hormonal replacement therapy reduces forearm fracture incidence in recent postmenopausal women —...
TRANSCRIPT

Maturitas 36 (2000) 181–193
Hormonal replacement therapy reduces forearm fractureincidence in recent postmenopausal women — results of the
Danish Osteoporosis Prevention Study
Leif Mosekilde a, Henning Beck-Nielsen b, Ole Helmer Sørensen c,Stig Pors Nielsen d, Peder Charles a, Peter Vestergaard a,*,
Anne Pernille Hermann a, Jeppe Gram b, Tony Bill Hansen b,Bo Abrahamsen b, Ebbe Nils Ebbesen b, Lis Stilgren b, Lars Bjørn Jensen c,Christine Brot c, Birgitte Hansen c, Charlotte Landbo Tofteng c, Pia Eiken d,
Niels Kolthoff d
a Department of Endocrinology and Metabolism, The Osteoporosis Clinic, Aarhus Amtssygehus, Aarhus Uni6ersity Hospital,Tage Hansens Gade 2, DK-8000 AarhusC, Denmark
b Department of Endocrinology, Odense Uni6ersity Hospital, Odense, Denmarkc Copenhagen Municipal Hospital, Copenhagen, Denmark
d Hillerød Hospital, Hillerød, Denmark
Received 10 March 2000; accepted 10 July 2000
Abstract
Objecti6es: To study the fracture reducing potential of hormonal replacement therapy (HRT) in recent post-menopausal women in a primary preventive scenario. Methods: Prospective controlled comprehensive cohort trial:2016 healthy women aged 45–58 years, from three to 24 months past last menstrual bleeding were recruited from arandom sample of the background population. Mean age was 50.892.8 years, and the number of person yearsfollowed was 9335.3. There were two main study arms: a randomised arm (randomised to HRT; n=502, or not;n=504) and a non-randomised arm (on HRT; n=221, or not; n=789 by own choice). First line HRT was oralsequential oestradiol/norethisterone in women with intact uterus and oral continuous oestradiol in hysterectomisedwomen. Results: After five years, a total of 156 fractures were sustained by 140 women. There were 51 forearmfractures in 51 women. By intention-to-treat analysis (n=2016), overall fracture risk was borderline statisticallysignificantly reduced (RR=0.73, 95% CI: 0.50–1.05), and forearm fracture risk was significantly reduced (RR=0.45,95% CI: 0.22–0.90) with HRT. Restricting the analysis to women who had adhered to their initial allocation of eitherHRT (n=395) or no HRT (n=977) showed a significant reduction in both the overall fracture risk (RR=0.61, 95%CI: 0.39–0.97) and the risk of forearm fractures (RR=0.24, 95% CI: 0.09–0.69). Compliance with HRT was 65%
www.elsevier.com/locate/maturitas
* Corresponding author. Tel.:+45-89-497681; fax: +45-89-497684.E-mail address: [email protected] (P. Vestergaard).
0378-5122/00/$ - see front matter © 2000 Elsevier Science Ireland Ltd. All rights reserved.
PII: S 0378 -5122 (00 )00158 -4
L. Mosekilde et al. / Maturitas 36 (2000) 181–193182
after five years. Conclusions: It is possible to reduce the number of forearm fractures and possibly the total numberof fractures in recent postmenopausal women by use of HRT as primary prevention. © 2000 Elsevier Science IrelandLtd. All rights reserved.
Keywords: Hormonal replacement therapy; Fractures; Oestrogen
1. Introduction
Osteoporosis is a frequent condition [1] leadingto substantial morbidity and mortality. Os-teoporosis is more frequent in women than in menprimarily due to the loss of endogenous oestrogenproduction after menopause [1].
Several studies have pointed towards a protec-tive effect of hormonal replacement therapy(HRT) against postmenopausal bone loss [2,3]and fracture occurrence [4–7]. However, mostprevious fracture studies except one [7] have beenobservational. Two recent prospective studies onoestrogen use to prevent fractures showed a re-duction [8] and no reduction [9] in fracture occur-rence respectively.
HRT may be used in a general way to preventfractures in postmenopausal women independentof prior risk factors (primary prevention), it maybe used in women with prevalent risk factors (e.g.low bone mineral density — secondary preven-tion [9]), or as done by Lufkin et al. [7] to preventnew fractures in women with prevalent fractures(tertiary prevention).
The Danish Osteoporosis Prevention Study(DOPS) was designed to study primary preventionof fractures in recent postmenopausal womenthrough the use of HRT during a total follow-upperiod of 20 years [10]. Compliance is of concernwith HRT [11–14] particularly due to inductionof menstrual bleeding and shifts in drug regimensmay be necessary. As these factors preclude blind-ing, the DOPS was designed as an open trial. Thestudy was designed with a randomised arm (HRTor no HRT) and a non-randomised arm (HRT orno HRT by own choice) to overcome some of thedifficulties with subjects not accepting randomisa-tion and thus not being included in a randomisedtrial. The study was thus partly randomised witha classical randomised controlled trial as one ofthe study arms and an observational study arm asthe other.
In order to be able to prevent any acceleratedperimenopausal bone loss, the women were in-cluded as close as possible to the menopause, toensure that HRT would maintain as much of thepeak bone mass as possible.
In this article we present the results concerningfracture risk during the first five years of the studyperiod.
