injuries to the phrenic nerve resulting in diaphragmatic paralysis with special reference to stretch...
TRANSCRIPT

Injuries to the Phrenic Nerve Resulting in Diaphragmatic
Paralysis with Special Reference to Stretch Trauma
Leigh I. G. Iverson, MD,’ Oakland, California
Arun Mlttal, MD,* Torrance, California
David J. Dugan, MD, Oakland, California
Paul C. Samson, MD, Oakland, California
The incidence of phrenic nerve injury with resulting diaphragmatic paralysis or eventration in the adult is not accurately known. This syndrome is certainly much more common than clinically recognized. Bisgard [I] defined eventration as “an abnormally high elevated position of one leaf of the intact dia- phragm as a result of paralysis, aplasia or atrophy of varying degrees of the muscle fibers.” In his review of eventration, Thomas [2] further separated the condition into congenital (nonparalytic) and ac- quired (paralytic). Traumatic eventration of the di- aphragm was first mentioned by Cruveilhier [3] in the middle of the last century. There have been only sporadic reports (perhaps 15) of this injury in the literature since that time [4-71. We have now re- viewed our own group of patients with traumatic diaphragmatic paralysis and this summary concerns their clinical presentation and treatment. To our certain knowledge this is the largest series of person&l cases so far reported. Emphasis is given to our pa- tients who have had stretch injuries of the phrenic nerve.
Injuries to the phrenic nerve may be classified as follows:
A. Direct (Seddon’s neurotmesis or neuraprax- ia)
1. Stab wound-knife, ice pick 2. Missile wound-gunshot or shell fragment 3. Iatrogenic
a. Deliberate-phrenic nerve crush (Sed- don’s axonotmesis), phrenic exeresis, radical cancer resection
b. Accidental-pericardiectomy, pleurec- tomy, empyemectomy, lysis of adhesions
From the Division of Thwacic end Cardiac Swgwy, Samuel Merritt Hospital, and the DepMnwnt of Ttwxacic Sugery, Ht#dad General Hospital, D&land, Callfomia.
Reprint requests shouM be addressed to David J. Dugan, MD, 3300 Webster Street, Oaklend. California 94609.
Presented at the Forty-Seventh Annual Meeting of the Pacific Coast Surgical Association, Monterey, California, February 15-18. 1976.
B. Indirect (Seddon’s axonotmesis, neurotmesis, or neurapraxia)
1. Crush injury of the chest (predominantly stretch injury)
2. Stretch injury (traction) of the neck (Sed- don’s axonotmesis or neurotmesis)
a. Cervical plexus b. Cervical and brachial plexus
The mechanism of injury may be penetrating or nonpenetrating trauma. The penetrating injuries, although uncommon, have obvious mechanisms. Depending on the degree of contusion, laceration, or transection, the injury may be self-limited, with gradual return of function, or it may be permanent. When phrenic crush procedures were performed in treating tuberculosis, the majority of patients had return of diaphragmatic motion over the following six months. The extent of injury and resultant disa- bility may also be modified by an accessory phrenic nerve. This nerve may arise from the fifth cervical root or from the nerve to the subclavius.
The accessory phrenic nerve may escape injury that involves the main phrenic nerve.
Nonpenetrating injuries may be less evident as to cause. In cervical strain, forced flexion or rotation of the occiput toward a fixed depressed shoulder can cause a stretch (traction) injury or even an avulsion of any part or all of the cervical and brachial plexus. Theoretically, at least hyperextension, hyperflexion injuries of the cervical spine (so-called whiplash) should cause phrenic paralysis frequently, but this has not been the case in our small series. In only one instance was a hyperextension cervicobrachial injury indicated.
Crushing chest injuries have far less obvious spe- cific causes. It is entirely possible and indeed prob- able that a severe traction or stretch injury has many times been hidden in the crushed chest.
The exquisite descriptions by Seddon [8] of the types of peripheral nerve injury are most instructive.
Volume 132, Au~d 1976 263
lverson et al
For instance, the term “axonotmesis” is a convenient name for the type of phrenic crush we used to apply therapeutically. Firm pressure is necessary, and it must be repeated several times at one spot to have axons and their myelin sheaths broken. The stroma of the nerve, however, remains in continuity; the Schwann basement membranes persist.
“Neurotmesis” implies a separation of parts .and can well be applied to stretch or traction injuries which are permanent. The term is more inclusive than mechanical division because it also embraces lesions in which the nerve preserves an appearance of continuity but is, in fact, totally destroyed over a longer or shorter distance.
The phrenic nerve is an “internal” peripheral nerve and is not subject to the usual methods of ex- amination. Since there is ordinarily no emergency about open exploration, the differential between “neurotmesis” (a permanent paralysis) and “neu- rapraxia” (“the nerve being out of action” for a pe- riod) is generally a matter of time. If the paralysis lasts more than six months, it should be assumed to be permanent. Surgical imbrication then depends upon the symptoms. Operation, however, should be prompt if signs and symptoms warrant.
