molecular, cellular, and tissue responses following photodynamic therapy
TRANSCRIPT

Lasers in Surgery and Medicine 8:450-463 (1988)
Molecular, Cellular, and Tissue Responses Following Photodynamic Therapy
Charles J. Gomer, PhD, Angela Ferrario, PhD, Naganobu Hayashi, MD, PhD, Natalie Rucker, BS, Bernard C. Szirth, PAV, and A. Linn Murphree, MD
Clayton Ocular Oncology Center, Children’s Hospital of Los Angeles (C.J.G., A.F., N. H., N. R., B.C.S., A. L. M.) and Departments of Pediatrics (Division of Hematology-Oncology) (C. J. G.), Radiation Oncology (C. J.G.), Ophthalmology (A. L. M.), USC School of Medicine,
Los Angeles
Photodynamic therapy (PDT) is being utilized in the treatment of a wide variety of malignant tumors. Results using PDT have been en- couraging, and controlled clinical trials are currently being performed. The procedure exploits both the tumor-localizing and -photosensitizing properties of hematoporphyrin derivative or its purified component, Photofrin 11. When this porphyrin mixture is administered systemi- cally, it is retained preferentially in tumor tissue as compared to sur- rounding normal tissue. Localized tumor destruction induced by PDT results from the photochemical generation of cytotoxic oxygen species within the tumor. This review will provide a summary of historical and current research pertaining to molecular, cellular, and tissue responses induced by PDT. Emphasis is placed on information related to the chemistry of current photosensitizers, subcellular targets, preclinical treatment parameters, and clinical responses following PDT.
Key words: hematoporphyrin derivative, laser, photosensitization, tumor
INTRODUCTION
The initial biomedical use of porphyrins was in the area of tumor diagnosis. Hematoporphyrin (Hp) was shown to be taken up in tumor tissue (following systemic administration), and these le- sions could then be visualized by fluorescence when exposed to violet light [l]. An improved tu- mor localizer containing a mixture of monomeric and aggregated porphyrins was produced in 1961 by first acetylating and then reducing the crude hematoporphyrin [ 21. This mixture exhibited more reproducible tumor-localizing properties than Hp and was called hematoporphyrin derivative (HpD). HpD fluorescence as a diagnostic tool was exten- sively examined in the late 1960s and early 1970s 131. The current availability of image intensifiers and endoscopes have played a major role in the successful use of porphyrins in the diagnosis of sputum-positive but X-ray-negative carcinoma in situ of the bronchus [4).
The documentation in the early 1970s that porphyrins were efficient photosensitizers of tu- mor tissue initiated the current interest in the field of photodynamic therapy [5,6]. Interestingly,
there was little chemical information available regarding the active localizing and photosensitiz- ing components of HpD even though this mixture was used in numerous basic and clinical studies during the 1970s and 1980s. The acetylation pro- cedure utilized in the production of HpD yields several species of porphyrins including monoace- tates and diacetates of hematoporphyrin as well as hydroxyethylvinyldeuteroporphyrin and proto- porphyrin (71. When the monoacetates and diace- tates of Hp are treated with sodium hydroxide, a polymeric fraction is formed, which constitutes the active material of HpD [8]. The monomeric por- phyrins that are found in HpD are not efficient in vivo tumor photosensitizers 171. In the early 1980s, Dougherty separated HpD utilizing gel exclusion chromatography and observed that approximately 45% of the initial HpD was responsible for the
Accepted for publication June 22, 1988. Address reprint requests to Dr. Charles J. Gomer, Clayton Ocular Oncology Center, Children’s Hospital of Los Angeles, 4650 Sunset Boulevard, Los Angeles, CA 90027.
0 1988 Alan R. Liss, Inc.

Responses to Photodynamic Therapy 451
w 0 z
v)
4
: m
drug's tumor-photosensitizing properties [9]. The active fraction of HpD is now thought to be an aggregated mixture of hematoporphyrin mole- cules linked by either ether or ester bonds, as shown in Figure 1 [10,11]. Photofrin I1 is the com- mercial name for the di-hematoporphyrin ether andor ester (DHE) material. This drug is cur- rently available from Quadra Logic Technologies, Inc. Vancouver, British Columbia.
Porphyrins such as HpD and Photofrin I1 pos- sess absorption spectra that make them excellent in vitro photosensitizers, but they are only mod- erately effective in vivo photosensitizers. These chromophores have an intense absorption in the violet region around 400 nm (termed the soret band) and four additional absorption bands (with decreasing intensity) between 500 and 630 nm [ 121. The evaluation of porphyrin photosensitiza- tion in solutions and in cells can utilize light throughout the visible light spectrum. Unfortu- nately, in vivo and clinical photodynamic therapy (PDT) must utilize wavelengths of light corre- sponding to the weakest porphyrin absorption band. Attenuation of light in tissue decreases with increasing wavelengths [ 131, and therefore light at 630 nm is normally used in PDT. Optical pene- tration depths in tumor tissue (defined as the depth at which light intensity is reduced to 37% of its initial value) are typically less than 1 mm for wavelengths of light below 600 nm and approxi- mately 2.5-4.5 mm for light at 630 nm [14]. The soret absorption band (370-410 nm) is routinely utilized only to activate porphyrin fluorescence for tumor diagnostic studies. The next generation of photosensitizers will undoubtedly possess a major absorption peak at a wavelength above 650 nm. These properties will provide improved penetra- tion depth of delivered light as well as enhanced photon absorption by the drug. Absorption spectra for two new photosensitizers (from the chlorin and phthalocyanine families) are shown in Figure 2 along with the corresponding spectrum for DHE.
Porphyrin photosensitizers can undergo sev- eral photochemical reactions. Cellular and tissue damage induced by PDT is believed to result from the formation of singlet oxygen (l02) via the pho- tochemical type I1 reaction shown in Figure 3 [15]. The absorption of a photon of light will excite the porphyrin molecule to an excited and short-lived (lop9 to seconds) singlet state. From the ex- cited singlet state, the photosensitizer can decay back to the ground state and emit light in the form of fluorescence. Kinetic studies have demon- strated that most effective photodynamic sensitiz-
1": I , I , I , I I
DHE - .-.-a NPe6 ---- APCS I 1
I ' I 1 I 0 I 1 I ' I I
I I I !
/ . ' I !'. I
I
Fig. 1. Proposed chemical structures of the active compo- nents of Photofrin 11. Di-hematoporphyrin ether (A) and di- hematoporphyrin ester (B).
