pulmonary activation of coagulation and inhibition of fibrinolysis after burn injuries and...
TRANSCRIPT
ORIGINAL ARTICLE
Pulmonary Activation of Coagulation and Inhibition of FibrinolysisAfter Burn Injuries and Inhalation Trauma
Jorrit J. Hofstra, MD, Alexander P. Vlaar, MD, PhD, Paul Knape, MD, Dave P. Mackie, MD,Rogier M. Determann, MD, PhD, Goda Choi, MD, PhD, Tom van der Poll, MD, PhD, Marcel Levi, MD, PhD,
and Marcus J. Schultz, MD, PhD, FCCP
Background: Pulmonary coagulopathy is intrinsic to pneumonia and other formsof acute lung injury. We hypothesized patients with burn injuries and inhalationtrauma to have similar alterations in pulmonary coagulation and fibrinolysis.Methods: We performed a prospective study on changes in pulmonary andsystemic thrombin generation and fibrinolytic activity in patients with burninjuries and inhalation trauma requiring mechanical ventilation. Nondirectedbronchial lavage was performed on alternate days. Patients requiring me-chanical ventilation for nonpulmonary reasons who did not meet the NorthAmerican European Consensus Conference criteria for acute lung injuryfunctioned as control patients.Results: We studied 13 patients with burn injuries and inhalation trauma and15 control patients. On admission, patients with burn injuries and inhalationtrauma showed a significant increase in thrombin generation in the airwayscompared with control patients, as reflected by increased lavage fluid levelsof thrombin-antithrombin complexes and fibrin degradation products, anddecreased lavage fluid levels of activated protein C and antithrombin.Simultaneously, burn patients showed a significant decrease in fibrinolyticactivity, as reflected by decreased lavage fluid levels of plasminogen acti-vator activity. Pulmonary coagulopathy persisted throughout the period ofmechanical ventilation and was accompanied by similar changes in systemiccoagulation and fibrinolysis. There was no significant correlation betweenchanges in coagulation and fibrinolysis and the extent of burn injury.Conclusions: Patients with burn injuries and inhalation trauma requiringmechanical ventilation show a distinct and sustained procoagulant andantifibrinolytic shift in the pulmonary compartment. Pulmonary coagulopa-thy could be an important therapeutic target in these patients.Key Words: Burn injuries, Inhalation trauma, Coagulation, Fibrinolysis.
(J Trauma. 2011;70: 1389–1397)
In the United States, each year �50,000 patients are hospi-talized after burn injuries. Concomitant inhalation trauma is
reported in 20% to 35% of burn patients requiring hospital-
ization,1,2 and it is most frequently encountered after housefires, explosions, and other disasters involving fire withsmoke formation. Inhalation trauma is an important indepen-dent predictor of morbidity and mortality in patients withburn injuries and increases mortality by 20% to 60%. Al-though advanced care for burn injuries has improved out-come, respiratory complications of inhalation trauma remaina serious threat.3 To date, no specific intervention is availablefor the treatment of inhalation trauma and therapy is merelysupportive (i.e., intubation and mechanical ventilation).
Pulmonary coagulopathy is intrinsic to pneumonia andother forms of acute lung injury (ALI) or acute respiratorydistress syndrome (ARDS).4 Alveolar fibrin depositions inpneumonia and ALI/ARDS are the result of local activationof coagulation on the one hand and inhibition of fibrinolysison the other. Preclinical studies in models of ALI that specifi-cally targeted pulmonary coagulopathy have demonstrated thattreatment with anticoagulants has the potential to attenuatepulmonary coagulopathy and to reduce inflammation.5
We hypothesized burn patients with inhalation traumato show similar alterations in pulmonary coagulation andfibrinolysis as patients with pneumonia or ALI/ARDS. Ifpresent, systemic or maybe even local anticoagulant or pro-fibrinolytic therapies could benefit these patients. In thisobservational clinical study, we investigated pulmonary andsystemic coagulation and fibrinolysis in patients with burninjuries and concomitant inhalation trauma during mechani-cal ventilation.
PATIENTS AND METHODS
StudyAn observational study was performed in the intensive
care units (ICUs) of an academic hospital and a regionalteaching hospital specialized in care for burn patients in theNetherlands. The study protocol was reviewed and approvedby the local medical ethics committee. Admissions werescreened from January 2006 to December 2008, and writteninformed consent was obtained from patients or their closestrelatives before enrollment.
SubjectsPatients older than 18 years with burn injuries and
inhalation trauma, expected to need mechanical ventilationfor �72 hours, were eligible for participation. The clinical
Submitted for publication December 24, 2009.Accepted for publication January 10, 2011.Copyright © 2011 by Lippincott Williams & WilkinsFrom the Departments of Intensive Care Medicine (J.J.H., A.P.V., M.J.S.),
Anesthesiology (J.J.H.), and Internal Medicine (R.M.D., G.C., T.v.d.P., M.L.)and Center for Experimental and Molecular Medicine (T.v.d.P.), AcademicMedical Center, University of Amsterdam, Amsterdam, The Netherlands; andDepartment of Anesthesiology (P.K., D.P.M.), Rode Kruis Ziekenhuis, Brand-wonden Centrum Beverwijk, Beverwijk, The Netherlands.