2. Material and methods
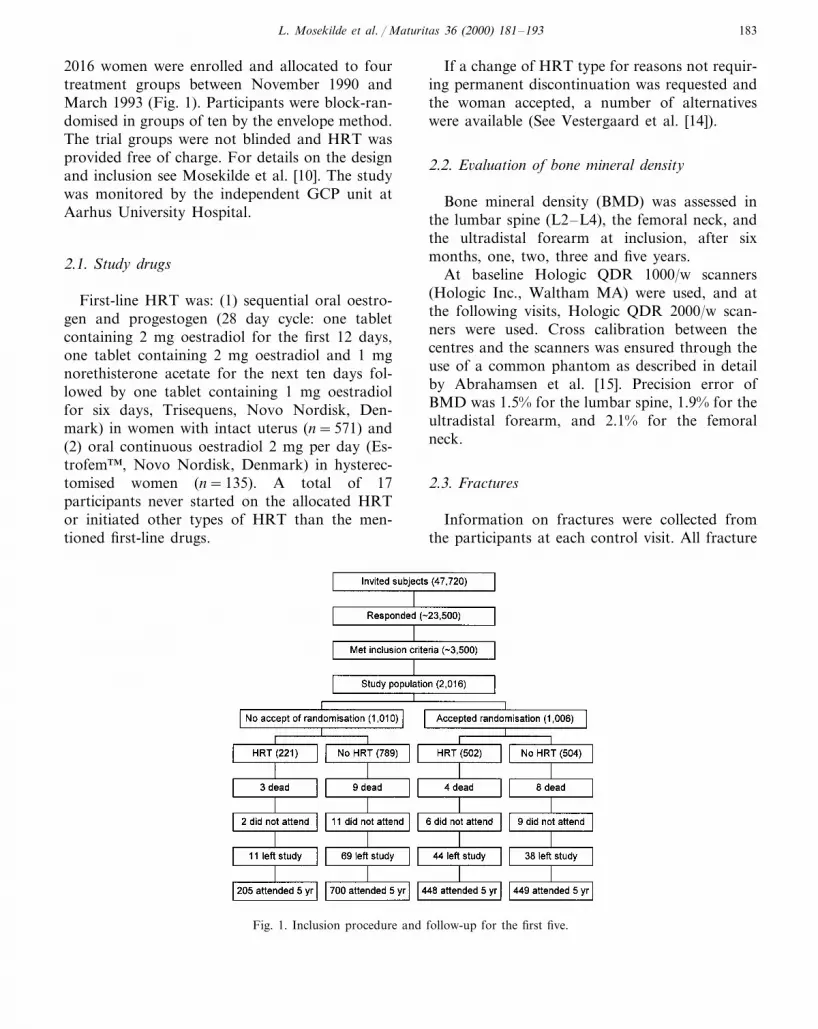
DOPS is an ongoing long-term comprehensivecohort multicentre study of osteoporotic fractureprevention in postmenopausal women through theuse of HRT. The study was approved by theregional ethics committee (no. 1990/1821). Theparticipants were recruited by a short question-naire concerning menopausal status mailed to arandom sample of women 45–58 years old (Fig.1). Women returning the questionnaires, willingto participate and fulfilling the inclusion criteriawere invited to receive further information andclinical examination. Inclusion criteria were: (1)women with an intact uterus aged 45–58 yearsand three–24 months past last menstrual bleedingor experiencing perimenopausal symptoms (in-cluding irregular menstruations) — the lattercombined with elevated serum follicular stimulat-ing hormone (FSH); and (2) hysterectomisedwomen aged 45–52 years and having elevatedFSH. Exclusion criteria were: (1) metabolic bonedisease, including osteoporosis defined as non-traumatic vertebral fractures on X-ray; (2) currentoestrogen use or oestrogen use within the pastthree months; (3) current or past treatment withglucocorticoids \six months; (4) current orpast malignancy; (5) newly diagnosed or uncon-trolled chronic disease; or (6) alcohol or drugaddiction.
After written informed consent (Helsinki II)
L. Mosekilde et al. / Maturitas 36 (2000) 181–193 183
2016 women were enrolled and allocated to fourtreatment groups between November 1990 andMarch 1993 (Fig. 1). Participants were block-ran-domised in groups of ten by the envelope method.The trial groups were not blinded and HRT wasprovided free of charge. For details on the designand inclusion see Mosekilde et al. [10]. The studywas monitored by the independent GCP unit atAarhus University Hospital.
2.1. Study drugs
First-line HRT was: (1) sequential oral oestro-gen and progestogen (28 day cycle: one tabletcontaining 2 mg oestradiol for the first 12 days,one tablet containing 2 mg oestradiol and 1 mgnorethisterone acetate for the next ten days fol-lowed by one tablet containing 1 mg oestradiolfor six days, Trisequens, Novo Nordisk, Den-mark) in women with intact uterus (n=571) and(2) oral continuous oestradiol 2 mg per day (Es-trofem™, Novo Nordisk, Denmark) in hysterec-tomised women (n=135). A total of 17participants never started on the allocated HRTor initiated other types of HRT than the men-tioned first-line drugs.
If a change of HRT type for reasons not requir-ing permanent discontinuation was requested andthe woman accepted, a number of alternativeswere available (See Vestergaard et al. [14]).
2.2. E6aluation of bone mineral density
Bone mineral density (BMD) was assessed inthe lumbar spine (L2–L4), the femoral neck, andthe ultradistal forearm at inclusion, after sixmonths, one, two, three and five years.
At baseline Hologic QDR 1000/w scanners(Hologic Inc., Waltham MA) were used, and atthe following visits, Hologic QDR 2000/w scan-ners were used. Cross calibration between thecentres and the scanners was ensured through theuse of a common phantom as described in detailby Abrahamsen et al. [15]. Precision error ofBMD was 1.5% for the lumbar spine, 1.9% for theultradistal forearm, and 2.1% for the femoralneck.
2.3. Fractures
Information on fractures were collected fromthe participants at each control visit. All fracture
Fig. 1. Inclusion procedure and follow-up for the first five.
L. Mosekilde et al. / Maturitas 36 (2000) 181–193184
reports were verified through files from hospitals,emergency rooms, X-ray departments, generalpractitioners and other relevant sources. Fractureswere defined as definite incident fractures verifiedon X-rays that had occurred no later than thelatest attended control visit.
According to the participants’ accounts and theinformation from files, the fractures were evalu-ated and divided into low energy or high energyfractures by a blinded observer. Low energy frac-tures were fractures occurring after traumas lessor equal to a fall at the same level, while highenergy fractures were fractures following anytraumas with higher energy (e.g. a fall from onelevel to another, automobile accidents etc.).
There were 156 confirmed incident fractures in140 subjects stemming from 153 independent inci-dents (three participants had two simultaneousfractures following high energy traumas). A totalof 127 subjects experienced one fracture, ten hadtwo fractures, and three had three fractures. Therewere 51 verified forearm fractures in 51 women. Afurther 15 fracture reports by the participantscould not be verified (three rib fractures, three toefractures, two vertebral fractures, two finger frac-tures, a fracture of the knee cap, of the orbitalmargin, the upper arm, the elbow, and the coc-cygeal bone). Only the 156 fractures which couldbe verified were included in the analysis.
2.4. X-rays of spine
These were obtained as lateral projections ofthe spine covering Th4 to L5 at inclusion andafter five years. The images were reviewed bytrained radiologists who were blinded to the treat-ment status of the participants. A fracture wasdefined as more than 20% reduction in the heightof a vertebrae compared to the highest verticaldistance of that vertebrae [16].
2.5. Statistical analyses
The effect of HRT was analysed primarily ac-cording to intention-to-treat (all 2016 partici-pants), and secondarily according to unchangedadherence to the initial allocation of HRT or noHRT (causal analysis). The intention-to-treat
analysis included all allocated to HRT includingthe 17 who never initiated HRT.
The observed fracture incidence was comparedto the incidence observed by Tuppurainen et al.[17]. The number of forearm fractures [18], verte-bral fractures [19], and breast cancers [20] werecompared to the expected number in an agematched sample from the general Danishpopulation.