ers (including porphyrins) will undergo inter- system crossing from the excited singlet state to the more stable and longer-lived seconds) triplet state of the molecule. The excited triplet state has a high probability of interacting with ground state oxygen. The transfer of energy from the triplet photosensitizer to ground state oxygen generates highly reactive singlet oxygen [ 161. Sin- glet oxygen is electrophilic and reacts with elec- tron-rich regions of biomolecules to produce oxidized forms of the molecules [ 171. However, the excited triplet state of the porphyrin molecule can

452 Gomer et a1
also react directly with a biomolecule of interest a role in inducing tolerance to PDT or in cellular by electron or hydrogen atom transfer to produce repair following oxidative stress. radical forms of the sensitizer and substrate. Once While a large spectrum of specific types of formed, the porphyrin radical can interact with subcellular damage has been documented follow- oxygen in a reaction that regenerates the ground ing PDT, the actual target site(s> for cytotoxicity state of the porphyrin molecule and produces hy- have not been satisfactorily identified. In fact, the drogen peroxide, hydroxyl radical, or superoxide targets for in vitro PDT-induced cytotoxicity will [18-201. The actual biological significance of spe- probably vary as a function of the porphyrin incu- cies other than singlet oxygen and hydroxyl radi- bation conditions utilized in individual exper- cals in PDT is still unclear. However, the absolute iments. Short porphyrin incubation time periods requirement for oxygen in the photosensitizing (less than 1 hour) followed by light exposure leads action of clinically used porphyrins has been doc- primarily to plasma membrane damage, whereas umented in solution, in culture, and in vivo [21- extended time periods of porphyrin incubation 23). These results suggest that extremely hypoxic (which may more closely mimic the clinical situa- tumor tissue may be resistant to the direct effects tion) followed by light exposure induces damage of PDT. However, if the tumor vasculature is ac- to cytoplasmic organelles [34]. Standard mamma- tually a primary target in PDT (as suggested by lian cell culture studies have demonstrated that several recent investigations), then the degree of in vitro PDT is neither mutagenic nor carcino- tumor hypoxia at the time of treatment may not genic [27,35]. In addition, porphyrin PDT has been play a major role in the effectiveness of this found to induce comparable levels of cytotoxicity modality. in normal human fibroblasts and in DNA repair-
deficient fibroblasts from ataxia telangiectasia and
IN VITRO PORPHYRIN PHOTOBIOLOGY xeroderma pigmentosum patients [36]. These re- sults provide evidence that nuclear damage andl
Numerous studies have demonstrated that or repair is not a dominant factor in the cytotoxic- PDT is extremely effective in generating cytotoxic ity induced by porphyrin photosensitization. damage to subcellular organelles and biomole- Several basic parameters related to por- cules [ 17,241. Photodegradation of lipids, proteins, phyrin-induced photosensitization of mammalian and nucleic acids can routinely be observed follow- cells have been described. The quantitative depen- ing porphyrin photosensitization. Unsaturated dence of oxygen for porphyrin-induced photoinac- fatty acids can be photooxidized by a singlet oxy- tivation of mammalian cells has been examined gen type I1 mechanism. Lipid peroxidation as well by several investigators. A 1% oxygen concentra- as protein crosslinking of membranes have been tion reduced the quantum yield of photoinactiva- observed in mammalian cells following photosen- tion by approximately 50%, and anoxic cells were sitization. Membrane damage can then lead to found to be resistant to porphyrin photosensitiza- inhibited membrane transport of amino acids and tion [21,221. In addition, normal mouse skin ren- nucleosides, increased permeability and rupture dered anoxic by clamping is resistant to photo- of lysosomes, as well as marked contraction and dynamic therapy [23]. These results indicate that rupture of mitochondria [25]. At the level of the areas of hypoxia may be resistant to direct PDT- nucleus, PDT can produce single-strand breaks induced photosensitization. and alkali-labile sites in DNA, sister chromatid The expression and repair of potentially le- exchanges, and chromosome aberrations [26-281. thal damage can be observed in mammalian cells Enzymes bound to hydrophobic regions of mito- treated with porphyrin photodynamic therapy chondria (membrane-bound) are more sensitive to [37]. Hypothermic exposure (4°C) or incubation of PDT than enzymes located in the hydrophilic mi- PDT-treated cells with caffeine can potentiate the tochondrial matrix [29]. Interestingly, cytosol en- lethal effects of PDT. Recovery from potentially zymes including lactate dehydrogenase, pyruvate lethal damage expressed by post-treatment hypo- kinase, and glucose phosphate isomerase are only thermia is complete within 1 hour of treatment, moderately sensitive to PDT [30]. However, both while recovery from potentially lethal damage ex- RNA-dependent DNA polymerase and DNA-de- pressed by post-treatment caffeine exposure re- pendent RNA polymerase can be inactivated by quires time periods of up to 24 hours. Classical HpD-induced photosensitization [31,32]. Recently, split-dose studies have demonstrated that cells PDT has been shown to activate a variety of cel- treated with PDT can repair sublethal damage lular stress proteins 1331. These proteins may play 1381. However, in vitro and in vivo studies indicate

Responses to Photodynamic Therapy 453
that the efficiency of porphyrin photosensitization is not effected by nonthermal variations in dose rates of delivered light 1391. Clonigenic assays us- ing Chinese hamster cells have shown that maxi- mal photosensitization utilizing clinically relevant red light is obtained within the narrow range of 630-6325 nm [40]. The action spectra for cell kill- ing matches the absorption spectra for porphyrin bound to cells rather than the absorption spec- trum of porphyrin dissolved in aqueous solution (which is blue shifted). Similar action spectra have been reported for in vivo inactivation of tumors as well as for PDT-induced normal skin damage [7].
Several studies have indicated that malig- nant and normal cells accumulate similar levels of porphyrin during in vitro incubation [41]. In addition, differences in cell photosensitivity are usually not observed for normal and transformed cell lines [41]. However, significant variations in cellular photosensitivity have recently been ob- served when components of the vasculature were examined [36]. Specifically, bovine cells of endo- thelial, smooth muscle, and fibroblast origin were compared for porphyrin retention, toxicity, and photosensitization. Bovine endothelial cells were considerably more sensitive than smooth muscle or fibroblast cells treated under identical condi- tions when assayed for viability using clonigenic- ity. All bovine cells accumulated similar levels of porphyrin, and therefore the increased sensitivity of the endothelial cells was not due to differences in porphyrin retention. These results indicate that endothelial cell photosensitivity may play a role in the vascular damage observed following por- phyrin photodynamic therapy.
To begin examining the molecular basis for the observed differential photosensitivity of cellu- lar components of the vasculature, we performed a kinetic analysis of stress protein synthesis fol- lowing isoeffect doses of PDT. PDT doses that in- duced 10% survival (315, 420, and 525 J/m2 for endothelial, fibroblast, and smooth muscle cells, respectively) were delivered to cells incubated for 16 hours with DHE. Control cells as well as cells treated with DHE alone, light alone, or hyperther- mia were also analyzed. Following treatment, the cells were incubated at 37°C in complete growth medium for designated time intervals (0-12 hours) and then incubated for 2 hours in minimum essen- tial medium (MEM) media supplemented with 35S- methionine. The cells were then collected, and ali- quots were taken for determination of radioactiv- ity, protein concentration, and cell number. Samples were then analyzed by sodium dodecyl
sulfate (SDS) polyacrylamide gel electrophoresis with each lane being loaded with equal levels of radioactivity. Autoradiographs obtained from these gels are shown in Figure 4. Kinetic evalua- tions of protein synthesis are shown in Figure 5 and were obtained using densitometry readings of specific proteins from the autoradiographs. Con- trols as well as light alone samples had compara- ble protein gel patterns. Treatment with heat induced a characteristic increase in the 70,000 MW heat shock protein (HSP-70), indicating that all three cell lines were capable of inducing this stress protein. Interestingly, all three cell lines also demonstrated induction of a 34,000 MW pro- tein (presumably a stress protein) when the cells were incubated with DHE in the absence of light as well as after PDT. Smooth muscle and fibro- blasts demonstrated a large increase in the amounts of HSP-70 (peaking at about 6-8 hours post-treatment). A 78,000 MW glucose regulated protein (GRP-78) was also induced at extended time periods after treatment for these two cell lines. However, the protein patterns for the most sensitive cell type (endothelial cells) demonstrated only minimal levels of HSP-70 protein production. The significance of these findings is currently un- clear. However, HSP-70 is believed to play a role in the induction of cellular tolerance and/or repair.
PORPHYRIN PHOTOCHEMISTRY
1 Ssnr + h v ----.) 'Sons ABSORPTION
2 S m s .........- Sans t hv FLUORESCENCE EMISSION
3 , 1 sen. _......__, Sen* NONRADIATIVE DECAY
, , 1 Sen. ..._ ....., 3sen1 INTERSYSTEM CROSSOVER
5 . Sans -----.---m Sans + h v PHOSPHORESCENCE EMISSION
6 l S a n r t ' 0 2 --.- Sans + '02 ENERGY TRANSFER
7 . 1 0 2 ___.._____) 3 0 2 SINGLET OXYGEN DECAY
8 . ' 0 + A -.----> SUBSTRATE OXIDATION (CELL DEATH)
AO.
