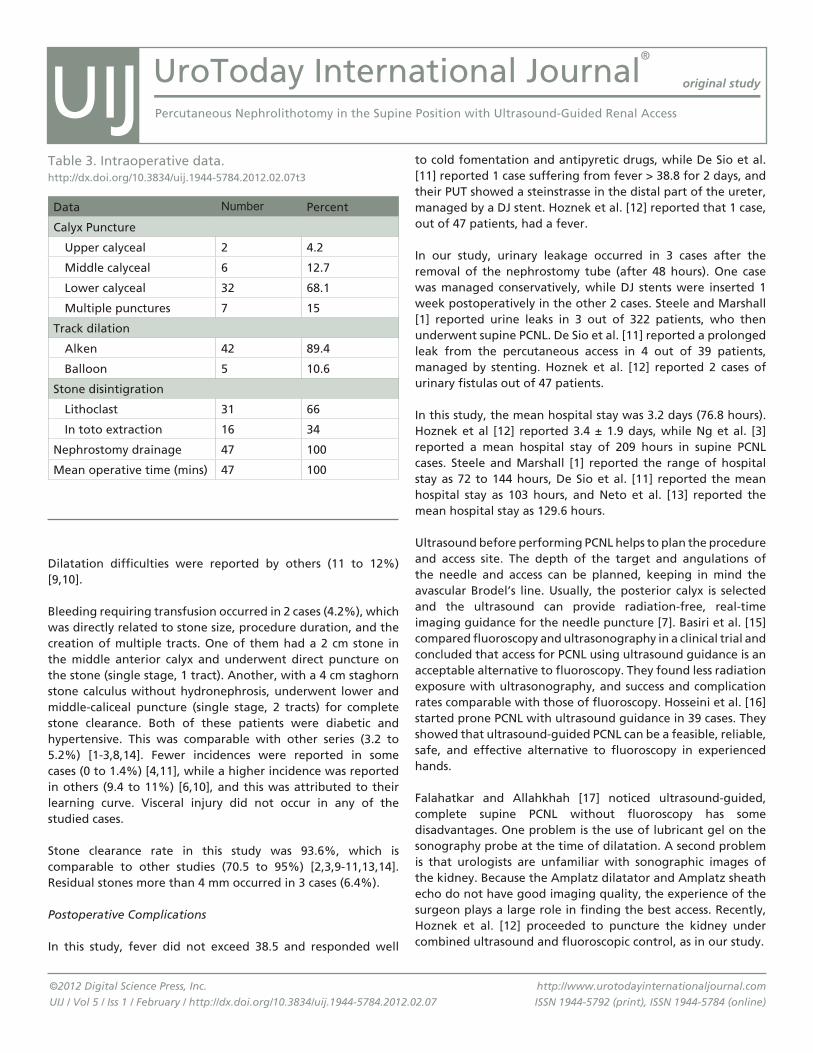
UroToday International Journal®
original study
Percutaneous Nephrolithotomy in the Supine Position with Ultrasound-Guided Renal Access
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.07
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
Dilatation difficulties were reported by others (11 to 12%) [9,10].
Bleeding requiring transfusion occurred in 2 cases (4.2%), which was directly related to stone size, procedure duration, and the creation of multiple tracts. One of them had a 2 cm stone in the middle anterior calyx and underwent direct puncture on the stone (single stage, 1 tract). Another, with a 4 cm staghorn stone calculus without hydronephrosis, underwent lower and middle-caliceal puncture (single stage, 2 tracts) for complete stone clearance. Both of these patients were diabetic and hypertensive. This was comparable with other series (3.2 to 5.2%) [1-3,8,14]. Fewer incidences were reported in some cases (0 to 1.4%) [4,11], while a higher incidence was reported in others (9.4 to 11%) [6,10], and this was attributed to their learning curve. Visceral injury did not occur in any of the studied cases.
Stone clearance rate in this study was 93.6%, which is comparable to other studies (70.5 to 95%) [2,3,9-11,13,14]. Residual stones more than 4 mm occurred in 3 cases (6.4%).
Postoperative Complications
In this study, fever did not exceed 38.5 and responded well
to cold fomentation and antipyretic drugs, while De Sio et al. [11] reported 1 case suffering from fever > 38.8 for 2 days, and their PUT showed a steinstrasse in the distal part of the ureter, managed by a DJ stent. Hoznek et al. [12] reported that 1 case, out of 47 patients, had a fever.
In our study, urinary leakage occurred in 3 cases after the removal of the nephrostomy tube (after 48 hours). One case was managed conservatively, while DJ stents were inserted 1 week postoperatively in the other 2 cases. Steele and Marshall [1] reported urine leaks in 3 out of 322 patients, who then underwent supine PCNL. De Sio et al. [11] reported a prolonged leak from the percutaneous access in 4 out of 39 patients, managed by stenting. Hoznek et al. [12] reported 2 cases of urinary fistulas out of 47 patients.
In this study, the mean hospital stay was 3.2 days (76.8 hours). Hoznek et al [12] reported 3.4 ± 1.9 days, while Ng et al. [3] reported a mean hospital stay of 209 hours in supine PCNL cases. Steele and Marshall [1] reported the range of hospital stay as 72 to 144 hours, De Sio et al. [11] reported the mean hospital stay as 103 hours, and Neto et al. [13] reported the mean hospital stay as 129.6 hours.
Ultrasound before performing PCNL helps to plan the procedure and access site. The depth of the target and angulations of the needle and access can be planned, keeping in mind the avascular Brodel’s line. Usually, the posterior calyx is selected and the ultrasound can provide radiation-free, real-time imaging guidance for the needle puncture [7]. Basiri et al. [15] compared fluoroscopy and ultrasonography in a clinical trial and concluded that access for PCNL using ultrasound guidance is an acceptable alternative to fluoroscopy. They found less radiation exposure with ultrasonography, and success and complication rates comparable with those of fluoroscopy. Hosseini et al. [16] started prone PCNL with ultrasound guidance in 39 cases. They showed that ultrasound-guided PCNL can be a feasible, reliable, safe, and effective alternative to fluoroscopy in experienced hands.
Falahatkar and Allahkhah [17] noticed ultrasound-guided, complete supine PCNL without fluoroscopy has some disadvantages. One problem is the use of lubricant gel on the sonography probe at the time of dilatation. A second problem is that urologists are unfamiliar with sonographic images of the kidney. Because the Amplatz dilatator and Amplatz sheath echo do not have good imaging quality, the experience of the surgeon plays a large role in finding the best access. Recently, Hoznek et al. [12] proceeded to puncture the kidney under combined ultrasound and fluoroscopic control, as in our study.
Data Number Percent
Calyx Puncture
Upper calyceal 2 4.2
Middle calyceal 6 12.7
Lower calyceal 32 68.1
Multiple punctures 7 15
Track dilation
Alken 42 89.4
Balloon 5 10.6
Stone disintigration
Lithoclast 31 66
In toto extraction 16 34
Nephrostomy drainage 47 100
Mean operative time (mins) 47 100
Table 3. Intraoperative data.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.07t3
UIJ
UroToday International Journal®
original study
Percutaneous Nephrolithotomy in the Supine Position with Ultrasound-Guided Renal Access
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.07
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
Published studies from different centers have shown that supine PCNL is safe, and it has several benefits for the patient and several technical advantages for the surgeon [9-11,18]. Patient positioning is less demanding and time-consuming because a change is not required from the lithotomy to the prone position during the procedure [19].
The supine position also allows greater versatility during stone management since ureteroscopy can be performed if there are contralateral ureteral stones, or simultaneous procedures for renal, ureteral, and bladder stones in the same single supine lithotomy position. A final advantage of the supine PCNL position is that urologists are more comfortable adopting a sitting posture during stone management. Although supine percutaneous nephrolithotomy is routine in some surgical centers throughout the world, its popularity in the field of urology, due to a deficiency in its training in educational centers, as a whole, is still minimal [20].
Lastly, systematic literature review was performed by Wu and his colleagues [21] who concluded, for general patients with kidney calculi, PCNL in the supine position has similar, stone-free rates compared with the prone position. Supine PCNL does not increase related complications. The operative times significantly decrease in the supine position. However, there is still no consensus on the optimal position for PCNL.
CONCLUSION
PCNL in the supine position, under ultrasound-guided puncture, is feasible, safe, and successful, with minimal complications. ACKNOWLEDgEMENTS
The authors are grateful to the residents in the urology department of Benha University Hospital, Benha, Egypt, for help in patient recruitment and follow-up.
REfERENCES
1. Steele D, Marshall V. Percutaneous nephrolithotomy in the supine position: A neglected approach? J Endourol. 2007;21(12):1433-1437. PubMed ; CrossRef
2. Manohar T, Jain P, Desai M. Supine percutaneous nephrolithotomy: Effective approach to high-risk and morbidly obese patients. J Endourol. 2007;21(1):44-49. PubMed ; CrossRef
3. Ng MT, Sun WH, Cheng CW, Chan ES. Supine position is safe and effective for percutaneous nephrolithotomy. J Endourol. 2004;18(5):469-474. PubMed ; CrossRef
4. Valdivia Uria JG, Valle Gerhold J, López López JA, et al. Technique and complications of percutaneous nephroscopy: Experience with 557 patients in the supine position. J Urol.1998;160(6 pt 1):1975-1978. PubMed ; CrossRef
5. Hopper KD, Sherman JL, Luethke JM, Ghaed N. The retrorenal colon in the supine and prone patient. Radiology.1987;162(2):443-446. PubMed
6. Zhou X, Gao X, Wen J, Xiao C. Clinical value of minimally Invasive percutaneous nephrolithotomy in the supine position under the guidance of real-time ultrasound: report of 92 cases. Urol Res. 2008;36(2):111-114. PubMed ; CrossRef
7. Kang PS, Paspulati RM. Ultrasound-Guided Genitourinary Interventions. Ultrasound Clin. 2007;2(1):115-120. CrossRef
8. Falahatkar S, Neiroomand H, Enshaei A, Kazemzadeh M, Allahkhah A, Jalili MF. Totally ultrasound versus fluoroscopically guided complete supine percutaneous nephrolithotripsy: a first report. J Endourol. 2010;24(9):1421-1426. PubMed ; CrossRef
9. Rana AM, Bhojwani JP, Junejo NN, Das Bhagia S. Tubeless PCNL with patients in supine position: procedure for all seasons? with comprehensive technique. Urology. 2008;71(4):581-585. PubMed ; CrossRef
10. Shoma AM, Eraky I, El-Kenawy MR, El-Kappany HA. Percutaneous nephrolithotomy in the supine position: technical aspects and functional outcome compared with the prone technique. Urology. 2002;60(3):388-392. PubMed ; CrossRef
11. De Sio M, Autorino R, Quarto G, et al. Modified supine versus prone position in percutaneous nephrolithotomy for renal stones treatable with a single percutaneous access: a prospective randomized trial. Eur Urol. 2008;54(1):196-202. PubMed ; CrossRef
12. Hoznek A, Rode J, Ouzaid I, et al. Modified Supine Percutaneous Nephrolithotomy for Large Kidney and Ureteral Stones: Technique and Results. Eur Urol. 2012;61(1):164-170. PubMed ; CrossRef
UIJ
UroToday International Journal®
original study
Percutaneous Nephrolithotomy in the Supine Position with Ultrasound-Guided Renal Access
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.07
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
13. Neto EA, Mitre AI, Gomes CM, Arap MA, Srougi M. Percutaneous nephrolithotripsy with the patient in a modified supine position. J Urol. 2007;178(1):165-168. PubMed ; CrossRef
14. Basiri A, Sichani MM, Hosseini SR, et al. X-ray-free percutaneous nephrolithotomy in supine position with ultrasound guidance. World J Urol. 2010;28(2):239-244. PubMed ; CrossRef
15. Basiri A, Ziaee AM, Kianan HR, Mehrabi S, Karami H, Moghaddam SM. Ultrasonographic versus fluoroscopic access for percutaneous nephrolithotomy: a randomized clinical trial. J Endourol. 2008;22(2):281-284. PubMed ; CrossRef
16. Hosseini MM, Hassanpour A, Farzan R, Yousefi A, Afrasiabi MA. Ultrasonography-guided percutaneous nephrolithotomy. J Endourol. 2009;23(4):603-607. PubMed ; CrossRef
17. Falahatkar S, Allahkhah A. Recent Developments in Percutaneous Nephrolithotomy: Benefits of the Complete Supine Position. UroToday Int J. 2010;3(2):1944-5784. CrossRef
18. Domenech A, Vivaldi B, Diaz C, et al. Complications in percutaneous nephrolithotomy: A comparative study between the supine and prone positions using the modified clavien system. Urology. 2008;72(5 suppl 1):S16. CrossRef
19. de la Rosette JJ, Tsakiris P, Ferrandino MN, Elsakka AM, Rioja J, Preminger GM. Beyond prone position in percutaneous nephrolithotomy: a comprehensive review. Eur Urol. 2008;54(6):1262-1269. PubMed ; CrossRef
20. Falahatkar S, Farzan A, Allahkhah A. Is complete supine percutaneous nephrolithotripsy feasible in all patients? Urol Res. 2011;39(2):99-104. PubMed ; CrossRef
21. Wu P, Wang L, Wang K. Supine versus prone position in percutaneous nephrolithotomy for kidney calculi: a meta-analysis. Int Urol Nephrol. 2011;43(1):67-77. PubMed ; CrossRef
UIJ
Bikash Bawri,1 Rajeev T Puthenveetil,2 Saumar J Baruah,3 Sasanka K Barua,4 Puskal K Bagchi4
1Department of Urology, Gauhati Medical College Hospital, Guwahati, Assam, India2Associate Professor, Department of Urology, Gauhati Medical College Hospital, Guwahati, Assam, India3Professor and HOD, Department of Urology, Gauhati Medical College Hospital, Guwahati, Assam, India4Assistant Professor, Department of Urology, Gauhati Medical College Hospital, Guwahati, Assam, IndiaSubmitted September 9, 2011 - Accepted for Publication November 9, 2011
www.urotodayinternationaljournal.comVolume 5 - February 2012
A Rare Cause of Acute Urinary Retention in a Young Female: Leiomyoma Bladder
ABSTRACT
Leiomyoma represents the largest subgroup of benign mesenchymal tumors that may arise anywhere within the genitourinary tract. Usual presenting symptoms include voiding symptoms such as obstruction and irritation. It can be diagnosed by careful physical examination assisted with ultrasound and endoscopic evaluation, but the confirmatory diagnosis is always histological. Bladder-conservative surgery is usually contemplated as the treatment of choice, be it transurethral resection or open surgery. This can include partial cystectomy due to the benign nature of the disease. Although the occurrence of this tumor is rare, it should be suspected with any urinary bladder tumor presenting with benign features. The prognosis is good with bladder preservative protocols.
KEYWORDS: Leiomyoma; Genitourinary tract; Obstruction; Partial cystectomy
CORRESPONDENCE: Bikash Bawri, MD, RK Singh Apartment, House No 54, Ashram Road, Kasturba Nagar, Ulubari, Guwahati-781007, Assam, India ([email protected]).
CITATION: UroToday Int J. 2012 Feb;5(1):art 83. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.01
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.01
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
INTRODuCTION
Benign mesenchymal tumors make up 1 to 5% of all bladder neoplasms, with leiomyoma representing the largest subgroup of these benign tumors (.04 to .5%) [1,3]. A leiomyoma is a benign, smooth muscle tumor most often located in the uterus or gastrointestinal tract. However, these tumors may arise anywhere within the genitourinary tract and are usually asymptomatic unless urinary tract function is affected [2]. They are predominantly found in women, although men can also be affected. Approximately 250 cases have been reported to date, including patients who had leiomyoma in a urethral location
[4]. Typically, it occurs in the fourth and fifth decades of life.
The most common presenting complaints are urinary voiding
symptoms, such as obstruction and irritation. Surgery is the
standard treatment, and the surgical approach depends on
tumor size and localization at the bladder wall. Prognosis is
good due to the benign behavior of these lesions. We describe
a case of urinary bladder leiomyoma in a young woman with
acute urinary retention. Although not initially suspected, the
diagnosis of urinary bladder leiomyoma was subsequently,
histologically confirmed.
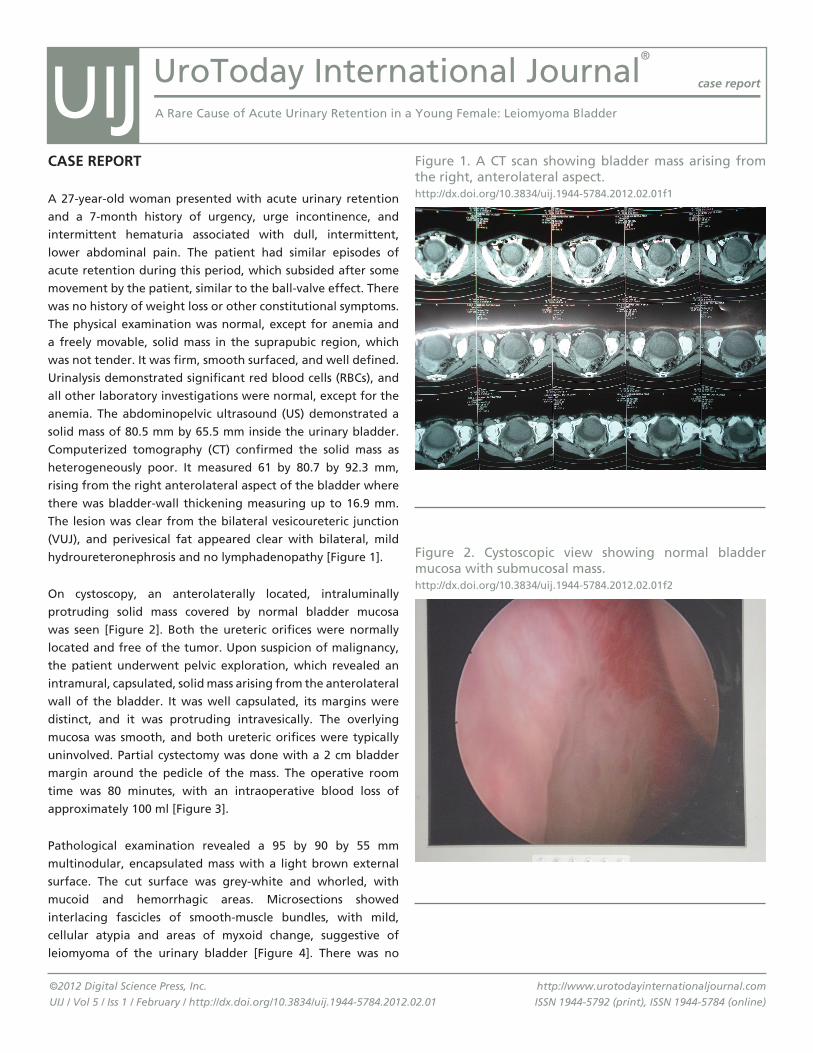
UroToday International Journal®
case report
A Rare Cause of Acute Urinary Retention in a Young Female: Leiomyoma Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.01
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
CASE REPORT
A 27-year-old woman presented with acute urinary retention
and a 7-month history of urgency, urge incontinence, and
intermittent hematuria associated with dull, intermittent,
lower abdominal pain. The patient had similar episodes of
acute retention during this period, which subsided after some
movement by the patient, similar to the ball-valve effect. There
was no history of weight loss or other constitutional symptoms.
The physical examination was normal, except for anemia and
a freely movable, solid mass in the suprapubic region, which
was not tender. It was firm, smooth surfaced, and well defined.
Urinalysis demonstrated significant red blood cells (RBCs), and
all other laboratory investigations were normal, except for the
anemia. The abdominopelvic ultrasound (US) demonstrated a
solid mass of 80.5 mm by 65.5 mm inside the urinary bladder.
Computerized tomography (CT) confirmed the solid mass as
heterogeneously poor. It measured 61 by 80.7 by 92.3 mm,
rising from the right anterolateral aspect of the bladder where
there was bladder-wall thickening measuring up to 16.9 mm.
The lesion was clear from the bilateral vesicoureteric junction
(VUJ), and perivesical fat appeared clear with bilateral, mild
hydroureteronephrosis and no lymphadenopathy [Figure 1].
On cystoscopy, an anterolaterally located, intraluminally
protruding solid mass covered by normal bladder mucosa
was seen [Figure 2]. Both the ureteric orifices were normally
located and free of the tumor. Upon suspicion of malignancy,
the patient underwent pelvic exploration, which revealed an
intramural, capsulated, solid mass arising from the anterolateral
wall of the bladder. It was well capsulated, its margins were
distinct, and it was protruding intravesically. The overlying
mucosa was smooth, and both ureteric orifices were typically
uninvolved. Partial cystectomy was done with a 2 cm bladder
margin around the pedicle of the mass. The operative room
time was 80 minutes, with an intraoperative blood loss of
approximately 100 ml [Figure 3].
Pathological examination revealed a 95 by 90 by 55 mm
multinodular, encapsulated mass with a light brown external
surface. The cut surface was grey-white and whorled, with
mucoid and hemorrhagic areas. Microsections showed
interlacing fascicles of smooth-muscle bundles, with mild,
cellular atypia and areas of myxoid change, suggestive of
leiomyoma of the urinary bladder [Figure 4]. There was no
Figure 1. A CT scan showing bladder mass arising from the right, anterolateral aspect. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.01f1
Figure 2. Cystoscopic view showing normal bladder mucosa with submucosal mass.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.01f2
UIJ
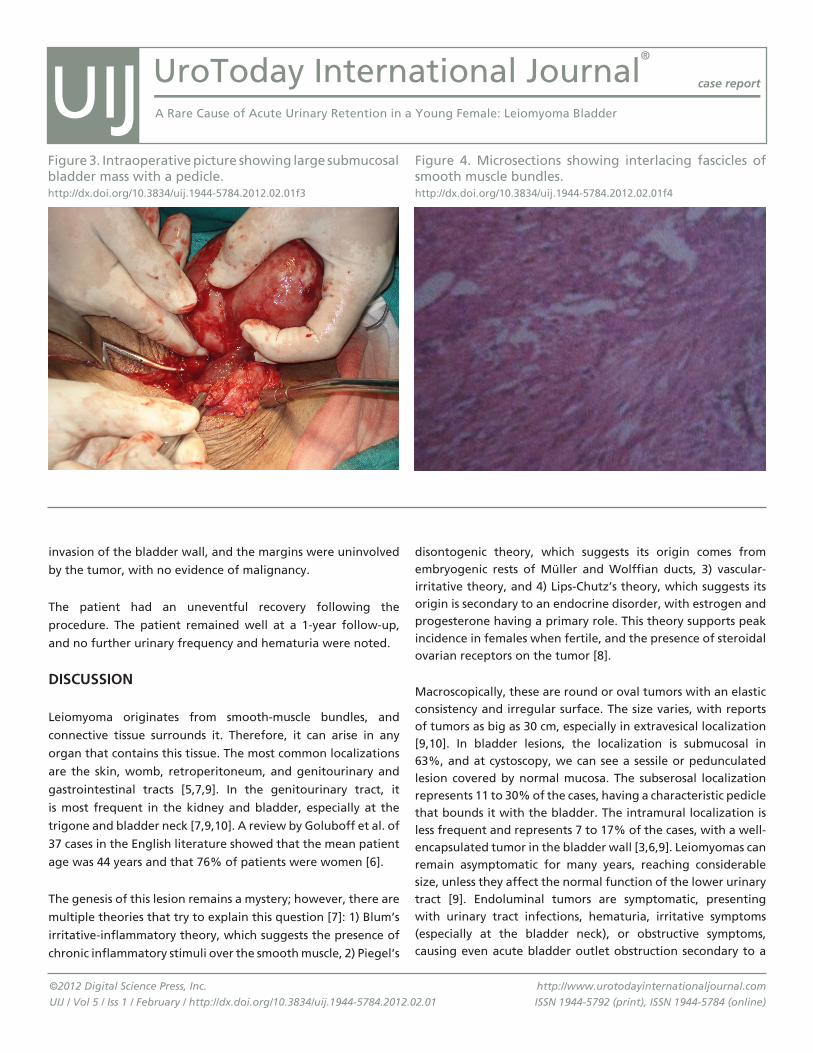
UroToday International Journal®
case report
A Rare Cause of Acute Urinary Retention in a Young Female: Leiomyoma Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.01
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
invasion of the bladder wall, and the margins were uninvolved
by the tumor, with no evidence of malignancy.
The patient had an uneventful recovery following the
procedure. The patient remained well at a 1-year follow-up,
and no further urinary frequency and hematuria were noted.
DISCuSSION
Leiomyoma originates from smooth-muscle bundles, and
connective tissue surrounds it. Therefore, it can arise in any
organ that contains this tissue. The most common localizations
are the skin, womb, retroperitoneum, and genitourinary and
gastrointestinal tracts [5,7,9]. In the genitourinary tract, it
is most frequent in the kidney and bladder, especially at the
trigone and bladder neck [7,9,10]. A review by Goluboff et al. of
37 cases in the English literature showed that the mean patient
age was 44 years and that 76% of patients were women [6].
The genesis of this lesion remains a mystery; however, there are
multiple theories that try to explain this question [7]: 1) Blum’s
irritative-inflammatory theory, which suggests the presence of
chronic inflammatory stimuli over the smooth muscle, 2) Piegel’s
disontogenic theory, which suggests its origin comes from embryogenic rests of Müller and Wolffian ducts, 3) vascular-irritative theory, and 4) Lips-Chutz’s theory, which suggests its origin is secondary to an endocrine disorder, with estrogen and progesterone having a primary role. This theory supports peak incidence in females when fertile, and the presence of steroidal ovarian receptors on the tumor [8].
Macroscopically, these are round or oval tumors with an elastic consistency and irregular surface. The size varies, with reports of tumors as big as 30 cm, especially in extravesical localization [9,10]. In bladder lesions, the localization is submucosal in 63%, and at cystoscopy, we can see a sessile or pedunculated lesion covered by normal mucosa. The subserosal localization represents 11 to 30% of the cases, having a characteristic pedicle that bounds it with the bladder. The intramural localization is less frequent and represents 7 to 17% of the cases, with a well-encapsulated tumor in the bladder wall [3,6,9]. Leiomyomas can remain asymptomatic for many years, reaching considerable size, unless they affect the normal function of the lower urinary tract [9]. Endoluminal tumors are symptomatic, presenting with urinary tract infections, hematuria, irritative symptoms (especially at the bladder neck), or obstructive symptoms, causing even acute bladder outlet obstruction secondary to a
Figure 3. Intraoperative picture showing large submucosal bladder mass with a pedicle. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.01f3
Figure 4. Microsections showing interlacing fascicles of smooth muscle bundles. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.01f4
UIJ