The first two authors contributed equally to this work.Address for reprints: Alexander P.J. Vlaar, MD, Department of Intensive Care Medicine,
C3-329, Academic Medical Center, University of Amsterdam, Meibergdreef 9, 1105AZ Amsterdam, The Netherlands; email: [email protected].
DOI: 10.1097/TA.0b013e31820f85a7
The Journal of TRAUMA® Injury, Infection, and Critical Care • Volume 70, Number 6, June 2011 1389

diagnosis of inhalation trauma traditionally rests on indirectobservation: inhalation trauma was suspected in patients whowere trapped in a confined space or who lost consciousnessduring a fire, the presence of soot in throat or sputum, andpresence of facial and upper cervical burns, singed eyebrows,and nasal vibrissae. For the purpose of this study, the clinicaldiagnosis had to be confirmed with bronchoscopy showingsoot or infralaryngeal mucosal damage, indicating exposureof the tracheobronchial tree to the physical products ofcombustion.
Patients older than 18 years with neither burn injuriesnor inhalation trauma who did not meet the North AmericanEuropean Consensus Conference (NAECC) criteria for ALI/ARDS and were expected to require mechanical ventilationfor �72 hours functioned as control patients. Participation ininterventional trials, pregnancy, increased intracranial pres-sure, and preexisting severe chronic respiratory disease (de-fined as a forced expiratory volume in 1 second to forced vitalcapacity ratio �0.64 and daily medication), and suspectedpneumonia were exclusion criteria in addition to the use ofcorticosteroids or other immunosuppressive agents and intra-venously administered heparin. Treatment of patients (i.e.,ventilator settings, fluid resuscitation, use of vasopressors,and antibiotic treatment) was based on local guidelines thatwere in accordance with international guidelines.
All patients were ventilated with Evita 4 ventilators(Drager, Zoetermeer, The Netherlands) in volume-controlledmode, with tidal volumes of 6 mL/kg predicted body weight.The levels of positive end-expiratory pressure (PEEP) andinspired oxygen (FIO2) were titrated on PaO2 according to thelocal mechanical ventilation guideline. The ventilator wasroutinely (3 times/d) switched to the pressure support mode.If the pressure support mode was tolerated, this mode wasused for further mechanical ventilation.
Data CollectionDemographic data, admission diagnosis, the Acute
Physiology and Chronic Health Evaluation (APACHE) IIscores and data on the extent of burn injury, expressed as apercentage of the total body surface area (TBSA), werecalculated using Lund-Bowder charts. On ICU admission andeach alternate day, ventilator settings, blood gas parameters,and chest radiographs data were recorded until the patientwas completely weaned from the mechanical ventilator.
The oxygenation index was calculated from the venti-lator and blood gas analyses data using the following for-mula: mean airway pressure � FIO2 � 100%/PaO2. Meanairway pressure was measured by the ventilator. The lunginjury score (LIS) was calculated.6
All patients were monitored for development of ALI/ARDS. ALI/ARDS was diagnosed if a patient met theNAECC criteria. Two independent physicians who wereblinded to patient or group identity scored chest radiographsfor the presence of bilateral interstitial changes. During thereview process, they had access to echocardiography resultsand data on fluid balance and pulmonary capillary wedgepressures if measured. When interpretation differed, consen-sus was obtained while reviewing the patients together.
Specimen CollectionBlood sample collection followed by nondirected bron-
chial lavage was performed on ICU admission and eachalternate day throughout the period of mechanical ventilation.Blood samples were drawn into sterile Vacutainer tubescontaining citrate, using an already in place arterial catheter.Lavage was performed by instilling 20 mL of sterile 0.9%saline via a standard 50 cm, 14-French tracheal suctioncatheter as described previously.7 In short, the distal end ofthe catheter was introduced via the endotracheal tube andadvanced until significant resistance was encountered. Imme-diately after instillation over 10 seconds, fluid was aspiratedbefore withdrawal of the catheter. Generally, 4 mL to 8 mL offluid was recovered.
Specimen ProcessingThe lavage fluids and blood samples were centrifuged
at 1,500 � g for 10 minutes at 4°C. The specimens werecentrifuged at 1,500 g for 10 minutes at 4°C. The superna-tants were stored at �80°C until assays were performed.Blood samples were centrifuged at 1,500 g for 10 minutes at4°C and supernatants were stored at �80°C until assays wereperformed.