Mean and standard deviations were used fordescriptive statistics. Groups were compared byindependent samples t-test, and Fisher’s exact testwhen appropriate. Incidences were analysed usingMantel–Haenszel type statistics. Kaplan–Meieranalysis and log-rank test were used to test frac-ture-free survival. Multiple comparisons were per-formed using Cox regression. Logistic regressionwas applied in the analysis of spine fractureswhere an exact fracture date was not alwaysknown. A significance level of 0.05 was applied.All calculations were performed using SPSS 6.1.3.
3. Results
Table 1 gives baseline characteristics of the2016 participants. Compliance with HRT duringfollow-up was equal in those randomised to HRTand in those on HRT by their own choice (Fig. 2).Of the 723 initially allocated to HRT, 653 at-tended the five year visit, and of these 395 (60%)were on unchanged HRT, 115 (18%) had changedthe type of HRT (of these 31 had continued HRTwithout interruption), and 143 (22%) had stoppedHRT. Among the 1293 initially allocated to noHRT, 1149 attended the five year visit, and ofthese 977 (85%) had never initiated HRT, whereas169 (15%) had started HRT because of climactericsymptoms or other reasons. Among the lattergroup, 33 (19.5%) had later stopped HRT again,and 65 (38.5%) had changed the type of HRT. Inthree participants (B1%) information on HRTuse was missing.
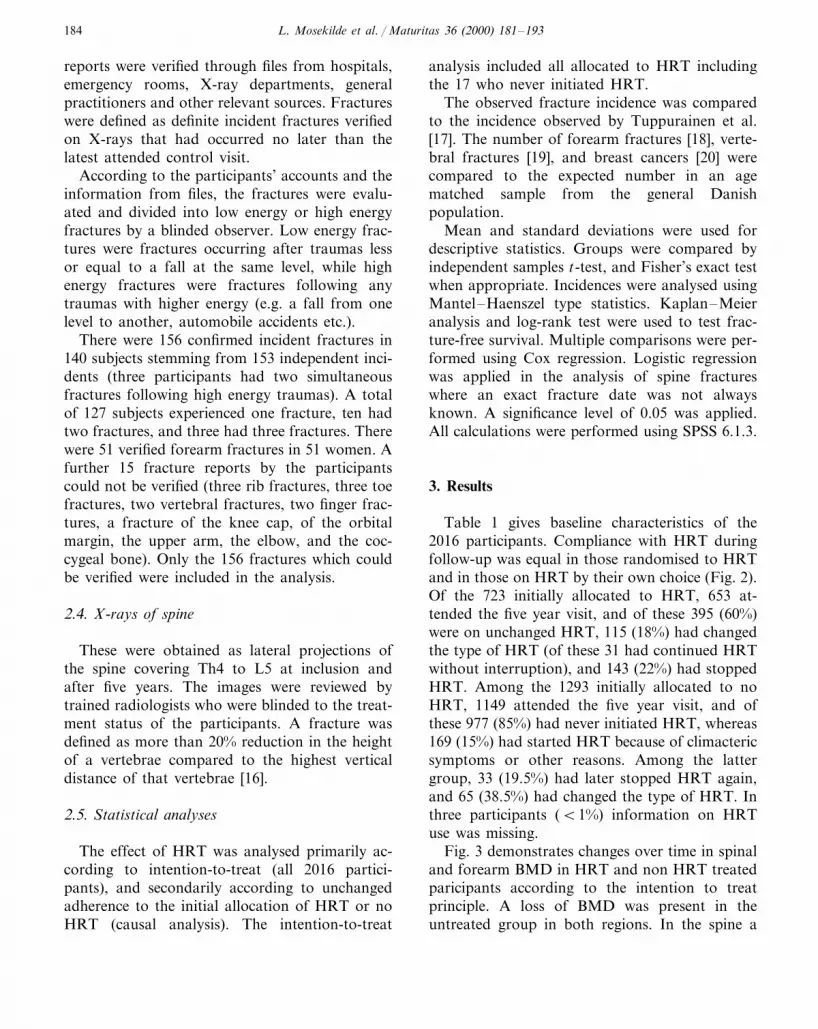
Fig. 3 demonstrates changes over time in spinaland forearm BMD in HRT and non HRT treatedparicipants according to the intention to treatprinciple. A loss of BMD was present in theuntreated group in both regions. In the spine a
L. Mosekilde et al. / Maturitas 36 (2000) 181–193 185
Table 1Baseline characteristics (mean and SD)
Randomised to Randomised to noParameter HRT by own No HRT by own choiceHRT (n=504)HRTa (n=502) choice (n=221) (n=789)
49.592.7*Age (years) 50.092.8* 50.192.6** 50.592.9**68.3911.9Weight (kg) 68.1912.6 64.9910.1** 68.5912.3**
164.596.1 164.695.9164.595.8 164.796.0Height (cm)25.394.3BMI (kg/m2) 25.294.5 23.993.6** 25.394.4**
106 (21%) 51 (23%)**106 (21%) 134 (17%)**Previous fracture107 (21%) 44 (20%)Maternal fracture historyb 152 (19%)95 (19%)8459339 88793348559333 8639341Daily calcium intake (mg)c
3.092.8Daily vitamin D intake (IU)c 3.092.7 2.992.3 3.393.5225 (45%) 102 (46%)**213 (43%) 293 (37%)**Current smokers
95 (19%)Hysterectomised 97 (19%) 40 (18%)** 88 (11%)**0.790.6Time since menopause (years) 0.790.6**0.790.6 0.990.7**
5.894.8 5.994.9 6.295.8Hours of physical activity per 6.195.0week
1.04190.141* 1.01690.127*BMD of lumbar spine (L2–L4, 1.01990.143** 1.03090.144**g/cm2)
0.79390.111BMD of femoral neck (g/cm2) 0.78690.1170.80790.114 0.79890.115BMD of ultradistal forearm 0.39990.051* 0.39190.048* 0.38690.048 0.39190.049
(g/cm2)
a HRT: hormonal replacement therapy.b Maternal fracture of hip or forearm.c From dietary records.* Significant difference between randomised groups (2pB0.05 by independent samples t-test).** Significant difference between non-randomised groups (2pB0.05 by independent samples t-test).
gain in BMD was seen, while a small but statisti-cally significant loss of BMD was seen in theforearm among the HRT treated. In the intention-to-treat analysis, BMD of the hip declined from0.91690.121 to 0.8790.123 g/cm2 (2PB0.01) af-ter five years, whereas it remained stable amongthe treated (0.92090.114 at inclusion and0.91790.118 g/cm2 after five years, 2P=0.20).
