pre-hospital trauma care resources for road traffic injuries in a middle-income country—a province...
TRANSCRIPT

Injury, Int. J. Care Injured 42 (2011) 879–884
Contents lists available at ScienceDirect
Injury
journa l homepage: www.e lsevier .com/ locate / in jury
Pre-hospital trauma care resources for road traffic injuries in a middle-incomecountry—A province based study on need and access in Iran
Hassan Haghparast Bidgoli a,b,d,*, Lennart Bogg a,c, Marie Hasselberg a
a Department of Public Health Sciences, Division of Global Health, Karolinska Institute, Swedenb Health Management and Economics Research Centre, Isfahan University of Medical Sciences, Iranc School of Sustainable Development of Society and Technology, Malardalen University, Swedend The Swedish Research School for Global Health, Partnership between Umea University and Karolinska Institute, Sweden
A R T I C L E I N F O
Article history:
Accepted 26 April 2010
Keywords:
Traffic related mortality and morbidity
Pre-hospital trauma care facilities
Need
Access
Low- and middle-income countries
A B S T R A C T
Background: Access to pre-hospital trauma care can help minimize many of traffic related mortality and
morbidity in low- and middle-income countries with high rate of traffic deaths such as Iran. The aim of
this study was to assess if the distribution of pre-hospital trauma care facilities reflect the burden of road
traffic injury and mortality in different provinces in Iran.
Methods: This national cross-sectional study is based on ecological data on road traffic mortality (RTM),
road traffic injuries (RTIs) and pre-hospital trauma facilities for all 30 provinces in Iran in 2006. Lorenz
curves and Gini coefficients were used to describe the distributions of RTM/RTIs and pre-hospital trauma
care facilities across provinces. Spearman rank-order correlation was performed to assess the
relationship between RTM/RTI and pre-hospital trauma care facilities.
Results: RTM and RTIs as well as pre-hospital trauma care facilities were distributed unequally between
different provinces. There was no significant association between the rate of RTM and RTIs and the
number of pre-hospital trauma care facilities across the country.
Conclusions: The distribution of pre-hospital trauma care facilities does not reflect the needs in terms of
RTM and RTIs for different provinces. These results suggest that traffic related mortality and morbidity
could be reduced if the needs in terms of RTM and RTIs were taken into consideration when distributing
pre-hospital trauma care facilities between the provinces.
� 2010 Elsevier Ltd. All rights reserved.
Introduction
Road traffic injuries (RTIs) are a major public health problemglobally causing more than a million deaths and almost 50 millionsinjuries every year, disproportionately distributed in low andmiddle-income countries (LMICs).25 Road traffic mortality (RTM) ispredicted to increase by 83% in LMICs, unless preventive efforts areundertaken.25 Iran has one of the highest RTM rates in the world.2
RTIs are considered to be the third greatest cause of mortality, aftermyocardial infarction and cerebral vascular diseases, in Iran withover 27,000 deaths and almost 0.8 million injured people (1.1% ofthe population).2,21
Several studies have mentioned the inadequacy of the publichealth infrastructure and poor access to health services, includingpre-hospital trauma services, as major reasons for the high burden
* Corresponding author at: Department of Public Health Sciences, Division of
Global Health, Karolinska Institutet, Nobels vag 9, SE-171 77, Stockholm, Sweden.
Tel.: +46 8 52483391; fax: +46 8 311 590.
E-mail address: [email protected] (H.H. Bidgoli).
0020–1383/$ – see front matter � 2010 Elsevier Ltd. All rights reserved.
doi:10.1016/j.injury.2010.04.024
of RTM in LMICs.10,16,19,22,23 As the majority of trauma deaths inLMICs occur in the pre-hospital setting,16,20 it is suggested thataccess to an effective pre-hospital trauma care can help minimizemany of traffic related mortality and morbidity.1,16,17,27,29 ButMost LMICs have insufficient pre-hospital trauma services.25,35 Inthe absence of well-organized pre-hospital care, injured people areoften cared for by untrained laypeople and transported to thenearest medical facility in commercial vehicles.13,25,35 Data from2002 indicates that 60% of the deaths in Iran occurred at the crashscene or on the way to the hospital.21 Furthermore, the data showsthat only 14% of the injured people are transported to hospitals byambulance and only 10% are transported by trained people (withknowledge of first aid or medical training).21
The reasons for the high burden of traffic related mortality andmorbidity in LMICs have been discussed in many studies,19,22,25
but very little research has been done in order to assess the role ofpre-hospital trauma care in terms of physical and humanresources.16
Emergency Medical Services (EMS) in Iran, which is mainlybased on a Basic Life Support (BLS) system,27 is centralized in theMinistry of Health and Medical Education (MOHME). Provincial

H.H. Bidgoli et al. / Injury, Int. J. Care Injured 42 (2011) 879–884880
centres are affiliated to the Medical Sciences and Health ServicesUniversities in the provinces. According to EMS policy, thedistribution of pre-hospital trauma care facilities is based on thenumber of inhabitants in a city and also on the distance betweenthe ambulance dispatch sites on roads between cities.15 Although,the overall number of ambulance dispatch sites, ambulances andeducated staff for treating RTIs has increased considerably duringrecent years, the levels of traffic related morbidity and mortalityhave not decreased noticeably in Iran.2,12
The current study examines accessibility of pre-hospital traumacare facilities (including dispatch sites, ambulances and staff)using inequality measures, the Lorenz curve and Gini coefficient.These two measures have traditionally been used to analyze thedistribution of income and wealth.5 A number of researchers haveused these methods within new fields e.g. to analyze thedistribution of physicians within different geographical areas.4,8,32
The use of these two measures make it possible to illustrategeographical variations and equality in the distribution of pre-hospital trauma care facilities, RTM and RTIs in Iran.