UroToday International Journal®
case report
A Rare Cause of Acute Urinary Retention in a Young Female: Leiomyoma Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.01
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
valve effect [5,6,9,10], as in our case. Intramural and subserosal tumors are, in general, asymptomatic and the diagnosis is incidental. At cystoscopy, submucosal tumors appear as a sessile or pedunculated lesion covered by normal mucosa, but it could be normal if the tumor is intramural or subserosal. The same situation can occur in the intravenous pyelography (IVP), showing a filling defect in the bladder wall if the lesion is submucosal. Ultrasound allows us to define the solid or cystic nature of the lesion, showing, in these cases, a solid, smooth wall lesion with homogeneous echoes. Transvaginal ultrasound is an excellent option in female posterior bladder-wall tumors in subserosal localization [6,9]. Computed tomography gives us information about the size, position, and relationship between the tumor and bladder wall. An MRI shows a leiomyoma with an intermediate signal on T1 weighted images, with contrast between the tumor and the urine, which has a low-signal intensity. Nevertheless, imaging tests add important data that suggest the benign nature of these tumors, like the presence of a well-circumscribed lesion with homogeneous density, poor enhancement with contrast media, and normal, perivesical fat. There is no test that allows us to differentiate a leiomyoma from leiomyosarcoma; therefore, pathologic diagnosis is mandatory [5]. Leiomyomas are firm and rubbery in consistency, appear as whitish-gray, round to ovoid nodules with a spiral appearance of smooth-muscle fibers, and eosinophilic cytoplasm with less than 2 mitotic figures per high-power field. They are surrounded by a variable amount of connective tissue, and there is no necrosis or cellular atypia [6].
In a literature review by Silva-Ramos et al., 90 bladder leiomyomas where analyzed, 28 of which where biopsied before the definitive treatment. All samples obtained with a Tru-Cut needle and transurethral resection (TUR) were diagnostic, whereas the cold-cup biopsy samples showed a 50% false negative. Fine-needle aspiration biopsy was the least useful diagnostic tool [5].
The treatment depends on the tumor size, localization, and relationship with the bladder wall [6]. Surgery is indicated because of the potential growing capacity of these tumors [9]. Given the benign nature of these lesions, the surgery must be as conservative as possible. Submucosal tumors can be managed by transurethral resection, noting the size is an important issue. Subserosal and huge submucosal lesions can be managed by enucleation or with partial cystectomy. In Goluboff’s review of the literature, 62% were treated by open resection, whereas
30% were removed by transurethral resection [6]. Prognosis is good and recurrence is rare if the resection is adequate; therefore, it seems unnecessary to establish follow-up protocols. However, Lake, in 1981, described what is, to date, the only case of a leiomyoma with malignant degeneration [7]. The laparoscopic approach is an excellent option for tumors located at the mobile wall of the bladder, allowing an easy and safe procedure. Bladder-wall edges are simple to identify, especially if simultaneous cystoscopic control is used, which adds the option of resecting the tumor with the resectoscope [11].
Leiomyoma of the urinary bladder is actually not an uncommon disease for middle-aged women presenting with obstructive and irritative voiding symptoms. Careful physical examination and ultrasound may occasionally discover it. It is readily and successfully treated with TUR or open surgery, in most cases. It should be considered for its successfully diagnosable and treatable nature in any pelvic mass involving the bladder wall. Although only 250 cases have been reported to date, our case presented at a very young age, with typical symptoms of ball-valve-type acute retention with a large-sized leiomyoma.
REfERENCES
1. Campbell EW, Gislason GJ, et al. Benign mesothelial tumors of the urinary bladder: Review of literature and a report of a case of leiomyoma. J Urol. 1953;70(5):733-741. PubMed
2. Knoll LD, Sergura JW, Scheithauer BW. Leiomyoma of the bladder. J Urol. 1986;136(4):906-908. PubMed
3. Ojea Calvo A, Núñez López A, Alonso Rodrigo A, et al. [Bladder leiomyoma]. Actas Urol Esp. 2001;25(10):759-763. PubMed
4. Cornella JL, Larson TR, Lee RA, Magrina JF, Kammerer-Doak D. Leiomyoma of the female urethra and bladder: report of twenty-three patients and review of the literature. Am J Obstet Gynecol. 1997;176(6):1278-1285. PubMed ; CrossRef
5. Silva-Ramos M, Massó P, Versos R, et al. [Leiomyoma of the bladder. Analysis of a collection of 90 cases]. Actas Urol Esp. 2003;27(8):581-586. PubMed ; CrossRef
UIJ
UroToday International Journal®
case report
A Rare Cause of Acute Urinary Retention in a Young Female: Leiomyoma Bladder
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.01
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
6. Goluboff E, O´Toole K, Sawczuk IS. Leiomyoma of bladder: Report of case and review of literature. Urology. 1994;43(2):238-241. PubMed ; CrossRef
7. Rubio Muñoz A, Bono Ariño A, Berné Manero JM, et al. [Leiomyoma of the bladder]. Arch Esp Urol. 2000;53(10):934-937. PubMed
8. Furuhashi M, Suganuma N. Recurrent bladder leiomyoma with ovarian steroid hormone receptors. J Urol. 2002;167(3):1399-1400. PubMed ; CrossRef
9. Jiménez Aristu JI, Lozano Uruñuela F, de Pablo Cárdenas A, et al. [Leiomyoma of the bladder. Report of a case]. Actas Urol Esp. 2001;25(3):223-225. PubMed ;
10. Belis JA, Post GJ, Rochman SC, Milam DF. Genitourinary leiomyomas. Urology. 1979;13(4):424-429. PubMed ; CrossRef
11. Jeschke K, Wakonig J, Winzely M, Henning K. Laparoscopic partial cystectomy for leiomyoma of the bladder wall. J Urol. 2002;168(5):2115-2116. PubMed ; CrossRef
UIJ

