osteomyelitis of jaws
TRANSCRIPT
Osteomyelitis of the jaws
DR. ABHITOSH DEBATA, DEPT OF OMFS, C.I.D.S
11
CONTENTS• INTRODUCTION – DEFINITION• NORMAL ANATOMY OF BONE – IN BRIEF• PREDISPOSING FACTORS• ETIOLOGY• PATHOGENESIS• CLASSIFICATION• CLINICAL TYPES• COMPLICATIONS OF OSTEOMYELITIS• DIAGNOSTIC METHODS• TREATMENT
2
INTRODUCTION• “Osseous” in Latin means – Bony
• “Osteon” in Greek means – Bone
• “myelos” means marrow
• “itis” means inflammation
3
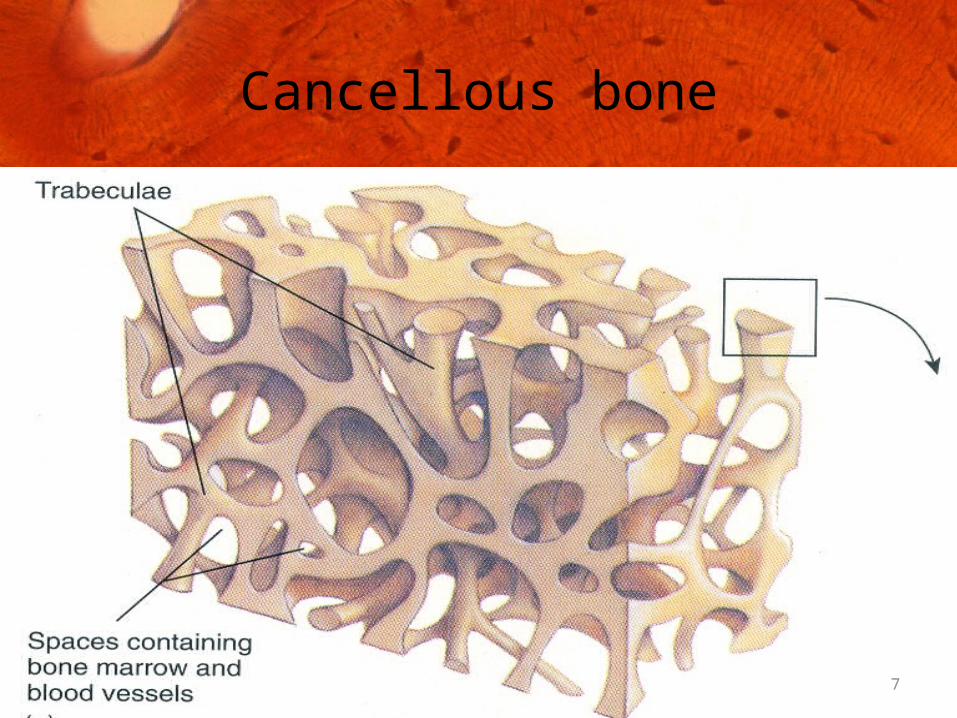
Definition :• Osteomyelitis is an extensive inflammation of a bone. It involves the cancellous portion, bone marrow, cortex, and periosteum.
(Laskin 1989)
• Osteomyelitis is defined as an inflammatory condition of bone primarily involving the soft tissues
(Archer)
4
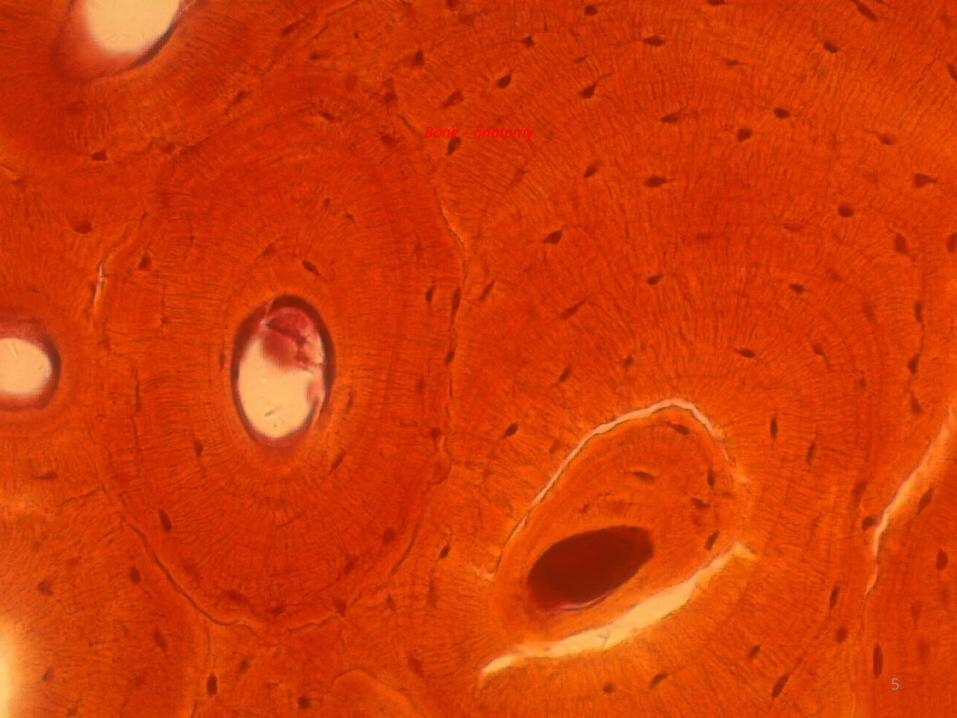
Bone – anatomy
5
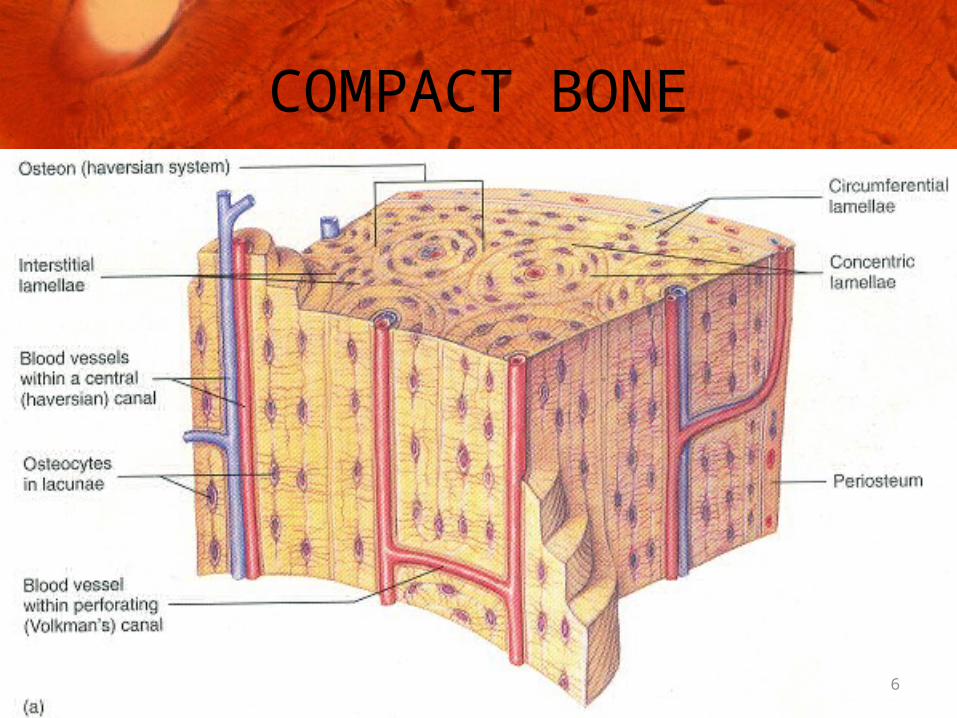
COMPACT BONE
6
7
Cancellous bone
Predisposing factorsConditions that alter HOST IMMUNITY
- Leukemia- Severe anemia- Malnutrition- AIDS- IV- drug abuse- Chronic alcoholism- Febrile illnesses- Malignancy- Autoimmune disease- Diabetes mellitus- Arthritis- Agranulocytosis
8
Conditions that alter vascularity of bone
- Osteoporosis
- Paget’s disease
- Fibrous dysplasia
- Bone malignancy- Radiation
9
Virulence of the organisms
• Certain organisms precipitate thrombi formation by virtue of their destructive lysosomal enzymes.
• Organisms proliferate in enriched host medium while protected from host immunity.
• Marx et al (1992) identified Actinomyces, Eikenella & Arachnia in some refractile forms
10
etiology Odontogenic infections
Trauma
Infections of oro facial region
Infections derived from hematogenous route
Compound fractures of the jaws.
11
RELATIONSHIP OF EXODONTIA WITH OSTEOMYELITIS
12

