plga-based nanoparticles: an overview of biomedical applications
TRANSCRIPT

Journal of Controlled Release 161 (2012) 505–522
Contents lists available at SciVerse ScienceDirect
Journal of Controlled Release
j ourna l homepage: www.e lsev ie r .com/ locate / jconre l
Review
PLGA-based nanoparticles: An overview of biomedical applications
Fabienne Danhier a, Eduardo Ansorena a, JoanaM. Silva a,b, Régis Coco a, Aude Le Breton a, Véronique Préat a,⁎a Université Catholique de Louvain, Louvain Drug Research Institute, Pharmaceutics and Drug Delivery, Avenue Mounier, B1 73.12, 1200 Brussels, Belgiumb Nanomedicine & Drug Delivery Systems Group, iMed, Faculty of pharmacy, University of Lisbon, Lisbon, 1619-003, Portugal
⁎ Corresponding author at: Université Catholique deBelgium. Tel.: +32 2 7647320; fax: +32 2 7647398.
E-mail address: [email protected] (V. Pr
0168-3659/$ – see front matter © 2012 Elsevier B.V. Alldoi:10.1016/j.jconrel.2012.01.043
a b s t r a c t
a r t i c l e i n f oArticle history:Received 14 October 2011Accepted 30 January 2012Available online 4 February 2012
Keywords:Poly(lactic-co-glycolic acid)NanoparticlesTargetingDrug delivery
Poly(lactic-co-glycolic acid) (PLGA) is one of the most successfully developed biodegradable polymers.Among the different polymers developed to formulate polymeric nanoparticles, PLGA has attracted consider-able attention due to its attractive properties: (i) biodegradability and biocompatibility, (ii) FDA and EuropeanMedicine Agency approval in drug delivery systems for parenteral administration, (iii) well described formu-lations and methods of production adapted to various types of drugs e.g. hydrophilic or hydrophobic smallmolecules or macromolecules, (iv) protection of drug from degradation, (v) possibility of sustained release,(vi) possibility to modify surface properties to provide stealthness and/or better interaction with biologicalmaterials and (vii) possibility to target nanoparticles to specific organs or cells. This review presents whyPLGA has been chosen to design nanoparticles as drug delivery systems in various biomedical applicationssuch as vaccination, cancer, inflammation and other diseases. This review focuses on the understanding ofspecific characteristics exploited by PLGA-based nanoparticles to target a specific organ or tissue or specificcells.
© 2012 Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5062. PLGA-based nanoparticles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 507
2.1. Methods of formulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5072.2. Physico-chemical properties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5072.3. Pitfalls . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5082.4. Encapsulation of small hydrophobic drugs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5092.5. Encapsulation of proteins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5092.6. Encapsulation of nucleic acids . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 509
3. Vaccination with PLGA-based nanoparticles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5103.1. PLGA as a vaccine delivery system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5103.2. Targeting of the immune system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5103.3. Cancer immunotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 511
4. Cancer treatment with PLGA-based nanoparticles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5124.1. Passive targeting by EPR effect and active targeting of specific receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5124.2. Cancer chemotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5124.3. Proteins delivery for cancer treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5144.4. Cancer gene therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5144.5. Cancer diagnosis and imaging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5144.6. Theragnostics of cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5144.7. Specific pitfalls of nanoparticles in cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 515
5. Inflammatory diseases treated by PLGA-based nanoparticles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5155.1. Targeting of inflammation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5155.2. Inflammatory bowel diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5155.3. Rheumatoid arthritis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 515
Louvain, Louvain Drug Research Institute, Pharmaceutics and Drug Delivery, Avenue Mounier B1 73.12, B-1200 Brussels,
éat).
rights reserved.

506 F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
5.4. Inflammatory lung diseases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5155.5. Ophthalmic inflammatory disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 516
6. Treatment of cerebral diseases with PLGA-based nanoparticles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5167. Regenerative medicine and PLGA-based nanoparticles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5168. Treatment of cardiovascular diseases with PLGA-based nanoparticles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5179. Infection treatment by PLGA-based nanoparticles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 518
10. Treatment of other diseases with PLGA-based nanoparticles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51811. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 518References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 518
1. Introduction
Nanoparticles are solid and spherical structures ranging around100 nm in size and prepared from natural or synthetic polymers. Awide variety of drugs can be delivered using nanoparticles suchas hydrophilic small drugs, hydrophobic small drugs, vaccinesand biological macromolecules. Nanoparticles also allow a targetedadministration to specific organs or cells or controlled drug delivery[1,2].
Poly(lactic-co-glycolic acid) (PLGA) is one of the most successfullyused biodegradable polymers because its hydrolysis leads to metabo-lite monomers, lactic acid and glycolic acid (Fig. 1). Because these twomonomers are endogenous and easily metabolized by the body viathe Krebs cycle, a minimal systemic toxicity is associated with theuse of PLGA for drug delivery or biomaterial applications [3]. PLGAis approved by the US FDA and European Medicine Agency (EMA)in various drug delivery systems in humans. The polymers are com-mercially available with different molecular weights and copolymercompositions. The degradation time can vary from several monthsto several years, depending on the molecular weight and copolymerratio [4,5]. The forms of PLGA are usually identified by the monomersratio used. For example, PLGA 50:50 identifies a copolymer whosecomposition is 50% lactic acid and 50% glycolic acid. Poly(lactic acid)(PLA) has also been used to a lesser extent than PLGA due to thelower degradation rate.
PLGA-nanoparticles are internalized in cells partly through fluidphase pinocytosis and also through clathrin-mediated endocytosis.PLGA-nanoparticles rapidly escape the endo-lysosomes and enterthe cytoplasm within 10 min of incubation (Fig. 2). This facilitates in-teractions of nanoparticles with the vesicular membranes leading totransient and localized destabilization of the membrane resulting inthe escape of nanoparticles into the cytosol [6].
The body recognizes hydrophobic particles as foreign. Thereticulo-endothelial system (RES) eliminates these from the bloodstream and takes them up in the liver or the spleen. This process isone of the most important biological barriers to nanoparticles-basedcontrolled drug delivery [3]. The binding of opsonin proteins presentin the blood serum to injected nanoparticles leads to attachment ofopsonized particles to macrophages and subsequently to their inter-nalization by phagocytosis [8].
Fig. 1. Hydrolysis of PLGA [3].
To address these limitations, several methods of surface modifica-tions have been developed to produce nanoparticles not recognizedby the RES. Nanoparticles can be coated with molecules that hidethe hydrophobicity by providing a hydrophilic layer at the surface.The most common moiety for surface modification is the hydrophilicand non-ionic polymer polyethylene glycol (PEG) (Fig. 3A). It hasbeen largely demonstrated that the “PEGylation” increases theirblood circulation half-life by several orders of magnitude [8]. More-over, PEG exhibits an excellent biocompatibility. Poloxamer, poloxa-mines or chitosan have also been studied for surface modification[1,3]. These groups can block the electrostatic and hydrophobic inter-actions that help opsonins to bind to particles surfaces.
Another application of surface modification is the targeting of tu-mors or organs to increase selective cellular binding and internaliza-tion through receptor-mediated endocytosis. Targeting ligands areoften grafted at the nanoparticles surface via a linkage on PEG chains[9]. Ligands need to be optimally conjugated on nanoparticles tomaintain their affinity for receptors binding. As a sufficient PEG coatingis essential for avoiding recognition by the RES, ligands should beextended away from the nanoparticle surfaces to avoid shielding bythe PEG chains [10].
Surface charges of nanoparticles also have an important influenceon their interaction with cells and on their uptake. Positively chargednanoparticles seem to allow higher extent of internalization, appar-ently as a result of the ionic interactions established between posi-tively charged particles and negatively charged cell membranes[11,12]. Moreover, positively charged nanoparticles seem to be ableto escape from lysosomes after being internalized and exhibit peri-nuclear localization, whereas the negatively and neutrally chargednanoparticles prefer to colocalize with lysosomes [13]. PLGA nano-particles have negative charges which can be shifted to neutral orpositive charges by surface modification, for example by PEGylationof the PLGA polymer [14] or chitosan coating [15], respectively.
Fig. 2. Schematic representation of nanoparticle internalization in cells [7].
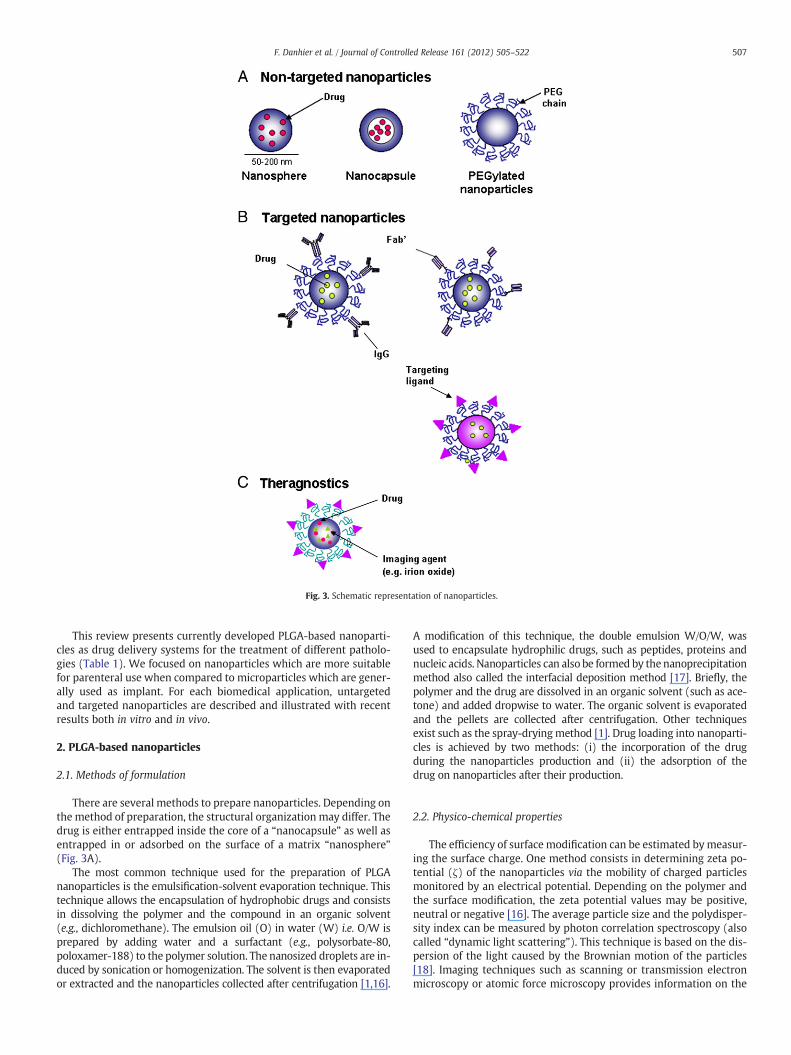
Fig. 3. Schematic representation of nanoparticles.
507F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
This review presents currently developed PLGA-based nanoparti-cles as drug delivery systems for the treatment of different patholo-gies (Table 1). We focused on nanoparticles which are more suitablefor parenteral use when compared to microparticles which are gener-ally used as implant. For each biomedical application, untargetedand targeted nanoparticles are described and illustrated with recentresults both in vitro and in vivo.
2. PLGA-based nanoparticles
2.1. Methods of formulation
There are several methods to prepare nanoparticles. Depending onthe method of preparation, the structural organization may differ. Thedrug is either entrapped inside the core of a “nanocapsule” as well asentrapped in or adsorbed on the surface of a matrix “nanosphere”(Fig. 3A).
The most common technique used for the preparation of PLGAnanoparticles is the emulsification-solvent evaporation technique. Thistechnique allows the encapsulation of hydrophobic drugs and consistsin dissolving the polymer and the compound in an organic solvent(e.g., dichloromethane). The emulsion oil (O) in water (W) i.e. O/W isprepared by adding water and a surfactant (e.g., polysorbate-80,poloxamer-188) to the polymer solution. The nanosized droplets are in-duced by sonication or homogenization. The solvent is then evaporatedor extracted and the nanoparticles collected after centrifugation [1,16].
A modification of this technique, the double emulsion W/O/W, wasused to encapsulate hydrophilic drugs, such as peptides, proteins andnucleic acids. Nanoparticles can also be formed by the nanoprecipitationmethod also called the interfacial deposition method [17]. Briefly, thepolymer and the drug are dissolved in an organic solvent (such as ace-tone) and added dropwise to water. The organic solvent is evaporatedand the pellets are collected after centrifugation. Other techniquesexist such as the spray-dryingmethod [1]. Drug loading into nanoparti-cles is achieved by two methods: (i) the incorporation of the drugduring the nanoparticles production and (ii) the adsorption of thedrug on nanoparticles after their production.
2.2. Physico-chemical properties
The efficiency of surface modification can be estimated bymeasur-ing the surface charge. One method consists in determining zeta po-tential (ζ) of the nanoparticles via the mobility of charged particlesmonitored by an electrical potential. Depending on the polymer andthe surface modification, the zeta potential values may be positive,neutral or negative [16]. The average particle size and the polydisper-sity index can be measured by photon correlation spectroscopy (alsocalled “dynamic light scattering”). This technique is based on the dis-persion of the light caused by the Brownian motion of the particles[18]. Imaging techniques such as scanning or transmission electronmicroscopy or atomic force microscopy provides information on the

Table 1Examples of currently developed PLGA-based nanoparticles as drug delivery systems for the treatment of different pathologies.
Receptors Ligands Therapeutic compounds Study design Ref
VaccinationTargeted nanoparticles
Toll-like receptors MPLA OVA Preclinical (mice) [71]C-type lectins Mannan OVA Preclinical (mice) [73]Siglec Anti-Siglec-7 polyclonal antibody – In vitro [79]Claudins CPE30 Influenza hemagglutinin Preclinical (mice) [82]αvβ1 integrins RGD/RGDp
LDV/LDVpOVA Preclinical (mice) [84]
STAT3 JSI-124 – Preclinical [90]
CancerUntargeted nanoparticles
Paclitaxel Preclinical (mice) [98]9-nitro-camptothecin In vitro [20]Rh-G-CSF In vitro [111]siRNA targeting MBD1 In vitro [113]shRNA targeting AnxA2 Preclinical (mice) [116]
Targeted nanoparticlesICAM-1 cLABL Doxorubicin In vitro [99]Folate receptor Folate Paclitaxel Preclinical [101]Specific receptor of lymphatic metastatic tumors LyP-1 – Preclinical [102]Prostate specific receptor PSMA Cisplatin Preclinical [103]αvβ3 integrins RGD Paclitaxel Preclinical (mice) [107]Nucleolin AS1411 Paclitaxel In vivo [104]HER-2 rhuMAbHER2 PE38KDL Preclinical (mice) [112]
InflammationUntargeted nanoparticles
Diclofenac In vivo [144]Flubiprofen Preclinical (rabbit) [145]Rolipram Preclinical [130]Tacrolimus Preclinical (rats) [131]Betamethasone Preclinical (rabbit) [135]PS-341 Preclinical [137]
Cerebral diseasesUntargeted nanoparticles
Superoxide dismutase Preclinical (rats) [150]Targeted nanoparticles
Transferrin receptor Lactoferrin Urocortin Preclinical (rats) [153]Opioid receptor Simil-opioid peptide (g7) Loperamide Preclinical [154]Opioid receptor Simil-opioid peptide (g7) Sialic acid Preclinical [155]Specific brain receptor Pep TGN – Preclinical [157]
Regenerative medicineGDNF Preclinical (rats) [160]VEGF Preclinical (mice) [178]FGF-2 Preclinical (mice) [180]BMP-7/BMP-2 In vitro [188]
Cardiovascular diseasesUntargeted nanoparticles
DNA Preclinical (pig coronary arteries) [192]
InfectionsUntargeted nanoparticles
Sparfloxacin Preclinical (rabbits) [202]Gentamycin In vivo [199]
OsteoporosisUntargeted nanoparticles
Calcitonine In vivo [203]
DiabetesUntargeted nanoparticles
Insulin Preclinical [212]
508 F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
morphology and size of the nanoparticles. Typically, the size of thenanoparticles is in the range of 100 to 250 nm.
2.3. Pitfalls
Nanoparticles need to have a high encapsulation efficiency (i.e.percentage of loaded amount of drug relative to the total amount of
drug used for the formulation) and a high drug loading (i.e. percent-age of loaded amount of drug relative to the total amount of nanopar-ticles). Precise determination of the drug content is not easy becausenanoparticles are colloidal systems [3]. Therefore, the most relevantway to separate nanoparticles from non encapsulated or nonadsorbed drug is the ultracentrifugation. Encapsulation efficiency ofdrugs varies from 6% to 90% for dexamethasone and paclitaxel,