This study, specifically focuses on the following researchquestions: are pre-hospital trauma care facilities distributedequally between different provinces? Does the distribution ofpre-hospital trauma care facilities reflect RTM and RTIs in allprovinces?
Materials and methods
Study setting
Iran, a lower-middle-income country, is located in the EasternMediterranean Region and covers 1,648,000 sq km. The countryhas 30 provinces, 293 districts, 885 cities, and approximately68,000 villages. With an estimated population of 71.4 million, Iranis the most populous country in the region, and the 16th mostpopulous in the world.36 Within the population, 66% live in urbanareas33 and the average annual growth rate of the urbanpopulation was 2.5% between the years 1990 and 2006.33 Vehicleownership is significantly higher in Iran compared to othercountries with similar income levels.2 Based on estimates from the2006 Census, Iran had almost six million cars and over five millionmotorized two-wheelers.2 The total length of roads is 72,013 km.31
Data sources and definitions
Information about RTM and RTIs is based on data from theForensic Medicine Organization (FMO), which is an affiliatedorganization of the Judicial Authority in Iran. The FMO is the mostreliable source of mortality data in Iran.20 According to Iranian law,all deaths due to external causes, including RTIs, should be reportedto FMO for examination and recording and to issue the deathcertificate. The recorded variables for deaths due to RTIs in FMOinclude: name of victim, age, gender, education level, occupationtype, vehicle type, place of accident, place of death, date of accident,date of death, date of post mortem, cause of death and localization ofinjury. The variables are recorded using ICD10 guidelines.28,37
Moreover, FMO collects data about RTIs from all victims referred tothe FMO centres all over the country. The victims need FMO approvalto claim for compensations from the insurance agencies, and theymainly contact FMO by themselves or are sent by hospitals andsometimes by police and insurance agencies. The recorded variablesfor RTIs victims are similar to the deceased victims and are collectedby the coroners using the same questionnaire in all FMO centres.
Information about pre-hospital care facilities and infrastructureis based on data from the National EMS Centre in MOHME. TheCentre collects information from the Medical Universities in theprovinces regarding ambulances, ambulance dispatch sites and staff.
Data about the total number of kilometres of roads (all roadsexcept local rural roads) and highways in different provinces wasextracted from the Road Maintenance and Transportation Orga-nization’s annual reports. Moreover, data about population sizeand number of registered vehicles (all kind of motorized vehiclesincluding public transport) was obtained from the StatisticalCentre of Iran.
In the current study, access was defined as physical availabilityof pre-hospital trauma care facilities and need was defined asnumber of injuries and deaths due to road traffic crashes in eachprovince. Three variables were used as indicators for access to pre-hospital trauma care; number of ambulance dispatch sites(including urban and road-side sites with 1–2 ambulances andnecessary trained staff), number of ambulances (mostly equippedwith basic life support equipments) and number of on duty staff(including physicians, nurses, emergency medical technicians andother paramedics working in the centres). The following twovariables were used as indicators for population health need, RTMand RTIs. RTM was defined as deaths occurring at crash site orwithin 30 days after the crash.19 In addition, two proxies for trafficexposure were used: the mean number of registered vehiclesduring 10 years and the proportion of highways (out of total kmroads) in each province were included in the analyses.
