antibiotics for treating chronic osteomyelitis in adults
TRANSCRIPT
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 1
Antibiotics for treating chronic osteomyelitis in adultsReview informationAuthors
Lucieni O Conterno1, Carlos Rodrigues da Silva Filho1
1Department of General Internal Medicine and Clinical Epidemiology Unit, Marilia Medical School, Marilia, Brazil
Citation example: Conterno LO, da Silva Filho CRodrigues. Antibiotics for treating chronic osteomyelitis in adults. Cochrane Database of Systematic Reviews 2003, Issue 4. Art. No.: CD004439. DOI: 10.1002/14651858.CD004439.
Contact personLucieni O ConternoDepartment of General Internal Medicine and Clinical Epidemiology UnitMarilia Medical SchoolAvenida Monte Carmelo 800Fragata17519-030 MariliaSão PauloBrazil
E-mail: [email protected]
DatesAssessed as Up-to-date: 01 December 2008
Date of Search: 30 September 2008
Next Stage Expected: 08 July 2011
Protocol First Published: Issue 4, 2003
Review First Published: Not specified
Last Citation Issue: Issue 4, 2003
What's new
Date / Event Description
History
Date / Event Description
23 October 2008Amended
Converted to new review format.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 2
AbstractBackgroundChronic osteomyelitis is generally treated with antibiotics and surgical debridement but can persist intermittently for years with frequent therapeutic failure. Despite advances in both antibiotics and surgical treatment, the long-term recurrence rate remains at approximately 20% to 30%.
ObjectivesTo determine the effects of different systemic antibiotic treatment regimens for treating chronic osteomyelitis in adults.
Search methodsWe searched the Cochrane Bone, Joint and Muscle Trauma Group Specialised Register (October 2008), the Cochrane Central Register of Controlled Trials (The Cochrane Library 2008, Issue 3), MEDLINE (January 1966 to October 2008), EMBASE (January 1980 to October 2008), LILACS (October 2008) and reference lists of relevant articles.
Selection criteriaRandomised or quasi-randomised controlled trials addressing the effects of different antibiotic treatments given after surgical debridement for chronic osteomyelitis in adults.
Data collection and analysisTwo authors independently screened papers for inclusion, extracted data and appraised the quality of included trials. Where appropriate, we pooled data using the fixed-effect model.
ResultsWe included eight small trials (257 participants in total, with data available from 228). Study quality was often inadequate: in particular, concealment of allocation was not confirmed and there was an absence of blinding of outcome assessment. The antibiotic regimens, duration of treatment and follow-up varied between trials. Five trials compared oral versus parenteral antibiotics. There was no statistically significant difference between the two groups in the remission rate 12 or more months after treatment (risk ratio 0.94, 95% confidence interval 0.78 to 1.13; 3 trials). Antibiotic treatment for osteomyelitis was associated with moderate or severe adverse events in 4.8% of patients allocated oral antibiotics and 15.5% patients allocated parenteral antibiotics (risk ratio: 0.40, 95% confidence interval 0.13 to 1.22; 4 trials). Single trials with very few participants found no statistical significant differences for remission or adverse events for the following three comparisons: parenteral plus oral versus parenteral only administration; two oral antibiotic regimens; and two parenteral antibiotic regimens. No trials compared different durations of antibiotic treatment for chronic osteomyelitis, or adjusted the remission rate for bacteria species or severity of disease.
Authors' conclusionsLimited evidence suggests that the method of antibiotic administration (oral versus parenteral) does not affect the rate of disease remission if the bacteria are sensitive to the antibiotic used. However, this and the lack of statistically significant differences in adverse effects need confirmation. No or insufficient evidence exists for other aspects of antibiotic therapy for chronic osteomyelitis.
Plain language summaryAntibiotics for treating chronic osteomyelitis in adults
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 3
Osteomyelitis is an inflammation of the bone and bone marrow caused by pus-forming bacteria, mycobacteria or fungi. All bone infection that is long-standing is called chronic osteomyelitis. Antibiotics can be administered either orally or parenterally (i.e. by any route other than the mouth or bowel). This review identified eight small randomised trials which presented results for a total of 228 patients, most of whom were reported to have had surgical removal of the infected tissue (debridement) before starting on antibiotic therapy. There were four comparisons but pooling of results was only possible for the comparison of oral versus parenteral administration of antibiotics. Pooled results from three trials showed no statistically significant differences in the numbers of people who were without symptoms (in 'remission') at 12 months or more follow-up; nor in numbers with adverse effects or with a superinfection (another infection that is not sensitive to the antibiotic being used). This evidence suggests that the method of antibiotic administration does not have an impact on the rate of disease remission if the bacteria causing the infection are sensitive to the antibiotic used. However, confirmation is needed. There was either no or insufficient evidence to inform on the optimal duration of antibiotic therapy and on types of antibiotics.
BackgroundOsteomyelitis is an inflammation of the bone and bone marrow caused by pyogenic bacteria, mycobacteria or fungi. Based on aetiological considerations, traditionally osteomyelitis has been classified as either hematogenous, secondary to a contiguous focus (adjacent areas are in contact) of infection or those associated with peripheral vascular disease (Cunha 2002; Mader 1997a; Mader 1999a; Waldvogel 1970). In hematogenous osteomyelitis, blood-born bacteria reach bone from a remote portal of entry. It is predominantly encountered in paediatric populations. Osteomyelitis secondary to a contiguous focus of infection results either from a direct inoculation of bacteria into the bone at the time of trauma, or during surgical reduction and internal fixation of fractures, or from an adjacent focus (e.g. decubitus ulcer, soft tissue trauma). Whatever the route of access, in order to start the infection, the microorganism, for example Staphylococcus aureus, adheres to fibronectin's receptors or other membrane proteins of the bone marrow. Subsequently bacteria is covered by a layer of fibrinogen (slimy coat) and protected from host defence mechanism and antibiotics. In osteomyelitis resulting from contiguous spread of infection, injury from local inflammation or trauma may devitalise the bone and tissue, providing an inert matrix upon which microorganisms thrive (Ciampolini 2000; Gristina 1990; Haas 1996; Mader 1997a; Waldvogel 1970). Bacteria can also elude host defence mechanisms by hiding intracellularly and by acquiring a very slow metabolic rate.
Another classification of osteomyelitis is based on anatomic stage of disease and is related to prognosis: medullary (confined to medullary cavity), superficial (involve just cortical bone), localized (involves both the cortical and medullary bone, but not the entire bone diameter), diffuse (involves the entire thickness of the bone). In this classification system, the patients are classified as A, B or C according to the presence and severity of underlying diseases (Cierny 2003).
All aetiological classes of osteomyelitis may progress to a chronic process. Chronic osteomyelitis occurs when bone tissue dies as a result of the lost blood supply; fragments of dead bone (sequestra) or metal implants can perpetuate the infection by exposing sites to which pathogenic bacteria can bind. The infection can persist intermittently for years with frequent therapeutic failure (Huber 2002; Mader 1993). Therefore the classification of osteomyelitis into acute or chronic based just on duration of disease is inaccurate, because the hallmark of chronic osteomyelitis is the simultaneous presence of microorganisms and necrotic bone (Bamberger 1993; Haas 1996; Mader 1997a; Mader 1997b), independent of time.
Chronic osteomyelitis usually occurs in adults, generally secondary to an open injury to the bone, or after surgery for reconstruction of the bone (Holtom 1999; Lazzarini 2002; Mader 1999b). In these situations the bone is devitalized from the outset by the trauma. Infection associated with prostheses are also common (Carek 2001; Haas 1996; Lew 1997). Chronic osteomyelitis may present as a recurrent or intermittent disease, with periods of quiescence of variable duration. These tend to relapse, after apparently successful therapy, with a major impact on the quality of life and a substantial financial burden to health system (Huber 2002).
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 4
From cultures of operative specimens, Staphylococcus aureus is the main causative agent of chronic osteomyelitis, followed by Pseudomonas spp and Enterobacteriaceae (Carek 2001; Mader 1992; Waldvogel 1980).
Chronic osteomyelitis is generally treated with antibiotics and surgical debridement to remove all the dead bone tissue. Microorganisms residing in the dead bone, if not removed along with sequestra (dead bone), can cause flare-ups many years after the initial attack. The goal of debridement is to reach healthy, viable tissue. Laser doppler flowmetry can be used to ensure that the remaining bone is viable (Swiontkoski 1990). Adequate debridement may leave a large bone defect known as dead space. The dead space should be filled with local tissue flaps, or free flaps, bone graft or temporarily with polymethylmethacrylate beads. The goal of dead space management is to replace dead bone and scar tissue with durable vascularised tissue. If necessary, measures must be taken to achieve permanent stability of the bone. Skin grafting is used to cover wound sites involving bone that has undergone surgery, or to cover muscle flaps or graft of cancellous bone (bone that has a spongy structure) (Ciampolini 2000; Eckardt 1994; Lew 1997; Mader 1997a; Mader 1999b; Waldvogel 1980).
Despite advances in both antibiotics and surgical treatment, the long-term recurrence rate remains at approximately 20% to 30% (Gentry 1990; Mader 1990; Rissing 1997; Waldvogel 1970; Waldvogel 1980). Evaluating the success of treatment is difficult as many studies show promising initial results but long-term follow up data are frequently lacking (Mader 1992). According to some authors, the tendency for infection to relapse, sometimes years after apparently successful therapy, suggests remission (or arrest) rather than cure of treated osteomyelitis (Haas 1996; Mader 1999b).
The optimal duration of antibiotic therapy has not been well defined. Four to six weeks of parenteral (non-oral administration such as an intravenous injection) antibiotic therapy after surgery has become the standard treatment of chronic osteomyelitis. The rationale behind this regimen is the recognition that three to four weeks are required for the bone to revascularise, and from the experience obtained in treating children with acute osteomyelitis (Carek 2001; Gentry 1990; Lazzarini 2002; Lazarini 2005; Mader 1992; Mader 1999a; Waldvogel 1970). However, because the failure rates in clinical studies, some authors advocate longer treatment with six to eight weeks of intravenous therapy followed by a course of three months or longer of oral therapy. Besides the doubts related to the duration of chronic osteomyelitis treatment, there are some controversies about the best method of antibiotic administration to treat it. Some reports suggest that short-term parenteral therapy followed by oral antibiotic therapy for six weeks or oral antibiotic alone may be an effective strategy with more economic benefits than parenteral therapy alone (Gentry 1990; Greenberg 2000; Mader 2001; Rissing 1997; Swiontkowski 1999).
Nonspecific blood tests like erythrocyte sedimentation rate, C-reactive protein, alpha-1 acid glycoprotein, are widely employed in assessing chronic osteomyelitis. They are usually elevated but have low sensitivity and specificity. Some authors suggest that they can be helpful to assist the early diagnosis of post-operative bone infection; and assess effectiveness during the course of antibiotic therapy (Bourguignat 1996; Ferard 2002).
Nowadays the increasing antibiotic resistance is of great concern worldwide. Therefore the length of antibiotic therapy for the treatment of chronic osteomyelitis has to be defined based on good quality research.
ObjectivesTo determine the effects of systemic antibiotics in the treatment of chronic osteomyelitis in adults.
We aimed to compare different antibiotic treatment regimens that differed in duration and methods of administration. Secondly, we aimed to assess whether remission differed according to the causative agent (e.g. different bacteria) for osteomyelitis.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 5
MethodsCriteria for considering studies for this reviewTypes of studiesRandomised and quasi-randomised (e.g. date of birth, alternation) controlled trials were included. Trials were included irrespective of publication status and blinding.
Types of participantsAdults diagnosed with chronic osteomyelitis were included.
The diagnosis of chronic osteomyelitis could be defined by: clinical pattern evolved over months or years and characterised by low-grade inflammation, presence of pus, microorganisms, and presence of dead bone (sequestra), demonstrated by plain film, computed tomography or magnetic resonance imaging, and isolation of bacteria from the bone lesion (Lew 1997). Trial participants should have undergone surgical management of infection with adequate and extensive debridement of all necrotic tissue. The failure to describe prior treatment was not, however, a reason for exclusion. Trials specifically focusing on the treatment of diabetic foot osteomyelitis, implant-associated osteomyelitis, sternal or vertebral osteomyelitis were excluded. Mixed population trials primarily focusing on chronic osteomyelitis were included only if the proportion of participants with otherwise excluded conditions was low.
Types of interventionsComparative studies of systemic antibiotic treatment of chronic osteomyelitis. Trials comparing different antibiotics, different antibiotic routes of administration (oral or parenteral and/or combination of parenteral and oral) or different duration of treatment were included. We defined parenteral route of administration as any route other than the mouth or bowel. We did not include studies addressing local antibiotic treatment. The bacteria should have had documented sensitivity to the antibiotics used. The participants should have had surgical management of infection with adequate and extensive debridement of all necrotic tissue. Obliteration of dead space, stabilisation of the bone and adequate soft tissue coverage should be done if necessary.
Types of outcome measures
Primary outcomesSustained remission of infection (where 'sustained remission' was defined as the resolution of all signs and symptoms of active infection at the end of therapy and after a minimal post-treatment observation period of one year (Carek 2001; Gentry 1990; Mader 1992);Number of participants who present resolution of all signs and symptoms of active infection at the end of therapy;Number of participants who present resolution of disease at least one year after therapy.
Secondary outcomesNumber of participants with failure (defined as a lack of apparent response to therapy as evidenced by one or more of the following: persistence of drainage, recurrence of sinus tract or failure of sinus tract to close, persistence of systemic signs of infection (chills, fever, weight loss, bone pain), or progression of bone infection shown by imaging methods) (Gentry 1990; Mader 1992). Treatment failure also includes early termination of treatment, such as for adverse effects or disease complications like amputation;Number of participants with early relapse (defined as recurrence of signs and symptoms plus isolation of the same pathogen(s) within 4 to 6 weeks after discontinuation of antibacterial therapy) (Gentry 1990; Mader 1992);
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 6
Number of participants with late relapse (defined as recurrence occurring after six weeks and up to 12 months after the end of therapy) (Gentry 1990; Mader 1992);
Adverse events
Adverse events related to antibiotic useOrthopaedic sequels like residual pain, residual non-unionSuperinfectionNumber of amputations doneCost of different antibiotics used for treatmentNumber of days of hospitalisationSquamous cell carcinomaDeath
Search methods for identification of studies
Electronic searchesWe searched the Cochrane Bone, Joint and Muscle Trauma Group Specialised Register (October 2008), the Cochrane Central Register of Controlled Trials (The Cochrane Library 2008, Issue 3), MEDLINE (January 1966 to October 2008), EMBASE (January 1980 to October 2008), LILACS (Latin America and Caribbean Health Sciences - accessed 24 October 2008). No language restrictions were applied.
