tuberculous osteomyelitis of the cuboid: a report of four cases
TRANSCRIPT
CASE REPORTS
Tuberculous Osteomyelitis of theCuboid: A Report of Four Cases
Mandeep S. Dhillon, MS, MNAMS,1 Paramjit Singh, MD,2 Rajan Sharma, MS,3Shivinder S. Gill, MS, MNAMS,4 and Onkar N. Nagi, MS, MSc (Oxon), FAMS5
Osteoarticular tuberculosis, although rare, has shown a resurgence in recent times, especially inimmunocompromised patients. Involvement of the foot is infrequent, and the differential diagnosis isconfusing, leading to diagnostic delays. We reviewed four cases of tuberculosis of the cuboid wherethe infection was limited to the bone without articular involvement. All four cases were adults anddiagnostic delays were observed in all. Three of the cases had an osteolytic lesion on radiographsresembling a space-occupying lesion. Magnetic resonance imaging (MRI) or Computed tomography(CT) scans were helpful in three cases, and post-treatment MRI helped in evaluating outcome in onecase. Antitubercular chemotherapy was sufficient to cause resolution of the lesion in three cases, whilein one case surgical intervention was necessary. Since isolated osteomyelitis is usually seen only in theearly stages of the disease process, early diagnosis and appropriate therapy are imperative to get goodlong-term results. Concomitant extraskeletal lesions are not always seen, nor is the organism culturedin a majority of the cases. Thus a high index of suspicion is mandatory in high-risk groups (immigrants,immunocompromised cases or those with history of contact); clinical and radiologic features, alongwith histopathologic evidence of granulomatous pathology should be sufficient to initiate therapy. (TheJournal of Foot & Ankle Surgery 39(5):329-335, 2000)
Key words: cuboid, osteomyelitis, tarsals, tuberculosis
Extrapulmonary tuberculosis, when it presents withosteoarticular involvement, accounts for less than 3% ofpatients. In a previous study from our institute (1), as wellas seen from a literature review (2-6), the foot was foundto be involved in less than 10% of the cases with skeletaltuberculosis. This renders tuberculosis of a foot bone arare event. The ability of tuberculosis to mimic otherdiseases (7-8), combined with a lack of awareness of footand ankle surgeons, often leads to diagnostic delays. This
From the Post Graduate Institute of Medical Education and Research,Chandigarh, India. Address correspondence to: Dr. M. S. Dhillon,1090/2 Sector 39-8, Chandigarh, 160037 India; e-mail: [email protected].
1Associate Professor, Department of Orthopaedics.2Assistant Professor, Department of Radiodiagnosis.3Senior Resident, Department of Orthopaedics.4Additional Professor, Department of Orthopaedics.5Professor and Head, Department of Orthopaedics.Received for publication December 16, 1999; accepted in revised
form for publication June 22, 2000.The Journal of Foot & ankle Surgery 1067-2516/00/3905-0329$4.00/0Copyright © 2000 by the American College of Foot and Ankle Surgeons
is unfortunate, as in many cases, the disease starts as abony focus, with the subsequent development of eithera sinus to the exterior or involvement of the adjacentjoint. Both these extraosseous extension patterns rendera prognosis that is worse than the purely osteomyeliticstage, either in the form of secondary infections with otherorganisms or decreased joint motion.
Hindfoot tuberculosis is most commonly seen in thecalcaneus (1, 9). The lesser tarsals are infrequently involved, and problems in their management are rarely discussed. We present a series of four cases involving the cuboid.In addition to the usual diagnostic maneuvers, the role ofspecialized radiologic techniques as well as the role ofMRI in the evaluation of therapy are discussed.