Intention-to-treat analysis of the effect of HRTon fracture occurrence is given in Table 2 andTable 3. For most fracture types, the relative risk(RR) of fracture was almost identical for therandomised and the non-randomised arms whencomparing those on HRT initially with those noton HRT. The unadjusted overall fracture risk didnot differ between treatment groups. However,the risk tended to be reduced in the HRT group(RR=0.73, 95% CI: 0.50–1.05, P=0.09) afteradjustment for age and spinal BMD at the studystart (Table 3). The forearm fracture risk wasmarkedly reduced (RR=0.43, 95% CI: 0.22–0.85, P=0.01) in the two treatment groups com-
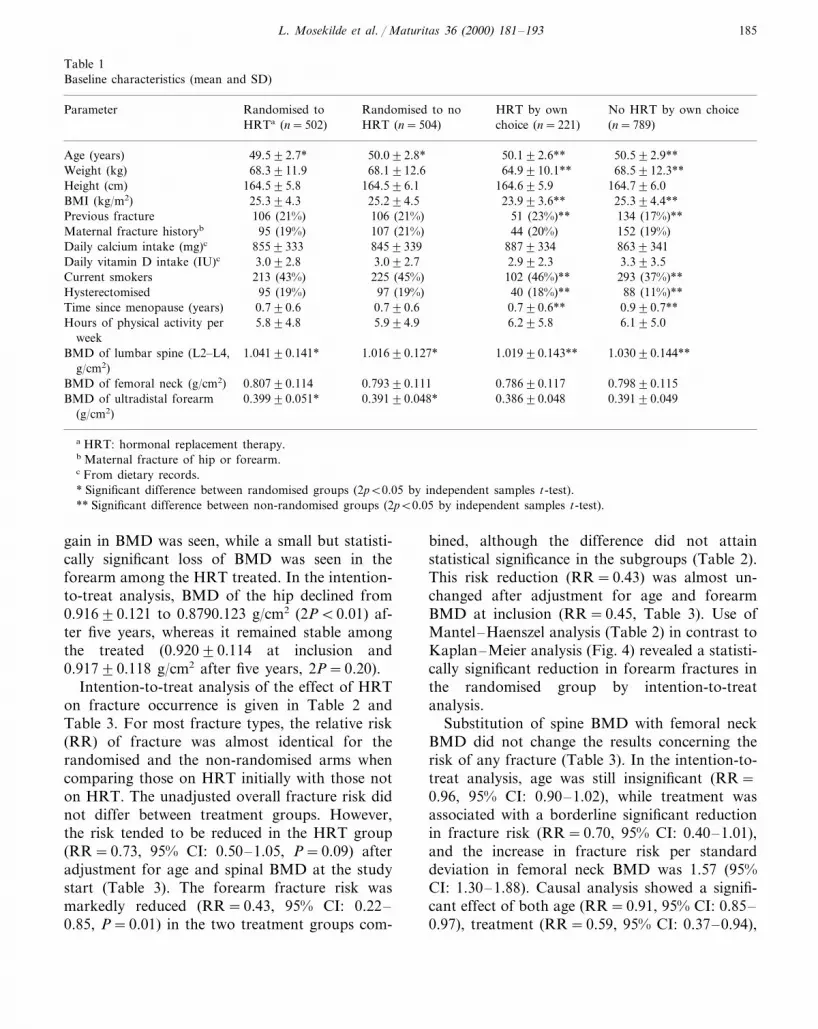
bined, although the difference did not attainstatistical significance in the subgroups (Table 2).This risk reduction (RR=0.43) was almost un-changed after adjustment for age and forearmBMD at inclusion (RR=0.45, Table 3). Use ofMantel–Haenszel analysis (Table 2) in contrast toKaplan–Meier analysis (Fig. 4) revealed a statisti-cally significant reduction in forearm fractures inthe randomised group by intention-to-treatanalysis.
Substitution of spine BMD with femoral neckBMD did not change the results concerning therisk of any fracture (Table 3). In the intention-to-treat analysis, age was still insignificant (RR=0.96, 95% CI: 0.90–1.02), while treatment wasassociated with a borderline significant reductionin fracture risk (RR=0.70, 95% CI: 0.40–1.01),and the increase in fracture risk per standarddeviation in femoral neck BMD was 1.57 (95%CI: 1.30–1.88). Causal analysis showed a signifi-cant effect of both age (RR=0.91, 95% CI: 0.85–0.97), treatment (RR=0.59, 95% CI: 0.37–0.94),

L. Mosekilde et al. / Maturitas 36 (2000) 181–193186
and a significant increase in fracture risk perstandard deviation decrease in femoral neck BMD(RR=1.60, 95% CI: 1.30–1.97).
The risk of spinal deformities or symptomaticspinal fractures did not differ between the treat-ment groups (Table 2 and Table 3). Adjusting forcompliance with HRT reduced the odds ratio(OR) of fracture associated with HRT from 1.80to 0.74 (Table 3). Only three of 26 incident verte-bral fractures presented with symptoms (11.5%,95% CI: 2.4–30.2%).
Causal analysis (Table 3) including only thosewho continued unchanged with their initial HRTor stayed without HRT revealed not only a moremarked reduction in forearm fracture occurrence(RR=0.24, 95% CI: 0.09–0.69) after adjustmentfor age and forearm BMD at inclusion, but also areduction in overall fracture risk (RR=0.61, 95%CI: 0.39–0.97). Analysis of those who were onlycompliant with HRT during part of the follow-uptime yielded risk reduction estimates intermediateto the intention-to-treat and the causal analysis.Adding a term to the Cox regression separatingbetween randomised and non-randomised subjectsdid not change the results concerning the effect ofHRT.
Including a prior fracture as a risk factor in theanalyses in Table 3 did not change the outcomes
Fig. 3. Changes in lumbar spine BMD (L2–L4, g/cm2) inHRT allocated (n=723) and non HRT allocated (n=1293)— intention-to-treat. Figures are mean and one S.E.M.. *denotes a significant difference between treated and untreated(2PB0.05 by independent samples t-test).
concerning the effects of age, BMD and treat-ment. However, any prior fracture from birthuntil time of inclusion was associated with anincreased risk of any incident fracture duringfollow-up, in both the intention-to-treat (RR=1.52, 95% CI: 1.04–2.20) and the causal analysis(RR=1.65, 95% CI: 1.08–2.52).
Neither any prior fracture nor any prior fore-arm fracture was not linked to the risk of anincident forearm fracture during follow-up.
There was no difference between the proportionof low and high energy fractures in the intentionto treat analysis (29% high energy fractures in theHRT treated group vs 26% in the untreatedgroup, 2P=0.90) or the causal analysis (37 vs32%, 2P=0.66). Furthermore, the proportion ofhigh energy fractures was the same at any skeletalsite.
Restricting the analysis to the low energy frac-tures revealed risk reductions with HRT in the
Fig. 2. Compliance with HRT in all participants initiallyallocated to HRT. Compliance was defined as time untilpermanent cessation of any type of HRT, i.e. a change toanother type of HRT was not counted as an event. Nodifference between own choice of HRT and randomisation toHRT (p=0.54 by log-rank test). Due to malfunctioning ofone of the scanners, a participant was first examined aftermore than six years when the scanner was repaired.