PATHOGENESIS DEV OF INFECTION BACTERIAL INVASION PUS FORMATION SPREAD OF INFECTION INCREASED INTRAMEDULLARY PRESSURE , BLOOD FLOW , OSTEOCLASTIC ACTIVITY INFLAMMATORY RESPONSES INCREASED PERIOSTEAL PRESSURE PROCESS BECOMES CHRONIC
GRANULATION TISSUE FORMATION LYSIS OF BONE
SEQUESTRUM FORMATION
13
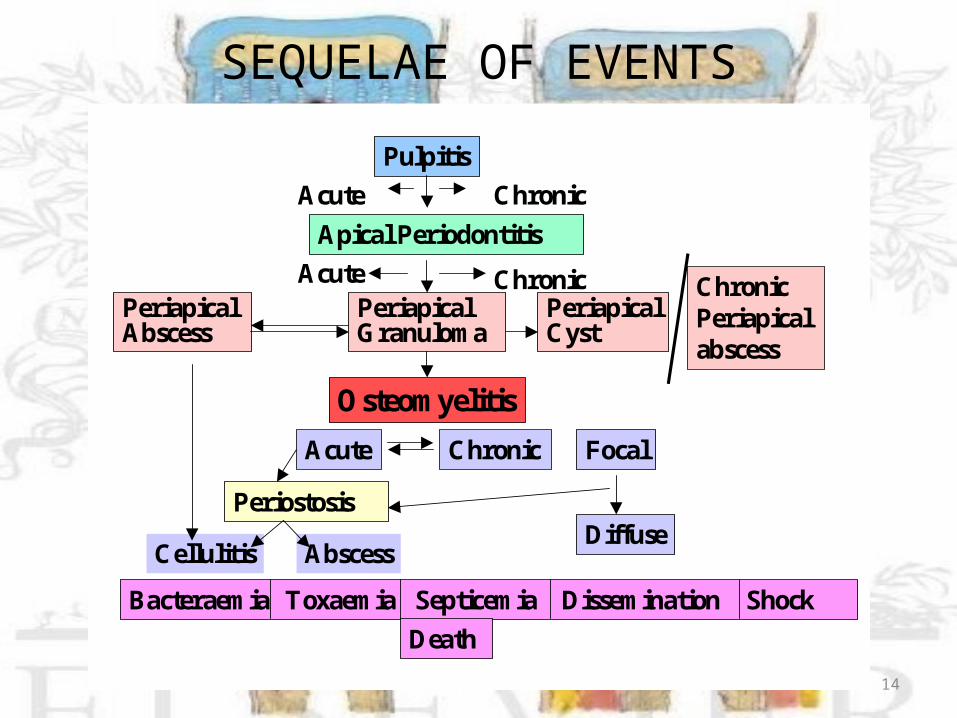
SEQUELAE OF EVENTSPulpitis
Acute ChronicApical Periodontitis
Acute ChronicPeriapical Abscess
Periapical Granulom a
Periapical Cyst
O steom yelitisAcute Chronic Focal
DiffusePeriostosis
Cellulitis AbscessBacteraem ia Toxaem ia Septicem ia Dissem ination Shock
Death
Chronic Periapical abscess
14
In the jaws…Osteomyelitis in maxilla
Osteomyelitis in mandible
15
16
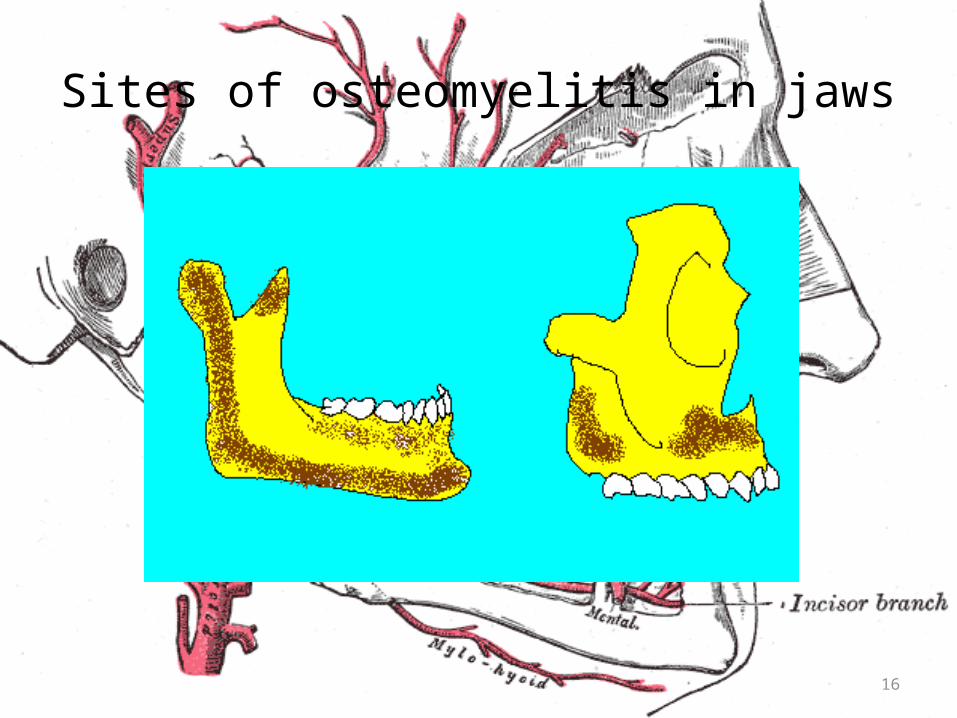
Sites of osteomyelitis in jaws

