international journal of leprosy
TRANSCRIPT
INTERNATIONAL JOURNAL OF LEPROSY^
Volume 62, Number IPrinted in the U.S.A.
(ISSN 0148-9I6X)
INTERNATIONALJOURNAL OF LEPROSY
And Other Mycobacterial Diseases
VOLUME 62, NUMBER 1^ MARCH 1994
An Epidemiological Study of Leprosy Infection bySerology and Polymerase Chain Reaction'
Stella M. van Beers, Shinzo Izumi, Baedah Madjid,Yumi Maeda, Rosmini Day, and Paul R. Klatser 2
Although the prevalence of leprosy hasdeclined worldwide over the past decades,the incidence has not declined in many de-veloping countries (22 ). Apart from socialstigma and economic loss, the sequelae ofleprosy involve severe deformities. An es-timated 2 to 3 million individuals are hand-icapped as a result of having ever contractedleprosy ( 18).
The generally accepted concept is thatovert leprosy patients are the main sourceof transmission. If one accepts this view thena control strategy based on case finding andtreatment would ultimately lead to the erad-ication of leprosy. However, the effective-ness of this approach in the reduction ofleprosy incidence is difficult to assess ( 10 ).
' Received for publication on 3 August 1993; ac-cepted for publication on 26 October 1993.
= S. M. van Beers, M.Sc.; B. Madjid, M.D., Depart-ment of Microbiology, Hasanuddin University, UjungPadang, South Sulawesi, Indonesia. S. lzumi, Ph.D.;Y. Maeda, Technician, National Institute for LeprosyResearch, Tokyo, Japan. R. Day, M.D., M.P.H., Lep-rosy Control, Directorate General of CommunicableDisease Control and Environmental Health, Ministryof Health, Jakarta, Indonesia. P. R. Klatser, Ph.D.,Department of Biomedical Research, Royal TropicalInstitute, Meibergdreef 39, 1105 AZ Amsterdam, TheNetherlands.
Reprint requests to Dr. Klatser.
Little is known about the distribution andtransmission of infection and the factorsleading to disease, mainly due to the in-ability to grow the causative organism ofleprosy, Mycobacterium leprac.
The employment of serological assaysbased on the detection of antibodies to spe-cies-specific antigens of Al. leprac haveopened new possibilities to study Al. lepraeinfection. It is generally assumed that an-tibody levels are associated with the inten-sity of exposure to Al. leprae ( 2 '). It also hasbecome clear that infection with AI. lepraeis more prevalent than disease. On the otherhand, serological assays do not reflect allclinical infections, since the majority ofpaucibacillary patients do not elicit a de-tectable humoral response ( 2 ). In addition,follow-up studies have shown that new casesof leprosy are also found in the scronegativegroups ( 21 ), suggesting that neither are allsubclinical infections necessarily reflectedby a serological response. Another limita-tion of serology may be that it cannot dis-tinguish between past and present infection.With these provisos in mind, serology maystill give valuable information on the extentof infection in a population and on thetransmission of the infection. Assuming thatthe prevalence of seropositivity in a popu-lation roughly reflects exposure/infection
International Journal of Leprosy^ 1994
rates, the effect of control measures maythus be evaluated upon repeated serologicalscreening. The polymerise chain reaction(PCR) for the detection of Al. leprae hasgiven new opportunities in the study of theepidemiology of leprosy, since the presenceof Al. leprae DNA is proof of the presenceof bacilli ( 7 . 13, ' 4 ).
South Sulawesi is an area with one of thehighest prevalences of leprosy in Indonesia( 5 ). The factors that determine such a highendemicity are not known. In order to getinsight into such determinants it is first nec-essary to collect basic data on infection (car-riage?) rates in the population in additionto data based on clinically diagnosed pa-tients rates.
The use of PCR and serological assays,either alone or in combination, could leadto a better understanding of the epidemi-ology of Al. leprac infection. We performeda population-based study in this high en-demic area in which the prevalence of an-tibodies to M. leprae antigens in serum wasmeasured in conjunction with the presenceof Al. leprae in the nose as determined byPCR.
MATERIALS AND METHODSField study. Two isolated adjacent vil-
lages in a rural area of South Sulawesi, In-donesia, highly endemic for leprosy ( 5 ) wereselected for the survey. The village of Ban-timala had 1193 inhabitants and Tondong-kura had 738. Multidrug therapy (MDT)had not yet been introduced in the area andthe registered patients all received, often atirregular intervals, dapsone monotherapy.The villages shared similar characteristicsin terms of geographical, socioeconomic andcultural conditions. The population con-sisted mainly of subsistent farmers; cash in-come was received from sales of surplus andfrom relatives working elsewhere. Most vil-lagers were living in wooden houses builton stilts. The facilities for drinking waterand sanitation were poor. Health care wasprovided by one health center in Bantimalaand a small village health post in Ton-dongkura, both of which were staffed onlyby paramedical personnel.
Before the study was undertaken the vil-lages were informed of the purpose of thestudy and consent was obtained from all
participants. Only residents living for at least3 months in the villages were included inthe study.