Raj Kumar Sharma, Vir Kumar Jain, S Mukherjee, SN Mondal, D KarmakarCalcutta National Medical College, Kolkata, IndiaSubmitted November 5, 2011 - Accepted for Publication December 9, 2011
www.urotodayinternationaljournal.comVolume 5 - February 2012
Inflammatory Pseudotumor of the Urachus
ABSTRACT
Urachal diseases often create serious diagnostic dilemmas owing to their uncommon occurrences and the diversity of
their presentations. We present a rare case of inflammatory pseudotumor of the urachus. The rarity and confusing
nature of this condition prompted us to submit the present information.
KEYWORDS: Inflammatory pseudotumor; Urachus
CORRESPONDENCE: Raj Kumar Sharma, MBBS, MS, MCh, Department of Urology, Calcutta National Medical College, Kolkata, West Bengal, India 700046 ([email protected]).
CITATION: UroToday Int J. 2012 Feb;5(1):art 94. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.12
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/ 10.3834/uij.1944-5784.2012.02.12
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
INTRODuCTION
Urachal diseases often create serious diagnostic dilemmas owing to their uncommon occurrences and the diversity of their presentations. This is especially true for its tumors. Malignant tumors are common among all the tumors of the urachus, of which adenocarcinoma is the most common. Benign tumors, however, are uncommon in this vestigial organ [1]. Inflammatory pseudotumor is a benign, fibromuscular tumorous growth in which there is proliferation of plasma cells, lymphocytes, and histiocytes in a benign-looking, spindle-shaped stroma (myofibroblasts). It is commonly seen in abdominal and pelvic structures. Its occurrence in the urachus has been reported only a couple of times in the literature. We present a rare case of inflammatory pseudotumor of the urachus, which was also unique for the diagnostic dilemmas it created for the treating team. The rarity and confusing nature of this condition
prompted us to submit the present information.
CASE REPORT
A male child of 12 years of age presented at our surgical department with complaints of a lump in the lower abdomen for 2 months, and pain over the lower abdomen for the previous 3 days. There was no history of vomiting, alteration of bowel habit, or urinary symptoms. On abdominal examination, a single intra-abdominal lump of approximately 10 cm by 8 cm in size was found occupying the mainly hypogastric and umbilical regions, along with adjacent areas of iliac fossae, which did not move with respiration. Palpation revealed a non-tender mass, which was of normal temperature and firm-to-hard in consistency. It had a bosselated surface and ill-defined margins in its lower part. Percussion revealed dullness over the lump. The liver was not enlarged, the spleen was not palpable, and

UroToday International Journal®
case report
Inflammatory Pseudotumor of the Urachus
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.12
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
there was no other apparent abnormal finding.
On routine investigation, total and differential white blood-cell counts were normal, as was the routine examination of urine. Fine-needle aspiration was done and the cytology report was inconclusive. Ultrasound examination revealed a solid, multinodular mass of 63 mm by 71 mm by 63 mm in the right iliac fossa, extending up to the umbilicus. On CT scan, a large, solid, lobulated mass of 11 cm by 6 cm was seen in the pelvis (more towards the right side), which was slightly hypodense in attenuation. The mass was seen displacing bowels and indenting the bladder. It was continuous with anterior abdominal wall muscle. On IV contrast administration, the mass showed heterogeneous enhancement with sparing of the central region (dense fibrosis).
Based on these findings, an exploratory laparotomy was performed. The laparotomy revealed a large lobulated mass, which was free from adjacent bowel loops and mesenteries. Its lower part was attached to a dome of the urinary bladder in a pedunculated form (Figure 1). It was excised after securing hemostasis and was sent for histopathological examination. Postoperative recovery was uneventful.
Histopathological examination of the specimen grossly revealed a greyish-white, soft-to-firm mass. On microscopic examination, the section revealed a spindle-cell tumor composed of loose fibromyxoid stroma with spindle-and-stellate-shaped cells mixed with dense lymphoplasmacytic and mononuclear infiltrate. Although the spindle cells showed mild pleomorphism, there was no mitotic activity. A focus of ischemic necrosis was also seen. The final pathological diagnosis came out to be a spindle cell tumor suggestive of inflammatory pseudotumor.
DISCuSSION
The urachus is a vestigial remnant of 2 embryonic structures, which are urogenital sinus (the precursor of urinary bladder) and allantois (the derivative of yolk sack). Normally, it is obliterated before birth, leaving a fibrous band extending from the dome of the urinary bladder to the umbilicus. Common pathologies of this structure are congenital anomalies and infections [2]. Tumors are rare findings in the urachus. The majority of tumors in the urachus are malignant (0.5% of all bladder carcinomas), adenocarcinomas constituting the majority of this group (80%) [1]. Benign tumors of the urachus are extremely uncommon. This group consists of adenomas, fibromas, fibroadenomas, fibromyomas, and hamartomas [2]. These benign tumors must be thoroughly evaluated owing to the potential confusion they create in the diagnosis of abdominal lumps as a whole [3,4,9].
Inflammatory pseudotumor of the urachus is one such tumor, which runs a benign clinical course. The most common site for this pseudotumor is the lung and mediastinum, followed by extrapulmonary sites, the list of which includes almost every organ in the body [5,6].
Despite its common predilection for abdominal and pelvic organs, including the urinary bladder, bowel, liver, and peritoneum [6,7], it has been rarely reported in the urachal remnant [8,9]. Along with the rarity of this tumor, our case is a good example of the diagnostic confusion the lumps of the urachus can create for a clinician. It resisted complete diagnosis until imaging investigations, exploratory laparotomy, and histopathology were correlated. Thus, the importance of investigations in urachal lumps is again underscored here, which was stressed previously [4,5].
Finally, regarding the treatment of inflammatory pseudotumor, 2 schools of thought are advocated. Our treatment of simple excision was due to the history, clinically as well as preoperatively, which was more in favor of a benign tumor. Simple excision has been used previously in similar cases [10]. A second school of thought also advocates that in cases where preoperative findings are inconclusive or in favor of malignancy, aggressive surgery should be the choice [9]. The best intervention frequently depends on the discretion of the
Figure 1. Inflammatory pseudotumor on right hand and urinary bladder with Foley catheter bulb on left hand.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.12f1
UIJ
UroToday International Journal®
case report
Inflammatory Pseudotumor of the Urachus
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.12
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
individual surgeon; however, aggressive surgery is preferred over simple excision if there is any doubt about the presence of malignancy.
REfERENCES
1. Sheldon CA, Clayman RV, Gonzalez R, et al. Malignant urachal lesions. J Urol. 1984;131(1):1-8. PubMed
2. Yu JS, Kim KW, Lee HJ, et al. Urachal Remnant Diseases: Spectrum of CT and US Findings. Radiographics. 2001;21(2):451-461. PubMed
3. Eble JN, Hull MT, Rowland RG, Hostetter M. Villous adenoma of the urachus with mucusuria: a light and electron microscopic study. J Urol. 1986;135(6):1240-1244. PubMed
4. Narumi Y, Sato T, Kuniyama K, et al. Vesical Dome Tumors: Significance of Extravesical Extension on CT. Radiology. 1988;169(2):383-385. PubMed
5. Narla LD, Newman B, Spottswood SS, Narla S, Kolli R. Inflammatory Pseudotumor. Radiographics. 2003;23(3):719-729. PubMed ; CrossRef
6. Coffin CM, Humphrey PA, Dehner LP. Extrapulmonary inflammatory myofibroblastic tumor: a clinical and pathological survey. Semin Diagn Pathol. 1998;15(2):85-101. PubMed
7. Bonnet JP, Basset T, Dijoux D. Abdominal inflammatory myofibroblastic tumors in children: report of an appendiceal case and review of the literature. J Pediatr Surg. 1996;31(9): 1311-1314. PubMed ; CrossRef
8. Nascimento AF, Dal Cin P, Cilento BG, et al. Urachal inflammatory myofibroblastic tumor with ALK gene rearrangement: a study of urachal remnants. Urology. 2004;64(1):140-144. PubMed ; CrossRef
9. Tunca F, Sanli O, Demirkol K, et al. Inflammatory pseudotumor of urachus mimicking invasive carcinoma of bladder. Urology. 2006;67(3):623.e1-623.e3. PubMed
10. Lee HJ, Kim JS, Choi YS, et al. Treatment of Inflammatory Myofibroblastic Tumor of the Chest: The Extent of Resection. Ann Thorac Surg. 2007;84(1):221-224. PubMed ; CrossRef
UIJ
Eng Hong Goh,1 Akhavan Adel,1 Praveen Singam,1 Christopher Chee Kong Ho,1 Guan Hee Tan,1 Badrulhisham Bahadzor,1 Zulkifli Md Zainuddin,1 Isa Mohamed Rose2
1Urology Unit, Department of Surgery, Universiti Kebangsaan Malaysia Medical Centre2Department of Pathology, Universiti Kebangsaan Malaysia Medical CentreSubmitted June 12, 2011 - Accepted for Publication August 12, 2011
www.urotodayinternationaljournal.comVolume 5 - February 2012
Lymphoepithelioma-like Carcinoma of the Bladder: Is the Prognosis Different from Conventional Bladder Carcinoma?
ABSTRACT
Recognition of other histological variants of urothelial carcinoma of the bladder is important because they may
mimic benign lesions or have different clinical implications and associated prognoses, as well as treatment protocols.
We report a case of lymphoepithelioma-like carcinoma (LELCA) in the bladder and discuss this rare entity with a
review of other articles. Although we could not draw a conclusion on this particular disease, it is hoped that by
adding cases with sufficient detail into literature, we will enable a more thorough and meaningful study where
characteristics of the disease and the appropriate treatment regime could be facilitated.
KEYWORDS: Bladder; Lymphoepithelioma-like carcinoma; Cancer
CORRESPONDENCE: Eng Hong Goh, Urology Unit, Department of Surgery, Universiti Kebangsaan Malaysia Medical Centre, Jalan Yaacob Latif, Bandar Tun Razak, Kuala Lumpur, 56000, Malaysia ([email protected]).
CITATION: UroToday Int J. 2012 Feb;5(1):art 84. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.02
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.02
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
INTRODuCTION
Lymphoepithelioma is a form of undifferentiated carcinoma that was identified primarily in the nasopharynx in Asian patients. In this location, it is in close pathogenetic relation to Epstein-Barr virus (EBV), although such an association has not been documented for lymphoepithelioma-like carcinoma (LELCA) of the urinary bladder. In addition to the bladder, LELCA has been documented in other organs, including salivary glands, the thymus, lungs, skin, the stomach, the uterine cervix, and breasts [1]. First reported by Zuckerberg et al. in 1991 [2], LELCA of the urinary bladder has gradually gained recognition worldwide, but it seems that there is still no unanimous agreement on its subtypes or its prognosis. Our
case has given us an opportunity to review the various papers and make a discussion on this interesting disease.
CASE REPORT
A 71-year-old Chinese woman had repeatedly presented with a history of suprapubic pain, dysuria, and intermittent hematuria for the last 7 years. All of these episodes were treated as urinary tract infections by her general practitioner. However, after a severe bout at the end of 2009, she developed a fever, chills, and rigors, in addition to the usual urinary symptoms aforementioned. She was admitted to a private hospital in another district, and it was during this admission that she was found to have a growth at the posterior wall of her bladder.