WHERE:
%a. GROUND STATE OF PORPHYRIN PHOTOSENSITIZER
lS.ns. EXCITED SINGLET STATE
3Ssnr - EXCITED TRIPLET STATE
3 0 ~ - GROUND TRIPLET STATE OF OXYGEN
'02. EXCITED SINGLET STATE OF OXYGEN
Fig. 3. Type I1 (energy transfer) photochemistry involved in the cytotoxic action of PDT.

454 Gomer et al
BOVINE FIBROBLAST CELLS BOVINE ENDOTHELIAL CELLS
*+ -34 31.0 -
I -1
DHE: 25 UGIML; 16 HR HEAT: 15 MIN. ; 45 C PDT: 420 JOULES/SQ M
A
21.5 -
DHE: 25 UCML; 16 HR HEAT: 15 MIN. ; 45 C
C PDT: 315 JOULESSQ M
Fig. 4. Patterns of protein synthesis in exponentially grow- ing fibroblasts (A), smooth muscle (B), and endothelial cells (C) of bovine origin. Cells were exposed to either control incubation conditions (MEM media supplemented with 10% or 5% fetal calf serum); Photofrin I1 (DHE) alone (16-hour incubation with a drug concentration of 25 pg/ml in MEM media supplemented with 5 8 FCS, followed by a 30-minute washout incubation in fresh MEM media containing 10% FCS); light exposure alone (630 Jim'); heat (15 minutes at 45°C) or PDT (25 p g DHE/ml and a light dose that produced 10% clonogenic survival [see 361 At selected time intervals following treatment, cells were pulse-labeled for 2 hours with 75SS-methionine. Lysates of cells containing equal levels of radioactivity were size-separated using polyacrylamide gel electrophoresis. Resulting gels were stained with Coomassie blue and dried. Autoradiographs of the gels are presented with molecular weight markers shown on the left and the major stress proteins induced by heat and/or PDT shown on
BOVINE SMOOTH MUSCLE CELLS
& #
-i> I = r r c ( r c r : ~ $ E g g g;* N * I X x I I- - .- N p (D m Z 9 z 5 ,,j 1 C t ,= L- ,-+. ,= ~ ~ ~ P ~ w w o o ~ o ~ ~ U U O - I ~ X ~ P ~ P P ~ ~
R E - I n
97 4 . 66 2 . the right.
42 6 -
IN VIVO AND PRECLINICAL PHOTODYNAMIC THERAPY 3 1 0 -
Interest in porphyrin PDT for the treatment of solid tumors started in the early 1970s. Initial work in 1972 showed that Hp combined with white light induced extensive damage to glioma tumors
21.5 -
8 DHE: 25 UG/ML; 16 HR HEAT: 15 MIN. ; 45 C PDT: 525 JOULESISQ M
transplanted in rats [ 5 I . Long-term cures were re- ported in 1975 when HpD, combined with red light, was used to treat spontaneous and transplanted

Responses to Photodynamic Therapy 455
mammary carcinomas in mice 161. The initial studies from Dougherty's group at Roswell Park Memorial Institute (Buffalo, NY) have had a ma- jor impact on the extensive growth and utilization of PDT during the last 10 years [7].
Pharmacokinetics of HpD have been ana- lyzed utilizing radiolabeled materials (14C-HpD and 3H-HpD) in tumor-bearing mice [42]. Hema- toporphyrin derivative and subsequently Pho- tofrin I1 have been shown to be retained in tumor tissue a t higher concentrations than in normal tissues such as skin, muscle, brain, and lungs. However, significantly greater quantities of these porphyrins are taken up and retained in organs such as liver, spleen, and kidney. While the actual mechanism for the delivery and retention of por- phyrins in tumor tissues is not known, recent re- ports indicate that there is a high porphyrid lipoprotein affinity [43,44]. Porphyrins such as HpD and Photofrin I1 can bind to various lipopro- tein fractions in the serum including low-density lipoproteins (LDL). It is interesting to note that the number of LDL receptor sites is elevated in neoplastic cells as well as in the various organs in which there are relatively high concentrations of porphyrin. In agreement with these observations is the report that there is a significant enhance- ment in the preferential uptake of Hp in tumor tissue when Hp is bound to LDL prior to systemic administration in tumor-bearing mice [45].
While the photochemical properties of photo- dynamic therapy indicate that singlet oxygen is a primary agent in the induction of tumoricidal ef- fects, the actual targets of PDT at the tissue level have still not been clearly defined. A number of studies have indicated that both normal and tu- mor vasculature can be severely damaged follow- ing photodynamic therapy. Sophisticated in vivo/ in vitro studies have demonstrated that the cloni- genicity of EMT-6 and RIF tumor cells is not re- duced if the cells are taken from treated mouse tumors immediately following PDT treatments that would normally lead to significant cytotoxic- ity if the tumors were left in situ [46]. In separate studies, blood flow was reduced to almost zero in transplantable rat bladder tumors following PDT [47]. Taken together, these and other studies sug- gest that vascular damage plays an important role in the mechanism of tumor response following PDT.
Experiments were performed to determine if PDT could destroy experimentally induced ocular blood vessels [48]. For these experiments, corneal neovascularization was induced in albino rabbits using paracentral silk sutures with exposed knots.
0 a a l-
U W
t- W a
v)
z W 0
A
o_ a t-
a w c W I : m z W n
6
P a I-
U U w t- W a 2 v)
z w 0
C
3 1
'1
GRP-78 / ACTIN
c 2 4 6 8 1 0 ' 7 ' 4
TtME (hours afler irradiation)
HSP-70 / ACTIN
2 -
-1 6 8 : 3 : 2 'J - " TIME (hours alter irradialion)
34 KD / ACTIN
-0 Srnootti MLSC t?
+ Fibroblas! * Endolhclial
0 2 4 6 8 1 0 12 1 4
TIME (hours after irradiation)
Fig. 5. Kinetics of stress protein synthesis as a function of time following isoeffect doses of PDT. Densitometer readings were obtained from scanning the autoradiographs described in Figure 4 and are ratios of (A) 78-kD stress proteins (GRP- 78) vs. actin, (B) 70-kD stress proteins (HSP-70) vs. actin; and (C) 34-kD stress proteins vs. actin. Ratios for fibroblasts (+I, smooth muscle (21, and endothelial cells (0 ) are shown for each stress protein.
Using this method, discrete corneal vessels ex- tending a n average of 3.5 mm into the clear cornea could be created. The model of neovascularization provided an excellent method for visualizing both the vessels and the effect of PDT on these vessels. Initial treatments utilized intravenously (1.V.) in-

Gomer et al
n.. LIGHT DELIVERI PLAQUE
Fig. 6. The ability of porphyrin photosensitization to destroy blood vessels is exploited in trans-scleral PDT for the treat- ment of experimental choroidal melanoma. A trans-scleral light delivery probe (emitting unidirectional light over a 0.78- cm2 area) is placed on the sclera. Light is delivered through the sclera and into the highly vascularized choroid. The sclera does not take up porphyrin, while the choroid contains high concentrations of porphyrin following I.V. administration. All blood and nutrients supplied to choroidal melanomas come from the choroidal vessels directly under the scleral probe.
jected HpD (5 mgkg). At various time periods fol- lowing injection individual quadrants of vas- cularized cornea were exposed to either krypton (407 nm), argon (488 and 514 nm), or dye laser (630 nm) light. Pre- and post-treatment fluorescein an- giograms were performed to document the vascu- lar integrity of the treated vessels. These initial studies indicated that PDT could induce a regres- sion in the neovascularization. Histological exam- ination was performed 48 hours after treatment in select animals, and these studies revealed destruc- tion of the vascular endothelium. Violet light, which is absorbed more efficiently by porphyrins than red light, induced complete vascular destruc- tion at lower total light doses than that required for treatment with red light. Dose-response exper- iments and histopathological evaluations are cur- rently being completed.