Materials and Methods
Over a to-year period, four cases with tuberculousosteomyelitis limited to the cuboid were seen at ourinstitution. All cases were young adults (average age29 years), with three female and one male patient. The
VOLUME 39, NUMBER 5, SEPTEMBER/OCTOBER 2000 329
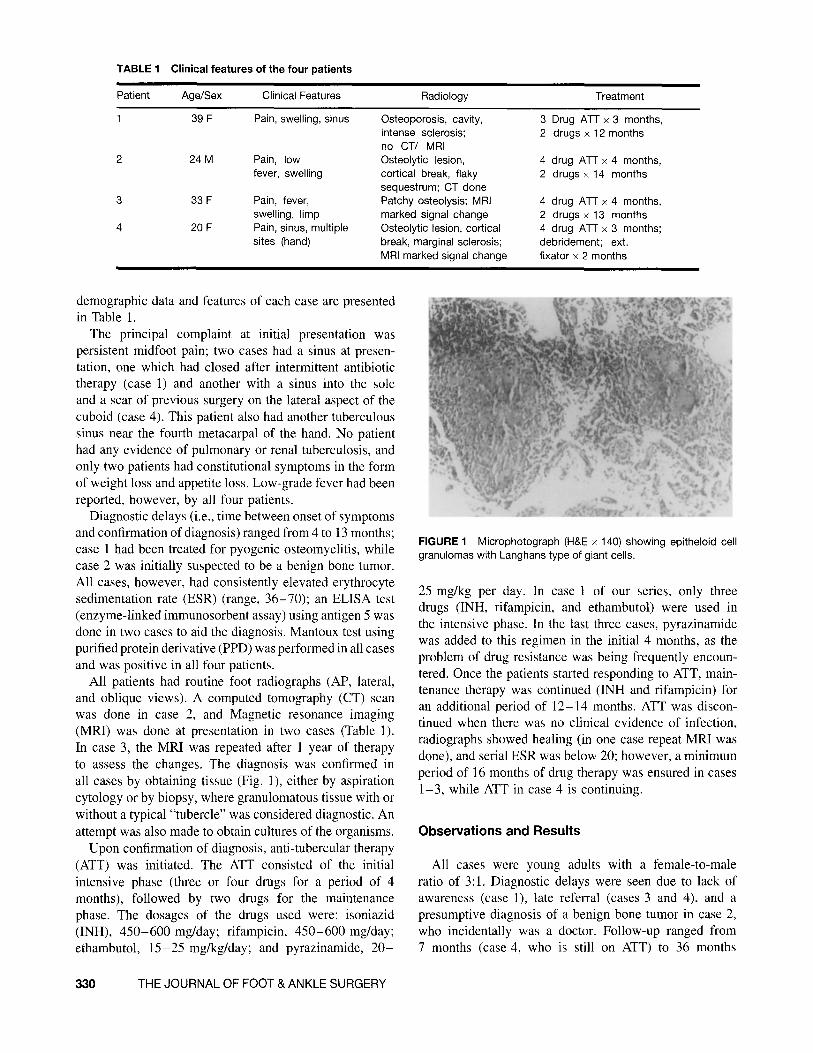
TABLE 1 Clinical features of the four patients
Patient Age/Sex Clinical Features Radiology Treatment
39 F Pain, swelling, sinus Osteoporosis, cavity, 3 Drug An x 3 months,intense sclerosis; 2 drugs x 12 monthsno CT/ MRI
2 24M Pain, low Osteolytic lesion, 4 drug An x 4 months,fever, swelling cortical break, flaky 2 drugs x 14 months
sequestrum; CT done3 33 F Pain, fever, Patchy osteolysis; MRI 4 drug An x 4 months,
swelling, limp marked signal change 2 drugs x 13 months4 20 F Pain, sinus, multiple Osteolytic lesion, cortical 4 drug An x 3 months;
sites (hand) break, marginal sclerosis; debridement; ext.MRI marked signal change fixator x 2 months
demographic data and features of each case are presentedin Table 1.
The principal complaint at initial presentation waspersistent midfoot pain; two cases had a sinus at presentation, one which had closed after intermittent antibiotictherapy (case 1) and another with a sinus into the soleand a scar of previous surgery on the lateral aspect of thecuboid (case 4). This patient also had another tuberculoussinus near the fourth metacarpal of the hand. No patienthad any evidence of pulmonary or renal tuberculosis, andonly two patients had constitutional symptoms in the formof weight loss and appetite loss. Low-grade fever had beenreported, however, by all four patients.
Diagnostic delays (i.e., time between onset of symptomsand confirmation of diagnosis) ranged from 4 to 13 months;case 1 had been treated for pyogenic osteomyelitis, whilecase 2 was initially suspected to be a benign bone tumor.All cases, however, had consistently elevated erythrocytesedimentation rate (ESR) (range, 36-70); an ELISA test(enzyme-linked immunosorbent assay) using antigen 5 wasdone in two cases to aid the diagnosis. Mantoux test usingpurified protein derivative (PPD) was performed in all casesand was positive in all four patients.