Clinical examination was carried out byexperienced leprosy workers and diagnosisbased on the Ridley-Jopling classification/19 , was confirmed by the provincial leprosymedical officer. The bacterial index (131) wasdetermined from slit-skin smears taken fromall patients. Household contacts of patientswere defined as those persons living in thesame house as the index case.
Blood was collected from individuals be-tween 5 and 65 years of age by venipunc-ture. Blood was left to clot and the serumwas separated by centrifugation in the vil-lages. Sodium azidc (0.01%) was added tothe sera, which were then stored at 4°C andtransported to the laboratory where theywere kept refrigerated until analyzed.
Nasal swab specimens were collected andexamined for the presence of Al. leprac bya polymerasc chain reaction (PCR) as de-scribed elsewhere (6 ).
Serological assays. The presence of an-tibodies to phenolic glycolipid I (PGL-I) wasestablished in a simple gelatin particle ag-glutination test (MLPA Serodia-leprae kit,Fujirebio, Japan) (IS). This test will be re-ferred to as MLPA.
In addition, the presence of IgM and IgGantibodies to PGL-I was measured in en-zyme-linked immunosorbent assays (ELI-SAs) as described previously ( 2 ). In theseassays, the semisynthetic trisaccharide an-alog, NT-P-BSA, of PGL-I was employedas antigen (' 2 )• These tests will be referredto as IgM-PGL and IgG-PGL, respectively.
The presence of IgG antibodies to li-poarabinomannan B (LAM-B) from Al. tu-berculosis H37Ra, kindly provided by Dr.P. J. Brennan, Colorado State University,Fort Collins, Colorado, U.S.A., were dem-onstrated in an ELISA as described previ-ously (8 ). This test will be referred to as IgG-LAM.
For each scrum sample the optical density(OD) obtained in the ELISA with uncoatedwells was subtracted from the value ob-tained with the antigen-coated wells. All se-rum samples were tested in duplicate and ifthe variance between the two wells was morethan 10%, the serum was retested. The plate-to-plate variation was controlled by using astandardized reference serum on each plate.
60
50-59-
30-39--
40-49--
L. 20-29 -¢
10-19-
0-9-
62, 1^van Beers, et al.: Epidemiology of Leprosy Infection^3
The positive threshold values were definedby using the 95-percentile of the OD valuesobtained with sera from nonendemic con-trols from Japan. This resulted in the fol-lowing cut-off values: for the MLPA, a titerof 1:32; for IgM-PGL, an OD of 0.380; forIgG-PGL, an OD of 0.380; for IgG-LAM,an OD of 0.250.
PCR. Treatment of the swab specimenswith lysis buffer and PCR was done as re-ported previously (6 ). Briefly, the specimenswere subjected to PCR for the species-spe-cific amplification of a fragment of the pragene of Al. leprae and subsequently wereanalyzed for the presence of a 531-bp am-plification product by agarose gel electro-phoresis followed by hybridization with a1.0 Kb EcoRI fragment comprising the pragene of Al. leprae as a DNA probe. To de-termine if the sample contained inhibitingcomponents that could have caused a neg-ative result, samples in which a 531-bp frag-ment was not detected were submitted to asecond PCR in which a 531-bp modifiedtemplate was added to the reaction mixture.DNA was purified from the samples whichwere found to inhibit amplification of themodified template. These samples were runagain in PCR. PCR reaction mixtures con-tained dUTP and uracil-DNA-glycosylaseto prevent false-positive reactions due tocross-contamination with amplified DNA.In each run, positive controls of chromo-somal Al. /epme DNA were included, as wellas five negative controls without target DNA(i.e., lysis buffer). A specimen was consid-ered positive when it revealed, with or with-out purification of DNA, a 531-bp fragmentby both agarose gel electrophoresis and sub-sequent hybridization. A sample was con-sidered negative when it did not show am-plification in the first PCR and did notinhibit the amplification of the modifiedtemplate. If a sample inhibited the ampli-fication of the modified template, even afterpurification, we could not determine wheth-er it contained M. leprae DNA or not. Atotal of 37 samples (2.9%) were excludedfrom analysis as being uninterpretable.
Data analysis. All data were entered ona personal computer and analyzed using Epi-Info version 5. Analysis of variance meth-ods were applied as indicated in the text.All probabilities presented are two-tailed,unless otherwise stated.