• Definition• Pre disposing factors• Etiology• Site
17

classification• Historically accepted classification –[Hudson’s classification]
I. Acute –
a. Contiguous focus – trauma, surgery & odontogenic infections
b. Progressive – burns, sinusitis, vascular insufficiency
c. Hematogenous – metastatic , dev skeleton(children)
18
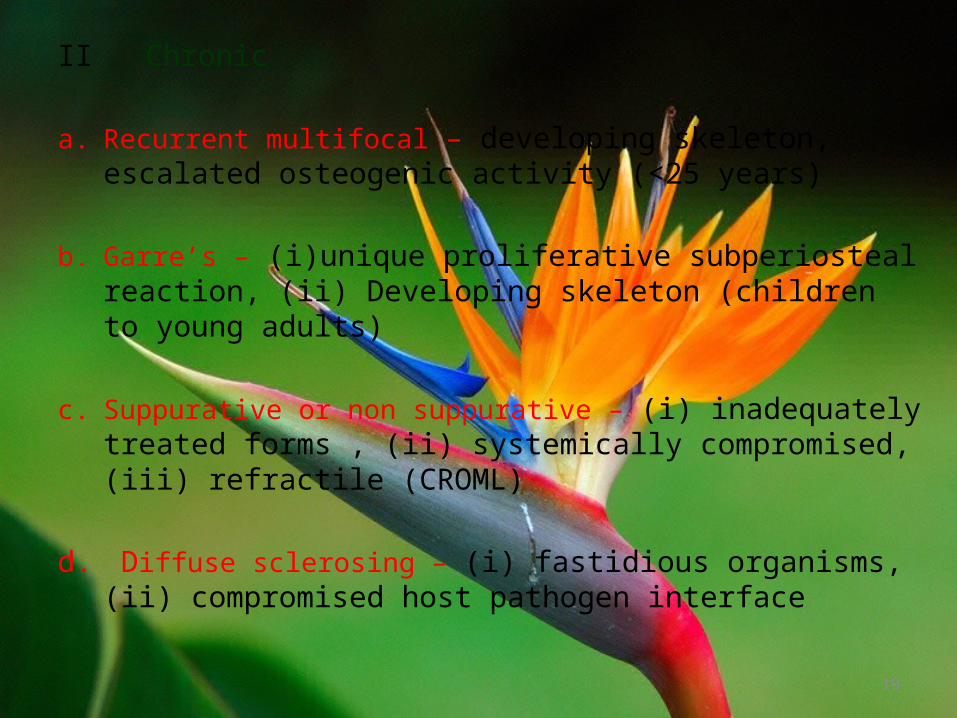
II Chronic
a. Recurrent multifocal – developing skeleton, escalated osteogenic activity (<25 years)
b. Garre’s – (i)unique proliferative subperiosteal reaction, (ii) Developing skeleton (children to young adults)
c. Suppurative or non suppurative – (i) inadequately treated forms , (ii) systemically compromised, (iii) refractile (CROML)
d. Diffuse sclerosing – (i) fastidious organisms, (ii) compromised host pathogen interface
19