AssaysThrombin generation was assessed by measuring
thrombin-antithrombin complex (TATc) levels by means ofan enzyme-linked immunosorbent assay (Behring, Marburg,Germany). Antithrombin (AT) levels were measured by anautomated amidolytic assay. Levels of activated protein C(APC) were measured with an enzyme capture assay, usingmonoclonal antibody HAPC 1555 and chromogenic substrateSpectrozyme PCa (American Diagnostica, Greenwich, CT).Plasminogen activator activity (PAA) and plasminogen acti-vator inhibitor (PAI)-1 activity were measured by amidolyticassays.
Statistical AnalysisData are expressed as mean � 95% confidence interval
or median with interquartile ranges, as appropriate. Compar-isons between groups on the different time points were madeby the Student’s t test or Mann-Whitney U test, as appropri-ate. Correlation between percentage of TBSA involved inburn injury and markers of coagulation and fibrinolysis wereassessed by linear regression analysis of mean, minimum, andmaximum values of each patient during the complete studyperiod. The balance between procoagulant and anticoagulantactivity was assessed by determination of the TATc to PAAratio. A two-tailed p value �0.05 was considered as statisti-cally significant. Data were analyzed using SPSS, version16.0 (SPSS Inc., Chicago, IL).
RESULTS
PatientsData and sample collection were completed for 28
patients; 13 patients with burn injuries and inhalation traumaand 15 control patients. Baseline characteristics are shown inTable 1. Burn patients were younger than control patients and
Hofstra et al. The Journal of TRAUMA® Injury, Infection, and Critical Care • Volume 70, Number 6, June 2011
© 2011 Lippincott Williams & Wilkins1390
had lower APACHE II scores. Two burn patients sufferedfrom ALI/ARDS on ICU admission and three burn patientsdeveloped ALI/ARDS during the course of mechanical ven-tilation (on days 2, 4, and 6, respectively). There was nodifference between groups with regard to the recovered vol-ume of lavage fluid.
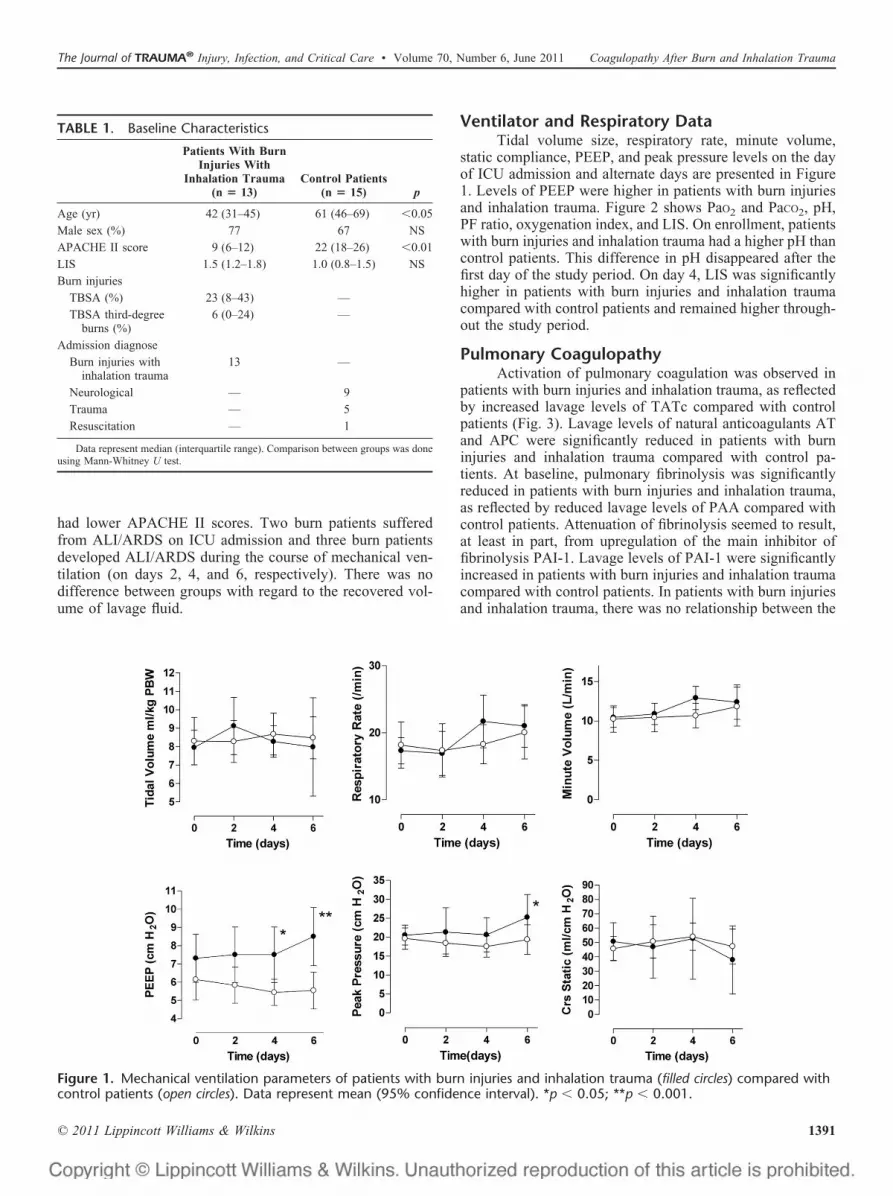
Ventilator and Respiratory DataTidal volume size, respiratory rate, minute volume,
static compliance, PEEP, and peak pressure levels on the dayof ICU admission and alternate days are presented in Figure1. Levels of PEEP were higher in patients with burn injuriesand inhalation trauma. Figure 2 shows PaO2 and PaCO2, pH,PF ratio, oxygenation index, and LIS. On enrollment, patientswith burn injuries and inhalation trauma had a higher pH thancontrol patients. This difference in pH disappeared after thefirst day of the study period. On day 4, LIS was significantlyhigher in patients with burn injuries and inhalation traumacompared with control patients and remained higher through-out the study period.