UroToday International Journal®
case report
Lymphoepithelioma-like Carcinoma of the Bladder: Is the Prognosis Different from Conventional Bladder
Carcinoma?
©2012 Digital Science Press, Inc.
UIJ / Vol 4 / Iss 6 / December / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.02
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
The initial transurethral resection of the bladder tumor (TURBT) revealed a histopathology finding of muscle-invasive, high-grade urothelial carcinoma, but the specimen was unavailable for another inspection at our institution due to logistics and costs. Her subsequent management at our hospital included a work-up computed tomography (CT) scan (Figure 1) and bone scans showing T4aN2M0 disease, with bladder growth infiltrating to the vagina and right vesicoureteric orifice. This resulted in right obstructive uropathy and regional lymphadenopathies. The patient refused any neoadjuvant therapy. She underwent an uneventful cystectomy, including removal of her anterior portion of the vagina, uterus, both fallopian tubes, and ovaries, as well as a lymphadenectomy to iliac level and ileal conduit creation in March 2010. The intraoperative frozen-section assessment at the ureteric margin needed repeating, as there was tremendous difficulty in identifying the malignant cellular margin in the first samples. The official histopathology result reported the presence of
diffusely infiltrating and rather undifferentiated malignant cells arranged in sheets, and trabeculae with pleomorphic nuclei and prominent nucleoli. There was also a prominent lymphoid infiltrate associated with the tumor sheets and clumps. The malignant cells infiltrated into the underlying muscularis propria up to the perivesical soft tissue and into the posterior cervical region. Fortunately, the surgical margin was clear, and there was no evidence of lymphovascular invasion. However, a 1 cm, right obturator node, out of 27 lymph nodes, harbored the malignant cells similar to those seen in the bladder. The malignant tissues stained positively for cytokeratin, CD3, CD20, p53, and Ki67 (90% high), but negatively for CK20 (Figures 2 and 3). A diagnosis of pure lymphoepithelioma-like carcinoma of the bladder was thus made. During her follow-up 14 months later, she was not given adjuvant therapy and was free of the disease, both clinically and radiologically.
DISCuSSION
There have been numerous studies on this particular disease. Given that it is an uncommon entity with an incidence of 0.4 to 1.3% of all bladder carcinomas [2], most studies are either case reports or a case series with a small number of patients. The largest study to date was performed by Williamson et al. who described 34 cases in the bladder in 2011 [3]. Other large case series included those by Tamas et al. [4] with 28 cases in 2007, Lopez-Beltran et al. [5], which reported 13 cases in 2000, Holmang et al. [6] with 9 cases in 1998, and Amin et al. with 11 cases in 1994 [1]. A report by Serrano et al. in 2008 compiled all cases of LELCA of the bladder by searching through PubMed in English literature. It produced very informative details and characteristics of the disease in the form of tables [7]. We actually attempted to compile all of these cases for the purpose of analysis, as well as comparison, with the large series of conventional, transitional-cell carcinoma, but the effort was hindered by inconsistency in classification and a lack of vital details.
It is unfortunate that we could not compare the 2 histological specimens of our patient, nor could we explain the differences, although there is a propensity of urothelial carcinoma for divergent variation and abundant variability in tumor morphology [3]. The histological pattern and the subclassification of LELCA of the bladder have been well described in many earlier papers [1,4,6]. Its importance lies in the fact that the prognosis of “pure” or “predominant” disease is considered better than the conventional carcinoma of the bladder, whereas the prognosis of the “focal” disease does not differ from the conventional type [1,2,5]. However, Tamas et al., who subclassified their cases into either “pure” or
Figure 1. CT scan of the abdomen showing a tumor at the right posterolateral aspect of the bladder infiltrating posteriorly as well as onto the right vesicoureteric junction. A DJ stent positioned in the right ureter is seen in the bladder.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.02f1
UIJ

UroToday International Journal®
case report
Lymphoepithelioma-like Carcinoma of the Bladder: Is the Prognosis Different from Conventional Bladder
Carcinoma?
©2012 Digital Science Press, Inc.
UIJ / Vol 4 / Iss 6 / December / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.02
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
“mixed” types, did not share their findings. They observed that the outcomes similarly disregarded subclassification. The paper also claimed that LELCA, as a whole, shared similar outcomes with conventional urothelial carcinoma [4]. In regards to the differing opinions, many of these papers reported that the T stage of the disease and the N status—crucial prognostic factors—were tremendously unknown. The latest and largest series by Williamson et al. included the N status in almost all of their cases and reported a favorable prognosis in “pure” or “predominant” cases, but the number of patients involved was quite small; i.e., only 5 [3]. Determining the prognosis is vital, as the arguments have primarily concentrated on whether or not bladder preservation therapy is appropriate [3,4]. Taking into account our patient, with a 7-year history of symptoms, a final stage of T4aN1M0, and the absence of neoadjuvant or adjuvant therapy while remaining disease-free until the present moment, the notion that “pure” or “predominant” LELCA has a favorable prognosis is perhaps true. Is there another prognosis determinant in LELCA of the bladder? Thus far, attention has been paid to the morphological pattern of the tumor, but the molecular abnormalities have not been studied thoroughly yet [3].
In conclusion, it is our opinion that “pure” or “predominant” LELCA carries a positive outcome based on our experience, as well as that of others, although current limited data could not prove the evidence sufficiently. By pooling cases of LELCA of the
bladder with adequate and comparable details in literature, a
more precise understanding of this disease and a comparison
with the conventional urothelial carcinoma can be facilitated.
Venturing out of the avenue of morphological patterns may
open up new insights into this particular disease.
REfERENCES
1. Amin MB, Ro JY, Lee KM, et al. Lymphoepithelioma-
like carcinoma of the urinary bladder. Am J Surg Pathol.
1994;18:466-473. PubMed ; CrossRef
2. Porcaro AB, Gilioli E, Migliorini F, Antoniolli SZ, Lannucci
A, Comunale L. Primary lymphoepithelioma like
carcinoma of the urinary bladder: Report of one case
with review and update of the literature after a pooled
analysis of 43 patients. Int Urol Nephrol. 2003;35:99-
106. PubMed ; CrossRef
3. Williamson SR, Zhang S, Lopez-Beltran A, et al.
Lymphoepithelioma-like carcinoma of the urinary
bladder: Clinicopathologic, immunohistochemical, and
molecular features. Am J Surg Pathol. 2011;35:474-483.
PubMed ; CrossRef
Figure 2. Clump of large, poorly differentiated malignant cells surrounded by an infiltrate of lymphocytes and occasional eosinophils (H and E x 200).http://dx.doi.org/10.3834/uij.1944-5784.2012.02.02f2
Figure 3. Immunostain showing positively stained malignant cells surrounded by infiltrate of unstained lymphocytes (cytokeratin x 200).http://dx.doi.org/10.3834/uij.1944-5784.2012.02.02f3
UIJ

UroToday International Journal®
case report
Lymphoepithelioma-like Carcinoma of the Bladder: Is the Prognosis Different from Conventional Bladder
Carcinoma?
©2012 Digital Science Press, Inc.
UIJ / Vol 4 / Iss 6 / December / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.02
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
4. Tamas EF, Nielsen ME, Schoenberg MP, Epstein JI. Lympoepithelioma-like carcinoma of the urinary tract: A clinicopathological study of 30 pure and mixed cases. Mod Pathol. 2007;20:828-834. PubMed ; CrossRef
5. Lopez-Beltran A, Luque RJ, Vicioso L, et al. Lymphoepithelioma-like carcinoma of the urinary bladder: A clinicopathologic study of 13 cases. Virchows Arch. 2001;438:552-557. PubMed ; CrossRef
6. Holmäng S, Borghede G, Johansson SL. Bladder carcinoma with lymphoepithelioma-like differentiation: A report of 9 cases. J Urol. 1998;159(3):779-782. PubMed ; CrossRef
7. Serrano GB, Fúnez FA, López RG, et al. Bladder lymphoepithelioma-like carcinoma. Bibliographic review and case report. Arch Esp Urol. 2008;61(6):723-729. PubMed
UIJ

Kapil Singla, Ashish Kumar Sharma, Sistla Bobby Viswaroop, Ganesh Gopalakrishnan, Sangam Vedanayagam KandasamiDepartment of Urology, Vedanayagam Hospital, Coimbatore, Tamil Nadu, IndiaSubmitted October 19, 2011 - Accepted for Publication November 23, 2011
www.urotodayinternationaljournal.comVolume 5 - February 2012
Mondor’s Disease of the Penis: A Forgotten Entity
ABSTRACT
Introduction: Thrombophlebitis of the superficial dorsal vein of the penis, known as Mondor’s disease of the penis,
was first described by Braun-Falco in 1955.
Case Presentation: An apparently healthy 37-year-old man presented with painful swelling of the dorsal aspect of
his penis. Doppler ultrasonography revealed a noncompressible portion of superficial dorsal vein of the penis, as
well as the lack of venous flow signals. The patient was treated conservatively.
Conclusion: Mondor’s disease of the penis is a rare clinical entity and a urologist should be aware of this condition.
KEYWORDS: Mondor’s disease; Superficial thrombophlebitis; Conservative management
CORRESPONDENCE: Kapil Singla, Department of Urology, Vedanayagam Hospital, Coimbatore, Tamil Nadu, India 641 002 ([email protected]).
CITATION: UroToday Int J. 2012 Feb;5(1):art 87. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.05
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/ 10.3834/uij.1944-5784.2012.02.05
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
INTRODuCTION
Superficial-vein thrombosis was first described by Mondor in 1939 when it involved subcutaneous veins of the anterolateral thoracoabdominal wall [1]. The most commonly involved vessel is the thoracoepigastric vessel. In 1955, Braun-Falco described penile participation, and, in 1958, Helm and Hodge described an isolated, superficial penile vein thrombosis [2,3]. Mondor’s disease of the penis is an under-reported condition. Although it is rare, proper diagnosis and consequent reassurance can help to dissipate the anxiety experienced by patients with the disease. This case report describes the symptomatology, diagnosis, and treatment of thrombosis of the superficial dorsal vein of the penis.
CASE PRESENTATION
A 37-year-old man presented with a painful dorsal induration of the penis for 4 days. The pain was of the throbbing type. There was no associated itching, discharge, hematuria, fever, or dysuria. He denied any history of recent trauma, vigorous sexual activity, or use of constriction devices. He also denied any history of fever or lower urinary tract symptoms. A physical examination revealed a physically healthy man with a tender, cord-like swelling on the dorsal surface of the penis, which was extending from the glans penis up to the suprapubic area (Figure 1). There was no associated inguinal lymphadenopathy. Routine blood tests and the coagulation profile were normal. Doppler ultrasonography of the penis revealed a noncompressible, superficial dorsal vein, as well as the lack of venous flow
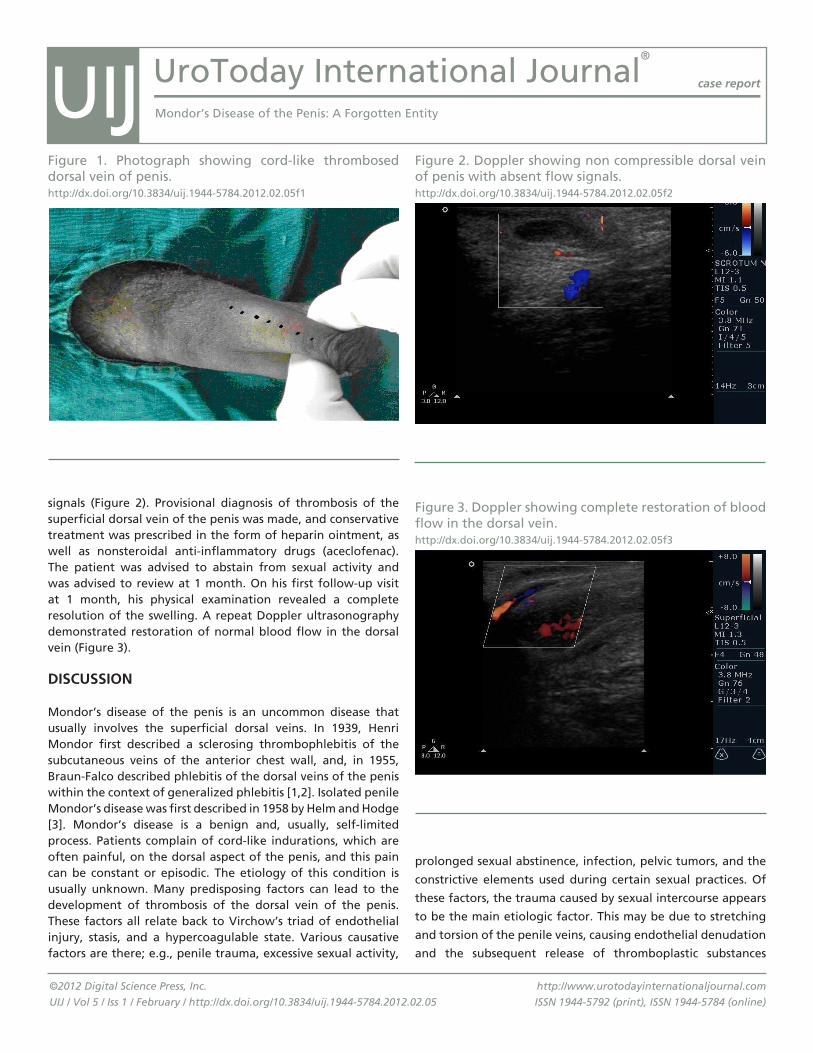
UroToday International Journal®
case report
Mondor’s Disease of the Penis: A Forgotten Entity
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.05
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
signals (Figure 2). Provisional diagnosis of thrombosis of the superficial dorsal vein of the penis was made, and conservative treatment was prescribed in the form of heparin ointment, as well as nonsteroidal anti-inflammatory drugs (aceclofenac). The patient was advised to abstain from sexual activity and was advised to review at 1 month. On his first follow-up visit at 1 month, his physical examination revealed a complete resolution of the swelling. A repeat Doppler ultrasonography demonstrated restoration of normal blood flow in the dorsal vein (Figure 3).
DISCuSSION
Mondor’s disease of the penis is an uncommon disease that usually involves the superficial dorsal veins. In 1939, Henri Mondor first described a sclerosing thrombophlebitis of the subcutaneous veins of the anterior chest wall, and, in 1955, Braun-Falco described phlebitis of the dorsal veins of the penis within the context of generalized phlebitis [1,2]. Isolated penile Mondor’s disease was first described in 1958 by Helm and Hodge [3]. Mondor’s disease is a benign and, usually, self-limited process. Patients complain of cord-like indurations, which are often painful, on the dorsal aspect of the penis, and this pain can be constant or episodic. The etiology of this condition is usually unknown. Many predisposing factors can lead to the development of thrombosis of the dorsal vein of the penis. These factors all relate back to Virchow’s triad of endothelial injury, stasis, and a hypercoagulable state. Various causative factors are there; e.g., penile trauma, excessive sexual activity,
prolonged sexual abstinence, infection, pelvic tumors, and the
constrictive elements used during certain sexual practices. Of
these factors, the trauma caused by sexual intercourse appears
to be the main etiologic factor. This may be due to stretching
and torsion of the penile veins, causing endothelial denudation
and the subsequent release of thromboplastic substances
Figure 1. Photograph showing cord-like thrombosed dorsal vein of penis.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.05f1
Figure 2. Doppler showing non compressible dorsal vein of penis with absent flow signals.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.05f2
Figure 3. Doppler showing complete restoration of blood flow in the dorsal vein.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.05f3
UIJ