Signs and symptoms may vary. The injury may be missed initially either because of the magnitude of associated trauma or because the patient is asymp- tomatic. Patients may remain asymptomatic for months or years. Many of these injuries may be mistaken for congenital (nonparalytic) eventration of the diaphragm. Thomas [9] has pointed out that in congenital eventration true paradoxical motion of the diaphragm is not present: “The initial passive upward movement of the redundant portion of the diaphragm, until the slack is taken up, is sometimes confused with paradoxical motion. The muscularized portion will contract simultaneously with the oppo- site diaphragm.” Symptoms may be dyspeptic, res- piratory, and circulatory or any combination of the three [IO]. The abdominal symptoms are determined by the particular diaphragm which has been injured. In right diaphragmatic paralysis the patient may develop symptoms of gallbladder dysfunction. In left-sided paralysis the symptoms may be those of gastric outlet obstruction, that is, nausea, vomiting’, bloating, and pain. Gastric symptoms can be relieved by lying on the left or right side, depending on which is necessary to improve gastric drainage [II]. Vol- vulus of the stomach has been reported in instances with a very high lying left diaphragm [12]. Respira- tory symptoms include dyspnea, pain, cough, and cyanosis. Cardiac symptoms include palpitation, tachycardia, and extrasystoles.
Pathophysiologically, the respiratory distress is due to a combination of events. The elevated dia- phragm results in atelectasis, and the mediastinum shifts toward the normal side on inspiration. Actual mediastinal flutter may be observed fluoroscopically. Gastric and gallbladder symptoms are due to eleva- tion of the ipsilateral diaphragm and consequent displacement of the intra-abdominal organs.
Physical findings are characteristic of loss of dia- phragmatic movement. Respiration may be labored. Breath sounds are absent, the percussion note is dull,
,and fremitus is increased over the lower chest wall. Bowel sounds may be heard instead of breath sounds in the region of the left lower lobe. Hoover’s sign may occur, that is, uninhibited movement of the costal margin away from the midline on the side of injury [13]. This is due to intercostal muscle contraction which is no longer opposed by the now paralyzed ipsilateral diaphragm. Associated brachial plexus injuries and more serious trauma of the cervical plexus may coexist. Skeletal injuries of the chest, neck, and shoulder girdle as well as more distant sites can accompany