In MEDLINE (OVID WEB) the search strategy was combined with the revised optimal trial search strategy (Higgins 2006), and modified for use in other databases (see Appendix 1).
Searching other resourcesWe searched reference lists of relevant articles.
Data collection and analysis
Selection of studiesTwo authors (LOC and CRSF) independently inspected each reference identified by the search and selected those that met the inclusion criteria. Full texts of selected studies were obtained and inspected independently by the two authors.
Data extraction and managementTwo authors (LOC and CRSF) independently extracted the data from trial reports. We used a tool based on the generic data extraction tool developed by the Cochrane Bone, Joint and Muscle Trauma Group. Disagreement was resolved by consensus.
Assessment of risk of bias in included studiesTrials that met the review inclusion criteria were independently assessed for methodological quality by both authors, and disagreement was resolved by consensus. Quality assessment was used only to assist the reader in interpreting the review (Higgins 2005). We used the Cochrane Bone, Joint and Muscle Trauma Group's former quality assessment tool (see Table 1). Although stipulated in the protocol, total quality scores were not calculated for the review, because there is no empirical evidence that these are useful.
Data analysisThe unit of analysis was each participant. We calculated risk ratios (RR) and 95% confidence intervals (CI) for
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 7
dichotomous outcomes. If studies with continuous outcomes are included in future updates we will calculate mean differences and 95% confidence intervals.
We pooled data using the fixed-effect model where appropriate.
We assessed heterogeneity by visual inspection of the forest plot and using the chi2 statistic (with significance
set at P < 0.10) in conjunction with the I2 statistic which describes the percentage of the variability in effect
estimates that are due to heterogeneity rather than sampling error (chance) (Higgins 2003). A value of I2
greater than 50% may be considered substantial heterogeneity. If there is heterogeneity in future updates we will investigate possible causes by exploring the impact of methodological quality, bacteria species, severity of the disease and treatment duration using subgroup analyses. We may consider pooling heterogeneous results using the random-effects model.
ResultsDescription of studies
Results of the searchThe search strategy retrieved 519 studies. After initial screening of titles and abstracts we selected 18 papers for possible inclusion.
Included studiesDetails of the individual trials are found in 'Characteristics of included studies'.
DesignOf the eight included trials, seven were randomised controlled trials and one was a quasi-randomised controlled trial (Mader 1990).Three trials (Gentry 1990; Gentry 1991; Norden 1986) were multicenter trials while the other five were probably conducted at a single site (Gomis 1999; Greenberg 1987; Greenberg 2000; Mader 1990; Sheftel 1986).
Sample sizes
The eight included trials included a total of 257 participants, with data available from 228. The number of participants enrolled in the individual studies ranged from 12 in Greenberg 2000 to 67 in Gentry 1990. The numbers in individual intervention groups ranged from five in Greenberg 2000 to 31 in Gentry 1990. It is notable that only one trial reported a sample-size calculation, but even for this trial the desired sample size was not achieved (Norden 1986).
Setting
All eight trials were conducted in a tertiary care (hospital) setting. Seven trials were conducted in the USA, two of these Gentry 1990; Gentry 1991) were also conducted in a hospital in Costa Rica. Gomis 1999 was conducted in Spain and an English translation of this trial obtained.
Participants
All trials had at least twice as many male as female participants. Where reported, the mean age of trial participants ranged from 33 years (Mader 1990) to 59 years (Gomis 1999).
The duration of chronic osteomyelitis was reported in just two trials (Mader 1990; Norden 1986) and ranged from two months to 28 years.
Two studies described the classification of osteomyelitis using the Cierny-Mader System (Mader 1990; Norden
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 8
1986) and Gomis 1999 used the classification based on aetiology. Post-traumatic osteomyelitis was the most frequent. Where reported, the location of the infection was mainly the tibia and femur.
In seven trials, the culture for microbiologic diagnosis was obtained by open biopsy or aspiration from infected bone. In one trial (Greenberg 1987), seven out of 30 patients had the microbiologic diagnosis by wound culture swabs. In all eight trials included in this review, the bacteria had proved sensitive to the antibiotic used.
In four trials (Gentry 1990; Gentry 1991; Gomis 1999; Mader 1990), Staphylococcus aureus was the most frequent bacteria isolated, but polymicrobial infections and infections caused by Pseudomonas aeruginosa were common among the trials. One trial included only chronic osteomyelitis caused by Staphylococcus aureus (Norden 1986) and another trial reported only infection caused by gram-negative bacteria (Sheftel 1986).
Debridement was mentioned as part of treatment in seven trials, but was not mentioned in Greenberg 1987. Details about the surgical proceedings were given in only two trials (Mader 1990; Norden 1986).
InterventionsFour comparisons were tested by the included trials. Five studies compared parenteral versus oral antibiotics (Gentry 1990; Gentry 1991; Gomis 1999; Greenberg 1987; Mader 1990). Oral antibiotics were compared in Greenberg 2000; a combination of parenteral and oral antibiotics was compared with parenteral antibiotics in Norden 1986; and Sheftel 1986 compared parenteral antibiotics.
The oral antibiotics used were quinolones in six trials (Gentry 1990; Gentry 1991; Gomis 1999; Greenberg 1987; Greenberg 2000; Mader 1990), rifampin in Norden 1986 and cloxacillin in Gentry 1991.
The parenteral antibiotics used were very diverse. Ceftazidime or cefazolin were used in five trials (Gentry 1990; Gentry 1991; Greenberg 1987; Norden 1986; Sheftel 1986), nafcillin in three (Gentry 1990; Mader 1990; Norden 1986), imipenem in one trial (Gomis 1999), and aminoglycoside in three trials (Gentry 1990; Mader 1990; Sheftel 1986).
The antibiotic regimens varied among the trials in terms of drugs used; even in each trial there were many different combinations of antibiotics. No comparison could be made to determine the best antibiotic for treating chronic osteomyelitis in adults.
The duration of treatment in the included studies varied within and between trials and ranged from less than seven days (Gomis 1999) to five months (Greenberg 1987). No trial specifically compared different durations of antibiotic treatment for chronic osteomyelitis.
OutcomesThere was variation between trials in the reported definition of the outcomes but we considered these definitions clinically consistent enough to permit pooling in some cases.
The outcomes were clinically and microbiologically based in two trials (Gentry 1990; Sheftel 1986) and clinically based in the remaining six trials.
Seven trials reported the complete resolution of symptoms of disease at the end of treatment and six trials after follow-up of at least 12 months (Gentry 1990; Gentry 1990; Greenberg 2000; Mader 1990; Norden 1986; Sheftel 1986). The length of follow-up, which varied between and within trials, ranged from one month (Greenberg 2000) to four years (Norden 1986).
Eight trials reported adverse events related to antibiotic therapy. The adverse events were reported as severe in five trials. Five trials reported the occurrence of superinfection during the treatment (Gentry 1990; Gentry 1991; Gomis 1999; Greenberg 1987; Sheftel 1986). This outcome was added to the 'Types of outcome measures'.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 9
Excluded studiesWe excluded 10 studies (see 'Characteristics of excluded studies' for details).
Risk of bias in included studiesThe results of the quality assessment for individual trials are shown in Table 2. A summary of the findings for individual items (see Table 1) of quality assessment is given below.
Allocation concealment (item A) was unclear in six trials (Gentry 1990; Gentry 1991; Greenberg 1987; Greenberg 2000; Norden 1986; Sheftel 1986), and inadequate in Gomis 1999, which used an open label method, and Mader 1990, which was quasi-randomised.
Withdrawn participants were excluded from analysis in four trials (Gentry 1990; Gentry 1991; Mader 1990; Norden 1986) (item B).
Outcome assessors (item C), participants (item E) and treatment providers (item F) were not blinded to intervention allocation in any of the included trials.
In general, the baseline characteristics of participants described by studies were age, gender and location of infection. Just two trials (Mader 1990; Norden 1986) mentioned duration of disease, and just two (Mader 1990; Sheftel 1986) gave the classification of disease using Cierny-Mader System. Baseline comparability (item D) was considered sufficient in three trials (Gomis 1999; Mader 1990; Norden 1986).
Apparently the participants in all trials received identical care programs (item G). Notably, however, there were no details given in terms of medical history, physical examination and laboratory investigations carried out during the study for the intervention and control groups separately.
There was some variation between trials in the definition of inclusion criteria (item H), outcome measures (item J) and outcome assessment (item K), but all trials gave sufficient information and were clinically consistent.
The trials reported active follow-up, but the length of follow-up was different for each participant within the trials, and not sufficiently long for all participants in three trials (Greenberg 1987; Greenberg 2000; Sheftel 1986) where some participants were followed up less than two months (item L).
Effects of interventionsThe results for the four comparisons made by the included trials are reported below. None of these addressed the impact of different bacteria species (e.g Staphylococcus aureus, Enterobacteriaceae, Pseudomonas spp) on the rate of remission.
Oral versus parenteral route of administration of antibioticsFive trials, presentating data from a total of 180 participants, compared oral quinolones to various parenteral antibiotics regimens (Gentry 1990; Gentry 1991; Gomis 1999; Greenberg 1987; Mader 1990).
The remission rates at the end of treatment with oral versus parenteral antibiotic were 82% with oral antibiotic and 80% with parenteral antibiotic, with no statistically significant difference between the two groups (see Analysis 1.1: risk ratio (RR) 1.00, 95% confidence interval (CI) 0.88 to 1.14). There was no statistical heterogeneity between trials.
Remission rates at 12 or more months after the end of treatment, pooled from three trials (Gentry 1990; Gentry 1991; Mader 1990) and including 118 participants were 77% with oral antibiotic and 81% with parenteral antibiotics. There was no statistically significant difference between groups (see Analysis 1.2: RR 0.94, 95% CI 0.78 to 1.13) and no statistical heterogeneity between trials.
Four trials reported a variety of mild adverse events relating to the antibiotic used (Gentry 1990; Gentry 1991; Greenberg 1987; Mader 1990) but no statistical difference was observed (see Analysis 1.3: RR 1.09, 95% CI
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 10
0.53 to 2.28). Moderate or severe adverse events, such as those requiring termination of treatment, occurred in 4.8% of participants in the oral antibiotic group and 15.5% in the parenteral groups but this was not statistically significant (see Analysis 1.4: RR 0.40 95% CI 0.13 to 1.22).
Superinfection occurred in participants of both groups (7.5% in the oral group versus 5.4% in the parenteral group) (see Analysis 1.5: RR 1.29, 95% CI 0.43 to 3.88).
Parenteral plus oral antibiotics versus parenteral antiobioticsRemission rate at least 12 months after the end of treatment was reported in only one trial with 19 participants (data available from 18) with chronic osteomyelitis caused by Staphylococcus aureus (Norden 1986). The remission rates were 80% in the parenteral plus oral antibiotic group and 50% in the parenteral antibiotic group. No statistically significant difference was observed (see Analysis 2.1: RR 1.60, 95% CI 0.75 to 3.42).
Significant neutrophenia occurred in one participant of the parenteral plus oral antibiotic group and three participants of the parenteral antibiotic group, all with spontaneous recovery (see Analysis 2.2: RR 0.27, 95% CI 0.03 to 2.10).
Oral antibioticsOne trial (Greenberg 2000) compared two different oral quinolones (ciprofloxacin and lomefloxacin) and included five and seven participants with chronic osteomyelitis respectively in the two groups. No statistically significant difference was observed in the remission rates after 12 months of follow-up between the groups (see Analysis 3.1: RR 1.40, 95% CI 0.29 to 6.86).
Adverse events were reported in three participants of the lomefloxacin group, but this difference was not statistically significant (see Analysis 3.2: RR 0.19, 95% CI 0.01 to 3.03).
Parenteral antibioticsSheftel 1986 compared regimens of parenteral antibiotics (ceftazidime versus ticarcillin plus tobramycin) in 18 participants with chronic osteomyelitis caused by gram negative bacilli. Pseudomonas aeruginosa and Enterobacter cloacae were the most common organisms isolated. The remission rates at 12 months after the end of treatment were 67% in the group that received ceftazidime and 89% in the group that received ticarcillin (see Analysis 4.1: RR 0.75, 95% 0.45 to 1.26).
The author reported one adverse event, a case of mild increase in serum hepatic enzyme level, in the ceftazidime group and none in the other group (see Analysis 4.2: RR 3.0, 95% 0.14 to 65.16).
Superinfection occurred in two participants of the ceftazidime group and none of ticarcillin plus tobramycin group (see Analysis 4.3: RR 5.0, 95% CI 0.27 to 91.52).
Discussion
Summary of main resultsThis review included only eight small and heterogeneous studies including 257 participants (data available from 228) adults with biopsy-proven chronic osteomyelitis caused by bacteria with confirmed sensitivity to the antibiotics used. The main finding of this review is the lack of evidence to inform practice. Only the route of antibiotic administration was evaluated by more than one trial. The review found that there was no evidence of a difference between oral antibiotics (quinolones in four trials and cloxacillin in the fifth trial) in rate of remission at the end of therapy (RR 1.00, 95% CI 0.80 to 1.14; 5 trials) and after 12 months or more of follow-up (0.94, 95% CI 0.78 to 1.13; 3 trials). These results were statistically homogeneous. Separately pooled results for mild and more serious adverse events again showed no statistical differences between the two routes of administration. Nor was there a difference between the two groups in the incidence of superinfection.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 11
Single trials with very few participants found no statistical significant differences for remission or adverse events for the following three comparisons: parenteral plus oral versus parenteral only administration (18 participants); two oral antibiotic regimens (12 participants); and two parenteral antibiotic regimens (18 participants).