Pulmonary CoagulopathyActivation of pulmonary coagulation was observed in
patients with burn injuries and inhalation trauma, as reflectedby increased lavage levels of TATc compared with controlpatients (Fig. 3). Lavage levels of natural anticoagulants ATand APC were significantly reduced in patients with burninjuries and inhalation trauma compared with control pa-tients. At baseline, pulmonary fibrinolysis was significantlyreduced in patients with burn injuries and inhalation trauma,as reflected by reduced lavage levels of PAA compared withcontrol patients. Attenuation of fibrinolysis seemed to result,at least in part, from upregulation of the main inhibitor offibrinolysis PAI-1. Lavage levels of PAI-1 were significantlyincreased in patients with burn injuries and inhalation traumacompared with control patients. In patients with burn injuriesand inhalation trauma, there was no relationship between the
TABLE 1. Baseline Characteristics
Patients With BurnInjuries With
Inhalation Trauma(n � 13)
Control Patients(n � 15) p
Age (yr) 42 (31–45) 61 (46–69) �0.05
Male sex (%) 77 67 NS
APACHE II score 9 (6–12) 22 (18–26) �0.01
LIS 1.5 (1.2–1.8) 1.0 (0.8–1.5) NS
Burn injuries
TBSA (%) 23 (8–43) —
TBSA third-degreeburns (%)
6 (0–24) —
Admission diagnose
Burn injuries withinhalation trauma
13 —
Neurological — 9
Trauma — 5
Resuscitation — 1
Data represent median (interquartile range). Comparison between groups was doneusing Mann-Whitney U test.
Figure 1. Mechanical ventilation parameters of patients with burn injuries and inhalation trauma (filled circles) compared withcontrol patients (open circles). Data represent mean (95% confidence interval). *p � 0.05; **p � 0.001.
The Journal of TRAUMA® Injury, Infection, and Critical Care • Volume 70, Number 6, June 2011 Coagulopathy After Burn and Inhalation Trauma
© 2011 Lippincott Williams & Wilkins 1391

Figure 3. Levels of TATc, AT, APC, PAA, and PAI-1 in lavage fluid of patients with burn injuries and inhalation trauma (filledcircles) compared with control patients (open circles). Data represent median with interquartile ranges. **p � 0.001 for all timepoints.
Figure 2. Respiratory values and lung injury score of patients with burn injuries and inhalation trauma (filled circles) comparedwith control patients (open circles). Data represent mean (95% confidence interval). *p � 0.05.
Hofstra et al. The Journal of TRAUMA® Injury, Infection, and Critical Care • Volume 70, Number 6, June 2011
© 2011 Lippincott Williams & Wilkins1392

extent of pulmonary coagulopathy and the presence or devel-opment ALI/ARDS.
Correlations between pulmonary coagulopathy and theextent of burn injury, expressed as percentage TBSA burn,were poor to medium (Fig. 4). Only the minimum level ofAPC in each patient was significantly associated with burnsize, similar to the correlations between pulmonary coagu-lopathy and the severity of the burn injury as measured bypercentage third-degree TBSA burn (data not shown).
Systemic CoagulopathyAll patients with burn injuries and inhalation trauma
had systemic hemostatic disturbances as reflected by in-creased plasma levels of TATc and reduced plasma levels ofPAA (Fig. 5). Correlations between systemic coagulopathyand the percentage TBSA burn (Fig. 6), and third-degreeTBSA burn (data not shown) were poor. The procoagulant-anticoagulant balance, expressed as TATc to PAA ratio, wassignificantly higher in the burn and inhalation trauma patientscompared with the control patients (0.04 � 0.02 vs. 0.009 �0.003, p � 0.0001).
DISCUSSIONIn this study, marked procoagulant and antifibrinolytic
changes were found in the airways of patients with burninjuries and inhalation trauma compared with patients with-out burn injuries and inhalation trauma and no ALI/ARDS.Pulmonary coagulopathy seems to be intrinsic to inhalationtrauma. All patients with burn injuries and inhalation traumademonstrated pulmonary coagulopathy to a similar degree,irrespective of the presence or development of ALI/ARDS orthe extent of burn injury, expressed as TBSA burn. This is thefirst study on the presence and extent of pulmonary coagu-lopathy in patients with burn injuries and inhalation trauma.