UroToday International Journal®
case report
Mondor’s Disease of the Penis: A Forgotten Entity
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.05
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
that can activate the coagulation cascade [4]. Furthermore, Mondor’s disease of the penis has also been reported after long-haul flights [5], as an unusual manifestation of metastatic pancreatic adenocarcinoma, and as an idiopathic condition. The diagnosis of the disease is mainly clinical, supplemented with Doppler ultrasonography [6]. The differential diagnosis includes sclerosing lymphangitis, Peyronie’s disease, and a fractured penis [7]. Treatment is essentially conservative. Several methods of treatment have been proposed for penile Mondor’s disease. Anticoagulation with aspirin, heparin, or other antiplatelet agents will not expedite healing and is not necessary to prevent additional thrombosis. Antibiotics can be used prophylactically. NSAIDs can be used for pain relief, as well as for their inflammatory action. Patients should also be informed about the avoidance of sexual intercourse or masturbation. In most of the cases, symptoms resolve completely within 6 to 8 weeks. In cases with no resolution, despite conservative treatment, thrombus excision or excision of the vein has to be done [4]. Such surgeries can relieve pain and diminish skin induration, and produce aesthetically pleasing results.
ACKNOWlEDgEmENT
Dr. S Boopathy Vijaya Raghavan (Consultant Radiologist)
REfERENCES
1. Mondor H, Tronculite Sons. Cutanee de la parvi thoracique antero-lateral. Mem Acad Chir.1939;65:1275-1278.
2. Braun-Falco O. [Clinical manifestations, histology and pathogenesis of the cordlike superficial phlebitis forms]. Dermatol Wochenschr. 1955;132:705-715. PubMed
3. Helm JD Jr, Hodge IG. Thrombophlebitis of a dorsal vein of the penis: report of a case treated by phenylbutazone (Butaolidin). J Urol. 1958;79:306-307. PubMed
4. Kraus S, Lüdecke G, Weidner W. Mondor’s disease of the penis. Urol Int. 2000;64:99-100. PubMed ; CrossRef
5. Day S, Bingham JS. Mondor’s disease of the penis following a long-haul flight. Int J STD AIDS. 2005;16(7):510-511. PubMed ; CrossRef
6. Yanik B, Conkbayir I, Oner O, Hekimoğlu B. Imaging findings in Mondor’s disease. J Clin Ultrasound. 2003;31(2):103-107. PubMed ; CrossRef
7. Nazir SS, Khan M. Thrombosis of the dorsal vein of the penis (Mondor’s Disease): A case report. Indian J Urol. 2010;26:431-433. PubMed ; CrossRef
UIJ

Rahul Devraj, Vedamurthy Pogula Reddy, Surya Prakash Vaddi, Ajit Vikram, Sreedhar DDept of Urology and Renal Transplantation, Narayana Medical College, Nellore, IndiaSubmitted May 9, 2011 - Accepted for Publication July 25, 2011
www.urotodayinternationaljournal.comVolume 5 - February 2012
Retroperitoneal Textiloma Mimicking an Adrenal Tumor
ABSTRACT
We describe a case with a perirenal-retained sponge presenting as an adrenal tumor in a patient who had undergone
surgery for urolithiasis 10 years prior. It was incidentally diagnosed during an evaluation of left flank pain.
KEYWORDS: Retained sponge; Textiloma; Adrenal tumor
CORRESPONDENCE: Vedamurthy Pogula Reddy, MCh, Dept of Urology and Renal Transplantation, Narayana Medical College, Nellore, Andhra Pradesh, India, 524 002 ([email protected]).
CITATION: UroToday Int J. 2012 Feb;5(1):art 85. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.03
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/ 10.3834/uij.1944-5784.2012.02.03
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
INTRODuCTION
Despite the widespread use of radio-opaque-labeled surgical sponges, retained sponges, or so-called textilomas from previous surgical procedures, are still causing diagnostic and therapeutic problems. We present an unusual case and late discovery of a retained sponge, 10 years after pyelolithotomy, mimicking an adrenal tumor.
CASE REPORT
A 52-year-old man was admitted to the hospital with the complaint of left flank pain. He was a known hypertensive. He underwent left pyelolithotomy 10 years before this admission. On physical examination, a left flank incision scar and left flank tenderness were noted. His serum creatinine was 1.8 mg. An ultrasound of the abdomen and a plain CT scan of the abdomen showed a left adrenal tumor (Figure.1). Biochemical evaluation revealed normal urinary catecholamine metabolites and serum
cortisol levels. A left retroperitoneal adrenalectomy was planned.
During the operation, the left adrenal gland was normal and a
6 cm by 5 cm mass was seen lateral to the left suprarenal gland.
Dense adhesions were present between the mass, the left adrenal
gland, and left kidney. The mass was excised in toto. A cut section
revealed a surgical sponge encapsulated by a thick, fibrous wall
(Figure 2).
DISCuSSION
The abdomen, pelvis, and retroperitoneum are the most common
locations associated with retained surgical foreign bodies (RSFB)
[1]. RSFB in these anatomic areas can vary from an asymptomatic,
retained foreign body detected accidentally on diagnostic imaging
to sepsis, bowel obstruction, and fistula formation. Asymptomatic
soft-tissue mass suspicious for an abscess or a soft-tissue tumor
has also been described as presenting features of RSFB in the
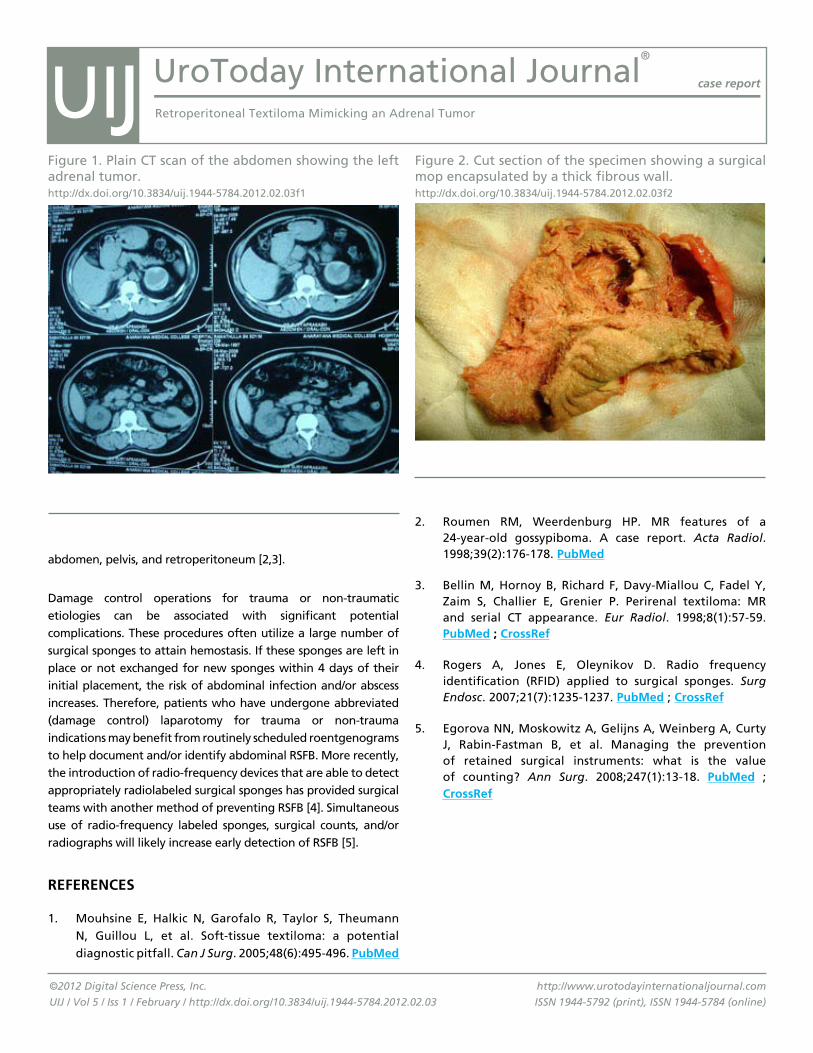
UroToday International Journal®
case report
Retroperitoneal Textiloma Mimicking an Adrenal Tumor
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.03
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
abdomen, pelvis, and retroperitoneum [2,3].
Damage control operations for trauma or non-traumatic etiologies can be associated with significant potential complications. These procedures often utilize a large number of surgical sponges to attain hemostasis. If these sponges are left in place or not exchanged for new sponges within 4 days of their initial placement, the risk of abdominal infection and/or abscess increases. Therefore, patients who have undergone abbreviated (damage control) laparotomy for trauma or non-trauma indications may benefit from routinely scheduled roentgenograms to help document and/or identify abdominal RSFB. More recently, the introduction of radio-frequency devices that are able to detect appropriately radiolabeled surgical sponges has provided surgical teams with another method of preventing RSFB [4]. Simultaneous use of radio-frequency labeled sponges, surgical counts, and/or radiographs will likely increase early detection of RSFB [5].
REfERENCES
1. Mouhsine E, Halkic N, Garofalo R, Taylor S, Theumann N, Guillou L, et al. Soft-tissue textiloma: a potential diagnostic pitfall. Can J Surg. 2005;48(6):495-496. PubMed
2. Roumen RM, Weerdenburg HP. MR features of a 24-year-old gossypiboma. A case report. Acta Radiol. 1998;39(2):176-178. PubMed
3. Bellin M, Hornoy B, Richard F, Davy-Miallou C, Fadel Y, Zaim S, Challier E, Grenier P. Perirenal textiloma: MR and serial CT appearance. Eur Radiol. 1998;8(1):57-59. PubMed ; CrossRef
4. Rogers A, Jones E, Oleynikov D. Radio frequency identification (RFID) applied to surgical sponges. Surg Endosc. 2007;21(7):1235-1237. PubMed ; CrossRef
5. Egorova NN, Moskowitz A, Gelijns A, Weinberg A, Curty J, Rabin-Fastman B, et al. Managing the prevention of retained surgical instruments: what is the value of counting? Ann Surg. 2008;247(1):13-18. PubMed ; CrossRef
Figure 1. Plain CT scan of the abdomen showing the left adrenal tumor.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.03f1
Figure 2. Cut section of the specimen showing a surgical mop encapsulated by a thick fibrous wall.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.03f2
UIJ

Jameel Hisham Bardesi, Ahmed Jalal Al-SayyadKing Abdulaziz University, Jeddah, Saudi ArabiaSubmitted October 15, 2011 - Accepted for Publication December 6, 2011
www.urotodayinternationaljournal.comVolume 5 - February 2012
Teratoid Wilms Tumor in a Child: A Case Report
ABSTRACT
Teratoid Wilms is a very rare histopathological variant of Wilms tumors that is characterized by the predominance
of heterologous components, and is described by many to be a nonaggressive, nonmetastatic tumor with a
favorable prognosis. We report a case of a 4-year-old boy with a rare, aggressive metastatic variant of teratoid
Wilms tumor. The boy presented with abdominal pain and a palpable abdominal mass. The computed tomography
scan demonstrated a large, cystic, multiloculated left renal mass and a single left pulmonary metastasis. The patient
had a 5-week course of neoadjuvant chemotherapy. As a result, the size of the metastatic lesion decreased, but
there was no change in the size of the renal mass. Subsequently, a left radical nephrectomy and left pulmonary
metastectomy were performed where the pathology report showed metastatic teratoid Wilms tumor. The patient
received adjuvant chemotherapy and radiotherapy. One year following the initial surgery, the child developed
bilateral pulmonary metastases where he is currently having an aggressive regimen of chemotherapy. Although
teratoid Wilms has been described as a nonaggressive tumor with a favorable prognosis, it can present with more
aggressive forms, with a tendency for metastasis.
KEYWORDS: Wilms tumor; Teratoid Wilms; Rare Wilms
CORRESPONDENCE: Jameel Hisham Bardesi, King Abdulaziz University, Jeddah 21589, Saudi Arabia ([email protected]).
CITATION: UroToday Int J. 2012 Feb;5(1):art 90. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.08
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/ 10.3834/uij.1944-5784.2012.02.08
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
INTRODuCTION
Wilms tumor is an embryonic tumor of mesodermal origin. It is typically characterized by a display of a triphasic histological pattern of blastemal, stromal, and epithelial cells. Heterologous mesodermal components, such as adipose tissue, skeletal muscle, cartilage, and neurological tissue, may be seen in small foci throughout the neoplasm [1-3]. In 1984, a rare variant with heterologous predominance was described by Variend et al., who introduced the term “teratoid Wilms” [1]. Teratoid Wilms
has been described by many as a nonaggressive, nonmetastatic tumor with a favorable prognosis [1-3,5]. Review of 17—including 15 cases without metastases and 2 with metastases—cases showed that 12 of them had no evidence of disease after receiving treatment [3]. Similar outcomes were reported in other cases [5,8]. Conversely, Myers et al. [8] stated that 50% of those with teratoid Wilms presented at stage III or higher. They also reported an incidence of bilateral disease in 38%. According to the available data, a total of 3 cases of metastases and 4 deaths—2 of them linked to progression—have been