Overall completeness and applicability of evidenceAlthough the data are still too few to draw robust conclusions, only the comparison of oral versus parenteral antibiotics merits consideration here. The data suggest that provided the infective bacteria show sensitivity to the antibiotic used, the method of administration does not affect rate of disease remission. However, it is also likely that the small numbers of participants in the included trials and pooled results is insufficient to detect a difference between different routes of antibiotic administration to treat chronic osteomyelitis if this exists.
Other considerations include length of follow-up, the relative importance of debridement and currency of the trial evidence.
Chronic osteomyelitis usually occurs in adults, generally secondary to an open injury to the bone, or after surgery for reconstruction of the bone (Holtom 1999; Lazzarini 2002; Mader 1999b). It may present as a recurrent or intermittent disease, with periods of quiescence of variable duration. Because of these aspects of disease, the term 'remission' is preferable to 'cure' and the time of post-treatment follow up should be at least 12 months to assume a sustained remission of disease. While we have applied the 12 months definition here some authors suggest a follow-up of five years as ideal (Mader 1990). Additionally, others recommend a survival analysis to provide information about the length of time free of relapse (Simpson 2001; Walenkamp 1997).
The treatment of chronic osteomyelitis includes complete surgical debridement of necrotic bone and antibiotic therapy. The contribution of each component for clinical success in the treatment of osteomyelitis is not known. However, some researchers argue that the surgical intervention is the most important (Eckardt 1994; Gentry 1990; Stengel 2001) and that is not possible to conclude whether antibiotics have substantial influence on the progress of chronic osteomyelitis. The necessity of surgical debridement is unquestionable, but we hypothesised that antibiotics contribute to the control of the infection and if the bacteria show sensitivity to the antibiotic used, the methods of administration, the duration of therapy and the types of bacteria involved could influence the rate of sustained remission of infection. Only the method of administration has been tested here.
The trial participants were treated with many different antibiotics and surgical debridement. Since the trials did not give details about the surgical intervention, it was not possible to know if this aspect of treatment was adequate and comparable among the trials. Some trials did, however, attribute some treatment failures to inadequate debridement (e.g. Gentry 1990). Nonetheless, the available data preclude any conclusion about the exact contribution of surgery on the rate of remission.
If oral antibiotics have the same success rates as parenteral antibiotics, with the perhaps the potential for milder even if more numerous adverse effects, then these have the attraction of being easier to administer and avoiding the costs and inconvenience of prolonged hospital stays and medical treatment associated with parenteral administration. This is not proven here and the variation in the trial characteristics and lack of evidence for aspects of administration such as duration of treatment are also unhelpful.
Finally, many of the included trials were conducted over 20 years ago and nowadays we are faced with higher prevalence of resistant bacteria to many avaliable antibiotics, mainly when the infections are associated with healthcare procedures. For instance, the rates of methicillin resistant S.aureus are much higher now than in the past two decades, and we have a very limited number of antibiotics to treat infection by this bacteria. This continuously evolving bacterial resistance represents another challenge to the choice of antibiotics to treat chronic osteomyelitis.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 12
Quality of the evidenceThere was a moderate to high risk of bias for these trials given various deficiencies in trial design and conduct. There was a probable failure to conceal allocation, a lack of blinding, often poor or unknown comparability of baseline characteristics, inadequate follow-up, and post-randomisation exclusions in some trials. There is, however, a lack of finding of statistically significant differences for the pooled results of trials comparing oral versus parenteral antibiotics and thus exaggerated effects, that may be associated with these biases, were not apparent.
Potential biases in the review processThe key potential bias in our review is that we have not included all the evidence from randomised trials. Although our database search was comprehensive, it is likely that we have missed trials reported in conference proceedings. However, such reports are likely to be unavailable if these were contemporaneous with most of the studies in this review. The dated nature of the trials and trial reports meant that we decided not to request information from trial authors, including separate data for patients with chronic osteomyelitis in several excluded trials with mixed populations.
Agreements and disagreements with other studies or reviewsWe have located two published systematic reviews on the clinical efficacy of antibiotic for treating bone and joint infection including chronic osteomyelitis (Lazarini 2005; Stengel 2001). These differ from our review in terms of types of participants, types of infections and study designs included. In this review, we included just randomised and quasi-randomised controlled trials of adult patients with chronic osteomyelitis treated with systemic antibiotics. Stengel 2001 again just included randomised and quasi-randomised trials, but also included local antibiotic therapy and joint infection. Stengel 2001 concluded that no reliable inferences could be made from the data analysed for antibiotic therapy for osteomyelitis and septic arthritis.
A more recent review (Lazarini 2005) evaluated antibiotic treatment for acute and chronic osteomyelitis in children and adults and included uncontrolled studies. The authors' conclusion was that the optimal duration of antibiotic therapy remains undefined and that the data available could not determine the best agent, route or duration of antibiotic therapy.
Authors' conclusionsImplications for practiceThere is insufficient evidence to confirm the lack of statistically significant differences in remission and adverse events between oral versus parenteral administration of systemic antibiotics for treating chronic osteomyelitis in adults. There is either insufficient or no evidence from randomised trials to inform on other aspects such as duration of treatment or type of antibiotic.
Implications for researchThere is need for well designed adequately powered randomised controlled trials comparing antibiotic treatment for chronic osteomyelitis in terms of route of administration, therapy duration and adjusted for groups of bacteria (gram positive, gram negative, polymicrobial) and severity of disease. Such trials are likely to be multi-centre, should ensure adequate surgical debridement prior to starting the trial interventions; and actively record remission and adverse affects of treatment for at least 12 months.
AcknowledgementsWe are very grateful to Dr Karla Soares Weiser for her suggestions on the protocol and the Iberoamerican Cochrane Centre for assistance during the review. We are very grateful to Lesley Gillespie for searching for the studies and help during the editorial process, to Joanne Elliott for updating the search and to Lindsey
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 13
Elstub, Helen Handoll, Lesley Gillespie, Vicki Livingstone, Janet Wale and Geert Walenkamp for valuable comments and guidance provided during this review.
Contributions of authorsProf Lucieni Oliveira Conterno: responsible for screening studies for inclusion, data extraction and analysis, interpretation of results and writing of the review. Prof Conterno is the guarantor of the review.Prof Carlos Rodrigues da Silva Filho: responsible for screening studies for inclusion, data extraction and analysis, and interpretation of results.
Declarations of interestNone known.
Differences between protocol and reviewAdditions to 'Types of outcome measures':a) Treatment failure also includes early termination of treatment, such as for adverse effects or disease complications like amputation.b) Superinfection.
Although stipulated in the protocol, total quality scores from the methodological quality assessment tool were not calculated for the review.
Published notes
Characteristics of studiesCharacteristics of included studiesGentry 1990
Methods Randomised controlled trial. Participants, treatment providers, outcome assessors not blinded.
Follow-up was 12 months after the end of treatment.
Participants Two-site trial conducted in USA and Costa Rica (1980 to 1987).
Enrolled 67 adults with chronic osteomyelitis. Data available from 59: 51 male, 8 female; mean age 37 years. Location of infection (listed only for treatment failures): femur (6); ischium (1); tibia (6).
Interventions Debridement and remotion of all foreign material plus: oral ciprofloxacin (28 to 96 days) versus ceftazidime or nafcillin and aminoglycoside (parenteral administration) (8 to77 days).
Outcomes Clinical outcomes: all signs and symptoms related to infection absent on completion of therapy and at 12 months follow up; relapse of infection (same pathogen) or reinfection (different pathogen) within 12 months of completion of therapy. Adverse outcomes, superinfection.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 14
Notes Microbiologic diagnosis were obtained by open biopsy and were repeated during and after therapy completion. Excluded MRSA infection. S.aureus accounted for 25% of isolates and Pseudomonas aeruginosa for 21%.
Risk of bias table
Item Judgement Description
Allocation concealment? Unclear B - Unclear
Gentry 1991
Methods Randomised controlled trial. Participants, treatment providers, outcome assessors not blinded.
Follow-up was 18 months.
Participants Two-site trial conducted in USA and Costa Rica.
Enrolled 42 adults with chronic osteomyelitis. Data available from 33 (23 male, 10 female). Location of infection not mentioned.
Interventions Debridement if necessary plus: oral ofloxacin (21 to 86 days) versus cefazolin or ceftazidime (15 to 55 days) plus cloxacillin.
Outcomes Clinical outcomes: all signs and symptoms related to infection absent on completion of therapy and at 18 months of follow-up; relapse of infection (same pathogen) or reinfection (different pathogen) within 18 months of completion of therapy. Adverse outcomes, superinfection.
Notes Microbiologic diagnosis were obtained by open biopsy or aspirate.
S.aureus accounted for 40% of isolates.
Risk of bias table
Item Judgement Description
Allocation concealment? Unclear B - Unclear
Gomis 1999
Methods Randomised open-label controlled trial. Participants, treatment providers, outcome assessors not blinded.
Follow-up was 6 months.
Participants Trial conducted in Spain (1993-1996).
Enrolled 32 adults with chronic osteomyelitis (22 male and 10 female); mean age 59 years. Types of chronic osteomyelitis: contiguous (14); post traumatic (8); post surgical (4); associated with foot in diabetes patients (4); associated with a prosthetic device (1). Location of infection: tibia (9); foot (7); ankle (4); femur (4);
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 15
hand (3); radius (2); sacrum (1); femur and tibia (1); femur and sacrum (1).
Interventions Debridement as indicated plus oral ofloxacin (7 to 50 days) versus imipenem-cilastin (1 to 42 days). Clindamycin added if anaerobic organism isolated or suspected.
Outcomes Clinical outcomes: cure (resolution of all signs and symptoms of active infection at the end of therapy and follow up); failure (lack of apparent response to therapy or recurrence of signs and symptoms plus isolation of the same pathogen four to six weeks after discontinuation of antibacterial therapy).
Microbiologic response: eradication, presumptive eradication, eradication with relapse, persistence, superinfection, undetermined. Adverse events.
Notes Microbiologic diagnosis were obtained by open biopsy.
S. aureus accounted for 32% of isolates; Pseudomonas aeruginosa accounted for 17% of isolates.
Risk of bias table
Item Judgement Description
Allocation concealment? No C - Inadequate
Greenberg 1987
Methods Randomised controlled trial. Participants, treatment providers, outcome assessors not blinded.
Follow-up was from 1 to 13 months.
Participants Trial conducted in USA.
Enrolled 30 adults with chronic osteomyelitis (20 male and 10 female); mean age 52 years. Location of infection not mentioned.
Interventions Debridement not mentioned. Oral ciprofloxacin (44 to 73 days) versus another appropriate antimicrobial therapy (19 to 150 days).
Outcomes Clinical outcomes: cure (complete healing of the wound drainage site at the end of therapy); improvement (marked decrease in inflammation at the infection site, but without total healing); relapse (reappearance of signs and symptoms of infection at the infection site after resolution of signs and symptoms). Adverse events. Superinfection.
Notes Microbiologic diagnosis were obtained by open biopsy or aspiration from infected bone (seven obtained by swab). Pseudomonas aeruginosa accounted for 34% of isolates and S.aureus for 6%.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 16
Risk of bias table
Item Judgement Description
Allocation concealment? Unclear B - Unclear
Greenberg 2000
Methods Randomised controlled trial. Participants, treatment provider, outcome assessor not blinded.
Follow-up was from 0 to 36 months.
Participants Trial conducted in USA.
Enrolled 12 adults with chronic osteomyelitis. Together with 15 other patients given levofloxacin in an open trial: 20 male; 7 female; mean age 38 years. Location of infection: tibia (4); femur (3); knee (1); finger (1); ulna (1); fibula (1); disc (1).
Interventions Debridement plus oral ciprofloxacin (52 -110 days) versus oral lomefloxacin (2-59 days)
Outcomes Clinical outcomes: cure (healed wound without any drainage or swelling); improved (signs and symptoms markedly reduced at the end of therapy); failure (no response during the therapy). Adverse events.
Notes Microbiologic diagnosis were obtained by open biopsy or aspiration from infected bone. S.aureus accounted for 75% of isolates.
Patients from open trial were not included in the review.
Risk of bias table
Item Judgement Description
Allocation concealment? Unclear B - Unclear
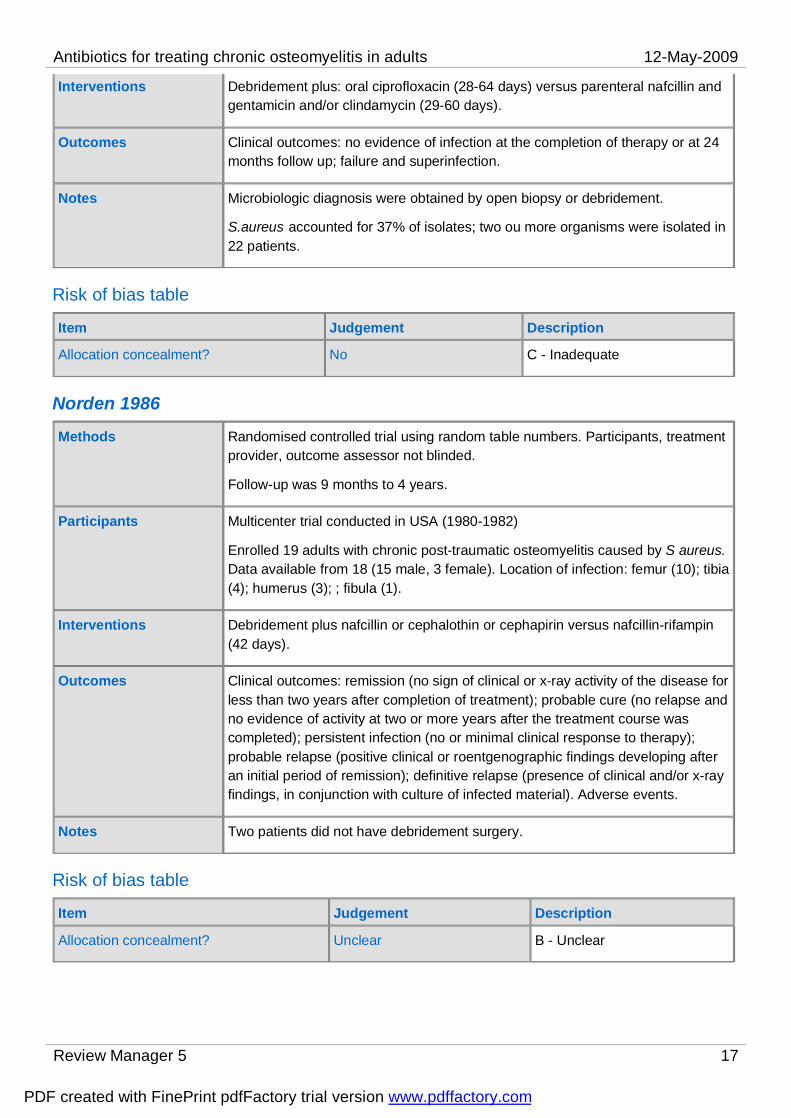
Mader 1990
Methods Quasi-randomised controlled trial. Participants were sequentially assigned. Participants, treatment provider, outcome assessor not blinded.