Lorenz curve and Gini index
The Lorenz curve compares the distribution of a specificvariable with the uniform distribution that represents equali-ty.4,8,32 This equality distribution is shown by a diagonal line, andthe greater the deviation of the Lorenz curve from this line, thegreater the inequality.32 The cumulative proportion of thepopulation is generally shown on the X axis, and the cumulativeproportion of the health variable on the Y axis. The Gini coefficientis derived from the Lorenz curve and calculated as the ratio of thearea between the Lorenz curve and the diagonal line, to the wholearea below the diagonal line.5,32 Gini index represents a value from0 (perfect equality) to 1 (maximum possible inequality) andprovides a quantitative measure to enable comparison of relativeinequality of distribution across different settings.
Data analysis
RTM and RTIs rates per 100,000 population and pre-hospitaltrauma care facilities per 100,000 population were calculated forall the provinces. Also, the proportion of highways and the meannumber of registered vehicles (during 10 years from 1997 to 2006)per 100,000 population in each province was calculated. Theproportion of highways was calculated by dividing the kilometresof highway with the total km of all roads.
The Lorenz curve and Gini coefficient were used to measure thelevel of inequality in the distribution of pre-hospital trauma carefacilities and RTIs and RTM across the country.
Spearman rank-order correlation analysis was used in order tosee if pre-hospital trauma care facilities were distributed based onRTIs and RTM rates and possible association with traffic exposuremeasured as mean number of vehicles and proportion of highwaysin the 30 provinces.
All statistical analyses were carried out using the softwarepackage Stata version 10. The study was undertaken with thepermission of the National Ethics Committee of the Ministry ofHealth.
Results
Table 1 shows the distribution of pre-hospital trauma carefacilities (including ambulance, dispatch sites and staff), RTIs and
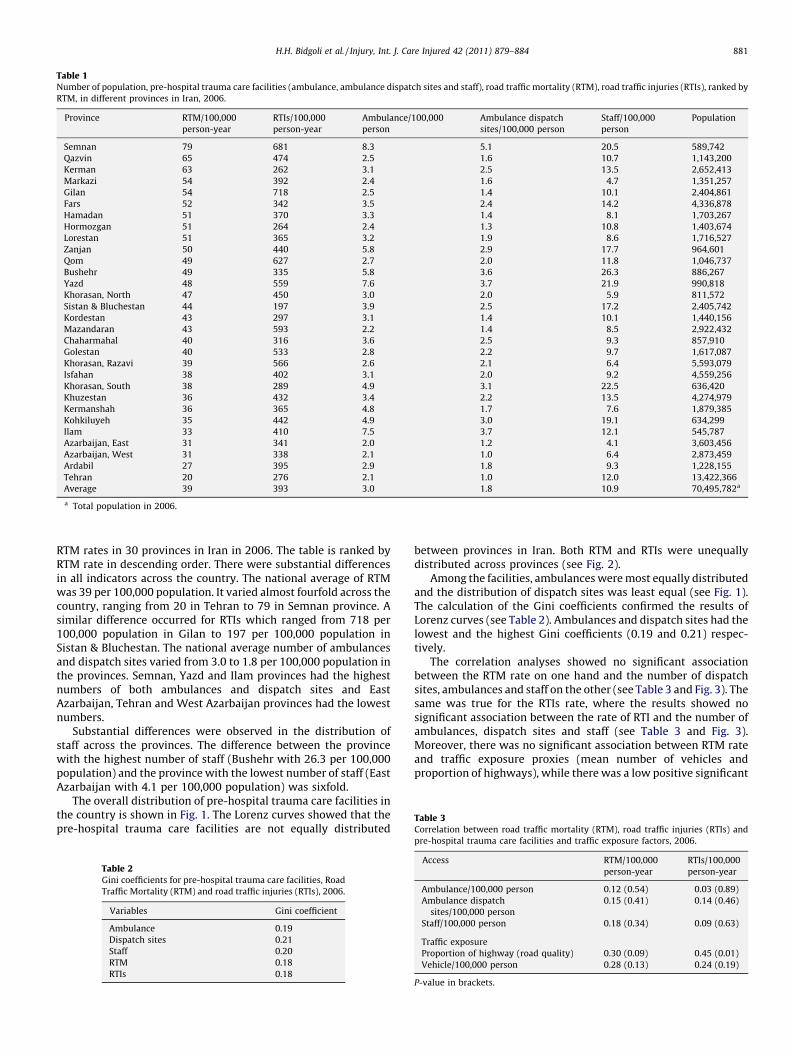
Table 1Number of population, pre-hospital trauma care facilities (ambulance, ambulance dispatch sites and staff), road traffic mortality (RTM), road traffic injuries (RTIs), ranked by
RTM, in different provinces in Iran, 2006.