As described above, there is considerable evi- dence that PDT can effectively destroy blood ves- sels in both tumor tissue and normal tissue. This phenomenon is currently being exploited in the preclinical evaluation of trans-scleral PDT for the treatment of choroidal melanomas. The concept of trans-scleral light delivery for ocular PDT is at- tractive for several reasons (Fig. 6). First, HpD pharmacology data indicates that the choroid con- tains high levels of HpD immediately after I.V.
injection 1491. Of equal importance is the fact that the sclera does not take up significant amounts of HpD. A second attraction of trans-scleral light de- livery is that porphyrin-activating red light can be delivered precisely and selectively to specific areas of the vascular choroid. This structure sup- plies all oxygen and nutrients to choroidal melanoma.
Preliminary experiments have been per- formed using pigmented rabbits to determine the effectiveness of trans-scleral PDT for destroying a select area of the choroid. Initial results indicate that this procedure can produce complete and lo- calized choroidal damage with vascular occlusion. Rabbits were injected I.V. with Photofrin I1 (5 mg/ kg followed either 1 hour or 24 hours later by localized trans-scleral PDT. The diameter of the light delivery probe was 10 mm, and the dose of 630-nm light was 200 J/cm2. The light dose rate utilized in these experiments was 100 mW/cm2. Complete choroidal and retinal necrosis was ob- served in the treatment field, while areas outside the light delivery field appeared normal. Of equal importance in these preliminary studies was the observation that the sclera within the treatment field was not damaged as documented by light microscopy and visual examination. The lack of scleral damage was expected since we have ob- served and reported that HpD is not localized in this structure. Control eyes, which received light alone, appeared normal both inside and outside of the treatment field. PDT treatments initiated soon after porphyrin injection were significantly more effective as compared to those initiated 24 hours after injection.
The examination of hypoxic cell cytotoxic agents combined with PDT has been initiated as a result of the observed vascular damage and result- ing induction of hypoxic tumor tissue following PDT. Enhancements in tumor growth delays have been obtained in rat prostate tumors treated with a combination of PDT and misonidazole, and this potentiation is thought to result from direct mi- sonidazole-induced cytotoxicity of hypoxic cells [50,51]. These observations indicate that hypoxic cell cytotoxins could be utilized to enhance the effectiveness of PDT. However, while vascular ef- fects of PDT continue to be documented, there are also in vivo studies indicating that direct tumor cell inactivation via PDT can be exploited. Murine ascites tumors have been effectively treated with interperitoneal U.P.) PDT 1521. Tumor cures reach- ing a n 85% level have been obtained utilizing a total of 4 PDT treatments given at 2-day intervals

Responses to Photodynamic Therapy 457
in C3H mice containing ascitic malignant tera- toma cells. Treatment of the same tumor with chemotherapy (adriamycin) induced less than 20% cures.
Examination of tumor metastasis induced by PDT was evaluated because this treatment is being suggested for use in early-stage clinical ma- lignancies and because of the continued observa- tion of direct vascular injury following PDT [53]. Studies were performed to determine whether lo- calized PDT treatment of subcutaneously growing Lewis lung carcinoma influenced the formation of distant metastasis. Mice exposed to localized PDT treatment had significantly reduced numbers of metastatic lung colonies compared to controls. In addition, PDT-treated mice had equal or decreased numbers of metastatic lung colonies than compa- rable mice treated with local surgery. These re- sults indicate that local PDT does not enhance the metastatic spread of Lewis lung carcinoma follow- ing treatment.
Recent investigations have examined various immunological responses following PDT. This treatment has been shown to induce systemic im- munosuppression related to inhibition of contact hypersensitivity of dinitrofluorobenzene in mice [ 541. The immunosuppression induced by PDT may be mediated by the activation of the complement system 155, 561. We have recently examined the natural killer (NK) cell activity in non-tumor- bearing mice treated with localized photodynamic therapy. A correlation has been reported between NK cell activity and the in vivo capacity to elimi-
PDT: Melanotic Melanoma
W
2 0 U 0
c c z W 0 U W
a
I
n
-+ 300
0 2 0 0 4 0 0 6 0 0
LIGHT DOSE (Joulesisq.crn.)
Fig. 7. Tumor response curves for C57BU6 mice implanted with a B-16 melanotic melanoma and treated with PDT. Tu- mors (5-7 mm in diameter) were exposed to 630-nm light 24 hours following a 10 mgKg I.P. injection of Photofrin 11. Total light doses ranged from 0 to 500 J/cm*, and light dose rates were 150 (P), 300 (+), 450 (01, or 600 (0) m (W/crnZ. Percent cure was determined from animals that were disease-free 45 days following treatment. Each point represents the average of ten animals.
nate circulating tumor cells [57j. There is also increasing evidence to suggest that NK cells play a significant role in the resistance to progressive growth and metastasis of tumors 1581. It was therefore of interest to determine the effect of PDT on NK cell activity and to see whether this re- sponse correlated with the lack of metastatic in- duction observed with PDT 1531. C57BL/6 mice were used to evaluate NK cell activity as well as to document spleen weight following porphyrin administration and light exposure. Splenic NK cell activity was determined utilizing the proce- dure of Pollock et al. [59]. The YAC-1 lymphoma cell line was labeled with 5'Cr sodium chromate
PDT: AMELANOTIC MELANOMA
100 , -
a 0
F 5 5 W 0
W a a
. 9 600
40 1
20+ 0 0 1 0 0 2 0 0 3 0 0 4 0 0 5 0 0 600
LIGHT DOSE (Joulesisq cm )
Fig. 8. Tumor response curves for C57BL/6 mice implanted with a B-16 amelanotic melanoma and treated with PDT. Other details as per Figure 7.
MELANOTIC MELANOMA, 630 NM, 2 mm DEPTH
30 , I
W
E W
I-
w
u i-
a a a a
i!