Follow-up was 24 to 39 months after the end of treatment.
Participants Trial conducted in USA
Enrolled 37 adults with post traumatic chronic osteomyelitis. Data available from 26 (19 male, 7 female); mean age 33 years. Location of infection: tibia (18); femur (4); ulna (1); hip (2) humerus (1). Classification using the Cierny-Mader system: type1 (2); type 2 (1); type 3 (11); type 4 (12) and the physiologic class of the host: A (16); B (10).
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 17
Interventions Debridement plus: oral ciprofloxacin (28-64 days) versus parenteral nafcillin and gentamicin and/or clindamycin (29-60 days).
Outcomes Clinical outcomes: no evidence of infection at the completion of therapy or at 24 months follow up; failure and superinfection.
Notes Microbiologic diagnosis were obtained by open biopsy or debridement.
S.aureus accounted for 37% of isolates; two ou more organisms were isolated in 22 patients.
Risk of bias table
Item Judgement Description
Allocation concealment? No C - Inadequate
Norden 1986
Methods Randomised controlled trial using random table numbers. Participants, treatment provider, outcome assessor not blinded.
Follow-up was 9 months to 4 years.
Participants Multicenter trial conducted in USA (1980-1982)
Enrolled 19 adults with chronic post-traumatic osteomyelitis caused by S aureus. Data available from 18 (15 male, 3 female). Location of infection: femur (10); tibia (4); humerus (3); ; fibula (1).
Interventions Debridement plus nafcillin or cephalothin or cephapirin versus nafcillin-rifampin (42 days).
Outcomes Clinical outcomes: remission (no sign of clinical or x-ray activity of the disease for less than two years after completion of treatment); probable cure (no relapse and no evidence of activity at two or more years after the treatment course was completed); persistent infection (no or minimal clinical response to therapy); probable relapse (positive clinical or roentgenographic findings developing after an initial period of remission); definitive relapse (presence of clinical and/or x-ray findings, in conjunction with culture of infected material). Adverse events.
Notes Two patients did not have debridement surgery.
Risk of bias table
Item Judgement Description
Allocation concealment? Unclear B - Unclear
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 18
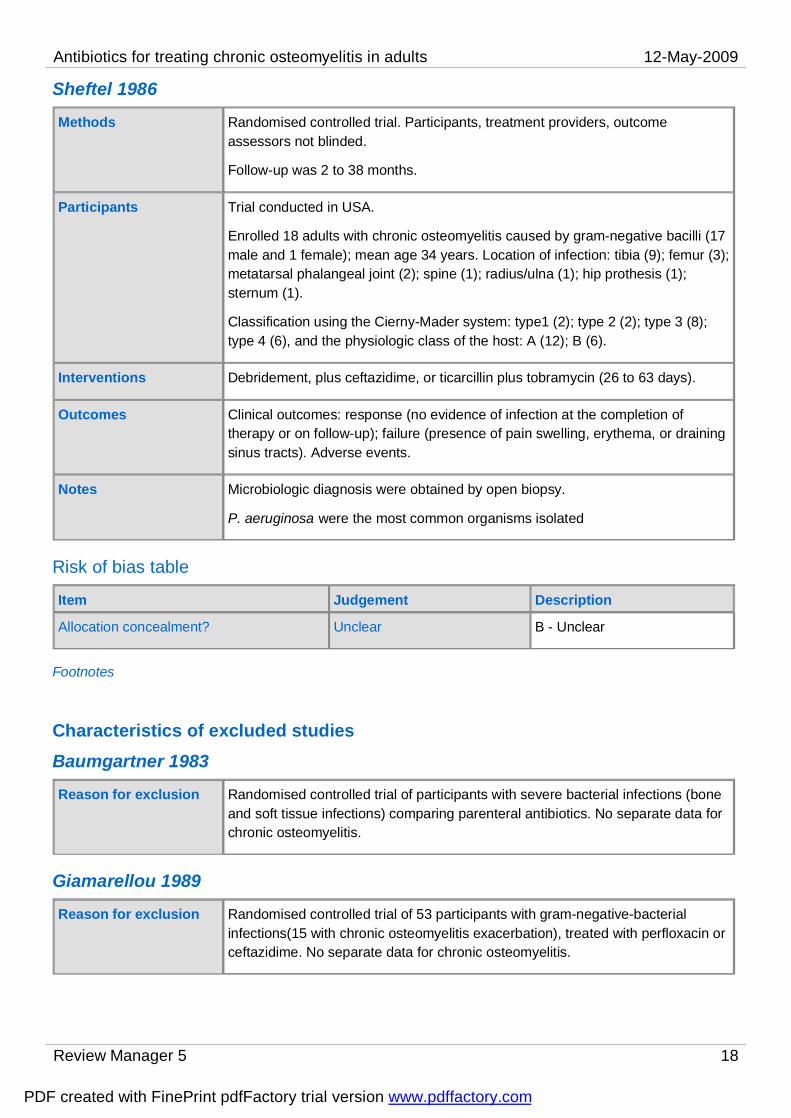
Sheftel 1986
Methods Randomised controlled trial. Participants, treatment providers, outcome assessors not blinded.
Follow-up was 2 to 38 months.
Participants Trial conducted in USA.
Enrolled 18 adults with chronic osteomyelitis caused by gram-negative bacilli (17 male and 1 female); mean age 34 years. Location of infection: tibia (9); femur (3); metatarsal phalangeal joint (2); spine (1); radius/ulna (1); hip prothesis (1); sternum (1).
Classification using the Cierny-Mader system: type1 (2); type 2 (2); type 3 (8); type 4 (6), and the physiologic class of the host: A (12); B (6).
Interventions Debridement, plus ceftazidime, or ticarcillin plus tobramycin (26 to 63 days).
Outcomes Clinical outcomes: response (no evidence of infection at the completion of therapy or on follow-up); failure (presence of pain swelling, erythema, or draining sinus tracts). Adverse events.
Notes Microbiologic diagnosis were obtained by open biopsy.
P. aeruginosa were the most common organisms isolated
Risk of bias table
Item Judgement Description
Allocation concealment? Unclear B - Unclear
Footnotes
Characteristics of excluded studiesBaumgartner 1983
Reason for exclusion Randomised controlled trial of participants with severe bacterial infections (bone and soft tissue infections) comparing parenteral antibiotics. No separate data for chronic osteomyelitis.
Giamarellou 1989
Reason for exclusion Randomised controlled trial of 53 participants with gram-negative-bacterial infections(15 with chronic osteomyelitis exacerbation), treated with perfloxacin or ceftazidime. No separate data for chronic osteomyelitis.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 19
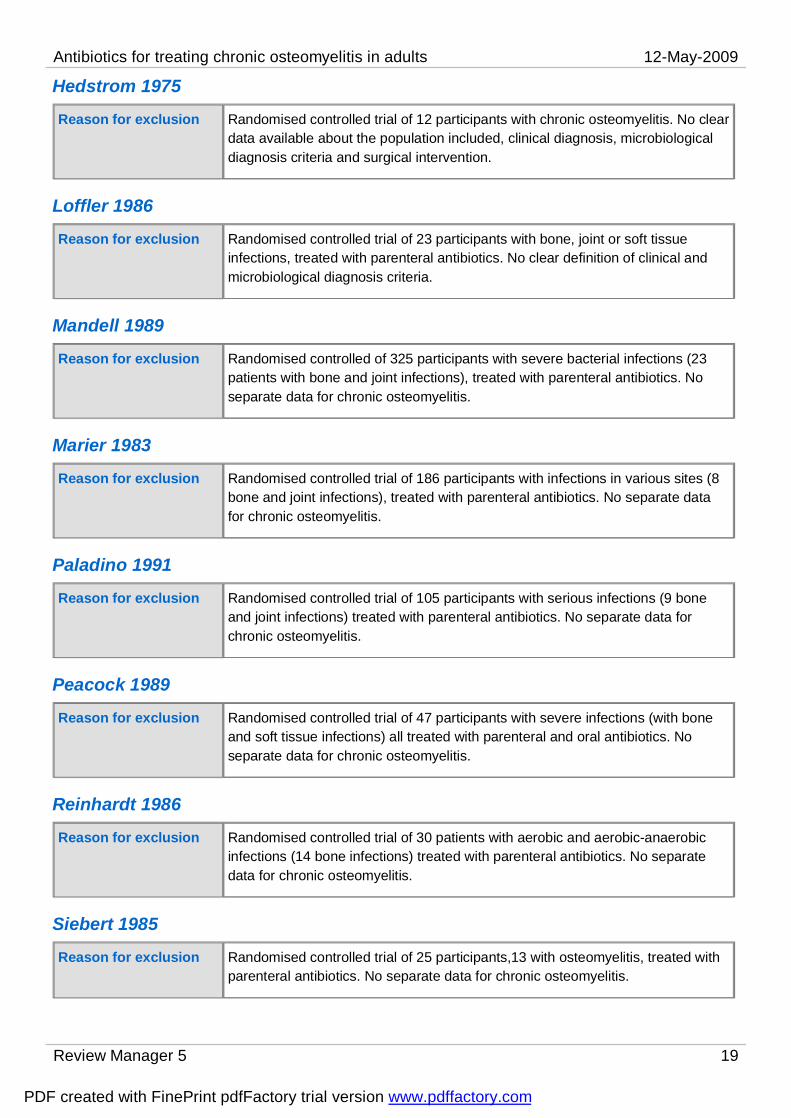
Hedstrom 1975
Reason for exclusion Randomised controlled trial of 12 participants with chronic osteomyelitis. No clear data available about the population included, clinical diagnosis, microbiological diagnosis criteria and surgical intervention.
Loffler 1986
Reason for exclusion Randomised controlled trial of 23 participants with bone, joint or soft tissue infections, treated with parenteral antibiotics. No clear definition of clinical and microbiological diagnosis criteria.
Mandell 1989
Reason for exclusion Randomised controlled of 325 participants with severe bacterial infections (23 patients with bone and joint infections), treated with parenteral antibiotics. No separate data for chronic osteomyelitis.
Marier 1983
Reason for exclusion Randomised controlled trial of 186 participants with infections in various sites (8 bone and joint infections), treated with parenteral antibiotics. No separate data for chronic osteomyelitis.
Paladino 1991
Reason for exclusion Randomised controlled trial of 105 participants with serious infections (9 bone and joint infections) treated with parenteral antibiotics. No separate data for chronic osteomyelitis.
Peacock 1989
Reason for exclusion Randomised controlled trial of 47 participants with severe infections (with bone and soft tissue infections) all treated with parenteral and oral antibiotics. No separate data for chronic osteomyelitis.
Reinhardt 1986
Reason for exclusion Randomised controlled trial of 30 patients with aerobic and aerobic-anaerobic infections (14 bone infections) treated with parenteral antibiotics. No separate data for chronic osteomyelitis.