Province RTM/100,000
person-year
RTIs/100,000
person-year
Ambulance/100,000
person
Ambulance dispatch
sites/100,000 person
Staff/100,000
person
Population
Semnan 79 681 8.3 5.1 20.5 589,742
Qazvin 65 474 2.5 1.6 10.7 1,143,200
Kerman 63 262 3.1 2.5 13.5 2,652,413
Markazi 54 392 2.4 1.6 4.7 1,351,257
Gilan 54 718 2.5 1.4 10.1 2,404,861
Fars 52 342 3.5 2.4 14.2 4,336,878
Hamadan 51 370 3.3 1.4 8.1 1,703,267
Hormozgan 51 264 2.4 1.3 10.8 1,403,674
Lorestan 51 365 3.2 1.9 8.6 1,716,527
Zanjan 50 440 5.8 2.9 17.7 964,601
Qom 49 627 2.7 2.0 11.8 1,046,737
Bushehr 49 335 5.8 3.6 26.3 886,267
Yazd 48 559 7.6 3.7 21.9 990,818
Khorasan, North 47 450 3.0 2.0 5.9 811,572
Sistan & Bluchestan 44 197 3.9 2.5 17.2 2,405,742
Kordestan 43 297 3.1 1.4 10.1 1,440,156
Mazandaran 43 593 2.2 1.4 8.5 2,922,432
Chaharmahal 40 316 3.6 2.5 9.3 857,910
Golestan 40 533 2.8 2.2 9.7 1,617,087
Khorasan, Razavi 39 566 2.6 2.1 6.4 5,593,079
Isfahan 38 402 3.1 2.0 9.2 4,559,256
Khorasan, South 38 289 4.9 3.1 22.5 636,420
Khuzestan 36 432 3.4 2.2 13.5 4,274,979
Kermanshah 36 365 4.8 1.7 7.6 1,879,385
Kohkiluyeh 35 442 4.9 3.0 19.1 634,299
Ilam 33 410 7.5 3.7 12.1 545,787
Azarbaijan, East 31 341 2.0 1.2 4.1 3,603,456
Azarbaijan, West 31 338 2.1 1.0 6.4 2,873,459
Ardabil 27 395 2.9 1.8 9.3 1,228,155
Tehran 20 276 2.1 1.0 12.0 13,422,366
Average 39 393 3.0 1.8 10.9 70,495,782a
a Total population in 2006.
Table 3Correlation between road traffic mortality (RTM), road traffic injuries (RTIs) and
H.H. Bidgoli et al. / Injury, Int. J. Care Injured 42 (2011) 879–884 881
RTM rates in 30 provinces in Iran in 2006. The table is ranked byRTM rate in descending order. There were substantial differencesin all indicators across the country. The national average of RTMwas 39 per 100,000 population. It varied almost fourfold across thecountry, ranging from 20 in Tehran to 79 in Semnan province. Asimilar difference occurred for RTIs which ranged from 718 per100,000 population in Gilan to 197 per 100,000 population inSistan & Bluchestan. The national average number of ambulancesand dispatch sites varied from 3.0 to 1.8 per 100,000 population inthe provinces. Semnan, Yazd and Ilam provinces had the highestnumbers of both ambulances and dispatch sites and EastAzarbaijan, Tehran and West Azarbaijan provinces had the lowestnumbers.
Substantial differences were observed in the distribution ofstaff across the provinces. The difference between the provincewith the highest number of staff (Bushehr with 26.3 per 100,000population) and the province with the lowest number of staff (EastAzarbaijan with 4.1 per 100,000 population) was sixfold.
The overall distribution of pre-hospital trauma care facilities inthe country is shown in Fig. 1. The Lorenz curves showed that thepre-hospital trauma care facilities are not equally distributed
Table 2Gini coefficients for pre-hospital trauma care facilities, Road
Traffic Mortality (RTM) and road traffic injuries (RTIs), 2006.
Variables Gini coefficient
Ambulance 0.19
Dispatch sites 0.21
Staff 0.20
RTM 0.18
RTIs 0.18
between provinces in Iran. Both RTM and RTIs were unequallydistributed across provinces (see Fig. 2).
Among the facilities, ambulances were most equally distributedand the distribution of dispatch sites was least equal (see Fig. 1).The calculation of the Gini coefficients confirmed the results ofLorenz curves (see Table 2). Ambulances and dispatch sites had thelowest and the highest Gini coefficients (0.19 and 0.21) respec-tively.
The correlation analyses showed no significant associationbetween the RTM rate on one hand and the number of dispatchsites, ambulances and staff on the other (see Table 3 and Fig. 3). Thesame was true for the RTIs rate, where the results showed nosignificant association between the rate of RTI and the number ofambulances, dispatch sites and staff (see Table 3 and Fig. 3).Moreover, there was no significant association between RTM rateand traffic exposure proxies (mean number of vehicles andproportion of highways), while there was a low positive significant
pre-hospital trauma care facilities and traffic exposure factors, 2006.