20
• Classification based on clinical picture by Marx 1991; Mercuri1991;Koorbusch1992.
• Classification based on pathogenesis by Vibhagool 1993.
• Classification based on pathological anatomy and pathophysiology from Vibhagool 1993 and Cierny 1985.
• Zurich classification of osteomyelitis
Classification based on clinical picture,radiology, and etiology - Topazian
Suppurative osteomyelitis• 1. Acute suppurative osteomyelitis• 2. Chronic suppurative osteomyelitis
• – Primary chronic suppurative osteomyelitis
• – Secondary chronic suppurative• osteomyelitis• 3. Infantile osteomyelitis
21
Nonsuppurative osteomyelitis• 1. Chronic sclerosing osteomyelitis
• – Focal sclerosing osteomyelitis
• – Diffuse sclerosing osteomyelitis
• 2. Garre's sclerosing osteomyelitis
• 3. Actinomycotic osteomyelitis• 4. Radiation osteomyelitis and necrosis
22
Acute suppurative osteomyelitis
• Serious sequela of periapical infection.
• Leads to spread of pus through the medullary cavities of bone.
• Depending upon the main site of involvement of bone, can be of two types-
i. Acute intramedullary
ii. Acute subperiosteal
23
Acute Intramedullary Osteomyelitis
CLINICAL FEATURES:• Patient experiences dull , continuous pain , indurated swelling forms over the affected region of jaw involving the cheek , febrile.
• When mandible involved, loss of sensation occurs on lower lip on affected side due to involvement of inferior alveolar nerve.
• Teeth become loose later along with tender on percussion
• Pus discharge , trismus , foul smell , regional lymphadenopathy , weakness
24
RADIOGRAPHIC FEATURES
• Earliest radiographic change is that trabeculae in involved area are thin, of poor density & slightly blurred.
• Subsequently multiple radiolucencies appear which become apparent on radiograph.
• In some cases there is saucer shaped area of destruction with irregular margins.
• Loss of continuity of lamina dura, seen in more than one tooth.
25
HISTOLOGIC FEATURES:
• Dense infiltration of marrow by polymorphonuclear leukocytes.
• Bone trabeculae in involved site (sequestrum) are devoid of cells in the lacunae.
• separation of considerable portions of devitalized bone.
26
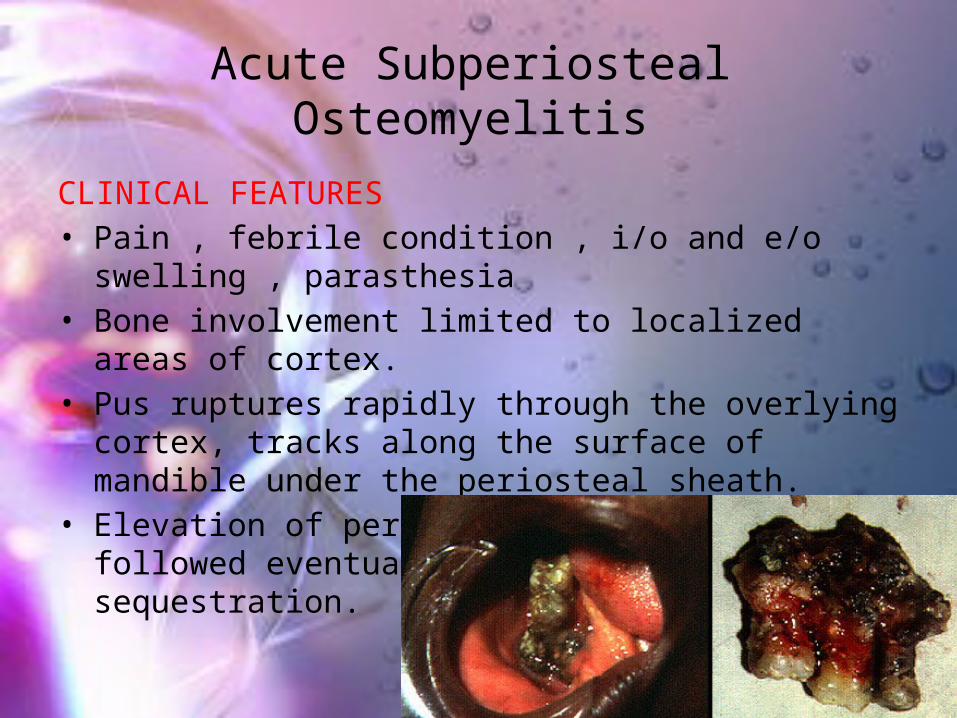
Acute Subperiosteal Osteomyelitis
CLINICAL FEATURES• Pain , febrile condition , i/o and e/o swelling , parasthesia
• Bone involvement limited to localized areas of cortex.
• Pus ruptures rapidly through the overlying cortex, tracks along the surface of mandible under the periosteal sheath.
• Elevation of periosteum from cortex is followed eventually by minute cortical sequestration.
27
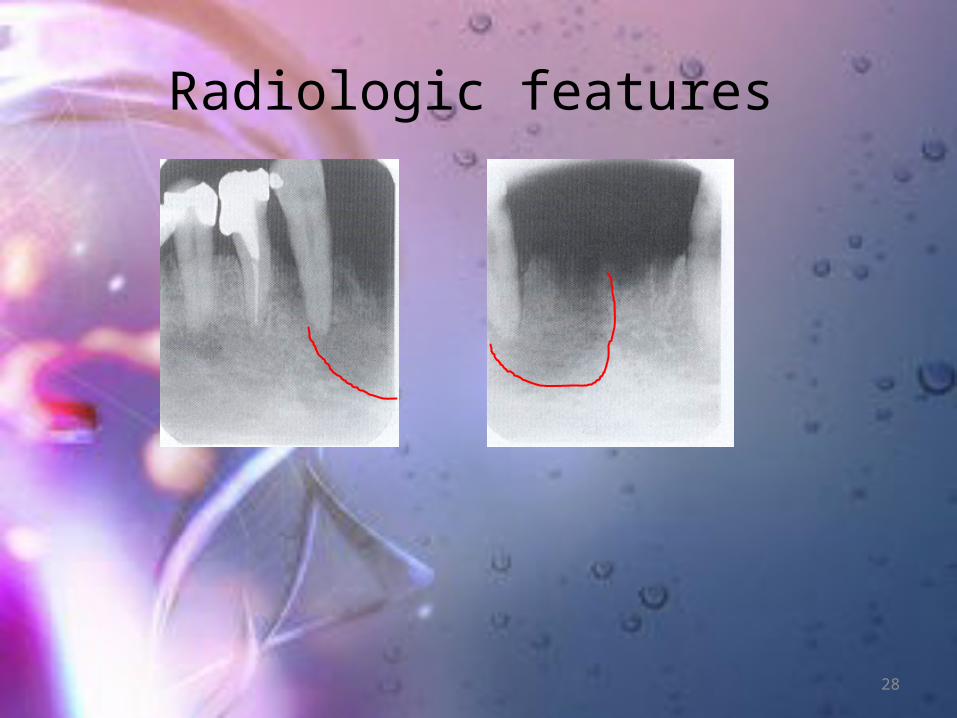
Radiologic features
28

-
Radiologic features
29

Histologic picture
• Devitalized scalloped edges
• Absence of osteoblasts and
osteocytes
30
Chronic Osteomyelitis• As soon as pus drains intra or extraorally, condition ceases to spread and chronic phase commences.
• Infection is localized but persistent as bacteria are able to grow in dead bone inaccessible to body’s defenses.
31
Clinical features• Primary – insidious in onset , slight pain , gradual increase in jaw size.
• Secondary - Pain is deep pain and intermittent, temperature fluctuations , pyrexia , cellulitis eventually leading to abscess
• New bone formation leads to thickening causing facial asymmetry.
• Thickened or “wooden” character of bone in cr sec osteomyelitis.
• Eventually cures itself as the last sequestra is discharged.
32
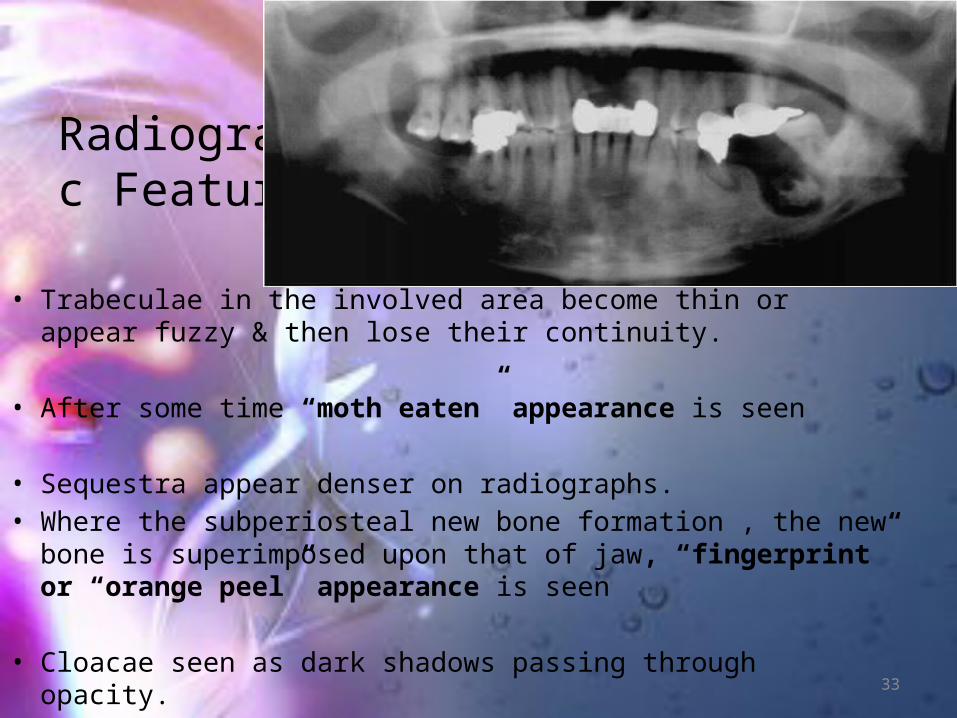
Radiographic Features
• Trabeculae in the involved area become thin or appear fuzzy & then lose their continuity.
• After some time “moth eaten” appearance is seen
• Sequestra appear denser on radiographs.• Where the subperiosteal new bone formation , the new bone is superimposed upon that of jaw, “fingerprint” or “orange peel” appearance is seen
• Cloacae seen as dark shadows passing through opacity. 33