^I ^III
^250 200 150 100 50^0^50 100 150 200 250MALES (N) FEMALES (N)
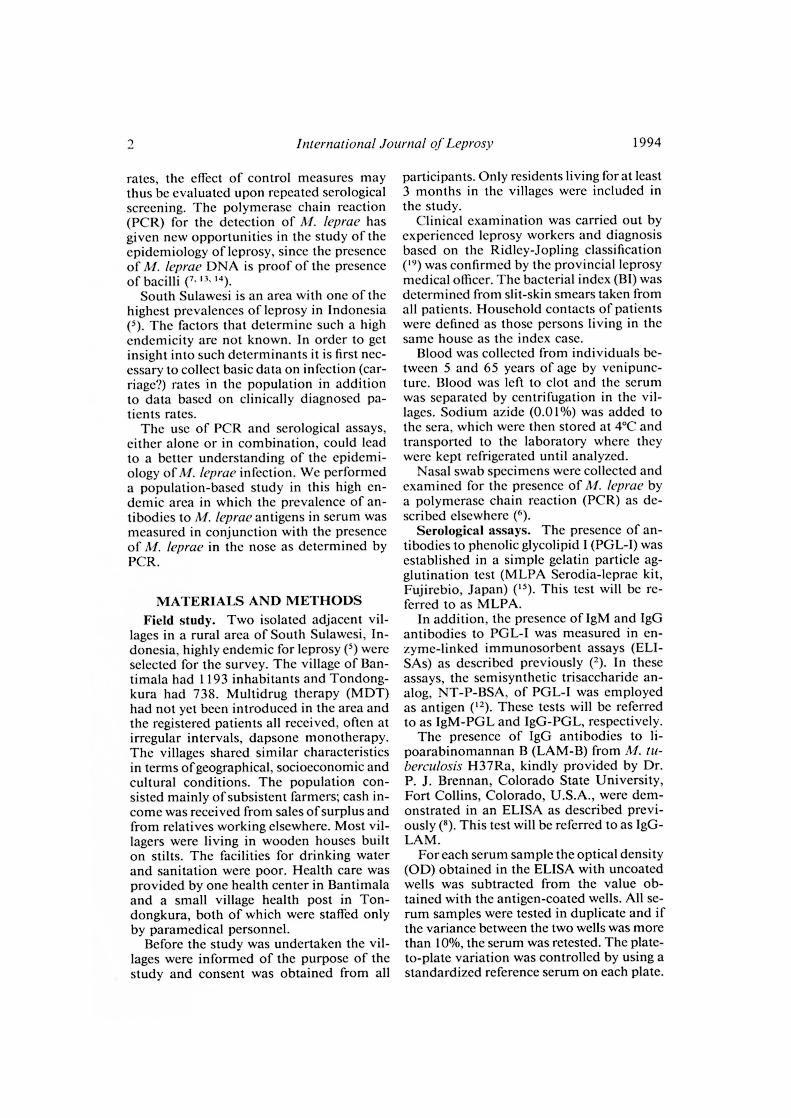
FIG. 1. Distribution of the registered and testedpopulation according to age and sex. (^) = registered;(•) = tested (tested group comprised only persons be-tween 5 and 65 years of age).
To examine whether the distribution of scr-opositivity was equal among all households,we compared the observed and expectednumber of seropositives among householdsin a goodness-of-fit test (1:R0—EY/ED. Theexpected frequency of seropositivity in house-holds was calculated for each household sizeusing the formula (p + q)", whereby p =overall seropositivity rate, q = p — 1 andn = number of persons tested in the house-hold. The expected number of householdswith each frequency of seropositivity wasthen obtained by multiplication of the ex-pected frequency with the number of house-holds in each size category.
RESULTSSurvey. A total of 954 males and 977
females were registered in the two villages.Figure 1 illustrates the age and sex distri-bution of the registered and serologicallytested population. In the 20-50 age cohortthe sex ratio was 0.8, reflecting that a num-ber of males had left the village in searchof work elsewhere.
A total of 1302 persons were clinicallyexamined, representing 67.4% of the regis-tered population. The male : female ratio inthe examined population was 0.83 com-pared to 0.98 in the registered population.
During the survey a total of 13 leprosypatients were diagnosed, 10 new and 3 oldpatients, giving a prevalence in these twovillages of 10/1000. Of the 13 leprosy pa-tients three were females (23.1%), which isa significantly lower prevalence of leprosy

30 35 40 45 50 55 60 65
50
40 -
30 -
2 20 -e
10 -
0^,^5^10 15 20 25
4^ International Journal of Leprosy^ 1994
TABLE 1. Seropositivity rates of MLPA, IgM-PGL, IgG-PGL and IgG-LAM for leprosypatients, their contacts and noncontacts.
Total
Test Patients^ContactsN = 13^N = 45
NoncontactsN = 957 Males Females
N = 434 N = 581
MLPA 23.1 (3)' 33.3 (15) 32.0 (306) 24.7 (107) 37.3 (217)1gM-PGL 23.1 (3) 28.9 (13) 31.0 (297) 24.4 (106) 35.6 (207)IgG-PGL 23.1 (3) 2.2 (1) 6.7 (64) 6.5 (28) 6.9 (38)IgG-LAM 38.5 (5) 13.3 (6) 11.2 (107) 15.2 (66) 9.0 (52)All' 38.5 (5) 44.4 (20) 45.9 (439) 41.4 (180) 48.9 (284)
Seropositivity is shown as percentage, the number of positives are in parentheses.Seropositivity in any of the four tests.
in females than in males in this population(Fisher's exact test, p < 0.01). The clinicalclassification of 4 patients was BL (BIs ofthe slit-skin smears ranging from 1.0 to 3.5);3 were diagnosed as BT and 6 as TT. Theage of the patients ranged between 16 and55 years.
A total of 1015 sera were examined forthe presence of antibodies using the fourdifferent serological assays, representing78.0% of the number of persons clinicallyexamined.
Serology. The seropositivity rates of thefour tests for leprosy patients, their contactsand noncontacts are shown in Table 1. Thethree multibacillary patients from whom se-rum was obtained were seropositive, whilefour paucibacillary patients were negativein all tests. Two more paucibacillary pa-tients were positive in the IgG-LAM.