the phrenic paralysis. Visceral in- juries within the thorax and abdomen may occur and often interfere with recognition of the diaphragmatic injury. X-ray films and fluoroscopy remain the cor- nerstone in making the definitive diagnosis. Both inspiratory and expiratory fiis are required to show the degree of movement of the diaphragm. The sine qua non of the diagnosis is fluoroscopic evidence of paradoxical motion of the involved diaphragm (Kienback’s phenomenon). The patient exhales slowly and sniffs vigorously in the performance of this test. Pulmonary function studies will show a restrictive defect of varying severity.
Treatment must be individualized and depends on the incapacity of the individual. Most often the pa- tient will improve with time as diaphragmatic motion returns. Residual symptoms depend on the com- pleteness of return to normal function by the phrenic nerve and whether or not isolated segments of the diaphragm remain paralyzed. In those who are in- capacitated by their symptoms a straightforward but effective operative procedure is available. Through a low thoracotomy the adhesions between diaphragm and chest wall are freed circumferentially down to the normal attachments. The diaphragm is then incised anterolaterally to posteromedially and imbricated so as to flatten it out at the lowest possible part of the thoracic cavity. Redundant and attenuated dia- phragmatic tissue is excised as necessary. The effects of this in returning the enteric organs to their normal positions as well as the consequent relief of com- pression atelectasis are obvious. Sarnoff and co-
264 The American Journal of Surgery
Phrenic Nerve injuries
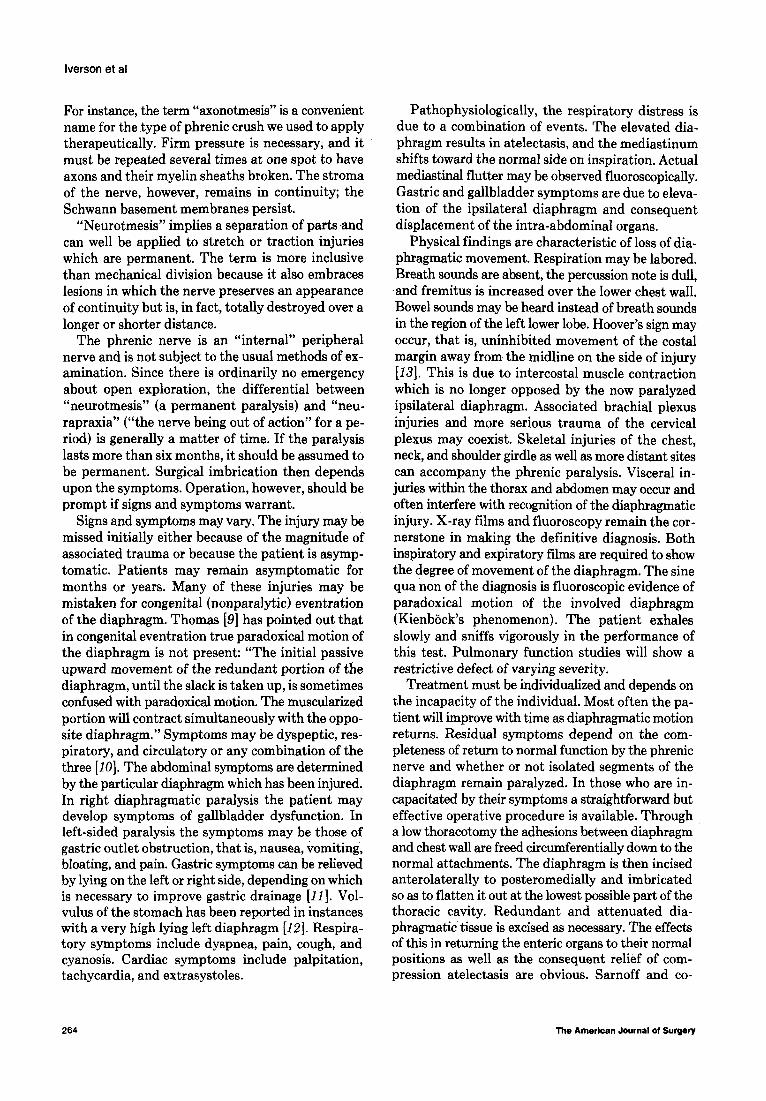
Figure 1. Complete transection of left phrenic nerve found at thoracotomy. (Reprinted from [16] by permlssion of publisher.)
workers [14,15) in animal experiments as well as man have demonstrated that this also significantly im- proves ventilation dynamics. Studies of arterial gases and oxygen uptake as well as differential spirometry in these patients showed that the contralateral lung was functioning normally. Presumably then, if a hi& lying diaphragm is surgically corrected to lie in a more normal position, the patient’s respiratory function will return to normal as the atelectasis caused by malposition of the diaphragm is corrected and ventilation perfusion defects return toward normal.
Case Reports
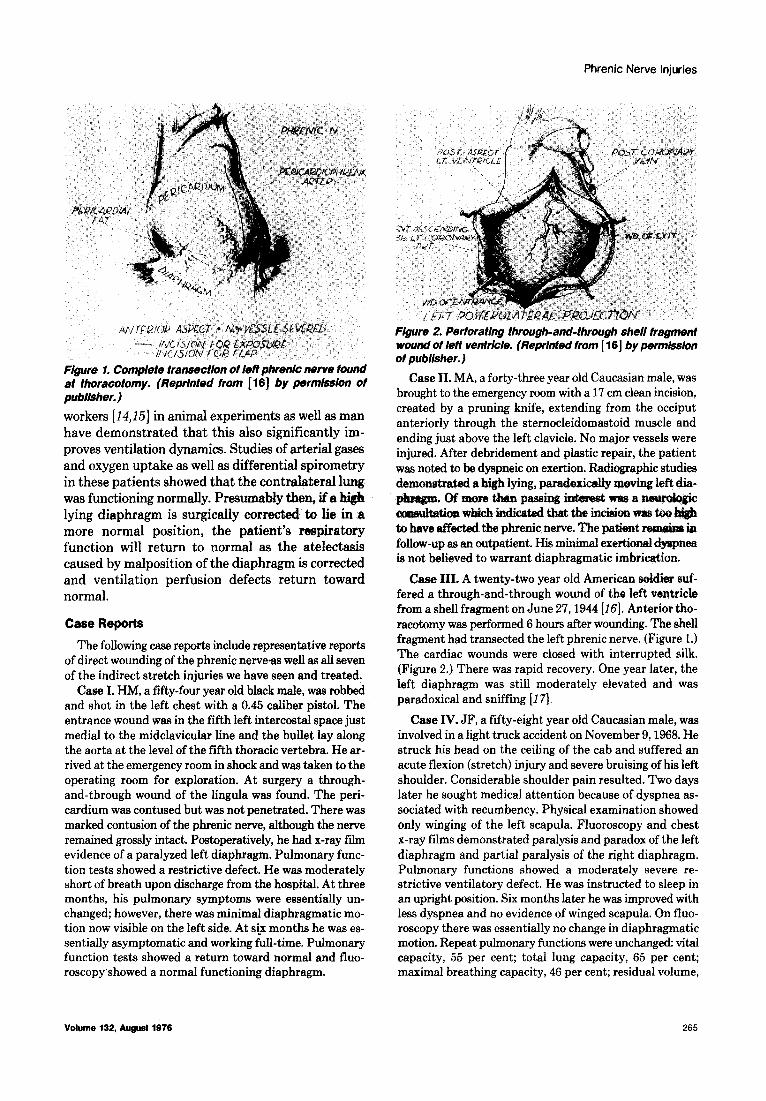
Figure 2. Perforating through-and-through shell fragment wound of left ventricle. (Rep&ted from [ 161 by permission of publisher.)