Histologic features• Areas of acute and subacute inflammation in the cancellous spaces of the necrotic bone.
• Foci of acute inflammation
• Active osteoclastic resorption of bone noted in peripheral portions
34
Chronic Subperiosteal Osteomyelitis
• Cortical plate deprived of its blood supply undergoes necrosis, underlying medullary bone is slightly affected.
• Multiple small sequestra form, eventually discharged through sinuses with pus.
• Following extrusion of sequestra, healing occurs.
• Spontaneous drainage poor in submassetric area.
• Much of body of mandible is lost due to poor central blood supply of the region.
35

D/D• Paget’s disease – particularly wen periosteal bone is involved
• Fibrous dysplasia• Osteosarcoma
36

Chronic sclerosing osteomyelitis – focal
- diffuse
37
Focal Sclerosing Osteomyelitis
38
Clinical features• Most commonly in children and young adults, rarely in older individuals.
• Tooth most commonly involved is the mandibular third molar presenting with a large carious lesion.
• No signs or symptoms other than mild pain associated with infected pulp.
39
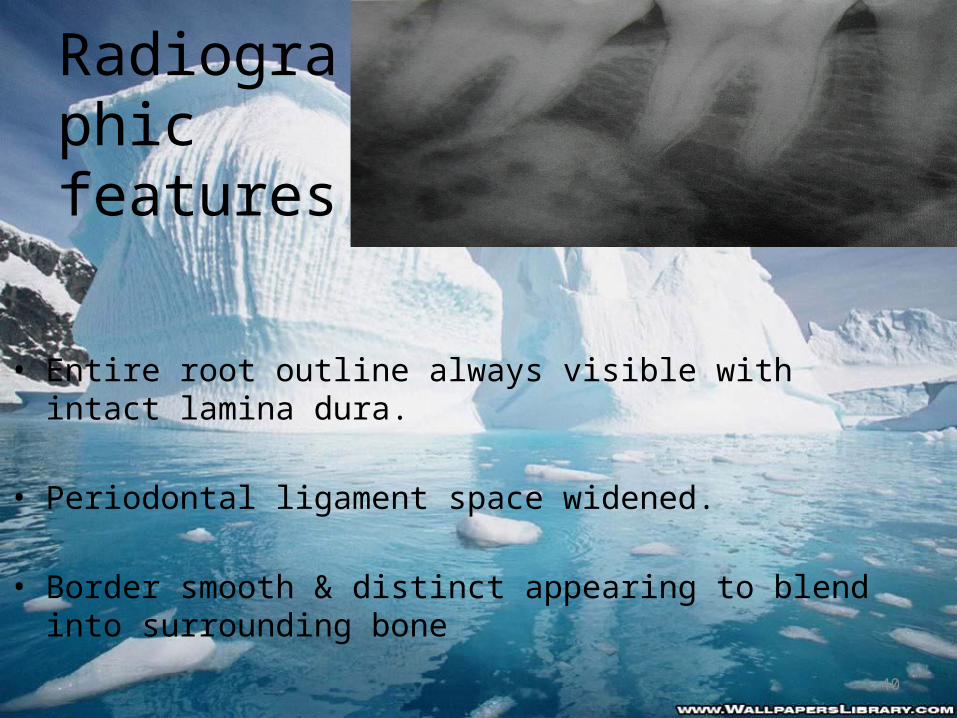
Radiographic features
• Entire root outline always visible with intact lamina dura.
• Periodontal ligament space widened.
• Border smooth & distinct appearing to blend into surrounding bone
40
D/D for focal sclerosing osteomyelitis• Local bone sclerosis
• Sclerosing cementoma
• Gigantiform cementoma
41
Treatment & prognosis• Affected tooth may be treated endodontically or extracted.
• Sclerotic bone not attached to tooth and remains behind after tooth is removed.
• This dense area may not get remodeled.
• Recognizable on bone years later and is referred as bone scar.
42
Diffuse Sclerosing Osteomyelitis
• May occur at any age, most common in older persons, esp in edentulous mandibles
• vague pain, unpleasant taste.
• Many times spontaneous formation of fistula seen opening onto mucosal surface to establish drainage
• Slowly progressive, not particularly dangerous since it is non destructive & seldom produces complications
43
Radiographic features• Diffuse patchy, sclerosis of bone – “cotton wool” appearance
• Radiopacity may be extensive and bilateral.
• Due to diffuse nature, border between sclerosis & normal bone is often indistinct.
44
D/D for DIFFUSE sclerosing osteomyelitis
FLORID OSSEOUS DYSPLASIA
SCLEROTIC CEMENTAL MASSES
TRUE CHR DIFFUSE SCLEROSING OSTEOMYELITIS
FIBROUS DYSPLASIA
45
Treatment & Prognosis• Resolution of adjacent foci of chronic infection often leads to improvement.
• Usually too extensive to be removed surgically,
• Acute episodes treated with antibiotics.
46
Initial results of the treatment of diffuse sclerosing osteomyelitis of the mandible
with bisphosphonates Sophie C.C. Kuijpers Journal of Cranio-Maxillo-Facial Surgery 39 (2011) 65e68
• Study design: Seven patients suffering from treatment resistant DSO were treated with intravenous bisphosphonates. Diagnosis was based on clinical, radiological and histopathological examination.
• Follow-up varied from 18 to 46 months (mean 30).
47
• Results: In all patients, symptoms and the need for analgesic drugs diminished considerably. One patient remained free of symptoms after one treatment. In two patients a switch in bisphosphonate was made based on a decreased response.
• Conclusion: In therapy-resistant DSO bisphosphonate treatment may be a good option
48