The seropositivity rates obtained with allassays did not differ between the householdcontacts and the nonhousehold contacts
AGE
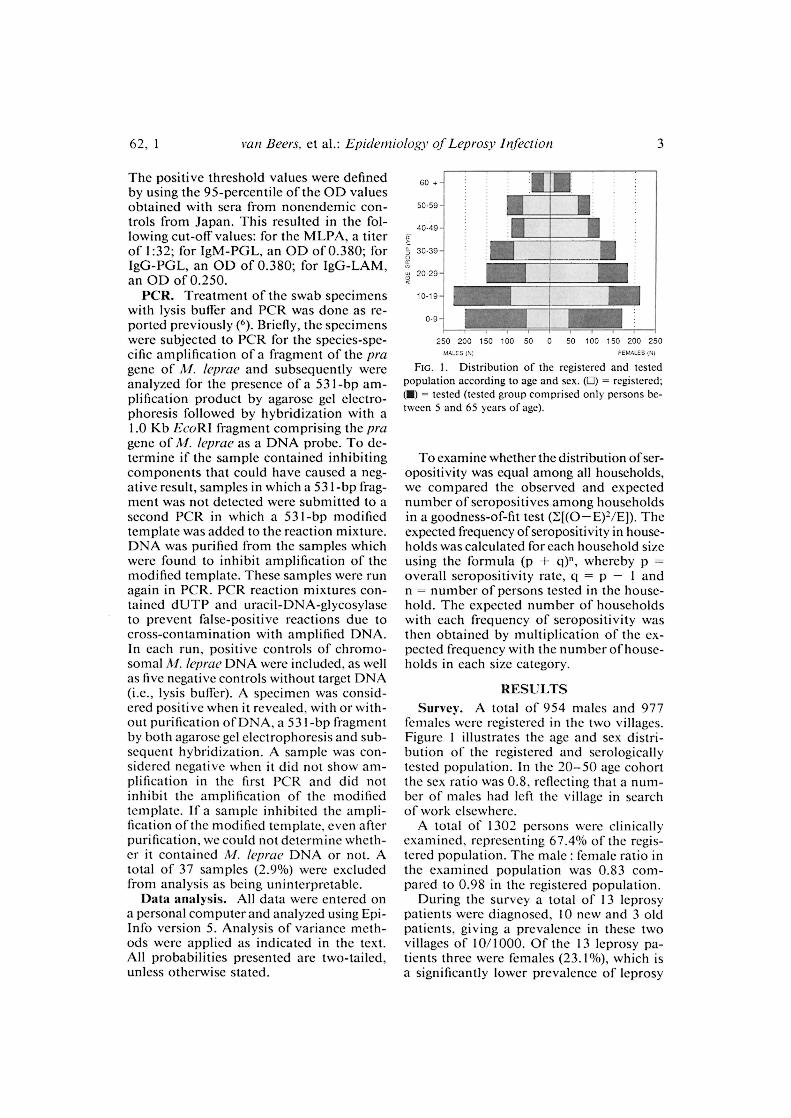
FIG. 2. Frequency of seropositives according to age.(-) - MLPA; (^ ) = IgM-PGL; (---) = IgG-PGL; (^) = IgG-LAM.
(Chi-squared test, p > 0.05). Therefore, infurther analysis no distinction was made be-tween contacts and noncontacts.
The overall seropositivity rates were32.0% for MLPA, 30.8% for IgM-PGL, 6.7%for IgG-PGL, and 11.6% for IgG-LAM.
When the seropositivities of the differentassays were combined, the overall percent-age of persons being seropositive in any ofthe four tests was 45.8%.
The seropositivity rates of MLPA andIgM-PGL were significantly higher in fe-males compared to males (Mantel-Haenszelsummary Chi-squared test stratified for age,MLPA = p < 0.001, IgM-PGL = p < 0.001).Seropositivity was found to be higher inmales than in females with IgG-LAM (Man-tel-Haenszel summary Chi-squared teststratified for age, p < 0.001). With IgG-PGL the difference in seropositivity be-tween males and females was small and in-significant. However, the mean test values(OD or titer) of the tested persons was notdifferent in males and females for any ofthese tests (Kruskal-Wallis test for IgM-PGL, p = 0.22; Chi-squared test for trendfor MLPA, p = 0.17; result not shown).
Figure 2 shows the seropositivity ratesobtained with the four assays according tothe age of the tested population. The prev-alence of MLPA and IgM-PGL seropositiv-ity was highest in the younger age groupsand declined with increasing age. No suchclear pattern could be observed with IgG-PGL and IgG-LAM.
No significant relationship was found be-tween the presence of a BCG scar and sero-positivity in any of the tests (results notshown).

62, 1^van Beers, et al.: Epidemiology of Leprosy Infection^5
TABLE 2. MLPA seropositivity accordingto household size.