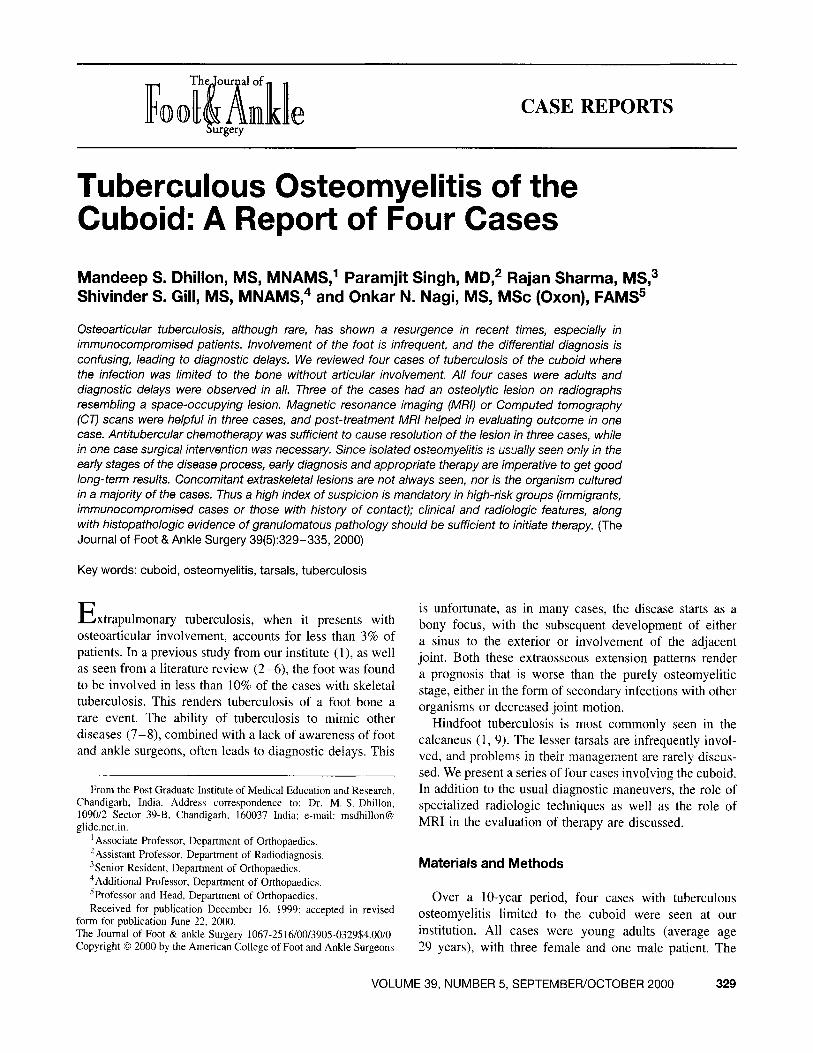
All patients had routine foot radiographs (AP, lateral,and oblique views). A computed tomography (CT) scanwas done in case 2, and Magnetic resonance imaging(MRI) was done at presentation in two cases (Table 1).In case 3, the MRI was repeated after 1 year of therapyto assess the changes. The diagnosis was confirmed inall cases by obtaining tissue (Fig. 1), either by aspirationcytology or by biopsy, where granulomatous tissue with orwithout a typical "tubercle" was considered diagnostic. Anattempt was also made to obtain cultures of the organisms.
Upon confirmation of diagnosis, anti-tubercular therapy(ATT) was initiated. The ATT consisted of the initialintensive phase (three or four drugs for a period of 4months), followed by two drugs for the maintenancephase. The dosages of the drugs used were: isoniazid(INH), 450-600 mg/day; rifampicin, 450-600 mg/day;ethambutol, 15-25 mg/kg/day; and pyrazinamide, 20-
330 THEJOURNAL OF FOOT& ANKLESURGERY
FIGURE 1 Microphotograph (H&E x 140) showing epitheloid cellgranulomas with Langhans type of giant cells.
25 mg/kg per day. In case 1 of our series, only threedrugs (INH, rifampicin, and ethambutol) were used inthe intensive phase. In the last three cases, pyrazinamidewas added to this regimen in the initial 4 months, as theproblem of drug resistance was being frequently encountered. Once the patients started responding to ATT, maintenance therapy was continued (INH and rifampicin) foran additional period of 12-14 months. ATT was discontinued when there was no clinical evidence of infection,radiographs showed healing (in one case repeat MRI wasdone), and serial ESR was below 20; however, a minimumperiod of 16 months of drug therapy was ensured in cases1-3, while ATT in case 4 is continuing.
Observations and Results
All cases were young adults with a female-to-maleratio of 3:1. Diagnostic delays were seen due to lack ofawareness (case I), late referral (cases 3 and 4), and apresumptive diagnosis of a benign bone tumor in case 2,who incidentally was a doctor. Follow-up ranged from7 months (case 4, who is still on ATT) to 36 months
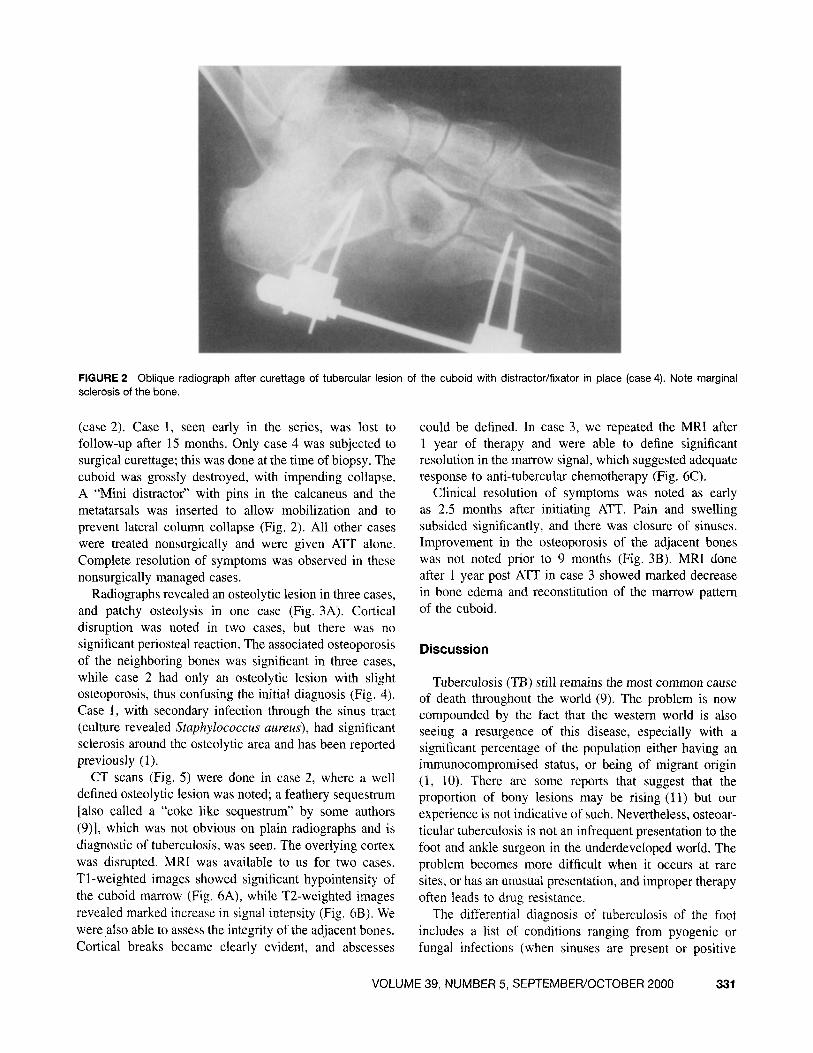
FIGURE 2 Oblique radiograph after curettage of tubercular lesion of the cuboid with distractor/fixator in place (case 4). Note marginalsclerosis of the bone.
(case 2). Case 1, seen early in the series, was lost tofollow-up after 15 months. Only case 4 was subjected tosurgical curettage; this was done at the time of biopsy. Thecuboid was grossly destroyed, with impending collapse.A "Mini distractor" with pins in the calcaneus and themetatarsals was inserted to allow mobilization and toprevent lateral column collapse (Fig. 2). All other caseswere treated nonsurgically and were given ATT alone.Complete resolution of symptoms was observed in thesenonsurgically managed cases.