Access RTM/100,000
person-year
RTIs/100,000
person-year
Ambulance/100,000 person 0.12 (0.54) 0.03 (0.89)
Ambulance dispatch
sites/100,000 person
0.15 (0.41) 0.14 (0.46)
Staff/100,000 person 0.18 (0.34) �0.09 (0.63)
Traffic exposure
Proportion of highway (road quality) 0.30 (0.09) 0.45 (0.01)
Vehicle/100,000 person 0.28 (0.13) 0.24 (0.19)
P-value in brackets.
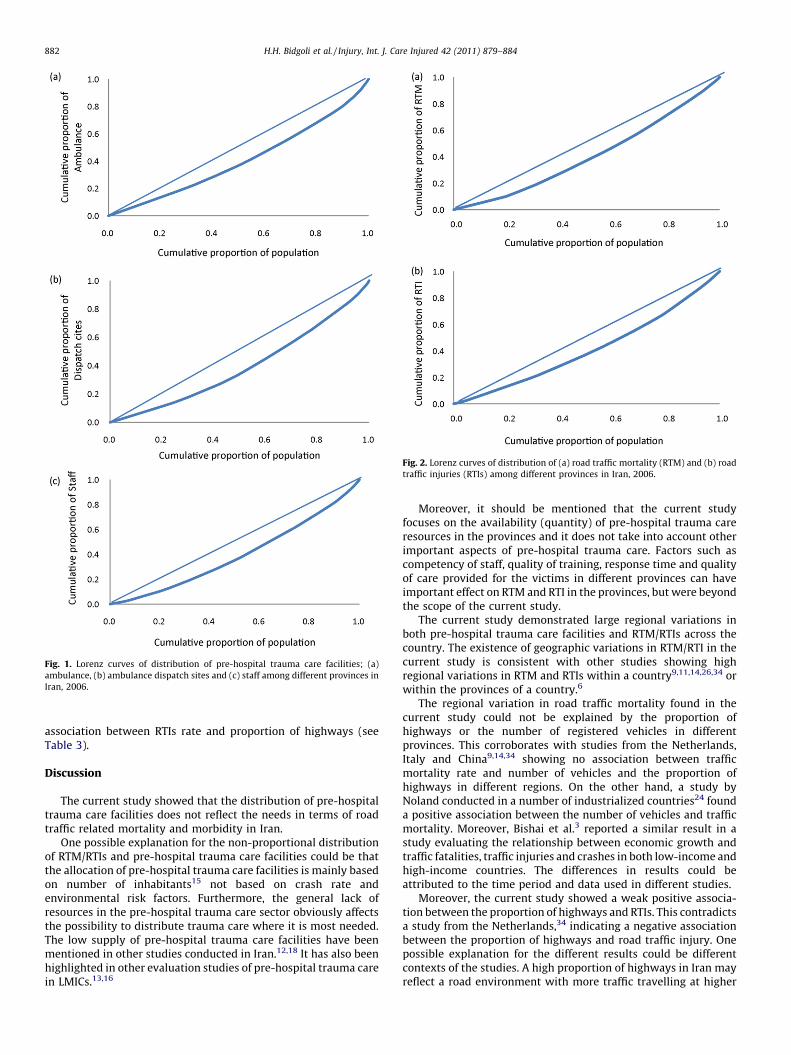
Fig. 1. Lorenz curves of distribution of pre-hospital trauma care facilities; (a)
ambulance, (b) ambulance dispatch sites and (c) staff among different provinces in
Iran, 2006.
Fig. 2. Lorenz curves of distribution of (a) road traffic mortality (RTM) and (b) road
traffic injuries (RTIs) among different provinces in Iran, 2006.
H.H. Bidgoli et al. / Injury, Int. J. Care Injured 42 (2011) 879–884882
association between RTIs rate and proportion of highways (seeTable 3).
Discussion
The current study showed that the distribution of pre-hospitaltrauma care facilities does not reflect the needs in terms of roadtraffic related mortality and morbidity in Iran.
One possible explanation for the non-proportional distributionof RTM/RTIs and pre-hospital trauma care facilities could be thatthe allocation of pre-hospital trauma care facilities is mainly basedon number of inhabitants15 not based on crash rate andenvironmental risk factors. Furthermore, the general lack ofresources in the pre-hospital trauma care sector obviously affectsthe possibility to distribute trauma care where it is most needed.The low supply of pre-hospital trauma care facilities have beenmentioned in other studies conducted in Iran.12,18 It has also beenhighlighted in other evaluation studies of pre-hospital trauma carein LMICs.13,16
Moreover, it should be mentioned that the current studyfocuses on the availability (quantity) of pre-hospital trauma careresources in the provinces and it does not take into account otherimportant aspects of pre-hospital trauma care. Factors such ascompetency of staff, quality of training, response time and qualityof care provided for the victims in different provinces can haveimportant effect on RTM and RTI in the provinces, but were beyondthe scope of the current study.