No. personsper
household
No. personsliving in
household
No.personstested
MLPApositivity
1-3 53 32 34.4%4-6 367 168 31.5%7-9 549 283 31.4%
10-12 625 345 31.9%13-15 255 139 34.5%16-17 82 48 27.1%
Total 1931 1015 31.9%
Distribution of seropositivity amonghouseholds. A total of 391 houses were oc-cupied, giving an average occupancy rate of4.9 persons. The average living space was9.1 square meters per person. Serum sam-ples of persons belonging to 346 householdswere examined. No influence of the house-hold size was found on the chance of beingseropositive for any of the serological assays(Chi-squared test for trend, p > 0.05 for alltests). This is illustrated in Table 2 forMLPA. Two-hundred-seven households(59.8%) contained one or more MLPA-pos-itive members.
In order to investigate whether the sero-positivity rates were equally distributedamong all households, the observed house-hold seropositivity rate was compared withthe expected household seropositivity ratefor each household size. Nonrandom dis-tribution of seropositivity was found forMLPA and IgM-PGL (Chi-squared = 60.8;p < 0.001 for MLPA; Chi-squared = 65.3,p < 0.001 for IgM-PGL), but not for theother two tests. Further analysis revealedthat this finding could be attributed to eighthouseholds. In five households there was anexcess of seropositive persons; these house-
holds comprised 21 seropositives among 24persons tested. In three households sero-negative persons were in excess; they con-sisted of 21 persons all of whom were neg-ative. There was no difference between ageor sex composition of the members of thesetwo household groups, excluding confound-ing by age and sex (results not shown). Theseropositivity rates among all other house-holds conformed with a random distribu-tion.
Comparison between serological tests.The results of the MLPA and the IgM-PGLto measure antibodies against the PGL-I an-tigen showed little differences. The MLPAtest demonstrated antibodies in 32.0% ofthe population and the IgM-PGL in 30.8%.The overall agreement was 91.4% (Table 3).The agreement increased for higher titers forMLPA; whereas 51 of 197 samples with atiter of 1:32 (positive) were lgM-PGL-neg-ative. There was only one serum with a titerhigher than 1:32 (i.e., 1:128) which was neg-ative in IgM-PGL.
Only weak correlations between the re-sults could be established between all tests(r ranging from 0.14 to 0.24, with the ex-ception of IgM-PGL versus MLPA [r = 0.82,p < 0.001]).
Relation serology and PCR. PCR resultswere obtained on 1228 nasal swab speci-mens. The overall positivity rate was 7.8%and did not show any relation to age or sex.Detailed results have been presented else-where (to). From 965 persons the results wereobtained by both serology and PCR. In thisgroup of persons the PCR positivity ratewas 7 .7%. No relationship could be detectedbetween PCR positivity and seropositivityin the four serological assays, nor was thereany correlation between PCR positivity andthe height of the values obtained in the se-rological assays.
TABLE 3. Comparison between MLPA and IgM-PGL according to different MLPA titers.
MLPAtiter No. sera tested
IgM-PGL OD No. 1gM-PGLAgreement
(mean ± S.D.) Positive Negative
16 691 0.185 ± 0.109 41 650 94.132 197 0.465 ± 0.124 146 51 74.164 91 0.679 ± 0.164 91 0 100.0
128 31 0.979 ± 0.228 30 1 96.8256 5 1.562 ± 0.381 5 0 100.0
6^ International Journal of Leprosy^ 1994
DISCUSSION
In this study we have applied four differ-ent serological assays and a PCR on speci-mens collected through a population-basedsurvey in a high endemic area for leprosy.The results indicate widespread Al. lepracinfection in the population.
During the survey five new active leprosypatients were detected in each village, re-sulting in a similar registered prevalence ofleprosy cases among the examined popu-lation of 10.7 and 9.9 per 1000 inhabitants,respectively. Therefore, results from the twovillages were analyzed together. Since thestudied population did not differ from thetotal population in its characteristics and,thus, was a representative sample thereof,it is justified to extrapolate the serologicaland PCR results of the whole populationfrom both villages.
The seropositivity rates in leprosy pa-tients in this study were similar to previousreports: high rates in multibacillary and lowin paucibacillary patients ( 2 ).
Antibodies to PGL-I were demonstratedin 30.8% and 32% of the tested populationby ELISA and the MLPA test. Assumingthat the height of a serological response toPGL-I reflects the intensity of exposure toAI. leprae ( 21 ), the large number of positivesindicates a high level of exposure in thiscommunity. This is in agreement with ourfinding that the positivity rates in householdcontacts were similar to those of noncon-tacts, suggesting a uniform risk of exposurein this population. The results of other scro-epidemiological studies performed in SouthSulawesi also implied a high risk of'expo-sure in this population ( 20 ).
The seropositivity rates in MLPA and1gM-PGL in the population showed a sim-ilar age-related pattern as demonstrated be-fore in other studies ("• 2°): seropositivitywas highest in the younger age groups anddeclined with increasing age. Noteworthy isthe large number of seropositives in the agegroup 5-9 years, which is further evidenceof widespread exposure. Our results showeda higher seropositivity rate among femalesthan males, in conformity with what hasbeen reported in a number of other studies(' ' ,2 '). The higher seropositivity rates amongfemales did not reflect a higher case rate inour population; 4 out of 14 patients were
female. Higher innate IgM levels among fe-males compared to males is the most simpleexplanation for this phenomenon (").