Radiographs revealed an osteolytic lesion in three cases,and patchy osteolysis in one case (Fig. 3A). Corticaldisruption was noted in two cases, but there was nosignificant periosteal reaction. The associated osteoporosisof the neighboring bones was significant in three cases,while case 2 had only an osteolytic lesion with slightosteoporosis, thus confusing the initial diagnosis (Fig. 4).Case I, with secondary infection through the sinus tract(culture revealed Staphylococcus aureus), had significantsclerosis around the osteolytic area and has been reportedpreviously (1).
CT scans (Fig. 5) were done in case 2, where a welldefined osteolytic lesion was noted; a feathery sequestrum[also called a "coke like sequestrum" by some authors(9)], which was not obvious on plain radiographs and isdiagnostic of tuberculosis, was seen. The overlying cortexwas disrupted. MRI was available to us for two cases.T'l-weighted images showed significant hypointensity ofthe cuboid marrow (Fig. 6A), while T2-weighted imagesrevealed marked increase in signal intensity (Fig. 68). Wewere also able to assess the integrity of the adjacent bones.Cortical breaks became clearly evident, and abscesses
could be defined. In case 3, we repeated the MRI after1 year of therapy and were able to define significantresolution in the marrow signal, which suggested adequateresponse to anti-tubercular chemotherapy (Fig. 6C).
Clinical resolution of symptoms was noted as earlyas 2.5 months after initiating ATT. Pain and swellingsubsided significantly, and there was closure of sinuses.Improvement in the osteoporosis of the adjacent boneswas not noted prior to 9 months (Fig. 3B). MRI doneafter 1 year post ATT in case 3 showed marked decreasein bone edema and reconstitution of the marrow patternof the cuboid.
Discussion
Tuberculosis (TB) still remains the most common causeof death throughout the world (9). The problem is nowcompounded by the fact that the western world is alsoseeing a resurgence of this disease, especially with asignificant percentage of the population either having animmunocompromised status, or being of migrant origin(1, 10). There are some reports that suggest that theproportion of bony lesions may be rising (11) but ourexperience is not indicative of such. Nevertheless, osteoarticular tuberculosis is not an infrequent presentation to thefoot and ankle surgeon in the underdeveloped world. Theproblem becomes more difficult when it occurs at raresites, or has an unusual presentation, and improper therapyoften leads to drug resistance.