UroToday International Journal®
case report
Teratoid Wilms Tumor in a Child: A Case Report
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.08
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
reported in those with teratoid Wilms [3,9,10]. We report a rare case of 4-year-old boy with an aggressive metastatic variant of teratoid Wilms tumor.
CASE REPORT
A 4-year-old healthy boy presented with abdominal pain and a palpable abdominal mass. A computed tomography (CT) scan of the abdomen showed a huge multiloculated cystic mass involving the left kidney (Figures 1 and 2). A CT chest revealed a single metastasis in the left lung (Figure 3). A diagnosis of Wilms tumor of the left kidney with pulmonary metastasis was made. The patient underwent chemotherapy for 5 consecutive weeks. The patient received carboplatin (450 mg/m², IV, day 1 only) and etoposide (100 mg/m², IV, once daily for 5 days) in week 0, vincristine (0.05 mg/kg, IV, day 1 only), and actinomycin-D (15 mcg/kg, IV, once daily for 5 days) in week 1, and weekly vincristine (0.05 mg/kg, IV, day 1 only) throughout the second, third, and fourth weeks. As a result, the size of the metastatic lesion decreased while there was no change in the size of the renal mass. Subsequently, a left radical nephrectomy in conjunction with a left pulmonary metastectomy was performed. Cut sections of the mass were multicystic in appearance, with areas of necrosis and hemorrhage, and showed no extension to the perinephric fat. Microscopically, sections of the kidney revealed a multicystic neoplastic process with wide areas of necrosis, hemorrhage, and hemosiderin-laden macrophages. The tumor was composed of nests and clusters of embryonal-looking cells, with enlarged hyperchromatic nuclei and occasional mitotic figures (Figure 4). Focal areas of spindle cells and smooth-muscle differentiation were also seen. Few cysts were lined by flattened epithelium while others were lined by stratified squamous epithelium and filled with keratin flakes (Figure 5). The left lung nodule was positive for metastases and had a blastemal component (Figure 6). A panel of immunohistochemical markers was performed on the lung nodule, including CK-Pan, vimentin, and WT-1. The tumor cells were positive for WT-1, focally positive for vimentin, and negative for CK-Pan (Figure 7). Postoperative radiotherapy (to the lung and abdomen) and chemotherapy in the form of actinomycin D (15 mcg/kg, IV, once daily for 5 days on weeks 12, 24, 36, 48, and 60 of initial treatment, and 30 mcg/kg day 1 only of weeks 6, 9, 18, 30, 42, 54, and 66 of initial treatment), vincristine (0.05 mg/kg, IV, day 1 only of weeks 6, 9, 28, 30, 42, 54, and 66, and 0.05 mg/kg, IV, once daily on days 1 and 5 in weeks 12, 24, 36, 48. 60), and doxorubicin (40 mg/m², IV, on day 1 of weeks 6 and 9, and 60 mg/m², IV, on day 1 of weeks 18, 30, 42, 54, and 66) were delivered.
One year following the initial surgery, a routine follow-up
Figure 1. Multicystic, multiloculated left renal mass.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.08f1
Figure 2. Coronal view of mass.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.08f2
CT of the chest demonstrated multiple small focal lesions in both lungs. There were no signs of local recurrence or residual disease in the abdomen.
The patient is currently alive 21 months after initial treatment.
UIJ
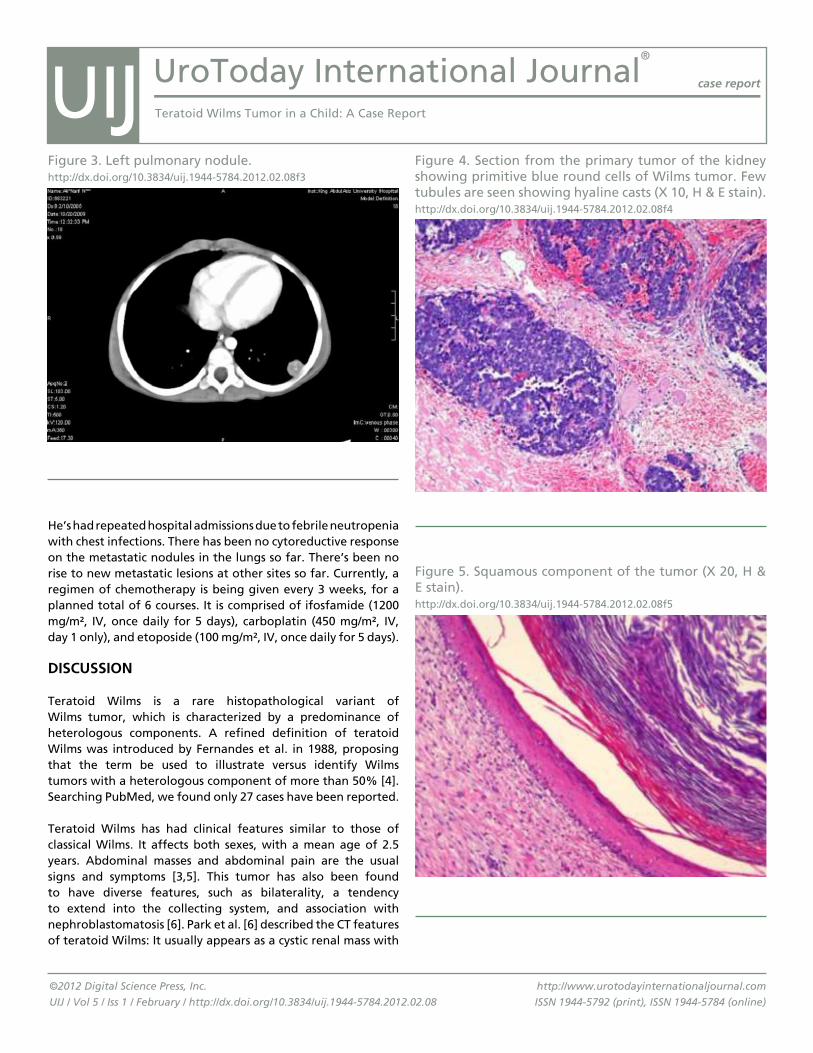
UroToday International Journal®
case report
Teratoid Wilms Tumor in a Child: A Case Report
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.08
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
He’s had repeated hospital admissions due to febrile neutropenia with chest infections. There has been no cytoreductive response on the metastatic nodules in the lungs so far. There’s been no rise to new metastatic lesions at other sites so far. Currently, a regimen of chemotherapy is being given every 3 weeks, for a planned total of 6 courses. It is comprised of ifosfamide (1200 mg/m², IV, once daily for 5 days), carboplatin (450 mg/m², IV, day 1 only), and etoposide (100 mg/m², IV, once daily for 5 days).
DISCuSSION
Teratoid Wilms is a rare histopathological variant of Wilms tumor, which is characterized by a predominance of heterologous components. A refined definition of teratoid Wilms was introduced by Fernandes et al. in 1988, proposing that the term be used to illustrate versus identify Wilms tumors with a heterologous component of more than 50% [4]. Searching PubMed, we found only 27 cases have been reported.
Teratoid Wilms has had clinical features similar to those of classical Wilms. It affects both sexes, with a mean age of 2.5 years. Abdominal masses and abdominal pain are the usual signs and symptoms [3,5]. This tumor has also been found to have diverse features, such as bilaterality, a tendency to extend into the collecting system, and association with nephroblastomatosis [6]. Park et al. [6] described the CT features of teratoid Wilms: It usually appears as a cystic renal mass with
Figure 4. Section from the primary tumor of the kidney showing primitive blue round cells of Wilms tumor. Few tubules are seen showing hyaline casts (X 10, H & E stain).http://dx.doi.org/10.3834/uij.1944-5784.2012.02.08f4
Figure 3. Left pulmonary nodule.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.08f3
Figure 5. Squamous component of the tumor (X 20, H & E stain).http://dx.doi.org/10.3834/uij.1944-5784.2012.02.08f5
UIJ

UroToday International Journal®
case report
Teratoid Wilms Tumor in a Child: A Case Report
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.08
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
tumors less than 550 grams, and have a favorable histology. Those with recurrent Wilms tumors may be treated with aggressive chemotherapy, such as the ICE regimen (ifosfamide, carboplatin, and etoposide) or other regimens studied in clinical trials [11]. No specific treatment strategy has been proposed to those with teratoid Wilms. Our patient, as well as 2 other patients who had disease progression, received the ICE regimen, with mortality being the end result of the latter 2 [3].
Taking into consideration the diverse biological behavior of teratoid Wilms tumors, with most of them demonstrating a nonaggressive, nonmetastatic behavior, whereas some variants—including our case—exhibit an aggressive metastatic behavior, a question is raised of whether or not the later variant is truly teratoid Wilms or a different entity. Probably a better description of the clinical, imaging, histopathological, immunohistochemical, and genetic characteristics of these tumors might help distinguish aggressive from nonaggressive variants to predict prognosis.
SummARY
We present a rare, aggressive variant of teratoid Wilms tumor with metastasis. Disease progression was evident, even after neoadjuvant chemotherapy, radical nephrectomy, pulmonary metastatectomy, and adujuvant chemoradiotherapy. Although teratoid Wilms has been described as a nonaggressive, nonmetastatic tumor with a favorable prognosis, it can present
multifocal, solid components containing fatty elements and occasional calcifications.
Teratoid Wilms tumor and renal teratoma have been hisologically similar. Beckwith proposed criteria to differentiate the 2 from each other. He stated that renal teratoids should be intrarenal and show attempts of heterotopic organ formation [7]. Cytogenic analysis for the deletion of the short arm of chromosome 11 has been helpful in complicated cases [2].
Although teratoid Wilms has been described as a nonaggressive, nonmetastatic tumor with a favorable prognosis [1-3,5], a total of 4 cases of metastases have been reported, including our case [3,10]. This rare variant of Wilms has been portrayed as chemo-resistant by many [1,2,10,9]. Neoadjuvant chemotherapy has been unable to produce a cytoreductive response in most cases [10,9]. This may be attributed to the well differentiated nature of the teratomatous elements in these cases [6,2]. In our patient, although downsizing could be achieved in the single pulmonary metastasis, no size reduction was observed in the primary tumor with neoadjuvant chemotherapy.
The American Cancer Society guidelines for the treatment of Wilms tumor advise surgery, followed by chemotherapy with actinomycin-D (dactinomycin) and vincristine for all stages, with the exception of those who are less than 2 years of age, have
Figure 6. Section from the metastatic tumor to the lung showing sheets of primitive round cells invading the lung parenchyma (X 10, H & E stain).http://dx.doi.org/10.3834/uij.1944-5784.2012.02.08f6
Figure 7. Blastema cells showing positive nuclear staining for WT-1 immunostaining (X 20).http://dx.doi.org/10.3834/uij.1944-5784.2012.02.08f7
UIJ
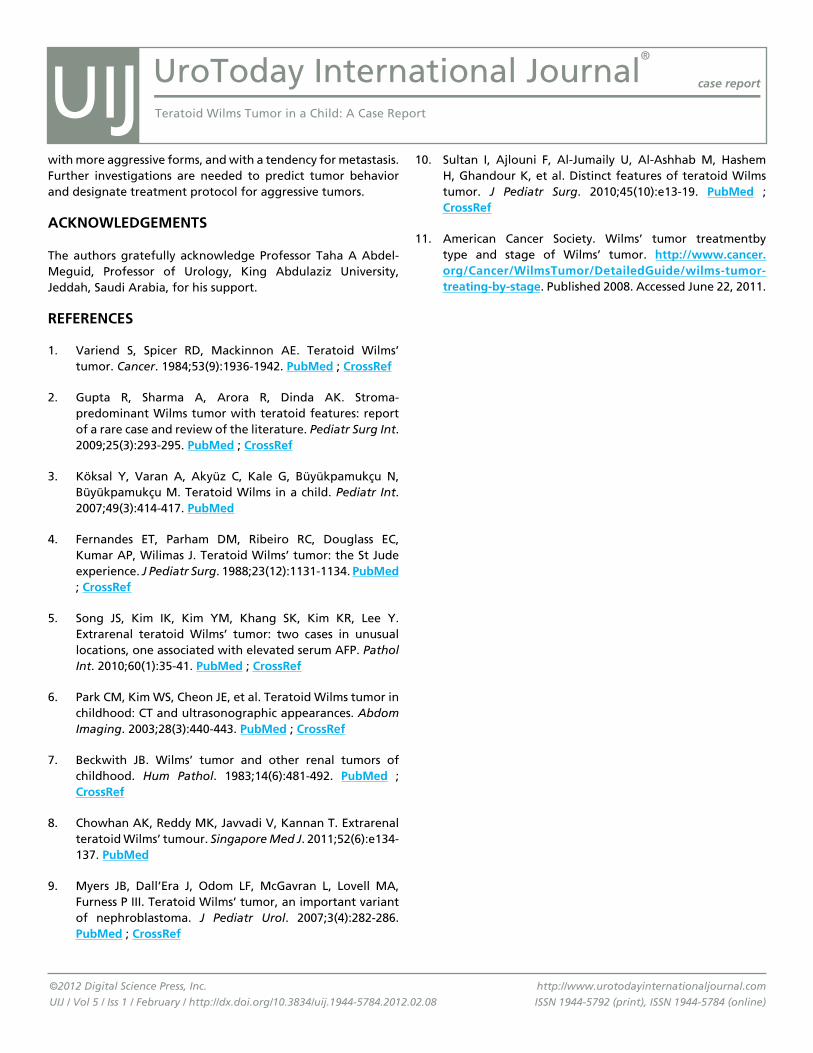
UroToday International Journal®
case report
Teratoid Wilms Tumor in a Child: A Case Report
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.08
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
with more aggressive forms, and with a tendency for metastasis. Further investigations are needed to predict tumor behavior and designate treatment protocol for aggressive tumors.
ACKNOWlEDgEmENTS
The authors gratefully acknowledge Professor Taha A Abdel-Meguid, Professor of Urology, King Abdulaziz University, Jeddah, Saudi Arabia, for his support.
REfERENCES
1. Variend S, Spicer RD, Mackinnon AE. Teratoid Wilms’ tumor. Cancer. 1984;53(9):1936-1942. Pubmed ; CrossRef
2. Gupta R, Sharma A, Arora R, Dinda AK. Stroma-predominant Wilms tumor with teratoid features: report of a rare case and review of the literature. Pediatr Surg Int. 2009;25(3):293-295. Pubmed ; CrossRef
3. Köksal Y, Varan A, Akyüz C, Kale G, Büyükpamukçu N, Büyükpamukçu M. Teratoid Wilms in a child. Pediatr Int. 2007;49(3):414-417. Pubmed
4. Fernandes ET, Parham DM, Ribeiro RC, Douglass EC, Kumar AP, Wilimas J. Teratoid Wilms’ tumor: the St Jude experience. J Pediatr Surg. 1988;23(12):1131-1134. Pubmed ; CrossRef
5. Song JS, Kim IK, Kim YM, Khang SK, Kim KR, Lee Y. Extrarenal teratoid Wilms’ tumor: two cases in unusual locations, one associated with elevated serum AFP. Pathol Int. 2010;60(1):35-41. Pubmed ; CrossRef
6. Park CM, Kim WS, Cheon JE, et al. Teratoid Wilms tumor in childhood: CT and ultrasonographic appearances. Abdom Imaging. 2003;28(3):440-443. Pubmed ; CrossRef
7. Beckwith JB. Wilms’ tumor and other renal tumors of childhood. Hum Pathol. 1983;14(6):481-492. Pubmed ; CrossRef
8. Chowhan AK, Reddy MK, Javvadi V, Kannan T. Extrarenal teratoid Wilms’ tumour. Singapore Med J. 2011;52(6):e134-137. Pubmed
9. Myers JB, Dall’Era J, Odom LF, McGavran L, Lovell MA, Furness P III. Teratoid Wilms’ tumor, an important variant of nephroblastoma. J Pediatr Urol. 2007;3(4):282-286. Pubmed ; CrossRef
10. Sultan I, Ajlouni F, Al-Jumaily U, Al-Ashhab M, Hashem H, Ghandour K, et al. Distinct features of teratoid Wilms tumor. J Pediatr Surg. 2010;45(10):e13-19. Pubmed ; CrossRef
11. American Cancer Society. Wilms’ tumor treatmentby type and stage of Wilms’ tumor. http://www.cancer.org/Cancer/WilmsTumor/Detailedguide/wilms-tumor-treating-by-stage. Published 2008. Accessed June 22, 2011.
UIJ