An interesting finding in this study wasthe observation that the seropositivity ratesin the MLPA and IgM-PGL were not ran-domly distributed among all households.Five households were identified with an ex-cess of seropositive members. In contrast,three other households had an excess of se-ronegati ve members. This observation isunlikely to be due to chance alone, and thecomposition of these households was sim-ilar with respect to age and sex. Clusteringofseropositivity to PGL-I has been reportedbefore among contacts of multibacillary in-dex cases; the increased ability to shed ba-cilli by some index cases and the consequentexposure of household members to largenumbers of bacilli has been put forward asone possible explanation for this clustering("). Such a phenomenon could account forour finding of excessive seropositivityamong certain households. A familial pre-disposition responsible for clustering, theother explanation, is in line with our ob-servation of large households with only se-ronegatives. The persistence of this ob-served pattern of clustering needs to beestablished before it can be ascertainedwhether either environmental or geneticfactors or both are the underlying causes.
The MLPA and IgM-PGL showed anoverall agreement of 91% and revealed asimilar seropositivity profile in all aspectsconfirming reports of other studies ( 15 ). Sincethe MLPA test is much simpler to carry out,this test could he the test of choice, es-pecially in less equipped laboratories. In ad-dition, the MLPA has the advantage overthe ELISA in that it is a standardized test,allowing a legitimate comparison betweenMLPA results of different seroepidemiolog-ical studies. The analysis of the results ofthe lgG-PGL and IgG-LAM did not revealclear patterns, except for a male predomi-nance of IgG-LAM seropositivity. The re-sults of IgG-PGL and IgG-LAM did notcorrelate well with the results of the assaysdetecting 1gM to PGL-I. It has been sug-gested that the LAM-based assays may de-tect additionally infected individuals com-pared to the PGL-I-based assays alone,assuming that certain individuals do reactto At leprae infection with predominantly

62, 1^van Beers, et al.: Epidemiology of Leprosy Infection^7
an IgG response to LAM and not with anIgM response to PGL-I ( 8 ). Indeed, we alsofound more seropositive individuals whenthe assays were combined. Although themeasurement of anti-LAM responses maybe useful in the study of leprosy patients ( 8 ),the crossreactive nature of LAM compli-cates the interpretation of our results ob-tained in the healthy population.
In this study we have compared Al. lep-rae-specific antibody responses and thepresence of Al. leprae in the nose as deter-mined by PCR at a population level. Norelationship between the two could be es-tablished. This finding may not be surpris-ing since the presence of A/. leprae in thenose does not necessarily imply infection.A transient state of carriership without col-onization resulting in infection may haveoccurred. On the other hand, the discrep-ancy between PCR positivity and seropos-itivity also may be due to a time lag betweenthe carriage of M. leprae in the nose and theonset of a serological response. Moreover,not every infection leads necessarily to aserological response, notably in those proneto get paucibacillary leprosy. Several follow-up studies have shown that new cases ofleprosy also are found in the seronegativegroups ( 1 ' 2 '). Whether measurement of na-sal immunity may be of value in this respecthas to be awaited (4 ). Since the nasal mucosais probably the main port of entry, nasalimmunity is likely to be an important de-fense against further dissemination of thebacilli.
It has been suggested that multibacillarycases are the main source of infection in acommunity. However, it is difficult to con-ceive how four multibacillary patients, twoof whom had been treated for prolongedperiods, would be responsible for an infec-tion rate of at least 3 0% in this community.This high exposure rate suggests that thereare important other sources of transmis-sion. The finding that 7.8% of the popula-tion harbors AL leprae in the nose adds tothat possibility.
SUMMARYA population-based study has been car-
ried out in two adjacent villages in a highlyleprosy-endemic area of South Sulawesi, In-donesia. The prevalence of clinical leprosywas 10.0 per 1000 inhabitants. A total of
1015 serum samples and 1228 nasal swabspecimens were collected. IgM antibodiesin blood to phenolic glycolipid-I (PGL-I) ofAlycobacterium leprae were demonstratedby the gelatin particle agglutination test(MLPA) and by indirect ELISA (IgM-PGL).IgG antibodies to PGL-I (IgG-PGL) andlipoarabinomannan-B (IgG-LAM) weremeasured by indirect ELISA. The presenceof AI. leprae in nasal swab specimens wasestablished by a polymerase chain reaction(PCR).
The seropositivity rates in the populationwere 32% for MLPA, 30.8% for IgM-PGL,6.7% for IgG-PGL, and 11.6% for IgG-LAM. Seropositivity rates for MLPA andIgM-PGL were highest in the younger agegroups. There was no difference in seropos-itivity in any of the tests between householdcontacts of leprosy patients and noncon-tacts. The scropositivity rates in the MLPAand IgM-PGL were not randomly distrib-uted among all households. The presence ofAl. leprae by PCR was demonstrated in 7.8%of the nasal swab specimens. No correlationwas found between the results of the PCRand serology. This study indicates that Al.leprae is widespread in the population, andthat in endemic areas many individuals car-ry A/. leprae in their nasal cavities withouthaving obvious symptoms of leprosy.