Siebert 1985
Reason for exclusion Randomised controlled trial of 25 participants,13 with osteomyelitis, treated with parenteral antibiotics. No separate data for chronic osteomyelitis.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 20
Footnotes
Characteristics of studies awaiting classificationFootnotes
Characteristics of ongoing studiesFootnotes
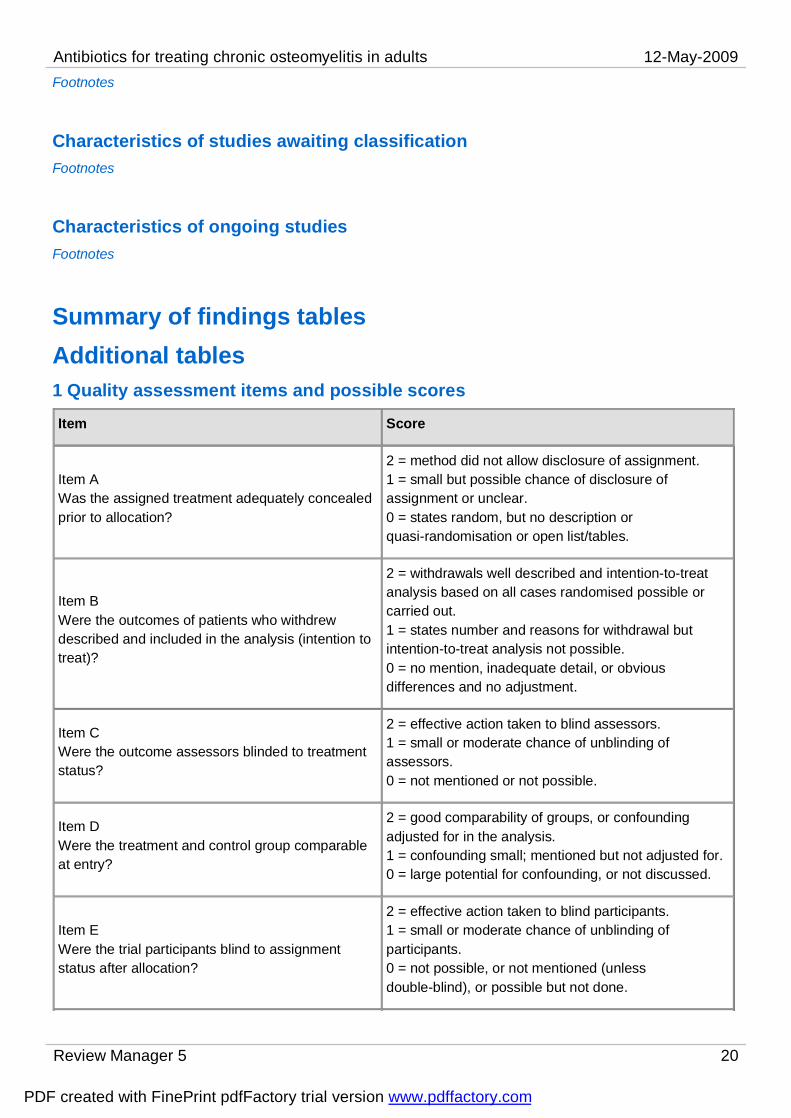
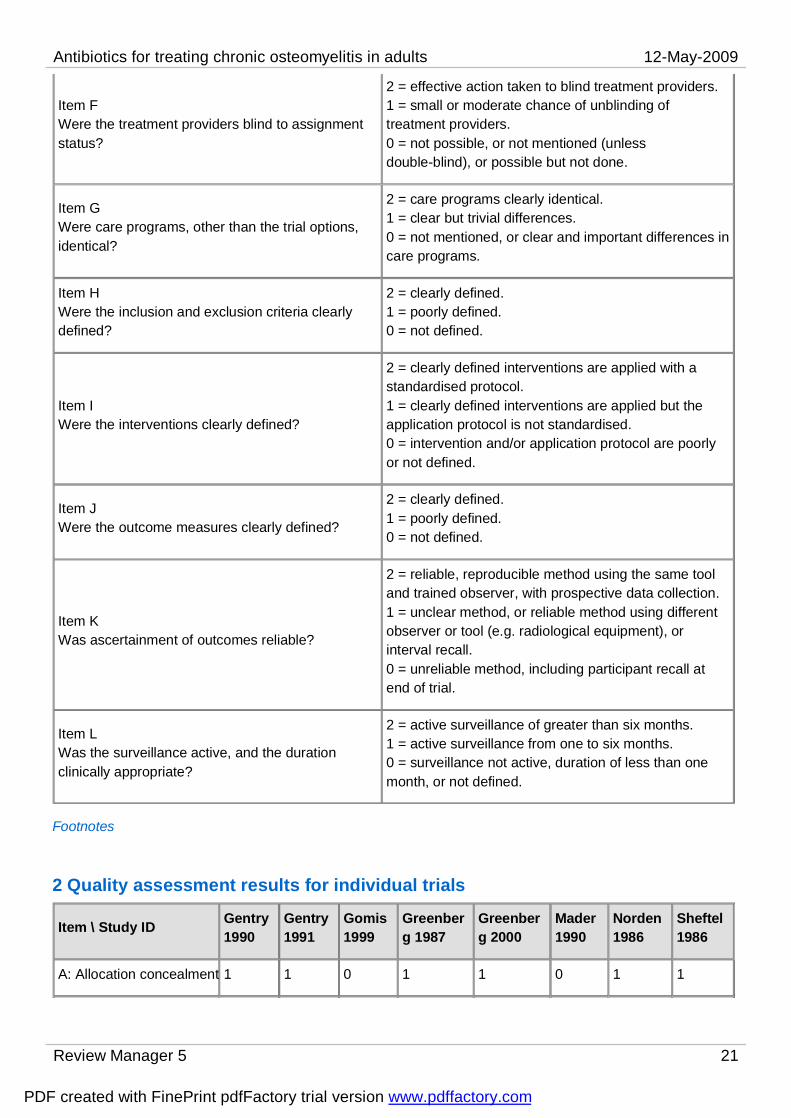
Summary of findings tablesAdditional tables1 Quality assessment items and possible scores
Item Score
Item AWas the assigned treatment adequately concealed prior to allocation?
2 = method did not allow disclosure of assignment.1 = small but possible chance of disclosure of assignment or unclear.0 = states random, but no description or quasi-randomisation or open list/tables.
Item BWere the outcomes of patients who withdrew described and included in the analysis (intention to treat)?
2 = withdrawals well described and intention-to-treat analysis based on all cases randomised possible or carried out.1 = states number and reasons for withdrawal but intention-to-treat analysis not possible.0 = no mention, inadequate detail, or obvious differences and no adjustment.
Item CWere the outcome assessors blinded to treatment status?
2 = effective action taken to blind assessors.1 = small or moderate chance of unblinding of assessors.0 = not mentioned or not possible.
Item DWere the treatment and control group comparable at entry?
2 = good comparability of groups, or confounding adjusted for in the analysis.1 = confounding small; mentioned but not adjusted for.0 = large potential for confounding, or not discussed.
Item EWere the trial participants blind to assignment status after allocation?
2 = effective action taken to blind participants.1 = small or moderate chance of unblinding of participants.0 = not possible, or not mentioned (unless double-blind), or possible but not done.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 21
Item FWere the treatment providers blind to assignment status?
2 = effective action taken to blind treatment providers.1 = small or moderate chance of unblinding of treatment providers.0 = not possible, or not mentioned (unless double-blind), or possible but not done.
Item GWere care programs, other than the trial options, identical?
2 = care programs clearly identical.1 = clear but trivial differences.0 = not mentioned, or clear and important differences in care programs.
Item HWere the inclusion and exclusion criteria clearly defined?
2 = clearly defined.1 = poorly defined.0 = not defined.
Item IWere the interventions clearly defined?
2 = clearly defined interventions are applied with a standardised protocol.1 = clearly defined interventions are applied but the application protocol is not standardised.0 = intervention and/or application protocol are poorly or not defined.
Item JWere the outcome measures clearly defined?
2 = clearly defined.1 = poorly defined.0 = not defined.
Item KWas ascertainment of outcomes reliable?
2 = reliable, reproducible method using the same tool and trained observer, with prospective data collection.1 = unclear method, or reliable method using different observer or tool (e.g. radiological equipment), or interval recall.0 = unreliable method, including participant recall at end of trial.
Item LWas the surveillance active, and the duration clinically appropriate?
2 = active surveillance of greater than six months.1 = active surveillance from one to six months.0 = surveillance not active, duration of less than one month, or not defined.
Footnotes
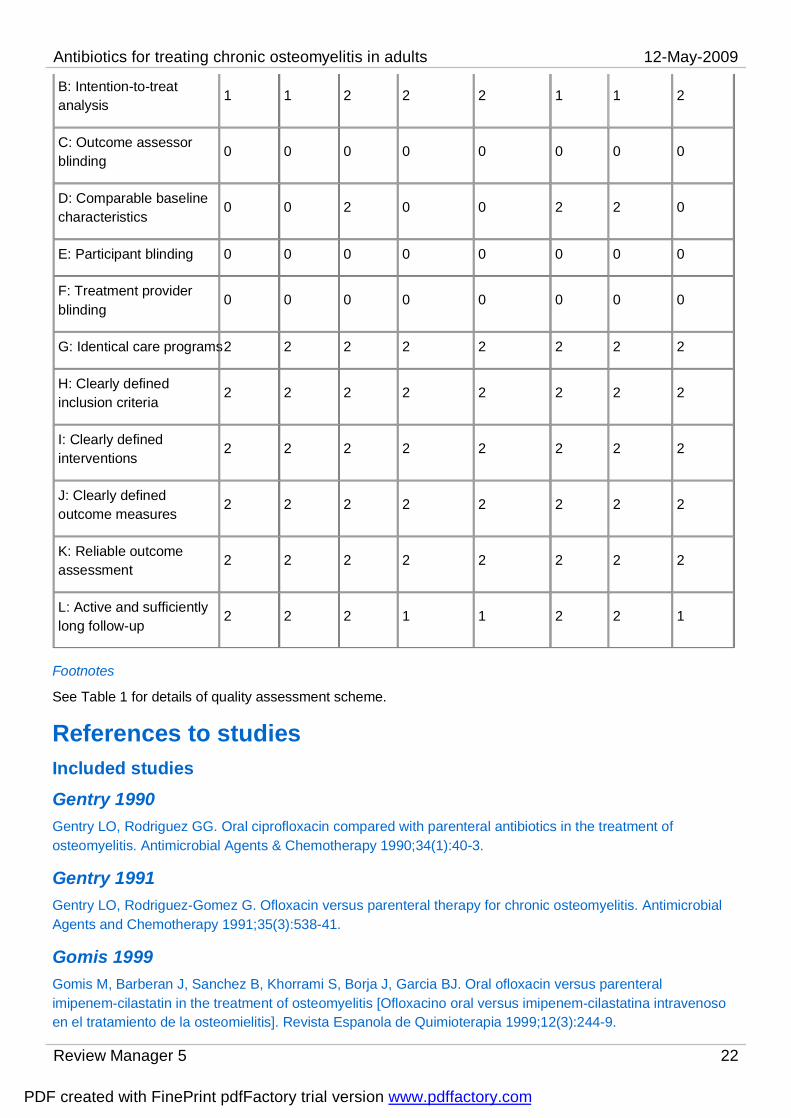
2 Quality assessment results for individual trials
Item \ Study ID Gentry 1990
Gentry 1991
Gomis 1999
Greenberg 1987
Greenberg 2000
Mader 1990
Norden 1986
Sheftel 1986
A: Allocation concealment 1 1 0 1 1 0 1 1
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 22
B: Intention-to-treat analysis
1 1 2 2 2 1 1 2
C: Outcome assessor blinding
0 0 0 0 0 0 0 0
D: Comparable baseline characteristics
0 0 2 0 0 2 2 0
E: Participant blinding 0 0 0 0 0 0 0 0
F: Treatment provider blinding
0 0 0 0 0 0 0 0
G: Identical care programs2 2 2 2 2 2 2 2
H: Clearly defined inclusion criteria
2 2 2 2 2 2 2 2
I: Clearly defined interventions
2 2 2 2 2 2 2 2
J: Clearly defined outcome measures
2 2 2 2 2 2 2 2
K: Reliable outcome assessment
2 2 2 2 2 2 2 2
L: Active and sufficiently long follow-up
2 2 2 1 1 2 2 1
Footnotes
See Table 1 for details of quality assessment scheme.
References to studiesIncluded studiesGentry 1990Gentry LO, Rodriguez GG. Oral ciprofloxacin compared with parenteral antibiotics in the treatment of osteomyelitis. Antimicrobial Agents & Chemotherapy 1990;34(1):40-3.
Gentry 1991Gentry LO, Rodriguez-Gomez G. Ofloxacin versus parenteral therapy for chronic osteomyelitis. Antimicrobial Agents and Chemotherapy 1991;35(3):538-41.
Gomis 1999Gomis M, Barberan J, Sanchez B, Khorrami S, Borja J, Garcia BJ. Oral ofloxacin versus parenteral imipenem-cilastatin in the treatment of osteomyelitis [Ofloxacino oral versus imipenem-cilastatina intravenoso en el tratamiento de la osteomielitis]. Revista Espanola de Quimioterapia 1999;12(3):244-9.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com

Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 23
Greenberg 1987Greenberg RN, Tice AD, Marsh PK, Craven PC, Reilly PM, Bollinger M et al. Randomized trial of ciprofloxacin compared with other antimicrobial therapy in the treatment of osteomyelitis. American Journal of Medicine 1987;82(4A):266-9.
Greenberg 2000Greenberg RN, Newman MT, Shariaty S, Pectol RW. Ciprofloxacin, lomefloxacin, or levofloxacin as treatment for chronic osteomyelitis. Antimicrobial Agents & Chemotherapy 2000;44(1):164-6.
Mader 1990Mader JT, Cantrell JS, Calhoun J. Oral ciprofloxacin compared with standard parenteral antibiotic therapy for chronic osteomyelitis in adults. Journal of Bone Joint Surgery - American Volume 1990;72(1):104-10.
Norden 1986* Norden CW, Bryant R, Palmer D, Montgomerie JZ, Wheat J. Chronic osteomyelitis caused by Staphylococcus aureus: controlled clinical trial of nafcillin therapy and nafcillin-rifampin therapy. Southern Medical Journal 1986;79(8):947-51.
Norden CW, Fierer J, Bryant RE. Chronic Staphylococcus osteomyelitis: treatment with regimens containing rifampin. Reviews of Infectious Diseases 1983;5 Suppl 3:S495-501.
Sheftel 1986Sheftel TG, Mader JT. Randomized evaluation of ceftazidime or ticarcillin and tobramycin for the treatment of osteomyelitis caused by gram-negative bacilli. Antimicrobial Agents & Chemotherapy 1986;29(1):112-5.
Excluded studiesBaumgartner 1983Baumgartner JD, Glauser MP. Comparative study of imipenem in severe infections. Journal of Antimicrobial Chemotherapy 1983;12 Suppl D:141-8.
Giamarellou 1989Giamarellou H, Perdikaris G, Galanakis N, Davoulos G, Mandragos K, Sfikakis P. Pefloxacin versus ceftazidime in the treatment of a variety of gram-negative-bacterial infections. Antimicrobial Agents & Chemotherapy 1989;33(8):1362-7.
Hedstrom 1975Hedstrom SA. Treatment of chronic staphylococcal osteomyelitis with cloxacillin and dicloxacillin - a comparative study in 12 patients. Scandinavian Journal of Infectious Diseases 1975;7(1):55-7.
Loffler 1986Loffler L, Bauernfeind A, Keyl W, Hoffstedt B, Piergies A, Lenz W. An open, comparative study of sulbactam plus ampicillin vs. cefotaxime as initial therapy for serious soft tissue and bone and joint infections. Reviews of Infectious Diseases 1986;8 Suppl 5:S593-8.