Previous studies have reported increased procoagulantactivity in the alveolar space in patients with pneumonia orALI/ARDS.4,8 Gunther et al.4 found disturbances in the alve-olar hemostatic balance in patients with severe pneumonia,both spontaneously breathing and those requiring mechanicalventilation. Schultz et al.8 demonstrated disturbances in thelocal hemostatic balance in mechanically ventilated patientswho developed ventilator-associated pneumonia. In thisstudy, there was a marked increase in procoagulant activitywith an increase in PAI-1 levels even before the diagnosis ofpneumonia was made clinically, suggesting that a shift in thehemostatic balance in the lungs toward a procoagulant state isan early feature of pulmonary inflammation. This studyconfirms the hypothesis that similar procoagulant changes arepresent in the lungs of patients with burn injuries and inha-lation trauma.
Interestingly, similar to the early procoagulant changesin pneumonia, the procoagulant changes after burn injuriesand inhalation trauma occur shortly after the insults. Al-though pulmonary coagulopathy was a consistent finding inburn patients, only a minority of the 13 patients developALI/ARDS. At first glance, this contradicts with the above-mentioned hypothesis; however, ALI/ARDS was diagnosedonly when patients fulfilled the NAECC criteria. These cri-teria may be difficult to interpret, especially when higher
levels of PEEP are being applied. Indeed, higher levels ofPEEP may erroneously give the impression that ALI/ARDSis not present or resolving. Hence, pulmonary coagulopathymay be present in patients not (yet) fulfilling the NAECCcriteria. The correlation data of coagulopathy and LIS under-line this hypothesis. The LIS corrects for level of PEEP andconsequently an increase in coagulopathy was correlated witha higher LIS. Notably, levels of PEEP were already higher onpostburn day 1 in the burn patients with inhalation comparedwith the control patients. Since mechanical ventilation pro-tocols were similar for burn patients and patients withoutburns, in particular with respect to the titration of levels ofPEEP and FIO2, this suggests that burn patients with inhala-tion already developed lung injury early after the insult.
Higher systemic levels of TAT and lower levels ofPAA were found in patients with burn and inhalationtrauma. With this design of the study, we were unable toanalyze whether this was caused by the burn or by theinhalation trauma.
Ware et al.9 demonstrated the degree of pulmonarycoagulopathy to be an independent risk factor for mortalityand adverse clinical outcomes of ALI/ARDS patients. Al-though being a precondition for secondary reparative pro-cesses, there is a substantial body of in vitro and in vivo data,suggesting that pulmonary coagulopathy and persistent depo-sition of fibrin in the alveolar compartment contribute to lunginjury. Thrombin exerts proinflammatory effects through itsregulation of cytokine transcription and release and is responsi-ble for the increased production of interleukin-6, interleukin-1beta, and monocyte chemotactic protein-1. Binding of fibrin tomonocytes activates the transcription of NF-kB and AP-1,which in turn regulates the production of various cytokines.10
Furthermore, the binding of fibrin to monocytes and othercells enhances the inflammatory response by facilitating andenhancing cell migration. Fibrin may also directly compro-mise lung function by inactivating surfactant leading to lossof lung compliance and atelectasis.11 Fibrin has been shownto be an important composite of obstructive cast material inan ovine model of combined smoke inhalation and burn.12,13