Infantile Osteomyelitis• Osteomyelitis Maxillaries Neonatarum, Maxillitis of infancy
• Osteomyelitis in the jaws of new born infants occurs almost exclusively in maxilla.
49
Etiology • Trauma – through break in mucosa cause during delivery.
• Infection of maxillary sinus
• Paunz & Ramon et al believe that disease caused through infection from the nose.
• Hematogenous spread through streptococci & pneumococci
50
Clinical features• Fever, anorexia & intestinal disturbances.• swelling or redness below the inner canthus of the eye in lacrimal region.
• Followed by marked edema of the eyelids on the affected side.
• Next, alveolus & palate in region of first deciduous molar become swollen.
• Pus discharge from affected sites
51
D/D for Infantile Osteomyelitis
• Dacrocystitis neonatarum
• Orbital cellulitis
• Ophthalmia neonatarum
• Infantile cortical hyperostosis
52

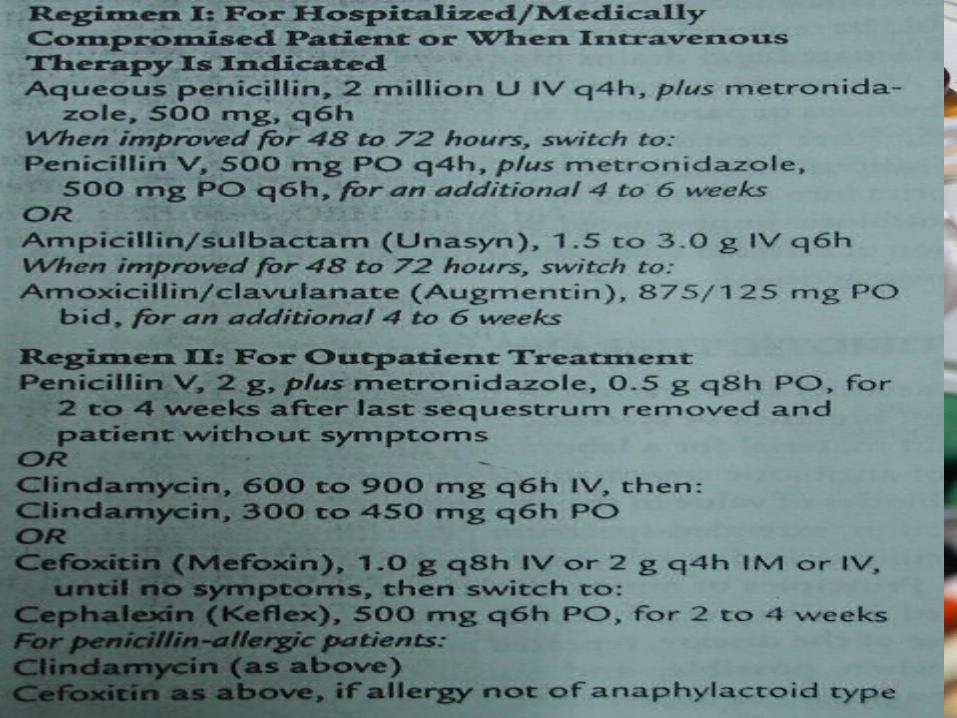
TREATMENT• Intravenous antibiotics, preferably penicillin.
• Culture & sensitivity testing
• Incision & drainage of fluctuant areas
• Sequestrectomy
• Supportive therapy
53
Garre’s Osteomyelitis (Chronic Osteomyelitis with Proliferative Perosteitis)• Chronic Non Suppurative Sclerosing Osteitis/ Periostitis Ossificans.
• Non suppurative productive disease characterized by a hard swelling.
• Occurs due to low grade infection and irritation• The infectious agent localizes in or beneath the periosteal covering of the cortex & spreads only slightly into the interior of the bone.
• Occurs primarily in young persons who possess great osteogenic activity of the periosteum.
54
Clinical Features• Uncommonly encountered, described in tibia and in the head and neck region, in the mandible.
• Typically involves the posterior mandible & is usually unilateral.
• Patients present with an asymptomatic bony, hard swelling with normal appearing overlying skin and mucosa.
• On occasion slight tenderness may be noted
• pain is most constant feature• The increase in the mass of bone may be due to mild toxic stimulation of periosteal osteoblasts by attenuated infection.
55
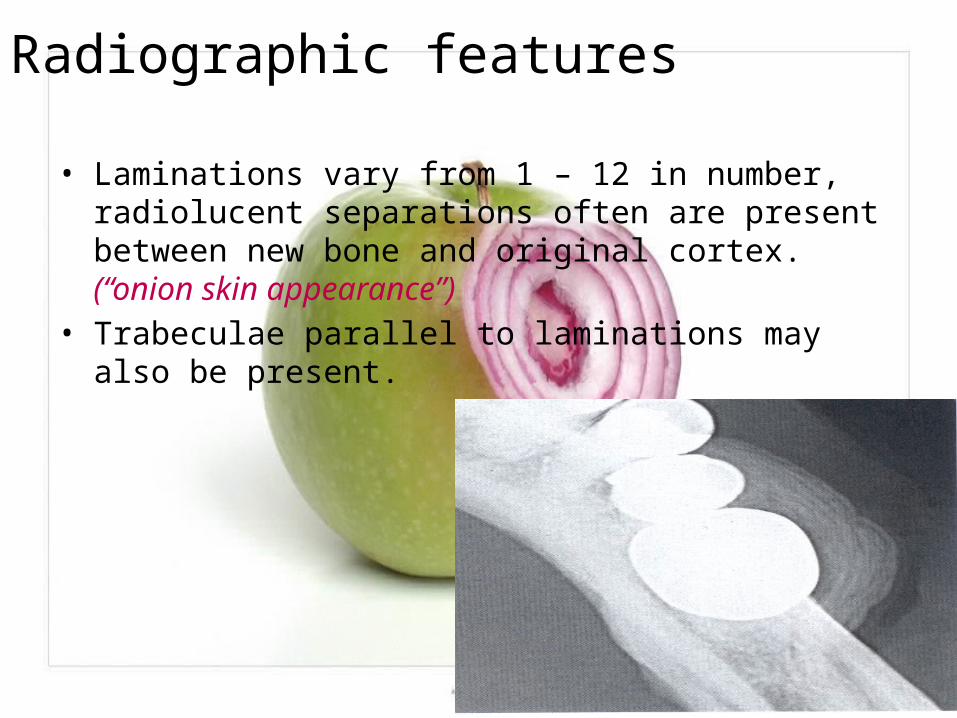
Radiographic features
• Laminations vary from 1 – 12 in number, radiolucent separations often are present between new bone and original cortex. (“onion skin appearance”)
• Trabeculae parallel to laminations may also be present.
56