L. Mosekilde et al. / Maturitas 36 (2000) 181–193 187
same range as those shown in Table 3 for the totalnumber of fractures, but the power was too lowto demonstrate statistical significance due to thereduced number of end-points.
Stratification of initial BMD into BMD belowmean and above mean revealed a fracture riskreduction of the same magnitude as presented inTable 2 at both high and low BMD values.
The overall number of fractures observed (156)was close to the number of fractures expectedfrom a fracture incidence of 1.7%/year in recentpostmenopausal women (158.6, P=0.84).
Furthermore, there were no differences betweenthe number of observed and expected forearmfractures (51 forearm fractures observed, 46.6 ex-pected, P=0.52), vertebral fractures (three ob-served, 4.7 expected, P=0.44), or breast cancers(18 observed, 20.0 expected, P=0.66).
Table 4 shows the number of serious adverseevents. There was no trend towards an increase inbreast cancers in the treatment groups.
4. Discussion
We have, for the first time in a comprehensivecohort study design, demonstrated a decrease inthe incidence of forearm fractures in recent post-menopausal women allocated to HRT. Further-more, employing a causal analysis withadjustment for age and BMD we have found areduction in overall fracture occurrence in HRTusers.
The observed differences between causal andintention-to-treat analyses with a more markedreduction in fracture risk in those adherent toinitial HRT, illustrates the issue of compliance
Table 2Fracture incidence stratified by treatment group and fracture site (intention to treat)
RR (95% CI)
Fractures Each groupaFracture site Both groupsb
All fracture typesc 0.86 (0.62–1.20)35/43Randomised9HRTd 0.82 (0.53–1.29)
Not randomised9HRT 0.89 (0.51-1.54)16/62Forearms (radius and ulna) 0.43 (0.22–0.85)*Randomised9HRT 6/15 0.40 (0.16–1.01)
0.53 (0.19–1.49)Not randomised9HRT 4/26Spinee
Vertebral fractures with symptoms 3.54 (0.37–33.52)Randomised9HRT –1/0
3.44 (0.25–46.71)1/1Not randomised9HRTAll vertebral fracturesf 1.52 (0.71–3.28)
2.00 (0.62–6.49)Randomised9HRT 8/44/10Not randomised9HRT 1.39 (0.44–4.42)
Femoral neck –1/0Randomised9HRT –
–1/0Not randomised9HRT1.04 (0.70–1.57)Other (clavicles, legs, upper arms, pelvis etc.)
27/28Randomised9HRT 0.96 (0.57–1.64)10/35 1.00 (0.49–2.01)Not randomised9HRT
a Unadjusted RR for HRT vs no HRT in randomised and non randomised separately, intention-to-treat.b Unadjusted RR, all HRT allocated (n=723) vs all non HRT allocated (n=1293), intention-to-treat.c Excluding symptomless vertebral fractures.d HRT: hormonal replacement therapy.e Counted as number of subjects with at least one incident spine fracture (th4–L5).f i.e. also fractures identified by the radiologist without the participant reporting symptoms.* pB0.05 by Mantel–Haenszel x2 test.
L. Mosekilde et al. / Maturitas 36 (2000) 181–193188
Table 3Factors of significance to fracture occurrence: risk estimates and 95% CI
ForearmsaParameter Spineb All fracturesc
Intention-to-treat (all participants)Age at inclusion (years) 1.16 (1.01–1.33)*0.97 (0.88–1.07) 0.95 (0.90–1.01)
1.85 (1.21–2.82)* 1.47 (1.23–1.76)*BMD (g/cm2)d 2.24 (1.69–2.97)*1.80 (0.81–3.96) 0.73 (0.50–1.05)0.45 (0.22–0.90)*Treatment (HRT vs no HRT)e
Causal f
1.11 (0.93–1.33)0.91 (0.82–1.02) 0.91 (0.85–0.98)*Age at inclusion (years)2.24 (1.63–3.08)*BMD (g/cm2)d 1.61 (0.94–2.77) 1.41 (1.15–1.72)*
0.74 (0.20–2.70)0.24 (0.09–0.69)* 0.61 (0.39–0.97)*Treatment (HRT vs no HRT)f
a Cox regression, all independent variables entered, BMD of ultradistal forearm. Adjusted RR and 95% confidence limits.b Logistic regression of all incident vertebral fractures (including symptomless ones), all independent variables entered, BMD of
lumbar spine (L2–L4). Adjusted OR and 95% confidence limits. The dependent variable was occurrence of at least one incidentvertebral fracture vs no vertebral fractures from baseline to the five year follow-up visit.
c Cox regression with all independent variables entered. All fractures excluding symptomless vertebral fractures, BMD of lumbarspine (L2–L4). Adjusted RR and 95% confidence limits.
d Increase in fracture risk per one standard deviation decrease in BMD in actual region.e Intention to treat (all 2016 participants).f Comparison of the 395 who continued unchanged with the same HRT type vs the 977 who never received HRT during the five
year follow-up.* PB0.05.