Pathology studies in this model have shown that obstructingmaterials are mainly composed of infiltrated neutrophils, shedbronchial epithelial cells, mucus, and fibrin.14,15 Indeed, inthis model, treatment with aerosolized tissue-plasminogenactivator significantly improved pulmonary function.16 Inter-estingly, nebulized tissue-plasminogen activator has alsobeen shown to be of benefit in the removal of mucous clots ina pediatric patient with plastic bronchitis.17
Activation of coagulation during inflammation is aphysiologic response, which helps containing inflammatoryactivity (or infection) at the site of injury. However, it mayalso aggravate inflammation and thus contribute to disease.Blocking coagulation or stimulating fibrinolysis could theo-retically dampen the inflammatory response thereby reducinglung injury. Moreover, many anticoagulant and profibrinolytic com-pounds have also been shown to have anti-inflammatory effectsthat seem to be independent of their anticoagulant and pro-fibrinolytic properties.5 Of interest, in our study, the extent ofburn injury, expressed as TBSA burn was associated with a
The Journal of TRAUMA® Injury, Infection, and Critical Care • Volume 70, Number 6, June 2011 Coagulopathy After Burn and Inhalation Trauma
© 2011 Lippincott Williams & Wilkins 1393
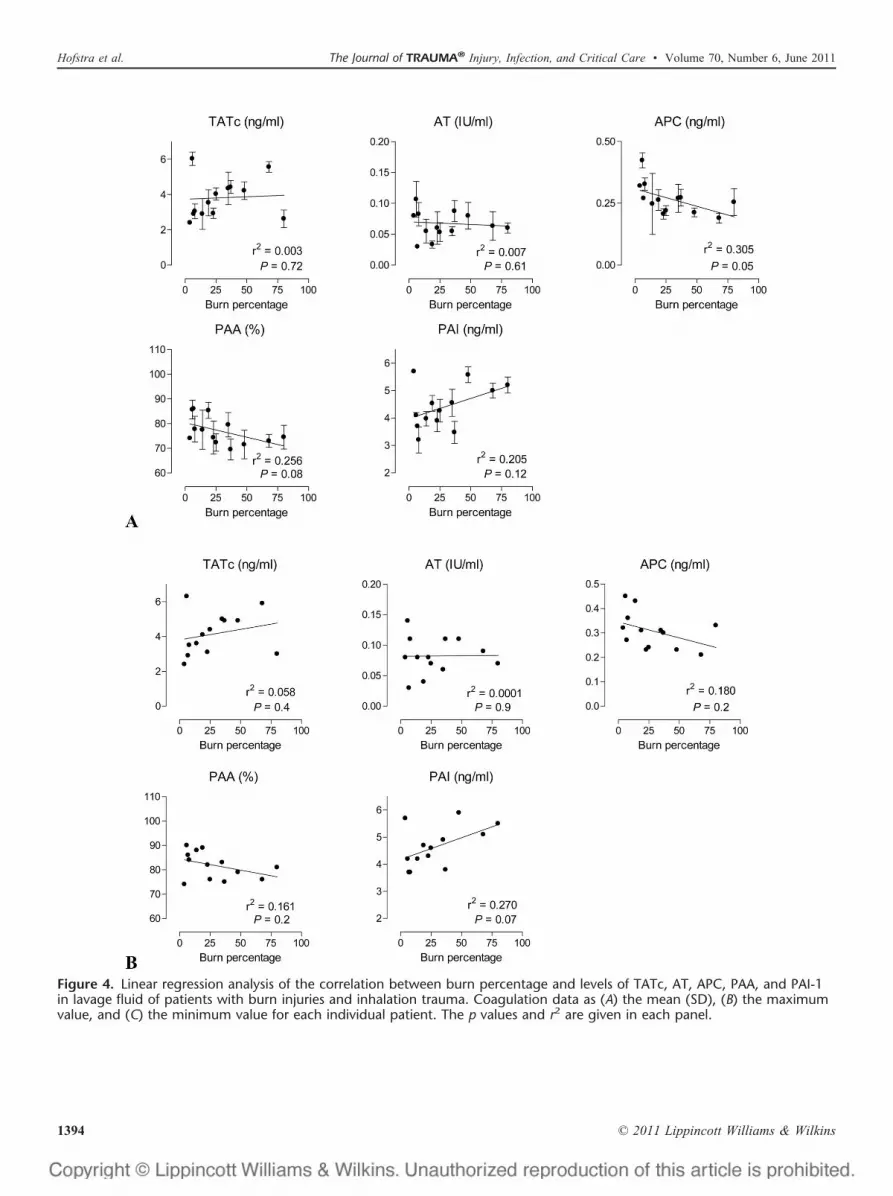
Figure 4. Linear regression analysis of the correlation between burn percentage and levels of TATc, AT, APC, PAA, and PAI-1in lavage fluid of patients with burn injuries and inhalation trauma. Coagulation data as (A) the mean (SD), (B) the maximumvalue, and (C) the minimum value for each individual patient. The p values and r2 are given in each panel.
Hofstra et al. The Journal of TRAUMA® Injury, Infection, and Critical Care • Volume 70, Number 6, June 2011
© 2011 Lippincott Williams & Wilkins1394

decrease in pulmonary APC levels, suggesting that burninjury results in a loss of anticoagulant function.
Several preclinical models of inhalation trauma inves-tigated the effects of anticoagulants on the formation ofairway obstructive casts. Infusion of unfractionated heparinsreduced pulmonary fibrin depositions and improved oxygen-ation in a combined ovine model of smoke inhalation andbarotraumas.18 However, inflammatory responses in lungswere similar to control patients. However, local administra-tion of heparin to the lungs through nebulization did show areduction in cellular infiltration of the lungs in an ovinemodel of smoke inhalation injury combined with intratrachealinstillation of bacteria.19 In an ovine model of smoke inhala-
tion injury combined with intratracheal administration ofbacteria, infusion of APC improved oxygenation but did notaffect pulmonary edema.20 Intravenously administered andaerosolized recombinant human AT in combination withaerosolized heparin in an ovine model of ALI/ARDS inducedby skin burn and cotton smoke inhalation attenuated allobserved pulmonary pathophysiology.21,22 It remains unclearto what extent the beneficial effects of these aerosolizedagents rest on the breakdown of central bronchial obstruc-tions or on the effects on alveolar fibrin, the end product ofcoagulation. To date, only one rather small clinical trialinvestigated the effect of anticoagulant therapy for inhalationtrauma. In pediatric patients suffering from inhalation injury,
Figure 4. (Continued).