The current study demonstrated large regional variations inboth pre-hospital trauma care facilities and RTM/RTIs across thecountry. The existence of geographic variations in RTM/RTI in thecurrent study is consistent with other studies showing highregional variations in RTM and RTIs within a country9,11,14,26,34 orwithin the provinces of a country.6
The regional variation in road traffic mortality found in thecurrent study could not be explained by the proportion ofhighways or the number of registered vehicles in differentprovinces. This corroborates with studies from the Netherlands,Italy and China9,14,34 showing no association between trafficmortality rate and number of vehicles and the proportion ofhighways in different regions. On the other hand, a study byNoland conducted in a number of industrialized countries24 founda positive association between the number of vehicles and trafficmortality. Moreover, Bishai et al.3 reported a similar result in astudy evaluating the relationship between economic growth andtraffic fatalities, traffic injuries and crashes in both low-income andhigh-income countries. The differences in results could beattributed to the time period and data used in different studies.
Moreover, the current study showed a weak positive associa-tion between the proportion of highways and RTIs. This contradictsa study from the Netherlands,34 indicating a negative associationbetween the proportion of highways and road traffic injury. Onepossible explanation for the different results could be differentcontexts of the studies. A high proportion of highways in Iran mayreflect a road environment with more traffic travelling at higher
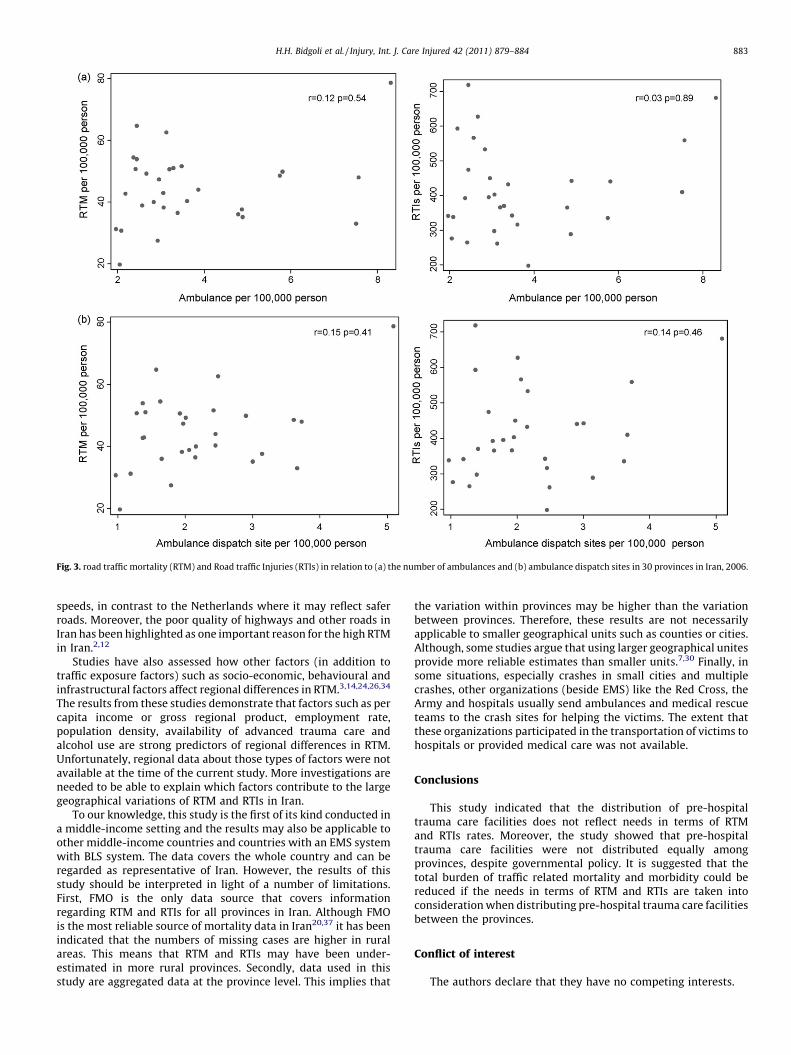
Fig. 3. road traffic mortality (RTM) and Road traffic Injuries (RTIs) in relation to (a) the number of ambulances and (b) ambulance dispatch sites in 30 provinces in Iran, 2006.