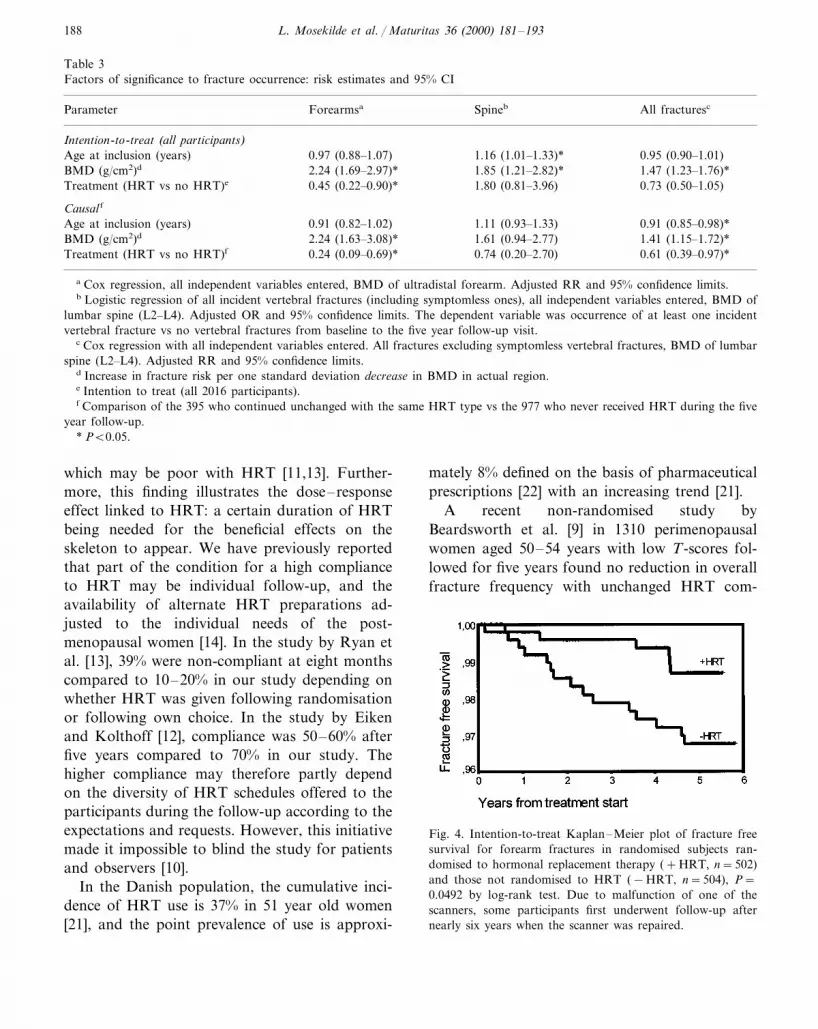
which may be poor with HRT [11,13]. Further-more, this finding illustrates the dose–responseeffect linked to HRT: a certain duration of HRTbeing needed for the beneficial effects on theskeleton to appear. We have previously reportedthat part of the condition for a high complianceto HRT may be individual follow-up, and theavailability of alternate HRT preparations ad-justed to the individual needs of the post-menopausal women [14]. In the study by Ryan etal. [13], 39% were non-compliant at eight monthscompared to 10–20% in our study depending onwhether HRT was given following randomisationor following own choice. In the study by Eikenand Kolthoff [12], compliance was 50–60% afterfive years compared to 70% in our study. Thehigher compliance may therefore partly dependon the diversity of HRT schedules offered to theparticipants during the follow-up according to theexpectations and requests. However, this initiativemade it impossible to blind the study for patientsand observers [10].
In the Danish population, the cumulative inci-dence of HRT use is 37% in 51 year old women[21], and the point prevalence of use is approxi-
mately 8% defined on the basis of pharmaceuticalprescriptions [22] with an increasing trend [21].
A recent non-randomised study byBeardsworth et al. [9] in 1310 perimenopausalwomen aged 50–54 years with low T-scores fol-lowed for five years found no reduction in overallfracture frequency with unchanged HRT com-
Fig. 4. Intention-to-treat Kaplan–Meier plot of fracture freesurvival for forearm fractures in randomised subjects ran-domised to hormonal replacement therapy (+HRT, n=502)and those not randomised to HRT (−HRT, n=504), P=0.0492 by log-rank test. Due to malfunction of one of thescanners, some participants first underwent follow-up afternearly six years when the scanner was repaired.

L. Mosekilde et al. / Maturitas 36 (2000) 181–193 189
Table 4Serious adverse events
Number RR (95% CI)
Serious adverse eventa Each groupb Both groupsc
Breast cancerd 0.68 (0.24–1.90)0.40 (0.08–1.98)2/5Randomised9HRTe
3/8Not randomised9HRT 1.29 (0.34–4.85)Other cancersf 1.18 (0.42–3.31)
1.52 (0.26–8.97)3/2Randomised9HRTNot randomised9HRT 3/7 1.47 (0.38–5.65)
1.01 (0.30–3.46)Cardiovascular incidents2/3Randomised9HRT 0.67 (0.11–3.99)2/4Not randomised9HRT 1.72 (0.32–9.20)
0.51 (0.11–2.36)Cerebrovascular incidents0.00 (–)Randomised9HRT 0/21.38 (0.27–7.04)2/5Not randomised9HRT
Hysterectomiesg 1.39 (0.70–2.75)10/6Randomised9HRT 1.69 (0.62–4.59)
1.16 (0.38–3.56)4/13Not randomised9HRTCholecystectomies 1.62 (0.72–3.65)
1.42 (0.45–4.44)7/5Randomised9HRT4/7Not randomised9HRT 1.97 (0.59–6.56)
Hyperthyroidism 0.97 (0.36–2.61)0.20 (0.03–1.50)1/5Randomised9HRT
5/6Not randomised9HRT 2.87 (0.92–8.91)Diabetesh 1.77 (0.52–6.01)
4.05 (0.54–30.60)4/1Randomised9HRT1/4Not randomised9HRT 0.86 (0.10–7.68)
Lung diseases 0.85 (0.45–1.62)0.88 (0.42–1.84)13/15Randomised9HRT
1/14Not randomised9HRT 0.24 (0.04–1.60)1.05 (0.68–1.62)Arthritis and joint diseasesi
26/28Randomised9HRT 0.94 (0.55–1.60)Not randomised9HRT 0.79 (0.30–1.93)6/26
a There were no reports of venous thromboembolism.b Unadjusted RR for HRT vs no HRT in randomised and non randomised separately, intention-to-treat.c Unadjusted RR, All HRT allocated vs all non HRT allocated, intention-to-treat.d All participants were offered a mammography at the five year visit.e HRT: hormonal replacement therapy.f Two of these were cancers of the endometrium, both in non HRT treated, two were cancers of the ovaries (one in a HRT treated,
and one in a non HRT treated subject)g RR calculated for the proportion of participants with intact uterus at baseline.h All new cases were non-insulin dependent.i Including rheumatoid arthritis and collagenoses; PB0.05 by Mantel-Haenszel x2 test.
pared to no HRT [9]. In contrast to these investi-gators, we found a reduction in overall fractureincidence when comparing those that continuedthe same HRT regimen to those who never tookHRT. However, on intention-to-treat analysis wedid not find a statistically significant reduction inoverall fracture incidence.
Komulainen et al. [8] did a randomised studycomparing four study groups of recent post-menopausal women (HRT; n=116; HRT+vita-min D supplementation, n=116; vitamin Dsupplementation, n=116; placebo, n=116). Af-ter adjustment for baseline femoral neck BMDthey found a significant reduction in non-vertebral

L. Mosekilde et al. / Maturitas 36 (2000) 181–193190
fractures after five years when comparing the jointHRT and HRT+vitamin D groups (n=232)with the placebo group (RR=0.44, 95% CI:0.21–0.93). Compliance with HRT was compara-ble to our study group (64% compliant after 5years [8]), but the risk reduction was higher.
It should be noted that the risk reduction wassimilar in both the randomised and the non-ran-domised group in our study (Table 2), indicatingthat in this setting randomisation did not alter theobserved risk reduction, i.e. this risk reductionmay with a high degree of probability be applieddirectly to the general population.
At baseline low T-score was neither a criterionfor entrance into the study, nor a criterion fortreatment with HRT, as the study was designed toevaluate the primary preventive effect of the deci-sion to initiate HRT. As the women in the actualage group have a low fracture risk [1,17,18], it isinteresting that it was possible to obtain a markedreduction in the risk of forearm fractures, and aborderline significant reduction in overall fracturerisk, demonstrating that when taken, HRT has arelatively strong antifracture potential even at ahigh bone density.