509F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
respectively while mean encapsulation efficiency is around 60 to 70%for various drugs such as estradiol or xanthones [3]. One of the majorpitfalls of PLGA-based nanoparticles relates to the poor loading. In-deed, while PLGA-based nanoparticles often present high encapsula-tion efficiencies, the drug loading is generally poor (around 1%which means that nanoparticles content 1 mg active ingredient per100 mg polymers of nanoparticles). This low drug loading constitutesa major problem for some drugs in the design of PLGA-basednanoparticles.
A second important pitfall consists in the high burst release ofdrug from nanoparticles. This phenomenon is described for most ofPLGA-based nanoparticles. Consequently, the drug might not be ableto reach the target tissue or cells, leading to a loss of efficacy. Becauseof the application of nanoparticles in sustained release drug delivery,the drug release mechanisms are also important to understand.According to Kumari and colleagues, five mechanisms of drug releaseexist: (i) desorption of drug bound to the surface, (ii) diffusionthrough the polymer matrix, (iii) diffusion through the polymerwall of nanocapsules, (iv) nanoparticles matrix erosion and (v) acombined erosion–diffusion process. Drug release mechanisms de-pend on the polymer used and on the loading efficiency. Generally,the rapid initial, or burst release is attributed to adsorbed drug tothe nanoparticles surface [3].
A new subdiscipline of nanotechnology called “nanotoxicology”has emerged. Indeed, the interactions of nanocarriers with biologicalsystems are extremely complex. As expected, the size and surfaceproperties of nanocarriers modify the behavior of these componentsin the body. More data are needed to understand their structure–property relationships. Some nanomedicines received regulatory ap-provals showing their biocompatibility while others were not tested.Toxicology studies and regulations are necessary in order to fully de-fine the biocompatibility of nanocarriers in humans. In most of case,in vitro studies provide encouraging results. Unfortunately, these re-sults are often far away from reality in vivo. In the same idea, animalmodels routinely used in preclinical trials are far from being repre-sentative for the clinical situation.
Finally, to commercialize a new drug delivery system, the financialaspect has to be taken in account, not only for the pharmaceutical in-dustry but also for patients. The production of GMP PLGA with welldefined properties can be expensive. Another limitation for the com-mercialization of nanoparticles is the scaling-up. Many steps in exper-imental production are impossible to reproduce industrially such asdialysis, ultracentrifugation, sonication, etc (Fig. 4).
2.4. Encapsulation of small hydrophobic drugs
PLGA nanoparticles loaded with hydrophobic poorly solubledrugs are most commonly formulated by nanoprecipitation. Drug re-lease and effective response of PLGA nanoparticles are influenced by(i) the surface modification, (ii) the method of preparation, (iii) theparticle size, (iv) the molecular weight of the encapsulated drug and(v) the ratio of lactide to glycolide moieties [3]. PLGA nanoparticles
Fig. 4. Potential pitfalls of PLGA-based nanoparticles.
are described in the literature as effective nanocarriers for the encapsu-lation of various anti-cancer agents such as paclitaxel [19], 9-nitrocamptothecin [20], cisplatin [21], etc. but also for the encapsulationof various drugs such as haloperidol [22], estradiol [23], etc.
2.5. Encapsulation of proteins
The administration of proteins alone represents a real challenge astheir oral bioavailability is limited by the epithelial barriers of the gas-trointestinal tract, their susceptibility to gastrointestinal degradationby digestive enzymes, their short half-life in vivo and the fact thatmost of them cannot diffuse across some biological barriers. Nowa-days, recombinant proteins are delivered mainly by invasive routessuch as subcutaneous injections and their delivery generally requiresrepeated injections to achieve effective therapeutic levels due to theirrapid degradation and elimination [24]. The encapsulation of thesetherapeutic proteins in PLGA nanoparticles has arisen as a promisingalternative to overcome all these problems as well as to contributewith specific extra benefits. The incorporation of the proteins intothe polymer matrix provide protection against its enzymatic and hy-drolytic degradation in vivo, maintain their integrity and activity,could improve their bioavailability and in some cases could targetthe therapeutic protein to the target area.
One of the most frequently employed technique for the encapsula-tion of proteins into PLGA nanoparticles is the double emulsion W/O/W solvent evaporation procedure, as proteins tend to be hydrophilicmacromolecules. The encapsulation of proteins into PLGA nanoparticlespresents some challenges as instability problems [25]. For example, inthefirst step of theW/O/W formulation procedure the protein dissolvedin the aqueous phase may aggregate or be denatured at the water/or-ganic solvent interface, adsorb to the hydrophobic polymer or unfoldbecause of the shear stress used for the formation of the primary emul-sion [26]. Denatured or aggregated protein specieswill not only be ther-apeutically inactive, but also may induce unpredictable side effects,such as toxicity or immunogenicity [27]. To overcome these problems,many studies have focused on optimizing the formulation process inorder to improve protein stability during classical W/O/W procedure.
Another factor to be considered is the acidification of the environ-ment induced by the degradation products (lactic acid and glycolicacid), as well as the presence of PLGA carboxylic acid end groups,which could interact with the positive charges of the encapsulatedprotein, altering or even blocking its release. This exposure of thetherapeutic protein to an acidic pH could induce its aggregation or af-fect its activity [25,28]. Diverse stabilizer agents, such as pluronic F68,trehalose, sodium bicarbonate, among others, have also been testedto increase protein stability [29,30].
2.6. Encapsulation of nucleic acids
Nucleic acids can either promote gene expression by bringing agene that is not or under-expressed into cells (cDNA), or silence ex-pression of genes (RNAi mediators). Nucleic acids are fragile andhave poor intrinsic transfection efficiency because of their large sizeand negative charge. As an alternative to viral delivery, polymer-based nanoparticles have been developed. Nucleic acids can be eitherentrapped into polymeric matrix [31], or adsorbed by electrostatic in-teractions on nanoparticle surface by using appropriate surfactants oradding cationic polymers to the matrix [32].
PLGA-based nanoparticles, loaded with nucleic acids, are formu-lated either by W/O/W solvent evaporation [33] or by modified nano-precipitation [34]. Among all studies on nucleic acid delivery based onPLGA nanoparticles, there are no major differences in methods usedto formulate DNA-loaded nanoparticles or siRNA-loaded nanoparti-cles. W/O/W method involves drastic conditions which can lead tonucleic acids degradation. The addition of acetylated bovin serum al-bumin in nucleic acid-containing aqueous phase as an emulsifier

510 F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
showed an effect on the stabilization of the first emulsion (W/O) andenhanced the encapsulation efficiency of hydrophilic molecules[35,36]. Modified-nanoprecipitation is a milder formulation process:nucleic acid and polymers are both dissolved in the same organic sol-vent (such as DMSO), the mixture is then added dropwise to an aque-ous surfactant solution. Tahara et al. showed that pre-complexingnucleic acid with a cationic moiety as DOTAP enhanced nucleic acidsolubility in organic solvent [37]. Other polymers can be added toPLGA matrix, as a constituent of the matrix or as surface coating, toextend the features of nanoparticles. Addition of cationic polymers,such as polyethyleneimine (PEI) [38] or chitosan [37] can be used toimprove encapsulation efficiency. Encapsulation efficiencies were re-spectively improved from 43% to 80% and from 28% to 44%, in thepresence of the PEI or chitosan moieties. Moreover, cationic moietiesalso promoted interaction between negatively charged cell mem-branes and positively charged nanoparticles and/or enhanced endo-somal escape. PLGA concentration and the volume had to beoptimized for obtaining an encapsulation efficiency higher than 70%[39]. It should be noticed that even if the encapsulation efficiencycan be up to approximately 80%, the nucleic acid loading remains rel-atively low, in the range of 0.1 to 1 mg per 100 mg nanoparticles.
3. Vaccination with PLGA-based nanoparticles
3.1. PLGA as a vaccine delivery system
Several studies have demonstrated that delivery nanosystemscould enhance the uptake of either antigens or adjuvants by AntigenPresenting Cells (APCs) and are associated with better immune re-sponses than those obtained with the soluble counterparts [40,41].Apart from the higher uptake by APCs, vaccines and cancer immuno-therapeutics based on nanotechnologies, and more specifically PLGAnanoparticles, provide several other advantages.
Numerous antigens as proteins, peptides, lipopeptides, cell lysates,viruses or plasmid DNA have been successfully formulated in PLGAnanoparticles [42–47]. In vaccination, prolonged release of antigenscan provide more effective immune responses. It can also avoid therisk of tolerance and substitute the need of several boosting adminis-trations typically required to induce protective immunity [48]. PLGAnanoparticles are able to provide continuous in vitro release ofentrapped antigens for long periods of time [46,49]. PLGA nanoparti-cles can function as delivery systems encapsulating an antigen, com-binations of different antigens or, more importantly, combination ofantigens and adjuvants in the same particle. It has been demonstratedthat antigens and adjuvants must be co-delivered by the same parti-cle in order to be internalized simultaneously by the same cell [50].Moreover, PLGA nanoparticles containing very low doses of antigensand adjuvants are able to induce strong T cell responses [51]. Theuse of lower doses of these molecules would be advantageous notonly for minimizing the potential side effects often associatedwith the use of adjuvants but also from an economical point ofview. Several antigens and adjuvants have been successfully encapsu-lated together into PLGA nanoparticles [52,53].
Presentation of antigens through MHC I complexes is essential forthe control of tumor and infectious diseases as it is the pathway thatcan stimulate CD8+ T cells to acquire a cytotoxic phenotype [54].PLGA nanoparticles used as vaccines and for cancer immunotherapycan deliver exogenous antigens that can be cross-presented throughMHC I complexes to CD8+ cells. PLGA nanoparticles seem to havethe special capability to reach the MHC I pathway after their internal-ization by dendritic cells (DCs) [55].
3.2. Targeting of the immune system
Functionalization of nanoparticles with ligands directed againstsurface receptors of cells can enhance the targeting the immune
system [56]. A multitude of ligands are currently being assessed tofunctionalize nanoparticles including peptides, antibodies, proteins,polysaccharides, glycolipids, glycoproteins, and lectins [57] (Fig. 2).
Uptake of nanoparticles by APCs can rely on relatively simplecharacteristics of the antigen delivery system. These characteristics,such as size, shape, surface charge, hydrophobicity and hydrophilicity,can be manipulated on PLGA nanoparticles [58].
Size is one of the most important factors affecting the uptake ofantigens-loaded nanoparticles by APCs, and also determining their in-tracellular fate. The optimal size for nanoparticles uptake by APCs isstill a matter of debate. It makes sense that APCs have evolved to ef-fectively process any antigen with dimensions that are similar topathogens, ranging from viruses (20–100 nm) to bacteria and evencells (in the micrometer range) [59].
Apart from the fact that peripheral APCs can uptake nanoparticlesat peripheral sites as epidermis and dermis, it seems to be advanta-geous to target directly nanoparticles to the lymph nodes where themajority of resident DCs have an immature phenotype and can re-spond to activator signals and mature in situ. When targeting thelymph nodes, additional size aspects must be taken into account. Ini-tial lymph vessels have diameters around 10–60 μm whereas the si-nusoids in the spleen vary from 150 to 200 nm [60]. Nanoparticlessmaller than 200 nm can reach the lymphoid organs directly withinhours after injection, while particles larger than 200–500 nm requireAPCs, which will take approximately 24 h to arrive in the lymphnodes [61]. In vivo, lymphatic uptake and retention in a rat modelindicated that 50 nm PLGA-PEG nanoparticles are ideal for sustainedregional delivery into the lymphatics for prevention/treatment ofoligometastases [62].
When targeting the immune system with functionalized nanopar-ticles, two specific goals may be achieved. First, introduction of li-gands for specific cell surface receptors may target defined celltypes of the immune system as DCs and enhance cellular uptake bythese cells [63]. Second, the recognition of some specific ligands bytheir receptors on APCs can further enhance the immunogenicity ofnanoparticulate vaccines, by providing an intrinsic “danger signal”that induces the activation of innate and adaptive immune mecha-nisms [64,65].
The ligands carried by a number of pathogens that can interactwith receptors on cells of the immune system constitute an importantissue for vaccine design. APCs possess a broad spectrum of cell surfacereceptors known as pattern recognition receptors (PRRs) that are in-volved in the initiation, promotion and execution of immune re-sponses. PRRs, such as Toll-like receptors (TLRs), nucleotideoligomerization domain (NOD)-like receptors, scavenger receptors,retinoic-acid inducible gene-like receptors (RLR) and C-type lectin re-ceptors (CLRs), recognize some conservative elements exclusivelyexpressed on pathogens, known as pathogen-associated molecularpatterns (PAMPs) [66–68]. Recognition of PAMPs by PRRs rapidly in-duces activation of APCs by triggering intracellular signaling path-ways that culminate in the induction of inflammatory cytokines,chemokines, interferons and upregulation of co-stimulatory mole-cules [69]. As many studies have demonstrated direct co-stimulatory effects of TLR agonists in CD4+, CD8+ T cells and B cells[70,71] enhancing proliferation, activation and effector functions,the use of TLR agonists as vaccine adjuvants is an attractive goal forresearch.
Among CLRs, the mannose receptor (MR/CD206), the prototype ofC-type lectins, recognizes specific sugars on a variety of foreignorganisms and certain endogenous glycoproteins, such as lysosomalhydrolases [72]. PLGA nanoparticles decorated with mannan, a natu-ral polymannose have demonstrated a strong binding affinity and in-creased CD4+ and CD8+ T cell responses compared to non-decoratednanoparticles [73]. DC-specific intracellular adhesion molecule-3grabbing non-integrin (DC-SIGN) is one of the most DC-restricted C-type lectin receptors in humans that specifically binds high-

Fig. 5. (A) Influence of ligand grafting on nanoparticle transport across mono- and co-cultures of Caco-2 cells. Cell monolayers were first apically pre-incubated with anti-β1integrin (inhibitor+) or without (inhibitor−) at 5 μg/ml in HBSS for 1 h at 37 °C, be-fore adding nanoparticle suspension at a final concentration of 2.7×1010 nanoparti-cles/ml. The number of transported nanoparticles was evaluated by flow cytometryand is expressed as apparent permeability coefficient (Papp) as a mean±standarderror of the mean (SEM). *pb0.05: vs. NP, **pb0.05: inhibitor vs. no inhibitor(n=24). (B) Influence of the ligand grafting at the nanoparticle surface on IgGtot con-centration in serum of mice immunized by intraduodenal administration with 2×50 μgof ovalbumin free or encapsulated (blood sampling 6 weeks after priming). Mice indi-vidual absorbance obtained after ELISA at the 1/320 dilution of the serum (n=6–10).*pb0.05 [84].
511F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
mannose glycans and Lewis-type antigens present on pathogens suchas HIV andMycobacterium [74]. Targeting the DC-SIGN receptor usingPLGA nanoparticles decorated with the humanized targeting antibodyhD1 improved antigen presentation of nanoparticles and inducedantigen-dependent T cell responses at 10–100 fold lower concentra-tions than non-targeted nanoparticles [75].
Another family of PRR that can be targeted by nanoparticles is theSiglec (sialic acid-binding immunoglobulin-like lectins) family [76].Siglecs bind specific sialic acid-containing carbohydrates [77]. Siglecreceptors are mainly expressed on leukocytes in a cell type-specificand differentiation-dependent manner and on other immune cells in-cluding APCs [78]. PLGA nanoparticles conjugated to antibodies rec-ognizing the Siglec-7 receptor were successfully internalized byfibroblasts expressing recombinant Siglec-7 receptor [79].
For mucosal immunization, targeting M-cells can be advantageousas these cells have an active role in antigen sampling and have directaccess to APCs. Hence, targeting receptors on these cells is also an at-tractive approach for the targeting of nanoparticles to the immunesystem [80]. Claudins are a family of integral membrane proteinsthat are found on tight junctions [81]. Claudin-4 is highly expressedon M-cells in the colon and nasopharynx surface epithelium. PLGAnanoparticles containing a recombinant protein which the C-terminal region has affinity to Claudin-4 demonstrated significantlyenhanced uptake by upper airway and intestinal M-cells on mice[82]. Another family of receptor that can be targeted on M-cells isthe family of integrins. β1-integrins mark the surface of M-cells andmediate uptake of bacteria. Garinot et al. demonstrated significant in-creased uptake in vitro of PEGylated PLGA nanoparticles grafted withthe β1 intregrin peptide ligand RGD (Arg-Gly-Asp) and in vivo studiesdemonstrated that those nanoparticles concentrated particularly inM-cells and induced an IgG response on mice against an encapsulatedmodel antigen [83]. As RGD peptide could be degraded during thetransport through the gastro-intestinal tract, novel non-peptidic andpeptidic analogs of the RGD peptide were tested by Fievez et al.RGD peptidomimetic (RGDp), LDV derivative (LDVd) and LDV pepti-domimetic (LDVp) as well as mannose were grafted on the PEGchain of PCL-PEG and incorporated in PLGA-based nanoparticles(Fig. 5). RGD and RGDp increased the transport of nanoparticlesacross an in vitro model of human M-cells. RGD, LDVp, LDVd andmannose enhanced nanoparticle uptake by macrophages in vitro.The intraduodenal immunization with RGDp-, LDVd- or mannose-labeled nanoparticles elicited a higher production of IgG antibodiesthan the intramuscular injection of free ovalbumin or intraduodenaladministration of either non-targeted or RGD-nanoparticles [84].
NKT cells are another attractive target of particulate vaccines andimmunotherapies as these cells are an effective bridge between theinnate and immune system. A number of lipid and glycolipid antigensthat can bind CD1d and activate NKT cells have been identified. Theprototypical antigen, KRN7000, an α-linked galactosylceramide (α-GalCer), has been encapsulated in PLGA nanoparticles to activateNKT cells in vitro and in vivo[85].
3.3. Cancer immunotherapy
PLGA nanoparticles have been tested as cancer vaccines by encap-sulating tumor-associated antigens (TAAs) either alone [86] or associ-ated with adjuvants as TLR ligands [53]. Tumor lysates have also beenencapsulated in PLGA nanoparticles [87]. Generally, theses strategiesgenerate stronger immune responses when compared to the admin-istration of soluble antigens and the use of adjuvants provides evenstronger and long lasting anti-tumor responses.
One of the drawbacks of cancer immunotherapy that contributesto its poor therapeutic outcome in clinic is the immunosuppressiveenvironment within the tumor [88]. Efforts have been made to devel-op new therapeutic strategies that can restore immunocompetence incancer patients. One example is the signal transducer and activator of
transcription-3 (STAT3) which is constitutively activated in tumorcells and DCs favoring the induction of immunosuppression in thetumor environment. PLGA nanoparticles have been used to targetthe inhibition of STAT3 either by the encapsulation of a STAT3 inhib-itor (JSI-124) alone [89] either combined with the TLR4 ligand 7-acyllipid A [90], or by the encapsulation of anti-STAT3 siRNA polyplexes[91] and all the strategies demonstrated to be able to restore DCsfunction in vitro.
Given the complexity of cancer microenvironment and cancer im-mune responses, the combination of several anti-tumor strategiesstarted to be combined in order to develop a stronger and more com-plete anti-tumor immune response. For example, formulations whichcould directly kill cancer cells as well as activate the immunosup-pressed tumor microenvironment to mount a robust anti-tumor im-mune response could be benefic. PLGA nanoparticles combiningPaclitaxel (PTX) and SP-LPS (nontoxic derivative of lipopolysaccha-ride) as anti-cancer drug and immunostimulant respectively demon-strated both cytotoxic and immunostimulatory effects in vitro andstrong tumor accumulation in vivo [92].
Future strategies might take advantage of the possibility to coordi-nate multiple functionalizations on PLGA nanoparticles in order toproduce a complete vector for cancer immunotherapy by combining:(i) the enhancement of nanoparticle uptake by targeting immunecells with ligands or Abs that recognize PRRs, as those targeting C-type lectin receptors on DCs; (ii) the fully activation of DCs by