Figure 5. Systemic levels of TATc and PAA in patients withburns and inhalation trauma (filled circles) compared withcontrol patients (open circles). Data represent medianwith interquartile ranges. **p � 0.001 for all time points.
Figure 6. Linear regression analysis of the correlation be-tween burn percentage and systemic levels of TATc and PAAin patients with burn injuries and inhalation trauma. Datarepresent the mean (SD) for each individual patient. The pvalues and r2 are given in each panel.
The Journal of TRAUMA® Injury, Infection, and Critical Care • Volume 70, Number 6, June 2011 Coagulopathy After Burn and Inhalation Trauma
© 2011 Lippincott Williams & Wilkins 1395

treatment with a combination of nebulized heparin reducedmortality.23 However, since treatment with heparin in this studywas combined with the mucolytic agent, N-acetylcystein, it isimpossible to determine the exact role of alveolar anticoagula-tion on mortality in these patients.
A limitation of our study is that we only comparedpatients with combined burn injuries and inhalation traumawith a control group of ventilated patients without lunginjury. Ideally, we should have compared patients with solelysmoke inhalation with patients with solely burns. However,burn patients without inhalation trauma frequently do notneed intubation and mechanical ventilation for several daysunless the burn is very large, and patients with solely inha-lation trauma have self-limited injury with fairly rapid extu-bation as well. As a consequence, we were only able to adda control group of ventilated patients without burns andinhalation trauma. This makes it difficult to analyze to whatextent burn injuries and inhalation trauma separately contrib-uted to the disturbances in pulmonary coagulation. The ef-fects of burn injuries on systemic coagulation and fibrinolysisas described previously may have contributed to pulmonarycoagulopathy.24 In other words, the changes in coagulationand fibrinolysis found in the pulmonary compartment (asmeasured in the lavage fluid) could be the result of leakagefrom the system. Indeed, we also observed increased activa-tion of coagulation in the systemic compartment. However,this seems unlikely for the following reasons: (1) with theused lavage technique, there is a �100-fold dilution ofalveolar concentrations, so the levels of coagulation andfibrinolysis markers were much higher in the pulmonarycompartment than systemic levels; and (2) the correlationbetween pulmonary coagulopathy and the extent and severityof the burn injuries was poor.
Another shortcoming is that because of the absence (inthe literature) of a satisfactory means to assess the severity ofinhalation injury, we were not able to quantify inhalationinjury in our patients.25 It can be speculated that morecoagulopathy exists with more severe inhalation trauma.
Another limitation of our study is that at baseline, thepatients in the control group differed from the patients withburn injuries and inhalation trauma with regard to age andAPACHE II scores. However, it is unlikely that age affectedpulmonary coagulation and fibrinolysis in our study. Thedifference in baseline APACHE II score seems to indicatethat the control patients were more severely ill than thepatients with burn injuries and inhalation trauma. However, itshould be noted that the APACHE II score is of limited usein burn patients with inhalation trauma since neurologic,metabolic, hemodynamic, and respiratory problems usuallydo not occur until hours after admission. Also, a considerablepart of difference in APACHE II scores was due to the factthat the control patients were mostly neurologic admissionswith a lower Glasgow Coma Score.
Finally, the samples obtained from these patientsmay not adequately reflect changes in coagulation andfibrinolysis in the alveoli because of the sampling strategy.We used a nondirected lavage technique to obtain samplesfrom the pulmonary compartment. This technique only
yields samples from the larger airways. Procoagulantchanges in larger airways may not reflect changes in thesmaller airways and alveoli.
In conclusion, pulmonary coagulopathy seems intrinsicto burn injury and inhalation trauma. It could be an importanttherapeutic target in these patients. Further clinical researchshould investigate whether anticoagulant interventions arebeneficial in patients with burn injuries and inhalationtrauma.
REFERENCES1. Dancey DR, Hayes J, Gomez M, et al. ARDS in patients with thermal
injury. Intensive Care Med. 1999;25:1231–1236.2. Barillo DJ, Goode R. Fire fatality study: demographics of fire victims.
Burns. 1996;22:85–88.3. Santaniello JM, Luchette FA, Esposito TJ, et al. Ten year experience of
burn, trauma, and combined burn/trauma injuries comparing outcomes.J Trauma. 2004;57:696–700.
4. Gunther A, Mosavi P, Heinemann S, et al. Alveolar fibrin formationcaused by enhanced procoagulant and depressed fibrinolytic capacitiesin severe pneumonia. Comparison with the acute respiratory distresssyndrome. Am J Respir Crit Care Med. 2000;161:454–462.