Although not all women may have been post-menopausal according to strict definitions [23],the short time interval from cessation of menstru-ations to inclusion in the study ensured that anyaccelerated perimenopausal bone loss was pre-vented [24] and thus a preservation of as much aspossible of the peak bone mass.
The decrease in femoral neck BMD amongthose allocated to HRT is in contrast to theresults of the PEPI trial [3], where an increase inhip of 1.7% was seen after three years among thetreated. However, the absolute difference betweenhip BMD in the treated and untreated was thesame in the PEPI trial after three years (approxi-mately 3.5%) [3] as in our study (3.2%). Theparticipants in the PEPI trial [3] were older thanthe participants in our study (mean 56 vs 50years), and longer after menopause (\1 year). Itmay, therefore, simply be that in our study theHRT treated participants maintained their peakbone mass (treatment was initiated before theaccelerated bone loss in menopause) while theHRT treated participants in the PEPI trial re-
gained already lost BMD because the HRT nor-malised the increased bone turnover.
The inclusion of the participants close tomenopause and thus to peak bone mass mayexplain some of the effect seen in this study: theearly initiation of HRT maintained a relativelyhigh BMD level as the accelerated post-menopausal bone loss was avoided.
We observed a pronounced reduction in fore-arm fractures, but not in spine fractures, despitethe observation that the difference in forearmBMD was only 5% between those on intention totreat and those on intention not to treat versus adifference of 8% in lumbar spine BMD. Thisdiscrepancy between response in forearm BMDand fracture reduction has also been observedwith other treatment schedules, e.g. the bisphos-phonates [16], and may be related to structuralchanges in trabecular bone or perhaps a reducedtendency to falls, for example [25].
The absence of a difference in fracture energiesbetween those on HRT and those not on HRTmay have several reasons: (1) the differences inBMD were too small in this narrow time span todetect any difference in fracture energies, but onlyin fracture occurrence or not; or (2) the number offall episodes and thus fracture producing traumaswere smaller in the HRT treated than in thenon-HRT treated. Unfortunately we did not havedata to support the latter hypothesis. Long-termfollow-up will have to determine whether a differ-ence in fracture energies emerges and the cause ofany such difference.
Tuppurainen et al. [17] found that overall frac-ture risk increased from 1.2% per year in pre-menopausal women less than 2.5 years beforemenopause, to 1.7% per year in women less than2.5 years after menopause. With a 100% compli-ance with HRT, we found a risk reduction of 39%(RR=0.61). It may thus be hypothesised that thelarger part of the increase in fractures aftermenopause is potentially reversible through theuse of HRT (0.61×1.7=1.04, which is close tothe rate observed by Tuppurainen et al. [17] be-fore the menopause). However, due to the sideeffects of HRT (bleeding disturbances etc.) a re-duction in fractures of this magnitude may not beachievable [11]. A further concern is the potential

L. Mosekilde et al. / Maturitas 36 (2000) 181–193 191
risk of breast cancer with prolonged use of HRT[26], although the reduction in cardiovascularevents following postmenopausal oestrogen use[27] may result in a reduced overall mortality inusers of HRT [6,28].
The number of serious adverse events in ourstudy was too small to draw definite conclusions.However, there was no trend towards an increasein the number of breast cancers, but previousstudies have suggested that such an increasewould first be expected after more than five yearsof HRT [26].
As no deviations between the observed andexpected number of fractures and breast cancerswere found, it seems that our study group wasrepresentative of the general population.
Previous observational studies have indicatedthat HRT may be beneficial in reducing the num-ber of cardiovascular events [6,27]. In our study,the participants were relatively close tomenopause and the incidence of cardiovascularevents thus too small to detect any positive oradverse effects of HRT, although there was atrend towards more cardiovascular events in thenon-randomised subjects allocated to HRT. Ourstudy may thus only during the long-term follow-up potentially contribute to the ongoing discus-sion that the reduction in cardiovascular risk seenwith HRT in observational studies may be due toselection bias — HRT users perhaps being‘‘healthier’’ than non-users [27]. The trend to-wards an excess risk of cardiovascular events inthe non-randomised group must at present beinterpreted with caution.
The subjects randomised to no HRT were alittle older than those randomised to HRT, andconsequently also had a little lower BMD. Athorough investigation revealed that inclusioncriteria had been followed and that the most likelyexplanation for the difference was a chance find-ing. The differences in forearm BMD did notseem to bias the results concerning the effect ofHRT, the fracture risk reduction with HRT in theforearms being almost unchanged after adjust-ment for BMD. However, as mentioned there wasan interaction between BMD, cessation of HRTand fractures in the spine, a discontinuation ofHRT being associated with a higher likelihood of
fracture. This may potentially be the effect of anaccelerated bone loss in a high turnover area suchas the spine following discontinuation of HRT.
The relative risks of fracture associated withdecreasing BMD were close to those observed byMarshall et al. [29].
Only a minor percentage of vertebral fracturespresented with symptoms (approximately 11%).This finding is partly in accordance with Black etal. [16] who found that approximately 50% ofincident vertebral fractures in women aged 65+years were without symptoms. The decline in ORof fracture associated with HRT from 1.80 in theintention to treat analysis to 0.74 in the causalanalysis probably represents a marked interactionbetween BMD, HRT and fracture risk: those whostopped HRT had an increase in risk of fracturesof the spine.
Our group was much younger than the studygroup of Black et al. [16] and it may be hypothe-sised that non-traumatic vertebral fractures areless likely to present with symptoms in youngerage groups or that the higher number of fallepisodes in older subjects leads to detection offractures who would otherwise have been un-recognised, whereby these fractures becomeclassified as fractures with symptoms. The lack ofan effect of HRT on fracture occurrence in thespine may be due to the low total number offractures with symptoms in this age group.
In conclusion it seems possible to reduce thenumber of forearm fractures and possibly thetotal number of fractures in recent post-menopausal women by the use of HRT as pri-mary prevention.
Acknowledgements
The participants are acknowledged for theirparticipation. Mrs Britta Malm, Ms Ilse Ras-mussen, Mrs Donna Lund, Mrs Birthe Weinell,Mrs Lisbeth Flyvbjerg, Mrs Liselotte Stenkjær,Mrs Kirsten Westermann, Mrs Else Rettmer, MrsAnne Mette Rasmussen, Mrs Zanne Henriksen,Mrs Hanne Kobbernagel, Mrs Elisabeth Stark,Mr Olaf Barenholdt, and Mr Jorg Andresen MDare acknowledged for skilful technical assistance.