H.H. Bidgoli et al. / Injury, Int. J. Care Injured 42 (2011) 879–884 883
speeds, in contrast to the Netherlands where it may reflect saferroads. Moreover, the poor quality of highways and other roads inIran has been highlighted as one important reason for the high RTMin Iran.2,12
Studies have also assessed how other factors (in addition totraffic exposure factors) such as socio-economic, behavioural andinfrastructural factors affect regional differences in RTM.3,14,24,26,34
The results from these studies demonstrate that factors such as percapita income or gross regional product, employment rate,population density, availability of advanced trauma care andalcohol use are strong predictors of regional differences in RTM.Unfortunately, regional data about those types of factors were notavailable at the time of the current study. More investigations areneeded to be able to explain which factors contribute to the largegeographical variations of RTM and RTIs in Iran.
To our knowledge, this study is the first of its kind conducted ina middle-income setting and the results may also be applicable toother middle-income countries and countries with an EMS systemwith BLS system. The data covers the whole country and can beregarded as representative of Iran. However, the results of thisstudy should be interpreted in light of a number of limitations.First, FMO is the only data source that covers informationregarding RTM and RTIs for all provinces in Iran. Although FMOis the most reliable source of mortality data in Iran20,37 it has beenindicated that the numbers of missing cases are higher in ruralareas. This means that RTM and RTIs may have been under-estimated in more rural provinces. Secondly, data used in thisstudy are aggregated data at the province level. This implies that
the variation within provinces may be higher than the variationbetween provinces. Therefore, these results are not necessarilyapplicable to smaller geographical units such as counties or cities.Although, some studies argue that using larger geographical unitesprovide more reliable estimates than smaller units.7,30 Finally, insome situations, especially crashes in small cities and multiplecrashes, other organizations (beside EMS) like the Red Cross, theArmy and hospitals usually send ambulances and medical rescueteams to the crash sites for helping the victims. The extent thatthese organizations participated in the transportation of victims tohospitals or provided medical care was not available.
Conclusions
This study indicated that the distribution of pre-hospitaltrauma care facilities does not reflect needs in terms of RTMand RTIs rates. Moreover, the study showed that pre-hospitaltrauma care facilities were not distributed equally amongprovinces, despite governmental policy. It is suggested that thetotal burden of traffic related mortality and morbidity could bereduced if the needs in terms of RTM and RTIs are taken intoconsideration when distributing pre-hospital trauma care facilitiesbetween the provinces.
Conflict of interest
The authors declare that they have no competing interests.

H.H. Bidgoli et al. / Injury, Int. J. Care Injured 42 (2011) 879–884884
Acknowledgement
We thank Dr. Hamid Reza Khankeh, Dr. Davoud KhorasaniZavareh, Dr. Dariush Nasrollahzadeh Nesheli, Mohammad Hajiza-deh and, Dr. Behrooz Hamzeh for their helpful comments. Thisstudy was supported by a research grant from the Iran Ministry ofHealth and Medical Education.
References
1. Arreola-Risa C, Mock CN, Lojero-Wheatly L, et al. Low-cost improvements inprehospital trauma care in a Latin American city. J Trauma 2000;48:119–24.
2. Bhalla K, Shahraz S, Naghavi M, et al. Road traffic injuries in Iran. HarvardUniversity Initiative for Global Health; 2008.
3. Bishai D, Quresh A, James P, Ghaffar A. National road casualties and economicdevelopment. Health Econ 2006;15:65–81.
4. Chang RK, Halfon N. Geographic distribution of pediatricians in the UnitedStates: an analysis of the fifty states and Washington, DC. Pediatrics1997;100:172–9.
5. De Maio FG. Income inequality measures. J Epidemiol Community Health2007;61:849–52.
6. Durkin M, McElroy J, Guan H, et al. Geographic analysis of traffic injury inWisconsin: impact on case fatality of distance to level I/II trauma care. WMJ2005;104:26–31.
7. Eksler V, Lassarre S, Thomas I. Regional analysis of road mortality in Europe.Public Health 2008;122:826–37.
8. Gravelle H, Sutton M. Inequality in the geographical distribution of generalpractitioners in England and Wales 1974–1995. J Health Serv Res Policy2001;6:6–13.
9. Hu G, Wen M, Baker TD, Baker SP. Road-traffic deaths in China, 1985–2005:threat and opportunity. Inj Prev 2008;14:149–53.
10. Hyder AA, Peden M. Inequality and road-traffic injuries: call for action. Lancet2003;362:2034–5.
11. Jones AP, Haynes R, Kennedy V, et al. Geographical variations in mortality andmorbidity from road traffic accidents in England and Wales. Health Place2008;14:519–35.