512 F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
providing additional “danger signals” as TLR ligands; (iii) immuno-competence restoration by providing agents that are able to block sig-nals responsible by the immunosuppressive tumor microenvironmentas STAT3 inhibitors; (iv) chemotherapeutic agents that are able toreduce tumor burden, enhance cross-priming of tumor antigens andmanipulate pathways of tumor tolerance and regulation; and (v) TAAsthat are broadly expressed on tumors and are efficiently recognizedby the T cells.
4. Cancer treatment with PLGA-based nanoparticles
4.1. Passive targeting by EPR effect and active targeting ofspecific receptors
Chemotherapeutic agents damage healthy tissues, leading to sys-temic toxicity and adverse effects that greatly limit the maximum tol-erated dose of anti-cancer drugs and thus restricts their therapeuticefficacy. To solve these problems, nanomedicines have attractedgreat attention in recent years. PLGA-based nanoparticles are current-ly under investigations for applications in cancer imaging and cancertherapy.
In general, nanoparticles can achieve tumors via an active or pas-sive targeting. Passive targeting (Fig. 6) takes advantage of the sizeof nanoparticles and exploits the unique anatomical and pathologicalabnormalities of the tumor vasculature. Nanoparticles can extrava-sate and accumulate inside the interstitial space. This contributes toan “enhanced permeability”. Moreover, lymphatic vessels are absentor ineffective in tumors, leading to inefficient drainage of the tumortissue. This contributes to an “enhanced retention”. Together thesetwo phenomena constitute the “Enhanced Permeability and Reten-tion” (EPR) effect. This effect is considered as a gold standard in thedesign of new anti-cancer drug delivery system and was first de-scribed by Maeda and colleagues [93].
In active targeting (Fig. 6), targeting ligands are grafted at thenanoparticles surface [14]. The ligand is chosen to bind specific recep-tors overexpressed by tumor cells or tumor vasculature and non-expressed by normal cells. Another important factor in the choice oftargeting ligands is the homogeneity of the expression of the receptoron all targeted cells. Nevertheless, this information is often deficient.Two cellular targets can be distinguished (Fig. 6): (i) cancer cells and(ii) tumoral endothelial cells. To target cancer cells, several overex-pressed receptors have been investigated e.g., the transferrin recep-tor, the folate receptor, glycoproteins, the epidermal growth factorreceptor (EGFR) or integrins. To target tumoral endothelium,
Fig. 6. Passive and active targeting of nanocarriers. Nanocarriers can reach tumors se-lectively through the leaky vasculature surrounding the tumors. Ligands grafted atthe surface of nanocarriers bind to receptors (over)-expressed by cancer cells (green)or angiogenic endothelial cells (pink).Adapted from [14].
targeting ligands have to recognize specific receptors such as the vas-cular endothelial growth factor receptors (VEGFR-1 and VEGFR-2),the integrins (αvβ3, α5β1), the vascular cell adhesion molecule-1(VCAM-1) or the matrix metalloproteinases (MMPs). The rationalebehind this targeting was firstly suggested by J. Folkman in 1971: de-struction of tumoral endothelium can result in the death of the tumordue to the lack of oxygen and nutrients [94]. Thus in this strategy, tar-geted nanocarriers aimed to directly kill angiogenic blood vessels andindirectly kill tumor cells [14].
The enhanced cellular internalization rather than an increasedtumor accumulation is responsible of the anti-tumoral efficacy of ac-tively targeted nanocarriers. This is the base of the design of deliverysystems targeted to endocytosis-prone surface receptors [95].Therefore, this receptor-mediated internalization constitutes amajor advantage of targeted nanoparticles in addition to the specifictargeting of nanoparticles.
4.2. Cancer chemotherapy
Many small anti-cancer drugs have been encapsulated in PLGA-based nanoparticles and have been evaluated in vitro and in vivo totreat various cancers. For example, long-term clinical use of doxorubi-cin (DOX), a highly potent anthracycline approved for use against awide spectrum of tumors is compromised by toxicities, cardiomyopa-thies and subsequent congestive heart failures. PEGylated PLGA nano-particles encapsulating DOX enhance DOX anti-tumoral efficacycompared with the free drug. Moreover, these nanoparticles wereshown to decrease drastically the cardiomyopathies compared toDoxil®, a liposomal formulation of DOX currently available on themarket [96]. Chemotherapy of glioblastoma is largely ineffective asthe blood–brain barrier prevents entry of most anti-cancer agents inthe brain. Non-targeted DOX-loaded PLGA nanoparticles coatedwith poloxamer 188 were found to cross the blood–brain barrierand to effectively decrease the tumor growth in rat model [97]. Pacli-taxel (PTX), a mitotic inhibitor used in the treatment of various can-cers, presents a low therapeutic index and a low aqueous solubility.Its current commercialized form, Taxol®, contains PTX at a concentra-tion of 6 mg/ml solubilized in a mixture of Cremophor® EL and etha-nol (1:1). However, serious side effects are associated withCremophor® EL. The encapsulation of PTX into PLGA nanoparticlesstrongly enhances the cytotoxic effect of the drug as compared toTaxol® in vitro [19] and in vivo [98]. 9-nitrocamptothecin (9-NC) isan anti-cancer drug which targets the Topoisomerase I nuclear en-zyme. Because of instability at biological pH and low water solubility,the delivery of this drug is quite challenging. 9-NC-loaded PLGA nano-particles, prepared by nanoprecipitation, have shown a sustained re-lease up to 160 h indicating the suitability of PLGA nanoparticles incontrolled 9-NC release [20].
PLGA-based nanoparticles targeting the tumor cells or tumor en-dothelium have been shown to be usually more active in preclinicalstudies than non targeted nanoparticles. A cyclic peptide, Cyclo-(1,12)-penITDGEATDSGC (cLABL), has been shown to inhibit LFA-1/ICAM-1 via the binding to ICAM-1. In addition, cLABL has beenshown to be internalized after binding to ICAM-1. This cyclic peptidewas conjugated to PLGA nanoparticles for the delivery of DOX. ThecLABL-nanoparticles were shown to be more rapidly taken intoA549 lung epithelial cells than non-targeted nanoparticles. The cyto-toxicity study of cLABL-nanoparticles and non-targeted nanoparticlescompared to free DOX showed similar IC50 values suggesting that theactivity of DOX was maintained [99]. Folate-decorated DOX-loadedPLGA nanoparticles induced a cellular uptake 1.5 times higher byMCF-7 cells than non-targeted nanoparticles [100]. Recently, otherfolate-decorated PTX-loaded PLGA-PEG nanoparticles showed agreater cytotoxicity against HEC-1A cancer cells both in vitro and invivo. The accumulation of folate-decorated nanoparticles dependson dual effects of passive and active targeting [101]. The peptide

513F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
LyP-1 has been recognized for its specific binding to tumors and theirlymphatics. LyP-1-PEG-PLGA nanoparticles have been studied fortheir targetability to tumor lymph metastases. In vivo, the uptake ofthese LyP-1-targeted nanoparticles in metastatic lymph nodes wasabout eight times higher than non-targeted nanoparticles, indicatingthat these nanoparticles are a promising carrier to lymphatic meta-static tumors [102]. The prostate-specific membrane antigen (PSMA)was used to functionalize PLGA-PEG nanoparticles for the delivery ofcisplatin (Pt(IV)). A comparison between Pt(IV)-encapsulated PSMA-nanoparticles and non targeted Pt(IV)-nanoparticles against humanprostate PSMA-overexpressing LNCaP cells revealed that the effective-ness of targeted nanoparticles is approximately one order of magnitudegreater than that of free cisplatin [103]. AS1411, a DNA aptamer whichbinds to nucleolin highly expressed in the plasma membrane of bothcancer cells and endothelial cells, was chosen to target gliomas. Thesenanoparticles prolonged circulation and enhanced PTX accumulation
Fig. 7. Fluorescent microscopy of TLT tumors grown in NMRI mice and harvested 2 h afterCD31 to label endothelial cells (red) and counterstained with DAPI for nucleus detectionPLGA signal from TLT tumors after NP and RGD-NP injection (n=4). ***pb0.001. (D) Fluoreof NP containing fluorescent-PLGA (green). Sections were stained with DAPI for nucleus deAdapted from [107].
at the tumor site [104]. The αvβ3 integrin a receptor for extracellularmatrix proteins is upregulated in both tumor cells and angiogenic en-dothelial cells [105]. The RGD peptide is the most studied peptidewhich binds to αvβ3 integrin. The surface of PLGA nanoparticles waslinked with PEG and the RGD peptide to realize both passive and activetargeting functions for the delivery of DOX. The nanoparticle targetingability was proven through strong affinity to various integrin-expressing cancer cells and much less affinity to the low integrin-expressing cancer cells [106]. Other PLGA-based nanoparticlesgrafted with the RGD peptide have been designed for the deliveryof PTX. The targeting to the tumoral endothelium was demonstratedboth in vitro and in vivo. Moreover, therapeutic efficacy has beendemonstrated by effective retardation of TLT tumor growth andprolonged survival times of mice treated by PTX-loaded RGD-nanoparticles when compared to non-targeted nanoparticles [107](Fig. 7).
injection of NP containing fluorescent-PLGA (green). Sections were stained with anti-(blue). (A) RGD-NP and (B) non-targeted NP. (C) Quantification of the fluorescent-scent microscopy of TLT tumors grown in NMRI mice and harvested 4 h after injectiontection (blue).

514 F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
In the past decades, increasing interest has been found in the liter-ature towards oral administration of cytotoxic agents. PTX was en-capsulated in nanoparticles composed of PLGA with vitamin E TPGSas emulsifier for oral administration. Its oral bioavailability was 10times higher compared with Taxol® [108]. Oral bioavailability oftamoxifen-loaded nanoparticles was increased 11 times as comparedto free tamoxifen base. In vivo oral anti-tumor efficacy of tamoxifen-nanoparticles was demonstrated in DMBA induced breast tumormodel with a marked reduction in hepatotoxicity when comparedwith free tamoxifen [109].
While numerous studies are described in the literature aboutPLGA-based nanoparticles, only few papers described active targetingusing PLGA-based nanoparticles. Moreover, the majority of thesepapers describe the characterization of their system in vitro only.Very few research articles report actively targeted PLGA-based nano-particles both in vitro and in vivo.
4.3. Proteins delivery for cancer treatment
Endostar, a 20 kDa anti-angiogenic peptide, is an endostatin whichshows activity against solid tumors but needs multiple injections at ahigh dose to achieve a therapeutic effect. Endostar-loaded PEG-PLGAnanoparticles showed longer half-life than free drug, higher amountin murine tumors and offered higher inhibition rate and strongeranti-angiogenic effect than free endostar.
Recombinant human granulocyte colony-stimulating factor (rh-G-CSF) was successfully loaded in PLGA nanoparticles and showed an invitro sustained release with 90% of encapsulated protein releasedfrom the nanoparticles over 1 week period [111].
PE38KDL, a model protein toxin, was loaded in PLGA nanoparticlesmodified on their surface by coating of Fab′ fragments of a humanizedanti-HER2 monoclonal antibody (rhuMAbHER2). In vitro and in vivodata showed that PE38KL-loaded nanoparticles presenting rhuMAb-HER2 (PE-NPs-HER2) have a better in vitro cytotoxicity againstHER2-overexpressing breast cancer lines than PE38KL-loaded nano-particles without rhuMAbHER2, demonstrating prominence of activetargeting. Furthermore, in vivo, a better anti-tumor activity and,above all, a higher maximal tolerated dose were observed for PE-NPs-HER2 than for the control, showing a decrease of non-specifictoxicity due to nanoencapsulation [112].
4.4. Cancer gene therapy
Gene-based therapy has become of great interest in the anti-cancer field. In the past years, several research papers have been pub-lished showing evidences of promising PLGA-based vector systemsloaded with plasmids or siRNA therapeutics against cancer-associated targets.
PLGA nanoparticles loaded with plasmid coding for siRNA se-quence targeting Methyl-CpG binding domain protein 1 (MBD1)were formulated with an encapsulation efficiency of 33%. In vitro,this system did not exhibit any cytotoxicity, and showed an uptakeby BxPC3 tumor cells up to 30% leading to cell growth inhibitionand inducing tumor cell apoptosis [113]. More complex PLGA-basednanoparticles involving cationic polymers have also been studied invitro. PEI or cetylated-PEI was added to the polymeric matrix to loadBCL-w (a member of BCL-2 family involved in cell survival) siRNAon nanoparticles [114]. No adsorption of siRNA was observed onpure PLGA nanoparticles, but addition of PEI or Cet-PEI allowed an ad-sorption up to 90%. The presence of PEI also dramatically enhancedcellular uptake and transfection efficiency: BCL-wmRNAwas silencedby more than 60% with BCL-w siRNA-loaded PLGA-PEI nanoparticles.Liver-targeted nanoparticles using asialofetuin as ligand were validat-ed in vitro[115]. These nanoparticles were carrying IL-12 coding plas-mids. HepG2 cells (expressing asialofetuin receptor) were bettertransfected with targeted nanoparticles than with non-targeted
nanoparticles. Moreover, the uptake mechanism of targeted nanopar-ticles was suggested to be receptor-mediated endocytosis.
Nucleic acids have also been successfully transfected by PLGA-based nanoparticles in in vivomodels. After intra-tumoral administra-tion of PLGA nanoparticles loaded with plasmid coding for AnxA2shRNA, expression of AnxA2, (Annexin 2 is involved in malignantphenotype of prostate cancer) was significantly reduced and tumorgrowth was inhibited [116]. Similar results were obtained after re-peated intra-peritoneal injection of plasmid coding for CLDN3shRNA in SKOV3 (ovarian carcinoma) subcutaneous tumor-bearingmice [36]. CLDN3 is known to be overexpressed in epithelial ovariantumors [117]. CLDN3 expression was reduced as well as angiogenesisand tumor cell proliferation. Apoptosis was increased, leading to a re-duced tumor growth. After intravenous injection, cDNA-loaded PLGAnanoparticles passively accumulated into PC3 subcutaneous tumor,reducing tumor growth and thus increasing survival rate among trea-ted mice [118]. Up to date, the only study describing active targetingof tumor in vivo by PLGA-based nanoparticles in the field of gene ther-apy has been published recently by Patil et al.[38]. Complex nanopar-ticles, made of a matrix of PLGA and PEI encapsulating siRNA andexhibiting biotin as a ligand for breast cancer cells, were able to effi-ciently silence P-glycoprotein and thus to restore sensitivity oftumor cells to drugs such as PTX.
Several studies provide the proof of concept of in vivo gene therapyby vectorizing plasmids or RNAi mediators in polymeric nanoparticlesmade of PLGA. Most studies only use passive targeting (by mean of in-jection in a restricted area, or EPR effect) to concentrate transfectionsystems at the tumor site.
4.5. Cancer diagnosis and imaging
Tumor imaging plays a key role in clinical oncology by helping toidentify solid tumors, determine recurrence and monitor therapeuticresponses. The development of non-invasive molecular imaging sys-tems able to detect tumors at early stages would represent a signifi-cant improvement over the current available clinical diagnosticmethods. The development of nanoparticles for the delivery of con-trast agents has emerged in recent years since the possibility of theproduction of multifunctional nanoparticles able to specifically targetthe tumor [7]. PLGA was used to formulate nanoparticles encapsulat-ing superparamagnetic iron oxides for MRI. This system improved theimaging effects along with increasing the half-life of nanoparticles inthe blood stream, thereby reducing their side effects [119]. Anotherexample consists in the encapsulation of a radiotracer, technetium-99m (99mTc), in PLGA nanoparticles for sentinel lymph node detec-tion. Biodistribution and scintigraphic imaging studies performed inWistar rats revealed localization of 99mTc-labeled PLGA nanoparticlesin the sentinel nodes [7].
4.6. Theragnostics of cancer
Theragnostics are defined by the combination of therapeutic anddiagnosis agents on a single platform (Fig. 2). Theragnostics maycombine passive and active targeting, environmentally responsivedrug release, molecular imaging and other therapeutic functionsinto a single platform [120]. For example, DOX was encapsulatedinto magnetic nanoparticles that were embedded in PLGA throughhydrophobic interactions. DOX was released sustainably withoutany inhibition due to the presence of magnetic nanocapsules. Thesenanoparticles were tested in mice, rats and in human [121,122].More recently, magnetic nanoparticles embedded in PLGA matriceswere designed as dual drug delivery and imaging system able to en-capsulate both hydrophilic (carboplatin) and hydrophobic drugs(PTX and rapamycin) in a 2:1 ratio. Magnetic resonance imagingshowed in vitro and in vivo that these nanoparticles present a bettercontrast effect than commercial contrast agents [123].