Histologic Features• Reactive new bone.
• Parallel rows of highly cellular & reactive woven bone in which the individual trabeculae are oriented perpendicular to surface.
• Osteoblasts predominate in this area.
57
D/D for Garre’s Osteomyelitis• Ewing's sarcoma
• Caffey’s disease
• Fibrous dysplasia
• Osteosarcoma
58
Treatment
• Removal of the offending cause.
• Once inflammation resolves, layers of the bone consolidate in 6 – 12 months, as the overlying muscle helps to remodel.
• If no focus of infection evident, biopsy recommended.
59

Infective osteomyelitis• Tuberculous osteomyelitis
• Syphilitic osteomyelitis
• Actinomycotic osteomyelitis
60
Tuberculous osteomyelitis
• Non healing sinus tract formation• Age group affected is around 15 – 40 years.
• Commonly seen in phalanges and dorsal and lumbar vertebrae.
• Usually occurs secondary to tuberculosis of lungs.
• Cases have been reported where mandibular lesions were not associated with pulmonary disease.
• Another common entrance is through a carious tooth via open pulp. 61
Syphilitic Osteomyelitis• Difficult to distinguish syphilitic osteomyelitis of the jaws from pyogenic osteomyelitis on clinical & radiographic examination.
• Main features are progressive course & failure to improve with usual treatment for pyogenic osteomyelitis.
• Massive sequestration may occur resulting in pathologic fracture.
• If unchecked, eventually causes perforation of the cortex.
62
Actinomycotic Osteomyelitis
• The organisms thrive in the oral cavity, especially tissues adjacent to mandible.
• May enter the bone through a fresh wound, carious tooth or a periodontal pocket at the gingival margin of erupting tooth.
• Soft or firm tissue masses on skin, which have purplish, dark red, oily areas with occasional zones of fluctuation.
• Spontaneous drainage of serous fluid containing granular material.
• Regional lymph nodes occasionally enlarged.• Mimics parotitis / parotid tumors
63

investigations
• CULTURE & SENSITIVITY TESTS • STAINING and microscopy• Biopsy • BLOOD INVESTIGATIONS• BONE MARROW ASPIRATION• IMAGING
64
Imaging CONVENTIONAL• IOPA• OCCLUSAL• OPG• LATERAL OBLIQUE• BONE SCAN• CT SCAN• MRI• POSITRON EMISSION TOMOGRAPHY
65
66
Follow-up of acute osteomyelitis in children: the possible role of PET/CT in selected cases Steven W. Warmann Journal of Pediatric Surgery (2011)
• Magnetic resonance imaging (MRI) and/or scintigraphy are commonly used for follow-up in children after treatment of acute osteomyelitis.
• The PET/CT was superior to MRI in distinguishing between infection and reparative activity within the musculoskeletal system in selected children after acute osteomyelitis. The termination of antibiotic treatment for children after acute osteomyelitis seems justified when laboratory parameters as well as clinical presentation are normal, and PET/CT scan is unsuspicious.

treatment• Goal of management
• Management includes – Conservative management Surgical management
67

Conservative Management• bed rest
• Rehydration
• Pain control
• Antimicrobial therapy
68
69

• Erythromycin• Neoporin irrigants• Antibiotics impregnated beads
70
Duration of post-surgical antibiotics in chronic osteomyelitis : empiric or evidence-based by Rachid Haidar et al.(International Journal of
Infectious Diseases , 2010) Despite all of the advances in antibiotic and operative treatment, osteomyelitis remains difficult to treat. This is because bacteria can elude host defense mechanisms by hiding intracellularly and by developing a protective slimy coat. By acquiring a very slow metabolic rate, bacteria become less sensitive to antibiotics. For all the above reasons, operative treatment is considered whenever possible. Osteomyelitis has traditionally been treated with 4–6 weeks of parenteral antibiotics after definitive debridement surgery. However, this time frame has no documented superiority over other time intervals, and there is no evidence that prolonged parenteral antibiotics will penetrate the necrotic bone.
Hence this review article questions the continuous and traditional use of long-term antibiotic treatment for chronic osteomyelitis in spite of the advances in surgical treatment using flaps. 71
Surgical Therapy• Incision & drainage• Extraction of loose teeth• Debridement • Decortication• Sequestrectomy• Saucerization• Trephination or fenestration• Resection• Immediate/ delayed reconstruction• Postoperative care
72