12. Khorasani-Zavareh D, Khankeh HR, Mohammadi R, et al. Post-crash manage-ment of road traffic injury victims in Iran. Stakeholders’ views on currentbarriers and potential facilitators. BMC Emerg Med 2009;9:8.
13. Kobusingye OC, Hyder AA, Bishai D, et al. Emergency medical systems in low-and middle-income countries: recommendations for action. Bull World HealthOrgan 2005;83:626–31.
14. La Torre G, Van Beeck E, Quaranta G, et al. Determinants of within-countryvariation in traffic accident mortality in Italy: a geographical analysis. Int JHealth Geogr 2007;6:49.
15. Ministry of Health and Medical Education. Universal access to pre-hospitalemergency care act. Tehran: Ministry of Health and Medical Education; 2007.
16. Mock C, Arreola-Risa C, Quansah R. Strengthening care for injured persons inless developed countries: a case study of Ghana and Mexico. Inj Control SafPromot 2003;10:45–51.
17. Mock C, Quansah R, Krishnan R, et al. Strengthening the prevention and care ofinjuries worldwide. Lancet 2004;363:2172–9.
18. Modaghegh MH, Roudsari BS, Sajadehchi A. Prehospital trauma care in Tehran:potential areas for improvement. Prehosp Emerg Care 2002;6:218–23.
19. Mohan D, Tiwari G, Khayesi M, Nafukho FM. Road traffic injury prevention:training manual. Geneva: World Health Organization; 2006.
20. Montazeri A. Road-traffic-related mortality in Iran: a descriptive study. PublicHealth 2004;118:110–3.
21. Naghavi M, Jafari N, Alaeddini F, Akbari ME. Injury Epidemiology caused byexternal cause of injury in the Islamic Republic of Iran. Tehran, Iran: Ministry ofHealth and Medical Education; 2005.
22. Nantulya VM, Reich MR. The neglected epidemic: road traffic injuries indeveloping countries. BMJ 2002;324:1139–41.
23. Nantulya VM, Sleet DA, Reich MR, et al. Introduction: the global challenge ofroad traffic injuries: can we achieve equity in safety? Inj Control Saf Promot2003;10:3–7.
24. Noland RB. Medical treatment and traffic fatality reductions in industrializedcountries. Accid Anal Prev 2003;35:877–83.
25. Peden M, Scurfield R, Sleet D, et al. World report on road traffic injury preven-tion. Geneva; 2004.
26. Rivas-Ruiz F, Perea-Milla E, Jimenez-Puente A. Geographic variability of fatalroad traffic injuries in Spain during the period 2002–2004: an ecological study.BMC Public Health 2007;7:266.
27. Roudsari BS, Nathens AB, Arreola-Risa C, et al. Emergency Medical Service(EMS) systems in developed and developing countries. Injury 2007;38:1001–13.
28. Sanaei Zadeh H. Modern forensic medicine and the medico-legal system in Iran.J Clin Forensic Med 2002;9:12–4.
29. Sasser SM, Varghese M, Joshipura M, Kellermann A. Preventing death anddisability through the timely provision of prehospital trauma care. Bull WorldHealth Organ 2006;84:507.
30. Shi L, Macinko J, Starfield B, et al. Primary care, social inequalities and all-cause,heart disease and cancer mortality in US counties: a comparison between urbanand non-urban areas. Public Health 2005;119:699–710.
31. Statistical Center of Iran. Iran Statistical year book. Statistical Center of Iran2008. Available at: http://www.sci.org.ir/portal/faces/public/sci_en/sci_en.Glance/sci_en.trans [accessed 15.04.09].
32. Theodorakis PN, Mantzavinis GD, Rrumbullaku L, et al. Measuring healthinequalities in Albania: a focus on the distribution of general practitioners.Hum Resour Health 2006;4:5.
33. UNICEF. At a glance: Iran, Islamic Republic of. UNICEF 2008. Available at: http://www.unicef.org/infobycountry/iran.html [accessed 15.04.09].
34. Van Beeck EF, Mackenbach JP, Looman CW, Kunst AE. Determinants of trafficaccident mortality in The Netherlands: a geographical analysis. Int J Epidemiol1991;20:698–706.
35. Von Elm E. Prehospital emergency care and the global road safety crisis. JAMA2004;292:923.
36. World Health Organization. Country profile of Iran. Regional Office for theEastern Mediterranean 2008. Available at: http://www.emro.who.int/iran/countryprofile.htm [accessed 20.09.09].
37. Zavareh DK, Mohammadi R, Laflamme L, et al. Estimating road traffic mortalitymore accurately: use of the capture-recapture method in the West Azarbaijanprovince of Iran. Int J Inj Control Saf Promot 2008;15:9–17.