515F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
4.7. Specific pitfalls of nanoparticles in cancer
One of the major pitfalls in the field of tumor-targeted drug deliv-ery relates to the fact that the EPR is often misinterpreted. The EPR ef-fect is a highly heterogenous phenomenon, which varies substantiallyfrom tumor model to tumor model, as well as from patient to patient.Another aspect relates to the overestimation of the potential useful-ness of active drug targeting. Theoretically, the benefit of targetednanoparticles is to be retained more efficiently and more rapidlythan non-targeted ones. However, the introduction of targeting moi-eties often leads to an increase in immunogenicity and in protein ad-sorption. The main advantage of actively targeted nanoparticles overpassively targeted formulations is that they are taken up by cancercells more efficiently [14].
5. Inflammatory diseases treated by PLGA-based nanoparticles
5.1. Targeting of inflammation
In order to avoid serious side effects resulting from systemic appli-cation and long-term treatment, a local delivery of anti-inflammatorydrugs might be an interesting approach. PLGA nanoparticles wereshown to be able to enhance drug localization in target site and torelease sustainably the entrapped compound [124].
After their systemic administration, PLGA-based drug deliverysystems are preferentially taken up by the RES and present a highand selective uptake in inflamed areas. This phenomenon might beexplained by increased presence of immune-related cells like macro-phages, lymphocytes or DCs and by disruption of epithelium in theseinflamed sites, resulting in a preferential accumulation of these nano-particles. These characteristics look like the well known “enhancedpermeability” from the cancer field [125].
The surface of nanoparticles can be also modified in order to graft,to coat or to conjugate with inflamed specific-targeting moieties. An-tigens, receptors on cells or tissues, overexpressed in inflamed areaswhich are not or poorly expressed in healthy areas (such as integrinαvβ3, ICAM-1 or E-selectin), can be recognized by grafted moleculesas antibodies, specific adhesion molecules or specific ligands [126].
5.2. Inflammatory bowel diseases
Although ulcerative colitis and Crohn's disease present differentpathogenesis, conventional treatment is similar for both inflammato-ry bowel diseases (IBD). 5-aminosalicylic acid and corticosteroids areused to induce andmaintain remission. However, a gradually increaseof daily intake is necessary to maintain pharmacological effect result-ing in severe side effects [127]. PLGA nanoparticles appear to be apromising candidate to deliver drugs to colon in an IBD. A size-dependency was observed in ulcerated regions with the highest de-position amount for 100 nm-sized nanoparticles, because (i) smallerparticles are taken up more easily by immune-related cells as macro-phages and DCs in areas of active inflammation [128]; and (ii) parti-cles adhesion to inflamed area is enhanced due to strong increasedmucus production leading to a thicker mucus layer. Another impor-tant factor is the charge of nanoparticles: high concentrations of pos-itively charged proteins in ulcerated tissues might attract negativelycharged particles as PLGA based drug systems. A study with confocallaser endomicroscopy revealed mucosal accumulation of PLGA-nanoparticles in ulcerous lesions of patients with inflammatorybowel diseases [129]. Finally, PLGA nanoparticles allow sustained re-lease of entrapped anti-inflammatory drugs.
Oral administration of rolipram-loaded PLGA nanoparticles to ratssuffering from trinitrobenzene sulfonic acid-induced colitis led to adecrease of clinical activity score as compared to administration ofrolipram in solution. Moreover, although control group of animalshowed a strong relapse after 5 days without treatment, rolipram-
loaded PLGA nanoparticles continuously reduced clinical activityscore. This could be explained by PLGA nanoparticles accumulationin inflamed regions of the colon associated to biodegradability ofPLGA polymer allowing a sustained release of the entrapped drug. Re-duction of neurotropic effects was observed after rolipram-loadedPLGA nanoparticles administration[130].
PLGA nanoparticles encapsulating tacrolimus were administeredin two different rat colitis models, either by oral or rectal routes.Whereas free tacrolimus was found in high concentrations in healthytissues, tacrolimus-loaded PLGA nanoparticles increased drugamounts in inflamed areas. PLGA nanoparticles protected tacrolimusfrom its mucosal metabolism and P-gp efflux [131]. When Y. Meissneret al. compared therapeutic effect of oral administration oftacrolimus-loaded PLGA or Eudragit P-4135F nanoparticles in a dex-tran sulfate colitis model in mice, a selective accumulation of PLGAnanoparticles was observed leading to higher drug concentration in-side the inflamed tissue even if lower total amount of drug reachedinflamed sites [132].
5.3. Rheumatoid arthritis
Rheumatoid arthritis (RA) is a chronic and systemic inflammatorydisorder that results in progressive cartilage and bone destruction. AsRA has no known cure, therapy is more focused on reducing symp-toms and relieving pain. Anti-inflammatory drugs as glucocorticoidshave been widely used but are associated to some serious systemicside effects [133]. Glucocorticoids can be delivered locally by anintra-articular way and rapidly disappear from the articular cavity.Therefore, different drug delivery systems have been developed inorder to achieve sustained release of anti-inflammatory drugs. Fur-thermore, it has been reported that non-biocompatible particlesmay induce an undesirable effect called “crystal-induced pain”. Be-cause they are biodegradable, biocompatible and nano-sized, PLGAnanocarriers might be adapted to develop an arthritic lesion deliverysystem for anti-inflammatory drugs as glucocorticoids. PLGA nano-particles directly injected inside the rat joint cavity were preferential-ly phagocytosed by macrophages and sent into underlying tissuewhereas PLGA microspheres stayed in synovium [134]. Betametha-sone sodium phosphate (BSP), a water-soluble steroid, has been en-capsulated in PLGA nanoparticles for sustained release. A sustaineddrug release was shown in vivo in different animal arthritis models[135,136]. Thus, whereas BSP introduced as aqueous solution has afast and short drug release, in vivo data showed that direct intra-articular injection of PLGA nanoparticles with a size of 300–490 nmprovided a sustained release of BSP in arthritic joints of rabbits,resulting in a prolonged pharmacological efficacy. Horisawa et al.also showed that this intra-articular administration was safe [136].
5.4. Inflammatory lung diseases
PS-341, a selective inhibitor of chymotryptic threonine proteasethat ameliorates the inflammatory physiopathology of cystic fibrosis(CF) was encapsulated in PLGA-PEG nanoparticles to enhance its invivo stability and half-life and to provide mucoadhesive propertiesby shielding the intrinsic negative charge of the PLGA polymer Sus-tained release and lung accumulation of the particles were observedby administration of fluorescent PLGA-PEG nanoparticles to Cftr−/−
mice, demonstrating mucus penetration of particles. In addition,Pseudomonas aeruginosa LPS-induced inflammation was controlledby PS-341-loaded PLGA-PEG nanoparticles whereas intranasal ad-ministration of free PS-341 did not decrease the number of inflamma-tory macrophages and neutrophil cells. These drug loadednanoparticles could provide sustained delivery of CF “correctors”and “anti-inflammatories” to the lungs [137].
PLGA nanoparticles encapsulating curcumin were synthesized andused to treat two different CF mouse strains in an effort to correct the

516 F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
defects associated with CF by improving bioavailability of curcumin.Oral administration of PLGA nanoparticles encapsulating curcuminenhanced the effects of curcumin therapy in CF mice, as comparedto delivery of nonencapsulated curcumin [138].
5.5. Ophthalmic inflammatory disorders
Topical administration of free drugs in the eyes is limited by thepoor bioavailability in this tissue due to rapid tear turnover or imper-meability of the drugs to the corneal epithelial membrane. As a result,free drug is rapidly eliminated from the eye after application and only5% of the applied dose reaches intraocular tissues after cornea pene-tration [139]. Frequent administration is needed to obtain the thera-peutic effects. An ideal ophthalmic drug delivery system shouldprovide sustained and controlled drug release. PLGA nanoparticlesare promising ocular delivery systems that have been mainly usedfor sustained drug delivery in treatment of ophthalmic inflammatorydisorders. They have a suitable size [140–142]. Moreover, PLGA andits degradation products are non-toxic, biodegradable and biocom-patible and thus present low irritation for ocular tissues [83].
Use of non-steroidal anti-inflammatory drugs, in ocular topical ad-ministration, helps to manage post-operative inflammation, treat-ment of seasonal allergic conjunctivitis, in decreasing bacterialcolonization of contact lenses and prevent bacterial adhesion tohuman corneal epithelial cells [143]. PLGA nanoparticles may providea sustained ocular delivery for this drug class. In vivo ocular irritancyof diclofenac-loaded PLGA nanoparticles was investigated by using amodified Draize test. The formulation showed no irritant effects invivo after topical administration [144]. Flurbiprofen was loaded inPLGA nanoparticles with Poloxamer 188 (P188). P188 was used inorder to graft cationic polymers on the anionic surface of the PLGAnanoparticles. The formulation was applied topically on a sodiumarachidonate-induced inflammation in rabbit eyes. The nanoparticlesshowed no toxicity and better anti-inflammatory efficacy than com-mercial product eye-drops (Ocuflur®) at the same concentration offlurbiprofen (0.03%). They presented a burst release followed by aslow release. Furthermore, flurbiprofen-loaded nanoparticles had ahigher precorneal residence time in inflamed ocular tissues than inhealthy ones probably due to the “enhanced permeability” of in-flamed areas [145,146].
PLGA can also be associated to others polymers in order to modifynanoparticle properties and target more specific sites in the eye. Afterocular instillation in rabbit eye, Ciprofloxacin-loaded PLGA/Eudragit®
RL (75:25) nanoparticles showed higher drug concentration in tearfilm than the marketed emulsion probably due to the associationwith cationic polymer Eudragit® RL which allowed the formulationto interact with the anionic mucins present in the mucus layer atthe eye surface [147]. These modified-PLGA nanoparticles modulatedthe sustained drug release specifically in the conjunctival sac-like for-mation. In case of ocular inflammation, PLGA nanoparticles lead to asustained release and may offer good perspective for topical delivery.
6. Treatment of cerebral diseases with PLGA-based nanoparticles
The blood–brain barrier (BBB) limits the delivery of drugs to thebrain. Endothelial cells of BBB linked to themselves by tight junctionsfilter the passage of most of the compounds from the bloodstream tothe brain parenchyma. However, specific receptors allow the trans-port of endogenous compounds through the BBB [148]. By promotingendocytosis and targeting of the BBB receptors, PLGA nanoparticlescan provide an efficient drug delivery system to the central nervoussystem [149].
Non-coated nanoparticles have been used for the passive delivery ofproteins to the brain, such as the superoxide dismutase (SOD) whoseadministration is limited by its short in vivo half-life (∼6 min) and itspoor permeability across the BBB. In vitro studies with primary cultures
of human fetal neurons challenged with hydrogen peroxide, demon-strated in a dose- and time-dependent manner the neuroprotective ef-ficacy of these SOD-loaded PLGA nanoparticles against oxidative stressthat was more effective than free SOD and to PEGylated SOD. It was at-tributed to a better stability of the encapsulated enzyme and its superiorneuronal uptake following encapsulation [150]. In ischemia-reperfusionmodel, the treated animals not only showed greater surviv-al than untreated control (75% vs. 0% at 28 days) and better results inthe reduction of infarct volume, but also regained most vital neurologi-cal functions with time, maintaining the BBB integrity, reducing thelevel of reactive oxygen species (ROS) formed following reperfusion,and protecting neurons from undergoing apoptosis [151].
Specific brain ligands can be coated on the surface of the polymericnanoparticle, allowing the binding to specific receptors to brain capil-lary endothelium. Lactoferrin (Lf), a glycoprotein belonging to trans-ferrin family, has a receptor in the BBB and has been proved to be apromising brain targetingmolecule [152]. Lf was therefore conjugatedto PEG-PLGA nanoparticles. One hour after intravenous injection,no PEG-PLGA nanoparticles were found in brain mice whereas Lf-PEG-PLGA nanoparticles were mainly found in the substantia nigra,cortex and striatum region, demonstrating efficiency of the transportacross the BBB and brain targeting by Lf. Urocortin a corticotrophin re-leasing hormone-related peptide that might be really useful againstParkinson's disease was then encapsulated. After intravenous injec-tion in the 6-OHDA model rats, urocortin-loaded Lf-nanoparticlesshowed a lower striatal lesion severity, a better tyrosine hydroxylaseimmunoreactivity and an enhanced dopamine content than untreatedgroup, showing a potential anti-parkinsonian activity [153].
Loperamide is an opioid drug without any anti-nociceptive effectafter intravenous injection, due to its inability to cross the BBB. Loper-amide was then chosen as model drug to treat chronic neuro-diseases[154]. A simil-opioid peptide (NH2-Gly-L-Phe-D-Thr-Gly-L-Phe-L-Leu-L-Ser(O-B-D-Glucose)-COOH, g7) was first grafted on PLGAnanoparticles. These modified nanoparticles were able to pass acrossthe BBB, reached all the brain areas examined ensuring a sustainedrelease of the embedded drug [155]. Nanoparticles decorated withtwo moieties: g7, to penetrate the BBB and a sialic acid (SA) deriva-tive, to target brain sialoadhesin receptors [156]. Nociceptive studiesdemonstrated ability of SA-g7 nanoparticles to cross the BBB and tosustain in the brain parenchyma probably due to g7 and SA residuerespectively. As the opioid effect of loperamide-loaded g7-nanoparticles lasted 5 h, double conjugated SA-g7 nanoparticles pre-sented anti-nociceptive effect lasting 24 h after intravenous injection.Loperamide solution and loperamide-loaded unmodified PLGA nano-particles did not show any central analgesic effect [157]. However,due to the fact that SA receptors are present in different organs,these modified nanoparticles accumulated in other organs such asliver and kidneys in a higher amount than g7- and unmodified PLGAnanoparticles, highlighting the limitations of SA derivative as a goodand above all specific brain ligand.
The sequence TGNYKALHPHNG, also known as Pep TGN, was identi-fied by phage display and successfully conjugated on the surface offluo-rescent PLGA nanoparticles and revealed a significantly higher brainuptake than unmodified nanoparticles in mice 24 h after intravenousinjection. Furthermore, the more PepTGN was present on the surfaceof the nanoparticles, the more brain transport was efficient, demon-strating the importance of the targeting for the brain delivery [158].
7. Regenerative medicine and PLGA-based nanoparticles
Tissue engineering and regenerative medicine are emerging disci-plines of biomedical research that promote the regeneration of tis-sues or the replacement of failing or malfunctioning organs. Theycombine the use of adequate cells, scaffolds (that support and directthe growth of cells, and present appropriate physicochemical proper-ties, mechanical strength and biodegradation profile) and bioactive