The differential diagnosis of tuberculosis of the footincludes a list of conditions ranging from pyogenic orfungal infections (when sinuses are present or positive
VOLUME 39, NUMBER 5, SEPTEMBER/OCTOBER 2000 331
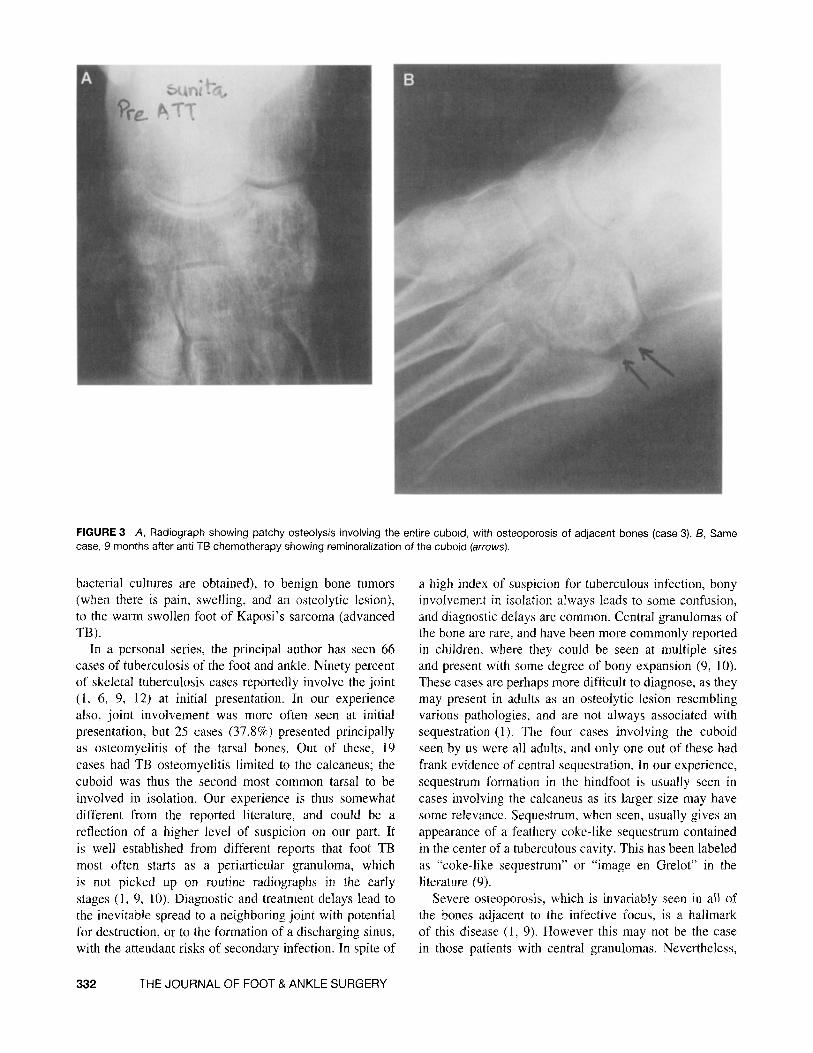
FIGURE 3 A, Radiograph showing patchy osteolysis involving the entire cuboid, with osteoporosis of adjacent bones (case 3). B, Samecase, 9 months after anti TB chemotherapy showing remineralization of the cuboid (arrows).
bacterial cultures are obtained), to benign bone tumors(when there is pain, swelling, and an osteolytic lesion),to the warm swollen foot of Kaposi's sarcoma (advancedTB).
In a personal series, the principal author has seen 66cases of tuberculosis of the foot and ankle. Ninety percentof skeletal tuberculosis cases reportedly involve the joint(l , 6, 9, 12) at initial presentation. In our experiencealso, joint involvement was more often seen at initialpresentation, but 25 cases (37.8%) presented principallyas osteomyelitis of the tarsal bones. Out of these, 19cases had TB osteomyelitis limited to the calcaneus; thecuboid was thus the second most common tarsal to beinvolved in isolation. Our experience is thus somewhatdifferent from the reported literature, and could be areflection of a higher level of suspicion on our part. Itis well established from different reports that foot TBmost often starts as a periarticular granuloma, whichis not picked up on routine radiographs in the earlystages (I, 9, 10). Diagnostic and treatment delays lead tothe inevitable spread to a neighboring joint with potentialfor destruction, or to the formation of a discharging sinus,with the attendant risks of secondary infection. In spite of
332 THE JOURNAL OF FOOT & ANKLE SURGERY
a high index of suspicion for tuberculous infection, bonyinvolvement in isolation always leads to some confusion,and diagnostic delays are common. Central granulomas ofthe bone are rare, and have been more commonly reportedin children, where they could be seen at multiple sitesand present with some degree of bony expansion (9, 10).These cases are perhaps more difficult to diagnose, as theymay present in adults as an osteolytic lesion resemblingvarious pathologies, and are not always associated withsequestration (I). The four cases involving the cuboidseen by us were all adults, and only one out of these hadfrank evidence of central sequestration. In our experience,sequestrum formation in the hindfoot is usually seen incases involving the calcaneus as its larger size may havesome relevance. Sequestrum, when seen, usually gives anappearance of a feathery coke-like sequestrum containedin the center of a tuberculous cavity. This has been labeledas "coke-like sequestrum" or "image en Grelot" in theliterature (9).