Omri Nativ, Sarel Halachmi, Boaz Moskovitz, Ofer NativDepartment of Urology, Bnei-Zion Medical Center, Haifa, IsraelSubmitted November 4, 2011 - Accepted for Publication December 13, 2011
www.urotodayinternationaljournal.comVolume 5 - February 2012
Treatment of Post, High-Intensity-Focused Ultrasound Urethral Stricture with Novel Long-term Stent
ABSTRACT
Urethral strictures (US) can be recurrent chronic illnesses leading to severe side effects and poor quality of life.
Several options to treat US exist, including repeated dilatations, stents, and open surgery. A urethral stent is a good,
minimally invasive option but has major limitations, such as stent migration, mucosal growth, and incontinence,
especially for bladder-neck strictures. Herein, we describe a new stent that, due to its design, may solve some of the
above-mentioned problems, enabling long-term use and safe removal.
KEYWORDS: High-intensity-focused ultrasound; Urethral stricture; Long-term urethral stent
CORRESPONDENCE: Sarel Halachmi, MD, Department of Urology, Bnai-Zion Medical Center, Haifa, Isreal ([email protected]).
CITATION: UroToday Int J. 2012 Feb;5(1):art 92. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.10
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/ 10.3834/uij.1944-5784.2012.02.10
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
CASE REPORT
A 66-year-old presented to us who, 3 years earlier, had undergone high-intensity-focused ultrasound (HIFU) treatment for organ-confined (Gleason score 3+4) prostate cancer. Approximately 3 months after the procedure, he presented to his local urologist with progressive obstructive voiding symptoms that were managed endoscopically via visual internal urethrotomy, followed by a transurethral resection of stenotic scar tissue. Afterwards, he underwent repeated endoscopic treatment for restenosis every 10 to 12 weeks. A typical pre- and post-treatment endoscopic view is shown in Figure 1. Upon arrival at our medical center, the patient underwent a urinary ultrasound that revealed a normal upper urinary tract, small prostate, and 240 ml of post-void residual urinary volume. Uroflowmetry demonstrated an obstructive pattern with maximal urinary flow of 5.6 ml/sec. A cystoscopy demonstrated a tiny opening
of the urethra at the level of the prostatic urethra/bladder-neck area. The patient was referred for an Allium round posterior urethral stent (RPS) placement.
Description of the Allium RPS Stent
The Allium RPS system is indicated for the management of bladder outlet obstruction in adult males. The stent, presented in Figure 2 and Figure 3, is a large-caliber, long-term, fully covered stent made of a self-expandable Nitinol skeleton covered with a thin membrane of biocompatible and biostable copolymer. The entire skeleton of the RPS is made of a single Nitinol wire. The copolymer covers the entire stent body and its anchor to prevent intraluminal tissue ingrowth. It has a single length of 40 mm, a 45 Fr round cross-section, and is composed of 3 segments: body (40 mm), anchor (14 mm), and trans-sphincteric wire, which connects the body to the anchor.
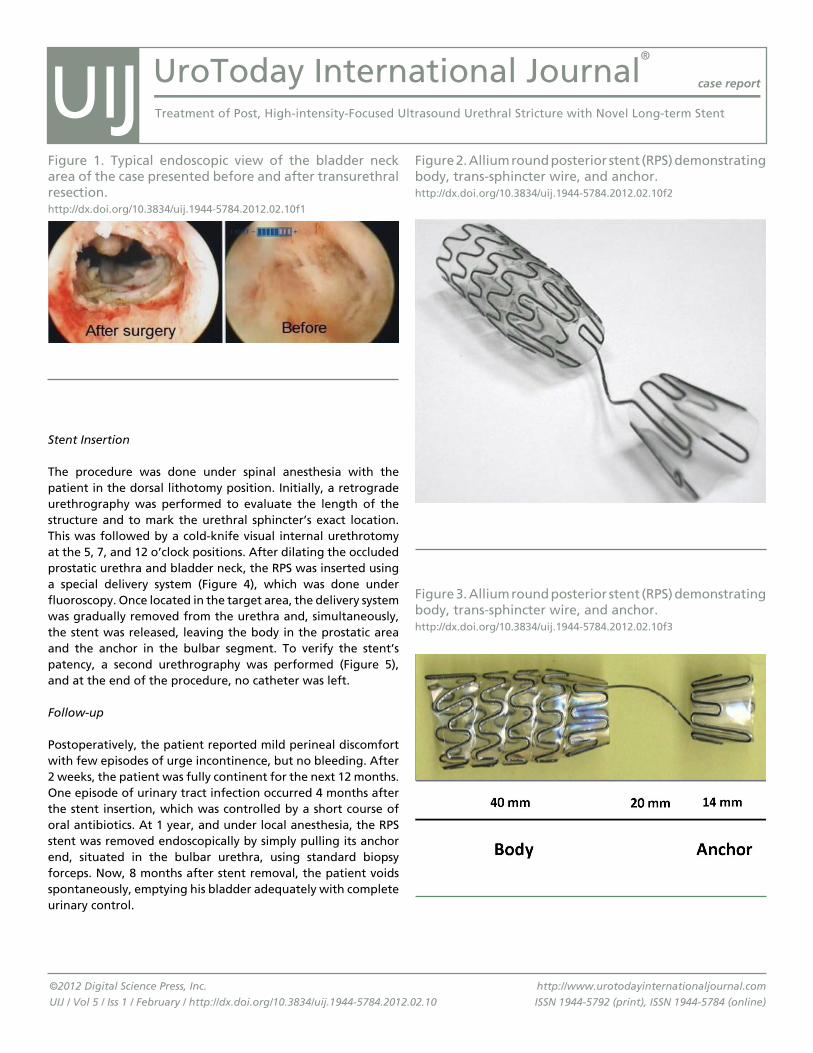
UroToday International Journal®
case report
Treatment of Post, High-intensity-Focused Ultrasound Urethral Stricture with Novel Long-term Stent
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.10
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
Stent Insertion
The procedure was done under spinal anesthesia with the patient in the dorsal lithotomy position. Initially, a retrograde urethrography was performed to evaluate the length of the structure and to mark the urethral sphincter’s exact location. This was followed by a cold-knife visual internal urethrotomy at the 5, 7, and 12 o’clock positions. After dilating the occluded prostatic urethra and bladder neck, the RPS was inserted using a special delivery system (Figure 4), which was done under fluoroscopy. Once located in the target area, the delivery system was gradually removed from the urethra and, simultaneously, the stent was released, leaving the body in the prostatic area and the anchor in the bulbar segment. To verify the stent’s patency, a second urethrography was performed (Figure 5), and at the end of the procedure, no catheter was left.
Follow-up
Postoperatively, the patient reported mild perineal discomfort with few episodes of urge incontinence, but no bleeding. After 2 weeks, the patient was fully continent for the next 12 months. One episode of urinary tract infection occurred 4 months after the stent insertion, which was controlled by a short course of oral antibiotics. At 1 year, and under local anesthesia, the RPS stent was removed endoscopically by simply pulling its anchor end, situated in the bulbar urethra, using standard biopsy forceps. Now, 8 months after stent removal, the patient voids spontaneously, emptying his bladder adequately with complete urinary control.
Figure 1. Typical endoscopic view of the bladder neck area of the case presented before and after transurethral resection.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.10f1
Figure 2. Allium round posterior stent (RPS) demonstrating body, trans-sphincter wire, and anchor.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.10f2
Figure 3. Allium round posterior stent (RPS) demonstrating body, trans-sphincter wire, and anchor.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.10f3
UIJ
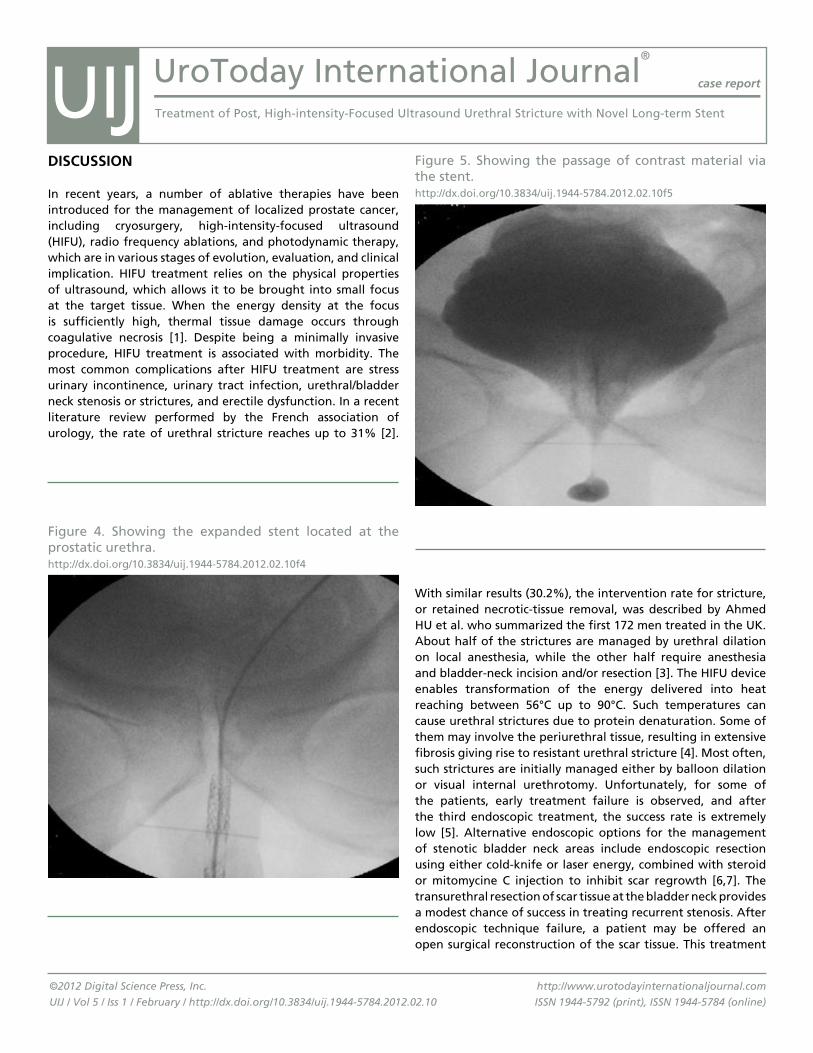
UroToday International Journal®
case report
Treatment of Post, High-intensity-Focused Ultrasound Urethral Stricture with Novel Long-term Stent
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.10
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
DISCuSSION
In recent years, a number of ablative therapies have been introduced for the management of localized prostate cancer, including cryosurgery, high-intensity-focused ultrasound (HIFU), radio frequency ablations, and photodynamic therapy, which are in various stages of evolution, evaluation, and clinical implication. HIFU treatment relies on the physical properties of ultrasound, which allows it to be brought into small focus at the target tissue. When the energy density at the focus is sufficiently high, thermal tissue damage occurs through coagulative necrosis [1]. Despite being a minimally invasive procedure, HIFU treatment is associated with morbidity. The most common complications after HIFU treatment are stress urinary incontinence, urinary tract infection, urethral/bladder neck stenosis or strictures, and erectile dysfunction. In a recent literature review performed by the French association of urology, the rate of urethral stricture reaches up to 31% [2].
With similar results (30.2%), the intervention rate for stricture, or retained necrotic-tissue removal, was described by Ahmed HU et al. who summarized the first 172 men treated in the UK. About half of the strictures are managed by urethral dilation on local anesthesia, while the other half require anesthesia and bladder-neck incision and/or resection [3]. The HIFU device enables transformation of the energy delivered into heat reaching between 56°C up to 90°C. Such temperatures can cause urethral strictures due to protein denaturation. Some of them may involve the periurethral tissue, resulting in extensive fibrosis giving rise to resistant urethral stricture [4]. Most often, such strictures are initially managed either by balloon dilation or visual internal urethrotomy. Unfortunately, for some of the patients, early treatment failure is observed, and after the third endoscopic treatment, the success rate is extremely low [5]. Alternative endoscopic options for the management of stenotic bladder neck areas include endoscopic resection using either cold-knife or laser energy, combined with steroid or mitomycine C injection to inhibit scar regrowth [6,7]. The transurethral resection of scar tissue at the bladder neck provides a modest chance of success in treating recurrent stenosis. After endoscopic technique failure, a patient may be offered an open surgical reconstruction of the scar tissue. This treatment
Figure 4. Showing the expanded stent located at the prostatic urethra.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.10f4
Figure 5. Showing the passage of contrast material via the stent.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.10f5
UIJ