20
10
0 0 1 0 2 0 3 0
TIME (minutes)
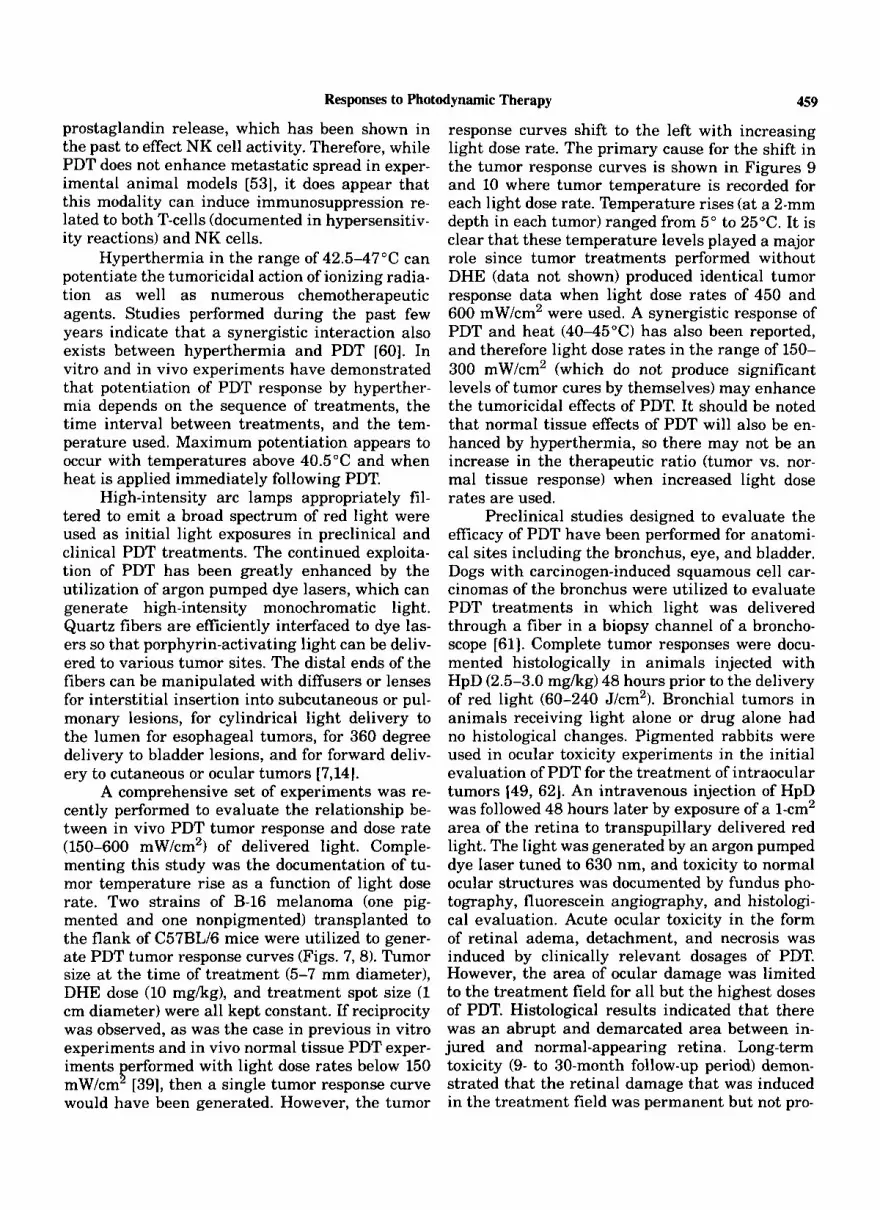
Fig. 9. B-16 melanotic melanoma tumor temperature as a function of time during 630-nm light exposure. Light was delivered at dose rates of 150 (E), 300 (+), 450, (E) or 600 (0) mW/cm2. The treatment spot diameter was 1 cm, and temper- atures were measured at a 2-mm depth from the tumor s ~ - face using a 21-gauge thermocouple hypodermic needle (Omega). Each point represents the average of five tumors.

458 Gomer et a1
TABLE 1. Natural Killer Cell Activity and Spleen Weight in C57RL16 Mice Following Photofrin I1 Administration
Spleen weight
Percent cell lysis at Days following effector: target ratioa photofrin I 1 Photofrin I1 No. administration dose (mgkg) of mice 1OO: l 50:l 25:l (mg)
1 0 5 24.2 17.4 11.8 60 10 4 22.0 16.2 11.0 65 50 4 18.5 13.0 8.0 69.2
3 0 8 23.3 17.0 11.6 65 10 7 19.2 13.6 8.8 75.8 50 7 19.2 14.4 9.5 92.8
10 7 28.4 20.4 13.1 87.8 50 7 27.4 16.1 10.7 106.5
14 0 4 21.5 16.2 9.7 50.2 10 7 25.0 20.0 13.2 82 50 4 15.0 11.5 7.0 75.2
7 0 7 26.1 18.7 12.2 55.4
"Effector cells were spleen cells; target cells were 2 x lo4 "Cr-labeled YAC-1 cells.
TABLE 2. Natural Killer Cell Activity and Spleen Weight in C57BL/6 Mice Following - Photodynamic Therapy*
Days following Percent cell lysis at Spleen photodynamic No. of effector: target ratio" . . weight
1 Control 7 20.5 18.8 10.0 73.5 PDT 10 3.7 2.5 1.2 40.3
3 Control 6 28.0 22.6 12.8 96.5 PDT 8 21.2 17.5 9.1 55
7 Cont.rol 4 30.0 22.7 12.2 63.5 PDT 8 26.6 21.6 10.6 88.1
14 Control 5 24.7 17.7 8.2 81 ._ - PDT 13 29.5 23.9 11.3 83
*Photofrin I1 (10 mgikg) administered 24 hours prior to PDT. PDT consisted of a 400 Jlcm' dose delivered over a 1-cm-diameter area of the right hindleg at a dose rate of 150 mW/cm2. "Effector cells were spleen cells; target cells were 2 x lo4 51Cr-labeled YAC-1 cells.
t h e r a p y . . Treatment . - mice 1OO:l 50:l 25:l (mg)..
and was then used as the target cell in NK assays. Splenic effector cells at various dilution ratios were incubated with 2 x lo4 YAC cells. Photofrin I1 alone at concentrations of 10 and 25 mgkg induced a significant increase in spleen size as indicated in Table 1. The maximum increase in spleen weight was observed 7 days following por- phyrin administration. While the spleen size in mice injected with Photofrin I1 increased, there was no change from control values for NK cell activities. However, alterations in both NK cell activity and in spleen weight were observed for mice treated with PDT, and results are shown in Table 2. PDT consisted of a 10 mgkg I.P. dose of Photofrin I1 followed 24 hours later by local expo-
sure of the right hindlimb to 400 J/cm2 of 630-nm light. A rapid decrease in both spleen size and NK cell activity was observed following PDT. Within 24 hours, the NK cell activity was reduced to levels near zero. Associated with this decrease in NK activity was a reduction in spleen weight to approximately one-half of control values. Both of these changes were transient in nature, with NK cell activity and spleen size returning to control values within 3 days.
The observed decrease in NK cell activity following PDT appears to be a systemic effect, since only the hindlimb of the experimental ani- mal received the light treatment. The observed decrease in NK activity could be the results of
Responses to Photodynamic Therapy 459
prostaglandin release, which has been shown in the past to effect NK cell activity. Therefore, while PDT does not enhance metastatic spread in exper- imental animal models [53], it does appear that this modality can induce immunosuppression re- lated to both T-cells (documented in hypersensitiv- ity reactions) and NK cells.
Hyperthermia in the range of 42.5-47"C can potentiate the tumoricidal action of ionizing radia- tion as well as numerous chemotherapeutic agents. Studies performed during the past few years indicate that a synergistic interaction also exists between hyperthermia and PDT [SO]. In vitro and in vivo experiments have demonstrated that potentiation of PDT response by hyperther- mia depends on the sequence of treatments, the time interval between treatments, and the tem- perature used. Maximum potentiation appears to occur with temperatures above 40.5"C and when heat is applied immediately following PDT.
High-intensity arc lamps appropriately fil- tered to emit a broad spectrum of red light were used as initial light exposures in preclinical and clinical PDT treatments. The continued exploita- tion of PDT has been greatly enhanced by the utilization of argon pumped dye lasers, which can generate high-intensity monochromatic light. Quartz fibers are efficiently interfaced to dye las- ers so that porphyrin-activating light can be deliv- ered to various tumor sites. The distal ends of the fibers can be manipulated with diffusers or lenses for interstitial insertion into subcutaneous or pul- monary lesions, for cylindrical light delivery to the lumen for esophageal tumors, for 360 degree delivery to bladder lesions, and for forward deliv- ery to cutaneous or ocular tumors [7,14].