Case II. MA, a forty-three year old Caucasian male, was brought to the emergency room with a 17 cm clean incision, created by a pruning knife, extending from the occiput anteriorly through the sternocleidomastoid muscle and ending just above the left clavicle. No major vessels were injured. After debridement and plastic repair, the patient was noted to be dyspneic on exertion. Radiographic studies demonstrated a high lying, paradoxically m&ng left dia-
r5orethanpassinginksestprasa wl&b indicated that the incision was
to have affected the phrenic nerve. The patient rem&88 in follow-up as an outpatient. His minimal exertional clysp~ is not believed to warrant diaphragmatic imbrication.
Case III. A twenty-two year old American s&dier euf- fered a through-and-through wound of the left ventricle from a shell fragment on June 27,1944 [16]. Anterior tho- racotomy was performed 6 hours after wounding. The shell
The following case reports include representative reports of direct wounding of the phrenic nerveas well as all seven of the indirect stretch injuries we have seen and treated.
Case I. HM, a fifty-four year old black male, was robbed and shot in the left chest with a 0.45 caliber nistol. The
fragment had transected the left phrenic nerve. (Figure 1.) The cardiac wounds were closed with interrupted silk. (Figure 2.) There was rapid recovery. One year later, the left diaphragm was still moderately elevated and was paradoxical and sniffing [17].
entrance wound was in the fifth left intercostal space just Case IV. JF, a fifty-eight year old Caucasian male, was medial to the midclavicular line and the bullet lay along involved in a light truck accident on November 9,1968. He the aorta at the level of the fifth thoracic vertebra. He ar- struck his head on the ceiling of the cab and suffered an rived at the emergency room in shock and was taken to the acute flexion (stretch) injury and severe bruising of his left operating room for exploration. At surgery a through- shoulder. Considerable shoulder pain resulted. Two days and-through wound of the lingula was found. The peri- later he sought medical attention because of dyspnea as- cardium was contused but was not penetrated. There was sociated with recumbency. Physical examination showed marked contusion of the phrenic nerve, although the nerve only winging of the left scapula. Fluoroscopy and chest remained grossly intact. Postoperatively, he had x-ray fii x-ray films demonstrated paralysis and paradox of the left evidence of a paralyzed left diaphragm. Pulmonary func- diaphragm and partial paralysis of the right diaphragm. tion tests showed a restrictive defect. He was moderately Pulmonary functions showed a moderately severe re- short of breath upon discharge from the hospital. At three strictive ventilatory defect. He was instructed to sleep in months, his pulmonary symptoms were essentially un- an upright position. Six months later he was improved with changed; however, there was minimal diaphragmatic mo- less dyspnea and no evidence of winged scapula. On fluo- tion now visible on the left side. At six months he was es- roscopy there was essentially no change in diaphragmatic sentially asymptomatic and working full-time. Pulmonary motion. Repeat pulmonary functions were unchanged: vital function tests showed a return toward normal and fluo- capacity, 55 per cent; total lung capacity, 65 per cent; roscopy showed a normal functioning diaphragm. maximal breathing capacity, 46 per cent; residual volume,