Loffler L, Bauernfeind A, Keyl W. Sulbactam/ampicillin versus cefotaxime as initial therapy in serious soft tissue, joint and bone infections. Drugs 1988;35(Suppl 7):46-52.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 24
Mandell 1989Mandell LA, Bergeron MG, Ronald AR, Vega C, Harding G, Saginur R et al. Once-day therapy with ceftriaxone compared with daily multiple-dose therapy with cefotaxime for serious bacterial infections: a randomized, double-blind study. Journal of Infectious Diseases 1989;160(3):433-41.
Marier 1983Marier RL, McCloskey RV, Dickenson G, Sanders CV, Aldridge KE, Hoffman T et al. Comparative clinical trial of imipenem-cilastatin (N-formimidoyl-thienamycin-dehydropeptidase inhibitor) and cefazolin. Journal of Antimicrobial Chemotherapy 1983;12(Suppl D):133-9.
Paladino 1991Paladino JA, Sperry HE, Backes JM, Gelber JA, Serrianne,DJ, Cumbo TJ et al. Clinical and economic evaluation of oral ciprofloxacin after an abbreviated course of intravenous antibiotics. American Journal of Medicine 1991;91(5):462-70.
Peacock 1989Peacock JE, Pegram PS, Weber SF, Leone PA. Prospective, randomized comparison of sequential intravenous followed by oral ciprofloxacin with intravenous ceftazidime in the treatment of serious infections. American Journal of Medicine 1989;87(Nov 30 Suppl):185S-90S.
Reinhardt 1986Reinhardt JF, Jonnston L, Ruane P, Johnson CC, Ingram-drake L, MacDonald K et al. A randomized, double-blind comparison of sulbactam/ampicillin and clindamycin for the treatment of aerobic and aerobic-anaerobic infections. Reviews of Infectious Diseases 1986;8(Suppl 5):S569-75.
Siebert 1985Siebert WT, Kopp PE. Ticarcillin plus clavulanic acid versus moxalactam therapy of osteomyelitis, septic arthritis, and skin and soft tissue infections. American Journal of Medicine 1985;79(5B):141-5.
Studies awaiting classificationOngoing studies
Other referencesAdditional referencesBamberger 1993Bamberger DM. Osteomyelitis. A commonsense approach to antibiotic and surgical treatment. Postgraduate Medicine 1993;94(5):177-82, 184.
Bourguignat 1996Bourguignat A, Ferard G, Jenny JY, Gaudias J, Kempf I. Diagnostic value of C-reactive protein and transthyretin in bone infections of lower limb. Clinica Chimica Acta 1996;255(1):27-38.
Carek 2001Carek PJ, Dickerson LM, Sack JL. Diagnosis and management of osteomyelitis. American Family Physician 2001;63(12):2413-20.
PDF created with FinePrint pdfFactory trial version www.pdffactory.com

Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 25
Ciampolini 2000Ciampolini J, Harding KG. Pathophysiology of chronic bacterial osteomyelitis. Why do antibiotics fail so often? Postgraduate Medical Journal 2000;76(898):479-83.
Cierny 2003Cierny G 3rd, Mader JT, Penninck JJ. A clinical staging system for adult osteomyelitis. Clinical Orthopaedic and Related Research 2003;414:7-24.
Cunha 2002Cunha BA. Osteomyelitis in elderly patients. Clinical Infectious Diseases 2002;35(3):287-93.
Eckardt 1994Eckardt JJ, Wirganowicz PZ, Mar T. An aggressive surgical approach to the management of chronic osteomyelitis. Clinical Orthopaedics and Related Research 1994;(298):229-39.
Ferard 2002Ferard G, Gaudias J, Bourguignat A, Ingenbleek Y. C-reactive protein to transthyretin ratio for the early diagnosis and follow-up of postoperative infection. Clinical Chemistry and Laboratory Medicine 2002;40(12):1334-8.
Greenberg 2000Greenberg RN, Newman MT, Shariaty S, Pectol RW. Ciprofloxacin, lomefloxacin, or levofloxacin as treatment for chronic osteomyelitis. Antimicrobial Agents & Chemotherapy 2000;44(1):164-6.
Gristina 1990Gristina AG, Naylor PT, Myrvik QN. Musculoskeletal infection, microbial adhesion, and antibiotic resistance. Infectious Disease Clinics of North America 1990;4(3):391-408.
Haas 1996Haas DW, McAndrew MP. Bacterial osteomyelitis in adults: evolving considerations in diagnosis and treatment. American Journal of Medicine 1996;101(5):550-61.
Higgins 2003Higgins JP, Tompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003;327(7414):557-60.
Higgins 2005Higgins JPT, Green S, editors. Assessement of study quality. Cochrane Handbook for Systematic Reviews of Interventions 4.2.5 [update May 2005)]; Section 6. In: The Cochrane Library 2005, Issue 3. Chichester, UK: John Wiley & Sons, Ltd.
Higgins 2006Higgins JPT, Green S, editors. Highly sensitive search strategies for identifying reports of randomized controlled trials in MEDLINE. Cochrane Handbook for Systematic Reviews of Interventions 4.2.6 [updated September 2006]; Appendix 5b. www.cochrane.org/resources/handbook/hbook.htm (accessed 01 May 2007).
Holtom 1999Holtom PD, Smith AM. Introduction to adult posttraumatic osteomyelitis of the tibia. Clinical Orthopaedics and
PDF created with FinePrint pdfFactory trial version www.pdffactory.com

Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 26
Related Research 1999;(360):6-13.
Huber 2002Huber AM, Lam PY, Duffy CM, Yeung RS, Ditchfield M, Laxer D et al. Chronic recurrent multifocal osteomyelitis: clinical outcomes after more than five years of follow-up. Journal of Pediatrics 2002;141(2):198-203.
Lazarini 2005Lazzarini L, Lipsky BA, Mader JT. Antibiotic treatment of osteomyelitis: what have we learned from 30 years of clinical trials? International Journal of Infectious Diseases 2005;9(3):127-38.
Lazzarini 2002Lazzarini L, De Lalla F, Mader JT. Long bone osteomyelitis. Current Infectious Disease Reports 2002;4(5):439-45.
Lew 1997Lew DP, Waldvogel FA. Osteomyelitis. New England Journal of Medicine 1997;336(14):999-1007.
Mader 1992Mader JT, Norden C, Nelson JD, Calandra GB. Evaluation of new anti-infective drugs for the treatment of osteomyelitis in adults. Infectious Diseases Society of America and the Food and Drug Administration. Clinical Infectious Diseases 1992;15(Suppl 1):S155-61.
Mader 1993Mader JT, Landon GC, Calhoun J. Antimicrobial treatment of osteomyelitis. Clinical Orthopaedics and Related Research 1993;(295):87-95.
Mader 1997aMader JT, Shirtliff M, Calhoun JH. Staging and staging application in osteomyelitis. Clinical Infectious Diseases 1997;25(6):1303-9.
Mader 1997bMader JT, Mohan D, Calhoun J. A practical guide to the diagnosis and management of bone and joint infections. Drugs 1997;54(2):253-64.
Mader 1999aMader JT, Shirtliff ME, Bergquist SC, Calhoun J. Antimicrobial treatment of chronic osteomyelitis. Clinical Orthopaedics and Related Research 1999;(360):47-65.