A comprehensive set of experiments was re- cently performed to evaluate the relationship be- tween in vivo PDT tumor response and dose rate (150-600 mW/cm2) of delivered light. Comple- menting this study was the documentation of tu- mor temperature rise as a function of light dose rate. Two strains of B-16 melanoma (one pig- mented and one nonpigmented) transplanted to the flank of C57BL/6 mice were utilized to gener- ate PDT tumor response curves (Figs. 7,8). Tumor size at the time of treatment (5-7 mm diameter), DHE dose (10 mgkg), and treatment spot size (1 cm diameter) were all kept constant. If reciprocity was observed, as was the case in previous in vitro experiments and in vivo normal tissue PDT exper- iments erformed with light dose rates below 150 mW/cm [39], then a single tumor response curve would have been generated. However, the tumor
E
response curves shift to the left with increasing light dose rate. The primary cause for the shift in the tumor response curves is shown in Figures 9 and 10 where tumor temperature is recorded for each light dose rate. Temperature rises (at a 2-mm depth in each tumor) ranged from 5" to 25°C. It is clear that these temperature levels played a major role since tumor treatments performed without DHE (data not shown) produced identical tumor response data when light dose rates of 450 and 600 mW/cm2 were used. A synergistic response of PDT and heat (4045°C) has also been reported, and therefore light dose rates in the range of 150- 300 mW/cm2 (which do not produce significant levels of tumor cures by themselves) may enhance the tumoricidal effects of PDT. It should be noted that normal tissue effects of PDT will also be en- hanced by hyperthermia, so there may not be an increase in the therapeutic ratio (tumor vs. nor- mal tissue response) when increased light dose rates are used.
Preclinical studies designed to evaluate the efficacy of PDT have been performed for anatomi- cal sites including the bronchus, eye, and bladder. Dogs with carcinogen-induced squamous cell car- cinomas of the bronchus were utilized to evaluate PDT treatments in which light was delivered through a fiber in a biopsy channel of a broncho- scope [61]. Complete tumor responses were docu- mented histologically in animals injected with HpD (2.5-3.0 mgkg) 48 hours prior to the delivery of red light (60-240 J/cm2). Bronchial tumors in animals receiving light alone or drug alone had no histological changes. Pigmented rabbits were used in ocular toxicity experiments in the initial evaluation of PDT for the treatment of intraocular tumors 149, 621. An intravenous injection of HpD was followed 48 hours later by exposure of a 1-cm2 area of the retina to transpupillary delivered red light. The light was generated by an argon pumped dye laser tuned to 630 nm, and toxicity to normal ocular structures was documented by fundus pho- tography, fluorescein angiography, and histologi- cal evaluation. Acute ocular toxicity in the form of retinal adema, detachment, and necrosis was induced by clinically relevant dosages of PDT. However, the area of ocular damage was limited to the treatment field for all but the highest doses of PDT. Histological results indicated that there was an abrupt and demarcated area between in- jured and normal-appearing retina. Long-term toxicity (9- to 30-month follow-up period) demon- strated that the retinal damage that was induced in the treatment field was permanent but not pro-

Gomer et al
AMELANOTIC MELANOMA, 630 NM. 2 mm DEPTH 30 7 I
I 20
10
0 0 1 0 2 0 3 0
TIME (minutes)
Fig. 10. B-16 amelanotic melanoma tumor temperature rise as a function of time during PDT light exposure. Other details as per Figure 9.
gressive. Lens opacities were not observed during the follow-up period, and the cornea, aqueous, and vitreous remained clear in all tested animals. The efficacy of PDT has also been examined in normal dog bladders as well as in rabbit bladders trans- planted with the Brown-Pearce carcinoma 163- 661. A 360 J/cm2 dose of 630-nm light delivered to a l-cm2 area of normal dog bladder 3 days after a 2.5 mgkg injection of Photofrin I1 produced a le- sion that extended to the muscle layer but did not induce a fistula. Light doses less than 360 J/cm2 produced only superficial damage to the exposed area. Results from rabbit experiments demon- strated that HpD was preferentially taken up in the transplanted bladder carcinoma and that PDT could effectively destroy the tumor without dam- age to normal urothelium.
CLINICAL PDT
The first use of prophyrin PDT for the clinical treatment of solid tumors was in 1976, and cur- rently more than 3,000 patients have received this therapy [7,14,24]. The only significant side effect associated with PDT has been transient skin pho- tosensitization. For some patients, the skin sensi- tivity can last more than 6 weeks after systemic injection of HpD or Photofrin I1 as a result of prolonged retention of the porphyrin in the skin. While there are anecdotal cases of PDT for almost every anatomical site and histological type of solid cancer, the use of PDT appears to be most encour- aging for solid tumors of the bronchus, esophagus, bladder, head and neck, skin, and eye. As with most new cancer therapies, the majority of pa- tients treated with PDT have been advanced cases in whom all conventional therapies have failed, and unfortunately there is little information re- lated to long-term response. Early-stage lesions (for which there are significantly fewer patients)
routinely have excellent initial tumor responses following PDT. Several extensive reviews on clin- ical PDT have been published [7,14], and therefore only recent clinical highlights will be presented.
PDT appears to be effective in superficial bladder cancer, and PDT may find an important role in the management of diffuse carcinoma in situ and in noninvasive transitional cell carci- noma [67]. Bladder tumors can be treated with PDT by delivering light directly into the bladder via an endoscope. Individual lesions can be ex- posed to unidirectional light emitted from a flat- tipped fiber, while a diffusing bulb can be used for whole-bladder illumination. An excellent correla- tion between HpD localization and histologically defined dysplasia and carcinoma in situ of the bladder has been reported [66]. In addition, PDT has been extremely effective against Ta and T1 disease for lesions less than 1 cm, but PDT has not been effective for lesions greater than 1.5 cm [68].
Obstructive endobronchial tumors are treated with PDT by using a fiberoptic broncho- scope. Good tumor responses and improvements in patient performance status are routinely observed provided that a clean-up bronchoscopy is per- formed 2-3 days following PDT [69,70]. These le- sions can receive PDT using either surface tumor illumination or by inserting a diffusing cylindrical fiber directly into the lesion for interstitial PDT (711. The use of PDT for obstructive esophageal tumors utilizes techniques similar to that used for endobronchial tumors. The early response for esophageal lesions are encouraging, and the pro- cedure appears to offer excellent palliation [72].
Primary and metastatic skin lesions have re- sponded favorably to PDT [ 141. Metastatic breast carcinomas recurrent to the chest wall can be treated with PDT using either surface or intersti- tial light delivery. Multiple PDT treatments are also possible. The primary problem in treating skin tumors has been to minimize PDT-induced normal skin toxicity. Basal cell carcinomas appear to be extremely sensitive to PDT, and this treat- ment has been used successfully in patients with nevoid basal cell carcinoma syndrome [73].
The optical characteristics of the eye com- bined with the relatively small size of intraocular tumors suggest that ocular PDT could be ex- tremely useful in the treatment of eye tumors. Transcorneal PDT delivered with high light dose rates (greater than 400 mW/cm2) is effective in reducing the height of pigmented choroidal mela- nomas. In the absence of pigment, as in the case of retinoblastoma or amelanotic melanoma of the iris or choroid, tumor kill attributed to PDT alone can be significant 1741.

Responses to Photodynamic Therapy 461
Clinical PDT trials utilizing Photofrin I1 have recently been reinitiated with the assistance of Lederle Laboratories, American Cyanamid and Quadra Logics Tech., Inc. Three major anatomical tumor sites are being evaluated. Non-small cell endobronchial carcinoma will be evaluated in two trials. First, in unilateral disease radiation ther- apy with or without PDT will be evaluated. The second lung trial will be performed in sympto- matic patients with metastatic disease, and in this case PDT will be compared to Nd:YAG laser ther- apy. For this study, endpoints will include time to first remission as well as relief of pain. Two trials are also being evaluated for esophageal carci- noma. The first trial will again compare Nd:YAG laser therapy to PDT. Endpoints will be time to first remission. The second study is a single-arm trial for completely obstructive esophageal tu- mors. Bladder carcinomas will be evaluated in the third group of clinical trials. For carcinoma in situ, PDT will be compared to standard thio-TEPA treatment. In addition, a second trial is planned in which prophylaxis treatment of bladder tumors will be evaluated.
ACKNOWLEDGMENTS
We thank Barbara Paul for assistance in the
This work was supported in part by USPHS preparation of this manuscript.
grants CA-31230, CA-43087, and CA-44733.