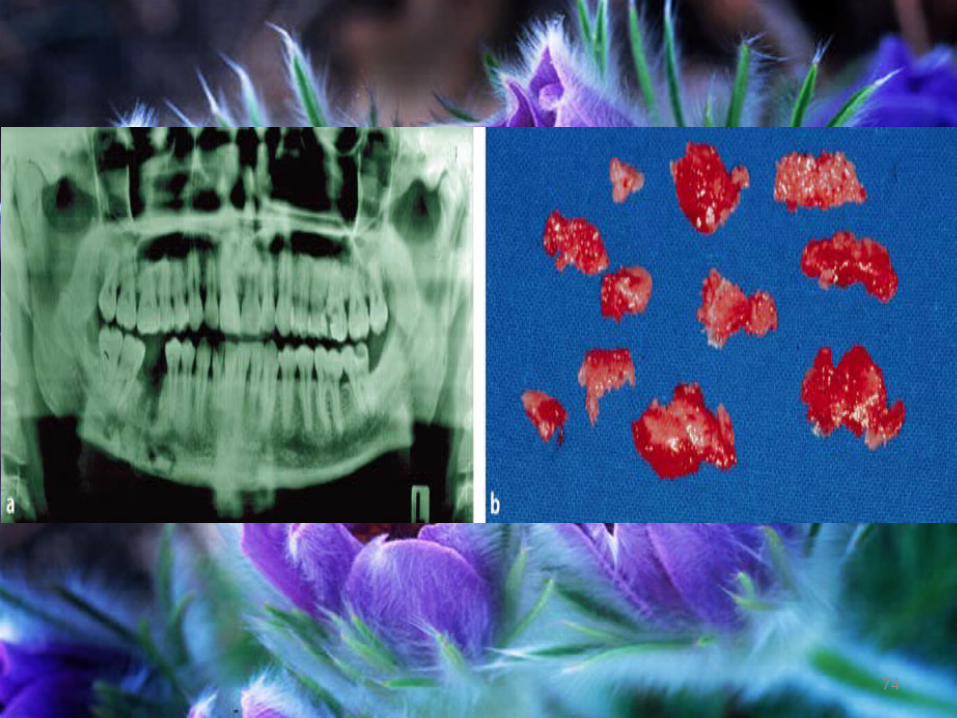
• SEQUESTRECTOMY• SAUCERIZATION• DECORTICATION• TREPHINATION
73
74
75

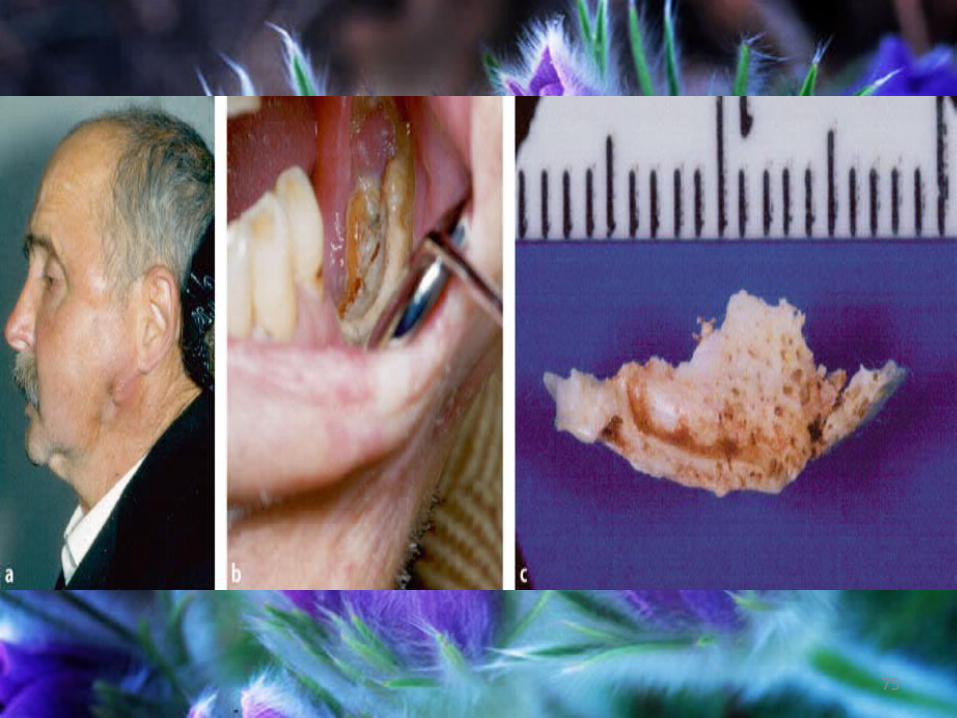
Osteoradionecrosis
• Defined as “exposure of non viable, non healing, non septic lesion in the irradiated bone, which fails to heal without intervention”.
• One of the most serious complications of radiation to the head and neck.
• Acute form of osteomyelitis caused by damage to intraosseous blood vessels.
• Seen in patients receiving more than 60Gy during radiation therapy
76

Factors leading to osteoradionecrosis
• Irradiation of area of previous surgery before healing occurs
• Irradiation of lesions in close proximity to bone
• High dose of radiation
• Combination of external radiation and intraoral implants
• Poor oral hygiene and continue use of irritants
77

Pathogenesis
• Not an infection itself, it is the bone’s reduced ability to heal resulting in lesions, pain and fragility
78
PATHOGENESIS
RADIATION - NORMAL CELLS DESTRUCTION ALONG WITH CANCER CELLS – ENDARTERITIS OBLITERANS – DECREASED MICROCICULATION – HYPOVASCULARITY – HYPOXIA - HYPOCELLULARITY
79
Clinical features• Mandible affected far more frequently than maxilla.
• Trismus , Foetid odour , Pyrexia , Pathologic fracture , Sequestration , Dull pain which may continue for weeks or months , Swelling of face when infection develops
• Soft tissue abscess & persistently draining sinuses
• Exposed bone, associated with intra or extraoral fistulae
80

Radiologic features• May appear radiolucent, with indefinite nonsclerotic borders & occasional areas of radiopacity.
• Sequestra & involucra occur late or not at all; due to severely compromised blood supply.
81
Steps to avoid Osteoradionecrosis
PRE THERAPY:
• All teeth with questionable prognosis should be extracted
• All restorable teeth should be restored. • Thorough prophylaxis & topical fluoride application.
• Oral hygiene measures & instructions should be demonstrated & reinforced.
• Any sharp cusps should be rounded to prevent mechanical irritation.
• Impressions for fabrication of custom fluoride trays to be used during treatment.
• Stop habits like tobacco use & alcohol consumption.
82
DURING THERAPY:
• Pt should rinse mouth with saline.• Chlorhexidine mouth rinses twice daily to minimize bacterial/ fungal levels within mouth.
• Weekly oral hygiene evaluation by dentist.• If overgrowth of candida albicans – nystatin or clotrimazole topical application.
• Monitor mouth opening.• Monitor nutritional status.
83
POST THERAPY
• Dental evaluation every 3 – 4 months.
• Oral prophylaxis.
• Topical fluoride application should be done using custom trays.
• Pt to be instructed in daily self administration of topical fluoride administration.
• Salivary substitutes should be prescribed.84
• Restore teeth developing post-radiotherapy caries using amalgam or composites.
• Extraction of teeth can be carried out with the use of
- Hyperbaric oxygen before & after extraction
- Prophylactic antibiotic
• Evaluate artificial dentures.
85

Treatment CONSERVATIVE METHOD:
• Systemic antibiotics• Selective rinsing with topical antiseptics• Selective removal of small sequestra• Curetting & local debridement• Burring of bone until normal bleeding bone appears.
86
RADICAL TREATMENT
• Debridement• Control of infection• Hydration & nutritional supplements• Analgesics• Maintaining good oral hygiene• Frequent irrigation of wounds• Sequestrectomy• Bone resection• Hyperbaric Oxygen therapy
87
Hyperbaric Oxygen Therapy
• Involves intermittent, usually daily, inhalation of 100% humidified oxygen under pressure greater than 1 absolute atmospheric pressure
• Patient is placed in a chamber, oxygen is given by mask or hood
• Each session, or dive, is 90 minutes in length.
• Treatment given 5 days per week for 30, 60 or more dives for 90 minutes while breathing 100% oxygen twice daily
• Free radicals of oxygen bactericidal to many pathogens.
• Many exotoxins liberated by microorganisma rendered inert by exposure to elevated partial pressure of oxygen.
88
Contraindications • As considered by the HBO Committee of the Undersea Medical Society, Fisher et al(1988) & Marx et al (1985)
Pneumothorax Severe COPD Acute viral infection Upper respiratory tract infection Uncontrolled acute seizures Malignant disease
89
• Evidence for osteomyelitis found in the fossil record is studied by paleopathologists, specialists in ancient disease and injury. It has been reported in fossils of the large carnivorous dinosaur Allosaurus fragilus
90

References • Textbook of Oral Surgery – Topazian• A textbook of oral pathology – 5th edition; Shafer, Hine & Levy
• Textbook of Oral & Maxillofacial Surgery – Neelima Anil Malik
• Textbook of Oral Medicine – Anil Govindrao Ghom
• Oral & Maxillofacial Pathology – Marx & Stern
• Osteomyelitis of the Jaws: Definition and Classification - Marc Baltensperger and Gerold Eyrich
91