Mader 1999bMader JT, Cripps MW, Calhoun JH. Adult posttraumatic osteomyelitis of the tibia. Clinical Orthopaedics and Related Research 1999;(360):14-21.
Mader 2001Mader JT, Wang J, Calhoun JH. Antibiotic therapy for musculoskeletal infections. The Journal of Bone & Joint Surgery - American Volume 2001;83(12):1878-90.
Rissing 1997Rissing JP. Antimicrobial therapy for chronic osteomyelitis in adults: role of the quinolones. Clinical Infectious
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 27
Diseases 1997;25(6):1327-33.
Simpson 2001Simpson AH, Deakin M, Latham JM. Chronic osteomyelitis. The effect of the extent of surgical resection on infection-free survival. Journal of Bone & Joint Surgery - British Volume 2001;83(3):403-7.
Stengel 2001Stengel D, Bauwens K, Sehouli J, Ekkernkamp A, Porzsolt F. Systematic review and meta-analysis of antibiotic therapy for bone and joint infections. The Lancet Infectious Diseases 2001;1(3):175-88.
Swiontkoski 1990Swiontkowski MF. Surgical approaches in osteomyelitis: use of laser Doppler flowmetry to determine nonviable bone. Infectious Disease Clinics of North America 1990;4(3):501-12.
Swiontkowski 1999Swiontkowski MF, Hanel DP, Vedder NB, Schwappach JR. A comparison of short- and long-term intravenous antibiotic therapy in the postoperative management of adult osteomyelitis. Journal of Bone and Joint Surgery - British Volume 1999;81(6):1046-50.
Waldvogel 1970Waldvogel FA, Medoff G, Swartz MN. Treatment of osteomyelitis. New England Journal of Medicine 1970;283(15):822.
Waldvogel 1980Waldvogel FA, Papageorgiou PS. Osteomyelitis: the past decade. New England Journal of Medicine 1980;303(7):360-70.
Walenkamp 1997Walenkamp GHIM. Chronic osteomyelitis. Acta Orthopaedica Scandinavica 1997;68(5):497-506.
Other published versions of this review
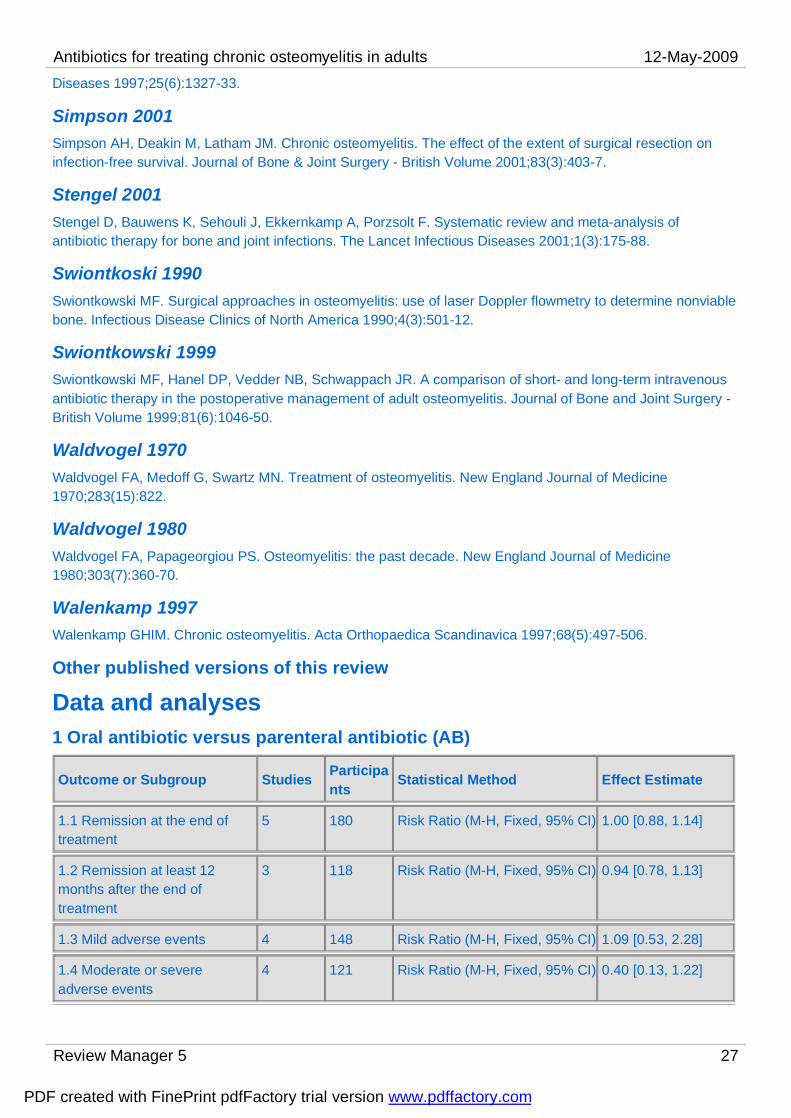
Data and analyses1 Oral antibiotic versus parenteral antibiotic (AB)
Outcome or Subgroup Studies Participants
Statistical Method Effect Estimate
1.1 Remission at the end of treatment
5 180 Risk Ratio (M-H, Fixed, 95% CI) 1.00 [0.88, 1.14]
1.2 Remission at least 12 months after the end of treatment
3 118 Risk Ratio (M-H, Fixed, 95% CI) 0.94 [0.78, 1.13]
1.3 Mild adverse events 4 148 Risk Ratio (M-H, Fixed, 95% CI) 1.09 [0.53, 2.28]
1.4 Moderate or severe adverse events
4 121 Risk Ratio (M-H, Fixed, 95% CI) 0.40 [0.13, 1.22]
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 28
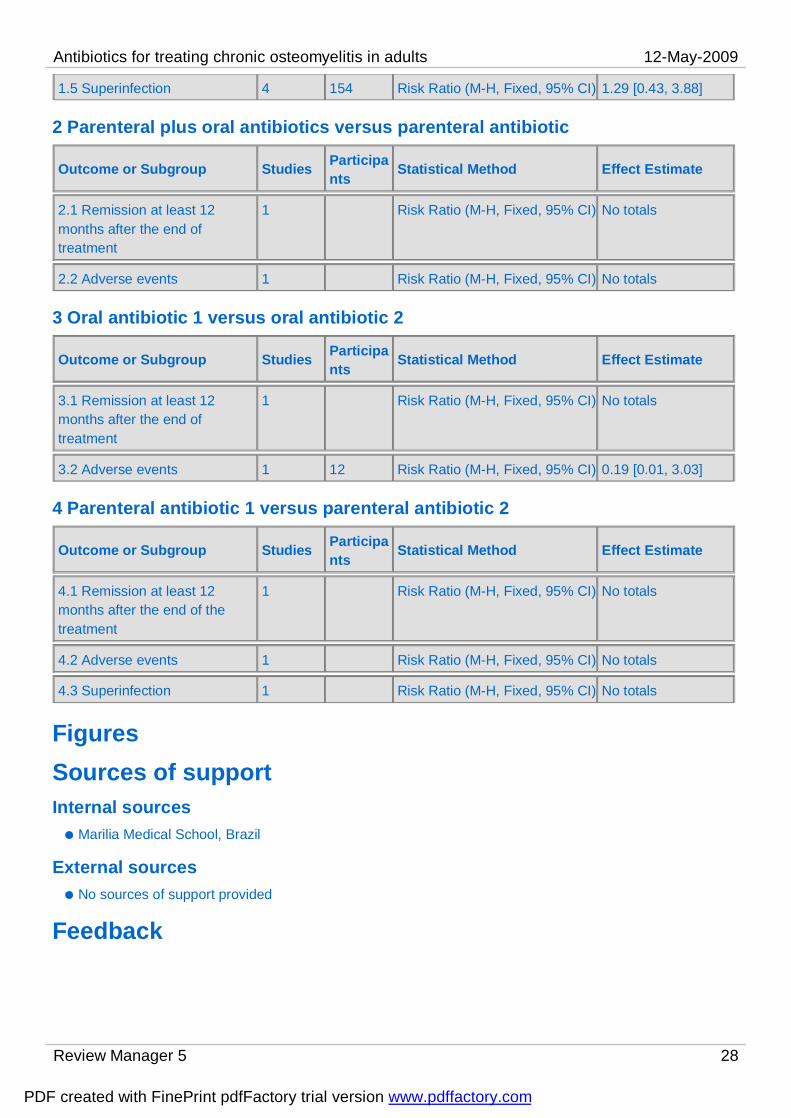
1.5 Superinfection 4 154 Risk Ratio (M-H, Fixed, 95% CI) 1.29 [0.43, 3.88]
2 Parenteral plus oral antibiotics versus parenteral antibiotic
Outcome or Subgroup Studies Participants
Statistical Method Effect Estimate
2.1 Remission at least 12 months after the end of treatment
1 Risk Ratio (M-H, Fixed, 95% CI) No totals
2.2 Adverse events 1 Risk Ratio (M-H, Fixed, 95% CI) No totals
3 Oral antibiotic 1 versus oral antibiotic 2
Outcome or Subgroup Studies Participants
Statistical Method Effect Estimate
3.1 Remission at least 12 months after the end of treatment
1 Risk Ratio (M-H, Fixed, 95% CI) No totals
3.2 Adverse events 1 12 Risk Ratio (M-H, Fixed, 95% CI) 0.19 [0.01, 3.03]
4 Parenteral antibiotic 1 versus parenteral antibiotic 2
Outcome or Subgroup Studies Participants
Statistical Method Effect Estimate
4.1 Remission at least 12 months after the end of the treatment
1 Risk Ratio (M-H, Fixed, 95% CI) No totals
4.2 Adverse events 1 Risk Ratio (M-H, Fixed, 95% CI) No totals
4.3 Superinfection 1 Risk Ratio (M-H, Fixed, 95% CI) No totals
FiguresSources of supportInternal sources
Marilia Medical School, Brazil
External sourcesNo sources of support provided
Feedback
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 29
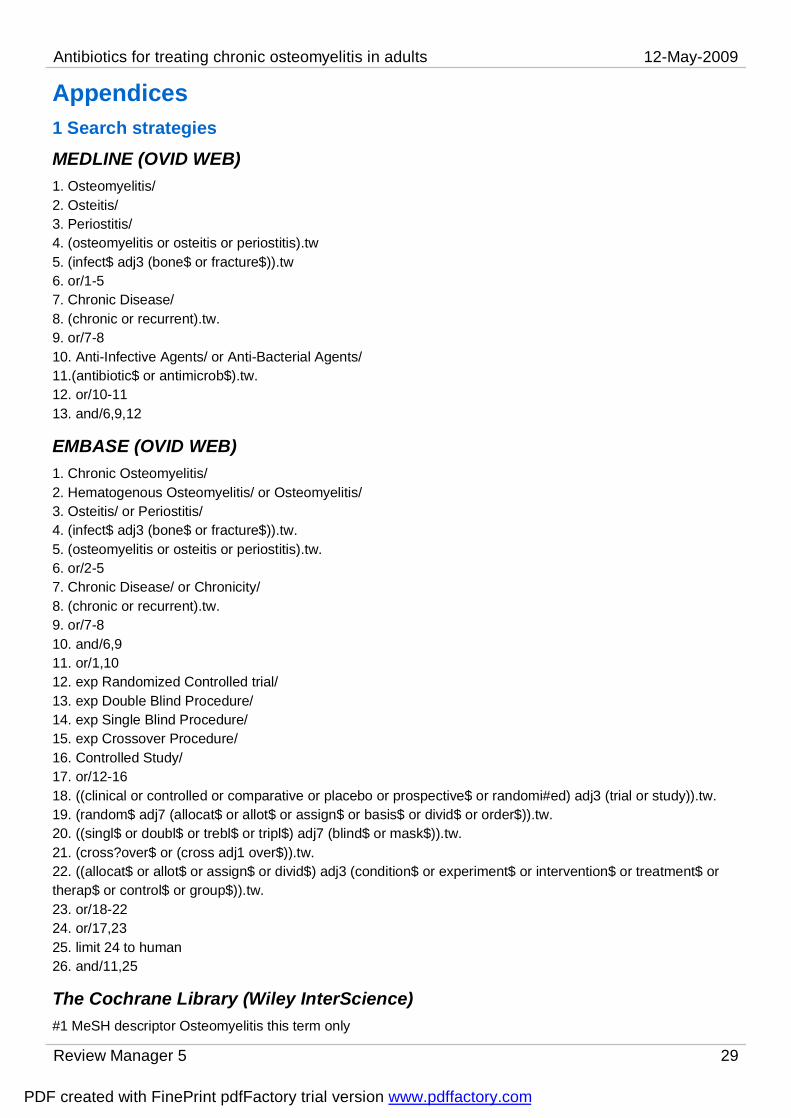
Appendices1 Search strategiesMEDLINE (OVID WEB)1. Osteomyelitis/2. Osteitis/3. Periostitis/4. (osteomyelitis or osteitis or periostitis).tw5. (infect$ adj3 (bone$ or fracture$)).tw6. or/1-57. Chronic Disease/8. (chronic or recurrent).tw.9. or/7-810. Anti-Infective Agents/ or Anti-Bacterial Agents/11.(antibiotic$ or antimicrob$).tw.12. or/10-1113. and/6,9,12
EMBASE (OVID WEB)1. Chronic Osteomyelitis/2. Hematogenous Osteomyelitis/ or Osteomyelitis/3. Osteitis/ or Periostitis/4. (infect$ adj3 (bone$ or fracture$)).tw.5. (osteomyelitis or osteitis or periostitis).tw.6. or/2-57. Chronic Disease/ or Chronicity/8. (chronic or recurrent).tw.9. or/7-810. and/6,911. or/1,1012. exp Randomized Controlled trial/13. exp Double Blind Procedure/14. exp Single Blind Procedure/15. exp Crossover Procedure/16. Controlled Study/17. or/12-1618. ((clinical or controlled or comparative or placebo or prospective$ or randomi#ed) adj3 (trial or study)).tw.19. (random$ adj7 (allocat$ or allot$ or assign$ or basis$ or divid$ or order$)).tw.20. ((singl$ or doubl$ or trebl$ or tripl$) adj7 (blind$ or mask$)).tw.21. (cross?over$ or (cross adj1 over$)).tw.22. ((allocat$ or allot$ or assign$ or divid$) adj3 (condition$ or experiment$ or intervention$ or treatment$ or therap$ or control$ or group$)).tw.23. or/18-2224. or/17,2325. limit 24 to human26. and/11,25
The Cochrane Library (Wiley InterScience)#1 MeSH descriptor Osteomyelitis this term only
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 30
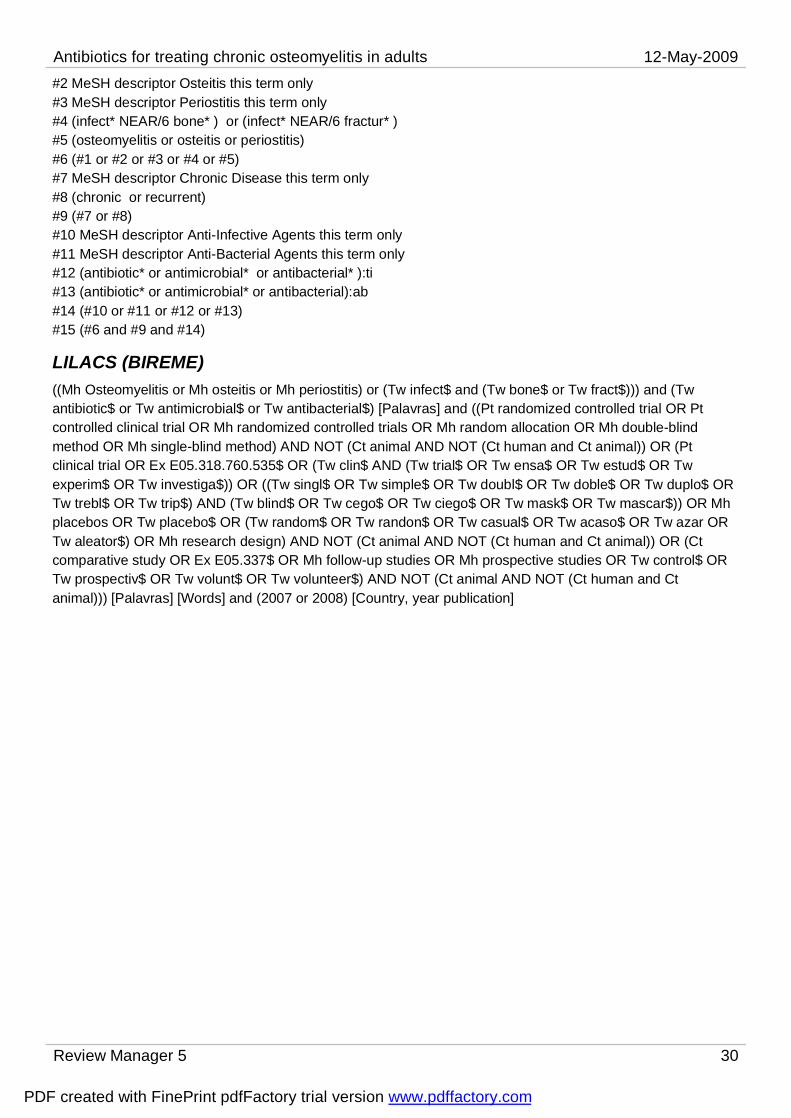
#2 MeSH descriptor Osteitis this term only#3 MeSH descriptor Periostitis this term only#4 (infect* NEAR/6 bone* ) or (infect* NEAR/6 fractur* )#5 (osteomyelitis or osteitis or periostitis)#6 (#1 or #2 or #3 or #4 or #5)#7 MeSH descriptor Chronic Disease this term only#8 (chronic or recurrent)#9 (#7 or #8)#10 MeSH descriptor Anti-Infective Agents this term only#11 MeSH descriptor Anti-Bacterial Agents this term only#12 (antibiotic* or antimicrobial* or antibacterial* ):ti#13 (antibiotic* or antimicrobial* or antibacterial):ab#14 (#10 or #11 or #12 or #13)#15 (#6 and #9 and #14)