Volume 132, August 1976 265
lverson et al
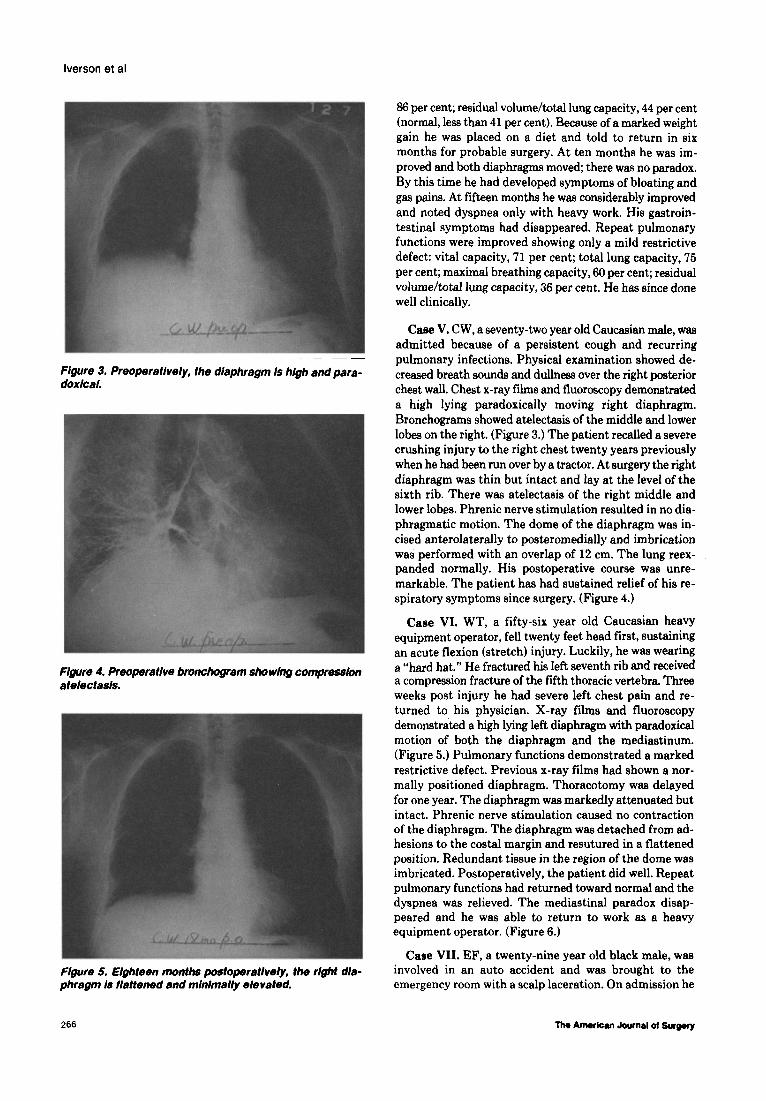
Figure 3. Preoperative/y, fhe diaphragm is high and para- doxical.
F lgure 4. Preopera five bronchogram sho wing compresskm atelectasls.
Flgure 5. Eighteen tmwths postoPeratively, the right dla- phragm Is flattened and minimally elevated.
66 per cent; residual volume/total lung capacity, 44 per cent (normal, less than 41 per cent). Because of a marked weight gain he was placed on a diet and told to return in six months for probable surgery. At ten months he was im- proved and both diaphragms moved; there was no paradox. By this time he had developed symptoms of bloating and gas pains. At fifteen months he was considerably improved and noted dyspnea only with heavy work. His gastroin- testinal symptoms had disappeared. Repeat pulmonary functions were improved showing only a mild restrictive defect: vital capacity, 71 per cent; total lung capacity, 75 per cent; maximal breathing capacity, 60 per cent; residual volume/t&al lung capacity, 36 per cent. He has since done well clinically.
Case V. CW, a seventy-two year old Caucasian male, was admitted because of a persistent cough and recurring pulmonary infections. Physical examination showed de- creased breath sounds and dullness over the right posterior chest wall. Chest x-ray films and fluoroscopy demonstrated a high lying paradoxically moving right diaphragm. Bronchograms showed atelectasis of the middle and lower lobes on the right. (Figure 3.) The patient recalled a severe crushing injury to the right chest twenty years previously when he had been run over by a tractor. At surgery the right diaphragm was thin but intact and lay at the level of the sixth rib. There was atelectasis of the right middle and lower lobes. Phrenic nerve stimulation resulted in no dia- phragmatic motion. The dome of the diaphragm was in- cised anterolaterally to posteromedially and imbrication was performed with an overlap of 12 cm. The lung reex- panded normally. His postoperative course was unre- markable. The patient has had sustained relief of his re- spiratory symptoms since surgery. (Figure 4.)
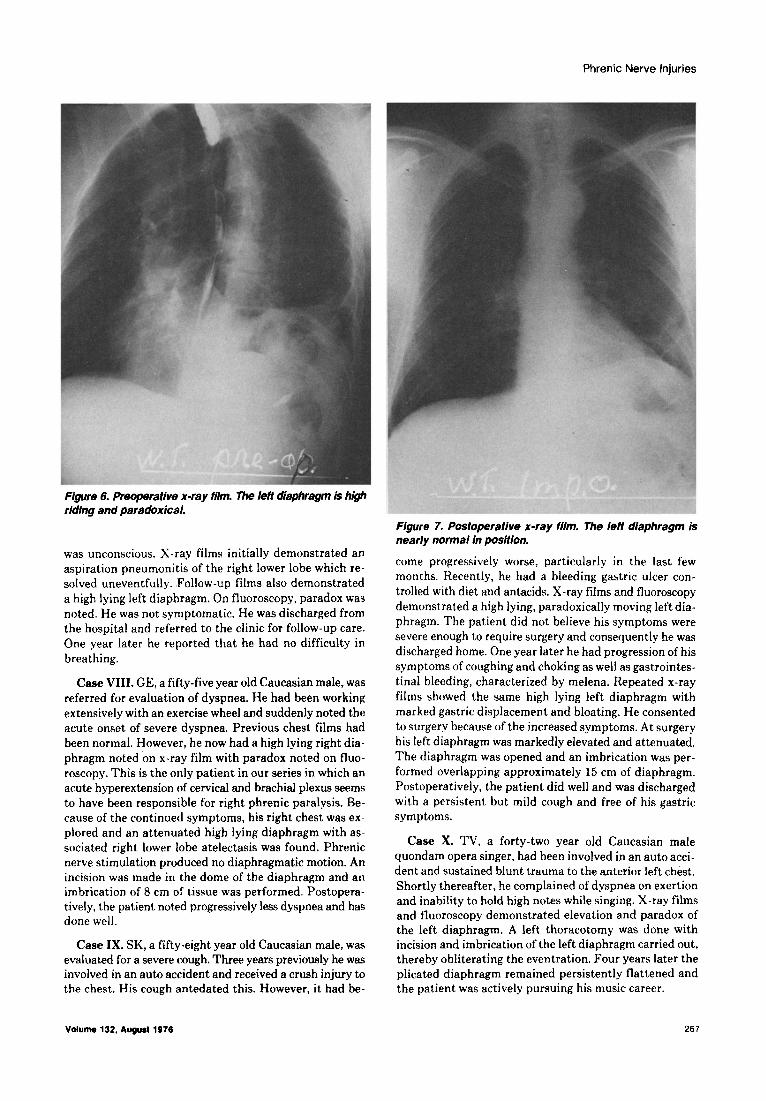
Case VI. WT, a fifty-six year old Caucasian heavy equipment operator, fell twenty feet head first, sustaining an acute flexion (stretch) injury. Luckily, he was wearing a “hard hat.” He fractured his left seventh rib and received a compression fracture of the fifth thoracic vertebra. Three weeks post injury he had severe left chest pain and re- turned to his physician. X-ray films and fluoroscopy demonstrated a high lying left diaphragm with paradoxical motion of both the diaphragm and the mediastinum. (Figure 5.) Pulmonary functions demonstrated a marked restrictive defect. Previous x-ray films had shown a nor- mally positioned diaphragm. Thoracotomy was delayed for one year. The diaphragm was markedly attenuated but intact. Phrenic nerve stimulation caused no contraction of the diaphragm. The diaphragm was detached from ad- hesions to the costal margin and resutured in a flattened position. Redundant tissue in the region of the dome was imbricated. Postoperatively, the patient did well. Repeat pulmonary functions had returned toward normal and the dyspnea was relieved. The mediastinal paradox disap- peared and he was able to return to work as a heavy equipment operator. (Figure 6.)