RESUMENSe efectu6 un estudio poblacional en dos comuni-
dades vecinas de un area de Sulawesi del Sur (Indo-nesia) con alta endemia de lepra, en donde Ia preva-
lencia de lepra clinica fue de 10 por 1000 habitantes.
Se colectaron un total de 1015 muestras de suero y1228 especimenes de exudado nasal. Se buscaron anti-
cuerpos IgM contra el glicolipido fenOlico I (PGL-1) deMycobacterium leprae usando Ia têcnica de aglutina-cian de particular de gelatina (MLPA) y un ELISA
indirecto (IgM-PGL). Los anticuerpos IgG anti PGL-I(IgG-PGL) y anti-lipoarabinomanana (IgG-LAM) se
midicron usando un ELISA indirecto. La presencia deM. leprae en los especimenes de exudado nasal se es-tablecia mediante una reacciOn en cadena de la poll-rnerasa (PCR).
Los grados de seropositividad en la poblacian fucrondel 32% para MLPA, del 30.8% para lgM-PGL, del
6.7% para IgG-PGL, y del 1 1.6% para IgM-LAM. Los
indices de seropositividad en las pruebas MLPA e IgM-
PGL no estuvicron distribuidos aleatoriamente entretodos los contactor familiares. La presencia de Al. lep-
rae por PCR se demostrO en el 7.8% de los especimenesde exudado nasal. No se encontrO correlaciOn entre losresultados por PCR y Ia serologia. Este estudio indica

8^ International Journal of Leprosy^ 1994
que M. Ieprae esta ampliamente distribuido en la po-blaciem y que en las areas endemicas muchos indivi-duos alojan al M. Ieprae en sus cavidadcs nasales sin^2.tener los sintomas obvios de Ia lepra.
RESUME
Une etude a ête realisee dans la population de deux
villages adjacents dans une region a haute endemicite
lepreuse de Sud-Sulawesi en Indonesie. La prevalencede la lepre clinique etait de 10,0 pour 1000 habitants.Un total de 1015 echantillons de serum et 1228 pre.-
levements en provenance des fosses nasales a ête
collecte. La presence clans le sang d'anticorps IgM vis-a-vis du glycolipide phenolique I (PGL-1) de Myco-
bacterium Ieprae a ete demontree par Ic test d'agglu-tination de particules de gelatine (MPLA) et par ELISA
indirect (IgM-PGL). Les anticorps IgG (IgG-PGL) etIc lipoarabinomannan-B (IgG-LAM) ont ete inesures
par ELISA indirect. La presence de M. Ieprae dans les
prelevemcnts en provenance des fosses nasales a ete&labile par une reaction de polymerase en chaine (PCR).
Les taux de seropositivite observes dans la popula-tion etaient de 32% pour MPLA, 30, 8% pour 1gM-
PGL, 6, 7% pour IgG-PGL, et 11, 6% pour IgG-LAM.
Les taux de seropositivite pour MPLA et IgM-PGL
etaient les plus eleves dans les grouper d'age jeunes. II
n'y avail pas de diErence de sêropositivité pour aucun
des tests entre les contacts domiciliaires de patientslepreux et les noncontacts. Les taux de seropositivitepour le MPLA et l'IgM-PGL n'etaient pas distribuês
de maniere aleatoire parmi l'ensemble des habitations.
La presence de M. Ieprae a Ia PCR a ete mise en evi-
dence dans 7, 8% des prelevements provenant des fos-ses nasales. On n'a pas trouve de correlation entre les
resultats de la PCR et Ia serologic. Cette etude indique
que M. Ieprae est largement repandu dans la popula-tion, et que dans les regions endemiques, de nom-
breuses personnes sont portcuses de Al. Ieprae danslours cavites nasales sans avoir de symptiimes evidents
do lepre.
Acknowledgment. We would like to express ourgratitude to the Head of the Regional Office of the
Ministry of Health, Republic of Indonesia in South
Sulawesi, and to the leprosy officers in the Ministry of
Health and in the Province of South Sulawesi for their
cooperation. We are obliged to Dr. Peter Lever andDr. Djumadi Achmed for their valuable help.
We are indebted to all of the people in the villageswho voluntarily cooperated in this study.
The financial support by the Netherlands LeprosyRelief Association (NSL) and the European Commu-
nities Directorate General for Science, Research and
Development (TS2-0275-NL) is greatly appreciated.
REFERENCESI. BAGSHAWE, A. F., GARSIA, R. J., BAUMGART, K.
and ASTBURY, L. IgM serum antibodies to phe-nolic glycolipid-I and clinical leprosy: two years'
observation in a community with hyperendemicleprosy. Int. J. Lepr. 58 (1990) 25-30.
CHO, S.-N., FUJIWARA, T., HUNTER, S. W., REA,
T. H., GELBER, R. H. and BRENNAN, P. J. Use of
an artificial antigen containing the 3,6-Di-0-
methyl-beta-D glucopyranosyl epitope for the se-rodiagnosis of leprosy. J. Infect. Dis. 150 (1984)
311-322.3. Ctio, S.-N., KIM, S. H., CELLONA, R. V., CHAN, G.
P., FAJARDO, T. T., WALSH, G. P. and KIM, J. D.Prevalence of IgM antibodies to phenolic glyco-
lipid 1 among household contacts and controls inKorea and The Philippines. Lepr. Rev. 63 (1992)12-20.