REFERENCES
1.
2.
3.
4.
5.
6.
Figge F, Wieland G, Mangiello L: Cancer detection and therapy. Affinity of neoplastic, embryonic and trauma- tized tissue for porphyrins and metalloporphyrins. Proc Soc Exp Biol Med 1948; 168:640-641. Lipson R, Baldes E, Olsen A: The use of a derivative of hematoporphyrin in tumor detection. JNCI 1961; 267:l- 8. Gregorie H, Horder E, Ward J, Green JF, Richards T, Robertson HC, Stevenson TB: Hematoporphyrin-deriva- tive fluorescence in malignant neoplasms. Ann Surg 1968; 672320-828. Balchum OJ, Profio AE, Doiron DK, Huth GC: Imaging fluorescence bronchoscopy for localizing bronchial cancer and carcinoma in-situ. In Doiron DR, Gomer CJ (eds): “Porphyrin Localization and Treatment of Tumors.” New York: Alan R. Liss, Inc., 1984: 847-861. Diamond I, Granelli S, McDonagh A, Neilsen S, Wilson CB, Jaenicke R: Photodynamic therapy of malignant tu- mors. Lancet 1973; 2:1175-1177. Dougherty TJ, Grindley GB, Fie1 R, Weishaupt KR, Boyle DG: Photoradiation therapy, 11. Cure of animal tumors with hematoporphyrin and light. JNCI 1975; 55:115-119.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24,
25.
26.
27.
Dougherty TJ: Photoradiation therapy (PRT) of malig- nant tumors. CRC Crit Rev Biochem 1984; 2233-116. Byrne CJ, Marshallsay LV, Ward AD: The structure of the active material in hematoporphyrin derivative. Pho- tochem Photobiol 1987; 46:575-580. Dougherty TJ: The structure of the active component of hematoporphyrin derivative. In Doiron DR, Gomer CJ (eds): “Porphyrin Localization and Treatment of Tu- mors.” New York: Alan R. Liss, Inc., 1984: 301-334, Dougherty TJ: Studies on the structure of porphyrins contained in Photofrin 11. Photochem Photobiol 1987;
Kessel D, Thompson P, Musselman B, Chang CK: Chem- istry of hematoporphyrin-derived photosensitizers. Pho- tochem Photobiol 1987; 46:563-568. Wijesekera TP, Dolphin D: Some preparations and prop- erties of porphyrins. In Kessel D (ed): “Methods in Porphyrin Photosensitization.” New York: Plenum Pub- lishing, 1985: 229-266. Wilson BC, Jeeves WP, Lowe DM: In-vivo and post-mor- tem measurements of the attenuation spectra of light in mammalian tissues. Photochem Photobiol 1985; 43:2153- 2159. Wilson BC, Jeeves WP: Photodynamic therapy of cancer. In Ben-Hur E, Rosenthal I (eds): “Photomedicine,” Vol. 11. Boca Raton, FL: CRC Press, 1987: 127-177. Weishaupt K, Gomer CJ, Dougherty T: Identification of singlet oxygen as the cytotoxic agent in photo-inactiva- tion of a murine tumor. Cancer Res 1976; 36:2326-2329. Foote CS: Mechanisms of photooxygenation. In Doiron DR, Gomer CJ (eds): “Porphyrin Localization and Treat- ment of Tumors.” New York: Alan R. Liss, Inc., 1984: 3- 22. Jori G, Spikes JD: Photobiochemistry of porphyrins. In Smith KC (ed): “Topics in Photomedicine.” New York: Plenum Press, 1984: 183-318. Buettner GR, Need MJ: Hydrogen peroxide and hydroxyl free radical production by hematoporphyrin derivative, ascorbate and light. Cancer Lett 1985; 25:297-304. Hariharan PV, Cortney J, Eleczko S: Production of hy- droxyl radicals in cell systems exposed to hematopor- phyrin and red light. Int J Radiat Biol 1980; 37:691-694. Van Steveninck J , Tijssen K, Boegheim JPJ, van der Zee J , Dubbelman TMAR: Photodynamic generation of hy- droxyl radicals by hematoporphyrin derivative and light. Photochem Photobiol 1986; 44:711-716. Moan J , Sommer S: Oxygen dependence of the photosen- sitizing effect of hematoporphyrin derivative in NHIK- 3025 cells. Cancer Res 1985; 45:1608-1610. Mitchell JB, McPhearson S, DeGraff W, Gamson J, Zabell A, Russo A: Oxygen dependence of hematoporphyrin de- rivative induced photoinactivation of Chinese hamster cells. Cancer Res 1985; 45:2008-2011. Gomer CJ, Razum NJ: Acute skin resonse in albino mice following porphyrin photosensitization under oxic and anoxic conditions. Photochem Photobiol 1984; 40:435- 439. Gomer CJ (ed): “Photodynamic Therapy.” Oxford: Perga- mon Press, 1987. Moan J Porphyrin-sensitized photodynamic inactivation of cells: A review. Lasers Med Sci 1986; 1:5-12. Gomer CJ: DNA damage and repair in CHO cells follow- ing hematoporphyrin photoradiation. Cancer Lett 1980:
Gomer CJ, Rucker N, Banerjee A, Benedict WF: Compar- ison of mutagenicity and induction of sister chromatid exchanges in Chinese hamster cells exposed to hemato-
46:569-573.
11: 161-167.

462 Gorner et a1
porphyrin derivative, photoradiation, ionizing radiation, or U.V. radiation. Cancer Res 1983; 43:2622-2627.
28. Moan J , Waksvik H, Christensen T: DNA single-strand breaks and sister chromatid exchanges induced by treat- ment with hematoprophyrin and light or by X-rays in human NHIK 3025 cells. Cancer Res 1980; 40:2915-2918.
29. Hilf R, Smail DB, Murant RS, Leakey PB, Gibson SL: Hematoporphyrin derivative-induced photosensitivity of mitochondria1 succinate dehydrogenase and selected cy- tosolic enzymes of R3230 AC mammary adenocarcinomas of rats. Cancer Res 1984; 44:1483-1488.
30. Hilf R, Warne NW, Smail DB, Gibson SL: Photodynamic inactivation of selected intracellular enzymes by hema- toporphyrin derivative and their relationship to tumor cell ability in-vitro. Cancer Lett 1984; 44:165-227.
31. Munson BR: Fie1 RJ: Hematoporphyrin-sensitized photo- dynamic inactivation of viral RNA-dependent DNA poly- merase. Res Commun Chem Pathol Pharmacol 1977;
32. Munson BR: Photodynamic inactivation of mammalian DNA-dependent RNA polymerase by hematoporphyrin a n visible light. Int J Biochem 1970; 10:957-960.
33. Mang TS, Dougherty TJ: Time and sequence dependent influence of in-vitro photodynamic therapy (PDT) sur- vival by hyperthermia. Photochem Photobiol 1980;
34. Kessel D: Photosensitization with derivatives of hemato- porphyrin. Int J Radiat Biol 1986; 49:901-907.
35. Gomer CJ, Rucker N, Murphree AL: Transformation and mutagenic potential of porphyrin photodynamic therapy in mammalian cells. Int J Radiat Biol 1988; 53:651-659.
36. Gomer CJ, Rucker N, Murphree AL: Differential cell photosensitivity following porphyrin photodynamic ther- apy. Cancer Res 1988; 48:4539-4542.
37. Gomer CJ, Rucker N, Ferrario A, Murphree AL: Expres- sion of potentially lethal damage in Chinese hamster cells exposed to hematoporphyrin derivative photody- namic therapy. Cancer Res 1986; 4613348-3352.