Severe osteoporosis, which is invariably seen in all ofthe bones adjacent to the infective focus, is a hallmarkof this disease (1, 9). However this may not be the casein those patients with central granulomas. Nevertheless,
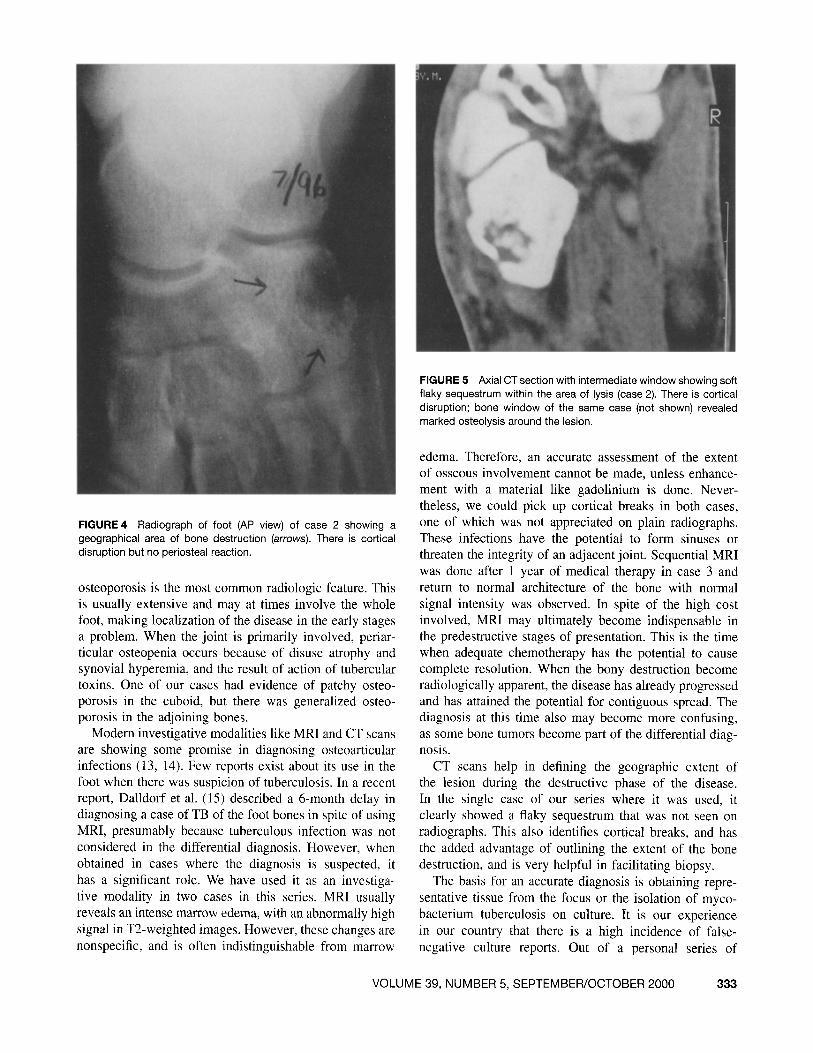
FIGURE 4 Radiograph of foot (AP view) of case 2 showing ageographical area of bone destruct ion (arrows). There is cort icaldisruption but no periosteal reaction.
osteoporosis is the most common radiologic feature. Thisis usually extensive and may at times involve the wholefoot, making localization of the disease in the early stagesa problem. When the joint is primarily involved, periarticular osteopenia occurs because of disuse atrophy andsynovial hyperemia, and the result of action of tuberculartoxins. One of our cases had evidence of patchy osteoporosis in the cuboid, but there was generalized osteoporosis in the adjoining bones.
Modem investigative modalities like MRI and CT scansare showing some promise in diagnosing osteoarticularinfections (13, 14). Few reports exist about its use in thefoot when there was suspicion of tuberculosi s. In a recentreport , Dalldorf et al. (15) described a 6-month delay indiagnosing a case of TB of the foot bones in spite of usingMRI, presumably because tuberculous infection was notconsidered in the differential diagnosis. However, whenobtained in cases where the diagnosis is suspected, ithas a significant role. We have used it as an investigative modality in two cases in this series. MRI usuallyreveals an intense marrow edema, with an abnormally highsignal in T2-weighted images. However, these changes arenonspecific, and is often indistinguishable from marrow
FIGURE 5 Axial CT section with intermediate window showing softflaky sequestrum within the area of lysis (case 2). There is cort icaldisruption ; bone window of the same case (not shown) revealedmarked osteolysis around the lesion.
edema. Therefore, an accurate assessment of the extentof osseous involvement cannot be made, unless enhancement with a material like gadolinium is done. Nevertheless, we could pick up cortical breaks in both cases,one of which was not appreciated on plain radiographs.These infection s have the potential to form sinuses orthreaten the integrity of an adjacent joint. Sequential MRIwas done after 1 year of medical therapy in case 3 andreturn to normal architecture of the bone with normalsignal intensity was observed. In spite of the high costinvolved, MRI may ultimately become indispensable inthe predestructive stages of presentation. This is the timewhen adequate chemotherapy has the potential to causecomplete resolution. When the bony destruction becomeradiologically apparent, the disease has already progre ssedand has attained the potential for contiguous spread. Thediagnosis at this time also may become more confusing,as some bone tumors become part of the differential diagnosis.