4. CREE, I. A., SHARPE, S., STURROCK, N. D. C.,COCHRANE, 1. H., SMITH, W. C. and BECK, J. S.Mucosal immunity to mycobacteria in leprosy pa-tients and their contacts. Lepr. Rev. 59 (1988)309-316.
5. DAY, R., LEVER, P. and ASRI, M. Leprosy controlin 7 districts of South Sulawesi, Indonesia, 1986-91. Lepr. Rev. 63 (1992) 247-254.
6. DE WIT, M. Y. L., DOUGLAS, J. T., MCFADDEN, J.and KLATSER, P. R. Polymerase chain reactionfor detection ofitircobaderium leprae in nasal swabspecimens. J. Clin. Microbiol. 31 (1993) 502-506.
7. DE WIT, M. Y. L., FABER, W. R., KRIEG, S. R.,
DOUGLAS, J. T., LUCAS, S. B., MONTREEWASUWAT,
N., PATTYN, S. R., HUSSAIN, R., PONNIGHAUS, J.M., HARTSKEERL, R. A. and KLATSER, P. R. Ap-
plication of a polymerase chain reaction for thedetection of Mycobacterium Ieprae in skin tissues.J. Clin. Microbiol. 29 (1991) 906-910.
8. DHANDAYUTHAPAN1, S., IZUMI, S., ANANDAN, D.and BHATIA, V. N. Specificity of IgG subclass
antibodies in different clinical manifestations ofleprosy. Clin. Exp. Immunol. 88 (1992) 253-257.
9. DOUGLAS, J. T., CELONA, R. V., ABALOS, R. M.,
MADARANG, M. G. and FAJARDO, T. Serological
reactivity and early detection of leprosy amongcontacts of lepromatous patients in Cebu, ThePhilippines. Int. J. Lepr. 55 (1987) 718-721.
10. FINE, P. E. M. Reflections on the elimination ofleprosy. Int. J. Lepr. 60 (1992) 71-80.
FINE, P. E., PONNIGHAUS, J. M., BURGESS, P.,
CLARKSON, J. A. and DRAPER, C. C. M. Seroepide-miological studies of leprosy in northern Malawi
based on an enzyme-linked immuno-sorbent as-
say using synthetic glycoconjugate antigen. Int. J.Lepr. 56 (1988) 243-254.
12. FUJIWARA T., ASPINALL, G. 0., HUNTER, S. W. andBRENNAN, P. J. Chemical synthesis of the trisae-
charide unit of the species-specific phenolic gly-colipid of Mtcobacterium leprae. CarbohydrateRes. 163 (1987) 41-52.
13. GILLIS, T. P. and WILLIAMS, D. L. Polymerasechain reaction and leprosy. Int. J. Lepr. 59 (1991)311-316.
14. HARTSKEERL, R. A., DE WIT M. Y. L. and KLATSER,
P. R. Polymerase chain reaction for the detection

62, 1^van Beers, et al.: Epidemiology of Leprosy Infection^9
of Afycobacteriztm leprae. J. Gen. Microbiol. 135(1989) 2357-2364.
15. lzumi, S., FUJIWARA, T., IKEDA, M., NISHIMURA,
Y., SUGIYAMA, K. and KAwATsu, K. Novel gel-atin particle agglutination tests for serodiagnosisofleprosy in the field. J. Clin. Microbiol. 28 (1990)525-529.
16. KLATSER, P. R., VAN BEERS, S., MADJID, B., DAY,
R. and DE WIT, M. Y. L. Detection of Afycobac-
terium leprae nasal carriage in leprosy endemicpopulations. J. Clin. Microbiol. 31 (1993) 2947—2951.
17. MADDISON, S. E., STEWART, C. C., FARSHY, C. E.
and REIMER, C. B. The relationship of race, sexand age to concentrations of serum immunoglob-ulins expressed in international units in healthyadults in the U.S.A. Bull. WHO 52 (1975) 179—185.
18. NORDEEN, S. K., LOPEZ-BRAVO, L. and SUNDARE-
SAN, T. K. Estimated number of leprosy cases inthe world. Lepr. Rev. 63 (1992) 255-262.
19. RIDLEY, D. S. and JOPLING, W. H. Classificationof leprosy according to immunity; a five-groupsystem. Int. J. Lepr. 34 (1966) 255-273.
20. SOEBONO, H. and KLATSER, P. R. A seroepide-miological study of leprosy in high- and low-en-demic Indonesian villages. Int. J. Lepr. 59 (1991)416-425.
21. ULRICH, M., SMITH, P. G., SAMPSON, C., ZUNIGA,
M., CENTENO, M., GARCIA, V., MANRIQUE, X.,SALGADO, A. and CONVIT, J. IgM antibodies tonative glycolipid-I in contacts of leprosy patientsin Venezuela: epidemiological observations and aprospective study of the risk of leprosy. Int. J.Lepr. 59 (1991) 405-415.
22. WHO EXPERT COMMITTEE ON LEPROSY. Sixth re-port. Geneva: World Health Organization, 1988.Tech. Rep. Ser. 768.