5. Hofstra JJ, Haitsma JJ, Juffermans NP, Levi M, Schultz MJ. The role ofbronchoalveolar hemostasis in the pathogenesis of acute lung injury.Semin Thromb Hemost. 2008;34:475–484.
6. Murray JF, Matthay MA, Luce JM, Flick MR. An expanded definition ofthe adult respiratory distress syndrome. Am Rev Respir Dis. 1988;138:720–723.
7. Millo JL, Schultz MJ, Williams C, et al. Compartmentalisation ofcytokines and cytokine inhibitors in ventilator-associated pneumonia.Intensive Care Med. 2004;30:68–74.
8. Schultz MJ, Millo J, Levi M, et al. Local activation of coagulation andinhibition of fibrinolysis in the lung during ventilator associated pneu-monia. Thorax. 2004;59:130–135.
9. Ware LB, Matthay MA, Parsons PE, et al. Pathogenetic and prognosticsignificance of altered coagulation and fibrinolysis in acute lung injury/acute respiratory distress syndrome. Crit Care Med. 2007;35:1821–1828.
10. Johnson K, Choi Y, DeGroot E, Samuels I, Creasey A, Aarden L.Potential mechanisms for a proinflammatory vascular cytokine responseto coagulation activation. J Immunol. 1998;160:5130–5135.
11. Seeger W, Elssner A, Gunther A, Kramer HJ, Kalinowski HO. Lungsurfactant phospholipids associate with polymerizing fibrin: loss ofsurface activity. Am J Respir Cell Mol Biol. 1993;9:213–220.
12. Herndon DN, Traber DL, Niehaus GD, Linares HA, Traber LD. Thepathophysiology of smoke inhalation injury in a sheep model. J Trauma.1984;24:1044–1051.
13. Basadre JO, Sugi K, Traber DL, Traber LD, Niehaus GD, Herndon DN.The effect of leukocyte depletion on smoke inhalation injury in sheep.Surgery. 1988;104:208–215.
14. Cox RA, Burke AS, Oliveras G, et al. Acute bronchial obstruction insheep: histopathology and gland cytokine expression. Exp Lung Res.2005;31:819–837.
15. Cox RA, Burke AS, Soejima K, et al. Airway obstruction in sheep withburn and smoke inhalation injuries. Am J Respir Cell Mol Biol. 2003;29:295–302.
16. Enkhbaatar P, Murakami K, Cox R, et al. Aerosolized tissue plasmino-gen inhibitor improves pulmonary function in sheep with burn andsmoke inhalation. Shock. 2004;22:70–75.
17. Costello JM, Steinhorn D, McColley S, Gerber ME, Kumar SP. Treatmentof plastic bronchitis in a Fontan patient with tissue plasminogen activator: acase report and review of the literature. Pediatrics. 2002;109:e67.
18. Cox CS Jr, Zwischenberger JB, Traber DL, Traber LD, Haque AK,Herndon DN. Heparin improves oxygenation and minimizes barotraumaafter severe smoke inhalation in an ovine model. Surg Gynecol Obstet.1993;176:339–349.
19. Murakami K, McGuire R, Cox RA, et al. Heparin nebulization attenu-ates acute lung injury in sepsis following smoke inhalation in sheep.Shock. 2002;18:236–241.
Hofstra et al. The Journal of TRAUMA® Injury, Infection, and Critical Care • Volume 70, Number 6, June 2011
© 2011 Lippincott Williams & Wilkins1396

20. Maybauer MO, Maybauer DM, Fraser JF, et al. Recombinant humanactivated protein C improves pulmonary function in ovine acute lunginjury resulting from smoke inhalation and sepsis. Crit Care Med.2006;34:2432–2438.
21. Enkhbaatar P, Esechie A, Wang J, et al. Combined anticoagulantsameliorate acute lung injury in sheep after burn and smoke inhalation.Clin Sci (Lond). 2008;114:321–329.
22. Enkhbaatar P, Cox RA, Traber LD, et al. Aerosolized anticoagulantsameliorate acute lung injury in sheep after exposure to burn and smokeinhalation. Crit Care Med. 2007;35:2805–2810.
23. Desai MH, Mlcak R, Richardson J, Nichols R, Herndon DN. Reductionin mortality in pediatric patients with inhalation injury with aerosolizedheparin/N-acetylcystine [correction of acetylcystine] therapy. J BurnCare Rehabil. 1998;19:210–212.
24. Lavrentieva A, Kontakiotis T, Bitzani M, et al. Early coagulationdisorders after severe burn injury: impact on mortality. Intensive CareMed. 2008;34:700–706.
25. Liffner G, Bak Z, Reske A, Sjoberg F. Inhalation injury assessed byscore does not contribute to the development of acute respiratory distresssyndrome in burn victims. Burns. 2005;31:263–268.
The Journal of TRAUMA® Injury, Infection, and Critical Care • Volume 70, Number 6, June 2011 Coagulopathy After Burn and Inhalation Trauma
© 2011 Lippincott Williams & Wilkins 1397