517F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
molecules. These bioactive molecules essentially include proteinsstimulating cell migration, proliferation or inducing cell differentia-tion, such as growth and neurotrophic factors [159].
The incorporation of these bioactive proteins in PLGA nanoparti-cles could present several advantages. The control over spatial andtemporal release of growth factors in tissue engineering scaffoldsand matrices, as well as their protection, is biologically highly rele-vant [159]. For instance, after the lesion occurred, there is an up-regulated proteolytic enzyme activity that would degrade the bioac-tive protein if administered alone. Repeated penetrating injectionsinto the lesion to ensure an efficient level of growing factors may ag-gravate tissue damage and hinder functional recovery, in certaincases [160]. Nanoparticles would protect the protein from degrada-tion and would deliver the bioactive compound in a controlled andsustained manner maintaining the therapeutic levels over the time,avoiding or reducing those frequent injections. Furthermore, theywould target the restorative molecule into the injured area. Thislocalized effect represents also an important benefit, because theadministration of these proteins could present undesired side effectswhen they activate non-target areas [161,162].
Glial cell-line derived neurotrophic factor (GDNF) is a potent neu-rotrophic factor originally described for dopaminergic neurons. Afterthe good results observed with its direct infusion in phase I clinicaltrials for the Parkinson's disease [163–165], a phase II clinical trialwas halted, at least in part, due to lack of efficacy probably becausethe protein did not reach the target area [166]. Therefore, researchgroups encapsulated this molecule in PLGA drug delivery systemsfor its stereotaxic implantation in animal models of the disease,obtaining promising results [167–169].
The administration of the neurotrophic factor also showed benefi-cial effects on neurons present in the spinal cord [170–173]. Wang etal. encapsulated GDNF in PLGA nanoparticles for its implantation intothe spinal cord. Neuronal cell viability studies confirmed that the re-leased neutrophic factor maintained its bioactivity. In vivo studies inrats have shown that the nanoparticles were taken up by glia andneuron cells [160]. More importantly, its injection in a contusionmodel of spinal cord injury induced an increase in neuronal survival,fiber regeneration and improved hind-limb locomotion function inthe treated rats. These results improved the ones obtained using abolus injection of GDNF [171].
In tissue engineering, vascularization is one of the first require-ments to achieve tissue regeneration. The delivery of angiogenic fac-tors from implants has been widely investigated for establishing avascular network within the developing tissue [174]. VEGF is agrowth factor that regulates blood and lymphatic vessel development(by signaling vascular endothelial cells to undergo proliferation, mi-gration and differentiation into new blood vessels) and it also pre-sents some effects on neural cells [175,176]. VEGF was incorporatedinto PLGA nanoparticles, arguing that nanoparticle encapsulationconfers several advantages over microparticle encapsulation, includ-ing a lower risk of embolization [33,177]. Even though the effectiveloading yield in VEGF-loaded nanoparticles fabrication was only 5%,the in vitro bioassay using an aortic ring confirmed that the proteinreleased was active. In vivo studies in a mouse femoral artery ische-mia model have shown that VEGF-loaded PLGA nanoparticles treat-ment had a significant increase in total vessel volume and vesselconnectivity compared to mice administered with free protein orsaline treatment [178]. VEGF-loaded PLGA nanoparticles have beenrecently formulated, optimized and incorporated in a thermo-sensitive hydrogel in porcine bladder acellular matrix, for bladderreconstruction therapy. Nanoparticles demonstrated, in an in vitroproliferative study, a sustained release of bioactive angiogenic factor,and the thermo-sensitive behavior (sol–gel transmission at appropri-ate temperature) of the system in nude mice [179].
Due to the growing interest in new blood vessels formation for tis-sue engineering as well as to treat vascular and ischemia-related
diseases, other pro-angiogenic growth factors (platelet derivedgrowth factor (PDGF-BB) and fibroblast growth factor (FGF-2)) havebeen encapsulated in PLGA-poloxamer blend nanoparticles preserv-ing its structure by the incorporation of the stabilizing agents: bovineserum albumine and heparin sodium salt. Furthermore, they also in-creased the encapsulation efficiency of PDGF-BB and FGF-2 to 87%and 63% respectively. Once the activity of the released FGF-2 was con-firmed by migration of human microvascular endothelial cells [180],nanoparticles were co-administered intra-arterially with microbub-bles in a mouse model of hind-limb arterial insufficiency. The ultra-sonic microbubble destruction induced microvessel disruptionswhich allowed intravascular constituents to be transported into theendothelium and interstitium of ultrasound-exposed tissues[181–183]. The delivery of the FGF-2-loaded PLGA nanoparticlesstimulated considerable arteriogenic remodeling in ischemic mousehind-limb adductor muscles. This response included an increase inthe total number of large and moderate diameter arterioles, as wellas a marked luminal expansion of both the pre-existing collateralarteries and the transverse arterioles [180].
Bone tissue engineering is also a field in development that in-cludes as well the use of 3-D systems combining bone forming cells,porous biodegradable scaffolds and growth factors (that guide theproliferation and differentiation of the cells). Bone morphogeneticproteins (BMPs) are a group of growth factors that promote bone for-mation by inducing the differentiation of mesenchymal stem cells to-ward chondroblastic and osteoblastic cells [184]. Among them, BMP-2 and BMP-7 have been described as the most effective to inducecomplete bone morphogenesis [185] and have been approved bythe FDA for their clinical applications [186,187]. During fracture heal-ing, BMP-2 has been described to be an early appearing factor, peak-ing at day 1 after fracture, while BMP-7 is being expressedapproximately 2 weeks later [188]. In order to provide this sequentialtime pattern of administration and also to increase the stability of thegrowth factors, BMP-2 was encapsulated in PLGA nanoparticles for anearly release, whereas BMP-7 was encapsulated in poly (3-hydroxy-butyrate-co-3-hydroxyvalerate) nanoparticles, for later release[189]. When tested in an in vitro bioassay of the osteogenic differen-tiation into osteoblasts of rat bone marrow mesenchymal stem cells,a synergistic effect was observed with the sequential delivery of theBMPs in contrast with their single and simultaneous (using PLGAnanoparticles for both BMPs) delivery [189]. These nanoparticleswere subsequently incorporated together with mesenchymal stemcells within different chitosan-based scaffolds that presented smoothand rough fiber surfaces. The best results in the in vitro studies weredescribed with the sequential delivery of the BMPs incorporatingthe nanoparticles on the fiber surface [190]. These nanoparticleswere also incorporated into poly (ε-caprolactone) (PCL) scaffolds.The effect of scaffold geometry and growth factor delivery from thescaffolds were investigated again using bone marrow mesenchymalstem cells. The positive effect of co-administration of BMP-2 andBMP-7 in a sequential manner was established as well in thismodel, as they increased the osteogenic activity. The 3-D architectureof the PLC scaffolds affected proliferation and differentiation of mes-enchymal stem cells. Better results were obtained with randomly or-ganized fibers scaffold [191].
The data reported in the literature indicate that PLGA nanoparti-cles are promising to achieve a sustained and spatially and temporallycontrolled delivery of growth factors required for cell growth and celldifferentiation. They can be incorporated with cells in solid scaffold orinjectable hydrogels.
8. Treatment of cardiovascular diseases withPLGA-based nanoparticles
Cardiovascular diseases (CVD) are still the major cause of mortal-ity among populations of developed countries. CVD research field is

518 F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
very productive and nanotechnologies such as PLGA-based nanopar-ticles have been investigated in this area to develop new possibilitiesin terms of diagnosis and treatment.
The first option to treat CVD is the placement of a stent. This pro-cedure can be ameliorated by the introduction of therapeutic com-pounds such as small molecules or biomolecules. This is possiblewith the use of nanotechnologies. Stents can be coated with PLGA-based nanoparticles encapsulating specific drugs, genes, or proteins,and allowing a slow release of these therapeutics. Among other ex-amples, DNA-loaded PLGA nanoparticles-coated stents have shownefficient DNA transfection in cultured smooth muscle cells, and inpig coronary arteries [192]. In this system, modification of PLGAwith denatured collagen enhanced 10 times transfection efficiency,by enhancing nanoparticles–cells interactions through specific recep-tor interactions [193].
Once cardiovascular tissue is too damaged to be only treated withdrugs, arterial replacement becomes necessary. Synthetic grafts areavailable but have a limited success in some cases [194]. Thus tissueengineered grafts are currently developed. To do so, biomaterialswith biodegradable, strong and elastic properties are needed, andPLGA-based systems offer this kind of biomechanical and biologicalfeatures [195]. Research in this area have led to the development ofpatterned cell sheets that can create vessels walls when layered[196], to the delivery and controlled release of specific drugs or mol-ecules [197], such as growth factors, to enhance interaction betweenthe graft scaffold and the vascular cells.
9. Infection treatment by PLGA-based nanoparticles
Several studies aimed at developing antibiotic-loaded PLGA nano-particles to improve the treatment of bacterial infections. To be moreeffective, plasma concentrations of most antibiotics need to be con-stant. Sustained release of drugs from PLGA-based nanoparticlescould thus potentially improve the treatment efficacy. Moreover, forsome intracellular pathogens, such as Chlamydia, nanoparticles canenhance the intracellular delivery of antibiotics.
Rifampicin and azithromycin were encapsulated in PLGA nanopar-ticles. Intracellular trafficking studies showed that nanoparticles effi-ciently concentrated in inclusions in both acutely and persistentlyChlamydia infected cells [110]. The nanoparticles enhanced the effec-tiveness of the antibiotics in reducing microbial burden.
Gentamycin, an aminoglycoside with poor cellular penetrationwas encapsulated in PLGA nanoparticles. Nanoparticles were endocy-tosed by murine monocytes and reached the spleen and liver, thetarget organs for brucellosis [198]. Pharmacokinetic parameter aftera single intravenous administration revealed higher AUCs for theliver and spleen and higher mean retention times, indicating success-ful uptake by phagocytic cells [199]. Ion pairing with an anionicsurfactant to enhance encapsulation did not modify the anti-bacterial activity [200].
Nafcillin-loaded PLGA nanoparticles killed or significantly reducedintracellular Staphylococcus aureus infecting osteoblasts suggestingtheir potential use for the treatment of osteomylitis [201].
Sparfloxacin is a poorly water-soluble fluoroquinolone used forthe treatment of bacterial conjunctivitis. Gupta et al. demonstratedby gamma scintigraphy that Tc-99m sparfloxacin-loaded nanoparti-cles were retained at the corneal surface for a longer duration thanthe marketed formulation of free sparfloxacin in albino rabbits. More-over, while marketed formulation was found in the systemiccirculation, no sparfloxacin-loaded PLGA nanosystem was found out-side the ocular tissues even after 6 h [202].
The preclinical examples clearly demonstrate that PLGA basednanoparticles have proven potential for the treatment of infection.(i) As nanoparticles are usually taken up by endocytosis in cells,antibiotic-loaded nanoparticles could be a promising delivery systemto target intracellular infections. (ii) As nanoparticle can achieve a
sustained delivery, antibiotic-loaded PLGA nanoparticles are helpfulto treat or prevent local infection.
10. Treatment of other diseases with PLGA-based nanoparticles
Calcitonine is a hormone that plays a crucial role in bone remodel-ing and calcium homeostasis [203]. It is generally administered by in-jection or intra-nasally for the treatment of osteoporosis. Thishormone has been incorporated into PLGA nanoparticles for its oraland pulmonary administration. Calcitonin-loaded PLGA nanoparticlescan increase the oral absorption [204]. The administration in lungs ofguinea pigs of calcitonin-loaded PLGA/chitosan nanoparticles using anebulizer revealed that the presence of chitosan in the surface signif-icantly decreased the elimination rate of the nanoparticles comparedto the unmodified nanospheres, due to the mucoadhesive propertiesof chitosan. Furthermore, it was confirmed that chitosan enhancedthe protein absorption by opening of the intercellular tight junctionsin the lung epithelium [205].
Due to its wide use in the treatment of diabetes mellitus (Type I),the encapsulation of insulin in PLGA nanoparticles has been exten-sively studied [206]. Insulin has been complexed with diverse com-pounds to increase its liposolubility, to facilitate its loadingefficiency [207–211] with drug entrapment efficiency values up to90% [212]. In the work of Liu et al. [213], the PLGA nanoparticleswere embedded into cross-linked poly-(vinyl alcohol) (PVA) hydro-gels, obtaining a reduction in the release rate and the total amountof protein released. The administration of the different formulationsin vivo significantly decreased the blood glucose levels of diabeticrats, mice, and guinea pigs [212,213]. However, the poor oral bioavail-ability, the poor control of the dose absorbed and the poor drug load-ing have hindered clinical trials with insulin-loaded PLGAnanoparticles.
11. Conclusions
PLGA-based nanoparticles present many advantages for drug de-livery. They can protect drugs from degradation and enhance theirstability. Moreover, due to their size, nanoparticles can penetrate spe-cific tissues via (i) the fenestrations present in the endothelium ofcancer and inflamed tissue or (ii) via receptors overexpressed by tar-get cells or in the blood brain barrier. This allows a specific delivery ofdrugs, proteins, peptides or nucleic acids to their target tissue. PLGA-based nanoparticles can increase the efficacy of treatments because ofthe sustained release of the therapeutic agent from stable nanoparti-cles. They can improve pharmacokinetic and pharmacodynamic pro-files. Another major advantage of PLGA over other polymers is thatPLGA is approved by the FDA and EMA in various drug delivery sys-tems, leading PLGA-based nanoparticles in a good position for clinicaltrials.
These systems present also some disadvantages such as the lowdrug loading described for many drugs, the high cost of productionand the difficulty of the scale-up. Even though this issue is seldomaddressed, the relatively low drug loading efficiency is probably themajor hurdle limiting the use of drug-loaded PLGA-based nanoparti-cles in clinical trials.
In this review, many examples of proof of concept of the potentialbenefit to use PLGA-based nanoparticles in the treatment of variousdiseases have been described both in vitro and when available invivo using as therapeutic strategy, untargeted and targeted nanopar-ticles (Table 1). These examples clearly illustrate the promise ofthese nanoparticles for novel treatments in the future.
References
[1] M.L. Hans, A.M. Lowman, Biodegradable nanoparticles for drug delivery and tar-geting, Curr. Opin. Solid State Mater. Sci. 6 (2002) 319–327.