UroToday International Journal®
case report
Treatment of Post, High-intensity-Focused Ultrasound Urethral Stricture with Novel Long-term Stent
©2012 Digital Science Press, Inc.
UIJ / Vol 5 / Iss 1 / February / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.10
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
option is technically demanding and would typically leave the patient incontinent. A completely different approach is the use of an intraurethral stent, which may be either permanent or temporary. Elliot SP et al. reported their experience with 10 cases, using the UroLume permanent stent. Unfortunately, this stent, if placed near the trigon, might cause urinary irritative symptoms, can be occluded by calcification or by scar tissue, and, once inserted, the endoprosthesis is extremely difficult to remove, requiring an open surgical approach [8]. Henderson et al. described their experience with the Spanner temporary urethral stent to relieve bladder outflow obstruction after prostate brachytherapy [9]. Although they were not treating resistant strictures, and no prior endoscopic treatment was performed, they reported early (after 7 days) stent removal due to severe discomfort, while the remaining 60% were able to hold the stent for the planned 30 days.
In the case presented, we describe successful management of post-HIFU, severe bladder-neck and prostatic urethral strictures using a new temporary urethral stent called the Allium RPS. It is a temporary long-term and temporary self-retaining intraurethral stent. Insertion of the stent is simple, and its positioning is under fluoroscopy while the removal can be done as an outpatient procedure under local anesthesia. Being covered by a thin copolymer, intraluminal ingrowth was prevented, allowing the stenotic area to remain open for the duration of 1 year in which no bladder discomfort or incontinence were reported. During 7 months of post-stent removal follow-up, no outflow obstruction developed and the patient is able to completely empty the bladder. This favorable outcome may be related to an extended duration (1 year) of the stent that enabled bladder neck remodeling and stabilization of the periurethral scar tissue. Finally, this minimally invasive treatment alternative is more efficient than current endoscopic treatments, is safe, tolerable by the patient, and more cost-effective.
REfERENCES
1. Illing RO, Leslie TA, Kennedy JE, Calleary JG, Ogden CW, Emberton M. Visually directed HIFU for organ confined prostate cancer – a proposed standard for the conduct of therapy. BJU Int. 2006;98(6):1187-1192. PubMed ; CrossRef
2 Rebillard X, Soulié M, Chartier-Kastler E, Davin JL, Mignard JP, Moreau JL, Coulange C, et al. High-intensity focused ultrasound in prostate cancer; a systematic literature review of the French Association of Urology. BJU Int. 2008;101(10):1205-1213. PubMed ; CrossRef
3 Ahmed HU, Zacharakis E, Dudderidge T, Armitage JN, Scott R, Calleary J, et al. High-Intensity-Focused Ultrasound in the treatment of primary prostate cancer: the first UK series. Br J Cancer. 2009;101(1):19-26. PubMed ; CrossRef
4 Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA. Campbell-Walsh Urology. 9th ed. Philadelphia, Pa: Saunders Elsevier; 2007:1023-1054.
5 Heyns CF, Steenkamp JW, De Kock ML, Whitaker P. Treatment of male urethral strictures: is repeated dilation or internal urethrotomy useful? J Urol. 1998;160(2):356-358. PubMed ; CrossRef
6 Vanni AJ, Zinman LN, Buckley JC. Radial Urethrotomy and Intra-lesion Mitomycin C for the Management of Recurrent Bladder Neck Contractures. J Urol. 2011;186(1):156-160. PubMed ; CrossRef
7 Eltahawy E, Gur U, Virasoro R, Schlossberg SM, Jordan GH. Management of recurrent anastomotic stenosis following radical prostatectomy using Holmium laser and Steroid injection. BJU Int. 2008;102(7):796-798. PubMed ; CrossRef
8 Elliott SP, McAninch JW, Chi T, Doyle SM, Master VA. Management of severe urethral complications of prostate cancer therapy. J Urol. 2006;176(6 pt 1):2508-2513. PubMed ; CrossRef
9 Henderson A, Laing RW, Langley SE. A Spanner in the works- the use of a new temporary urethral stent to relieve bladder outflow obstruction after prostate brachytherapy. Brachytherapy. 2002;1(4):211-218. PubMed ; CrossRef
UIJ
Sallami Satáa, Sami Ben Rhouma, Ali HorchaniDepartment of Urology, La Rabta Hospital-University, Tunis, TunisiaSubmitted September 1, 2011 - Accepted for Publication October 4, 2011
www.urotodayinternationaljournal.comVolume 4 - December 2011
Ureteral Diverticulum in Adults: Diagnostic Problems and Therapeutic Implications
ABSTRACT
Ureteral diverticulum is a rare anomaly and often gives rise to urinary complications. We report a case of a woman with bifid renal pelvis. She had a stone in the lower pelvis with cystic dilation of the upper ureter.
KEYWORDS: Diverticulum; Ureter; Abnormalities; Stone
CORRESPONDENCE: Sallami Satáa, MD, Department of Urology, La Rabta Hospital-University, Tunis, Tunisia ([email protected]).
CITATION: UroToday Int J. 2011 Dec;4(6):art 86. http://dx.doi.org/10.3834/uij.1944-5784.2012.02.04
UroToday International Journal®UIJ
©2012 Digital Science Press, Inc.
UIJ / Vol 4 / Iss 6 / December / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.04
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
INTRODuCTION
True ureteral diverticulum is a rare anomaly and often gives rise
to urinary complications [1].
Its etiology remains unknown, although many theories have
been proposed. It may be congenital or acquired [2]. Congenital
diverticula of the ureter are exceptional and only a few cases
were reported in the literature.
Herein we present a case with a view of surgical treatment and
long-term results.
CASE REPORT
A 36-year-old woman, with no significant medical history,
presented for chronic right lumbar pain. Her physical
examination was unremarkable. The urinalysis was normal and
so were the blood-count cells and plasma creatinine. The KUB
film (Figure 1) and renal ultrasonography showed a stone on
the right renal pelvis. On intravenous pyelography, the left
kidney, pelvicalyceal system, and the bladder looked normal.
The right kidney had a duplex system. The lower pelvis contained
a stone of 3 cm in size with mild hydronephrosis, and the ureter
of the lower pelvis showed an outpouching (Figure 2).
The patient underwent a surgical diverticular resection
with removal of the pelvic stone, and an end-to-end ureter
anastomosis with the insertion of a double J catheter.
The pathological study concluded true ureteral diverticulum,
with all the layers of a ureteral wall and with no sign of
malignancy. The recovery period was uneventful. The double
J catheter was removed 4 weeks later. By the 26-month
follow-up, the pain completely disappeared and radiological
investigations didn’t reveal any anomaly.
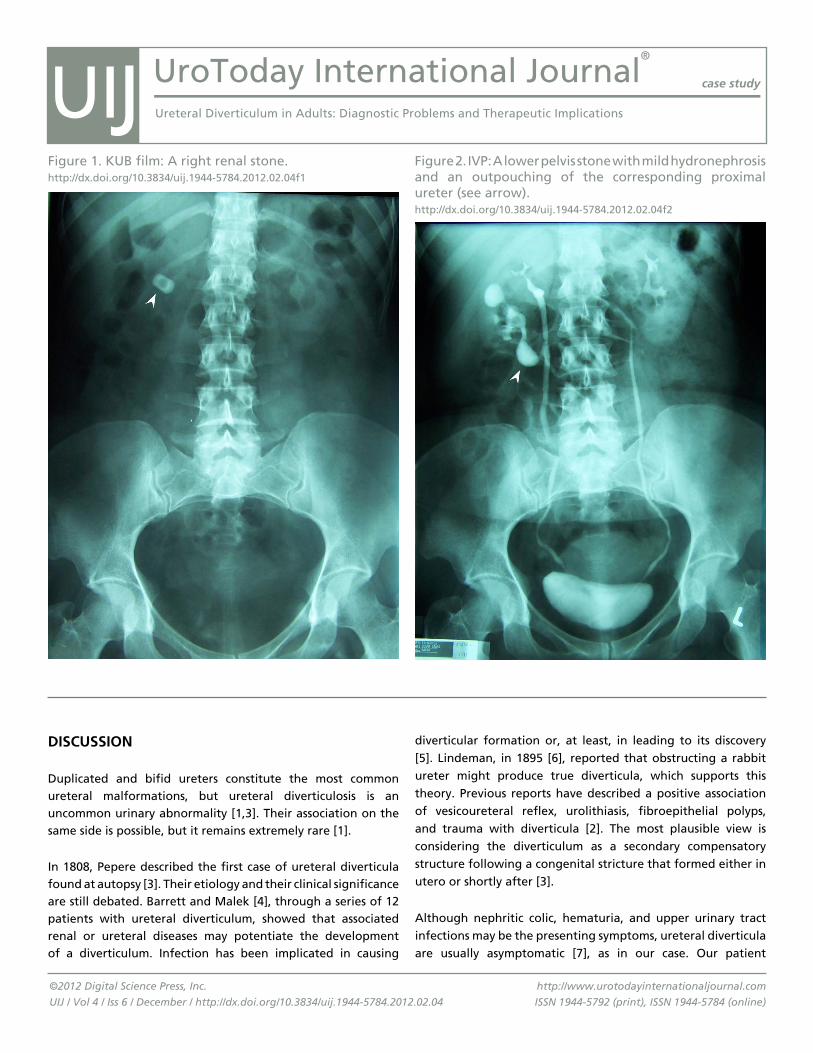
UroToday International Journal®
case study
Ureteral Diverticulum in Adults: Diagnostic Problems and Therapeutic Implications
©2012 Digital Science Press, Inc.
UIJ / Vol 4 / Iss 6 / December / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.04
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
DISCuSSION
Duplicated and bifid ureters constitute the most common ureteral malformations, but ureteral diverticulosis is an uncommon urinary abnormality [1,3]. Their association on the same side is possible, but it remains extremely rare [1].
In 1808, Pepere described the first case of ureteral diverticula found at autopsy [3]. Their etiology and their clinical significance are still debated. Barrett and Malek [4], through a series of 12 patients with ureteral diverticulum, showed that associated renal or ureteral diseases may potentiate the development of a diverticulum. Infection has been implicated in causing
diverticular formation or, at least, in leading to its discovery [5]. Lindeman, in 1895 [6], reported that obstructing a rabbit ureter might produce true diverticula, which supports this theory. Previous reports have described a positive association of vesicoureteral reflex, urolithiasis, fibroepithelial polyps, and trauma with diverticula [2]. The most plausible view is considering the diverticulum as a secondary compensatory structure following a congenital stricture that formed either in utero or shortly after [3].
Although nephritic colic, hematuria, and upper urinary tract infections may be the presenting symptoms, ureteral diverticula are usually asymptomatic [7], as in our case. Our patient
Figure 1. KUB film: A right renal stone.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.04f1
Figure 2. IVP: A lower pelvis stone with mild hydronephrosis and an outpouching of the corresponding proximal ureter (see arrow).http://dx.doi.org/10.3834/uij.1944-5784.2012.02.04f2
UIJ

UroToday International Journal®
case study
Ureteral Diverticulum in Adults: Diagnostic Problems and Therapeutic Implications
©2012 Digital Science Press, Inc.
UIJ / Vol 4 / Iss 6 / December / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.04
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
remained asymptomatic until adult age. Actually, this anomaly
is accidentally discovered via radiological investigations in
patients with lumbar pain or renal colic more and more. They
are occasionally detected during urography or retrograde
pyelography, they appear as small specula or as a saccade wall
outpouching, they are singular or more often in multiples, and
they are mostly limited to the upper third of the ureter (5).
Gray and Skandalakis had classified the diverticula of the ureter
into 3 categories: 1) abortive ureteral duplications (blind-
ending bifid ureters), 2) true congenital diverticula containing
all tissue layers of the normal ureter, and 3) acquired diverticula
representing mucosal herniations [8]. Congenital diverticula
possess the histological layers of the ureter (mucosa, muscularis,
and adventitia), and they connect with the other ureter
at an acute angle. Through these structural features, they
are distinguished from acquired diverticula (post traumatic
or infective), which have no ureteric wall proper [1]. The
histopathologic diagnosis in our case revealed these different
layers, which are typically seen in congenital cases.
When diagnosed, treatment of the diverticulum depends on
the clinical presentations [2]. Treatment is indicated if the
diverticulum is thought to be the cause of symptoms or if
complications ensue. Infection is the most common complication, but several cases of stone formation in a diverticulum have been reported, as in our case [5], and other cases that include ureteral strictures. A case of transitional-cell carcinoma in a diverticulum of the lower ureter was described [9].
The principal aim of treatment is to release the obstruction of the collecting system and the creation of a patent ureter with ureteroscopic maneuvers or open surgery. A nephrectomy is rarely necessary and should only be applied to infected and nonfunctioning kidneys [2,4]. Our patient underwent a diverticular resection with extraction of the stone by open surgery. In all cases, operated or nonoperated patients, the radiological follow-up is mandatory to detect later complications, such as secondary ureteral stenosis.
CONCLuSION
Ureteral diverticulum is a very rare urinary abnormality associated with an increased risk of local complications. Diagnosis is made during radiological investigations, especially the intravenous pyelogram. The treatment, if indicated, is surgical.
Figure 3. By open surgery, we performed a diverticular resection (diverticulectomy) with removal of the pelvic stone, and end-to-end ureter anastomosis with insertion of a double J catheter.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.04f3
Figure 4. Three different layers of the ureteral diverticulum after excision.http://dx.doi.org/10.3834/uij.1944-5784.2012.02.04f4
UIJ
UroToday International Journal®
case study
Ureteral Diverticulum in Adults: Diagnostic Problems and Therapeutic Implications
©2012 Digital Science Press, Inc.
UIJ / Vol 4 / Iss 6 / December / http://dx.doi.org/10.3834/uij.1944-5784.2012.02.04
http://www.urotodayinternationaljournal.com
ISSN 1944-5792 (print), ISSN 1944-5784 (online)
REfERENCES
1. Haberal A, Kovalak EE, Gökcü M, Çil AP, Topaloglu H. Diverticulum of the ureter presenting as an adnexal mass in a woman with familial adenomatous polyposis: A case report. J Turkish German Gynecol Assoc. 2006;7:59-61.
2. Hsieh DF, Wu HC. A Ureteral diverticulum mimicking pelvic cyst. JTUA. 2002;13:157-160.
3. Hale NG, Von Geldern CE. Ureteral diverticula. Cal State J Med. 1921;19(7):284-287. PubMed
4. Barrett DM, Malek RS. Ureteral diverticulum. J Urol. 1975;114(1):33-35. PubMed
5. Socher SA, Dewolf WC, Morgentaler A. Ureteral pseudodiverticulosis: the case for the retrograde urogram. Urology. 1996;47(6):924-927. PubMed ; CrossRef
6. Lindeman W. Divertikel am ureter bei atresie des letzteren. Zentralb Allg Path. 1895;6:801-802.
7. Schlussel RN, Retik AB. Ectopic ureter, ureterocele, and other anomalies of the ureter. In: Walsh PC, ed. Campbell’s Urology. 8th ed. Philadelphia, PA: Saunders; 2002;2007-2052.
8. Roodhooft AM, Boven K, Gentens P, Van Acker KJ. Abdominal colic due to ureteric diverticulum with stone formation. Pediatr Radiol. 1987;17(3):252-253. PubMed ; CrossRef
9. Harrison GS. Transitional cell carcinoma in a congenital ureteral diverticulum. J Urol. 1983;129(6):1231-1232. PubMed
UIJ