Case VII. EF, a twenty-nine year old black male, was involved in an auto accident and was brought to the emergency room with a scalp laceration. On admission he
266 lho Amwhan Journal of Surm
Phrenic Nerve Injuries
Figure 6. Preoperative x-ray film. The fefi diaphragm is high riding and paradoxical.
was unconscious. X-ray films initially demonstrated an aspiration pneumonitis of the right lower lobe which re- solved uneventfully. .Follow-up films also demonstrated a high lying left diaphragm. On fluoroscopy, paradox was noted. He was not symptomatic. He was discharged from the hospital and referred to the clinic for follow-up care. One year later he reported that he had no difficulty in breathing.
Case VIII. GE, a fifty-five year old Caucasian male, was referred for evaluation of dyspnea. He had been working extensively with an exercise wheel and suddenly noted the acute onset of severe dyspnea. Previous chest films had been normal. However, he now had a high lying right dia- phragm noted on x-ray film with paradox noted on fluo- roscopy. This is the only patient in our series in which an acute hyperextension of cervical and brachial plexus seems t.o have been responsible for right phrenic paralysis. Be- cause of the continued symptoms, his right chest was ex- plored and an attenuated high lying diaphragm with as- sociated right lower lobe atelectasis was found. Phrenic nerve stimulation produced no diaphragmatic motion. An incision was made in the dome of the diaphragm and an imbrication of 8 cm of tissue was performed. Postopera- tively, the patient noted progressively less dyspnea and has done well.
Case IX. SK, a fifty-eight year old Caucasian male, was evaluated for a severe cough. Three years previously he was involved in an auto accident and received a crush injury to the chest. His cough antedated this. However, it had be-
Figure 7. Postoperative x-ray film. The left diaphragm is nearly normal in posftion.
come progressively worse, particularly in the last few months. Recently, he had a bleeding gastric ulcer con- trolled with diet and antacids. X-ray films and fluoroscopy demons1 rated a high lying, paradoxically moving left dia- phragm. The patient did not believe his symptoms were severe enough to require surgery and consequently he was discharged home. One year later he had progression of his symptoms of coughing and choking as well as gastrointes- tinal bleeding, characterized by melena. Repeated x-ray films showed the same high lying left diaphragm with marked gastric displacement and bloating. He consented to surgery because of the increased symptoms. At surgery his left diaphragm was markedly elevated and attenuated. The diaphragm was opened and an imbrication was per- formed overlapping approximately 15 cm of diaphragm. Postoperatively, the patient did well and was discharged with a persistent but mild cough and free of his gastric symptoms.