LILACS (BIREME)((Mh Osteomyelitis or Mh osteitis or Mh periostitis) or (Tw infect$ and (Tw bone$ or Tw fract$))) and (Tw antibiotic$ or Tw antimicrobial$ or Tw antibacterial$) [Palavras] and ((Pt randomized controlled trial OR Pt controlled clinical trial OR Mh randomized controlled trials OR Mh random allocation OR Mh double-blind method OR Mh single-blind method) AND NOT (Ct animal AND NOT (Ct human and Ct animal)) OR (Pt clinical trial OR Ex E05.318.760.535$ OR (Tw clin$ AND (Tw trial$ OR Tw ensa$ OR Tw estud$ OR Tw experim$ OR Tw investiga$)) OR ((Tw singl$ OR Tw simple$ OR Tw doubl$ OR Tw doble$ OR Tw duplo$ OR Tw trebl$ OR Tw trip$) AND (Tw blind$ OR Tw cego$ OR Tw ciego$ OR Tw mask$ OR Tw mascar$)) OR Mh placebos OR Tw placebo$ OR (Tw random$ OR Tw randon$ OR Tw casual$ OR Tw acaso$ OR Tw azar OR Tw aleator$) OR Mh research design) AND NOT (Ct animal AND NOT (Ct human and Ct animal)) OR (Ct comparative study OR Ex E05.337$ OR Mh follow-up studies OR Mh prospective studies OR Tw control$ OR Tw prospectiv$ OR Tw volunt$ OR Tw volunteer$) AND NOT (Ct animal AND NOT (Ct human and Ct animal))) [Palavras] [Words] and (2007 or 2008) [Country, year publication]
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
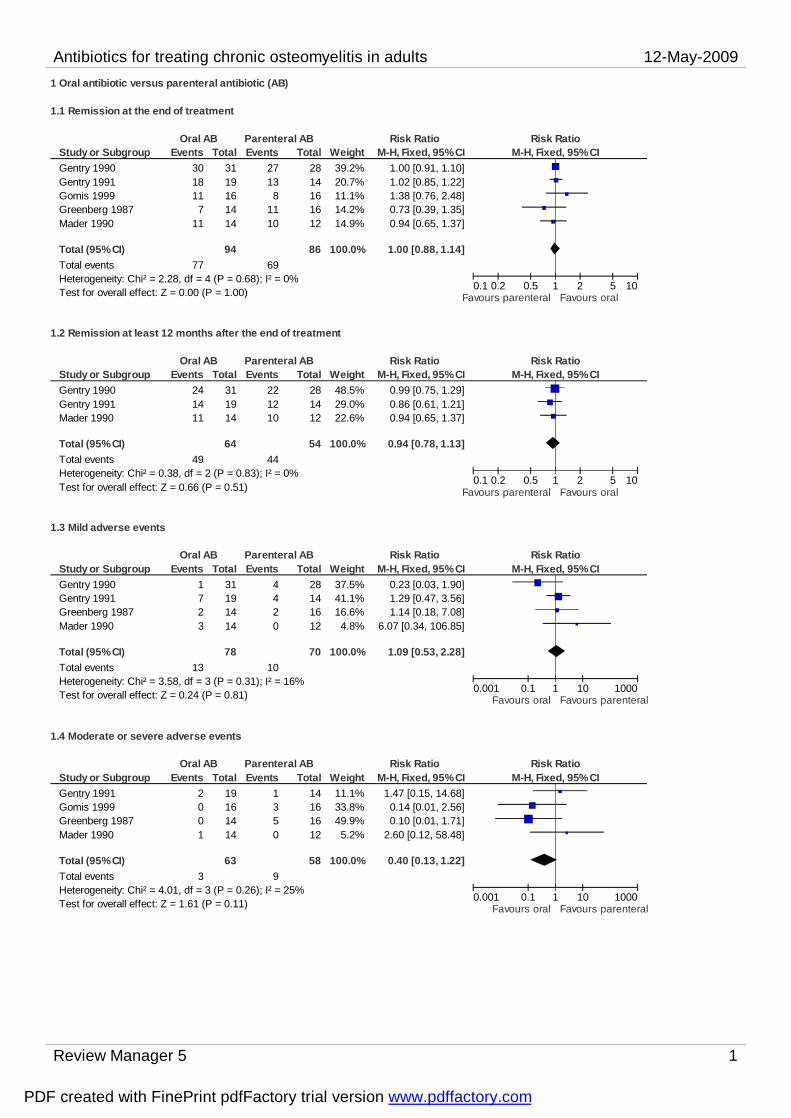
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 1
1 Oral antibiotic versus parenteral antibiotic (AB)
1.1 Remission at the end of treatment
Study or SubgroupGentry 1990Gentry 1991Gomis 1999Greenberg 1987Mader 1990
Total (95% CI)Total eventsHeterogeneity: Chi² = 2.28, df = 4 (P = 0.68); I² = 0%Test for overall effect: Z = 0.00 (P = 1.00)
Events3018117
11
77
Total3119161414
94
Events27138
1110
69
Total2814161612
86
Weight39.2%20.7%11.1%14.2%14.9%
100.0%
M-H, Fixed, 95% CI1.00 [0.91, 1.10]1.02 [0.85, 1.22]1.38 [0.76, 2.48]0.73 [0.39, 1.35]0.94 [0.65, 1.37]
1.00 [0.88, 1.14]
Oral AB Parenteral AB Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10Favours parenteral Favours oral
1.2 Remission at least 12 months after the end of treatment
Study or SubgroupGentry 1990Gentry 1991Mader 1990
Total (95% CI)Total eventsHeterogeneity: Chi² = 0.38, df = 2 (P = 0.83); I² = 0%Test for overall effect: Z = 0.66 (P = 0.51)
Events241411
49
Total311914
64
Events221210
44
Total281412
54
Weight48.5%29.0%22.6%
100.0%
M-H, Fixed, 95% CI0.99 [0.75, 1.29]0.86 [0.61, 1.21]0.94 [0.65, 1.37]
0.94 [0.78, 1.13]
Oral AB Parenteral AB Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10Favours parenteral Favours oral
1.3 Mild adverse events
Study or SubgroupGentry 1990Gentry 1991Greenberg 1987Mader 1990
Total (95% CI)Total eventsHeterogeneity: Chi² = 3.58, df = 3 (P = 0.31); I² = 16%Test for overall effect: Z = 0.24 (P = 0.81)
Events1723
13
Total31191414
78
Events4420
10
Total28141612
70
Weight37.5%41.1%16.6%4.8%
100.0%
M-H, Fixed, 95% CI0.23 [0.03, 1.90]1.29 [0.47, 3.56]1.14 [0.18, 7.08]
6.07 [0.34, 106.85]
1.09 [0.53, 2.28]
Oral AB Parenteral AB Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.001 0.1 1 10 1000Favours oral Favours parenteral
1.4 Moderate or severe adverse events
Study or SubgroupGentry 1991Gomis 1999Greenberg 1987Mader 1990
Total (95% CI)Total eventsHeterogeneity: Chi² = 4.01, df = 3 (P = 0.26); I² = 25%Test for overall effect: Z = 1.61 (P = 0.11)
Events2001
3
Total19161414
63
Events1350
9
Total14161612
58
Weight11.1%33.8%49.9%5.2%
100.0%
M-H, Fixed, 95% CI1.47 [0.15, 14.68]0.14 [0.01, 2.56]0.10 [0.01, 1.71]
2.60 [0.12, 58.48]
0.40 [0.13, 1.22]
Oral AB Parenteral AB Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.001 0.1 1 10 1000Favours oral Favours parenteral
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
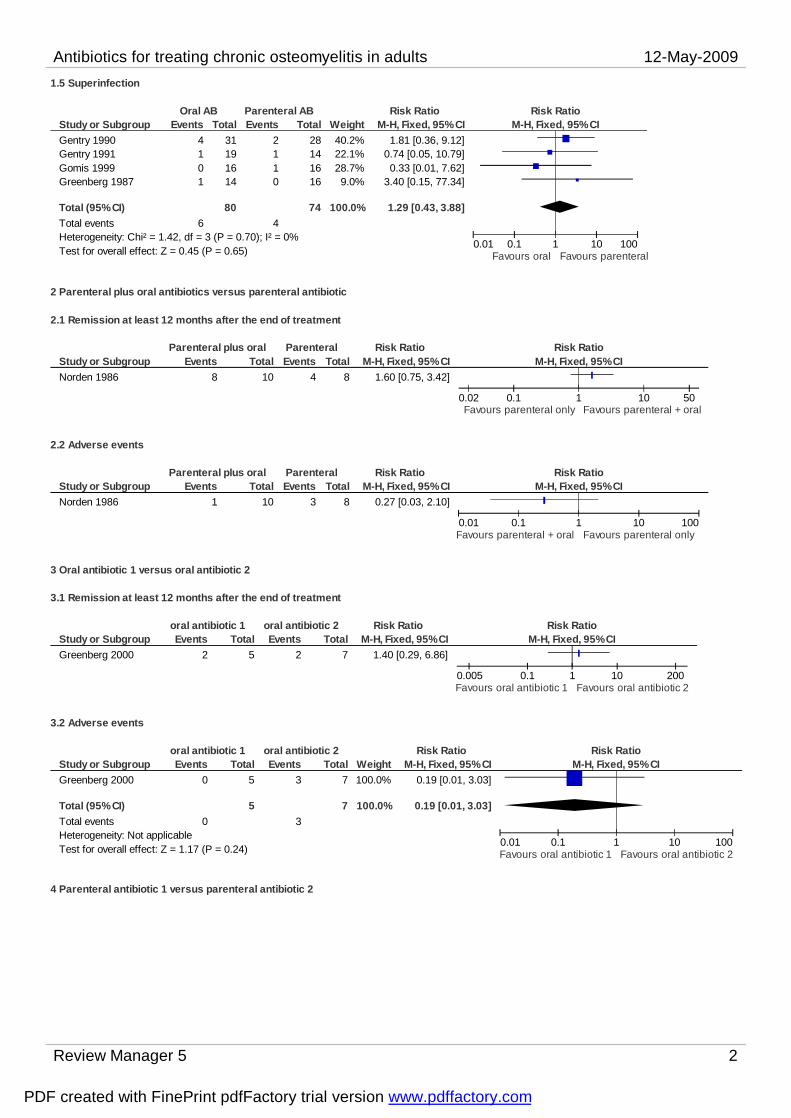
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 2
1.5 Superinfection
Study or SubgroupGentry 1990Gentry 1991Gomis 1999Greenberg 1987
Total (95% CI)Total eventsHeterogeneity: Chi² = 1.42, df = 3 (P = 0.70); I² = 0%Test for overall effect: Z = 0.45 (P = 0.65)
Events4101
6
Total31191614
80
Events2110
4
Total28141616
74
Weight40.2%22.1%28.7%9.0%
100.0%
M-H, Fixed, 95% CI1.81 [0.36, 9.12]
0.74 [0.05, 10.79]0.33 [0.01, 7.62]
3.40 [0.15, 77.34]
1.29 [0.43, 3.88]
Oral AB Parenteral AB Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours oral Favours parenteral
2 Parenteral plus oral antibiotics versus parenteral antibiotic
2.1 Remission at least 12 months after the end of treatment
Study or SubgroupNorden 1986
Events8
Total10
Events4
Total8
M-H, Fixed, 95% CI1.60 [0.75, 3.42]
Parenteral plus oral Parenteral Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.02 0.1 1 10 50Favours parenteral only Favours parenteral + oral
2.2 Adverse events
Study or SubgroupNorden 1986
Events1
Total10
Events3
Total8
M-H, Fixed, 95% CI0.27 [0.03, 2.10]
Parenteral plus oral Parenteral Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours parenteral + oral Favours parenteral only
3 Oral antibiotic 1 versus oral antibiotic 2
3.1 Remission at least 12 months after the end of treatment
Study or SubgroupGreenberg 2000
Events2
Total5
Events2
Total7
M-H, Fixed, 95% CI1.40 [0.29, 6.86]
oral antibiotic 1 oral antibiotic 2 Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.005 0.1 1 10 200Favours oral antibiotic 1 Favours oral antibiotic 2
3.2 Adverse events
Study or SubgroupGreenberg 2000
Total (95% CI)Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.17 (P = 0.24)
Events0
0
Total5
5
Events3
3
Total7
7
Weight100.0%
100.0%
M-H, Fixed, 95% CI0.19 [0.01, 3.03]
0.19 [0.01, 3.03]
oral antibiotic 1 oral antibiotic 2 Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours oral antibiotic 1 Favours oral antibiotic 2
4 Parenteral antibiotic 1 versus parenteral antibiotic 2
PDF created with FinePrint pdfFactory trial version www.pdffactory.com
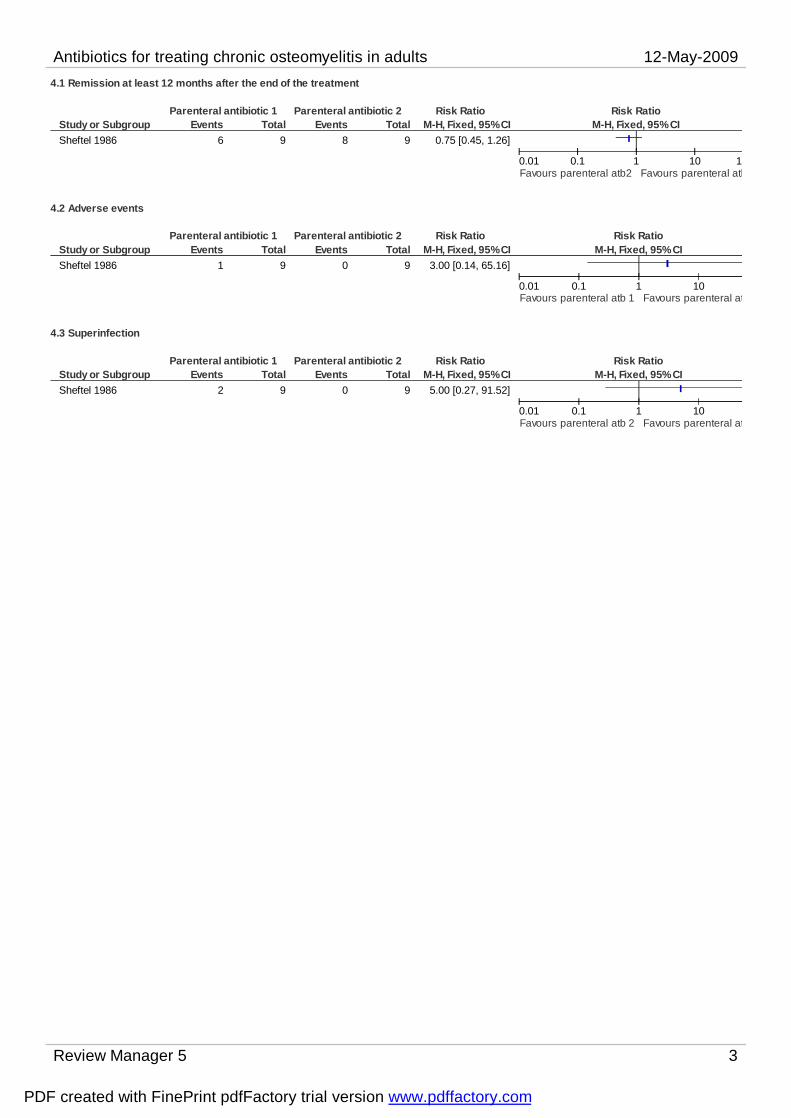
Antibiotics for treating chronic osteomyelitis in adults 12-May-2009
Review Manager 5 3
4.1 Remission at least 12 months after the end of the treatment
Study or SubgroupSheftel 1986
Events6
Total9
Events8
Total9
M-H, Fixed, 95% CI0.75 [0.45, 1.26]
Parenteral antibiotic 1 Parenteral antibiotic 2 Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours parenteral atb2 Favours parenteral atb
4.2 Adverse events
Study or SubgroupSheftel 1986
Events1
Total9
Events0
Total9
M-H, Fixed, 95% CI3.00 [0.14, 65.16]
Parenteral antibiotic 1 Parenteral antibiotic 2 Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours parenteral atb 1 Favours parenteral at
4.3 Superinfection
Study or SubgroupSheftel 1986
Events2
Total9
Events0
Total9
M-H, Fixed, 95% CI5.00 [0.27, 91.52]
Parenteral antibiotic 1 Parenteral antibiotic 2 Risk Ratio Risk RatioM-H, Fixed, 95% CI
0.01 0.1 1 10 100Favours parenteral atb 2 Favours parenteral at
PDF created with FinePrint pdfFactory trial version www.pdffactory.com