519F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
[2] H. Hillaireau, P. Couvreur, Nanocarriers' entry into the cell: relevance to drug de-livery, Cell. Mol. Life Sci. 66 (2009) 2873–2896.
[3] A. Kumari, S.K. Yadav, S.C. Yadav, Biodegradable polymeric nanoparticles baseddrug delivery systems, Colloids Surf. B Biointerfaces 75 (2010) 1–18.
[4] A. Prokop, J.M. Davidson, Nanovehicular intracellular delivery systems, J. Pharm.Sci. 97 (2008) 3518–3590.
[5] M. Vert, J. Mauduit, S. Li, Biodegradation of PLA/GA polymers: increasing com-plexity, Biomaterials 15 (1994) 1209–1213.
[6] J.K. Vasir, V. Labhasetwar, Biodegradable nanoparticles for cytosolic delivery oftherapeutics, Adv. Drug Deliv. Rev. 59 (2007) 718–728.
[7] S. Acharya, S.K. Sahoo, PLGA nanoparticles containing various anticancer agentsand tumour delivery by EPR effect, Adv. Drug Deliv. Rev. 63 (2011) 170–183.
[8] D.E. Owens III, N.A. Peppas, Opsonization, biodistribution, and pharmacokineticsof polymeric nanoparticles, Int. J. Pharm. 307 (2006) 93–102.
[9] T. Betancourt, J.D. Byrne, N. Sunaryo, S.W. Crowder, M. Kadapakkam, S. Patel, S.Casciato, L. Brannon-Peppas, PEGylation strategies for active targeting ofPLA/PLGA nanoparticles, J. Biomed. Mater. Res. 91A (2009) 263–276.
[10] M. Wang, M. Thanou, Targeting nanoparticles to cancer, Pharmacol. Res. 62(2010) 90–99.
[11] C. Foged, B. Brodin, S. Frokjaer, A. Sundblad, Particle size and surface charge af-fect particle uptake by human dendritic cells in an in vitro model, Int. J. Pharm.298 (2005) 315–322.
[12] J.K. Vasir, V. Labhasetwar, Quantification of the force of nanoparticle–cell mem-brane interactions and its influence on intracellular trafficking of nanoparticles,Biomaterials 29 (2008) 4244–4252.
[13] Z.G. Yue, W. Wei, P.P. Lv, H. Yue, L.Y. Wang, Z.G. Su, G.H. Ma, Surface charge af-fects cellular uptake and intracellular trafficking of chitosan-based nanoparti-cles, Biomacromolecules 12 (2011) 2440–2446.
[14] F. Danhier, O. Feron, V. Preat, To exploit the tumor microenvironment: passiveand active tumor targeting of nanocarriers for anti-cancer drug delivery, J. Con-trol. Release 148 (2010) 135–146.
[15] K. Tahara, T. Sakai, H. Yamamoto, H. Takeuchi, N. Hirashima, Y. Kawashima,Improved cellular uptake of chitosan-modified PLGA nanospheres by A549cells, Int. J. Pharm. 382 (2009) 198–204.
[16] K.S. Soppimath, T.M. Aminabhavi, A.R. Kulkarni, W.E. Rudzinski, Biodegradablepolymeric nanoparticles as drug delivery devices, J. Control. Release 70 (2001)1–20.
[17] H. Fessi, F. Puisieux, J.P. Devissaguet, N. Ammoury, S. Benita, Nanocapsule forma-tion by interfacial polymer deposition following solvent displacement, Int. J.Pharm. 55 (1989) R1–R4.
[18] M. Gaumet, A. Vargas, R. Gurny, F. Delie, Nanoparticles for drug delivery: theneed for precision in reporting particle size parameters, Eur. J. Pharm. Biopharm.69 (2008) 1–9.
[19] C. Fonseca, S. Simoes, R. Gaspar, Paclitaxel-loaded PLGA nanoparticles: prepara-tion, physicochemical characterization and in vitro anti-tumoral activity, J. Con-trol. Release 83 (2002) 273–286.
[20] K. Derakhshandeh, M. Erfan, S. Dadashzadeh, Encapsulation of 9-nitrocamptothecin, a novel anticancer drug, in biodegradable nanoparticles:factorial design, characterization and release kinetics, Eur. J. Pharm. Biopharm.66 (2007) 34–41.
[21] K. Avgoustakis, A. Beletsi, Z. Panagi, P. Klepetsanis, A.G. Karydas, D.S. Ithakissios,PLGA-mPEG nanoparticles of cisplatin: in vitro nanoparticle degradation, in vitrodrug release and in vivo drug residence in blood properties, J. Control. Release 79(2002) 123–135.
[22] A. Budhian, S.J. Siegel, K.I. Winey, Production of haloperidol-loaded PLGA nano-particles for extended controlled drug release of haloperidol, J. Microencapsul.22 (2005) 773–785.
[23] G. Mittal, D.K. Sahana, V. Bhardwaj, M.N. Ravi Kumar, Estradiol loaded PLGAnanoparticles for oral administration: effect of polymer molecular weight andcopolymer composition on release behavior in vitro and in vivo, J. Control. Re-lease 119 (2007) 77–85.
[24] J.E. Talmadge, The pharmaceutics and delivery of therapeutic polypeptides andproteins, Adv. Drug Deliv. Rev. 10 (1993) 247–299.
[25] M. van de Weert, W.E. Hennink, W. Jiskoot, Protein instability in poly(lactic-co-glycolic acid) microparticles, Pharm. Res. 17 (2000) 1159–1167.
[26] A. Giteau, M.C. Venier-Julienne, S. Marchal, J.L. Courthaudon, M. Sergent, C.Montero-Menei, J.M. Verdier, J.P. Benoit, Reversible protein precipitation to en-sure stability during encapsulation within PLGA microspheres, Eur. J. Pharm.Biopharm. 70 (2008) 127–136.
[27] J.L. Cleland, M.F. Powell, S.J. Shire, The development of stable protein formula-tions: a close look at protein aggregation, deamidation, and oxidation, Crit.Rev. Ther. Drug Carrier Syst. 10 (1993) 307–377.
[28] G. Zhu, S.R. Mallery, S.P. Schwendeman, Stabilization of proteins encapsulated ininjectable poly(lactide-co-glycolide), Nat. Biotechnol. 18 (2000) 52–57.
[29] P.S. Kumar, S. Ramakrishna, T.R. Saini, P.V. Diwan, Influence of microencapsula-tion method and peptide loading on formulation of poly(lactide-co-glycolide)insulin nanoparticles, Pharmazie 61 (2006) 613–617.
[30] P.S. Kumar, T.R. Saini, D. Chandrasekar, V.K. Yellepeddi, S. Ramakrishna, P.V.Diwan, Novel approach for delivery of insulin loaded poly(lactide-co-glycolide)nanoparticles using a combination of stabilizers, Drug Deliv. 14 (2007) 517–523.
[31] S. Ribeiro, N. Hussain, A.T. Florence, Release of DNA from dendriplexes encapsu-lated in PLGA nanoparticles, Int. J. Pharm. 298 (2005) 354–360.
[32] I.S. Kim, S.K. Lee, Y.M. Park, Y.B. Lee, S.C. Shin, K.C. Lee, I.J. Oh, Physicochemicalcharacterization of poly(L-lactic acid) and poly(D,L-lactide-co-glycolide) nano-particles with polyethylenimine as gene delivery carrier, Int. J. Pharm. 298(2005) 255–262.
[33] J. Davda, V. Labhasetwar, Characterization of nanoparticle uptake by endothelialcells, Int. J. Pharm. 233 (2002) 51–59.
[34] X. Niu, W. Zou, C. Liu, N. Zhang, C. Fu, Modified nanoprecipitation method to fab-ricate DNA-loaded PLGA nanoparticles, Drug Dev. Ind. Pharm. 35 (2009)1375–1383.
[35] S. Prabha, V. Labhasetwar, Critical determinants in PLGA/PLA nanoparticle-mediated gene expression, Pharm. Res. 21 (2004) 354–364.
[36] C. Sun, T. Yi, X. Song, S. Li, X. Qi, X. Chen, H. Lin, X. He, Z. Li, Y. Wei, X. Zhao,Efficient inhibition of ovarian cancer by short hairpin RNA targeting claudin-3,Oncol. Rep. 26 (2011) 193–200.
[37] K. Tahara, T. Sakai, H. Yamamoto, H. Takeuchi, Y. Kawashima, Establishing chit-osan coated PLGA nanosphere platform loaded with wide variety of nucleic acidby complexation with cationic compound for gene delivery, Int. J. Pharm. 354(2008) 210–216.
[38] Y.B. Patil, S.K. Swaminathan, T. Sadhukha, L. Ma, J. Panyam, The use ofnanoparticle-mediated targeted gene silencing and drug delivery to overcometumor drug resistance, Biomaterials 31 (2010) 358–365.
[39] D. Cun, D.K. Jensen, M.J. Maltesen, M. Bunker, P. Whiteside, D. Scurr, C. Foged,H.M. Nielsen, High loading efficiency and sustained release of siRNA encapsulatedin PLGA nanoparticles: quality by design optimization and characterization, Eur. J.Pharm. Biopharm. 77 (2011) 26–35.
[40] T.T. Beaudette, E.M. Bachelder, J.A. Cohen, A.C. Obermeyer, K.E. Broaders, J.M.Frechet, E.S. Kang, I. Mende, W.W. Tseng, M.G. Davidson, E.G. Engleman, Invivo studies on the effect of co-encapsulation of CpG DNA and antigen in acid-degradable microparticle vaccines, Mol. Pharm. 6 (2009) 1160–1169.
[41] S. de Jong, G. Chikh, L. Sekirov, S. Raney, S. Semple, S. Klimuk, N. Yuan, M. Hope,P. Cullis, Y. Tam, Encapsulation in liposomal nanoparticles enhances the immu-nostimulatory, adjuvant and anti-tumor activity of subcutaneously adminis-tered CpG ODN, Cancer Immunol. Immunother. 56 (2007) 1251–1264.
[42] C. Clawson, C.T. Huang, D. Futalan, D.M. Seible, R. Saenz, M. Larsson, W. Ma, B.Minev, F. Zhang, M. Ozkan, C. Ozkan, S. Esener, D. Messmer, Delivery of a peptidevia poly(D,L-lactic-co-glycolic) acid nanoparticles enhances its dendritic cell-stimulatory capacity, Nanomedicine 6 (2010) 651–661.
[43] M. Diwan, P. Elamanchili, H. Lane, A. Gainer, J. Samuel, Biodegradable nanopar-ticle mediated antigen delivery to human cord blood derived dendritic cells forinduction of primary T cell responses, J. Drug Target. 11 (2003) 495–507.
[44] S. Prasad, V. Cody, J.K. Saucier-Sawyer, W.M. Saltzman, C.T. Sasaki, R.L. Edelson,M.A. Birchall, D.J. Hanlon, Polymer nanoparticles containing tumor lysates as an-tigen delivery vehicles for dendritic cell-based antitumor immunotherapy,Nanomedicine 7 (2011) 1–10.
[45] C.M. Solbrig, J.K. Saucier-Sawyer, V. Cody, W.M. Saltzman, D.J. Hanlon, Polymernanoparticles for immunotherapy from encapsulated tumor-associated antigensand whole tumor cells, Mol. Pharm. 4 (2007) 47–57.
[46] C. Thomas, A. Rawat, L. Hope-Weeks, F. Ahsan, Aerosolized PLA and PLGA nano-particles enhance humoral, mucosal and cytokine responses to hepatitis B vac-cine, Mol. Pharm. 8 (2010) 405–415.
[47] J. Tian, J. Yu, Poly(lactic-co-glycolic acid) nanoparticles as candidate DNA vac-cine carrier for oral immunization of Japanese flounder (Paralichthys olivaceus)against lymphocystis disease virus, Fish Shellfish Immunol. 30 (2011) 109–117.
[48] W. Jiang, R.K. Gupta, M.C. Deshpande, S.P. Schwendeman, Biodegradablepoly(lactic-co-glycolic acid) microparticles for injectable delivery of vaccineantigens, Adv. Drug Deliv. Rev. 57 (2005) 391–410.
[49] B. Slutter, S. Bal, C. Keijzer, R. Mallants, N. Hagenaars, I. Que, E. Kaijzel, W. vanEden, P. Augustijns, C. Lowik, J. Bouwstra, F. Broere, W. Jiskoot, Nasal vaccinationwith N-trimethyl chitosan and PLGA based nanoparticles: nanoparticle charac-teristics determine quality and strength of the antibody response in miceagainst the encapsulated antigen, Vaccine 28 (2010) 6282–6291.
[50] R. Brunner, E. Jensen-Jarolim, I. Pali-Scholl, The ABC of clinical and experimentaladjuvants—a brief overview, Immunol. Lett. 128 (2010) 29–35.
[51] M. Diwan, P. Elamanchili, M. Cao, J. Samuel, Dose sparing of CpG oligodeoxynu-cleotide vaccine adjuvants by nanoparticle delivery, Curr. Drug Deliv. 1 (2004)405–412.
[52] P. Elamanchili, C.M. Lutsiak, S. Hamdy, M. Diwan, J. Samuel, “Pathogen-mimicking”nanoparticles for vaccine delivery to dendritic cells, J. Immunother. 30 (2007)378–395.
[53] S. Hamdy, O. Molavi, Z. Ma, A. Haddadi, A. Alshamsan, Z. Gobti, S. Elhasi, J.Samuel, A. Lavasanifar, Co-delivery of cancer-associated antigen and Toll-like re-ceptor 4 ligand in PLGA nanoparticles induces potent CD8+ T cell-mediatedanti-tumor immunity, Vaccine 26 (2008) 5046–5057.
[54] R. Arens, S.P. Schoenberger, Plasticity in programming of effector and memoryCD8 T-cell formation, Immunol. Rev. 235 (2010) 190–205.
[55] H. Shen, A.L. Ackerman, V. Cody, A. Giodini, E.R. Hinson, P. Cresswell, R.L.Edelson, W.M. Saltzman, D.J. Hanlon, Enhanced and prolonged cross-presentation following endosomal escape of exogenous antigens encapsulatedin biodegradable nanoparticles, Immunology 117 (2006) 78–88.
[56] F. Alexis, E. Pridgen, L.K. Molnar, O.C. Farokhzad, Factors affecting the clearanceand biodistribution of polymeric nanoparticles, Mol. Pharm. 5 (2008) 505–515.
[57] C. Kelly, C. Jefferies, S.A. Cryan, Targeted liposomal drug delivery to monocytesand macrophages, J. Drug Deliv. 2011 (2011) 727241.
[58] R.A. Jain, The manufacturing techniques of various drug loaded biodegradablepoly(lactide-co-glycolide) (PLGA) devices, Biomaterials 21 (2000)2475–2490.
[59] M.F. Bachmann, G.T. Jennings, Vaccine delivery: a matter of size, geometry, ki-netics and molecular patterns, Nat. Rev. Immunol. 10 (2010) 787–796.
[60] K. Cho, X. Wang, S. Nie, Z.G. Chen, D.M. Shin, Therapeutic nanoparticles for drugdelivery in cancer, Clin. Cancer Res. 14 (2008) 1310–1316.