Case X. TV, a forty-two year old Caucasian male quondam opera singer, had been involved in an auto acci- dent and sustained blunt trauma to the anterior left chest. Shortly thereafter, he complained of dyspnea on exertion and inability to hold high notes while singing. X-ray films and fluoroscopy demonstrated elevation and paradox of the left diaphragm. A left thoracotomy was done with incision and imbrication of the left diaphragm carried out, thereby obliterating the eventration. Four years later the plicated diaphragm remained persistently flattened and the patient was actively pursuing his music career.
Vdume 132, Aqusll976 267

lverson et al
Summary
Traumatic interruption of the phrenic nerve
causing diaphragmatic paralysis occurs much more commonly than realized. Patients present with symptoms referable to the respiratory, gastrointes- tinal, or ,cardiovascular systems as a result of ana- tomic displacement of the respective organ (even- tration). Symptoms often occur shortly after the in- jury but may be delayed for many years; conse- quently, prolonged follow-up of these patients is es- sential. If patients are symptomatic after trauma, judicious observation is dictated, since many will experience gradual return of normal diaphragmatic function over the succeeding six to twelve months. In those who remain significantly symptomatic, thoracotomy and imbrication of the eventration is a simple and effective surgical procedure.
Acknowledgment: We extend our thanks to Doc- tors Duane M. Merrill and W. James Eldred who furnished case reports.
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
Bfsgard JD: Congenital eventration of the diaphragm. Surgery 16: 484. 1947.
Thomas TV: Nonparalytic eventration of the dlaphragm. J 77wrac Cardlovasc Surg 55: 566, 1968.
Cruveilhier: Anatcmie pathologique du corps dumain Tracte d’anatomie pathologique general. Paris, JB Bailliere, 1829.
Wood WB, Wood FG: Ccngsnital eventratitm of the diaphragm. lancet 2: 392. 1931.
Reed JA, Borden DL: Eventration of the diaphragm. Arch Surg 31: 30, 1935.
Michelson E: EventratIon of the diaphragm. Surgery 49: 410, 1961.
~JJ,Paulscx~DL,UrscMHC,Razz&MD:Eventratbn of the dfaphragm. Surpry 64: 1014, 1988.
Seddcn H: Bt@cal DBordars of the Peripheral Nerves. London. Churchill LivIngstone, 1972.
Thomas TV: Congenital eventration of the dfaphragm: a col- lective review. Ann 7bmc Swg 10: 180,197O.
Christensen P: Eventratfcn of the diaphragm. 7horax 14: 311, 1959.
Chin EF, Lynn RB: Surgery of eventration of the diaphragm. J 7hcrac Cadiovasc Surg 32: 6, 1956.
Kirklln BR, Hkfgson JR: Rcentgenographic characteristics of diaphragnetic hernia. Am J Roentgs+md 58: 77, 1947.
Hoover CF: Functions of the diaphragm and their diagnostic importance. Arch tntern A&d 12: 214, 1913.
Samoff SJ, Gaensler EA, Maloney JV: Electrophrenk respi- ration. J 7huac Cardiovasc Surg 19: 929. 1950.
tiff 3J. Whlttenbsrger JL: ElecWo@renk respiratk~. Sug Oynecol Obstet 93: 190, 1951.
Samson PC Two unusual cases of war wounds of the heart. Surgery 20: 373, 1948.
DiscussIon
Howard A. Brown (San Francisco, CA): This paper presents a very interesting problem, and one which neu- rosurgeons very seldom see. The reasons for this would
appear to be that early recognition of phrenic nerve pa- ralysis is not always possible, particularly in severe crush-type injuries. Phrenic nerve injury may occur at any point from its root origin at the fourth cervical vertebra, and at times the fifth, down through its cervical course and intrathoracic extension to the diaphragm. In stretch in- juries involving the cervical and brachial plexus followed by respiratory difficulties, an early diagnosis could be made. Unfortunately, such injuries do not lend themselves well to real benefits from neurologic exploration and neu- rolysis.
In sharp instrument injuries in the neck with obvious phrenic nerve paralysis, exploration or possible suture of the nerve could be undertaken. The degree of nerve re- covery after such procedures would be in doubt for many months, and the pulmonary symptoms might be severe enough to require diaphragmatic surgery before sufficient time had elapsed to expect nerve regeneration to have reached its peripheral diaphragmatic destination.
There have been instances in which operations for cer- vical rib removal or even a scalenus an icus section have resulted in injury to the phrenic nerve. I do not have suf- ficient information in regard to a reasonable series of such patients to offer any prognosis from the standpoint of di- aphragmatic recovery. However, I believe that diaphrag- matic recovery would take place over a period of time in most cases unless the nerve was completely cut.