CT scans help in defining the geographic extent ofthe lesion during the destructive phase of the disease.In the single case of our series where it was used, itclearly showed a flaky sequestrum that was not seen onradiographs. This also identifies cortical breaks, and hasthe added advantage of outlining the extent of the bonedestruction, and is very helpful in facilitating biopsy.
The basis for an accurate diagnosis is obtainin g representative tissue from the focus or the isolation of mycobacterium tuberculo sis on culture . It is our experiencein our country that there is a high incidence of falsenegative culture reports. Out of a personal series of
VOLUME 39, NUMBER 5, SEPTEMBER/OCTOBER 2000 333
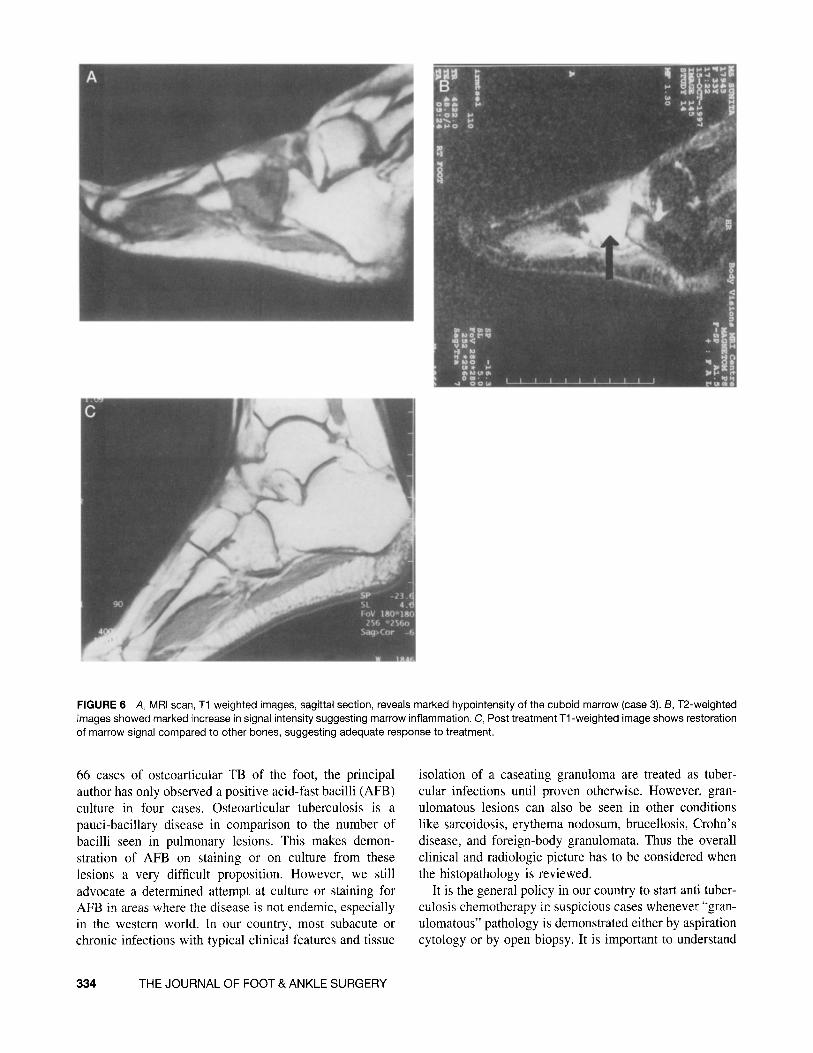
FIGURE 6 A, MRI scan, T1 weighted images, sagittal section , reveals marked hypointensity of the cubo id marrow (case 3). B, T2-weightedimages showed marked increase in signal intensity suggesting marrow inflammation. C, Post treatment T1-weighted image shows restorationof marrow signal compared to other bones, suggesting adequate response to treatment.
66 cases of osteoarticular TB of the foot, the principalauthor has only observed a positive acid-fast bacilli (AFB)culture in four cases. Osteoarticular tuberculosis is apauci-bacillary disease in comparison to the number ofbacilli seen in pulmonary lesions. This makes demonstration of AFB on staining or on culture from theselesions a very difficult propo sition . However, we stilladvocate a determined attempt at culture or staining forAFB in areas where the disease is not endemic, especiallyin the western world . In our country, most subacute orchronic infections with typical clinical features and tissue
334 THE JOURNAL OF FOOT & ANKLE SURGERY
isolation of a caseating granuloma are treated as tubercular infections until proven otherwise. However, granulomatous lesions can also be seen in other conditionslike sarcoidosis, erythema nodosum, brucellosis, Crohn ' sdisease, and foreign-body granulomata. Thus the overallclinical and radiologic picture has to be considered whenthe histopathology is reviewed .