520 F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
[61] V. Manolova, A. Flace, M. Bauer, K. Schwarz, P. Saudan, M.F. Bachmann, Nanopar-ticles target distinct dendritic cell populations according to their size, Eur. J.Immunol. 38 (2008) 1404–1413.
[62] U.N. Rao, S.J. Lee, W. Luo, M.C. Mihm Jr., J.M. Kirkwood, Presence of tumor-infiltrating lymphocytes and a dominant nodule within primary melanoma areprognostic factors for relapse-free survival of patients with thick (t4) primarymelanoma: pathologic analysis of the e1690 and e1694 intergroup trials, Am.J. Clin. Pathol. 133 (2010) 646–653.
[63] S. Burgdorf, C. Kurts, Endocytosis mechanisms and the cell biology of antigenpresentation, Curr. Opin. Immunol. 20 (2008) 89–95.
[64] E. Fernandez-Megia, R. Novoa-Carballal, E. Quinoa, R. Riguera, Conjugation ofbioactive ligands to PEG-grafted chitosan at the distal end of PEG, Biomacromo-lecules 8 (2007) 833–842.
[65] J.H. van den Berg, K. Oosterhuis, W.E. Hennink, G. Storm, L.J. van der Aa, J.F.Engbersen, J.B. Haanen, J.H. Beijnen, T.N. Schumacher, B. Nuijen, Shielding thecationic charge of nanoparticle-formulated dermal DNAvaccines is essential for an-tigen expression and immunogenicity, J. Control. Release 141 (2010) 234–240.
[66] N. Kadowaki, Dendritic cells: a conductor of T cell differentiation, Allergol. Int.56 (2007) 193–199.
[67] H. Kumar, T. Kawai, S. Akira, Pathogen recognition in the innate immune re-sponse, Biochem. J. 420 (2009) 1–16.
[68] O. Takeuchi, S. Akira, Pattern recognition receptors and inflammation, Cell 140(2010) 805–820.
[69] T. Kawai, S. Akira, TLR signaling, Semin. Immunol. 19 (2007) 24–32.[70] I. Bekeredjian-Ding, G. Jego, Toll-like receptors—sentries in the B-cell response,
Immunology 128 (2009) 311–323.[71] G. Liu, L. Zhang, Y. Zhao, Modulation of immune responses through direct activa-
tion of Toll-like receptors to T cells, Clin. Exp. Immunol. 160 (2010) 168–175.[72] U. Gazi, L. Martinez-Pomares, Influence of the mannose receptor in host immune
responses, Immunobiology 214 (2009) 554–561.[73] S. Hamdy, A. Haddadi, A. Shayeganpour, J. Samuel, A. Lavasanifar, Activation of
antigen-specific T cell-responses by mannan-decorated PLGA nanoparticles,Pharm. Res. 9 (2011) 2288–2301.
[74] M.D. Joshi, W.W. Unger, A.J. van Beelen, S.C. Bruijns, M. Litjens, B.L. van, H. Kalay,K.Y. van, G. Storm, DC-SIGN mediated antigen-targeting using glycan-modifiedliposomes: formulation considerations, Int. J. Pharm. 2 (2011) 426–432.
[75] L.J. Cruz, P.J. Tacken, R. Fokkink, B. Joosten, M.C. Stuart, F. Albericio, R. Torensma,C.G. Figdor, Targeted PLGA nano- but not microparticles specifically deliver an-tigen to human dendritic cells via DC-SIGN in vitro, J. Control. Release 144(2010) 118–126.
[76] M.K. O'Reilly, J.C. Paulson, Siglecs as targets for therapy in immune-cell-mediated disease, Trends Pharmacol. Sci. 30 (2009) 240–248.
[77] G.S. von, B.S. Bochner, Basic and clinical immunology of Siglecs, Ann. N. Y. Acad.Sci. 1143 (2008) 61–82.
[78] C. Jandus, H.U. Simon, G.S. von, Targeting Siglecs—a novel pharmacological strat-egy for immuno- and glycotherapy, Biochem. Pharmacol. 82 (2011) 323–332.
[79] C.J. Scott, W.M. Marouf, D.J. Quinn, R.J. Buick, S.J. Orr, R.F. Donnelly, P.A.McCarron, Immunocolloidal targeting of the endocytotic siglec-7 receptorusing peripheral attachment of siglec-7 antibodies to poly(lactide-co-glycolide)nanoparticles, Pharm. Res. 25 (2008) 135–146.
[80] A. des Rieux, V. Fievez, M. Garinot, Y.J. Schneider, V. Preat, Nanoparticles as po-tential oral delivery systems of proteins and vaccines: a mechanistic approach, J.Control. Release 116 (2006) 1–27.
[81] Y. Peter, D. Goodenough, Claudins, Curr. Biol. 14 (2004) R293–R294.[82] T.E. Rajapaksa, M. Stover-Hamer, X. Fernandez, H.A. Eckelhoefer, D.D. Lo, Claudin
4-targeted protein incorporated into PLGA nanoparticles can mediate M cell tar-geted delivery, J. Control. Release 142 (2010) 196–205.
[83] M. Garinot, V. Fievez, V. Pourcelle, F. Stoffelbach, A. des Rieux, L. Plapied, I.Theate, H. Freichels, C. Jerome, J. Marchand-Brynaert, Y.J. Schneider, V. Preat,PEGylated PLGA-based nanoparticles targeting M cells for oral vaccination,J. Control. Release 120 (2007) 195–204.
[84] V. Fievez, L. Plapied, A. des Rieux, V. Pourcelle, H. Freichels, V. Wascotte, M.L.Vanderhaeghen, C. Jerome, A. Vanderplasschen, J. Marchand-Brynaert, Y.J.Schneider, V. Preat, Targeting nanoparticles to M cells with non-peptidic ligandsfor oral vaccination, Eur. J. Pharm. Biopharm. 73 (2009) 16–24.
[85] E.M. Fernandez, J. Chang, J. Fontaine, E. Bialecki, F. Rodriguez, E. Werkmeister, V.Krieger, C. Ehret, B. Heurtault, S. Fournel, B. Frisch, D. Betbeder, C. Faveeuw, F.Trottein, Activation of invariant Natural Killer T lymphocytes in response tothe [alpha]-galactosylceramide analogue KRN7000 encapsulated in PLGA-based nanoparticles and microparticles, Int. J. Pharm. 423 (2012) 45–54.
[86] Z. Zhang, S. Tongchusak, Y. Mizukami, Y.J. Kang, T. Ioji, M. Touma, B. Reinhold,D.B. Keskin, E.L. Reinherz, T. Sasada, Induction of anti-tumor cytotoxic T cell re-sponses through PLGA-nanoparticle mediated antigen delivery, Biomaterials 32(2011) 3666–3678.
[87] D.J. Hanlon, P.B. Aldo, L. Devine, A.B. Alvero, A.K. Engberg, R. Edelson, G. Mor,Enhanced stimulation of anti-ovarian cancer CD8(+) T cells by dendritic cellsloaded with nanoparticle encapsulated tumor antigen, Am. J. Reprod. Immunol.65 (2011) 597–609.
[88] T. Yaguchi, H. Sumimoto, C. Kudo-Saito, N. Tsukamoto, R. Ueda, T. Iwata-Kajihara, H. Nishio, N. Kawamura, Y. Kawakami, The mechanisms of cancerimmunoescape and development of overcoming strategies, Int. J. Hematol. 93(2011) 294–300.
[89] O. Molavi, A. Mahmud, S. Hamdy, R.W. Hung, R. Lai, J. Samuel, A. Lavasanifar, De-velopment of a poly(D,L-lactic-co-glycolic acid) nanoparticle formulation ofSTAT3 inhibitor JSI-124: implication for cancer immunotherapy, Mol. Pharm. 7(2010) 364–374.
[90] O. Molavi, Z. Ma, S. Hamdy, A. Lavasanifar, J. Samuel, Immunomodulatory andanticancer effects of intra-tumoral co-delivery of synthetic lipid A adjuvantand STAT3 inhibitor, JSI-124, Immunopharmacol. Immunotoxicol. 31 (2009)214–221.
[91] A. Alshamsan, S. Hamdy, A. Haddadi, J. Samuel, A.O. El-Kadi, H. Uludag, A.Lavasanifar, STAT3 knockdown in B16 melanoma by siRNA lipopolyplexes in-duces bystander immune response in vitro and in vivo, Transl. Oncol. 4 (2011)178–188.
[92] A. Roy, M.S. Singh, P. Upadhyay, S. Bhaskar, Combined chemo-immunotherapyas a prospective strategy to combat cancer: a nanoparticle based approach,Mol. Pharm. 7 (2010) 1778–1788.
[93] Y. Matsumura, H. Maeda, A new concept for macromolecular therapeutics incancer chemotherapy: mechanism of tumoritropic accumulation of proteinsand the antitumor agent smancs, Cancer Res. 46 (1986) 6387–6392.
[94] J. Folkman, Tumor angiogenesis: therapeutic implications, N. Engl. J. Med. 285(1971) 1182–1186.
[95] D.B. Kirpotin, D.C. Drummond, Y. Shao, M.R. Shalaby, K. Hong, U.B. Nielsen, J.D.Marks, C.C. Benz, J.W. Park, Antibody targeting of long-circulating lipidic nano-particles does not increase tumor localization but does increase internalizationin animal models, Cancer Res. 66 (2006) 6732–6740.
[96] J. Park, P.M. Fong, J. Lu, K.S. Russell, C.J. Booth, W.M. Saltzman, T.M. Fahmy,PEGylated PLGA nanoparticles for the improved delivery of doxorubicin, Nano-medicine 5 (2009) 410–418.
[97] S. Wohlfart, A.S. Khalansky, S. Gelperina, O. Maksimenko, C. Bernreuther, M.Glatzel, J. Kreuter, Efficient chemotherapy of rat glioblastoma usingdoxorubicin-loaded PLGA nanoparticles with different stabilizers, PLoS One 6(2011) e19121.
[98] F. Danhier, N. Lecouturier, B. Vroman, C. Jerome, J. Marchand-Brynaert, O. Feron,V. Preat, Paclitaxel-loaded PEGylated PLGA-based nanoparticles: in vitro and invivo evaluation, J. Control. Release 133 (2009) 11–17.
[99] C. Chittasupho, S.X. Xie, A. Baoum, T. Yakovleva, T.J. Siahaan, C.J. Berkland, ICAM-1targeting of doxorubicin-loaded PLGA nanoparticles to lung epithelial cells, Eur. J.Pharm. Sci. 37 (2009) 141–150.
[100] Z. Zhang, L.S. Huey, S.S. Feng, Folate-decorated poly(lactide-co-glycolide)-vitamin ETPGS nanoparticles for targeted drug delivery, Biomaterials 28 (2007) 1889–1899.
[101] C. Liang, Y. Yang, Y. Ling, Y. Huang, T. Li, X. Li, Improved therapeutic effect offolate-decorated PLGA-PEG nanoparticles for endometrial carcinoma, Bioorg.Med. Chem. 19 (2011) 4057–4066.
[102] G. Luo, X. Yu, C. Jin, F. Yang, D. Fu, J. Long, J. Xu, C. Zhan, W. Lu, LyP-1-conjugatednanoparticles for targeting drug delivery to lymphatic metastatic tumors, Int. J.Pharm. 385 (2010) 150–156.
[103] S. Dhar, F.X. Gu, R. Langer, O.C. Farokhzad, S.J. Lippard, Targeted delivery of cis-platin to prostate cancer cells by aptamer functionalized Pt(IV) prodrug-PLGA-PEG nanoparticles, Proc. Natl. Acad. Sci. U. S. A. 105 (2008) 17356–17361.
[104] J. Guo, X. Gao, L. Su, H. Xia, G. Gu, Z. Pang, X. Jiang, L. Yao, J. Chen, H. Chen,Aptamer-functionalized PEG-PLGA nanoparticles for enhanced anti-gliomadrug delivery, Biomaterials 31 (2011) 8010–8020.
[105] J.S. Desgrosellier, D.A. Cheresh, Integrins in cancer: biological implications andtherapeutic opportunities, Nat. Rev. Cancer 10 (2010) 9–22.
[106] Z. Wang, W.K. Chui, P.C. Ho, Design of a multifunctional PLGA nanoparticulatedrug delivery system: evaluation of its physicochemical properties and antican-cer activity to malignant cancer cells, Pharm. Res. 26 (2009) 1162–1171.
[107] F. Danhier, B. Vroman, N. Lecouturier, N. Crokart, V. Pourcelle, H. Freichels, C.Jerome, J. Marchand-Brynaert, O. Feron, V. Preat, Targeting of tumor endotheliumby RGD-grafted PLGA-nanoparticles loaded with paclitaxel, J. Control. Release140 (2009) 166–173.
[108] L. Zhao, S.S. Feng, Enhanced oral bioavailability of paclitaxel formulated in vita-min E-TPGS emulsified nanoparticles of biodegradable polymers: in vitro and invivo studies, J. Pharm. Sci. 99 (2010) 3552–3560.
[109] A.K. Jain, N.K. Swarnakar, C. Godugu, R.P. Singh, S. Jain, The effect of the oral ad-ministration of polymeric nanoparticles on the efficacy and toxicity of tamoxi-fen, Biomaterials 32 (2011) 503–515.
[110] U.S. Toti, B.R. Guru, M. Hali, C.M. McPharlin, S.M. Wykes, J. Panyam, J.A.Whittum-Hudson, Targeted delivery of antibiotics to intracellular chlamydialinfections using PLGA nanoparticles, Biomaterials 32 (2011) 6606–6613.
[111] S.H. Choi, T.G. Park, G-CSF loaded biodegradable PLGA nanoparticles prepared bya single oil-in-water emulsion method, Int. J. Pharm. 311 (2006) 223–228.
[112] H. Chen, J. Gao, Y. Lu, G. Kou, H. Zhang, L. Fan, Z. Sun, Y. Guo, Y. Zhong, Prepara-tion and characterization of PE38KDEL-loaded anti-HER2 nanoparticles for tar-geted cancer therapy, J. Control. Release 128 (2008) 209–216.
[113] G. Luo, C. Jin, J. Long, D. Fu, F. Yang, J. Xu, X. Yu, W. Chen, Q. Ni, RNA interferenceof MBD1 in BxPC-3 human pancreatic cancer cells delivered by PLGA-poloxamernanoparticles, Cancer Biol. Ther. 8 (2009) 594–598.
[114] M.O. Andersen, A. Lichawska, A. Arpanaei, S.M. Rask Jensen, H. Kaur, D. Oupicky,F. Besenbacher, P. Kingshott, J. Kjems, K.A. Howard, Surface functionalisation ofPLGA nanoparticles for gene silencing, Biomaterials 31 (2010) 5671–5677.
[115] S. Diez, I. Migueliz, C. Tros de Ilarduya, Targeted cationic poly(D,L-lactic-co-glycolicacid) nanoparticles for gene delivery to cultured cells, CellMol. Biol. Lett. 14 (2009)347–362.
[116] A.R. Braden, M.T. Kafka, L. Cunningham, H. Jones, J.K. Vishwanatha, Polymericnanoparticles for sustained down-regulation of annexin A2 inhibit prostatetumor growth, J. Nanosci. Nanotechnol. 9 (2009) 2856–2865.
[117] L.B. Rangel, R. Agarwal, T. D'Souza, E.S. Pizer, P.L. Alo, W.D. Lancaster, L. Gregoire,D.R. Schwartz, K.R. Cho, P.J. Morin, Tight junction proteins claudin-3 andclaudin-4 are frequently overexpressed in ovarian cancer but not in ovariancystadenomas, Clin. Cancer Res. 9 (2003) 2567–2575.

521F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
[118] B. Sharma, W. Ma, I. Adjei, J. Panyam, S. Dimitrijevic, V. Labhasetwar, Nanoparti-cle-mediated p53 gene therapy for tumor inhibition, Drug Deliv. Transl. Res. 1(2011) 43–52.
[119] Y. Wang, Y.G. Ng, Y. Chen, B. Shuter, J. Yi, J. Ding, S. Wang, S.G. Feng, Formula-tion of superparamagnetic iron oxides by nanoparticles of biodegradablepolymers for magnetic resonance imaging, Adv. Funct. Mater. 18 (2008)308–318.
[120] S.M. Janib, A.S. Moses, J.A. Mackay, Imaging and drug delivery using theranosticnanoparticles, Adv. Drug Deliv. Rev. 62 (2010) 1052–1063.
[121] A.S. Lubbe, C. Bergemann, W. Huhnt, T. Fricke, H. Riess, J.W. Brock, D. Huhn,Preclinical experiences with magnetic drug targeting: tolerance and efficacy,Cancer Res. 56 (1996) 4694–4701.
[122] A.S. Lubbe, C. Bergemann, H. Riess, F. Schriever, P. Reichardt, K. Possinger, M.Matthias, B. Dorken, F. Herrmann, R. Gurtler, P. Hohenberger, N. Haas, R. Sohr,B. Sander, A.J. Lemke, D. Ohlendorf, W. Huhnt, D. Huhn, Clinical experienceswith magnetic drug targeting: a phase I study with 4′-epidoxorubicin in 14 pa-tients with advanced solid tumors, Cancer Res. 56 (1996) 4686–4693.
[123] A. Singh, F. Dilnawaz, S. Mewar, U. Sharma, N.R. Jagannathan, S.K. Sahoo, Com-posite polymeric magnetic nanoparticles for co-delivery of hydrophobic and hy-drophilic anticancer drugs andMRI imaging for cancer therapy, ACS Appl. Mater.Interfaces 3 (2011) 842–856.
[124] R. Gref, Y. Minamitake, M.T. Peracchia, V. Trubetskoy, V. Torchilin, R. Langer, Bio-degradable long-circulating polymeric nanospheres, Science 263 (1994)1600–1603.
[125] W. Ulbrich, A. Lamprecht, Targeted drug-delivery approaches by nanoparticu-late carriers in the therapy of inflammatory diseases, J. R. Soc. Interface 7(Suppl 1) (2010) S55–S66.
[126] E. Simone, B.S. Ding, V. Muzykantov, Targeted delivery of therapeutics to endo-thelium, Cell Tissue Res. 335 (2009) 283–300.
[127] Y. Meissner, A. Lamprecht, Alternative drug delivery approaches for the therapyof inflammatory bowel disease, J. Pharm. Sci. 97 (2008) 2878–2891.
[128] A. Lamprecht, U. Schafer, C.M. Lehr, Size-dependent bioadhesion of micro- andnanoparticulate carriers to the inflamed colonic mucosa, Pharm. Res. 18(2001) 788–793.
[129] C. Schmidt, E.M. Collnot, C. Bojarski, M. Schumann, J.D. Schulzke, C.M. Lehr,A. Stallmach, W1266 confocal laser endomicroscopy (CLE) reveals mucosalaccumulation of PLGA-nanoparticles in ulcerous lesions of patients with in-flammatory bowel diseases, Gastroenterology 138 (1-5-2010) S-687 (RefType: Abstract).
[130] A. Lamprecht, N. Ubrich, H. Yamamoto, U. Schafer, H. Takeuchi, P. Maincent, Y.Kawashima, C.M. Lehr, Biodegradable nanoparticles for targeted drug deliveryin treatment of inflammatory bowel disease, J. Pharmacol. Exp. Ther. 299(2001) 775–781.
[131] A. Lamprecht, H. Yamamoto, H. Takeuchi, Y. Kawashima, Nanoparticles enhancetherapeutic efficiency by selectively increased local drug dose in experimentalcolitis in rats, J. Pharmacol. Exp. Ther. 315 (2005) 196–202.
[132] Y. Meissner, Y. Pellequer, A. Lamprecht, Nanoparticles in inflammatory boweldisease: particle targeting versus pH-sensitive delivery, Int. J. Pharm. 316(2006) 138–143.
[133] S.J. Lee, A. Kavanaugh, Pharmacological treatment of established rheumatoid ar-thritis, Best Pract. Res. Clin. Rheumatol. 17 (2003) 811–829.
[134] E. Horisawa, K. Kubota, I. Tuboi, K. Sato, H. Yamamoto, H. Takeuchi, Y.Kawashima, Size-dependency of DL-lactide/glycolide copolymer particulatesfor intra-articular delivery system on phagocytosis in rat synovium, Pharm.Res. 19 (2002) 132–139.
[135] M. Higaki, T. Ishihara, N. Izumo, M. Takatsu, Y. Mizushima, Treatment of exper-imental arthritis with poly(D,L-lactic/glycolic acid) nanoparticles encapsulatingbetamethasone sodium phosphate, Ann. Rheum. Dis. 64 (2005) 1132–1136.
[136] E. Horisawa, T. Hirota, S. Kawazoe, J. Yamada, H. Yamamoto, H. Takeuchi, Y.Kawashima, Prolonged anti-inflammatory action of DL-lactide/glycolide copoly-mer nanospheres containing betamethasone sodium phosphate for an intra-articular delivery system in antigen-induced arthritic rabbit, Pharm. Res. 19(2002) 403–410.
[137] N. Vij, T. Min, R. Marasigan, C.N. Belcher, S. Mazur, H. Ding, K.T. Yong, I. Roy, De-velopment of PEGylated PLGA nanoparticle for controlled and sustained drugdelivery in cystic fibrosis, J. Nanobiotechnol. 8 (2010) 22.
[138] M.S. Cartiera, E.C. Ferreira, C. Caputo, M.E. Egan, M.J. Caplan, W.M. Saltzman, Par-tial correction of cystic fibrosis defects with PLGA nanoparticles encapsulatingcurcumin, Mol. Pharm. 7 (2010) 86–93.
[139] W. Zhang, M.R. Prausnitz, A. Edwards, Model of transient drug diffusion acrosscornea, J. Control. Release 99 (2004) 241–258.
[140] A.S. Guinedi, N.D. Mortada, S. Mansour, R.M. Hathout, Preparation and evalua-tion of reverse-phase evaporation and multilamellar niosomes as ophthalmiccarriers of acetazolamide, Int. J. Pharm. 306 (2005) 71–82.
[141] D.S. Kohane, J.Y. Tse, Y. Yeo, R. Padera, M. Shubina, R. Langer, Biodegradablepolymeric microspheres and nanospheres for drug delivery in the peritoneum,J. Biomed. Mater. Res. A 77 (2006) 351–361.
[142] V.B. Patravale, A.A. Date, R.M. Kulkarni, Nanosuspensions: a promising drug de-livery strategy, J. Pharm. Pharmacol. 56 (2004) 827–840.
[143] R. Schalnus, Topical nonsteroidal anti-inflammatory therapy in ophthalmology,Ophthalmologica 217 (2003) 89–98.
[144] S.M. Agnihotri, P.R. Vavia, Diclofenac-loaded biopolymeric nanosuspensions forophthalmic application, Nanomedicine 5 (2009) 90–95.
[145] J. Araujo, E. Vega, C. Lopes, M.A. Egea, M.L. Garcia, E.B. Souto, Effect of polymerviscosity on physicochemical properties and ocular tolerance of FB-loadedPLGA nanospheres, Colloids Surf. B Biointerfaces 72 (2009) 48–56.
[146] E. Vega, F. Gamisans, M.L. Garcia, A. Chauvet, F. Lacoulonche, M.A. Egea, PLGAnanospheres for the ocular delivery of flurbiprofen: drug release and interac-tions, J. Pharm. Sci. 97 (2008) 5306–5317.
[147] K. Dillen, J. Vandervoort, G. Van den Mooter, A. Ludwig, Evaluation ofciprofloxacin-loaded Eudragit RS100 or RL100/PLGA nanoparticles, Int. J.Pharm. 314 (2006) 72–82.
[148] R.H. Edwards, Drug delivery via the blood–brain barrier, Nat. Neurosci. 4 (2001)221–222.
[149] L. Costantino, F. Gandolfi, L. Bossy-Nobs, G. Tosi, R. Gurny, F. Rivasi, M.A.Vandelli, F. Forni, Nanoparticulate drug carriers based on hybrid poly(D,L-lac-tide-co-glycolide)-dendron structures, Biomaterials 27 (2006) 4635–4645.
[150] M.K. Reddy, L. Wu, W. Kou, A. Ghorpade, V. Labhasetwar, Superoxide dismutase-loaded PLGA nanoparticles protect cultured human neurons under oxidativestress, Appl. Biochem. Biotechnol. 151 (2008) 565–577.
[151] M.K. Reddy, V. Labhasetwar, Nanoparticle-mediated delivery of superoxide dis-mutase to the brain: an effective strategy to reduce ischemia-reperfusion injury,FASEB J. 23 (2009) 1384–1395.
[152] K. Hu, J. Li, Y. Shen, W. Lu, X. Gao, Q. Zhang, X. Jiang, Lactoferrin-conjugated PEG-PLA nanoparticles with improved brain delivery: in vitro and in vivo evaluations,J. Control. Release 134 (2009) 55–61.
[153] K. Hu, Y. Shi, W. Jiang, J. Han, S. Huang, X. Jiang, Lactoferrin conjugated PEG-PLGA nanoparticles for brain delivery: preparation, characterization and efficacyin Parkinson's disease, Int. J. Pharm. 415 (2011) 273–283.
[154] G. Tosi, L. Costantino, F. Rivasi, B. Ruozi, E. Leo, A.V. Vergoni, R. Tacchi, A.Bertolini, M.A. Vandelli, F. Forni, Targeting the central nervous system: in vivoexperiments with peptide-derivatized nanoparticles loaded with Loperamideand Rhodamine-123, J. Control. Release 122 (2007) 1–9.
[155] L. Costantino, F. Gandolfi, G. Tosi, F. Rivasi, M.A. Vandelli, F. Forni, Peptide-deri-vatized biodegradable nanoparticles able to cross the blood–brain barrier, J.Control. Release 108 (2005) 84–96.
[156] L. Bondioli, L. Costantino, A. Ballestrazzi, D. Lucchesi, D. Boraschi, F. Pellati, S.Benvenuti, G. Tosi, M.A. Vandelli, PLGA nanoparticles surface decorated withthe sialic acid, N-acetylneuraminic acid, Biomaterials 31 (2010) 3395–3403.
[157] G. Tosi, A.V. Vergoni, B. Ruozi, L. Bondioli, L. Badiali, F. Rivasi, L. Costantino, F.Forni, M.A. Vandelli, Sialic acid and glycopeptides conjugated PLGA nanoparti-cles for central nervous system targeting: in vivo pharmacological evidenceand biodistribution, J. Control. Release 145 (2010) 49–57.
[158] J. Li, L. Feng, L. Fan, Y. Zha, L. Guo, Q. Zhang, J. Chen, Z. Pang, Y. Wang, X. Jiang,V.C. Yang, L. Wen, Targeting the brain with PEG-PLGA nanoparticles modifiedwith phage-displayed peptides, Biomaterials 32 (2011) 4943–4950.
[159] K. Ladewig, Drug delivery in soft tissue engineering, Expert. Opin. Drug Deliv. 9(2011) 1175–1188.
[160] Y.C. Wang, Y.T. Wu, H.Y. Huang, H.I. Lin, L.W. Lo, S.F. Tzeng, C.S. Yang, Sustainedintraspinal delivery of neurotrophic factor encapsulated in biodegradable nanoparti-cles following contusive spinal cord injury, Biomaterials 29 (2008) 4546–4553.
[161] J.H. Kordower, S. Palfi, E.Y. Chen, S.Y. Ma, T. Sendera, E.J. Cochran, E.J. Cochran,E.J. Mufson, R. Penn, C.G. Goetz, C.D. Comella, Clinicopathological findings fol-lowing intraventricular glial-derived neurotrophic factor treatment in a patientwith Parkinson's disease, Ann. Neurol. 46 (1999) 419–424.
[162] J.G. Nutt, K.J. Burchiel, C.L. Comella, J. Jankovic, A.E. Lang, E.R. Laws Jr., A.M.Lozano, R.D. Penn, R.K. Simpson Jr., M. Stacy, G.F. Wooten, Randomized,double-blind trial of glial cell line-derived neurotrophic factor (GDNF) in PD,Neurology 60 (2003) 69–73.
[163] S.S. Gill, N.K. Patel, G.R. Hotton, K. O'Sullivan, R. McCarter, M. Bunnage, D.J.Brooks, C.N. Svendsen, P. Heywood, Direct brain infusion of glial cell line-derived neurotrophic factor in Parkinson disease, Nat. Med. 9 (2003) 589–595.
[164] N.K. Patel, M. Bunnage, P. Plaha, C.N. Svendsen, P. Heywood, S.S. Gill, Intraputa-menal infusion of glial cell line-derived neurotrophic factor in PD: a two-yearoutcome study, Ann. Neurol. 57 (2005) 298–302.
[165] J.T. Slevin, G.A. Gerhardt, C.D. Smith, D.M. Gash, R. Kryscio, B. Young, Improve-ment of bilateral motor functions in patients with Parkinson disease throughthe unilateral intraputaminal infusion of glial cell line-derived neurotrophic fac-tor, J. Neurosurg. 102 (2005) 216–222.
[166] A.E. Lang, S. Gill, N.K. Patel, A. Lozano, J.G. Nutt, R. Penn, D.J. Brooks, G. Hotton, E.Moro, P. Heywood, M.A. Brodsky, K. Burchiel, P. Kelly, A. Dalvi, B. Scott, M. Stacy,D. Turner, V.G. Wooten, W.J. Elias, E.R. Laws, V. Dhawan, A.J. Stoessl, J. Matcham,R.J. Coffey, M. Traub, Randomized controlled trial of intraputamenal glial cellline-derived neurotrophic factor infusion in Parkinson disease, Ann. Neurol. 59(2006) 459–466.
[167] E. Garbayo, C.N. Montero-Menei, E. Ansorena, J.L. Lanciego, M.S. Aymerich, M.J.Blanco-Prieto, Effective GDNF brain delivery using microspheres—a promisingstrategy for Parkinson's disease, J. Control. Release 135 (2009) 119–126.
[168] E. Garbayo, E. Ansorena, J. Luis Lanciego, M.J. Blanco Prieto, M.S. Aymerich, Long-term neuroprotection and neurorestoration by glial cell-derived neurotrophicfactor microspheres for the treatment of parkinson's disease, Mov. Disord. 10(2011) 1943–1947.
[169] C. Jollivet, A. Aubert-Pouessel, A. Clavreul, M.C. Venier-Julienne, S. Remy, C.N.Montero-Menei, J.P. Benoit, P. Menei, Striatal implantation of GDNF releasingbiodegradable microspheres promotes recovery of motor function in a partialmodel of Parkinson's disease, Biomaterials 25 (2004) 933–942.
[170] L. Cao, L. Liu, Z.Y. Chen, L.M. Wang, J.L. Ye, H.Y. Qiu, C.L. Lu, C. He, Olfactoryensheathing cells genetically modified to secrete GDNF to promote spinal cordrepair, Brain 127 (2004) 535–549.
[171] H. Cheng, J.P. Wu, S.F. Tzeng, Neuroprotection of glial cell line-derived neuro-trophic factor in damaged spinal cords following contusive injury, J. Neurosci.Res. 69 (2002) 397–405.