L. Mosekilde et al. / Maturitas 36 (2000) 181–193192
Contributors: Leif Mosekilde MD DMSc de-signed the study and was principal investigator.Henning Beck Nielsen MD DMSc, Ole HelmerSørensen MD DMSc, Stig Pors Nielsen MDDMSc, and Peder Charles MD DMSc were co-principal investigators. Peter Vestergaard MDPhD was study investigator, performed the statis-tical analysis, and drafted the paper. Study inves-tigators who all contributed to the writingprocess: Aarhus: Anne Pernille Hermann MDPhD, Odense: Jeppe Gram MD PhD, Tony BillHansen MD PhD, Bo Abrahamsen MD PhD,Ebbe Nils Ebbesen MD PhD, Lis Stilgren MD,Copenhagen: Lars Bjørn Jensen MD PhD,Christine Brot MD PhD, Birgitte Hansen MD,Charlotte Landbo Tofteng MD, Hillerød: PiaEiken MD PhD, Niels Kolthoff MD PhD. Finan-cial support: The study was made possiblethrough financial support by Karen Elise Jensen’sFoundation and the Danish Medical ResearchCouncil. Novo Nordisk Denmark, Novartis Den-mark, and Leo Denmark provided the study med-ication free of charge.
References
[1] Assessment of fracture risk and its application to screen-ing for postmenopausal osteoporosis: report of a WHOStudy Group. Geneva: WHO Technical Report Series843, 1994.
[2] Christiansen C, Christensen MS, Transbøl I. Bone massin postmenopausal women after withdrawal of oestrogen/gestagen replacement therapy. Lancet 1981;i:459–61.
[3] Effects of hormone therapy on bone mineral density:results from the postmenopausal estrogen/progestin inter-ventions (PEPI) trial. J.A.M.A. 1996; 276: 1389-96.
[4] Kiel DP, Felson DT, Anderson JJ, Wilson PWF,Moskowitz MA. Hip fracture and the use of estrogens inpostmenopausal women: the Framingham study. NewEngl J Med 1987;317:1169–74.
[5] Maxim P, Ettinger B, Spitalny GM. Fracture protectionprovided by long-term estrogen treatment. Osteoporos Int1995;5:23–9.
[6] Grady D, Rubin SM, Petitti DB, et al. Hormone therapyto prevent disease and prolong life in postmenopausalwomen. Ann Int Med 1992;117:1016–37.
[7] Lufkin EG, Wahner HW, O’Fallon WM, et al. Treatmentof postmenopausal osteoporosis with transdermal estro-gen. Ann Intern Med 1992;117:1–9.
[8] Komulainen MH, Kroger H, Tuppurainen MT, et al.HRT and Vit D in prevention of non-vertebral fractures
in postmenopausal women: a 5 year randomized trial.Maturitas 1998;31:45–54.
[9] Beardsworth SA, Kearney CE, Steel SA, Purdie DW. Afive year prospective study of BMD and fracture risk inHRT treated and untreated perimenopausal women. Cal-cif Tissue Int [Abstract] 1999;64 Suppl. 1:S43.
[10] Mosekilde L, Hermann AP, Beck-Nielsen H, Charles P,Nielsen SP, Sorensen OH. The Danish Osteoporosis Pre-vention Study (DOPS): Project design and inclusion of2016 normal perimenopausal women. Maturitas1999;31:207–19.
[11] Coope J, Marsh J. Can we improve compliance withlong-term HRT? Maturitas 1992;15:151–8.
[12] Eiken P, Kolthoff N. Compliance with long-term oralhormonal replacement therapy. Maturitas 1995;22:97–103.
[13] Ryan PJ, Harrison R, Blake GM, Fogelman I. Compli-ance with hormone replacement therapy (HRT) afterscreening for post menopausal osteoporosis. Br J ObstetGynaecol 1992;99:325–8.
[14] Vestergaard P, Hermann AP, Gram J, et al. Improvingcompliance with hormonal replacement therapy in pri-mary osteoporosis prevention. Maturitas 1997;28:137–45.
[15] Abrahamsen B, Gram J, Hansen TB, Beck-Nielsen H.Cross-calibration of QDR-2000 and QDR-1000 dual en-ergy X-ray densitometers for bone mineral and soft tissuemeasurements. Bone 1995;16:385–91.
[16] Black DM, Cummings SR, Karpf DB, et al. Randomisedtrial of the effect of alendronate on risk of fracture inwomen with existing vertebral fractures. Lancet1996;348:1535–41.
[17] Tuppurainen M, Honkanen R, Kroger H, Saarikoski S,Alhava E. Osteoporosis risk factors, gynaecological his-tory and fractures in perimenopausal women-the resultsof the baseline postal enquiry of the Kuopio OsteoporosisRisk Factor and Prevention Study. Maturitas1993;17:89–100.
[18] Solgaard S, Petersen VS. Epidemiology of distal radiusfractures. Acta Orthop Scand 1985;56:391–3.
[19] [Pattern of diseases in hospitalised patients and outpa-tients 1995 — Healthstatistics 1997:5]. Copenhagen: Na-tional Board of Health, 1997.
[20] Ankjaer-Jensen A, Johnell O. Prevention of osteoporosis:cost-effectiveness of different pharmaceutical treatments.Osteoporosis Int 1996;6:265–75.
[21] Køster A. Hormone replacement therapy: use patterns in51-year-old Danish Women. Maturitas 1990;12:345–56.
[22] Juul S, Sabroe S, Hansen EH. Det Danske Sund-hedsvæsen. Copenhagen: Fadl’s Forlag, 1989.
[23] Greendale GA, Lee NP, Arriola ER. The menopause.Lancet 1999;353:571–80.
[24] Riggs BL, Wahner HW, Melton LJ, III, Richelson LS,Judd HL, Offord KP. Rates of bone loss in the appendic-ular and axial skeletons of women: evidence of substantialvertebral bone loss before menopause. J Clin Invest1986;77:1487–91.

L. Mosekilde et al. / Maturitas 36 (2000) 181–193 193
[25] Torgerson DJ, Garton MJ, Reid DM. Falling and peri-menopausal women. Age Ageing 1993;22:59–64.
[26] Colditz GA, Hankinson SE, Hunter DJ, et al. The use ofestrogens and progestins and the risk of breast cancer inpostmenopausal women. New Engl J Med 1995;332:1589–93.
[27] Grodstein F, Stampfer MJ, Manson JE, et al. Post-menopausal estrogen and progestin use and the risk of
cardiovascular disease. New Engl J Med 1996;335:453–61.[28] Gorsky RD, Koplan JP, Peterson HB, Thacker SB. Rela-
tive risks and benefits of long-term estrogen replacementtherapy: a decision analysis. Obstet Gynecol 1994;83:161–6.
[29] Marshall D, Johnell O, Wedel H. Meta-analysis of how wellmeasures of bone mineral density predict occurrence ofosteoporotic fractures. BMJ 1996;312:1254–9.
.