It is the general policy in our country to start anti tuberculosis chemotherapy in suspicious cases whenever "granulomatous" pathology is demonstrated either by aspirationcytology or by open biopsy. It is important to understand

that the basic treatment of tuberculosis is adequate andprolonged multidrug chemotherapy, and surgical intervention is at best an adjunct to this. The standard regimensinclude both rifampicin and isoniazid in appropriate doses,and since the problem of drug resistance is becomingsignificant, we advocate the use of four drugs in combination for a minimum period of 3-4 months (initial intensive phase of the protocol). Laboratory investigations likeserial ESR and ELIZA tests could be used to monitor theprogress of the disease. When correlated with resolutionof clinical symptoms as well as the radiologic changes,the time to initiate the maintenance phase of the protocolbecomes evident. In cases with a purely osteolytic lesionwithout joint involvement, it may be wise to do openbiopsy as this allows us to do some debridement of thelocal area. In long-standing cases, the entire bone maybe just a hollow shell, and in case 4 we had to supplement the debridement by an external fixator to prevent thelate collapse of the cuboid bone. This may not be necessary in all cases, as the surrounding sclerosis may makethe bone strong enough in some cases. In these cases, aperiod of immobilization may be beneficial, although theadvantages are more obvious with articular extension.
Conclusions
The aim of this report was to draw attention to the factthat tuberculosis can present as an osteolytic lesion inthe tarsal bones. The cuboid is the second most involvedtarsal bone. The diagnosis is not always frankly evident,and a high index of suspicion has to be maintained. Thepotential for sinus formation or invasion of the neighboring joint increases with delays in adequate therapy.Surgical intervention should be limited to biopsy onlyas multidrug chemotherapy alone is sufficient to achievecomplete healing. In one case we applied an externalfixator in distraction mode to maintain the length of thelateral column of the foot, as we felt there as a possibilityof collapse of the destroyed cuboid. In our experience CT,and MRI, though expensive investigations, have a definiterole to play in defining the extent of the lesion, the state of
the adjacent joint, and even the marrow response to drugtherapy. It is important to note, however, that the organismmay not be cultured in all the cases. We feel justified instarting treatment with histopathologic evidence of typicalcaseating granulomatous pathology, in cases where otherinvestigations and clinical judgment suggest the diagnosis.We feel that tuberculosis must be strongly considered evenin osteolytic lesions limited to a bone, especially in highrisk groups and in endemic areas.
References
1. Dhillon, M. S., Sharma, S., Gill, S. S. Nagi, O. N. Tuberculosis ofbones and joints of the foot: an analysis of 22 cases. Foot Ankle14:505-513,1993.
2. Evanchick, C. c., Davis, D. E., Harrington, T. M. Tuberculosis ofperipheral joints; an often missed diagnosis. J. Rheumatol. 13:187191, 1986.
3. Garcia-Porrua, C., Gonzalez-Gay, M. A. Sanchez-Andrade, A.,Vaquez-Caruncho, M. Arthritis in the right great toe as the clinicalpresentation of tuberculosis. Arthritis Rheum. 41:374-375, 1998.
4. Watts, H. G., Lifeso, R. M. Current concepts review: Tuberculosisof bones and joints. J. Bone Joint Surg. 78-A:288- 298, 1996.
5. Werd, M. B. Mason, E. J., Landsman, A. S., Hanft, J. R., Kashuk,K. B. Peripheral skeletal tuberculosis of the foot. Etiologic reviewand case study. J. Am. Podiatr. Med. Assoc. 84:390-398, 1994.
6. Sobel, E., Levitz, S. Tuberculosis of the foot. A diagnostic challenge. J. Am. Podiatr. Med. Assoc. 85(2):83-90, 1995.
7. Naidoo, K. S. The great imitator. J. Bone Joint Surg. 62-B:279,1980.
8. Standish, W., Hyndman, J., Forsythe, M. Skeletal tuberculosis: thegreat imitator. J. Bone Joint Surg. 59-B:511, 1977.
9. Tuli, S. M. Tuberculosis of the skeletal system, 2nd ed. Jaypee Bros,New Delhi, 1997.
10. Jellis, J. In The Foot, pp. 614-623, edited by B. Helal and D. Wilson Churchill Livingstone, London, 1988.
11. Scott, J. E., Taor, W. S. The changing pattern of bone and jointtuberculosis. J Bone Joint Surg. 64-B:250, 1970.
12. Abdelwahab, I F., Kenan, S., Hermann, G. et al. Tuberculous peroneal tenosynovitis. 1. Bone Joint Surg. 75-A: 1687, 1993.
13. Boutin, R. D., Brossman, 1., Sartoris, D. 1., Reilly, D., Resnick, D.Update on imaging of orthopaedic infections. Orthop. Clin. NorthAm. 29:41-65,1998.
14. Ridley, N., Shaikh, M. I., Remedios, D., Mitchell, R. Review: radiology of skeletal tuberculosis. Orthopaedics 21:1213-1220, 1998.
15. Dalldorf, P. G. Tuberculosis of the foot: a case report. Foot Ankle156:505, 1993.
VOLUME 39, NUMBER 5, SEPTEMBER/OCTOBER 2000 335