522 F. Danhier et al. / Journal of Controlled Release 161 (2012) 505–522
[172] K.D. Foust, T.R. Flotte, P.J. Reier, R.J. Mandel, Recombinant adeno-associatedvirus-mediated global anterograde delivery of glial cell line-derived neuro-trophic factor to the spinal cord: comparison of rubrospinal and corticospinaltracts in the rat, Hum. Gene Ther. 19 (2008) 71–82.
[173] M.H. Tai, H. Cheng, J.P. Wu, Y.L. Liu, P.R. Lin, J.S. Kuo, C.J. Tseng, S.F. Tzeng, Genetransfer of glial cell line-derived neurotrophic factor promotes functional recov-ery following spinal cord contusion, Exp. Neurol. 183 (2003) 508–515.
[174] A. des Rieux, B. Ucakar, B.P.K. Mupendwa, D. Colau, O. Feron, P. Carmeliet, V.Préat, 3D systems delivering VEGF to promote angiogenesis for tissue engineer-ing, J. Control. Release 150 (2011) 272–278.
[175] P. Carmeliet, R.K. Jain, Molecular mechanisms and clinical applications of angio-genesis, Nature 473 (2011) 298–307.
[176] A.C. Ruiz de, D. Lambrechts, M. Mazzone, P. Carmeliet, Role and therapeutic po-tential of VEGF in the nervous system, Physiol. Rev. 89 (2009) 607–648.
[177] J. Panyam, V. Labhasetwar, Biodegradable nanoparticles for drug and gene deliv-ery to cells and tissue, Adv. Drug Deliv. Rev. 55 (2003) 329–347.
[178] J.S. Golub, Y.T. Kim, C.L. Duvall, R.V. Bellamkonda, D. Gupta, A.S. Lin, D. Weiss,T.W. Robert, R.E. Guldberg, Sustained VEGF delivery via PLGA nanoparticles pro-motes vascular growth, Am. J. Physiol. Heart Circ. Physiol. 298 (2010)H1959–H1965.
[179] H. Geng, H. Song, J. Qi, D. Cui, Sustained release of VEGF from PLGA nanoparticlesembedded thermo-sensitive hydrogel in full-thickness porcine bladder acellularmatrix, Nanoscale Res. Lett. 6 (2011) 312.
[180] J.C. Chappell, J. Song, C.W. Burke, A.L. Klibanov, R.J. Price, Targeted delivery ofnanoparticles bearing fibroblast growth factor-2 by ultrasonic microbubble de-struction for therapeutic arteriogenesis, Small 4 (2008) 1769–1777.
[181] R.J. Lee, M.L. Springer, W.E. Blanco-Bose, R. Shaw, P.C. Ursell, H.M. Blau, VEGFgene delivery to myocardium: deleterious effects of unregulated expression, Cir-culation 102 (2000) 898–901.
[182] R.J. Price, D.M. Skyba, S. Kaul, T.C. Skalak, Delivery of colloidal particles and redblood cells to tissue through microvessel ruptures created by targeted micro-bubble destruction with ultrasound, Circulation 98 (1998) 1264–1267.
[183] J. Song, J.C. Chappell, M. Qi, E.J. VanGieson, S. Kaul, R.J. Price, Influence of injec-tion site, microvascular pressureand ultrasound variables on microbubble-mediated delivery of microspheres to muscle, J. Am. Coll. Cardiol. 39 (2002)726–731.
[184] M.R. Urist, Bone: formation by autoinduction, Science 150 (1965) 893–899.[185] P.C. Bessa, M. Casal, R.L. Reis, Bone morphogenetic proteins in tissue engineering:
the road from the laboratory to the clinic, part I (basic concepts), J. Tissue Eng.Regen. Med. 2 (2008) 1–13.
[186] W.F. McKay, S.M. Peckham, J.M. Badura, A comprehensive clinical review of re-combinant human bone morphogenetic protein-2 (INFUSE Bone Graft), Int.Orthop. 31 (2007) 729–734.
[187] A.P. White, A.R. Vaccaro, J.A. Hall, P.G. Whang, B.C. Friel, M.D. McKee, Clinical ap-plications of BMP-7/OP-1 in fractures, nonunions and spinal fusion, Int. Orthop.31 (2007) 735–741.
[188] T.J. Cho, L.C. Gerstenfeld, T.A. Einhorn, Differential temporal expression of mem-bers of the transforming growth factor beta superfamily during murine fracturehealing, J. Bone Miner. Res. 17 (2002) 513–520.
[189] P. Yilgor, N. Hasirci, V. Hasirci, Sequential BMP-2/BMP-7 delivery from polyesternanocapsules, J. Biomed. Mater. Res. 93A (2010) 528–536.
[190] P. Yilgor, K. Tuzlakoglu, R.L. Reis, N. Hasirci, V. Hasirci, Incorporation of a sequen-tial BMP-2/BMP-7 delivery system into chitosan-based scaffolds for bone tissueengineering, Biomaterials 30 (2009) 3551–3559.
[191] P. Yilgor, R.A. Sousa, R.L. Reis, N. Hasirci, V. Hasirci, Effect of scaffold architectureand BMP-2/BMP-7 delivery on in vitro bone regeneration, J. Mater. Sci. Mater.Med. 21 (2010) 2999–3008.
[192] B.D. Klugherz, P.L. Jones, X. Cui, W. Chen, N.F. Meneveau, S. DeFelice, J. Connolly,R.L. Wilensky, R.J. Levy, Gene delivery from a DNA controlled-release stent inporcine coronary arteries, Nat. Biotechnol. 18 (2000) 1181–1184.
[193] I. Perlstein, J.M. Connolly, X. Cui, C. Song, Q. Li, P.L. Jones, Z. Lu, S. DeFelice, B.Klugherz, R. Wilensky, R.J. Levy, DNA delivery from an intravascular stent with
a denatured collagen-polylactic-polyglycolic acid-controlled release coating:mechanisms of enhanced transfection, Gene Ther. 10 (2003) 1420–1428.
[194] R.Y. Kannan, H.J. Salacinski, P.E. Butler, G. Hamilton, A.M. Seifalian, Current sta-tus of prosthetic bypass grafts: a review, J. Biomed. Mater. Res. B Appl. Biomater.74 (2005) 570–581.
[195] D.A. Vorp, T. Maul, A. Nieponice, Molecular aspects of vascular tissue engineering,Front. Biosci. 10 (2005) 768–789.
[196] S. Sarkar, G.Y. Lee, J.Y. Wong, T.A. Desai, Development and characterization of aporous micro-patterned scaffold for vascular tissue engineering applications,Biomaterials 27 (2006) 4775–4782.
[197] H.J. Lim, H.Y. Nam, B.H. Lee, D.J. Kim, J.Y. Ko, J.S. Park, A novel technique for load-ing of paclitaxel-PLGA nanoparticles onto ePTFE vascular grafts, Biotechnol.Prog. 23 (2007) 693–697.
[198] C. Lecaroz, C. Gamazo, M.J. Blanco-Prieto, Nanocarriers with gentamicin to treatintracellular pathogens, J. Nanosci. Nanotechnol. 6 (2006) 3296–3302.
[199] M.C. Lecaroz, M.J. Blanco-Prieto, M.A. Campanero, H. Salman, C. Gamazo, Poly(D,L-lactide-coglycolide) particles containing gentamicin: pharmacokinetics andpharmacodynamics in Brucella melitensis-infected mice, Antimicrob. AgentsChemother. 51 (2007) 1185–1190.
[200] E. Imbuluzqueta, E. Elizondo, C. Gamazo, E. Moreno-Calvo, J. Veciana, N. Ventosa,M.J. Blanco-Prieto, Novel bioactive hydrophobic gentamicin carriers for thetreatment of intracellular bacterial infections, Acta Biomater. 7 (2011)1599–1608.
[201] R.R. Pillai, S.N. Somayaji, M. Rabinovich, M.C. Hudson, K.E. Gonsalves, Nafcillin-loaded PLGA nanoparticles for treatment of osteomyelitis, Biomed. Mater. 3(2008) 034114.
[202] H. Gupta, M. Aqil, R.K. Khar, A. Ali, A. Bhatnagar, G. Mittal, Sparfloxacin-loadedPLGA nanoparticles for sustained ocular drug delivery, Nanomedicine 6 (2010)324–333.
[203] M.T. McDermott, G.S. Kidd, The role of calcitonin in the development and treat-ment of osteoporosis, Endocr. Rev. 8 (1987) 377–390.
[204] T.S. Jung, B.S. Kwon, H.E. Lee, A.Y. Kim, M.J. Lee, C.R. Park, H.K. Kang, Y.D. Kim,S.K. Lee, J.S. Kang, G.J. Choi, Enhanced oral absorption of salmon calcitonin-encapsulated PLGA nanoparticles by adding organic substances, Korean J.Chem. Eng. 26 (2009) 131–135.
[205] H. Yamamoto, Y. Kuno, S. Sugimoto, H. Takeuchi, Y. Kawashima, Surface-modi-fied PLGA nanosphere with chitosan improved pulmonary delivery of calcitoninby mucoadhesion and opening of the intercellular tight junctions, J. Control. Re-lease 102 (2005) 373–381.
[206] R. Tisch, H. McDevitt, Insulin-dependent diabetes mellitus, Cell 85 (1996)291–297.
[207] F.D. Cui, A.J. Tao, D.M. Cun, L.Q. Zhang, K. Shi, Preparation of insulin loaded PLGA-Hp55 nanoparticles for oral delivery, J. Pharm. Sci. 96 (2007) 421–427.
[208] K. Shi, F. Cui, H. Yamamoto, Y. Kawashima, Optimized preparation of insulin-lauryl sulfate complex loaded poly (lactide-co-glycolide) nanoparticles using re-sponse surface methodology, Pharmazie 63 (2008) 721–725.
[209] K. Shi, F. Cui, H. Yamamoto, Y. Kawashima, Investigation of drug loading and invitro release mechanisms of insulin-lauryl sulfate complex loaded PLGA nano-particles, Pharmazie 63 (2008) 866–871.
[210] K. Shi, F. Cui, H. Yamamoto, Y. Kawashima, Optimized formulation of high-payload PLGA nanoparticles containing insulin-lauryl sulfate complex, DrugDev. Ind. Pharm. 35 (2009) 177–184.
[211] S. Sun, N. Liang, H. Piao, H. Yamamoto, Y. Kawashima, F. Cui, Insulin-S.O (sodiumoleate) complex-loaded PLGA nanoparticles: formulation, characterization andin vivo evaluation, J. Microencapsul. 27 (2010) 471–478.
[212] F. Cui, K. Shi, L. Zhang, A. Tao, Y. Kawashima, Biodegradable nanoparticles loadedwith insulin-phospholipid complex for oral delivery: preparation, in vitro char-acterization and in vivo evaluation, J. Control. Release 114 (2006) 242–250.
[213] J. Liu, S.M. Zhang, P.P. Chen, L. Cheng, W. Zhou, W.X. Tang, Z.W. Chen, C.M. Ke,Controlled release of insulin from PLGA nanoparticles embedded within PVAhydrogels, J. Mater. Sci. Mater. Med. 18 (2007) 2205–2210.