I encountered a very interesting report by Doctors Hardy, Perret, and Meyers (J Neurosurg 14: 400, (1957) reporting on phrenicofacial anastomosis in patients who had acoustic tumors removed with resulting facial paral- ysis. After such a situation, these doctors proposed and carried out an anastomosis between the phrenic nerve and the facial nerve. Subsequent fluoroscopy revealed gradual recovery of diaphragmatic movement, and it was of further interest to know that in 20 to 30 per cent of the patients who had had the phrenicectomy subsequent fluoroscopy revealed a normal diaphragmatic motion. The explanation offered was that accessory contributions from sources in the thorax join the phrenic nerve below the cervicobrachial level. It was also believed that the disability was less than that resulting from using the spinal accessory or hypo- glossal nerve for the anastomosis. One interesting sidelight that these doctors reported was that after facial recovery, when these patients took a deep breath, the eye on the af- fected side would wink involuntarily.
In view of the very successful results with a plastic ap- proach to the diaphragm which has been so well described here, I am very doubtful that the neurosurgical approach has very much to offer. The only exception would be a clean severence of the phrenic nerve in a surgically accessible area, lending itself to correct suture. Again, the time ele- ment for possible regeneration is lengthy and always un- certain.
Lyman A. Brewer III (LOS Angeles, CA): Before World War II, phrenic nerve paralysis to elevate the diaphragm was an accepted treatment for pulmonary tuberculosis, currently rendered obsolete by effective drugs and pul-
266
Phrenic Nerve Injuries
monary resection. So we have now come full circle, with studies and surgery to combat the ill effects of the high paralyzed diaphragm.
We agree that plication of the diaphragm is indicated for pronounced symptoms resulting from severe physiologic impairment and have successfully operated on ten such patients. In a much larger series of patients with less severe symptoms, we have not performed surgery. In only one instance in an adult did an emergency operation seem in- dicated. This patient unfortunately refused surgery and ultimately died of a cardiac condition.
A case was presented in which the high paralyzed dia- phragm had markedly decreased the pulmonary arterial blood flow to the lower lobe and, to a lesser extent, the upper lobe. Thus, both perfusion and ventilation are de- creased in these cases.
In addition to plication, electrophrenic pacing has been used on a limited scale: (1) through a vena caval electrode to stimulate the right phrenic nerve; and (2) direct nerve stimulus through an implanted electrode using radiofre- quency induction current. Definite physiologic improve- ment has followed electrophrenic pacing, both in the ex- perimental laboratory and on clinical triak In the future, it should be hoped that electrophrenic pacing, which is more physiologic, may become the procedure of choice.
Richard D. Sloop (Salem, OR): The authors have pointed up the matter of phrenic nerve paralysis as being something that is probably with us considerably more than we have realized. Two years ago I had thrust upon me in a short period of time three instances of phrenic nerve in- jury by blunt trauma, two of which I would like to describe. They point up two extremes of the problem that phrenic neurapraxia may present.
In the first case, a garbageman turned his truck over and suffered multiple injuries including crush of the upper chest, with extensive mediastinal hematoma. He was in rather marked respiratory compromise on a mechanical basis, not because of flail chest but because neither side of his diaphragm was functioning. What was seen in observing
the man was gross paradox of the abdominal wall during inspiration. The net result of this was that despite not very severe chest injury and not very severe pulmonary injury, he required mechanical ventilatory support for six weeks. The normal position of his diaphragm returned in three months.
(Slide) In the next case, a dump truck tail gate felI off and hit the patient across the lower chest. He really was not in very bad shape. Our major finding was in the x-ray film seen here-marked elevation of the right hemidiaphragm. Fluoroscopy showed no motion on the right side. The next day we were still wrestling with what was going on here: was this paralyzed hemidiaphragm or was this liver up in the right chest? (Slide) Carbon dioxide was placed in the ab- dominal cavity. His diaphragm is seen to be intact above the liver; none of the gas passed into the right chest. As I said, the fellow was really not in trouble. (Slide) This pic- ture, taken five days later, revealed apparent complete recovery.
Paul C. Samson (closing): Almost always the operation of imbrication can wait until it is indicated whether or not the diaphragmatic paralysis might be permanent, and this usually takes about six months. However, on a few occa- sions we have operated within six months because of per- sistent troublesome symptoms, and we do not believe we should wait on these until the decision as to whether the permanency of the paralysis has been-satisfied. The neu- rapraxia if sudden is one instance of temporary paralysis, and we can wait on this if at all possible.
We have had a number of cases of “idiopathic paralysis” in which Doctor Dugan has been particularly interested and in which without any history of trauma the same symptoms occur, namely, gastrointestinal or respiratory problems. In such cases we have come more and more to prompt operation because of the possibility of an occult cancer. Luckily this has proved not to be the case.
Doctor Eugene Stern sends in a question as to the re- currence of eventration and of symptoms after meticulous surgical imbrication. This has not occurred in our series.
Volume 132, Aqu8i 1976 269