38. Bellnier D, Lin CW: Photosensitization and split-dose recovery in cultured human urinary bladder carcinoma cells containing nonexchangable hematoporphyrin deriv- ative. Cancer Res 1985; 45:2507-2511.
39. Gomer CJ, Rucker N, Razum NJ, Murphree AL: In-vitro and in-vivo light dose rate effects related to hematopor- phyrin derivative photodynamic therapy. Cancer Res
40. Gomer CJ, Doiron DR, Rucker N, Razum NJ, Fountain SW: Action spectrum (620-640 nm) for hematoporphyrin derivative induced cell killing. Photochem Photobiol 1984;
41. Moan J , Steen HB, Feren K, Christensen T: Uptake of hematoporphyrin derivative and sensitized photoinacti- vation of C3H cells with different oncogenic potential. Cancer Lett 1981; 14:291-296.
42. Gomer CJ, Dougherty TJ: Determination of [‘HI and [14C] hematoporphyrin derivative distribution in malignant and normal tissue. Cancer Res 1979; 39:146-151.
43. Reyftmann JP, Morliere P, Goldstein S, Santus R, Dub- ertret L, Lagrange D: Interaction of human serum low density lipoproteins with porphyrins. A spectroscopic and photochemical study. Photochem Photobiol 1984; 40:721- 729.
44. Jori G, Reddi E, Salvato B, Pagnan A, Ziron L: Evidence for a major role of plasma lipoproteins as hematopor- phyrin carriers in-vivo. Cancer Lett 1984; 24:291-297.
16:175-178.
42~533-540.
1985; 45~1973-1977.
39:365-368.
45. Barel A, Jori G, Perin A, Romandini P, Pagnan A, Buf- fanti S: Role of high, low and very low density lipopro- teins in the transport and tumor delivery of hema- toporphyrin in-vivo. Cancer Lett 1986; 32:145-150.
46. Henderson BW, Waldow SM, Mang “S, Potter WR, Ma- lone PB, Dougherty TJ: Tumor destruction and kinetics of tumor cell death in two experimental mouse tumors following photodynamic therapy. Cancer Res 1985; 572- 576.
47. Selman SH, Kreimer-Birnbaum M, Klaunig JE, Gold- blatt PJ , Keck RW, Britton SS: Blood flow in transplant- able bladder tumors treated with hematoporphyrin derivative and light. Cancer Res 1984; 44: 1924-1927.
48. York KK, Gomer CJ, Murphree AL, Schanzlin DR: He- matoporphyrin derivative photoradiation therapy for cor- neal neovascularization. Invest Ophthalmol Vis Sci \Supple] 26:180, 1985 (Abstract).
49. Gomer CJ, Jester JV, Razum NJ, Szirth BC, Murphree AL: Photodynamic therapy of intraocular tumors, exam- ination of hematoporphyrin derivative distribution and long-term damage in rabbit ocular tissue. Cancer Res 1985; 45:3718-3725.
50. Gonzalez S, Arnfield MR, Meeker BE, Tulip J , Lakey WH, Chapman JD, McPhee MS: Treatment of Dunning R3327-AT rat prostate tumors with photodynamic ther- apy in combination with misonidazole. Cancer Res 1986;
51. Hirsch BD, Walz NC, Meeker BE, Arnfield MR, Tulip J , McPhee MS, Chapman JD: Photodynamic therapy-in- duced hypoxia in rat tumors and normal tissues. Photo- chem Photobiol 1987; 46:847-852.
52. Tochner Z, Mitchell JB, Smith P, Harrington F, Glatstein E, Russo D, Russo A: Photodynamic therapy of ascites tumors within the peritoneal cavity. Br J Cancer 1986; 551733-736.
53. Gomer CJ, Ferrario A, Murphree AL: The effect of local- ized porphyrin photodynamic therapy on the induction of tumor metastasis. Br J Cancer 1987; 56:27-32.
54. Elmets CA, Bowen KD: Immunological suppression in mice treated with hematoporphyrin derivative photora- diation. Cancer Res 1986; 46:168-1611.
55. Lim HW, Young L, Hagan M, Gigli I: Delayed phase of hematoporphyrin-induced phototoxicity: Modulation by complement, leukocytes and antihistamines. J Invest Dermatol 1985; 84:114-117.
56. Lim HW, Pol-Fitzpatrick MB, Gigli I: Activation of the complement system in patients with porphyrins after ir- radiation in-vivo. J Clin Invest 1984; 74:1961-1965.
57. Hanna M, Fidler IJ: Rate of natural killer cells in the destruction of circulating tumor emboli. JNCI 1980; 65:801-809.
58. Herberman RB (ed): “NK Cells and Other Natural Effec- tor Cells.” New York: Academic Press, 1982.
59. Pollock RE, Babcock GF, Romschahl MM, Nishioka K: Surgical stress-mediated suppression of murine natural killer cell cytotoxicity. Cancer Res 1984; 44:3888-3891.
60. Waldow SM, Dougherty TJ: Interaction of hyperthermia and photoradiation therapy. Radiat Res 1984; 97:380- 385.
61. Hayata Y, Kato H, Konaka C, Hayashi N, Tahara M, Saitc T, Ono J: Fiberoptic bronchoscopic photoradiation in experimentally induced canine lung cancer. Cancer 1983; 5150.
62. Gomer CJ, Doiron DR, Jester JV, Szirth BC, Murphree AL: Hematoporphyrin derivative photoradiation therapy
46:2858-2866.

Responses to Photodynamic Therapy 463
for the treatment of intraocular tumors. Examination of acute normal ocular tissue toxicity. Cancer Res 1983; 43:721.
63. Dougherty TJ: Photodynamic therapy. Clin Chest Med
64. Hisazumi H, Misaki T, Misyoshi N: Photoradiation ther- apy of bladder tumors. J Urol 1983; 130:685.
65. Jocham D, Staehler G, Chaussey C, Unsold E: Integral dye-laser irradiation of photosensitized bladder tumors with the air of a light-scattering medium. In Doiron DR, Gomer C J (eds): “Porphyrin Localization and Treatment of Tumors.” New York: Alan R. Liss, Inc. New York 1984:
66. Benson R, Farrow G, Kinsey J, Cortese DA, Zincke H, Utz DC: Detection and localization of in-situ carcinoma of the bladder with hematoporphyrin derivative. Mayo Clin Proc 1982; 57:548-555.
67. Prout GR Jr, Lin CW, Benson R, et al.: Phototherapy with hematoporphyrin derivative in the treatment of su- perficial transitional-cell carcinoma of the bladder. N Engl J Med 1987; 317:1251-1255.
1985; 6:219-236.
249-256.
68. Benson RC Jr: Treatment of diffuse transitional cell car- cinoma in-situ by whole bladder hematoporphyrin deriv- ative photodynamic therapy. J Urol 1985; 134:675-678.
69. Balchum OJ, Doiron DR: Photoradiation therapy of en- dobronchial cancer. Clin Chest Med 1985; 6:255-275.
70. Lam S, Muller NL, Miller RR: Predicting the response of obstructive endobronchial tumors to photodynamic ther- apy. Cancer 1986; 58:2298-2306.
71. Cortese DA, Kinsey JH: Hematoporphyrin derivative phototherapy in the treatment of bronchogenic carci- noma. Chest 1984; 86:8-13.
72. McCaughan JS Jr: Overview of experiences with photo- dynamic therapy for malignancy in 192 patients. Photo- chem Photobiol 1987; 46:903-909.
73. Tse DT, Kersten RC, Anderson RL: Hematoporphyrin derivative photoradiation therapy in managing nevoid basal-cell carcinoma syndrome. A preliminary report. Arch Ophthalmol 1984; 102:990-994.
74. Murphree AL, Cote M, Gomer CJ: The evolution of pho- todynamic therapy techniques in the treatment of intra- ocular tumors. Photochem Photobiol 1987; 46:919-923.